UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
_______________
Form 10-K
_______________
|
|
| (Mark One) |
☑þ
| ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the Fiscal Year Ended December 31, 20172021
or
|
|
☐¨
| TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from _____ to _____
Commission File Number: 000-29959
Pain Therapeutics, CassavaSciences,Inc.
(Exact name of registrant as specified in its charter)
|
|
Delaware | 91-1911336 |
(State or other jurisdiction of | (I.R.S. Employer |
incorporation or organization) | Identification Number) |
7801 N. Capital of Texas Highway, Suite 260, Austin, TX 78731
(512) 501-2444
(Address, including zip code, of registrant's principal executive offices and
telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act: Common Stock, $0.001 par value
0 |
|
|
|
|
Title of each class |
| Trading Symbol(s) |
| Name of each exchange on which registered |
Common Stock, $0.001 par value |
| SAVA |
| NASDAQ Capital Market |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐þ No ☑¨
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐¨ No ☑þ
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☑þ No ☐¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☑þ No ☐.¨.
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act..Act. (Check one):
|
|
Large accelerated filer ☐þ | Accelerated filer ☐¨ |
Non-accelerated filer ☐¨ | Smaller reporting company ☑þ |
(Do not check if a smaller reporting company)
| Emerging growth company ☐¨ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐¨
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 USC. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. þ
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐¨ No ☑þ
The aggregate market value of the voting and non-voting common equity held by non-affiliates was $22,840,436approximately $3.2 billion computed by reference to the last sales price of $4.15$85.44 as reported on the Nasdaq Global SelectCapital Market, as of the last business day of the Registrant's most recently completed second fiscal quarter, June 30, 2017.2021. The number of shares outstanding of the Registrant's common stock, par value $0.001 per share, on January 19, 2018February 24, 2022 was 6,595,509, as adjusted to reflect a ratio of 7-for-1 reverse stock split effective May 10, 2017.40,016,792.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the Registrant's Proxy Statementproxy statement for its 20182022 Annual Meeting of Stockholders (the "Proxy Statement"“Proxy Statement”), to be filed with the U.S. Securities and Exchange Commission, no later than 120 days after the Registrant’s fiscal year ended December 31, 2021, are incorporated by reference to Part III of this Annual Report on Form 10-K Report.
10-K.
PAIN THERAPEUTICS,CASSAVA SCIENCES, INC.
FORM 10-K
INDEX
Signatures
PART I
FORWARD-LOOKING STATEMENTS
This annual report contains certain statements that are consideredAnnual Report on Form 10-K and the documents incorporated by reference contain forward-looking statements within the meaning of the Private Securities Reform Act of 1995. All statements other than statements of historical facts contained in this Annual Report are forward-looking statements. We intend that such statements be protected by the safe harbor created thereby. Forward-looking statements relate to expectations, beliefs, projections, future plans and strategies, anticipated events or trends and similar expressions concerning matters that are not historical facts. In some cases, you can identify forward-looking statements by terms such as “anticipate,” “believe,” “could,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “should,” “will” and “would” or the negatives of these terms or other comparable terminology.
The forward-looking statements are based on our beliefs, assumptions and expectations of our future performance, taking into account all information currently available to us. Forward-looking statements involve risks and uncertainties and our actual results and the timing of events may differ significantly from the results discussed in the forward-looking statements. Such forward-looking statements and our business are subject to numerous risks and uncertainties that you should consider before investing in our Company. These risks are described more fully in the section titled “Risk Factors.” Accordingly, you should not rely upon forward-looking statements as predictions of future events. Examples of such forward-looking statements include, but are not limited to statements about:
the number of patients with Alzheimer’s disease we expect to enroll in our on-going Phase 3 studies, the enrollment rates for and the length of time to complete our studies, the geographic areas for patient enrollment, and the expected safety profile or treatment benefits of simufilam for people with Alzheimer’s disease; our reliance on third-party contractors to conduct the clinical trials and make drug supply on a large-scale for our Phase 3 clinical program, or their ability to do so on-time or on-budget; limitations around the interpretation of improvements in cognition scores observed in interim analyses in our long-term open-label study, as compared to efficacy results from a fully completed, randomized controlled study design; the ability of clinical scales to assess cognition or health in our trials of Alzheimer’s disease; announcements or plans regarding any future interim analyses of our open-label study of simufilam and our estimated timeline for doing so; any significant changes we may make, or anticipate making, to the design of any of our on-going studies of simufilam in patients with Alzheimer’s disease; our ability to initiate, conduct or analyze additional clinical and non-clinical studies with our product candidates targeted at Alzheimer’s disease and other neurodegenerative diseases; the interpretation of results from our early clinical studies, such as Phase 1 and Phase 2 studies; our plans to further develop SavaDx, our investigational blood-based diagnostic, and to evaluate a non-antibody approach for SavaDx; our ability or willingness to expand therapeutic indications for simufilam outside of Alzheimer’s disease the safety, efficacy, or potential therapeutic benefits of our product candidates; the utility of protection, or the sufficiency, of our intellectual property; our potential competitors or competitive products; expected future sources of revenue and capital and increasing cash needs; our use of a Clinical Research Organization (CRO) to conduct clinical studies of our lead product candidate; expectations regarding trade secrets, technological innovations, licensing agreements and outsourcing of certain business functions; our expenses increasing or fluctuations in our financial or operating results; our operating losses, anticipated operating and capital expenditures and legal expenses;; expectations regarding the issuance of shares of common stock to employees pursuant to equity compensation awards, net of employment taxes; the development and maintenance of our internal information systems and infrastructure; our need to hire additional personnel and our ability to attract and retain such personnel; existing regulations and regulatory developments in the United States and other jurisdictions in which we operate; our plans to expand the size and scope of our operations and physical facilities; the sufficiency of our current resources to continue to fund our operations; | ·
| | The timing and topics of discussions with the U.S. Food and Drug Administration, or FDA, regarding the New Drug Application, or NDA, for REMOXY® ER (oxycodone capsules CII), or REMOXY;
|
| ·
| | the timing of the planned resubmission of the NDA for REMOXY;
|
| ·
| | the ability of REMOXY to capture a share of the market for extended release opioid drugs;
|
| ·
| | the status of products and potential products which are competitive with REMOXY and the implications of the FDA requirements for approval of such competitive products;
|
| ·
| | our plans to rely on third parties, including Durect Corporation, or Durect, and Noramco, Inc., or Noramco, to supply us with excipients and active pharmaceutical ingredients and to manufacture REMOXY;
|
| ·
| | discussions with potential strategic partners for the development and commercialization of REMOXY;
|
| ·
| | the outcome of research and development activities, including, without limitation, development activities for FENROCK™ and potential formulation of additional dosage forms of our drug candidates;
|
| ·
| | the potential benefits of our product candidates such as REMOXY, FENROCK, PTI-125 or PTI-125DX including the potential ability of PTI-125 to prevent or reverse amyloid-related Alzheimer’s damage or PTI-125DX to diagnose Alzheimer’s disease;
|
| ·
| | the utility of protection of our intellectual property;
|
| ·
| | expected future sources of revenue and capital and increasing cash needs;
|
| ·
| | potential competitors or competitive products;
|
| ·
| | market acceptance of our drug candidates and potential drug candidates;
|
| ·
| | expectations regarding trade secrets, technological innovations, licensing agreements and outsourcing of certain business functions;
|
| ·
| | expenses increasing, interest income decreasing or fluctuations in our operating results;
|
| ·
| | operating losses and anticipated operating and capital expenditures;
|
| ·
| | expected uses of capital resources;
|
| ·
| | expectations regarding the issuance of shares of common stock to employees pursuant to equity compensation awards net of employment taxes;
|
| ·
| | anticipated hiring and development of our internal systems and infrastructure;
|
| ·
| | the sufficiency of our current resources to fund our operations over the next twelve months; and
|
| ·
| | assumptions and estimates used for our disclosures regarding stock-based compensation.
|
Such
the accuracy of our estimates regarding expenses, capital requirements, and needs for additional financing;
assumptions and estimates used for our disclosures regarding stock-based compensation;
the expense, timing and outcome of pending or future litigation or other legal proceedings and claims, including U.S. government inquiries;
litigation, claims or other uncertainties that may arise from allegations made against us or our collaborators; and
the impact of COVID-19, a novel coronavirus first detected in 2019, on our operations and financial condition.
Drug development and commercialization involve a high degree of risk, and only a small number of research and development programs result in regulatory approval and subsequent commercialization of a product. Our clinical results from earlier-stage clinical trials may not be indicative of full results or results from later-stage or larger scale clinical trials and do not ensure regulatory approval. You should not place undue reliance on these statements or any scientific data we present or publish.
We cannot assure you that we will realize the results or developments we expect or anticipate or, even if substantially realized, that they will result in the consequences or affect us or our operations in the way we expect. The forward-looking statements involve risks and uncertainties, including, but not limited to, those risks and uncertainties relating to:
| ·
| | difficulties or delays in the preparation and filing of the NDA for REMOXY and in potentially obtaining regulatory approval of the NDA for REMOXY, including the potential for requests by the FDA for additional data which may require an extended period of time to obtain and submit;
|
| ·
| | unexpected adverse side effects or inadequate therapeutic efficacy or manufacturing or stability issue of our drug candidates that could slow or prevent product approval (including the risk that current and past results of clinical trials are not indicative of future results of clinical trials) or potential post-approval market acceptance;
|
| ·
| | having or obtaining sufficient resources for the successful development, manufacture and commercialization of REMOXY;
|
| ·
| | the quantity, quality or sufficiency of the data, materials and information transferred to us by Pfizer, Inc., or Pfizer regarding the REMOXY development program;
|
| ·
| | discussions with potential strategic partners for the development and commercialization of REMOXY;
|
| ·
| | the successful development of other drug candidates, independently as well as pursuant to our other collaboration agreements, and the continuation of such agreements;
|
| ·
| | difficulties or delays in development, testing, clinical trials (including patient enrollment), regulatory authorization or approval, production and commercialization of our drug candidates;
|
| ·
| | the uncertainty of protection of our intellectual property rights or trade secrets;
|
| ·
| | potential infringement of the intellectual property rights of third parties;
|
| ·
| | pursuing in-license and acquisition opportunities;
|
| ·
| | maintenance or third party funding of our collaboration and license agreements;
|
| ·
| | legislation or regulatory actions affecting product pricing, reimbursement or access;
|
| ·
| | significant breakdown or interruption of our information technology and infrastructure;
|
| ·
| | significant issues that may arise related to outsourcing certain preclinical studies, clinical trials and formation and manufacturing activities;
|
| ·
| | hiring and retaining personnel; and
|
| ·
| | our financial position and our ability to obtain additional financing if necessary.
|
In addition, such statements are subject to the risks and uncertainties discussed in the "Risk Factors" section and elsewhere in this document.
All informationincluded in this Annual Report on Form 10-K has been retroactively adjustedare made only as of the date hereof. We undertake no obligation to reflect the ratiopublicly update or revise any forward-looking statement as a result of a 7-for-1 reverse stock split that took effect on May 10, 2017,new information, future events or otherwise, except as otherwise described or as required by law. See “Part II-Item 1 Management’s Discussion
In addition, statements that “we believe” and Analysissimilar statements reflect our beliefs and opinions on the relevant subject. These statements are based upon information available to us as of Financial Conditionthe date of this report, and Resultswhile we believe such information forms a reasonable basis for such statements, such information may be limited or incomplete, and our statements should not be read to indicate that we have conducted an exhaustive inquiry into, or review of, Operations-Recent developmentsall potentially available relevant information. These statements are inherently uncertain and you are cautioned not to unduly rely upon these statements.
Our research programs in neurodegeneration have benefited from longstanding scientific and financial support from the National Institutes of Health (NIH).” The contents of this Annual Report are solely our responsibility and do not necessarily represent any official views of NIH.
Item 1.Business
Overview
Pain Therapeutics,Cassava Sciences, Inc. developsis a clinical-stage biotechnology company based in Austin, Texas. Our mission is to detect and treat neurodegenerative diseases, such as Alzheimer’s disease. Our novel science is based on stabilizing – but not removing – a critical protein in the brain.
Over the past 10 years, we have combined state-of-the-art technology with new insights in neurobiology to develop novel solutions for Alzheimer’s disease and other neurodegenerative diseases. Our strategy is to leverage our unique scientific/clinical platform to develop a first-in-class program for treating neurodegenerative diseases, such as Alzheimer’s.
We currently have two biopharmaceutical assets under development:
our lead therapeutic product candidate, called simufilam, is a novel treatment for Alzheimer’s disease; and
our lead investigational diagnostic product candidate, called SavaDx, is a novel way to detect the presence of Alzheimer’s disease from a small sample of blood.
Our scientific approach for the treatment of Alzheimer’s disease seeks to simultaneously suppress both neurodegeneration and neuroinflammation. We believe our ability to improve multiple vital functions in the brain represents a new, different and crucial approach to address Alzheimer’s disease.
Our lead therapeutic product candidate, simufilam, is a proprietary drugssmall molecule (oral) drug. Simufilam targets an altered form of a protein called filamin A (FLNA) in the Alzheimer’s brain. Published studies have demonstrated that offer significant improvementsthe altered form of FLNA causes neuronal dysfunction, neuronal degeneration and neuroinflammation.
We believe simufilam improves brain health by reverting altered FLNA back to patientsits native, healthy conformation, thus countering the downstream toxic effects of altered FLNA. We have generated and healthcare professionals. We generally focus our drug development effortspublished experimental and clinical evidence of improved brain health with simufilam. Importantly, simufilam is not dependent on disordersclearing amyloid from the brain. Since simufilam has a unique mechanism of action, we believe its potential therapeutic effects may be additive or synergistic with those of other therapeutic candidates aiming to treat neurodegeneration.
Simufilam has demonstrated a multitude of treatment effects in animal models of disease, including normalizing neurotransmission, decreasing neuroinflammation, suppressing neurodegeneration, and restoring memory and cognition.
Phase 2a Study
In 2019, we completed a small, first-in-patient, clinical-proof-of-concept, open-label Phase 2a study of simufilam in the U.S., with substantial support from the National Institute on Aging (NIA), a division of the nervous system. NIH. Treatment with simufilam for 28 days significantly improved certain key biomarkers of Alzheimer’s pathology, neurodegeneration and neuroinflammation (p<0.001). Biomarkers effects were seen in all patients in both cerebrospinal fluid (CSF) and plasma.
Our expertise consistsPhase 2b Study
In September 2020, we announced final results of developing newa Phase 2b study with simufilam in Alzheimer’s disease. In this clinical study funded by the NIH, Alzheimer’s patientstreated with 50 mg or 100 mg of simufilam twice-daily for 28 days showed statistically significant (p<0.05) improvements in CSF biomarkers of disease pathology, neurodegeneration and neuroinflammation, versusAlzheimer’s patients who took placebo. In addition, Alzheimer’s patientstreated with simufilam showed improvements in validated tests of episodic memory and spatial working memory,versus patients on placebo. Cognitive improvements correlated most strongly with decreases in levels of P-tau181, a biomarker that suggests brain changes from Alzheimer’s disease.
Open-label Study Strategy
Much of the value of our ongoing open-label study is to gain data to support simufilam’s long-term safety profile in patients.
Clinical data from an open-label study has limitations compared to safety and efficacy data from a fully completed, large, randomized controlled clinical trial. However, we believe there is logic to conducting an open-label study prior to conducting a large, expensive Phase 3 clinical testing program. First, this is a standard clinical method of demonstrating drug candidatessafety. Second, we believe that if an experimental drug for Alzheimer’s shows no treatment benefits in a well-designed, long-term open-label study, then there is no chance that drug will succeed in Phase 3 clinical testing. The opposite is not true: encouraging treatment effects in an open-label study is not proof of drug safety or efficacy, nor can encouraging treatment effects predict clinical success in a Phase 3 program.
We believe a well-designed, long-term, open-label study is an exercise in prudent risk-management. Clinical results may serve as a tool to help inform and guiding these through various regulatorymanage the inherent risks and development pathways in preparation for their eventual commercialization. By necessity, the conductuncertainties of drug development is complex, lengthy,prior to undertaking a large, expensive and risky. The FDA has not yet establishedPhase 3 clinical testing program.
We also believe the safety or efficacyuse of interim analyses in our drug candidates.
Reverse Stock Split
On May 4, 2017, following stockholder approval, our board of directors approved a reverse stock split at a ratio of 7-for-1. On May 4, 2017, we filed with the Secretary of State of the State of Delaware a Certificate of Amendment to the Company’s Amended and Restated Certificate of Incorporation to effect the 7-for-1 reverse stock split of our outstanding shares of common stock. The number of outstanding shares of common stock on the date of the reverse split was reduced from 46.1 million to 6.6 million shares. Our common stock began trading on the Nasdaq Global Market on a split-adjusted basis when the market opened for trading on May 10, 2017. As a result, all common stock share amounts included in this Annual Report on Form 10-K have been retroactively reduced by a factor of seven, and all common stock per share amounts have been increased by a factor of seven, with the exception of our common stock par value.
The followingopen-label study is a summaryrational approach to inform the design of ongoing, pending, or future clinical studies. An interim analysis is a form of preliminary scientific enquiry that evaluates clinical data before a study is concluded, before patient enrollment has been completed and before data validation procedures are conducted to ensure the final clinical dataset is valid and accurate. Interim, “top-line” and preliminary data from our pipeline of drug assets:open-label clinical trial that we announce or publish from time to time are likely to change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final clinical dataset.
REMOXY ER (extended-release oxycodone capsules CII) – REMOXY,Open-label Study Results
In March 2020, we initiated a long-term, open-label study to evaluate simufilam, our lead drug candidate, in patients with Alzheimer’s disease. This study is a proprietary abuse-deterrent, twice-daily, oral oxycodone to treat severe chronic pain. We plan to resubmit the REMOXY NDA to the FDA, with Priority Reviewfunded in Q1 2018. We own exclusive rights to develop and commercialize REMOXY worldwide, with a sales royalty obligation to one of our technology partners.
FENROCK™ (transdermal fentanyl patch CII) – FENROCK is a proprietary, abuse-deterrent fentanyl skin patch to treat severe pain. This is an early-stage program that is substantially fundedpart by a competitive research grant award from the National InstituteInstitutes of Health (NIH). The study is intended to monitor the long-term safety and tolerability of simufilam 100 mg twice daily for 12 or
more months. Another study objective is to measure changes in cognition and biomarkers. This study uses ADAS-Cog to measure changes in cognition and the Neuropsychiatric Inventory (NPI) to assess dementia-related behavior. Both scales are both standard clinical tools in trials of Alzheimer’s disease.
In September 2021, the open-label study reached its final target enrollment of approximately 200 subjects with mild-to-moderate Alzheimer’s disease. To date, drug is safe and well-tolerated.
The open-label study protocol has pre-specified interim analyses, including cognition measurements at 6, 9 and 12 months.
6-month Interim Analysis. In February 2021, we announced top-line results of a preplanned interim analysis of our open-label study with simufilam. This interim analysis summarized clinical data in the first 50 patients who had completed at least 6 months of drug treatment. Patients’ cognition and behavior scores improved following six months of simufilam treatment, with no safety issues. Six months of simufilam treatment improved cognition scores by 1.6 points on Drug Abuse (NIDA)ADAS-Cog11, a 10% mean improvement from baseline to month 6. In these same patients, simufilam also improved dementia-related behavior, such as anxiety, delusions and agitation, by 1.3 points on the Neuropsychiatric Inventory (NPI), a 29% mean improvement from baseline to month 6.
9-month Interim Analysis.In July 2021, we announced top-line results of a second preplanned interim analysis of our open-label study with simufilam. This interim analysis summarized clinical data on the primary agencyfirst 50 patients who had completed at least 9 months of drug treatment.Patients’ cognition and behavior scores improved following nine months of simufilam treatment, with no safety issues. Nine months of simufilam treatment improved cognition scores by 3.0 points on ADAS-Cog11, an 18% mean improvement from baseline to month 9 (p<0.001). Simufilam improved ADAS-Cog scores in 66% of patients at 9 months. An additional 22% of patients declined less than reported in the science literature at 9 months. Cognition outcomes suggest simufilam’s treatment effects were broad-based (Figure 1).
12-month Interim Analysis.In September 2021, we announced top-line results of a third preplanned interim analysis of our open-label study with simufilam. This interim analysis summarized clinical data on the first 50 patients who had completed at least 12 months of drug treatment.Patients’ cognition and behavior scores both improved following twelve months of simufilam treatment, with no safety issues. Twelve months of simufilam treatment improved cognition scores by 3.2 points on ADAS-Cog11 from baseline to month 12 (p<0.001). Sixty-eight percent (68%) of study subjects improved on ADAS-Cog at 12 months; these study subjects improved an average of 6.8 points (S.D. ± 3.8). An additional 20% of study subjects declined less than 5 points on ADAS-Cog at 12 months; these study subjects declined an average of 2.5 points (S.D. ± 1.3).
In 2022, we may conduct one or more ad hoc interim analyses as the open-label study progresses.
Figure 1. Individual Patient Changes in ADAS-Cog (N=50) at 9 months
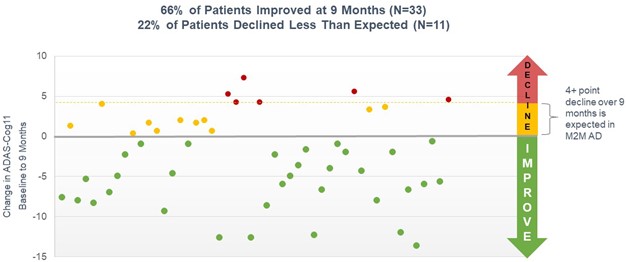
Interim analyses summarize clinical data on the first 50 patients who have completed 6, 9, and 12 months of open-label treatment. Baseline values for cognition for each 50-patient cohort will not be the same at months 6, 9 and 12 because some study participants may drop out of the U.S. government for research on drug abuse. We own exclusive, worldwide rights to FENROCK, with no royalty obligations to any third party.open-label study in-between interim analyses and dropouts are replaced, such that each interim analysis collects data from the first 50 patients who complete each specified time point.
Figure 2. Changes in ADAS-Cog (N=50) at 6, 9 and 12-month Interim Analyses
PTI-125 – PTI-125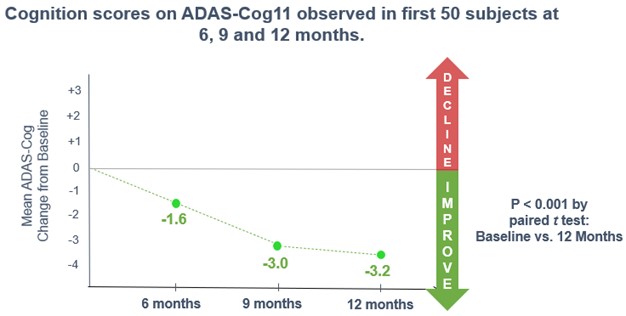
Historical Rates of Cognitive Decline - Alzheimer’s is a progressive disease. Cognition will always decline over time. Historical controls indicate that in patients with mild-to-moderate Alzheimer’s disease, cognition declines an average of 5.5 points on ADAS-Cog over 12 months amongst study subjects administered placebo in randomized, controlled trials, as reported by the science literature1. As an example of decline in an early Alzheimer’s disease population, in 2020, one of our competitors, Biogen, Inc., reported a 5.2-point decline over 18 months on ADAS-Cog amongst study subjects who were administered placebo in two Phase 3 randomized, controlled trials studies with their proprietary drug, aducanumab2.
1Disease Progression Meta-analysis Model in Alzheimer’s disease (Ito, et al., Pfizer Global Research), Alzheimer’s & Dementia 6 (2010) 39-53
2EMERGE and ENGAGE Topline Results (2020), available on-line.
Alzheimer’s is often accompanied by behavior disorders, such as anxiety, agitation or delusions. Such disorders may come and go over time, but they typically emerge or become more frequent as disease progresses. Simufilam reduced dementia-related behavior at 12 months on the Neuropsychiatric Inventory (NPI), a clinical tool used to measure changes in dementia-related behavior.
At baseline, 34% of study subjects had no neuropsychiatric symptoms.
At month 6, 38% of study subjects had no neuropsychiatric symptoms.
At month 9, over 50% of study subjects had no neuropsychiatric symptoms.
At month 12, over 50% of study subjects had no neuropsychiatric symptoms.
Biomarker Analysis. Biomarkers are objective biological data. There are no known placebo effects. A key objective of this study is to measure changes in levels of biomarkers in patients before and after 6 months and 12 months of open-label treatment with simufilam.
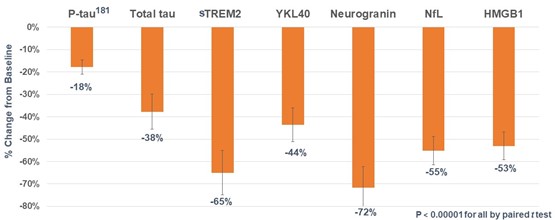
In July 2021, we announced positive biomarker data from our open-label study.Six months of open label treatment with simufilam robustly improved CSF biomarkers in a cohort of 25 patients with mild-to-moderate Alzheimer’s disease. Biomarker data were analyzed from cerebrospinal fluid (CSF) collected from 25 study participants in the open-label study who agreed to undergo a lumbar puncture at baseline and again after 6 months of treatment. CSF bioanalyses were conducted blind by City University of New York (CUNY).
Cerebrospinal fluid (CSF) biomarkers of disease pathology, t-tau and p-tau181, decreased 38% and 18%, respectively (both p<0.00001). CSF biomarkers of neurodegeneration, neurogranin and Nfl, decreased 72% and 55%, respectively (both p<0.00001). CSF biomarkers of neuroinflammation, sTREM2 and YKL-40, decreased 65% and 44% (both p<0.00001). All p-values are baseline vs. 6-month levels by paired t-test. Figure 3.
Core markers of Alzheimer’s pathology are total tau (T-tau), phosphorylated tau (P-tau181), and amyloid beta42 (Aβ42). In Alzheimer’s, tau levels are elevated and Aβ42 is low.
T-tau decreased 38% (p<0.00001)
P-tau181 decreased 18% (p<0.00001)
CSF Aβ42 increased 84% (p<0.00001)
Elevated CSF levels of two proteins, neurogranin (Ng) and neurofilament Light Chain (NfL) indicate neurodegeneration.
Ng decreased 72% (p<0.00001)
NfL decreased 55% (p<0.00001)
Elevated levels of marker YKL-40 indicate neuroinflammation.
YKL-40 decreased 44% (p<0.00001)
sTREM2 is a biomarker of microglia-induced neuroinflammation that has commanded substantial recent attention from researchers for its role in Alzheimer’s and frontotemporal dementia.
sTREM2 decreased 65% (p<0.00001)
HMGB1 protein, is a damage-related protein sometimes called a ‘danger molecule’ because it triggers additional neuroinflammation and loss of neurons.
HMGB1 decreased 53% (p<0.00001)
Figure 3. Significant Decreases in CSF Biomarkers at Month 6
In 2022, we expect to measure CSF biomarkers in approximately 25 study participants who complete 12 months of treatment with open label simufilam.
Cognition Maintenance Study (CMS)
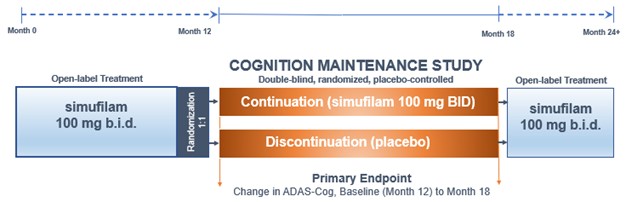
In May 2021, we initiated a Cognition Maintenance Study (CMS). This is a double-blind, randomized, placebo-controlled study of simufilam in patients with mild-to-moderate Alzheimer’s disease. Study subjects are randomized (1:1) to simufilam or placebo for six months. To enroll in the CMS, patients must have previously completed 12 months or more of open-label treatment with simufilam. The CMS is designed to evaluate simufilam’s effects on cognition and health outcomes in Alzheimer’s patients who continue with drug treatment versus patients who discontinue drug treatment. Figure 4.
The target enrollment for the CMS is approximately 100 subjects or more. As of February 2022, over 60 subjects have been enrolled in the CMS and 35 have completed the study.
Figure 4. Cognition Maintenance Study Design
End-of-Phase 2 (EOP2) Meeting with FDA
In January 2021, we held an End-of-phase 2 (EOP2) meeting for simufilam with the U.S. Food and Drug Administration (FDA). The purpose of this EOP2 meeting was to gain general agreement around key elements of a pivotal Phase 3 program to treat Alzheimer’s disease dementia. FDA attendees included Robert Temple, MD, Deputy Center Director for Clinical Science and Senior Advisor in the Office of New Drugs; Billy Dunn, MD, Director, Office of Neuroscience; Eric Bastings, MD, Director, Division of Neurology, and others.
In February 2021, we announced the successful completion of our EOP2 meeting. Official meeting minutes confirm that we and FDA are aligned on key elements of a Phase 3 clinical program for simufilam. FDA has agreed that the completed Phase 2 program, together with an ongoing and well-defined Phase 3 clinical program, are sufficient to show evidence of clinical efficacy for simufilam in Alzheimer’s disease. There is also agreement that the use of separate clinical scales to assess cognition (ADAS-cog1) and function (ADCS-ADL2) are appropriate co-primary endpoints of efficacy. A clinical scale that combines cognition and function, such as iADRS3, is a secondary efficacy endpoint.
1 ADAS-Cog = The Alzheimer’s Disease Assessment Scale – Cognitive Subscale, a measure of cognition
2 ADCS-ADL = Alzheimer’s Disease Cooperative Study – Activities of Daily Living, a measure of health function
3 iADRS = integrated Alzheimer’s Disease Rating Scale, a composite measure of cognition and health function
Special Protocol Assessments
In August 2021, we announced we had reached agreement with FDA under a Special Protocol Assessment (SPA) for both Phase 3 studies. These SPA agreements document that FDA has reviewed and agreed upon the key design features of our Phase 3 study protocols of simufilam for the treatment of patients with Alzheimer’s disease.
An SPA agreement indicates concurrence by the FDA with the adequacy and acceptability of specific critical elements of overall protocol design (e.g., entry criteria, dose selection, endpoints, etc.). These elements are critical to ensure that our planned Phase 3 studies of simufilam in Alzheimer’s disease can be considered adequate and well-controlled studies in support of a future regulatory submission and marketing application.
The first clinical study protocol under the SPA is titled “A Phase 3, Randomized, Double-Blind, Placebo-Controlled, Parallel-Group, 52-Week Study Evaluating the Safety and Efficacy of One Dose of Simufilam in Subjects with Mild-to-Moderate Alzheimer's Disease.”
The second clinical study protocol under the SPA is titled “A Phase 3, Randomized, Double-Blind, Placebo-Controlled, Parallel-Group, 76-Week Study Evaluating the Safety and Efficacy of Two Doses of Simufilam in Subjects with Mild-to-Moderate Alzheimer’s Disease.”
Phase 3 Drug Supply
In March 2021, we announced we had entered into a drug supply agreement with Evonik Industries AG for simufilam. Under the agreement, Evonik will supply us with large-scale, clinical-grade quantities of simufilam. Evonik is one of the world’s largest contract development and manufacturing organizations for pharmaceutical ingredients. Other vendors supply excipients, the finished dosage form (i.e., simufilam tablets), drug packaging, package labeling and other critical steps in the supply chain for Phase 3 drug supply.
Phase 3 Clinical Program Overview
The Phase 3 program consists of two large, double-blind, randomized, placebo-controlled studies of simufilam in patients with mild-to-moderate Alzheimer’s disease dementia. Figure 5. In 2021, the FDA granted each study a Special Protocol Assessment (SPA). In June 2021, we announced the selection of Premier Research International as our clinical research organization (CRO) to help conduct the Phase 3 clinical program of simufilam for Alzheimer’s disease.
Figure 5.

RETHINK-ALZ and REFOCUS-ALZ
On October 6, 2021, and November 18, 2021, we announced initiation of our two Phase 3 studies of simufilam, respectively.
The first Phase 3 study, called RETHINK-ALZ, is designed to evaluate the safety and efficacy of oral simufilam 100 mg in enhancing cognition and slowing cognitive and functional decline over 52 weeks. Secondary objectives include the assessment of simufilam's effect on neuropsychiatric symptoms and caregiver burden. This randomized, double-blind, placebo-controlled study plans to enroll approximately 750 patients with mild-to-moderate Alzheimer’s disease in the U.S. and Canada and, eventually, overseas.
Details of the RETHINK-ALZ Phase 3 study include:
Approximately 750 subjects with mild-to-moderate Alzheimer’s disease to be enrolled.
Subjects to be randomized (1:1) to simufilam 100 mg or placebo twice daily.
Subjects to be treated for 12 months.
The co-primary efficacy endpoints are ADAS-Cog1, a cognitive scale, and ADCS-ADL2, a functional scale; both are standard clinical tools in trials of Alzheimer’s disease.
A secondary efficacy endpoint is iADRS3, a standard clinical tool in trials of Alzheimer’s disease that combines cognitive and functional scores from ADAS-Cog & ADCS-ADL.
Other secondary endpoints include plasma biomarkers of disease and NPI4, a clinical tool that assesses the presence and severity of dementia-related behavior.
On November 18, 2021, we announced initiation of a second Phase 3 study, called REFOCUS-ALZ, designed to evaluate the safety and efficacy of oral simufilam 100 mg and 50 mg over 76 weeks. This randomized, double-blind, placebo-controlled study plans to enroll approximately 1,000 patients with mild-to-moderate Alzheimer’s disease in the U.S. and Canada and, eventually, overseas.
Details of the REFOCUS-ALZ Phase 3 study include:
Approximately 1,000 subjects with mild-to-moderate Alzheimer’s disease to be enrolled.
Subjects to be randomized (1:1:1) to simufilam 100 mg, 50 mg, or placebo BID.
Subjects to be treated for 76 weeks.
The co-primary efficacy endpoints are ADAS-Cog1, a cognitive scale, and ADCS-ADL2, a functional scale; both are widely used clinical tools in trials of Alzheimer’s disease.
A secondary efficacy endpoint is iADRS3, a widely used clinical tool in trials of Alzheimer’s disease that combines cognitive and functional scores from ADAS-Cog & ADCS-ADL.
Other secondary endpoints include CSF, plasma and imaging biomarkers of disease and NPI4, a clinical tool that assesses the presence and severity of dementia-related behavior.
_____________________________
1 ADAS-Cog = The Alzheimer’s Disease Assessment Scale – Cognitive Subscale, a measure of cognition
2 ADCS-ADL = Alzheimer’s Disease Cooperative Study – Activities of Daily Living, a measure of health function
3 iADRS = integrated Alzheimer’s Disease Rating Scale, a composite measure of cognition and health function
4 Neuropsychiatric Inventory (NPI)
SavaDx
Our investigational product candidate, called SavaDx, is early-stage program focused on detecting the presence of Alzheimer’s disease from a small sample of blood. For business, technical and personnel reasons, we continue to prioritize the development of simufilam, our novel drug candidate, over SavaDx, our novel diagnostic candidate.
The regulatory pathway for SavaDx may eventually include formal analytical validation studies and clinical studies that support evidence of sensitivity, specificity and other variables in various healthy and diseased patient populations. We have not conducted such studies and do not expect to conduct such studies in 2022.
SavaDx is currently designed as an antibody-based detection system for altered filamin A (FLNA). In 2022, we plan to evaluate a new approach to detect FLNA without the use of antibodies.
About Alzheimer’s Disease
Alzheimer’s disease is a progressive neurodegenerative disorder that affects cognition, function and behavior. As of 2021, there were approximately 55 million people worldwide living with dementia, a figure expected to increase to 139 million by 2050 according to outside sources. The annual global cost of dementia is now above $1 trillion, according to Alzheimer’s Disease International, a charitable organization. If this occurs, there is potential for Alzheimer's disease to cause a major financial drain on the national economy.
Our Scientific Approach is Different
Over the last ten years, we have developed a new and promising scientific approach for the treatment and diagnosis of neurodegenerative diseases, such as Alzheimer’s disease. Importantly, we do not seek to clear amyloid out of the brain. Rather, we seek to stabilize a critical protein in the brain that has many downstream effects.
Our scientific approach is to treat neurodegeneration by targeting an altered form of a scaffold protein called FLNA. Through years of basic research, we and our academic collaborators identified FLNA as a structurally altered protein in the Alzheimer’s brain. We have shown that the altered form of FLNA is pervasive in the Alzheimer’s brain and undetectable in healthy control brains.
Using scientific insight and advanced techniques in molecular biochemistry, bioinformatics and imaging, we have elucidated this protein dysfunction. Through this work, we have produced experimental evidence that altered FLNA plays a critical role in Alzheimer’s disease. We engineered a family of high-affinity, small molecules to target this structurally altered protein and restore its normal shape and function. This family of small molecules, including our lead therapeutic candidate, simufilam, was designed in-house and characterized by our academic collaborators.
Our lead therapeutic product candidate, simufilam, is a small molecule (oral) drug with a novel mechanism of action. The target of simufilam is altered FLNA, the brain protein we seek to stabilize. Importantly, since simufilam has a unique mechanism of action, we believe its potential therapeutic effects may be additive or synergistic with those of other therapeutic candidates aiming to treat neurodegeneration.
Given the biopharmaceutical industry’s challenging track record in Alzheimer’s research, we believe there is an urgent need to consider more recent and innovative approaches to combat this disease. We believe our scientific approach may broaden the range of possible treatment approaches for this complex disease.
Our science is based on stabilizing a critical protein in the brain
Proteins are essential for cell function because they participate in virtually every biological process. If protein function is impaired, the health consequences can be devastating. Technological advances in medicine and improvements in lifestyle are making our lives longer. But with age, genetic mutations and other factors conspire against healthy cells, resulting in altered proteins. Sometimes a cell can rid itself of altered proteins. However, when disease changes the shape and function of critical proteins, multiple downstream processes are impaired. There are many clinical conditions in which proteins become structurally altered and impair the normal function of cells, tissues and organs, leading to disease. Conversely, restoring altered proteins back to health –called proteostasis – is a well-accepted therapeutic strategy in clinical medicine.
For over 100 years, scientists have ascribed various neurodegenerative diseases to proteins that misfold and are rendered pathological. In Alzheimer’s disease, certain proteins, such as amyloid and tau, lose their normal shape and function. Such misfolded proteins can breakdown or aggregate in clumps and form plaque or tangles in the brain. Destruction of neuronal synapses, accelerated nerve cell death, and dysfunction of the brain support cells, are all widely believed to be direct consequences of misfolded proteins.
FLNA is a scaffolding protein found in high levels in the brain. A healthy scaffolding protein brings multiple proteins together, coordinating their interaction. However, an altered form of FLNA protein is found in the Alzheimer’s brain. Our experimental evidence shows that altered FLNA protein contributes to Alzheimer’s disease by disrupting the normal function of neurons, leading to neurodegeneration and brain inflammation. Our product candidate, simufilam, aims to counter the altered and toxic form of FLNA in the brain, thus restoring the normal function of this critical protein. Our novel science is based on stabilizing – but not removing – a critical protein in the brain.
One drug, multiple effects
Our lead therapeutic candidate, simufilam, binds to altered FLNA with very high (femtomolar) affinity. This drug effect restores the normal shape of FLNA and the normal function of key brain receptors, including: the alpha-7 nicotinic acetylcholine receptor; the N-methyl-D-aspartate (NMDA) receptor; and the insulin receptor. These receptors have pivotal roles in brain cell survival, cognition and memory.
In animal models, treatment with simufilam resulted in dramatic improvements in brain health, such as reduced amyloid and tau deposits, improved receptor signaling and improved learning and memory. In addition, simufilam has another beneficial treatment effect of significantly reducing inflammatory cytokines in the brain. In animal models of disease, treatment with simufilam greatly reduced levels of IL-6 and suppressed TNF-alpha and IL-1beta levels by 86% and 80%, respectively, illustrating a powerful anti-neuroinflammatory effect.
By restoring function to multiple receptors and exerting powerful anti-inflammatory effects, we believe our approach has potential to slow the progression of neurodegeneration in patients. Thus, we have designed simufilam to slow or, potentially, even reverse the deterioration of brain cells.
Our science is published in multiple peer-reviewed journals. In addition, our research has been supported by NIH under multiple research grant awards. Each grant was awarded following an in-depth, peer-reviewed evaluation of our approach for scientific and technical merit by a panel of outside experts in the field. Strong, long-term support from NIH has allowed us to advance our two product candidates for neurodegeneration, simufilam and SavaDx, into clinical development.
Currently marketed drug therapies for Alzheimer’s disease have limited therapeutic effect
There are currently no disease-modifying drug therapies to treat Alzheimer’s disease. The FDA has not approved any new drugs for Alzheimer’s disease since 2003, except, however, in June 2021, aducanumab received marketing approval from FDA for the treatment of Alzheimer’s disease (AD). In 2017, we completedusing the accelerated approval pathway “based on the drug’s effect on a first-in-human Phase I studysurrogate endpoint that is reasonably likely to predict a clinical benefit to patients, with PTI-125. This programa required post-approval trial to verify that the drug provides the expected clinical benefit.”1 Aducanumab has been beset by controversy about whether the drug is substantially funded by competitive research grant awards from the National Institutes of Health (NIH), the primary agency of the U.S. government for biomedical research. We own exclusive, worldwide rights to PTI-125, with no royalty obligations to any third party.
PTI-125DX – PTI-125effective in patients. Aducanumab is a proprietary blood-based diagnostic/biomarkerdrug of Biogen, Inc., a large biopharmaceutical company.
__________________
1 See: FDA Grants Accelerated Approval for Alzheimer’s Drug, June 07, 2021, https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-alzheimers-drug
Currently marketed drug therapies focus solely on treating symptoms, mostly in patients with mild-to-moderate Alzheimer's disease. At the time of diagnosis, patients are initiated on a class of drugs called cholinesterase inhibitors. The Alzheimer’s brain has low levels of a neurotransmitter called acetylcholine. Cholinesterase inhibitors prevent an enzyme in the brain, called acetylcholinesterase, from breaking down acetylcholine. Currently marketed cholinesterase inhibitors include donepezil (marketed by Eisai Co., Ltd. and Pfizer, Inc. as Aricept®), rivastigmine (marketed by Novartis AG as Exelon®) and galantamine (marketed by Janssen Pharmaceuticals, Inc. as Razadyne®). Cholinesterase inhibitors may benefit some patients for several months, after which the targeted brain receptors are desensitized, and drug efficacy is lost. To our knowledge, no drug for Alzheimer’s has shown an ability to detectstabilize cognition in patients, much less improve cognition, beyond a few months.
Simufilam is our Proprietary Drug Candidate for the Treatment of Alzheimer’s disease (AD). This clinical-stage programDisease.
We have generated and published experimental evidence of improved brain health by restoring altered FLNA with simufilam, our lead therapeutic product candidate. Simufilam is substantially funded by competitive research grant awards froma proprietary small molecule (oral) drug that represents an entirely new scientific approach to treat neurodegeneration. Published studies have demonstrated that simufilam targets an altered form of a protein called FLNA that is pervasive in the NIH.Alzheimer’s brain. Altered FLNA causes neuronal dysfunction, neuronal degeneration and neuroinflammation. We own exclusive, worldwide rights to PTI-125DX, with no royalty obligations to any third party.
REMOXY ER - a drug candidate for severe chronic pain
Ourbelieve our lead drug candidate, simufilam, improves brain health by reverting altered FLNA back to its native, healthy conformation, thus countering downstream toxic effects of altered FLNA. Importantly, simufilam is called REMOXY ER (extended-release). REMOXY is a proprietary, abuse-deterrent, twice-daily, capsule formulation of oral oxycodone, a strong opioid drug. REMOXY is intended to meet the needs of healthcare professionals who appropriately prescribe extended-release oxycodone and who seek to minimize the risks of drug diversion, abuse or accidental patient misuse. In particular, REMOXY’s thick, sticky, high viscosity formulation may deter unapproved routes of drug administration, such as injection, snorting or smoking. The proposed indication for REMOXY is for "the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate."
We own exclusive, worldwide rights to REMOXY.
Opioid drugs, such as oxycodone, are an important treatment option for patients with severe chronic pain. However, misuse, abuse and diversion of these prescription drugs remains a serious, persistent problem. For over a decade, we have pioneered technology, tools and techniques that enable the development of Abuse-Deterrent Formulations (ADFs). ADFs are intended to make opioid drugs difficult to abuse yet provide steady pain relief when used appropriately by patients. ADFs are intended to help in the fight against prescription drug abuse.
In March 2016, we resubmitted to the FDA a New Drug Application (NDA) for REMOXY. In September 2016, we received a Complete Response Letter, or CRL, not dependent on clearing amyloid from the FDA for the REMOXY NDA. The CRL informed us that REMOXY could not be approved in its present form and specified additional actions and data needed for drug approval. The CRL substantially focused on the need to conduct a clinical abuse-deterrent study via the nasal route of administration, and additional in vitro (non-clinical) studies to further characterize the abuse-deterrent properties of REMOXY. The 2016 CRL
made no mention of clinical safety, drug efficacy, manufacturing, stability, bioequivalence or any other issues from a prior CRL.
In February 2017, we met with the FDA regarding REMOXY. During this meeting, we reached written agreement with the FDA on a roadmap to resubmit the NDA for REMOXY. Final minutes of our FDA meeting confirmed two key requirements needed for the resubmission of the REMOXY NDA:
| ·
| | To support a potential drug label claim against abuse by injection: Repeat an injectability/syringeability study using thin films of drug, smaller volumes of solvents, additional mixed solvents and alternative extraction methods and syringe filter.
|
| ·
| | To support a potential drug label claim against abuse by snorting: Conduct an intranasal abuse potential study in human volunteers.
|
During 2017, we conducted these mandated studies with REMOXY. We believe positive results from these studies support label claims against abuse by injection and abuse by snorting. In November 2017, we concluded a pre-NDA meeting with the FDA. The purpose of this pre-NDA meeting was to agree on submission requirements for the REMOXY NDA under Section 505(b)(2) of the Federal Food, Drug, and Cosmetic Act. During the pre-NDA meeting, we received comments and clarification from the FDA on the acceptability of the data to be included in the REMOXY NDA resubmission, including a recent intranasal study. All questions were addressed and summarized in official minutes of the meeting issued by the FDA. There are no discrepancies or requests for clarifications following receipt of final meeting minutes.
As a result, we intend to resubmit the REMOXY NDA in Q1 2018 with Priority (six-month) Review.
Background on Uses and Abuse of Opioid Drugs
Opioid drugs are primarily used to relieve pain. They are among the world’s oldest known drugs. The term ‘opioid’ refers to an entire class of analgesic substances that are derived from the opium poppy plant. Drugs that fall within this class include oxycodone, hydrocodone, fentanyl, heroin, morphine and many other related substances.
In recent decades, oxycodone, a semi-synthetic opium derivative, has become a standard of care to treat severe chronic pain. Oxycodone is in Schedule II of the federal Controlled Substances Act of 1970, which means it has accepted medical use with severe restrictions, a high potential for abuse and regulations around its manufacture, possession, storage, use and distribution.
Oxycodone can provide significant therapeutic benefits for patients in pain when used as prescribed. In recent years, patients with severe chronic pain have benefited from oxycodone in long-acting formulations. Long-acting formulations contain a very high dose of oxycodone that is intended to release evenly over 12 hours. Long-acting oxycodone offers the convenience of less-frequent dosing intervals and improved compliance, a potential win-win for prescribers and for patients with severe chronic pain.
However, the emergence of long-acting oxycodone has also corresponded with a dramatic increase in opioid drug abuse. Drug abuse is the use of opioid drugs for reasons other than what the drug was prescribed for, and often via unapproved routes of administration, such as injection, snorting or smoking. Opioids such as oxycodone are primarily abused due to their ability to produce a strong, if fleeting, euphoric high.
Drug abusers have learned effective ways to tamper with, and defeat, long-acting oxycodone formulations. Defeating the long-acting properties of an oxycodone formulation can be as easy as crushing or grinding tablets, then swallowing, injecting, snorting or smoking the crushed substance. This release high levels of oxycodone faster than intended (called “dose-dumping”), resulting in an immediate and powerful euphoric high, as compared to swallowing an intact tablet as prescribed.
Misuse of oxycodone is not always intentional. According to a medical publication, about two-thirds of surveyed patients with chronic pain did not think that cutting, crushing, or grinding their medication would change the way it worked (Pergolizzi et al., 2014).
In addition, the pain-relieving effects of OxyContin® (oxycodone HCI), a widely used abuse-deterrent extended-release formulation of oxycodone, often wears off early, according to a lengthy investigation published by the Los Angeles Times in 2016. The Los Angeles Times investigation reports that a single dose of twice-daily oxycodone often does not last for the intended 12 hours and performs more like “an 8-hour drug.” This makes some patients take extra doses or stronger ones, raising the risk of abuse and addiction. An additional problem for physicians and patients alike can arise when insurance plans will not reimburse, and pharmacists will not dispense, more than two doses of OxyContin per day.
Opioid abuse is extremely dangerous. Opioid abuse can lead to drug-seeking behavior, tolerance and physical or psychological dependence. Even a single episode of opioid abuse can also lead to overdose, respiratory depression or death.
The Role of Abuse-deterrent Formulations
Policy makers have developed a multi-pronged approach aimed at combating opioid misuse, abuse and addiction. One targeted effort has been to encourage the pharmaceutical industry to develop ADFs. In April 2015, the FDA issued a final guidance to assist the pharmaceutical industry in developing ADF opioid drug products.
ADFs attempt to raise the bar on opioid abuse by making it more difficult, longer or aversive to tamper with a long-acting formulation, while recognizing that no drug or drug formulation can be made abuse-proof. In particular, an ADF drug can still be misused and result in overdose simply by ingesting the drug in higher than recommended doses. ADFs are not designed to prevent opioid-induced euphoria. ADF technology aims to decrease the likelihood that a long-acting opioid formulation will dose-dump under conditions of abuse or accidental misuse. By mitigating dose-dumping, the likelihood of overdose and death associated may decrease.
The intention of ADFs is to displace non-abuse-deterrent drug products. First-generation ADFs were introduced into the marketplace in 2010. However, we believe the relative weakness of first generation ADFs means opioid abuse continues to be a serious public health issue.In 2016, over 64,000 people died in the United States from opioid overdose, increasing from over 33,000 in 2015, according to the Centers for Disease Control Prevention. According to the FDA, “for each death [due to narcotic pain relievers], there are an additional ten treatment admissions, 32 emergency department visits and 825 nonmedical users of these drugs.” (Source: FDA’s Efforts to Address the Misuse and Abuse of Opioids, 2/6/2013).
As a pioneer in the design and development of ADFs, we believe a robust design for a novel ADF for twice-daily oxycodone revolves around four basic objectives: (i) safety and clinical efficacy over the entire 12-hours when used as prescribed; ii) abuse-deterrent when abused; (iii) ease of large scale manufacturing; and (iv) novel, non-infringing intellectual property. Many ADF programs may achieve three of these four objectives but the practical reality is that few ADFs achieve all four. We believe this is reflected in the industry’s relatively high failure rate with regards to ADFs developments for long-acting opioid formulations.
Market Opportunity for REMOXY ER
REMOXY targets the market for opioid therapy. The global opioid market has been estimated by third-parties to be valued at nearly $35 billion in 2015. North America dominates the global market, with about 60-65% market share, or about $20 billion. We estimate extended‑release opioid drugs are an approximately $4 billion market in the United States.
We believe REMOXY can capture a share of the approximately $4 billion market in the United States for extended‑release opioid drugs, including a portion of the existing multi-billion OxyContin (Purdue Pharma L.P.) franchise. OxyContin remains the largest selling extended‑release opioid in the United States by dollars. Despite OxyContin’s commercial success, we believe the drug carries a stigma due to widespread, well-documented cases of abuse and overdose; the persistence of negative media reports around this drug; the magnitude of the opioid epidemic and the sheer number of deaths associated with this problem; and on-going legal actions against Purdue by government agencies and private parties.
In addition to targeting the oxycodone market, REMOXY targets the approximately 10-15 million additional prescriptions for non‑abuse‑deterrent extended‑release opioids annually in the United States. Many of these opioids include active pharmaceutical ingredients, such as morphine, that may be perceived as having greater side effects than oxycodone‑based formulations.
Opioid prescriptions in the United States peaked in 2010 and have decreased each year through 2017. The reasons for this erosion are complex, but center around the fact that opioid abuse remains a serious, pervasive and persistent problem for physicians and patients alike. In particular, prescriptions for non-abuse deterrent opioids are likely to continue to drop significantly in the years ahead.
In addition, government actions serve to materially limit the market for opioid therapy to only those patients who have an appropriate need for such drugs. For example, in response to an epidemic of opioid overdoses, in 2017 the Center for Disease Control (CDC) released important new clinical guidelines for physicians treating adult patients for chronic pain. The CDC guidelines provide specific recommendations to clinicians about the appropriate prescribing of opioids to improve pain management and patient safety, including: “When opioids are started, the lowest possible effective dosage should be prescribed to reduce risks of opioid use disorder and overdose.” (Source: CDC Guideline for Prescribing Opioids for Chronic Pain). We believe these and other actions will continue to restrict the approvability, use, promotion and distribution of opioid drugs in the United States, and may serve to eliminate the market for non‑abuse‑deterrent opioids.
We own exclusive, worldwide rights to REMOXY. If approved and granted appropriate label claims, we believe REMOXY may have potential to distinguish itself from competitors with:
| ü
| | best-in-class abuse-deterrent properties;
|
| ü
| | true twice-daily dosing;
|
| ü
| | lowest initial starting dose;
|
| ü
| | lack of generic drug substitution; and
|
| ü
| | over 15 years of intellectual property protection.
|
We believe direct competitors to REMOXY will include the two ADFs of twice-daily oxycodone that are commercially available in the United States:
| ·
| | OxyContin ER (oxycodone HCI) from Purdue Pharma L.P. - A reformulated version of the original OxyContin OC, this drug received FDA approval in April 2010. According to its package insert, "OxyContin is formulated with inactive ingredients intended to make the tablet more difficult to manipulate for misuse and abuse." Some patients have complained that the new formulation is not as effective or causes gastrointestinal problems, according to Pain News Network (2016).
|
| ·
| | Xtampza® ER (oxycodone) from Collegium Pharmaceuticals, Inc. - Xtampza ERreceived FDA approved in April 2016 and is available in capsules containing microspheres formulated with oxycodone base and inactive ingredients that make the formulation more difficult to manipulate for the purpose of abuse. Each capsule contains 9, 13.5, 18, 27, or 36 mg of oxycodone (equivalent to 10, 15, 20, 30 or 40 mg of oxycodone HCl, respectively).
|
The FDA has approved two other extended-release, ADFs of oxycodone. However, neither of these two drugs were ever launched into the marketplace in the United States: a) in 2016, the FDA approved Troxyca® ER (Pfizer, Inc), a capsule combination of oxycodone HCL and naltrexone, an opioid antagonist; and b) in 2014, the FDA approved Targiniq® ER (Purdue Pharma LP), a tablet combination of oxycodone HCL and naloxone, an opioid antagonist.
REMOXY will compete against all extended‑release opioids, including generic drug products. In November 2017, the FDA issued final guidance on the regulatory pathway for generic abuse‑deterrent opioid products. Among other requirements, the new FDA guidance emphasizes that sponsors of generic abuse-deterrent oxycodone must ensure that a generic opioid drug is no less abuse deterrent than the original opioid and must also evaluate all potential routes of abuse, even those routes of abuse for which a generic sponsor does not seek a label-claim. We believe these new FDA requirements represents a high bar for generic drug developers in terms of added development time, expenses, technical expertise and regulatory risks.
Currently we have no capability to launch or to commercialize REMOXY. We continue to review potential launch and commercialization strategies for REMOXY. Options include a potential strategic transaction around all of our drug candidates; a commercial collaboration for REMOXY; or establishing commercial capabilities in-house to launch REMOXY on our own.
Chronology of REMOXY ER
We initiated the development of REMOXY over a decade ago, before any formal guidance was in place with regards to regulatory pathways for ADFs. As a result of our pioneering efforts with REMOXY, we have developed a foundation of practical and scientific experience with regard to regulatory and development pathways for ADFs.
brain. The following is a top-line reverse chronologyadditional detail on simufilam’s drug development program.
IND submission to FDA
Over the past ten years, we successfully conducted basic research, in vitro studies and preclinical studies in support of the development of REMOXY:
| ·
| | As a result of our pre-NDA meeting, we intend to resubmit the REMOXY NDA to the FDA in Q1 2018 with Priority (six-month) Review.
|
| ·
| | In November 2017, we concluded a pre-NDA meeting with the FDA.
|
| ·
| | In February 2017, we met with the FDA regarding REMOXY.
|
| ·
| | In September 2016, we received a CRL from the FDA regarding the NDA for REMOXY.
|
| ·
| | In March 2016, we resubmitted the NDA for REMOXY with the FDA.
|
| ·
| | In 2015, we generated additional abuse-deterrent data, continued an on-going stability study and made other preparations necessary to resubmit the NDA for REMOXY with the FDA.
|
| ·
| | In 2015, we and Pfizer concluded the transfer of the REMOXY program. We believe Pfizer has transferred to us its data, materials, capital equipment and other assets related to REMOXY.
|
| ·
| | In 2014, Pfizer provided us with written notice of termination of its development of REMOXY. We and Pfizer agreed on an orderly transfer of all rights, data, IP, etc.
|
| ·
| | From 2011-2014, Pfizer conducted fundamental investigations of the REMOXY formulation and its manufacture. As a result, Pfizer modified the REMOXY formulation and conducted successful studies to establish bioequivalence of the current formulation to the original formulation of REMOXY, to generate additional abuse-deterrent data and to provide manufacturing stability.
|
| ·
| | In 2011, Pfizer received a CRL on the REMOXY NDA filed by King. Once again, FDA cited manufacturing issues (specifically, in vitro drug stability). Once again, the CRL did not question REMOXY’s safety, clinical efficacy, abuse-deterrent properties or use of the reference listed drug.
|
| ·
| | In 2010, King resubmitted the REMOXY NDA with the FDA. In early 2011, Pfizer acquired King. References to Pfizer include references to Pfizer’s subsidiary King.
|
| ·
| | In 2009, King assumed sole control and responsibility for REMOXY.
|
| ·
| | In 2008, we filed an NDA for REMOXY with the FDA. Later that year, we received a CRL over manufacturing issues (specifically, in vitro drug stability). However, the CRL did not question REMOXY’s safety, clinical efficacy, abuse-deterrent properties or use of the reference listed drug.
|
| ·
| | In 2005, we and King Pharmaceuticals, Inc., or King, entered into an exclusive agreement to develop and commercialize REMOXY.
|
| ·
| | In 2003, we filed an Investigational New Drug application, or IND, for REMOXY with the FDA.
|
FENROCK™ -a drug candidate for severe pain
FENROCK is a proprietary transdermal patch that contains the prescription drug fentanyl to manage pain and incorporates novel abuse-deterrent technology. This is an early-stage, pre-IND program that is substantially funded by a competitive research grant award from the NIH’s NIDA.
Fentanyl is an opioid drug that is up to 100 times more potent than morphine. When used properly by patients under the care of a qualified physician, a fentanyl patch releases the drug slowly over 72 hours. This helps to manage pain that is severe enough to require daily around-the-clock, long-term treatment. However, fentanyl is also abused by non-patients for its euphoric effects. Abusers can chew on a fentanyl patch, or simply extract the fentanyl from a patch, then inject or ingest the contents. This practice is illicit and highly dangerous. It can quickly introduce into the body a massive amount of fentanyl, which can lead to addiction, overdose and death.
In November 2017, we announced a research and development grant from NIDA following a competitive, in-depth evaluation of FENROCK technology for scientific and technical merit. The grant of approximately $2.2 million provides us with funding to develop FENROCK.
We developed in-house the technology for FENROCK and own all development and commercial rights, without royalty or milestone obligations to any third-parties.
Fentanyl is a schedule II substance under the U.S. Controlled Substance Act.
PTI-125 -a drug candidate to treat Alzheimer’s Disease
PTI-125 is a proprietary, experimental drug for the treatment of Alzheimer’s disease (AD). AD is a progressive brain disorder that slowly destroys memory and thinking skills, and eventually the ability to carry out the simplest tasks. Damage to the brain starts a decade or more before problems appear. During this early stage of disease, people seem to be symptom-free, but toxic changes are taking place in the brain. Eventually, brain damage becomes widespread and affected people are often unable to care for themselves. Currently, AD cannot be detected until symptoms appear. Over five million Americans live with AD, a number that is expected to increase significantly in the coming years.
PTI-125 is a small molecule drug candidate that was designed by us and characterized by outside collaborators. PTI-125 has been shown to significantly improve AD neuropathologies in mouse models of the disease and in post-mortem brain tissue from AD patients, including receptor dysfunctions, neuroinflammation, tau hyperphosphorylation, insulin resistance and plaques and tangles that are hallmarks of AD.
PTI-125 works by binding to filamin A (FLNA), a protein critical to beta amyloid’s toxicity. Beta amyloid exerts multiple toxic effects, eventually causing the plaques and tangles found in the brains of people with AD. By binding to FLNA, PTI-125 may prevents and even reverse amyloid-related AD damage.
To date, the underlying science for PTI-125 has been published in Journal of Neuroscience, Neurobiology of Aging, Journal of Biological Chemistry, PLOS-One and other peer-reviewed scientific journals.
In June 2017, we announced that the NIH's National Institute on Aging awarded us a $1.7 million research grant following a competitive, in-depth evaluation of PTI-125 for scientific and technical merit. This NIH research grant enabled us to begin testing PTI-125 in human subjects. Subsequently, an Investigational New Drug (IND) applicationsubmission to FDA for PTI-125 was submittedsimufilam, including requisite studies around safety pharmacology, toxicology, genotoxicity and accepted by the FDA.
bioanalytical methods. In October 2017 we announced the successful completionfiled an IND with FDA for simufilam.
Clinical safety of simufilam in a Phase I clinical1 study for PTI-125. This study
Following FDA acceptance of our IND in 2017, we investigated for the first time the safety, dosing and pharmacokinetic profile of PTI-125simufilam in healthy human volunteers. The design of our first-in-human Phase 1 study was based on regulatory feedback, clinical and scientific rationale and observations from previously conducted preclinical and in vitro studies.
In this first-in-humana Phase 1 study, PTI-125simufilam was evaluated in 24 healthy human volunteers in a single-sitesingle site in the United StatesU.S. for safety, tolerability and pharmacokinetics. Study subjects were administered a single oral dose of 50, 100 or 200 mg of PTI-125. The drugsimufilam. Drug was well-tolerated in all subjects. Importantly, PTI-125simufilam showed no treatment-related adverse effects and no dose-limiting safety findings. Pharmacokinetic measurements showed PTI-125,demonstrated that simufilam, a small molecule, was rapidly absorbed. Dose-proportionality outcomes werewas observed over the entirefull dose range of 50 to 200 mg. There were two key findings for this Phase I Study:
| ·
| | PTI-125 was safe and well-tolerated at all doses studied; and
|
| ·
| | PTI-125 demonstrated favorable pharmacokinetics for further drug development.
|
Mean PTI-125 Plasma Concentration Concentration (ng/mL) 0 500 100 1500 0 4 8 12 16 g 200 mg Time (
Given the absence of any observable dose-limiting effects in healthy adults an excellent non-clinical safety database,in a Phase 1 study, a strong scientific rationale, and multiple peer-reviewed publications and research grant awards, we believe this program demonstrated favorable proof-of-principle for the development of simufilam in Alzheimer’s disease.
Phase 2a Clinical Study
In 2019, we completed a first-in-patient, clinical proof-of-concept study of simufilam in the U.S. Our Phase 2a was an open-label, multi-center, safety and pharmacokinetic study of simufilam. Thirteen (13) patients with mild-to-moderate Alzheimer’s disease, age 50-85, received 100 mg oral simufilam twice daily for 28 days. A diagnosis of Alzheimer’s disease was confirmed with Mini-Mental State Examination (MMSE) ≥ 16 and ≤ 24 and a cerebrospinal fluid (CSF) T-tau/Aβ42 ratio ≥ 0.30. Safety was assessed by ECGs, clinical labs, adverse event monitoring and physical examinations. CSF was drawn from patients before dosing started and again after 28 continuous days of dosing with simufilam. CSF samples were then analyzed for biomarkers of Alzheimer’s pathology (T-tau, P-tau, Aβ42); neurodegeneration (NfL, neurogranin); and neuroinflammation (YKL-40, IL-6, IL-1β and TNFα). A consultingbiostatistician conducted an independentanalysis of the data set.
A key objective of our Phase 2a study was to measure levels of CSF biomarkers in the brain. Key results of this study include (Figure 6):
Total tau (T-tau) decreased 20% (p<0.001)
Phosphorylated tau (P-tau) decreased 34% (p<0.0001)
Neurofilament light chain (NfL), a marker for neurodegeneration, decreased 22% (p<0.0001)
Neurogranin, a marker for cognitive decline, decreased 32% (p<0.0001)
Neuroinflammatory marker YKL-40, an indicator of microglial activation, decreased 9% (p<0.0001)
Proinflammatory Interleukin 6 (IL-6) decreased 14% (p<0.0001)
Proinflammatory Interleukin 1 beta (IL-1β) decreased 11% (p<0.0001)
Proinflammatory Tumor Necrosis Factor alpha (TNFα) decreased 5% (p<0.001)
The ratio of CSF P-tau to Aβ42, a widely accepted biochemical value of Alzheimer’s disease, improved in all patients (p<0.001)
Figure 6: Simufilam treatment reduces levels of CSF biomarkers in patients with Alzheimer’s in a Phase 2a study.
|
|
|
|
|
|
|
|
Neurogranin* | NfL* | T-tau+ | P-tau181* | YKL40* | IL-6* | IL-1β* | TNFα+ |
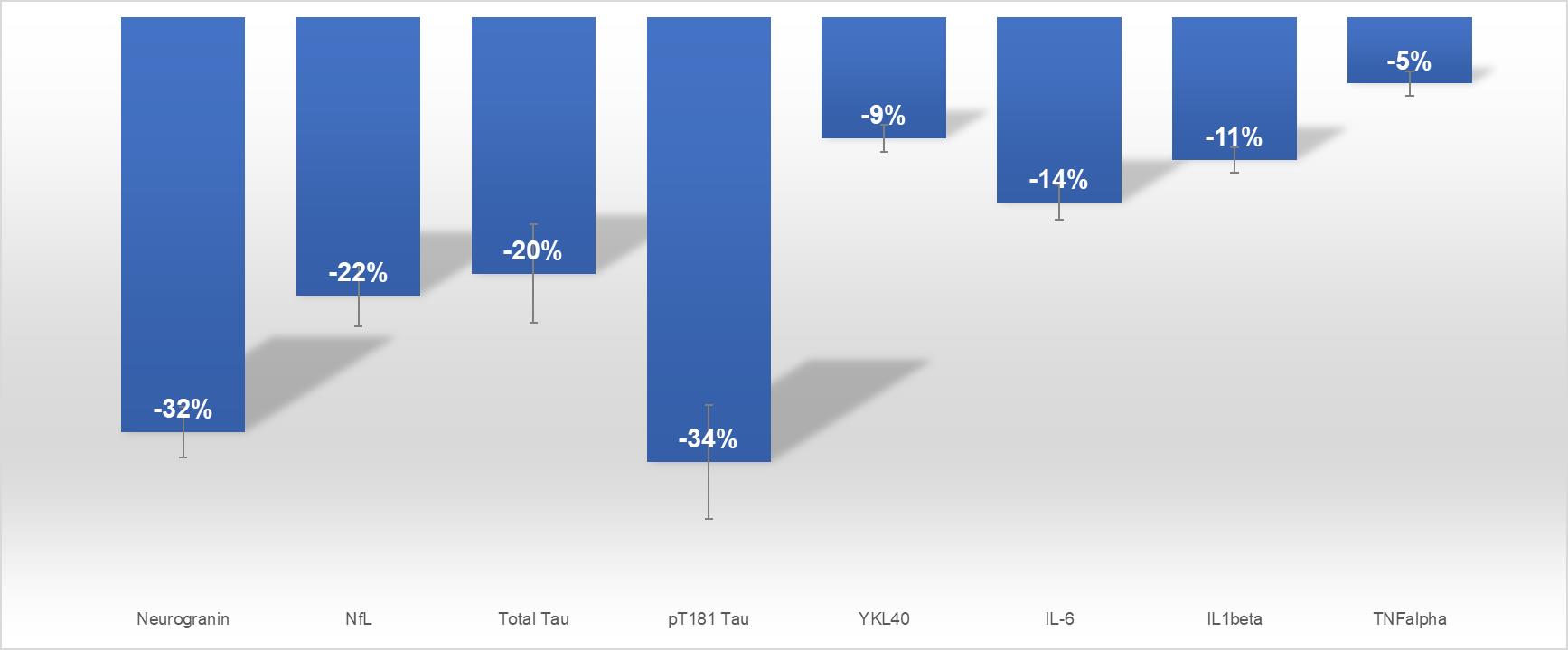
Neurogranin* NfL* T-tau+ P-tau181* YKL40* IL-6* IL-1β* TNFα+ -32% -22% -20% -34% -9% -14% -11% -5%
Figure 6. Percent change from baseline in CSF biomarkers measured by ELISA. Eight CSF biomarkers of disease in Alzheimer’s patients were significantly reduced with simufilam treatment. *p < 0.0001, +p < 0.001 in paired t test comparing Day 28 to pre-dose baseline.
Consistent with over 10 years of basic research and preclinical data, we believe our Phase 2a study showed clinical evidence of simufilam’s mechanism of action and drug-target engagement, including:
Improvements in biomarkers of Alzheimer’s disease in CSF, plasma and lymphocytes;
Consistency across biomarker improvements in CSF, plasma, and lymphocytes;
Significant reductions (p<0.01) in both nitrated and phosphorylated forms of tau protein;
Evidence that each individual patient showed biomarker responses to simufilam;
Evidence that simufilam reversed the shape of altered filamin A in lymphocytes;
Evidence that simufilam reduced levels of amyloid bound to alpha 7 nicotinic receptors in lymphocytes;
Early clinical validation of the drug target – altered filamin A – as a facilitator protein between amyloid beta and both neuroinflammation and tau pathology.
Cognition and function were not assessed in this small Phase 2a study. However, independent research has shown that high levels of CSF biomarkers of P-tau and total tau/Aβ42 ratio correlate with worse performance on a wide range of memory and attention tests. Conversely, we believe lowering a panel of CSF biomarkers of disease may benefit patients.
Phase 2b Clinical Study
In March 2020, we announced the completion of a double-blind, randomized, placebo-controlled, multi-center clinical study of simufilam. Sixty-four patients with mild-to-moderate Alzheimer’s disease, age 50-85, were randomized (1:1:1) to 100 mg or 50 mg oral simufilam or matching placebo. Treatment was administered twice daily for 28 days. Nine U.S. study sites enrolled patients. A clinical diagnosis was confirmed with the MMSE ≥16 and ≤26 and a CSF T-tau/Aβ42 ratio ≥0.28. Safety was assessed by ECGs, clinical labs, adverse event monitoring and physical examinations. This study was substantially funded by a research grant award from NIH.
The Phase 2b clinical study was designed to evaluate safety, tolerability and drug effects of simufilam on biomarkers of Alzheimer’s disease. The primary endpoint was improvement in biomarkers of Alzheimer’s disease from baseline to Day 28. CSF was drawn from patients before dosing started and again after 28 continuous days of dosing with simufilam. CSF samples were then analyzed for biomarkers of Alzheimer’s pathology (T-tau, P-tau, Aβ42); neurodegeneration (NfL, neurogranin); and neuroinflammation (YKL-40, IL-6, sTREM2, HMGB1) and BBB integrity (IgG, albumin). A consultingbiostatistician conducted an independentanalysis of the data set.
In May 2020, we announced that an outside lab with whom we had no prior work experience conducted a bioanalysis of CSF samples from our Phase 2b study. The data set from this initial bioanalysis showed unnaturally high variability and other problems. Overall, we believe data from the initial bioanalysis can be interpreted as anomalous and highly improbable. With its validity in question, we believe the initial bioanalysis serves no useful purpose. Backup CSF samples were subsequently sent to City University of New York (CUNY) for bioanalysis. All bioanalyses were conducted under blinded conditions to eliminate any possibility of bias.
In September 2020, we reported final positive Phase 2b clinical study results. Drug was safe and well-tolerated in this study. Simufilam significantly (P<0.05) improved an entire panel of biomarkers of disease in patients with Alzheimer’s disease compared to a placebo group. In addition, Alzheimer’s patients treated with simufilam showed directional improvements in validated tests of episodic memory and spatial working memory, versus patients on placebo. Cognitive improvements correlated most strongly (R=0.5) with decreases in levels of P-tau181 in CSF. The study achieved a 98% response rate, defined as the proportion of study participants taking simufilam who showed improvements in biomarkers. Importantly, we believe these data are consistent with prior clinical and preclinical results, the drug’s mechanism of action and over 10 years of basic research.
To our knowledge, no drug candidate has demonstrated the ability to reduce an entire panel of biomarkers of disease in patients with Alzheimer’s disease. For this reason, clinical data generated in our Phase 2a and Phase 2b studies may not be directly comparable to results generated by our competitors.
Key biomarker results include the following (all p-values versus placebo) (Figure 7):
Core markers of Alzheimer’s pathology are total tau (T-tau), phosphorylated tau (P-tau181), and amyloid beta42 (Aβ42). In Alzheimer’s, tau and P-tau levels are elevated and Aβ42 is low.
oT-tau decreased 15% (p<0.01) for patients in the 50 mg drug group.
oT-tau decreased 18% (p<0.01) for patients in the 100 mg drug group.
oP-tau decreased 8% (p<0.01) for patients in the 50 mg drug group.
oP-tau decreased 11% (p<0.01) for patients in the 100 mg drug group.
oAβ42 increased 17% (p<0.01) for patients in the 50 mg drug group.
oAβ42 increased 14% (p<0.01) for patients in the 100 mg drug group.
Elevated CSF levels of two proteins, Neurogranin (Ng) and Neurofilament Light Chain (NfL) indicate neurodegeneration.
oNg decreased 36% (p<0.01) for patients in the 50 mg drug group.
oNg decreased 43% (p<0.01) for patients in the 100 mg drug group.
oNfL decreased 28% (p<0.05) for patients in the 50 mg drug group.
oNfL decreased 34% (p<0.01) for patients in the 100 mg drug group.
Proinflammatory IL-6 (Interleukin 6) is produced in response to tissue stress and injury.
oIL-6 decreased 10% (p<0.01) for patients in the 50 mg drug group.
oIL-6 decreased 11% (p<0.01) for patients in the 100 mg drug group.
Elevated levels of neuroinflammatory marker YKL-40 indicate microglial activation.
oYKL-40 decreased 10% (p<0.01) for patients in the 50 mg drug group.
oYKL-40 decreased 12% (p<0.01) for patients in the 100 mg drug group.
sTREM2 is a neuroinflammation biomarker that has commanded substantial recent attention from researchersfor its role in Alzheimer’s disease and frontotemporal dementia.
osTREM2 decreased 43% (p<0.01)for patients in the 50 mg drug group.
osTREM2decreased 46% (P<0.01) forpatients in the 100 mg drug group.
Simufilam Significantly Reduced Levels of HMGB1 in CSF.
oHMGB1 decreased 33% (p<0.01) in patients treated with 50 mg simufilam
oHMGB1 decreased 32% (p<0.01) in patients treated with 100 mg simufilam
Simufilam Significantly Improved the Integrity of the Blood-brain Barrier (BBB).
oCSF IgG decreased 30% (p<0.05) in patients treated with 50 mg simufilam
oCSF IgG decreased 30% (p<0.05) in patients treated with 100 mg simufilam
oCSF albumin decreased 15% (p<0.05) in patients treated with 50 mg simufilam
oCSF albumin decreased 28% (p<0.05) in patients treated with 100 mg simufilam
Simufilam Improved the Albumin Ratio, a Test of Blood-brain Barrier (BBB) Permeability:
oBBB permeability can be clinically evaluated by comparing levels of albumin in CSF and plasma. The albumin ratio is a test for BBB permeability because albumin protein is not synthesized in CSF. Hence, albumin in CSF necessarily comes from plasma through the BBB. The albumin ratio is frequently elevated in patients with dementia and various other disorders.
oIn the Phase 2b study, the albumin ratio was unchanged for Alzheimer’s patients on placebo. The albumin ratio improved by approximately 5 and 7 points for patients treated with simufilam, 50 mg and 100 mg, respectively, over 28 days.
Changes in the Albumin Ratio by Treatment Group
|
|
|
|
|
|
|
|
Treatment | Day 0 | Day 28 | Change-Day 0 to 28 |
Placebo | 24 | 24 | No change |
50 mg simufilam | 25 | 20 | - 20% |
100 mg simufilam | 25 | 18 | - 28% |
Figure 7.Simufilam improved levels of CSF biomarkers in patients with Alzheimer’s in a Phase 2b study.
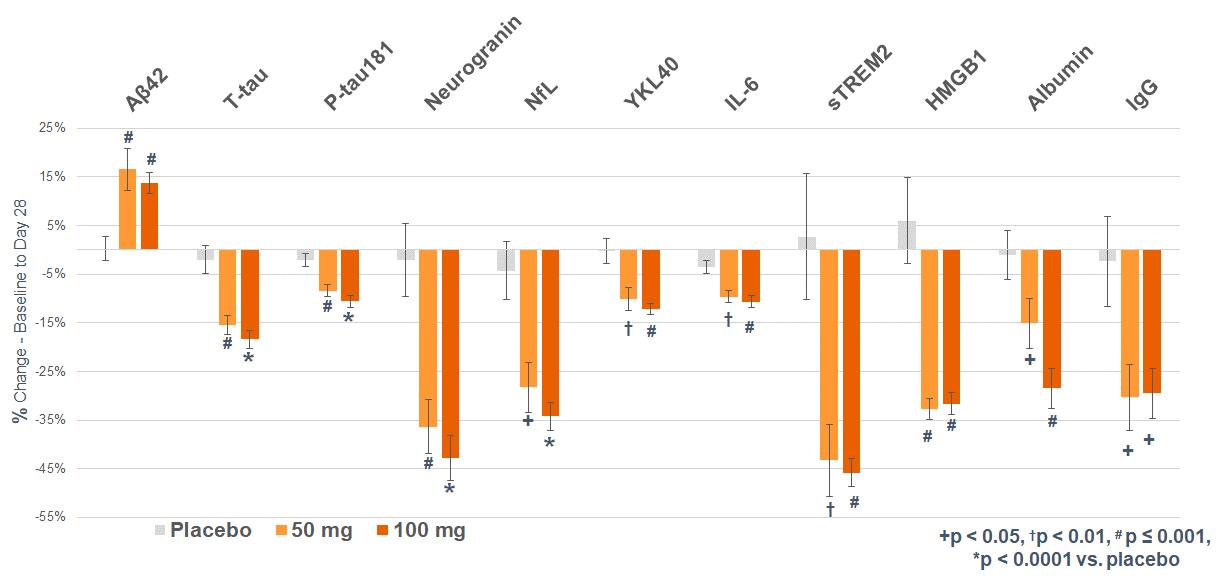
% Change Baseline to Day 28 -55% -45% -35% -25% -15% -5% 5% 15% 25% A42 T-tau P-tau181 Nurogranin NfL YKL-40 IL-6 sTREM2 HMGB1 Albumin IgG Placebo 50 mg 100 mg +p < 0.05 p < 0.01, # p < 0.001, p < 0.0001 vs. placebo
Figure 8. Study response rate, defined as the proportion of study participants taking simufilam who showed improvements in biomarkers.
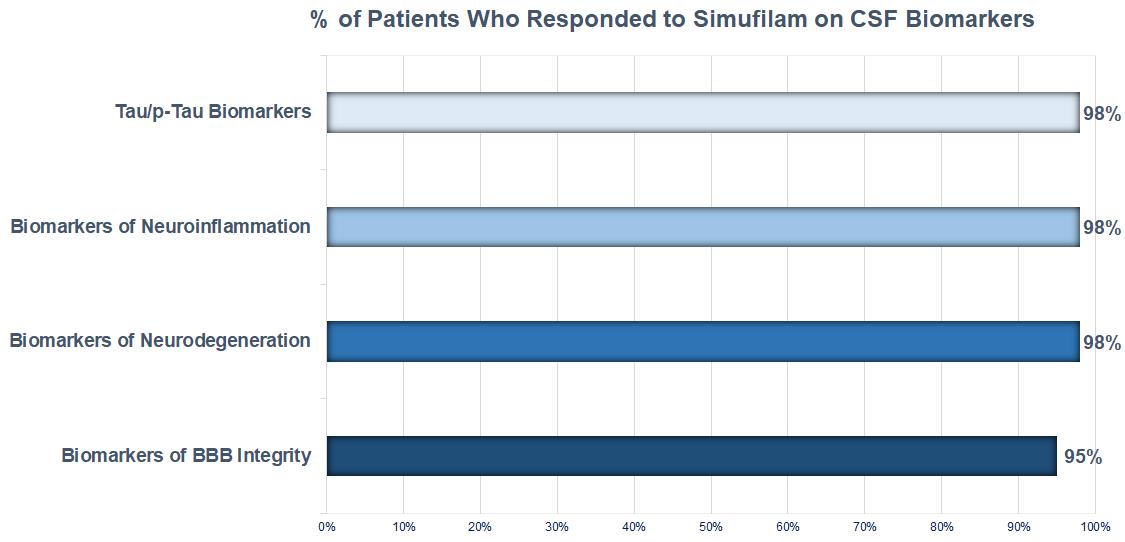
% of Patients Who Responded to Simufilam on CSF Biomarkets Tau/p- Tau Biomarkers 98% Biomarkers of Neuroinflammation 98% Biomarkers of Neurodegeneration 98% Biomarkers of BBB Integrity 95% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
A further objective of this study was to measure drug effects on cognition. Patients were tested at baseline and again on Day 28. Changes in episodic memory and spatial working memory were assessed on CANTAB, a validated, computer-based battery of tests. CANTAB is designed to measure cognitive skills regardless of the subject’s language skills, speed, gender or education.
Only directional trends are observed in memory improvements, due to limitations around study size (N=64). The final data analysis shown in Figure 9 excludes three patients who we subsequently learned showed no detectable level of simufilam in plasma and two patients who missed 25% or more of their doses by pill counts. In addition, outlier subjects with the most and fewest errors (by baseline score cutoffs) were removed from the final analysis of episodic memory (Figure 9):
Alzheimer’s patients in both drug groups showed directional improvements on tests of episodic memory and spatial memory after 28 days of treatment, versus patients on placebo.
Episodic memory improved by -5.7 (lower score is better) for Alzheimer’s patients in the 50 mg drug group, versus -1.5 for patients on placebo.
Episodic memory improved by -4.5 (lower score is better) for Alzheimer’s patients in the 100 mg drug group, versus -1.5 for patients on placebo.
Spatial memory improved by -2.31 (lower score is better) for Alzheimer’s patients in the 50 mg drug group, versus -0.4 for patients on placebo.
Spatial memory improved by -3.35 (lower score is better) for Alzheimer’s patients in the 100 mg drug group, versus -0.4 for patients on placebo.
Improvements in cognition correlated most strongly (statistical R=0.5) with decreases in CSF P-tau181, a biomarker that, when elevated, leads to tangles in the brain. Simufilam decreased brain levels of Ptau-181 by 8-11%, versus placebo.
Figure 9. Episodic Memory and Spatial Working Memory Improvements
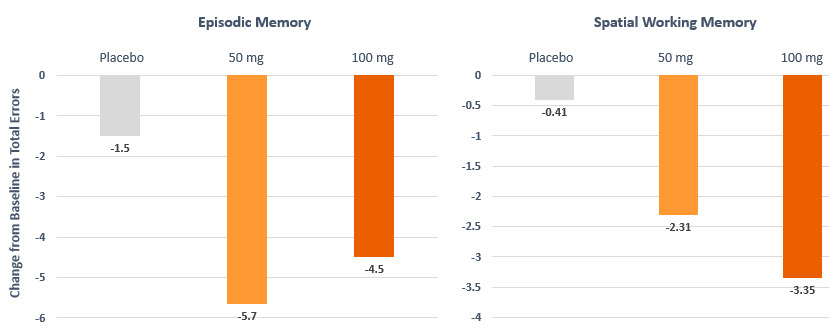
Change in Errors Baseline to Day 28 -6.0 -5.0 -4.0 -3.0 -2.0 -1.0 0.0 Placebo -1.5 50 mg -5.7 100 mg -4.5 37% Effect Size 2% Effect Size -3.5 -3.0 -2.5 -2.0 -1.5 -1.0 -0.5 0.0 Placebo -0.41 50 mg -1.65 100 mg -3.33
SavaDx
Our investigational diagnostic product candidate, called SavaDx, is early-stage program focused on detecting the presence of Alzheimer’s disease from a small sample of blood based. For business, technical and personnel reasons, we continue to prioritize the development of simufilam, our novel drug candidate, over SavaDx, our novel diagnostic candidate.
The regulatory pathway for SavaDx may eventually include formal analytical validation studies and clinical studies that support evidence of sensitivity, specificity and other variables in various healthy and diseased patient populations. We have not conducted such studies and do not expect to conduct such studies in 2022.
SavaDx is currently designed as an antibody-based detection system for altered filamin A (FLNA). In 2022, we plan to evaluate a new approach to detect FLNA without the use of antibodies.
Over the past ten years, we discovered that altered FLNA is a hallmark feature of brain pathology in patients with Alzheimer’s disease. We believe SavaDx may reveal early traces of the disease, potentially even before the overt appearance of disease symptoms, such as memory loss.
A diagnostic test usually measures one or more biomarkers, which are biological indicators of disease. A deep understanding of the biology of disease is required to identify and develop a diagnostic. A valid diagnostic has certain baseline characteristics to be functional and useful for clinical practice. It must detect disease in patients and, conversely, not detect disease in healthy subjects; and it is preferably quantitative, giving some indication of severity or stage of disease. Collectively, the ability to selectively detect disease indicators can be useful to provide diagnostic information (i.e., detect the disease) or prognostic information (i.e., predict the disease or its future course).
Currently, the most definitive method to diagnose Alzheimer’s disease is through autopsy after death, which is not particularly helpful. Methods to detect Alzheimer’s disease during its course can be expensive, invasive, subjective, risky or uncomfortable. Importantly, because of the expense and invasiveness of current tests, most people are not tested until they show obvious cognitive decline.
Current approaches for diagnosing Alzheimer’s disease include measurement of amyloid-β (specifically, Aβ42), total tau (T-tau) or phosphorylated tau (P-tau) levels in CSF or plasma; structural neuroimaging techniques, including magnetic resonance imaging (MRI) or computerized tomography (CT); positron-emission tomography (PET) imaging of brain amyloid (AmyVid®); and batteries of cognitive tests. Usually, a combination of more than one test is necessary to provide a working diagnosis. When such tests and techniques are used together, the totality of data can be sensitive and specific for the detection of Alzheimer’s disease. In practice, however, such tests and techniques are only used after overt symptoms of impaired memory.
We believe there is a profound need for a blood-based diagnostic test for Alzheimer’s disease. A quick, simple, inexpensive test may benefit the medical community in many ways. Advantages may include confirming the presence of Alzheimer’s disease earlier, when lifestyle changes and potential therapeutics may have the most impact, or conversely, to rule out Alzheimer’s disease at such early stages. Other potential benefits include discriminating Alzheimer’s disease from other causes of dementias; helping to identify stage of Alzheimer’s disease; selection and enrollment of appropriate patients into clinical studies of experimental product candidates; and better alignment of a patient’s specific diagnosis with a targeted therapeutic.
It is widely accepted that in Alzheimer’s disease, pathological changes in the brain occur at least 10-15 years before clinical symptoms appear. These “pre-symptomatic” changes include deposits of certain misfolded or impaired proteins in the brain. Our long-term goal with SavaDx is to identify people with Alzheimer’s disease, potentially long before clinical symptoms occur. Early detection may be critical for any intervention to cease - or at least slow down - brain damage before it is too late. Importantly, a non-invasive screen for latent Alzheimer’s disease prior to overt symptoms could be conducted as a general health screen, not just in patients at risk by family history or in patients already showing cognitive impairment. Once a disease-modifying treatment is found, early detection is likely to be critically important. Early detection and treatment may also be critical in identifying such a disease-modifying treatment, as many believe one reason for clinical study failures in Alzheimer’s disease is that treatment has routinely started too late in the course of disease to make any impact.
Moreover, with repeat measurements over time, SavaDx may provide a probability of cognitive decline or disease progression. Even if SavaDx does not provide a precise numerical cutoff value for Alzheimer’s disease, we believe it may be important to incorporate data from SavaDx into the overall diagnostic framework for neurodegeneration, and Alzheimer’s disease in particular. As with any diagnosis of disease, some people may embrace a way to detect Alzheimer’s disease long before clinical symptoms appear, while others may prefer not to know – at least until a treatment is found.
Diagnostic development program.
Diagnostic development differs from drug development in many important ways. As a result, diagnostic development requires substantial differences in planning, study design and study execution.
Some of the ways that diagnostic development differs from drug development include the following:
We may need to choose among a wider range of regulatory pathways for approval of SavaDx, depending on factors such as intended use and user, test type and complexity and role in patient-care decisions;
Drug studies usually deal primarily with one office within FDA, but the regulatory pathway for SavaDx may require us to consider the policies of multiple federal or state regulatory agencies and offices;
Unlike drug programs, statistical analysis with SavaDx does not focus on efficacy and safety endpoints. Rather, study endpoints for SavaDx will focus on sensitivity (true positives), specificity (true negatives), positive predictive value (percentage of correct positive diagnoses of known positive cases) and negative predictive value (percentage of correct negative diagnoses of known negative cases).
SavaDx is an investigational diagnostic product candidate that has not yet been reviewed by FDA. Clinical testing consists of collecting blood samples on a limited scale to test and validate SavaDx using antibodies. Our ability to test such samples depends on multiple factors, many of which are beyond our control. For example, optimal sample collection depends on risk of sample degradation, storage requirements to preserve samples, cost of sample storage and actual vs. predicted time of assay validation.
Over the past five years, we have conducted early validation tests using SavaDx. In three blinded studies of test samples, SavaDx detected more than a 10-fold separation between Alzheimer’s patients and normal healthy control subjects (N=232 test samples). In these three proof-of-concept studies, SavaDx demonstrated nearly 100% accuracy and specificity. The three studies deployed a research grade antibody manufactured by an outside vendor.
A fourth blinded study of SavaDx failed to generate meaningful diagnostic data. We believe the fourth study deployed a faulty research antibody sourced from an outside vendor. Commercially available research antibodies can present certain technical flaws, such as improper validation, significant meritbatch-to-batch variations or inconsistent storage, any of which can jeopardize results of studies and experiments. For these reasons, and in order to move thisincrease consistency of quality, reliability and availability, we have attempted to develop and validate a proprietary, fit-for-purpose, monoclonal antibody system for use with SavaDx. This effort remains a work-in-progress.
In July 2021, we announced positive clinical data with SavaDx when used to measure plasma levels of altered filamin A before and after simufilam treatment in patients with Alzheimer’s disease. In a Phase 2b randomized, controlled trial sponsored by the National Institutes of Health (NIH), simufilam significantly reduced plasma levels of altered filamin A in Alzheimer’s patients treated for 28 days. Plasma levels of p-tau181 also dropped significantly in these same patients.
The legal system for intellectual property around diagnostic methods is highly complex and uncertain. In the U.S., patent courts have struggled to define a clear means of patent eligibility for modern age diagnostics. Generally, a simple process involving correlations between blood test results and patient health is not eligible for patent claims because such processes incorporate “laws of nature”. However, different outcomes from different courts, including Federal Circuit, district court and Patent Trial and Appeal Board decisions, have continued to create a sometimes vague or conflicting legal framework for determining the eligibility of patent claims for diagnostic methods. As a result, we cannot be certain how SavaDx fits into the current U.S. legal framework for obtaining effective patent claims. Furthermore, claims for diagnostic methods can be complicated to enforce.
We currently have no issued patents in the United States with respect to SavaDx, which we believe may be protected in the United States by trade secrets, know-how and other proprietary rights technology.
Expansion of our science to other indications.
It is well-known that protein misfolds occur in a wide variety of biological processes and diseases. We may leverage our scientific insights in neurodegeneration and advanced tools in biochemistry, bioinformatics and imaging to expand our science
to other diseases. New indications and new drug programdevelopment approaches may complement our initial focus on Alzheimer’s disease.
Preclinical programs are always visionary, sometimes innovative and often of high biomedical potential. However, by definition such programs are exploratory and risky. Moreover, most preclinical programs fail for scientific or other reasons, regardless of the amount of effort or resources that are brought to the next levelbear upon such programs. For these reasons, in general we do not intend to disclose our preclinical programs until such time as they become material to our pipeline of development.product candidates.
We own exclusive, worldwide rights to PTI-125, with no royalty obligations to any third party.our neurodegeneration program.
PTI-125DX -a blood-based diagnostic to detect Alzheimer’s Disease
We are developing innovativeown intellectual property, including patents, patent applications, technology, to diagnose AD with a simple blood test. We believe finding a way to diagnose AD at an early-stage is vitally important. A blood test may help detect AD before symptoms occur, or rule out other possible causes of memory problems, or might be used as a biomarker to measuretrade secrets and know-how in the efficacy of drug candidates during clinical trials, or to define new potential therapies for AD.
Our diagnostic technology is related to PTI-125, our clinical-stage drug candidate for AD, whose underlying science has been published in Journal of Neuroscience, Neurobiology of Aging, Journal of Biological Chemistry, PLOS-OneU.S. and other peer-reviewed scientific journals. PTI-125DX is not a genetic based assay, nor does it rely on neuroimaging markers. PTI-125DX highlights critical changes that occur in the brain by detecting biochemical markers that are found in blood during the course of the disease.
The PTI-125DX assay is relatively quick, easy, non-hazardous and inexpensive, and can be repeated as necessary without contraindications. If successful, we believe the data generated by PTI-125DX can be used by clinicians or algorithms to classify patients at different stages of AD and/or to distinguish AD from other related diseases with better specificity or reliability than current methodologies.
PTI-125DX is an early-stage program. We have generated data from hundreds of blood samples using PTI-125DX. Results have not been published to date in order to better protect the intellectual property around this technology.
In September 2017, we announced a $1.8 million research grant from the NIH for PTI-125DX. The NIH's National Institute on Aging awarded us this research grant following a confidential, competitive and in-depth evaluation of PTI-125DX technology for scientific and technical merit. The research grant is a technical-milestone based award that will enable us to work collaboratively with leaders in the field to develop and test on clinical samples a blood-based diagnostic for AD.
PTI-125DX was designed by us and characterized by outside collaborators. We own worldwide commercial rights to PTI-125DX and related technology, without royalty or milestone obligations to any third parties.
Strategy
Our corporate strategy has changed little over the years: to spend carefully but to keep innovation at the top of our agenda. Elements of our corporate strategy include:
Focus on Clinical Development Stage Products. We believe this focus will enable us to generate product revenues earlier than if we were focused on early-stage research and discovery activities.
Retain Significant Rights to Our Drugs. We currently retain worldwide commercialization rights to all of our technology and drug candidates in all markets and indications, including REMOXY. In general, we intend to independently develop our drug candidates through late-stage clinical trials.
Outsource Key Functions. We intend to continue to outsource preclinical studies, clinical trials and formulation and manufacturing activities. We believe outsourcing permits significant time savings and allows for more efficient deployment of our resources.
We also conduct basic research and development in collaboration with academic and other partners. Our research and development expenses were $7.6 million and $9.2 million for the year ended December 31, 2017 and 2016, respectively. See “Item 7 Management’s Discussion and Analysis of Financial Condition and Results of Operations” for additional details regarding our research and development activities.
Our Intellectual Property
countries. The protection of patents, designs, trademarks and other proprietary rights that we own or license is critical to our success and competitive position. We own or license a number of U.S. and foreign patents, patent applications and rights to patents covering our products and technology. We consider the overall protection of our patents and other intellectual property rights to be of material value and act to protect these rights from infringement.
We seek to protect our technology by, among other methods, filing and prosecuting U.S. and foreign patents and patent applications with respect to our technology and products and their uses. The focus of our patent strategy is to secure and maintain intellectual property rights to technology for our program in neurodegeneration.
Simufilam and SavaDx were both discovered and designed in-house and were characterized by our academic collaborators during research activities that were conducted from approximately 2008 to date. We own exclusive, worldwide rights to these drug assets and related technologies, without royalty obligations to any third party. Our patent protection with respect to simufilam and use of simufilam for Alzheimer’s disease and other neurodegenerative disease currently runs through 2033 and includes six issued patents and related patent filings and applications. In addition, we have patent protection with respect to simufilam for use in treating certain cancers that runs through 2034. We currently have no issued patents in the following categoriesUnited States with respect to SavaDx, which we believe may be protected in the United States by trade secrets, know-how and other proprietary rights technology.
Our Development Team
Our product development team is led by seasoned professionals with a proven track record of innovation in drug discovery and development, as well as substantial business expertise.
Our Founder and Chief Executive Officer, Remi Barbier, has over 25 years of biopharmaceutical industry experience and has led teams responsible for pioneering several pharmaceutical innovations, including abuse-deterrent drugs; the clinical development of multiple pain drugs; an innovative antibody program in cancer; and other programs in neuroscience and other therapeutics areas. Before founding Cassava Sciences, he held leadership roles and was founder or co-founder of four life science companies, three of which are now publicly traded or acquired.
Our Chief Medical Officer, Nadav Friedmann PhD, MD, has eight prior FDA drug approvals and previously served as CEO of Daiichi Pharmaceuticals USA and Head of Johnson & Johnson’s Biotechnology Research Center.
Our Chief Clinical Development Officer, James Kupiec, MD, has two prior FDA drug approvals and previously served as VP, Global Clinical Leader for Parkinson’s Disease and Clinical Head of the Neuroscience Research Unit for Pfizer, Inc. and also held leadership roles at Sanofi and Ciba-Geigy Pharmaceuticals.
Lindsay Burns, PhD, SVP, Neuroscience, worked on the development of several product candidates in neuroscience and other therapeutics areas while at Neurex (acquired by Elan Pharmaceuticals) and Abgenix (acquired by Amgen).
Michael Zamloot, SVP of Technology Operations, has four prior FDA drug approvals and has worked in drug operations and supply chain management at Boehringer Mannheim (acquired by Roche Diagnostics), Athena Neuroscience (acquired by Elan Pharmaceuticals) and Ciba-Geigy (acquired by Novartis).
Michael Marsman, PharmD, SVP of Regulatory Affairs previously held senior positions at Impax Laboratories, Millennium Pharmaceuticals, and Syntex, where he had shared responsibility for the regulatory approval of several high-profile drugs. He also previously led regulatory affairs for our Company for nearly a decade until 2019.
George (Ben) Thornton, PhD, SVP of Technology, has led research and development teams at Johnson & Johnson as well as translated basic science to the clinical setting at biotechnology start-ups such as GeneMedicine and Apovia.
Our management team is further supported by scientific advisors who are leading experts in the field and share our commitment to advancing new treatments for neurodegenerative diseases, including Alzheimer’s disease.
Our Strategy
Our goal is to develop product candidates to diagnose and treat neurodegeneration, such as Alzheimer’s disease. Key elements of our business:business strategy to achieve this mission include:
building a lean company that is narrowly focused on developing innovative product candidates for Alzheimer’s disease and other areas of neurodegeneration; validating our unique scientific approach with competitive research grants and publishing our scientific data in peer-reviewed journals; applying our development capabilities to advance our product candidates through clinical proof-of-concept studies and beyond; using our expertise and experience to continue to focus on discovering new indications and product candidates, validated by experimental evidence and leading experts in the field; and continuing to outsource preclinical studies, clinical studies and formulation development activities in order to allow more efficient deployment of our resources
We also conduct basic research and development in collaboration with academic and other partners. Our research and development expenses were $24.8 million and $3.1 million for the year ended December 31, 2021 and 2020, respectively. These amounts are net of significant reimbursement received from NIH. See “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations” for additional details regarding our research and development activities.
Competition
The drug discovery and development industry is characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. We face potential competition from many different sources, including pharmaceutical and biotechnology companies, academic institutions and governmental agencies and public and private research institutions. Any product candidates that we successfully develop and commercialize, such as simufilam or SavaDx, may compete with existing therapies and new therapies that may become available in the future.
Historically, the drug industry has attempted to treat Alzheimer’s disease by developing drugs that block the synthesis of, or remove or dis-aggregate, beta amyloid and, more recently, another protein in the brain called tau. Essentially, the prevailing doctrine says amyloid (or tau) must be cleared out of the brain. This scientific approach – known as the amyloid hypothesis - has been repeatedly tested by our competitors in late-stage clinical studies using a variety of antibody backbones, epitopes, target conformations, biomarkers and in various stages of disease. While this approach may yet work, to date the amyloid hypothesis has failed to generate unambiguous therapeutic benefit in patients with Alzheimer’s disease. More recent competitors in Alzheimer’s research are focused on modulating proteins in the brain that have anti-inflammatory or other properties, an approach known as immunotherapy.
In contrast, our scientific approach seeks to simultaneously improve neurodegeneration and neuroinflammation. We believe improving multiple vital functions in the brain represents a new, different and crucial approach to address Alzheimer’s disease.
Regardless of scientific approach, improvements in cognition and function remains a key criterion for FDA approval of a new drug in Alzheimer’s disease, a hurdle which, to date, no drug candidate has met with clear and compelling clinical data in nearly two decades.
Our competitors may have significantly greater financial resources, an established presence in the market, expertise in research and development, manufacturing, preclinical and clinical testing, obtaining regulatory approvals and reimbursement and marketing-approved products. These competitors also compete with us in recruiting and retaining qualified scientific and | ·
| | the technology that forms the basis of REMOXY and FENROCK, our other abuse-deterrent drug candidates;
|
| ·
| | the technologies related to PTI-125 and PTI-125DX product candidates; and
|
| ·
| | the manufacture and use of our product candidates.
|
technical personnel, establishing clinical study sites and patient registration for clinical studies, as well as in acquiring or developing technologies complementary to, or necessary for, our programs. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies.
However,
The key competitive factors affecting the success of simufilam, and any other product candidates that we develop to address neurodegenerative disorders, if approved, are likely to be their efficacy, safety, convenience, price, the level of generic competition, patient and physician acceptance and the availability of reimbursement from government and other third-party payors. Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are more effective, have fewer or less severe side effects, are more convenient or are less expensive than any products that we may relydevelop.
Our competitors also may obtain FDA approval for their products more rapidly than we may obtain approval for ours. For example, in June 2021, Biogen, Inc., a large biopharmaceutical company, received FDA approval for aducanumab (human monoclonal antibody) for the treatment of Alzheimer’s disease using an accelerated approval pathway. Aducanumab’s safety and efficacy profile is complex and subject to debate. Since its approval in 2021, aducanumab has had modest clinical utilization due to its high cost, lack of widespread reimbursement and other reasons. We are also aware that Eli Lilly, a large biopharmaceutical company, has announced that in 2022 it plans to petition the FDA for accelerated approval of donanemab, its monoclonal antibody drug candidate for the proposed treatment of Alzheimer’s disease.
In recent years, we have observed ramped-up worldwide efforts aimed at developing blood-based techniques to detect and monitor Alzheimer’s disease. The key competitive factors affecting the success of SavaDx, and any other product candidates that we develop to diagnose neurodegeneration, if approved, are likely to be their measure of accuracy, such as specificity and sensitivity, as well as their convenience, patient acceptance, price and the availability of reimbursement from government and other third-party payors. Our competitors in the diagnostic area are pharmaceutical and biotechnology companies, academic institutions and governmental agencies and public and private research institutions. Despite increased research effort, the field has generally been hampered by lack of reproducibility and an unclear path on certain proprietary technologies and know-how thathow to move academic discoveries into clinical utilization.
In addition to blood-based techniques to detect Alzheimer’s disease, competitors are not patentable. We protect our proprietary information, in part, byexamining the use of confidentiality agreements with our employees, consultants,novel tracing agents and certainimaging techniques to map the course of our contractors.
We plan to prosecute and defend our patent applications, allowed patents, issued patents and proprietary information. Our competitive position and potential future revenues will depend in large part upon our ability to protect our intellectual property from challenges and to enforce our patent rights against potential infringements.
Patents expire, onneurodegeneration. In 2012, FDA approved Amyvid® (Eli Lilly Pharmaceuticals), which is a country by country basis, at various times depending on various factors, including the filing dateradioactive diagnostic agent for brain imaging of corresponding patent applications. Our patents and the patents we license from third parties include the following issued U.S. Patents: 8,168,217; 8,153,152; 8,147,870; 8,133,507; 8,354,124; 8,415,401; 8,420,120; 8,974,821; 8,945,614; 8,951,556; 9,233,160; 9,517,271; 9,555,113; 9,592,204; 9,855,333; and 9,572,885.
Our issued U.S. patent for REMOXY with the longest patent term extends to March 2034. Outside the United States, our granted patent with the longest patent term for REMOXY extends to 2028. Patents may have their term extended for various reasons including the grant of patent term adjustments, patent term extensions,amyloid plaque. Amyvid can rule out Alzheimer’s disease but does not confirm its presence. That is, a negative scan means little or supplemental protection certificates, or may have their term shortened for various reasons including by terminal disclaimers. Certain United States patent applications and patent applications outside the United states are pending.
no plaque is present; however, a positive scan does not necessarily indicate Alzheimer’s disease. In addition, we use a uniqueAmyvid cannot be used to stage Alzheimer’s disease because some people take years to show cognitive decline after amyloid plaque develops, while other others rapidly develop advanced Alzheimer’s disease within months. Since its approval in 2012, Amyvid has had modest clinical utilization due to its high cost, lack of widespread reimbursement and complex process to manufacture REMOXY. We also protect as trade secrets the significant pharmaceutical know-how and detailed knowledge of a complex supply chain to manufacture REMOXY.need for specialized training.
REMOXY, REMOXY ERand FENROCK are trademarks of Pain Therapeutics, Inc.Manufacturing
Formulation Agreement with Durect Corporation
We have an exclusive, worldwide Development and License Agreement, or the Durect Agreement, with Durect to use a patented controlled-release technology that forms the basis for REMOXY.
Under the terms of the Durect Agreement, we are solely responsible for clinical development, Durect is responsible for furnishing suitable laboratory facilities, equipment and personnel during pre-clinical phases of development and we and Durect are jointly responsible for certain pre-clinical activities. We reimburse Durect’s expenses and have made milestone payments based on the achievement of certain clinical or regulatory milestones. We paid Durect approximately $40.4 million from the inception of the Durect Agreement to December 31, 2017. We could pay another $1.5 million milestone payment to Durect under the Durect Agreement.
We are obligated to pay Durect royalties on commercial sales of REMOXY. These royalties range from 6.0% to 11.5% of net sales, depending on the volume of sales of REMOXY in a given calendar year. There are no minimum payments, and the royalty rate resets back to 6.0% at the beginning of each calendar year.
The Durect Agreement terminates on a country-by-country basis upon the later of the expiration of the last to expire of the patents licensed under such agreement or a certain number of years following first commercial sale in such country. Currently, the last to expire patent covered by such agreement expires in 2034. However, such date may be extended by the issuance of any additional patents pursuant to pending patent applications. We can terminate the Durect Agreement with notice to Durect, and we and Durect can terminate such agreement under certain circumstances, including material breach and insolvency.
Prior Agreements with Pfizer
Between 2005 and 2014, Pfizer paid us a total of $290 million, including $155 million in upfront fees, $30 million in milestone payments and $105 million to reimburse expenses we incurred under the agreements we had with Pfizer. Pfizer has no further obligations to us. We have no further obligations to Pfizer, except that we will owe Pfizer a one-time payment of $200,000, payable at the time REMOXY is approved by the FDA, related to certain commercial manufacturing equipment we purchased from Pfizer.
Manufacturing
We do not own or lease any manufacturing facilities. We outsource formulation, manufacturing and related activities to third parties. For the foreseeable future, we will continue to rely on third parties to conduct certain quality control and assurance testing, shipping or storage of our product candidates.
We currently rely on one non affiliated contract development and manufacturing organization (CDMO) to manufacture simufilam and expect to continue to do so.
We believe our manufacturing strategy is on-track to ensure sufficient drug supply for a Phase 3 program, including both drug substance (i.e., active ingredient) and drug product (i.e., oral tablets). In March 2021, we entered into an agreement with Evonik Corporation to supply large-scale, clinical-grade quantities of drug substance for simufilam. The goal is to ensure the integrity of the drug supply chain on a worldwide basis, in compliance with FDA standards.
We believe raw materials for our drug product are readily available from reliable sources. To date, we have experienced minimal drug supply chain disruption due to COVID-19 but this may change at any time.
Our suppliers must comply with current good manufacturing practices or GMP,(cGMP) enforced by the FDA and other government agencies such as the U.S. Drug Enforcement Administration, or DEA.agencies. Our suppliers are subject to unannounced inspection by regulators, including pre-approval inspections by the FDA, and the DEA, to
ensure they are in strict compliance with government regulations and standards. Our suppliers may be forced to stop producing, storing, shipping or testing our drug products if they fall out of compliance with government regulations and standards.
We have no control over our suppliers’ compliance, or lack thereof, with the multitude of regulations and standards that affect our drug products. We cannot control decisions by our suppliers that affect their ability or willingness to continue to supply us on acceptable terms, or at all.
We may not be able to replace a commercial supplier on commercially reasonable terms, or at all. Replacing any of our commercial suppliers will be expensive and time consuming. Further, if REMOXY is approved, our commercial suppliers may encounter difficulties in achieving high volumes of production to satisfy commercial demands. Failure by any of our suppliers to perform as expected could delay or prevent commercialization of REMOXY or result in shortages, cost overruns, or other problems and would materially harm our business.Government Regulation
Commercial supply of certain excipients from Durect
We will rely on Durect as the sole source of certain excipients in REMOXY. Durect has limited experience manufacturing pharmaceutical products and maintaining GMP-compliant operations. A Pre-Approval Inspection, or PAI, by the FDA officials is often integral to the FDA approval process. A PAI is an unannounced evaluation of a manufacturing or test site for readiness for commercial scale manufacturing, conformance with commitments made in an NDA and data integrity. To our knowledge, the FDA has never conducted a PAI of any Durect facility. We do not and cannot know whether Durect’s manufacturing or test facilities could pass a PAI inspection related to REMOXY, or whether Durect has invested in the necessary systems to pass a PAI inspection.
We rely on Durect to supply to us certain excipients for the REMOXY formulation. Under the Durect Agreement, these excipients are supplied to us at Durect’s cost, plus thirty (30) percent. We currently do not have a long-term commercial supply agreement in place with Durect. We expect that we and Durect will negotiate a supply agreement for these excipients. We may not be able to establish a commercial supply agreement on acceptable terms. Until a commercial supply agreement is in place with Durect, we expect to obtain excipients from Durect via individual purchase orders.
If we receive marketing approval for REMOXY, Durect may need to materially expand its manufacturing capacity. Durect may not be able to increase its manufacturing capacity for REMOXY in a timely or economic manner, or at all. Moreover,
significant scale up of manufacturing will require additional validation studies, whichOur operations are subject to the FDA reviewvarious levels of governmental controls and approval.
Commercial supply of oxycodone with Noramco
We expect to rely on Noramco as the sole source of the oxycodone base used in REMOXY. We currently do not have a long-term commercial supply agreement in place with Noramco. We expect to negotiate with Noramco a commercial supply agreement to supply us with oxycodone base. We may not be able to establish a commercial supply agreement on acceptable terms, or at all. Until we have a commercial supply agreement in place with Noramco, we expect to obtain oxycodone base from Noramco via individual purchase orders.
Commercial drug supply agreement with Mallinckrodt
Our sole supplier for commercial supplies of REMOXY is Mallinkcrodt Pharmaceuticals, or Mallinckrodt. In October 2007, we and Mallinckrodt entered into a long-term supply agreement, or the Mallinckrodt Agreement when Pfizer was responsible for commercialization of REMOXY. Pfizer assigned the Mallinckrodt Agreement to us upon the termination of the Pfizer Agreements. In March 2010, we and Mallinckrodt entered into an amended and restated long-term supply agreement. In a letter dated February 21, 2017, Mallinckrodt alleged a breach of contract because REMOXY had not yet been approved by the FDA. However, since then we and Mallinkcrodt have continued to work towards the approvability of REMOXY and commercial readiness. We continue to rely on our agreement with Mallinkcrodt to move forward with the REMOXY program.
We expect to continue to rely on Mallinckrodt as the sole-source drug product manufacturer of REMOXY pursuant to the Mallinckrodt Agreement. In addition to drug product manufacturing, Mallinckrodt is responsible for sourcing excipients in REMOXY other than those provided by the Durect Agreement.
Commercial manufacturing and supply agreements
We will rely on third parties to conduct certain quality control and assurance testing, shipping or storage of REMOXY.
Government Regulation
Regulation by governmental authoritiesregulations in the United States and in Canada. We attempt to comply with all legal requirements in the conduct of our operations and employ business practices that we consider to be prudent under the circumstances in which we operate. Government authorities in the U.S. at the federal, state and local level and in Canada and other countries isregulate, among other things, the research, development, testing, manufacture, quality control, approval, labeling, packaging, storage, record-keeping, promotion, advertising, distribution, post-approval monitoring and reporting, marketing and export and import of drug and diagnostic products. Generally, before a significant factor innew drug or diagnostic can be marketed, considerable data demonstrating its quality, safety and efficacy and/or specificity must be obtained, organized into a format specific for each regulatory authority, submitted for review and approved by each regulatory authority.
U.S. Drug Development
In the manufactureU.S., FDA regulates drugs under the Food, Drug, and marketing of pharmaceuticalsCosmetic Act (FDCA). Both drugs and in our ongoing research and development activities. All of our products will require regulatory approval by governmental agencies prior to commercialization. In particular, human therapeutic productsdiagnostics also are subject to rigorous preclinical testingother federal, state and clinical trialslocal statutes and other pre-marketing approval requirements byregulations. The process of obtaining regulatory approvals and the FDAsubsequent compliance with appropriate federal, state, local and regulatory authorities in other countries. In the United States, various federal, and in some cases state,foreign statutes and regulations also governrequires the expenditure of substantial time and financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or impactpost-market may subject an applicant to administrative or judicial sanctions. These sanctions could include, among other actions, FDA’s refusal to approve pending applications, withdrawal of an approval, a clinical hold, untitled or warning letters, product recalls or market withdrawals, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement and civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on us.
Product candidates must be approved by FDA before they may be commercialized in the U.S. The drug approval process generally involves the following:
Completion of extensive preclinical studies in accordance with applicable regulations, including studies conducted in accordance with good laboratory practice;
Submission to FDA of an IND, which must become effective before human clinical studies may begin;
Approval by an independent institutional review board (IRB) or ethics committee before each study may be initiated;
Performance of adequate and well-controlled human clinical studies in accordance with applicable IND regulations, code of good clinical practice (cGCP), requirements and other clinical trial-related regulations to establish the safety and efficacy of the investigational product for each proposed indication;
Submission to FDA of an NDA;
A determination by FDA within 60 days of its receipt of an NDA to accept the filing for review;
Satisfactory completion of an FDA pre-approval inspection of the manufacturing safety, labeling, storage, record keeping and marketing of our products. The lengthy process of seeking required approvals andfacility or facilities where the continuing need fordrug will be produced to assess compliance with applicable statutescGMP, requirements to assure that the facilities, methods and regulations require uscontrols are adequate to spendpreserve the drug’s identity, strength, quality and purity;
Potential FDA audit of the preclinical study and/or clinical study sites that generated the data in support of the NDA;
FDA review and approval of the NDA, including consideration of the views of any FDA advisory committee, prior to any commercial marketing or sale of the drug in the U.S.; and
Compliance with any post-approval requirements, including the potential requirement to conduct post-approval studies.
The data required to support an NDA are generated in two distinct developmental stages: preclinical and clinical. The preclinical and clinical testing and approval process requires substantial resources. Regulatory approval, whentime, effort and if obtained, mayfinancial resources, and we cannot be limited in scope which may significantly limit the indicated usescertain that any approvals for which our products mayany future product candidates will be marketed. Further, approved drugs,granted on a timely basis, or at all.
Preclinical Studies and IND
The preclinical developmental stage generally involves laboratory evaluations of drug chemistry, formulation and stability, as well as their manufacturers, are subjectstudies to ongoing reviewevaluate toxicity in animals, which support subsequent clinical testing. As sponsor, we must submit the results of the preclinical studies, together with manufacturing information, analytical data, any available clinical data or literature and discoverya proposed clinical protocol, to FDA as part of previously unknown problems with such products thatthe IND. An IND is a request for authorization from FDA to administer an investigational product to humans and must become effective before human clinical studies may result in restrictions on their manufacture, sale or use or in their withdrawal from the market.begin.
Applicable FDA regulations require the filing of an NDA or a Biologic License Application, or BLA and approval by the FDA prior to commercialization of any of our drug candidates in the United States.
The Drug Approval Process
We will be required to complete several activities before we can market any of our drug candidates for human use in the United States, including:
| ·
| | submission to the FDA of an IND which must become effective before human clinical trials commence;
|
| ·
| | adequate and well-controlled human clinical trials to establish the safety and efficacy of the drug candidate;
|
| ·
| | submission to the FDA of an NDA; and
|
| ·
| | FDA approval of the NDA prior to any commercial sale or shipment of the drug.
|
Preclinical testsstudies include laboratory evaluation of product chemistry and formulation, as well asin vitro and animal studies to assess the potential safetyfor adverse events and in some cases to establish a rationale for therapeutic use. The conduct of the product. Preclinical safety testspreclinical studies is subject to federal regulations and requirements, including cGCP regulations for safety/toxicology studies. An IND sponsor must be conducted by laboratories that comply with the FDA regulations regarding Good Laboratory Practice. We submittedsubmit the results of the preclinical tests, together with manufacturing information, analytical data, any available clinical data or literature and plans for clinical studies, among other things, to the FDA as part of our INDs prior to commencing clinical trials. We may be required to conduct additional toxicology studies.
Based onan IND. Some long-term preclinical testing, ansuch as long-term toxicity tests, animal tests of reproductive adverse events and carcinogenicity, may continue after the IND is filed with thesubmitted. An IND automatically becomes effective 30 days after receipt by FDA, to begin human testingunless before that time FDA raises concerns or questions about any aspect of the drugprogram. In such a case, the IND sponsor and FDA must resolve any outstanding concerns before the clinical study can begin.
Clinical Studies
The clinical stage of development involves the administration of the investigational product to healthy volunteers or patients under the supervision of qualified investigators, generally physicians not employed by or under the study sponsor’s control, in accordance with cGCP requirements, which include the United States. The IND becomes effective if not rejectedrequirement that all research subjects provide their informed consent for their participation in any clinical trial. Clinical studies are conducted under protocols detailing, among other things, the objectives of the clinical trial, dosing procedures, subject selection and exclusion criteria and the parameters to be used to monitor subject safety and assess efficacy. Each protocol, and any subsequent amendments to the protocol, must be submitted to FDA as part of the IND. Furthermore, each clinical study must be reviewed and approved by an IRB for each institution at which the FDA within 30 days. The IND must indicate the results of previous experiments, how, where and by whom the new clinical trialsstudy will be conducted to ensure that the chemical structurerisks to individuals participating in the clinical studies are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the informed consent form that must be provided to each clinical study subject or his or her legal representative and must monitor the clinical study until completed. There also are requirements governing the reporting of ongoing clinical studies and completed clinical study results to public registries.
A sponsor who wishes to conduct a clinical study outside of the compound,U.S. may, but need not, obtain FDA authorization to conduct the method by which itclinical study under an IND. If a foreign clinical study is believednot conducted under an IND, the sponsor may submit data from the clinical study to workFDA in support of an NDA. The FDA may accept a well-designed and well-conducted foreign clinical study not conducted under an IND if the human body, any toxic effects of the compound found in the animal studies and how the compound is manufactured. All clinical trials must bestudy was conducted in accordance with Good cGCP requirements and FDA is able to validate the data through an onsite inspection if deemed necessary. We launched clinical sites in Canada in 2021 and plan to perform additional clinical studies outside of the U.S. and Canada in the future.
Clinical Practice. In addition,studies in the U.S. generally are conducted in three sequential phases, known as Phase 1, Phase 2 and Phase 3, and may overlap.
Phase 1 clinical studies generally involve a small number of healthy volunteers or disease-affected patients who are initially exposed to a single dose and then multiple doses of the product candidate. The primary purpose of these clinical studies is to assess the metabolism, pharmacologic action, tolerability and safety of a drug candidate.
Phase 2 clinical studies involve studies in disease-affected patients to determine the proper dose required to produce the desired benefits. At the same time, safety and further pharmacokinetic and pharmacodynamic information is collected, possible adverse effects and safety risks are identified, and a preliminary evaluation of efficacy may be observed.
Phase 3 clinical studies generally involve many patients at multiple sites and are designed to provide the data necessary to demonstrate the effectiveness of the product for its intended use, its safety in use and to establish the overall benefit/risk relationship of the product and provide an Institutional Review Board, adequate basis for product approval. These studies may include comparisons with placebo and/or IRB, generally comprisedother comparator treatments. The duration of physicians attreatment is often extended to mimic the hospital or clinic where the proposedactual use of a product during marketing.
Post-approval studies, sometimes referred to as Phase 4 clinical trials willstudies, may be conducted must review and approveafter initial marketing approval. These studies are used to gain additional experience from the IND. The IRB also continues to monitortreatment of patients in the intended therapeutic indication. In certain instances, FDA may mandate the performance of Phase 4 clinical trial. We must submit progressstudies as a condition of approval of an NDA.
Progress reports detailing the results of the clinical trialsstudies, among other information, must be submitted at least annually to FDA. Written safety reports and the investigators for serious and unexpected adverse events, or any other findings suggesting a significant risk to humans exposed to the drug must be submitted to FDA.
Phase 1, Phase 2, and Phase 3 clinical studies may not be completed successfully within any specified period, if at all. The FDA at least annually. In addition,or the FDAsponsor may suspend or terminate a clinical study at any time duringon various grounds, including a finding that the 30-day periodresearch subjects or at any time thereafter, impose a clinical hold on proposed or ongoing clinical trials. If the FDA imposes a clinical hold, clinical trials under the IND cannot commence or recommence without the FDA authorization and then only under terms authorized by the FDA. An FDA imposed clinical hold on an IND application can result in substantial delay and large, unforeseen expenses, and it may cancel the viability of developing a new drug candidate in the United States.
Clinical trials are typically conducted in three sequential phases that may overlap. Phase I clinical trials typically study a drug’s safety profile and may include the safe dosage range. Phase I clinical trials also determine how a drug is absorbed, distributed, metabolized and excreted by the body, and the duration of its action. In addition, we may, to the extent feasible, assess early indicators of a drug’s efficacy in our Phase I clinical trials. In Phase II clinical trials, controlled studies are conducted on volunteer patients with the targeted disease or condition. The primary purpose of these tests is to evaluate the effectiveness of the drug on the volunteer patients as well as to determine a drug’s side effect profile. These clinical trials may be conducted concurrently with Phase I clinical trials. In addition, Phase I/II clinical trials may be conducted to evaluate not only the efficacy of the drug on the patient population, but also its safety. During Phase III clinical trials, the drug is studied in an expanded patient population and in multiple sites. Physicians monitor the patients to determine efficacy and to observe and report adverse events that may result from use of the drug.
Our clinical trials are designed to produce clinical information about how our drugs perform compared to placebo or compared to existing drugs where appropriate. We have designed most Phase II and Phase III clinical trials to date as randomized, double-blind, placebo-controlled, dose-ranging studies. A randomized clinical trial is one in which patients are randomly assigned to the various study treatment arms. A double-blind clinical trial is one in which the patient, the physician and our trial monitor are unaware if the patient is receiving placebo or study drug in order to preserve the integrity of the clinical trial and reduce bias. A placebo-controlled clinical trial is one in which a subset of patients is purposefully given inactive medication.
We may not successfully complete Phase I, Phase II or Phase III clinical trials within any specified time period, or at all, with respect to any of our drug candidates. Furthermore, we or the FDA may suspend clinical trials at any time in response to concerns that participants arebeing exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical study at its institution if the clinical study is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients. Additionally, some clinical studies are overseen by an independent group of qualified experts organized by the clinical study sponsor, known as a data safety monitoring board. This group provides authorization for whether a study may move forward at designated check-points based on access to certain data from the trial. Concurrent with clinical studies, companies usually complete additional animal studies and must develop additional information about the chemistry and physical characteristics of the drug as well as finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the product and, among other things, companies must develop methods for testing the identity, strength, quality and purity of the final product. Additionally, appropriate packaging must be selected and tested, and stability studies must be conducted to demonstrate that our product candidates do not undergo unacceptable deterioration over their shelf life.
After theNDA Review Process
Following completion of the clinical trials, if therestudies, data is substantial evidence thatanalyzed to assess whether the druginvestigational product is safe and effective for the proposed indicated use or uses. The results of preclinical studies and clinical studies are then submitted to FDA as part of an NDA, along with proposed labeling, chemistry and manufacturing information to ensure product quality and other relevant data. In short, the NDA is a request for approval to market a drug for one or more specified indication and must contain proof of safety and efficacy for a drug’s purity and potency. The application may include both negative and ambiguous results of preclinical studies and clinical studies, as well as positive findings. Data may come from company-sponsored clinical studies intended to test the safety and efficacy of a product’s use or from several alternative sources, including studies initiated by investigators. To support marketing approval, the data submitted must be sufficient in quality and quantity to establish the safety and efficacy of the investigational product to the satisfaction of FDA. FDA approval of an NDA must be obtained before a drug may be marketed in the U.S.
Under the Prescription Drug User Fee Act (PDUFA), as amended, each NDA must be accompanied by a user fee. FDA adjusts the PDUFA user fees on an annual basis. According to FDA’s fiscal year 2022 fee schedule, effective through September 30, 2022, the user fee for an application requiring clinical data, such as an NDA, is filed with the FDA. The NDA must contain allapproximately $3.1 million. Fee waivers or reductions are available in certain circumstances, including a waiver of the informationapplication fee for the first application filed by a small business. Additionally, no user fees are assessed on NDAs for products designated as orphan drugs, unless the drug gathered to that date, including data from the clinical trials. NDAs often exceed 100,000 pages in length.product also includes a non-orphan indication.
The FDA reviews all submitted NDAs before it accepts them for filing and may request additional information beforerather than accept the NDA for filing. The FDA must decide on accepting an NDA. In such an event, the NDA must be resubmitted with the additional information and, again, is subject to review before filing.for filing within 60 days of receipt. Once the submission is accepted for filing, the FDA begins an in-depth review of the NDA. Under the Federal Food, Druggoals and Cosmetic Act,policies agreed to by FDA under PDUFA, FDA has 10 months, from the FDA reviews thefiling date, in which to complete its initial review of a new molecular-entity NDA and respondsrespond to the applicant.applicant, and six months from the filing date of a new molecular-entity NDA designated for priority review. The FDA does not always meet its PDUFA goal dates for standard and priority NDAs, and the review process is typicallyoften extended for significant amounts of time by the FDA’sFDA requests for additional information or clarification regarding information already providedclarification.
Before approving an NDA, FDA may conduct a pre-approval inspection of the manufacturing facilities for the new product to determine whether they comply with cGMP requirements. The FDA will not approve the product unless it determines that the manufacturing processes and facilities fully comply with cGMP requirements and are adequate to assure
consistent production of the product within required specifications. The FDA also may audit data from clinical studies to ensure compliance with cGCP requirements. Additionally, FDA may refer applications for novel product candidates which present difficult questions of safety or efficacy to an advisory committee, typically a panel that includes clinicians and other experts, for review, evaluation and a recommendation as to whether the application should be approved and under what conditions, if any. The FDA is not bound by recommendations of an advisory committee, but it considers such recommendations when making decisions on approval. The FDA likely will reanalyze the clinical study data, which could result in extensive discussions between FDA and the submission.
It is FDA policy to convene an expert Advisory Committee meetingapplicant during the review cycle for opioid drug products. The purpose ofprocess. After FDA evaluates an Advisory Committee is to provide third-party input on key regulatory decisions, including approval and labeling of abuse-deterrent products, and whether the totality of the data submitted by a sponsor is sufficient to support marketing approval in the United States and labeling of the product with claims on abuse-deterrence. Advisory Committee meetings are non-binding, that is, the FDA is not legally bound to follow any recommendation, vote or input of an Advisory Committee on any matter.
If the FDA’s evaluations of the NDA, and the manufacturing facilities are favorable, the FDA mayit will issue either a CRL indicating either an approval letter or may identify conditions that must be met in order to secure final approval of the NDA. When and if those conditions have been met to the FDA’s satisfaction, the FDA will issue ana Complete Response Letter (CRL). An approval letter authorizingauthorizes commercial marketing of the drug with specific prescribing information for certainspecific indications. If theA CRL indicates that FDA’s evaluationreview of the application is complete and the application cannot be approved in its present form. A CRL usually describes the specific deficiencies in the NDA submission identified by FDA. The CRL may require additional clinical data, additional pivotal Phase 3 clinical trial(s) and/or manufacturing facilitiesother significant and time-consuming requirements related to clinical studies, preclinical studies or manufacturing. If a CRL is not favorable,issued, the applicant may either resubmit the NDA, addressing all the deficiencies identified in the CRL, or withdraw the application. Even if such data and information are submitted, FDA may refuse to approvedecide that the NDA or issue adoes not approvable letter.
Ifsatisfy the FDA approves the NDA, the drug becomes availablecriteria for physicians to prescribe. Periodic reports must be submitted to the FDA, including descriptions of any reported adverse reactions. Theapproval. Data obtained from clinical studies are not always conclusive and FDA may request additional post-marketing studies, or Phase IV clinical trials, to evaluate long-term effects ofinterpret data differently than we interpret the approved drug.same data.
Risk Evaluation and Mitigation Strategy (REMS)
The FDA requires a Risk Evaluation and Mitigation Strategy, or REMS, as a condition of the approval of an NDA or after approval to ensure that the benefits of a drug outweigh its risks. In determining whether a REMS is necessary, the FDA considers the size of the population likely to use the drug, the seriousness of the disease or condition to be treated, the expected benefit of the drug, the duration of treatment, the seriousness of known or potential adverse events, and whether the drug is a new molecular entity. If the FDA determines a REMS is necessary for a new drug, the drug sponsor must submit a proposed REMS plan as part of its NDA prior to approval. A REMS for a newly approved drug can include medication guides, communication plans for healthcare professionals, and Elements To Assure Safe Use, or ETASU. ETASU can include, but are not limited to, special training or certification for prescribing or dispensing, dispensing only under certain circumstances, special monitoring, and the use of patient registries. In addition, the REMS must include a timetable to periodically assess the strategy, at a minimum, at 18 months, three years, and seven years after the REMS approval. The requirement for a REMS can materially affect the potential market and profitability of a drug.
The FDA has initiated efforts to develop a standardized REMS for opioid medications to ensure their safe use. In July 2012, the FDA approved a class‑wide REMS for extended‑release formulations of oxycodone. Manufacturers subject to this class‑wide REMS must work together to implement the REMS as part of a single shared system to reduce the burden of the REMS on the healthcare system. The central component of the extended release/long acting opioid REMS program is an education program for prescribers and patients. REMS include a Medication Guide available for distribution to patients who are dispensed the drug, as well as ETASU. ETASU include training for healthcare professionals who prescribe the drug; information provided to prescribers that they can use to educate patients in the safe use, storage, and disposal of opioids; and information provided to prescribers of the existence of the REMS and the need to successfully complete the necessary training. Prescriber training required as part of the REMS is conducted by accredited, independent continuing education providers, without cost to healthcare professionals, under unrestricted grants funded by opioid analgesic manufacturers. Moreover, REMS assessments must be submitted on an annual basis to assess the extent to which ETASU are meeting the goals of the REMS and whether the goals or elements should be modified.
Advertising and Promotion
The FDA and other federal regulatory agencies closely regulate the marketing and promotion of drugs through, among other things, standards and regulations for direct‑to‑direct-to-consumer advertising, communications regarding unapproved uses, industry‑industry-sponsored scientific and educational activities, and promotional activities involving the Internet. Our lead drug candidate, REMOXY, cannotNone of our product candidates can be commercially promoted before receiving FDA approval. After approval, product promotion can include only those claims relating to safety and effectiveness that are consistent with the labeling approved by the FDA. Healthcare providers are permitted to prescribe drugs for “off‑“off-label” uses — that is, uses not approved by the FDA and therefore not described in the drug’s labeling — because the FDA does not regulate the practice of medicine. However, FDA
regulations impose stringent restrictions on manufacturers’ communications regarding off‑off-label uses. Failure to comply with applicable FDA requirements and restrictions in this area may subject us to adverse publicity and enforcement action by the FDA, the U.S. Department of Justice, or the Office of the Inspector General of the HHS,Health and Human Services, as well as state authorities. This could subject us to a range of penalties that could have a significant commercial impact, including civil and criminal fines and agreements that materially restrict the manner in which we promote or distribute REMOXY.our product candidates.
Post‑Post-Approval Requirements
Once an NDAAfter a product candidate receives regulatory approval, it is approved, REMOXY will beoften subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to drug listing and registration, recordkeeping, periodic reporting, product sampling and distribution, adverse event reporting and advertising, marketing and promotion restrictions.
Adverse event reporting and submission of periodic reports is required following FDA approval of an NDA. The FDA also may require post‑post-market testing, known as Phase 4 testing, REMS, and surveillance to monitor the effects of an approved product, or the FDA may place conditions on an approval that could restrict the distribution or use of the product. In addition, quality control, drug manufacture, packaging, and labeling procedures must continue to conform to Current Good Manufacturing Practices (cGMPs)cGMP after approval. Drug manufacturers and certain of their subcontractors are required to register their establishments with the FDA and certain state agencies. Registration subjects entities tomay result in periodic announced or unannounced inspections by the FDA or these state agencies, during which the agency inspects manufacturing facilities to assess compliance with cGMPs.cGMP. Accordingly, manufacturers must continue to expend time, money, and effort in the areas of production and quality control to maintain compliance with cGMPs.cGMP. Regulatory authorities may withdraw product approvals or request product recalls if a company fails to comply with regulatory standards, if it encounters problems following initial marketing, or if previously unrecognized problems are subsequently discovered. In addition, other regulatory actions may be taken, including, among other things, warning letters, the seizure of products, injunctions, consent decrees placing significant restrictions on or suspending manufacturing operations, refusal to approve pending applications or supplements to approved applications, civil penalties, and criminal prosecution.
The FDA may require post‑post-approval clinical studies and clinical trials ifto help assure continued safety or effectiveness of the FDA finds that scientific data, including information regarding related drugs, deem it appropriate. The purpose of such studies would be to assess a known serious risk or signals of serious risk related to the drug or to identify an unexpected serious risk when available data indicate the potential for a serious risk.approved drug. The FDA may also require a labeling change if it becomes aware of new safety information that it believes should be included in the labeling of a drug.
The Hatch‑Hatch-Waxman Amendments
Orange Book Listing
In seeking approval for REMOXYour product candidates through an NDA, we will be required to list with the FDA each patent whose claims cover the drug product. Upon receiving regulatory approval, of REMOXY, each of the patents listed in the application for this drug is then published in the FDA’s Approved Drug Products with Therapeutic Equivalence Evaluations, commonly known as the “Orange Book”. Drugs listed in the Orange Book can, in turn, be cited by potential generic competitors in support of approval of an abbreviated NDA, or ANDA. An ANDA provides for marketing of a drug product that has the same active ingredient in the same strengths and dosage form as the listed drug and has been shown through bioequivalence testing to be therapeutically equivalent to the listed drug. Other than the requirement for bioequivalence testing, ANDA applicants are not required to conduct, or submit results of, preclinical or clinical tests to prove the safety or efficacy of their drug product. However, in November 2017, the FDA issued final guidance on the regulatory pathway for generic abuse‑deterrent opioid products. Among other requirements, the new FDA guidance emphasizes that sponsors of generic abuse-deterrent oxycodone must ensure that a generic opioid drug is no less abuse deterrent than the original opioid and must also evaluate all potential routes of abuse, even those routes of abuse for which a generic sponsor does not seek a label-claim. Drugs approved in this way are commonly referred to as “generic equivalents” to the listed drug, and can often be substituted by pharmacists under prescriptions written for the original listed drug.
The ANDA applicant is required to make certain certifications to the FDA concerning any patents listed for the approved product in the FDA’s Orange Book. Specifically, the applicant must certify that: (i) the required patent information has not
been filed; (ii) the listed patent has expired; (iii) the listed patent has not expired but will expire on a particular date and approval is sought after patent expiration; or (iv) the listed patent is invalid or will not be infringed by the new product. The ANDA applicant may also elect to submit a section viii statement certifying that its proposed ANDA label does not contain (or carves out) any language regarding the patented method‑of‑method-of-use rather than make certifications concerning a listed method‑of‑method-of-use patent. If the applicant does not challenge the listed patents, the ANDA application will not be approved until all the listed patents claiming the referenced product have expired.
A certification that the new product will not infringe the already approved product’s listed patents, or that such patents are invalid, is called a Paragraph IV certification. If the ANDA applicant has provided a Paragraph IV certification to the FDA, the applicant must also send notice of the Paragraph IV certification to the NDA and patent holders once the ANDA has been accepted for filing by the FDA. The NDA and patent holders may then initiate a patent infringement lawsuit in response to the notice of the Paragraph IV certification. The filing of a patent infringement lawsuit within 45 days of the receipt of a Paragraph IV certification automatically prevents the FDA from approving the ANDA until the earlier of 30 months, expiration of the patent, settlement of the lawsuit, or a decision in the infringement case that is favorable to the ANDA applicant. The ANDA application also will not be approved until any applicable non‑non-patent exclusivity listed in the Orange Book for the referenced product has expired.
Exclusivity
Upon NDA approval of a new chemical entity, or NCE, which is a drug that contains no active moiety that has been approved by the FDA in any other NDA, that drug receives five years of marketing exclusivity during which the FDA cannot receive any ANDA seeking approval of a generic version of that drug or any Section 505(b)(2) NDA that relies on the FDA’s findings regarding that drug. A drug may obtain a three‑year period of exclusivity for a change to the drug, such as the addition of a new indication to the labeling or a new formulation, during which the FDA cannot approve an ANDA or any Section 505(b)(2) NDA, if the supplement includes reports of new clinical trials (other than bioavailability clinical trials) essential to the approval of the supplement.
An ANDA may be submitted one year before NCE exclusivity expires if a Paragraph IV certification is filed. If there is no listed patent in the Orange Book, there may not be a Paragraph IV certification, and, thus, no ANDA may be filed before the expiration of the exclusivity period.
Section 505(b)(2) NDAs
Generally, drug products obtain FDA marketing approval pursuant to an NDA or an ANDA. A third alternative is a Section 505(b)(2) NDA, which enables the applicant to rely, in part, on data not developed by the applicant, such as the FDA’s findings of safety and efficacy in the approval of a similar product or published literature in support of its application.
Section 505(b)(2) NDAs may provide an alternate path to FDA approval for new or improved formulations or new uses of previously approved products. Section 505(b)(2) permits the filing of an NDA where at least some of the information required for approval comes from clinical trials not conducted by, or for, the applicant and for which the applicant has not obtained a right of reference. If the Section 505(b)(2) applicant can establish that reliance on the FDA’s previous findings of safety and efficacy is scientifically appropriate, it may eliminate the need to conduct certain preclinical or clinical trials of the new product. The FDA may also require companies to perform additional clinical trials or provide additional materials to support the change from the approved product. The FDA may then approve the new product candidate for all, or some, of the label indications for which the referenced product has been approved, as well as for any new indication sought by the Section 505(b)(2) applicant.
To the extent that the Section 505(b)(2) applicant is relying on the FDA’s findings of safety and effectiveness for an already approved product, the applicant is required to certify to the FDA concerning any patents listed for the approved product in the Orange Book to the same extent that an ANDA applicant would. Therefore, approval of a Section 505(b)(2) NDA can be stalled until all the listed patents claiming the referenced product have expired; until any non‑patent exclusivity, such as exclusivity for obtaining approval of a new chemical entity, listed in the Orange Book for the referenced product has expired; and, in the case of a Paragraph IV certification and subsequent patent infringement suit, until the earlier of 30 months, settlement of the lawsuit or a decision in the infringement case that is favorable to the Section 505(b)(2) applicant. In the interim period, the FDA may grant tentative approval. Tentative approval indicates that the FDA has determined that the applicant meets the standards for approval as of the date that the tentative approval is granted. Final regulatory approval can
only be granted if the FDA is assured that there is no new information that would affect final regulatory approval. As with traditional NDAs, a Section 505(b)(2) NDA may be eligible for three‑year marketing exclusivity, assuming the NDA includes reports of new clinical trials (other than bioavailability clinical trials) essential to the approval of the NDA.
Disclosure of Clinical TrialStudy Information
Sponsors of clinical trialsstudies of FDA‑FDA-regulated products, including drugs, are required to register and disclose certain clinical trialstudy information. Information related to the product, patient population, phase of investigation, clinical trialstudy sites and investigators, and other aspects of the clinical trialstudy is then made public as part of the registration. Sponsors are also obligated to post certain information regarding the results of their clinical trialsstudies after completion. Disclosure of the results of these trialsstudies can be delayed until the new product or new indication being studied has been approved. Competitors may use this publicly available information to gain knowledge regarding the progress of development programs.
DEAOther Regulatory Requirements
Our lead drug candidate, REMOXY, is regulated as a controlled substance under the Controlled Substances Act, or CSA. CSA establishes registration, security, recordkeeping, reporting, storage, distribution, importation, exportation and other requirements administered by the DEA. The DEA regulates the handling of controlled substances through a closed chain of distribution. This control extends to the equipment and raw materials used in their manufacture and packaging of REMOXY, in order to prevent loss and diversion into illicit channels of commerce.
REMOXY, an abuse‑deterrent oral formulation of oxycodone, is listed by the DEA as a Schedule II controlled substance under the CSA. Consequently, the manufacturing, shipping, storing, selling and use of the products is subject to a high degree of regulation. Schedule II drugs are subject to the strictest requirements for registration, security, recordkeeping and reporting. Also, distribution and dispensing of these drugs are highly regulated. For example, all Schedule II drug prescriptions must be signed by a physician, physically presented to a pharmacist andWe may not be refilled without a new prescription.
Annual registration is required for any facility that manufactures, distributes, dispenses, imports or exports any controlled substance. The registration is specific to the particular location, activity and controlled substance schedule. For example, separate registrations are needed for import and manufacturing, and each registration will specify which schedules of controlled substances are authorized.
The DEA typically inspects a facility to review its security measures prior to issuing a registration. Security requirements vary by controlled substance schedule, with the most stringent requirements applying to Schedule I and Schedule II substances. Required security measures include background checks on employees and physical control of inventory through measures such as cages, surveillance cameras and inventory reconciliations. Records must be maintained for the handling of all controlled substances, and periodic reports made to the DEA, for example distribution reports for Schedule I and II controlled substances, Schedule III substances that are narcotics, and other designated substances. Reports must also be made for thefts or losses of any controlled substance, and to obtain authorization to destroy any controlled substance. In addition, special permits and notification requirements apply to imports and exports of narcotic drugs.
In addition, a DEA quota system controls and limits the availability and production of controlled substances in Schedule I or II. Distributions of any Schedule I or II controlled substance must also be accompanied by special order forms, with copies provided to the DEA. Because REMOXY is regulated as a Schedule II controlled substance, it will be subject to federal, state and local environmental laws and regulations, including the DEA’s productionEnvironmental Protection Act and procurement quota scheme. The DEA establishes annuallythe Clean Air Act. Although we believe that our safety procedures for handling and disposing of controlled materials comply with the standards prescribed by state and federal regulations, accidental contamination or injury from these materials may occur. In the event of such an aggregate quotaoccurrence, we could be held liable for how much oxycodone may be produced in total in the United States based on the DEA’s estimate of the quantity needed to meet legitimate scientificany damages that result and medicinal needs. The limited aggregate amount of opioids that the DEA allows to be produced in the United States each year is allocated among individual companies, who must submit applications annually to the DEA for individual production and procurement quotas. We andany such liability could exceed our contract manufacturers must receive an annual quota from the DEA in order to produce or procure any Schedule I or Schedule II substance, including oxycodone base for use in manufacturing REMOXY. The DEA may adjust aggregate production quotas and individual production and procurement quotas from time to time during the year, although the DEA has substantial discretion in whether or not to make such adjustments.resources.
To enforce these requirements, the DEA conducts periodic inspections of registered establishments that handle controlled substances. Failure to maintain compliance with applicable requirements, particularly as manifested in loss or diversion, can result in administrative, civil or criminal enforcement action that could have a material adverse effect on our business, results of operations and financial condition. The DEA may seek civil penalties, refuse to renew necessary registrations or initiate administrative proceedings to revoke those registrations. In certain circumstances, violations could result in criminal proceedings. In addition, individual states also independently regulate controlled substances. We and our contract manufacturers will be subject to state regulation on distribution of these products.
Other Regulatory Requirements
We may also be subject to regulations under other federal, state, and local laws, including the Occupational Safety and Health Act, the Environmental Protection Act, the Clean Air Act, national restrictions on technology transfer, and import, export, and customs regulations. It is possible that any portion of the regulatory framework under which we operate may change and that such change could have a negative impact on our current and anticipated operations. Failure to comply with these requirements could result, among other things, in suspension of regulatory approval, recalls, injunctions or civil or criminal sanctions.
Third‑Third-Party Payor Coverage and Reimbursement
The commercial success of REMOXY,our product candidates, if approved, will depend, in part, upon the availability of coverage and adequate reimbursement from third‑third-party payors at the federal, state and private levels. Third‑Third-party payors include governmental programs such as Medicare or Medicaid, private insurance plans and managed care plans. These third‑third-party payors may deny coverage or reimbursement for REMOXYour product candidates in whole or in part if they determine that our drug product iscandidates are not medically appropriate or necessary. Also, third partythird-party payors attempt to control costs by limiting coverage through the use of formularies and other cost‑cost-containment mechanisms and the amount of reimbursement for particular procedures or drug treatments.
Some third‑third-party payors also require pre‑pre-approval of coverage for new or innovative devices or drug therapies before they will reimburse healthcare providers who use such therapies. While we cannot predict whether any proposed cost‑cost-containment measures will be adopted or otherwise implemented in the future, these requirements or any announcement or adoption of such proposals could have a material adverse effect on our ability to obtain adequate prices for REMOXYour approved product candidates to operate profitably.
CompetitionHuman Capital
Our success will depend,approach to human capital resource management starts with our mission to detect and treat neurodegenerative diseases, such as Alzheimer’s disease. Our industry exists in part, upona complex regulatory environment. The unique demands of our industry, together with the challenges of running an enterprise focused on the discovery, development, manufacture and commercialization of innovative medicines, require talent that is highly educated and/or has significant industry experience. Additionally, for certain key functions, we require specific scientific expertise to oversee and conduct research and development activities and the complex manufacturing requirements for biopharmaceutical products.
We consider our ability to achieve market share atrecruit, retain and motivate our employees to be critical to our success. We are an equal opportunity employer, and we are fundamentally committed to creating and maintaining a work environment in which employees are treated with respect and dignity. All human resources policies, practices and actions related to hiring, promotion, compensation, benefits and termination are administered in accordance with the expenseprincipal of existingequal employment opportunity, meaning that they are made on the basis of individual skills, knowledge, abilities, job performance and establishedother legitimate criteria and future productswithout regard to race, color, religion, sex, sexual orientation, gender expression or identity, ethnicity, national origin, ancestry, age, mental or physical disability, genetic information, any veteran status, any military status or application for military service, or membership in any other category protected under applicable law. By focusing on employee retention and engagement, we also improve our target markets. Existingability to support our clinical trials, our pipeline, business and future products, therapies, technological approaches or delivery systems will compete directly with REMOXY. Competing products may provide greater therapeutic benefits foroperations, and also protect the long-term interests of our stockholders. Our success also depends on our ability to attract, engage and retain a specific indication, or may offer comparable performance at a lower cost. Companies that currently sell generic or proprietary opioid formulations indiverse group of employees.
Our base pay program aims to compensate management and staff members relative to the United States may include, but are not limitedvalue of the contributions of their role, which takes into account the skills, knowledge and abilities required to Purdue Pharma, Collegium, Inc., Roxane Laboratories, Mylan, Abbott Laboratories, Endo Pharmaceuticals, Teva Pharmaceuticals, Elkins-Sinn, Watson Laboratories, Hikma Pharmaceuticals, Pernix, Mallinckrodt, Eaglet Pharmaceuticals, Ortho-McNeil Pharmaceutical and Forest Pharmaceuticals,perform each position, as well as several generic companies.
Alternative technologies are being developedthe experience brought to address the issuejob. We also provide cash incentive programs to reward our management team and staff members in alignment with achievement of abuse or misuse of opioid painkillers or increase opioid potency, as well as alternatives to opioid therapy for pain management, several of which are in clinical trials or are awaiting approval from the FDA.
We compete with fully integrated pharmaceutical companies, smaller companiesCompany-wide goals that are collaborating with larger pharmaceutical companies, academic institutions, government agenciesdesigned to drive aspects of our strategic priorities that support and other publicadvance our strategy across our Company. Our management team and private research organizations. Manystaff members are eligible for the grant of equity awards under our long-term incentive program that are designed to align the experience of these competitors have opioid drugs already approved bystaff with that of our stockholders.
Our benefit programs are also generally broad-based, promote health and overall well-being and emphasize saving for retirement. All management team and regular staff members are eligible to participate in the FDA or in developmentsame core health and operate larger researchwelfare and development programs in these fields than we do. In addition, manyretirement savings plans. Other employee benefits include medical plans, dental plans, vacation and sick-pay plans, flexible spending accounts, life and accident insurance and short and long-term disability benefits.
Our Compensation Committee provides oversight of these competitors, either alone or together with their collaborative partners, have substantially greater financial resources than we do, as well as significantly greater experience in:
| ·
| | undertaking preclinical testing and human clinical trials;
|
| ·
| | obtaining FDA and other regulatory approvals of drugs;
|
| ·
| | formulating and manufacturing drugs; and
|
| ·
| | launching, marketing, distributing and selling drugs.
|
our executive compensation plans, policies and programs.
Developments by competitors may render our drug candidates or technologies obsolete or non-competitive. We also compete with these companies for qualified personnel and opportunities for product acquisitions, joint ventures or other strategic alliances.
Incorporation
We were incorporated in Delaware in May 1998.
Employees
As of December 31, 2017,2021, we had 924 full-time employees. None of our employees are represented by a labor union or covered under a collective bargaining agreement. We also engage numerous consultants from time to time to perform services on retainer, a per diem or an hourly basis.
Impact of COVID-19 on our Business
Available
During the COVID-19 pandemic, our top priorities are to protect the health, well-being, and safety of our employees and partners, while still focusing on the key drivers of our business. Despite COVID-19, we believe we may be on-track to achieve our major strategic objectives for 2022 with simufilam. We have generally not experienced major disruptions across our drug manufacturing operations or supply of materials. We have experienced some disruptions across certain investigational clinical study sites because of pandemic effects on job-loss, employment and other factors. Our broad spectrum of technical consultants, scientific advisors and service providers continue to provide timely services. We have adapted flexible business practices, such as remote work arrangements and temporary travel restrictions, to insure we continue to operate safety and cautiously while also meeting our public health responsibilities. We recognize the pandemic has created a dynamic and uncertain situation in the national economy. We continue to closely monitor the latest information to make timely, informed business decisions and public disclosures regarding the potential impact of pandemic on our operations. However, the scope of pandemic is unprecedented and its long-term impact on our operations cannot be reasonably estimated at this time.
Publication Corrections
An erratum or corrigendum is a correction of a published text, generally a production or author's error, that was not caught in proofing. Such errors generally do not impact data conclusions. We note the following corrections in our published works.
In July 2021, we presented clinical data for SavaDx in a poster presentation titled, “SavaDx, a Novel Plasma Biomarker to Detect Alzheimer’s Disease, Confirms Mechanism of Action of Simufilam” at the Alzheimer’s Association International Conference (AAIC) in Denver, CO and virtually. Publication correction: the AAIC data and data analysis are correct, however, visual errors that were not caught in proofing were disclosed by the Company in September 2021. This error does not impact data conclusions.
In 2017, we published in Neurobiology of Aging an article titled “PTI-125 binds and reverses an altered conformation of filamin A to reduce Alzheimer’s disease pathogenesis” (Vol 55, July 2017, Pages 99–114). Publication correction: Figure 12 contains an image showing 12 control bands. It should show 13. The data analysis was based on all 13 control bands. Other human errors in this publication have been noted and are expected to be corrected and published. These errors do not impact data conclusions.
In 2012, we published in the Journal of Neuroscience an article titled, “Reducing Amyloid-Related Alzheimer's Disease Pathogenesis by a Small Molecule Targeting Filamin A” (JNeurosci 2012;32:9773-9784). Publication correction: a duplicated panel appears in Figure 8B of the article. This error does not impact data conclusions and the publisher is expected to print a correction.
Citizen Petitions Filed with FDA
Four Citizen Petitions regarding our research program in Alzheimer’s disease were submitted to FDA during August through November 2021, by various third parties.
In August 2021, an attorney representing anonymous clients submitted a Citizen Petition to the FDA requesting an immediate halt to the clinical development of simufilam, our lead drug candidate. The attorney subsequently disclosed in a press release that his clients are “short-sellers”, that is, investors who earn a profit from a decline in our stock price. FDA did not halt the clinical development of simufilam. In February 2022, FDA denied this Citizen Petition and its four supplements.
In September 2021, the same attorney representing short-sellers clients submitted a Citizen Petition requesting that FDA immediately rescind previously granted Special Protocol Assessments (SPAs) for our Phase 3 clinical program with simufilam. FDA did not rescind our SPAs. In February 2022, FDA denied this Citizen Petition and its supplement.
In October 2021, an individual not previously known to us submitted a Citizen Petition to FDA requesting “FDA [approve] Simufilam and immediate initiation of Phase 4 trials for further efficacy, safety assessment and, most critically, to address one of the greatest needs in modern science.” FDA has not ruled on this Citizen Petition.
In November 2021, an academic physician not previously known to us submitted a Citizen Petition to FDA requesting “Accelerated Approval of Simufilam for the most significant medical need in the United States of America.” The FDA has not ruled on this Citizen Petition.
No assurance can be given that FDA will grant, deny, dismiss, defer or otherwise act upon these or any other Citizen Petition or supplements within any timeframe, if ever.
Corporate Information
We were incorporated as a Delaware corporation in May 1998 under the name Pain Therapeutics, Inc. In March 2019, we changed our company name to Cassava Sciences, Inc. Our principal offices are located at 7801 N. Capital of Texas Highway, Suite 260, Austin, TX, 78731. Our telephone number is 512-501-2444. Our website address is www.CassavaSciences.com. Information contained on our website is not a part of this Annual Report on Form 10-K and the inclusion of our website address in this Annual Report on Form 10-K is an inactive textual reference only.
We use Cassava Sciences, the Cassava Sciences logo, artwork and other marks as trademarks in the United States and other countries. Solely for convenience, trademarks and trade names referred to in this Annual Report, including logos, artwork, and other visual displays, may appear without the ® or TM symbols, but such references are not intended to indicate in any way that we will not assert, to the fullest extent under applicable law, our rights, or the rights of the applicable licensor to these trademarks and trade names. We do not intend our use or display of other entities’ trade names, trademarks, or service marks to imply a relationship with, or endorsement or sponsorship of us by, any other entity.
We file electronically with the Securities and Exchange Commission, or SEC, our annual reports on Form 10-K, quarterly reports on Form 10-Q and current reports on Form 8-K pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934. The public may read or copy any materials we file with the SEC at the SEC’s Public Reference Room at 450 Fifth Street, NW, Washington, DC 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. The SEC maintains an Internet site that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC. The address of thatthe site is http://www.sec.gov.www.sec.gov.
You may obtain a free copy of our annual reports on Form 10-K, quarterly reports on Form 10-Q and current reports on Form 8-K and amendments to those reports on the day of filing with the SEC on our website at http://www.paintrials.com,www.cassavasciences.com, by contacting our corporate offices by calling 512-501-2444512-501-2450 or by sending an e-mail message to IR@paintrials.com.IR@cassavasciences.com.
Item 1A.Risk Factors
RISK FACTORS
Investing in our common stock involves a high degree of risk.
You should carefully consider the risks described below, as well as all other information contained in this Annual Report on Form 10-K, including our consolidated financial statements and the related notes thereto and the section entitledtitled “Management’s Discussion and Analysis of Financial Condition and Results of Operations.Operations,” Ifbefore deciding whether to invest in our common stock. The occurrence of any of the following risks occur,events or developments described below could harm our business, financial condition, operating results prospectsof operations, and ability to accomplish our strategic objectives could be materially harmed. As a result,growth prospects. In such an event, the tradingmarket price of our common stock could quickly decline, by a material amount, and you couldmay lose all or part of your investment.
Below is a summary of the principal factors that make an investment in our common stock speculative or risky. Additional risks and uncertainties not presently known to us or that we currently deem immaterial also may also impair our business operations and the market price of our common stock.
Risks Related to the Discovery, Development, and Commercialization of Our Product Candidates
Clinical
Since 2017, we have concentrated a substantial portion of our research and Regulatory Risksdevelopment efforts on the treatment of Alzheimer’s disease, an area of research that has seen significant failure rates. Further, our product candidates are based on new scientific approaches and novel technology, which makes it difficult to predict the time and cost of product candidate development and likelihood of success.
We are heavily dependent on the success of simufilam, our product candidate which is still under development. If this product candidate does not receive regulatory approval, we will be unable to generate product revenue and our business will be harmed.
We have a limited operating history in our business targeting Alzheimer’s disease and no history of product approvals for commercial sale, which may make it difficult to evaluate our current business and predict our future success and viability.
We cannot give any assurance that any of our product candidates will receive regulatory approval, which is necessary before they can be commercialized.
There can be no assurance that results of smaller Phase 1 and Phase 2 clinical trials or open-label study with simufilam will be reproduced in our large Phase 3 studies that are required to demonstrate safety and efficacy in order to potentially receive regulatory approval.
We may encounter substantial delays in our clinical studies or may not be able to conduct or complete our clinical studies on the timelines we expect, if at all.
If physicians and patients do not accept and use our drugs, we will not achieve sufficient product revenues and our business will suffer.
Risks Related to Government Regulation and Other Legal Compliance Matters
Our success depends in large part on receiving FDAfinancial condition and operating results could be adversely impacted by unfavorable results of legal proceedings, government investigations or allegations and other claims.
If we are ultimately unable to obtain regulatory approval for our product candidates, we will be unable to generate product revenue and our business will be substantially harmed.
Our ability to market and promote our product candidates will be determined and limited by FDA-approved labeling.
Our employees, independent contractors, consultants, commercial partners, and vendors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements.
If we fail to comply with the complex federal, state, local and foreign laws and regulations that apply to our business, we could suffer severe consequences that could materially and adversely affect our operating results and financial condition.
Government agencies may establish and promulgate usage guidelines that could limit the use of our product candidates.
Risks Related to Our Intellectual Property
If we are unable to obtain and maintain sufficient patent protection for any product candidates we develop, our competitors could develop and commercialize products similar or identical to ours, and our ability to successfully commercialize any product candidates we may develop may be adversely affected.
U.S. intellectual property rights around diagnostic methods is a complex, evolving area of law and effective patent claims may not be available to us for our investigational diagnostic product candidate, SavaDx, in the United States.
Issued patents covering our product candidates and other technologies could be found invalid or unenforceable if challenged in court or before administrative bodies in the U.S. or abroad.
If we do not obtain patent term extension and data exclusivity for any product candidates we may develop, our business may be materially harmed.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position would be materially harmed.
Risks Related to Our Business and Operations
Our reputation and operations could be adversely impacted by allegations, regardless of their merits.
Our ability to continue to operate without any significant disruptions will, in part, depend on our ability to source raw materials and clinical supplies via our product supply chains.
The worldwide outbreak of the COVID-19 virus and associated mutations or variants may materially and adversely affect our business operations and our ability to conduct clinical studies.
Our reliance on third parties for both the supply and manufacture of materials for our product candidates carries the risk that we will not have sufficient quality or quantities of such materials or product candidates, or that such supply will not be available to us at an acceptable cost, which could delay, prevent, or impair our development or commercialization efforts.
We expect to grow the size and capabilities of our organization, including accessing new physical facilities, and we may experience difficulties in effectively managing this growth.
Ownership of our corporate headquarters and property leasing to third parties are subject to numerous risks and uncertainties.
Our internal computer systems, or those used by third parties on whom we rely, may fail or suffer other breakdowns, cyberattacks, or information security breaches that could compromise the confidentiality, integrity, and availability of such systems and data, result in material disruptions of our development programs and business operations, risk disclosure of confidential, financial, or proprietary information, and affect our reputation.
Our business involves environmental risks that may result in liability for us.
Business disruptions and lack of appropriate levels of commercial insurance could seriously harm our future revenue and financial condition and increase our costs and expenses.
Social media platforms present risks and challenges.
Risks Related to Financial Condition and Capital Requirements
We have incurred significant net losses in each period since our inception and anticipate that we will continue to incur net losses for the foreseeable future.
We have broad discretion in the use of the net proceeds from any of our financing transactions and may not use them effectively.
We have no product revenues and may never achieve revenues or profitability based on product revenues.
Risks Related to the Ownership of Our Common Stock
We do not know whether a sufficient market will continue to develop for our common stock or what the market price of our common stock will be, and, as a result, it may be difficult for investors to sell shares of our common stock.
The market price of our common stock has historically been highly volatile and we expect it to continue to be volatile, which could result in substantial losses for investors who purchase our shares.
If we are unable to maintain effective internal controls, our business, financial position, and results of operations could be adversely affected.
Anti-takeover provisions in our charter documents and Delaware law may prevent or delay removal of incumbent management or a change of control.
Changes in our ownership could limit our ability to utilize net operating loss carryforwards.
Risks Related to the Discovery, Development, and Commercialization of Our Product Candidates
Since 2017, we have concentrated a substantial portion of our research and development efforts on the treatment of Alzheimer’s disease, an area of research that has seen significant failure rates. Further, our product candidates are based on new scientific approaches and novel technology, which makes it difficult to predict the time and cost of product candidate development and likelihood of success.
Since 2017, we have concentrated a substantial portion of our research and development efforts on experimental methods for the treatment of Alzheimer’s disease. Prior efforts by biopharmaceutical companies to develop new treatments for Alzheimer’s disease have seen very limited clinical success. Since 2003, several large Phase 3 clinical studies in Alzheimer’s disease have been completed, yet no drug candidate has shown clear evidence of safety and clinical efficacy. There are no FDA-approved disease modifying therapeutics available for patients with Alzheimer’s disease. Notwithstanding these substantial challenges to date, we seek to improve brain health by addressing the neurodegeneration and neuroinflammation components of Alzheimer’s disease. Our lead drug candidate for Alzheimer’s disease is based on a new approach of stabilizing – but not removing – a critical protein in the brain. We cannot be certain that our novel technologies will lead to an approvable or marketable product. In addition, because FDA has limited comparators to evaluate our lead drug candidate, we could experience a longer than expected regulatory review process and increased development costs.
We are heavily dependent on the success of simufilam, our product REMOXY.candidate which is still under development. If this product candidate does not receive regulatory approval, we will be unable to generate product revenue and our business may be harmed.
Since inception, we have not succeeded in getting regulatory approval for our product candidates and we may never do so. In recent years, we have invested a significant portion of our efforts and financial resources in the development of simufilam and, to a lesser extent, SavaDx, for the treatment and detection of Alzheimer’s disease, respectively. Our future success is substantially dependent on our ability to successfully complete clinical development and obtain regulatory approval for simufilam, which may never occur. We expect that a substantial portion of our efforts and expenditures over the next few years will be devoted to simufilam and, to a lesser extent, SavaDx. This will require additional clinical development, management of clinical and manufacturing activities, regulatory approval in one or more national jurisdictions and obtaining commercial-scale manufacturing supply. Substantial investment and significant efforts will be required before we can generate any revenues from any commercial sales. We cannot be certain that we will be able to successfully complete any of these activities.
We have a limited operating history in our business targeting Alzheimer’s disease and no history of product approvals for commercial sale, which may make it difficult to evaluate our current business and predict our future success and viability.
We are a clinical-stage biopharmaceutical company with a limited operating history in our business targeting Alzheimer’s disease. Since we commenced operations in 1998, we have had no product candidates approved for commercial sale and have not generated any revenue from product sales. Drug development is a highly uncertain undertaking and involves a substantial degree of risk. To date, we have not completed a pivotal clinical study involving Alzheimer’s disease, obtained marketing approval for any product candidates, or conducted sales and marketing activities necessary for successful product commercialization. Our long operating history as a company without product revenue makes any assessment of our future success and viability subject to significant uncertainty.
We will continue to encounter risks and difficulties frequently experienced by clinical-stage biopharmaceutical companies in rapidly evolving fields. We have not yet demonstrated an ability to successfully overcome such risks and difficulties. If we do not successfully address these risks and difficulties, our business, results of operations and financial condition will suffer materially.
We cannot give any assurance that any of our product candidates will receive regulatory approval, which is necessary before they can be commercialized.
To date, we have invested substantial effort and financial resources to identify, procure intellectual property for, and develop our programs in neurodegeneration, including conducting preclinical and clinical studies for our product candidates, simufilam and SavaDx, and providing general and administrative support for these operations. Our future success is dependent on our ability to successfully develop, obtain regulatory approval for, and then successfully commercialize our product candidates, and we may fail to do so for many reasons, including the development of following:
our lead product REMOXY. Despite these investments, candidates may not successfully complete preclinical studies or clinical studies;
a product candidate may, on further study, be shown to have harmful side effects or other characteristics that indicate it is unlikely to be effective or otherwise does not meet applicable regulatory criteria;
our competitors may develop products that render our product candidates obsolete or less attractive;
the REMOXY NDA received CRL from product candidates that we develop may not be sufficiently covered by intellectual property;
the FDA in 2008, 2011 and 2016 indicating our drug was not yet ready for approval. Collectively, these CRLs have resulted in long delays to product revenue; sudden, severe and prolonged drops in our stock price; loss of our initial competitive advantages in candidates that we develop may be challenged by third parties’ patents or other intellectual property or exclusive rights;
the market for abuse-deterrent opioid drugs;our product candidates may change so that the continued development of a product candidate is no longer reasonable or commercially attractive;
our product candidates may not be capable of being produced in commercial quantities at an acceptable cost, or at all;
if a product candidate obtains regulatory approval, we may be unable to establish sales and dwindling cash balances. Accordingly,marketing capabilities, or successfully market such approved product candidate, to gain market acceptance; and
a product candidate may not be accepted as safe, effective or useful by patients, the medical community or third-party payors, if applicable.
If any of these events occur, we may be forced to abandon our development efforts for a program or programs, which would have a material adverse effect on our business and could potentially cause us to cease operations.
We may not be successful in our efforts to further develop our product candidates. We are not permitted to market or promote any of our product candidates before we receive regulatory approval from FDA or comparable foreign regulatory authorities, and we may never receive such regulatory approval for any of our product candidates. SavaDx is in the early stages of development. Simufilam, our late-stage product candidate, will require significant additional clinical development, management of preclinical, clinical, and manufacturing activities, regulatory approval, adequate manufacturing supply, a commercial organization, and significant marketing efforts before we generate any revenue from product sales, if at all.
We have never completed a product development program in neurodegeneration. Further, we cannot assure yoube certain that any of our product candidates will be successful in clinical studies. We may in the future advance product candidates into clinical studies and terminate such studies prior to their completion.
If any of our product candidates successfully complete clinical studies, we may seek regulatory approval to market our product candidates in the U.S., Japan, Canada, the United Kingdom or the European Union, and in additional foreign countries where we believe there is a viable commercial opportunity. We may never receive regulatory approval to market any product candidates anywhere even if such product candidates successfully complete clinical studies, which would adversely affect our viability. To obtain regulatory approval in countries outside the U.S., we would need to comply with numerous and varying regulatory requirements of such other countries regarding safety, efficacy, manufacturing and controls, clinical studies, commercial sales, pricing, and distribution of our product candidates. Even if we are successful in obtaining approval in one jurisdiction, we cannot ensure that we will obtain approval in any other jurisdictions. If we are unable to obtain approval for our product candidates in multiple jurisdictions, our business, financial condition, results of operations, and our growth prospects could be negatively affected.
Even if we receive regulatory approval to market any of our product candidates, whether for the treatment or diagnosis of neurodegenerative diseases or other diseases, we cannot provide assurance that any such product candidate will be successfully commercialized, widely accepted in the marketplace or more effective than other commercially available alternatives.
Investment in biopharmaceutical product development involves significant risk that any product candidate will fail to demonstrate adequate efficacy or an acceptable safety profile, gain regulatory approval, and become commercially viable. We cannot provide any assurance that we will be able to successfully advance any of our product candidates through the development process or, if approved, successfully commercialize any of our product candidates.
There can be no assurance that results of smaller Phase 1 and Phase 2 clinical trials or open-label study with simufilam will be reproduced in our large Phase 3 studies that are required to demonstrate safety and efficacy in order to potentially receive FDAregulatory approval.
Results of our Phase 1, Phase 2 and open-label safety studies with simufilam may not be predictive of the results of later-stage clinical trials. Simufilam may fail to show the desired safety and efficacy in later clinical trials despite having progressed through preclinical studies and initial clinical trials. Many companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. In addition, conclusions based on data from analyses of Phase 1 and Phase 2 clinical studies and open-label results may not be reproduced when implemented in large, well-controlled, randomized clinical trials. Even if our clinical trials for simufilam are completed as planned, we cannot be certain that their results will support the safety and efficacy sufficient to obtain regulatory approval.
We may encounter substantial delays in our clinical studies or may not be able to conduct or complete our clinical studies on the timelines we expect, if at all.
Clinical testing is expensive, time consuming, and subject to uncertainty. We cannot guarantee that any clinical studies will be conducted as planned, enroll patients as planned or be completed on schedule, if at all. Moreover, even after our studies begin, safety or other issues may arise that could suspend or terminate such clinical studies. A failure of one or more clinical studies can occur at any stage of testing, and our future clinical studies may not be successful. Events that may prevent successful or timely initiation or completion of clinical studies include:
inability to generate sufficient preclinical, toxicology, or other in vivo or in vitro data to support the initiation or continuation of clinical studies;
delays in confirming target engagement, patient selection, or other relevant biomarkers to be utilized in preclinical and clinical product candidate development;
delays in reaching a consensus with regulatory agencies on study design;
delays in reaching an agreement on acceptable terms with prospective and clinical study sites, the terms of which can be subject to extensive negotiation and may vary significantly among different clinical study sites;
delays in identifying and recruiting suitable clinical investigators;
delays in obtaining required IRB approval for REMOXY,each clinical study site;
a new safety finding that presents unreasonable risk to clinical study participants;
a negative finding from an inspection of our clinical research organization (CRO), clinical study operations or study sites; or
the finding that the investigational protocol or plan is deficient to meet its stated objectives;
delays in identifying, recruiting, and enrolling suitable patients to participate in our clinical studies, and delays caused by patients withdrawing from clinical studies, or failing to return for post-treatment follow-up;
delays caused by disease epidemics or pandemics, such as COVID-19;
difficulty collaborating with patient groups and investigators;
failure by our CRO or other third parties, or us to adhere to clinical study requirements;
failure to perform in accordance with FDA’s or any other regulatory authority’s Code of Good Clinical Practice (GCPs) requirements, or other regulatory guidelines in other countries;
occurrence of adverse events associated with the product candidate that are viewed to outweigh its potential benefits;
changes in regulatory requirements and guidance that require amending or submitting new clinical protocols;
changes in the standard of care on which a clinical development plan was based, which may require new or additional studies;
the cost of clinical studies of our product candidates being greater than we anticipate;
clinical studies of our product candidates producing negative or inconclusive results, which may result in our deciding, or regulators requiring us, to conduct additional clinical studies or abandon product development programs; and
delays in manufacturing, testing, releasing, validating, or importing/exporting sufficient stable quantities of our product candidates for use in clinical studies or the inability to do any of the foregoing.
Any inability to successfully initiate or complete clinical studies could result in additional costs to us or impair our ability to generate revenue. In addition, if we make manufacturing or formulation changes to our product candidates, we may be required to, or we may elect, to conduct additional studies to bridge our modified product candidates to earlier versions. Clinical study delays could also shorten any periods during which our products have patent protection and may allow our competitors to bring products to market before we do, which could impair our ability to successfully commercialize thisour product candidates and may harm our business and results of operations.
We may in the future advance product candidates into clinical studies and terminate such studies prior to their completion, which could adversely affect our business.
Delays in the completion of any clinical study of our product candidates will increase our costs, slow down our product candidate development and approval process and delay, or potentially jeopardize our ability to commence product sales and generate revenue. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical studies may also ultimately lead to the denial of regulatory approval of our product candidates.
The FDA or other regulatory agency may put a clinical hold on our clinical studies and our business will suffer.
A clinical hold is an order issued by FDA or other regulatory agency to suspend an ongoing clinical trial, typically due to newly identified deficiencies with our studies or our drug candidate. For example, we are aware that in 2022, FDA has placed clinical holds on drug candidates for Alzheimer’s disease from two competitors, Cortexzyme Inc. and Denali Therapeutics Inc. The grounds for imposition of a clinical hold are complex, variable and somewhat arbitrary. If FDA imposes a clinical hold on us, no new subjects may be enrolled and study subjects already in a study may be taken off our drug candidate unless treatment is specifically permitted by FDA in the interest of patient safety. If we cannot do so,are issued a clinical hold, FDA will expect us to address the cited deficiencies and submit a detailed, written response. A clinical hold may require us to spend significant resources over many months to address the root causes of FDA’s concerns. We may not find and successfully address such root causes, which could adversely affect our business. Our response may not be adequate to lift such clinical hold, or we may disagree with FDA’s assessments of deficiencies. If we are significantly delayedon clinical hold for 1 year or longer, the FDA may consider our IND for simufilam to fall into Inactive Status, which may result in doing so,termination of the clinical program for simufilam. To the extent we are not successful in lifting an FDA clinical hold, our results of operations and business will be materially harmed,adversely affected.
If physicians and patients do not accept and use our drugs, we will not achieve sufficient product revenues and our business will suffer.
Even if FDA approves our drugs, physicians and patients may not accept and use them. Acceptance and use of our drugs will depend on a number of factors including:
when the drug is launched into the market and related competition;
approved label claims;
perceptions by members of the healthcare community, including physicians, about the safety and effectiveness of our drugs;
perceptions by physicians regarding the cost-benefit of our product candidates;
published studies demonstrating the cost effectiveness of our drugs relative to competing products;
availability of reimbursement for our products from government or healthcare payers;
effectiveness of marketing and distribution efforts by us and other licensees and distributors.
Because we expect to rely on sales generated by our current lead product candidates for substantially all of our revenues for the foreseeable future, the failure of any of these drugs to find market acceptance would harm our business and could require us to seek additional financing.
We may not be successful in developing our product candidates in neurodegeneration.
Our product candidates in neurodegeneration are still in development and will take several more years to develop and must undergo extensive clinical and scientific validations.Even if we are successful in developing any of our product candidates through clinical and scientific validation, we may not be able to survive asdevelop a business.drug or a diagnostic that:
The FDA may not approve product labeling for REMOXY that would permit us to marketmeets applicable regulatory standards, in a timely manner or at all;
successfully competes with other technologies and promote this drug intests;
avoids infringing the United Statesproprietary rights of others;
is adequately reimbursed by describing their abuse-deterrent features.third-party payors;
There can be no assurance that REMOXY will receive final FDA-approved product labeling that adequately describes its abuse deterrent features. We have invested substantial time and money conducting abuse deterrence studies to ensure that REMOXY complies with the FDA’s guidance regarding opioid abuse deterrence. If the FDA does not approve product labeling containing abuse deterrence claims for REMOXY, we will not be able to promote REMOXY based on its abuse deterrent features and may not be able to differentiate our drug from other opioid products containing the same active pharmaceutical ingredients. This would make REMOXY less competitive,performed at commercial levels or even un-competitive, in the market. Furthermore, the FDA’s April 2015 final guidance on abuse deterrent opioids expects sponsors to compare their formulations against approved abuse deterrent versions of the same opioid based on the relevant categories of testing. If the FDA decides that REMOXY is less resistant to manipulation than an approved product, our lead drug candidate may not be approvedat reasonable cost; or may lack product labeling containing abuse deterrence claims
Even if REMOXY is approved for marketing with certain abuse-deterrence claims, the April 2015 final FDA guidance on abuse-deterrent opioids is not binding law and may be superseded or modified at any time. Also, if the FDA determines that our post-marketing data do not demonstrate that REMOXY’s abuse-deterrent properties do in fact result in reduction of abuse, or demonstrate a shift to routes of abuse that present a greater risk, the FDA may find that product labeling revisions are needed, and potentially may require the removal of any abuse-deterrence claims.
If we fail to obtain the necessary regulatory approvals, or if such approvals are limited, we and our collaborators will not be allowed to commercialize our drug candidates, and we will not generate product revenues.
Satisfaction of all regulatory requirements for commercialization of a drug candidate typically takes many years, is dependent upon the type, complexity and novelty of the drug candidate, and requires the expenditure of substantial resources for research and development. In December 2008, we received from the FDA a CRL for the REMOXY NDA. In this CRL, the FDA indicated that additional non-clinical data was required to support the approval of REMOXY. However, the FDA did not request or recommend additional clinical efficacy studies prior to approval. In March 2009, King Pharmaceuticals, Inc., or King, assumed sole responsibility for the regulatory approval of REMOXY. In December 2010, King resubmitted the NDA for REMOXY. In June 2011, we and Pfizer announced that King received a CRL from the FDA in response to King’s
resubmission of the REMOXY NDA. The FDA’s CRL raised concerns related to, among other matters, the Chemistry, Manufacturing, and Controls section of the NDA for REMOXY. Certain drug lots showed inconsistent release performance during in vitro testing. Pfizer completed work designed to address the June 2011 CRL. On April 21, 2015, we announced that we resumed responsibility for REMOXY under the terms of a letter agreement with Pfizer. The letter agreement was entered into within the scope of the previously disclosed provisions of the Collaboration Agreement between us and Pfizer relating to the return of REMOXY.
We believe Pfizer has now transferred to us its data, materials, capital equipment and other assets related to REMOXY. Pfizer and the FDA had discussed and agreed to a regulatory plan to refile the NDA for REMOXY. The FDA had agreed that we may follow this plan for the NDA for REMOXY.
In March 2016, we resubmitted to the FDA the NDA for REMOXY. In April 2016, the FDA determined that the NDA for REMOXY was sufficiently complete to permit a substantive review. On May 19, 2016, we announced that the FDA planned to hold an Advisory Committee meeting to review the NDA for REMOXY. On July 1, 2016, we announced that the FDA had determined that an Advisory Committee meeting for REMOXY was unnecessary and would not be held.
In September 2016, we received a CRL from the FDA on the resubmission of NDA for REMOXY. The CRL informed us that the NDA for REMOXY could not be approved in its present form and specifies additional actions and data that are needed for drug approval. The CRL focuses on the abuse-deterrent properties of REMOXY and proposed drug labeling.
On February 13, 2017, we met with the FDA regarding REMOXY. During this meeting, we reached agreement with the FDA on a roadmap to resubmit the NDA for REMOXY. Final minutes of our FDA meeting confirmed two key requirements needed for the resubmission of the REMOXY NDA: a) to conduct a clinical abuse potential study via the intranasal route of abuse; and b) to conduct a non-clinical abuse potential study using household solvents.
During 2017, we conducted these mandated studies with REMOXY. In November 2017, we concluded a regulatory meeting with the FDA. The purpose of this pre-New Drug Application (NDA) meeting was to agree on submission requirements for the REMOXY NDA under 505(b)(2) of the Federal Food, Drug, and Cosmetic Act. We received comments and clarification from the FDA on the acceptability of the data to be included in the REMOXY NDA resubmission, including a recent intranasal study. All questions were addressed and summarized in official minutes of the meeting issued by the FDA. There are no discrepancies or requests for clarifications following receipt of final meeting minutes. As a result, we intend to resubmit the REMOXY NDA in Q1 2018 with Priority (six-month) Review.
There can be no assurance thatsuccessfully marketed.
To the FDA will approve an NDA for REMOXY or that the FDA will not require submission of additional clinical or non-clinical data. Obtaining data from such studies (even if completed) that is insufficient to support approval of REMOXY, or any adverse decisions by the FDA (including any decision by the FDA to require additional clinical or non-clinical data) may significantly delay or prevent the potential approval of REMOXY.
Our research and clinical approaches may not lead to drugs that the FDA considers safe for humans and effective for indicated uses we are studying. The FDA may require additional studies, in which case we or our collaborators would have to expend additional time and resources and would likely delay the date of potentially receiving regulatory approval. The approval process may also be delayed by changes in government regulation, future legislation or administrative action or changes in FDA policy that occur prior to or during our regulatory review. Delays in obtaining regulatory approvals would:
| ·
| | delay commercialization of, and product revenues from, our drug candidates; and
|
| ·
| | diminish the competitive advantages that we may have otherwise enjoyed, which would have an adverse effect on our operating results and financial condition.
|
Even if we or our collaborators comply with all FDA regulatory requirements, our drug candidates may never obtain regulatory approval. If we or our collaborators fail to obtain regulatory approval for any of our drug candidates we will have fewer commercial products, if any, and corresponding lower product revenues, if any. Even if our drug candidates receive regulatory approval, such approval may involve limitations on the indications and conditions of use or marketing claims for our products. Further, later discovery of previously unknown problems or adverse events could result in additional regulatory restrictions, including withdrawal of products. The FDA may also require us or our collaborators to commit to perform lengthy Phase IV post-approval clinical efficacy or safety studies. Our expending additional resources on such trials would have an adverse effect on our operating results and financial condition.
In jurisdictions outside the United States, we must receive marketing authorizations from the appropriate regulatory authorities before commercializing our drugs. Regulatory approval processes outside the United States generally include all of the aforementioned requirements and risks associated with FDA approval.
If we are unable to design, conduct and complete preclinical and clinical trials successfully, our drug candidates will not be able to receive regulatory approval.
In order to obtain FDA approval for any of our drug candidates, we must submit to the FDA an NDA that demonstrates with substantive evidence that the drug candidate is both safe and effective in humans for its intended use. This demonstration requires significant research and animal tests, which are referred to as preclinical studies, as well as human tests, which are referred to as clinical trials.
Preclinical studies may not provide results we believe are sufficient to support the filing of an IND. Success in early preclinical studies does not ensure success in later preclinical or clinical studies. The FDA may disagree with the design of our preclinical studies or our interpretations of data from preclinical studies. The FDA may not accept an IND for our product candidate and may require additional preclinical studies to support the filing of an IND.
Success in preclinical studies and early clinical trials does not ensure that later clinical trials will be successful. Results from Phase I clinical programs may not support moving a drug candidate to Phase II or Phase III clinical trials. Phase III clinical trials may not demonstrate the safety or efficacy of our drug candidates. Results of later clinical trials may not replicate the results of prior clinical trials and preclinical studies. Even if the results of Phase III clinical trials are positive, we or our collaborators may have to commit substantial time and additional resources to conducting further preclinical studies and clinical trials before obtaining FDA approval for any of our drug candidates.
Clinical trials are very expensive and difficult to design and implement, in part because they are subject to rigorous requirements. The clinical trial process also consumes a significant amount of time. Furthermore, if patients in clinical trials suffer drug-related adverse reactions during the course of such clinical trials, or if we, our collaborators or the FDA believe that participating patients are being exposed to unacceptable health risks, such clinical trials will have to be suspended or terminated. Failure can occur at any stage of the clinical trials, and we or our collaborators could encounter problems that cause abandonment or repetition of clinical trials.
Clinical trials with REMOXY and our potential future clinical trials for other drug candidates for treatment of pain measure clinical symptoms, such as pain and physical dependence, that are not biologically measurable. The success in these clinical trials depends on reaching statistically significant changes in patients’ symptoms based on clinician-rated scales. Due in part to a lack of consensus on standardized processes for assessing clinical outcomes, these scores may or may not be reliable, useful or acceptable to regulatory agencies.
In addition, completion of clinical trials can be delayed by numerous factors, including:
| ·
| | delays in identifying and agreeing on acceptable terms with prospective clinical trial sites;
|
| ·
| | slower than expected rates of patient recruitment and enrollment;
|
| ·
| | unanticipated patient dropout rates;
|
| ·
| | increases in time required to complete monitoring of patients during or after participation in a clinical trial; and
|
| ·
| | unexpected need for additional patient-related data.
|
Any of these delays could significantly impact the timing, approval and commercialization of our drug candidates and could significantly increase our overall costs of drug development.
Even if clinical trials are completed as planned, their results may not support expectations or intended marketing claims. The clinical trials process may fail to demonstrate that our drug candidates are safe and effective for indicated uses. Such failure would cause us to abandon a drug candidate and could delay development of other drug candidates.
Clinical trial designs that were discussed with regulatory authorities prior to their commencement may subsequently be considered insufficient for approval at the time of application for regulatory approval.
We discuss with and obtain guidance from regulatory authorities on certain of our clinical development activities. With the exception of our Special Protocol Assessment (SPA), these discussions are not binding obligations on the part of regulatory authorities.
Regulatory authorities may revise previous guidance or decide to ignore previous guidance at any time during the course of our clinical activities or after the completion of our clinical trials. Even with successful clinical safety and efficacy data, including such data from a clinical trial conducted pursuant to a SPA, we or our collaborators may be required to conduct additional, expensive clinical trials to obtain regulatory approval.
Developments by competitors may establish standards of care that affect our ability to conduct our clinical trials as planned.
We have conducted clinical trials of our drug candidates comparing our drug candidates to both placebo and other approved drugs. Changes in standards related to clinical trial design could affect our ability to design and conduct clinical trials as planned. For example, regulatory authorities may not allow us to compare our drug candidates to placebo in a particular clinical indication where approved products are available. In that case, both the cost and the amount of time required to conduct a clinical trial could increase.
The U.S. Drug Enforcement Agency, or DEA, limits the availability of the active ingredients in certain of our current drug candidates and, as a result, quotas for these ingredients may not be sufficient to complete clinical trials, or to meet commercial demand, or may result in clinical delays.
The DEA regulates chemical compounds as Schedule I, II, III, IV or V substances, with Schedule I substances considered to present the highest risk of substance abuse and Schedule V substances the lowest risk. Certain active ingredients in our current drug candidates, such as oxycodone, are listed by the DEA as Schedule II under the Controlled Substances Act of 1970. Consequently, their manufacture, research, shipment, storage, sale and use are subject to a high degree of oversight and regulation. For example, all Schedule II drug prescriptions must be signed by a physician, physically presented to a pharmacist and may not be refilled without a new prescription. Furthermore, the amount of Schedule II substances that can be obtained for clinical trials and commercial distribution is limited by the DEA and quotas for these substances may not be sufficient to complete clinical trials or meet commercial demand. There is a risk that DEA regulations may interfere with the supply of the drugs used in clinical trials for our product candidates, and, in the future, the ability to produce and distribute our products in the volume needed to meet commercial demand.
Conducting clinical trials of our drug candidates or potential commercial sales of a drug candidate may expose us to expensive product liability claims, and we may not be able to maintain product liability insurance on reasonable terms or at all.
The risk of product liability is inherent in the testing of pharmaceutical products. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit or terminate testing of one or more of our drug candidates. Our inability to obtain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims could prevent or inhibit the commercialization of our drug candidates. We currently carry clinical trial insurance but do not carry product liability insurance. If we successfully commercialize one or more of our drug candidates, we may face product liability claims, regardless of FDA approval for commercial manufacturing and sale. We may not be able to obtain such insurance at a reasonable cost, if at all. Even if our agreements with any current or future corporate collaborators entitle us to indemnification against product liability losses, such indemnification may not be available or adequate should any claim arise.
If our drug candidates receive regulatory approval, we and our collaborators will be subject to ongoing FDA obligations and continued regulatory review, such as continued safety reporting requirements, and we and our collaborators may also be subject to additional FDA post-marketing obligations or new regulations, all of which may result in significant expense and limit our and our collaborators’ ability to commercialize our potential drugs.
Any regulatory approvals that our drug candidates receive may also be subject to limitations on the indicated uses for which the drug may be marketed or contain requirements for potentially costly post-marketing follow-up studies. In addition, if the FDA approves any of our drug candidates, the labeling, packaging, adverse event reporting, storage, advertising, promotion and record keeping for the drug will be subject to extensive regulatory requirements. The subsequent discovery of previously unknown problems with the drug, including but not limited to adverse events of unanticipated severity or frequency, or the discovery that adverse events previously observed in preclinical research or clinical trials that were believed to be minor actually constitute much more serious problems, may result in restrictions on the marketing of the drug, and could include withdrawal of the drug from the market.
The FDA’s policies may change and additional government regulations may be enacted that could prevent or delay regulatory approval of our drug candidates. We cannot predict the likelihood, nature or extent of adverse government regulation that may arise from future legislation or administrative action, either in the United States or abroad. If we are not able to maintain regulatory compliance, we may be subject to fines, suspension or withdrawal of regulatory approvals, product recalls, seizure of products, operating restrictions and criminal prosecution. Any of these events could prevent us from marketing our drugs and our business could suffer.
We may not be able to successfully develop or commercialize FENROCK, a proprietary abuse-deterrent transdermal pain patch (fentanyl), designed to prevent common methods of abuse of fentanyl.
We have no history of developing transdermal patches. We do not know whether any of our planned development activities for FENROCK will result in approval of such drug candidate by the FDA, or, if FENROCK is approved, it will be a commercially viable product.
We may not be able to successfully develop or commercialize PTI-125, a proprietary drug candidate to treat Alzheimer’s disease.
We have no history of developing treatment for AD. The biopharmaceutical industry as a whole has a poor track record in developing drugs for AD. Drug candidates aimed at AD have almost universally failed in every attempt to show late-stage efficacy in clinical studies. We do not know whether any of our planned development activities for AD will result in approval of such drug candidate by the FDA, or, if PTI-125 is approved, it will be a commercially viable product.
We may not be able to successfully develop or commercialize PTI-125DX, a blood-based test to detect Alzheimer’s disease.
We have no history of developing diagnostics. The biopharmaceutical industry as a whole has a poor track record in developing blood-based diagnostics for AD. Diagnostics aimed at detecting AD have almost universally failed in large studies despite evidence of success in early testing. We do not know whether any of our planned development activities for AD will result in approval of a diagnostic by the FDA, or, if PTI-125DX is approved, it will be a commercially viable product.
Risks Relating to our Collaboration Agreements
If Pfizer did not transfer to us all data and documentation or the quality of the data and documentation transferred is insufficient, our ability to achieve approval of the NDA for REMOXY will be negatively impacted and our business will suffer.
In April 2015, we announced that we resumed responsibility for REMOXY under the terms of a letter agreement with Pfizer. The letter agreement was entered into within the scope of the previously disclosed provisions of the Collaboration Agreement between us and Pfizer relating to the return of REMOXY.
We believe Pfizer has transferred to us data, materials, capital equipment and other assets related to REMOXY. In preparing to resubmit the NDA for REMOXY, we may find that there are additional data, materials or agreements that Pfizer should have transferred to us. If Pfizer did not meet its obligations to transfer all such materials or if the quality of the data and documentation transferred is insufficient, we would be significantly delayed in our ability to achieve FDA approval of the NDA for REMOXY, and may need to conduct further development activities or clinical trials to prepare any potential resubmission. As a result, any further development, regulatory approval and product introduction for REMOXY would be delayed or prevented and our business would suffer.
If outside collaborators fail to devote sufficient time and resources to drug development programs related to our product candidates, or to the manufacture of our products, or if their performance is substandard, regulatory submissions and introductions for our products may be delayed.
We rely on Durect as the sole-source provider of certain components of REMOXY. Durect’s failure for any reason to provide these components could result in delays or failures in product testing or delivery, cost overruns or other problems that could materially harm our business.
We depend on independent investigators and collaborators, such as universities and medical institutions, to conduct our clinical trials under agreements with us. These investigators and collaborators are not our employees, and we cannot control the amount or timing of resources that they devote to our programs. They may not assign as great a priority to our programs or pursue them as diligently as we would if we were undertaking such activities ourselves. If these investigators or collaborators fail to devote sufficient time and resources to our drug development programs, or if their performance is substandard, the approval of our regulatory submissions and our introductions of new drugs will be delayed or prevented.
Our collaborators may also have relationships with other commercial entities, some of which may compete with us. If outside collaborators assist our competitors to our detriment, the approval of our regulatory submissions will be delayed and the sales from our products, if any are commercialized, will be less than expected.
If we fail to enter into or maintain collaboration agreements and licenses for REMOXY and other drugs designed to reduce potential risks of unintended use, we may have to reduce or delay our drug candidate development.
Our plan for developing, manufacturing and commercializing REMOXY currently requires us to successfully maintain our license from Durect. If we are unable to meet the obligations necessary to maintain our license with Durect for one or more potential products we may lose the rights to utilize Durect’s technology for such potential products, our potential future revenues may suffer and we may have to reduce or delay development of our other drug candidates. In addition, we expect to seek a new corporate collaborator with respect to REMOXY. If we do not enter into a new collaboration with respect to the continued development and potential commercialization of REMOXY, we will be required to undertake and fund such activities ourselves and may need to seek additional capital (which may not be available on acceptable terms, if at all), personnel or other resources. If we are not successful in such efforts, developmentdeveloping our new product candidates in neurodegeneration, our results of operations and commercializationbusiness will be materially adversely affected.
Interim, “top-line” and preliminary data from our clinical trials that we announce or publish from time to time are likely to change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final dataset.
From time to time, we may publish interim, “top-line” or preliminary data from our clinical trials. Interim data from clinical trials that we may complete are subject to the risk that one or more of REMOXYthe clinical outcomes may materially change as patient enrollment continues and our other drug candidates wouldmore patient data become available. Preliminary or “top-line” data also remain subject to audit and verification procedures that may result in the final data being materially different from the preliminary data we previously published. As a result, interim and preliminary data should be delayedviewed with caution until the final data is available. Differences between preliminary or prevented,interim data and final data could significantly harm our business would suffer.prospects and may cause the trading price of our common stock to fluctuate significantly.
Our collaborative agreements may not succeed or may give rise to disputes over intellectual property, disputes concerning the scope of collaboration activities or other issues.
Our collaborative agreements with third parties, such as our license agreement with Durect, are generally complex and contain provisions that could give rise to legal disputes, including potential disputes concerning ownership of intellectual property under collaborations or disputes concerning the scope of collaboration activities. Such disputes can delay or prevent the development of potential new drug products, or can lead to lengthy, expensive litigation or arbitration. Other factors relating to collaborative agreements may adversely affect our business, including:
| ·
| | the development of parallel products by our collaborators or by a competitor;
|
| ·
| | arrangements with collaborative partners that limit or preclude us from developing certain products or technologies;
|
| ·
| | premature termination of a collaborative or license agreement; or
|
| ·
| | failure by a collaborative partner to provide required funding, to devote sufficient resources to the development of or legal defense of our potential products or to provide data or other information to us as required by our collaborative agreements.
|
Risks Relating to Commercialization
We currently have no in-house capabilities to manufacture or commercialize our product candidates and we rely on third-party commercial drug products.manufacturers for clinical drug supplies. If we are unable to develop our own manufacturing, sales, marketing and distribution capabilities, or if we are not successful in contracting with third parties for these services on favorable terms, or at all, our product revenues could be disappointing.adversely impacted.
We currently rely on Mallinckrodt as the sole manufacturer for REMOXYvarious third parties to manufacture, fill, label, store, test and commercialization of REMOXY is dependentship our product candidates. We plan to continue to outsource formulation, manufacturing and related activities. These suppliers must comply with cGMP regulations enforced by FDA and other government agencies, and are subject to ongoing periodic unannounced inspection, including preapproval inspections by FDA and corresponding state and foreign government agencies to ensure strict compliance with cGMP and other standards. These manufacturers may subsequently be stopped from producing, manufacturing, filling, labeling, storing, testing and shipping our product candidates due to their non-compliance with federal, state or local regulations. We do not have control over our suppliers’ compliance with these regulations and standards and we cannot control decisions by our suppliers that affect their ability or willingness to continue to supply us on continuation of such relationship. acceptable terms, or at all.
Disputes in the past have arisen with Mallinckrodtsome of these third parties with respect to us fulfilling our obligations under the Mallinckrodt Agreement.certain conditions and obligations. There can be no guarantee that such disputes will not arise again in the future, which may lead to Mallinckrodt terminating the Mallinckrodt Agreement.termination of an agreement. If the Mallinckrodt Agreementan agreement is terminated, we would not be able to commercialize REMOXYour product candidates until another manufacturer is identified and we have entered into a manufacturing agreement with such manufacturer. If we are requiredWe may not be able to replace Mallinckrodta commercial supplier on commercially reasonable terms, or at all. Replacing any of our commercial suppliers would be expensive and time consuming. Failure by any of our suppliers to perform as expected could delay or prevent the manufacturercommercialization or potential regulatory approval of REMOXY, it is likely to delay commercialization of REMOXYour product candidates for an extended period of time.time, result in shortages, cost overruns or other problems and would materially harm our business.
We currently have no sales, marketing or distribution capabilities. We have not established commercial strategies regarding any of our product candidates, including REMOXY.candidates. In order to commercialize our products, if any are approved by the FDA, we will either have to develop such capabilities internally or collaborate with third parties who can perform these services for us.
If we decide to commercialize any of our drugs ourselves, we may not be able to
| ·
| | hire and retain the necessary experienced personnel;
|
| ·
| | build sales, marketing and distribution operations in a cost-effective manner which are capable of successfully launching new drugs;
|
| ·
| | obtain access to adequate numbers of physicians to prescribe our products; or
|
| ·
| | generate sufficient product revenues.
|
hire and retain the necessary experienced personnel;
build sales, marketing and distribution operations in a cost-effective manner which are capable of successfully launching new drugs;
obtain access to adequate numbers of physicians to prescribe our products; or
generate sufficient product revenues.
In addition, establishing such operations on our own will take time and involve significant expense. If our commercial operations lack complementary products, we may not be able to compete in a cost-effective manner with competitors with more products to sell. If we engage third-party collaborators to perform any commercial operations, our future revenues may depend significantly upon the performance of those collaborators.
If we decide to enter into new co-promotion or other licensing arrangements with third parties, we may be unable to locate acceptable collaborators because the number of potential collaborators is limited and because of competition from others for similar alliances with potential collaborators.alliances. Even if we are able to identify one or more acceptable new collaborators, we may not be able to enter into any collaborative arrangements on favorable terms, or at all.
In addition, due to the nature of the market for our drugproduct candidates, it may be necessary for us to license all or substantially all of our drugproduct candidates to a single collaborator, thereby eliminating our opportunity to commercialize these other products independently. If we enter into any such new collaborative arrangements, our revenues are likely to be lower than if we marketed and sold our products ourselves.
In addition, any revenues we receive would depend upon our collaborators’ efforts which may not be adequate due to lack of attention or resource commitments, management turnover, change of strategic focus, business combinations or other factors outside of our control. Depending upon the terms of our collaboration, the remedies we have against an under-performing collaborator may be limited. If we were to terminate the relationship, it may be difficult or impossible to find a replacement collaborator on acceptable terms, or at all.
Nearly every attempt at drug approval for Alzheimer’s disease has failed.
Despite billions of dollars invested by NIH and the biopharmaceutical industry in research programs to develop novel therapeutics for Alzheimer’s disease, the FDA has not approved any new drugs for Alzheimer’s disease since 2003, except, however, that in June 2021, aducanumab (Biogen, Inc) received approval from FDA for the treatment of Alzheimer’s disease using the accelerated approval pathway. Since 2003, many new types and classes of drugs have been developed and tested in Alzheimer’s disease, including monoclonal antibodies, gamma secretase modulators and inhibitors, β-site amyloid precursor protein cleaving enzyme (BACE) inhibitors, receptor for advanced glycation end-products (RAGE) inhibitors, nicotinic partial agonists and allosteric modulators, serotonin subtype receptor (5HT6) antagonists, and others. Virtually all of these scientific programs have failed in clinical testing.
We may not be successful in our efforts to expand our technology or product candidates in other indications.
Our drug development strategy is to clinically test and seek regulatory approval for our product candidates in Alzheimer’s disease, our primary indication. We may expand our research efforts outside of this primary indication and into other areas of clinical medicine based on genetic, biological or mechanistic overlap with the primary indication. Conducting clinical studies for additional indications for our product candidates will require substantial technical, financial and human resources and is prone to the inherent risks of failure in drug development. We cannot provide any assurance that we will be successful in our effort to expand our technology or our product candidates in additional indications, even if we obtain approval for our product candidate in Alzheimer’s disease.
If physicianswe fail to successfully identify and develop additional product candidates, our commercial opportunity will be limited to Alzheimer’s disease or other neurodegenerations.
Identifying, developing, obtaining regulatory approval, and commercializing additional product candidates requires substantial expertise and funding and is prone to the risks of failure inherent in drug development. We cannot provide any assurance that we will be able to successfully identify or acquire additional product candidates, advance any additional product candidates through the development process, or assemble sufficient resources to identify, acquire, or develop additional product candidates. If we are unable to successfully identify, acquire, develop, and commercialize additional product candidates, our commercial opportunity may be limited.
Early indications of safety and tolerability from our small clinical studies with simufilam may not predict the results of later studies.
Results of a Phase 1 clinical study with simufilam demonstrated safety, tolerability and pharmacokinetics in 24 healthy subjects exposed to 50-200 mg in a single ascending dose study. However, this was a small, “first-in-human” Phase 1 study designed to assess the initial safety characteristics of simufilam in healthy subjects and this study was not designed to, and did not, evaluate safety, tolerability and efficacy of simufilam in patients. Additional large, well-controlled, multi-dose studies will be required to evaluate the safety, tolerability and efficacy of simufilam to treat patients with any indication, including Alzheimer’s disease. There can be no assurance that such future studies will demonstrate the safety, tolerability or efficacy of simufilam.
Phase 2 clinical studies with simufilam were designed to assess the safety characteristics of simufilam in patients. Our Phase 2 program was not designed to, and did not, evaluate large-scale or long-term safety, tolerability and efficacy of simufilam in patients. Additional large, well-controlled, multi-dose studies will be required to evaluate the safety, tolerability and efficacy of simufilam to treat patients with any indication, including Alzheimer’s disease. There can be no assurance that such future studies will demonstrate the safety, tolerability or efficacy of simufilam. The failure of simufilam to show safety, tolerability or efficacy in any future clinical studies would significantly harm our business.
We have never obtained FDA approval for a diagnostic test and we may not be able to secure such approval in a timely manner or at all.
We are developing a blood-based diagnostic test for Alzheimer’s disease, called SavaDx, which will require FDA approval prior to commercialization. Our diagnostic product candidate, marketing, sales and development activities and manufacturing processes are subject to extensive and rigorous regulation by FDA pursuant to the FDCA, by comparable agencies in foreign countries, and by other regulatory agencies and governing bodies. Under the FDCA, a diagnostic must
receive FDA clearance or approval before it can be commercially marketed in the U.S. The process of obtaining marketing approval or clearance from FDA or by comparable agencies in foreign countries for new products could:
take a significant period of time;
require the expenditure of substantial resources;
involve rigorous preclinical testing, as well as increased post-market surveillance;
require changes to products; and
result in limitations on the indicated uses of products.
If we do not acceptcompete effectively with scientific and usecommercial competitors, we may not be able to successfully develop our drugs,diagnostic test for Alzheimer’s disease.
The field of clinical laboratory testing is highly competitive. Diagnostic tests that are developed are characterized by rapid technological change. Our competitors in the U.S. and abroad are numerous and include, among others, major diagnostic companies, reference laboratories, molecular diagnostic firms, universities and other research institutions. Most of our potential competitors have considerably greater financial, technical, marketing and other resources than we do, which may allow these competitors to discover important biological markers and determine their function before we do. We could be adversely affected if we do not discover proteins or biomarkers and characterize their function, develop diagnostic and pharmaceutical and clinical services based on these discoveries, obtain required regulatory and other approvals and launch these tests and their related services before our competitors. We also expect to encounter significant competition with respect to any diagnostic tests that we may develop or commercialize. Those companies that bring to market new diagnostic tests before we do may achieve a significant competitive advantage in marketing and commercializing their tests. We may not be able to develop additional diagnostic tests successfully and we may not obtain or enforce patents, if any, covering these tests that provide protection against our competitors. Moreover, our competitors may succeed in developing diagnostic tests that circumvent our technologies or tests. Furthermore, our competitors may succeed in developing technologies or tests that are more effective or less costly than those developed by us or that would render our technologies or tests less competitive or obsolete. We expect competition to intensify in the fields in which we are involved as technical advances in these fields occur and become more widely known and changes in intellectual property laws generate challenges to our intellectual property position.
We will need to develop our own proprietary antibodies or find alternative approaches that do not achieve sufficient product revenuesinvolve antibodies to advance our SavaDx and our business will suffer.diagnostic program.
Even ifSavaDx currently relies on the FDA approves our drugs, physicians and patients may not accept and use them. Acceptance and use of our drugs will depend on a number of factors including:
| ·
| | when the drug is launched into the market and related competition;
|
| ·
| | perceptions by members of the healthcare community, including physicians, about the safety and effectiveness of our drugs, and, in particular, the effectiveness of REMOXY in reducing potential risks of unintended use;
|
| ·
| | perceptions by physicians regarding the cost benefit of REMOXY in reducing potential risks of unintended use;
|
| ·
| | published studies demonstrating the cost-effectiveness of our drugs relative to competing products;
|
| ·
| | availability of reimbursement for our products from government or healthcare payers;
|
| ·
| | our or our collaborators’ ability to implement a risk management plan prior to the distribution of any Schedule II drug; and
|
| ·
| | effectiveness of marketing and distribution efforts by us and other licensees and distributors.
|
Because we expectcommercially available antibodies, which are complex molecules that can recognize and bind to rely on sales generated by our current lead drug candidates for substantially all of our revenues for the foreseeable future, the failure ofan intended protein. Commercially available antibodies present certain technical flaws, such as improper validation, significant batch-to-batch variations or inconsistent storage, any of these drugswhich can jeopardize our studies and experiments. Because antibody underperformance can be a significant drain on time and resources, we have attempted to find market acceptance would harmdevelop and validate our businessown, fit-for-purpose antibody for use with SavaDx. The complexity of developing our own antibody gives rise to many technical issues that are challenging to solve, and could require us to seek additional financing.
The science of abuse-deterrence is relatively new.
The analytical, clinical, and statistical methods for evaluating abuse-deterrent technologies and study results are new and rapidly evolving. Although we believe the FDA will take a flexible, adaptive approach to the evaluation and labeling of potentially abuse-deterrent products, such as REMOXY, we cannot be certain that we will be able to successfully complete any of these activities, in which case our program may be harmed. We are also evaluating an alternative approach to detect Alzheimer’s disease that does not involve antibodies. The complexity of such an alternative approach also gives rise to many technical issues that are challenging to solve. We cannot be certain that we will be able to successfully complete the development of a detection system for Alzheimer’s disease that does or does not involve antibodies.
We have concentrated a substantial portion of our research and development efforts on the treatment and detection of Alzheimer’s disease, an area of research that has seen significant failure rates. Further, our product candidates are based on new scientific approaches and novel technology, which makes it difficult to predict the time and cost of product candidate development.
We focus substantially all of our research and development efforts on addressing neurodegenerations, such as Alzheimer’s disease. Collectively, efforts by biopharmaceutical companies in the field of neurodegenerative diseases have seen many failures and limited success in drug development. Our future success is highly dependent on the successful development of our product candidates for treating Alzheimer’s disease. Developing and, if approved, commercializing our product candidates for treatment of Alzheimer’s disease subjects us to many challenges, including obtaining regulatory approval from FDA and other regulatory authorities who have only a limited set of precedents to rely on. We cannot be sure that our approach will yield satisfactory therapeutic products that are safe and effective, scalable, or profitable.
Our Phase 2 clinical studies with simufilam in patients with Alzheimer’s disease are generally not designed to show a statistically meaningful difference in cognition or other health functions between those patients who receive placebo and those who receive drug.
Clinical research data is often analyzed with statistical probability (p-value) to address the question of whether a clinical observation is related to a treatment effect, a random effect or something else. This, in turn, requires a clinical study to incorporate a sufficiently large sample patient population to infer the appropriate statistical analysis. By design, our Phase 2 clinical studies with simufilam generally do not include a sufficiently large patient population to generate statistical probability on measures of cognition or other health functions. This feature may make it difficult for investors to properly interpret whether clinical observations in those Phase 2 studies with simufilam are important or meaningful. Conversely, our clinical studies may generate statistically significant data (i.e., p<0.05) with regard to biomarkers, or other endpoints, that have unknown or no clinical importance. In general, the distinction between statistically significant and clinically meaningful is a complex area of research that continues to evolve and may be subject to differences of opinion among scientists, clinicians and other professionals.
We may encounter difficulties enrolling patients in our clinical studies, and our clinical development activities could thereby be delayed or otherwise adversely affected.
The timely completion of clinical studies in accordance with their protocols depends, among other things, on our ability to enroll enough patients who remain in the study until its conclusion. We may experience difficulties in patient enrollment in our clinical studies for a variety of reasons, including:
the size and severity of disease in the patient population;
the patient eligibility criteria defined in the protocol, including biomarker-driven identification and/or certain highly-specific criteria related to stage of disease progression, which may limit the patient populations eligible for our clinical studies to a greater extent than competing clinical studies for the same indication that do not have biomarker-driven patient eligibility criteria;
the size of the study population required for analysis of the trial’s primary endpoints;
the design of our study protocol;
our ability to recruit clinical study investigators with the appropriate competencies and experience;
competing clinical studies for similar therapies or targeting patient populations meeting our patient eligibility criteria;
clinicians’ and patients’ perceptions as to the potential advantages and side effects of the product candidate being studied in relation to other available therapies and product candidates;
our ability to obtain and maintain patient consents;
physicians’ patient referral practices that are out of our control;
our ability to adequately monitor patients and their caregivers during and after treatment; and
the risk that patients enrolled in clinical studies will not complete such studies, for any reason.
Our clinical studies may fail to demonstrate substantial evidence of the safety and efficacy of our product candidates, which would prevent, delay, or limit the scope of regulatory approval and commercialization.
Before obtaining regulatory approvals for any of our product candidates, we must demonstrate through lengthy, complex, and expensive preclinical experiments and clinical studies that our product candidates are both safe and effective for use in an intended population. Each product candidate must demonstrate an adequate risk versus benefit profile in its intended patient population and for its intended use.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical study process. The results of preclinical studies of our product candidates may not be predictive of the results of early-stage or later-stage clinical studies, and results of early clinical studies of our product candidates may not be predictive of the results of later-stage clinical studies. The results of clinical studies in one set of patients or disease indications may not be predictive of those obtained in another. In some instances, there can be significant variability in safety or efficacy results between different clinical studies of the same product candidate due to numerous factors, including changes in study procedures set forth in protocols, differences in the size and type of the patient populations, changes in and adherence to the dosing regimen, and other clinical study protocols and the rate of dropout among clinical study participants.
Open-label extension studies may also extend the timing and cost of a clinical study substantially. Product candidates in later stages of clinical studies may fail to show the desired safety and efficacy profile despite having progressed through preclinical studies and initial clinical studies. Many companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical studies due to lack of efficacy or unacceptable safety issues, notwithstanding promising results in earlier studies. This is particularly true in neurodegenerative diseases, where failure rates historically have been higher than in many other disease areas. Most product candidates that begin clinical studies are never approved by regulatory authorities for commercialization.
We have limited experience in designing clinical studies in neurodegeneration and may be unable to design and execute a clinical study to support marketing approval. We cannot be certain that our current clinical studies or any other future clinical studies will be successful. Additionally, any safety concerns observed in any one of our clinical studies in our targeted indications could limit the prospects for regulatory approval of our product candidates in those and other indications, which could have a material adverse effect on our business, financial condition, and results of operations.
In addition, even if such clinical studies are successfully completed, we cannot guarantee that FDA or foreign regulatory authorities will interpret the results as we do, and more studies could be required before we submit our product candidates for approval. To the extent that the results of the studies are not satisfactory to FDA or foreign regulatory authorities for support of a marketing application, we may be required to expend significant resources, which may not be available to us, to conduct additional studies in support of potential approval of our product candidates. Even if regulatory approval is secured for any of our product candidates, the terms of such approval may limit the scope and use of our product candidates, which may also limit its commercial potential.
If our drug candidate causes or contribute to a death or a serious injury before or after approval, we will be subject to medical reporting regulations, which can result in voluntary corrective actions or agency enforcement actions.
Our drug candidate in Alzheimer’s disease is aimed at frail, elderly patients who are in a state of cognitive decline. Under FDA medical reporting regulations, we are required to report to the FDA information that our drug candidate has or may have caused or contributed to a death or serious injury. Any such serious adverse event involving our drug could result in future FDA action, such as an inspection, enforcement action or warning, or in more serious cases, a complete shutdown of our clinical program. In the context of our ongoing clinical trials, we report adverse events to the FDA in accordance with applicable national and local regulations. Any corrective action, whether voluntary or involuntary, and either pre- or post-market, needed to address any serious adverse events will require the dedication of our time and capital, distract management from operating our business, and may harm our reputation and financial results.
The market opportunities for simufilam and SavaDx, if approved, may be smaller than we anticipate.
If our clinical development programs succeed, we expect to seek regulatory approval of simufilam and SavaDx for patients with Alzheimer’s disease. Our projections of the number of patients with Alzheimer’s disease is based on our beliefs and estimates. These estimates have been derived from a variety of outside sources, including scientific literature, patient foundations and market research, and may prove to be incorrect. The actual number of patients may turn out to be lower than expected. Additionally, the potential patient population for our current programs or future product candidates may be limited. Even if we obtain significant market share for any product candidate, if approved, if the potential target populations are smaller than anticipated, we may never achieve profitability without obtaining marketing approval for additional indications.
We face significant competition in an environment of rapid technological and scientific change, and there is a possibility that additional competitors may achieve regulatory approval before us or develop therapies that are safer, more advanced, or more effective than ours, any of which may harm our business operations.
Drug discovery and development is highly competitive. Moreover, the neurodegenerative field is characterized by intense and increasing competition, and a strong emphasis on intellectual property. We may face competition with respect to any of our product candidates that we seek to develop or commercialize in the future from major pharmaceutical companies, specialty pharmaceutical companies, and biotechnology companies worldwide. Potential competitors also include academic institutions, government agencies, and other public and private research organizations that conduct research, seek patent protection, and establish collaborative arrangements for research, development, manufacturing, and commercialization.
In addition to Biogen and Eli Lilly, several large pharmaceutical and biotechnology companies are currently pursuing the development of products for the treatment of neurodegenerative diseases, including Alzheimer’s disease. Many of these current or potential competitors, either alone or with their strategic partners, have significantly greater financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical studies, obtaining regulatory approvals, and marketing approved products than we do.
Our commercial opportunity could be reduced or eliminated if other competitors develop and commercialize products that are safer, more effective, have fewer or less severe side effects, are more convenient, or are less expensive than any products that we may develop. Furthermore, currently approved products could be discovered to have application for treatment of neurodegenerative disease indications, which could give such products significant advantages over any of our product candidates. Competitors other than Biogen may also obtain FDA or other regulatory approval for their products more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market. For example, Eli Lilly, a large pharmaceutical company, announced it plans to petition the FDA for accelerated approval of donanemab, its monoclonal antibody drug candidate for the proposed treatment of Alzheimer’s disease. Additionally, products or technologies developed by our competitors may render our potential product candidates uneconomical or obsolete, and we may not be successful in marketing any product candidates we may develop against competitors.
In addition, we could face litigation or other proceedings with respect to the scope, ownership, validity, and/or enforceability of our patents relating to our competitors’ products and our competitors may allege that our products infringe, misappropriate, or otherwise violate their intellectual property. The availability of our competitors’ products could limit the demand, and the price we are able to charge, for any products that we may develop and commercialize.
Risks Related to Government Regulation and Other Legal Compliance Matters
Our financial condition and operating results could be adversely impacted by unfavorable results of legal proceedings, government investigations or allegations and other claims.
We are subject to various claims, legal proceedings and government investigations that have arisen in the ordinary course of business and have not yet been fully resolved, and new matters may arise in the future.
We are currently managing U.S. government inquiries, as well as civil claims under federal and state laws, relating to and/or arising out of our disclosures regarding our research and development of simufilam. New claims or inquiries may arise in the future. Regardless of the merit of particular claims and inquiries, defending against litigation or responding to government investigations is expensive, time-consuming, disruptive to our operations and distracting to management. In recognition of these considerations, we may enter into agreements or other arrangements to settle such matters and resolve such challenges. No assurance can be given that such agreements can be obtained on acceptable terms or that litigation will not occur.
The outcome of legal proceedings, academic inquiries or government investigations is inherently uncertain. If one or more such matters were resolved against us, our financial condition and operating results could be materially adversely affected. Further, such an outcome could result in significant compensatory, punitive or trebled monetary damages, disgorgement of revenue or profits, remedial corporate measures or injunctive relief against us, all of which could materially adversely affect our financial condition and operating results.
While we maintain insurance coverage for certain types of claims, such insurance coverage may be insufficient to cover all losses or all types of claims that may arise.
Additional future litigation against us could be costly and time-consuming to defend.
Innovative drug development is highly litigious, and we may become subject, from time to time, to additional legal proceedings, claims and allegations that arise in the ordinary course of business or pursuant to governmental or regulatory enforcement activity. Regardless of merit, any lawsuits against us, individually or in the aggregate, may have a material adverse effect on our business, financial condition, results of operations or cash flows. In addition, any litigation to which we subsequently become a party might result in substantial costs and divert management's attention, time and resources, which
might seriously harm our business, financial condition, results of operations and cash flows. Our insurance policies might not cover such claims, might not provide sufficient payments to cover all of the costs to resolve one or more such claims, and might not continue to be available on terms acceptable to us. In particular, any claim could result in potential liability for us if the claim is outside the scope of the indemnification agreement we have with our third-party partners, or our third-party partners do not abide by the indemnification agreement as required, or the liability exceeds the amount of any applicable indemnification limits or available insurance coverage. A claim brought against us that is uninsured or underinsured could result in unanticipated costs and could have a material adverse effect on our financial condition, results of operations, cash flows or reputation.
If we are ultimately unable to obtain regulatory approval for our product candidates, we will be unable to generate product revenue and our business will be substantially harmed.
The time required to obtain approval by FDA and comparable foreign regulatory authorities is unpredictable, typically takes many years following the commencement of clinical studies, and depends upon numerous factors, including the type, complexity, and novelty of the product candidates involved. In addition, approval policies, regulations, or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions, which may cause delays in the approval or the decision not to approve an application. Regulatory authorities have substantial discretion in the approval process and may refuse to accept any application or may decide that our data are insufficient for approval and require additional preclinical, clinical, or other studies. We have not obtained regulatory approval for any product candidate, including our product candidates aimed at Alzheimer’s disease, and it is possible that none of our existing product candidates or any product candidates we may seek to develop in the future will ever obtain regulatory approval.
Applications for our product candidates could fail to receive regulatory approval in an initial or subsequent indication for many reasons, including but not limited to the following:
FDA or comparable foreign regulatory authorities may disagree with the design, implementation, or results of our clinical studies;
FDA or comparable foreign regulatory authorities may determine that our product candidates are not safe and effective, only moderately effective or have undesirable or unintended side effects, toxicities, or other characteristics that preclude our obtaining marketing approval or prevent or limit commercial use;
the population studied in the clinical program may not be sufficiently broad or representative to assure efficacy and safety in the full population for which we seek approval;
we may be unable to demonstrate to FDA or comparable foreign regulatory authorities that a product candidate’s risk-benefit ratio when compared to the standard of care is acceptable;
FDA or comparable foreign regulatory authorities may disagree with our interpretation of abuse-deterrent data for REMOXY is consistent with from preclinical studies or clinical studies;
the viewsdata collected from clinical studies of the FDA. In our opinion, the FDA has limited data correlating the potentially abuse-deterrent properties of certain opioid drug products, such as REMOXY, with actual reduction in abuse or adverse events associated with abuse. In addition, the FDA has stated it isproduct candidates may not able to provide specific guidance on the magnitude of effect that would be sufficient to support the submission of a new drug application (NDA), or other submission or to obtain regulatory approval in the United States or elsewhere;
FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes, test procedures, and specifications, or facilities of third-party manufacturers with which we contract for clinical and commercial supplies; and
the approval policies or regulations of FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval.
This lengthy approval process, as well as the unpredictability of the results of clinical studies, may result in our failing to obtain regulatory approval to market any particular type of label claim for abuse-deterrence.our product candidates, which would significantly harm our business, results of operations, and growth prospects.
Our ability to market and promote REMOXY and its abuse-deterrent featuresour product candidates will be determined and limited by FDA-approved labeling.
The commercial success of REMOXY and certain of our other product candidates will depend upon our ability to obtain FDA-approved labeling describing their abuse-deterrent features. Our failure to achieve FDA approval of product labeling containing such information will prevent us from advertising and promoting the abuse-deterrentkey features of our product candidates in order to differentiate them from other similar products. This would make our products less competitive in the market.
Abuse-deterrent label claims
Our employees, independent contractors, consultants, commercial partners, and vendors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements.
We are exposed to the risk of fraud, misconduct, or other illegal activity by our employees, independent contractors, consultants, commercial partners, and vendors. Misconduct by these parties could include intentional, reckless, and negligent conduct that fails to:
comply with the laws of FDA and other comparable foreign regulatory authorities;
provide true, complete, and accurate information to FDA and other comparable foreign regulatory authorities;
comply with manufacturing standards we have established;
comply with healthcare fraud and abuse laws in the U.S. and similar foreign fraudulent misconduct laws; or
report financial information or data accurately or to disclose unauthorized activities to us.
Activities subject to laws also involve the improper use of information obtained in the course of patient recruitment for REMOXYclinical studies, which could result in regulatory sanctions and cause serious harm to our reputation. Further, it is not always possible to identify and deter misconduct by employees and third parties, and the precautions we take to detect and prevent this activity may not be broad enougheffective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to demonstratecomply with such laws. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a substantial benefitsignificant impact on our business, including the imposition of significant fines or other sanctions.
If we fail to health care providerscomply with the complex federal, state, local and patients.foreign laws and regulations that apply to our business, we could suffer severe consequences that could materially and adversely affect our operating results and financial condition.
Our operations are subject to extensive federal, state, local and foreign laws and regulations, all of which are subject to change. These laws and regulations currently include, among other things:
The Clinical Laboratory Improvement Amendments (CLIA) of 1988, which are United States federal regulatory standards that apply to all clinical laboratory testing performed on humans in the United States, requires that laboratories obtain certification from the federal government, and state licensure laws;
FDA approval is required in order to make claims that a product has an abuse-deterrent effect. In April 2015, the FDA published final guidancelaws and regulations;
The Health Insurance Portability and Accountability Act (HIPAA), which imposes comprehensive federal standards with regardrespect to the evaluationprivacy and labelingsecurity of abuse-deterrent opioids. The guidance provides direction asprotected health information and requirements for the use of certain standardized electronic transactions, including penalties for violators, enforcement authority to state attorneys general and requirements for breach notification;
state laws regulating testing and protecting the studies and data required for obtaining abuse-deterrent claims in a product label. FDA guidance describes three categoriesprivacy of pre-market studies that may lead to an abuse-deterrent claim:
Category 1 – laboratory manipulation and extraction studies;
Category 2 – pharmacokinetic studies; and
Category 3 – human abuse potential studies.
According to the FDA guidance, label claims for abuse-deterrence should describe the product’s specific abuse-deterrent propertiestest results, as well as state laws protecting the specific routesprivacy and security of health information and personal data and mandating reporting of breaches to affected individuals and state regulators;
the federal anti-kickback law, or the Anti-Kickback Statute, which prohibits knowingly and willfully offering, paying, soliciting, receiving, or providing remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual, or the furnishing, arranging for, or recommending of an item or service that is reimbursable, in whole or in part, by a federal health care program;
the federal False Claims Act (FCA), which imposes liability on any person or entity that, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment to the federal government;
the federal Civil Monetary Penalties Law, which prohibits, among other things, the offering or transfer of remuneration to a Medicare or state health care program beneficiary if the person knows or should know it is likely to influence the beneficiary’s selection of a particular provider, practitioner, or supplier of services reimbursable by Medicare or a state health care program, unless an exception applies;
other federal and state fraud and abuse laws, such as anti-kickback laws, prohibitions on self-referral, and false claims acts, which may extend to services reimbursable by any third-party payor, including private insurers;
the federal Physician Payments Sunshine Act, which requires manufacturers to track and report to the federal government certain payments and other transfers of value made to physicians and teaching hospitals and ownership or investment interests held by physicians and their immediate family members;
Section 216 of the federal Protecting Access to Medicare Act of 2014 (PAMA), which requires applicable laboratories to report private payer data in a timely and accurate manner every three years (and in some cases annually);
state laws that impose reporting and other compliance-related requirements; and
similar foreign laws and regulations that will apply to us in foreign countries in which we may choose to operate in the future.
Government agencies may establish and promulgate usage guidelines that could limit the use of our product has been developedcandidates.
Government agencies, professional and medical societies, and other groups may establish usage guidelines that apply to deter. When data predictour product candidates. These guidelines could address such matters as usage and dose, among other factors. Application of such guidelines could limit the clinical use or showcommercial appeal of our product candidates.
Our product candidates may cause undesirable side effects or have other properties that a product’s potentially abuse-deterrent properties can be expectedcould halt their clinical development, prevent their regulatory approval, limit their commercial potential, or result in significant negative consequences.
During the conduct of clinical trials, study participants report changes in their health to their doctor, including illnesses, injuries and discomforts. Often, it is not possible to determine whether our product candidate caused these conditions. Regulatory authorities may draw different conclusions and may require us to pause our clinical trials or actually do,require additional testing to confirm these determinations, if they occur. In addition, we have not yet completed long-term safety studies with simufilam to determine if this product candidate is safe for humans. Adverse events or other undesirable side effects caused by simufilam could cause us or regulatory authorities to interrupt, delay, or halt clinical studies and could result in a significant reductionmore restrictive label or the delay or denial of regulatory approval by FDA or other comparable foreign regulatory authorities. Drug-related side effects could affect patient recruitment, the ability of enrolled patients to complete the study, and/or result in that product’s abuse potential these data, together with an accurate characterization of what the data mean,claims.
Our insurance policies may be included ininadequate and potentially expose us to unrecoverable risks.
Although we maintain product labeling.
Ifliability insurance coverage, such insurance may not be adequate to cover all liabilities that we may incur. We anticipate that we will need to increase our insurance coverage each time we commence a clinical trial and if we successfully commercialize any product is approved by the FDAcandidate. Insurance availability, coverage terms and pricing continue to include such claims in its label, the applicantvary with market conditions. We endeavor to obtain appropriate insurance coverage for insurable risks that we identify; however, we may use the approved labeling information about the abuse-deterrent features of the product in its marketing effortsfail to physicians.
Althoughcorrectly anticipate or quantify insurable risks, we may not be able to obtain appropriate insurance coverage and insurers may not respond as we intend to provide datacover insurable events that may occur. Conditions in the insurance markets relating to the FDAnearly all areas of traditional corporate insurance change rapidly and may result in higher premium costs, higher policy deductibles and lower coverage limits. For some risks, we may not have or maintain insurance coverage because of cost or availability.
We are required to support approval of abuse-deterrence label claims for REMOXY, there can be no assurance that REMOXY or anymaintain product liability insurance pursuant to certain of our development and commercialization agreements. We may not be able to maintain insurance coverage at a reasonable cost or in sufficient amounts to protect us against losses due to liability. A successful product liability claim or series of claims brought against us could adversely affect our results of operations, business, and reputation. In addition, regardless of merit or eventual outcome, product liability claims may result in impairment of our business reputation, withdrawal of clinical study participants, costs due to related litigation, distraction of management’s attention from our primary business, initiation of investigations by regulators, substantial monetary awards to patients or other claimants, the inability to commercialize our product candidates, and decreased demand for our product candidates, if approved for commercial sale.
If our product candidates receive regulatory approval, we and our collaborators will receive FDA-approved labeling that describes the abuse-deterrent featuresbe subject to ongoing FDA obligations and continued regulatory review, such as continued safety reporting requirements, and we and our collaborators may also be subject to additional FDA post-marketing obligations or new regulations, all of such products. The FDAwhich may find thatresult in significant expense and limit our studies and data do not support abuse-deterrent labeling orour collaborators’ ability to commercialize our potential drugs.
Any regulatory approvals that our product candidates doreceive may also be subject to limitations on the indicated uses for which the drug may be marketed or contain requirements for potentially costly post-marketing follow-up studies. In addition,
if FDA approves any of our product candidates, the labeling, packaging, adverse event reporting, storage, advertising, promotion and record keeping for the drug will be subject to extensive regulatory requirements. The subsequent discovery of previously unknown problems with the drug, including but not provide substantial abuse-deterrence because, for example, their deterrence mechanisms do not addresslimited to adverse events of unanticipated severity or frequency, or the way they are most likelydiscovery that adverse events previously observed in preclinical research or clinical studies that were believed to be abused. Further,minor actually constitute much more serious problems, may result in restrictions on the FDA is not required to follow its guidancemarketing of the drug, and could include withdrawal of the drug from the market.
The FDA’s policies may change, this guidance, whichand additional government regulations may be enacted that could require us to conduct additional studiesprevent or generate additional data.delay regulatory approval of our product candidates. We cannot predict the likelihood, nature or extent of adverse government regulation that may arise from future legislation or administrative action, either in the U.S. or abroad. If the FDA doeswe are not approve abuse-deterrent labeling, we will not be able to promote suchmaintain regulatory compliance, we may be subject to fines, suspension or withdrawal of regulatory approvals, product recalls, seizure of products, based on their abuse-deterrent featuresoperating restrictions and criminal prosecution. Any of these events could prevent us from marketing our products and our business maycould suffer.
Even if we do receive FDA approval for abuse-deterrent claims, the claims may not be broad enough to demonstrate a substantial benefit to health care providers and patients. For instance, the claims may not encompass the more common forms of abuse for products like our product candidates. Moreover, continued investigation in Phase IV studies following product approval, if required, is expensive and may not support the continued use of abuse-deterrent claims.
If we cannot compete successfully for market share against other drug companies, we may not achieve sufficient product revenues and our business will suffer.
The market for our drug candidates is characterized by intense competition and rapid technological advances. If our drug candidates receive FDA approval, they will compete with a number of existing and future drugs and therapies developed, manufactured and marketed by others. Existing or future competing products may provide greater therapeutic convenience or clinical or other benefits for a specific indication than our products, or may offer comparable performance at a lower cost. If our products are unable to capture and maintain market share, we may not achieve sufficient product revenues and our business will suffer.
We and our collaborators will compete for market share against fully integrated pharmaceutical companies or other companies that are collaborating with larger pharmaceutical companies, academic institutions, government agencies and other public and private research organizations. Many of these competitors have drugs already approved or drug candidates in development that will or may compete against our approved drug candidates. In addition, many of these competitors, either alone or together with their collaborative partners, operate larger research and development programs and have substantially greater financial resources than we do, as well as significantly greater experience in:
| ·
| | conducting preclinical testing and human clinical trials;
|
| ·
| | obtaining FDA and other regulatory approvals of drugs;
|
| ·
| | formulating and manufacturing drugs; and
|
| ·
| | launching, marketing, distributing and selling drugs.
|
If we fail to obtain acceptable prices or an adequate level of reimbursement for our products from healthcare payers, our ability to generate product revenues will be diminished.
Our ability to commercialize drugs we (alone or with other collaborators) may develop will depend in part on the extent to which reimbursement can be obtained for such drugs from:
| ·
| | government and health administration authorities;
|
| ·
| | private health maintenance organizations and health insurers; and
|
| ·
| | other healthcare payers.
|
Significant uncertainty exists as to the reimbursement status of newly approved healthcare products. Healthcare payers, including Medicare, health maintenance organizations and managed care organizations, are challenging the prices charged for medical products and services and/or are seeking pharmacoeconomic data to justify formulary acceptance and reimbursement practices. We currently have not generated pharmacoeconomic data on any of our drug candidates. Government and other healthcare payers increasingly are attempting to contain healthcare costs by limiting both coverage and the level of reimbursement for drugs, and by refusing, in some cases, to provide coverage for uses of approved products for disease indications for which the FDA has or has not granted labeling approval. Adequate third-party insurance coverage may not be available to patients for any products we discover and develop, alone or with collaborators. If government and other healthcare payers do not provide adequate coverage and reimbursement levels for our products, market acceptance of our drug candidates could be limited.
Enacted and future legislation may increase the difficulty and cost for us to commercialize our product candidates and may reduce the prices we are able to obtain for our product candidates.
Legislative and regulatory changes and future changes regarding the healthcare system could prevent or delay marketing approval of our product candidates, restrict or regulate post-approval activities or affect our ability to profitably sell any product candidates for which we obtain marketing approval.
In the United States,U.S., the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 or the(the Medicare Modernization Act,Act) established the Medicare Part D program and provided authority for limiting the number of drugs that will be covered in any therapeutic class thereunder. The Medicare Modernization Act, including its cost reduction initiatives, could limit the coverage and reimbursement rate that we receive for any of our approved products. Private payors may follow Medicare coverage policies and payment limitations in setting their own reimbursement rates resulting in similar limits in payments from private payors.
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or collectively, the Affordable Care Act, among other things, imposes a significant annual fee on companies that manufacture or import branded prescription drug products.product candidates. It also contains substantial provisions intended to, among other things, broaden access to health insurance, reduce or constrain the growth of health care spending, enhance remedies against healthcare fraud and abuse, add new transparency requirements for the healthcare and health insurance industries, and impose additional health policy reforms, any of which could have a material adverse effect on our business. A significant number of provisions are not yet, or have only recently become, effective, but the Affordable Care Act may result in downward pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase our regulatory burdens and operating costs.
The Affordable Care Act, as well as other healthcare reform measures that have been and may be adopted in the future, may result in more rigorous coverage criteria and in additional downward pressure on the price that we receive for any approved product, and could seriously harm our future revenues. Any reduction in reimbursement from Medicare or other government programs may result in a similar reduction in payments from private payors. The implementation of cost containment measures or other healthcare reforms may compromise our ability to generate revenue, attain profitability or commercialize our products.
The Affordable Care Act is a highly complex piece of legislation that continues to evolve. We do not and cannot understand or anticipate the full impact and potential implications of the Affordable Care Act on our business or on our drugs.
If the FDA or other applicable regulatory authorities approve generic products with abuse-deterrent claims that compete with any of our product candidates, it could reduce our sales of those product candidates.
Once an NDA, including a Section 505(b)(2) application, is approved, the product covered thereby becomes a "listed drug" which can, in turn, be cited by potential competitors in support of approval of an abbreviated NDA, or ANDA. Potential competitors may create modified, non-infringing versions of a drug to facilitate the approval of an ANDA or other application for generic substitutes. These competitors might only be required to conduct a relatively inexpensive study to show that their product has the same active ingredients, dosage form, strength, route of administration, and conditions of use, or labeling, as our products and that the generic product is absorbed in the body at the same rate and to the same extent as, or is bioequivalent to, our products. These generic equivalents would be significantly less costly than ours to bring to market and companies that produce generic equivalents are generally able to offer their products at lower prices. Thus, after the introduction of a generic competitor, a significant percentage of the sales of any branded product are typically lost to the generic product. Accordingly, competition from generic equivalents to our products would substantially limit our ability to generate revenues and therefore to obtain a return on the investments we have made in our product candidates.
Our relationships with customers and payors will be subject to applicable anti-kickback, fraud and abuse, transparency, and other healthcare laws and regulations, which could expose us to criminal sanctions, civil penalties, exclusion from government healthcare programs, contractual damages, reputational harm, administrative burdens, and diminished profits and future earnings.
Healthcare providers, physicians and payors play a primary role in the recommendation and prescription of any product candidates for which we may obtain marketing approval. Our future arrangements with payors and customers may expose us to broadly applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we market, sell and distribute any product candidates for which we may obtain marketing approval. Even though we do not and will not control referrals of healthcare services or bill directly to Medicare, Medicaid or other third-party payors, federal and state healthcare laws and regulations pertaining to fraud and abuse and patients' rights are and will be applicable to our business. Restrictions under applicable federal, state and foreign healthcare laws and regulations may affect our ability to operate and expose us to areas of risk, including:
| ·
| | the federal Anti-Kickback Statute, which prohibits, among other things, knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under federal and state healthcare programs such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation;
|
| ·
| | the federal False Claims Act, which imposes criminal and civil penalties, including through civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government. In addition, the government may assert that a claim including items and services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the False Claims Act;
|
| ·
| | the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, which imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute to defraud any healthcare benefit program or specific intent to violate it in order to have committed a violation;
|
| ·
| | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH, and its implementing regulations, which also imposes obligations on certain covered entity healthcare providers, health plans, and healthcare clearinghouses as well as their business associates that perform certain services involving the use or disclosure of individually identifiable health information, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information;
|
| ·
| | federal laws requiring drug manufacturers to report information related to payments and other transfers of value made to physicians and other healthcare providers, as well as ownership or investment interests held by physicians and their immediate family members, including under the federal Open Payments program, commonly known as the Sunshine Act, as well as other state and foreign laws regulating marketing activities; and
|
| ·
| | state and foreign equivalents of each of the above laws, including state anti-kickback and false claims laws, which may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental payors, including private insurers; state laws which require pharmaceutical companies to comply with the pharmaceutical industry's voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government or otherwise restricting payments that may be made to healthcare providers; and state and foreign laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
|
the federal Anti-Kickback Statute, which prohibits, among other things, knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under federal and state healthcare programs such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation;
the FCA, which imposes criminal and civil penalties, including through civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government. In addition, the government may assert that a claim including items and services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the FCA;
HIPAA, which imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute to defraud any healthcare benefit program or specific intent to violate it in order to have committed a violation;
HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009 and its implementing regulations, which also imposes obligations on certain covered entity healthcare providers, health plans, and healthcare clearinghouses as well as their business associates that perform certain services involving the use or disclosure of individually identifiable health information, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information;
federal laws requiring drug manufacturers to report information related to payments and other transfers of value made to physicians and other healthcare providers, as well as ownership or investment interests held by physicians and their immediate family members, including under the federal Open Payments program, commonly known as the Sunshine Act, as well as other state and foreign laws regulating marketing activities; and
state and foreign equivalents of each of the above laws, including state anti-kickback and false claims laws, which may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental payors, including private insurers; state laws which require pharmaceutical companies to comply with the pharmaceutical industry's voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government or otherwise restricting payments that may be made to healthcare providers; and state and foreign laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. Nonetheless, it is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, imprisonment, exclusion from participation in government funded healthcare programs, such as Medicare and Medicaid, and the curtailment or restructuring of our operations.
A recent federal court ruling may establishmandate significant new disclosure requirements for clinical data dating back over a decade which may lead to costly or burdensome disclosures.
A federal court ruling may require all clinical study sponsors to report a decade’s worth of previously exempted clinical study data to the federal government for publication on ClinicalTrials.gov. In February 2020, the U.S. District Court for the Southern District of New York invalidated a prior interpretation of NIH regulations that had exempted many clinical studies conducted between 2007 and promulgate usage guidelines that2017 from reporting requirements mandated by the Food and Drug Administration Amendments Act. If this court ruling takes effect without appeal, or if it is upheld on appeal, it could limitrequire us to submit an onerous amount of old clinical data to the usefederal government. In many cases, we were the responsible party for generating such clinical data, but such prior data may be difficult or not feasible for us to access as a result of our strategic shift away from analgesic drug candidates.
Government agencies, professional and medical societies, and other groupsdevelopment in 2019. We may establish usage guidelinesno longer have control over, or access to, prior clinical data that we may legally be required to report to NIH in the future. Furthermore, it is unclear whether such new disclosure requirements apply to inactive, failed or abandoned drug development programs. As a result of these uncertainties, the government’s recent ruling may leave us in a conflicted position or out of compliance with new disclosure requirements. We currently do not and cannot understand or anticipate the full impact and potential implications of this court ruling on our drug candidates. These guidelines could address such matters as usage and dose, among other factors. Application of such guidelines could limit the clinical use or commercial appeal of our drug candidates.business.
Risks RelatingRelated to ourOur Intellectual Property
OurIf we are unable to obtain and maintain sufficient patent protection for any product candidates we develop, our competitors could develop and commercialize products similar or identical to ours, and our ability to successfully commercialize our drugany product candidates will dependwe may develop may be adversely affected.
Our success depends in large part on our ability to sell such products without infringingobtain and maintain patent protection in the U.S. and other countries with respect to our proprietary product candidates and other technologies we may develop. We seek to protect our proprietary position by filing patent applications in the U.S. and abroad relating to our core programs and product candidates, as well as other technologies that are important to our business. Given that our product candidates are in in early or proprietary rightsclinical stages of third parties. If we are sued for infringing thedevelopment, our intellectual property rightsportfolio with respect to certain aspects of third parties, such litigation will be costly and time consuming andour product candidates is also at an unfavorable outcome wouldearly stage. For example, we have a significant adverse effectfiled or intend to file patent applications on our business.
Our ability to commercialize our drug candidates will depend on our ability to sell such products without infringing the patents or other proprietary rightsaspects of third parties. Intellectual property rights in the areas of controlled-releaseour technology and pharmaceutical ingredients are complicated and are continuously evolving. Holders of patent rights in these areas may allege that the commercialization of REMOXY or our other drug candidates infringes such patent rights. While we believe that we would have valid defenses to any claim of infringement,core product candidates; however, there can be no assurance that any such patent applications will issue as granted patents. Furthermore, in some cases, we have only filed provisional patent applications on certain aspects of our technology and product candidates and each of these orprovisional patent applications is not eligible to become an issued patent until, among other third-party patents will not limit ourthings, we file a non-provisional patent application within 12 months of the filing date of the applicable provisional patent application. Any failure to file a non-provisional patent application within this timeline could cause us to lose the ability to commercialize REMOXY orobtain patent protection for the inventions disclosed in the associated provisional patent applications.
Furthermore, in some cases, we may not be able to obtain issued claims covering compositions relating to our core programs and product candidates, as well as other drug candidates.
In addition, becausetechnologies that are important to our business, and instead may need to rely on filing patent applications are published sometime after filing,with claims covering a method of use and/or method of manufacture for protection of such core programs, product candidates, and because applications can take several years to issue, there may be currently pending third party patent applications that are unknown to us, which may later result in issued patents. If a third party claims that we infringe on its patents or other proprietary rights, we could face a number of issues that could seriously harm our competitive position, including:
| ·
| | infringement claims that, with or without merit, can be costly and time consuming to litigate, can delay the regulatory approval process and can divert management’s attention from our core business strategy;
|
| ·
| | substantial damages for past infringement which we may have to pay if a court determines that our products or technologies infringe upon a competitor’s patent or other proprietary rights;
|
| ·
| | a court order prohibiting us from commercializing our products or technologies unless the holder licenses the patent or other proprietary rights to us, which such holder is not required to do;
|
| ·
| | if a license is available from a holder, we may have to pay substantial royalties or grant cross licenses to our patents or other proprietary rights; and
|
| ·
| | redesigning our process so that it does not infringe third party intellectual property rights, which may not be possible, or which may require substantial time and expense including delays in bringing our own products to market. Such actions could harm our competitive position and our ability to generate revenue and could result in increased costs.
|
If we are unable to protect our intellectual property, our competitors could develop and market products with similar features that may reduce demand for our drug candidates.
Our success, competitive position and potential future revenues will depend in part on our ability to protect our intellectual property. If we or our collaborators fail to file, prosecute, obtain or maintain certain patents, our competitors could market products that contain features and clinical benefits similar to those of our products, and demand for our products could decline as a result.
We and our collaborators have filed patent applications in the United States and select international jurisdictions to protect our intellectual property. The coverage sought in a patent application can be denied or significantly reduced before or after the patent is issued. Consequently, we do not know whether any of our pending applications will result in the issuance of patents, or if any existing or future patents will provide significant protection or commercial advantage or will be circumvented by others.technologies. There can be no assurance that patentsany such patent applications will issue as granted patents, and even if they do issue, such patent claims may be insufficient to prevent third parties, such as our competitors, from utilizing our pendingtechnology. Any failure to obtain or futuremaintain patent protection with respect to our core programs and product candidates could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
U.S. intellectual property rights around diagnostic methods is a complex, evolving area of law and effective patent claims may not be available to us for our investigational diagnostic product candidate, SavaDx, in the United States.
The legal system for intellectual property around diagnostic methods is highly complex, remains uncertain and continues to evolve. In the U.S., patent courts have struggled to define a clear means of patent eligibility for modern age diagnostics. Case law interpretations from the U.S. Supreme Court has left certain important scientific advances in the area of diagnostics without effective patent claims. In 2012, the Supreme Court held that a simple process involving correlations between blood test results and patient health is not eligible for patent claims because such processes incorporate “laws of nature”. Since then, different outcomes from different courts, including Federal Circuit, district court and Patent Trial and Appeal Board decisions, have continued to create a sometimes vague or conflicting legal framework for determining the eligibility of patent claims for diagnostic methods. As a result, we cannot be certain how SavaDx fits into the current U.S. legal framework for obtaining
effective patent claims. We currently have no U.S. patents or patent applications with respect to SavaDx, and we believe it may only be protected in the United States by trade secrets, know-how and other proprietary rights technology. Furthermore, claims for diagnostic methods can be complicated to enforce. For patent infringement to occur with a protected diagnostic, the patented method must generally either be performed by one person in its entirety or performed by multiple parties all under the control or direction of a single party. Accordingly, even if effective patent claims are issued for SavaDx, it may be impractical, impossible or even undesirable to enforce potential infringement claims.
Issued patents covering our product candidates and other technologies could be found invalid or unenforceable if challenged in court or before administrative bodies in the U.S. or abroad.
If we initiated legal proceedings against a third party to enforce a patent covering our product candidates or other technologies, the defendant could counterclaim that such patents will be of commercial benefit to us, afford us adequate protection from competing products,patent is invalid or not be challengedunenforceable. In patent litigation in the U.S., defendant counterclaims alleging invalidity or declared invalid. Thus, if these patent applications do not result in issued patents or result inunenforceability are commonplace. Grounds for a patent that is challenged by others, the duration or scope of our patent rights may be limited and our future revenuesvalidity challenge could be lower asan alleged failure to meet any of several statutory requirements, including lack of novelty, obviousness, or non-enablement. Grounds for an unenforceability assertion could be an allegation that someone connected with prosecution of the patent withheld relevant information from the USPTO, or made a result.
Wemisleading statement, during prosecution. Third parties may be involved in challenges to our intellectual property. If our competitors are able to successfully challengeraise claims challenging the validity or scopeenforceability of our patent rights, based onpatents before administrative bodies in the existenceU.S. or abroad, even outside the context of prior art or otherwise, they might be able to market products that contain featureslitigation. Such mechanisms include re-examination, post-grant review, inter partesreview, interference proceedings, derivation proceedings, and clinical benefits similar to those of our drug candidates, and demand for our drug candidates could decline as a result. An adverse outcome of a challenge to our intellectual propertyequivalent proceedings in foreign jurisdictions (e.g., opposition proceedings). Such proceedings could result in the revocation of, cancellation of, or amendment to our patents in such a way that they no longer cover our product candidates or other technologies. The outcome following legal assertions of invalidity and unenforceability is unpredictable. With respect to the validity question, for example, we cannot be certain that there is no invalidating prior art, of which we or our licensing partners and the patent examiner were unaware during prosecution. If a third party were to prevail on a legal assertion of invalidity or unenforceability, we would lose at least part, and perhaps all, of the patent protection on our product candidates or other technologies. Such a loss of claims of patents or other intellectual property rights that pertain to certain drugs we currently have under development and couldpatent protection would have a material adverse impact on our future revenues.business, financial condition, results of operations, and growth prospects.
We intend to file additionalIf we do not obtain patent applications relating to our technology, productsterm extension and processes. We may direct our collaborators to file additional patent applications relating to the licensed technology ordata exclusivity for any product candidates we may do so ourselves. However, our competitors may challenge, invalidate or circumvent any of our current or future patents. These patents may also fail to provide us with meaningful competitive advantages.
We may become involved in expensive litigation or other legal proceedings related to our existing intellectual property rights, including patents.
We expect that we will rely upon patents, trade secrets, know-how, continuing technological innovations and licensing opportunities to develop, and maintain our competitive position. While we use confidentiality agreements with our employees, consultants and certain of our contractors, if trade secrets or other confidential information is made public, our business may be harmedmaterially harmed.
Depending upon the timing, duration, and our legal remediesspecifics of any FDA marketing approval of any product candidates we may be limited or insufficient. Others may independently develop, substantially equivalent proprietary information or be issued patents that may prevent the sale of our products or know-how or require us to license such information and pay significant fees or royalties in order to produce our products.
Our technology could infringe upon claims of patents owned by others. If we were found to be infringing on a patent held by another, we might have to seek a license to use the patented technology. In that case, we might not be able to obtain such a license on terms acceptable to us, or at all. If a legal action were to be brought against us or our licensors, we could incur substantial defense costs, and any such action might not be resolved in our favor. If such a dispute were to be resolved against us, we could have to pay the other party large sums of money and our use of our technology and the testing, manufacture, marketing or sale of one or more of our proposed productsU.S. patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984 (Hatch-Waxman Act). The Hatch-Waxman Act permits a patent term extension of up to five years as compensation for patent term lost during FDA regulatory review process. A patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval, only one patent may be extended and only those claims covering the approved drug, a method for using it, or a method for manufacturing it may be extended. Similar extensions as compensation for patent term lost during regulatory review processes are also available in certain foreign countries and territories, such as in Europe under a Supplementary Patent Certificate. However, we may not be granted an extension in the U.S. and/or foreign countries and territories because of, for example, failing to exercise due diligence during the testing phase or regulatory review process, failing to apply within applicable deadlines, failing to apply prior to expiration of relevant patents, or otherwise failing to satisfy applicable requirements. Moreover, the applicable time period or the scope of patent protection afforded could be restrictedless than we request. If we are unable to obtain a patent term extension or prohibited.the term of any such extension is shorter than what we request, our competitors may obtain approval of competing products following our patent expiration, and our business, financial condition, results of operations, and growth prospects could be materially harmed.
If we are unable to protect the confidentiality of our intellectual property, the valuetrade secrets, our business and competitive position would be harmed.
In addition to seeking patents for our product candidates and other technologies, we also rely on trade secrets and confidentiality agreements to protect our unpatented know-how, technology, and other proprietary information and to maintain our competitive position. We consider trade secrets and know-how to be one of our primary sources of intellectual property couldproperty. Trade secrets and know-how can be materially adversely affecteddifficult to protect. We expect our trade secrets and our business wouldknow-how to over time be harmed.disseminated within the industry through independent development, the publication of journal articles describing the methodology, and the movement of personnel from academic to industry scientific positions.
We seek to protect our intellectual property,these trade secrets and other proprietary technology, in part, by entering into non-disclosure and confidentiality agreements with parties who have access to them, such as our employees, corporate collaborators, outside scientific collaborators, CROs, CDMOs, consultants, advisors, and other third parties. We also enter into confidentiality and invention or patent assignment agreements with our employees and consultants scientific advisors, contractorsas well as train our employees not to bring or use proprietary information or technology from former employers to us or in their work, and collaborators. However, there can be no assuranceremind former employees when they leave their employment of their confidentiality obligations. We cannot guarantee that our intellectual property will not be disclosedwe have entered into such agreements with each party that may have or that competitors will not otherwise gainhave had access to our intellectual propertytrade secrets or independently develop
substantially equivalent intellectual property. For example, ifproprietary technology and processes. Despite our confidentialefforts, any of these parties may breach the agreements and disclose our proprietary information, were disclosed in violation ofincluding our confidentiality agreements,trade secrets, and we may not be able to obtain adequate remedies for such breaches. We also seekEnforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive, and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside the U.S. are less willing or unwilling to protect our intellectual property by maintaining physical security of our premises and physical and electronic security of our information technology systems, but it is possible that these security measures could be breached.trade secrets. If any of our intellectual propertytrade secrets were to be lawfully obtained or independently developed by a competitor or other third party, we would have no right to prevent such competitorthem from using that intellectual propertytechnology or information to compete with us, whichus. If any of our trade secrets were to be disclosed to or independently developed by a competitor or other third party, our competitive position would be materially and adversely harmed.
If any of our patent applications do not issue as patents in any jurisdiction, we may not be able to compete effectively.
Changes in either the patent laws or their interpretation in the U.S. and other countries may diminish our ability to protect our inventions, obtain, maintain, and enforce our intellectual property rights and, more generally, could harmaffect the value of our business.
Risks Relatingintellectual property or narrow the scope of our patents with respect to our Businessproduct candidates. With respect to our intellectual property related to our product candidates, we cannot predict whether the patent applications we are currently pursuing will issue as patents in any particular jurisdiction or whether the claims of any issued patents will provide sufficient protection from competitors or other third parties.
The patent prosecution process is expensive, time-consuming, and Strategy
Our businesscomplex, and we may not be able to file, prosecute, maintain, or enforce all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail without a new equity incentive plan.
We depend heavily on equity incentives to retain the services of allidentify patentable aspects of our personnel, without whichresearch and development output in time to obtain patent protection. Although we enter into nondisclosure and confidentiality agreements with parties who have access to confidential or patentable aspects of our research and development output, such as our employees, outside scientific collaborators, CROs, CDMOs, consultants, advisors, and other third parties, any of these parties may breach the agreements and disclose such output before a patent application is filed, thereby jeopardizing our ability to seek patent protection. In addition, our ability to obtain and maintain valid and enforceable patents depends on whether the differences between our inventions and the prior art allow our inventions to be patentable. Furthermore, publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the U.S. and other jurisdictions are typically not ablepublished until 18 months after filing, or in some cases not at all. Therefore, we cannot be certain that we were the first to retainmake the inventions claimed in any of our patents or hire qualified personnelpending patent applications, or board members. In particular,that we were the first to file for patent protection of such inventions.
If the scope of any patent protection we obtain is not sufficiently broad, or if we lose any of our independent board members receive no formpatent protection, our ability to prevent our competitors from commercializing similar or identical technology and product candidates would be adversely affected.
The patent position of compensation for their services other than new equity incentives every year. The 2008 Equity Plan expiredbiotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions, and has been the subject of much litigation in December 2017. Furthermore, in 2017, shareholders rejected a proposal to renew an equity incentive plan.recent years. As a result, going-forwardthe issuance, scope, validity, enforceability, and commercial value of our patent rights are highly uncertain. Our pending and future patent applications may not result in patents being issued which protect our product candidates or other technologies or which effectively prevent others from commercializing competitive technologies and product candidates.
Moreover, the coverage claimed in a patent application can be significantly reduced before the patent is issued, and its scope can be reinterpreted after issuance. Even if patent applications we own currently or in the future issue as patents, they may not issue in a form that will provide us with any meaningful protection, prevent competitors or other third parties from competing with us, or otherwise provide us with any competitive advantage. Any patents to which we have rights may be challenged, narrowed, circumvented, or invalidated by third parties. Consequently, we do not know whether product candidates or other technologies will be protectable or remain protected by valid and enforceable patents. Our competitors or other third parties may be able to circumvent our patents by developing similar or alternative technologies or products in a
non-infringing manner which could materially adversely affect our business, financial condition, results of operations and growth prospects.
The issuance of a patent is not conclusive as to its inventorship, scope, validity, or enforceability, and our patents may be challenged in the courts or patent offices in the U.S. and abroad. We may be subject to a third-party pre-issuance submission of prior art to the United States Patent and Trademark Office (USPTO) or become involved in opposition, derivation, revocation, reexamination, post-grant and inter partes review, or interference proceedings or other similar proceedings challenging our patent rights. An adverse determination in any such submission, proceeding, or litigation could reduce the scope of, or invalidate or render unenforceable, such patent rights, allow third parties to commercialize our product candidates or other technologies and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize products without infringing third-party patent rights. Moreover, we may have to participate in interference proceedings declared by the USPTO to determine priority of invention or in post-grant challenge proceedings, such as oppositions in a foreign patent office, that challenge our priority of invention or other features of patentability with respect to our patents and patent applications. Such challenges may result in loss of patent rights, loss of exclusivity, or in patent claims being narrowed, invalidated, or held unenforceable, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our product candidates and other technologies. Such proceedings also may result in substantial cost and require significant time from our scientists and management, even if the eventual outcome is favorable to us. If we are no longer ableunsuccessful in any such proceeding or other priority or inventorship dispute, we may be required to grant new equity incentivesobtain and maintain licenses from third parties, including parties involved in any such interference proceedings or other priority or inventorship disputes. Such licenses may not be available on commercially reasonable terms or at all or may be non-exclusive. If we are unable to anyobtain and maintain such licenses, we may need to cease the development, manufacture, and commercialization of our personnel, including new potential hires and board members, until and unless shareholders approve a new equity incentive plan.one or more of the product candidates we may develop. The loss of personnel and board members, and our potential inability to hire replacement personnel, will materially delayexclusivity or disrupt our operations and will put us out of compliance with various legal standards and regulations for listed companies, all of which may force us to curtail or cease operations.
If we are not successful in attracting and retaining qualified personnel, we could experience delays in completing necessary clinical trials, in the regulatory approval process or in formulating, manufacturing, marketing and selling our potential products.
We depend on the servicesnarrowing of our key personnel, including Remi Barbier,owned and licensed patent claims could limit our Chairman, Presidentability to stop others from using or commercializing similar or identical technology and Chief Executive Officer. On February 14, 2017, Peter S. Roddy resigned, effective March 9, 2017, as Vice President, Chief Financial Officerproducts.
In addition, given the amount of time required for the development, testing, and Secretary. Remi Barbier, President and Chief Executive Officer, has assumed the roleregulatory review of Principal Financial Officer untilnew product candidates, patents protecting such time asproduct candidates might expire before or shortly after such product candidates are commercialized. As a new Chief Financial Officer is appointed.
The loss of key personnel, including members of executive management as well as key bioengineering, product development, and technical personnel, could disruptresult, our operations and have an adverse effect on our business. We will need to hire additional qualified personnel with expertise in clinical research, preclinical testing, government regulation, formulation and manufacturing and sales and marketing. We compete for qualified individuals with numerous biopharmaceutical companies, universities and other research institutions. Competition for such individuals is intense, and our search for such personnelintellectual property may not be successful. Attracting and retaining qualified personnel is criticalprovide us with sufficient rights to our success.exclude others from commercializing products similar or identical to ours.
We have employees whose equity ownership in the Company could result in a substantial increase in personal wealth if the fair value of our common stock increases. Over time, this increase in personal wealth may make it more challenging to retain these employees.
If third-party manufacturers of our drug candidates fail to devote sufficient time and resources to our concerns, or if their performance is substandard, our clinical trials and product introductions may be delayed and our costs may be higher than expected.
We have no manufacturing facilities and have limited experience in drug product development and commercial manufacturing. We lack the resources and expertise to formulate, manufacture or test the technical performance of our drug candidates. We rely on and expect to continue to rely on a limited number of experienced personnel and a small number of contract manufacturers and other vendors to formulate, test, supply, store and distribute drug supplies for our preclinical studies and clinical trials. Our reliance on a limited number of vendors exposes us to the following risks, any of which could delay our clinical trials, and, consequently, FDA approval of our drug candidates and commercialization of our products, result in higher costs, or deprive us of potential product revenues:
| ·
| | Contract commercial manufacturers, their sub-contractors or other third parties we rely on and expect to rely on, may encounter difficulties in achieving the volume of production needed to satisfy preclinical and clinical needs or commercial demand, may experience technical issues that impact quality or compliance with applicable and strictly enforced regulations governing the manufacture of pharmaceutical products, and may experience shortages of qualified personnel to adequately staff production operations.
|
| ·
| | Our contract manufacturers could default on their agreements with us to provide supplies or meet our requirements for commercialization of our products.
|
| ·
| | For certain of our drug candidates, the use of alternate manufacturers may be difficult because the number of potential manufacturers that have the necessary governmental licenses to produce narcotic products is limited. Additionally, the FDA and the DEA must approve any alternative manufacturer of our products before we may use the alternative manufacturer to produce our supplies.
|
| ·
| | It may be difficult or impossible for us to find a replacement manufacturer on acceptable terms quickly, or at all. Our contract manufacturers and vendors may not perform as agreed or may not remain in the contract manufacturing business for the time required to successfully produce, store and distribute our products.
|
| ·
| | If any contract manufacturer makes improvements in the manufacturing process for our products, we may not own, or may have to share, the intellectual property rights to such innovation.
|
We may not be able to successfullyprotect our intellectual property and proprietary rights throughout the world.
Filing, prosecuting, and defending patents on our product candidates and other technologies in all countries throughout the world would be prohibitively expensive, and the laws of foreign countries may not protect our rights to the same extent as the laws of the U.S.
Consequently, we may not be able to prevent third parties from practicing our inventions in all countries outside the U.S., or from selling or importing products made using our inventions in and into the U.S. or other jurisdictions. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products, and, further, may export otherwise infringing products to territories where we have patent protection, but enforcement is not as strong as that in the U.S. These products may compete with our products, and our patents or other intellectual property rights may not be effective or sufficient to prevent them from competing.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents, trade secrets, and other intellectual property protection, particularly those relating to biotechnology products, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our intellectual property and proprietary rights generally. Proceedings to enforce our intellectual property and proprietary rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly, could put our patent applications at risk of not issuing, and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate, and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property and proprietary rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or commercializelicense.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment, and other requirements imposed by government patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees, and various other government fees on patents and applications will be due to be paid to the USPTO and various government patent agencies outside of the U.S. over the lifetime of our owned or licensed patents and applications. The USPTO and various non-U.S. government agencies require compliance with several procedural, documentary, fee payment, and other similar provisions during the patent application process. In some cases, an inadvertent lapse can be cured by payment of a late fee or by other means in accordance with the applicable rules. There are situations, however, in which non-compliance can result in abandonment or lapse of the patent or patent application, resulting in a partial or complete loss of patent rights in the relevant jurisdiction. In such an event, potential drugcompetitors might be able to enter the market with similar or identical products or technology, which could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
Changes in U.S. patent law could diminish the value of patents in general, thereby impairing our ability to protect our products.
Changes in either the patent laws or interpretation of the patent laws in the U.S. could increase the uncertainties and costs surrounding the prosecution of patent applications and the enforcement or defense of issued patents. Assuming that other requirements for patentability are met, prior to March 2013, in the U.S., the first to invent the claimed invention was entitled to the patent, while outside the U.S., the first to file a patent application was entitled to the patent. After March 2013, under the Leahy-Smith America Invents Act (the America Invents Act) enacted in September 2011, the U.S. transitioned to a first inventor to file system in which, assuming that other requirements for patentability are met, the first inventor to file a patent application will be entitled to the patent on an invention regardless of whether a third party was the first to invent the claimed invention. A third party that files a patent application in the USPTO after March 2013, but before us could therefore be awarded a patent covering an invention of ours even if we had made the invention before it was made by such third party. This will require us to be cognizant going forward of the time from invention to filing of a patent application. Since patent applications in the U.S. and most other countries are confidential for a period of time after filing or until issuance, we cannot be certain that we were the first to either (i) file any patent application related to our product candidates or other technologies or (ii) invent any of the inventions claimed in our patents or patent applications.
The America Invents Act also includes a number of significant changes that affect the way patent applications will be prosecuted and also may affect patent litigation. These include allowing third party submission of prior art to the USPTO during patent prosecution and additional procedures to attack the validity of a patent by USPTO administered post-grant proceedings, including post-grant review, inter partesreview, and derivation proceedings. Because of a lower evidentiary standard in USPTO proceedings as compared to the evidentiary standard in U.S. federal courts necessary to invalidate a patent claim, a third party could potentially provide evidence in a USPTO proceeding sufficient for indicationsthe USPTO to hold a claim invalid even though the same evidence would be insufficient to invalidate the claim if first presented in a district court action. Accordingly, a third party may attempt to use the USPTO procedures to invalidate our patent claims that would not have been invalidated if first challenged by the third party as a defendant in a district court action. Therefore, the America Invents Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents, all of which could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
In addition, the patent positions of companies in the development and commercialization of pharmaceuticals are particularly uncertain. Various U.S. Supreme Court rulings have narrowed the scope of patent protection available in certain circumstances and weakened the rights of patent owners in certain situations. This combination of events has created uncertainty with respect to the validity and enforceability of patents, once obtained. Depending on future actions by the U.S. Congress, the federal courts, and the USPTO, the laws and regulations governing patents could change in unpredictable ways that could have a material adverse effect on our existing patent portfolio and our ability to protect and enforce our intellectual property in the future.
We may be subject to claims challenging the inventorship of our patents and other than pain.intellectual property.
OurWe may be subject to claims that former employees, scientific collaborators or other third parties have an interest in our patents, trade secrets, or other intellectual property as an inventor or co-inventor. For example, we may have inventorship
disputes arise from conflicting obligations of employees, consultants, or others who are involved in developing our product candidates or other technologies. Litigation may be necessary to defend against these and other claims challenging inventorship or ownership of our patents, trade secrets, or other intellectual property. If the defense of any such claims fails, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, intellectual property that is important to our product candidates and other technologies. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees. Any of the foregoing could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
We may not be successful in obtaining necessary rights to our product candidates or other technologies.
Many pharmaceutical companies, biotechnology companies, and academic institutions that compete with us in the field of neurodegeneration therapy may have patents filed and are likely filing patent applications potentially relevant to our business. In order to avoid infringing these third-party patents, we may find it necessary or prudent to obtain licenses to such patents from such third-party intellectual property holders. We may also require licenses from third parties for certain technologies for use with future product candidates. In addition, with respect to any patents we co-own with third parties, we may wish to obtain licenses to such co-owner’s interest to such patents. However, we may be unable to secure such licenses or otherwise acquire any compositions, methods of use, processes, or other intellectual property rights from third parties that we identify as necessary for our future product candidates. The licensing or acquisition of third-party intellectual property rights is a competitive area, and several more established companies may pursue strategies to license or acquire third-party intellectual property rights that we may consider attractive or necessary. These established companies may have a competitive advantage over us due to their size, capital resources, and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment or at all. If we are unable to successfully obtain rights to required third-party intellectual property rights or maintain the existing intellectual property rights we have, we may have to abandon development of the relevant program or product candidate, which could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
We may be subject to claims that our employees, consultants, or advisors have wrongfully used or disclosed alleged trade secrets of their current or former employers or claims asserting ownership of what we regard as our own intellectual property which may prevent or delay the development of our product candidates.
The field of developing innovations for neurodegenerative diseases is highly competitive and dynamic. Due to the focused research and development activities include development of potential drug candidates for indicationsthat is taking place by several companies, including us and our competitors, the intellectual property landscape in this field is in flux, and it may remain uncertain in the future. Additionally, no products utilizing our underlying science and technology have yet reached the market. As such, there may be significant intellectual property related litigation and proceedings relating to our, and other than pain. We have no history of developing such drug candidates. We do not know whether any of our planned development activities will resultthird party, intellectual property and proprietary rights in marketable products. We do not anticipate that our drug candidates in these areas will reach the market for at least several years, if at all.future.
Our employees and consultants are generally subject to confidentiality or other agreements with their former employers and they may inadvertently or otherwise violate those agreements.
Many of our employees, consultants, and consultantsadvisors are currently or were previously employed at universities or other biotechnology or pharmaceutical companies. Whilecompanies, including our competitors and potential competitors. Although we requiretry to ensure that our employees, consultants, and consultants to honor any agreements they may have entered into prior to working withadvisors do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we inadvertently or otherwisethese individuals have used or disclosed intellectual property, including trade secrets or other confidentialproprietary information, belonging toof any such individual’s current or former employers. Failureemployer. Litigation may be necessary to defend against these claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we are successful in defending against such claims, litigation could result in losssubstantial costs and be a distraction to management.
In addition, while it is our policy to require our employees and contractors who may be involved in the conception or development of valuableintellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who, in fact, conceives or develops intellectual property that we regard as our own. The assignment of intellectual property rights may not be self-executing, or personnel,the assignment agreements may be breached, and we may be forced to bring claims against third parties, or defend claims that they may bring against us, to determine the ownership of what we regard as our intellectual property. Such claims could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
Our commercial success depends in part on our ability to develop, manufacture, market, and sell any product candidates that we develop and to use our proprietary technologies without infringing, misappropriating, and otherwise violating the patents and other intellectual property rights of third parties. There is a substantial amount of complex litigation involving patents and other intellectual property rights in the biotechnology and pharmaceutical industries, as well as administrative proceedings for challenging patents, including interference, derivation, and reexamination proceedings before the USPTO or oppositions and other comparable proceedings in foreign jurisdictions. We may become party to, or threatened with, such actions in the future, regardless of their merit. As discussed above, recently, due to changes in U.S. law referred to as patent reform, new procedures including inter partes review and post-grant review have been implemented. As stated above, this reform adds uncertainty to the possibility of challenge to our patents in the future.
Numerous U.S. and foreign issued patents and pending patent applications owned by third parties exist in the fields in which we are developing our product candidates. As the biotechnology and pharmaceutical industries expand and more patents are issued, the risk increases that our product candidates and other technologies may give rise to claims of infringement of the patent rights of others. Although we believe that we do not infringe on any third parties’ patents or other intellectual property, we cannot assure you that our product candidates and other technologies that we have developed, are developing or may develop in turnthe future will not infringe existing or future patents owned by third parties. We may not be aware of patents that have already been issued to a third party, such as a competitor in the fields in which we are developing product candidates, who might assert infringement of patents it may hold by our current or future product candidates or other technologies, including claims to compositions, formulations, methods of manufacture or methods of use or treatment that cover our product candidates or other technologies. It is also possible that patents owned by third parties of which we are aware, but which we do not believe are relevant to our product candidates or other technologies, could harmbe found to be infringed by our product candidates or prevent commercializationother technologies. In addition, because patent applications can take many years to issue, there may be currently pending patent applications that may later result in issued patents that our product candidates or other technologies may infringe.
Engaging in litigation to defend against third parties alleging that we have infringed, misappropriated, or otherwise violated their patents or other intellectual property rights is very expensive, particularly for a company of our drug candidates. Successful defensesize, and time-consuming. Some of our competitors may be able to sustain the costs of litigation or administrative proceedings more effectively than we can because of greater financial resources. Patent litigation and other proceedings may also absorb significant management time. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings against us could impair our ability to compete in the marketplace. The occurrence of any of the foregoing could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
We may become involved in lawsuits to protect or enforce our patents and other intellectual property rights, which could be expensive, time consuming, and unsuccessful.
Competitors may infringe on our patents or the patents of our licensing partners, or we may be required to defend against claims of infringement. In addition, our patents or the patents of our licensing partners also may become involved in inventorship, priority, or validity disputes. To counter or defend against such claims can be expensive and time consuming. In an infringement proceeding, a court may decide that a patent in which we have an interest is invalid or unenforceable, the other party’s use of our patented technology falls under the safe harbor to patent infringement, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation proceeding could put one or more of our patents at risk of being invalidated or interpreted narrowly. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation.
Even if resolved in our favor, litigation or other legal proceedings relating to intellectual property claims may cause us to incur significant expenses and could distract our personnel from their normal responsibilities. In addition, there could be public announcements of the results of hearings, motions, or other interim proceedings or developments, and if securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of our common stock. Such litigation or proceedings could substantially increase our operating losses and reduce the resources available for development activities or any future sales, marketing, or distribution activities. We may not have sufficient financial or other resources to conduct such litigation or proceedings adequately. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their greater financial resources and more mature and developed intellectual property portfolios. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material adverse effect on our ability to compete in the marketplace.
Intellectual property rights do not necessarily address all potential threats.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations and may not adequately protect our business or permit us to maintain our competitive advantage. For example:
others may be able to make products that are similar to our product candidates or utilize similar technology but that are not covered by the claims of the patents that we may own;
we might distractnot have been the first to make the inventions covered by the issued patent or pending patent application that we own now or in the future;
we might not have been the first to file patent applications covering certain of our inventions;
others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our owned intellectual property rights;
it is possible that our current or future pending patent applications will not lead to issued patents;
issued patents that we hold rights to may be held invalid or unenforceable, including as a result of legal challenges by our competitors or other third parties;
our competitors or other third parties might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive products for sale in our major commercial markets;
we may not develop additional proprietary technologies that are patentable;
the patents of others may harm our business; and
we may choose not to file a patent in order to maintain certain trade secrets or know-how, and a third party may subsequently file a patent covering such intellectual property.
Should any of these events occur, they could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
Risks Related to Our Business and Operations
Our reputation and operations could be adversely impacted by allegations, regardless of their merits.
We believe that our reputation has significantly contributed to the success of our business. We also believe that maintaining and enhancing our reputation is critical to many of our core operations, such as conducting studies, working with outside vendors, hiring qualified employees, members of our Board of Directors or science collaborators, raising funds for future operations, or working with potential industry and government collaborators. Maintaining and enhancing our reputation will depend largely on our ability to develop innovative drug products, continue to generate credible scientific data and respond appropriately to our critics, which we may not do successfully.
Our reputation may be injured by published false statements purporting to be fact, or by hostile actions made by or paid for by parties who represent investors who seek a decline in the price of our securities (“short-sellers”). Such allegations and statements may be published on internet forums over which we have no control, such as social media, and may be adopted by the editors of scientific or technical journals that have published our research, potentially resulting in retractions or expressions of concern by the journals. Regardless of merit, allegations and false statements may spread quickly and erode confidence in our reputation. Maintaining and enhancing our reputation may require us from executingto make substantial investments in legal actions or other activities, and these investments could be expensive, time consuming, and unsuccessful. If we fail to successfully maintain our strategies.reputation, or if we incur excessive expenses in this effort, our business, operations, future prospects, cash flows, and financial position may be adversely affected.
Law enforcement concerns over Our ability to continue to operate without any significant disruptions will in part depend on our ability to source raw materials and clinical supplies via our product supply chains.
The widespread outbreak of COVID-19 has generally not significantly impacted our ability to source raw materials and clinical supplies to date. However, we are broadly aware of some general supply chain disruptions in certain markets due primarily to the restriction of employee movements and, in North America, due to labor shortages, supply chain disruptions and transportation constraints. In addition, uncertainty in the duration and scope of the pandemic, the emergence of new
mutations or variants of the virus, the likelihood of a resurgence of positive cases, the speed at which treatments and vaccines are administered or mandated and governmental actions in response to the pandemic could result in an unforeseen disruption to our operations. In addition, our ability to conduct clinical trials require the use of a host of critical ancillary supplies. Clinical ancillary supplies are general consumable or disposable products, such as sample collection tubes, latex gloves, instruments and other products routinely used in a medical or clinical research setting. We rely on independent vendors globally to supply us or our clinical collaborators with ancillary supplies. Any disruptions, gaps or shortages in the global supply chain for ancillary supplies could increase the cost or complexity of our supply chain management and delay the completion of our Phase 3 clinical program.
We cannot reasonably predict disruptions, gaps or shortages across our product supply-chains. With prolonged disruptions, there exists the possibility of a material adverse impact on our business, clinical operations, future prospects, cash flows, and financial position. Should we be unable to obtain key raw materials and clinical supplies on a timely basis, it could have a material adverse effect on our business, financial condition, results of operations, and growth prospects.
The worldwide outbreak of the COVID-19 virus and associated mutations or variants may materially and adversely affect our business operations and our ability to conduct clinical studies.
A widespread outbreak of COVID-19 has been declared by the World Health Organization to be a “public health emergency of international concern”; a national emergency by the President of the U.S; and a major disaster by several states in which we operate. This unprecedented spread of disease may affect our operations by causing a period of business disruption, including the potential interruption or halt of our clinical study activities and delays or disruptions in the supply of our products and product candidates, or the inability of our employees to continue their normal course of work due to disease, quarantine or leave requirements, or the possibility of legal claims and actions against us for claims of loss arising out of COVID-19. As a small company that operates with a limited number of employees, the impact of disease may disproportionately hurt our operations. Further, our business insurance may not provide coverage against economic loss or claims specifically tied to COVID-19 or any other disease.
COVID-19 presents many challenges that are without precedent. As such, we cannot presently assess or predict all current and potential uncertainties around the scope and severity of COVID-19 on our business operations with any meaningful precision. There is no assurance that COVID-19 will not have a material adverse impact on our future results. For example, the continued spread of COVID-19 could adversely impact our clinical study operations, including our ability to recruit and retain patients and principal investigators and site staff who, as healthcare providers, may have heightened exposure to COVID-19 if an outbreak occurs in their geography. COVID-19 could also negatively affect our manufacturing operations, which could result in delays or disruptions in the supply of our product candidates. A greater number of our employees working remotely during this outbreak of disease may expose us to greater risks related to cybersecurity and cyber-liability. Our study participants, vendors, employees, suppliers or others may allege they became sick due to our negligence. In addition, there could be a potential effect of a slowdown at FDA, which could result in delays of regulatory correspondence that are necessary for us to maintain or advance our product candidates in clinical studies. Further, the COVID-19 outbreak may adversely impact our ability to file on a routine and timely basis our obligations under federal securities laws, present new data at annual scientific meetings and professional conferences, reach out to institutional investors through in-person meetings, advance simufilam in a Phase 3 efficacy program, add an international component to our clinical studies, obtain additional financing as needed, engage in partnering discussions or conduct other activities necessary to the success of our business.
The extent to which the COVID-19 pandemic may impact our business with respect to research and development and clinical trials will depend on future developments, which are highly uncertain and cannot be predicted with confidence, such as the ultimate geographic spread of the disease, vaccine distribution, variants of the virus, the duration of the outbreak, travel restrictions and social distancing in the United States and other countries, business closures or business disruptions, and the effectiveness of actions taken in the United States and other countries to contain and treat the disease. As the COVID-19 pandemic continues to spread around the globe, we will likely experience disruptions that could severely impact our business with respect to research and development and clinical trials, including:
•delays or difficulties in enrolling patients or maintaining scheduled study visits in our clinical trials;
•delays or difficulties in clinical site initiation, including difficulties in recruiting clinical site investigators and clinical site staff;
•negative impact on interactions necessary for clinical testing, due to restricted access for industry employees;
•challenges in providing clinical study education with respect to our Phase 3 program in a virtual setting, and restrictions on clinician and provider travel;
•diversion of opioidshealthcare resources, clinical staff, physicians and social issues around abuseadvanced practice providers in neurology, including clinical sites serving as our clinical trial sites, away from the conduct of opioidsour clinical trials;
•interruption of key clinical trial activities, such as clinical trial site monitoring, due to limitations on travel imposed or recommended by federal or state governments, employers and others;
•limitations in employee resources that would otherwise be focused on the conduct of our business with respect to research and development or clinical trials, including due to illness of our employees or their families, an increase in childcare responsibilities for certain employees, the desire of our employees to avoid close contact or contact with large groups of people or because of governmental imposition of stay-at-home orders or similar working restrictions;
•delays in receiving approval from local regulatory authorities to initiate our planned clinical trials;
•delays in clinical sites receiving the supplies and materials needed to conduct clinical trials;
•interruption in domestic or global shipping that may makeaffect the transport of clinical trial materials;
•changes in regulations as part of a response to the COVID-19 pandemic, which may require us to change the ways in which our clinical trials are conducted, which may result in unexpected costs, or discontinuing clinical trials altogether;
•delays in necessary interactions and anticipated timelines with local and federal regulators (including the FDA), ethics committees and other important agencies and contractors due to limitations in employee resources or forced furlough of government employees; and
•refusal of the FDA to accept data from clinical trials in affected geographies outside the United States.
If we or any of the third parties with whom we engage were to experience shutdowns or other business disruptions related to COVID-19, our ability to conduct our business in the manner and on the timelines presently planned could be materially and negatively impacted, which could have a material adverse effect on our business, results of operations and financial condition.
Our dependence on single source suppliers for our drug substance and drug product could materially adversely affect our ability to manufacture our product candidates and materially increase our costs.
We rely on single source suppliers for materials that are critical to the manufacturing of simufilam, our lead product candidate. This reliance subjects us to risks related to our potential inability to obtain an adequate supply of required materials. Our operating results could be materially adversely affected if we were unable to obtain adequate supplies of simufilam in a timely manner or if their cost increased significantly.
Further, it would likely result in production and delivery delays if we needed to find alternative suppliers for simufilam, which could lead to delays in our clinical trials and have a material adverse effect on our business, results of operations and financial condition.
Changes in funding for the FDA and other government agencies could hinder their ability to hire and retain key leadership and other personnel, or otherwise prevent our product candidates from being developed or commercialized in a timely manner, which could negatively impact our business.
We rely on the FDA to assist with the development our product candidates. The ability of the FDA to review and approve new drug products can be affected by a variety of factors outside of our control, including government budget and funding levels, ability to hire and retain key personnel and accept the payment of user fees, and statutory, regulatory, and policy changes. Average review times at the agency have fluctuated in recent years as a result. In addition, government funding of other government agencies that fund research and development activities is subject to the political process, which is inherently fluid and unpredictable.
Disruptions at the FDA and other agencies may also slow the time necessary for our product candidates to be reviewed and/or potentially approved by necessary government agencies, which would adversely affect our business. For example, over the last several years, including for 35 days beginning on December 22, 2018, the U.S. government has shut down several times and certain regulatory agencies, such as the FDA, have had to furlough critical FDA employees and stop critical activities. If a prolonged government shutdown occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business. If the timing of FDA’s
review and approval process and commercializationof new products is delayed, the estimated timing of our drug candidates very difficult.
Law enforcement agencies or regulatory agenciesdevelopment program may apply policies that seek to limit the availabilitybe delayed which would materially increase costs of opioids. Such efforts may adversely affect the regulatory approval and commercialization of our drug candidates.
Developments by competitors may render our products or technologies obsolete or non-competitive.
Alternative technologies and products are being developed to improve or replace the use of opioids for pain management, several of which are in clinical trials or are awaiting approval from the FDA. In addition, the active ingredients in nearly all opioid drugs are available in generic form. Drug companies that sell generic opioid drugs represent substantial competition. Many of these organizations competing with us have substantially greater capital resources, larger research and development staffs and facilities, greater experience in drug development and in obtaining regulatory approvalsharm our operations or business.
Our reliance on third parties for both the supply and greater manufacturing and marketing capabilities thanmanufacture of materials for our product candidates carries the risk that we do. Our competitors may market less expensivewill not have sufficient quality or more effective drugs that would compete with our drugquantities of such materials or product candidates, or reach marketthat such supply will not be available to us at an acceptable cost, which could delay, prevent, or impair our development or commercialization efforts.
We do not have any manufacturing facilities. We currently rely on CDMOs for all of the manufacture of our materials for preclinical studies and clinical studies and expect to continue to do so for preclinical studies, clinical studies, and for commercial supply of any product candidates that we may develop. We currently have established relationships with competing drugs beforeseveral CDMOs for the manufacturing of our product candidates. We may be unable to establish any further agreements with CDMOs or to do so on acceptable terms. Even if we are able to reach marketestablish agreements with third-party manufacturers, reliance on CDMOs entails additional risks, including:
the possible breach of the manufacturing agreement by the third party;
the possible termination or nonrenewal of the agreement by the third party at a time that is costly or inconvenient for us;
reliance on the third party for regulatory compliance, quality assurance, safety, and pharmacovigilance and related reporting; and
the inability to produce required volume in a timely manner and to quality standards.
Third-party manufacturers may not be able to comply with cGMP regulations or similar regulatory requirements outside the U.S. Our failure, or the failure of our drug candidates. These organizations alsoCDMOs, to comply with applicable regulations could result in clinical holds on our studies, sanctions being imposed on us, including fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, seizures, or recalls of product candidates or product candidates, operating restrictions, and criminal prosecutions, any of which could significantly and adversely affect supplies of our product candidates and harm our business, financial condition, results of operations, and growth prospects.
Any product candidates that we may develop may compete with usother product candidates and products for access to attract qualified personnelmanufacturing facilities. There are a limited number of manufacturers that operate under cGMP regulations and partnersthat might be capable of manufacturing for acquisitions, joint venturesus.
Any performance failure on the part of our existing or other collaborations.future third-party manufacturers could delay clinical development or marketing approval. If any one of our current contract manufacturers cannot perform as agreed, we may be required to replace that manufacturer and may incur added costs and delays in identifying and qualifying any such replacement. Furthermore, securing and reserving production capacity with contract manufacturers may result in significant costs.
Business interruptions could limitWe also rely on third-parties for the supply of the raw materials required for the production of our product candidates, and we expect to continue to rely on third party manufacturers for the commercial supply of any of our product candidates for which we obtain marketing approval. Our current and anticipated future dependence upon others for the manufacture of any product candidates we may develop may adversely affect our future profit margins and our ability to operatecommercialize any medicines that receive marketing approval on a timely and competitive basis.
Our employees, principal investigators, consultants and vendors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements and insider trading.
We are exposed to the risk of fraud or other misconduct by our business.
Our operations, as well asemployees, principal investigators, consultants and vendors. Misconduct by these parties could include intentional failures, reckless and/or negligent conduct or unauthorized activities that violate (i) the laws and regulations of FDA and other regulatory authorities, including those laws requiring the reporting of our collaborators on which we depend, are vulnerabletrue, complete and accurate information to damagesuch authorities, (ii) manufacturing standards, (iii) federal and state data privacy, security, fraud and abuse and other healthcare laws and regulations in the United States and abroad and (iv) laws that require the true, complete and accurate reporting of financial information or interruption from computer viruses, human error, natural disasters, electrical and telecommunication failures, international acts of terror and similar events. We have not established a formal disaster recovery plan and our back-up operationsdata. In particular, clinical and business interruption insurancearrangements in the biotechnology and healthcare industries are subject to extensive laws and regulations intended to prevent fraud, misconduct, kickbacks, self-dealing and other abusive practices. These laws and regulations restrict or prohibit a wide range of financial arrangements, incentive programs and other business arrangements. Such misconduct also could involve
the improper use of individually identifiable information, including, without limitation, information obtained in the conduct of clinical trials, creating fraudulent data in our preclinical studies or clinical trials or illegal misappropriation of drug product, which could result in regulatory sanctions and cause serious harm to our reputation. It is not always possible to identify and deter misconduct by employees and other third parties, and the precautions we take to detect and prevent this activity may not be adequateeffective in controlling unknown or unmanaged risks or losses or in protecting us from government investigations or other actions or lawsuits stemming from a failure to compensatecomply with these laws or regulations.
Additionally, we are subject to the risk that a person or government could allege such fraud or other misconduct, even if none occurred. If any such actions are instituted against us for lossesand we may suffer. A significant business interruptionare not successful in defending ourselves or asserting our rights, those actions could result in lossessignificant civil, criminal and administrative penalties, damages, fines, disgorgement, imprisonment, exclusion from participating in government-funded healthcare programs, such as Medicare and Medicaid, additional reporting requirements and oversight if we become subject to a corporate integrity agreement or similar agreement to resolve allegations of noncompliance with these laws, contractual damages, incurred by usreputational harm and require us to ceasethe curtailment or curtail our operations.
Cyber-attacks or other failures in telecommunications or information technology systems could result in information theft, data corruption and significant disruptionrestructuring of our operations, any of which could have a negative impact on our business, operations.financial condition, results of operations and prospects.
We use information technology, computerexpect to grow the size and capabilities of our organization, including accessing new physical facilities, and we may experience difficulties in effectively managing this growth.
As our development plans and strategies develop, we expect to add a significant number of additional managerial, operational, financial, and other personnel. Future growth will impose significant added responsibilities on members of management, including:
identifying, recruiting, integrating, retaining, and motivating additional employees;
executing a planned move to our new corporate headquarters in 2022;
increasing employee headcount;
managing our internal development efforts effectively, including the clinical and FDA review process for our current and future product candidates, while complying with our contractual obligations to contractors and other third parties;
expanding our operational, financial and management controls, reporting systems, and networksprocedures; and
managing increasing operational and managerial complexity.
Our future financial performance and our ability to process, transmitcontinue to develop and, store electronic informationif approved, commercialize our product candidates will depend, in connection withpart, on our businessability to effectively manage any future growth. Our management may also have to divert a disproportionate amount of its attention away from day-to-day activities in order to manage these growth activities. Cyber incidents, including deliberate attacks
We currently rely, and attemptsfor the foreseeable future will continue to gain unauthorized accessrely, in substantial part on certain independent organizations, advisors, and consultants to computer systemsprovide certain services. There can be no assurance that the services of these independent organizations, advisors, and networks, have increased in frequency, scopeconsultants will continue to be available to us on a timely basis when needed, or that we can find qualified replacements. In addition, if we are unable to effectively manage our outsourced activities or if the quality or accuracy of the services provided by consultants is compromised for any reason, our clinical studies may be extended, delayed, or terminated, and sophistication in every industry. These threats pose a riskwe may not be able to the securityobtain regulatory approval of our systems and networks and the confidentiality, availability and integrity ofproduct candidates or otherwise advance our data, and may cause a disruption in our operations, harm our reputation and increase our stock trading risk.business. There can be no assurance that we will be successfulable to manage our existing consultants or find other competent outside contractors and consultants on economically reasonable terms, if at all.
If we are not able to effectively expand our organization by hiring new employees and expanding our groups of consultants and contractors, we may not be able to successfully implement the tasks necessary to further develop our product candidates and, accordingly, may not achieve our research, development, and commercialization goals.
Ownership of our corporate headquarters and property leasing are subject to numerous risks and uncertainties.
In August 2021, we made an all-cash purchase of an office complex in preventing cyber-attacksAustin, Texas, that we anticipate will serve as our corporate headquarters for the long term. Title to this property is held by Austin Innovation Park, LLC, a Texas limited liability company wholly owned by Cassava Sciences. The purchase required a substantial upfront cash investment and may require further commitments of our resources in the future. We have assumed or successfully mitigating their effects. Similarly, there canentered into lessor commitments with independent third parties for portions of our office complex and will continue to do so in the future. Commercial property ownership and
related leasing activity are subject to many factors that pose substantial financial risks and uncertainties, including tenant default or non-payment of lease obligations by tenants. Macro-economic or other factors outside of our control could have an adverse effect on the demand for leased office space in our locale or may cause a decline in the market value of our corporate headquarters. If we fail to lease unoccupied office space at favorable rates, or if we incur excessive expenses in this effort or incur excessive leasehold improvements or property ownership expenses, our business, operations, future prospects, cash flows, and financial position may be no assuranceadversely affected.
Our internal computer systems, or those used by third parties on whom we rely, may fail or suffer other breakdowns, cyberattacks, or information security breaches that could compromise the confidentiality, integrity, and availability of such systems and data, result in material disruptions of our third-party collaborators, distributorsdevelopment programs and business operations, risk disclosure of confidential, financial, or proprietary information, and affect our reputation.
In the ordinary course of our business, we collect and store sensitive data, including legally protected patient health information, personally identifiable information about our employees, intellectual property, and proprietary business information. We manage and maintain our applications and data utilizing on-site systems. These applications and data encompass a wide variety of business-critical information including research and development information, commercial information and business and financial information. Despite the implementation of security measures, our internal computer systems and those of our current or future Clinical Research Organizations (CROs) and other contractors and consultants willmay be successfulvulnerable to damage from computer viruses and unauthorized access. As the cyber-threat landscape evolves, these attacks are growing in protecting our data that is stored on their systems. Afrequency, sophistication, and intensity, and are becoming increasingly difficult to detect. Such attacks could include the use of key loggers or other harmful and virulent malware, including ransomware or other denials of service, and can be deployed through malicious websites, the use of social engineering, and/or other means. If a breakdown, cyberattack, or destructionother information security breach were to occur and cause interruptions in our operations, it could result in a misappropriation of confidential information, including our intellectual property or financial information, and a material disruption of our development programs and our business operations. For example, the loss of clinical study data from completed, ongoing, or future clinical studies could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. Likewise, we rely on our third-party research institution collaborators for research and development of our product candidates and other third parties for the manufacture of our product candidates and to conduct clinical studies, and similar events relating to their computer systems could also have a material adverse effect on our business. To the extent that any disruption or security breach were to result in a loss of, or damage to, our data or systems, or inappropriate disclosure of confidential, financial, or proprietary information, including data related to our personnel, we could incur liability or risk disclosure of confidential, financial, or proprietary information, and the further development and commercialization of our product candidates could be delayed. There can be no assurance that we and our business and prospects. In addition, we may suffer reputational harmcounterparties will be successful in efforts to detect, prevent, or face litigationfully recover systems or adverse regulatory action as a resultdata from all breakdowns, service interruptions, attacks, or breaches of cyber-attacks or other data security breaches and may incur significant additional expense to implement further data protection measures.
Unfavorable media coverage of opioid pharmaceuticalssystems that could negatively affect our business.
Opioid drug abuse receives a high degree of media coverage. Unfavorable publicity regarding, for example, the use or misuse of oxycodone or other opioid drugs, the limitations of ADFs, public inquiries and investigations into prescription drug abuse, litigation or regulatory activity could adversely affect our reputation. Such negative publicity could have an adverse effect on the potential size of the market for our drug candidates and decrease revenues and royalties, which would adversely affect our business and operations and/or result in the loss of critical or sensitive data, which could result in financial, results.legal, business, or reputational harm to us.
Our business involves environmental risks that may result in liability for us.
Risks Relating
In connection with our research and development activities, we, and our collaborators and vendors, are subject to Manufacturingfederal, state and local laws, rules, regulations and policies governing the use, generation, manufacture, storage, air emission, effluent discharge, handling and disposal of certain materials, biological specimens, chemicals and wastes. Although we believe that we comply with such applicable laws, regulations and policies in all material respects and have not been required to correct any material noncompliance, we may incur significant costs to comply with environmental and health and safety regulations in the future. Although we believe that our safety procedures for handling and disposing of controlled materials comply with the standards prescribed by state and federal regulations, accidental contamination or injury from these materials may occur. In the event of such an occurrence, we could be held liable for any damages that result and any such liability could exceed our resources.
Business disruptions and lack of appropriate levels of commercial insurance could seriously harm our future revenue and financial condition and increase our costs and expenses.
Our operations, and those of our third-party research institution collaborators, CROs, CDMOs, suppliers, and other contractors and consultants, could be subject to earthquakes, power shortages, telecommunications failures, water shortages, floods, hurricanes, typhoons, fires, extreme weather conditions, disease epidemics or pandemics, such as COVID-19, a novel coronavirus first detected in 2019, and other natural or man-made disasters or business interruptions, for which we are partly
or entirely uninsured. In addition, we rely on our third-party research institution collaborators for conducting research and development of our product candidates, and they may be affected by government shutdowns or withdrawn funding. The occurrence of any of these business disruptions could seriously harm our operations and financial condition and increase our costs and expenses. We rely on third party manufacturers to produce and process our product candidates. Our ability to obtain clinical supplies of our product candidates could be disrupted if the operations of these suppliers are affected by a man-made or natural disaster or other business interruption.
Our day-to-day operations are located in a single office facility in Austin, Texas. Damage or extended periods of interruption to our corporate, development, or research facilities could cause us to cease or delay development of some or all our product candidates. Our insurance might not cover losses under such circumstances and our business may be seriously harmed by such delays and interruption.
Social media platforms present risks and challenges.
As social media continues to expand, it also presents us with new challenges. The inappropriate or unauthorized use of our confidential information on media platforms could cause brand damage or information leakage, which would cause legal or regulatory issues for us. In addition, negative, inappropriate or inaccurate posts or comments about us or our product candidates on social media internet sites could quickly and irreversible damage our reputation, brand image and goodwill. Further, the accidental or intentional disclosure of non-public sensitive information by our workforce or others through media channels could lead to information loss or could lead to legal or regulatory issues for us.
We expect to rely on third parties to conduct our studies and some aspects of our research, and such third parties may not perform satisfactorily, which could delay or harm our studies, research, and testing.
We substantially rely and expect to continue to rely on third parties, such as CROs, clinical data management organizations, medical institutions, and clinical investigators, to conduct some aspects of our research and preclinical testing and our clinical studies. Any of these third parties may terminate their engagements with us or be unable to fulfill their contractual obligations. If we need to enter into alternative arrangements, it will delay our product development activities.
Our reliance on these third parties for research and development activities reduces our control over these activities but does not relieve us of our responsibilities. For example, we remain responsible for ensuring that all of our clinical studies are conducted in accordance with the general investigational plan and protocols for the trial. Moreover, FDA requires us to comply with the norms of Good Clinical Practice (GCPs) for conducting, recording, and reporting the results of clinical studies to assure that data and reported results are credible, reproducible, and accurate and that the rights, integrity, and confidentiality of study participants are protected. We also are required to register ongoing clinical studies and post the results of completed clinical studies on a government-sponsored database within certain timeframes. Failure to do so can result in fines, adverse publicity, and civil and criminal sanctions.
If our third-party vendors do not successfully carry out their contractual duties, meet expected deadlines, or conduct studies in accordance with regulatory requirements or our stated protocols, we will not be able to obtain, or may be delayed in obtaining, marketing approvals for any product candidates we may develop and will not be able to, or may be delayed in our efforts to, successfully commercialize our product candidates. For example, one of our vendors failed to fully comply with certain Good Laboratory Practice (GLP) norms in its research facility, which required us to repeat a lab study at a different research site.
We also rely on other third parties to label, store and distribute drug supplies for our clinical studies. Any performance failure on the part of our distributors, including with the shipment of any drug supplies, could delay clinical development or marketing approval of any product candidates we may develop or commercialization of our product candidates, producing additional losses and depriving us of potential product revenue.
We do not own any manufacturing facilities and we rely on third-party commercial drug manufacturers for clinical drug supply.
We do not own any manufacturing facilities. We plan to continue to outsource formulation, manufacturing and related activities.
We rely on a limited number of third-party suppliers to formulate, manufacture, fill, label, ship or store all of our drugproduct candidates. These suppliers must comply with current good manufacturing practices, or GMP,cGMP regulations enforced by the FDA and other government
agencies, and DEA regulations, and are subject to ongoing periodic unannounced inspection, including preapproval inspections by the FDA and DEA and corresponding state and foreign government agencies to ensure
strict compliance with cGMP and other government regulations and corresponding foreign standards. These manufacturers may subsequently be stopped from producing, storing, shipping or testing our drug products due to their non-compliance with federal, state or local regulations. We do not have control over our suppliers’ compliance with these regulations and standards.
If REMOXY is approved, our commercial suppliers may encounter difficulties in achieving high volumes of production to satisfy commercial demands.
We cannot control decisions by our suppliers that affect their ability or willingness to continue to supply us on acceptable terms, or at all.
We may not be able to replace a commercial supplier on commercially reasonable terms, or at all. Replacing any of our commercial suppliers would be expensive and time consuming.
Failure by any of our suppliers to perform as expected could delay or prevent commercialization of REMOXYour product candidates or result in shortages, cost overruns, or other problems and would materially harm our business.
We will relyare a small company with a limited number of employees. We are highly dependent on Durect as the sole source of certain excipientsour key personnel, and if we are not successful in REMOXY. Durect has limited experience manufacturing pharmaceutical productsattracting, motivating, and maintaining GMP-compliant operations. We currently do not have a long-term commercial supply agreement in place with Durect. We expect thatretaining highly qualified personnel, we and Durect will negotiate a supply agreement for these excipients. We may not be able to establish a commercial supply agreementsuccessfully implement our business strategy.
Our ability to compete in the highly competitive biotechnology and pharmaceutical industries depends upon our ability to attract, motivate, and retain highly qualified managerial, scientific, and medical personnel. We are highly dependent on acceptable terms, or at all.
If we receive marketing approval forour management, particularly our President and commercially launch REMOXY, Durect may needChief Executive Officer, Remi Barbier, and our scientific and technical personnel. The loss of the services provided by any of our executive officers, other key employees, and other scientific and medical advisors, and our inability to materially expand its manufacturing capacity. Durect may not be able to increase its manufacturing capacity for REMOXYfind suitable replacements, could result in a timely or economic manner, or at all. Moreover, significant scale updelays in the development of manufacturing will require additional validation studies, which are subject to FDA reviewour product candidates and approval. If Durect is unable to successfully increase the manufacturing capacity, at an acceptable cost or otherwise, and we are unable to establish alternative manufacturing capabilities, there may be a shortage in supply, which would harm our future revenuesbusiness.
Competition for skilled personnel is intense and causethe turnover rate can be high, which may limit our businessability to suffer.
If Durect fails to supply excipients to us, they may be in breach of their supply obligations. With or without a commercial supply agreement, Durect’s failure for any reason to supply these excipients, including failure resulting from Durect relying on sole source providers, could delay or prevent commercialization of REMOXY or result in shortages, delays, unexpected costs or other problemshire and would materially harm our business.
We expect to rely on Noramco as the sole source of the oxycodone in REMOXY. We currently do not have a long-term commercial supply agreement in place with Noramco. Effective July 1, 2016, Noramco is owned by SK Capital Partners, a private investment firm. We expect to negotiate with Noramco a commercial supply agreement to supply us with oxycodone. We may not be able to establish a commercial supply agreementretain highly qualified personnel on acceptable terms or at all. UntilWe expect that we may need to recruit talent from outside of our region in Austin, Texas, and doing so may be costly and difficult.
To induce valuable employees to remain at our company, in addition to salary and cash incentives, we have provided equity option grants that vest over time or a commercial supply agreementcash bonus plan. The value to employees of these equity grants that vest over time or cash bonus plans may be significantly affected by movements in placeour stock price that are beyond our control and may at any time be insufficient to counteract more lucrative offers from other companies. Although we have employment agreements with Noramco,our key employees, these employment agreements provide for at-will employment, which means that any of our employees could leave our employment at any time, with or without notice. If we expectare unable to obtain oxycodone from Noramco via purchase orders. There can be no assurance that Noramco will accept our purchase ordersattract and incentivize quality personnel on acceptable terms, or at all. With or withoutall, it may cause our business and operating results to suffer.
We may need to cease our operations if we are unable to attract and retain key personnel.
We are engaged in developing early-stage technologies and will continue to do so for the foreseeable future. Unlike larger organizations, we rely on a commercial supply agreement, Noramco’s failurevery small number of highly skilled, and highly sought after, employees to continue the advancement of our development stage technologies. The knowledge and skills contributed by our key employees may be irreplaceable and the loss of a key employee may cause substantial negative financial, operational and scientific consequences for any reason to supply us with oxycodone could delay or prevent commercializationour business. As an example, our research grant awards from NIH depend in part on the continued participation of REMOXY orcertain key employees, known as a Principal Investigator. The loss of a Principal Investigator may result in shortages, cost overrunsthe loss of one or other problemsmore research grant awards from NIH, which would have significant adverse effects on our ability to continue to conduct, conclude or fund our research programs in Alzheimer’s disease. Likewise, the intellectual property that would materially harmis intended to protect our business.
Wedevelopment stage technologies is still evolving and its evolution remains highly dependent on a small number of employees with specific expertise. The loss of a key employee may jeopardize our existing or pending intellectual property or may prevent us from accessing the technical information and knowledge necessary to extend our portfolio of intellectual property. Furthermore, we believe the adverse effects that may result from losing a key employee’s participation cannot be compensated with any specific insurance policies, such as “key person” or “business life” insurance. If we are not successful in retaining key employees, our business and financial condition will suffer, and we may need to identifycease our operations.
If our current research collaborators or scientific advisors terminate their relationships with us or develop relationships with a third-partycompetitor, our ability to manufacture commercial suppliescontinue our business operations could be adversely affected.
We have relationships with unaffiliated research collaborators at academic and other institutions who conduct research at our request. These research collaborators are not our employees. As a result, we have limited control over their activities and,
except as otherwise required by our collaboration agreements, can expect only limited amounts of REMOXY. Without a commercial manufacturer,their time to be dedicated to our activities. Our ability to discover drugs and biomarkers involved in human disease and validate and commercialize diagnostic tests will depend in part on the continuation of these collaborations. If any of these collaborations are terminated, we may not be able commercialize REMOXY. To date, we have not identified such third-party manufacturer and we may never find a viable source of commercial supplies of REMOXY. We expect to rely on such third party as the sole-source drug product manufacturer of REMOXY pursuant to a supply agreement.enter into other acceptable collaborations. In addition, our existing collaborations may not be successful. Our research collaborators and scientific advisors may have relationships with other commercial entities, some of which could compete with us. Our research collaborators and scientific advisors sign agreements which provide for the confidentiality of our proprietary information and the results of studies conducted at our request. We may not, however, be able to drug product manufacturing, this third-part manufacturer will needmaintain the confidentiality of our technology and other confidential information related to all collaborations. The dissemination of our confidential information could have a material adverse effect on our business.
Our business may be responsibleimpacted by political events, war, terrorism, business interruptions and other geopolitical events and uncertainties beyond our control.
War, terrorism, geopolitical uncertainties and other business interruptions could cause damage to, disrupt or cancel the conduct of our clinical studies on a global or regional basis, which could have a material adverse effect on our business, clinical sites or vendors with which we do business. Such events could also decrease patient demand to enroll in our clinical studies or make it difficult or impossible for sourcing excipientsus to deliver products and services to our clinical investigational sites. In addition, territorial invasions can lead to cybersecurity attacks on technology companies, such as ours, located far outside of the conflict zone. In the event of prolonged business interruptions due to geopolitical events, we could incur significant losses, require substantial recovery time and experience significant expenditures in REMOXY other than those provided byorder to resume our business or clinical operations. We have no operations in Russia or the Durect Agreement. Failure for any reasonUkraine, but we do not and cannot know if the current uncertainties in these geopolitical areas, which are unfolding in real-time, may escalate and result in broad economic and security conditions or rationing of medical supplies, which could limit our ability to manufacture and supply REMOXY could delay or prevent commercialization of REMOXYconduct clinical trials outside the U.S. or result in shortages, product recalls or withdrawals, delays or failuresmaterial implications for our business. In addition, our insurance policies typically contain a war exclusion of some description and we do not know how our insurers are likely to respond in product testing or delivery, cost overruns or other problemsthe event of a loss alleged to have been caused by geopolitical uncertainties.
Risks Related to Financial Condition and Capital Requirements
We have incurred significant net losses in each period since our inception and anticipate that would materially harm our business.
If we cannot formulate and scale-up additional dosage forms of REMOXY, the commercial opportunity for REMOXY might be diminished.
We plan to formulate and scale-up additional dosage forms of REMOXY. We may not be able to successfully complete our formulation or scale-up activities or we may determine that the commercial opportunity for REMOXY in certain dosage forms is too limited to warrant further investment. If we are unsuccessful in our formulation or scale-up activities with REMOXY, our future revenue may be less than expected and our operations may suffer.
We rely solely on Durect to provide us with certain components of drug candidates and will continue to rely on Durect as the sole-source providerof these components.
We rely on Durect as the sole-source provider of certain components of REMOXY and other drug candidates designed to reduce the potential risks of unintended use, and will rely solely on Durect to produce commercial supplies of these components. Durect’s failure for any reason to provide these components or to achieve and maintain satisfactory manufacturing standards could result in product recalls or withdrawals, delays or failures in product testing or delivery, cost overruns or other problems that could materially harm our business.
Durect may encounter manufacturing difficulties involving production yields, quality control and quality assurance. Durect is subject to ongoing periodic unannounced inspection by the FDA and corresponding state and foreign agencies to ensure strict compliance with government regulations and corresponding foreign standards. We cannot control Durect’s compliance with these regulations and standards.
If we receive marketing approval for and commercially launch REMOXY, Durect may need to materially expand its manufacturing capacity. Durect may not be able to increase its manufacturing capacity for REMOXY in a timely or economic manner, or at all. Moreover, significant scale up of manufacturing will require additional validation studies, which are subject to FDA review and approval. If Durect is unable to successfully increase the manufacturing capacity for such components of REMOXY, at an acceptable cost or otherwise, and we are unable to establish alternative manufacturing capabilities, commercialization of REMOXY may be delayed, prevented or impaired or there may be a shortage in supply, which would harm our future revenues and cause our business to suffer.
We expect to rely on Noramco as the sole source of the oxycodone in REMOXY.
We expect to rely on Noramco as the sole source of the oxycodone in REMOXY. We expect we and Noramco will negotiate a supply agreement to supply us with the oxycodone in REMOXY. Noramco’s operation is subject to regulation by the DEA and the Controlled Substances Act. Noramco’s failure for any reason to manufacture and supply us with the oxycodone in REMOXY could result in shortages, cost overruns or other problems that could materially harm our business.
Risks Relating to our Financial Position and Need for Financing
Our operating history may make it difficult for you to evaluate our business to date and to assess its future viability.
Our operations from our inception to date have been limited to organizing and staffing our company, acquiring, developing and securing our technology, undertaking preclinical studies and clinical trials of our drug candidates and forming collaborations. We have not yet demonstrated our ability to obtain regulatory approval, formulate and manufacture our drug candidates on a commercial scale or conduct sales and marketing activities. Consequently, any predictions you make about our future success or viability may not be as accurate as they could be if we had a longer operating history.
We have a history ofincur net losses and expect to incur substantial losses and negative operating cash flows for the foreseeable future.
Although we were profitable in some years in the past based on payments received pursuant to collaboration agreements and interest income, we have yet to generate any revenues from product sales. We have incurred net losses in each reporting period since our inception, including a net loss of $32.4 million for the year ended December 31, 2021. As of December 31, 2021, we had an accumulated deficit of $157 million$207.3 million.
We have invested significant financial resources in research and development activities for product candidates. We do not expect to generate revenue from product sales for several years, if at December 31, 2017. Even if we succeed in developing and commercializing one or moreall. The amount of our drug candidates, wefuture net losses will depend, in part, on the level of our future expenditures and revenue. Moreover, our net losses may fluctuate significantly from quarter to quarter and year to year, such that a period-to-period comparison of our results of operations may not be a good indicator of our future performance.
We expect to continue to useincur significant cash resources in our operationsexpenses and higher operating losses for the foreseeable future.
We anticipate that our expenses will increase substantially as we:
continue our research and discovery activities;
advance our current and any future product candidates through preclinical and clinical development;
initiate and conduct additional preclinical, clinical, or other studies for our product candidates;
work with our CDMO’s to scale up the manufacturing processes for our product candidates;
seek regulatory approvals and marketing authorizations for our product candidates;
obtain, maintain, protect, defend and enforce our intellectual property portfolio;
attract, hire, and retain qualified personnel;
provide additional internal infrastructure to support our continued research and development operations and any planned commercialization efforts in the foreseeablefuture;
experience any delays or encounter other issues related to our operations; and
meet the requirements and demands of being a public company.
Our prior losses and expected future as we:
| ·
| | continue to conduct preclinical studies and clinical trials for our drug candidates;
|
| ·
| | seek regulatory approvals for our drug candidates;
|
| ·
| | develop, formulate, manufacture and commercialize our drug candidates;
|
| ·
| | implement additional internal systems and develop new infrastructure;
|
| ·
| | acquire or in-license additional products or technologies, or expand the use of our technology;
|
| ·
| | maintain, defend and expand the scope of our intellectual property; and
|
| ·
| | hire additional personnel.
|
losses have had and will continue to have an adverse effect on our stockholders’ equity and working capital. In any quarter, our operating results could be below the expectations of securities analysts or investors, which could cause our stock price to decline.
We have broad discretion in the use of the net proceeds from any of our financing transactions and may not use them effectively.
We have broad discretion in the application of the net proceeds from our financing transactions, and investors will neednot have the opportunity to generateassess whether the net proceeds are being used appropriately. We could spend the net proceeds from offerings in ways that vary substantially from their intended use, do not improve our results of operations or enhance the value of our common stock. Our failure to apply these funds effectively could result in financial losses that could have a material adverse effect on our business, cause the price of our common stock to decline and delay the development of our product candidates. Pending their use, we may invest the net proceeds from our financing transactions in a manner that does not produce income or that loses value.
We have no product revenues and may never achieve revenues or profitability based on product revenues.
We have no products approved for commercial sale. To obtain revenues from the sales of our product candidates that are significant revenuesor large enough to achieve and maintain profitability. Ifprofitability, we must succeed, either alone or our collaborators cannot successfully develop, obtainwith third parties, in developing, obtaining regulatory approval for, manufacturing, and commercializemarketing product candidates with significant commercial value. This is a significant endeavor that few early-stage biopharmaceutical companies can successfully achieve. Our ability to generate revenue and achieve profitability depends on many factors, including:
completing research and preclinical and clinical development of our product candidates;
obtaining regulatory approvals and marketing authorizations for product candidates for which we successfully complete clinical development;
developing a sustainable and scalable manufacturing process for our product candidates, as well as establishing and maintaining commercially viable supply relationships with third parties that can provide adequate products and services to support clinical activities and commercial demand for our product candidates;
identifying, assessing, acquiring, and/or developing new product candidates;
negotiating favorable terms in any collaboration, licensing, or other arrangements into which we may enter;
addressing any competing technological and market developments;
maintaining, protecting, expanding, and enforcing our portfolio of intellectual property rights, including patents, trade secrets, and know-how; and
attracting, hiring, and retaining qualified personnel.
Because of the numerous risks and uncertainties associated with drug candidates,development, we are unable to predict the timing or amount of our expenses, or when we will not be able to generate such revenuesany meaningful revenue or achieve profitability in the future. Our failure to achieve or maintain profitability, would have a material adverse impact on the market priceif ever. In addition, our expenses could increase beyond our current expectations if we are required by FDA or foreign regulatory agencies to perform studies in addition to those that we currently anticipate, or if there are any delays in any of our common stock.clinical studies or the development of any of our product candidates.
If we cannot raiseWe may require additional capital to fund our operations and to complete the development of our product candidates. A failure to obtain this necessary capital on acceptable terms, or at all, could force us to delay, limit, reduce, or terminate our commercialization efforts, product development, or other operations.
Our operations have required substantial amounts of cash since inception, and we may be unableexpect our expenses to complete planned clinical trials of any or some of our drug candidates or to pursue attractive business opportunities.
Weincrease significantly in the foreseeable future. To date, we have funded all offinanced our operations and capital expenditures withprimarily through the proceeds from our publicsale of equity securities, research grants and private stock offerings, payments received under collaboration agreementsfrom prior third-party collaborations. Developing our product candidates and interest earnedconducting clinical studies for the treatment of neurodegenerative diseases, including Alzheimer’s disease, will require substantial amounts of capital. We will also require a significant amount of capital to commercialize any approved products.
As of December 31, 2021, we had cash and cash equivalents of $233.4 million. Based on our investments. We expectcurrent operating plan, we believe that our currentexisting cash and cash equivalents and marketable securities will be sufficient to meetfund our working capital and capital expenditure needsprojected operations for at least the next twelve12 months. However,Our estimate as to how long we expect our existing cash and cash equivalents to be available to fund our operations
is based on assumptions that may prove inaccurate, and we could use our available capital resources sooner than we currently expect. In addition, changing circumstances may cause us to increase our spending significantly faster than we currently anticipate, and we may electneed to raise additional funds within such twelve-month period orspend more money than currently expected because of circumstances beyond our control. We may need to raise additional funds thereafter andsooner than we anticipate if we choose to expand more rapidly than we presently anticipate.
We may require additional financingcapital for the further development of our product candidates. Additional capital may not be available when we need it, or on favorable terms ifacceptable to us or at all. EvenWe have no committed source of additional capital. If adequate capital is not available to us on a timely basis, we may be required to significantly delay, limit, reduce or terminate our research and development programs or the commercialization of product candidates, if we succeed in selling additional securitiesapproved, or be unable to raise funds,continue or expand our existing stockholders’ ownership percentage would be reducedoperations, or otherwise capitalize on our business opportunities, as desired, which could materially affect our business, financial condition, results of operations, and new investors may demand rights, preferences or privileges seniorgrowth prospects and cause the price of our common stock to those of existing stockholders. Ifdecline.
To the extent that we raise additional capital through the sale of equity or convertible debt securities, the ownership interest of our stockholders will be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect your rights as a common stockholder. Debt financing, if available, such financings may involve agreements that include covenants that restrictlimiting or restricting our business activities.ability to take specific actions, such as incurring additional debt, making capital expenditures, or declaring dividends. If we raise additional capitalfunds through collaborations, strategic alliance and licensealliances, or licensing arrangements with pharmaceutical partners, we may have to trade ourrelinquish valuable rights to our technology, intellectual propertytechnologies, future revenue streams, research programs, or drugproduct candidates, to others in such arrangementsor grant licenses on terms that may not be favorable to us.
If we determine that we needGlobal credit and financial market conditions could negatively impact the value of our portfolio of cash equivalents and our ability to raise additional fundsmeet our financing objectives.
Our cash and cash equivalents are generally maintained in highly liquid investments with original maturities of 90 days or less at the time of purchase. While, as of the date of this filing, we are not successfulaware of any downgrades, material losses, or other significant deterioration in doing so, wethe fair value of our cash equivalents since December 31, 2021, no assurance can be given that deterioration in conditions of the global credit and financial markets would not negatively impact our current portfolio of cash equivalents or our ability to meet our financing objectives.
Risks Related to the Ownership of Our Common Stock
We do not know whether a sufficient market will continue to develop for our common stock or what the market price of our common stock will be, and, as a result, it may be unabledifficult for investors to complete the clinical development of some or allsell shares of our drug candidates orcommon stock.
If a market for our common stock is not sustained, it may be difficult to seek or obtain FDA approvalsell shares of our drug candidates.common stock at an attractive price or at all. We then could be forced to discontinue product development, enter into a relationship with an additional strategic partner earlier than currently intended, relinquish or license on unfavorable terms our rights to technologies or drug candidates that we would seek to develop ourselves or significantly delay, scale-back or curtail our operations.
Our forecast ofcannot predict the period of time throughprices at which our financial resourcescommon stock will be adequate to supporttrade. It is possible that in one or more future periods our results of operations is a forward-looking statement and involves risksprogression of our product pipeline may not meet the expectations of public market analysts and uncertainties,investors, and, actual results could vary as a result of these and other factors, the price of our common stock may fall.
The market price of our common stock has historically been highly volatile, and we expect it to continue to be volatile, which could result in substantial losses for investors who purchase our shares.
For example, the closing price of our common stock has fluctuated from a numberlow of factors, including$32.15 to a high of $135.30 over the 12 months preceding the filing date of this Annual Report on Form 10-K. Some of the factors discussed elsewhere in this “Risk Factors” section. We have based this estimate on assumptions that may provecause the market price of our common stock to fluctuate include:
the success of existing or new competitive products or technologies;
the timing and results of clinical studies for our current product candidates and any future product candidates that we may develop;
failure or discontinuation of any of our product development and research programs;
results of preclinical studies, clinical studies, or regulatory approvals of product candidates of our competitors, or announcements about new research programs or product candidates of our competitors;
regulatory or legal developments in the United States and other countries;
developments or disputes concerning patent applications, issued patents, or other proprietary rights;
the recruitment or departure of key personnel;
the level of expenses related to any of our research programs, clinical development programs, or product candidates that we may develop;
the results of our efforts to develop additional product candidates or products;
actual or anticipated changes in estimates as to financial results or development timelines;
announcement or expectation of additional financing efforts;
sales of our common stock by us, our insiders, or other stockholders;
variations in our financial results or those of companies that are perceived to be wrong,similar to us;
changes in estimates or recommendations by securities analysts, if any, that cover our stock;
market conditions in the pharmaceutical and we could utilize our available capital resources sooner than we currently expect. biotechnology sectors;
general economic, industry, and market conditions; and
securities litigation, regardless of merit.
Risks Relating to an Investment
In recent years, the stock market in our Common Stock
Our stock price has been volatilegeneral, Nasdaq, and could experience a sudden decline in value.
Our common stockthe markets for early stage companies and pharmaceutical and biotechnology companies, has experienced significant price and volume fluctuations and may continuethat have often been unrelated or disproportionate to experience volatilitychanges in the future. You may not be able to sell your shares quickly or atoperating performance of the latest market price if trading in ourcompanies whose stock is not active or theexperiencing those price and volume is low.
The followingfluctuations. Broad market and industry factors in addition to other risk factors described in this section, may have a significant impact onseriously affect the market price of our common stock:
| ·
| | results of or delays in efforts to seek regulatory approval for REMOXY, and in preclinical studies and clinical trials for our other drug candidates;
|
| ·
| | publicity regarding products under development by us or others, including with respect to actual or potential medical results relating to such matters;
|
| ·
| | announcements of technological innovations or new commercial products by us or others;
|
| ·
| | developments in patent or other proprietary rights by us or others;
|
| ·
| | comments or opinions by securities analysts or major stockholders;
|
| ·
| | adverse media coverage related to opioid pharmaceuticals;
|
| ·
| | future sales of our common stock by existing stockholders;
|
| ·
| | developments with respect to potential merger and acquisition activity of companies with whom we have strategic alliances or other agreements;
|
| ·
| | regulatory developments or changes in regulatory guidance enacted by applicable governmental or other authorities;
|
| ·
| | litigation or threats of litigation;
|
| ·
| | economic and other external factors or other disaster or crises;
|
| ·
| | the departure of any of our officers, directors or key employees;
|
| ·
| | period-to-period fluctuations in financial results;
|
| ·
| | announcement or expectations of additional financing efforts;
|
| ·
| | changes in accounting practices;
|
| ·
| | changes in the structure of the healthcare payment system;
|
| ·
| | market conditions in the biopharmaceutical industry;
|
| ·
| | publication of research reports about us, our competitor or our industry, or positive or negative recommendations or withdrawal of research coverage by securities analysts; and
|
| ·
| | limited daily trading volume.
|
stock, regardless of our actual operating performance. Following periods of such volatility in the market price of a company’s securities, securities class action litigation has often been brought against that company. Because of the potential volatility of our stock price, we are currently and may become the target of securities litigation in the future. Securities litigation could result in substantial costs and divert management’s attention and resources from our business.
If securities analysts do not publish research or reports about our business, or we are the subject of negative publicity, the price of our stock could decline.
The trading market for our common stock depends, in part, on the research and reports that securities or industry analysts publish about us or our business. We do not control these analysts. If one or more of the analysts who cover us downgrade our stock or publish inaccurate or unfavorable evaluations of our company or our stock, the price of our stock could decline. If one or more of these analysts cease coverage of our company or fail to publish reports covering our company regularly, our stock may lose visibility in the market, which in turn could cause our stock price to decline. In addition, if we are athe subject of negative publicity, whether from an analyst, academic, social media, industry group or the general or financial press, our stock price may decline.
Effective December 31, 2021, we no longer qualify as “a smaller reporting companycompany” and we cannot be certain if the reduced disclosure requirements applicable to smaller reporting companies no longer apply beginning with ourquarterly report for the three-month period ended March 31, 2022, which will makeincrease our costs and demands on management.
As a result of our public float (the market value of our common stock less attractive to investors.
We are currentlyshares held by non-affiliates) as of June 30, 2021, we became a large accelerated filer as of December 31, 2021 and, therefore, no longer qualify as a “smaller reporting company” as defined under the Exchange Act. However, we are not required to reflect the change in our smaller reporting company status until our quarterly report for the three-month period ended March 31, 2022.
As a smaller reporting company, we have had the option to take advantage of certain exemptions from various reporting requirements that are applicable to other public companies, including, but not limited to, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements and exemptions related to certain “Say-on-Pay” rules under Section 14A of the Exchange Act, including requirements to hold a nonbinding advisory vote on named executive officer compensation, the frequency of such votes and arrangements with named executive officers regarding compensation based on or related to an acquisition, merger, or similar transaction.
General Risk Factors
If we are unable to maintain effective internal controls, our business, financial position, and results of operations could be adversely affected.
As a public company, we are subject to reporting and other obligations under the Securities Exchange Act of 1934, and are thus allowed to provide simplified executive compensation disclosures inas amended (Exchange Act), including the requirements of Section 404(a) of SOX, which require annual management assessments of the effectiveness of our filings, are exempt from the provisions of internal control over financial reporting. Section 404(b) of the Sarbanes-Oxley Act requiring(“SOX”) also requires our independent auditors to attest to, and report on, the effectiveness of our internal control over financial reporting.
The rules governing the standards that anmust be met for management to assess our internal control over financial reporting are complex and require significant documentation, testing and possible remediation to meet the detailed standards under the rules. During testing, our management may identify material weaknesses or deficiencies which may not be remedied in time to meet the deadline imposed by SOX. These reporting and other obligations place significant demands on our management and administrative and operational resources, including accounting resources.
Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of consolidated financial statements for external purposes in accordance with accounting principles generally accepted in the U.S. Any failure to maintain effective internal controls, or if our independent registered public accounting firm provide an attestation report onis unable to attest to the effectiveness of our internal control over financial reporting and have certain other reduced disclosure obligations with respect to our SEC filings. We will remain a “smaller reporting company” until the aggregate market value of our outstanding common stock held by non-affiliates as of the last business day our recently completed second fiscal quarter is $75 million or more. We cannot predict whether investors will find our common stock less attractive because of our reliance on any of these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile.
We have in the past and may in the future fail to meet all applicable listing requirements, our common stock may be delisted from The Nasdaq Global Market, which, could have an adverse impacteffect on the liquidityour business, financial position, and market priceresults of our common stock.operations.
Our common stock is currently listed on The Nasdaq Global Market, which has qualitative and quantitative listing criteria. If we are unable to meet any of the Nasdaq listing requirements in the future, such as the corporate governance requirements, the minimum closing bid price requirement, the minimum market value of listed securities requirement, total assets and total revenues, net income from continuing operations, the number of publicly held shares or any other Nasdaq requirements. Nasdaq could determine to delist our common stock. A delisting of our common stock could adversely affect the market
liquidity of our common stock, decrease the market price of our common stock, adversely affect our ability to obtain financing for the continuation of our operations and result in the loss of confidence in our company. On November 16, 2016, we received notice from the Listing Qualifications Department of the Nasdaq Stock Market (the “Staff”) indicating that, for the previous 30 consecutive business days, the bid price for our common stock closed below the minimum $1.00 per share required for continued inclusion on The Nasdaq Global Market. The notification letter stated that we would be afforded 180 calendar days, or until May 15, 2017, to regain compliance with the minimum bid price requirement. In order to regain compliance, on May 4, 2017, our board of directors and stockholders approved the Charter Amendment to effect the Reverse Stock Split. On May 10, 2017, our common stock began trading on The Nasdaq Global Market on a split-adjusted basis at a ratio of 7-for-1. On May 24, 2017, we received a letter from the Staff indicating that we had regained compliance with the $1.00 minimum closing bid price requirement. Despite effecting the Reverse Stock Split, there can be no assurance that the market price per share of our common stock will remain in excess of the $1.00 minimum closing bid price requirement in the future. The continuing effect of the Reverse Stock Split on the market price of our common stock cannot be predicted with any certainty, and the history of similar stock split combinations for companies in like circumstances is varied.
Anti-takeover provisions in our charter documents and Delaware law may prevent or delay removal of incumbent management or a change of control.
Anti-takeover provisions of our amended and restated certificate of incorporation and amended and restated bylaws and Delaware law may have the effect of deterring or delaying attempts by our stockholders to remove or replace management, engage in proxy contests and effect changes in control. The provisions of our charter documents include:
| ·
| | a classified board so that only one of the three classes of directors on our board of directors is elected each year;
|
| ·
| | elimination of cumulative voting in the election of directors;
|
| ·
| | procedures for advance notification of stockholder nominations and proposals;
|
| ·
| | the ability of our board of directors to amend our bylaws without stockholder approval; and
|
| ·
| | the ability of our board of directors to issue up to 10,000,000 shares of preferred stock without stockholder approval upon the terms and conditions and with the rights, privileges and preferences as our board of directors may determine.
|
a classified board so that only one of the three classes of directors on our Board of Directors (the “Board”) is elected each year;
elimination of cumulative voting in the election of directors;
procedures for advance notification of stockholder nominations and proposals;
the ability of the Board to amend our bylaws without stockholder approval; and
the ability of the Board to issue up to 10,000,000 shares of preferred stock without stockholder approval upon the terms and conditions and with the rights, privileges and preferences as the Board may determine.
In addition, as a Delaware corporation, we are subject to Delaware law, including Section 203 of the Delaware General Corporation Law. In general, Section 203 prohibits a Delaware corporation from engaging in any business combination with any interested stockholder for a period of three years following the date that the stockholder became an interested stockholder unless certain specific requirements are met as set forth in Section 203.
These provisions, alone or together, could have the effect of deterring or delaying changes in incumbent management, proxy contests or changes in control.
Our share ownership is concentrated,amended and restated bylaws provide that the federal district courts of the United States of America shall be the exclusive forum for the resolution of any complaint asserting a cause of action arising under the Securities Laws of 1933, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us or our directors, officers directorsor employees.
Our amended and principal stockholders can exert significant control over matters requiringrestated bylaws provide that the federal district courts of the United States of America shall be the exclusive forum for the resolution of any complaint asserting a cause of action arising under the Securities Act of 1933.
While the Delaware courts have determined that such choice of forum provisions are factually valid, a stockholder approval.
Duemay nevertheless seek to their combined stock holdings, our officers, directorsbring a claim in a venue other than those designated in the exclusive forum provisions. In such instance, we would expect to vigorously assert the validity and principal stockholders (stockholders holding greater than 5%enforceability of the exclusive forum provisions of our common stock) acting collectivelyamended and restated bylaws. This may haverequire significant additional costs associated with resolving such action in other jurisdictions and there can be no assurance that the provisions will be enforced by a court in those other jurisdictions.
These exclusive-forum provisions may limit a stockholder’s ability to exercisebring a claim in a judicial forum that it finds favorable for disputes with us or our directors, officers or other employees, which may discourage these types of lawsuits. Furthermore, the enforceability of similar choice of forum provisions in other companies’ certificates of incorporation or bylaws has been challenged in legal proceedings, and it is possible that a court could find these types of provisions to be inapplicable or unenforceable. If a court were to find the exclusive-forum provision contained in our amended and restated bylaws to be inapplicable or unenforceable in an action, we may incur further significant influence over matters requiring stockholder approval including the electionadditional costs associated with resolving such action in other jurisdictions, all of directors and approvalwhich could harm our business.
Changes in our ownership could limit our ability to utilize net operating loss carryforwards.
As of significant corporate transactions. In particular, Remi Barbier, our founder, ChairmanDecember 31, 2021, we had aggregate federal net operating loss carryforwards of approximately $118.0 million, which begin to expire in 2029. Under Section 382 of the BoardInternal Revenue Code of Directors, President and Chief Executive Officer, owns or controls a significant1986, as amended, changes in our ownership may limit the amount of our net operating loss carryforwards that could be utilized annually to offset our future taxable income, if any. This limitation would generally apply in the voting powerevent of a cumulative change in ownership of our outstanding capital stock. This concentrationcompany of ownershipmore than 50% within a rolling three-year period. Any such limitation may delay or prevent a change in controlsignificantly reduce our ability to utilize our net operating loss carryforwards and tax credit carryforwards. Any such limitation, whether as the result of the Company and may make some transactions, including but not limited to any merger, consolidation, or sale of substantially all of our assets, more difficult or impossible to complete without the support of key stockholders.
Publicly available information regarding stockholders’ ownership may not be comprehensive because the SEC does not require certain large stockholders to publicly disclose their stock ownership positions.
If the fair value of our stock increases and outstanding Performance Awards vest, we expect to use substantial amounts of cash to fund employee tax liabilities.
We have Performance Awards outstanding. If these Performance Awards vest, we expect to issue our employees sharespast offerings, sales of our common stock net of statutory employment taxes. This net issuance results in fewer shares issued and usesby our cash to
fund these taxes. The use of cash could be substantially higher, depending on the fair valueexisting stockholders or additional sales of our common stock on the date the Performance Awards vest. If our use of cash to fund these taxes is substantial, our cash balance could substantially decline and our stock price could also decline.
We mayby us in the future seekcould have a material adverse effect on our results of operations in future years. We have not completed a study to assess whether an ownership change for purposes of Section 382 has occurred, or whether there have been multiple ownership changes since our inception, nor do we plan to do so due to the significant costs and complexities associated with such study.
We may sell additional equity or debt securities to fund the cash usedour operations, and have outstanding securities exercisable for Performance Awards through the sale of our common stock. However, we may not be successful in selling shares of our common stock, to fund the cash used for Performance Awards. If the number of shares we sell to fund the cash used for Performance awards is significant, our stock price could decline.
Volatility in the stock prices of other companieswhich may contribute to volatility in our stock price.
The stock market in general, Nasdaq and the market for technology companies in particular, have experienced significant price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of those companies. Further, there has been particular volatility in the market prices of securities of early stage life sciences companies. These broad market and industry factors may seriously harm the market price of our common stock, regardless of our operating performance. In the past, following periods of volatility in the market price of a company’s securities, securities class action litigation has often been instituted. A securities class action suit against us could result in substantial costs, potential liabilitiesdilution to our stockholders and the diversion of management’s attention and resources.impose restrictions on our business.
Our operating results may fluctuate from quarter to quarter and this fluctuation may cause our stock price to decline.
Our quarterly operating results have fluctuated in the past and are likely to fluctuate in the future. Factors contributing to these fluctuations include, among other items, the timing and enrollment rates of clinical trials for our drug candidates, our need for clinical supplies and the valuation of stock-based compensation. Thus, quarter-to-quarter comparisons of our operating results may not be not indicative of what we might expect in the future. As a result, in some future quarters our clinical, financial or operating results may not meet the expectations of securities analysts and investors and could result in a decline in the price of our stock.
If securities or industry analysts publish inaccurate or unfavorable research about our business or product candidates, our stock price could decline.
Securities or industry analysts publish research and reports about our business or product candidates. An analyst’s conclusions regarding prospects for product candidates in the biopharmaceutical industry can include judgments based on the limited publicly-available data. If one or more analysts issues unfavorable research about our business or our product candidates, including a downgrade of our common stock, the price of our stock may decline.
You may experience future dilution as a result of future equity offerings.
In order to raise additional capital to support our operations, we may in the future offersell additional shares of our common stock or other securities convertible into or exchangeable for our common stock. stock which could result in dilution our stockholders.
We cannot assure you that we will be able to sell shares or other securities in any other offering at a price per share that is equal to or greater than the price per share paid by investors in prior offerings, and investors purchasing our shares or other securities in the future could have rights superior to existing shareholders. The price per share at which we sell additional shares of our common stock or securities convertible into or exchangeable for our common Stockstock in future transactions may be higher or lower than the price per share in prior offerings.
There You may notalso be an active, liquid trading market for our common stock.
There is no guarantee that an active trading market fordiluted upon the exercise of outstanding stock options as of December 31, 2021 to purchase 2,663,727 shares of our common stock will be maintained on Nasdaq. Investorsat a weighted average price of $11.56 per share, and the future issuance of up to 152,188 compensatory equity awards authorized under our 2018 Omnibus Incentive Plan and up to 58,017 shares we may not be able to sell their shares quickly or at the latest market price if trading inunder our stock is not active.Employee Stock Purchase Plan.
Item 1B.Unresolved Staff Comments
None.
Item 2.Properties
We lease approximately 6,000 square feet of office space pursuant to a non-cancelable operating lease in Austin, TXTexas that expires April 30, 2024. We also lease an additional 3,600 square feet of office space in Austin, Texas that expires on April 30, 2022.
On August 4, 2021, we completed the purchase of a two-building office complex in Austin, Texas, which will serve as our future corporate headquarters. The seller was a third party not affiliated with us. This property is intended to accommodate our anticipated growth and expansion of our operations in the coming years. Maintenance, physical facilities, leasing, property management and other key responsibilities related to property ownership are being outsourced to professional real-estate
managers. The purchase price of the property was $22.0 million, including closing costs, funded with cash on hand. The office complex measures approximately 90,000 rentable square feet. At acquisition and December 2020. We believe that our facilities are adequate and suitable for our current needs.31, 2021, the property was 59% leased. The Company is planning to occupy approximately 25% of the property in 2022.
Item 3.Legal Proceedings
None.From time to time, we may become involved in litigation or other legal proceedings and claims, including U.S. government inquiries, investigations and Citizen Petitions submitted to FDA. The outcome of these proceedings is inherently uncertain. Regardless of outcome, legal proceedings can have an adverse impact on us because of defense and settlement costs, diversion of management resources, and other factors. At this time, no assessment can be made as to their likely outcome or whether the outcome will be material to us. No information is available to indicate that it is probable that a loss has been incurred or can be reasonably estimated as of the date of the consolidated financial statements and, as such, no accrual for these matters has been recorded within the consolidated financial statements.
Government Investigations
Certain government agencies have asked us to provide them with corporate information and documents. We have been cooperating and will continue to cooperate with government authorities. No government agency has informed us that any wrongdoing has occurred by any party. We cannot predict the outcome or impact of any these ongoing matters, including whether a government agency may pursue an enforcement action against us or others.
FDA Citizen Petitions
In August 2021, an attorney representing anonymous clients submitted a Citizen Petition to the FDA. This Citizen Petition requested that the FDA Commissioner immediately halt the clinical development of simufilam, our drug candidate for Alzheimer’s disease. The attorney subsequently disclosed that his clients are short sellers, that is, investors who earn a profit from a decline in our stock price. In September 2021, the same attorney filed another Citizen Petition, which requested that the FDA Commissioner immediately rescind previously granted Special Protocol Assessments (SPAs) for our Phase 3 clinical program with simufilam. FDA has not halted the clinical development of simufilam and has not rescinded our SPAs.
In February 2022, FDA denied both Citizen Petitions and their supplements. As of February 23, 2022, FDA’s denial letter could be found at: https://www.regulations.gov/document/FDA-2021-P-0930-0228.
In October 2021, a Citizen Petition was submitted to FDA by an individual unknown to us. This Citizen Petition requests FDA “…approval of simufilam and immediate initiation of Phase 4 trials for further efficacy, safety assessment and, most critically, to address one of the greatest needs in modern medicine.” The FDA has not engaged with us regarding this Citizen Petition.
In November 2021, an academic physician not previously known to us submitted a Citizen Petition to FDA requesting “Accelerated Approval of Simufilam for the most significant medical need in the United States of America.” The FDA has not ruled on this Citizen Petition.
No assurance can be given that FDA will grant, deny, dismiss, defer or otherwise act upon these or any other Citizen Petition or supplements within any timeframe, if ever.
Securities Class Actions and Shareholder Derivative Action
Between August 27 and October 26, 2021, four putative class action lawsuits were filed alleging violations of the federal securities laws by us and certain named officers. The complaints rely on allegations contained in two Citizen Petitions that were submitted to FDA, and allege that various statements made by the defendants regarding simufilam were rendered materially false and misleading. The two Citizen Petitions were subsequently denied by FDA. These actions were filed in the U.S. District Court for the Western District of Texas. The complaints seek unspecified compensatory damages and other relief on behalf of a purported class of purchasers of our securities between September 14, 2020 and August 27, 2021. We expect that the cases will be consolidated and that a lead plaintiff and lead counsel will be appointed and thereafter that a consolidated amended complaint will be filed. We believe the lawsuit claims are without merit and intend to defend against these lawsuits vigorously. We are unable to estimate the possible loss or range of loss, if any, associated with these lawsuits.
On November 4, 2021, a related shareholder derivative action was filed, purportedly on behalf of the Company, in the U.S. District Court for the Western District of Texas, asserting claims under the U.S. securities laws and state fiduciary duty laws against certain named officers and the members of the Company’s board of directors. The complaint relies on allegations made in two Citizen Petitions that were submitted to FDA. The two Citizen Petitions, which were subsequently denied by FDA, allege, among other things, that the individual defendants exposed the Company to unspecified damages and securities law liability by causing it to make materially false and misleading statements, in violation of the U.S. securities laws and in breach of their fiduciary duties to the Company. The derivative case seeks, among other things, to recover unspecified compensatory damages on behalf of the Company arising out of the individual defendant’s alleged wrongful conduct. Although the plaintiffs in the derivative cases does not seek relief against the Company, we have certain indemnification obligations to the individual defendants. Since November 4, 2021, three additional shareholder derivative actions were filed alleging substantially similar claims, two in the U.S. District Court for the Western District of Texas, and one in Texas state court (Travis County District Court). The state court action has been stayed pending the resolution of the motions to dismiss in the securities class actions. The parties to the three federal court actions have filed a motion, which the court has not yet ruled on, to consolidate and stay pending the resolution of motions to dismiss in the securities class actions. We are unable to estimate the possible loss or range of loss, if any, associated with these lawsuits.
Item 4.Mine Safety Disclosures
Not applicable.
PART II
Item 5.Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Price of and Dividends of the Registrants Common Equity and Related Stockholder Matters
Our common stock is quoted on Nasdaq, under the symbol "PTIE."SAVA." The following table sets forth the high and low sales prices per share
As of February 23, 2022, there were approximately 30 registered holders of record of our common stock as reported on Nasdaq for the periods indicated.stock. The actual number of stockholders is greater than this number of record holders and includes stockholders who are beneficial owners but whose shares are held in street name by brokers and other nominees.
| | | | | |
| Sales Prices |
| High | | Low |
Fiscal 2016: | | | | | |
First Quarter | $ | 2.40 | | $ | 1.55 |
Second Quarter | $ | 2.63 | | $ | 1.95 |
Third Quarter | $ | 3.00 | | $ | 0.96 |
Fourth Quarter | $ | 1.04 | | $ | 0.51 |
Fiscal 2017: | | | | | |
First Quarter | $ | 9.31 | | $ | 3.71 |
Second Quarter | $ | 7.42 | | $ | 3.38 |
Third Quarter | $ | 4.30 | | $ | 3.10 |
Fourth Quarter | $ | 6.49 | | $ | 3.10 |
| | | | | |
Dividend Policy
We currently expect to retain future earnings, if any, for use in the operation and expansion of our business and, notwithstanding our special nondividendnon-dividend distributions in December 2012 (of $0.75 per share of common stock totaling $34.0 million) and December 2010 (of $2.00 per share of common stock totaling $85.7 million), we have not paid and do not anticipate paying any cash dividends in the foreseeable future. As of January 12, 2018, there were approximately 48 holders of record of our common stock.
Item 6.Selected Financial Data[Reserved]
Item 7.Management’s Discussion and Analysis of Financial Condition and Results of Operations
This discussion and analysisof our financial condition and results of operations should be read in conjunction with our consolidated financial statements and accompanying notes included elsewhere in this report. Annual Report on Form 10-K. This discussion contains forward-looking statements that involve risk and uncertainties, such as statements of our plans, objectives, expectations, and intentions, that are based on the beliefs of our management. Operating results are not necessarily indicative of results that may occur in future periods.Factors that could cause or contribute to such differences include, but are not limited to, those discussed in the “Risk Factors” section of this Annual Report on Form 10-K.
Overview
Overview
We are a clinical-stage biotechnology company based in Austin, Texas. Our mission is to detect and treat neurodegenerative diseases, such as Alzheimer’s disease. Our novel science is based on stabilizing – but not removing – a critical protein in the brain.
Pain Therapeutics, Inc. develops proprietary drugs that offer significant improvements
Over the past 10 years, we have combined state-of-the-art technology with new insights in neurobiology to patientsdevelop novel solutions for Alzheimer’s disease and healthcare professionals. other neurodegenerative diseases. Our strategy is to leverage our unique scientific/clinical platform to develop a first-in-class program for treating neurodegenerative diseases, such as Alzheimer’s.
We generally focus currently have two biopharmaceutical assets under development:
our drug development efforts on disorders of the nervous system.
Our expertise consists of developing new drug candidates and guiding these through various regulatory and development pathways in preparation for their eventual commercialization. By necessity, the conduct of drug development is complex, lengthy, expensive and risky. The FDA has not yet established the safety or efficacy of our drug candidates.
The followinglead therapeutic product candidate, called simufilam, is a summary of our pipeline of drug assets:novel treatment for Alzheimer’s disease; and
REMOXY ER (extended-release oxycodone capsules CII) – REMOXY, our lead druginvestigational diagnostic product candidate, called SavaDx, is a proprietary abuse-deterrent, twice-daily, oral oxycodonenovel way to treat severe chronic pain. We plan to resubmitdetect the REMOXY NDA to the FDA, with Priority Review in Q1 2018. We own exclusive rights to develop and commercialize REMOXY worldwide, withpresence of Alzheimer’s disease from a sales royalty obligation to onesmall sample of our technology partners.blood.
FENROCK™ (transdermal fentanyl patch CII) – FENROCK is a proprietary, abuse-deterrent fentanyl skin patch to treat severe pain. This is an early-stage program that is substantially funded by a competitive research grant award from the National Institute on Drug Abuse (NIDA), the primary agency of the U.S. government for research on drug abuse. We own exclusive, worldwide rights to FENROCK, with no royalty obligations to any third party.
PTI-125 – PTI-125 is a proprietary small molecule drugOur scientific approach for the treatment of Alzheimer’s disease (AD). In 2017, we completedseeks to simultaneously suppress both neurodegeneration and neuroinflammation. We believe our ability to improve multiple vital functions in the brain represents a first-in-human Phase I study with PTI-125. This program is substantially funded by competitive research grant awards from the National Institutes of Health (NIH), the primary agency of the U.S. government for biomedical research. We own exclusive, worldwide rightsnew, different and crucial approach to PTI-125, with no royalty obligations to any third party.address Alzheimer’s disease.
PTI-125DX – PTI-125Our lead therapeutic product candidate, simufilam, is a proprietary blood-based diagnostic/biomarkersmall molecule (oral) drug. Simufilam targets an altered form of a protein called filamin A (FLNA) in the Alzheimer’s brain. Published studies have demonstrated that the altered form of FLNA causes neuronal dysfunction, neuronal degeneration and neuroinflammation.
We believe simufilam improves brain health by reverting altered FLNA back to detectits native, healthy conformation, thus countering the downstream toxic effects of altered FLNA. We have generated and published experimental and clinical evidence of improved brain health with simufilam. Importantly, simufilam is not dependent on clearing amyloid from the brain. Since simufilam has a unique mechanism of action, we believe its potential therapeutic effects may be additive or synergistic with those of other therapeutic candidates aiming to treat neurodegeneration.
On October 6, 2021, and November 18, 2021, we announced initiation of our two Phase 3 studies of simufilam, respectively.
The first Phase 3 study, called RETHINK-ALZ, is designed to evaluate the safety and efficacy of oral simufilam 100 mg in enhancing cognition and slowing cognitive and functional decline over 52 weeks. Secondary objectives include the assessment of simufilam's effect on neuropsychiatric symptoms and caregiver burden. This randomized, double-blind, placebo-controlled study plans to enroll approximately 750 patients with mild-to-moderate Alzheimer’s disease (AD).in the U.S. and Canada and, eventually, overseas.
The second Phase 3 study, called REFOCUS-ALZ, is designed to evaluate the safety and efficacy of oral simufilam 100 mg and 50 mg over 76 weeks. This clinical-stagerandomized, double-blind, placebo-controlled study plans to enroll approximately 1,000 patients with mild-to-moderate Alzheimer’s disease in the U.S. and Canada and, eventually, overseas.
Our investigational diagnostic product candidate, called SavaDx, is an early-stage program focused on detecting the presence of Alzheimer’s disease from a small sample of blood. The goal is substantially funded by competitive research grant awards fromto make the NIH. We own exclusive, worldwide rights to PTI-125DX, with no royalty obligations to any third party.detection of Alzheimer’s disease as simple as getting a blood test.
Financial Overview
We have yet to generate any revenues from product sales. We have an accumulated deficit of $157$207.3 million at December 31, 2017.2021. These losses have resulted principally from costs incurred in connection with research and development activities, salaries and other personnel-related costs and general corporate expenses. Research and development activities include costs of preclinical and clinical trialsstudies as well as clinical supplies associated with our drugproduct candidates. Salaries and other personnel-related costs include non-cash stock-based compensation associated with options and other equity awards granted to employees and non-employees. Our operating results may fluctuate substantially from period to period as a result of the timing of preclinical activities, enrollment rates of clinical trialsstudies for our drugproduct candidates and our need for clinical supplies.
We believe that our cash and cash equivalents at December 31, 2017,2021, will enable us to fund our operating expenses for at least the next 12 months. In addition, we willmay seek in the future to fund our operations through additional public or private equity or debt financings or other sources. However, we may be unable to raise additional funds or enter into such other arrangements when needed on favorable terms or at all. If we are unable to obtain financing or increasereach profitability, the related lack of liquidity will have a material adverse effect on our operations and future prospects.prospects, and we may have to significantly delay, scale back or discontinue the development and commercialization of simufilam, our lead drug candidate, or delay our efforts to expand our product pipeline.
We expect to continue to use significant cash resources in our operations for the next several years. Our cash requirements for operating activities and capital expenditures may increase substantially in the future as we:
| ·
| | conduct preclinical and clinical trials for our drug candidates;
|
| ·
| | seek regulatory approvals for our drug candidates;
|
| ·
| | develop, formulate, manufacture and commercialize our drug candidates;
|
| ·
| | implement additional internal systems and develop new infrastructure;
|
| ·
| | acquire or in-license additional products or technologies, or expand the use of our technology;
|
| ·
| | maintain, defend and expand the scope of our intellectual property; and
|
| ·
| | hire additional personnel.
|
continue our ongoing Phase 3 program with simufilam;
manufacture large-scale supplies for simufilam;
conduct other preclinical and clinical studies for our product candidates;
seek regulatory approvals for our product candidates;
develop, formulate, manufacture and commercialize our product candidates;
implement additional internal systems and develop new infrastructure;
acquire or in-license additional products or technologies, or expand the use of our technology;
maintain, defend and expand the scope of our intellectual property; and
hire additional personnel.
Product revenue will depend on our ability to receive regulatory approvals for, and successfully market, our drugproduct candidates. If our development efforts result in regulatory approval and successful commercialization of our drugproduct candidates, we willexpect to generate revenue from direct sales of our drugs and/or, if we license our drugs to future collaborators, from the receipt of license fees and royalties from sales of licensed products. We conduct our research and development programs through a combination of internal and collaborative programs. We rely on arrangements with universities, ourcertain collaborators, contract research organizationsCDMOs, CROs and clinical research sites for a significant portion of our product development efforts.
Components of Operating Results
Operating Expenses
Research and Development Expenses
We focus substantially all our research and development efforts on research and development in the areas of neurology. The following table summarizes expenses by category for research and development efforts (in thousands):
| | | | | |
|
|
|
|
|
| | | | | |
|
|
|
|
|
| Years ended December 31, | Year ended |
| 2017 | | 2016 | December 31, |
| | | | | | 2021 |
| 2020 |
Compensation | $ | 2,913 | | $ | 3,561 | $ | 5,935 |
| $ | 1,575 |
Contractor fees and supplies | | 3,989 | | | 4,842 |
| 17,970 |
|
| 980 |
Other common costs | | 713 | | | 773 |
| 908 |
|
| 498 |
| $ | 7,615 | | $ | 9,176 | $ | 24,813 |
| $ | 3,053 |
| | | | | |
|
|
|
|
|
Research and development expenses include compensation, contractor fees and supplies as well as allocated common costs. Contractor fees and supplies generally include expenses for preclinicalclinical studies and clinical trialspreclinical studies and costs for formulation and manufacturing activities. Other common costs include the allocation of common costs such as facilities. During the years ended December 31, 2021 and 2020, we received $3.9 million and $4.2 million in research grants from the NIH, respectively. These reimbursements were recorded as a reduction to our research and development expenses.
Our technology has been applied across certain of our portfolio of drugproduct candidates. Data, know-how, personnel, clinical results, research results and other matters related to the research and development of any one of our drugproduct candidates also relate to, and further the development of, our other drugproduct candidates. As a result, costs allocated to a specific drugproduct candidate may not necessarily reflect the actual costs surrounding research and development of that drugsuch product candidate due to cross application of the foregoing.
Estimating the dates of completion of clinical development, and the costs to complete development, of our drugproduct candidates would be highly speculative, subjective and potentially misleading. Pharmaceutical products take a significant amount of time to research, develop and commercialize. The clinical trialstudy portion of the development of a new drug alone usually spans several years. We expect our research and development expenses to increase substantially during the next few years as we seek to advance our product candidates through the clinical development process and, potentially to seek regulatory approval of simufilam. Over the next few years, we expect our preclinical, clinical and contract manufacturing expenses to increase significantly relative to what we have incurred to date. We expect to reassess our future research and development plans based on our review of data we receive from our current research and development activities. The cost and pace of our future research and development activities are linked and subject to change.
Critical Accounting PoliciesEstimates
The preparation of our consolidated financial statements in accordance with United StatesU.S. generally accepted accounting principles requires us to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenues, expenses and interest income in our consolidated financial statements and accompanying notes. We evaluate our estimates on an ongoing basis, including those estimates related to agreements and research collaborations and investments.collaborations. We base our estimates on historical experience and various other assumptions that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual
results may differ from these estimates under different assumptions or conditions. The following items in our consolidated financial statements require significant estimates and judgments:
Research Contracts and Accruals. We have entered into various research and development contracts with research institutions and other third-party vendors. Related payments are recorded as research and development expenses as incurred. We record accruals for estimated ongoing research costs. When evaluating the adequacy of the accrued liabilities, we analyze progress of the studies including the phase or completion of events, invoices received and contracted costs. Significant judgments and estimates are made in determining the accrued balances at the end of any reporting period. Actual results could differ from our estimates. Our historical accrual estimates have not been materially different from actual costs.
Legal and other contingencies. The Company is subject to lawsuits, claims, allegations and investigations regarding simufilam. The Company believes the claims are without merit and intends to defend against these lawsuits vigorously. The Company is unable to estimate the possible loss or range of loss, if any, associated with these lawsuits. However, litigation is subject to inherent uncertainties, and unfavorable rulings could occur. If an unfavorable ruling were to occur, it may cause a material adverse impact on the results of operations, cash flows, or financial condition for the period in which the ruling occurs, or future periods. Refer to Note 12 to the Consolidated Financial Statements for further information on contingencies.
2020 Cash Incentive Bonus Plan. In 2020, we established the 2020 Cash Incentive Bonus Plan (the “Plan”) to incentivize Plan participants. Awards under the Plan are accounted for as liability awards under ASC 718, “Stock-based Compensation”. The fair value of each potential Plan award will be determined once a grant date occurs and will be remeasured each reporting period. Compensation expense associated with the Plan will be recognized over the expected achievement period for each Plan award, when a Performance Condition is considered probable of being met.
| ·
| | Stock-based compensation.
The Plan was established to promote the long-term success of the Company by creating an “at-risk” cash bonus program that rewards Plan participants with additional cash compensation in lockstep with significant increases in our market capitalization. The Plan is considered “at-risk” because Plan participants will not receive a cash bonus unless our market capitalization increases significantly and (1) we complete a merger or acquisition transaction that constitutes a sale of ownership of the Company or its assets (a Merger Transaction) or (2) the Compensation Committee of the Board (the Compensation Committee) determines the Company has sufficient cash on hand, as defined in the Plan, to render payment (each, a “Performance Condition”), neither of which may ever occur. Because of the inherent discretion and uncertainty regarding these requirements, we have concluded that a Plan grant date has not occurred as of December 31, 2021. No actual cash payments were authorized or made to participants under the Plan through December 31, 2021.
Stock-based Compensation. We recognize non-cash expense for the fair value of all stock options and other share-based awards. We use the Black-Scholes option valuation model to calculate the fair value of stock options, using the single-option award approach and straight-line attribution method. For options granted to employees and directors, we recognize the resulting fair value as expense on a straight-line basis over the vesting period of each respective stock option, generally four years. For options granted to non-employees, we remeasure the fair value expense using Black-Scholes each reporting period.
|
We have granted share-based awards that vest upon achievement of certain performance criteria, or Performance Awards. We multiply the number of Performance Awards by the fair market value of our common stock on the date of grant to calculate the fair value of each award. We estimate an implicit service periodstock options, using the single-option award approach and straight-line attribution method. Significant judgments and estimates are made in determining inputs to the Black-Scholes option valuation model. See Note 7 to our Consolidated Financial Statements for achieving performance criteria for each award. We recognize the resulting fair value as expense over the implicit service period when we conclude that achieving the performance criteria is probable. We periodically review and update as appropriate our estimates of implicit service periods and determinations on achievement of the performance criteria. Performance Awards vest and common stock is issued upon achievement of the performance criteria.
| ·
| | Income Taxes. We make estimates and judgments in determining the need for a provision for income taxes, including the estimation of our taxable income or loss for each full fiscal year.We have accumulated significant deferred tax assets that reflect the tax effects of net operating loss and tax credit carryovers and temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Realization of deferred tax assets is dependent upon future earnings, if any. We are uncertain as to the timing and amount of any future earnings. Accordingly, we offset these deferred tax assets with a valuation allowance. We may in the future determine that our deferred tax assets will likely be realized, in which case we will reduce our valuation allowance in the quarter in which such determination is made. If the valuation allowance is reduced, we may recognize a benefit from income taxes in our statement of operations in that period. We classify interest recognized in connection with our tax positions as interest expense, when appropriate.
|
significant assumptions regarding stock-based compensation.
Recent Accounting Pronouncements
In August 2016,See Note 2. Summary of Significant Accounting Policies, in Notes to the FASB issued ASU No. 2016-15, StatementConsolidated Financial Statements in Item 8 of Cash Flows (Topic 230): Classification of Certain Cash Receipts and Cash Payments. This ASU provides guidance on statement of cash flows presentation for eight specific cash flow issues where diversity in practice exists. This ASU is effective for fiscal years beginning after December 15, 2017, and interim periods within those fiscal years. The Company expects that the adoption will not have a material impact on its financial statements.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842). The core principle of Topic 842 is that a lessee should recognize the assets and liabilities that arise from leases. For operating leases, a lessee is required to recognize a right-of-use asset and a lease liability, initially measured at the present value of the lease payments, in the statement of financial position. This ASU is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. The Company is evaluating the effect that the adoptionPart II of this ASU will haveAnnual Report on itsForm 10-K for a full description of recent accounting pronouncements, including the expected dates of adoption and estimated effects on financial statements. The Company currently expects that its operating lease commitment will be subject to the new standardcondition and recognized as right-of-use asset and operating lease liability upon adoptionresults of ASU 2016-02,operations, which will increase the total assets and total liabilities that it reports relative to such amounts prior to adoption.is incorporated herein by reference.
Results of Operations
Research and Development Expense
Research and development expense consistsconsist primarily of costs of drug development work associated with our drugproduct candidates, including:
| ·
| | clinical supplies and related formulation and design costs, and
|
| ·
| | compensation and other personnel-related expenses.
|
clinical studies,
preclinical testing,
clinical supplies and related formulation and design costs, and
compensation and other personnel-related expenses.
Research and development expenses decreasedincreased to $7.6$24.8 million in 20172021 from $9.2$3.1 million in 2016,2020, representing a 713% increase. This increase was due primarily due to decreases in REMOXYcosts related expensesto manufacture of clinical trial supplies for and non-cash Performance Award relatedthe initiation of a Phase 3 clinical program with simufilam, costs of an on-going open-label study and cognition maintenance study with simufilam, as well as increased personnel expenses in the year ended 2017 as compared to the same periodprior year. Research and development expenses also included stock-based compensation expenses of $1.3 million in 2016. 2021 compared to $0.5 million in 2020.
We received a $1.4NIH reimbursement of $3.9 million from research grantgrants in 2017 from the NIH that we2021 recorded as a reduction to our research and development expense, as compared to a $1.5 million research grant in 2016.
Research and development expenses included non-cash stock-related compensation expenses of $1.2$4.2 million in 2017 compared to $1.8 million in 2016.2020.
We expect research and development expense to fluctuateover the next several yearsincreasein future periods as we manufacture drug supply and continue our development efforts. We expect our development efforts to result in our drug candidates progressing through various stages ofPhase 3 clinical trials. Our research and development expenses may fluctuate from period to period due to the timing and scope of our development activities and the results of clinical trials and preclinical studies.program with simufilam.
General and Administrative Expense
General and administrative expenses consist of personnel costs, allocated expenses and other expenses for outside professional services, including legal, human resources, audit and accounting services. Personnel costs consist of salaries, bonus, benefits and stock-based compensation. Allocated expenses consist primarily of existing facility costs. We incur insurance, audit, investor relations, SOX compliance and other administrative and professional services expenses associated with operating as a public company, including expenses related to compliance with the rules and regulations of the SEC and Nasdaq. General and administrative expense consists primarily of compensation and other general corporate expenses. General and administrative expense decreasedincreased to $4.3$8.1 million in 20172021 from $5.8$3.7 million in 20162020. The 115% increase was due primarily due to decreases in non-cash Performance Award relatedhigher legal fees, personnel costs and insurance expenses and the departure of our CFO in 2017 as compared in 2016.
General and administrative expenses included non-cash stock-related compensation expenses of $1.8 million in 2017 compared to $2.6 millionthe prior year. In addition, 2021 expense included $500,000 of depreciation and amortization for the two-building office complex in 2016.Austin, Texas, purchased in third quarter 2021.
We expect other general and administrative expense for 20182022 will be consistent with 2017.increase in the foreseeable future compared to 2021 due primarily to anticipated higher legal and professional fees related to ongoing securities class action and derivative lawsuits, governmental investigations as well as higher operating costs such as compliance costs and depreciation and amortization.
Gain on Sale of Property and Equipment
There were no sales of property and equipment during the year ended December 31, 2021.
During the year ended December 31, 2020, we sold surplus manufacturing equipment to an non-affiliated third party and received proceeds totaling $360,000. The original cost of the property and equipment was $892,000 and accumulated depreciation was $878,000, resulting in a gain on sale of property and equipment of $346,000 during the year ended December 31, 2020.
Interest Income
Interest and other income, net, was $38,000$49,000 in 20172021 compared to $107,000$112,000 in 2016. We expect our2020. The decrease in interest income was due to decreaselower interest rates, which more than offset additional interest from increases in our cash balances compared to the futureprior period.
Other income, net
We record the activities related to leasing office space to third parties in buildings we own as other income, net, as leasing is not core to the Company’s operations. Other income, net, was $434,000 during the year ended December 31, 2021. There was no other income, net, during the year ended December 31, 2020 as we use cash to fund our operations.acquired the two-building office complex in August 2021.
Liquidity and Capital Resources
Since inception, we have financed our operations primarily through public and private stock offerings, payments received under collaborative agreements and interest earned on our investments.cash and cash equivalents balances. We intend to continue to use our capital resources to fund research and development activities, capital expenditures, working capital requirements and other general corporate purposes. As of December 31, 2017,2021, cash and cash equivalents totaled $233.4 million.
2021 Registered Direct Offering
On February 12, 2021, we completed a common stock offering pursuant to which certain investors purchased 4,081,633 shares of common stock at a price of $49.00 per share. Net proceeds of the offering were approximately $189.7 million after deducting offering expenses.
2020 Follow-on Public Offering
On November 13, 2020, we completed the sale of 9,375,000 shares of our common stock in an underwritten public offering at a price of $8.00 per share. We received net proceeds from the offering of approximately $70.3 million after deducting underwriting discounts and marketable securitiesoffering expenses.
Common Stock Warrants
In August 2018, we issued warrants to purchase up to an aggregate of 9.1 million shares of its common stock in conjunction with an offering of our common stock.
During 2021, we received proceeds of $0.7 million from the exercise of 0.6 million shares pursuant to warrants. During 2020, we received proceeds of $4.9 million from the exercise of 4.0 million shares pursuant to warrants.
There were $10.5no warrants outstanding following the 2021 exercises.
At the Market (ATM) Common Stock Issuance
On March 27, 2020, we established an at-the-market offering program (ATM) to sell, from time to time, shares of our common stock having an aggregate offering price of up to $100 million in transactions pursuant to a shelf registration statement that was declared effective by the U.S. Securities and Exchange Commission (the SEC) on May 5, 2020. We are obligated to pay a commission of 3.0% of the gross proceeds from the sale of shares of common stock in the offering. We are not obligated to sell any shares in the offering.
There were no common stock sales under the ATM during the years ended December 31, 2021 and 2020.
NIH Research Grant Awards
Our research has been supported by NIH under multiple research grant awards. Strong, long-term support from NIH has allowed us to advance our two lead product candidates, simufilam and SavaDx, into clinical development.
In May 2021, we were awarded a new research grant award from NIH of up to $2.7 million to support clinical readiness activities for a Phase 3 program with simufilam. In April 2020, we were awarded a research grant from NIH of up to $2.5 million. In March 2020, we were awarded a supplemental research funding grant from NIH of up to $374,000. These non-dilutive research grants are intended to strengthen our clinical program of simufilam, our investigational drug to treat Alzheimer’s disease. All of our NIH research grant awards are paid out on a reimbursement basis and require milestone-based technical progress.
2020 Cash Incentive Bonus Plan Obligations
In August 2020, the Board approved the 2020 Cash Incentive Bonus Plan (the Plan). The Plan was established to promote the long-term success of the Company by creating an “at-risk” cash bonus program that rewards Plan participants with additional cash compensation in lockstep with significant increases in the Company’s market capitalization. The Plan is considered “at-risk” because Plan participants will not receive a cash bonus unless the Company’s market capitalization increases significantly and certain other conditions specified in the Plan are met. Specifically, Plan participants will not be paid any cash bonuses unless (1) the Company completes a merger or acquisition transaction that constitutes a sale of ownership of the Company or its assets (a Merger Transaction) or (2) the Compensation Committee determines the Company has sufficient cash on hand, as defined in the Plan. Plan participants will be paid all earned cash bonuses in the event of a Merger Transaction.
The Company’s market capitalization, including all outstanding stock options, was $89.4 million at the inception of the Plan in August 2020. If the Company were to exceed a $5 billion market capitalization for no less than 20 consecutive trading days, and conditions noted above for payment are met, all Plan milestones would be deemed achieved, in which case total cash bonus awards would range from a minimum of $139.1 million up to a hypothetical maximum of $322.3 million.
The Company’s potential financial obligation to plan participants at December 31, 2021 totaled $7.3 million, based upon the achievement of one Plan milestone in the Company’s market capitalization in 2020. No actual cash bonus payments have been made to any Plan participant, as the Company has not yet satisfied all the conditions necessary for amounts to be paid under the Plan. During the year ended December 31, 2021, the Company’s market capitalization increased substantially. These increases triggered the achievement of 11 additional Plan milestones. Collectively, the achievement of such milestones could trigger potential Company obligations to Plan participants ranging from a minimum of $93.7 million up to a hypothetical
maximum of $225.0 million, with exact amounts to be determined by the Compensation Committee and contingent upon future satisfaction of a Performance Condition.
No actual cash payments were authorized or made to participants under the Plan as of December 31, 2021, or through the filing date of this Annual Report on Form 10-K.
Use of Cash
Net cash used in operating activities was $8.2$30.2 million for 2017 compared to $12.2the year ended December 31, 2021, resulting primarily from the net loss reported of $32.4 million and an increase in prepaid and other assets of $11.0 million, partially offset by an increase in accounts payable of $6.2 million, accrued development expense of $2.1 million, accrued compensation and benefits of $1.8 million, other current liabilities of $0.7 million and stock-based compensation expense of $1.8 million.
Net cash used in operating activities was $5.4 million for the year ended December 31, 2020, resulting primarily from the net loss reported of $6.3 million and a gain on sale of property and equipment of $0.3 million, partially offset by stock-based compensation expense of $1.0 million and changes in 2016. The decreaseoperating assets and liabilities of $0.3 million.
Net cash used in investing activities during the year ended December 31, 2021 was $22.2 million related primarily due to lower research and development expenses during 2017the purchase of a two-building office complex in Austin, Texas, which will serve as compared in 2016.our future corporate headquarters.
Net cash provided by investing activities during the year ended December 31, 2020 was $2.1 million in 2017 compared to net cash used in investing activities$360,000 for proceeds received from the sale of $2.2 million in 2016. Investing activities for both years consisted primarily of the purchaseproperty and maturities of marketable securities.equipment.
Net cash usedprovided by financing activities during the year ended December 31, 2021 was $192.3 million, consisting of $189.8��million in proceeds from our registered direct offering of common stock in February 2021, $1.8 million from the exercise of stock options and $0.7 million in proceeds from the exercise of common stock warrants.
Net cash provided by financing activities during the year ended December 31, 2020 was $75.4 million consisting of $70.3 million proceeds from our follow-on public offering of common stock in November 2020, $4.9 million proceeds from exercise of common stock warrants and $0.3 million in 2016 resulting primarily from issuing sharesexercise of our common stock to employees for vested Performance Awards net of statutory employment taxes.options.
Realization of our deferred tax assets is dependent on future earnings, if any. We are uncertain about the timing and amount of any future earnings. Accordingly, we offset these net deferred tax assets with a valuation allowance.
We lease approximately 6,000 square feet of office space pursuant to a non-cancelable operating lease in Austin, TXTexas that expires in 2020.April 2024. We also lease an additional 3,600 square feet of office space in Austin, Texas that expires on April 30, 2022. Future minimum lease payments are $0.3 million at December 31, 2017.as follows (in thousands):
We have license agreements that require us to make milestone payments upon the successful achievement of milestones, including clinical milestones. Our license agreements also require us to pay certain royalties to our licensors if we succeed in
|
|
|
|
For the year ending December 31, |
|
|
|
2022 |
|
| 123 |
2023 |
|
| 107 |
2024 |
|
| 36 |
Total future lease payments |
| $ | 266 |
|
|
|
|
49
fully commercializing products under these license agreements. All of these potential future payments are cancelable as of December 31, 2017. Our formulation agreement with Durect Corporation obligates us to make certain milestone payments upon achieving clinical milestones and regulatory milestones.
We have an accumulated deficit of $157$207.3 million at December 31, 2017.2021. We expect our cash requirements to be significant in the future. The amount and timing of our future cash requirements will depend on regulatory and market acceptance of our drugproduct candidates and the resources we devote to researching and developing, formulating, manufacturing, commercializing and supporting our products. We believe that our current resources should be sufficient to fund our operations for at least the next 12 months. We may seek additional future funding through public or private financing within this timeframe,in the future, if such funding is available and on terms acceptable to us.
Off-balance Sheet Arrangements
As of December 31, 2017,If we did not have any relationships with unconsolidated entitiesraise additional funds by issuing debt financing or financial partnerships, such as entities often referredequity securities, our stockholders will experience dilution. Any future debt financing into which we enter may impose upon us additional covenants that restrict our operations, including limitations on our ability to as structured financeincur liens or special purpose entities, which would have been established for the purpose of facilitating off-balance sheet arrangements or other contractually narrow or limited purposes. In addition, we do notadditional debt, pay dividends, repurchase our common stock, make certain investments and engage in trading activities involving non-exchange traded contracts. Therefore,certain merger, consolidation or asset sale transactions. Any debt financing or additional equity that we raise may contain terms that are not materially exposedfavorable to financing, liquidity, market or credit risk that could arise if we had engaged in these relationships. We do not have relationships or transactions with persons or entities that derive benefits from their non-independent relationship with us or our related parties.stockholders. If we are unable to raise additional funds
when needed, we may be required to delay, reduce, or terminate some or all of our development programs and clinical trials. We may also be required to sell or license to others rights to our drug candidates in certain territories or indications that we would prefer to develop and commercialize ourselves.
Item 7A.Quantitative and Qualitative Disclosures about Market Risk
The primary objectivePursuant to Item 305(e) of our cash investment activitiesRegulation S-K, the information called for by Item 7A is to preserve principal while at the same time maximizing the income we receive from our investments without significantly increasing risk. Some of the securities that we invest in may be subject to market risk. This means that a change in prevailing interest rates may cause the principal amount of the investment to fluctuate. For example, if we hold a security that was issued with a fixed interest rate at the then-prevailing rate and the interest rate later rises, the principal amount of our investment will probably decline. A hypothetical 50 basis point increase in interest rates reduces the fair value of our available-for-sale securities at December 31, 2017 by approximately $2,000. To minimize this risk in the future, we intend to maintain our portfolio of cash equivalents and marketable securities in a variety of securities, including commercial paper, government and non-government debt securities and/or money market funds that invest in such securities. We have no holdings of derivative financial or commodity instruments. As of December 31, 2017, our investments consisted of investments in commercial paper, corporate notes and obligations or in money market accounts and checking funds with variable market rates of interest. We believe our credit risk is immaterial.not required.
Item 8.Consolidated Financial Statements and Supplementary Data
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Report of Independent Registered Public Accounting Firm
TheTo the Stockholders and the Board of Directors and Stockholders of Pain Therapeutics,Cassava Sciences, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Pain Therapeutics,Cassava Sciences, Inc. (the Company) as of December 31, 20172021 and 2016,2020, the related consolidated statements of operations, comprehensive income (loss), stockholders' equity and cash flows for each of the two years in the period ended December 31, 2017,2021, and the related notes (collectively referred to as the “financial“consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 20172021 and 2016,2020, and the results of its operations and its cash flows for each of the two years in the period ended December 31, 2017,2021, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company's internal control over financial reporting as of December 31, 2021, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework)and our report dated February 28, 2022 expressed an unqualified opinion thereon.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB)PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company's internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the financial statements that were communicated or required to be communicated to the audit committee and that: (1) relate to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing separate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
|
|
Description of the Matter | Accrued Development Expenses – Patient Clinical Trials As explained in Note 2 to the consolidated financial statements, the Company has various research and development contracts with research institutions and other third-party vendors to assist in the conducting of patient clinical trials, the costs for which are recorded as research and development expenses as incurred. At December 31, 2021, accrued development expense for patient clinical trials totaled $988 thousand.
Auditing the Company’s accrued development expense for patient clinical trials was challenging because the accrual involved a higher degree of management judgment to estimate costs incurred but not yet billed at the end of the reporting period. An estimate of the costs incurred was necessary due to the long duration of the clinical trials and the delayed timing of invoices received from third parties. |
|
|
How We Addressed the Matter in Our Audit | We obtained an understanding, evaluated the design, and tested the operating effectiveness of controls over the Company’s accounting for accrued development expenses for the patient clinical trials process, including controls over management’s review of clinical trial activity progress in comparison to budgets and invoices received from third parties.
To evaluate the adequacy of the Company’s accrued development expense for patient clinical trials, our audit procedures included, among others, testing the accuracy and completeness of the underlying data used in the estimate, evaluating the significant assumptions used by management to estimate the accrual, and evaluating other factors that could impact the accrual such as invoices received. To evaluate the significant assumptions (i.e., progress of patient clinical trials, estimating costs incurred), on a sample basis, we: (i) obtained confirmation directly from third parties of key clinical trial contract terms and conditions, the number of patients enrolled, and costs incurred, (ii) agreed information used in the estimate to the contracts with third parties and any amendments thereto, and (iii) corroborated the progress of clinical trials through inquiry of Company personnel who oversee research and development efforts. We also obtained and reviewed subsequent invoices received from third parties to corroborate the accrual at the end of the reporting period. |
|
|
Description of the Matter | Loss Contingencies The Company is subject to lawsuits, claims, allegations and investigations regarding simufilam. As described in Note 12 to the consolidated financial statements, such allegations and claims could result in adverse consequences. As further described in Note 12, at December 31, 2021, the Company was unable to estimate the possible loss or range of loss, if any, associated with these lawsuits and investigations.
Auditing management’s accounting for and disclosure of loss contingencies related to the lawsuits and investigations was challenging because management’s evaluation of the likelihood of losses required significant judgment. |
|
|
How We Addressed the Matter in Our Audit | We obtained an understanding, evaluated the design, and tested the operating effectiveness of controls over the evaluation of the accounting for and disclosure of these matters. This included controls over management’s assessment of the probability of incurrence of a loss and whether the loss or range of loss was reasonably estimable, and the development of related disclosures.
Our audit procedures included gaining an understanding of the status of ongoing lawsuits and investigations, reading the minutes of the meetings of the committees of the board of directors, reading summaries of the proceedings and related correspondence, requesting inquiry letters from external legal counsel, meeting with external legal counsel to discuss developments related to the lawsuits and investigations together with our forensic professionals, and obtaining written representations from the Company on these matters. We also evaluated the Company’s disclosures in relation to these matters. |
/s/ Ernst & Young LLP
We have served as the Company’s auditor since 2002.
Austin, Texas
February 6, 201828, 2022
| | | | |
|
|
|
|
|
|
| | | | |
|
|
|
|
|
|
PAIN THERAPEUTICS, INC. | |
CASSAVA SCIENCES, INC. | | CASSAVA SCIENCES, INC. |
| | | | |
|
|
|
|
|
|
BALANCE SHEETS | |
(in thousands, except share and per share data) | |
CONSOLIDATED BALANCE SHEETS | | CONSOLIDATED BALANCE SHEETS |
(In thousands, except share and par value data) | | (In thousands, except share and par value data) |
| | | | |
|
| December 31, | December 31, |
|
| 2017 | 2016 | 2021 |
|
| 2020 |
|
| | | | |
|
|
|
|
|
|
ASSETS | ASSETS | ASSETS |
Current assets: | | | | |
|
|
|
|
|
|
Cash and cash equivalents | $ | 10,479 | $ | 16,615 | $ | 233,437 |
| $ | 93,506 |
|
Marketable securities | | — | | 2,099 | |
Other current assets | | 184 | | 356 | |
Prepaid expenses and other current assets | |
| 11,045 |
|
| 488 |
|
Total current assets | | 10,663 | | 19,070 |
| 244,482 |
|
| 93,994 |
|
Operating lease right-of-use assets | |
| 210 |
|
| 295 |
|
Property and equipment, net | | 156 | | 232 |
| 20,616 |
|
| 11 |
|
Intangible assets, net | |
| 1,075 |
|
| — |
|
Other assets | | 12 | | — |
| 399 |
|
| — |
|
Total assets | $ | 10,831 | $ | 19,302 | $ | 266,782 |
| $ | 94,300 |
|
| | | | |
|
|
|
|
|
|
LIABILITIES AND STOCKHOLDERS' EQUITY | LIABILITIES AND STOCKHOLDERS' EQUITY | LIABILITIES AND STOCKHOLDERS' EQUITY |
Current liabilities: | | | | |
|
|
|
|
|
|
Accounts payable | $ | 424 | $ | 303 | $ | 7,126 |
| $ | 911 |
|
Accrued development expense | | 399 | | 27 |
| 2,803 |
|
| 719 |
|
Accrued compensation and benefits | | 309 | | 335 |
| 1,877 |
|
| 83 |
|
Operating lease liabilities, current | |
| 97 |
|
| 58 |
|
Other current liabilities | |
| 631 |
|
| 94 |
|
Total current liabilities | | 1,132 | | 665 |
| 12,534 |
|
| 1,865 |
|
Noncurrent liabilities | | — | | — | |
Operating lease liabilities, non-current | |
| 139 |
|
| 235 |
|
Other non-current liabilities | |
| 194 |
|
| — |
|
Total liabilities | | 1,132 | | 665 |
| 12,867 |
|
| 2,100 |
|
Commitments and contingencies | | | | | |
Commitments and contingencies (Notes 10, 11 and 12) | |
| |
|
| |
|
Stockholders' equity: | | | | |
|
|
|
|
|
|
Preferred stock, $.001 par value; 10,000,000 shares authorized, none issued and outstanding | | — | | — | |
Common stock, $.001 par value; 120,000,000 shares authorized; 6,595,509 and 6,591,705 | | | | | |
shares issued and outstanding at December 31, 2017 and 2016, respectively | | 7 | | 7 | |
Preferred stock, $0.001 par value; 10,000,000 shares authorized, NaN issued and outstanding | |
| — |
|
| — |
|
Common stock, $0.001 par value; 120,000,000 shares authorized; 40,016,792 and 35,237,987 shares issued and outstanding at December 31, 2021 and 2020, respectively | |
| 40 |
|
| 35 |
|
Additional paid-in capital | | 167,091 | | 164,118 |
| 461,181 |
|
| 267,086 |
|
Accumulated other comprehensive income | | — | | — | |
Accumulated deficit | | (157,399) | | (145,488) |
| (207,306) |
|
| (174,921) |
|
Total stockholders' equity | | 9,699 | | 18,637 |
| 253,915 |
|
| 92,200 |
|
Total liabilities and stockholders' equity | $ | 10,831 | $ | 19,302 | $ | 266,782 |
| $ | 94,300 |
|
| | | | |
|
|
|
|
|
|
See accompanying notes to consolidated financial statements.
|
|
|
|
|
|
|
|
|
|
|
|
CASSAVA SCIENCES, INC. |
|
|
|
|
|
|
CONSOLIDATED STATEMENTS OF OPERATIONS |
(In thousands, except per share data) |
|
| Year ended |
| December 31, |
| 2021 |
| 2020 |
Operating expenses: |
|
|
|
|
|
Research and development, net of grant reimbursement | $ | 24,813 |
| $ | 3,053 |
General and administrative |
| 8,055 |
|
| 3,739 |
Gain on sale of property and equipment |
| — |
|
| (346) |
Total operating expenses |
| 32,868 |
|
| 6,446 |
Operating loss |
| (32,868) |
|
| (6,446) |
Interest income |
| 49 |
|
| 112 |
Other income, net |
| 434 |
|
| — |
Net loss | $ | (32,385) |
| $ | (6,334) |
Net loss per share, basic and diluted | $ | (0.82) |
| $ | (0.24) |
Shares used in computing net loss per share, basic and diluted |
| 39,405 |
|
| 26,105 |
|
|
|
|
|
|
| | | | | |
| | | | | |
PAIN THERAPEUTICS, INC. |
| | | | | |
STATEMENTS OF OPERATIONS |
(in thousands, except per share data) |
| | | | | |
| | | | | |
| Years ended December 31, |
| 2017 | | 2016 |
Operating expenses: | | | | | |
Research and development | $ | 7,615 | | $ | 9,176 |
General and administrative | | 4,334 | | | 5,781 |
Total operating expenses | | 11,949 | | | 14,957 |
Operating loss | | (11,949) | | | (14,957) |
Interest income | | 38 | | | 107 |
Net loss | $ | (11,911) | | $ | (14,850) |
Net loss per share, basic and diluted | $ | (1.82) | | $ | (2.28) |
Shares used in computing net loss per share, basic and diluted | | 6,537 | | | 6,520 |
| | | | | |
See accompanying notes to consolidated financial statements.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASSAVA SCIENCES, INC. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY |
(In thousands) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Accumulated |
|
|
|
|
|
|
|
|
|
|
|
| other |
|
|
|
| Total |
| Common stock |
| Additional |
| comprehensive |
| Accumulated |
| stockholders' |
| Shares |
| Par value |
| paid-in capital |
| income |
| deficit |
| equity |
Balance at December 31, 2019 | 21,841,810 |
| $ | 22 |
| $ | 190,664 |
| $ | — |
| $ | (168,587) |
| $ | 22,099 |
Stock-based compensation for: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stock options for employees | — |
|
| — |
|
| 961 |
|
| — |
|
| — |
|
| 961 |
Stock options for non-employees | — |
|
| — |
|
| 27 |
|
| — |
|
| — |
|
| 27 |
Issuance of common stock pursuant to exercise of stock options | 71,105 |
|
| — |
|
| 256 |
|
| — |
|
| — |
|
| 256 |
Issuance of common stock pursuant to exercise of warrants | 3,950,072 |
|
| 4 |
|
| 4,936 |
|
| — |
|
| — |
|
| 4,940 |
Common stock issued in conjunction with follow-on public offering, net of issuance costs | 9,375,000 |
|
| 9 |
|
| 70,242 |
|
| — |
|
| — |
|
| 70,251 |
Net loss | — |
|
| — |
|
| — |
|
| — |
|
| (6,334) |
|
| (6,334) |
Balance at December 31, 2020 | 35,237,987 |
|
| 35 |
|
| 267,086 |
|
| — |
|
| (174,921) |
| $ | 92,200 |
Stock-based compensation for: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stock options for employees | — |
|
| — |
|
| 1,706 |
|
| — |
|
| — |
|
| 1,706 |
Stock options for non-employees | — |
|
| — |
|
| 53 |
|
| — |
|
| — |
|
| 53 |
Issuance of common stock pursuant to exercise of stock options | 143,153 |
|
| — |
|
| 1,824 |
|
| — |
|
| — |
|
| 1,824 |
Issuance of common stock pursuant to exercise of warrants | 554,019 |
|
| 1 |
|
| 691 |
|
| — |
|
| — |
|
| 692 |
Common stock issued in conjunction with registered direct offering, net of issuance costs | 4,081,633 |
|
| 4 |
|
| 189,821 |
|
| — |
|
| — |
|
| 189,825 |
Net loss | — |
|
| — |
|
| — |
|
| — |
|
| (32,385) |
|
| (32,385) |
Balance at December 31, 2021 | 40,016,792 |
| $ | 40 |
| $ | 461,181 |
| $ | — |
| $ | (207,306) |
| $ | 253,915 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| | | | | |
| | | | | |
PAIN THERAPEUTICS, INC. |
| | | | | |
STATEMENTS OF COMPREHENSIVE INCOME (LOSS) |
(in thousands) |
| | | | | |
| | | | | |
| Years ended December 31, |
| 2017 | | 2016 |
Net loss | $ | (11,911) | | $ | (14,850) |
Other comprehensive income (loss): | | | | | |
Net unrealized gains (losses) on marketable securities | | — | | | — |
Comprehensive loss | $ | (11,911) | | $ | (14,850) |
| | | | | |
See accompanying notes to consolidated financial statements.
|
|
|
|
|
|
|
|
|
|
|
|
CASSAVA SCIENCES, INC. |
|
|
|
|
|
|
CONSOLIDATED STATEMENTS OF CASH FLOWS |
(In thousands) |
|
|
|
|
|
|
|
|
| Year ended December 31, |
| 2021 |
| 2020 |
Cash flows from operating activities: |
|
|
|
|
|
Net loss | $ | (32,385) |
| $ | (6,334) |
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
Stock-based compensation |
| 1,759 |
|
| 988 |
Depreciation |
| 310 |
|
| 22 |
Amortization of intangible assets |
| 224 |
|
| — |
Gain on sale of property and equipment |
| — |
|
| (346) |
Changes in operating assets and liabilities: |
|
|
|
|
|
Prepaid and other assets |
| (10,956) |
|
| (220) |
Operating lease right-of-use assets and liabilities |
| 28 |
|
| (2) |
Accounts payable |
| 6,215 |
|
| 458 |
Accrued development expense |
| 2,084 |
|
| (58) |
Accrued compensation and benefits |
| 1,794 |
|
| 25 |
Other liabilities |
| 731 |
|
| 85 |
Net cash used in operating activities |
| (30,196) |
|
| (5,382) |
Cash flows from investing activities: |
|
|
|
|
|
Purchase of property and equipment |
| (22,214) |
|
| — |
Proceeds from sale of property and equipment |
| — |
|
| 360 |
Net cash (used in) provided by investing activities |
| (22,214) |
|
| 360 |
Cash flows from financing activities: |
|
|
|
|
|
Proceeds from issuance of common stock upon exercise of stock options |
| 1,824 |
|
| 256 |
Proceeds from issuance of common stock upon exercise of common stock warrants |
| 692 |
|
| 4,940 |
Proceeds from common stock offering, net of issuance costs |
| 189,825 |
|
| 70,251 |
Net cash provided by financing activities |
| 192,341 |
|
| 75,447 |
Net increase in cash and cash equivalents |
| 139,931 |
|
| 70,425 |
Cash and cash equivalents at beginning of period |
| 93,506 |
|
| 23,081 |
Cash and cash equivalents at end of period | $ | 233,437 |
| $ | 93,506 |
|
|
|
|
|
|
| | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | |
PAIN THERAPEUTICS, INC. |
| | | | | | | | | | | | | | | | |
STATEMENTS OF STOCKHOLDERS' EQUITY |
(in thousands) |
| | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | |
| | | | | | | | | Accumulated | | | | | | |
| | | | | | other | | | | | Total |
| Common stock | | Additional | | comprehensive | | Accumulated | | stockholders' |
| Shares | | Par value | | paid-in capital | | income | | deficit | | equity |
Balance at December 31, 2015 | 6,536,588 | | | 7 | | | 159,998 | | | — | | | (130,638) | | | 29,367 |
Non-cash stock-related compensation for: | | | | | | | | | | | | | | | | |
Stock options for employees | — | | | — | | | 3,467 | | | — | | | — | | | 3,467 |
Stock options for non-employees | — | | | — | | | 25 | | | — | | | — | | | 25 |
Performance Awards and related non-cash stock-related compensation | 69,286 | | | — | | | 842 | | | — | | | — | | | 842 |
Performance Awards related to statutory taxes | (14,169) | | | — | | | (214) | | | — | | | — | | | (214) |
Other comprehensive loss | — | | | — | | | — | | | — | | | — | | | — |
Net loss | — | | | — | | | — | | | — | | | (14,850) | | | (14,850) |
Balance at December 31, 2016 | 6,591,705 | | | 7 | | | 164,118 | | | — | | | (145,488) | | | 18,637 |
Non-cash stock-related compensation for: | | | | | | | | | | | | | | | | |
Stock options for employees | — | | | — | | | 2,954 | | | — | | | — | | | 2,954 |
Stock options for non-employees | — | | | — | | | 19 | | | — | | | — | | | 19 |
Issuance of common stock pursuant to 7 to 1 Reverse stock split round up | 3,804 | | | — | | | — | | | — | | | — | | | — |
Net loss | — | | | — | | | — | | | — | | | (11,911) | | | (11,911) |
Balance at December 31, 2017 | 6,595,509 | | $ | 7 | | $ | 167,091 | | $ | — | | $ | (157,399) | | $ | 9,699 |
| | | | | | | | | | | | | | | | |
See accompanying notes to financial statements.
| | | | | |
| | | | | |
PAIN THERAPEUTICS, INC. |
| | | | | |
STATEMENTS OF CASH FLOWS |
(in thousands) |
| | | | | |
| | | | |
| Years ended December 31, |
| 2017 | | 2016 |
Cash flows from operating activities: | | | | | |
Net loss | $ | (11,911) | | $ | (14,850) |
Adjustments to reconcile net loss to net cash used in operating activities: | | | | | |
Non-cash stock-based compensation | | 2,973 | | | 4,334 |
Depreciation and amortization | | 68 | | | 58 |
Non-cash net interest income | | (2) | | | (8) |
Changes in operating assets and liabilities: | | | | | |
Other current assets | | 172 | | | 86 |
Other non-current assets | | (12) | | | 12 |
Accounts payable | | 129 | | | (711) |
Accrued development expense | | 372 | | | (867) |
Accrued compensation and benefits | | (26) | | | (288) |
Net cash used in operating activities | | (8,237) | | | (12,234) |
Cash flows from investing activities: | | | | | |
Purchases of property and equipment | | — | | | (75) |
Purchases of marketable securities | | (399) | | | (4,141) |
Sales of marketable securities | | 400 | | | — |
Maturities of marketable securities | | 2,100 | | | 2,050 |
Net cash provided (used in) investing activities | | 2,101 | | | (2,166) |
Cash flows from financing activities: | | | | | |
Cash used for statutory taxes for net exercise of Performance Awards | | — | | | (214) |
Deferred financing costs | | — | | | (70) |
Net cash used in financing activities | | — | | | (284) |
Net decrease in cash and cash equivalents | | (6,136) | | | (14,684) |
Cash and cash equivalents at beginning of period | | 16,615 | | | 31,299 |
Cash and cash equivalents at end of period | $ | 10,479 | | $ | 16,615 |
| | | | | |
See accompanying notes toconsolidated financial statements.
PAIN THERAPEUTICS,CASSAVA SCIENCES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. General, Liquidity and LiquidityBasis of Presentation
Pain Therapeutics,Cassava Sciences, Inc. and its wholly-owned subsidiary (collectively referred to as the “Company”) discovers and develops proprietary drugspharmaceutical product candidates that may offer significant improvements to patients and healthcare professionals. WeThe Company generally focus our drugfocuses its product discovery and development efforts on disorders of the nervous system, such as chronic pain.system.
On November 16, 2016, we receivedCoronavirus Disease 2019 (COVID-19)
The widespread outbreak of a letter from the Listing Qualifications staff of Nasdaq (the “Staff”) notifying us that, for the previous 30 consecutive business days, the bid price for our common stock had closed below the minimum $1.00 per share requirement (the “Minimum Price Requirement”) under Nasdaq’s Listing Rule 5450(a)(1) for continued listing on The Nasdaq Global Market. In accordance with Nasdaq Listing Rule 5810(c)(3)(A), if during the 180 calendar days following the date of the notification,novel infectious disease called Coronavirus Disease 2019, or prior to May 15, 2017, the closing bid price of our common stock is at or above $1.00 for a minimum of 10 consecutive business days, the Staff will provide us with written confirmation of compliance. On May 24, 2017, we received a letter from the Staff indicating that we had regained compliance with the $1.00 minimum closing bid requirement following completion of the reverse stock split described below.
On May 4, 2017, following stockholder approval, our board of directors approved a reverse stock split at a ratio of 7-for-1. On May 4, 2017, we filed with the Secretary of State of the State of Delaware a Certificate of Amendment toCOVID-19, has not significantly impacted the Company’s Amendedoperations or financial condition as of February 28, 2022. However, this pandemic has created a dynamic and Restated Certificateuncertain situation in the national economy. The Company continues to closely monitor the latest information to make timely, informed business decisions and public disclosures regarding the potential impact of Incorporation to effect the 7-for-1 reverse stock splitpandemic on its operations and financial condition. The scope of our outstanding shares of common stock. The number of outstanding shares of common stockpandemic is unprecedented and its long-term impact on the dateCompany’s operations and financial condition cannot be reasonably estimated at this time.
Basis of the reverse split was reduced from 46.1 million to 6.6 million shares. Our common stock began trading on the Nasdaq Global Market on a split-adjusted basis when the market opened for trading on May 10, 2017. As a result, all common stock share amounts included in theseConsolidation
The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiary. All intercompany transactions have been retroactively reduced by a factor of seven, and all common stock per share amounts have been increased by a factor of seven, with the exception of our common stock par value.eliminated in consolidation.
Liquidity
The Company has incurred significant net losses and negative cash flows since inception, and as a result has an accumulated deficit of $157$207.3 million at December 31, 2017. We expect our2021. The Company expects its cash requirements to be significant in the future. The amount and timing of ourthe Company’s future cash requirements will depend on regulatory and market acceptance of our drugits product candidates and the resources we devoteit devotes to researching and developing, formulating, manufacturing, commercializing and supporting ourits products. WeThe Company may seek additional future funding through public or private financing within this timeframe,in the future, if such funding is available and on terms acceptable to us.the Company. There are no assurances that additional financing will be available on favorable terms, or at all. However, management believes that the current working capital position will be sufficient to meet the Company’s working capital needs for at least the next 12 months.
2. Summary of Significant Accounting Policies
Use of Estimates
The preparation ofCompany makes estimates and assumptions in preparing its consolidated financial statements in conformity with accounting principles generally accepted in the United States of America requires that management makeStates. These estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amount of revenue earned and expenses incurred during the reporting period. The Company evaluates its estimates on an ongoing basis, including those estimates related to manufacturing agreements and research collaborations. Actual results could differ from those estimates.these estimates and assumptions.
Proceeds from Grants
In 2017, we2021, the Company received $1.4$3.9 million of reimbursement from the National Institutes of Health and National Institute on Drug Abuse and $4.2 million in research grants from the NIH and NIDA and $1.5 million in 2016. We record2020. The Company records the proceeds from the grantthese grants as a reductionreductions to ourits research and development expenses.
Cash and Cash Equivalents Marketable Securities and Concentration of Credit Risk
We investThe Company invests in cash equivalents and marketable securities. We considercash equivalents. The Company considers highly-liquid financial instruments with original maturities of three months or less to be cash equivalents. Our marketable securitiesHighly liquid investments that are considered cash equivalents include interest-bearing financial instruments, generally consistingmoney market accounts and funds, certificates of corporate or governmentdeposit and U.S. Treasury securities.
Our investment policy allows for investments in marketable securities with active secondary or resale markets, establishes diversification The Company maintains its cash and credit quality requirements and limits investments by maturity and issuer. We maintain our investmentscash equivalents at one financial institution.
A changeFair Value Measurements
The Company recognizes financial instruments in prevailing interest rates may causeaccordance with the authoritative guidance on fair value measurements and disclosures for financial assets and liabilities. This guidance defines fair value, establishes a framework for measuring fair value in accordance with GAAP, and expands disclosures about fair value measurements. The guidance also establishes a three-tier fair value hierarchy, which prioritizes the inputs used in measuring fair value. These tiers include:
Level 1 includes quoted prices in active markets.
Level 2 includes significant observable inputs, such as quoted prices for identical or similar securities, or other inputs that are observable and can be corroborated by observable market data for similar securities. The Company uses market pricing and other observable market inputs obtained from third-party providers. It uses the bid price to establish fair value where a bid price is available. The Company does not have any financial instruments where the fair value of the investment to fluctuate. We dois based on Level 2 inputs.
Level 3 includes unobservable inputs that are supported by little or no market activity. The Company does not recognize an impairment charge related to this type of fluctuation because the fluctuation is temporary and eliminated by the time an investment matures. We would recognize an impairment charge if and when we determine that a decline in have any financial instruments where the fair value belowis based on Level 3 inputs.
If a financial instrument uses inputs that fall in different levels of the amortized costhierarchy, the instrument will be categorized based upon the lowest level of an investmentinput that is other-than-temporary. We consider various factors in determining whethersignificant to recognize an impairment charge, including any adverse changes in the investees’ financial condition, how long the fair value has been below the amortized costcalculation. The fair value of cash and whether it is more likely than not that we would elect to or be required to sell the marketable security before its anticipated recovery.
We may elect to sell marketable securities before they mature. We hold these investments as “available for sale” and include these investments in our Balance Sheets as current assets, even though the contractual maturity of a particular investment may be beyond one year.
Fair Value Measurements
We report our cash equivalents and marketable securities at fair value aswas based on Level 1 Level 2 or Level 3 using the following inputs:
| ·
| | Level 1 includes quoted prices in active markets. We base the fair value of money market funds and U.S. treasury securities on Level 1 inputs.
|
| ·
| | Level 2 includes significant observable inputs, such as quoted prices for identical or similar investments, or other inputs that are observable and can be corroborated by observable market data for similar securities. We use market pricing and other observable market inputs obtained from third-party providers. We use the bid price to establish fair value where a bid price is available. We base the fair value of our marketable securities on Level 2 inputs.
|
| ·
| | Level 3 includes unobservable inputs that are supported by little or no market activity. We do not have any investments where the fair value is based on Level 3 inputs.
|
inputs at December 31, 2021 and 2020.
We include unrealized gains or losses on our investments as Accumulated other comprehensive income (loss) in the Stockholders’ equity section of our Balance Sheets. We include changes in net unrealized gains or losses in our Statements of Comprehensive Income (Loss). We would recognize significant realized gains and losses on a specific identification basis as other income in our Statements of Operations.
Business Segments
We reportThe Company reports segment information based on how weit internally evaluateevaluates the operating performance of ourits business units, or segments. OurThe Company’s operations are confined to one1 business segment: the development of novel drugs.drugs and diagnostics.
Stock-based Compensation
We recognizeThe Company recognizes non-cash expense for the fair value of all stock options and other share-based awards. We useThe Company uses the Black-Scholes option valuation model (“Black-Scholes”) to calculate the fair value of stock options, using the single-option award approach and straight-line attribution method. This model requires the input of subjective assumptions including expected stock price volatility, expected life and estimated forfeitures of each award. These assumptions consist of estimates of future market conditions, which are inherently uncertain, and therefore, are subject to management's judgment. For all options granted, to employees and directors, we recognizeit recognizes the resulting fair value as expense on a straight-line basis over the vesting period of each respective stock option, generally four years. For options granted to non-employees, we remeasure the fair value expense using Black-Scholes each reporting period.
We haveThe Company has granted share-based awards that vest upon achievement of certain performance criteria or (“Performance Awards. We multiplyAwards”). The Company multiplies the number of Performance Awards by the fair market value of ourits common stock on the date of grant to calculate the fair value of each award. We estimateIt estimates an implicit service period for achieving performance criteria for each award. We recognizeThe Company recognizes the resulting fair value as expense over the implicit service period when we concludeit concludes that achieving the performance criteria is probable. WeIt periodically reviewreviews and updateupdates as appropriate ourits estimates of implicit
service periods and conclusions on achieving the performance criteria. Performance Awards vest and common stock is issued upon achievement of the performance criteria.
Net Loss per Share
BasicThe Company computes basic net loss per share is computed on the basis of the weighted-average number of common shares outstanding for the reporting period. Diluted net loss per share is computed on the basis of the weighted-average number of common shares outstanding plus potential dilutive potential common shares outstanding using the treasury-stock method. Potential dilutive common shares consist of outstanding equity awardscommon stock options and warrants. There is no difference between the Company’s net loss and comprehensive loss. The numerators and denominators in the calculation of basic and diluted net loss per share were as follows (in thousands)thousands, except net loss per share data):
| |
|
|
|
|
|
| | | | | |
|
|
|
|
|
| | | | | | Year ended |
| Years ended December 31, | December 31, |
| 2017 | | 2016 | 2021 |
| 2020 |
Numerator: | | | | | |
|
|
|
|
|
Net loss | $ | (11,911) | | $ | (14,850) | $ | (32,385) |
| $ | (6,334) |
Denominator: | | | | | |
|
|
|
|
|
Shares used in computing net loss per share, basic and diluted | | 6,537 | | | 6,520 |
| 39,405 |
|
| 26,105 |
Net loss per share, basic and diluted | $ | (1.82) | | $ | (2.28) | $ | (0.82) |
| $ | (0.24) |
Dilutive common shares excluded from net loss per share, diluted | | 2,497 | | | 2,535 | |
| | | | | |
|
|
|
|
|
Dilutive common stock options excluded from net loss per share, diluted | |
| 2,211 |
|
| 2,145 |
Common stock warrants excluded from net loss per share, diluted | |
| — |
|
| 554 |
| |
|
|
|
|
|
WeThe Company excluded weighted equity awards outstanding to purchase common stock options and warrants outstanding from the calculation of diluted net loss per share, diluted, because the effect of including these sharesoutstanding options and warrants would have been anti-dilutive.
Fair Value of Financial Instruments
Financial instruments include accounts payable and accrued liabilities. The estimated fair value of certain financial instruments may be determined using available market information or other appropriate valuation methodologies. However, considerable judgment is required in this calculationinterpreting market data to develop estimates of fair value; therefore, the estimates are not necessarily indicative of the amounts that could be realized or would be anti-dilutive.paid in a current market exchange. The effect of using different market assumptions and/or estimation methodologies may be material to the estimated fair value amounts. The carrying amounts of accounts payable and accrued liabilities are at cost, which approximates fair value due to the short maturity of those instruments.
Income TaxesResearch Contract Costs and Accruals
We makeThe Company has entered into various research and development contracts with research institutions and other third-party vendors. These agreements are generally cancelable. Related payments are recorded as research and development expenses as incurred. The Company records accruals for estimated ongoing research costs. When evaluating the adequacy of the accrued liabilities, the Company analyzes progress of the studies including the phase or completion of events, invoices received and contracted costs. Significant judgments and estimates and judgmentsare made in determining the needaccrued balances at the end of any reporting period. Actual results could differ from the Company’s estimates. The Company’s historical accrual estimates have not been materially different from actual costs.
Incentive Bonus Plan
In 2020, the Company established the 2020 Cash Incentive Bonus Plan (the “Plan”) to incentivize Plan participants. Awards under the Plan are accounted for as liability awards under Accounting Standards Codification (ASC) 718 “Stock-based Compensation”. The fair value of each potential Plan award will be determined once a provisiongrant date occurs and will be remeasured each reporting period. Compensation expense associated with the Plan will be recognized over the expected achievement period for each Plan award, when a Performance Condition (as defined below) is considered probable of being met. See Note 11 for further discussion of the Plan.
Leases
The Company recognizes assets and liabilities that arise from leases. For operating leases, the Company is required to recognize a right-of-use asset and a lease liability, initially measured at the present value of the lease payments during the lease term, in the consolidated balance sheets. The Company elected the short-term lease recognition exemption for all leases that qualify. This means, for those leases that qualify, the Company does not recognize right-of-use assets or lease liabilities. As the Company`s leases do not provide an implicit rate, it uses its incremental borrowing rate based on the information available at the commencement date in determining the present value of lease payments. Lease expense for lease payments is recognized on a straight-line basis over the lease term.
Property and equipment
Property and equipment is recorded at cost, net of accumulated depreciation. Depreciation is recorded using the straight-line method over the estimated useful lives of the assets. Buildings and site improvements have estimated useful lives of 39 years and 9 years, respectively. Tenant improvements are amortized using the straight-line method over the useful lives of the improvements or the remaining term of the corresponding leases, whichever is shorter. The remaining term of the corresponding leases is approximately 2.8 years.
Property and equipment are reviewed for impairment when events or changes in circumstances indicate the carrying amount of an asset may not be recoverable. If property and equipment are considered to be impaired, an impairment loss is recognized.
Intangible assets
Acquired intangible assets are recorded at fair value at the date of acquisition and primarily consist of lease-in-place agreements and leasing commissions. Intangible assets are amortized over the estimated life of the lease-in-place agreements, which approximates 2.7 years.
Intangible assets are reviewed for impairment on an annual basis, and when there is reason to believe that their values have been diminished or impaired. If intangible assets are considered to be impaired, an impairment loss is recognized.
Income Taxes
The Company accounts for income taxes includingunder the estimationasset and liability method. Deferred tax assets and liabilities are recognized for the estimated future tax consequences attributable to differences between the financial statement carrying amounts of our taxable income or loss for each full fiscal year.
We haveexisting assets and liabilities and their respective tax bases. Deferred tax balances are adjusted to reflect tax rates based on currently enacted tax laws, which will be in effect in the years in which the temporary differences are expected to reverse. The Company has accumulated significant deferred tax assets that reflect the tax effects of net operating loss and tax credit carryovers and temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Realization of certain deferred tax assets is dependent upon future earnings. We areThe Company is uncertain about the timing and amount of any future earnings. Accordingly, we offsetthe Company offsets these deferred tax assets with a valuation allowance.
We mayThe Company accounts for uncertain tax positions in accordance with ASC 740, “Income Taxes”, which clarifies the accounting for uncertainty in tax positions. These provisions require recognition of the impact of a tax position in the future determineCompany’s financial statements only if that certain deferredposition is more likely than not of being sustained upon examination by taxing authorities, based on the technical merits of the position. Any interest and penalties related to uncertain tax assetspositions will likely be realized, in which case we will reduce our valuation allowance in the period in which such determination is made. If the valuation allowance is reduced, we may recognizereflected as a benefit fromcomponent of income taxes in our Statement of Operations in that period.tax expense.
We classify interest recognized pursuant to our deferred tax assets as interest expense, when appropriate.
Recent Accounting Pronouncements
WeThe Company reviewed recently issued accounting pronouncements and plan to adopt those that are applicable to us. We doit, and does not expect the adoption of these pronouncements to have a material impact on ourits financial position, results of operations or cash flows.
In AugustJune 2016, the FASBFinancial Accounting Standards Board (FASB) issued Accounting Standards Update No. 2016-13 (“ASU No. 2016-15, Statement2016-13”) Financial Instruments—Credit Losses (Topic 326): Measurement of Cash Flows (Topic 230): Classification of Certain Cash Receipts and Cash Paymentscredit losses on financial instruments. This ASU provides guidance on statement of cash flows presentation2016-13 introduces the current expected credit losses methodology for eight specific cash flow issues where diversity in practice exists. This ASUestimating allowances for credit losses. The standard is effective forin fiscal years and interim periods beginning after December 15, 2017,2020. The adoption of adoption of ASU 2016-13 in the first quarter of 2021 did not have a material impact on its consolidated financial statements and related disclosures.
In December 2019, the FASB issued Accounting Standards Update No. 2019-12 (“ASU 2019-12”), Income Taxes (Topic 740) Simplifying Accounting for Income Taxes, as part of its initiative to reduce complexity in the accounting standards. The guidance amended certain disclosure requirements that had become redundant, outdated or superseded. Additionally, this guidance amends accounting for the interim period effects of changes in tax laws or rates, and simplifies aspects of the accounting for franchise taxes. The guidance is effective for annual periods beginning after December 15, 2020, including interim periods within those fiscal years.therein. The Company expects thatadoption of ASU 2019-12 in the adoption willfirst quarter of 2021 did not have a material impact on itsthe Company’s consolidated financial statements.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842). The core principle of Topic 842 is that a lessee should recognize the
3.Prepaid and Other Current Assets
Prepaid and other current assets at December 31, 2021 and liabilities that arise from leases. For operating leases, a lessee is required to recognize a right-of-use asset and a lease liability, initially measured at the present value of the lease payments, in the statement of financial position. This ASU is effective for fiscal years beginning after December 15, 2018, including
interim periods within those fiscal years. The Company is evaluating the effect that the adoption of this ASU will have on its financial statements. The Company currently expects that its operating lease commitment will be subject to the new standard and recognized as right-of-use asset and operating lease liability upon adoption of ASU 2016-02, which will increase the total assets and total liabilities that it reports relative to such amounts prior to adoption.
3. Collaboration Agreements
Durect Corporation
We have an exclusive, worldwide Development and License Agreement, or the Durect Agreement, with Durect to use a patented controlled-release technology that forms the basis for REMOXY. Under the terms of the Durect Agreement, we are solely responsible for clinical development, Durect is responsible for furnishing suitable laboratory facilities, equipment and personnel during pre-clinical phases of development and we and Durect are jointly responsible for certain pre-clinical activities. We reimburse Durect’s expenses and have made milestone payments based on the achievement of certain clinical or regulatory milestones.
4. Cash and Cash Equivalents and Marketable Securities
Cash, cash equivalents and marketable securities held as available-for-sale2020 consisted of the following (in thousands):
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
| Cash, Cash Equivalents and Marketable Securities |
| Amortized Cost | | Unrealized Gains | | Unrealized Losses | | Estimated Fair Value | | Accrued Interest | | Total Value |
December 31, 2017 | | | | | | | | | | | | | | | | | |
Cash | $ | 158 | | $ | — | | $ | — | | $ | 158 | | $ | — | | $ | 158 |
Cash equivalents | | 10,321 | | | — | | | — | | | 10,321 | | | — | | | 10,321 |
Total cash and cash equivalents | $ | 10,479 | | $ | — | | $ | — | | $ | 10,479 | | $ | — | | $ | 10,479 |
Reported as: | | | | | | | | | | | | | | | | | |
Cash and cash equivalents | $ | 10,479 | | | — | | | — | | $ | 10,479 | | $ | — | | $ | 10,479 |
Marketable securities | | — | | | — | | | — | | | — | | | — | | | — |
| $ | 10,479 | | $ | — | | $ | — | | $ | 10,479 | | $ | — | | $ | 10,479 |
Maturities: | | | | | | | | | | | | | | | | | |
Matures in one year or less | $ | 10,479 | | $ | — | | $ | — | | $ | 10,479 | | $ | — | | $ | 10,479 |
Matures one to three years | | — | | | — | | | — | | | — | | | — | | | — |
| $ | 10,479 | | $ | — | | $ | — | | $ | 10,479 | | $ | — | | $ | 10,479 |
| | | | | | | | | | | | | | | | | |
December 31, 2016 | | | | | | | | | | | | | | | | | |
Cash | $ | 1,434 | | $ | — | | $ | — | | $ | 1,434 | | $ | — | | $ | 1,434 |
Cash equivalents | | 12,783 | | | — | | | — | | | 12,783 | | | — | | | 12,783 |
Commercial paper | | 4,497 | | | — | | | — | | | 4,497 | | | — | | | 4,497 |
Total cash and cash equivalents | $ | 18,714 | | $ | — | | $ | — | | $ | 18,714 | | $ | — | | $ | 18,714 |
Reported as: | | | | | | | | | | | | | | | | | |
Cash and cash equivalents | $ | 16,615 | | | — | | | — | | $ | 16,615 | | $ | — | | $ | 16,615 |
Marketable securities | | 2,099 | | | — | | | — | | | 2,099 | | | — | | | 2,099 |
| $ | 18,714 | | $ | — | | $ | — | | $ | 18,714 | | $ | — | | $ | 18,714 |
Maturities: | | | | | | | | | | | | | | | | | |
Matures in one year or less | $ | 18,714 | | $ | — | | $ | — | | $ | 18,714 | | $ | — | | $ | 18,714 |
Matures one to three years | | — | | | — | | | — | | | — | | | — | | | — |
| $ | 18,714 | | $ | — | | $ | — | | $ | 18,714 | | $ | — | | $ | 18,714 |
| | | | | | | | | | | | | | | | | |
|
|
|
|
|
|
|
|
|
|
|
|
|
| December 31, |
|
| 2021 |
|
| 2020 |
Prepaid insurance | $ | 662 |
| $ | 457 |
Contract research organization and other deposits |
| 10,330 |
|
| — |
Other |
| 53 |
|
| 31 |
Total prepaid expenses and other current assets | $ | 11,045 |
| $ | 488 |
To date we have not recorded any impairment charges on marketable securitiesContract research organization and other deposits represent cash payments made to vendors in excess of expenses incurred.
4. Real Property Acquisition
On August 4, 2021, the Company completed the all-cash purchase of a two-building office complex in Austin, Texas, which will serve as its future corporate headquarters. This property is intended to accommodate the Company’s anticipated growth and expansion of its operations in the coming years. Maintenance, physical facilities, leasing, property management and other key responsibilities related to other-than-temporary declinesproperty ownership are being outsourced to professional real-estate managers. The purchase price of the property was $22.0 million, including transaction costs. The office complex measures approximately 90,000 rentable square feet. At acquisition and December 31, 2021, the property was 59% leased. The Company is planning to occupy approximately 25% of the property in market value.2022. The seller was a third party not affiliated with the Company.
Our assets measured atThe purchase was accounted for as an asset acquisition under ASC 805, Business Combinations. As substantially all of the fair value of the gross assets acquired were concentrated into a single identifiable asset, the Company concluded that the screen was met, and the transaction is considered an asset acquisition rather than an acquisition of a business. Pursuant to the cost accumulation method as prescribed in ASC 805, the cost of the acquisition, including certain transaction costs, is allocated to the assets acquired on the basis of relative fair values. The value of acquired in-place leases is measured as the sum of lost revenues that would be incurred during a prospective lease-up period that would be necessary to achieve occupancy similar to that at the time of acquisition. The value is calculated as the average number of months of lease-up multiplied by the gross monthly market rental rate (base rent plus reimbursements) for each particular suite.
The assets acquired are summarized as follows (in thousands):
| | | | | | | | | | | |
| | | | | | | | | | | |
| Level 1 | | Level 2 | | Level 3 | | Total |
December 31, 2017 | | | | | | | | | | | |
Cash and cash equivalents | $ | 10,479 | | $ | — | | $ | — | | $ | 10,479 |
Commercial paper | | — | | | — | | | — | | | — |
| $ | 10,479 | | $ | — | | $ | — | | $ | 10,479 |
December 31, 2016 | | | | | | | | | | | |
Cash and cash equivalents | $ | 14,217 | | $ | — | | $ | — | | $ | 14,217 |
Commercial paper | | — | | | 4,497 | | | — | | | 4,497 |
| $ | 14,217 | | $ | 4,497 | | $ | — | | $ | 18,714 |
| | | | | | | | | | | |
|
|
|
|
|
|
|
|
Land | $ | 3,734 |
Buildings |
| 15,980 |
Site improvements |
| 453 |
Tenant improvements |
| 567 |
Total tangible assets | $ | 20,734 |
|
|
|
Lease-in-place agreements | $ | 1,053 |
Leasing commissions and other |
| 246 |
Total intangible assets | $ | 1,299 |
|
|
|
Consideration paid | $ | 22,033 |
|
|
|
The Company records the net income from building operations and leases as other income, net, as leasing is not core to the Company’s operations. Building depreciation and amortization is included in general and administrative expense. Components of other income, net, for the years ended December 31, 2021 and 2020 were as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
| Year ended |
| December 31, |
| 2021 |
| 2020 |
Lease revenue | $ | 911 |
| $ | — |
Property operating expenses |
| (477) |
|
| — |
Other income, net | $ | 434 |
| $ | — |
|
|
|
|
|
|
5. Property and Equipment
PropertyThe components of property and equipment, includes furniturenet, as of December 31, 2021 and 2020 were as follows (in thousands):
|
|
|
|
|
|
|
|
|
|
|
|
|
| December 31, |
| 2021 |
| 2020 |
Land | $ | 3,734 |
| $ | — |
Buildings |
| 15,980 |
|
| — |
Site improvements |
| 470 |
|
| — |
Tenant improvements |
| 567 |
|
| — |
Furniture and equipment |
| 178 |
|
| 97 |
Construction in progress |
| 83 |
|
| — |
Gross property and equipment | $ | 21,012 |
| $ | 97 |
Accumulated depreciation |
| (396) |
|
| (86) |
Property and equipment, net | $ | 20,616 |
| $ | 11 |
|
|
|
|
|
|
Depreciation expense for property and equipment with a purchase value of $1.0 million atwas $310,000 and $22,000 for the years ended December 31, 20172021 and 2016. Depreciation is recognized using2020, respectively.
There were 0 sales of property and equipment during the straight-line method overyear ended December 31, 2021.
During the expected lifeyear ended December 31, 2020, the Company sold surplus manufacturing equipment to an independent third party and received proceeds totaling $360,000. The original cost of the property and equipment. Accumulatedequipment was $892,000 and accumulated depreciation was $0.8 million at$878,000, resulting a gain on sale of property and equipment of $346,000 during the year ended December 31, 2017 and $0.7 million at2020.
6. Intangible assets
The components of intangible assets, net, as of December 31, 2016.2021 and 2020 were as follows (in thousands):
6.
|
|
|
|
|
|
|
|
|
|
|
|
| December 31, |
| 2021 |
| 2020 |
Lease-in-place agreements | $ | 1,053 |
| $ | — |
Leasing commissions and other |
| 246 |
|
| — |
Gross intangible assets | $ | 1,299 |
| $ | — |
Accumulated amortization |
| (224) |
|
| — |
Intangible assets, net | $ | 1,075 |
| $ | — |
|
|
|
|
|
|
Amortization expense for intangible assets was $224,000 for the year ended December 31, 2021. There was no amortization expense for the year ended December 31, 2020.
Amortization expense for finite-lived intangible assets is expected to be as follows (in thousands):
|
|
|
|
|
|
|
|
For the year ending December 31, |
|
|
|
2022 |
|
| 464 |
2023 |
|
| 464 |
2024 |
|
| 147 |
Total amortization |
| $ | 1,075 |
|
|
|
|
7. Stockholders' Equity and Stock-Based Compensation
Preferred Stock
OurThe Company’s Board of Directors (the “Board”) has the authority to issue preferred stock in one or more series and to fix the rights, preferences, privileges, restrictions and the number of shares constituting any series or the designation of the series.
2021 Registered Direct Offering
On February 12, 2021, the Company completed a common stock offering pursuant to which certain investors purchased 4,081,633 shares of common stock at a price of $49.00 per share. Net proceeds of the offering were approximately $189.8 million after deducting offering expenses.
2020 Follow-on Public Offering
On November 13, 2020, the Company completed the sale of 9,375,000 shares of Cassava common stock in an underwritten public offering at a price of $8.00 per share. The Company received net proceeds from the offering of approximately $70.3 million after deducting underwriting discounts and offering expenses.
Common Stock Warrants
In August 2018, the Company issued warrants to purchase up to an aggregate of 9.1 million shares of its common stock in conjunction with an offering of its common stock.
During 2021, the Company received proceeds of $0.7 million from the exercise of 0.6 million shares pursuant to common stock warrants. There were no common stock warrants outstanding following the 2021 exercises.
During 2020, the Company received proceeds of $4.9 million from the exercise of 4.0 million shares pursuant to common stock warrants.
At the Market (ATM) Common Stock Issuance
On March 27, 2020, the Company established an at-the-market offering program (ATM) to sell, from time to time, shares of Company common stock having an aggregate offering price of up to $100 million in transactions pursuant to a shelf registration statement that was declared effective by the U.S. Securities and Exchange Commission (the SEC) on May 5, 2020. The Company is obligated to pay a commission of 3.0% of the gross proceeds from the sale of shares of common stock in the offering. The Company is not obligated to sell any shares in the offering.
There were 0 common stock sales under the ATM during the years ended December 31, 2021 and 2020.
2008 Equity Incentive Plan
Under ourthe Company’s 2008 Equity Incentive Plan, or 2008 Equity Plan, ourits employees, directors and consultants received share-based awards, including grants of stock options and Performance Awards. Our Board of Directors or a designated Committee of the Board is responsible for administration of the 2008 Equity Plan and determined the terms and conditions of each option granted, consistent with the terms of the plan.performance awards. The 2008 Equity Plan expired in December 2017. Share-based awards generally expire ten years from the date of grant.
2018 Equity Incentive Plan
In January 2018, the Company’s Board approved the Company’s 2018 Omnibus Incentive Plan (the 2018 Plan). The Company’s Board or a designated Committee of the Board is responsible for administration of the 2018 Plan and determined the terms and conditions of each option granted, consistent with the terms of the 2018 Plan. The Company’s employees, directors, and consultants are eligible to receive awards under the 2018 Plan, including grants of stock options and performance awards. Share-based awards generally expire ten years from the date of grant. The 2018 Plan provides for issuance of up to 1,000,000 shares of common stock, par value $0.001 per share under the 2018 Plan, subject to adjustment as provided in the 2018 Plan.
When stock options or Performance Awardsperformance awards are exercised net of the exercise price and taxes, the number of shares of stock issued is reduced by the number of shares equal to the amount of taxes owed by the award recipient and that number of shares are cancelled. WeThe Company then use ouruses its cash to pay tax authorities the amount of statutory taxes owed by and on behalf of the award recipient.
Stock Options
The following summarizes information about stock option activity during 2017:2021:
| | | | | | | | | | | |
| | | Number of Options | | Weighted Average Exercise Price | | Weighted Average Remaining Contractual Term | | Aggregate Intrinsic Value |
| | | | | | | | In years | | In millions |
| Outstanding as of December 31, 2016 | | 2,435,249 | | $ | 25.19 | | 4.8 | | $ | — |
| Options granted | | 1,026,410 | | $ | 3.68 | | | | | |
| Options exercised | | — | | $ | — | | | | | |
| Options forfeited/canceled | | (479,504) | | | 31.73 | | | | | |
| Outstanding as of December 31, 2017 | | 2,982,155 | | $ | 16.74 | | 6.2 | | $ | 0.4 |
| Vested and expected to vest at December 31, 2017 | | 2,982,155 | | $ | 16.74 | | 6.2 | | $ | 0.4 |
| Exercisable at December 31, 2017 | | 1,757,688 | | $ | 24.02 | | 4.1 | | $ | — |
| | | | | | | | | | | |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Number of Options |
|
| Weighted Average Exercise Price |
| Weighted Average Remaining Contractual Term in Years |
| Aggregate Intrinsic Value in Millions |
|
|
|
|
|
|
|
|
|
|
|
| Outstanding as of December 31, 2020 |
| 2,817,504 |
| $ | 11.30 |
| 5.60 |
| $ | 6.4 |
| Options granted |
| 100,000 |
|
| 69.20 |
|
|
|
|
|
| Options exercised |
| (241,638) |
|
| 30.75 |
|
|
|
|
|
| Options forfeited/canceled |
| (12,139) |
|
| 44.01 |
|
|
|
|
|
| Outstanding as of December 31, 2021 |
| 2,663,727 |
|
| 11.56 |
| 5.13 |
| $ | 88.2 |
| Vested and expected to vest at December 31, 2021 |
| 2,663,727 |
|
| 11.56 |
| 5.13 |
| $ | 88.2 |
| Exercisable at December 31, 2021 |
| 2,294,190 |
| $ | 10.52 |
| 4.63 |
| $ | 76.5 |
|
|
|
|
|
|
|
|
|
|
|
|
The following summarizes information about stock options at December 31, 20172021 by a range of exercise prices:
| | | | | | | | | | | | | | | | | |
| | | | | | | Options outstanding | | Options exercisable |
| | | | | | | | | Weighted | | | | | | | | |
| | | | | | | | | average | | Weighted | | | | Weighted |
| | | | | | | Number of | | remaining | | average | | Number of | | average |
| Range of exercise prices | | outstanding | | contractual | | exercise | | vested | | exercise |
| From | | To | | options | | life (in years) | | price | | options | | price |
| $ | 3.24 | | $ | 4.09 | | 933,200 | | 9.8 | | $ | 3.59 | | 46,458 | | $ | 3.25 |
| $ | 4.10 | | $ | 15.61 | | 620,243 | | 7.5 | | $ | 11.63 | | 345,168 | | $ | 12.51 |
| $ | 16.31 | | $ | 23.38 | | 628,411 | | 3.9 | | $ | 19.05 | | 597,399 | | $ | 19.16 |
| $ | 23.59 | | $ | 35.00 | | 656,841 | | 2.9 | | $ | 30.41 | | 626,841 | | $ | 30.24 |
| $ | 36.40 | | $ | 53.55 | | 143,460 | | 3.4 | | $ | 51.66 | | 141,822 | | $ | 51.82 |
| | | | | | | 2,982,155 | | 6.2 | | $ | 16.74 | | 1,757,688 | | $ | 24.02 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Options outstanding |
| Options exercisable |
|
|
|
|
|
|
|
|
| Weighted |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| average |
| Weighted |
|
|
| Weighted |
|
|
|
|
|
|
| Number of |
| remaining |
| average |
| Number of |
| average |
| Range of exercise prices |
| outstanding |
| contractual |
| exercise |
| vested |
| exercise |
| From |
| To |
| options |
| life (in years) |
| price |
| options |
| price |
| $ | 0.95 |
| $ | 1.88 |
| 657,813 |
| 7.4 |
| $ | 1.47 |
| 415,363 |
| $ | 1.37 |
| $ | 3.24 |
| $ | 3.24 |
| 550,000 |
| 5.6 |
| $ | 3.24 |
| 550,000 |
| $ | 3.24 |
| $ | 4.09 |
| $ | 12.04 |
| 547,576 |
| 5.2 |
| $ | 7.06 |
| 506,638 |
| $ | 7.02 |
| $ | 12.39 |
| $ | 23.38 |
| 597,746 |
| 2.3 |
| $ | 16.77 |
| 597,746 |
| $ | 16.77 |
| $ | 23.59 |
| $ | 77.00 |
| 310,592 |
| 4.6 |
| $ | 45.53 |
| 224,443 |
| $ | 36.50 |
|
|
|
|
|
|
| 2,663,727 |
| 5.1 |
| $ | 11.56 |
| 2,294,190 |
| $ | 10.52 |
We useThe Company uses Black-Scholes to estimate the fair value of options granted. Black-Scholes considers a number of factors, including the market price of ourthe Company’s common stock. For options granted to employees and directors, we used certain factorsFactors utilized in Black-Scholes to value each stock option granted, which resulted in aand the weighted average fair value of options granted during 2017the years ended December 31, 2021 and 2016,2020 were as follows:
| | | | |
| | 2017 | | 2016 |
| Volatility | 79% to 83% | | 72% |
| Risk-free interest rates | 2% to 2.4% | | 1% to 2% |
| Expected life of option | 7 years | | 7 years |
| Dividend yield | zero | | zero |
| Forfeiture rate | zero | | zero |
| Weighted average fair value of stock options granted | $2.74 | | $1.60 |
| | | | |
|
|
|
|
|
|
| 2021 |
| 2020 |
| Volatility | 147% to 151% |
| 123% to 139% |
| Risk-free interest rates | 1.12% to 1.42% |
| 0.46% to 0.78% |
| Expected life of option | 7.0 years |
| 7.0 years |
| Dividend yield | 0 |
| 0 |
| Forfeiture rate | 0 |
| 0 |
| Weighted average fair value of stock options granted | $65.83 |
| $6.69 |
|
|
|
|
|
Volatility is based on reviews of the historical volatility of ourthe Company’s common stock. Risk-free interest rates are based on yields of U.S. treasury notes in effect at the date of grant. Expected life of option is based on actual historical option exercises. Dividend yield is zero0 because we dothe Company does not anticipate paying cash dividends in the foreseeable future. We estimate forfeitures and adjust this estimate periodically based in part on the extent to which actual forfeitures differ from our estimates.
For options granted to non-employees, we estimate the fair value of stock options granted using factors similar to those used for stock options granted to employees and directors and appropriate for the terms underlying the stock options granted to non-employees. We re-measure the compensation expense for options granted to non-employees each reporting period.
As of December 31, 2017, we expect2021, the Company expects to recognize compensation expense of $5.3$6.2 million related to non-vested options held by employees and directorsequity plan participants over the weighted average remaining recognition period of 3.22.1 years.
Performance Awards
The following summarizes information about Performance Awardperformance award activity during 2017:2021:
|
|
|
|
| Number of Performance Awards |
Outstanding as of December 31, 20162020 | | 222,060 |
Granted
| | —138,055
|
Vested Performance AwardsGranted
|
| — |
Forfeited/CanceledVested
|
| (69,720)— |
Forfeited/canceled |
| — |
Outstanding as of December 31, 20172021 |
| 152,340 138,055 |
|
|
|
If and when outstanding Performance Awardsperformance awards vest, wethe Company would recognize $2.5$2.3 million in non-cash stock-based compensation expense. These Performance Awardsperformance awards expire between 2022 and 2026.2026.
Stock-Based Compensation Expense
The following summarizes information about non-cash stock-based compensation expense, in thousands:
| | | | | |
| | | | | |
| Years ended December 31, |
| 2017 | | 2016 |
| | | | | |
Research and development | | | | | |
Vesting of stock options | $ | 1,205 | | $ | 1,313 |
Vesting of Performance Awards | | — | | | 438 |
| | 1,205 | | | 1,751 |
General and administrative | | | | | |
Vesting of stock options | | 1,768 | | | 2,179 |
Vesting of Performance Awards | | — | | | 404 |
| | 1,768 | | | 2,583 |
Total non-cash stock-based compensation expenses | | | | | |
Vesting of stock options | | 2,973 | | | 3,492 |
Vesting of Performance Awards | | — | | | 842 |
| $ | 2,973 | | $ | 4,334 |
| | | | | |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Year ended |
|
| December 31, |
|
| 2021 |
| 2020 |
|
Research and development | $ | 1,302 |
| $ | 453 |
|
|
|
|
|
|
|
|
General and administrative |
| 457 |
|
| 535 |
|
|
|
|
|
|
|
|
Total stock-based compensation expense | $ | 1,759 |
| $ | 988 |
|
|
|
|
|
|
|
|
Non-cash stock-related compensation expense related to vesting of Performance Awards was associated with the resubmission of the NDA for REMOXY.
7.
8. Employee 401(k) Benefit Plan
We haveThe Company has a defined-contribution savings plan under Section 401(k) of the Internal Revenue Code. The plan covers substantially all employees. Employees are eligible to participate in the plan the first day of the month after hire and may contribute up to the current statutory limits under Internal Revenue Service regulations. The 401(k) plan permits usthe Company to make additional matching contributions on behalf of all employees. Through December 31, 2017, we have2021, the Company has not made any matching contributions to the 401(k) plan.
8.9. Income Taxes
U.S. Tax Reform
On December 22, 2017, legislation commonly known as the Tax Cuts and Jobs Act, or the Act, was signed in to law. The Tax Act, among other changes, reduces the U.S. federal corporate tax rate from 35% to 21%, requires taxpayers to pay a one-time transition tax on earnings of certain foreign subsidiaries that were previously tax deferred and creates new taxes on certain foreign sourced earnings. On December 31, 2017, the Company did not have any foreign subsidiaries and the international aspects of the Tax Act are not applicable.
In connection with the initial analysis of the impact of the Tax Act, the Company remeasured certain deferred tax assets and liabilities based on the rates at which they are expected to reverse in the future, which is generally 21%. The remeasurement of the Company's deferred tax balance was primarily offset by application of its valuation allowance. The Company is still in the process of analyzing the impact to the Company of the Tax Act. Where the Company has been able to make reasonable estimates of the effects for which its analysis is not yet complete, the Company has recorded provisional amounts. Where the Company has not yet been able to make reasonable estimates of the impact of certain elements, the Company has not recorded any amounts related to those elements and has continued accounting for them in accordance with ASC 740 on the basis of the tax laws in effect immediately prior to the enactment of the Tax Act.
We did not provide for income taxes in 20172021 and 20162020 because weit had a net operating loss for tax purposesbook and federal taxable losses in those years and the tax benefit that would have resulted from the statutory ratepre-tax losses was fully offset by a change in the valuation allowance.
The reconciliation of the statutory federal income tax rate to the Company’s effective tax rate for the years ended December 31, 2021 and 2020 was as follows:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Year ended December 31, |
|
|
|
|
|
|
| 2021 | 2020 |
|
|
Tax at federal statutory rate |
|
|
|
| 21.0 | % |
| 21.0 | % |
|
State tax, net of federal benefit |
|
|
|
| — |
|
| — |
|
|
Share-based compensation |
|
|
|
| 1.2 |
|
| (42.8) |
|
|
Research and development credits |
|
|
|
| 2.3 |
|
| 1.6 |
|
|
Section 162(m) limitation |
|
|
|
| (0.5) |
|
| — |
|
|
Other |
|
|
|
| (0.2) |
|
| — |
|
|
Change in valuation allowance |
|
|
|
| (23.8) |
|
| 20.2 |
|
|
Effective income tax rate |
|
|
|
| — | % |
| — | % |
|
|
|
|
|
|
|
|
|
|
|
|
Deferred tax assets and valuation allowance
Deferred tax assets reflect the tax effects of net operating loss and tax credit carryforwards and temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. We reduced ourThe Company’s deferred taxes assets at December 31, 2017 for2021 and 2020 were valued at the reduced corporate tax rate toof 21% in recently enacted tax legislations. We offset our. The Company offsets its deferred tax assets by a valuation allowance because we areit is uncertain about the timing and amount of any future profits. Significant components of ourits deferred tax assets are as follows (in thousands):
| | | | | |
|
|
|
|
|
| December 31, | December 31, |
| 2017 | | 2016 | 2021 |
| 2020 |
Deferred tax assets: | | | | | |
|
|
|
|
|
Net operating loss carryforwards | $ | 15,600 | | $ | 22,300 | $ | 24,777 |
| $ | 18,333 |
Stock-related compensation | | 5,300 | | | 9,100 | |
Research & development credit carryforwards | | 6,400 | | | 6,200 | |
Share-based compensation | |
| 2,870 |
|
| 3,230 |
Research and development credit carryforwards | |
| 7,439 |
|
| 6,687 |
Other | | 200 | | | 200 |
| 1,130 |
|
| 264 |
Total deferred tax assets | |
| 36,216 |
|
| 28,514 |
Valuation allowance | |
| (36,166) |
|
| (28,447) |
Net deferred tax assets | |
| 50 |
|
| 67 |
Deferred tax liabilities: | |
|
|
|
|
|
Property and equipment | |
| — |
|
| (5) |
Operating lease right-of-use assets | |
| (50) |
|
| (62) |
Total deferred tax liabilities | |
| (50) |
|
| (67) |
Net deferred tax asset (liability) | | $ | — |
| $ | — |
| | 27,500 | | | 37,800 |
|
|
|
|
|
Valuation allowance | | (27,500) | | | (37,800) | |
| $ | — | | $ | — | |
| | | | | | |
As of the beginning of 2017, we increased both our net operating loss carryforwards and ourThe valuation allowance increased by $0.9$7.7 million when we adopted ASU 2016-09 for certain tax deductions associated with stock option transactions greater than the stock-related compensation expense in our financial statements. 2021 due primarily to continuing operations.
The valuation allowance decreased by $10.3$1.3 million in 2017 and increased by $3.6 million in 2016. 2020 due to continuing operations.
Our pre-taxThe Company’s net operating loss carryforwards of $74$118.0 million are federal, of which $74.1 million expires between 2029and expire between 20292037 and 2036.$43.9 million carries forward indefinitely. As of December 31, 2017, we2021, the Company had federal research and development tax credits of approximately $10.7$12.4 million, which expire in the years 20232024 through 2036. 2041.
Unrecognized tax benefits
We haveAs of December 31, 2021 and 2020, the Company has unrecognized tax benefits related to tax credits. We added to ourcredits of $5.0 million and $4.5 million, respectively. None of the unrecognized tax benefits in 2017as of December 31, 2021, if recognized, would impact the effective tax rate due to the valuation allowance and 2016no interest or penalties have been recognized. A reconciliation of the beginning and ending balance of unrecognized tax benefits is as follows (in thousands):
| |
|
|
|
|
|
| | | | | |
|
|
|
|
|
| | | | | |
| Year ended December 31, |
| 2017 | | 2016 | 2021 |
| 2020 |
Beginning balance | $ | 4,200 | | $ | 4,000 | $ | 4,500 |
| $ | 4,400 |
Additions based on tax positions related to the current year | | 100 | | | 200 |
| 501 |
|
| 100 |
Ending balance | $ | 4,300 | | $ | 4,200 | $ | 5,001 |
| $ | 4,500 |
| | | | | |
|
|
|
|
|
9.As of December 31, 2021, there were no unrecognized tax benefits that we expect would change significantly over the next 12 months.
The Company files U.S. and Texas income tax returns. In the United States, the statute of limitations with respect to the federal income tax returns for tax years after 2017 are open to audit; however, since the Company has net operating losses, the taxing authority has the ability to review tax returns prior to the 2018 tax year and make adjustments to these net operating loss carryforwards. We are not under audit in any taxing jurisdiction at this time.
10. Leases and Commitments
WeRight-of-use Asset and Liability
The Company has a non-cancelable operating lease for approximately 6,000 square feet of office space pursuant to a non-cancelable operating lease in Austin, TXTexas, which is used for the development of novel products. On September 4, 2020, the Company entered into a lease amendment that extended the lease termination date to April 30, 2024 and set new rental rates effective as of January 1, 2021. The Company also has a short-term lease agreement for an additional 3,600 square feet of office space in Austin, Texas that expires in December 2020.on April 30, 2022. Future minimum lease payments are (in thousands).
| | | | | | | | | | | | |
| | | | | | | | | | | | |
| | 2018 | | 2019 | | 2020 | | Total |
Minimum lease payments | | $ | 91 | | $ | 95 | | $ | 99 | | $ | 285 |
| | | | | | | | | | | | |
|
|
|
|
|
|
|
|
|
|
| 2022 | 2023 | 2024 | Total future lease payments | Less: imputed interest |
| Total |
|
|
|
|
|
|
|
|
|
Operating leases | $ | 102 | 107 | 36 | 245 | (9) | $ | 236 |
Short-term operating lease | $ | 21 | — | — | 21 | — | $ | 21 |
We believe that our facilities are adequate and suitable for our current needs. Rent expense was $0.1 million bothfor the year ended December 31, 2021 and 2020.
There were 0 right-of-use assets exchanged for operating lease liabilities during the year ended December 31, 2021. The Company recorded a right-of-use asset and lease liability of $316,000 as a result of the lease modification in 2017September 2020. The Company utilized a discount rate of 3.25% for the modified lease to determine the present value of the future lease payments, which approximated the Company’s incremental borrowing rate in September 2020.
Cash paid for operating lease liabilities totaled $109,000 and 2016.$99,000 during the years ended December 31, 2021 and 2020, respectively.
We conduct ourOther Commitments
The Company conducts its product research and development programs through a combination of internal and collaborative programs that include, among others, arrangements with universities, contract research organizations and clinical research sites. We haveIt has contractual arrangements with these organizations however these contractsthat are cancelable on thirty days’ notice and ourgenerally cancelable. The Company’s obligations under these contracts are largely based on services performed. The Company had non-cancellable commitments for preclinical and clinical studies as well as the manufacture of simufilam totaling approximately $4.7 million at December 31, 2021.
The Company is dependent on contract development and manufacturing organizations for the manufacture of all our materials for clinical studies.
Note 11. 2020 Cash Incentive Bonus Plan
In August 2020, the Board approved the Plan. The Plan was established to promote the long-term success of the Company by creating an “at-risk” cash bonus program that rewards Plan participants with additional cash compensation in lockstep with significant increases in the Company’s market capitalization. The Plan is considered “at-risk” because Plan participants will not receive a cash bonus unless the Company’s market capitalization increases significantly and certain other conditions specified in the Plan are met. Specifically, Plan participants will not be paid any cash bonuses unless (1) the Company completes a merger or acquisition transaction that constitutes a sale of ownership of the Company or its assets (a Merger Transaction) or (2) the Compensation Committee of the Board (the Compensation Committee) determines the Company has sufficient cash on hand, as defined in the Plan. Because of the inherent discretion and uncertainty regarding these requirements, the Company has concluded that a Plan grant date has not occurred as of December 31, 2021.
Plan participants will be paid all earned cash bonuses in the event of a Merger Transaction.
The Company’s market capitalization for purposes of the Plan is determined based on either (1) the Company’s closing price of one share on the Nasdaq Capital Market multiplied by the total issued and outstanding shares and options
to purchase shares of the Company, or (2) the aggregate consideration payable to security holders of the Company in a Merger Transaction. This constitutes a market condition under applicable accounting guidance.
The Plan triggers a potential cash bonus each time the Company’s market capitalization increases significantly, up to a maximum $5 billion in market capitalization. The Plan specifies 14 incremental amounts between $200 million and $5 billion (each increment, a “Valuation Milestone”). Each Valuation Milestone triggers a potential cash bonus award in a pre-set amount defined in the Plan. Each Valuation Milestone must be achieved and maintained for no less than 20 consecutive trading days for Plan participants to be eligible for a potential cash bonus award. Approximately 58% of each cash bonus award associated with a Valuation Milestone is subject to adjustment and approval by the Compensation Committee. Any amounts not awarded by the Compensation Committee are no longer available for distribution.
If the Company were to exceed a $5 billion market capitalization for no less than 20 consecutive trading days, all Valuation Milestones would be deemed achieved, in which case cash bonus awards would range from a minimum of $139.1 million up to a hypothetical maximum of $322.3 million. Payment of cash bonuses is deferred until such time as (1) the Company completes a Merger Transaction, or (2) the Compensation Committee determines the Company has sufficient cash on hand to render payment (each, a “Performance Condition”), neither of which may ever occur. Accordingly, there can be no assurance that Plan participants will ever be paid a cash bonus that is awarded under the Plan, even if the Company’s market capitalization increases significantly.
The Plan is accounted for as a liability award. The fair value of each Valuation Milestone award will be determined once a grant date occurs and will be remeasured each reporting period. Compensation expense associated with the Plan will be recognized over the expected achievement period for each of the 14 Valuation Milestones, when a Performance Condition is considered probable of being met.
In October 2020, the Company achieved the first Valuation Milestone. Subsequently, the Compensation Committee approved a potential cash bonus award of $7.3 million in total for all Plan participants, subject to future satisfaction of a Performance Condition.
During the year ended December 31, 2021, the Company achieved 11 additional Valuation Milestones triggering potential Company obligations to all Plan participants from a minimum of $93.7 million up to a hypothetical maximum of $225.0 million, to be determined by the Compensation Committee and contingent upon future satisfaction of a Performance Condition. However, no compensation expense has been recorded since no grant date has occurred and no Performance Conditions are considered probable of being met. There is no continuing service requirement for Plan participants once the Compensation Committee approves a cash bonus award.
NaN actual cash payments were authorized or made to participants under the Plan through December 31, 2021.
12. Contingencies
Securities Class Actions and Shareholder Derivative Action
Between August 27 and October 26, 2021, four putative class action lawsuits were filed alleging violations of the federal securities laws by the Company and certain named officers. The complaints rely on allegations contained in two Citizen Petitions submitted to FDA, and allege that various statements made by the defendants regarding simufilam were rendered materially false and misleading. The two Citizen Petitions were subsequently denied by FDA. These actions were filed in the U.S. District Court for the Western District of Texas. The complaints seek unspecified compensatory damages and other relief on behalf of a purported class of purchasers of the Company’s securities between September 14, 2020, and August 27, 2021. The Company expects that the cases will be consolidated and that a lead plaintiff and lead counsel will be appointed and thereafter that a consolidated amended complaint will be filed. The Company believes the lawsuit claims are without merit and intends to defend against these lawsuits vigorously. The Company is unable to estimate the possible loss or range of loss, if any, associated with these lawsuits.
On November 4, 2021, a related shareholder derivative action was filed, purportedly on behalf of the Company, in the U.S. District Court for the Western District of Texas, asserting claims under the U.S. securities laws and state fiduciary
duty laws against certain named officers and the members of the Company’s board of directors. The complaint relies on the allegations made in two Citizen Petitions that were submitted to FDA. The two Citizen Petitions, which were subsequently denied by FDA, allege, among other things, that the individual defendants exposed the Company to unspecified damages and securities law liability by causing it to make materially false and misleading statements, in violation of the U.S. securities laws and in breach of their fiduciary duties to the Company. The derivative case seeks, among other things, to recover unspecified compensatory damages on behalf of the Company arising out of the individual defendant’s alleged wrongful conduct. Although the plaintiffs in the derivative cases does not seek relief against the Company, it has certain indemnification obligations to the individual defendants. Since November 4, 2021, three additional shareholder derivative actions were filed alleging substantially similar claims, two in the U.S. District Court for the Western District of Texas, and one in Texas state court (Travis County District Court). The state court action has been stayed pending the resolution of the motions to dismiss in the securities class actions. The parties to the three federal court actions have filed a motion, which the court has not yet ruled on, to consolidate and stay pending the resolution of motions to dismiss in the securities class actions. The Company is unable to estimate the possible loss or range of loss, if any, associated with these lawsuits.
Item 9.Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None.
Item 9A.Controls and Procedures
Evaluation of disclosure controls and procedures.
Our management, with the participation of our Chief Executive Officer and our Chief Financial Officer, evaluated the effectiveness of our disclosure controls and procedures as of the end of the period covered by this Annual Report on Form 10-K. Based on this evaluation, our Chief Executive Officer (as Principle Executiveand our Chief Financial Officer and Principal Financial Officer)hashave concluded that our disclosure controls and procedures arewere effective to ensure that information we are required to disclose in reports that we file or submit under the Securities Exchange Act of 1934, as amended, is recorded, processed, summarized and reported within the time periods specified in the Securities and Exchange Commission, or SEC, rules and forms and that such information is accumulated and communicated to management as appropriate to allow timely decisions regarding required disclosures.
Management’s annual report on internal control over financial reporting. We are Our management is responsible for establishing and maintaining adequate internal control over our financial reporting. We haveOur management has assessed the effectiveness of internal control over financial reporting as of December 31, 2017.2021. Our assessment was based on criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission, or COSO, in Internal Control-Integrated Framework (2013 Framework).
Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of consolidated financial statements for external purposes in accordance with generally accepted accounting principles. Our internal control over financial reporting includes those policies and procedures that:
| (1)
| | pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect our transactions and dispositions of our assets;
|
| (2)
| | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and board of directors; and
|
| (3)
| | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of our assets that could have a material effect on the financial statements.
|
(1)pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect our transactions and dispositions of our assets;
(2)provide reasonable assurance that transactions are recorded as necessary to permit preparation of consolidated financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and board of directors; and
(3)provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of our assets that could have a material effect on the consolidated financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Based on the COSO criteria, we believe our internal control over financial reporting as of December 31, 20172021 was effective.
Changes in internal control over financial reporting.
As previously announced,There was no change in our internal control over financial reporting that occurred during the quarter ended December 31, 2021 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
The effectiveness of our internal control over financial reporting as of December 31, 2021 has been audited by Ernst & Young LLP, an independent registered public accounting firm, as stated in their report which is included herein.
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Cassava Sciences, Inc.
Opinion on Internal Control Over Financial Reporting
We have audited Cassava Sciences, Inc.’s internal control over financial reporting as of December 31, 2021, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (the COSO criteria). In our opinion, Cassava Sciences, Inc. (the Company) maintained, in all material respects, effective internal control over financial reporting as of December 31, 2021, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the consolidated balance sheets of Cassava Sciences, Inc. (the Company) as of December 31, 2021 and 2020, the related consolidated statements of operations, stockholders' equity and cash flows for each of the two years in the period ended December 31, 2021, and the related notes and our report dated February 14, 2017, Peter S. Roddy resigned,28, 2022 expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective March 9, 2017,internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management's Annual Report on Internal Controls over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects.
Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as Vice President, Chiefwe considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial OfficerReporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and Secretary. Remi Barbier, Presidentthe preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and Chief Executive Officer, has assumedprocedures that (1) pertain to the rolemaintenance of Principal Financial Officer until such timerecords that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a new Chief Financial Officer is appointed.material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ Ernst & Young LLP
Austin, Texas
February 28, 2022
Item 9B.Other Information
None.
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspection
PART III
Item 10.Directors and Executive Officers and Corporate Governance
The information regarding our directors, executive officers, director nomination process and the audit committee of our board of directorsthe Board is incorporated by reference from "Directors and Executive Officers" in our Proxy Statement for our 20182022 Annual Meeting of Stockholders.
Section 16(a) Beneficial Ownership Reporting Compliance
Section 16(a) of the Securities Exchange Act of 1934, as amended requires our executive officers and directors and persons who own more than ten percent (10%) of a registered class of our equity securities to file reports of ownership and changes in ownership with the SEC. Executive officers, directors and greater than ten percent (10%) stockholders are required to furnish us with copies of all Section 16(a) forms they file. We believe all of our executive officers and directors complied with all applicable filing requirements during 2017.2021.
Code of Ethics
We have adopted a Code of Ethics that applies to all of our directors, officers and employees, including our principal executive officer principal financial officer and principal accountingfinancial officer. We publicize the Code of Ethics through posting the policy on our website, http://www.paintrials.com.www.cassavasciences.com. We will disclose on our website any waivers of, or amendments to, our Code of Ethics.
Item 11.Executive Compensation
The information required by this Item is incorporated by reference from our definitive Proxy Statement referred to in Item 10 above where it appears under the heading "Executive Compensation and Other Matters."
Item 12.Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required by this Item regarding security ownership of certain beneficial owners and management is incorporated by reference from our definitive Proxy Statement referred to in Item 10 above where it appears under the heading "Security Ownership of Certain Beneficial Owners and Management."
The following table summarizes the securities authorized for issuance under our equity compensation plans as of December 31, 2017:2021:
| | | | | | | |
|
|
|
|
|
|
|
|
| | Number of
Securities to be
Issued Upon
Exercise of
Outstanding
Options, Warrants
and Rights | | | Weighted Average
Exercise Price of
Outstanding
Options,
Warrants
and Rights | | Number of Securities
Remaining Available
for Future Issuance
Under Equity
Compensation
Plans |
| Number of
Securities to be
Issued Upon
Exercise of
Outstanding
Options, Warrants
and Rights |
|
| Weighted Average
Exercise Price of
Outstanding
Options,
Warrants
and Rights |
| Number of Securities
Remaining Available
for Future Issuance
Under Equity
Compensation
Plans |
|
Equity compensation plans approved by stockholders | | 3,134,495 | | $ | 15.92 | | 58,017 |
| 2,801,782 | (1) | $ | 10.99 | (2) | 210,205 | (3) |
Equity compensation plans not approved by stockholders | | — | | | — | | — |
| — |
|
| — |
| — |
|
| | 3,134,495 | | $ | 15.92 | | 58,017 |
| 2,801,782 |
| $ | 10.99 |
| 210,205 |
|
| | | | | | | |
|
|
|
|
|
|
|
|
(1)Includes outstanding stock options and awards for 1,976,885 shares of our common stock under the 2008 Plan and 824,897 shares of our common stock under the 2018 Plan.
(2)Includes the weighted average stock price for outstanding stock options of $12.18 under the 2008 Plan and $10.16 for the 2018 Plan.
(3)Represents 152,188 shares of our common stock for the 2018 Plan and 58,017 for the Employee Stock Purchase Plan. No future awards shall occur under the 2008 Plan.
Item 13.Certain Relationships and Related Transactions and Director Independence
The information required by this Item is incorporated by reference from our definitive Proxy Statement referred to in Item 10 above where it appears under the heading "Certain Relationships and Related Transactions."
Item 14.Principal Accountant Fees and Services
The information required by this Item is incorporated by reference from our definitive Proxy Statement referred to in Item 10 above where it appears under the heading “Principal Accountant Fees and Services.”
PART IV
Item 15.Exhibits and Financial Statement Schedules
(a)The following documents are filed as part of this Form 10-K:
(1)Consolidated Financial Statements (included in Part II of this report):
Report of Independent Registered Public Accounting Firm
Consolidated Balance Sheets
Consolidated Statements of Operations
Statements of Comprehensive Income
Consolidated Statements of Stockholders' Equity
Consolidated Statements of Cash Flows
Notes to Consolidated Financial Statements
(2)Consolidated Financial Statement Schedules:
All consolidated financial statement schedules are omitted because the information is inapplicable or presented in the notes to the consolidated financial statements.
(3)Management Contracts, Compensatory Plans and Arrangements.
Management contracts, compensatory plans and arrangements are indicated by the symbol “*” in the applicable exhibits listed in Item 15(b), below.
(b)Exhibits
The exhibits listed below are filed as part of this Form 10-K other than Exhibit 32.1, which shall be deemed furnished.
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | Incorporated by Reference | | |
Exhibit
No. | | Description | | Form | | Filing
Date | | Exhibit
No. | | Filed
Herewith |
3.1 | | | Amended and Restated Certificate of Incorporation. | | 10-Q | | 7/29/2005 | | 3.1 | | |
3.2 | | | Amended and Restated Bylaws. | | 10-Q | | 4/24/2013 | | 3.2 | | |
3.3 | | | Amended and Restated Certificate of Incorporation | | 8-K | | 5/8/2017 | | 3.1 | | |
4.1 | | | Specimen Common Stock Certificate. | | 10-Q | | 7/29/2005 | | 4.1 | | |
10.1 | * | | Form of Indemnification Agreement between Pain Therapeutics and each of its directors and officers. | | S-1 | | 3/14/2000 | | 10.1 | | |
10.3 | * | | Employment Agreement dated October 23, 2001, between Registrant and Nadav Friedmann, PhD. M.D. | | 10-K | | 3/22/2002 | | 10.5 | | |
10.4 | + | | Development and License Agreement dated December 19, 2002 between Registrant and DURECT Corporation and Southern Biosystems, Inc. | | 10-K | | 2/24/2006 | | 10.10 | | |
10.5 | + | | Amendment dated December 15, 2005 to Development and License Agreement dated December 19, 2002 between Registrant and DURECT Corporation and Southern Biosystems, Inc. | | 10-K | | 2/24/2006 | | 10.11 | | |
10.11 | * | | Employment Agreement dated July 1, 1998 and amended December 17, 2008 between Registrant and Remi Barbier. | | 10-K | | 2/13/2009 | | 10.12 | | |
10.12 | * | | 2000 Employee Stock Purchase Plan, as amended and restated. | | 10-Q | | 7/29/2010 | | 10.1 | | |
10.13 | | | Lease agreement, dated as of February 14, 2011 between Registrant and StoneCliff Office, L.P. | | 10-Q | | 4/27/2011 | | 10.1 | | |
10.14 | * | | Amendment Number 1 to the 2008 Equity Incentive Plan. | | 10-Q | | 8/1/2013 | | 10.1 | | |
10.15 | * | | Amendment No. 2 to Employment Agreement between Registrant and Remi Barbier. | | 10-Q | | 8/1/2013 | | 10.2 | | |
10.16 | | | Second Amendment to Lease Agreement, dated as of April 8, 2014 between Registrant and StoneCliff Office, L.P. | | 10-Q | | 8/6/2014 | | 10.1 | | |
10.17 | | | Third Amendment to Lease Agreement, dated as of November 3, 2017 between Registrant US REIF Eurus Austin, LLC dba StoneCliff Building as successor in interest to StoneCliff Office, L.P. | | | | | | | | X |
23.1 | | | Consent of Independent Registered Public Accounting Firm. | | | | | | | | X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Incorporated by Reference |
|
|
Exhibit
No. |
| Description |
| Form |
| Filing
Date |
| Exhibit
No. |
| Filed
Herewith |
3.1 |
|
| Amended and Restated Certificate of Incorporation. |
| 10-Q |
| 7/29/2005 |
| 3.1 |
|
|
3.2 |
|
| Certificate of Amendment of Restated Certificate of Incorporation. |
| 8-K |
| 5/8/2017 |
| 3.1 |
|
|
3.3 |
|
| Certificate of Amendment of Restated Certificate of Incorporation. |
| 10-K |
| 3/29/2019 |
| 3.3 |
|
|
3.4 |
|
| Amended and Restated Bylaws of Cassava Sciences, Inc. |
| 8-K |
| 12/11/2020 |
| 3.1 |
|
|
4.1 |
|
| Specimen Common Stock Certificate. |
| 10-Q |
| 8/12/2019 |
| 4.1 |
|
|
4.2 |
|
| Description of Registrant’s Securities. |
| 10-K |
| 3/26/2020 |
| 4.2 |
|
|
10.2 | * |
| Employment Agreement, dated October 23, 2001, between Registrant and Nadav Friedmann, PhD. M.D. |
| 10-K |
| 3/22/2002 |
| 10.5 |
|
|
10.5 | * |
| Employment Agreement, dated July 1, 1998 and amended December 17, 2008, between Registrant and Remi Barbier. |
| 10-K |
| 2/13/2009 |
| 10.12 |
|
|
10.6 | * |
| 2000 Employee Stock Purchase Plan, as amended and restated. |
| 10-Q |
| 7/29/2010 |
| 10.1 |
|
|
10.7 | * |
| 2008 Equity Incentive Plan. |
| 8-K |
| 5/29/2008 |
| 10.1 |
|
|
10.8 | * |
| Amendment Number 1 to the 2008 Equity Incentive Plan. |
| 10-Q |
| 8/1/2013 |
| 10.1 |
|
|
10.9 | * |
| Amendment No. 2 to Employment Agreement between Registrant and Remi Barbier. |
| 10-Q |
| 8/1/2013 |
| 10.2 |
|
|
10.10 |
|
| Lease Agreement, dated as of February 14, 2011 between Registrant and StoneCliff Office, L.P. |
| 10-Q |
| 4/27/2011 |
| 10.1 |
|
|
10.11 | * |
| First Amendment to Lease Agreement, dated September 21, 2011. |
| 10-K |
| 2/9/2012 |
| 10.20 |
|
|
10.12 |
|
| Second Amendment to Lease Agreement, dated as of April 3, 2014 between Registrant and StoneCliff Office, L.P. |
| 10-Q |
| 8/6/2014 |
| 10.1 |
|
|
10.13 |
|
| Third Amendment to Lease Agreement, dated as of November 3, 2017 between Registrant US REIF Eurus Austin, LLC dba StoneCliff Building as successor in interest to StoneCliff Office, L.P. |
| 10-K |
| 2/6/2018 |
| 10.17 |
|
|
10.14 |
|
| Fourth Amendment to Lease Agreement, dated September 4, 2020 between Registrant US REIF Eurus Austin, LLC dba StoneCliff Building as successor in interest to StoneCliff Office, L.P. |
| 8-K |
| 9/10/2020 |
| 10.1 |
|
|
10.15 | * |
| 2018 Omnibus Incentive Plan. |
| 8-K |
| 5/11/2018 |
| 10.1 |
|
|
10.16 |
|
| Sales Agreement, Dated March 27, 2020, between Registrant and SVB Leerink LLC. |
| S-3 |
| 3/27/2020 |
| 1.1 |
|
|
10.17 | * |
| Cassava Sciences, Inc. 2020 Cash Incentive Bonus Plan |
| 8-K |
| 9/1/2020 |
| 10.1 |
|
|
10.18 | * |
| Employment Agreement, executed on October 9, 2018, by and between Registrant and Eric Schoen. |
| 8-K |
| 10/11/2018 |
| 10.1 |
|
|
10.19 | * |
| Employment Agreement, executed on January 1, 2020, by and between Registrant and Dr. James Kupiec. |
| 8-K |
| 1/6/2021 |
| 10.1 |
|
|
10.20 |
|
| Form of Securities Purchase Agreement, dated February 10, 2021, by and between Cassava Sciences, Inc. and the purchasers named therein. |
| 8-K |
| 2/12/2021 |
| 10.1 |
|
|
10.21+ |
|
| Master Services Agreement between Cassava Sciences, Inc. and Evonik Corporation, dated February 22, 2021. |
| 8-K |
| 3/11/2021 |
| 10.1 |
|
|
10.22+ |
|
| Master Services Agreement between Cassava Sciences, Inc. and Premier Research International LLC, dated June 11, 2021 |
| 10-Q |
| 8/4/2021 |
| 10.3 |
|
|
10.23+ |
|
| Agreement of Sale and Purchase Between DWF IV Lakewood, LP and Cassava Sciences, Inc. dated July 2, 2021 |
| 10-Q |
| 11/15/2021 |
| 10.4 |
|
|
10.1 | * |
| Form of Indemnification Agreement between Registrant and each of its directors and officers. |
|
|
|
|
|
|
| X |
21.1 |
|
| Subsidiaries of the Registrant. |
|
|
|
|
|
|
| X |
23.1 |
|
| Consent of Independent Registered Public Accounting Firm. |
|
|
|
|
|
|
| X |
31.1 |
|
| Certification of Principal Executive Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. |
|
|
|
|
|
|
| X |
31.2 |
|
| Certification of Principal Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. |
|
|
|
|
|
|
| X |
32.1 |
|
| Certifications of the Chief Executive Officer and the Chief Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. |
|
|
|
|
|
|
| X |
101.INS |
|
| XBRL Instance Document. |
|
|
|
|
|
|
| X |
101.SCH |
|
| XBRL Taxonomy Extension Schema Document. |
|
|
|
|
|
|
| X |
101.CAL |
|
| XBRL Taxonomy Extension Calculation Linkbase Document. |
|
|
|
|
|
|
| X |
101.DEF |
|
| XBRL Taxonomy Extension Definition Linkbase Document. |
|
|
|
|
|
|
| X |
101.LAB |
|
| XBRL Taxonomy Extension Labels Linkbase Document. |
|
|
|
|
|
|
| X |
101.PRE |
|
| XBRL Taxonomy Extension Presentation Linkbase Document. |
|
|
|
|
|
|
| X |
104 |
|
| The cover page from the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2021, formatted in Inline XBRL (included in Exhibit 101). |
|
|
|
|
|
|
| X |
* Management contract, compensatory plan or arrangement. +Confidential portions of this document have been redacted as permitted by applicable regulations. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(c)Consolidated Financial Statement Schedules
All consolidated financial statement schedules are omitted because the information is inapplicable or presented in the notes to the consolidated financial statements.
Item 16.Form 10-K Summary
The Company has elected not to includedinclude summary information.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
(Principal Executive |
|
|
| Pain Therapeutics,Cassava Sciences, Inc.
|
|
| (Registrant) |
|
|
| /s/ REMI BARBIER |
|
| Remi Barbier, |
| Chairman of the Board of Directors, |
| President and Chief Executive Officer |
|
|
Dated: February 6, 201828, 2022
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Remi Barbier his true and lawful attorneys-in-fact, with full power of substitution, for him in any and all capacities, to sign any amendments to this Annual Report on Form 10-K and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-in-fact or their substitute or substitutes may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
|
|
|
|
|
|
|
|
|
Signature |
| Title |
| Date |
|
|
|
|
|
/s/ REMI BARBIER |
| President, Chief Executive Officer and |
| February 6, 201828, 2022 |
Remi Barbier |
| Chairman of the Board of Directors |
|
|
|
| (Principal Executive Officer and Principal Financial Officer) |
|
|
|
|
|
|
|
/s/ ERIC J. SCHOEN |
| Chief Financial Officer |
| February 28, 2022 |
Eric J. Schoen |
| (Principal Financial Officer) |
|
|
|
|
|
|
|
/s/ NADAV FRIEDMANN, PH.D., M.D. |
| Chief Operating and Medical Officer |
| February 6, 201828, 2022 |
Nadav Friedmann, Ph.D., M.D. |
| and Director |
|
|
|
|
|
|
|
/s/ RICHARD J. BARRY |
| Director |
| February 28, 2022 |
Richard J. Barry |
|
|
|
|
|
|
|
|
|
/s/ ROBERT Z. GUSSIN, PH.D. |
| Director |
| February 6, 201828, 2022 |
Robert Z. Gussin, Ph.D. |
|
|
|
|
|
|
|
|
|
/s/ MICHAEL J. O'DONNELL, ESQ. |
| Director |
| February 6, 201828, 2022 |
Michael J. O'Donnell, Esq. |
|
|
|
|
|
|
|
|
|
/s/ SAIRA RAMASASTRY
| | Director
| | February 6, 2018
|
Saira Ramasastry
| | | | |
| | | | |
/s/ SANFORD R. ROBERTSON |
| Director |
| February 6, 201828, 2022 |
Sanford R. Robertson |
|
|
|
|
|
|
|
|
|
/s/ PATRICK SCANNON, M.D,M.D., PH.D. |
| Director |
| February 6, 201828, 2022 |
Patrick Scannon, M.D., Ph.D. |
|
|
|
|
|
|
|
|
|