NOTE REGARDING FORWARD-LOOKING STATEMENTS Unless the context requires otherwise, in this Annual Report on Form 10-K10‑K the terms “Ardelyx”, “we,” “us,” “our” and “the Company” refer to Ardelyx, Inc. This Annual Report on Form 10-K10‑K contains forward-looking statements that involve risks and uncertainties. Any statements contained herein that are not statements of historical facts may be deemed to be forward-looking statements. In some cases, you can identify forward-looking statements by terminology such as “aim,” “anticipate,” “assume,” “believe,” “continue,” “could,” “due,” “estimate,” “expect,” “goal,” “intend,” “may,” “objective,” “plan,” “predict,” “potential,” “positioned,” “seek,” “should,” “target,” “will,” “would,” and other similar expressions that are predictions of or indicate future events and future trends, or the negative of these terms or other comparable terminology. These forward-looking statements include, but are not limited to, statements about: | · | | our expectation regarding the timing of our filing of a New Drug Application with the U.S.Federal Food and Drug Administration requesting approval to market tenapanor for patients with irritable bowel syndrome with constipation, or IBS-C; |
| · | | our expectation regarding the timing of receipt of results from our second Phase 3 clinical trial evaluating tenapanor for the treatment of hyperphosphatemia in patients with end-stage renal disease, or ESRD, on dialysis; |
| · | | our expectations regarding our plans for and our participation in the commercialization of tenapanor for the treatment of hyperphosphatemia in ESRD patients on dialysis, including our expectations regarding our plans to build our own sales and marketing organization to market and sell tenapanor for such indication; |
| · | | our plans to seek one or more collaboration partners to commercialize tenapanor for IBS-C; |
| · | | our expectations regarding the potential market size and the size of the patient populations for our product candidates; |
| · | | our plans with respect to our pre-clinical programs; |
| · | | our ability to identify and validate targets and novel drug candidates using our proprietary drug discovery and design platform including the Ardelyx Primary Enterocyte and Colonocyte Culture System; |
| · | | the implementation of our business model and strategic plans for our business, product candidates and technology; |
| · | | estimates of our expenses, future revenue, capital requirements, our needs for additional financing and our ability to obtain additional capital; |
| · | | our expectations regarding the time during which we will be an emerging growth company under the Jumpstart Our Business Startups Act of 2012; |
| · | | our financial performance; and |
| · | | the timing of receipt of results for the Phase 3 clinical trials evaluating tenapanor in patients with IBS-C;
the timing of the receipt of results for a Phase 2b clinical trial evaluating tenapanor for the treatment of hyperphosphatemia in ESRD patients;
the possibility that we may seek approval from the FDA to consider the tenapanor Phase 2b hyperphosphatemia clinical study as the first of two well-controlled studies;
the timing of the initiation of a Phase 3 clinical program for RDX022;
our expectation regarding the availability of the 505(b)(2) regulatory pathway for RDX022;
the timing of the filing of an IND for RDX009;
our expectations regarding our plans for and our participation in the commercialization of our products candidates;
our expectations regarding the potential market size and the size of the patient populations for our product candidates, if approved for commercial use;
our plans with respect to our pre-clinical programs;
our ability to identify and validate targets and novel drug candidates using our proprietary drug discovery and design platform including APECCS;
our ability to develop, acquire and advance product candidates into, and successfully complete, clinical trials;
the timing or likelihood of regulatory filings, approvals and commercialization for our product candidates, including tenapanor and RDX022;
the implementation of our business model and strategic plans for our business, product candidates and technology;
estimates of our expenses, future revenue, capital requirements, our needs for additional financing and our ability to obtain additional capital;
our expectations regarding the time during which we will be an emerging growth company under the Jumpstart Our Business Startups Act of 2012, JOBS Act;
our financial performance; and
developments and projections relating to our competitors and our industry. |
Factors that could cause actual results or conditions to differ from those anticipated by these and other forward-looking statements include those more fully described in the “ITEM“ITEM 1A. RISK FACTORS”FACTORS” section and elsewhere in this Annual Report on Form 10-K.10‑K. Except as required by law, we assume no obligation to update any forward-looking statement publicly, or to revise any forward-looking statement to reflect events or developments occurring after the date of this Annual Report on Form 10-K,10‑K, even if new information becomes available in the future. Thus, you should not assume that our silence over time means that actual events are bearing out as expressed or implied in any such forward-looking statement. ITEM 1. BUSINESS COMPANY OVERVIEWCompany overview
We are a clinical-stagespecialized biopharmaceutical company focused on developing first-in-class, disruptive medicines for the discovery, developmenttreatment of renal diseases. Our primary therapeutic focus is on treating people with renal diseases, which affect both the heart and commercialization of innovative, minimally-systemic therapeutic drugs that work exclusively in the gastrointestinal, or GI, tract to treat GI and cardio-renal diseases. We have developed a proprietary drug discovery and design platform enabling us, in a rapid and cost-efficient manner, to discover and design novel drug candidates. Utilizing our platform, we discovered and designed our lead product candidate, tenapanor, which is currently being evaluated in two pivotal Phase 3 clinical studies in patients with constipation-predominant irritable bowel syndrome, or IBS-C. In a Phase 2b clinical study, tenapanor demonstrated the ability to improve the symptoms of IBS-C. In a separate Phase 2b clinical trial, tenapanor demonstrated the ability to lower elevated serum phosphorus levels inkidneys. This includes patients with end-stage renal disease, or ESRD.ESRD, who suffer from elevated serum phosphorus, or hyperphosphatemia; patients with chronic kidney disease, or CKD, and/or heart failure patients with elevated serum potassium, or hyperkalemia. We have initiated an additionalalso developed a number of programs directed toward treating gastrointestinal, or GI, disorders, including the treatment of irritable bowel syndrome with constipation, or IBS-C. Our portfolio is led by the development of tenapanor, a first-in-class inhibitor of NHE3. In our renal pipeline, tenapanor is being evaluated in a second Phase 2b clinical3 trial for the treatment of hyperphosphatemia in patients with ESRD who are on dialysis. This registration trial follows a successful first Phase 3 trial completed in 2017, which achieved statistical significance for the primary endpoint. We are also advancing a small molecule potassium secretagogue program, RDX013, for the potential treatment of hyperkalemia. We believe that both tenapanor and RDX013 have the potential to evaluate dosing regimensprovide treatment options that are differentiated significantly from binders, the current standards of care in both of these markets. We believe our small molecule approach to treating these conditions could significantly reduce the pill burden for patients, leading to higher compliance, and offer completely new mechanisms of action that interact with receptors in the gut, potentially allowing improved efficacy in some patients. In addition to the development for renal diseases, we have developed tenapanor for the treatment of hyperphosphatemia,patients with IBS-C. In 2017, we completed the T3MPO program for this indication, including two Phase 3 studies, both of which achieved statistical significance for the primary endpoint, and a long-term safety extension study. We believe that data from the T3MPO program collectively demonstrated the ability of tenapanor to provide sustained relief of constipation and reduced abdominal pain with a generally favorable tolerability profile. Based on the results of the T3MPO clinical program in IBS-C, we are preparing to submit our first New Drug Application, or elevated serum phosphorus, in ESRD patients,NDA, to the United States Food and we expect to receive results from this trialDrug Administration, or FDA, in the second half of 2016. We are developing another drug candidate, RDX022,2018 for tenapanor for the treatment of hyperkalemia, or elevated serum potassium. In January 2016, we announced the results of an open label clinical study evaluating the pharmacodynamic activity of RDX022 in healthy adult volunteers. The study demonstratedIBS-C. Our Commercial Strategy We aim to build a multi-product company that RDX022 was generally well-tolerated at all doses evaluated and effectively binds to potassium in the GI tract, supporting our plans to proceed with a Phase 3 clinical program, which we currently expect to initiate in the second half of 2016. We are pursuing a 505(b)(2) regulatory pathway for RDX022. We have additional drug candidates in earlier stages of research and development focused in GI and cardio-renal diseases including RDX009, a secretagogue of glucagon-like peptide-1, or GLP-1, and glucagon-like peptide-2, or GLP-2, and RDX013, a potassium secretagogue. We currently expect to file an investigational new drug application, or IND, for RDX009 in the second half of 2016. Tenapanor is a minimally-systemic small molecule that acts locally in the GI tract to inhibit the sodium transporter NHE3 and reduce sodium and phosphorus uptake from the gut. In human studies of orally- administered tenapanor, the drug was detected in the blood in only 0.7% of more than 3,000 collected serum samples, and even in those, at very low levels (< 1.5 ng/mL). We have evaluated tenapanor in fourteen human clinical studies in over 1,000 individuals to date. We are currently evaluating tenapanor in two different programs:
| • | | IBS-C: In the fourth quarter 2015, we initiated two pivotal Phase 3 clinical trials evaluating tenapanor in patients with IBS-C, and we currently expect results from those trials in 2017. In a Phase 2b clinical study, tenapanor demonstrated the ability to improve symptoms of IBS-C. In that study, the twice daily 50 mg dose of tenapanor met the primary efficacy endpoint of an increase in the complete spontaneous bowel movement (CSBM) responder rate. Most secondary endpoints, including abdominal pain, the overall responder rate and other abdominal and IBS-C symptoms, demonstrated statistically significant and clinically meaningful improvements. |
| • | | Hyperphosphatemia in ESRD patients: In the fourth quarter 2015, we initiated a second Phase 2b clinical study to evaluate the optimal dosing regimen for tenapanor for the treatment of hyperphosphatemia in ESRD patients, and we expect results from this trial in the second half of 2016. We have designed the clinical trial and the statistical analysis plan so that, assuming positive results, there is the potential that the FDA may agree that this trial could be considered the first of two well-controlled studies to support an NDA for our hyperphosphatemia indication. Results from the first Phase 2b clinical study in this indication were announced in 2015. In that study, there was a statistically significant dose-related decrease in serum phosphate levels for tenapanor-treated patients compared to patients receiving placebo (p=0.012). It was noted, however, that the rate of diarrhea and the rate of discontinuations due to diarrhea were higher than expected based on previous clinical trials. Higher discontinuations rates due to diarrhea were observed primarily in the 30 mg once daily and 30 mg twice daily dose groups. The overall safety profile remained consistent with that observed in previous tenapanor trials. |
We believe the market opportunity for tenapanor for these two potential patient populations may be significant. Based on reports in the literature regarding the prevalence of IBS in the U.S. population and the percentage of individuals who have IBS-C as compared to other forms of IBS, we believe that 1.4% of the U.S. population, or approximately 4.4 million individualscommercializes its renal products in the United States haveStates. Our strategy is to leverage ex-U.S. collaborations with established industry leaders to efficiently bring our renal medicines to patients outside the United States. Additionally, our goal is to bring tenapanor for IBS-C to market by leveraging domestic and ex-U.S. collaborations.
In November 2017, we entered into a license agreement that approximately 1.0 million of those patients have been diagnosedprovides Kyowa Hakko Kirin Co., Ltd., or KHK, with IBS-C. Additionally, we estimate that there are about 6.6 million IBS-C patients in Europeexclusive rights to develop and about 3.4 million in Japan. We are developing RDX022commercialize tenapanor for the treatment of hyperkalemia. RDX022 is our proprietary oral, non-absorbed potassium-binder. It iscardiorenal diseases, including hyperphosphatemia, in Japan. Under the terms of the license agreement, we received a $30 million upfront payment and are eligible to receive up to $130 million in development and commercialization milestones based on polystyrene sulfonate, a well-known and well-characterized polymer, used to treat hyperkalemia. We have made numerous improvements toupon currency exchange rates as of the polymer by engineering into RDX022 several key physical and chemical modifications in an effort to improve various properties. We also changedeffective date of the counter-ion from sodium to calcium to be more consistent with standard of care in these patients. We have filed a patent application covering the composition of matter for these modifications. Data from the literaturelicense agreement, as well as independent market research suggests that hyperkalemia affects about 900,000 individualshigh-teen royalties on net sales throughout the term of the agreement.
In December 2017, we entered into a license agreement with CKD Stage 3bShanghai Fosun Pharmaceutical Industrial Development Co. Ltd., or Stage 4, about 900,000Fosun Pharma, providing Fosun Pharma with the exclusive rights to develop and commercialize tenapanor in China for the treatment of patients with HFhyperphosphatemia related to CKD and about 200,000 patients with ESRD. In January 2016,IBS-C. Under the terms of the agreement, we announced resultsreceived an upfront payment of $12 million and are eligible to receive additional milestones of up to $113 million, as well as tiered royalties on net sales ranging from an open-label pharmacodynamic study of RDX022 in healthy adult volunteers. In this study, RDX022 was administered at 4.6 g BID (9.2 g/day), 6.9 g BID (13.8 g/day), 4.6 g TID (13.8 g/day) and 9.2 g TID (27.5 g/day), and resulted in a mean increase of fecal potassium from baseline of 888 mg/day, 1,791 mg/day, 1,408 mg/day, and 1,670 mg/day, respectively. RDX022 was generally well-tolerated at all doses and demonstrated comparable resultsthe mid-teens to those observed with sodium polystyrene sulfonate. Other fecal electrolytes were monitored during the study and no unexpected changes were observed; in particular, fecal magnesium remained unchanged from baseline. We currently expect to begin a Phase 3 clinical study with RDX022 in the second half of 2016.20%. Utilizing our proprietary drug discovery and design platform, we are pursuing other internal discovery and lead-development programs that are currently in the research phase.
RDX009 Program: Our focus is the discovery and development of minimally-systemic TGR5 agonists that stimulate GLP-1 and GLP-2 secretion. We are evaluating RDX009 in animal models for its effect in multiple indications. In December 2015, we declared a development candidate for RDX009 and currently expect to file an IND for RDX009 in the second half of 2016.
RDX013 Program: We are continuing to research RDX013, a small molecule drug candidate for hyperkalemia. This agent, a potential potassium secretagogue, is intended to enhance potassium secretion or prevent potassium absorption with a much lower pill burden than potassium binders and may provide significant advantages as a stand-alone agent or used in combination with potassium binders, including RDX022.
RDX011 Program: We intend to leverage our knowledge of NHE3 inhibitors and their effect on phosphate management as we seek to further understand tenapanor’s phosphate lowering mechanism of action. We also intend to evaluate new indications for tenapanor and other NHE3 inhibitors in order to exploit the unique capabilities and tools we have developed to modulate ion transport channels located on mucosal surfaces.
OUR PROPRIETARY DRUG DISCOVERY AND DESIGN PLATFORM Our platform, comprised of proprietary know-howIn line with our overall strategy and drug discovery and design tools, provides us with a competitive advantage in drug development. This platform enables us, in a rapid and cost-efficient manner,transition to discover and design novel drug candidates that work exclusively in the GI tract to treat GI and cardio-renal diseases. By targeting receptors and transporters localized in the GI tract, we can modulate certain important functions of the gut, such as absorption of specific nutrients and minerals, or the gut’s various hormonal functions, to treat and prevent diseases while avoiding systemic toxicities.
The pillars offocus solely on our drug discovery and design platform include the following:
Medicinal Chemistry to develop minimally-systemic products: our medicinal chemistry team has developed the tools, expertise and approach to ensure that our small molecule drug candidates are potent, have appropriate drug properties, are able to be readily manufactured, and are minimally- systemic, a property that we believe is not generally targeted for most other drug programs;
| • | | In vivopharmacology: Ourin vivopharmacology group has developed animal models and expertise in-house that allow it to rapidly assess the minimally-systemic nature of our drug candidates as well as test the hypotheses that our drug candidates can treat and prevent diseases and conditions in our targeted therapeutic fields; |
GI Informatics: With genetic and proteomic informatics tools,renal pipeline, we have identified over 3,800 human GI tract-specific RNA transcriptsshifted our research focus to support our preclinical and proteins on the inner surface of the gut, many of which we believe may be drug targets.clinical development candidates including tenapanor and RDX013, as well as other potential renal opportunities. We intend to become leading experts in human and rodent gut physiology and the molecular pathways that leadcontinue to disease inutilize our targeted therapeutic areas;
| • | | In vitroexpertise: We have developed a cell-culture system that simulates gut tissue. We call this component of our discovery platform Ardelyx Primary Enterocyte and Colonocyte Culture System, or APECCS. APECCS involves the biopsy of various segments of the gut and the growth of those cells under proprietary conditions to maintain, to the extent possible, the integrity and functionality of the various cell types and substructures. We have developed this into a miniaturized format that allows us to utilize it for cell based drug screening. In addition to using APECCS in the design of our small molecule drug candidates, we use the APECCS technology to measure epithelial transport of ions and nutrients and to screen compounds to identify potential disease modulators such as inhibitors or activators using phenotypic screening. APECCS has the potential to allow us to identify novel targets, mechanisms of action and physiology as well as provide us an early understanding of how identified compounds may interact with specific gut tissues. In addition, we believe that APECCS may also provide us with a clear path to translate cell-based observations into in vivo rodent models and ultimately into human clinical studies. |
OUR STRATEGY
We are a biotechnology company with a clinical pipeline of drug candidates in the fields of GI and cardio-renal diseases. We are currently advancing the clinical development of our two product candidates, tenapanor and RDX022, and we currently expect to file an IND for RDX009 in the second half of 2016.
Our goal is to use our proprietary drugunique discovery and design platform to discover new minimally-systemic drug candidates that preventhelp
elucidate first-in-class mechanisms of action, as with tenapanor, and treat important diseases in these same therapeutic areas of GI and cardio-renal diseases. To date, all ofto inform preclinical experiments to help advance our drug candidates have resulted fromproduct candidates. We also use our internal research. If our drug candidates are approved for marketing byplatform to further support the U.S. Food and Drug Administration, or FDA, we expect to participate in thepotential commercialization of our programs, which is valuable to us and future partners. We believe that our platform, and early pipeline, represent additional collaborative opportunities, market potential and downstream value-creation.
Using our platform, we have been able to discover targets found in the GI tract that regulate important processes in the body and design products candidates that act upon those targets to take advantage of the gut’s ability to communicate with other organs. Our platform integrates two critical concepts: (i) our own specialty-based sales force, initially targeting gastroenterologistsproprietary chemistry capabilities that enable us to design and nephrologists. optimize gut-restricted compounds that can provide a higher margin of safety than systemically absorbed compounds, and (ii) our stem cell-based translational technology called the Ardelyx Primary Enterocyte and Colonocyte Culture System, or APECCS, that enables us to discover targets in the GI tract which control health and disease processes, to optimize drug candidates and to understand their mechanisms of action. Our executive management team, and in particular our President and Chief Executive Officer, Michael Raab, has extensive experience in developing and commercializing therapeutic drugsplatform can be applied across the entire GI tract, allowing for the CKD and ESRD markets, and we expectbroadest evaluation of disease targets to leverage this expertise in a manner that will allowdevelop medicines optimized for specific diseases. The predictive ability of our platform enables us to create and retain significant value from our marketed products.better assess, at a very early stage, the potential for small molecule compounds to treat specific diseases. OUR PRODUCT PIPELINE Tenapanor: A New Approach for Treating Hyperphosphatemia in ESRD Patients on Dialysis The following table summarizes key information aboutlead product candidate in our product candidates as of December 31, 2015: 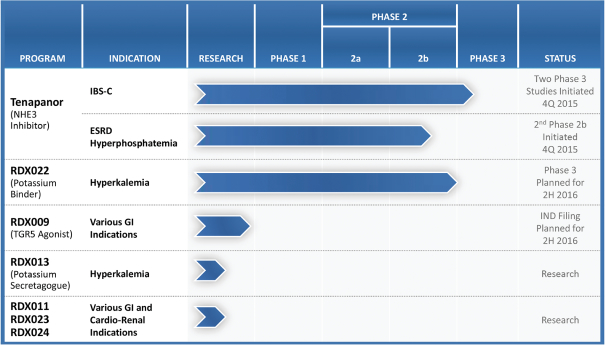
Tenapanor
Tenapanorrenal portfolio is a minimally-systemic small molecule that acts locally in the GI tract to inhibit the sodium transporter NHE3 and reduce sodium and phosphorus uptake from the gut. In human studies of orally- administered tenapanor, the drug was detected in the blood in only 0.7% of more than 3,000 collected serum samples, and even in those, at very low levels (< 1.5 ng/mL) confirming that tenapanor is minimally-systemic. We have evaluated tenapanor in fourteen human clinical studies in over 1,000 individuals to date. We are currently evaluating tenapanor for the treatment of constipation and pain in IBS-C patients and for the treatmenthyperphosphatemia, or high levels of hyperphosphatemiablood phosphorus, in ESRD patients.
Tenapanor for treating IBS-C
IBS-Cpatients on dialysis. Hyperphosphatemia is a GI disorder in which abdominal pain or discomfort is associated with constipation, which significantly affects the health and quality of life of affected patients. In a recent study led by Dr. Joel J. Heidelbaugh (published in 2015), over 50% of IBS-Csignificant problem among dialysis patients rated their pain, constipation and straining as being “extremely bothersome.” In the same study, GI symptoms led to an average 4.9 days of “disrupted productivity” and 0.8 days of missed work per month. Additionally, IBS-C led to over 50% of patients seeking physician care in the past 12 months and over a third were “a little or not at all satisfied” with their physician care. It is currently unknown what causes IBS-C. There is no specific test or biomarker for IBS-C and therefore, its presence is diagnosed by symptoms and by eliminating other disorders. IBS-C is very similar to chronic constipation and it is clinically distinguished by a significant pain component.
Clinical data supporting tenapanor in IBS-C
We conducted a Phase 2b clinical trial in IBS-C patients and announced results from that study in October 2014. The clinical trial was a randomized, double blind, placebo-controlled, multi-center study to evaluate the safety and efficacy of three dose levels of tenapanor in 371 subjects with IBS-C as defined by the Rome III criteria and who had active disease as determined during a two-week screening period. Subjects who qualified
and who were randomized into the study received 5, 20, or 50 mg of tenapanor or placebo twice daily for 12 consecutive weeks. At the end of this treatment period, subjects were followed for an additional 4 weeks. The results were reported on an intent-to-treat basis.
The primary endpoint, CSBM responder rate, was achieved in 60.7% of patients receiving tenapanor 50 mg twice daily versus 33.7% receiving placebo (p<0.001). A CSBM responder was defined as a patient who had an increase of greater than or equal to one CSBM from baseline during 6 out of 12 weeks. We also measured a more stringent CSBM response where a responder was defined as a patient who an increase of greater than or equal to one CSBM from baseline and had three or more CSBMs per week during 9 out of 12 weeks. The CSBM 9 of 12 week responder rate was achieved in 23.8% of patients receiving tenapanor 50 mg twice daily versus 7.9% receiving placebo (p<0.004).
An abdominal pain responder was achieved in 65.5% of patients receiving tenapanor 50 mg twice daily versus 48.3% receiving placebo (p<0.026). An abdominal pain responder was defined as a patient who experienced at least a 30% decrease in abdominal pain from baseline for 6 of 12 weeks. We also measured a more stringent abdominal pain responder rate where a responder was defined as a patient who experienced at least a 30% decrease in abdominal pain from baseline for 9 of 12 weeks. For this more stringent abdominal pain measurement, the abdominal pain 9 of 12 responder rate was achieved in 48.8% of patients receiving tenapanor 50 mg twice daily versus 31.5% receiving placebo (p<0.022).
The overall responder rate, or dual composite endpoint percent, was achieved in 50% of patients receiving tenapanor 50 mg twice daily versus 23.6% receiving placebo (p<0.001). An overall responder was defined as a patient who was a CSBM responder and an abdominal pain responder during the same week for 6 of 12 weeks. We also measured a more stringent overall responder rate where a responder was defined as a patient who was both a CSBM responder and an abdominal pain responder during the same week for 9 of 12 weeks. The overall 9 of 12 week responder rate was achieved in 20.2% of patients receiving tenapanor 50 mg twice daily versus 6.7% receiving placebo (p<0.01).
Most other secondary endpoints measured also demonstrated significant improvements for patients receiving 50 mg tenapanor twice daily compared to placebo-treated patients.
A dose response relationship among all doses was observed in the primary endpoint, as well as in most secondary endpoints, although statistical significance was not achieved at the 5 mg or 20 mg doses. Additionally, the activity of tenapanor was maintained throughout the entire 12-week treatment period.
Tenapanor was well-tolerated in these patients, and the safety results were consistent with those observed in previous tenapanor trials. The most common adverse events at 50 mg twice daily (greater than or equal to 5%) that occurred more frequently in tenapanor-treated patients compared to placebo-treated patients were diarrhea at 11.2% vs. 0%, and urinary tract infections at 5.6% vs. 4.4%. Overall rates of discontinuation due to adverse events were 4.5% for the tenapanor-treated patients (50 mg twice daily) and 3.3% for the placebo-treated patients. Based on the analysis of plasma samples tested as part of the study, the minimally-systemic nature of tenapanor was confirmed.
In the fourth quarter of 2015, we initiated two pivotal Phase 3, randomized, placebo-controlled clinical trials evaluating tenapanor in IBS-C patients. We expect to enroll approximately 600 patients in each trial, and we currently expect results from these two Phase 3 clinical trials in 2017. The primary endpoint in each of the trials is the 6 of 12 week overall responder rate. An overall responder is defined as a weekly responder for 6 of 12 weeks where both an abdominal pain response and a CSBM response criteria are met during the same week. An abdominal pain responder is defined as a patient with a 30% or greater reduction in average weekly worst abdominal pain compared to baseline during the week, and a CSBM responder is defined as a patient who has an increase of one or more in average weekly CSBMs compared to baseline during the week. We are also evaluating other endpoints in these studies, including CSBM and abdominal pain responder rates for 6 of 12 weeks as well as for 9 of 12 weeks, abdominal symptoms and other clinically relevant endpoints.
The IBS-C market opportunity
Numerous treatments exist for the constipation component of IBS-C, many of which are over-the-counter. We are aware of two prescription products marketed for IBS-C, Linzess (linaclotide) marketed by Ironwood Pharmaceuticals and Allergan and Amitiza (lubiprostone) marketed by Sucampo and Takeda. In Phase 3 clinical trials of Linzess in IBS-C patients, up to 20% more patients receiving Linzess than placebo reached the primary endpoint, overall responder rate, indicating a significant response during 6 out of 12 weeks of treatment. In these studies, Linzess caused diarrhea in up to 17% more patients than placebo.
We believe that tenapanor may offer a significant benefit over currently marketed drugs like Amitiza and Linzess, due in part to the potential to adjust the dose and/or dose frequency of tenapanor in order to optimize its efficacy and minimize diarrhea. The data we have generated in both animal and human studies have suggested that the effect of tenapanor for the treatment of IBS-C can be modulated by adjusting its dose and dose frequency.
Based on reports in the literature regarding the prevalence of IBS in the U.S. population and the percentage of individuals who have IBS-C as opposed to other forms of IBS, we estimate that approximately 1.4% of the U.S. population has IBS-C, or about 4.4 million individuals, and that approximately 1.0 million of those patients have been diagnosed with IBS-C. Additionally, we estimate there are about 6.6 million IBS-C patients in Europe and about 3.4 million in Japan.
Tenapanor for treating hyperphosphatemia in ESRD patientsworldwide.
CKD is the progressive deterioration of renal function that can occur over several months or years. The symptoms of worsening kidney function are nonspecific, and can include having less energy, reduced appetite, dry itchy skin, swollen feet and ankles or generally just not feeling well. If the deterioration continues and is not halted by either changes in lifestyle or with the assistance of pharmacological intervention, the disease will likely cause significant cardiovascular morbidity, and can progress to ESRD, the final stage of CKD, where kidney function will be lost entirely. Current management of ESRD includes hemodialysis and peritoneal dialysis as a means to filter toxins from the blood once kidneys have failed. Unless this intervention occurs, kidney failure results in the accumulation of waste products that may ultimately cause death. Hemodialysis, the most common form of dialysis, generally requires a patient to visit a dialysis center at least three times per week for a three- to five-hour session, significantly reducing quality of life. Phosphorus, a vital element required for most cellular processes, is present in almost every food in the Western diet, and, in individuals with normal kidney function, any excess dietary phosphorus is efficiently removed by the kidneykidneys and excreted in urine. In adults with functioning kidneys, normal serum phosphorus levels are 2.62.5 to 3.84.5 mg/dL. With kidney failure, elevated phosphorus becomes harmful and is diagnosed as hyperphosphatemia when serum phosphorus levels are greater than 5.0 mg/dL. Although patients with ESRD rely on dialysis to eliminate harmful agents, phosphorus is not readily removed by the procedure and other means of managing phosphorus levels must be employed. In ESRD patients, excess levels of phosphorus have been shown to lead to an increase in cardiovascular disease risk, as well as increases in serum FGF-23,FGF‑23, an important serum endocrine hormone that regulates phosphorus metabolism,regulator of phosphate and vitamin D metabolism. Highly elevated levels of FGF23 is an independent risk factor for adverse cardiac clinical outcomes as well as the development of secondary hyperparathyroidism, or SHPT, marked by elevated parathyroid hormone, also known as secondary hyperparathyroidism. These endocrine changes in ESRD patients are a concern as elevated parathyroid hormone leads to the development ofhormone. SHPT is associated with renal osteodystrophy, a condition of abnormal bone growth characterized by brittle bones. Since dialysis is unable to efficiently eliminate excess phosphorus, ESRD patients are put on restrictive low phosphorus diets and are currently prescribed medications called phosphate binders, the only pharmacologic interventions currently marketed for the treatment of hyperphosphatemia. Binders are a collection of drugs whose function is to bind, or absorb,Phosphate binders act by binding dietary phosphorus and arecommonly need to be taken in conjunction with meals and snacks. They include calcium, iron or lanthanum, a rare-earth metal, which bind to and precipitate with dietary phosphate in the GI tract. The goal of these elemental phosphorusphosphate binders is for patients to eliminate,
through their stool, the precipitated phosphorus in their stool. A limitationthat comes from the food they ingest. Phosphate binders have a number of this approach is the systemic excess absorption of calcium, iron or lanthanum, resulting in side effects and other unintended consequences for ESRD patients.limitations, including: | · | | systemic excess absorption of calcium, iron or lanthanum, resulting in side effects and other unintended consequences for ESRD patients, and |
| · | | significant challenges with patient compliance because of the large quantity and/or mass of the binders that must be taken each day. |
Safety and tolerability have also been significant concerns with many approved phosphate binders, with side effects that include long-term vascular calcification with calcium-based binders and iron-overload with iron-based binders. The more common side effects of certain approved phosphate binders include long-term vascular calcification,GI-related adverse events such as nausea, and vomiting, diarrhea, or constipation and ileus or disruption of the normal propulsive ability of the GI tract.dyspepsia as well as hypercalcemia for calcium-based binders and discolored feces for iron-based binders. ESRD patients, take on average 10-14 oral medications each day, and theywho generally are severely restricted in their fluid intake. In addition, to control their serum phosphorus, their phosphate binder-related pill burden is significant, typically consisting of nineintake, are prescribed as many as 12 or more phosphate binder pills a day.per day, among other medications. The amount of phosphatephosphorus a binder can remove is limited by its binding capacity, and therefore, increasing the dose, and thereforehence the pill burden, of the binder is the only way to increase the amount of phosphatephosphorus being bound and excreted. As a result of pill burden and mass, as well as a number of side effects, prescribed phosphate binder doses are intolerable for many patients. Clinical data supporting tenapanor in hyperphosphatemia
In February 2015, we announced results frompatients, leading to a Phase 2b clinical trial evaluating tenapanor for the control of hyperphosphatemia in ESRD patients. This Phase 2b trial was a randomized, double blind, placebo-controlled, multi-center, international study evaluating the safety and efficacy of six dose levels of tenapanor (3 and 30 mg once daily, and 1, 3, 10, and 30 mg twice daily) in 161 ESRD patients with hyperphosphatemia. The primary efficacy endpoint was the change from baseline of serum phosphate levels to the endlack of treatment adherence and the endpoint was analyzed using an analysis of covariance model (ANCOVA). The study met its primary endpoint by demonstrating a statistically significant dose-related decrease in serum phosphate levels for tenapanor-treated patients compared to patients receiving placebo (p=0.012).compliance.
The Effect of Tenapanor on Serum Phosphate in ESRD Patients with Hyperphosphatemia
| | | | | | | | | | | | | Group | | n | | | LSMean* (mg/dL) | | | 95% CI | | 1 mg BID | | | 23 | | | | -0.47 | | | | (-1.18, 0.24 | ) | 3 mg BID | | | 21 | | | | -1.18 | | | | (-1.93, -0.44 | ) | 10 mg BID | | | 23 | | | | -1.70 | | | | (-2.41, -0.99 | ) | 30 mg BID | | | 24 | | | | -1.98 | | | | (-2.67, -1.28 | ) | 3 mg QD | | | 22 | | | | -0.56 | | | | (-1.28, 0.17 | ) | 30 mg QD | | | 21 | | | | -1.11 | | | | (-1.85, -0.37 | ) | Placebo | | | 26 | | | | -0.54 | | | | (-1.21, 0.13 | ) |
* | LSMean = least square mean |
As shown in the table, a dose-response relationship was observed in the primary endpoint and twice daily dosing had better pharmacodynamic activity than once daily dosing.
As expected, due to its pharmacological actions, the most frequent adverse event was diarrhea. The rate of diarrhea and the discontinuation rate due to diarrhea at the highest doses were higher than expected based on previous clinical trials. Higher discontinuations rates due to diarrhea were observed primarily in the 30 mg once daily and 30 mg twice daily dose groups. There were no other notable gastrointestinal adverse events that appeared to be tenapanor related. The overall safety profile remains consistent with that observed in previous tenapanor trials in this patient population.
Phase 2b ESRD Hyperphosphatemia: Discontinuations Due to Adverse Events
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | Adverse Event Term | | 1 mg BID | | | 3 mg BID | | | 10 mg BID | | | 30 mg BID | | | 3 mg QD | | | 30 mg QD | | | Placebo | | n/group | | | 23 | | | | 21 | | | | 23 | | | | 25 | | | | 22 | | | | 21 | | | | 26 | | Discontinuations due to AE/group* | | | 3 | | | | 3 | | | | 3 | | | | 9 | | | | 1 | | | | 7 | | | | 2 | | Abdominal Pain | | | | | | | | | | | | | | | 1 | | | | | | | | | | | | | | Diarrhea** | | | 2 | | | | 3 | | | | 3 | | | | 8 | | | | | | | | 6 | | | | | | Nausea | | | | | | | | | | | | | | | | | | | | | | | 1 | | | | | | Vomiting | | | | | | | | | | | | | | | | | | | | | | | 1 | | | | | | Serum Calcium Decrease | | | | | | | | | | | | | | | | | | | 1 | | | | | | | | | | Hyperphosphatemia | | | 1 | | | | | | | | | | | | | | | | 1 | | | | | | | | 2 | | Dizziness | | | | | | | | | | | | | | | | | | | | | | | 1 | | | | | | Atherosclerosis | | | | | | | 1 | | | | | | | | | | | | | | | | | | | | | |
* | There may be multiple reasons for a single discontinuation |
** | Personal assessment reported by the patient |
In December 2015, we initiated a Phase 2b clinical trial to evaluate the optimal dosing regimen forWe are developing tenapanor for the treatment of hyperphosphatemia in ESRD patients on dialysis, as we believe it has the potential to address certain of the key limitations of current treatments and we expectoffer a completely new mechanism of action. If approved, tenapanor would be the first small molecule/non-binder approach to receive results from this trialtreating hyperphosphatemia, with a unique mechanism of action that acts by inhibiting, or blocking, the NHE3 transporter in the second halfGI tract to reduce the absorption of 2016.
dietary sodium. When tenapanor blocks the NHE3 sodium transporter in the GI tract, it reduces the absorption of dietary sodium, resulting in an increase in protons within the cells. This increase in protons causes a selective reduction in phosphate uptake by tightening junctions or pores that are involved in the regulation of phosphate homeostasis, which then limits the amount of dietary phosphate that can pass from the gut into the blood. We have not observed this impact on other ions, nutrients or macromolecules in our clinical trials. We have submitted a manuscript for publication of this mechanism in a scientific peer-reviewed journal. This unique mechanism of action allows tenapanor to be active in many patients at a dose of 10mg to 30mg twice daily as opposed to the multiple gram quantities per day required of the phosphate binders. Over the course of a week, the amount of tenapanor required would be less than 500mg, or a total of 14 small pills, whereas the amount of phosphate binder required, based on package inserts, would be 10 to 30 grams, or up to 64 large pills, depending on the phosphate binder. We believe this significant pill burden advantage will result in better adherence and compliance which could lead to more consistent efficacy in ESRD patients on dialysis. Tenapanor has been specifically designed thisto work exclusively within the GI tract, thereby significantly reducing the amount of drug that is absorbed into the bloodstream and the potential side effects that could occur. In human studies of orally-administered tenapanor, the drug was detected in the blood in less than 1% in thousands of collected serum samples, and even in those, at very low levels (< 1.5 ng/mL). We have evaluated tenapanor across 20 clinical studies in over 2,500 individuals to date. Clinical data supporting tenapanor in hyperphosphatemia In February 2017, we announced data from our first Phase 2b3 clinical trial and the statistical analysis plan so that, assuming positive results, there is potential that the FDA may agree that this trial could be considered the first of two well-controlled studies to support an NDA forevaluating tenapanor for the treatment of hyperphosphatemia in ESRD patients.patients on dialysis. SizeThe Phase 3 trial was an eight-week, double-blind, randomized trial, with a four-week placebo-controlled randomized withdrawal period. We enrolled a total of 219 ESRD patients with hyperphosphatemia who are on dialysis. Enrolled patients were randomized evenly into three arms, in which all groups received tenapanor for eight weeks.
Tenapanor was administered at doses of 3 mg or 10 mg twice-daily and in a dose-titration arm starting at 30 mg twice-daily with the option to down-titrate once a week during the first four weeks to 20, 15, 10 and 3 mg twice-daily, based on GI tolerability. After the end of the eight-week treatment period, patients were re-randomized 1:1 to either remain on their current tenapanor dose or switch to placebo for a four-week, placebo-controlled, randomized withdrawal period. The primary endpoint of the trial was the difference in change in serum phosphorus between the pooled tenapanor-treated patients and placebo-treated patients from the end of the eight-week treatment period to the end of the four-week randomized withdrawal period, in the responder population. The responder population, which was reviewed by the FDA, is defined as patients who demonstrate a greater than or equal to 1.2 mg/dL decrease in serum phosphorus from baseline during the initial eight-week treatment period. The study demonstrated a statistically significant difference in serum phosphorus levels from the end of the eight-week treatment period to the end of the four-week randomized withdrawal period between the tenapanor-treated group and the placebo-treated group in the responder patient population (mean -1.01 mg/dL, median of -1.3 mg/dL) and met its primary endpoint (95% confidence interval, -1.44, -0.21, LSmean -0.82 mg/dL, p=0.01). The responder population (n=80 out of 164) had a mean reduction in serum phosphorus from baseline to the end of the eight-week treatment period of 2.56 mg/dL, with a reduction of up to 5.7 mg/dL. Notably, in this group, 33% of patients had a reduction in serum phosphorus of greater than 3 mg/dL. Tenapanor was well-tolerated in the trial. In the eight-week treatment period, the only adverse event that affected more than five percent of patients treated with tenapanor was diarrhea (39%), a patient-reported side effect of loosened stool or increased frequency in bowel movements regardless of magnitude. In the four-week randomized withdrawal period, there was a diarrhea rate of 1.2% for patients treated with tenapanor compared with 2.4% on placebo. Treatment discontinuations due to diarrhea for patients on tenapanor was 7.8% (n=17). There were no discontinuations due to diarrhea in the randomized withdrawal period. In order to fully assess GI tolerability, patients used an eDiary to record the frequency of daily bowel habits, as well as stool form using the Bristol Stool Form Scale, or BSFS. During the eight-week treatment period, there was an average 0.4 per day increase in bowel movement frequency from baseline, and during the four-week randomized withdrawal period, there was an average 0.29 per day increase as compared to placebo. Average bowel movement frequency was within the normal range in all groups. During the eight-week treatment period, there was an average 0.87 point increase in BSFS from a baseline score of 4.2, out of a maximum of seven, where seven is liquid stool. During the four-week randomized withdrawal period, there was an average 0.7 point difference in BSFS between placebo (4.4) and tenapanor treatment (5.1). We have initiated a second Phase 3 study of tenapanor for the treatment of hyperphosphatemia in ESRD patients on dialysis. The study's design, shown in the figure, will include a 26‑week open-label treatment period, with a 12-week randomized withdrawal period followed by an additional 14‑week safety extension. Results from this study are expected in 2019. We currently intend to build our own sales and marketing organization to market and sell tenapanor for hyperphosphatemia in the United States. 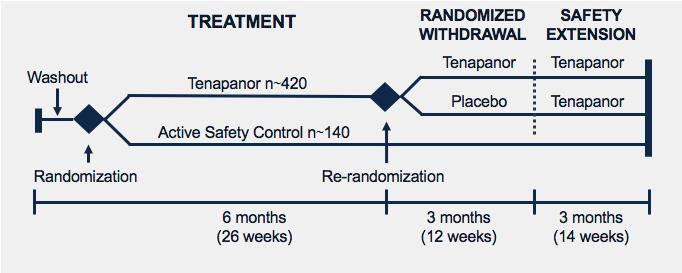
The hyperphosphatemia market Phosphate binders are the only pharmacologic interventions currentlydrugs marketed for the treatment of hyperphosphatemia. Calcium-based binders are the least expensive option to treat hyperphosphatemia. In hemodialysis patients, sevelamer has a 35% patient share versus 45% for calcium-based binders, 15% for lanthanum and 12% for iron-based binders.hyperphosphatemia in ESRD patients. The various types of phosphate binders commercialized in the United States include the following: | · | | Calcium carbonate (many over-the-counter brands including Tums and Caltrate) |
| · | | Calcium acetate (several prescription brands including PhosLo and Phoslyra) |
| · | | Lanthanum carbonate (Fosrenol marketed by Shire) |
| · | | Sevelamer hydrochloride (Renagel, marketed by Sanofi) |
| · | | Sevelamer carbonate (Renvela, marketed by Sanofi) |
| · | | Sucroferric oxyhydroxide (Velphoro, marketed by Vifor Fresenius) |
| · | | Ferric citrate (Auryxia, marketed by Keryx) |
Generic sevelamer was expected to enter the U.S. market in early 2014 after expiration of Sanofi’s patent, but as of early 2016, no generic sevelamer has yet been approved. Generic sevelamer was approved, however, in certain jurisdictions in Europe in 2015.
Each of these agents has certain limitations. Calcium carbonate and calcium acetate can cause long term vascular calcification.
Lanthanum carbonate (Fosrenol) entered the market in 2004 as an alternative to calcium and aluminum based agents, but nephrologists’ concerns about the long term toxicity from the absorption of metals such as lanthanum and its GI side effect profile have limited its market penetration. Sevelamer hydrochloride (Renagel) is an acidic formulation of sevelamer that has been linked with worsening of metabolic acidosis in patients. Sevelamer carbonate (Renvela) was developed as an improved formulation of sevelamer to reduce incidence of acidosis. The active ingredient of both products, sevelamer, is associated long-term with vomiting (22%), nausea (20%), diarrhea (19%), dyspepsia (16%), abdominal pain (9%), and flatulence (8%).
Ferric citrate (Auryxia), an iron-based phosphate binder, was approved by FDA in September 2014. While iron is often deficient in ESRD patients because of CKD-associated anemia and lack of sufficient dietary iron, the FDA has required Auryxia to add a warning of iron-overload in the label.
The hydrochloride form of sevelamer, Renagel, was launched in the United States by Genzyme Corporation in 1998 prior to its acquisition by Sanofi, and the carbonate form, Renvela, was launched in 2008. Renvela is currently priced in the United States at a cost of more than $7,000 per patient per year, Fosrenol (lanthanum carbonate) is priced at about $7,500 and calcium-based binders are approximately $900. Sevelamer is the leading phosphate binder product in the hemodialysis market with 35% patient share (versus 45% split among several calcium-based binders). Sanofi booked €935reported €922 million ($1.041.05 billion) in worldwide sales of sevelamer during 2015. The2016 and €802 million ($0.98 billion) in 2017. Generic sevelamer carbonate has been approved in certain jurisdictions in Europe since 2015 and in the U.S. patents for sevelamer expired in February 2014 and generic launch was allowed in March 2014.market since June 2017. In addition to the currently marketed phosphate binders, we are aware of at least two other binders in development, including fermagate (Alpharen), an iron-based binder in Phase 23 studies being developed by Opko Health, Inc., and PT20, an iron-based binder in Phase 23 being developed by PhosphateShield Therapeutics. According to the most recent data available from the U.S. Renal Data System, in 20132015 there were 421,349444,337 patients on hemodialysis in the United States. Additionally, according to the European ERA-EDTA Registry 20122015 Annual Report and a study in 20102014 by the Japanese Society for Dialysis Therapy, there were approximately 280,000317,000 patients on hemodialysis in Europe and about 250,000255,000 in Japan. We estimate, based on phosphate binder utilization, the only approved therapies for hyperphosphatemia, that there are approximately 290,000, 225,000310,000, 250,000 and 220,000260,000 ESRD patients with hyperphosphatemia in the United States, countries in Europe and Japan, respectively.respectively, resulting in approximately 820,000 ESRD patients with hyperphosphatemia in such countries. Because many ESRD patients with hyperphosphatemia are unable to lower serum phosphorus levels to below 5.5 mg/dL with currently marketed phosphate binders, we believe there is a significant opportunitymedical need for new agents with new mechanisms, demonstrated efficacy, a strong safety profile, and significantly lower pill burden. We believe that tenapanor, if approved, has the potential to have the lowest pill burden and mass among any currently marketed hyperphosphatemia drugs,products, with milligram rather than gram quantities dosed once or twice daily.quantities. In addition, we may evaluate whether tenapanor has the potential to be used in combination with phosphate binders for those patients who cannot achieve adequate phosphate control with a single agent. RDX022Our intention is to build a United States-focused, highly efficient, specialized sales and marketing organization focused on nephrology. The nephrology market is a concentrated market strongly influenced by key opinion leaders. There were 10,083 nephrologists in the United States in 2015 and 6,620 dialysis facilities in the United States that offer in-center dialysis. Based on the experience of our management team, we believe that a specialty salesforce is appropriate for treating hyperkalemia
this marketplace. We are developing RDX022believe that tenapanor for the treatment of hyperkalemia. RDX022 is our proprietary oral, non-absorbed potassium-binder. It based on polystyrene sulfonate,hyperphosphatemia could represent a well-knownmarket opportunity of between $500 million and well-characterized polymer. We have made numerous improvements to the polymer by engineering into RDX022 several key physical and chemical modifications in an effort to improve various properties. We have filed a patent application covering the composition of matter for these modifications. Clinical data supporting RDX022 in hyperkalemia
In January 2016, we announced results from an open-label pharmacodynamic study of RDX022 in healthy adult volunteers. The study consisted of a two-day treatment-free baseline period and a four-day treatment
period. The study included four cohorts, and in each cohort 12 subjects received RDX022 and three subjects received a similar dose of sodium polystyrene sulfonate, or SPS for a total of 60 subjects. RDX022 was administered at 4.6 g BID (9.2 g/day), 6.9 g BID (13.8 g/day), 4.6 g TID (13.8 g/day) and 9.2 g TID (27.5 g/day), and resulted in a mean increase of fecal potassium from baseline of 888 mg/day, 1,791 mg/day, 1,408 mg/day, and 1,670 mg/day, respectively. RDX022 was generally well-tolerated at all doses and demonstrated comparable results to those observed with SPS. Other fecal electrolytes were monitored during the study and no unexpected changes were observed; in particular, fecal magnesium remained unchanged from baseline.
Sodium is currently used as a counter-ion in SPS products marketed$700 million in the United StatesStates.
As a first-in-class treatment, and certain other products under development. We formulated RDX022as the first non-binder option with a calcium counter-ion, rather thanwell-tolerated safety profile, we believe tenapanor could address the significant pill burden challenges and intolerability that patients experience with today’s binder treatments. After the second Phase 3 study readout, if successful, we intend to submit a sodium counter- ion, as adding sodiumNew Drug Application to the daily intakeFDA in 2019 and would plan for a potential launch 2020. To bring tenapanor to patients outside the United States, we intend to establish strategic collaborations with industry leading pharmaceutical companies with established commercial infrastructures. In 2017, we entered into two collaboration partnerships, and the revenues recorded from those collaboration partnerships in 2017 accounted for more than 10% of total revenues recorded during the year ended December 31, 2017. License agreement with KHK In November 2017, we entered into a license agreement (“KHK License Agreement”) with KHK under which we granted KHK an exclusive license to develop and commercialize tenapanor in Japan for the treatment of cardiorenal diseases and conditions, excluding cancer (“KHK Field”). We retained the rights to tenapanor outside of Japan, and also retained the rights to tenapanor in Japan for indications other than those in the KHK Field. Pursuant to the KHK License Agreement, KHK is responsible for all of the targetdevelopment and commercialization costs for tenapanor in the KHK Field in Japan. Under the KHK License Agreement, we are responsible for supplying the tenapanor drug product for KHK’s use in development and during commercialization until KHK has assumed such responsibility. Additionally, we are responsible for supplying the tenapanor drug substance for KHK’s use in development and commercialization throughout the term of the KHK License Agreement, provided that KHK may exercise an option to manufacture the tenapanor drug substance under certain conditions. Under the terms of the KHK License Agreement, we have received a $30.0 million upfront payment and are eligible to receive up to an additional $130.0 million in development and commercialization milestones, based upon currency exchange rates as of the effective date of KHK License Agreement. We are also eligible to receive royalties based on aggregate annual net sales of the licensed products at a high teen percentage, subject to certain single digit reductions under certain circumstances described in the KHK License Agreement. The KHK License Agreement will continue until all of KHK’s applicable payment obligations under the KHK License Agreement have been performed or have expired, or the agreement is earlier terminated. Under the terms of the KHK License Agreement, we and KHK each have the right to terminate the agreement for material breach by the other party. In addition, KHK may terminate the agreement for convenience; for certain safety reasons or if certain primary endpoints under an applicable development plan are not met despite KHK’s commercially reasonable efforts and KHK reasonably determines that it cannot obtain regulatory approval. KHK may also terminate the agreement if certain pivotal clinical trials conducted by us do not meet their primary endpoints. We may terminate the KHK License Agreement if KHK challenges any patents licensed to KHK under the agreement. License agreement with Fosun In December 2017, we entered into a license agreement (the “Fosun License Agreement”) with Fosun Pharma under which we granted Fosun Pharma an exclusive license to develop and commercialize tenapanor in China for the treatment, diagnosis or prevention of (i) irritable bowel syndrome with constipation and chronic idiopathic constipation, (ii) hyperphosphatemia related to chronic kidney disease and (iii) other diseases or conditions for which we obtain marketing approval in either the US or China (collectively, “Fosun Field”). The Fosun Field excludes the treatment of cancer. We retained the rights to tenapanor outside of China, and also retained the rights to tenapanor in China for indications other than those in the Field. Pursuant to the terms of the Fosun License Agreement, Fosun Pharma is responsible for all of the development and commercialization costs for tenapanor in the Fosun Field in China. Under the terms of the Fosun License Agreement, we are responsible for supplying the tenapanor drug product for Fosun Pharma’s use in development and during commercialization until Fosun Pharma has assumed such responsibility. Additionally, we are responsible for supplying the tenapanor drug substance for Fosun Pharma’s use in development and commercialization throughout the term of the Fosun License Agreement. Under the terms of the Fosun License Agreement, we received an upfront payment of $12 million and are eligible to receive additional milestones of up to $113 million in the aggregate, as well as tiered royalty payments on aggregate net sales ranging from the mid-teen percent to twenty percent, subject to certain reductions under certain circumstances, as described in the Fosun License Agreement. The Fosun License Agreement will continue until all of Fosun Pharma’s applicable payment obligations under the License Agreement have been performed or have expired, or the agreement is earlier terminated. Under the terms of the Fosun License Agreement, we and Fosun Pharma each have the right to terminate the agreement for material breach by the other party or in the event of insolvency by the other party. In addition, Fosun Pharma may terminate the agreement for convenience and we may terminate the agreement if Fosun Pharma challenges any patents licensed to it under the agreement. RDX013 Program: Small Molecule for Treating Hyperkalemia RDX013 is our novel, small molecule program for the potential treatment of hyperkalemia. Our RDX013 approach works by tapping into the GI tract’s natural ability to secrete potassium into the lumen of the gut to reduce serum potassium levels. This mechanism differs significantly from the potassium binders currently on or approaching the market. For a potassium binder to work, it must be present when dietary potassium is ingested so that the agent can bind the potassium and prevent its absorption in the gut. This results in the need for large quantities of binder in order to bind the large amounts of potassium in the diets of most individuals. In contrast, we observed in our preclinical models that a small amount of RDX013 could cause potassium to be secreted into the lumen of the gut. In this way, we believe that RDX013 may have the potential to lower serum potassium whether or not potassium is present in the diet and could result in a very low pill burden, potentially allowing better patient population runs countercompliance, longer-term use and potentially better efficacy than potassium binders. As described below, certain medications commonly administered to best clinical practice. In patients with CKD and/or HF,heart failure can also cause hyperkalemia. With the standardsuccessful development of care is a low-sodium diet as sodium can contributean effective potassium secretagogue to fluid overload and edema, a common experience for these patients. In addition, excess sodium diminishes the beneficial effects of blood pressure drugs that inhibit the renin-angiotensin-aldosterone system, or RAAS. We have also improved both the physical properties of polystyrene sulfonate and the formulationtreat hyperkalemia in a manner that we expect may lead to improved patient adherence and compliance. Notably, in a single center, randomized, crossover study to evaluate various oral formulations of RDX022 in healthy subjects, RDX022 consistently outperformed SPS in all aspects of the taste assessments, including mouth feel, texture and flavor. We currently expect to initiate a Phase 3 clinical trial for RDX022 in the second half of 2016. The Phase 3 clinical trial will enroll patients with CKD, with or without HF, who are taking RAAS inhibitors and are diagnosed with hyperkalemia, a common side effect that occurs in patients taking RAAS inhibitors. Based on discussions with the FDA,small, convenient pill format, we believe we will be ableour RDX013 approach may allow nephrologists and cardiologists with an opportunity to submit an application for RDX022 undertreat hyperkalemia chronically without reducing the 505(b)(2) regulatory pathway.
Sizedose of the hyperkalemia marketthese medications.
Hyperkalemia is generally defined as the presence of blood potassium levels greater than 5.0mEq/5.0 mEq/L. Normal levels are 3.5 to 5.0 mEq/L. When hyperkalemia is severe, or above 7.0mEq/7.0 mEq/L, there is a significantly increased risk of death because of the potential for heart conductance problems. Hyperkalemia can be caused by a variety of sources.issues. Kidney disease can result in the build-upelevation of potassium in the blood. Also, certainCertain drugs such as the common blood pressurehypertension medications known as RAAS inhibitors, or inhibitors ofwhich inhibit the renin-angiotensin-aldosterone system, can cause hyperkalemia. As a result, the dosage of RAAS inhibitors though quite effective for controlling blood pressure, aremust often be significantly reduced in patients suchwhose potassium levels are elevated (such as in those with CKD and HF whose potassium levels are elevated becauseheart failure). Because of the fearrisk of hyperkalemia, several published guidelines have suggested that elevated potassium can cause significantly worse problems thanphysicians should reduce and possibly discontinue RAAS inhibitors in order to manage the risk of hyperkalemia in CKD and heart failure patients. The alternative medications used to control hypertension, including sudden cardiac arrestdiuretics and calcium channel blockers, are less effective than RAAS inhibitors, particularly in patients with failing kidneys and severe cases.hypertension. According to the 2015 publication Market Dynamix: Hyperkalemia, released by Spherix Global Insights, U.S. cardiologists reported that of the patients who would benefit from RAAS inhibition, up to 38% of patients with heart failure and up to 55% of patients with both heart failure and CKD are being administered a sub-optimal dose or none at all. Nephrologists reported that at least one-third of patients who would benefit from RAAS inhibition receive a sub-optimal dose or none at all. We believe there is clearly a strong medical need for new medications that control hyperkalemia in order to allow for optimal use of RAAS inhibitors to control hypertension in these patient populations. The hyperkalemia market Of the people with CKD and/or heart failure in the United States, we estimate that there are approximately 2.1 million people who also have occurrences of hyperkalemia. According to a retrospective observational study conducted in 2005 of a national cohort of 246,000 veteranspatients cared for in the Veterans Health Administration, about 21% and 42% of patients with CKD Stage 3b and Stage 4, respectively, had a hyperkalemic event during a 12-month period, suggesting that hyperkalemia affects about 900,000 individuals with CKD Stage 3b or Stage 4 in the United States. According to the United States Renal Data System 2014 Atlas of CKD & ESRD, over 50% of CKD Stage 3b and Stage 4 patients are prescribed RAAS inhibitors because of their efficacy in controllingto control hypertension and success in slowingto slow the clinical course of CKD. Additionally, according to the American Heart Association, 5.7 million Americans arenumber of adults in the U.S. living today with heart failure.failure is about 6.5 million, based on data collected in the National Health and Nutrition Examination Survey, which is taken in stages over multiple years. Our proprietary research suggests that up to 16%, or approximately 900,000,1,000,000, of these patients had hyperkalemia during a 12-month period. Over half of heart failure patients are prescribed RAAS inhibitors. Despite the success of RAAS inhibitors in both of these populations, several published guidelines have suggested that physicians should reduce and possibly discontinue RAAS inhibitors in order to manage the risk of hyperkalemia in CKD and heart failure patients. The alternative medications used to control hypertension, including diuretics and calcium channel blockers, are significantly less effective than RAAS inhibitors, particularly in patients with failing kidneys and severe hypertension. According to the publication Market
Dynamix: Hyperkalemia recently released by Spherix Global Insights, U.S. cardiologists reported that of the patients who would benefit from RAAS inhibition, up to 38% of patients with heart failure and up to 55% of patients with both heart failure and CKD are being administered a sub-optimal dose or none at all, and nephrologists reported that at least one-third of patients who would benefit from RAAS inhibition receive a sub- optimal dose or none at all. We believe there is a strong medical need for new medications that control hyperkalemia in order to allow for continued use of RAAS inhibitors to control hypertension in these patient populations.
An additional market not currently addressed by any product on the market is hyperkalemia in ESRD patients. Our proprietary research also suggests that up to 48% of patients on dialysis have at least one intervention for hyperkalemia during a 12-month period despite being dialyzed, resulting in a 7% mortality rate. This suggests up to 200,000 patients with ESRD thatin the U.S. could benefit from an agent that treats hyperkalemia.
We are aware of at least two drugs approaching or on the market for the treatment of hyperkalemia. Veltassa (patiromer FOS), an oral, polymer-based potassium binder, was approved for marketing by the FDA in October 2015 and was just recently commercially launched by Relypsa. Relypsa, which was acquired by Galenica AG for $1.5 billion in September 2016. However, according to a 2017 survey of more than 200 nephrologists and cardiologists, conducted by Spherix Global Insights, about half of those surveyed note that, even with Veltassa available, there remains a high unmet need for new treatments for hyperkalemia. Additionally, a new drug application, orZS Pharma submitted an NDA was submitted in June 2015 for ZS-9, a sodium zirconium cyclosilicate-based oral potassium binder being developedbinder. ZS Pharma was acquired by AstraZeneca in December 2015 for $2.7 billion. We believe that, unlike these agents which require large amounts of drug for the desired effect, RDX013 may have the potential to lower serum potassium whether or not potassium is present in the diet and could result in very low pill burden, allowing better compliance, longer-term use and potentially better efficacy than potassium binders. If we are successful in developing RDX013 and obtaining marketing authorization from the FDA, we would expect to leverage the renal sales and marketing organization that we intend to build to support commercialization in the United States of tenapanor for treating hyperphosphatemia in dialysis patients. Tenapanor: NHE3 Inhibitor for Treating IBS-C In addition to its development for hyperphosphatemia, we have completed development of tenapanor for the treatment of hyperkalemia by AstraZeneca after its acquisition of ZS PharmaIBS-C and are pursuing strategic collaborations to bring it to market in December 2015. OTHER DEVELOPMENT PROGRAMS
Other product candidatesthis indication. We have completed two Phase 3 clinical trials in our pipeline include the following:
RDX009 Program
Our focus is the discoverypatients with IBS-C (T3MPO-1 and development of minimally-systemic TGR5 agonists that stimulate GLP-1T3MPO-2) along with a long-term safety study (T3MPO-3) and GLP-2 secretion for various indications. In December 2015, we declared a development candidate for RDX009, and we currently expect to filesubmit an IND for RDX009NDA to the FDA in the second half of 2016. We are evaluating RDX009 in animal models for its effect in multiple indications.2018.
TGR5IBS-C is a receptor present onGI disorder in which abdominal pain or discomfort is associated with constipation, and which significantly impacts the membranehealth and quality of certain cells withinlife of affected patients. A study published in the American Journal of Gastroenterology in 2015, showed that over 50% of IBS-C patients rated their pain, constipation and straining as being
“extremely bothersome.” In the same study, GI symptoms led to an average 4.9 days of “disrupted productivity” and 0.8 days of missed work per month. There is no specific test or biomarker for IBS-C and therefore its presence is diagnosed by symptoms and by eliminating other disorders. IBS-C is very similar to chronic constipation and is clinically distinguished by a significant abdominal pain component. Tenapanor is a minimally-systemic small molecule that acts locally in the GI tract to inhibit the sodium transporter NHE3 and reduce sodium uptake from the gut. Part of its mechanism to treat constipation caused by IBS-C is an osmotic effect in the intestines – water follows salt and stool is gently loosened by the body’s own fluids. In addition to this mechanism, data from nonclinical studies, which were presented in November 2017 at the American Society of Nephrology Annual Meeting, suggest that respondstenapanor reduced abdominal pain caused by IBS-C through the inhibition of TRPV-1 dependent signaling. TRPV-1, better known as the "hot chili pepper receptor," is a well-established pain target known for transmitting painful stimuli from a variety of sources including heat, protons and inflammatory molecules. Using an established rodent model of IBS-like colonic hypersensitivity, preclinical data showed that tenapanor treatment reduced visceral hypersensitivity (pain in the internal organs) and normalized colonic sensory neuronal excitability and TRPV-1 currents. Treatment with tenapanor also increased stool excretion and stool water content. In these nonclinical studies, tenapanor had a superior effect on visceral hypersensitivity than placebo or PEG, a well-known laxative not known to bile acids secretedhave an analgesic effect. Phase 3 clinical data supporting tenapanor in response to food.IBS-C At the end of 2017, we completed our Phase 3 program, the T3MPO program, for tenapanor for the treatment of IBS-C. This included two Phase 3 studies, T3MPO-1 and T3MPO-2, and a long-term safety extension study, T3MPO-3. In the normal physiological response, bindingdiscussion below, statistical significance is denoted by p-values. The p-value is the probability that the reported result was achieved purely by chance (e.g., a p-value <0.001 means that there is a less than a 0.1% probability that the observed change was purely due to chance). Generally, a p-value less than 0.05 is considered statistically significant. In May 2017, we reported data from the first Phase 3 study, T3MPO-1. T3MPO-1 was a 12-week, double-blind, placebo-controlled, multi-center, randomized trial with a four-week, randomized withdrawal period conducted in a total of bile acids610 patients meeting the ROME III criteria for the diagnosis of IBS-C. Patients were randomized one to TGR5 stimulatesone to receive either 50 mg of tenapanor or placebo twice-daily. The trial included a two-week screening period, during which patients with active disease, based on bowel movement frequency and abdominal pain score recorded in a daily phone diary, were randomized into the productiontrial. The study achieved statistical significance for the primary endpoint and seven of hormones such as glucagon- like peptides 1eight secondary endpoints. The primary endpoint, the combined responder rate for six of 12 weeks, showed that a greater proportion of tenapanor-treated patients compared to placebo-treated patients (27.0% vs 18.7%, p=0.02) had at least a 30% reduction in abdominal pain and 2 (GLP-1 and GLP-2). GLP-1 is involvedan increase of one or more complete spontaneous bowel movements, or CSBM, in maintaining insulin sensitivity and in aiding glucose and lipid metabolism. GLP-2 is involved in maintenancethe same week for at least six of the structural integrity12 weeks of the guttreatment period. The CSBM responder rate in the six of 12 weeks (defined as having an increase of at least one CSBM from baseline during a week for six of 12 weeks) did not reach statistical significance (33.9% vs. 29.4%, p=0.27); however, the abdominal pain responder rate in the six of 12 weeks (defined as having at least a 30% decrease in abdominal pain from baseline during a week for six of 12 weeks) did achieve statistical significance (44.0% vs. 33.1%, p=0.008). In the nine of 12 treatment weeks, the study achieved statistical significance for the combined responder rate (13.7% vs. 3.3%, p<0.001), in which patients must have had an increase of at least one CSBM from baseline and at least three CSBMs during a week for nine of 12 weeks as well as its growth.a 30% or greater reduction in abdominal pain for nine of the 12 weeks. In addition, for the nine of 12 weeks, the study achieved statistical significance for the individual CSBM responder rate (16.9% vs. 5%, p<0.001) and the abdominal pain responder rate (30.3% vs. 19.4%, p=0.003). Tenapanor was well-tolerated in the study. The only adverse events observed in more than two percent of patients treated with tenapanor, as compared with placebo, were diarrhea (14.6% vs 1.7%) and nausea (2.6% vs 1.7%). The placebo adjusted discontinuation rate due to diarrhea was 5.3%. In October 2017, we reported results from the second Phase 3 study of tenapanor for the treatment of IBS-C, T3MPO-2, a 26-week, double-blind, placebo-controlled, multi-center, randomized trial in 593 patients. Patients were randomized one to one to receive either 50 mg of tenapanor or placebo twice-daily. The trial included a two-week screening period, during which patients with active disease, based on bowel movement frequency and abdominal pain score recorded in a daily phone diary, were randomized into the trial. The study achieved statistical significance for the primary endpoint and all secondary endpoints evaluated for the topline results and demonstrated the ability to normalize bowel movements. The primary endpoint, the combined responder rate for six of 12 weeks, showed that a greater proportion of tenapanor-treated patients compared to placebo-treated patients (36.5% vs. 23.7%, p<0.001) had at least a 30% reduction in abdominal pain and an increase of one or more CSBMs in the same week for at least six of the 12 weeks of the treatment period. The study achieved statistical significance for the CSBM and abdominal pain responder rates in the six of 12 weeks (47.4% vs. 33.3%, p<0.001; 49.8% vs. 38.3%, p=0.004). In the nine of 12 treatment weeks, the study achieved statistical significance for the combined responder rate (18.4% vs. 5.3%, p<0.001), in which patients must have had an increase of at least one bowel movement from baseline and at least three per week and a 30% reduction in abdominal pain for nine of the 12 weeks. In addition, for the nine of 12 weeks, the study achieved statistical significant for the individual CSBM responder rate (22.2% vs. 6.0%, p<0.001) and the abdominal pain responder rate (35.8% vs. 26.7%, p=0.015). The study also achieved statistical significance for all three durable responder endpoints, the combined responder rate (18.1% vs. 5.0%, p<0.001), CSBM responder rate (21.2% vs. 5.7%, p<0.001) and abdominal pain responder rate (34.8% vs. 26.7%, p=0.028), which are identical to the nine of 12-week responder endpoints, except the response must also occur in three of the last four treatment period weeks. Tenapanor was well-tolerated in the T3MPO-2 study. The only adverse events observed in more than two percent of patients in the tenapanor-treated group that were also greater than placebo were diarrhea (16.0% vs. 3.7%), flatulence (3.1% vs. 1.0%), nasopharyngitis (4.4% vs. 3.7%) and abdominal distension (3.4% vs. 0.3%). The placebo adjusted discontinuation rate due to diarrhea was 5.8%. Patients who completed T3MPO-1 and T3MPO-2 were eligible to enter T3MPO-3, our open-label, long-term safety trial where patients could continue to receive tenapanor for up to one year. In late 2017, we completed T3MPO-3 and have reported results that tenapanor had a mean compliance rate of approximately 98%, and that tenapanor was well-tolerated among the 240 patients treated. Of patients treated, 9.2% reported experiencing diarrhea, with 1.7% of patients discontinuing treatment due to diarrhea. The overall discontinuation rate in the study was 2.1%. Based on the positive results from the T3MPO program, we are preparing to submit an NDA to the FDA to request marketing approval of tenapanor for the treatment of IBS-C in the United States. To support the global commercialization of tenapanor for IBS-C, we are pursuing strategic collaborations to bring tenapanor to patients. In December 2017, we entered into a license agreement to provide Fosun Pharma with the exclusive rights to develop and commercialize tenapanor in China for the treatment of patients with IBS-C and hyperphosphatemia related to chronic kidney disease. The IBS-C market Numerous treatments exist for the constipation component of IBS-C, many of which are over-the-counter. There are three prescription products marketed for IBS-C: (i) Linzess (linaclotide), marketed by Ironwood Pharmaceuticals and Allergan, (ii) Amitiza (lubiprostone), marketed by Takeda and Sucampo, a wholly-owned subsidiary of Mallinckrodt, and (iii) Trulance (plecanatide), marketed by Synergy Pharmaceuticals. We believe that endogenoustenapanor may offer a significant benefit over currently marketed drugs like Amitiza, Linzess and local secretionTrulance in part because of GLP-1 and GLP-2 triggered by the stimulationprofile demonstrated in our Phase 3 program, which showed best-in-class efficacy results for the 9-of-12 week combined responder rates. Within the United States, there are approximately 11 million patients that suffer that suffer from IBS-C. There is significant unmet need for prescription medications, where, according a 2015 American Gastroenterological Association report, only 1 in 4 treated patients are very satisfied with the current FDA approved treatments in IBS-C. Other GI Programs In addition to tenapanor for IBS-C, we have an early GI pipeline comprised of RDX8940, a minimally absorbed, oral TGR5 agonist may have significant therapeutic potential for the treatment of several conditions. An injectable, stabilized form of GLP-2, called teduglutide (Gattex), is marketed for short bowel syndromewhich we submitted an investigational new drug application, or IND, in late 2016; RDX011, our second-generation NHE3 inhibitor; and has been studied in Crohn’s disease. GLP-2 is hypothesized to work in inflammatory bowel disease, or IBD, such as Crohn’s disease and ulcerative colitis, or UC, by stimulating the repair of the gut and improving the structural integrity of gut wall that is damaged in patients with IBD. Additionally, GLP-2 and its analogs have been shown to prevent chemotherapy-induced diarrhea in animal models. Injectable stabilized GLP-1 analogs that are commercially available, such as exenatide (Byetta) and liraglutide (Victoza), are commonly used to treat type 2 diabetes, among other metabolic conditions. Additionally, injectable GLP-1 analogs are being evaluated in the treatment of NASH because they are known to improve lipid metabolism in the liver. In all of these cases, GLP-1 and GLP-2 analogs are injectable thus we believe an oral agent that can emulate these effects would be welcome. Historically one of the limitationsour RDX023 program for the development of TGR5 agonists has been the observation with systemic compounds that stimulation of TGR5 in the gallbladder results in excess gallbladder filling, potentially increasing the risk of gallstones. Utilizing our approachgut-biased farnesoid X receptor, or FXR, agonists. While we are not currently actively developing these programs, they represent potential collaboration opportunities to design small molecules, we have created novel TGR5 agonist candidates that have extremely low systemic exposure and we have shown that these agents do not result in excess gallbladder filling in preclinical animal models.
We have selected a development candidate for the RDX009 program. This compound, in combination with a DPP-IV inhibitor, has demonstrated proof-of-concept in an animal efficacy model of IBD, and analogs of this compound have shown activity in animal models of chemotherapy-induced diarrhea and short bowel syndrome. We continue to evaluate the development candidate in several animal models of disease as we complete our pre-clinical studies with the intent of filing an IND in the second half of 2016.
RDX013 Program
Our RDX013 program is aimed at discovering and evaluating small molecule, orally-administered drug candidates that modulate the transport of potassium in the GI tract. Our agents will be designed to enhance potassium secretion or prevent potassium absorption in the colon and correct hyperkalemia disorders in CKD patients. We believe that specific potassium transporters in the intestines may serve as useful targets for our program. We believe that such agents may be used as stand-alone agents or used in combination with potassium binders to boost efficacy or to reduce the pill burden of the potassium binders. Several agents we have developed have demonstrated significant activity in animals.
RDX011 Program
We intend to leverage our knowledge of NHE3 inhibitors andsupport their effect on phosphate management as we seek to further understand tenapanor’s phosphate lowering mechanism of action. We also intend to evaluate new indications for tenapanor and other NHE3 inhibitors in order to exploit the unique capabilities and tools we have developed to modulate ion transport channels located on mucosal surfaces.continued development.
INTELLECTUAL PROPERTY Our commercial success depends in part on our ability to obtain and maintain proprietary protection for our drug candidates, manufacturing and process discoveries, and other know-how, to operate without infringing the proprietary rights of others and to prevent others from infringing our proprietary rights. Our policy is to seek to protect our proprietary positionintellectual property by, among other methods, filing U.S. and foreign patent applications related to our proprietary technology inventions and improvementsinventions that are important to the development and implementationoperation of our business. We also rely on trade secrets and careful monitoring of our proprietary information to protect aspects of our business that are not amenable to, or that we do not consider appropriate for, patent protection. As a normal course of business, we pursue composition-of-matter and method-of-use patents for our product candidates in key therapeutic areas. We also seek patent protection for broader structural and functional attributes of our product candidates that enable a minimally-systemic or minimally-systemic profile.
The patent positions of biopharmaceutical companies like us are generally uncertain and involve complex legal, scientific and factual questions. In addition, the coverage claimed in a patent application can be significantly reduced before the patent is issued, and its scope can be reinterpreted after issuance. Consequently, we do not know whether any of our product candidates will be protectable or remain protected by enforceable patents. We cannot predict whether the patent applications we are currently pursuing will issue as patents in any particular jurisdiction or whether the claims of our issued patents will provide sufficient proprietary protection from competitors. Any patents that we hold may be challenged, circumvented or invalidated by third parties. If third parties prepare and file patent applications in the United States that also claim technology or therapeutics to which we have rights, we may have to participate in interference proceedings in the U.S. Patent and Trademark Office, or USPTO, to determine priority of invention, which would result in substantial costs to us even if the eventual outcome is favorable to us. The term of individual patents depends upon the legal term of the patents in countries in which they are obtained. In most countries, including the United States, the patent term is generally 20 years from the earliest date of filing a non-provisional patent application in the applicable country. In the United States, a patent’s term may, in certain cases, be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the USPTO in examining and granting a patent, or may be shortened if a patent is terminally disclaimed over a commonly owned patent or a patent naming a common inventor and having an earlier expiration date. In addition, in the United States, the Hatch-Waxman Act permits a patent term extension of up to five years beyond the expiration of a U.S. patent as partial compensation for the patent term lost during the FDA regulatory review process occurring while the patent is in force. A patent extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval, and only one patent applicable to each regulatory review period may be extended and only those claims covering the approved drug, a method for using it or a method for manufacturing it may be extended. Similar provisions are available in the European Union and certain other foreign jurisdictions to extend the term of a patent that covers an approved drug. We may rely, in some circumstances, on trade secrets to protect our technology. Although we take steps to protect our proprietary information and trade secrets, including through contractual means with our employees and consultants, third parties may independently develop substantially equivalent proprietary information and techniques or otherwise gain access to our trade secrets or disclose our technology. Thus, we may not be able to meaningfully protect our trade secrets. It is our policy to require our employees, consultants, outside scientific collaboration partners, sponsored researchers and other advisors to execute confidentiality agreements upon the commencement of employment or consulting relationships with us. These agreements provide that all confidential information concerning the business or financial affairs developed or made known to the individual during the course of the individual’s relationship with us is to be kept confidential and not disclosed to third parties except in specific circumstances. In the case of employees, the agreements provide that all inventions conceived by the individual, and which are related to our current or planned business or research and development or made during the normal working hours, on our premises or using our equipment or proprietary information, are our exclusive property. NHE3 patents Our NHE3 patent portfolio is wholly owned by us. This portfolio includes threefour issued U.S. patents, two issued Japanese patents, two issued Korean patents and one issued Mexican patent.patent in each of the following territories: Australia, China, the European Union, Mexico, and Israel. These issued patents cover the composition and methods of using tenapanor and are predicted, without extension or adjustment, to expire in 2029. We have related national patent applications pending in Europe, China, India, Israel and a number of other countries. Any patents issuing from these patent applications are also predicted without extension or adjustment to expire in 2029. Additional U.S. and international patent applications are pending covering additional methods of using tenapanor, and composition of matter and methods of using compounds that we believe may be follow on compounds to tenapanor. Other program patents We have patent applications pending in the United States covering the composition of or methods of using tenapanor, or its backup compounds. NaP2b Patents
We have a portfolio of patents and patent applications claiming the compositions and methods of using our proprietary NaP2b inhibitor compounds. NaP2b is an intestinal transporter of dietary phosphorus. Our portfolio is wholly owned by us and includes four issued U.S. patents and three allowed U.S. applications covering the composition of or methods of using our NaP2b inhibitor compounds. The issued patents, and if issued, the allowed applications are predicted to expire in 2031. Numerous related patents have issued in Europe, Hong Kong and Japan Any patents resulting from these patent applications, if issued, are also predicted to expire in 2031.
RDX022
We have filed a PCT application covering the compositions and methods of using RDX022.
RDX009
We have filed a provisional application coveringinternationally that cover the compositions and methods of using our TGR5 agonists.agonists, our FXR agonists and compounds in our RDX013 program.
MANUFACTURING To date, we have relied upon third-party contract manufacturing organizations, or CMOs, to manufacture both the active pharmaceutical ingredient and final drug product dosage forms of our potential drug candidates used as clinical trial material. We expect that we will continue to rely upon CMOs for the manufacture of our clinical trial materials and for our own internal programs.commercial product requirements, when and if regulatory approval is received. Our license agreements with KHK and Fosun Pharma require us to supply active pharmaceutical ingredient and final drug product dosage forms of tenapanor for their use in the development of tenapanor in each of their respective territories, and we are further obligated to continue to supply active pharmaceutical ingredient to support their commercialization of tenapanor in each of their territories. We expect that we will use CMOs to satisfy our supply obligations to our collaboration partners. GOVERNMENT REGULATION/FDA The FDA and comparable regulatory authorities in state and local jurisdictions and in other countries impose substantial and burdensome requirements upon companies involved in the clinical development, manufacture, marketing and distribution of drugs. These agencies and other federal, state and local entities regulate research and development activities and the testing, manufacture, quality control, safety, effectiveness, labeling, storage, record keeping, approval, advertising and promotion, distribution, post-approval monitoring and reporting, sampling, and export and import of our product candidates. In the United States, the FDA regulates drug products under the Federal Food, Drug, and Cosmetic Act, or FFDCA, and the FDA’s implementing regulations. If we fail to comply with applicable FDA or other requirements at any time during the drug development process, the approval process or after approval, we may become subject to administrative or judicial sanctions. These sanctions could include the FDA’s refusal to approve pending applications, license suspension or revocation, withdrawal of an approval, warning letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, civil penalties or criminal prosecution. Any FDA enforcement action could have a material adverse effect on us. FDA approval is required before any new unapproved drug or dosage form, including a new use of a previously approved drug, can be marketed in the United States. The process required by the FDA before a drug may be marketed in the United States generally involves: | · | | completion of extensive preclinical laboratory tests, preclinical animal studies and formulation studies, some performed in accordance with the FDA’s current Good Laboratory Practice, or GLP, regulations; |
| · | | submission to the FDA of an Investigational New Drug, or IND, application which must become effective before human clinical trials in the United States may begin; |
| · | | approval by an independent institutional review board, or IRB, or ethics committee at each clinical trial site before each trial may be initiated; |
| · | | performance of adequate and well-controlled human clinical trials in accordance with Good Clinical Practice, or GCP, regulations to establish the safety and efficacy of the drug candidate for each proposed indication; |
| · | | submission to the FDA of a new drug application, or NDA; |
| · | | satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the drug is produced to assess compliance with current Good Manufacturing Practice, or cGMP, regulations; |
| · | | satisfactory completion of a potential review by an FDA advisory committee, if applicable; and |
| · | | completion of extensive preclinical laboratory tests, preclinical animal studies and formulation studies, some performed in accordance with the FDA’s current Good Laboratory Practice, or GLP, regulations;
submission to the FDA of an Investigational New Drug, or IND, application which must become effective before human clinical trials in the United States may begin;
approval by an independent institutional review board, or IRB, or ethics committee at each clinical trial site before each trial may be initiated;
performance of adequate and well-controlled human clinical trials in accordance with Good Clinical Practice, or GCP, regulations to establish the safety and efficacy of the drug candidate for each proposed indication;
submission to the FDA of a new drug application, or NDA;
satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the drug is produced to assess compliance with current Good Manufacturing Practice, or cGMP, regulations;
satisfactory completion of a potential review by an FDA advisory committee, if applicable; and
FDA review and approval of the NDA prior to any commercial marketing, sale or commercial shipment of the drug. |
The preclinical and clinical testing and approval process requires substantial time, effort and financial resources, and we cannot be certain that any approvals for our product candidates will be granted on a timely basis, if at all. Nonclinical tests include laboratory evaluation of product chemistry, formulation, stability and toxicity, as well as animal studies to assess the characteristics and potential safety and efficacy of the product. The results of preclinical tests, together with manufacturing information, analytical data and a proposed clinical trial protocol and other information, are submitted as part of an IND to the FDA. Some preclinical testing may continue even after the IND is submitted. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day30‑day time period, raises concerns or questions relating to the IND and places the clinical trial on a clinical hold, including concerns that human research subjects will be exposed to unreasonable health risks. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. A separate submission to an existing IND must also be made for each successive clinical trial conducted during product development. Clinical trials involve the administration of the investigational drug to human subjects under the supervision of qualified investigators. Clinical trials are conducted under protocols detailing, among other things, the objectives of the clinical trial, the parameters to be used in monitoring safety and the effectiveness criteria to be used. Each protocol must be submitted to the FDA as part of the IND. An independent IRB or ethics committee for each medical center proposing to conduct a clinical trial must also review and approve a plan for any clinical trial before it can begin at that center and the IRB must monitor the clinical trial until it is completed. The FDA, the IRB, or the sponsor may suspend or discontinue a clinical trial at any time on various grounds, including a finding that the subjects are being exposed to an unacceptable health risk. Clinical testing also must satisfy extensive GCP requirements, including the requirements for informed consent. All clinical research performed in the United States in support of an NDA must be authorized in advance by the FDA under the IND regulations and procedures described above. However, a sponsor who wishes to conduct a clinical trial outside the United States may, but need not, obtain FDA authorization to conduct the clinical trial under an IND. If a foreign clinical trial is not conducted under an IND, the sponsor may submit data from the clinical trial to the FDA in support of an NDA so long as the clinical trial is conducted in compliance with GCP and if the FDA is able to validate the data from the study through an onsite inspection, if necessary. GCP includes review and approval by an independent ethics committee, such as an IRB, and obtaining and documenting the freely given informed consent of the subject before study initiation. If the applicant seeks approval of an NDA solely on the basis of foreign data, the FDA will only accept such data if they are applicable to the U.S. population and U.S. medical practice, the studies have been performed by clinical investigators of recognized competence, and the data may be considered valid without the need for an on-site inspection by the FDA, or if the FDA considers such an inspection to be necessary, the FDA is able to validate the data through an on-site inspection or through other appropriate means. Clinical trials The clinical investigation of a new drug is typically conducted in three or four phases, which may overlap or be combined, and generally proceed as follows. | •· | | Phase 1: Clinical trials are initially conducted in a limited population of subjects to test the drug candidate for safety, dose tolerance, absorption, metabolism, distribution and excretion in healthy humans or, on occasion, in patients with severe problems or life-threatening diseases to gain an early indication of its effectiveness. |
| •· | | Phase 2: Clinical trials are generally conducted in a limited patient population to evaluate dosage tolerance and appropriate dosage, identify possible adverse effects and safety risks, and evaluate preliminarily the efficacy of the drug for specific targeted indications in patients with the disease or condition under study. |
| • | | · | | Phase 3: Clinical trials are typically conducted when Phase 2 clinical trials demonstrate that a dose range of the product candidate is effective and has an acceptable safety profile. Phase 3 clinical trials are commonly referred to as “pivotal” studies, which typically denotes a study which presents the data that the FDA or other relevant regulatory agency will use to determine whether or not to approve a |
| drug. Phase 3 clinical trials are generally undertaken with large numbers of patients, such as groups of several hundred to several thousand, to further evaluate dosage, to provide substantial evidence of clinical efficacy and to further test for safety in an expanded and diverse patient population at multiple, geographically-dispersed clinical trial sites. |
| •· | | Phase 4: In some cases, the FDA may condition approval of an NDA for a product candidate on the sponsor’s agreement to conduct additional clinical trials after NDA approval. In other cases, a sponsor may voluntarily conduct additional clinical trials post approval to gain more information about the drug. Such post approval trials are typically referred to as Phase 4 clinical trials. |
Concurrent with clinical trials, companies usually complete additional preclinicalnonclinical studies and must also develop additional information about the chemistry and physical characteristics of the drug and finalize a process for manufacturing the drug in commercial quantities in accordance with GMP requirements. The manufacturing process must be capable of consistently producing quality batches of the drug candidate and, among other things, the manufacturer must develop methods for testing the identity, strength, quality and purity of the final drug product. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the drug candidate does not undergo unacceptable deterioration over its shelf life. The FDA, the IRB or the clinical trial sponsor may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research subjects are being exposed to an unacceptable health risk. Additionally, some clinical trials are overseen by an independent group of qualified experts organized by the clinical trial sponsor, known as a data safety monitoring board or committee. This group provides authorization for whether or not a trial may move forward at designated check points based on access to certain data from the study. We may also suspend or terminate a clinical trial based on evolving business objectives and/or competitive climate.
New drug applications The results of preclinical studies and of the clinical trials, together with other detailed information, including extensive manufacturing information and information on the composition of the drug, are submitted to the FDA in the form of an NDA requesting approval to market the drug for one or more specified indications. The FDA reviews an NDA to determine, among other things, whether a drug is safe and effective for its intended use. Under the Prescription Drug User Fee Act, the FDA has a goal of responding to standard review NDAs of new molecular entities within ten months after the 60 60‑day filing review period, or six months after the 60 60‑day filing review period for priority review NDAs, but this timeframe is often extended by FDA requests for additional information or clarification. The FDA may refer the application to an advisory committee for review, evaluation and recommendation as to whether the application should be approved. The FDA is not bound by the recommendation of an advisory committee, but it generally follows such recommendations. Before approving an application, the FDA will inspect the facility or the facilities at which the finished drug product, and sometimes the active pharmaceutical ingredient, or API, is manufactured, and will not approve the drug unless cGMP compliance is satisfactory. The FDA may also inspect the sites at which the clinical trials were conducted to assess their compliance, and will not approve the drug unless compliance with cGCP requirements is satisfactory. After the FDA evaluates the NDA and conducts inspections of manufacturing facilities where the drug product and/or its API will be produced, it may issue an approval letter or a Complete Response Letter. An approval letter authorizes commercial marketing of the drug with specific prescribing information for specific indications. A Complete Response Letter indicates that the review cycle of the application is complete and the application is not ready for approval. A Complete Response Letter may require additional clinical data and/or an additional pivotal Phase 3 clinical trial(s), and/or other significant, expensive and time-consuming requirements related to clinical trials, preclinical studies or manufacturing. Even if such additional information is submitted, the FDA may ultimately decide that the NDA does not satisfy the criteria for approval. The FDA could also approve the NDA with a Risk Evaluation and Mitigation Strategy, or REMS, plan to mitigate risks, which could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA also may condition approval on, among other things, changes to proposed labeling, development of adequate controls and specifications, or a commitment to conduct one or more post-market studies or clinical trials. Such post-market testing may include Phase 4 clinical trials and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization. The FDA has the authority to prevent or limit further marketing of a drug based on the results of these post-marketing programs. Once the FDA approves an NDA, or supplement thereto, the FDA may withdraw the approval if ongoing regulatory requirements are not met or if safety problems are identified after the drug reaches the market. Drugs may be marketed only for the FDA approved indications and in accordance with the provisions of the approved labeling. Further, if there are any modifications to the drug, including changes in indications, labeling, or manufacturing processes or facilities, the applicant may be required to submit and obtain FDA approval of a new NDA or NDA supplement, which may require the applicant to develop additional data or conduct additional preclinical studies and clinical trials. The testing and approval processes require substantial time, effort and financial resources, and each may take several years to complete. The FDA may not grant approval on a timely basis, or at all. Even if we believe a clinical trial has demonstrated safety and efficacy of one of our drug candidates for the proposed indication, the results may not be satisfactory to the FDA. Nonclinical and clinical data may be interpreted by the FDA in different ways, which could delay, limit or prevent regulatory approval. We may encounter difficulties or unanticipated costs in our efforts to secure necessary governmental approvals which could delay or preclude us from marketing drugs. The FDA may limit the indications for use or place other conditions on any approvals that could restrict the commercial application of the drugs. After approval, certain changes to the approved drug, such as adding new indications, manufacturing changes, or additional labeling claims are subject to further FDA review and approval. Depending on the nature of the change proposed, an NDA supplement must be filed and approved before the change may be implemented. For many proposed post-approval changes to an NDA, but excluding efficacy supplements to an NDA, the FDA has up to 180 days to review the application. As with new NDAs, the review process is often significantly extended by the FDA requests for additional information or clarification.
Other regulatory requirements Any drugs manufactured or distributed by us or our collaboration partners pursuant to FDA approvals would be subject to continuing regulation by the FDA, including recordkeeping requirements and reporting of adverse experiences associated with the drug. Drug manufacturers and their subcontractors are required to register their establishments with the FDA and certain state agencies, and are subject to periodic announced and unannounced inspections by the FDA and certain state agencies for compliance with ongoing regulatory requirements, including cGMP, which impose certain procedural and documentation requirements upon us and our third partythird-party manufacturers. Failure to comply with the statutory and regulatory requirements can subject a manufacturer to possible legal or regulatory action, such as warning letters, suspension of manufacturing, seizure of product, injunctive action or possible civil penalties. We cannot be certain that we or our present or future third partythird-party manufacturers or suppliers will be able to comply with the cGMP regulations and other ongoing FDA regulatory requirements. If we or our present or future third partythird-party manufacturers or suppliers are not able to comply with these requirements, the FDA may, among other things, halt our clinical trials, require us to recall a drug from distribution or withdraw approval of the NDA for that drug. The FDA closely regulates the post-approval marketing and promotion of drugs, including standards and regulations for direct-to-consumer advertising, off-label promotion, industry-sponsored scientific and educational activities and promotional activities involving the Internet. A company can make only those claims relating to safety and efficacy that are approved by the FDA. Failure to comply with these requirements can result in, among other things, adverse publicity, warning letters, corrective advertising and potential civil and criminal penalties. Physicians may prescribe legally available drugs for uses that are not described in the product’s labeling and that differ from those tested by us and approved by the FDA. Such off-label uses are common across medical specialties. Physicians may believe that such off-label uses are the best treatment for many patients in varied circumstances. The FDA does not regulate the behavior of physicians in their choice of treatments. The FDA does, however, impose stringent restrictions on manufacturers’ communications regarding off-label use. Hatch-Waxman Act Section 505 of the FFDCA describes three types of marketing applications that may be submitted to the FDA to request marketing authorization for a new drug. A Section 505(b)(1) NDA is an application that contains full reports of investigations of safety and efficacy. A 505(b)(2) NDA is an application that contains full reports of investigations of safety and efficacy but where at least some of the information required for approval comes from investigations that were not conducted by or for the applicant and for which the applicant has not obtained a right of reference or use from the person by or for whom the investigations were conducted. This regulatory pathway enables the applicant to rely, in part, on the FDA’s prior findings of safety and efficacy for an existing product, or published literature, in support of its application. Section 505(j) establishes an abbreviated approval process for a generic version of approved drug products through the submission of an Abbreviated New Drug Application, or ANDA. An ANDA provides for marketing of a generic drug product that has the same active ingredients, dosage form, strength, route of administration, labeling, performance characteristics and intended use, among other things, to a previously approved product. ANDAs are termed “abbreviated” because they are generally not required to include nonclinical (animal) and clinical (human) data to establish safety and efficacy. Instead, generic applicants must scientifically demonstrate that their product is bioequivalent to, or performs in the same manner as, the innovator drug through in vitro, in vivo, or other testing. The generic version must deliver the same amount of active ingredients into a subject’s bloodstream in the same amount of time as the innovator drug and can often be substituted by pharmacists under prescriptions written for the reference listed drug. In seeking approval for a drug through an NDA, applicants are required to list with the FDA each patent with claims that cover the applicant’s drug or a method of using the drug. Upon approval of a drug, each of the patents listed in the application for the drug is then published in the FDA’s Approved Drug Products with Therapeutic Equivalence Evaluations, commonly known as the Orange Book. Drugs listed in the Orange Book can, in turn, be cited by potential competitors in support of approval of an ANDA or 505(b)(2) NDA. Upon submission of an ANDA or a 505(b)(2) NDA, an applicant must certify to the FDA that (1) no patent information on the drug product that is the subject of the application has been submitted to the FDA; (2) such patent has expired; (3) the date on which such patent expires; or (4) such patent is invalid or will not be infringed upon by the manufacture, use or sale of the drug product for which the application is submitted. Generally, the ANDA or 505(b)(2) NDA cannot be approved until all listed patents have expired, except where the ANDA or 505(b)(2) NDA applicant challenges a listed patent through the last type of certification, also known as a paragraph IV certification. If the applicant does not challenge the listed patents or indicates that it is not seeking approval of a patented method of use, the ANDA or 505(b)(2) NDA application will not be approved until all of the listed patents claiming the referenced product have expired. If the ANDA or 505(b)(2) NDA applicant has provided a Paragraph IV certification to the FDA, the applicant must send notice of the Paragraph IV certification to the NDA and patent holders once the application has been accepted for filing by the FDA. The NDA and patent holders may then initiate a patent infringement lawsuit in response to the notice of the paragraph IV certification. If the paragraph IV certification is challenged by an NDA holder or the patent owner(s) asserts a patent challenge to the paragraph IV certification, the FDA may not approve that application until the earlier of 30 months from the receipt of the notice of the paragraph IV certification, the expiration of the patent, when the infringement case concerning each such patent was favorably decided in the applicant’s favor or settled, or such shorter or longer period as may be ordered by a court. This prohibition is generally referred to as the 30‑month stay. In instances where an ANDA or 505(b)(2) NDA applicant files a paragraph IV certification, the NDA holder or patent owner(s) regularly take action to trigger the 30‑month stay, recognizing that the related patent litigation may take many months or years to resolve. Thus, approval of an ANDA or 505(b)(2) NDA could be delayed for a significant period of time depending on the patent certification the applicant makes and the reference drug sponsor’s decision to initiate patent litigation. The Hatch-Waxman Act establishes periods of regulatory exclusivity for certain approved drug products, during which the FDA cannot approve (or in some cases accept) an ANDA or 505(b)(2) application that relies on the branded reference drug. For example, the holder of an NDA, including a 505(b)(2) NDA, may obtain five years of exclusivity upon approval of a new drug containing new chemical entities, or NCEs, that have not been previously approved by the FDA. A drug is a new chemical entity if the FDA has not previously approved any other new drug containing the same active moiety, which is the molecule or ion responsible for the therapeutic activity of the drug substance. During the exclusivity period, the FDA may not accept for review an ANDA or a 505(b)(2) NDA submitted by another company that contains the previously approved active moiety. However, an ANDA or 505(b)(2) NDA may be submitted after four years if it contains a certification of patent invalidity or non-infringement. The Hatch-Waxman Act also provides three years of marketing exclusivity to the holder of an NDA (including a 505(b)(2) NDA) for a particular condition of approval, or change to a marketed product, such as a new formulation for a previously approved product, if one or more new clinical studies (other than bioavailability or bioequivalence studies) was essential to the approval of the application and was conducted/sponsored by the applicant. This three-year exclusivity period protects against FDA approval of ANDAs and 505(b)(2) NDAs for the condition of the new drug’s approval. As a general matter, the three-year exclusivity does not prohibit the FDA from approving ANDAs or 505(b)(2) NDAs for generic versions of the original, unmodified drug product. Five-year and three-year exclusivity will not delay the submission or approval of a full NDA; however, an applicant submitting a full NDA would be required to conduct or obtain a right of reference to all of the preclinical studies and adequate and well-controlled clinical trials necessary to demonstrate safety and efficacy. Fraud and abuse laws In the United States, the research, manufacturing, distribution, sale and promotion of drug products and medical devices are potentially subject to regulation by various federal, state and local authorities in addition to the FDA, including the Centers for Medicare & Medicaid Services, or CMS, other divisions of the U.S. Department of Health and Human Services (e.g., the Office of Inspector General), the U.S. Department of Justice, state Attorneys General, and other state and local government agencies. These laws include but are not limited to, the Anti-Kickback Statute, the federal False Claims Act, the federal Physician Payments Sunshine Payment Act, and other state and federal laws and regulations. The Anti-Kickback Statute makes it illegal for any person, including a prescription drug manufacturer (or a party acting on its behalf) to knowingly and willfully solicit, receive, offer, or pay any remuneration that is intended to induce the referral of business, including the purchase, order, or prescription of a particular drug, for which payment may be made under a federal healthcare program, such as Medicare or Medicaid. Violations of this law are punishable by up to five years in prison, criminal fines, administrative civil money penalties, and exclusion from participation in federal healthcare programs. In addition, the Affordable Care Act, among other things, amends the intent requirement of the federal Anti-Kickback Statute and federal criminal healthcare fraud statutes. Aa person or entity no longer needsdoes not need to have actual knowledge of the statute or specific intent to violate it.it in order to have committed a violation. Moreover, the Affordable Care Act provides that the government may assert that a claim including items or services resulting from a violation of the federal anti-kickback statuteAnti-Kickback Statute constitutes a false or fraudulent claim for purposes of the False Claims Act. The federal False Claims Act prohibits anyone from knowingly presenting, or causing to be presented, for payment to federal programs (including Medicare and Medicaid) claims for items or services, including drugs, that are false or fraudulent, claims for items or services not provided as claimed, or claims for medically unnecessary items or services. Although we would not submit claims directly to payors, manufacturers can be held liable under these laws if they are deemed to “cause” the submission of false or fraudulent claims by, for example, providing inaccurate billing or coding information to customers or promoting a product off-label. In addition, our future activities relating to the reporting of wholesaler or estimated retail prices for our products, the reporting of prices used to calculate Medicaid rebate information and other information affecting federal, state, and third-party reimbursement for our products, and the sale and marketing of our products, are subject to scrutiny under this law. For example, pharmaceutical companies have been prosecuted under the federal False Claims Act in connection with their off-label promotion of drugs. Penalties for a False Claims Act violation include three times the actual damages sustained by the government, plus mandatory civil penalties of between $5,500$11,181 and $11,000$22,363 for each separate false claim, the potential for exclusion from participation in federal healthcare programs, and, although the federal False Claims Act is a civil statute, conduct that results in a False Claims Act violation may also implicate various federal criminal statutes. If the government were to allege that we were, or convict us of, violating these false claims laws, we could be subject to a substantial fine and may suffer a decline in our stock price. In addition, private individuals have the ability to bring actions under the federal False Claims Act and certain states have enacted laws modeled after the federal False Claims Act. In addition to the laws described above, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively known as the Affordable Care Act, also imposed new reporting requirements on drug manufacturers for payments made to physicians and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members. Failure to submit required information may result in civil monetary penalties of up to an aggregate of $150,000$165,786 per year (or up to an aggregate of $1$1.105 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately and completely reported in an annual submission. The period between August 1, 2013 and December 31, 2013 was the first reporting period and manufacturers were required to report aggregate payment data by March 31, 2014, and will be required to report detailed payment data and submit legal attestation to the accuracy of such data during Phase 2 of the program (which begins in May 2014 and extends for at least 30 days). Thereafter, manufacturersManufacturers must submit reports by the 90th day of each subsequent calendar year.
Many states have also adopted laws similar to the federal laws discussed above. Some of these state prohibitions apply to the referral of patients for healthcare services reimbursed by any insurer, not just federal healthcare programs such as Medicare and Medicaid. There has also been a recent trend of increased regulation of payments made to physicians and other healthcare providers. Certain states mandate implementation of compliance programs, impose restrictions on drug manufacturers’ marketing practices and/or require the tracking and reporting of pricing and marketing information as well as gifts, compensation and other remuneration to physicians. Many of these laws contain ambiguities as to what is required to comply with such laws, which may affect our sales, marketing, and other promotional activities by imposing administrative and compliance burdens on us. In addition, given the lack of clarity with respect to these laws and their implementation, our reporting actions could be subject to the penalty provisions of the pertinent state and perhaps federal, authorities. Because we intend to commercialize products that could be reimbursed under a federal healthcare program and other governmental healthcare programs, we plan to develop a comprehensive compliance program that establishes internal controls to facilitate adherence to the rules and program requirements to which we will or may become subject. Although compliance programs can mitigate the risk of investigation and prosecution for violations of these laws, the risks cannot be entirely eliminated. Due to the breadth of these laws, the absence of guidance in the form of regulations or court decisions, and the potential for additional legal or regulatory change in this area, it is possible that our future sales and marketing practices and/or our future relationships with physicians and other healthcare providers might be challenged under such laws. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business.
Third-party coverage and reimbursement Sales of pharmaceutical products depend in significant part on the availability of coverage and adequate reimbursement by third-party payors, such as state and federal governments, including Medicare and Medicaid, and commercial managed care providers. In the United States, no uniform policy of coverage and reimbursement for drug products exists among third-party payors. Accordingly, decisions regarding the extent of coverage and amount of reimbursement to be provided for our product candidates, if approved, will be made on a payor by payor basis. As a result, the coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our product candidates to each payor separately, with no assurance that coverage and adequate reimbursement will be obtained. Third-party payors may limit coverage to specific drug products on an approved list, or formulary, which might not include all of the FDA-approved drugs for a particular indication. A decision by a third-party payor not to cover our product candidates could reduce physician utilization of our products once approved and have a material adverse effect on our future sales, results of operations and financial condition. Moreover, a payor’s decision to provide coverage for a drug product does not imply that an adequate reimbursement rate will be approved. Adequate third-party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on our investment in product development. In addition, in July 2010, CMS released its final rule to implement a bundled prospective payment system for the treatment of ESRD patients as required by the Medicare Improvements for Patients and Providers Act, or MIPPA. The bundled payment includes all renal dialysis services furnished for outpatient maintenance dialysis, including ESRD-related drugs and biologicals. The final rule delayed the inclusion of oral medications without intravenous equivalents in the bundled payment until January 1, 2014 and in April 2014, President Obama signed the Protecting Accessdue to Medicare Act of 2014, which further extends this implementation date tosubsequent legislative amendments, CMS provided that such inclusion will remain delayed until January 1, 2024. As a result of the recent legislation,2025. Unless additional Congressional action is taken, beginning in 2024,2025 ESRD-related drugs will be included in the bundle and separate Medicare reimbursement will no longer be available for such drugs, as it is today under Medicare Part D. While it is too early to project the full impact that bundling may have on drugs for the phosphate binder industry,treatment of hyperphosphatemia, the impact could potentially cause dramatic price reductions for tenapanor, if approved. Healthcare reform In March 2010, Congress passed and President Obama signed into law, the Patient Protection and Affordable Care Act, a healthcare reform measure, often called, the Affordable Care Act. The Affordable Care Act substantially changes the way healthcare will beis financed by both governmental and private insurers, and significantly impacts the pharmaceutical industry. The Affordable Care Act contains a number of provisions, including those governing enrollment in federal healthcare programs, reimbursement changes and fraud and abuse measures, which will impacthave impacted existing government healthcare programs and will resulthave resulted in the development of new programs, including Medicare payment for performance initiatives and improvements to the physician quality reporting system and feedback program. Additionally, the Affordable Care Act: | · | | increases the minimum level of Medicaid rebates payable by manufacturers of brand-name drugs from 15.1% to 23.1%; |
| · | | requires collection of rebates for drugs paid by Medicaid managed care organizations; |
| · | | increases the minimum level of Medicaid rebates payable by manufacturers of brand-name drugs from 15.1% to 23.1%;
requires collection of rebates for drugs paid by Medicaid managed care organizations;
expands eligibility criteria for Medicaid programs by, among other things, allowing states to offer Medicaid coverage to additional individuals and by adding new mandatory eligibility categories for certain individuals with income at or below 133% of the federal poverty level, thereby potentially increasing a manufacturer’s Medicaid rebate liability; |
| · | | expands access to commercial health insurance coverage through new state-based health insurance marketplaces, or exchanges; |
| · | | requires manufacturers to participate in a coverage gap discount program, under which they must agree to offer 50 percent point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D, beginning January 2011; and |
| · | | imposes a non-deductible annual fee on pharmaceutical manufacturers or importers who sell “branded prescription drugs” to specified federal government programs. |
Since its enactment, there have been judicial and Congressional challenges to certain aspects of the federal poverty level, thereby potentially increasing a manufacturer’s Medicaid rebate liability; expands accessAffordable Care Act. We expect that the new presidential administration and U.S. Congress will likely continue to commercial health insuranceseek to modify, repeal, or otherwise invalidate all or certain provisions of, the Affordable Care Act. There is still uncertainty with respect to the impact President Trump’s administration and the U.S. Congress may have, if any, and any changes will likely take time to unfold, and could have an impact on coverage through new state-based health insurance marketplaces, or exchanges;
requires manufacturers to participate in a coverage gap discount program, under which they must agree to offer 50 percent point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a conditionand reimbursement for healthcare items and services covered by plans that were authorized by the manufacturer’s outpatient drugs to be covered under Medicare Part D, beginning January 2011; and
Affordable Care Act. imposes a non-deductible annual fee on pharmaceutical manufacturers or importers who sell “branded prescription drugs” to specified federal government programs.
In addition, other legislative changes have been proposed and adopted in the United States since the Affordable Care Act was enacted. InFor example, in August 2011, the Budget Control Act of 2011, among other things, created the Joint Select Committee on Deficit Reduction to recommend proposals in spending reductions to Congress. The Joint Select Committee did not achieve its targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, triggering the legislation’s automatic reduction to several government programs. This includesincluded aggregate reductions to Medicare payments to providers of 2 percent per fiscal year, which went into effect on April 1, 2013.2013, and, due to subsequent legislative amendments, will remain in effect through 2025 unless additional Congressional action is taken. In January 2013, the ATRA was enacted, which,American Taxpayer Relief Act, among other things, further reduced Medicare payments to several providers, including hospitals, imaging centers and cancer treatment centers.centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. Additionally, individual states have also become increasingly active in passing legislation and implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access, and to encourage importation from other countries and bulk purchasing. Recently, there has also been heightened governmental scrutiny over the manner in which drug manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed bills designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drug products. These new laws and the regulations and policies implementing them, as well as other healthcare reform measures that may be adopted in the future, may have a material adverse effect on our industry generally and on our ability to successfully develop and commercialize our products. Other regulations We are also subject to numerous federal, state and local laws relating to such matters as safe working conditions, manufacturing practices, environmental protection, fire hazard control, and disposal of hazardous or potentially hazardous substances. We may incur significant costs to comply with such laws and regulations now or in the future. EMPLOYEES As of December 31, 2015,2017, we had 6175 full-time employees, including a total of 2015 employees with Ph.D. degrees. Within our workforce, 4854 employees are engaged in research and development and the remaining 1321 in general management and administration, including finance, legal, and business development. None of our employees are represented by labor unions or covered by collective bargaining agreements. We believe that we maintain good relations with our employees. RESEARCH AND DEVELOPMENT The costs were $39.9 million, $25.9 million and $28.1 million inOur research and development costs were $75.5 million, $94.2 million and $39.9 million in the years 2015, 2014ended December 31, 2017, 2016 and 2013,2015, respectively. See “ITEM“ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS”OPERATIONS” for additional detail regarding our research and development activities.
CORPORATE INFORMATION We were incorporated in Delaware on October 17, 2007, under the name Nteryx and changed our name to Ardelyx, Inc. in June 2008. We operate in only one business segment, which is the research, development and commercialization of biopharmaceutical products. See Note 1 to our financial statements included in this Annual Report on Form 10-K.10‑K. Our principal offices are located at 34175 Ardenwood Blvd., Suite 200, Fremont, CA 94555, and our telephone number is (510) 745-1700.745‑1700. Our website address is www.ardelyx.com. We file electronically with the Securities and Exchange Commission, or SEC, our annual reports on Form 10-K,10‑K, quarterly reports on Form 10-Q10‑Q and current reports on Form 8-K8‑K pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934, as amended. We make available on our website at www.ardelyx.com, free of charge, copies of these reports, as soon as reasonably practicable after we electronically file such material with, or furnish it to, the SEC. The public may read or copy any materials we file with the SEC at the SEC’s Public Reference Room at 100 F Street NE, Washington, D.C. 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330.1‑800‑SEC‑0330. The SEC maintains a website that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC. The address of that website iswww.sec.gov. www.sec.gov. ITEM 1A. RISK FACTORS Our business involves significant risks, some of which are described below. You should carefully consider these risks, as well as other information in this Annual Report on Form 10-K,10‑K, including our financial statements and the related notes and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” The occurrence of any of the events or developments described below could harm our business, financial condition, results of operations, cash flows, the trading price of our common stock and our growth prospects. Additional risks and uncertainties not presently known to us or that we currently deem immaterial may also impair our business operations. Risks Related to Our Limited Operating History, Financial Condition and Capital Requirements We have a limited operating history, have incurred significant losses since our inception and we will incur losses in the future, which makes it difficult to assess our future viability. We are a clinical-stage biopharmaceutical company with a limited operating history. Biopharmaceutical product development is a highly speculative undertaking and involves a substantial degree of risk. To date, we have focused substantially all of our efforts on our research and development activities, including developing our clinical product candidates, tenapanor and RDX022, and developing our proprietary drug discovery and design platform. To date, we have not commercialized any products or generated any revenue from the sale of products. We are not profitable and have incurred losses in each year since our inception in October 2007, and we do not know whether or when we will become profitable. We have only a limited operating history upon which to evaluate our business and prospects. We continue to incur significant research, development and other expenses related to our ongoing operations. As of December 31, 2015,2017, we had an accumulated deficit of $101.5$278.2 million. We expect that our operating losses will substantially increase for the foreseeable future as we continueprepare for the potential commercialization of, and incur manufacturing and development ofcosts for, tenapanor, and RDX022. Inincluding costs associated with completing the fourth quarter of 2015, we initiated twoongoing Phase 3 clinical trials to evaluate tenapanor for the treatmentdevelopment of IBS-C, and in December 2015, we initiated a Phase 2b clinical trial evaluating tenapanor for the treatment of hyperphosphatemia in end stage renal disease patients. In addition, we expect our operating lossesESRD patients on dialysis, preparing the new drug application, or NDA, for submission to substantially increase as we incur manufacturing coststhe U.S. Food and Drug Administration, or FDA, to request marketing authorization for tenapanor for the treatment of patients with IBS-C, and RDX022, advance RDX022 into a Phase 3 clinical program which we expect to initiate in the second half of 2016, and as we continuecontinuing our discovery research, development, manufacturing and commercializationresearch activities. Our prior losses, combined with expected future losses, have had and will continue to have an adverse effect on our stockholders’ equity and working capital. Further, the net losses we incur may fluctuate significantly from quarter to quarter and year to year, such that a period-to-period comparison of our results of operations may not be a good indication of our future performance.
We have substantial net operating loss and tax credit carryforwards for Federal and California income tax purposes. Such net operating losses and tax credits carryforwards may be reduced as a result of certain intercompany restructuring transactions. In addition, the future utilization of such net operating loss and tax credit carryforwards and credits will be subject to limitations, pursuant to Internal Revenue Code Sections 382 and 383, as a result of ownership changes that have occurred previously and additional limitations may be applicable as a result of ownership changes that could occur in the future. We have never generated any revenue from product sales and may never be profitable. We have no products approved for sale and have never generated any revenue from product sales. Our ability to generate revenue from product sales and achieve profitability depends on our ability to successfully complete the development of and obtain the regulatory and marketing approvals necessary to commercialize tenapanor for one or more ofindications, either on our product candidates.own, or with one or more collaboration partners. We do not anticipate generating revenue from product sales for the foreseeable future. Our ability to generate future revenue from product sales or pursuant to milestone payments depends heavily on many factors, including but not limited to: | · | | the successful completion of nonclinical and clinical development of tenapanor; |
| · | | obtaining regulatory approvals for tenapanor, either on our own, or with one or more collaboration partners; |
| · | | our ability to successfully commercialize tenapanor, either on our own, or with one or more collaboration partners; |
| · | | developing a sustainable and scalable manufacturing process for tenapanor and establishing and maintaining supply and manufacturing relationships with third parties that can provide an adequate (in amount and quality) supply of product to support the market demand for tenapanor, if approved; |
| · | | obtaining market acceptance of tenapanor, if approved, as a viable treatment option for the indications for which it is approved; |
| · | | addressing any competing technological and market developments; |
| · | | identifying, assessing, acquiring, in-licensing and/or developing new product candidates; |
| · | | negotiating favorable terms in any collaboration partnership, licensing or other arrangements into which we may enter; |
| · | | maintaining, protecting, and expanding our portfolio of intellectual property rights, including patents, trade secrets, and know-how, and our ability to develop, manufacture and commercialize our product candidates and products without infringing intellectual property rights of others; and |
| · | | the completion of nonclinical and clinical development of our product candidates;
obtaining regulatory approvals for our product candidates, either on our own, or with one or more collaboration partners;
our ability to successfully commercialize our product candidates, either on our own, or with one or more collaboration partners;
developing a sustainable and scalable manufacturing process for any approved product candidates and establishing and maintaining supply and manufacturing relationships with third parties that can provide an adequate (in amount and quality) supply of product to support clinical development and the market demand for our product candidates, if approved;
obtaining market acceptance of our product candidates, if approved, as viable treatment options;
addressing any competing technological and market developments;
identifying, assessing, acquiring, in-licensing and/or developing new product candidates;
negotiating favorable terms in any collaboration partnership, licensing or other arrangements into which we may enter;
maintaining, protecting, and expanding our portfolio of intellectual property rights, including patents, trade secrets, and know-how, and our ability to develop, manufacture and commercialize our product candidates and products without infringing intellectual property rights of others; and
attracting, hiring, and retaining qualified personnel. |
In cases where we are successful in obtaining regulatory approvals to market tenapanor for one or more of our product candidates,indications, our revenue will be dependent, in part, upon the size of the markets in the territories for which regulatory approval is granted, the accepted price for the product, the ability to get reimbursement at any price and whether we are commercializing the product or the product is being commercialized by a collaboration partner, and in such case, whether we have royalty and/or co-promotion rights for that territory. If the number of patients suitable for our product candidatestenapanor is not as significant as we estimate, the indicationindications approved by regulatory authorities isare narrower than we expect, or the reasonably accepted population for treatment is narrowed by competition, physician choice or treatment guidelines, we may not generate significant revenue from the sale of such products,tenapanor, even if approved. Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods. Our failure to generate revenue from product sales would likely depress our market value and could impair our ability to raise capital, expand our business, discover or develop other product candidates or continue our operations. A decline in the value of our common stock could cause our stockholders to lose all or part of their investment. We will require substantial additional financing to achieve our goals, and a failurethe inability to obtainaccess this necessary capital when needed on acceptable terms, or at all, could force us to delay, limit, reduce or terminate our planned clinical programspre-commercialization efforts for tenapanor and RDX022, or our other product development and platform development activities. Since our inception, most of our resources have been dedicated to our research and development activities, including developing our clinical product candidates,candidate tenapanor and RDX022, and developing our proprietary drug discovery and design platform. We believe that we will continue to expend substantial resources for the foreseeable future, including costs associated with conductingcompleting the Phase 3 clinical programsprogram for tenapanor and RDX022,for the treatment of hyperphosphatemia in ESRD patients on dialysis, research and development, conducting preclinical studies and clinical trials for our other programs, obtaining regulatory approvals, developing and maintaining scalable manufacturing processes for our product candidates and sales and marketing. Because the outcome of any clinical trial and/or regulatory approval process is highly uncertain, we cannot reasonably estimate the actual amounts necessary to successfully complete the development, regulatory approval process and commercialization or co-promotion of any of our product candidates. Our future funding requirements will depend on many factors, including, but not limited to: | · | | the progress, timing, scope, results and costs of our Phase 3 clinical trial programs evaluating tenapanor for the treatment of hyperphosphatemia in ESRD patients on dialysis, the submission of an NDA with the FDA to request marketing authorization for tenapanor for the treatment of IBS-C, as well as our decision whether or not to pursue other indications for tenapanor; |
| · | | our ability to successfully commercialize tenapanor, either alone or with one or more collaboration partners; |
| · | | the manufacturing costs of our product candidates, and the availability of one or more suppliers for our product candidates at reasonable costs, both for clinical and commercial supply; |
| · | | the selling and marketing costs associated with tenapanor, including the cost and timing of building our sales and marketing capabilities, should we elect to do so; |
| · | | our ability to maintain our existing collaboration partnerships and to establish additional collaboration partnerships, in-license/out-license, joint ventures or other similar arrangements and the financial terms of such agreements; |
| · | | the timing, receipt, and amount of sales of, or royalties on, tenapanor, if any; |
| · | | the sales price and the availability of adequate third-party reimbursement for tenapanor, if approved; |
| · | | the cash requirements of any future acquisitions or discovery of product candidates; |
| · | | the number and scope of preclinical and discovery programs that we decide to pursue or initiate, and any clinical trials we decide to pursue for other product candidates; |
| · | | the time and cost necessary to respond to technological and market developments; and |
| · | | the costs of filing, prosecuting, maintaining, defending and enforcing any patent claims and other intellectual property rights, including litigation costs and the outcome of such litigation, including costs of defending any claims of infringement brought by others in connection with the development, manufacture or commercialization of tenapanor or any of our product candidates. |
the progress, timing, scope, results and coststhe progress, timing, scope, results and costs of our clinical program for RDX022;
the time and cost necessary to obtain regulatory approvals for our product candidates and the costs of post-marketing studies that could be required by regulatory authorities;
our ability to successfully commercialize our product candidates, either alone or with one or more collaboration partners;
the manufacturing costs of our product candidates, and the availability of one or more suppliers for our product candidates at reasonable costs, both for clinical and commercial supply;
the selling and marketing costs associated with product candidates, including the cost and timing of building our sales and marketing capabilities;
our ability to establish and maintain collaboration partnerships, in-license/out-license or other similar arrangements and the financial terms of such agreements;
the timing, receipt, and amount of sales of, or royalties on, our future products, if any;
the sales price and the availability of adequate third-party reimbursement for our product candidates;
the cash requirements of any future acquisitions or discovery of product candidates;
the number and scope of preclinical and discovery programs that we decide to pursue or initiate, and any clinical trials we decide to pursue for other product candidates;
the time and cost necessary to respond to technological and market developments; and
the costs of filing, prosecuting, maintaining, defending and enforcing any patent claims and other intellectual property rights, including litigation costs and the outcome of such litigation, including costs of defending any claims of infringement brought by others in connection with the development, manufacture or commercialization of our product candidates.
Additional funds may not be available when we need them on terms that are acceptable to us, or at all. If adequate funds are not available to us on a timely basis, we may be required to delay, the clinical development of tenapanor and/or RDX022, delay, limit, reduce or terminate our research activities, preclinical and clinical trials for our other product candidates and our establishment and maintenance of sales and marketing capabilities or other activities that may be necessary to commercialize our product candidates,tenapanor, either alone or with collaboration partners. Additionally, our inability to access capital on a collaboration partner.timely basis and on terms that are acceptable to us may force us to restructure certain aspects of our business or identify and complete one or more strategic collaborations or other transactions in order to fund the development or commercialization of tenapanor or certain of our product candidates through the use of alternative structures. Risks Related to Our Business We are substantially dependent on the success of our lead product candidate, tenapanor, which may not be successful in further nonclinical studies or clinical trials, receive regulatory approval or be successfully commercialized. To date, we have invested a significant amount of our efforts and financial resources in the research and development of tenapanor, which is currently our lead product candidate and one of only two product candidates in clinical trials.candidate. The clinical and commercial success of tenapanor will depend on a number of factors, including the following: | · | | our ability to, in a timely manner and under terms that are acceptable to us, establish a collaborative relationship for the commercialization of tenapanor for the treatment of IBS-C in the United States; |
| · | | the ability of the third-party manufacturers we contract with to successfully execute and scale up the manufacturing processes for tenapanor, which has not yet been demonstrated, and to manufacture supplies of tenapanor and to develop, validate and maintain commercially viable manufacturing processes that are compliant with cGMP, requirements; |
| · | | whether the FDA or foreign regulatory authorities require additional nonclinical and/or clinical studies, which could delay the commercialization of tenapanor; |
| · | | whether the FDA or foreign regulatory authorities require us to conduct clinical trials in addition to those anticipated prior to approval to market tenapanor; |
| · | | whether we will be required to conduct clinical trials in addition to those anticipated to obtain adequate commercial pricing; |
| · | | the prevalence and severity of adverse side effects of tenapanor; |
| · | | whether tenapanor’s safety and efficacy profile is satisfactory to the FDA and foreign regulatory authorities to gain marketing approval; |
| · | | the timely receipt of necessary marketing approvals from the FDA and foreign regulatory authorities; |
| · | | our ability, either alone, or with a collaboration partner, to successfully commercialize tenapanor, if approved for marketing and sale by the FDA or foreign regulatory authorities, including educating physicians and patients about the benefits, administration and use of tenapanor; |
| · | | achieving and maintaining compliance with all regulatory requirements applicable to tenapanor; |
| · | | acceptance of tenapanor as safe, effective and well-tolerated by patients and the medical community; |
| · | | our ability, alone or with collaboration partners, to manage the complex pricing and reimbursement negotiations associated with marketing the same product at different doses for separate indications, if |
our ability to, in a timely manner and under terms that are acceptable to us, to establish one or more collaborative relationships for the commercializationtenapanor is approved for marketing and sale by the FDA or foreign regulatory authorities for both IBS-C and hyperphosphatemia in dialysis patients; |
| · | | the availability, perceived advantages, relative cost, relative safety and relative efficacy of tenapanor compared to alternative and competing treatments; |
| · | | obtaining and sustaining an adequate level of coverage and reimbursement for tenapanor by third-party payors; |
| · | | enforcing intellectual property rights in and to tenapanor; |
| · | | avoiding third-party interference, opposition, derivation or similar proceedings with respect to our patent rights, and avoiding other challenges to our patent rights and patent infringement claims; and |
| · | | the ability of the third-party manufacturers we contract with, to successfully execute and scale up the manufacturing processes for tenapanor, which has not yet been demonstrated, and to manufacture supplies of tenapanor and to develop, validate and maintain a commercially viable manufacturing processes that are compliant with current good manufacturing practice, or cGMP, requirements;
whether the specifications for tenapanor drug product and drug substance will be acceptable to the FDA for use in the clinical development of tenapanor as planned, or whether we will be required to produce such material to different specifications, which if required, could delay the development of tenapanor, and result in substantial additional costs;
whether the long-term rat carcinogenicity study required for regulatory approval of tenapanor, which is currently ongoing, will provide data acceptable to the FDA, or whether we will be required to start a new long-term rat carcinogenicity study, which if required, could delay the development of tenapanor;
whether, as a result of the observation of the absorption of inactive metabolites of tenapanor seen in our radiolabeled human ADME study, the FDA or foreign regulatory authorities require additional nonclinical and/or clinical studies, which could delay the commercialization of tenapanor;
whether FDA or foreign regulatory authorities require additional clinical trials than those anticipated prior to approval to market tenapanor;
the prevalence and severity of adverse side effects of tenapanor;
whether tenapanor’s safety and efficacy profile is satisfactory to the FDA and foreign regulatory authorities to gain marketing approval;
the timely receipt of necessary marketing approvals from the FDA and foreign regulatory authorities;
our ability, either alone, or with a collaboration partner, to successfully commercialize tenapanor, if approved for marketing and sale by the FDA or foreign regulatory authorities, including educating physicians and patients about the benefits, administration and use of tenapanor;
achieving and maintaining compliance with all regulatory requirements applicable to tenapanor;
acceptance of tenapanor as safe, effective and well-tolerated by patients and the medical community;
our ability to manage the complex pricing and reimbursement negotiations associated with marketing the same product at different doses for separate indications, if tenapanor is approved for marketing and sale by the FDA or foreign regulatory authorities for both IBS-C and hyperphosphatemia in dialysis patients;
the availability, perceived advantages, relative cost, relative safety and relative efficacy of alternative and competing treatments;
obtaining and sustaining an adequate level of coverage and reimbursement for tenapanor by third-party payors;
enforcing intellectual property rights in and to tenapanor;
avoiding third-party interference, opposition, derivation or similar proceedings with respect to our patent rights, and avoiding other challenges to our patent rights and patent infringement claims; and
a continued acceptable safety and tolerability profile of tenapanor following approval. |
As tenapanor is a first-in-class drug, there is a higher likelihood that approval may not be attained as compared to a class of drugs with approved products. We cannotWhile tenapanor met the primary endpoint in two Phase 3 clinical studies evaluating tenapanor for the treatment of patients with IBS-C, there can be certainno assurance that our NDA that we plan to submit for this indication, once submitted, will be accepted by FDA or that we will receive marketing authorization from FDA. Although tenapanor met the primary endpoint in the first Phase 3 clinical trial for the treatment of hyperphosphatemia in ESRD patients on dialysis, there can be no assurances that the second Phase 3 trial of tenapanor in this indication will achieve the primary endpoint, or that tenapanor will be successful in non-clinical safety studies or clinical trials, or that it will receive regulatory approval.approval for this indication. Further, it may not be possible or practicable to demonstrate, or if approved, to market tenapanor on the basis of certain of the benefits we believe tenapanor possesses. For example, the reduction of serum phosphorus is currently an approvable endpoint in CKDESRD patients on dialysis, but not for the broader CKD patient population in the United States. If the number of patients in the market for tenapanor or the price that the market can bear is not as significant as we estimate, we may not generate sufficient revenue from sales of tenapanor, if approved. Accordingly, there can be no assurance that tenapanor will ever be successfully commercialized or that we will ever generate income from sales of tenapanor. If we are not successful in completing the development of, obtaining approval for, and commercializing tenapanor, or are significantly delayed in doing so, our business will be materially harmed. Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and we may encounter substantial delays in our Phase 3 clinical studies.study of tenapanor for the treatment of hyperphosphatemia. Furthermore, results of earlier studies and trials may not be predictive of future trial results. Before obtaining marketing approval from regulatory authorities for the sale of our product candidates, we must conduct extensive clinical studies to demonstrate the safety and efficacy of the product candidates in humans. Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The results of preclinical and clinical studies of our product candidates may not be predictive of the results of later-stage clinical trials. For example, the positive results generated to date in preclinical and clinical studies for tenapanor do not ensure that the ongoing Phase 3 clinical trials for tenapanor, or future clinical trials, will demonstrate similar results. An unexpected adverse event profile, or the results of drug-drug interaction studies, may present challenges for the future development and commercialization of a product candidate for a particular condition despite receipt of positive efficacy data in a clinical study. For example,Although tenapanor met the primary endpoint in athe first Phase 2b study evaluating tenapanor3 clinical trial for the treatment of hyperphosphatemia in end stage renal disease, or ESRD patients we observedon dialysis, there can be no assurances that the study met its primary endpoint by demonstrating a statistically significant dose-related decreasesecond Phase 3 trial results of tenapanor in serum phosphate levels for tenapanor-treated patients compared to patients receiving placebo, while also observing that the rate of diarrhea and the discontinuation rate due to diarrhea at the highest doses were higher than expected based upon previous clinical trials. Product candidates in later stages of clinical trials may fail toindication will show the desired safety and efficacy despite having progressed through preclinical studies and initial clinical trials.efficacy. A number of companies in the pharmaceutical, biopharmaceutical and biotechnology industries have suffered significant setbacks in advanced clinical trials for similar indications that we are pursuing due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier studies, and we cannot be certain that we will not face similar setbacks. Even if our clinical trials arePhase 3 program for tenapanor for the treatment of hyperphosphatemia is completed, and despite the completion of our Phase 3 program for tenapanor for IBS-C, the results for one or both indications may not be sufficient to obtain regulatory approval for our product candidates,tenapanor, or if such regulatory approval is obtained, the content of the label approved by regulatory authorities may materially and adversely impact our ability to commercialize the product.product for the approved indication. We do not know whether futureour second Phase 3 clinical trialstrial for tenapanor for the treatment of hyperphosphatemia will begin on time, or whether our ongoing or future clinical trials will need to be redesigned, enroll an adequate number of patients on time or be completed on schedule, if at all. Clinical trials can be delayed or terminated for a variety of reasons, including delay or failure to: | · | | reach agreement on acceptable terms with prospective contract research organizations, or CROs, and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
| · | | obtain institutional review board, or IRB, approval at each site; |
| · | | recruit suitable patients in a timely manner to participate in our trials; |
| · | | have patients complete a trial or return for post-treatment follow-up; |
| · | | ensure that clinical sites observe trial protocol, comply with good clinical practices, or GCPs, or continue to participate in a trial; |
| · | | address any patient safety concerns that arise during the course of a trial; |
| · | | address any conflicts with new or existing laws or regulations; or |
| · | | manufacture sufficient quantities of product candidate meeting specified quality standards for use in clinical trials;
obtain regulatory approval to commence a trial, if applicable;
reach agreement on acceptable terms with prospective contract research organizations, or CROs, and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites;
obtain institutional review board, or IRB, approval at each site;
recruit suitable patients in a timely manner to participate in our trials;
have patients complete a trial or return for post-treatment follow-up;
ensure that clinical sites observe trial protocol, comply with good clinical practices, or GCPs, or continue to participate in a trial;
address any patient safety concerns that arise during the course of a trial;
address any conflicts with new or existing laws or regulations; or
initiate or add a sufficient number of clinical trial sites. |
Patient enrollment is a significant factor in the timing of clinical trials and is affected by many factors, including the size and nature of the patient population, the proximity of patients to clinical sites, the eligibility criteria for the trial, the design of the clinical trial, competing clinical trials and clinicians’ and patients’ perceptions as to the potential advantages of the drug being studied in relation to other available therapies, including any new drugs or treatments that may be approved for the indications we are investigating. We could also encounter delays if aour Phase 3 clinical trial is suspended or terminated by us, by the IRBs of the institutions in which such trials arethe trial is being conducted, by an independent data safety monitoring board for such trial or by the FDA or other regulatory authorities. Such authorities may suspend or terminate a clinical trial due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA or other regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a drug, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial. Further, conducting clinical trials in foreign countries presents additional risks that may delay completion of clinical trials. These risks include the failure of physicians or enrolled patients in foreign countries to adhere to clinical protocol as a result of differences in healthcare services or cultural customs, managing additional administrative burdens associated with foreign regulatory schemes and political and economic risks relevant to such foreign countries. In addition, the FDA may determine that the clinical trial results obtained in foreign subjects do not represent the safety and efficacy of a product candidate when administered in U.S. patients and are thus not supportive of New Drug Application, or NDA, approval in the United States. Ifif there are delays in the completion of, or termination of, anythe Phase 3 clinical trial for tenapanor for the treatment of our product candidates,hyperphosphatemia, the commercial prospects of our product candidatestenapanor for such indication may be harmed, and our ability to generate revenue from product sales from any of these product candidatestenapanor for such indication will be delayed. In addition, any delays in completing the clinical trialstrial will increase costs, slow down our product candidate development and approval process for tenapanor for hyperphosphatemia and jeopardize the ability to commence product sales and generate revenue from product sales.sales for this indication. Any of these occurrences may significantly harm our business, financial condition and prospects. In addition, many of the factors that may cause, or lead to, a delay in the commencement or completion of the Phase 3 clinical trialstrial may also ultimately lead to the denial of regulatory approval. Even if we successfully obtain regulatory approval for tenapanor, it may never achieve market acceptance, sufficient third-party coverage or reimbursement, or commercial success, which will depend, in part, upon the degree of our product candidates.acceptance among physicians, patients, patient advocacy groups, health care payors and the medical community. We intend to devote significant resources to the development of RDX022 whichEven if tenapanor obtains FDA or other regulatory approvals, and is ultimately commercialized for one or more indications, it may not be successfulachieve market acceptance among physicians, patients, third-party payors, patient advocacy groups, and the medical community. Market acceptance of tenapanor, in nonclinical studiesthe event that marketing approval is obtained, depends on a number of factors, including:
| · | | with respect to tenapanor for IBS-C in the United States, our ability to obtain a collaboration partner for commercialization and the strength of such collaboration partner’s marketing and distribution organizations; |
| · | | the efficacy demonstrated in clinical trials; |
| · | | the prevalence and severity of any side effects and overall safety and tolerability profile of the product; |
| · | | the clinical indications for which it is approved; |
| · | | advantages over new or traditional or existing therapies, including recently approved therapies or therapies that the physician community anticipate will be approved; |
| · | | acceptance by physicians, major operators of clinics and patients of tenapanor as a safe, effective and well-tolerated treatment; |
| · | | relative convenience and ease of administration of tenapanor; |
| · | | the potential and perceived advantages of tenapanor over current treatment options or alternative treatments, including future alternative treatments; |
| · | | the cost of treatment in relation to alternative treatments and willingness to pay for tenapanor, if approved, on the part of physicians and patients; |
| · | | the availability of alternative products and their ability to meet market demand; and |
| · | | the quality of our relationships with patient advocacy groups; and |
Any failure by us to obtain a collaboration partner for the commercialization of tenapanor in the United States for IBS-C and any failure of tenapanor to achieve market acceptance, sufficient third-party coverage or clinical trials,reimbursement, or commercial success, should it receive regulatory approval, or be successfully commercialized.would adversely affect our results of operations. With the advancement of RDX022 into human studies in June 2015, and the expected initiation of a Phase 3 clinical program for RDX022 in the second half of 2016, we expect to invest a significant amount of our efforts and financial resources in the development of RDX022. We are pursuing a 505(b)(2) regulatory path for approval of RDX022, which, among other things allows us to rely on the FDA’s previous findings of safety and efficacy and may eliminate the need to conduct certain nonclinical and clinical studies of our product candidate. This regulatory pathway, which can accelerate development, may not be available to us if a pharmaceutically equivalent product to RDX022 were approved prior to the approval of our 505(b)(2) application.currently have no sales organization. If we are unable to rely uponestablish sales capabilities on our own or through third parties, we may not be able to commercialize tenapanor or any of our other product candidates.
We currently do not have a 505(b)(2)sales organization. In order to commercialize or co-promote tenapanor or any of our other product candidates, we must enter collaborative relationships with one or more third parties, or build internal marketing, sales, distribution, managerial and other non-technical capabilities. There can be no assurances that we will be successful in establishing collaborative relationships in a timely manner or on terms that are acceptable to us. If tenapanor receives regulatory pathwayapproval and we have not entered collaborative relationships for the approvalcommercialization of RDX022,tenapanor in the United States, we would have to establish appropriate sales organizations with technical expertise supporting distribution capabilities to commercialize the product candidate, which will be expensive and time consuming, or delay the commercial launch of tenapanor for such indication. As a company, we have no prior experience in the marketing, sale and distribution of pharmaceutical products and there are significant risks involved in building and managing a sales organization, including our ability to secure the capital necessary to fund such efforts on acceptable terms, hire, retain, and incentivize qualified individuals, generate sufficient sales leads, provide adequate training to sales and marketing personnel, comply with regulatory requirements applicable to the marketing and sale of drug products and effectively manage a geographically dispersed sales and marketing team. If we are unable to enter collaborative relationships a timely manner, or on acceptable terms, and/or we fail or are delayed in the development of RDX022 may be substantially delayed orour internal sales, marketing and distribution capabilities, we may choose to delay the commercialization of our products and/or the commercialization of our products could be required to abandon such development. The clinicaladversely impacted, and commercial success of RDX022 will depend on a number of factors, including the following:
the ability of the third-party manufacturers we contract with, to successfully develop and scale up the manufacturing processes for RDX022, which hasmay not yet been demonstrated, to manufacture supplies of RDX022 and to develop, validate and maintain a commercially viable manufacturing process that is compliant with current good manufacturing practice, or cGMP, requirements;
the significant expansion of the market for the treatment of hyperkalemia beyond its currently limited size, including the success of commercial launches of new hyperkalemia products and the use of any such products by nephrologists and cardiologists in the chronic setting; our ability to successfully obtain labeling claims necessary or desirable for the commercial success of RDX022;
our ability to successfully obtain labeling claims necessary or desirable for the commercial success of RDX022;
the availability, perceived advantages regarding relative palatability, relative cost, relative safety, relative tolerance and relative efficacy of alternative and competing treatments;
whether we arebe able to obtain intellectual property protection for RDX022, and the strength of such protection if granted
the timely receipt of necessary marketing approvals and exclusivity periods, if any, from the FDA and foreign regulatory authorities;
our ability to successfully commercialize RDX022, if approved for marketing and sale by the FDA or foreign regulatory authorities, including educating physicians and patients about the benefits, administration and use of RDX022;
obtaining and sustaining an adequate level of coverage and reimbursement for RDX022 by third-party payors; and
the effectiveness of our marketing, sales and distribution strategy and operations.
As a result of pursuing a 505(b)(2) path for RDX022, we will not evaluate the efficacy of RDX022 in patients with hyperkalemia prior to the initiation of the Phase 3 clinical program. We cannot be certain that clinical trials evaluating RDX022 will establish a safety and efficacy profile sufficient to enable RDX022 to gain approval by the FDA, or if approved, compete effectively with alternative and competing treatments. Further, it
product candidates.may not be possible or practicable to demonstrate, or if approved, to market on the basis of, certain of the benefits we believe RDX022 may possess. Accordingly, there can be no assurance that RDX022 will ever be successfully commercialized or that we will ever generate revenue from sales of RDX022. If we are not successful in completing the development of, obtaining approval for, and commercializing RDX022, or are significantly delayed in doing so, our business will be materially harmed.
We may not be successful in our efforts to develop our product candidates that are at an early stage of development, including RDX009, or expand our pipeline of product candidates.candidates, as a result of numerous factors, which may include the inability to access capital necessary to fund such efforts on acceptable terms. A key element of our strategy is to expandhas been focused on the expansion of our pipeline of product candidates utilizing our proprietary drug discovery and design platform and to advance such product candidates through clinical development. In December 2015,2016, we selectedfiled an IND to commence clinical development of RDX8940 in the United States. In August 2017, we completed a comprehensive strategic review of our operations, assessing several core areas, to optimally position the company to advance towards delivering on multiple significant opportunities with our late-stage portfolio and execute on our strategic objectives. This review resulted in the prioritization of resources to focus on the upcoming milestones for the late-stage programs, a delay in the development candidate for our RDX009 program. This product candidate,of a number of earlier-stage programs, including RDX8940, and a reduction in workforce. RDX8940 and those product candidates that are in the discovery and lead identification stages of preclinical development will require substantial preclinical and clinical development, testing and regulatory approval prior to commercialization. In particular, tenapanorcommercialization, and RDX022 arewe may not be able to access the capital necessary to fund such efforts on acceptable terms. Our inability to access capital in a timely manner or on acceptable terms to fund our onlyearly stage product candidates in clinical trials and allmay force us to consider certain restructuring activities to enable the funding of our other product candidates are inthose early assets through the preclinical stage with significant research and development required before we could begin clinical studies. Ofuse of alternative structures. In addition, of the large number of drugs in development, only a small percentage of such drugs successfully complete the FDA regulatory approval process and are commercialized. Accordingly, even if we are able to continue to fund our research and early stage development programs, there can be no assurance that any product candidates will reach the clinic or be successfully developed or commercialized. Research programs to identify product candidates require substantial technical, financial and human resources, whether or not any product candidates are ultimately identified. Although our research and development efforts to date have resulted in several development programs, we may not be able to develop product candidates that are safe, effective and well-tolerated. Our research programs may initially show promise in identifying potential product candidates, and we may select candidates for development, yet we may fail to yieldadvance product candidates forto clinical development or commercialization for many reasons, including the following: | · | | we may be unable to access sufficient capital on acceptable terms to fund the development of all of our assets and as a result we may be forced to delay or terminate the development of certain product candidates, or to consider restructuring efforts to secure alternate funding for those assets; |
| · | | the research methodology used and our drug discovery and design platform may not be successful in identifying potential product candidates; |
| · | | competitors may develop alternatives that render our product candidates obsolete or less attractive; |
| · | | product candidates we develop may nevertheless be covered by third parties’ patents or other exclusive rights; |
| · | | the market for a product candidate may change during our program so that the continued development of that product candidate is no longer reasonable; |
the research methodology used and our drug discovery and design platform may not be successful in identifying potential product candidates;competitors may develop alternatives that render our product candidates obsolete or less attractive; | · | | a product candidate may on further study be shown to have harmful side effects or other characteristics that indicate it is unlikely to be effective, well- tolerated or otherwise does not meet applicable regulatory or commercial criteria; |
| · | | a product candidate may not be capable of being produced in commercial quantities at an acceptable cost, or at all; and |
| · | | product candidates we develop may nevertheless be covered by third parties’ patents or other exclusive rights;
the market for a product candidate may change during our program so that the continued development of that product candidate is no longer reasonable;
a product candidate may on further study be shown to have harmful side effects or other characteristics that indicate it is unlikely to be effective, well-tolerated or otherwise does not meet applicable regulatory criteria;
a product candidate may not be capable of being produced in commercial quantities at an acceptable cost, or at all; and
a product candidate may not be accepted as safe, effective and well-tolerated by patients, the medical community or third-party payors, if applicable. |
Even if we are successful in continuing to expand our pipeline, through our own research and development efforts, or by pursuing in-licensing or acquisition of product candidates, the potential product candidates that we identify or for which we identify or acquire rights may not be suitable for clinical development, including as a result of being shown to have harmful side effects or other characteristics that indicate that they are unlikely to receive marketing approval and achieve market acceptance. If we do not successfully develop and commercialize a product pipeline, we may not be able to generate revenue from product sales in future periods or ever achieve profitability. Our proprietary drug discovery and design platform, and, in particular, APECCS, is a new approach to the discovery, design and development of new product candidates and may not result in any products of commercial value. We have developed a proprietary drug discovery and design platform to enable the identification, screening, testing, design and development of new product candidates, and have developed APECCS as a component of this of this platform. We utilize APECCS in the design of our small molecules and to identify new and potentially novel targets in the GI tract. However, there can be no assurance that APECCS will be able to identify new targets in the GI tract or that any of these potential targets or other aspects of our proprietary drug discovery and design platform will yield product candidates that could enter clinical development and, ultimately, be commercially valuable. Although we expect to continue to enhance the capabilities of our APECCS system by advancing the cell culture and screening process and/or acquiring new technologies to broaden the scope of APECCS, we may not be successful in any of our enhancement and development efforts. In addition, we may not be able to enter into agreements on suitable terms to utilize technologies required to exploit certain capabilities of APECCS, and in such case, we may be forced to limit our use or further development of APECCS, or to modify APECCS for continued use. It may not be possible to modify APECCS in manner that avoids the utilization of certain technologies, without materially and adversely affecting the performance of APECCS or without incurring substantial cost and delay in advancement of the system. In addition, we may not be successful in developing the conditions necessary to grow multiple segments of intestine or from multiple species, or otherwise develop assays or cell cultures necessary to expand these capabilities. If our enhancement or development efforts are unsuccessful, or if we are forced to limit our use or further development of APECCS due to the inability to enter into agreements on suitable terms to permit the utilization of technologies required to exploit APECCS, we may not be able to advance our drug discovery capabilities as quickly as we expect or identify as many potential drugable targets as we desire.
We rely on third parties to conduct some of our preclinical and nonclinical studies and all of our clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may be unable to obtain regulatory approval for or commercialize our product candidates. We do not have the ability to independently conduct clinical trials and, in some cases, preclinical or nonclinical studies. We rely on medical institutions, clinical investigators, contract laboratories, and other third parties, such as CROs, to conduct clinical trials on our product candidates. The third parties with whom we contract for execution of the clinical trials play a significant role in the conduct of these trials and the subsequent collection and analysis of data. However, these third parties are not our employees, and except for contractual duties and obligations, we control only certain aspects of their activities and have limited ability to control the amount or timing of resources that they devote to our programs. Although we rely, and will continue to rely, on these third parties to conduct some of our preclinical and nonclinical studies and all of our clinical trials, we remain responsible for ensuring that each of our studies and clinical trials is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards and our reliance on third parties does not relieve us of our regulatory responsibilities. We, and these third parties are required to comply with current good laboratory practices, or GLPs for preclinical and nonclinical studies, and good clinical practices, or GCPs, for clinical studies. GLPs and GCPs are regulations and guidelines enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area, or EEA, and comparable foreign regulatory authorities for all of our products in preclinicalnonclinical and clinical development, respectively. Regulatory authorities enforce GCPs through periodic inspections of trial sponsors, principal investigators and trial sites. If we or any of our third partythird-party contractors fail to comply with applicable regulatory requirements, including GCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA, the European Medicines Agency, or EMA, or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. There can be no assurance that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials comply with GCP regulations. In addition, our clinical trials must be conducted with product produced under current good manufacturing practices or cGMP regulations. Our failure to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process. Even if our product candidates obtain regulatory approval, they may never achieve market acceptance or commercial success, which will depend, in part, upon the degree of acceptance among physicians, patients, patient advocacy groups, health care payors and the medical community.30
Even if our product candidates obtain FDA or other regulatory approvals, and are ultimately commercialized, our product candidates may not achieve market acceptance among physicians, patients, third-party payors, patient advocacy groups, health care payors and the medical community. Market acceptance of our product candidates for which marketing approval is obtained depends on a number of factors, including:
the prevalence and severity of any side effects and overall safety and tolerability profile of the product;
the clinical indications for which the product is approved;
advantages over new or traditional or existing therapies, including recently approved therapies or therapies that the physician community anticipate will be approved;
acceptance by physicians, major operators of clinics and patients of the product as a safe, effective and well-tolerated treatment;
relative convenience and ease of administration of our products;
the potential and perceived advantages of our product candidates over current treatment options or alternative treatments, including future alternative treatments;
the cost of treatment in relation to alternative treatments and willingness to pay for our products, if approved, on the part of physicians and patients;
the availability of alternative products and their ability to meet market demand;
the strength of our or our collaboration partners’ marketing and distribution organizations;
the quality of our relationships with patient advocacy groups; and
sufficient third-party coverage or reimbursement.
Any failure by our product candidates that obtain regulatory approval to achieve market acceptance or commercial success would adversely affect our results of operations.
Our product candidates may cause undesirable side effects or have other properties that could delay our clinical trials, or delay or prevent regulatory approval, limit the commercial profile of an approved label, or result in significant negative consequences following regulatory approval, if any. If tenapanor or any of our other product candidates receives marketing approval and we or others later identify undesirable side effects caused by the product candidate, the ability to market the product candidates could be compromised. Undesirable side effects caused by our product candidates could cause us or regulatory authorities to interrupt, delay or halt clinical trials, result in the delay or denial of regulatory approval by the FDA or other comparable foreign regulatory authorities or limit the commercial profile of an approved label. To date, patients treated with tenapanor have experienced drug-related side effects including diarrhea, nausea, vomiting, flatulence, abdominal discomfort, abdominal pain, abdominal distention and changes in electrolytes, and in the a Phase 2b clinical trial evaluating tenapanor for the treatment of hyperphosphatemia in ESRD patients, we observed that the rate of diarrhea and the discontinuation rate due to diarrhea at the highest doses was higher than expected based upon the results of previous clinical trials.electrolytes. In the event that trials conducted by us with tenapanor or trials we conduct with our other product candidates, reveal an unacceptable severity and prevalence of these or other side effects, such trials could be suspended or terminated and the FDA or comparable foreign regulatory authorities could order us to cease further development of or deny approval of tenapanor, or any such other product candidate, for any or all targeted indications. Additionally, despite a positive efficacy profile, the prevalence and/or severity of these or other side effects could cause us to cease further development of a product candidate for a particular indication, or entirely. The drug-related side effects could affect patient recruitment or the ability of enrolled patients to complete the trial or result in potential product liability claims. Any of these occurrences may harm our business, financial condition and prospects significantly. In addition, in the event that any of our product candidates receives regulatory approval and we or others later identify undesirable side effects caused by one of our products, a number of potentially significant negative consequences could occur, including: | · | | regulatory authorities may withdraw their approval of the product or seize the product; |
| · | | we, or a collaboration partner, may be required to recall the product; |
| · | | additional restrictions may be imposed on the marketing of the particular product or the manufacturing processes for the product or any component thereof, including the imposition of a Risk Evaluation and Mitigation Strategies, or REMS, plan that may require creation of a Medication Guide outlining the risks of such side effects for distribution to patients, as well as elements to assure safe use of the product, such as a patient registry and training and certification of prescribers; |
| · | | we, or a collaboration partner, may be subject to fines, injunctions or the imposition of civil or criminal penalties; |
| · | | regulatory authorities may require the addition of labeling statements, such as a “black box” warning or a contraindication; |
| · | | we could be sued and held liable for harm caused to patients; |
| · | | the product may become less competitive; and |
| · | | regulatory authorities may withdraw their approval of the product or seize the product;
we may be required to recall the product;
additional restrictions may be imposed on the marketing of the particular product or the manufacturing processes for the product or any component thereof, including the imposition of a Risk Evaluation and Mitigation Strategies, or REMS, plan that may require creation of a Medication Guide outlining the risks of such side effects for distribution to patients, as well as elements to assure safe use of the product, such as a patient registry and training and certification of prescribers;
we may be subject to fines, injunctions or the imposition of civil or criminal penalties;
regulatory authorities may require the addition of labeling statements, such as a “black box” warning or a contraindication;
we could be sued and held liable for harm caused to patients;
the product may become less competitive; and
our reputation may suffer |
Any of the foregoing events could prevent us, or a collaboration partner, from achieving or maintaining market acceptance of a particular product candidate, if approved, and could result in the loss of significant revenue to us, which would materially and adversely affect our results of operations and business.
We face substantial competition and our competitors may discover, develop or commercialize products faster or more successfully than us. The biotechnology and pharmaceutical industries are highly competitive, and we face significant competition from companies in the biotechnology, pharmaceutical and other related markets that are researching and marketing products designed to address diseases that we are currently developing products to treat. If approved for marketing by the FDA or other regulatory agencies, tenapanor, and RDX022, as well as our other product candidates, would compete against existing treatments. For example, tenapanor will, if approved, compete directly with phosphate binders for the treatment of hyperphosphatemia in ESRD patients on dialysis. The various types of phosphate binders commercialized in the United States include the following: | · | | Calcium carbonate (many over-the-counter brands including Tums and Caltrate) |
| · | | Calcium acetate (several prescription brands including PhosLo and Phoslyra) |
| · | | Lanthanum carbonate (Fosrenol marketed by Shire) |
| · | | Sevelamer hydrochloride (Renagel, marketed by Sanofi) |
| · | | Sevelamer carbonate (Renvela, marketed by Sanofi) |
| · | | Sucroferric oxyhydroxide (Velphoro, marketed by Vifor Fresenius) |
| · | | Ferric citrate (Auryxia, marketed by Keryx) |
The hydrochloride form of sevelamer, hydrochloride (Renagel)Renagel, was launched in the United States by Genzyme Corporation in 1998 prior to its acquisition by Sanofi, and the carbonate form, Renvela, was launched in 2008. Sanofi booked €802 million ($0.98 billion) in worldwide sales of sevelamer during 2017. Generic sevelamer carbonate (Renvela), which were launched by Genzyme. Synthon announced the successful completion of a Phase 3 multicenter, randomized, double-blind, multiple-dose, crossover trialhas been approved in certain jurisdictions in Europe to compare safetysince 2015 and demonstrate equivalence of serum phosphate control of Synthon sevelamer carbonate tablets to Renvela tablets in chronic kidney disease patients on hemodialysis in April 2014. Currently, several pharmaceutical companies are distributing Synthon manufactured sevelamer carbonate tablets in multiple European countries including, but not limited to, the United Kingdom, Spain, Sweden and Denmark.U.S. market since June 2017. In addition to the currently marketed phosphate binders, Keryx has received FDA approval for ferric citrate (Auryxia), an iron-based binder, that is also approved in Japan and we are aware of at least two other binders in development, including fermagate (Alpharen), an iron-based binder in Phase 23 being developed by Opko Health. Additionally, RDX022, if approved, will compete directly with KayexalateHealth, Inc., and its generic equivalents, known as sodium polystyrene sulfonate, on the marketPT20, an iron-based binder in the United States. In addition, Relypsa just recently commercially launched patiromer (Veltassa) for the treatment of hyperkalemia, and a new drug application, or NDA, was submitted in June 2015, for a sodium zirconium cyclosilicate-based oral potassium binderPhase 3 being developed for the treatment of hyperkalemia by AstraZeneca after its acquisition of ZS Pharma in December 2015.Shield Therapeutics. Numerous treatments exist for constipation and the constipation component of IBS-C, many of which are over-the-counter. These include psyllium husk (such as Metamucil), methylcellulose (such as Citrucel), calcium polycarbophil (such as FiberCon), lactulose (such as Cephulac), polyethylene glycol (such as MiraLax), sennosides (such as Exlax), bisacodyl (such as Ducolax), docusate sodium (such as Colace), magnesium hydroxide (such as Milk of Magnesia), saline enemas (such as Fleet) and sorbitol. These agents are generally inexpensive and work well to temporarily relieve temporary constipation. We are also aware of twothree prescription drugs currently on the U.S. market that are approved to treat IBS-C,products marketed for IBS-C: (i) Linzess (linaclotide), which was developedmarketed by Ironwood Pharmaceuticals and is approved for IBS-C and chronic constipation in both the United States and in Europe, andAllergan, (ii) Amitiza (lubiprostone), which was first approved in the United States in 2006 and is currently marketed by Takeda and Sucampo, a wholly-owned subsidiary of Mallinckrodt, and Takeda for treatment of chronic idiopathic constipation, or CIC, IBS-C and opioid induced constipation, or OIC. Additionally,(iii) Trulance (plecanatide), marketed by Synergy filed an NDA for Plecanatide for the treatment of CIC in January 2016, and is currently conducting two Phase 3 clinical trials of Plecanatide for the treatment of IBS-C.Pharmaceuticals. It is possible that our competitors will develop and market drugs or other treatments that are less expensive and more effective than our product candidates, or that will render our product candidates obsolete. It is also possible that our competitors will commercialize competing drugs or treatments before we, or our collaboration partners, can launch any products developed from our product candidates. We also anticipate that we will face increased competition in the future as new companies enter into our target markets. Many of our competitors have materially greater name recognition and financial, manufacturing, marketing, research and drug development resources than we do. Additional mergers and acquisitions in the biotechnology and pharmaceutical industries may result in even more resources being concentrated in our competitors. Large pharmaceutical companies in particular have extensive expertise in preclinical and clinical testing and in obtaining regulatory approvals for drugs. In addition, academic institutions, government agencies, and other public and private organizations conducting research may seek patent protection with respect to potentially competitive products or technologies. These organizations may also establish exclusive collaboration partnerships or licensing relationships with our competitors. We may experience difficulties in managing our current activities and growth given our level of managerial, operational, financial and other resources. On August 7, 2017, our Board of Directors approved a restructuring plan, pursuant to which we reduced our workforce by 29%, resulting in 75 remaining employees. We will need to manage our operations and clinical trials, and continue our development and pre-commercial activities for our product candidates with this reduced workforce. Our management and personnel, and systems currently have no sales organization. in place may not be adequate to support our current activities or future growth. Our need to effectively execute our business strategy requires that we: | · | | manage our clinical trials effectively, including the Phase 3 trial of tenapanor which is being conducted at multiple trial sites; |
| · | | manage our internal research and development efforts effectively while carrying out our contractual obligations to licensors, contractors, collaborators, government agencies and other third parties; |
| · | | continue to improve our operational, financial and management controls, reporting systems and procedures; and |
| · | | retain and motivate our remaining employees and potentially identify, recruit, and integrate additional employees. |
If we are unable to establish sales capabilities onmaintain or expand our own or through third parties, we may not be able to commercialize tenapanor and RDX022, or any of our other product candidates. We currently do not have a sales organization. In order to promote tenapanor and RDX022, either alone, or with a collaboration partner, and in order to commercialize or co-promote any of our other product candidates, we must build our marketing, sales, distribution, managerial, operational, financial and other non-technical capabilities or make arrangements with third partiesresources to perform these services,the extent required to manage our development and we may not be successful in doing so. In order to commercialize tenapanor or RDX022 outside of the United States, we expect to enter into collaborative relationships with one or more third parties. Additionally, in order to commercialize tenapanor for IBS-C, we expect to enter into a collaborative relationship with one or more third parties in the United States to address the primary care market. There can be no assurances that wepre-commercialization activities, our business will be successful in establishing such relationships in a timely manner or on terms that are acceptable to us. If one or more of our product candidates receives regulatory approval, we expect to establish a specialty sales organization with technical expertise and supporting distribution capabilities to commercialize our product candidates, which will be expensive and time consuming. As a company, we have no prior experience in the marketing, sale and distribution of pharmaceutical products and there are significant risks involved in building and managing a sales organization, including our ability to hire, retain, and incentivize qualified individuals, generate sufficient sales leads, provide adequate training to sales and marketing personnel, comply with regulatory requirements applicable to the marketing and sale of drug products and effectively manage a geographically dispersed sales and marketing team. Any failure or delay in the development of our internal sales, marketing and distribution capabilities wouldmaterially adversely impact the commercialization of these products.affected.
We may choose to collaborate with third parties that have direct sales forces and established distribution systems, either to augment our own sales force and distribution systems or in lieu of our own sales force and distribution systems. If we are unable to enter into such arrangements on acceptable terms or at all, we may not be able to successfully commercialize our product candidates.
We rely completely on third parties to manufacture our preclinicalnonclinical and clinical drug supplies, and we intend to rely on third parties to produce commercial supplies of any approved product candidate.tenapanor, if approved. Our business would be harmed if those third parties fail to obtain approval of the FDA, Competent Authorities of the Member States of the EEA or comparable regulatory authorities, fail to provide us with sufficient quantities of drug product, or fail to do so at acceptable quality levels or prices. We do not currently have, nor do we plan to acquire, the infrastructure or capability internally to manufacture tenapanor or any of other our preclinical and clinicalproduct candidates on a commercial scale, or to manufacture our drug supplies for use in the conduct of our preclinicalnonclinical and clinical studies, and we lack the resources and the capability to manufacture any of our product candidates on a clinical or commercial scale.studies. The facilities used by our contract manufacturers to manufacture any drug products must be approved by the FDA pursuant to inspections that will be conducted after an NDA is submitted to the FDA. We do not control the manufacturing process of our product candidates, and we are completely dependent on our contract manufacturing partners for compliance with the regulatory requirements, known as cGMPs, for manufacture of both active drug substances and finished drug products. If our contract manufacturers cannot successfully manufacture material that conforms to our specifications and the strict regulatory requirements of the FDA or others, they will not be able to secure and/or maintain regulatory approval for their manufacturing facilities. In addition, we have no control over the ability of our contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. If the FDA or a comparable foreign regulatory authority does not approve these facilities for the manufacture of our product candidates or if it withdraws any such approval in the future, we may need to find alternative manufacturing facilities, which would significantly impact our ability to develop, obtain regulatory approval for or market our product candidates, if approved. We rely on our manufacturers to purchase from third-party suppliers the materials necessary to produce our product candidates for our clinical studies. There are a limited number of suppliers for raw materials that we use to manufacture our drugs, and there may be a need to identify alternate suppliers to prevent a possible disruption of the manufacture of the materials necessary to produce our product candidates for our clinical studies, and, if approved, ultimately for commercial sale. We do not have any control over the process or timing of the acquisition of these raw materials by our manufacturers. Although we generally do not begin a clinical study unless we believe we have on hand, or will be able to manufacture, a sufficient supply of a product candidate to complete such study, any significant delay or discontinuity in the supply of a product candidate, or the raw material components thereof, for an ongoing clinical study due to the need to replace a third-party manufacturer could considerably delay completion of our clinical studies, product testing, and potential regulatory approval of our product candidates, which could harm our business and results of operations. Third-party payor coverage and reimbursement status of newly-approved products is uncertain. Failure to obtain or maintain adequate coverage and reimbursement for our products, if approved, could limit our ability to market those products and decrease our ability to generate revenue. The pricing, coverage and reimbursement of our product candidates, if approved, must be adequate to support a commercial infrastructure. The availability and adequacy of coverage and reimbursement by governmental and private payors are essential for most patients to be able to afford treatments such as ours, assuming approval. Sales of our product candidates will depend substantially, both domestically and abroad, on the extent to which the costs of our product candidates will be paid for by health maintenance, managed care, pharmacy benefit, and similar healthcare management organizations, or reimbursed by government authorities, private health insurers, and other third-party payors. If coverage and reimbursement are not available, or are available only to limited levels, we may not be able to successfully commercialize our product candidates. Even if coverage is provided, the approved reimbursement amount may not be high enough to allow us to establish or maintain pricing sufficient to realize a return on our investment. There is significant uncertainty related to the insurance coverage and reimbursement of newly approved products. In the United States, the principal decisions about coverage and reimbursement for new drugs are typically made by the Centers for Medicare & Medicaid Services, or CMS, an agency within the U.S. Department of Health and Human Services responsible for administering the Medicare program, as CMS decides whether and to what extent a new drug will be covered and reimbursed under Medicare. Private payors tend to follow the coverage reimbursement policies established by CMS to a substantial degree. It is difficult to predict what CMS will decide with respect to reimbursement for products such as ours. In July 2010, CMS released its final rule to implement a bundled prospective payment system for the treatment of ESRD patients as required by the Medicare Improvements for Patients and Providers Act, or MIPPA. The bundled payment covers a bundle of items and services routinely required for dialysis treatments furnished to Medicare beneficiaries in Medicare-certified ESRD facilities or at their home, including the cost of certain routine drugs. The final rule delayed the inclusion of oral medications without intravenous equivalents in the bundled payment until January 1, 2014 and in April 2014, President Obama signed the Protecting Access to Medicare Act of 2014, which further extendsextended this implementation date to January 1, 2024. Additionally, section 204 of the Stephen Beck, Jr., Achieving a Better Life Experience Act of 2014, or ABLE, provides that payment for oral-only ESRD drugs cannot be made under the ESRD Prospective Payment System prior to January 1, 2025. As a result of the recent legislation, beginning in 2024,2025, ESRD-related drugs willmay be included in the bundle and separate Medicare reimbursement will no longer be available for such drugs, as it is today under Medicare Part D. While it is too early to project the full impact that bundling may have on the industry, the impact could potentially cause dramatic price reductions for tenapanor, and RDX022, if approved. We may be unable to sell tenapanor, and/or RDX022, if approved, to dialysis providers on a profitable basis if third-party payors reduce their current levels of payment, or if our costs of production increase faster than increases in reimbursement levels. Outside the United States, international operations are generally subject to extensive governmental price controls and other market regulations, and we believe the increasing emphasis on cost-containment initiatives in Europe, Canada, Japan, China and other countries has and will continue to put pressure on the pricing and usage of our product candidates. In many countries, the prices of medical products are subject to varying price control mechanisms as part of national health systems. Other countries allow companies to fix their own prices for medicinal products, but monitor and control company profits. Additional foreign price controls or other changes in pricing regulation could restrict the amount that we are able to charge for our product candidates. Accordingly, in markets outside the United States, the reimbursement for our products may be reduced compared with the United States and may be insufficient to generate commercially reasonable revenue and profits. Moreover, increasing efforts by governmental and third-party payors in the United States and abroad to cap or reduce healthcare costs may cause such organizations to limit both coverage and the level of reimbursement for newnewly approved products approved and, as a result, these caps may not cover or provide adequate payment for our product candidates. We expect to experience pricing pressures in connection with the sale of any of our product candidates due to the trend toward managed healthcare, the increasing influence of health maintenance organizations, and additional legislative changes. The downward pressure on healthcare costs in general, particularly prescription drugs and surgical procedures and other treatments, has become very intense. As a result, increasingly high barriers are being erected to the entry of new products. If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of our product candidates. We face an inherent risk of product liability as a result of the clinical testing of our product candidates and will face an even greater risk if we commercialize any products. For example, we may be sued if any product we develop allegedly causes injury or is found to be otherwise unsuitable during product testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability, and a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our product candidates. Even successful defense would require significant financial and management resources. Regardless of the merits or eventual outcome, liability claims may result in: | · | | decreased demand for our product candidates; |
| · | | injury to our reputation; |
| · | | withdrawal of clinical trial participants; |
| · | | costs to defend the related litigation; |
| · | | a diversion of management’s time and our resources; |
| · | | substantial monetary awards to trial participants or patients; |
| · | | regulatory investigations, product recalls or withdrawals, or labeling, marketing or promotional restrictions; |
| · | | decreased demand for our product candidates;
injury to our reputation;
withdrawal of clinical trial participants;
costs to defend the related litigation;
a diversion of management’s time and our resources;
substantial monetary awards to trial participants or patients;
regulatory investigations, product recalls or withdrawals, or labeling, marketing or promotional restrictions;
loss of revenue; and
the inability to commercialize or co-promote our product candidates. |
Our inability to obtain and maintain sufficient product liability insurance at an acceptable cost and scope of coverage to protect against potential product liability claims could prevent or inhibit the commercialization of any products we develop. We currently carry product liability insurance covering use in our clinical trials in the amount of $10.0 million in the aggregate. Although we maintain such insurance, any claim that may be brought against us could result in a court judgment or settlement in an amount that is not covered, in whole or in part, by our insurance or that is in excess of the limits of our insurance coverage. Our insurance policies also have various exclusions and deductibles, and we may be subject to a product liability claim for which we have no coverage. We will have to pay any amounts awarded by a court or negotiated in a settlement that exceed our coverage limitations or that are not covered by our insurance, and we may not have, or be able to obtain, sufficient capital to pay such amounts. Moreover, in the future, we may not be able to maintain insurance coverage at a reasonable cost or in sufficient amounts to protect us against losses. We are highly dependent on the services of our President and Chief Executive Officer, Michael Raab, our Executive Vice President and Chief ScientificOperating Officer, Jeremy Caldwell, Ph.D.,Reginald Seeto, MBBS, and our Senior Vice President of DrugChief Development Officer, David Rosenbaum, Ph.D. If we are not able to retain these members of our management team, or recruit additional management, clinical and scientific personnel, our business will suffer. Our success depends in part on our continued ability to attract, retain and motivate highly qualified personnel. In particular, we are highly dependent upon Michael Raab, our President and Chief Executive Officer, Jeremy Caldwell, Ph.D.,Reginald Seeto, MBBS, our Chief ScientificOperating Officer and David Rosenbaum, Ph.D., our Senior Vice President of Drug Development.Chief Development Officer. The loss of services of any of these individuals could delay or impair the successful development of our product pipeline, completion of our planned clinical trials or the commercialization of our product candidates. Although we have entered into employment agreements with our senior management team, including Mr. Raab and Drs. CaldwellSeeto and Rosenbaum, these agreements are terminable at will with or without notice and, therefore, we may not be able to retain their services as expected. Although we have not historically experienced unique difficulties attracting and retaining qualified employees, we could experience such problems in the future. For example, competition for qualified personnel in the biotechnology and pharmaceuticals field is intense due to the limited number of individuals who possess the skills and experience required by our industry. In addition to the competition for personnel, the San Francisco Bay area in particular is characterized by a high cost of living. As such, we could have difficulty attracting experienced personnel to our company and may be required to expend significant financial resources in our employee recruitment and retention efforts. We will need to continue to increase the sizeOur internal computer systems, or those of our organization, and weCROs or other contractors or consultants, may experience difficulties in managing growth.
We will need to continue to expand our clinical, managerial, operational, finance and other resources in order to manage our operations, preclinical and clinical trials, research and development activities, regulatory filings, manufacturing and supply activities, and any marketing and commercialization activities. Our management, personnel, systems and facilities currently in place may not be adequate to support this future growth. Our need to effectively execute our growth strategy requires that we:
expand our general and administrative functions;
establish and build a marketing and commercial organization;
identify, recruit, retain, incentivize and integrate additional employees;
manage our internal development efforts effectively while carrying out our contractual obligations to third parties; and
continue to improve our operational, legal, financial and management controls, reporting systems and procedures.
If we are not able to attract, retain and motivate necessary personnel to accomplish our business objectives, we may experience constraints that will significantly impede the achievement of our development objectives, our ability to raise additional capital and our ability to implement our business strategy.
Significant disruptions of information technology systemsfail or breaches ofsuffer data security breaches, which could adversely affect our business.
Our business is increasingly dependent on critical, complex and interdependent information technology systems to support business processes as well as internal and external communications. TheDespite the implementation of security measures, the size and complexity of our internal computer systems, and those of our CROs and other contractors, make them vulnerable to breakdown, malicious intrusiondamage from computer viruses, unauthorized access, natural disasters, terrorism, war and computer viruses. We have developed systemstelecommunication and processes that are designed to protect our information and prevent data loss and other security breaches, including systems and processes designed to reduce the impact of a security breach; however, such measures cannot provide absolute security, andelectrical failures. While we have taken,not experienced any such system failure, accident or security breach to date, if such an event were to occur and will take, additional security measures to protect against any future intrusion. Any failure to protect against breakdowns, malicious intrusions and computer viruses maycause interruptions in our operations, it could result in a material disruption of our programs. For example, the impairmentloss of productionclinical trial data from completed or ongoing clinical trials for any of our product candidates could result in delays in our regulatory approval efforts and key business processes.significantly increase our costs to recover or reproduce the data. In addition, our systems are potentially vulnerable to data security breaches, whether by employees or others, which may expose sensitive data to unauthorized persons. Such data security breaches could lead to the loss of trade secrets or other intellectual property, or could lead to the public exposure of personal information of our employees, clinical trial patients, customers, and others. Such disruptions and breaches of security could expose us to liability and have a material adverse effect on the operating results and financial condition of our business. We incur significant costs as a result of operating as a public company, and our management will devote substantial time to new compliance initiatives. We may fail to comply with the rules that apply to public companies, including Section 404 of the Sarbanes-Oxley Act of 2002, which could result in sanctions or other penalties that would harm our business. We incur significant legal, accounting and other expenses as a public company, including costs resulting from public company reporting obligations under the Securities Exchange Act of 1934, as amended, or the Exchange Act, and regulations regarding corporate governance practices. The listing requirements of The NASDAQNasdaq Global Market require that we satisfy certain corporate governance requirements relating to director independence, distributing annual and interim reports, stockholder meetings, approvals and voting, soliciting proxies, conflicts of interest and a code of conduct. Our management and other personnel will need to devote a substantial amount of time to ensure that we comply with all of these requirements. Moreover, the reporting requirements, rules and regulations will increase our legal and financial compliance costs and will make some activities more time consuming and costly. Any changes we make to comply with these obligations may not be sufficient to allow us to satisfy our obligations as a public company on a timely basis, or at all. These reporting requirements, rules and regulations, coupled with the increase in potential litigation exposure associated with being a public company, could also make it more difficult for us to attract and retain qualified persons to serve on our board of directors or board committees or to serve as executive officers, or to obtain certain types of insurance, including directors’ and officers’ insurance, on acceptable terms. In addition, we are in the process of implementing an enterprise resource planning, or ERP, system for our company. An ERP system is intended to combine and streamline the management of our financial, accounting, human resources, sales and marketing and other functions, enabling us to manage operations and track
performance more effectively. However, an ERP system will require us to complete many processes and procedures for the effective use of the system or to run our business using the system, which may result in substantial costs. Additionally, during the conversion process, we may be limited in our ability to convert any business that we acquire to the ERP. Any disruptions or difficulties in implementing or using an ERP system could adversely affect our controls and harm our business, including our ability to forecast or make sales and collect our receivables. Moreover, such disruption or difficulties could result in unanticipated costs and diversion of management attention.
We are subject to Section 404 of The Sarbanes-Oxley Act of 2002, or Section 404, and the related rules of the Securities and Exchange Commission, or SEC, which generally require our management and independent registered public accounting firm to report on the effectiveness of our internal control over financial reporting. Section 404 requires an annual management assessment of the effectiveness of our internal control over financial reporting. However, for so long as we remain an emerging growth company as defined in the Jumpstart Our Business Startups Act of 2012, or JOBS Act, we intend to take advantage of certain exemptions from various reporting requirements that are applicable to public companies that are emerging growth companies, including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404. Once we are no longer an emerging growth company or, if prior to such date, we opt to no longer take advantage of the applicable exemption, we will be required to include an opinion from our independent registered public accounting firm on the effectiveness of our internal controls over financial reporting. We will remain an emerging growth company until the earlier of (1) the last day of the fiscal year following the fifth anniversary of the completion of our IPO (December 31, 2019), (2) the last day of the fiscal year in which we have total annual gross revenue of at least $1.0 billion, or (3) the last day of the fiscal year in which we are deemed to be a large accelerated filer, which means the market value of our common stock that is held by non-affiliates exceeds $700 million as of the prior June 30th,30th, and (4) the date on which we have issued more than $1.0 billion in non-convertible debt during the prior three-year period. During the course of our review and testing of our internal controls, we may identify deficiencies and be unable to remediate them before we must provide the required reports. Furthermore, if we have a material weakness in our internal controls over financial reporting, we may not detect errors on a timely basis and our financial statements may be materially misstated. We or our independent registered public accounting firm may not be able to conclude on an ongoing basis that we have effective internal control over financial reporting, which could harm our operating results, cause investors to lose confidence in our reported financial information and cause the trading price of our stock to fall. In addition, as a public company we are required to file accurate and timely quarterly and annual reports with the SEC under the Exchange Act. Any failure to report our financial results on an accurate and timely basis could result in sanctions, lawsuits, delisting of our shares from The NASDAQNasdaq Global Market or other adverse consequences that would materially harm our business. We have formed in the past, and may form collaboration partnerships in the future, collaboration partnerships, joint ventures and/or licensing arrangements, and we may not realize the benefits of such collaborations. We mayhave current collaboration partnerships for the commercialization of tenapanor in certain foreign countries, and we currently expect to form additional collaboration partnerships, create joint ventures or enter into additional licensing arrangements with third parties in the United States and abroad that we believe will complement or augment our existing business. In particular, we have formed collaboration partnerships with Kyowa Hakko Kirin Co., Ltd. for commercialization of tenapanor for hyperphosphatemia in Japan and with Shanghai Fosun Pharmaceutical Industrial Development Co. Ltd. for commercialization of tenapanor for hyperphosphatemia and IBS-C in China and related territories. We also expect to form one or more additional collaboration partnerships in connection with the commercialization of tenapanor, outside of the United States, and in the United States for IBS-C to address the primary care market, if approved. We face significant competition in seeking appropriate collaboration partners, and the negotiation process to secure appropriate terms is time-consuming and complex. Any delays in identifying suitable additional collaboration partners and entering into agreements to develop our product candidates could also delay the commercialization of our product candidates, which may reduce their competitiveness even if they reach the market. Moreover, we may not be successful in our efforts to establish such aadditional collaboration partnershippartnerships for tenapanor for IBS-C commercialization or for any future product candidates and programs on terms that are acceptable to us, or at all. ThisWith respect to tenapanor, this may be because third parties may not view tenapanor for the treatment of IBS-C as having sufficient potential to be successfully commercialized. If we are unable to establish a collaboration partnership for the commercialization of IBS-C in the United States, the commercialization of tenapanor for IBS-C, if approved, could be materially and adversely impacted, which could have a material adverse effect on our business, results of operations, financial condition and prospects. Additionally, we may not be successful in our efforts to establish collaboration partnerships for our other product candidates because our product candidates and programs may be deemed to be at too early of a stage of development for collaborative effort, our research and development pipeline may be viewed as insufficient, and/or third parties may not view oursuch other product candidates and programs as having sufficient potential for commercialization, including the likelihood of an adequate safety and efficacy profile. Even if we are successful in entering into a collaboration partnership or license arrangement, thereThere is no guarantee that our current collaboration partnerships or any such arrangements we enter into in the collaboration partnershipfuture will be successful, or that any future collaboration partner will commit sufficient resources to the development, regulatory approval, and commercialization effort for such products, or that such alliances will result in us achieving revenues that justify such transactions.
We may engage in strategic transactions that could impact our liquidity, increase our expenses and present significant distractions to our management. We intend tomay consider strategic transactions, such as acquisitions of companies, asset purchases, and or in-licensing of products, product candidates or technologies. In addition, if we are unable to access capital on a timely basis and on terms that are acceptable to us, we may be forced to restructure certain aspects of our business or identify and complete one or more strategic collaborations or other transactions in order to fund the development or commercialization of tenapanor or certain of our product candidates through the use of alternative structures. Additional potential transactions that we may consider include a variety of different business arrangements, including spin-offs, spin outs, collaboration partnerships, joint ventures, restructurings, divestitures, business combinations and investments. Any such transaction may require us to incur non-recurring or other charges, may increase our near- and long-term expenditures and may pose significant integration challenges or disrupt our management or business, which could adversely affect our operations and financial results. For example, these transactions may entail numerous operational and financial risks, including: | · | | up-front, milestone and royalty payments, equity investments and financial support of new research and development candidates including increase of personnel, all of which may be substantial; |
| · | | exposure to unknown liabilities; |
| · | | disruption of our business and diversion of our management’s time and attention in order to develop acquired products, product candidates or technologies; |
| · | | incurrence of substantial debt or dilutive issuances of equity securities to pay for acquisitions; |
| · | | higher-than-expected acquisition and integration costs; |
| · | | write-downs of assets or goodwill or impairment charges; |
| · | | increased amortization expenses; |
| · | | difficulty and cost in combining the operations and personnel of any acquired businesses with our operations and personnel; |
| · | | impairment of relationships with key suppliers or customers of any acquired businesses due to changes in management and ownership; and |
| · | | inability to retain key employees of any acquired businesses. |
up-front, milestone and royalty payments, equity investments and financial supportexposure to unknown liabilities;
disruption of our business and diversion of our management’s time and attention in order to develop acquired products, product candidates or technologies;
incurrence of substantial debt or dilutive issuances of equity securities to pay for acquisitions;
higher-than-expected acquisition and integration costs;
write-downs of assets or goodwill or impairment charges;
increased amortization expenses;
difficulty and cost in combining the operations and personnel of any acquired businesses with our operations and personnel;
impairment of relationships with key suppliers or customers of any acquired businesses due to changes in management and ownership; and
inability to retain key employees of any acquired businesses.
Accordingly, although there can be no assurance that we will undertake or successfully complete any transactions of the nature described above, any transactions that we do complete may be subject to the foregoing or other risks and could have a material adverse effect on our business, results of operations, financial condition and prospects. If we seek and obtain approval to commercialize our product candidates outside of the United States, or otherwise engage in business outside of the United States, a variety of risks associated with international operations could materially adversely affect our business. WeIn addition to Japan and China, we or our collaboration partners may decide to seek marketing approval for certain of our product candidates outside the United States or otherwise engage in business outside the United States, including entering into contractual agreements with third-parties. We expect that we will be subject to additional risks related to entering into these international business markets and relationships, including:
| · | | different regulatory requirements for drug approvals in foreign countries; |
| · | | differing United States and foreign drug import and export rules; |
| · | | reduced protection for intellectual property rights in foreign countries; |
| · | | unexpected changes in tariffs, trade barriers and regulatory requirements; |
| · | | different reimbursement systems, and different competitive drugs; |
| · | | economic weakness, including inflation, or political instability in particular foreign economies and markets; |
| · | | compliance with tax, employment, immigration and labor laws for employees living or traveling abroad; |
| · | | foreign taxes, including withholding of payroll taxes; |
| · | | foreign currency fluctuations, which could result in increased operating expenses and reduced revenues, and other obligations incident to doing business in another country; |
| · | | workforce uncertainty in countries where labor unrest is more common than in the United States; |
| · | | production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad; |
| · | | potential liability resulting from development work conducted by these distributors; and |
| · | | business interruptions resulting from geopolitical actions, including war and terrorism, or natural disasters. |
differing United States and foreign drug import and export rules;
reduced protection for intellectual property rights in foreign countries;
unexpected changes in tariffs, trade barriers and regulatory requirements;
different reimbursement systems, and different competitive drugs;
economic weakness, including inflation, or political instability in particular foreign economies and markets;
compliance with tax, employment, immigration and labor laws for employees living or traveling abroad;
foreign taxes, including withholding of payroll taxes;
foreign currency fluctuations, which could result in increased operating expenses and reduced revenues, and other obligations incident to doing business in another country;
workforce uncertainty in countries where labor unrest is more common than in the United States;
production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad;
potential liability resulting from development work conducted by these distributors; and
business interruptions resulting from geopolitical actions, including war and terrorism, or natural disasters.
Our business involves the use of hazardous materials and we and third-parties with whom we contract must comply with environmental laws and regulations, which can be expensive and restrict how we do business. Our research and development activities involve the controlled storage, use and disposal of hazardous materials, including the components of our product candidates and other hazardous compounds. We and manufacturers and suppliers with whom we may contract are subject to laws and regulations governing the use, manufacture, storage, handling and disposal of these hazardous materials. In some cases, these hazardous materials and various wastes resulting from their use are stored at our and our manufacturers’ facilities pending their use and disposal. We cannot eliminate the risk of contamination, which could cause an interruption of our commercialization efforts, research and development efforts and business operations, environmental damage resulting in costly clean-up and liabilities under applicable laws and regulations governing the use, storage, handling and disposal of these materials and specified waste products. We cannot guarantee that that the safety procedures utilized by third-party manufacturers and suppliers with whom we may contract will comply with the standards prescribed by laws and regulations or will eliminate the risk of accidental contamination or injury from these materials. In such an event, we may be held liable for any resulting damages and such liability could exceed our resources and state or federal or other applicable authorities may curtail our use of certain materials and/or interrupt our business operations. Furthermore, environmental laws and regulations are complex, change frequently and have tended to become more stringent. We cannot predict the impact of such changes and cannot be certain of our future compliance. We do not currently carry biological or hazardous waste insurance coverage. Our internal computer systems, or those of our CROs or other contractors or consultants, may fail or suffer security breaches, which could result in a material disruption of our product development programs.
Despite the implementation of security measures, our internal computer systems and those of our CROs and other contractors and consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. While we have not experienced any such system failure, accident or security breach to date, if such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our programs. For example, the loss of clinical trial data from completed or ongoing clinical trials for any of our product candidates could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach results in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development of our product candidates could be delayed.
We may be adversely affected by the current global economic environment. Our ability to attract and retain collaboration partners or customers, invest in and grow our business and meet our financial obligations depends on our operating and financial performance, which, in turn, is subject to numerous factors, including the prevailing economic conditions and financial, business and other factors beyond our control, such as the rate of unemployment, the number of uninsured persons in the United States, presidential elections, other political influences and inflationary pressures. Our results of operations could be adversely affected by general conditions in the global economy and in the global financial markets. The recent2008 global financial crisis caused extreme volatility and disruptions in the capital and credit markets. We cannot anticipate all the ways in which the current global economic climate and global financial market conditions could adversely impact our business.business in the future. We are exposed to risks associated with reduced profitability and the potential financial instability of our collaboration partners or customers, many of which may be adversely affected by volatile conditions in the financial markets. For example, unemployment and underemployment, and the resultant loss of insurance, may decrease the demand for healthcare services and pharmaceuticals. If fewer patients are seeking medical care because they do not have insurance coverage, our collaboration partners or customers may experience reductions in revenues, profitability and/or cash flow that could lead them to reduce their support of our programs or financing activities. If collaboration partners or customers are not successful in generating sufficient revenue or are precluded from securing financing, they may not be able to pay, or may delay payment of, accounts receivable that are owed to us. In addition, the volatility in the financial markets could cause significant fluctuations in the interest rate and currency markets. We currently do not hedge for these risks. The foregoing events, in turn, could adversely affect our financial condition and liquidity. In addition, if economic challenges in the United States result in widespread and prolonged unemployment, either regionally or on a national basis, prior to the effectiveness ofor if certain provisions of the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively known as the Affordable Care Act, are repealed, a substantial number of people may become uninsured or underinsured. To the extent economic challenges result in fewer individuals pursuing or being able to afford our product candidates once commercialized, our business, results of operations, financial condition and cash flows could be adversely affected. We may be adversely affected by earthquakes or other natural disasters and our business continuity and disaster recovery plans may not adequately protect us from a serious disaster. Our corporate headquarters and other facilities are located in the San Francisco Bay Area, which in the past has experienced severe earthquakes. We do not carry earthquake insurance. Earthquakes or other natural disasters could severely disrupt our operations, and have a material adverse effect on our business, results of operations, financial condition and prospects. If a natural disaster, power outage or other event occurred that prevented us from using all or a significant portion of our headquarters, that damaged critical infrastructure, such as our enterprise financial systems or manufacturing resource planning and enterprise quality systems, or that otherwise disrupted operations, it may be difficult or, in certain cases, impossible for us to continue our business for a substantial period of time. The disaster recovery and business continuity plans we have in place currently are limited and are unlikely to prove adequate in the event of a serious disaster or similar event. We may incur substantial expenses as a result of the limited nature of our disaster recovery and business continuity plans, which, particularly when taken together with our lack of earthquake insurance, could have a material adverse effect on our business. Risks Related to Government Regulation The regulatory approval processes of the FDA and comparable foreign authorities are lengthy, time consuming and inherently unpredictable. If we are ultimately unable to obtain regulatory approval for our product candidates, our business will be substantially harmed. The research, testing, manufacturing, labeling, approval, selling, import, export, marketing and distribution of drug products are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries, which regulations differ from country to country. Neither we nor any of our collaboration partners is permitted to market any drug product in the United States until we receive marketing approval from the FDA. We have not submitted an application or obtained marketing approval for any of our product candidates anywhere in the world. Obtaining regulatory approval of a NDA can be a lengthy, expensive and uncertain process. In addition, failure to comply with FDA and other applicable United States and foreign regulatory requirements may subject us to administrative or judicially imposed sanctions or other actions, including: | · | | civil and criminal penalties; |
| · | | withdrawal of regulatory approval of products; |
| · | | product seizure or detention; |
| · | | total or partial suspension of production; and |
| · | | warning letters;
civil and criminal penalties;
injunctions;
withdrawal of regulatory approval of products;
product seizure or detention;
product recalls;
total or partial suspension of production; and
refusal to approve pending NDAs or supplements to approved NDAs. |
Prior to obtaining approval to commercialize a drug candidate in the United States or abroad, we or our collaboration partners must demonstrate with substantial evidence from well-controlled clinical trials, and to the satisfaction of the FDA or other foreign regulatory agencies, that such drug candidates are safe and effective for their intended uses. The number of nonclinical studies and clinical trials that will be required for FDA approval varies depending on the drug candidate, the disease or condition that the drug candidate is designed to address, and the regulations applicable to any particular drug candidate. Results from nonclinical studies and clinical trials can be interpreted in different ways. Even if we believe the nonclinical or clinical data for our drug candidates are promising, such data may not be sufficient to support approval by the FDA and other regulatory authorities. Administering drug candidates to humans may produce undesirable side effects, which could interrupt, delay or halt clinical trials and result in the FDA or other regulatory authorities denying approval of a drug candidate for any or all targeted indications. The time required to obtain approval by the FDA and comparable foreign authorities is unpredictable, typically takes many years following the commencement of clinical studies, and depends upon numerous factors. The FDA and comparable foreign authorities have substantial discretion in the approval process and we may encounter matters with the FDA or such comparable authorities that requires us to expend additional time and resources and delay or prevent the approval of our product candidates. For example, the FDA may require us to conduct additional studies or trials for drug product either prior to or post-approval, such as additional drug-drug interaction studies or safety or efficacy studies or trials, or it may object to elements of our clinical development program such as the number of subjects in our current clinical trials from the United States. In addition, approval policies, regulations or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions, which may cause delays in the approval or result in a decision not to approve an application for regulatory approval. Despite the time and expense exerted, failure can occur at any stage. Applications for our product candidates could fail to receive regulatory approval for many reasons, including but not limited to the following: | · | | the FDA or comparable foreign regulatory authorities may disagree with the design or implementation of our, or our collaboration partners’, clinical studies; |
| · | | the population studied in the clinical program may not be sufficiently broad or representative to assure safety in the full population for which approval is sought; |
| · | | the FDA or comparable foreign regulatory authorities may disagree with the interpretation of data from preclinical studies or clinical studies; |
| · | | the data collected from clinical studies of our product candidates may not be sufficient to support the submission of a NDA or other submission or to obtain regulatory approval in the United States or elsewhere; |
| · | | we or our collaboration partners may be unable to demonstrate to the FDA or comparable foreign regulatory authorities that a product candidate’s risk-benefit ratio for its proposed indication is acceptable; |
| · | | the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes, test procedures and specifications, or facilities of third-party manufacturers responsible for clinical and commercial supplies; and |
| · | | the FDA or comparable foreign regulatory authorities may disagree with the design or implementation of our, or our collaboration partners’, clinical studies;
the population studied in the clinical program may not be sufficiently broad or representative to assure safety in the full population for which approval is sought;
the FDA or comparable foreign regulatory authorities may disagree with the interpretation of data from preclinical studies or clinical studies;
the data collected from clinical studies of our product candidates may not be sufficient to support the submission of a NDA or other submission or to obtain regulatory approval in the United States or elsewhere;
we or our collaboration partners may be unable to demonstrate to the FDA or comparable foreign regulatory authorities that a product candidate’s risk-benefit ratio for its proposed indication is acceptable;
the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes, test procedures and specifications, or facilities of third-party manufacturers responsible for clinical and commercial supplies; and
the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval. |
This lengthy approval process, as well as the unpredictability of the results of clinical studies, may result in our failure and/or that of our collaboration partners to obtain regulatory approval to market any of our product candidates, which would significantly harm our business, results of operations, and prospects. Additionally, if the FDA requires that we conduct additional clinical studies, places limitations in our label, delays approval to market our product candidates or limits the use of our products, our business and results of operations may be harmed. In addition, even if we were to obtain approval, regulatory authorities may approve any of our product candidates for fewer or more limited indications than we request, may not approve the price we intend to charge for our products, may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve a product candidate with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that product candidate. Any of the foregoing scenarios could materially harm the commercial prospects for our product candidates. Even if we receive regulatory approval for a product candidate, we will be subject to ongoing regulatory obligations and continued regulatory review, which may result in significant additional expense. Additionally, any product candidates, if approved, could be subject to labeling and other restrictions and market withdrawal, and we may be subject to penalties if we fail to comply with regulatory requirements or experience unanticipated problems with our products. Even if a drug is approved by the FDA or foreign regulatory authorities, the manufacturing processes, labeling, packaging, distribution, adverse event reporting, storage, advertising, promotion and recordkeeping for the product will be subject to extensive and ongoing regulatory requirements. These requirements include submissions of safety and other post-marketing information and reports, registration, as well as continued compliance with cGMPs and GCPsGCP regulations for any clinical trials that we conduct post-approval. As such, we and our third partythird-party contract manufacturers will be subject to continual review and periodic inspections to assess compliance with regulatory requirements. Accordingly, we and others with whom we work must continue to expend time, money, and effort in all areas of regulatory compliance, including manufacturing, production, and quality control. Regulatory authorities may also impose significant restrictions on a product’s indicated uses or marketing or impose ongoing requirements for potentially costly post-marketing studies. Furthermore, any new legislation addressing drug safety issues could result in delays or increased costs to assure compliance. We will also be required to report certain adverse reactions and production problems, if any, to the FDA, and to comply with requirements concerning advertising and promotion for our products. Promotional communications with respect to prescription drugs are subject to a variety of legal and regulatory restrictions and must be consistent with the information in the product’s approved label. As such, we may not promote our products for indications or uses for which they do not have FDA approval. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with our third-party manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may result in, among other things: | · | | warning letters, fines or holds on clinical trials; |
| · | | restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market or voluntary or mandatory product recalls; |
| · | | injunctions or the imposition of civil or criminal penalties; |
| · | | suspension or revocation of existing regulatory approvals; |
| · | | suspension of any of our ongoing clinical trials; |
| · | | refusal to approve pending applications or supplements to approved applications submitted by us; |
| · | | restrictions on our or our contract manufacturers’ operations; or |
| · | | warning letters, fines or holds on clinical trials;
restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market or voluntary or mandatory product recalls;
injunctions or the imposition of civil or criminal penalties;
suspension or revocation of existing regulatory approvals;
suspension of any of our ongoing clinical trials;
refusal to approve pending applications or supplements to approved applications submitted by us;
restrictions on our or our contract manufacturers’ operations; or
product seizure or detention, or refusal to permit the import or export of products. |
Any government investigation of alleged violations of law could require us to expend significant time and resources in response, and could generate negative publicity. Any failure to comply with ongoing regulatory requirements may significantly and adversely affect our ability to commercialize our product candidates. If regulatory sanctions are applied or if regulatory approval is withdrawn, the value of our company and our operating results will be adversely affected. In addition, the FDA’s policies may change and additional government regulations may be enacted that could prevent, limit or delay regulatory approval of our product candidates. If we are slow or unable to adapt to changes in existing requirements or the adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we may lose any marketing approval that we may have obtained, which would adversely affect our business, prospects and ability to achieve or sustain profitability. We also cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative or executive action, either in the United States or abroad. For example, certain policies of the Trump administration may impact our business and industry. Namely, the Trump administration has taken several executive actions, including the issuance of a number of Executive Orders, that could impose significant burdens on, or otherwise materially delay, the FDA’s ability to engage in routine regulatory and oversight activities such as implementing statutes through rulemaking, issuance of guidance, and review and approval of marketing applications. It is difficult to predict how these Executive Orders will be implemented, and the extent to which they will impact the FDA’s ability to exercise its regulatory authority. If these executive actions impose constraints on FDA’s ability to engage in oversight and implementation activities in the normal course, our business may be negatively impacted. We and our contract manufacturers are subject to significant regulation with respect to manufacturing our product candidates. The manufacturing facilities on which we rely may not continue to meet regulatory requirements or may not be able to meet supply demands. All entities involved in the preparation of product candidates for clinical studies or commercial sale, including our existing contract manufacturers for our product candidates are subject to extensive regulation. Components of a finished therapeutic product approved for commercial sale or used in late-stage clinical studies must be manufactured in accordance with cGMP.cGMP regulations. These regulations govern manufacturing processes and procedures (including record keeping) and the implementation and operation of quality systems to control and assure the quality of investigational products and products approved for sale. Poor control of production processes can lead to the introduction of contaminants or to inadvertent changes in the properties or stability of our product candidates that may not be detectable in final product testing. We or our contract manufacturers must supply all necessary documentation in support of an NDA or comparable regulatory filing on a timely basis and must adhere to cGMP regulations enforced by the FDA and other regulatory agencies through their facilities inspection programs. The facilities and quality systems of some or all of our third-party contractors must pass a pre-approval inspection for compliance with the applicable regulations as a condition of regulatory approval of our product candidates. In addition, the regulatory authorities may, at any time, audit or inspect a manufacturing facility involved with the preparation of our product candidates or our other potential products or the associated quality systems for compliance with the regulations applicable to the activities being conducted. Although we oversee the contract manufacturers, we cannot control the manufacturing process of, and are completely dependent on, our contract manufacturing partners for compliance with the regulatory requirements. If these facilities do not pass a pre-approval plant inspection, regulatory approval of the products may not be granted or may be substantially delayed until any violations are corrected to the satisfaction of the regulatory authority, if ever. In addition, we have no control over the ability of our contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. The regulatory authorities also may, at any time following approval of a product for sale, audit the manufacturing facilities of our third-party contractors. If any such inspection or audit identifies a failure to comply with applicable regulations or if a violation of our product specifications or applicable regulations occurs independent of such an inspection or audit, we or the relevant regulatory authority may require remedial measures that may be costly and/or time consuming for us or a third party to implement, and that may include the temporary or permanent suspension of a clinical study or commercial sales or the temporary or permanent suspension of production or closure of a facility. Any such remedial measures imposed upon us or third parties with whom we contract could materially harm our business. If we or any of our third-party manufacturers fail to maintain regulatory compliance, the FDA or other applicable regulatory authority can impose regulatory sanctions including, among other things, refusal to approve a pending application for a new drug product, withdrawal of an approval, or suspension of production. As a result, our business, financial condition, and results of operations may be materially harmed. Additionally, if supply from one approved manufacturer is interrupted, an alternative manufacturer would need to be qualified through an NDA, a supplemental NDA or equivalent foreign regulatory filing, which could result in further delay. The regulatory agencies may also require additional studies if a new manufacturer is relied upon for commercial production. Switching manufacturers may involve substantial costs and is likely to result in a delay in our desired clinical and commercial timelines. These factors could cause us to incur higher costs and could cause the delay or termination of clinical studies, regulatory submissions, required approvals, or commercialization of our product candidates. Furthermore, if our suppliers fail to meet contractual requirements and we are unable to secure one or more replacement suppliers capable of production at a substantially equivalent cost, our clinical studies may be delayed or we could lose potential revenue.
If we fail to comply or are found to have failed to comply with FDA and other regulations related to the promotion of our products for unapproved uses, we could be subject to criminal penalties, substantial fines or other sanctions and damage awards. The regulations relating to the promotion of products for unapproved uses are complex and subject to substantial interpretation by the FDA and other government agencies. If tenapanor RDX022 or our other product candidates receive marketing approval, we and our collaboratingcollaboration partners, if any, will be restricted from marketing the product outside of its approved labeling, also referred to as off-label promotion. However, physicians may nevertheless prescribe an approved product to their patients in a manner that is inconsistent with the approved label, which is an off-label use. We intend to implement compliance and training programs designed to ensure that our sales and marketing practices comply with applicable regulations regarding off-label promotion. Notwithstanding these programs, the FDA or other government agencies may allege or find that our practices constitute prohibited promotion of our product candidates for unapproved uses. We also cannot be sure that our employees will comply with company policies and applicable regulations regarding the promotion of products for unapproved uses. Over the past several years, a significant number of pharmaceutical and biotechnology companies have been the target of inquiries and investigations by various federal and state regulatory, investigative, prosecutorial and administrative entities in connection with the promotion of products for unapproved uses and other sales practices, including the Department of Justice and various U.S. Attorneys’ Offices, the Office of Inspector General of the Department of Health and Human Services, the FDA, the Federal Trade Commission and various state Attorneys General offices. These investigations have alleged violations of various federal and state laws and regulations, including claims asserting antitrust violations, violations of the Food, Drug and Cosmetic Act, the False Claims Act, the Prescription Drug Marketing Act, anti-kickback laws, and other alleged violations in connection with the promotion of products for unapproved uses, pricing and Medicare and/or Medicaid reimbursement. Many of these investigations originate as “qui tam” actions under the False Claims Act. Under the False Claims Act, any individual can bring a claim on behalf of the government alleging that a person or entity has presented a false claim, or caused a false claim to be submitted, to the government for payment. The person bringing a qui tam suit is entitled to a share of any recovery or settlement. Qui tam suits, also commonly referred to as “whistleblower suits,” are often brought by current or former employees. In a qui tam suit, the government must decide whether to intervene and prosecute the case. If it declines, the individual may pursue the case alone. If the FDA or any other governmental agency initiates an enforcement action against us or if we are the subject of a qui tam suit and it is determined that we violated prohibitions relating to the promotion of products for unapproved uses, we could be subject to substantial civil or criminal fines or damage awards and other sanctions such as consent decrees and corporate integrity agreements pursuant to which our activities would be subject to ongoing scrutiny and monitoring to ensure compliance with applicable laws and regulations. Any such fines, awards or other sanctions would have an adverse effect on our revenue, business, financial prospects and reputation. If approved, tenapanor RDX022 and our other product candidates may cause or contribute to adverse medical events that we are required to report to regulatory agencies and if we fail to do so we could be subject to sanctions that would materially harm our business. Some participants in clinical studies of tenapanor have reported adverse effects after being treated with tenapanor, including diarrhea, nausea, flatulence, abdominal discomfort, abdominal pain, abdominal distention and changes in electrolytes and in the Phase 2b evaluating tenapanor for the treatment of hyperphosphatemia in ESRD patients, we observed that the rate of diarrhea and the discontinuation rate due to diarrhea at the highest doses was higher than expected based upon the results of previous clinical trials.electrolytes. If we are successful in commercializing any products, FDA and foreign regulatory agency regulations require that we report certain information about adverse medical events if those products may have caused or contributed to those adverse events. The timing of our obligation to report would be triggered by the date we become aware of the adverse event as well as the nature of the event. We may fail to report adverse events we become aware of within the prescribed timeframe. We may also fail to appreciate that we have become aware of a reportable adverse event, especially if it is not reported to us as an adverse event or if it is an adverse event that is unexpected or removed in time from the use of our products. If we fail to comply with our reporting obligations, the FDA or a foreign regulatory agency could take action, including criminal prosecution, the imposition of civil monetary penalties, seizure of our products or delay in approval or clearance of future products.
Our employees, independent contractors, principal investigators, CROs, collaboration partners, consultants and vendors may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements. We are exposed to the risk that our employees, independent contractors, principal investigators, CROs, collaboration partners, consultants and vendors may engage in fraudulent conduct or other illegal activity. Misconduct by these parties could include intentional, reckless and/or negligent conduct or unauthorized activities that violate: (1) FDA regulations, including those laws that require the reporting of true, complete and accurate information to the FDA; (2) manufacturing standards; (3) federal and state healthcare fraud and abuse laws and regulations; or (4) laws that require the reporting of true and accurate financial information and data. Specifically, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. These activities also include the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter misconduct by employees and other third parties, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliancecomply with such laws or regulations. Additionally, we are subject to the risk that a person or government could allege such fraud or other misconduct, even if none occurred. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant civil, criminal and administrative penalties, damages, monetary fines, disgorgements, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, individual imprisonment, other sanctions, contractual damages, reputational harm, diminished profits and future earnings, and curtailment of our operations, any of which could adversely affect our ability to operate our business and our results of operations. Failure to obtain regulatory approvals in foreign jurisdictions would prevent us from marketing our products internationally. In order to market any product in the EEA (which is composed of the 28 Member States of the European Union plus Norway, Iceland and Liechtenstein), and many other foreign jurisdictions, separate regulatory approvals are required. In the EEA, medicinal products can only be commercialized after obtaining a Marketing Authorization, or MA. Before granting the MA, the EMA or the competent authorities of the Member States of the EEA make an assessment of the risk-benefit balance of the product on the basis of scientific criteria concerning its quality, safety and efficacy. The approval procedures vary among countries and can involve additional clinical testing, and the time required to obtain approval may differ from that required to obtain FDA approval. Clinical trials conducted in one country may not be accepted by regulatory authorities in other countries. Approval by the FDA does not ensure approval by regulatory authorities in other countries, and approval by one or more foreign regulatory authorities does not ensure approval by regulatory authorities in other foreign countries or by the FDA. However, a failure or delay in obtaining regulatory approval in one country may have a negative effect on the regulatory process in others. The foreign regulatory approval process may include all of the risks associated with obtaining FDA approval. We may not be able to file for regulatory approvals or to do so on a timely basis, and even if we do file we may not receive necessary approvals to commercialize our products in any market. We and our collaboration partners if any, may be subject to healthcare laws, regulation and enforcement; our failure or the failure of any such collaboration partners to comply with these laws could have a material adverse effect on our results of operations and financial conditions. Although we do not currently have any products on the market, once we begin commercializing our products, we and our collaboration partners if any, may be subject to additional healthcare statutory and regulatory requirements and enforcement by the federal government and the states and foreign governments in which we conduct our business. The laws that may affect our ability to operate as a commercial organization include: | · | | the federal Anti-Kickback Statute, which prohibits, among other things, persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual for, or the purchase, order or recommendation of, any good or service for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs; |
| · | | federal false claims laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent; |
| · | | federal criminal laws that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters; |
| · | | the federal Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act, which governs the conduct of certain electronic healthcare transactions and protects the security and privacy of protected health information; |
| · | | the federal physician sunshine requirements under the Affordable Care Act, which requires manufacturers of drugs, devices, biologics, and medical supplies to report annually to the CMS information related to payments and other transfers of value to physicians, other healthcare providers, and teaching hospitals, and ownership and investment interests held by physicians and other healthcare providers and their immediate family members; |
| · | | state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers; |
| · | | state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the applicable compliance guidance promulgated by the federal government, or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; |
| · | | state laws that require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or pricing information and marketing expenditures; and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways, thus complicating compliance efforts; and |
| · | | the federal Anti-Kickback Statute, which prohibits, among other things, persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual for, or the purchase, order or recommendation of, any good or service for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs;
federal false claims laws which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid, or other third-party payors that are false or fraudulent;
federal criminal laws that prohibit executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters;
the federal Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act, which governs the conduct of certain electronic healthcare transactions and protects the security and privacy of protected health information;
the federal physician sunshine requirements under the Affordable Care Act, which requires manufacturers of drugs, devices, biologics, and medical supplies to report annually to the CMS information related to payments and other transfers of value to physicians, other healthcare providers, and teaching hospitals, and ownership and investment interests held by physicians and other healthcare providers and their immediate family members;
state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers;
state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the applicable compliance guidance promulgated by the federal government, or otherwise restrict payments that may be made to healthcare providers and other potential referral sources;
state laws that require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways, thus complicating compliance efforts; and
European and other foreign law equivalents of each of the laws, including reporting requirements detailing interactions with and payments to healthcare providers. |
Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available, it is possible that some of our business activities could be subject to challenge under one or more of such laws. The risk of our being found in violation of these laws is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. Further, the Affordable Care Act, among other things, amends the intent requirement of the federal anti-kickback and criminal health care fraud statutes. A person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it. In addition, the Affordable Care Act provides that the government may assert that a claim including items or services resulting from a violation of the federal anti-kickback statuteAnti-Kickback Statute constitutes a false or fraudulent claim for purposes of the false claims statutes. Any action against us for violation of these laws, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. If our operations are found to be in violation of any of the laws described above or any other governmental laws and regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines, the curtailment or restructuring of our operations, the exclusion from participation in federal and state healthcare programs and imprisonment, any of which could adversely affect our ability to market our products and adversely impact our financial results. Legislative or regulatory healthcare reforms in the United States may make it more difficult and costly for us to obtain regulatory clearance or approval of our product candidates and to produce, market and distribute our products after clearance or approval is obtained. From time to time, legislation is drafted and introduced in Congress that could significantly change the statutory provisions governing the regulatory clearance or approval, manufacture, and marketing of regulated products or the reimbursement thereof. In addition, FDA regulations and guidance are often revised or reinterpreted by the FDA in ways that may significantly affect our business and our products. Any new regulations or revisions or reinterpretations of existing regulations may impose additional costs or lengthen review times of our product candidates. We cannot determine what effect changes in regulations, statutes, legal interpretation or policies, when and if promulgated, enacted or adopted may have on our business in the future. Such changes could, among other things, require: | · | | additional clinical trials to be conducted prior to obtaining approval; |
| · | | changes to manufacturing methods; |
| · | | recall, replacement, or discontinuance of one or more of our products; and |
| · | | additional clinical trials to be conducted prior to obtaining approval;
changes to manufacturing methods;
recall, replacement, or discontinuance of one or more of our products; and
additional record keeping. |
Each of these would likely entail substantial time and cost and could materially harm our business and our financial results. In addition, delays in receipt of or failure to receive regulatory clearances or approvals for any future products would harm our business, financial condition and results of operations. In addition, the full impact of recent healthcare reform and other changes in the healthcare industry and in healthcare spending is currently unknown, and may adversely affect our business model. In the United States, the Affordable Care Act was enacted in 2010 with a goal of reducing the cost of healthcare and substantially changing the way healthcare is financed by both government and private insurers. The Affordable Care Act, among other things, increased the minimum Medicaid rebates owed by manufacturers under the Medicaid Drug Rebate Program and extended the rebate program to individuals enrolled in Medicaid managed care organizations, established annual fees and taxes on manufacturers of certain branded prescription drugs, and created a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D. In addition, other legislative changes have been proposed and adopted in the United States since the Affordable Care Act was enacted. On August 2, 2011, the Budget Control Act of 2011 created measures for spending reductions by Congress. A Joint Select Committee on Deficit Reduction, tasked with recommending a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, was unable to reach required goals, thereby triggering the legislation’s automatic reduction to several government programs. This included aggregate reductions of Medicare payments to providers of 2% per fiscal year, which went into effect on April 1, 2013. On January 2, 2013, the ATRA was signed into law, which, among other things, further reduced Medicare payments to several providers, including hospitals.
It is likelyWe currently expect that federal and state legislatures within the United States and foreign governments will continue to consider changes to existing healthcare legislation. Welegislation, and we currently expect that the current Presidential Administration and U.S. Congress will seek to modify, or repeal all, or certain provisions of, the Affordable Care Act. There is still uncertainty with respect to any regulatory changes, and such regulatory changes could have an impact on coverage and reimbursement for healthcare items and services covered by plans that were otherwise authorized by the Affordable Care Act. However, we cannot predict the reform initiatives that may be adopted in the future or whether initiatives that have been adopted will be repealed or modified. The continuing efforts of the government, insurance companies, managed care organizations and other payors of healthcare services to contain or reduce costs of healthcare may adversely affect the demand for any drug products for which we may obtain regulatory approval, our ability to set a price that we believe is fair for our products, our ability to obtain coverage and reimbursement approval for a product, our ability to generate revenues and achieve or maintain profitability, and the level of taxes that we are required to pay.
Other legislative changes have been proposed and adopted in the United States since the Affordable Care Act was enacted. These new laws, among other things, included aggregate reductions of Medicare payments to providers of 2% per fiscal year that will remain in effect through 2025 unless additional action is taken by Congress, additional specific reductions in Medicare payments to several types of providers, including hospitals, imaging centers and cancer treatment centers, and an increase in the statute of limitations period for the government to recover overpayments to providers from three to five years. Additionally, individual states have become increasingly active in passing legislation and implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access, and to encourage importation from other countries and bulk purchasing. Recently, there has also been heightened governmental scrutiny over the manner in which drug manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed bills designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drug products. Risks Related to Intellectual Property We may become subject to claims alleging infringement of third parties’ patents or proprietary rights and/or claims seeking to invalidate our patents, which would be costly, time consuming and, if successfully asserted against us, delay or prevent the development and commercialization of tenapanor RDX022 or our other product candidates, or prevent or delay the continued use of our drug discovery and development platform, including APECCS. There have been many lawsuits and other proceedings asserting infringement or misappropriation of patents and other intellectual property rights in the pharmaceutical and biotechnology industries. There can be no assurances that we will not be subject to claims alleging that the manufacture, use or sale of tenapanor RDX022 or any other product candidates, or that the use of our drug discovery and development platform, including APECCS, infringes existing or future third-party patents, or that such claims, if any, will not be successful. Because patent applications can take many years to issue and may be confidential for 18 months or more after filing, and because pending patent claims can be revised before issuance, there may be applications now pending which may later result in issued patents that may be infringed by the manufacture, use or sale of tenapanor RDX022 or other product candidates or by the use of APECCS. Moreover, we may face patent infringement claims from non-practicing entities that have no relevant product revenue and against whom our own patent portfolio may thus have no deterrent effect. We may be unaware of one or more issued patents that would be infringed by the manufacture, sale or use of tenapanor RDX022 or our other product candidates, or by the use of APECCS. We may be subject to third-party patent infringement claims in the future against us or our that would cause us to incur substantial expenses and, if successful against us, could cause us to pay substantial damages, including treble damages and attorney’s fees if we are found to be willfully infringing a third party’s patents. We may be required to indemnify future collaboration partners against such claims. We are not aware of any threatened or pending claims related to these matters, but in the future litigation may be necessary to defend against such claims. If a patent infringement suit were brought against us we could be forced to stop or delay research, development, manufacturing or sales of the product or product candidate that is the subject of the suit. In addition, if a patent infringement suit were brought against us regarding the use of APECCS, we could be forced to stop our use of APECCS or modify our processes to avoid infringement, which may not be possible at a reasonable cost, if at all, and which could result in substantial delay in our use of APECCS for the discovery of new product candidates or potential targets. As a result of patent infringement claims, or in order to avoid potential claims, we may choose to seek, or be required to seek, a license from the third party and would most likely be required to pay license fees or royalties or both. These licenses may not be available on acceptable terms, or at all. Even if we were able to obtain a license, we may be unable to maintain such licenses and the rights may be nonexclusive, which would give our competitors access to the same intellectual property. Ultimately, we could be prevented from commercializing a product, or forced to redesign it, or to cease our use of APECCS or some other aspect of our business operations if, as a result of actual or threatened patent infringement claims, we are unable to enter into licenses on acceptable terms.terms, or unable to maintain such licenses when granted. Even if we are successful in defending against such claims, such litigation can be expensive and time consuming to litigate and would divert management’s attention from our core business. Any of these events could harm our business significantly. In addition to infringement claims against us, if third parties prepare and file patent applications in the United States that also claim technology similar or identical to ours, we may have to participate in interference or derivation proceedings in the United States Patent and Trademark Office, or the USPTO, to determine which party is entitled to a patent on the disputed invention. We may also become involved in similar opposition proceedings in the European Patent Office or similar offices in other jurisdictions regarding our intellectual property rights with respect to our products and technology. Since patent applications are confidential for a period of time after filing, we cannot be certain that we were the first to file any patent application related to our product candidates. If our intellectual property related to our product candidates is not adequate or if we are not able to protect our trade secrets or our confidential information, we may not be able to compete effectively in our market. We rely upon a combination of patents, trade secret protection and confidentiality agreements to protect the intellectual property related to our product candidates, our drug discovery and development platform and our development programs. Any disclosure to or misappropriation by third parties of our confidential or proprietary information could enable competitors to quickly duplicate or surpass our technological achievements, thus eroding our competitive position in our market. The strength of patents in the biotechnology and pharmaceutical field involves complex legal and scientific questions and can be uncertain. The patent applications that we own or license may fail to result in issued patents in the United States or in foreign countries. Additionally, our research and development efforts may result in product candidates for which patent protection is limited or not available. Even if patents do successfully issue, third parties may challenge the validity, enforceability or scope thereof, which may result in such patents being narrowed, invalidated or held unenforceable. For example, U.S. patents can be challenged by any person before the new USPTO Patent Trial and Appeals Board at any time before one year after that person is served an infringement complaint based on the patents. Patents granted by the European Patent Office may be similarly opposed by any person within nine months from the publication of the grant. Similar proceedings are available in other jurisdictions, and in the United States, Europe and other jurisdictions third parties can raise questions of validity with a patent office even before a patent has granted. Furthermore, even if they are unchallenged, our patents and patent applications may not adequately protect our intellectual property or prevent others from designing around our claims. For example, a third party may develop a competitive product that provides therapeutic benefits similar to one or more of our product candidates but has a sufficiently different composition to fall outside the scope of our patent protection. If the breadth or strength of protection provided by the patents and patent applications we hold or pursue with respect to our product candidates is successfully challenged, then our ability to commercialize such product candidates could be negatively affected, and we may face unexpected competition that could have a material adverse impact on our business. Further, if we encounter delays in our clinical trials, the period of time during which we or our collaboration partners could market tenapanor or other product candidates under patent protection would be reduced. Even where laws provide protection, costly and time-consuming litigation could be necessary to enforce and determine the scope of our proprietary rights, and the outcome of such litigation would be uncertain. If we or one of our collaboration partners were to initiate legal proceedings against a third party to enforce a patent covering the product candidate, the defendant could counterclaim that our patent is invalid and/or unenforceable. In patent litigation in the United States, defendant counterclaims alleging invalidity and/or unenforceability are commonplace. Grounds for a validity challenge could be an alleged failure to meet any of several statutory requirements, including lack of novelty, obviousness or non-enablement. Grounds for an unenforceability assertion could be an allegation that someone connected with prosecution of the patent withheld relevant information from the USPTO, or made a misleading statement, during prosecution. The outcome following legal assertions of invalidity and unenforceability is unpredictable. With respect to validity, for example, we cannot be certain that there is no invalidating prior art, of which we and the patent examiner were unaware during prosecution. If a defendant were to prevail on a legal assertion of invalidity and/or unenforceability against our intellectual property related to a product candidate, we would lose at least part, and perhaps all, of the patent protection on such product candidate. Such a loss of patent protection would have a material adverse impact on our business. Moreover, our competitors could counterclaim that we infringe their intellectual property, and some of our competitors have substantially greater intellectual property portfolios than we do. We also rely on trade secret protection and confidentiality agreements to protect proprietary know-how that may not be patentable, processes for which patents may be difficult to obtain and/or enforce and any other elements of our drug discovery and development processes that involve proprietary know-how, information or technology that is not covered by patents. Although we require all of our employees, consultants, advisors and any third parties who have access to our proprietary know-how, information or technology, to assign their inventions to us, and endeavor to execute confidentiality agreements with all such parties, we cannot be certain that we have executed such agreements with all parties who may have helped to develop our intellectual property or who had access to our proprietary information, nor can we be certain that our agreements will not be breached by such consultants, advisors or third parties, or by our former employees. The breach of such agreements by individuals or entities who are actively involved in the discovery and design of our potential drug candidates, or in the development of our discovery and design platform, including APECCS, could require us to pursue legal action to protect our trade secrets and confidential information, which would be expensive, and the outcome of which would be unpredictable. If we are not successful in prohibiting the continued breach of such agreements, our business could be negatively impacted. We cannot guarantee that our trade secrets and other confidential proprietary information will not be disclosed or that competitors will not otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. Further, the laws of some foreign countries do not protect proprietary rights to the same extent or in the same manner as the laws of the United States. As a result, we may encounter significant problems in protecting and defending our intellectual property both in the United States and abroad. If we are unable to prevent material disclosure of the intellectual property related to our technologies to third parties, we will not be able to establish or maintain a competitive advantage in our market, which could materially adversely affect our business, results of operations and financial condition. If we do not obtain patent term extension in the United States under the Hatch-Waxman Act and in foreign countries under similar legislation, thereby potentially extending the term of marketing exclusivity for our product candidates, our business may be materially harmed. Depending upon the timing, duration and specifics of FDA marketing approval of our product candidates, if any, one of the U.S. patents covering each of such approved product(s) or the use thereof may be eligible for up to five years of patent term restoration under the Hatch-Waxman Act. The Hatch-Waxman Act allows a maximum of one patent to be extended per FDA approved product. Patent term extension also may be available in certain foreign countries upon regulatory approval of our product candidates. Nevertheless, we may not be granted patent term extension either in the United States or in any foreign country because of, for example, failing to apply within applicable deadlines, failing to apply prior to expiration of relevant patents or otherwise failing to satisfy applicable requirements. Moreover, the term of extension, as well as the scope of patent protection during any such extension, afforded by the governmental authority could be less than we request. If we are unable to obtain patent term extension or restoration, or the term of any such extension is less than we request, the period during which we will have the right to exclusively market our product will be shortened and our competitors may obtain approval of competing products following our patent expiration, and our revenue could be reduced, possibly materially. Changes in U.S. patent law could diminish the value of patents in general, thereby impairing our ability to protect our products. As is the case with other biopharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involve both technological and legal complexity. Therefore, obtaining and enforcing biopharmaceutical patents is costly, time consuming and inherently uncertain. In addition, the United States has recently enacted and is currently implementing wide-ranging patent reform legislation, including the Leahy-Smith America Invents Act signed into law on September 16, 2011. That Act includes a number of significant changes to U.S. patent law. These include provisions that affect the way patent applications are prosecuted and new venues and opportunities for competitors to challenge patent portfolios. Because of that Act, the U.S. patent system is now a “first to file” system, which may make it more difficult to obtain patent protection for inventions and increase the uncertainties and costs surrounding the prosecution of our or our collaboration partners’ patent applications and the enforcement or defense of our or our collaboration partners’ issued patents, all of which could materially adversely affect our business, results of operations and financial condition. The United States Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents once obtained. Depending on future actions by the U.S. Congress, the federal courts, and the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future. Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements. The USPTO and various foreign patent agencies require compliance with a number of procedural, documentary, fee payment and other provisions to maintain patent applications and issued patents. Noncompliance with these requirements can result in abandonment or lapse of a patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. In such an event, competitors might be able to enter the market earlier than would otherwise have been the case. We may not be able to enforce our intellectual property rights throughout the world. The laws of some foreign countries do not protect intellectual property rights to the same extent as the laws of the United States. Many companies have encountered significant problems in protecting and defending intellectual property rights in certain foreign jurisdictions. The legal systems of some countries, particularly developing countries, do not favor the enforcement of patents and other intellectual property protection, especially those relating to life sciences. This could make it difficult for us to stop the infringement of our patents or the misappropriation of our other intellectual property rights. For example, many foreign countries have compulsory licensing laws under which a patent owner must grant licenses to third parties. Proceedings to enforce our patent rights in foreign jurisdictions, whether or not successful, could result in substantial costs and divert our efforts and attention from other aspects of our business. Furthermore, while we intend to protect our intellectual property rights in our expected significant markets, we cannot ensure that we will be able to initiate or maintain similar efforts in all jurisdictions in which we may wish to market our products. Accordingly, our efforts to protect our intellectual property rights in such countries may be inadequate. In addition, changes in the law and legal decisions by courts in the United States and foreign countries may affect our ability to obtain and enforce adequate intellectual property protection for our technology. We may be subject to claims that we or our employees have misappropriated the intellectual property, including know-how or trade secrets, of a third party, or claiming ownership of what we regard as our own intellectual property. Many of our employees, consultants and contractors were previously employed at or engaged by other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Some of these employees, consultants and contractors, executed proprietary rights, non-disclosure and non-competition agreements in connection with such previous employment. Although we try to ensure that our employees, consultants and contractors do not use the intellectual property and other proprietary information or know-how or trade secrets of others in their work for us, and do not perform work for us that is in conflict with their obligations to another employer or any other entity, we may be subject to claims that we or these employees, consultants and contractors have used or disclosed such intellectual property, including know-how, trade secrets or other proprietary information. In addition, an employee, advisor or consultant who performs work for us may have obligations to a third party that are in conflict with their obligations to us, and as a result such third party may claim an ownership interest in the intellectual property arising out of work performed for us. We are not aware of any threatened or pending claims related to these matters, but in the future litigation may be necessary to defend against such claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel, or access to consultants and contractors. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management. In addition, while we typically require our employees, consultants and contractors who may be involved in the development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who in fact develops intellectual property that we regard as our own, which may result in claims by or against us related to the ownership of such intellectual property. If we fail in prosecuting or defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights. Even if we are successful in prosecuting or defending against such claims, litigation could result in substantial costs and be a distraction to our management and scientific personnel. Risks Related to Our Common Stock Our stock price may be volatile and our stockholders may not be able to resell shares of our common stock at or above the price they paid. The trading price of our common stock is highly volatile and could be subject to wide fluctuations in response to various factors, some of which are beyond our control. These factors include those discussed in this “Risk Factors” section and others such as: | · | | results from, or any delays in, clinical trial programs relating to our product candidates, including the ongoing Phase 3 clinical trial for tenapanor for hyperphosphatemia; |
| · | | the success of our efforts to establish a collaboration partnership for the commercialization of tenapanor for IBS-C in the United States; |
| · | | our ability, alone or with collaboration partners, to commercialize or obtain regulatory approval for tenapanor, or delays in commercializing or obtaining regulatory approval; |
| · | | announcements of regulatory approval, a complete response letter or a refuse to file letter to tenapanor, or specific label restrictions or patient populations for its use, or changes or delays in the regulatory review process; |
| · | | announcements relating to our current or future collaboration partnerships; |
| · | | announcements of therapeutic innovations or new products by us or our competitors; |
| · | | adverse actions taken by regulatory agencies with respect to our clinical trials, manufacturing supply chain or sales and marketing activities; |
| · | | changes or developments in laws or regulations applicable to our product candidates; |
| · | | the success of our testing and clinical trials; |
| · | | failure to meet any of our projected timelines or goals with regard to the clinical development of any of our product candidates, including the Phase 3 clinical trial for tenapanor for hyperphosphatemia; |
| · | | failure to meet any of our projected timelines with regard to the filing of the NDA for tenapanor for IBS-C; |
| · | | the success of our efforts to acquire or license or discover additional product candidates; |
results from, or any delays in, clinical trial programs relating to our product candidates, including the ongoing and planned clinical trials for tenapanor and RDX022;ability to commercialize or obtain regulatory approval for our product candidates, or delays in commercializing or obtaining regulatory approval; | · | | any intellectual property infringement actions in which we may become involved; |
| · | | the success of our efforts to obtain adequate intellectual property protection for our product candidates; |
| · | | announcements concerning our competitors or the pharmaceutical industry in general; |
| · | | achievement of expected product sales and profitability; |
| · | | manufacture, supply or distribution shortages; |
| · | | actual or anticipated fluctuations in our operating results; |
| · | | FDA or other U.S. or foreign regulatory actions affecting us or our industry or other healthcare reform measures in the United States; |
| · | | changes in financial estimates or recommendations by securities analysts; |
| · | | trading volume of our common stock; |
| · | | sales of our common stock by us, our executive officers and directors or our stockholders in the future; |
| · | | general economic and market conditions and overall fluctuations in the United States equity markets; and |
| · | | announcements of regulatory approval or a complete response letter to tenapanor or RDX022, or specific label indications or patient populations for its use, or changes or delays in the regulatory review process;
announcements relating to future collaboration partnerships;
announcements of therapeutic innovations or new products by us or our competitors;
adverse actions taken by regulatory agencies with respect to our clinical trials, manufacturing supply chain or sales and marketing activities;
changes or developments in laws or regulations applicable to our product candidates;
the success of our testing and clinical trials;
the success of our efforts to acquire or license or discover additional product candidates;
any intellectual property infringement actions in which we may become involved;
the success of our efforts to obtain adequate intellectual property protection for our product candidates;
announcements concerning our competitors or the pharmaceutical industry in general;
achievement of expected product sales and profitability;
manufacture, supply or distribution shortages;
actual or anticipated fluctuations in our operating results;
FDA or other U.S. or foreign regulatory actions affecting us or our industry or other healthcare reform measures in the United States;
changes in financial estimates or recommendations by securities analysts;
trading volume of our common stock;
sales of our common stock by us, our executive officers and directors or our stockholders in the future;
general economic and market conditions and overall fluctuations in the United States equity markets; and
the loss of any of our key scientific or management personnel. |
In addition, the stock markets in general, and the markets for pharmaceutical, biopharmaceutical and biotechnology stocks in particular, have experienced extreme volatility that may have been unrelated to the operating performance of the issuer. These broad market fluctuations may adversely affect the trading price or liquidity of our common stock. In the past, when the market price of a stock has been volatile, holders of that stock have sometimes instituted securities class action litigation against the issuer. If any of our stockholders were to bring such a lawsuit against us, we could incur substantial costs defending the lawsuit and the attention of our management would be diverted from the operation of our business, which could seriously harm our financial position. Any adverse determination in litigation could also subject us to significant liabilities. One of our principal stockholders ownowns a significant percentage of our stock and, together with our other principal stockholders and management, will be able to exert significant control over matters subject to stockholder approval. As of December 31, 2015,2017, entities affiliated with New Enterprise Associates, or NEA, a venture capital fund associated with one of our directors, collectively beneficially holdowned approximately 39.65%29.6% of our common stock, and NEA together with our executive officers and directors beneficially owned approximately 34.5% of our capital stock, including outstanding restricted stock units that will vest within 60 days of December 31, 2017, and warrants and stock options exercisable for shares of our common stock and together our executive officers, directors, and affiliated stockholders beneficially owned approximately 42.39%within 60 days of our capital stock, including warrants exercisable for shares of our common stock.December 31, 2017. Therefore, these stockholders may be able to determine all matters requiring stockholder approval, and the entities affiliated with New Enterprise AssociatesNEA alone will have significant ability to influence decisions through their ownership position. For example, these stockholders may be able to influence or control elections of directors, amendments ofto our organizational documents, or approval of any merger, sale of assets, or other major corporate transaction. This may prevent or discourage unsolicited acquisition proposals or offers for our common stock that certain stockholders may feel are in their best interest as one of our stockholders.
If we sell shares of our common stock in future financings, stockholders may experience immediate dilution and, as a result, our stock price may decline. We may from time to time issue additional shares of common stock at a discount from the current trading price of our common stock. As a result, our stockholders would experience immediate dilution upon the purchase of any shares of our common stock sold at such discount. In addition, as opportunities present themselves, we may enter into financing or similar arrangements in the future, including the issuance of debt securities, preferred stock or common stock. If we issue common stock or securities convertible into common stock, our common stockholders would experience additional dilution and, as a result, our stock price may decline. Sales of a substantial number of shares of our common stock in the public market could cause our stock price to fall. If our existing stockholders sell, or indicate an intention to sell, substantial amounts of our common stock in the public market, the trading price of our common stock could decline. As of December 31, 2015,2017, we had 25,964,88647,534,979 shares of common stock outstanding. Of those shares, approximately 10.514.4 million were held by current directors, executive officers and other affiliates, or may otherwise be subject to Rule 144 under the Securities Act of 1933, or the Securities Act. In addition, asAs of December 31, 2015,2017, approximately 1.30.7 million shares of common stock that are subject toissuable upon vesting of outstanding restricted stock units and approximately 4.0 million shares of common stock issuable upon exercise of outstanding options were eligible for sale in the public market to the extent permitted by the provisions of variousthe applicable vesting schedules, and Rule 144 and Rule 701 under the Securities Act. In addition, as of December 31, 2017, approximately 2.2 million shares that are subject toof common stock issuable upon exercise of outstanding warrants arewere eligible for sale in the public market. If these additional shares of common stock are issued and sold, or if it is perceived that they will be sold, in the public market, the trading price of our common stock could decline.
TheAs of December 31, 2017, the holders of approximately 9.05.6 million shares of our outstanding common stock as of December 31, 2015, are entitled to rights with respect to the registration of their shares under the Securities Act. Registration of these shares under the Securities Act would result in the shares becoming freely tradable without restriction under the Securities Act, except for shares purchased by affiliates. Any sales of securities by these stockholders could have a material adverse effect on the trading price of our common stock.
Provisions in our charter documents and under Delaware law could discourage a takeover that stockholders may consider favorable and may lead to entrenchment of management. Our amended and restated certificate of incorporation and amended and restated bylaws contain provisions that could significantly reduce the value of our shares to a potential acquirer or delay or prevent changes in control or changes in our management without the consent of our board of directors. The provisions in our charter documents include the following: a classified board of directors with three-year staggered terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors;
no cumulative voting in the election of directors, which limits the ability of minority stockholders to elect director candidates;
the exclusive right of our board of directors to elect a director to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from being able to fill vacancies on our board of directors;
| •· | | a classified board of directors with three-year staggered terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors; |
| · | | no cumulative voting in the election of directors, which limits the ability of minority stockholders to elect director candidates; |
| · | | the exclusive right of our board of directors to elect a director to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from being able to fill vacancies on our board of directors; |
| · | | the required approval of at least 66 2⁄3%two-thirds of the shares entitled to vote to remove a director for cause, and the prohibition on removal of directors without cause; |
the ability of our board of directors to alter our bylaws without obtaining stockholder approval;
| •· | | the ability of our board of directors to authorize the issuance of shares of preferred stock and to determine the price and other terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquirer; |
| · | | the ability of our board of directors to alter our bylaws without obtaining stockholder approval; |
| · | | the required approval of at least 66 2⁄3%two-thirds of the shares entitled to vote at an election of directors to adopt, amend or repeal our bylaws or repeal the provisions of our amended and restated certificate of incorporation regarding the election and removal of directors; |
| · | | a prohibition on stockholder action by written consent, which forces stockholder action to be taken at an annual or special meeting of our stockholders; |
| · | | the requirement that a special meeting of stockholders may be called only by the chairman of the board of directors, the chief executive officer, the president or the board of directors, which may delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors; and |
advance notice procedures that stockholders must comply with in order to nominate candidates to our board of directors or to propose matters to be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquiror from conducting a solicitation of proxies to elect the acquiror’s | · | | advance notice procedures that stockholders must comply with in order to nominate candidates to our board of directors or to propose matters to be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquirer from conducting a solicitation of proxies to elect the acquirer’s own slate of directors or otherwise attempting to obtain control of us. |
In addition, these provisions would apply even if we were to receive an offer that some stockholders may consider beneficial. We are also subject to the anti-takeover provisions contained in Section 203 of the Delaware General Corporation Law. Under Section 203, a corporation may not, in general, engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other exceptions, the board of directors has approved the transaction. Claims for indemnification by our directors and officers may reduce our available funds to satisfy successful third-party claims against us and may reduce the amount of money available to us. Our amended and restated certificate of incorporation and amended and restated bylaws provide that we will indemnify our directors and officers, in each case to the fullest extent permitted by Delaware law. In addition, as permitted by Section 145 of the Delaware General Corporation Law, our amended and restated bylaws and our indemnification agreements that we have entered into with our directors and officers provide that: | · | | We will indemnify our directors and officers for serving us in those capacities or for serving other business enterprises at our request, to the fullest extent permitted by Delaware law. Delaware law provides that a corporation may indemnify such person if such person acted in good faith and in a manner such person reasonably believed to be in or not opposed to the best interests of the registrant and, with respect to any criminal proceeding, had no reasonable cause to believe such person’s conduct was unlawful. |
| · | | We may, in our discretion, indemnify employees and agents in those circumstances where indemnification is permitted by applicable law. |
| · | | We are required to advance expenses, as incurred, to our directors and officers in connection with defending a proceeding, except that such directors or officers shall undertake to repay such advances if it is ultimately determined that such person is not entitled to indemnification. |
We will indemnify our directors and officers for serving us in those capacities or for serving other business enterprises at our request, to the fullest extent permitted by Delaware law. Delaware law provides that a corporation may indemnify such person if such person acted in good faith and in a manner such person reasonably believed to be in or not opposed to the best interests | · | | We will not be obligated pursuant to our amended and restated bylaws to indemnify a person with respect to proceedings initiated by that person against us or our other indemnitees, except with respect to proceedings authorized by our board of directors or brought to enforce a right to indemnification. |
| · | | The rights conferred in our amended and restated bylaws are not exclusive, and we are authorized to enter into indemnification agreements with our directors, officers, employees and agents and to obtain insurance to indemnify such persons. |
| · | | We may not retroactively amend our amended and restated bylaw provisions to reduce our indemnification obligations to directors, officers, employees and agents. |
We may, in our discretion, indemnify employees and agents in those circumstances where indemnification is permitted by applicable law.
We are required to advance expenses, as incurred, to our directors and officers in connection with defending a proceeding, except that such directors or officers shall undertake to repay such advances if it is ultimately determined that such person is not entitled to indemnification.
We will not be obligated pursuant to our amended and restated bylaws to indemnify a person with respect to proceedings initiated by that person against us or our other indemnitees, except with respect to proceedings authorized by our board of directors or brought to enforce a right to indemnification.
The rights conferred in our amended and restated bylaws are not exclusive, and we are authorized to enter into indemnification agreements with our directors, officers, employees and agents and to obtain insurance to indemnify such persons.
We may not retroactively amend our amended and restated bylaw provisions to reduce our indemnification obligations to directors, officers, employees and agents.
We do not currently intend to pay dividends on our common stock, and, consequently, our stockholders’ ability to achieve a return on their investment will depend on appreciation in the price of our common stock. We do not currently intend to pay any cash dividends on our common stock for the foreseeable future. We currently intend to invest our future earnings, if any, to fund our growth. Additionally, the terms of our loan and security agreements could restrict our ability to pay dividends. Therefore, our stockholders are not likely to receive any dividends on our common stock for the foreseeable future. Since we do not intend to pay dividends, our stockholders’ ability to receive a return on their investment will depend on any future appreciation in the market value of our common stock. There is no guarantee that our common stock will appreciate or even maintain the price at which our holders have purchased it. ITEM 1B. UNRESOLVED STAFF COMMENTS None. ITEM 2. PROPERTIES Our headquarters is currently located in Fremont, California, and consists of approximately 39,78161,784 square feet, plus a further 10,716 square feet beginning in September 2019, of leased office and laboratory space under a lease that currently expires in September 2019.2021. In addition, we lease 3,814 square feet of office space in Boston, Massachusetts, under a lease that currently expires in June 2018. We expectbelieve that during 2016,our existing facilities are adequate for our current needs. If we will either increasedetermine that additional or new facilities are needed in the square footagefuture, we believe that sufficient options would be available to us in our existing facility or obtain additional space in another location in order to accommodate our anticipated needs. We may also require additional space and facilities as our business expands.on commercially reasonable terms. ITEM 3. LEGAL PROCEEDINGS From time to time, we may be involved in legal proceedings arising in the ordinary course of business. We believe that as of December 31, 2015,2017, there is no litigation pending that would reasonably be expected to have a material adverse effect on our results of operations and financial condition. ITEM 4. MINE SAFETY DISCLOSURES Not applicable. PART II ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES Price Range of Common Stock Our common stock commenced trading on The NASDAQNasdaq Global Select Market under the symbol “ARDX” on June 19, 2014. Prior to that date, there was no public trading market for our common stock. The following table sets forth, for the periods indicated, the high and low reported sales prices of our common stock as reported on The NASDAQNasdaq Global Select Market: | | | | | | | | | High | | Low | 2017: | | | | | | | First Quarter | | $ | 15.40 | | $ | 10.95 | Second Quarter | | $ | 14.10 | | $ | 4.05 | Third Quarter | | $ | 6.20 | | $ | 4.28 | Fourth Quarter | | $ | 8.65 | | $ | 4.75 |
| | | | | | | | | | | | | | High | | | Low | | | High | | Low | Year ended December 31, 2015: | | | | | | 2016: | | | | | | | | First Quarter | | $ | 27.99 | | | $ | 13.00 | | | $ | 17.90 | | $ | 6.84 | Second Quarter | | $ | 17.66 | | | $ | 7.95 | | | $ | 9.81 | | $ | 6.36 | Third Quarter | | $ | 22.48 | | | $ | 15.00 | | | $ | 13.29 | | $ | 8.42 | Fourth Quarter | | $ | 21.27 | | | $ | 15.13 | | | $ | 16.30 | | $ | 10.55 | | | | | High | | | Low | | | Year Ended December 31, 2014: | | | | | | Second Quarter (from June 19, 2014) | | $ | 16.00 | | | $ | 14.05 | | | Third Quarter | | $ | 21.60 | | | $ | 11.37 | | | Fourth Quarter | | $ | 35.48 | | | $ | 15.10 | | |
As of March 2, 2016,December 31, 2017, there were 3840 holders of record of our common stock. The last reported sale price of the common stock on March 2, 20168, 2018, on The Nasdaq Global Market was $10.54$5.55 per share. Dividends We have never declared or paid cash dividends on our capital stock. We currently intend to retain any future earnings to finance the growth and development of our business. Recent Sales of Unregistered Securities On June 2, 2015, we entered into a Securities Purchase Agreement, or the Purchase Agreement, with the investors named therein, or the Investors. Pursuant to the Purchase Agreement, on June 5, 2015 we sold an aggregate of 7,242,992 shares of common stock, or the Shares, and warrants, or the Warrants, to purchase 2,172,899 shares of common stock, or Warrant Shares, for aggregate gross proceeds of approximately $77.8 million, or net proceeds, after deducting issuance costs, of approximately $74.3 million. The purchase price for each Share was $10.70, which was equal to the consolidated closing bid price on the NASDAQ Global Market on the day of pricing, June 2, 2015. The purchase price for each Warrant was equal to $0.125 for each Warrant Share, consistent with NASDAQ Global Market requirements for an “at the market” offering, and the Warrants are exercisable at an exercise price of $13.91 per share. Investors participating in the offering include entities associated with New Enterprise Associates, a venture capital firm that is one of our significant stockholders, and a combination of new and existing investors, including RA Capital Management, Broadfin Capital LLC, Cormorant Asset Management LLC, Foresite Capital Management, LLC, Rock Springs Capital Management LP, and a fund managed by Sabby Capital, LLC. Leerink Partners LLC acted as the sole placement agent of the offering and Wedbush PacGrow acted as a financial advisor in connection with the offering. We expect to use the net proceeds from the offering to develop our drug candidates, tenapanor and RDX022.
In connection with the Purchase Agreement, we entered into a Registration Rights Agreement, or the Registration Rights Agreement, with the Investors. Pursuant to the Registration Rights Agreement, we agreed to prepare and file a registration statement with the Securities and Exchange Commission, or SEC, by July 20, 2015 for purposes of registering the resale of the Shares, the Warrant Shares, and any shares of common stock issued as a dividend or other distribution with respect to the Shares or Warrant Shares. We filed the registration
statement on July 13, 2015 and it was declared effective by the SEC on July 20, 2015. We also agreed, among other things, to indemnify the selling holders under the registration statements from certain liabilities and to pay all fees and expenses (excluding underwriting discounts and selling commissions and all legal fees of any selling holder) incident to our obligations under the Registration Rights Agreement.
The financing is exempt from registration pursuant to the exemption for transactions by an issuer not involving any public offering under Section 4(2) the Securities Act of 1933, as amended, and Regulation D under the Securities Act of 1933, as amended.None.
Use of Proceeds Not applicable. Issuer Purchases of Equity Securities Not applicable. Stock Price Performance Graph The following stock performance graph compares our total stock return with the total return for (i) the NASDAQNasdaq Composite Index (depicted in the graph as “IXIC”) and the (ii) the NASDAQNasdaq Biotechnology Index (depicted in the graph as “NBI”) for the period from June 19, 2014 (the date our common stock commenced trading on The NASDAQNasdaq Global Market) through December 31, 2015.2017. The figures represented below assume an investment of $100 in our common stock at the closing price of $14.11 on June 19, 2014 and in the NASDAQNasdaq Composite Index and the NASDAQNasdaq Biotechnology Index on June 19, 2014 and the reinvestment of dividends into shares of common stock. The comparisons in the table are required by the Securities and Exchange Commission, or SEC, and are not intended to forecast or be indicative of possible future performance of our common stock. This graph shall not be deemed “soliciting material” or be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, or the Exchange Act, or otherwise subject to the liabilities under that Section, and shall not be deemed to be incorporated by reference into any of our filings under the Securities Act whether made before or after the date hereof and irrespective of any general incorporation language in any such filing. 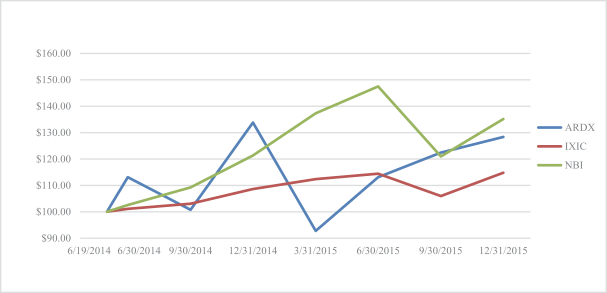 
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | $100 invested in stock or index | | Ticker | | | 6/19/14 | | | 6/30/14 | | | 9/30/14 | | | 12/31/14 | | | 3/31/15 | | | 6/30/15 | | | 9/30/15 | | | 12/31/15 | | Ardelyx, Inc | | | ARDX | | | $ | 100.00 | | | $ | 113.18 | | | $ | 100.71 | | | $ | 133.88 | | | $ | 92.77 | | | $ | 113.18 | | | $ | 122.47 | | | $ | 128.42 | | NASDAQ Composite Index | | | IXIC | | | $ | 100.00 | | | $ | 101.12 | | | $ | 103.08 | | | $ | 108.64 | | | $ | 112.42 | | | $ | 114.40 | | | $ | 105.98 | | | $ | 114.87 | | NASDAQ Biotechnology Index | | | NBI | | | $ | 100.00 | | | $ | 102.62 | | | $ | 109.22 | | | $ | 121.38 | | | $ | 137.41 | | | $ | 147.63 | | | $ | 121.06 | | | $ | 135.24 | |
| | | | | | | | | | | | | | | | | | $100 invested in stock or index | | Ticker | | 6/19/2014 | | 12/31/2014 | | 12/31/2015 | | 12/31/2016 | | 12/31/2017 | Ardelyx, Inc | | ARDX | | $ | 100.00 | | $ | 133.88 | | $ | 128.42 | | $ | 100.64 | | $ | 46.78 | Nasdaq Composite Index | | IXIC | | $ | 100.00 | | $ | 108.64 | | $ | 114.87 | | $ | 123.49 | | $ | 158.36 | Nasdaq Biotechnology Index | | NBI | | $ | 100.00 | | $ | 121.38 | | $ | 135.24 | | $ | 105.92 | | $ | 128.22 |
ITEM 6. SELECTED FINANCIAL DATA The data set forth below is not necessarily indicative of the results of future operations and should be read in conjunction with the financial statements and the notes included elsewhere in this annual report on Form 10-K10‑K and also with “ITEM“ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS”OPERATIONS” and our financial statements and the related notes included in this Annual Report on Form 10-K.10‑K. | | | | | | | | | | | | | | | | | | Year Ended December 31, | Statement of Operations Data: | | 2017 | | 2016 | | 2015 | | 2014 | | 2013 | | | (in thousands, except share and per share amounts) | Revenue: | | | | | | | | | | | | | | | | Licensing revenue | | $ | 42,000 | | $ | — | | $ | 21,611 | | $ | 18,394 | | $ | 8,063 | Collaborative development revenue | | | — | | | — | | | 2,415 | | | 13,229 | | | 20,865 | Total revenue | | | 42,000 | | | — | | | 24,026 | | | 31,623 | | | 28,928 | Cost of revenue | | | 8,400 | | | — | | | — | | | — | | | — | Gross profit | | | 33,600 | | | — | | | 24,026 | | | 31,623 | | | 28,928 | Operating expenses: | | | | | | | | | | | | | | | | Research and development | | | 75,484 | | | 94,161 | | | 39,885 | | | 25,900 | | | 28,093 | General and administrative | | | 23,231 | | | 18,734 | | | 13,530 | | | 7,287 | | | 3,700 | Total operating expenses | | | 98,715 | | | 112,895 | | | 53,415 | | | 33,187 | | | 31,793 | Loss from operations | | | (65,115) | | | (112,895) | | | (29,389) | | | (1,564) | | | (2,865) | Other income (expense), net | | | 1,955 | | | 508 | | | (261) | | | 10 | | | (52) | Change in fair value of preferred stock warrant liability | | | — | | | — | | | — | | | (1,593) | | | (3,506) | Loss before provision for income taxes | | | (63,160) | | | (112,387) | | | (29,650) | | | (3,147) | | | (6,423) | Provision for (benefit from) income taxes | | | 1,179 | | | — | | | (29) | | | 67 | | | 141 | Net loss | | $ | (64,339) | | $ | (112,387) | | $ | (29,621) | | $ | (3,214) | | $ | (6,564) | Net loss per common share, basic and diluted | | $ | (1.36) | | $ | (2.80) | | $ | (1.29) | | $ | (0.31) | | $ | (5.82) | Shares used in computing net loss per share - basic and diluted | | | 47,435,331 | | | 40,118,522 | | | 22,892,640 | | | 10,248,337 | | | 1,127,948 |
| | | | | | | | | | | | | | | | | | | | Year Ended December 31, | | | | | 2015 | | | 2014 | | | 2013 | | | 2012 | | | | | (in thousands, except share and per share amounts) | | Statement of Operations Data: | | | | | Revenue: | | | | | | | | | | | | | | | | | Licensing revenue | | $ | 21,611 | | | $ | 18,394 | | | $ | 8,063 | | | $ | 3,182 | | Collaborative development revenue | | | 2,415 | | | | 13,229 | | | | 20,865 | | | | 2,228 | | | | | | | | | | | | | | | | | | | Total revenue | | | 24,026 | | | | 31,623 | | | | 28,928 | | | | 5,410 | | Operating expenses: | | | | | | | | | | | | | | | | | Research and development | | | 39,885 | | | | 25,900 | | | | 28,093 | | | | 10,184 | | General and administrative | | | 13,530 | | | | 7,287 | | | | 3,700 | | | | 4,031 | | | | | | | | | | | | | | | | | | | Total operating expenses | | | 53,415 | | | | 33,187 | | | | 31,793 | | | | 14,215 | | | | | | | | | | | | | | | | | | | Loss from operations | | | (29,389 | ) | | | (1,564 | ) | | | (2,865 | ) | | | (8,805 | ) | Other (expense) income, net | | | (261 | ) | | | 10 | | | | (52 | ) | | | (30 | ) | Change in fair value of preferred stock warrant liability | | | — | | | | (1,593 | ) | | | (3,506 | ) | | | (950 | ) | | | | | | | | | | | | | | | | | | Loss before provision for income taxes | | | (29,650 | ) | | | (3,147 | ) | | | (6,423 | ) | | | (9,785 | ) | Benefit from (provision for) income taxes | | | 29 | | | | (67 | ) | | | (141 | ) | | | — | | | | | | | | | | | | | | | | | | | Net loss and comprehensive loss | | $ | (29,621 | ) | | $ | (3,214 | ) | | $ | (6,564 | ) | | $ | (9,785 | ) | | | | | | | | | | | | | | | | | | Net loss per common share, basic and diluted | | $ | (1.29 | ) | | $ | (0.31 | ) | | $ | (5.82 | ) | | $ | 11.32 | | | | | | | | | | | | | | | | | | | Shares used to compute net loss per common share, basic and dilute | | | 22,892,640 | | | | 10,248,337 | | | | 1,127,948 | | | | 864,020 | | | | | | | | | | | | | | | | | | | | | | | | As of December 31, | | | | | 2015 | | | 2014 | | | 2013 | | | 2012 | | | | | (in thousands) | | Balance Sheet Data: | | | | | | | | | | | | | | | | | Cash and cash equivalent | | $ | 107,004 | | | $ | 107,286 | | | $ | 34,435 | | | $ | 32,903 | | Total assets | | | 116,946 | | | | 113,414 | | | | 42,904 | | | | 37,884 | | Deferred revenue | | | — | | | | 47,053 | | | | 40,298 | | | | 32,662 | | Convertible preferred stock warrant liability | | | — | | | | — | | | | 6,456 | | | | 2,950 | | Convertible preferred stock | | | — | | | | — | | | | 56,155 | | | | 56,155 | | Accumulated deficit | | | (101,488 | ) | | | (71,867 | ) | | | (68,653 | ) | | | (62,089 | ) | Total stockholders’ equity ( deficit) | | | 108,901 | | | | 60,682 | | | | (63,479 | ) | | | (57,392 | ) |
| | | | | | | | | | | | | | | | | | As of December 31, | Balance Sheet Data: | | 2017 | | 2016 | | 2015 | | 2014 | | 2013 | | | (in thousands) | Cash, cash equivalents and short-term investments | | $ | 133,976 | | $ | 200,823 | | $ | 107,004 | | $ | 107,286 | | $ | 34,435 | Total assets | | | 157,903 | | | 213,131 | | | 116,946 | | | 113,414 | | | 42,904 | Deferred revenue | | | — | | | — | | | — | | | 47,053 | | | 40,298 | Convertible preferred stock warrant liability | | | — | | | — | | | — | | | — | | | 6,456 | Convertible preferred stock | | | — | | | — | | | — | | | — | | | 56,155 | Accumulated deficit | | | (278,214) | | | (213,875) | | | (101,488) | | | (71,867) | | | (68,653) | Total stockholders' equity (deficit) | | | 139,312 | | | 193,151 | | | 108,901 | | | 60,682 | | | (63,479) |
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS You should read the following discussion and analysis of our financial condition and results of operations together with the section of this report entitled “Selected Financial Data” and our financial statements and related notes included elsewhere in this report. This discussion and other parts of this report contain forward-lookingforward- looking statements that involve risk and uncertainties, such as statements of our plans, objectives, expectations and intentions. Our actual results could differ materially from those discussed in these forward-looking statements. Factors that could cause or contribute to such differences include, but are not limited to, those discussed in the section of this report entitled “Risk Factors.” OVERVIEW We are a clinical-stagespecialized biopharmaceutical company focused on developing first-in-class, disruptive medicines for the discovery, developmenttreatment of renal diseases, which affect both the heart and commercializationthe kidneys. This includes patients with end-stage renal disease, or ESRD, who suffer from elevated serum phosphorus, or hyperphosphatemia; and chronic kidney disease, or CKD, and/or heart failure patients with elevated serum potassium, or hyperkalemia. We have also developed a number of innovative, minimally-systemic therapeutic drugs that work exclusively in theprograms directed toward treating gastrointestinal, or GI, tractdisorders, including the treatment of irritable bowel syndrome with constipation, or IBS-C. Our portfolio is led by the development of tenapanor, a first-in-class inhibitor of NHE3. In our renal pipeline, tenapanor is being evaluated in a second Phase 3 trial for the treatment of hyperphosphatemia in patients with ESRD who are on dialysis. We are also advancing a small molecule potassium secretagogue program, RDX013, for the potential treatment of hyperkalemia. We have also developed tenapanor for the treatment of people with irritable bowel syndrome with constipation, or IBS-C. In 2017, we completed the T3MPO program for this indication, including two Phase 3 studies, both of which achieved statistical significance for the primary endpoint, and a long-term safety extension study. Based on the results of the T3MPO clinical program in IBS-C, we currently plan to treat cardio-renalsubmit our first New Drug Application, or NDA, to the United States Food and GI diseases. Drug Administration, or FDA, in the second half of 2018 for tenapanor for the treatment of IBS-C. We have developed a proprietary drug discovery and design platform enabling us, in a rapid and cost-efficient manner, to discover and design novel drug candidates. Utilizing our platform, we discovered and designed our lead product candidate, tenapanor, which is currently being evaluated in two pivotal Phase 3 clinical studies in patients with constipation-predominant irritable bowel syndrome, or IBS-C, and we currently expect to receive results from those trials in 2017. In a Phase 2b clinical study, tenapanor demonstrated the ability to improve the symptoms of IBS-C. In a separate Phase 2b clinical trial, tenapanor demonstrated the ability to lower elevated serum phosphorus levels in patients with end-stage renal disease, or ESRD. We have initiated an additional Phase 2b clinical trial to evaluate dosing regimens of tenapanor for the treatment of hyperphosphatemia, or elevated serum phosphorus, in ESRD patients, and we expect to receive results from this trial in the second half of 2016. We are developing another drug candidate, RDX022, for the treatment of hyperkalemia, or elevated serum potassium. In January 2016, we announced the results of an open label clinical study evaluating the pharmacodynamic activity of RDX022 in healthy adult volunteers. The study demonstrated that RDX022 was generally well-tolerated at all doses evaluated and effectively binds to potassiumtargets found in the GI tract supporting our plans to proceed with a Phase 3 clinical program, which we currently expect to initiatethat regulate processes in the second halfbody and design products candidates that act upon those targets to take advantage of 2016. We are pursuing a 505(b)(2) regulatory pathway for RDX022. We have additional drug candidates in earlier stages of research and development focused in GI and cardio-renal diseases including RDX009, a secretagogue of glucagon-like peptide-1, or GLP-1, and glucagon-like peptide-2, or GLP-2, and RDX013, a potassium secretagogue. We currently expectthe gut’s ability to file an investigational new drug application, or IND, for RDX009 in the second half of 2016.communicate with other organs. Since commencing operations in October 2007, substantially all our efforts have been dedicated to our research and development activities, including developing our clinical product candidates,candidate tenapanor and RDX022, and developing our proprietary drug discovery and design platform. We have not generated any revenues from product sales and have no products approved for commercialization. Our only revenue has been pursuant to our collaboration partnerships with AstraZenaca and Sanofi, each of which has been terminated. As of December 31, 2015,2017, we had an accumulated deficit of $101.5$278.2 million. We expect that ourto incur operating losses will substantially increase for the foreseeable future as we as we continueprepare for the developmentcommercialization of tenapanor, and RDX022, including costs associated with conductingcompleting the on-going Phase 3 clinical programsdevelopment program for tenapanor and RDX022, research and development, conducting preclinical studies and clinical trials for our other programs, obtaining regulatory approvals, and developing and maintaining scalable manufacturing processes for our product candidates.the treatment of hyperphosphatemia in patients with ESRD on dialysis. To date, we have funded our operations from the sale and issuance of common stock, convertible preferred stock, funds from our former collaboration partnerships with AstraZeneca AB, or AstraZeneca, and Sanofi SA, or Sanofi, and funds from our collaborations. On June 24, 2014, we completed our initial public offeringrecent license agreements with Kyowa Hakko Kirin Co., Ltd., or KHK, and sold 4,928,900 shares of our common stock, which included 642,900 shares of common stock purchased by the underwriters upon the full exercise of their option to purchase additional shares of common stock. We received cash proceeds of $61.2 million, net of underwriting discounts and commissions and expenses paid by us.Shanghai Fosun Pharmaceutical Industrial Development Co. Ltd., or Fosun Pharma.
In June 2015, we closedsold and issued 7,242,992 shares of common stock and warrants to purchase 2,172,899 shares of common stock at an exercise price of $13.91 per share in a private placement financingtransaction in which we raised approximately $77.8 million in gross proceeds orproceeds. We received $74.3 million in net proceeds, after deducting issuance costs. OnIn January 13, 2016, we completed a registeredan underwritten public offering and sold an aggregate of 8,625,000 shares of common stock which included 1,125,000at an offering price of $10.00 per share for gross proceeds of $86.3 million. This offering was completed under our shelf
registration statement filed on July 13, 2015, and we received net proceeds from the offering of approximately $80.8 million, after deducting the underwriters’ discounts and commissions and offering expenses. In July 2016, we sold and issued an aggregate of 12,600,230 shares of common stock purchased by the underwriters upon the full exercisein a private placement transaction at an offering price of their option to purchase additional shares$8.73 per share for gross proceeds of stock.$110.0 million. We received net proceeds from the offering of approximately $80.4$109.8 million, netafter deducting offering expenses. FINANCIAL OPERATIONS OVERVIEW Revenue We have not generated any revenue from product sales. Prior to 2017, our revenue to date had been generated from non-refundable license payments and reimbursements for research and development expenses under license agreements with AstraZeneca and Sanofi, both of underwriting discountswhich were terminated in 2015. We recognized revenue from upfront payments ratably over the term of our estimated period of performance under those agreements, which we recorded as licensing revenue. Reimbursements from AstraZeneca for development costs incurred under our license and commissions and expenses paid by us. collaboration agreement with them were classified as collaborative development revenue. There has been no recognition of collaborative development revenue since the termination of the AstraZeneca AB (“AstraZeneca”)agreement in 2015. In October 2012,2017, we entered into a collaboration partnershipexecuted license agreements with AstraZenecaKHK and Fosun Pharma for the worldwide development, commercialization and commercializationdistribution of tenapanor.tenapanor for certain uses in Japan and China, respectively. Under the terms of the AstraZeneca collaboration partnership agreement, orKHK and Fosun Pharma license agreements, the AstraZeneca Agreement, weCompany received an aggregate of $30.0 million and $12.0 million, respectively, in up-front license fee of $35.0 million in October 2012, a $15.0 million payment in December 2013 and a $25.0 million payment in May 2014. Thefees. These amounts were recorded as deferred revenue when received andthe contracts were recognizedexecuted. These agreements also contain milestone payments, which will be recorded as revenue on a straight-line basis overwhen we achieve the remaining estimated periodunderlying milestone. See “ITEM 1. BUSINESS—OUR PRODUCT PIPELINE—TENAPANOR: A NEW APPROACH FOR TREATING HYPERPHOSPHATEMIA IN ESRD PATIENTS ON DIALYSIS” for additional detail regarding the KHK and Fosun Pharma license agreements. Cost of performanceRevenue Cost of revenue currently represents license payments due to AstraZeneca, who under the AstraZeneca Agreement, which during the three months ended March 31, 2015, we estimated to be December 2017. In June 2015, we entered intoterms of a termination agreement with AstraZeneca (the “Termination Agreement”) pursuantentered into in 2015 are entitled to which all licenses granted to AstraZeneca to our portfolio of NHE3 inhibitors, including our lead product candidate, tenapanor, were terminated, except for the limited purpose of allowing AstraZeneca to satisfy its obligations under the Termination Agreement. Under the terms of the Termination Agreement, we agreed to pay AstraZeneca certain amounts for the return of the licenses granted to it, including (a) an upfront fee of $15.0 million, (b)(i) future royalties at a royalty rate of 10% of net sales of tenapanor or other NHE3 products by us or our licensees, and (c)(ii) 20% of non-royalty revenue received from a new collaboration partner should we elect to license, or otherwise provide rights to develop and commercialize tenapanor or another NHE3 inhibitor. The amounts described in (a)-(c) are capped at the aggregate amount of $90.0 million. We also paid AstraZeneca $10.0 million as reimbursement for certain research and development expenses incurred by AstraZeneca under the collaboration agreement during 2015, and for the acceleration of the transfer of information and materialsinhibitor, up to us. Under the Termination Agreement, AstraZeneca was obligated to complete the manufacturing of clinical trial material necessary for the Phase 3 clinical program for tenapanor in IBS-C, and we agreed to pay AstraZeneca a maximum amount of $10 million for such clinical trial material, which maximum amount was subsequently reduced to $8.0 million pursuant to an amendment to the Termination Agreement (“Amendment Number One”).
As the AstraZeneca Agreement was terminated in June 2015, we recognized the remaining deferred revenue balance of $43.1 million during the three months ended June 30, 2015. In the three months ended June 30, 2015, we recorded the $15.0 million upfront payment for the return of the licenses as well as the $10.0 million payment for reimbursement of research and development expenses and the acceleration of the transfer of information and materials as a reduction in licensing revenue in the condensed statements of operations and comprehensive loss. We recorded $7.3$75.0 million in expenses incurredaggregate for the tenapanor clinical trial material from AstraZeneca during the year ended December 31, 2015.
Sanofi SA (“Sanofi”)
In February 2014, we entered into an option(i) and license agreement with Sanofi, or the Sanofi Agreement, under which we granted Sanofi an exclusive worldwide license to conduct research utilizing our program evaluating small molecule NaP2b inhibitors for the treatment of hyperphosphatemia in CKD patients on dialysis. In addition, Sanofi had the option under the Sanofi Agreement to obtain an exclusive license to develop, manufacture and commercialize our NaP2b inhibitors. Under the Sanofi Agreement, we received an upfront payment of $1.25 million in March 2014, which was fully recognized as licensing revenue in May 2014 after we completed our obligation to provide Sanofi the background know-how, listed patents, and materials described in the Sanofi Agreement.
The Sanofi Agreement was terminated effective September 30, 2015 and all rights were returned to Ardelyx. There was no payment associated with termination and the return of rights to Ardelyx.
FINANCIAL OPERATIONS OVERVIEW
Revenue
We have not generated any revenue from product sales. Our revenue to date has been generated from non-refundable license payments and reimbursements for research and development expenses under our license
agreements with AstraZeneca and Sanofi, both of which were terminated in 2015.(ii). We recognize revenue from upfront payments ratably over the termthese expenses as cost of our estimated period of performance under the agreement, which we consider to be licensing revenue. Should any of our agreements contain event based payments, such payments are recorded as revenue when we achieverecognize the underlying milestone if it is deemed to be a substantive milestone at the date the arrangement is entered into. To the extentrevenue that non-substantive milestones are achieved and we have remaining performance obligations, milestones are deferred and recognized as revenue over the estimated remaining period of performance. Reimbursements from AstraZenecagenerates our liability for development costs incurred under ourthese license and collaboration agreement with them were classified as collaborative development revenue.payments.
Research and Development Expenses Research and development expenses represent costs incurred to conduct research, such as the discovery and development of our unpartnered product candidates, and prior to the termination of the AstraZeneca Agreement, research and development expenses also included costs we incurred in connection with the development of tenapanor pursuant to our license agreement with AstraZeneca. We recognize all research and development expenses as they are incurred.
incurred to support the discovery, development and manufacturing of our product candidates. Research and development expenses consist of the following: | · | | external research and development expenses incurred under agreements with consultants, third-party contract research organizations and investigative sites where a substantial portion of our clinical studies are conducted, and with contract manufacturing organizations where our clinical supplies are produced; |
| · | | expenses associated with supplies and materials consumed in connection with our research operations; |
| · | | employee-related expenses, which include salaries, benefits, travel and stock-based compensation; |
| · | | other costs associated with regulatory, clinical and non-clinical development activities; and |
| · | | facilities and other allocated expenses, which include direct and allocated expenses for rent and maintenance of facilities, depreciation and amortization expense, information technology expense and expenses for supplies. |
We expect to continue to make substantial investments in research and development expenses incurred under agreements with consultants, third-party contract research organizations and investigative sites where a substantial portion of our clinical studies are conducted, and with contract manufacturing organizations where our clinical supplies are produced; expenses associated with supplies and materials consumed in connection with our research operations;
employee-related expenses, which include salaries, benefits and stock-based compensation; and
facilities and other allocated expenses, which include direct and allocated expenses for rent and maintenance of facilities, depreciation and amortization expense and other supplies.
We expect our research and development expenses will increase substantially in the futureactivities as we progress the development of tenapanor, andas well as our other our internal product candidates, advance our discovery research projectsprograms into the preclinical stage and continue our early stage research including further development of our APECCS cell-culture system.proprietary drug discovery and design platform. The process of conducting preclinical studies and clinical trials necessary to obtain regulatory approval is costly and time consuming. We or our collaboration partner(s), if any, may never succeed in achieving marketing approval for any of our product candidates.candidates, including tenapanor. Additionally, if marketing approval is received for tenapanor for the treatment of IBS-C, we may not be successful in securing one or more collaboration partners to commercialize tenapanor in the United States and other territories. The probability of success of each of the product candidates may be affected by numerous factors, including preclinical data, clinical data, market acceptance, sufficient third-party coverage or reimbursement, our ability to access capital on acceptable terms, our ability to enter into collaboration partnerships on acceptable terms, competition, manufacturing capability and commercial viability.
The successful development of our product candidates is highly uncertain and may not result in approved products. Completion dates and completion costs can vary significantly for each product candidate and are difficult to predict. Given the uncertainty associated with clinical trial enrollment and the risks inherent in the development process, we are unable to determine the duration and completion costs of current or future clinical trials of our product candidates or if and to what extent we will generate revenues from the commercialization and sale of any of our product candidates. We anticipate that we will make determinations as to which programs to pursue and how much funding to direct to each program on an ongoing basis in response to the scientific and clinical success of each product candidate, as well as an ongoing assessment as to each product candidate’s commercial potential.potential, and our ability to access capital on acceptable terms. We will need to raise additional capital and will seek additional collaboration partnerships in the future in order to complete the development and commercialization of tenapanor. If we are unable to access capital on a timely basis and on terms that are acceptable to us, we may be forced to restructure certain aspects of our business or identify and complete one or more strategic collaborations or other transactions in order to fund the development or commercialization of tenapanor or certain of our product candidates including tenapanor.through the use of alternative structures.
General and Administrative General and administrative expenses consist primarily of salaries and related costs, including stock-based compensation. Other general and administrative expenses include facility related costs and professional fees for legal, accounting, investor relations and other consulting services. We anticipate that our selling, general and administrative expenses will increase substantially in the future primarily because of (i) increased pre-commercial activities and personnel costs travelto support the potential launch of tenapanor for the treatment of hyperphosphatemia in ESRD patients on dialysis and (ii) expenses and other expenses for outside professional services, including legal, human resources, audit and accounting services. Personnelrelated to costs includes salaries, bonus, benefits and stock-based compensation. Since becomingof operating as a public company in 2014, we have incurred and expect to continue to incur expenses required of public companies, including costs to comply with the rules and regulations applicable to companies listed on a national securities exchange and costs related to compliance and reporting obligations pursuant to the rules and regulations of the SEC. Other related public company costs include increased expensespreparing for additional insurance, investor relations and professional services.future integrated audits.
Income Taxes We recorded a foreign income tax benefit forcharge of $1.2 million in the year ended December 31, 20152017, due to a withholding tax in China on our license revenue from Fosun Pharma. All other income tax charges and benefits in the three years ended December 31, 2017, have not been material, primarily due to the provision to return true-up for the year ended December 31, 2014.net loss in each year. For each of the tax years ended December 31, 2014 and 2013, the Company recorded an income tax provision due to the minimum taxes which resulted from upfront and milestone payments received from AstraZeneca.
Due to the history of cumulative losses, the Company’sOur deferred taxesassets continue to be subject to full valuation allowance for the tax years ended December 31, 2015, 2014,2017 and 2013.2016. A valuation allowance is recorded when it is more likely than not that all or some portion of the deferred income tax assets will not be realized. We regularly assess the need for a valuation allowance against our deferred income tax assets by considering both positive and negative evidence related to whether it is more likely than not that our deferred income tax assets will be realized. In evaluating our ability to recover our deferred income tax assets within the jurisdiction from which they arise, we consider all available positive and negative evidence, including scheduled reversals of deferred income tax liabilities, future tax rates, projected future taxable income, tax-planning strategies, and results of recent operations.
CRITICAL ACCOUNTING POLICES AND ESTIMATES A detailed discussion of our significant accounting policies can be found in Note 1 of the Notes to Consolidated Financial Statements in Part II, Item 8, and the impact and risks associated with our accounting policies are discussed throughout this Annual Report on Form 10-K10‑K and in the footnotes to the financial statements. Critical accounting policies are those that require significant judgment and/or estimates by management at the time that financial statements are prepared such that materially different results might have been reported if other assumptions had been made. We consider certain accounting policies related to revenue recognition, accrued liabilities, and use of estimates to be critical policies. These estimates form the basis for making judgments about the carrying values of assets and liabilities. We base our estimates and judgments on historical experience and on various other assumptions that we believe to be reasonable under the circumstances. Actual results could differ materially from these estimates. We believe the following policies to be the most critical to an understanding of our financial condition and results of operations because they require us to make estimates, assumptions and judgments about matters that are inherently uncertain. Revenue Recognition Research Activities Revenue from research activities madeconducted under collaboration partnership agreements are recognized as the services are provided and when there is persuasive evidence that an arrangement exists, delivery has occurred, the price is fixed or determinable, and collectability is reasonably assured. Revenue generated from research and license agreements typically includes up-front signing or license fees, cost reimbursements, research services, minimum sublicense fees, milestone payments, and royalties on future licensees’ product sales. Multiple-Element Arrangements For revenue agreements with multiple-element arrangements, such as license and development agreements, we allocate revenue to each non-contingent unit of accounting based on the relative selling price of each unit. When applying the relative selling price method, we determine the selling price for each deliverable using vendor-specific objective evidence or third-party evidence. If neither exists, we use the best estimate of selling price for that deliverable. Revenue allocated is then recognized when the four basic revenue recognition criteria are met for each unit. Our obligations under the agreements may include the transfer of intellectual property rights in the form of licenses, obligations to provide research and development services and obligations to participate on certain development committees with the collaboration partner. We make judgments that affect the period over which we recognize revenue. On a quarterly basis, we review our estimated period of performance for our license revenue based on the progress under the arrangement and account for the impact of any changes in estimated periods of performance, on a prospective basis.basis, if applicable given the facts and circumstances of the agreement. Cost Reimbursement We recognize cost reimbursement revenue under collaboration partnership agreements as the related research and development costs for services are rendered. Deferred revenue represents the portion of research or license payments received that have not been earned. Milestone A milestone is considered substantive when the consideration earned from the achievement of the milestone (i) is commensurate with either our performance to achieve the milestone or the enhancement of value of the item delivered as a result of a specific outcome resulting from our performance to achieve the milestone, (ii) relates solely to past performance and (iii) is reasonable relative to all deliverables and payment terms in the arrangement. Such payments that are contingent upon the achievement of a substantive milestone are recognized entirely as revenue in the period in which the milestone is achieved. To the extent that non-substantive milestones are achieved and we have remaining performance obligations, milestones are deferred and recognized as revenue over the estimated remaining period of performance. If there were no remaining performance obligations, we recognize the revenue in the period it is earned. Accrued Research and Development ExpenseExpenses As part of the process of preparing our financial statements, we are required to estimate our accrued expenses. This process involves reviewing open contracts and Accruals Researchpurchase orders, communicating with our personnel to identify services that have been performed on our behalf and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of the actual cost. The majority of our service providers invoice us monthly in arrears for services performed or when contractual milestones are met. We make estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy of our estimates with the service providers and make adjustments if necessary. Examples of estimated accrued research and development expenses include employee-relatedfees paid to:
| · | | CROs in connection with clinical studies; |
| · | | investigative sites in connection with clinical studies; |
| · | | vendors related to product manufacturing, development and distribution of clinical supplies; |
| · | | collaborator entities in connection with our collaboration agreements; and |
| · | | vendors in connection with preclinical development activities. |
We record expenses related to clinical trial costs, consultant fees, supplies,studies and manufacturing costs for research and development programs and allocations of corporate costs. All such costs are charged to research and development expense as incurred. These expenses result from our independent research and development efforts as well as efforts associated with collaborations. Our expense accruals for clinical trials areactivities based on our estimates of the services received and efforts expended pursuant to contracts with our CROs and manufacturing vendors that conduct and manage these activities on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract, and may result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the expense. Payments under some of these contracts depend on factors such as the successful enrollment of subjects and the completion of clinical trial centersmilestones. In accruing service fees, we estimate the time period over which services will be performed, enrollment of subjects, number of sites activated and clinical research organizations.the level of effort to be expended in each period. If possible,the actual timing of the performance of services or the level of effort varies from our estimate, we obtain information regarding unbilledadjust the accrued or prepaid expense balance accordingly. Although we do not expect our estimates to be materially different from amounts actually incurred, if our estimates of the status and timing of services directlyperformed differ from service providers. However,the actual status and timing of services performed, we may be requiredreport amounts that are too high or too low in any particular period. To date, there have been no material differences from our estimates to estimate these services based on information available to our product development or administrative staff. If we underestimate or overestimate the activity associated with a study or service at a given point in time, adjustments to research and development expenses may be necessary in future periods. Historically, our estimated accrued liabilities have approximated actual expenseamounts actually incurred. Stock-Based Compensation We estimate the fair value of stock options and Employee Stock Purchase Plan, (ESPP)or ESPP, shares using the Black-Scholes valuation model. The Black-Scholes model requires the input of highly subjective assumptions. The most significant assumptions are our estimates of the expected volatility and the expected term of the award. The Black-Scholes option-pricing model requires the use of highly subjective assumptions which determine the fair value of stock-based awards. These assumptions include: Expected Term—The Company hasTerm—We have very limited historical information to develop reasonable expectations about future exercise patterns and post-vesting employment termination behavior for itsour stock-option grants. As such, the expected term wasis estimated using the simplified method whereby the expected term equals the arithmetic average of the vesting term and the original contractual term of the option. Expected Volatility—Since January 1, 2017, we have used the Company has limited information on thehistoric volatility of its commonour own stock dueover the retrospective period corresponding to no significant trading history, the expected remaining term of the options, or the period since our shares were first quoted on The Nasdaq Global Market, if that is shorter, to compute our expected stock price volatility. Prior to December 31, 2016, our stock had not been publicly traded for a sufficient period to enable us to use our own historic volatility, so the expected volatility was calculated based on the average volatility for comparable publicly traded biopharmaceutical companies over a period equal to the expected term of the stock option grants. The comparable companies were chosen based on their similar size, stage in the life cycle, and financial leverage of the Company. Risk-Free Interest Rate—The risk-free interest rate assumption is based on the zero-coupon U.S. Treasury instruments on the date of grant with a maturity date consistent with the expected term of the Company’sour stock option grants. Expected Dividend—To date, the Company haswe have not declared or paid any cash dividends and doesdo not have any plans to do so in the future. Therefore, the Company usedwe use an expected dividend yield of zero. As required, we review our valuation assumptions at each grant date and, as a result, we are likely to change our valuation assumptions used to value employee stock-based awards granted in future periods. Employee and director stock-based compensation costs are to be recognized over the vesting period of the award, and we have elected to use the straight-line attribution method. Forfeitures are to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. We estimate forfeitures based on historical experience. Restricted stock units, (RSUs)or RSUs, are measured at the fair value of our common stock on the date of grant and expensed over the period of vesting using the straight-line attribution approach. Prior to our IPO in June 2014, our board of directors, with the assistance of management and independent consultants, performed fair value analyses for the valuation of our common stock. For grants made on dates for which there was no contemporaneous valuation to utilize in setting the exercise price of our common stock, and given the absence of an active market for our common stock prior to our IPO in June 2014, our board of directors determined the fair value of our common stock on the date of grant based on several factors, including:
progress of our research and development efforts;
our operating results and financial condition, including our levels of available capital resources;
rights and preferences of our common stock compared to the rights and preferences of our other outstanding equity securities;
material risks related to our business;
equity market conditions affecting comparable public companies;
the likelihood of achieving a liquidity event for the shares of common stock, such as an initial public offering given prevailing market and biotechnology sector conditions; and
that the grants involved illiquid securities in a private company.
For valuations after the completion of our initial public offering on June 18, 2014, our board of directors determined the fair value of each share of underlying common stock based on the closing price of our common stock as reported on the date of grant.
Estimated Fair Value of Convertible Preferred Stock Warrants
Freestanding warrants for shares that were contingently redeemable were classified as a liability on the balance sheet at their estimated fair value. At the end of each reporting period, the change in estimated fair value during the period was recorded in change in fair value of convertible preferred stock warrant liability in the statement of operations and comprehensive loss. Beginning in 2013, we estimated the fair value of the warrant liability using a hybrid of the options pricing method, or OPM, and the probability-weighted return method, or PWERM. The hybrid method applied the PWERM utilizing the probability of two exit scenarios, going public or being acquired, and the OPM was utilized in the remaining private scenario. The scenarios were weighted based on our estimate of the assigned probability. We continued to adjust the carrying value of the warrants until the completion of our initial public offering in June 2014, at which time the liability was reclassified to additional paid-in capital and is no longer subject to remeasurement.
RESULTS OF OPERATIONS Comparison of the Years Ended December 31, 20152017 and 20142016 Revenue | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | | (in thousands) | Licensing revenue | | $ | 42,000 | | $ | — | Dollar change from prior year | | | 42,000 | | | | Percent change from prior year | | | N/A | | | |
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2015 | | | 2014 | | | Dollar Change | | | | | | | | (in thousands) | | | | | Revenue: | | | | | | | | | | | | | Licensing revenue | | $ | 21,611 | | | $ | 18,394 | | | $ | 3,217 | | Collaborative development revenue | | | 2,415 | | | | 13,229 | | | | (10,814 | ) | | | | | | | | | | | | | | Total revenue | | $ | 24,026 | | | $ | 31,623 | | | $ | (7,597 | ) |
Licensing revenue for the year ended December 31, 20152017, was $21.6$42.0 million, an increase of $3.2$42.0 million or 17%, compared to $18.4the year ended December 31, 2016, when we generated no licensing revenue. Licensing revenue for 2017 was related to the recognition of revenue from upfront payments under our KHK and Fosun Pharma agreements. Cost of revenue | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | | (in thousands) | Cost of revenue | | $ | 8,400 | | $ | — | Dollar change from prior year | | | 8,400 | | | | Percent change from prior year | | | N/A | | | |
Cost of revenue for the year ended December 31, 2017, was $8.4 million, an increase of $8.4 million compared to the year ended December 31, 2016, when we generated no revenue and therefore incurred no related costs. Cost of revenue represents license payments due to AstraZeneca, which under the terms of a termination agreement entered into in 2015 are entitled to (i) future royalties at a royalty rate of 10% of net sales of tenapanor or other NHE3 products by us or our licensees, and (ii) 20% of non-royalty revenue received from a new collaboration partner should we elect to license, or otherwise provide rights to develop and commercialize tenapanor or another NHE3 inhibitor, with the maximum amount due AstraZeneca for royalties and non-royalty revenue not to exceed $75.0 million in aggregate for (i) and (ii). Research and Development | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | | (in thousands) | Research and development | | $ | 75,484 | | $ | 94,161 | Dollar change from prior year | | | (18,677) | | | | Percent change from prior year | | | (20) | % | | |
Research and development expenses were $75.5 million for the year ended December 31, 2014. 2017, a decrease of $18.7 million, or 20%, compared to $94.2 million for the year ended December 31, 2016. The decrease consisted of a $23.8 million decrease in our external program costs, partially offset by a $5.1 million increase in our internal program costs. The decrease in our external program costs of $23.8 million was primarily due to a decrease of $22.3 million in expenses incurred for clinical development activities related to the completion of our T3MPO Phase 3 clinical program for tenapanor, our first Phase 3 clinical trial evaluating tenapanor for the treatment of hyperphosphatemia patients with ESRD on dialysis and a decrease in manufacturing development activities related to tenapanor. In addition, expenses incurred for clinical development activities, clinical manufacturing and process development activities associated with RDX8940 decreased by $3.2 million. These decreases were offset by an increase of $1.7 million in expenses incurred primarily for clinical development activities associated with RDX7675, including costs associated with the termination of that program. The increase reflectsin our internal costs of $5.1 million was primarily due to an increase in salaries and related costs, including stock-based compensation, facilities-related costs, principally related to supporting the impactgrowth of our development team and severance costs relating to our reduction in workforce in the third quarter 2017. General and Administrative | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | | (in thousands) | General and administrative | | $ | 23,231 | | $ | 18,734 | Dollar change from prior year | | | 4,497 | | | | Percent change from prior year | | | 24 | % | | |
General and administrative expenses were $23.2 million for the year ended December 31, 2017, an increase of $4.5 million, or 24%, compared to $18.7 million for the year ended December 31, 2016. The increase was primarily due to increases in salaries and related costs, including stock-based compensation and facilities costs including depreciation expense, due to an increase in headcount and an expansion of facilities late in 2016, increased legal fees, and severance costs due to the refocusing of resources towards late-stage programs and subsequent reduction in the workforce in the third quarter of 2017, offset by reductions in certain professional services. Comparison of the Years Ended December 31, 2016 and 2015 Revenue | | | | | | | | | Year Ended December 31, | | | 2016 | | 2015 | | | (in thousands) | Licensing revenue | | $ | — | | $ | 21,611 | Dollar change from prior year | | | (21,611) | | | | Percent change from prior year | | | (100) | % | | |
Licensing revenue for the year ended December 31, 2016 was zero, a decrease of $21.6 million, or 100%, compared to $21.6 million for the year ended December 31, 2015. Licensing revenue for 2015 was related to the recognition of $3.9 million of licensing revenue forfrom upfront and milestone payments under the three months ended March 31,AstraZeneca agreement. Because the AstraZeneca agreement was terminated in June 2015, and thethere has been no further recognition of revenue related to the remaining deferred revenue balance of $43.1 million during the three months ended June 30, 2015upfront and as a result of the Termination Agreement with AstraZeneca. This recognition of deferred revenue was primarily offset by an aggregate of $25.0 million in upfrontmilestone payments made to AstraZeneca in connection with the Termination Agreement.under such agreement since that time. | | | | | | | | | Year Ended December 31, | | | 2016 | | 2015 | | | | (in thousands) | Collaborative development revenue | | $ | — | | $ | 2,415 | Dollar change from prior year | | | (2,415) | | | | Percent change from prior year | | | (100) | % | | |
Collaborative development revenue consists of our development expenses that were reimbursable to us by AstraZeneca as part of our licenseunder the AstraZeneca agreement. Collaborative development revenue for the year ended December 31, 20152016 was $2.4 million,zero, a decrease of $10.8$2.4 million, or 82%100%, compared to $13.2$2.4 million for the year ended December 31, 2014.2015. The decrease was due to the reductiontermination of our collaboration with AstraZeneca in the development activities that we performed for tenapanor in the first half of 2015 and due to the Termination Agreement with AstraZeneca.related cessation of reimbursement of research and development expenses. Research and Development | | | | | | | | | Year Ended December 31, | | | 2016 | | 2015 | | | (in thousands) | Research and development | | $ | 94,161 | | $ | 39,885 | Dollar change from prior year | | | 54,276 | | | | Percent change from prior year | | | 136 | % | | |
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2015 | | | 2014 | | | Dollar Change | | | | | | | | (in thousands) | | | | | Research and development | | $ | 39,885 | | | $ | 25,900 | | | $ | 13,985 | |
Research and development expenses were $94.2 million for the year ended December 31, 2016, an increase of $54.3 million, or 136%, compared to $39.9 million for the year ended December 31, 2015, an2015. The increase consisted of $14.0a $44.1 million or 54%, compared to $25.9increase in our external program costs and a $10.2 million for the year ended December 31, 2014.increase in our internal program costs. The changeincrease in external program costs of $44.1 million was primarily due to the $7.3 million in expenses incurred for the tenapanor clinical trial material from AstraZeneca as well as an increase of $6.7 million in expenses incurred for clinical development activities associated with tenapanor including the commencement of two Phase 3 clinical trials in IBS-C, a long-term safety trial, and RDX022,one Phase 3 clinical trial in hyperphosphatemia, as well as clinical manufacturing and manufacturing process development for RDX022.activities associated with tenapanor, RDX7675 and RDX8940. The increase in our internal costs of $10.2 million was primarily due to an increase in personnel, facility and other costs, primarily related to an increase in research and development headcount to support the growth of our development activities. General and Administrative | | | | | | | | | Year Ended December 31, | | | 2016 | | 2015 | | (in thousands) | General and administrative | | $ | 18,734 | | $ | 13,530 | Dollar change from prior year | | | 5,204 | | | | Percent change from prior year | | | 38 | % | | |
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2015 | | | 2014 | | | Dollar Change | | | | | | | | (in thousands) | | | | | General and administrative | | $ | 13,530 | | | $ | 7,287 | | | $ | 6,243 | |
General and administrative expenses were $18.7 million for the year ended December 31, 2016, an increase of $5.2 million, or 38%, compared to $13.5 million for the year ended December 31, 2015, an increase of $6.2 million, or 86%, compared to $7.3 million for the year ended December 31, 2014.2015. The increase was primarily due to an increaseincreases of $2.7 million in professional services fees, personnel and public company costs. Change in Fair Value of Preferred Stock Warrant Liability
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2015 | | | 2014 | | | Dollar Change | | | | | | | | (in thousands) | | | | | Change in Fair Value of Preferred Stock Warrant Liability | | $ | — | | | $ | (1,593 | ) | | $ | 1,593 | |
Change in fair value of preferred stock warrant liability was zero for the year ended December 31, 2015 compared to $(1.6) million for the year ended December 31, 2014. The preferred stock warrants were net exercised upon the completion of our initial public offering (IPO) in June 2014 and are no longer subject to remeasurement.
Comparison of the Years Ended December 31, 2014 and 2013
Revenue
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2014 | | | 2013 | | | Dollar Change | | | | | | | | (in thousands) | | | | | Revenue: | | | | | | | | | | | | | Licensing revenue | | $ | 18,394 | | | $ | 8,063 | | | $ | 10,331 | | Collaborative development revenue | | | 13,229 | | | | 20,865 | | | | (7,636 | ) | | | | | | | | | | | | | | Total revenue | | $ | 31,623 | | | $ | 28,928 | | | $ | 2,695 | |
Licensing revenue for the year ended December 31, 2014 was $18.4 million, an increase of $10.3 million, or 128%, compared to $8.1 million for the year ended December 31, 2013. The increase was primarily due to the amortization of deferred revenue from the $15.0 million development milestone payment we received in December 2013 related to the amendment to the AstraZeneca agreement and the $25.0 million development milestone payment we received in May 2014 related to the dosing of the first patient in the Phase 2b ESRD clinical trial in hyperphosphatemia in April 2014, which were both recognized ratably over the expected period of performance under the agreement. The estimated period of performance was based on the completion of all of the Phase 2 clinical trials for tenapanor, which we estimated to be December 2017. This estimated period was extended during the third quarter of 2014 from December 2016 to December 2017 due to the extension of the estimated completion date of the remaining Phase 2 clinical trials. The remaining increase was due to the $1.25 million we recognized in May 2014 pursuant to the Option and License Agreement with Sanofi upon the completion of our performance obligations.
Collaborative development revenue consists of our development expenses that are reimbursable to us by AstraZeneca as part of our license agreement. Collaborative development revenue for the year ended December 31, 2014 was $13.2 million, a decrease of $7.6 million, or 37%, compared to $20.9 million for the year ended December 31, 2013. The decrease was due to a decrease in our development activities primarily related to the clinical trials that are a part of the AstraZeneca agreement.
Research and Development
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2014 | | | 2013 | | | Dollar Change | | | | | | | | (in thousands) | | | | | Research and development | | $ | 25,900 | | | $ | 28,093 | | | $ | (2,193 | ) |
Research and development expenses were $25.9 million for the year ended December 31, 2014, a decrease of $2.2 million, or 8%, compared to $28.1 million for the year ended December 31, 2013. The change was due to a decrease in AstraZeneca collaboration development expense of $7.2 million which was primarily driven by the
decrease in development activities related to tenapanor conducted by us under the license agreement with AstraZeneca. The decrease was offset by a $5.0 million increase in discovery research expenses primarily due to an increase in our personnelother costs of $1.2 million, an increase in ourincluding stock-based compensation, expense of $1.2 million primarily driven by the acceleration of stock option vesting related to the separation agreement with Dr. Charmot, an increase in CRO consultant service fees and other temporary consultant fees of $0.9 million, and an increase in lab supply expenses from increased research activities for unpartnered programs of $0.8 million.
General and Administrative
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2014 | | | 2013 | | | Dollar Change | | | | | | | | (in thousands) | | | | | General and administrative | | $ | 7,287 | | | $ | 3,700 | | | $ | 3,587 | |
General and administrative expenses were $7.3 million for the year ended December 31, 2014, an increase of $3.6 million, or 97%, compared to $3.7 million for the year ended December 31, 2013. The increase was primarily due to an increase in professional services fees, personnel and operational costs as a result of our being a public company.
Change in Fair Value of Preferred Stock Warrant Liability
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | | | | 2014 | | | 2013 | | | Dollar Change | | | | | | | | (in thousands) | | | | | Change in fair value of preferred stock warrant liability | | $ | (1,593 | ) | | $ | (3,506 | ) | | $ | 1,913 | |
Change in fair value of preferred stock warrant liability was $1.6 million for the year ended December 31, 2014 compared to $3.5 million for the year ended December 31, 2013. The amounts recorded in each of 2014 and 2013 were due to increases in the fair value of our convertible preferred stock as compared with the prior year. The smaller amount recorded in 2014 was due to a smalleran increase in the value of the underlying stock as compared with the prior year. The preferred stock warrants were net exercised upon the completion of the IPOheadcount, $1.4 million in professional fees and are no longer subject to remeasurement.$1.1 million in market research and pre-commercialization activities.
LIQUIDITY AND CAPITAL RESOURCES | | | | | | | | | December 31, | | | 2017 | | 2016 | | | (in thousands) | Cash and cash equivalents | | | 75,383 | | | 74,598 | Short-term investments | | | 58,593 | | | 126,225 | Total liquid funds | | $ | 133,976 | | $ | 200,823 |
| | | | | | | | | | | | December 31,
2015 | | | December 31,
2014 | | Cash and cash equivalents | | $ | 107,004 | | | $ | 107,286 | |
As of December 31, 2015,2017, we had cash, and cash equivalents and short-term investments totaling $107.0 million, which reflects a general ledger overdraft resulting from outstanding checks in the amount of $1.5 million which is included in accounts payable in the balance sheet.$134.0 million. On July 13, 2015, we filed a shelf registration statement on Form S-3S‑3 (File No. 333‑205631) with the SEC, under which we may sell an aggregate of up to $200.0 million of common stock, preferred stock, debt securities, warrants, purchase contractcontracts and/or units. The S-3S‑3 shelf registration statement included a prospectus covering the offering, issuance and sale of up to $50.0 million of shares of common stock from time to time in “at the market,” or “ATM offerings” pursuant to an At the Market Issuancea Controlled Equity Offering Sales Agreement, or Sales Agreement, entered into with Cantor Fitzgerald & Co. on July 13, 2015. No shares of common stock have been sold to date in ATM offerings, and on February 6, 2017 we gave notice to Cantor Fitzgerald & Co. of our termination of the Sales Agreement, effective February 16, 2017. OnIn January 13, 2016, we completed a registeredan underwritten public offering pursuant to our S-3 shelf registration statement and sold an aggregate of 8,625,000 shares of common stock which included 1,125,000
sharesat an offering price of common stock purchased by the underwriters upon the full exercise$10.00 per share for gross proceeds of their option to purchase additional shares of stock. We$86.3 million. This offering was completed under our shelf registration statement filed on July 13, 2015, and we received net proceeds from the offering of approximately $80.4$80.8 million, net ofafter deducting the underwriters’ discounts and commissions and expensesoffering expenses.
In July 2016, we sold and issued an aggregate of 12,600,230 shares of common stock in a private placement transaction at an offering price of $8.73 per share for gross proceeds of $110.0 million. We received net proceeds from the offering of approximately $109.8 million, after deducting offering expenses. In November and December 2017, we executed license agreements with KHK and Fosun Pharma for the development, commercialization and distribution of tenapanor for certain indications in Japan and China, respectively, under which we were entitled to an aggregate of $30.0 million and $12.0 million, respectively, in up-front license fees. The $30.0 million was collected by December 31, 2017 and the remaining $12.0 million, less $1.2 million of withholding taxes, was collected in January 2018. We accrued a liability of $8.4 million to AstraZeneca in accordance with the terms of our termination agreement with AstraZeneca entered into in 2015, of which $6.0 million was paid us.by December 31, 2017 and the remainder of which was paid in February 2018. Our primary uses of cash are to fund operating expenses, primarily research and development expenditures. We intend to use our existing cash and cash equivalents, including the net proceeds from our January equity offering to support the tenapanor and RDX022 Phase 3 clinical programs, including manufacturing of clinical trial materials, as well as to support the IND filing for RDX009 and to fund additional research and development for our earlier stage programs. Cash used to fund operating expenses is impacted by the timing of when we pay these expenses, as reflected in the change in our outstanding accounts payable and accrued expenses. We believe that our existing capital resources as of December 31, 2015, and2017, combined with the net proceedsupfront payment from theFosun Pharma received in January 2016 stock offering,2018, will be sufficient to meet our projected operating requirements for at least the next 12 months.12-month period following the filing date of this Annual Report on Form 10-K. We have based this estimate on assumptions that may prove to be wrong, and we could utilize our available capital resources sooner than we currently expect. Further, our operating plan maycan change, and we may needrequire significant additional fundscapital to meet operational needsfund our operations, including to support the development, commercialization and manufacturing efforts for tenapanor. We may seek to obtain such additional capital requirements for clinical trials and other research and development expenditures.through debt financings, credit facilities, additional equity offerings and/or strategic collaborations. We currently have no credit facility or committed sources of capital.capital, and there can be no assurances that such sources of capital will be available to us when needed or on acceptable terms. Because of the numerous risks and uncertainties associated with the development and commercialization of our product candidates, and the extent to which we may enter into additional collaboration partnerships with third partiesthird-parties to participate in their development and commercialization, we are unable to estimate the amounts of increased capital outlays and operating expenditures associated with our current and anticipated clinical studies.studies, manufacturing requirements and commercial plans. Our future funding requirements will depend on many factors, including the following: | · | | the progress, timing, scope, results and costs of our clinical trial programs evaluating tenapanor for the treatment of hyperphosphatemia in ESRD patients on dialysis and the submission of an NDA to the FDA to request marketing authorization for tenapanor in patients with IBS-C, as well as our decision whether or not to pursue other indications for tenapanor; |
| · | | our ability to successfully commercialize tenapanor, either alone or with one or more collaboration partners; |
| · | | the manufacturing costs of tenapanor, and the availability of one or more suppliers for tenapanor at reasonable costs; |
| · | | the selling and marketing costs associated with tenapanor, including the cost and timing of building our sales and marketing capabilities; |
| · | | our ability to maintain our existing collaboration partnerships and to establish additional collaboration partnerships, in-license/out-license, joint ventures or other similar arrangements and the financial terms of such agreements; |
| · | | the timing, receipt, and amount of sales of, or royalties on, tenapanor, if any; |
| · | | the sales price and the availability of adequate third-party reimbursement for tenapanor; |
| · | | the cash requirements of any future acquisitions or discovery of product candidates; |
| · | | the number and scope of research programs that we decide to pursue or initiate, and any clinical trials we decide to pursue for other product candidates; |
| · | | the time and cost necessary to respond to technological and market developments; and |
| · | | the costs of filing, prosecuting, maintaining, defending and enforcing any patent claims and other intellectual property rights, including litigation costs and the outcome of such litigation, including costs of defending any claims of infringement brought by others in connection with the development, manufacture or commercialization of tenapanor or any of our product candidates. |
the progress, timing, scope, results and coststhe progress, timing, scope, results and costs of our clinical program for RDX022;
the time and cost necessary to obtain regulatory approvals for our product candidates and the costs of post-marketing studies that could be required by regulatory authorities;
our ability to successfully commercialize our product candidates, either alone or with one or more collaboration partners;
the manufacturing costs of our product candidates, and the availability of one or more suppliers for our product candidates at reasonable costs, both for clinical and commercial supply;
the selling and marketing costs associated with our product candidates, including the cost and timing of building our sales and marketing capabilities;
our ability to establish and maintain collaboration partnerships, in-license/out-license or other similar arrangements and the financial terms of such agreements;
the timing, receipt, and amount of sales of, or royalties on, our future products, if any;
the sales price and the availability of adequate third-party reimbursement for our product candidates;
the cash requirements of any future acquisitions or discovery of product candidates;
the number and scope of preclinical and discovery programs that we decide to pursue or initiate, and any clinical trials we decide to pursue for other product candidates;
the time and cost necessary to respond to technological and market developments; and
the costs of filing, prosecuting, maintaining, defending and enforcing any patent claims and other intellectual property rights, including litigation costs and the outcome of such litigation, including costs of defending any claims of infringement brought by others in connection with the development, manufacture or commercialization of our product candidates.
The following table summarizes our cash flows for the periods indicated (in thousands):indicated: | | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | | | (in thousands) | Cash used in operating activities | | $ | (65,190) | | $ | (92,534) | | $ | (71,840) | Cash provided by (used in) investing activities | | | 65,290 | | | (131,076) | | | (3,454) | Cash provided by financing activities | | | 685 | | | 191,204 | | | 75,012 | Net increase (decrease) in cash and cash equivalents | | $ | 785 | | $ | (32,406) | | $ | (282) |
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | 2015 | | | 2014 | | | 2013 | | Cash (used in) provided by operating activities | | $ | (71,840 | ) | | $ | 13,397 | | | $ | 1,811 | | Cash used in investing activities | | | (3,454 | ) | | | (1,856 | ) | | | (278 | ) | Cash provided by (used in) financing activities | | | 75,012 | | | | 61,310 | | | | (1 | ) |
Cash Flows from Operating Activities Net cash used in operating activities during the year ended December 31, 2017, was approximately $65.2 million. The net loss of $64.3 million was adjusted for (i) non-cash charges of $3.2 million for depreciation and amortization and $9.6 million for stock-based compensation, (ii) an increase of $10.8 million in accounts receivable, solely related to the Fosun Pharma license up front fee after withholding taxes, (iii) an increase of $2.1 million in prepaid expenses, primarily advances to vendors for clinical development and manufacturing activities, and (iv) a decrease in accounts payable and accrued liabilities of $0.7 million primarily due to expenses incurred for the clinical manufacturing, process development, and clinical development activities for tenapanor and RDX7675. Net cash used in operating activities during the year ended December 31, 2016, was approximately $92.5 million. The net loss of $112.4 million was adjusted for (i) an increase of accounts payable and accrued liabilities of $11.2 million primarily due to expenses incurred for the clinical manufacturing, process development, and clinical development activities for tenapanor, RDX7675 and RDX8940, (ii) non-cash charges of $1.8 million for depreciation and amortization and $5.3 million for stock-based compensation and (iii) pre-payments of $1.6 million to vendors for clinical development and manufacturing activities. Net cash used in operating activities during the year ended December 31, 2015, was approximately $71.8 million. The net loss of $29.6 million comparedwas adjusted for (i) the recognition of deferred revenues of $47.1 million related to upfront payments from AstraZeneca, (ii) an increase of accounts payable and accrued liabilities of $2.3 million due to expenses incurred for the clinical manufacturing, process development, and clinical development activities for tenapanor, RDX7675 and RDX8940, (iii) non-cash charges of $1.3 million for depreciation and amortization and $2.6 million for stock-based compensation, (iv) advance payments of $4.1 million to vendors for clinical development and manufacturing activities, and (v) a decrease accounts receivable of $2.6 million due to the termination of our collaboration with AstraZeneca. Cash Flows from Investing Activities Net cash provided by operatinginvesting activities of $13.4was $65.3 million during 2014.The change wasfor the year ended December 31, 2017, primarily due a decreaseto maturities and sales, less purchases, of $47.1short-term investments of $67.7 million. This was offset by the acquisition of property and equipment of $2.4 million in deferred revenue duerelated to the Termination Agreement with AstraZeneca, net losspurchase of laboratory equipment and leasehold improvements. Net cash used by investing activities was $131.1 million for each respective period adjusted for stock-based compensation, depreciation expensethe year ended December 31, 2016, and other changes in working capital. Cash provided by operating activities during 2014 was approximately $13.4 million, compared to cash provided by operating activities of $1.8 million during 2013. The change was primarily due to purchases of marketable securities of $133.8 million and acquisition of property and equipment of $4.9 million related to the expansion of our net loss adjusted for movements in working capital, stock-based compensationlaboratory and depreciation expense.related equipment. These uses of cash were partially offset by maturities of short-term investments of $7.6 million. Cash Flows from Investing Activities
CashNet cash used in investing activities for the years ended December 31, 2015, 2014 and 2013 was related to our acquisition of property and equipment of $3.5 million, $1.9 million and $0.3 million, respectively. Purchases of property and equipment are primarily related to expansion of our laboratory and related equipment.
Cash Flows from Financing Activities CashNet cash provided by financing activities for the yearsyear ended December 31, 2015 and 20142017, was approximately $75.0$0.7 million, and $61.3 million, respectively, and was primarily due to proceeds from issuance of common stock under stock plans.
Net cash provided by financing activities for the year ended December 31, 2016, was $191.2 million and was primarily due to net proceeds of $190.6 million from public and private offerings of our common stock. Net cash provided by financing activities for the year ended December 31, 2015, was $75.0 million and was primarily due to net proceeds of $74.3 million from a private offering of our common stock. CONTRACTUAL OBLIGATIONS AND OTHER COMMITMENTS The following table summarizes our contractual obligations as of December 31, 2015 (in thousands):
| | | | | | | | | | | | | | | | | | | | | | | | Payments Due by Period | | Contractual Obligation: | | Less than
1 year | | | 1 to 3
Years | | | 4 to 5
Years | | | More Than 5
Years | | | Total | | Purchase commitments (1) | | $ | 2,324 | | | $ | — | | | $ | — | | | $ | — | | | $ | 2,324 | | Operating leases (2) | | | 868 | | | | 1,816 | | | | 653 | | | | — | | | | 3,337 | | | | | | | | | | | | | | | | | | | | | | | Total contractual obligations | | $ | 3,192 | | | $ | 1,816 | | | $ | 653 | | | $ | — | | | $ | 5,661 | | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | Payments Due by Period (in thousands) | | | Less than | | 1 to 3 | | 3 to 5 | | More Than 5 | | | | Contractual Obligation: | | 1 year | | Years | | Years | | Years | | Total | Operating leases (1) | | $ | 1,615 | | $ | 3,739 | | $ | 1,440 | | $ | — | | $ | 6,794 | | | | | | | | | | | | | | | | | Total contractual obligations | | $ | 1,615 | | $ | 3,739 | | $ | 1,440 | | $ | — | | $ | 6,794 |
(1) | At December 31, 2015, we had non-cancelable purchase commitments of approximately $2.3 million arising from manufacturing agreements for our clinical candidates and for tenapanor clinical trial material arising from the Termination Agreement with AstraZeneca. |
(2)(1) | | Operating leases include total future minimum rent payments under non-cancelable operating lease agreements. |
OFF-BALANCE SHEET ARRANGEMENTS As of December 31, 2015,2017, we did not have any off-balance sheet arrangements as defined in Item 303(a)(4) of Regulation S-K as promulgated by the SEC. RECENT ACCOUNTING PRONOUNCEMENTS ForRefer to Note 2 in the notes to our consolidated financial statements in Part I, Item 8 of this Annual Report on Form 10‑K, for a discussion of new accounting pronouncements refer toNOTE 2, SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES, to our financial statements appearing elsewhere in this Annual Report on Form 10-K.pronouncements.
JOBS ACT ACCOUNTING ELECTION We are an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act. Under the JOBS Act, emerging growth companies can delay adopting new or revised accounting standards issued subsequent to the enactment of the JOBS Act until such time as those standards apply to private companies. We have irrevocably elected not to avail ourselves of this exemption from new or revised accounting standards, and, therefore, are subject to the same new or revised accounting standards as other public companies that are not emerging growth companies. In addition, as an emerging growth company, we have reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK Interest Rate Risk We are exposed to market risks in the ordinary course of our business. These risks primarily include risk related to interest rate sensitivities. We had cash, and cash equivalents and short-term investments of $107.0$134.0 million as of December 31, 2015,2017, which consist of bank deposits and money market funds.funds, as well as high quality fixed income instruments including corporate bonds, commercial paper, and asset-backed securities collateralized by non-mortgage consumer receivables. The credit rating of our short-term investments must be rated A‑1/P‑1, or better by Standard and Poor’s and Moody’s Investors Service. The credit rating of our long-term securities must be rated at least A- by Standard & Poor’s or A3 by Moody’s. Asset-backed securities must be rated AAA/Aaa. Money Market funds must be rated AAAm/Aaa. Such interest-earning instruments carry a degree of interest rate risk. However, because our investments are high quality and primarily short-term in duration, we believe that our exposure to interest rate risk is not significant and a 10% movement in market interest rates would not have a significant impact on the total value of our portfolio. We do not enter into investments for trading or speculative purposes.
Foreign Currency Exchange Risk Certain expensesexpenditures and receipts related to our international activities are payable in foreign currencies. As a result, factors such as changes in foreign currency exchange rates or weak economic conditions in foreign markets will affect our financial results. We recognized net foreign currency exchange transactiongains of $0.5 million for the year ended December 31, 2017, compared to losses of $0.1 million for the year ended December 31, 2015. We currently2016. For most contracts payable in a foreign currency, we have generally purchased the total expected payable amount of foreign currency at the execution of the contract. Because we only have $6.2 million in foreign currency cash holdings, all in stable European currencies, we do not hedge foreign currency exchange rate exposure. Althoughexpect that the impact of currency fluctuations on our financial results has been immaterial in the past, there can be no guarantee the impact of currency fluctuations related to our international activities will not be material in the future. ITEM 8. CONSOLIDATED FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA ARDELYX, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Report of Independent Registered Public Accounting FirmREPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM TheTo the Stockholders and the Board of Directors and Stockholders
of Ardelyx, Inc. Opinion on the Financial Statements We have audited the accompanying consolidated balance sheets of Ardelyx, Inc. (the Company) as of December 31, 20152017 and 2014,2016, and the related consolidated statements of operations and comprehensive loss, convertible preferred stock and stockholders’ equity (deficit), and cash flows for each of the three years in the period ended December 31, 2015. 2017, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2017 and 2016, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2017, in conformity with U.S. generally accepted accounting principles. Basis for Opinion These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on thesethe Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB. We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States).PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. Wemisstatement, whether due to error or fraud. The Company is not required to have, nor were notwe engaged to perform, an audit of the Company’sits internal control over financial reporting. OurAs part of our audits included considerationwe are required to obtain an understanding of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence supportingregarding the amounts and disclosures in the financial statements, assessingstatements. Our audits also included evaluating the accounting principles used and significant estimates made by management, andas well as evaluating the overall presentation of the financial statement presentation.statements. We believe that our audits provide a reasonable basis for our opinion. In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of Ardelyx, Inc. at December 31, 2015 and 2014, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2015, in conformity with U.S. generally accepted accounting principles.
/s/ Ernst & Young LLP We have served as the Company’s auditor since 2009. Redwood City, California March 4, 2016 14, 2018
ARDELYX, INC. CONSOLIDATED BALANCE SHEETS (in thousands, except share and per share amounts) | | | | | | | | | | | | | | December 31, | | | December 31, | | | | 2015 | | 2014 | | | 2017 | | 2016 | Assets | | | | | | | | | | | Current assets: | | | | | | | | | | | Cash and cash equivalents | | $ | 107,004 | | | $ | 107,286 | | | $ | 75,383 | | $ | 74,598 | Short-term investments | | | | 58,593 | | | 126,225 | Accounts receivable | | | — | | | 2,584 | | | | 10,796 | | | — | Prepaid expenses and other current assets | | | 5,027 | | | 1,209 | | | | 4,940 | | | 3,169 | | | | | | | | | Total current assets | | | 112,031 | | | 111,079 | | | | 149,712 | | | 203,992 | Property and equipment, net | | | 4,711 | | | 2,131 | | | | 8,032 | | | 8,991 | Other assets | | | 104 | | | 104 | | | | 159 | | | 148 | Restricted cash | | | 100 | | | 100 | | | | | | | | | | | Total assets | | $ | 116,946 | | | $ | 113,414 | | | $ | 157,903 | | $ | 213,131 | | | | | | | | | Liabilities and stockholders’ equity | | | | | | | | | | | Current liabilities: | | | | | | | | | | | Accounts payable | | $ | 2,777 | | | $ | 3,129 | | | $ | 3,933 | | $ | 5,635 | Accrued compensation and benefits | | | 2,366 | | | 1,648 | | | | 3,229 | | | 3,161 | Accrued and other liabilities | | | 2,580 | | | 780 | | | | 10,709 | | | 10,405 | Deferred revenue, current portion | | | — | | | 15,979 | | | | | | | | | | | Total current liabilities | | | 7,723 | | | 21,536 | | | | 17,871 | | | 19,201 | Other long-term liabilities | | | 322 | | | 122 | | | | 720 | | | 779 | Deferred revenue, non-current | | | — | | | 31,074 | | | | | | | | | | | Total liabilities | | | 8,045 | | | 52,732 | | | | 18,591 | | | 19,980 | | | | | | | | | Commitments and contingencies (Note 12) | | | | | | Commitments and contingencies (Note 13) | | | | | | | | Stockholders’ equity: | | | | | | | | | | | Preferred stock, $0.0001 par value; 5,000,000 shares authorized as of December 31, 2015 and December 31, 2014, respectively; no shares issued and outstanding as of December 31, 2015 and December 31, 2014, respectively. | | | — | | | | — | | | Common stock, $0.0001 par value; 300,000,000 shares authorized as of December 31, 2015 and December 31, 2014, respectively; 25,964,886 and 18,589,245 shares issued and outstanding as of December 31, 2015 and December 31, 2014, respectively. | | | 3 | | | 2 | | | Preferred stock, $0.0001 par value; 5,000,000 shares authorized; no shares issued and outstanding as of December 31, 2017 and December 31, 2016 | | | | — | | | — | Common stock, $0.0001 par value; 300,000,000 shares authorized; 47,534,979 and 47,309,422 shares issued and outstanding as of December 31, 2017 and December 31, 2016, respectively | | | | 5 | | | 5 | Additional paid-in capital | | | 210,386 | | | 132,547 | | | | 417,568 | | | 407,092 | Accumulated deficit | | | (101,488 | ) | | (71,867 | ) | | | (278,214) | | | (213,875) | | | | | | | | | Accumulated other comprehensive loss | | | | (47) | | | (71) | Total stockholders’ equity | | | 108,901 | | | 60,682 | | | | 139,312 | | | 193,151 | | | | | | | | | Total liabilities and stockholders’ equity | | $ | 116,946 | | | $ | 113,414 | | | $ | 157,903 | | $ | 213,131 | | | | | | | | |
See accompanying notes. ARDELYX, INC. CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS (in thousands, except share and per share amounts) | | | | | | | | | | | | | | | | Year Ended December 31, | | | | | 2015 | | | 2014 | | | 2013 | | | | | (in thousands, except share and per share amounts) | | Revenue: | | | | | | | | | | | | | Licensing revenue | | $ | 21,611 | | | $ | 18,394 | | | $ | 8,063 | | Collaborative development revenue | | | 2,415 | | | | 13,229 | | | | 20,865 | | | | | | | | | | | | | | | Total revenue | | | 24,026 | | | | 31,623 | | | | 28,928 | | Operating expenses: | | | | | | | | | | | | | Research and development | | | 39,885 | | | | 25,900 | | | | 28,093 | | General and administrative | | | 13,530 | | | | 7,287 | | | | 3,700 | | | | | | | | | | | | | | | Total operating expenses | | | 53,415 | | | | 33,187 | | | | 31,793 | | | | | | | | | | | | | | | Loss from operations | | | (29,389 | ) | | | (1,564 | ) | | | (2,865 | ) | Other income (expense), net | | | (261 | ) | | | 10 | | | | (52 | ) | Change in fair value of preferred stock warrant liability | | | — | | | | (1,593 | ) | | | (3,506 | ) | | | | | | | | | | | | | | Loss before provision for income taxes | | | (29,650 | ) | | | (3,147 | ) | | | (6,423 | ) | Benefit from (provision for) income taxes | | | 29 | | | | (67 | ) | | | (141 | ) | | | | | | | | | | | | | | Net loss and comprehensive loss | | $ | (29,621 | ) | | $ | (3,214 | ) | | $ | (6,564 | ) | | | | | | | | | | | | | | Net loss per common share, basic and diluted | | $ | (1.29 | ) | | $ | (0.31 | ) | | $ | (5.82 | ) | | | | | | | | | | | | | | Shares used to compute net loss per common share, basic and diluted | | | 22,892,640 | | | | 10,248,337 | | | | 1,127,948 | | | | | | | | | | | | | | |
| | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | Revenue: | | | | | | | | | | Licensing revenue | | $ | 42,000 | | $ | — | | $ | 21,611 | Collaborative development revenue | | | — | | | — | | | 2,415 | Total revenue | | | 42,000 | | | — | | | 24,026 | Cost of revenue | | | 8,400 | | | — | | | — | Gross profit | | | 33,600 | | | — | | | 24,026 | Operating expenses: | | | | | | | | | | Research and development | | | 75,484 | | | 94,161 | | | 39,885 | General and administrative | | | 23,231 | | | 18,734 | | | 13,530 | Total operating expenses | | | 98,715 | | | 112,895 | | | 53,415 | Loss from operations | | | (65,115) | | | (112,895) | | | (29,389) | Other income (expense), net | | | 1,955 | | | 508 | | | (261) | Loss before provision for income taxes | | | (63,160) | | | (112,387) | | | (29,650) | Provision for (benefit from) income taxes | | | 1,179 | | | — | | | (29) | Net loss | | $ | (64,339) | | $ | (112,387) | | $ | (29,621) | Net loss per common share, basic and diluted | | $ | (1.36) | | $ | (2.80) | | $ | (1.29) | Shares used in computing net loss per share - basic and diluted | | | 47,435,331 | | | 40,118,522 | | | 22,892,640 | Comprehensive Loss: | | | | | | | | | | Net loss | | $ | (64,339) | | $ | (112,387) | | $ | (29,621) | Unrealized gain (loss) on available-for-sale securities, net of tax | | | 24 | | | (71) | | | — | Comprehensive loss | | $ | (64,315) | | $ | (112,458) | | $ | (29,621) |
See accompanying notes.
ARDELYX, INC. CONSOLIDATED STATEMENTS OF CONVERTIBLE PREFERRED STOCK AND STOCKHOLDERS’ EQUITY (DEFICIT) (in thousands, except share amounts) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Convertible
Preferred Stock | | | | | Common Stock | | | | | | | | | | | Shares | | | Amount | | | | | Shares | | | Amount | | | Additional
Paid-In
Capital | | | Accumulated
Deficit | | | Total
Stockholders’
( Deficit)
Equity | | Balance as of December 31, 2012 | | | 11,517,222 | | | $ | 56,155 | | | | | | 1,001,616 | | | $ | — | | | $ | 4,697 | | | $ | (62,089 | ) | | $ | (57,392 | ) | Exercise of stock options and vesting of early exercised stock options, net of repurchases | | | — | | | | — | | | | | | 223,865 | | | | — | | | | 125 | | | | — | | | | 125 | | Stock-based compensation | | | — | | | | — | | | | | | — | | | | — | | | | 352 | | | | — | | | | 352 | | Net loss | | | — | | | | — | | | | | | — | | | | — | | | | | | | | (6,564 | ) | | | (6,564 | ) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Balance as of December 31, 2013 | | | 11,517,222 | | | | 56,155 | | | | | | 1,225,481 | | | | — | | | | 5,174 | | | $ | (68,653 | ) | | $ | (63,479 | ) | Conversion of convertible preferred stock to common stock in connection with initial public offering | | | (11,517,222 | ) | | | (56,155 | ) | | | | | 11,517,222 | | | | 1 | | | | 56,154 | | | | — | | | | 56,155 | | Net exercise and conversion of preferred stock warrants to common stock in connection with initial public offering | | | — | | | | — | | | | | | 571,244 | | | | — | | | | 8,049 | | | | — | | | | 8,049 | | Exercise of stock options and vesting of early exercised stock options, net of repurchases | | | — | | | | — | | | | | | 336,398 | | | | — | | | | 238 | | | | — | | | | 238 | | Issuance of common stock in connection with initial public offering, net of offering costs | | | — | | | | — | | | | | | 4,928,900 | | | | 1 | | | | 61,240 | | | | — | | | | 61,241 | | Issuance of common stock for services | | | — | | | | — | | | | | | 10,000 | | | | — | | | | 208 | | | | — | | | | 208 | | Stock-based compensation | | | — | | | | — | | | | | | — | | | | — | | | | 1,484 | | | | — | | | | 1,484 | | Net loss | | | — | | | | — | | | | | | — | | | | — | | | | — | | | | (3,214 | ) | | | (3,214 | ) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Balance as of December 31, 2014 | | | — | | | | — | | | | | | 18,589,245 | | | | 2 | | | | 132,547 | | | | (71,867 | ) | | | 60,682 | | Issuance of common stock upon exercise of options | | | — | | | | — | | | | | | 77,784 | | | | — | | | | 111 | | | | — | | | | 111 | | Issuance of common stock under employee stock purchase plan | | | — | | | | — | | | | | | 41,580 | | | | — | | | | 548 | | | | — | | | | 548 | | Issuance of common stock and warrants in connection with the private placement, net of expenses of $3,449 | | | — | | | | — | | | | | | 7,242,992 | | | | 1 | | | | 74,322 | | | | — | | | | 74,323 | | Stock-based compensation | | | — | | | | — | | | | | | — | | | | — | | | | 2,634 | | | | — | | | | 2,634 | | Issuance of common stock for services | | | — | | | | — | | | | | | 13,285 | | | | — | | | | 194 | | | | — | | | | 194 | | Other | | | — | | | | — | | | | | | — | | | | — | | | | 30 | | | | — | | | | 30 | | Net loss | | | — | | | | — | | | | | | — | | | | — | | | | — | | | | (29,621 | ) | | | (29,621 | ) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Balance as of December 31, 2015 | | | — | | | $ | — | | | | | | 25,964,886 | | | $ | 3 | | | $ | 210,386 | | | $ | (101,488 | ) | | $ | 108,901 | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
See accompanying notes.
ARDELYX, INC.
STATEMENTS OF CASH FLOWS
(in thousands)
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | 2015 | | | 2014 | | | 2013 | | Operating activities | | | | | | | | | Net loss | | $ | (29,621 | ) | | $ | (3,214 | ) | | $ | (6,564 | ) | Adjustments to reconcile net loss to net cash used in operating activities: | | | | | | | | | Depreciation expense | | | 829 | | | | 302 | | | | 592 | | Amortization of deferred financing costs | | | 351 | | | | — | | | | — | | Amortization of deferred compensation for services | | | 107 | | | | — | | | | — | | Stock-based compensation | | | 2,634 | | | | 1,692 | | | | 352 | | Change in fair value of preferred stock warrant liability | | | — | | | | 1,593 | | | | 3,506 | | Loss from disposal of fixed assets | | | 65 | | | | — | | | | — | | Changes in operating assets and liabilities: | | | | | | | | | Accounts receivable | | | 2,584 | | | | 3,852 | | | | (3,364 | ) | Prepaid expenses and other assets | | | (4,083 | ) | | | 96 | | | | (438 | ) | Accounts payable | | | (371 | ) | | | 831 | | | | 1,138 | | Accrued compensation and benefits | | | 718 | | | | 721 | | | | (38 | ) | Accrued and other liabilities | | | 2,000 | | | | 647 | | | | (1,009 | ) | Deferred revenue | | | (47,053 | ) | | | 6,755 | | | | 7,636 | | Other long-term liabilities | | | — | | | | 122 | | | | — | | | | | | | | | | | | | | | Net cash (used in) provided by operating activities | | | (71,840 | ) | | | 13,397 | | | | 1,811 | | | | | | | | | | | | | | | Investing activities | | | | | | | | | Purchases of property and equipment | | | (3,454 | ) | | | (1,856 | ) | | | (278 | ) | | | | | | | | | | | | | | Net cash used in investing activities | | | (3,454 | ) | | | (1,856 | ) | | | (278 | ) | | | | | | | | | | | | | | Financing activities | | | | | | | | | Proceeds from issuance of common stock, net | | | 74,323 | | | | 61,241 | | | | — | | Proceeds from issuance of common stock from exercise of options | | | 659 | | | | 71 | | | | 1 | | Other | | | 30 | | | | (2 | ) | | | (2 | ) | | | | | | | | | | | | | | Net cash provided by (used in) financing activities | | | 75,012 | | | | 61,310 | | | | (1 | ) | | | | | | | | | | | | | | Net increase in cash and cash equivalents | | | (282 | ) | | | 72,851 | | | | 1,532 | | Cash and cash equivalents at beginning of period | | | 107,286 | | | | 34,435 | | | | 32,903 | | | | | | | | | | | | | | | Cash and cash equivalents at end of period | | $ | 107,004 | | | $ | 107,286 | | | $ | 34,435 | | | | | | | | | | | | | | | Supplementary disclosure of cash flow information | | | | | | | | | Income taxes paid | | $ | 69 | | | $ | — | | | $ | 160 | | Supplementary disclosure of non-cash financing information: | | | | | | | | | Acquisition of property and equipment included in accounts payable and accrued liabilities | | $ | — | | | $ | — | | | $ | — | | Services settled through the issuance of common stock | | $ | — | | | $ | 208 | | | $ | — | | Reclassification of convertible preferred warrant liability to additional paid-in capital | | $ | — | | | $ | 8,049 | | | $ | — | | Conversion of convertible preferred stock to common stock at closing of initial public offering | | $ | — | | | $ | 56,155 | | | $ | — | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | Accumulated | | | | | | | | | | | Additional | | | | | Other | | Total | | | Common Stock | | Paid-In | | Accumulated | | Comprehensive | | Stockholders' | | | Shares | | Amount | | Capital | | Deficit | | Income (Loss) | | Equity | Balance as of December 31, 2014 | | 18,589,245 | | $ | 2 | | $ | 132,547 | | $ | (71,867) | | $ | — | | $ | 60,682 | Issuance of common stock and warrants in connection with the private placement, net of expenses of $3,449 | | 7,242,992 | | | 1 | | | 74,322 | | | — | | | — | | | 74,323 | Issuance of common stock upon exercise of options | | 77,784 | | | — | | | 111 | | | — | | | — | | | 111 | Issuance of common stock under employee stock purchase plan | | 41,580 | | | — | | | 548 | | | — | | | — | | | 548 | Issuance of common stock for services | | 13,285 | | | — | | | 194 | | | — | | | — | | | 194 | Stock-based compensation | | — | | | — | | | 2,634 | | | — | | | — | | | 2,634 | Other | | — | | | — | | | 30 | | | — | | | — | | | 30 | Net loss | | — | | | — | | | — | | | (29,621) | | | — | | | (29,621) | Balance as of December 31, 2015 | | 25,964,886 | | $ | 3 | | $ | 210,386 | | $ | (101,488) | | $ | — | | $ | 108,901 | Issuance of common stock in connection with PIPE, net of expenses of $263 | | 12,600,230 | | | 1 | | | 109,735 | | | — | | | — | | | 109,736 | Issuance of common stock in connection with public offering, net of expenses of $5,413 | | 8,625,000 | | | 1 | | | 80,836 | | | — | | | — | | | 80,837 | Issuance of common stock under employee stock purchase plan | | 69,054 | | | — | | | 576 | | | — | | | — | | | 576 | Issuance of common stock for services | | 20,118 | | | — | | | 187 | | | — | | | — | | | 187 | Issuance of common stock upon exercise of options | | 25,134 | | | | | | 55 | | | | | | | | | 55 | Issuance of common stock upon vesting of restricted stock units | | 5,000 | | | — | | | — | | | — | | | — | | | — | Stock-based compensation | | — | | | — | | | 5,317 | | | — | | | — | | | 5,317 | Other comprehensive loss | | — | | | — | | | — | | | — | | | (71) | | | (71) | Net loss | | — | | | — | | | — | | | (112,387) | | | — | | | (112,387) | Balance as of December 31, 2016 | | 47,309,422 | | $ | 5 | | $ | 407,092 | | $ | (213,875) | | $ | (71) | | $ | 193,151 | Issuance of common stock under employee stock purchase plan | | 99,343 | | | — | | | 623 | | | — | | | — | | | 623 | Issuance of common stock for services | | 46,858 | | | — | | | 201 | | | — | | | — | | | 201 | Issuance of common stock upon exercise of options | | 35,759 | | | | | | 62 | | | | | | | | | 62 | Issuance of common stock upon vesting of restricted stock units | | 43,597 | | | — | | | — | | | — | | | — | | | — | Stock-based compensation | | — | | | — | | | 9,590 | | | — | | | — | | | 9,590 | Other comprehensive income | | — | | | — | | | — | | | — | | | 24 | | | 24 | Net loss | | — | | | — | | | — | | | (64,339) | | | — | | | (64,339) | Balance as of December 31, 2017 | | 47,534,979 | | $ | 5 | | $ | 417,568 | | $ | (278,214) | | $ | (47) | | $ | 139,312 |
See accompanying notes. ARDELYX, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS (in thousands) | | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | Operating activities | | | | | | | | | | Net loss | | $ | (64,339) | | $ | (112,387) | | $ | (29,621) | Adjustments to reconcile net loss to net cash used in operating activities: | | | | | | | | | | Depreciation expense | | | 2,639 | | | 1,295 | | | 829 | Amortization of deferred financing costs | | | 375 | | | 346 | | | 351 | Amortization of deferred compensation for services | | | 192 | | | 194 | | | 107 | Amortization of premium on investment securities | | | 11 | | | (86) | | | — | Stock-based compensation | | | 9,590 | | | 5,317 | | | 2,634 | Loss from disposal of fixed assets | | | — | | | — | | | 65 | Changes in operating assets and liabilities: | | | | | | | | | | Accounts receivable | | | (10,796) | | | — | | | 2,584 | Prepaid expenses and other assets | | | (2,148) | | | 1,562 | | | (4,083) | Accounts payable | | | (1,027) | | | 2,148 | | | (371) | Accrued compensation and benefits | | | 68 | | | 795 | | | 718 | Accrued and other liabilities | | | 245 | | | 8,282 | | | 2,000 | Deferred revenue | | | — | | | — | | | (47,053) | Net cash used in operating activities | | | (65,190) | | | (92,534) | | | (71,840) | Investing activities | | | | | | | | | | Proceeds from maturities of investments | | | 133,701 | | | 7,600 | | | — | Sales and redemptions of investments | | | 17,957 | | | — | | | — | Purchases of investments | | | (84,013) | | | (133,810) | | | — | Purchases of property and equipment | | | (2,355) | | | (4,866) | | | (3,454) | Net cash provided by (used in) investing activities | | | 65,290 | | | (131,076) | | | (3,454) | Financing activities | | | | | | | | | | Proceeds from issuance of common stock, net of issuance costs | | | — | | | 190,573 | | | 74,323 | Proceeds from issuance of common stock under stock plans | | | 685 | | | 631 | | | 659 | Other | | | — | | | — | | | 30 | Net cash provided by financing activities | | | 685 | | | 191,204 | | | 75,012 | Net increase (decrease) in cash and cash equivalents | | | 785 | | | (32,406) | | | (282) | Cash and cash equivalents at beginning of period | | | 74,598 | | | 107,004 | | | 107,286 | Cash and cash equivalents at end of period | | $ | 75,383 | | $ | 74,598 | | $ | 107,004 | Supplementary disclosure of cash flow information: | | | | | | | | | | Income taxes paid | | $ | 3 | | $ | — | | $ | 69 | Supplementary disclosure of non-cash financing information: | | | | | | | | | | Acquisition of property and equipment included in accounts payable and accrued liabilities | | $ | 55 | | $ | 730 | | $ | — | Services settled through the issuance of common stock | | $ | 201 | | $ | 187 | | $ | 194 |
See accompanying notes. ARDELYX, INC.
NOTES CONSOLIDATED TO FINANCIAL STATEMENTS 1. ORGANIZATION AND BASIS OF PRESENTATION Ardelyx, Inc. (the “Company”), or “the Company,” is a clinical-stagespecialized biopharmaceutical company focused on developing first-in-class, disruptive medicines for the discovery, developmenttreatment of renal diseases, which affect both the heart and commercializationthe kidneys. Tenapanor, a first-in-class inhibitor of innovative, minimally-systemic therapeutic drugs that work exclusively in the gastrointestinal, or GI, tract to treat GI and cardio-renal. The Company has developed a proprietary drug discovery and design platform enabling it, in a rapid and cost-efficient manner, to discover and design novel drug candidates. Utilizing its platform, the Company discovered and designed its lead product candidate, tenapanor, whichNHE3, is currently being evaluated in two pivotala second Phase 3 clinical studiestrial for the treatment of hyperphosphatemia in patients with constipation-predominant irritable bowel syndrome, or IBS-C. In a Phase 2b clinical study, tenapanor demonstrated the ability to lower elevated serum phosphorus levels in patients with end-stage renal disease, or ESRD.ESRD who are on dialysis. The Company has initiated an additional Phase 2b clinical trial to evaluate dosing regimensis also advancing a small molecule potassium secretagogue program, RDX013, for the potential treatment of hyperkalemia as well as tenapanor for the treatment of hyperphosphatemia,people with irritable bowel syndrome with constipation, or elevated serum phosphorus in ESRD patients. TheIBS-C, for which the Company is developing another drug candidate, RDX022, forpreparing to submit a New Drug Application (“NDA”) to the treatmentUnited States Food and Drug Administration (“FDA”) in the second half of hyperkalemia, or elevated serum potassium. The Company is pursuing a 505(b)(2) regulatory pathway for RDX022. The Company has additional drug candidates in earlier stages of research and development focused in GI and cardio-renal diseases including RDX009, a secretagogue of glucagon-like peptide-1, or GLP-1, and glucagon-like peptide-2, or GLP-2, and RDX013, a potassium secretagogue.2018. The Company was incorporated in Delaware on October 17, 2007, under the name Nteryx and changed its name to Ardelyx, Inc. in June 2008. The Company operates in only one business segment, which is the development of biopharmaceutical products.
Initial Public Offering
On June 18, 2014, the Company’s registration statement on Form S-1 (File No. 333-196090) relating to the initial public offering (the “IPO”) of its common stock was declared effective by the SEC, and the IPO closed on June 24, 2014. The Company sold 4,928,900 shares of its common stock, which included the exercise in full by the underwriters of the IPO of their option to purchase 642,900 additional shares of the Company’s common stock, and the Company received cash proceeds of $61.2 million from the IPO, net of $7.8 million underwriting discounts and commissions and expenses paid by the Company.
On June 24, 2014, prior to the closing of the IPO, all outstanding shares of convertible preferred stock converted into 11,517,222 shares of common stock with the related carrying value of $56.2 million being reclassified to common stock and additional paid-in capital. In addition, all convertible preferred stock warrants were net exercised and the related convertible preferred stock warrant liability was reclassified to additional paid-in capital.
On June 24, 2014, the Company’s Amended and Restated Certificate of Incorporation became effective and the number of shares of capital stock the Company is authorized to issue was increased to 305,000,000 shares, of which 300,000,000 shares may be common stock and 5,000,000 shares may be preferred stock. Both the common stock and preferred stock have a par value of $0.0001 per share. There are no shares of preferred stock outstanding at December 31, 2015 or 2014.
2. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES Basis of Presentation The Company’saccompanying consolidated financial statements have been prepared in accordance with U.S. generally accepted accounting principles (“U.S. GAAP”). Use of Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America (“U.S. GAAP”).
Principles of Consolidation The accompanying consolidated financial statements include the accounts of Ardelyx and its wholly-owned subsidiary, Ardelyx Cayman Islands, which was placed into voluntary liquidation in December 2017. Intercompany transactions and balances have been eliminated in consolidation. Use of Estimates The preparation of consolidated financial statements in conformity with U.S. GAAP requires management to make estimates and judgments that affect the amounts reported in the consolidated financial statements and accompanying notes. On an ongoing basis, management evaluates its estimates, including those related to recognition of revenue, recognition, clinical trial accruals, contract manufacturing accruals, fair value of assets and liabilities, income taxes and stock-based compensation. Management bases its estimates on historical experience and on various other market-specific and relevant assumptions that management believes to be reasonable under the circumstances. Actual results maycould differ from those estimates. Liquidity The Company has never been profitable on an annual basis and, as of December 31, 2017, the Company has an accumulated deficit of $278.2 million. The Company has incurred net losses of approximately $64.3 million, $112.4 million and $29.6 million in the years ended December 31, 2017, 2016 and 2015, respectively. The Company expects to continue to incur net operating losses for the foreseeable future, as the Company continues the development of, seeks regulatory approval for, and if approved, begins to commercialize and manufacture tenapanor, either directly by the Company or through one or more of its collaboration partners. The Company will need additional funding to support its future operating activities and adequate funding may not be available to the Company on acceptable terms, or at all. The Company’s failure to obtain sufficient funds on acceptable terms when needed could have a material adverse effect on the business, results of operations, and financial condition. The Company will need to generate significant revenues to achieve profitability and may never do so. Cash and Cash Equivalents The Company considers all highly liquid investments purchased with an original maturity date of 90 days or less on the date of purchase to be cash equivalents. The Company invests its cash in bank deposits and money market funds. Cash overdraftsShort-Term Investments
An overdraft totaling $1.5 million wasShort-term investments consist of debt securities classified as accounts payableavailable-for-sale and have maturities greater than 90 days, but less than one year, from the date of acquisition. Short-term investments are carried at December 31, 2015.fair value based upon quoted market prices. Unrealized gains and losses on available-for-sale securities are excluded from earnings and are reported as a component of accumulated other comprehensive loss. The Company’s policycost of available-for-sale securities sold is to reportbased on the change in overdrafts as an operating activity in the Statements of Cash Flows.specific-identification method.
Restricted Cash
The Company is required to guarantee the credit limit on its corporate credit card with a certificate of deposit of $0.1 million. The collateral will be released upon the cancellation of the corporate credit card.
Concentration of Credit Risk Financial instruments that potentially subject the Company to significant concentrations of credit risk consist primarily of cash, and cash equivalents. Cash and cash equivalents, short-term investments and accounts receivable. The Company is exposed to credit risks in the event of default by the counterparties to the extent of the amount recorded in its consolidated balance sheet. Cash, cash equivalents and short-term investments are invested through banks and other financial institutions in the United States. Such deposits may Accounts Receivable An allowance for doubtful accounts will be in excessrecorded based on a combination of insured limits. The Company maintains cashhistorical experience, aging analysis, and cash equivalentsinformation on specific accounts. Account balances will be written off against the allowance after all means of collection have been exhausted and investments with various high credit quality and capitalized financial institutions.the potential for recovery is considered remote. No provision was made for doubtful accounts as of December 31, 2017 or 2016. Property and Equipment Property and equipment are stated at cost, less accumulated depreciation and amortization. Depreciation is computed using the straight-line method over the estimated useful lives of the respective assets, generally three to five years. Leasehold improvements are amortized over the lesser of the estimated useful lives or the related remaining lease term. Impairment of Long-Lived Assets The carrying value of long-lived assets, including property and equipment, are reviewed for impairment whenever events or changes in circumstances indicate that the asset may not be recoverable. An impairment loss is recognized when the total of estimated future undiscounted cash flows, expected to result from the use of the asset and its eventual disposition, are less than its carrying amount. Impairment, if any, would be assessed using discounted cash flows or other appropriate measures of fair value. Through December 31, 2015,2017, there have been no such impairment losses. Income Taxes The Company uses the asset and liability method of accounting for income taxes. Under this method, deferred tax assets and liabilities are determined based on the differences between the financial reporting and the tax bases of assets and liabilities and are measured using the enacted tax rates and laws that will be in effect when the differences are expected to reverse. A valuation allowance is provided when it is more likely than not that some portion or all of a deferred tax asset will not be realized.
Revenue Recognition Revenue from research activities made under collaboration partnership agreements areis recognized as the services are provided and when there is persuasive evidence that an arrangement exists, delivery has occurred, the price is fixed or determinable, and collectability is reasonably assured. Revenue generated from research and licensing agreements typically includes up-front signing or license fees, cost reimbursements, research services, minimum sublicense fees, milestone payments, and royalties on future licensees’ product sales. For revenue agreements with multiple-element arrangements, such as license and development agreements, the Company allocates revenue to each unit of accounting based on the relative selling price of each unit. When applying the relative selling price method, the Company determines the selling price for each deliverable using vendor-specific objective evidence or third-party evidence. If neither exists, the Company uses its best estimate of selling price for that deliverable. Revenue allocated is then recognized when the four basic revenue recognition criteria are met for each deliverable. The Company recognizes revenue from upfront payments under license agreements on contract execution if the license payment is a separate unit of accounting and the Company has no continuing performance obligations under the license, as is the case with the Company’s license agreements with KHK and Fosun Pharma. If the license is not a separate unit of accounting, the Company recognizes revenue from upfront payments ratably over the term of its estimated period of performance under the agreement which is recorded as licensing revenue. Reimbursements for development costs incurred under the Company’s license agreementcontract with AstraZeneca, areuntil it was terminated, were classified as collaborative development revenue. The Company recognizes cost reimbursement revenue under collaboration partnership agreements as the related research and development costs for services are rendered. Deferred revenue represents the portion of research or license payments received which has not been earned. Revenues from milestones, if they are nonrefundable and deemed substantive, are recognized upon successful accomplishment of the milestones. To the extent that non-substantive milestones are achieved and the Company has remaining performance obligations, milestones are deferred and recognized as revenue over the estimated remaining period of performance. The Company will recognize revenue associated with the non-substantive milestones upon achievement of the milestone if there are no undelivered units and it has no remaining performance obligations. The Company will account for sales-based milestones as royalties that will be recognized as revenue upon achievement of the milestone. Revenue subject to governmental withholding taxes is recognized on a gross basis with the withholding taxes recorded as a component of income tax expense. Research and Development Costs Research and development costs are charged to expense as incurred and consist of costs incurred to further the Company’s research and development activities including salaries and related employee benefits, costs associated with clinical trials, costs related to pre-commercialization manufacturing activities such as manufacturing process validation activities and the manufacturing of clinical drug supply, nonclinical research and development activities, regulatory activities, research-related overhead expenses and fees paid to external service providers and contract research and manufacturing organizations that conduct certain research and development activities on behalf of the Company. Accrued Research and Development Expenses As part of the process of preparing our financial statements, the Company is required to estimate its accrued expenses. This process involves reviewing open contracts and purchase orders, communicating with its personnel to identify services that have been performed on its behalf and estimating the level of service performed and the associated cost incurred for the service when the Company has not yet been invoiced or otherwise notified of the actual cost. The majority of the Company’s service providers invoice the Company monthly in arrears for services performed or when contractual milestones are met. The Company makes estimates of its accrued expenses as of each balance sheet date in its financial statements based on facts and circumstances known to the Company at that time. The Company periodically confirms the accuracy of its estimates with the service providers and make adjustments if necessary. Examples of estimated accrued research and development expenses include fees paid to: | · | | contract research organizations (“CROs”) in connection with clinical studies; |
| · | | investigative sites in connection with clinical studies; |
| · | | vendors related to product manufacturing, development and distribution of clinical supplies; and |
| · | | vendors in connection with preclinical development activities. |
The Company records expenses related to clinical studies and manufacturing development activities based on its estimates of the services received and efforts expended pursuant to contracts with multiple CROs and manufacturing vendors that conduct and manage these activities on its behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract, and may result in uneven payment flows. There may be instances in which payments made to the Company’s vendors will exceed the level of services provided and result in a prepayment of the expense. Payments under some of these contracts depend on factors such as the successful enrollment of subjects and the completion of clinical trial milestones. In accruing service fees, the Company estimates the time period over which services will be performed, enrollment of subjects, number of sites activated and the level of effort to be expended in each period. If the actual timing of the performance of services or the level of effort varies from the Company’s estimate, the Company will adjust the accrued or prepaid expense balance accordingly. To date, there have been no material differences from the Company’s estimates to the amounts actually incurred. Stock-Based Compensation The Company measures itsrecognizes compensation expense for all stock-based payment awards made to employees and directors based on the estimated fair valuesvalues. For employee stock options, the Company determines the grant date fair value of the awards using the Black-Scholes option-pricing model and generally recognizes the fair value as stock-based compensation expense on a straight-line basis over the vesting period of the respective awards. For restricted stock, the compensation cost for these awards is based on the closing price of the Company’s common stock on the date of grant and recognized as compensation expense on a straight-line basis over the requisite service period. The Company has selected the Black-Scholes option-pricing model to estimate the fair value of its stock-based awards. Stock-based compensation expense is recognized using the straight-line method. Stock-based compensation expense is based on the value of the portion of stock-based payment awards that is ultimately expected to vest. As such, the Company’s stock-based compensation is reduced for the estimated forfeitures at the date of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. The Company accounts for compensation expense relatedequity instruments issued to stocknonemployees based on their fair values on the measurement dates using the Black-Scholes option-pricing model. The estimated fair values of the options granted to non-employees based onnonemployees are remeasured as they vest. As a result, the noncash charge to operations for nonemployee options with vesting conditions is affected each reporting period by changes in the fair values estimated using the Black-Scholes model. Stock options granted to non-employees are remeasured at each reporting date until the award is vested. Research and Development Costs
Research and development expenditures are expensed as incurred. Major components of research and development expenses consist of personnel costs, materials and supplies, and allocations of facilities-related costs, as well as fees paid to consultants and third parties that conduct certain research and development activities
on the Company’s behalf. Payments made to other entities are under agreements that are generally cancelable by the Company. Nonrefundable advance payments for goods or services to be rendered in the future for use in research and development activities are deferred and capitalized. The capitalized amounts are expensed as the related goods are delivered or the services are performed.
Convertible Preferred Stock Warrant Liability
The Company accounted for freestanding warrants to purchase shares of convertible preferred stock that were contingently redeemable as liabilities in the balance sheets at their estimated fair value. Convertible preferred stock warrants were subject to remeasurement at each balance sheet date, and any change in fair value was recognized as a component of other expense, net in the statements of operations and comprehensive loss. The Company continued to adjust the carrying value of the warrants until the closing of the IPO, at which time the warrants were net exercised for shares of the Company’s common stock and the liability was reclassified to stockholders’ equity (deficit).stock.
Comprehensive Loss Comprehensive loss is composed of two components: net loss and other comprehensive loss.income (loss). Other comprehensive income (loss) refers to gains and losses that under U.S. GAAP are recorded as an element of stockholders’ equity, (deficit), but are excluded from net loss. The Company did not record any transactions within other comprehensive income (loss) in the periods presented and, therefore, the net loss and comprehensive loss were the same for all periods presented. Net Loss per Share Basic net loss per common share is calculated by dividing the net loss by the weighted-average number of common shares outstanding during the period, without consideration of potential common stock equivalents.shares. Diluted net loss per common share in the periods presented is the same as basic net loss per common share, since the effects of potentially dilutive securities are antidilutive.antidilutive due to the net loss for all periods presented.
Recent Accounting Pronouncements In May 2014, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2014-09,2014‑09, Revenue from Contracts with Customers (“ASU 2014-09”2014‑09”). This standard outlines a single comprehensive model for entities to use in accounting for revenue arising from contracts with customers and supersedes most current revenue recognition guidance, including industry-specific guidance. The main principle of ASU 2014-09 is, which requires an entity to recognize revenues whenthe amount of revenue to which it expects to be entitled for the transfer of promised goods or services are transferred to customerscustomers. ASU 2014‑09 will replace most existing revenue recognition guidance in an amount that reflectsU.S. GAAP when it becomes effective. In July 2015, the consideration that is expectedFASB voted to be receivedapprove a deferral of the effective date of this ASU by one year, and to permit entities to adopt up to one year earlier if they choose. Therefore, the new standard becomes effective for those goodsthe Company on January 1, 2018, with early application permitted for periods beginning on or services. ASU 2014-09 provides companies withafter January 1, 2017. The standard permits the use of two implementation methods: (i) apply the standardtransition methods on adoption, either retrospectively to each prior reporting period presented (full retrospective application);method), or (ii) apply the standard retrospectively with the cumulative effect of initially applying the standard as an adjustment to the opening balance of retained earnings of the annual reporting period that includes the date of initial application (modified retrospective application)method). This guidance is effective for annual reporting periods beginning after December 15, 2017,Since the issuance of ASU 2014‑09, the FASB has issued several amendments which clarify certain points in the new Topic 606 - Revenue from Contracts with Customers, including interim periods within that reporting period.ASU 2016‑08 (“Principal versus Agent Considerations—Reporting Revenue Gross versus Net”), ASU 2016‑10 (“Identifying Performance Obligations and Licensing”), ASU 2016‑11 (“Rescission of SEC Guidance Because of Accounting Standards Updates 2014‑09 and 2014‑16 Pursuant to Staff Announcements at the March 3, 2016 EITF Meeting”) and ASU 2016‑12 (“Narrow-Scope Improvements and Practical Expedients”). The Company has not yet selected an implementation date or a transitionplans to adopt all these standards using the modified retrospective method nor has it determinedon January 1, 2018, and will modify its accounting policies to reflect the effectrequirements of the standard on its ongoing financial reporting. In August 2014, the FASB issued ASU No. 2014-15,Presentation of Financial Statements—Going Concern: Disclosure of Uncertainties about an Entity’s Ability to Continue as a Going Concern (“ASU 2014-15”). ASU 2014-15 is intended to define management’s responsibility to evaluate whether there is substantial doubt about an organization’s ability to continue as a going concern and to provide related footnote disclosures, if required. ASU 2014-15 is effective for annual reporting periods ending after December 15, 2016, and applies to annual and interim periods thereafter.these standards. The Company is evaluatingexpects to record an increase in current assets of $5.0 million related to the impact thatfirst milestone under the adoption of ASU 2014-15 will have on its financial statements and related disclosures.
In November 2015, the FASB issued ASU No. 2015-17,Income Taxes (Topic 740): Balance Sheet Classification of Deferred TaxesCompany’s license with Kyowa Hakko Kirin Co., Ltd. (“KHK”), which eliminates the Company believes is not materially at risk, an increase in current requirementliabilities of $1.0 million related to present deferred tax assets and liabilities as current and noncurrentthe corresponding payment to AstraZeneca AB (“AstraZeneca”), in a classified balance sheet. Instead, entities will be required to classify all deferred tax assets and liabilities as noncurrent. The Company early adopted this accounting standard update, on a prospective basis as of December 31, 2015. All deferred tax assets and liabilities, as of December 31, 2015, have been classified as noncurrent in the accompanying Balance Sheets and the notes thereto. The adoption had no material impact onaccordance with the Company’s balance sheet. No prior periods were retrospectively adjusted.termination agreement and a related decrease in its accumulated deficit of approximately $4.0 million when it adopts the new standards on January 1, 2018, as Topic 606 permits revenue from certain milestones to be recognized earlier than Topic 605, the U.S. GAAP that is being superseded.
In February 2016, the FASB issued ASU No. 2016-02,2016‑02, Leases (Topic 842). Under, which replaces most current lease guidance when it becomes effective. This standard update intends to increase the transparency and improve comparability by requiring entities to recognize assets and liabilities on the balance sheet for all leases, with certain exceptions. The new guidance, lesseesstandard states that a lessee will be required to recognize a lease liability for the obligation to make lease payments and a right-of-use asset for all leases (withthe right to use the underlying asset for the lease term. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the consolidated statements of operations. The new guidance will be effective for the Company starting in the first quarter of fiscal 2019. Early adoption is permitted. The Company plans to adopt the new guidance effective January 1, 2019, and is currently evaluating the effect that this guidance will have on its consolidated financial statements and related disclosures. In October 2016, the FASB issued ASU No. 2016‑16, Income Taxes: Intra-Entity Transfers of Assets Other Than Inventory (ASU 2016‑16). This update is to improve the accounting for the income tax consequences of intra-entity transfers of assets other than inventory. ASU 2016‑16 amends the guidance to recognize the income tax consequences of an intra-entity transfer of an asset other than inventory when the transfer occurs. Consequently, the amendments in this update eliminate the exception for an intra-entity transfer of short-term leases) atan asset other than inventory. The amendments in this update do not include new disclosure requirements; however, existing disclosure requirements might be applicable when accounting for the commencement date. Lessor accounting undercurrent and deferred income taxes for an intra-entity transfer of an asset other than inventory. ASU 2016-02 is largely unchanged. ASU 2016-022016‑16 is effective for the Company’s interim and annual reporting periods during the year ending December 31, 2018, and all annual and interim reporting periods beginningthereafter. Early adoption is permitted. The adoption of ASU 2016‑16 is not expected to have a material effect on the Company’s consolidated financial statements. In May 2017, FASB issued ASU No. 2017‑09, Compensation-Stock Compensation (Topic 718) - Scope of Modification Accounting (ASU 2017‑09). The amendments included in this update provide guidance about which changes to the terms or conditions of a share-based payment award require an entity to apply modification accounting. The amendments in this update will be applied prospectively to an award modified on or after the adoption date. The amendments in ASU 2017‑09 are effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2018 and early2017. The adoption of this standard is permitted. Under ASU 2016-02, lessees (for capital and operating leases) and lessors (for sales-type, direct financing, and operating leases) must applynot expected to have a modified retrospective transition approach for leases existing at, or entered into after,material impact on the beginning of the earliest comparative period presented in theCompany’s consolidated financial statements. Lessees and lessors may not apply a full retrospective transition approach. The Company has not yet selected an implementation date nor has it determined the effect The Company has reviewed all other significant newly-issued accounting pronouncements and concluded that they either are not applicable to the Company’s operations or that no material effect is expected on its consolidated financial statements as a result of future adoption. 3. CASH, CASH EQUIVALENTS AND INVESTMENTS Securities classified as cash, cash equivalents and short-term investments as of December 31, 2017 and December 31, 2016 are summarized below (in thousands). Estimated fair value is based on quoted market prices for these investments. | | | | | | | | | | | | | | | December 31, 2017 | | | Amortized | | Gross Unrealized | | | | | | Cost | | Gains | | Losses | | Fair Value | Cash and cash equivalents: | | | | | | | | | | | | | Cash | | $ | 5,882 | | $ | — | | $ | — | | $ | 5,882 | Money market funds | | | 68,651 | | | — | | | — | | | 68,651 | Commercial paper | | | 850 | | | — | | | — | | | 850 | Total cash and cash equivalents | | | 75,383 | | | — | | | — | | | 75,383 | Short-term investments | | | | | | | | | | | | | U.S. treasury securities | | | 3,994 | | | — | | | (1) | | | 3,993 | Corporate bonds | | | 26,853 | | | — | | | (26) | | | 26,827 | Commercial paper | | | 19,584 | | | — | | | (14) | | | 19,570 | Asset-backed securities | | | 8,209 | | | — | | | (6) | | | 8,203 | Total short-term investments | | | 58,640 | | | — | | | (47) | | | 58,593 | Total cash equivalents and investments | | $ | 134,023 | | $ | — | | $ | (47) | | $ | 133,976 |
| | | | | | | | | | | | | | | December 31, 2016 | | | Amortized | | Gross Unrealized | | | | | | Cost | | Gains | | Losses | | Fair Value | Cash and cash equivalents: | | | | | | | | | | | | | Cash | | $ | 3,638 | | $ | — | | $ | — | | $ | 3,638 | Money market funds | | | 68,561 | | | — | | | — | | | 68,561 | Commercial paper | | | 2,399 | | | — | | | — | | | 2,399 | Total cash and cash equivalents | | | 74,598 | | | — | | | — | | | 74,598 | Short-term investments | | | | | | | | | | | | | Corporate bonds | | | 58,464 | | | 2 | | | (56) | | | 58,410 | Commercial paper | | | 62,946 | | | 5 | | | (20) | | | 62,931 | Asset-backed securities | | | 4,886 | | | — | | | (2) | | | 4,884 | Total short-term investments | | | 126,296 | | | 7 | | | (78) | | | 126,225 | Total cash equivalents and investments | | $ | 200,894 | | $ | 7 | | $ | (78) | | $ | 200,823 |
Cash equivalents consist of money market funds and other debt securities with original maturities of three months or less at the time of purchase, and the carrying amount is a reasonable approximation of fair value. The Company invests its cash in high quality securities of financial and commercial institutions. These securities are carried at fair value, which is based on readily available market information, with unrealized gains and losses included in “accumulated other comprehensive income (loss)” within stockholders’ equity on the Company’s consolidated balance sheets. The Company uses the specific identification method to determine the amount of realized gains or losses on sales of marketable securities. Realized gains or losses to date have been insignificant and are included in “other income, net” in the consolidated statements of operations. All available-for-sale securities held as of December 31, 2017 and 2016, had contractual maturities of less than one year. The Company’s available-for-sale securities are subject to a periodic impairment review. The Company considers a debt security to be impaired when its fair value is less than its carrying cost, in which case the Company would further review the investment to determine whether it is other-than-temporarily impaired. When the Company evaluates an investment for other-than-temporary impairment, the Company reviews factors such as the length of time and extent to which fair value has been below cost basis, the financial condition of the issuer and any changes thereto, intent to sell, and whether it is more likely than not the Company will be required to sell the investment before the recovery of its cost basis. If an investment is other-than-temporarily impaired, the Company writes it down through the statement of operations to its fair value and establishes that value as a new cost basis for the investment. The Company did not identify any of its available-for-sale securities as other-than-temporarily impaired in any of the periods presented. As of December 31, 2017 and 2016, no investment was in a continuous unrealized loss position for more than one year, the unrealized losses were not due to a change in credit risk, and the Company believes that is more likely than not the investments will be held until maturity or a forecasted recovery of fair value. 4. FAIR VALUE MEASUREMENTS Fair value is defined as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. Valuation techniques used to measure fair value must maximize the use of observable inputs and minimize the use of unobservable inputs. The three-level hierarchy for the inputs to valuation techniques is briefly summarized as follows: Level 1 – Valuations are based on quoted prices in active markets for identical assets or liabilities. Examples of assets and liabilities utilizing Level 1 inputs are certain money market funds, U.S. Treasuries and trading securities with quoted prices on active markets. | | | | | Level 1
Level 2 – Valuations based on inputs other than the quoted prices in active markets that are observable, either directly or indirectly, such as quoted prices for similar assets or liabilities; quoted prices in markets that are not active; or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities. Examples of assets and liabilities utilizing Level 2 inputs are corporate bonds, commercial paper, certificates of deposit and over-the-counter derivatives. Level 3 – Valuations based on unobservable inputs in which there is little or no market data, which require the Company to develop its own assumptions. | | – | | Valuations are based on quoted prices in active markets for identical assets or liabilities and readily accessible by us at the reporting date. Examples of assets and liabilities utilizing Level 1 inputs are certain money market funds, U.S. Treasuries and trading securities with quoted prices on active markets. | | | | Level 2
| | – | | Valuations based on inputs other than the quoted prices in active markets that are observable either directly or indirectly in active markets. Examples of assets and liabilities utilizing Level 2 inputs are U.S. government agency bonds, corporate bonds, commercial paper, certificates of deposit and over-the-counter derivatives. | | | | Level 3
| | – | | Valuations based on unobservable inputs in which there is little or no market data, which require us to develop our own assumptions. |
The following table sets forth the fair value of the Company’s financial assets and liabilities measured on a recurring basis by level within the fair value hierarchy: | | | | | | | | | | | | | | | December 31, 2017 | | | Total | | Level 1 | | Level 2 | | Level 3 | Assets: | | | | | | | | | | | | | Money market funds | | $ | 68,651 | | $ | 68,651 | | $ | — | | $ | — | U.S. treasury securities | | | 3,993 | | | 3,993 | | | — | | | — | Corporate bonds | | | 26,827 | | | — | | | 26,827 | | | — | Commercial paper | | | 20,420 | | | — | | | 20,420 | | | — | Asset-backed securities | | | 8,203 | | | — | | | 8,203 | | | — | Total | | $ | 128,094 | | $ | 72,644 | | $ | 55,450 | | $ | — |
| | | | | | | | | | | | | | | | | | | | December 31, 2015 | | | | | Total | | | Level 1 | | | Level 2 | | | Level 3 | | | | | (in thousands) | | Assets: | | | | | | | | | | | | | | | | | Money market funds | | $ | 105,819 | | | $ | 105,819 | | | $ | — | | | $ | — | | Certificates of deposit | | | 100 | | | | — | | | | 100 | | | | — | | | | | | | | | | | | | | | | | | | Total | | $ | 105,919 | | | $ | 105,819 | | | $ | 100 | | | $ | — | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | December 31, 2014 | | | | | Total | | | Level 1 | | | Level 2 | | | Level 3 | | | | | (in thousands) | | Assets: | | | | | | | | | | | | | | | | | Money market funds | | $ | 105,410 | | | $ | 105,410 | | | $ | — | | | $ | — | | Certificates of deposit | | | 100 | | | | — | | | | 100 | | | | — | | | | | | | | | | | | | | | | | | | Total | | $ | 105,510 | | | $ | 105,410 | | | $ | 100 | | | $ | — | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | December 31, 2016 | | | Total | | Level 1 | | Level 2 | | Level 3 | Assets: | | | | | | | | | | | | | Money market funds | | $ | 68,561 | | $ | 68,561 | | $ | — | | $ | — | Corporate bonds | | | 58,410 | | | — | | | 58,410 | | | — | Commercial paper | | | 65,330 | | | — | | | 65,330 | | | — | Asset-backed securities | | | 4,884 | | | — | | | 4,884 | | | — | Total | | $ | 197,185 | | $ | 68,561 | | $ | 128,624 | | $ | — |
Where quoted prices are available in an active market, securities are classified as Level 1. The Company classifies money market funds, U.S. treasury securities and U.S. government-sponsored agency bonds as Level 1. When quoted market prices are not available for the specific security, then the Company estimates fair value by using benchmark yields, reported trades, broker/dealer quotes and issuer spreads. The Company classifies certificates of depositcorporate bonds, commercial paper and asset-backed securities as Level 2. In certain cases, where there is limited activity or less transparency around inputs to valuation, securities are classified as Level 3. There were no transfers between Level 1 and Level 2 during the periods presented. The carrying amounts reflected in the balance sheets for cash equivalents, short-term investments, accounts receivable, prepaid expenses and other current assets, accounts payable and accrued expenses approximate their fair values at both December 31, 20152017 and December 31, 2014,2016, due to their short-term nature. 4.5. PROPERTY AND EQUIPMENT
Property and equipment consist of the following: | | | | | | | | | December 31, | | | 2017 | | 2016 | | | (in thousands) | Laboratory equipment | | $ | 6,857 | | $ | 5,487 | Office equipment and furniture | | | 815 | | | 824 | Leasehold improvements | | | 7,949 | | | 7,783 | Property and equipment, gross | | | 15,621 | | | 14,094 | Less: accumulated depreciation | | | (7,589) | | | (5,103) | Total property and equipment, net | | $ | 8,032 | | $ | 8,991 |
| | | | | | | | | | | | December 31, | | | | | 2015 | | | 2014 | | | | | (in thousands) | | Laboratory equipment | | $ | 4,471 | | | $ | 3,039 | | Office equipment and furniture | | | 134 | | | | 229 | | Construction in progress | | | — | | | | 362 | | Leasehold improvements | | | 3,914 | | | | 2,135 | | | | | | | | | | | Property and equipment, gross | | | 8,519 | | | | 5,765 | | Less: accumulated depreciation | | | (3,808 | ) | | | (3,634 | ) | | | | | | | | | | Total property and equipment, net | | $ | 4,711 | | | $ | 2,131 | | | | | | | | | | |
Depreciation and amortization expense totaled $0.8$2.6 million, $0.3$1.3 million and $0.6$0.8 million for the years ended December 31, 2017, 2016 and 2015, 2014respectively. 6. ACCRUED AND OTHER LIABILITIES Accrued and 2013.other liabilities consist of the following (in thousands): | | | | | | | | | December 31, | | | 2017 | | 2016 | Accrued clinical and non-clinical expenses | | $ | 5,447 | | $ | 6,694 | Accrued contract manufacturing | | | 3,980 | | | 2,705 | Accrued professional and consulting services | | | 530 | | | 322 | Other | | | 752 | | | 684 | | | $ | 10,709 | | $ | 10,405 |
5.
7. COLLABORATION AND LICENSING AGREEMENTS KHK In November 2017, the Company entered into an exclusive license agreement with KHK (the “KHK Agreement”) for the development, commercialization and distribution of tenapanor in Japan. Under the terms of the KHK Agreement, the Company received an aggregate of $30.0 million in up-front license fees which was recognized as revenue when the agreement was executed. In addition, the Company may be entitled to receive up to $130 million in additional development and commercialization milestones based upon currency exchange rates as of the effective date of license agreement, as well as reimbursement of cost plus a reasonable overhead for the supply of product and high-teen royalties on net sales throughout the term of the agreement. Shanghai Fosun Pharmaceutical Industrial Development Co. Ltd. (“Fosun Pharma”) In December 2017, the Company entered into an exclusive license agreement with Fosun Pharma (the “Fosun Agreement”) for the development, commercialization and distribution of tenapanor in China. Under the terms of the Fosun Agreement, the Company will receive an aggregate of $12.0 million in up-front license fees which was recognized as revenue when the agreement was executed. In addition, the Company may be entitled to additional milestones of up to $113 million, as well as reimbursement of cost plus a reasonable overhead for the supply of product and tiered royalties on net sales ranging from the mid-teens to 20%. AstraZeneca AB (“AstraZeneca”) In October 2012, the Company entered into a collaboration partnership with AstraZeneca for the worldwide development and commercialization of tenapanor. Under the terms of the AstraZeneca collaboration partnership agreement, or the AstraZeneca Agreement, the Company received an aggregate of $75 million in up-front license fee of $35.0 million in October 2012, a $15.0 million payment in December 2013 and a $25.0 million payment in May 2014.milestone fees. The amounts were recorded as deferred revenue when received and were recognized as revenue on a straight-line basis over the remaining estimated period of performance under the AstraZeneca Agreement, which during the three months ended March 31, 2015, the Company estimated to extend to December 2017.Agreement. In June 2015, the Company entered into a termination agreement with AstraZeneca (the “Termination Agreement”) pursuant to which all licenses granted to AstraZeneca to the Company’s portfolio of NHE3 inhibitors, including the Company’s lead product candidate, tenapanor, were terminated, except for the limited purpose of allowing AstraZeneca to satisfy its obligations under the Termination Agreement. Under the terms of the Termination Agreement, the Company agreed to pay AstraZeneca certain amounts for the return of the licenses granted to it, including (a) an upfront fee of $15.0 million, (b) future royalties at a royalty rate of 10% of net sales of tenapanor or other NHE3 products by the Company or its licensees, and (c) 20% of non-royalty revenue received from a new collaboration partner should the Company elect to license, or otherwise provide rights to develop and commercialize tenapanor, or another NHE3 inhibitor. The amounts payable by the Company as described in (a)-(c) are capped at the aggregate amount of $90.0 million. The Company also paid AstraZeneca $10.0 million as reimbursement for certain research and development expenses incurred by AstraZeneca under the collaboration agreement during 2015 and in consideration of the acceleration of the transfer of information and materials to the Company. In addition, AstraZeneca was obligated to supply the Company with clinical trial materials, drug substance and drug product. The maximum amount that the Company was obligated to pay for such materials was set at $10 million in the Termination Agreement, which maximum amount was subsequently reduced to $8.0 million pursuant to an amendment to the Termination Agreement (“Amendment Number One”). As the AstraZeneca Agreement was terminated in June 2015, the Company recognized the remaining deferred revenue balance of $43.1 million during the three months ended June 30, 2015. Also inIn the three months ended June 30, 2015, the Company recorded thea $15.0 million upfront payment for the return of the licenses as well as thea $10.0 million payment for reimbursement of research and development expenses and the acceleration of the transfer of information and materials as a reduction in licensing revenue. revenue in the consolidated statements of operations. There has been no recognition of licensing revenue or collaborative development revenue since the termination of the AstraZeneca Agreement in 2015. The Company recorded $7.3remains liable to pay AstraZeneca license fees for (i) future royalties at a royalty rate of 10% of net sales of tenapanor or other NHE3 products by us or our licensees, and (ii) 20% of non-royalty revenue received from a new collaboration partner should we elect to license, or otherwise provide rights to develop and commercialize tenapanor or another NHE3 inhibitor, up to a maximum of $75.0 million in expenses incurredaggregate for (i) and (ii). We recognized $8.4 million, being 20% of the tenapanor clinical trial material from AstraZeneca duringcombined license revenue recognized under the KHK Agreement and Fosun Agreement, as cost of revenue in the year ended December 31, 2015.2017. Sanofi SA (“Sanofi”)
In February 2014, the Company entered into a license option and license agreement with Sanofi (the“Sanofi Agreement”) for its phosphate transport NaP2b inhibitor program. Under the terms
The Sanofi Agreement was terminated effective September 30, 2015 and all rights were returned to the Company. There was no payment associated with termination and the return of rights to the Company.
6. CONVERTIBLE PREFERRED STOCK
On June 24, 2014, prior to the closing of the IPO, all outstanding shares of convertible preferred stock converted into 11,517,222 shares of common stock with the related carrying value of $56.2 million reclassified to common stock and additional paid-in capital.
7. PREFERRED STOCK WARRANTS
In connection with the closing of the Series B financing in August 2011, the Company issued warrants for the purchase of 574,953 shares of Series B convertible preferred stock. The exercise price of the warrants was $0.09 per share. The preferred stock warrant liability was measured at fair value on a recurring basis. Changes in fair value were recorded in change in fair value of preferred stock warrant liability in the Statements of Operations and Comprehensive Loss. As of December 31, 2013 and for the period in 2014 up to the IPO date, the Company revalued the warrants using a hybrid of the option pricing method and the probability-weighted expected return method. The hybrid methodology was applied to reflect two exit scenarios, IPO and merger using a market approach and the income approach was used in the stay private scenario. The scenarios were weighted
based on the Company’s estimate of the probability of each scenario: 20% for IPO; 10% for merger and 70% for stay private for the year ended December 31, 2013. As of December 31, 2013, the fair value of this convertible preferred stock warrant liability amounted to $6.5 million. Just prior to the IPO close date of June 24, 2014, the preferred stock warrant liability was remeasured prior to the net exercise of the warrants using the IPO price.
8. EQUITY INCENTIVE PLANS 2008 Plan The Company granted options under its 2008 Stock Incentive Plan (the “2008 Plan”) until June 2014 when it was terminated as to future awards, although it continues to govern the terms of options that remain outstanding under the 2008 Plan. The 2008 Plan provided for the granting of incentive and nonstatutorynon-qualified stock options, and stock purchase rights to employees, directors and consultants at the discretion of the Board of Directors. Stock options granted generally vest over a period of four years from the date of grant. In connection with the Board of Directors and stockholdersstockholders’ approval of the 2014 Plan, all remaining shares available for future award under the 2008 Plan were transferred to 2014 Plan, and the 2008 Plan was terminated. 2014 Plan The 2014 Equity Incentive Award Plan (“2014(the “2014 Plan”) became effective on June 18, 2014, immediately prior to the time the Company’s Registration Statement on Form S-1 became effective.2014. Under the 2014 Plan, 1,419,328 shares of common stock were initially reserved for issuance pursuant to a variety of stock-based compensation awards, including stock options, stock appreciation rights, or SARs, restricted stock awards, service-based restricted stock unit (“RSU”) awards, performance-based restricted stock unit (“PRSU”) awards, deferred stock awards, deferred stock unit awards, dividend equivalent awards, stock payment awards and performance awards. In addition, 35,221 shares that had been available for future awards under the 2008 Plan as of June 18, 2014, were added to the initial reserve available under the 2014 Plan, bringing the total reserve upon the effective date of the 2014 Plan to 1,454,549. The number of shares initially reserved for issuance or transfer pursuant to awards under the 2014 Plan will be increased by (i) the number of shares represented by awards outstanding under 2008 Plan on June 18, 2014, that are either forfeited or lapse unexercised or that are repurchased for the original purchase price thereof, up to a maximum of 1,153,279 shares, and (ii) if approved by the Administrator of the 2014 Plan, an annual increase on the first day of each fiscal year ending in 2024 equal to the lesser of (A) four percent (4.0%) of the shares of stock outstanding (on an as converted basis) on the last day of the immediately preceding fiscal year and (B) such smaller number of shares of stock as determined by our board of directors; provided, however, that no more than 10,683,053 shares of stock may be issued upon the exercise of incentive stock options. Effective January 1, 2016,2018, the 2014 Plan share reserve was increased by 1,038, 5951,901,399 shares. 2016 Plan In November 2016, the Company’s board of directors approved the 2016 Employment Commencement Incentive Plan (the “Inducement Plan”) under which 1,000,000 shares were reserved. As of December 31, 2017, no shares of the Company’s common stock were subject to inducement grants that were issued pursuant to the Inducement Plan.
Stock Plan Activity The following table summarizes activity under the 2008 Plan and the 2014 Plan, including grants issued to nonemployees, and restricted stock issued:in the three years ended December 31, 2017: | | | | | | | | | | | | | | | | | Options Issued and Outstanding | | Weighted | | | | | | | | | | Weighted-Average | | Average | | | | | | Shares Available | | | | Exercise Price per | | Remaining | | Aggregate | | | for Grant | | Number of Shares | | Share | | Contractual Term | | Intrinsic Value | | | | | | | | | | (in Years) | | (in thousands) | Balance at December 31, 2014 | | 1,265,282 | | 1,007,724 | | $ | 5.51 | | | | | | Options authorized | | 743,569 | | — | | $ | — | | | | | | Options granted | | (379,709) | | 379,709 | | $ | 19.60 | | | | | | Options exercised | | — | | (77,784) | | $ | 1.42 | | | | | | Options canceled | | 28,563 | | (28,563) | | $ | 12.41 | | | | | | Issuance of common stock for services and restricted stock units | | (23,285) | | — | | | — | | | | | | Balance at December 31, 2015 | | 1,634,420 | | 1,281,086 | | $ | 9.78 | | | | | | Options authorized | | 1,038,595 | | — | | $ | — | | | | | | Options granted | | (1,524,014) | | 1,524,014 | | $ | 11.42 | | | | | | Options exercised | | — | | (25,134) | | $ | 2.19 | | | | | | Options canceled | | 67,743 | | (67,743) | | $ | 16.67 | | | | | | Issuance of common stock for services and restricted stock units, net of 5,000 forfeitures | | (189,507) | | — | | $ | — | | | | | | Balance at December 31, 2016 | | 1,027,237 | | 2,712,223 | | $ | 10.60 | | | | | | Options authorized | | 1,892,376 | | — | | $ | — | | | | | | Options granted | | (1,723,906) | | 1,723,906 | | $ | 11.73 | | | | | | Options exercised | | — | | (35,759) | | $ | 1.70 | | | | | | Options canceled | | 445,029 | | (445,029) | | $ | 14.15 | | | | | | Issuance of common stock for services and restricted stock units, net of 79,850 forfeitures | | (601,008) | | — | | $ | — | | | | | | Balance at December 31, 2017 | | 1,039,728 | | 3,955,341 | | $ | 10.78 | | 7.67 | | $ | 4,393 | Vested and expected to vest at December 31, 2017 | | | | 3,840,963 | | $ | 10.74 | | 7.63 | | $ | 4,363 | Exercisable at December 31, 2017 | | | | 1,978,711 | | $ | 9.74 | | 6.55 | | $ | 3,767 |
| | | | | | | | | | | | | | | | | | | | | | | Options Issued and Outstanding | | | | | | | | Shares Available for
Grant | | | Number of Shares | | | Average Exercise
Price per Share | | | Aggregate
Intrinsic Value | | | | | | | | | | | | | | (in thousands) | | Balance at December 31, 2012 | | | 96,841 | | | | 1,293,767 | | | $ | 0.77 | | | | | | Options granted | | | (99,552 | ) | | | 99,552 | | | | 3.42 | | | | | | Options exercised | | | — | | | | (223,865 | ) | | | 0.56 | | | | | | Options canceled | | | 6,625 | | | | (6,625 | ) | | | 2.23 | | | | | | | | | | | | | | | | | | | | | | | Balance at December 31, 2013 | | | 3,914 | | | | 1,162,829 | | | $ | 1.03 | | | | | | Options authorized | | | 1,452,661 | | | | — | | | | | | | | | | Options granted | | | (188,888 | ) | | | 188,888 | | | | 24.41 | | | | | | Options exercised | | | — | | | | (336,398 | ) | | | 0.71 | | | | | | Options canceled | | | 4,084 | | | | (4,084 | ) | | | 2.21 | | | | | | Options repurchased | | | 3,511 | | | | (3,511 | ) | | | 0.55 | | | | | | Issuance of common stock for services | | | (10,000 | ) | | | — | | | | — | | | | | | | | | | | | | | | | | | | | | | | Balance at December 31, 2014 | | | 1,265,282 | | | | 1,007,724 | | | $ | 5.51 | | | | | | Options authorized | | | 743,569 | | | | — | | | | | | | | | | Options granted | | | (379,709 | ) | | | 379,709 | | | | 19.60 | | | | | | Options exercised | | | — | | | | (77,784 | ) | | | 1.42 | | | | | | Options canceled | | | 28,563 | | | | (28,563 | ) | | | 12.41 | | | | | | Issuance of common stock for services | | | (13,285 | ) | | | — | | | | — | | | | | | | | | | | | | | | | | | | | | | | Balance at December 31, 2015 | | | 1,644,420 | | | | 1,281,086 | | | $ | 9.78 | | | $ | 13,129 | | | | | | | | | | | | | | | | | | | Vested and expected to vest at December 31, 2015 | | | | | | | 1,259,972 | | | $ | 9.59 | | | $ | 13,096 | | | | | | | | | | | | | | | | | | | Vested at December 31, 2015 | | | | | | | 835,860 | | | $ | 4.36 | | | $ | 12,075 | | | | | | | | | | | | | | | | | | |
The aggregate intrinsic value represents the difference between the total pre-tax value (i.e., the difference between the Company’s stock price and the exercise price) of stock options outstanding as of December 31, 2017, based on the Company’s common stock closing price of $6.60 per share, which would have been received by the option holders had all their in-the-money options been exercised as of that date. The intrinsic value of options exercised during the years ended December 31, 2017, 2016 and 2015, was $0.3 million, $0.3 million and $1.1 million, respectively. The weighted-average grant-date estimated fair value of options granted during the years ended December 31, 2017, 2016 and 2015 2014was $8.19, $7.69 and 2013 was $12.91 $18.53 and $2.68 per share.share, respectively. The aggregate intrinsicestimated grant date fair value of employee stock options was calculated asusing the difference betweenBlack-Scholes option-pricing model, based on the following weighted-average assumptions: | | | | | | | | | | Year Ended December 31, | | | | 2017 | | 2016 | | 2015 | | Expected term (years) | | 5.93 | | 5.99 | | 5.89 | | Expected volatility | | 82 | % | 77 | % | 75 | % | Risk-free interest rate | | 2.08 | % | 1.62 | % | 1.64 | % | Dividend yield | | — | % | — | % | — | % |
Expected Term—The Company has very limited historical information to develop reasonable expectations about future exercise pricepatterns and post-vesting employment termination behavior for its stock-option grants. As such, the expected term was estimated using the simplified method whereby the expected term equals the arithmetic average of the vesting term and the original contractual term of the option. Expected Volatility—Since January 1, 2017, the Company has used the historic volatility of its own stock over the retrospective period corresponding to the expected remaining term of the options, or the period since its shares were first quoted on The Nasdaq Global Market, if that is shorter, to compute its expected stock price volatility. Prior to December 31, 2016, the expected stock price volatility was calculated based on the average historical volatility for comparable publicly traded pharmaceutical companies. The Company selected companies with comparable characteristics, including enterprise value, risk profiles, position within the industry, and with historical share price information sufficient to meet the estimatedexpected life of the Company’s stock-based awards. Risk-Free Interest Rate—The risk-free interest rate assumption is based on the zero-coupon U.S. Treasury instruments on the date of grant with a maturity date consistent with the expected term of the Company’s stock option grants. Dividend Yield—To date, the Company has not declared or paid any cash dividends and does not have any plans to do so in the future. Therefore, the Company used an expected dividend yield of zero. Restricted Stock Units The following table summarizes restricted stock unit activity under the 2014 Plan in the three years ended December 31, 2017: | | | | | | | | | | | | | | | | | | | Weighted- | | | | | Weighted-Average | | Number of | | Average Grant | | | Number of Service- | | Grant Date Fair | | Performance- | | Date Fair Value | | | Based RSUs | | Value Per Share | | Based RSUs | | Per Share | Non-vested restricted stock units at December 31, 2014 | | — | | $ | — | | — | | $ | — | Granted | | 10,000 | | $ | 18.04 | | — | | $ | — | Non-vested restricted stock units at December 31, 2015 | | 10,000 | | $ | 18.04 | | — | | $ | — | Granted | | 174,389 | | $ | 14.34 | | — | | $ | — | Vested | | (5,000) | | $ | 18.04 | | — | | $ | — | Forfeited | | (5,000) | | $ | 18.04 | | — | | $ | — | Non-vested restricted stock units at December 31, 2016 | | 174,389 | | $ | 14.34 | | — | | $ | — | Granted | | 472,135 | | $ | 4.70 | | 161,865 | | $ | 13.90 | Vested | | (43,597) | | $ | 14.34 | | — | | $ | — | Forfeited | | (61,865) | | $ | 13.36 | | (17,985) | | $ | 13.90 | Non-vested restricted stock units at December 31, 2017 | | 541,062 | | $ | 6.04 | | 143,880 | | $ | 13.90 |
RSUs are generally subject to forfeiture if employment terminates prior to the release of vesting restrictions. The related compensation expense, which is based on the grant date fair value of the Company’s common stock multiplied by the number of $18.12 per share asunits granted, is recognized ratably over the period during which the vesting restrictions lapse. In January 2017, the Company granted PRSU awards to senior management which vest upon the achievement of certain performance conditions, subject to each employee’s continued service relationship with the Company. None of the PRSUs vested during the year ended December 31, 2015.2017. When achievement of the performance conditions is considered probable, the related compensation expense, which is based on the grant date fair value of the Company’s common stock multiplied by the number of units granted, is recognized ratably over the estimated vesting period. The Company recognized $1.0 million of related expense during the year ended December 31, 2017. The total estimated fair value of options thatRSUs vested during the years ended December 31, 2017, 2016 and 2015 was $0.4 million, $0.1 million and nil, respectively. Issuance of Common Stock for Services During the years ended December 31, 2017, 2016 and 2015, the Company issued 46,858, 20,118 and 13,285 shares of common stock under the 2014 and 2013 was $2.4Plan in exchange for services performed, respectively, valued at $0.2 million, $0.5$0.2 million and $0.2 million, respectively.respectively, based on the fair value of the common stock on the date of grant. Employee Stock Purchase Plan The Company adopted the 2014 Employee Stock Purchase Plan (ESPP)(“ESPP”) and initially reserved 202,762 shares of common stock as of its effective date of June 18, 2014. If approved by the Administrator of the ESPP, on the first day of each calendar year, ending in 2024, the number of shares in the reserve will increase by an amount equal to the lesser of (i) one percent (1.0%) of the shares of common stock outstanding on the last day of the immediately preceding fiscal year and (ii) such number of shares of common stock as determined by the board of directors; provided, however, no more than 2,230,374 shares of our common stock may be issued under the ESPP. Effective January 1, 2015, The following table summarizes ESPP activity in the ESPP share reserve was increased by 185,892. Under the ESPP, participants are offered the option to purchase shares of the Company’s common stock at a discount during a series of successive offering periods normally commencing on March 1 and September 1 of each year. The initial offering period commenced on September 1, 2014 and will end on February 27, 2015. The number of shares authorized for issuance under the ESPP as ofthree years ended December 31, 2015 was 388,654, of which 347,074 shares were available for future issuance.2017: | | | | | | | | | | | | | Shares Available | | Number of Shares | | Purchase Price | | | | | | for Grant | | Purchased | | per Share | | Gross Proceeds | | | | | | | | | | (in thousands) | Balance at December 31, 2014 | | 202,762 | | — | | | | | | | Shares authorized | | 185,892 | | — | | | | | | | Shares purchased | | (41,580) | | 41,580 | | $ | 13.25 | | $ | 551 | Balance at December 31, 2015 | | 347,074 | | 41,580 | | | | | | | Shares purchased | | (69,054) | | 69,054 | | $ | 8.34 | | $ | 576 | Balance at December 31, 2016 | | 278,020 | | 110,634 | | | | | | | Shares purchased | | (99,343) | | 99,343 | | $ | 6.27 | | $ | 623 | Balance at December 31, 2017 | | 178,677 | | 209,977 | | | | | | |
The following table illustrates the weighted-average assumptions for the Black-Scholes option-pricing model used in determining the fair value of ESPP purchase rights granted to employees: | | | | | | | | | | Year Ended December 31, | | | | 2017 | | 2016 | | 2015 | | Expected term (years) | | 0.5 | | 0.5 | | 0.5 | | Expected volatility | | 80 | % | 76 | % | 97 | % | Risk-free interest rate | | 0.97 | % | 0.48 | % | 0.16 | % | Dividend yield | | — | % | — | % | — | % |
| | | | | | | | | | | | Year Ended December 31, 2015 | | | | | 2015 | | | 2014 | | Expected term ( years) | | | 0.5 | | | | 0.5 | | Volatility | | | 97 | % | | | 73 | % | Risk-free interest rate | | | 0.16 | % | | | 0.05 | % | Dividend yield | | | — | % | | | — | % |
There were no shares issued during the year endedStock-based Compensation
Total stock-based compensation recognized was as follows (in thousands): | | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | | | (in thousands) | Research and development | | $ | 4,585 | | $ | 2,786 | | $ | 1,327 | General and administrative | | | 5,005 | | | 2,531 | | | 1,307 | Total stock-based compensation | | $ | 9,590 | | $ | 5,317 | | $ | 2,634 |
As of December 31, 2014 under the ESPP. In 2015,2017, the Company sold 41,580 shareshad $14.5 million, $2.5 million, $0.9 million and $0.1 million of its commontotal unrecognized compensation expense, net of estimated forfeitures, related to stock under the ESPP. The shares were purchased at a weighted-average purchase priceoptions, RSUs, PRSUs and ESPP, respectively, that will be recognized over an average vesting period of $13.25 with proceeds of approximately $0.6 million.2.43 years, 1.55 years, 0.83 years and 0.16 years, respectively. Modification of Stock Awards9. WARRANTS
During September 2014, the Company entered into a Transition and Separation Agreement with its Chief Scientific Officer, Dominique Charmot, under which certain restricted shares that were subject to vesting and repurchase by the Company have become fully vested as of Dr. Charmot’s separation from the Company as an employee and director on December 23, 2014. This resulted in the acceleration of the vesting for 58,969 shares of restricted stock. As a result of the acceleration, the Company has recorded a stock-based compensation charge of $0.8 million during the year ended December 31, 2014 to reflect the revised service period for the restricted stock and related vesting of shares that would otherwise not have vested.
Offering of Common Stock and Warrants In June 2015, the Company sold and issued an aggregate of 7,242,992 shares of its common stock and warrants to purchase 2,172,899 shares of common stock for aggregate gross proceeds of approximately $77.8 million or net proceeds, after deducting issuance costs, of approximately $74.3 million. The purchase price for the common stock was $10.70 per share and the purchase price for the warrants was $0.125 per warrant. The warrants are exercisable for an exercise price of $13.91 per share at any time prior to the earlier of (i) 5 years from the date of issuance or (ii) certain changes in control of the Company. The Company has determined that the warrants should be classified as equity. In July 2015, the Company filed a registration statement with the SEC with respect to the common stock and warrants. Other than with respect to warrants issued to holders affiliated with New Enterprise Associates, the warrants contain limitations that prevent each holder of warrants from acquiring shares upon exercise of the warrants that would cause the number of shares beneficially owned by it and its affiliates to exceed 9.99% of the total number of shares of the Company’s common stock then issued and outstanding. In addition, upon certain changes in control of the Company, each holder of a warrant can elect to receive, subject to certain limitations and assumptions, securities in a successor entity. None of the warrants issued in June 2015 have been exercised during the year ended December 31, 2015. Stock-based Compensation
Total stock-based compensation recognized was as follows (in thousands):
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | 2015 | | | 2014 | | | 2013 | | | | | (in thousands) | | Research and development | | $ | 1,327 | | | $ | 1,376 | | | $ | 200 | | General and administrative | | | 1,307 | | | | 316 | | | | 152 | | | | | | | | | | | | | | | Total stock-based compensation | | $ | 2,634 | | | $ | 1,692 | | | $ | 352 | | | | | | | | | | | | | | |
Aseach of December 31, 2015, the Company had $5.6 million and $0.1 million of total unrecognized compensation expense, net of estimated forfeitures, related to stock option grants and purchase rights, respectively, that will be recognized over an average vesting period of 2.6 years and 0.2 years, respectively.
The estimated grant date fair value of employee stock options was calculated using the Black-Scholes option-pricing model, based on the following weighted assumptions:
| | | | | | | | | | | | | | | | Year Ended December 31, | | | | | 2015 | | | 2014 | | | 2013 | | Expected term (years) | | | 5.89 | | | | 5.97 | | | | 6.07 | | Volatility | | | 75 | % | | | 94 | % | | | 98 | % | Risk-free interest rate | | | 1.64 | % | | | 1.79 | % | | | 1.35 | % | Dividend yield | | | — | % | | | — | % | | | — | % |
Expected Term—The Company has very limited historical information to develop reasonable expectations about future exercise patterns and post-vesting employment termination behavior for its stock-option grants. As such, the expected term was estimated using the simplified method whereby the expected term equals the arithmetic average of the vesting term and the original contractual term of the option.
Expected Volatility—Since the Company has limited information on the volatility of its common stock due to no significant trading history, the expected stock price volatility was calculated based on the average volatility for comparable publicly traded biopharmaceutical companies over a period equal to the expected term of the stock option grants. The comparable companies were chosen based on their similar size, stage in the life cycle, and financial leverage to the Company.
Risk-Free Interest Rate—The risk-free interest rate assumption is based on the zero-coupon U.S. Treasury instruments on the date of grant with a maturity date consistent with the expected term of the Company’s stock option grants.
Expected Dividend—To date, the Company has not declared or paid any cash dividends and does not have any plans to do so in the future. Therefore, the Company used an expected dividend yield of zero.
Options Granted to Nonemployees
The Company has granted options to purchase shares of common stock to consultants in exchange for services performed. The Company granted options to purchase 5,000, 10,000 and 3,333 shares with average exercise prices of $18.58, $20.77 and $3.43 per share, respectively, during the years ended December 31, 2015, 20142016 and 2013, respectively. These options vest upon grant or various terms up to three years. 2017.
10. INCOME TAXES The Company recognized non-employees stock compensation expense of $0.2 million, $0.1 million and insignificant during the years ended December 31, 2015, 2014 and 2013, respectively. The fair value of non-employees’ options was measured using the Black-Scholes option-pricing model reflecting the same assumptions as applied to employee options in eachcomponents of the reported years, other than the expected life, which is assumed to be the remaining contractual life of the option. Issuance of Common Stockprovision for Services
Duringincome taxes for the year ended December 31, 2017, 2016 and 2015, the Company issued 13,285 shares of common stock in exchange for services performed. The shares issued were valued at $0.2 million based on the fair value of the common stock on the date of grant. During the year ended December 31, 2014, the Company issued 10,000 shares of common stock in exchange for services performed. The shares issued were valued at $0.2 million based on the fair value of the common stock on the date of grant.are as follows (in thousands):
| | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | Current: | | | | | | | | | | Federal | | $ | — | | $ | — | | $ | (7) | State | | | 5 | | | — | | | (22) | Foreign | | | 1,204 | | | — | | | — | Total current | | | 1,209 | | | — | | | (29) | Deferred: | | | | | | | | | | Federal | | | (30) | | | — | | | — | State | | | — | | | — | | | — | Foreign | | | — | | | — | | | — | Total deferred | | | (30) | | | — | | | — | Provision for (benefit from) income taxes | | $ | 1,179 | | $ | — | | $ | (29) |
9. INCOME TAXES
The following is a reconciliation of the statutory federal income tax rate to the Company’s effective tax rate: | | | | | | | | | | December 31, | | | | 2017 | | 2016 | | 2015 | | Income tax at the federal statutory rate | | 35.0 | % | 35.0 | % | 35.0 | % | State taxes, net of federal benefit | | 0.5 | | 0.3 | | (3.8) | | Net impact related to foreign subsidiary | | (1.2) | | — | | — | | Change in valuation allowance | | 19.9 | | (36.2) | | (30.7) | | Impact of tax reform rate change | | (56.4) | | — | | — | | Tax credits | | 1.0 | | 0.3 | | 1.3 | | Other | | (0.7) | | 0.6 | | (1.7) | | Income tax provision | | (1.9) | % | — | % | 0.1 | % |
| | | | | | | | | | | | | | | | December 31, | | | | | 2015 | | | 2014 | | | 2013 | | Expected income tax provision at the federal statutory rate | | | 35.0 | % | | | 35.0 | % | | | 35.0 | % | State taxes, net of federal benefit | | | (3.8 | ) | | | 4.6 | | | | (1.4 | ) | Change in valuation allowance | | | (30.7 | ) | | | (17.9 | ) | | | (22.6 | ) | Nondeductible expenses | | | — | | | | (20.6 | ) | | | (20.8 | ) | Tax credits | | | 1.3 | | | | — | | | | 7.3 | | Other | | | (1.7 | ) | | | (3.2 | ) | | | 0.3 | | | | | | | | | | | | | | | Income tax provision | | | 0.1 | % | | | (2.1 | %) | | | (2.2 | %) | | | | | | | | | | | | | |
Deferred income taxes reflect the tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Significant components of the Company’s deferred tax assets are as follows:follows as of December 31, 2017 and 2016 (in thousands): | | | | | | | | | December 31, | | | 2017 | | 2016 | | | (in thousands) | Deferred tax assets: | | | | | | | Fixed assets and intangibles | | $ | 30,804 | | $ | — | Net operating loss carryforwards | | | 22,355 | | | 68,639 | Research credits | | | 5,209 | | | 2,643 | Stock-based compensation | | | 3,159 | | | 2,583 | Other | | | 754 | | | 1,558 | Gross deferred tax assets | | | 62,281 | | | 75,423 | Valuation allowance | | | (61,911) | | | (74,520) | Deferred tax assets net of valuation allowance | | | 370 | | | 903 | Deferred tax liabilities | | | (370) | | | (903) | Net deferred tax assets | | $ | — | | $ | — |
| | | | | | | | | | | | December 31, | | | | | 2015 | | | 2014 | | | | | (in thousands) | | Deferred tax assets: | | | | | | | | | Net operating loss carryforwards | | $ | 30,572 | | | $ | 11,262 | | Deferred revenue | | | — | | | | 11,099 | | Research credits | | | 1,919 | | | | 1,260 | | Other | | | 1,582 | | | | 1,201 | | | | | | | | | | | Gross deferred tax assets | | | 34,073 | | | | 24,822 | | Valuation allowance | | | (33,845 | ) | | | (24,741 | ) | | | | | | | | | | Total deferred tax assets | | | 228 | | | | 81 | | Deferred tax liabilities | | | (228 | ) | | | (81 | ) | | | | | | | | | | Net deferred tax assets | | $ | — | | | $ | — | | | | | | | | | | |
The Company assesses the available positive and negative evidence to estimate whether sufficient future taxable income will be generated to permit use of the existing deferred tax assets. A significant piece of objective negative evidence evaluated was the cumulative loss incurred over the three-year periods ended December 31, 2017, 2016 and December 31, 2015. Such objective evidence limits the ability to consider other subjective evidence, such as the Company’s projections for future growth. On the basis of this evaluation, as of December 31, 2017 and 2016, a full valuation allowance has been recorded against Company’s net deferred tax asset. The amount of the deferred tax asset considered realizable, however, could be adjusted if estimates of future taxable income during the carryforward period are reduced or increased or if objective negative evidence in the form of cumulative losses is no longer present and additional weight is given to subjective evidence such as our projections for growth. Realization of deferred tax assets is dependent on future earnings,taxable income, if any, the timing and the amount of which are uncertain. Accordingly,The valuation allowance decreased by approximately $12.6 million during the year ended December 31, 2017, and increased by approximately $40.7 million and $9.1 million during the years ended December 31, 2016 and 2015, respectively. The decrease in the valuation allowance in the year ended December 31, 2017 primarily relates to the re-measurement of the deferred tax assets have been fully offset byand liabilities due to the U.S. government’s enactment of comprehensive tax legislation commonly referred to as the Tax Cuts and Jobs Act (“TCJA”) on December 22, 2017, as discussed below. The TCJA makes broad and complex changes to the U.S. tax code, including, but not limited to, reducing the U.S. federal corporate tax rate from 35% to 21%, effective January 1, 2018. The Company is able to determine a valuation allowance. Thereasonable estimate of certain effects of the TCJA and has therefore recognized the provisional tax impacts related to the revaluation of deferred tax assets and liabilities. As a result, the Company has recorded a decrease related to net deferred tax assets of $35.6 million, with an offsetting change in valuation allowance increased by approximately $9.1of $35.6 million for the year ended December 31, 2015.2017. The valuation allowance decreased by approximately $0.3 million forSecurities and Exchange Commission has provided accounting and reporting guidance that allows the Company to report provisional amounts within a measurement period of up to one year ended December 31, 2014.from the date of enactment due to the complexities inherent in adopting the TCJA. The ultimate impact may differ from provisional amounts, possibly materially, due to, among other things, additional analysis, changes in interpretations and assumptions the Company has made, additional regulatory guidance that may be issued, and actions the Company may take as a result of the TCJA. At December 31, 2015,2017, the Company had net operating loss carryforwards for federal income tax purposes of approximately $85.2$149.4 million that expire beginning in 2030 if not utilized, and federal research and development tax credit carryforwards of approximately $2.7$4.4 million that expire beginning in 2027 if not utilized, and foreign tax credit carryforwards of approximately $1.2 million that expire in 2027 if not utilized. In addition, the Company had net operating loss carryforwards for California income tax purposes of approximately $32.3$88.3 million that expire beginning in 2030 if not utilized, and state research and development tax credit carryforwards of approximately $3.0$4.6 million which can be carried forward indefinitely. Finally, theThe Company had other state net operating losses of approximately $1.9 million that begin to expire in 2025. The Company had approximately insignificant and $0.2$0.1 million of minimum tax credit carryovers for federal and California income tax purposes, respectively.purposes. The minimum tax credits have no expiration date. As a result of certain realization requirements of ASC 718, the table of deferred tax assets and liabilities does not include certain deferred tax assets as of December 31, 2015, and December 31, 2014, that arose directly from tax deductions related to equity compensation that are greater than the compensation recognized for financial reporting.
Equity will be increased by approximately $0.7 million if and when such deferred tax assets are ultimately realized. We use ASC 740 ordering when determining when excess tax benefits have been realized.
The future utilization of the net operating loss and tax credit carryforwards and credits may be subject to an annual limitation, pursuant to Internal Revenue Code Sections 382 and 383, as a result of ownership changes that may have occurred previously or that could occur in the future. The Company has previously completed a study in order to assess whether any ownership changes had arisen through December 31, 2014. As a result of the study, it was determined that the Company experienced an ownership change, as defined in Section 382, during May 2008. As a result of the analysis, it was determined that approximately $1.0 million of net operating losses and $49,000 of credit carryovers generated through May 2008 would expire prior to being utilized. No other ownership changes were identified through December 31, 2014. The Company is currently updating its Section 382 analysis but this analysis was not completed by year end. Preliminarily, it appears that there may be an additional ownership change in January 2016 which would impose further annual limitations on the utilization of operating loss and credit carryforwards. Due to the existence of the valuation allowance, future changeslimitations under SectionsSection 382 and 383 will not impact the Company’s effective tax rate. A reconciliation of the beginning and ending amount of unrecognized tax benefits is as follows: | | | | | | | | | | | | December 31, | | | 2017 | | 2016 | | 2015 | | | (in thousands) | Balance at beginning of year | | $ | 3,892 | | $ | 3,298 | | $ | 2,815 | Additions (subtractions) based on tax positions related to prior year | | | 16,103 | | | 45 | | | (58) | Additions based on tax positions related to current year | | | 739 | | | 549 | | | 541 | Balance at end of year | | $ | 20,734 | | $ | 3,892 | | $ | 3,298 |
| | | | | | | | | | | | | | | | December 31, | | | | | 2015 | | | 2014 | | | 2013 | | | | | (in thousands) | | Balance at beginning of year | | $ | 2,815 | | | $ | 1,411 | | | $ | 1,064 | | Additions (subtractions) based on tax positions related to prior year | | | (58 | ) | | | 405 | | | | — | | Additions based on tax positions related to current year | | | 541 | | | | 999 | | | | 347 | | | | | | | | | | | | | | | Balance at end of year | | $ | 3,298 | | | $ | 2,815 | | | $ | 1,411 | | | | | | | | | | | | | | |
The unrecognized tax benefits, if recognized and in absence of full valuation allowance, would impact the income tax provision by $3.3$8.6 million, $2.8$3.5 million and $1.4$2.9 million as of December 31, 2015, 20142017, 2016 and 2013,2015, respectively. The Company has elected to include interest and penalties as a component of tax expense. During the years ended December 31, 2015, 20142017, 2016 and 2013,2015, the Company did not recognize accrued interest and penalties related to unrecognized tax benefits. Although the timing and outcome of an income tax audit is highly uncertain, the Company does not anticipate that the amount of existing unrecognized tax benefits will change significantly change during the next 12 months. The Company files income tax returns in the U.S. federal, California, Maryland, Massachusetts, New Hampshire, New Jersey and MassachusettsOregon tax jurisdictions. Due to the Company’s net operating loss and tax credit carryforwards, the income tax returns remain open to U.S. federal and California state tax examinations. The Company is not currently under examination in any tax jurisdiction. 11.GEOGRAPHIC INFORMATION AND CONCENTRATIONS 10.Revenue by geographic areas for the years ended December 31, 2017, 2016 and 2015, are as follows (in thousands):
| | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | United States | | $ | — | | $ | — | | $ | — | International: | | | | | | | | | | Asia Pacific (1) | | | 42,000 | | | — | | | — | Europe (2) | | | — | | | — | | | 24,026 | Total revenue | | $ | 42,000 | | $ | — | | $ | 24,026 |
(1)Revenues from Asia Pacific in 2017 included $30.0 million from Japan in accordance with the KHK Agreement and $12.0 million from China in accordance with the Fosun Agreement. (2)Revenues from Europe in 2015 comprised $24.0 million from Sweden in accordance with the AstraZeneca Agreement. Revenues are attributed to geographical areas based on the domicile of the Company’s collaboration partners. Revenues recorded in the years ended December 31, 2017, 2016 and 2015, were wholly from collaboration partnerships. Collaboration partnerships accounting for more than 10% of total revenues during the years ended December 31, 2017, 2016 and 2015, are as follows: | | | | | | | | | | Year Ended December 31, | | | | 2017 | | 2016 | | 2015 | | KHK | | 71 | % | — | | — | | Fosun Pharma | | 29 | % | — | | — | | AstraZeneca | | — | | — | | 100 | % |
12. NET LOSS PER SHARE Basic net loss per share is calculated by dividing net loss by the weighted-average number of common shares outstanding during the period, less shares subject to repurchase, and excludes any dilutive effects of share-basedstock-based awards and warrants. Diluted net loss per common share is computed giving effect to all potential dilutive common shares, including common stock issuable upon exercise of stock options, and unvested restricted common stock and stock units. As the Company had net losses for the years ended December 31, 2015, 20142017, 2016 and 2013,2015, all potential common shares were determined to be anti-dilutive. The following table sets forth the computation of net loss per common share (in thousands, except share and per share amounts): | | | | | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | Numerator: | | | | | | | | | | Net loss | | $ | (64,339) | | $ | (112,387) | | $ | (29,621) | Denominator: | | | | | | | | | | Weighted average number of shares outstanding—basic and diluted | | | 47,435,331 | | | 40,118,522 | | | 22,892,640 | Net loss per share - basic and diluted | | $ | (1.36) | | $ | (2.80) | | $ | (1.29) |
| | | | | | | | | | | | | | | | December 31, | | | | | 2015 | | | 2014 | | | 2013 | | Numerator: | | | | | | | | | | | | | Net loss | | $ | (29,621 | ) | | $ | (3,214 | ) | | $ | (6,564 | ) | | | | | | | | | | | | | | Denominator: | | | | | | | | | | | | | Weighted average number of shares outstanding—basic and diluted | | | 22,892,640 | | | | 10,248,337 | | | | 1,127,948 | | | | | | | | | | | | | | | Net loss per share—basic and diluted | | $ | (1.29 | ) | | $ | (0.31 | ) | | $ | (5.82 | ) | | | | | | | | | | | | | |
Potentially dilutive securities that were not included in the diluted per share calculations because they would be anti-dilutive were as follows:
| | | | | | | | | | | | | | | | December 31, | | | | | 2015 | | | 2014 | | | 2013 | | Convertible preferred stock | | | — | | | | — | | | | 11,517,222 | | Options to purchase common stock | | | 1,244,442 | | | | 1,007,724 | | | | 1,162,829 | | Warrants to purchase convertible preferred stock | | | — | | | | — | | | | 574,953 | | Warrants to purchase common stock | | | 300,302 | | | | — | | | | — | | | | | | | | | | | | | | | Total | | | 1,544,744 | | | | 1,007,724 | | | | 13,255,004 | | | | | | | | | | | | | | |
There were no related party transactions in 2015.
As part of the consulting arrangement with the spouse of an executive of the Company to provide research and development services related to clinical operations, the Company incurred expenses of $0.2 million for services rendered during each ofFor the years ended December 31, 20142017, 2016 and 2013,2015, the total numbers of securities that could potentially dilute net income per share in the future that were not considered in the diluted net loss per share calculations because the effect would have been anti-dilutive were as follows:
| | | | | | | | | Year Ended December 31, | | | 2017 | | 2016 | | 2015 | Options to purchase common stock | | 3,977,160 | | 2,464,089 | | 1,241,741 | Warrants to purchase common stock | | 2,172,899 | | 2,172,899 | | 1,268,021 | Restricted stock units | | 323,819 | | 87,079 | | 603 | Performance-based restricted stock units | | 148,216 | | — | | — | ESPP shares issuable | | 60,524 | | 37,227 | | 21,077 | Total | | 6,682,618 | | 4,761,294 | | 2,531,442 |
The number of potential common shares that would have been included in diluted income per share were it not for the anti-dilutive effect caused by the net loss, computed by converting these securities using the treasury stock method during the years ended December 31, 2017, 2016 and 2015, was approximately 1.0 million, 0.8 million and 1.0 million, respectively. 12.
13. COMMITMENTS AND CONTINGENCIES Leases The Company has a lease agreement for a facility in Fremont, California that was amended in December 2012 to extend the lease agreement to September 2016. In September 2014, the Company signed the second amendment to its facility lease agreement in Fremont, California to add space and to extend the lease term through September 2019. In addition, the amended lease agreement provides for a tenant improvement allowance of up to $0.6 million. In May 2016, the Company signed a third amendment to its facility lease agreement in Fremont, California to add space and to extend the lease term through September 2021 (the “Third Amendment”). The Third Amendment provides for a tenant improvement allowance of up to $0.4 million and the extended lease has rent escalation clauses throughthroughout the lease term. It also provides a lease extension option for five years on the entire premises at the higher of (i) a 3% annual escalation of the then-current base rent and (ii) the then-current fair market value for comparable premises. Rent increases, including the impact of a rent holiday and leasehold improvement allowance from the landlord, will be recognized as deferred rent and amortized on a straight-line basis over the term of the lease. Under the terms of the lease agreement, the Company provided the lessor with a security deposit in the amount of $0.1 million. The lessor shall be entitled to draw on the security deposit in the event of any uncured default by the Company under the terms of the lease. The future minimum payments under the noncancelable operating leaseleases at December 31, 2015,2017, are as follows (in thousands): | | | | Year Ended December 31, | | Amounts | 2018 | | $ | 1,615 | 2019 | | | 1,713 | 2020 | | | 2,026 | 2021 | | | 1,440 | Thereafter | | | — | Total | | $ | 6,794 |
| | | | | Year ending December 31, | | Amounts | | 2016 | | | 868 | | 2017 | | | 895 | | 2018 | | | 921 | | 2019 | | | 653 | | | | | | | Total | | $ | 3,337 | | | | | | |
Rent expense under operating leases was $0.9$1.7 million, $0.6$1.3 million and $0.5$0.9 million for the years ended December 31, 2015, 20142017, 2016 and 2013,2015, respectively. The Company entered into a series
Guarantees and Indemnifications The Company indemnifies each of ourits officers and directors for certain events or occurrences, subject to certain limits, while the officer or director is or was serving at our request in such capacity, as permitted under Delaware law and in accordance with our certificate of incorporation and bylaws. The term of the indemnification period lasts as long as an officer or director may be subject to any proceeding arising out of acts or omissions of such officer or director in such capacity. The maximum amount of potential future indemnification is unlimited; however, the Company currently holds director and officer liability insurance. This insurance allows the transfer of risk associated with our exposure and may enable the Company to recover a portion of any future amounts paid. The Company believes that the fair value of these indemnification obligations is minimal. Accordingly, the Company has not recognized any liabilities relating to these obligations for any period presented. 13.Legal Proceedings and Claims
From time to time the Company may be involved in claims arising in connection with its business. Based on information currently available, the Company believes that the amount, or range, of reasonably possible losses in connection with any pending actions against it in excess of established reserves, in the aggregate, not to be material to its consolidated financial condition or cash flows. However, losses may be material to the Company’s operating results for any particular future period, depending on the level of income or loss for such period. 14. SELECTED QUARTERLY FINANCIAL DATA (UNAUDITED) Selected quarterly financial results from operations for the years ended December 31, 20152017 and 20142016 are as follows (in thousands, except per share amounts): | | | | | | | | | | | | | | | 2017 Quarter End | | | March 31 | | June 30 | | September 30 | | December 31 | Total revenue | | $ | — | | $ | — | | $ | — | | $ | 42,000 | Gross profit | | | — | | | — | | | — | | | 33,600 | Operating expenses | | | 28,434 | | | 26,418 | | | 21,225 | | | 22,638 | Net income (loss) | | | (28,008) | | | (25,721) | | | (20,724) | | | 10,114 | Net income (loss) per share - basic | | $ | (0.59) | | $ | (0.54) | | $ | (0.44) | | $ | 0.21 | Net income (loss) per share - diluted | | $ | (0.59) | | $ | (0.54) | | $ | (0.44) | | $ | 0.21 |
| | | | | | | | | | | | | | | | | | | | 2015 Quarter End | | | | | March 31, | | | June 30 | | | September 30 | | | December 31 | | Total revenue | | $ | 5,883 | | | $ | 18,143 | | | $ | — | | | $ | — | | Operating expenses | | | 9,373 | | | | 9,087 | | | | 18,079 | | | | 16,876 | | Net (loss) income | | | (3,502 | ) | | | 9,007 | | | | (18,126 | ) | | | (17,000 | ) | Net (loss) income per share: | | | | | | | | | | | | | | | | | Basic | | | (0.19 | ) | | | 0.43 | | | | (0.70 | ) | | | (0.65 | ) | Diluted | | | (0.19 | ) | | | 0.42 | | | | (0.70 | ) | | | (0.65 | ) | | | | | | 2014 Quarter End | | | | | March 31, | | | June 30 | | | September 30 | | | December 31 | | Total revenue | | $ | 8,550 | | | $ | 9,137 | | | $ | 7,598 | | | $ | 6,338 | | Operating expenses | | | 9,014 | | | | 6,386 | | | | 7,517 | | | | 10,270 | | Net (loss) income | | | (3,071 | ) | | | 3,753 | | | | 74 | | | | (3,970 | ) | Net (loss) income per share: | | | | | | | | | | | | | | | | | Basic | | | (2.44 | ) | | | 0.20 | | | | — | | | | (0.21 | ) | Diluted | | | (2.44 | ) | | | 0.18 | | | | — | | | | (0.21 | ) |
| | | | | | | | | | | | | | | 2016 Quarter End | | | March 31 | | June 30 | | September 30 | | December 31 | Total revenue | | $ | — | | $ | — | | $ | — | | $ | — | Operating expenses | | | 23,529 | | | 28,690 | | | 29,200 | | | 31,476 | Net loss | | | (23,467) | | | (28,613) | | | (29,031) | | | (31,276) | Net loss per share - basic and diluted | | $ | (0.70) | | $ | (0.83) | | $ | (0.65) | | $ | (0.66) |
14. SUBSEQUENT EVENTS
In January 2016, the Company completed the sale and issuance
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE None. ITEM 9A. CONTROLS AND PROCEDURES Conclusions Regarding the Effectiveness of Disclosure Controls and Procedures As of December 31, 2015,2017, management, with the participation of our Chief Executive Officer and Chief Financial Officer, performed an evaluation of the effectiveness of the design and operation of our disclosure controls and procedures as defined in Rules 13a-15(e)13a‑15(e) and 15d-15(e)15d‑15(e) of the Exchange Act. Our disclosure controls and procedures are designed to ensure that information required to be disclosed in the reports we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the Securities and Exchange Commission’s rules and forms, and that such information is accumulated and communicated to our management, including the Chief Executive Officer and the Chief Financial Officer, to allow timely decisions regarding required disclosures. Any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objective and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on this evaluation, our Chief Executive Officer and Chief Financial Officer concluded that, as of December 31, 2015,2017, the design and operation of our disclosure controls and procedures were effective at a reasonable assurance level. Management’s Annual Report on Internal Control Over Financial Reporting Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is a process designed by, or under the supervision of, our CEO and CFO, and effected by our Board of Directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that: | · | | Pertain to the maintenance of records that accurately and fairly reflect in reasonable detail the transactions and dispositions of the assets of our company; |
| · | | Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and |
| · | | Pertain to the maintenance of records that accurately and fairly reflect in reasonable detail the transactions and dispositions of the assets of our company;
Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and
Provide reasonable assurances regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material adverse effect on our financial statements. |
Our management assessed our internal control over financial reporting as of December 31, 2015,2017, the end the period covered by this Annual Report on Form 10-K.10‑K. Management based its assessment on criteria established in “Internal Control—Integrated Framework (2013)” issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on management’s assessment of our internal control over financial reporting, management concluded that, as of December 31, 2015,2017, our internal control over financial reporting was effective. Internal control over financial reporting has inherent limitations. Internal control over financial reporting is a process that involves human diligence and compliance and is subject to lapses in judgment and breakdowns resulting from human failures. Internal control over financial reporting also can be circumvented by collusion or improper management override. Because of such limitations, there is a risk that material misstatements will not be prevented or detected on a timely basis by internal control over financial reporting. However, these inherent limitations are known features of the financial reporting process. Therefore, it is possible to design into the process safeguards to reduce, though not eliminate, this risk. Attestation Report of the Registered Public Accounting Firm This Annual Report on Form 10-K10‑K does not include an attestation report of our registered public accounting firm due to an exemption established by the JOBS Act for “emerging growth companies.” Changes in Internal Control over Financial Reporting There were no changes in our internal controls over financial reporting during the quarter ended December 31, 20152017, identified in connection with the evaluation required by Rule 13a-15(d)13a‑15(d) and 15d-15(d)15d‑15(d) of the Exchange Act that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting. ITEM 9B. OTHER INFORMATION None.On March 14, 2018, the Company appointed Jan M. Lundberg, Ph.D., as a member of its board of directors (the “Board”), effective March 23, 2018, to serve in Class I until the 2018 Annual Meeting of Stockholders and until his successor is duly elected and qualified, or until his earlier death, resignation or removal. In connection with Dr. Lundberg’s appointment, the Board increased the authorized number of members of the Board from seven to eight members. Following the effective date of Dr. Lundberg’s appointment, Class I will consist of William Bertand, Jr., Annalisa Jenkins and Dr. Lundberg.
Dr. Lundberg was also appointed to serve as a member of the Compensation Committee of the Board effective March 23, 2018. Following the effective date of Dr. Lundberg’s appointment, the Compensation Committee will consist of David Mott, as chairman, Richard Rodgers, Robert Bazemore and Dr. Lundberg. The Board has determined that Dr. Lundberg is independent as defined in Listing Rule 5605 of The Nasdaq Stock Market LLC for purposes of serving on the Board and the Compensation Committee. Pursuant to the Company’s compensation program for its non-employee directors, (the “Director Compensation Program”), Dr. Lundberg will receive an option to purchase 30,000 shares of the Company’s common stock. Dr. Lundberg’s options will have a per share exercise price equal to the last reporting sale price reported by The Nasdaq Stock Market on the date of grant, and the option will vest over three years in substantially equal installments on each monthly anniversary of the grant date so long as Dr. Lundberg remains on the Board through each such vesting date. In addition, Dr. Lundberg will be entitled to receive annual cash retainers in the amount of $40,000 per year for his service on the Board and $7,500 per year for his service on our Compensation Committee any other compensation provided pursuant to the Director Compensation Program. The Company intends to enter into its standard form of indemnification agreement with Dr. Lundberg. PART III ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE Information required by this item will be contained in our definitive proxy statement to be filed with the Securities and Exchange Commission on Schedule 14A in connection with our 20162018 Annual Meeting of Stockholders (the “Proxy Statement”), which will be filed not later than 120 days after the end of our fiscal year ended December 31, 2015,2017, under the headings “Executive Officers,” “Election of Directors,” “Corporate Governance,” and “ Section 16(a) Beneficial Ownership Reporting Compliance,” and is incorporated herein by reference. We have adopted a Code of Business Conduct and Ethics that applies to our officers, directors and employees which is available on our website at www.ardelyx.com. The Code of Business Conduct and Ethics is intended to qualify as a “code of ethics” within the meaning of Section 406 of the Sarbanes-Oxley Act of 2002 and Item 406 of Regulation S-K. In addition, we intend to promptly disclose (1) the nature of any amendment to our Code of Business Conduct and Ethics that applies to our principal executive officer, principal financial officer, principal accounting officer or controller or persons performing similar functions and (2) the nature of any waiver, including an implicit waiver, from a provision of our code of ethics that is granted to one of these specified officers, the name of such person who is granted the waiver and the date of the waiver on our website in the future. ITEM 11. EXECUTIVE COMPENSATION The information required by this item regarding executive compensation will be incorporated by reference to the information set forth in the sections titled “Executive Compensation” in our Proxy Statement. ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS The information required by this item regarding security ownership of certain beneficial owners and management will be incorporated by reference to the information set forth in the section titled “Security Ownership of Certain Beneficial Owners and Management” and “Equity Compensation Plan Information” in our Proxy Statement. ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE The information required by this item regarding certain relationships and related transactions and director independence will be incorporated by reference to the information set forth in the sections titled “Certain Relationships and Related Party Transactions” and “Election of Directors”, respectively, in our Proxy Statement. ITEM 14. PRINCIPAL ACCOUNTING FEES AND SERVICES The information required by this item regarding principal accountant fees and services will be incorporated by reference to the information set forth in the section titled “Principal Accountant Fees and Services” in our Proxy Statement. PART IV ITEM 15. EXHIBITS, FINANCIAL STATEMENT SCHEDULES (a) The following documents are filed as part of this report:
| 1.(a) | | The following documents are filed as part of this report: |
See Index to Financial Statements at Item 8 herein. | 2. | | Financial Statement Schedules |
All schedules are omitted because they are not applicable or the required information is shown in the financial statements or notes thereto. See the Exhibit Index immediately following the signature pagethis page. ITEM 16. FORM 10-K SUMMARY None. | | | | | | | | | | | Exhibit | | | | Incorporated by Reference | | Filed | Number | | Exhibit Description | | Form | | Date | | Number | | Herewith | 3.1 | | Amended and Restated Certificate of Incorporation | | 8‑K | | 6/24/2014 | | 3.1 | | | 3.2 | | Amended and Restated Bylaws | | 8‑K | | 6/24/2014 | | 3.2 | | | 4.1 | | Reference is made to Exhibits 3.1 and 3.2 | | | | | | | | | 4.2 | | Form of Common Stock Certificate | | S‑1/A | | 6/18/2014 | | 4.2 | | | 4.3 | | Form of Warrant issued pursuant to the Securities Purchase Agreement by and among Ardelyx, Inc. and the purchasers signatory thereto, dated June 2, 2015 | | S‑3 | | 7/13/2015 | | 4.3 | | | 10.1 | | Termination Agreement, dated June 2, 2015, by and between AstraZeneca AB and Ardelyx, Inc. | | 10‑Q | | 8/12/2015 | | 10.1 | | | 10.2 | | Amendment No. 1 to Termination Agreement and to Manufacturing and Supply Agreement, dated November 2, 2015 by and between AstraZeneca AB and Ardelyx, Inc. | | 10‑K | | 3/4/2016 | | 10.1(d) | | | 10.3 | | Amended and Restated Investor’s Rights Agreement dated June 23, 2011, by and among Ardelyx, Inc. and the investors listed therein | | S‑1 | | 5/19/2014 | | 10.3 | | | 10.4(a) | | Lease, dated August 8, 2008, by and between 34175 Ardenwood Venture, LLC and Ardelyx, Inc. | | S‑1 | | 5/19/2014 | | 10.4(a) | | | 10.4(b) | | First Amendment to Lease, dated December 20, 2012, by and between 34175 Ardenwood Venture, LLC and Ardelyx, Inc. | | S‑1 | | 5/19/2014 | | 10.4(b) | | | 10.4(c) | | Second Amendment to Lease, dated September 5, 2014, by and between Ardelyx, Inc. and 34175 Ardenwood Venture, LLC | | 8‑K | | 9/9/2014 | | 10.1 | | | 10.4(d) | | Third Amendment to Lease, dated April 28, 2016, by and between Ardelyx, Inc. and 34175 Ardenwood Venture, LLC | | 10‑Q | | 8/8/2016 | | 10.3 | | | 10.5(a)# | | Ardelyx, Inc. 2008 Stock Incentive Plan, as amended | | S‑1 | | 5/19/2014 | | 10.5(a) | | | 10.5(b)# | | Form of Stock Option Grant Notice and Stock Option Agreement under the 2008 Stock Incentive Plan, as amended | | S‑1 | | 5/19/2014 | | 10.5(b) | | | 10.5(c)# | | Form of Restricted Stock Purchase Grant Notice and Restricted Stock Purchase Agreement under the 2008 Stock Incentive Plan, as amended | | S‑1 | | 5/19/2014 | | 10.5(c) | | | 10.6(a)# | | Ardelyx, Inc. 2014 Equity Incentive Award Plan | | S‑8 | | 7/14/2014 | | 99.3 | | | 10.6(b)# | | Form of Stock Option Grant Notice and Stock Option Agreement under the 2014 Equity Incentive Award Plan | | S‑1/A | | 6/9/2014 | | 10.6(b) | | | 10.6(c)# | | Form of Restricted Stock Award Agreement and Restricted Stock Unit Award Grant Notice under the 2014 Equity Incentive Award Plan | | S‑1/A | | 6/9/2014 | | 10.6(c) | | | 10.7# | | Form of Indemnification Agreement for directors and officers | | S‑1/A | | 6/9/2014 | | 10.7 | | | 10.8# | | Amended and Restated Executive Employment Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Michael Raab | | S‑1/A | | 6/9/2014 | | 10.8 | | | 10.9# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Mark Kaufmann | | S‑1/A | | 6/9/2014 | | 10.15 | | |
| | | | | | | | | | | Exhibit | | | | Incorporated by Reference | | Filed | Number | | Exhibit Description | | Form | | Date | | Number | | Herewith | 10.10# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Elizabeth Grammer, Esq. | | S‑1/A | | 6/9/2014 | | 10.16 | | | 10.11# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Jeffrey Jacobs, Ph.D. | | S‑1/A | | 6/9/2014 | | 10.17 | | | 10.12# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and David Rosenbaum, Ph.D. | | S‑1/A | | 6/9/2014 | | 10.19 | | | 10.13# | | Offer Letter, dated August 11, 2011, by and between Ardelyx, Inc. and Mark Kaufmann | | S‑1/A | | 6/9/2014 | | 10.10 | | | 10.14# | | Offer Letter, dated May 2, 2008, by and between Ardelyx, Inc. and Jeff Jacobs, Ph.D. | | S‑1/A | | 6/9/2014 | | 10.12 | | | 10.15# | | Offer Letter, dated December 28, 2009, by and between Ardelyx, Inc. and David Rosenbaum, Ph.D. | | S‑1/A | | 6/9/2014 | | 10.13 | | | 10.16# | | Offer Letter, dated November 21, 2012, by and between Ardelyx, Inc. and Elizabeth Grammer, Esq. | | S‑1/A | | 6/9/2014 | | 10.14 | | | 10.19# | | Offer Letter, dated November 21, 2014, by and between Ardelyx, Inc. and Jeremy S. Caldwell, Ph.D. | | 10‑K | | 3/5/2015 | | 10.22 | | | 10.20# | | Change in Control Severance Agreement, dated December 19, 2014, by and between Ardelyx, Inc. and Jeremy S. Caldwell, Ph.D. | | 10‑K | | 3/4/2016 | | 10.23 | | | 10.21# | | Offer Letter, dated December 12, 2015, by and between Ardelyx, Inc. and Paul Korner, MD, MBA | | 10‑K | | 3/4/2016 | | 10.21 | | | 10.22# | | Ardelyx, Inc. 2014 Employee Stock Purchase Plan | | S‑8 | | 7/14/2014 | | 99.6 | | | 10.23(a)# | | Non-Employee Director Compensation Program | | S‑1/A | | 6/9/2014 | | 10.21 | | | 10.23(b)# | | Description of amendments to Non-Employee Director Compensation Program | | 8‑K | | 3/9/2017 | | N/A | | | 10.24 | | Securities Purchase Agreement by and among Ardelyx, Inc. and the purchasers signatory thereto, dated June 2, 2015 | | 10‑Q | | 8/12/2015 | | 10.2 | | | 10.25 | | Registration Rights Agreement by and among Ardelyx, Inc. and the investors signatory thereto, dated June 2, 2015 | | S‑3 | | 7/13/2015 | | 99.1 | | | 10.26 | | Securities Purchase Agreement by and among Ardelyx, Inc. and the purchasers signatory thereto, dated July 14, 2016 | | 10‑Q | | 8/8/2016 | | 10.1 | | | 10.27 | | Registration Rights Agreement by and among Ardelyx, Inc. and the investors signatory thereto, dated July 14, 2016 | | 10‑Q | | 8/8/2016 | | 10.2 | | | 10.28(a)# | | Ardelyx, Inc. 2016 Employment Commencement Incentive Plan | | S‑8 | | 11/10/2016 | | 99.1 | | | 10.28(b)# | | Form of Stock Option Grant Notice and Stock Option Agreement under the 2016 Employment Commencement Incentive Plan | | S‑8 | | 11/10/2016 | | 99.2 | | | 10.28(c)# | | Form of Restricted Stock Unit Award Grant Notice and Restricted Stock Unit Award Agreement under the 2016 Employment Commencement Incentive Plan | | S‑8 | | 11/10/2016 | | 99.3 | | | 10.28(d)# | | Form of Restricted Stock Award Grant Notice and Restricted Stock Award Agreement under the 2016 Employment Commencement Incentive Plan | | S‑8 | | 11/10/16 | | 99.4 | | |
| | | | | | | | | | | Exhibit | | | | Incorporated by Reference | | Filed | Number | | Exhibit Description | | Form | | Date | | Number | | Herewith | 10.29# | | Change in Control Severance Agreement, dated January 4, 2016, by and between Ardelyx, Inc. and Paul Korner, MD, MBA | | 10‑K | | 2/17/2017 | | 10.29 | | | 10.30# | | Offer Letter, dated October 1, 2016, by and between Ardelyx, Inc. and Reginald Kim Seeto, MB.BS; B.Sc. | | 10‑K | | 2/17/2017 | | 10.30 | | | 10.31# | | Change in Control Severance Agreement, dated October 22, 2016, by and between Ardelyx, Inc. and Reginald Kim Seeto, MB.BS; B.Sc. | | 10‑K | | 2/17/2017 | | 10.31 | | | 10.32# | | Offer Letter, dated November 15, 2016, by and between Ardelyx, Inc. and Bryan Shaw | | 10‑K | | 2/17/2017 | | 10.32 | | | 10.33# | | Change in Control Severance Agreement, dated December 6, 2016, by and between Ardelyx, Inc. and Bryan Shaw | | 10‑K | | 2/17/2017 | | 10.33 | | | 10.34# | | Transition and Separation Agreement dated August 21, 2017, by and between the Company and Dr. Paul Korner | | 10‑Q | | 11/7/2017 | | 10.1 | | | 10.35†† | | License Agreement, dated November 27, 2017, by and between Kyowa Hakko Kirin Co., Ltd. and Ardelyx, Inc. | | | | | | | | X | 10.36†† | | License Agreement, dated December 11, 2017, by and between Shanghai Fosun Pharmaceutical Industrial Development Co. Ltd. and Ardelyx, Inc. | | | | | | | | X | 12.1 | | Statement of Computation of Ratio of Earnings to Fixed Charges | | | | | | | | X | 21.1 | | Subsidiaries of the Registrant | | | | | | | | X | 23.1 | | Consent of Independent Registered Public Accounting Firm | | | | | | | | X | 31.1 | | Certification of Principal Executive Officer Required Under Rule 13a‑14(a) and 15d‑14(a) of the Securities Exchange Act of 1934, as amended | | | | | | | | X | 31.2 | | Certification of Principal Financial Officer Required Under Rule 13a‑14(a) and 15d‑14(a) of the Securities Exchange Act of 1934, as amended | | | | | | | | X | 32.1 | | Certification of Principal Executive Officer and Principal Financial Officer Required Under Rule 13a‑14(b) of the Securities Exchange Act of 1934, as amended, and 18 U.S.C §1350 | | | | | | | | X | 101.INS | | XBRL Instance Document | | | | | | | | X | 101.SCH | | XBRL Taxonomy Extension Schema Document | | | | | | | | X | 101.CAL | | XBRL Taxonomy Extension Calculation Linkbase Document | | | | | | | | X | 101.DEF | | XBRL Taxonomy Extension Definition Linkbase Document | | | | | | | | X | 101.LAB | | XBRL Taxonomy Extension Label Linkbase Document | | | | | | | | X | 101.PRE | | XBRL Taxonomy Extension Presentation Linkbase Document | | | | | | | | X |
†Confidential treatment granted as to portions of this Annual Report on Form 10-K. Exhibit. The confidential portions of this Exhibit have been omitted and are marked by asterisks.††Certain portions have been omitted pursuant to a confidential treatment request. Omitted information has been filed separately with the Securities and Exchange Commission. #Indicates management contract or compensatory plan. SIGNATURES Pursuant to the requirements of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized. | | | | | | Ardelyx, Inc. | | | | | Ardelyx, Inc. | | | | | Date: March 4, 201614, 2018 | | By: | | By: | | /s/ Michael Raab | | | | | | | Michael Raab | | | | | | | President Chief Executive Officer and Director | | | | | | | (Principal Executive Officer) |
POWER OF ATTORNEY Each person whose individual signature appears below hereby authorizes and appoints Michael Raab and Mark Kaufmann, and each of them, with full power of substitution and resubstitution and full power to act without the other, as his or her true and lawful attorney-in-fact and agent to act in his or her name, place and stead and to execute in the name and on behalf of each person, individually and in each capacity stated below, and to file any and all amendments to this annual report on Form 10-K10‑K and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing, ratifying and confirming all that said attorneys-in-fact and agents or any of them or their or his substitute or substitutes may lawfully do or cause to be done by virtue thereof. Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated. | | | | | Signature | | Title | | Date | | | | | | /s/ Michael Raab Michael Raab
| | President, Chief Executive Officer and Director |
| March 14, 2018 | Michael Raab | | (Principal Executive Officer) | | March 4, 2016 | | | | | | /s/ Mark Kaufmann Mark Kaufmann
| | Chief Financial Officer |
| March 14, 2018 | Mark Kaufmann | | (Principal Financial and Accounting Officer) | | March 4, 2016 | | | | /s/ Narani Arasaratnam
Narani Arasaratnam
| | VP, Corporate Controller
(Principal Accounting Officer)
| | March 4, 2016 | | | | /s/ David Mott | David Mott
| | Chairman of the Board of Directors | | March 4, 201614, 2018 | David Mott | | | | | | | | | | /s/ Robert Bazemore | | Director | | March 14, 2018 | Robert Bazemore | | | | | | | | | | /s/ William Bertrand, Jr. | | Director | | March 14, 2018 | William Bertrand, Jr. | | Director | | March 4, 2016 | | | | | | /s/ Annalisa Jenkins, MBBS, MRCPFRCP | | Director | | March 14, 2018 | Annalisa Jenkins, MBBS, MRCPFRCP | | Director | | March 4, 2016 | | | | | | /s/ Gordon Ringold, Ph.D. | | Director | | March 14, 2018 | Gordon Ringold, Ph.D. | | Director | | March 4, 2016 | | | | | | /s/ Richard Rodgers | | Director | | March 14, 2018 | Richard Rodgers | | Director | | March 4, 2016 |
Exhibit Index
| | | | | | | | | | | | | | | | Incorporated by Reference | Exhibit Number | | Exhibit Description | | Form | | Date | | Number | | Filed Herewith | | | | | | | | 3.1 | | Amended and Restated Certificate of Incorporation. | | 8-K | | 6/24/2014 | | 3.1 | | | | | | | | | | 3.2 | | Amended and Restated Bylaws. | | 8-K | | 6/24/2014 | | 3.2 | | | | | | | | | | 4.1 | | Reference is made to exhibits 3.1 and 3.2. | | | | | | | | | | | | | | | | 4.2 | | Form of Common Stock Certificate. | | S-1/A | | 6/18/2014 | | 4.2 | | | | | | | | | | 4.3 | | Form of Warrant issued pursuant to the Securities Purchase Agreement by and among Ardelyx, Inc. and the purchasers signatory thereto, dated June 2, 2015 | | S-3 | | 7/13/2015 | | 4.3 | | | | | | | | | | 10.1(a)† | | License Agreement, dated as of October 4, 2012, by and among AstraZeneca AB and Ardelyx, Inc. | | S-1/A | | 6/5/2014 | | 10.1(a) | | | | | | | | | | 10.1(b)† | | Amendment Number One to License Agreement, dated as of December 23, 2013, by and between AstraZeneca AB and Ardelyx, Inc. | | S-1/A | | 6/5/2014 | | 10.1(b) | | | | | | | | | | 10.1(c) | | Termination Agreement, dated June 2, 2015, by and between AstraZeneca AB and Ardelyx, Inc. | | 10-Q | | 8/12/2015 | | 10.1 | | | | | | | | | | 10.1(d) | | Amendment No. 1 to Termination Agreement and to Manufacturing and Supply Agreement, dated November 2, 2015 by and between AstraZeneca AB and Ardelyx, Inc. | | | | | | | | X | | | | | | | | 10.2† | | License and Option Agreement, dated February 21, 2014, by and between Sanofi and Ardelyx, Inc. | | S-1/A | | 6/5/2014 | | 10.2 | | | | | | | | | | 10.3 | | Amended and Restated Investor’s Rights Agreement dated June 23, 2011, by and among Ardelyx, Inc. and the investors listed therein. | | S-1 | | 5/19/2014 | | 10.3 | | | | | | | | | | 10.4(a) | | Lease, dated August 8, 2008, by and between 34175 Ardenwood Venture, LLC and Ardelyx, Inc. | | S-1 | | 5/19/2014 | | 10.4(a) | | | | | | | | | | 10.4(b) | | Amendment to Lease, dated December 20, 2012, by and between 34175 Ardenwood Venture, LLC and Ardelyx, Inc. | | S-1 | | 5/19/2014 | | 10.4(b) | | | | | | | | | | 10.4(c) | | Second Amendment to Lease, dated September 5, 2014, by and between Ardelyx, Inc. and 34175 Ardenwood Venture, LLC. | | 8-K | | 9/9/2014 | | 10.1 | | | | | | | | | | 10.5(a)# | | Ardelyx, Inc. 2008 Stock Incentive Plan, as amended. | | S-1 | | 5/19/2014 | | 10.5(a) | | | | | | | | | | 10.5(b)# | | Form of Stock Option Grant Notice and Stock Option Agreement under the 2008 Stock Incentive Plan, as amended. | | S-1 | | 5/19/2014 | | 10.5(b) | | | | | | | | | | 10.5(c)# | | Form of Restricted Stock Purchase Grant Notice and Restricted Stock Purchase Agreement under the 2008 Stock Incentive Plan, as amended. | | S-1 | | 5/19/2014 | | 10.5(c) | | | | | | | | | | 10.6(a)# | | Ardelyx, Inc. 2014 Equity Incentive Award Plan. | | S-8 | | 7/14/2014 | | 99.3 | | |
| | | | | | | | | | | | | | | Incorporated by Reference | Exhibit
Number
| | Exhibit Description
| | Form
| | Date
| | Number
| | Filed
Herewith
| | | | | | | 10.6(b)# | | Form of Stock Option Grant Notice and Stock Option Agreement under the 2014 Equity Incentive Award Plan. | | S-1/A | | 6/18/2014 | | 10.6(b) | | | | | | | | | 10.6(c)# | | Form of Restricted Stock Award Agreement and Restricted Stock Unit Award Grant Notice under the 2014 Equity Incentive Award Plan. | | S-1/A | | 6/18/2014 | | 10.6(c) | | | | | | | | | 10.7# | | Form of Indemnification Agreement for directors and officers. | | S-1/A | | 6/9/2014 | | 10.7 | | | | | | | | | 10.8# | | Amended and Restated Executive Employment Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Michael Raab. | | S-1/A | | 6/9/2014 | | 10.8 | | | | | | | | | 10.9# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Mark Kaufmann. | | S-1/A | | 6/9/2014 | | 10.15 | | | | | | | | | 10.10# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Elizabeth Grammer, Esq. | | S-1/A | | 6/9/2014 | | 10.16 | | | | | | | | | 10.11# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and Jeffrey Jacobs, Ph.D. | | S-1/A | | 6/9/2014 | | 10.17 | | | | | | | | | 10.12# | | Amended and Restated Change in Control Severance Agreement, dated June 6, 2014, by and between Ardelyx, Inc. and David Rosenbaum, Ph.D. | | S-1/A | | 6/9/2014 | | 10.19 | | | | | | | | | 10.13# | | Offer Letter, dated August 11, 2011, by and between Ardelyx, Inc. and Mark Kaufmann. | | S-1/A | | 6/9/2014 | | 10.10 | | | | | | | | | 10.14# | | Offer Letter, dated May 2, 2008, by and between Ardelyx, Inc. and Jeff Jacobs, Ph.D. | | S-1/A | | 6/9/2014 | | 10.12 | | | | | | | | | 10.15# | | Offer Letter, dated December 28, 2009, by and between Ardelyx, Inc. and David Rosenbaum, Ph.D. | | S-1/A | | 6/9/2014 | | 10.13 | | | | | | | | | 10.16# | | Offer Letter, dated November 21, 2012, by and between Ardelyx, Inc. and Elizabeth Grammer, Esq. | | S-1/A | | 6/9/2014 | | 10.14 | | | | | | | | | 10.17# | | Offer Letter, dated October 15, 2014, by and between Ardelyx, Inc. and Narani Arasaratnam. | | 10-K | | 3/5/2015 | | 10.20 | | | | | | | | | 10.18# | | Change in Control Severance Agreement, dated November 26, 2014, by and Between Ardelyx, Inc. and Narani Arasaratnam. | | 10-K | | 3/5/2015 | | 10.21 | | | | | | | | | 10.19# | | Offer Letter, dated November 21, 2014, by and between Ardelyx, Inc. and Jeremy S. Caldwell, Ph.D. | | 10-K | | 3/5/2015 | | 10.22 | | | | | | | | | 10.20# | | Change in Control Severance Agreement, dated December 19, 2014, by and between Ardelyx, Inc. and Jeremy S. Caldwell, Ph.D. | | 10-K | | 3/5/2015 | | 10.23 | | | | | | | | | 10.21# | | Offer Letter, dated December 12, 2015, by and between Ardelyx, Inc. and Paul Korner, MD, MBA | | | | | | | | X |
107 | | | | | | | | | | | | | | | | Incorporated by Reference | Exhibit Number | | Exhibit Description | | Form | | Date | | Number | | Filed Herewith | | | | | | | | 10.22# | | Ardelyx, Inc. 2014 Employee Stock Purchase Plan. | | S-8 | | 7/14/2014 | | 99.6 | | | | | | | | | | 10.23# | | Non-Employee Director Compensation Program. | | S-1/A | | 6/9/2014 | | 10.21 | | | | | | | | | | 10.24 | | Securities Purchase Agreement by and among Ardelyx, Inc. and the purchasers signatory thereto, dated June 2, 2015 | | 10-Q | | 8/12/15 | | 10.2 | | | | | | | | | | 10.25 | | Registration Rights Agreement by and among Ardelyx, Inc. and the investors signatory thereto, dated June 2, 2015 | | S-3 | | 7/13/15 | | 99.1 | | | | | | | | | | 12.1 | | Statement Regarding the Computation of Ratio of Earnings to Fixed Charges | | | | | | | | X | | | | | | | | 23.1 | | Consent of Ernst & Young LLP, Independent Registered Public Accounting Firm | | | | | | | | X | | | | | | | | 31.1 | | Certification of Principal Executive Officer Required Under Rule 13a-14(a) and 15d-14(a) of the Securities Exchange Act of 1934, as amended. | | | | | | | | X | | | | | | | | 31.2 | | Certification of Principal Financial Officer Required Under Rule 13a-14(a) and 15d-14(a) of the Securities Exchange Act of 1934, as amended. | | | | | | | | X | | | | | | | | 32.1 | | Certification of Principal Executive Officer and Principal Financial Officer Required Under Rule 13a-14(b) of the Securities Exchange Act of 1934, as amended, and 18 U.S.C §1350. | | | | | | | | X | | | | | | | | 101.INS | | XBRL Instance Document | | | | | | | | X | | | | | | | | 101.SCH | | XBRL Taxonomy Extension Schema Document | | | | | | | | X | | | | | | | | 101.CAL | | XBRL Taxonomy Extension Calculation Linkbase Document | | | | | | | | X | | | | | | | | 101.DEF | | XBRL Taxonomy Extension Definition Linkbase Document | | | | | | | | X | | | | | | | | 101.LAB | | XBRL Taxonomy Extension Label Linkbase Document | | | | | | | | X | | | | | | | | 101.PRE | | XBRL Taxonomy Extension Presentation Linkbase Document | | | | | | | | X |
† | Confidential treatment granted as to portions of this Exhibit. The confidential portions of this Exhibit have been omitted and are marked by asterisks. |
# | Indicates management contract or compensatory plan. |
102
|
|