WASHINGTON, D.C. 20549
"SAFE HARBOR" STATEMENTSPECIAL NOTE REGARDING FORWARD LOOKING STATEMENTS
Some of the information contained in this annual report may includeThis Annual Report on Form 10-K includes forward-looking statements that reflect our current views with respect to our development programs, business strategy, business plan, financial performance and other future events. These statements include forward-looking statements both with respect to us, specifically, and our industry, in general. We make theseSuch forward-looking statements pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. Statements that include the words “expect,"expect," "intend,” “intend,"plan," "believe," "project," "estimate,” “plan,"may,” “believe,” “project,” “estimate,” “may,” “should,” “anticipate,” “will”"should," "anticipate," "will" and similar statements of a future or forward-looking nature identify forward-looking statements and include, without limitation, statements regarding:
•our future financial and business performance;
•strategic plans for purposesour business and product candidates;
•our ability to develop or commercialize products;
•the expected results and timing of clinical trials and nonclinical studies;
•our ability to comply with the terms of our license agreements;
•developments and projections relating to our competitors and industry;
•our expectations regarding our ability to obtain, develop and maintain intellectual property protection and not infringe on the rights of others;
•our ability to retain and attract highly-skilled executive officers and employees;
•our future capital requirements and the timing of those requirements and sources and uses of cash;
•our ability to obtain funding for our operations; and
•changes in applicable laws or regulations.
These statements are subject to known and unknown risks, uncertainties and assumptions that could cause actual results to differ materially from those projected or otherwise implied by the forward-looking statements, including the following:
•risks associated with preclinical or clinical development and trials;
•changes in the assumptions underlying our expectations regarding our future business or business model;
•our ability to develop, manufacture and commercialize product candidates;
•general economic, financial, legal, political and business conditions and changes in domestic and foreign markets;
•changes in applicable laws or regulations;
•the impact of natural disasters, including climate change, and the impact of health epidemics, on our business;
•the size and growth potential of the federal securities lawsmarkets for our products, and otherwise.our ability to serve those markets;
•market acceptance of our planned products;
•our ability to raise capital;
•the possibility that we may be adversely affected by other economic, business, and/or competitive factors; and
•other risks and uncertainties set forth in this report in the section entitled “Risk Factors.”
Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based only on our current beliefs, expectations and assumptions regarding the future of our business, future plans and strategies, projections, anticipated events and trends, the economy and other future conditions. Because forward-lookingForward-looking statements relate to the future, they are subject to inherent uncertainties, risks and changes in circumstances that are difficult to predict and many of which are outside of our control. There are or will be important factors that could cause actual results to differ materially from those indicated inGiven these statements. These factors include, but are not limited to, those factors set forth in the sections entitled “Business,” “Risk Factors,” “Legal Proceedings,” “Management’s Discussionrisks and Analysis of Financial Condition and Results of Operations,” “Quantitative and Qualitative Disclosures About Market Risk” and “Controls and Procedures” in this annual report, all of whichuncertainties, you should review carefully. Please consider ournot place undue reliance on these forward-looking statements in light of those risks as you read this annual report.statements. We undertake no obligation to publicly update or review any forward-looking statement, whether as a result of new information, future developments or otherwise, except as required by law.
If one
SELLAS LIFE SCIENCES GROUP, INC.
FORM 10-K - Annual Report
For the Year Ended December 31, 2023
TABLE OF CONTENTS
| | | | | | | | | | | |
| | | Page |
| | | |
| | PART I | |
| Item 1 | | | |
| Item 1A | | | |
| Item 1B | | | |
| Item 1C | | | |
| Item 2 | | | |
| Item 3 | | | |
| Item 4 | | | |
| | PART II | |
| Item 5 | | | |
| Item 6 | | | |
| Item 7 | | | |
| Item 7A | | | |
| Item 8 | | | |
| Item 9 | | | |
| Item 9A | | | |
| Item 9B | | | |
| Item 9C | | | |
| | PART III | |
| Item 10 | | | |
| Item 11 | | | |
| Item 12 | | | |
| Item 13 | | | |
| Item 14 | | | |
| | PART IV | |
| Item 15 | | | |
| Item 16 | | | |
| | | |
| | | |
Unless the context otherwise indicates, references in these notes to the “Company,” “we,” “us” or more“our” refer to SELLAS Life Sciences Group, Inc. and its wholly owned subsidiaries. The names “SELLAS Life Sciences Group, Inc.,” “SELLAS,” the SELLAS logo, and other trademarks or service marks of SELLAS Life Sciences Group, Inc. appearing in this Annual Report on Form 10-K are the property of SELLAS Life Sciences Group, Inc. Other trademarks, service marks or trade names appearing in this prospectus are the property of their respective owners. We do not intend the use or display of other companies’ trade names, trademarks or service marks to imply a relationship with, or endorsement or sponsorship of or by either, of these or other companies.
SUMMARY OF PRINCIPAL RISK FACTORS
This summary briefly lists the principal risks orand uncertainties materializes, or iffacing our underlying assumptions prove to be incorrect, actual results may vary materially from what we anticipate. All subsequent writtenbusiness, which are only a select portion of those risks. A more complete discussion of those risks and oral forward-looking statements attributableuncertainties is set forth in Part I, Item 1A of this Annual Report on Form 10-K, entitled “Risk Factors.” Additional risks not presently known to us or individuals actingthat we currently deem immaterial may also affect us. If any of these risks occur, our business, financial condition or results of operations could be materially and adversely affected. Our business is subject to the following principal risks and uncertainties:
•We have incurred substantial losses since our inception and anticipate that we will continue to incur substantial and increasing losses for the foreseeable future as we continue development and, subject to positive data and regulatory approval, the commercialization of our product candidates.
•We currently have no source of product revenues. We may never generate such revenues or achieve profitability.
•We will need additional financing to fund our operations and complete the development and, subject to positive data and regulatory approval, the commercialization of our product candidates. If we are unable to raise capital when needed, or our licensing partners are unable to make milestone or other payments in accordance with relevant agreements, we could be forced to delay, reduce or eliminate our development programs or commercialization efforts.
•Our lead product candidate galinpepimut-S, or GPS, represents a new therapeutic approach that presents significant challenges.
•Our business, in particular our clinical development programs, has been and may continue to be adversely affected by global health crises.
•Clinical drug development involves a lengthy and expensive process with an uncertain outcome. Our existing product candidates in clinical trials, and any other product candidates that may advance into clinical trials, may not have favorable results in later clinical trials or receive regulatory approval.
•Our current and future product candidates, the methods used to deliver them or their dosage levels may cause undesirable side effects or have other properties that could delay or prevent their regulatory approval, limit the commercial profile of an approved label or result in significant negative consequences following any regulatory approval.
•Our current and future product candidates could fail to receive regulatory approval from the U.S. Food and Drug Administration, or FDA.
•Failure to obtain regulatory approval in international jurisdictions would prevent our product candidates from being marketed abroad.
•We have limited to no manufacturing, sales, marketing or distribution capability and must rely upon third parties for such.
•If any of the clinical manufacturing facilities of our contract manufacturing organizations, or CMOs, are damaged or destroyed or production at such facilities is otherwise interrupted, our business and prospects would be negatively affected.
•We rely on third parties to conduct our behalfpreclinical studies and clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, or if we lose any of our contract research organizations, or CROs, or other key third-party vendors, we may not be able to obtain regulatory approval for or commercialize our current or future product candidates on a timely basis, if at all.
•We have in-licensed a significant portion of our intellectual property from Memorial Sloan Kettering Cancer Center, or MSK, and GenFleet Therapeutics (Shanghai), Inc, or GenFleet. If we breach either or both of our
license agreements with MSK and GenFleet, respectively, we could lose the ability to continue the development and potential commercialization of GPS or SLS009 (formerly GFH009), our second product candidate which we in-licensed from GenFleet.
•We may not be able to obtain and enforce patent rights or other intellectual property rights that cover our product candidates and that are expressly qualifiedof sufficient breadth to prevent third parties from competing against us.
•Our pending and future patent applications, and any collaboration or commercialization partner’s pending and future patent applications, may not result in their entirety by this “Safe Harbor” Statement.patents being issued which protect our technology or products, in whole or in part, or which effectively prevent others from commercializing competitive technologies and products.
•Our product candidates may face biosimilar competition sooner than expected after the expiration of our composition of matter patent protection for such products.
•Our commercial success depends upon attaining significant market acceptance of our current and future product candidates, if approved, among physicians, patients, health care payors and cancer treatment centers.
•Even if we are able to commercialize our current or future product candidates, the products may not receive coverage and adequate reimbursement from third-party payors in the United States and in other countries in which we seek to commercialize our products, which could harm our business.
•We have been involved in multiple legal and governmental proceedings, including securities class action litigation, relating to our predecessor in the past, and may in the future be involved in any such proceedings, that could divert management’s attention and adversely affect our financial condition and our business.
•If we fail to maintain an effective system of internal control over financial reporting, we may not be able to accurately report our financial results or prevent fraud. As a result, stockholders could lose confidence in our financial and other public reports, which would harm our business, the trading price of our common stock and our ability to raise additional capital in the future.
•We face substantial competition, which may result in others discovering, developing or commercializing products before or more successfully than we do.
•Significant disruptions of information technology systems, computer system failures or cybersecurity incidents could adversely affect our business.
•We will need to secure additional capital which may cause dilution to you and our existing stockholders, provide subsequent investors with rights and preference that are senior to yours, restrict our operations or require us to relinquish rights to our product candidates on unfavorable terms to us.
•Our failure to meet the continued listing requirements of The Nasdaq Capital Market could result in a delisting of our common stock.
PART I
ITEM 1. BUSINESS
Overview
Galena Biopharma, Inc. (“
We are a late-stage clinical biopharmaceutical company focused on the development of novel therapeutics for a broad range of cancer indications. Our product candidates currently include galinpepimut-S, or GPS, a peptide immunotherapy directed against the Wilms tumor 1, or WT1, antigen, and SLS009 (formerly, GFH009), a highly selective small molecule cyclin-dependent kinase 9, or CDK9, inhibitor.
Galinpepimut-S
Our lead product candidate, GPS, is a cancer immunotherapeutic agent licensed from Memorial Sloan Kettering Cancer Center, or MSK, that targets the WT1 protein, which is present in 20 or more cancer types. Based on its mechanism of action as a directly immunizing agent, GPS has potential as a monotherapy or in combination with other immunotherapeutic agents to address a broad spectrum of hematologic, or blood, cancers, and solid tumor indications.
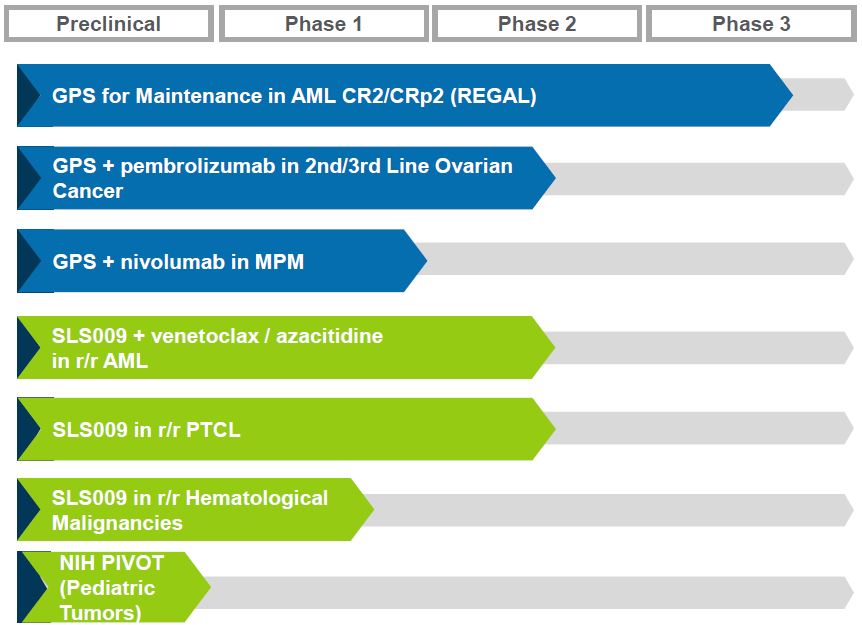
In January 2020, we” “us,” “our,” “Galena” commenced in the United States an open label randomized Phase 3 clinical trial, the REGAL study, for GPS monotherapy in patients with acute myeloid leukemia, or AML, in the maintenance setting after achievement of second complete remission, or CR2, following successful completion of second-line antileukemic therapy. Patients are randomized to receive either GPS or best available treatment, or BAT. We expect this study will be used as the basis for submission of a Biologics License Application, or BLA, subject to a statistically significant and clinically meaningful data outcome and agreement with the U.S. Food and Drug Administration, or the “Company”)FDA. The primary endpoint of the REGAL study is overall survival, or OS. We planned to enroll approximately 125 to 140 patients at approximately 95 clinical sites in North America, Europe and Asia with a planned interim safety, efficacy and futility analysis after 60 events (deaths). In March 2024, we announced the completion of enrollment. Under our current assumptions with respect to enrollment and the estimated survival times for both the treated and control groups in the study, we believe, after discussions with our external statisticians and experts, that the planned interim analysis after 60 events (deaths) per the protocol will occur in the first half of 2024 and the final analysis after 80 events will occur by the end of 2024. Because these analyses are event driven, they are difficult to predict with any certainty and may occur at a different time than currently expected.
In December 2020, we entered into an exclusive license agreement with 3D Medicines Inc., or 3D Medicines, a China-based biopharmaceutical company developing hematology and oncology therapeutics that address unmet medical needs. The Company’s pipeline consists of multiple mid- to late-stage clinical assets, including our hematology asset, GALE-401, and our novel cancer immunotherapy programs including NeuVax™ (nelipepimut-S), GALE-301 and GALE-302. GALE-401 is a controlled release version of the approved drug anagrelidenext-generation immuno-oncology drugs, for the development and commercialization of GPS, as well as the Company’s next generation heptavalent immunotherapeutic GPS+, which is at preclinical stage, across all therapeutic and diagnostic uses in mainland China, Hong Kong, Macau and Taiwan, which we refer to as Greater China. We have retained sole rights to GPS and GPS+ outside of Greater China. In November 2022, we announced that we had agreed with 3D Medicines for 3D Medicines to participate in the REGAL study through the inclusion of approximately 20 patients from mainland China. Although the REGAL study has completed enrollment as announced in March 2024, in accordance with the predetermined statistical analysis plan, 3D Medicines may still enroll patients in mainland China. The timing of such participation and patient enrollment by 3D Medicines, if at all, cannot be predicted with certainty. In December 2023, we announced that we had commenced a binding arbitration proceeding against 3D Medicines to resolve a dispute regarding, among other things, the trigger and payment of relevant milestone payments due to us under the 3D Medicines Agreement. See Item 3. Legal Proceedings. As of March 15, 2024, we have received an aggregate of $10.5 million in upfront and milestone payments under our license agreement with 3D Medicines, or the 3D Medicines Agreement, and a total of $191.5 million in potential future development, regulatory and sales milestones, not including future royalties, remains under the license agreement, which milestones are variable in nature and not under our control.
In December 2018, pursuant to a Clinical Trial Collaboration and Supply Agreement, we initiated a Phase 1/2 multi-arm "basket" type clinical study of GPS in combination with Merck & Co., Inc.’s anti-PD-1 therapy, pembrolizumab (Keytruda®). In 2020, we, together with Merck, determined to focus on ovarian cancer (second or third line). In November 2022, we reported topline clinical and initial immune response data from this study, which showed that treatment with the combination of elevated plateletsGPS and pembrolizumab compared favorably to treatment with anti-PD-1 therapy alone in a similar patient population. In November 2023, additional immunobiological and clinical data from the
study was presented at the International Gynecologic Cancer Society 2023 Annual Global Meeting which showed a correlation between immune response and progression free survival, or PFS.
In February 2020, a Phase 1 open-label investigator-sponsored clinical trial of GPS, in combination with Bristol-Myers Squibb’s anti-PD-1 therapy, nivolumab (Opdivo®), in patients with myeloproliferative neoplasms. GALE- 401malignant pleural mesothelioma, or MPM, who harbor relapsed or refractory disease after having received frontline standard of care multimodality therapy was commenced at MSK. Enrollment of a target total of 10 evaluable patients was completed at the end of 2022. We reported positive topline safety and efficacy data from this study in June 2023 and positive follow-up immune response and survival data in December 2023.
GPS was granted Orphan Drug Designations, or ODD, from the FDA, as well as orphan medicines designations from the European Medicines Agency, or EMA, for GPS in AML, MPM, and multiple myeloma, or MM, as well as Fast Track designations for AML, MPM, and MM from the FDA.
SLS009
On March 31, 2022, we entered into an exclusive license agreement, or the GenFleet Agreement, with GenFleet Therapeutics (Shanghai), Inc., or GenFleet, a clinical-stage biotechnology company developing cutting-edge therapeutics in oncology and immunology, that grants rights to us for the development and commercialization of SLS009, a highly selective small molecule CDK9 inhibitor, across all therapeutic and diagnostic uses worldwide, except for Greater China.
CDK9 activity has been shown to correlate negatively with OS in a number of cancer types, including hematologic cancers, such as AML and lymphomas, as well as solid cancers, such as osteosarcoma, pediatric soft tissue sarcomas, melanoma, endometrial, lung, prostate, breast and ovarian. As demonstrated in preclinical and clinical data, to date, SLS009’s high selectivity has the potential to reduce toxicity as compared to older CDK9 inhibitors and other next-generation CDK9 inhibitors currently in clinical development and to potentially be more efficacious.
We completed a Phase 21 dose-escalating clinical trial in the United States and China for SLS009 in mid-2023 and reported positive safety and efficacy data for both patient cohorts, that is relapsed and/or refractory AML and refractory lymphoma. We also established in the trial a recommended Phase 2 dose, or RP2D, of 60 mg for AML and 100 mg for lymphomas.
In the second quarter of 2023, we commenced an open label, single arm, multi-center Phase 2a clinical trial of SLS009 in combination with venetoclax and azacitidine, or aza/ven, in AML patients who failed or did not respond to treatment with venetoclax-based therapies. The Phase 2a trial is evaluating safety, tolerability and efficacy at two dose levels, 45 mg once weekly, and 60 mg once weekly or 30 mg twice a week. In the fourth quarter of 2023, we announced the dosing of the first patient in a Phase 1b/2 open-label, single arm trial in relapsed/refractory, or r/r, peripheral T-cell lymphoma, or PTCL, which will enroll up to 95 patients to evaluate safety and efficacy and, based on results, may serve as a registrational study. This study is funded by GenFleet and is being conducted in China.
In March 2024, we announced positive topline data from the Phase 2a clinical trial of SLS009 in combination with aza/ven in r/r/ AML. A total of 21 patients were enrolled in the study as of March 15, 2024: 10 in the 45 mg safety cohort and 11 in the 60 mg cohort (30 mg twice a week or 60 mg once a week). Response rates observed in the three cohorts were 10% in the 45 mg once a week safety dose cohort (dose level below the RP2D), 20% in the 60 mg once a week dose cohort, and 50% in the 30 mg twice a week dose cohort. Additionally, we observed strong anti-leukemic activity, which is defined as 50% or more bone marrow blast reduction in 67% of patients across all dose levels. Median OS has not been reached in any of the cohorts and the asset is ready to advance intofirst patient enrolled in the study who achieved a pivotalCR continues on the study and remains leukemia-free 9 months after enrollment. During the trial, we identified potential biomarkers currently undergoing testing as predictive markers in the most recent portion of the study. Patients with the identified biomarkers exhibited significantly higher response rates: 100% response rate at the optimal dose level (30 mg twice a week) and 57% response rate across all dose levels. Furthermore, we have clarified the proposed biological basis and mechanism of action for SLS009 activity in patients with essential thrombocythemia (ET). NeuVax is currentlythese biomarkers. The relevant biomarkers are present in multiple investigator-sponsored Phase 2 clinical trials in breast cancer. GALE-301hematologic and GALE-302 have completed early stage trials in ovarian, endometrial and breast cancers.
We are seeking to build value for shareholders through pursuit of the following objectives:
Develop hematology and oncology assets through clinical developmentsolid cancer indications, with a focus in areas of unmet medical need. Our hematology asset is targeting the treatmentsubstantial proportion of patients with ETexhibiting them in additional indications, ranging up to reduce elevated platelet counts. Our immunotherapy programs are currently targeting two key areas: secondary prevention intended to significantly decrease~50% of patients in some indications.
SLS009 was granted ODD for AML and PTCL and Fast Track designations for r/r AML and r/r PTCL by the risk of disease recurrence in breast, gastric, and ovarian cancers; and primary prevention intended to prevent ductal carcinoma in situ (DCIS) from becoming invasive breast cancer.
FDA.Evaluating strategic alternatives that may include continuing to advance the clinical programs as a stand-alone entity, a sale of the company, a business combination, merger or reverse merger, and a license or other disposition of corporate assets of the company.
Leverage partnerships and collaborations, as well as investigator-sponsored trial arrangements, to maximize the scope of potential clinical opportunities in a cost effective and efficient manner.
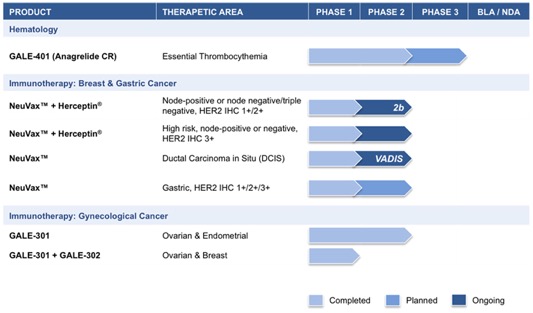
The chart below summarizes the current status of our clinical development pipeline:
HematologyOur Strategy
GALE-401 (anagrelide controlled release (CR))
GALE-401 contains the active ingredient anagrelide, an FDA-approvedOur overall goal is to develop multiple oncology product for the treatment of patients with myeloproliferative neoplasms (“MPNs”)candidates in order to lower abnormally elevated platelet levels. The currently available immediate release (“IR”) version of anagrelide causes adverse events that are believed to be dose and plasma concentration dependent, and may limit the use of the IR version of the drug. Therefore, reducing the maximum concentration (“Cmax”) and increasing the half-life of the drug is hypothesized to reduce the side effects, while preserving the efficacy, potentially allowing a broader use of the drug.
Multiple Phase 1 studies in 98 healthy subjects have shown GALE-401 reduces the Cmax of anagrelide and increases the half-life following oral administration, appears to be well tolerated at the doses administered, and to be capable of reducing platelet levels effectively. The Phase 1 program provided the desired PK/PD (pharmacokinetic/pharmacodynamic) profile to enable the initiation of the Phase 2 proof-of-concept trial. The Phase 2, open label, single arm, proof-of concept trial enrolled 18 patientsachieve marketing authorization in the United States and the rest of the world. We are particularly focused on developing better treatments for AML, the lead indication for both GPS and SLS009, which will allow us to leverage our clinical development expertise in hematology/oncology and to build a single streamlined commercial infrastructure sufficient for both of our current product candidates.
Products/Pipeline
Galinpepimut-S (GPS): Innovative WT1 Targeting Immunotherapy
Overview
GPS is a WT1-targeting peptide-based cancer immunotherapeutic being developed as a monotherapy and in combination with other therapeutic agents to treat different types of cancers that result from uninhibited tumor cell growth. GPS targets malignancies and tumors characterized by an overexpression of the WT1 protein. The WT1 protein is one of the most widely expressed cancer proteins in multiple malignancies. A 2009 pilot project regarding the prioritization of cancer antigens (substances that evoke an immune response) conducted by the National Cancer Institute, or NCI, a division of the National Institutes of Health, or NIH, ranked the WT1 protein as a top priority for immunotherapy.
WT1 is a protein that resides in the cell’s nucleus and participates in the process of cancer formation and progression. As such, WT1 is classified as an “oncogene.” WT1 plays a key role in the development of the kidneys in fetal life, but then almost disappears from normal organs and tissues. In approximately 20 cancer types, WT1
becomes detectable again in at least 50% of tumor pathology specimens in the cells of these cancers. WT1 appears in large amounts (i.e., becomes “overexpressed”) in numerous hematological malignancies, including AML, MM and chronic myeloid leukemia, as well as in many solid malignancies such as MPM, gastrointestinal cancers (such as colorectal cancer), glioblastoma multiforme, triple negative breast cancer, or TNBC, ovarian cancer and small cell lung cancer, or SCLC.
Mechanism of Action in Immune System
GPS is a multi-peptide product that has been modified to enhance the degree and duration of the immune response against the WT1 protein. Two of the four peptides in the peptide mixture comprising GPS are deliberately mutated in a single amino acid residue. These mutated peptides are recognized by the immune system as non-self entities and are therefore less likely to induce immune tolerance. These mutated peptides are designed using artificial intelligence (AI) to elicit strong T-cell response against both mutated peptides and naturally occurring peptides in cancer cells. This concept is called the heteroclitic principle.
We believe that GPS has a mechanism of action that involves direct activation of the patient’s immune system specifically and solely against the WT1 protein. Although the immune system is designed to identify foreign or abnormal proteins expressed on tumor cells, this process is often defective in cancer patients. Typically, patients harboring WT1-positive malignancies have very few or no T-cells specifically reactive or responsive to, and therefore activated by, WT1. T-cells are involved in both sensing and killing abnormal cells, in addition to coordinating the activation of other cells in an immune response. T-cells can be classified into two major subsets, CD4 cells and CD8 cells. CD8 cells, often called cytotoxic T-cells, are characterized by the expression of the CD8 protein on their cell surface. Once activated, cytotoxic T-cells recognize, bind and kill cancer cells marked by abnormal proteins. CD4 cells, known as helper T-cells, are critical to providing the signals necessary for sustained CD8 cell responses and are also capable of exerting direct anti-tumor activity. GPS is designed to elicit both CD4 and CD8 cell immune responses. We believe that the activation of CD8 cells by GPS could lead to direct cancer cell killing, or cytotoxicity, and the eventual establishment of immunologic memory against a WT1-expressing cancer. This occurs by two mechanisms: (i) conversion of some of the activated CD8 cells to memory CD8 cells, and (ii) activation of CD4 cells and the eventual creation of CD4 terminal effector memory cells.
We further believe that cytotoxic CD8 T-cells activated by GPS have been shown to be able to kill up to 10 to 20 WT1-positive cancer cells. Further, with respect to the activation of CD4 cells, we believe that CD4 cells are stimulated to produce WT1-specific helper T-cells, which are able, in turn, to activate cytotoxic T-cells and B-cells. The B-cells “helped” by the helper T-cells produce antibodies to specific WT1 epitopes. The anti-cancer effect is considered to be a result of a combination of all of the above actions, as well as possible additional, less clear, mechanisms involving other immune cell types (e.g., natural killer cells) that are not as widely understood.
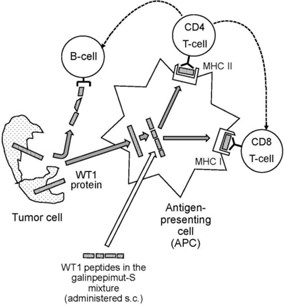
The following diagram illustrate GPS’ mechanism of action:
GPS cannot be administered to patients in a water-soluble form, and so it is given under the skin, or subcutaneously. If administered on its own, GPS would rapidly degrade and would not have the opportunity to activate the immune system. Therefore, GPS is mixed with Montanide™, a commercially available, non-specific immune adjuvant composed of a natural metabolizable oil and a very refined emulsifier, creating a water in oil emulsion. The GPS and Montanide emulsion is administered by subcutaneous injection to optimally activate cellular and humoral immune responses in vaccinated patients. Additionally, prior to the administration of GPS, patients receive another immune adjuvant, granulocyte-macrophage colony-stimulating factor, or GM-CSF, to non-specifically stimulate and activate antigen-presenting cells, or APCs, in the vicinity of the subcutaneously injected GPS.
After subcutaneous injection, the WT1 peptides within GPS disperse locally underneath the injection site and at local lymph nodes and are ingested by APCs. Digested peptide fragments are then presented on the surface of APCs to CD8 and CD4 T-cells while simultaneously associated on the cell membrane with major histocompatibility complexes, or MHC, human leukocyte antigen, or HLA, molecules. This process activates the CD4 and CD8 cells and sensitizes them to the key 25 epitopes of WT1, thus initiating the process of short- and long-term T-cell-mediated immunity against WT1.
Key Features
The following table summarizes the key features of GPS:
| | | | | | | | |
Key features of an Optimal Cancer Active Immunizer Therapeutic | | GPS Properties and Clinical Strategy |
Selecting the right target antigen and
epitopes within that antigen | | Four peptides and 25 epitopes selected optimally with the objective of ensuring: - optimal MHC complex presentation; - specificity across different HLA types; - activation of both CD4 and CD8 T-cells; and - enhancing immune response and overcoming tolerance (the heteroclitic principle). |
| | |
Optimal T-cell engagement leading to
cancer cell destruction | | Immune response data from the final analysis of the Phase 1 clinical study of GPS in MM in 12 evaluable patients that were presented at the 44th Annual Meeting of the European Society for Blood and Marrow Transplantation, or EBMT, in 2018 (Dr. Kohne et al.) showed 75% frequency of either CD8+ or CD4+ responses to an all-pool mixture of WT1-derived antigens after completion of the 12 vaccinations per the study protocol. This evidence of multi-epitope, broad cross-reactivity along the full-length of the WT1 protein is suggestive of epitope spreading, as it emerged across epitopes against which the patients were not specifically immunized. These data corroborate the results of an earlier analysis in mid-2017 and strongly suggest stimulation of T-cells towards intracellular antigen fragments from GPS-induced destruction of tumor cells, which effect is a hallmark of an effective vaccine, e.g., that it is targeting the right epitopes chosen by design. |
| | |
Overcoming the barriers of an
adverse/immunosuppressive tumor
micro-environment, or TME | | The GPS monotherapy clinical studies are in the setting of complete remission, or CR, and minimal residual disease, or MRD, whereby no bulky or measurable tumor deposits exist. This is typically seen after successful frontline therapy in select cancer types for which such debulking standard therapies exist (e.g., AML or MPM). In these settings, the tumor micro-environment, or TME, is substantially absent. We are also pursuing combination therapy with checkpoint inhibitors in tumor settings whereby measurable disease exists, as contemporaneous checkpoint inhibition would abrogate the immunosuppressive effects of the TME. |
| | |
Overcoming or mitigating immune
tolerance | | Heteroclitic peptides are those in which mutations have been deliberately introduced in the amino acid sequence. The use of heteroclitic peptide in an active immunizer, such as GPS, increases immunogenicity without changes in the antigenicity profile, as well as strengthens MHC binding of the peptide to produce cytotoxic CD8 cells that continue to recognize the corresponding native peptide sequence. This is believed to be a key factor differentiating GPS from essentially all previously developed peptide vaccines, and applies a highly innovative technology platform, peptide heteroclicity, in a clinical late-stage cancer immunotherapeutic candidate product. |
| | |
Addressing the broadest possible
candidate patient population | | GPS has activity across multiple HLA types that could allow treatment of a vast majority of global patient populations harboring WT1-positive malignancies. |
Potential Key Differentiators
GPS’ potential key differentiators as compared to other active immunization or vaccine-type approaches, as well as compared to immunotherapy approaches more generally, are as follows:
•heteroclitic peptides may offer increased immune response and less potential for tolerance;
•multivalent oligopeptide mixture potentially drives differentiated immunotherapeutic efficacy, targeting 25 key epitopes of WT1;
•potentially applicable to 20 or more cancer types worldwide and the vast majority of HLA types;
•CR or MRD status (after initial tumor debulking with preceding standard therapy) is the preferred setting for GPS monotherapy;
•not directly competitive with current clinical standard of care therapies, but rather believed to complement them in the maintenance setting;
•potential for combination approaches with other cancer immunotherapies, due to tolerable adverse event profile;
•anticipated cost-effective manufacturing; allogeneic, “off-the-shelf,” vialed subcutaneously administered drug that is not patient-specific; and
•positive Phase 2 clinical data on effectiveness (based on OS in AML and PFS in MM) with good tolerability and a favorable safety profile.
Development Program for GPS
GPS has the potential as a monotherapy or in combination with other immunotherapeutic agents to address a broad spectrum of hematologic, or blood, cancers and solid tumor indications. We are currently exploring the potential role for GPS in both monotherapy and in combination therapy with checkpoint inhibitors such as PD-1 inhibitors as set forth in the table below:
| | | | | |
| Program | Status |
| |
| GPS Monotherapy | |
| |
•Registrational Phase 3 REGAL open-label randomized clinical trial in AML patients who have achieved hematologic complete remission, with or without thrombocytopenia (CR2/CRp2), after second-line antileukemic therapy and who are deemed ineligible for, or unable to undergo, allogeneic stem-cell transplantation | Ongoing |
| |
•Phase 1 clinical trial of 3D189 (GPS) in China (our licensee, 3D Medicines is the sponsor) | Ongoing |
| |
•Phase 1 clinical trial in patients with hematologic and thoracic malignancies with no demonstrable residual/recurrent disease after debulking therapy | Completed; final data reported |
| |
•Phase 2 clinical trial in patients with AML with first complete remission (CR1) patients | Completed; final data reported |
| |
•Phase 2 clinical trial in patients with high-risk MDS or AML patients with ≥2 lines of prior therapy (CR2) | Completed; final data reported |
| |
•Phase 2 clinical trial in MM patients | Completed; final data reported |
| |
•Phase 2 randomized, double-blind, placebo-controlled clinical trial in MPM patients | Completed; final data reported |
| |
| GPS Combination Therapy | |
| |
•Phase 1/2 clinical trial of GPS in combination with the anti-PD-1 therapy pembrolizumab (Keytruda) in ovarian cancer (second or third line) in collaboration with a Merck & Co., Inc., Kenilworth, N.J., U.S. subsidiary (known as MSD outside the United States and Canada), or Merck | Completed; final data reported |
| |
•Phase 1 open-label investigator-sponsored clinical trial of GPS, in combination with Bristol-Myers Squibb’s anti-PD-1 therapy, nivolumab (Opdivo), in patients with MPM who harbor relapsed or refractory disease after having received frontline standard of care multimodality therapy | Completed; final data reported |
| |
•Phase 1/pilot open-label, non-randomized clinical trialof GPS in combination with nivolumab in patients with WT1-expressing, or WT1+, recurrent ovarian, fallopian tube or primary peritoneal cancer who were in second or greater clinical remission (after their successful first or subsequent “salvage” therapy) | Completed; final data reported |
| |
Current AML Treatment Therapies
AML is an aggressive and potentially lethal blood cancer characterized by the rapid growth of abnormal white blood cells that build up in the bone marrow and interfere with the production of normal blood cells. Its symptoms include fatigue, shortness of breath, bruising and bleeding, and increased risk of infection. The cause of AML is unknown, and the disease is typically fatal within weeks or months if untreated. AML most commonly affects adults, and its incidence increases with age.
A June 2021 report from Delvelnsight estimates a global market size for AML of $5.09 billion by the end of 2030, with a compound annual growth rate, or CAGR, of 21.85% from 2018 to 2030. The total number of newly diagnosed patients with AML per year in the United States is approximately 20,050 (2022 epidemiological data: American Cancer Society). According to PharmaIntelligence (Informa, April 2022) as AML patients progress through their individual journeys and experience disease progression, the number of patients that ultimately receive a second-line treatment of thrombocytosis,any kind in the U.S. is roughly 36% (about 7,500 patients) of the stated incident population. The corresponding numbers of second-line treated patients in the key markets of the European Union (Germany, France, Italy and Spain) is approximately 6,520 and of Japan is approximately 3,482. According to CD DiNardo (N Engl J Med 2018; 378:2386-2398) and D Verma (Leuk Lymphoma 2010 May;51(5):778-82), about 50% of patients in second-line achieve complete remission, or elevated platelet counts,CR2 (our Phase 3 REGAL patient population). These figures would substantiate a total of approximately 8,750 clinically appropriate patients for GPS in patients with MPNs. Final safety and efficacy data from this Phase 2 trial were presented in December 2015 and demonstrated a prolonged clinical benefit with a potentially improved safety profile.the referenced key markets.
We have analyzed our data and
Until recently, the overall treatment landscape for MPNs,AML had remained static for decades, as numerous targeted and antiproliferative agents were unsuccessful in providing meaningful long-term clinical benefits, including increments in survival. In recent years, additional drugs have been approved and current standard treatments include chemotherapy (including the fixed molar ratio combination chemotherapy Vyxeos), hypomethylating agents, or HMAs, drugs that target mutations of the isocitrate dehydrogenase type-1 and -2 and the FMS-like tyrosine-protein kinase, FLT3, in patients whose disease harbors these genetic aberrations, the B-cell lymphoma 2 inhibitor venetoclax (in combination with chemotherapy or HMAs), the CD33-targeting antibody-drug conjugate gemtuzumab ozogamicin, and the sonic hedgehog signaling inhibitor glasdegib. Select patients could also undergo an allogeneic hematopoietic, or blood-forming, stem cell transplant, referred to as allo-HSCT. One of the fundamental goals of therapy for AML, both in the upfront and salvage settings, is for the patient to achieve a state of complete remission. Complete remission is defined per consensus criteria by the European Leukemia Net, or ELN, whereby the hematologic and clinical features of the disease are no longer detected. In the first line setting, AML patients who achieve a status of first complete remission, or CR1, have two options for a meaningful long-term benefit: allo-HSCT and maintenance therapy with the oral form of the HMA azacitidine, which the FDA approved for use in the second half of 2020. In the second line setting, i.e., in AML patients who have relapsed and are receiving salvage antileukemic therapy, we are not aware of any therapies, other than allo-HSCT, that have shown through rigorous blinded, randomized, controlled clinical trials to offer a meaningful long-term benefit (either relapse-free or OS) when used as maintenance after patients achieve a status of CR2. Once the disease relapses after second-line therapy, patients have limited options which currently include off-label administration of HMAs, venetoclax in combination with either HMAs or low-dose cytarabine or investigational agents in the context of a Phase 1/2 clinical trial.
AML as lead indication for GPS Program
We chose AML, for which we have been granted Fast Track and ODD by the FDA, as our lead indication for GPS for the reasons outlined below:
•AML presents a clinical setting in which complete remission status (specifically CR1 and/or CR2) can be achieved with standard antileukemic therapy;
•the high degree of unmet medical need in recurrent/relapsed AML and the absence of an effective maintenance therapy over the decades after salvage re-induction until and immediately after achievement of CR2 status, especially considering that most patients in this clinical scenario are older than 60 years of age;
•the almost universal expression of WT1 in leukemic blasts, which are AML’s replicating malignant cells, as well as leukemic stem cells, or LSCs, cells that are or become extremely resistant to standard chemotherapy or targeted agent approaches and which can be realistically eradicated only with immunotherapy methods (including allo-HSCT). LSCs have been shown to be susceptible to targeting by cytotoxic T-cells (CD8 and CD4 cells) stimulated against leukemia-associated antigens and we believe this will be the case for GPS;
•the fact that WT1 has been associated with the actual development of leukemia;
•the positive correlation between the level of expression of WT1 and the prognosis in AML;
•the fact that the level of expression of WT1 can be followed over time in patients during and after therapy, including immunotherapy, as a method of monitoring for MRD;
•early evidence from mouse models that vaccination with peptides against select WT1 antigenic epitopes leads to detection of immune response;
•early evidence that human immunocytes sensitized ex-vivo to peptides contained in GPS were able to recognize naturally presented WT1 peptides on the surface of several leukemia cell lines;
•early anecdotal (at the time) clinical data showing antileukemic activity of WT1 monovalent vaccines in the CR1 maintenance setting in the Japanese population (albeit restricted to HLA-A*2401 type), as well as a dendritic cell vaccine in the Netherlands (independent of HLA haplotype) in the same setting;
•a predictive assumption of very low to negligible degree of clinical toxicity with a current focus on Essential Thrombocythemia (“ET”). SubjectWT1-targeted immunotherapy such as GPS, due to completionthe fact that WT1 in normal, non-cancerous, tissues is both expressed at extremely low levels and limited in number of organs and tissues, but also due to the fact that WT1 fragments, or peptide epitopes, in normal cells are presented to host APCs in a different manner than are WT1 fragments produced in cancer cells; of note, WT1 expression in normal tissues of adults is limited to the podocyte layer of the manufacturingglomerulus (kidney), Sertoli cells (testis), granulosa cells (ovary), decidual cells (uterus), mesothelial cells (peritoneum, pleura), mammary duct and lobule (breast), and blood-forming (hematopoietic) progenitor cells (CD34+ cells in the bone marrow);
•the advent of modern immunotherapeutics in cancer and the new formulationpromise of an innovative, off-the-shelf potentially effective, low adverse event burden immunotherapy to prevent or delay relapse in patients once they achieve complete remission status in AML, a disease that has historically been associated with dearth of deep and other internal work, GALE-401sustained responses to checkpoint inhibitors; and
•evidence from our completed Phase 1 and Phase 2 clinical trials that administration of GPS can lead to extended relapse free survival and OS especially in patients who demonstrated clear WT1 specific CD4 and/or CD8 immune response to GPS administration.
Furthermore, we believe that there is readya significant unmet medical need for a clinically safe and effective therapy as maintenance after AML patients achieve CR1 and/or CR2 status following successful first-line or second-line (salvage) therapies, as a significant percentage of these patients are ineligible for, or unable to advance into a Phase 3undergo, allo-HSCT. No third-line therapies have shown demonstrable clinical impact to date in AML patients after their second relapse and eventually AML patients in second relapse generally succumb to AML or complications associated therewith.
Our Clinical Data in AML CR1 and CR2 Patients
In an initial pilot clinical trial in ETAML, a total of nine adult patients of all ages with de novo AML were treated with upfront standard chemotherapy and were able to achieve CR1. Administration of GPS resulted in a median OS that was at least 35 months from the time of GPS administration. In this study, specifically for patients who are intolerantwere 60 years and older (n=5), median OS was at least 33 months from the time of GPS administration or resistant to hydroxyurea.approximately 43 months from the time of initial AML diagnosis. The trial is designed to compare GALE-401 (drug arm) versus best available therapy (BAT) to include a sizable populationmean time of patients treated with anagrelide IR. A productive meeting withfollow-up was 30 months from the U.S. Food and Drug Administration (FDA) in December 2016 confirmed that the GALE-401 development program is appropriate for a New Drug Application (NDA) filing using the 505(b)(2) regulatory pathway.time of diagnosis
Essential Thrombocythemia is a myeloproliferative blood disorder, and is characterized by the overproduction
at the time of diagnosis. However, manythis analysis for all patients. Of the eight patients develop symptoms duringtested for immunologic response, seven, or 87.5%, demonstrated a WT1-specific immune response.
In a subsequent Phase 2 clinical trial in AML, a total of 22 adult patients of all ages with de novo AML were treated with upfront standard chemotherapy and were able to achieve CR1. Most patients also received one to four cycles of “consolidation” chemotherapy per standard AML treatment guidelines. GPS was then administered within three months from the coursecompletion of the consolidation chemotherapy regimen in up to 12 total doses: six initial doses (priming immunization) followed by six additional “booster” immunizations over a total period of up to 15 months to qualifying patients (i.e., patients who were clinically stable and did not show disease recurrence after the first six injections). This Phase 2 clinical trial met its primary endpoint of an actual OS rate of at least 34%, measured three years into the clinical trial (i.e., percentage of patients alive after three years of follow-up). An actual OS rate of 47.4% was demonstrated at three years post-GPS treatment, exceeding historical published data of OS of 20% to 25% by 2.4- to 1.9-fold (or 240% to 190%), respectively.
GPS administration was also shown to improve OS in comparison to historical data in patients in CR1. Administration of GPS resulted in a median OS that affectwas poised to exceed 67.6 months from the qualitytime of life.initial AML diagnosis in patients of all ages, which represents a substantial improvement compared to best standard therapy. Only five of the 22 patients underwent allo-HSCT and an ad hoc statistical analysis failed to show a significant effect of the transplant upon OS (either in median survival times or survival rates at specific landmark time-points). In this study, the patients’ median age was 64 years old. Importantly, a preplanned subgroup analysis for the cohort of 13 patients within the clinical trial who were 60 years of age or older demonstrated a median OS of 35.3 months from time of initial diagnosis. Comparable historical populations have a median OS ranging from 9.5 to 16.8 months from initial diagnosis, which represents a 2.25 to 3.75-fold improvement in OS associated with GPS therapy in the CR1 maintenance setting as contrasted to these historical cohorts of broadly comparable patients.
NovelThe most frequent toxicities were mild to moderate local skin reactions and inflammation, as well as fatigue, which were self-limited and responded to local supportive measures and analgesics. None of the patients developed significant serious or high grade systemic adverse reactions (including anaphylaxis) attributable to GPS. GPS elicited WT1-specific immune responses in 88% of patients, including CD4 and CD8 T-cell responses. Further, the heteroclitic principle was confirmed, in that immune responses were seen against the native version of the two mutated WT1 peptides within the GPS mixture. The results showed a trend in improved clinical outcomes in patients who mounted an immune response with GPS compared to those patients who did not.
An additional Phase 2 clinical trial of GPS was performed at the H. Lee Moffitt Cancer ImmunotherapiesCenter & Research Institute, or Moffitt. This Phase 2 trial included 10 AML patients who had received first-line therapy for their disease, who then experienced relapse and were subsequently treated with second-line chemotherapy and achieved a CR2. This group of patients had a more advanced disease in comparison to those treated in the Phase 2 clinical trial in CR1 patients discussed above, and typically demonstrated a historical OS of less than ~8 months, even with post-CR2 allo-HSCT. In the Moffitt trial, the efficacy of GPS (measured as median OS, from the time of achievement of CR2 until death from any cause) was compared with that of “watchful waiting” in a cohort of 15 contemporaneously treated (but not matched by randomization) broadly comparable patients treated by the same clinical team at Moffitt. Initial data, at a median follow-up of 19.3 months, showed that GPS administration resulted in a median OS of 16.3 months (495 days) compared to 5.4 months (165 days) from the time of achievement of CR2. This was a statistically significant difference (p=0.0175). Two of 14 AML patients demonstrated relapse-free survival of more than one year. Both of these patients were in CR2 at time of GPS administration, with duration of their second remission exceeding duration of their CR1, strongly suggesting a potential benefit based on immune response mechanisms.
Our targeted cancer immunotherapy approach
Final data, at a median follow-up of 30.8 months, showed a median OS of 21.0 months in patients receiving GPS therapy compared to 5.4 months in the AML CR2 patients treated with best standard care resulting in a statistically significant difference (p-value < 0.02). GPS was well-tolerated in this clinical trial.
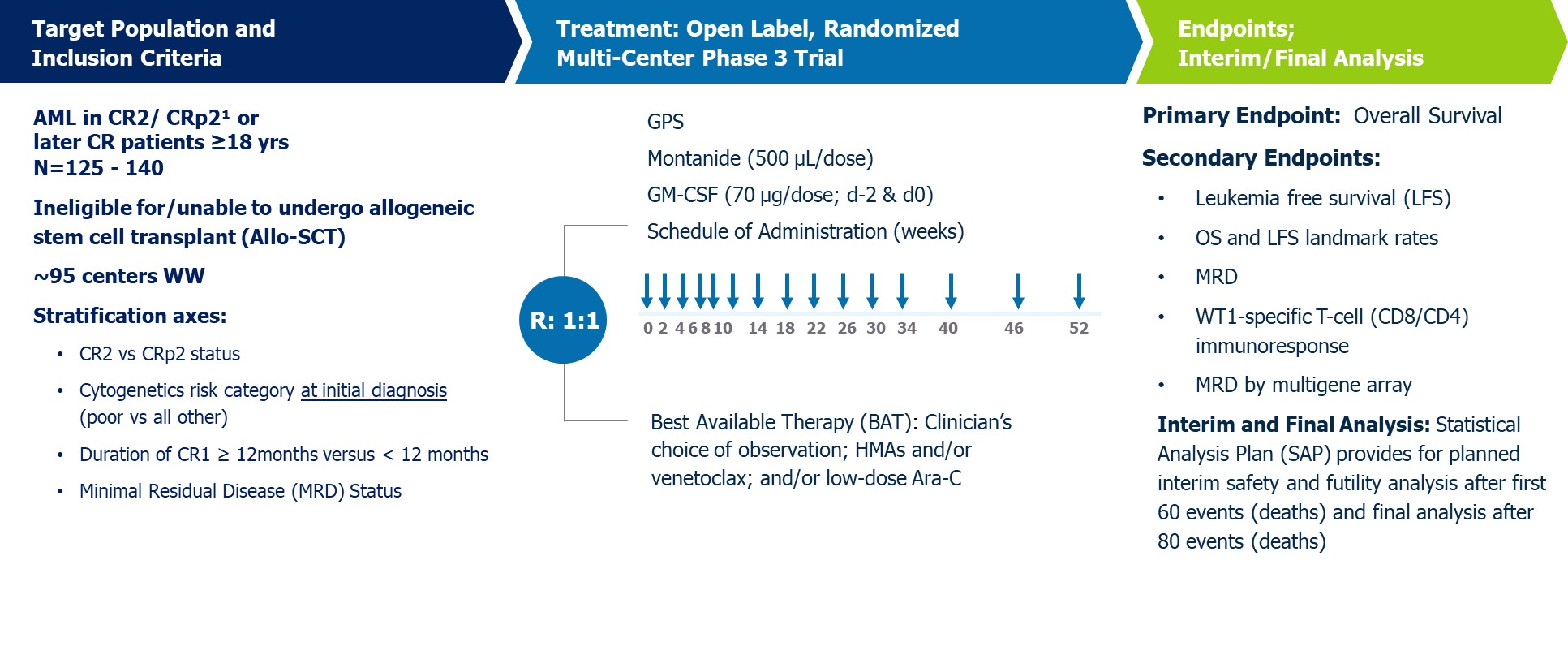
Phase 3 REGAL Clinical Trial
Building on the Phase 2 study in AML CR2 patients, which showed a median OS of 21.0 months, at a median follow-up of 30.8 months, in patients receiving GPS compared to 5.4 months in contemporaneously treated patients
with best standard therapy, in January 2020, we commenced a Phase 3 pivotal registration-enabling study for GPS in AML patients in CR2, including those in complete remission with incomplete platelet recovery. This study, which we refer to as the REGAL study, is currently based upon two key areas: preventinga 1:1 randomized, open-label study comparing GPS in the maintenance setting to investigators’ choice of best available treatment, or BAT, in adult AML patients (age >18 years) who have achieved their second or later hematologic (morphological) complete remission, with or without thrombocytopenia, after second-line antileukemic therapy and who are deemed ineligible for, or unable to undergo, allo-HSCT. The primary endpoint is OS and secondary recurrenceendpoints include leukemia-free survival, or LFS, landmark OS and LFS rates, and achievement of cancer, which is becoming increasingly importantMRD negativity. Exploratory endpoints include antigen-specific T-cell immune response dynamics over time. We expect this study will be used as the basis for a BLA submission, subject to a statistically significant and clinically meaningful data outcome and agreement with the FDA.
The REGAL study was expected to enroll approximately 125 to 140 patients (not including potentially 20-25 patients from mainland China) at approximately 95 clinical sites in North America, Europe and Asia. In the fourth quarter of 2023, we announced that we had exceeded our target enrollment of 105 patients (excluding the approximately 20-25 patients intended for enrollment in mainland China) and exceeded the number of cancer survivors continues to grow; and, primary prevention intended to prevent ductal carcinoma in situ (DCIS) from becoming invasive breast cancer. Once a patient’s tumor becomes metastatic, the outcome is often fatal, making the prevention of recurrence a potentially critical component of overall patient care. Our secondary recurrence programs primarily target patients in the adjuvant (after-surgery) setting who have relatively healthy immune systems, but may still have residual disease. Minimal residual disease, or micrometastasis, that are undetectable by current radiographic scanning technologies, can result in disease recurrence.
Our therapies utilize an immunodominant peptide combined with the immune adjuvant, recombinant human granulocyte macrophage-colony stimulating factor (rhGM-CSF), and work by harnessing the patient’s own immune system to seek out and attack any residual cancer cells. Using peptide immunogens has many potential clinical advantages, including a favorable safety profile, since these drugs may lack the toxicities typical of most cancer therapies. They also have the potential to induce immunologic memory and provide long-lasting protection with a convenient, intradermal mode of delivery.
NeuVax™ (nelipepimut-S)
NeuVax™ (nelipepimut-S) is a cancer immunotherapy targeting human epidermal growth factor receptor (HER2) expressing cancers. NeuVax is the immunodominant nonapeptide derived from the extracellular domain of the HER2 protein, a well-established and validated targetneeded for therapeutic intervention in breast and gastric carcinomas. The NeuVax vaccine is combined with GM-CSF for injection under the skin, or intradermal administration. Data has shown that an increased presence of circulating tumor cells (CTCs) may predict reduced Disease Free Survival (DFS) and Overall Survival (OS) suggesting a presence of isolated micrometastases, not detectable clinically, but, over time, can lead to recurrence of cancer, most often in distant sites. After binding to the specific HLA molecules on antigen presenting cells, the nelipepimut-S sequence stimulates specific cytotoxic T lymphocytes, or CTLs, causing significant clonal expansion. These activated CTLs recognize, neutralize and destroy, through cell lysis, HER2 expressing cancer cells, including occult cancer cells and micrometastatic foci. The nelipepimut immune response can also generate CTLs to other immunogenic peptides through inter- and intra-antigenic epitope spreading.
Breast Cancer: According to the National Cancer Institute (NCI), over 230,000 women in the U.S. are diagnosed with breast cancer annually. While improved diagnostics and targeted therapies have decreased breast cancer mortality in the U.S., metastatic breast cancer remains incurable. Approximately 75% to 80% of breast cancer patients have tissue test positive for some increased amount of the HER2 receptor, which is associated with disease progression and decreased survival. Only approximately 20% to 30% of all breast cancer patients-those with HER2 immunohistochemistry (IHC) 3+ disease, or IHC 2+ and fluorescence in situ hybridization (FISH) amplified-have a HER2 directed, approved treatment option available after their initial standard of care. This leaves the majority of breast cancer patients with low-to-intermediate HER2 expression (IHC 1+, 2+) ineligible for therapy and without an effective targeted treatment option to prevent cancer recurrence.
We currently have two investigator-sponsored trials (IST) ongoing with NeuVax in combination with trastuzumab (Herceptin®; Genentech/Roche). The combination of trastuzumab and NeuVax has been shown pre-clinically and in a pilot study to be synergistic. Our Phase 2b clinical trial is a randomized, multicenter, investigator-sponsored, 300 patient study enrolling HER2 1+ and 2+, HLA A2+, A3+, A24 and/or A26, node positive, and high-risk node negative patients. Eligible patients are randomized to receive NeuVax + GM-CSF + trastuzumab or trastuzumab + GM-CSF alone. The primary endpoint of the study is disease-free survival. Genentech/Roche is providing the trastuzumab and partial funding for this trial. Data presented in October 2016 demonstrated that this novel combination of trastuzumab and NeuVax with HER2 low-expressing patients is well tolerated and the cardiac effects of trastuzumab are not impacted by the addition of NeuVax. In February 2017, the Data Safety Monitoring Board (DSMB) reported that there were no safety concerns with the trial and the trial is not futile. The recommendation from the DSMB was to continue the trial with one revision to the statistical analysis plan regarding the timing of the pre-specified interim analysis. Givenand final analyses (60/80). In March 2024, we announced the lengthy durationcompletion of enrollment for the trial, the DSMB determinedenrollment.
The protocol specifies that the pre-specified interim efficacy analysis be moved up from 12 months to 6 months after the last patient is enrolled. Completion of enrollment is expected in the second quarter of 2017; therefore, the DSMB expects to perform the interim efficacy analysis near the end of 2017.
Our second combination IST isstudy will have a Phase 2 in HER2 3+ breast cancer patients who have completed neoadjuvant therapy with an approved regimen that includes trastuzumab and fail to achieve a pathological complete response, meaning they have microscopic evidence of residual disease and are therefore at an increased risk of disease recurrence. This multi-center, prospective, randomized, single-blinded Phase 2 trial is enrolling approximately 100 patients with a diagnosis of HER2 3+ breast cancer who are HLA A2+ or HLA A3+ and are determined to be at high-risk for recurrence. High-risk is defined as having received neoadjuvant therapy with an approved regimen that includes trastuzumab but not obtaining a pathological complete response at surgery, or those who undergo surgery as a first intervention and are found to be pathologically node-positive. These high-risk patients are known to have higher recurrence rates than other HER2 3+ breast cancer patients. Eligible patients will be randomized to receive NeuVax + GM-CSF + trastuzumab or trastuzumab + GM-CSF alone. The primary endpoint of the study is disease-free survival. Funding for this trial was awarded through the Congressionally Directed Medical Research Program (CDMRP), funded through the Department of Defense (DoD), via a Breast Cancer Research Program (BCRP) Breakthrough Award. In February 2017, the Data Safety Monitoring Board (DSMB) reported that there were no safety concerns with the trial and the trial is not futile. The pre-specifiedplanned interim safety, efficacy and futility analysis was also completed on n=50 patients and demonstrated thatafter 60 events (deaths). In addition, the agent is well tolerated with no increased cardiotoxicity associated with giving NeuVax in combination with trastuzumab. The recommendation from the DSMB was to continue the HER2 3+ trial unmodified.
A Phase 2 trial clinical with NeuVax as a single agent in patients with ductal carcinoma in situ, or DCIS, is opencharter for enrollment. The trial is being run in collaboration with the NCI, potentially positioning NeuVax as a treatment for earlier stage disease. The trial has an immunological endpoint evaluating NeuVax peptide-specific cytotoxic T lymphocyte (CTL; CD8+ T-cell) response in vaccinated patients. DCIS is defined by the NCI as a noninvasive condition in which abnormal cells are found in the lining of a breast duct and have not spread outside the duct to other tissues in the breast. DCIS is the most common type of breast cancer. In some cases, DCIS may become invasive cancer and spread to other tissues, and at this time, there is no way to know which lesions could become invasive. Current treatment options for DCIS include breast-conserving surgery and radiation therapy with or without tamoxifen, breast-conserving surgery without radiation therapy, or total mastectomy with or without tamoxifen. According to the American Cancer Society, in 2015 there were over 60,000 diagnoses of DCIS.
A Phase 3 PRESENT (Prevention of Recurrence in Early-Stage, Node- Positive Breast Cancer with Low to Intermediate HER2 Expression with NeuVax Treatment) study enrolled 758 HER2 1+/2+ patients who are node-positive and HLA A2 or A3 positive. On June 27, 2016, the Independent Data Monitoring Committee, or IDMC, recommendedfor the REGAL study provides that the IDMC may conduct risk-benefit assessments at earlier points in the clinical trial. The IDMC has met several times to perform these prespecified risk-benefit assessments of unblinded data from the study and have recommended in each instance that the trial continue without modifications. Based upon our current assumptions with respect to completion of enrollment and the estimated survival times for both the treated and control groups, we believe, after discussions with our external statisticians and experts, that the planned interim analysis after 60 events per the protocol will occur in the first half of 2024 and that the final analysis after 80 events will occur by the end of 2024. Because these analyses are event driven, they are difficult to predict with any certainty and may become available at different times than currently expected.
We have agreed with our partner in China, 3D Medicines, for 3D Medicines to participate in the REGAL study through the inclusion of approximately 20-25 patients from mainland China. Although the REGAL study has completed enrollment as announced in March 2024, in accordance with the predetermined statistical analysis plan, 3D Medicines may still enroll patients in mainland China. The timing of such participation and patient enrollment by 3D Medicines, if at all, cannot be predicted with certainty. In December 2023, we announced that we had commenced a binding arbitration proceeding administered by the Hong Kong International Arbitration Centre, which proceeding will be governed by New York law as per the terms of the 3D Medicines Agreement. We commenced the proceeding after having exhausted the dispute resolution provisions in the 3D Medicines Agreement to resolve a dispute regarding, among other things, the trigger and payment of relevant milestone payments due to us under the 3D Medicines Agreement as well as 3D Medicines' failure to use commercially reasonable best efforts to develop GPS in accordance with the terms of the agreement. See Item 3. Legal Proceedings.
The key features and schema of this study are shown in the following graphic:
Phase 3 PRESENT1 clinical trial be stoppedof 3D189 in China
In January 2022, 3D Medicines submitted an Investigational New Drug, or IND, application to initiate the first clinical trial in China for futility.3D189, also known as GPS. The PRESENTIND for the Phase 1 clinical trial, which is investigating safety, was stopped,accepted by China’s National Medical Products Administration, or NMPA, and the trial commenced in mid-2022. 3D Medicines is responsible for all expenses related to executing the trial in China. In the second quarter of 2022, we initiated an investigation intoreceived a $1.0 million milestone payment which was triggered by the causesNMPA’s approval of the recommendation. Our analysisIND. Enrollment in this study has been completed.
Expanded Access Program
At the request of several investigators, in 2022 we instituted an Expanded Access Program that allows qualified physicians to treat patients who do not meet currently required study entry criteria for the ongoing REGAL trial with GPS. This access is provided on a case-by-case basis to patients in the United States and Germany. Patients treated under the Expanded Access Program are not considered participants in the REGAL study.
GPS Combination Therapy with Checkpoint Inhibitors
Phase 1/2 Clinical Trial of GPS in Combination with Pembrolizumab
Given the potential immunobiologic and pharmacodynamic synergy between GPS and an immune check-point inhibitor (e.g., PD-1 inhibitor), we entered into a Clinical Trial Collaboration and Supply Agreement with Merck (known as MSD outside the United States and Canada), to assess the efficacy and safety of GPS in combination with Merck’s anti-PD-1 therapy pembrolizumab with exploratory long-term follow-up for OS and safety. In December 2018, we, in collaboration with Merck, initiated a Phase 1/2 open-label, non-comparative, multicenter, multi-arm clinical trial of GPS in combination with pembrolizumab in patients with WT1-positive advanced cancers, including both hematologic malignancies and solid tumors. We, together with Merck, determined to focus on 2nd or 3rd line WT1+ relapsed or refractory ovarian metastatic cancer as the primary indication for the study.
Ovarian cancer represents an intriguing opportunity to study both the clinical and immunologic effects of GPS in this solid tumor. Additionally, therapeutic targeting of WT1 through immune pathways has largely not been pursued by others to date for this indication and ovarian cancer remains “incurable” once it advances and becomes disseminated, even in the face of significant advances in the field. Ovarian cancer was chosen as a target indication for the following reasons:
•ovarian cancer presents a clinical setting whereby MRD status can be achieved with standard upfront therapy both immediately after first line therapy, but also after effective debulking of the data showed“first relapse.” The latter subgroup of patients (after successful second line treatment/first salvage, lacking demonstrable macroscopic residual disease) would be optimal candidates for GPS therapy, as no standard maintenance therapy exists for such patients and the subsequent relapse patterns and metrics are known and predictable;
•the high levels of expression of WT1 in ovarian cancer cells. In fact, WT1 expression is so frequent that there waspathologists routinely use immunohistochemical stains for WT1 (with a separationstandardized convention for describing expression and determining as “positive” or “negative”) to help distinguish epithelial ovarian cancers from other tumors;
•preliminary evidence, in a previous study of GPS with nivolumab in ovarian cancer, that WT1 expression may be linked to prognosis in ovarian cancer and that it may play an anti-apoptotic role in ovarian cancer cell lines;
•the high degree of unmet medical need in ovarian cancer patients after first (or subsequent) successful “salvage” debulking therapy and the absence of effective therapies for such patients; and
•a predictive assumption of very low to negligible degree of clinical toxicity with a WT1-targeted immunotherapy such as GPS due to the fact that WT1 in normal, non-cancerous tissues is both expressed at extremely low levels and limited in number of organs and tissues, but also due to the fact that WT1 fragments, or peptide epitopes, in normal cells are presented to host APCs in a different manner than are WT1 fragments produced in cancer cells.
Epithelial cancer of the curves, albeit not statistically significant,ovary, or ovarian cancer, is a relatively common gynecologic cancer that develops insidiously, and hence is associated with vague or no symptoms that would urge patients to seek medical attention. Not surprisingly, most women with ovarian cancer present with advanced (at least locally or regionally, and often systemically spread) disease. Ovarian cancer is managed with initial surgical resection followed by platinum-based chemotherapy. During the control arm performing better than expectedpast decade, incremental advances in chemotherapy, and the NeuVax arm performing consistentintroduction of targeted therapies (such as poly-ADP-ribose polymerase inhibitors and several others) and specially formulated compounds (such as liposomal anthracyclines) have resulted in improved survival and in more effective treatment of relapsed disease. In addition, a better understanding of genetic risk factors, along with our protocol assumptionsaggressive screening, has permitted a tailored approach to preventive strategies, such as bilateral salpingo-oophorectomy in selected women along in specific patient populations genetically predisposed to this cancer (such as those harboring genetic alterations of the BRCA gene family). Although a complete clinical remission following initial chemotherapy can be anticipated for the control group. Becausemany patients, a review of “second-look” laparotomy, when it was often performed as a matter of routine care, indicates that less than 50% of patients are actually free of disease. Furthermore, nearly half of patients with a negative “second-look” procedure relapse and require additional treatment. Many patients will achieve a CR2 clinical response with additional chemotherapy. However, almost all patients will relapse after a short remission interval of nine to 11 months, with median OS of nine to 12 months. Effective strategies, such as introduction of novel immunotherapies, to prolong remission or to prevent relapse are required, as subsequent remissions are of progressively shorter duration until chemotherapy resistance broadly develops, leading to eventual disease-related demise.
The purpose of the study was deemed futile,to determine if the administration of GPS in combination with pembrolizumab has the potential to demonstrate clinical activity in the presence of macroscopic disease, where monotherapy with either agent would have a more limited effect. This study was the first clinical trial of GPS in a patient population harboring overt bulky disease. The negative influence of TME factors on the immune response is predicted to be mitigated by PD1 inhibition (by pembrolizumab), thus allowing the patient's own immune cells to invade and destroy cancerous growth deposits specifically sensitized against WT1 (by concomitantly-administered GPS). The endpoints of the study were safety, immunobiological response, overall response rate (as measured by “response evaluation criteria in solid tumors”, or RECIST), progression free survival and OS and other analyses of interest. GPS has been designed as maintenance therapy in order to provide an OS benefit after patients reach MRD status or complete remission. The final topline data from this study demonstrated that the combination of GPS and pembrolizumab could halt or slow down the progression in highly active disease refractory to other therapies.
On February 1, 2022, we closedannounced the PRESENTcompletion of enrollment in the study.
On November 10, 2022, we reported the following confirmatory topline data from 17 evaluable patients in the study.
•Median OS was 18.4 months compared to 13.8 months with pembrolizumab alone in a in a checkpoint inhibitor single agent study in a similar patient population treated with checkpoint inhibitor alone.
•Median progression-free survival, or PFS, was 12 weeks compared to 8 weeks in a checkpoint inhibitor single agent study in a similar patient population treated with checkpoint inhibitor alone.
•The overall response rate of the trial and we expect to present the datawas 6.3 percent with a DCR of 50.1 percent at a future medical conference.median follow-up of 14.4 months. In a checkpoint inhibitor single agent study in a similar platinum-resistant ovarian cancer patient population treated with a checkpoint inhibitor alone, the observed DCR was 37.2 percent, consistent with a DCR rate increase of approximately 45 percent in the GPS combination with pembrolizumab over that seen for checkpoint inhibitors alone.
Gastric Cancer: According
•Survival and disease control benefits were observed in patients harboring tumors with any level of detectable PD-L1 expression, i.e., those with Combined Positive Score, or CPS, of 1 or higher. The DCR is 63.6% in patients with a CPS of 1 or higher. Patients with a CPS score of less than 1 showed a median OS of 3.2 months vs. patients with a CPS greater than or equal to 1 who had a median OS of 18.4 months and, as it relates to time to progression, patients with a CPS score of less than 1 had a median PFS of 1.9 months and patients with a CPS score of greater than or equal than 1 showed a median PFS of 3.8 months.
•In 16 evaluable patients in whom serial peripheral blood samples were available, a correlation was observed between PFS and OS and WT1-specific immune response after GPS vaccination across more than 1 channel with intracellular cytokine flow-cytometry assays in peripheral blood lymphocytes assaying reactivity against the NCI, gastric (stomach) cancer isfour pooled WT1 antigens comprising GPS. The data were consistent with those seen in previous studies of GPS.
•The safety profile of GPS in combination with pembrolizumab was similar to pembrolizumab alone, with only the addition of low-grade rapidly resolving local reactions at the GPS injection site, consistent with observations from other GPS clinical studies.
In November 2023, additional immunobiological and clinical data from the study for 16 safety and efficacy evaluable patients who had follow-up cross-sectional imaging (CT/MRI) were presented at the International Gynecologic Cancer Society 2023 Annual Global Meeting:
•WT1-specific T-cell (CD8 and CD4) immune response data showed a positive trend over time post-baseline with highest consistency and potential biomarkers for consistency being IFNγ and MIP1β.
•GPS in combination with pembrolizumab was strongly immunogenic, as evidenced by the positive T-cell responses seen post-vaccination.
◦42.8% of patients (6/14) achieved CD8 T-cell immune response.
◦85.7% of patients (12/14) achieved CD4 T-cell immune response.
•A correlation between WT1 specific T-cell immune responses (CD8 or CD4) and PFS was observed in a subset of analyzed patients with 41% longer PFS in patients with recorded immune response vs without (p=0.025).
GPS Combination Therapy with Nivolumab for MPM
A single-center, open-label, single-arm, non-randomized investigator-sponsored Phase 1 trial of concomitant administration of GPS in combination with Bristol-Myers Squibb’s anti-PD-1 therapy, nivolumab (Opdivo) was initiated in February 2020 at MSK in patients with MPM who have previously received treatment with pemetrexed-
based chemotherapy and have measurable disease on imaging, either due to residual disease after prior treatment or recurrent disease. We provided GPS and Bristol-Myers Squibb provided nivolumab for this study.
The principal investigator for the study was Dr. Marjorie G. Zauderer, MD, Co-Director, Mesothelioma Program and Associate Attending Physician in the Thoracic Oncology Service, Department of Medicine at MSK. The purpose of the trial was to determine if the administration of GPS in combination with nivolumab has the potential to demonstrate antitumor immune responses and meaningful clinical activity in the presence of macroscopic disease in MPM patients. The study also investigated the tolerability of the combination, evaluated the immunogenicity of the two agents administered together, by CD4+ and CD8+ T-lymphocytes (both peripherally and at the tumor site), and gauged the degree of clinical benefit by assessment of the overall response rate with the combination in comparison with that reported with nivolumab alone in historical comparable patient populations.
With approximately 3,300 cases in the United States each year, accompanied by a rising incidence in developing countries, MPM is notoriously difficult to treat and can lead to poor clinical outcomes with respect to both OS and progression-free survival, especially for those patients with the sarcomatoid variant who show a median OS of approximately 4.0 to 5.0 months. In relapsed and refractory patients who progressed after the first line standard of care pemetrexed, a similar patient population to that in the GPS nivolumab combination trial, the common treatment regimen is vinorelbine and OS in those patients is reported to be between 4.5 and 6.2 months. In patients treated with other chemotherapy regimens, such as carboplatin and irinotecan, median OS is reported to be approximately 7.0 months.
In a randomized, controlled, blinded Phase 2 clinical trial in MPM patients completed in 2017, GPS monotherapy given as maintenance after first line tumor-debulking multimodality treatment demonstrated meaningful clinical activity with median survival of 22.8 months vs. 18.3 months in the control group (n=41) and with associated sustained immune responses (both CD4+ and CD8+) against the WT1 antigen while adverse events were mainly comprised of low grade reactions at the site of the injection. See GPS Monotherapy: Completed Clinical Trials in Other Indications.
Study enrollment (target total n=10) was completed at the end of 2022. In June 2023, we reported positive topline safety and efficacy data from the study:
•Nine of the 10 patients enrolled received at least three doses of GPS, with the third GPS dose given in combination with nivolumab.
•All enrolled patients had either received and progressed with or were refractory to frontline pemetrexed-based chemotherapy.
•Median OS in patients who received the combination therapy (9/10 patients) was 70.3 weeks (17.6 months) and 54.1 weeks (13.5 months) for all 10 patients (nine patients with combination therapy and one GPS only patient). Median OS for patients who entered the study as Stage IV patients was 62.3 weeks (15.6 months). OS was calculated as the time from cessation of the most recent previous therapy until confirmed death or most recent data update for patients who still alive.
•Median PFS for all patients was 11.9 weeks.
•DCR was 30% with three patients achieving stable disease per RECIST criteria with the tumor volume decrease of up to 17%.
•As expected in this high-risk advanced cancer population, all patients experienced adverse events, unrelated and related. Seven out of 10 patients (70%) had treatment related toxicities and six (60%) had nivolumab related toxicities. Grade 3, or G3, and higher toxicities were observed in three patients (30%). None of the G3 and higher toxicities were related to GPS. GPS related toxicities were observed in three patients (30%), all were Grade 1, or G1, and included G1 skin induration at the site of injection/injection site reaction and/or fatigue in two patients and G1 dizziness and non-cardiac chest pain, each in one patient.
•Of the 10 evaluable patients, eight were male and two were female, with a median age of 69 years. Sixty percent of entered the study as Stage III or IV patients. Initial tumor stages were I (one patient), II (three patients), III (two patients) and IV (four patients).
•All patients had MPM epithelioid and/or sarcomatoid variant, a tumor which malignant (cancer) cells formuniversally expresses WT1.
In December 2023, we reported positive follow-up immune response and survival data:
•The median OS among patients who did not have an immune response to GPS was 9.0 months; the median OS for patients who had an immune response to GPS was 27.8 months, which was more than three times longer (208.3% increase) than for those patients without an immune response. Among the nine evaluable patients, four patients had a CD4+ immune response (44.4%) and three patients had a CD8+ immune response (33.3%) to GPS. Three patients had both CD4+ and CD8+ immune responses (33.3%).
•Among patients who had a full immune response (both CD4+ and CD8+) to GPS, two patients achieved an objective response (66.7%), while among the patients who did not have an immune response to GPS one patient achieved an objective response (14.3%).
GPS Monotherapy: Completed Clinical Trials in Other Indications
MPM
MPM is an asbestos-related cancer that forms on the protective tissues that cover many of the internal organs. The most common area affected is the lining of the stomach. Almost all gastriclungs and abdomen, though it can also form around the lining of the heart. Most cases are traced to job-related exposures to asbestos and it can take approximately 40 years between exposure and cancer formation. Symptoms may include shortness of breath, a swollen abdomen, chest wall pain, cough, feeling tired, and weight loss. MPM is generally resistant to radiation and chemotherapy, and long-term survival is rare, even in cases where aggressive upfront debulking multimodality therapy (i.e., extirpative surgery, chemotherapy and in some cases radiotherapy, often described as “trimodality therapy” when used to treat MPM) are used.
A randomized, double-blind, placebo-controlled Phase 2 clinical trial in MPM patients enrolled a total of 41 patients at MSK and MDACC. Data from this Phase 2 clinical trial was presented in 2016. Based on an initial analysis of 40 patients who were eligible at the time with a median follow-up of 16.3 months, a median OS of 24.8 months was seen for GPS-treated MPM patients, compared to a median OS of 16.6 months for patients in the control arm. For patients with a basic reproductive ratio tumor resection and subsequent treatment with GPS, a significant survival benefit was observed compared to those who received a placebo, with a median OS of 39.3 months compared to 24.8 months (HR: 0.415) in favor of GPS. In a subsequent analysis for the entire cohort (n=41) in August 2016, with a median follow-up of 17.2 months, a median OS of 22.8 months was observed for GPS-treated MPM patients, compared to a median OS of 18.3 months for patients in the control arm. In the datasets from both of these analyses, GPS was shown to induce WT1-specific CD8 and CD4 T-cell activation. There were no clinically significant severe adverse events in this study.
Multiple Myeloma (MM)
MM is a cancer formed by malignant plasma cells, and its cause is unknown. The overgrowth of plasma cells in the bone marrow crowds out normal blood-forming cells, causing low blood counts and anemia (a shortage of red blood cells). MM can also cause a shortage of platelets (cells responsible for normal blood clotting) and lead to increased bleeding and bruising, along with problems fighting infections due to low white cell counts and/or lower levels of infection-fighting antibodies. MM causes a host of organ problems and symptoms, including fatigue, bone pain, fractures, circulatory problems (in small vessels of the brain, eye retina, heart, bowel, etc.) and kidney failure. Treatment for MM includes chemotherapy, glucocorticoids, drugs that modulate the immune system (immunomodulatory drugs, or IMiDs), proteasome inhibitors, histone deacetylase inhibitors, targeted monoclonal antibodies, radiation and autologous stem cell transplants, or ASCTs. The prognosis in MM is highly variable and depends on numerous risk factors, some related to the biology of the disease, others to the host (e.g., age and functional status). Consequently, median survival can vary from up to at least 15 years in non-high-risk patients who achieve complete remission, as defined by the International Myeloma Working Group, or IMWG, criteria, to
approximately three years (from time of initial treatment) in patients with MM who achieve less than partial response, or PR, after ASCT. There are patients with MM who fare even more poorly than described above. For example, those in the immediately aforementioned group who also have high-risk cytogenetics at baseline may survive on average less than three years. Similarly, patients who are ineligible for ASCT and are managed only with chemotherapy and long-term IMiD maintenance (with up to nine cycles of lenalidomide) who also achieve less than complete remission and remain MRD-positive demonstrate a three-year OS rate of only about 55%; these landmark three-year OS rates decrease by approximately 40 to 50% in patients who also have high-risk cytogenetics at baseline. Despite significant therapeutic advances in the management of MM, the prognosis of patients with high-risk cytogenetics at the time of diagnosis remains quite poor, even when they successfully complete an ASCT, particularly if such patients continue to have evidence of MRD.
We have reported comprehensive final data from a Phase 2 study for GPS in 19 patients with MM. All non-progression events were confirmed and remained ongoing as of the time of the latest presentation (median follow-up at 20 months for survivors). The data indicate promising clinical activity among MM patients with high-risk cytogenetics at initial diagnosis who also remain MRD(+) after successful frontline therapy (induction regimen followed by ASCT). This subgroup of MM patients, when serially assessed per IMWG criteria, typically relapse/progress within 12 to 14 months after ASCT, even when they receive maintenance therapy with IMiDs such as thalidomide or proteasome inhibitors such as bortezomib - 18 of the 19 patients received lenalidomide maintenance starting after the first three GPS administrations following ASCT; the remaining single patient received bortezomib under the same schedule. All patients had evidence of at least MRD (MRD+) after ASCT, while 15 of the 19 also had high-risk cytogenetics at diagnosis. Combined, these characteristics typically result in low PFS rates that do not exceed 12 to 14 months following ASCT, even while on maintenance therapy with IMiDs or proteasome inhibitors, which are the current standards of care. At June 2017, median PFS with GPS was 23.6 months, while median OS had not been reached. Our results compare favorably with an unmatched cohort of broadly comparable MM patients with high-risk cytogenetics published by the Spanish PETHEMA group from the PETHEMA Network No. 2005-001110-41 trial. Our GPS therapy demonstrated a 1.87-fold increase in median PFS, as well as a 1.34-fold increase in the PFS rate at 18 months compared to the aforementioned historical cohort, which included MM patients with high-risk cytogenetics and MRD(+) post-ASCT and on continuous intensive maintenance with thalidomide +/- bortezomib. The safety profile was devoid of grade 3/4/5 treatment-related adverse events. Immune response data showed that up to 91% of patients had successfully developed T-cell (CD8 or CD4) reactivity to any of the four peptides within the GPS mixture, while up to 64% of patients demonstrated immune response positivity (CD4/CD8) against more than one WT1 peptide (multivalent responses). Moreover, multifunctional cross-epitope T-cell reactivity was observed in 75% of patients to antigenic epitopes against which hosts were not specifically immunized, in a pattern akin to epitope spreading. Further, a distinctive link was shown between the evolution of immune responses and changes in clinical response status (achievement of CR/very good partial response clinical status per IMWG criteria) over time following treatment with GPS, with each patient being used as his or her own control for each longitudinal comparison. This association has not been previously described for a peptide vaccine in MM. We believe that these results offer mechanistic underpinnings for immune activation against WT1 in patients with aggressive, high-risk MM, and support the potential antimyeloma activity of GPS.
GPS Combination Therapy: Completed Clinical Trial in Ovarian Cancer
GPS was studied in combination with nivolumab in an open-label, non-randomized Phase 1/pilot clinical trial, which was independently sponsored by MSK. The aim of the study was to evaluate the safety and efficacy of this combination in patients with WT1+ recurrent ovarian, fallopian tube or primary peritoneal cancer who were in second or greater clinical remission (after their successful first or subsequent “salvage” therapy). Eligible patients were devoid of macroscopic residual or recurrent disease, i.e., were free of locally or distantly metastatic deposits detectable by imaging modalities (CT, MRI and/or PET scan). This Phase 1/pilot clinical trial enrolled 11 patients with recurrent ovarian cancer who were in second or greater clinical remission at MSK, of whom 10 were evaluable. Patients enrolled in the clinical trial received the combination therapy during a 14-week treatment period. Individuals who had not progressed by the end of this period also received a maintenance course of GPS. In this study, treatment was continued until disease progression or toxicity. Information on the primary endpoint of this clinical trial, which was the safety of repeated GPS administrations, for a total of six doses, in combination with seven infusions of nivolumab was presented at the American Society of Clinical Oncology, or ASCO, 2018 annual meeting (O’Cearbhaill RE, et al). The secondary endpoint of the study was immune response, and the exploratory endpoints included landmark one-year PFS rate compared to historical controls and correlative analyses between clinical and
immune responses. Exploratory efficacy interim data from this pilot trial showed that GPS, when combined with a PD-1 inhibitor, in this case nivolumab, demonstrated PFS of 64% at one year in an intent to treat the group of 11 evaluable patients with WT1+ ovarian cancer in second or greater remission. Among patients who received at least three doses of GPS in combination with nivolumab, PFS at one year was 70% (7/10). The historical rates with best standard treatment do not exceed 50% in this disease setting. The most common adverse events were Grade 1 or 2, including fatigue and injection site reactions. Dose limiting toxicity was observed in one patient, following the second dose of the combination. No additional adverse event burden was observed for the combination as compared to nivolumab monotherapy. The combination induced a high frequency of T- and B-cell immune responses.
Follow-up data now show that three of the 11 patients enrolled in the study have continued to show no signs of disease progression. The mean PFS for these three patients is 35.4 months from the initiation of salvage chemotherapy, or mean PFS of 30.1 months from the first administration of GPS plus nivolumab. Based on this follow-up information, the estimated two-year PFS rate for this study is now 27.3% for the intent-to-treat, or ITT, patients (n=11) and approximately 30% for patients who received greater than two doses of GPS and nivolumab (n=10), as compared to a historical 3% to 10% PFS rate for patients receiving only salvage chemotherapy. No new serious adverse events were noted during the longer follow-up period.
SLS009: Highly Selective Next Generation CDK9 Inhibitor
Overview
SLS009 is a next generation highly selective CDK9 inhibitor which we in-licensed from GenFleet in March 2022. We have worldwide development and commercialization rights, except for Greater China. See Strategic Collaborations and License Agreements -Exclusive License Agreement with GenFleet Therapeutics (Shanghai), Inc. CDK9 activity has been shown to correlate negatively with OS in several cancer types, including hematologic cancers, are adenocarcinomas (cancers that beginsuch as AML and lymphomas, as well as solid cancers, such as osteosarcoma, pediatric soft tissue sarcomas, melanoma, endometrial, lung, prostate, breast and ovarian cancer.
Mechanism of Action
CDK9 is a major cancer target. CDK9, together with cyclin T1, forms positive transcription elongation factor b, or P-TEFb, which plays an important role in cells that make and release mucus and other fluids). Other types of gastric cancer are gastrointestinal carcinoid tumors, gastrointestinal stromal tumors, and lymphomas. Infection with bacteria called Helicobacter pylori (H. pylori) is thoughtallowing long RNA strands to be quickly transcribed. P-TEFb is crucial for the causesynthesis of gastricsome of the key proteins necessary for survival of cancer cells, including short-lived proteins such as MCL-1, which is a key anti-apoptotic (preventing programmed cell death) protein, and age, diet,oncogenes such as c-MYC. These proteins must be constantly replenished for cancer cells to survive. Inhibition of CDK9 can decrease the levels of MCL-1 and stomach diseasec-MYC which can affectresult in apoptosis and cell cycle arrest. Cyclin-dependent kinases, or CDKs, play a role not only in cancer cells but also healthy cells. Drug candidates that broadly target CDKs, i.e., those with lower specificity, can have issues with toxicity because healthy cells as well as cancer cells are targeted. The first generation of CDK9 inhibitors worked across many CDK targets in addition to CDK9. These first-generation drug candidates showed some clinical activity but had significant toxicity due to low specificity. Next generation CDK9 inhibitors, including SLS009, have potential for higher specificity for CDK9 and lack of binding to other CDKs, potentially resulting in less toxicity and more consistent clinical activity.
Key Attributes
Higher selectivity: In preclinical studies, SLS009 has demonstrated higher selectivity for CDK9 than other members of the riskhuman kinome when compared to other non-oral CDK9 inhibitors currently in active clinical development in the United States for hematological cancers, including AZD-4573 being developed by AstraZeneca and enitociclib (VIP152) being developed by Vincerx Pharma. The human kinome is a set of developing gastric cancer. Gastricall 538 kinases, which are enzymes that play essential functions by catalyzing protein phosphorylation. SLS009 has been shown to block activity of fewer kinases, other than CDK9, than these competing development candidates which, as demonstrated in clinical trials, has resulted in a better safety profile with fewer treatment related adverse events.
Higher anti-cancer activity: The preclinical data below is a comparison of SLS009 and an exact molecular copy of enitociclib (VIP152) (shown in the graphs as GFC002). The top table shows the maximal inhibitory concentration, which is the amount of drug that is needed to inhibit survival of cancer cells, across different cell lines of cancer in
vitro. Across multiple cancer cell line histologies, a smaller concentration of SLS009 is needed to achieve the same inhibitory effect as compared to the exact molecular copy of enitociclib (VIP152). In a mouse AML xenograft model, the lowest tumor growth and the highest AML cell killing was achieved by SLS009. In this mouse model, there was significantly more toxicity, including weight loss, observed with enitocliclib (VIP152) treated mice.
| | | | | | | | |
| Cell lines | SLS009 IC50 (72h) | VIP152 IC50 (72h) |
| AML | 4.8 ~33 nM | 15.9 ~136 nM |
| Lymphoma | 10.6~77.9 nM | 16.6 ~138 nM |
| MM | 33.6 ~151 nM | 51.4 ~397 nM |
| ALL | 13.4~35.7 nM | 42.3 ~68.6 nM |
| CLL | 25 nM | 40.7 nM |
Pharmacokinetic, or PK, Data: PK data observed from the completed Phase 1 trial are shown below. PK data show the relationship between the dosing regimen and the body’s exposure to a drug as indicated by the concentration time curve. An important component of the mechanism of CDK9 inhibition in cancer is often diagnosedto achieve very high concentration immediately which then shuts down the cancer cell and leads to apoptosis, while quickly ramping down so that there is not apoptosis of neutrophils. PK analyses were made for both twice a week dosing regimen (BIW cohorts) and once a week dosing regimen (QW cohorts).
BIW cohorts: The PK analysis result showed that after intravenous infusion of 2.5 mg (N=1), 4.5 mg (N=5), 9 mg (N=8), 15 mg (N=11), 22.5 mg (N=7), 30 mg (N=8), and 40 mg (N=3) of SLS009 twice a week (BIW, administered on the first and second days of each week for one hour), the plasma concentration reached peak at the end of the infusion. The exposure parameters (Cmax and AUC) of SLS009 increased in an advanced stage becauseapproximately proportional manner in the dose range 2.5 mg to 40 mg. The PK profiles in single and repeated administration were comparable.
QW cohorts: After intravenous infusion of 30 mg (N=7), 45 mg (N=8), and 60 mg (N=9) of SLS009 once a week (QW, administered on the first day of each week for four hours), the plasma concentration-time profiles were comparable to those of BIW administration, indicating a similar characterization of distribution and metabolism. The plasma concentration reached peak at the end of the infusion. The exposure parameters (Cmax and AUC) of SLS009 increased in an approximately proportional manner with the dose range 30 mg~60 mg. After QW administration, there was no obvious accumulation of SLS009.
Comparison of twice a week and once a week dosing regimens is shown below.
Pharmacodynamic, or PD, Data: The graphs below show certain correlative pharmacodynamic data from the completed Phase 1 study. At higher dose levels, a pattern of drug induced decreases in two biomarkers commonly used for assessing pharmacodynamics of CDK9 inhibitors, MCL1 and MYC, is seen. These data are no early signsimportant in that we believe they demonstrate that SLS009 is translating CDK9 inhibition into a meaningful suppression of cancer associated proteins. MCL1 is a key antiapoptotic protein which is difficult to inhibit directly. It is postulated that CDK9 inhibitors can indirectly inhibit MCL1. We believe that these PD data demonstrate that SLS009 does inhibit MCL1. MYC is a key driver in many cancers, both hematological and solid tumors. We believe that the data presented below demonstrate meaningful MYC suppression.
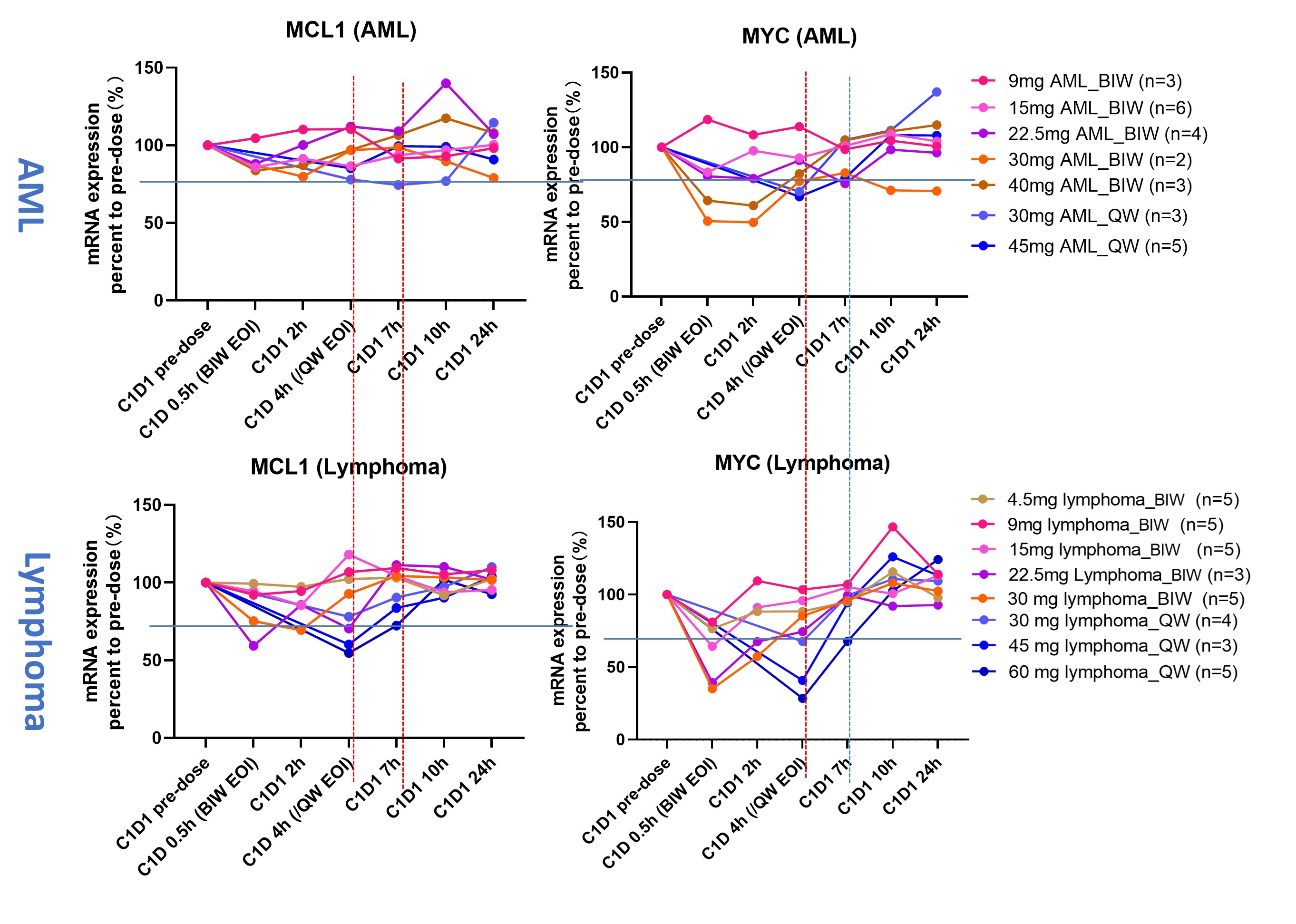
Efficacy in venetoclax resistant disease: Venetoclax, in combination with hypomethylating agents, is a key component of treatment for AML across all patient categories, especially older patients, who are the vast majority of AML patients. We believe that SLS009 has potential as a treatment option for AML patients who are r/r to venetoclax. We observed in the Phase 1 study that a r/r AML patient achieved a complete response and four additional r/r AML patients achieved greater than or symptoms, andequal to 50% decrease in bone marrow blasts which includes patients who had prior treatment with venetoclax. To our knowledge, as of March 1, 2024, SLS009 is the second-most commononly CDK9 inhibitor for which a complete response as monotherapy in r/r AML has been reported. See Phase 1 Clinical Trial.
Phase 1 Clinical Trial
The Phase 1 dose-escalating clinical trial in the United States and China for SLS009 was completed in 2023. The study evaluated both twice-a-week and once-a-week dosing and the indications were r/r AML, chronic lymphocytic leukemia, or CLL, small lymphocytic leukemia, or SLL, and lymphoma. The primary goal of the trial was to establish the RP2D which was established at 60 mg for AML and 100mg for lymphomas.
Two dosing regimens were tested in incremental SLS009 dose levels from 2.5 mg to 100 mg, either twice a week, or BIW, dosing regimen or once a week, or QW, dosing regimen. A total of 34 patients were treated in the AML cohort and 52 patients in the r/r lymphoma cohort. Among the 52 r/r lymphoma patients, 15 were diagnosed with PTCL.
For the cohort of patients with AML and with lymphomas, all key study objectives regarding PK, PD, safety and clinical activity data were met:
Efficacy:
AML cohort:
•Anti-tumor activity and clinical responses across groups and dose levels were observed, indicating a broad therapeutic index. Meaningful cell killing activity was defined as ≥50% reduction in blasts in the bone marrow.
◦AML cohort: cell killing activity observed at the following dose levels:
▪9 mg BIW: 50.0% bone marrow blast (BMB) reduction;
▪15 mg BIW: 53.8% BMB reduction;
▪30 mg QW: 57.1% BMB reduction;
▪45 mg QW: 61.3% BMB reduction;
▪60 mg QW: 77.3% BMB reduction.
◦Durable complete remission (CR) with no MRD in one patient with AML who had failed prior aza/ven therapy was achieved. The duration of the CR was eight months. Historic, best available therapy median OS for patients relapsed after aza/ven is estimated at 2.5 months.
Lymphomas cohort:
•Among34 evaluable r/r lymphoma patients, five (14.7%) achieved a clinical response with a reduction in tumor burden of up to 62%.
•An additional seven patients (20.6%) achieved stable disease, or SD, resulting in an overall DCR of 35.3%.
•In the subgroup of PTCL patients, four out of 11 (36.4%) evaluable patients achieved a clinical response.
Safety:
AML cohort:
•No dose limiting toxicities and no higher grade non-hematologic toxicities of any kind were observed.
•Some hematologic toxicities were difficult to determine in patients with hematologic cancers but were short in duration and reversible.
Lymphomas cohort:
•There were no drug-related fatalities at any dose level, and the drug was well tolerated.
•In patients treated with BIW dosing regimen, no significant safety events appeared to be dose-dependent.
•In patients receiving the QW dosing regimen, ≥ G3 treatment-related adverse events, or TRAEs, occurred, primarily hematologic events, at higher dose levels.
•Non-hematologic toxicities were rare across all dose levels with five out of 52 patients (9.6%) experiencing higher grade toxicities, including hypokalemia (3/52 patients, 5.8%), upper respiratory tract infection (1/52 patients, 1.9%) and increase in bilirubin (1/52 patients, 1.9%).
•Maximum Tolerated Dose, or MTD, was not reached with only 1/5 patients at the highest dose level studied (100 mg) experiencing a dose-limiting toxicity, or DLT.
•No DLTs were observed at any other dose level, and there were no unexpected toxicities across the study.
PK Data:
AML cohort:
•Achieved desired 24 hours > IC90 peripheral blood concentrations after the first infusion, with IC90 concentrations resulting in up to 97% cancer cells killed.
Lymphomas cohort:
•Exposure parameters (maximum concentration, or Cmax, and area under curve, or AUC) increased in an approximately proportional manner with the dose range of 30 mg~60 mg QW. The exposure of 100 mg was the highest, and the mean plasma concentration remained above IC90 for the longest time period (nearly 50 hours).
PD Data:
AML cohort:
•Achieved desired levels of MCL1 and MYC suppression in peripheral blood with decrease in MCL1 or MYC observed in 97% (66/68) of analyzed patients. A trend of proportionally increased maximum inhibition of MCL1 and MYC observed among maleshigher doses (22.5 mg to 60 mg) in both AML and third-most common among femaleslymphoma patients, which is more prominent in AsiaQW cohorts compared to BIW cohorts. QW regimen was able to induce longer sustained inhibition (at least 6 hours) of MCL1 and worldwideMYC than BIW treatment, allowing longer period for CDK9 inhibition to induce cancer cell apoptosis.
Lymphomas cohort:
•Desired levels of suppression in peripheral blood were achieved, leading to a decrease in MCL1 or MYC biomarkers in all (100%) studied patients. Biomarker suppression was dose-dependent in patients receiving QW dosing. The biomarkers studied included MYC and MCL1 with over 63,000 new casesSLS009 administration resulted in biomarkers suppression across dose levels in both administration regimens (BIW and QW) and a yeardose-dependent decrease in India, whereQW groups. 100mg QW dose level resulted in the longest sustained inhibition of both MCL1 and MYC.
Phase 2 Development Program
Phase 2a clinical trial in AML patients
In the second quarter of 2023, we commenced an initialopen label, single arm, multi-center Phase 2a clinical trial of NeuVaxSLS009 in combination with aza/ven in AML patients who failed or did not respond to treatment with venetoclax-based therapies. The trial is planned. Overexpressiondesigned to evaluate safety, tolerability, and efficacy at two dose levels of SLS009, 45 mg QW, and 60 mg QW or 30 mg BIW, in combination with aza/ven. In addition to safety and tolerability of SLS009 in combination with aza/ven, the primary endpoints are complete response composite rate and duration of response. Additional endpoints include event free survival, OS, and PK and PD assessments. The trial includes several sites in the United States, will enroll a minimum of 20 patients and, based on initial results, may be expanded into a registrational trial.
In the fourth quarter of 2023, we completed enrollment in the 45 mg QW dose cohort in the Phase 2a study and reported positive initial topline data. We also commenced enrollment of the HER2 receptor occurs60 mg dose cohort with patients
randomized to one of two groups, 60 mg fixed dose QW or 30 mg fixed dose BIW. Each group will enroll approximately five to 10 patients.
In March 2024, we announced positive topline data from the Phase 2a STUDY of SLS009 in approximately combination with aza/ven in r/r AML. As of March 15, 2024 data cutoff, 21 patients were treated. All patients were diagnosed with AML refractory to or relapsed after venetoclax containing regimens. 20 out of 21 (95%) enrolled patients had adverse/high-risk cytogenetics and 1 patient (5%) had intermediate cytogenetics. Median age was 70 and 19/21 (90.5%) of patients were older than 60.
Efficacy:
A total of 21 patients were enrolled in the study as of March 15, 2024: 10 in the 45 mg safety cohort and 11 in the 60 mg cohort (2 x 30 mg twice a week or 60 mg once a week).
•10% response rate in the 45 mg QW safety cohort (dose level below the RP2D).
•20% response rate in the 60 mg QW cohort.
•50% response rate in the 60 mg, 2 x 30 mg BIW cohort.
•Observed strong anti-leukemic activity, defined as 50% or more bone marrow blast reduction in 67% of gastric and gastro-esophageal junction adenocarcinomas, predominantly thosepatients across all dose levels.
•Median survival rate has not been reached in any of the intestinal type. Overall, without regarddose levels.
•The first patient enrolled in the study who achieved a complete response (CR) continues on the study and remains leukemia-free 9 months after enrollment.
Biomarkers:
•During the trial, we identified potential biomarkers currently undergoing testing as predictive markers in the most recent portion of the study.
•Patients with the identified biomarkers exhibited significantly higher response rates:
•100% response rate at the optimal dose level (30 mg BIW).
•57% response rate across all dose levels.
•Furthermore, we have clarified the proposed biological basis and mechanism of action for SLS009 activity in patients with these biomarkers.
•The relevant biomarkers are present in multiple hematologic and solid cancer indications, with a substantial proportion of patients exhibiting them in additional indications, ranging up to ~50% of patients in some indications.
Safety:
•SLS009 in combination with aza/ven has been well-tolerated at all tested dose levels.
•No DLTs at any of the studied dose levels and no treatment-related high-grade (≥G3) toxicities were observed.
•Hematologic toxicities profile was consistent with aza/ven standalone treatment.
Patients with AML that fail venetoclax-based therapies have limited treatment options and a poor prognosis with a median OS of approximately 2.5 months. See Current AML Treatment Therapies for more information on the AML treatment landscape.
Additional data from the 60 mg dose cohort are expected in the second quarter of 2024.
Phase 1b/2 in PTCL
The first patient in a Phase 1b/2 trial evaluating SLS009 in r/r PTCL was dosed in the fourth quarter of 2023. The open-label, single-arm trial will enroll up to 95 patients to evaluate safety and efficacy and, based on the results,
may serve as a registrational study. This initial PTCL study is fully funded by GenFleet and is being conducted in China. We expect to report initial topline data from the study in the second quarter of 2024.
Phase 1b/2 in Combination with Brukinsa® in Diffuse Large B-Cell Lymphoma (DLBCL)
In March 2024, GenFleet announced that it entered into a collaboration and supply agreement with BeiGene Switzerland GmbH to initiate a combination study of SLS009 and Brukinsa (zanubrutinib), a BTK inhibitor, in r/r DLBCL and the first patient was dosed in the trial. The open-label, single-arm multi-center trial will be conducted in two parts. In the Phase 1b portion, 6-18 patients will be enrolled. In the Phase 2 portion, approximately 45 patients will be enrolled. This study is funded by GenFleet and is being conducted in China.
Preclinical Studies
In August 2022, we announced results from preclinical in vitro studies for SLS009 in AML cell lines. The in vitro studies were conducted at an independent third-party contract research organization, and utilized the following cell lines based on their unique characteristics in combination with SLS009’s mechanism of action: RH30, a pediatric soft tissue sarcoma cell line that is a model for studying high-risk pediatric rhabdomyosarcoma, NCI-H209, a small cell lung cancer cell line characterized by the loss of function of two major tumor suppressor genes, RB1 and TP53, and which also expresses MCL-1, a major target of CDK9 inhibition, SKOV-3, an ovarian cancer cell line containing the wild type BRCA1 gene and highly expresses CDK9, and OCI-AML-2, an AML cell line that develops resistance to venetoclax. The data showed that SLS009 demonstrated significant anti-tumor effects in all four selected cell lines. In three out of the four cell lines, SLS009 inhibited cancer cell growth by 90 to 100 percent.
In August, we announced results from a new preclinical in vitro study for SLS009 in neuroendocrine prostate cancer, or NEPC. The data shows that SLS009 demonstrated significant anti-tumor effects in the selected cell line at nanomolar concentrations and, in certain samples, complete growth inhibition with no viable cancer cells. Additionally, in December 2022, we announced results from a preclinical in vivo study for SLS009 that demonstrated robust inhibition of tumor growth in a mouse xenograft model of SCLC. SLS009 was tested against NCI-H209 SCLC xenografts in athymic nude mice in four treatment groups of eight mice each (n=32) consisting of SLS009 alone, olaparib (a PARP inhibitor) alone, a combined regimen of SLS009 and olaparib, and a vehicle control. Treatments were initiated after tumor xenograft volumes exceeded 120 mm3 in each animal group and mice were subsequently sacrificed after mean tumor volume exceeded 1,500 mm3 in the control group.SLS009 treated mice exhibited a 40.4% decrease in mean tumor growth compared to the stagecontrol group in this very aggressive cancer model which had a tenfold increase in average tumor volume over 20 days. Strongest effects were observed with SLS009 in combination with olaparib, with mean tumor growth decreased by 72.3%. Treatment with olaparib alone resulted in a 30.2% mean decrease in tumor growth. No significant toxicity or safety concerns were observed in any of the treatment groups.
PIVOT Program
In December 2022, we announced that SLS009 will be evaluated in pediatric solid tumors and leukemia models through the NCI Pediatric Preclinical in Vivo Testing, or PIVOT, program. SLS009 testing through the program involves a three-phase research plan for PK, tolerability, and efficacy in pediatric tumors. In the first phase, PIVOT principal investigators will conduct PK experiments to confirm the appropriate dose and route administration for SLS009. In the second phase, tolerability of the dose and route of administration selected from the PK phase will be determined. In the last phase, monotherapy in vivo efficacy testing for SLS009 will be performed by PIVOT investigators. Studies will be supported through cooperative agreement grants from the NCI to the seven PIVOT research programs performing the testing and a centralized coordinating center.
The PIVOT program is a comprehensive program to systematically evaluate novel agents against genomically characterized pediatric solid tumor and leukemia models at eight participating research institutions. By supporting a more reliable agent prioritization process, the PIVOT program contributes to the goal of accelerating discovery of more effective treatments for children with cancer.
Each PIVOT principal investigator has expertise in preclinical testing of childhood cancer only approximately 28%in vivo models. These models utilize patient derived xenografts, many of which are refractory to current standard of care treatments, from
high-risk childhood cancers and have undergone comprehensive genomic characterization to demonstrate close resemblance to genetic alterations seen in the respective human cancers. Research strategies are based on a substantial body of data showing that preclinical testing in the appropriate pediatric cancer models, combined with expertise on relative drug exposures tolerated in mice and humans, provides powerful insights into likely clinical utility of investigational agents.
PIVOT Program participating institutions and relevant pediatric cancer models are as follows:
•Jackson Laboratory which serves as PIVOT Coordinating Center
•St. Jude Children’s Research Hospital for soft tissue sarcomas including rhabdomyosarcoma
•MD Anderson Cancer Center for osteosarcoma
•University of Texas Health Science Center San Antonio for Ewing sarcoma rhabdomyosarcoma, kidney, and liver cancers
•Memorial Sloan Kettering Cancer Center for pediatric sarcomas and other solid tumors
•Children's Hospital of Chicago for orthotopic CNS tumors
•Children’s Cancer Inst Australia for acute lymphoblastic leukemia
•Children’s Hospital of Philadelphia for neuroblastoma
The first phase of the program, pharmacokinetics, has been successfully completed and dosing regimens have been developed. The second phase of the program, tolerability, is currently in progress and is projected to be completed at all sites in the first half of 2024. The final phase of the program, efficacy, is in progress at certain sites and will have commenced at all sites by the second quarter of 2024. We expect to report relevant data from the program in the second half of 2024.
Strategic Collaborations and License Agreements
Exclusive License Agreement-Memorial Sloan Kettering Cancer Center
In September 2014, we entered into a license agreement with MSK under which we were granted an exclusive license to develop and commercialize MSK’s WT1 peptide vaccine technology. The MSK original license agreement was first amended in October 2015, further amended in August 2016, amended and restated in May 2017 and again amended and restated in October 2017. In connection with the entry of the original license agreement and its amendments, MSK was issued or assigned an aggregate of 4,846 ordinary shares of the privately held Bermuda exempted company, Sellas Life Sciences Group Ltd., or Private SELLAS, common stock for the year ended December 31, 2017. These common stock shares were converted into our common stock shares upon the business combination with Private SELLAS on December 29, 2017.
Under the terms of the current amended and restated MSK license agreement, we agreed to pay minimum royalty payments in the amount of $0.1 million each year commencing in 2015 and research funding costs of $0.2 million in each year and for three years commencing in January 2016. We also agreed to pay MSK a mid-six digit amount over a one year period in exchange for MSK’s agreement to further amend and restate the MSK license agreement in October 2017. In addition, to the extent certain development and commercial milestones are achieved, we also agreed to pay MSK up to $17.4 million in aggregate milestone payments for each licensed product, and for each additional patent licensed product, up to $2.8 million in additional milestone payments. We also agreed to pay MSK a tiered royalty in the mid-single digits in the event of commercial sales of any licensed products and agreed to raise $25.0 million in gross proceeds no later than December 31, 2018. We raised this amount from the proceeds received from the sale of our Series A Convertible Preferred stock in March 2018 and our underwritten public offering of shares of common stock, pre-funded warrants to purchase shares of common-stock, and warrants to purchase shares of common stock in July 2018. Under the terms of the agreement, we achieved a clinical
development milestone at the end of the fourth quarter of 2018, triggering a $0.5 million payment in the first quarter of 2019.
Unless terminated earlier in accordance with its terms, the MSK license agreement as amended and restated, will continue on a country-by-country and licensed product-by-licensed product basis, until the later, of: (a) expiration of the last valid claim embracing such licensed product; (b) expiration of any market exclusivity period granted by law with respect to such licensed product; or (c) ten years from the first commercial sale in such country.
Merck & Co., Inc. Clinical Trial Collaboration and Supply Agreement
In September 2017, we entered into a clinical trial collaboration and supply agreement through a Merck subsidiary, whereby we agreed with the Merck subsidiary to collaborate on a clinical program to evaluate GPS as it is administered in combination with their PD-1 inhibitor pembrolizumab in a Phase 1/2 clinical trial enrolling patients in up to five cancer indications, including both hematologic malignancies and solid tumors.
The Phase 1/2 clinical trial was designed to explore the combination of GPS plus pembrolizumab in patients with stomachWT1+ relapsed or refractory tumors in both solid tumor and hematological cancer liveindications and to assess the efficacy and safety of the combination, comparing overall response rates and immune response markers achieved with the combination compared to prespecified rates based on those seen with pembrolizumab alone in comparable patient populations. This trial was initiated in December 2018. In 2020, we, together with Merck determined to focus on ovarian cancer (second or third line). We reported updated clinical and initial immune response data from this study in June 2021. In February 2022 we reported that we had completed enrollment of 17 evaluable patients in this study. In November 2022, we reported topline clinical and initial immune response data from this study, which showed that treatment with the combination of GPS and pembrolizumab compared favorably to treatment with anti-PD-1 therapy alone in a similar patient population and presented final data from this study at least fivethe International Gynecologic Cancer Society 2023 Annual Global Meeting in November 2023.
Exclusive License Agreement with 3D Medicines Inc.
In December 2020, we, together with our wholly-owned subsidiary, SLSG Limited, LLC, entered into an Exclusive License Agreement (the “3D Medicines Agreement”) with 3D Medicines pursuant to which we granted 3D Medicines a sublicensable, royalty-bearing license, under certain intellectual property owned or controlled by us, to develop, manufacture and have manufactured, and commercialize GPS and heptavalent GPS, or GPS-Plus, product candidates, or the GPS Licensed Products, for all therapeutic and other diagnostic uses in Greater China, or the 3DMed Territory. The license is exclusive, except with respect to certain know-how that has been non-exclusively licensed to us and is sublicensed to 3D Medicines on a non-exclusive basis. We have retained development, manufacturing and commercialization rights with respect to the GPS Licensed Products in the rest of the world.
In partial consideration for the rights granted by us, 3D Medicines agreed to pay us (i) a one-time upfront cash payment of $7.5 million in order to reimburse us for certain expenses incurred with respect to the development of the GPS Licensed Products prior to execution of the 3D Medicines Agreement, and (ii) milestone payments totaling up to $194.5 million in the aggregate upon the achievement of certain technology transfer, development and regulatory milestones, as well as certain net sales thresholds of GPS Licensed Products in the 3DMed Territory in a given calendar year.
3D Medicines also agreed to pay tiered royalties based upon a percentage of annual net sales of GPS Licensed Products in the 3DMed Territory ranging from the high single digits to the low double digits. The royalties are payable on a GPS Licensed Product-by- GPS Licensed Product and region-by-region basis commencing on the first commercial sale of a GPS Licensed Product in a region and continuing until the latest of (i) the date that is 15 years from the receipt of marketing authorization for such GPS Licensed Product in such region and (ii) the date that is 10 years from the expiration of the last valid claim of a licensed patent covering or claiming such GPS Licensed Product in such region. The royalty rate is subject to reduction under certain circumstances, including when generic competition for a GPS Licensed Product exists in a particular region.
3D Medicines is responsible for all costs related to developing, obtaining regulatory approval of and commercializing the GPS Licensed Products in the 3DMed Territory. 3D Medicines is required to use commercially reasonable best efforts to develop and obtain regulatory approval for, and upon receipt of regulatory approval, commercialize the
GPS Licensed Products in the 3DMed Territory. A joint development committee has been established between 3D Medicines and us to coordinate and review the development, manufacturing and commercialization plans with respect to the GPS Licensed Products in the 3DMed Territory. We and 3D Medicines also agreed to negotiate in good faith the terms and conditions of a clinical supply agreement, a commercial supply agreement, and related quality agreements pursuant to which we will manufacture or have manufactured and supply 3D Medicines with all quantities of the GPS Licensed Product necessary for 3D Medicines to develop and commercialize the GPS Licensed Products in the 3DMed Territory until 3D Medicines has received all approvals required for 3D Medicines or its designated contract manufacturing organization to manufacture the GPS Licensed Products in the 3DMed Territory.
The 3D Medicines Agreement will expire on a GPS Licensed Product-by-GPS Licensed Product and region-by-region basis on the date of the expiration of all of 3D Medicines’ payment obligations to us. Upon expiration of the 3D Medicines Agreement, the license granted to 3D Medicines will become fully paid-up, perpetual and irrevocable. Either party may terminate the 3D Medicines Agreement for the other party’s material breach following diagnosisa cure period or upon certain insolvency events. We may terminate the 3D Medicines Agreement if 3D Medicines or its affiliates or sublicensees challenge the validity or enforceability of the licensed patents. At any time following the two-year anniversary of the effective date, 3D Medicines has the right to terminate the 3D Medicines Agreement for convenience, subject to certain requirements. 3D Medicines may terminate the 3D Medicines Agreement upon prior notice to us if the grant of the license to 3D Medicines is prohibited or delayed for a period of time due to a change of U.S. export laws and new adjuvant treatments are neededregulations.
The 3D Medicines Agreement includes customary representations and warranties, covenants and indemnification obligations for a transaction of this nature.
Under the 3D Medicines Agreement, we achieved regulatory milestones relating to prevent disease recurrence. agreement upon and completion of a technology transfer plan in March 2021 and June 2021, respectively, for $1.0 million each and upon approval by the NMPA in March 2022 of an IND for a Phase 1 study, which triggered a $1.0 million milestone payment to us.A total of $191.5 million in potential future development, regulatory and sales milestones, not including future royalties, remains under the 3D Medicines Agreement.
We currently have anentered into a Side Letter Agreement with 3D Medicines, dated December 5, 2022, or Side Letter, arising from our agreement with Dr. Reddy’s Laboratories3D Medicines for 3D Medicines to conduct a Phase 2 investigational study in gastric cancer in India.
GALE-301 and GALE-302
Our second immunotherapy franchise targets folate binding protein (FBP) receptor-alpha. FBP is a well-validated therapeutic target that is highly over-express in ovarian, endometrial and breast cancers, and is the source of immunogenic peptides that can stimulate cytotoxic T lymphocytes (CTLs) to recognize and destroy FBP-expressing cancer cells. Current treatments after surgery for these diseases are principally with platinum based chemotherapeutic agents. These patients suffer a high recurrence rate and most relapse with an extremely poor prognosis. GALE-301 and GALE-302 are immunogenic peptides that consist of a peptide derived from FBP combined with GM-CSF for the prevention of cancer recurrenceparticipate in the adjuvant setting. GALE-301 isREGAL study through the E39 peptide, while GALE-302 is an attenuated versioninclusion of this peptide, knownapproximately 20 patients from mainland China. The Side Letter, together with the 3D Medicines Agreement, details the terms and conditions of 3D Medicines' participation in the REGAL study.
In December 2023, we announced that we had commenced a binding arbitration proceeding against 3D Medicines regarding, among other things, the trigger and payment of relevant milestone payments due to us as E39’well as 3D Medicines' failure to use commercially reasonable best efforts to develop GPS in accordance with the terms of the agreement. See Item 3. Legal Proceedings. Two early stage clinical trials
Exclusive License Agreement with GenFleet Therapeutics (Shanghai), Inc.
On March 31, 2022, or the GenFleet Agreement Effective Date, we entered into a License Agreement, or the GenFleet Agreement, with GenFleet pursuant to which GenFleet granted to us a sublicensable, royalty-bearing license, under certain of its intellectual property, to develop, manufacture and have been completed with our FBP peptides in ovarian, endometrial,manufactured, and breast cancers. In June 2016,commercialize a small molecule CDK9 inhibitor, or the U.S. Food and Drug Administration (FDA) granted two orphan-drug designationsCDK9 Licensed Product, for the treatment, (includingdiagnosis or prevention of recurrence) of ovarian cancer: one for GALE-301 (E39),disease in humans and one for GALE-301 (E39) and GALE-302 (E39’).
Ovarian Cancer: According toanimals in all territories other than Greater China, or the NCI Surveillance, Epidemiology, and End Results (SEER) Program, new cases of ovarian cancer occur at an annual rate of 11.9 per 100,000 womenSLS009 Territory. The CDK9 inhibitor, known as SLS009, is currently in the U.S., with an estimated 22,280 new cases and 14,240 deaths in 2016. Only 46.2% of ovarian cancer patients are expected to survive five years after diagnosis. Approximately 1.3% of women will be diagnosed with ovarian cancer at some point during their lifetime (2011 - 2013 data). The prevalence data from 2013 showed an estimated 195,767 women living with ovarian cancera Phase 1 clinical trial in the United States. DueStates and China.
In consideration for these rights, we agreed to pay to GenFleet (i) an initial payment of $10.0 million as an upfront license fee and for a technology transfer, $4.5 million of which was paid within 30 days of the GenFleet Agreement Effective Date and $5.5 million of which is due upon the first day of the 15th calendar month following the GenFleet Agreement Effective Date, (ii) development and regulatory milestone payments for up to three indications totaling up to $48.0 million in the aggregate, and (iii) milestone payments totaling up to $92.0 million in the aggregate upon the achievement of certain net sales thresholds of CDK9 Licensed Products in the SLS009 Territory in a given calendar year.
We also agreed to pay GenFleet tiered royalties based upon a percentage of annual net sales of CDK9 Licensed Products in the SLS009 Territory ranging from the low to high single digits. The royalties are payable on a CDK9 Licensed Product-by-CDK9 Licensed Product and region-by-region basis commencing on the first commercial sale of a CDK9 Licensed Product in a region and continuing until the later of (i) the date that is 10 years following the date of first commercial sale for such CDK9 Licensed Product in such region and (ii) the date of the expiration of the last valid claim of a licensed patent covering or claiming such CDK9 Licensed Product in such region. The royalty rate is subject to reduction under certain circumstances, including when generic competition for a CDK9 Licensed Product exists in a particular region.
We are responsible for all costs related to developing, obtaining regulatory approval of and commercializing the CDK9 Licensed Products in the SLS009 Territory and we are required to use commercially reasonable efforts to develop and obtain regulatory approval for, and upon receipt of regulatory approval, commercialize the CDK9 Licensed Products in the SLS009 Territory. We and GenFleet have established a joint steering committee to coordinate and review the development, manufacturing and commercialization plans with respect to the lack of specific symptoms,CDK9 Licensed Products in the majority of ovarian cancer patients are diagnosed at later stagesSLS009 Territory. We and GenFleet also have entered into a supply agreement and related quality agreement pursuant to which GenFleet is manufacturing, or having manufactured, and supplying us with all quantities of the disease,CDK9 Licensed Product necessary for us to develop and commercialize the CDK9 Licensed Products in the SLS009 Territory.
The GenFleet Agreement will expire on a CDK9 Licensed Product-by-CDK9 Licensed Product and region-by-region basis on the date of the expiration of all of our payment obligations to GenFleet. Upon expiration of the GenFleet Agreement, the license granted to us will become fully paid-up, perpetual and irrevocable. Either party may terminate the GenFleet Agreement for the other party’s material breach following a cure period or upon certain insolvency events. During the period from the first anniversary of the GenFleet Agreement Effective Date until the first regulatory approval of a CDK9 Licensed Product in any country within the SLS009 Territory, we will have the right to terminate the GenFleet Agreement upon 180 days’ prior written notice to GenFleet if a clinical failure, as described in the GenFleet Agreement, occurs. If we terminate the GenFleet Agreement before the first day of the 15th calendar month following the GenFleet Agreement Effective Date, then we will be required to pay to GenFleet the remainder of the $10 million initial payment upon the first day of the 15th calendar month following the GenFleet Agreement Effective Date. Upon receipt of the first regulatory approval of a CDK9 Licensed Product and continuing throughout the term of the GenFleet Agreement, we will have the right to terminate the GenFleet Agreement upon one year’s prior written notice to GenFleet. In addition, we may terminate the GenFleet Agreement upon 90 days’ notice to GenFleet upon the occurrence of certain safety events described in the GenFleet Agreement.
GenFleet may terminate the GenFleet Agreement upon notice to us if we become in arrears in any payments due pursuant to the GenFleet Agreement and we fail to make the required payment within 60 days after the delivery of written notice from GenFleet. In addition, if we fail to meet the deadline for a diligence milestone event (as described in the GenFleet Agreement), GenFleet may treat such failure as a material breach which has not been cured and GenFleet will be entitled to terminate the GenFleet Agreement if such material breach is not cured within 90 days of receiving notice of such material breach.
At GenFleet’s request within 30 days of termination of the GenFleet Agreement, other than termination by us for GenFleet’s material breach following a cure period, we will grant GenFleet an option to enter into negotiations with us with respect to a license agreement pursuant to which we would grant GenFleet a non-exclusive, royalty-bearing, worldwide license for certain of our intellectual property that is necessary and used to develop, commercialize and manufacture the terminated products.
Manufacturing
We do not own or operate manufacturing facilities for the production of our product candidates, nor do we have plans to develop our own manufacturing operations in the foreseeable future. We currently depend on third-party contract manufacturers for all of our required raw materials, active pharmaceutical ingredients, and finished product candidate for our clinical trials. We do not have any current contractual arrangements for the manufacture of commercial supplies of any product candidates. We currently employ internal resources and third-party consultants to manage our manufacturing contractors.
GPS
Our sole CMO for GPS drug substance peptides is Polypeptide Group. Our sole CMO for GPS drug product is Lyophilization Services of New England, Inc., or LSNE. Our CMOs comply with cGMP requirements and manufacture product batches used in ongoing clinical trials. We anticipate the same CMOs to manufacture commercial batches. All batches for clinical trials meet release criteria and are monitored for long-term and accelerated stability.
We have significantly advanced the chemistry, manufacturing, and controls, or CMC, objectives in support of the GPS clinical development program and for licensure, including:
•Manufacturing lyophilized clinical GMP batches;
•Qualifying processes;
•Validating analytical methods; and
•Monitoring the stability program.
In the third quarter of 2023, based upon this work, we concluded a Type C meeting with the FDA regarding the CMC sections in a potential BLA for GPS. We had submitted a briefing package to FDA which provided an estimated 80%up-to-date overview of women presentingthe extensive work we have completed for the GPS CMC program, including commercial manufacturing and regulatory plans. Following review of the package and accompanying questions to FDA, the FDA responded with advanced-stage (III or IV) disease. These patients have their tumors routinely surgically debulkedpositive guidance, including agreement on our proposed potency assay and manufacturing processes validation and our stability data generation plan for the commercial presentation of GPS. The current storage condition of GPS drug product is -20°C and we are collecting stability data to minimal residual disease,allow GPS to be stored in 2-8°C (36° – 46°F), which would be more optimal for supply chain logistics and then are treatedwould make it more accessible for end-users.
SLS009
In October 2022, we entered into a Clinical Supply Agreement with platinum-GenFleet pursuant to which GenFleet will manufacture and/or taxane-based chemotherapy. While many patients respondhave manufactured through third parties (with which GenFleet entered into agreements and to this treatment regimenwhich we have access, as necessary), and become clinically free-of-disease,supply SLS009 and any back-up molecule or intermediary related to SLS009 (including all methods, forms, presentations, dosage strengths, dosage forms, and formulations), for our use in all research and development activities necessary to obtain, maintain or expand regulatory approval worldwide, except Greater China.
Sales and Marketing
The infrastructure required to commercialize oncology products is market and product dependent. For a rare disease, such as AML, a relatively focused infrastructure may be sufficient which would make it cost-effective for us to internally develop a marketing, access and reimbursement function, and field-based sales force. We will potentially build the majorityinfrastructure to commercialize our product candidates in North America and, possibly, Europe, if GPS or our other product candidates are approved by the FDA and other regulatory authorities. However, we will remain opportunistic in seeking strategic partnerships in these and other markets when advantageous and increase shareholder value.
The commercial infrastructure of these patients will relapse. Depending upon their levelspecialty oncology products typically consists of residual disease, the risk for recurrence after completion of primary therapy is approximately 70%. Unfortunately, for these women, once the disease recurs, treatment options area targeted, specialty sales force that calls on a limited and focused group of physicians supported by sales management, internal sales support, an internal marketing group, and distribution support. As GPS and our other product candidates may initially be developed for orphan indications with a relatively small number of treating physicians, we anticipate that a reduced infrastructure, including a small, targeted sales force, will be sufficient to support our sales and marketing objectives. We continue to assess the disease is most likely incurable.infrastructure and resources needed to establish our commercial operations and support other relevant commercial matters, such as pricing and market access.
Alliance Partners in Therapeutic Areas
We leveragemay elect in the future to utilize strategic partners, distributors, or contract sales forces and clinical nurse educators to assist in the commercialization of our technology platforms by working with pharmaceuticalproducts.
In December 2020, we entered into the 3D Medicines Agreement for the development and biotechnology partnerscommercialization of GPS, as well as the Company’s next generation heptavalent immunotherapeutic GPS+, which is at preclinical stage, across all therapeutic and diagnostic uses in a numberGreater China. We have retained sole rights to GPS and GPS+ outside of therapeutic areas in oncology.Greater China. See Strategic Collaborations and License Agreements.
Intellectual Property
PatentsOur commercial success depends in part on our ability to avoid infringing the proprietary rights of third parties, our ability to obtain and maintain proprietary protection for our product candidates, technologies and know-how, and our ability to prevent others from infringing our proprietary rights. We seek to protect our proprietary position by, among other methods, evaluating relevant patents, establishing defensive positions, monitoring European Union, or EU, oppositions and pending intellectual property rights, preparing litigation strategies in view of the U.S. legislative framework, filing U.S. and international patent applications on technologies, inventions and improvements that are crucialimportant to our success. It isbusiness and maintaining our policy to protect our intellectual property rights through available means, including filing and prosecuting patent applications in the U.S. and other countries, protecting trade secrets, and utilizing regulatory protections such as data exclusivity.issued patents. We also include restrictions regarding use and disclosure of our proprietary information in our contracts with third parties, and utilize customary confidentiality and invention assignment agreements with our employees, consultants, clinical investigators and scientific advisors to protect our confidential information and know-how. Together with our licensors, we also rely on trade secrets to protect our combined technology especially where we do not believe patent protection is appropriate or obtainable. It is our policy to operate without knowingly infringing on, or misappropriating, the proprietary rights of others.
The following chart summarizes our intellectual property rights:term of individual patents depends upon the legal term of the patents in countries in which they are obtained. In most countries, including the United States, the patent term is generally 20 years from the earliest date of filing a non-provisional patent application in the applicable country. In the United States, a patent’s term may, in certain cases, be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the U.S. Patent and Trademark Office in examining and granting a patent or may be shortened if a patent is terminally disclaimed over a commonly owned patent or a patent naming a common inventor and having an earlier expiration date.
|
| | | |
Drug Candidate | Indication | Scope | Estimated
Exclusivity
Period
|
GALE-401 (Anagrelide Controlled Release) | Platelet Lowering | Pending and/or issued | 2029 |
NeuVax™ (nelipepimut-S) | Breast cancer recurrence | Pending and/or issued | 2028 |
NeuVax™ (nelipepimut-S) | Gastric | Pending and/or issued | 2028 |
NeuVax™ (nelipepimut-S) | DCIS | Pending and/or issued | 2028 |
NeuVax™ in combination with trastuzumab | Breast cancer | Pending and/or issued | 2026 |
NeuVax™ in combination with other compounds | Breast cancer | Pending and/or issued | 2037 |
GALE-301 & GALE-302 | Breast, ovarian and endometrial cancer | Pending and/or issued | 2036 |
Out-License Agreements
Teva Pharmaceuticals
Effective December 3, 2012, we entered intoThe patent term of a license and supply agreement with ABIC Marketing Limited, a subsidiary of Teva Pharmaceuticals (“ABIC”). Under the agreement, we granted ABIC exclusive rights to seek marketing approval in Israelpatent that covers an FDA-approved drug may also be eligible for our NeuVax product candidatepatent term extension, which permits patent term restoration as compensation for the treatmentpatent term lost during the FDA regulatory review process. The Drug Price Competition and Patent Term Restoration Act of breast cancer following its1984, or the Hatch-Waxman Act, permits a patent term extension of up to five years beyond the expiration of the patent. The length of the patent term extension is related to the length of time the drug is under regulatory review. Patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval, and only one patent applicable to an approved drug may be extended. Similar provisions are available in the EU and certain other foreign jurisdictions to extend the term of a patent that covers an approved drug. In the future, if and when our product candidates receive approval by the FDA or foreign regulatory authorities, we expect to apply for patent term extensions on issued patents covering those products, depending upon the European Medicines Agency,length of the clinical trials for each drug and to market, sellother factors.
Our patent portfolio includes the following:
Patents and distribute NeuVax in Israel assuming such approval is obtained. ABIC’s rights also includepatent applications covering GPS and WT1-targeting peptides:
•Patent application co-owned by us and MSK:
◦Patent applications covering a rightheptavalent (7-peptide) immunotherapy composition and methods of first refusal in Israeluse for all future indications for which NeuVax may be approved.
Undertreating, reducing the license and supply agreement, ABIC will assume responsibility for regulatory registrationincidence of, NeuVax in Israel, provide financial support for local development, and commercialize the productor inducing an immune response against a WT1-expressing cancer pending in the regionUnited States, Australia, Canada, China, Europe, Hong Kong, India, Israel, Japan, South Korea, Mexico and Russia, which, if granted, are expected to expire in exchange for making royalty payments to us based on future sales2040.
•Patents and patent applications in-licensed from MSK:
◦Composition-of-matter patents covering certain WT1-targeting peptides and methods of NeuVax. ABIC also agreesuse in the licenseUnited States, which are expected to expire in 2034; and supply agreement to purchase all suppliesa composition-of-matter patent covering
Dr. Reddy’s Laboratories Ltd.
Effective January 14, 2014, we entered into a strategic developmentadditional WT1-targeting peptides and commercialization partnership with Dr. Reddy’s Laboratories Ltd. (“Dr. Reddy’s”), under which we licensed commercial rights in India to Dr. Reddy’s for NeuVax in breast and gastric cancers. We currently have an agreement with Dr. Reddy's to conduct a Phase 2 investigational study in gastric cancer in India. To date, Dr. Reddy's has not initiated the Phase 2 study with NeuVax.
Kwang Dong Pharmaceutical Co., Ltd.
Effective April 30, 2009, we entered into a license agreement with Kwang Dong Pharmaceutical Co, Ltd (Kwang Dong). Under the agreement, we granted Kwang Dong exclusive rights to seek marketing approval in The Republicmethods of Korea (South Korea) for our NeuVax product candidate for the treatment of breast cancer following its approval by the FDA or the European Medicines Agency, and to market, sell and distribute NeuVax in South Korea assuming such approval is obtained.
Recent Developments (in reverse chronological order)
Evaluation of Strategic Alternatives and Resignation of President and Chief Executive Officer.
On January 31, 2017, the Board of Directors announced that it isuse in the process of engaging an outside advisor to evaluate strategic alternatives for the company focused on maximizing stockholder value. On March 9, 2017, it was announced that Canaccord Genuity, Inc. was engaged as the Company's financial advisor to assist in the review process. Potential strategic alternatives that may be explored or evaluated as part of this review include continuing to advance the clinical programs as a stand-alone entity, a sale of the company, a business combination, merger or reverse merger, and a license or other disposition of corporate assets of the company. There is no set timetable for this process and there can be no assurance that this process will result in a transaction. On January 31, 2017, the Company also announced the resignation of Mark W. Schwartz, Ph.D., from his position as President and Chief Executive Officer and as a member of the board of directors of each of Galena Biopharma, Inc. and our Apthera, Inc. and Mills Pharmaceutical, LLC and subsidiaries.
Appointment of Interim Chief Executive Officer
On February 21, 2017, our Board of Directors appointed Mr. Stephen Ghiglieri to be our Interim Chief Executive Officer (CEO). Mr. Ghiglieri previously held the position of Executive Vice President and Chief Financial Officer (CFO). He will continue to serve as the Company’s CFO, a position to which he was appointed in November 2016.
Closed a Public Offering of Common Stock and Warrants
On February 13, 2017, we closed the previously announced underwritten public offering of common stock and warrants. The net proceeds to us were approximately $15.5 million.
Positive Outcome from the Data Safety Monitoring Board on the Two NeuVax Clinical Trials in Combination with Trastuzumab
On February 6, 2017, we reported the results from a meeting of the Data Safety Monitoring Board (DSMB) for the two investigator-sponsored (IST) combination clinical trials with NeuVax plus trastuzumab. The DSMB reported that there are no safety concerns with either trial and neither was found to be futile. For the Phase 2b trial in patients with low-to-intermediate HER2 expression (HER2 1+/2+), n=242 patients were evaluated, and the recommendation from the DSMB is to continue the trial with one revision to the statistical analysis plan regarding the timing of the pre-specified interim analysis. Given the lengthy duration of enrollment for the trial, the DSMB determined that the pre-specified interim efficacy analysis be moved up from 12 months to 6 months after the last patient is enrolled. Completion of enrollment is expected in the second quarter of 2017; therefore, the DSMB expects to perform the interim efficacy analysis near the end of 2017. For the Phase 2 trial in high-risk, HER2 3+ patients, and per the trial protocol, the pre-specified interim safety analysis was also completed on n=50 patients and demonstrated that the agent is well tolerated with no increased cardiotoxicity associated with giving NeuVax in combination with trastuzumab. These findings were similar to the findings presented in October 2016 from the HER2 1+/2+ trial. The recommendation from the DSMB is to continue the HER2 3+ trial unmodified.
FDA Confirms 505(b)(2) regulatory pathway for GALE-401 Phase 3 Trial
On December 28, 2017, we announced that after a productive meeting with the U.S. Food and Drug Administration (FDA), the Agency confirmed that the GALE-401 development program is appropriate for a New Drug Application (NDA) filing using the 505(b)(2) regulatory pathway in patients with ET who are intolerant to or failed to achieve an optimal response with hydroxyurea.
Settlement with the Securities and Exchange Commission
On December 22, 2016, Galena and its former CEO reached an agreement in principle to a proposed settlement that would resolve an investigation by the staff of the Securities and Exchange Commission (SEC) involving conduct in the period 2012-2014 regarding the commissioning of internet publications by outside promotional firms. The proposed settlement is subject to approval by the Commission and would acknowledge our cooperation in the investigation and confirm our voluntary undertaking to continue that cooperation. If the Commission does not approve the settlement, we may need to enter into further discussions with the SEC staff to resolve the investigated matters on different terms and conditions. As a result, there can be no assurance as to the final terms of any resolution including its financial impact or any future adjustment to the financial statements.
Announced the Phase 2 Clinical Trial of NeuVax in DCIS is Open for Enrollment and Screening Patients
On December 14, 2016, the Company announced the NeuVax Phase 2 clinical trial entitled VADIS: Phase 2 trial of the Nelipepimut-S Peptide VAccine in Women with DCIS of the Breast is now open for enrollment and screening patients. The trial is being run in collaboration with the National Cancer Institute (NCI) and The University of Texas MD Anderson Cancer Center Phase I and II Chemoprevention Consortium.
Presented Two Posters at the San Antonio Breast Cancer Symposium
On December 12, 2016, we announced that two posters were presented at the San Antonio Breast Cancer Symposium (SABCS). The poster, entitled, “ VADIS trial: Phase 2 trial of the nelipepimut-S peptide vaccine in women with DCIS of the breast,” presented the trial design for the planned, Phase 2 investigator-sponsored clinical trial with NeuVax in patients with DCIS. The poster, entitled, “ Determining the optimal vaccination strategy using a combination of the folate binding protein (FBP) peptide vaccine (E39+GM-CSF) and an attenuated version (E39’) to maximize the immunologic response in breast cancer patients,” was presented on the breast cancer patients in the Company’s GALE-301 (E39) and GALE-302 (E39’) Phase 1b clinical trial targeting Folate Binding Protein. In the trial, both the E39 and E39’ peptide vaccines were noted to be well tolerated and immunogenic with no clinicopathologic differences between groups. Local reaction increased in all groups with administration of the vaccine as measured and assessed using orthogonal means. The greatest increase was seen in the treatment arm that administered GALE-301 followed by GALE-302, which approached statistical significance, and this arm was also the only arm with a statistically significant increase in DTH.
Presented GALE-301/GALE-302 Phase 1b Data
On November 14, 2016, data from our GALE-301/GALE-302 clinical program was presented at the Society for Immunotherapy of Cancer Conference 2016 in National Harbor, Maryland. The presentation, entitled, “Phase Ib Trial of Two Folate Binding Protein (FBP) Peptide Booster Vaccines (E39 and E39’) in Breast and Ovarian Cancer Patients,” reported the peptide-specific immune response to E39 and E39’ after different combinations of vaccination and boosting. The data showed that both E39 and E39’ are well tolerated with all related adverse events at grade 1 or grade 2. Though numbers were small, patients boosted with the attenuated peptide showed increased CTL response to boosting regardless of significant residual immunity (SRI) resulting from the primary vaccination series (PVS). While this data needs to be confirmed with a larger sample size, this is consistent with the theoretical advantage of boosting with an attenuated peptide,United States, which is expected to induce less antigen-induced cell deathexpire in 2035;
◦Composition-of-matter patents covering certain WT1-targeting peptides and methods of CTLs.use in Australia, China, Hong Kong, several countries of the EU and Japan, which are expected to expire in 2034;
Announced◦Patent applications covering certain WT1-targeting peptides and methods of use pending in the United States, Australia, EU, Canada, China, Hong Kong, and Japan, which, if granted, are expected to expire in 2034;
◦Patents covering methods for treating, reducing the incidence of, or inducing an immune response against a Reverse Stock SplitWT1-expressing cancer, using the peptides of GPS in combination with anti-PD-1 antibody checkpoint inhibitors in the United States, Australia, China, Hong Kong, several countries in the EU and Japan, which are expected to expire in 2037 (United States) and 2036 (Australia, China, Hong Kong, EU and Japan);
On October 31, 2016, we announced◦Patent applications covering methods for treating, reducing the incidence of, or inducing an immune response against a reverse stock splitWT1-expressing cancer, using the peptides of our sharesGPS in combination with immune checkpoint inhibitors pending in the United States, Australia, Canada, China, Hong Kong, EU, South Korea, and Japan, which, if granted, are expected to expire in 2036;
◦Composition-of-matter patents covering the WT1-A1 peptide of common stock atGPS in the United States, Canada, Australia, and several countries of the EU, which are expected to expire in the United States in 2026 and elsewhere in 2024;
◦Composition-of-matter patent covering the WT1-427 long and WT1-331 long peptides of GPS issued in the United States, which is expected to expire in 2031, and patents covering the methods of use in the United States, which are expected to expire in 2026; a ratiopatent covering peptide conjugates of 1-for-20 as approved by the BoardWT1-427 long peptide or WT1-331 long peptide in the United States, which is expected to expire in 2027; and a patent application covering peptide conjugates of Directors on October 26, 2016. The reverse stock split was authorized by the Company’s stockholders atWT1-427 long peptide or WT1-331 long peptide pending in the Special MeetingUnited States, which, if granted, is expected to expire in 2026;
◦Composition-of-matter patents covering the WT1-427 long peptide of Stockholders held on October 21, 2016. The reverse stock split became effective on November 11, 2016GPS and WT1-331 long peptide of GPS, and methods of use, in Australia and several countries of the EU, which are expected to expire in 2026; composition-of-matter patent covering the WT1-427 long peptide of GPS and method of use in Canada, which is expected to expire in 2026;
◦Composition-of-matter patent application covering the WT1-331 long peptide of GPS and the Company’s common stock commenced trading onWT1-427 long peptide of GPS and method of use pending in Canada, which, if granted, is expected to expire in 2026;
◦Composition-of-matter patent covering a split-adjusted basis on Wednesday, November 14, 2016 underWT1-specific peptide in the symbol “GALE” but underUnited States, which is expected to expire in 2026;
◦Composition-of-matter patent covering the new CUSIP number 363256504.WT1-122A1 long peptide of GPS in the United States which is expected to expire in 2033; patent covering the WT1-122A1 long peptide of GPS and methods of use in the United States, which is expected to expire in 2029; and patent application covering the WT1-122A1 long peptide of GPS and methods of use pending in the United States, which, if granted, is expected to expire in 2027; and
◦Composition-of-matter patent covering the WT1-122A1 long peptide of GPS and methods of use in several countries of the EU, which is expected to expire in 2027, and patent applications covering the WT1-122A1 long peptide of GPS and methods of use pending in the EU, Hong Kong and Canada, which, if granted, are expected to expire in 2027.
Presented GALE-301/GALE-302 Phase 1b Data
On October 20, 2016, Dr. Doreen Jackson delivered
Patents and patent applications covering SLS009:
•Patents and patent applications in-licensed from GenFleet:
◦Composition-of-matter patents covering SLS009 and use thereof in the treatment or amelioration of cancer in the United States, Australia, Canada, Japan, Russia, South Korea, the United Kingdom, and several countries of the EU, which are expected to expire in 2038; and a podium presentation on our GALE-301patent application covering SLS009 and GALE-302 clinical program atuse thereof in the American Collegetreatment or amelioration of Surgeons Clinical Congress 2016. The Phase 1bcancer pending in Brazil, which, if granted, is expected to expire in 2038; and
◦Patents covering maleate and fumarate crystal salts and polymorphs of SLS009, syntheses thereof, and use thereof in prevention or treatment of CDK9-related diseases, including cancer, in Australia and Japan, which are expected to expire in 2040; patent applications covering maleate and fumarate salt forms and polymorphs of SLS009, syntheses thereof, and use thereof in prevention or treatment of CDK9-related diseases, including cancer, pending in the United States, Brazil, Canada, South Korea, the United Kingdom and the EU (via the European Patent Office), and several former Soviet bloc countries, including Russia (via the Eurasian Patent Office), which, if granted, are expected to expire in 2040.
Competition
Oncology in general, and specifically, cancer immunotherapy, is a single-center, randomized, single-blinded, three-arm study in patientssignificant growth area for the biopharmaceutical industry, attracting large pharmaceutical companies as well as small niche players. While we believe that our scientific knowledge, assets, development experience and ability to attract experienced commercial professionals provide us with breast or ovarian cancer diagnosis who were treated with standard of care and were without evidence of disease. The presentation was entitled, “A Phase Ib Trial Comparing Different Doses/Schedules of a Folate Binding Protein (FBP)-derived Peptide Vaccine, E39, and its Attenuated Version, E39’, to Induce Long-term FBP- specific Immunity in Disease-free Cancer Patients.” In this trial, which enrolled mostly breast cancer patients who have lower FBP exposure than ovarian patients, the 500mcg dose appears to provide a more optimal immunological response. This differscompetitive advantages, we face potential competition from the results in ovarian cancer patients, who have much higher FBP expression, with potential secondary immune tolerance, where 1000mcg was the optimal dose. E39’ (GALE-302) given after E39 (GALE-301) was able to induce long-term immunity in both dosing cohorts, underscoring the potential importance of attenuated peptides in relatively antigen-naïve patients.
Presented NeuVax plus Trastuzumab Interim Safety Data
On October 10, 2016, we presented interim safety data from the NeuVax Phase 2b combination study with trastuzumab at the European Society for Medical Oncology (ESMO) 2016. The clinical trial is a randomized, multicenter, investigator-sponsored, 300 patient Phase 2b study enrolling HER2 1+ and 2+ node positive, and high-risk node negative patients. The poster, entitled “Interim safety analysis of a phase II trial combining trastuzumab and NeuVax, a HER2-targeted peptide vaccine, to prevent breast cancer recurrence in HER2 low expression,” demonstrated that this novel combination of trastuzumab and NeuVax in HER2 low-expressing patients is well-tolerated and the cardiac effects of trastuzumab are not impacted by the addition of NeuVax.
Competition
The biotechnology industry,many different sources, including cancer immunotherapy vaccines and hematology therapies, is intensely competitive and involves a high degree of risk. Potential competitors in the U.S. and worldwide are numerous and includemajor pharmaceutical, specialty pharmaceutical and biotechnology companies, educational institutionswhich either alone or together with their collaborative partners, have substantially greater resources than we have.
Generally, our competitors in the oncology therapeutic market are large and research foundations. Wemid-sized companies with approved oncology therapeutic products and companies currently engaged in clinical development of such products. Any product candidates that we successfully develop and commercialize may compete with these existing therapies and new therapies that may become available in the future.
Companies developing novel products with similar indications to those we are pursuing and may pursue are expected to influence our ability to penetrate and maintain market share. Principal competitors for AML broadly include companies with currently marketed products, such as AbbVie/Genentech (Venclexta), Pfizer (Mylotarg), Daiichi-Sankyo (Vanflyta), Rigel Pharmaceuticals (Rezlidhia) and Bristol Myers Squibb (Vidaza), among others. There are also companies developing therapies to treat AML in the r/r setting, which are in earlier stages of clinical development, including emavusertib, which is in a Phase 1/2 trial in AML and being developed by Curis, and later-stage clinical development candidates which may enter the market before our potential products, such as GlycoMimetics (uproleselan), Delta-Fly Pharma (DFP-10917), and AROG Pharmaceuticals (crenolanib). Actinium Pharmaceuticals, which announced in late 2022 / early 2023 positive results in its Phase 3 trial of Iomab-B in adults aged 55 and above with r/r AML, may be a key competitor.
With respect to WT1-targeting therapies, we do not believe GPS has direct competition in AML in the maintenance setting after CR2 at this time. While there are companies engaged in the clinical development of WT-1 targeting therapies including Astellas (ASP7517) and Cue Biopharma (CUE-102), they are not currently focused on AML.
With respect to SLS009, we anticipate competition from companies who are currently engaged in the clinical development of selective CKD9-targeting therapies. MEI Pharma is in Phase 1 clinical development for voruciclib alone and in combination with venetoclax for adults with r/r AML. Vincerx Pharma may also be a potential competitor in our other indication, PTCL, with enitociclib, its CDK9 inhibitor, as a monotherapy and in combination with venetoclax. There are other companies which are in early development stages for their CDK9 inhibitors and targeting other hematologic malignancies or solid tumors, including Kronos Bio (KB-0742), Sumitomo Dainippon Pharma (TP-1287), Adastra Pharmaceuticals (zotiraciclib) and Prelude Therapeutics (PRT2527).
With regard to both GPS and SLS009, many of these companies whoour competitors, either alone or with their strategic partners, have farsubstantially greater experience, capital resources research and technical resources, marketing experience,expertise in research and development, staffsmanufacturing, preclinical testing, obtaining regulatory approvals, and facilitiesmarketing approved products than us. Somewe have. Mergers and acquisitions in the biotechnology, pharmaceutical and diagnostics industries may result in even more resources being concentrated among a smaller number of our competitors. These competitors may develop and commercialize products that compete directly with those incorporating our technology, and they may introduce products to market earlier than our products or on a more cost effective basis. We may be unable to effectively develop our technology or any other applications on a cost effective basis or otherwise. In addition, our technology may be subject to competition from other technology or methods developed using techniques other than those developed by traditional biotechnology methods. Our competitorsalso compete with us in recruiting and retaining qualified scientific and management personnel, as well asthe ability to work with specific clinical contract organizations due to conflict of interest, and also the conduct of trials in acquiring technologies complementarythe ability to recruit clinical trial sites and subjects for our technology. clinical trials. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These activities may lead to consolidated efforts that allow for more rapid development of cancer immunotherapy product candidates.
We expect the key competitive factors that could affect the success of any products that we develop and our collaborators, may facecommercialize are likely to be efficacy, safety, price, level of generic competition, with respect to product efficacyplacement (or lack thereof) in clinical treatment guidelines and safety, ease of use and adaptability to various modes of administration, acceptance by physicians, the timing and scope of regulatory approvals, availability of resources, reimbursement coverage, price,from government and patentother third-party payors. Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize products that are viewed as safer, more convenient or less expensive than any products that we may develop. Our competitors also may obtain FDA or other regulatory approval for their products more rapidly than we may obtain approval for our current product candidates or any other future product candidate, which could result in our competitors establishing a strong market position including potentially dominant patent positions of others.
For patients with myeloproliferative neoplasms (MPNs), current treatment options include Agrylin® (anagrelide hydrochloride) and its generic equivalents, hydorxyurea and interferon alpha. Agents currently being studied in patients with MPNs include investigational JAK2 inhibitors (e.g., LY2784544 (Eli Lily), momelotinib (Gilead Sciences) and pegylated interferon alfa-2a (Pegasys, Genentech/Roche)).
For patients with early stage breast cancer, adjuvant therapy is often givenbefore we are able to prevent recurrence and increaseenter the chance of long-term disease free survival. Adjuvant therapy for breast cancer can include chemotherapy, hormonal therapy, radiation therapy, or combinations thereof.market. In addition, the HER2 targeted drug trastuzumab (Herceptin®)our ability to complete may be givenaffected by insurers or other third-party payors seeking to encourage the use of generic or biosimilar products. If our therapeutic product candidates are approved, we believe that they would be priced at a premium over competitive generic products.
Employees and Human Capital
We have assembled a management team of biopharmaceutical experts with extensive experience in building and operating organizations that develop and deliver innovative medicines to patients with tumors with high expression of HER2 (IHC 3+), as well as other novel targets such as MUC1 which may be usefulcancer. Our management team has broad expertise and successful track records in treating breast cancer.
There are a numberclinical development and approval of cancer vaccinestherapies.
As of March 1, 2024, we had 16 full time employees. In addition to our full-time employees, we engage various independent consultants and advisors to support key areas of our business. None of our employees are represented by a labor union or covered by collective bargaining agreements. We believe our relationship with our employees is good.
We are committed to creating and maintaining a diverse, inclusive and safe work environment which encourages collaboration and integrity and inspires high performance and achievement. Our employees have various backgrounds, experience and perspectives. For example, as of March 1, 2024, of our 16 employees, 56% self-identify as women, 25% self-identify as racial or ethnic minorities and 62% have advanced degrees. In addition, two of our six Board of Director members self-identify as women, including the Chair. We believe we have built and continue to build a strong culture of cooperation, respect and acceptance.
We also invest in development for breast cancer, including but not limitedour employees and are able to Lapuleucel-T (Dendreon), AE-37 (Antigen Express),recruit talented individuals through our competitive benefits, compensation packages and Stimuvax (Merck KgA). While these development candidateshealth and wellness initiatives, which are aimed at a number of different targets, and AE-37 has published data in the HER2 breast cancer patient population, there is no guarantee that any of the these compounds will not in the future be indicated for treatment of low-to-intermediate HER2 breast cancer patients and become directly competitive with NeuVax.based on peer company benchmarks.
A number of chemotherapeutic agents have demonstrated activity in gynecological carcinomas (ovarian and endometrial), particularly platinum based regimens. New chemotherapy agents are being evaluated including trabectedin (Yondelis) and belotecan as well as targeted agents such as bevacizumab (Avastin) and pazopanib (Avotrient). Monoclonal antibodies are also being developed including farletuzumab and catumaxomab. The Company is not aware of any of these agents being evaluated in the adjuvant setting where GALE-301 is being considered for further development. TPIV200 (TapImmune) is in development targeting FBP in ovarian cancer.
Government Regulation
The U.S.FDA and other developedregulatory authorities at federal, state, and local levels, as well as in foreign countries, extensively regulate, among other things, the preclinical and clinicalresearch, development, testing, manufacturing,manufacture, quality control, import, export, safety, effectiveness, labeling, packaging, storage, record-keeping,distribution, record keeping, approval, advertising, promotion, export, marketing, post-approval monitoring, and distributionpost-approval reporting of drugs and biologics such as those we are developing. Along with our third-party contractors, we will be required to navigate the various preclinical, clinical and commercial approval requirements of the governing regulatory agencies of the countries in which we wish to conduct studies or seek approval or licensure of its current or future product candidates. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local, and foreign statutes and regulations require the expenditure of substantial time and financial resources. A company can make
only those claims relating to safety and efficacy, purity and potency that are approved by the FDA and in accordance with the provisions of the approved label.
A biologic products.candidate is licensed by the FDA through approval of a biologics license application, or BLA.Assuming we receive positive data from our REGAL clinical trial of GPS for monotherapy in patients with AML, we will submit a BLA to the FDA. A drug candidate must be approved by the FDA through a new drug application, or NDA. For SLS009, we will seek marketing approval through the submission of an NDA to the FDA. The process required by the FDA regulates pharmaceuticalbefore drug or biological product candidates may be marketed in the United States generally involves the following:
•completion of extensive nonclinical laboratory tests and biologic products underanimal studies performed in accordance with the FederalFDA’s current good laboratory practice, or GLP, regulations and other applicable regulations;
•submission to the FDA of an IND application, which must become effective before clinical trials may begin and must be updated annually or when significant changes are made;
•approval by an institutional review board, or IRB, or ethics committee at each clinical site before the trial is initiated at such sites;
•performance of adequate and well-controlled human clinical trials in accordance with good clinical practice, or GCP, and other clinical-trial related regulations to establish the safety and efficacy of the investigational product candidate for its proposed indication;
•preparation of and submission to the FDA of an NDA or BLA, after completion of all pivotal clinical trials;
•satisfactory completion of an FDA Advisory Committee review, if applicable;
•a determination by the FDA within 60 days of its receipt of an NDA or BLA to file the application for review;
•satisfactory completion of an FDA pre-approval inspection of the manufacturing facility or facilities at which the proposed product is produced to assess compliance with current good manufacturing practice, or cGMP, regulations and to assure that the facilities, methods and controls are adequate to preserve the product’s continued identity, strength, quality and purity for a drug and safety, purity and potency for a biologic;
•potential audit of selected clinical trial sites to assess compliance with GCP and the integrity of the clinical data submitted in support of the NDA or BLA; and
•FDA review and approval of the NDA or BLA to permit commercial marketing of the product for particular indications for use in the United States.
The testing and approval process requires substantial time, effort and financial resources, and we cannot be certain that any approvals for our current or future product candidates will be granted on a timely basis, if at all.
Preclinical testing
Before testing any drug or biological product candidate, including our product candidates, in humans, the product candidate must undergo rigorous preclinical testing. Nonclinical studies during the preclinical development stage include laboratory evaluation of product chemistry and formulation and typically include in vitro and animal studies to assess the potential for adverse events and in some cases to establish a rationale for therapeutic use. The
Consolidated Appropriations Act for 2023, signed into law on December 29, 2022, (P.L. 117-328) amended the Food, Drug, and Cosmetic Act, or the FDCA, and the Public Health Service Act to specify that nonclinical testing for drugs and biologics may, but is not required to, include in vivo animal testing. According to the amended language, a sponsor may fulfill nonclinical testing requirements by completing various in vitro assays (e.g., cell-based assays, organ chips, or microphysiological systems), in silico studies (i.e., computer modeling), other human or nonhuman biology-based tests (e.g., bioprinting), or in vivo animal tests. The conduct of preclinical studies is subject to federal statutesregulations and regulations.requirements, including GLP regulations for safety/toxicology studies. Some long-term preclinical testing, such as animal tests of reproductive adverse events and carcinogenicity, may continue after an IND for an investigational drug or biologic candidate is submitted to the FDA and human clinical trials have been initiated.
To obtain approval of our futurePrior to beginning the first clinical trial with a product candidatescandidate, we must submit an IND to the FDA. An IND is a request for authorization from the FDA weto administer an investigational new drug product to humans. The central focus of an IND submission is on the general investigational plan and the protocol(s) for clinical studies. The IND also includes the results of the nonclinical studies of the product candidate, together with manufacturing information, analytical data, any available clinical data or literature. An IND must become effective before human clinical trials may begin. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day time period, issues a notice expressly authorizing the proposed trial to proceed or raises safety concerns or questions about the proposed clinical trial. If the FDA raises concerns or places the trial on clinical hold, the IND may be placed on clinical hold and the IND sponsor and the agency must resolve any outstanding concerns or questions before the proposed trial can begin. Submission of an IND therefore may or may not result in FDA authorization to begin a clinical trial.
Human clinical trials in support of an NDA or BLA
Clinical trials involve the administration of the investigational product to human subjects under the supervision of qualified investigators in accordance with GCP, which include the requirement that all research subjects provide their informed consent for their participation in any clinical trial. Clinical trials are conducted under protocols detailing, among other requirements, submit data supportingthings, the objectives of the clinical trial, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated. A separate submission to the existing IND must be made for each successive clinical trial conducted during product development and for any subsequent protocol amendments. Furthermore, an IRB for each site proposing to conduct the clinical trial must review and approve the plan for any clinical trial and its informed consent form before the clinical trial begins at that site and must monitor the clinical trial until completed. Regulatory authorities, the IRB or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the subjects are being exposed to an unacceptable health risk or that the trial is unlikely to meet its stated objectives. Some studies also include oversight by an independent data safety monitoring board, or DSMB, organized by the clinical trial sponsor, which at designated check points based on access to certain data from the clinical trial may recommend the sponsor to halt the trial if the DSMB determines that there is an unacceptable safety risk for subjects or other grounds, such as no demonstration of efficacy.
Information about certain clinical trials, including details of the protocol and eventually study results, also must be submitted within specific timeframes to the NIH for public dissemination on the ClinicalTrials.gov data registry. Information related to the product, patient population, phase of investigation, study sites and investigators and other aspects of the clinical trial is made public as part of the registration of the clinical trial. Sponsors are also obligated to disclose the results of their clinical trials after completion. Disclosure of the results of these trials can be delayed in some cases for up to two years after the date of completion of the trial. Competitors may use this publicly available information to gain knowledge regarding the progress of development programs. Failure to timely register a covered clinical trial or to submit study results as provided for in the law can give rise to civil monetary penalties and also prevent the non-compliant party from receiving future grant funds from the federal government. The NIH Final Rule on ClinicalTrials.gov registration and reporting requirements became effective in 2017, and both NIH and FDA have brought enforcement actions against non-compliant clinical trial sponsors.
For purposes of NDA or BLA approval, human clinical trials are typically conducted in three sequential phases that may overlap.
•Phase 1-The investigational product is initially introduced into healthy human subjects or patients with the target disease or condition. These studies are designed to test the safety, dosage tolerance, absorption,
metabolism, distribution, and excretion of the investigational product in humans, the side effects associated with increasing doses, and, if possible, to gain early evidence on effectiveness.
•Phase 2-The investigational product is administered to a limited patient population with a specified disease or condition to evaluate the preliminary efficacy, optimal dosages and dosing schedule and to identify possible adverse side effects and safety risks. Multiple Phase 2 clinical trials may be conducted to obtain information prior to beginning larger and more expensive Phase 3 clinical trials.
•Phase 3-The investigational product is administered to an expanded patient population to further evaluate dosage, to provide statistically significant evidence of clinical efficacy and to further test for safety, generally at multiple geographically dispersed clinical trial sites. These clinical trials are intended to establish the overall risk/benefit ratio of the investigational product and to provide an adequate basis for product approval and labeling. These trials may include comparisons with placebo and/or other comparator treatments. The duration of treatment is often extended to mimic the actual use of a product during marketing.
•Phase 4-In some cases, the FDA may require, or companies may voluntarily pursue, additional clinical trials after a product is approved to gain additional information and experience from the treatment of patients in the intended therapeutic indication, particularly for long-term safety follow up. These so-called Phase 4 studies may be made a condition to approval of the BLA or NDA.
In the Consolidated Appropriations Act for 2023, Congress amended the FDCA to require sponsors of a Phase 3 clinical trial, or other “pivotal study” of a new drug to support marketing authorization, to submit a diversity action plan for such clinical trial. The action plan must include the sponsor’s diversity goals for enrollment, as well as detaileda rationale for the goals and a description of how the sponsor will meet them. A sponsor must submit a diversity action plan to FDA by the time the sponsor submits the trial protocol to the agency for review. The FDA may grant a waiver for some or all of the requirements for a diversity action plan. To grant a waiver, FDA must determine that the prevalence or incidence of the disease or condition being studied makes it impracticable to conduct a clinical trial in accordance with a diversity action plan, or that a waiver is necessary to protect public health during a public health emergency. Our Phase 3 REGAL trial of GPS for AML patients who have achieved CR2 was initiated before this requirement became effective, but for any future Phase 3 trials we plan to conduct, we must submit a diversity action plan to the FDA by the time we submit plans for such Phase 3, or pivotal study, protocol to the agency for review as part of an IND, unless we are able to obtain a waiver for some or all of the requirements for a diversity action plan. It is unknown at this time how the diversity action plan may affect Phase 3 trial planning and timing or what specific information FDA will expect in such plans, but if FDA objects to a sponsor’s diversity action plan and requires the sponsor to amend the plan or take other actions, it may delay trial initiation.
Phase 1, Phase 2 and Phase 3 testing may not be completed successfully within a specified period, if at all, and there can be no assurance that the data collected will support FDA approval or licensure of the product.
Progress reports detailing the results of the clinical trials must be submitted at least annually to the FDA and more frequently if unexpected serious adverse events, or SAEs, occur. The FDA or the sponsor may suspend or terminate a clinical trial at any time on various grounds, including a finding that the manufactureresearch subjects or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the clinical protocol, GCP, or other IRB requirements or if the drug has been associated with unexpected serious harm to patients.
Concurrent with clinical trials, companies may complete additional nonclinical studies and compositiondevelop additional information about the biological characteristics of the product candidate. In most cases, this will require extensive laboratory testscandidate and must finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the product candidate and, among other things, must incorporate methods for testing the identity, strength, quality and purity of the final product, or for biologics, the safety, purity and potency. Additionally, appropriate packaging must be selected and tested, and stability studies must be conducted to demonstrate that the product candidate does not undergo unacceptable deterioration over its shelf life.
Marketing Application Submission and Review by the FDA
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, the results of product development, preclinical studies and clinical trials are submitted to the FDA as part of an NDA or BLA requesting approval to market the product for one or more indications. The NDA or BLA must contain proof of the product candidate’s safety and substantial evidence of effectiveness for its proposed indication or indications in the form of relevant data available from pertinent preclinical and clinical trials. The collection of these data,studies, including negative or ambiguous results as well as positive findings, together with detailed information relating to the preparation of applicationsproduct’s chemistry, manufacturing, controls, and proposed labeling, among other things. In particular, a marketing application must demonstrate that the manufacturing methods and quality controls used to produce the drug or biological product are adequate to preserve the drug’s identity, strength, quality, and purity for review by the FDA involve significant timean NDA or a biologic’s safety, purity, and expense. The FDA may require post-marketing testingpotency for a BLA. Data can come from company-sponsored clinical studies intended to monitortest the safety and efficacyeffectiveness of approved products or place conditions on any product approvals that could restrict the therapeutic claims and commercial applications of these products. Regulatory authorities may withdraw product approvals if we fail to comply with regulatory standards and or the conditionsa use of the regulatory approval at any time following initial marketingproduct, or from a number of our products.
The amount of time takenalternative sources, including studies initiated by theinvestigators. FDA for approval of an NDA or Biologics License Application (BLA) will depend uponBLA must be obtained before the corresponding drug or biologic may be marketed in the United States.
Under federal law, the fee for the submission of an NDA or BLA for which clinical data is submitted and analyzed is substantial, and the sponsor of an approved NDA or BLA is also subject to an annual program fee. These fees are typically increased annually, but exemptions and waivers may be available under certain circumstances (such as a numberwaiver for the first human drug application submitted by a qualifying small business and exemptions for orphan products).
The FDA reviews all submitted NDAs and BLAs to determine if they are substantially complete before it accepts them for filing and may request additional information rather than accepting a submission for filing. The FDA must make a decision on accepting an NDA or BLA for filing within 60 days of factors, includingreceipt and must inform the sponsor by the 74th day after the FDA’s receipt of the submission whether the application is sufficiently complete to permit substantive review. The FDA may refuse to file any submission that it deems incomplete or not properly reviewable at the time of submission and may request additional information. In this event, the marketing application must be resubmitted with the additional information requested by the agency. The resubmitted application is also subject to review before the FDA accepts it for filing.
Once an NDA or BLA is accepted for filing, the FDA’s goal is to review the application within 10 months after it accepts the application for filing, or, if the application meets the criteria for “priority review”, six months after the FDA accepts the application for filing. The review process is often significantly extended by FDA requests for additional information or clarification after the NDA or BLA has been accepted for filing. The review process may be extended by the FDA for three additional months to consider new information or in the case of a clarification provided by the applicant to address an outstanding deficiency identified by the FDA following the original submission.
During the review process, the FDA reviews the NDA or BLA to determine, among other things, whether the product candidate has received priority review or fast track designation, the quality of the submissionis safe, effective, pure and studies presented,potent and the workload atfacility in which it is manufactured, processed, packed, or held meets standards designed to assure the FDA.product’s continued safety, purity and potency. The FDA may refer any NDA or BLA, including applications for novel drug or biologic candidates which present difficult questions of safety or efficacy, to an advisory committee to provide clinical insight on application review questions. Typically, an advisory committee is a panel of independent experts, including clinicians and other scientific experts that reviews, evaluates and provides a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendation of an advisory committee, but it considers such recommendations carefully when making final decisions on approval.
We anticipate that our products will be manufactured by our strategic partners, licensees or other third parties. Before approving an NDA or BLA, the FDA will typically inspect the facility or facilities at whichwhere the product is manufactured andmanufactured. The FDA will not approve the productan application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the FDA’s current goodproduct within required specifications. Additionally, before approving an NDA or BLA, the FDA will typically inspect one or more clinical sites to assure compliance with GCP and integrity of the clinical data. If the FDA determines that the application, manufacturing practice (“cGMP”),process or manufacturing facilities are not acceptable, it will outline the deficiencies as part of the review process and often will request additional testing or information. Notwithstanding the submission of
any requested additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval.
Under the Pediatric Research Equity Act, or PREA, amendments to the FDCA, an NDA or BLA or supplement to such applications must contain data that are adequate to assess the safety and efficacy of the product candidate for the claimed indications in all relevant pediatric populations and to support dosing and administration for each pediatric population for which the product is safe and effective. The FDA may grant deferrals for submission of pediatric data or full or partial waivers. The PREA requires a sponsor that is planning to submit a marketing application for a product that includes a new active ingredient, new indication, new dosage form, new dosing regimen or new route of administration to submit an initial Pediatric Study Plan, or PSP, within sixty days of an end of-Phase 2 meeting or, if there is no such meeting, as early as practicable before the initiation of the Phase 3 or Phase 2/3 clinical trial. The initial PSP must include an outline of the pediatric study or studies that the sponsor plans to conduct, including trial objectives and design, age groups, relevant endpoints and statistical approach, or a justification for not including such detailed information, and any request for a deferral of pediatric assessments or a full or partial waiver of the requirement to provide data from pediatric studies along with supporting information. The FDA and the sponsor must reach an agreement on the PSP. A sponsor can submit amendments to an agreed upon initial PSP at any time if changes to the pediatric plan need to be considered based on data collected from preclinical studies, early-phase clinical trials or other clinical development programs.
The testing and approval process requires substantial time, effort and financial resources, and each may take several years to complete. The FDA may not grant approval on a timely basis, or at all, and we may encounter difficulties or unanticipated costs in our efforts to secure necessary governmental approvals, which could delay or preclude us from marketing our products. After the FDA evaluates an NDA or BLA and conducts inspections of the manufacturing facilities where the investigational product and/or its drug substance will be produced, the FDA may issue an approval letter or a Complete Response Letter, or CRL. An approval letter authorizes commercial marketing of the product with specific prescribing information for specific indications. A CRL indicates that the review cycle of the application is complete and the application will not be approved in its present form. A CRL generally outlines the deficiencies in the submission and may require substantial additional testing, information or clarification for FDA to reconsider the application. The FDA may delay or refuse approval of an NDA or BLA if applicable regulatory criteria are regulations that govern the manufacture, holdingnot satisfied, require additional testing or information and/or require post-marketing testing and distributionsurveillance to monitor safety or efficacy of a product. ManufacturersIf a CRL is issued, the applicant may either resubmit the NDA or BLA, addressing all of biologics also must comply withthe deficiencies identified in the letter, or withdraw the application. If and when the deficiencies have been addressed to the FDA’s general biologicalsatisfaction in a resubmission of the marketing application, the FDA will issue an approval letter. The FDA has committed to reviewing such resubmissions in response to an issued CRL in either two or six months depending on the type of information included. Even if such data and information are submitted, the FDA may ultimately decide that the NDA or BLA does not satisfy the criteria for approval.
If regulatory approval of a product standards. Our manufacturers also willis granted, such approval is limited to the conditions of use (e.g., patient population, indication) described in the application and may entail further limitations on the indicated uses for which such product may be subjectmarketed. For example, the FDA may approve the NDA or BLA with a Risk Evaluation and Mitigation Strategy, or REMS, plan to regulation under the Occupational Safety and Health Act, the Nuclear Energy and Radiation Control Act, the Toxic Substance Control Act and the Resource Conservation and Recovery Actmitigate risks, which could include medication guides, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other applicable environmental statutes. Following approval,risk minimization tools. The FDA determines the requirement for a REMS, as well as the specific REMS provisions, on a case-by-case basis. If the FDA periodically inspects drugconcludes a REMS plan is needed, the sponsor of the NDA or BLA must submit a proposed REMS. The FDA will not approve an NDA or BLA without a REMS, if one is required. The FDA also may condition approval on, among other things, changes to proposed labeling (e.g., adding contraindications, warnings or precautions) or the development of adequate controls and biologic manufacturing facilities to ensure continued compliance withspecifications. Once approved, the good manufacturing practices regulations. Our manufacturers will have to continue to comply with those requirements. Failure to comply with these requirements subjects the manufacturer to possible legal or regulatory action, such as suspension of manufacturing or recall or seizure of product. Adverse patient experiences withFDA may withdraw the product must be reported to the FDA and could result in the imposition of marketing restrictions through labeling changes or market removal. Product approvals may be withdrawnapproval if compliance with pre- and post-marketing regulatory requirementsstandards is not maintained or if problems concerningoccur after the product reaches the marketplace. The FDA may require one or more Phase 4 post-market studies and surveillance to further assess and monitor the product’s safety or efficacyand effectiveness after commercialization and may limit further marketing of the product occur followingbased on the results of these post-marketing studies. After approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further testing requirements and FDA review and approval. In addition, new government requirements, including those resulting from new legislation,
may be established, or the FDA’s policies may change, which could delay or prevent regulatory approval of our products under development.
Fast Track, Priority Review, and Breakthrough Therapy Designations
A sponsor may seek approval of its product candidate under programs designed to accelerate FDA’s review and approval of new drugs and biological products that meet certain criteria. Specifically, new drugs and biological products are eligible for Fast Track designation if they are intended to treat a serious or life-threatening condition and demonstrate the potential to address unmet medical needs for the condition. Fast Track designation provides increased opportunities for sponsor interactions with the FDA during preclinical and clinical development, in addition to the potential for rolling review once a marketing application is filed, meaning that the FDA may consider for review sections of the NDA or BLA on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the NDA or BLA, the FDA agrees to accept sections of the marketing application and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the application. A Fast Track designated product candidate may also qualify for accelerated approval (described below) or priority review, under which the FDA sets the target date for FDA action on the NDA or BLA at six months after the FDA accepts the application for filing. We have obtained Fast Track designation for GPS in AML, MPM and MM, and for SLS009 in r/r AML and r/r PTCL.
Priority review is granted when there is evidence that the proposed product would be a significant improvement in the safety or effectiveness of the treatment, diagnosis, or prevention of a serious condition. Significant improvement may be illustrated by evidence of increased effectiveness in the treatment of a condition, elimination or substantial reduction of a treatment-limiting drug reaction, documented enhancement of patient compliance that may lead to improvement in serious outcomes, or evidence of safety and effectiveness in a new subpopulation. If criteria are not met for priority review, the application is subject to the standard FDA review period of ten months after FDA accepts the application for filing.
In addition, a sponsor may seek FDA designation of its product candidate as a Breakthrough Therapy, if the product candidate is intended, alone or in combination with one or more other drugs or biologics, to treat a serious or life-threatening disease or condition and preliminary clinical evidence indicates that the therapy may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. Breakthrough Therapy designation provides all the features of Fast Track designation in addition to intensive guidance on an efficient development program beginning as early as Phase 1, and FDA organizational commitment to expedited development, including involvement of senior managers and experienced review and regulatory staff in a proactive, collaborative, cross-disciplinary review, where appropriate. A drug designated as Breakthrough Therapy is also eligible for accelerated approval if the relevant criteria are met.
Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review or approval will not be shortened. Fast Track, priority review and Breakthrough Therapy designations do not change the scientific or medical standards for approval or the quality of evidence necessary to support approval but may expedite the development or approval process.
Accelerated Approval
In addition, products studied for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may receive accelerated approval from the FDA and may be approved on the basis of adequate and well-controlled clinical trials establishing that the drug product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit. The labeling, advertising, promotion, marketingFDA may also grant accelerated approval for such a drug or biologic when it has an effect on an intermediate clinical endpoint that can be measured earlier than an effect on irreversible morbidity or mortality, or IMM, and distributionthat is reasonably likely to predict an effect on IMM or other clinical benefit, taking into account the severity, rarity, or prevalence of the condition and the availability or lack of alternative treatments. As a condition of approval, the FDA may require that a sponsor of a drug or biologic receiving accelerated approval perform post-marketing clinical trials to verify and
describe the predicted effect on IMM or other clinical endpoint, and the product may be subject to expedited withdrawal procedures. Drugs and biologics granted accelerated approval must meet the same statutory standards for safety and effectiveness as those granted traditional approval.
For the purposes of accelerated approval, a surrogate endpoint is a marker, such as a laboratory measurement, radiographic image, physical sign, or other measure that is thought to predict clinical benefit but is not itself a measure of clinical benefit. Surrogate endpoints can often be measured more easily or more rapidly than clinical endpoints. An intermediate clinical endpoint is a measurement of a therapeutic effect that is considered reasonably likely to predict the clinical benefit of a drug or biologic, such as an effect on IMM. The FDA has limited experience with accelerated approvals based on intermediate clinical endpoints but has indicated that such endpoints generally may support accelerated approval when the therapeutic effect measured by the endpoint is not itself a clinical benefit and basis for traditional approval, if there is a basis for concluding that the therapeutic effect is reasonably likely to predict the ultimate long-term clinical benefit of a drug or biologic.
The accelerated approval pathway is most often used in settings in which the course of a disease is long and an extended period of time is required to measure the intended clinical benefit of a drug, even if the effect on the surrogate or intermediate clinical endpoint occurs rapidly. For example, accelerated approval has been used extensively in the development and approval of drugs and biologics for treatment of a variety of cancers in which the goal of therapy is generally to improve survival or decrease morbidity and the duration of the typical disease course requires lengthy and sometimes large clinical trials to demonstrate a clinical or survival benefit.
The accelerated approval pathway is usually contingent on a sponsor’s agreement to conduct, in a diligent manner, additional post-approval confirmatory studies to verify and describe the product candidate’s clinical benefit. As a result, a product candidate approved on this basis is subject to rigorous post-marketing compliance requirements, including the completion of Phase 4 or post-approval clinical trials to confirm the effect on the clinical endpoint. Failure to conduct required post-approval studies, or to confirm the predicted clinical benefit of the product during post-marketing studies, would allow the FDA to withdraw approval of the product. As part of the Consolidated
Appropriations Act for 2023, Congress provided FDA additional statutory authority to mitigate potential risks to
patients from continued marketing of ineffective drugs or biologics previously granted accelerated approval. Under
the act’s amendments to the FDCA, FDA may require the sponsor of a product granted accelerated approval to have a confirmatory trial underway prior to approval. The sponsor must also submit progress reports on a confirmatory trial every six months until the trial is complete, and such reports are published on FDA’s website. The amendments also give FDA the option of using expedited procedures to withdraw product approval if the sponsor’s confirmatory trial fails to verify the claimed clinical benefits of the product.
All promotional materials for product candidates being considered and approved under the accelerated approval program are subject to prior review by the FDA.
Orphan Drugs
Under the Orphan Drug Act, the FDA may grant Orphan Drug Product Designation to a drug or biologic intended to treat a rare disease or condition, defined as a disease or condition with a patient population of fewer than 200,000 individuals in the United States, or a patient population greater than 200,000 individuals in the United States and when there is no reasonable expectation that the cost of developing and making available the drug or biologic in the United States will be recovered from sales in the United States for that drug or biologic. Orphan Drug Product Designation must be requested before submitting an NDA or BLA. After the FDA grants Orphan Drug Product Designation, the generic identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA.
If a drug or biologic product that has Orphan Drug Product Designation subsequently receives the first FDA approval for a particular active ingredient for the disease for which it has such designation, the product is entitled to orphan product exclusivity, which means that the FDA may not approve any other applications, including a full NDA or BLA, to market the same drug or biologic for the same indication for seven years, except in compliancelimited circumstances, such as a showing of clinical superiority to the product with orphan product exclusivity or if FDA finds that the holder of the orphan product exclusivity has not shown that it can assure the availability of sufficient
quantities of the orphan product to meet the needs of patients with the disease or condition for which the drug or biologic was designated. Orphan product exclusivity does not prevent the FDA from approving a different drug or biologic for the same disease or condition, or the same drug or biologic for a different disease or condition. Among the other benefits of Orphan Drug Product Designation are tax credits for certain research and Federal Trade Commissiona waiver of the BLA application user fee.
A drug or biologic with Orphan Drug Product Designation may not receive orphan product exclusivity if it is approved for a use that is broader than the indication for which it received Orphan Drug Product Designation. In addition, orphan product exclusive marketing rights in the United States may be lost if the FDA later determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantities of the product to meet the needs of patients with the rare disease or condition.
Recent court cases have challenged FDA’s approach to determining the scope of orphan drug exclusivity; however, at this time the agency continues to apply its long-standing interpretation of the governing regulations and has stated that it does not plan to change any orphan drug implementing regulations.
We have obtained Orphan Drug Product Designation in the United States for GPS in AML, MPM and MM and for SLS009 for AML and PTCL.
Pediatric exclusivity
Pediatric exclusivity is a type of non-patent marketing exclusivity available in the United States and, if granted, it provides for the attachment of an additional six months of marketing protection to the term of any existing regulatory exclusivity or listed patents. This six-month exclusivity may be granted if an NDA or BLA sponsor submits pediatric data that fairly respond to a written request from the FDA for such data. The data do not need to show the product to be effective in the pediatric population studied; rather, if the clinical trial is deemed to fairly respond to the FDA’s request, the additional protection is granted. If reports of requested pediatric studies are submitted to and accepted by the FDA within the statutory time limits, whatever statutory or regulatory periods of exclusivity or patent protection cover the product are extended by six months. This is not a patent term extension, but it effectively extends the regulatory period during which the FDA cannot approve another application. The issuance of a written request does not require the sponsor to undertake the described studies.
Patent term restoration
Depending upon the timing, duration and specifics of FDA approval of the use of our product candidates, some of our United States patents may be eligible for limited patent term extension under the Hatch-Waxman Act. The Hatch-Waxman Act permits a patent restoration term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, patent term restoration cannot extend the remaining term of a patent beyond a total of 14 years from the product candidate’s approval date. The patent term restoration period is generally one half of the time between the effective date of an IND and the submission date of an NDA or BLA, plus the time between the submission date of the NDA or BLA and the approval of that application, except that the review period is reduced by any time during which the applicant failed to exercise due diligence. Only one patent applicable to an approved product candidate is eligible for the extension and the application for extension must be made prior to expiration of the patent. The USPTO, in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In the future, we intend to apply for restorations of patent term for some of our currently owned or licensed patents to add patent life beyond their current expiration date, depending on the expected length of clinical trials and other factors involved in the submission of the relevant NDA or BLA.
Abbreviated new drug applications for generic drugs
In 1984, with passage of the Drug Price Competition and Patent Term Restoration Act, or Hatch-Waxman Act, which established an abbreviated regulatory scheme authorizing the FDA to approve generic drugs based on an innovator or “reference” product, Congress also enacted Section 505(b)(2) of the FDCA, which provides a hybrid pathway combining features of a traditional NDA and a generic drug application. To obtain approval of a generic
drug, an applicant must submit an abbreviated new drug application, or ANDA, to the agency. ANDAs are “abbreviated” because they do not include preclinical and clinical data to demonstrate safety and effectiveness.
Instead, in support of such applications, a generic manufacturer may rely on the preclinical and clinical testing previously conducted for a drug product previously approved under an NDA, known as the reference-listed drug, or RLD.
Specifically, in order for an ANDA to be approved, the FDA must find that the generic version is identical to the RLD with respect to the active ingredients, the route of administration, the dosage form, and the strength of the drug. At the same time, the FDA must also determine that the generic drug is “bioequivalent” to the innovator drug. Under the statute, a generic drug is bioequivalent to an RLD if “the rate and extent of absorption of the drug do not show a significant difference from the rate and extent of absorption of the listed drug.”
Upon approval of an ANDA, the FDA indicates whether the generic product is “therapeutically equivalent” to the RLD in its publication Approved Drug Products with Therapeutic Equivalence Evaluations, also referred to as the Orange Book. Clinicians and pharmacists consider a therapeutic equivalent generic drug to be fully substitutable for the RLD. In addition, by operation of certain state laws and numerous health insurance programs, the FDA’s designation of therapeutic equivalence often results in substitution of the generic drug without the knowledge or consent of either the prescribing clinicians or patient.
In contrast, Section 505(b)(2) permits the filing of an NDA where at least some of the information required for approval comes from studies not conducted by or for the applicant and for which the applicant has not obtained a right of reference. A Section 505(b)(2) applicant may eliminate the need to conduct certain preclinical or clinical studies, if it can establish that reliance on studies conducted for a previously approved product is scientifically appropriate. Unlike the ANDA pathway used by developers of bioequivalent versions of innovator drugs, the 505(b)(2) regulatory pathway does not preclude the possibility that a follow-on applicant would need to conduct additional clinical trials or nonclinical studies; for example, they may be seeking approval to market a previously approved drug for new indications or for a new patient population that would require new clinical data to demonstrate safety or effectiveness.
In addition, under the Hatch-Waxman Act, the FDA might not approve an ANDA or 505(b)(2) NDA until any applicable period of non-patent exclusivity for the RLD has expired. These market exclusivity provisions under the FDCA also can delay the submission or the approval of certain applications. The FDCA provides a period of five years of non-patent data exclusivity for a new drug containing a new chemical entity. For the purposes of this provision, a new chemical entity, or NCE, is a drug that contains no active moiety that has previously been approved by the FDA in any other NDA. An active moiety is the molecule or ion responsible for the physiological or pharmacological action of the drug substance. In cases where such NCE exclusivity has been granted, an ANDA or 505(b)(2) NDA may not be filed with the FDA until the expiration of five years unless the submission is accompanied by a Paragraph IV certification (described below), in which case the applicant may submit its application four years following the original product approval.
The FDCA also provides for a period of three years of exclusivity for an NDA, 505(b)(2) NDA or supplement thereto if one or more new clinical investigations, other than bioavailability or bioequivalence studies, that were conducted by or for the applicant are deemed by the FDA to be essential to the approval of the application. This three-year exclusivity period often protects changes to a previously approved drug product, such as a new dosage form, route of administration, combination or indication. The three-year exclusivity covers only the conditions of use associated with the new clinical investigations and does not prohibit the FDA from approving follow-on applications for drugs containing the original active agent. Five-year and three-year exclusivity also will not delay the submission or approval of a traditional NDA filed under Section 505(b)(1) of the FDCA. However, an applicant submitting a traditional NDA would be required to either conduct or obtain a right of reference to all of the preclinical studies and
adequate and well-controlled clinical trials necessary to demonstrate safety and effectiveness.
Hatch-Waxman patent certification and the 30-month stay
Upon approval of an NDA or a supplement thereto, NDA sponsors are required to list with the FDA each patent with claims that cover the applicant’s product or an approved method of using the product. Each of the patents listed by
the NDA sponsor is published in the Orange Book. When an ANDA applicant files its application with the FDA, the applicant is required to certify to the FDA concerning any patents listed for the reference product in the Orange Book, except for patents covering methods of use for which the ANDA applicant is not seeking approval. To the extent that the Section 505(b)(2) NDA applicant is relying on studies conducted for an already approved product, the applicant is required to certify to the FDA concerning any patents listed for the approved product in the Orange Book to the same extent that an ANDA applicant would.
Specifically, the applicant must certify with respect to each patent that:
I.the required patent information has not been filed by the original applicant;
II.the listed patent has expired;
III.the listed patent has not expired, but will expire on a particular date and approval is sought after patent expiration; or
IV.the listed patent is invalid, unenforceable or will not be infringed by the manufacture, use or sale of the new product.
If a Paragraph I or II certification is filed, the FDA may make approval of the application effective immediately upon completion of its review. If a Paragraph III certification is filed, the approval may be made effective on the patent expiration date specified in the application, although a tentative approval may be issued before that time. If an application contains a Paragraph IV certification, a series of events will be triggered, the outcome of which will determine the effective date of approval of the ANDA or 505(b)(2) application.
If the follow-on applicant has provided a Paragraph IV certification to the FDA, the applicant must also send notice of the Paragraph IV certification to the NDA and patent holders once the follow-on application in question has been accepted for filing by the FDA. The NDA and patent holders may then initiate a patent infringement lawsuit in response to the notice of the Paragraph IV certification. The filing of a patent infringement lawsuit within 45 days after the receipt of a Paragraph IV certification automatically prevents the FDA from approving the ANDA or 505(b)(2) NDA until the earlier of 30 months after the receipt of the Paragraph IV notice, expiration of the patent, or a decision in the infringement case that is favorable to the ANDA or 505(b)(2) applicant. Alternatively, if the listed patent holder does not file a patent infringement lawsuit within the required 45-day period, the follow-on applicant’s ANDA or 505(b)(2) NDA will not be subject to the 30-month stay.
Reference a product exclusivity for biological products
The Biologics Price Competition and Innovation Act of 2009, or BPCIA, amended the PHSA to authorize the FDA to approve similar versions of innovative biologics such as ours, which are also known as “reference biological products.” The new pathway authorized under the BPCIA allows FDA to approve, under an abbreviated application, a biological product that are demonstrated to be “biosimilar” or “interchangeable” with an FDA-licensed reference biological product. Biosimilarity to an approved reference product requires that there be no differences in mechanism of action for the conditions of use, route of administration, dosage form, and strength, and no clinically meaningful differences between the follow-on biological product and the reference product in terms of safety, purity, and potency. Biosimilarity is demonstrated in steps beginning with rigorous analytical studies or “fingerprinting,” in vitro studies, in vivo animal studies, and generally at least one clinical study, absent a waiver from the FDA. The biosimilarity exercise tests the hypothesis that the investigational product and the reference product are the same. If at any point in the stepwise biosimilarity process a significant difference is observed, then the products are not biosimilar, and the development of a standalone BLA for the follow-on biological product is necessary. In order to meet the higher hurdle of interchangeability, a sponsor must demonstrate that the biosimilar product can be expected to produce the same clinical result as the reference product, and for a product that is administered more than once, that the risk of switching between the reference product and biosimilar product is not greater than the risk of maintaining the patient on the reference product. Complexities associated with the larger, and often more complex, structures of biological products, as well as the process by which such products are manufactured, pose significant hurdles to implementation that are still being evaluated by the FDA.
Under the BPCIA, a reference biological product is granted 12 years of data exclusivity from the date of first licensure of the product, which means that the FDA is barred from approving biosimilar applications for 12 years after the reference biological product receives initial marketing approval. The first approved interchangeable
biological product will be granted an exclusivity period of up to one year after it is first commercially marketed, and as part of the Consolidated Appropriations Act for 2023, Congress amended the PHSA in order to permit multiple interchangeable products approved on the same day to receive and benefit from this one-year exclusivity period. In addition, the FDA will not accept an application for a biosimilar or interchangeable product based on the reference biological product until four years after the date of first licensure of the reference product. “First licensure” typically means the initial date the particular product at issue was licensed in the United States. Date of first licensure does not include the date of licensure of (and a new period of exclusivity is not available for) a supplement for the reference product for a subsequent application filed by the same sponsor or manufacturer of the reference product (or licensor, predecessor in interest or other related entity) for a change (not including a modification to the structure of the biological product) that results in a new indication, route of administration, dosing schedule, dosage form, delivery system, delivery device or strength or for a modification to the structure of the biological product that does not result in a change in safety, purity or potency. Therefore, one must determine whether a new product includes a modification to the structure of a previously licensed product that results in a change in safety, purity or potency to assess whether the licensure of the new product is a first licensure that triggers its own period of exclusivity. Whether a subsequent application, if approved, warrants exclusivity as the “first licensure” of a biological product is determined on a case-by-case basis with data submitted by the sponsor.
The BPCIA is complex and continues to be interpreted and implemented by the FDA. In addition, recent government proposals have sought to reduce the 12-year reference product exclusivity period. Other aspects of the BPCIA, some of which may impact the BPCIA exclusivity provisions, have also been the subject of recent litigation. As a result, the ultimate impact, implementation and meaning of the BPCIA continues to be subject to significant uncertainty.
Post-approval requirements
Following approval of a new product, the manufacturer and the approved product are subject to pervasive and continuing regulation by the FDA, including, among other things, monitoring and recordkeeping activities, reporting of adverse experiences with the product, product sampling and distribution restrictions, complying with promotion and advertising requirements, which include among others, standardsrestrictions on promoting drugs for unapproved uses or patient populations (i.e., “off-label use”) and regulations for off-label promotion, industry sponsoredlimitations on industry-sponsored scientific and educational activities, promotional activities involvingactivities. The manufacturer and its products are also subject to similar post-approval requirements by regulatory authorities comparable to FDA in jurisdictions outside of the internet,United States where the products are approved. Although physicians may prescribe legally available products for off-label uses, manufacturers may not market or promote such uses. The FDA and direct-to-consumer advertising.other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant liability. If there are any modifications to the product, including changes in indications, labeling or manufacturing processes or facilities, the applicant may be required to submit and obtain FDA approval of a new NDA or BLA or a supplement thereto, which may require the applicant to develop additional data or conduct additional preclinical studies and clinical trials. The FDA may also place other conditions on approvals including the requirement for a REMS to assure the safe use of the product. A REMS could include medication guides, physician communication plans or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. Any of these limitations on approval or marketing could restrict the commercial promotion, distribution, prescription or dispensing of products. Product approvals may be withdrawn for non-compliance with regulatory standards or if problems occur following initial marketing.
FDA regulations require that products be manufactured in specific approved facilities and in accordance with cGMP. The cGMP regulations include requirements relating to organization of personnel, buildings and facilities, equipment, control of components and drug product containers and closures, production and process controls, packaging and labeling controls, holding and distribution, laboratory controls, records and reports and returned or salvaged products. The manufacturing facilities for our product candidates must meet applicable cGMP requirements to the FDA’s or comparable foreign regulatory authorities’ satisfaction before any product is approved and our commercial products can be manufactured. We rely, and expect to continue to rely, on third parties for the production of clinical and commercial quantities of our products in accordance with cGMP regulations. These manufacturers must comply with cGMP regulations that require, among other things, quality control and quality assurance, the maintenance of records and documentation and the obligation to investigate and correct any deviations from cGMP. Manufacturers and other entities involved in the manufacture and distribution of approved
drugs or biologics are required to register their establishments with the FDA and certain state agencies and are subject to periodic prescheduled or unannounced inspections by the FDA and certain state agencies for compliance with cGMP and other laws. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain cGMP compliance. Future inspections by the FDA and other regulatory agencies may identify compliance issues at the facilities of our CMOs that may disrupt production or distribution or require substantial resources to correct. In addition, wethe discovery of conditions that violate these rules, including failure to conform to cGMP, could result in enforcement actions, and the discovery of problems with a product after approval may result in restrictions on a product, manufacturer or holder of an approved BLA, including voluntary recall and regulatory sanctions as described below.
Once an approval of a drug or biologic is granted, the FDA may withdraw the approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in mandatory revisions to the approved labeling to add new safety information; imposition of post-market or clinical trials to assess new safety risks; or imposition of distribution or other restrictions under a REMS program. Other potential consequences include, among other things:
•restrictions on the marketing or manufacturing of the product, complete withdrawal of the product from the market or product recalls;
•fines, warning letters or other enforcement-related letters or clinical holds on post-approval clinical trials;
•refusal of the FDA to approve pending NDAs or BLAs or supplements to approved marketing authorizations, or suspension or revocation of product approvals;
•product seizure or detention, or refusal to permit the import or export of products;
•injunctions or the imposition of civil or criminal penalties; and
•consent decrees, corporate integrity agreements, debarment, or exclusion from federal health care programs; or mandated modification of promotional materials and labeling and the issuance of corrective information.
In addition, the distribution of prescription pharmaceutical products is subject to the Prescription Drug Marketing Act, or PDMA, which regulates the distribution of drugs and drug samples at the federal level and sets minimum standards for the registration and regulation of drug distributors by the states. Both the PDMA and state laws limit the distribution of prescription pharmaceutical product samples and impose requirements to ensure accountability in distribution. Furthermore, the Drug Supply Chain Security Act, or DSCSA, was enacted with the aim of building an electronic system to identify and trace certain prescription drugs distributed in the United States, including most biological products. The DSCSA mandates phased-in and resource-intensive obligations for pharmaceutical manufacturers, wholesale distributors, and dispensers over a ten-year period, which culminated in November 2023. Most recently, the FDA announced a one-year stabilization period to November 2024, giving entities subject to the DSCSA additional time to finalize interoperable tracking systems and to ensure supply chain continuity. From time to time, new legislation and regulations may be implemented that could significantly change the statutory provisions governing the approval, manufacturing and marketing of products regulated by the FDA. It is impossible to predict whether further legislative or regulatory changes will be enacted, whether FDA regulations, guidance or interpretations will be changed or what the impact of such changes, if any, may be.
Other Health Care Laws and Compliance Requirements
Our sales, promotion, medical education and other activities following product approval will be subject to variousregulation by numerous regulatory and law enforcement authorities in the United States in addition to FDA, including potentially the Federal Trade Commission, or FTC, the Department of Justice, or DOJ, the Centers for Medicare and Medicaid Services, or CMS, other divisions of the Department of Health and Human Services, or DHHS, and state and local governments. Our promotional and scientific/educational programs must comply with the federal
Anti-Kickback Statute, the Foreign Corrupt Practices Act, the False Claims Act, or FCA, the Veterans Health Care Act, physician payment transparency laws, privacy laws, security laws, and additional state laws similar to the foregoing.
The federal Anti-Kickback Statute prohibits, among other things, persons from knowingly and willfully soliciting, offering, receiving, or paying remuneration, directly or indirectly, in cash or in kind, in exchange for or to induce or reward either the referral of patients for, or the purchase, order or recommendation of, any good or service that may be paid for in whole or part by Medicare, Medicaid or other federal health care programs. Remuneration has been broadly defined to include anything of value, including cash, improper discounts, and free or reduced-price items and services. The government has enforced the Anti-Kickback Statute to reach large settlements with health care companies based on sham research or consulting and other financial arrangements with physicians. Further, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it to have committed a violation. In addition, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the FCA. Many states have similar laws that apply to their state health care programs as well as private payors.
The FCA imposes liability on persons who, among other things, (i) knowingly present or cause to be presented false or fraudulent claims for payment or approval by a federal health care program, (ii) knowingly make, use, or cause to be made or used a false record or statement material to a false or fraudulent claim to the federal government, or (iii) avoid, decrease, or conceal an obligation to pay money to the federal government. The FCA has been used to prosecute persons submitting claims for payment that are inaccurate or fraudulent, that are for services not provided as claimed, or for services that are not medically necessary. Actions under the FCA may be brought by the U.S. Attorney General or as a qui tam action by a private individual in the name of the government. Violations of the FCA can result in significant monetary penalties and treble damages. The federal government is using the FCA, and the accompanying threat of significant liability, in its investigation and prosecution of pharmaceutical and biotechnology companies throughout the country, for example, in connection with the promotion of products for unapproved uses and other sales and marketing practices. The government has obtained multi-million and multi-billion dollar settlements under the FCA in addition to individual criminal convictions under applicable criminal statutes. Conviction or civil judgment for violating the FCA may result in exclusion from federal health care programs, and suspension and debarment from government contracts, and refusal of orders under existing government contracts. In addition, companies have been forced to implement extensive corrective action plans and have often become subject to consent decrees or corporate integrity agreements, restricting the manner in which they conduct their business. The federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, also created federal criminal statutes that prohibit, among other things, knowingly and willfully executing a scheme to defraud any health care benefit program, including private third-party payors and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for health care benefits, items or services. Given the significant size of actual and potential settlements, it is expected that the government will continue to devote substantial resources to investigating health care providers’ and manufacturers’ compliance with applicable fraud and abuse laws.
In addition, there has been a recent trend of increased federal and state regulation of payments made to physicians and other health care providers. The federal Physician Payments Sunshine Act, enacted as part of the Patient Protection and Affordable Care Act of 2010, or the ACA, requires manufacturers of FDA-approved drugs, devices, biologics and medical supplies covered by Medicare, Medicaid or the Children’s Health Insurance Program to report, on an annual basis, to CMS information related to payments or other transfers of value made by them to U.S.-licensed physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors), certain advanced non-physician health care practitioners and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members. Failure to submit required information may result in civil monetary penalties. Certain states also mandate implementation of commercial compliance programs, impose restrictions on drug manufacturer marketing practices and/or require the tracking and reporting of gifts, compensation and other remuneration to physicians and other health care professionals.
The federal criminal statutes enacted under HIPAA impose criminal liability for knowingly and willfully executing, or attempting to execute, a scheme to defraud any health care benefit program, including private third-party payors, or obtain, by means of false or fraudulent pretenses, representations, or promises, any of the money or property owned by, or under the custody or control of, any health care benefit program; knowingly and willfully embezzling or
stealing from a health care benefit program; willfully preventing, obstructing, misleading, or delaying a criminal investigation of a health care offense; and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statements in connection with the delivery of or payment for health care benefits, items or services. Similar to the federal Anti-Kickback Statute, a person or entity need not have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
We may also be subject to data privacy and security regulation by both the federal government and the states in which it conducts its business. HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH, and their respective implementing regulations impose specific requirements on covered entities relating to the privacy, security and transmission of individually identifiable health information, known as protected health information. Among other things, HITECH makes HIPAA’s privacy and security standards directly applicable to “business associates,” defined as independent contractors or agents of covered entities that create, receive, maintain or transmit protected health information in connection with providing a service for or on behalf of a covered entity for a function or activity regulated by HIPAA. HITECH also increased the civil and criminal penalties that may be imposed against covered entities, business associates and possibly other persons, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorney’s fees and costs associated with pursuing federal civil actions. We are not a covered entity or a business associate under HIPAA; however, we are indirectly affected by HIPAA because the protected health information held by investigators conducting our clinical trials is subject to HIPAA and can only be used for our clinical research consistent with HIPAA requirements imposed on those investigators. In addition, state laws, such as the California Consumer Privacy Act, or the CCPA, govern the privacy and security of the personal information of individuals residing in such states, and may in certain circumstances, apply to health information. In addition to California, other states have implemented laws protecting identifiable health and personal information, and many of these laws differ from each other in significant ways and may not be preempted by HIPAA, thus complicating compliance efforts.
We may also be subject to analogous state and foreign laws and regulations, governing laboratory practicessuch as state anti-kickback and false claims laws, which may apply to sales or marketing arrangements and claims involving health care items or services reimbursed by non-governmental third-party payors, including private insurers, and may be broader in scope than their federal equivalents. The laws of some U.S. states and foreign jurisdictions require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the experimentalrelevant compliance guidance promulgated by the federal government or otherwise restrict payments that may be made to health care providers. In addition, certain state and foreign laws and regulations require disclosures to regulatory agencies and/or commercial purchasers with respect to certain price increases that exceed a certain level as identified in the relevant statutes, require drug manufacturers to report information related to payments and other transfers of value to physicians and other health care providers, and restrict marketing practices or require disclosure of marketing expenditures and pricing information. Some U.S. states also require registration of pharmaceutical sales representatives.
If our operations are found to be in violation of any of such laws or any other governmental regulations that apply to it, we may be subject to penalties, including, without limitation, civil and criminal penalties, damages, fines, the curtailment or restructuring of our operations, exclusion from participation in federal and state health care programs and imprisonment, any of which could adversely affect our ability to operate our business and our financial results. Also, the U.S. Foreign Corrupt Practices Act and similar worldwide anti-bribery laws generally prohibit companies and their intermediaries from making improper payments to foreign officials for the purpose of obtaining or retaining business. We cannot assure you that our internal control policies and procedures will protect us from reckless or negligent acts committed by our employees, future distributors, partners, collaborators or agents. Violations of these laws, or allegations of such violations, could result in fines, penalties or prosecution and have a negative impact on our business, results of operations and reputation.
General Data Protection Regulation
The collection, use, disclosure, transfer, or other processing of personal data regarding individuals in the EU, including personal health data, is subject to the EU’s General Data Protection Regulation, or GDPR, which became effective on May 25, 2018. The GDPR is wide-ranging in scope and imposes numerous requirements on companies that process personal data, including requirements relating to processing health and other sensitive data, obtaining
consent of the individuals to whom the personal data relates, providing information to individuals regarding data processing activities, implementing safeguards to protect the security and confidentiality of personal data, providing notification of data breaches, and taking certain measures when engaging third-party processors. The GDPR also imposes strict rules on the transfer of personal data to countries outside the EU, including the U.S., and permits data protection authorities to impose large penalties for violations of the GDPR, including potential fines of up to €20 million or 4% of annual global revenues, whichever is greater. The GDPR also confers a private right of action on data subjects and consumer associations to lodge complaints with supervisory authorities, seek judicial remedies, and obtain compensation for damages resulting from violations of the GDPR. The Company must comply with the GDPR in the performance of its clinical trials in the EU and relies on its CROs to implement appropriate safeguards and procedures relating to informed consent in order to ensure that trials are conducted in a manner consistent with the GDPR.
In July 2023, the European Commission adopted an adequacy decision for a new mechanism for transferring personal data from the EU to the United States – the EU-U.S. Data Privacy Framework, which provides EU individuals with several new rights, including the right to obtain access to their data, or obtain correction or deletion of incorrect or unlawfully handled data. In addition, the EU-U.S. Data Privacy Framework offers additional redress avenues for violations, including free of charge independent dispute resolution mechanisms and an arbitration panel. The adequacy decision followed the U.S.' signing of an executive order introducing new binding safeguards to address the points raised by the Court of Justice of the EU in its decision on a case known as Schrems II, which invalidated the previous EU-U.S. Privacy Shield. Notably, the new obligations were geared to ensure that data can be accessed by U.S. intelligence agencies only to the extent necessary and proportionate and to establish an independent and impartial redress mechanism to handle complaints from Europeans concerning the collection of their data for national security purposes. The European Commission will continually review developments in the United States along with its adequacy decision. Adequacy decisions can be adapted or even withdrawn in the event of developments affecting the level of protection in the applicable jurisdiction. Future actions of EU data protection authorities are difficult to predict. Some customers or other service providers may respond to these evolving laws and regulations by asking us to make certain privacy or data-related contractual commitments that we are unable or unwilling to make. This could lead to the loss of current or prospective customers or other business relationships.
Coverage and Reimbursement
Sales of our products approved for marketing by the FDA and foreign regulatory authorities will depend, in part, on the extent to which our products will be covered by third-party payors, such as government health programs, commercial or private insurance and managed care organizations. The process for determining whether a payor will provide coverage for a drug or biological product may be separate from the process for setting the price or reimbursement rate that the payor will pay for the drug or biological product. Third-party payors may limit coverage to specific drug or biological products on an approved list, or formulary, which might not include all of the FDA-approved drug or biological products for a particular indication. Third-party payors are increasingly challenging drug prices and examining the medical necessity and cost-effectiveness of medical products and services, in addition to their safety and efficacy.
In order to secure coverage and reimbursement for any product that might be approved for sale, a company may need to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost-effectiveness of the product, in addition to the costs required to obtain FDA or other comparable regulatory approvals. Our drug or biological candidates may or may not be considered medically necessary or cost-effective or may require prior authorizations before use. A payor’s decision to provide coverage for a product does not imply that an adequate reimbursement rate will be approved. Moreover, eligibility for reimbursement may not be available at a rate that covers our costs, including research, development, manufacture, sale and distribution. Interim payments for new products, if applicable, may also not be sufficient to cover our costs and may not be made permanent. Reimbursement rates may vary according to the use of animals.the product and the clinical setting in which it is used, may be based on reimbursement levels already set for lower cost products and may be incorporated into existing payments for other services. Net prices for products may be reduced by mandatory discounts or rebates required by third-party payors and by any future relaxation of laws that presently restrict imports of products from countries where they may be sold at lower prices than in the United States. In the United States, third-party payors often rely upon CMS coverage policy and payment limitations in setting their own reimbursement policies, but they also have their own methods and approval process apart from CMS coverage and reimbursement determinations.
Accordingly, one third-party payor’s determination to provide coverage for a product does not assure that other payors will also provide coverage for the product.
The coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our products to each payor separately, with no assurance that coverage and adequate reimbursement will be applied consistently or granted at all. The process for determining whether a payor will cover and provide reimbursement for a product may be separate from the process of seeking approval for or setting the price of the product. Even if reimbursement is provided, market acceptance of our products may be adversely affected if the amount of payment for our products proves to be unprofitable for health care providers or less profitable than alternative treatments or if administrative burdens make our products less desirable to use.
Additionally, the United States government, state legislatures and foreign governments have shown significant interest in implementing cost containment programs to limit the growth of government-paid health care costs, including price controls, restrictions on reimbursement and requirements for substitution of generic products for branded prescription drugs. For example, the ACA contains provisions that may reduce the profitability of drug products through increased rebates for drugs reimbursed by Medicaid programs, extension of Medicaid rebates to Medicaid managed care plans, mandatory discounts for certain Medicare Part D beneficiaries and annual fees based on biopharmaceutical companies’ share of sales to federal health care programs. Adoption of general controls and measures, coupled with the tightening of restrictive policies in jurisdictions with existing controls and measures, could limit payments for drugs and biologics. The Medicaid Drug Rebate Program requires biopharmaceutical manufacturers to enter into and have in effect a national rebate agreement with the Secretary of the DHHS as a condition for states to receive federal matching funds for the manufacturer’s outpatient therapeutic products furnished to Medicaid patients. The ACA made several changes to the Medicaid Drug Rebate Program, including increasing biopharmaceutical manufacturers’ rebate liability by raising the minimum basic Medicaid rebate on most branded prescription drugs from 15.1% of average manufacturer price, or AMP, to 23.1% of AMP and adding a new rebate calculation for “line extensions” (i.e., new formulations, such as extended release formulations) of solid oral dosage forms of branded products, as well as potentially impacting their rebate liability by modifying the statutory definition of AMP. The ACA also expanded the universe of Medicaid utilization subject to drug rebates by requiring biopharmaceutical manufacturers to pay rebates on Medicaid managed care utilization and by enlarging the population potentially eligible for Medicaid drug benefits. As another example, the 2021 Consolidated Appropriations Act, signed into law on December 27, 2020, incorporated extensive health care provisions and amendments to existing laws, including a requirement that all manufacturers of drugs and biological products covered under Medicare Part B report the product’s average sales price, or ASP, to the DHHS beginning on January 1, 2022, subject to enforcement via civil money penalties.
Under currently applicable U.S. law, certain products that are not self-administered by the patient (including injectable drugs) may be eligible for coverage under Medicare through Medicare Part B. Medicare Part B is administered by Medicare Administrative Contractors, which generally have the responsibility of making coverage decisions. Subject to certain payment adjustments and limits, Medicare generally pays for a Part B-covered drug or biologic based on a percentage of manufacturer-reported Average Sales Price, which is regularly updated. For a drug or biological product to receive federal reimbursement under the Medicaid or Medicare Part B programs or to be sold directly to U.S. government agencies, the manufacturer must extend discounts to entities eligible to participate in the 340B Drug Pricing Program. The maximum amount that a manufacturer may charge a 340B covered entity for a given product is the AMP reduced by the rebate amount paid by the manufacturer to Medicaid for each unit of that product. As 340B drug pricing is determined based on AMP and Medicaid rebate data, the revisions to the Medicaid rebate formula and AMP definition described above could cause the required 340B discount to increase.
There has been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drug products. For example, the 2021 Consolidated Appropriations Act signed into law on December 27, 2020 incorporated extensive health care provisions and amendments to existing laws, including new requirements for (1) all manufacturers of drugs and biological products covered under Medicare Part B to report the product’s ASP, to the DHHS beginning on January 1, 2022, subject to enforcement via civil money penalties, (2)
certain Medicare plans to develop tools to display Medicare Part D prescription drug benefit information in real time, and (3) for group and health insurance issuers to report information on pharmacy benefit and drug costs to the Secretaries of the DHHS, the Department of Labor and the Department of the Treasury.
More recently, in August 2022, President Biden signed into the law the Inflation Reduction Act of 2022, or the IRA. Among other things, the IRA has multiple provisions that may impact the prices of drug products that are both sold into the Medicare program and throughout the United States. Starting in 2023, a manufacturer of a drug or biological product covered by Medicare Parts B or D must pay a rebate to the federal government if the drug product’s price increases faster than the rate of inflation. This calculation is made on a drug product by drug product basis and the amount of the rebate owed to the federal government is directly dependent on the volume of a drug product that is paid for by Medicare Parts B or D. Additionally, starting in payment year 2026, CMS will negotiate drug prices annually for a select number of single-source Part D drugs without generic or biosimilar competition. CMS will also negotiate drug prices for a select number of Part B drugs starting for payment year 2028. If a drug product is selected by CMS for negotiation, it is expected that the revenue generated from such drug will decrease. CMS has begun to implement these new authorities and entered into the first set of agreements with pharmaceutical manufacturers to conduct price negotiations in October 2023. However, the IRA’s impact on the pharmaceutical industry in the United States remains uncertain, in part because multiple large pharmaceutical companies and other stakeholders (e.g., the U.S. Chamber of Commerce) have initiated federal lawsuits against CMS arguing the program is unconstitutional for a variety of reasons, among other complaints. Those lawsuits are currently ongoing.
At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control drug and biological product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. For example, in recent years, several states have formed prescription drug affordability boards, or PDABs. Much like the IRA’s drug price negotiation program, these PDABs have attempted to implement upper payment limits, or UPLs, on drugs sold in their respective states in both public and commercial health plans. For example, in August 2023, Colorado’s PDAB announced a list of five prescription drugs that would undergo an affordability review. The effects of these areas,efforts remain uncertain pending the outcomes of several federal lawsuits challenging state authority to regulate prescription drug payment limits. We expect that federal, state and local governments in the United States will continue to consider legislation directed at lowering the total cost of health care. In December 2020, the U.S. Supreme Court held unanimously that federal law does not preempt the states’ ability to regulate pharmacy benefit managers, or PBMs, and other members of the health care and pharmaceutical supply chain, an important decision that may lead to further and more aggressive efforts by states in this area. The Federal Trade Commission in mid-2022 also launched sweeping investigations in the practices of the PBM industry that could lead to additional federal and state legislative or regulatory proposals targeting such entities’ operations, pharmacy networks, or financial arrangements. Significant efforts to change the PBM industry as it currently exists in the United States may affect the entire pharmaceutical supply chain and the business of other stakeholders, including biopharmaceutical developers like us.
As noted above, the FDAmarketability of any products for which we receive regulatory approval for commercial sale may suffer if the government and third-party payors fail to provide adequate coverage and reimbursement. An increasing emphasis on cost containment measures in the United States has broadincreased and we expect will continue to increase the pressure on drug or biological product pricing. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which we receive regulatory approval, less favorable coverage policies and enforcement powers, includingreimbursement rates may be implemented in the abilityfuture.
In some foreign countries, proposed pricing for drug and biological products must be approved before the product may be lawfully marketed. The requirements governing drug pricing vary widely from country to levy finescountry. Some countries provide that drug and civil penalties, suspendbiological products may be marketed only after agreement on a reimbursement price has been reached. Some countries may require additional studies that compare the cost-effectiveness of our product candidate to currently available therapies (so called health technology assessment, or delay issuanceHTA) in order to obtain reimbursement or pricing approval. For example, the EU provides options for its member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicines. A member state may approve a specific price for the product approvals, seize or recallit may instead adopt a
system of direct or indirect controls on the profitability of the company placing the product on the market. Other member states allow companies to fix their own drug prices but monitor and control prescription volumes and issue guidance to physicians to limit prescriptions. There can be no assurance that any country that has price controls or reimbursement limitations for drug and biological products will allow favorable reimbursement and deny or withdraw approvals.pricing arrangements for any of our products. Historically, products launched in the EU do not follow price structures of the United States and generally tend to be priced significantly lower.
WeForeign Regulation
In addition to regulations in the United States, we are and will also be subject, either directly or through our distribution partners, to a variety of regulations in other jurisdictions governing, among other things, clinical trials and commercial sales and distribution of our products, outside the U.S. if approved in such jurisdiction.
Whether or not we obtain FDA approval has been obtained, approval offor a product, candidate bywe must obtain the comparablerequisite approvals from regulatory authorities of foreignin non-U.S. countries and regions must be obtained prior to the commencement of clinical trials or marketing of the product in those countries. The time required to obtain approval process variesin other countries and jurisdictions might differ from one regulatory authority to another and the time may be longer or shorter than that required forto obtain FDA approval. Regulatory approval in one country or jurisdiction does not ensure regulatory approval in another, but a failure or delay in obtaining regulatory approval in one country or jurisdiction may negatively impact the regulatory process in others.
Similar to the United States, the various phases of non-clinical and clinical research that takes place in other countries are subject to significant regulatory controls. For example, the EU’s Clinical Trials Regulation, which took effect in January 2022, was enacted to simplify and streamline the approval of clinical trials in the region. The main characteristics of the regulation include: a streamlined application procedure via a single entry point, the “EU portal” or Clinical Trial Information System; a single set of documents to be prepared and submitted for the application as well as simplified reporting procedures for clinical trial sponsors; and a harmonized procedure for the assessment of applications for clinical trials, which is divided in two parts. Part I, which contains scientific and medicinal product documentation, is assessed by the competent authorities of all EU member states in which an application for authorization of a clinical trial has been submitted. Part II, which contains the national and patient-level documentation, will be assessed individually by each such EU member state. Any substantial changes to the trial protocol or other information submitted with the CTA must be notified to or approved by the relevant competent authorities and ethics committees. Medicines used in clinical trials must be manufactured in accordance with applicable cGMP requirements. Other national and EU-wide regulatory requirements may also apply. Currently, the extent to which clinical trials will be governed by the Clinical Trials Regulation will depend on when the clinical trial is initiated or on the duration of an ongoing trial. As of January 2023, all new clinical trials must comply with the Clinical Trials Regulation. In addition, any clinical trial that was already under way as of January 1, 2023, and continues for more than three years from the day on which the Clinical Trials Regulation becomes applicable (i.e., January 31, 2025), the Clinical Trials Regulation will at that time begin to apply to the clinical trial.
The requirements and processes governing the conduct of clinical trials, product licensing, pricing and reimbursement in Europe vary from country to country, even though there is already some degree of legal harmonization in the EU member states resulting from the national implementation of underlying EU legislation. In all cases, the clinical trials are conducted in accordance with GCP and other applicable regulatory requirements. To obtain regulatory approval of a new drug or medicinal product in the EU, a sponsor must obtain approval of a marketing authorization application. The way in which a medicinal product can be approved in the EU depends on the nature of the medicinal product.
The centralized procedure results in a single marketing authorization granted by the European Commission that is valid across the EU, as well as in Iceland, Liechtenstein and Norway, or the European Economic Area. The centralized procedure is compulsory for human medicines that are: (i) derived from biotechnology processes, such as genetic engineering, (ii) contain a new active substance indicated for the treatment of certain diseases, such as HIV/AIDS, cancer, diabetes, neurodegenerative diseases, autoimmune and other immune dysfunctions and viral diseases, (iii) officially designated as orphan medicinal product and (iv) advanced-therapy medicines, such as gene-therapy, somatic cell-therapy or tissue-engineered medicines. The centralized procedure may at the request of the applicant also be used for human medicines which do not fall within the above mentioned categories if the medicinal product contains a new active substance which has not been previously authorized in the European Economic
Area, or the EEA, the product constitutes a significant therapeutic, scientific or technical innovation, or where the granting of authorization in the centralized procedure is in the interests of public health in the EEA.
Under the centralized procedure in the EU, the maximum timeframe for the evaluation of a marketing authorization application by the EMA is 210 days (excluding clock stops, when additional written or oral information is to be provided by the applicant in response to questions asked by the Committee for Medicinal Products for Human Use, or CHMP, with adoption of the actual marketing authorization by the European Commission thereafter. Accelerated evaluation might be granted by the CHMP in exceptional cases, when a medicinal product is expected to be of a major public health interest from the point of view of therapeutic innovation, defined by three cumulative criteria: the seriousness of the disease to be treated; the absence of an appropriate alternative therapeutic approach, and anticipation of exceptional high therapeutic benefit. In this circumstance, EMA ensures that the evaluation for the opinion of the CHMP is completed within 150 days, excluding clock stops, and the opinion issued thereafter.
There are also two other possible routes to authorize medicinal products in several EU countries, which are available for investigational medicinal products for which the centralized procedure is not obligatory: the decentralized procedure and the mutual recognition procedure, or MRP. Using the decentralized procedure, an applicant may apply for simultaneous authorization in more than one EU country of a medicinal product that has not yet been authorized in any EU country and that does not fall within the mandatory scope of the centralized procedure.
The MRP is applicable to the majority of conventional medicinal products and is based on the principle of recognition of an already existing national marketing authorization by one or more member states. In the MRP process, a marketing authorization for a drug already exists in one or more member states of the EU and subsequently marketing authorization applications are made in other EU member states by referring to the initial marketing authorization. The member state in which the marketing authorization was first granted will then act as the reference member state. The member states where the marketing authorization is subsequently applied for act as concerned member states. After the reference state completes its medicinal product assessment, copies of the report are sent to all member states, together with the approved summary of product characteristics, labeling and package leaflet. The concerned member states then have 90 days to recognize the decision of the reference member state and the summary of product characteristics, labeling and package leaflet. National marketing authorizations shall be granted within 30 days after acknowledgement of the agreement.
Should any EU member state refuse to recognize the marketing authorization by the reference member state, on the grounds of potential serious risk to public health, the issue will be referred to a coordination group. Within a timeframe of 60 days, member states shall, within the coordination group, make all efforts to reach a consensus. If this fails, the procedure is submitted to an EMA scientific committee for arbitration. The opinion of this EMA Committee is then forwarded to the European Union, CanadaCommission, for the start of the decision-making process. As in the centralized procedure, this process entails consulting various European Commission Directorates General and Australia,the EU member states Standing Committee on Human Medicinal Products.
In the EU, new chemical entities, sometimes referred to as new active substances, qualify for eight years of data exclusivity upon marketing authorization and an additional two years of market exclusivity. The data exclusivity, if granted, prevents regulatory requirementsauthorities in the EU from referencing the innovator’s data to assess a generic or biosimilar application for eight years, after which generic marketing authorization can be submitted, and approval processesthe innovator’s data may be referenced, but not approved for two years. The overall ten-year period can be extended to a maximum of 11 years if, during the first eight years of those ten years, the marketing authorization holder obtains an authorization for one or more new therapeutic indications which, during the scientific evaluation prior to their authorization, are determined to bring a significant clinical benefit in comparison with currently approved therapies.
The criteria for designating an orphan medicinal product in the EU are similar in principle to those in the U.S.United States. Under Article 3 of Regulation (EC) 141/2000, a medicinal product may be designated as orphan if (1) it is intended for the diagnosis, prevention or treatment of a life-threatening or chronically debilitating condition; (2) either (a) such condition affects no more than five in 10,000 persons in the EU when the application is made, or (b) the product, without the benefits derived from orphan status, would not generate sufficient return in the EU to justify investment; and (3) there exists no satisfactory method of diagnosis, prevention or treatment of such condition authorized for marketing in the EU, or if such a method exists, the product will be of significant benefit to those
Financial Conditionaffected by the condition, as defined in Regulation (EC) 847/2000. Orphan medicinal products are eligible for financial incentives such as reduction of fees or fee waivers and are, upon grant of a marketing authorization, entitled to ten years of market exclusivity for the approved therapeutic indication. The application for orphan designation must be submitted before the application for marketing authorization. The applicant will receive a fee reduction for the marketing authorization application if the orphan designation has been granted, but not if the designation is still pending at the time the marketing authorization is submitted. Orphan designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process.
The 10-year market exclusivity for orphan products in the EU may be reduced to six years if, at the end of the fifth year, it is established that the product no longer meets the criteria for orphan designation, for example, if the product is sufficiently profitable not to justify maintenance of market exclusivity. Additionally, marketing authorization may be granted to a similar product for the same indication at any time if:
•the second applicant can establish that its product, although similar, is safer, more effective or otherwise clinically superior;
•the applicant consents to a second orphan medicinal product application; or
•the applicant cannot supply enough orphan medicinal product.
We had cashhave obtained Orphan Medicinal Product Designations from the EMA for GPS in AML, MPM and cash equivalentsMM.
For other countries outside of approximately $29.1 million as of February 28, 2017. We believe that our existing cash and cash equivalents, funding available under our Lincoln Park Capital, LLC (LPC) purchase agreement and At The Market Issuance Sales Agreements (ATM), should be sufficient to fund our operations for at least one year. This projection is based on our current limited operations and estimates of legal expenses associated with the ongoing government investigation and legal matters pending against the company, and is subject to changes in our operating plans, resolutions of such government investigation and legal matters, uncertainties inherent in our business, strategic alternatives outcomes,United States and the needEU, such as countries in Eastern Europe, Latin America or Asia, the requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary from country to seek to replenish our existing cashcountry. In all cases, again, the clinical trials are conducted in accordance with GCP and cash equivalents sooner than we project and in greater amounts that we had projected. There is no guarantee that any debt, additional equity orthe other funding will be available to us on acceptable terms, or at all. applicable regulatory requirements.
If we fail to obtain additional funding when needed,comply with applicable foreign regulatory requirements, we wouldmay be forcedsubject to, scale back,among other things, fines, suspension of clinical trials, suspension or terminate, our operations orwithdrawal of regulatory approvals, product recalls, seizure of products, operating restrictions and criminal prosecution.
Health Care Reform in the U.S. and Potential Changes to seek to merge with orHealth Care Laws
In the United States and some foreign jurisdictions, there have been, and continue to be, acquiredseveral legislative and regulatory changes and proposed changes regarding the health care system that could prevent or delay marketing approval of product and therapeutic candidates, restrict or regulate post-approval activities, and affect the ability to profitably sell product and therapeutic candidates that obtain marketing approval. The FDA’s and other regulatory authorities’ policies may change and additional government regulations may be enacted that could prevent, limit or delay regulatory approval of our product and therapeutic candidates.
As previously mentioned, the primary trend in the US health care industry and elsewhere is cost containment. Government authorities and other third-party payors have attempted to control costs by another company.
On February 13, 2017,limiting coverage and the Company closed an underwritten public offeringamount of 17,000,000 shares of common stockreimbursement for particular medical products and warrants to purchase 17,000,000 shares of common stock priced at $1.00 per shareservices, implementing reductions in Medicare and accompanying warrant. The warrants are immediately exercisable with a strike price of $1.10other health care funding and will expire on the fifth anniversary of the date of issuance. The net proceeds of the February 2017 Offering were $15.5 million, after deducting underwriting discounts and commissions and offering expenses paid by the Company.
applying new payment methodologies. In addition to the proceeds fromsweeping reforms contained in the February 2017 Offering,ACA (summarized above in Januarythe section entitled “Coverage and February 2017Reimbursement”), other legislative changes have been proposed and adopted in the holderUnited States that may affect health care expenditures. For example, the 2020 Further Consolidated Appropriations Act (P.L. 116-94) included a piece of bipartisan legislation called the Creating and Restoring Equal Access to Equivalent Samples Act of 2019, or the CREATES Act. The CREATES Act aims to address the concern articulated by both the FDA and others in the industry that some brand manufacturers have improperly restricted the distribution of their products, including by invoking the existence of a REMS for certain products, to deny generic and biosimilar product developers access to samples of brand products. Because generic and biosimilar product developers need samples to conduct certain comparative testing required by the FDA, some have attributed the inability to timely obtain samples as a cause of delay in the entry of generic and biosimilar products. To remedy this concern, the CREATES Act establishes a private cause of action that permits a generic or biosimilar product developer to sue the brand manufacturer to compel it to furnish the necessary samples on “commercially reasonable, market-based terms.” Whether and how generic and biosimilar product developments will use this new pathway, as well as the likely outcome of any legal challenges to provisions of the Debenture redeemed $3.95 millionCREATES Act, remain highly uncertain and its potential effects on our future commercial products are unknown. The Consolidated
Appropriations Act of 2021 also includes, among other things, a new requirement for patent information to be submitted to the FDA and published in a “Purple Book” that was satisfiedcontains detailed information about each FDA-licensed biological product, analogous to the Orange Book that provides information about approved small-molecule drug products and their patent and exclusivity information under the Hatch-Waxman Act.
In addition to the IRA’s drug price negotiation provisions summarized above, President Biden’s Executive Order 14087, issued in October 2022, called for the CMS Innovation Center to prepare and submit a report to the White House on potential payment and delivery modes that would complement the IRA, lower drug costs, and promote access to innovative drugs. In February 2023, CMS published its report which described three potential models focusing on affordability, accessibility and feasibility of implementation for further testing by the Company with 3,518,663 sharesCMS Innovation Center. As of our common stock. The Company was ableJanuary 2024, the CMS Innovation Center continues to transfertest the $3.95 million outproposed models and develop implementation plans.
In the EU, many member states have increased the amount of restricted cashdiscounts required on pharmaceuticals and cash equivalentsthese efforts could continue as countries attempt to manage health care expenditures, especially in light of the severe fiscal and into unrestricted cash and cash equivalents to be used to fund the Company's ongoing operations. The outstanding principal balance as of March 15, 2017 is $13,617,702.
On January 31, 2017, the Company announced that it isdebt crises experienced by many countries in the processEU. The downward pressure on health care costs in general, particularly prescription products, has become intense. As a result, increasingly high barriers are being erected to the entry of evaluating strategic alternatives focused on maximizing stockholder value. Potential strategic alternatives thatnew medicinal products. Political, economic and regulatory developments may be explored or evaluated as part of this review include continuing to advance the clinical programs as a stand-alone entity, a sale of the company, a business combination, merger or reverse merger,further complicate pricing negotiations, and a license or other disposition of corporate assets of the company.pricing negotiations may continue after reimbursement has been obtained. Reference pricing used by various EU member states, and parallel trade, i.e., arbitrage between low-priced and high-priced member states, can further reduce prices. There is no set timetable for this process and there can be no assurance that this processany country that has price controls or reimbursement limitations for medicinal products will resultallow favorable reimbursement and pricing arrangements for any products, if approved in a transaction. Whilethose countries.
We cannot predict the Company evaluates its strategic alternatives, Galena’s investigator-sponsored immunotherapy trials will remain ongoing. With the confirmationlikelihood, nature or extent of government regulation that may arise from the FDA that the GALE-401 development program is appropriate for a New Drug Application (NDA) filing using the 505(b)(2) regulatory pathway in patients with ET who are intolerantfuture legislation or resistant to hydroxyurea, we have developed a clear path forward for GALE-401administrative or executive action, either in the treatment of ET. Subject to completing the manufacturing of the new formulationUnited States or abroad. We expect that additional state and the internal work to prepare the Phase 3 trial for initiation, the Company is evaluating the appropriate time to commence enrollment of the GALE-401 trial and anticipates making a definitive determinationfederal health care reform measures will be adopted in the second halffuture, any of 2017. The Company has focused on reducing expenditureswhich could limit the amounts that federal and state governments will pay for health care products and services. Moreover, if we are slow or unable to adapt to changes in orderexisting requirements or the adoption of new requirements or policies, or if we are not able to preserve liquidity while pursuing a strategic alternative.
In addition to the funds raised through underwritten public offeringsmaintain regulatory compliance, our therapeutic candidates may lose any marketing approval that may have been obtained and the debenture, we maintain a purchase agreement with LPC and ATM with future availability of $2.0 million and $19.1 million, respectively subject to certain terms and conditions. On February 6, 2017, the Company and LPC amended the Purchase Agreement, as amended, to decrease the value of Common Stock that the Company may sell to LPC from $42.2 million to $2.0 million, a reduction of $39.4 million of availability. We may also continue to use the ATM,not achieve or other instruments, in order to fund our operations going forward.
We expect to continue to incur operating losses as we advance our product candidates through the drug development and the regulatory process. In the absence of revenue, our potential sources of operational funding are proceeds from the sale of equity, funded research and development payments, debt financing arrangements, and payments received under partnership and collaborative agreements.
Environmental Compliance
Our development programs involve the controlled use of potentially harmful biological materials as well as hazardous materials, chemicals and various radioactive compounds. We are subject to federal, state and local laws and regulations governing the use, storage, handling and disposal of these materials and specific waste products. We are also subject to numerous environmental, health and workplace safety laws and regulations. The cost of compliance with these laws and regulations could be significant and maysustain profitability, which would adversely affect capital expenditures to the extent we are required to procure expensive capital equipment to meet regulatory requirements.our business, prospects, financial condition and results of operations.
Human Resources
As of March 15, 2017, the Company had 14 full-time employees. None of our employees are represented by a labor union or covered by a collective bargaining agreement, nor have we experienced any work stoppages.
Corporate Information
Our principal executive offices are located at 2000 Crow Canyon Place,7 Times Square, Suite 380, San Ramon, CA 94583,2503, New York, NY 10036, and our phone number is (855) 855-4253.(646) 200-5278. Our website address is www.galenabiopharma.com.www.sellaslifesciences.com. We do not incorporate the information on our website into this annual report,Annual Report on Form 10-K, and you should not consider such information part of this annual report.Annual Report on Form 10-K.
We were incorporated on April 3, 2006 in Delaware as Argonaut Pharmaceuticals, Inc. On November 28, 2006, we changed our name to RXi Pharmaceuticals Corporation and began operations January 2007. On September 26, 2011, we changed our name to Galena Biopharma, Inc., or Galena. In December 2017, we completed a business combination, or the Merger, with SELLAS Life Sciences Group, Ltd., a privately held Bermuda exempted company, or Private SELLAS, and changed our name to “SELLAS Life Sciences Group, Inc.”
A copy of our Corporate Governance Guidelines, Code of Business Conduct and Ethics and the charters of the Audit Committee, Compensation Committee and Nominating and Corporate Governance Committee are posted on our website, www.sellaslifesciences.com, under “Investors – Corporate Governance.”
ITEM 1A. RISK FACTORS
Our business is subject to numerous risks. We caution you that
You should carefully consider the following important factors, among others, could cause our actual results to differ materially from those expressed in statements made by us or on our behalf in filingsrisks and uncertainties described below, together with the SEC, press releases or communications with investors and others. Any or all of our statementsthe other information in this annual reportAnnual Report on Form 10-K. We operate in a dynamic and in any other public statements we make may turn out to be wrong. They can be affected by inaccurate assumptions or by known or unknownrapidly changing industry that involves numerous risks and uncertainties. The factors mentioned inrisks and uncertainties described below are not the discussiononly ones we face. Other risks and uncertainties, including those that we do not currently consider material, may impair our business.
If any of the risks discussed below willactually occur, our business, financial condition, operating results or cash flows could be important in determining future results. Consequently,materially adversely affected. This Annual Report on Form 10-K also contains forward-looking statements that involve risks and uncertainties. Our actual future results may varycould differ materially from those anticipated in these forward-looking statements as a result of certain factors, including the risks we face as described below and elsewhere in this annual report or our other public statements.Annual Report on Form 10-K.
Risks RelatingRelated to Our Former Commercial OperationsFinancial Position and Capital Needs
We have incurred substantial losses since our inception and anticipate that we will continue to incur substantial and increasing losses for the foreseeable future.
Investment in biopharmaceutical product development is highly speculative because it entails substantial upfront capital expenditures and significant risk that a product candidate will fail to prove effective, gain regulatory approval or become commercially viable. We do not have any products approved by regulatory authorities, have not generated any product revenues to date, and have incurred significant research, development and other expenses related to our ongoing operations. As a result, we have not been profitable and have incurred significant operating losses in every reporting period since our inception. For the years ended December 31, 2023 and 2022, we reported a net loss of $37.3 million and $41.3 million, respectively. As of December 31, 2023 and 2022, we had an accumulated deficit of $217.2 million and $179.9 million, respectively.
We do not expect to generate product revenues for many years, if at all. We expect to continue to incur significant expenses and operating losses for the foreseeable future. We anticipate these losses to increase as we continue to research, develop and seek regulatory approvals for our product candidates and any additional product candidates we may acquire, and potentially begin to commercialize product candidates that may achieve regulatory approval. We may also encounter unforeseen expenses, difficulties, complications, delays and other unknown factors that may adversely affect our business. The size of our future net losses will depend, in part, on the rate of future growth of our expenses and our ability to generate revenues. Our expenses will further increase as we:
•conduct additional clinical trials of our lead product, GPS, including the Phase 3 clinical trial evaluating GPS for AML, and our second clinical candidate, SLS009;
•seek marketing approval for any of our product candidates that successfully complete clinical trials;
•develop our outsourced manufacturing activities and establish sales, marketing and distribution capabilities, if we receive, or expect to receive, marketing approval for any product candidates;
•in-license or acquire the rights to, and pursue development of, other products, product candidates or technologies;
•maintain, expand and protect our intellectual property portfolio;
•hire additional personnel, including clinical, manufacturing, quality control, quality assurance and other scientific personnel, sales and marketing personnel and general and administrative personnel; and
•add operational, financial and management information systems and personnel.
We currently have no source of revenues from product sales. We may never generate such revenues or achieve profitability.
Currently, we do not generate any revenues from product sales or otherwise. Even if we are subjectable to successfully achieve regulatory approval for our product candidates, we do not know when we will generate revenues or become profitable, if at all. Our ability to generate revenues from product sales and achieve profitability will depend on our ability to successfully commercialize products, including our current product candidates, and other product candidates that we may develop, in-license or acquire in the future. Our ability to generate revenues and achieve profitability also depends on a number of additional factors, including our ability to:
•successfully complete development activities, including the necessary clinical trials;
•complete and submit BLAs and NDAs to the FDA and obtain U.S. federalregulatory approval for indications for which there is a commercial market;
•complete and state health care fraudsubmit applications to foreign regulatory authorities in Europe, Asia and abuseother jurisdictions;
•obtain regulatory approval in territories with viable market sizes;
•obtain coverage and false claims lawsadequate reimbursement from third parties, including government and regulations,private payors;
•set commercially viable prices for our products, if any;
•establish and maintain supply and manufacturing relationships with reliable third parties and/or build our own manufacturing facility and ensure adequate, legally globally compliant manufacturing of bulk drug substances and drug products to maintain that supply;
•develop distribution processes for our product candidates;
•develop commercial quantities of our product candidates, once approved, at acceptable cost levels;
•obtain additional funding, if required to develop and commercialize our product candidates;
•develop a commercial organization capable of sales, marketing and distribution for any products we intend to sell ourselves, in the markets in which we choose to commercialize on our own, and successfully enter into arrangements with third parties to sell, market, and distribute our products in markets where we choose not to commercialize on our own;
•achieve market acceptance of our products;
•attract, hire and retain qualified personnel; and
•protect our rights in our intellectual property portfolio.
Our revenues for any product candidate for which regulatory approval is obtained will be dependent, in part, upon the size of the markets in the territories for which it gains regulatory approval, the accepted price for the product, the ability to get reimbursement at any price, and whether we own the commercial rights for that territory. If the number of our addressable disease patients is not as significant as our estimates, the indication approved by regulatory authorities is narrower than we expect, or the reasonably accepted population for treatment is narrowed by competition, physician choice or treatment guidelines, we may not generate significant revenues from sales of such products, even if approved. In addition, we anticipate incurring significant costs associated with commercializing any approved product candidate. As a result, even if we generate revenues, we may not become profitable and may need to obtain additional funding to continue operations. If we fail to become profitable or are unable to sustain profitability on a continuing basis, then we may be unable to continue our operations at planned levels and may be forced to reduce our operations.
We will need additional financing to fund our operations and complete the development and, if approved, the commercialization of our product candidates. If we are unable to raise capital when needed, we could be forced to delay, reduce or eliminate our product development programs or commercialization efforts.
We expect to expend substantial resources for the foreseeable future to continue the clinical development and manufacturing of GPS, in particular the Phase 3 study of GPS in AML, and SLS009. Our existing cash will not be sufficient to complete such development activities and obtain regulatory approval for our product candidates and, if we receive regulatory approval for our product candidates, commence commercialization activities, and we recently have been subpoenaed in connection with marketing and promotional practices relatedwill need to Abstral® (fentanyl) sublingual tablets. Prosecutions under such laws have increased in recent yearsraise significant additional capital to help us do so. In addition, our operating plan may change as a result of factors currently unknown to us, and we may become subject to such prosecutions or related litigation under these laws.need additional funds sooner than planned. If we have not fully complied with such laws,are unable to obtain
sufficient funding for our operations, we could face substantial penalties.
Our former commercial operations andmay be delayed in pursuing our development programs are subject to various U.S. federalfor GPS and state fraudSLS009.
Our future capital requirements depend on many factors, including:
•the scope, progress, results and abuse laws, including, without limitation, the federal False Claims Act, federal Anti-Kickback Statute,costs of our ongoing and the federal Sunshine Act. A federal investigation led by the U.S. Attorney’s Officeplanned development programs for the Southern District of Alabama (SDAL) of two of the high-prescribing physicians for Abstral has resulted in the criminal prosecution of the two physicians for alleged violations of the federal False Claims Act and other federal statutes. On April 28, 2016, a second superseding indictment was filed in the criminal case, which added additional information about the defendant physicians and provided information regarding the facts and circumstances involving a rebate agreement between the Company and the defendant physicians’ pharmacyour product candidates, as well as their ownershipany additional clinical trials we undertake to obtain data sufficient to seek marketing approval for our product candidates in any indication;
•the timing of, and the costs involved in, obtaining regulatory approvals for our product candidates if our clinical trials are successful;
•the cost of commercialization activities for our product candidates, if any of these product candidates are approved for sale, including marketing, sales and distribution costs;
•the cost of manufacturing our product candidates for clinical trials in preparation for regulatory approval, including the cost and timing of process development, manufacturing scale-up and validation activities;
•our ability to establish and maintain strategic licensing or other arrangements and the financial terms of such agreements;
•the costs to in-license future product candidates or technologies;
•the costs involved in preparing, filing, prosecuting, maintaining, expanding, defending and enforcing patent claims, including litigation costs and the outcome of such litigation;
•the costs in defending and resolving future derivative and securities class action litigation;
•our operating expenses; and
•the emergence of competing technologies or other adverse market developments.
Additional funds may not be available when we need them on terms that are acceptable to us, or at all. Moreover, global and domestic events, such as public health crises, geopolitical unrest and domestic political events, have caused and could continue to cause uncertainty and volatility in the capital markets which could impact our ability to raise capital. If adequate funds are not available to us on a timely basis, we may not be able to continue as a going concern or we may be required to delay, limit, reduce or terminate preclinical studies, clinical trials or other development activities for one or more of our product candidates or target indications, or delay, limit, reduce or terminate our establishment of sales and marketing capabilities or other activities that may be necessary to commercialize our product candidates.
Raising additional capital may cause dilution to our existing stockholders, restrict our operations or require us to relinquish rights to our product candidates on unfavorable terms to us.
We may seek additional capital through a variety of means, including through private and public equity offerings and debt financings, collaborations, strategic alliances and marketing, distribution or licensing arrangements. To the extent that we raise additional capital through the sale of equity or convertible debt securities, or through the issuance of shares under management or other types of contracts, or upon the exercise or conversion of outstanding derivative securities, the ownership interests of our stockholders will be diluted, and the terms of such financings may include liquidation or other preferences, anti-dilution rights, conversion and exercise price adjustments and other provisions that adversely affect the rights of our stockholders, including rights, preferences and privileges that are senior to those of our holders of common stock in the event of a liquidation. In such event, there is a possibility that once all senior claims are settled, there may be no assets remaining to pay out to the holders of our common stock. The criminal trial,Debt financing, if available, could include covenants limiting or restricting our ability to take certain actions, such as incurring additional debt, making capital expenditures, entering into licensing arrangements, or declaring dividends and may require us to grant security interests in our assets, including our
intellectual property, and for our subsidiaries to guarantee our obligations. If we are unable to raise additional funds through equity or debt financings when needed, we may be required to grant rights to develop and market products or product candidates that we would otherwise prefer to develop and market ourselves. If we raise additional funds through collaborations, strategic alliances, or marketing, distribution or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, products or product candidates or grant licenses on terms that may not be favorable to us.
Our cash and cash equivalents balance as of December 31, 2023 will fund our operations for less than one year.
As of December 31, 2023, we had a cash and cash equivalents balance of approximately $2.5 million. We expect our existing cash and cash equivalents balance as of December 31, 2023, will be insufficient to fund current planned operations for at least the next 12 months from the date of issuance of our consolidated financial statements for the year ended December 31, 2023, and that we will need to raise additional capital in order to continue our operations as currently planned. In the event that we are unable to obtain additional financing, we may be unable to continue as a going concern. There is no guarantee that we will be able to secure additional financing. Changes in our operating plans, our existing and anticipated working capital needs, the acceleration or modification of our development activities, any near-term or future expansion plans, increased expenses, potential acquisitions or other events may further affect our ability to continue as a going concern. See Note 2 to our consolidated financial statements included elsewhere in this Annual Report on Form 10-K for additional information on our assessment. Similarly, the report of our independent registered public accounting firm on our consolidated financial statements as of and for the year ended December 31, 2023 includes an Emphasis of Matter paragraph indicating that there is substantial doubt about our ability to continue as a going concern. Our consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty. If we cannot continue as a viable entity, our security holders may lose some or all of their investment in us.
Adverse developments affecting the financial services industry, such as actual events or concerns involving liquidity, defaults or non-performance by financial institutions or transactional counterparties, could adversely affect our current and projected business operations and its financial condition and results of operations.
Actual events involving limited liquidity, defaults, non-performance or other adverse developments that affect financial institutions, transactional counterparties or other companies in the financial services industry or the financial services industry generally, or concerns or rumors about any events of these kinds or other similar risks, have in the past and may in the future lead to market-wide liquidity problems. For example, on March 10, 2023, Silicon Valley Bank, or SVB, was closed by the California Department of Financial Protection and Innovation, which beganappointed the Federal Deposit Insurance Corporation, or the FDIC, as receiver. Similarly, on January 4, 2017, concludedMarch 12, 2023, Signature Bank and Silvergate Capital Corp. were each swept into receivership. If any of our counterparties to any credit agreements, letters of credit or certain other financial instruments that we may enter into in the future were to be placed into receivership, we may be unable to access such funds. In addition, if any parties with whom we conduct business are unable to access funds pursuant to such instruments or lending arrangements with such a jury verdict on February 23, 2017 finding these physicians guilty on 19financial institution, such parties’ ability to pay their obligations to us or to enter into new commercial arrangements requiring additional payments to us could be adversely affected. Similar impacts have occurred in the past, such as during the 2008-2010 financial crisis.
Inflation and rapid increases in interest rates have led to a decline in the trading value of 20 counts; sentencingpreviously issued government securities with interest rates below current market interest rates. There is scheduled for May 2017. Atno guarantee that the endU.S. Department of Treasury, FDIC and Federal Reserve Board will provide access to uninsured funds in the future in the event of the SDAL case, SDAL dismissed count 18closure of other banks or financial institutions, or that they would do so in a timely fashion.
Although we assess our banking relationships as we believe necessary or appropriate, our access to funding sources and other credit arrangements in amounts adequate to finance or capitalize our current and projected future business operations could be significantly impaired by factors that affect us, the financial institutions with which we have arrangements directly, or the financial services industry or economy in general. These factors could include, among others, events such as liquidity constraints or failures, the ability to perform obligations under various types of financial, credit or liquidity agreements or arrangements, disruptions or instability in the financial
services industry or financial markets, or concerns or negative expectations about the prospects for companies in the financial services industry. These factors could involve financial institutions or financial services industry companies with which we have financial or business relationships, but could also include factors involving financial markets or the financial services industry generally.
In addition, investor concerns regarding the U.S. or international financial systems could result in less favorable commercial financing terms, including higher interest rates or costs and tighter financial and operating covenants, or systemic limitations on access to credit and liquidity sources, thereby making it more difficult for us to acquire financing on acceptable terms or at all. Any decline in available funding or access to our cash and liquidity resources could, among other risks, adversely impact our ability to meet our operating expenses, financial obligations or fulfill our other obligations, result in breaches of our financial and/or contractual obligations or result in violations of federal or state wage and hour laws. Any of these impacts, or any other impacts resulting from the factors described above or other related or similar factors not described above, could have material adverse impacts on our liquidity and our current and/or projected business operations and financial condition and results of operations.
In addition, any further deterioration in the macroeconomic economy or financial services industry could lead to losses or defaults by parties with whom we conduct business, which in turn, could have a material adverse effect on our current and/or projected business operations and results of operations and financial condition. For example, a party with whom we conduct business may fail to make payments when due, default under their agreements with us, become insolvent or declare bankruptcy. Any bankruptcy or insolvency, or the failure to make payments when due, of any counterparty of ours, or the loss of any significant relationships, could have material adverse impacts on our liquidity and our current and/or projected business operations and financial condition and results of operations.
Risks Related to the Development and Regulatory Approval of Our Product Candidates
Clinical-stage biopharmaceutical companies with product candidates in clinical development face a wide range of challenging activities which may entail substantial risk.
The success of our product candidates will depend on several factors, including the following:
•designing, conducting and successfully completing preclinical development activities, including preclinical efficacy and IND-enabling studies, for our product candidates or product candidates we are interested in in-licensing or acquiring;
•designing, conducting and completing clinical trials for our product candidates with positive results;
•receipt of regulatory approvals from applicable authorities;
•obtaining and maintaining patent and trade secret protection and regulatory exclusivity for our product candidates;
•making arrangements with third-party manufacturers, receiving regulatory approval of our manufacturing processes and our third-party manufacturers’ facilities from applicable regulatory authorities and ensuring adequate supply of drug product;
•manufacturing our product candidates at an acceptable cost;
•effectively launching commercial sales of our product candidates, if approved, whether alone or in collaboration with others;
•achieving acceptance of our product candidates, if approved, by patients, the medical community and third-party payors;
•effectively competing with other therapies;
•if our products candidates are approved, obtaining and maintaining coverage and adequate reimbursement by third-party payors, including government payors, for our product candidates;
•complying with all applicable regulatory requirements, including FDA GCP and cGMP requirements, as well as, standards, rules and regulations governing promotional and other marketing activities;
•maintaining a continued acceptable safety profile of the indictment chargingproducts during development and following approval; and
•maintaining and growing an organization of scientists and businesspeople who can develop and commercialize our product candidates.
If we do not achieve one or more of these factors in a timely manner or at all, we could experience significant delays or an inability to successfully develop and commercialize our product candidates, which could materially harm our business.
Our lead product candidate, GPS, represents a new therapeutic approach that presents significant challenges.
Our future success is substantially dependent on the physicians conspired, throughsuccessful development of WT1 peptide immunotherapies in general and GPS in particular. Because this program represents a new approach to cancer immunotherapy for the C&R Pharmacy,treatment of cancer and other diseases, developing and commercializing GPS subjects us to receive illegal kickbacks in exchange for prescribing Abstral. Though certain former employees received trial subpoenas to appear at the trial and provide oral testimony, only one former employee testified at the trial. We agreed to reimburse those former employees’ attorney’s fees. To our knowledge, we were not a target or subjectnumber of that investigation.challenges, including:
There have also been federal and state investigations of a company that has a product that competes with Abstral in the same therapeutic class, and we have learned that
•obtaining regulatory approval from the FDA and other governmental agenciesregulatory authorities, which have very limited experience with the development and commercialization of WT1 cancer immunotherapies;
•obtaining the components required for the administration of GPS (i.e., GPS, GM-CSF, and Montanide) from three separate sources, the subsequent separate storage requirements for each of these components and the separate delivery of these components to the administration location;
•utilizing GPS in combination with other therapies, which may increase the risk of adverse side effects;
•sourcing clinical and, if approved, commercial supplies for the materials used to manufacture and process GPS;
•developing a manufacturing process used in connection with GPS that will yield a satisfactory product that is safe, effective, scalable and profitable;
•establishing sales and marketing capabilities after obtaining any regulatory approval to gain market acceptance; and
•obtaining coverage and adequate reimbursement from third-party payors and government authorities.
Moreover, public perception of safety issues, including adoption of new therapeutics or novel approaches to treatment, may adversely influence the willingness of subjects to participate in clinical trials, or if approved, of physicians to subscribe to the novel treatment mechanics. Physicians, hospitals and third-party payors often are investigatingslow to adopt new products, technologies and treatment practices that require additional educational upfront costs and training. Physicians may not be willing to undergo training to adopt this novel therapy, may decide the therapy is too complex to adopt without appropriate training and may choose not to administer the therapy. Based on these and other factors, hospitals and payors may decide that the benefits of this new therapy do not or will not outweigh their costs.
The limited number of patients who have the diseases for which our Abstral promotion practices. On December 16, 2015,product candidates are being studied, has made it more difficult to enroll patients in our clinical trials, which could delay or prevent the start of clinical trials for our product candidates.
Identifying and qualifying patients to participate in clinical trials of our current and future product candidates is essential to our success. The timing of our clinical trials depends in part on the rate at which we receivedcan recruit patients to participate in clinical trials of our product candidates, and we may experience delays in our clinical trials if we encounter difficulties in enrollment. If we experience delays in our clinical trials, the timeline for obtaining regulatory approval of our product candidates will most likely be delayed.
Many factors may affect our ability to identify, enroll and maintain qualified patients, including the following:
•shortages of personnel at our clinical sites;
•eligibility criteria of our ongoing and planned clinical trials with specific characteristics appropriate for inclusion in our clinical trials;
•design of the clinical trial;
•size and nature of the patient population;
•patients’ perceptions as to risks and benefits of the product candidate under study and the participation in a subpoena issuedclinical trial generally in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating;
•the availability and efficacy of competing therapies and clinical trials;
•pendency of other trials underway in the same patient population;
•willingness of physicians to participate in our planned clinical trials;
•severity of the disease under investigation;
•proximity of patients to clinical sites;
•patients who do not complete the trials for personal reasons; and
•issues with contract research organizations, or CROs, and/or with other vendors that handle our clinical trials.
The indication being studied in our Phase 3 clinical trial for GPS, i.e., patients with AML who have achieved CR2, is an orphan indication. In addition, only those CR2 patients who meet specific inclusion criteria are eligible to participate in the study. Primary entry restrictions include demonstrating adequate hematologic recovery and not being candidates for bone marrow transplants. The estimated prevalence of newly diagnosed AML patients is approximately 20,000 cases in the United States annually (across all ages) with only a subset of this group having achieved CR2 and only a further subset of the CR2 subset satisfying the enrollment criteria for our AML Phase 3 clinical trial.
We may not be able to initiate or continue to support clinical trials of our product candidates for one or more indications, or any future product candidates if we are unable to locate and enroll a sufficient number of eligible participants in these trials as required by the U.S. Attorney’s OfficeFDA or other regulatory authorities. Even if we are able to enroll a sufficient number of patients in our clinical trials, if the pace of enrollment is slower than we expect, the development costs for our product candidates may increase and the Districtcompletion of New Jersey requestingour trials may be delayed or our trials could become too expensive to complete.
Congress also recently amended the productionFDCA to require sponsors of a broad rangePhase 3 clinical trial, or other “pivotal study” of documents pertaininga new drug or biologic to oursupport marketing authorization, to design and promotional practicessubmit a diversity action plan for Abstral. We have been in contact with the U.S. Attorney’s Officesuch clinical trial. The action plan must describe appropriate diversity goals for the District of New Jersey and are cooperating in the production of the requested documents. We have come to understand that the investigation being undertaken by the U.S. Attorney’s Office for the District of New Jersey and Department of Justice is a criminal investigation in addition to a civil investigation that could ultimately involve the companyenrollment, as well as a rationale for the goals and a description of how the sponsor will meet them. Our Phase 3 REGAL trial of GPS for AML patients who
have achieved CR2 was initiated before this requirement became effective, but for any future Phase 3 trials we plan to conduct, including any registrational study for SLS009, we must submit a diversity action plan to the FDA by the time we submit plans for such Phase 3, or pivotal study, protocol to the agency for review as part of an IND, unless we are able to obtain a waiver for some or all of the requirements for a diversity action plan. It is unknown at this time how the diversity action plan may affect the planning and timing of any future Phase 3 trial for our product candidates or what specific information FDA will expect in such plans. However, initiation of such trials may be delayed if the FDA objects to our proposed diversity action plans for any future Phase 3 trial for our product candidates, and we may experience difficulties recruiting a diverse population of patients in attempting to fulfill the requirements of any approved diversity action plan.
If we experience delays in the completion of, or termination of, any clinical trials of our current or future product candidates, the commercial prospects of our product candidates could be harmed, and our ability to generate product revenue from any of these product candidates could be delayed or prevented. In addition, any delays in completing our clinical trials would likely increase our overall costs, impair product candidate development and jeopardize our ability to obtain regulatory approval relative to our current plans. Any of these occurrences may harm our business, financial condition, and prospects significantly.
The results of preclinical studies or earlier clinical trials are not necessarily predictive of future results. Our existing product candidates in clinical trials, and any other product candidates that may advance into clinical trials, may not have favorable results in later clinical trials or receive regulatory approval.
Success in preclinical studies and early clinical trials does not ensure that later clinical trials will generate adequate data to demonstrate the efficacy and safety of an investigational drug. A number of companies in the pharmaceutical and biotechnology industries, including those with greater resources and experience than us, have suffered significant setbacks in clinical trials, even after seeing promising results in earlier preclinical studies or clinical trials. Any of our product candidates that are in, or may advance to, clinical trials may not succeed in clinical trials despite promising preclinical data. For example, with respect to GPS, a broadly similar anti-cancer peptide immunotherapeutic against melanoma-specific antigen being developed by GlaxoSmithKline for advanced unresectable melanoma initially produced positive efficacy data in a Phase 2 clinical study, but subsequently failed to prove more beneficial than placebo in a controlled, blinded and randomized Phase 3, registration-enabling clinical trial in the same indication in patients after tumor resection.
Despite the results reported in earlier preclinical studies or clinical trials for our product candidates, we do not know whether the clinical trials we may conduct will demonstrate adequate efficacy and safety to result in regulatory approval to market any of our product candidates for a particular indication, either as a monotherapy or in combination, in any particular jurisdiction. Efficacy data from prospectively designed trials may differ significantly from those obtained from retrospective subgroup analyses. If later-stage clinical trials do not produce favorable results, our ability to achieve regulatory approval for our product candidates may be adversely impacted. Even if we believe that we have adequate data to support an application for regulatory approval to market any of our current or future product candidates, the FDA or other regulatory authorities may not agree and may require that we conduct additional clinical trials.
Interim, topline and preliminary data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final data.
From time to time, we may publicly disclose preliminary, interim or topline data from our clinical trials. These interim updates are based on a preliminary analysis of then-available data, and the results and related findings and conclusions are subject to change following a more comprehensive review of the data related to a particular study or trial. We also make assumptions, estimations, calculations and conclusions as part of our analyses of data, and we may not have received or had the opportunity to fully evaluate all data. As a result, the topline results or preliminary data that we report may differ from future results of the same studies, or different conclusions or considerations may qualify such results, once additional data have been received and fully evaluated. Topline data also remain subject to audit and verification procedures that may result in the final data being materially different from the preliminary data we previously published. As a result, topline data should be viewed with caution until the final data are available. In addition, we may report interim analyses of only certain endpoints rather than all
endpoints. Interim data from clinical trials that we complete are subject to the risk that one or more former employees. Pursuantof the clinical outcomes may materially change as more patient data becomes available. Adverse changes between interim data and final data could adversely affect our business and prospects and could result in volatility in the price of our common stock.
We are developing and may continue to develop our programs in combination with other therapies, which exposes us to additional risks.
We are currently investigating SLS009 in combination with aza/ven ina Phase 2a clinical trial and we may continue to develop clinical candidates in combination with one or more currently approved cancer therapies or therapies currently in clinical development. Patients may not be able to tolerate our product candidates in combination with other therapies or dosing of our product candidates in combination with other therapies may have unexpected consequences. Even if any of our product candidates were to receive marketing approval or be commercialized for use in combination with other existing therapies, we would continue to be subject to the Company’s charter,risks that the FDA, EMA or other comparable foreign regulatory authorities could revoke approval of the therapy used in combination with any of our product candidates, or safety, efficacy, manufacturing or supply issues could arise with these existing therapies. In addition, it is possible that existing therapies with which our product candidates are approved for use could themselves fall out of favor or be relegated to later lines of treatment. This could result in the need to identify other combination therapies for our product candidates or our own products being less successful commercially.
We may also evaluate our product candidates in combination with one or more other cancer therapies that have not yet been approved for marketing by the FDA, EMA or comparable foreign regulatory authorities. If the FDA, EMA or other comparable foreign regulatory authorities do not approve or revoke their approval of these other therapies, or if safety, efficacy, commercial adoption, manufacturing or supply issues arise with the therapies we choose to evaluate in combination with our product candidates, we may be unable to obtain approval of or successfully market our product candidates.
Additionally, if the third-party providers of therapies or therapies in development used in combination with our product candidates are unable to produce sufficient quantities for clinical trials or commercialization of our product candidates, or if the cost of combination therapies are prohibitive, our development and commercialization efforts would be impaired, which would have an adverse impact on our business, financial condition, results of operations and growth prospects.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome.
Clinical testing is expensive and can take many years to complete, with the outcome inherently uncertain. Failure can occur at any time during the clinical trial process. Before obtaining approval from regulatory authorities for the sale of any product candidate, we must conduct extensive clinical trials to demonstrate the safety and efficacy of our product candidates in humans. Prior to initiating clinical trials, a sponsor must complete extensive preclinical testing of a product candidate, including, in most cases, preclinical efficacy experiments as well IND-enabling toxicology studies. These experiments and studies may be time-consuming and expensive to complete. The necessary preclinical testing may not be completed successfully for a preclinical product candidate and a potentially promising product candidate may therefore never be tested in humans. Once it commences, clinical testing is expensive, difficult to design and implement, can take many years to complete and is uncertain as to outcome. A failure of one or more clinical trials can occur at any stage of testing. The outcome of preclinical testing and early clinical trials may not be predictive of the success of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses, and many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval of their products. We may experience numerous unforeseen events during drug development that could delay or prevent our ability to receive marketing approval or commercialize our product candidates. In particular, clinical trials of our product candidates may produce inconclusive or negative results. We have limited data regarding the safety, tolerability and efficacy of GPS administered as monotherapy or in combination with PD-1 inhibitors or for SLS009 as monotherapy and in combination with other therapeutics, including aza/ven. For a further discussion of the safety risks in our trials, see the risk factor herein entitled "Our current and future product candidates, the methods used to deliver them or their dosage levels may cause undesirable side effects or have other properties that could delay or
prevent their regulatory approval, limit the commercial profile of an approved label or result in significant negative consequences following any regulatory approval."
Clinical trials also require the review and oversight of an IRB. An inability or delay in obtaining IRB approval could prevent or delay the initiation and completion of clinical trials, and the FDA may decide not to consider any data or information derived from a clinical investigation not subject to initial and continuing IRB review and approval.
We may experience delays in our ongoing or future clinical trials, and we do not know whether planned clinical trials will begin or enroll subjects on time, will need to be redesigned or will be completed on schedule, if at all. There can be no assurance that the FDA will not put clinical trials of any of our product candidates on clinical hold in the future. Clinical trials may be delayed, suspended or prematurely terminated for a variety of reasons, such as:
•delay or failure in reaching agreement with the FDA or a comparable foreign regulatory authority on a clinical trial design that we are currently reimbursing any former employees’ attorney’s feesable to execute;
•delay or failure in obtaining authorization to commence a trial or inability to comply with respectconditions imposed by a regulatory authority regarding the scope or design of a trial;
•delay or failure in reaching agreement on acceptable terms with prospective contract research organizations, or CROs, and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites;
•delay or failure in obtaining IRB approval or the approval of other reviewing entities, including comparable foreign regulatory authorities, to conduct a clinical trial at each site;
•withdrawal of clinical trial sites from our clinical trials or the ineligibility of a site to participate in our clinical trials;
•clinical sites and investigators deviating from trial protocol, failing to conduct the trial in accordance with regulatory requirements, or dropping out of a trial;
•inability to identify and maintain a sufficient number of trial sites, many of which may already be engaged in other clinical trial programs, including some that may be for the same indication;
•failure of our third-party clinical trial managers, CROs, clinical trial sites, contracted laboratories or other third-party vendors to satisfy their contractual duties, meet expected deadlines or return trustworthy data;
•delay or failure in adding new trial sites;
•delay or failure in recruiting and enrolling suitable subjects to participate in a trial;
•delay or failure in subjects completing a trial or returning for post-treatment follow-up;
•interim results or data that are ambiguous or negative or are inconsistent with earlier results or data;
•alteration of trial design necessitated by re-evaluation of design assumptions based upon observed data;
•feedback from the FDA, or foreign regulatory authority, the IRB, or DSMB, or results from earlier stage or concurrent preclinical studies and clinical trials, that might require modification to the investigation. We are cooperatingprotocol for a trial;
•a decision by the FDA or foreign regulatory authority, the IRB, or us, or a recommendation by a DSMB or comparable foreign regulatory authority, to suspend or terminate clinical trials at any time for safety issues or for any other reason;
•unacceptable risk-benefit profile, unforeseen safety issues or adverse side effects;
•failure to demonstrate a benefit from using a product candidate;
•difficulties in manufacturing or obtaining from third parties sufficient quantities of a product candidate to start or to use in clinical trials;
•lack of adequate funding to continue a trial, including the incurrence of unforeseen costs due to enrollment delays, requirements to conduct additional studies or increased expenses associated with the civilservices of our CROs and criminal investigationother third parties; or
•changes in governmental regulations or administrative actions or lack of adequate funding to continue a clinical trial.
If we experience delays in the completion or termination of any clinical trial of our product candidates, the approval and throughcommercial prospects of such product candidates will be harmed, delaying our outside counselability to generate product revenues from such product candidate and our costs will most likely increase. The required regulatory approvals may also be delayed, thereby jeopardizing our ability to commence product sales and generate revenues and the period of commercial exclusivity for our products may be decreased. Regulatory approval of our product candidates may be denied for the same reasons that caused the delay.
Risks associated with operating in foreign countries could materially adversely affect our product development.
For certain of our clinical trials, we have recently begun preliminary discussions with the government aimed at the ultimate resolutionclinical sites in countries outside of the investigation regarding the Company.
WeUnited States. Consequently, we may be subject to risks related to operating in foreign countries. Risks associated with conducting operations in foreign countries include:
•differing regulatory requirements for drug approvals and regulation of approved drugs in foreign countries; more stringent privacy requirements for data to be supplied to our operations in the United States, e.g., GDPR in the EU;
•unexpected changes in tariffs, trade barriers and regulatory requirements; economic weakness, including inflation, or political instability in particular foreign economies and markets; compliance with tax, employment, immigration and labor laws for employees living or traveling abroad; foreign taxes, including withholding of payroll taxes;
•differing payor reimbursement regimes, governmental payors or patient self-pay systems and price controls;
•foreign currency fluctuations, which could result in increased operating expenses or reduced revenues, and other obligations incident to doing business or operating in another country;
•workforce uncertainty in countries where labor unrest is more common than in the United States;
•continued uncertainties related to the withdrawal of the United Kingdom from the EU (known as "Brexit") and its financial, trade, regulatory and legal implications, which could lead to legal uncertainty and potentially divergent national laws and regulations as the United Kingdom determines which EU laws to replace or administrativereplicate, and which may further create global economic uncertainty, which could materially adversely affect our business, business opportunities, results of operations, financial condition, and cash flows;
•production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad, including those that may result from the recent coronavirus outbreak; and
•business interruptions resulting from geopolitical actions, including war and terrorism.
Global, market and economic conditions may negatively impact our business, financial condition and share price.
The results of our operations could be adversely affected by general conditions in the global economy, the global financial markets and the global political conditions. The United States and global economies have recently faced growing inflation, higher interest rates and a potential recession. Furthermore, a prolonged economic downturn, including a recession or depression resulting from public health crises such as a pandemic or ongoing political disruption such as the war between Ukraine and Russia and the conflict involving Israel and Hamas could result in a variety of risks to our business, including weakened demand for our programs and development candidates, if approved, relationships with any vendors or business partners located in affected geographies and our ability to raise additional capital when needed on acceptable terms, if at all. A weak or declining economy or political disruption, including any international trade disputes, particularly between the United States and China, could also strain our existing or future partnerships, manufacturers or suppliers, possibly resulting in disruption to our clinical trials or supply, or cause our customers to delay making payments for our potential products. Any of the foregoing could seriously harm our business, and we cannot anticipate all of the ways in which the political or economic climate and financial market conditions could seriously harm our business.
Although we do not currently have any clinical study sites in Russia or Ukraine, economic, political and social conditions resulting from Russia’s invasion of Ukraine could materially disrupt our clinical trials, increase our costs and may disrupt planned clinical development activities. For example, we currently have clinical sites for our REGAL study in Poland, a country that borders Ukraine and has been impacted by an influx of Ukrainian refugees resulting from Russia’s invasion of Ukraine. Furthermore, we rely on suppliers in the EU. To the extent the conflict between Ukraine and Russia adversely impacts the ability of our suppliers to distribute the supplies we need for our clinical trials, or such distribution cannot be done on a timely basis, the timing for completing our clinical trials may be adversely impacted.
Continued increases in inflation could raise our costs for commodities, labor, materials and services and other costs required to grow and operate our business, and failure to secure these on reasonable terms may adversely impact our financial condition. Additionally, increases in inflation, along with the uncertainties surrounding geopolitical developments and global supply chain disruptions, have caused, and may in the future cause, global economic uncertainty and uncertainty about the interest rate environment. A failure to adequately respond to these risks could have a material adverse impact on our financial condition, results of operations or cash flows. In response to high levels of inflation and recession fears, the U.S. Federal Reserve, the European Central Bank, and the Bank of England have raised, and may continue to raise, interest rates and implement fiscal policy interventions. Even if these interventions lower inflation, they may also reduce economic growth rates, create a recession, and have other similar effects.
The U.S. debt ceiling and budget deficit concerns have increased the possibility of credit-rating downgrades and economic slowdowns, or a recession in the United States. Although U.S. lawmakers have previously passed legislation to raise the federal debt ceiling on multiple occasions, there is a history of ratings agencies lowering or threatening to lower the long-term sovereign credit rating on the United States given such uncertainty. On August 1, 2023, Fitch Ratings downgraded the United States’ long-term foreign currency issuer default rating to AA+ from AAA as a result of these matters, or therepeated debt ceiling and budget deficit concerns. The impact of such matters. this or any further downgrades to the U.S. government’s sovereign credit rating or its perceived creditworthiness could adversely affect the U.S. and global financial markets and economic conditions.
If the equity and credit markets deteriorate, it may make any necessary equity or debt financing more difficult to secure, more costly or more dilutive. Failure to secure any necessary financing in a timely manner and on favorable terms could harm our growth strategy, financial performance and stock price and could require us to delay or abandon plans with respect to our business, including clinical development plans. Further, recent developments in the banking industry could adversely affect our business. If the financial institutions with which we are found to bedo business enter receivership or become insolvent in violationthe future, there is no guarantee that the Department of the False Claims Act, Anti-Kickback Statute, Patient ProtectionTreasury, the Federal Reserve and Affordable Care Act,the FDIC will intercede to provide us and other depositors with access to balances in excess of the $250,000 FDIC insurance limit, that we would be able to access our existing cash, cash equivalents and investments, that we would be able to maintain any required letters of credit or any other applicable statecredit support arrangements, or any federal fraud and abuse laws,that we maywould be subjectable to penalties, such as civil and criminal penalties, damages, fines, or an administrative actionadequately fund our business for a prolonged period of exclusion from government health care reimbursement programs. We can make no assurances as to the time or resources that will need to be devoted to these matters or their outcome, or the impact, ifat all, any that these matters or any resulting legal or administrative proceedings may have on our business or financial condition.
Many of the regulatory provisions that we are subject to include criminal provisions. If we are unable to comply with these provisions in the operation of our business we may become subject to civil and criminal investigations and proceedings thatwhich could have a material adverse effect on our business, financial condition and prospects.
The federal False Claims Act prohibits persons from knowingly filing, or causing to be filed, a false claim to, orresults of operations. We cannot predict the knowing use of false statements to obtain payment from,impact that the federal government. Qui tam suits filed under the False Claims Act can be brought by any individual on behalfhigh market volatility and instability of the governmentbanking sector more broadly could have on economic
activity and such individuals, commonly known as “relators”our business in particular. In addition, there is a risk that one or “whistleblowers,”more of our current service providers, manufacturers or other third parties with which we conduct business may share in any amounts paid bynot survive difficult economic times, the entity toongoing conflict between Russia and Ukraine, the government in fines or settlement. The frequency of filing qui tam actions has increased significantly in recent years, causing greater numbers of health care companies to have to defend such qui tam actionswar between Israel and pay substantial sums to settle such actions. The federal Anti-Kickback Statute prohibits persons from knowingly and willfully soliciting, offering, receiving, or providing remuneration, directly or indirectly, in exchange for or to induce eitherHamas, the referral of an individual, or the furnishing or arranging for a good or service, for which payment may be made under a federal health care program such as the Medicare and Medicaid programs. Several courts have interpreted the statute’s intent requirement to mean that if any one purpose of an arrangement involving remuneration is to induce referrals of federal health care covered business, the statute has been violated. The Anti-Kickback Statute is broad, and despite a series of narrow safe harbors, prohibits many arrangements and practices that are lawful in businesses outsideinstability of the health care industry. Penalties for violations ofbanking sector, and the federal Anti-Kickback Statute include criminal penaltiesuncertainty associated with current worldwide economic conditions, which could directly affect our ability to attain our operating goals on schedule and civilon budget.
Our partnerships in China subject us to risks and administrative sanctions such as fines, imprisonment and possible exclusion from Medicare, Medicaid and other federal health care programs. An alleged violation ofuncertainties relating to the Anti- Kickback Statute may be used as a predicate offense to establish liability pursuant to other federal laws and regulations of China and the changes in relations between the United States and China.
Under its current leadership, the government of China has been pursuing economic reform policies, including by encouraging foreign trade and investment. However, there is no assurance that the Chinese government will continue to pursue such aspolicies, that such policies will be successfully implemented, that such policies will not be significantly altered, or that such policies will be beneficial to our partnerships in China. China’s system of laws can be unpredictable, especially with respect to foreign investment and foreign trade. The U.S. government has called for substantial changes to foreign trade policy with China and has raised, and has proposed to further raise in the federal False Claims Act. Many states have alsofuture, tariffs on several Chinese goods. China has retaliated with increased tariffs on U.S. goods. Moreover, China’s legislature has adopted laws similara national security law to substantially change the federal Anti-Kickback Statute, someway Hong Kong has been governed since the territory was handed over by the United Kingdom to China in 1997. This law increases the power of which apply to the referralcentral government in Beijing over Hong Kong, limit the civil liberties of patients for health care items or services reimbursed by any source, not only Medicareresidents of Hong Kong and Medicaid programs.
The federal Patient Protection and Affordable Care Act includes provisions expandingcould restrict the ability of certain relatorsbusinesses in Hong Kong to bring actionscontinue to conduct business or to continue to with business as previously conducted. The U.S. State Department has indicated that would have been dismissed under prior law. When an entity is determinedthe United States no longer considers Hong Kong to have violatedsignificant autonomy from China. The U.S. State Department also previously enacted sanctions related to China’s governing of Hong Kong, and the federal False ClaimsUnited States may impose the same tariffs and other trade restrictions on exports from Hong Kong that it places on goods from mainland China. Any further changes in U.S. trade policy could trigger retaliatory actions by affected countries, including China, resulting in trade wars. For example, the Uyghur Forced Labor Prevention Act bans imports from China’s Xinjiang Uyghur Autonomous Region unless it can be shown that the goods were not produced using forced labor and this legislation may be required to pay up to three timeshave an adverse effect on global supply chains which could adversely impact our business and results of operations. Additionally, the actual damages sustainedbiopharmaceutical industry in particular in China is strictly regulated by the government, plus civil penalties for each separate false claim. The Deficit Reduction ActChinese government. Changes to Chinese regulations affecting biopharmaceutical companies are also unpredictable. Any regulatory changes and changes in United States and China relations may have a material adverse effect on our partnerships in China which could materially harm our business and financial condition.
Climate change or legal, regulatory or market measures to address climate change may negatively affect our business, results of 2005 encouraged statesoperations, cash flows and prospects.
Climate change may potentially negatively affect our business and results of operations, cash flows and prospects in the future. We could be exposed to enactphysical risks (such as extreme weather conditions or modify their state false claims actsrising sea levels), risks in transitioning to a low-carbon economy (such as additional legal or regulatory requirements, changes in technology, market risk and reputational risk), and social and human effects (such as population dislocations and harm to health and well-being) associated with climate change. These risks can be at leasteither acute (short-term) or chronic (long-term).
Extreme weather and sea-level rise could pose physical risks to facilities of our suppliers. Such risks include losses incurred as effective as the federal False Claims Acta result of physical damage to facilities, loss or spoilage of inventory, and business interruption caused by granting states a portion of any federal Medicaid funds recovered through Medicaid-related actions. Most states have enacted state false claims laws,such natural disasters and many of those states included laws including qui tam provisions. The federal Patient Protectionextreme weather events which could disrupt our operations and Affordable Care Act includes provisions known as the Physician Payments Sunshine Act, which requires manufacturers of drugs, biologics, devices and medical supplies covered under Medicare and Medicaid to record any transfers of value to physicians and teaching hospitals and to report this data beginning in 2013 to the Centers for Medicare and Medicaid Services for subsequent public disclosures. Manufacturers must also disclose investment interests held by physicians and their family members. Failure to submit the required informationsupply chains that may result in civil monetary penaltiesincreased costs.
New legal or regulatory requirements may be enacted to prevent, mitigate, or adapt to the implications of up to $1 million per year for knowing violationsa changing climate and its effects on the environment. These regulations, which may differ across jurisdictions, could result in liability underus being subject to new or expanded carbon pricing or taxes, increased compliance costs, restrictions on greenhouse gas emissions, investment in new technologies, increased carbon disclosure and transparency, upgrade of facilities to meet new building codes, and the redesign of utility systems, which could increase our operating costs, including the cost of electricity and energy used by us. Our supply chain would likely be subject to these same transitional risks and would likely pass along any increased costs to us.
Our current and future product candidates, the methods used to deliver them or their dosage levels may cause undesirable side effects or have other federal lawsproperties that could delay or regulations. Similar reporting requirements have also been enacted onprevent their regulatory approval, limit the state levelcommercial profile of an approved label or result in significant negative consequences following any regulatory approval.
Undesirable side effects caused by our current or future product candidates, their delivery methods or dosage levels could cause us, the IRB, DSMB, or the FDA or comparable regulatory authorities to interrupt, delay or halt clinical trials and could result in a more restrictive label or the delay or denial of regulatory approval or termination of clinical trials. For example, although no high-grade delayed type hypersensitivity in the U.S.,skin or systemic anaphylaxis events have been noted after GPS administration in patients treated in our clinical studies to date, it is theoretically possible that such toxicities, or other type of adverse events, may occur in future clinical studies. As a result of safety or toxicity issues that we may experience in our clinical trials, or negative or inconclusive results from the clinical trials of others for drug candidates similar to our own, we may not receive approval to market any product candidates, which could prevent us from ever generating revenues or achieving profitability. Results of our trials could reveal an unacceptably high severity and incidence of side effects. In such an increasing numberevent, our trials could be suspended or terminated, and the FDA or comparable foreign regulatory authorities could order us to cease further development of countries worldwide either have adopted or are considering similar laws requiring transparencydeny approval of interactions with health care professionals. In addition, some states such as Massachusetts and Vermont imposed an outright ban on certain gifts to physicians. These laws could affect our product promotional activities by limitingcandidates for any or all targeted indications. The drug-related side effects could also affect patient recruitment or the kindsability of interactions we could have with hospitals, physiciansenrolled subjects to complete the trial or otherresult in potential purchasers or users of our system. Both the disclosure laws and gift bans also will impose administrative, cost and compliance burdens on us.
We face product liability exposure and, if successful claims are brought against us, we may incur substantial liability if our insurance coverage for those claims is inadequate.
The commercial sale of our products after they are approved as well as the use of our products in clinical trials exposes us to possible product liability claims. This risk exists even if a product is approved for commercial sale by the FDA and manufactured in facilities licensed and regulated by the FDA, if our products were sold to third parties, or if our products are provided in clinical trials. Our products are designed to affect important bodily functions and processes. Any side effects, manufacturing defects, misuse or abuse associated with our products could result in injury to a patient or even death. For example, because the placeboof these occurrences may have performed better than NeuVax in the PRESENT Trial, the use of NeuVax may have worsened the patient’s condition.
Product liability claims may be brought against us by consumers, health care providers, pharmaceutical companies or others selling or otherwise coming into contact with our products or generic versions of our products. If we cannot successfully defend ourselves against product liability claims we could incur substantial liabilities. Because we have sold Abstral and Zuplenz® (ondansetron) oral soluble film and provided NeuVax as a study drug in the PRESENT Trial and other clinical trials, regardless of merit or eventual outcome, product liability claims may result in:
impairment of our business reputation;
costs of related litigation;
distraction of management’s attention from our primary business; or
substantial monetary awards to patients or other claimants.
We have obtained product liability insurance coverage for commercial product sales with a $10 million per occurrence and a $10 million annual aggregate coverage limit. Our insurance coverage may not be sufficient to cover all of our product liability related expenses or losses and may not cover us for any expenses or losses we may suffer. Moreover, insurance coverage is becoming increasingly expensive and, in the future, we may not be able to maintain insurance coverage at a reasonable cost, in sufficient amounts or upon adequate terms to protect us against losses due to product liability. If we determine that it is prudent to increase our product liability coverage based on sales of our products, we may be unable to obtain this increased product liability insurance on commercially reasonable terms or at all. Large judgments have been awarded in class action or individual lawsuits based on drugs that had unanticipated side effects, including side effects that may be less severe than those of our products. A successful product liability claim or series of claims brought against us could cause our stock price to decline and, if judgments exceed our insurance coverage, could decrease our cash and have a material adverse effect on our business, results of operations, financial condition, cash flows and future prospects.
Additionally, if any of our product candidates receives regulatory approval, and we or others later identify undesirable side effects caused by such product, a number of potentially significant negative consequences could result, including that:
•we may be forced to suspend marketing of such product;
•regulatory authorities may withdraw their approvals of such product;
•regulatory authorities may require additional warnings on the label that could diminish the usage or otherwise limit the commercial success of such product;
•we may be required to conduct post-marketing studies;
•we may be required to change or the health care setting in which the way the product is administered;
•we could be sued and held liable for harm caused to subjects or patients; and
•our reputation may suffer.
Any of these events could prevent us from achieving or maintaining market acceptance of the particular product candidate, if approved.
Our product development program may not uncover all possible adverse events that patients who take our product candidates may experience. The number of subjects exposed to product candidates and the average exposure time in the clinical development program may be inadequate to detect rare adverse events or chance findings that may only be detected once the product is administered to more patients and for greater periods of time.
Clinical trials by their nature utilize a sample of the potential patient population. However, with a limited number of subjects and limited duration of exposure, we cannot be fully assured that rare and severe side effects of our product candidates will be uncovered. Such rare and severe side effects may only be uncovered with a significantly larger number of patients exposed to our product candidates. If such safety problems occur or are identified after any of our product candidates reaches the market, the FDA may require that we amend the labeling of the product or recall the product, or may even withdraw approval for the product, any of which could subject us to substantial product liability claims and related litigation.
Our future success is dependent on the regulatory approval of our product candidates.
Our business is dependent on our ability to obtain regulatory approval for our product candidates in a timely manner. We cannot commercialize product candidates in the United States without first obtaining regulatory approval for the product from the FDA. Similarly, we cannot commercialize product candidates outside of the United States without obtaining regulatory approval from comparable foreign regulatory authorities. Before obtaining regulatory approvals for the commercial sale of any product candidate for a target indication, we must demonstrate with substantial evidence gathered from preclinical studies and well-controlled clinical trials that the product candidate is safe and effective for use for that target indication and that the manufacturing facilities, processes and controls are adequate with respect to such product candidate.
The time required to obtain approval by the FDA and comparable foreign regulatory authorities is unpredictable but typically takes many years following the commencement of preclinical studies and clinical trials and depends upon numerous factors, including the substantial discretion and available resources of the regulatory authorities. In addition, approval policies, regulations, or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions.
Even if a product candidate were to successfully obtain approval from the FDA and comparable foreign regulatory authorities, any approval might contain significant limitations related to use restrictions for specified age groups, warnings, precautions or contraindications, or may be subject to burdensome post-approval study or risk management requirements. Also, any regulatory approval of our current or future product candidates, once obtained, may be withdrawn.
Our current and future product candidates could fail to receive regulatory approval from the FDA or comparable foreign regulatory authorities.
We have not obtained regulatory approval for any product candidate and it is possible that our existing product candidates or any future product candidates will not obtain regulatory approval, for many reasons, including:
•disagreement with the regulatory authorities regarding the scope, design or implementation of our clinical trials;
•failure to demonstrate that a product candidate is safe and effective for our proposed indication;
•failure of clinical trials to meet the level of statistical significance required for approval;
•failure to demonstrate that a product candidate’s clinical and other benefits outweigh its safety risks;
•disagreement with our interpretation of data from preclinical studies or clinical trials;
•the insufficiency of data collected from clinical trials of our product candidates to support the submission and filing of a BLA, NDA or other submission or to obtain regulatory approval;
•the insufficiency of a single Phase 3 clinical trial of GPS in AML for regulatory approval in that indication;
•failure to obtain approval of our manufacturing processes or facilities of third-party manufacturers with whom we contract for clinical and commercial supplies or our own manufacturing facility; or
•changes in the approval policies or regulations that render our preclinical and clinical data insufficient for approval.
The FDA or a comparable foreign regulatory authority may require more information, including additional preclinical or clinical data to support approval or additional studies, to support a marketing approval decision, which may delay or prevent approval and our commercialization plans, or we may decide to abandon the development program. If we were to obtain approval, regulatory authorities may approve any of our product candidates for fewer or more limited
indications than we request (including failing to approve the most commercially promising indications), may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve a product candidate with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that product candidate.
If we are unable to obtain regulatory approval for one of our product candidates in one or more jurisdictions, or any approval contains significant limitations, we may not be able to obtain sufficient funding to continue the development of that product or generate revenues attributable to that product candidate.
We currently have ODD designation for GPS and SLS009 for certain indications, which might not provide the intended benefit thereof.
Regulatory authorities in some jurisdictions, including the United States and Europe, may designate drugs for relatively small patient populations as Orphan Drug Products. Under the Orphan Drug Act, the FDA may designate a product as an Orphan Drug Product if it is a drug intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals annually in the United States. We have received ODD from the FDA for GPS in AML, MPM and MM as well as Orphan Medicinal Product designations from the EMA for GPS in AML, MPM and MM. In addition, we have received ODD from the FDA for SLS009 for the treatment of AML and PTCL. Although we have received ODD for GPS and SLS009, there is no guarantee that any of these indications for GPS or SLS009 will be successfully approved by the FDA or the EMA, that GPS or SLS009 will be commercially successful in the marketplace, or that another product will not be approved for the same indication ahead of our product candidate.
Even if we obtain orphan product exclusivity for a product, that exclusivity may not effectively protect the product from competition because different drugs can be approved for the same disease or condition. Even after an Orphan Drug Product is approved, the FDA can subsequently approve another drug or biologic for the same disease or condition if the FDA concludes that the later product is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care. In addition, Orphan product exclusivity may be lost if the FDA or EMA determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug to meet the needs of patients with the rare disease or condition.
We currently have Fast Track designation for GPS and SLS009 and may seek Fast Track designation for additional product candidates, or indications, which might not be received or provide the intended benefits thereof.
If a product candidate is intended for the treatment of a serious condition and nonclinical or clinical data demonstrate the potential to address unmet medical need for this condition, a product sponsor may apply to the FDA for Fast Track designation, which may or may not be granted by the FDA. We have received Fast Track designation from the FDA for GPS in AML, MPM and MM and Fast Track designation for SLS009 for the treatment of r/r AML and r/r PTCL.
However, Fast Track designation does not ensure that we will receive marketing approval or that approval will be granted within any particular timeframe. We may not experience a faster development or regulatory review or approval process with Fast Track designation compared to conventional FDA procedures. In addition, the FDA may withdraw Fast Track designation if it believes that the designation is no longer supported by data from our clinical development program. Fast Track designation alone does not guarantee qualification for the FDA’s accelerated approval or priority review procedures.
Failure to obtain regulatory approval in international jurisdictions would prevent our product candidates from being marketed abroad.
In addition to regulations in the United States, to market and sell our product candidates in the EU, United Kingdom, many Asian countries and other jurisdictions, we must obtain separate regulatory approvals and comply with numerous and varying regulatory requirements. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions, and approval by one regulatory authority outside the United States does not ensure approval by regulatory authorities in other countries or jurisdictions or by the FDA. The regulatory
approval process outside the United States generally includes all of the risks associated with obtaining FDA approval as well as risks attributable to the satisfaction of local regulations in foreign jurisdictions. The approval procedures vary among countries and can involve additional nonclinical or clinical testing. The time required to obtain approval may differ substantially from that required to obtain FDA approval. We may not be able to obtain approvals from regulatory authorities outside the United States on a timely basis, if at all. Clinical trials accepted in one country may not be accepted by regulatory authorities in other countries. In addition, many countries outside the United States require that a product be approved for reimbursement before it can be approved for sale in that country. A product candidate that has been approved for sale in a particular country may not receive reimbursement approval in that country, or may receive reimbursement at a level that is not commercially viable.
We may not be able to file for regulatory approvals and may not receive necessary approvals to commercialize our products in any market. If we are unable to obtain approval of any of our current or future product candidates by regulatory authorities in the EU, United Kingdom, Asia or elsewhere, the commercial prospects of that product candidate may be significantly diminished, our business prospects could decline and this could materially adversely affect our business, results of operations and financial condition.
Even if our current and future product candidates receive regulatory approval, they may still face future development and regulatory difficulties.
Any regulatory approvals we receive for any of our product candidates may be subject to limitations on the approved indicated uses for which the product candidate may be marketed or to the conditions of approval, or contain requirements for potentially costly post-marketing testing, including Phase 4 clinical trials. In addition, any such regulatory approvals would be subject to ongoing requirements by the FDA and comparable foreign regulatory authorities governing the manufacture, quality control, further development, labeling, packaging, storage, distribution, adverse event reporting, safety surveillance, import, export, advertising, promotion, recordkeeping and reporting of safety and other post-marketing information. These requirements include submissions of safety and other post-marketing information and reports, registration, as well as continued compliance by us and/or our CMOs with respect to product quality and manufacturing operations and our CROs for any post-approval clinical trials that we may conduct. The safety profile of any product will continue to be closely monitored by the FDA and comparable foreign regulatory authorities after approval. If the FDA or comparable foreign regulatory authorities become aware of new safety information after approval of any of our product candidates, they may require labeling changes or establishment of a REMS, impose significant restrictions on a product’s indicated uses or marketing or impose ongoing requirements for potentially costly post-approval studies or post-market surveillance. Any new legislation addressing drug safety issues could result in delays in product development or commercialization, or increased costs to assure compliance. If our original marketing approval for a product candidate was obtained through an accelerated approval pathway, we could be required to conduct a successful post-marketing clinical trial to confirm the clinical benefit for our products. An unsuccessful post-marketing clinical trial or failure to complete such a trial could result in the withdrawal of marketing approval.
In addition, manufacturers and manufacturers’ facilities are required to continuously comply with FDA and comparable foreign regulatory authority requirements, including ensuring quality control and manufacturing procedures conform to cGMP, regulations and corresponding foreign regulatory manufacturing requirements. Accordingly, we and our contract manufacturers will be subject to continual review and inspections to assess compliance with cGMP and adherence to commitments made in any BLA or NDA submission to the FDA or any other type of domestic or foreign marketing authorization application. We or our third-party manufacturers may not be able to comply with cGMP regulations or similar regulatory requirements outside of the United States. If any of our third-party suppliers fails to comply with cGMP or other applicable manufacturing regulations, our ability to develop and commercialize our product candidates could suffer significant interruptions. If we or a regulatory agency discover previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where the product is manufactured, a regulatory agency may impose restrictions on that product, the manufacturing facility or us, including requiring recall or withdrawal of the product from the market or suspension of manufacturing. If we, our product candidates or the manufacturing facilities for our product candidates fail to comply with applicable regulatory requirements, a regulatory agency may take the following actions, any of which could significantly and adversely affect supplies of our products:
•issue Form 483 notices of observations, warning letters or untitled letters;
•mandate modifications to promotional materials or require us to provide corrective information to health care practitioners;
•require us to enter into a consent decree, which can include imposition of various fines, reimbursements for inspection costs, required due dates for specific actions and penalties for noncompliance;
•seek an injunction or impose civil or criminal penalties or monetary fines;
•suspend or withdraw regulatory approval;
•suspend any ongoing clinical trials;
•refuse to approve pending applications or supplements to applications filed by us;
•suspend or impose restrictions on operations, including costly new manufacturing requirements; or
•seize or detain products, refuse to permit the import or export of products, or require us to initiate a product recall.
Any government investigation of alleged violations of law would require us to expend significant time and resources in response and could generate adverse publicity. The occurrence of any event or penalty described above may inhibit our ability to successfully commercialize our products and generate revenues.
Advertising and promotion of any product candidate that obtains approval in the United States will be heavily scrutinized by the FDA, the DOJ, the Office of Inspector General for the DHHS, state attorneys general, members of Congress and the public. A company can make only those claims relating to safety and efficacy, purity and potency that are approved by the FDA and in accordance with the provisions of the approved label. Additionally, advertising and promotion of any product candidate that obtains approval outside of the United States will be heavily scrutinized by comparable foreign regulatory authorities. Violations, including actual or alleged promotion of our products for unapproved or off-label uses, are subject to enforcement letters, inquiries and investigations, and civil and criminal sanctions by the FDA, as well as potential prosecution under the federal False Claims Act. Any actual or alleged failure to comply with labeling and promotion requirements may have a negative impact on our business.
Risks Related to Our Manufacturing
We have limited to no manufacturing or distribution capability and must rely upon third parties for such.
We currently have direct or indirect agreements or arrangements with various third-party manufacturing facilities for production of our product candidates for research and development and testing purposes. For example, for SLS009 we are party to a supply agreement with GenFleet who has agreements with third-party manufacturers for the manufacture of SLS009. We depend on these manufacturers to meet our deadlines, quality standards and specifications. Reliance on third-party providers may expose us to more risk than if we were to manufacture our product candidates ourselves. We do not control the manufacturing processes of the CMOs we rely on and are dependent on those third parties for the production of our product candidates in accordance with relevant applicable regulations, such as cGMP, which includes, among other things, quality control, quality assurance and the maintenance of records and documentation. Our reliance on third parties for the manufacture of our active pharmaceutical ingredients and investigational drug products and, in the future, any approved products, creates a dependency that could severely disrupt our research and development, our clinical testing, and ultimately our sales and marketing efforts if the source of such supply proves to be unreliable or unavailable. If the contracted manufacturing source is unreliable or unavailable, we may not be able to manufacture clinical supplies of our product candidates, and our preclinical and clinical testing programs may not be able to move forward and our entire business plan could fail.
The third-party manufacturers we rely on for the manufacture of our product candidates are subject to inspection and approval by regulatory authorities before we can commence the manufacture and sale of any of our product
candidates, and thereafter are subject to ongoing inspection from time to time. Our third-party manufacturers may not be able to comply with applicable cGMP regulations or similar regulatory requirements outside of the United States. In complying with the manufacturing regulations of the FDA and other comparable foreign regulatory authorities, we and our third-party suppliers must spend significant time, money and effort in the areas of design and development, testing, production, record-keeping and quality control to assure that the products meet applicable specifications and other regulatory requirements. If either we or the CMOs we rely on fail to comply with these requirements, our ability to develop and commercialize our product candidates could suffer significant interruptions, and we may be subject to regulatory enforcement action, including the seizure of products and shutting down of production.
Both the active pharmaceutical ingredient and drug product for our product candidates are currently single-sourced. We believe these single sources are currently capable of supplying all anticipated needs of our proposed clinical studies, as well as initial commercial introduction should such product candidates received regulatory approval. If we are able to commercialize our products in the future, there is no assurance that our manufacturers will be able to meet commercialized scale production requirements in a timely manner or in accordance with applicable standards or cGMP. Once the nature and scope of additional indications and their commensurate drug product demands are established, we will seek secondary suppliers of both the active pharmaceutical ingredients and drug products for our product candidates, but we cannot assure that such secondary suppliers will be found on terms acceptable to us, or in a timely manner, or at all.
We are subject to a multitude of manufacturing risks, any of which could substantially increase our costs and limit supply of our product candidates.
We and the CMOs we rely on will need to conduct significant development work for each product candidate for each target indication for studies, trials and commercial launch readiness. We intend to improve the existing processes for GPS in connection with more advanced clinical trials or commercialization efforts we may undertake in the future. Developing commercially viable manufacturing processes is a difficult, expensive and uncertain task, and there are risks associated with scaling to the level required for advanced clinical trials or commercialization, including cost overruns, potential problems with process scale-up, process reproducibility, stability issues, storage issues, consistency and timely availability of reagents or raw materials. The manufacturing facilities in which our product candidates will be made could be adversely affected by the recent coronavirus outbreak, other pandemics, earthquakes and other natural disasters, equipment failures, labor shortages, lack of adequate temperature controls, power failures, and numerous other factors. We currently estimate that we have sufficient clinical supplies to support our clinical trials, however, this estimate is dependent on patient enrollment rates and a number of other factors and, accordingly, could change. Moreover, current clinical supplies may not be adequate for future clinical studies.
Additionally, the process of manufacturing our product candidates is complex, highly regulated and subject to several risks, including but not limited to:
•product loss due to contamination, equipment failure or improper installation or operation of equipment, or vendor or operator error;
•product loss or manufacturing failure due to failure of temperature controls in production, storage or transit;
•product loss, which may not be covered by insurance, due to global conflict and unrest, including related inoperability of shipping lanes;
•reduced production yields, product defects, and other supply disruptions due to deviations, even minor, from normal manufacturing and distribution processes;
•inability to procure or delay in procuring raw materials and reagents for manufacturing products;
•unexpected product defects;
•microbial, viral, or other contaminations in our product candidates or in the manufacturing facilities in which our product candidates are made, which may result in the closure of such manufacturing facilities for an extended period of time to allow for the investigation and remediation of the contamination;
•adverse impact on the active ingredient of GPS as a result of potential contamination from the presence of heavy metals which can lead to higher than acceptable rates of impurities resulting in the active ingredient being unacceptable for use; and
•adverse impact on the manufacturing of GPS as a result of potential contamination from excess humidity and oxygen which can lead to higher than acceptable levels of impurities resulting in the drug product being unacceptable for use.
Any adverse developments affecting manufacturing operations for our product candidates may result in shipment delays, inventory shortages, lot failures, withdrawals or recalls or other interruptions in the supply of our drug substance and drug product, which could delay the development of our product candidates. We may also have to write off inventory, incur other charges and expenses for supply of drug product that fails to meet specifications, undertake costly remediation efforts, or seek more costly manufacturing alternatives. Inability to meet the demand for our product candidates could damage our reputation and the reputation of our products among physicians, health care payors, patients or the medical community, and cancer treatment centers, which could adversely affect our ability to operate our business and our results of operations.
In our GPS clinical trials, GM-CSF and Montanide are also administered in addition to GPS and their availability is dependent upon third-party manufacturers, which may or may not reliably provide GM-CSF or Montanide, thus jeopardizing the completion of the trials.
GPS is administered in combination with GM-CSF, which is available exclusively from one manufacturer, and Montanide, which is exclusively available from another supplier. We will continue to be dependent on these manufacturers for our supply of these materials in connection with the ongoing GPS trials and the potential commercial manufacture of GPS. We have not entered into a dedicated supply agreement with the manufacturers for GM-CSF or Montanide, and instead rely on purchase orders to meet our supply needs. Any temporary interruptions or discontinuation of the availability of these materials, or any determination by us to change their use with GPS, could have a material adverse effect on our clinical trials and any commercialization of the assets.
If any of the clinical manufacturing facilities of CMOs we rely on for clinical supply are damaged or destroyed or production at such facilities is otherwise interrupted, our business and prospects would be negatively affected.
If the manufacturing facilities of the CMOs we rely on for clinical supply or the equipment in them is damaged or destroyed, we may not be able, quickly or inexpensively, to replace such manufacturing capacity or replace it at all. In the event of a temporary or protracted loss of a facility or equipment, we might not be able to transfer manufacturing to another CMO. Even if we could transfer manufacturing to another CMO, the shift would likely be expensive and time-consuming, particularly because the new facility would need to comply with the necessary regulatory requirements, and we would need FDA approval before selling any products manufactured at that facility. Such an event could delay our clinical trials or reduce our product sales.
Although we currently maintain insurance coverage against damage to our property and to cover business interruption and research and development restoration expenses, our insurance coverage may not reimburse us, or may not be sufficient to reimburse us, for any expenses or losses we may suffer. In addition, our clinical trials insurance coverage has exclusions for global conflict and unrest of the type currently ongoing in Ukraine. We may be unable to meet our requirements for our product candidates if there were a catastrophic event or failure of our current manufacturing facility or processes.
Risks Related to Our Dependence on Third Parties and Our License Agreements
We rely on third parties to conduct our preclinical studies and clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, or if we lose any of our CROs or
other key third-party vendors, we may not be able to obtain regulatory approval for or commercialize our current or future product candidates on a timely basis, if at all.
Our internal capacity for clinical trial execution and management is limited and therefore we rely heavily on third parties. We have relied upon and plan to continue to rely upon third-party CROs, vendors and contractors to monitor and manage data for our ongoing preclinical and clinical programs. We currently rely on and plan to continue to rely on a CRO for our Phase 3 trial for GPS in AML and well as all of our ongoing and contemplated clinical studies, with services to be rendered by such CROs and vendors ranging from specific and need-tailored (e.g., data management and biostatistics) to, in the case of our Phase 3 trial for GPS in AML, all-encompassing. We rely on these parties for the execution of our preclinical studies and clinical trials, including the proper and timely conduct of our clinical trials, and we control only some aspects of their activities. Outsourcing these functions involves risk that third parties may not perform to our standards, may not produce results or data in a timely manner or may fail to perform at all.
While we have agreements governing the commitments of our third-party vendor services, we have limited influence over their actual performance. Nevertheless, we are responsible for ensuring that each of our trials is conducted in accordance with the applicable protocol and legal, regulatory and scientific standards, and our reliance on the CROs does not relieve us of our regulatory responsibilities.
If we or any of our partners or CROs fail to comply with applicable regulations and GCP, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our regulatory applications. Upon inspection by a given regulatory authority, such regulatory authority could determine that any of our clinical trials are not in compliance with applicable requirements. In addition, our clinical trials must be conducted with product candidates produced under cGMP and other requirements. We are also required to register ongoing clinical trials and post the results of completed clinical trials on a government-sponsored database, ClinicalTrials.gov, within a specified timeframe. Failure to comply also would violate federal requirements in the United States and could result in other penalties, which would delay the regulatory approval process and result in adverse publicity.
Our CROs, third-party vendors and contractors are not our employees, and except for remedies available to us under our agreements with such CROs, third-party vendors and contractors, we cannot control whether or not they devote sufficient time and resources, including experienced staff, to our ongoing clinical, nonclinical and preclinical programs. They may also have relationships with other entities, some of which may be our competitors. If CROs, third-party vendors and contractors do not successfully carry out their contractual duties or obligations or meet expected deadlines or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to obtain regulatory approval for or successfully commercialize our current or future product candidates. CRO, vendor or contractor errors could cause our results of operations and the commercial prospects for our current or future product candidates to be harmed, our costs to increase and our ability to generate revenues to be delayed.
In addition, the use of third-party service providers requires us to disclose our proprietary information to these parties, which could increase the risk that this information will be misappropriated. We currently have a small number of employees, which limits the internal resources we have available to identify and monitor our third-party providers. To the extent we are unable to identify and successfully manage the performance of third-party service providers in the future, our business may be adversely affected. Though we carefully manage our relationships with our CROs, there can be no assurance that we will not encounter challenges or delays in the future or that these delays or challenges will not have a material adverse impact on our business, financial condition and prospects.
If any of our relationships with our third-party CROs, third-party vendors or contractors terminate, we may not be able to enter into arrangements with alternative CROs, third-party vendors or contractors on a timely basis, on commercially reasonable terms or at all.
Our CROs, third-party vendors and contractors have the right to terminate their agreements with us in the event of an uncured material breach. In addition, some of our CROs, third-party vendors and contractors have an ability to terminate their respective agreements with us if it can be reasonably demonstrated that the safety of the subjects
participating in our clinical trials warrants such termination, if we make a general assignment for the benefit of our creditors or if we are liquidated. Identifying, qualifying and managing performance of third-party service providers can be difficult, time consuming and cause delays in our development programs. In addition, there is a natural transition period when a new CRO, third-party vendor or contractor commences work and the new CRO, third-party vendor or contractor may not provide the same type or level of services as the original provider.
We have in-licensed a significant portion of our intellectual property from MSK. If we breach our license agreement with MSK, we could lose the ability to continue the development and potential commercialization of GPS.
GPS is in-licensed from MSK and includes an exclusive license to U.S. and foreign patent applications. Under the MSK license agreement, we are subject to various obligations, including diligence obligations with respect to funding, development and commercialization activities, payment obligations upon achievement of certain milestones and royalties on product sales, as well as other material obligations. If there is any conflict, dispute, disagreement or issue of nonperformance between us and MSK regarding our rights or obligations under the license agreements, including any such conflict, dispute or disagreement arising from our failure to satisfy diligence or payment obligations under any such agreement, we may be liable to pay damages and MSK may have a right to terminate the affected license. The loss of our license agreement with MSK could materially adversely affect our ability to proceed to utilize the affected intellectual property in our development efforts, our ability to enter into future collaboration, licensing and/or marketing agreements for GPS and our ability to commercialize GPS.
We rely on a license agreement with GenFleet for the development of SLS009, and if this license is breached or otherwise terminated, we could lose the ability to continue the development and potential commercialization of SLS009.
We have entered into a license agreement with GenFleet under which we have an exclusive license to develop and commercialize SLS009 worldwide, other than in mainland China, Hong Kong, Macau and Taiwan. Under the license agreement, we are subject to various obligations, including diligence obligations with respect to development and commercialization activities, payment obligations upon achievement of certain milestones, and royalties on annual net sales (if the product candidate is ultimately commercialized), as well as other material obligations. If there is any conflict, dispute, disagreement, or issue of nonperformance between us and GenFleet regarding our rights or obligations under the license agreement, including any such conflict, dispute, or disagreement arising from our failure to satisfy diligence or payment obligations under the license agreement, we may be liable to pay damages and GenFleet may have a right to terminate the license. The loss of the license agreement could prevent us from developing, commercializing, or entering into future strategic transactions relating to SLS009.
The risks described elsewhere pertaining to our patents and other intellectual property rights also apply to the intellectual property rights that we license, and any failure by us or our licensors to obtain, maintain and enforce these rights could have a material adverse effect on our business. In addition, our business depends on our ability to license additional therapeutic compounds from third parties. If we fail to meet our obligations under our current license agreements, we may lose the ability to enter into licenses for the development of additional product candidates in the future, which would adversely affect our business.
We may not realize the benefits of our strategic alliances that we may form in the future.
We may form strategic alliances, create joint ventures or collaborations or enter into licensing arrangements with third parties that we believe will complement or augment our existing business, such as our license agreement with 3D Medicines and our license agreement with GenFleet. These relationships, or those like them, may require us to incur nonrecurring and other charges, increase our near- and long-term expenditures, issue securities that dilute our existing stockholders or disrupt our management and business. In addition, we face significant competition in seeking appropriate strategic alliances and the negotiation process is time-consuming and complex. Moreover, we may not be successful in our efforts to establish a strategic alliance or other alternative arrangements for any future product candidates and programs because our research and development pipeline may be insufficient, our product candidates and programs may be deemed to be at too early a stage of development for collaborative effort and third parties may not view our product candidates and programs as having the requisite potential to demonstrate safety and efficacy. If we license products or acquire businesses, we may not be able to realize the benefit of such
transactions if we are unable to successfully integrate them with our existing operations and company culture. We cannot be certain that, following a strategic transaction or license, we will achieve the revenues or specific net income that justifies such transaction. Any delays in entering into new strategic alliances or license agreements related to our product candidates could also delay the development and commercialization of our product candidates and reduce their competitiveness even if they reach the market.
Our business involves the use of hazardous materials and we and our third-party manufacturers and suppliers must comply with environmental, health and safety laws and regulations, which can be expensive and restrict how we do business.
Our third-party manufacturers and supplierssuppliers’ activities involve the controlled storage, use and disposal of hazardous materials. We and our manufacturers and suppliers are subject to laws and regulations governing the use, manufacture, storage, handling and disposal of these hazardous materials even after we sell or otherwise dispose of the products. In some cases, these hazardous materials and various wastes resulting from their use will be stored at our contractors or manufacturers’ facilities pending use and disposal. We cannot completely eliminate the risk of contamination, which could cause injury to our employees and others, environmental damage resulting in costly cleanup and liabilities under applicable laws and regulations governing the use, storage, handling and disposal of these materials and specified waste products. Although we expect that the safety procedures utilized by our third-partythird party contractors and manufacturers for handling and disposing of these materials will generally comply with the standards prescribed by these laws and regulations, we cannot guarantee that this will be the case or eliminate the risk of accidental contamination or injury from these materials. In such an event, we may be held liable for any resulting damages and such liability could exceed our resources. We do not currently carry biological or hazardous waste insurance coverage and our property and casualty, and general liability insurance policies specifically exclude coverage for damages and fines arising from biological or hazardous waste exposure or contamination.
We will continue to be responsible for certain liabilities and obligations related to Abstral and Zuplenz, and if unknown liabilities were to arise it could have a material adverse effect on us.
Under our respective asset purchase agreements with Sentynl Therapeutics, Inc. and Midatech Pharma PLC, our future obligations under our former agreements with Orexo AB and MonoSol Rx have been assumed by Sentynl and Midatech, respectively, except that we will continue to be responsible for chargebacks, rebates, patient assistance and certain other product distribution channel liabilities related to Abstral and Zuplenz for a specified period of time post-closing. We also will be responsible for any pre-closing liabilities and obligations related to Abstral and Zuplenz, including unknown liabilities, and have agreed in the respective asset purchase agreements to indemnify Sentynl and Midatech for any breach of our representations, warranties and covenants in the respective asset purchase agreements up to a certain agreed to amount. We cannot quantify these responsibilities to Sentanyl and Midatech, but if substantial unknown liabilities were to arise, it could have a material adverse effect on our financial condition.
Risks Relating to Our Development Programs
Our drug candidates may not receive regulatory approval or be successfully commercialized.
Before they can be marketed, our products in development must be approved by the FDA or similar foreign governmental agencies. The process for obtaining FDA approval is both time-consuming and costly, with no certainty of a successful outcome. Before obtaining regulatory approval for the sale of any drug candidate, we must conduct extensive preclinical tests and clinical trials to demonstrate the safety and efficacy in humans of our product candidates. Although our drug candidates have exhibited no serious adverse events (“SAEs”) in the Phase 1 and 1/2 clinical trial, SAEs or other unexpected side effects may arising during further testing and development, and A failure of any preclinical study or clinical trial can occur at any stage of testing. The results of preclinical and initial clinical testing of these products may not necessarily indicate the results that will be obtained from later or more extensive testing. It also is possible to suffer significant setbacks in advanced clinical trials, even after obtaining promising results in earlier trials.
Our Phase 3 PRESENT clinical trial has been stopped due to futility and though we have conducted an investigation of the causes for the failure of the clinical trial, we are not certain that the investigation has identified the reason(s) for the failure.
On June 27, 2016, the Independent Data Monitoring Committee conducting the pre-planned interim analysis of the PRESENT Trial recommended that we stop the clinical trial because of futility. We have conducted an investigation of the causes of the failure of the trial. As a result, our observations are that a phenomenon known as pseudoprogression likely had a meaningful impact on the events assessed as NeuVax recurrences in the trial. The purpose of the NeuVax vaccine is to generate a HER2 directed T cell-based immune response targeting those undetected micrometastases and eradicate them before they grow into a clinically detectable tumor. Pseudoprogression is a phenomenon that occurs when radiographic scans in patients responding to treatment with immunotherapy give the appearance of progression due to increased tumor size or swelling from tumor-infiltrating lymphocytes, or TILs, and other immune cells. In simple terms, the cancer looks like it has progressed on radiographic images, but in reality, the immunotherapy has done its job to create an immune response via inflammation around a micrometastasis. Therefore, a growing tumor or a new tumor detected via imaging isn’t always progressing cancer and may simply represent an immune system response to an undetectable micrometastasis that would not otherwise be seen on the scan. In the trial, we believe that the low rate of recurrences in the control arm resulted from an overall improvement in the standard of care. In addition, proactive imaging led to the discovery of lesions, some of which may not have had any clinical significance at the time of identification. Finally, the inflammation caused by TILs within the micrometastases and more specifically the NeuVax-induced cytotoxic T-cells, made them visible on scans in the NeuVax group and not in the control group. We now believe that causing this inflammation may have identified lesions via proactive scanning that may have never progressed to a clinical tumor. Because patients were discontinued from this study at the time they were identified as having DFS event, we do not know if some of these patients who were diagnosed with a recurrence on the CT scan would have progressed to have metastatic cancer. In summary, though we are applying the knowledge and observations to our other immunotherapy programs, we may not have identified the reason(s) for the failure of the clinical trial.
Our products, GALE-301 and GALE-302 have the same mechanism of action as NeuVax and may not be a viable product to prevent the recurrence of ovarian cancer or other types of cancers.
GALE-301 and GALE-302, which have a similar mechanism of action as NeuVax, may no longer be a viable product to prevent the recurrence of ovarian cancer or other types of cancer, depending upon the reasons for the causes of the failure of NeuVax.
A number of different factors could prevent us from obtaining regulatory approval or commercializing our product candidates on a timely basis, or at all.
We, the FDA or other applicable regulatory authorities, an Independent Data Safety Monitoring Board or “IDSMB” governing our clinical trials, or an institutional review board, or “IRB,” which is an independent committee registered with and overseen by the U.S. Department of Health and Human Services, or “HHS,” that functions to approve, monitor and review biomedical and behavioral research involving humans, may suspend clinical trials of a drug candidate at any time for various reasons, including if we or it believe the subjects or patients participating in such trials are being exposed to unacceptable health risks. Among other reasons, adverse side effects of a drug candidate on subjects or patients in a clinical trial could result in the FDA or other regulatory authorities suspending or terminating the trial and refusing to approve a particular drug candidate for any or all indications of use.
Clinical trials of a new drug candidate require the enrollment of a sufficient number of patients, including patients who are suffering from the disease the drug candidate is intended to treat and who meet other eligibility criteria. Rates of patient enrollment are affected by many factors, and delays in patient enrollment can result in increased costs and longer development times than we expect at present. Patients who are enrolled at the outset of this standard of care also may eventually choose for personal reasons not to participate in the study. We also compete for eligible patients with other clinical trials underway from time to time, and we may experience delays in patient enrollment due to the dependency of other large trials underway in the same patient population.
Clinical trials also require the review and oversight of IRBs, which approve and continually review clinical investigations to protect the rights and welfare of human subjects. An inability or delay in obtaining IRB approval could prevent or delay the initiation and completion of clinical trials, and the FDA may decide not to consider any data or information derived from a clinical investigation not subject to initial and continuing IRB review and approval.
In addition, cancer vaccines are a relatively new form of therapeutic treatment and a very limited number of such products have received regulatory approval. Therefore, the FDA or other regulatory authority may apply standards for approval of a new cancer vaccine that is different from past experience.
Numerous factors could affect the timing, cost or outcome of our drug development efforts, including the following:
difficulties or delays in enrolling patients in our planned clinical trials in conformity with required protocols or projected timelines;
conditions imposed on us by the FDA or comparable foreign authorities regarding the scope or design of our clinical trials;
difficulties or delays in arranging for third parties to conduct clinical trials of our product candidates;
problems in engaging IRBs to oversee trials or problems in obtaining or maintaining IRB approval of studies;
third-party contractors failing to comply with regulatory requirements or meet their contractual obligations to us in a timely manner;
our drug candidates having very different chemical and pharmacological properties in humans than in laboratory testing and interacting with human biological systems in unforeseen, ineffective or harmful ways, and the possibility that our previous Phase 1 or Phase 2 trials will not be indicative of our drug candidates’ performance in larger patient populations;
the need to suspend or terminate our clinical trials if the participants are being exposed to unacceptable health risks;
insufficient or inadequate supply or quality of our drug candidates or other necessary materials necessary to conduct our clinical trials;
disruption at our clinical trial sites resulting from local social or political unrest or other geopolitical factors;
effects of our drug candidates not having the desired effects or including undesirable side effects or the drug candidates having other unexpected characteristics;
negative or inconclusive results from our clinical trials or the clinical trials of others for drug candidates similar to our own or inability to generate statistically significant data confirming the efficacy of the product being tested;
adverse results obtained by other companies developing similar drugs;
modification of the drug during testing;
our capital resources; and
reallocation of our financial and other resources to other clinical programs.
It is possible that none of the product candidates that we develop will obtain the appropriate regulatory approvals necessary for us to begin selling them or that any regulatory approval to market a product may be subject to limitations on the indicated uses for which we may market the product. The time required to obtain FDA and other approvals is unpredictable but often can take years following the commencement of clinical trials, depending upon the complexity of the drug candidate. Any analysis we perform of data from clinical activities is subject to confirmation and interpretation by regulatory authorities, which could delay, limit or prevent regulatory approval. Any delay or failure in obtaining required approvals could have a material adverse effect on our ability to generate revenue from the particular drug candidate.
In addition, the length of time to develop the product candidates as well as any regulatory delays in the development and regulatory approval process could cause the patent exclusivity to be unavailable or greatly reduced for each product candidate. The lack of patent exclusivity could have a material adverse effect on our ability to generate revenue from the particular drug candidate.
We are also subject to numerous foreign regulatory requirements governing the conduct of clinical trials, manufacturing and marketing authorization, pricing and third-party reimbursement. The foreign regulatory approval process includes all of the risks associated with the FDA approval described above as well as risks attributable to the satisfaction of local regulations in foreign jurisdictions. Approval by the FDA does not assure approval by regulatory authorities outside of the U.S.
We are dependent upon contract manufacturers for clinical supplies of our product candidates.
We do not have the facilities or expertise to manufacture supplies of any of our product candidates for clinical trials. Accordingly, we are dependent upon contract manufacturers for these supplies. There can be no assurance that we will be able to secure needed supply arrangements on reasonable terms, or at all. Our failure to secure these arrangements as needed could have a materially adverse effect on our ability to complete the development of our product candidates or, if we obtain regulatory approval for our product candidates, to commercialize them.
Our current plans call for the manufacture of our compounds by contract manufacturers offering research grade, Good Laboratory Practices grade and Good Manufacturing Practices grade materials for preclinical studies (e.g., toxicology studies) and for clinical use. Certain of our product candidates are complex molecules requiring many synthesis steps, which may lead to challenges with purification and scale-up. These challenges could result in increased costs and delays in manufacturing. For GALE-401, we will change contract manufacturers for the supply of the clinical study drug and the commercial product, which may lead to delays in the initiation and completion of the Phase 3 trial and filing for regulatory approval.
In the clinical trials using NeuVax, Leukine is also administered and its availability is dependent upon a third-party manufacturer, which may or may not reliably provide Leukine, thus jeopardizing the completion of the trials.
NeuVax is administered in combination with Leukine, a “GM-CSF” available in both liquid and lyopholyzed forms exclusively from Genzyme Corporation, or “Genzyme,” a subsidiary of Sanofi-Aventis. We will continue to be dependent on Genzyme for our supply of Leukine in connection with the ongoing NeuVax and GALE-301/GALE-302 trials and the potential commercial manufacture of these programs. Any temporary interruptions or discontinuation of the availability of Leukine, or any determination by us to change the GM-CSF used with NeuVax or GALE-301/GALE-302, may have a material adverse effect on our clinical trials and any commercialization of the assets.
We may not be able to establish or maintain the third-party relationships that are necessary to develop or potentially commercialize some or all of our product candidates.candidates, including our relationship with 3D Medicines.
We expect to depend on collaborators, partners, licensees, clinical research organizations and other third parties to support our discovery efforts, to formulate product candidates, to manufacture our product candidates, and to conduct clinical trials for some or all of our product candidates.candidates and to commercialize our product candidates if approved. For example, in December 2020 we entered into an Exclusive License Agreement with 3D Medicines pursuant to which we granted commercialization rights in Greater China to 3D Medicines. In accordance with the 3D Medicines Agreement and Side Letter, we expected that 3D Medicines would begin enrolling patients in mainland China in the REGAL study in the second half of 2023. To date, no patients have been enrolled in mainland China. However, patients were enrolled in the REGAL study in Taiwan, which is part of the Greater China territory, prior to the second half of 2023. Thus, we and 3D Medicines are currently engaged in a dispute regarding, among other things, the trigger and payment of the relevant milestone payments due to us as well as 3D Medicines’ failure to use commercially reasonable best efforts to develop GPS in the Greater China territory, and particularly in mainland China. Over the last three to four months of 2023, we attempted to resolve the aforementioned matters in good faith under the dispute resolution provisions of the 3D Medicines Agreement with 3D Medicines but we were unable to reach a resolution. Accordingly, we commenced a binding arbitration proceeding administered by the Hong Kong International Arbitration Centre governed by New York State law as per the 3D Medicines Agreement in December 2023. We are unable at this time to predict with certainty the outcome of the arbitration proceeding, or the timing of the receipt of any milestone payments and other damages it is seeking in the arbitration proceeding, if at all.
Additionally, we cannot guarantee that we will be able to successfully negotiate future agreements for or maintain relationships with collaborators, partners, licensees, clinical investigators, vendors and other third parties on favorable terms, if at all. Our ability to successfully negotiate such agreements will depend on, among other things, potential partners’ evaluation of the superiority of our technology over competing technologies and the quality of the preclinical and clinical data that we have generated, and the perceived risks specific to developing our product candidates. If we are unable to obtain or maintain these agreements, we may not be able to clinically develop, formulate, manufacture, obtain regulatory approvals for or commercialize our product candidates. Under certain license agreements that we have already entered into, we have minimum dollar amounts per year that we are obligated to spend on the development of the technology we have licensed from our contract partners and other obligations to maintain certain licenses. If we fail to meet this requirement under any of our licenses that contain such requirements or any other obligations under these licenses, we may be in breach of our obligations under such agreement, which may result in the loss of the technology licensed. We cannot necessarily control the amount or timing of resources that our contract partners, including 3D Medicines, will devote to our research and development programs, product candidates or potential product candidates, and we cannot
guarantee that these parties will fulfill itstheir obligations to us under these arrangements in a timely fashion.fashion, if at all. We may not be able to readily terminate any such agreements with contract partners even if such contract partners do not fulfill itstheir obligations to us.
In addition, we may receive notices from third parties from time to time alleging that our technology or product candidates infringe upon the intellectual property rights of those third parties. Any assertion by third parties that our activities or product candidates infringe upon itsthe intellectual property rights of third parties may adversely affect our ability to secure strategic partners or licensees for our technology or product candidates or our ability to secure or maintain manufacturers for our compounds.
We are subject to competition and may not be able to compete successfully.
The biotechnology industry, including the cancer immunotherapy market, is intensely competitive and involves a high degree of risk. We compete with other companies that have far greater experience and financial, research and technical resources than us. Potential competitors in the U.S. and worldwide are numerous and include pharmaceutical and biotechnology companies, educational institutions and research foundations, many of which have substantially greater capital resources, marketing experience, research and development staffs and facilities than us. Some of our competitors may develop and commercialize products that compete directly with those incorporating our technology, introduce products to market earlier than our products or on a more cost effective basis. In addition, our technology may be subject to competition from other technology or methods developed using techniques other than those developed by traditional biotechnology methods. Our competitors compete with us in recruiting and retaining qualified scientific and management personnel as well as in acquiring technologies complementary to our technology. We and our collaborators may face competition with respect to product efficacy and safety, ease of use and adaptability to various modes of administration, acceptance by physicians, the timing and scope of regulatory approvals, availability of resources, reimbursement coverage, price and patent position, including the potentially dominant patent positions of others. An inability to successfully complete our product development could lead to us having limited prospects for establishing market share or generating revenue from our technology.
GALE-401 must successfully complete a Phase 3 clinical trial and obtain regulatory approval before we can market the product and our competitors may obtain a successful clinical trial result and regulatory approval before we do.
GALE-401 contains the active ingredient, anagrelide, an FDA-approved product, for the treatment of patients with myeloproliferative neoplasms (MPNs) to lower abnormally elevated platelet levels. The currently available immediate release (IR) version of anagrelide causes adverse events that are believed to be dose and plasma concentration dependent. These adverse events may limit the use of the IR version of the drug. Therefore, reducing the maximum concentration (Cmax) is hypothesized to reduce the side effects, while preserving efficacy, potentially allowing a broader use of the drug. We have analyzed our data and the treatment landscape for MPNs, with a current focus on Essential Thrombocythemia (ET) where we see an unmet medical need in patients who are intolerant to the current standard of care. We may be advancing GALE-401 into a pivotal trial. The risks include but are not limited to regulatory (agreement with regulatory agency on the development plan), operational (rate of enrollment), and statistical confirmation of the safety and efficacy endpoints. In addition, there are other potential competitors whose clinical trials may be successful and obtain regulatory approval prior to our regulatory approval, if our pivotal trial is successful.
We are dependent on technologies we license, and if we lose the right to license such technologies or we fail to license new technologies in the future, our ability to develop new products would be harmed.
We currently are dependent on licenses from third parties for technologies relating to our product candidates. Our current licenses impose, and any future licenses we enter into are likely to impose, various development, funding, royalty, diligence, sublicensing, insurance and other obligations on us. If our license with respect to any of these technologies is terminated for any reason, the development of the products contemplated by the licenses would be delayed, or suspended altogether, while we seek to license similar technology or develop new non-infringing technology. The costs of obtaining new licenses are high.
Risks associated with operating in foreign countries could materially adversely affect our product development.
We may conduct future studies in countries outside of the United States. Consequently, we may be subject to risks related to operating in foreign countries. Risks associated with conducting operations in foreign countries include:
differing regulatory requirements for drug approvals and regulation of approved drugs in foreign countries;
unexpected changes in tariffs, trade barriers and regulatory requirements; economic weakness, including inflation, or political instability in particular foreign economies and markets; compliance
with tax, employment, immigration and labor laws for employees living or traveling abroad; foreign taxes, including withholding of payroll taxes;
foreign currency fluctuations, which could result in increased operating expenses or reduced revenues, and other obligations incident to doing business or operating in another country;
workforce uncertainty in countries where labor unrest is more common than in the U.S.;
production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad; and
business interruptions resulting from geopolitical actions, including war and terrorism.
Risks Relating to Our Financial Position and Capital Requirements
We are conducting a review of strategic alternatives for the Company, including evaluating potential paths forward for NeuVax, GALE 301/302 and GALE 401 that could significantly impact our future operations and financial position.
In January 2017, we announced that our board of directors had initiated a review of strategic alternatives that could result in changes to our business strategy and future operations. As part of this process, our board of directors is reviewing alternatives with the goal of maximizing stockholder value. Potential strategic alternatives that we may explore and evaluate during the ongoing review process include, among others, a sale of the company, a reverse merger, a business combination or a sale, license or other disposition of corporate assets of the company. Pending any decision to change strategic direction, we have limited our research and development activities to manage our cash position. We cannot provide any commitment as to the timing of our determination or the strategy we may adopt. If we determine to change our business strategy or to seek to engage in a strategic transaction, our future business, prospects, financial position and operating results could be significantly different than those in historical periods or projected by our management. If we determine to further develop NeuVax, GALE 301/302 and GALE 401, or all of the products, we will need to obtain substantial additional funding. Because of the significant uncertainty regarding our future plans, we are not able to accurately predict the impact of a potential change in our business strategy and future funding requirements.
We may not be able to obtain sufficient financing, and may not be able to develop our product candidates.
We had cash and cash equivalents of approximately $29.1 million as of February 28, 2017. We had no revenue during the year ended December 31, 2016, and our cash burn from operations for the quarter ending December 31, 2016 was approximately $8.0 million. We believe that our existing cash and cash equivalents should be sufficient to fund our operations for at least one year from the date of issuance of the Company's consolidated financial statements. This projection is based on our current limited planned operations, anticipated payments for defense costs for the governmental investigation, and estimates of potential resolution of the SEC investigation, and is also subject to changes in our operating plans, resolution of and unanticipated developments in the ongoing government investigation and other legal matters and uncertainties inherent in our business. We may need to seek to replenish our existing cash and cash equivalents prior over the next year.
In addition, we have approximately $13.7 million of restricted cash as of February 28, 2017. We negotiated an amendment with the holder of the debt that reduces the restricted cash amount to the lesser of $18.5 million or the outstanding balance of the amended debenture under certain conditions. We also have limited funding available under our amended purchase agreement with Lincoln Park Capital Fund, LLC and sales agreements with FBR & Co. and Maxim Group LLC. There is no guarantee that such funding will be available to us on favorable terms or will be sufficient to meet all of our future funding needs.
At our annual meeting of stockholders adjourned on July 15, 2016, our stockholders approved an increase in our authorized common stock from 275,000,000 to 350,000,000. In addition, our shareholders authorized the Board of Directors to approve a reverse stock split within twelve months of October 21, 2016 at a ratio between 1:2 and 1:20. There was no reduction in the amount of authorized shares. The Board of Directors approved a reverse stock split at a ratio of 1:20, effective on November 11, 2016. We are not able to predict whether volume of shares post reverse stock split will be sufficient based upon the reverse stock split price to meet the Company’s ongoing financing requirements to maintain the Company’s operations.
If we fail to obtain additional future funding when needed, we could be forced to scale back or terminate our operations, or to seek to merge with or to be acquired by another company. We may not be able to meet our obligations as they come due, raising substantial doubts as to our ability to continue as a going concern. Any such inability to continue as a going concern may result in our common stock holders losing their entire investment. There is no guaranty that we will become profitable or secure additional financing.
We expect to continue to incur significant operating and non-operating expenses, which may make it difficult for us to secure sufficient financing, and may lead to uncertainty about our ability to continue as a going concern.
Substantial funds were expended to develop our technologies and product candidates, and additional substantial funds will be required for further preclinical testing and clinical trials of our product candidates, and to manufacture and market any products that are approved for commercial sale. Because the successful development of our products is uncertain, we are unable to precisely estimate the actual funds we will require to develop and potentially commercialize them. In addition, we may not be able to generate enough revenue, even if we are able to commercialize any of our product candidates, to become profitable.
In the event that we are unable to obtain additional financing if needed or if we incur significant expense related to the resolution of the ongoing government investigation, we may not be able to meet our obligations as they come due, that in turn may raise substantial doubts as to our ability to continue as a going concern. Any such inability to continue as a going concern may result in our common stock holders losing their entire investment. There is no guaranty that we will secure additional financing if we need such financing. Our financial statements contemplate that we will continue as a going concern and do not contain any adjustments that might result if we were unable to continue as a going concern. Changes in our operating plans, our existing and anticipated working capital needs, defense costs related to the recent securities lawsuits, resolution of the ongoing government investigation, the acceleration or modification of our expansion plans, increased expenses, potential acquisitions or other events may affect our ability to continue as a going concern. Future financing may be obtained through, and future development efforts may be paid for by, the issuance of debt or equity, which may have an adverse effect on our security holders or may otherwise adversely affect our business.
If we raise funds through the issuance of debt or equity, any debt securities or preferred stock issued will have rights, preferences and privileges senior to those of holders of our common stock in the event of a liquidation. In such event, there is a possibility that once all senior claims are settled, there may be no assets remaining to pay out to the holders of common stock. In addition, if we raise funds through the issuance of additional equity, whether through private placements or additional public offerings, such an issuance would dilute your ownership in us.
The terms of debt securities may also impose restrictions on our operations, which may include limiting our ability to incur additional indebtedness, to pay dividends on or repurchase our capital stock, or to make certain acquisitions or investments. In addition, we may be subject to covenants requiring us to satisfy certain financial tests and ratios, and our ability to satisfy such covenants may be affected by events outside of our control.
You may have difficulty evaluating our business, and our historical financial information may not be representative of our future results.
We have closed our PRESENT trial due to futility, are evaluating the appropriate time to commence the GALE-401 trial and anticipate making a definitive determination in the second half of 2017, and plan to continue to support the investigator-sponsored immunotherapy trials. As a result, we will have no recurring revenues unless and until we are able to obtain marketing approval of one or more of our other product candidates and our historical financial information may not be representative of our future results.
We may be unable to comply with our reporting and other requirements under federal securities laws.
As a publicly traded company, we are subject to the reporting requirements of the Securities Exchange Act of 1934, as amended, or the “Exchange Act,” and the Sarbanes-Oxley Act of 2002, or the “Sarbanes-Oxley Act.” In addition, the Exchange Act requires that we file annual, quarterly and current reports. Our failure to prepare and disclose this information in a timely manner could subject us to penalties under federal securities laws, expose us to lawsuits and restrict our ability to access financing. The Sarbanes-Oxley Act requires that we, among other things, establish and maintain effective internal controls and procedures for financial reporting. From time to time we evaluate our existing internal controls in light of the standards adopted by the Public Company Accounting Oversight Board. It is possible that we, or our independent registered public accounting firm, may identify significant deficiencies or material weaknesses in our internal control over financial reporting in the future. Any failure or difficulties in implementing and maintaining these controls could cause us to fail to meet the periodic reporting obligations or result in material misstatements in our financial statements.
Section 404 of the Sarbanes-Oxley Act requires annual management and independent auditor assessments of the effectiveness of our internal control over financial reporting. Our failure to satisfy the requirements of Section 404 on a timely basis could result in the loss of investor confidence in the reliability of our financial statements, which in turn could have a material adverse effect on our business and our common stock.
Risks Related to Our Intellectual Property
We may not be able to obtain and enforce patent rights or other intellectual property rights that cover our product candidates and that are of sufficient breadth to prevent third parties from competing against us.us.
Our success with respect to our product candidates will depend in part on our ability to obtain and maintain patent protection in the U.S.United States and abroad, to preserve our trade secrets, and to prevent third parties from infringing upon our proprietary rights. Our patentsWe seek to protect our proprietary position by filing in the United States and in certain foreign jurisdictions patent applications however, may not be sufficientrelated to provide protection for NeuVax or our other productsnovel technologies and product candidates against commercial competition.
The active peptide found in NeuVax, the E75 peptide, has been known and studied for many years. We have one issued U.S. patent, US 6,514,942, covering the composition of matter of the E75 peptide, which expired in mid-2015, prior to any potential commercialization of NeuVax. We do not have and will not be able to obtain any composition of matter patent protection for E75, the active peptide in NeuVax. We also have a license from The Henry M. Jackson Foundation to issued U.S., European, Japanese, Korean, Mexican and Australian method of use patents, which expire in 2028, that are directedimportant to a method of inducing immunity against breast cancer recurrence by administering a composition comprising the E75 peptide to patients who have both an immunohistochemistry (IHC) rating of 1+ or 2+ for HER2/neu protein expression, as well as a fluorescence in situ hybridization (FISH) rating of less than about 2.0 for HER2/neu gene expression.our business. The license further includes an issued U.S. method of use patent directed to a method of inducing immunity against recurrence of any HER2/neu expressing tumors by administering the E75 peptide to patients with tumors having a FISH rating of less than about 2.0 for HER2/neu gene expression; an allowed U.S application which includes claims to the use of E75 to reduce the risk of cancer recurrence, including bone only recurrence;prosecution process is expensive and pending applications with similar claims in a number of foreign jurisdiction, all of which expire in 2028. Also included in the license is a method of use patent, which expires in 2026, that is directed to the use of NeuVax in combination with Herceptin® (trastuzumab) to treat any HER2/neu expressing cancer. Thus, our method of use patents may not prevent competitors from seeking to developtime-consuming, and market NeuVax for use in cancer patients who do not meet these criteria. If any such alternative uses were approved, this could lead to off-label use and price erosion for our NeuVax product. We may seek FDA approval for use of NeuVax to treat cancer patients who fall outside the claimed IHC and FISH ranges and for other cancers as well. Although we are pursuing additional patent protection for NeuVax through pending patent applications, we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain additionalpatent protection. In addition, we may not pursue or obtain patent protection in all major markets. Moreover, in some circumstances, we do not have the right to control the preparation, filing or prosecution of patent applications, or to maintain the patents, covering technology that would providewe license from third parties or covering technology that a collaboration or commercialization partner may develop. In some circumstances, our licensors have the right to prosecute and/or enforce the licensed patents without our involvement or consent, or to decide not to enforce or to allow us to enforce the licensed patents. Therefore, these patents and applications may not be prosecuted and enforced in a manner consistent with the best interests of our business. If any such licensors fail to maintain such patents, or lose rights to those patents, the rights that we have licensed may be reduced or eliminated and our ability to develop and commercialize any of our products that are the subject of such licensed rights could be adversely affected.
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions and has in recent years been the subject of much litigation. In addition, the laws of foreign jurisdictions may not protect our rights to the same extent as the laws of the United States. For example, European patent law restricts the patentability of methods of treatment of the human body more than U.S. law does. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until 18 months after filing, or in some cases not at all. Therefore, we cannot be certain that we or our licensors were the first to make the inventions claimed in our owned or licensed patents or pending patent applications, or that we or our licensors were the first to file for patent protection of such inventions. Moreover, the U.S. Patent and Trademark Office, or USPTO, might require that the term of a significant commercial advantage.
Anagrelide hydrochloride,patent issuing from a pending patent application be disclaimed and limited to the sole active pharmaceutical ingredient,term of another patent that is commonly owned or “API,” in GALE-401, has been approved for many years and, thus, it is not possible to obtain composition of matter patents that cover anagrelide hydrochloride.names a common inventor. As a result, competitors who obtain the requisite regulatory approval can offer products with the same 43 API as GALE-401, so long as the competitors do not infringe any formulation patents that we may have or may obtain or license, if any. The onlyissuance, scope, validity, term, enforceability and commercial value of our patent protection that we have orrights are likely to obtain covering GALE-401 are patents relating to specific formulations, methods using these formulations,highly uncertain.
Our pending and methods of manufacturing and packaging. We have an issued U.S. Patent, which expires in 2020, covering methods of using anagrelide to reduce platelet count in patients subject to veno-occlusive events. We have granted patents in the U.S., United Kingdom and Japan, which expire in 2029, covering controlled release formulations of anagrelide and methods of use. We also are prosecuting pendingfuture patent applications, in other territories including, but not limited to, the U.S., Europe, India, and Japan, whichany collaboration or commercialization partner’s pending and future patent applications, may not issue priorresult in patents being issued which protect our technology or products, in whole or in part, or which effectively prevent others from commercializing competitive technologies and products.
During prosecution of any patent application, the issuance of any patents based on the application may depend upon our or our partners’ ability to generate additional preclinical or clinical data that support the patentability of our proposed claims. We or any potentialcollaboration or commercialization of GALE-401. We may seek FDA approval for use of GALE-401 to treat patients with myeloproliferative neoplasms that include several hematological disorders, including essential thrombocythemia. Although we are pursuing additional patent protection for GALE-401 through pending patent applications, wepartner may not be able to obtaingenerate sufficient additional patent protection that would provide us withdata on a significant commercial advantage.
The active peptides found in GALE-301 and GALE-302 are derived from Folate Binding Protein. One of the active peptides, E39, has been known and studied for many years. The other active peptide, GALE-302, is a derivative of E39. We have a license from The Henry M. Jackson Foundation to issued and granted patents in the U.S., Europe, Canada, and Japan, covering composition of matter for the E39 derivative peptides, including GALE-302, alone and in combination with E39, as well as the use of these compositions for the treatment of cancer. These patents are expected to expire in 2022, prior to any potential commercialization of GALE-301. We do not have and will not be able to obtain any composition of matter patent protection for the E39 peptide in any territory. The license we have from The Henry M. Jackson Foundation grants us the right to develop and market GALE-301 for any use, including methods of treating cancer. Our patents may not prevent competitors from seeking to develop and market the E39 peptide alone. If any such alternative uses of compositions containing the E39 peptide were approved, this could lead to off label use and price erosion for GALE-301. We may seek FDA approval for use of GALE-301, alonetimely basis, or in combination with GALE-302, to treat cancer patients with ovarian and endometrial cancers and for other cancers, as well. Although we are pursuing additional patent protection for GALE-301 and the combination of GALE-301 and GALE-302 through pending patent applications, we may not be able to obtain additional patent protection that would provide us with a significant commercial advantage.
Our ability to obtain, maintain and enforce patents is uncertain and involves complex legal and factual questions. Accordingly, rights under any patents we have or may obtain or license may not provide us with sufficient protection for our commercial product and product candidates to afford a commercial advantage against competitive products or processes, including those from branded and generic pharmaceutical companies. In addition, we cannot guarantee that any patents will issue from any pending or future patent applications owned by or licensed to us. Nor can we guarantee that the claims of these patents will be held valid or enforceable by the courts or will provide us with any significant protection against competitive products or otherwise be commercially valuable to us.
Changesat all. Moreover, changes in either the patent laws or ininterpretation of the interpretationspatent
laws in the U.S.United States or other countries may diminish the value of our or a collaboration or commercialization partner’s patents or narrow the scope of our or their patent protection.
Changes in the patent laws, regulations, or interpretations thereof in the United States or abroad may diminish the value of our intellectual property. In addition, on September 16, 2011,
The following are potential factors that could affect the Leahy-Smith America Invents Act,scope our intellectual property:
Patent Reform Legislation: The United States Congress periodically considers patent reform legislation aimed at modifying the standards for patentability, patent enforcement procedures, or the Leahy-Smith Act, was signed into law. The Leahy-Smith Act includesrights of patent holders. Such legislative changes could introduce stricter requirements for patent eligibility, limit the scope of patent protection, or streamline patent challenges. Any of these changes may weaken the enforceability or value of our existing patents or make it more difficult to obtain new patents for our products or technologies.
Judicial Interpretations: Court decisions, particularly those from the United States Supreme Court and the Federal Circuit, play a number of significant changescrucial role in shaping patent law and practice. Shifts in judicial interpretations, such as alterations to the U.S.criteria for patent law. These include provisions that affecteligibility or the waystandard for proving patent applications will be prosecutedinfringement, may impact prosecution, defense, and enforcement of certain patent claims in our patent portfolio.
International Harmonization: Changes in patent laws or regulations in foreign jurisdictions where we hold or seek patent protection may also affect patent litigation. Accordingly, it is not clear what, if any, impact the Leahy-Smith Act will have on the operationvalue of our business. However,intellectual property. Harmonization efforts or shifts in international standards for patentability criteria, enforcement mechanisms, or patent term extensions could affect our ability to protect and monetize our intellectual property in key markets outside the Leahy-Smith Act,United States.
Patent Regulations and Patent Office Practices: Alterations in particularpatent examination procedures or policies at the first-to-file provisionUnited States Patent and its implementationTrademark Office, or USPTO, or foreign patent offices could increaseinfluence the uncertaintiesstrength and costs surrounding the prosecutionscope of our patent applicationsrights. Changes in patent office practices related to patent eligibility or patentability standards, or the handling of post-grant proceedings such as inter partes reviews, or IPRs, may weaken our ability to obtain some patent claims or to enforce patents that may issue to us in the future. Moreover, changes in regulations governing patent rights, such as those related to government-funded programs, may affect our current or future intellectual property rights.
While we continuously monitor developments in patent laws and regulations, there can be no assurance that changes in patent laws, regulations, or interpretations thereof will not adversely affect the enforcement of or defensevalue of our issued patents, all of which could have a material adverse effect on our business and financial condition. Accordingly, we cannot predict the breadth of claims that may be allowed or enforced in our patents or in third-party patents.intellectual property.
While we intend to take actions reasonably necessary to enforce our patent rights, we may not be able to detect infringement of our own or in-licensed patents, which may be especially difficult for methods of manufacturing or formulation products, and weproducts.
We depend, in part, on our licensors and collaborators to protect a substantial portion of our proprietary rights. In addition, third parties may challenge our in-licensed patents and any of our own patents that we may obtain, which could result in the invalidation or unenforceability of some or all of the relevant patent claims. Litigation or other proceedings to enforce or defend intellectual property rights is very complex, expensive, and may divert our management’s attention from our core business and may result in unfavorable results that could adversely affect our ability to prevent third parties from competing with us.
If another party has reason to assert a substantial new question of patentability against any of our claims in our own and in-licensed patents, the third party can request that the patent claims be reexamined, which may result in a loss of scope of some claims or a loss of the entire patent. In addition to potential infringement suits, and interference and reexamination proceedings, we may become a party to inter partes and post-grant review proceedings in the United States and patent opposition proceedings outside the United States, where either the patentability of the inventions subject of our patents areis challenged, or we are challenging the patents of others. The costs of these proceedings could be substantial, and it is possible that such efforts would be unsuccessful. As the medical device, biotechnology and pharmaceutical industries expand and more patents are issued, the risk increases that others may assert our commercial product and/or product candidates infringe their patent rights. If a third-party’s patents were found to
cover our commercial product and product candidates, proprietary technologies, or itsour uses, we or our collaborators could be enjoined by a court and required to pay damages and could be unable to continue to commercialize our products or use our proprietary technologies unless we or itsuch collaborators obtained a license to the patent. A license may not be available to us or our collaborators on acceptable terms, if at all. In addition, during litigation, the patent holder could obtain a preliminary injunction or other equitable relief, which could prohibit us from making, using or selling our commercial product and product candidates pending a trial on the merits, which could be years away.
Proprietary
SLS009 may face generic competition sooner than expected before the expiration of our composition of matter patent protection.
Even if we are successful in achieving regulatory approval to commercialize SLS009, our product candidate may face generic competition. Once an NDA is approved, the product covered thereby becomes a “reference listed drug” in the FDA’s Orange Book. In the United States, manufacturers may seek approval of generic versions of reference listed drugs through submission of an ANDA or approval through a 505(b)(2) NDA. In support of an ANDA, a generic manufacturer need not conduct clinical trials to assess safety and efficacy. Rather, the applicant generally must show that its product has the same active ingredient(s), dosage form, strength, route of administration and conditions of use or labelling as the reference listed drug and that the generic version is bioequivalent to the reference listed drug, meaning it is absorbed in the body at the same rate and to the same extent. Generic products may be significantly less costly to bring to market than the reference listed drug and companies that produce generic products are generally able to offer them at lower prices. Thus, following introduction of a generic drug, a significant percentage of the sales of any branded drug is typically lost to the generic product. In contrast, Section 505(b)(2) enables the applicant to rely, in part, on the FDA’s prior findings of safety and efficacy data for an existing product, or published literature, in support of its application. Section 505(b)(2) provides an alternate path to FDA approval for new or improved formulations or new uses of previously approved products; for example, a follow-on applicant may be seeking approval to market a previously approved drug for new indications or for a new patient population that would require new clinical data to demonstrate safety or effectiveness. Competition that our products could face from follow-on versions of our products could materially and adversely affect our future revenue, profitability and cash flows and substantially limit our ability to obtain a return on the investments we have made in those products. Because SLS009 has not been previously approved as an active ingredient, we expect the Hatch-Waxman Act to provide a five-year period of new chemical entity, or NCE, exclusivity following its approval during which time generic competitors cannot file an ANDA for a generic version of SLS009 or a 505(b)(2) NDA for SLS009, unless the submission contains a Paragraph IV Certification that one or more patents listed in the Orange Book for SLS009 are invalid, unenforceable or will not be infringed by a proposed ANDA product, in which case the submission may be made four years following the original drug approval. If a Paragraph IV Certification is made, the follow-on applicant is required to provide a Paragraph IV Notice Letter advising of the certification. If that occurs, we will have the opportunity to bring a patent infringement action against the follow-on applicant. If such a suit is filed within the 45-day period following receipt of the Paragraph IV Notice Letter, the Hatch-Waxman Act provides for a 30-month stay on FDA’s ability to grant final approval of the proposed follow-on product. The 30-month stay generally runs from the date the Paragraph IV Notice Letter is received. However, when a Paragraph IV certification is received during the five-year period of NCE exclusivity following the date of first NDA approval, the 30-month stay extends from five years after the date that product was first approved. The 30-month stay may be shortened or lengthened, including due to a settlement of a lawsuit, a court order (including a decision by the district court on the merits of the case), or patent expiration. The party filing the ANDA or 505(b)(2) NDA may also counterclaim in the litigation that one or more of our patents are invalid, unenforceable, and/or not infringed. If all of the asserted SLS009 patents were found invalid, enforceable, and/or not infringed, a competing generic product could be marketed prior to expiration of those patents, our business could be harmed.
Settlements and related licensing agreements resulting from Hatch-Waxman litigation can be challenged and have the potential to generate additional litigation which can be costly. The success of such litigation depends on the strength of the patents covering our branded products and our ability to prove that the follow-on applicant’s product would infringe one or more such patents. The outcome of such litigation is inherently uncertain and may result in potential loss of market exclusivity for SLS009, which may have a significant financial impact on our business. Furthermore, the Federal Trade Commission, or FTC, has brought successful lawsuits challenging Hatch-Waxman litigation settlements as anti-competitive, and such decisions have been upheld by federal circuit courts. If we engage in Hatch-Waxman litigation, we may also face an FTC challenge with respect to any proposed settlement related to such litigation, which may result in additional expense or penalty. The FTC also has more recently been questioning pharmaceutical company patent listings in the Orange Book and raising concerns about “improper”
listings that may be intended to discourage competition by follow-on drug developers, and certain members of Congress have been investigating similar issues. Accordingly, there could be future changes to federal laws, regulations, or guidelines related to Hatch-Waxman requirements or procedures that could have a material adverse impact on all pharmaceutical innovators, including us.
If the FDA, EMA or other foreign regulatory authorities approve generic or biosimilar versions of any of our product candidates that receive marketing approval, or such authorities do not grant our products appropriate periods of exclusivity before approving generic or biosimilar versions of those products, the sales of our products, if approved, could be adversely affected.
Even if we are successful in achieving regulatory approval to commercialize a biologic product candidate ahead of our competitors, our product candidates may face competition from biosimilar and generic products. Most biological products are licensed for marketing by FDA via a BLA, under authorities in the Public Health Service Act, or PHSA. Assuming that we receive positive data from the REGAL trial, we will file a BLA in order to obtain marketing authorization for GPS. In 2010, the BPCIA, enacted as Title VII of the ACA, established an abbreviated pathway under the PHSA for licensure of biosimilar biologics (i.e., biosimilars, sometimes referred to as follow-on biologics). A biosimilar is a biological product that is demonstrated to be “highly similar” (i.e., biosimilar), but not identical, to an FDA-licensed biological product (i.e., the reference product).
The BPCIA also establishes periods of exclusivity for a brand-name biologic (the reference product), one with a duration of four years and the other with a duration of 12 years. These periods of regulatory exclusivity initiate upon licensure of the new biological product if certain requirements are met. During the four-year exclusivity period, an abbreviated BLA for a biosimilar referencing the protected brand-name biologic may not be submitted to FDA. During the 12-year exclusivity period, approval of an abbreviated BLA for a biosimilar referencing the protected brand-name biologic may not be made effective, which means FDA may not approve the biosimilar application until 12 years after the date on which the reference product was first licensed.
In addition, the BPCIA provides for a process for disclosure and negotiation between the biosimilar applicant and reference product sponsor, sometimes referred to as the “patent dance.” Although not mandatory on the party of the biosimilar applicant, the dance involves several rounds of informational exchanges concerning potential disputes over the biosimilar applicant’s infringement of the reference product sponsor’s patents. Also, biosimilar licensure under the BPCIA is not contingent upon resolution of patent disputes. Therefore, the FDA may approve a biosimilar despite unresolved patent issues between the reference product sponsor and the biosimilar applicant.
We believe that GPS will qualify for four years of data exclusivity and 12 years of market exclusivity under the BPCIA. The law is complex and continues to be interpreted and implemented by the FDA. As a result, its ultimate impact, implementation, and meaning are subject to uncertainty. While it is uncertain when such processes intended to implement BPCIA may be fully adopted by the FDA, any such processes could have a material adverse effect on the future commercial prospects for our product candidates. There is also a risk that the U.S. Congress could amend the BPCIA to shorten the 12-year market exclusivity period or that the FDA will not consider our product candidates to be reference biological products pursuant to its interpretation of the exclusivity provisions of the BPCIA for competing products, potentially creating the opportunity for biosimilar competition sooner than anticipated after the expiration of our patent protection. Moreover, the extent to which a biosimilar, once approved, will be substituted for any reference product in a way that is similar to traditional generic substitution for non-biological products is not yet clear, and will depend on a number of marketplace and regulatory factors that are still developing. Under the BPCIA as well as state pharmacy laws, only interchangeable biosimilar products are considered substitutable for the reference biological product without the intervention of the health care provider who prescribed the original biological product. However, as with all prescribing decisions made in the context of a patient-provider relationship and a patient’s specific medical needs, health care providers are not restricted from prescribing biosimilar products in an off-label manner.
Even if, as we expect, GPS is considered to be reference products eligible for 12 years of exclusivity under the BPCIA, a competitor could decide to forego the abbreviated approval pathway available for biosimilar products and to submit a full BLA for product licensure after completing its own preclinical studies and clinical trials. In such a situation, any exclusivity to which we may be eligible under the BPCIA would not prevent the competitor from marketing its biological product as soon as it is approved.
In Europe, the European Commission has granted marketing authorizations for several biosimilar products pursuant to a set of general and product class-specific guidelines for biosimilar approvals issued over the past few years. In addition, companies may be developing biosimilar products in other countries that could compete with our products, if approved.
The regulatory, or non-patent, exclusivity available to drugs or biologics in some countries is less than that provided by the United States. For instance, Canada currently provides for an eight-year period of exclusivity for new biological products, and Mexico provides for a five-year period of exclusivity. Furthermore, in some countries outside of the United States, peptide vaccines, such as GPS, are regulated as chemical drugs rather than as biologics and may or may not be eligible for non-patent exclusivity.
If competitors are able to obtain marketing approval for biosimilars referencing our therapeutic candidates, if approved, our future products may become subject to competition from such biosimilars, whether or not they are designated as interchangeable, with the attendant competitive pressure and potential adverse consequences. Such competitive products may be able to immediately compete with us in each indication for which our therapeutic candidates may have received approval.
If we are sued for infringing the intellectual property rights of third parties, such litigation could be costly and time-consuming and could prevent or delay our development and commercialization efforts.
Our commercial success depends, in part, on us and our collaborators not infringing the patents and proprietary rights of third parties. There is a substantial amount of litigation and other adversarial proceedings, both within and outside the United States, involving patent and other intellectual property rights in the biotechnology and pharmaceutical industries, including patent infringement lawsuits, interference or derivation proceedings, oppositions, and inter partes and post-grant review proceedings before the USPTO and non-U.S. patent offices. Numerous U.S. and non-U.S. issued patents and pending patent applications owned by third parties exist in the fields in which we are developing and may develop our current and future product candidates. As the biotechnology and pharmaceutical industries expand and more patents are issued, and as our product pipeline grows, the risk increases that our product candidates may be subject to claims of infringement of third parties’ patent rights as it may not always be clear to industry participants, including us, which patents cover various types of products or methods of use. The coverage of patents is subject to interpretation by the courts, and the interpretation is not always uniform or predictable.
If we are sued for patent infringement, we would need to demonstrate that our product candidates, products and methods either do not infringe the patent claims of the relevant patent or that the patent claims are invalid, and we may not be able to do this. Proving that a patent is invalid is difficult. If any issued third-party patents were held by a court of competent jurisdiction to cover aspects of our materials, formulations, methods of manufacture or methods for treatment, we could be forced, including by court order, to cease developing, manufacturing or commercializing the relevant product candidate until such patent expired. Alternatively, we may be required to obtain a license from such third party in order to use the infringing technology and to continue developing, manufacturing or marketing the infringing product candidate. We could be prevented from commercializing a product candidate or be forced to cease some aspect of our business operations, if, as a result of actual or threatened patent infringement claims, we are unable to enter into licenses on acceptable terms. In addition, parties making claims against us may also obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our product candidates.
Defending against claims of patent infringement or misappropriation of trade secrets could be costly and unpatented know-howtime consuming, regardless of the outcome. Thus, even if we were to ultimately prevail, or to settle at an early stage, such litigation could burden us with substantial unanticipated costs. In addition, litigation or threatened litigation could result in significant demands on the time and attention of our management team, distracting them from the pursuit of other company business. In the event of a successful claim of infringement against us, we may have to pay substantial damages, including treble damages and attorneys’ fees if we are found to have willfully infringed a patent, or to redesign our infringing product candidates, which may be impossible or require substantial time and monetary expenditure. We may also very importantelect to enter into license agreements in order to settle patent infringement claims prior to litigation, and any such license agreement may require us to pay royalties and other fees that could
be significant. During the course of any patent or other intellectual property litigation, there could be public announcements of the results of hearings, rulings on motions, and other interim proceedings in the litigation. If securities analysts or investors regard these announcements as negative, the perceived value of our product candidates, programs or intellectual property could be diminished. Accordingly, the market price of our shares of common stock may decline.
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting, enforcing and defending patents on our current and future product candidates in all countries throughout the world would be prohibitively expensive. We or our licensors’ intellectual property rights in certain countries outside the United States may be less extensive than those in the United States. In addition, the laws of certain foreign countries do not protect intellectual property rights to the same extent as laws in the United States. Consequently, we and our licensors may not be able to prevent third parties from practicing our and our licensors’ inventions in countries outside the United States, or from selling or importing infringing products made using our and our licensors’ inventions in and into the United States or other jurisdictions. Competitors may use our and our licensors’ technologies in jurisdictions where we have not obtained patent protection or where we do not have exclusive rights under the relevant patent(s) to develop their own products and, further, may export otherwise infringing products to territories where we and our licensors have patent protection but where enforcement is not as strong as that in the United States. These infringing products may compete with our product candidates in jurisdictions where we or our licensors have no issued patents or where we do not have exclusive rights under the relevant patent(s), or our patent claims and other intellectual property rights may not be effective or sufficient to prevent them from so competing.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents and other intellectual property protection, particularly those relating to drugs and biologics, which could make it difficult for us and our licensors to stop the infringement of our and our licensors’ patents or marketing of competing products in violation of our and our licensors’ proprietary rights generally. Certain governments outside the United States have indicated that compulsory licenses to patents may be sought to further their domestic policies or on the basis of national emergencies. Proceedings to enforce our and our licensors’ patent rights in foreign jurisdictions could result in substantial costs and divert our attention from other aspects of our business, could put our and our licensors’ patents at risk of being invalidated or interpreted narrowly, could put our and our licensors’ patent applications at risk of not issuing, and could provoke third parties to assert claims against us or our licensors. We or our licensors may not prevail in any lawsuit that we or our licensors initiate, and even if we or our licensors are successful the damages or other remedies awarded, if any, may not be commercially meaningful.
We may become involved in lawsuits to protect or enforce our intellectual property, which could be expensive, time-consuming and unsuccessful and have a material adverse effect on the success of our business and on our stock price.
Third parties may infringe our patents, the patents of our licensors, or misappropriate or otherwise violate our or our licensors’ intellectual property rights. We and our licensors’ patent applications cannot be enforced against third parties practicing the technology claimed in such applications unless and until a patent is issued from such applications, and then only to the extent the issued claims cover the technology. In the future, we or our licensors may elect to initiate legal proceedings to enforce or defend our or our licensors’ intellectual property rights, to protect our or our licensors’ trade secrets or to determine the validity or scope of intellectual property rights we own or control. Any claims that we assert against perceived infringers could also provoke these parties to assert counterclaims against us alleging that we infringe their intellectual property rights or that our intellectual property rights are invalid. In addition, third parties may initiate legal proceedings against us or our licensors to challenge the validity or scope of intellectual property rights we own or control. The proceedings can be expensive and time-consuming. Many of our or our licensors’ adversaries in these proceedings may have the ability to dedicate substantially greater resources to prosecuting these legal actions than we or our licensors can. Accordingly, despite our or our licensors’ efforts, we or our licensors may not be able to prevent third parties from infringing upon or misappropriating intellectual property rights we own or control, particularly in countries where the laws may not protect our rights as fully as in the United States. Litigation could result in substantial costs and diversion of
management resources, which could harm our business and financial results. In addition, in an infringement proceeding, a court may decide that a patent owned by or licensed to us is invalid or unenforceable, in whole or in part, or may refuse to stop the other party from using the technology at issue on the grounds that our or our licensors’ patents do not cover the technology in question. An adverse result in any litigation proceeding could put one or more of our or our licensors’ patents at risk of being invalidated, held unenforceable or interpreted narrowly.
Interference or derivation proceedings provoked by third parties, brought by us or our licensors or collaborators, or brought by the USPTO or any non-U.S. patent authority may be necessary to determine the priority of inventions or matters of inventorship with respect to our business. or our licensors’ patents or patent applications. We may also become involved in other proceedings, such as reexamination, reissue, or opposition proceedings, inter partes review, post-grant review or other pre-issuance or post-grant proceedings in the USPTO or its foreign counterparts relating to our intellectual property or the intellectual property of others. An unfavorable outcome in any such proceeding could require us or our licensors to cease using the related technology and commercializing the affected product candidate, or to attempt to license rights to it from the prevailing party.
Our business could be harmed if the prevailing party does not offer us or our licensors a license on commercially reasonable terms if any license is offered at all. Even if we or our licensors obtain a license, it may be non-exclusive, thereby giving our competitors access to the same technologies licensed to us or our licensors. In addition, if the breadth or strength of protection provided by our or our licensor’s patents and patent applications is threatened, it could dissuade companies from collaborating with us to license, develop or commercialize current and future product candidates. Even if we successfully defend such litigation or proceeding, we may incur substantial costs and it may distract our management and other employees. We could be found liable for monetary damages, including treble damages and attorneys’ fees, if we are found to have willfully infringed a patent.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of shares of our common stock. Furthermore, under Title XI of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003, or MMA, certain agreements, including patent litigation settlement agreements between brand and generic drug companies, must be filed with the FTC and DOJ. The Patient Right to Know Drug Prices Act amended MMA Title XI, expanding the reporting requirements to include agreements between biosimilar product applicants and biologic companies.
Although we have taken steps to protect our trade secrets and unpatented know-how by entering into confidentiality agreements with third parties and proprietary information and invention agreements with our employees and certain employees, consultants and advisors, third parties may still obtain this information or we may be unable to protect our rights. We also have limited control over the protection of trade secrets used by our licensors, collaborators and suppliers.
There can be no assurance that binding agreements will not be breached, that we would have adequate remedies for any breach, or that our trade secrets and unpatented know-how will not otherwise become known or be independently discovered by our competitors. If trade secrets are independently discovered, we would not be able to prevent their use. Enforcing a claim that a third party illegally obtained and is using our trade secrets or unpatented know-how is expensive and time consuming,time-consuming, and the outcome is unpredictable.
We may be subject to claims that our employees, consultants or independent contractors have wrongfully used or disclosed to us alleged trade secrets of their other clients or former employers. As is common in the biotechnology and pharmaceutical industry, certain of our employees were formerly employed by other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Moreover, we engage the services of consultants to assist us in the development of our commercial product and product candidates, many of whom were previously employed at or may have previously been or are currently providing consulting services to, other biotechnology or pharmaceutical companies, including our competitors or potential competitors. We may be subject to claims that these employees and consultants or we have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers or their former or current customers. Litigation may be necessary to defend against these types of claims. Even if we are successful in defending against any such
claims, any such litigation would likely be protracted, expensive, a distraction to our management team, not viewed favorably by investors and other third parties, and may potentially result in an unfavorable outcome.
If we are unable to protect the confidentiality of our trade secrets and other proprietary information, the value of our technology could be materially adversely affected, and our business could be harmed.
Proprietary trade secrets and unpatented know-how are also very important to our business. We have limited control over the protection of trade secrets used by our licensors, collaborators and suppliers. We rely on trade secret protection and confidentiality agreements to protect proprietary know-how that is not patentable or that we elect not to patent, processes for which patents are difficult to enforce, and other elements of our technology, discovery and development processes that involve proprietary know-how, information or technology that is not covered by patents. Any disclosure to or misappropriation by third parties of our confidential proprietary information could enable competitors to quickly duplicate or surpass our technological achievements, including by enabling them to develop and commercialize products substantially similar to or competitive with our current or future product candidates, thus eroding our competitive position in the market. Trade secrets can be difficult to protect. We seek to protect our proprietary technology and processes, in part, by entering into confidentiality agreements and invention assignment agreements with our employees, consultants, and outside scientific advisors, contractors and collaborators. These agreements are designed to protect our proprietary information. Although we use reasonable efforts to protect our trade secrets, our employees, consultants, contractors, or outside scientific advisors might intentionally or inadvertently disclose our trade secrets or confidential, proprietary information to competitors. In addition, competitors may otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. If any of our confidential proprietary information were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent such competitor from using that technology or information to compete with us, which could harm our competitive position.
Enforcing a claim that a third party illegally obtained and is using any of our trade secrets is expensive and time consuming, and the outcome is unpredictable. In addition, the laws of certain foreign countries do not protect proprietary rights such as trade secrets to the same extent or in the same manner as the laws of the United States. Misappropriation or unauthorized disclosure of our trade secrets to third parties could impair our competitive advantage in the market and could materially adversely affect our business, results of operations and financial condition.
Some intellectual property that we have in-licensed, if created as a result of government funded programs, may be subject to certain federal regulations.
Some of the agreements covering the intellectual property rights we have licensed provide that to the extent that such rights are derived from the use of U.S. government funding, those rights may therefore be subject to certain federal regulations. As a result, the U.S. government may have certain rights to intellectual property embodied in our current or future product candidates pursuant to the Bayh-Dole Act of 1980, or Bayh-Dole Act. These U.S. government rights in certain inventions developed under a government-funded program include a non-exclusive, non-transferable, irrevocable worldwide license to use inventions for any governmental purpose. In addition, the U.S. government has the right to require us to grant exclusive, partially exclusive or non-exclusive licenses to any of these inventions to a third party if it determines that: (i) adequate steps have not been taken to commercialize the invention, (ii) government action is necessary to meet public health or safety needs or (iii) government action is necessary to meet requirements for public use under federal regulations (also referred to as "march-in rights"). The U.S. government also has the right to take title to these inventions if we, or the applicable licensor, fail to disclose the invention to the government and fail to file an application to register the intellectual property within specified time limits. Intellectual property generated under a government funded program is also subject to certain reporting requirements, compliance with which may require us or the applicable licensor to expend substantial resources. In addition, the U.S. government requires that any products embodying the subject invention or produced through the use of the subject invention be manufactured substantially in the United States. The manufacturing preference requirement can be waived if the owner of the intellectual property can show that reasonable but unsuccessful efforts have been made to grant licenses on similar terms to potential licensees that would be likely to manufacture substantially in the United States or that under the circumstances domestic manufacture is not commercially feasible. This preference for U.S. manufacturers may limit our ability to contract with non-U.S. product manufacturers for products covered by such intellectual property. To the extent any of our current or future intellectual property is generated through the use of U.S. government funding, the provisions of the Bayh-Dole Act
may similarly apply. Moreover, changes in regulations related to government-funded programs may affect how the government may exercise march-in rights and affect any of our current or future intellectual property rights derived from U.S. government funding.
Risks Related to Competition and Commercialization of Our Current and Future Product Candidates
We face substantial competition, which may result in others discovering, developing or commercializing products before or more successfully than we do.
Our product candidates may face competition sooner than expected afterfuture success depends on our ability to demonstrate and maintain a competitive advantage with respect to the expiration of our composition of matter patent protection for such products.
Our composition of matter patents for manydesign, development, and commercialization of our product candidates. Our competitors may succeed in developing competing products before we do for the same indications we are pursuing, obtaining regulatory approval for products, or gaining acceptance for the same markets that we are targeting. If we are not “first to market” with a product candidate, thereby effecting our order of entry, our competitive position could be compromised via reduced market share and higher hurdles to regulatory approval.
We expect any product candidate which we commercialize will compete with products from other companies in the biotechnology and pharmaceutical industries. There are several biopharmaceutical companies which have approved treatments options in the United States for AML broadly, with different mechanisms of action, including AbbVie/Genentech (Venclexta), Pfizer (Mylotarg), Daiichi-Sankyo (Vanflyta), Rigel Pharmaceuticals (Rezlidhia) and Bristol Myers Squibb (Vidaza).
Key late-stage pipeline agents that are different from GPS have been granted ODD or Fast Track designation due to the unmet need in AML. Therefore, clinical late-stage companies developing late-stage clinical candidates to treat r/r AML may enter the market before our potential products, such as GlycoMimetics (uproleselan), Delta-Fly Pharma (DFP-10917), and AROG Pharmaceuticals (crenolanib). A key competitor may be Iomab-b, which is being developed by Actinium Pharmaceuticals. In late 2022 / early 2023, Actinium announced positive results in its pivotal Phase 3 trial in adults aged 55 and above with active r/r AML.
With respect to WT1-targeting therapies, we do not believe GPS currently has direct competition in AML in the maintenance setting after CR2. There are companies engaged in the clinical development of WT-1 targeting therapies; however, they are not focused on AML at this time, including Astellas (ASP7517) and Cue Biopharma (CUE-102), or are in earlier stages, such as NexImmune (NEXI-001).
With respect to our SLS009 program, we anticipate competition with MEI Pharma, whose voruciclib is in a Phase 1 clinical trial as a monotherapy and in combination with venetoclax for adults with r/r AML. There may also be competition in one of our other indications, PTCL, from enitociclib, a CDK9 inhibitor under development by Vincerx Pharma as a monotherapy and in combination with venetoclax for the treatment of PTCL. Furthermore, there are other companies which are in early development stages for their CDK9 inhibitors and targeting other hematological malignancies or solid tumors, including Kronos Bio (KB-0742), Sumitomo Dainippon Pharma (TP-1287),Adastra Pharmaceuticals (zotiraciclib), and Prelude Therapeutics (PRT2527).
Many of our competitors have expiredsubstantially greater commercial infrastructures and financial, technical and personnel resources than we have. In addition, some are farther along in their clinical development programs or in collaboration with larger, established pharmaceutical companies. We may not be able to compete unless we successfully:
•design and develop products that are superior to other products in the market;
•conduct successful preclinical and clinical trials;
•attract qualified scientific, medical, sales and marketing and commercial personnel;
•obtain patent and/or other proprietary protection for our processes and product candidates;
•obtain required regulatory approvals; and
•collaborate with others in the design, development, and commercialization of new products.
Established competitors may invest heavily to quickly discover and develop novel compounds that could make our product candidates obsolete. In addition, any new product that competes with an approved product must
demonstrate compelling advantages in efficacy, convenience, tolerability, and safety to overcome price competition and to be commercially successful. If we are not able to compete effectively against our current and future competitors, our business will expirenot grow, and our financial condition and operations will suffer.
If we obtain marketing approval, our commercial success depends on establishing or implementing our own sales, marketing, access and reimbursement, and distribution capabilities or entering into licensing or collaboration agreements for these purposes, and the timing of these.
With the exception of very few employees, including our executive officers, we have not yet built a broader team with any significant sales, marketing, access and reimbursement, or distribution experience. If we progress toward regulatory approval, we will take an efficient and measured approach to building an appropriately sized commercial infrastructure depending on whether we choose to commercialize our current and any future product candidates on our own or through licensing, distribution or collaboration agreements. We will have to invest significant amounts of financial and management resources, some of which will be committed prior to the receipt of positive data if we choose to commercialize on our own. We may need to successfully recruit, retain and train a broad complement of effective commercial staff, including, but not limited to, sales, access and reimbursement, business analytics, and diagnostics. As AML is a highly competitive space, we would expect some personnel to be sought by our competitors. Any delays in hiring an adequate number of experienced sales personnel (including support staff), inability to obtain access to key markets, and unforeseen time, cost and expenses associated with creating a separate and high performing sales and marketing organization could adversely impact commercialization of any product for which we obtain marketing approval.
We intendmay elect to seek data exclusivityutilize other means of commercialization should the economics of the approach be deemed appropriate. This could include contract sales forces or market exclusivitystrategic partners to support in the commercialization of our product candidates. If we enter into arrangements with third parties to perform sales, marketing and distribution services for our NeuVaxproducts, the resulting revenues or the profitability from these revenues to us are likely to be lower than if we had sold, marketed and distributed our products ourselves. In addition, we may not be successful in entering into arrangements with third parties to sell, market and distribute our product candidates, or do so in a timely manner, or may be unable to do so on terms that are favorable to us. We may also need the infrastructure and resources to maintain the contractual relationships and external support. If we are not able to timely and properly establish a commercial organization on our own or in collaboration with third parties, then we may not be profitable.
Our commercial success depends upon attaining significant market acceptance of our current and future product candidates, if approved, among health care providers, third-party payors and operators of major cancer clinics.
Even if we obtain regulatory approval for any of our current or future product candidates, the products may not gain market acceptance among physicians, third-party payors, patients or the medical community. For example, current cancer treatment such as chemotherapy and radiation therapy are well-established in the medical community, and health care providers may continue to rely on these treatments. The degree of market acceptance of any product candidates for which we receive approval depends on a number of factors, including:
•the efficacy and safety of such product candidates as demonstrated in clinical trials, and acceptance of such by physicians, major cancer treatment centers, and patients;
•the potential and perceived advantages and disadvantages of product candidates over alternative treatments, including the degree of clinically meaningful improvement in care, ease of administration and prevalence and severity of side effects;
•the clinical indications and patient populations for which the product candidate is approved and the willingness of the target patient population to try new therapies and of physicians to prescribe these therapies;
•the ability to garner placement of our therapeutics in widely accepted clinical practice treatment guidelines;
•the placement, or the lack of placement, of our therapeutics in reputable and highly regarded clinical treatment guidelines;
•product labeling or product insert requirements of the FDA or other regulatory authorities and any restrictions on use with other medications;
•the timing of market introduction of our products as well as competitive products;
•the cost of treatment and coverage and reimbursement status;
•development and effectiveness of our GALE-301sales and GALE-302marketing, manufacturing and distribution efforts for commercial scale; and
•new healthcare legislation that could adversely affect the payor profile of our marketed assets.
If any of our current and future product candidates providedare approved but fail to achieve market acceptance, we will not be able to generate significant revenues, which would compromise our ability to become profitable.
Even if we are able to commercialize our current or future product candidates, the products may become subject to unfavorable pricing regulations, third-party reimbursement practices or health care reform initiatives, which could harm our business.
Significant uncertainty exists as to the coverage and reimbursement status of any drug or biological candidates for which we obtain regulatory approval. The regulations that govern marketing approvals, pricing and reimbursement (public and private) for new drug products vary widely from country to country. In the United States, recently passed legislation may significantly change the approval requirements in ways that could involve additional costs and cause delays in obtaining approvals. Some countries require approval of the sale price of a drug before it can be marketed. In many countries, the pricing review period begins after marketing or product licensing approval is granted. In some foreign markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain marketing approval for a product in a particular country, but then be subject to price regulations that delay our commercial launch of the product, possibly for lengthy time periods, and negatively impact the revenues we are able to generate from the sale of the product in that country. Adverse pricing limitations may hinder our ability to recoup our investment in one or more product candidates, even if our product candidates obtain marketing approval.
Our ability to commercialize any product successfully will also depend, in part, on the extent to which reimbursement for these products and related treatments will be available from government health administration authorities, private health insurers and other organizations. Government authorities and third-party payors, such as private health insurers and health maintenance organizations, decide which medications they will cover and how much they will pay. A primary trend in the U.S. health care industry and elsewhere is cost containment. Government authorities and third-party have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. We cannot be sure that reimbursement will be available for any product that we commercialize and, if reimbursement is available, the level of reimbursement. Reimbursement may impact the demand for, or the price of, any product candidate for which we obtain marketing approval. Obtaining reimbursement for our products may be particularly difficult because of the higher prices often associated with drugs administered under the Federal Food, Drugsupervision of a physician. If reimbursement is not available or is available only to limited levels, we may not be able to successfully commercialize any product candidate for which we obtain marketing approval.
There may be significant delays in obtaining reimbursement for newly approved drugs, and Cosmetic Act,coverage may be more limited than the purposes for which the drug is approved by the FDA or FDCA,similar foreign regulatory authorities outside the United States. Moreover, eligibility for coverage does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and similardistribution. Reimbursement rates may vary according to the use of the drug and the clinical setting in which it is used, may be based on
reimbursement levels already set for lower cost drugs and may be incorporated into existing payments for other services. Net prices for drugs may be reduced by mandatory discounts or rebates required by government health care programs or private payors and by any future relaxation of laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the United States. Third-party commercial payors often follow CMS coverage policy and payment limitations in setting their own reimbursement policies. Our inability to promptly obtain coverage and profitable payment rates from both government-funded and private payors for any approved products that we develop could have a material adverse effect on our operating results, our ability to raise capital needed to commercialize products and our overall financial condition.
Further, there have been, and may continue to be, legislative and regulatory proposals at the U.S. federal and state levels and in foreign jurisdictions directed at broadening the availability and containing or lowering the cost of health care. The continuing efforts of the government, insurance companies, managed care organizations and other countries. We believethird-party payors to contain or reduce costs of health care may adversely affect our ability to set prices for our products that would allow us to achieve or sustain profitability. In addition, governments may impose price controls on any of our products that obtain marketing approval, which may adversely affect our future profitability.
More recently, in August 2022, President Biden signed into the law the IRA. Among other things, the IRA has multiple provisions that may impact the prices of drug products that are both sold into the Medicare program and throughout the United States. Starting in 2023, a manufacturer of drugs or biological products covered by Medicare Parts B or D must pay a rebate to the federal government if their drug product’s price increases faster than the rate of inflation. This calculation is made on a drug product-by-drug product basis and the amount of the rebate owed to the federal government is directly dependent on the volume of a drug product that is paid for by Medicare Parts B or D. Additionally, starting for payment year 2026, CMS will negotiate drug prices annually for a select number of single source Part D drugs without generic or biosimilar competition. CMS will also negotiate drug prices for a select number of Part B drugs starting for payment year 2028. If a drug product is selected by CMS for negotiation, it is expected that the revenue generated from such drug will decrease. Additional state and federal health care reform measures are expected to be adopted in the future, any of which could limit the amounts that federal and state governments will pay for health care products and services, which could result in reduced demand for certain biopharmaceutical products or additional pricing pressures.
In some foreign countries, particularly the member states of the EU, the pricing of prescription pharmaceuticals is subject to governmental control. In these product candidates will qualifycountries, pricing negotiations with governmental authorities can be a long and expensive process after the receipt of marketing approval for 12 years of data exclusivity under the Biologics Price Competitiona drug candidate. In addition, there can be considerable pressure by governments and Innovation Act of 2009, or BPCIA, which was enactedother stakeholders on prices and reimbursement levels, including as part of cost containment measures. Political, economic and regulatory developments may further complicate pricing negotiations, and pricing negotiations may continue after reimbursement has been obtained. Reference pricing used by various EU member states and parallel distribution, or arbitrage between low-priced and high-priced member states, can further reduce prices. In some countries, we may be required to conduct additional clinical trials that compare the cost-effectiveness of our drug candidates to other available therapies in order to obtain reimbursement or pricing approval. Publication of discounts by third-party payors or authorities may lead to further pressure on prices or reimbursement levels within the country of publication and other countries. If reimbursement of our products is unavailable or limited in scope or amount in a particular country, or if pricing is set at unsatisfactory levels, we may be unable to successfully commercialize and achieve or sustain profitability for sales of any of our drug candidates that are approved for marketing in that country and our business could be adversely affected.
Health care policy changes may have a material adverse effect on our business and results of operations.
Our business may be affected by the efforts of government and third-party payors to contain or reduce the cost of health care through various means. For example, the recently enacted IRA requires drug manufacturers to pay a rebate to the federal government if prices for single-source drugs and biologicals covered under Medicare Part B and nearly all covered drugs under Part D increase faster than the rate of inflation (CPI-U Penalty). The Patient Protection and Affordable Care Act, and the Health Care and Education Affordability Reconciliation Act of 2010, (collectively,or collectively, the Affordable Care Act or ACA)ACA, enacted in March 2010. Under2010, substantially changed the BPCIA,way health care is financed by both governmental and private insurers, and significantly impacted the pharmaceutical industry, by among other things, increasing the minimum Medicaid rebates owed by most manufacturers under the Medicaid Drug Rebate Program;
introducing a new methodology by which rebates owed by manufacturers under the Medicaid Drug Rebate Program are calculated for drugs that are inhaled, infused, instilled, implanted or injected; extending the Medicaid Drug Rebate Program to utilization of prescriptions of individuals enrolled in Medicaid managed care plans; imposing mandatory discounts for certain Medicare Part D beneficiaries as a condition for manufacturers’ outpatient drugs coverage under Medicare Part D; and establishing a Center for Medicare Innovation at the CMS to test innovative payment and service delivery models to lower Medicare and Medicaid spending. Regardless of whether or not the ACA is changed or modified by Congress or the U.S. Supreme Court, we expect both government and private health plans to continue to require health care providers, including health care providers that may one day purchase our products, to contain costs and demonstrate the value of the therapies they provide.
In addition to the IRA’s drug price negotiation provisions summarized above (see the risk factor herein entitled “Even if we are able to commercialize our current or future product candidates, the products may become subject to unfavorable pricing regulations, third-party reimbursement practices or health care reform initiatives, which could harm our business.”), President Biden’s Executive Order 14087, issued in October 2022, called for the CMS Innovation Center to prepare and submit a report to the White House on potential payment and delivery modes that would complement the IRA, lower drug costs, and promote access to innovative drugs. In February 2023, CMS published its report which described three potential models focusing on affordability, accessibility and feasibility of implementation for further testing by the CMS Innovation Center. As of January 2024, the CMS Innovation Center continues to test the proposed models and develop implementation plans. Such models, if implemented, may have a significant impact on the distribution of and reimbursement for our product candidates that receive FDA approval, if any.
Additionally, there has been heightened governmental scrutiny in the United States of pharmaceutical pricing practices considering the rising cost of prescription drugs and biologics. Such scrutiny has resulted in several congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for products. For example, in May 2019, CMS issued a final rule to allow Medicare Advantage plans the option to use step therapy for Part B drugs beginning January 1, 2020. This final rule codified CMS’s policy change that was effective January 1, 2019. In addition, the 2021 Consolidated Appropriations Act signed into law on December 27, 2020, incorporated extensive health care provisions and amendments to existing laws, including a requirement that all manufacturers of drug products covered under Medicare Part B report the product’s average sales price to CMS beginning on January 1, 2022, subject to enforcement via civil money penalties.
Individual states in the United States have also increasingly passed legislation and implemented regulations designed to control biopharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. For example, in recent years, several states have formed PDABs. Much like the IRA’s drug price negotiation program, these PDABs have attempted to implement upper payment limits on drugs sold in their respective states in both public and commercial health plans. For example, in August 2023, Colorado’s PDAB announced a list of five prescription drugs that would undergo an applicationaffordability review. The effects of these efforts remain uncertain pending the outcomes of several federal lawsuits challenging state authority to regulate prescription drug payment limits. In December 2020, the U.S. Supreme Court held unanimously that federal law does not preempt the states’ ability to regulate pharmacy benefit managers, or PBMs, and other members of the health care and pharmaceutical supply chain, an important decision that may lead to further and more aggressive efforts by states in this area. In addition, the FTC in mid-2022 also launched sweeping investigations into the practices of the PBM industry that could lead to additional federal and state legislative or regulatory proposals targeting such entities’ operations, pharmacy networks, or financial arrangements. Significant efforts to change the PBM industry as it currently exists in the United States may affect the entire pharmaceutical supply chain and the business of other stakeholders, including biopharmaceutical developers like us.
We expect that these and other health care reform measures that may be adopted in the future may result in additional reductions in Medicare and other health care funding, more rigorous coverage criteria, new payment methodologies and additional downward pressure on the price that we receive for any approved product. We cannot predict the initiatives that may be adopted in the future. The continuing efforts of the government, insurance
companies, managed care organizations and other payors of health care services to contain or reduce costs of health care and/or impose price controls may adversely affect:
•the demand for our product candidates, if we obtain regulatory approval;
•our ability to receive or set a price that we believe is fair for our products;
•our ability to generate revenue and achieve or maintain profitability;
•our ability to enjoy or maintain market exclusivity;
•the level of taxes that we are required to pay; and
•the availability of capital.
On January 5, 2024, the FDA granted approval to Florida for the importation of specific prescription medications from Canada. This initiative aims to provide residents of Florida with access to more affordable drug prices comparable to those paid by Canadians. The noteworthy aspect of this announcement lies in it being the inaugural instance where the FDA has officially sanctioned a state to securely import prescription drugs from an international source. Should this trend of parallel importing grow within the U.S. markets, net revenues could be adversely affected.
Price controls may be imposed in foreign markets, which may adversely affect our future profitability.
In some countries, particularly member states of the EU, the pricing of prescription drugs is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after receipt of regulatory approval for a biosimilarproduct. In addition, there can be considerable pressure by governments and other stakeholders on prices and reimbursement levels, including as part of cost containment measures. Political, economic and regulatory developments may further complicate pricing negotiations, and pricing negotiations may continue after reimbursement has been obtained. Global reference pricing used by most (if not all) EU member states and parallel distribution, or arbitrage between low-priced and high-priced member states, can further reduce prices. In some countries, we or our collaborators may be required to conduct a clinical trial or other studies that compare the cost-effectiveness of our product candidates to other available therapies in order to obtain or BLA cannot be submittedmaintain reimbursement or pricing approval. Publication of discounts by third-party payors or authorities may lead to further pressure on the FDA until four years,prices or reimbursement levels within the country of publication and other countries. If reimbursement of our products is unavailable or limited in scope or amount, or if approved by the FDA, until 12 years, after the original brand product identified as the reference productpricing is approved under a BLA. The BPCIA provides an abbreviated pathway for the approval of biosimilarset at unsatisfactory levels, our business could be adversely affected.
Risks Related to Health Care Compliance Regulations
Our relationships with customers and interchangeable biological products. The new abbreviated regulatory pathway establishes legal authority for the FDAthird-party payors will be subject to reviewapplicable anti-kickback, fraud and approve biosimilar biologics, including the possible designation of a biosimilar as “interchangeable” based on its similarityabuse and other health care laws and regulations, which could expose us to an existing brand product. The new law is complexcriminal sanctions, civil penalties, contractual damages, reputational harm and is only beginningdiminished profits and future earnings. If we or they are unable to be interpretedcomply with these provisions, we may become subject to civil and implemented by the FDA. While it is uncertain when any such processes may be fully adopted by the FDA, any such processescriminal investigations and proceedings that could have a material adverse effect on our business, financial condition and prospects.
Health care providers, physicians and third-party payors will play a primary role in the recommendation and prescription of any product candidates for which we obtain regulatory approval. Our current and future arrangements with health care providers, health care entities, third-party payors and customers may expose us to broadly applicable fraud and abuse and other health care laws and regulations that may constrain the business or financial arrangements and relationships through which we research, develop and will market, sell and distribute our products. As a biopharmaceutical company, even though we do not and will not control referrals of health care services or bill directly to Medicare, Medicaid or other third-party payors, federal and state health care laws and regulations pertaining to fraud and abuse and patients’ rights are applicable to our business. Restrictions under applicable federal and state health care laws and regulations that may affect our ability to operate include the following:
•the federal health care Anti-Kickback Statute which prohibits, among other things, individuals and entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, overtly or covertly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made, in whole or in part, under a federal health care program such as Medicare or Medicaid;
•federal civil and criminal false claims laws, including the FCA that can be enforced through civil whistleblower or qui tam actions, and civil monetary penalty laws, prohibit individuals or entities from knowingly presenting, or causing to be presented, to the federal government, including the Medicare and Medicaid programs, claims for payment or approval that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government;
•HIPAA, which imposes criminal and civil liability for executing a scheme to defraud any health care benefit program and also created federal criminal laws that prohibit knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statements in connection with the delivery of or payment for health care benefits, items or services, and further, as amended by HITECH, imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information on entities subject to the law, such as certain health care providers, health plans, and health care clearinghouses, known as covered entities, and their respective business associates that perform services for them that involve the creation, use, maintenance or disclosure of, individually identifiable health information;
•the federal physician sunshine requirements under the ACA which requires certain manufacturers of drugs, devices, biologics and medical supplies, with certain exceptions, to report annually to HHS information related to payments and other transfers of value to physicians, certain advanced non-physician health care practitioners, and teaching hospitals, and ownership and investment interests held by physicians and other health care providers and their immediate family members and applicable group purchasing organizations;
•analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws, which may apply to sales or marketing arrangements and claims involving health care items or services reimbursed by non-governmental third-party payors, including private insurers; some state laws which require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and may require drug manufacturers to report information related to payments and other transfers of value to physicians and other health care providers, marketing expenditures or pricing information; and certain state and local laws which require the registration of pharmaceutical sales representatives; and
•state and foreign laws govern the privacy and security of health information in specified circumstances, including the GDPR, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts.
Efforts to ensure that our business arrangements with third parties will comply with applicable health care laws and regulations will involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other health care laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, imprisonment, disgorgement, exclusion from government funded health care programs, such as Medicare and Medicaid, integrity oversight and reporting obligations, and the curtailment or restructuring of our operations. If any physicians or other health care providers or entities with whom we expect to do business are found to not be in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded health care programs. Many health care laws and regulations are rapidly changing and legislative bodies and regulatory agencies are regularly considering amendments and supplements to existing laws and regulations, and as a result interpretations of rules and confirmation of our compliance with such rules can be ambiguous.
We may be subject to, or may in the future commercial prospectsbecome subject to, U.S. federal and state, and international laws and regulations imposing obligations on how we collect, use, disclose, store and process personal information. Our actual or perceived failure to comply with such evolving privacy and data protection laws could adversely affect our business, results of operations, and financial condition.
New privacy and data security laws have been proposed in more than half of the states in the United States and in the U.S. Congress, reflecting a trend toward more stringent privacy legislation in the U.S., which trend may accelerate with increasing concerns about individual privacy. The existence of comprehensive privacy laws in different states in the U.S. may make our compliance obligations more complex and costly, may require us to modify our data processing practices and policies, and may require us to incur substantial costs and potential liability in an effort to comply.
In California, the CCPA, which became effective in 2020, broadly defines personal information, gives California residents expanded individual privacy rights and protections, provides for civil penalties for violations, and gives California residents a private right of action for data breaches in certain cases. Further, the California Privacy Rights Act, or the CPRA, which became effective in 2023 and amends the CCPA, imposes additional obligations on covered businesses, including additional consumer rights processes, limitations on data uses, new audit requirements for higher risk data, and opt outs for certain uses of sensitive data. It also created a new California Privacy Protection Agency authorized to issue substantive regulations and is expected to result in increased privacy and information security enforcement. The CPRA also extends the provisions of both the CCPA and the CPRA to the personal information of California-based employees. While there is an exception for certain health information, including protected health information that is subject to HIPAA, and clinical trial data, the CCPA may impact our business activities if we become a “Business” regulated by the CCPA. Further, there continues to be some uncertainly about how certain provisions of the CCPA will be interpreted and how some areas of the law will be enforced. We will continue to monitor developments related to the CCPA and anticipate additional costs and expenses associated with compliance.
In addition to the CCPA, broad consumer privacy laws recently went into effect in Virginia on January 1, 2023, in Colorado and Connecticut on July 1, 2023, and in Utah on December 31, 2023. New privacy laws will also become effective in Florida, Montana, Oregon, and Texas in 2024, in Delaware, Iowa, New Hampshire, New Jersey, and Tennessee in 2025, and in Indiana in 2026. In addition, numerous other states are considering new comprehensive privacy laws.
Other U.S. states, such as New York and Massachusetts have enacted stringent data security laws and numerous other states have proposed similar laws. Additionally, various states, such as California and Massachusetts, have implemented similar privacy laws and regulations, such as the California Confidentiality of Medical Information Act, that impose restrictive requirements regulating the use and disclosure of health information and other personally identifiable information. These laws and regulations are not necessarily preempted by HIPAA, particularly if a state affords greater protection to individuals than HIPAA. Where state laws are more protective, we have to comply with the stricter provisions. In addition to fines and penalties imposed upon violators, some of these state laws also afford private rights of action to individuals who believe their personal information has been misused. California’s patient privacy laws, for example, provide for penalties of up to $250,000 and permit injured parties to sue for damages. Similarly, as discussed above, the CCPA allows consumers a private right of action when certain personal information is subject to unauthorized access and exfiltration, theft or disclosure due to a business’ failure to implement and maintain reasonable security procedures.
Furthermore, over the past few years, the number of privacy-related enforcement actions in the U.S., and in many cases the fines, have steadily increased. Failure to comply with these current and future laws, policies, industry standards, or legal obligations. or any data breach involving personal information, may result in government enforcement actions, litigation, fines, and penalties, private litigation, or adverse publicity, and could cause our customers, business partners, and investors to lose trust in us which could have a material adverse impact on our business, results of our operations, and our financial condition. We continue to face uncertainty as to the exact interpretation of the new requirements on our clinical trials and we may be unsuccessful in implementing all measures required by data protection authorities or courts in interpretation of the new law.
The interplay of federal and state laws may be subject to varying interpretations by courts and government agencies, creating complex compliance issues for us and data we receive, use and share, potentially exposing us to additional expense, adverse publicity and liability. Further, as regulatory focus on privacy issues continues to increase and laws and regulations concerning the protection of personal information expand and become more complex, these potential risks to our business could intensify. Changes in laws or regulations associated with the enhanced protection of certain types of sensitive data, for the treatment of genetic data, along with increased customer demands for enhanced data security infrastructure, could greatly increase our cost of providing our products, decrease demand for our biological product candidates. Thereproducts, reduce our revenues and/or subject us to additional liabilities.
In many activities, including the conduct of clinical trials and our regulatory and commercial operations in the EEA and the United Kingdom, or UK, we are subject to international laws and regulations governing data privacy and the protection of health-related and other personal information. The regulatory framework for collecting, using, safeguarding, sharing, transferring and other processing of information worldwide is alsorapidly evolving and is likely to remain uncertain for the foreseeable future. The withdrawal of the UK from the EU and the subsequent separation of the data protection regimes of these territories means we are required to comply with separate data protection laws in the EU and the UK, which may lead to additional compliance costs and could increase our overall risk. Similar laws and regulations govern our processing of personal data, including the collection, access, use, analysis, modification, storage, transfer, security breach notification, destruction and disposal of personal data. For example, the collection, use, disclosure, transfer, or other processing of personal data regarding individuals in the EU, including personal health data, is subject to the GDPR, which took effect across all Member States of the EEA on May 25, 2018, and as still in effect in the UK as the UK GDPR. On June 28, 2021, the EU Commission adopted decisions on the UK’s adequacy under the EU GDPR, and the UK continues to operate under this adequacy decision. The GDPR applies to any company established in the EU as well as to those outside the EU that process personal data in connection with the offering of goods or services to individuals in the EU or the monitoring of their behavior. We currently conduct clinical trials and engage in regulatory and commercial operations in the EEA and the UK. As a result, we are subject to privacy laws, including the GDPR and UK GDPR. The GDPR imposes a broad range of data protection obligations on controllers and/or processors, as applicable, that must be complied with when processing personal data subject to the GDPR, including, for example, providing expanded disclosures about how their personal data will be used; higher standards for organizations to demonstrate that they have obtained valid consent or have another legal basis in place to justify their data processing activities; the obligation to appoint data protection officers in certain circumstances; new rights for individuals to be “forgotten” and rights to data portability, as well as enhanced current rights (e.g., access requests); the principal of accountability and demonstrating compliance through policies, procedures, training and audit; limitations on retention of information; mandatory data breach notification requirements; ; safeguards to protect the security and confidentiality of personal data; restrictions on transfers of personal data outside of the EU to third countries deemed to lack adequate privacy protections (such as the U.S.), and onerous new obligations and liabilities on services providers or data processors. .In particular, medical or health data, genetic data and biometric data are all classified as “special category” data under the GDPR and afford greater protection and require additional compliance obligations. Further, the UK and EU member states have a broad right to impose additional conditions—including restrictions—on these data categories. This is because the GDPR allows EU member states to derogate from the requirements of the GDPR mainly in regard to specific processing situations (including special category data and processing for scientific or statistical purposes). Non-compliance with the GDPR may result in monetary penalties of up to €20 million or 4% of worldwide revenue, whichever is greater. Moreover, data subjects can claim damages resulting from infringement of the GDPR. The GDPR further grants non-profit organizations and consumer organizations the right to bring claims on behalf of data subjects. The GDPR and other changes in laws or regulations associated with the enhanced protection of certain types of personal data, such as healthcare data or other sensitive information, could greatly increase our cost of providing our products and services or even prevent us from offering certain services in jurisdictions that we may operate in. The GDPR may increase our responsibility and liability in relation to personal data that we process where such processing is subject to the GDPR, and we may be required to put in place additional mechanisms to ensure compliance with the GDPR, including as implemented by individual EU Member States. Compliance with the GDPR is a rigorous and time-intensive process that may increase our cost of doing business or require us to change our business practices, and despite those efforts, there is a risk that we may be subject to fines and penalties, litigation, and reputational harm in connection with our EU activities.
Further, as referenced above, following the UK’s withdrawal from the EU (i.e., Brexit), and the expiry of the Brexit transition period, which ended on December 31, 2020, the EU GDPR has been implemented in the UK (as the UK
GDPR). The UK GDPR sits alongside the UK Data Protection Act 2018 which implements certain derogations in the EU GDPR into UK law. Under the UK GDPR, companies not established in the UK but who process personal data in relation to the offering of goods or services to individuals in the UK, or to monitor their behavior will be subject to the UK GDPR – the requirements of which are (at this time) largely aligned with those under the EU GDPR and as such, may lead to similar compliance and operational costs. Non-compliance with the UK GDPR may result in monetary penalties of up to £17.5 million or 4% of worldwide revenue, whichever is higher.
In addition, we may be unable to transfer personal data from the EU, UK, and other jurisdictions to U.S or other countries due to limitations on cross-border data flows. In particular, the EEA and the UK have significantly regulated the transfer of personal data to the U.S and other countries whose privacy laws it believes are inadequate. Other jurisdictions may adopt similarly stringent interpretations of their data localization and cross-border data transfer laws. Although there are currently various mechanisms that may be used to transfer personal data from the EEA and the UK to the U.S. Congressin compliance with law, such as the EEA and UK’s standard contractual clauses and the newly-adopted Data Privacy Framework, these mechanisms are subject to legal challenges, and there is no assurance that we can satisfy or rely on these measures to lawfully transfer personal data to the U.S.. If there is no lawful manner for us to transfer personal data from the EEA, the UK or other jurisdictions to the U.S., or if the requirements for a legally-compliant transfer are too onerous, we could amendface significant adverse consequences, including the BPCIA to shorten this exclusivity period, potentially creating the opportunity for biosimilar competition sooner than anticipated after the expirationinterruption or degradation of our patent protection. Moreover,operations, the extentneed to relocate part of or all of our business or data processing activities to other jurisdictions at significant expense, increased exposure to regulatory actions, substantial fines and penalties, the inability to transfer data and work with partners, vendors and other third parties, and injunctions against our processing or transferring of personal data necessary to operate our business. Additionally, companies that transfer personal data out of the EEA and the UK to other jurisdictions, particularly to the U.S., are subject to increased scrutiny from regulators, individual litigants, and activist groups.
If we are investigated by an EEA or UK data protection authority, we may face fines and other penalties, which could have a biosimilar, once approved, willnegative effect on our existing business and on our ability to attract and retain new clients or pharmaceutical partners. We may also experience hesitancy, reluctance, or refusal by EEA, UK, or multi-national clients or pharmaceutical partners to continue to use our products due to the potential risk exposure because of the current (and future) data protection obligations imposed on them by certain data protection authorities in interpretation of current law, including the GDPR and UK GDPR. Such clients or pharmaceutical partners may also view any alternative approaches to compliance as being too costly, too burdensome, too legally uncertain, or otherwise objectionable and therefore decide not to do business with us. Any of the foregoing could materially harm our business, prospects, financial condition, and results of operations.
In addition, many jurisdictions outside of the EEA and the UK are also considering and/or enacting comprehensive data protection legislation. For example, as of August 2020, the Brazilian General Data Protection Law imposes stringent requirements similar to GDPR with respect to personal information collected from individuals in Brazil.
In China, there have also been recent significant developments concerning privacy and data security. The Data Security Law of the People’s Republic of China (Data Security Law), which took effect on September 1, 2021, requires data processing (which includes the collection, storage, use, processing, transmission, provision and publication of data), to be substituted for any reference productconducted in a waylegitimate and proper manner. The Data Security Law imposes data security and privacy obligations on entities and individuals carrying out data processing activities and also introduces a data classification and hierarchical protection system based on the importance of data in economic and social development and the degree of harm it may cause to national security, public interests, or legitimate rights and interests of individuals or organizations if such data are tampered with, destroyed, leaked, illegally acquired or illegally used. The appropriate level of protection measures is required to be taken for each respective category of data.
Also in China, the Personal Information Protection Law, which took effect on November 1, 2021, introduced stringent protection requirements for processing personal information, which are in many ways akin to the requirements of the GDPR. We may be required to make further significant adjustments to our business practices to comply with the personal information protection laws and regulations in China including the Personal Information Protection Law.
We also continue to see jurisdictions imposing data localization laws. These regulations may interfere with our intended business activities, inhibit our ability to expand into those markets or prohibit us from continuing to offer services in those markets without significant additional costs.
Because the interpretation and application of many domestic and international privacy and data protection laws, commercial frameworks, and standards are uncertain, it is possible that these laws, frameworks, and standards may be interpreted and applied in a manner that is inconsistent with our existing data management practices and policies. It is also possible that by complying with one law, we may be violating another. In addition to the possibility of fines, lawsuits, breach of contract claims, and other claims and penalties, we could be required to fundamentally change our business activities and practices or modify our solutions, which could have an adverse effect on our business. Failure to comply with current and future privacy and data protection laws and regulations could result in government enforcement actions (including the imposition of significant penalties), criminal and civil liability for us and our officers and directors, private litigation and/or adverse publicity that negatively affects our business. Any inability to adequately respond to privacy and security concerns, even if unfounded, or to comply with applicable privacy and data protection laws, regulations, and policies, could result in additional cost and liability to us, damage our reputation, inhibit our ability to conduct trials, and adversely affect our business.
Our employees may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements, which could cause significant liability for us and harm our reputation.
We are exposed to the risk of employee fraud or other misconduct, including intentional failures to comply with FDA regulations or similar regulations of comparable foreign regulatory authorities, provide accurate information to traditional generic substitution for non-biological productsthe FDA or comparable foreign regulatory authorities, comply with manufacturing standards we have established, comply with federal and state health care fraud and abuse laws and regulations and similar laws and regulations established and enforced by comparable foreign regulatory authorities, report financial information or data accurately or disclose unauthorized activities to us. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not yet clear,always possible to identify and deter employee misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business and results of operations, including the imposition of significant civil, criminal and administrative penalties, damages, fines, imprisonment, exclusion from government funded health care programs, such as Medicare and Medicaid, and integrity oversight and reporting obligations.
Product liability lawsuits against us could cause us to incur substantial liabilities and to limit commercialization of any products that we may develop.
We face an inherent risk of product liability exposure related to the testing of our current or future product candidates in human clinical trials and will depend on a number of marketplace and regulatory factorsface an even greater risk if we commercially sell any products that are still developing.
we may develop. Product liability claims may be brought against us by subjects enrolled in our clinical trials, patients, health care providers or others using, administering or selling our products. If we cannot successfully defend ourselves against claims that our product candidates are not considered biologicsor products caused injuries, we could incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
•decreased demand for any product candidates or products that would qualifywe may develop;
•termination of clinical trial sites or entire clinical trial programs;
•injury to our reputation and significant negative media attention;
•withdrawal of clinical trial participants;
•significant costs to defend the related litigation;
•substantial monetary awards to trial subjects or patients;
•loss of revenue;
•diversion of management and scientific resources from our business operations; and
•the inability to commercialize any products that we may develop.
We currently hold product liability insurance coverage at a level that we believe is customary for exclusivity under the BPCIA, they may be eligiblesimilarly situated companies and adequate to provide us with insurance coverage for market exclusivity as drugs under the FDCA. The FDCA provides a five-year period of non-patent marketing exclusivity within the U.S. to the first applicant to gain approval of an NDA for a new chemical entity. A drug is a new chemical entity if the FDA has not previously approved any other new drug containing the same active moiety,foreseeable risks, but which is the molecule or ion responsible for the action of the drug substance. During the exclusivity period, the FDA may not accept for review an abbreviated new drug application, or ANDA, or a 505(b)(2) NDA, submitted by another company for another version of such drug where the applicant does not own or have a legal right of reference to all the data required for approval. However, an application may be submitted after four years if it contains a certification of patent invalidity or non-infringement. The FDCA also provides three years of marketing exclusivity for an NDA, 505(b)(2) NDA or supplement to an existing NDA if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant are deemed by FDA to be essential to the approval of the application, for example, for new indications, dosages, or strengths of an existing drug. This three-year exclusivity covers only the conditions associated with the new clinical investigations and does not prohibit the FDA from approving ANDAs for drugs containing the original active agent.
Even if, as we expect, NeuVax, GALE-301 and GALE-302 are considered to be reference products eligible for 12 years of exclusivity under the BPCIA or five years of exclusivity under the FDCA, another company could market competing products if the FDA approves a full BLA or full NDA for such product containing the sponsor’s own preclinical data and data from adequate and well-controlled clinical trials to demonstrate the safety, purity and potency of the products.
In some countries outside of the U.S., peptide vaccines, such as NeuVax, GALE-301 and GALE-302, are regulated as chemical drugs rather than as biologics and may or may not be eligibleadequate to cover all liabilities that we may incur. Insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise. We intend to expand our insurance coverage for non-patent exclusivity.
Althoughproducts to include the sale of commercial products if we obtain regulatory approval for our product candidates in development, but we may be unable to obtain commercially reasonable product liability insurance for any products that receive regulatory approval. Large judgments have been awarded in class action lawsuits based on drugs that had unanticipated side effects. A successful product liability claim or series of claims brought against us, particularly if judgments exceed our insurance coverage, could decrease our cash and adversely affect our business. In addition, even in instances where we have received orphan drug designationinsurance coverage, our insurance carriers may deny coverage, which could lead to the inability to recover for both GALE-301,certain losses and costly insurance coverage disputes with our carriers.
Risks Related to our Business Operations
If we fail to maintain an effective system of internal control over financial reporting, we may not be able to accurately report our financial results or prevent fraud. As a result, stockholders could lose confidence in our financial and other public reports, which would harm our business, the trading price of our common stock and our ability to raise additional capital in the future.
Effective internal controls over financial reporting are necessary for us to provide reliable financial reports and, together with adequate disclosure controls and procedures, are designed to prevent fraud. Any failure to implement required new or improved controls, or difficulties encountered in their implementation, could cause us to fail to meet our reporting obligations. Ineffective internal controls could also cause investors to lose confidence in our reported financial information, which could have a negative effect on the trading price of our common stock, and which could impact our ability to raise capital in the future. In addition, any future testing by us conducted in connection with Section 404 of the Sarbanes-Oxley Act of 2002, as amended, or SOX, or any required subsequent testing by our independent registered public accounting firm, may reveal deficiencies in our internal controls over financial reporting that are deemed to be material weaknesses or that may require prospective or retroactive changes to our consolidated financial statements or identify other areas for further attention or improvement.
We are required, pursuant to Section 404 of SOX, to furnish a report by management on, among other things, the effectiveness of our internal control over financial reporting as of December 31, 2023. However, our independent registered public accounting firm is not required to attest to the effectiveness of our internal control over financial reporting pursuant to Section 404. Under the supervision and with the participation of our Chief Executive Officer and Chief Financial Officer, our management conducted an evaluation of the effectiveness of our internal control over financial reporting based on the guidelines in the Internal Control-Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on that evaluation, our management concluded that our internal control over financial reporting was effective as of December 31, 2023. An independent assessment of the effectiveness of our internal controls could detect problems that our management’s assessment might not. Undetected material weaknesses in our internal controls could lead to financial statement restatements and require us to incur the expense of remediation.
We enter into various contracts in the normal course of our business in which we may be required to indemnify the other party to the contract under certain specific scenarios. In the event we have to perform under these indemnification provisions, it could have a material adverse effect on our business, financial condition and results of operations.
In the normal course of business, we periodically enter into academic, commercial, service, collaboration, licensing, consulting and other agreements that contain indemnification provisions. With respect to our academic and other research agreements, we typically agree to indemnify the institution and related parties from losses arising from claims relating to the products, processes or services made, used, sold or performed pursuant to the agreements for which we have secured licenses, and from claims arising from our or our sublicensees’ exercise of rights under the agreement. With respect to our collaboration agreements, we indemnify our collaborators from any third-party product liability claims that could result from the production, use or consumption of the product, as well as GALE-301for alleged infringements of any patent or other intellectual property right by a third party. With respect to consultants, we indemnify them from claims arising from the good faith performance of their services.
Should our obligations under an indemnification provision exceed applicable insurance coverage or if we were denied insurance coverage for any claim, our business, financial condition and GALE-302, thereresults of operations could be adversely affected. Similarly, if we are relying on a collaborator to indemnify us and the collaborator is no guarantee that the drugs will be successfully approved by the FDA, that they will be commercially successful in the marketplace, or that another drug will not be approveddenied insurance coverage for the same indication aheadclaim or the indemnification obligation exceeds the applicable insurance coverage, and if the collaborator does not have other assets available to indemnify us, our business, financial condition and results of our drugs.operations could be adversely affected.
Significant disruptions of information technology systems, computer system failures or breaches of information securitycybersecurity incidents could adversely affect our business.
We rely to a large extent upon sophisticated information technology networks and systems to operate our business. In the ordinary course of business, we collect, store and transmit large amounts of confidential information (including, but not limited to, personal information and intellectual property). We also have outsourced significant elements of our operations to third parties, including significant elements of our information technology infrastructure and, as a result, we are managing many independent vendor relationships withrely on third parties who may or could have access tothat process confidential information on our confidential information.behalf. This includes information technology systems of MSK, our CROs, our CMOs, and other business vendors on which we rely. The size and complexity of our information technology and information security systems, and those of our third-party vendors with whom we contract, (andand the large amounts of confidential information that is present on them),and data stored or processed thereon, make such systems potentially vulnerable to service interruptionscomputer viruses, bugs, worms, or to security breaches from inadvertent or intentional actions by our employees or vendors, or fromother malicious codes, malware, including as a result of advanced persistent threat intrusions, and other attacks by third parties.computer hackers, cracking, application security attacks, social engineering, including through phishing attacks, supply chain attacks and vulnerabilities through our third-party service providers, denial-of-service attacks, such as credential stuffing, credential harvesting, personnel misconduct or error, supply-chain attacks, software bugs, server malfunctions, software or hardware failures, loss of data or other information technology assets, adware, telecommunications failures, earthquakes, fires, floods, and other similar threats. Such attacks are of ever-increasing levels of sophistication and are made by groups, including nation states and organized crime, and individuals with a wide range of motives (including, but not limited to, industrial espionage and market manipulation) and expertise. These threats pose a risk to the security of our systems and networks and the confidentiality, availability and integrity of our data. While we have invested significantly in the protection of data and information technology, there can be no assurance that we will be able to detect any such disruption or cybersecurity incident in a timely manner or at all, or that our efforts will prevent service interruptions or cybersecurity incidents.
While we have implemented security breaches.measures, there can be no assurances that a cybersecurity incident or any other previously identified threats will not occur. Any such event could have a material adverse effect upon our reputation, business, operations, or financial condition. For example, if such an event were to occur and cause interruptions in our operations or those of our third-parties on which we rely, it could result in a material disruption of our drug development programs and the development of our services and technologies could be delayed. Any such interruption or breach in our systems could adversely affect our business operations and/or result in the loss of critical or sensitive confidential information or intellectual property, and could result in financial, legal, business and reputational harm to us or allow third parties to gain material, inside information that they use to trade in our securities. For example, the loss of clinical trial data from completed or ongoing clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or cybersecurity incident results in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability, the further development of our current and future product candidates could be delayed and our business could be otherwise adversely affected.
The costs related to significant cybersecurity incidents or disruptions could be material and could exceed the limits of the cybersecurity insurance we maintain against such risks. If the information technology systems of our third-party vendors and other contractors and consultants become subject to disruptions or cybersecurity incidents, we may have insufficient recourse against such third parties and may have to expend significant resources to mitigate the impact of such an event, and to develop and implement protections to prevent future events of this nature from occurring.
Furthermore, significant disruptions of our internal information technology systems or those of our third-party vendors and other contractors and consultants, or cybersecurity incidents could result in the loss, misappropriation, and/or unauthorized access, use, or disclosure of, or the prevention of access to, confidential information (including trade secrets or other intellectual property, proprietary business information, and personal information), which could result in financial, legal, business, and reputational harm to us. For instance, any such event that leads to unauthorized access to, or use, acquisition, or disclosure of personal information, including personal information regarding our customers, employees or other individuals, could harm our reputation, subject us to liability under and require us to comply with federal and/or state breach notification laws and international law equivalents, domestic or international privacy, data protection, and data security laws such as HIPAA and HITECH, subject us to mandatory corrective action, and otherwise subject us to liability under laws and regulations that protect the privacy and security of personal information. Such incidents could also result in legal claims or proceedings. Certain cybersecurity incidents require notice to the affected individuals, contractual partners, regulatory authorities such as the Secretary of HHS and attorneys general, and in some cases, require notice to the media. Such notice could harm our reputation and our ability to compete, result in significant legal and financial exposure and reputational damages, and loss of confidence in us, all of which could potentially have an adverse effect on our business.
Although we have implemented security measures, there is no guarantee we can protect our data from cybersecurity incidents. Cybersecurity incidents could also damage our reputation or disrupt our operations, including our ability to conduct our analyses, conduct research and development activities, collect, process and prepare company financial information, and manage the administrative aspects of our business.
Penalties for violations of these laws vary. For instance, penalties for failure to comply with a requirement of HIPAA and HITECH vary significantly, and include significant civil monetary penalties and, in certain circumstances, criminal penalties with fines up to $250,000 per violation and/or imprisonment. A person who knowingly obtains or discloses individually identifiable health information in violation of HIPAA may face a criminal penalty of up to $50,000 and up to one-year imprisonment. The criminal penalties increase if the wrongful conduct involves false pretenses or the intent to sell, transfer or use identifiable health information for commercial advantage, personal gain or malicious harm.
Artificial intelligence presents risks and challenges that can impact our business including by posing security risks to our confidential information, proprietary information, and personal data.
Issues in the development and use of artificial intelligence, combined with an uncertain regulatory environment, may result in reputational harm, liability, or other adverse consequences to our business operations. As with many technological innovations, artificial intelligence presents risks and challenges that could impact our business. Our vendors may incorporate generative artificial intelligence tools into their offerings without disclosing this use to us, and the providers of these generative artificial intelligence tools may not meet existing or rapidly evolving regulatory or industry standards with respect to privacy and data protection and may inhibit our or our vendors’ ability to maintain an adequate level of service and experience. If we, our vendors, or our third-party partners experience an actual or perceived breach or privacy or security incident because of the use of generative artificial intelligence, we may lose valuable intellectual property and confidential information and our reputation and the public perception of the effectiveness of our security measures could be harmed. Further, bad actors around the world use increasingly sophisticated methods, including the use of artificial intelligence, to engage in illegal activities involving the theft and misuse of personal information, confidential information, and intellectual property. Any of these outcomes could damage our reputation, result in the loss of valuable property and information, and adversely impact our business.
A pandemic, epidemic, or outbreak of an infectious disease, such as the COVID-19 pandemic, could materially and adversely affect our business.
Public health crises such as pandemics or similar outbreaks could adversely impact our business. Previously, our clinical trial operations were directly and indirectly adversely impacted by the COVID-19 pandemic. A new pandemic or a resurgence of the COVID-19 pandemic could have adverse economic impacts to us.
We will need to grow the size of our organization in the future, and we may experience difficulties in managing this growth.
As of March 1, 2024, we had 16 full-time employees. As our development and commercialization plans and strategies continue to develop, our need for additional managerial, operational, manufacturing, regulatory, sales, marketing, financial and other resources may increase. We will need to grow the size of our organization in order to support our continued development and potential commercialization of our product candidates to complement our management and employees currently in place and to support our future growth. Future growth would impose significant added responsibilities on members of management, including:
•managing our clinical trials effectively;
•identifying, recruiting, maintaining, motivating, integrating and retaining additional employees;
•managing our internal development efforts effectively while complying with our contractual obligations to licensors, licensees, contractors and other third parties;
•improving our managerial, development, operational, information technology, human resources and finance systems; and
•expanding our facilities.
If our operations expand, we will also need to manage additional relationships with various strategic partners, suppliers and other third parties. Our future financial performance and our ability to commercialize our product candidates and to compete effectively will depend, in part, on our ability to manage any future growth effectively, as well as our ability to develop a sales and marketing force when appropriate for our company. To that end, we must be able to manage our development efforts and preclinical studies and clinical trials effectively and hire, train and integrate additional management, research and development, manufacturing, administrative and sales and marketing personnel. The failure to accomplish any of these tasks could prevent us from successfully growing our company.
The requirements of being a public company may strain our resources, divert management’s attention and affect our ability to attract and retain qualified board members.
As a public company, we are subject to the reporting requirements of the Exchange Act, the Sarbanes-Oxley Act, the Dodd-Frank Act, the listing requirements of Nasdaq and other applicable securities rules and regulations. Compliance with these rules and regulations has increased, and will likely continue to increase, our legal and financial compliance costs, make some activities more difficult, time-consuming or costly, and place significant strain on our personnel, systems and resources. In addition, changing laws, regulations and standards relating to corporate governance and public disclosure are creating uncertainty for public companies, increasing legal and financial compliance costs and making some activities more time consuming. These laws, regulations and standards are subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time. This could result in continuing uncertainty regarding compliance matters, higher administrative expenses and a diversion of management’s time and attention. Further, if our compliance efforts differ from the activities intended by regulatory or governing bodies due to ambiguities related to practice, regulatory authorities may initiate legal proceedings against us and our business may be harmed. Being a public company that is subject to these rules and regulations also makes it more expensive for us to obtain and retain director and officer liability insurance, and we may in the future be required to accept reduced coverage or incur substantially higher costs to obtain or retain adequate coverage. These factors could also make it more difficult for us to attract and retain qualified members of our board of directors and qualified executive officers.
Our future success depends on our ability to retain our executive officers and to attract, retain and motivate qualified personnel.
We are highly dependent upon our personnel, including Dr. Angelos M. Stergiou M.D., Sc.D. h.c., our President and Chief Executive Officer, and member of our board of directors. Our employment agreement with Dr. Stergiou does not prevent him from terminating his employment with us at any time. The loss of Dr. Stergiou’s services could impede the achievement of our research, development and commercialization objectives. We have not obtained, do not own, nor are we the beneficiary of, key-person life insurance. We employ our executive officers, other than Dr. Stergiou, on an at-will basis and their employment can be terminated by them or us at any time, for any reason and without notice. The loss of any member of our senior management team or the inability to hire or retain experienced senior management personnel could compromise our ability to execute our business plan and harm our operating results.
In order to retain valuable employees at our company, in addition to salary and discretionary non-equity incentive plan compensation, we provide stock options and restricted stock units, or RSUs, that vest over time. The value to our employees of stock options and RSUs could be significantly affected by movements in our stock price that are beyond our control and may at any time be insufficient to counteract offers from other companies.
Our future growth and success depend not only on our ability to retain, manage and motivate our employees but also on our ability to recruit new employees which is key to our growth. We might not be able to attract or retain qualified management and other key personnel in the future due to the intense competition for qualified talent among biotechnology, pharmaceutical and other businesses. We could have difficulty attracting experienced personnel to our company and may be required to expend significant financial resources in our employment recruitment and retention efforts. Many pharmaceutical and biotechnology companies with whom we compete for qualified personnel have greater financial and other resources, different risk profiles and longer histories in the industry than we do.
Legislation or other changes in U.S. tax law could adversely affect our business and financial condition.
The rules dealing with U.S. federal, state and local income taxation are constantly under review by persons involved in the legislative process and by the Internal Revenue Service and the U.S. Treasury Department. Changes to tax laws (which changes may have retroactive application) could adversely affect us or holders of our common stock. In recent years, many changes have been made to applicable tax laws and changes are likely to continue to occur in the future.
For example, legislation enacted in 2017 informally titled, the Tax Cuts and Jobs Act, or the TCJA, made significant changes to corporate taxation, including the reduction of the corporate tax rate from a top marginal rate of 35% to a flat rate of 21%, the limitation of the tax deduction for net interest expense to 30% of adjusted taxable income (except for certain small businesses), the limitation of the deduction for net operating losses from taxable years beginning after December 31, 2017 to 80% of current year taxable income and the elimination of net operating loss carrybacks generated in taxable years ending after December 31, 2017 (though any such net operating losses may be carried forward indefinitely) and the modification or repeal of many business deductions and credits. In addition, on March 27, 2020, former President Trump signed into law the “Coronavirus Aid, Relief, and Economic Security Act” or the CARES Act, which included certain changes in tax law intended to stimulate the U.S. economy in light of the COVID-19 public health emergency, including providing temporary relief from certain aspects of the TCJA that had imposed limitations on the utilization of certain losses, interest expense deductions, and minimum tax credits and provided temporary deferral of certain payroll taxes.
It cannot be predicted whether, when, in what form or with what effective dates new tax laws may be enacted, or regulations and rulings may be enacted, promulgated or issued under existing or new tax laws, which could result in an increase in our or our shareholders’ tax liability or require changes in the manner in which we operate in order to minimize or mitigate any adverse effects of changes in tax law or in the interpretation thereof.
Our ability to use net operating losses to offset future taxable income may be subject to limitations.
As of December 31, 2023, we had federal and state net operating loss carryforwards of approximately $57.1 million and $3.6 million, respectively. Our NOLs generated in tax years ending on or prior to December 31, 2017 are only permitted to be carried forward for 20 years under applicable U.S. tax laws, and will begin to expire, if not utilized, beginning in 2027. These NOL carryforwards could expire unused and be unavailable to offset future income tax liabilities. Under the Tax Act, federal NOLs incurred in tax years ending after December 31, 2017 may be carried forward indefinitely, but the deductibility of such federal NOLs is limited. In addition, under Section 382 of the Internal Revenue Code of 1986, as amended, and certain corresponding provisions of state law, if a corporation undergoes an “ownership change,” which is generally defined as a greater than 50% change, by value, in the ownership of its equity over a three-year period, the corporation’s ability to use its pre-change NOL carryforwards and other pre-change tax attributes to offset its post-change income may be limited. The Merger constituted an ownership change and as such, our ability to use our NOL carryforwards is materially limited, which may harm our future operating results by effectively increasing our future tax obligations.
Risks RelatingRelated to Ownership of Our Common Stock
Our common
We will likely need to secure additional capital which may cause dilution to you and our existing stockholders, provide subsequent investors with rights and preference that are senior to yours, restrict our operations or require us to relinquish rights to our product candidates on unfavorable terms to us.
We will likely need to raise additional capital in the future. If we raise funds through the issuance of debt or equity, any debt securities or preferred stock trades at prices less than $1.00 which is the minimum bid price requirement under NASDAQ’s continued listing standards, as such our common stock may be subjectissued will have rights, preferences and privileges senior to delisting from the NASDAQ Capital Market.
The continued listing requirementsthose of the NASDAQ Capital Market require that the closing bid priceholders of our common stock not be less than $1.00 for 30 consecutive trading days. On March 14, 2017in the last reported sale priceevent of our common stock on the NASDAQ Capital Market was $0.55 per share and has been below the $1.00 closing bid price since February 8, 2017. If our trading price falls below $1.00 for 30 consecutive trading days or more, we may receive a notice from NASDAQ informing usliquidation. In such event, there is a possibility that weonce all senior claims are settled, there may be delisted unless our trading price is above $1.00 for more than 10 consecutive trading days. In accordance with NASDAQ Listing Rule 5810(c)(3)(A), we would have 180 calendar daysno assets remaining to regain compliance with the $1.00 minimum bid price requirement. We can regain compliance with the $1.00 minimum bid listing requirement if the closing bid price is at least $1.00 per share for a minimum of ten consecutive trading days during this initial 180-day compliance period. If compliance is not achieved within the 180-day period, NASDAQ would provide written notification to us that our common stock is subject to delisting. In the event that we fail to regain compliance with NASDAQ continued listing standards by the expiration of the applicable cure period or any extension period, NASDAQ will commence suspension and delisting procedures with respect to our common stock, which could impair the value of your investment.
On January 18, 2017, we received an inquiry from NASDAQ Listing Qualifications Department seeking information in connection with the subpoenas issuedpay out to the Company by the US Attorney’s Office for the Districtholders of New Jersey and the U.S. Attorney’s Office for the Southern District of Alabama. We responded to the inquiry on February 1, 2017. If we are not in compliance with the listing requirements under NASDAQ Listing Rule 5502(a)(2), we could be delisted by NASDAQ.
If our common stock is delisted from NASDAQ Capital Market in the future, such securities may be traded over-the-counter on the “pink sheets.” Such alternative market, however, is generally considered to be less efficient than, and not as broad as, NASDAQ. Accordingly, delisting of our common stock from NASDAQ could have a significant negative effect on the trading volume, liquidity and market price of our common stock. In addition, if we raise funds through the delistingissuance of additional equity, whether through private placements or additional public offerings, such an issuance would dilute our stockholders and, similar to some of our common stockpast financings, may contain terms that could adversely affectresult in additional further significant dilution in the future. Debt financing, if available, could include covenants limiting or restricting our ability to raisetake certain actions, such as incurring additional debt, making capital on terms acceptableexpenditures, entering into licensing arrangements, or declaring dividends, and may require us to us or at allgrant security interests in our assets, including our intellectual property and could reduce the number of investors willingfor our subsidiaries to hold or acquireguarantee our common stock.obligations.
The market price and trading volume of shares of our common stock may be volatile.
The market price of shares of our common stock has exhibited substantial volatility recently.volatility. Between January 1, 20163, 2023 and February 28, 2017,December 29, 2023, the saledaily closing price of shares of our common stock as reported on The NASDAQ Capital MarketNasdaq ranged from a low of $0.62$0.88 to a high of $49.80 as adjusted for the reverse stock split effected in November 2016.$3.86. The market price of shares of our common stock could continue to fluctuate significantly for many reasons, including the following factors:
•reports of the results of our clinical trials regarding the safety or efficacy of our product candidates and surrogate markers;
•announcements of regulatory developments or technological innovations by us or our competitors;
•announcements of business or strategic transactions or our success in finalizing such a transaction;
•announcements of legal or regulatory actions against us or any adverse outcome of any such actions;
•changes in our relationshiprelationships with our licensors, licensees and other strategic partners;
•low volume in the number of shares of our common stock traded on Nasdaq;
•our quarterly operating results;
•announcements of dilutive financing;
•announcements of additional potential reverse stock split;
•developments in patent or other technology ownership rights;
•additional funds may not be available on terms that are favorable to us and, in the case of equity financings, may result in dilution to our stockholders;
•government regulation of drug pricing; and
•general changes in the economy, the financial marketsmarket conditions and other factors unrelated to our operating performance or the pharmaceutical or biotechnology industries.operating performance of our competitors, including deteriorating market conditions due to investor concerns regarding inflation and hostilities between Russia and Ukraine and Israel and Hamas.
Factors beyond our control may also have an impact on the market price of shares of our common stock. For example, to the extent that other companies within our industry experience declines in their stock prices, the market price of shares of our common stock price may decline as well.
We are,Inadequate funding for the FDA, the SEC and other domestic and foreign government agencies could hinder their ability to hire and retain key leadership and other personnel, prevent new products and services from being developed or commercialized in a timely manner or otherwise prevent those agencies from performing normal business functions on which the futureoperation of our business may be, subject to legal or administrative actions thatrely, which could adversely affect our financial condition andnegatively impact our business.
On December 22, 2016, Galena Biopharma, Inc.
The ability of the FDA or foreign regulatory authorities to review and its former CEO reached an agreementapprove new products can be affected by a variety of factors, including government budget and funding levels, ability to hire and retain key personnel and accept the payment of user fees, and statutory, regulatory, and policy changes. Average review times at the agency have fluctuated in principle torecent years as a proposed settlement that would resolve an investigation by the staffresult. In addition, government funding of the SEC involving conduct in the period 2012-2014 regarding the commissioning of internet publications by outside promotional firms. Under the terms of the proposed settlement framework, Galena and the former CEO would consent to the entry of an administrative order requiringother government agencies on which our operations may rely, including those that wefund research and the former CEO cease and desist from any future violations of Sections 5(a), 5(b), 5(c), 17(a), and 17(b) of the Securities Act of 1933, as amended, and Section 10(b), 13(a), and 13(b)(2)(A) of the Securities Exchange Act of 1934, as amended, and various rules thereunder, without admitting or denying the findings in the order. Based upon the proposed settlement framework, the Company will make a $200,000 penalty payment. In addition to other remedies, the proposed settlement framework would require the former CEO to make a disgorgement and prejudgment interest payment as well as a penalty payment to the Commission. To address the issues raised by the SEC staff’s investigation, in addition to previous governance enhancements we have implemented, we have voluntarily undertaken to implement a number of remedial actions relating to securities offerings and our interactions with investor relations and public relations firms. The proposed settlementdevelopment activities is subject to approval by the Commission and would acknowledge our cooperation in the investigation and confirm our voluntary undertaking to continue that cooperation. If the Commission does not approve the settlement, we may need to enter into further discussions with the SEC staff to resolve the investigated matters on different terms and conditions. As a result, there can be no assurance as to the final terms of any resolution including its financial impact or any future adjustment to the financial statements. A special committee of the Board of Directors has determined in response to an indemnification claim by the former CEO that we are required under Delaware law to indemnify our former CEO for the disgorgement and prejudgment interest payment of approximately $750,000 that he would be required to pay if and when the settlement is approved by the Commission. Any penalty payment that the former CEO will be required to make in connection with this matter ($600,000 under the proposed settlement framework) will be the responsibility of the former CEO. In the event the Commission does approve the proposed settlement, the Company may not have available certain exemptions and safe harbor protections under the securities laws.
On February 13, 2017, a putative shareholder securities class action complaint was filed in the U.S. District Court for the District of New Jersey entitled, Miller v. Galena Biopharma, Inc., et al. On February 15, 2017, a putative shareholder securities class action complaint was filed in the U.S. District Court for the District of New Jersey entitled, Kattuah v Galena Biopharma, Inc., et al. Within the time allowed under the federal rules and statutes, the Company and the other defendants, former and current officers, will respond to the complaints through an appropriate pleading or motion.
A federal investigation of two of the high-prescribing physicians for Abstral (former commercial product) has resulted in the criminal prosecution of the two physicians for alleged violations of the federal False Claims Act and other federal statutes. The criminal trial began in January 2017 and is ongoing. We have received a trial subpoena for documents in connection with that investigation and we have been in contact with the U.S. Attorney’s Office for the Southern District of Alabama,political process, which is handling the criminal trial,inherently fluid and are cooperating in the production of documents. On April 28, 2016, a second superseding indictment was filed in the criminal case, which added additional information about the defendant physicians and provided information regarding the facts and circumstances involving a rebate agreement between the Company and the defendant physicians’ pharmacy as well as their ownership of our stock. The criminal trial, which began on January 4, 2017, concluded with a jury verdict on February 23, 2017 finding these physicians guilty on 19 of 20 counts; sentencing is scheduled for May 2017. At the end of the SDAL case, SDAL dismissed count 18 of the indictment charging that the physicians conspired, through the C&R Pharmacy, to receive illegal kickbacks in exchange for prescribing Abstral. Though certain former employees received trial subpoenas to appearunpredictable.
Disruptions at the trial and provide oral testimony, only one former employee testified at the trial. We agreed to reimburse those former employees’ attorney’s fees. To our knowledge, we were not a target or subject of that investigation.
There also have been federal and state investigations of a company that has a product that competes with Abstral in the same therapeutic class, and we have learned that the FDA and other governmental agencies are investigatingmay also slow the time necessary for new drugs to be reviewed and/or approved by necessary government agencies, which would adversely affect our Abstral promotion practices. On December 16, 2015, we received a subpoena issued bybusiness. For example, over the last several years the U.S. Attorney’s Office forgovernment has shut down several times and certain regulatory agencies, such as the District of New Jersey requestingFDA and the production ofSEC, have had to furlough critical FDA, SEC and other government employees and stop critical activities. If a broad range of documents pertainingprolonged government shutdown were to our marketing and promotional practices for Abstral. We have been in contact withoccur, it could significantly impact the U.S. Attorney’s Office for the District of New Jersey and are cooperating in the productionability of the requested documents. We have comeFDA to understand that the investigation being undertaken by the U.S. Attorney’s Office for the District of New Jerseytimely review and Department of Justice is a criminal investigation in addition to a civil investigation that could ultimately involve the company as well as one or more former employees. Pursuant to the Company’s charter, we are currently reimbursing any former employees’ attorney’s fees with respect to the investigation. We are cooperating with the civil and criminal investigation and throughprocess our outside counsel we have recently begun preliminary discussions with the government aimed at the ultimate resolution of the investigation regarding the Company.
We may be subject to legal or administrative actions as a result of these matters, or the impact of such matters. If we are found to be in violation of the False Claims Act, Anti-Kickback Statute, Patient Protection and Affordable Care Act, or any other applicable state or any federal fraud and abuse laws, we may be subject to penalties, such as civil and criminal penalties, damages, fines, or an administrative action of exclusion from government health care reimbursement programs. We can make no assurances as to the time or resources that will need to be devoted to these matters or their outcome, or the impact, if any, that these matters or any resulting legal or administrative proceedings may have on our business or financial condition.
Litigation is inherently uncertain. We have incurred and may continue to incur substantial unreimbursed legal fees and other expenses in connection with these or other legal and regulatory proceedings that may not qualify for coverage under, or may exceed the limits of, our applicable directors and officers liability insurance policies andsubmissions, which could have a material adverse effect on our financial condition, liquidity, and results of operations. These matters also may distract the time and attention of our officers and directors or divert our other resources away from our ongoing development programs. An unfavorable outcome in any of these matters could damage our business and reputation or resultcould impact our ability to access the public markets and obtain necessary capital in additional claims or proceedings against us.order to properly capitalize and continue our operations.
Future sales of substantial amounts of our common stock, or the possibility that such sales could occur, could adversely affect the market price of our common stock.
Future sales in the public market of shares of our common stock, including shares referred to in the foregoing risk factors or shares issued upon exercise of our outstanding stock options or warrants, or the perception by the market that these sales could occur, could lower the market price of our common stock or make it difficult for us to raise additional capital.
As of December 31, 2016,2023, we had reserved for issuance 560,92515,853,773 shares of our common stock issuable upon the exercise of outstanding warrants at a weighted-average exercise price of $1.95 per share, 1,606,803 shares of our common stock issuable upon the exercise of outstanding stock options at a weighted-average exercise price of $41.50$5.92 per share, and 2,569,751338,141 shares of our common stock issuable upon the exercisevesting of outstanding warrants atrestricted stock units with a weighted-average exercise priceweighted average grant date fair value of $29.12$2.99 per share. Upon exercise of these options and warrants,or conversion, the underlying shares, similar to those issued as the settlement payment, may be resold into the public market. In the case of outstanding options and warrantssecurities that have exercise or conversion prices that are below the market price of our common stock from time to time, our stockholders would experience dilution upon the exercise or conversion of these options.securities.
Our outstanding warrants may result in dilution
Certain of our securityholders have registration rights and they can require us, subject to our stockholders.
Our outstanding April 2011 warrantscertain limitations, to purchase a total of 12,900 shares of common stock as of December 31, 2016 at a current exerciseregister their securities for resale and to maintain such registration. Any such resales into the public market could place downward pressure on the price of $1.00 per share contain so-called full-ratchet anti-dilution provisions. Our outstanding December 2012 warrants to purchase 151,565 shares of common stock as of December 2016 with a current exercise price of $10.32 per share contain so-called weighted-average anti-dilution provisions. These anti-dilution provisions may be triggered by the issuance of the shares being offered hereby or upon any future issuance by us of shares of our common stock or common stock equivalents at a price per share below the then-exercise price of the warrants, subject to some exceptions. The share and per share amounts described above are presented on a post-split basis that was effected November 11, 2016.stock.
To the extent that these anti-dilution provisions are triggered in the future, we would be required to reduce the exercise price of all of the warrants on either a full-ratchet or weighted-average basis, which would have a dilutive effect on our stockholders.
We have issued and may issue additional preferred stock in the future, and the terms of the preferred stock may reduce the value of our common stock.
We are authorized to issue up to 5 million5,000,000 shares of preferred stock in one or more series. Our Boardboard of Directorsdirectors may determine the terms of future preferred stock offerings without further action by our stockholders. If we issue shares of preferred stock, it could affect stockholder rights or reduce the market value of our outstanding common stock. In particular, specific rights granted to future holders of preferred stock may include voting rights, preferences as to dividends and liquidation, conversion and redemption rights, sinking fund provisions, and restrictions on our ability to merge with or sell our assets to a third party.
We have settled in the past and may in the future settle legal claims through the issuance of freely tradable shares of our common stock, which results in dilution to holders of our common stock and may adversely affect the market price of our common stock.
We have settled in the past and may in the future settle legal claims through the issuance of freely tradable shares of our common stock. We may issue additional shares of common stock as settlement payments in the future. Payment of these amounts in our common stock could cause significant dilution to our stockholders, and the amount of that dilution will vary depending on the price of our common stock at the time of the payment. In addition, the issuance of such a significant number of shares of our common stock may cause a decrease in the trading price of our common stock.
Anti-takeover provisions of our amendedAmended and restated certificateRestated Certificate of incorporationIncorporation and amendedour Amended and restated bylawsRestated Bylaws and provisions of Delaware law could delay or prevent a change of control.
Anti-takeover provisions of our amendedAmended and restated certificateRestated Certificate of incorporationIncorporation and amendedour Amended and restated bylawsRestated Bylaws may discourage, delay or prevent a merger or other change of control that stockholders may consider favorable or may impede the ability of the holders of our common stock to change our management and may be constrained by other contractual agreements with third parties. These provisions of our amendedAmended and restated certificateRestated Certificate of incorporationIncorporation and amendedour Amended and restated bylaws,Restated Bylaws, among other things:
•divide our boardBoard of directorsDirectors into three classes, with members of each class to be elected for staggered three-year terms;
•limit the right of security holderssecurityholders to remove directors;
•prohibit stockholders from acting by written consent;
•regulate how stockholders may present proposals or nominate directors for election at annual meetings of stockholders; and
•authorize our board of directorsBoard to issue preferred stock in one or more series, without stockholder approval.
In addition, Section 203 of the Delaware General Corporation Law provides that, subject to limited exceptions, persons that acquire, or are affiliated with a person that acquires, more than 15% of the outstanding voting stock of a Delaware corporation such as our company shall not engage in any business combination with that corporation, including by merger, consolidation or acquisitions of additional shares for a three-year period following the date on which that person or itsour affiliate crosses the 15% stock ownership threshold. Section 203 could operate to delay or prevent a change of control of us.
If our company.common stock becomes subject to the penny stock rules, it may be more difficult to sell our common stock.
The SEC has adopted rules that regulate broker-dealer practices in connection with transactions in penny stocks. Penny stocks are generally equity securities with a price of less than $5.00 (other than securities registered on certain national securities exchanges or authorized for quotation on certain automated quotation systems, provided that current price and volume information with respect to transactions in such securities is provided by the exchange or system). The OTC Bulletin Board does not meet such requirements and if the price of our common stock is less than $5.00 and our common stock is no longer listed on a national securities exchange such as Nasdaq, our stock may be deemed a penny stock. The penny stock rules require a broker-dealer, at least two business days prior to a transaction in a penny stock not otherwise exempt from those rules, to deliver to the customer a standardized risk disclosure document containing specified information and to obtain from the customer a signed and date acknowledgment of receipt of that document. In addition, the penny stock rules require that prior to effecting any transaction in a penny stock not otherwise exempt from those rules, a broker-dealer must make a special written determination that the penny stock is a suitable investment for the purchaser and receive: (i) the purchaser’s written acknowledgment of the receipt of a risk disclosure statement; (ii) a written agreement to transactions involving penny stocks; and (iii) a signed and dated copy of a written suitability statement. These disclosure requirements may have the effect of reducing the trading activity in the secondary market for our common stock, and therefore stockholders may have difficulty selling their shares.
Our failure to meet the continued listing requirements of The Nasdaq Capital Market could result in a delisting of our common stock.
Our shares of common stock are currently listed on The Nasdaq Capital Market. If we fail to satisfy the continued listing requirements of Nasdaq, such as the corporate governance requirements, minimum bid price requirement or the minimum stockholder's equity requirement, The Nasdaq Stock Market LLC may take steps to delist our common stock. A delisting of our common stock from The Nasdaq Capital Market could materially reduce the liquidity of our common stock and result in a corresponding material reduction in the price of our common stock. In addition, delisting could harm our ability to raise capital through alternative financing sources on terms acceptable to us, or at all, and may result in the potential loss of confidence by investors, suppliers, customers and employees and fewer business development opportunities.
On December 6, 2023, we received a letter from Nasdaq notifying us that we no longer met Nasdaq's requirements for continued listing on The Nasdaq Capital Market under Nasdaq Listing Rule 5550(b)(2), or the MVLS Rule, because, for a period of 30 consecutive business days, the market value of our common stock, calculated based upon the most recent total shares outstanding multiplied by the closing bid price per share, had not maintained a minimum of $35.0 million.
In accordance with Nasdaq Listing Rule 5810(c)(3)(C), we were provided a period of 180 calendar days, or until June 3, 2024, in which to regain compliance with the MVLS Rule. To regain compliance, the market value of our common stock must meet or exceed $35.0 million for a minimum of 10 consecutive business days during the 180-day compliance period. If we have not regained compliance with the MVLS Rule by June 3, 2024, Nasdaq will provide notice to us that our securities will be subject to delisting, in which case we may appeal the delisting determination to a Nasdaq Hearings Panel.
On March 5, 2024, we received a letter from Nasdaq stating that we have regained compliance under the MVLS Rule by maintaining a market value of our common stock of greater than $35 million for 10 consecutive business, and that the matter is now closed.
On February 14, 2024, we received a letter from Nasdaq notifying us that we no longer met Nasdaq's requirements for continued listing on The Nasdaq Capital Market under Nasdaq Listing Rule 5550(a)(2), or the Minimum Bid Price Requirement, because, for the preceding 30 consecutive business days, our common stock did not maintain a minimum closing bid price of $1.00 per share.
In accordance with Nasdaq Listing Rule 5810(c)(3)(A), we were provided a period of 180 calendar days, or until August 12, 2024, to regain compliance with the Minimum Bid Price Requirement. Compliance can be achieved automatically and without further action if the closing bid price of our common stock is at or above $1.00 for a minimum of 10 consecutive business days at any time during the 180-day compliance period, in which case Nasdaq
will notify us of our compliance and the matter will be closed. If, however, we do not achieve compliance with the Minimum Bid Price Requirement by August 12, 2024, we may be eligible for additional time to comply. In order to be eligible for such additional time, we will be required to meet the continued listing requirement for market
value of publicly held shares and all other initial listing standards for The Nasdaq Capital Market, with the exception of the Minimum Bid Price Requirement, and must notify Nasdaq in writing of our intention to cure the deficiency during the second compliance period, by effecting a reverse stock split, if necessary.
On March 11, 2024, we received a letter from Nasdaq stating that we have regained compliance under the Minimum Bid Price Requirement by maintaining a minimum closing bid price of our common stock of $1.00 per share for 10 consecutive business days, from February 26, 2024 to March 8, 2024, and that the matter is now closed.
Our common stock currently remains listed on The Nasdaq Capital Market under the symbol SLS.
We have never declared or paid cash dividends on our capitalcommon stock and we do not anticipate paying cash dividends on our common stock in the foreseeable future.
Our business requires significant funding. We currently plan to invest all available funds and future earnings in the development and growth of our business and do not anticipate paying any cash dividends on our common stock in the foreseeable future, and are prohibited by the terms of our outstanding indebtedness from paying dividends on any common stock, except with the prior consent of our lenders.future. As a result, capital appreciation, if any, of our common stock will be our stockholders’ sole source of potential gain for the foreseeable future.
The terms
We are prohibited by the terms of our outstanding indebtedness from disposing of any of our business or property, except with the consent of our lenders or if we were to prepay the outstanding indebtedness and related fees in accordance with the loan security agreement. Our outstanding indebtedness may inhibit potential acquirers or other interested parties from seeking to acquire all or a part of our business or assets, and there is no assurance that our lenders would consent to any proposed future transaction that might be beneficial to our stockholders.
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
ITEM 1C. CYBERSECURITY
We have received no unresolved written comments fromrecognize the staffcritical importance of maintaining the trust and confidence of business partners, such as CROs and CMOs, clinical trial investigators, patients and employees toward our business and are committed to protecting the confidentiality, integrity and availability of our business operations and systems. Our board of directors is actively involved in oversight of our risk management activities, and cybersecurity represents an important element of our overall approach to risk management. In general, we seek to address cybersecurity risks through a comprehensive, cross-functional approach that is focused on preserving the confidentiality, security and availability of the SECinformation that we collect and store by identifying, preventing and mitigating cybersecurity threats and effectively responding to cybersecurity incidents when they occur.
Cybersecurity Risk Management and Strategy; Effect of Risk
We face risks related to cybersecurity, such as unauthorized access, cybersecurity attacks, and other security incidents, including perpetration by hackers and unintentional damage or disruption to hardware and software systems, loss of data, and misappropriation of confidential information. To identify and assess material risks from cybersecurity threats, we, together with our contracted third-party cybersecurity advisors, maintain a comprehensive cybersecurity program to ensure our systems are effective and prepared for information security risks, including regular oversight of our programs for security monitoring of internal and external threats to ensure the confidentiality and integrity of our information assets. We consider risks from cybersecurity threats alongside other company risks as part of our overall risk assessment process. As discussed in more detail under “Cybersecurity Governance” below, our audit committee provides oversight of our cybersecurity risk management and strategy processes, which are led by management.
We, with assistance from our contracted third-party cybersecurity advisors, identify our cybersecurity threat risks by comparing our processes to standards set by the National Institute of Standards and Technology, or NIST. To provide for the availability of critical data and systems, maintain regulatory compliance, manage our material risks from cybersecurity threats, and protect against and respond to cybersecurity incidents, we undertake the following activities:
•monitor emerging data protection laws and implement changes to our processes that are designed to comply with such laws;
•through our policies, practices, and contracts (as applicable), require employees, as well as third parties that provide services on our behalf, to treat confidential information and data with care;
•employ technical safeguards that are designed to protect our information systems from cybersecurity threats, including firewalls, intrusion prevention and detection systems, anti-malware functionality and access controls;
•provide regular, mandatory training for our employees and contractors regarding cybersecurity threats as a means to equip them with effective tools to address cybersecurity threats, and to communicate our evolving information security policies, standards, processes and practices;
•conduct regular phishing email simulations for all employees and contractors with access to our email systems to enhance awareness and responsiveness to possible threats;
•conduct cybersecurity management and incident training for employees involved in our systems and processes that handle sensitive data;
•leverage the NIST incident handling framework to help us identify, protect, detect, respond and recover when there is a potential cybersecurity incident; and
•carry information security risk insurance that provides protection against the potential losses arising from a cybersecurity incident.
Our processes also address cybersecurity threat risks associated with our selection and oversight of third-party service providers, including our suppliers and manufacturers or those who have access to patient and employee data or our systems. We generally require those third parties that could introduce significant cybersecurity risk to us to agree by contract to manage their cybersecurity risks in specified ways.
We describe whether and how risks from identified cybersecurity threats, including as a result of any previous cybersecurity incidents, have materially affected or are reasonably likely to materially affect us, including our business strategy, results of operations, or financial condition, under the heading Significant disruptions of information technology systems, computer system failures or cybersecurity incidents could adversely affect our business, which disclosures are incorporated by reference herein.
In the last three fiscal years, we have not experienced any material cybersecurity incidents.
Cybersecurity Governance; Management
Cybersecurity is an important part of our risk management processes and an area of focus for our Board of Directors and management. Management is responsible for the operational oversight of company-wide cybersecurity strategy, policy, and standards across relevant departments to assess and help prepare us to address cybersecurity risks.
The Audit Committee of the Board of Directors, or the Audit Committee, provides direct oversight over cybersecurity risk and periodically updates our Board of Directors on such matters. The Audit Committee receives periodic updates from management regarding cybersecurity matters, and is notified between such updates regarding any significant new cybersecurity threats or current reports.incidents.
Our cybersecurity risk management and strategy processes, which are discussed in greater detail above, are led by our Chief Financial Officer and Vice President, Associate General Counsel and Head of Compliance, with the assistance of our contracted third-party cybersecurity advisors. These management team members are informed about and monitor the prevention, mitigation, detection, and remediation of cybersecurity incidents through their management of, and participation in, the cybersecurity risk management and strategy processes described above, including incident response processes. As discussed above, these management team members periodically report to the Audit Committee about cybersecurity threat risks, among other cybersecurity related matters.
ITEM 2. PROPERTIES
On July 10, 2015, we entered into aWe lease with Legacy III SR Crow Canyon, LLCour headquarters in New York, New York. The lease covers approximately 8,455 square feet of office space, which includes additional space beginning on February 22, 2022, and expires in September 2025. We believe that our facility is adequate for our facility located at 2000 Crow Canyon Place, Suite 380, San Ramon, CA 94583. The facility is approximately 8,100 square feet and is used for our general and administrative offices. The monthly rent is approximately $20,000.current needs.
ITEM 3. LEGAL PROCEEDINGS
On June 24, 2016, the U.S. District Court for the District of OregonIn December 2020, we entered a final order and judgment in into 3D Medicines Agreement. In re Galena Biopharma, Inc. Derivative Litigation, granting final approval to the settlement awarding attorney’s fees of $4.5 million plus costs, which was paid by our insurance carriers. The settlement included a payment of $15 million in cash by our insurance carriers, whichNovember 2022, we used to fund a portion of the class action settlement, and cancellation of 1,200,000 outstanding director stock options. The settlement also requiredannounced that we adopt and implement certain corporate governance measures. The settlement did not include any admission of wrongdoing or liability on the part of us or the individual defendants and included a full release of us and the current and former officers and directors in connectionhad agreed with the allegations made3D Medicines for 3D Medicines to participate in the consolidated federal derivative actions and state court derivative actions.REGAL study through the inclusion of approximately 20 patients from mainland China.
On June 24, 2016, the U.S. District Court for the District of Oregon entered a final order and partial judgment in In re Galena Biopharma, Inc. Securities Litigation, granting final approval of the settlement awarding attorney’s fees of $4.5 million plus costs, which was paid out of the settlement funds. The settlement agreement provided for a payment of $20 million to the class and the dismissal of all claims against us and our current and former officers and directors in connection with the consolidated federal securities class actions. Of the $20 million settlement payment to the class, $16.7 million was paid by our insurance carriers and $2.3 million in cash was paid by us on July 1, 2016, along with $1 million in shares of our common stock (24,002 shares) issued by us on July 6, 2016. We are responsible for defense costs and any settlements or judgments incurred for any related opt-out lawsuits.
In July 2016, we resolved claims brought by shareholders that relate to the securities litigation mentioned above in one case for $150,000 plus $150,000 in shares (14,563 shares) of our common stock, and in another case for $1.5 million in shares of our common stock (168,337 shares). The shares issued in connectionaccordance with such settlements are included in the secondary offering filed on July 25, 2016. The settlements did not include any admission of wrongdoing or liability on the part of us or any of the current or former directors and officers and included a full release of us and the current and former directors and officers in connection with the allegations made. We are not aware of any other claims made by shareholders who have opted out of the securities litigation.
On October 13, 2016, we filed a complaint in the Circuit Court for the County of Multnomah for the State of Oregon against Aon Risk Insurance Services West, Inc. where we are seeking attorney's fees, costs and expenses incurred by us related to our coverage dispute with a certain insurer and for amounts we were required to contribute to the settlements of In re Galena Biopharma, Inc. Derivative Litigation and In re Galena Biopharma, Inc. Securities Litigation as a direct result of certain insurer's failure to pay its full policy limits of liability and other relief. We are currently engaged in written discovery.
On December 22, 2016, Galena and its former CEO during the period March 2011 to August 2014 reached an agreement in principle to a proposed settlement that would resolve an investigation by the staff of the Securities and Exchange Commission (SEC) involving conduct in the period 2012-2014 regarding the commissioning of internet publications by outside promotional firms. Under the terms of the proposed settlement framework, Galena3D Medicines Agreement and the former CEOSide Letter, we had expected that 3D Medicines would consentbegin enrolling patients in mainland China in the REGAL study in the second half of 2023 and subsequently make two development milestone payments totaling $13.0 million. Patients were enrolled in the REGAL study in Taiwan, which is part of the 3DMed Territory, prior to the entrysecond half of an administrative order requiring that2023.
On December 20, 2023, we commenced a binding arbitration proceeding against 3D Medicines, administered by the Hong Kong International Arbitration Centre and governed by New York State law as per the former CEO cease3D Medicines
Agreement. The arbitration proceeding involves, among other things, the trigger and desist from any future violations of Sections 5(a), 5(b), 5(c), 17(a), and 17(b)payment of the Securities Act of 1933, as amended, and Section 10(b), 13(a), and 13(b)(2)(A) of the Securities Exchange Act of 1934, as amended, and various rules thereunder, without admitting or denying the findings in the order. Based upon the proposed settlement framework, the Company will make a $200,000 penalty payment. In additionrelevant milestone payments due to other remedies, the proposed settlement framework would require the former CEO to make a disgorgement and prejudgment interest paymentus as well as a penalty payment3D Medicines’ failure to the Commission. To address the issues raised by the SEC staff’s investigation, in additionuse commercially reasonable best efforts to previous governance enhancements we have implemented, we have voluntarily undertaken to implement a number of remedial actions relating to securities offerings and our interactions with investor relations and public relations firms. The proposed settlement is subject to approval by the Commission and would acknowledge our cooperationdevelop GPS in the investigation3DMed Territory, and confirm our voluntary undertakingparticularly in mainland China.
We have engaged an international law firm with expertise in mainland China to continue that cooperation. If the Commission does not approve the settlement, we may need to enter into further discussionsassist us with the SEC staffarbitration proceeding. While we are unable at this time to resolvepredict with certainty the investigated matters on different terms and conditions. As a result, there can be no assurance as tooutcome of the final termsarbitration proceeding, or the timing of the receipt of any resolution including its financial impact or any future adjustment to the financial statements. A special committee of the Board of Directors has determined in response to an indemnification claim by the former CEO that we are required under Delaware law to indemnify our former CEO for the disgorgementmilestone payments and prejudgment interest payment of approximately $750,000 that he would be required to pay if and when the settlementother damages it is approved by the Commission. Any penalty payment that the former CEO will be required to make in connection with this matter ($600,000 under the proposed settlement framework) will be the responsibility of the former CEO.
On February 13, 2017, a putative shareholder securities class action complaint was filedseeking in the U.S. District Court for the District of New Jersey entitled, Miller v. Galena Biopharma, Inc., et al. On February 15, 2017, a putative shareholder securities class action complaint was filed in the U.S. District Court for the District of New Jersey entitled, Kattuah v Galena Biopharma, Inc., et al. Within the time allowed under the federal rules and statutes, the Company and the other defendants, former and current officers, will respond to the complaints through an appropriate pleading or motion.arbitration proceeding, if at all, we believe that our claims are meritorious.
A federal investigation of two of the high-prescribing physicians for Abstral (former commercial product) has resulted in the criminal prosecution of the two physicians for alleged violations of the federal False Claims Act and other federal statutes. We received a trial subpoena for documents in connection with that investigation and we have been in contact with the U.S. Attorney’s Office for the Southern District of Alabama (SDAL), which is handling the criminal trial, and are cooperating in the production of documents. On April 28, 2016, a second superseding indictment was filed in the criminal case, which added additional information about the defendant physicians and provided information regarding the facts and circumstances involving a rebate agreement between the Company and the defendant physicians’ pharmacy as well as their ownership of our stock. The criminal trial, which began on January 4, 2017, concluded with a jury verdict on February 23, 2017 finding these physicians guilty on 19 of 20 counts; sentencing is scheduled for May 2017. At the end of the SDAL case, SDAL dismissed count 18 of the indictment charging that the physicians conspired, through the C&R Pharmacy, to receive illegal kickbacks in exchange for prescribing Abstral. Though certain former employees received trial subpoenas to appear at the trial and provide oral testimony, only one former employee testified at the trial. We agreed to reimburse those former employees’ attorney’s fees. To our knowledge, we were not a target or subject of that investigation.
There also have been federal and state investigations of a company that has a product that competes with Abstral in the same therapeutic class, and we have learned that the FDA and other governmental agencies are investigating our Abstral promotion practices. On December 16, 2015, we received a subpoena issued by the U.S. Attorney’s Office for the District of New Jersey requesting the production of a broad range of documents pertaining to our marketing and promotional practices for Abstral, the commercial product we sold in the fourth quarter of 2015. We have been in contact with the U.S. Attorney’s Office for the District of New Jersey and Department of Justice, and we have come understand that the investigation being undertaken by the U.S. Attorney’s Office for the District of New Jersey and Department of Justice is a criminal investigation in addition to a civil investigation that could ultimately involve the Company as well as one or more former employees. Pursuant to the Company’s charter, we are currently reimbursing certain former employees’ attorney’s fees with respect to the investigation. We are cooperating with the civil and criminal investigation, and through our outside counsel we have recently begun preliminary discussions with the government aimed at the ultimate resolution of the investigation regarding the Company.
ITEM 4. Mine Safety DisclosuresMINE SAFETY DISCLOSURES
Not applicable.
PART II
ITEM 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information
Our common stock is listed on The NASDAQNasdaq Capital Market under the symbol “GALE ” The following table shows the high and low per-share sale prices of our common stock for the periods indicated:SLS.
|
| | | | | | | |
| | High | | Low |
| 2015 | | | |
| First Quarter | $ | 42.40 |
| | $ | 26.60 |
|
| Second Quarter | 47.80 |
| | 25.40 |
|
| Third Quarter | 38.40 |
| | 22.00 |
|
| Fourth Quarter | 36.60 |
| | 27.40 |
|
| 2016 | | | |
| First Quarter | $ | 30.00 |
| | $ | 11.80 |
|
| Second Quarter | 49.80 |
| | 5.60 |
|
| Third Quarter | 15.40 |
| | 6.20 |
|
| Fourth Quarter | 7.00 |
| | 1.84 |
|
Holders
As of February 28, 2017,March 27, 2024, there were approximately 18935 holders of record of our common stock. Because many of our shares are held by brokers and other institutions on behalf of stockholders, we are unable to estimate the total number of individual stockholders represented by these holders of record.
Dividends
We have never paid any cash dividends on our common stock and do not anticipate paying any cash dividends on our common stock in the foreseeable future. We expect to retain future earnings, if any, for use in our development activities and the operation of our business. The payment of any future dividends will be subject to the discretion of our Board of Directors and will depend, among other things, upon our results of operations, financial condition, cash requirements, prospects and other factors that our boardBoard of directorsDirectors may deem relevant. Additionally, ourOur ability to pay future dividends may be restricted by the terms of any debt financing.future securities we may issue.
Equity Compensation Plan
The following table sets forth certain information as of December 31, 2016, regarding securities authorized for issuance under our equity compensation plans:
|
| | | | | | | | | |
| | (a) | | (b) | | Number of Securities Remaining Available for Issuance Under Equity Compensation Plans (Excluding Securities Reflected in Column (a)) |
| Plan Category | Number of Securities to be Issued Upon Exercise of Outstanding Options, Warrants and Rights | | Weighted- Average Exercise Price of Outstanding Options, Warrants and Rights | |
| Equity compensation plans approved by our security holders: | | | | | |
| Amended and Restated 2016 Incentive Plan | 560,925 |
| | $ | 41.50 |
| | 500,692 |
|
| Equity compensation plans not approved by our security holders: | | | | | |
| Employee Stock Purchase Plan | NA |
| | NA |
| | 20,930 |
|
Outstanding warrants (1) | 124,109 |
| | $ | 20.15 |
| | — |
|
| Total | 685,034 |
| | $ | 37.63 |
| | 521,622 |
|
| |
(1)
| The warrants shown were issued in discrete transactions from time to time as compensation for services rendered by consultants, advisers or other third parties, and do not include warrants sold in private placement or public offering transactions. The material terms of such warrants were determined based upon arm’s-length negotiations with the services providers. The warrant exercise prices approximated the market price of our common stock at or about the date of grant, and the warrant terms range from three to ten years from the grant date. |
Performance Graph
The following graph shows the value of an investment of $100 on December 31, 2011 in each of Galena Biopharma, Inc. common stock, the NASDAQ Composite Index, the NASDAQ Biotechnology Index, and Standard & Poor's Index (S&P 500). All values assume reinvestment of pretax value of dividends and are calculated as of December 31 of each year. The historical stock price performance of our common stock shown in the performance graph is not necessarily indicative of future stock performance.
COMPARISON OF FIVE YEAR CUMULATIVE RETURNS
|
| | | | | | | | | | | | | | | | | | | | | | | |
| | As of December 31, |
| | 2011 | | 2012 | | 2013 | | 2014 | | 2015 | | 2016 |
Galena Biopharma, Inc.(1) | $ | 100.00 |
| | $ | 325.53 |
| | $ | 1,055.32 |
| | $ | 321.28 |
| | $ | 312.77 |
| | $ | 20.64 |
|
| S&P 500 | 100.00 |
| | 115.88 |
| | 153.01 |
| | 173.68 |
| | 176.07 |
| | 196.78 |
|
| NASDAQ Composite | 100.00 |
| | 117.70 |
| | 164.65 |
| | 188.87 |
| | 202.25 |
| | 220.13 |
|
| NASDAQ Biotechnology | 100.00 |
| | 132.72 |
| | 220.22 |
| | 202.25 |
| | 330.71 |
| | 260.12 |
|
(1) The cumulative return depicted above for Galena Biopharma, Inc. does not include the value of our former subsidiary, RXi Pharmaceuticals Corporation ("RXi"), which we spun off to our stockholders in April 2012.
Recent Sales of Unregistered Securities
During the period covered by this annual report,Annual Report on Form 10-K, there were no sales by us of unregistered securities that were not previously reported by us in a Quarterly Report on Form 10-Q or Current Report on Form 8-K.
Purchases of Equity SecuritiesITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
Further analysis of the changes and trends in our operating results are discussed below.
The following table summarizes our cash flows from operating, investing, and financing activities for the yearyears ended December 31, 20162023 and 2015 ($ in2022 (in thousands):
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
The primary objective of our investment activities is to preserve capital. We do not utilize hedging contracts or similar instruments.
In addition, we are exposed to foreign currency exchange rate fluctuations relating to payments we make to certain vendors and suppliers and license partners using foreign currencies. We do not hedge against foreign currency risks. Consequently, changes in exchange rates could adversely affect our operating results and stock price. Such losses have not been significant to date.