UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
☒ Annual Report under Section 13 or 15(d) of the Securities Exchange Act of 1934
For the fiscal year ended December 31, 20212023
or
☐Transitional Report under Section 13 or 15(d) of the Securities Exchange Act of 1934
Commission File Number 001-39531
Processa Pharmaceuticals, Inc.
(Exact name of registrant as specified in its charter)
| Delaware | 45-1539785 | |
(State or other jurisdiction of incorporation or organization) | (IRS Employer Identification No.) |
7380 Coca Cola Drive, Suite 106,
Hanover, Maryland 21076
((443)443) 776-3133
Securities registered pursuant to Section 12(b) of the Exchange Act:
| Title of Each Class | Trading Symbol(s) | Name of each exchange on which registered | ||
| Common Stock, $0.0001 par value per share | PCSA | The Nasdaq Stock Market LLC |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or emerging growth company. See definition of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ☐ | Accelerated filer | ☐ |
| Non-accelerated filer | ☐ | Smaller reporting company | ☒ |
| Emerging growth company | ☐ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its managements’ assessment of the effectiveness of its internal controls over financial reporting under Section 404(b) of the Sarbanes Oxley Act (15 U.S.C 7262(b)) by the registered public accounting firm that prepared or issued its audit report ☐
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No No☒ ☒
The aggregate market value of the voting and non-voting common equity held by non-affiliates on June 30, 2021,2023, the last business day of the most recently completed second quarter, based upon the closing price of Common Stock on such date as reported on Nasdaq Capital Market, was approximately $95.410.2 million.
The number of outstanding shares of the registrant’s common stock as of March 24, 202221, 2024 was .
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the Proxy Statement for the registrant’s 20222024 Annual Meeting of Stockholders (the “Proxy Statement”) to be filed within 120 days of the end of the fiscal year ended December 31, 20212023 are incorporated by reference into Part III hereof. Except with respect to information specifically incorporated by reference in this Form 10-K, the Proxy Statement is not deemed to be filed as a part hereof.
Table of Contents
| 2 |
GLOSSARY OF CERTAIN SCIENTIFIC TERMS
The medical and scientific terms used in this Annual Report on Form 10-K have the following meanings:
“Active metabolite” means a drug that is processed by the body into an altered form which effects the body.
“Agonist” means a chemical/drug that binds to a receptor in the body and activates that receptor to produce a biological response.
“Analog” means a compound having a structure similar to that of an approved drug but differing from it with respect to a certain component of the molecule which may cause it to have similar or different effects on the body.
“cGCP” means current Good Clinical Practices. The FDA and other regulatory agencies promulgate regulations and standards, commonly referred to as current Good Clinical Practices, for designing, conducting, monitoring, auditing and reporting the results of clinical trials to ensure that the data and results are accurate and that the rights and welfare of trial participants are adequately protected.
“cGMP” means current Good Manufacturing Practices. The FDA and other regulatory agencies promulgate regulations and standards, commonly referred to as current Good Manufacturing Practices, which include requirements relating to quality control and quality assurance, as well as the corresponding maintenance of records and documentation.
“CMO” means Contract Manufacturing Organization.
“CRO” means Contract Research Organization.
“Deuterated analog” means a small molecule in which one or more of the hydrogen atoms are replaced by deuterium.
“EMA” means the European Medicines Agency.
“FDA” means the Food and Drug Administration.
“FPI” means First Patient In (enrolled into the clinical trial).
“IND” means an Investigational New Drug Application. Before testing a new drug on human subjects, the company must file an IND with the FDA. Information must be produced on the absorption, distribution, metabolism, and excretion properties of the drug and detailed protocols for testing on human subjects must be submitted.
“Indication” means a condition which makes a particular treatment or procedure advisable.
“Moiety” means an active or functional part of a molecule.
“NDA” means a New Drug Application submitted to the FDA. Under the Food, Drug, and Cosmetic Act of 1938, an NDA is submitted to the FDA enumerating the uses of the drug and providing evidence of its safety.
“NGC” means Next Generation Chemotherapy, referring to the drugs in our pipeline that have active cancer killing metabolites that are the same or have very similar chemical structure to existing FDA-approved chemotherapy treatments, resulting in our NGCs killing cancer cells following the same mechanism as the FDA-approved treatments.
“NL” means Necrobiosis Lipoidica, a rare chronic and granulomatous disorder.
“Osteonecrosis” means the death of bone cells due to decreased blood flow. It can lead to pain and collapse of areas of bone.
| 3 |
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS AND RISK FACTOR SUMMARY
This Annual Report on Form 10-K contains forward-looking statements that involve risks and uncertainties. All statements other than statements of historical facts contained in this Form 10-K are forward-looking statements. In some cases, you can identify forward-looking statements by words such as “anticipate,” “believe,” “contemplate,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,” “project,” “seek,” “should,” “target,” “will,” “would,” or the negative of these words or other comparable terminology. We have based these forward-looking statements on our current expectations and projections about future events and trends that we believe may affect our financial condition, results of operations, strategy, short- and long-term business operations and objectives, and financial needs. These forward-looking statements are subject to a number of risks, uncertainties and assumptions, including those described in “Risk Factors” and elsewhere in this Form 10-K. Moreover, we operate in a very competitive and rapidly changing environment, and new risks emerge from time to time. It is not possible for our management to predict all risks, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements we may make. In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed in this Form 10-K may not occur, and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. Given these uncertainties, you should not place undue reliance on these forward-looking statements. These risks are discussed more fully in the “Risk Factors” section of this Annual Report on Form 10-K.10-K and are summarized below under the “Summary Risk Factors” section. These risks include, but are not limited to, the following:
| ● | our ability to obtain funding for our future | |
| ● | our ability to obtain and maintain regulatory approval of our product candidates; | |
| ● | our ability to contract with third-party suppliers, manufacturers and other service providers and their ability to perform adequately; | |
| ● | our ability to meet obligations under our license agreements; | |
| ● | the potential market size, opportunity and growth potential for our product candidates, if approved; | |
| ● | our ability to build our own sales and marketing capabilities, or seek collaborative partners, to commercialize our product candidates, if approved; | |
| ● | our ability to retain the continued service of our key professionals and to identify, hire and retain additional qualified professionals; | |
| ● | our ability to advance product candidates into, and successfully complete, clinical trials; | |
| ● | our ability to recruit and enroll suitable patients in our clinical trials; | |
| ● | the initiation, timing, progress and results of clinical trials and pre-clinical studies for our NGC drugs; | |
| ● | the timing or likelihood of the accomplishment of various scientific, clinical, regulatory filings and approvals and other product development objectives; | |
| ● | the pricing and reimbursement of our product candidates, if approved; | |
| ● | the rate and degree of market acceptance of our product candidates by physicians, patients, third-party payors and others in the medical community, if approved; | |
| ● | the implementation of our business model, strategic plans for our business, product candidates and technology; | |
| ● | the scope of protection we are able to establish and maintain for intellectual property rights covering our product candidates and technology; | |
| ● | developments relating to our competitors and our industry; | |
| ● | the accuracy of our estimates regarding expenses, capital requirements and needs for additional financing; | |
| ● | our financial | |
| ● | other risks and uncertainties, including those described under part I, Item 1A. Risk Factors of this Annual Report. |
You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable as of the date of this Form 10-K, we cannot guarantee that the future results, levels of activity, performance or events and circumstances reflected in the forward-looking statements will be achieved or occur. We undertake no obligation to update publicly any forward-looking statements for any reason after the date of this Form 10-K to conform these statements to new information, actual results or to changes in our expectations, except as required by law.
You should read this Form 10-K and the documents that we reference in this Form 10-K and have filed with the SEC as exhibits with the understanding that our actual future results, levels of activity, performance, and events and circumstances may be materially different from what we expect.
In this Form 10-K, “we,” “us”, “our”, “Processa” and “the Company” refer to Processa Pharmaceuticals, Inc. and its subsidiary.
| 4 |
SUMMARY RISK FACTORS
We are providing the following summary of the risk factors contained in our Form 10-K to enhance the readability and accessibility of our risk factor disclosures. We encourage our stockholders to carefully review the full risk factors contained in this Form 10-K in their entirety for additional information regarding the risks and uncertainties that could cause our actual results to vary materially from our recent results or from our anticipated future results.
Risks Related to Our Financial Position and Need for Additional Capital
| ● | We have a history of losses and we may never become profitable. | |
| ● | We have limited cash resources and will require additional financing. | |
| ● | Our financial statements contain a statement regarding a substantial doubt about our ability to continue as a going concern. | |
| ● | Our ability to use our net operating loss carryforwards and other tax attributes may be limited. |
Risks Relating to Clinical Development and Commercialization of Our Product Candidates
| ● | We currently do not have, and may never develop, any FDA-approved, licensed or commercialized products. | |
| ● | Our licenses are subject to termination by the licensor in certain circumstances. | |
| ● | If we fail to comply with our obligations contained in the agreements under which we license intellectual property rights from third parties, we could lose important license rights. | |
| ● | We depend entirely on the successful development of our product candidates, which have not yet demonstrated efficacy for their target indications in clinical trials. We may never be able to demonstrate efficacy for our product candidates, thus preventing us from licensing, obtaining marketing approval by any regulatory agency, and/or commercializing our product(s). | |
| ● | We must successfully complete clinical trials for our product candidates before we can apply for marketing approval. | |
| ● | We have little corporate history of conducting clinical trials. Our planned clinical trials or those of our collaborators may reveal significant adverse events, toxicities or other side effects not seen in our preclinical studies and may result in a safety profile that could inhibit regulatory approval or market acceptance of any of our product candidates. | |
| ● | Even if we receive regulatory approval for any of our product candidates, we may not be able to successfully license or commercialize the product and the revenue that we generate from its sales, if any, may be limited. | |
| ● | We are completely dependent on third parties to manufacture our product candidates, and our commercialization of our product candidates could be halted, delayed or made less profitable if those third parties fail to obtain manufacturing approval from the FDA or comparable foreign regulatory authorities, fail to provide us with sufficient quantities of our product candidates or fail to do so at acceptable quality levels or prices. | |
| ● | Even if we obtain marketing approval for any of our product candidates, we will be subject to ongoing obligations and continued regulatory review, which may result in significant additional expenses. | |
| ● | Obtaining and maintaining regulatory approval of our product candidates in one jurisdiction does not mean that we will be successful in obtaining regulatory approval of our product candidates in other jurisdictions. | |
| ● | Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of and commercialize our product candidates and affect the prices we may obtain. | |
| ● | We could face competition from other biotechnology and pharmaceutical companies, and our operating results would suffer if we fail to innovate and compete effectively. | |
| ● | We rely on third parties to conduct clinical trials for our product candidates. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize any of our product candidates and our business would be substantially harmed. | |
| ● | Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results. | |
| ● | Even though we may apply for orphan drug designation for a product candidate, we may not be able to obtain orphan drug marketing exclusivity. | |
| ● | Although we may pursue expedited regulatory approval pathways for a product candidate, it may not qualify for expedited development or, if it does qualify for expedited development, it may not actually lead to a faster development, regulatory review or approval process. | |
| ● | Third-party coverage and reimbursement, health care cost containment initiatives and treatment guidelines may constrain our future revenues. | |
| ● | Legal, regulatory and legislative changes with respect to reimbursement, pricing and contracting may adversely affect our business and future prospects. | |
| ● | We may face product liability exposure, and if successful claims are brought against us, we may incur substantial liability if our insurance coverage for those claims is inadequate. | |
| ● | If any of our product candidates are approved for marketing and we are found to have improperly promoted off-label uses, or if physicians misuse our products or use our products off-label, we may become subject to prohibitions on the sale or marketing of our products, product liability claims and significant fines, penalties and sanctions, and our brand and reputation could be harmed. | |
| ● | We may choose not to continue developing or commercializing any of our product candidates at any time during development or after approval, which would reduce or eliminate our potential return on investment for those product candidates. |
Risks Relating to Our Intellectual Property Rights
| ● | We depend on rights to certain pharmaceutical compounds that are or will be licensed to us. We do not own the intellectual property rights to these pharmaceutical compounds and any loss of our rights to them could prevent us from selling our products. | |
| ● | We cannot ensure protection of our licensed intellectual property rights. | |
| ● | Our product candidates may infringe the intellectual property rights of others, which could increase our costs and delay or prevent our development and commercialization efforts. | |
| ● | Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements. |
General Company-Related Risks
| ● | We will need to grow the size of our organization, and we may experience difficulties in managing this growth. | |
| ● | If we lose key management personnel, or if we fail to recruit additional highly skilled personnel, our ability to identify and develop new or next generation product candidates will be impaired, could result in loss of markets or market share and could make us less competitive. | |
| ● | If our information technology systems or data, or those of third parties upon which we rely, are or were compromised, we could experience adverse consequences resulting from such compromise, including but not limited to regulatory investigations or actions, interruptions or disruptions to operations or clinical trials, reputational harm, litigation, fines and penalties. | |
| ● | We are exposed to cyber-attacks and data breaches, including the risks and costs associated with protecting our systems and maintaining integrity and security of our business information, as well as personal data of our guests, employees and business partners. |
Risks Related to Ownership of Our Common Stock
| ● | Our failure to maintain compliance with Nasdaq’s continued listing requirements could result in the delisting of our common stock. | |
| ● | Future equity offerings, license transactions or acquisitions may dilute our existing stockholders’ ownership and/or have other adverse effects on our operations. | |
| ● | Our common stock price is expected to be volatile. | |
| ● | We are a “smaller reporting company,” and the reduced disclosure requirements applicable to us as such may make our common stock less attractive to our stockholders and investors. | |
| ● | We do not currently intend to pay dividends to our stockholders in the foreseeable future, and consequently, your ability to achieve a return on your investment will depend on appreciation in our value. | |
| ● | If securities or industry analysts do not publish research or reports about our business, or if they publish negative evaluations of our stock or negative reports about our business, our stock price and trading volume could decline. | |
| ● | Provisions in our corporate documents and Delaware law could have the effect of delaying, deferring, or preventing a change in control of us, even if that change may be considered beneficial by some of our stockholders. | |
| ● | Provisions in our bylaws provide for indemnification of officers and directors, which could require us to direct funds away from our business and the development of our product candidates. |
| 5 |
Part I
Item 1. Business
Overview
We are a clinical-stage biopharmaceutical company focused on utilizing our “regulatory science” approach, including the principles associated with FDA’s Project Optimus Oncology initiative and the related FDA Draft Guidance, in the development of Next Generation Chemotherapy (“NGC”) oncology drug products. Our mission is to provide better treatment options than those that presently exist by extending a patient’s survival and/or improving a patient’s quality of life. This is achieved by improving upon FDA-approved, widely used oncology drugs or the cancer-killing metabolites of these drugs by altering how they are metabolized and/or distributed in the body, including how they are distributed to the actual cancer cells.
Our regulatory science approach was conceived in the early 1990s when the founders of Processa and other faculty at the University of Maryland worked with the FDA to develop multiple FDA Guidances. Regulatory science is the science of developing new tools, standards, and approaches to assess the safety, efficacy, quality, and performance of all FDA-regulated products. Over the last 30 years, two of our founders, Dr. David Young and Dr. Sian Bigora, have expanded the original regulatory science concept by including the pre-clinical and clinical studies to justify the benefit-risk assessment required for FDA approval when designing the development programs of new drug products.
Our regulatory science approach defines the scientific information that the FDA requires to determine if the benefit outweighs the risk of a drug in a specific population of patients and at a specific dosage regimen for a specific drug product. The studies are designed to obtain the necessary scientific information to support the regulatory decision.
Recently, the FDA has taken steps to define some of the regulatory science required for the FDA approval of oncology products. Through the FDA’s Project Optimus Oncology Initiative and the related Draft Guidance on determining the “optimal” dosage regimen for an oncology drug, the FDA has chosen to make the development of oncology drugs more science-based than in the past. Since the principles of the FDA’s Project Optimus and the related Draft Guidance have been used by our regulatory science approach in a number of non-oncology drugs, our experience with the principles of Project Optimus differentiates us from other biotechnology companies by focusing us not only on the clinical science, but also on the equally important regulatory process. We believe utilizing our regulatory science approach provides us with three distinct advantages:
| ● | greater efficiencies (e.g., the right trial design and trial readouts); | |
| ● | greater possibility of drug approval by the FDA or other regulatory authorities; and | |
| ● | greater ability to evaluate the benefit-risk of a drug compared to existing therapy, which allows prescribers to provide better treatment options for each patient. |
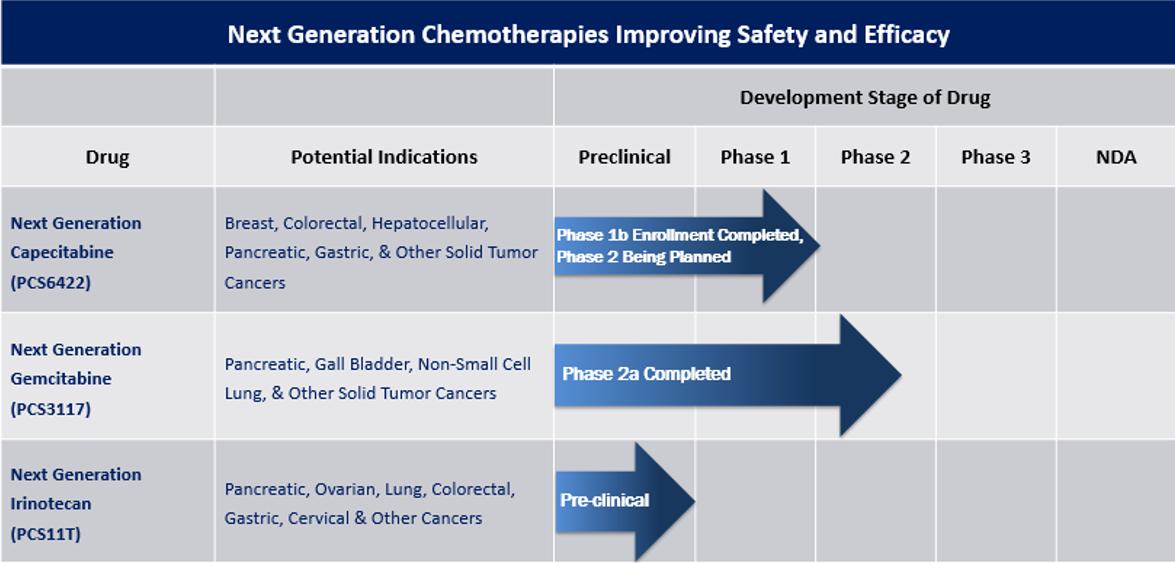
Our strategic prioritization is to advance our pipeline of NGC proprietary small molecule oncology drugs. The NGC products are new chemical entities, but they work by changing the metabolism, distribution and/or elimination of already FDA-approved cancer drugs or their active metabolites while maintaining the mechanism of how the drug kills cancer cells. We believe our NGC treatments will provide improved safety-efficacy profiles when compared to their currently marketed counterparts – capecitabine, gemcitabine, and irinotecan. All future studies of these drugs are subject to availability of capital to conduct the trials.
The three NGC treatments in our pipeline are as follows:
| ● | NGC-Capecitabine (also referred to as NGC-Cap) is a combination of PCS6422 and capecitabine, capecitabine being the oral prodrug of the cancer drug 5-fluorouracil (5-FU). PCS6422, without having any clinically meaningful biological effect itself, alters the metabolism of 5-FU, resulting in more 5-FU distribution to the cancer cells. In clinical trials, NGC-Cap has shown a safety profile different than capecitabine when administered alone. Side effects such as Hand-Foot Syndrome (HFS) and cardiotoxicity typically occur in up to 50-70% of patients treated with capecitabine and are caused by specific capecitabine metabolites. These types of toxicities frequently result in decreased doses, interrupted doses, or discontinuation of treatment with capecitabine. Since a much smaller amount of these metabolites are formed with NGC-Cap, these side effects appear in less patients and are less severe when they do occur. In addition, NGC-Cap has been found to be up to 50 times more potent than capecitabine based on the systemic exposure of the capecitabine metabolite 5-FU, which is metabolized to the cancer-killing metabolites. Like capecitabine, NGC-Cap could potentially be used to treat patients with various cancers, such as metastatic breast, colorectal, gastrointestinal, and pancreatic. On December 11, 2023, we had a successful meeting with the FDA regarding the next Phase 2 study supporting the advancement of NGC-Cap for cancer patients. The meeting with the FDA was supported by the interim results from the ongoing Phase 1B study that was fully enrolled in the first quarter of 2024. Following the meeting with the FDA, we decided the next NGC-Cap trial would be a Phase 2 trial in breast cancer. This decision was supported through discussions with the FDA where we agreed with the FDA that the development of NGC-Cap in breast cancer would be a more efficient development program than metastatic colorectal cancer and improve the likelihood of FDA approval. The FDA has agreed that the data from past and existing studies could be used to directly support the Phase 2 trial in breast cancer. Breast cancer is the most diagnosed cancer, representing approximately 15% of all new cancer patients in 2023. It has a prevalence of more than 3.8 million patients, with nearly 300,000 new diagnoses last year. Over 150,000 women are currently living with advanced or metastatic breast cancer. The NGC-Cap annual newly diagnosed incidence rate for breast, colorectal and other cancers is greater than 250,000 patients per year. |
| 6 |
| ● | PCS3117, also referred to as NGC-Gemcitabine (NGC-Gem), is an oral analog of gemcitabine that is converted to its active metabolite by a different enzyme system than gemcitabine resulting in a positive response in gemcitabine patients as well as some gemcitabine treatment-resistant patients. Like gemcitabine, NGC-Gem could be used to treat patients with various cancers such as pancreatic, biliary tract, lung, ovarian, and breast. We estimate more than 275,000 patients in the United States were newly diagnosed in 2022 with pancreatic, biliary tract, lung, ovarian, and breast cancer. We plan to meet with the FDA to discuss potential study designs including implementation of the Project Optimus initiative as part of the design in 2024. | |
| ● | PCS11T, also referred to as NGC-Irinotecan (NGC-Iri), is a prodrug of the active metabolite of irinotecan (SN-38). The chemical structure of NGC-Iri influences the uptake of the drug into cancer cells, resulting in more NGC-Iri entering cancer cells than normal cells in mice. These levels were significantly greater than those seen with irinotecan, resulting in lower doses of NGC-Iri having greater efficacy than irinotecan and improved safety in animal models. Like irinotecan, NGC-Iri could be used to treat patients with various cancers such as lung, colorectal, gastrointestinal, and pancreatic cancer. We estimate at least 200,000 patients in the United States were newly diagnosed in 2022 with lung, colorectal, gastrointestinal, and pancreatic cancer. We plan to conduct IND-enabling and toxicology studies in 2024-2025. |
We have completed our Phase 2A trial for PCS12852 in gastroparesis patients with positive results. Additionally, in February 2023, due primarily to the inability to identify and enroll patients in our rare disease Phase 2 trial for PCS499 in ulcerative Necrobiosis Lipoidica (uNL), we decided to cease further enrollment in the PCS499 trial and terminated the trial. We did not experience any safety concerns during the conduct of either the PCS12852 or PCS499 trial. We are currently evaluating options to monetize these non-core drug assets, which may include out-licensing or partnering these assets with one or more third parties.
Our shift in prioritization to NGC oncology drugs does not change our mission. We continue to be focused on drug products that improve the survival and/or quality of life for patients by improving the safety and/or efficacy of the drug in a targeted patient population, while providing a more efficient and probable path to FDA approval and differentiating our drugs from those on the market or are currently being developed.
Historically, much of oncology drug development has searched for novel or different ways to treat cancer. Our approach is to take three current FDA-approved cancer drugs and modify and improve how the human body metabolizes and/or distributes these NGC treatments compared to their presently approved counterpart chemotherapy drugs while maintaining the cancer-killing mechanism of action; thus, our reason for calling our drugs Next Generation Chemotherapy (or NGC) treatments. Part of the development includes determining the optimal dosage regimen based on the dose-response relationship as described in the FDA’s Project Optimus Initiative and Draft Optimal Dosage Regimen Oncology Guidance. To date, we have data that we believe suggests our NGC treatments are likely to have a better safety-efficacy profile than the current widely used marketed counterpart drugs, not only potentially making the development and approval process more efficient, but also clearly differentiating our NGC treatments from the existing treatment. We believe our NGC treatments have the potential to extend the survival and/or quality of life for more patients diagnosed with high unmet medical need conditions for which few or no treatment options currently exist. We are a clinical-stage development company, not a discovery company, that seeks to identify and develop drugs forcancer while decreasing the number of patients who need betterare required to dose-adjust or discontinue treatment options. In orderbecause of side effects or lack of response.
| 7 |
Our Strategy
Our strategy is to develop our pipeline of NGC proprietary small molecule oncology drugs using our regulatory science approach to determine the optimal dosage regimen of our oncology drugs. By changing either the metabolism, distribution, and/or elimination of already FDA-approved cancer drugs (e.g., capecitabine, gemcitabine, and irinotecan) or their active metabolites, we believe that our three new oncology drugs represent the next generation of chemotherapy with an improved safety profile, improved efficacy profile and/or potentially benefiting more patients while maintaining the mechanism of how the drug kills cancer cells. By combining these modified approved cancer treatments with our regulatory science approach and our experience using the principles of FDA’s Project Optimus initiative, we anticipate that we will be able to increase the probability of development success,FDA approval, improve the safety-efficacy profile over the existing counterparts of our pipeline only includesNGC drugs, which have previously demonstrated some efficacy in the targeted population or a drug with very similar pharmacological properties that has been shown to be effective in the population.
Our screening criteria for identifying and selecting new candidates include:
In many instances, these clinical candidates have significant pre-clinical and clinical data that we may leverage to high value inflection points while de-risking the programs and adding in optionality to potential future indications. Our regulatory science approach developed by our team over decades of work with regulatory authorities attempts to balance the “benefit/risk” equation to identify a regulatory path with higher clinical benefit and/or lower clinical risk with shorter timelines to deliver better treatment options to patients, physicians and caregivers.more efficiently develop each drug.
Our pipeline includes drugs thatof NGCs (i) already have clinical proof-of-concepthas data demonstrating the desired pharmacological activity in humans or minimally, clinical evidenceappropriate animal models and is able to provide improved safety and/or efficacy by some modification in the formformation and/or distribution of case studies or clinical experience demonstratingthe active moieties associated with the drug or a similar drug pharmacologically can successfully treat patients with the targeted indication;and (ii) target indicationstargets cancers for which a single positive pivotal studytrial demonstrating efficacy might provide enough evidence that the clinical benefits of the drug and its approval outweighs the risks associated with the drug or the present standard of care (e.g., some orphan indications, many serious life-threatening conditions, some serious quality of life conditions); and/or (iii) target indications where the prevalence of the condition and the likelihood of patients enrolling in a study meet the desired timeframe to demonstrate that the drug can, at some level, treat or potentially treat patients with the condition.drug.
To advance our mission, we have assembled an experienced and successful development team with a track record of drug approvals and successful exits. Our team is experienced in developing drug products through all principal regulatory tiers from IND enabling studies to NDA submission. The combined scientific, development and regulatory experience of our team members has resulted in more than 30 drug approvals by the FDA, over 100 meetings with the FDA and involvement with more than 50 drug development programs, including drug products targeted to patients who have an unmet medical need. Although we believe that the skills and experience of our team members in drug development and commercialization is an important indicator of our future success, the past successes of our team members in developing and commercializing pharmaceutical products does not guarantee that they will successfully develop and commercialize drugs in our current pipeline. In addition, the growth in revenues of companies at which our executive officers and directors served in was due to many factors and does not guarantee that they will successfully operate or manage us or that we will experience similar growth in revenues, even if they continue to serve as executive officers and/or directors.
Our ability to generate meaningful revenue from any products depends on our ability to out-license the drugs before or after we obtain FDA NDA approval. Even if our products are authorized and approved by the FDA, it should be noted that the products must still meet the challenges of successful marketing, distribution and consumer acceptance.
Our Strategy
Our strategy is to obtain and develop drugs that will not only treat patients with unmet medical need conditions but, with our regulatory science approach, also have the potential to be more efficiently developed with a greater probability of development success than what typically occurs in the biotech-pharma industry and a better return on investment given lower development costs, more efficient development and high commercial value. Given the prior successes of our regulatory science approach, we have selected drugs for our portfolio which may have greater chance for approval in a population of patients who desperately need better treatment options. We have applied rigorous standards to identify drugs for our portfolio, namely:
Our Team
Our drug development efforts are guided by our knowledge and experience in applying rigorousour regulatory science approach to decrease manageable risks, costs, and time toward achieving marketing authorization from regulatory authorities including the FDA. We have assembled a seasoned management team and development team with extensive experience in developing therapies, including advancing product candidates from preclinical research through clinical development and ultimately regulatory approval and commercialization. Our team is led by our ChairmanPresident of Research and CEODevelopment and Founder David Young, Pharm.D., Ph.D. who has extensive experience in research, regulatory approval and business development and who served at Questcor Pharmaceuticals for eight years, initially as an independent director on its Board of Directors and, subsequently, as its Chief Scientific Officer. Dr. Young’s guidance led
To execute our strategy, we assembled an experienced and development team with a successful track record of drug approvals and successful exits. Our team is experienced in developing drug products through all principal regulatory tiers from IND-enabling studies to New Drug Application (NDA) submission. Throughout their careers, the approvalcombined scientific, development and regulatory experiences of Actharour team members have resulted in Infantile Spasmsmore than 30 drug approvals in indications reviewed by almost every division of the FDA including the oncology divisions, over 100 meetings with the FDA and involvement with more than 50 drug development programs, including drug products targeted to patients who have an unmet medical need and cancer patients. In addition, the ultimate sale of Questcor in 2014.FDA Project Optimus Oncology initiative and recent FDA Oncology Guidance applies our regulatory science approach and principles used and refined by our Founders over the last 30 years.
| 8 |
Our Drug Pipeline
WeOur pipeline currently have five drugs: four in various stagesconsists of clinical development (PCS499, PCS12852,NGC-Cap, NGC-Gem and NGC-Iri (also identified as PCS6422, PCS3117 and PCS6422)PCS11T, respectively) and onetwo non-oncology drugs (PCS12852 and PCS499). The non-oncology drugs are not included in nonclinical development (PCS11T). We groupthe pipeline chart above, as we are exploring our options for those drugs, into non-oncology (PCS499 and PCS12852) and oncology (PCS3117, PCS6422 and PCS11T).which may include out-licensing or partnership opportunities. A summary of each drug is provided below:

below.
* Cleared by FDA for Clinical TrialNext Generation Chemotherapy Pipeline
PCS499
PCS499, an oral tablet of a deuterated analog of one of the major metabolites of pentoxifylline (PTX or Trental®), is classified by FDA as a new molecular entity. PCS499 and its metabolites act on multiple pharmacological targets that are important in a variety of conditions. We have targeted ulcerative Necrobiosis Lipoidica (uNL) as our lead indication for PCS499. NL is a chronic, disfiguring condition affecting the skin and tissue under the skin typically on the lower extremities with no currently approved FDA treatments. NL presents more commonly in women than in men and occurs more often in people with diabetes. Ulceration has been reported to occur in up to 30% of NL patients, which can lead to more severe complications, such as deep tissue infections and osteonecrosis threatening the life of the limb. Approximately 65,000 people in the United States and more than 120,000 people outside the United States are affected with uNL.
The degeneration of tissue occurring at the NL lesion site may be caused by a number of pathophysiological changes, which make it extremely difficult to develop effective treatments for this condition. Because PCS499 and its metabolites appear to affect most of the biological pathways that contribute to the pathophysiology associated with NL, PCS499 may provide a novel treatment solution for NL.
On June 18, 2018, the FDA granted orphan-drug designation for PCS499 for the treatment of NL. On September 28, 2018, the IND for PCS499 in NL became effective, such that we initiated and completed a Phase 2A multicenter, open-label prospective trial designed to determine the safety and tolerability of PCS499 in patients with NL. The study initially had a six-month treatment phase and a six-month optional extension phase. In December 2019, we informed patients and sites that the study would conclude after the treatment phase and there would no longer be an extension phase. The first enrolled NL patient in this Phase 2A clinical trial was dosed on January 29, 2019 and the study completed enrollment on August 23, 2019. The last patient visit took place in February 2020.
The primary objective of the Phase 2A trial was to evaluate the safety and tolerability of PCS499 in patients with NL (ulcerated and non-ulcerated patients) and to use the safety and efficacy data to design future clinical trials. Based on toxicology studies and healthy human volunteer studies, we and the FDA agreed that a PCS499 dose of 1.8 grams/day would be the highest dose administered to NL patients in this Phase 2A trial. As anticipated, the PCS499 dose of 1.8 grams/day, 50% greater than the maximum tolerated dose of PTX, appeared to be well tolerated with no serious adverse events (SAEs) reported. All adverse events (AEs) reported in the study were mild in severity. As expected, gastrointestinal symptoms were the most frequent AEs and reported in four patients, all of which resolved within 1-2 weeks of starting dosing.
Two of the twelve patients in the study presented with uNL and had ulcers for more than two months prior to dosing. At baseline, the reference ulcer in one of the two patients measured 3.5 cm2 and had completely closed by Month 2 of treatment. The second patient had a baseline reference ulcer of 1.2 cm2 which completely closed by Month 9 during the patient’s treatment extension period. In addition, while in the trial, both patients also developed small ulcers at other sites, possibly related to contact trauma, and these ulcers resolved within one month. The other ten patients, presenting with mild to moderate NL and did not have ulceration, had more limited improvement of the NL lesions during treatment. Historically, 13 - 20% of all the patients with NL naturally progress to complete healing over many years after presenting with NL. Although the natural healing of the uNL patients has not been evaluated independently, medical experts who treat NL patients suggest that the natural progression of an open ulcerated wound to complete closure may be significantly less than 13% over 1-2 years and probably close to 0% in patients with the larger ulcers.
On March 25, 2020, we met with the FDA and discussed the clinical program, as well as the nonclinical and clinical pharmacology plans to ultimately support the submission of the PCS499 New Drug Application (NDA) in the U.S. for the treatment of ulcers in NL patients. With input from the FDA, we designed the next trial as a randomized, placebo-controlled Phase 2B study to evaluate the ability of PCS499 to completely close ulcers in patients with NL and better understand the potential response of NL patients on drug and on placebo. We currently have selected six clinical trial sites in the United States and are evaluating additional sites to add to our study. We had four sites in Europe, but these sites were unable to recruit patients timely, largely due to COVID-19, so we decided to close them and concentrate our efforts on recruiting patients within the United States.
We began recruiting for the clinical trial in the first half of 2021. On May 19, 2021, we dosed our first patient in the randomized, placebo-controlled trial and are planning to complete an interim analysis of the data from this trial by the end of 2022. After obtaining the results from this Phase 2B study, we expect to have an end of Phase 2 meeting with the FDA to agree on the design of the Phase 3 study, with the intent to define a Special Protocol Assessment for the Phase 3 study and to agree on the next steps to obtain approval.
PCS12852
On August 19, 2020, we in-licensed PCS12852 (formerly known as YH12852) from Yuhan Corporation (“Yuhan”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS12852 globally, excluding South Korea.
PCS12852 is a novel, potent and highly selective 5-hydroxytryptamine 4 (5-HT4) receptor agonist. Other 5-HT receptor agonists with less 5-HT4 selectivity have been shown to successfully treat gastrointestinal (GI) motility disorders such as gastroparesis, chronic constipation, constipation-predominant irritable bowel syndrome and functional dyspepsia. Less selective 5-HT4 agonists, such as cisapride, have been either removed from the market or not approved because of the cardiovascular side effects associated with the drugs binding to other receptors, especially receptors other than 5-HT4.
Two clinical studies, both which have demonstrated the effectiveness of PCS12852 on GI motility, have been previously conducted by Yuhan with PCS12852. In a Phase 1 trial (Protocol YH12852-101), the initial safety and tolerability of PCS12852 were evaluated after single and multiple oral doses in healthy subjects. PCS12852 was shown to increase GI motility in this study, increasing stool frequency with faster onset when compared to prucalopride, a less specific 5-HT4 agonist FDA-approved drug for the treatment of chronic idiopathic constipation. Based on an increase of ≥1 spontaneous bowel movement (SBM)/week from baseline during 7-day multiple dosing, the PCS12852 dose group had a higher percent of patients with an increase than the prucalopride group. All doses of PCS12852 were safe and well tolerated and no SAEs occurred during the study. The most frequently reported AEs were headache, nausea and diarrhea which were temporal, manageable and reversible within 24 hours. There were no clinically significant changes in platelet aggregation and ECG parameters including a change in QTc prolongation in the study. In a Phase 1/2A clinical trial (Protocol YH12852-102), the safety, tolerability, gastric emptying rate and pharmacokinetics of multiple doses of a PCS12852 immediate release (IR) formulation and a delayed release (DR) formulation were evaluated. PCS12852 was safe and well tolerated after single and multiple administrations. The most frequent AEs for both the IR and DR formulations of PCS12852 were headache, nausea and diarrhea, but the incidences of these AEs were comparable with those of the 2mg prucalopride group. These AEs, which were transient and mostly mild in severity, are also commonly observed with other 5-HT4 agonists. Both formulations of PCS12852 also increased the gastric emptying rate and increased GI motility.
Yuhan had also conducted extensive toxicological studies for the product that demonstrated that the product is safe for use and can be moved into Phase 2 studies.
We received guidance from the FDA in the first half of 2021 and in October 2021 we received notice of safe to proceed for PCS12852 evaluation in a Phase 2A randomized, placebo-controlled study in patients with gastroparesis. We anticipate beginning to enroll patients in the first half of 2022, with expected completion in the first half of 2023. The purpose of the Phase 2A trial is to evaluate the safety, efficacy and pharmacokinetics of two different dosing regimens for PCS12852. Data obtained from this study will be used to better design a future Phase 2/3 efficacy study. Since patients with gastroparesis have an abnormal pattern of upper GI motility in the absence of mechanical obstruction, the Phase 2A study was designed to evaluate the change in gastric emptying in patients with gastroparesis from two different dosing regimens of PCS12852 compared to placebo. The only FDA-approved drug to treat gastroparesis is metoclopramide, a dopamine D2 receptor antagonist that has documented serious side effects which limit dosing to no more than 12 weeks. Other 5-HT4 drugs have been used clinically but the side effects, caused mainly by binding to other receptors, has resulted in these drugs not being a viable option to treat patients with gastroparesis. It should be noted that PCS12852 is a highly specific 5-HT4 agonist that has been shown in nonclinical studies to have a cardiovascular side effect only at concentrations greater than 1,000 times the maximum concentration seen in humans.
PCS3117
On June 16, 2021, we executed a License Agreement with Ocuphire Pharma, Inc. (“Ocuphire Agreement”) under which we received a license to research, develop and commercialize PCS3117 (formerly RX-3117) globally, excluding Republic of Singapore, China, Hong Kong, Macau and Taiwan.
PCS3117 is a novel, investigational, oral small molecule nucleoside compound. PCS3117 is an analog of the endogenous nucleoside, cytidine, and an analog of the cancer drug gemcitabine. Once intracellularly activated (phosphorylated) by the enzyme UCK2, it is incorporated into the DNA or RNA of cells and inhibits both DNA and RNA synthesis, which induces apoptotic cell death of tumor cells. PCS3117 has received orphan drug designation from the FDA and the European Commission for the treatment of patients with pancreatic cancer.
Gemcitabine is usually used as second line therapy for metastatic pancreatic cancer and non-small cell lung cancer, as well as used as second line therapy for other types of cancer. The difference between PCS3117 and gemcitabine is how they are activated to cancer killing nucleotides. PCS3117 also has additional pharmacological pathways which will result in cancer cell apoptosis. Since 45% - 85% of pancreatic cancer and non-small cell lung cancer patients are inherently resistant or acquire resistance to gemcitabine, the differences between PCS3117 and gemcitabine could potentially provide a therapeutic alternative to patients who do not or will not respond to gemcitabine.
Resistance to gemcitabine or PCS3117 is likely caused by:
| ● | ||
| a | ||
PCS3117 has shown broad spectrum anti-tumor activity against over 100 different humanCapecitabine, as presently prescribed and FDA-approved, forms the cancer cell linesdrug 5-FU which is then further metabolized to anabolites (which kill both cancer cells and efficacy in 17 different mouse xenograft models. In preclinical trials, PCS3117 retained its anti-tumor activity in humannormal duplicating cells) and catabolites (which cause side effects and have no cancer cell lines made resistant to the anti-tumor effects of gemcitabine. In August 2012, the completion of an exploratory Phase 1 clinical trial of PCS3117 in cancer patients to investigate the oral bioavailability, safety and tolerability of the compound was reported. In that study, oral administration of a 50 mg dose of PCS3117 indicated an oral bioavailability of 56% and a plasma half-life (T1/2) of 14 hours. In addition, PCS3117 appeared to be well tolerated in all subjects throughout the dose range tested.
Final results from a Phase 1B clinical trial of PCS3117 were presented in June 2016 showing evidence of single agent activity. Patients in the study had generally received four or more cancer therapies prior to enrollment. In this study, 12 patients experienced stable disease persisting for up to 276 days and three patients showed evidence of tumor burden reduction. A maximum tolerated dose of 700 mg was identified in the study. At the doses tested, PCS3117 appeared to be well tolerated with a predictable pharmacokinetic profile following oral administration.
In March 2016, a multi-center Phase 2A clinical trial of PCS3117 in patients with relapsed or refractory pancreatic cancer was initiated to further evaluate safety and efficacy. The study was designed as a two-stage study with 10 patients in stage 1 and an additional 40 patients in stage 2. According to pre-set criteria, if greater than 20% of the patients had an increase in progression free survival of more than four months, or an objective clinical response rate and reduction in tumor size, additional pancreatic cancer patients would be enrolled into stage 2. Secondary endpoints included time to disease progression, overall response rate and duration of response, as well as pharmacokinetic assessments and safety parameters. In January 2018, the final data from this trial showed evidence of tumor shrinkage in some patients with metastatic pancreatic cancer that was resistant to gemcitabine and who had failed on multiple prior treatments was presented. In this study, 31% of patients experienced progression free survival for two months or more and five patients, or 12%, had disease stabilization for greater than four months. Although the pre-set criteria of 20% of the patients having an increase in progression free survival for four months was not met, some of the gemcitabine refractory patients did respond to PCS3117. However, an evaluation of why patients were resistant to PCS3117 was not undertaken within the study.
In November 2017, a Phase 2A trial of PCS3117killing properties). When capecitabine is given in combination with ABRAXANEPCS6422 in patients newly diagnosed with metastatic pancreatic cancer was initiated. The multicenter, single-arm, open-label study was designed to evaluate PCS3117NGC-Cap, PCS6422 significantly changes the metabolism of 5-FU, which results in combination with ABRAXANE in first line metastatic pancreatic cancer patients. In February 2019, the target enrollment of 40 evaluable patients in this trial was reached. An overall response rate of 23% had been observed in 40 patients that had at least one scan on treatment. Preliminary and unaudited data indicated that the median progression free survival for patientsa change in the study was approximately 5.6 months. The most commonly reported related adverse events were nausea, diarrhea, fatigue, alopecia, decreased appetite, rash, vomitingdistribution of 5-FU within the body. Due to this change in metabolism and anemia. Again, evaluationthe overall metabolite profile of anabolites and catabolites, the causeside effect and efficacy profile of treatment resistance to PCS3117 was not undertaken.
In order to identify patients who would more likely respond to PCS3117 than gemcitabine, we will be refining existing assays and developing new assays of biological molecules (i.e., biomarkers) over the next 6-12 months that could help to identify which patients are more likely to respond to or activate PCS3117 over gemcitabine.
PCS6422
On August 23, 2020, we in-licensed PCS6422 from Elion Oncology, Inc. (“Elion”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS6422 globally.
PCS6422 is an oral, potent, selective and irreversible inhibitor of dihydropyrimidine dehydrogenase (DPD), the enzyme that rapidly metabolizes a common chemotherapy drug known as 5-FU, into inactive metabolites, such as α-fluoro-β-alanine (F-Bal). F-Bal is a metabolite thatNGC-Cap has no anti-cancer activity but causes unwanted side effects, which notably leads to dose interruptions and significantly affect a patient’s quality of life. F-Bal is thought to cause the neurotoxicity and Hand–Foot Syndrome (HFS) associated with 5-FU, and greater formation of F-Bal appearsbeen found to be associated with a decrease indifferent from capecitabine given without PCS6422. Since the antitumor activitypotency of 5-FU. HFS can affect activities of daily living, quality of life, and requires dose interruptions/adjustments and even therapy discontinuation resulting in suboptimal tumor effects. We believe that the inhibition of DPD by PCS6422 will significantly reduce 5-FU side effects related to a decrease in F-Bal, although the timeframe and magnitude for DPD inhibition has been shown to vary, ranging from 2-14 days depending on the de novo formation of DPD within a patient and the dosage regimen of PCS6422. With the inhibition of DPD, the level of the 5-FU anti-cancer metabolites couldNGC-Cap is also be potentially higher within cancer and normal cells leading to an improved efficacy profile and/or increased side effects associated with these antimetabolites such as neutropenia. By combininggreater than FDA-approved capecitabine (oral pro-drug form of 5-FU) with PCS6422, the change in 5-FU metabolism should result in an increase in the systemic exposure of 5-FU based on the 5-FU Area Under the Plasma Concentration Curve (AUC)systemic exposure per mg of capecitabine dosed. This resultsadministered, the amount of capecitabine anabolites formed from 1 mg of capecitabine administered in needing less capecitabine to kill cancer cells and treat each patient, makingNGC-Cap will, therefore, be much greater than formed from the combinationadministration of PCS6422 and capecitabine (the “Next Generation Capecitabine”) more potent than current FDA approved1 mg of existing capecitabine.
Fluoropyrimidines (e.g., 5-FU, capecitabine) remain the cornerstone of treatment for many different types of cancers, either as monotherapy or in combination with other chemotherapy agents by an estimated two million patients annually. Xeloda®, the brand name of capecitabine, is an oral pro-drug of 5-FU and approved as first-line therapy for metastatic colorectal and breast cancer. However, its use is limited by adverse effects such as the development of HFS in up to 60% of patients.
Elion evaluated the potential for the combination of PCS6422 with capecitabine as a treatment of advanced gastrointestinal (GI) tumors. Nonclinical efficacy data indicated that in colorectal cancer models, pretreatment with PCS6422 enhanced the antitumor activity of capecitabine. PCS6422 dramatically increased the antitumor potency of capecitabine without increasing the toxicity. The antitumor efficacy of the combination of PCS6422 and capecitabine was tested in several xenograft animal models with human breast, pancreatic and colorectal cancer cells. These preclinical xenograft models demonstrate that PCS6422 potentiates the antitumor activity of capecitabine and significantly reduces the dose of capecitabine required to be efficacious.
Other DPD enzyme inhibitors (e.g. Gimeracil used in Teysuno® approved only outside the US) act as competitive reversible inhibitors. These agents must be present when 5-FU or capecitabine are administered to inhibit 5-FU breakdown by DPD in order to improve the efficacy and safety profiles of 5-FU. Given the reversible nature of their effect on DPD, over time 5-FU metabolism to F-Bal will return if the reversible inhibitor is not present, decreasing the amount of 5-FU in the cancer cells and decreasing the potential cytotoxicity on the cancer cells. There is also evidence that administering large amounts of DPD inhibitors directly with 5-FU may also decrease the antitumor effect of the 5-FU. Because PCS6422 is an irreversible inactivator of DPD, it is dosed the day before capecitabine administration and its effect on DPD can last longer than the reversible DPD inhibitors and beyond the time 5-FU exists in the cancer cell, even after PCS6422 has been completely eliminated out of the body. We believe this can optimize the potential cytotoxic effect of the 5-FU nucleotide metabolites and minimize the catabolism of 5-FU to F-Bal.
Prior to Elion’s involvement, two multicenter Phase 3 studies were conducted in patients with colorectal cancer with PCS6422 administered in 10-fold excess to 5-FU and administered with the 5-FU. Unfortunately, we believe the dose of PCS6422 during these trials was not optimal and that PCS6422 was not administered early enough to irreversibly affect the DPD enzyme, thus the regimen tended to produce less antitumor benefit than the control arm with the standard regimen of 5-FU/leucovorin (LV) without PCS6422. Later preclinical work suggested that when PCS6422 was present at the same time as and in excess to 5-FU, it diminished the antitumor activity of 5-FU, which we believe supports the proposed dosing PCS6422 several hours before 5-FU to allow PCS6422 to be cleared before the administration of 5-FU.
Elion met with the FDA in 2019 and agreed upon the clinical development program required for the combination of PCS6422 and capecitabine as first-line therapy for metastatic colorectal cancer when treatment with fluoropyrimidine therapy alone is preferred. On May 17, 2020, an IND for the Phase 1B study was granted safe to proceed by the FDA. This Phase 1B study was designed to evaluate: i) the safety and tolerability of PCS6422 and several doses of capecitabine in advanced GI tumor patients; ii) the pharmacokinetics of PCS6422, capecitabine, 5-FU and selected metabolites; iii) the activity of DPD over time after PCS6422 administration; and iv) the maximum tolerated dose in up to 30 patients over multiple cycles. The study began patient recruitment in the second half of 2021. On August 2, 2021, we enrolled the first patient in the study.
Theour Phase 1B dose-escalation maximum tolerated dose trial in patients with advanced refractory gastrointestinal (GI) tract tumors. Our interim analysis of Cohorts 1 and 2 was recently conducted. DLTs, drug related2A of the ongoing clinical trial found no dose-limiting toxicities (DLTs), no drug-related adverse events of greater than Grade 1, and hand-foot syndrome were not observed in these patients. Also, this Next Generation Capecitabine effectively inhibited DPD enzyme activity 24-48 hours after PCS6422 administrationno adverse events associated with <10%the catabolites of 5-FU metabolized to F-Balsuch as compared to ~80% with the FDA approved capecitabine. Additionally, 5-FU potency based on the 5-FU AUC systemic exposure per mg of capecitabine dosed was 50 times greater with Next Generation Capecitabine. The interim analysis showed, however, that the improved metabolic profile and increased potency was not sustained at Day 7 after PCS6422 single dose administration.HFS. In February 2022, we submitted a modifiedthis Phase 1B trial, protocolit was demonstrated that the irreversible inhibition of DPD by PCS6422 could alter the metabolism, distribution and elimination of 5-FU, making NGC-Cap significantly (up to 50 times) more potent than capecitabine alone and potentially leading to higher levels of anabolites which can kill replicating cancer and normal cells. By administering NGC-Cap to cancer patients, the balance between anabolites and catabolites changes depending on the dosage regimens of PCS6422 and capecitabine used, making the efficacy-safety profile of NGC-Cap different than that of FDA-approved capecitabine and requiring further evaluation of the PCS6422 and capecitabine regimens to determine the optimal NGC-Cap regimens for patients.
| 9 |
In order for NGC-Cap to provide a safer and more efficacious profile for cancer patients compared to existing chemotherapy, understanding how the different regimens of PCS6422 and capecitabine may affect the systemic and tumor exposure to the FDAanabolites, as well as the systemic exposure to not only determine the MTDcatabolites, is required. This can be achieved by following the timeline of capecitabine but alsoDPD irreversible inhibition and the formation of new DPD using the plasma concentrations of 5-FU and its catabolites.
In an effort to further evaluatebetter estimate the timeline of DPD inhibition and de novo formation of new DPD, we modified the protocol for the Phase 1B trial and began enrolling patients in the amended Phase 1B trial in April 2022. On November 1, 2022, we announced that data from the Phase 1B trial identified multiple dosage regimens with potentially better safety and efficacy profiles than currently existing chemotherapy regimens. Since 5-FU exposure is dependent on both the PCS6422 regimen and the capecitabine regimen, safe regimens were identified as well as regimens that cause DLTs. One of the regimens in the Phase 1B trial did cause DLTs in two patients, one of whom died. The Phase 1B trial is continuing to enroll patients and is expected to complete enrollment in early 2024. The next trial will be a functionPhase 2 trial to determine which regimens provide an improved efficacy-safety profile over present therapy using the principles of PCS6422 dosing.the FDA’s Project Optimus initiative to help guide the design of the trial. This FDA initiative requires us to consider NGC regimens that are not at the maximum tolerated dose or exposure level.
We anticipate that this additional data will allow us to select PCS6422 dosage regimens that will maintain DPD inhibition throughout capecitabine dosing for each patient treated with this Next Generation Capecitabine. After interactingDiscussions with the FDA in April 2023 have clarified that the major goal for the next Phase 2 trial will be to evaluate and making protocol modifications,understand the dose- and exposure-response relationship for anti-tumor activity and safety. The specific dosage regimens for the trial will be defined following the determination of the MTD from our ongoing Phase 1B trial. Cohort 3 in the Phase 1B trial, which dosed patients with PCS6422 in combination with capecitabine at 150 mg BID (twice a day), completed with no dose-limiting toxicities. Enrollment in Cohort 4 was expanded to include six patients to further evaluate the safety at this dose. Enrollment in this cohort is now complete and to date, no DLTs have been observed in this cohort, but safety evaluation for this cohort is still ongoing. Once the cohort and the safety evaluation is complete, the need for any additional cohorts will be further evaluated. Following the FDA meeting on December 11, 2023, we have decided the next NGC-Cap trial would be a Phase 2 trial in breast cancer. This decision was supported through discussions with the FDA where we agreed with the FDA that the development of NGC-Cap in breast cancer would be a more efficient development program than metastatic colorectal cancer and improve the likelihood of FDA approval. The FDA has agreed that the data generated from past and existing studies could be used to directly support the Phase 2 trial in breast cancer. Capecitabine is already approved as both monotherapy and combination therapy in breast cancer, which contributes to the logic and efficiency of our current direction. In addition, the FDA’s agreement that our present data would support a Phase 2 trial in breast cancer makes the expansion seamless. The objective for the Phase 2 trial will be to provide safety-efficacy data to preliminarily demonstrate the benefit of NGC-Cap over capecitabine and other treatment options. Based on this expansion to breast cancer, we expanded our Oncology Advisory Board to include key breast cancer oncologists. We have already determined the Phase 2 study design, which we expect to restartshare with the Phase 1B studyFDA soon, and plan to use the funding from our January 2024 public offering to begin enrolling patients in the secondthird quarter of 2022 while defining the Next Generation Capecitabine regimens by the end of 2022. Although we are making modifications to the existing Phase 1B protocol, we expect that our overall timeline has not changed with a Phase 2B or 3 trial starting in 2023-2024 and NDA submission in 2027-2028.2024.
Our license agreement with Elion Oncology, Inc. (“Elion”) for NGC-Cap requires us to use commercially reasonable efforts, at our sole cost and expense, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that include dosing a first patient with a product in a Phase 2 or 3 clinical trial on or before October 2, 2024. We are currently conducting pre-trial activities and planning to dose the first patient in our Phase 2 trial in the third quarter of 2024.
| 10 |
| ● | NGC-Gem is a cytidine analog similar to gemcitabine (Gemzar®), but different enough in chemical structure that some patients are more likely to respond to PCS3117 than gemcitabine. In addition, we believe those patients inherently resistant or who acquire resistance to gemcitabine are likely not to be resistant to NGC-Gem. The difference in response occurs because NGC-Gem is metabolized to its active metabolite through a different enzyme system than gemcitabine. We continue to evaluate the potential use of NGC-Gem in patients with pancreatic and other potential cancers and to evaluate ways to identify patients who are more likely to respond to NGC-Gem than gemcitabine. We plan to meet with the FDA in 2024 to discuss potential trial designs including implementation of the Project Optimus initiative as part of the design. Similar to NGC-Cap, we will need to obtain additional funding before we can begin the Phase 2 trial for NGC-Gem. |
PCS11TOur license agreement with Ocuphire Pharma, Inc. (“Ocuphire”) for NGC-Gem requires us to use commercially reasonable efforts, at our sole cost and expense to oversee such commercialization efforts, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) dosing a patient in a clinical trial prior to June 16, 2024; and (ii) dosing a patient in a pivotal clinical trial or in a clinical trial for a second indication of the drug prior to June 16, 2026. We are currently in discussions with Ocuphire to extend these deadlines.
| ● | NGC-Iri is an analog of SN38 (SN38 is the active metabolite of irinotecan) and should have an improved safety/efficacy profile in every type of cancer that irinotecan is presently used. The manufacturing process and sites for drug substance and drug product are presently being evaluated and IND-enabling toxicology studies will then be initiated. In addition, we are defining the potential paths to approval, which include defining the targeted patient population and the type of cancer. We plan to conduct IND enabling and toxicology studies in 2024, subject to available funding. |
On May 24, 2020, we in-licensed PCS11T (formerly known as ATT-11T) from Aposense, Ltd. (“Aposense”), pursuant to which we were granted Aposense’s patent rights and Know-How to develop and commercialize their next generation irinotecan cancer drug, PCS11T.
Non-Oncology Pipeline for Out-licensing or Partnership
PCS11T is a novel lipophilic anti-cancer pro-drug that is being developed for the treatment of the same solid tumors as prescribed for irinotecan. This pro-drug is a conjugate of a specific proprietary Aposense molecule connected to SN-38, the active metabolite of irinotecan. The proprietary molecule in PCS11T has been designed to allow PCS11T to bind to cell membranes to form an inactive pro-drug depot on the cell with SN-38 preferentially accumulating in the membrane of tumors cells and the tumor core. This unique characteristic may make the therapeutic window of PCS11T wider than other irinotecan products such that the antitumor effect of PCS11T could occur at a much lower dose with a milder adverse effect profile than irinotecan. Despite the widespread use of commercially marketed irinotecan products in the treatment of metastatic colorectal cancer and other cancers resulting in peak annual sales of approximately $1.1 billion, irinotecan has a narrow therapeutic window and includes an FDA “Black Box” warning for both neutropenia and severe diarrhea. There is, therefore, a substantial unmet need to overcome the limitations of the current commercially marketed irinotecan products, improving efficacy and reducing the severity of treatment emergent AEs. We believe the potential wider therapeutic window of PCS11T will likely lead to more patients responding with less side effects when on PCS11T compared to other irinotecan products.
| ● | PCS12852 is a highly specific and potent 5HT4 agonist that has already been evaluated in clinical studies in South Korea for gastric emptying and gastrointestinal motility in healthy volunteers and volunteers with a history of constipation. In October 2021, the FDA cleared our IND application to proceed with a Phase 2A trial for the treatment of gastroparesis. We enrolled our first patient on April 5, 2022 and completed enrollment of the trial on September 2, 2022. Results from this Phase 2A trial, which included 25 patients with moderate to severe gastroparesis, demonstrated improvements in gastric emptying in patients receiving 0.5 mg of PCS12852 as compared to placebo. The results indicated that for the patients in the PCS12852 group, the mean time for 50% of the gastric contents to empty (t50) compared to their baseline value (±SD) decreased by -31.90 min (±50.53) (compared to the change seen in the placebo group of only -9.36 min (±42.43). Significant gastric emptying differences were not observed between the placebo and the 0.1 mg dose. Adverse events associated with the administration of PCS12852 were generally mild to moderate as expected, limited in duration, and quickly resolved without any sequelae. There were no cardiovascular safety events or serious adverse events reported during the trial. Additionally, the 0.5 mg of PCS12852 showed a greater improvement than placebo in the gastroparesis symptomology scales used in the trial, including both total scores in the scales, as well as sub-scores such as nausea, vomiting and abdominal pain. With the trial now complete, we have the data necessary to finalize the development plan for the treatment of diabetic gastroparesis patients. We are exploring options for PCS12852, which may include licensing, partnering and/or collaborating opportunities. |
Pre-clinical studies conducted to date showed that PCS11T demonstrated tumor eradication at much lower doses than irinotecan across various tumor xenograft models. PCS11T does not affect acetyl choline esterase (AChE) activity in human and rat plasma in vitro, which would suggest that PCS11T will show an improved safety profile, compared to irinotecan, which is known for its cholinergic-related side effects.
| ● | PCS499 is an oral tablet of the deuterated analog of one of the major metabolites of pentoxifylline (PTX or Trental®). PCS499 is a drug that can be used to treat unmet medical need conditions caused by multiple pathophysiological changes. We completed a Phase 2A trial for PCS499 in patients with ulcerative and non-ulcerative necrobiosis lipoidica (uNL and NL, respectively) in late 2020, and in May 2021, we enrolled the first patient in our Phase 2B trial for the treatment of uNL. Although we initiated several recruitment programs to enroll patients in this trial, we were only able to recruit four patients. We experienced extremely slow enrollment in the trial given the extreme rarity of the condition (rarer than reported in the literature), the impact of COVID-19, and the reluctance of patients to be in a clinical trial. We completed the Phase 2B uNL trial for those currently enrolled but halted further efforts to enroll new patients in the trial and have terminated the trial. There were no safety concerns during the conduct of the trial. Although we believe that PCS499 can be effective in treating uNL, preliminary data indicated that the placebo response was likely to be much greater than the literature and clinical experts believe; thus, a much larger sample size would be required in a pivotal trial for an indication where it was extremely difficult to enroll even four patients. We are exploring options for PCS499 in other indications, which may include licensing, partnering and/or collaborating opportunities. |
We are currently planning to manufacture the product at a GMP facility, conduct the required toxicological studies required to file the IND in 2023 and initiate the Phase 1B study in oncology patients with solid tumors.
| 11 |
Manufacturing and Clinical Supplies
We do not own or operate, and currently have no plans to establish, any manufacturing facilities. We currently rely, and expect to continue to rely, on multiple third partythird-party contract manufacturing organizations (CMOs), for the supply of cGMP-gradecurrent Good Manufacturing Practices (cGMP)-grade clinical trial materials and commercial quantities of our product candidates and products, if approved. We require all of our CMOs to conduct manufacturing activities in compliance with cGMP. We have assembled a team of experienced employees and consultants to provide the necessary technical, quality and regulatory oversight of our CMOs.
We anticipate that these CMOs will have the capacity to support both clinical supply and commercial-scale production, but we do not have any formal agreements at this time with any of these CMOs to cover commercial production.
We also may elect to pursue additional CMOs for manufacturing supplies of drug substance and finished drug product in the future. We believe that our standardized manufacturing process can be transferred to a number of other CMOs for the production of clinical and commercial supplies of our product candidates in the ordinary course of business.
Competition
Many of our potential competitors may have significantly greater financial resources, a more established presence in the market, and more expertise in research and development, manufacturing, pre-clinical and clinical testing, obtaining regulatory approvals and reimbursement, and marketing approved products than we do. Mergers and acquisitions in the pharmaceutical, biotechnology and diagnostic industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These potential competitors may also compete with us in recruiting and retaining top qualified scientific, sales, marketing and management personnel and establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
The key competitive factors affecting each of our products, if approved, are likely to include the efficacy, safety, convenience and price of the products relative to other approved products used on-labelon- or off-label for each unmet medical need condition. Although preliminary clinical data exists to support the possibility of improved efficacy and safety profiles for our drugs, more in-depth randomized, controlled studies are required for our products to determine if our preliminary findings will support the approval in the designated unmet medical need indication.
For PCS499,NGC-Cap, the competitive factors will be related to the efficacy and safety of the product when compared to capecitabine. The market penetration will depend on how much improvement will occur in the efficacy and/or safety profiles when administered in combination with PCS6422. Currently, there are no other reversible or irreversible enzyme inhibitor products approved in the US and no irreversible enzyme inhibitors approved ex-US, which may make PCS6422 the first DPD irreversible inhibitor available.
For NGC-Gem, the competitive factors will include establishing market penetration against other cytidine analogues, such as gemcitabine, which is currently no FDA-approved drugsused as first or second line chemotherapy either alone or in combination with other chemotherapy agents. The market penetration will depend on the potential for an improved efficacy profile in patients who have developed tolerance to other agents.
For NGC-Iri, the treatmentcompetitive factors will include establishing marketing penetration against the existing irinotecan product (Camptosar®) and the newer liposomal irinotecan product (Onivyde®). The establishment of patients with NL, and few drugs are used off-label for NL given the lack ofthat market will be based upon improved efficacy and/or side effect concerns.safety of NGC-Iri.
For PCS12852, the competitive factors will include establishing marketing penetration against the metoclopramide products (the only approved drug to treat gastroparesis) and other 5-HT4 receptor agonists used off label. The market penetration will depend on the potential for an improved safety profile due to the very selective 5-HT4 receptor binding by PCS12852 and similar or greater efficacy in the treatment of gastroparesis.
For PCS3117, the competitive factors will include establishing market penetration against other cytidine analogues, such as gemcitabine which is currently used as first or second line chemotherapy either alone or in combination with other chemotherapy agents. The market penetration will depend on the potential for an improved efficacy profile in patients who have developed tolerance to other agents.
For PCS6422,PCS499, there are currently no FDA-approved drugs for the competitive factors will be related totreatment of patients with NL, and few drugs are used off-label for NL given the efficacy and safetylack of the product when used in combination with existing cytotoxic drugs such as capecitabine and fluoropyrimidines compared to the efficacy and safety when these cytotoxic agents are administered without PCS6422 or with reversible enzyme inhibitors. The market penetration will depend on how much improvement will occur in the efficacy and/or safety profiles when administered in combination with PCS6422. Currently, there are no other reversible or irreversible enzyme inhibitor products approved in the US and no irreversible enzyme inhibitors approved ex-US, which may make PCS6422 the first DPD irreversible inhibitor available.side effect concerns.
For PCS11T, the competitive factors will include establishing marketing penetration against the existing irinotecan product (Camptosar®) and the newer liposomal irinotecan product (Onivyde®). The establishment of that market will be based upon improved efficacy and/or safety of PCS11T.
| 12 |
Our commercial opportunity for any of our product candidates could be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, less expensive, more convenient or easier to administer, or have fewer or less severe side effects, than any products that we may develop. Our competitors also may obtain FDA, EMA or other regulatory approval for their products more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we are able to enter the market.
Intellectual Property
Our success will depend in large part on our ability and that of our licensors to:
| ● | obtain and maintain international and domestic patent and other legal protections for the proprietary technology, inventions and improvements we consider important to our business; | |
| ● | prosecute and defend our existing and future patents, once obtained; | |
| ● | preserve confidentiality of our own and our licensed methods, processes and know-how; and | |
| ● | operate without infringing the patents and proprietary rights of other parties. |
Although we rely extensively on licensing patents from third parties, we intend to seek appropriate patent protection for product candidates in our research and development programs, where applicable, and their uses by filing patent applications in the United States and other selected countries. We intend for these patent applications to cover, where possible, claims for compositions of matter, medical uses, processes for preparation and formulations.
Our current patent portfolio consists of the number of patents related to our drug candidates licensed from each third-party licensor. In addition to the international patents and/or international and U.S. patent applications licensed from our third-party licensors, we have licensed at least the following number of U.S. patents:
| CoNCERT | Yuhan | Aposense | Elion | Ocuphire | Total | |||||||||||||||||||
| U.S. patents | 9 | 4 | 3 | 3 | 6 | 25 | ||||||||||||||||||
| CoNCERT | Yuhan | Aposense | Elion | Ocuphire | Total | ||||||||
| U.S. patents | 9 | 5 | 3 | 2 | 6 | 25 |
We have filed aA provisional patent for PCS6422 and are evaluating another patent for PCS499.NGC-Cap has been filed.
Besides relying on patents, we may also rely on trade secrets, proprietary know-how and continuing innovation to develop and maintain our competitive position, especially when we do not believe that patent protection is appropriate or can be obtained. In addition, we continuously evaluate opportunities to obtain exclusivity through our regulatory filings with the FDA. We seek protection of these trade secrets, proprietary know-how and any continuing innovation, in part, through confidentiality and proprietary information agreements. However, these agreements may not provide meaningful protection for, or adequate remedies to protect, our technology in the event of unauthorized use or disclosure of information. Furthermore, our trade secrets may otherwise become known to, or be independently developed by, our competitors.
| 13 |
License Agreements
The following descriptions of our license agreements are only summaries. You should also refer to the copies of such agreements which have been filed as exhibits to this Annual Report.
License Agreement with Elion Oncology, Inc.
On August 23, 2020, we entered into a condition precedent License Agreement with Elion Oncology (“Elion License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS6422 globally. The license grant was conditioned on the following being satisfied by October 30, 2020: (i) our closing on an equity financing of at least $15 million in gross proceeds and (ii) successful up-listing to Nasdaq.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS6422 to our portfolio, and we paid $100,000 cash and issued 41,250 shares of our common stock to Elion. As part of the Elion License Agreement, we agreed to issue to Elion 5,000 shares of our common stock on each of the first and second anniversary dates of the Elion License Agreement.
As additional consideration, we will pay Elion development and regulatory milestone payments (a portion of which are payable in shares of our common stock and a portion of which are payable in cash) upon the achievement of certain milestones, which include FDA or other regulatory approval and dosing a patient. In addition, we must pay Elion one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any milestone payments received with Elion based on any sub-license agreement we may enter.
On May 17, 2022, we amended the third Milestone Event of Section 6.4 of our License Agreement with Elion Oncology, Inc. changing the third Milestone Event from “1st Patient in Dose Confirmation Study” to (a) determination of the maximum tolerated dose (MTD) or (b) determination of the recommended Phase 2 Dose. Prior to this amendment, the third milestone was not considered probable since it was unknown when, or if a dose confirmation study was going to be conducted. As a result of the modification, we consider it probable that the recommended Phase 2 dosage regimen could be determined in connection with our current Phase 1B trial for NGC-Cap. We recorded an expense and related liability of $189,000 representing the value of the shares we anticipate issuing to Elion at the fair value on the date of modification. No other terms or conditions of the License Agreement were modified. We determined the dosage for our Phase 2 study on January 25, 2024 and issued 5,000 shares of common stock to Elion for meeting this milestone.
We are required to use commercially reasonable efforts, at our sole cost and expense to research, develop and commercialize products in one or more countries, including dosing a first patient with a product in a Phase 2 or 3 clinical trial by October 2, 2024. We are currently on track to dose our first patient in a Phase 2 clinical trial by the deadline. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 90-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
| 14 |
License Agreement with Ocuphire Pharma, Inc.
On June 16, 2021, we executed a License Agreement with Ocuphire Pharma, Inc. (“Ocuphire Agreement”) under which we received a license to research, develop and commercialize PCS3117 globally, excluding the Republic of Singapore, China, Hong Kong, Macau and Taiwan.
As consideration for the Ocuphire Agreement, we issued 2,235 shares of our common stock to Ocuphire, a cash payment of $200,000 and assumed $66,583 in certain liabilities. Additional consideration includes future development and regulatory milestones payments to Ocuphire upon our achievement of certain defined clinical milestones, such as dosing a patient in pivotal trials and receiving marketing authorization by a regulatory authority in the United States or another country. In addition, we are required to pay Ocuphire one-time sales milestone payments based on the achievement during a calendar year of the highest annual Net Sales for products made and pay royalties based on annual Net Sales, as defined in the Ocuphire Agreement.
We are required to use commercially reasonable efforts, at our sole cost and expense to oversee such commercialization efforts, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) first patient administered drug in a Clinical Trial of a Product prior to June 16, 2024 and (ii) first patient administered drug in a Pivotal Clinical Trial of a Product or first patient administered drug in a Clinical Trial for a Second Indication of a Product prior to June 16, 2026. We are currently in discussions with Ocuphire to extend these deadlines. Although we do not anticipate having any issues in extending the deadlines, there can be no assurance that such negotiations will be successful. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 120-day opportunity to cure such breach.
License Agreement with Aposense, Ltd.
On May 24, 2020, we entered into a condition precedent License Agreement with Aposense, Ltd. (“Aposense License Agreement”), pursuant to which we were granted Aposense’s patent rights and Know-How to develop and commercialize their next generation irinotecan cancer drug, PCS11T. The Aposense License Agreement provides us with an exclusive worldwide license (excluding China), to research, develop and commercialize products comprising or containing PCS11T. The license grant was conditioned on the following being satisfied within nine months of May 24, 2020 (or the Aposense License Agreement shall terminate): (i) our closing of an equity financing and successful up-listing to Nasdaq and (ii) Aposense obtaining the approval of the Israel Innovation Authority for the consummation of the transactions contemplated by the Aposense License Agreement.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS11T to our portfolio, and we issued 31,250 shares of our common stock to Aposense. As additional consideration, we will pay Aposense development and regulatory milestone payments (up to $3.0 million per milestone) upon the achievement of certain milestones, which primarily consist of having a drug indication approved by a regulatory authority in the United States or another country. In addition, we will pay Aposense one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any sales milestone payments or royalties we receive with Aposense based on any sub-license agreement we may enter.
License Agreement with Yuhan Corporation
On August 19, 2020, we entered into a License Agreement with Yuhan Corporation (“Yuhan License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS12852 globally, excluding South Korea.
As consideration for the Yuhan License Agreement and related Share Issuance Agreement, we issued to Yuhan 25,000 shares of common stock. As additional consideration, we will pay Yuhan development and regulatory milestone payments (a portion of which are payable in shares of our common stock based on the volume weighted average trading price during the period prior to such achievement and a portion of which are payable in cash) upon the achievement of certain milestones, based on a Yuhan affiliate purchasing 37,500 shares of common stock for $3,000,000 in our October 2020 underwritten public offering. The milestones primarily consist of dosing a patient in pivotal trials or having a drug indication approved by a regulatory authority in the United States or another country. In addition, we must pay Yuhan one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any milestone payments received with Yuhan based on any sub-license agreement we may enter.
We are required to use commercially reasonable efforts, at our sole cost and expense, in conjunction with a joint Processa-Yuhan Board to oversee such commercialization efforts, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) preparing a first draft of the product development plan within 90 days; (ii) requesting an FDA pre-IND meeting for a product within 6 months; (iii) dosing a first patient in a Phase 2A clinical trial with a product within 24 months; and (iv) dosing a first patient with a product in a Phase 2B clinical trial, Phase 3 clinical trial or other pivotal clinical trial with a product by August 19, 2024. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 60-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
| 15 |
License Agreement with CoNCERT Pharmaceuticals, Inc.
On October 4, 2017, Promet entered into a License Agreement with CoNCERT (“CoNCERT License Agreement”). On March 19, 2018, we, Promet, and CoNCERT entered into an Amended Option Licensing Agreement (“March Amendment”) that, among other things, assigned the CoNCERT Agreement from Promet to us and we exercised the exclusive commercial license option for the PCS499 compound from CoNCERT.
The CoNCERT License Agreement provides us with an exclusive (including as to CoNCERT) royalty-bearing license to CoNCERT’s patent rights and Know-How to develop, manufacture, use, sub-license and commercialize compounds (PCS499 and each metabolite thereof) and pharmaceutical products with such compounds worldwide. We are required to pay CoNCERT royalties, on a product–by-product basis, on future worldwide net sales, or pay a percentage of any sublicense revenue.
We will incur royalty obligations to CoNCERT on a country-by-country and product-by-product basis that expire on a country-by-country and product-by-product basis on the later of (i) expiration or invalidation of the last patent rights covering such product in such country or (ii) the tenth anniversary of the date of the first commercial sale to a non-sublicensee third party of such product in such country.
We are required to use commercially reasonable efforts, at our sole cost and expense, to develop and obtain regulatory approval for one product in the U.S. and at least one other major market and, subject to obtaining regulatory approval in the applicable major market, commercialize one product in the U.S. and at least one other major market. CoNCERT may terminate the agreement if, following written notice and a 60 day60-day opportunity to demonstrate a plan to cure, it believes that we are not using commercially reasonable efforts to develop and obtain regulatory approval for one product in the U.S. and in at least one other major market for any consecutive nine monthnine-month period.
The term of the CoNCERT License Agreement continues in full force and effect until the expiration of the last royalty term. On a country-by-country and product-by-product basis, upon the expiration of the royalty term in such country with respect to such product, we shall have a fully paid-up, perpetual, irrevocable license to such intellectual property with respect to such product in such country. In the event of a material breach of the CoNCERT Agreement, either party may terminate the agreement provided such breach is not cured in the 90 days following written notice of the breach (which is shortened to 15 days for a payment breach). In addition, either party may terminate the agreement upon an assignment for the benefit of creditors or the filing of an insolvency proceeding by or against the other party that is not dismissed within 90 days of such filing.
| 16 |
License Agreement with Yuhan Corporation
On August 19, 2020, we entered into a License Agreement with Yuhan Corporation (“Yuhan License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS12852 globally, excluding South Korea.
As consideration for the Yuhan License Agreement and related Share Issuance Agreement, we issued to Yuhan 500,000 shares of common stock. As additional consideration, we will pay Yuhan development and regulatory milestone payments (a portion of which are payable in shares of our common stock based on the volume weighted average trading price during the period prior to such achievement and a portion of which are payable in cash) upon the achievement of certain milestones, based on a Yuhan affiliate purchasing 750,000 shares of common stock for $3,000,000 in our October 2020 underwritten public offering. The milestones primarily consist of dosing a patient in pivotal trials or having a drug indication approved by a regulatory authority in the United States or another country. In addition, we must pay Yuhan one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any milestone payments received with Yuhan based on any sub-license agreement we may enter into.
In conjunction with a joint Processa-Yuhan Board to oversee such commercialization efforts, we are required to use commercially reasonable efforts, at our sole cost and expense, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) preparing a first draft of the product development plan within 90 days; (ii) requesting an FDA pre-IND meeting for a product within 6 months; (iii) dosing a first patient in a Phase 2A clinical trial with a product within 24 months; and (iv) dosing a first patient with a product in a Phase 2B clinical trial, Phase 3 clinical trial or other pivotal clinical trial with a product within 48 months. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 60-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
License Agreement with Ocuphire Pharma, Inc.
On June 16, 2021, we executed a License Agreement with Ocuphire Pharma, Inc. (“Ocuphire Agreement”) under which provided us with a license to research, develop and commercialize PCS3117 globally, excluding the Republic of Singapore, China, Hong Kong, Macau and Taiwan.
As consideration for the Ocuphire Agreement, we issued 44,689 shares of our common stock to Ocuphire, a cash payment of $200,000 and assumed certain liabilities. Additional consideration includes future development and regulatory milestones payments to Ocuphire upon our achievement of certain defined clinical milestones, such as dosing a patient in pivotal trials and receiving marketing authorization by a regulatory authority in the United States or another country. In addition, we are required to pay Ocuphire one-time sales milestone payments based on the achievement during a calendar year of the highest annual Net Sales for products made and pay royalties based on annual Net Sales, as defined in the Ocuphire Agreement.
We are required to use commercially reasonable efforts, at our sole cost and expense to oversee such commercialization efforts, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) first patient administered drug in a Clinical Trial of a Product prior to June 16, 2024; and (ii) first patient administered drug in a Pivotal Clinical Trial of a Product or first patient administered drug in a Clinical Trial for a Second Indication of a Product prior to June 16, 2026. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 120-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
License Agreement with Elion Oncology, Inc.
On August 23, 2020, we entered into a condition precedent License Agreement with Elion Oncology (“Elion License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS6422 globally. The grant of license was conditioned on the following being satisfied by October 30, 2020: (i) our closing on an equity financing of at least $15 million in gross proceeds and (ii) successful up-listing to Nasdaq.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS6422 to the Processa portfolio, and we paid $100,000 cash and issued 825,000 shares of our common stock to Elion. Such shares are subject to a lock-up, with 50% of such shares released from such lock up after six months and the remaining 25% tranches to be released following 9 months and 12 months, respectively.
As part of the Elion License Agreement, we have agreed to issue to Elion 100,000 shares of our common stock on each of the first and second anniversary dates of the Elion License Agreement. We issued 100,000 shares on the first anniversary and believe the payment on the second anniversary is probable and represent seller financing since the only condition related to their payment is the passage of time, which management does not believe is substantive. We valued the shares at $4.00 per share based on the underwritten public offering price on October 6, 2020, which is the date the conditions precedent in the license agreement were met.
As additional consideration, we will pay Elion development and regulatory milestone payments (a portion of which are payable in shares of our common stock and a portion of which are payable in cash) upon the achievement of certain milestones, which include FDA or other regulatory approval and dosing a patient. In addition, we must pay Elion one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any milestone payments received with Elion based on any sub-license agreement we may enter into.
We are required to use commercially reasonable efforts, at our sole cost and expense, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) dosing a first patient in a Phase 1B clinical trial with a product within 12 months; and (ii) dosing a first patient with a product in a Phase 2 or 3 clinical trial within 48 months. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 90-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
License Agreement with Aposense, Ltd.
On May 24, 2020, we entered into a condition precedent License Agreement with Aposense, Ltd. (“Aposense License Agreement”), pursuant to which we were granted Aposense’s patent rights and Know-How to develop and commercialize their next generation irinotecan cancer drug, PCS11T (formerly known as ATT-11T). The Aposense License Agreement provides us with an exclusive worldwide license (excluding China) to research, develop and commercialize products comprising or containing PCS11T. The grant of license was conditioned on the following being satisfied within nine months of May 24, 2020: (i) our closing of an equity financing and successful up-listing to Nasdaq and (ii) Aposense obtaining the approval of the Israel Innovation Authority for the consummation of the transactions contemplated by the Aposense License Agreement.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS11T to the Processa portfolio, and we issued 625,000 shares of our common stock to Aposense. Such shares are subject to a lock-up, with 40% of such shares released from such lock up after six months and the remaining two 30% tranches to be released upon completion of the next two subsequent quarters. As additional consideration, we will pay Aposense development and regulatory milestone payments (up to $3.0 million per milestone) upon the achievement of certain milestones, which primarily consist of having a drug indication approved by a regulatory authority in the United States or another country. In addition, we will pay Aposense one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any sales milestone payments or royalties we receive with Aposense based on any sub-license agreement we may enter into.
Government Regulation
The FDA and comparable regulatory authorities in state and local jurisdictions and in other countries impose substantial and burdensome requirements upon companies involved in the clinical development, manufacture, marketing and distribution of drugs, such as those we are developing. These agencies and other federal, state and local entities regulate, among other things, the research and development, testing, manufacture, quality control, safety, effectiveness, labeling, storage, record keeping, approval, advertising and promotion, distribution, post-approval monitoring and reporting, sampling and export and import of our product candidates.
U.S. Government Regulation
In the United States, the FDA regulates drugs under the Federal Food, Drug, and Cosmetic Act, or FDCA, and its implementing regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations requires the expenditure of substantial time and financial resources. Failure to comply with the applicable U.S. requirements at any time during the product development process, approval process or after approval, may subject an applicant to a variety of administrative or judicial sanctions, such as the FDA’s refusal to approve pending NDAs, withdrawal of an approval, imposition of a clinical hold, issuance of warning letters, product recalls, product seizures, total or partial suspension of production or distribution, injunctions, fines, refusals of government contracts, restitution, disgorgement or civil or criminal penalties.
The process required by the FDA before a drug may be marketed in the United States generally involves the following:
| ● | completion of pre-clinical laboratory tests, animal studies and formulation studies in compliance with the FDA’s good laboratory practice (GLP) regulations; | |
| ● | submission to the FDA of an IND application, which must become effective before human clinical trials may begin; |
| ● | approval by an independent Institutional Review Board (IRB), at each clinical site before each trial may be initiated; | |
| ● | performance of adequate and well-controlled human clinical trials in accordance with good clinical practices (GCP) requirements to establish the safety and efficacy of the proposed drug product for each indication; | |
| ● | submission to the FDA of an NDA; | |
| ● | satisfactory completion of an FDA advisory committee review, if applicable; | |
| ● | satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the product is produced to assess compliance with cGMP requirements and to assure that the facilities, methods and controls are adequate to preserve the drug’s identity, strength, quality and purity; | |
| ● | FDA review and approval of the NDA, including consideration of the views of any FDA advisory committee, prior to commercial marketing or sale of the drug in the United States; and | |
| ● | compliance with any post-approval requirements, including the potential requirement to implement a Risk Evaluation and Mitigation Strategy (REMS) or to conduct a post-approval study. |
Pre-clinical studies
Before testing any biological product candidate in humans, including our product candidates, the product candidate must undergo rigorous pre-clinical testing. The pre-clinical developmental stage generally involves laboratory evaluations of drug chemistry, formulation and stability, as well as studies to evaluate toxicity in animals, to assess the potential for adverse events and, in some cases, to establish a rationale for therapeutic use. The conduct of pre-clinical studies is subject to federal regulations and requirements, including GLP regulations for safety/toxicology studies. An IND sponsor must submit the results of the pre-clinical studies, together with manufacturing information, analytical data, any available clinical data or literature and a proposed clinical protocol, to the FDA as part of the IND.
An IND is a request for authorization from the FDA to administer an investigational product to humans and must become effective before human clinical trials may begin. Some long-term pre-clinical testing, such as animal tests of reproductive adverse events and carcinogenicity, may continue after the IND is submitted. An IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA raises concerns or questions before that time related to one or more proposed clinical trials and places the trial on clinical hold. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. As a result, submission of an IND may not result in the FDA allowing clinical trials to commence.
| 17 |
Clinical trials
The clinical stage of development involves the administration of the investigational product to healthy volunteers or patients under the supervision of qualified investigators, generally physicians not employed by, or under control of, the trial sponsor, in accordance with GCPs, which include the requirement that all research patients provide their informed consent for their participation in any clinical trial. Clinical trials are conducted under protocols detailing, among other things, the objectives of the clinical trial, dosing procedures, subject selection and exclusion criteria and the parameters to be used to monitor subject safety and assess efficacy. Each protocol, and any subsequent amendments to the protocol, must be submitted to the FDA as part of the IND. Furthermore, each clinical trial must be reviewed and approved by an IRB for each institution at which the clinical trial will be conducted to ensure that the risks to individuals participating in the clinical trials are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the informed consent form that must be provided to each clinical trial subject or his or her legal representative and must monitor the clinical trial until completed. There also are requirements governing the reporting of ongoing clinical trials and completed clinical trial results to public registries. Information about most clinical trials must be submitted within specific timeframes for publication on www.clinicaltrials.gov. Information related to the product, patient population, phase of investigation, study sites and investigators and other aspects of the clinical trial is made public as part of the registration of the clinical trial. Sponsors are also obligated to disclose the results of their clinical trials after completion. Disclosure of the results of these trials can be delayed in some cases for up to two years after the date of completion of the trial. Competitors may use thisthe publicly available information to gain knowledge regarding the progress of development programs.
Human clinical trials are typically conducted in three sequential phases, which may overlap or be combined:
| ● | Phase 1 clinical trials generally involve a small number of healthy volunteers or disease-affected patients who are initially exposed to a single dose and then multiple doses of the product candidate. The primary purpose of these clinical trials is to assess the metabolism, pharmacologic action, side effect tolerability and safety of the drug. | |
| ● | Phase 2 clinical trials involve studies in disease-affected patients to determine the dose required to produce the desired benefits. At the same time, safety and further pharmacokinetic and pharmacodynamic information is collected, possible adverse effects and safety risks are identified, and a preliminary evaluation of efficacy is conducted. The goal of the Phase 2 trial is to also determine the “best” dosage regimen(s) to evaluate in the Phase 3 trial. The “best” regimen(s) means the regimen(s) that is(are) most likely to provide a safe-efficacious regimen that appropriately balances the risk-benefit analysis that the FDA is required to evaluate in each drug approval. The ideal way to define this “best” regimen for FDA is to evaluate the adverse event-drug exposure and efficacy-drug exposure relationships, which has also been previously called dose-response relationships or studies, and which has now become the foundation for both the FDA’s Project Optimus Oncology initiative and the draft Guidance to determine the optimal dose for an oncology drug. | |
| ● | Phase 3 clinical trials generally involve a larger number of patients at multiple sites and are designed to provide the data necessary to demonstrate the effectiveness of the product for its intended use, its safety in use and to establish the overall benefit/risk relationship of the product and provide an adequate basis for product approval. These trials may include comparisons with placebo and/or other comparator treatments. The duration of treatment is often extended to mimic the actual use of a product during marketing. |
Post-approval trials, sometimes referred to as Phase 4 clinical trials, may be conducted after initial marketing approval. These trials are used to gain additional experience from the treatment of patients in the intended therapeutic indication, particularly for long-term safety follow up. In certain instances, the FDA may mandate the performance of Phase 4 clinical trials as a condition of approval of a biologics license application (BLA).
Progress reports detailing the results of the clinical trials must be submitted at least annually to the FDA and more frequently if serious adverse events occur. The FDA or the sponsor may suspend or terminate a clinical trial at any time, or the FDA may impose other sanctions on various grounds, including a finding that the research patients are being exposed to an unacceptable health risk. Similarly, an IRB can refuse, suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients.
Concurrently with clinical trials, companies usually complete additional pre-clinical studies and must also develop additional information about the physical characteristics of the biological product as well as finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the product candidate and, among other things, the sponsor must develop methods for testing the identity, strength, quality, potency and purity of the final biological product. Additionally, appropriate packaging must be selected and tested, and stability studies must be conducted to demonstrate that the biological product candidate does not undergo unacceptable deterioration over its shelf life.
| 18 |
Marketing Approval
Assuming successful completion of the required clinical testing, the results of the pre-clinical studies and clinical trials, together with detailed information relating to the product’s chemistry, manufacture, controls and proposed labeling, among other things, are submitted to the FDA as part of an NDA requesting approval to market the product for one or more indications. In most cases, the submission of an NDA is subject to a substantial application user fee.
The review process typically takes twelve months from the date the NDA is submitted to the FDA. The FDA conducts a preliminary review of all NDAs within the first 60 days after submission to determine whether they are sufficiently complete to permit substantive review before accepting them for “filing.” The FDA may request additional information rather than accept an NDA for filing. In this event, the application must be resubmitted with the additional information. The resubmitted application is also subject to review before the FDA accepts it for filing. Once the submission is accepted for filing, the FDA begins an in-depth substantive review. The FDA reviews an NDA to determine, among other things, whether the drug is safe and effective and whether the facility in which it is manufactured, processed, packaged or held meets standards designed to assure the product’s continued safety, quality and purity. Under the current guidelines in effect in the Prescription Drug User Fee Act (PDUFA), the FDA has a goal to review and act on the submission within ten months from the completion of the preliminary review of a standard NDA for a new molecular entity.
In addition, under the Pediatric Research Equity Act of 2003, as amended and reauthorized, certain NDAs or supplements to an NDA must contain data that are adequate to assess the safety and effectiveness of the drug for the claimed indications in all relevant pediatric subpopulations, and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The FDA may, on its own initiative or at the request of the applicant, grant deferrals for submission of some or all pediatric data until after approval of the product for use in adults, or full or partial waivers from the pediatric data requirements.
The FDA also may require submission of a REMS plan to ensure that the benefits of the drug outweigh its risks. The REMS plan could include medication guides, physician communication plans, assessment plans, and/or elements to assure safe use, such as restricted distribution methods, patient registries, or other risk minimization tools.
The FDA may refer an application for a novel drug to an advisory committee. An advisory committee is a panel of independent experts, including clinicians and other scientific experts, that reviews, evaluates and provides a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions.
Before approving an NDA, the FDA typically will inspect the facility or facilities where the product is manufactured. The FDA will not approve an application unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving an NDA, the FDA may inspect one or more clinical trial sites to assure compliance with GCP requirements.
After evaluating the NDA and all related information, including the advisory committee recommendation, if any, and inspection reports regarding the manufacturing facilities and clinical trial sites, the FDA may issue an approval letter, or, in some cases, a complete response letter. A complete response letter generally contains a statement of specific conditions that must be met in order to secure final approval of the NDA and may require additional clinical trials or pre-clinical studies in order for FDA to reconsider the application. Even with submission of this additional information, the FDA ultimately may decide that the application does not satisfy the regulatory criteria for approval. If and when those conditions have been met to the FDA’s satisfaction, the FDA will typically issue an approval letter. An approval letter authorizes commercial marketing of the drug with specific prescribing information for specific indications.
| 19 |
Orphan drug designation
Under the Orphan Drug Act, the FDA may grant orphan designation to a drug or biologic product intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States, or more than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making the product available in the United States for this type of disease or condition will be recovered from sales of the product in the United States. Orphan drug designation must be requested before submitting a BLA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process. Orphan drug designation entitles a party to financial incentives such as opportunities for grant funding towards clinical trial costs, tax advantages and user-fee waivers.
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug exclusivity, which means that the FDA may not approve any other applications to market the same drug for the same indication for seven years from the date of such approval, except in limited circumstances, such as a showing of clinical superiority to the product with orphan exclusivity by means of greater effectiveness, greater safety, by providing a major contribution to patient care or in instances of drug supply issues. Competitors, however, may receive approval of either a different product for the same indication or the same product for a different indication that could be used “off-label” by physicians in the orphan indication, even though the competitor’s product is not approved in the orphan indication. Orphan drug exclusivity also could block the approval of one of our products for seven years if a competitor obtains approval before we do of the same product, as defined by the FDA, for the same indication we are seeking, or if our product candidate is determined to be contained within the scope of the competitor’s product for the same indication or disease. If one of our products designated as an orphan drug receives marketing approval for an indication broader than that which is designated, it may not be entitled to orphan drug exclusivity. Orphan drug status in the European Union, or EU, has similar, but not identical, requirements and benefits.
Expedited review and approval
The FDA has various programs, including fast track designation, accelerated approval, priority review and breakthrough therapy designation, which are intended to expedite or simplify the process for the development and FDA review of drugs that are intended for the treatment of serious or life-threatening diseases or conditions and demonstrate the potential to address unmet medical needs. The purpose of these programs is to provide important new drugs to patients earlier than under standard FDA review procedures.
To be eligible for a fast track designation, the FDA must determine, based on the request of a sponsor, that a product is intended to treat a serious or life-threatening disease or condition and demonstrates the potential to address an unmet medical need. The FDA will determine that a product will fill an unmet medical need if it will provide a therapy where none exists or provide a therapy that may be potentially superior to existing therapy based on efficacy or safety factors. The FDA may review sections of the NDA for a fast track product on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the NDA, the FDA agrees to accept sections of the NDA and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the NDA.
The FDA may give a priority review designation to drugs that offer major advances in treatment or provide a treatment where no adequate therapy exists. A priority review means that the goal for the FDA to review an application is six months, rather than the standard review of ten months under current PDUFA guidelines. Under the new PDUFA agreement, these six- and ten-month review periods are measured from the “filing” date rather than the receipt date for NDAs for new molecular entities, which typically adds approximately two months to the timeline for review and decision from the date of submission. Most products that are eligible for fast track designation are also likely to be considered appropriate to receive a priority review.
In addition, products studied for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may be eligible for accelerated approval and may be approved on the basis of adequate and well-controlled clinical trials establishing that the drug product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit, or on a clinical endpoint that can be measured earlier than irreversible morbidity or mortality, that is reasonably likely to predict an effect on irreversible morbidity or mortality or other clinical benefit, taking into account the severity, rarity or prevalence of the condition and the availability or lack of alternative treatments. As a condition of approval, the FDA may require a sponsor of a drug receiving accelerated approval to perform post-marketing studies to verify and describe the predicted effect on irreversible morbidity or mortality or other clinical endpoint, and the drug may be subject to accelerated withdrawal procedures.
| 20 |
Moreover, under the provisions of the Food and Drug Administration Safety and Innovation Act, a sponsor can request designation of a product candidate as a “breakthrough therapy.” A breakthrough therapy is defined as a drug that is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening disease or condition, and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. Drugs designated as breakthrough therapies are also eligible for accelerated approval. The FDA must take certain actions, such as holding timely meetings and providing advice, intended to expedite the development and review of an application for approval of a breakthrough therapy.
Even if a product qualifies for one or more of these programs, the FDA may later decide that the product no longer meets the conditions for qualification or decide that the time period for FDA review or approval will not be shortened. Furthermore, fast track designation, priority review and breakthrough therapy designation do not change the standards for approval, but may expedite the development or approval process. We may explore some of these opportunities for our product candidates as appropriate.
Post-approval requirements
Drugs manufactured or distributed pursuant to FDA approvals are subject to pervasive and continuing regulation by the FDA, including, among other things, requirements relating to recordkeeping, periodic reporting, product sampling and distribution, advertising and promotion and reporting of adverse experiences with the product. After approval, most changes to the approved product, such as adding new indications or other labeling claims are subject to prior FDA review and approval. There are also are continuing annual user fee requirements for any marketed products and the establishments at which such products are manufactured, as well as new application fees for supplemental applications with clinical data.
The FDA may impose a number of post-approval requirements as a condition of approval of an NDA. For example, the FDA may require post-marketing testing, including Phase 4 clinical trials, and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization.
In addition, drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are required to register their establishments with the FDA and state agencies, and are subject to periodic unannounced inspections by the FDA and these state agencies for compliance with cGMP requirements. Changes to the manufacturing process are strictly regulated and often require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from cGMP requirements and impose reporting and documentation requirements upon the sponsor and any third-party manufacturers that the sponsor may decide to use. Accordingly, manufacturers must continue to expend time, money, and effort in the area of production and quality control to maintain cGMP compliance.
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory requirements and standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with manufacturing processes, or failure to comply with regulatory requirements, may result in mandatory revisions to the approved labeling to add new safety information; imposition of post-market studies or clinical trials to assess new safety risks; or imposition of distribution or other restrictions under a REMS program. Other potential consequences include, among other things:
| ● | restrictions on the marketing or manufacturing of the product; | |
| ● | complete withdrawal of the product from the market or product recalls; | |
| ● | safety alerts, Dear Healthcare Provider letters, press releases or other communications containing warning or other safety information about the product; | |
| ● | fines, warning letters or holds on post-approval clinical trials; | |
| ● | refusal of the FDA to approve pending NDAs or supplements to approved NDAs, or suspension or revocation of product approvals; product seizure or detention, or refusal to permit the import or export of products; or | |
| ● | injunctions or the imposition of civil or criminal penalties. |
| 21 |
The FDA strictly regulates marketing, labeling, advertising and promotion of products that are placed on the market. Drugs may be promoted only for the approved indications and in accordance with the provisions of the approved label. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant liability.
In addition, the distribution of prescription pharmaceutical products is subject to the Prescription Drug Marketing Act (PDMA), which regulates the distribution of drugs and drug samples at the federal level and sets minimum standards for the registration and regulation of drug distributors by the states. Both the PDMA and state laws limit the distribution of prescription pharmaceutical product samples and impose requirements to ensure accountability in distribution.
Other Regulatory Matters
Pharmaceutical companies are subject to additional healthcare regulation and enforcement by the federal government and by authorities in the states and foreign jurisdictions in which they conduct their business. Manufacturing, sales, promotion and other activities following product approval are subject to regulation by numerous regulatory authorities in the United States in addition to the FDA, including Centers for Medicare and Medicaid Services (CMS), other divisions of the Department of Health and Human Services, the Department of Justice, the Drug Enforcement Administration, the Consumer Product Safety Commission, the Federal Trade Commission, the Occupational Safety & Health Administration, the Environmental Protection Agency, and state and local governments.
For example, in the United States, sales, marketing and scientific and educational programs also must comply with state and federal fraud and abuse laws, false claims laws, transparency laws, government price reporting, and health information privacy and security laws. These laws include the following:
| ● | the federal Anti-Kickback Statute, which makes it illegal for any person, including a prescription drug manufacturer (or a party acting on its behalf), to knowingly and willfully solicit, receive, offer or pay any remuneration that is intended to induce or reward referrals, including the purchase, recommendation, order or prescription of a particular drug, for which payment may be made under a federal healthcare program, such as Medicare or Medicaid. Moreover, the Patient Protection and Affordable Care Act of 2010, as amended by the Health Care and Education Reconciliation Act of 2010 (collectively, the ACA), provides that the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the civil False Claims Act; | |
| ● | federal civil and criminal false claims and civil monetary penalties laws, including the civil False Claims Act that can be enforced by private citizens through civil whistleblower or qui tam actions, prohibit individuals or entities from, among other things, knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| ● | the Federal Health Insurance Portability and Accountability Act of 1996 (HIPAA) which prohibits, among other things, executing or attempting to execute a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters;
| |
| ● | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act and their implementing regulations, which also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; | |
| ● | federal consumer protection and unfair competition laws, which broadly regulate marketplace activities and activities that potentially harm consumers; |
| 22 |
| ● | the FDCA, which prohibits, among other things, the adulteration or misbranding of drugs, biologics and medical devices; | |
| ● | the federal Physician Payments Sunshine Act, which requires applicable manufacturers of covered drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, with specific exceptions, to annually report to CMS information regarding payments and other transfers of value to physicians and teaching hospitals as well as information regarding ownership and investment interests held by physicians and their immediate family members; and | |
| ● | analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws which may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third-party payors, including private insurers; state laws that require biotechnology companies to comply with the biotechnology industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and may require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; state laws that require biotechnology companies to report information on the pricing of certain drug products; and state and foreign laws that govern the privacy and security of health information in some circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts. |
Pricing and rebate programs must also comply with the Medicaid rebate requirements of the U.S. Omnibus Budget Reconciliation Act of 1990 and more recent requirements in the ACA. If products are made available to authorized users of the Federal Supply Schedule of the General Services Administration, additional laws and requirements apply. Products must meet applicable child-resistant packaging requirements under the U.S. Poison Prevention Packaging Act. Manufacturing, sales, promotion and other activities also are potentially subject to federal and state consumer protection and unfair competition laws.
The distribution of pharmaceutical products is subject to additional requirements and regulations, including extensive record-keeping, licensing, storage and security requirements intended to prevent the unauthorized sale of pharmaceutical products.
The failure to comply with any of these laws or regulatory requirements subjects firms to possible legal or regulatory action. Depending on the circumstances, failure to meet applicable regulatory requirements can result in significant civil, criminal and administrative penalties, including damages, fines, disgorgement, individual imprisonment, exclusion from participation in government funded healthcare programs, such as Medicare and Medicaid, integrity oversight and reporting obligations, contractual damages, reputational harm, diminished profits and future earnings, injunctions, requests for recall, seizure of products, total or partial suspension of production, denial or withdrawal of product approvals or refusal to allow a firm to enter into supply contracts, including government contracts.
U.S. Patent-Term Restoration and Marketing Exclusivity
Depending upon the timing, duration and specifics of FDA approval of any future product candidates, some of our U.S. patents may be eligible for limited patent term extension under the Hatch-Waxman Act. The Hatch-Waxman Act permits restoration of the patent term of up to five years as compensation for patent term lost during product development and FDA regulatory review process. Patent-term restoration, however, cannot extend the remaining term of a patent beyond a total of 14 years from the product’s approval date. The patent-term restoration period is generally one-half the time between the effective date of an IND or the issue date of the patent, whichever is later, and the submission date of an NDA plus the time between the submission date of an NDA or the issue date of the patent, whichever is later, and the approval of that application, except that the review period is reduced by any time during which the applicant failed to exercise due diligence. Only one patent applicable to an approved drug is eligible for the extension and the application for the extension must be submitted prior to the expiration of the patent. The United States Patent and Trademark Office, in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In the future, we may apply for restoration of patent term for our currently owned or licensed patents to add patent life beyond its current expiration date, depending on the expected length of the clinical trials and other factors involved in the filing of the relevant NDA.
| 23 |
Market exclusivity provisions under the FDCA also can delay the submission or the approval of certain applications. The FDCA provides a five-year period of non-patent marketing exclusivity within the United States to the first applicant to gain approval of an NDA for a new chemical entity. A drug is a new chemical entity if the FDA has not previously approved any other new drug containing the same active moiety, which is the molecule or ion responsible for the action of the drug substance. During the exclusivity period, the FDA may not accept for review an abbreviated new drug application (ANDA) or a 505(b)(2) NDA submitted by another company for another version of such drug where the applicant does not own or have a legal right of reference to all the data required for approval. However, an application may be submitted after four years if it contains a certification of patent invalidity or non-infringement. The FDCA also provides three years of marketing exclusivity for an NDA, 505(b)(2) NDA or supplement to an existing NDA if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant are deemed by the FDA to be essential to the approval of the application, for example, new indications, dosages or strengths of an existing drug. This three-year exclusivity covers only the conditions of use associated with the new clinical investigations and does not prohibit the FDA from approving ANDAs for drugs containing the original active agent. Five-year and three-year exclusivity will not delay the submission or approval of a full NDA. However, an applicant submitting a full NDA would be required to conduct or obtain a right of reference to all of the preclinical studies and adequate and well-controlled clinical trials necessary to demonstrate safety and effectiveness.
European Union Drug Development
Similar to the United States, the various phases of preclinical and clinical research in the European Union are subject to significant regulatory controls. Although the European Union Clinical Trials Directive 2001/20/EC has sought to harmonize the EU clinical trials regulatory framework, setting out common rules for the control and authorization of clinical trials in the EU, the EU Member States have transposed and applied the provisions of the Directive differently. This has led to significant variations in the member state regimes. Under the current regime, before a clinical trial can be initiated, it must be approved in each of the EU countries where the trial is to be conducted by two distinct bodies: the National Competent Authority (NCA) and one or more Ethics Committees (ECs). Under the current regime, all suspected unexpected serious adverse reactions to the investigated drug that occur during the clinical trial have to be reported to the NCA and ECs of the Member State where they occurred.
The EU clinical trials legislation is currently is undergoing a transition process mainly aimed at harmonizing and streamlining clinical-trial authorization , simplifying adverse-event reporting procedures, improving the supervision of clinical trials and increasing their transparency. Recently enacted Clinical Trials Regulation EU No 536/2014 ensures that the rules for conducting clinical trials in the EU will be identical. In the meantime, Clinical Trials Directive 2001/20/EC continues to govern all clinical trials performed in the EU.
European Union Drug Review and Approval
In the European Economic Area (EEA), which is comprised of the 26 Member States of the European Union (including Norway and excluding Croatia), Iceland and Liechtenstein, medicinal products can only be commercialized after obtaining a Marketing Authorization (MA). There are two types of marketing authorizations:
| ● | The Community MA is issued by the European Commission through the Centralized Procedure, based on the opinion of the Committee for Medicinal Products for Human Use (CHMP) of the EMA, and is valid throughout the entire territory of the EEA. The Centralized Procedure is mandatory for certain types of products, such as biotechnology medicinal products, orphan medicinal products, advanced-therapy medicines such as gene-therapy, somatic cell-therapy or tissue-engineered medicines and medicinal products containing a new active substance indicated for the treatment of HIV, AIDS, cancer, neurodegenerative disorders, diabetes, auto-immune and other immune dysfunctions and viral diseases. The Centralized Procedure is optional for products containing a new active substance not yet authorized in the EEA, or for products that constitute a significant therapeutic, scientific or technical innovation or which are in the interest of public health in the European Union. |
| 24 |
| ● | National MAs, which are issued by the competent authorities of the Member States of the EEA and only cover their respective territory, are available for products not falling within the mandatory scope of the Centralized Procedure. Where a product has already been authorized for marketing in a Member State of the European Union, this National MA can be recognized in another Member State through the Mutual Recognition Procedure. If the product has not received a National MA in any Member State at the time of application, it can be approved simultaneously in various Member States through the Decentralized Procedure. Under the Decentralized Procedure, an identical dossier is submitted to the competent authorities of each of the Member States in which the MA is sought, one of which is selected by the applicant as the Reference Member State (RMS). The competent authority of the RMS prepares a draft assessment report, a draft summary of the product characteristics (SmPC), and a draft of the labeling and package leaflet, which are sent to the other Member States (referred to as the Member States Concerned) for their approval. If the Member States Concerned raise no objections, based on a potential serious risk to public health, to the assessment, SmPC, labeling or packaging proposed by the RMS, the product is subsequently granted a national MA in all the Member States (i.e., in the RMS and the Member States Concerned). |
Under the above describedabove-described procedures, before granting the MA, EMA or the competent authorities of the Member States of the European Union make an assessment of the risk-benefit balance of the product on the basis of scientific criteria concerning its quality, safety and efficacy. Similar to the U.S. patent term-restoration, Supplementary Protection Certificates (SPCs) serve as an extension to a patent right in Europe for up to five years. SPCs apply to specific pharmaceutical products to offset the loss of patent protection due to the lengthy testing and clinical trials these products require prior to obtaining regulatory marketing approval.
Coverage and Reimbursement
Sales of our products will depend, in part, on the extent to which our products will be covered by third-party payors, such as government health programs, commercial insurance, and managed healthcare organizations. There is significant uncertainty related to third-party payor coverage and reimbursement of newly approved products. In the United States, for example, principal decisions about reimbursement for new products are typically made by CMS. CMS decides whether and to what extent a new product will be covered and reimbursed under Medicare, and private third-party payors often follow CMS’s decisions regarding coverage and reimbursement to a substantial degree. However, no uniform policy of coverage and reimbursement for drug products exists. Accordingly, decisions regarding the extent of coverage and amount of reimbursement to be provided for any of our products will be made on a payor-by-payor basis.
Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. Further, such payors are increasingly challenging the price, examining the medical necessity and reviewing the cost effectiveness of medical product candidates. There may be especially significant delays in obtaining coverage and reimbursement for newly approved drugs. Third-party payors may limit coverage to specific product candidates on an approved list, known as a formulary, which might not include all FDA-approved drugs for a particular indication. We may need to conduct expensive pharmaco-economic studies to demonstrate the medical necessity and cost effectiveness of our products. As a result, the coverage determination process is often a time-consuming and costly process that will require us to provide scientific and clinical support for the use of our products to each payor separately, with no assurance that coverage and adequate reimbursement will be obtained.
In addition, in most foreign countries, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing and reimbursement vary widely from country to country. For example, the European Union provides options for its Member States to restrict the range of medicinal products for which their national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A Member State may approve a specific price for the medicinal product, or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products. Historically, products launched in the European Union do not follow price structures of the United States and generally prices tend to be significantly lower.
| 25 |
Healthcare Reform
The United States government, state legislatures, and foreign governments have shown significant interest in implementing cost containment programs to limit the growth of government-paid healthcare costs, including price-controls, restrictions on reimbursement, and requirements for substitution of generic products for branded prescription drugs. For example, the ACA was passed in March 2010 whichand substantially changed the way healthcare is financed by both the government and private insurers, and significantly impacts the U.S. pharmaceutical industry. The ACA contains provisions that may reduce the profitability of drug products through increased rebates for drugs reimbursed by Medicaid programs, extension of Medicaid rebates to Medicaid managed care plans, mandatory discounts for certain Medicare Part D beneficiaries and annual fees based on pharmaceutical companies’ share of sales to federal health care programs.
The Medicaid Drug Rebate Program requires pharmaceutical manufacturers to enter into and have in effect a national rebate agreement with the HHS Secretary as a condition for states to receive federal matching funds for the manufacturer’s outpatient drugs furnished to Medicaid patients. The ACA made several changes to the Medicaid Drug Rebate Program, including increasing pharmaceutical manufacturers’ rebate liability by raising the minimum basic Medicaid rebate on most branded prescription drugs from 15.1% of average manufacturer price (AMP), to 23.1% of AMP and adding a new rebate calculation for “line extensions” (i.e., new formulations, such as extended release formulations) of solid oral dosage forms of branded products, as well as potentially impacting their rebate liability by modifying the statutory definition of AMP. The ACA also expanded the universe of Medicaid utilization subject to drug rebates by requiring pharmaceutical manufacturers to pay rebates on Medicaid managed care utilization and by enlarging the population potentially eligible for Medicaid drug benefits. Effective April 1, 2020, Medicaid rebate liability will be expanded to include the territories of the United States as well. Additionally, for a drug product to receive federal reimbursement under the Medicaid or Medicare Part B programs or to be sold directly to U.S. government agencies, the manufacturer must extend discounts to entities eligible to participate in the 340B drug pricing program. The required 340B discount on a given product is calculated based on the AMP and Medicaid rebate amounts reported by the manufacturer.
Some of the provisions of the ACA have yet to be implemented, and there have been judicial, Congressional and executive branch challenges to certain aspects of the ACA. Additionally, there has been heightened governmental scrutiny recently over the manner in which drug manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed and enacted federal and state legislation designed to, among other things, bring more transparency to product pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drug products. For example, at the federal level, there is a “Blueprint” to lower prescription drug prices and reduce out-of-pocket costs of drugs that contains additional proposals to increase manufacturer competition, increase the negotiating power of certain federal healthcare programs, incentivize manufacturers to lower the list price of their products and reduce the out-of-pocket costs of drug products paid by consumers. At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical and biological product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
Further, on August 16, 2022, President Biden signed the Inflation Reduction Act of 2022 (“IRA”) into law, which among other things, extends enhanced subsidies for individuals purchasing health insurance coverage in ACA marketplaces through plan year 2025. The IRA also eliminates the “donut hole” under the Medicare Part D program beginning in 2025 by significantly lowering the beneficiary maximum out-of-pocket cost and creating a new manufacturer discount program. It is possible that the Affordable Care Act will be subject to judicial or Congressional challenges in the future. It is unclear how such challenges and the healthcare reform measures of the current administration will impact the Affordable Care Act and our business.
Moreover, the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) established the Medicare Part D program to provide a voluntary prescription drug benefit to Medicare beneficiaries. Under Part D, Medicare beneficiaries may enroll in prescription drug plans offered by private entities that provide coverage of outpatient prescription drugs. Unlike Medicare Part A and B, Part D coverage is not standardized. While all Medicare drug plans must give at least a standard level of coverage set by Medicare, Part D prescription drug plan sponsors are not required to pay for all covered Part D drugs, and each drug plan can develop its own drug formulary that identifies which drugs it will cover and at what tier or level. However, Part D prescription drug formularies must include drugs within each therapeutic category and class of covered Part D drugs, though not necessarily all the drugs in each category or class. Any formulary used by a Part D prescription drug plan must be developed and reviewed by a pharmacy and therapeutic committee. Government payment for some of the costs of prescription drugs may increase demand for products for which we receive marketing approval. However, any negotiated prices for our products covered by a Part D prescription drug plan likely will be lower than the prices we might otherwise obtain. Moreover, while the MMA applies only to drug benefits for Medicare beneficiaries, private third-party payors often follow Medicare coverage policy and payment limitations in setting their own payment rates.
| 26 |
EmployeesHuman Capital
As of March 24, 2022,21, 2024, we had 15 full13 full- and part timepart-time employees. None of our employees is subject to a collective bargaining agreement or represented by a trade or labor union and we believe our relationships with our employees are good.
We are highly dependent upon the principal members of our small management team and staff, including David Young, Pharm.D., Ph.D, our Chief Executive Officer, George Ng; President of Research and Development, David Young, Pharm.D., Ph.D; and our Chief Development and Regulatory Officer, Sian Bigora, Pharm.D., our Chief Development Officer. Despite our efforts to retain valuable employees, members of our management, scientific and development teams may terminate their employment with us on short notice. Although we expect to have employment agreements with our key employees, these employment agreements may still allow these employees to leave our employment at any time, for or without cause. Our success also depends on our ability to continue to attract, retain and motivate highly skilled junior, mid-level and senior managers as well as junior, mid-level and senior scientific and medical and scientific personnel.
Corporate Information
We were incorporated under the laws of the State of Delaware on March 29, 2011. Our principal executive office is located at 7380 Coca Cola Drive, Suite 106, Hanover, MD 21076. Our telephone number is (443) 776-3133.
We make available free of charge on or through our Internet website (http://www.processapharmaceuticals.com) our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and, if applicable, amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act, as well as our Code of Ethics and Code of Conduct, as soon as reasonably practicable after we electronically file such material with, or furnish it to, the Securities and Exchange Commission (SEC). The SEC also maintains a website which provides online access to reports and other information regarding registrants that file electronically with the SEC at: www.sec.gov.
The information contained on our website and social media channels is not included as a part of, or incorporated by reference into, this report.
Information about our Executive Officers
Our executive officers as of March 24, 2022 are as follows:
David Young, Pharm.D., Ph.D.- Dr. Young has served as our Chairman and Chief Executive Officer since October 4, 2017 and has over 30 years of pharmaceutical research, drug development and corporate experience. He served as our interim CFO from October 4, 2017 to September 1, 2018. From 2006 to 2009, prior to joining the Questcor executive management team, Dr. Young served as an independent Director on the Questcor Board of Directors. As an independent director, Dr. Young, representing Questcor, worked with the FDA in developing a process to obtain approval for Acthar (the only commercial product owned by Questcor) in Infantile Spasms (IS), a deadly and debilitating very rare orphan indication. In 2009, Dr. Young joined the Questcor executive management team as Chief Scientific Officer (CSO) in order to obtain IS FDA approval and market exclusivity by completing the New Drug Application (NDA) process, working with FDA on modernizing the label, and leading all aspects of approval including the Advisory Committee Meeting that voted to approve the NDA for IS. During the eight years that Dr. Young was involved with Questcor as an independent director and as its CSO, Questcor transitioned to an orphan drug specialty pharmaceutical company, moving from an outdated Acthar label and near bankruptcy in 2007 to a modernized Acthar label that helped it to achieve sales greater than $750 million per year and the ultimate sale of the company for approximately $5.6 billion in 2014. While serving on Questcor’s Board of Directors, Dr. Young was Executive Director & President, U.S. Operations of AGI Therapeutics plc. Dr. Young has also served as the Executive Vice President of the Strategic Drug Development Division of ICON plc, an international CRO, and was the Founder and CEO of GloboMax LLC, a CRO specializing in FDA drug development, purchased by ICON plc in 2003. Prior to forming GloboMax, Dr. Young was a Tenured Associate Professor at the School of Pharmacy, University of Maryland at Baltimore (UMAB), where he led a group of 30 faculty, scientists, postdocs, graduate students and technicians in evaluating the biological properties of drugs and drug delivery systems in animals and humans.
Dr. Young is an expert in small molecule and protein non-clinical and clinical drug development. He has served on FDA Advisory Committees, was Co-Principal Investigator on an FDA-funded Clinical Pharmacology contract, was responsible for the analytical and pharmacokinetic evaluation of all oral products manufactured in the UMAB-FDA contract which led to the Scale-up and Post-Approval Changes (SUPAC) and in-vitro in-vivo correlation (IVIVC) FDA Guidance, taught FDA reviewers as part of the UMAB-FDA contract for five years, has served on National Institutes of Health (NIH) grant review committees, and was Co-Principal Investigator on a National Cancer Institute contract to evaluate new oncology drugs. Dr. Young has met with the FDA over 100 times on more than 50 drug products and has been a key team member on more than 30 NDA/supplemental NDA approvals. Dr. Young has more than 150 presentations-authored publications-book chapters, including formal presentations to the FDA, FDA Advisory Committees, and numerous invited presentations at both scientific and investment meetings. Dr. Young received his B.S. in Physiology from the University of California at Berkeley, his M.S. in Medical Physics from the University of Wisconsin at Madison, and his Pharm.D. - Ph.D. with emphasis in Pharmacokinetics and Pharmaceutical Sciences from the University of Southern California.
Sian Bigora, Pharm.D.- Dr. Bigora has served as our Chief Development Officer since October 4, 2017 and has over 20 years of pharmaceutical research, regulatory strategy and drug development experience working closely with Dr. Young. From 2009 to 2015 Dr. Bigora was Vice President of Regulatory Affairs at Questcor Pharmaceuticals (acquired by Mallinckrodt Pharmaceuticals in 2014), including leading efforts on modernizing the Acthar Gel label and in obtaining FDA approval in Infantile Spasms, events of material importance to Questcor’s subsequent success. During her time at Questcor, she assisted in building an expert regulatory group to address both commercial and development needs for complex products such as Acthar. Dr. Bigora’s role at Questcor included heading up the development of a safety pharmacovigilance group and a clinical quality group. Prior to her position at Questcor, Dr. Bigora was Vice President of Clinical and Regulatory Affairs, U.S. Operations of AGI Therapeutics, plc. In this role, she was responsible for the development and implementation of Global Phase 3 studies and interactions with regulatory authorities. Previously, she operated her own consulting company, serving as the regulatory and drug development expert team member for multiple small and mid-sized pharmaceutical companies. Dr. Bigora held multiple positions in regulatory affairs, operations and project management ending as VP of Regulatory Affairs at the Strategic Drug Development Division of ICON, plc, an international CRO, and at GloboMax LLC, a CRO specializing in FDA drug development, purchased by ICON plc in 2003. Prior to GloboMax, she worked in the Pharmacokinetics and Biopharmaceutics Laboratory at the School of Pharmacy, University of Maryland on the FDA funded Clinical Pharmacology contract and UMAB-FDA contract as a clinical scientist and instructor for FDA reviewers. Dr. Bigora received a Pharm.D. from the School of Pharmacy at the University of Maryland at Baltimore. She also completed a Fellowship in Pharmacokinetics and Pediatric Infectious Diseases at the University of Maryland at Baltimore.
Michael Floyd – Mr. Floyd has served as our Chief Operating Officer since October 6, 2020. Mr. Floyd has been a serial entrepreneur with over 15 years of experience with early-stage biopharma businesses in infectious diseases, oncology and rare diseases. In 1996, he founded Neurologic, an early-stage enterprise that in-licensed technology from the National Institutes of Health for a diagnostic test for Alzheimer’s disease. Mr. Floyd was the co-author of the plan that created the Blanchette Rockefeller Neurosciences Institute in 1998 with the Honorable Jay Rockefeller and Johns Hopkins University. In 2006, Mr. Floyd was the Chief Executive Officer for the North American subsidiary of Arpida Ltd. where he organized the Phase 3 program for an MRSA drug and organized the NDA submission. Mr. Floyd subsequently led the US efforts to remediate the NDA for Gentium, SpA for defibrotide beginning in 2011. Mr. Floyd was the Founder of Bio-AIM, which is developing monoclonal antibodies for Acinetobacter baumannii and a Co-Founder of Exbaq, which is developing therapies for Gram negative pathogens. In 2016, Mr. Floyd co-founded Elion Oncology and served as its Chief Executive officer until joining Processa. Mr. Floyd received a BSBA in Accounting from Georgetown University and is a Certified Public Accountant (inactive).
Wendy Guy- Ms. Guy has served as our Chief Administrative Officer since October 4, 2017 and has more than 20 years of experience in business operations. She has worked closely with Dr. Young in the past in corporate management and operations, human resources, and finance roles. From 2009 to 2014, Ms. Guy was employed at Questcor Pharmaceuticals (acquired by Mallinckrodt Pharmaceuticals in 2014) as Senior Manager, Business Operation in charge of the Maryland Office for Questcor. During the five years she spent at Questcor, she built a dynamic administrative and contracts team, grew the Maryland Office from two employees to just under 100, and expanded the facility from 1,200 sq. ft. to 15,000 sq. ft. Prior to her position at Questcor, Ms. Guy was Senior Manager, U.S. Operations of AGI Therapeutics, plc. In this role, she was responsible for the day-to-day business and administrative operations of the company. Previously, she held multiple senior level positions with the Strategic Drug Development Division of ICON, GloboMax, and Mercer Management Consulting. Ms. Guy received an A.A. from Mount Wachusett Community College.
Patrick Lin - Mr. Lin has served as our Chief Business & Strategy Officer since October 4, 2017 and has over 20 years of financing and investing experience in the Biopharm Sector. He is founder and, for more than 15 years, Managing Partner of Primarius Capital, a family office that manages public and private investments focused on small capitalization companies. For 10 years prior to forming Primarius Capital, Mr. Lin worked at several Wall Street banking and brokerage firms including Robertson Stephens & Co., E*Offering, and Goldman Sachs & Co. Mr. Lin was Co-Founding Partner of E*Offering. Mr. Lin received an MBA from Kellogg Graduate School of Management, a Master of Engineering Management, and a Bachelor of Science in Business Administration from the University of Southern California.
James Stanker - Mr. Stanker has served as our Chief Financial Officer since September 5, 2018. Mr. Stanker has over 30 years of financial and executive leadership experience in the areas of accounting principles and audit standards, regulatory reporting, and fiscal management and strategy. He has served in a financial leadership role as an audit partner at Grant Thornton from February 2000 until his retirement in August 2016. His responsibilities included managing the audit quality in the Atlantic Coast Market Territory. From 2009 to 2012, he served as the Global Head of Audit Quality for Grant Thornton International. Prior to joining Grant Thornton, Mr. Stanker served as the Chief Financial Officer for a Nasdaq listed company and for a privately-held life science company. Mr. Stanker is a Certified Public Accountant. He has a Bachelors degree in Aeronautics from San Jose State University and a Masters in Business Administration from California State University, East Bay. He previously served on the Board of Directors of GSE Systems, Inc. Mr. Stanker is also a visiting professor in the George B. Delaplaine School of Business at Hood College.
Item 1A. Risk Factors
An investment in our common stock involves a high degree of risk. If any of the following risks actually occur, our business, financial condition, or results of operations could be materially adversely affected, the trading price of our common stock could decline, and you may lose all or part of your investment. You should also refer to the other information contained in this Form 10-K, including our consolidated financial statements and the notes to those statements, and the information set forth under the caption “Special Note Regarding Forward-Looking Statements and Risk Factor Summary.” The risks described below and contained in our other periodic reports are not the only ones that we face. Additional risks not presently known to us or that we currently deem immaterial may also adversely affect our business operations.
Risks Related to Our Financial Position and Need for Additional Capital
We have a history of losses and we may never become profitable.
We are a clinical stage biopharmaceutical company. Processa itself as an organization has never had a drug approved by the FDA or any regulatory agency. The likelihood of success of our business plan must be considered in light of the challenges, substantial expenses, difficulties, complications and delays frequently encountered in connection with developing and expanding early-stage businesses and the regulatory and competitive environment in which we operate. Biopharmaceutical product development is a highly speculative undertaking, involves a substantial degree of risk, and is a capital-intensive business. If we cannot successfully execute our plan to develop our drug pipeline, our business may not succeed.
At December 31, 2021,2023, the accumulated deficit was approximately $36.8$75.4 million. We will incur additional losses as we continue our research and development activities, seek regulatory approvals for our product candidates and engage in clinical trials. These losses will cause, among other things, our stockholders’ equity and working capital to decrease. Any future earnings and cash flow from the operations of our business are dependent on our ability to further develop our products and on revenues and profitability from sales of products or successful joint venture relationships.
| 27 |
There can be no assurance that we will be able to generate sufficient product revenue to become profitable at all or on a sustained basis. Even if we generate revenues, we expect to have quarter-to-quarter fluctuations in revenues and expenses, some of which could be significant, due to research, development, clinical trial, and marketing and manufacturing expenses and activities. We also expect to incur substantial expenses without corresponding revenues, unless and until we are able to obtain regulatory approval and successfully license or commercialize our product candidates. If our product candidates fail in clinical trials or do not gain regulatory approval, or if our products do not achieve market acceptance, we may never become profitable.
We may never be able to obtain regulatory approval for the marketing of our product candidates in any indication in the United States or internationally. As we commercialize and market products, we will need to incur expenses for product marketing and brand awareness and conduct significant research, development, testing and regulatory compliance activities that, together with general and administrative expenses, could result in substantial operating losses for the foreseeable future. Even if we do achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our stock price may decline, and you may lose all or a substantial part of your investment in us.
We have limited cash resources and will require additional financing.
Since inception, we have not generated any revenue, have incurred net losses, have used net cash in our operations and have funded our business and operations primarily through proceeds from the sale of our securities. We expect to continue to require significant future financing to fund our operating activities and to use cash in operating activities for the foreseeable future as we continue our research and development activities to develop products that can be commercialized to generate revenue. Our ability to obtain additional financing will be subject to many factors, including market conditions, our operating performance and investor sentiment. If we are unable to raise additional capital when required or on acceptable terms, we may have to significantly delay, scale back or discontinue the development or commercialization of one or more of our product candidates, restrict our operations or obtain funds by entering into agreements on unattractive terms, which would likely have a material adverse effect on our business, stock price and our relationships with third parties with whom we have business relationships, at least until additional funding is obtained. If we do not have sufficient funds to continue operations, we could be required to seek bankruptcy protection or other alternatives that would likely result in our stockholders losing some or all of their investment in us.
We may seek additional capital through a combination of private and public equity offerings, debt financings and strategic collaborations, including sales of our common stock under ourthe existing or a future equity line of credit or through a future at-the-market sales agreement and/or our agreement with Lincoln Park, LLC.offering. If we raise additional funds through the issuance of equity or convertible debt securities, the percentage ownership of our stockholders could be significantly diluted, and these newly issued securities may have rights, preferences or privileges senior to those of existing stockholders. Debt, receivables and royalty financings may be coupled with an equity component, such as warrants to purchase stock, which could also result in dilution of our existing stockholders’ ownership. The incurrence of indebtedness would result in increased fixed payment obligations and could also result in certain restrictive covenants, such as limitations on our ability to incur additional debt, limitations on our ability to acquire or license intellectual property rights and other operating restrictions that could adversely impact our ability to conduct our business and may result in liens being placed on our assets and intellectual property. If we were to default on such indebtedness, we could lose such assets and intellectual property. If we raise additional funds through strategic partnerships and alliances and licensing arrangements with third parties, we may have to relinquish valuable rights to our product candidates or grant licenses on terms that are not favorable to us.
| 28 |
The ongoing COVID-19 pandemic or another pandemic may disrupt our operations and affect
Our financial statements contain a statement regarding a substantial doubt about our ability to successfully conduct clinical studies and raise capital.
The COVID-19 pandemic has negatively impacted the global economy, disrupted global supply chains, and created significant volatility and disruption in the financial and capital markets. We are unable to accurately predict the full impact that the ongoing COVID-19 pandemic will have on our results from operations, financial condition, and scientific and clinical activities due to numerous factors that are not within our control, including the duration and severity of the outbreak, stay-at-home orders, business closures, travel restrictions, supply chain disruptions and employee illness or quarantines, which could result in disruptions to our operations and adversely impact our results from operations and financial condition. In addition, the COVID-19 pandemic has resulted in ongoing volatility in the financial and capital markets. If our access to capital is restricted or associated borrowing costs increasecontinue as a result of developments in financial markets relating to the COVID-19 pandemic, our operations and financial condition could be adversely impacted.
We have experienced delays in the enrollment of patients in our PCS499 Phase 2B trial due to COVID-19. Potential patients have died of COVID-19 prior to screening and continue to be reluctant to travel to our testing sites for fear of contracting COVID-19. Delays in enrollment lengthen the time of studies and increase their costs. While we are hopeful the infection rate of COVID-19 will continue to decline, we cannot predict the future impact COVID-19 or future pandemics from other viruses will have on our current and future clinical trials.
We have a significant amount of intangible assets related to our acquisition of PCS499 recorded on our balance sheet, which may lead to potentially significant impairment charges in the future.going concern.
We review long-lived assets, including intangible assets,had no revenue during the year ended December 31, 2023 or in prior years, and do not have any revenue under contract or any immediate sales prospects. Our primary uses of cash are to fund our planned clinical trials, research and development expenditures and for impairment whenever events or changes in estimatesoperating expenses. Cash used to fund operating expenses is impacted by the timing of when we incur and circumstances indicate that the related carrying amounts may not be recoverablepay these expenses. Our consolidated financial statements have been prepared using U.S. GAAP, and are based on the existenceassumption that we will continue as a going concern, which contemplates the realization of assets and liquidation of liabilities in the normal course of business. We face certain triggering events. Intangible assetsrisks and uncertainties that are also subject to an impairment assessment at least annually. The amount of identifiable intangible assetspresent in our consolidated balance sheet is related to our acquisition of PCS499many emerging pharmaceutical companies regarding product development, limited working capital, recurring losses and our right of use assets. At December 31, 2021, net intangible assets recorded on our consolidated balance sheet was $8.1 million. Any impairment of our assets could have a negative impact on our stock price andcash flow from operations, future profitability, ability to seek additional financing.obtain future capital, protection of patents, technologies and property rights, competition, rapid technological change, navigating the domestic and major foreign markets’ regulatory and clinical environment, recruiting and retaining key personnel, dependence on third party manufacturing organizations, third party collaboration and licensing agreements, lack of sales and marketing activities. We currently have no customers or pharmaceutical products to sell or distribute. These risks and other factors raise substantial doubt about our ability to continue as a going concern.
Our ability to continue as a going concern is dependent on our ability to obtain the necessary financing to meet our obligations and repay our liabilities arising from the ordinary course of business operations when they become due. The substantial doubt about our ability to continue as a going concern may affect the price of our common stock, may impact our relationship with third parties with whom we do business, may impact our ability to raise additional capital and may impact our ability to comply going forward with covenants in our debt agreements.
Our ability to use our net operating loss carryforwards and other tax attributes may be limited.
As of December 31, 2023, we had net operating loss (NOL) carryforwards of approximately $28.7 million for federal and state income tax available to offset future taxable income, and federal and state research and development tax credits of approximately $1.2 million, prior to consideration of annual limitations that may be imposed under Section 382 of the Internal Revenue Code of 1986, as amended (Section 382). NOL carryforwards prior to 2018 will expire in 2037 if not utilized.
Our NOL and tax credit carryforwards could expire unused and be unavailable to offset future income tax liabilities. Under Section 382, and corresponding provisions of state law, if a corporation undergoes an “ownership change,” generally defined as a greater than 50% change, by value, in its equity ownership over a three-year period, the corporation’s ability to use its pre-change NOLs and other pre-change tax attributes, such as research and development tax credits, to offset its post-change income may be limited. We have not completed a Section 382 study and as such our net operating loss carryforwards may be subject to such limitation.
In addition, we may experience additional ownership changes in the future as a result of subsequent shifts in our stock ownership, including through completed or contemplated financings, some of which may be outside of our control. If we determine that a future ownership change has occurred and our ability to use our historical net operating loss and tax credit carryforwards is materially limited, it would harm our future operating results by effectively increasing our future tax obligations.
Risks Relating to Clinical Development and Commercialization of Our Product Candidates
We currently do not have, and may never develop, any FDA-approved, licensed or commercialized products.
We have not yet sought to obtain any regulatory approvals for any product candidates in the United States or in any foreign market. For us to develop any products that might be licensed or commercialized, we will have to invest further time and capital in research and product development, regulatory compliance and market development. Therefore, we and our licensors, prospective business partners and other collaborators may never develop any products that can be licensed or commercialized. All of our development efforts will require substantial additional funding, none of which may result in any revenue.
Our licenses are subject to termination by the licensor in certain circumstances.
Our rights to practice the inventions claimed in the licensed patents and patent applications are subject to our licensors abiding by the terms of those licenses and not terminating them. Our licenses may be terminated by the licensor if we are in material breach of certain terms or conditions of the license agreement or in certain other circumstances. Our license agreements each include provisions that allow the licensor to terminate the license if (i) we breach any payment obligation or other material provision under the agreement and fail to cure the breach within a fixed time following written notice of termination; (ii) we or any of our affiliates, licensees or sublicensees directly or indirectly challenge the validity, enforceability, or extension of any of the licensed patents; or (iii) we declare bankruptcy or dissolve. The majority of license agreements require us to satisfy due diligence milestones that relate to the development of new products containing the licensed drug or the agreement may be terminated by such counterparty. Our rights under thesesthese licenses are subject to our continued compliance with the terms of the license, including the payment of royalties due under the licenses. Termination of any of these licenses could prevent us from marketing some or all of our products. Because of the complexity of our products and the patents we have licensed, determining the scope of the license and related royalty obligations can be difficult and can lead to disputes between us and the licensor. An unfavorable resolution of such a dispute could lead to an increase in the royalties payable pursuant to the license. If a licensor believed we were not paying the royalties due under the license or were otherwise not in compliance with the terms of the license, the licensor might attempt to revoke the license. If such an attempt were successful, we might be barred from producing and selling some or all of our products.
If we fail to comply with our obligations contained in the agreements under which we license intellectual property rights from third parties, we could lose important license rights.
Our license agreements have various requirements. For example, our license agreement with Elion Oncology, Inc. (“Elion”) for NGC-Cap (also known as PCS6422) requires us to administer the drug to the first patient in a Phase 2 or Phase 3 trial for NGC-Cap on or before October 2, 2024. Our license agreement with Ocuphire Pharma, Inc. (“Ocuphire”) for NGC-Gem (also known as PCS3117) imposes two future obligations on us. The first diligence obligation requires that the first patient must be administered the drug in a clinical trial on or before June 16, 2024, and the second obligation requires that the first patient is administered the drug (i) in a pivotal clinical trial, or (ii) in a clinical trial for a second indication of the drug on or before June 16, 2026. We are in the process of requesting an extension of these obligations with Ocuphire, and there is no assurance that we will be able to obtain such extension.
Should we fail to meet any of the obligations under our license agreements, absent extensions, other arrangements or other extenuating circumstances, the licensor may be able to terminate the license agreement, which would have a material effect on the value of our intellectual property portfolio, our financial condition, future prospects, and results of operations.
| 29 |
We depend entirely on the successful development of our product candidates, which have not yet demonstrated efficacy for their target indications in clinical trials. We may never be able to demonstrate efficacy for our product candidates, thus preventing us from licensing, obtaining marketing approval by any regulatory agency, and/or commercializing our product(s).
Our product candidates are either in the early stages of clinical development or late stages of preclinical development. Significant additional research and development activity and clinical testing are required before we will have a chance to achieve a viable product for licensing or commercialization from such candidates. Our research and development efforts remain subject to all the risks associated with the development of new biopharmaceutical products and treatments. Development of the underlying technology may be affected by unanticipated technical or other problems, among other research and development issues, and the possible insufficiency of funds needed in order to complete development of these product candidates. Safety, regulatory and efficacy issues, clinical hurdles or other challenges may result in delays and cause us to incur additional expenses that would increase our losses. If we and our collaborators cannot complete, or if we experience significant delays in developing, our potential therapeutics or products for use in potential commercial applications, particularly after incurring significant expenditures, our business may fail, and investors may lose the entirety of their investment.
When we submit an IND or foreign equivalent to the FDA or international regulatory authorities seeking approval to initiate clinical trials in the United States and other countries, we may not be successful in obtaining acceptance from the FDA or comparable foreign regulatory authorities to start our clinical trials. If we do not obtain such acceptance, the time in which we expect to commence clinical programs for any product candidate will be extended and such extension will increase our expenses and increase our need for additional capital. Moreover, there is no guarantee that our clinical trials will be successful or that we will continue clinical development in support of an approval from the FDA or comparable foreign regulatory authorities for any indication. We note that most drug candidates never reach the clinical development stage and even those that do commence clinical development have only a small chance of successfully completing clinical development and gaining regulatory approval. Therefore, our business currently depends entirely on the successful development, regulatory approval, and licensing or commercialization of our product candidates, which may never occur.
We must successfully complete clinical trials for our product candidates before we can apply for marketing approval.
Even if we complete our clinical trials, it does not assure marketing approval. Our clinical trials may be unsuccessful, which would materially harm our business. Even if our initial clinical trials are successful, we are required to conduct additional clinical trials to establish our product candidates’ safety and efficacy before submitting an NDA. Clinical testing is expensive, is difficult to design and implement, can take many years to complete and is uncertain as to the outcome. Success in early phases of pre-clinical and clinical trials does not ensure that later clinical trials will be successful, and interim results of a clinical trial do not necessarily predict final results. A failure of one or more of our clinical trials can occur at any stage of testing. We may experience numerous unforeseen events during, or as a result of, the clinical trial process that could delay or prevent our ability to receive regulatory approval or commercialize our product candidates. The research, testing, manufacturing, labeling, packaging, storage, approval, sale, marketing, advertising and promotion, pricing, export, import and distribution of drug products are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries, which regulations differ from country to country.
We are not permitted to market our product candidates as prescription pharmaceutical products in the United States until we receive approval of an NDA from the FDA, or in any foreign countries until we receive the requisite approval from such countries.
| 30 |
We have little corporate history of conducting clinical trials. Our planned clinical trials or those of our collaborators may reveal significant adverse events, toxicities or other side effects not seen in our preclinical studies and may result in a safety profile that could inhibit regulatory approval or market acceptance of any of our product candidates.
Our operations to date have been limited to financing and staffing, conducting research and developing our core technologies, identifying and optimizing our lead product clinical candidates, performing due diligence on other potential drug in-licensing opportunities and further moving the clinical product candidates through the development programs identified. Some of the activities in the development programs include receiving FDA orphan designation on PCS499 in Necrobiosis Lipoidica (NL), improving the manufacturing of PCS499 final product, receiving FDA IND clearance on one indication for two product candidates, completing a Phase 2A trial for PCS12852 in gastroparesis patients, conducting a Phase 1B trial for NGC-Cap in patients with advanced gastrointestinal tumors, completing a Phase 1 healthy human volunteer trial, completing a Phase 2A clinical trial and conducting a Phase 2 clinical trial in patients with NL initiating a Phase 2A trialand receiving FDA orphan designation on PCS499 in NL. Other activities include improving the manufacturing of PCS499, PCS6422 and PCS11T final products and developing regulatory strategy plans for PCS12852 in gastroparesis patients and conducting a Phase 1B trial for PCS6422 in patients with advanced gastrointestinal tumors.each of the products including expedited review plans, as applicable. Although we have recruited a team that has experience with clinical trials in the United States and outside the United States, as a company, we have only conducted twofour clinical trials in any jurisdiction and have not had previous experience commercializing product candidates through the FDA or similar submissions to initiate clinical trials or obtain marketing authorization to foreign regulatory authorities. We cannot be certain that other planned clinical trials will begin or be completed on time, if at all; that our development program and studies would be acceptable to the FDA or other regulatory authorities; or that, if regulatory approval is obtained, our product candidates can be successfully commercialized. Clinical trials and commercializing our product candidates will require significant additional financial and management resources, and reliance on third-party clinical investigators, CROs, consultants and collaborators. Relying on third-party clinical investigators, CROs or collaborators may result in delays that are outside of our control.
Furthermore, we may not have the financial resources to continue development of, or to enter into collaborations for, a product candidate if we experience any problems or other unforeseen events that delay or prevent regulatory approval of, or our ability to commercialize, product candidates.
Through our IND for PCS499, we are evaluated the safety tolerability of PCS499 in patients with NL in a Phase 2A clinical trial. Based on toxicologySome preclinical studies and healthy human volunteer studies, we administered a PCS499 dose of 1.8 grams/day to patients participating in the study. As anticipated, the 1.8 grams/day of PCS499 was generally well tolerated with no serious adverse events reported. All adverse events reported in the study were mild in severity. As expected, gastrointestinal symptoms were the most frequent adverse events and reported in four patients, all of which resolved within 1-2 weeks of starting dosing. We are currently evaluating the ability of PCS499 to completely close ulcers in patients with NL and better understand the potential response of NL patients on drug and on placebo in a Phase 2early clinical trial.
The FDA also cleared our IND for PCS12852 in October 2021 to proceed with a Phase 2A clinical trial for the treatment of gastroparesis. We anticipate beginning to enroll patients in the first half of 2022, complete enrollment in the second half of 2022 and complete final analysis in the first half of 2023.
We have initiated the Phase 1B trial for PCS6422 in patients with advance GI tumors. This trial will determine the maximum tolerated dose of capecitabine when administered with different dosage regimes of PCS6422. This trial was initiated in the second half of 2021 and is expected to complete enrollment in the second half of 2022.
Some preclinical studies of our product candidates have been completed, but we do not know the predictive value of these studies for our targeted population of patients, and we cannot guarantee that any positive results in preclinicalthese studies will translate successfully to ourthe larger targeted population of patients. It is not uncommon to observe results in human clinical trials that are unexpected based on preclinical testing or early clinical studies, and many product candidates fail in clinical trials despite promising preclinical or early clinical results. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses, and many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval for their products. Human patients in clinical trials may suffer significant adverse events or other side effects not observed in our preclinical studies, including, but not limited to, immunogenic responses, organ toxicities such as liver, heart or kidney or other tolerability issues or possibly even death. The observed potency and kinetics of our planned product candidates in preclinical studies may not be observed in human clinical trials. If clinical trials of our planned product candidates fail to demonstrate efficacy to the satisfaction of regulatory authorities or do not otherwise produce positive results, we may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our planned product candidates which may result in complete loss of expenditures which we devote to those products.
We may have difficulty recruiting patients to the clinical trial, patients may drop out of our trial, or we may be required to abandon the trial or our development efforts of that product candidate altogether. We, the FDA, an Institutional Review Board (“IRB”), or other applicable regulatory authorities may suspend clinical trials of a product candidate at any time for various reasons, including a belief that subjects in such trials are being exposed to unacceptable health risks or adverse side effects. Some potential therapeutics developed in the biotechnology industry that initially showed therapeutic promise in early-stage studies have later been found to cause side effects that prevented their further development. Even if the side effects do not preclude the drug from obtaining or maintaining marketing approval, undesirable side effects may inhibit market acceptance of the approved product due to its tolerability versus other therapies. Any of these developments could materially harm our business, financial condition, and prospects.
Further, if any of our product candidates obtains marketing approval, toxicities associated with our product candidates may also develop after such approval and lead to a requirement to conduct additional clinical safety trials, additional warnings being added to the labeling, significant restrictions on the use of the product or the withdrawal of the product from the market. We cannot predict whether our product candidates will cause toxicities in humans that would preclude or lead to the revocation of regulatory approval based on preclinical studies or early stageearly-stage clinical testing. However, any such event, were it to occur, would cause substantial harm to our business and financial condition and would result in the diversion of our management’s attention.
| 31 |
Even if we receive regulatory approval for any of our product candidates, we may not be able to successfully license or commercialize the product and the revenue that we generate from its sales, if any, may be limited.
If approved for marketing, the commercial success of our product candidates will depend upon each product’s acceptance by the medical community (including physicians, patients and health care payors) and the potential competitive products available to the patients upon commercialization. The degree of market acceptance for any of our product candidates will depend on a number of factors, including:
| ● | demonstration of clinical safety and efficacy; | |
| ● | relative convenience, dosing burden and ease of administration; | |
| ● | the prevalence and severity of any adverse effects; | |
| ● | the willingness of physicians to prescribe our product candidates, and the target patient population to try new therapies; | |
| ● | efficacy of our product candidates compared to competing products; | |
| ● | the introduction of any new products that may in the future become available targeting indications for which our product candidates may be approved; | |
| ● | new procedures or therapies that may reduce the incidences of any of the indications in which our product candidates may show utility; | |
| ● | pricing and cost-effectiveness; | |
| ● | the inclusion or omission of our product candidates in treatment guidelines; | |
| ● | the effectiveness of our own or any future collaborators’ sales and marketing strategies; | |
| ● | limitations or warnings contained in approved labeling from regulatory authorities; | |
| ● | our ability to obtain and maintain sufficient third-party coverage or reimbursement from government health care programs, including Medicare and Medicaid, private health insurers and other third-party payors or to receive the necessary pricing approvals from government bodies regulating the pricing and usage of therapeutics; and | |
| ● | the willingness of patients to pay out-of-pocket in the absence of third-party coverage or reimbursement or government pricing approvals. |
If any of our product candidates are approved, but do not achieve an adequate level of acceptance by physicians, health care payors and patients, we may not generate sufficient revenue and we may not be able to achieve or sustain profitability. Our efforts to educate the medical community and third-party payors on the benefits of our product candidates may require significant resources and may never be successful.
In addition, even if we obtain regulatory approvals, the timing or scope of any approvals may prohibit or reduce our ability to commercialize our product candidates successfully. For example, if the approval process takes too long, we may miss market opportunities and give other companies the ability to develop competing products or establish market dominance. Any regulatory approval we ultimately obtain may be limited or subject to restrictions or post-approval commitments that render our product candidates not commercially viable.
| 32 |
We are completely dependent on third parties to manufacture our product candidates, and our commercialization of our product candidates could be halted, delayed or made less profitable if those third parties fail to obtain manufacturing approval from the FDA or comparable foreign regulatory authorities, fail to provide us with sufficient quantities of our product candidates or fail to do so at acceptable quality levels or prices.
We do not currently have, nor do we plan to acquire, the capability or infrastructure to manufacture the active pharmaceutical ingredient, or API, in our product candidates for use in our clinical trials or for commercial product.products. In addition, we do not have the capability to formulate any of our product candidates into a finished drug product for commercial distribution. As a result, we will be obligated to rely on contract manufacturers, if and when any of our product candidates are approved for commercialization. We have not entered into an agreement with any contract manufacturers for commercial supply and may not be able to engage a contract manufacturer for commercial supply of any of our product candidates on favorable terms to us, or at all.
The facilities used by our contract manufacturers to manufacture our product candidates must be approved by the FDA or comparable foreign regulatory authorities pursuant to inspections that will be conducted after we submit an NDA or BLA to the FDA or their equivalents to other relevant regulatory authorities. We will not control the manufacturing process of, and will be completely dependent on, our contract manufacturing partners for compliance with cGMPs to manufacture both active drug substances and finished drug products. These cGMP regulations cover all aspects of the manufacturing, testing, quality control and record keeping relating to our product candidates. If our contract manufacturers do not successfully manufacture material that conforms to our specifications and the strict regulatory requirements of the FDA or others, they will not be able to secure and/or maintain regulatory approval for their manufacturing facilities. If the FDA or a comparable foreign regulatory authority does not approve these facilities for the manufacture of our product candidates or if it withdraws any such approval in the future, we may need to find alternative manufacturing facilities, which would significantly impact our ability to develop, obtain regulatory approval for or market our product candidates, if approved.
Our contract manufacturers will be subject to ongoing periodic unannounced inspections by the FDA and corresponding state and foreign agencies for compliance with cGMPs and similar regulatory requirements. We will not have control over our contract manufacturers’ compliance with these regulations and standards. Failure by any of our contract manufacturers to comply with applicable regulations could result in sanctions being imposed on us, including fines, injunctions, civil penalties, failure to grant approval to market any of our product candidates, delays, suspensions or withdrawals of approvals, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect our business. In addition, we will not have control over the ability of our contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. Failure by our contract manufacturers to comply with or maintain any of these standards could adversely affect our ability to develop, obtain regulatory approval for or market any of our product candidates.
If, for any reason, these third parties are unable or unwilling to perform, we may not be able to terminate our agreements with them, and we may not be able to locate alternative manufacturers or formulators or enter into favorable agreements with them and we cannot be certain that any such third parties will have the manufacturing capacity to meet future requirements. If these manufacturers or any alternate manufacturer of finished drug product experiences any significant difficulties in its respective manufacturing processes for our API or finished products or should cease doing business with us, we could experience significant interruptions in the supply of any of our product candidates or may not be able to create a supply of our product candidates at all. Were we to encounter manufacturing issues, our ability to produce a sufficient supply of any of our product candidates might be negatively affected. Our inability to coordinate the efforts of our third-party manufacturing partners, or the lack of capacity available at our third-party manufacturing partners, could impair our ability to supply any of our product candidates at required levels. Because of the significant regulatory requirements that we would need to satisfy in order to qualify a new bulk or finished product manufacturer, if we face these or other difficulties with our current manufacturing partners, we could experience significant interruptions in the supply of any of our product candidates if we decided to transfer the manufacture of any of our product candidates to one or more alternative manufacturers in an effort to deal with the difficulties.
Any manufacturing problem or the loss of a contract manufacturer could be disruptive to our operations and result in lost sales. Additionally, we rely on third parties to supply the raw materials needed to manufacture our potential products. Any reliance on suppliers may involve several risks, including a potential inability to obtain critical materials and reduced control over production costs, delivery schedules, reliability and quality. Any unanticipated disruption to a future contract manufacturer caused by problems atwith suppliers could delay shipment of any of our product candidates, increase our cost of goods sold and result in lost sales.
| 33 |
We cannot guarantee that our future manufacturing and supply partners will be able to reduce the costs of commercial scale manufacturing of any of our product candidates over time. If the commercial-scale manufacturing costs of any of our product candidates are higher than expected, these costs may significantly impact our operating results. In order to reduce costs, we may need to develop and implement process improvements. However, in order to do so, we will need, from time to time, to notify or make submissions withto regulatory authorities, and the improvements may be subject to approval by such regulatory authorities. We cannot be sure that we will receive these necessary approvals or that these approvals will be granted in a timely fashion. We also cannot guarantee that we will be able to enhance and optimize output in our commercial manufacturing process. If we cannot enhance and optimize output, we may not be able to reduce our costs over time.
Even if we obtain marketing approval for any of our product candidates, we will be subject to ongoing obligations and continued regulatory review, which may result in significant additional expense.expenses.
Even if we obtain regulatory approval for any of our product candidates for an indication, the FDA or foreign equivalent may still impose significant restrictions on their indicated uses or marketing or the conditions of approval or impose ongoing requirements for potentially costly and time-consuming post-approval studies, including Phase 4 clinical trials, and post-market surveillance to monitor safety and efficacy. Our product candidates will also be subject to ongoing regulatory requirements governing the manufacturing, labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, recordkeeping and reporting of adverse events and other post-market information. These requirements include registration with the FDA, as well as continued compliance with current Good Clinical Practices (cGCPs) for any clinical trials that we conduct post-approval. In addition, manufacturers of drug products and their facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with cGMP regulations, requirements relating to quality control, quality assurance and corresponding maintenance of records and documents. Compliance with such regulations may result in significant costs and expenses.
Obtaining and maintaining regulatory approval of our product candidates in one jurisdiction does not mean that we will be successful in obtaining regulatory approval of our product candidates in other jurisdictions.
Obtaining and maintaining regulatory approval of our product candidates in one jurisdiction does not guarantee that we will be able to obtain or maintain regulatory approval in any other jurisdiction, but a failure or delay in obtaining regulatory approval in one jurisdiction may have a negative effect on the regulatory approval process in others. For example, even if the FDA grants marketing approval of a product candidate, comparable regulatory authorities in foreign jurisdictions must also approve the manufacturing, marketing and promotion of the product candidate in those countries. Approval procedures vary among jurisdictions and can involve requirements and administrative review periods different from those in the United States, including additional preclinical studies or clinical trials, as clinical studies conducted in one jurisdiction may not be accepted by regulatory authorities in other jurisdictions. In many jurisdictions outside the United States, a product candidate must be approved for reimbursement before it can be approved for sale in that jurisdiction. In some cases, the price that we intend to charge for our products is also subject to approval.
Obtaining foreign regulatory approvals and compliance with foreign regulatory requirements could result in significant delays, difficulties and costs for us and could delay or prevent the introduction of our products in certain countries. If we fail to comply with the regulatory requirements in international markets and/or to receive applicable marketing approvals, our target market will be reduced and our ability to realize the full market potential of our product candidates will be harmed.
Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of and commercialize our product candidates and affect the prices we may obtain.
In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay marketing approval for our product candidates, restrict or regulate post-approval activities and affect our ability to profitably sell our product candidates. Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products.
In the United States, the Medicare Modernization Act (MMA) changed the way Medicare covers and pays for pharmaceutical products. The legislation expanded Medicare coverage for drug purchases by the elderly and introduced a new reimbursement methodology based on average sales prices for drugs. In addition, this legislation authorized Medicare Part D prescription drug plans to use formularies where they can limit the number of drugs that will be covered in any therapeutic class. As a result of this legislation and the expansion of federal coverage of drug products, we expect that there will be additional pressure to contain and reduce costs. These cost reduction initiatives and other provisions of this legislation could decrease the coverage and price that we receive for our product candidates and could seriously harm our business. While the MMA applies only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates, and any reduction in reimbursement that results from the MMA may result in a similar reduction in payments from private payors.
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act of 2010 or, collectively, the ACA, is a sweeping law intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms. The ACA revised the definition of “average manufacturer price” for reporting purposes, which could increase the amount of Medicaid drug rebates to states. The law also imposed a significant annual fee on companies that manufacture or import branded prescription drug products. Further, on August 16, 2022, President Biden signed the Inflation Reduction Act of 2022 (IRA), into law which, among other things, extends enhanced subsidies for individuals purchasing health insurance coverage in ACA marketplaces through plan year 2025. The IRA also eliminates the “donut hole” under the Medicare Part D program beginning in 2025 by significantly lowering the beneficiary maximum out-of-pocket cost and creating a new manufacturer discount program. It is unclear how such challenges, and the healthcare reform measures of the Biden administration will impact the ACA and our business.
We do not know whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our product candidates, if any, may be. In addition, increased scrutiny by the U.S. Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
We could face competition from other biotechnology and pharmaceutical companies, and our operating results would suffer if we fail to innovate and compete effectively.
Our products are used for indications where we believe that there is an unmet medical need. If existing or newly approved drug products, whether approved by the FDA for the indication or not, are able to successfully treat the same patients, it may be more difficult to perform clinical studies, to develop our product and/or to commercialize our product, adversely affecting our business. Since the biopharmaceutical industry is characterized by intense competition and rapid innovation, our competitors may be able to develop other compounds or drugs that are able to achieve similar or better results than our product candidates. Our competitors may include major multinational pharmaceutical companies, established biotechnology companies, specialty pharmaceutical companies, and universities and other research institutions. Many of our competitors have substantially greater financial, technical and other resources, such as a larger research and development staff and experienced marketing and manufacturing organizations, established relationships with CROs and other collaborators, as well as established sales forces. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large, established companies. Mergers and acquisitions in the biotechnology and pharmaceutical industries may result in even more resources being concentrated in our competitors. Competition may increase further as a result of advances in the commercial applicability of technologies and greater availability of capital for investment in these industries. Our competitors, either alone or with collaborative partners, may succeed in developing, acquiring or licensing on an exclusive basis drug or biologic products that are more effective, safer, more easily commercialized or less costly than our product candidates, or may develop proprietary technologies or secure patent protection and, in turn, exclude us from technologies that we may need for the development of our technologies and potential products.
Even if we obtain regulatory approval of any of our product candidates, we may not be the first to market and that may negatively affect the price or demand for our product candidates. Additionally, we may not be able to implement our business plan if the acceptance of our product candidates is inhibited by price competition or the reluctance of physicians to switch from existing methods of treatment to our product candidates, or if physicians switch to other new drug or biologic products or choose to reserve our product candidates for use in limited circumstances. Furthermore, for drugs that receive orphan drug designation at the FDA, a competitor could obtain orphan product approval from the FDA with respect to such competitor’s drug product. If such competitor drug product is determined to be the same product as one of our product candidates, we may be prevented from obtaining approval from the FDA for such product candidate for the same indication for seven years, except in limited circumstances, and we may be subject to similar restrictions under non-U.S. regulations.
We rely on third parties to conduct clinical trials for our product candidates. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize any of our product candidates and our business would be substantially harmed.
We have entered into agreements with third-party CROs to conduct and manage our clinical programs including contracting with clinical sites to perform our clinical studies. We rely heavily on these parties for execution ofto execute clinical studies for our product candidates and will control only certain aspects of their activities. Nevertheless, we will be responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards, and our reliance on CROs and clinical sites will not relieve us of our regulatory responsibilities. We and our CROs will be required to comply with cGCPs, which are regulations and guidelines enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area and comparable foreign regulatory authorities for any products in clinical development. The FDA and its foreign equivalents enforce these cGCP regulations through periodic inspections of trial sponsors, principal investigators and trial sites. If we or our CROs fail to comply with applicable cGCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that, upon inspection, the FDA or other regulatory authorities will determine that any of our clinical trials comply with cGCPs. In addition, our clinical trials must be conducted with products produced under cGMP regulations and will require a large number of test subjects. Our failure or the failure of our CROs or clinical sites to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process and could also subject us to enforcement action up to and including civil and criminal penalties.
| 35 |
Although we design the clinical trials for our product candidates in consultation with CROs, the CROs will manage all of the clinical trials conducted at contracted clinical sites. As a result, many important aspects of our drug development programs would be outside of our direct control. In addition, the CROs and clinical sites may not perform all of their obligations under arrangements with us or in compliance with regulatory requirements. If the CROs or clinical sites do not perform clinical trials in a satisfactory manner, breach their obligations to us or fail to comply with regulatory requirements, the development and commercialization of any of our product candidates for the subject indication may be delayed or our development program materially and irreversibly harmed. We cannot control the amount and timing of resources these CROs and clinical sites will devote to our program or any of our product candidates. If we are unable to rely on clinical data collected by our CROs, we could be required to repeat, extend the duration of, or increase the size of our clinical trials, which could significantly delay commercialization and require significantly greater expenditures.
If any of our relationships with these third-party CROs or clinical sites terminate, we may not be able to enter into arrangements with alternative CROs or clinical sites. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, any such clinical trials may be extended, delayed or terminated, and we may not be able to obtain regulatory approval for or successfully commercialize our product candidates. As a result, our financial results and the commercial prospects for any of our product candidates would be harmed, our costs could increase and our ability to generate revenue could be delayed.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results.
Clinical testing of drug product candidates is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The results of pre-clinical studies and early clinical trials may not be predictive of the results of later-stage clinical trials. We cannot assure you that the FDA or comparable foreign regulatory authorities will view the results as we do or that any future trials of any of our product candidates will achieve positive results. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through pre-clinical studies and initial clinical trials. A number of companies in the biopharmaceutical industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. Any future clinical trial results for our product candidates may not be successful.
In addition, a number of factors could contribute to a lack of favorable safety and efficacy results for any of our product candidates. For example, such trials could result in increased variability due to varying site characteristics, such as local standards of care, differences in evaluation period and surgical technique, and due to varying patient characteristics including demographic factors and health status.
Even though we may apply for orphan drug designation for a product candidate, we may not be able to obtain orphan drug marketing exclusivity.
There is no guarantee that the FDA, EMA or their foreign equivalents will grant any future application for orphan drug designation for any of our product candidates, which would make us ineligible for the additional exclusivity and other benefits of orphan drug designation. Even where orphan drug designation or equivalent status is granted, there is no guarantee of orphan drug marketing exclusivity.
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making a drug available in the Unites States for this type of disease or condition will be recovered from sales of the product. Orphan drug designation must be requested before submitting an NDA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan product designation does not convey any advantage in or shorten the duration of regulatory review and approval process.
| 36 |
If a product that has orphan designation subsequently receives the first FDA approval for the disease or condition for which it has such designation, the product is entitled to orphan drug exclusivity, which means the FDA may not approve any other applications to market the same drug for the same indication for seven years, except in limited circumstances, such as (i) the drug’s orphan designation is revoked; (ii) its marketing approval is withdrawn; (iii) the orphan exclusivity holder consents to the approval of another applicant’s product; (iv) the orphan exclusivity holder is unable to assure the availability of a sufficient quantity of drug; or (v) a showing of clinical superiority to the product with orphan exclusivity by a competitor product. If a drug designated as an orphan product receives marketing approval for an indication broader than what is designated, it may not be entitled to orphan drug exclusivity. While the FDA granted orphan-drug designation to PCS499 for the treatment of NL and to PCS3117 for the treatment of pancreatic cancer, there can be no assurance that we will receive orphan drug designation for any additional product candidates in the indications for which we think they might qualify, if we elect to seek such applications.
Although we may pursue expedited regulatory approval pathways for a product candidate, it may not qualify for expedited development or, if it does qualify for expedited development, it may not actually lead to a faster development, regulatory review or approval process.
Although we believe there may be an opportunity to accelerate the development of certain of our product candidates through one or more of the FDA’s expedited programs, such as fast track, breakthrough therapy, accelerated approval or priority review, we cannot be assured that any of our product candidates will qualify for such programs.
For example, a drug may be eligible for designation as a breakthrough therapy if the drug is intended, alone or in combination with one or more other drugs, to treat a serious or life-threatening condition and preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints. Although breakthrough designation or access to any other expedited program may expedite the development or approval process, it does not change the standards for approval. If we apply for an expedited program for our product candidates, the FDA may determine that our proposed target indication or other aspects of our clinical development plans do not qualify for such expedited program. Even if we are successful in obtaining access to an expedited program, we may not experience faster development timelines or achieve faster review or approval compared to conventional FDA procedures. Access to an expedited program may also be withdrawn by the FDA if it believes that the designation is no longer supported by data from our clinical development program. Additionally, qualification for any expedited review procedure does not ensure that we will ultimately obtain regulatory approval for such product candidate.
Third-party coverage and reimbursement, health care cost containment initiatives and treatment guidelines may constrain our future revenues.
Our ability to successfully market our product candidates will depend in part on the level of reimbursement that government health administration authorities, private health coverage insurers and other organizations provide for the cost of our products and related treatments. Countries in which any of our product candidates may be sold through reimbursement schemes under national health insurance programs frequently require that manufacturers and sellers of pharmaceutical products obtain governmental approval of initial prices and any subsequent price increases. In certain countries, including the United States, government-funded and private medical care plans can exert significant indirect pressure on prices. We may not be able to sell our product candidates profitably if adequate prices are not approved or coverage and reimbursement is unavailable or limited in scope.
Legal, regulatory and legislative changes with respect to reimbursement, pricing and contracting may adversely affect our business and future prospects.
Federal and state governments may adopt policies affecting drug pricing and contracting practices outside of the context of federal programs such as Medicare and Medicaid, which may adversely affect our business. For example, several states have adopted laws that require drug manufacturers to provide advance notice of certain price increaseincreases and to report information relating to those price increases. On May 11, 2018, the Department of Health and Human Services requested comments on a “Blueprint to Lower Drug Prices and Reduce Out-of-Pocket Costs,” which outlines a wide range of proposals and policy considerations intended to improve competition; lower patient out-of-pocket costs; enhance negotiation; and provide incentives for lower manufacturer list prices. Some of the proposals would require Congressional approval, while others could be adopted administratively. There can be no assurances that future changes to Medicare and/or Medicaid prescription drug reimbursement policies, drug pricing and contracting practices, or government drug price regulation programs such as the Medicaid Drug Rebate Program or 340B Drug Pricing Program will not have an adverse impact on our business and future prospects.
| 37 |
We cannot predict what healthcare reform initiatives may be adopted in the future. Further federal, state and foreign legislative and regulatory developments are likely, and we expect ongoing initiatives to increase pressure on drug pricing. Such reforms could have an adverse effect on anticipated revenues from product candidates and may affect our overall financial condition and ability to develop product candidates.
We may face product liability exposure, and if successful claims are brought against us, we may incur substantial liability if our insurance coverage for those claims is inadequate.
We face an inherent risk of product liability as a result of the clinical testing of our product candidates and will face an even greater risk if we commercialize any products. This risk exists even if a product is approved for commercial sale by the FDA and manufactured in facilities licensed and regulated by the FDA or an applicable foreign regulatory authority. Our products and product candidates are designed to affect important bodily functions and processes. Any side effects, manufacturing defects, misuse or abuse associated with our product candidates could result in injury to a patient or even death. We cannot offer any assurance that we will not face product liability suits in the future, or that our insurance coverage will be sufficient to cover our liability underin any such cases.
In addition, a liability claim may be brought against us even if our product candidates merely appear to have caused an injury. Product liability claims may be brought against us by consumers, health care providers, pharmaceutical companies or others selling or otherwise coming into contact with our product candidates, among others. If we cannot successfully defend ourselves against product liability claims, we will incur substantial liabilities and reputational harm. In addition, regardless of merit or eventual outcome, product liability claims may result in:
| ● | withdrawal of clinical trial participants; | |
| ● | termination of clinical trial sites or entire trial programs; | |
| ● | the inability to commercialize our product candidates; | |
| ● | decreased demand for our product candidates; | |
| ● | impairment of our business reputations; | |
| ● | product recall or withdrawal from the market or labeling, marketing or promotional restrictions; | |
| ● | substantial costs of any related litigation or similar disputes; | |
| ● | distractions of management’s attention and other resources from our primary business; | |
| ● | substantial monetary awards to patients or other claimants against us that may not be covered by insurance; or | |
| ● | loss of revenue. |
We have obtained product liability insurance coverage for our clinical trials. However, large judgments have been awarded in class action or individual lawsuits based on drugs that had unanticipated side effects and our insurance coverage may not be sufficient to cover all of our product liability related expenses or losses and may not cover us for any expenses or losses we may suffer. Moreover, insurance coverage is becoming increasingly expensive, and, in the future, we may not be able to maintain insurance coverage at a reasonable cost, in sufficient amounts or upon adequate terms to protect us against losses due to product liability. We will need to increase our product liability coverage if any of our product candidates receive regulatory approval, which will be costly, and we may be unable to obtain this increased product liability insurance on commercially reasonable terms, or at all. A successful product liability claim, or series of claims, brought against us could cause our stock price to decline and, if judgments exceed our insurance coverage, could decrease our cash and could harm our business, financial condition, operating results and prospects.
If any of our product candidates are approved for marketing and we are found to have improperly promoted off-label uses, or if physicians misuse our products or use our products off-label, we may become subject to prohibitions on the sale or marketing of our products, product liability claims and significant fines, penalties and sanctions, and our brand and reputation could be harmed.
The FDA and other regulatory agencies strictly regulate the marketing and promotional claims that are made about drug products. In particular, a product may not be promoted for uses or indications that are not approved by the FDA or such other regulatory agencies as reflected in the product’s approved labeling and comparative safety or efficacy claims cannot be made without direct comparative clinical data. If we are found to have promoted off-label uses of any of our product candidates, we may become subject to significant liability, which would materially harm our business. Both federal and state governments have levied large civil and criminal fines against companies for alleged improper promotion and have enjoined several companies from engaging in off-label promotion. If we become the target of such an investigation or prosecution based on our marketing and promotional practices, we could face similar sanctions, which would materially harm our business. In addition, management’s attention could be diverted from our business operations, significant legal expenses could be incurred, and our brand and reputation could be damaged.
The FDA has also requested that companies enter into consent decrees or permanent injunctions under which specified promotional conduct is changed or curtailed. If we are deemed by the FDA to have engaged in the promotion of our products for off-label use, we could be subject to FDA regulatory or enforcement actions, including the issuance of an untitled letter, a warning letter, injunction, seizure, civil fine or criminal penalties. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our business activities constitute promotion of an off-label use, which could result in significant penalties, including criminal, civil or administrative penalties, damages, fines, disgorgement, exclusion from participation in government healthcare programs and the curtailment or restructuring of our operations.
We cannot, however, prevent a physician from using our product candidates outside of those indications for use when in the physician’s independent professional medical judgment he or she deems appropriate. Physicians may also misuse our product candidates or use improper techniques, potentially leading to adverse results, side effects or injury, which may lead to product liability claims. If our product candidates are misused or used with improper technique, we may become subject to costly litigation by physicians or their patients. Furthermore, the use of our product candidates for indications other than those cleared by the FDA may not effectively treat such conditions, which could harm our reputation among physicians and patients.
We may choose not to continue developing or commercializing any of our product candidates at any time during development or after approval, which would reduce or eliminate our potential return on investment for those product candidates.
At any time, we may decide to discontinue the development of any of our product candidates or not to continue commercializing one or more of our approved product candidates for a variety of reasons, including changes in our internal product, technology or indication focus, the appearance of new technologies that make our product obsolete, competition from a competing product or changes in or failure to comply with applicable regulatory requirements. If we terminate a program in which we have invested significant resources, we will not receive any return on our investment, and we will have missed the opportunity to have allocated those resources to potentially more productive uses.
| 39 |
Risks Relating to Our Intellectual Property Rights
We depend on rights to certain pharmaceutical compounds that are or will be licensed to us. We do not own the intellectual property rights to these pharmaceutical compounds and any loss of our rights to them could prevent us from selling our products.
Within our present pipeline and potentially future pipeline of drugs, our drugs are in-licensed from other biotech or pharmaceutical companies. We do not currently own any intellectual property rights, including the patents that underlie these licenses. Our rights to use the pharmaceutical compounds we license are subject to the negotiation of, continuation of and compliance with the terms of those licenses. Thus, these patents and patent applications are not written by us or our attorneys, and we did not have control over the drafting and prosecution. The former patent owners and our licensors might not have given the same attention to the drafting and prosecution of these patents and applications as we would have if we had been the owners of the patents and applications and had control over the drafting. Moreover, under certain of our licenses, patent prosecution activities remain under the control of the licensor. We cannot be certain that drafting of the licensed patents and patent applications, or patent prosecution, by the licensors have been or will be conducted in compliance with applicable laws and regulations or will result in valid and enforceable patents and other intellectual property rights.
Significant additional research and development activity, pre-clinical testing, and/or clinical testing of our drug product candidates are required before we will have a chance to achieve a viable product for licensing or commercialization. Our business currently depends entirely on the successful development, regulatory approval, and licensing or commercialization of our product candidates, which may never occur.
Enforcement of our licensed patents or defense of any claims asserting invalidity of these patents is often subject to the control or cooperation of our licensors. Legal action could be initiated against the owners of the intellectual property that we license and an adverse outcome in such legal action could harm our business because it might prevent such companies or institutions from continuing to license intellectual property that we may need to operate our business. In addition, such licensors may resolve such litigation in a way that benefits them but adversely affects our ability to have freedom to operate to develop and commercialize our product candidates.
We cannot ensure protection of our licensed intellectual property rights.
Our commercial success will depend, in part, on the ability of our licensors to obtain and maintain patent protection for our licensed technologies, products and processes, successfully defend these licensed patents against third-party challenges and successfully enforce these patents against third partythird-party competitors. The patent positions of pharmaceutical companies can be highly uncertain and involve complex legal, scientific and factual questions for which important legal principles remain unresolved. Changes in either the patent laws or in interpretations of patent laws may diminish the value of our licensed intellectual property rights. Accordingly, we cannot predict the breadth of claims that may be allowable or enforceable in our patents. The existing patents and patent applications relating to our drug product candidates may be challenged, invalidated or circumvented by third parties and might not protect us against competitors with similar products or technologies.
The degree of future protection for our proprietary rights is uncertain. We may not be able to adequately protect our rights, gain or keep our competitive advantage, or provide any competitive advantage at all. For example, others have filed, and in the future are likely to file, patent applications covering products and technologies that are similar, identical or competitive to any of our product candidates, or important to our business. We cannot be certain that any patent application owned by a third party will not have priority over patent applications licensed or filed by us, or that our licensed intellectual property or intellectual property that we develop in the future will not be involved in interference, opposition or invalidity proceedings before United States or foreign patent offices.
In the future, we may rely on know-how and trade secrets to protect technology, especially in cases when we believe patent protection is not appropriate or obtainable. However, know-how and trade secrets are difficult to protect. While we intend to require employees, academic collaborators, consultants and other contractors to enter into confidentiality agreements, we may not be able to adequately protect our trade secrets or other proprietary or licensed information. Typically, research collaborators and scientific advisors have rights to publish data and information in which we may also have rights. If we cannot maintain the confidentiality of our licensed or owned proprietary technology and other confidential information, our ability to protect valuable information licensed or owned by us may be imperiled. Enforcing a claim that a third-party entity illegally obtained and is using any of our licensed or owned know-how and trade secrets is expensive and time consuming, and the outcome is unpredictable. In addition, courts are sometimes less willing to protect trade secrets than patents. Moreover, our competitors may independently develop equivalent knowledge, methods and know-how.
| 40 |
If we fail to obtain or maintain patent or trade secret protection for our product candidates or our technologies, third parties could use our licensed or owned intellectual property, which could impair our ability to compete in the market and adversely affect our ability to generate revenues and attain profitability.
We may also rely on the trademarks we may develop to distinguish our products from the products of our competitors. We cannot guarantee that any trademark applications filed by our licensors, us, or our business partners will be approved. Third parties may also oppose such trademark applications, or otherwise challenge our use of the trademarks. In the event that the trademarks we use are successfully challenged, we could be forced to rebrand our products, which could result in loss of brand recognition, and could require us to devote resources to advertising and marketing new brands. Further, we cannot provide assurance that competitors will not infringe the trademarks we use, or that we, our licensors, or business partners will have adequate resources to enforce these trademarks.
Our product candidates may infringe the intellectual property rights of others, which could increase our costs and delay or prevent our development and commercialization efforts.
Our success depends in part on avoiding infringement of the proprietary technologies of others. The pharmaceutical industry has been characterized by frequent litigation regarding patent and other intellectual property rights. Identification of third-party patent rights that may be relevant to our licensed technology is difficult because patent searching is imperfect due to differences in terminology among patents, incomplete databases and the difficulty in assessing the meaning of patent claims. Additionally, because patent applications are maintained in secrecy until the application is published, we may be unaware of third-party patents that may be infringed by commercialization of any of our licensed product candidates or any future product candidate. There may be certain issued patents and patent applications claiming subject matter that we may be required to license in order to research, develop or commercialize any of our product candidates, and we do not know if such patents and patent applications would be available to license on commercially reasonable terms, or at all. Any claims of patent infringement asserted by third parties would be time-consuming and may divert the time and attention of our technical personnel and management.
Third parties may hold proprietary rights that could prevent any of our licensed product candidates from being marketed. Any patent-related legal action against us claiming damages and seeking to enjoin commercial activities relating to any of our product candidates or our processes could subject us to potential liability for damages and require us to obtain a license and pay royalties to continue to manufacture or market any of our product candidates or any future product candidates. We cannot predict whether we would prevail in any such actions or that any license required under any of these patents would be made available on commercially acceptable terms, if at all. In addition, we cannot be sure that we could redesign our product candidates or any future product candidates or processes to avoid infringement, if necessary. Accordingly, an adverse determination in a judicial or administrative proceeding, or the failure to obtain necessary licenses, could prevent us from developing and commercializing any of our product candidates or a future product candidate, which could harm our business, financial condition and operating results.
A number of companies, including several major pharmaceutical companies, have conducted, or are conducting, research within the licensed fields in which we intend to operate, which has resulted, or may result, in the filing of many patent applications related to this research. If we were to challenge the validity of these or any issued United States patent in court, we would need to overcome a statutory presumption of validity that attaches to every issued United States patent. This means that, in order to prevail, we would have to present clear and convincing evidence as to the invalidity of the patent’s claims. If we were to challenge the validity of these or any issued United States patent in an administrative trial before the Patent Trial and Appeal Board in the United States Patent and Trademark Office (USPTO), we would have to prove that the claims are unpatentable by a preponderance of the evidence. There is no assurance that a jury and/or court would find in our favor on questions of infringement, validity or enforceability.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees, renewal fees, annuity fees and various other governmental fees on patents and applications are required to be paid to the USPTO and various governmental patent agencies outside of the U.S. in several stages over the lifetime of the patents and applications. The USPTO and various non-U.S. governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process and after a patent has issued. There are situations in which non-compliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction.
| 41 |
General Company-Related Risks
We will need to grow the size of our organization, and we may experience difficulties in managing this growth.
As our development and commercialization plans and strategies develop, we may need to expand the size of our employee and consultant/contractor base. Future growth would impose significant added responsibilities on members of management, including the need to identify, recruit, maintain, motivate and integrate additional employees. In addition, our management may have to divert a disproportionate amount of its attention away from our day-to-day activities and devote a substantial amount of time to managing these growth activities. Our future financial performance and our ability to compete effectively will depend, in part, on our ability to manage any future growth effectively. To that end, we must be able to:
| ● | manage all our development efforts effectively, especially our clinical trials; | |
| ● | integrate additional management, administrative, scientific, operation and regulatory personnel; | |
| ● | maintain sufficient administrative, accounting and management information systems and controls; and | |
| ● | hire and train additional qualified personnel. |
We may not be able to accomplish these tasks, and our failure to accomplish any of them could harm our financial results.
If we lose key management personnel, or if we fail to recruit additional highly skilled personnel, our ability to identify and develop new or next generation product candidates will be impaired, could result in loss of markets or market share and could make us less competitive.
We are highly dependent upon the principal members of our small management team and staff, including George Ng, our Chief Executive Officer; David Young, Pharm.D., Ph.D, our Chief Executive Officer,President of Research and Development; and Sian Bigora, Pharm.D., our Chief Development and Regulatory Officer. The employment of Drs. Young and Bigora may be terminated at any time by either us or Dr. Young or Dr. Bigora. The loss of any current or future team member could impair our ability to design, identify, and develop new intellectual property and product candidates and new scientific or product ideas. Additionally, if we lose the services of any of these persons, we would likely be forced to expend significant time and money in the pursuit of replacements, which may result in a delay in the development of our product candidates and the implementation of our business plan and plan of operations and diversion of our management’s attention. We can give no assurance that we couldcan find satisfactory replacements for our current and future key scientific and management employees on terms that would not be unduly expensive or burdensome to us.
Despite our efforts to retain valuable employees, members of our management, scientific and development teams may terminate their employment with us on short notice. Although we expect to have employment agreements with our key employees, these employment agreements may still allow these employees to leave our employment at any time, for or without cause. We do not maintain “key man” insurance policies on the lives of these individuals or the lives of any of our other employees. Our success also depends on our ability to continue to attract, retain and motivate highly skilled junior, mid-level and senior managers as well as junior, mid-level and senior scientific and medical and scientific personnel.
If our information technology systems or data, or those of third parties upon which we rely, are or were compromised, we could experience adverse consequences resulting from such compromise, including but not limited to regulatory investigations or actions, interruptions or disruptions to operations or clinical trials, reputational harm, litigation, fines and penalties.
In the ordinary course of our business, we, or the third parties upon which we rely, process, collect, receive, store, use, transmit, transfer, make accessible, protect, secure, dispose of, disclose and share proprietary, confidential, and sensitive data, including personal data (such as health-related data), intellectual property, and trade secrets.
Cyberattacks, malicious internet-based activity, online and offline fraud and other similar activities threaten the confidentiality, integrity, and availability of our sensitive information and information technology systems, and those of the third parties upon which we rely.
We and the third parties upon which we rely are subject to a variety of evolving threats, including but not limited to, social engineering attacks (including through phishing attacks), malicious code (such as viruses and worms), malware (including as a result of advanced persistent threat intrusions), denial-of-service attacks (such as credential stuffing), personnel misconduct or error, ransomware attacks, supply-chain attacks, software bugs, server malfunction, software or hardware failures, loss of data or other information technology assets, adware, telecommunications failures, earthquakes, fire, flood, and other similar threats.
We rely on third-party service providers and technologies to operate critical business systems to process sensitive information in a variety of contexts, including, without limitation, cloud-based infrastructure, drug suppliers, data center facilities, encryption and authentication technology, employee email, content delivery to customers, and other functions. Our ability to monitor these third parties’ information security practices is limited, and these third parties may not have adequate information security measures in place.
Any of the previously identified or similar threats could cause a security incident or other interruption that could result in unauthorized, unlawful, or accidental acquisition, modification, destruction, loss, alteration, encryption, disclosure of, or access to our sensitive information or our information technology systems, or those of the third parties upon whom we rely. A security incident or other interruption could disrupt our ability (and that of third parties upon whom we rely) to perform our research and development activities.
| 42 |
We are exposed to cyber-attacks and data breaches, including the risks and costs associated with protecting our systems and maintaining integrity and security of our business information, as well as personal data of our guests, employees and business partners.
We are subject to cyber-attacks. These cyber-attacks can vary in scope and intent from attacks with the objective of compromising our systems, networks and communications for economic gain to attacks with the objective of disrupting, disabling or otherwise compromising our operations. The attacks can encompass a wide range of methods and intent, including phishing attacks, illegitimate requests for payment, theft of intellectual property, theft of confidential or non-public information, installation of malware, installation of ransomware and theft of personal or business information. The breadth and scope of these attacks, as well as the techniques and sophistication used to conduct these attacks, have grown over time.
A successful cyber-attack may target us directly, or it may be the result of a third party’s inadequate care. In either scenario, we may suffer damage to our systems and data that could interrupt our operations, adversely impact our reputation and brand and expose us to increased risks of governmental investigation, litigation and other liability, any of which could adversely affect our business. Furthermore, responding to such an attack and mitigating the risk of future attacks could result in additional operating and capital costs in systems technology, personnel, monitoring and other investments.
In addition, we are also subject to various risks associated with the collection, handling, storage and transmission of sensitive information. In the course of doing business, we collect employee, customer and other third-party data, including personally identifiable information and individual credit data, for various business purposes. These laws continue to develop and may be inconsistent from jurisdiction to jurisdiction. If we fail to comply with the various applicable data collection and privacy laws, we could be exposed to fines, penalties, restrictions, litigation or other expenses, and our business could be adversely impacted.
Any breach, theft, loss, or fraudulent use of employee, third-party or company data, could adversely impact our reputation and expose us to risks of data loss, business disruption, governmental investigation, litigation and other liability, any of which could adversely affect our business. Significant capital investments and other expenditures could be required to remedy the problem and prevent future breaches, including costs associated with additional security technologies, personnel, experts and credit monitoring services for those whose data has been breached. Further, if we or our vendors experience significant data security breaches or fail to detect and appropriately respond to significant data security breaches, we could be exposed to government enforcement actions and private litigation.
Risks Related to Ownership of Our Common Stock
Our failure to maintain compliance with Nasdaq’s continued listing requirements could result in the delisting of our Common Stock.
Our common stock is currently listed for trading on The Nasdaq Capital Market. We must satisfy The Nasdaq Capital Market’s continued listing requirements, including, among other things, a minimum bid price requirement of $1.00 per share or risk delisting, which would have a material adverse effect on our business. A delisting of our common stock from The Nasdaq Capital Market could materially reduce the liquidity of our common stock and result in a corresponding material reduction in the price of our common stock. In addition, delisting could harm our ability to raise capital through alternative financing sources on terms acceptable to us, or at all, and may result in the potential loss of confidence by investors, suppliers, customers and employees and fewer business development opportunities.
Although we have not been delisted from Nasdaq and currently meet the minimum listing requirements, on March 22, 2023, we received notice from the Listing Qualifications Staff of Nasdaq indicating that, based upon the closing bid price of our common stock for the prior 30 consecutive business days, we were not in compliance with the requirement to maintain a minimum bid price of $1.00 per share for continued listing on Nasdaq as set forth in Nasdaq Listing Rule 5550(a)(2). Nasdaq granted us an extension until March 18, 2024 to regain compliance with the minimum closing bid requirement, and we regained compliance with such requirement as of February 2, 2024.
If our common stock were delisted from Nasdaq, trading of our common stock would most likely take place on an over-the-counter market established for unlisted securities, such as the OTCQB or the Pink Market maintained by OTC Markets Group Inc. An investor would likely find it less convenient to sell, or to obtain accurate quotations in seeking to buy, our common stock on an over-the-counter market, and many investors would likely not buy or sell our common stock due to difficulty in accessing over-the-counter markets, policies preventing them from trading in securities not listed on a national exchange or other reasons. In addition, as a delisted security, our common stock would be subject to SEC rules as a “penny stock,” which impose additional disclosure requirements on broker-dealers. The regulations relating to penny stocks, coupled with the typically higher cost per trade to the investor of penny stocks due to factors such as broker commissions generally representing a higher percentage of the price of a penny stock than of a higher-priced stock, would further limit the ability of investors to trade in our common stock. In addition, delisting could harm our ability to raise capital through alternative financing sources on terms acceptable to us, or at all, and may result in the potential loss of confidence by investors, suppliers, customers and employees and fewer business development opportunities. For these reasons and others, delisting would adversely affect the liquidity, trading volume and price of our common stock, causing the value of an investment in us to decrease and having an adverse effect on our business, financial condition and results of operations, including our ability to attract and retain qualified employees and to raise capital.
Future equity offerings, license transactions or acquisitions may dilute our existing stockholders’ ownership and/or have other adverse effects on our operations.
In order to raise additional capital, we may in the future offer additional shares of our common stock or other securities convertible into or exchangeable for our common stock at prices that may be higher or lower than what our existing stockholders paid and other securities in the future could have rights superior to existing stockholders.
In addition, we may engage in one or more potential license transactions or acquisitions in the future, which could involve issuing our common stock as some or all of the consideration payable by us to complete such transactions. If we issue common stock or securities linked to our common stock, the newly issued securities may have a dilutive effect on the interests of the holders of our common stock. Additionally, future sales of newly issued shares used to effect a transaction could depress the market price of our common stock.stock and have a dilutive effect on our existing stockholders.
We may also issue equity securities that provide rights, preferences and privileges senior to those of our common stock. If we raise additional funds by issuing debt securities, these debt securities would have rights senior to those of our common stock and the terms of the debt securities issued could impose significant restrictions on our operations, including liens on our assets. If we raise additional funds through collaborations and licensing arrangements, we may be required to relinquish some rights to our technologies or candidate products, or to grant licenses on terms that are not favorable to us.
| 43 |
Our common stock price is expected to be volatile.
The market price of our common stock could be subject to significant fluctuations. Market prices for securities of early-stage pharmaceutical, biotechnology and other life sciences companies have historically been particularly volatile. Some of the factors that may cause the market price of our common stock to fluctuate include:
| ● | relatively low trading volume, which can result in significant volatility in the market price of our common stock based on a relatively smaller number of trades and dollar amount of transactions; | |
| ● | changes in estimates or recommendations by securities analysts, if any, who cover our common stock; | |
| ● | the timing and results of our current and any future preclinical or clinical trials of our product candidates; | |
| ● | the entry into or termination of key agreements, including, among others, key collaboration and license agreements; | |
| ● | the results and timing of regulatory reviews relating to the approval of our product candidates; | |
| ● | the initiation of, material developments in, or conclusion of, litigation to enforce or defend any of our intellectual property rights; | |
| ● | failure of any of our product candidates, if approved, to achieve commercial success; | |
| ● | general and industry-specific economic conditions that may affect our research and development expenditures; | |
| ● | the results of clinical trials conducted by others on products that would compete with our product candidates; | |
| ● | issues in manufacturing our product candidates or any approved products; | |
| ● | the introduction of technological innovations or new commercial products by our competitors; | |
| ● | developments or disputes concerning patent applications, issued patents or other proprietary rights; | |
| ● | future sales of our common stock by us, our insiders or our other stockholders; | |
| ● | a negative outcome in any litigation or potential legal proceeding; | |
| ● | additions and departures of key personnel; | |
| ● | negative publicity or announcements regarding regulatory developments relating to our products; | |
| ● | actual or anticipated fluctuations in our financial condition and operating results, including our cash and cash equivalents balance, operating expenses, cash burn rate or revenue levels; | |
| ● | our filing for protection under federal bankruptcy laws; or | |
| ● | the other factors described in this “Risk Factors” section. |
The stock markets in general have experienced substantial volatility that has often been unrelated to the operating performance of individual companies. These broad market fluctuations may also adversely affect the trading price of our common stock, especially in light of the COVID-19 pandemic.stock. In the past, following periods of volatility in the market price of a company’s securities, stockholders have often instituted class action securities litigation against those companies. Such litigation, if instituted, could result in substantial costs and diversion of management attention and resources, which could significantly harm our profitability and reputation.
We are a “smaller reporting company,” and the reduced disclosure requirements applicable to us as such may make our common stock less attractive to our stockholders and investors.
We are a “smaller reporting company” under the federal securities laws and, as such, are subject to scaled disclosure requirements afforded to such companies. For example, as a smaller reporting company, we are subject to reduced executive compensation disclosure requirements. Our stockholders and investors may find our common stock less attractive as a result of our status as a “smaller reporting company” and our reliance on the reduced disclosure requirements afforded to these companies. If some of our stockholders or investors find our common stock less attractive, as a result, there may be a less active trading market for our common stock and the market price of our common stock may be more volatile.
| 44 |
Our executive officers, directors and principal stockholders and their affiliates, if they choose to act together, have the ability to exercise significant influence over all matters submitted to stockholders for approval, which will limit your ability to influence corporate matters and could delay or prevent a change in corporate control.
Our executive officers and directors, combined with our stockholders who owned more than 5% of our outstanding common stock and their respective affiliates, in the aggregate, beneficially own shares representing approximately 27.0% of our outstanding capital stock. As a result, if these stockholders were to choose to act together, they would be able to influence our management and affairs and potentially control the outcome of matters submitted to our stockholders for approval, including the election of directors and any sale, merger, consolidation, or sale of all or substantially all of our assets. This concentration of voting power may adversely affect the market price of our common stock by:
We do not currently intend to pay dividends to our stockholders in the foreseeable future, and consequently, your ability to achieve a return on your investment will depend on appreciation in our value.
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the growth and development of our business. In addition, the terms of any future debt agreements may preclude us from paying dividends. As a result, capital appreciation, if any, of our common stock will be your sole source of gain for the foreseeable future. There is no guarantee that our valuation will appreciate in value or even maintain the valuation at which our stockholders have purchased their shares.
If securities or industry analysts do not publish research or reports about our business, or if they publish negative evaluations of our stock or negative reports about our business, our stock price and trading volume could decline.
The trading market for our common stock will depend in part on the research and reports that securities or industry analysts publish about us or our business. We do not have any control over these analysts. We may never obtain research coverage by industry or financial analysts. If no or few analysts commence coverage of us, the trading price of our stock would likely decrease. Even if we do obtain analyst coverage, there can be no assurance that analysts will cover us or provide favorable coverage. If one or more of the analysts who coverscover us downgrades our stock or changes his or her opinion of our stock, our stock price would likely decline. If one or more of these analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which could cause our stock price or trading volume to decline.
Provisions in our corporate documents and Delaware law could have the effect of delaying, deferring, or preventing a change in control of us, even if that change may be considered beneficial by some of our stockholders.
The existence of some provisions of our certificate of incorporation or our bylaws or Delaware law could have the effect of delaying, deferring, or preventing a change in control of us that a stockholder may consider favorable. These provisions include:
| ● | providing that the number of members of our Board is limited to a range fixed by our bylaws; | |
| ● | establishing advance notice requirements for nominations of candidates for election to our Board of Directors or for proposing matters that can be acted on by stockholders at stockholder meetings; and | |
| ● | authorizing the issuance of “blank check” preferred stock, which could be issued by our Board of Directors to issue securities with voting rights and thwart a takeover attempt. |
| 45 |
As a Delaware corporation, we are also subject to provisions of Delaware law, including Section 203 of the General Corporation Law of the State of Delaware. Section 203 prevents some stockholders holding more than 15% of our voting stock from engaging in certain business combinations unless the business combination or the transaction that resulted in the stockholder becoming an interested stockholder was approved in advance by our Board of Directors, results in the stockholder holding more than 85% of our voting stock (subject to certain restrictions), or is approved at an annual or special meeting of stockholders by the holders of at least 66 2/3% of our voting stock not held by the stockholder engaging in the transaction. Any provision of our certificate of incorporation or our bylaws or Delaware law that has the effect of delaying or deterring a change in control could limit the opportunity for our stockholders to receive a premium for their shares of our common stock and affect the price that some investors are willing to pay for our common stock.
Provisions in our bylaws provide for indemnification of officers and directors, which could require us to direct funds away from our business and the development of our product candidates.
Our bylaws provide for the indemnification of our officers and directors. We may in the future be required to advance costs incurred by an officer or director and to pay judgments, fines and expenses incurred by an officer or director, including reasonable attorneys’ fees, as a result of actions or proceedings in which our officers and directors are involved by reason of being or having been an officer or director of our company. Funds paid in satisfaction of judgments, fines and expenses may be funds we need for the operation of our business and the development of our product candidates, thereby affecting our ability to attain profitability.
Item 1B. Unresolved Staff Comments
None.
Item 1C. Cybersecurity
Cybersecurity Risk Management and Strategy
We have established processes to assess, identify, and manage cybersecurity risks. These processes are integrated into our overall risk management program and are designed to protect our information assets from internal and external cyber threats and include:
| ● | implementing physical, procedural, and technical safeguards; | |
| ● | developing and maintaining comprehensive response plans; | |
| ● | engaging with external cybersecurity experts to enhance our oversight and keep pace with evolving threats; and | |
| ● | considering the cybersecurity capabilities of partners and third-party service providers, both prior to engaging them and on an ongoing basis. |
Cybersecurity Governance and Oversight
Our Board of Directors provides direct oversight of cybersecurity risk and has delegated to its audit committee the responsibility of reviewing and discussing with management our risk exposures relating to cybersecurity. The Board of Directors and the audit committee will receive regular updates from management on cybersecurity matters and are promptly informed by management about any significant new threats or incidents. In the future, management and our third-party service providers will conduct reviews at least once annually of our cybersecurity readiness to ensure continuous improvement in our cybersecurity strategies.
We have implemented mechanisms to monitor and manage cybersecurity threats and incidents, including utilization of tools for continuous monitoring of our IT environment to detect and mitigate threats, a fundamental plan for responding to cyber incidents and training for employees to recognize and report potential cybersecurity incidents and to foster a culture of cybersecurity awareness and vigilance. Our Chief Administrative Officer, along with a third-party service provider, are responsible for operational oversight of our cybersecurity strategy and policies. Any identified cybersecurity incident is reported to our Chief Administrative Officer who evaluates the severity of the incident. Based on this assessment, further steps are taken involving other members of management and, depending on the severity, the audit committee and the Board of Directors. We believe this structured approach allows us to effectively manage and mitigate cybersecurity risks, safeguarding our systems and data against various digital threats. Additionally, our proactive stance is supported by cybersecurity insurance, which further reinforces our preparedness against potential cyber threats.
Cybersecurity Incident Reporting and Management
During the years ended December 31, 2022 and 2023, we have not identified any risks from cybersecurity threats that have materially affected or are reasonably likely to materially affect us, including our business strategy, results of operations, or financial condition. However, we remain vigilant and prepared to respond effectively to any incidents, should they arise.
Item 2. Properties.
Our principal executive office is located at 7380 Coca Cola Drive, Suite 106, Hanover, MD 21076. We currently lease approximately 6,500 square feet of office space at this location until September 2022.2025.
Item 3. Legal Proceedings.
From time to time, we may become involved in litigation or other legal proceedings. We are not currently a party to any litigation or legal proceedings. Regardless of outcome, any litigation that we may become involved in can have an adverse impact on us because of defense and settlement costs, diversion of management resources and other factors.
Item 4. Mine Safety Disclosures.
None.
Part II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and issuer Purchases of Equity Securities.
Our common stock commenced tradingis traded on the Nasdaq Capital Market on October 2, 2020 under the symbol “PCSA.” Prior to October 2, 2020, we traded on the OTCQB.
On January 1, 2022,June 29, 2023, we amended our Certificate of Incorporation to increase the number of authorized shares of our common stock from 30,000,00050,000,000 to 50,000,000.100,000,000. The number of authorized shares of preferred stock remains unchanged at 1,000,000 shares.
On January 22, 2024, we effected a 1-for-20 reverse stock split, reducing the number of our common shares issued on that date from 24,706,474 shares to 1,291,000 shares. There was no corresponding reduction in the number of authorized shares of common stock and no change in the par value per share. All share and per share amounts and conversion and exercise prices presented herein have been adjusted retroactively to reflect this change.
Holders
As of March 24, 2022,21, 2024, there were 15,843,6212,855,981 shares of common stock outstanding and 215187 shareholders of record. One of these holders of record is Cede & Co, a nominee for Depository Trust Company (“DTC”). All of the shares of common stock held by brokerage firms and other financial institutions as nominees for beneficial owners are deposited into participant accounts at DTC and are therefore considered to be held of record by Cede & Co. as one stockholder. The actual number of stockholders is greater than the number of record holders and includes stockholders who are beneficial owners but whose shares are held in street name by brokers and other nominees.
Transfer Agent and Registrar
The transfer agent and registrar for our common stock is EquinitiContinental Stock Transfer & Trust Company.
| 47 |
Dividend Policy
We have not previously declared or paid any dividends on our common stock and do not intend to do so in the near future. We intend to retain any future earnings to fund ongoing operations and future capital requirements of our business. Any future determination to pay cash dividends will be at the discretion of the Board of Directors and will be dependent upon our financial condition, results of operations, capital requirements and such other factors as the Board of Directors deems relevant.
Securities Authorized for Issuance under Equity Compensation Plans
The table below provides information as to our 2019 Omnibus Incentive Plan as of December 31, 2021.2023.
| Number of securities to be issued upon exercise of outstanding options, warrants and rights | Weighted-average exercise price of outstanding options, warrants and rights | Number of securities remaining available for issuance under equity compensation plans (excluding securities reflected in column (a)) | Number of securities to be issued upon exercise of outstanding options, warrants and rights | Weighted-average exercise price of outstanding options, warrants and rights | Number of securities remaining available for issuance under equity compensation plans (excluding securities reflected in column (a)) | |||||||||||||||||||
| (a) | (b) | (c) | (a) | (b) | (c) | |||||||||||||||||||
| Equity compensation plans approved by security holders | 280,724 | (1) | $ | 11.45 | 1,899,696 | 315,159 | (1) | $ | 223.89 | 27,326 | ||||||||||||||
| Equity compensation plans not approved by security holders | 47,772 | 19.88 | - | 2,389 | 397.60 | - | ||||||||||||||||||
| Total | 328,496 | 1,899,696 | (2) | 317,548 | 27,326 | (2) | ||||||||||||||||||
| (1) | Includes stock options to purchase | |
| (2) | Consists of shares available for issuance under the 2019 Omnibus Incentive Plan. |
Recent Sales of Unregistered Securities
During the fourth quarter
We had no sales of 2021, we didunregistered securities during 2023 that have not issue any securities that were not registered under the Securities Act.been previously disclosed in a Current Report on Form 8-K or Quarterly Report on Form 10-Q.
Repurchases of Equity Securities
We did not repurchase any shares of our common stock during the year ended December 31, 2021.in 2023.
Item 6. [Reserved]
| 48 |
Item 7. Management’s Discussion and Analysis of the Results of Operations
You should read the following discussion and analysis of our financial condition and results of operations together with our consolidated financial statements and the related notes and other financial information included elsewhere in this Annual Report on Form 10-K. Some of the information contained in this discussion and analysis contains forward-looking statements that involve risks and uncertainties. You should review the section titled “Risk Factors” in this Annual Report on Form 10-K for a discussion of important factors that could cause actual results to differ materially from the results described below.
Overview
We are a clinical-stage biopharmaceutical company focused on utilizing our “regulatory science” approach, including the principles associated with FDA’s Project Optimus Oncology initiative and the related FDA Draft Guidance, in the development of Next Generation Chemotherapy (“NGC”) oncology drug products. Our mission is to provide better treatment options than those that presently exist by extending a patient’s survival and/or improving a patient’s quality of life. This is achieved by improving upon FDA-approved, widely used oncology drugs or the cancer-killing metabolites of these drugs by altering how they are metabolized and/or distributed in the body, including how they are distributed to the actual cancer cells.
Our mission isregulatory science approach was conceived in the early 1990s when the founders of Processa and other faculty at the University of Maryland worked with the FDA to develop multiple FDA Guidances. Regulatory science is the science of developing new tools, standards, and approaches to assess the safety, efficacy, quality, and performance of all FDA-regulated products. Over the last 30 years, two of our founders, Dr. David Young and Dr. Sian Bigora, have expanded the original regulatory science concept by including the pre-clinical and clinical studies to justify the benefit-risk assessment required for FDA approval when designing the development programs of new drug products that improve the survival and/or quality of life for patients with high unmet medical need conditions for which few or no treatment options currently exist. We are a clinical-stage development company, not a discovery company, that seeks to identify and develop drugs for patients who need better treatment options. In order to increase the probability of development success, our pipeline only includes drugs which have previously demonstrated some efficacy in the targeted population or a drug with very similar pharmacological properties that has been shown to be effective in the population.
products.
Our regulatory science approach defines the scientific information that the FDA requires to determine if the benefit outweighs the risk of a drug in a specific population of patients and at a specific dosage regimen for a specific drug product. The studies are designed to obtain the necessary scientific information to support the regulatory decision.
Our screening criteria
Recently, the FDA has taken steps to define some of the regulatory science required for identifyingthe FDA approval of oncology products. Through the FDA’s Project Optimus Oncology Initiative and selecting new candidates include:the related Draft Guidance on determining the “optimal” dosage regimen for an oncology drug, the FDA has chosen to make the development of oncology drugs more science-based than in the past. Since the principles of the FDA’s Project Optimus and the related Draft Guidance have been used by our regulatory science approach in a number of non-oncology drugs in the past, our experience with the principles of Project Optimus differentiates us from other biotechnology companies by focusing us not only on the clinical science, but also on the equally important regulatory process. We believe utilizing our regulatory science approach provides us with three distinct advantages:
| ● | ||
| ● | ||
| ● |
In many instances, these clinical candidates have significant pre-clinical and clinical data that we may leverage to high value inflection points while de-risking the programs and adding in optionality to potential future indications. Our regulatory science approach developed by our team over decades of work with regulatory authorities attempts to balance the “benefit/risk” equation to identify a regulatory path with higher clinical benefit and/or lower clinical risk with shorter timelines to deliver better treatment options to patients, physicians and caregivers.
Our pipeline includes drugs that (i) already have clinical proof-of-concept data demonstrating the desired pharmacological activity in humans or, minimally, clinical evidence in the form of case studies or clinical experience demonstrating the drug or a similar drug pharmacologically can successfully treat patients with the targeted indication; (ii) target indications for which a single positive pivotal study demonstrating efficacy might provide enough evidence that the clinical benefits of the drug and its approval outweighs the risks associated with the drug or the present standard of care (e.g., some orphan indications, many serious life-threatening conditions, some serious quality of life conditions); and/or (iii) target indications where the prevalence of the condition and the likelihood of patients enrolling in a study meet the desired timeframe to demonstrate that the drug can, at some level, treat or potentially treat patients with the condition.
To advance our mission, we have assembled an experienced and successful development team with a track record of drug approvals and successful exits. Our team is experienced in developing drug products through all principal regulatory tiers from IND enabling studies to NDA submission. The combined scientific, development and regulatory experience of our team members has resulted in more than 30 drug approvals by the FDA, over 100 meetings with the FDA and involvement with more than 50 drug development programs, including drug products targeted to patients who have an unmet medical need. Although we believe that the skills and experience of our team members in drug development and commercialization is an important indicator of our future success, the past successes of our team members in developing and commercializing pharmaceutical products does not guarantee that they will successfully develop and commercialize drugs in our current pipeline. In addition, the growth in revenues of companies at which our executive officers and directors served in was due to many factors and does not guarantee that they will successfully operate or manage us or that we will experience similar growth in revenues, even if they continue to serve as executive officers and/or directors.
Our ability to generate meaningful revenue from any products depends on our ability to out-license the drugs before or after we obtain FDA NDA approval. Even if our products are authorized and approved by the FDA, it should be noted that the products must still meet the challenges of successful marketing, distribution and consumer acceptance.
Our Strategystrategic prioritization is to advance our pipeline of NGC proprietary small molecule oncology drugs. The NGC products are new chemical entities, but they work by changing the metabolism, distribution and/or elimination of already FDA-approved cancer drugs or their active metabolites while maintaining the mechanism of how the drug kills cancer cells. We believe our NGC treatments will provide improved safety-efficacy profiles when compared to their currently marketed counterparts – capecitabine, gemcitabine, and irinotecan. All future studies of these drugs are subject to availability of capital to conduct the trials.
| 49 |
Our strategy is to obtain and develop drugs that will not only treat patients with unmet medical need conditions, but, with
The three NGC treatments in our regulatory science approach, also have the potential to be more efficiently developed with a greater probability of development success than what typically occurs in the biotech-pharma industry and a better return on investment given lower development costs, more efficient development and high commercial value. Given the prior successes of our regulatory science approach, we have selected drugs for our portfolio which may have greater chance for approval in a population of patients who desperately need better treatment options. We have applied rigorous standards to identify drugs for our portfolio, namely:pipeline are as follows:
| PCS11T, also referred to as NGC-Irinotecan (NGC-Iri), is a prodrug of the active metabolite of irinotecan (SN-38). The |
In orderOur shift in prioritization to add significant valueNGC oncology drugs does not change our mission. We continue to our in-licensed drugs within 2 to 4 years,be focused on drug products that improve the drugs must besurvival and/or quality of life for patients by improving the safety and/or efficacy of the drug in the clinical development stage and not in discovery stage, and during those 2 to 4 years we must be able to obtain clinical data to support the added value. The additional clinical data could range from a clinical proof-of-concept data to further demonstrate that the proposed pharmacology occurs clinically in the targeted patient population, while providing a more efficient and probable path to a pivotal well-designed randomized controlled trial.FDA approval and differentiating our drugs from those on the market or are currently being developed.
Historically, much of oncology drug development has searched for novel or different ways to treat cancer. Our approach is to take three current FDA-approved cancer drugs, e.g. capecitabine, gemcitabine and irinotecan, and modify and improve how the human body metabolizes and/or distributes these NGC treatments compared to their presently approved counterpart chemotherapy drugs while maintaining the cancer-killing mechanism of action; thus, our reason for calling our drugs Next Generation Chemotherapy (or NGC) treatments. Part of the development includes determining the optimal dosage regimen based on the dose-response relationship as described in the FDA’s Project Optimus Initiative and Draft Optimal Dosage Regimen Oncology Guidance. To date, we have data that we believe suggests our NGC treatments are likely to have a better safety-efficacy profile than the current widely used marketed counterpart drugs, not only potentially making the development and approval process more efficient, but also clearly differentiating our NGC treatments from the existing treatment. We believe our NGC treatments have the potential to extend the survival and/or quality of life for more patients diagnosed with cancer while decreasing the number of patients who are required to dose-adjust or discontinue treatment because of side effects or lack of response.
In 2023, we completed our Phase 2A trial for PCS12852 in gastroparesis patients with positive results. Additionally, in February 2023, due primarily to the inability to identify and enroll patients in our rare disease Phase 2 trial for PCS499 in ulcerative Necrobiosis Lipoidica (uNL), we decided to cease further enrollment in the PCS499 trial and terminated the trial. We did not experience any safety concerns during the conduct of either the PCS12852 or PCS499 trial. We continue to evaluate options to monetize these non-core drug assets, which may include out-licensing or partnering these assets with one or more third parties.
| 50 |
Recent Developments
License Agreement with Ocuphire Pharma, Inc. – Reverse Stock SplitOn June 16, 2021, we executed a License Agreement with Ocuphire Pharma, Inc. (“Ocuphire Agreement”) under which we received a license to research, develop and commercialize PCS3117 (formerly RX-3117) globally, excluding the Republic of Singapore, China, Hong Kong, Macau and Taiwan.
Shelf Registration Statement - On June 30, 2021,January 22, 2024, we filedeffected a shelf registration statement1-for-20 reverse stock split, reducing the number of our common shares issued on Form S-3, which became effectivethat date from 24,706,474 shares to 1,291,000 shares. There is no corresponding reduction in July 2021. The shelf registration statement permits the offering, issuance and salenumber of up to $75.0 millionauthorized shares of common stock preferred stock, warrants and/or unitsand no change in one or more offeringsthe par value per share. All share and in any combination of the foregoing.per share amounts and conversion and exercise prices presented herein have been adjusted retroactively to reflect this change.
Public Offering
“At-the-Market” (ATM) Offering –
On August 20, 2021,January 30, 2024, we entered into an equity distribution agreement (the “Sales Agreement”) with Oppenheimer & Co. Inc. (the “Sales Agent”) under which we may issue and sell in a registered “at-the-market” offeringraised gross proceeds of $7.0 million (net proceeds of $6.3 million) from the sale of 476,000 shares of our common stock, having an aggregate offering price ofpre-funded warrants to purchase up to $30.0 million from time1,079,555 shares of our common stock and warrants to time through orpurchase 1,555,555 shares of our common stock in a public offering, as described in Note 13. Simultaneously with the closing of the sale, the pre-funded warrants were exercised in exchange for 1,079,555 shares of our common stock. We plan to our Sales Agent under our shelf registration statement (the “ATM Offering”). We expect to use the net proceeds from the ATM Offering over time as a sourcethis financing for continued research and development for NCG-Cap, and working capital and general corporate purposes. We are not obligated to make any sales of our common stock under the Sales Agreement and no assurance can be given as to the price or amount of shares that we will sell, or the dates on which any such sales will take place. We will pay the Sales Agent an aggregate of up to 3.0% of the gross proceeds of the sales price per share of common stock sold through the Sales Agent under the Sales Agreement. The shares under the ATM Offering will be sold and issued pursuant to our S-3 shelf registration statement. During the fourth quarter of 2021, we sold 21,597 shares of our common stock for $174 thousand in net proceeds after paying $5 thousand in commissions to the Sales Agent.
Lincoln Park Capital Fund, LLC Purchase Agreement - On March 23, 2022, we entered into a purchase agreement (the “Purchase Agreement”) with Lincoln Park Capital Fund, LLC (“Lincoln Park”), pursuant to which Lincoln Park has committed to purchase up to $15.0 million of shares (the “Purchase Shares”) of our common stock, $0.0001 par value per share (“Common Stock”), subject to the terms and conditions in the Purchase Agreement. We issued 123,609 shares of common stock (valued at $450,000) to Lincoln Park as a commitment fee in connection with entering into the Purchase Agreement and agreed to reimburse Lincoln Park $25,000 for fees incurred in connection with the Purchase Agreement. Concurrently with entering into the Purchase Agreement, we also entered into a registration rights agreement with Lincoln Park (the “Registration Rights Agreement”), pursuant to which we agreed to take certain actions relating to the registration under the Securities Act of 1933, as amended, of the offer and sale of the shares of common stock available for issuance under the Purchase Agreement. See Note 14 for additional details concerning the Purchase Agreement.
Impact of COVID-19
The COVID-19 pandemic continues to create uncertainties in the expected timelines for clinical stage biopharmaceutical companies such as ours, including causing delays in clinical trials and disruptions in the supply chain for raw materials used in clinical trial work. We have experienced delays in the enrollment of patients in our PCS499 Phase 2B trial due to COVID-19. Potential patients have died from COVID-19 prior to screening and continue to be reluctant to travel to our testing sites for fear of contracting COVID-19. Delays in enrollment lengthen the time of studies and increase their costs. While we are hopeful the infection rate of COVID-19 will continue to decline, we cannot predict the future impact COVID-19 will have on our current and future clinical trials. Continued delays could materially impact our business in future periods and further extend our timelines.
For more information on the risks associated with COVID-19, refer to Part I, Item 1A, “Risk Factors” herein.
Results of Operations
Comparison of the year ended December 31, 20212023 and 20202022
The following table summarizes our operations loss during the periods indicated:
| Year Ended December 31, | ||||||||||||
| 2021 | 2020 | Change | ||||||||||
| Operating Expenses | ||||||||||||
| Research and development costs | $ | 6,878,021 | $ | 3,172,385 | $ | 3,705,636 | ||||||
| Acquisition of in-process research and development | 566,583 | 8,700,000 | (8,133,417 | ) | ||||||||
| General and administrative expenses | 4,688,939 | 3,264,474 | 1,424,465 | |||||||||
| Operating Loss | (12,133,543 | ) | (15,136,859 | ) | ||||||||
| Other Income (Expense) | ||||||||||||
| Forgiveness of Payroll Protection Program loan and related accrued interest | 163,771 | - | 163,771 | |||||||||
| Interest expense | (362 | ) | (281,122 | ) | 280,760 | |||||||
| Interest income | 11,989 | 3,174 | 8,815 | |||||||||
| Total other income (expense) | 175,398 | (277,948 | ) | |||||||||
| Net Operating Loss Before Income Tax Benefit | (11,958,145 | ) | (15,414,807 | ) | 3,456,662 | |||||||
| Income Tax Benefit | 530,611 | 1,001,019 | (470,408 | ) | ||||||||
| Net Loss | $ | (11,427,534 | ) | $ | (14,413,788 | ) | ||||||
| Year Ended December 31, | ||||||||||||
| 2023 | 2022 | Change | ||||||||||
| Operating Expenses | ||||||||||||
| Research and development costs | $ | 5,799,518 | $ | 11,494,230 | $ | (5,694,712 | ) | |||||
| General and administrative expenses | 5,657,543 | 8,763,058 | (3,105,515 | ) | ||||||||
| Impairment of intangible asset | - | 7,268,143 | (7,268,143 | ) | ||||||||
| Operating Loss | (11,457,061 | ) | (27,525,431 | ) | ||||||||
| Other Income (Expense) | ||||||||||||
| Interest income, net | 335,541 | 101,202 | 234,339 | |||||||||
| Net Loss | $ | (11,121,520 | ) | $ | (27,424,229 | ) | ||||||
| 51 |
Revenues.
We had no revenue during the years ended December 31, 20212023 and 2020.2022. We do not currently have any revenue under contract or any immediate sales prospects.
Research and Development Expenses.
Our research and development costs are expensed as incurred. Research and development expenses include (i) amortization of the exclusive PCS499 license intangible asset used in research and development activities, (ii) program and testing related expenses including external consulting and professional fees related to the product testing and our development activities and (iii)(ii) internal research and development staff related salaries and other payroll costs including stock-based compensation, payroll taxes and employee benefits. In 2022, we also had expenses related to the amortization of the exclusive PCS499 license intangible asset. Non-refundable advance payments for goods and services to be used in future research and development activities are recorded as prepaid expenses and expensed when the research and development activities are performed.
Research and development costs for the years ended December 31, 20212023 and 20202022 were as follows:
| Year ended December 31, | Year ended December 31, | |||||||||||||||
| 2021 | 2020 | 2023 | 2022 | |||||||||||||
| Amortization of intangible assets | $ | 790,488 | $ | 795,328 | ||||||||||||
| Preclinical, clinical trial and other costs | 4,171,836 | 972,711 | $ | 3,817,669 | $ | 6,269,006 | ||||||||||
| Research and development salaries and benefits | 1,915,697 | 1,404,346 | 1,981,849 | 4,436,729 | ||||||||||||
| Amortization of intangible assets | - | 788,495 | ||||||||||||||
| Total | $ | 6,878,021 | $ | 3,172,385 | $ | 5,799,518 | $ | 11,494,230 | ||||||||
During the year ended December 31, 2021,2023, our research and development expenses increaseddecreased by $3,705,636$5.7 million to $6,878,021$5,799,518 when compared to $3,172,385$11,494,230 for the year ended December 31, 2020.2022. The increase was primarily due to an increasedecrease in preclinical, clinical trial and other costs of $3,199,125, which areduring 2023 when compared to 2022 was attributable to expenses we incurred as we commencedthe completion of our Phase 2B clinical trial for PCS499, Phase 1BPCS12852 and the early termination of our clinical trial for PCS6422 and for pre-INDPCS499. Expenses include costs for PCS12852. Expenses included paymentsrelated to contract research organizations, for regulatory filingsfiling and maintenance fees, drug product testing and stability, consulting, and other clinical fees. During the same periodWe also did not have any amortization expense in 2020, we were completing the patient portion of our Phase 2A clinical trial for PCS499 and incurring regulatory filing and consulting fees2023, as we preparedfully impaired our PCS499 intangible asset at December 31, 2022. In 2022, we had three active clinical trials and amortization expense for our meeting with the FDA. Additionally, duringintangible asset. We also experienced decreases in stock-based compensation of $2.5 million as a result of a reduction in stock awards granted. During 2023, we also experienced a decrease in salaries and related expenses of $29,000. While we have promoted and/or increased salary rates for some personnel, we have fewer full-time R&D employees in 2023 than 2022.
During the year ended December 31, 2021,2022, we experienced increases in payroll and related costsamended the third Milestone Event of $511,351 resulting from hiring additional development personnel and increased employee salary rates, when compared toour License Agreement with Elion changing the same period in 2020. These increases were offset bythird Milestone Event. As a decrease of $4,840 in amortization expense, as the capitalized software was fully amortized during the year ended December 31, 2021.
We anticipate ourresult, we recorded research and development expense and a related liability of $189,000, which represents the value of the 5,000 shares of our common stock we issued to Elion in 2024 in satisfaction of the third Milestone Event (as modified) at the fair value on the date of modification.
On January 30, 2024, we raised net proceeds of $6.3 million, which we intend to use for continued research and development for NCG-Cap and for working capital. We are also incurring costs to continue to increase significantly in 2022 as we: (i) continuepreparation for our clinical trials for PCS499 and PCS6422 and begin our clinicalplanned Phase 2 trial for PCS12852,NGC-Cap, including the cost of having drug product manufactured; (ii) complete a biomarker assaymanufactured and other pre-trial tasks, as well as costs we may incur in connection with the submission of any Phase 2B protocol for PCS3117;NGC-Gem. In early 2025, we will need to raise additional capital to fund our operations and (iii) obtain IND enabling data for PCS11T.continue our planned development of our NGC drugs.
| 52 |
The funding necessary to bring a drug candidate to market is subject to numerous uncertainties. Once a drug candidate is identified, the further development of that drug candidate may be halted or abandoned at any time due to a number of factors. These factors include, but are not limited to, funding constraints, safety or a change in market demand. For each of our drug candidate programs, we periodically assess the scientific progress and merits of the programs to determine if continued research and development is economically viable. Some programs may be terminated due to the lack of scientific progress and lack of prospects for ultimate commercialization. As noted above, weWe anticipate our research and development costs to increase in the future, subject to obtaining sufficient financing, as we finalize our clinical trials; plan/conduct future clinical trials, including the Phase 2B trial to evaluatecost of having drug product manufactured; continue our evaluation of the ability of PCS499 to completely close ulcers in patients with NL and to continue with an amended Phase 1B clinical trial for PCS6422. On May 19, 2021, we dosed the first patientremaining drugs in our PCS499 randomized, placebo-controlled trial, but have experienced delays in patient enrollment;portfolio; and while we dosed the first patient inexpand our PCS6422 trial on August 2, 2021, we submitted a modified Phase 1B trial protocol in February 2022 to determine the maximum tolerated dose of capecitabine and provide us with data on the timeline of DPD inhibition and de novo formation. We expect to restart the PCS6422 Phase 1B trial in the second quarter of 2022.development team.
Our clinical trial cost accruals are based on estimates of patient enrollment and related costs at clinical investigator sites, as well as estimates for the services received and efforts expended pursuant to contracts with multiple research institutions and CROs that conduct and manage clinical trials on our behalf.
We estimate preclinical and clinical trial expenses based on the services performed, pursuant to contracts with research institutions and clinical research organizations that conduct and manage preclinical studies and clinical trials on our behalf. In accruing service fees, we estimate the time period over which services will be performed and the level of patient enrollment and activity expended in each period. If the actual timing of the performance of services or the level of effort varies from the estimate, we will adjust the accrual accordingly. Payments made to third parties under these arrangements in advance of the receipt of the related series are recorded as prepaid expenses until the services are rendered.
Acquisition of In-Process Research and Development.
In connection with the Ocuphire Agreement, At December 31, 2023, we have recorded $566,583 of acquired in-process research and development expense$570,000 in 2021. The total acquisition cost includes the issuance of 44,689 shares (with a fair value of $300,000) ofprepaid expenses for advanced payments made to our common stock we issued to Ocuphire, a cash payment of $200,000 and $66,583 in expenses we agreed to pay on behalf of Ocuphire. During the same period in 2020, we recorded $8.7 million of acquired in-process research and development expense in connection withCRO for our license agreements with Yuhan, Aposense and Elion. We believe the in-process research and development assets acquired have no alternative future use.NGC-Cap clinical trial.
General and Administrative Expenses.
Our general and administrative expenses for the year ended December 31, 2021 increased2023 decreased by $1,424,465$3.1 million to $4,688,939$5,657,543 when compared to $3,264,474$8,763,058 for the same period in 2020.2022. The majority of the increasedecrease was mostly due to increased professional and other consulting feesemployee stock-based compensation of $1,086,673 (which includes$4.9 million as a $620,793 increaseresult of fees paida reduction in stock compensation); increased payroll and related costs of $174,115 from hiring additional personnel, increased salary rates and health insurance premiums; and a $110,410 increase in employee stock-based compensation.awards granted. We also experienced an increasenet decreases in our insurance of $116,024, mostly due to increased insurance premiums; an increase intaxes, travel and other miscellaneous office and repairs and maintenance expenses of $113,465 as we purchased new/replacement computers for our new and existing employees and replaced outdated hardware and old cabling in the office; and an increase of $10,825 in other miscellaneous expenses. These increased expenses$38,000. The decreases were primarily offset by decreasesincreases in depreciation, equipment rent, taxesprofessional fees of $1.3 million related to the warrants we issued to Spartan Capital as compensation for services provided under a consulting agreement and travelfor salaries and related expenses of $179,724.$493,000. We share office space with CorLyst, a related party, and during the years ended December 31, 20212023 and 2020,2022, they reimbursed us $126,324$112,000 and $119,001,$124,000, respectively, for rent and other costs we incurred on their behalf.
Impairment of Intangible Asset.
Our gross intangible assets consisted primarily of costs we capitalized related to the acquisition of license rights to PCS499 from CoNCERT Pharmaceuticals. Inc. (“CoNCERT”) for shares of our common stock. We expectcapitalized $8.0 million, which was the general and administrative expensesfair value of the common stock we issued to continueCoNCERT when we acquired the license rights to PCS499 on March 19, 2018.
We review amounts previously capitalized for impairment whenever events or changes in circumstances indicate to us that the carrying value of the assets might not be recoverable. In May 2021, we enrolled our first patient in our Phase 2B trial for the treatment of ulcerative NL with PCS499. Although we initiated a number of recruitment programs to increase asthe enrollment of patients in this study, we add staffwere only able to support our growing research and development activitiesrecruit four patients by December 31, 2022. We experienced extremely slow enrollment in the study given the extreme rarity of the condition (rarer than reported in the literature), the impact of COVID-19, and the administration requiredreluctance of patients to operatebe in a clinical study. As a result, we terminated the trial early. At December 31, 2022, as a public company.result of our decision to halt future enrollment and terminate our PCS499 clinical trial for ulcerative necrobiosis lipoidica, we recognized an impairment of the remaining book value of the intangible asset of $7.3 million, thereby reducing the value of our intangible asset to zero. Our assessment was based on the uncertainty of determining whether we will be able to out-license PCS499 or enter into a partnering/collaborating arrangement for its future development.
Other Income and (Expense)Income.
Net other income consisting primarily of interest income was $335,541 and (expense) was $175,398 and ($277,948)$101,202 for the years ended December 31, 20212023 and 2020,2022, respectively. During 2021, we recognized $163,771 as other income for the principal amount and related accrued interest related to the forgiveness of our Paycheck Protection Program loan. Interest income represents interest earned on money market funds. Interest expense in 2021 was related to our Paycheck Protection Program loan while interest expense in 2020 was related to our $805,000 8% Senior Notes sold in 2019 and 2020 and borrowings on a related party LOC. Included in interest expense is the amortization of debt issuance costs totaling $199,900 for the year ended December 31, 2020.
| 53 |
Income Tax Benefit.
AnWe did not recognize any income tax benefit of $530,611 and $1,001,019 was recognized for the yearsyear ended December 31, 2021 and 2020, respectively. A deferred tax liability was created as a result of our acquisition of CoNCERT’s license and “Know-How” in exchange for Processa stock that had been issued in the Internal Revenue Code Section 351 transaction on March 19, 2018. The Section 351 transaction treated the acquisition of the Know-How for stock as a tax-free exchange. As a result, under ASC 740-10-25-51 Income Taxes, Processa2023 or 2022. At December 31, 2023, we recorded a deferred tax liability of $3,037,147 for the acquired temporary difference between the financial reporting basis of $11,038,929 and the tax basis of $1,782. The deferred tax liability will be reduced for the effect of the non-deductibility of the amortization of the intangible asset and may be offset by the deferred tax assets resulting fromtotaling $17,639,071, including $7,685,377 of net operating tax losses (see Note 4 – Income Taxes). Thisthat are fully offset results in the recognition ofby a deferred tax benefit shown in the consolidated statements of operations.valuation allowance.
Liquidity
Sources of Liquidity
At December 31, 20212023, we had $16.5$4.7 million in cash and cash equivalents.
equivalents and raised an additional $6.3 million net proceeds in January 2024. On February 24, 2021,January 30, 2024, we closed a private placement for the salesold, pursuant to securities purchase agreements (the “Purchase Agreement”), 476,000 shares of 1,321,132common stock, pre-funded warrants to purchase up to 1,079,555 shares of common stock in lieu of shares of common stock (the “Pre-Funded Warrants”), and warrants to purchase up to 1,555,555 shares of our common stock (the “Common Warrants’) pursuant to a public offering (the “Offering”). The Common Warrants have an exercise price of $4.50, are immediately exercisable and will remain exercisable until the date that is five years after their original issuance. The Shares were offered at a purchasecombined public offering price of $7.75$4.50 per share to accredited and institutional investorsaccompanying Common Warrant and $4.4999 per Pre-Funded Warrant and accompanying Common Warrant. The Pre-Funded Warrants had an exercise price of $0.0001 and were exercised in full simultaneously with the closing of the Offering in exchange for gross1,079,555 shares of our common stock. Gross proceeds of $10.2 million. Net proceeds fromin connection with the offeringOffering were $9.9$7.0 million. We also completed an underwritten public offeringreceived $6.3 million in late 2020 where we raised net proceeds from the offeringOffering, after deducting the fees of approximately $17.1 million.
On August 20, 2021, we entered into the Sales Agreement under which we may issueplacement agent and sell shares of our common stock in a registered ATM Offering having an aggregate offering price of up to $30.0 million from time to time through or to our Sales Agent.other offering-related expenses. We expect to use net proceeds from the ATM Offering over time as a source for working capital and general corporate purposes. We are not obligated to make any sales of our common stock under the Sales Agreement and no assurance can be given asalso issued to the price or amount of shares that we will sell, or the dates on which any such sales will take place. We will pay the Sales Agent an aggregate of upplacement agent warrants to 3.0% of the gross proceeds of the sales price per share of common stock sold through the Sales Agent under the Sales Agreement. The shares under the ATM Offering will be sold and issued pursuant to our S-3 shelf registration statement. During the fourth quarter of 2021, we sold 21,597purchase 62,222 shares of common stock, under the ATM Offering for net proceeds of $174 thousand. We have not yet sold any shares under the ATM Offering in 2022.
On March 23, 2022, we entered into a Purchase Agreement (the “Purchase Agreement”) with Lincoln Park Capital Fund, LLC (“Lincoln Park”) under which we have the right, but not the obligation, to sell to Lincoln Park, and Lincoln Park is obligated to purchase up to $15,000,000 of our shares of common stock, par value $0.0001exercisable at $5.625 per share subject to the terms and conditions in the Purchase Agreement, during the term of the Purchase Agreement as more fully described in Note 14 to the Consolidated Financial Statements.that expire on February 1, 2027.
We have incurred losses and net cash used in our operating activities during the year ended December 31, 2021,2023, which we expect to continue for the foreseeable future. We do not currently nor have since our inception had any sales. We have incurred losses since our inception, devoting substantially all of our efforts toward research and development, and have an accumulated deficit of approximately $36.8$75.4 million at December 31, 2021.2023. During the year ended December 31, 2021,2023, we generated a net loss of approximately $11.4$11.1 million, of which $4.5$2.4 million arewere non-cash expenses. Based on our current business plans, we believe these funds will satisfy our current cash balance is adequate for at least the next twelve months without considering amounts available from the Lincoln Park Purchase Agreement or potential sales under our ATM Offering.capital needs into early 2025. Our ability to execute our longer-term operating plans, including unplanned future clinical trials for our portfolio of drugs depend on our ability to obtain additional funding from the sale of equity and/or debt securities, a strategic transaction or other funding transactions. We plan to continue to actively pursue financing alternatives, but there can be no assurance that we will obtain the necessary funding in the future when necessary.needed.
Our estimate of future cash needs is based on assumptions that may prove to be wrong, and we could utilize our available cash sooner than we currently expect. Our ultimate success depends on the outcome of our planned clinical trials and our research and development activities, as disclosed above. We expect to incur additional losses in the future, and we will need to raise additional capital to fully implement our business plan if the costcosts of our clinical trials are greater than we expect or they take longer than anticipated. We also expect to incur increased general and administrative expenses in the future. We also plan to develop a biomarker assay for PCS3117 and obtain IND enabling data for PCS11T. In addition, there may be costs we incur as we develop these drug products that we do not currently anticipate, requiring us to need additional capital sooner than currently expected.
Our future capital requirements will depend on many factors, including:
| ● | the cost of our current and future clinical trials | |
| ● | the initiation, progress, timing, costs and results of drug manufacturing, pre-clinical studies, and clinical trials of | |
| ● | the number and characteristics of product candidates that we pursue; | |
| ● | the outcome, timing, and costs of seeking regulatory approvals; | |
| ● | the costs associated with hiring additional personnel and consultants | |
| activities; | ||
| ● | the emergence of competing therapies and other adverse market developments; | |
| ● | the costs involved in preparing, filing, prosecuting, maintaining, expanding, defending, and enforcing patent claims, including litigation costs and the outcome of such litigation; | |
| ● | the extent to which we in-license or acquire other products and technologies; and | |
| ● | the costs of operating as a public company. |
Until such time as we can generate substantial product revenues to support our capital requirements, if ever, we expect to finance our cash needs through a combination of public or private equity offerings, debt financings, collaborations and licensing arrangements or other capital sources. We alsocurrently have an effective S-3 shelf registration statement on Form S-3 on file with the SEC, which provides us flexibility and optionality to raise capital, including pursuant to the ATM Offering and thea Purchase Agreement with Lincoln Park Purchase Agreement,Capital or a future at-the-market offering, but there can be no assurance that capital will continue to be available to us on acceptable terms, won’t be limited, or be available at all. To the extent that we raise additional capital through the sale of equity or convertible debt securities, the ownership interest of our stockholders will be or could be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect the rights of our common stockholders.
| 54 |
Cash Flows
The following table sets forth our sources and uses of cash and cash equivalents for the years ended December 31, 20212023 and 2020:2022:
| For the Year Ended December 31, | For the Year Ended December 31, | |||||||||||||||
| 2021 | 2020 | 2023 | 2022 | |||||||||||||
| Net cash provided by (used in): | ||||||||||||||||
| Net cash (used in) provided by: | ||||||||||||||||
| Operating activities | $ | (8,717,291 | ) | $ | (3,143,196 | ) | $ | (8,063,346 | ) | $ | (9,605,143 | ) | ||||
| Investing activities | (2,776 | ) | - | |||||||||||||
| Financing activities | 9,798,648 | 17,867,884 | 6,268,724 | (388,843 | ) | |||||||||||
| Net increase in cash and cash equivalents | $ | 1,081,357 | $ | 14,724,688 | ||||||||||||
| Net decrease in cash and cash equivalents | $ | (1,797,398 | ) | $ | (9,993,986 | ) | ||||||||||
Net cash used in operating activities
We used net cash in our operating activities of $8,717,291$8,063,346 and $3,143,196$9,605,143 during the years ended December 31, 20212023 and 2020,2022, respectively. The increase in cash used in operating activities during the year ended December 31, 2021 compared to the comparable period in 2020 was primarily related to costs we incurred related to our Phase 2B clinical study for PCS499, Phase 1B clinical study for PCS6422, pre-clinical costs for PCS12852, as well as increased professional fees and salaries. Our prepaid expenses increased by $1.2 million during the year ended December 31, 2021, primarily due to deposits paid to our CROs for clinical trial related costs. Of this amount, $186,491 represents deferred offering costs which impacted net cash provided by financing activities. As a result, the change in prepaid expenses impacting net cash used in operating activities is $1.0 million.
As we continue our clinical trials for PCS499 and PCS6422, begin a Phase 2A clinical trial for PCS12852,NGC-Cap and continue to evaluate and develop the other NGC drugs in our portfolio, we anticipate our research and development efforts and ongoing general and administrative costs will continue to generate negative cash flows from operating activities for the foreseeable future. We expect these amountsUntil we begin our Phase 2 clinical trial for NGC-Cap, we anticipate clinical trial costs will decrease when compared to increaseprior periods since we are only conducting one clinical trial for NGC-Cap.
At December 31, 2023, our prepaid expense and other consisted primarily of $570,000 for advanced payments we made to our NGC-Cap CRO that have not yet been applied to our clinical trial and $212,000 in the future.various insurance policies, such as directors’ and officers’ insurance and product liability insurance for conducting our clinical trials. Our prepaid expense and other at December 31, 2022 also included an additional $394,000 for advanced payments made to CROs for our PCS499 and PCS12852 clinical trials; an unamortized non-cash commitment fee we paid to Lincoln Park of approximately $334,000; and unamortized ATM offering related costs of $186,000.
Net cash used in investing activities
We used net cash in our investing activities of $2,776 during year ended December 31, 2023 to purchase property and equipment. We did not have a similar expense during the same period in 2022.
Net cash provided by (used in) financing activities
During the year ended December 31, 2021,2023, we received $9,875,550 inraised net proceeds from our February 2021 private placement transaction and $173,987 in net proceedsof $6.4 million from the sale of 21,597421,611 shares of our common stock under our ATM Offering. We incurred $186,941and used $31,000 in legal expenses related to our ATM Offering, $186,493January 2024 raise and $53,000 for the settlement of which we have capitalized and will amortize as we sell additional shares under our ATM Offering.
Net cash provided by financing activities duringa stock award. During the year ended December 31, 20202022, we used net cash in financing activities of $17,867,884 ($17.1 million$300,000 to purchase 5,000 shares of our common stock from a licensee in net proceeds) was from our 2020 underwritten public offering, borrowings totaling $700,000 under a related-party LOC Agreement,early 2022 and $162,459 we received from the Bank of America pursuant$89,000 to a promissory note under the Paycheck Protection Program.pay income taxes owed on vested stock-based compensation.
Contractual Obligations and Commitments
The following table summarizes our contractual obligations at December 31, 2021:2023:
| Payments Due by Period | Payments Due by Period | |||||||||||||||||||||||||||||||||||||||
| Less than | 1-3 | 3-5 | More than | Less than | 1-3 | 3-5 | More than | |||||||||||||||||||||||||||||||||
| Total | 1 Year | Years | Years | 5 Years | Total | 1 Year | Years | Years | 5 Years | |||||||||||||||||||||||||||||||
| Operating lease obligations | $ | 83,754 | $ | 75,969 | $ | 7,785 | $ | - | $ | - | $ | 160,737 | $ | 90,697 | $ | 70,040 | $ | - | $ | - | ||||||||||||||||||||
| Total | $ | 83,754 | $ | 75,969 | $ | 7,785 | $ | - | $ | - | $ | 160,737 | $ | 90,697 | $ | 70,040 | $ | - | $ | - | ||||||||||||||||||||
| 55 |
We enter into contracts in the normal course of business with CROs, clinical supply manufacturers and vendors for pre-clinical studies, research supplies and other services and products for operating purposes. These contracts generally provide for termination after a notice period, and, therefore, are cancelable contracts and not included in the table above.
We have also entered into license and collaboration agreements with third parties, which are in the normal course of business. We have not included future payments under these agreements in the table of contractual obligations above since obligations under these agreements are contingent upon future events such as our achievement of specified development, regulatory, and commercial milestones, or royalties on net product salessales.
Off Balance Sheet Arrangements
During the periods presented we did not have, nor do we currently have, any off-balance sheet arrangements as defined under SEC rules.
Critical Accounting Policies and Use of Estimates
Our management’s discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with U.S. GAAP. The preparation of these consolidated financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, and expenses and the disclosure of contingent assets and liabilities. On an ongoing basis, we evaluate our estimates and judgments, including those related to accrued expenses and stock-based compensation. We base our estimates on historical experience, known trends and events, and various other factors that are believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
We believe the following accounting policies and estimates are most critical to aid in understanding and evaluating our financial results reported in our consolidated financial statements.
ValuationImpairment of Intangible AssetsPCS499 In-process Research and Development Asset
Our intangible assets consistIn February 2023, we suspended further enrollment in our PCS499 trial for uNL due to difficulties we encountered in enrolling the trial, along with our limited resources. In May 2021, we enrolled our first patient in our Phase 2B trial for the treatment of ulcerative NL with PCS499. Although we initiated a number of recruitment programs to increase the enrollment of patients in this study, we were only able to recruit four patients by December 31, 2022. We experienced extremely slow enrollment in the study given the extreme rarity of the capitalized costscondition (rarer than reported in the literature), the impact of $20,500 for a software license and $11,038,929 associated with the exercise of the option to acquire the exclusive license from CoNCERT related to patent rights and Know-How to develop and commercialize compounds and products for PCS499 and each metabolite thereofCOVID-19, and the related income tax effects. The capitalized costsreluctance of patients to be in a clinical study. We completed the study for the license rightsthose currently enrolled and halted further efforts to PCS499, in addition to the fair valueenroll new patients. As a result, we recognized a non-cash expense of the common stock issued, also includes $1,782 in transaction costs and $3,037,147 associated with the initial recognition$7.3 million as of an offsetting deferred tax liabilityDecember 31, 2022 related to the acquired temporary difference for an asset purchased that is not a business combination and has a nominal tax basis in accordance with ASC 740-10-25-51 Income Taxes. In accordance with ASC Topic 730, Research and Development, we capitalized the costs of acquiring the exclusive license rights to PCS499 as the exclusive license rights represent intangible assets to be used in research and development activities that have future alternative uses.
We used a market approach to estimate the fair valueimpairment of the common stock issued tointangible asset for PCS499. We originally recognized this intangible asset in conjunction with its acquisition from CoNCERT Pharmaceuticals, Inc. in this transaction. Our estimate was based on the final negotiated number of shares of stock issued and the volume weighted average market price over a 45-day period preceding the mid-February 2018 finalized negotiation of the modification to the option and license agreement with CoNCERT. We believe the fair values used to record intangible assets acquired in this transaction are based upon reasonable estimates and assumptions given the facts and circumstances as of the related valuation dates.
We determined our intangible assets to have finite useful lives and review them for impairment when facts or circumstances suggest that the carrying value of these assets may not be recoverable.2018.
Clinical Trial Accruals / Research and Development
As part of the process of preparing our consolidated financial statements, we are required to estimate expenses resulting from our obligations under contracts with vendors, CROs and consultants and under clinical site agreements related to conducting our clinical trials. The financial terms of these contracts vary and may result in payment flows that do not match the period over which materials or services are provided under such contracts.
Our clinical trial accruals are based on estimates of patient enrollment and related costs at clinical investigator sites as well as estimates for the services received and efforts expended pursuant to contracts with multiple research institutions and CROs that conduct and manage clinical trials on our behalf. During a clinical trial, we will adjust the clinical expense recognition if actual results differ from estimates. We make estimates of accrued expenses as of each balance sheet date based on the facts and circumstances known at that time. Our clinical trial accruals are partially dependent on the accurate reporting by the CRO and other third-party vendors. Although we do not expect estimates to differ materially from actual amounts, our understanding of the status and timing of services performed relative to the actual status and timing of services performed may vary and may result in reporting amounts that may be too high or too low for any reporting period.
| 56 |
Payments made to third parties under these arrangements in advance of the receipt of the related services are recorded as prepaid expenses until the services are rendered. We expense research and development costs as they are incurred.
Stock-Based Compensation
Stock-based compensation expense is based on the grant-date fair value estimated in accordance with the provisions of ASC 718, Compensation-Stock Compensation. We expense stock-based compensation over the requisite service period based on the estimated grant-date fair value of the awards. Stock-based awards with graded-vesting schedules are recognized on a straight-line basis over the requisite service period for each separately vesting portion of the award. No expense is recognized for stock-based awards with performance-vesting conditions until management believes it is probable the performance-vesting condition will be met. We value restricted stock awards (RSAs) and restricted stock units (RSUs) based on the closing share price on the date of grant. We estimate the fair value of stock option and warrant grants using the Black-Scholes option pricing model, and the assumptions used in calculating the fair value of stock-based awards represent management’s best estimates and involve inherent uncertainties and the application of management’s judgment. We account for forfeitures in the period in which they occur, rather than estimate expected forfeitures.
See Note 53 – Stock-Based Compensation for information concerning certain of the specific assumptions we used in applying the Black-Scholes option pricing model to determine the estimated fair value of our stock optionswarrants granted during the yearsyear ended December 31, 2021 and 2020.2023.
All stock-based compensation costs are recorded in general and administrative or research and development costs in the consolidated statements of operations based upon the underlying individual’s or entity’s role.
Income Taxes
We account for income taxes in accordance with ASC Topic 740, Income TaxesTaxes.. Under the asset and liability method, deferred Deferred income taxes are recognizedrecorded for the futureexpected tax consequences attributable toof temporary differences between the financial statement carrying amountsbasis of existing assets and liabilities for financial reporting purposes and their respectiveamounts recognized for income tax basispurposes. We have recorded a valuation allowance equal to the full recorded amount of our net deferred tax assets since it was more-likely-than-not that benefits from our deferred tax assets would not be realized. The valuation allowance is reviewed quarterly and is maintained until sufficient positive evidence exists to support its reversal. As part of an evaluation of our tax attributes in 2022, we recharacterized approximately $7.4 million of startup costs previously capitalized as an IRC Section 195 asset as net operating loss carryforwards.losses. The recharacterization has no impact on total deferred tax assets since we had previously and will continue to provide a full valuation allowance on our unutilized net deferred tax assets. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the year in which those temporary differences are expected to be recovered or settled. The effect of changes in tax rates on deferred tax assets and liabilities is recognized in income in the period such changes are enacted. A valuation allowanceNo income tax benefit or expense was recorded for any periods presented nor is provided againstexpected in the foreseeable future since we expect to generate future taxable net deferred tax assets if recoverability is uncertain on a more likely than not basis. As of December 31, 2021 and 2020, we have established a valuation allowance to offset certain deferred tax assets.operating losses.
We recognize the impact of an uncertain tax position if the position will more likely than not be sustained upon examination by a taxing authority, based on the technical merits of the position. Our policy is to record interest and penalties related to income taxes as part of its income tax provision. As ofAt December 31, 2021,2023, we had no unrecognized tax benefits and as such, no liability, interest or penalties were required to be recorded. We do not expect this to change significantly in the next twelve months.
Recently Issued Accounting Pronouncements
See Note 2 of our consolidated financial statements for new accounting pronouncements or changes to the recent accounting pronouncements during the year ended December 31, 2021.2023.
Item 7A. Quantitative and Qualitative Disclosures about Market Risk
Item 7A is not applicable to us as a smaller reporting company and has been omitted.
Item 8. Financial Statements and Supplementary Data
| 57 |
INDEX TO FINANCIAL STATEMENTS
| F-1 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM

To the Board of Directors and Stockholders of
Processa Pharmaceuticals, Inc.
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheets of Processa Pharmaceuticals, Inc. (the “Company”) as of December 31, 20212023 and 2020,2022, the related consolidated statements of operations, stockholders’ equity, and cash flows, for the years then ended, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 20212023 and 2020,2022, and the results of its operations and its cash flows for the years then ended, in conformity with accounting principles generally accepted in the United States of America.
The Company’s Ability to Continue as a Going Concern
The accompanying consolidated financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 1 to the financial statements, the Company has suffered recurring losses from operations and has stated that substantial doubt exists about the Company’s ability to continue as a going concern. Management’s evaluation of the events and conditions and management’s plans regarding these matters are described in Note 1. The consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty.
Basis for Opinion
These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s consolidated financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (“PCAOB”) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the consolidated financial statements that were communicated or required to be communicated to the audit committee and that: (1) relate to accounts or disclosures that are material to the consolidated financial statements and (2) involvedinvolve our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing a separate opinionsopinion on the critical audit matters or on the accountsaccount or disclosures to which they relate.
Intangible AssetGoing Concern
As discussed in Note 1 to the consolidated financial statements, the Company has determined that there is substantial doubt about its ability to continue as a going concern.
We identified the going concern as a critical audit matter due to the difficulty the Company experienced raising funds. Additionally, it has no source of cash beyond equity and debt financing.
Equity Related Matters
As discussed in Notes 2, 3, 4 and 105 to the consolidated financial statements, the Company has capitalized costs of $8,056,638 related to the acquisitionsubstantial equity activity, including financing transactions and stock compensation. The volume and complexity of the exclusive license rights to PCS499. This intangible asset is tested at least annually for impairment or when events indicate it is more likely than not that the carrying amount of the asset may not be recoverable.activity have resulted in a complex earnings per share calculation.
We identified the analysis for potential impairment of this intangible assetequity as a critical audit matter due to the materiality of the asset. To test the impairment of the asset, we reviewed management’s analysis and tested the significant assumptions used by management.
Acquisition of In-Process Research and Development
As discussed in Note 10 to the consolidated financial statements, the Company has acquired one additional license in addition to the four licenses acquired in prior years to develop, manufacture and commercialize drugs. The Company determined there were no alternative future use and therefore expensed the cost of acquiring the drug as acquisition of in-process research and development.
We identified the treatment of this license as a critical audit matter due to the materiality of the transactiontransactions as well as the added complexity involvingof the issuance of common stock in conjunction with acquiring the license.related calculations. To test the appropriatenesscompleteness and accuracy of expensing the license,transactions, we read the agreementall relevant agreements and reviewedtested management’s analysis.calculations.
/s/ BD & CoCompany, Inc.
Owings Mills, MD
March 30, 202229, 2024
We have served as the Company’s auditor since 2017.
| F-2 |
Processa Pharmaceuticals, Inc.
Consolidated Balance Sheets
| December 31, 2021 | December 31, 2020 | December 31, 2023 | December 31, 2022 | |||||||||||||
| ASSETS | ||||||||||||||||
| Current Assets | ||||||||||||||||
| Cash and cash equivalents | $ | 16,497,581 | $ | 15,416,224 | $ | 4,706,197 | $ | 6,503,595 | ||||||||
| Due from related party | - | 154,730 | ||||||||||||||
| Due from tax agencies | 70,274 | 77,024 | ||||||||||||||
| Prepaid expenses and other | 1,759,296 | 554,708 | 926,300 | 1,883,134 | ||||||||||||
| Total Current Assets | 18,327,151 | 16,202,686 | 5,632,497 | 8,386,729 | ||||||||||||
| Property and Equipment | ||||||||||||||||
| Software | 19,740 | 19,740 | ||||||||||||||
| Office equipment | 9,327 | 9,327 | ||||||||||||||
| Total Cost | 29,067 | 29,067 | ||||||||||||||
| Less: accumulated depreciation | 29,067 | 28,583 | ||||||||||||||
| Property and equipment, net | - | 484 | ||||||||||||||
| Property and Equipment, net | 2,554 | - | ||||||||||||||
| Other Assets | ||||||||||||||||
| Operating lease right-of-use assets, net | 74,181 | 158,558 | 146,057 | 227,587 | ||||||||||||
| Intangible assets, net | 8,056,638 | 8,847,126 | ||||||||||||||
| Security deposit | 5,535 | 5,535 | ||||||||||||||
| Other | 5,535 | 5,535 | ||||||||||||||
| Total Other Assets | 8,136,354 | 9,011,219 | 151,592 | 233,122 | ||||||||||||
| Total Assets | $ | 26,463,505 | $ | 25,214,389 | $ | 5,786,643 | $ | 8,619,851 | ||||||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY | ||||||||||||||||
| Current Liabilities | ||||||||||||||||
| Note payable – Paycheck Protection Program, current portion | $ | - | $ | 117,574 | ||||||||||||
| Current maturities of operating lease liability | 71,078 | 87,200 | $ | 83,649 | $ | 78,896 | ||||||||||
| Accrued interest | - | 950 | ||||||||||||||
| Accounts payable | 218,905 | 320,694 | 311,617 | 327,548 | ||||||||||||
| Due to licensor | 400,000 | 400,000 | 189,000 | 189,000 | ||||||||||||
| Due to related parties | 1,772 | 69,858 | 39 | 51 | ||||||||||||
| Accrued expenses | 279,265 | 224,676 | 146,274 | 403,061 | ||||||||||||
| Total Current Liabilities | 971,020 | 1,220,952 | 730,579 | 998,556 | ||||||||||||
| Non-current Liabilities | ||||||||||||||||
| Note payable – Paycheck Protection Program | - | 44,885 | ||||||||||||||
| Non-current operating lease liability | 7,385 | 78,463 | 66,905 | 150,554 | ||||||||||||
| Non-current due to licensor | - | 400,000 | ||||||||||||||
| Net deferred tax liability | - | 530,611 | ||||||||||||||
| Total Liabilities | 978,405 | 2,274,911 | 797,484 | 1,149,110 | ||||||||||||
| Commitments and Contingencies | - | - | - | - | ||||||||||||
| Stockholders’ Equity | ||||||||||||||||
| Common stock, par value $, shares authorized; and issued and outstanding at December 31, 2021 and 2020, respectively | 1,571 | 1,419 | ||||||||||||||
| Common stock, par value $, shares authorized; issued and outstanding at December 31, 2023 and issued and outstanding at December 31, 2022 | 129 | 80 | ||||||||||||||
| Additional paid-in capital | 62,306,861 | 48,333,857 | 80,658,111 | 72,018,222 | ||||||||||||
| Treasury stock | (300,000 | ) | (300,000 | ) | ||||||||||||
| Accumulated deficit | (36,823,332 | ) | (25,395,798 | ) | (75,369,081 | ) | (64,247,561 | ) | ||||||||
| Total Stockholders’ Equity | 25,485,100 | 22,939,478 | 4,989,159 | 7,470,741 | ||||||||||||
| Total Liabilities and Stockholders’ Equity | $ | 26,463,505 | $ | 25,214,389 | $ | 5,786,643 | $ | 8,619,851 | ||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-3 |
Processa Pharmaceuticals, Inc.
Consolidated Statements of Operations
| 2021 | 2020 | 2023 | 2022 | |||||||||||||
| Years Ended December 31, | Years Ended December 31, | |||||||||||||||
| 2021 | 2020 | 2023 | 2022 | |||||||||||||
| Operating Expenses | ||||||||||||||||
| Research and development expenses | $ | 6,878,021 | $ | 3,172,385 | $ | 5,799,518 | $ | 11,494,230 | ||||||||
| Acquisition of in-process research and development | 566,583 | 8,700,000 | ||||||||||||||
| General and administrative expenses | 4,688,939 | 3,264,474 | 5,657,543 | 8,763,058 | ||||||||||||
| Impairment of intangible asset | - | 7,268,143 | ||||||||||||||
| Operating Loss | (12,133,543 | ) | (15,136,859 | ) | (11,457,061 | ) | (27,525,431 | ) | ||||||||
| Other Income (Expense) | ||||||||||||||||
| Forgiveness of Payroll Protection Program loan and related accrued interest | 163,771 | - | ||||||||||||||
| Interest expense | (362 | ) | (281,122 | ) | ||||||||||||
| Interest income | 11,989 | 3,174 | ||||||||||||||
| Interest income, net | 335,541 | 101,202 | ||||||||||||||
| Net Operating Loss Before Income Tax Benefit | (11,958,145 | ) | (15,414,807 | ) | (11,121,520 | ) | (27,424,229 | ) | ||||||||
| Income Tax Benefit | 530,611 | 1,001,019 | - | - | ||||||||||||
| Net Loss | $ | (11,427,534 | ) | $ | (14,413,788 | ) | $ | (11,121,520 | ) | $ | (27,424,229 | ) | ||||
| Net Loss Per Common Share - Basic and Diluted | $ | (0.75 | ) | $ | (2.54 | ) | $ | ) | $ | ) | ||||||
| Weighted Average Common Shares Used to Compute | ||||||||||||||||
| Net Loss Per Common Shares - Basic and Diluted | 15,319,463 | 7,499,678 | ||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-4 |
Processa Pharmaceuticals, Inc.
Consolidated StatementStatements of Changes in Stockholders’ Equity
Years Ended December 31, 20212023 and 20202022
| Shares | Amount | Additional Paid in Capital | Stock Dividend Payable | Accumulated Deficit | Total | |||||||||||||||||||
| Balance, January 1, 2020 | 5,486,595 | $ | 549 | $ | 18,994,008 | $ | 3 | $ | (10,982,010 | ) | $ | 8,012,550 | ||||||||||||
| Shares issued in connection with our 2020 offering, net of transaction costs of $2,099,363 | 4,800,000 | 480 | 17,100,157 | - | �� | - | 17,100,637 | |||||||||||||||||
| Shares issued in connection with license agreements | 1,950,000 | 195 | 7,799,805 | - | - | 7,800,000 | ||||||||||||||||||
| Shares issued due to full-ratchet anti-dilution adjustment | 1,156,487 | 116 | (116 | ) | - | - | - | |||||||||||||||||
| Conversion of LOC Agreement into shares of common stock | 199,537 | 19 | 718,314 | - | - | 718,333 | ||||||||||||||||||
| Conversion of 8% Senior Convertible Notes into shares of common stock | 247,088 | 25 | 889,488 | - | - | 889,513 | ||||||||||||||||||
| Stock dividend distributed due to full-ratchet anti-dilution adjustment | 28,971 | 3 | - | (3 | ) | - | - | |||||||||||||||||
| Fair value of warrants issued in the sale of our 2019 Senior Notes | - | - | 197,403 | - | 197,403 | |||||||||||||||||||
| Stock-based compensation | 336,860 | 34 | 2,730,008 | - | - | 2,730,042 | ||||||||||||||||||
| Shares issued in private placement, net of transaction costs | ||||||||||||||||||||||||
| Shares issued in private placement, net of transaction costs, shares | ||||||||||||||||||||||||
| Shares withheld to pay income tax on stock-based compensation | (23,804 | ) | (2 | ) | (95,210 | ) | - | (95,212 | ) | |||||||||||||||
| Shares issued in ATM purchases, net of transaction costs | ||||||||||||||||||||||||
| Shares issued in ATM purchases, net of transaction costs, shares | ||||||||||||||||||||||||
| Net loss | - | - | - | - | (14,413,788 | ) | (14,413,788 | ) | ||||||||||||||||
| Balance, December 31, 2020 | 14,181,734 | 1,419 | 48,333,857 | - | (25,395,798 | ) | 22,939,478 | |||||||||||||||||
| Stock-based compensation | 50,270 | 5 | 3,288,010 | - | - | 3,288,015 | ||||||||||||||||||
| Shares issued in private placement, net of transaction costs | 1,321,132 | 132 | 9,875,418 | - | - | 9,875,550 | ||||||||||||||||||
| Shares issued in connection with license agreements | 144,689 | 14 | 699,986 | - | - | 700,000 | ||||||||||||||||||
| Shares withheld to pay income taxes on stock-based compensation | (9,176 | ) | (1 | ) | (64,395 | ) | - | - | (64,396 | ) | ||||||||||||||
| Shares issued in ATM purchases, net of transaction costs | 21,597 | 2 | 173,985 | - | - | 173,987 | ||||||||||||||||||
| Net loss | - | - | - | - | (11,427,534 | ) | (11,427,534 | ) | ||||||||||||||||
| Balance, December 31, 2021 | 15,710,246 | $ | 1,571 | $ | 62,306,861 | $ | - | $ | (36,823,332 | ) | $ | 25,485,100 | ||||||||||||
| Shares | Amount | Capital | Shares | Amount | Deficit | Total | ||||||||||||||||||||||
| Additional | ||||||||||||||||||||||||||||
| Common Stock | Paid-In | Treasury Stock | Accumulated | |||||||||||||||||||||||||
| Shares | Amount | Capital | Shares | Amount | Deficit | Total | ||||||||||||||||||||||
| Balance at January 1, 2022 | 785,512 | $ | 79 | $ | 62,308,353 | $ | - | $ | - | $ | (36,823,332 | ) | $ | 25,485,100 | ||||||||||||||
| Acquisition of treasury stock | - | - | - | (5,000 | ) | (300,000 | ) | - | (300,000 | ) | ||||||||||||||||||
| Stock-based compensation | 11,890 | 1 | 8,948,712 | - | - | - | 8,948,713 | |||||||||||||||||||||
| Shares issued in connection with the Purchase Agreement with Lincoln Park | 6,181 | 1 | 449,999 | - | - | - | 450,000 | |||||||||||||||||||||
| Shares issued in connection with license agreement | 5,000 | - | 400,000 | - | - | - | 400,000 | |||||||||||||||||||||
| Shares withheld to pay income taxes on stock-based compensation | (1,809 | ) | (1 | ) | (88,842 | ) | - | - | - | (88,843 | ) | |||||||||||||||||
| Net loss | - | - | - | - | - | (27,424,229 | ) | (27,424,229 | ) | |||||||||||||||||||
| Balance, January 1, 2023 | 806,774 | 80 | 72,018,222 | (5,000 | ) | (300,000 | ) | (64,247,561 | ) | 7,470,741 | ||||||||||||||||||
| Balance | 806,774 | 80 | 72,018,222 | (5,000 | ) | (300,000 | ) | (64,247,561 | ) | 7,470,741 | ||||||||||||||||||
| Stock-based compensation | 6,945 | 1 | 1,060,338 | - | - | - | 1,060,339 | |||||||||||||||||||||
| Shares issued in connection with capital raises, net of transaction costs | 421,611 | 42 | 6,352,035 | - | - | - | 6,352,077 | |||||||||||||||||||||
| Warrant granted in connection with a consulting agreement | - | - | 1,310,875 | - | - | - | 1,310,875 | |||||||||||||||||||||
| Settlement of stock award | - | - | (52,746 | ) | - | - | - | (52,746 | ) | |||||||||||||||||||
| Other | 55,670 | 6 | (30,613 | ) | - | - | - | (30,607 | ) | |||||||||||||||||||
| Net loss | - | - | - | - | - | (11,121,520 | ) | (11,121,520 | ) | |||||||||||||||||||
| Balance, December 31, 2023 | 1,291,000 | $ | 129 | $ | 80,658,111 | (5,000 | ) | $ | (300,000 | ) | $ | (75,369,081 | ) | $ | 4,989,159 | |||||||||||||
| Balance | 1,291,000 | $ | 129 | $ | 80,658,111 | (5,000 | ) | $ | (300,000 | ) | $ | (75,369,081 | ) | $ | 4,989,159 | |||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-5 |
Processa Pharmaceuticals, Inc.
Consolidated Statements of Cash Flows
| 2023 | 2022 | |||||||||||||||
| Years Ended December 31, | Years Ended December 31, | |||||||||||||||
| 2021 | 2020 | 2023 | 2022 | |||||||||||||
| Cash Flows From Operating Activities | ||||||||||||||||
| Net Loss | $ | (11,427,534 | ) | $ | (14,413,788 | ) | $ | (11,121,520 | ) | $ | (27,424,229 | ) | ||||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||||||||||
| Depreciation | 484 | 8,446 | 222 | - | ||||||||||||
| Non-cash lease expense for right-of-use assets | 84,377 | 78,288 | 81,530 | 85,518 | ||||||||||||
| Non-cash acquisition of in-process research and development | 300,000 | 8,600,000 | ||||||||||||||
| Non-cash milestone expense in connection with license agreement | - | 189,000 | ||||||||||||||
| Amortization of debt issuance costs | - | 199,900 | - | 115,613 | ||||||||||||
| Amortization of intangible asset | 790,488 | 795,328 | - | 788,495 | ||||||||||||
| Deferred income tax (benefit) expense | (530,611 | ) | (1,001,019 | ) | ||||||||||||
| Impairment of intangible asset | - | 7,268,143 | ||||||||||||||
| Stock-based compensation | 3,408,015 | 2,730,042 | 1,060,339 | 8,828,713 | ||||||||||||
| Forgiveness of Payroll Protection Program loan and related accrued interest | (163,771 | ) | - | |||||||||||||
| Warrants issued to purchase 158,007 shares of common stock | 1,310,875 | - | ||||||||||||||
| Net changes in operating assets and liabilities: | ||||||||||||||||
| Prepaid expenses and other | (1,018,095 | ) | (239,103 | ) | 956,834 | 210,549 | ||||||||||
| Operating lease liability | (87,200 | ) | (77,491 | ) | (78,896 | ) | (87,937 | ) | ||||||||
| Accrued interest, including amounts converted into common stock | 362 | 81,894 | ||||||||||||||
| Accounts payable | (101,789 | ) | 245,082 | (15,931 | ) | 108,643 | ||||||||||
| Due (from) to related parties | 86,644 | (85,188 | ) | (12 | ) | (1,721 | ) | |||||||||
| Other receivables | 6,750 | (77,024 | ) | - | 70,274 | |||||||||||
| Accrued expenses | (65,411 | ) | 11,437 | (256,787 | ) | 243,796 | ) | |||||||||
| Net cash (used in) operating activities | (8,717,291 | ) | (3,143,196 | ) | (8,063,346 | ) | (9,605,143 | ) | ||||||||
| Cash Flows From Investing Activities | ||||||||||||||||
| Purchase of property and equipment | (2,776 | ) | - | |||||||||||||
| Net cash (used in) provided by investing activities | (2,776 | ) | - | |||||||||||||
| Cash Flows From Financing Activities | ||||||||||||||||
| Net proceeds from common stock sold | 10,049,537 | 17,100,637 | ||||||||||||||
| Line of credit payable from related party | - | 700,000 | ||||||||||||||
| Proceeds from our Paycheck Protection Program note payable | - | 162,459 | ||||||||||||||
| Shares withheld to pay taxes on stock based compensation | (64,396 | ) | (95,212 | ) | ||||||||||||
| Other | (186,493 | ) | - | |||||||||||||
| Net cash provided by financing activities | 9,798,648 | 17,867,884 | ||||||||||||||
| Net proceeds from issuance of stock | 6,321,470 | - | ||||||||||||||
| Shares withheld to pay taxes on stock-based compensation | - | (88,843 | ) | |||||||||||||
| Settlement of stock award | (52,746 | ) | - | |||||||||||||
| Acquisition of treasury stock | - | (300,000 | ) | |||||||||||||
| Net cash (used in) provided by financing activities | 6,268,724 | (388,843 | ) | |||||||||||||
| Net Increase in Cash and Cash Equivalents | 1,081,357 | 14,724,688 | ||||||||||||||
| Net (Decrease) Increase in Cash and Cash Equivalents | (1,797,398 | ) | (9,993,986 | |||||||||||||
| Cash and Cash Equivalents - Beginning of Year | 15,416,224 | 691,536 | 6,503,595 | 16,497,581 | ||||||||||||
| Cash and Cash Equivalents - End of Year | $ | 16,497,581 | $ | 15,416,224 | $ | 4,706,197 | $ | 6,503,595 | ||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-6 |
Processa Pharmaceuticals, Inc.
Consolidated Statements of Cash Flows (continued)
| Years Ended December 31, | ||||||||||||||||
| Years Ended December 31, | 2023 | 2022 | ||||||||||||||
| Supplemental Cash Flow Information: | 2021 | 2020 | ||||||||||||||
| Cash paid for interest | $ | - | $ | - | $ | - | $ | - | ||||||||
| Cash paid for income taxes | - | - | - | - | ||||||||||||
| Non-Cash Investing and Financing Activities: | ||||||||||||||||
| Non-Cash Financing Activities | ||||||||||||||||
| Issuance of shares of common stock in satisfaction of accrued director fees | $ | - | $ | 120,000 | ||||||||||||
| Issuance of shares of common stock in connection with a licensing agreement which had previously been recorded as a due to licensor | $ | - | $ | 400,000 | ||||||||||||
| Issuance of shares of common stock in connection with the Purchase Agreement with Lincoln Park | $ | - | $ | 450,000 | ||||||||||||
| - | ||||||||||||||||
| Right-of-use asset obtained in exchange for operating lease liability | $ | - | $ | (17,772 | ) | $ | - | $ | (238,924 | ) | ||||||
| Operating lease liability | - | 17,772 | - | 238,924 | ||||||||||||
| Net | $ | - | $ | - | $ | - | $ | - | ||||||||
| Issuance of shares of common stock in connection with a licensing agreement which had previously been recorded as a due to licensor | $ | 400,000 | $ | - | ||||||||||||
| Conversion of $805,000 of Senior Convertible Debt and related accrued interest of $84,513 into shares of common stock | $ | - | $ | 805,000 | ||||||||||||
| Conversion of $700,000 of Line of Credit Payable with related party and related accrued interest of $18,333 into shares of common stock | $ | - | $ | 700,000 | ||||||||||||
| Issuance of 1,185,458 shares of common stock due to triggering the full-ratchet anti-dilution provision of common stock sold in our 2018 Private Placement Transactions | $ | - | $ | 119 | ||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-7 |
Processa Pharmaceuticals, Inc.
Notes to Consolidated Financial Statements
Note 1 – Organization and Description of the Business
Business Activities and Organization
We are a clinical-stage biopharmaceutical company focused on incorporating our Regulatory Science Approach into the development of drug productsour Next Generation Chemotherapy (NGC) drugs to improve the safety and efficacy of cancer treatment. Our NGC drugs are modifications of existing FDA-approved oncology drugs resulting in an alteration of the metabolism and/or distribution while maintaining the well-known and established existing mechanisms of killing the cancer cells. By modifying the NGC drugs in this manner, we believe our three NGC treatments will provide improved safety-efficacy profiles when compared to their currently marketed counterparts.
On January 22, 2024, we filed a Certificate of Amendment to our Certificate of Incorporation, as amended with the Secretary of State of Delaware that are intendedeffected a 1-for-20 reverse stock split of our common stock, par value $ per share (the “Reverse Stock Split”). Pursuant to provide treatment for patients who have a high unmet medical need condition that effects survivalthe Certificate of Amendment, our issued common stock decreased from shares to shares and our outstanding common stock decreased from to . The Reverse Stock Split did not affect our authorized common stock of shares or our common stock par value. All shares of common stock, including common stock underlying warrants, stock options, and restricted stock units, as well as exercise prices and per share information in these consolidated financial statements give retroactive effect to the patient’s quality of life and for which few or no treatment options currently exist. We currently have five drugs: four in various stages of clinical development (PCS499, PCS12852, PCS3117 and PCS6422) and one in nonclinical development (PCS11T). We group our drugs into non-oncology (PCS499 and PCS12852) and oncology (PCS3117, PCS6422 and PCS11T). A summary of each drug is provided below:Reverse Stock Split.
Liquidity
Our consolidated financial statements have been prepared on a going concern basis, which contemplates the continuity of operations, realization of assets and the satisfaction of liabilities and commitments in the ordinary course of business. We have incurred losses since inception, currently devoting substantially all of our efforts toward research and development of our next generation chemotherapy drug product candidates, including conducting clinical trials and providing general and administrative support for these operations, and have an accumulated deficit of $75.4 million at December 31, 2023. During the year ended December 31, 2023, we generated a net loss of $11.1 million and used $8.1 million in net cash for operating activities from continuing operations. To date, none of our drug candidates have been approved for sale, and therefore we have not generated any product revenue and do not expect positive cash flow from operations in the foreseeable future.
We have financed our operations primarily through public equity issuances, including an offering we closed on January 30, 2024 where we sold shares of our common stock, pre-funded warrants to purchase up to 1,079,555 shares of our common stock, and warrants for the purchase of up to 1,555,555 shares of our common stock for net proceeds of $6.3 million, after deducting placement agent fees and offering-related expenses (see Note 13 for additional details). Simultaneously with the closing of the sale, the pre-funded warrants were exercised in exchange for shares of our common stock. We will continue to be dependent upon equity and/or debt financing until we are able to generate positive cash flows from its operations.
At December 31, 2023, we had cash and cash equivalents totaling $4.7 million. Together with the $6.3 million net proceeds we raised in January 2024, and based on our current business plans, we believe these funds will satisfy our capital needs into early 2025. Our ability to execute our longer-term operating plans, including future preclinical studies and clinical trials for our portfolio of drugs depend on our ability to obtain additional funding from the sale of equity and/or debt securities, a strategic transaction or other funding transactions.
We plan to raise additional funds in the future through a combination of public or private equity offerings, debt financings, collaborations, strategic alliances, licensing arrangements and other marketing and distribution arrangements, but will only do so if the terms are acceptable to us. If we are unable to obtain adequate financing when needed, we may have to delay, reduce the scope of, or suspend our current or planned future clinical trial plans, or research and development programs. This may also cause us to not meet obligations contained in certain of our license agreements and put these assets at risk. To the extent that we raise additional capital through marketing and distribution arrangements or other collaborations, strategic alliances or licensing arrangements with third parties, we may have to relinquish valuable rights to our product candidates, future revenue streams, research programs or product candidates or to grant licenses on terms that may not be favorable to us. If we raise additional capital through public or private equity offerings, the ownership interest of our existing stockholders will be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect our stockholders’ rights. If we raise additional capital through debt financing, we may be subject to covenants limiting or restricting our ability to take specific actions, such as incurring additional debt or making capital expenditures. There can be no assurance that future funding will be available when needed.
Absent additional funding, we believe that our cash and cash equivalents will not be sufficient to fund our operations for a period of one year or more after the date that these consolidated financial statements are available to be issued based on the timing and amount of our projected net loss from continuing operations and cash to be used in operating activities during that period of time. As a result, substantial doubt exists about our ability to continue as a going concern within one year after the date that these consolidated financial statements are available to be issued. The accompanying consolidated financial statements do not include any adjustments to reflect the possible future effects on the recoverability and classification of recorded assets, or the amounts and classification of liabilities that might be different should we be unable to continue as a going concern based on the outcome of these uncertainties described above.
| F-8 |
Impact of COVID-19
We have experienced delays in the enrollment of patients in our PCS499 Phase 2B trial due to COVID-19. Potential patients have died from COVID-19 prior to screening and continue to be reluctant to travel to our testing sites for fear of contracting COVID-19. Delays in enrollment lengthen the time of studies and increase their costs. The COVID-19 pandemic has created uncertainties in the expected timelines for clinical stage biopharmaceutical companies such as ours, including possible delays in clinical trials and disruptions in the supply chain for raw materials used in clinical trial work. Such delays could materially impact our business in future periods. Furthermore, the spread of COVID-19, which has caused a broad impact globally, may materially affect us economically. For more information on the risks associated with COVID-19, refer to Part I, Item 1A, “Risk Factors.”
Note 2 – Basis of Presentation and Summary of Significant Accounting Policies
Basis of Presentation
The accompanying consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”) and pursuant to the rules and regulations of the United States Securities and Exchange Commission (the “SEC”), and reflect all of our activities, including those of our wholly-owned subsidiary. All material intercompany accounts and transactions have been eliminated in consolidation.
Liquidity
We have incurred losses since inception, devoting substantially all of our efforts toward research and development, and have an accumulated deficit of approximately $36.8 million at December 31, 2021. During Operating results for the year ended December 31, 2021, we generated a net loss2023 are not necessarily indicative of approximately $11.4 million and we expect to continue to generate operating losses and negative cash flow from operations for the foreseeable future. Based on our current plans, we believe our current cash balances is adequate for at least the next twelve months without considering amounts available from the Lincoln Park Purchase Agreement (see Note 14) or potential sales under our ATM Offering. Our ability to execute our longer-term operating plans, including unplanned future clinical trials for our portfolio of drugs depend on our ability to obtain additional funding from the sale of equity and/or debt securities, a strategic transaction or other funding transactions. We plan to continue to actively pursue financing alternatives, but there can be no assurance that we will obtain the necessary funding in the future when necessary.results.
We had 0 revenue during the year ended December 31, 2021 and do not have any revenue under contract or any immediate sales prospects. Our primary uses of cash are to fund our planned clinical trials, research and development expenditures and operating expenses. Cash used to fund operating expenses is impacted by the timing of when we incur and pay these expenses.
On August 20, 2021, we entered into an equity distribution agreement (the “Sales Agreement”) with Oppenheimer & Co. Inc. (the “Sales Agent”) under which we may issue and sell in a registered “at-the-market” offering shares of our common stock having an aggregate offering price of up to $ million from time to time through or to our Sales Agent (the “ATM Offering”). We expect to use net proceeds from the ATM Offering over time as a source for working capital and general corporate purposes.
On March 23, 2022, we entered into a Purchase Agreement (the “Purchase Agreement”) with Lincoln Park Capital Fund, LLC (“Lincoln Park”) under which we have the right, but not the obligation, to sell to Lincoln Park, and Lincoln Park is obligated to purchase up to $15,000,000of our shares of common stock, par value $per share, subject to the terms and conditions in the Purchase Agreement, during the term of the Purchase Agreement. See Note 14 for additional details concerning the Purchase Agreement.
Use of Estimates
In preparing our consolidated financial statements and related disclosures in conformity with GAAP and pursuant to the rules and regulations of the SEC, we make estimates and judgments that affect the amounts reported in the consolidated financial statements and accompanying notes. Estimates are used for, but not limited to:to stock-based compensation, intangible assets, future milestone payments and income taxes. These estimates and assumptions are continuously evaluated and are based on management’s experience and knowledge of the relevant facts and circumstances. While we believe the estimates to be reasonable, actual results could differ materially from those estimates and could impact future results of operations and cash flows.
Cash and Cash Equivalents
Cash and cash equivalents include cash on hand and money market funds. We consider all highly liquid investments with a maturity atmaturing within three months from the date of purchase of three months or less to beas cash equivalents.
Property and Equipment
Property is stated at cost, less accumulated depreciation. Costs of renewals and improvements that extend the useful lives of the assets are capitalized. Expenditures for maintenance and routine repairs are charged to expense as incurred. Depreciation is recognized on a straight-line basis over the estimated useful lives of the assets, which generally range from3 to 5 years. We amortize leasehold improvements over the shorter of the estimated useful life of the asset or the term of the related lease. Upon retirement or disposition of assets, the costs and related accumulated depreciation are removed from the accounts with the resulting net gain or loss, if any, reflected in the consolidated statement of operations.
Intangible Assets
Intangible assets acquired individually or with a group of other assets from others (other than in a business combination) are recognized at cost, including transaction costs, and allocated to the individual assets acquired based on relative fair values and no goodwill is recognized. Cost is measured based on cash consideration paid. If consideration given is in the form of non-cash assets, liabilities incurred, or equity interests issued, measurement of cost is based on either the fair value of the consideration given or the fair value of the assets (or net assets) acquired, whichever is more clearly evident and more reliably measurable. Costs of internally developing, maintaining or restoring intangible assets that are not specifically identifiable, have indeterminate lives or are inherent in a continuing business are expensed as incurred.
| F-9 |
Intangible assets purchased from others for use in research and development activities and that have alternative future uses (in research and development projects or otherwise) are capitalized in accordance with ASC Topic 350, Intangibles – Goodwill and Other. Those that have no alternative future uses (in research and development projects or otherwise), and therefore no separate economic value, are considered research and development costs and are expensed as incurred (see Note 10).incurred. Amortization of intangibles used in research and development activities is a research and development cost.
Intangibles with a finite useful life are amortized using the straight-line method unless the pattern in which the economic benefits of the intangible assets are consumed or used up are reliably determinable. The useful life is the best estimate of the period over which the asset is expected to contribute directly or indirectly to our future cash flows.flow. The useful life is based on the duration of the expected use of the asset by us and the legal, regulatory or contractual provisions that constrain the useful life and future cash flows of the asset, including regulatory acceptance and approval, obsolescence, demand, competition and other economic factors. We evaluate the remaining useful life of intangible assets each reporting period to determine whether any revision to the remaining useful life is required. If the remaining useful life is changed, the remaining carrying amount of the intangible asset will be amortized prospectively over the revised remaining useful life. If an income approach is used to measure the fair value of an intangible asset, we consider the period of expected cash flows used to measure the fair value of the intangible asset, adjusted as appropriate for company-specific factors discussed above, to determine the useful life for amortization purposes.
If no regulatory, contractual, competitive, economic or other factors limit the useful life of the intangible to us, the useful life is considered indefinite. Intangibles with an indefinite useful life are not amortized until its useful life is determined to be no longer indefinite. If the useful life is determined to be finite, the intangible is tested for impairment and the carrying amount is amortized over the remaining useful life in accordance with intangibles subject to amortization. Indefinite-lived intangibles are tested for impairment annually and more frequently if events or circumstances indicate that it is more-likely-than-not that the asset is impaired.
Impairment of Long-Lived Assets and Intangibles Other Than Goodwill
We account for the impairment of long-lived assets in accordance with ASC 360, Property, Plant and Equipment and ASC 350, Intangibles – Goodwill and Other, which require that long-lived assets and certain identifiable intangibles be reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to its expected future undiscounted net cash flows generated by the asset. If such assets are considered to be impaired, the impairment to be recognized is measured as the amount by which the carrying amounts of the assets exceed the fair value of the assets based on the present value of the expected future cash flows associated with the use of the asset. Assets to be disposed of are reported at the lower of the carrying amount or fair value less costs to sell. Based on management’s evaluation, there was 0we recorded an impairment loss recordedof $7.3 million during the yearsyear ended December 31, 2021 and 2020.2022 (see Note 8).
Fair Value Measurements and Disclosure
We apply ASC 820, Fair Value Measurements and Disclosures, which expands disclosures for assets and liabilities that are measured and reported at fair value on a recurring basis. Fair value is defined as an exit price, representing the amount that would be received upon the sale of an asset or payment to transfer a liability in an orderly transaction between market participants.
Fair value is a market-based measurement that is determined based on assumptions that market participants would use in pricing an asset or liability. A three-tier fair value hierarchy is used to prioritize the inputs in measuring fair value as follows:
Level 1 – Quoted market prices (unadjusted) in active markets for identical assets or liabilities that the reporting entity has the ability tocan access at the measurement date.
Level 2 – Quoted market prices for similar assets or liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, or other inputs that are observable, either directly or indirectly. Fair value determined through the use ofusing models or other valuation methodologies.
Level 3 – Significant unobservable inputs for assets or liabilities that cannot be corroborated by market data. Fair value is determined by the reporting entity’s own assumptions utilizing the best information available and includes situations where there is little market activity for the asset or liability.
| F-10 |
The asset’s or liability’s fair value measurement within the fair value hierarchy is based upon the lowest level of any input that is significant to the fair value measurement. Our policy is to recognize transfers between levels of the fair value hierarchy in the period the event or change in circumstances that caused the transfer. There were no transfers into or out of Level 1, 2, or 3 during the periods presented.
We measure compensation expense for stock options and other stock awards in accordance with ASC 718, Compensation—Stock Compensation. Stock-based compensation is measured at fair value on grant date and recognized as compensation expense over the requisite service period. Generally, we issue stock options and other stock awards with service-based and/or performance-based vesting conditions. For awards with only service-based vesting conditions, we record compensation cost for these awards using the straight-line method over the service period. For awards that contain performance vesting conditions, we do not recognize compensation expense until achieving the performance condition is probable. We estimate the fair value of stock option and warrant grants using the Black-Scholes option pricing model, and the assumptions used in calculating the fair value of stock-based awards represent management’s best estimates and involve inherent uncertainties and the application of management’s judgment. We value restricted stock awards (RSAs) and restricted stock units (RSUs) based on the closing share price of our common stock on the date of grant. Stock-based compensation costs are recorded as general and administrative or research and development costs in the statements of operations based upon the underlying individual’s or consultant’sentity’s role.
When evaluating the assumptions required for the Black-Scholes model, we recognized that our previous volatility computation was based on a basket of peer companies, which was no longer representative of the actual measure of the distribution of returns of our common stock. We concluded in the third quarter of 2021 that it would be appropriate for us to compute volatility based on the behavior of our own common stock since we have been a public company for more than three years and listed on the Nasdaq Capital Market for one year. As such, we adjusted the expected volatility for new grants issued on or after September 1, 2021 to %, which is not significantly different from our previous volatility computation of %.
Estimates of fair value are not intended to predict actual future events or the value ultimately realized by employees or consultants who receive these awards, and subsequent events are not indicative of the reasonableness of our original estimates of fair value. We account for forfeitures in the period in which they occur, rather than estimate expected forfeitures.
Basic net loss per share is computed by dividing our net loss available to common shareholders by the weighted average number of shares of common stock outstanding during the period.(which excludes unvested RSAs) and vested, but unissued RSUs. Diluted loss per share is computed by dividing our net loss available to common shareholders by the diluted weighted average number of shares of common stock outstanding during the period. Since we have experienced a net loss for all periods presented, basic and diluted net loss per share are the same. As such, diluted loss per share for the years ended December 31, 20212023 and 20202022 excludes the impact of potentially dilutive common shares related to outstanding stock options, unvested restricted stock awards (RSAs), unvested restricted stock units (RSUs)RSUs and purchase warrants.
As more fully described in Note 7 and 8, we have determined that each of the underwritten public offering in October 2020 and the sale of the 2019 Senior Notes in late 2019 triggered the full ratchet anti-dilution provision of the common stock we sold in 2018 Private Placement Transactions. For purposes of computing our basic and diluted earnings per share (EPS) for the year ended December 31, 2020, we increased our net loss available for common shareholders by the fair value of the additional shares issued since they did not affect all our common shareholders equally and there were no contingencies related to the issuance of these shares. We also included the related shares in the weighted number of shares of common stock outstanding for the year ended December 31, 2020.
Our diluted net loss per share for the years ended December 31, 20212023 and 20202022 excluded and of potentially dilutive common shares, respectively, related to outstanding stock options, unvested RSAs, unvested RSUs and warrants since those shares would have had an anti-dilutive effect on loss per share during the years then ended.
| F-11 |
Segments
We operate in one segment. Management uses one measurement of profitability and does not segregate its business for internal reporting. All ourOur assets are all located within the United States.
Fair Value of Financial Instruments
The carrying amounts of cash and cash equivalents, accounts receivable and accounts payable approximate their fair value because of the short-term maturity of these instruments.
Debt Issuance Costs
We recognized the debt issuance costs incurred related to our 2019 Senior Notes as a reduction of the carrying amount of the 2019 Senior Notes. The debt issuance costs were amortized to interest expense using the straight-line method over the term of the 2019 Senior Notes and at December 31, 2020 were fully amortized.
Research and development
Research and development costs are expensed as incurred and consistedconsist of direct and overhead-related expenses.expenses related primarily to clinical trials, including development personnel salaries and related costs. Research and development costs totaled $6,878,0215,799,518 and $3,172,385 11,494,230for the years ended December 31, 20212023 and 2020,2022, respectively. Expenditures to acquire technologies, including licenses, which are utilized in research and development and that have no alternative future use are expensed as the acquisition of in-process research and development when incurred. Technology we develop for use in our products is expensed as incurred until technological feasibility has been established after which it is capitalized and depreciated. No research and development costs were capitalized during the years ended December 31, 20212023 and 2020.2022.
Income Taxes
We account for income taxes in accordance with ASC Topic 740, Income TaxesTaxes.. Under the asset and liability method, deferred Deferred income taxes are recognizedrecorded for the futureexpected tax consequences attributable toof temporary differences between the financial statement carrying amountsbasis of existing assets and liabilities for financial reporting purposes and their respectiveamounts recognized for income tax basispurposes. As of December 31, 2023 and operating loss carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the year in which those temporary differences are expected to be recovered or settled. The effect of changes in tax rates on deferred tax assets and liabilities is recognized in income in the period such changes are enacted. A2022, we recorded a valuation allowance is provided againstequal to the full recorded amount of our net deferred tax assets if recoverabilitysince it is uncertain on a more likely thanmore-likely-than-not that benefits from our deferred tax assets will not basis. As of December 31, 2021 and 2020, we have established abe realized. The valuation allowance is reviewed quarterly and is maintained until sufficient positive evidence exists to offset certainsupport its reversal. As part of an evaluation of our tax attributes in 2022, we recharacterized approximately $7.4 million of startup costs previously capitalized as an IRC Section 195 asset as net operating losses. The recharacterization has no impact on total deferred tax assets since we had previously and will continue to provide a full valuation allowance on our unutilized net deferred tax assets.
We recognize the impact of an uncertain tax position if the position will more likely than not be sustained upon examination by a taxing authority, based on the technical merits of the position. Our policy is to record interest and penalties related to income taxes as part of its income tax provision. As of December 31, 2021,2023, we had no unrecognized tax benefits and as such, no liability, interest or penalties were required to be recorded. We do not expect this to change significantly in the next twelve months.
Recent Accounting Pronouncements
From time to time, the Financial Accounting Standards Board (“FASB”) or other standard setting bodies issue new accounting pronouncements. Updates to the FASB Accounting Standards Codification are communicated through issuance of an Accounting Standards Update (“ASU”). We have implemented all new accounting pronouncements that are in effect and that may impact our financial statements. We have evaluated recently issuedconsidered all recent accounting pronouncements and determinedissued since the last audit of our consolidated financial statements. We believe that there is nothese recent pronouncements will not have a material impacteffect on our consolidated financial position or results of operations.statements.
| F-12 |
Intangible assets atThe Processa Pharmaceuticals Inc. 2019 Omnibus Equity Incentive Plan (the “2019 Plan”) allows us to make grants of stock options, restricted and unrestricted stock and other stock-based awards to employees, including our executive officers, consultants and directors. The 2019 Plan originally provided for the aggregate issuance of shares of our common stock. On July 11, 2022, our shareholders approved an increase in the aggregate number of shares of our common stock available for issuance under our 2019 plan by shares to shares in total. As of December 31, 2021 and 2020 consisted of the following:2023, shares were available for future grants.
Summary of Intangible Assets
| 2021 | 2020 | |||||||
| Gross intangible assets | $ | 11,059,429 | $ | 11,059,429 | ||||
| Less: accumulated amortization | (3,002,791 | ) | (2,212,303 | ) | ||||
| Total intangible assets, net | $ | 8,056,638 | $ | 8,847,126 | ||||
Stock Compensation Expense
Schedule of Stock-based Compensation Expense
| 2023 | 2022 | |||||||
| Year Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Research and development | $ | 363,956 | $ | 2,895,653 | ||||
| General and administrative | 2,007,258 | 5,933,060 | ||||||
| Total | $ | 2,371,214 | $ | 8,828,713 | ||||
No tax benefits were attributed to the stock-based compensation expense in the accompanying consolidated statements of operations. As of December 31, 2021, estimated amortization expense will be approximately $788,000 per yearbecause a valuation allowance was maintained for the next 10 years.all net deferred tax assets relating to this expense.
Our gross intangible assets consist primarily of costs we capitalized related to the acquisition of license rights to PCS499 from CoNCERT Pharmaceuticals. Inc. (“CoNCERT”) for shares of our common stock that had an issue date fair value of $8Stock Options million, $1,782 in transaction costs and $3,037,147 associated with the initial recognition of an offsetting deferred tax liability related to the acquired temporary difference for an asset purchased that is not a business combination and has a tax basis of $1,782 in accordance with ASC 740-10-25-51 Income Taxes. In accordance with ASC Topic 730, Research and Development, we capitalized the costs of acquiring the exclusive license rights to PCS499 from CoNCERT, as the exclusive license rights represented intangible assets to be used in research and development activities that management believed had future alternative uses.
DuringThe following table summarizes our stock option activity during the years ended December 31, 20212022 and 2020, we incurred financial net operating losses before income tax benefit2023:
Schedule of Stock Option Activity
| Total options Outstanding | Weighted average exercise price | Weighted average remaining contractual life (in years) | ||||||||||
| Outstanding as of January 1, 2022 | 8,943 | $ | 341.34 | |||||||||
| Options granted | - | |||||||||||
| Forfeited | - | |||||||||||
| Outstanding as of December 31, 2022 | 8,943 | 341.34 | ||||||||||
| Options granted | - | |||||||||||
| Forfeited or expired | (1,951 | ) | 257.28 | |||||||||
| Outstanding and exercisable as of December 31, 2023 | 6,992 | $ | 364.72 | |||||||||
No forfeiture rate was applied to these stock options. The aggregate intrinsic value of outstanding options, all of which are exercisable, was $ at both December 31, 2023 and 2022. and $15,414,807, respectively, and federal taxable losses of $5,740,342 and $2,648,248, respectively. Forstock options were exercised during the years ended December 31, 20212023 or 2022 and 2020, we did not record any income tax benefits fromthere is no unamortized expense at either December 31, 2023 or 2022 since the following:options are fully vested.
Restricted Stock Awards
We have recorded the benefit of our 2021 and 2020 net operating losses in our consolidated financial statements to the extent possible as a reduction in the deferred tax liability created by the future financial statement amortization of the intangible asset from the acquired CoNCERT license and Know-How. The benefit associated with the net operating loss carry forward will more-likely-than-not go unrealized unless future operations are successful except for their offset against the deferred tax liability created by the acquired CoNCERT license and Know-How, which will decrease over time leading to an increase to the valuation allowance.
A deferred tax liability was recorded on March 19, 2018 when Processa received CoNCERT’s license and Know-How in exchange for Processa stock that had been issued in an Internal Revenue Code Section 351 Transaction. The Section 351 Transaction treats the acquisition of the license and Know-How for stock as a tax-free exchange. As a result, under ASC 740-10-25-51 Income Taxes, Processa recorded a deferred tax liability of $3,037,147 for the acquired temporary difference between intangible assets for the financial reporting basis of $11,038,929 and the tax basis of $1,782. The deferred tax liability has been reduced for the effect of non-deductibility of the amortization of the intangible asset to $2,145,620 at December 31, 2021 and offset by deferred tax assets resulting from net operating tax losses.
Schedule of Restricted Stock Awards (“RSAs”) Activity
| Number of shares | Weighted- average grant-date fair value per share | |||||||
| Unvested as of January 1, 2022 | 4,555 | $ | 157.81 | |||||
| Granted | 9,358 | 74.27 | ||||||
| Forfeited | (1,676 | ) | 110.62 | |||||
| Vested and issued | (9,142 | ) | 100.88 | |||||
| Unvested as of December 31, 2022 | 3,095 | 94.44 | ||||||
| Granted | 10,750 | 14.59 | ||||||
| Forfeited | (1,250 | ) | 133.00 | |||||
| Cancelled | (2,555 | ) | 22.13 | |||||
| Vested and issued | (8,790 | ) | 24.44 | |||||
| Unvested as of December 31, 2023 | 1,250 | $ | 9.26 | |||||
| F-13 |
As of December 31, 2023, unrecognized stock-based compensation expense for RSAs of $ is expected to be fully recognized in 2024.
On January 1, 2023, we granted RSAs totaling shares of common stock to three directors for their service for the six-month period ending June 30, 2023 to align their compensation plan with their service period and $1,001,019, respectively, aschanged the annual service period to begin and end on the date of respective Annual Meetings rather than the calendar year. Our directors are compensated through a resultcombination of offsetting our deferred tax liability (relatedcash and equity. On March 8, 2023, the directors increased the cash component and decreased the equity component of their compensation by equal amounts on a retroactive basis, to the CoNCERT asset) bybeginning of their respective service periods. Accordingly, we cancelled RSAs representing shares of previously issued, but unvested common stock.
On July 14, 2023, we granted RSAs totaling shares of common stock to a consultant (of which vested and were issued as of December 31, 2023) for services to be provided through March 18, 2024. RSAs for up to 2,500 shares of common stock are subject to regaining Nasdaq compliance, with RSAs for only 1,250 shares of common stock vesting if we regain Nasdaq compliance through a reverse stock split. Because we effected a reverse stock-split on January 22, 2024 (which we have retroactively applied to all share counts reported in this Annual Report on Form 10-K) and regained Nasdaq compliance on February 2, 2024. Effective December 31, 2023, we cancelled the deferred tax assets resulting fromRSAs for 1,250 shares of common stock that will not vest. On August 31, 2023, in connection with the resignation of our net operating lossChief Operating Officer, unvested RSAs representing shares of common stock were forfeited and we reversed previously recognized expense of $72,733.
Restricted Stock Units
Schedule of the intangible asset Restricted Stock Units (“RSUs”) Activity
| Number of shares | Weighted- average grant-date fair value per share | |||||||
| Outstanding at January 1, 2022 | 22,008 | $ | 155.29 | |||||
| Granted | 121,439 | 61.50 | ||||||
| Forfeited | (3,431 | ) | 101.73 | |||||
| Cancelled | (1,876 | ) | 171.58 | |||||
| Issued | (2,399 | ) | 79.07 | |||||
| Outstanding at December 31, 2022 | 135,741 | 73.81 | ||||||
| Granted | 116,078 | 14.18 | ||||||
| Forfeited | (12,296 | ) | 21.69 | |||||
| Cancelled | (16,801 | ) | 71.36 | |||||
| Outstanding at December 31, 2023 | 222,722 | 45.82 | ||||||
| Vested and unissued | (115,145 | ) | 71.90 | |||||
| Unvested at December 31, 2023 | 107,577 | $ | 17.90 | |||||
As of December 31, 2023, unrecognized stock-based compensation expense for RSUs of $ is expected to be fully recognized over a weighted average period of years. The unrecognized expense excludes $related to CoNCERT.certain RSUs with a performance milestone that is not currently probable of occurring.
| F-14 |
Our provision (benefit) for income taxes forDuring the yearsyear ended December 31, 20212023, we granted RSUs related to the future issuance of shares of our common stock to employees and 2020 wasdirectors, which have service vesting requirements.On August 8, 2023, we also granted RSUs related to the future issuance of shares of our common stock as follows:
Schedulepart of Provisionthe compensation package to our new Chief Executive Officer, George Ng. Vesting for Income Taxes RSUs occurs ratably over a three-year period. The remaining
RSUs will vest upon the achievement of certain performance metrics, with the first
| 2021 | 2020 | |||||||
| Year Ended December 31, | ||||||||
| 2021 | 2020 | |||||||
| Current: | ||||||||
| Federal | $ | - | $ | - | ||||
| State | - | - | ||||||
| Total deferred tax benefit | - | - | ||||||
| Deferred: | ||||||||
| Federal | (2,853,937 | ) | (3,068,218 | ) | ||||
| State | (624,844 | ) | (907,504 | ) | ||||
| Total deferred tax benefit | (3,478,781 | ) | (3,975,722 | ) | ||||
| Valuation allowance | 2,948,170 | 2,974,703 | ||||||
| Net deferred tax benefit | (530,611 | ) | (1,001,019 | ) | ||||
| Total tax provision (benefit) | $ | (530,611 | ) | $ | (1,001,019 | ) | ||
performance-based RSUs vesting when gross proceeds of $10,000,000 is raised, and the second performance-based RSUs vesting when additional gross proceeds of $10,000,000 is raised.
A reconciliationHolders of our effective income tax rate and statutory income tax rate forvested RSUs will be issued shares of our common stock upon the years ended December 31, 2021 and 2020 is as follows:satisfaction of the distribution restrictions contained in their Restricted Stock Unit Award Agreement. The distribution restrictions are typically different (longer) than the vesting schedule, imposing an additional restriction on the holder. Unlike RSAs, while employees may hold fully vested RSUs, the individual does not hold any shares or have any rights of a shareholder until the distribution restrictions are met. Upon distribution to the employee, each RSU converts into one share of our common stock. The RSUs contain dividend equivalent rights.
Schedule
On January 1, 2024, we granted RSUs totaling $1.3 million, contingent upon receiving shareholder approval to increase the number of Effective Income Tax Rate Reconciliationshares available under our 2019 Omnibus Incentive Plan (“Incentive Plan”), which we plan to obtain in June 2024. The number of shares to be issued under the RSUs will be based on the greater of: (i) $ per share or (ii) the closing price per share on the day we receive shareholder approval to increase the number of shares available under the Incentive Plan. We will grant a maximum of shares under these RSU grants.
| 2021 | 2020 | |||||||
| Year Ended December 31, | ||||||||
| 2021 | 2020 | |||||||
| Federal statutory income tax rate | 21.00 | % | 21.00 | % | ||||
| State tax rate, net | 1.05 | % | 1.54 | % | ||||
| Permanent differences | (0.18 | )% | (2.03 | )% | ||||
| Federal orphan drug tax credit | 3.04 | % | 0.94 | % | ||||
| Deferred tax asset valuation allowance | (20.48 | )% | (14.96 | )% | ||||
| Effective income tax rate | 4.43 | % | 6.49 | % | ||||
At December 31, 2021 and 2020, we had available federal and state net operating loss carryforwards of approximately $12.5 Warrantsmillion and $6.7 million, respectively. The federal net operating loss generated in 2021 and 2020 of $5.7 million and $2.6 million, respectively, will carry forward indefinitely. Net operating losses generated prior to 2018 will expire 2037. We are evaluating our qualified research expenditures for the federal orphan drug credit and the federal and state credit for increasing research activities to offset potential future tax liabilities. The federal research and development tax credits have a 20-year carryforward period. We have not recognized any deferred tax assets related to research and development tax credits as of December 31, 2021 or 2020. All federal and state net operating loss and credit carryforwards listed above are reflected after the reduction for amounts effectively eliminated under Section 382.
We recorded a valuation allowancewarrant activity during the years ended December 31, 20212022 and 2020 equal2023.
Schedule of Warrants Activity
| Total warrants outstanding | Weighted average exercise price | Weighted average remaining contractual life (in years) | ||||||||||
| Outstanding as of January 1, 2022 | 15,190 | $ | 213.22 | |||||||||
| Expired | (907 | ) | 343.28 | |||||||||
| Outstanding as of December 31, 2022 | 14,283 | 205.01 | ||||||||||
| Granted | 173,007 | 19.27 | ||||||||||
| Expired | (6,783 | ) | 266.96 | |||||||||
| Not exercisable | ) | |||||||||||
| Outstanding and exercisable as of December 31, 2023 | 173,007 | $ | 25.41 | |||||||||
In February 2023, we amended our financial consulting agreement with Spartan by extending the term until February 10, 2024. We compensated Spartan for financial consulting services provided under the amendment by granting warrants to the full recorded amountpurchase 158,007 shares of our net deferred tax assets relatedcommon stock on April 17, 2023, with an exercise price of $20.40. The warrants expire on April 17, 2026, and contain both call and cashless exercise provision. We also granted warrants to deferred start-up costs, federal orphan drug tax credit and other temporary differences since it is more-likely-than-not that such benefits will not be realized. The valuation allowance is reviewed quarterly and is maintained until sufficient positive evidence existspurchase shares of our common stock to support its reversal.a consultant on November 18, 2023, of which warrants to purchase 7,500 shares of our common stock were exercisable, with an exercise price of $7.40. These warrants expire on November 18, 2025.
Schedule of Stock Option Warrant Valuation Assumption
| Average risk-free rate of interest | 4.32-4.88 | % | ||
| Expected term (years) | 2.00–3.00 | |||
| Expected stock price volatility | 82.85-108.47 | % | ||
| Dividend yield | 0 | % |
| F-15 |
The significant components of our deferred tax assets and liabilities for Federal and state income taxes consisted of the following:
Schedule of Deferred Tax Assets and Liabilities
| 2021 | 2020 | |||||||
| December 31, | ||||||||
| 2021 | 2020 | |||||||
| Deferred tax assets: | ||||||||
| Non-current: | ||||||||
| Net operating loss carry forward – Federal | $ | 2,615,518 | $ | 1,410,046 | ||||
| Net operating loss carry forward – State | 760,897 | 437,618 | ||||||
| Stock compensation expense | 593,365 | 178,053 | ||||||
| Depreciation | 13,200 | 12,958 | ||||||
| Purchased in-process R&D | 2,481,070 | 2,405,997 | ||||||
| Federal orphan drug credits | 791,151 | 427,343 | ||||||
| Start-up expenditures and amortization | 1,978,418 | 1,171,162 | ||||||
| Total non-current deferred tax assets | 9,233,619 | 6,043,177 | ||||||
| Valuation allowance for deferred tax assets | (7,087,999 | ) | (4,139,829 | ) | ||||
| Total deferred tax assets | 2,145,620 | 1,903,348 | ||||||
| Deferred Tax Liabilities: | ||||||||
| Non-current: | ||||||||
| Intangible asset | (2,145,620 | ) | (2,433,959 | ) | ||||
| Total non-current deferred tax liabilities | (2,145,620 | ) | (2,433,959 | ) | ||||
| Total deferred tax asset (liability) | $ | - | $ | (530,611 | ) | |||
The ultimate realization of deferred tax assets is dependent upon the generation of future taxable income during the periods in which those temporary differences become deductible. Management considers the scheduled reversal of deferred tax liabilities, the projected future taxable income and tax planning strategies in making this assessment. Based on management’s analysis, a reserve has been established against the deferred tax assets related to deferred start-up expenditures and certain other deductible expenses. The change in the valuation allowance in 2021 and 2020 was $2,948,170 and $2,974,703, respectively.
Our total deferred tax asset as of December 31, 2021 and 2020 primarily includes $7,428,810 and $4,256,064 ($1,978,418 and $1,171,162 tax effected, respectively) of general and administrative expenses treated as deferred start-up expenditures for tax purposes, respectively, $12,454,846 and $6,714,504 ($3,376,415and $1,847,664 tax effected, respectively) of tax losses, respectively, resulting in tax loss carryforwards; $ and $, respectively, of stock-based compensation expense ($593,365 and $178,053 tax effected, respectively); $9,316,230 and $8,743,517, respectively,of purchased in-process research and development ($2,481,070 and $2,405,997 tax effected, respectively); and $791,151 and $427,343 of federal orphan drug tax credits, respectively. We have had no revenues and recognized cumulative loses since inception. Due to the uncertainty regarding future profitability and recognition of taxable income to utilize the amortization of deferred start-up expenditures, purchased in-process research and development, federal orphan drug tax credits and the tax loss carryforwards, except for their offset against the deferred tax liability created by our acquisition of the CoNCERT license, a valuation allowance against the deferred tax assets has been recognized for the years ended December 31, 2021 and 2020.
We recognize potential liabilities for uncertain tax positions using a two-step process. The first step is to evaluate the tax position for recognition by determining if the weight of available evidence indicates that it is more likely than not that the position will be sustained on audit, including resolution of related appeals or litigation processes, if any. The second step is to measure the tax benefit as the largest amount that is more than 50% likely of being realized upon settlement. We have not recorded any uncertain tax positions.
We file U.S. Federal income and California and Maryland state tax returns. There are currently no income tax examinations underway for these jurisdictions. However, tax years from and including 2017 remain open for examination by federal and state income tax authorities.
Note 5 - Stock-based Compensation
On June 19, 2019, our stockholders approved, and we adopted the Processa Pharmaceuticals Inc. 2019 Omnibus Equity Incentive Plan (the “2019 Plan”). The 2019 Plan allows us, under the direction of our Board of Directors or a committee thereof, to make grants of stock options, restricted and unrestricted stock and other stock-based awards to employees, including our executive officers, consultants and directors. The 2019 Plan provides for the aggregate issuance of shares of our common stock, with shares available for future grants at December 31, 2021.
Schedule of Stock-based Compensation Expense
| Years Ended December 31, | ||||||||
| 2021 | 2020 | |||||||
| Research and development | $ | 809,839 | $ | 863,069 | ||||
| General and administrative | 2,598,176 | 1,866,973 | ||||||
| Total | $ | 3,408,015 | $ | 2,730,042 | ||||
No tax benefits were attributed to the stock-based compensation expense because a valuation allowance was maintained for all net deferred tax assets relating to this expense.
As of December 31, 2021, there was a total of $unrecognized compensation expense, related to the unvested stock options, restricted stock awards (RSAs), restricted stock units (RSUs) and warrants which are expected to be recognized over a weighted average period of years, excluding the impact of RSUs for the future issuance of shares for which meeting the criteria is not yet probable.
Restricted Stock Awards
During the years ended December 31, 2021 and 2020, we issued and RSAs, respectively, under the 2019 Omnibus Incentive Plan to our employees and directors. We valued the RSAs based on the closing share price on the date of grant. RSAs are “shares that the recipient receives, but the rights to sell or transfer the shares are restricted until the vesting condition passes.” Recipients of RSAs are entitled to voting and dividend rights, even if they have not vested, so we consider these shares to be issued and outstanding once they have been granted.
At December 31, 2021, RSAs have vested as follows:
During the years ended December 31, 2021 and 2020, and vested RSAs, respectively, were forfeited to pay for federal, state and local income taxes, and an additional unvested RSAs were forfeited upon employment termination during the year ended December 31, 2021. The remaining unvested RSAs vest over time with years of employment.
Schedule of Information About RSA Outstanding
Number of shares | Weighted-average grant-date fair value per share | |||||||
| Unvested as of January 1, 2020 | - | $ | - | |||||
| Granted | 336,860 | 8.33 | ||||||
| Vested and Issued | (190,274 | ) | 8.50 | |||||
| Forfeited | (23,804 | ) | 8.50 | |||||
| Unvested as of December 31, 2020 | 122,782 | 8.04 | ||||||
| Granted | 37,500 | 6.65 | ||||||
| Vested and Issued | (58,467 | ) | 7.90 | |||||
| Forfeited | (10,706 | ) | 6.54 | |||||
| Unvested as of December 31, 2021 | 91,109 | $ | 7.74 | |||||
Included in accrued expenses at December 31, 2021 is $120,000 in fees earned by our Directors, which will be satisfied with the issuance of RSAs for shares of our common stock in 2022. This expense was accounted for as stock-based compensation in 2021.
Restricted Stock Units
During the year ended December 31, 2021, we granted restricted stock units (RSUs) related to the future issuance of shares of our common stock as follows:
Schedule of Information About RSU Outstanding
| Number of shares | Weighted-average grant-date fair value per share | |||||||
| Outstanding at January 1, 2021 | - | $ | - | |||||
| Granted | 457,593 | 7.75 | ||||||
| Forfeited | (4,000 | ) | 8.61 | |||||
| Shares issued | (14,000 | ) | 7.12 | |||||
| Outstanding at December 31, 2021 | 439,593 | $ | 7.76 | |||||
| Vested and unissued | (190,493 | ) | $ | 7.41 | ||||
| Unvested at December 31, 2021 | 249,100 | $ | 8.03 | |||||
Holders of our vested RSUs have our promise to issue shares of our common stock upon the earlier to occur of the distribution restrictions contained in their Restricted Stock Unit Award Agreement. The distribution restrictions are different (longer) than the vesting schedule, imposing an additional restriction on the holder. Unlike RSAs, while certain employees may hold fully vested RSUs, the individual does not hold any shares or have any rights of a shareholder until the distribution restrictions are met. The RSUs contain dividend equivalent rights.
Stock Options
We made one stock option grant to a consultant for the purchase of shares during the year ended December 31, 2021 and did not grant any stock options during the same period in 2020.
The fair value of each stock option grant was estimated using the Black-Scholes option-pricing model at the date of grant. We lacked company-specific historical and implied volatility information and therefore, we determined our expected stock volatility based on the historical volatility of a publicly traded set of peer companies. The expected volatility of stock option granted on or after September 1, 2021 will be calculated using the Company’s historical closing stock prices. The expected term of our stock options was determined utilizing the “simplified” method for awards that qualify as “plain-vanilla” options. The risk-free interest rate was determined by reference to the U.S. Treasury yield curve in effect at the time of grant of the award for time periods approximately equal to the expected term of the award. Expected dividend yield is based on the fact that we have never paid cash dividends and do not expect to pay any cash dividends in the foreseeable future.
Schedule of Stock Option Valuation Assumption
Schedule of Stock Option Activity
| Total options Outstanding | Weighted average exercise price | Weighted average remaining contractual life (in years) | ||||||||||
| Outstanding as of January 1, 2020 | 176,962 | $ | 17.93 | |||||||||
| Forfeited | (24,156 | ) | 16.80 | |||||||||
| Outstanding as of December 31, 2020 | 152,806 | 18.11 | ||||||||||
| Options granted | 30,000 | 11.70 | ||||||||||
| Forfeited | (4,310 | ) | 16.80 | |||||||||
| Outstanding as of December 31, 2021 | 178,496 | 17.07 | ||||||||||
| Exercisable (vested) at December 31, 2021 | 154,398 | $ | 17.14 | |||||||||
The weighted average grant-date fair value per share of options granted during the year ended December 31, 2021 was $. No forfeiture rate was applied to these stock options. The aggregate fair value of stock options vested at December 31, 2021 and 2020 was $and $, respectively.
Stock Option [Member]
stock options were exercised during the years ended December 31, 2021 or 2020.
Warrants
Schedule of Warrants Activity
| Total warrants outstanding | Weighted average exercise price | Weighted average remaining contractual life (in years) | ||||||||||
| Outstanding as of January 1, 2020 | 534,674 | $ | 18.34 | |||||||||
| Warrants granted | - | - | - | |||||||||
| Outstanding as of December 31, 2020 | 534,674 | 18.34 | ||||||||||
| Warrants granted | 229,268 | 8.09 | ||||||||||
| Forfeited | (460,217 | ) | 18.31 | |||||||||
| Outstanding as of December 31, 2021 | 303,725 | 10.66 | ||||||||||
| Exercisable (vested) at December 31, 2021 | 278,725 | $ | 10.90 | |||||||||
Our outstanding warrants expire at various dates through September 1, 2024.
On January 26, 2021, we issued a warrant for the purchase of 100,000 shares of our common stock to a consultant in exchange for service to be provided in 2021. The warrant expires on January 11, 2023 and has an exercise price of $7.18 per share. There were no vesting conditions associated with this warrant.
On September 1, 2021, we also issued a warrant for the purchase of 50,000 shares of our common stock to another consultant in exchange for service to be provided in 2021 and 2022. The warrant expires on September 1, 2024 and has an exercise price of $8.00 per share. The warrant vests options on each of September 30, 2021, December 31, 2021, March 31, 2022, and June 30, 2022, subject to continued service.
We determined the fair value of the warrants granted at the date of grant to be $, respectively, using the Black-Scholes option pricing model with the following assumptions:
We recognize expense based on the fair value of the warrants over their service or vesting periods and recorded $391,108 related to these warrants during the year ended December 31, 2021.
On February 16, 2021, we also issued warrants for the purchase of 79,268shares of our common stock to our placement agent in connection with a private placement of shares of our common stock as described in Note 7. These warrants are exercisable for cash at $9.30 per share and expire on February 16, 2023.
Note 6 – Paycheck Protection Program Loan
In May 2020, we entered into a $162,459 Paycheck Protection Promissory Note (the “PPP Loan”) with the Bank of America. The PPP Loan was made under, and is subject to the terms and conditions of, the PPP which was established under the CARES Act and is administered by the U.S. Small Business Administration. The original terms of the loan was two years with a maturity date of May 5, 2022 and it contained a favorable fixed annual interest rate of 1.00%. Payments of principal and interest on the PPP Loan were deferred for the first six months of the term of the PPP Loan until November 5, 2020. We used the proceeds of our PPP Loan for payroll costs. On January 18, 2021, we applied for full forgiveness of the loan and in August 2021, we received notice from the Small Business Administration that our loan had been forgiven.
Note 74 – Stockholders’ Equity
On January 1, 2022, we amended our Certificate of Incorporation increased the number of authorized shares of our common stock from to . We believe authorized shares of common stock better aligns our capital structure with our future needs.
Preferred Stock
There were issued or outstanding shares of preferred stock at either December 31, 20212023 or 2020.2022.
Common Stock
Increase in Our Authorized Number of Shares
Subsequent to receiving shareholder approval on June 27, 2023, we amended our Certificate of Incorporation to increase the number of authorized shares of our common stock from to . We believe authorized shares of common stock better aligns our capital structure with our future needs and have shown this retroactively in the consolidated financial statements.
Financings
During the year ended December 31, 2021,2023, we had the following grants and issuances:issued shares of our common stock through several fundraising efforts described below:
| ● | ATM Offering – On | |
| ● | Lincoln Park Capital Fund, LLC Purchase Agreement– During the year ended December 31, 2023, we sold shares at an average price of $per share for aggregate gross proceeds of $54,000 under the purchase agreement with Lincoln Park. | |
| ● | Registered Direct Offering – On February 14, 2023, we closed a registered direct offering (the “Offering”) for the sale of shares of common stock at a purchase price of $per share for gross proceeds of $6.3 million (net proceeds of $5.6 million). |
We paid the placement agent, Spartan Capital Securities, LLC, (“Spartan”) a cash fee of 8.0% of the gross proceeds from the Offering, excluding proceeds received from our insiders, and reimbursed Spartan for legal fees of $60,000. The engagement agreement with Spartan required us to indemnify Spartan and certain of its affiliates against certain customary liabilities. On February 14, 2023, we amended the consulting agreement with Spartan originally entered into on August 24, 2022, extending the term of the consulting agreement until February 10, 2024. As compensation for services under the agreement, on April 17, 2023, we granted Spartan warrants to purchase 158,007 shares of our common stock with an exercise price of $20.40. The warrants will expire April 17, 2026 and contain both call and cashless exercise provisions.
During the year ended December 31, 2022, we had the following activity:
| ● | On |
| F-16 |
We have the right to present Lincoln Park with a purchase notice (a “Regular Purchase Notice”), directing Lincoln Park to purchase up to shares of our common stock (the “Regular Purchase Amount”) provided that the closing sale price of the common stock on the purchase date is not below a threshold price of $1.00, set forth in the Purchase Agreement (a “Regular Purchase”). The Regular Purchase Amount may be increased to up to shares if the closing sale price of our common stock on the applicable purchase date equals or exceeds certain higher threshold prices set forth in the Purchase Agreement. If the share price of the Regular Purchase Amount is less than $ per share of common stock, we can sell additional shares (defined in the Purchase Agreement as the “Alternate Adjusted Regular Purchase Share Limit”) up to $150,000, subject to the Exchange Cap limitation (defined below). We and Lincoln Park may mutually agree to increase the Regular Purchase Amount with respect to any Regular Purchase under the Purchase Agreement, provided that Lincoln Park’s maximum committed purchase obligation under any single Regular Purchase shall not exceed $1,250,000. The above-referenced share amount limitations and closing sale price thresholds are subject to adjustment for any reorganization, recapitalization, non-cash dividend, stock split, reverse stock split or other similar transaction as provided in the Purchase Agreement. The purchase price per share for each Regular Purchase will be based on prevailing market prices of the common stock immediately preceding the time of sale as computed in accordance with the terms set forth in the Purchase Agreement. There are no upper limits on the price per share that Lincoln Park must pay for shares of common stock under the Purchase Agreement. Lincoln Park may not assign or transfer its rights and obligations under the Purchase Agreement.
The aggregate number of shares that we can issue to Lincoln Park under the Purchase Agreement may not exceed shares (subject to proportional adjustments for stock splits, reverse stock splits and similar events as described above), which is equal to 19.99% of the outstanding shares of common stock immediately prior to the execution of the Purchase Agreement (the “Exchange Cap”), unless (i) stockholder approval is obtained to issue shares of common stock in excess of the Exchange Cap, in which case the Exchange Cap will no longer apply, or (ii) the average price of all sales of shares of our common stock to Lincoln Park under the Purchase Agreement equals or exceeds the lower of (i) the Nasdaq official closing price immediately preceding the execution of the Purchase Agreement or (ii) the arithmetic average of the five Nasdaq official closing prices for the common stock immediately preceding the execution of the Purchase Agreement, plus an incremental amount to take into account the issuance of the commitment shares to Lincoln Park under the Purchase Agreement, such that the transactions contemplated by the Purchase Agreement are exempt from the Exchange Cap limitation under applicable Nasdaq rules. In all instances, we may not sell shares of our common stock to Lincoln Park under the Purchase Agreement if it would result in Lincoln Park beneficially owning more than 9.99% of the outstanding shares of common stock.
We may terminate the Purchase Agreement at any time, at our sole discretion, without any cost or penalty, by giving one business day notice to Lincoln Park to terminate the Purchase Agreement. Lincoln Park has covenanted not to cause or engage in any manner whatsoever, any direct or indirect short selling or hedging of the common stock.
There are no limitations on use of proceeds, financial or business covenants, restrictions on future financings (other than restrictions on our ability to enter into variable rate transactions described in the Purchase Agreement), rights of first refusal, participation rights, penalties or liquidated damages in the Purchase Agreement. We may deliver Purchase Notices under the Purchase Agreement, subject to market conditions, and in light of our capital needs from time to time and under the limitations contained in the Purchase Agreement. Any proceeds that we receive under the Purchase Agreement are expected to be used for working capital and general corporate purposes.
| ● | We issued shares to Elion | ||
Treasury Stock - Repurchase of Shares from Aposense, Ltd.
Also during the year ended December 31, 2021,On March 29, 2022, we purchased vested RSAs were forfeited to pay for federal, state and local income taxes and an additional unvested RSAs were forfeited upon employment termination.
On December 15, 2020, the holders of all our outstanding 2019 Senior 8% Convertible Notes converted their notes and accrued interest into shares of our common stock based onfrom Aposense Ltd. for $300,000 in a conversion price of $3.60private transaction per share, which, pursuant toand are holding these shares as treasury stock until they are reissued or retired at the 2019 Senior Note Agreement, is a 10% discount on the public offering price of $ per share received on our underwritten offering in October 2020.
We closed on our underwritten public offering of shares of common stock for a public offering price of $per share on October 6, 2020. Net proceeds from the offering were approximately $17.1 million. The following additional transactions occurred in connection with the closingdiscretion of our underwritten public offering:Board of Directors.
| F-17 |
We determinedBasic net loss per share is computed by dividing net loss by the sale of the 2019 Senior Notes triggered the full ratchet anti-dilution provision ofweighted average common stock we sold in our 2018 Private Placement Transactions. As a result, those stockholders were entitled to shares ofoutstanding (which excludes unvested RSAs) and vested, but unissued RSUs. Diluted net loss per share is computed by dividing net loss by the diluted weighted average common stock inoutstanding, which includes potentially dilutive effect of stock options, unvested RSAs, unvested RSUs and warrants. The treasury-stock method is used to determine the fourth quarterdilutive effect of 2019, whichour stock options and warrants grants. Since we issuedexperienced a loss for both periods presented, basic and diluted net loss per share are the same and, as they would have an anti-dilutive impact on June 18, 2020. We had accounteddiluted net loss per share, any dilutive common shares outstanding were excluded from the computation shown below.
Schedule of Net Loss Per Share Basic and Diluted
| 2023 | 2022 | |||||||
| Basic and diluted net loss per share: | ||||||||
| Net loss available to common shareholders | $ | (11,121,520 | ) | $ | (27,424,229 | ) | ||
| Weighted-average number of common shares-basic and diluted | ||||||||
| Basic and diluted net loss per share | $ | ) | $ | ) | ||||
| 2023 | 2022 | |||||||
| Weighted-average number of common shares outstanding – basic and diluted | ||||||||
| Weighted-average number of vested RSUs– basic and diluted | ||||||||
| Weighted-average number of common shares-basic and diluted | ||||||||
As described in Note 3, we issued various equity instruments during the years ended December 31, 2023 and 2022 which impact our EPS calculation. All granted RSAs are considered issued and outstanding for purposes of our financial statements. Unvested RSAs are included as dilutive securities, but are excluded from our denominator of basic EPS. At December 31, 2023 and 2022, and RSAs, respectively, were not vested and were excluded from the EPS calculation. Vested RSUs are included in our computation of the weighted average shares for basic EPS and unvested RSUs are included as dilutive securities. At December 31, 2023 and 2022, and unvested RSUs were excluded from the EPS calculation.
Schedule of Anti-dilutive Securities Excluded from Computation of Earnings Per Share
| 2023 | 2022 | |||||||
| Stock options, unvested RSAs, unvested RSUs and purchase warrants | 296,326 | 128,943 | ||||||
Note 6 – Leases
We lease our office space under an operating lease agreement. This lease does not have significant rent escalation, concessions, leasehold improvement incentives, or other build-out clauses. Further, the lease does not contain contingent rent provisions. Our office space lease includes both lease (e.g., fixed payments including rent, taxes, and insurance costs) and non-lease components (e.g., common-area or other maintenance costs), which are accounted for as a single lease component as we have elected the practical expedient to group lease and non-lease components for all leases. We also lease office equipment under an operating lease. Our leases do not provide an implicit rate and, as such, we have used our incremental borrowing rate of 8% to determine the present value of the lease payments based on the information available at the lease commencement date.
Lease costs included in our consolidated statements of operations totaled $97,000 for the years ended December 31, 2023 and 2022. The weighted average remaining lease terms and discount rate for our operating leases at December 31, 2023 were as follows:
Schedule of Weighted Average Remaining Lease Terms and Discount Rate for Operating Leases
| Remaining lease term (years) for our office lease | 1.8 | |||
| Remaining lease term (years) for our equipment lease | 0.3 | |||
| Weighted average remaining lease term (years) for our facility and equipment leases | 1.7 | |||
| Weighted average discount rate for our facility and equipment leases | 8.0 | % |
| F-18 |
Annual lease liabilities for all operating leases were as follows as of December 31, 2023:
Schedule of Annual Lease Liabilities for all Operating Leases
| 2024 | $ | 92,389 | ||
| 2025 | 70,040 | |||
| Total lease payments | 162,429 | |||
| Less: Interest | (11,875 | ) | ||
| Present value of lease liabilities | 150,554 | |||
| Less: current maturities | (83,649 | ) | ||
| Non-current lease liability | $ | 66,905 |
Note 87 – Net Loss per Share of Common StockLicense Agreements
Basic net loss per share is computed by dividing net loss by the weighted average common stock outstanding (which excludes unvested RSAs) and vested RSUs. Diluted net loss per share is computed by dividing net loss by the diluted weighted average common stock outstanding, which includes potentially dilutive effect of stock options, unvested RSAs, unvested RSUs and warrants. Since we experienced a loss for both periods presented, basic and diluted net loss per share are the same and, as they would have an anti-dilutive impact on diluted net loss per share, any dilutive common shares outstanding were excluded from the computation shown below.Elion Oncology, Inc.
The computation of net loss per share for the year ended December 31, 2021On August 23, 2020, we entered into a condition precedent License Agreement with Elion Oncology (“Elion License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and 2020 was as follows:
Schedule of Net Loss Per Share Basic and Diluted
| 2021 | 2020 | |||||||
| Basic and diluted net loss per share: | ||||||||
| Net loss | $ | (11,427,534 | ) | $ | (14,413,788 | ) | ||
| Value of the full ratchet anti-dilution shares | - | (4,625,948 | ) | |||||
| Net loss available to common shareholders | $ | (11,427,534 | ) | $ | (19,039,736 | ) | ||
| Weighted-average number of common shares-basic and diluted | 15,319,463 | 7,499,678 | ||||||
| Basic and diluted net loss per share | $ | (0.75 | ) | $ | (2.54 | ) | ||
We determined the sale of our common stock in our 2020 underwritten offering and the sale of our 2019 Senior Notes, which are convertible into common stock at a conversion rate of $per share, both triggered the full ratchet anti-dilution provision in 2020commercialize PCS6422 globally. As part of the common stockElion License Agreement, we sold in 2018 Private Placement Transactions. We issuedagreed to issue to Elion shares of our common stock in connection with triggering the full-ratchet anti-dilution provisions to shareholders who purchased these shares as a result of closing our underwritten offering in 2020. We valued these shares at $, which is the closing priceon each of the offeringfirst and second anniversary dates of $per share. This increased our weighted-average numberAs additional consideration, we will pay Elion development and regulatory milestone payments (a portion of shares shownwhich are payable in the table above by . We also issued shares of our common stock to these shareholdersand a portion of which are payable in June 2020 related tocash) upon the deemed dividendachievement of certain milestones, which include FDA or other regulatory approval and dosing a patient. In addition, we recorded at the end of 2019. We determined the value of these shares at $506,993 must pay Elion one-time sales milestone payments based on the achievement during a price per sharecalendar year of $which represents the closing price per shareone or more thresholds for annual sales for products made and pay royalties based on October 18, 2019, the last day investors hadannual licensing sales. We are also required to rescind their investment.split any milestone payments received with Elion based on any sub-license agreement we may enter.
For purposesOn May 17, 2022, we amended the third Milestone Event of computingSection 6.4 of our basicLicense Agreement with Elion Oncology, Inc. changing the third Milestone Event from “1st Patient in Dose Confirmation Study” to (a) determination of the maximum tolerated dose (MTD) or (b) determination of the recommended Phase 2 Dose. Prior to this amendment, the third milestone was not considered probable since it was unknown when, or if a dose confirmation study was going to be conducted. As a result of the modification, we consider it probable that the recommended Phase 2 dosage regimen could be determined in connection with our current Phase 1B trial for NGC-Cap. We recorded an expense and diluted EPS forrelated liability of $189,000 representing the year ended December 31, 2020,value of the shares we increased our net loss available for common shareholders byanticipate issuing to Elion at the fair value on the date of modification. No other terms or conditions of the additionalLicense Agreement were modified. We determined the dosage for our Phase 2 study on January 25, 2024 and issued shares issued related to the anti-dilution provision since they did not affect allof our common shareholders equally and there were no contingencies related to the issuance of these shares at December 31, 2020.
As described in Note 5, we issued various equity instruments during the years ended December 31, 2021 and 2020 which impact our EPS calculation. All granted RSAs are considered issued and outstandingstock for purposes of our financial statements. Unvested RSAs are included as dilutive securities, but are excluded from our denominator of basic EPS. At December 31, 2021 and 2020, and RSAs, respectively, were not vested and were excluded from the EPS calculation. Vested RSUs are include in our computation of the weighted average shares for basic EPS and unvested RSUs are included as dilutive securities. At December 31, 2021, unvested RSUs were excluded from the EPS calculation.
Schedule of Antidilutive Securities Excluded from Computation of Earnings Per Share
| 2021 | 2020 | |||||||
| Stock options, unvested RSAs, unvested RSUs and purchase warrants | 822,430 | 816,512 | ||||||
Basic net loss per share is computed by dividing net loss by the weighted average common shares outstanding. Diluted net loss per share is computed by dividing net loss by the weighted average common shares outstanding without the impact of potential dilutive common shares outstanding because they would have an anti-dilutive impact on diluted net loss per share. The treasury-stock method is used to determine the dilutive effect of our stock options and warrants grants, and the if-converted method is used to determine the dilutive effect of the 2019 Senior Notes in 2020.
Note 9 – Leasesmeeting this milestone.
We leaseare required to use commercially reasonable efforts, at our office space under an operating lease agreement. This lease does not have significant rent escalation, concessions, leasehold improvement incentives,sole cost and expense to research, develop and commercialize products in one or other build-out clauses. Further,more countries, including dosing a first patient with a product in a Phase 2 or 3 clinical trial within 48 months from when we entered into the lease does not contain contingent rent provisions.License Agreement. We also lease office equipment under an operating lease. Our office space lease includes both lease (e.g., fixed payments including rent, taxes, and insurance costs) and non-lease components (e.g., common-areaare currently on track to dose our first patient in a Phase 2 clinical trial on or other maintenance costs), which are accounted for asbefore October 2, 2024. Either party may terminate the agreement in the event of a single lease component as we have elected the practical expedient to group lease and non-lease components for all leases. Our leases do not provide an implicit rate and, as such, we have used our incremental borrowing rate of 8% in determining the present valuematerial breach of the lease payments based on the information available at the lease commencement date.agreement that has not been cured following written notice and a 90-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
Lease costs included in our consolidated statement of operations totaled $94,263 and $97,545 for the years ended December 31, 2021 and 2020, respectively. The weighted average remaining lease terms and discount rate for our operating leases were as follows at December 31, 2021:
Schedule of Weighted Average Remaining Lease Terms and Discount Rate for Operating Leases
Maturities of our lease liabilities for all operating leases were as follows as of December 31, 2021:
Schedule of Maturities of Lease Liabilities for all Operating Leases
| 2022 | ||||
| 2022 | $ | 75,969 | ||
| 2023 | 6,228 | |||
| 2024 | 1,557 | |||
| Total lease payments | 83,754 | |||
| Less: Interest | (5,291 | ) | ||
| Present value of lease liabilities | 78,463 | |||
| Less: current maturities | (71,078 | ) | ||
| Non-current lease liability | $ | 7,385 |
Note 10 – License Agreements
Ocuphire Pharma, Inc.
On June 16, 2021, we executed a License Agreement with Ocuphire Pharma, Inc. (“Ocuphire Agreement”) under which we received a license to research, develop and commercialize PCS3117 (formerly RX-3117) globally, excluding the Republic of Singapore, China, Hong Kong, Macau and Taiwan.
As consideration for the Ocuphire Agreement, we issued shares of our common stock to Ocuphire, a cash payment of $200,000and assumed $66,583in certain liabilities. Additional consideration includes future development and regulatory milestones payments to Ocuphire upon our achievement of certain defined clinical milestones, such as dosing a patient in pivotal trials and receiving marketing authorization by a regulatory authority in the United States or another country. In addition, we are required to pay Ocuphire one-time sales milestone payments based on the achievement during a calendar year of the highest annual Net Sales for products made and pay royalties based on annual Net Sales, as defined in the Ocuphire Agreement.
| F-19 |
We are required to use commercially reasonable efforts, at our sole cost and expense to oversee such commercialization efforts, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) first patient administered drug in a Clinical Trial of a Product prior to June 16, 2024;2024 and (ii) first patient administered drug in a Pivotal Clinical Trial of a Product or first patient administered drug in a Clinical Trial for a Second Indication of a Product prior to June 16, 2026. We are currently in discussions with Ocuphire to extend these deadlines. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 120-day opportunity to cure such breach.
Aposense, Ltd.
On May 24, 2020, we entered into a condition precedent License Agreement with Aposense, Ltd. (“Aposense License Agreement”), pursuant to which we were granted Aposense’s patent rights and Know-How to develop and commercialize their next generation irinotecan cancer drug, PCS11T. The Aposense License Agreement provides us with an exclusive worldwide license (excluding China), to research, develop and commercialize products comprising or containing PCS11T. The license grant was conditioned on the following being satisfied within nine months of May 24, 2020 (or the Aposense License Agreement shall terminate): (i) our closing of an equity financing and successful up-listing to Nasdaq and (ii) Aposense obtaining the approval of the Israel Innovation Authority for the consummation of the transactions contemplated by the Aposense License Agreement.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS11T to our portfolio, and we issued shares of our common stock to Aposense. As additional consideration, we will pay Aposense development and regulatory milestone payments (up to $3.0 million per milestone) upon the achievement of certain milestones, which primarily consist of having a drug indication approved by a regulatory authority in the United States or another country. In addition, we will pay Aposense one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any sales milestone payments or royalties we receive with Aposense based on any sub-license agreement we may enter.
Yuhan Corporation
On August 19, 2020, we entered into a License Agreement with Yuhan Corporation (“Yuhan License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS12852 (formerly known as YH12852) globally, excluding South Korea.
As consideration for the Yuhan License Agreement and related Share Issuance Agreement, we issued to Yuhan shares of common stock. As additional consideration, we will pay Yuhan development and regulatory milestone payments (a portion of which are payable in shares of our common stock based on the volume weighted average trading price during the period prior to such achievement and a portion of which are payable in cash) upon the achievement of certain milestones, based on a Yuhan affiliate purchasing 750,00037,500 shares of common stock for $3,000,000in our October 2020 underwritten public offering. The milestones primarily consist of dosing a patient in pivotal trials or having a drug indication approved by a regulatory authority in the United States or another country. In addition, we must pay Yuhan one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any milestone payments received with Yuhan based on any sub-license agreement we may enter intoenter..
We are required to use commercially reasonable efforts, at our sole cost and expense, in conjunction with a joint Processa-Yuhan Board to oversee such commercialization efforts, to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) preparing a first draft of the product development plan within 90 days; (ii) requesting an FDA pre-IND meeting for a product within 6 months; (iii) dosing a first patient in a Phase 2A clinical trial with a product within 24 months; and (iv) dosing a first patient with a product in a Phase 2B clinical trial, Phase 3 clinical trial or other pivotal clinical trial with a product within 48 monthsby August 19, 2024.. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 60-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
Elion Oncology, Inc.
On August 23, 2020, we entered into a condition precedent License Agreement with Elion Oncology (“Elion License Agreement”), pursuant to which we acquired an exclusive license to develop, manufacture and commercialize PCS6422 globally. The grant of license was conditioned on the following being satisfied by October 30, 2020: (i) our closing on an equity financing of at least $15 million in gross proceeds and (ii) successful up-listing to Nasdaq.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS6422 to the Processa portfolio, and we paid $100,000 cash and issued shares of our common stock to Elion. Such shares are subject to a lock-up, with 50% of such shares released from such lock up after six months and the remaining 25% tranches to be released following 9 months and 12 months, respectively.
As part of the Elion License Agreement, we have agreed to issue to Elion shares of our common stock on each of the first and second anniversary dates of the Elion License Agreement. We believe the payment of these amounts is probable and represent seller financing since the only condition related to their payment is the passage of time, which management does not believe is substantive. We valued the shares at $per share based on the underwritten public offering price on October 6, 2020, which is the date the conditions precedent in the license agreement were met.
As additional consideration, we will pay Elion development and regulatory milestone payments (a portion of which are payable in shares of our common stock and a portion of which are payable in cash) upon the achievement of certain milestones, which include FDA or other regulatory approval and dosing a patient. On October 6, 2021, shares were issued to Elion for the first milestone payment. In addition, we must pay Elion one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any milestone payments received with Elion based on any sub-license agreement we may enter into.
We are required to use commercially reasonable efforts, at our sole cost and expense to research, develop and commercialize products in one or more countries, including meeting specific diligence milestones that consist of: (i) dosing a first patient in a Phase 1B clinical trial with a product within 12 months; and (ii) dosing a first patient with a product in a Phase 2 or 3 clinical trial within 48 months. Either party may terminate the agreement in the event of a material breach of the agreement that has not been cured following written notice and a 90-day opportunity to cure such breach (which is shortened to 15 days for a payment breach).
Aposense, Ltd.
On May 24, 2020, we entered into a condition precedent License Agreement with Aposense, Ltd. (“Aposense License Agreement”), pursuant to which we were granted Aposense’s patent rights and Know-How to develop and commercialize their next generation irinotecan cancer drug, PCS11T (formerly known as ATT-11T). The Aposense License Agreement provides us with an exclusive worldwide license (excluding China), to research, develop and commercialize products comprising or containing PCS11T. The grant of license was conditioned on the following being satisfied within nine months of May 24, 2020 (or the Aposense License Agreement shall terminate): (i) our closing of an equity financing and successful up-listing to Nasdaq and (ii) Aposense obtaining the approval of the Israel Innovation Authority for the consummation of the transactions contemplated by the Aposense License Agreement.
On October 6, 2020, all conditions were satisfied, resulting in the addition of PCS11T to the Processa portfolio, and we issued shares of our common stock to Aposense. Such shares are subject to a lock-up, with 40% of such shares released from such lock up after six months and the remaining two 30% tranches to be released upon completion of the next two subsequent quarters. As additional consideration, we will pay Aposense development and regulatory milestone payments (up to $3.0 million per milestone) upon the achievement of certain milestones, which primarily consist of having a drug indication approved by a regulatory authority in the United States or another country. In addition, we will pay Aposense one-time sales milestone payments based on the achievement during a calendar year of one or more thresholds for annual sales for products made and pay royalties based on annual licensing sales. We are also required to split any sales milestone payments or royalties we receive with Aposense based on any sub-license agreement we may enter into.
CoNCERT Pharmaceuticals, Inc.
On March 19, 2018, Promet, Processa and CoNCERT amended the CoNCERT Agreement executed in October 2017. The Amendment assigned the CONCERT Agreement to us and we exercised the exclusive option for the PCS499 compound in exchange for CoNCERT receiving, in part, $88.0 million of our common stock that was held by Promet (shares at $per share)shares), for the benefit of Processa in satisfaction of the obligation due for the exclusive license for PCS499 acquired by us. There was no change in the total shares issued and outstanding of . Promet contributed the payment of the obligation due for the exclusive license to us without consideration paid to them. As a result of the transaction, we recognized an exclusive license intangible asset with a fair value of $88.0 million and an offsetting increase in additional paid-in capital resulting from the exchange.
We estimatedfully impaired the fair value of the common stock issued based on the market approach and CoNCERT’s requirement to receive shares valued at $8 million. The market approach was based on the final negotiated number of shares of stock determined on a volume weighted average price of our common stock over a 45 day period preceding the mid-February 2018 finalized negotiation of the modification to the option and license agreement with CoNCERT, an unrelated third party, for the exclusive license rights to PCS499. The total cost recognized for the exclusive license acquired represents the allocated fair value related to the stock transferred to CoNCERT plus the recognition of the deferred tax liability related to the acquired temporary difference and the transaction costs incurred to complete the transaction as discussed above.intangible asset in 2022.
We are required to pay CoNCERT royalties, on a product–by-product basis, on future worldwide net sales, or pay a percentage of any sublicense revenue, as described in the License Agreement with CoNCERT.
Note 8 - Intangible Assets
Our gross intangible assets consisted primarily of costs we capitalized related to the acquisition of license rights to PCS499 from CoNCERT Pharmaceuticals. Inc. (“CoNCERT”) for shares of our common stock that had an issue date fair value of $8.0 million, $1,782 in transaction costs and $3,037,147 associated with the initial recognition of an offsetting deferred tax liability related to the acquired temporary difference for an asset purchased that is not a business combination and has a tax basis of $1,782 in accordance with ASC 740-10-25-51 Income Taxes. In accordance with ASC Topic 730, Research and Development, we capitalized the costs of acquiring the exclusive license rights to PCS499 from CoNCERT, as the exclusive license rights represented intangible assets to be used in research and development activities that management believed had future alternative uses.
Intangible assets at December 31, 2023 and 2022 consisted of the following:
Summary of Intangible Assets
| 2023 | 2022 | |||||||
| Gross intangible assets | $ | - | $ | 11,059,429 | ||||
| Less: accumulated amortization | - | (3,791,286 | ) | |||||
| Less: impairment of intangible asset | - | (7,268,143 | ) | |||||
| Total intangible assets, net | $ | - | $ | - | ||||
Amortization expense was $788,495for the year ended December 31, 2022 and is included within research and development expense in the accompanying consolidated statements of operations. We did not have a similar expense during the year ended December 31, 2023. At December 31, 2022, following the difficulty we experienced to enroll patients in our Phase 2B clinical trial in PCS499, we terminated the trial for uNL. We recognized an impairment for remaining book value of the intangible asset of $7.3 million, thereby reducing the value of our intangible asset to zero. Our assessment was based on the uncertainty of determining whether we will be able to out-license PCS499 or enter a partnering/collaborating arrangement for its future development. We believe the rarity of the disease, along with other factors, makes enrollment not feasible for us due to time and cost constraints.
| F-21 |
Note 9 - Income Taxes
We have incurred net operating losses since inception. At December 31, 2023 and 2022, we had available federal and state net operating loss carryforwards of $28.6 and $24.0 million, respectively. The federal net operating losses generated in 2018 and later of $29.3 million will carry forward indefinitely. Net operating losses generated prior to 2018 will expire 2037. We have not recognized any deferred tax assets related to the federal orphan drug or other research and development tax credits as of December 31, 2023 or 2022. The federal research and development tax credits have a 20-year carryforward period.
Pursuant to Code Sec. 382 of the Internal Revenue Code (“the Code”), the utilization of our net operating loss carryforwards could be limited as a result of a cumulative change in stock ownership of more than 50% over a three-year period. We have not completed a Sec. 382 study and as such our net operating loss carryforwards may be subject to such limitation.
A reconciliation of our effective income tax rate and statutory income tax rate for the years ended December 31, 2023 and 2022 is as follows:
Schedule of Effective Income Tax Rate Reconciliation
| 2023 | 2022 | |||||||
| Year Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Federal statutory income tax rate | 21.00 | % | 21.00 | % | ||||
| State tax rate, net | 5.77 | % | 5.72 | % | ||||
| Permanent differences | (0.25 | )% | (0.55 | )% | ||||
| Federal orphan drug tax credit | 1.41 | % | 0.93 | % | ||||
| Deferred tax asset valuation allowance | (27.93 | )% | (27.10 | )% | ||||
| Effective income tax rate | 0.00 | % | 0.00 | % | ||||
The significant components of our deferred tax assets and liabilities for Federal and state income taxes consisted of the following:
Schedule of Deferred Tax Assets and Liabilities
| 2023 | 2022 | |||||||
| December 31, | ||||||||
| 2023 | 2022 | |||||||
| Deferred tax assets: | ||||||||
| Non-current: | ||||||||
| Net operating loss carry forward – Federal | $ | 6,012,941 | $ | 5,048,175 | ||||
| Net operating loss carry forward – State | 1,672,436 | 1,431,839 | ||||||
| Stock compensation expense | 3,453,799 | 2,590,890 | ||||||
| Depreciation and other | 999 | 976 | ||||||
| Purchased in-process R&D | 2,500,562 | 2,494,829 | ||||||
| Federal orphan drug credits | 1,202,955 | 1,046,539 | ||||||
| Capitalized research and development costs | 2,795,379 | 1,929,462 | ||||||
| Start-up expenditures and amortization | - | - | ||||||
| Total non-current deferred tax assets | 17,639,071 | 14,542,710 | ||||||
| Valuation allowance for deferred tax assets | (17,639,071 | ) | (14,542,710 | ) | ||||
| Total deferred tax assets | - | - | ||||||
| Deferred Tax Liabilities: | ||||||||
| Non-current: | ||||||||
| Intangible asset | - | - | ||||||
| Total non-current deferred tax liabilities | - | - | ||||||
| Total deferred tax asset (liability) | $ | - | $ | - | ||||
| F-22 |
Beginning in 2022, the Tax Cuts and Jobs Act of 2017 (TCJA) eliminated the option to deduct research and development expenditures in the current year and requires taxpayers to amortize them over five or fifteen years pursuant to IRC Section 174. During 2023 and 2022, for income tax purposes, we capitalized approximately $3.2 million and $7.2 million of research and development expenditures, net of amortization of these costs in each year.
In 2022, as part of an evaluation of our tax attributes, we recharacterized approximately $7.4 million of startup costs previously capitalized as an IRC Section 195 asset as net operating losses. The recharacterization has no impact on total deferred tax assets since we had previously and will continue to provide a full valuation allowance on our unutilized net deferred tax assets.
The valuation allowance generally reflects limitations on our ability to use the tax attributes and reduces the value of such attributes to the more-likely-than-not realizable amount. We assessed the available positive and negative evidence to estimate if sufficient taxable income will be generated to use the existing net deferred tax assets. Based on a weighing of the objectively verifiable negative evidence primarily in the form of cumulative operating losses, we believe that it is not more-likely-than-not that the deferred tax assets will be realized and, accordingly, a full valuation allowance has been established. The valuation allowance increased by $3.1 million and $7.4 million for the years ended December 31, 2023 and 2022, respectively.
We recognize potential liabilities for uncertain tax positions using a two-step process. The first step is to evaluate the tax position for recognition by determining if the weight of available evidence indicates that it is more-likely-than-not that the position will be sustained on audit, including resolution of related appeals or litigation processes, if any. The second step is to measure the tax benefit as the largest amount that is more than 50% likely to be realized upon settlement. We have not recorded any uncertain tax positions. As of December 31, 2023 and 2022, we had no accrued penalties or interest related to uncertain tax positions.
We file U.S. Federal income tax returns, as well as state tax returns for California, Florida and Maryland. There are currently no income tax examinations underway for these jurisdictions. However, tax years from and including 2017 remain open for examination by federal and state income tax authorities.
Note 1110 – Related Party Transactions
CorLyst, LLC (“CorLyst”) reimburses us for shared costs related to payroll, health insurance and rent based on actual costs incurred, which are recognized as a reduction of our general and administrative operating expenses being reimbursed in our consolidated statementstatements of operations. We recorded $126,324 112,000and $119,001 124,000of in reimbursements during the years ended December 31, 20212023 and 2020,2022, respectively. NaNNo amounts were due from CorLyst at December 31, 20212023 or 2022. Our President, Research and 2020. In September 2020, CorLyst prepaid shared expenses to us for the fourth quarter of 2020 through the second quarter of 2021. At December 31, 2021 and 2020, we recognized $1,772 and $69,858 in prepaid reimbursements as due to related parties in the accompanying consolidated balance sheet. Our CEODevelopment is also the CEO of CorLyst, and CorLyst is a shareholder.
At December 31, 2020, we had $154,730due from certain employees for federal, state and local income taxes related to the restricted stock awards that vested in October 2020. We did not have a similar receivable at December 31, 2021.
Note 1211 – Commitments and Contingencies
Purchase Obligations
We enter into contracts in the normal course of business with CROscontract research organizations and subcontractors to further develop our products. The contracts are cancellable, with varying provisions regarding termination. If we terminated a cancellable contract with a specific vendor, we would only be obligated for products or services that we received as of the effective date of the termination and any applicable cancellation fees. AtAs of December 31, 2021,2023, we are contractually obligated forto pay up to approximately $5.31.4 million offor future services under the agreementsagreement with the CROs, butCRO for our clinical trial in NGC-Cap. Our actual contractual obligations will also vary depending on the progress and results of the remaining clinical trials.
Note 1312 – Concentration of Credit Risk
Financial instruments that potentially subject us to significant concentration of credit risk consist primarily of our cash and cash equivalents. We utilize only well-established banks and financial institutions with high credit ratings. Balances on deposit are insured by the Federal Deposit Insurance Corporation (FDIC) up to specified limits. Total cash held by our banks at December 31, 2021,2023, exceeded FDIC limits.
Note 1413 – Subsequent Events
Lincoln Park Capital Fund, LLC Purchase Agreement
On March 23, 2022,January 30, 2024, we entered into asold, pursuant to securities purchase agreementagreements (the “Purchase Agreement”) with Lincoln Park Capital Fund, LLC (“Lincoln Park”), pursuant to which Lincoln Park has committed to purchase up to $ million of shares (the “Purchase Shares”) of our common stock, $ par value per share, subject to the terms and conditions in the Purchase Agreement. We issued shares of common stock, (valued at $450,000) to Lincoln Park as a commitment fee in connection with entering into the Purchase Agreement and agreed to reimburse Lincoln Park $25,000 for fees incurred in connection with the Purchase Agreement. Concurrently with entering into the Purchase Agreement, we also entered into a registration rights agreement with Lincoln Park (the “Registration Rights Agreement”), pursuant to which we agreed to take certain actions relating to the registration under the Securities Act of 1933, as amended, of the offer and sale of the shares of common stock available for issuance under the Purchase Agreement.
Beginning on March 23, 2022, we have the right to present Lincoln Park with a purchase notice (a “Regular Purchase Notice”), directing Lincoln Parkpre-funded warrants to purchase up to 25,0001,079,555 Purchase Shares (the “Regular Purchase Amount”) provided that the closing sale price of the common stock on the purchase date is not below a threshold price set forth in the Purchase Agreement (a “Regular Purchase”). The Regular Purchase Amount may be increased to up to shares if the closing sale price of our common stock on the applicable purchase date equals or exceeds certain higher threshold prices set forth in the Purchase Agreement. We and Lincoln Park may mutually agree to increase the Regular Purchase Amount with respect to any Regular Purchase under the Purchase Agreement, provided that Lincoln Park’s maximum committed purchase obligation under any single Regular Purchase shall not exceed $1,250,000. The above-referenced share amount limitations and closing sale price thresholds are subject to adjustment for any reorganization, recapitalization, non-cash dividend, stock split, reverse stock split or other similar transaction as provided in the Purchase Agreement. The purchase price per share for each Regular Purchase will be based on prevailing market prices of the common stock immediately preceding the time of sale as computed in accordance with the terms set forth in the Purchase Agreement. There are no upper limits on the price per share that Lincoln Park must pay for shares of common stock under the Purchase Agreement. Lincoln Park may not assign or transfer its rights and obligations under the Purchase Agreement.
The aggregate number of shares that we can issue to Lincoln Park under the Purchase Agreement may in no case exceed shares (subject to proportional adjustments for stock splits, reverse stock splits and similar events as described above), which number of shares is equal to 19.99% of the outstanding shares of common stock immediately prior to the execution of the Purchase Agreement (the “Exchange Cap”), unless (i) stockholder approval is obtained to issue shares of common stock in excesslieu of the Exchange Cap, in which case the Exchange Cap will no longer apply, or (ii) the average price of all sales of Purchase Shares to Lincoln Park under the Purchase Agreement equals or exceeds the lower of (i) the Nasdaq official closing price immediately preceding the execution of the Purchase Agreement or (ii) the arithmetic average of the five Nasdaq official closing prices for the common stock immediately preceding the execution of the Purchase Agreement, plus an incremental amount to take into account the issuance of the commitment shares to Lincoln Park under the Purchase Agreement, such that the transactions contemplated by the Purchase Agreement are exempt from the Exchange Cap limitation under applicable Nasdaq rules. In all instances, we may not sell shares of our common stock to Lincoln Park under the Purchase Agreement if it would result in Lincoln Park beneficially owning more than 9.99% of the outstanding shares of common stock.
We may terminate the Purchase Agreement at any time, at our sole discretion, without any cost or penalty, by giving one business day noticestock (the “Pre-Funded Warrants”), and warrants to Lincoln Parkpurchase up to terminate the Purchase Agreement. Lincoln Park has covenanted not to cause or engage in any manner whatsoever, any direct or indirect short selling or hedging of the common stock.
There are no limitations on use of proceeds, financial or business covenants, restrictions on future financings (other than restrictions on our ability to enter into variable rate transactions described in the Purchase Agreement), rights of first refusal, participation rights, penalties or liquidated damages in the Purchase Agreement. We may deliver Purchase Notices under the Purchase Agreement, subject to market conditions, and in light of our capital needs from time to time and under the limitations contained in the Purchase Agreement. Any proceeds that we receive under the Purchase Agreement are expected to be used for working capital and general corporate purposes.
Repurchase of Shares from Aposense, Ltd.
On March 29, 2022, we purchased shares of our common stock (the “Common Warrants’) pursuant to a public offering (the “Offering”). The Common Warrants have an exercise price of $4.50, are immediately exercisable and will remain exercisable until the date that is five years after their original issuance. The Shares were offered at a combined public offering price of $4.50 per share and accompanying Common Warrant and $ per Pre-Funded Warrant and accompanying Common Warrant. The Pre-Funded Warrants had an exercise price of $0.0001 and were exercised in full simultaneously with the closing of the Offering in exchange for shares of our common stock. Gross proceeds in connection with the Offering were $7.0 million. We received $6.3 million in net proceeds from Aposense Ltd. forthe Offering, after deducting the fees of the placement agent and other offering-related expenses. We also issued to the placement agent warrants to purchase 62,222 shares of common stock, exercisable at $300,0005.625 in a private transaction.per share that expire on February 1, 2027.
Item 9. Changes in and Disagreements with Accountants
None.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that information required to be disclosed in our reports under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure. In designing and evaluating the disclosure controls and procedures, management recognized that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives, as our controls are designed to do, and management was required to apply its judgment in evaluating the risks related to controls and procedures.
In connection with the preparation of this Annual Report on Form 10-K, as of December 31, 2021,2023, an evaluation was performed by management, including the Chief Executive Officer and Chief Financial Officer, of the effectiveness of the design and operation of our disclosure controls and procedures (as defined in Rule 13a-15(e) under the Exchange Act). Our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures were effective as of December 31, 20212023 to provide reasonable assurance that information required to be disclosed by us in reports we file or submit under the Exchange Act is (i) recorded, processed, summarized and reported within the time periods specified in the SEC rules and forms and (ii) accumulated and communicated to our management, including our principal executive officer and principal financial officer, as appropriate to allow timely decisions regarding required disclosure.
Inherent Limitations on Effectiveness of Controls
Our internal control over financial reporting is designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with U.S. generally accepted accounting principles (“GAAP”). Our internal control over financial reporting includes those policies and procedures that: (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of our assets; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with GAAP, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of our assets that could have a material effect on the financial statements.
Management, including our Chief Executive Officer and Chief Financial Officer, does not expect that our internal controls will prevent or detect all errors and all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of internal controls can provide absolute assurance that all control issues and instances of fraud, if any, have been detected. Also, any evaluation of the effectiveness of controls in future periods areis subject to the risk that those internal controls may become inadequate because of changes in business conditions, or that the degree of compliance with the policies or procedures may deteriorate.
| 58 |
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) to provide reasonable assurance regarding the reliability of our financial reporting and the preparation of consolidated financial statements for external purposes in accordance with GAAP.
Management assessed our internal control over financial reporting as of December 31, 2021.2023. Management based its assessment on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework). Management’s assessment included evaluation of elements such as the design and operating effectiveness of key financial reporting controls, process documentation, accounting policies, and our overall control environment.
Based on this assessment, management has concluded that, as of December 31, 2021,2023, our internal control over financial reporting was effective to provide reasonable assurance regarding the reliability of financial reporting and the preparation of consolidated financial statements for external reporting purposes in accordance with GAAP.
This Annual Report on Form 10-K does not include an attestation report of our independent registered public accounting firm, BD & Company, Inc., regarding internal controls over financial reporting. Management’s report was not subject to attestation by our registered public accounting firm as we are a smaller reporting company. We are not currently subject to Section 404(b) of the Sarbanes-Oxley Act of 2002.
Changes in Internal Control Over Financial Reporting
Other than those noted below, thereThere were no changes to our internal control over financial reporting identified in connection with the evaluation required by Rules 13a-15(d) and 15d-15(d) of the Exchange Act that occurred during the year ended December 31, 20212023 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Material Weaknesses Remediation
In our Annual Report on Form 10-K for our fiscal year ended December 31, 2020, management identified material weaknesses in internal control over financial reporting. During 2021, we took steps to address the internal control deficiencies that contributed to the material weaknesses, including:
We believe implementation of the above remediated our previously reported material weaknesses. However, as part of our commitment to maintaining a strong internal control environment, we plan to continue to strengthen our internal controls over financial reporting during 2022 as follows:
Item 9B. Other Information
During the quarter ended December 31, 2023, none of our directors or executive officers Not applicable.adopted or terminated a Rule 10b5-1 trading plan or a non-Rule 10b5-1 trading arrangement (as defined in Item 408(c) of Regulation S-K).
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections
Not applicable.
Part III
Item 10. Directors and Executive Officers of the Registrant
The information required by this Item 10 of Form 10-K will be in our 20212024 Proxy Statement to be filed with the SEC in connection with the solicitation of proxies for the Company’s 2022our 2024 Annual Meeting of Stockholders (“20222024 Proxy Statement”) is incorporated herein by reference to our 20222024 Proxy Statement. The 20222024 Proxy Statement will be filed with the SEC within 120 days after the end of the fiscal year to which this report relates. For information with respect to our executive officers, see “Executive Officers” at the end of Part I, Item 1 of this report.
Item 11. Executive Compensation
The information required by this Item 11 of Form 10-K is incorporated herein by reference to our 20222024 Proxy Statement.
| 59 |
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required by this Item 12 of Form 10-K is incorporated herein by reference to our 20222024 Proxy Statement.
Item 13. Certain Relationships and Related Transactions
The information required by this Item 13 of Form 10-K is incorporated herein by reference to our 20222024 Proxy Statement.
Item 14. Principal Accounting Fees and Services
The information required by this Item 14 of Form 10-K is incorporated herein by reference to our 20222024 Proxy Statement.
Part IV
Item 15. Exhibits, Financial Statement Schedules
(a)(1) and (2) Financial Statements and Schedules:
See Part II, Item 8, of this Annual Report on Form 10-K.
(3) Exhibits
| 60 |
| + | Indicates a management contract or compensatory plan or arrangement. |
| * |
Item 16. Form 10-K Summary
None.
| 61 |
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, hereunto duly authorized.
| PROCESSA PHARMACEUTICALS, INC. | ||
| By: | /s/ | |
Chief Executive Officer (Principal Executive Officer) | ||
| Dated: | March | |
| By: | /s/ James Stanker | |
| James Stanker | ||
Chief Financial Officer (Principal Financial and Accounting Officer) | ||
| Dated: | March | |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons in the capacities and on the dates indicated.
| Name | Capacity | Date | ||
| /s/ | Chief Executive Officer | March | ||
| /s/ James Stanker | Chief Financial Officer | March | ||
| James Stanker | ||||
| /s/ | President of Research and Development and Director | March 29, 2024 | ||
| David Young | ||||
| /s/ Khoso Baluch | Director | March | ||
| /s/ James Neal | Director | March 29, 2024 | ||
| James Neal | ||||
| /s/ Geraldine Pannu | Director | March | ||
| Geraldine Pannu | ||||
| /s/ Justin Yorke | Director | March | ||
| Justin Yorke |
| 62 |