UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 20172023
or
☐ TRANSITION REPORT PURSUANT OR SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from ___________ to ______
Commission File Number: 001-36612


ReWalk Robotics Ltd.
(Exact name of registrant as specified in charter)
Israel | Not applicable | |
(State or other jurisdiction of incorporation or organization) | (I.R.S. employer identification no.) | |
3 Hatnufa Street, Floor 6, Yokneam | 2069203 | |
(Address of principal executive offices) | (Zip Code) |
Securities registered pursuant to Section 12(b) of the Act:
Title of Each Class | Trading Symbol(s) | Name of Each Exchange on Which Registered | ||
Ordinary Shares, par value NIS | LFWD | Nasdaq |
Securities Registered Pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act.
Yes o☐ No x☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes o No x
Yes ☐ No ☒
Indicate by a check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the Registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days.
Yes x☒ No o☐
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files).
Yes x☒ No o☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or emerging growth company. See the definitions of “large accelerated filer”, “accelerated filer”, “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
Large accelerated filer | Accelerated filer | ||
Non-accelerated | Smaller reporting company | ||
Emerging growth company |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. x☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 USC. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☐
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act).
Yes o☐ No x☒
The aggregate market value of the Ordinary Shares held by non-affiliates of the Registrant based upon the closing priceof the Ordinary Shares as reported by theThe Nasdaq Capital Market on June 30, 20172023 (the last business day of the Registrant’s most recently completed second fiscal quarter) was $29,744,250.$35,050,478.
As of March 5, 2018,February 27, 2024, the Registrant had outstanding 30,006,575 59,480,132 Ordinary Shares, par value NIS 0.010.25 per share.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of our proxy statement for our 20182024 Annual Meeting of Shareholders, which is to be filed within 120 days after the end of our 20172023 fiscal year, are incorporated by reference into Part III of this annual report on Form 10-K.10-K.
REWALK ROBOTICS LTD.
FORM 10-K FOR THE YEAR ENDED DECEMBER 31,
2023
TABLE OF CONTENTS
TABLE OF CONTENTS
| Page No | ||||
| PART I | ||||
| 24 | ||||
| 55 | ||||
| 55 | ||||
| 56 | ||||
| 56 | ||||
| PART II | ||||
| 57 | ||||
| 58 | ||||
| 58 | ||||
| 71 | ||||
| 71 | ||||
| 71 | ||||
| 71 | ||||
| 72 | ||||
| 72 | ||||
| PART III | ||||
| 73 | ||||
| 74 | ||||
| 74 | ||||
| 74 | ||||
| 74 | ||||
| PART IV | ||||
| 75 | ||||
| 77 | ||||
| 78 | ||||
| 79 | ||||
| F -1 | ||||
i
Definitions and Introduction
Our legal and commercial name is ReWalk Robotics Ltd. As of January 29, 2024, we began doing business as “Lifeward”. We are a company limited by shares organized under the laws of the State of Israel and were founded in 2001. In September 2014, we listed our shares on theThe Nasdaq Global Market, and in
May 2017, we transferred our listing to theThe Nasdaq Capital Market. We have irrevocably appointed Lifeward, Inc. (formerly ReWalk Robotics, Inc.) as our agent to receive service of process in any action against us in any United States federal or state court. The address of ReWalk Robotics,Lifeward, Inc. is 200 Donald Lynch Blvd., Marlborough, Massachusetts 01752. As used herein, and unless the context clearly indicates otherwise, the terms “ReWalk”, “the Company”“Lifeward”, the “Company”, “we”, “us”, “our” or “ours” refer to ReWalk Robotics Ltd. Ltd. DBA Lifeward and its subsidiaries.
Special Note Regarding Forward-Looking Statements and Risk Factors Summary
This annual report on Form 10-K or (“annual report,report”) contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended, or the Securities Act, Section 21E of the Securities Exchange Act of 1934, as amended, or the Exchange Act, and the safe harbor provisions of the U.S. Private Securities Litigation Reform Act of 1995, that are based on our management’s beliefs and assumptions and on information currently available to our management. Forward-looking statements include information concerning our possible or assumed future results of operations, business strategies, financing plans, competitive position, industry environment, potential growth opportunities, potential market opportunities and the effects of competition. Forward-looking statements may include projections regarding our future performance and, in some cases, can be identified by words likesuch as “anticipate,” “assume,” “believe,” “could,” “seek,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,” “project,” “future,” “should,” “will,” “would” or similar expressions that convey uncertainty of future events or outcomes and the negatives of those terms. These statements may be found in this sectionthe sections of this quarterlyannual report titled “Part I,I. Item 2.1. Business,” “Part I. Item 1A. Risk Factors,” “Part II. Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in this quarterlyannual report. These statements include, but are not limited to, statements regarding:
These factors include those listed in “Part I. Item 1A. Risk Factors"Factors,” including those factors summarized below.
our expectations regarding future growth, including our ability to increase sales in this annual report.our existing geographic markets and expand to new markets;
our ability to maintain and grow our reputation and the market acceptance of our products;
our ability to achieve reimbursement from third-party payors or advance Centers for Medicare & Medicaid Services (“CMS”) coverage for our products;
our ability to regain and maintain compliance with the continued requirements of The Nasdaq Capital Market and the risk that our ordinary shares will be delisted if we fail to regain and maintain compliance with such requirements;
our ability to successfully integrate the operations of AlterG, Inc. into our organization, and realize the anticipated benefits therefrom;
our ability to have sufficient funds to meet certain future capital requirements, which could impair our efforts to develop and commercialize existing and new products;
our ability to leverage our sales, marketing and training infrastructure;
our ability to grow our business through acquisitions of businesses, products or technologies, and the failure to manage acquisitions, or the failure to integrate them with our existing business;
our expectations as to our clinical research program and clinical results;
our ability to obtain certain components of our products from third-party suppliers and our continued access to our product manufacturers;
our ability to improve our products and develop new products;
our compliance with medical device reporting regulations to report adverse events involving our products, which could result in voluntary corrective actions or enforcement actions such as mandatory recalls, and the potential impact of such adverse events on our ability to market and sell our products;
our ability to gain and maintain regulatory approvals and to comply with any post-marketing requests;
the risk of a cybersecurity attack or incident relating to our information technology systems significantly disrupting our business operations;
our ability to maintain adequate protection of our intellectual property and to avoid violation of the intellectual property rights of others;
ii
the impact of substantial sales of our shares by certain shareholders on the market price of our ordinary shares;
our ability to use effectively the proceeds of our offerings of securities;
the impact of the market price of our ordinary shares on the determination of whether we are a passive foreign investment company;
market and other conditions, including the extent to which inflation or global instability may disrupt our business operations or our financial condition or the financial condition of our customers and suppliers, including the outbreak of war between Israel and Hamas and the ongoing tension between China and Taiwan; and
other factors discussed in “Part I. Item 1A. Risk Factors.”
You should not rely upon forward-looking statements as predictions of future events. Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee that future results, levels of activity, performance and events and circumstances reflected in the forward-looking statements will be achieved or will occur.
You should not put undue reliance on any forward-looking statements. Any forward-looking statement in this annual report speaks only as of the date hereof. Except as required by law, we undertake no obligation to update publicly any forward-looking statements for any reason after the date of this annual report, to conform these statements to actual results or to changes in our expectations.
Where You Can Find Other Information
Our principal executive offices are located at 3 Hatnufa Street, Floor 6, Yokneam IlitIllit 2069203, Israel, and our telephone number is +972 (4) 959-0123. Our website is www.rewalk.comgolifeward.com. Information contained, or that can be accessed through, our website does not constitute a part of this annual report and is not incorporated by reference herein. We have included our website address in this annual report solely for informational purposes. Information that we furnish with or file with the Securities and Exchange Commission or the SEC,(the “SEC”), including annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and any amendments to, or exhibits included in, these reports are available for download, free of charge, on our website as soon as reasonably practicable after such materials are filed or furnished with the SEC. The SEC also maintains a website at www.SEC.gov that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC. Our SEC filings, including exhibits filed or furnished therewith, are also available on the SEC’s website at SEC.gov. You may obtain and copy any document we furnish to or file with the SEC at the SEC’s public reference room at 100 F Street, NE, Room 1580, Washington, D.C. 20549. You may obtain information on the operation of the SEC’s public reference facilities by calling the SEC at 1-800-SEC-0330. You may request copies of these documents, upon payment of a duplicating fee, by writing to the SEC at its principal office at 100 F Street, NE, Room 1580, Washington, D.C. 20549.this website.
iii
PART I
ITEM 1.BUSINESS
Overview
We are an innovativea medical device company that is designing, developingdesigns, develops, and commercializingcommercializes life-changing solutions that span the continuum of care in physical rehabilitation and recovery, delivering proven functional and health benefits in clinical settings as well as in the home and community. Our initial product offerings were the ReWalk Personal and ReWalk Rehabilitation Exoskeleton devices for individuals with spinal cord injury (“SCI Products”). These devices are robotic exoskeletons that allow individuals with mobility impairments or other medical conditions the ability to stand and walk once again. We have developed and are continuing to commercialize ReWalk, an exoskeleton designed for individuals with paraplegia that usesuse our patented tilt-sensor technology and an on-boardonboard computer and motion sensors to drive motorized legs that power movement. Additionally,These SCI Products allow individuals with spinal cord injury (“SCI”) the ability to stand and walk again during everyday activities at home or in the community. In March 2023, we are developingreceived clearance of our premarket notification (“510(k)”) from the U.S. Food and intendDrug Administration (“FDA”) for the ReWalk Personal Exoskeleton with stair and curb functionality, which adds usage on stairs and curbs to commercializethe indication for use for the device in the United States (U.S.). The clearance permits U.S. customers to participate in more walking activities in real-world environments in their daily lives where stairs or curbs may have previously limited them when using the exoskeleton for its intended, FDA-indicated uses. This feature has been available in Europe since initial CE Clearance, and real-world data from a cohort of 47 European users throughout a period of over seven years consisting of over 18,000 stair steps was collected to demonstrate the safety and efficacy of this feature and support the FDA submission.
We have sought to expand our product offerings beyond the SCI Products through internal development and distribution agreements and acquisitions. We have developed our ReStore Exo-Suit device, which we began commercializing in June 2019. The ReStore is a powered, lightweight soft suit exoskeleton, designed to support mobilityexo-suit intended for use during the rehabilitation of individuals suffering from otherwith lower limb disabilities due to stroke. During the second quarter of 2020, we finalized and moved to implement two separate agreements to distribute additional product lines in the United States. We are the exclusive distributor of the MYOLYN MyoCycle FES Pro cycles to U.S. rehabilitation clinics and for the MyoCycle Home cycles available to US veterans through the Veterans Health Administration (“VHA”) hospitals. In the second quarter of 2020, we also became the exclusive distributor of the MediTouch Tutor movement biofeedback systems in the United States; however, due to unsatisfactory sales performance of the MediTouch product lines, we terminated this agreement as of January 31, 2023. We refer to the MediTouch and MyoCycle devices as our “Distributed Products.”
On August 11, 2023, we made our first acquisition to supplement our internal growth when we acquired AlterG, Inc. (“AlterG”), a leading provider of Anti-Gravity systems for use in physical and neurological rehabilitation. Our AlterG Anti-Gravity systems use patented, National Aeronautics and Space Administration (“NASA”) derived differential air pressure (“DAP”) technology to reduce the effects of gravity and allow patients to rehabilitate with finely calibrated support and reduced pain. AlterG Anti-Gravity systems are utilized in over 4,000 facilities globally in more than 40 countries. We will continue to evaluate other products for distribution or acquisition that can broaden our product offerings further to help individuals with neurological injury and disability.
We are in the research stage of ReBoot, a personal soft exo-suit for home and community use by individuals post-stroke, and we are currently evaluating the reimbursement landscape and the potential clinical impact of this device. This product would be a complementary product to ReStore as it provides active assistance to the ankle during plantar flexion and dorsiflexion for gait and mobility improvement in the home environment, and it received Breakthrough Device Designation from the FDA in November 2021. Further investment in the development path of the ReBoot was paused in 2023 pending determination regarding the clinical and commercial opportunity of this device.
Our principal markets are primarily in the United States and Europe with some lesser sales in Asia, the Middle East and South America. We sell our products primarily directly in the United States, through a combination of direct sales and distributors (depending on the product line) in Germany, Canada, and Australia, and primarily through distributors in other markets. In markets where we sell direct to consumers, we have established relationships with clinics and rehabilitation centers, professional and college sports teams, and individuals and organizations in the SCI community, and in markets where we do not sell direct to consumers, our distributors maintain these relationships. We have primary offices in Marlborough, Massachusetts, Fremont, California, Berlin, Germany and Yokneam, Israel, from where we operate our business.
We have in the past generated and expect to generate in the future revenue from a combination of clinics and rehabilitation centers, commercial distributors, third-party payors (including private and government payors), professional and college sports teams, and self-pay individuals. While a broad uniform policy of coverage and reimbursement by third-party commercial payors currently does not exist in the United States for exoskeleton technologies such as stroke, multiple sclerosis, cerebral palsy, Parkinson's diseasethe ReWalk Personal Exoskeleton, we are pursuing various paths of reimbursement and elderly assistance.support fundraising efforts by institutions and clinics, such as the VHA policy that was issued in December 2015 for the evaluation, training, and procurement of ReWalk Personal Exoskeleton systems for all qualifying veterans living with SCI across the United States.
We have also pursued updates with the CMS to clarify the Medicare coverage category (i.e., benefit category) applicable for personal exoskeletons. In 2022, the National Spinal Cord Injury Statistical Center (“NSCISC”) reported that CMS is the primary payor for approximately 57% of the SCI population which are at least five years post their injury date, with Medicare representing a majority of this percentage. In July 2020, following a successful submission and hearing process, a code was issued for ReWalk Personal Exoskeleton, which may be used for purposes of claim submission to Medicare, Medicaid, and other payors.
1
On November 1, 2023, CMS released the Calendar Year 2024 Home Health Prospective Payment System Final Rule, CMS-1780-F (“Final Rule”), which was adopted through the notice and comment rulemaking process. The Final Rule includes a policy confirming that personal exoskeletons are included in the Medicare brace benefit category, as of January 1, 2024. Medicare personal exoskeleton claims with dates of service on or after January 1, 2024 that are billed using HCPCS code K1007 are assigned to the brace benefit category. CMS reimburses items classified under the brace benefit category using a lump sum payment methodology.
On November 29, 2023, CMS included the “ReWalk Personal Prosthetic Exoskeleton System” in the HCPCS public meeting where it solicited feedback on a preliminary payment determination of $94,617 for HCPCS code K1007. The preliminary payment determination was made by CMS by applying a “gap filling” process, which was used in light of CMS determining that the code describing the technology has no fee schedule pricing history and that lower extremity exoskeletons incorporate “revolutionary features” that cannot be described by or considered comparable to any other existing code or combination of codes. As part of gap-filling, CMS utilizes verifiable supplier or commercial pricing information and adjusts this pricing information according to a deflation and update factor methodology. In applying this formula to the K1007 code describing the ReWalk Personal Exoskeleton, CMS says that it relied on information about average prices from 2020 market transactions for which CMS had data.
CMS solicited information on updated verifiable market transactions from ReWalk, as well as any other makers of similar bilateral, lower limb exoskeletons, to “ensure that the Medicare payment amount for this code accurately reflects the full market of devices that would be classified in this code.” We participated in the HCPCS meeting process on November 29, 2023 to provide additional information to help ensure that the final payment determination accurately reflects current pricing information related to the market of lower-limb exoskeleton devices, including the current ReWalk Personal Exoskeleton. A final Medicare payment determination is expected from CMS in first quarter of 2024 with an April 1, 2024, effective date.
In Germany, we continue to make progress toward achieving coverage from the various government, private and worker’s compensation payors for our SCI products. In September 2017, each of German insurer BARMER GEK (“BARMER”) and national social accident insurance provider Deutsche Gesetzliche Unfallversicherung (“DGUV”), indicated that they will provide coverage to users who meet certain inclusion and exclusion criteria. In February 2018, the head office of German Statutory Health Insurance (“SHI”) Spitzenverband (“GKV”) confirmed their decision to list the ReWalk Personal Exoskeleton system in the German Medical Device Directory. This decision means that ReWalk is listed among all medical devices for compensation, which SHI providers can procure for any approved beneficiary on a case-by-case basis. During the year 2020 and 2021, we announced several new agreements with German SHIs, including TK and DAK Gesundheit, as well as the first German Private Health Insurer (“PHI”), which outline the process of obtaining our devices for eligible insured patients. We are also currently working with several additional SHIs on securing a formal operating contract that will establish the process of obtaining a ReWalk Personal Exoskeleton for their beneficiaries within their system. Additionally, to date, several private insurers in the United States and Europe are providing reimbursement for ReWalk in certain cases.
ReWalk Personal Exoskeleton and ReWalk Rehabilitation Exoskeleton
Development of ReWalkour SCI Products took over a decade and was spurred by the experiences of our founder, Dr. Amit Goffer, who became a quadriplegic due to an accident. Current ReWalk designs are intended for people with paraplegia, a spinal cord injuryan SCI resulting in complete or incomplete paralysis of the legs, who have the use of their upper bodies and arms. We currently offer two products:products in this category: the ReWalk Personal Exoskeleton and the ReWalk Rehabilitation.Rehabilitation Exoskeleton. The ReWalk Rehabilitation Exoskeleton is substantially similar to the ReWalk Personal Exoskeleton system except that it is currently designed for everyday use by paraplegic individuals at home and in their communities, and is custom fitted for each user. ReWalk Rehabilitation is currently designed for use by paraplegia patients insold with multiple sizes of our adjustable parts to allow different users the clinical rehabilitation environment, where it provides valuable exercise and therapy. It also enables individualsability to evaluate their capacity for usingtrain within a clinic.
The ReWalk Personal in the future. In 2011, we launched ReWalk Rehabilitation for use in hospitals and rehabilitation centers in the United States and Europe. We began marketing ReWalk Personal in Europe with CE mark clearance at the end of 2012 and received U.S. Food and Drug Administration, or FDA, clearance to market it in the United States in June 2014. Additionally, we have received regulatory approval to sell the ReWalk device in other countries. In the future we intend to seek approval from the applicable regulatory agencies in other jurisdictions where we seek to market ReWalk.
2
● ReWalk Personal Exoskeleton: intended for everyday use at home, at work or in the community with a trained companion. We began marketing ReWalk Personal Exoskeleton in Europe with CE mark clearance at the end of 2012. We received FDA clearance to market the ReWalk Personal Exoskeleton in the United States in June 2014. ReWalk Personal Exoskeleton units are all manufactured according to the same mechanical specifications. Each unit is then permanently sized to fit the individual user and the software is configured for the user’s specifications by the rehabilitation center, clinic, or distributor. We are currently offering our 6th generation device (6.0) with current research and development for our 7th generation device (7.0). ● ReWalk Rehabilitation Exoskeleton: the current offering for clinics who wish to implement exoskeleton training is composed of our Rewalk Personal Exoskeleton unit along with multiple sizing of different parts, enabling multiple patient use. The ReWalk Rehabilitation Exoskeleton provides a valuable means of exercise, training, and therapy. Use of the ReWalk Rehabilitation Exoskeleton in the clinic also enables individuals to evaluate their capacity for using the ReWalk Personal Exoskeleton in the future. | ReWalk Personal Exoskeleton | |
 |
Additionally, we have received regulatory approval to sell the ReWalk Personal Exoskeleton device in other countries. In the future we intend to seek approval from the applicable regulatory agencies in other jurisdictions where we may seek to market ReWalk Personal Exoskeleton. For more information about the safety of using our SCI products see “Part I, Item 1A. Risk Factors—Risks Related to our Business and our Industry— Defects in our products or the software that drives them could adversely affect the results of our operations.”
Overview of Spinal Cord Injury
Spinal Cord Injury
The spine is the central core of the human skeleton and provides structural support, alignment, and flexibility to the body. The spinal cord, housed inside the bones of the spinal column, is a complex bundle of nerves serving as the main pathway for information connecting the brain, and nervous system. Spinal cord injury is a serious medical condition that occurs as a result of physical damage to the nerves of the spinal cord, resulting in a loss of function, such as mobility or feeling. In most people who have spinal cord injury, the spinal cord is intact. Spinal cord injury is not the same as back injury, which may result from pinched nerves or ruptured disks. Even when a person sustains a break in a vertebra or vertebrae, there may not be any spinal cord injury if the spinal cord itself is not affected. There are two types of spinal cord injury – complete and incomplete. In a complete injury, a person loses all ability to feel and voluntarily move below the level of the injury. In an incomplete injury, there is some functioning below the level of the injury.
Upon medical examination, a patient is assigned a level of injury depending on the location of the spinal cord injury. Cervical level injuries cause paralysis or weakness in both arms and legs and is referred to as quadriplegia. Sometimes this type of injury is accompanied by loss of physical sensation, respiratory issues, bowel, bladder, and sexual dysfunction. Thoracic level injuries can cause paralysis or weakness of the legs (paraplegia) along with loss of physical sensation, bowel, bladder, and sexual dysfunction. In most cases, arms and hands are not affected. Lumbar level injuries result in paralysis or weakness of the legs (paraplegia). Loss of physical sensation, bowel, bladder, and sexual dysfunction can occur. The shoulder, arm, and hand functions are usually unaffected. Sacral level injuries primarily cause loss of bowel and bladder function as well as sexual dysfunction.
3
Clinical Evidence
Published clinical studies demonstrate ReWalk’sindicate the ReWalk Personal Exoskeleton’s ability to deliver a functional walking speed. In addition, our experience working withcertain potential secondary health benefits have been reported by healthcare practitioners and ReWalk users, including reports by study participants,participants. Although these benefits have not been established as well as recently releasedconclusive clinical data suggest that ReWalk may have the potential to providein randomized controlled trials, these reported secondary health benefits. These potential benefits may include reducing pain and spasticity, improving bowel and urinary tract function, enhancing metabolism and physical fitness, and reducing hospitalizations and dependence on medications, as well as emotional and psychological benefits. Because of these potential secondary medical benefits, weinclude:
| ● | reduced pain; |
| ● | improved bowel and urinary tract function; |
| ● | reduced spasticity; |
| ● | increases in joint range of motion for the hip and ankle joints; |
| ● | improved sleep and reduced fatigue; |
| ● | increase in oxygen uptake and heart rate as a result of walking as opposed to sitting and standing; |
| ● | ability to ambulate at a speed greater than 0.4 meters per second, which is considered to be conducive to outdoor related community ambulation; and |
| ● | reduced hospitalizations. |
We believe that ReWalkusing our SCI Products may have the ability to reduce the lifetime healthcare costs of individuals with spinal cord injuries, making itwhich we believe will make our SCI Products economically attractive for individuals and third-party payors. While we believe that ReWalkusing our SCI Products could potentially offer significant advantages over competing technologies and therapies, disadvantages include the time it takes for a user to put on ReWalk,the device, the slower pace of ReWalkthe device compared to a wheelchair, the training required by the user and companion to use the device, the weight of ReWalkthe device when carried, which makes it more burdensome for a companion to transport than a wheelchair, and the requirement that users be accompanied by a trained companion.
Market Opportunity
Current and 317 personal units innear-term market opportunities include providing a home or community use, compared to 112 units and 214 units, respectively, as of December 31, 2016. Furthermore, 44 of the units we placed during the year ended December 31, 2017 were paidsolution for by insurance reimbursement compared to 51 units during the prior year period. In the near future, we intend to continue focusing on our reimbursement efforts, with our streamlined staffing, by pursuing insurance claims on a case-by-case basis, managing claims through the review process, and investing in efforts to expand commercial reimbursement coverage. As of December 31, 2017, there were 224 pending insurance claims relating to coverage for our product, compared to 199 as of December 31, 2016.
 | |
The NSCISC estimates as of 2017according to its 2023 SCI Data Sheet that there were 285,000are 302,000 people in the United States living with spinal cord injury or SCI, with an annual incidence of approximately 17,50018,000 new cases per year. Approximately 44,000According to the VHA data there are approximately 42,000 of such patients who are veterans and are eligible for medical care and other benefits from the VA.VHA, out of which the VHA states that 27,000 veterans are receiving SCI treatment annually. With 24 VA25 VHA spinal cord injury centers designated SCI/D Hub locations, the VAVHA has the largest single network of spinal cord injury care in the United States.
The University of Alabama-Birmingham Department of Physical Medicine and Rehabilitation operates the NSCISC, which maintains the world’s largest database on spinal cord injury research. Since 2010,2015, motor vehicle crashes have been the leading cause of reported spinal cord injury cases (38%), followed by falls (31%(32%), acts of violence (14%(15%) and sports injuries (9%(8%). 81%Approximately 79% of spinal cord injuries occur among the male population. According to NSCISC data, upon hospital discharge, 87% of persons with spinal cord injuries are sent to private, non-institutional residence (in most cases, their homes prior to injury).
Based on information from a 2016the 2022 annual report published by the NSCISC, 40.6%40% of the total U.S. population of SCI patients suffered injuries between levels T4 and L5. ThreeFour published ReWalk trials for SCI patients had an aggregate screening acceptance rate of 79%50% considering all current FDA limitations, resulting in an estimated 33%20% of the total population of SCI patients beingcan be considered as candidates for current ReWalk products.Personal Exoskeleton or ReWalk Rehabilitation Exoskeleton according to the device instructions for use. For important qualifying information about this determination, see “Part I.I, Item 1A. Risk Factors-TheFactors—Risks Related to our Business and our Industry—The market for medical exoskeletons, isincluding soft exo-suit devices, remains relatively new and unproven, and important assumptions about the potential market for our current and future products may be inaccurate.”
4
 | ||
 | ||
United States
In the United States rehabilitation centers generallyU.S., individuals typically obtain a ReWalk Personal Exoskeleton for home use through third-party medical coverage. For an individual who suffered an SCI through a work-related incident, workers’ compensation insurance can be a source of funding to purchase the ReWalk Rehabilitation unit and then charge patientsdevice. Similarly, for ReWalk therapy on a per-session basis. These institutionsU.S. veterans, an individual may then seek reimbursement from insurance companiesbe covered by the VHA for each session.the purchase of the device regardless of whether the SCI occurred during active military service.
In December 2015,2014, the VAVHA issued a national policy or standard operating procedure (“SOP”) for the evaluation, training, and procurement of ReWalk Personal exoskeletonExoskeleton systems for all qualifying veterans across the United States.States and U.S. Territories. The VA policyVHA SOP is the first national coverage policy in the United States for qualifying individuals who have sufferedare living with spinal cord injury. In June 2018, the VHA updated the SOP, in part, to expand training options for individuals who could not complete the mandatory training due to excessive distance/drive times from a VHA-designated site. As of December 31, 2023, we had placed 42 units as part of the VHA policy. The VHA accounted for 12% of our total revenue for the year ended December 31, 2023.
We continue to work with the VHA to both accelerate the pace of implementation of the current VHA policy nationally, and to again expand opportunities for veterans to gain access to assessments, training, and devices in facilities outside VHA’s traditional spinal cord injury “hub and spoke” infrastructure. Community-based, non-VHA clinics are also being leveraged to allow veterans to be trained closer to their homes, while still being reimbursed by the VHA as part of the VHA’s Community Care Network program.
Successful commercialization depends in significant part on adequate coverage and reimbursement from third party payors, which may include government payors (such as Medicare and Medicaid programs in the United States), managed care organizations, and private health insurers. In general, each third-party payor decides which devices will be covered and reimbursed, establishes reimbursement and co-pay levels and sets conditions for coverage and reimbursement.
While no broad uniform policy of coverage and reimbursement for electronic exoskeleton medical technology exists among commercial insurance payors in the United States, reimbursement may be achievedevaluated by the payor on a case-by-case basis. To date, payments for the ReWalk Personal deviceExoskeleton have been made primarily through case-by-case determinations by third-party payors, including commercial insurers in the United States, by self-payors and donations and, to a lesser extent, through the use of funds from insurance and/or accident settlements.
As of December 31, 2017,2023, we had 8121 cases pending in the United States for private insurance and CMS coverage decisions.
According to the NSCISC 2022 annual report, approximately 57% of the spinal cord injury population received primary coverage from Medicare and Medicaid within five years after their injury date, with Medicare representing the larger primary payor.
In order to be covered and reimbursed by Medicare, the ReWalk Personal Exoskeleton must, among other things, be classified into an applicable Medicare benefit category. In addition, appropriate codes describing the technology must also be established to facilitate billing and claims processing.
In December 2019, we submitted the first application for a unique code to describe the ReWalk Personal Exoseleton and, in July 2020, a unique code was issued for ReWalk Personal Exoskeleton. On November 1, 2023, CMS released the Final Rule, which was adopted through the notice and comment rulemaking process. The Final Rule includes a policy confirming that personal exoskeletons are included in the Medicare brace benefit category Medicare personal exoskeleton claims with dates of service on or after January 1, 2024 that are billed using HCPCS code K1007 will be assigned to the brace benefit category. CMS reimburses items classified under the brace benefit category using a lump sum payment methodology.
On November 29, 2023, CMS included the “ReWalk Personal Prosthetic Exoskeleton System” in the HCPCS public meeting, where the agency had proposed a preliminary payment determination of $94,617 for HCPCS code K1007. The preliminary payment determination was made by CMS by applying a “gap filling” process, which was used in light of CMS determining that the code describing the technology has no fee schedule pricing history and that lower extremity exoskeletons incorporate “revolutionary features” that cannot be described by or considered comparable to any other existing code or combination of codes. As part of gap-filling, CMS stated that it relied on information about average prices from 2020 market transactions for which CMS had data. In the agenda describing the preliminary payment determination, CMS noted that it would welcome information on updated verifiable market transactions. We participated in the HCPCS meeting process to provide additional information to help ensure that the final payment determination accurately reflects current pricing information related to the market of lower-limb exoskeleton devices, including the current ReWalk Personal Exoskeleton. A final Medicare payment determination is expected from CMS in first quarter of 2024 with an April 1, 2024, effective date.
5
For more information about coverage and reimbursement risk factors, see “Part I.I, Item 1A. Risk Factors-RisksFactors—Risks Related to Ourour Business and Our Industry-We may fail to secure or maintain adequate insurance coverage or reimbursement for ReWalk by third-party payors….our Industry.”
As part of our plan for growth, we intend to continue working with both national and regional commercial insurance companies, health care practitioners, physicians, researchers, and the SCI community to support efforts to demonstrate the benefits and the caseof our SCI Products. In addition, we plan to securepursue potential coverage policies with third party payors based on supportive data and appeal rulings that have deemed exoskeleton devices a “medically necessary” under the standard of care for individuals with SCI. As part of this ongoing initiative, during 2017 we submitted a proposal to a large U.S. national insurance provider for a broader coverage policy for the ReWalk Personal device. While we believe there was support for a change, the insurer was unable to reach internal consensus and therefore elected not change its existing non-coverage policy. We will continue to work with this insurer and others on coverage policies. We have already submitted data to three additional U.S. commercial insurance groups for policy review and, ourOur efforts in the future will be focused on submitting applicationscontinued education of third-party payors through data application, supporting clinical trials to a substantial numberdemonstrate the clinical benefits of nationalusing the SCI Products, working with advocacy groups, ongoing communication as well continuing to seek greater clarity regarding Medicare coverage and regional insurance providers and workers' compensation groups for policy review.reimbursement standards applicable to the ReWalk Personal Exoskeleton.
Reimbursement for ReWalk in Europe varies by country and historically certain third-party payors have provided reimbursement for our products in certain cases in Germany and Italy.
We initially focused our European efforts in Europe in Germany where we continue to make progress toward achieving ReWalk coverage from the various government, private, and worker'sworkers’ compensation payers.payors. Specifically:
| ● | In September 2017, the German insurer BARMER confirmed it will provide ReWalk systems to all qualifying beneficiaries. BARMER provides coverage for nearly nine million people in Germany, as a member of the SHI network and one of the most significant national insurers in the country. Exoskeletons are provided to users that meet certain inclusion criteria and assessment by the German Health Insurance Medical Service (Medizinischer Dienst der Krankenversicherungen) before and after training. We remain in discussion with BARMER regarding a contract based on their 2017 decision. |
| ● | In September 2017 Germany’s national social accident insurance provider, DGUV, indicated that the DGUV’s member payors, including the health insurance association Berufsgenossenschaft (also known as BG) and state insurers, will approve the supply of exoskeleton systems for qualifying beneficiaries on a case-by-case basis. DGUV is comprised of 36 different insurers, which provide coverage for more than 80 million individuals in Germany. Per the agreement, eligible individuals go to BG clinics for evaluation as a part of the procurement. In May 2020 the DGUV agreed to a binding offer to the evaluation, training, and supply of the ReWalk Personal Exoskeleton to qualified individuals. |
| ● | In February 2018, the GKV-Spitzenverband (Central Federal Association of (the) Statutory Health Insurance Funds) confirmed its decision to list the ReWalk Personal Exoskeleton system in the German MDD, a comprehensive list of all medical devices which are principally and regularly reimbursed by German SHI and PHI providers. The ReWalk Personal was added to the official German list of medical aids, code number 23.29.01.2001, in June 2018. This decision means that ReWalk Personal Exoskeleton is listed among all medical devices for compensation, which SHI providers can procure for any approved beneficiary on a case-by-case basis. |
| ● | During the year 2020 we announced several new agreements with SHIs such as TK and DAK-Gesundheit and others as well as the first PHI that chose to enter into an agreement with us that outline the process to obtaining a device for eligible insured patients. |
| ● | In March 2021 we entered into a contract with BKK Mobile Oil health insurance to supply ReWalk’s Personal Exoskeleton to eligible persons in Germany. |
| ● | In June 2020, BARMER appealed the decision of the State Social Court, which ordered the supply of the SHI’s insured SCI person with ReWalk. The State Social Court ruled and deemed ReWalk as the medical aid which will directly compensate the plaintiff’s disability. BARMER initially appealed this ruling with the Federal Social Court (Bundessozialgericht), but later, in November 2022, withdrew its pending case and accepted the prior ruling from the state court that exoskeletons are considered as a direct disability compensation. This outcome means that an eligible insured person with spinal cord injury (SCI) in Germany has a legal basis for the supply of an exoskeleton as an orthopedic aid for direct disability compensation. Patients in Germany who are covered under these contracts and policies must be medically evaluated for their eligibility to use the ReWalk Personal Exoskeleton device. If medically qualified, the patient, along with his or her physician, must apply for coverage of the device. If a patient is found eligible and medically fit to use our ReWalk Personal Exoskeleton device, we first enter into a rental agreement which allows the patient the necessary period to train on how to use the device which usually takes between 3 to 6 months and then after approval from the insurer the patient receives a personal device to use at home or in the community. We are currently working with several additional SHIs and PHIs on securing a formal operating contract that will establish the process of obtaining a ReWalk Personal Exoskeleton for their beneficiaries within their system. |
6
We continue to support clinical research and academic publications, which we believe will further support the case for coverage.
We arehave distribution agreements in several European countries where we also pursuinghad success with reimbursement by private insurers and worker’s compensationcompensation. One of the examples was achieved in various European countries.March 2018, when the Italian Ministry of Labor and Social Policy’s statutory insurance corporation put in place a coverage policy that will provide exoskeleton systems for all qualifying beneficiaries. This policy, the first of its kind in Italy, provides individuals with spinal cord injury access to obtain their own ReWalk Personal Exoskeleton device so that they can stand and walk again. Since the initiation of coverage, we have supplied 10 units through our Italian distributor to individuals covered by this policy.
Other Funding Sources
In addition to being funded by third-party payors, including private insurance plans, government programs such as the VA,VHA, and Worker's Compensation,workers’ compensation plans, ReWalk Personal Exoskeleton is also funded by self-payers.self-payors. This includes individuals who purchase ReWalk with funds from legal settlements with insurance companies or third parties.
AlterG Anti-Gravity System

The DAP technology that underpins our AlterG Anti-Gravity systems was originally developed by researchers at the NASA Moffet Field Research Center to help astronauts maintain their muscle strength and Developmentbone density during extended periods in space outside of the effects of earth’s gravity. The DAP technology was used to create a pressurized bubble that could exert pressure on an astronaut while exercising to simulate the impact of gravity. While the technology ultimately was never implemented by NASA, it also had promise for use on earth.
The DAP technology was modified by the founders of AlterG, Inc. for the opposite purpose of using the buoyancy of a pressurized air chamber to investinguniformly reduce gravitational load and body weight. With subsequent product development, the initial AlterG Anti-Gravity system design was supplemented with other complementary features. Our current models utilize a precise air calibration system which modulates the air pressure supporting the user 100 times a second to ensure precise and consistent weight displacement that allows for modification of the pressurized support in one-percent increments of each user’s weight. Additionally, the AlterG systems can be fitted with cameras for live video monitoring and pressure sensors that track the user’s gait pattern.
Our proprietary Stride Smart software can provide real-time data and analytics so that the user can watch and self-correct gate abnormalities. Clinicians also can simultaneously read and respond to five gait assessment key performance indicators (“KPIs”). The five KPIs include:
| ● | weight-bearing symmetry; |
| ● | step length symmetry; |
| ● | stance time symmetry; |
| ● | cadence (stepping frequency); and |
| ● | pain level. |
The Stride Smart software provides clinicians with clear, objective data with which to assess, adjust, and modify a robust researchpatient’s rehabilitation progress. Since Stride Smart collects and development programpresents patient gait data automatically, clinicians can focus their efforts rehabbing the patient and selecting the data most useful to enhance our current ReWalk productstheir gait analysis and to develop our pipelinecorrection recommendations.
Based on usage patterns and feedback of new and complementary products, andclinicians, we believe that ongoing researchthe AlterG Anti-Gravity system provides a versatile tool for the rehabilitation of lower extremity injuries and development efforts are essentialconditions. By treating a broad range of conditions and facilitating faster recovery times, the AlterG Anti-Gravity system enables rehabilitation clinics the opportunity to our success. Our researchgain more referrals, increase the throughput of the facility, and development team consistsimprove the productivity of both in-house and external staff, including engineers, machinists, researchers, marketing, quality, manufacturing, regulatory and clinical personnel, who work closely together to design, enhance and validate our technologies. This research and development team conceptualizes technologies and then builds and tests prototypes before refining and/or redesigning as necessary. Our regulatory and clinical personnel work in parallel with engineers and researchers, allowing us to anticipate and resolve potential issues at early stages in the development cycle.staff.
7
FIT – This is the entry-level and most affordable model of anti-gravity system. In addition to the standard DAP technology, the FIT also includes live video monitoring. The treadmill is equipped to run at up to 12 miles per hour (“mph”) in part, through funding fromforward and 3 mph in reverse with a maximum incline of 15 degrees;
VIA – The mid-range model has the Israel Innovation Authority, or the IIA (formerly known as Officefeatures of the Chief ScientistFIT, plus the inclusion of the Stride Smart analytics and the AlterG Assistant; and
PRO – The PRO is our top-of-the-line model for sports medicine applications with utilization by professional and collegiate athletes. The PRO includes all the features of the VIA, plus several additional features that add durability and accommodate elite user performance. The treadmill is a high-performance slat belt design equipped to run at up to 18 m.p.h in forward and 10 m.p.h in reverse.
In addition to sales of the Israel MinistryAlterG Anti-Gravity systems, we also provide consumables and services that support the utilization of Economy), and from the BIRD Foundation. From our inception through December 31, 2017, we received funding totaling $1.77 million frominstalled base. For example, the IIA and $500 thousand fromAlterG systems require the BIRD Foundation. Our research and development expenses, net were approximately $6.0 million, $9.0 million and $5.9 million forusers to wear proprietary shorts that zip the fiscal years ended December 31, 2017, December 31, 2016 and December 31, 2015, respectively. For more information regarding our research and development financing arrangements and expenses, see “Part II. Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations - Components of Our Statements of Operations - Operating Expenses," "—Liquidity and Capital Resources” and “—Grants and Other Funding.”
The Collaboration Agreement will expirepotential market for AlterG Anti-Gravity systems is large and fragmented with several types of facilities that treat patients with conditions who could benefit from rehabilitation using partial weight displacement. According to the MedPAC 2021 Report, there are approximately 1,150 inpatient rehabilitation facilities in the U.S. These facilities treat patients with a range of conditions including stroke, lower extremity fractures, joint replacements, neurological conditions and brain injury, cardiac conditions, and other types of orthopaedic conditions. Depending on May 16, 2021. Subjectthe specific details of each case, many of these patients are candidates for therapy using partial weight displacement. Globally, we estimate that there are approximately 3,500 inpatient rehabilitation facilities that are comparable in budget and quality of care to payment of a minimum funding commitment under applicable circumstances, we may terminatethose in the agreement if there is a loss of Harvard’s principal investigator or if we do not believe that we have or can secure sufficient funding to proceed. The Collaboration Agreement may also be terminated by either Harvard or us due to a material uncured breach by the other party or upon termination of the Harvard License Agreement.U.S.
The Harvard License Agreement will continue in full force and effect untillargest potential market for the expiration of the last-to-expire valid claim of the licensed patents. We may terminate License the Agreement for any reason upon 60 days’ prior written notice, while Harvard may terminate the Agreement if we do not obtain requisite insurance, becomes insolvent or fail to meet certain development milestones. The Harvard License Agreement may also be terminated by Harvard or us due to the other party’s material uncured breach.
8
ReStore Exo-Suit In June 2017 we unveiled our lightweight exo-suit ReStore system designed initially for rehabilitation of stroke patients. The patented soft exo-suit technology was originally developed at Harvard University’s Wyss Institute for Biologically Inspired Engineering (“Harvard”), where it also underwent initial clinical testing that demonstrated potential to improve walking for stroke survivors. ReWalk and Harvard entered into a multi-year research collaboration agreement in 2016 which provides ReWalk license to intellectual property relating to lightweight exo-suit system technologies for lower limb disabilities and provides access to future innovations that emerge from this collaboration and may be relevant to additional stroke products or other therapies. The development and regulatory clearance process for ReStore took us approximately three years. We received FDA clearance for ReStore in June 2019 and CE clearance in May 2019. Following the regulatory clearances, we began to commercialize the ReStore product. For more information on the collaboration with Harvard, see “Research and Development-Research and Development Collaborations.” |  ReStore Exo-Suit |
The ReStore product consists of a soft, fabric-based design that connects to a lightweight waist pack and mechanical cables that help lift the patient’s affected leg in synchronized timing with their natural walking pattern. The lightweight structure wraps around the waist and supports an actuator with a motor, computer, and cable, along with sensors attached to a stable point on the user’s calf and footplate in the user’s shoe. This design provides targeted mechanical assistance to the patient’s ankle during forward propulsion (plantarflexion) and ground clearance (dorsiflexion), two key phases of the gait cycle. The ReStore system is designed to provide advantages to stroke rehabilitation clinics and therapists as compared to other traditional therapies and devices by enabling the therapist to specifically target and train for improved bowelpropulsion symmetry, which is a key contributor to improved walking speed and urinary tract function;efficiency for patients recovering from stroke.
9
The main market for ReStore is rehabilitation clinics with a stroke therapy program or clinics that would like to broaden their stroke presence. This product is marketed and sold directly to rehabilitation clinics for use during the hiptreatment of their patients which is generally reimbursed by commercial and ankle joints;
Stroke incidence rate in our other markets. In our direct markets,the United States is approximately 800,000 incidences per year and the survival rate is approximately 80%. Of this stroke population, 80% are left with some type of lower limb disability. This patient population seeks treatment in one of the approximately 1,600 primary and comprehensive inpatient, outpatient, and rehabilitation clinics providing therapy to stroke patients. With the clinical evidence we have established relationshipsto date on ReStore, its unique design and its cost-effectiveness compared to other products, we believe the ReStore soft exosuit has an opportunity to be adopted by clinics for use in therapy of their stroke patients. However, we also recognize that the process to achieve that might be long and will likely only occur once national or regional healthcare providers include the device within their stroke therapy programs. We also believe that to accelerate adoption, further clinical evidence is required as well as continued education on the new ReStore design and its unique advantages compared to current therapies and products.
As of December 31, 2023, and December 31, 2022, we had placed 42 and 33 ReStore units, respectively.
ReBoot Product
We are also in the research stage of ReBoot, a soft exoskeleton for stroke home and community use, and are currently evaluating the reimbursement landscape and the potential clinical impact of this device. This product would be a complementary product to ReStore, and it received Breakthrough Device Designation from the FDA in November 2021. The ReBoot is a lightweight, battery-powered exo-suit intended to assist ambulatory functions in individuals with reduced ankle function related to neurological injuries, such as stroke. The ReBoot is a customizable personalized device intended for home and community use with an estimated market of approximately 400,000 annual stroke patients who require walking assistance after being discharged home. Further investment in the development path of the ReBoot was paused in 2023 pending further determination about the clinical and commercial opportunity of this device.
Sales and Marketing Activities
With added resources from the AlterG acquisition, we have created a U.S. commercial team that we believe has the capacity and capabilities to support a broad range of physical and neurological rehabilitation products for use in facilities, the home and the community. As part of this integration, we have rebranded our company under the name Lifeward, to emphasize our commitment to pioneering a portfolio of innovative technologies to empower the pursuit of life’s ambitions in the face of physical limitation or disability. For the sake of clarity, we will continue to use the ReWalk name to designate our line of Exoskeleton products and the AlterG name to describe our line of anti-gravity systems.
In the U.S., our commercial efforts are direct sales focused generally on rehabilitation centers, hospitals, rehabilitation clinics, and similar facilities that treat patients who could benefit from offerings within our portfolio of products. We market our facility-based products, such as the AlterG and the spinal cord injury community, andMyoCycle Pro to these institutions for their use in providing care to their patients. We also market our indirect markets, our distributors maintain these relationships. Sales ofhome-based products, such as the ReWalk Personal Exoskeleton or MyoCycle Home, to physicians and physical therapists for referrals to individuals who could benefit from these devices as part of a home-based activity regimen that elevates the health and wellness of these individuals. Additionally, some sales of the ReWalk Personal Exoskeleton or MyoCycle Home are also generated primarily from the patient base at our rehabilitation centers, referrals through the spinal cord injury community and direct inquiries from potential users. The VA accounted for 35.2%users through our different marketing efforts. Beyond healthcare facilities, we also market our AlterG systems to professional and 33.3%college sports teams who use the systems to help their athletes recover from lower extremity sports injuries.
Outside the U.S., our distribution varies depending on the product and the geographic market. We market our ReWalk Personal Exoskeleton product directly in Germany and primarily through third-party distributors, who maintain the customer relationships, in our other markets. We market our AlterG systems directly in Canada and Australia, and in other territories utilize a network of our total revenues for the years endedover 40 third-party distributors who generally have exclusivity in their respective geographic territories.
As of December 31, 20172023, we had placed 131 ReWalk Rehabilitation Exoskeleton units in use at rehabilitation centers and 2016, respectively.598 ReWalk Personal Exoskeleton units in a home or community use, compared to 128 ReWalk Rehabilitation Exoskeleton units and 572 ReWalk Personal Exoskeleton units as of December 31, 2022. We estimate the installed base of AlterG systems is over 6,000 installed units worldwide as of December 31, 2023. With the anticipated finalization of the Medicare payment rates for exoskeletons which will be effective April 1, 2024, we intend to aggressively target the eligible Medicare customer base for growth while also continuing to focus on expanding commercial and other reimbursement coverage. Additionally, with our increased direct sales resources and distributor network, we also expect to greater penetrate the base of facilities which could utilize AlterG systems for rehabilitation of their patients.
10
Competition
The market in which we operate is characterized by active competition and rapid technological change, and we expect competition to increase. Competition arises from providers of other mobility systems and prosthetic devices.devices used in the clinic and/or home settings.
We are aware of a number ofseveral other companies developing competing technology and devices, and some of these competitors may have greater resources, greater name recognition, broader product lines, or larger customer bases than we do.
Our principal competitors in the medical exoskeleton market consist of Ekso Bionics (OTC:(NASDAQ: EKSO), Rex Bionics Pty, Cyberdyne (Tokyo Stock Exchange: 7779), Parker Hannifin (NYSE: PH)FREE Bionics, DIH (formerly known as Hocoma), Hocoma, AlterG,Wandercraft, and Bioness.Bioness (acquired by Bioventus (NASDAQ: BVS). The competitors’ products may also compete with the ReStore soft exo-suit, as well as manual forms of gait training which do not involve robotic assistive devices.
We believe that our ReWalk Personal deviceExoskeleton possesses key competitive advantages over these companies,companies’ products, such as our tilt-sensor technology that provides a self-initiated walking experience, six degrees of freedom which enable a more natural gait, and faster functional walking speed, the ability to support its own weight, and broad user specifications. In addition, ReWalk Personal Exoskeleton is the firstonly medical exoskeleton cleared bywith FDA and CE clearance for use on stairs and curbs, which greatly improves the FDA for personalability to use the device in the United States.everyday real-world environments.
We believe that our RestoreReStore soft exo-suit device will have keyhas several competitive advantages over the products of our competitors, including a lightweight soft-suit, of approximately 4 kilograms, a design that facilitates a natural, functional walking pattern mimicking the movement of a healthy leg,through flexible materials, sensors, and powered plantarflexion in addition toas well as dorsiflexion, making it the only solution of its type of which we are aware to supportof that supports such movement.movements, achieving that with a lower cost and weight than rigid exoskeletal devices.
In addition, we compete with alternative devices and alternative therapies, including treadmill-based gait therapies, such as those offered by Hocoma, AlterG,Tyromotion, Boost, Aretech, BTL, and Reha Technology. Other medical device or robotics companies, academic and research institutions, or others may develop new technologies or therapies that provide a superior walking experience, are more effective in treating the secondary medical conditions that we target or are less expensive than our current or future products. Our technologies and products could be rendered obsolete by such developments.
We may also compete with other treatments and technologies that address the secondary medical conditions that ReWalk seeks to mitigate.
Community Engagement and Education
We devote significant resources to engagement with and education of the spinal cord injury community with respect to the benefits of our SCI Products, as well as for our ReStore device. We actively seek opportunities to partner with hospitals, rehabilitation centers and key opinion leaders to engage in research and development and clinical activities. We also seek to educate and gain support from organizations such as patient advocacy groups and clinician societies with the goal of promoting adoption of exoskeleton technology from patient, clinician, and payor communities. We believe that our success has been and will continue to be driven in part by our reputation and acceptance within the spinal cord injury community.
To date, multiple advocacy groups have issued public endorsements of the ReWalk Personal Exoskeleton, including leading United States-based national organizations such as the United Spinal Association and the Dana and Christopher Reeves Foundation, as well as others. In addition, the National Institute for Health and Care excellence in the United Kingdom (also known as “NICE”), has issued a public announcement regarding the ReStore device.
11
Services and Customer Support
Our centers of operations in Marlborough, Massachusetts, Fremont, California, and Berlin, Germany coordinate all customer support and product service functions for North America and Europe, respectively, through dedicated technical service personnel who provide product services and customer support through training to healthcare providers and support to product users.
Research and Development
We are committed to investing in a robust research and development program to support our current product line and to potentially develop our pipeline of new and complementary products, and we believe that ongoing research and development efforts are essential to our success. Our research and development team consists of both in-house and external staff, including engineers, machinists, researchers and marketing, quality, manufacturing, regulatory and clinical personnel, which we employ as efficiently as possible meet our current and future needs, and who work closely together to design, enhance, and validate our technologies. This research and development team conceptualizes technologies and then builds and tests prototypes before refining and/or redesigning, as necessary. Our regulatory and clinical personnel work in parallel with engineers and researchers, allowing us to anticipate and resolve potential issues at early stages in the development cycle. Our level of research and development investment depends on our available resources, business plans, and future needs. For more information, see “Part I, Item 1A. Risk Factors — Risks Related to Our Business and Our Industry — Our future growth and operating results will depend on our ability to develop, receive regulatory clearance for, and commercialize new products and penetrate new product and geographic markets.”
We are working on product design improvements and expanded labeling for the ReWalk Personal Exoskeleton product which we plan to launch following obtaining regulatory clearance and approvals. In the longer term we are conducting research for our next generation exoskeleton with design improvements and advanced robotic technologies as part of the Human Robot Interaction Consortium research program. New medical indications impacting the ability to walk that we may pursue include multiple sclerosis, cerebral palsy, Parkinson’s disease, and elderly assistance.
We are also developing new generations of anti-gravity systems utilizing our DAP technology. We plan to introduce a new model of the AlterG system in mid-2024 that reduces the cost of manufacturing which in turn will allow us to make it more affordable for independent rehabilitation clinics, thereby expanding the potential market opportunity. Additionally, we are evaluating other applications for DAP technology to create entirely new rehabilitation systems for our facility-based customers.
We conduct our research and development efforts mainly at our facility in Yokneam, Israel. We believe that the close interaction among our research and development and manufacturing groups allows for timely and effective realization of our new product concepts.
Our research and development efforts have been financed, in part, through funding from the Israel Innovation Authority (formerly known as Office of the Chief Scientist in the Israel Ministry of Economy) (the “IIA”). From our inception through December 31, 2023, we received funding totaling $2.6 million from the IIA. For more information regarding our research and development financing arrangements, see “Part II. Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources” and “—Grants and Other Funding.”
Research and Development Collaborations
On April 1, 2022, we entered a research and development cooperation agreement with several companies and universities in the Human Robot Interaction (“HRI”) Consortium, part of the IIA’s MAGNET incentive program. This incentive program provides grants for R&D collaboration as part of a consortium comprised of private businesses and leading academic centers. The goals of the HRI consortium are to “develop advanced technologies aimed at providing robots with social capabilities, enabling them to carry out various tasks and effective interactions with different users in diverse operational environments.” The total program has a budget of NIS 57 million, which includes funding for research and development grants to help drive technological innovation. The Consortium is a 3-year program which has allocated NIS 1.745 million to fund ReWalk-specific projects over the first 18-month period of the program. As of December 31, 2023, the Company spent total funds in the amount of NIS 1.571 million which has allocated for the first 18-month period. In November 2023, we entered the second 18-month period of the program, the Consortium has allocated NIS 1.336 million to fund ReWalk-specific projects over the second 18-month period. As a member of the HRI Consortium, we collaborate with several universities to develop advanced technologies aimed at improving the human-exoskeleton interaction. This research collaboration with top researchers in the fields of robotics, behavioral sciences and human-computer interaction will seek to make the use of exoskeletons easier and more natural to promote wider adoption of the technology.
12
On May 16, 2016, we entered into the Research Collaboration Agreement (“Collaboration Agreement”) and the Exclusive License Agreement (“Harvard License Agreement”) with Harvard. Under the Collaboration Agreement, we and Harvard agreed to collaborate on research regarding the development of lightweight soft suit exoskeleton system technologies for lower limb disabilities, which are intended to treat stroke, multiple sclerosis, mobility limitations for the elderly and other medical applications. Under the Collaboration Agreement, we paid Harvard quarterly installment payments to help fund the research. Subject to the terms of the Collaboration Agreement, we and Harvard were required to report our respective research results and findings to each other on a regular basis. The Collaboration Agreement governed ownership of the research results and inventions generated in performance of the research collaboration and provided us the option to negotiate with Harvard for a license to certain new inventions of Harvard conceived in performance of the collaboration. The Collaboration Agreement concluded on March 31, 2022.
Under the Harvard License Agreement, we have been granted an exclusive, worldwide royalty-bearing license under certain patents of Harvard relating to lightweight “soft suit” exoskeleton system technologies for lower limb disabilities, a royalty-free license under certain related know-how and the option to obtain a license to certain inventions conceived under our joint research collaboration. Harvard retains the right to practice the patents for research, educational and scholarly purposes. We are required to use commercially reasonable efforts to develop products under the Harvard License Agreement in accordance with an agreed-upon development plan and to introduce and market such products commercially. In addition to an upfront fee and royalties on net sales, we are obligated to pay Harvard certain milestone payments upon the achievement of certain product development and commercialization milestones. We have also agreed to reimburse Harvard for expenses incurred in connection with the filing, prosecution, and maintenance of the licensed patents.
The Harvard License Agreement will continue in full force and effect until the expiration of the last-to-expire valid claim of the licensed patents, or it is terminated in accordance with its terms. We may terminate the License Agreement for any reason upon 60 days’ prior written notice, while Harvard may terminate the License Agreement if we do not maintain requisite insurance or become insolvent. The Harvard License Agreement may also be terminated by Harvard or us due to the other party’s material uncured breach.
The Harvard License Agreement contains, as applicable, customary representations and warranties and customary enforcement, indemnification, and insurance provisions. For further discussion of the Collaboration Agreement and Harvard License Agreement, see Note 10 to our consolidated financial statements for the fiscal year ended December 31, 2023 included elsewhere in this annual report.
Intellectual Property
Protection of our intellectual property is important to our business. We seek to protect our intellectual property through a combination of patents, trademarks, confidentiality, and assignment agreements with our employees and certain of our contractors and confidentiality agreements with certain of our consultants, scientific advisors and other vendors and contractors. In addition, we rely on trade secrets law to protect our proprietary software and product candidates/products in development.
In addition to ReWalk'sour portfolio of issued patents and pending patent applications, the Company licenseswe license certain patented and patented pending technology from a third party as described above under the "Research“Research and Development"Development” section.
As of February 1, 2018,December 31, 2023, we have five11 issued patents in the United States and ten19 issued patents outside of the United States, as well as 2813 pending patent applications in various countries around the world for our technology includingin the United States, China, and Europe. For our patents associated with DAP and other AlterG technology, we have 25 issued patents in the United States and Europe. As such,21 patents issued outside the United States, as well as 10 pending patent applications for anti-gravity associated technology in the United States.
In the United States and Europe, we have apparatus patent claims in the United States and Europe covering aspects of ReWalkboth our exoskeleton and our anti-gravity products and similar devices or systems, which use a pluralityfocus on protecting our products in terms of sensors to empower tilt-sensor technology. In addition, in the United Statesstructural characteristics and Europe,functionality. Moreover, we also have method patent claims covering certain methods of user activationoperation and control of systems such as ReWalk, including by sensing the user's torso lean or weight shifts. While our apparatus claims focus on protecting ReWalk in terms of its physicalexoskeleton and structural characteristics, we believe that our method claims,anti-gravity products, which protect the process behind how ReWalk is controlled by the user, provide additional protection for our tilt sensor technology. We do not currently license any of the technology contained in our currently commercialized ReWalk and AlterG products, other than with respect to technology that is generally publicly available, but we may do so in the future.
Patents filed both in the United States and Europe (as well as other countries) generally have a lifeterm of 20 years from thetheir earliest effective filing date. Asdate, although they can be slightly longer depending upon a local jurisdiction’s rules and laws. For example, the oldest of our issued patents relating to our tilt-sensor technology was filed in May 2001 our patents on that technology do not beginin the United States and would typically expire in May 2021. However, this patent actually expired in April of 2023 due to expire until May 2021.patent term adjustment (PTA) of 689 days for delays in examination by the United States Patent and Trademark Office.
13
We currently hold a registered trademark in the United States, Europe, Israel, and Israelthe United Kingdom, for the mark “ReWalk”“ReWalk.” We currently hold a registered trademark in United States, Europe and the United Kingdom for the mark “ReStore”. We are in the process of registering the mark “Restore”currently hold a registered trademark in the United States, Europe, Israel, and the United Kingdom for the mark “Alter G.” We have also recently sought trademark registration of “Lifeward” in the United States, Europe, and Israel.
We cannot be sure that our intellectual property will provide us with a competitive advantage especially as some of our older patents begin to expire, or that we will not infringe on the intellectual property rights of others. In addition, we cannot be sure that any patents will be granted in a timely manner or at all with respect to any of our patent pending applications. For a more comprehensive discussion of the risks related to our intellectual property, see “Item“Part I, Item 1A. Risk Factors—Risks Related to Our Intellectual Property.”
Government Regulation
U.S. Regulation
Our medical products and manufacturing operations are regulated by the FDA and other federal and state agencies. Our products are regulated as medical devices in the United States under the Federal Food, Drug, and Cosmetic Act, or the FFDCA, as implemented and enforced by the FDA. The FDA regulates the development, testing, manufacturing, labeling, storage, installation, servicing, advertising, promotion, marketing, distribution, import, export, and market surveillance of our medical devices.
Premarket Regulatory Requirements
Unless an exemption applies, each medical device commercially distributed in the United States requires either a substantial equivalence determination underFDA clearance of a 510(k) premarket notification, submission, or an approval of a premarket approval application (PMA)., or issuance of a de novo classification order. Under the FFDCA, medical devices are classified into one of three classes—Class I, Class II or Class III—depending on the degree of risk associated with each medical device and the extent of control needed to provide reasonable assurance of safety and effectiveness. Classification of a device is important because the class to which a device is assigned determines, among other things, the necessity and type of FDA review required prior to marketing the device. Class I devices are those for which reasonable assurance of safety and effectiveness can be assured by adherence to general controls that include compliance with the applicable portions of the FDA’s Quality System Regulation, or QSR, facility registration and product listing, reporting of adverse medical events, and appropriate, truthful and non-misleading labeling, advertising, and promotional materials. Class I also includes devices for which there is insufficient information to determine that general controls are sufficient to provide reasonable assurance of the safety and effectiveness of the device or to establish special controls to provide such assurance, but that are not life-supporting or life-sustaining or for a use which is of substantial importance in preventing impairment of human health, and that do not present a potential unreasonable risk of illness of injury.
Class II devices are those for which general controls alone are insufficient to provide reasonable assurance of safety and effectiveness and there is sufficient information to establish “special controls.” These special controls can include performance standards, postmarketpost-market surveillance, and patient registries and FDA guidance documents.registries. While most Class I devices are exempt from the 510(k) premarket notification requirement, most Class II devices require a 510(k) premarket notification to be marketed in the U.S. As a result, manufacturers of most Class II devices are required to submit to the FDA premarket notifications under Section 510(k) of the FFDCA requesting classification of their devices in order to market or commercially distribute those devices. To obtain a 510(k), a substantial equivalence determination for their devices, clearance, manufacturers must submit to the FDA premarket notifications demonstratingdemonstrate that the proposed device is “substantially equivalent” to a predicate device already on the market. A predicate device is a legally marketed device that is not subject to premarket approval, or PMA, meaning, (i) a device that was legally marketed prior to May 28, 1976 (pre-amendments device) and for which a PMA is not required, (ii) a device that has been reclassified from Class III to Class II or I, or (iii) a device that was found substantially equivalent through the 510(k) process. If the FDA agrees that the device is substantially equivalent to a predicate device currently on the market, it will grant 510(k) clearance to commercially market the device. If the device is not “substantially equivalent” to a previously cleared device, the device is automatically a Class III device. The device sponsor must then fulfill more rigorous premarket approval requirements or can request a risk-based classification determination for the device in accordance with the “de novo”“de novo” classification process, which is a route to market for medical devices that are low to moderate risk but are not substantially equivalent to a predicate device.
14
Devices that are intended to be life sustaining or life supporting, devices that are implantable, devices that present a potential unreasonable risk of harm or are of substantial importance in preventing impairment of health, and devices that are not substantially equivalent to a predicate device are placed in Class III and generally require approval of a PMA, unless the device is a pre-amendment device not yet subject to a regulation requiring premarket approval. The PMA process is more demanding than the 510(k) premarket notification process. In a PMA, the manufacturer must demonstrate that the device is safe and effective, and the PMA must be supported by extensive data, including data from preclinical studies and clinical trials. The PMA must also contain a full description of the device and its components, a full description of the methods, facilities and controls used for manufacturing, and proposed labeling. Following receipt of a PMA, the FDA determines whether the application is sufficiently complete to permit a substantive review. If the FDA accepts the application for review, it has 180 days under the FFDCA to complete its review of a PMA, although in practice, the FDA’s review often takes significantly longer, and can take up to several years.one year or even longer.
Clinical trials are almost always required to support PMAs and are sometimes required to support 510(k) submissions. All clinical investigations of devices to determine safety and effectiveness must be conducted in accordance with the FDA’s investigational device exemption, or IDE, regulations that govern investigational device labeling, prohibit promotion of the investigational device, and specify recordkeeping, reporting and monitoring responsibilities of study sponsors and study investigators. If the device presents a “significant risk,” as defined by the FDA, the agency requires the device sponsor to submit an IDE application to the FDA, which must become effective prior to commencing human clinical trials. The IDE will automatically become effective 30 days after receipt by the FDA, unless the FDA denies the application or notifies the company that the investigation is on hold and may not begin. If the FDA determines that there are deficiencies or other concerns with an IDE that require modification of the study, the FDA may permit a clinical trial to proceed under a conditional approval. In addition, the study must be approved by, and conducted under the oversight of, an Institutional Review Board, or IRB, for each clinical site. If the device presents a non-significant risk to the patient, a sponsor may begin the clinical trial after obtaining approval for the trial by one or more IRBs without separate approval from the FDA, but must still comply with abbreviated IDE requirements, such as monitoring the investigation, ensuring that the investigators obtain informed consent, and labeling and record-keeping requirements.
In June 2014, the FDA granted our petitionrequest for “de novo”“de novo” classification, which provides a route to market for medical devices that are low to moderate risk, but are not substantially equivalent to a predicate device, and classified ReWalk as a Class II powered exoskeleton device subject to special controls. The ReWalk is intended to enable individuals with spinal cord injuries to perform ambulatory functions under supervision of a specially trained companion, and inside rehabilitation institutions. The special controls established in the de novo classification order for all powered exoskeleton devices include the following: compliance with medical device consensus standards; clinical testing to demonstrate safe and effective use considering the level of supervision necessary and the use environment; non-clinical safety and performance testing, including durability testing to demonstrate that the device performs as intended under anticipated conditions of use; a training program; and labeling related to device use and user training. The special controls of this de novo order also apply to competing powered exoskeleton products seeking FDA clearance.
In June 2019, the FDA issued a 510(k) clearance for ReStore, which means that the device can be marketed in the U.S. ReStore is intended to be used to assist ambulatory functions in rehabilitation institutions under the supervision of a trained therapist for people with hemiplegia or hemiparesis due to stroke. ReStore complies with special controls for powered exoskeletons as described above. In order for us to market ReStore and ReWalk, we must comply with both these special controls as well as general controls, including controls related to quality, facility registration, reporting of adverse events and labeling. Failure to comply with the general and special controls could lead to removal of ReStore or ReWalk from the market, which would have a material adverse effect on our business.
In June 2022, we submitted a 510(k) premarket notification for ReWalk Personal Exoskeleton seeking to enable the stairs functionality and add uses on stairs and curbs to the indication for use for the device in the US. In March 2023, the FDA issued the 510(k) clearance.
For more information, see Part I.“Part I, Item 1A. Risk Factors-Risks Related to Government Regulation-We are subject to extensive governmental regulations relating to the manufacturing, labeling and marketing of our products, and a failure to comply with such regulations could lead to withdrawal or recall of our products from the market.”
Expedited Development and Review Programs
FDA’s Breakthrough Devices Program is a voluntary program offered to manufacturers of certain medical devices and device-led combination products that may provide for more effective treatment or diagnosis of life-threatening or irreversibly debilitating diseases or conditions. The goal of the program is to provide patients and health care providers with more timely access to qualifying devices by expediting their development, assessment and review, while preserving the statutory standards for marketing authorization.
15
The program is available to medical devices that meet certain eligibility criteria, including that the device provides more effective treatment or diagnosis of life-threatening or irreversibly debilitating diseases or conditions, and that the device meets one of the following criteria: (i) the device represents a breakthrough technology, (ii) no approved or cleared alternatives exist, (iii) the device offers significant advantages over existing approved or cleared alternatives, or (iv) the availability of the device is in the best interest of patients. Breakthrough Device designation provides certain benefits to device developers, including more interactive and timely communications with FDA staff, use of post market data collection, when scientifically appropriate, to facilitate expedited and efficient development and review of the device, opportunities for efficient and flexible clinical study design, and prioritized review of premarket submissions.
Post-Market Regulatory Requirements
After a device is cleared for marketing, and prior to marketing, numerous regulatory requirements apply. These include:
| ● | establishment registration and device listing; |
| ● | development of a quality assurance system, including establishing and implementing procedures to design and manufacture devices; |
| ● | labeling regulations that prohibit the promotion of products for unapproved or “off-label” uses and impose other restrictions on labeling; |
| ● | FDA’s Unique Device Identification requirements that call for a unique device identifier (UDI) on device labels and packages and submission of data to the FDA’s Global Unique Device Identification Database (GUDID); |
| ● | medical device reporting regulations that require manufacturers to report to the FDA if a device may have caused or contributed to a death or serious injury or malfunctioned in a way that would likely cause or contribute to a death or serious injury if it were to recur; and corrections and removal reporting regulations that require manufacturers report to the FDA field corrections and product recalls or removals if undertaken to reduce a risk to health posed by the device or to remedy a violation of the FFDCA that may present a risk to health; and |
| ● | post-market surveillance. |
Our manufacturing processes are required to comply with the applicable portions of the FDA’s Quality System Regulation (“QSR”) that covers the methods and the facilities and controls for the design, manufacture, testing, production, processes, controls, quality assurance, labeling, packaging, distribution, installation, and servicing of finished devices intended for human use. In February 2024, the FDA issued the Quality Management System Regulation (“QMSR”) Final Rule to amend the QSR, incorporating by reference the international standard for medical device quality management systems set by the International Organization for Standardization (ISO), ISO 13485:2016. The rule will become effective on February 2, 2026. Until then, manufacturers are required to comply with the QSR. We actively maintain compliance with the FDA’s Quality System Regulation, 21 CFR Part 820,QSR, and the European Union’s Quality Management Systems requirements, ISO 13485:2003.2016.
As a manufacturer, we are subject to periodic scheduled or unscheduled inspections by the FDA. If the FDA believes we or any of our contract manufacturers are not in compliance with the quality system requirements, or other postmarketpost-market requirements, it has significant enforcement authority. Specifically, if the FDA determines that we failed to comply with applicable regulatory requirements, it can take a variety of compliance or enforcement actions, which may result in any of the following sanctions:
| ● | untitled letters, warning letters, fines, injunctions, consent decrees and civil penalties; |
| ● | customer notifications or repair, replacement, or refunds; |
| ● | recalls, withdrawals, or administrative detention or seizure of our products; |
| ● | operating restrictions or partial suspension or total shutdown of production; |
| ● | refusing or delaying requests for approval of pre-market approval applications relating to new products or modified products; |
| ● | withdrawing PMA approval or reclassifying our devices; |
| ● | refusal to grant export approvals for our products; or |
| ● | pursuing criminal prosecution. |
Any such action by the FDA would have a material adverse effect on our business. In addition, these regulatory controls, as well as any changes in FDA policies, can affect the time and cost associated with the development, introduction, and continued availability of new products. Where possible, we anticipate these factors in our product development processes.
16
Regulation outsideOutside of the U.S.
In addition to the United States regulations, we are subject to a variety of foreign regulations governing clinical trials and commercial sales and distribution of our products. In particular, wethe E.U., medical devices are subject to regulationregulated by the European Union Medical Devices Regulation (EU) 2017/745 or MDR, which became applicable on 26 May 2021 and replaced the EU Medical Devices Directive 93/42/EEC, or MDD. The MDR and its associated guidance documents and harmonized standards, govern, among other things, device design and development, preclinical and clinical or performance testing, premarket conformity assessment, registration and listing, manufacturing, labeling, storage, claims, sales and distribution, export and import and post-market surveillance, vigilance, and market surveillance.
Before a device can be placed on the market in the E.U., which has directives and standards regulating the design, manufacture, clinical trials, labeling and adverse event (i.e. vigilance) reporting for medical devices. Devices that complycompliance with the MDR requirements of a relevant directive are entitledmust be demonstrated in order to bearaffix the CE conformity marking, indicating that the device conformsMark to the essential requirements of the applicable directive and, accordingly, can be commercially distributed throughout Europe.product. The method of assessing conformity varies depending on the class of the product, but normally involves a combination of self-assessment by the manufacturer and a third partythird-party assessment by a “Notified Body.” This third partythird-party assessment may consist of an audit of the manufacturer’s quality system or specific testing of the manufacturer’s product. The Notified Body issues a CE Certificate of Conformity to confirm successful completion of a conformity assessment procedure conducted in relation to the medical device and its manufacturer and their conformity with the essential requirements provided in the MDR. Under transitional provisions provided in the MDR, medical devices that had valid CE Certificates of Conformity issued under the MDD prior to May 26, 2021 and that remained valid (and not withdrawn) on March 20, 2023, can continue to be placed on the EEA market until the end of December 2027 or 2028 (depending on the class of device), provided the device’s manufacturer complies with certain requirements, including that there are no significant changes in the design and intended purpose of the applicable device. After the expiry of any applicable transitional period, only devices that have been CE marked on the basis of the MDR may be placed on the market in the EEA. We comply with the E.U. requirements and have received ta Notified Body Certificate of Conformity under the CE markMDD for all of our ReWalk systems including the ReStore device which are distributed in the E.U. This allows us to continue to apply the CE mark to our products and place them on the market throughout the E.U. during the transition period or until we have completed an appropriate conformity assessment procedure under the MDR.
Following the U.K.’s exit from the E.U. (known as “Brexit”), the MDR does not apply in the United Kingdom (except for Northern Ireland, which under the Northern Ireland Protocol is bound by certain E.U. laws). The medical device legislative framework in the United Kingdom is set out in the Medical Devices Regulations 2002, as amended. These regulations are based on the previous medical device directives of the E.U. but have been amended so that they function properly now the United Kingdom is no longer part of the E.U. The Medical Devices Regulations 2002 have introduced several changes including (but not limited to) replacing the CE mark with a UKCA marking (although E.U. CE marks will be recognized potentially up until June 2030), requiring manufacturers outside of the E.U.United Kingdom to appoint a “UK Responsible Person” if they place devices on the Great Britain market and more wide-ranging device registration requirements.
Sales in other jurisdictions are subject to the foreign government regulations of the relevant jurisdiction, and in most cases, we must obtain approval by the appropriate regulatory authorities before we can commence clinical trials or marketing activities in those countries. The approval process varies from country to country, and the time may be longer or shorter than that required to obtain a marketing authorization in the UnitesUnited States or the CE mark in the E.U. The requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary greatly from country to country.
The policies of the FDA and foreign regulatory authorities may change, and additional government regulations may be enacted that could prevent or delay regulatory approval of our products and could also increase the cost of regulatory compliance. We cannot predict the likelihood, nature, or extent of adverse governmental regulation that might arise from future legislative or administrative action, either in the United States or abroad.
U.S. Anti-kickback,Anti-Kickback, False Claims and Other Healthcare Fraud and Abuse Laws
In the United States, there are federal and state anti-kickback laws that prohibit the payment or receipt of kickbacks, bribes or other remuneration intended to induce the purchase or recommendation of healthcare products and services. Violations of these laws can lead to civil and criminal penalties, including exclusion from participation in federal healthcare programs. These laws apply to manufacturers of products, such as us, with respect to our financial relationship with hospitals, physicians and other potential purchasers or acquirers of our products. The U.S. government has published regulations that identify “safe harbors” or exemptions for certain practices from enforcement actions under the federal anti-kickback statute, and we will seek to comply with the safe harbors where possible. To qualify for a safe harbor, the activity must fit squarely within the safe harbor. Arrangements that do not meet a safe harbor are not necessarily illegal but must be evaluated on a case by casecase-by-case basis. Other provisions of state and federal law provide civil and criminal penalties for presenting, or causing to be presented, to third-party payers for reimbursement claims that are false or fraudulent, or for items or services that were not provided as claimed. False claims allegations under federal and some state laws may be brought on behalf of the government by private persons, “whistleblowers,” who then receive a share of any recovery.
17
The PPACA also imposes new reporting and disclosure requirements on device manufacturerscivil FCA prohibits, among other things, any person or entity from knowingly presenting, or causing to be presented, a false or fraudulent claim for any “transfer of value”payment to, or approval by, the federal government, knowingly making, using, or causing to be made or distributedused a false record or statement material to physiciansa false or fraudulent claim to the federal government, or avoiding, decreasing, or concealing an obligation to pay money to the federal government. A claim includes “any request or demand” for money or property presented to the U.S. government. The civil FCA has been used to assert liability on the basis of kickbacks and teaching hospitals. Device manufacturers will also beother improper referrals, improper use of Medicare provider or supplier numbers when detailing a provider of services, improper promotion of off-label uses not covered by a device’s clearance or approval, and allegations as to misrepresentations with respect to products, contract requirements, and services rendered. In addition, private payors have been filing follow-on lawsuits alleging fraudulent misrepresentation, although establishing liability and damages in these cases is more difficult than under the FCA. Intent to deceive is not required to reportestablish liability under the civil FCA. Civil FCA actions may be brought by the government or may be brought by private individuals on behalf of the government, called “qui tam” actions. If the government decides to intervene in a qui tam action and discloseprevails in the lawsuit, the individual will share in the proceeds from any fines or settlement funds. If the government declines to intervene, the individual may pursue the case alone. The civil FCA provides for treble damages and a civil penalty for each false claim, such as an invoice or pharmacy claim for reimbursement, which can aggregate into millions of dollars. For these reasons, FCA lawsuits against biopharmaceutical and device companies have increased significantly in volume and breadth, leading to several substantial civil and criminal settlements, as much as $3.0 billion, regarding certain sales practices and promoting off label uses. Civil FCA liability may further be imposed for known Medicare or Medicaid overpayments that are not refunded within 60 days of discovering the overpayment, even if the overpayment was not caused by a false or fraudulent act. In addition, conviction or civil judgment for violating the FCA may result in exclusion from federal health care programs, and suspension and debarment from government contracts, and refusal of orders under existing government contracts.
The government may further prosecute conduct constituting a false claim under the criminal FCA. The criminal FCA prohibits the making or presenting of a claim to the government knowing such claim to be false, fictitious, or fraudulent and, unlike the civil FCA, requires proof of intent to submit a false claim.
The civil monetary penalties statute is another statute under which medical device companies may potentially be subject to enforcement. Among other things, the civil monetary penalties statue imposes fines against any person who offers to provide remuneration to any individual eligible for benefits under Medicare or Medicaid that the offerer knows or should know is likely to influence the individual to order or receive from a particular provider or supplier of any item or service reimbursable under those programs.
The federal Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) also created federal criminal statutes that prohibit, among other actions, knowingly and willfully executing, or attempting to execute, a scheme to defraud or to obtain, by means of false or fraudulent pretenses, representations or promises, any of the money or property owned by, or under the custody or control of, a healthcare benefit program, regardless of whether the payor is public or private, in connection with the delivery or payment for health care benefits, knowingly and willfully embezzling or stealing from a health care benefit program, willfully obstructing a criminal investigation of a health care offense and knowingly and willfully falsifying, concealing, or covering up by any trick or device a material fact or making any materially false statements in connection with the delivery of, or payment for, healthcare benefits, items, or services relating to healthcare matters. Additionally, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act, or collectively the “ACA”, amended the intent requirement of certain of these criminal statutes under HIPAA so that a person or entity no longer needs to have actual knowledge of the statute, or the specific intent to violate it, to have committed a violation.
The Physician Payments Sunshine Act (“Sunshine Act”) requires annual reporting, by applicable device and drug manufacturers, of covered products, payments, and other transfers of value to certain health care providers, and ownership and investment interests held by physicians and their immediate family members duringmembers.
18
Further, we may be subject to data privacy and security regulation by both the preceding calendar year. A numberfederal government and the states in which we conduct our business. HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act (“HITECH”) and its respective implementing regulations imposes certain requirements on covered entities relating to the privacy, security, and transmission of provisionscertain individually identifiable health information, known as protected health information. Among other things, HITECH, through its implementing regulations, makes HIPAA’s security standards and certain privacy standards directly applicable to business associates, defined as a person or organization, other than a member of PPACAa covered entity’s workforce, that creates, receives, maintains, or transmits protected health information on behalf of a covered entity for a function or activity regulated by HIPAA. HITECH also reflect increased focusstrengthened the civil and criminal penalties that may be imposed against covered entities, business associates, and individuals, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorneys’ fees and costs associated with pursuing federal civil actions. In addition, other federal and state laws may govern the privacy and security of health and other information in certain circumstances, many of which differ from each other in significant ways and may not be pre-empted by HIPAA, thus complicating compliance efforts.
Many states have also adopted laws similar to each of the above federal laws, which may be broader in scope and apply to items or services reimbursed by any third-party payor, including commercial insurers. Certain states also require implementation of commercial compliance programs and compliance with the medical device industry’s voluntary compliance guidelines and the applicable compliance guidance promulgated by the federal government, or otherwise restrict payments or the provision of other items of value that may be made to healthcare providers and other potential referral sources; impose restrictions on marketing practices; or require companies to track and fundingreport information related to payments, and other items of value to physicians and other healthcare providers.
If our operations are found to be in violation of any of the laws or regulations described above or any other applicable laws, we may be subject to penalties or other enforcement actions, including criminal and significant civil monetary penalties, damages, fines, disgorgement, imprisonment, exclusion from participation in government healthcare programs, corporate integrity agreements, suspension and debarment from government contracts, and refusal of orders under existing government contracts, reputational harm, diminished profits and future earnings, and the curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business and our results of operations. Enforcement actions can be brought by federal or state governments, or as “qui tam” actions brought by individual whistleblowers in the name of the government under the civil FCA if the violations are alleged to have caused the government to pay a false or fraudulent claim.
To the extent that any of our products are sold in a foreign country, we may be subject to similar foreign laws and regulations, which may include, for instance, applicable post-marketing requirements, including safety surveillance, anti-fraud and abuse laws, and implementation of corporate compliance programs and reporting of payments or transfers of value to healthcare professionals.
Coverage and Reimbursement
The commercial success of our product candidates and our ability to commercialize any approved product candidates successfully will depend in part on the extent to which governmental payor programs at the federal and state levels, including Medicare and Medicaid, private health insurers, and other third-party payors provide coverage for and establish adequate reimbursement levels for our products. Government authorities, private health insurers, and other organizations generally decide which products and services they will pay for and establish reimbursement levels for healthcare. Medicare is a federally funded program managed by CMS through local fiscal intermediaries and carriers that administer coverage and reimbursement for certain healthcare items and services furnished to the elderly and disabled. Medicaid is an insurance program for certain categories of patients whose income and assets fall below state defined levels and who are otherwise uninsured that is both federally and state funded and managed by each state. In the United States, private health insurers and other third-party payors often provide reimbursement for products and services based on the level at which the government provides reimbursement through the Medicare or Medicaid programs for such products and services.
In the United States, the European Union, and other potentially significant markets for our products, government authorities and third-party payors are increasingly attempting to limit or regulate the price of medical products and services, particularly for new and innovative products and therapies, which often has resulted in average selling prices lower than they would otherwise be. In the United States, it is also common for certain government and private health plans to use coverage determinations to leverage rebates from labelers to reduce the plans’ net costs. These restrictions and limitations influence the purchase of healthcare fraud enforcement.
19
Federal programs also impose price controls through mandatory ceiling prices on purchases by federal agencies and federally funded hospitals and clinics. These restrictions and limitations influence the purchase of healthcare services and products. Legislative proposals to reform healthcare or reduce costs under government programs may result in lower reimbursement for our products or exclusion of our products.
Private payors often rely on the lead of the PPACA. Although this proposed legislation ultimately failedgovernmental payors in rendering coverage and reimbursement determinations. Therefore, achieving favorable CMS coverage and reimbursement is usually a significant gating issue for successful introduction of a new product.
Further, the increased emphasis on managed healthcare in the United States and on country and regional pricing and reimbursement controls in the European Union will put additional pressure on product pricing, reimbursement, and utilization, which may adversely affect our future product sales and results of operations. These pressures can arise from rules and practices of managed care groups, competition from other products, judicial decisions and governmental laws and regulations related to pass, Congress succeededMedicare, Medicaid, and healthcare reform, and pricing in repealinggeneral. Patients who are prescribed treatments for their conditions and providers performing the PPACA’s individual mandate asprescribed services generally rely on third-party payors to reimburse all or part of the U.S. Tax Cutsassociated healthcare costs. Sales of our product candidates will therefore depend substantially, both domestically and Jobs Act of 2017. Thus, in light of the stated policies of the new U.S. presidential administration, and actions of certain members of the U.S. Congress, there is uncertainty with respect to the impact, if any,abroad, on the provisionsextent to which the costs of our products will be paid by health maintenance, managed care, and similar healthcare management organizations, or reimbursed by government health administration authorities, such as Medicare and Medicaid, private health insurers, and other third-party payors.
Moreover, a payor’s decision to provide coverage for a product does not imply that an adequate reimbursement rate will be approved or that significant price concessions will not be required to avoid restrictive conditions. High health plan co-payment requirements may result in patients seeking alternative therapies. Adequate third-party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on our investment. Legislative proposals to reform healthcare or reduce costs under government insurance programs may result in lower reimbursement for our products or exclusion of our products from coverage. The cost containment measures that healthcare payors and providers are instituting and any healthcare reform could significantly reduce our revenue from the PPACA affecting us. Whilesale of any approved product candidates.
Healthcare Reform Measures
The United States and many foreign jurisdictions have enacted or proposed legislative and regulatory changes will likely take timeaffecting the healthcare system. The United States government, state legislatures and foreign governments also have shown significant interest in implementing cost-containment programs to develop,limit the growth of government-paid healthcare costs, including price controls, restrictions on reimbursement and mayrequirements for substitution of generic products for branded prescription drugs.
The ACA substantially changed the way healthcare is financed by both governmental and private insurers, and significantly impacts the pharmaceutical industry. The ACA is intended to broaden access to health insurance, reduce or mayconstrain the growth of healthcare spending, enhance remedies against healthcare fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on pharmaceutical and medical device manufacturers, and impose additional health policy reforms.
The ACA has been subject to challenges in the courts. On December 14, 2018, a Texas U.S. District Court Judge ruled that the ACA is unconstitutional in its entirety because the “individual mandate” was repealed by Congress. On December 18, 2019, the Fifth Circuit U.S. Court of Appeals held that the individual mandate is unconstitutional, but did not have an impactinvalidate the entire law, and remanded the case to the Texas District Court to reconsider its earlier invalidation of the entire ACA. An appeal was taken to the U.S. Supreme Court, which ruled on June 17, 2021, that the plaintiffs lacked standing to challenge the law as they had not alleged personal injury traceable to the allegedly unlawful conduct. As a result, the Supreme Court did not rule on the constitutionality of the ACA or any of its provisions.
Other legislative changes have been proposed and adopted since passage of the ACA. The Budget Control Act of 2011, among other things, created the Joint Select Committee on Deficit Reduction to recommend proposals in spending reductions to Congress. The Joint Select Committee did not achieve its targeted deficit reduction of an amount greater than $1.2 trillion for the fiscal years 2012 through 2021, triggering the legislation’s automatic reductions to several government programs. These reductions included aggregate reductions to Medicare payments to healthcare providers of up to 2.0% per fiscal year. The Bipartisan Budget Act of 2018 retained the federal budget “sequestration” Medicare payment reductions of 2% and extended it through 2027 unless congressional action is taken. On January 2, 2013, the American Taxpayer Relief Act was signed into law, which, among other things, reduced Medicare payments to several types of providers, including hospitals, imaging centers and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
20
Further legislative and regulatory regimechanges under the ACA remain possible, although President Biden indicated that he intends to which we are subject, we cannot predictuse executive orders to undo changes to the ultimate content, timingACA made by the Trump administration and would advocate for legislation to build on the ACA. It is unknown what form any such changes or effect of any law would take, and how or whether it may affect our business in the future. We expect that changes or additions to the ACA or the Medicare and Medicaid programs, and changes stemming from other healthcare reform measures, especially with regard to healthcare access, financing or other legislation in individual states, could have a material adverse effect on the healthcare industry.
At the state level, legislatures may also increasingly pass legislation and implement regulations designed to control product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures.
We expect that additional federal, state, and foreign healthcare reform measures will be adopted in the impactfuture, any of potential legislation on us.which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in limited coverage and reimbursement and reduced demand for our products, or additional pricing pressures.
Environmental Matters
We are subject to various environmental, health and safety laws and regulations, including those governing air emissions, water and wastewater discharges, noise emissions, the use, transport, management and disposal of chemicals and hazardous materials, the import, export and registration of chemicals, and the cleanup of contaminated sites. Based on information currently available to us, we do not expect environmental costs and contingencies to have a material adverse effect on us. The operation of our business and facilities, however, entails risks in these areas. Significant expenditures could be required in the future to comply with environmental or health and safety laws, regulations, or requirements.
In Israel, where our contract manufacturer produces all of our ReWalk and ReStore products, businesses storing or using certain hazardous materials (including materials necessary for our manufacturing process) are required, pursuant to the Israeli Dangerous Substances Law, 5753-1993, to obtain a toxin permit from the Ministry of Environmental Protection. In the U.S., where we manufacture our AlterG products in our Fremont, California facility, we do not utilize chemicals which require a toxic materials license. We have a hazardous waste disposal license with the County of Alameda and dispose of our expired and empty containers through a process in accordance with the license.
In the European marketplace, electrical and electronic equipment is required to comply with the Directive on Waste Electrical and Electronic Equipment, which aims to prevent waste by encouraging reuse and recycling, and the Directive on Restriction of Use of Certain Hazardous Substances, which restricts the use of sixten hazardous substances in electrical and electronic products. Our products and certain components of such products “put on the market” in the EUE.U. (whether or not manufactured in the EU)E.U.) are subject to these directives. Additionally, we are required to comply with certain laws, regulations, and directives, including the Toxic Substances Control Act in the United States and REACH in the EU,E.U., governing chemicals. These and similar laws and regulations require the testing, reporting and registration of certain chemicals we use and ship. We believe we are in compliancecomply in all material respects with applicable environmental laws and regulations.
Manufacturing
Our ReWalk includesexoskeletons, ReStore exo-suits, and AlterG Anti-Gravity systems include off-the-shelf and custom-made components produced to our specifications by various third parties, for technical and cost effectiveness.cost-effectiveness. We have contracted with Sanmina Corporation ("Sanmina"(“Sanmina”), a well-established contract manufacturer with expertise in the medical device industry, for the manufacture of all of our products. Pursuant to this contract, Sanmina manufactures ReWalkSCI Products and ReStore at its facility in Ma’alot, Israel. All ReWalk Personal units areWe manufacture the AlterG product ourselves at our facility in Fremont, California. Each product line is manufactured pursuant to the same applicable set of specifications, and all ReWalk Rehabilitation units are manufactured pursuant to another set.specifications. We place our manufacturing orders with Sanmina and other suppliers pursuant to purchase orders or by providing forecasts for future requirements. We may terminate our relationship with Sanmina or our other suppliers at any time upon written notice. Either we or Sanmina may terminate the relationship in the event of a material breach, subject to a 30-day cure period. Our agreement with Sanmina contains a limitation on liability that applies equally to both us and Sanmina.
We believe that this contract manufacturing relationship with Sanmina allows us to operate our business efficiently by focusing our internal efforts on the development and commercialization of our technology and our products and provides us with substantial scale-up capacity. We regularly test quality on-site at Sanmina’s facility and we obtain full quality inspection reports. We maintain a non-disclosure agreement with Sanmina.
21
We develop certain of the software components internally and license other software components that are generally available for commercial use as open sourceopen-source software.
We manufacture products based upon internal sales forecasts. We deliver products to customers and distributors based upon purchase orders received, and our goal is to fulfill each customer’s order for products in regular production within two weeks of receipt of the order.
Suppliers
We have contracted with Sanmina for the sourcing of all components and raw materials necessary for the manufacture of our ReWalk and ReStore products, although there are instances that we purchase raw materials ourselves. In addition, we directly source all components and raw materials necessary for the manufacture of our AlterG products. Components of our products and raw materials come from suppliers in the United States, Europe, China, Taiwan, and Israel, and we depend on certain of these components and raw materials, including certain electronic parts, for the manufacture of our products. To date, we have not experienced significant volatility in the prices of these components and raw materials. However, suchduring the COVID-19 pandemic several specific parts, mainly electronic parts, experienced temporary price increases which have returned to more normal levels. Such prices are subject to a number of factors, including purchase volumes, general economic conditions, currency exchange rates, industry cycles, production levels, and scarcity of supply.
We believe that our andin-house manufacturing, Sanmina’s facilities, our contracted manufacturing arrangement, and our supply arrangements are sufficient to support our potential capacity needs for the foreseeable future.
Human Capital
Employees
As of December 31, 2017,2023, we had 65108 employees (including full-time and hourly employees), of whom 27 are located in the United States, 26 were located in Israel and 12 were located in Germany. As of December 31, 2016, we had 94 employees, of whom 3674 were located in the United States, 4120 were located in Israel and 17 are located in Germany, and as of December 31, 2015, we had 87 employees, of whom 3214 were located in the United States, 39 were located in Israel and 16 were located in Germany.Europe. The majority of our employees are, and have been, engaged in sales and marketing and research and development activities. We do not employ a significant number of temporary or part time employees. The decline in total employees at the end of 2017 versus 2016 is a result of our efforts to reduce operating expenses announced in January 2017. We will continue to evaluate spending and organizational requirements as our business develops.
We are subject to labor laws and regulations within our locations mainly in the U.S. ,Germany, Germany, and Israel. These laws and regulations principally concern matters such as pensions, paid annual vacation, paid sick days, length of the workday and work week, minimum wages, overtime pay, insurance for work-related accidents, severance pay and other conditions of employment. Our employees are not represented by a labor union. We consider our relationship with our employees to be good. To date, we have not experienced any work stoppages.
Compensation and Benefits
We provide our employees with competitive salaries and bonuses, opportunities for equity ownership, and a robust employment package that promotes well-being across all aspects of our employees’ lives, including health care, retirement planning, and paid time off. We also invest in the ongoing development of our employees through our internal training programs.
Diversity and Inclusion
We value the diversity of our employees and take pride in our commitment to diversity and inclusion across all levels of our organizational structure. We encourage a diversity of views and strive to create an equal opportunity workplace, including working with managers to develop strategies for building diverse teams and promoting the advancement of employees from diverse backgrounds.
Financial Information about Geographic Areas and Significant Customer Information
The following table sets forth the geographical breakdown of our revenuesrevenue for each of the years ended December 31, 2017, 2016, 2015:2023, and 2022 (in thousands):
| Year Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Revenue based on customer’s location: | ||||||||
| United States | 7,636 | 2,303 | ||||||
| Europe | 5,044 | 3,057 | ||||||
| Asia-Pacific | 387 | 115 | ||||||
| Rest of the world | 787 | 36 | ||||||
| Total revenue | $ | 13,854 | $ | 5,511 | ||||
22
| Year Ended December 31, | |||||||||||
| 2017 | 2016 | 2015 | |||||||||
| Revenues based on customer’s location: | |||||||||||
| Israel | $ | — | $ | — | $ | — | |||||
| United States | 4,598 | 3,741 | 2,439 | ||||||||
| Europe | 3,094 | 1,144 | 820 | ||||||||
| Asia-Pacific | 61 | 984 | 487 | ||||||||
| Total revenues | $ | 7,753 | $ | 5,869 | $ | 3,746 | |||||
Additional discussion of financial information by reportable segment and geographic area and sales in excess of 10% of total revenuesrevenue to certain of our customers is contained in Note 1213 to our consolidated financial statements set forth in “Part II. Item 8. Financial Statements and Supplementary Data” of this annual report.
| ● | In March 2023, the ReWalk Personal Exoskeleton technology received clearance from the FDA for use on stairs and curbs in the United States, making it the only personal exoskeleton to receive FDA clearance for this indication. The clearance follows the FDA’s designation of the device as a "Breakthrough Device" in recognition of its unprecedented ability to provide ambulatory access to environments containing stairs and curbs for paralyzed individuals with SCI. |
| ● | In August 2023, we completed the acquisition of AlterG, which adds significant scale to our revenue base, extensive sales and service capabilities to our commercial team, and innovative systems that utilize DAP technology to our portfolio of rehabilitation solutions that facilitate mobility and wellness in rehabilitation and daily life. |
| ● | In November 2023, CMS released the Final Rule, which explicitly includes exoskeletons within a Medicare brace benefit category. The rule went into effect on January 1, 2024. |
| ● | In November 2023, CMS included the ReWalk Personal Exoskeleton system in the agenda for the November 29, 2023 HCPCS public meeting. The agency also proposed a preliminary payment determination of $94,617 for HCPCS code K1007 based on a “gap filling” process applied to 2020 market data. At the meeting, CMS solicited additional information for updated market transactions for use in developing a final payment determination. We participated in the HCPCS meeting process to provide additional information to help ensure that the final payment determination accurately reflects current pricing information related to the market of lower-limb exoskeleton devices, including the current ReWalk Personal Exoskeleton. A final Medicare payment determination is expected from CMS in first quarter of 2024 with an April 1, 2024, effective date. |
| ● | In December 2023, our first claim with Medicare for reimbursement for a ReWalk Personal Exoskeleton was paid; |
| ● | Record annual revenue for 2023 was $13.9 million, compared to $5.5 million in 2022, an increase of 151%. |
| ● | Our cash position remained strong with $28.1 million as of December 31, 2023, with no debt. |
23
ITEM 1A.RISK FACTORS
Our business faces significant risks. You should carefully consider all of the information set forth in this annual report and in our other filings with the SEC, including the following risk factors which we face and which are faced by our industry. Our business, financial condition and results of operations could be materially and adversely affected by any of these risks. In that event, the trading price of our ordinary shares would likely decline and you might lose all or part of your investment. This report also contains forward-looking statements that involve risks and uncertainties. Our results could materially differ from those anticipated in these forward-looking statements, as a result of certain factors including the risks described below and elsewhere in this report and our other SEC filings. See also “Special Note Regarding Forward-Looking Statements”Statements and Risk Factors Summary” on page (iii)(ii).
Risks Related to Our Business and Our Industry
We currently rely,may fail to realize the benefits expected from our acquisition of AlterG, which could adversely affect the price of our ordinary shares.
As discussed above in “Part I. Item 1. Business - Overview”, on August 11, 2023, we completed the acquisition of AlterG which became an indirect and wholly-owned subsidiary of the Company.
The anticipated benefits from our acquisition of AlterG are based on projections and assumptions about the combined businesses of ReWalk and AlterG, which may not materialize as expected or which may prove to be inaccurate. The value of our ordinary shares could be adversely affected if we are unable to realize the anticipated benefits from the acquisition on a timely basis or at all. Achieving the benefits of the acquisition will depend, in part, on our ability to integrate the business, operations and products of AlterG successfully and efficiently with our business. The process of integrating the operations of ReWalk and AlterG could encounter unexpected costs and delays, which include: the loss of key personnel; the loss of key customers; the loss of key suppliers; inability to properly identify, acquire or obtained required regulatory approvals; and unanticipated issues in integrating sales, marketing and administrative functions. In addition, the acquired AlterG business, products and technologies may not achieve anticipated revenues and income growth.
Further, the integration of AlterG may involve a number of additional risks, including diversion of management’s attention away from the rest of the business, which could adversely affect our results of operations. In addition, our failure to identify or accurately assess the magnitude of certain liabilities we assumed in the acquisition could result in unexpected litigation or regulatory exposure, unfavorable accounting charges, unexpected increases in taxes due, a loss of anticipated tax benefits or other adverse effects on our business, operating results or financial condition. If we do not realize the expected benefits or synergies of the acquisition, such as revenue gains or cost reductions, there could be a material adverse effect on our business, results of operations, and financial condition.
Global, regional, and local economic weakness and uncertainty could adversely affect our demand for our products and services and our business and financial performance.
Our business and financial performance depends on worldwide economic conditions and the demand for our products and services in the markets in which we compete. Ongoing economic weakness, including an economic slowdown or recession, uncertainty in markets throughout the world and other adverse economic conditions, including inflation, changes in monetary policy and increased interest rates, have resulted, and may result in the future, will rely, on sales of our ReWalk systems and related service contracts and extended warrantiesin decreased demand for our revenue. Additionally, we are developingproducts and intendservices and increased expenses and difficulty in managing inventory levels and accurately forecasting revenue, gross margin, cash flows and expenses. Ongoing U.S. federal government spending limits may continue to commercialize a lightweight soft suit exoskeleton, designed to support mobilityreduce demand for individuals sufferingour products and services from other lower limb disabilities, and aim to begin marketing an initial indication for stroke patients in the first half of 2019 after applying for and receiving mandatory regulatory clearances.We have sold only a limited number of ReWalk systems, and market acceptance and adoption depend on educating people with limited upright mobility and health care providers as to the distinct features, ease-of-use, positive lifestyle impact and other benefits of ReWalk compared to alternative technologies and treatments. ReWalk may not be perceived to have sufficient potential benefits compared with these alternatives. Users may also choose other therapies due to disadvantages of ReWalk, including the time it takes for a user to put on ReWalk, the slower pace of ReWalk compared to a wheelchair, the weight of ReWalk when carried, which makes it more burdensome for a companion to transport than a wheelchair, and the requirementorganizations that users be accompanied by a trained companion. Also, we believe that healthcare providers tend to be slow to change their medical treatment practices because of perceived liability risks arisingreceive funding from the use of new productsU.S. government and the uncertainty of third-party reimbursement. Accordingly, healthcare providers may not recommend ReWalk until there is sufficient evidence to convince them to alter the treatment methods they typically recommend, such as prominent healthcare providers or other key opinion leaders in the spinal cord injury community recommending ReWalk as effective in providing identifiable immediate and long-term health benefits.
Prolonged or more severe economic weakness and uncertainty could also cause our expenses to date,vary materially from our expectations. Any financial turmoil affecting the VA maintains its coverage policy for qualifying veterans acrossbanking system and financial markets or any significant financial services institution failures could negatively impact our treasury operations, as the United Statesfinancial condition of such parties may deteriorate rapidly and German insurers Barmerwithout notice. Poor financial performance of asset markets and DGUV have issued broad coverage decisions, no broad uniform policythe adverse effects of coveragefluctuating currency exchange rates could lead to higher pension and reimbursement for electronic exoskeleton medical technology exists among third-party payors in the United States. Additionally, health insurance companiespost-retirement benefit expenses. Interest and other third-party payorsexpenses could vary materially from expectations depending on changes in the future may not deliver adequate coverage or reimbursement for our products. The VA, Barmer or DGUV may cancel or materially curtail their current policy of providing coverage in the United States for qualifying individuals who have suffered spinal cord injury, or we may not place enough units through the VA to make our sales profitable under the VA policy. Additionally, any future government measures to restrict healthcare spending could limit or eliminate our ability to provide products to, and gain revenues from insurance reimbursements. We may be unable to sell ReWalk systems on a profitable basis if third-party payors deny coverage, limit reimbursement or reduce their levels of payment, or if ourinterest rates, borrowing costs, currency exchange rates, costs of production increase faster than increases in reimbursement levels. In addition, we may not obtain coverage and reimbursement approvals in a timely manner. Our failure to receive such approvals would negatively impact market acceptance of ReWalk.
24
We may not have sufficient funds to meet certain future operating needs or capital requirements, which could impair our efforts to develop and commercialize existing and new products, and as a result, we may need to take advantage of various forms ofin the future consider one or more capital-raising transactions, Futureincluding future equity or debt financings, strategic transactions, or borrowings which may also further dilute our shareholders or place us under restrictive covenants limiting our ability to operate.operate freely.
We intend to finance our business by close management of our operating costs over the next 12 months withexpenses until we reach profitable operation using existing cash on hand, issuances of equity and/or debt securities, including issuances under the Company's ATM Offering Program,and other future public or private issuances of securities, including the recently signed private placementcash exercised of ordinary shares to Timwell,outstanding warrants, or through a combination of the foregoing. However,foregoing, though we may also consider additional capital raising alternatives, such as entering into a credit facility, if the foregoing alternatives are not available to us or unavailable on reasonable terms. Although we had a cash and cash equivalents of $28.1 million as of December 31, 2023, which we believe will needbe sufficient to seek additional sources of financing if we require more funds than anticipated duringfund our planned operations through at least the next 12twelve months or in later periods, including if we cannot make our loan repayments under our Kreos Loan Agreement, or if we cannot raise sufficient funds from equity issuances, such as the ATM Offering Program. In addition, due to limitations under the rules of Form S-3, which have applied to us since we filed our Form 10-K in February 2017, we may only sell up to approximately $13.7 million in primary offerings under our effective registration statement on Form S-3 (the “Form S-3”), including our ATM Offering Program, during any 12-month period while we remain subject to these limitations. As of the date of this annual report, if we have sold approximately $9.3 millionare incorrect in securitiesour assumptions, we may need to raise additional capital sooner than expected or on less favorable terms than what might otherwise be available. Raising additional capital through one or more of these alternatives may further dilute our shareholders or place us under restrictive covenants limiting our ability to operate freely.
Raising additional capital in the public markets could also entail certain downsides. Although we are currently eligible to use our Form S-3, during the last 12 months, when we were subjectare limited to these restrictions. We will recalculate the amountselling no more than one-third of this limitation if we terminate our ongoing takedown and conduct another takedown underunaffiliated market capitalization, or public float, on Form S-3 in a 12-month period unless our Form S-3.public float rises above $75 million. For more information on our inability to use Form S-3, see “Part II,II. Item 7.2, Management’s Discussion and Analysis of Financial Condition and Results of Operations-LiquidityOperations—Liquidity and Capital Resources-Equity Raises.”
We may also need to pursue strategic transactions, such as joint ventures, in-licensing transactions, or the sale of our business, or all, or substantially all, of our assets.assets if our financial stability is uncertain, and we are unable to raise additional capital effectively. These private financings and strategic transactions have in the past and could in the future require significant management attention, disrupt our business, adversely affect our financial results, be unsuccessful or fail to achieve the desired results. We are in discussions routinely with such possible sources of additional funding. As another alternative,
Overall, if we cannot raise the required funds, or cannot raise them on terms acceptable to us or investors, we may choosebe forced to refinance upcurtail substantially our current operations or cease operations altogether.
We face economic and political risks associated with doing business in Taiwan, particularly due to the geopolitical tension between Taiwan and China, and in Russia that could negatively affect our business and hence the value of your investment.
Currently, we rely on third party suppliers in Taiwan for a substantial portion of the components we use in our indebtedness underAlterG products. Accordingly, our Kreos Loan Agreement, which we have considered with Kreosbusiness, financial condition and results of operations and the market price of our securities may be affected by changes in governmental policies, taxation, growth rate, inflation rate or interest rates and by social instability and diplomatic and social developments in or affecting Taiwan. In particular, the unique political status of Taiwan and its internal political movement cause sustained tension between China and Taiwan. Past developments related to the interactions between China and Taiwan, especially in relation to trade activities such as bans on exports of goods from time to time, have on occasions depressed the transactions and business operations of certain Taiwanese companies and overall economic environment. We cannot predict whether there will be escalation of the tensions between China and Taiwan, which would lead to new bans or borrowtariffs on exports or even conflict. Any conflict which threatens the military, political or economic stability in Taiwan could have a material adverse effect on our current or future business and financial conditions and results of operations.
In addition, we also sell our AlterG products in Russia. The current invasion of Ukraine by Russia has escalated tensions among the United States, the North Atlantic Treaty Organization (“NATO”) and Russia. The United States and other NATO member states, as well as non-member states, have announced new sanctions against Russia and certain Russian banks, enterprises and individuals. AlterG prior to the acquisition and Lifeward subsequent to the acquisition has remained in compliance with these sanctions by obtaining export licenses for each shipment to our distributor that serves Russia. These and any future additional funds. sanctions and any resulting conflict between Russia, the United States and NATO countries could have an adverse impact on our current operations.
25
Further, such invasion, ongoing military conflict, resulting sanctions and related countermeasures by NATO states, the United States and other countries are likely to lead to market disruptions, including significant volatility in commodity prices, credit and capital markets, as well as supply chain interruptions for equipment, which could have an adverse impact on our operations and financial performance.
We do not satisfy all requirements for continued listing on The Nasdaq Capital Market. We can provide no assurance that we will be able to comply with the continued listing requirements over time or that our ordinary shares will continue to be listed on The Nasdaq Capital Market.
As previously disclosed, on October 10, 2022, we received a notification letter (the “Bid Price Letter”) from Nasdaq that we failed to evidence a minimum closing bid price of $1.00 per share for the prior 30-consecutive business day period in contravention of Nasdaq Listing Rule 5550(a) (“Rule 5550(a)”). We were provided an initial period of 180 days to regain compliance with Rule 5550(a). On April 11, 2023, we received a second notification letter from Nasdaq indicating that we had been provided with an additional period of 180 calendar days, or until October 9, 2023, to regain compliance with Rule 5550(a). The bid price of our ordinary shares did not close at $1.00 per share or more for a minimum of 10 consecutive business days by October 5, 2023, and on October 6, 2023 we were notified by Nasdaq that, based upon our non-compliance with Rule 5550(a), as of October 5, 2023, our securities were subject to delisting unless we timely requested a hearing before the Nasdaq Hearings Panel (the “Panel”). We participated in an expedited review with the Panel, which first granted us an extension until January 31, 2024, to regain compliance with Rule 5550(a), including by implementing a reverse share split should such action be necessary to regain compliance.
We thereafter requested a further extension, through March 30, 2024, to allow for additional time for the finalization and implementation of the home health rule administrative proposal by CMS that explicitly includes exoskeletons within a Medicare benefit category. Our updated compliance plan continues to include the possible implementation of a reverse share split should such action be deemed necessary to maintain our listing on Nasdaq. On December 8, 2023, we were notified that the Panel had granted us the requested extension through March 30, 2024, to regain compliance with Rule 5550(a)(2). To do so, we must evidence a closing bid price of at least $1.00 per share for a minimum of 10 consecutive business days by March 30, 2024.
If we were to carry out these transactions usingare not successful in regaining compliance with Rule 5550(a)(2) during the extension period, our ordinary shares will be removed from trading on The Nasdaq Capital Market. Any delisting determination could seriously decrease or eliminate the value of an investment bank we previously engagedin our ordinary shares and other securities linked to assist usour ordinary shares. While an alternative listing on an over-the-counter exchange could maintain some degree of a wide range of strategic transactions,market in our ordinary shares, we could incur advisory fees determinedface substantial material adverse consequences, including, but not limited to, the following: limited availability for market quotations for our ordinary shares; reduced liquidity with respect to our ordinary shares; a determination that our ordinary shares are “penny stock” under SEC rules, subjecting brokers trading our ordinary shares to more stringent rules on disclosure and the class of investors to which the broker may sell the ordinary shares; limited news and analyst coverage, in part due to the “penny stock” rules; decreased ability to issue additional securities or obtain additional financing in the future; and potential breaches under or terminations of our agreements with current or prospective large shareholders, strategic investors and banks. The perception among investors that we are at heightened risk of delisting could also negatively affect the market price of our securities and trading volume of our ordinary shares. In the event of a delisting, we can provide no assurance that any action taken by us to restore compliance with the listing requirements would allow our ordinary shares to become listed again, stabilize the market price or improve the liquidity of our ordinary shares, prevent our ordinary shares from dropping below the Nasdaq minimum bid price requirement, or prevent future non-compliance with Nasdaq’s listing requirements.
Our future growth and operating results will depend on our ability to develop, receive regulatory clearance for and commercialize new products and penetrate new product and geographic markets.
We are currently engaged in research and development efforts to address the needs of patients with mobility impairments besides paraplegia, such as stroke, and, in the future, we may engage in efforts to address these needs in patients with other conditions such as multiple sclerosis, cerebral palsy, Parkinson’s disease and elderly assistance. In 2019, we commercialized our first product for stroke patients, the ReStore Exo-Suit. For more information, see “Part, Item 1. Business—ReStore Products” above. While our Collaboration Agreement with Harvard for the design, research and develop lightweight exoskeleton system technologies for lower limb disabilities intended to treat stroke, multiple sclerosis, mobility limitations for the elderly and other medical applications successfully concluded on March 31, 2022, Harvard has licensed to us certain of its intellectual property relating to lightweight exoskeleton system technologies for lower limb disabilities. We are obligated to use commercially reasonable efforts to develop products under the license in accordance with an agreed-upon development plan and to introduce and market such products commercially.
26
We expect that a percentageportion of total proceeds,our revenue will be derived, in the next few years, from the ReStore soft exo-suit product, other new products utilizing DAP, and, in later years, if we choose to advance the current designs, from other potential new products, such as ReBoot, a home use device for stroke patients, or new products aimed at addressing other medical indications which affect the ability to walk, including multiple sclerosis, cerebral palsy, Parkinson’s disease and elderly assistance. As such, our future results will depend on our ability to successfully develop and commercialize such new products and to penetrate our targeted markets with our existing ReStore product in larger scale than we have done to date. We cannot ensure that we will be able to introduce new products, products currently under development or products contemplated for future development for additional indications in a timely manner, or at all, as it depends on our available resources to fund such projects, as well as our ability to conduct clinical trials and testing. While we received governmental clearance to market our ReStore product on the anticipated timetable in 2019, obtaining clearance for any other products we may develop could be an extensive, costly, and time-consuming process, which could delay any planned commercialization timelines. For more information on the clearance processes for our products, see “Part I, Item 1. Business—Government Regulation” above.
Harvard may terminate its License Agreement with us if we fail to maintain the requisite insurance or become insolvent. Any such termination of this aspect of the collaboration with Harvard could impair our research and development efforts into lightweight soft suit exoskeleton system technologies for lower limb disabilities such as the ReBoot device which is intended to be used at home by people who suffered a stroke. In addition, we may not be able to clinically demonstrate the medical benefits of our products for new indications. We have limited clinical data demonstrating the benefits of our products and we might not be able to support the economic benefits our products have for our potential customers. We may also be unable to gain necessary regulatory clearances or approvals to enable us to market new products for additional indications or the regulatory process may be more costly and time-consuming than expected, which could adversely impact us given our cash position and ongoing capital requirements.
Even if we are successful in the design and development of new products, our growth and results of operations will depend on our ability to penetrate new markets and gain acceptance and reimbursement coverage in non-SCI markets such as the stroke rehabilitation market, and, in the longer term, the home use device market for stroke-caused lower limb disability, multiple sclerosis, elderly assistance and cerebral palsy patients. We may not be able to gain such market acceptance and coverage for these indications in a timely manner, or at all.
While our new products currently under development will share some aspects of the core technology platform of our current products, their design features and components may differ from our current products. Accordingly, these products will also be subject to negotiationthe risks described in the risk factor immediately below entitled “We rely on sales of our ReWalk Personal Exoskeletons, ReStore Exo-Suits, and AlterG Anti-Gravity systems and related service contracts and extended warranties for other potentially-owed fees. Agreements governing any borrowing arrangementour revenue. We may contain covenants that could restrictnot be able to achieve or maintain market acceptance of our ReWalk, ReStore, or AlterG Anti-Gravity products, or to generate sufficient revenue from these current and future products to sustain our operations. In sum, if” To the extent we are unable to obtain additional funds on reasonable terms, it could impair our efforts tosuccessfully develop and commercialize products beyond our existing commercial product portfolio, we will not meet our operating and financial objectives.
We rely on sales of our ReWalk Personal Exoskeletons, ReStore Exo-Suits, and AlterG Anti-Gravity systems and related service contracts and extended warranties for our revenue. We may not be able to achieve or maintain market acceptance of our ReWalk, ReStore, or AlterG Anti-Gravity products or to generate sufficient revenue from these current and future products to sustain our operations.
We currently rely, and expect in the future to rely, on sales of our ReWalk Personal Exoskeleton, ReStore Exo-Suit, and AlterG Anti-Gravity systems, and related service contracts and extended warranties for our revenue. We began marketing the ReStore lightweight soft exo-suit in 2019 in the United States and the E.U. (following the receipt of FDA and CE mark clearance) to support mobility for individuals suffering from other lower limb disabilities. Several factors could negatively affect our ability to achieve and maintain market acceptance of our ReWalk, AlterG, or ReStore systems, which could in turn materially impair our business, financial condition, and operating results, as follows:
| • | ReWalk. We have sold a limited number of ReWalk systems, and market acceptance and adoption depend on educating people with limited upright mobility and health care providers as to the distinct features, ease-of-use, positive lifestyle impact, and other benefits of ReWalk compared to alternative technologies. ReWalk may not be perceived to have sufficient potential benefits compared with these alternatives. Users may also choose other alternatives due to disadvantages of ReWalk, including the time it takes for a user to put on the device, the slower pace of ReWalk compared to a wheelchair, the weight of ReWalk when carried, which makes it more burdensome for a companion to transport than a wheelchair, the required training, and the requirement that users be accompanied by a trained companion. Also, we believe that healthcare providers tend to be slow to change their medical treatment practices because of perceived liability risks arising from the use of new products and the uncertainty of third-party reimbursement. Accordingly, healthcare providers may not recommend ReWalk until there is sufficient support for the device to convince them to alter the treatment methods they typically recommend, such as expanded reimbursement coverage by payors, and/or recommendations by prominent healthcare providers or other key opinion leaders in the spinal cord injury community that ReWalk is effective in providing identifiable immediate and long-term health benefits. |
27
In the United States, many private third-party payors use coverage decisions and payment amounts determined by CMS as guidelines in setting their coverage and reimbursement policies. In July 2020, CMS issued a Healthcare Common Procedure Coding System Level II Code for ReWalk Personal Exoskeleton. These codes are used to identify medical products and supplies and to repayfacilitate insurance claim submissions and processing for these items. On November 1, 2023, CMS issued Calendar Year 2024 Home Health Prospective Payment System Rule CMS-1780, which explicitly included exoskeletons within a Medicare brace benefit category. The rule went into effect on January 1, 2024. However, even with a positive coverage and reimbursement response from CMS regarding a product of ours, future action by CMS or other government agencies may diminish possible payments to clinicians, outpatient centers and/or hospitals that provide training to the patients so that they can operate the ReWalk Personal Exoskeletons satisfactorily before they take them home, which would discourage access to training sites to prospective users of ReWalk Personal Exoskeletons. Additionally, any decision by CMS regarding reimbursement could influence other payors, including private insurers. If CMS declines to provide for reimbursements of our liabilitiesproducts, or if its reimbursement price is lower than that of other payors, our products may not be reimbursed at a cost-effective level or at all. Those private third-party payors that do not follow the Medicare guidelines may adopt different coverage and reimbursement policies for purchase of our products or their use in a hospital or rehabilitative setting. In addition, we expect that the purchase of ReWalk Rehabilitation Exoskeleton systems and the ReStore system, as they become due, materially harmingit is currently being sold for use in rehabilitative settings, will require the approval of senior management at hospitals or rehabilitation facilities, inclusion in the hospitals’ or rehabilitation facilities’ budget process for capital expenditures, and in the case of ReWalk Personal Exoskeleton, fundraising, and financial planning or assistance.
| • | ReStore. The ReStore system is designed to provide advantages to stroke rehabilitation clinics and therapists as compared to other traditional therapies and devices by minimizing setup time, improving patients’ clinical results during therapy, supplying real-time analytics to optimize session productivity, and generating ongoing data reports to assist with tracking patient progress Since the ReStore device is currently only indicated for use in the rehabilitative clinical setting, its market reception will depend heavily on our ability to demonstrate to clinics and therapists the systemic and economic benefits of using the ReStore device, its clinical advantage when compared to other devices or manual therapy, the functionality of the device for a significant portion of the patients that they treat and the overall advantages that the device provides to their patients compared to other technologies. Because the ReStore system is only indicated for use in a clinical setting and we received FDA approval and CE clearance in 2019, close in time to the start of the COVID-19 pandemic, the overall sales of the system have been lower than originally anticipated, as many healthcare providers and rehabilitation centers have shifted focus from the clinical setting to at-home therapies and are generally less open for introduction of new technologies such as the ReStore |
| . | AlterG. The AlterG Anti-Gravity system has broad clinical utility for treating a wide variety of lower extremity conditions where partial displacement of a patient’s weight can enable exercise which facilitates healing and recovery of improved function. The potential of the AlterG Anti-Gravity systems to achieve greater penetration of the addressable market of rehabilitation hospitals, clinics, and sports medicine practices will depend upon the continued expansion of conditions for which clinicians utilize the AlterG and the ability for greater numbers of these facilities to afford the initial capital outlay for these devices. We are developing and hope to introduce in 2024 a new, lower-cost AlterG system, which we believe will make it more affordable for smaller, independent rehabilitation clinics. However, there can be no assurance that the introduction of this product can expand the size of the addressable market or will not reduce the sales of the existing, higher-priced models. |
As a general matter, achieving and maintaining market acceptance of our current or future products could be negatively impacted by many other factors, including, but not limited to the following: contribution to death or serious injury or malfunction, results of operationsclinical studies relating to our or similar products; claims that our products, or any of their components, infringe on patent or other intellectual property rights of third parties; our ability to support financially and leverage our sales, marketing and training infrastructure, as well as our level of research and development efforts; our ability to enhance and broaden our research and development efforts and product offerings in response to the evolving demands of people with paraplegia and lower limb disability and healthcare providers; our estimates regarding our current or future addressable market; perceived risks associated with the use of our products or similar products or technologies; the introduction of new competitive products or greater acceptance of competitive products; adverse regulatory or legal actions relating to our products or similar products or technologies; and problems arising from the outsourcing of our manufacturing capabilities, or our existing manufacturing and supply relationships. Any or all of these factors could materially and negatively impact our business, financial condition.condition and operating results.
28
The market for medical exoskeletons, including soft suit devices, isremains relatively new and unproven, and important assumptions about the potential market for our current and future products may be inaccurate.
The market for medical exoskeletons, isincluding lightweight exo-suit devices, remains relatively new and unproven. Accordingly, it is difficult to predict the future size and rate of growth of the market. We cannot be certain whether the market will continue to develop or if medical exoskeletons will achieve and sustain a level of market acceptance and demand sufficient for us to continue to generate revenue and achieve profitability.
We obtained FDA clearance for our ReWalk Personal Exoskeleton device in June 2014. This clearance permits us to market the device for use by individuals with spinal cord injury at levels T7 to L5 and for use by individuals in rehabilitation institutions with spinal cord injury at levels T4 to L5. The FDA’sT6. We obtained FDA clearance requires users offor our ReStore system in June 2019. This clearance permits us to market the device to meet the following criteria: healthy hands and shoulders that can support crutches, healthy bone density, no skeletal fractures,be used to assist ambulatory functions in good general health, ability to standrehabilitation institutions under supervision of a trained therapist for people with a stander device, weight of less than 220 pounds/100 kilograms and height between 5 feet 3 inches and 6 feet 2 inches/1.60 meters and 1.88 meters. Additionally, the FDA clearance contraindicates psychiatrichemiplegia or cognitive conditions that could interfere with a user’s proper operation of the device and various other clinical conditions, including pregnancy, severe concurrent medical diseases, a history of severe neurological injuries other than spinal cord injury, impaired joint mobility, unhealed limbs or pelvic fractures or unstable spine, severe spasticity and significant and chronic loss of joint mobilityhemiparesis due to structural changes in non-bony tissue. stroke who can ambulate at least 1.5 meters (5 feet) with no more than minimal to moderate levels of assistance.
Future products for those with paraplegia or other mobility impairments or spinal cord injuries such as our Restore product for stroke patients, may have the same or other restrictions.
Our business strategy is based, in part, on our estimates of the number of mobility impaired individuals with physical limitations and disability and considers the incurrenceoccurrence of spinal cord injuries, strokes, lower-extremity orthopedic injury or surgery, neurological disease, and obesity in our target markets, and the percentage of those groups that would be able to use our current and future products. Limited sources exist to obtain reliable market data with respect to the number of mobility-impaired individuals and the incurrence of spinal cord injuries and strokes in our target markets. In addition, there are no third-party reports or studies regarding what percentage of those with limited mobility and/or spinal cord injuries would be able to use exoskeletons, in general, or our current or planned future products, in particular. Our assumptions may be inaccurate and may change.
The NSCISC estimates according to its 2023 SCI Data Sheet that as of 2017 there were 285,000are 302,000 people in the United States living with SCI, and that thewith an annual incidence of SCI cases is approximately 17,50018,000 new cases per year. Based on information from a 2016the 2022 annual report published by the NSCISC, 40.6%40% of the total U.S. population of SCI patients suffered injuries between levels T4 and L5. ThreeFour published ReWalk trials with respect to such eligible SCI patients had an aggregate screening acceptance rate of 79%50% considering all current FDA limitations, resulting in an estimated 33%20% of the total population of SCI patentspatients being qualified candidates for current ReWalk products.products under its medical labeling criteria. There may be other permanent or short-term factors that affect the market size such as the ability to participate in the training program, the ability to use the device in the user’s current home environment as well as available companion support. With regards to our ReStore product for stroke rehabilitation, as the indication of use is currently in rehabilitation clinics our target market is based on the number of current and future clinics who treat stroke patients. Although there are thousands of inpatient, outpatient and rehabilitation clinics providing therapy in the U.S. for example, we currently see that only a limited portion of the clinics have decided to include ReStore in their stroke rehab program. For more information on our expectations regarding these plans, see “-Our“—Our future growth and operating results will depend on our ability to develop, receive regulatory clearance for and commercialize new products and penetrate new product and geographic markets” below. For more information regarding the potential market for future products, including our lightweight soft suit exoskeleton, see “Item“Part I, Item 1. Business-Market Opportunity.”Business—ReWalk Personal and ReWalk Rehabilitation Products—Market Opportunity” above.
We cannot assure you that our estimate regarding our current products is accurate or that our estimate regarding future products will remain the same. FDA or CE mark clearance for such products, if received at all, may contain different limitations from the ones the FDA or EU has placed on the devices we currently market for paraplegia patients.paraplegia. If our estimates of our current or future addressable market are incorrect, our business may not develop as we expect, and the price of our securities may suffer.
29
We may fail to secure or maintain adequate insurance coverage or reimbursement for ReWalkour products by third-party payors, which risk may be heightened if insurers find ReWalkthe products to be investigational or experimental or if new government regulations change existing reimbursement policies. Additionally, such coverage or reimbursement, even if maintained, may not produce revenuesrevenue that are high enough to allow us to sell our products profitably.
We expect that in the future a significant source of payment for ReWalk systems will be private insurance plans and managed care programs, government programs such as the VA, Medicare and Medicaid, worker’sVHA, CMS, workers’ compensation plans, and other third-party payors.
In December 2015, the VAVHA issued a national reimbursement policy for the ReWalk system, which entails the evaluation, training and procurement of ReWalk Personal exoskeletonExoskeleton systems for all qualifying veterans across the United States. Additionally, in September 2017, German insurer Barmer and national social accident insurance provider DGUV each signed a confirmation and letter of agreement regarding the provision of ReWalk systems for all qualifying beneficiaries.beneficiaries and the German national social accident insurance provider DGUV indicated that its member payors will approve the supply of exoskeleton systems for qualifying beneficiaries on a case-by-case basis. However, no broad uniform policy of coverage and reimbursement for electronic exoskeleton medical technology exists among third-party payors in the United States, although reimbursement may be achieved on a case-by-case basis. To date, payments for our products, which are largely for our ReWalk systems, have been made primarily through case-by-case determinations by third-party payors (including several private insurers in the United States), by self-payors and, to a lesser extent, through the use of funds from insurance and/or accident settlements.
Generally, private insurance companies in the United States do not cover or provide reimbursement for any medical exoskeleton products for personal use, including ReWalk Personal Exoskeleton, and may ultimately provide no coverage at all. For instance, during 2017 we submitted a proposal to a large U.S. national insurance provider for a broader coverage policy for the ReWalk Personal device. While we believe there was support for a change, the insurer was unable to reach internal consensus and therefore elected not change its existing non-coverage policy. Additionally, there is limited clinical data related to the ReWalk and ReStore systems, and third-party payors may consider use of ReWalkthem to be experimental and therefore refuse to cover it. For example, Aetna has determined that certain lower-limb prostheses, including ReWalk, are experimental and investigational because there is inadequate evidenceany or all of their effectiveness.them. Additionally, the majority of independent medical review decisions to date made following the denial of ReWalk coverage have determined that ReWalk is experimental and/or investigational, citing a lack of clinical data.
However, even with a positive coverage and reimbursement response from CMS will broaden coverage by private insurers, we cannot currently predict how long it would take for us to receiveregarding a decision from CMS. Even with a positive decision from CMS regarding ReWalk Personal,product of ours, future action by CMS or other government agencies may diminish possible payments to physicians, outpatient centers and/or hospitals that purchase ReWalk Rehabilitation,our products for use by their patients and possible payments to individuals who purchase the ReWalk Personal.Personal Exoskeleton for their own use. Additionally, a decision by CMS to provide reimbursement could influence other payors, including private insurers. If CMS declines to provide for reimbursements of ReWalkour products or if its reimbursement price is lower than that of other payors, ReWalkour products may not be reimbursed at a cost-effective level or at all. Those private third-party payors that do not follow the Medicare guidelines may adopt different coverage and reimbursement policies for purchase of ReWalk,our products or their use of ReWalk Rehabilitation atin a hospital or rehabilitation center.rehabilitative setting. In addition, we expect that the purchase of ReWalk Rehabilitation Exoskeleton systems and the ReStore system, as it is currently being sold for use in rehabilitative settings, will require the approval of senior management at hospitals or rehabilitation facilities, inclusion in the hospitals’ or rehabilitation facilities’ budget process for capital expenditures, and in the case of ReWalk Personal Exoskeleton, fundraising, and financial planning or assistance.
Third-party payors are developing increasingly sophisticated methods of controlling healthcare costs. These cost control methods include prospective payment systems, capitated rates, benefit redesigns and an exploration of other cost-effective methods of delivering healthcare. These cost control methods potentially limit the amount that healthcare providers may be willing to pay for electronic exoskeleton medical technology if they provide coverage at all. We may be unable to sell ReWalk systemsour products on a profitable basis if third-party payors deny coverage or provide insufficient levels of reimbursement.
Future legislation could result in modifications to the existing public and private health care insurance systems that would have a material adverse effect on the reimbursement policies discussed above. It is uncertain what impact the new U.S. presidential administration will have on healthcare spending. If enacted and implemented, any measures to restrict health care spending could result in decreased revenue from our products and decrease potential returns from our research and development initiatives.
Defects in our products or the software that drives them could adversely affect the results of Contents
our operations.In addition, our products incorporate sophisticated computer software and hardware. Complex software frequently contains errors, especially when first introduced. Our software may experience errors or performance problems in the future. If any part of our product’s hardware or software were to fail, the user could experience death or serious injury. For example, in 2021 ReWalk submitted medical device reports to the FDA and medical device vigilance reports to the European regulatory authorities and initiated a correction in response to two complaints regarding battery thermal runaway events. The correction that includes clarification of previous instructions and additional information on battery operation and storage is closed in Europe until 2012. We began selling ReWalk Personaland in the United StatesStates. ReWalk has separately initiated a design project to improve power management and battery operation during charge and discharge, and this project remains in process. Additionally, users may not use or maintain our products in accordance with safety, storage, and training protocols, which could enhance the risk of death or injury. Any such occurrence could cause delay in market acceptance of our products, damage to our reputation, the need for additional regulatory filings, product recalls, increased service and warranty costs, product liability claims, and loss of revenue relating to hardware or software defects.
The medical device industry has historically been subject to extensive litigation over product liability claims. We have been and anticipate that as part of our ordinary course of business we may be subject to product liability claims alleging defects in the third quarterdesign, manufacture, or labeling of 2014, asany of our products which has resulted in an injury or death. A product liability claim, regardless of its merit or eventual outcome, could result in significant legal defense costs and high punitive damage payments. Although we received FDA clearancemaintain product liability insurance, the coverage is subject to do so in June 2014. Therefore, we have limited operating history upon which you can evaluate our business plandeductibles and prospects. Our business planlimitations, and prospects must be considered in light of the potential problems, delays, uncertainties and complications encountered in connection with a more newly established business. The risks include, but are not limited to, that:
If we are unable to leverage our sales, marketing, and training infrastructure including in light of our reduced corporate spending, we may fail to increase our sales.
A key element of our long-term business strategy is the continued leveraging of our sales, marketing, training, and reimbursement
infrastructure, through the training, retainingretention, and motivatingmotivation of skilled sales and marketing representatives and reimbursement personnel with industry experience and knowledge. Our ability to derive revenue from sales of our products depends largely on our ability to market the products and obtain reimbursements for them. In order to continue growing our business efficiently, we must therefore coordinate the development of our sales, marketing, training and reimbursement infrastructure with the timing of regulatory approvals, decisions regarding reimbursements, limited resources consideration and other factors in various geographies. Managing and maintaining our sales and marketing infrastructure is expensive and time consuming, and an inability to leverage such an organization effectively, or in coordination with regulatory or other developments, could inhibit potential sales and the penetration and adoption of ReWalkour products into both existing and new markets. In addition, in early 2017 we announced our plans to reduce operation expenses by up to 30% compared to 2016, in part through a realignment of and reduction in staffing to match our 2017 business goals. We intend to continue funding field sales, service and training efforts for our ReWalk products. However, certain decisions we make regarding staffing in these areas in our efforts to decrease expensesmaintain an adequate spending level could have unintended negative effects on our revenues,revenue, such as by weakening our sales infrastructure, impairing our reimbursement efforts and/or harming the quality of our customer service. For instance, the number of our staff focused on reimbursement has decreased, and in 2017, we consolidated the functions of two employees that previously focused on reimbursement into the roles of certain executive officers and employees in other departments. Additionally, our Chief Commercial Officer recently passed away in October 2017 and her position was divided between several existing management functions. Throughout 2018, we will continue to evaluate spending to reduce where possible.
31
Additionally, we expect to face significant challenges as we manage and continue to improve our sales and marketing infrastructure and work to retain the individuals who make up those networks. Newly hired sales representatives require training and take time to achieve full productivity. If we fail to train new hires adequately, or if we experience high turnover in our sales force in the future, we cannot be certain that new hires will become as productive as may be necessary to maintain or increase our sales. Likewise, following our acquisition of AlterG in August 2023 and in connection with integrating AlterG with ReWalk, each set of sales representatives had to learn how to sell new products and services. In addition, if we are not able to retain subjectexisting and recruit new trainers to our plans to cut operating expenses, and continue to recruit our network of internal trainers,clinical staff, we may not be able to successfully train customers on the use of ReWalk, ReStore, or AlterG systems which could inhibit new sales and harm our reputation. If we are unable to expand our sales, marketing, and training capabilities, we may not be able to effectively commercialize ReWalk,our products, or enhance the strength of our brand, which could have a material adverse effect on our operating results.
The potential health benefits of our ReWalk products have not been substantiated by long-term clinical data, which could limit sales.sales of such products.
Although study participantspublished research and otherusers of our ReWalk usersproducts have reported the potential secondary health benefits of our ReWalk products such as a reduction in pain and spasticity, improved bowel and urinary tract functions and emotional and psychosocial benefits, among others, currently there is no conclusivelarge scale, randomized clinical datatrial establishing anythe secondary health benefits of ReWalk.ReWalk products due to the relatively small size of the applicable user population. There is also a lack of randomized clinical data for such health benefits of the ReStore-specifically its long-term benefits following the usage of the product within the clinic as the trials conducted to date using this product are limited.
As a result, potential customers and healthcare providers may be slower to adopt or recommend ReWalk products or ReStore and third-party payors may not be willing to provide coverage or reimbursement for our products. In addition, future studies or clinical experience may indicate that treatment with our current or future ReWalk products is not superior to treatment with alternative products or therapies. Such results could slow the adoption of our products and significantly reduce our sales.
We depend on a single third partythird-party supplier to manufacture ReWalksome of our products, and we rely on a limited number of third-party suppliers for certain components of ReWalk.our products.
We have contracted with Sanmina, Corporation, a well-established contract manufacturer with expertise in the medical device industry, for the manufacture of all of our productsReWalk and ReStore systems and the sourcing of all of our components and raw materials. Pursuant to this contract, Sanmina manufactures ReWalk, pursuant to our specifications, at its facility in Ma’alot, Israel.materials for those products. We may terminate our relationship with Sanmina at any time upon written notice. In addition, either we or Sanmina may terminate the relationship in the event of a material breach, subject to a 30-day cure period. For our business strategy to be successful, Sanmina must be able to manufacture our products in sufficient quantities, in compliance with regulatory requirements and quality control standards, in accordance with agreed upon specifications, at acceptable costs and quality levels, and on a timely basis. Increases in our product sales, whether forecasted or unanticipated, could strain the ability of Sanmina to manufacture an increasingly large supply of our current or future products in a manner that meets these various requirements. In addition, although we are not restricted from engaging an alternative manufacturer, and potentially have the capabilities to manufacture ReWalkour products in-house, the process of moving our manufacturing activities would be time consuming and costly, and may limit our ability to meet our sales commitments, which could harm our reputation and could have a material adverse effect on our business. Moreover, the failure of Sanmina to comply with applicable regulatory requirements could expose us to regulatory action including warning letters, product recalls, termination of distribution, product seizures or civil penalties.
We also rely on third-party suppliers, many of which contract directly with Sanmina, to supply certain components of ReWalk.our products, and in some cases, we purchase these components ourselves. In our factory in Fremont, California, where we manufacture our AlterG products, we also rely on third-party suppliers for key components of our products. Neither Lifeward nor Sanmina does not havehas long-term supply agreements with most of itsthe suppliers and, in many cases, makesmake purchases on a purchase order basis. Sanmina’sbasis and our ability to secure adequate quantities of such products may be limited. Suppliers may encounter problems that limit their ability to manufacture components for our products, including financial difficulties or damage to their manufacturing equipment or facilities. If Lifeward or Sanmina fails to obtain sufficient quantities of high qualityhigh-quality components to meet demand on a timely basis, we could lose customer orders, our reputation may be harmed, and our business could suffer.
Our results of operations and liquidity could be adversely impacted by supply chain disruptions and operational challenges faced by our manufacturer or suppliers. Sanmina generally uses a small number of suppliers for ReWalk.ReWalk and ReStore. Our manufacturing operations for AlterG also utilize a limited number of suppliers, some of which are the sole suppliers to us of such supplies. Depending on a limited number of suppliers exposes us to risks, including limited control over pricing, availability, quality, and delivery schedules. Such risks were heightened in light of the interruptions in supply chains and distribution networks related to the COVID-19 pandemic. For example, as a result of the COVID-19 pandemic, several components, mainly electronic parts, experienced price increases. If any one or more of our suppliers ceases to provide sufficient quantities of components in a timely manner or on acceptable terms, we or Sanmina would have to seek alternative sources of supply.supply or accept price increase as we saw during the pandemic. It may be difficult to engage additional or replacement suppliers in a timely manner. Failure of these suppliers to deliver products at the level our business requires would limit our ability to meet our sales commitments, which could harm our reputation and could have a material adverse effect on our business. We or Sanmina also may have difficulty obtaining similar components from other acceptable suppliers, that are acceptable to the FDA or other regulatory agencies, and the failure of Sanmina’s suppliers to comply with strictly enforced regulatory requirementswhich could expose us to regulatory action including warning letters, product recalls, termination of distribution, product seizures or civil penalties. It could also require Sanmina or us to cease using the components, seek alternative components or technologies and we could be forced to modify our products to incorporate alternative components or technologies, which could result in a requirement to seek additional regulatory clearances or approvals. Any disruption of this nature or increased expenses could harm our commercialization efforts and adversely affect our operating results.
We operate in a competitive industry that is subject to rapid technological change, and we expect competition to increase.
There are several other companies developing technology and devices that compete with ReWalk.our products. Our principal competitors in the medical exoskeleton market consist of Ekso Bionics, Parker Hannifin, Rex Bionics, Cyberdyne, FREE Bionics, Wandercraft, and others. These companies have products currently available for institutional use and in some cases personal use. We expect some of such products to become available for personal use in the next few years.years, especially as we continue to expand coverage by different payors and geographies. In addition, we compete with alternative devices and alternative therapies, including treadmill-based gait therapies, such as those offered by Hocoma, AlterG,DIH (formerly known as Hocoma), Boost, Aretech, BTL, Reha Technology, and Reha Technology.Bioness, which is a unit of Bioventus. Our competitor base may change or expand as we make effortscontinue to develop and commercialize our soft suit exoskeleton product in the future. These or other medical device or robotics companies, academic and research institutions, or others, may develop new technologies or therapies that provide a superior walking and usage experience, are more effective in treating the secondary medical conditions that we target or are less expensive than ReWalk, ReStore, AlterG, or future products. Our technologies and products could be rendered obsolete by such developments. We may also compete with other treatments and technologies that address the secondary medical conditions that ReWalk seeksour products seek to mitigate.
Our competitors may respond more quickly to new or emerging technologies, undertake more extensive marketing campaigns, have greater financial, marketing, and other resources than we do or may be more successful in attracting potential customers, employees, and strategic partners. In addition, potential customers, such as hospitals and rehabilitation centers, could have long-standing or contractual relationships with competitors or other medical device companies. Potential customers may be reluctant to adopt ReWalk, ReStore, or AlterG, particularly if it competes with or has the potential to compete with or diminish the need/utilization of products or treatments supported through these existing relationships. If we are not able to compete effectively, our business and results of operations will be negatively impacted.
33
In addition, because we operate in a new market, the actions of our competitors could adversely affect our business. Adverse events such as product defects or legal claims with respect to competing or similar products could cause reputational harm to the exoskeleton market on the whole. Further, adverse regulatory findings or reimbursement-related decisions with respect to other exoskeleton products could negatively impact the entire market and, accordingly, our business.
We have incurred net losses since our inception.
While we expect that the percentage of our sales generated from independent distributors will decrease over time as we continue to focus our resources on achieving reimbursement within our direct markets in the United States in response to the receipt of FDA clearance for ReWalk Personal and in Europe, with the CE mark clearance, we believe that a meaningful percentageindependent distributors of our salesthe ReWalk or ReStore products will continue to be generated by independent distributorsan important distribution channel for us in the future. None of our independent distributors has been required to sell our products exclusively. Our distributor agreements with these distributors generally have one-year initial terms and automatic renewals for an additional year. If any of our key independent distributors of the ReWalk or ReStore products were to cease to distribute our products, our sales could be adversely affected. In such a situation, we may need to seek alternative independent distributors or increase our reliance on our other independent distributors or our direct sales representatives, which may not prevent our sales from being adversely affected. Additionally, to the extent that we enter into additional arrangements with independent distributors to perform sales, marketing, or distribution services, the terms of the arrangements could cause our product margins to be lower than if we directly marketed and sold our products.
We may receive a significant number of warranty claims or our ReWalk, systemReStore, or AlterG systems may require significant amounts of service after sale.
Sales of ReWalk generally include a two-yearfive-year warranty for parts and services, other than for normal wear and tear. We alsoSome of our active devices were delivered prior to 2019 with a two-year warranty so we provide these customers with the option to purchase an extended warranty for up to an additional three years. In the beginning of 2018 we updated our service policyOur ReStore product offering includes a two-year warranty for new devicesparts and services. The AlterG Anti-Gravity systems are sold to include 5 years warranty.with a one-year factory warranty covering parts and services. If product returns or warranty claims are significant or exceed our expectations, we could incur unanticipated expenditures for parts and services, which could have a material adverse effect on our operating results.
We may not be able to enhance our exoskeleton product offerings through our research and development efforts.
In order to increase our sales and our market share in the exoskeleton market, we mustare working to enhance and broaden our research and development efforts and product offerings in response to the evolving demands of people with paraplegia, or paralysis, other medical conditions and healthcare providers, as well as competitive technologies. We are also currently involved in ongoing research and development efforts directed to the needs of patients with other mobility impairments, such as stroke, and multiple sclerosis. In thebegan commercializing our ReStore product for stroke patients in 2019. Depending on our future resources and business focus, we plan to address these needs in patients with other conditions or devices for stroke patients to be used at home, improving our current products, or developing products to address additional medical conditions such as multiple sclerosis, Parkinson’s disease or cerebral palsy and support elderly assistanceassistance. We may decide to invest our business development resources in partnerships, licensing agreements, business acquisition and cerebral palsy.other ways that will provide us new product offerings without significant research and development activities. We may not be successful in developing, obtaining regulatory approval for, or marketing our currently proposed products, andor our approved products for additional indications, products proposed to be created in the future.future or products that will be available for us through business acquisitions. In addition, notwithstanding our market research efforts, our future products may not be accepted by consumers, their caregivers, healthcare providers or third-party payors who reimburse consumers for our products. The success of any proposed product offerings will depend on numerous factors, including our ability to:
identify the product features that people with paraplegia or paralysis, their caregivers, and healthcare providers are seeking in a medical device that restores upright mobility and successfully incorporate those features into our products;
identify the product features that people with stroke, multiple sclerosis or other similar indications require while the products are used at home as well as what items are valuable to the clinics that provide them rehabilitation;
develop and introduce proposed products in sufficient quantities and in a timely manner;
adequately protect our intellectual property and avoid infringing upon the intellectual property rights of third-parties;
34
demonstrate the safety, efficacy, and health benefits of proposed products; and
obtain the necessary regulatory clearances and approvals for proposed products.
If we fail to generate demand by developing products that incorporate features desired by consumers, their caregivers or healthcare providers, or if we do not obtain regulatory clearance or approval for proposed products in time to meet market demand, we may fail to generate sales sufficient to achieve or maintain profitability. We have in the past experienced, and we may in the future experience, delays in various phases of product development, including during research and development, manufacturing, limited release testing, marketing, and customer education efforts. Such delays could cause customers to delay or forgo purchases of our products, or to purchase our competitors’ products. Even if we are able to successfully develop proposed products when anticipated, these products may not produce sales in excess of the costs of development, and they may be quickly rendered obsolete by changing consumer preferences or the introduction by our competitors of products embodying new technologies or features.
We may enter into collaborations, in-licensing arrangements, joint ventures, strategic alliances, business acquisitions or partnerships with third-partiesthird parties that may not result in the development of commercially viable products or the generation of significant future revenues.revenue.
In the ordinary course of our business, in the future we may enter into collaborations, in-licensing arrangements, joint ventures, strategic alliances, business acquisitions, partnerships or partnershipsother arrangements to develop ReWalkour products and to pursue new geographic or product markets. Proposing, negotiating, and implementing collaborations, in-licensing arrangements, joint ventures, strategic alliances, or partnerships may be a lengthy and complex process. Other companies, including those with substantially greater financial, marketing, sales, technology or other business resources, may compete with us for these opportunities or arrangements. We may not identify, secure, or complete any such transactions or arrangements in a timely manner, on a cost-effective basis, on acceptable terms or at all. We have limited institutional knowledge and experience with respect to these business development activities, and we may also not realize the anticipated benefits of any such transaction or arrangement. In particular, these collaborations may not result in the development of products that achieve commercial success or result in significant revenuesrevenue and could be terminated prior to developing any products. For example, we have entered into arrangementsagreements with YaskawaMediTouch and MYOLYN for the distribution of ourtheir products in certain Asian markets. We alsothe U.S. After several years of commercial collaboration, we determined that the agreement with MediTouch would not yield commercially acceptable results for us and we terminated the agreement as of January 31, 2023. Similarly, the distribution arrangement with MYOLYN or other new future arrangements may not be as productive or successful as we hope.
On May 16, 2016, we entered into the Collaboration Agreement and License Agreement with Harvard. Pursuant to the Collaboration Agreement, we have agreed to collaborate with Harvard University’s Wyss Institute for Biologically Inspired Engineering for the research, design, development, and commercialization of lightweight exoskeleton system technologies for lower limb disabilities, aimed to treat stroke, multiple sclerosis, mobility limitations for the elderly and other medical applications. Additionally,The Collaboration Agreement concluded on March 6, 2018, as part31, 2022. The License Agreement will continue in full force and effect until the expiration of our private placementthe last-to-expire valid claim of ordinary shares to Timwell, a Hong Kong entity, we agreed to collaborate with an affiliate of Timwell in forming a joint venture in China for the purposes of assembly, registration, operations, sales, and marketing of our products in China (including Hong Kong and Macau), and to grant to the joint venture, in accordance with the terms of an agreed form of license agreement, an exclusive license for certain of our patent rights marks and a non-exclusive sublicense for certain Company-controlled know-how.licensed patents. For more information on the collaboration with Harvard, see “Part I. Item 1. Business-Timwell Investment AgreementBusiness - Research and Related Transactions.”
Additionally, as we pursue these arrangements and choose to pursue other collaborations, in-licensing arrangements, joint ventures, strategic alliances, or partnerships in the future, we may not be in a position to exercise sole decision makingdecision-making authority regarding the transaction or arrangement. This could create the potential risk of creating impasses on decisions, and our collaborators may have economic or business interests or goals that are, or that may become, inconsistent with our business interests or goals. It is possible that conflicts may arise with our collaborators. Our collaborators or any future collaborators may act in their self-interest, which may be adverse to our best interest, and they may breach their obligations to us. Any such disputes couldDisputes between us and our collaborators or any future collaborators may result in litigation or arbitration which would increase our expenses and divert the attention of our management. Further, these transactions and arrangements are contractual in nature and may be terminated or dissolved under the terms of the applicable agreements.
35
We may seek to grow our business through acquisitions of complementarybusinesses, products or technologies, and the failure to manage acquisitions, or the failure to integrate them with our existing business, could have a material adverse effect on our business, financial condition, and operating results.
From time to time, we may consider opportunities to acquire or license other products or technologies that may enhance our product platform or technology, expand the breadth of our markets or customer base, or advance our business strategies. For example, as discussed above in “Part I. Item 1. Business - Overview”, on August 11, 2023, we completed the acquisition of AlterG, and AlterG became an indirect and wholly-owned subsidiary of the Company. Potential acquisitions involve numerous risks, including:
| ● | problems assimilating the acquired products or technologies; |
| ● | issues maintaining uniform standards, procedures, controls and policies; |
| ● | problems integrating employees from an acquired organization into our company and integrating each company’s accounting, management information, human resources and other administrative systems; |
| ● | unanticipated costs associated with acquisitions; |
| ● | diversion of management’s attention from our existing business operations; |
| ● | potential incurrence of debt, contingent liabilities or amortization expenses, or write-offs of goodwill; |
| ● | risks associated with entering new markets in which we have limited or no experience; and |
| ● | increased legal and accounting costs relating to the acquisitions or compliance with regulatory matters. |
We have no current commitments with respect to any acquisition.acquisition or licensing. We do not know if we will be able to identify such acquisitions or licensing we deem suitable, whether we will be able to successfully complete any such acquisitionstransactions on favorable terms, or at all, or whether we will be able to successfully integrate any acquired products or technologies. Our potential inability to integrate any acquired products or technologies effectively may adversely affect our business, operating results, and financial condition.
For more information, see Note 7ethe risk factor above entitled “Risks Related to Our Business and Our Industry – We may fail to realize the benefits expected from our consolidated financial statements set forth in "Part II. Item 8. Financial Statements and Supplementary Data"acquisition of this annual report.
Risks Related to Government Regulation
However, achieving Breakthrough Device Designation status does not guarantee regulatory clearance or approval or a speedier clearance or approval timeline. We have not yet submitted a premarket submission to the FDA or any incident in which our product may have caused or contributed to a death or serious injury or in which our product malfunctioned and, if the malfunction were to recur, our product or a similar device marketed by us would be likely to cause or contribute to death or serious injury. In addition, all manufacturers placing medical devices in European Union markets are legally bound to report any serious or potentially serious incidents involving devices they produce or sell to the relevant authority in whose jurisdiction the incident occurred. Since 2013, we have submitted nine MDRs to report incidents in which ReWalk Personal users sustained falls or fractures; 4 of these were submitted in 2017. The FDA sent us letters requesting additional information relating to these MDRs submitted in 2017, including a requestforeign regulatory agency for a failure analysis. We initiated a voluntary correction for the ReWalk device that related to certain use instructions to reduce the risk of fractures and submitted a report to the FDA under 21 CFR Part 806, (“Part 806”). Under Part 806, manufacturers and importers are required to make a report to the FDA of any correction or removal of a device if the correction or removal was initiated to reduce a risk to health posed by the device or to remedy a violation of the FFDCA caused by the device which may present a risk to health. We are currently evaluating potential labeling and design modifications to the ReWalk to mitigate the risk of fractures, and believe the implementation of these modifications will trigger the need for a new 510(k).
U.S. healthcare reform measures and other potential legislative initiatives could adversely affect our business.
Recent political changes in the United States could result in significant changes in, and uncertainty with respect to, legislation, regulation, global trade, and government policy that could substantially impact our business and the medical device industry generally. Certain proposals, if enacted into law, could impose limitations on the prices we will be able to charge for our ReWalk system or any products we may develop and offer in the futire,future, or the amounts of reimbursement available for such products from governmental agencies or third-party payers.payors. Additionally, any reduction in reimbursement from Medicare or other government-funded federal programs, including the VA,VHA, or state healthcare programs could lead to a similar reduction in payments from private commercial payors. The FDA’s policies may also change, and additional government regulations may be issued that could prevent, limit, or delay regulatory approval of our future products, or impose more stringent product labeling and post-marketing testing and other requirements. For instance,
We expect that changes or additions to the ACA or the Medicare and Medicaid programs, changes allowing the federal government to directly negotiate drug prices and changes stemming from other healthcare reform measures, especially with regard to healthcare access, financing or other legislation in September 2017, membersindividual states, could have a material adverse effect on the healthcare industry.
36
Other legislative changes have been proposed and adopted since passage of the U.S. Congress introduced legislation with the announced intention to repeal and replace major provisions of the PPACA. Although this proposed legislation ultimately failed to pass, Congress succeeded in repealing the PPACA’s individual mandate as part of the U.S. Tax Cuts and JobsACA. The Budget Control Act of 2017.2011, among other things, created the Joint Select Committee on Deficit Reduction to recommend proposals in spending reductions to Congress. The Joint Select Committee did not achieve its targeted deficit reduction of an amount greater than $1.2 trillion for the fiscal years 2012 through 2021, triggering the legislation’s automatic reductions to several government programs. These reductions included aggregate reductions to Medicare payments to healthcare providers of up to 2% per fiscal year. This 2% reduction was temporarily suspended during the pandemic, but has since been reinstated and, unless Congress and/or the Administration take additional action, will begin to increase gradually starting in April 2030, reaching 4% in April 2031, until sequestration ends in October 2031. On January 2, 2013, the American Taxpayer Relief Act was signed into law, which, among other things, reduced Medicare payments to several types of providers, including hospitals, imaging centers, and cancer treatment centers, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. The 2022 Inflation Reduction Act, among other things, directs CMS to engage in price-capped negotiation for certain drugs and biologics that CMS reimburses under Medicare Part B and Part D, penalizes drug manufacturers that increase prices of Medicare Part B and Part D drugs at a rate greater than the rate of inflation, and redesigns the Part D drug benefit, effective in 2025.
The implementation of cost containment measures or other healthcare reforms may thus prevent us from being able to generate revenue, attain profitability or further commercialize our existing ReWalk systems or future ReWalk products. We are currently unable to predict what additional legislation or regulation, if any, relating to the health care industry may be enacted in the future or what effect recently enacted federal legislation or any such additional legislation or regulation would have on our business. The pendency or approval of such proposals or reforms could result in a decrease in our stock price or limit our ability to raise capital or to enter into collaboration agreements for the further development and commercialization of our programs and products.
Our sales and Cosmetic Act (the “FFDCA”), based on our failuremarketing efforts, as well as promotions, are subject to initiate a postmarket surveillance study by the September 28, 2015 deadline, our allegedly deficient protocol for that study,various laws and the lack of progressregulations. Medical device promotions must be consistent with and communication regarding the study. Between June 2014 and our receipt of the September 2015 Warning Letter, we had responded latenot contrary to certain FDA’s requests related to our study protocol. In February 2016, the FDA sent us an additional information request, or the February 2016 Letter, requesting additional changes to our study protocol and asking that we amend the study within 30 days. This letter also discussed the FDA’s request, as further discussed in later communications with the FDA, for a new premarket notification for our ReWalk device, or a special 510(k), linked to what the FDA viewed as changes to the labeling and the indication for use, be truthful and not false or misleading, and be adequately substantiated. In addition to the requirements applicable to 510(k)-cleared products, we may also be subject to enforcement action in connection with any promotion of an investigational new device. A sponsor or investigator, or any person acting on behalf of a sponsor or investigator, may not represent in a promotional context that an investigational new device including to a computer included withis safe or effective for the purposes for which it is under investigation or otherwise promote the device. In late March 2016, following multiple discussions
Our marketing and promotional materials are subject to FDA scrutiny to ensure that the device is being marketed in compliance with these requirements. If the FDA including an in-person meeting, the FDA confirmedinvestigates our marketing and promotional materials and finds that the agency would permit the continued marketing of the ReWalk device conditioned upon our timely submitting a special 510(k) and initiating our postmarket surveillance study by June 1, 2016. The special 510(k) was timely submitted on April 8, 2016, and the FDA’s substantial equivalence determination was received by us on July 22, 2016, granting us permission to continue marketing the ReWalk device. Additionally, we submitted a protocol to the FDA for the postmarket surveillance study that was approved by the FDA on May 5, 2016.
We are subject to extensive governmental regulations relating to the manufacturing, labeling, and marketing of our products, and a failure to comply with such regulations could lead to withdrawal or recall of our products from the market.
Our medical products and manufacturing operations are subject to regulation by the FDA, the European Union, and other governmental authorities both inside and outside of the United States. These agencies enforce laws and regulations that govern the development, testing, manufacturing, labeling, storage, installation, servicing, advertising, promoting, marketing, distribution, import, export and market surveillance of ReWalk.our products.
Our products are regulated as medical devices in the United States under the FFDCA as implemented and enforced by the FDA. Under the FFDCA, medical devices are classified into one of three classes (Class I, Class II or Class III) depending on the degree of risk associated with the medical device, what is known about the type of device, and the extent of control needed to provide reasonable assurance of safety and effectiveness. Classification of a device is important because the class to which a device is assigned determines, among other things, the necessity and type of FDA review required prior to marketing the device. For more information, see “Part I.I, Item 1. Business-Government Regulation” above.
37
In June 2014, the FDA granted our petitionrequest for “de novo”“de novo” classification, which provides a route to market for medical devices that are low to moderate risk, but are not substantially equivalent to a predicate device, and classified ReWalk as Class II powered exoskeleton device subject to certain special controls. In March 2023 the FDA granted 510(k) clearance for the ReWalk Personal Exoskeleton with stair and curb functionality, which adds usage on stairs and curbs to the indication for use for the device in the U.S. The ReWalk is intended to enable individuals with spinal cord injuries to perform ambulatory functions under supervision of a specially trained companion, and inside rehabilitation institutions. The special controls established in the de novo order for all powered exoskeletons include the following: compliance with medical device consensus standards; clinical testing to demonstrate safe and effective use considering the level of supervision necessary and the use environment; non-clinical safety and performance testing, including durability testing to demonstrate that the device performs as intended under anticipated conditions of use; a training program; and labeling related to device use and user training. In order for us to market ReWalk, we must comply with both general controls, including controls related to quality, facility registration, reporting of adverse events and labeling, and the special controls established for the device. Failure to comply with the general and special controlsthese requirements could lead to removal of ReWalk from the market,an FDA enforcement action, which would have a material adverse effect on our business.
In June 2019, the FDA issued a 510(k) clearance for our ReStore device. ReStore is intended to be used to assist ambulatory functions in rehabilitation institutions under the supervision of a trained therapist for people with hemiplegia or hemiparesis due to stroke who have a specified amount of ambulatory function. In order for us to market ReStore and ReWalk, we must comply with both general controls, including controls related to quality, facility registration, reporting of adverse events and labeling, and the special controls established for powered exoskeleton devices as described above. Failure to comply with these requirements could lead to an FDA enforcement action, which would have a material adverse effect on our business.
In the E.U. we are subject to regulations and standards regulating the design, manufacture, clinical trials, labeling and adverse event (i.e., vigilance) reporting for medical devices. The Medical Devices Regulation (EU) 2017/745 (MDR) became fully applicable on May 26, 2021, repealing and replacing the pre-existing E.U. Medical Devices Directive 93/42/EEC. Devices that comply with the requirements of the MDR, subject to certain transitional provisions that allow continued compliance of certain products to the Directive, are entitled to bear the CE mark, indicating that the device conforms to the essential requirements of the MDR and, accordingly, can be commercially distributed throughout the European Economic Area (i.e., the E.U. Member States plus Norway, Iceland, and Lichtenstein). We comply with the E.U. requirements and have received the CE mark for all of our ReWalk systems including the ReStore device which are distributed in the E.U. As compared with the Directive, the MDR includes additional premarket and post-market requirements, as well as potential product reclassifications and more stringent commercialization requirements that could adversely affect our CE mark. Failure to comply with these new requirements could lead to substantial penalties, including fines, revocation or suspension of CE mark and criminal sanctions.
Following the introduction of a product, the governmental agencies will periodically reviewinspect our manufacturing processes and product performance,quality controls, and we are under a continuing obligation to ensure that all applicable regulatory requirements continue to be met. The process of complying with the applicable good manufacturing practices, adverse event reporting and other requirements can be costly and time consuming, and could delay or prevent the production, manufacturing, or sale of the ReWalk.our devices. In addition, if we fail to comply with applicable regulatory requirements, it could result in fines, or delays of regulatory clearances, closure of manufacturing sites, seizures or recalls of products and damage to our reputation. Recent changes inreputation, as well as enforcement practice byactions against us. For example, the FDA European Union and other agencies have resulted in increased enforcement activity, which increases the compliance riskcould request that we and other companiesrecall our ReWalk Personal Exoskeleton or ReStore device in our industry are facing.case of product defects or require us to conduct post-market surveillance studies. If we fail to recall the device and/or conduct requested post-market surveillance studies to FDA’s satisfaction, we could be subject to FDA enforcement action.
In addition, governmental agencies may impose new requirements regarding registration labeling or prohibited materialslabeling that may require us to modify or re-register ReWalk once it is already on the marketour products or otherwise impact our ability to market ReWalkour products in those countries.countries, such as the May 2021 Medical Device Regulation changes in the European Union. The process of complying with these governmental regulations can be costly and time consuming, and could delay or prevent the production, manufacturing, or sale of ReWalk. Failure to comply with governmental requirements could result in enforcement actions against us or our products. For example, the FDA could request that we recall our ReWalk Personal 6.0 device. For more information on certain deficiencies previously identified by the FDA in our mandatory post-market surveillance study on our ReWalk Personal 6.0, see “-While we addressed the observations that FDA cited in a 2015 warning letter related to our mandatory postmarket surveillance study and initiated the study, we are currently experiencing enrollment issues that make our study progress inadequate. . . ” above.
If we or our third-party manufacturers or suppliers fail to comply with the FDA’s Quality System Regulation, or QSR, our manufacturing operations could be interrupted.
We Sanmina and some of our suppliersmanufacturer Sanmina are required to comply with the FDA’s QSR which covers the methods and documentation of the design, testing, production, control, quality assurance, labeling, packaging, sterilization, storage, and shipping of our products. We, Sanmina, and our suppliers are also subject to the regulations of foreign jurisdictions regarding the manufacturing process if we or our distributors market our products abroad. We continue to monitor our quality management in order to improvemaintain our overall level of compliance. Our facilities are subject to periodic and unannounced inspection by U.S. and foreign regulatory agencies to audit compliance with the QSR and comparable foreign regulations. If our facilities or those of Sanmina or our suppliers are found to be in violation of applicable laws and regulations, or if we, Sanmina, or our suppliers fail to take satisfactory corrective action in response to an adverse inspection, the regulatory authority could take enforcement action, including any of the following sanctions:
| ● | untitled letters, warning letters, fines, injunctions, consent decrees and civil penalties; |
| ● | customer notifications or repair, replacement, or refunds; |
| ● | operating restrictions or partial suspension or total shutdown of production; |
| ● | recalls, withdrawals, or administrative detention or seizure of our products; |
| ● | denials or delays of approvals for pre-market approval applications relating to new products or modified products; |
| ● | withdrawals of a PMA approvals; |
| ● | refusal to provide Certificates for Foreign Government; |
| ● | refusal to grant export approval for our products; or |
| ● | pursuit of |
Any of these sanctions could impair our ability to produce ReWalkour products in a cost-effective and timely manner in order to meet our customers’ demands and could have a material adverse effect on our reputation, business, results of operations, and financial condition. We may also be required to bear other costs or take other actions that may have a negative impact on our future sales and our ability to generate profits.
We are subject to various laws and regulations, including “fraud and abuse” laws and anti-bribery laws, which, if violated, could subject us to substantial penalties.
Medical device companies such as ours have faced lawsuits and investigations pertaining to alleged violations of numerous statutes and regulations, including anti-corruption laws and health care “fraud and abuse” laws, such as the federal False Claims Act, the federal Anti-Kickback Statute, and the U.S. Foreign Corrupt Practices Act, or the FCPA. See Item 1. “Business-Government Regulation” above.
U.S. federal and state laws, including the federal Physician Payments Sunshine Act, or the Sunshine Act, and the implementation of Open Payments regulations under the Sunshine Act, require medical device companies to disclose certain payments or other transfers of value made to certain healthcare providers and teaching hospitals or funds spent on marketing and promotion of medical device products. It is widely believed that public reporting under the Sunshine Act and implementing Open Payments regulations results in increased scrutiny of the financial relationships between industry,Further, some state laws require medical device companies to report information related to payments to physicians and teaching hospitals. These anti-kickback, anti-bribery, public reporting and aggregate spending laws affect our sales,other health care providers or marketing and other promotional activities by limiting the kinds of financial arrangements, including sales programs, we may have with hospitals, rehabilitation centers, physicians or other potential purchasers or users of ReWalk.expenditures. They also impose additional administrative and compliance burdens on us. In particular, these laws influence, among other things, how we structure our sales offerings and other interactions with health care providers, including discount practices, customer support, education and training programs and physician consulting and other service arrangements.arrangements, including those with marketers and sales agents. We may face significant costs in attempting to comply with these laws and regulations. If we are found to be in violation of any of these requirements or any actions or investigations are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could be costly to defend and could have a significant impact on our business, including the imposition of significant criminal and civil fines and penalties, exclusion from federal healthcare programs or other sanctions.sanctions, and damage to our reputation or business.
The FCPA applies to companies, including ours, with a class of securities registered under the Exchange Act. The FCPA and other anti-bribery laws to which various aspects of our operations may be subject generally prohibit companies and their employees, agents, and other intermediaries from authorizing, promising, offering, providing, or making, directly or indirectly, improper payments or anything else of value to government officials for the purpose of obtaining or retaining business. The FCPA also requires covered companies such as ours to make and keep books and records that accurately and fairly reflect the transactions of the corporation and to devise and maintain an adequate system of internal accounting controls. In various jurisdictions, our operations require that we and third parties acting on our behalf routinely interact with government officials, including medical personnel who may be considered government officials for purposes of these laws because they are employees of state-owned or controlled facilities. Other anti-bribery laws to which various aspects of our operations may be subject, including the United Kingdom Bribery Act, also prohibit improper payments to private parties and prohibit receipt of improper payments. Our policies prohibit our employees from making or receiving corrupt payments, including, among other things, to require compliance by third parties engaged to act on our behalf. Our policies mandate compliance with these anti-bribery laws; however, we operaterecent years have seen an increase in many partsthe global enforcement of anti-corruption laws and our international operations could increase the world that have experienced governmental and/or private corruption to some degree.risk of such violations. As a result, the existence and implementation of a robust anti-corruption program cannot eliminate all risk that unauthorized reckless or criminalimproper acts have been or will be committed by our employees or agents. Violations of these anti-corruption laws, or allegations of such violations, could disruptresult in civil or criminal sanctions or other adverse consequences, including disruption of our business and harmharming our financial condition, results of operations, cash flows and reputation.
39
If we are found to have violated laws protecting the confidentiality of patient health information, we could be subject to civil or criminal penalties, which could increase our liabilities and harm our reputation or our business.
There are a number of federal, state and foreign laws protecting the confidentiality of certain patient health information, including patient records, and restricting the use and disclosure of that protected information. In particular, the U.S. Department of Health and Human Services, or HHS, promulgated patient privacy rules under the Health Insurance Portability and Accountability Act of 1996, or HIPAA. These privacy rules protect medical records and other personal health information by limiting their use and disclosure, giving individuals the right to access, amend and seek accounting of their own health information and limiting most use and disclosures of health information to the minimum amount reasonably necessary to accomplish the intended purpose. Additionally, the E.U. General Data Protection Regulation (the “GDPR”), which is intended to strengthen and unify data protection and address the export of personal data outside the E.U., will become effective in May 2018. Once effective and implemented, the GDPR will imposeimposes more stringent data protection requirements and will provideprovides for greater penalties for noncompliance. WithThus, with respect to our operations in Europe, the GDPR willmay increase our responsibility and liability in relation to personal data that we process and we may be required to put in place additional mechanisms ensuring compliance with the GDPR. This may be onerous and adversely affect our business, financial condition, results of operations and prospects. Additionally, if we or any of our service providers are found to be in violation of the promulgated patient privacy rules under HIPAA or once enforced, the GDPR, we could be subject to civil or criminal penalties, which could be substantial and could increase our liabilities, harm our reputation and have a material adverse effect on our business, financial condition and operating results.
In addition, a number of U.S. states have enacted data privacy and security laws and regulations that govern the collection, use, disclosure, transfer, storage, disposal, and protection of sensitive personal information, such as social security numbers, financial information and other personal information. For example, several U.S. territories and all 50 states now have data breach laws that require timely notification to individual victims, and at times regulators, if a company has experienced the unauthorized access or acquisition of sensitive personal data. Other state laws include the California Consumer Privacy Act (“CCPA”) which, among other things, contains new obligations for businesses that collect personal information about California residents and affords those individuals new rights relating to their personal information that may affect our ability to use personal information or share it with our business partners. Meanwhile, other states have enacted or are considering enacting privacy laws like the CCPA. Furthermore, it is anticipated that the California Privacy Rights Act of 2020, effective January 1, 2023, expands the CCPA’s requirements, including applying to personal information of business representatives and employees and establishing a new regulatory agency to implement and enforce the law. We will continue to monitor and assess the impact of state law developments, which may impose substantial penalties for violations, impose significant costs for investigations and compliance, allow private class-action litigation and carry significant potential liability for our business.
The interpretation and enforcement of the laws and regulations described above are uncertain and subject to change and may require substantial costs to monitor and implement compliance with any additional requirements. Failure to comply with U.S. or international data protection laws and regulations could result in government enforcement actions (which could include substantial civil and/or criminal penalties), private litigation, and/or adverse publicity and could negatively affect our operating results and business.
Compliance with various regulations, including those related to our status as a U.S. public company and the manufacturing, labeling, and marketing of our products, may result in heightened general and administrative expenses and costs, divert management’s attention from revenue-generating activities and pose challenges for our management team, which has limited time, personnel and finances to devote to regulatory compliance.
As a U.S. public company, we are subject to various regulatory and reporting requirements, including those imposed by the SEC, the Sarbanes-Oxley Act of 2002, or the Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010, or the Dodd-Frank Act, the listing requirements of theThe Nasdaq Capital Market and other applicable securities rules and regulations. Additionally, our medical products and manufacturing operations are regulated by the FDA, the European Union and other governmental authorities both inside and outside of the United States. Compliance with the rules and regulations applicable to us as a publicly traded company in the United States and medical device manufacturer has greatly increased, and may continue to increase, our legal, general and administrative and financial compliance costs and has made, and may continue to make, some activities more difficult, time-consuming or costly. Additionally, these regulatory requirements have diverted, and may continue to divert, management’s attention from revenue-generating activities and may increase demands on management’s already-limited resources.
Our management team consists of few employees, as the majority of our employees are engaged in sales and marketing and research and development activities. As part of our previously announced plan to reduce our operating expenses by up to 30% in 2017 as compared to 2016, During 2017 our gross profit as a percentage of revenue increased to 40% as compared to 13% in 2016 and operating expenses decreased by 20% versus 2016. During 2017, we reduced the number of employees worldwide from 94 to 65. In 2018, we will continue to evaluate spending to reduce where possible. For more information, see “Part I, Item 1. Business-Employees.”Business—Employees” above. In light of such constraints on its time, personnel and finances, our management may not be able to implement programs and policies in an effective and timely manner to respond adequately to the heightened legal, regulatory and reporting requirements applicable to us. In the past, for example, we have not always been able to respond on a timely basis to requests from regulators, although we have not to date experienced any long-term material adverse consequences as a result. For more information, see “-The FDA previously sent us letters regarding potential regulatory action for deficiencies in our mandatory post-market surveillance study on our ReWalk Personal 6.0…” above. Similar deficiencies, weaknesses, or lack of compliance with public company, medical device and other regulations could harm our reputation in the capital markets or for quality and safety, negatively affect our ability to maintain our public company status and to develop, commercialize or continue selling our products on a timely and effective basis, and cause us to incur sanctions, including fines, injunctions, and penalties.
In addition, complying with public disclosure rules makes our business more visible, which we believe may result in threatened or actual litigation, including by competitors and other third parties. If such claims are successful, our business and operating results could be harmed, and even if the claims do not result in litigation or are resolved in our favor, these claims, and the time and resources necessary to resolve them, could divert the resources of our management and harm our business and operating results.
We are also subject to the requirement of Section 1502 of the Dodd-Frank Act and SEC rules related thereto to conduct due diligence and disclose and report on whether certain minerals and metals, known as “conflict minerals,” are contained in our products and whether they originate from the Democratic Republic of Congo and certain adjoining countries. Each year our management team devotes significant time to conduct the required due diligence, and we may face reputational challenges if we determine that certain of our products contain minerals not determined to be conflict free or if we are unable to sufficiently verify the origins of all conflict minerals used in our products through the procedures we implement.
Risks Related to Our Intellectual Property and Information Technology
We depend on computer and telecommunications systems we do not own or control and failures in our systems or a cybersecurity attack or incident relating to our IT systems or technology could significantly disrupt our business operations or result in sensitive customer information being compromised which would negatively materially affect our reputation and/or results of operations.
We have entered into agreements with third parties for hardware, software, telecommunications, and other information technology services in connection with the operation of our business. It is possible we or a third party that we rely on could incur interruptions from a loss of communications, hardware or software failures, a cybersecurity attack or an incident relating to our IT systems or technology, ransomware, phishing attacks, computer viruses or malware. We believe that we have positive relations with our vendors and maintain adequate anti-virus and malware software and controls; however, any interruptions to our arrangements with third parties, to our computing and communications infrastructure, or to our information systems or any of those operated by a third party that we rely on could significantly disrupt our business operations.
In the current environment, there are numerous and evolving risks to cybersecurity and privacy, including criminal hackers, hacktivists, state-sponsored intrusions, industrial espionage, employee malfeasance and human or technological error. High-profile cybersecurity incidents at other companies and in government agencies have increased in recent years, and security industry experts and government officials have warned about the risks of hackers and cyberattacks targeting businesses such as ours. Computer hackers and others routinely attempt to breach the security of technology products, services, and systems, and to fraudulently induce employees, customers, or others to disclosure information or unwittingly provide access to systems or data. A cyberattack of our systems or networks that impairs our information technology systems could disrupt our business operations and result in loss of service to customers, including technical support for our ReWalk devices. While we have certain cybersecurity safeguards in place designed to protect and preserve the integrity of our information technology systems, we have experienced and expect to continue to experience actual or attempted cyberattacks of our IT systems or networks. However, none of these actual or attempted cyberattacks has had a material effect on our operations, business strategy, or financial condition.
41
Additionally, we have access to sensitive customer information in the ordinary course of business. If a significant cybersecurity incident occurred, our reputation may be adversely affected, customer confidence may be diminished, or we may be subject to legal claims, any of which may contribute to the loss of customers and have a material adverse effect on us. For more information, see “—Risks Related to Government Regulation” above. If we are found to have violated laws protecting the confidentiality of patient health information, we could be subject to civil or criminal penalties, which could increase our liabilities and harm our reputation or our business.” above.
Our success depends in part on our ability to obtain and maintain protection for the intellectual property relating to or incorporated into our products.
Our success depends in part on our ability to obtain and maintain protection for the intellectual property relating to or incorporated into our products. We seek to protect our intellectual property through a combination of patents, trademarks, confidentiality, and assignment agreements with our employees and certain of our contractors, and confidentiality agreements with certain of our consultants, scientific advisors, and other vendors and contractors. In addition, we rely on trade secret law to protect our proprietary software and product candidates/products in development. For more information, see Part I.“Part I, Item 1. Business-Intellectual Property.”Business—Intellectual Property” above.
Litigation to establish or challenge the validity of patents, or to defend against or assert against others infringement, unauthorized use, enforceability, or invalidity, can be lengthy and expensive and may result in our patents being invalidated or interpreted narrowly and restricting our ability to be granted new patents related to our pending patent applications. Even if we prevail, litigation may be time consuming,force us to incur significant costs, and could divert management’s attention from managing our business while any damages or other remedies awarded to us may not be valuable. In addition, U.S. patents and patent applications may be subject to interference proceedings, and U.S. patents may be subject to re-examination and review proceedings in the U.S. Patent and Trademark Office. Foreign patents may also be subject to opposition or comparable proceedings in the corresponding foreign patent offices. Any of these proceedings may be expensive and could result in the loss of a patent or denial of a patent application, or the loss or reduction in the scope of one or more of the claims of a patent or patent application.
In addition, we seek to protect our trade secrets, know-how, and confidential information that is not patentable by entering into confidentiality and assignment agreements with our employees and certain of our contractors and confidentiality agreements with certain of our consultants, scientific advisors, and other vendors and contractors. However, we may fail to enter into the necessary agreements, and even if entered into, these agreements may be breached or otherwise fail to prevent disclosure, third-party infringement, or misappropriation of our proprietary information, may be limited as to their term and may not provide an adequate remedy in the event of unauthorized disclosure or use of proprietary information. Enforcing a claim that a third party illegally obtained or is using our trade secrets without authorization may be expensive and time consuming, and the outcome is unpredictable. Some of our employees or consultants may own certain technology which they license to us for a set term. If these technologies are material to our business after the term of the license, our inability to use them could adversely affect our business and profitability.
We also have taken precautions to initiate reasonable safeguards to protect our information technology systems. However, these measures may not be adequate to safeguard our proprietary information, which could lead to the loss or impairment thereof or to expensive litigation to defend our rights against competitors who may be better funded and have superior resources. In addition, unauthorized parties may attempt to copy or reverse engineer certain aspects of our products that we consider proprietary, or our proprietary information may otherwise become known or may be independently developed by our competitors or other third parties. If other parties are able to use our proprietary technology or information, our ability to compete in the market could be harmed. Further, unauthorized use of our intellectual property may have occurred, or may occur in the future, without our knowledge.
If we are unable to obtain or maintain adequate protection for intellectual property, or if any protection is reduced or eliminated, competitors may be able to use our technologies, resulting in harm to our competitive position.
42
Our patents and proprietary technology and processes may not provide us with a competitive advantage.
Robotics, exoskeletons, and exoskeletonanti-gravity system technologies have been developing rapidly in recent years. We are aware of several other companies developing competing exoskeleton devices for individuals with limited mobility and we expect the level of competition and the pace of development in our industry to increase. Likewise, we are aware of several companies with commercial anti-gravity or treadmill-based gait therapy systems. For more information, see “Part I.I, Item 1. Business-Competition”Business—Competition” above. While we believe our tilt-sensor technology provides a more natural and superior method of exoskeleton activation, which creates a better user experience, as well as that our licensed technology used in our ReStore device is unique and provides better results when compared to other products, a variety of other activation and control methods exist for exoskeletons, several of which are being developed by our competitors, or may be developed in the future. Additionally, while our DAP technology provides what we believe is a superior method for partial weight displacement with strong market acceptance, there may be competitors developing innovative alternative gait therapies that could be introduced in the future. As a result, our patent portfolio and proprietary technology and processes may not provide us with a significant advantage over our competitors, and competitors may be able to design and sell alternative products that are equal to or superior to our products without infringing on our patents. In addition, upon the expiration ofas our current patents begin to expire, we may lose a competitive advantage over our competitors as we will no longer be able to keep our competitors from practicing the technology covered by the claim of the expired patents. We may also be unable to adequately develop new technologies and obtain future patent protection to preserve oura competitive advantage. If we are unable to maintain a competitive advantage, our business and results of operations may be materially adversely affected.
Even in instances where others are found to infringe on our patents, many countries have laws under which a patent owner may be compelled to grant licenses for the use of the patented technology to other parties. In addition, many countries limit the enforceability of patents against other parties, including government agencies or government contractors. In these countries, a patent owner may have limited remedies, which could diminish the value of a patent in those countries. Further, the laws of some countries do not protect intellectual property rights to the same extent as the laws of the United States, particularly in the field of medical products, and effective enforcement in those countries may not be available. The ability of others to market comparable products could adversely affect our business.
We are not able to protect our intellectual property rights in all countries.
Filing, prosecuting, maintaining, and defending patents on each of our products in all countries throughout the world would be prohibitively expensive, and thus our intellectual property rights outside the United States and Europe are limited. In addition, the laws of some foreign countries, especially developing countries, such as China, do not protect intellectual property rights to the same extent as federal and state laws in the United States. Also, it may not be possible to effectively enforce intellectual property rights in some countries at all or to the same extent as in the United States and other countries. Consequently, we are unable to prevent third parties from using our inventions in all countries, or from selling or importing products made using our inventions in the jurisdictions in which we do not have (or are unable to effectively enforce) patent protection. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop, market or otherwise commercialize their own products, and we may be unable to prevent those competitors from importing those infringing products into territories where we have patent protection, but enforcement may not be as strong as in the United States. These products may compete with our products and our patents and other intellectual property rights may not be effective or sufficient to prevent them from competing in those jurisdictions. Moreover, strategic partners, competitors, or others in the chain of commerce may raise legal challenges against our intellectual property rights or may infringe upon our intellectual property rights, including through means that may be difficult to prevent or detect. For instance, if our planned China JV were to infringe our licensed intellectual property in violation of the Timwell License Agreement, we could face difficulty effectively enforcing our rights in China or elsewhere. For more information on the Timwell License Agreement, see “Part I. Item 1. Business-Timwell Investment Agreement and Related Transactions.”
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. Proceedings to enforce our patent rights in the United States or foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing, and could provoke third parties to assert patent infringement or other claims against us. We may not prevail in any lawsuits that we initiate, and the damages or other remedies awarded, if any, may not be commercially meaningful. Accordingly, our efforts to enforce our intellectual property rights in the United States and around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we develop or license from third parties.
We may be subject to patent infringement claims, which could result in substantial costs and liability and prevent us from commercializing our current and future products.
The medical device industry is characterized by competing intellectual property and a substantial amount of litigation over patent rights. In particular, ourOur competitors in both the United States and abroad, many of which have substantially greater resources and have made substantial investments in competing technologies, have been issued patents and filed patent applications with respect to their products and processes and may apply for other patents in the future. The large number of patents, the rapid rate of new patent issuances, and the complexities of the technology involved increase the risk of patent litigation.
Determining whether a product infringes a patent involves complex legal and factual issues and the outcome of patent litigation is often uncertain. Even though we have conducted research of issued patents, no assurance can be given that patents containing claims covering our products, technology or methods do not exist, have not been filed or could not be filed or issued. In addition, because patent applications can take years to issue and because publication schedules for pending applications vary by jurisdiction, there may be applications now pending of which we are unaware, and which may result in issued patents that our current or future products infringe. Also, because the claims of published patent applications can change between publication and patent grant, published applications that initially do not appear to be problematic may issue with claims that potentially cover our products, technology, or methods.
Infringement actions and other intellectual property claims brought against us, whether with or without merit, may cause us to incur substantial costs and could place a significant strain on our financial resources, divert the attention of management, and harm our reputation. We cannot be certain that we will successfully defend against any allegations of infringement. If we are found to infringe another party’s patents, we could be required to pay damages. We could also be prevented from selling our infringing products, unless we can obtain a license to use the technology covered by such patents or can redesign our products so that they do not infringe. A license may be available on commercially reasonable terms or none at all, and we may not be able to redesign our products to avoid infringement. Further, any modification to our products could require us to conduct clinical trials and revise our filings with the FDA and other regulatory bodies, which would be time consuming and expensive. In these circumstances, we may not be able to sell our products at competitive prices or at all, and our business and operating results could be harmed.
We rely on trademark protection to distinguish our products from the products of our competitors.
We rely on trademark protection to distinguish our products from the products of our competitors. We have registered the trademark “ReWalk” in Israel and in the United States. The trademark “ReStore” is registered in Europe, the United States and are in the process of registering theUnited Kingdom. The trademark “Restore”“Alter G” is registered in the United States, Europe, Israel, and the United Kingdom. We have also recently sought trademark registration of “Lifeward” in the United States, Europe, and Israel. In jurisdictions where we have not registered our trademark and are using it, and as permitted by applicable local law, we rely on common law trademark protection. Third parties may oppose our trademark applications, or otherwise challenge our use of the trademarks, and may be able to use our trademarks in jurisdictions where they are not registered or otherwise protected by law. If our trademarks are successfully challenged or if a third party is using confusingly similar or identical trademarks in particular jurisdictions before we do, we could be forced to rebrand our products, which could result in loss of brand recognition, and could require us to devote additional resources to marketing new brands. If others are able to use our trademarks, our ability to distinguish our products may be impaired, which could adversely affect our business. Further, we cannot assure you that competitors will not infringe upon our trademarks, or that we will have adequate resources to enforce our trademarks.
We may be subject to damages resulting from claims that our employees or we have wrongfully used or disclosed alleged trade secrets of their former employers.
Many of our employees were previously employed at other medical device companies, including our competitors or potential competitors, and we may hire employees in the future that are so employed. We could in the future be subject to claims that these employees, or we, have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers. If we fail in defending against such claims, a court could order us to pay substantial damages and prohibit us from using technologies or features that are found to incorporate or be derived from the trade secrets or other proprietary information of the former employers. If any of these technologies or features that are important to our products, this could prevent us from selling those products and could have a material adverse effect on our business. Even if we are successful in defending against these claims, such litigation could result in substantial costs and divert the attention of management.
Risks Related to the Timwell Investment Agreement and Related Transactions
Sales of a substantial number of ordinary shares by us or our large shareholders, and holders of our warrants and other derivative securities, certain of whom may have registration rights, or dilutive exercises of a substantial number of warrants by our warrant-holders could have an adverse effect onadversely affect the value of our ordinary shares.
Sales by us or our shareholders of a substantial number of ordinary shares in the public market, or the perception that these sales might occur, could cause the value of our ordinary shares to decline or could impair our ability to raise capital through a future sale of or pay for acquisitions using, our equity securities. Additionally, dilutive exercises of a substantial number of warrants by our warrant-holders, or the perception that such exercises may occur, could put downward price on the market price of our ordinary shares.
As of December 31, 2017, 403,804 ordinary shares were issuable pursuant to the exercise of outstanding warrants granted as part of our Series E Preferred investment round in July 2014 at an exercise price of $10.08 and 2,437,500February 27, 2024, 19,135,096 ordinary shares were issuable pursuant to the exercise of warrants, with exercise prices ranging from $1.25 to $9.375 per warrant, issued in our follow-on offeringprivate and registered offerings of ordinary shares and warrants in November 2016,April 2019, June 2019, February 2020, July 2020, December 2020, February 2021 and September 2021. We have registered with an exercise pricethe SEC all of $4.75.these warrants and/or the resale of the shares issuable upon their exercise. There were also 167,0126,679 ordinary shares issuable pursuant to the exercise of warrants granted to Kreos Capital V (Expert Fund) Limited (“Kreos”), in connection with the Loan Agreementloan agreement we signed with Kreos on December 30, 2015 (the “Loan Agreement”) in January and December 2016, with an exercise price that is set to $7.50 per warrant. For more information, “Part I, Item 2. Management’s Discussion and Analysis of $9.64,Financial Condition and 2,523,660 ordinary shares issuable pursuant to the conversionResults of the Kreos Convertible Note at a conversion price of $1.268 per share (subject to customary anti-dilution adjustments).Operations—Liquidity and Capital Resources—Equity Raises”, below.
All shares sold pursuant to an offering covered by a registration statement would be freely transferable. With respect to the outstanding warrants, there may be certain restrictions on the holders to sell the underlying ordinary shares to the extent they are restricted securities, held by “affiliates” or would exceed certain ownership thresholds. Certain of our largest shareholders,, may also have limitations under Rule 144 under the Securities Act on the resale of certain ordinary shares they hold unless they are registered for resale under the Securities Act. Despite these limitations and the liquidity that we may gain from cash exercises of outstanding warrants, if we, our existing shareholders, or their affiliates sell a substantial number of the above-mentioned ordinary shares in the public market, the market price of our ordinary shares could decrease significantly. Shareholders may also incur substantial dilution if holders of our warrants exercise their warrants to purchase ordinary shares, which could lower the market price of our ordinary shares. Any such decrease could impair the value of your investment in us.
Future grants of ordinary shares under our equity incentive plans to our employees, non-employee directors and consultants, or sales by these individuals in the public market, could result in substantial dilution, thus decreasing the value of your investment in our ordinary shares, and certain grants may also require shareholder approval. In addition, stockholders will experience dilution upon the exercise of outstanding warrants.
We have historically used, and continue to use, our ordinary shares as a means of both rewarding our employees, non-employee directors, and consultants and aligning their interests with those of our shareholders. As of December 31, 2017, 3,148,3182023, 4,824,530 ordinary shares remained available for issuance to our and our affiliates’ respective employees, non-employee directors, and consultants under our equity incentive plans, including 1,846,7973,805,585 ordinary shares subject to outstanding awards (consisting of outstanding options to purchase 1,277,72633,171 ordinary shares and 569,0713,772,414 ordinary shares underlying unvested restricted share units (“RSUs”)).RSUs, and we may seek to increase the number of shares available under our equity incentive plans in the future. For more information, Seesee Note 8b9b to our consolidated financial statements set forth in "Part II. Item 8. Financial Statements and Supplementary Data" of this annual report.
Additionally, to the extent registered on a Form S-8, ordinary shares granted or issued under our equity incentive plans will, subject to vesting provisions, lock-up restrictions, and Rule 144 volume limitations applicable to our “affiliates,” be available for sale in the open market immediately upon registration. Further, as of December 31, 2023, there were 19,187,375 ordinary shares underlying issued and outstanding warrants, which if exercised for ordinary shares, could decrease the net tangible book value of our ordinary shares and cause dilution to our existing shareholders. Sales of a substantial number of the above-mentioned ordinary shares in the public market could result in a significant decrease in the market price of our ordinary shares and have a material adverse effect on an investment in our ordinary shares.
If we do not meet the expectations of equity research analysts, if they doany, if the sole remaining equity analyst following our business does not continue to publish research or reports about our business, or if they issuethe analyst issues unfavorable commentary or downgrade our ordinary shares, the price of our ordinary shares could decline. Additionally, we may fail to meet publicly announced financial guidance or other expectations about our business, which would cause our ordinary shares to decline in value.
45
From time to time, we have also faced difficulty accurately projecting our earnings and have missed certain of our publicly announced guidance. If our financial results for a particular period do not meet our guidance or if we reduce our guidance for future periods, the market price of our ordinary shares may decline.
We are an “emerging growtha “smaller reporting company” and “smaller reporting company,” and we cannot be certain whether the reduced reporting requirements applicable to emerging growthsuch companies and smaller reporting companies willmay make our ordinary shares less attractive to investors.
We are an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act. As a result, we may take advantage of certain exemptions from various requirements that are applicable to other public companies that are not “emerging growth companies.” For instance, we are subject to reduced compensation disclosure obligations under the JOBS Act, and we are not required to conduct votes seeking shareholder approval on an advisory basis of (i) the compensation of our named executive officers or the frequency with which such votes must be conducted or (ii) compensation arrangements and understandings in connection with merger transactions, known as “golden parachute” arrangements. Additionally, we are not required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act for up to five fiscal years after the date of our initial public offering.
We cannot predict or otherwise determine if investors will find our securities less attractive as a result of our reliance on exemptions under the JOBS Act or as a smaller reporting company.company and/or “non-accelerated filer.” If some investors find our securities less attractive as a result, there may be a less active trading market for our ordinary shares and the price of our ordinary shares may be more volatile.
We are subject to ongoing costs and risks associated with determining whether our existing internal controls over financial reporting systems are compliant with Section 404 of the Sarbanes-Oxley Act, and if we fail to achieve and maintain adequate internal controls it could have a material adverse effect on our stated results of operations and harm our reputation.
We are required to comply with the internal control, evaluation, and certification requirements of Section 404 of the Sarbanes-Oxley Act and the Public Company Accounting Oversight Board. Unless we lose our status as an emerging growth company underBoard, which requires us to furnish a report by management on, among other things, the JOBS Act prior to the end of the fiscal year in which the fifth anniversaryeffectiveness of our initial public offering occurred, we will not be required to obtain an auditor attestation under Section 404 of the Sarbanes-Oxley Act until the year ended December 31, 2019. However onceinternal control over financial reporting. Once we no longer qualify as an emerging growth company under the JOBS Acta “smaller reporting company” and “non-accelerated filer,” our independent registered public accounting firm will need to attest to the effectiveness of our internal control over financial reporting under Section 404.
our internal control over financial reporting, the cost of our compliance with Section 404 will correspondingly increase. Our compliance with applicable provisions of Section 404 will require that we incur substantial accounting expense and expend significant management time on compliance-related issues as we implement additional corporate governance practices and comply with reporting requirements. Moreover, if we are not able to comply with the requirements of Section 404 applicable to us in a timely manner, or if we or our independent registered public accounting firm identifies deficiencies in our internal control over financial reporting that are deemed to be material weaknesses, the market price of our stock could decline and we could be subject to sanctions or investigations by the SEC or other regulatory authorities, which would require additional financial and management resources.
The process of determining whether our existing internal controls over financial reporting systems are compliant with Section 404 and whether there are any material weaknesses or significant deficiencies in our existing internal controls requires the investment of substantial time and resources, including by our Chief Financial Officer and other members of our senior management. This determination and any remedial actions required could divert internal resources and take a significant amount of time and effort to complete and could result in us incurring additional costs that we did not anticipate, including the hiring of outside consultants. We could experience higher than anticipated operating expenses and higher independent auditor fees during and after the implementation of these changes.
Irrespective of compliance with Section 404, any failure of our internal controls could have a material adverse effect on our stated results of operations and harm our reputation. If we are unable to implement any of the required changes to our internal control over financial reporting effectively or efficiently or are required to do so earlier than anticipated, it could adversely affect our operations, financial reporting and/or results of operations and could result in an adverse opinion on internal controls from our management and once we lose our emerging growth company status, our independent auditors. Further, if our internal control over financial reporting is not effective, the reliability of our financial statements may be questioned, and our share price may suffer.
46
U.S. holders of our ordinary shares may suffer adverse U.S. tax consequences if we are characterized as a passive foreign investment company, or a PFIC, under Section 1297(a) of the Code.
Generally, if for any taxable year 75% or more of our gross income is passive income, or at least 50% of the average quarterly value of our assets (which may be determined in part by the market value of our ordinary shares, which is subject to change) are held for the production of, or produce passive income, we would be characterized as a passive foreign investment company, or PFIC, for U.S. federal income tax purposes. Passive income for this purpose generally includes, among other things, certain dividends, interest, royalties, rents, and gains from commodities and securities transactions and from the sale or exchange of property that gives rise to passive income. Passive income also includes amounts derived by reason of the temporary investment of funds, including those raised in an offering. In determining whether a non-U.S. corporation is a PFIC, a proportionate share of the income and assets of each corporation in which it owns, directly or indirectly, at least a 25% interest (by value) is taken into account.
The determination of whether we are a PFIC will depend on the nature and composition of our income and the nature, composition, and value of our assets from time to time. The 50% passive asset test described above is generally based on the fair market value of each asset, with the value of goodwill and going concern value determined in large part by reference to the market value of our ordinary shares, which may be volatile. If we are characterized as a “controlled foreign corporation,” or a “CFC”, under Section 957(a) of the Code and not considered publicly traded throughout the relevant taxable year, however, the passive asset test may be applied based on the adjusted tax bases of our assets instead of the fair market value of each asset (as described above). However, if we are treated as publicly traded for at least 20 trading days during the relevant taxable year, our assets would generally be required to be measured at their fair market value, even if we are a CFC.
Based on our gross income and assets, the market price of our ordinary shares, and the nature of our business, we believe that we were not a PFIC for the taxable year ended December 31, 2023. However, this determination is subject to uncertainty. In addition, there is a significant risk that we may be a PFIC for future taxable years, unless the market price of our ordinary shares increases, or we reduce the amount of cash and other passive assets we hold relative to the amount of non-passive assets we hold. Accordingly, no assurances can be made regarding our PFIC status in one or more subsequent years, and our U.S. counsel expresses no opinion with respect to our PFIC status in the taxable year ended December 31, 2023, or the current year 2024, and also expresses no opinion with respect to our predictions or past determinations regarding our PFIC status in the past or in the future.
If we are characterized as a PFIC, U.S. holders of our ordinary shares may suffer adverse tax consequences, including having gains realized on the sale of our ordinary shares treated as ordinary income, rather than capital gain, the loss of the preferential tax rate applicable to dividends received on our ordinary shares by individuals who are U.S. holders and having interest charges apply to distributions by us and to the proceeds of sales of our ordinary shares. In addition, special information reporting may be required. Certain elections exist that may alleviate some of the adverse consequences of PFIC status and would result in an alternative treatment (such as mark-to-market treatment or being able to make a qualified electing fund election). However, we do not intend to provide the information necessary for U.S. Holders to make qualified electing fund elections if we are classified as a PFIC.
Additionally, if we are characterized as a PFIC, for any taxable year during which a U.S. holder holds ordinary shares, we generally will continue to be treated as a PFIC with respect to such U.S. holder for all succeeding years during which such U.S. holder holds ordinary shares unless we cease to be a PFIC and such U.S. holder makes a “deemed sale” election with respect to such ordinary shares. If such election is made, such U.S. holder will be deemed to have sold such ordinary shares held by such U.S. holder at their fair market value on the last day of the last taxable year in which we qualified as a PFIC, and any gain from such deemed sale would be treated as described above.
Each U.S. holder of our ordinary shares is strongly urged to consult his, her or its tax advisor regarding the application of these rules and the availability of any potential elections.
47
The price of our ordinary shares may be volatile, and you may lose all or part of your investment.
Our ordinary shares were first publicly offered in our initial public offering in September 2014, at a price of $300.00 The market price of our ordinary shares has been in the past, and could continue to be, highly volatile and may fluctuate substantially as a result of many factors. Moreover, while there is no established public trading market for the warrants offered in our follow-on public offerings, and we do not expect one to develop, our ordinary shares will be issuable pursuant to exercise of these warrants. Because the warrants are exercisable into our ordinary shares, volatility, or a reduction in the market price of our ordinary shares could have an adverse effect on the trading price of the warrants. Factors which may cause fluctuations in the price of our ordinary shares include, but are not limited to:
| ● | actual or anticipated fluctuations in our growth rate or results of operations or those of our competitors; |
| ● | customer acceptance of our products; |
| ● | announcements by us or our competitors of new products or services, commercial relationships, acquisitions, or expansion plans; |
| ● | announcements by us or our competitors of other material developments; |
| ● | our involvement in litigation; |
| ● | changes in government regulation applicable to us and our products; |
| ● | sales, or the anticipation of sales, of our ordinary shares, warrants and debt securities by us, or sales of our ordinary shares by our insiders or other shareholders, including upon expiration of contractual lock-up agreements; |
| ● | developments with respect to intellectual property rights; |
| ● | competition from existing or new technologies and products; |
| ● | changes in key personnel; |
| ● | the trading volume of our ordinary shares; |
| ● | changes in the estimation of the future size and growth rate of our markets; |
| ● | changes in our quarterly or annual forecasts with respect to operating results and financial conditions; |
| ● | general economic and market conditions and; |
| ● | announcements regarding business acquisitions. |
In addition, the stock markets have experienced extreme price and volume fluctuations. Broad market and industry factors may materially harm the market price of our ordinary shares, regardless of our operating performance. Technical factors in the public trading market for our ordinary shares may produce price movements that may or may not comport with macro, industry or Company-specific fundamentals, including, without limitation, the sentiment of retail investors (including as may be expressed on financial trading and other social media sites), the amount and status of short interest in our securities, access to margin debt, trading in options and other derivatives on our ordinary shares and any related hedging or other technical trading factors. In the past, following periods of volatility in the market price of a company’s securities, securities class action litigation has often been instituted against that company, as was the case for ReWalk in a securities class action dismissed in full in November 2020. If we become involved in any similar litigation, we could incur substantial costs and our management’s attention and resources could be diverted.
Risks RelatingRelated to Our Incorporation and Location in Israel
Conditions in Israel, including Israel’s war against Hamas and other terrorist organizations in the Gaza Strip and a potential escalation of the conflict on Israel’s northern border, may materially and adversely affect our business and results of operations.
In early October 2023, Hamas terrorists based in the Gaza Strip attacked cities and villages inside Israel, murdering approximately 1,400 Israelis, wounding thousands, and abducting more than 200. The attack was accompanied by numerous rocket attacks on central and southern Israel. These rocket attacks continue through the date of this annual report. Israel called up substantial numbers of reservists and responded with extensive aerial attacks and a broad ground attack on terrorist targets in Gaza.
Following the attack by Hamas on Israel’s southern border, Hezbollah in Lebanon has also launched missile, rocket, and shooting attacks against Israeli military sites, troops, and civilian areas in northern Israel. In response to these attacks, the Israeli army has carried out a number of targeted strikes on Hezbollah in southern Lebanon and targets in Syria. It is possible that other terrorist organizations, including those located in the West Bank, as well as other countries hostile to Israel, such as Iran, will join the hostilities. Terrorist groups have also attacked U.S. military targets in the Middle East. These clashes have recently intensified and may escalate into a greater regional conflict.
48
Although we continue to monitor the situation closely, to date our operations in Israel – consisting primarily of the operations, quality, and R&D functions of the legacy ReWalk business and some finance functions – have continued without material interruption. In 2023, sales to customers in Israel accounted for less than 2% of our total revenues, and as of the date of this filing, approximately 80% of our employees are located outside of Israel. With the acquisition of AlterG in August 2023 and the anticipated shift in our sources of revenue in connection therewith, our Israel operations have become a less significant portion of our consolidated ReWalk operations. Our Israeli facilities are based in northern Israel, in an area that to date has seen minor disruptions from rocket attacks. Although to date none of our Israeli employees have been mobilized for emergency military service, we cannot predict whether there will be further mobilization of reservists and any further mobilization could further impact our employees, including employees who serve in critical roles in our company, which could adversely affect our ability to operate and our results of operations.
Sanmina, a well-established contract manufacturer with expertise in the medical device industry, manufactures all of our legacy ReWalk products at its facility in northern Israel. There has been no disruption to date to Sanmina’s business. If this facility were to be damaged or destroyed, or if Sanmina were otherwise unable to operate this facility, this could affect the supply of our legacy ReWalk products, and our business and our operating results would be negatively affected.
This is a rapidly changing situation, and we cannot predict how events will develop over the coming weeks and months. There can be no assurance that a significant expansion or worsening of the war will not have a material adverse effect on our ongoing development efforts, our business and our operating results.
Our technology development and quality headquarters and the manufacturing facility for our products are located in Israel and, therefore, our results may be adversely affected by economic restrictions imposed on, and political and military instability in, Israel.
Our technology development and quality headquarters, which houses substantially all of our research and development and our core research and development team, including engineers, machinists, researchers, and clinicalquality and regulatory personnel, as well as the facility of our contract manufacturer, Sanmina, are located in Israel. Many of our employees, directors and officers are residents of Israel. Accordingly, political, economic, and military conditions in Israel and the surrounding region may directly affect our business. Since the establishment of the State of Israel in 1948, a number of armed conflicts have taken place between Israel and its Arab neighbors, Hamas, (an Islamist militia and political group in the Gaza Strip), Hezbollah (an Islamist militia and political group in Lebanon) and other armed groups. Any hostilities involving Israel or the interruption or curtailment of trade within Israel or between Israel and its trading partners could materially and adversely affect our business, financial condition and results of operations and could make it more difficult for us to raise capital. In particular, an interruption of operations at the Tel Aviv airport related to the conflict in the Gaza Strip or otherwise could prevent or delay shipments of our components or products. Although we maintain inventory in the United States and Germany, an extended interruption could materially and adversely affect our business, financial condition, and results of operations.
Recent political uprisings, social unrest, and violence in various countries in the Middle East and North Africa, including Israel’s neighbors Lebanon, Egypt, and Syria, are affecting the political stability of those countries. This instability may lead to deterioration of the political relationships that exist between Israel and these countries and has raised concerns regarding security in the region and the potential for armed conflict. Our commercial insurance doescovers some, but not coverall, losses that may occur as a result of an event associated with the security situation in the Middle East. Any losses or damages incurred by us could have a material adverse effect on our business. In addition, Iran has threatened to attack Israel and is widely believed to be developing nuclear weapons. Iran is also believed to have a strong influence among parties hostile to Israel in areas that neighbor Israel, such as the Syrian government, Hamas in Gaza and Hezbollah in Lebanon. Any armed conflicts, terrorist activities or political instability in the region could materially and adversely affect our business, financial condition, and results of operations.
Our operations and the operations of our contract manufacturer, Sanmina, may be disrupted as a result of the obligation of Israeli citizens to perform military service.
Many Israeli citizens are obligated to perform one month, and in some cases more, of annual military reserve duty until they reach the age of 45 (or older, for reservists with certain occupations) and, in the event of a military conflict, may be called to active duty. In response to terrorist activity, there have been periods of significant call-ups of military reservists. For example, the Israeli armed forces called up a significant number of reservists to active duty in connection with the recent conflict in the Gaza Strip. It is possible that there will be additional military reserve duty call-ups in the future in connection with this conflict or otherwise. Some of our executive officers and employees, as well as those of Sanmina, the manufacturer of all of our products, are required to perform annual military reserve duty in Israel and may be called to active duty at any time under emergency circumstances. As described in the risk factor above entitled “Conditions in Israel, including Israel’s war against Hamas and other terrorist organizations in the Gaza Strip and a potential escalation of the conflict on Israel’s northern border, may materially and adversely affect our business and results of operations,” in response to the attack by Hamas on Israel in October 2023 Israel has called up substantial numbers of reservists. Although to date these call-ups have not had a material impact on our operations or on Sanmina’s ability to manufacture our products, we cannot predict whether there will be further mobilization of reservists and our operations and the operations of Sanmina could be disrupted by such call-ups.
Our sales may be adversely affected by boycotts of Israel.
Several countries, principally in the Middle East, restrict doing business with Israel and Israeli companies, and additional countries may impose restrictions on doing business with Israel and Israeli companies whether as a result of hostilities in the region or otherwise. In addition, there have been increased efforts by activists to cause companies and consumers to boycott Israeli goods based on Israeli government policies. Such actions, particularly if they become more widespread, may adversely impact our ability to sell our products.
The tax benefits that are available to us require us to continue to meet various conditions and may be terminated or reduced in the future, which could increase our costs and taxes.
Some of our operations in Israel, referred to as “Beneficiary Enterprises,” carry certain tax benefits under the Israeli Law for the Encouragement of Capital Investments, 5719-1959, or the Investment Law. Substantially all of our future income before taxes can be attributed to these programs. If we do not meet the requirements for maintaining these benefits or if our assumptions regarding the key elements affecting our tax rates are rejected by the tax authorities, they may be reduced or cancelled, and the relevant operations would be subject to Israeli corporate tax at the standard rate. In addition to being subject to the standard corporate tax rate, we could be required to refund any tax benefits that we may receive in the future, plus interest and penalties thereon. Even if we continue to meet the relevant requirements, the tax benefits that our current “Beneficiary Enterprises” receive may not be continued in the future at their current levels or at all. If these tax benefits were reduced or eliminated, the amount of taxes that we pay would likely increase, as all of our Israeli operations would consequently be subject to corporate tax at the standard rate, which could adversely affect our results of operations. Additionally, if we increase our activities outside of Israel, for example, by way of acquisitions, our increased activities may not be eligible for inclusion in Israeli tax benefit programs. For a discussion of our current tax obligations, see “Part 2.II. Item 7. “Management’s7, Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
We have received Israeli government grants for certain of our research and development activities and we may receive additional grants in the future. The terms of those grants restrict our ability to manufacture products or transfer technologies outside of Israel, and we may be required to pay penalties in such cases or upon the sale of our company.
From our inception through December 31, 2017,2023, we received a total of $1.77$2.6 million from the IIA. We may in the future apply to receive additional grants from the IIA to support our research and development activities. With respect to suchsome grants that were royalty-bearing grants, we are committed to paypaying royalties at a rate of 3.0% to 3.5% on sales proceeds up to the total amount of grants received, linked to the dollar, and bearing interest at an annual rate of LIBOR applicable to dollar deposits. Even after payment in full of these amounts, we will still be required to comply with the requirements of the Israeli Encouragement of Industrial Research, Development and Technological Innovation Law, 1984, or the R&D Law, and related regulations, with respect to those past grants. When a company develops know-how, technology or products using IIA grants, the terms of these grants and the R&D Law restrict the transfer outside of Israel of such know-how, and of the manufacturing or manufacturing rights of such products, technologies, or know-how, without the prior approval of the IIA. Therefore, if aspects of our technologies are deemed to have been developed with IIA funding, the discretionary approval of an IIA committee would be required for any transfer to third parties outside of Israel of know-how or manufacturing or manufacturing rights related to those aspects of such technologies. Furthermore, the IIA may impose certain conditions on any arrangement under which it permits us to transfer technology or development out of Israel or may not grant such approvals at all.
In addition to the above, any non-Israeli citizen, resident or entity that, among other things, (i) becomes a holder of 5% or more of our share capital or voting rights, (ii) is entitled to appoint one or more of our directors or our chief executive officer or (iii) serves as one of our directors or as our chief executive officer (including holders of 25% or more of the voting power, equity or the right to nominate directors in such direct holder, if applicable) is required to notify the IIA and undertake to comply with the rules and regulations applicable to the grant programs of the IIA, including the restrictions on transfer described above. Such notification will be required in connection with the investment being made by Investor.an investor which may discourage or limit investments from foreign investors in our company.
50
We may become subject to claims for remuneration or royalties for assigned service invention rights by our employees, which could result in litigation and adversely affect our business.
A significant portion of our intellectual property has been developed by our employees in the course of their employment for us. Under the Israeli Patent Law, 5727-1967 or the Patent Law,(the “Patent Law”) and recent decisions by the Israeli Supreme Court and the Israeli Compensation and Royalties Committee, a body constituted under the Patent Law, employees may be entitled to remuneration for intellectual property that they develop for us unless they explicitly waive any such rights, although the validity of any such waivers remains open to judicial review.rights. Although we enter into agreements with our employees pursuant to which they agree that any inventions created in the scope of their employment or engagement are owned exclusively by us, we may face claims demanding remuneration. As a consequence of such claims, we could be required to pay additional remuneration or royalties to our current and former employees, or be forced to litigate such claims, which could negatively affect our business.
Provisions of Israeli law and our Articles of Association may delay, prevent, or otherwise impede a merger with, or an acquisition of, us, even when the terms of such a transaction are favorable to us and our shareholders.
Israeli corporate law regulates mergers, requires tender offers for acquisitions of shares above specified thresholds, requires special approvals for transactions involving directors, officers or significant shareholders and regulates other matters that may be relevant to such types of transactions. For example, a tender offer for all of a company’s issued and outstanding shares can only be completed if the acquirer receives positive responses from the holders of at least 95% of the issued share capital. Completion of the tender offer also requires approval of a majority of the offerees that do not have a personal interest in the tender offer, unless at least 98% of the company’s outstanding shares are tendered. Furthermore, the shareholders, including those who indicated their acceptance of the tender offer (unless the acquirer stipulated in its tender offer that a shareholder that accepts the offer may not seek appraisal rights), may, at any time within six months following the completion of the tender offer, petition an Israeli court to alter the consideration for the acquisition. Israeli law also requires a “special tender offer” in certain cases where a shareholder crosses the 25% or 45% holding threshold, and it imposes procedural and special voting requirements for the approval of a merger in certain cases.
Our Articles of Association provide that our directors (other than external directors)directors, a requirement of Israeli corporate law from which we have opted out in accordance with an exemption for which we are currently eligible) are elected on a staggered basis, such that a potential acquirer cannot readily replace our entire board of directors at a single annual general shareholder meeting. This could prevent a potential acquirer from receiving board approval for an acquisition proposal that our board of directors opposes.
Furthermore, Israeli tax considerations may make potential transactions unappealing to us or to our shareholders whose country of residence does not have a tax treaty with Israel exempting such shareholders from Israeli tax. For example, Israeli tax law does not recognize tax-free share exchanges to the same extent as U.S. tax law. With respect to mergers involving an exchange of shares, Israeli tax law allows for tax deferral in certain circumstances but makes the deferral contingent on the fulfillment of a number of conditions, including, in some cases, a holding period of two years from the date of the transaction during which sales and dispositions of shares of the participating companies are subject to certain restrictions. Moreover, with respect to certain share swap transactions, the tax deferral is limited in time, and when such time expires, the tax becomes payable even if no disposition of the shares has occurred. These and other similar provisions could delay, prevent or impede an acquisition of us or our merger with another company, even if such an acquisition or merger would be beneficial to us or to our shareholders.
It may be difficult to enforce a judgment of a U.S. court against us, our officers, and directors, to assert U.S. securities laws claims in Israel or to serve process on our officers and directors.
We are incorporated in Israel. Although the majority of our directors and executive officers reside within the United States and most of the assets of these persons are also likely located within the United States, some of our directors and executive officers reside and may have the majority of their assets outside the United States. Additionally, most of our assets are located outside of the United States. Therefore, a judgment obtained against us, or those of our directors and executive officers residing outside of the United States, including a judgment based on the civil liability provisions of the U.S. federal securities laws, may not be collectible in the United States and may not be enforced by an Israeli court. It also may be difficult for you to effect service of process in the United States on those directors and executive officers residing outside of the United States or to assert U.S. securities law claims in original actions instituted in Israel. Israeli courts may refuse to hear a claim based on an alleged violation of U.S. securities laws reasoning that Israel is not the most appropriate forum in which to bring such a claim. In addition, even if an Israeli court agrees to hear a claim, it may determine that Israeli law and not U.S. law is applicable to the claim. If U.S. law is found to be applicable, the content of applicable U.S. law must be proven as a fact by expert witnesses, which can be a time-consuming and costly process. Certain matters of procedure will also be governed by Israeli law. There is little binding case law in Israel that addresses the matters described above. As a result of the difficulty associated with enforcing a judgment against us in Israel, you may be able to collect only limited, or may be unable to collect any, damages awarded by either a U.S. or foreign court.
51
In April 2021, we amended our articles of association such that, unless we consent in writing to the selection of an alternative forum, (i) the federal courts of the United States will be the exclusive forum for the resolution of any claim arising under the Securities Act, and (ii) the Tel-Aviv District Court will be the exclusive forum for (a) a derivative action or derivative proceeding that is filed in the name of the Company; (b) any action grounded in a breach of fiduciary duty of a director, officeholder or other employee towards us or our shareholders; or (c) any action the cause of which results from any provision of the Companies Law or the Israel Securities Law, 5728-1968. We have retained the ability to consent to an alternative forum in circumstances if we determine shareholder interests are best served by permitting a particular dispute to proceed in a forum other than the federal district courts or State of Israel, as applicable. However, there is uncertainty as to whether a court would enforce these provisions.
Your rights and responsibilities as a shareholder will be governed by Israeli law, which differs in some material respects from the rights and responsibilities of shareholders of U.S. companies.
The rights and responsibilities of the holders of our ordinary shares are governed by our Articles of Association and by Israeli law. These rights and responsibilities differ in some material respects from the rights and responsibilities of shareholders in U.S.-based corporations. In particular, a shareholder of an Israeli company has a duty to act in good faith and in a customary manner in exercising its rights and performing its obligations towards the company and other shareholders, and to refrain from abusing its power in the company, including, among other things, in voting at a general meeting of shareholders on matters such as amendments to a company’s articles of association, increases in a company’s authorized share capital, mergers and acquisitions and related party transactions requiring shareholder approval. In addition, a shareholder who is aware that it possesses the power to determine the outcome of a shareholder vote or to appoint or prevent the appointment of a director or executive officer in the company has a duty of fairness toward the company. There is limited case law available to assist us in understanding the nature of this duty or the implications of these provisions. These provisions may be interpreted to impose additional obligations and liabilities on holders of our ordinary shares that are not typically imposed on shareholders of U.S. corporations.
Our business could be negatively affected as a result of actions of activist shareholders, and such activism could impact the trading value of our securities.
In recent years, certain Israeli issuers listed on United States exchanges have been faced with governance-related demands from activist shareholders, unsolicited tender offers and proxy contests. Given our relatively low market cap and cash balance we might be an attractive target for such activists, in connection with our 2022 Annual General Meeting of Shareholders, Creative Value Capital Limited Partnership (“CVC”), which claimed to hold approximately three percent of our outstanding shares, nominated two candidates for election to our board of directors and submitted two additional proposals (including amendments to our Articles of Association) for approval at our 2022 Annual General Meeting of Shareholders held on July 27, 2022. Although none of CVC’s proposals were approved at the meeting, addressing and responding to such proposals was significantly costly and time-consuming, and diverted the attention of our management and employees.
Responding to these types of actions by activist shareholders could be costly and time-consuming, disrupting our operations and diverting the attention of management and our employees. Such activities could interfere with our ability to execute our strategic plan. In addition, a proxy contest for the election of directors at our annual meeting would require us to incur significant legal fees and proxy solicitation expenses and require significant time and attention by management and our board of directors. The perceived uncertainties as to our future direction also could affect the market price and volatility of our securitiessecurities.
Exchange rate fluctuations between the U.S. dollar, the euro and the NIS may negatively affect our earnings.
The U.S. dollar is our functional and reporting currency. However, we pay a significant portion of our expenses in NIS and in euro, and we expect this to continue. As a result, we are exposed to exchange rate risks that may materially and adversely affect our financial results. Accordingly, any appreciation of the NIS or euro relative to the U.S. dollar would adversely impact our net loss or net income, if any. For example, if the NIS appreciates against the U.S. dollar or if the value of the NIS declines against the U.S. dollar at a time when the rate of inflation in the cost of Israeli goods and services exceeds the rate of decline in the relative value of the NIS, then the U.S. dollar cost of our operations in Israel would increase and our results of operations could be materially and adversely affected.
52
Our operations also could be adversely affected if we are unable to effectively hedge against currency fluctuations in the future.
We cannot predict any future trends in the rate of inflation in Israel or the rate of devaluation (if any) of the NIS against the U.S. dollar. For example, while the NIS devalued against the U.S. dollar at a rate of approximately 3.1% and 4% during the fiscal year 2023 and 2022, respectively, during the fiscal year 2021 the NIS appreciated against the U.S. dollar at a rate of approximately 3%, respectively. The Israeli annual rate of inflation amounted to 2.96%, 5.3%, and 1.5% for the years ended December 31, 2023, 2022 and 2021, respectively.
We have in the past engaged in limited hedging activities, and we may enter into other hedging arrangements with financial institutions from time to time. Any hedging strategies that we may implement in the future to mitigate currency risks, such as forward contracts, options and foreign exchange swaps related to transaction exposures may not eliminate our exposure to foreign exchange fluctuations.
We are subject to certain regulatory regimes that may affect the way that we conduct business internationally, and our failure to comply with applicable laws and regulations could materially adversely affect our reputation and result in penalties and increased costs.
We are subject to a complex system of laws and regulations related to international trade, including economic sanctions and export control laws and regulations. We also depend on our distributors and agents for compliance and adherence to local laws and regulations in the markets in which they operate. Significant political or regulatory developments in the jurisdictions in which we sell our products, such as those stemming from the presidential administration in the United States or the U.K.’s exit from the E.U., are difficult to predict and may have a material adverse effect on us. For example, in the United States, the Trump administration-imposed tariffs on imports from China, Mexico, Canada, and other countries, and expressed support for greater restrictions on free trade and increase tariffs on goods imported into the United States. Changes in U.S. political, regulatory, and economic conditions or in its policies governing international trade and foreign manufacturing and investment in the United States could adversely affect our sales in the United States.
We are also subject to the FCPA and may be subject to similar worldwide anti-bribery laws that generally prohibit companies and their intermediaries from making improper payments to government officials for the purpose of obtaining or retaining business. Despite our compliance and training programs, we cannot be certain that our procedures will be sufficient to ensure consistent compliance with all applicable international trade and anti-corruption laws, or that our employees or channel partners will strictly follow all policies and requirements to which we subject them. Any alleged or actual violations of these laws may subject us to government scrutiny, investigation, debarment, and civil and criminal penalties, which may have an adverse effect on our results of operations, financial condition and reputation.
Our business may be materially affected by changes to fiscal and tax policies. Potentially negative or unexpected tax consequences of these policies, or the uncertainty surrounding their potential effects, could adversely affect our results of operations and share price.
The rules dealing with U.S. federal, state and local income taxation are constantly under review by persons involved in the legislative process and by the Internal Revenue Service (the “IRS”) and the U.S. Treasury Department. Changes to tax laws (which changes may have retroactive application) could adversely affect us or holders of our ordinary shares. In recent years, many such changes have been made, and changes are likely to continue to occur in the future. It cannot be predicted whether, when, in what form or with what effective dates tax laws, regulations and rulings may be enacted, promulgated or issued, which could result in an increase in our or our shareholders’ tax liability or require changes in the manner in which we operate in order to minimize or mitigate any adverse effects of changes in tax law.
In addition, foreign governments may enact tax laws in response to the changes in the rules dealing with U.S. federal, state and local income taxation or otherwise that could result in further changes to global taxation and materially affect our financial position and results of operations. The uncertainty surrounding the effect of the reforms on our financial results and business could also weaken confidence among investors.
Certain U.S. holders of our ordinary shares may suffer adverse U.S. tax consequences if we are characterized as a controlled foreign corporation, or a CFC, under Section 957 of the Code.
Each “Ten Percent Shareholder” (as defined below) in a non-U.S. corporation that is classified as a “controlled foreign corporation,” or a CFC, for U.S. federal income tax purposes generally is required to include in income for U.S. federal tax purposes such Ten Percent Shareholder’s pro rata share of the CFC’s “Subpart F income,” global intangible low-taxed income, and investment of earnings in U.S. property, even if the CFC has made no distributions to its shareholders. Subpart F income generally includes dividends, interest, rents and royalties, gains from the sale of securities and income from certain transactions with related parties. In addition, a Ten Percent Shareholder that realizes gain from the sale or exchange of shares in a CFC may be required to classify a portion of such gain as dividend income rather than capital gain. A non-U.S. corporation generally will be classified as a CFC for U.S. federal income tax purposes if Ten Percent Shareholders own, directly or indirectly, more than 50% of either the total combined voting power of all classes of stock of such corporation entitled to vote or of the total value of the stock of such corporation. A “Ten Percent Shareholder” is a United States person (as defined by the Code), who owns or is considered to own 10% or more of (1) the total combined voting power of all classes of stock entitled to vote or (2) the value of all classes of stock of such corporation. The determination of CFC status is complex and includes attribution rules, the application of which is not entirely certain.
53
During our 2023 taxable year, we believe that we had one shareholder that was a Ten Percent Shareholder for U.S. federal income tax purposes. However, our CFC status for the taxable year ending on December 31, 2023, and our current taxable year is unknown, and we may be a CFC for the taxable year ending on December 31, 2023, our current taxable year or a following year. In addition, recent changes to the attribution rules relation to the determination of CFC status may make it difficult to determine our CFC status for any taxable year or the CFC status of any of our subsidiaries. U.S. holders should consult their own tax advisors with respect to the potential adverse U.S. tax consequences of becoming a Ten Percent Shareholder in a CFC. If we are classified as both a CFC and a passive foreign investment company, or PFIC, we generally will not be treated as a PFIC with respect to those U.S. holders that meet the definition of a Ten Percent Shareholder during the period in which we are a CFC.
If there are significant disruptions in our information technology systems, our business, financial condition, and operating results could be adversely affected.
The efficient operation of our business depends on our information technology systems. We rely on our information technology systems to effectively manage sales and marketing data, accounting and financial functions, inventory management, product development tasks, research and development data, customer service and technical support functions. Our information technology systems are vulnerable to damage or interruption from earthquakes, fires, floods and other natural disasters, terrorist attacks, attacks by computer viruses or hackers, power losses, and computer system or data network failures. In addition, our data management application is hosted by a third-party service provider whose security and information technology systems are subject to similar risks, and our products’ systems contain software which could be subject to computer virus or hacker attacks or other failures.
The failure of our or our service providers’ information technology systems or our products’ software to perform as we anticipate or our failure to effectively implement new information technology systems could disrupt our entire operation or adversely affect our software products and could result in decreased sales, increased overhead costs, and product shortages, all of which could have a material adverse effect on our reputation, business, financial condition, and operating results.
If we fail to properly manage our anticipated growth, our business could suffer.
Our growth and product expansion has placed, and we expect that it will continue to place, a significant strain on our management team and on our financial resources. Failure to manage our growth effectively could cause us to misallocate management or financial resources, and result in losses or weaknesses in our infrastructure, which could materially adversely affect our business. Additionally, our anticipated growth will increase the demands placed on our suppliers, resulting in an increased need for us to manage our suppliers and monitor for quality assurance. Any failure by us to manage our growth effectively could have an adverse effect on our ability to achieve our business objectives.
We are highly dependent on the knowledge and skills of our senior management, and if we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our business strategy.
Our ability to compete in the highly competitive medical devices industry depends upon our ability to attract and retain highly qualified managerial, scientific, sales and medical personnel. We are highly dependent on our senior management team and have benefited substantially from the leadership and performance of our senior management. For example, we depend on our Chief Executive Officer’s experience successfully scaling an early-stage medical device company, as well as the experience of other members of management. The loss of the services of any of our executive officers and other key employees, and our inability to find suitable replacements could result in delays in product development and harm our business. Competition for senior management in our industry is intense and we cannot guarantee that we will be able to retain our personnel. Additionally, we do not carry key man insurance on any of our current executive officers. The loss of the services of certain members of our senior management could prevent or delay the implementation and completion of our strategic objectives or divert management’s attention to seeking qualified replacements.
54
Shutdowns of the U.S. federal government could materially impair our business and financial condition.
Development of our product candidates and/or regulatory approval may be delayed for reasons beyond our control. For example, in 2018 and 2019 the U.S. government shut down several times and certain regulatory agencies, such as the FDA and the SEC, had to furlough critical FDA, SEC, and other government employees and stop critical activities. If a prolonged government shutdown or budget sequestration occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business. Further, in our operations as a public company, future government shutdowns could impact our ability to access the public markets, such as through the declaration of effectiveness of registration statements and obtain necessary capital in order to properly capitalize and continue our operations.
ITEM 1B.UNRESOLVED STAFF COMMENTS
None.
Cybersecurity Risk Management and Strategy
The Company relies on information systems and the data stored on them to conduct its operations. We have adopted and maintain a cybersecurity risk management program in accordance with our risk profile and business that is informed by and incorporates elements of industry standards.
Our cybersecurity risk management program incorporates multiple components, including, but not limited to, ongoing monitoring of critical risks from cybersecurity threats using automated tools. Additionally, we have implemented an employee education and training program, which we provide on an annual basis, that is designed to raise awareness of cybersecurity threats. To support our cybersecurity risk management program, we leverage managed service providers and other third-party information technology and cybersecurity providers and consultants, including to perform regular system scans and threat intelligence analysis. Additionally, we require certain third-party providers and consultants to adhere to contractual requirements relating to privacy and cybersecurity standards.
We have not identified any cybersecurity incidents or threats that have materially affected us or are reasonably likely to materially affect us, including our business strategy, results of operations, or financial condition. However, like other companies in our industry, we and our third-party vendors have from time to time experienced threats and security incidents that could affect our information or systems. For more information, please see the section entitled “Risk Factors” in this Annual Report on Form 10-K.
Governance
Our audit committee, which reports directly to the board of directors, is responsible for overseeing our cybersecurity risk management program. The audit committee receives periodic updates on cybersecurity risks, mitigation strategies, and, in the event of a cybersecurity incident, incident response strategies from our Chief Financial Officer (“CFO”). The audit committee updates the full board of directors on matters relating to cybersecurity risk management and critical cybersecurity risks as appropriate.
Our Chief Technology Officer (“CTO”), who reports directly to our Vice President of Finance and, ultimately, our Chief Financial Officer, is responsible for the day-to-day management of our cybersecurity risk management program. The individual currently serving in this position is a third-party consultant who maintains 20 years of experience advising similarly situated companies on information technology and cybersecurity risk management. Our CTO provides regular cybersecurity updates to our Vice President of Finance and Chief Financial Officer on matters relating to our cybersecurity program and cybersecurity risk management.
55
ITEM 2.PROPERTIES
Our corporate headquarters are located in Yokneam, Israel, our U.S. headquarters are located in Marlborough, Massachusetts, with additional offices in Fremont, California, and Queens, New York, and our European headquarters are located in Berlin, Germany.
All of our facilities are leased, and we do not own any real property. The table below sets forth details of the square footage of our current leased properties, all of which are fully utilized. We have no material tangible fixed assets apart from the properties described below.
| Square feet (approximate) | ||||
| Fremont, California | 40,320 | |||
| Marlborough, Massachusetts | 11,850 | |||
| Yokneam, Israel | 11,500 | |||
| Queens, New York | 1,105 | |||
| Berlin, Germany | 950 | |||
| Total | 65,725 | |||
We believe our facilities are adequate and suitable for our current needs.
ITEM 3.LEGAL PROCEEDINGS
Occasionally the Company iswe are involved in various claims, lawsuits, regulatory examinations, investigations and other legal matters arising, for the most part, in the ordinary course of business. The outcome of litigation and other legal matters is inherently uncertain. In making a determination regarding accruals, using available information, the Company evaluateswe evaluate the likelihood of an unfavorable outcome in legal or regulatory proceedings to which the Company iswe are a party and records a loss contingency when it is probable a liability has been incurred and the amount of the loss can be reasonably estimated.
Where the Company determineswe determine an unfavorable outcome is not probable or reasonably estimable, the Company doeswe do not accrue for any potential litigation loss. These subjective determinations are based on the status of such legal or regulatory proceedings, the merits of our defenses and consultation with legal counsel. Actual outcomes of these legal and regulatory proceedings may materially differ from the Company’sour current estimates. It is possible that resolution of one or more of the legal matters currently pending or threatened could result in losses material to the Company’sour consolidated results of operations, liquidity, or financial condition.
ITEM 4. MINE SAFETY DISCLOSURES.
Not applicable.
PART II
ITEM 5. MARKET FOR REGISTRANT'SREGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information
Our ordinary shares began trading publicly on The Nasdaq Global Market on September 12, 2014 under the symbol “RWLK” and were transferred for listing on The Nasdaq Capital Market effective May 25, 2017. The following table sets forth,In January 2024, the symbol for the periods indicated, the high and low sales prices of our ordinary shares as reported by the Nasdaq.
| High | Low | ||||||
| 2017 | |||||||
| Fourth quarter 2017 | $ | 1.60 | $ | 1.05 | |||
| Third quarter 2017 | $ | 2.00 | $ | 1.30 | |||
| Second quarter 2017 | $ | 3.20 | $ | 1.10 | |||
| First quarter 2017 | $ | 3.60 | $ | 1.85 | |||
| 2016 | |||||||
| Fourth quarter 2016 | $ | 6.50 | $ | 2.55 | |||
| Third quarter 2016 | $ | 7.85 | $ | 5.55 | |||
| Second quarter 2016 | $ | 10.79 | $ | 6.00 | |||
| First quarter 2016 | $ | 15.81 | $ | 7.41 | |||
was changed to “LFWD”. As of February 1, 2018, there were 32 record holders23, 2024, we had approximately 278,478 shareholders of our ordinary shares.record.
Dividend Policy
We have never declared or paid any cash dividends on our ordinary shares. We do not anticipate paying any cash dividends in the foreseeable future. We currently intend to retain future earnings, if any, to finance operations and expand our business. Any future determination relating to our dividend policy will be made at the discretion of our board of directors and will depend on a number of factors, including future earnings, capital requirements, financial condition and future prospects and other factors our board of directors may deem relevant. The distribution of dividends may also be limited by Israeli law, which permits the distribution of dividends only out of retained earnings or otherwise upon the permission of an Israeli court.
Israeli Taxes Applicable to U.S. Holders
A non-Israeli resident who derives capital gains from the sale of shares in an Israeli resident company that were purchased after the company was listed for trading on a stock exchange outside of Israel will be exempt from Israeli tax so long as (amongst other things) the shares were not held through a permanent establishment that the non-resident maintains in Israel. A partial exemption may be available for non-Israeli resident shareholders who acquired their shares prior to the issuer’s initial public offering.
However, non-Israeli corporations will not be entitled to the foregoing exemption if Israeli residents (i) have a controlling interest of more than 25% in such non-Israeli corporation or (ii) are the beneficiaries of, or are entitled to, 25% or more of the revenuesrevenue or profits of such non-Israeli corporation, whether directly or indirectly. Such exemption is not applicable to a person whose gains from selling or otherwise disposing of the shares are deemed to be a business income. Additionally, under the United States-Israel Tax Treaty, or the treaty, the sale, exchange or other disposition of shares by a shareholder who (i) is a U.S. resident (for purposes of the treaty), (ii) holds the shares as a capital asset, and (iii) is entitled to claim the benefits afforded to such person by the treaty, is generally exempt from Israeli capital gains tax. Such exemption will not apply if: (i) the capital gain arising from the sale, exchange or other disposition can be attributed to a permanent establishment in Israel; (ii) the shareholder holds, directly or indirectly, shares representing 10% or more of the voting capital during any part of the 12-month period preceding the disposition, subject to certain conditions; or (iii) such U.S. resident is an individual and was present in Israel for 183 days or more during the relevant taxable year. In such case, the sale, exchange, or disposition of our ordinary shares should be subject to Israeli tax, to the extent applicable; however, under the treaty, the taxpayer would be permitted to claim a credit for such taxes against the U.S. federal income tax imposed with respect to such sale, exchange, or disposition, subject to the limitations under U.S. law applicable to foreign tax credits. The treaty does not relate to U.S. state or local taxes.
In some instances where our shareholders may be liable for Israeli tax on the sale of their ordinary shares, the payment of the consideration may be subject to the withholding of Israeli tax at source. If the above exemptions from capital gains tax are not available, individuals will be subject to a 25% tax rate on real capital gains derived from the sale of shares as long as the individual is not a substantial shareholder of the corporation issuing the shares (in which case the individual will be subject to a 30% tax rate), and corporations will be subject to a 24%23% corporate tax rate for 2017. Under an amendment enacted in December 2016 to the Israel Income Tax Ordinance 1961-5721, or the ordinance, the corporate tax rate will decrease to 23% for 2018 and thereafter.rate. A substantial shareholder is generally a person who alone or together with such person’s relative or another person who collaborates with such person on a permanent basis, holds, directly or indirectly, at least 10% of any of the means of control of the corporation, including the right to vote, receive profits, nominate a director or an executive officer, receive assets upon liquidation, or order someone who holds any of the aforesaid rights how to act, regardless of the source of such right. A substantial shareholder will be subject to tax at a rate of 30% in respect of capital gains derived from the sale of shares issued by a corporation in which he or she is a substantial shareholder. The determination of whether the individual is a substantial shareholder will be made on the date on which the securities are sold. In addition, the individual will be deemed to be a substantial shareholder if at any time during the 12 months preceding the date of the sale he or she was a substantial shareholder.
57
Dividends paid on publicly traded shares, like our ordinary shares, to non-Israeli residents are generally subject to Israeli income tax at the rate of 25%, or 30% if the recipient of the dividend was a substantial shareholder at the time of distribution or at any time during the prior 12-month period. Such dividends are generally subject to Israeli withholding tax at a rate of 25% if the shares are registered with a nominee company (whether the recipient is a substantial shareholder or not), unless a different rate is provided under an applicable tax treaty, provided that a certificate from the Israeli Tax Authority allowing for a reduced withholding tax rate is obtained in advance. Under the treaty,United States-Israel Tax Treaty, the maximum rate of tax withheld at source in Israel on dividends paid to a holder of our ordinary shares who is a U.S. resident (for purposes of the treaty) is 25%. The treaty provides for reduced tax rates on dividends if (a) the shareholder is a U.S. corporation holding at least 10% of our issued voting power during the part of the tax year that precedes the date of payment of the dividend and held such minimal percentage during the whole of its prior tax year, and (b) not more than 25% of the Israeli company’s gross income consists of interest or dividends, other than dividends or interest received from subsidiary corporations or corporations 50% or more of the outstanding voting shares of which is owned by the Israeli company. The reduced treaty rate, if applicable, is 15% in the case of dividends paid from income derived from a Beneficiary or Preferred Enterprise (which is entitled to corporate tax benefits) or 12.5% otherwise. We cannot assure you that in the event we declare a dividend we will designate the income out of which the dividend is paid in a manner that will reduce shareholders’ tax liability. If the dividend is attributable partly to income derived from a Beneficiary or Preferred Enterprise and partly to other sources of income, the withholding rate will be a blended rate reflecting the relative portions of the two types of income. U.S. residents who are subject to Israeli withholding tax on a dividend may be entitled to a credit or deduction for U.S. federal income tax purposes in the amount of the taxes withheld.
Individuals who are individuals with a taxable income that exceeds NIS 800,000subject to tax in a tax year (linked to the Israeli consumer price index each year, which equaled NIS 807,143 in the 2017 tax year) will beIsrael are also subject to an additional tax referred to as High Income Tax, at the rate of 2%3% on their taxable income for such tax year that is in excess of such threshold. For this purpose, taxable income includes taxable capital gains from the sale of our shares and taxable income from dividend distributions. Under an amendment enacted in December 2016 to the ordinance, for 2017 and thereafter the rate of High Income Tax will increase to 3% and will be applicable to annual income exceeding NIS 640,000 (linkeda certain threshold (NIS 721,560 for 2024, linked to the annual change in the Israeli consumer price index each year)Consumer Price Index), which equaled 641,880 in 2018.
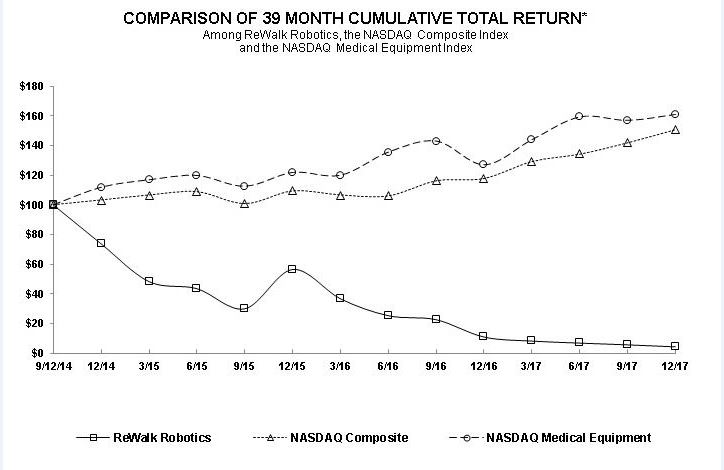
Recent Sales of Unregistered Equity Securities
Purchases of Equity Securities by the Issuer and Affiliated Purchasers
None.
ITEM 6. SELECTED FINANCIAL DATA[RESERVED]
| Year ended December 31 | |||||||||||||||||||
| (In thousands, except share and per share data) | |||||||||||||||||||
| 2017 | 2016 | 2015 | 2014 | 2013 | |||||||||||||||
| Revenues | $ | 7,753 | $ | 5,869 | $ | 3,746 | $ | 3,951 | $ | 1,588 | |||||||||
| Cost of revenues | 4,652 | 5,133 | 3,532 | 4,106 | 2,017 | ||||||||||||||
| Expense related to settlement of BIRD Foundation grants | — | — | — | 466 | — | ||||||||||||||
| Gross profit | 3,101 | 736 | 214 | (621 | ) | (429 | ) | ||||||||||||
| Operating expenses: | |||||||||||||||||||
| Research and development, net | 6,042 | 9,028 | 5,937 | 8,563 | 2,463 | ||||||||||||||
| Sales and marketing | 11,360 | 13,961 | 13,056 | 7,389 | 4,091 | ||||||||||||||
| General and administration | 7,691 | 8,188 | 6,395 | 3,352 | 1,762 | ||||||||||||||
| Total operating expenses | 25,093 | 31,177 | 25,388 | 19,304 | 8,316 | ||||||||||||||
| Operating loss | (21,992 | ) | (30,441 | ) | (25,174 | ) | (19,925 | ) | (8,745 | ) | |||||||||
| Loss on extinguishment of debt | 313 | — | — | — | — | ||||||||||||||
| Financial expenses, net | 2,293 | 2,059 | 188 | 1,698 | 3,410 | ||||||||||||||
| Loss before income taxes | (24,598 | ) | (32,500 | ) | (25,362 | ) | (21,623 | ) | (12,155 | ) | |||||||||
| Income taxes | 119 | 3 | 53 | 45 | 22 | ||||||||||||||
| Net loss | $ | (24,717 | ) | $ | (32,503 | ) | $ | (25,415 | ) | $ | (21,668 | ) | $ | (12,177 | ) | ||||
| Net loss per ordinary share, basic and diluted | $ | (1.22 | ) | $ | (2.47 | ) | $ | (2.10 | ) | $ | (6.34 | ) | $ | (74.53 | ) | ||||
| Weighted average number of shares used in computing net loss per ordinary share, basic and diluted | 20,214,895 | 13,178,107 | 12,115,038 | 3,766,694 | 185,688 | ||||||||||||||
| As of December 31, | |||||||||||||||||||
| (in thousands) | |||||||||||||||||||
| 2017 | 2016 | 2015 | 2014 | 2013 | |||||||||||||||
| Balance Sheet Data: | |||||||||||||||||||
| Cash and cash equivalents | $ | 14,567 | $ | 23,678 | $ | 17,689 | $ | 41,829 | $ | 8,860 | |||||||||
| Total assets | 22,863 | 31,763 | 25,574 | 47,665 | 11,059 | ||||||||||||||
| Accumulated deficit | (131,220 | ) | (106,492 | ) | (73,989 | ) | (48,574 | ) | (26,906 | ) | |||||||||
| Total shareholders’ equity | $ | 3,707 | $ | 8,260 | $ | 20,920 | $ | 43,853 | $ | 5,631 | |||||||||
ITEM 7. MANAGEMENT'SMANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion and analysis should be read in conjunction with “Part I. Item 6. Selected Financial Data” and our audited consolidated financial statements and the related notes included elsewhere in this annual report. This discussion contains forward-looking statements that are based on our management’s current expectations, estimates and projections for our business, which are subject to a number of risks and uncertainties. Our actual results may differ materially from those anticipated in these forward-looking statements as a result of many factors, including those set forth under “Special Note Regarding Forward-Looking Statements and “Part I. Item 1A. Risk Factors.”
Overview
We are an innovativea medical device company that is designing, developingdesigns, develops, and commercializingcommercializes life-changing solutions that span the continuum of care in physical rehabilitation and recovery, delivering proven functional and health benefits in clinical settings as well as in the home and community. Our initial product offerings were the ReWalk Personal and ReWalk Rehabilitation Exoskeleton devices for individuals with spinal cord injury (“SCI Products”). These devices are robotic exoskeletons that alloware designed for individuals with mobility impairments or other medical conditions the ability to stand and walk once again. We have developed and are continuing to commercialize ReWalk, an exoskeletonparaplegia that usesuse our patented tilt-sensor technology and an onboard computer and motion sensors to drive motorized legs that power movement. Additionally,These SCI Products allow individuals with spinal cord injury (“SCI”) the ability to stand and walk again during everyday activities at home or in the community. In March 2023, we are developingreceived clearance of our premarket notification (“510(k)”) from the U.S. Food and intendDrug Administration (“FDA”) for the ReWalk Personal Exoskeleton with stair and curb functionality, which adds usage on stairs and curbs to commercializethe indication for use for the device in the United States (U.S.). The clearance permits U.S. customers to participate in more walking activities in real-world environments in their daily lives where stairs or curbs may have previously limited them when using the exoskeleton for its intended, FDA-indicated uses. This feature has been available in Europe since initial CE Clearance, and real-world data from a cohort of 47 European users throughout a period of over seven years consisting of over 18,000 stair steps was collected to demonstrate the safety and efficacy of this feature and support the FDA submission.
58
We have sought to expand our product offerings beyond the SCI Products through internal development and distribution agreements and acquisitions. We have developed our ReStore Exo-Suit device, which we began commercializing in June 2019. The ReStore is a powered, lightweight soft suit exoskeleton, designed to support mobilityexo-suit intended for use during the rehabilitation of individuals suffering from otherwith lower limb disabilities suchdue to stroke. During the second quarter of 2020, we finalized and moved to implement two separate agreements to distribute additional product lines in the United States. We are the exclusive distributor of the MYOLYN MyoCycle FES Pro cycles to U.S. rehabilitation clinics and for the MyoCycle Home cycles available to US veterans through the Veterans Health Administration (“VHA”) hospitals. In the second quarter of 2020, we also became the exclusive distributor of the MediTouch Tutor movement biofeedback systems in the United States; however, due to unsatisfactory sales performance of the MediTouch product lines, we terminated this agreement as stroke, multiple sclerosis, cerebral palsy, Parkinson's diseaseof January 31, 2023. We refer to the MediTouch and elderly assistance.MyoCycle devices as our “Distributed Products.”
On August 11, 2023, we made our first acquisition to supplement our internal growth when we acquired AlterG, Inc. (“AlterG”), a leading provider of Anti-Gravity systems for use in physical and neurological rehabilitation. Our AlterG Anti-Gravity systems use patented, National Aeronautics and Space Administration (“NASA”) derived differential air pressure (“DAP”) technology to reduce the effects of gravity and allow patients to rehabilitate with finely calibrated support and reduced pain. AlterG Anti-Gravity systems are utilized in over 4,000 facilities globally in more than 40 countries. We will continue to evaluate other products for distribution or acquisition that can broaden our product offerings further to help individuals with neurological injury and disability.
We are in the research stage of ReBoot, a personal soft exo-suit for home and community use by individuals post-stroke, and we are currently evaluating the reimbursement landscape and the potential clinical impact of this device. This product would be a complementary product to ReStore as it provides active assistance to the ankle during plantar flexion and dorsiflexion for gait and mobility improvement in the home environment, and it received Breakthrough Device Designation from the FDA in November 2021. Further investment in the development path of the ReBoot was paused in 2023 pending determination regarding the clinical and commercial opportunity of this device.
Our principal markets are primarily in the United States and Europe with some lesser sales in Asia, the Middle East and South America. We sell our products primarily directly in the United States, through a combination of direct sales and distributors (depending on the product line) in Germany, Canada, and Australia, and primarily through distributors in other markets. In markets where we sell direct to consumers, we have established relationships with clinics and rehabilitation centers, professional and college sports teams, and individuals and organizations in the SCI community, and in markets where we do not sell direct to consumers, our distributors maintain these relationships. We have primary offices in Marlborough, Massachusetts, Fremont, California, Berlin, Germany and Yokneam, Israel, from where we operate our business.
We have in the past generated and expect to generate in the future expect to generate revenuesrevenue from a combination of clinics and rehabilitation centers, commercial distributors, third-party payors self-payors, including(including private and government employers,payors), professional and institutions.college sports teams, and self-pay individuals. While a broad uniform policy of coverage and reimbursement by third-party commercial payors currently does not exist in the United States for electronic exoskeleton technologies such as the ReWalk Personal Exoskeleton, we are pursuing various paths of reimbursement and support fundraising efforts by institutions and clinics. Inclinics, such as the VHA policy that was issued in December 2015 the Veterans' Administration (the “VA”) issued a national policy for the evaluation, training, and procurement of ReWalk Personal exoskeletonExoskeleton systems for all qualifying veterans living with SCI across the United States. The VA policy
We have also pursued updates with the Centers for Medicare & Medicaid Services (“CMS”) to clarify the Medicare coverage category (i.e., benefit category) applicable for personal exoskeletons. In 2022, the National Spinal Cord Injury Statistical Center (“NSCISC”) reported that CMS is the first national coverageprimary payor for approximately 57% of the SCI population which are at least five years post their injury date, with Medicare representing a majority of this percentage. In July 2020, following a successful submission and hearing process, a code was issued for ReWalk Personal Exoskeleton, which may be used for purposes of claim submission to Medicare, Medicaid, and other payors.
On November 1, 2023, CMS released the Calendar Year 2024 Home Health Prospective Payment System Final Rule, CMS-1780-F (“Final Rule”), which was adopted through the notice and comment rulemaking process. The Final Rule includes a policy confirming that personal exoskeletons are included in the United States for qualifying individuals who have suffered spinal cord injury. Additionally,Medicare brace benefit category, as of January 1, 2024. Medicare personal exoskeleton claims with dates of service on or after January 1, 2024 that are billed using HCPCS code K1007 are assigned to date several private insurersthe brace benefit category. CMS reimburses items classified under the brace benefit category using a lump sum payment methodology.
On November 29, 2023, CMS included the “ReWalk Personal Prosthetic Exoskeleton System” in the United StatesHCPCS public meeting where it solicited feedback on a preliminary payment determination of $94,617 for HCPCS code K1007. The preliminary payment determination was made by CMS by applying a “gap filling” process, which was used in light of CMS determining that the code describing the technology has no fee schedule pricing history and Europe have provided reimbursementthat lower extremity exoskeletons incorporate “revolutionary features” that cannot be described by or considered comparable to any other existing code or combination of codes. As part of gap-filling, CMS utilizes verifiable supplier or commercial pricing information and adjusts this pricing information according to a deflation and update factor methodology. In applying this formula to the K1007 code describing the ReWalk Personal Exoskeleton, CMS says that it relied on information about average prices from 2020 market transactions for which CMS had data.
59
CMS solicited information on updated verifiable market transactions from ReWalk, as well as any other makers of similar bilateral, lower limb exoskeletons, to “ensure that the Medicare payment amount for this code accurately reflects the full market of devices that would be classified in certain cases,this code.” We participated in the HCPCS meeting process on November 29, 2023 to provide additional information to help ensure that the final payment determination accurately reflects current pricing information related to the market of lower-limb exoskeleton devices, including the current ReWalk Personal Exoskeleton. A final Medicare payment determination is expected from CMS in first quarter of 2024 with an April 1, 2024, effective date.
In Germany, we continue to make progress toward achieving coverage from the various government, private and inworker’s compensation payors for our SCI products. In September 2017, each of German insurer BARMER GEK ("Barmer"(“BARMER”) and national social accident insurance provider Deutsche Gesetzliche Unfallversicherung (“DGUV”), signed a confirmationindicated that they will provide coverage to users who meet certain inclusion and letter of agreement, respectively, regarding the provision of ReWalk systems for all qualifying beneficiaries.exclusion criteria. In February 2018, the head office of German statutory health insurance, or SHI,Statutory Health Insurance (“SHI”) Spitzenverband (“GKV”) confirmed their decision to list the ReWalk Personal 6.0 Exoskeleton Systemsystem in the German Medical Device Directory. This decision means that ReWalk will beis listed among all medical devices for compensation, which SHI providers can procure for any approved beneficiary on a case-by-case basis.
During the year 2020 and 2021, we announced several new agreements with German SHIs, including TK and DAK Gesundheit, as well as the first German Private Health Insurer (“PHI”), which outline the process of obtaining our devices for eligible insured patients. We have incurred net losses and negative cash flow from operations since inception and anticipate thisare also currently working with several additional SHIs on securing a formal operating contract that will establish the process of obtaining a ReWalk Personal Exoskeleton for their beneficiaries within their system. Additionally, to continuedate, several private insurers in the near term. In early 2017 we initiated a process to reduce expenses by up to 30% as compared to 2016. During 2017 our gross profit as a percentage of revenue increased to 40% as compared to 13%United States and Europe are providing reimbursement for ReWalk in 2016 and operating expenses decreased by 20% versus 2016. In 2018 we will continue to evaluate spending to reduce where possible while continuing to focus resources on achieving commercial reimbursement coverage decisions, commercialization activities, clinical studies including the FDA 522 postmarket study and the Restore clinical studies to support regulatory clearance and activities to commercialize the Restore device for stroke patients in the first half of 2019.certain cases.
Components of Our Statements of Operations
Revenue
We currently rely, and in the future will rely, on sales and rentals of our ReWalk Personal and ReWalk Rehabilitation Exoskeleton devices, sales and rentals of our AlterG Anti-Gravity systems and related consumables and services, and sales of our ReStore exo-suit device, additional Distributed Products such as the MyoCycle, and related extended service contracts and extended warranties for our revenue.the SCI Products. Our revenue is generated from a combination of third-party payors, institutions and self-payors, including private and government employers.employers, institutions, and self-payors. Payments for our products by third party payors have been made primarily through case-by-case determinations. Third-party payors include, without limitation, private insurance plans, andworkers’ compensation programs, managed care programs,organizations, and government programs including the US Department of Veterans Affairs, worker's compensationVHA and Medicare and Medicaid.Medicare. We expect that third-party payors will be an increasingly important source of revenue in the future.future as we increase the volume of sales of ReWalk Personal systems to Medicare-eligible beneficiaries following establishment of a benefit category and anticipated pricing. In December 2015, the VAVHA issued a national policy for the evaluation, training, and procurement of ReWalk Personal exoskeletonExoskeleton systems for all qualifying veterans across the United States. The VAVHA policy is the first national coverage policy in the United States for qualifying individuals who have suffered spinal cord injury.
ReWalk Personal and ReWalk Rehabilitation Exoskeleton systems sold until the end of the current year are generally covered by a two-yearfive-year warranty from the date of purchase, which is included in the purchase price. We offer customers the ability to purchase, any time during the initialThe warranty period, an extended warranty for up to three additional years. Both warranties covercovers all elements of the ReWalk system,systems, including the batteries, other than normal wear and tear. InOur ReStore device is sold with a two-year warranty. The AlterG Anti-Gravity systems are sold with a one-year factory warranty covering parts and services in the beginning of 2018 we updated our service policy for new devices sold to includeU.S. and a five-year warranty.
Cost of RevenuesRevenue and Gross Profit (Loss)
For ReWalk and ReStore, cost of revenue consists primarily of complete systems purchased from our outsourced manufacturer, Sanmina,Sanmina. For these products, cost of revenue also includes internal costs such as salaries and related personnel costs including non-cash share basedshare-based compensation, associated withfunctions that support manufacturing and inventory management, training and inspection, service activities, freight costs, and reserves for warranty and service costs, shipping and handling and manufacturing startup and transition costs. Prior to the first quarter of 2014, when we completed the manufacturing transition to Sanmina,inventory condition. The cost of revenues also included costs of components, compensation related costs associated with manufacturing and costs to transition manufacturing to Sanmina. Cost of revenuesrevenue also includes royalties and expenses related to royalty-bearing research and development grantsgrants.
60
For our AlterG systems, which we manufacture ourselves at our facility in Fremont, California, cost of revenue consists primarily of raw materials, direct labor, indirect labor, and salesother factory overhead costs such as rent and marketing grants.utilities. In addition, cost of revenue also includes field service costs, shipping expenses and reserves for warranty and inventory condition.
For Distributed Products such as the MyoCycle cost of revenue consists primarily of complete systems purchased from MYOLYN. In addition, the cost of revenue also includes field service costs and shipping expenses.
Our gross profit (loss) and gross margin (defined as gross profit as a percentage of sales isrevenue) are influenced by a number of factors, including primarily the volume and price of our products sold, fluctuations in the mix of products sold, and fluctuationsvariability in our cost of revenues. Certain one-time expenses also impact gross margins including a 2014 expense relating to the early settlement, at a discount, of a royalty-bearing grant to the BIRD Foundation and 2015 and 2016 costs to transition manufacturing to the ReWalk Personal 6.0 model.revenue. We expect gross profit (loss) as a percentage of salesand gross margin will improveexpand in the future as we increase our salesrevenue volumes and decreaserealize operating efficiencies associated with greater scale which will reduce the product manufacturing costs.cost of revenue as a percentage of revenue.
Operating Expenses
Research and Development Expenses, Net
Research and development expenses, net consist primarily of salaries and related personnel costs including share-based compensation, supplies, materials, and consulting expenses relatedassociated with to product design and development, clinical studies, regulatory submissions, patent costs, sponsored research costs and other expenses related to our product development and research programs.activities. We expense all research and development expenses as they are incurred. We believe that continued investment in research and development is crucial to attaining our strategic product objectives.
Research and development expenses are presented net of the amount of any grants we receive for research and development in the period in which we receive the grant. We previously received grants and other funding from the BIRD Foundation and the Israel Innovation Authority, or “IIA” (formerly known as the Office of the Chief Scientist).IIA. Certain of those grants require us to pay royalties on sales of ReWalkcertain systems, which are recorded as cost of revenues.revenue. We may receive additional funding from these entities or others in the future. See “Grants and Other Funding” below.
Sales and Marketing Expenses
Our sales and marketing expenses consist primarily of salaries and related personnel costs including share-based compensation for sales, sales support, marketing, and reimbursement personnel,related activities, travel, marketing, advertisement, tradeshows and conferences, lobbying, and public relations activities and consulting costs. Also included in the sales and marketing expenses are the costs associated with our reimbursement activities in the United States and Germany.activities.
General and Administrative Expenses
Our general and administrative expenses consist primarily of salaries and related personnel costs including share-based compensation for our administrative, finance, and general management personnel, professional services, and insurance.
Financial Income (Expenses)Expenses (Income), Net
Financial income and expenses consist of bank commissions, foreign exchange gains and losses, interest earned on investments in short term deposits and revaluation of the fair value of warrants to purchase our preferred shares and expenses related to our convertible loans, which were issued in 2013 and are no longer outstanding.royalty income.
Interest income consists of interest earned on our cash and cash equivalent balances. Interest expense consists of interest accrued on, and certain other costs with respect to any indebtedness. Foreign currency exchange changes reflect gains or losses related to transactions denominated in currencies other than the U.S. dollar.
Taxes on Income
As of December 31, 2017,2023, we had not yet generated taxable income in Israel. As of that date, our net operating loss carry forwardscarryforwards for Israeli tax purposes amounted to approximately $108.6$242.6 million. After we utilize our net operating loss carry forwards,carryforwards, we are eligible for certain tax benefits in Israel under the Law for the Encouragement of Capital Investments, 1959. Our benefit period currently ends ten years after the year in which we first have taxable income in Israel provided that the benefit period will not extend beyond 2024. AlterG had federal net operating loss carry forwards totalling $31.4 million and state net operating loss carry forwards of $47.2 million, set to expire in 2025 and 2028, respectively.
Our taxable income generated outside of Israel will be subject to the regular corporate tax rate in the applicable jurisdictions. As a result, our effective tax rate will be a function of the relative proportion of our taxable income that is generated in those locations compared to our overall net income.
61
Grants and Other Funding
Israel Innovation Authority (formerly known as the Office of the Chief Scientist)
From our inception through December 31, 20172023, we have received a total of $1.77$2.6 million in funding from the IIA, $1.37$1.6 million of which are royalty-bearing grants, while $400 thousand were received in consideration for an investment in our preferred shares. Out ofshares while $570 thousand was received without future obligation. Of the royalty-bearing grants received, we have paid royalties to the IIA in the total amount of $50$110 thousand. We may apply to receive additional grants to support our research and development activities in 2017. The agreements with IIA require us to pay royalties at a rate of 3%-3.5% on sales of ReWalkcertain systems and related services up to the total amount of funding received for the development of these systems, linked to the dollar, and bearing interest at an annual rate of LIBOR applicable to dollar deposits. If we transfer IIA-supported technology or know-how outside of Israel, we will be liable for additional payments to IIA depending upon the value of the transferred technology or know-how, the amount of IIA support, the time of completion of the IIA-supported research project and other factors. As of December 31, 2017,2023, the aggregate contingent liability to the IIA was $1.4$1.6 million. For more information, see “Part I, Item 1A. Risk Factors-We have received Israeli government grants for certain of our research and development activities and we may receive additional grants in the future. The terms of those grants restrict our ability to manufacture products or transfer technologies outside of Israel...Israel and we may be required to pay penalties in such cases or upon the sale of our company.”
Results of Operations
Year Ended December 31, 20172023 Compared to Year Ended December 31, 20162022
Revenue
Our revenuesrevenue for 20172023 and 20162022 were as follows (dollars in thousands, except unit amounts):
| Years Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Revenue | $ | 13,854 | $ | 5,511 | ||||
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| Personal units placed | 103 | 109 | |||||
| Rehabilitation units placed | 4 | 10 | |||||
| Total units placed | 107 | 119 | |||||
| Personal unit revenues | $ | 7,463 | $ | 5,197 | |||
| Rehabilitation unit revenues | $ | 290 | $ | 672 | |||
| Revenues | $ | 7,753 | $ | 5,869 | |||
Revenues increased by $1.9consist of SCI Products, AlterG Anti-Gravity systems, ReStore and Distributed Products.
62
Revenue was $13.9 million, an increase of $8.3 million, or 32%51%, during 20172023 as compared to 2016 driven by our increased sales2022. Of this increase, $7.7 million was attributable to the AlterG business, which was acquired on August 11, 2023. The remaining increase of ReWalk Personal devices$0.7 million was a result of $2.3 million, or 44%, offset by decrease ina higher revenues from ReWalk Rehabilitation units of $382 thousand, or 57% during 2017 compared to 2016, The increase in revenue was primarily due to sales mix, including higher sales to the VA for use in an ongoing clinical study, reaching, as of December 31, 2017, 60 units placed as part of the study since its inception in the fourth quarter of 2015,Personal Exoskeletons and an increase in conversion of rental units into purchases.MyoCycles.
In the future, we expect our growth to be driven by sales of our ReWalk Personal device tothrough expansion of coverage and reimbursement by commercial and government third-party payors, as we continue to focusand our resources on broader commercial coverage policies with third-party payorsAlterG Anti-Gravity systems, as well as sales of Distributed Products, and the RestoreReStore device to rehabilitation institutes.clinics and personal users.
Gross Profit
Our gross profit for 20172023 and 20162022 were as follows (in thousands):
| Years Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Gross profit | $ | 4,453 | $ | 1,905 | ||||
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| Gross profit | $ | 3,101 | $ | 736 | |||
Gross profit was 40%$4.5 million, or 32% of revenue, for 2017,2023, as compared to a gross profit of 13%$1.9 million, or 35% of revenue for 2016.2022. The increase inAlterG business contributed $2.1 million of gross profit for 2023. Gross profit for 2023 also included the impact of $1.5 million for the amortization of intangible assets and purchase accounting inventory adjustments from the acquisition of AlterG. Excluding the impact of these factors resulting from the acquisition of AlterG, gross profit was driven by sales mix, the$2.4 million, or 38% of revenue for 2023, as compared to $1.9 million, or 35% of revenue for 2022. This increase was a result of a higher average selling price in 2023 due to new features in our ReWalk Personal Exoskeleton and MyoCycles.
We expect gross profit and gross margin will increase in the conversion of rental units into purchases, our cost reduction efforts and lower product costs.
Research and Development Expenses,Expense, Net
Our research and development expenses,expense, net for 20172023 and 2016 were2022 was as follows (in thousands):
| Years Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Research and development expense, net | $ | 4,148 | $ | 4,031 | ||||
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| Research and development expenses, net | $ | 6,042 | $ | 9,028 | |||
Research and development expenses, net, decreased by $3.0expense was $4.1 million in 2023, an increase of $0.1 million, or 33%3%, during 20172023 as compared to 2016.2022. The decrease in expenses is primarily attributable to a one-time chargeAlterG business contributed $0.8 million of $1.1 million recorded in 2016 related to the Collaboration Agreement and License Agreement with Harvard, grants received from the IIA which were credited to research and development expenses, and a decrease in personnel costs and personnel-related costs as a result of our cost reduction efforts, partially offset by an increase in costs related to developmentspending for 2023. Excluding the impact of the Restore device.acquisition of AlterG, research and development declined by $0.7 million, or 17% for the year ended December 31, 2023. The decrease is attributable to the conclusion of the stairs capability project and the gradual reduction of spend on the ReWalk 7 development project as it approached conclusion.
We intend to focus the rest of our research and development expenses in the near term primarilymainly on the Restore system for stroke patients and in the longer term on a “soft suit” exoskeleton for additional indications affecting the ability to walk, including multiple sclerosis, cerebral palsy, Parkinson’s disease and elderly assistance and the next generation of our current product support, as well as to advance the FDA submission for clearance of the ReWalk device.7 next-generation exoskeleton model. We have ongoing product development activity with our AlterG Anti-Gravity systems, including a program to develop a new entry level model of AlterG Anti-Gravity system aimed to improve the affordability to price-conscious customers.
63
Sales and Marketing ExpensesExpense
Our sales and marketing expense for 2023 and 2022 was as follows (in thousands):
| Years Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Sales and marketing expense | $ | 13,922 | $ | 9,842 | ||||
Sales and marketing expense was $13.9 million in 2023, an increase of $4.1 million, or 41%, during 2023 as compared to 2022. The AlterG business contributed $2.0 million of sales and marketing expenses for 2017 and 2016 were as follows (in thousands):
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| Sales and marketing expenses | $ | 11,360 | $ | 13,961 | |||
2023. Sales and marketing expenses decreased by $2.6for 2023 also included $0.6 million of amortization of intangible assets from the acquisition of AlterG. Excluding the impact of these factors resulting from the acquisition of AlterG, sales and marketing expenses increased $1.5 million, or 19%15%, during 2017 compared to 2016. This decrease isfor 2023. The remaining increase was primarily driven by lower personnel and personnel-related costs and reducedhigher consulting expenses as result of our cost reduction efforts.related to the CMS reimbursement process and market access initiatives.
In the near term our sales and marketing expensesexpense are expected to be driven by our commercialization efforts and reimbursement for the ReWalk Personal device as we continue to pursue insurance claims on a case- by- case basis, manage claims through the review process and invest in efforts to expand the reimbursement coverage as well as commercialization expenses forof our ReWalk Personal Exoskeleton device, to integrate and unify the Restore device.combined sales and marketing resources of the ReWalk and AlterG organizations, and to support our current commercial product activities.
General and Administrative ExpensesExpense
Our general and administrative expense for 2023 and 2022 was as follows (in thousands):
| Years Ended December 31, | ||||||||
| 2023 | 2021 | |||||||
| General and administrative | $ | 9,995 | $ | 7,134 | ||||
General and administrative expense was $10.0 million, an increase of $2.9 million, or 40%, during 2023 as compared to 2022. The AlterG business contributed $1.1 million of general and administrative expenses for 2017 and 2016 were as follows (in thousands):
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| General and administrative | $ | 7,691 | $ | 8,188 | |||
2023. General and administrative expenses also included $2.5 million of M&A-related expenses, and $0.1 million of amortization of intangible assets from the acquisition of AlterG offset partially by $0.3 remeasurement of earn out liability. Excluding the impact of these factors resulting from the acquisition of AlterG, general and administrative expenses decreased by $497 thousand,$0.6 million, or 6%7%, during 2017 compared to 2016.for 2023. The decrease in expenses is primarily attributable towas mainly driven by lower professional expenses and personnel-related costs.services expenses.
Financial Expenses, Netincome, net
Our financial expenses,income, net for 20172023 and 2016 were as follows (in thousands):
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| Financial expenses, net | $ | 2,293 | $ | 2,059 | |||
| Years Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Financial income, net | $ | 1,467 | $ | *) | ||||
| Years Ended December 31, | |||||||
| 2017 | 2016 | ||||||
| Income tax | $ | 119 | $ | 3 | |||
*) Represents an amount lower than $1.
Income taxes increasedTax
Our income tax for 2023 and 2022 was as follows (in thousands):
| Years Ended December 31, | ||||||||
| 2023 | 2022 | |||||||
| Taxes on income (benefit) | $ | (12 | ) | $ | 467 | |||
Income tax decreased by $116 thousand or 3,867%$0.5 million during 20172023 as compared to 2016. This increase is2022, mainly related to a deferred tax expense as a result of the tax rate change in the U.S due to the TCJA.utilization of net operation losses forward arising from the acquisition of AlterG.
64
Year Ended December 31, 20162022 Compared to Year Ended December 31, 20152021
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| Personal units placed | 109 | 53 | |||||
| Rehabilitation units placed | 10 | 20 | |||||
| Total units placed | 119 | 73 | |||||
| Personal unit revenues | $ | 5,197 | $ | 2,766 | |||
| Rehabilitation unit revenues | $ | 672 | $ | 980 | |||
| Revenues | $ | 5,869 | $ | 3,746 | |||
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| Gross profit | $ | 736 | $ | 214 | |||
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| Research and development expenses, net | $ | 9,028 | $ | 5,937 | |||
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| Sales and marketing expenses | $ | 13,961 | $ | 13,056 | |||
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| General and administrative | $ | 8,188 | $ | 6,395 | |||
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| Financial expenses, net | $ | 2,059 | $ | 188 | |||
| Years Ended December 31, | |||||||
| 2016 | 2015 | ||||||
| Income tax | $ | 3 | $ | 53 | |||
Critical Accounting Policies
Our consolidated financial statements are prepared in accordance with United States generally accepted accounting principles. The preparation of our financial statements requires us to make estimates, judgments and assumptions that can affect the reported amounts of assets and liabilities, disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenuesrevenue and expenses during the reporting period. We base our estimates, judgments and assumptions on historical experience and other factors that we believe to be reasonable under the circumstances. Materially different results can occur as circumstances change and additional information becomes known. Besides the estimates identified above that are considered critical, we make many other accounting estimates in preparing our financial statements and related disclosures. See Note 2 to our audited consolidated financial statements presented elsewhere in this annual report for a description of the significant accounting policies that we used to prepare our consolidated financial statements. The critical accounting policies that were impacted by the estimates, judgments and assumptions used in the preparation of our consolidated financial statements are discussed below.
Revenue Recognition
Our revenue is recognized in accordance with ASC 605, “Revenue Recognition,”Topic 606 when delivery has occurred, persuasive evidenceobligations under the terms of an agreement exists,a contract with our customer are satisfied; generally, this occurs with the feetransfer of control of our products or services. Revenue is fixedmeasured as the amount of consideration to which we expect to be entitled in exchange for transferring products or providing services. To achieve this core principle, we apply the following five steps:
1. identify the contract with a customer;
2. identify the performance obligations in the contract;
3. determine the transaction price;
4. allocate the transaction price to performance obligations in the contract; and determinable, collectability is reasonably assured and no further obligations exist.
5. recognize revenue when or as we satisfy a performance obligation.
Provisions are made at the time of revenue recognition for any applicable warranty cost expected to be incurred. The timing for revenue recognition among the various products and customers is dependent upon satisfaction of such criteria and generally varies from either shipment or delivery to the customer depending on the specific shipping terms of a given transaction, as stipulated in the agreement with each customer. Other than pricing terms which may differ due to the different volumes of purchases between distributors and end-users, there are no material differences in the terms and arrangements involving direct and indirect customers. Our products sold through agreements with distributors are non-exchangeable, non-refundable, non-returnable and without any rights of price protection or stock rotation. Accordingly, we consider all the distributors as end-users. We generally do not grant a right of return for our products. There have been a few occasionsproducts except in which we experienced a return of our products. Therefore,rare circumstances, and in those cases we record reductions to revenue for expected future product returns based on our historical experience.experience and estimates.
65
For the majority of sales of ReWalk Rehabilitation Exoskeleton systems, we include insignificant training and consider the elements in the arrangement to be a single unit of accounting. In accordance with ASC 605, we have concluded thatperformance obligation. Therefore, the training is essential to the functionality of our systems. Therefore, we recognizeCompany recognizes revenue for the system and training only when control is transferred after delivery and when the training has been completed, in accordance with the agreement delivery terms towith the customer, and after the training has been completed, once all other revenue recognition criteria have been met. For sales of ReWalk Personal Exoskeleton systems to end users, and for sales of ReWalk Personal Exoskeleton or ReWalk Rehabilitation Exoskeleton systems to third party distributors, we do not provide training to the end user as this training is completed by the rehabilitation centers or by the distributor that have previously completed the ReWalk Training program. In certain cases, when
Warranties are classified as either assurance type or service type warranty. A warranty is considered an assurance type warranty if it provides the consumer with assurance that the product arrangementswill function as intended for a limited period of time.
SCI Products include a five-year warranty. The first two years are bundled withconsidered as an assurance type warranty and the additional period is considered an extended service arrangement, which is a service type warranty. A service type warranty is either sold with a unit or separately for a unit for which the separation of the extended warranty falls under the scope of ASC 605-20-25-1 through 25-6,has expired. A service type warranty is accounted as a separate performance obligation and the separate price of the extended warranty stated in the agreementrevenue is deferred and recognized ratably over the extended warranty period. Deferred revenue includes primarily unearned amounts received in respect of service contracts but not yet recognized as revenues. The Company also offers a rent-to-purchase option for its ReWalk Personal device. Those transactions provide potential customers the option to lease the device for a short term, after which they can choose whether to purchase it. In such cases, the Company recognizes revenues over the period of the rent once all other revenue criteria are met.
The ReStore device is sold with a two-year warranty which is considered as assurance type warranty.
The Distributed Products are sold with an assurance type warranty ranging from between three years to ten years, depending on the specific part.
The AlterG Anti-Gravity systems are sold with a one-year assurance type warranty for parts and do not presently plan to pay cash dividendslabor in the foreseeable future. Consequently,US and with a two-year assurance type warranty for parts for distributors. We also sell extended warranties for AlterG Anti-Gravity systems for the periods after the expiration of the original warranty. These are accounted for as separate performance obligations from the AlterG Anti-Gravity system.
We rent our AlterG Anti-Gravity systems to customers for a fixed monthly fee over the rental term, which typically ranges from 2 to 3 years. Rental revenues accounted for under ASC Topic 842 and are recorded as earned on a monthly basis. We also offer for the SCI Products a rent-to-purchase model in which we used an expected dividend yield of zero.
Income Taxes
As part of the process of preparing our consolidated financial statements, we are required to estimate our taxes in each of the jurisdictions in which we operate. We account for income taxes in accordance with ASC Topic 740, “Income Taxes,” or ASC Topic 740. ASC Topic 740 prescribes the use of an asset and liability method whereby deferred tax asset and liability account balances are determined based on the difference between book value and the tax bases of assets and liabilities and carryforward tax losses. Deferred taxes are measured using the enacted tax rates and laws that are expected to be in effect when the differences are expected to reverse. We exercise judgment and provide a valuation allowance, if necessary, to reduce deferred tax assets to their estimated realizable value if it is more likely than not that some portion or all of the deferred tax asset will not be realized. We have established a full valuation allowance with respect to our deferred tax assets.
ASU 2015-17, “Balance Sheet Classification of Deferred Taxes"Taxes” provides presentation requirements to classify deferred tax assets and liabilities, along with any related valuation allowance, are classified as non-current on the balance sheet .sheet. We account for uncertain tax positions in accordance with ASC 740 and recognize the tax benefit from an uncertain tax position only if it is more likely than not that the tax position will be sustained on examination by the taxing authorities, based on the technical merits of the position. The tax benefits recognized in the financial statements from such a position should be measured based on the largest benefit that has a greater than 50% likelihood of being realized upon ultimate settlement. Accordingly, we report a liability for unrecognized tax benefits resulting from uncertain tax positions taken or expected to be taken in a tax return. We recognize interest and penalties, if any, related to unrecognized tax benefits in tax expense.
66
Recently Issued and Adopted Accounting Pronouncements
A discussion of recent accounting pronouncements is included in Note 2u,2w, New Accounting Pronouncements, to our consolidated financial statements included elsewhere in this annual report.
Liquidity and Capital Resources
Sources of Liquidity and Outlook
Since inception, we have funded our operations primarily through the sale of certain of our equity securities and convertible notes to investors in private placements, the sale of our ordinary sharesequity securities in public offerings, cash exercises of outstanding warrants and the incurrence of bank debt.
For the full year ended December 31, 2017, the Company2023, we incurred a consolidated net loss of $22.1 million and had cash and cash equivalents of $14.6 million. The Company has an accumulated deficit in the total amount of $131.2 million as of$235.9 million. Our cash and cash equivalents on December 31, 20172023, totalled $28.1 million. Our negative operating cash flow for the full year ended December 31, 2023, was $20.7 million. We have sufficient funds to support our operation for more than 12 months following the approval of our consolidated financial statements for the fiscal year ended December 31, 2023.
We expect to incur future net losses and further losses are anticipated in the development of its business. Those factors raise substantial doubt about the Company’s abilityour transition to continue as a going concern. The ability to continue as a going concernprofitability is dependent upon, among other things, the Company obtainingsuccessful development and commercialization of our products and product candidates, the necessary financingestablishment of contracts for the distribution of new product lines, or the acquisition of additional product lines, any of which, or in combination, would contribute to meet its obligations and repay its liabilities arisingthe achievement of a level of revenue adequate to support our cost structure. Until we achieve profitability or generate positive cash flows, we will continue to need to raise additional cash from normal businesstime to time.
We intend to fund future operations when they come due.
Our anticipated primary uses of cash are funding (i) sales, marketing, and reimbursement expensespromotion activities related to market development activitiesfor our ReWalk Personal Exoskeleton device and AlterG Anti-Gravity system, broadening third-party payor and CMS coverage for our ReWalk Personal Exoskeleton device and commercializing our new product lines added through distribution agreements; (ii) researchdevelopment of future generation designs for our ReWalk device, new AlterG products utilizing DAP technology, and development costs related to, in the shorter term, our Restore device that will assist patients who had stroke,lightweight exo-suit technology for potential home personal health utilization for multiple indications; (iii) routine product updates; (iv) potential acquisitions of businesses, such as our recent acquisition of AlterG, and in the longer term, developing our next generation of ReWalk with design improvements and building upon our technological platform to address new medical indications that affect the ability to walk(v) general corporate purposes, including cerebral palsy, Parkinson’s disease and elderly assistance.working capital needs. Our future cash requirements will depend on many factors, including our rate of revenue growth, the expansion of our sales and marketing activities, the timing and extent of our spending on research and development efforts, the attractiveness of potential acquisition candidates and international expansion. If our current estimates of revenue, expenses or capital or liquidity requirements change or are inaccurate, we may seek to sell additional equity or debt securities, arrange for additional bank debt financing, or refinance our indebtedness. There can be no assurance that we will be able to raise such funds on acceptable terms. For more information, see “Part I, Item 1A. Risk Factors-We have concluded that there are substantial doubts as to our ability to continue as a going concern.”
Equity Raises
Beginning with the filing of ordinary shares, warrants and/or debt securities and up to 4,388,143 ordinary shares offered by selling shareholders named therein. On May 10, 2016, we entered into our Equity Distribution Agreement with Piper Jaffray, pursuant to which we may offer and sell, from time to time, ordinary shares having an aggregate offering price of up to $25.0 million through Piper Jaffray acting as our agent. The ordinary shares issued under the Equity Distribution Agreement may be registered under the Securities Act using our Form S-3.
67
Equity Offerings and costly, including due to potential SEC review. We may also conduct such offerings in the form of private placements, potentially with registration rights or priced at a discount to the market value of our ordinary shares, which could require shareholder approval under the rules of the NASDAQ. Any such transactions could result in substantial dilution of shareholders’ interests.Warrant Exercises
On May 10, 2016, we entered into our Equity Distribution Agreement with Piper Jaffray, pursuant to which we may offer and sell, from time to time, ordinary shares having an aggregate offering price of up to $25.0 million through Piper Jaffray acting as our agent. Subject to the terms and conditions of the Equity Distribution Agreement, Piper Jaffray will use its commercially reasonable efforts to sell on our behalf all of the ordinary shares requested to be sold by us, consistent with its normal trading and sales practices. Piper Jaffray may also act as principal in the sale of ordinary shares under the Equity Distribution Agreement. Such sales may be made under our Form S-3 in what may be deemed “at-the-market” equity offerings as defined in Rule 415 promulgated under the Securities Act, directly on or through the Nasdaq Capital Market, to or through a market maker other than on an exchange or otherwise, in negotiated transactions at market prices prevailing at the time of sale or at prices related to such prevailing market prices, and/or any other method permitted by law, including in privately negotiated transactions.
On September 27, 2021, we signed a purchase agreement with certain institutional investors for the Company's follow-on public offeringissuance and sale of 6,857,00015,403,014 ordinary shares.shares, pre-funded warrants to purchase up to an aggregate of 610,504 ordinary shares and ordinary warrants to purchase up to an aggregate of 8,006,759 ordinary shares at an exercise price of $2.00 per share. The pre-funded warrants have an exercise price of $0.001 per ordinary share and are immediately exercisable and can be exercised at any time after their original issuance until such pre-funded warrants are exercised in full. Each ordinary share was sold at an offering price of $2.035 and each pre-funded warrant was sold at an offering price of $2.034 (equal to the public at apurchase price per ordinary share minus the exercise price of $1.05 per share. On November 22, 2017 Nationalthe pre-funded warrant). The offering of the ordinary shares, the pre-funded warrants and the ordinary shares that are issuable from time to time upon exercise of the pre-funded warrants was made pursuant to our shelf registration statement on Form S-3 initially filed with the SEC on May 9, 2019, and declared effective by the SEC on May 23, 2019, and the ordinary warrants were issued in a concurrent private placement. The ordinary warrants are exercisable at any time and from time to time, in whole or in part, following the date of issuance and ending five and one-half years from the date of issuance. All of the pre-funded warrants were exercised in full its optionon September 27, 2021, and the offering closed on September 29, 2021. Additionally, we issued warrants to purchase 1,028,550 additionalup to 960,811 ordinary shares, at the public offeringwith an exercise price of $1.05$2.5438 per share, lessexercisable from September 27, 2021, until September 27, 2026, to certain representatives of H.C. Wainwright as compensation for its role as the underwriting discount.placement agent in our September 2021 private placement offering.
As of December 31, 2023, warrants to purchase a total of 9,814,754 ordinary shares with exercise prices ranging from $1.25 to $1.79 were exercised, for total gross proceeds of approximately $13.8 million. During the twelve months that ended December 31, 2023, no warrants were $8.3 million. The Company's net aggregate proceeds, after deducting underwriting discounts and commissions and expenses, were$7.2 million.exercised.
On March 6, 2018, we entered into an investment agreement with Timwell, pursuantJune 2, 2022, our board of directors approved a share repurchase program to which we agreed, in return for aggregate gross proceedsrepurchase up to us of $20$8.0 million to issue to Timwell an aggregate of 16,000,000 of our ordinary shares . On July 21, 2022, we received approval from an Israeli court for the share repurchase program. The program was scheduled to expire on the earlier of January 20, 2023, or reaching $8.0 million of repurchases. On December 22, 2022, our board of directors approved an extension of the repurchase program, with such extension to be in the aggregate amount of up to $5.8 million. The extension was approved by an Israeli court on February 9, 2023, and it expired on August 9, 2023.
As of December 31, 2023, pursuant to the share repurchase program, we had repurchased a total of 4,022,607 of our outstanding ordinary shares at a price per sharetotal cost of $1.25, Timwell will make the investment in three tranches, including $5 million for 4,000,000 shares in the first tranche, $10 million for 8,000,000 shares in the second tranche and $5 million for 4,000,000 shares in the third tranche. We intend to use the net proceeds from this agreement primarily for (i) sales, marketing activities related to market development in our existing markets as well as expanding into China and reimbursement expenses related to broadening third-party payor coverage and (ii) research and development costs related to developing our lightweight “soft suit” exoskeleton technology for various lower limb disabilities, including stroke and other indications affecting the ability to walk, while using the remainder for general corporate purposes. We will have broad discretion in the way that we use the net proceeds of this agreement.$3.5 million.
| Years Ended December 31, | ||||||||||||
| 2023 | 2022 | 2021 | ||||||||||
| Net cash used in operating activities | $ | (20,667 | ) | $ | (17,891 | ) | $ | (11,469 | ) | |||
| Net cash used in investing activities | (18,149 | ) | (25 | ) | (47 | ) | ||||||
| Net cash (used in) provided by financing activities | (992 | ) | (2,500 | ) | 79,512 | |||||||
| Effect of Exchange rate changes on Cash, Cash Equivalents and Restricted Cash | 45 | (79 | ) | — | ||||||||
| Net cash flow | $ | (39,763 | ) | $ | (20,495 | ) | $ | 67,996 | ||||
68
Year Ended December 31, 2018 and no later than April 1, 2019. For more information, see “Part I. Item 1. Business-Timwell Investment Agreement and Related Transactions.”
| Years Ended December 31, | |||||||||||
| 2017 | 2016 | 2015 | |||||||||
| Net cash used in operating activities | $ | (22,498 | ) | $ | (27,537 | ) | $ | (25,180 | ) | ||
| Net cash provided by (used in) investing activities | (21 | ) | (437 | ) | 1,083 | ||||||
| Net cash provided by financing activities | 13,408 | 33,783 | 137 | ||||||||
| Net cash flow | $ | (9,111 | ) | $ | 5,809 | $ | (23,960 | ) | |||
Net Cash Used in Operating Activities
Net cash used in operating activities decreased from $27.5was $20.7 million in 20162023, an increase of $2.8 million as compared to $22.5 million in 2017,2022 mainly due to higher consulting and professional services fees primarily as a resultassociated with the acquisition of increased revenue, lower operating expenses as result of cost reduction efforts, a decrease in expenses related to Collaboration AgreementAlterG and the Harvard License Agreement and additional grants received from the IIA.CMS reimbursement process, as well as increased inventory purchases.
Net Cash Provided by (Used in)Used in Investing Activities
Net cash used in investing activities decreased from $0.4increased to $18.1 million in 20162023 as compared to $21 thousand$0.03 million in 2017,2022, primarily as a resultdue to the acquisition of decreased use of cash for the purchase of property and equipment.AlterG.
Net Cash Provided byUsed in Financing Activities
Net cash used in financing activities was $0.9 million in 2017, which reflects $7.22023, a decrease of $1.5 million, net proceeds fromas compared to 2022. The decrease was due to the issuancerepurchase of our ordinary shares under our share repurchase program, which expired on August 9, 2023.
Year Ended December 31, 2022 Compared to Year Ended December 31, 2021
A discussion of changes in our cash flows in 2022 compared to 2021 has been omitted from this annual report on Form 10-K but may be found in “Part I. Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations” of our Form 10-K for the follow-on offeringfiscal year ended December 31, 2022, filed with the SEC on February 23, 2023, which is available free of charge on the SECs website at www.sec.gov and $9.3 million net proceeds from the issuance of ordinary shares in the ATM, which was offsetat golifeward.com, and is incorporated by $3.1 million in capital repayments and debt issuance costs related to the Loan Agreement with Kreos. We generated $33.8 million from financing activities in 2016, which reflects $20.0 million from the Loan Agreement entered into with Kreos, $11.1 million net proceeds from the issuance of ordinary shares in the follow-on offering and $4.1 million net proceeds from the issuance of ordinary shares in the ATM, which was offset by $1.4 million in capital repayments and debt issuance costs related to the Loan Agreement with Kreos.reference herein.
Obligations and Commercial Commitments
Set forth below is a summary of our contractual obligations as of December 31, 2017.2023:
Payments due by period (in dollars, in thousands) | ||||||||||||
| Contractual obligations | Total | Less than 1 year | 1-3 years | |||||||||
| Purchase obligations (1) | $ | 8,551 | $ | 8,551 | $ | — | ||||||
| Collaboration Agreement and License Agreement obligations (2) | 34 | 34 | — | |||||||||
| Operating lease obligations (3) | 2,050 | 1,364 | 686 | |||||||||
| Earnout liability (4) | 3,292 | 576 | 2,716 | |||||||||
| Total | $ | 13,927 | $ | 10,525 | $ | 3,402 | ||||||
| (1) | We depend on one contract manufacturer, Sanmina Corporation, for both the SCI products and the ReStore Products. We place our manufacturing orders with Sanmina pursuant to purchase orders or by providing forecasts for future requirements. The AlterG Anti-Gravity systems are produced in Fremont, California by us. Purchase orders are executed with suppliers based on our sales forecast. |
| (2) | Under the Collaboration Agreement, we were required to pay in quarterly installments the funding of our joint research collaboration with Harvard, subject to a minimum funding commitment under applicable circumstances. Our License Agreement with Harvard consists of patent reimbursement expenses payments and a license upfront fee payment. There are also several milestone payments contingent upon the achievement of certain product development and commercialization milestones and royalty payments on net sales from certain patents licensed to Harvard. All product development milestones contemplated by the License Agreement have been met as of December 31, 2023; however, there are still outstanding commercialization milestones under the License Agreement that depend on us reaching certain sales amounts, some or all of which may not occur. Our Collaboration Agreement with Harvard was concluded on March 31, 2022. |
| Payments due by period (in dollars, in thousands) | |||||||||||||||||||
| Contractual obligations | Total | Less than 1 year | 1-3 years | 3-5 years | More than 5 years | ||||||||||||||
| Purchase obligations (1) | $ | 745 | $ | 745 | $ | — | $ | — | $ | — | |||||||||
| Collaboration Agreement and License Agreement obligations (2) | 3,879 | 1,303 | 2,025 | 551 | — | ||||||||||||||
| Operating lease obligations (3) | 4,129 | 643 | 1,182 | 1,196 | 1,108 | ||||||||||||||
| Long-term debt obligations (4) | 18,456 | 6,441 | 12,015 | — | — | ||||||||||||||
| Total | $ | 27,209 | $ | 9,132 | $ | 15,222 | $ | 1,747 | $ | 1,108 | |||||||||
| (3) | Our operating leases consist of leases for our facilities in the United States, Israel and Germany and motor vehicles in Israel. |
| (4) | Earnout payments based on AlterG’s revenue growth during the two consecutive trailing twelve-month periods following closing of the acquisition. |
We calculated the payments due under our operating lease obligation for our Israeli office that are to be paid in NIS at a rate of exchange of NIS 3.467:3.627:$1.00, and the payments due under our operating lease obligation for our German subsidiary that are to be paid in euros at a rate of exchange of €1.00 :$1.129, both of which were the applicable exchange ratesrate as of December 31, 2017. We calculated the payments due under our Loan Agreement with Kreos according to the current schedule of repayment of principal and interest, taking into account the two tranches of debt drawn down under the Loan Agreement. For information on this repayment schedule, see “-Liquidity and Capital Resources-Loan Agreement with Kreos and Related Warrant to Purchase Ordinary Shares” above.2023.
Off-Balance Sheet Arrangements
We had no off-balance sheet arrangements or guarantees of third-party obligations during the periods presented.
Trend Information
For information on significant known trends, please see “Part I,ItemI-Item 1. “Business -– Overview” in this annual report.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Currency Exchange Risk
Our results of operations and cash flows are affected by fluctuations in foreign currency exchange rates. In 2017, 2016 andSince 2015, most of our revenuesexpenses were denominated in U.S. dollars and the remaining expenses were denominated in NIS and euro, until 2018 most of our revenue was denominated in U.S. dollars and the remainder of our revenuesrevenue was denominated in euroseuro and British pounds, and most ofpound whereas in the last four years our expenses were also denominated in U.S. dollars, and the remainder ofeuro revenue is higher than our expenses were denominated in NIS and euros.U.S dollar revenue. Accordingly, changes in the value of the NIS and euroEuro relative to the U.S. dollar in each of the years 2015, 20162023, 2022, and 20172021 impacted amounts recorded on our consolidated statements of operations for thosethese periods. We expect that the denominations of our revenue and expenses in 20182024 will be consistent with what we experienced in 2017.2023.
The following table presents information about the changesdevaluation in the exchange rates of the NIS and euro against the U.S. dollar in 2015, 20162023, 2022 and 2017:2021:
| Change in Average Exchange Rate | ||||||||
| Period | NIS against the U.S. Dollar (%) | Euro against the U.S. Dollar (%) | ||||||
| 2023 | (9.00 | ) | 2.67 | |||||
| 2022 | 3.70 | 10.84 | ||||||
| 2021 | (6.38 | ) | 3.46 | |||||
| Change in Average Exchange Rate | ||||||
| Period | NIS against the U.S. Dollar (%) | Euro against the U.S. Dollar (%) | ||||
| 2015 | (8.24 | ) | (16.44 | ) | ||
| 2016 | 1.34 | (0.23 | ) | |||
| 2017 | 6.81 | 1.96 | ||||
The figures above represent the change in the average exchange rate in the given period compared to the average exchange rate in the immediately preceding period. Negative figures represent depreciationthe devaluation of the U.S. dollar compared to the NIS or the euro. A 10% increase or decrease in the value of the NIS against the U.S. dollar would have decreased or increased our net loss by approximately $968$513 thousand in 2017.2023. A 10% increase or decrease in the value of the euro against the U.S. dollar would have decreased or increased our net loss by approximately $148$14 thousand in 2017.2023.
Other Market Risks
We do not believe that we have material exposure to interest rate risks or to inflationary risks.
ITEM 8.FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
The information required hereunder is set forth under Report of Independent Registered Public Accounting Firm, Consolidated Balance Sheets, Consolidated Statements of Operations, Statements of Changes in Shareholders’ Equity, Consolidated Statements of Cash Flows and Notes to Consolidated Financial Statements included in the Consolidated Financial Statements that are a part of this annual report. Other financial information is included in the Consolidated Financial Statements that are a part of this annual report.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A.CONTROLS AND PROCEDURES
Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that information required to be disclosed in
our Exchange Act reports is recorded, processed, summarized, and reported within the time periods specified in the SEC’s rules
and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required financial disclosure.
As of the end of the period covered by this Report,annual report, we carried out an evaluation, under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, of the effectiveness of the design and operation of our disclosure controls and procedures (as defined in Rule 13a-15(e) and Rule 15d-15(e) of the Exchange Act). Based upon, and as of the date of, this evaluation, the Chief Executive Officer and the Chief Financial Officer concluded that our disclosure controls and procedures were effective such that the information required to be disclosed by us in our SEC reports is recorded, processed, summarized and reported within the time periods specified in SEC rules and forms, and is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosure.
71
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with U.S. GAAP.
Our internal control over financial reporting includes those policies and procedures that:
| ● | pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of our assets; |
| ● | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with U.S. GAAP, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and |
| ● | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of our assets that could have a material effect on our financial statements. |
Management has assessed the effectiveness of our internal control over financial reporting as of December 31, 2017.2023. In making its assessment, management used the criteria described in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission.
We have excluded from the scope of our assessment of internal control over financial reporting the operations and related assets of AlterG, which we acquired on August 11, 2023. Based on management’s assessment, management has concluded that our internal control over financial reporting was effective as of December 31, 20172023 to provide reasonable assurance regarding the reliability of financial reporting and the preparation of consolidated financial statements for external reporting purposes in accordance with U.S. GAAP.
This annual report does not include an attestation report of our independent registered public accounting firm regarding internal controls over financial reporting because the JOBS Act provides an exemption from such requirement as we qualify as an emerging growth company. We are also exempt from this requirement as we are a smaller reporting company.company and non-accelerated filer.
Changes in Internal Control over Financial Reporting
During the fourth quarterquarter of the fiscal year ended December 31, 2017,2023, there were no changes in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) of the Exchange Act) that materially affected, or that are reasonably likely to materially affect, our internal control over financial reporting.
ITEM 9B.OTHER INFORMATION
Not applicable
ITEM 9C.DISCLOSURE REGARDING FOREIGN JURISDICTIONS THAT PREVENT INSPECTIONS
Not applicable
PART III
ITEM 10.DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The following table sets forth the name, age and position of each of our executive officers as of March 5, 2018:February 27, 2024:
| Name | Age | Position | ||
| Larry Jasinski | Chief Executive Officer and Director | |||
| Chief Financial Officer | ||||
Chief Sales Officer | ||||
| Jeannine Lynch | 59 | Vice President | ||
| Almog Adar | 40 | Vice President of Finance |
Larry Jasinskihas served as our Chief Executive Officer and as a member of our board since February 2012. From 2005 until 2012, Mr. Jasinski served as the President and Chief Executive Officer of Soteira, Inc., a company engaged in development and commercialization of products used to treat individuals with vertebral compression fractures, which was acquired by Globus Medical in 2012. From 2001 to 2005, Mr. Jasinski was President and Chief Executive Officer of Cortek, Inc., a company that developed next-generation treatments for degenerative disc disease, which was acquired by Alphatec in 2005. From 1985 until 2001, Mr. Jasinski served in multiple sales, research and development, and general management roles at Boston Scientific Corporation. Mr. Jasinski has served on the board of directors of Massachusetts Bay Lines since 2015 and of LeMaitre Vascular, Inc. since 2003. Mr. Jasinski holds a B.Sc. in marketing from Providence College and an MBA from the University of Bridgeport.
Michael Lawless has served as our Chief Financial Officer effective February 22, 2018, when he succeeded Kevin Hershberger.since September 2022. Prior to Lifeward, Mr. Lawless served as a CFO consultant for Danforth Advisors, LLC, a provider of financial consulting services to the life sciences industry. From 2015 to 2018,2020, Mr. Gon served as our Corporate Controller. Prior to ReWalk RoboticsLawless held several financial leadership positions including Division CFO at Azenta, Inc. (formerly Brooks Automation, Inc.), a worldwide provider of management solutions for biological samples. Previously, Mr. Gon served as Corporate ControllerLawless also held financial leadership roles for AECOM Technology, Inc., PerkinElmer, Inc., Momenta Pharmaceuticals, Inc. and CTI Molecular Imaging, Inc. Mr. Lawless has a Bachelor of Arts degree in Economics from Swarthmore College, a Master of Business Administration degree from the Tuck School of Business at Oti Ltd from 2012 to 2015. Mr. GonDartmouth College and is a Certified Public AccountantAccountant.
Charles Remsberg has served as our Chief Sales Officer since August 2023. Prior to Lifeward, Mr. Remsberg served as CEO of AlterG from March 2017 until the acquisition of AlterG in IsraelAugust 2023. An industry veteran of over 30 years, Charles has been responsible for bringing innovative rehabilitation technology to physical therapy, neuro-rehabilitation, sports medicine, and wellness customers. Prior to serving at AlterG, Mr. Remsberg served in both executive and commercial leadership roles for Tibion (for which he served as the CEO from December 2009 to April 2013, when it was acquired by AlterG), Hocoma (for which he served as the U.S. CEO and Global Head of Sales from September 2003 to November 2009), and Biodex Medical Systems (for which he served as the Head of Worldwide Sales from January 1997 to October 2002). He holds a B.A.an AS in EconomicsBusiness Administration from Hebrew University of Jerusalem.Suffolk County Community College.
Jeannine Lynch has served as our Vice President Research & Developmentof Market Access and RegulatoryStrategy since February 2017,and was previously our Vice President Research and Development since he joined us in February 2013. Mr. Koren has alsoAugust 2021. Prior to Lifeward, Ms. Lynch served as General ManagerSenior Director of ReWalk Robotics Ltd. in Israel since October 2017. FromPatient Access Services at BioMarin Pharmaceuticals from April 2009 to 2013, Mr. Koren servedSeptember 2021. In addition to her work with BioMarin, Ms. Lynch has worked for industry leaders such as General ManagerGenentech and Pfizer/Agouron. She has held leadership roles in commercial management, product launches and built customized patient services to address several different rare and ultrarare medical conditions. Ms. Lynch also sits on the Board of RuggedCOM Israel,Directors for MVP, a developernon-profit organization to help young people of communications equipment. From 2007 to 2009, he served ascolor prepare, perform, progress, and prosper in their education, leadership and early professional careers. Ms. Lynch is a graduate of the Vice PresidentUniversity of ResearchCalifornia Berkeley and Development of Alvarion Technologies Ltd., an Israeli provider of wireless services. Mr. Koren holds a B.Sc. in electrical engineering from Tel Aviv University and an MBAMaster of Public Health from the University of Herriot Watt, Scotland.Michigan.
Almog Adar has served as our Vice President of Finance since December 2022. From 2020 to 2022, Mr. Adar served as our Director of Finance and Corporate Financial Controller. Prior to Lifeward, Mr. Adar served as Controller of Infinya Recycling Ltd. (previously Amnir Recycling) from January 2018 until December 2019. From January 2016 until December 2017, Mr. Adar served as Assistant Controller of Delta Galil Industries. Mr. Adar has a Bachelor of Arts degree in Accounting and Economics from the Open University of Israel and is a Certified Public Accountant licensed by the Israeli Ministry of Justice.
73
The remaining information required by this Item will be included in, and is incorporated herein by reference from, our definitive proxy statement for our 20182024 Annual Meeting of Shareholders to be filed with the SEC pursuant to Regulation 14A within 120 days after the end of our fiscal year ended December 31, 20172023 (the “Proxy Statement”).
ITEM 11.EXECUTIVE COMPENSATION
The information required by this Item 11 will be included in, and is incorporated herein by reference from, our Proxy Statement.
ITEM 12.SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this Item 12 will 12 be included in and is incorporated herein by reference from, our Proxy Statement.
ITEM 13.CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this Item 13 will be included in and is incorporated herein by reference, from our Proxy Statement.
ITEM 14.PRINCIPAL ACCOUNTINGACCOUNTANT FEES AND SERVICES
The information required by this Item 14 will be included in and is incorporated herein by reference, from our Proxy Statement.
PART IV
ITEM 15. EXHIBITS, FINANCIAL STATEMENT SCHEDULES
(a)(1) Financial Statements.
The Consolidated Financial Statements filed as part of this annual report are identified in the Index to Consolidated Financial Statements on page F-1 hereto.
(a)(2) Financial Statement Schedules.
Financial Statement Schedules have been omitted because the information required to be set forth therein is not applicable or is shown in the financial statements or notes thereto.
(a)(3) Exhibits.
See accompanying Exhibit Index included after the signature page of this report for a list of the exhibits filed or furnished with or incorporated by reference in this report.
EXHIBIT INDEX
75
76
| 10.14 | |
| 10.17 |
| 101.INS | XBRL Instance Document. |
| 101.SCH | XBRL Taxonomy Extension Schema Document. |
| 101.PRE | XBRL Taxonomy Presentation Linkbase Document. |
| 101.CAL | XBRL Taxonomy Calculation Linkbase Document. |
| 101.LAB | XBRL Taxonomy Label Linkbase Document. |
| 101.DEF | XBRL Taxonomy Extension Definition Linkbase Document. |
| + | Schedules have been omitted pursuant to Item 601(b)(2) of Regulation S-K. |
| * | Certain identified information in the exhibit has been omitted because it is the type of information that (i) the Company customarily and actually treats as private and confidential, and (ii) is not material. |
| ** | Management contract or compensatory plan, contract or arrangement. |
| *** | Furnished herewith. |
ITEM 16. FORM 10-K SUMMARY
Not applicable.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| ReWalk Robotics Ltd. | ||
| By: | /s/ Larry Jasinski | |
| Name: Larry Jasinski | ||
| Title: Chief Executive Officer | ||
Date: March 8, 2018February 27, 2024
78
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENT: That the undersigned officers and directors of ReWalk Robotics Ltd. do hereby constitute and appoint Larry Jasinski and Ori GonMike Lawless the lawful attorney and agent with power and authority to do any and all acts and things and to execute any and all instruments which said attorney and agent determines may be necessary or advisable or required to enable ReWalk Robotics Ltd. to comply with the Securities and Exchange Act of 1934, as amended, and any rules or regulations or requirements of the Securities and Exchange Commission in connection with this report. Without limiting the generality of the foregoing power and authority, the powers granted include the power and authority to sign the names of the undersigned officers and directors in the capacities indicated below to this report or amendments or supplements thereto, and each of the undersigned hereby ratifies and confirms all that said attorneys and agents, or either of them, shall do or cause to be done by virtue hereof. This Power of Attorney may be signed in several counterparts.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature | Title | Date | ||
| /s/ Larry Jasinski | Director and Chief Executive Officer | |||
| Larry Jasinski | (Principal Executive Officer) | |||
| /s/ | Chief Financial Officer | February 27, 2024 | ||
| Mike Lawless | (Principal Financial | |||
| /s/ Almog Adar | Vice President of Finance | February 27, 2024 | ||
| Almog Adar | (Principal Accounting Officer) | |||
| /s/ Jeff Dykan | Chairman of the Board | |||
| Jeff Dykan | ||||
| /s/ Dr. John William Poduska | Director | |||
| Dr. John William Poduska | ||||
| /s/ | Director | |||
| /s/ | Director | |||
| /s/ | Director | |||
79
PART IV
REWALK ROBOTICS LTD
CONSOLIDATED FINANCIAL STATEMENTS
U.S. DOLLARS IN THOUSANDS
INDEX
  | Kost Forer Gabbay & Kasierer | Tel: Fax: ey.com |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Shareholders and the Board of Directors of
REWALK ROBOTICS LTD.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Rewalk Robotics Ltd. ("RRL") and subsidiaries (the "Company")Company) as of December 31, 20172023 and 2016, and2022, the related consolidated statements of operations, shareholders' deficiencychanges is shareholders’ equity and cash flows for each of the three years in the period ended December 31, 2017,2023, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 20172023 and 2016,2022, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2017,2023, in conformity with U.S. generally accepted accounting principles.
Basis for Opinion
These financial statements are the responsibility of the Company'sCompany’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company'sCompany’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the financial statements that were communicated or required to be communicated to the audit committee and that: (1) relate to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of the critical audit matters does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing separate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
F - 2
Revenue recognition | |
Description of the Matter | As described in Note 2 to the consolidated financial statements, the Company generates revenues from sales of its medical devices. Revenue is recognized when obligations under the terms of a contract with the Company's customers are satisfied. Revenue is measured as the Auditing the Company’s evaluation of the allocation of the transaction price to the distinct performance obligations was challenging due to the effort and assumptions required to evaluate the standalone selling price of the SCI products service type warranty. The assumptions used in determining the standalone selling price of the service type warranty included costs allocation, inflation rates and expected margins. |
How We Addressed the Matter in Our Audit | To test the management’s determination of standalone selling prices of the SCI products service type warranty, our audit procedures included, among others, evaluating the methodology applied and testing the calculations as well as the completeness and accuracy of the underlying data including the costs allocation, inflation rates and expected margins used by the Company in its estimates. We also evaluated the Company’s disclosures included in notes to the consolidated financial statements. Business Combinations – Valuation |
Description of the Matter | |
As discussed in Notes 2 and 5 to the consolidated financial statements, the Company completed an acquisition of AlterG Inc. during 2023 for consideration of $22.1 million. The Company accounted for this acquisition as a business combination. The acquisition resulted in the recognition of intangible assets amounting to $14.1 million, which consisted of technology, customer relationship, trademark assets and backlog of $6.1 million, $6.9 million, $0.8 million and $0.3 million respectively. Auditing the Company’s estimation of the fair value of the acquired intangible assets was complex due to the estimation and uncertainty in the Company’s determination of the fair value of acquired identifiable intangible assets. The estimation uncertainty for the acquired intangible assets was primarily due to the underlying assumptions about the future performance of the acquired business, which were utilized in determining the fair value of the acquired intangible assets. The significant assumptions used by management included discount rates and certain assumptions that form the basis of the forecasted results, including revenue growth rates. These significant assumptions were forward-looking and could be affected by future economic and market conditions. | |
How We Addressed the Matter in Our Audit | To test the estimated fair value of the acquired intangible assets, our audit procedures included, among others, assessing the fair value methodology used by the Company and testing the significant assumptions and the underlying data used by the Company in its analyses. We also performed sensitivity analyses over the significant assumptions used to evaluate the change in the fair value resulting from changes in the assumptions. Additionally, we tested the completeness and accuracy of the underlying data used in the valuation. We involved our valuation specialists to assist us in our evaluation of the Company’s valuation model, related assumptions and output of the valuation model. |
KOST FORER GABBAY & KASIERER
We have served as the Company’s auditor since 2014.
Tel-Aviv, Israel
February 27, 2024
F - 3
REWALK ROBOTICS LTD. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
U.S. dollars in thousands
December 31, | ||||||||
2023 | 2022 | |||||||
ASSETS | ||||||||
CURRENT ASSETS: | ||||||||
Cash and cash equivalents | $ | 28,083 | $ | 67,896 | ||||
Trade receivable, net of credit losses of $328 and $26, respectively | 3,120 | 1,036 | ||||||
Prepaid expenses and other current assets | 2,366 | 649 | ||||||
Inventories | 5,653 | 2,929 | ||||||
Total current assets | 39,222 | 72,510 | ||||||
LONG-TERM ASSETS | ||||||||
Restricted cash and other long-term assets | 784 | 694 | ||||||
Operating lease right-of-use assets | 1,861 | 836 | ||||||
Property and equipment, net | 1,262 | 196 | ||||||
Intangible assets | 12,525 | - | ||||||
Goodwill | 7,538 | - | ||||||
Total long-term assets | 23,970 | 1,726 | ||||||
Total assets | $ | 63,192 | $ | 74,236 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
F - 4
REWALK ROBOTICS LTD. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
U.S. dollars in thousands (except share and per share data)
December 31, | ||||||||
2023 | 2022 | |||||||
LIABILITIES AND SHAREHOLDERS’ EQUITY | ||||||||
CURRENT LIABILITIES: | ||||||||
Trade payables | $ | 5,069 | $ | 1,950 | ||||
Employees and payroll accruals | 2,034 | 1,282 | ||||||
Deferred revenue | 1,504 | 301 | ||||||
Current maturities of operating leases liability | 1,296 | 564 | ||||||
Earnout liability | 576 | - | ||||||
Other current liabilities | 1,316 | 685 | ||||||
Total current liabilities | 11,795 | 4,782 | ||||||
LONG-TERM LIABILITIES | ||||||||
Earnout liability | 2,716 | - | ||||||
Deferred revenues | 1,506 | 890 | ||||||
Non-current operating leases liability | 607 | 333 | ||||||
Other long-term liabilities | 58 | 66 | ||||||
Total long-term liabilities | 4,887 | 1,289 | ||||||
Total liabilities | 16,682 | 6,071 | ||||||
COMMITMENTS AND CONTINGENT LIABILITIES | ||||||||
Shareholders’ equity: | ||||||||
Share capital | ||||||||
Ordinary share of NIS 0.25 par value-Authorized: 120,000,000 shares at December 31, 2023 and December 31, 2022; Issued: 64,132,706 and 63,023,506 shares at December 31, 2023 and December 31, 2022, respectively; Outstanding: 60,110,099 and 60,090,298 shares as of December 31, 2023 and December 31, 2022 respectively | 4,487 | 4,489 | ||||||
Additional paid-in capital | 281,109 | 279,857 | ||||||
Treasury Shares at cost, 4,022,607 and 2,933,208 ordinary shares at December 31, 2023 and December 31, 2022, respectively | (3,203 | ) | (2,431 | ) | ||||
Accumulated deficit | (235,883 | ) | (213,750 | ) | ||||
Total shareholders’ equity | 46,510 | 68,165 | ||||||
Total liabilities and shareholders’ equity | $ | 63,192 | $ | 74,236 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
F - 5
REWALK ROBOTICS LTD. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
U.S. dollars in thousands (except share and per share data)
Year ended December 31, | ||||||||||||
2023 | 2022 | 2021 | ||||||||||
Revenue | $ | 13,854 | $ | 5,511 | $ | 5,966 | ||||||
Cost of revenue | 9,401 | 3,606 | 3,063 | |||||||||
Gross profit | 4,453 | 1,905 | 2,903 | |||||||||
Operating expenses: | ||||||||||||
Research and development, net | 4,148 | 4,031 | 2,939 | |||||||||
Sales and marketing | 13,922 | 9,842 | 6,993 | |||||||||
General and administrative | 9,995 | 7,134 | 5,626 | |||||||||
Total operating expenses | 28,065 | 21,007 | 15,558 | |||||||||
Operating loss | (23,612 | ) | (19,102 | ) | (12,655 | ) | ||||||
Financial income, net | 1,467 | * | ) | 13 | ||||||||
Loss before income taxes | (22,145 | ) | (19,102 | ) | (12,642 | ) | ||||||
Taxes on income (benefit) | (12 | ) | 467 | 94 | ||||||||
Net loss | $ | (22,133 | ) | $ | (19,569 | ) | $ | (12,736 | ) | |||
Net loss per ordinary share, basic and diluted | $ | (0.37 | ) | $ | (0.31 | ) | $ | (0.27 | ) | |||
Weighted average number of shares used in computing net loss per ordinary share, basic and diluted | 59,719,064 | 62,378,797 | 47,935,652 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
*) Represents an amount lower than $1.
F - 6
REWALK ROBOTICS LTD. AND SUBSIDIARIES
STATEMENTS OF CHANGES IN SHAREHOLDERS’ EQUITY
U.S. dollars in thousands (except share data)
Ordinary Share | Additional paid-in | Treasury | Accumulated | Total shareholders’ | ||||||||||||||||||||
Number | Amount | capital | Shares | deficit | equity | |||||||||||||||||||
Balance as of December 31, 2020 | 25,332,225 | 1,827 | 201,392 | - | (181,445 | ) | 21,774 | |||||||||||||||||
Share-based compensation to employees and non-employees | - | - | 833 | - | - | 833 | ||||||||||||||||||
Issuance of ordinary shares upon vesting of RSUs by employees and non-employees | 398,164 | 31 | (31 | ) | - | - | - | |||||||||||||||||
Issuance of ordinary shares in a “Best Efforts” offering, net of issuance expenses in the amount of $3,679 (1) | 10,921,502 | 832 | 35,489 | - | - | 36,321 | ||||||||||||||||||
Exercise of pre-funded warrants and warrants (1)(2) | 10,425,258 | 772 | 14,288 | - | - | 15,060 | ||||||||||||||||||
Issuance of ordinary shares in a “registered direct” offering, net of issuance expenses in the amount of $3,215 (1) | 15,403,014 | 1,199 | 26,932 | - | - | 28,131 | ||||||||||||||||||
Net loss | - | - | - | - | (12,736 | ) | (12,736 | ) | ||||||||||||||||
Balance as of December 31, 2021 | 62,480,163 | 4,661 | 278,903 | (194,181 | ) | 89,383 | ||||||||||||||||||
Share-based compensation to employees and non-employees | - | - | 993 | - | - | 993 | ||||||||||||||||||
Issuance of ordinary shares upon vesting of RSUs by employees and non-employees | 543,343 | 39 | (39 | ) | - | - | - | |||||||||||||||||
Treasury shares at cost | (2,933,208 | ) | (211 | ) | - | (2,431 | ) | - | (2,642 | ) | ||||||||||||||
Net loss | - | - | - | - | (19,569 | ) | (19,569 | ) | ||||||||||||||||
Balance as of December 31, 2022 | 60,090,298 | $ | 4,489 | $ | 279,857 | $ | (2,431 | ) | $ | (213,750 | ) | $ | 68,165 | |||||||||||
Share-based compensation to employees and non-employees | - | - | 1,328 | - | - | 1,328 | ||||||||||||||||||
Issuance of ordinary shares upon vesting of RSUs by employees and non-employees | 1,109,200 | 76 | (76 | ) | - | - | - | |||||||||||||||||
Treasury shares at cost | (1,089,399 | ) | (78 | ) | - | (772 | ) | - | (850 | ) | ||||||||||||||
Net loss | - | - | - | - | (22,133 | ) | (22,133 | ) | ||||||||||||||||
Balance as of December 31, 2023 | 60,110,099 | 4,487 | 281,109 | (3,203 | ) | (235,883 | ) | 46,510 | ||||||||||||||||
(1) See Note 9a.
(2) See Note 9f.
The accompanying notes are an integral part of these consolidated financial statements.
F - 7
REWALK ROBOTICS LTD. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
STATEMENTS OF CASH FLOWS
U.S. dollars in thousands
| Year ended December 31, | ||||||||||||
| 2023 | 2022 | 2021 | ||||||||||
| Cash flows used in operating activities: | ||||||||||||
| Net loss | $ | (22,133 | ) | $ | (19,569 | ) | $ | (12,736 | ) | |||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||||||
| Depreciation | 239 | 202 | 266 | |||||||||
Amortization of intangible assets | 1,608 | - | - | |||||||||
| Share-based compensation | 1,328 | 993 | 833 | |||||||||
| Deferred taxes | - | 316 | (29 | ) | ||||||||
| Remeasurement of earnout liability | (315 | ) | - | - | ||||||||
| Interest income | (11 | ) | - | - | ||||||||
| Exchange rate fluctuations | (45 | ) | 79 | - | ||||||||
| Changes in assets and liabilities: | ||||||||||||
| Trade receivables, net | (311 | ) | (408 | ) | 99 | |||||||
| Prepaid expenses, operating lease right-of-use assets and other assets | (531 | ) | 94 | 592 | ||||||||
| Inventories | (277 | ) | (117 | ) | 432 | |||||||
| Trade payables | 1,037 | 566 | (884 | ) | ||||||||
| Employees and payroll accruals | (14 | ) | 140 | 275 | ||||||||
| Deferred revenues | (269 | ) | (34 | ) | 74 | |||||||
| Operating lease liabilities and other liabilities | (973 | ) | (153 | ) | (391 | ) | ||||||
| Net cash used in operating activities | (20,667 | ) | (17,891 | ) | (11,469 | ) | ||||||
| Cash flows used in investing activities: | ||||||||||||
| Acquisition of a business, net of cash acquired | (18,068 | ) | - | - | ||||||||
| Purchase of property and equipment | (81 | ) | (25 | ) | (47 | ) | ||||||
| Net cash used in investing activities | (18,149 | ) | (25 | ) | (47 | ) | ||||||
| Cash flows from financing activities: | ||||||||||||
| Issuance of ordinary shares in a private placement, net of issuance expenses paid in the amount of $3,679 (1) | - | - | 36,321 | |||||||||
| Issuance of ordinary shares in a “registered direct” offering, net of issuance expenses in the amount of $3,215 (1) | - | - | 28,131 | |||||||||
| Exercise of pre-funded warrants and warrants (1)(2) | - | - | 15,060 | |||||||||
| Purchase of treasury shares | (992 | ) | (2,500 | ) | - | |||||||
| Net cash (used in) provided by financing activities | (992 | ) | (2,500 | ) | 79,512 | |||||||
| Effect of Exchange rate changes on Cash, Cash Equivalents and Restricted Cash | 45 | (79 | ) | - | ||||||||
| Increase (decrease) in cash, cash equivalents, and restricted cash | (39,763 | ) | (20,495 | ) | 67,996 | |||||||
| Cash, cash equivalents, and restricted cash at beginning of period | 68,555 | 89,050 | 21,054 | |||||||||
| Cash, cash equivalents, and restricted cash at end of period | $ | 28,792 | $ | 68,555 | $ | 89,050 | ||||||
| December 31, | |||||||
| 2017 | 2016 | ||||||
| ASSETS | |||||||
| CURRENT ASSETS: | |||||||
| Cash and cash equivalents | $ | 14,567 | $ | 23,678 | |||
| Trade receivable, net | 1,103 | 1,254 | |||||
| Prepaid expenses and other current assets | 1,625 | 1,139 | |||||
| Inventories | 3,643 | 3,264 | |||||
| Total current assets | 20,938 | 29,335 | |||||
| LONG-TERM ASSETS | |||||||
| Other long term assets | 1,085 | 1,170 | |||||
| Property and equipment, net | 840 | 1,258 | |||||
| Total long-term assets | 1,925 | 2,428 | |||||
| Total assets | $ | 22,863 | $ | 31,763 | |||
(1) See Note 9a.
(2) See Note 9f.
The accompanying notes are an integral part of these consolidated financial statements.
F - 8
REWALK ROBOTICS LTD. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
STATEMENTS OF CASH FLOWS
U.S. dollars in thousands (except share and per share data)
| December 31, | |||||||
| 2017 | 2016 | ||||||
| LIABILITIES AND SHAREHOLDERS’ EQUITY | |||||||
| CURRENT LIABILITIES: | |||||||
| Current maturities of long term loan | $ | 6,441 | $ | 7,495 | |||
| Trade payables | 1,811 | 3,424 | |||||
| Employees and payroll accruals | 872 | 1,019 | |||||
| Deferred revenues and customers advances | 123 | 54 | |||||
| Other current liabilities | 480 | 406 | |||||
| Total current liabilities | 9,727 | 12,398 | |||||
| LONG-TERM LIABILITIES | |||||||
| Long term loan, net of current maturities | 8,911 | 10,518 | |||||
| Deferred revenues | 262 | 284 | |||||
| Other long-term liabilities | 256 | 303 | |||||
| Total long-term liabilities | 9,429 | 11,105 | |||||
| Total liabilities | 19,156 | 23,503 | |||||
| COMMITMENTS AND CONTINGENT LIABILITIES | |||||||
| Shareholders’ equity: | |||||||
| Share capital | |||||||
| Ordinary share of NIS 0.01 par value-Authorized: 250,000,000 shares at December 31, 2017 and 2016; Issued and outstanding: 30,003,639 and 16,338,257 shares at December 31, 2017 and 2016, respectively | 84 | 45 | |||||
| Additional paid-in capital | 134,843 | 114,707 | |||||
| Accumulated deficit | (131,220 | ) | (106,492 | ) | |||
| Total shareholders’ equity | 3,707 | 8,260 | |||||
| Total liabilities and shareholders’ equity | $ | 22,863 | $ | 31,763 | |||
| Year ended December 31, | ||||||||||||
| 2023 | 2022 | 2021 | ||||||||||
| Supplemental disclosures of non-cash flow information | ||||||||||||
| Classification of other current assets to property and equipment, net | $ | - | $ | 22 | $ | 34 | ||||||
| Classification of inventory to property and equipment | $ | 481 | $ | 67 | $ | 32 | ||||||
| Amounts related to shares re-purchase not yet paid | $ | - | $ | 142 | $ | - | ||||||
| ROU assets obtained from new lease liabilities | $ | 513 | $ | - | $ | - | ||||||
| Supplemental disclosures of cash flow information: | ||||||||||||
| Cash paid for income taxes | $ | 126 | $ | 113 | $ | 40 | ||||||
| Cash received from interest | $ | 1,341 | - | - | ||||||||
| Reconciliation of cash, cash equivalents and restricted cash as shown in the consolidated statements of cash flows | ||||||||||||
| Cash and cash equivalents | $ | 28,083 | $ | 67,896 | $ | 88,337 | ||||||
| Restricted cash included in other long-term assets | $ | 709 | $ | 659 | $ | 713 | ||||||
| Total Cash, cash equivalents, and restricted cash | $ | 28,792 | $ | 68,555 | $ | 89,050 | ||||||
(1) See Note 9a.
(2) See Note 9f.
The accompanying notes are an integral part of these consolidated financial statements.
F - 9
REWALK ROBOTICS LTD. AND SUBSIDIARIES
Notes to Consolidated Financial Statements
U.S. dollars in thousands
Year ended December 31 | |||||||||||
| 2017 | 2016 | 2015 | |||||||||
| Revenues | $ | 7,753 | $ | 5,869 | $ | 3,746 | |||||
| Cost of revenues | 4,652 | 5,133 | 3,532 | ||||||||
| Gross profit | 3,101 | 736 | 214 | ||||||||
| Operating expenses: | |||||||||||
| Research and development, net | 6,042 | 9,028 | 5,937 | ||||||||
| Sales and marketing | 11,360 | 13,961 | 13,056 | ||||||||
| General and administration | 7,691 | 8,188 | 6,395 | ||||||||
| Total operating expenses | 25,093 | 31,177 | 25,388 | ||||||||
| Operating loss | (21,992 | ) | (30,441 | ) | (25,174 | ) | |||||
| Loss on extinguishment of debt | 313 | — | — | ||||||||
| Financial expenses, net | 2,293 | 2,059 | 188 | ||||||||
| Loss before income taxes | (24,598 | ) | (32,500 | ) | (25,362 | ) | |||||
| Income taxes | 119 | 3 | 53 | ||||||||
| Net loss | $ | (24,717 | ) | $ | (32,503 | ) | $ | (25,415 | ) | ||
| Net loss per ordinary share, basic and diluted | $ | (1.22 | ) | $ | (2.47 | ) | $ | (2.10 | ) | ||
| Weighted average number of shares used in computing net loss per ordinary share, basic and diluted | 20,214,895 | 13,178,107 | 12,115,038 | ||||||||
Ordinary Share (1)(2) | Additional paid-in capital | Accumulated deficit | Total shareholders’ equity | ||||||||||||
| Number | Amount | ||||||||||||||
| Balance as of December 31, 2014 | 11,978,554 | 32 | 92,395 | (48,574 | ) | 43,853 | |||||||||
| Share-based compensation to employees and non employees | — | — | 2,345 | — | 2,345 | ||||||||||
| Issuance of ordinary share upon exercise of stock options and RSUs by employees and non employees | 194,345 | 1 | 136 | — | 137 | ||||||||||
| Cashless exercise of warrants into ordinary shares | 49,684 | *) | *) | — | — | ||||||||||
| Net loss | — | — | — | (25,415 | ) | (25,415 | ) | ||||||||
| Balance as of December 31, 2015 | 12,222,583 | 33 | 94,876 | (73,989 | ) | 20,920 | |||||||||
| Share-based compensation to employees and non-employees | — | — | 3,398 | — | 3,398 | ||||||||||
| Issuance of ordinary shares upon exercise of options to purchase ordinary shares and RSUs by employees and non-employees | 128,496 | 1 | 17 | — | 18 | ||||||||||
| Issuance of ordinary shares in at-the-market offering, net of issuance expenses in the amount of $468 | 692,062 | 2 | 4,097 | — | 4,099 | ||||||||||
| Issuance of warrants to purchase ordinary shares | — | — | 1,239 | — | 1,239 | ||||||||||
| Cashless exercise of warrants into ordinary shares | 45,116 | *) | *) | — | — | ||||||||||
| Issuance of ordinary shares and warrants to purchase ordinary shares in follow-on public offering, net of issuance expenses in an amount of $1,099 | 3,250,000 | 9 | 11,080 | — | 11,089 | ||||||||||
| Net loss | — | — | — | (32,503 | ) | (32,503 | ) | ||||||||
| Balance as of December 31, 2016 | 16,338,257 | 45 | 114,707 | (106,492 | ) | 8,260 | |||||||||
| Cumulative effect to stock based compensation from adoption of a new accounting standard | — | — | 11 | (11 | ) | — | |||||||||
| Share-based compensation to employees and non-employees | — | — | 3,654 | — | 3,654 | ||||||||||
| Issuance of ordinary shares upon exercise of options to purchase ordinary shares and RSUs by employees and non-employees | 166,748 | 1 | 37 | — | 38 | ||||||||||
| Issuance of ordinary shares in at-the-market offering, net of issuance expenses in the amount of $467 (3) | 5,613,084 | 16 | 9,293 | — | 9,309 | ||||||||||
| Issuance of ordinary shares in follow-on public offering, net of issuance expenses in an amount of $1,117 (4) | 7,885,550 | 22 | 7,141 | — | 7,163 | ||||||||||
| Net loss | — | — | — | (24,717 | ) | (24,717 | ) | ||||||||
| Balance as of December 31, 2017 | 30,003,639 | 84 | 134,843 | (131,220 | ) | 3,707 | |||||||||
| NOTE 1:- | |
GENERAL |
Year ended December 31 | |||||||||||
| 2017 | 2016 | 2015 | |||||||||
| Cash flows from operating activities: | |||||||||||
| Net loss | $ | (24,717 | ) | $ | (32,503 | ) | $ | (25,415 | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: | |||||||||||
| Depreciation | 642 | 696 | 438 | ||||||||
| Share-based compensation to employees and non employees | 3,654 | 3,398 | 2,345 | ||||||||
| Deferred taxes | 73 | (5 | ) | (61 | ) | ||||||
| Loss on extinguishment of debt | 313 | — | — | ||||||||
| Financial expenses related to long term loan | 128 | 675 | — | ||||||||
| Capital Gain | — | (8 | ) | — | |||||||
| Changes in assets and liabilities: | |||||||||||
| Trade receivables, net | 151 | 892 | (191 | ) | |||||||
| Prepaid expenses and other current assets | (474 | ) | (607 | ) | (613 | ) | |||||
| Inventories | (582 | ) | (911 | ) | (2,525 | ) | |||||
| Trade payables | (1,613 | ) | 950 | 1,084 | |||||||
| Employees and payroll accruals | (147 | ) | (202 | ) | 349 | ||||||
| Deferred revenues and advances from customers | 47 | (32 | ) | 121 | |||||||
| Other liabilities | 27 | 120 | (712 | ) | |||||||
| Net cash used in operating activities | (22,498 | ) | (27,537 | ) | (25,180 | ) | |||||
| Cash flows from investing activities: | |||||||||||
| Maturities of short-term deposits | — | — | 1,667 | ||||||||
| Purchase of property and equipment | (21 | ) | (452 | ) | (584 | ) | |||||
| Proceeds from sale of property and equipment | — | 15 | — | ||||||||
| Net cash provided by (used in) investing activities | (21 | ) | (437 | ) | 1,083 | ||||||
| Cash flows from financing activities: | |||||||||||
| Proceeds from long term loan | — | 20,000 | — | ||||||||
| Debt issuance cost | — | (501 | ) | — | |||||||
| Repayment of long term loan | (3,102 | ) | (922 | ) | — | ||||||
Issuance of ordinary shares in at-the-market offering, net of issuance expenses paid in the amount of $467 | 9,309 | 4,099 | — | ||||||||
Issuance of ordinary shares and warrants in follow-on offering, net of issuance expenses in an amount of $1,117 | 7,163 | 11,089 | — | ||||||||
| Issuance of ordinary share upon exercise of stock options by employees and non employees | 38 | 18 | 137 | ||||||||
| Net cash provided by financing activities | 13,408 | 33,783 | 137 | ||||||||
| Increase (decrease) in cash and cash equivalents | (9,111 | ) | 5,809 | (23,960 | ) | ||||||
| Cash and cash equivalents at beginning of period | 23,678 | 17,869 | 41,829 | ||||||||
| Cash and cash equivalents at end of period | $ | 14,567 | $ | 23,678 | $ | 17,869 | |||||
Year ended December 31 | |||||||||||
| 2017 | 2016 | 2015 | |||||||||
| Supplemental disclosures of non-cash flow information | |||||||||||
| Classification of inventory to property and equipment | $ | 203 | $ | 181 | $ | 768 | |||||
| Supplemental disclosures of cash flow information: | |||||||||||
| Cash paid for income taxes | $ | 21 | $ | 45 | $ | 163 | |||||
| Cash paid for interest | $ | 2,300 | $ | 1,301 | $ | — | |||||
| a. | ReWalk Robotics Ltd. (“RRL”, and together with its subsidiaries, the “Company”) was incorporated under the laws of the State of Israel on June 20, 2001 and commenced operations on the same date. |
| b. | RRL has |
| c. | The Company is a medical device company that is designing, developing, and commercializing innovative technologies that enable mobility and wellness in rehabilitation and daily life for individuals with physical and neurological conditions. The Company’s initial product offerings were the ReWalk |
The Company has sought to expand the product offerings beyond the SCI Products through internal development and distribution agreements. The Company has developed its ReStore Exo-Suit device, which it began commercializing in June 2019. The ReStore is a powered, lightweight soft exo-suit intended for use during the rehabilitation of individuals with lower limb disability due to stroke. During the second quarter of 2020, the Company signed two separate agreements to distribute additional product lines in the United States. The Company is the exclusive distributor of the MYOLYN MyoCycle FES Pro cycles to United States (“U.S.”) rehabilitation clinics and for the MyoCycle Home cycles available to US veterans through VA hospitals. In the second quarter of 2020, the Company also became the exclusive distributor of the MediTouch Tutor movement biofeedback systems in the United States; however, due to unsatisfactory sales performance of the MediTouch product lines, the Company terminated this agreement as of January 31, 2023. We refer to the MediTouch and MyoCycle devices as the Company’s “Distributed Products.”
On August 11, 2023, pursuant to an Agreement and Plan of Merger among RRI, AlterG, Atlas Merger Sub, Inc., a wholly owned subsidiary of RRI (“Merger Sub”), and Shareholder Representative Services LLC, dated August 11, 2023, RRI acquired AlterG and AlterG became a wholly owned subsidiary of the Company.
For accounting purposes, RRI was considered the acquirer and AlterG was considered the acquiree. The acquisition was accounted for using the acquisition method of accounting. See Note 5 for additional information.
The Company made its first acquisition to supplement its internal growth when it acquired AlterG, a leading provider of AlterG Anti-Gravity systems for use in physical and neurological rehabilitation. The Company paid a cash purchase price of $19.0 million at closing and additional cash earnouts may be paid based upon a percentage of AlterG’s year-over-year revenue growth over the two years following the closing. The AlterG Anti-Gravity systems use patented, NASA-derived Differential Air Pressure (“DAP”) technology to reduce the effects of gravity and allow people to rehabilitate with finely calibrated support and reduced pain. The Company will continue to evaluate other products for distribution or acquisition that can broaden its product offerings further to help individuals with physical and neurological injury and disability.
The Company markets and sells its products directly to institutions and individuals and through third-party distributors. The Company sells its products directly primarily in the United States, through a combination of direct sales and distributors (depending on the product line) in Germany, Canada, and Australia, and primarily through distributors in other markets. In its direct markets, the Company has established relationships with clinics and rehabilitation centers, professional and college sports teams, and individuals and organizations in the spinal cord injury community, and in its indirect markets, the Company’s distributors maintain these relationships. RRI and AlterG market and sell products mainly in the United States. RRG markets and sells the Company’s products mainly in Germany and Europe.
F - 10
| d. |
The Company depends on one contract manufacturer to manufacture the ReWalk and the ReStore products in its portfolio, Sanmina. Reliance on this vendor makes the Company vulnerable to possible capacity constraints and |
| e. | For the |
The Company expects to incur future net losses and the transition to profitability is dependent upon, among other things, the successful development and commercialization of the Company’s products and product candidates, the establishment of contracts for the distribution of new product lines, or the acquisition of additional product lines, any of which, or in combination, would contribute to the achievement of a level of revenue adequate to support the cost structure. Until the Company achieves profitability or generates positive cash flows, it will continue to need to raise additional cash. The Company intends to finance operating costs over the next twelve months withfund future operations through existing cash on hand, reducing operating spend, issuances under the Company's ATM Offering Program, additional private and/or other future issuancespublic offerings of debt or equity and debt securities, including the recently signed private placementcash exercises of ordinary shares to Timwell,outstanding warrants or through a combination of the foregoing. However,In addition, the Company may seek additional capital through arrangements with strategic partners or from other sources and will continue to address its cost structure. Notwithstanding, there can be no assurance that the Company will needbe able to seekraise additional sources of financing if the Company require more funds than anticipated during the next 12 months or in later periods.achieve or sustain profitability or positive cash flows from operations.
| NOTE 2:- | ||
SIGNIFICANT ACCOUNTING POLICIES |
The consolidated financial statements are prepared according toin accordance with accounting principles generally accepted in the United States generally accepted accounting principles (“U.S. GAAP”), applied on a consistent basis, as follows:
| a. | Use of Estimates |
The preparation of the consolidated financial statements in conformity with U.S. generally accepted accounting principlesGAAP requires management to make estimates, judgments, and assumptions. The Company’s management believes that the estimates, judgments, and assumptions used are reasonable based upon information available at the time they are made. These estimates, judgments, and assumptions can affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the dates of the financial statements, and the reported amounts of revenuesrevenue and expenses during the reporting period. Actual results could differ from those estimates. On an ongoing basis, the Company’s management evaluates estimates, including those related to inventories, fair values of share-based awards, and warrants, contingent liabilities, provision for warranty, allowance for doubtful accountcredit losses and sales return reserve. Such estimates are based on historical experience and on various other assumptions that are believed to be reasonable, the results of which form the basis for making judgments about the carrying values of assets and liabilities.
| b. | Financial Statements in U.S. Dollars: |
The functional currency is the currency that best reflects the economic environment in which the Company and its subsidiaries operate and conduct their transactions. Most of the revenues and costs of the Company are denominated in United States dollars (“dollars”). Some of the Company’s and its subsidiaries’ revenues and costs are incurred in Euros and New Israeli Shekels (“NIS”), however, the selling prices are linked toU.S. dollar. In addition, the Company’s price list which is determined in dollars, the budget is managed in dollars, financing activities including loans and cash investments, are madeincurred in U.S. dollars and thedollars. The Company’s management believes that the dollar is the primary currency of the economic environment in which the Company and each of its subsidiaries operate. Thus, the dollar is the Company’s and its subsidiaries’subsidiary's functional and reporting currency.
Accordingly, transactions denominatedmonetary accounts maintained in currencies other than the functional currencyU.S. dollar are re-measured to the functional currencyremeasured into U.S. dollars in accordance with Accounting Standards Codification (“ASC”) No.ASC 830 “Foreign Currency Matters” at the exchange rate at the dateMatters.” All transaction gains and losses of the transaction or the average exchange rate in the relevant reporting period. At the end of each reporting period, financial assets and liabilities are re-measured to the functional currency using exchange rates in effect at theremeasured monetary balance sheet date. Non-financial assets and liabilitiesitems are re-measured at historical exchange rates. Gains and losses related to re-measurement are recorded as financial income (expense)reflected in the consolidated statements of operations as financing income or expenses as appropriate.
F - 11
| c. | Principles of Consolidation: |
The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiaries, RRI and RRG. All intercompany transactions andwholly owned subsidiaries. Intercompany balances have been eliminated upon consolidation.
| d. | Cash Equivalents: |
Cash equivalents are short-term highly liquid investments that are readily convertible to cash with original maturities of three months or less, at the date acquired.
| e. | Inventories: |
Inventories are stated at the lower of cost or marketnet realizable value. Inventory reserves are provided to cover risks arising from slow-moving items or technological obsolescence.
The Company periodically evaluates the quantities on hand relative to historical, current, and projected sales volume. Based on this evaluation, an impairment charge is recorded when required to write-down inventory to its marketnet realized value.
Cost is determined as follows:
Finished products - based on the basis of raw materials and manufacturing costs on an average basis.
Raw materials - The weighted average cost method.
The Company regularly evaluates the ability to realize the value of inventory based on a combination of factors, including historical usage rates and forecasted sales according to outstanding backlogs. Purchasing requirements and alternative usage are explored within these processes to mitigate inventory exposure. When recorded, the reserves are intended to reduce the carrying value of inventory to its net realizable value. In the years ended December 31, 2017, 2016 and 2015, the Company wrote off inventory in the amount of $131 thousand, $237 thousand and $127 thousand, respectively. If actual demand for the Company’s products deteriorates, or market conditions are less favorablefavourable than those projected, additional inventory reserves may be required.
| f. |
Property and Equipment: |
Property and equipment are stated at cost, net of accumulated depreciation. Depreciation is calculated using the straight-line method over the estimated useful lives of the assets at the following annual rates:
% | |
Computer equipment | 20-33 (mainly 33) |
Office furniture and equipment | 6 - 10 (mainly 10) |
Machinery and laboratory equipment | 15 |
Field service units | 20-50 |
Leasehold improvements | Over the shorter of the lease term or estimated useful life |
| g. | Business Combinations |
The Company accounts for business combinations in accordance with ASC 805, “Business Combinations” (“ASC 805”). For business combinations accounted for under the acquisition method, ASC 805 requires recognition of assets acquired, liabilities assumed, and any non-controlling interest at the acquisition date, measured at their fair values as of that date. The Company determines the recognition of intangible assets based on the following criteria: (i) the intangible asset arises from contractual or other rights; or (ii) the intangible asset is separable or divisible from the acquired entity and capable of being sold, transferred, licensed, returned or exchanged.
The excess of the fair value of the purchase price over the fair values of the identifiable assets and liabilities is recorded as goodwill. Determining the fair value of the identifiable assets and liabilities requires management to use significant judgment and estimates including the forecasted revenue and revenues growth rates, discount rates, customer contract renewal rates and customer attrition rates. The process of estimating the fair values requires significant estimates, especially with respect to intangible assets. Management’s determination of fair value of assets acquired and liabilities assumed at the acquisition date is based on the best information available in the circumstances and incorporates management’s own assumptions and involves a significant degree of judgment.
Acquisition related costs include legal fees, consulting and success fees, and other non-recurring integration related costs. Acquisition-related costs are expensed as incurred.
F - 12
| h. | Goodwill and Other Intangibles |
For business combinations, the purchase prices are allocated to the tangible assets and intangible assets acquired and liabilities assumed based on their estimated fair values on the acquisition dates, with the remaining unallocated purchase prices recorded as goodwill.
The Company has no indefinite-lived intangible assets other than goodwill. Acquired identifiable finite-lived intangible assets include identifiable acquired technology, customer relationships, trademarks and backlog and are amortized on a straight-line basis over the estimated useful lives of the assets. The Company routinely reviews the remaining estimated useful lives of finite-lived intangible assets.
Goodwill is not amortized and is tested for impairment at least annually.
The Company operates as one reporting unit and the fair value of the reporting unit is estimated using quoted market prices of the Company’s stock in active markets. The Company tests goodwill for impairment annually in the fourth quarter and whenever events or changes in circumstances indicate the carrying amount of goodwill may not be recoverable.
When testing goodwill for impairment, the Company may first perform a qualitative assessment. If the Company determines it is not more likely than not the reporting unit’s fair value is less than its carrying value, then no further analysis is necessary. If the Company determines that it is more likely than not that the fair value of its reporting unit is less than its carrying amount, then the quantitative impairment test will be performed. The Company may elect to bypass the qualitative assessment and proceed directly to performing a quantitative analysis. Under the quantitative impairment test, if the carrying amount of the Company’s reporting unit exceeds its fair value, the Company recognizes an impairment of goodwill for the amount of this excess.
As of December 31, 2023, no impairments of goodwill have been recognized.
| i. | Impairment of Long-Lived |
The Company’s long-lived assets, including right-of-use (“ROU”) assets and identifiable intangible assets that are subject to amortization, are reviewed for impairment in accordance with ASC No. 360, “Property, Plant and Equipment” whenever events or changes in circumstances indicate that the carrying amount of an asset (or asset group) may not be recoverable. Recoverability of assets (or asset group) to be held and used is measured by a comparison of the carrying amount of an asset to the future undiscounted cash flows expected to be generated by the assets. If such assets are considered to be impaired, the impairment to be recognized is measured by the amount by which the carrying amount of the assets exceeds the fair value of the assets. During the years ended December 31, 2017, 20162023, 2022 and 2015,2021, no impairment losses have been recorded.
Restricted cash and Other |
Other long termlong-term assets include long-term prepaid expenses and restricted cash deposits for offices and cars leasing.leasing based upon the term of the remaining restrictions.
Treasury shares |
The Company repurchased its ordinary shares and its subsidiaries generateholds them as treasury shares. The Company presents the cost to repurchase treasury shares as a reduction of shareholders' equity.
F - 13
| l. | Revenue Recognition: |
The Company generates revenues from sales of products. The Company andsells its subsidiaries sell their products through a direct sales forcedirectly to end customers and through distributors. The Company sells its products to clinics and rehabilitation centres, professional and college sports teams, private individuals (who finance the purchases by themselves, through fundraising or reimbursement coverage from insurance companies), and distributors.
| 1. | Identify the contract with a customer |
The Company generally considers a purchase order or a signed quote to be a contract with a customer. In evaluating the contract with a customer, the Company analyzes the customer’s intent and ability to pay the amount of promised consideration (credit risk) and considers the probability of collecting substantially all of the consideration.
| 2. | Identify the performance obligations in the contract |
At a contract’s inception, the Company assesses the goods or services promised in a contract with a customer and identifies the performance obligations.
| 3. | Determine the transaction price |
The transaction price is determined based on the consideration to which the Company will be entitled in exchange for transferring products or services to the customer.
The Company does not offer extended payment terms beyond one year to customers.
| 4. | Allocate the transaction price to performance obligations in the contract |
If the contract contains a single performance obligation, the entire transaction price is allocated to the single performance obligation. Contracts that contain multiple performance obligations require an allocation of the transaction price to each performance obligation based on a relative standalone selling price basis.
| 5. | Recognize revenue when or as the Company satisfies a performance obligation |
Revenue is recognized when or as performance obligations are satisfied by transferring control of a promised good or service to a customer. Control either transfers over time or at a point in time, which affects when revenue is recorded.
The Company has occurred, persuasive evidence of an agreement exists,elected to apply the fee is fixedpractical expedient for financing component for transactions in which the difference between the payment date and determinable, collectability is reasonably assured and no further obligations exist. Provisions are made at the time of revenue recognition for any applicable warranty cost expectedtiming is up to be incurred.12 months.
Year Ended December 31, | ||||||||||||
2023 | 2022 | 2021 | ||||||||||
Product | $ | 10,681 | $ | 4,175 | $ | 4,916 | ||||||
Rental | 1,033 | 859 | 533 | |||||||||
Service and warranty | 2,140 | 477 | 517 | |||||||||
Total Revenues | $ | 13,854 | $ | 5,511 | $ | 5,966 | ||||||
For systems sold to rehabilitation facilities, the Company includes insignificant training and considers the elements in the arrangement to be a single unit of accounting. In accordance with ASC 605, the Company has concluded that the training is essential to the functionality of the Company’s systems.performance obligation. Therefore, the Company recognizes revenue for the system and training only when control is transferred after delivery in accordance with the agreement delivery terms to the customer and afterwhen the training has been completed, once all other revenue recognition criteria have been met.in accordance with the agreements terms with the customer.
F - 14
For sales of ReWalk Personal Exoskeleton systems to end users, and for sales of ReWalk Personal or ReWalk Rehabilitation Exoskeleton systems to third party distributors, the Company does not provide training to the end user as this training is completed by the Rehabilitation centersrehabilitation center or by the distributor that have previously completed the ReWalk Training program. Therefore, the Company recognizes revenue in such sales upon delivery, assumingdelivery.
The Company generally does not grant a right of return for its products. In rare circumstances when the other conditionsCompany provides a right of return for its products. the Company records reductions to revenue recognition have been met.for expected future product returns based on the Company’s historical experience and estimates.
Rental revenue
Rental revenue for the AlterG Anti-Gravity systems is accounted for under ASC Topic 842, Leases. The Company rents its products to customers for a fixed monthly fee over the rental term, which typically ranges from 2 to 3 years. Rental revenues are bundledrecorded as earned on a monthly basis. See Note 2x for additional information.
For the SCI Products, the Company also offers a rent-to-purchase model in which the Company recognizes revenue ratably according to the agreed rental monthly fee for a limited period prior to selling its products.
Service and warranties
The Company services its products after expiration of the initial warranty. Service revenue, consisting of time and materials to perform the repairs, is recorded as services are rendered.
Determining the transaction price requires of level judgment, which is discussed by revenue category in further detail below.
Warranties are classified as either an assurance type or a service type warranty. A warranty is considered an assurance type warranty if it provides the customer with assurance that the product will function as intended for a limited period of time. An assurance type warranty is not accounted for as a separate performance obligation under the revenue model.
SCI Products include a five -year warranty. The first two years are considered as an assurance type warranty and the additional period is considered an extended service arrangement, which is a service type warranty. A service type warranty is either sold with a unit or separately for a unit for which the warranty has expired. A service type warranty is accounted as a separate performance obligation and revenue is recognized ratably over the life of the warranty.
The ReStore device is sold with a two-year warranty which is considered as assurance type warranty.
The Distributed Products are sold with assurance type warranty ranging between three years to ten years, depending on the specific product and part.
For AlterG Anti-Gravity Products, the Company offers customers extended warranty contracts that extend or enhance the separationtechnical support, parts, and labor coverage offered as part of the extendedbase warranty falls underincluded with the scope of ASC 605-20-25-1 through 25-6, and the separately price of the extendedAnti-Gravity system products. Extended warranty stated in the agreementrevenue is deferred and recognized ratably over the extended warranty coverage period. The Company offers a one-year assurance type warranty to customers in the U.S. and two years assurance type warranty for spare parts only to its international distributors. For these products, the Company determines standalone selling price based on the price at which the performance obligation is sold separately.
F - 15
Contract balances (in thousands):
December 31, | December 31, | |||||||
2023 | 2022 | |||||||
Trade receivable, net of credit losses (1) | $ | 3,120 | $ | 1,036 | ||||
Deferred revenues (1) (2) | $ | 3,010 | $ | 1,191 | ||||
| (1) | Balance presented net of unrecognized revenue that was not yet collected. |
| (2) | $435 thousands of the December 31, 2022 deferred revenue balance was recognized as revenue during the year ended December 31, 2023. |
Deferred revenue includes primarilywhich represent a contract liability, include unearned amounts related to service type warranty obligations as well as other advances and payments which the Company received in respect of service contracts butfrom customers prior to satisfying the performance obligation, for which revenue has not yet been recognized. The Company's unearned performance obligations as of December 31, 2023 and the estimated revenue expected to be recognized as revenues. The Company also offers a rent-to-purchase option of its ReWalk Personal device. Those transactions provide potential customersin the optionfuture related to lease the device for a short term, afterservice type warranty amounts to $3.1 million, which they can choose whetherwill be fulfilled over one to purchase it. In such cases the Company recognize revenues over the period of the rent once all other revenue criteria are met.five years.
Accounting for Share-Based Compensation: |
The Company accounts for share-based compensation in accordance with ASC No. 718, “Compensation-Stock Compensation” (“ASC No. 718”). ASC No. 718 requires companies to estimate the fair value of equity-based payment awards on the date of grant using an Option-Pricing Model (“OPM”). The value of the portion of the award that is ultimately expected to vest is recognized as an expense over the requisite service periods in the Company’s consolidated statements of operations.
The Company recognizes compensation expenses for the value of its awards granted based on the straight-line method over the requisite service period of each of the awards.
The Company selected the Black-Scholes-Merton option pricing model as the most appropriate fair value method for its share-option awards. The option-pricing model requires a number of assumptions, of which the most significant are the fair market value of the underlying ordinary share, expected share price volatility and the expected option term. Expected volatility wasis calculated based uponon actual historical stock price movements over the most recent periods ending on the grant date, equal to the expected term of the options, or based on certain peer companies that the Company considered to be comparable. The expected option term represents the period of time that options granted are expectedcomparable, in case there is no sufficient trading volume to be outstanding.rely on market volatility. The expected option term is determined based on the simplified method, in accordance with Staff Accounting Bulletin No. 110, as adequate historical experience is not available to provide a reasonable estimate. The simplified method will continue to apply until enough historical experience is available to provide a reasonable estimate of the expected term. The risk-free interest rate is based on the yield from U.S. treasury bonds with an equivalent term. The Company has historically not paid dividends and has no foreseeable plans to pay dividends.
The fair value of Restricted Stock Units (RSUs)(“RSUs”) granted is determined based on the price of the Company'sCompany’s ordinary shares on the date of grant.
| December 31, | |||||
| 2017 | 2016 | 2015 | |||
| Expected volatility | 55% - 59% | 53% - 60% | 60% | ||
| Risk-free rate | 1.78% - 2.07% | 1.16% - 1.60% | 1.60% - 1.95% | ||
| Dividend yield | —% | —% | —% | ||
| Expected term (in years) | 5.31 - 6.11 | 5.31 - 6.11 | 5.73 - 6.11 | ||
| Share price | $1.30 - $2.00 | $6.80 - $11.88 | $7.30 - $20.97 | ||
The Company accounts for options granted to consultants and other service providers under ASC No. 718 and ASC No. 505, “Equity-based payments to non-employees.”718. The fair value of these options was estimated using a Black-Scholes-Merton option-pricing model. In 2017 the non-cash compensation expenses related to nonemployees were $45 thousand, in 2016 and 2015 the non-cash compensation expenses related to nonemployees were immaterial.
| n. | Warrants to Acquire Ordinary Shares: |
During the yearstwelve -month ended December 31, 2017, 20162021, the Company issued warrants to acquire up to 15,083,611 ordinary shares. There were no issued warrants during the twelve months ended December 31, 2023 and 2015 amounted2022. The Company assessed the warrants pursuant to $3,654 thousand, $3,398 thousandASC 480 "Distinguishing Liabilities from Equity" and $2,345 thousand respectively.ASC 815 "Derivatives and Hedging" and determined that the warrants should be accounted for as equity and not as a derivative liability. Refer to Note 9f for additional information.
| o. | ||
Research and Development Costs: |
Research and development costs are charged to the consolidated statement of operations as incurred and are presented net of the amount of any grants the company receiveCompany received for research and development in the period in which the grant was received.