● | our ability to obtain and maintain regulatory approvals for our product candidates, including TG-1701, TG-1801, and Azercabtagene Zapreleucel (azer-cel), as well as any other product candidates, and our ability to maintain regulatory approval of BRIUMVI® (ublituximab) for the treatment of relapsing forms of multiple sclerosis (RMS) in the United States (U.S.), the European Union (EU) and the United Kingdom (UK); |
● | our ability to adapt and expand our commercial infrastructure to successfully launch, market and sell BRIUMVI and our other product candidates; |
● | our ability to maintain a reliable supply of our products that meets market demand; |
● | the success of the ongoing commercialization of BRIUMVI or any future products or combinations of products, including the anticipated rate and degree of market acceptance and pricing and reimbursement; |
● | the initiation, timing, progress and results of our pre-clinical studies and clinical trials; |
● | our ability to advance drug candidates into, and successfully complete, clinical trials; | |
| ● | our ability to develop, formulate, manufacture and commercialize our product candidates; |
● | our ability to establish and maintain contractual relationships and partnerships, on commercially reasonable terms, with third parties for manufacturing, distribution, marketing and supply and a range of other support functions for our clinical development and commercialization efforts; |
● | the implementation of our business model and strategic plans for our business and drug candidates; |
● | the scope of protection we are able to establish and maintain for intellectual property rights covering our product and product candidates; |
● | estimates of our expenses, future revenues, capital requirements and our needs for additional financing; |
● | our ability to maintain and establish collaborations and enter into strategic arrangements, if desired; |
● | our ability to meet any of our financial projections or guidance, including without limitation short and long-term revenue projections or guidance and changes to the assumptions underlying those projections or guidance; |
● | our ability to obtain sufficient capital to fund our planned operations; |
● | our financial performance and cash burn management; | |
| ● | our ability to maintain or obtain adequate product liability and other insurance coverage; and |
● | developments relating to our competitors and our industry. |
Our business is subject to a number of risks of which you should be aware before making an investment decision. The risks described below are a summary of the principal risks associated with an investment in us and are not the only risks we face. You should carefully consider these risks, the risk factors in Item 1A, and the other reports and documents that we have filed with the Securities and Exchange Commission (SEC).
Risks Related to Commercialization
| ● | If we are unable to maintain current approval of BRIUMVI, our business will be materially harmed. |
| ● | We cannot predict when or if we will obtain regulatory approval to commercialize our product candidates, including TG-1701 and TG-1801 in B-cell disorders or azer-cel in non-oncology indications. |
| ● | We have limited experience operating as a commercial company, and, as a result, the marketing and sale of BRIUMVI for the treatment of RMS may be less successful than anticipated. |
| ● | If BRIUMVI or any of our future product candidates (if approved) do not achieve broad market acceptance among physicians, patients, payors or the medical community, the revenues that we generate from product sales will be limited. |
| ● | If the market opportunities for BRIUMVI and any future products for which we may receive approval, including TG-1701 or TG-1801 in B-cell disorders or azer-cel in non-oncology indications, are smaller than we estimate or if any approval we obtain is based on a narrower patient population or the labeling includes warnings or limitations that are not acceptable to patients or healthcare providers, our revenue will be adversely affected. |
| ● | We face substantial competition for treatments for our target indications, including from companies with greater resources than we have, which may result in others commercializing drugs before or more successfully than we do, which could result in the reduction or elimination of our commercial opportunity. |
| ● | If we are unable to generate sufficient revenue, we may need to raise substantial additional capital to sustain our business. |
| ● | Product liability lawsuits could cause us to incur substantial liabilities and limit product commercialization. |
Risks Related to Drug Development and Regulatory Approval
● | If we are unable to obtain or maintain regulatory approval for our product or product candidates and ultimately cannot commercialize one or more of them, or if we experience significant delays in doing so, our business will be materially harmed |
● | Our product and product candidates may cause undesirable side effects that could delay or prevent their regulatory approval or significantly limit their commercial profile following marketing approval, if any, or result in withdrawal from the market if approved |
● | Because results of preclinical studies and early clinical trials are not necessarily predictive of future results, any product candidate we advance may not have favorable results in later clinical trials. Moreover, interim, “top-line,” and preliminary data from our clinical trials that we announce or publish may change, or the perceived product profile may be impacted, as more patient data or additional endpoints are analyzed. |
● | Any products or product candidates we may advance through clinical development are subject to extensive regulation, which can be costly and time consuming, cause unanticipated delays, or prevent the receipt of the required approvals. |
Risks Related to Governmental Regulation of the Pharmaceutical Industry
● | We are subject to extensive regulation, including new legislative and regulatory proposals, including efforts to control, set or cap pricing for approved drugs, which may increase our costs and adversely affect our ability to market our products, obtain collaborators and raise capital. |
● | If we fail to comply with various healthcare laws and regulations, we may incur losses or be subject to liability. |
● | If we fail to comply with regulatory requirements, any product candidate may fail to receive regulatory approval and any product for which we obtain marketing approval could be subject to restrictions or withdrawal from the market and we may be subject to penalties. |
Risks Related to our Dependence on Third Parties
● | Our reliance on third parties for commercial and clinical supply of raw materials and our product and product candidates increases the risk that we will not have sufficient quantities of our product or product candidates or such quantities at an acceptable cost or quality, which could delay, prevent or impair our development or commercialization efforts. |
● | If the third parties on which we rely to conduct our clinical trials and generate clinical, preclinical, and other data necessary to support our regulatory applications do not perform their services as required, we may not be able to obtain regulatory approval for or commercialize our product or product candidates when expected or at all. |
● | Because we have in-licensed our product and product candidates from third parties, any dispute with, or non-performance by our licensors will adversely affect our ability to develop and commercialize the applicable product. |
Risks Related to Intellectual Property
| ● | Our success depends upon our ability to obtain and protect our intellectual property, and if the scope of our patent protection obtained is not sufficiently broad, our competitors could develop and commercialize products similar or identical to ours, and our ability to successfully commercialize our products may be impaired. |
| ● | Our patent protection could be reduced or eliminated for non-compliance with various procedural and other requirements imposed by governmental patent agencies. |
| ● | We may need to license certain intellectual property from third parties, and such licenses may not be available or may not be available on commercially reasonable terms. |
| ● | If we or our partners are sued for infringing intellectual property rights of third parties, it will be costly and time consuming to defend against such lawsuits, and an unfavorable outcome in any such lawsuit would have a material adverse effect on our business. |
| ● | If we are unable to protect the confidentiality of our trade secrets, our business may be significantly harmed. |
Risks Related to our Financial Position and Need for Additional Capital
● | We have incurred significant operating losses since our inception, and we may incur losses in the future. |
● | While we do not expect to need to raise additional capital, we may need to do so. If we are unable to raise capital, if needed, we may be required to delay, limit, reduce or eliminate some of our drug development programs or commercialization efforts. |
● | Our level of indebtedness and debt service obligations could adversely affect our financial condition and may make it more difficult for us to fund our operations. |
General Risk Factors
● | Public health issues including an epidemic or global pandemic, including the pandemic caused by COVID-19, could have an adverse impact on our financial condition and results of operations and other aspects of our business. |
● | Patients and healthcare providers have raised concerns that immunosuppressive products, like anti-CD20 antibodies and other B-cell targeted agents, may increase the risk of acquiring COVID-19 or lead to more severe complications upon infection. These concerns may impact the commercial potential for BRIUMVI and other immunosuppressive products that we have in development. |
● | We will need to develop and expand our business, and we may encounter difficulties in managing this development and expansion. |
● | Our ability to continue our clinical development and commercialization activities will depend on our ability to attract and maintain key management and other personnel. |
● | Certain of our executive officers, directors and other stockholders own more than 5% of our outstanding common stock and may be able to influence our management and the outcome of matters submitted to shareholders for approval. |
● | Certain anti-takeover provisions in our charter documents and Delaware law could make a third-party acquisition more difficult, which could limit the price investors might be willing to pay for our common stock. |
● | Our stock price is, and we expect it to remain, volatile, which could limit investors’ ability to sell stock at a profit and could subject us to securities and shareholder derivative litigation. |
● | Significant disruptions of information technology systems, breaches of data security or unauthorized disclosures of sensitive data could harm our business and subject us to liability or reputational damage. |
The foregoing is only a summary of some of our risks. These and other risks are discussed more fully in the section entitled “Risk Factors” in Part I, Item 1A and elsewhere in this Annual Report on Form 10-K (our Risk Factors).
Unless the context requires otherwise, references in this report to “TG,“TG,” “Company,“Company,” “we,“we,” “us”“us” and “our”“our” refer to TG Therapeutics, Inc. and our subsidiaries.
OVERVIEW
TG Therapeutics is a fully-integrated, commercial stage, biopharmaceutical company focused on the acquisition, development and commercialization of novel treatments for B-cell malignanciesmediated diseases. In addition to a research pipeline including several investigational medicines, TG has received approval from the U.S. Food and autoimmune diseases. Currently, we are developing two therapies targeting hematologic malignancies. TG-1101 (ublituximab) is a novel, glycoengineered monoclonal antibody that targets a unique epitope onDrug Administration (FDA) for BRIUMVI® (ublituximab-xiiy) for the CD20 antigen found on mature B-lymphocytes. We are also developing TGR-1202 (umbralisib), an orally available PI3K delta inhibitor. The delta isoformtreatment of PI3K is strongly expressed in cells of hematopoietic origin and is believed to be important in the proliferation and survival of B-lymphocytes. Both TG-1101 and TGR-1202, or the combination which is referred to as "U2," are in Phase 3 clinical development foradult patients with hematologic malignancies, with TG-1101 alsorelapsing forms of multiple sclerosis (RMS), to include clinically isolated syndrome, relapsing-remitting disease and active secondary progressive disease, in Phase 3 clinical developmentadults, as well as approval by the European Commission (EC) and the Medicines and Healthcare products Regulatory Agency (MHRA) for BRIUMVI to treat adult patients with multiple sclerosis. Additionally,RMS who have active disease defined by clinical or imaging features in Europe and the Company has recently brought its anti-PD-L1 monoclonal antibody into Phase 1 development and aims to bring additional pipeline assets into the clinic in the future.
Business Highlights
FDA Approval and U.S. Launch of BRIUMVI
On December 28, 2022, we announced that the FDA granted approval of ublituximab, now referred to as BRIUMVI, for the treatment of RMS, to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults. BRIUMVI is an anti-CD20 monoclonal antibody approved for patients with RMS that can be administered in a one-hour infusion following the starting dose. Approval was granted for this indication based on data from the ULTIMATE I & II Phase 3 trials, which demonstrated superiority over teriflunomide in significantly reducing the annualized relapse rate (ARR, the primary endpoint), the number of T1 Gd-enhancing lesions and the number of new or enlarging T2 lesions. Results from the ULTIMATE I & II trials were published in August 2022 in The New England Journal of Medicine.
On January 26, 2023, we announced the commercial launch of BRIUMVI, making it available to physicians and patients. We are committed to helping patients access BRIUMVI through the BRIUMVI Patient Support Program, which we launched following the approval, additional information can be found at www.briumvi.com.
Ex-U.S. Commercialization of BRIUMVI
On June 1, 2023, we announced that the EC granted approval of BRIUMVI for the treatment of adult patients with RMS who have notactive disease defined by clinical or imaging features.
On August 1, 2023, we announced an agreement with Neuraxpharm Pharmaceuticals, S.L. (Neuraxpharm), a leading European specialty pharmaceutical company focused on the treatment of central nervous system (CNS) disorders, for the ex-U.S. commercialization of BRIUMVI.
On November 1, 2023, we announced that we also received approval by the MHRA for BRIUMVI to treat adult patients with RMS with active disease defined by clinical or imaging features in the UK.
On February 26, 2024, we announced the commercial launch of BRIUMVI in the European Union (EU) by Neuraxpharm, with BRIUMVI made available for commercial sale in Germany, with additional EU markets expected to follow.
Pipeline Expansion
On January 9, 2024, we entered into an agreement with Precision BioSciences, Inc. (Precision) to acquire a worldwide license to Precision’s Azercabtagene Zapreleucel (azer-cel), an allogeneic CD19 CAR T cell therapy program for autoimmune diseases and all other non-oncology indications. Azer-cel is an allogeneic (off the shelf) CAR T program, and the Company has near term plans to evaluate the program in multiple autoimmune indications.
CORPORATE INFORMATION
We were incorporated in Delaware in 1993. Our executive offices are located at 2 Gansevoort St., 9th Floor, New York, New York 10014.3020 Carrington Mill Blvd, Suite 475, Morrisville, North Carolina, 27560. Our telephone number is 212-554-4484,1-877-575-TGTX(8489), and our e-mail address is info@tgtxinc.com.
We maintain a website with the address www.tgtherapeutics.com.www.tgtherapeutics.com and maintain various social media accounts, including but not limited to X (formerly Twitter) and LinkedIn. We also maintain websites related to BRIUMVI, including but not limited to www.BRIUMVI.com, and www.BRIUMVIPATIENTSUPPORT.com. We make available free of charge through our Internetcorporate website our annual reports on Form 10-K, quarterly reports on Form 10-Q and current reports on Form 8-K, andas well as any amendments to these reports, as soon as reasonably practicable after we electronically file such material with, or furnish such material to, the SEC. We are not including the information on our website or our social media accounts as a part of, nor incorporating iteither by reference into, this report. You may read and copy any such reports and amendments thereto at the SEC’s Public Reference Room at 100 F Street, N.E., Washington, D.C. 20549 on official business days during the hours of 10:00 a.m. to 3:00 p.m. Please call the SEC at 1-800-SEC-0330 for information on the Public Reference Room. Additionally, theThe SEC maintains a website that contains annual, quarterly, and current reports, proxy statements, and other information that issuers (including us) file electronically with the SEC. The SEC’s website address ishttp://www.sec.gov.
In addition, we intend to use our media and investor relationscorporate website, SEC filings, press releases, public conference calls and webcasts as well as social media to communicate with our subscribers and the public about the Company, its services and other issues.public. It is possible that the information we post on social media could be deemed to be material information. Therefore, in light of the SEC’s guidance, we encourage investors, the media and others interested in the Companyus to review the information we post on the U.S. social media channels listed on our website.
STRATEGY
As a chimeric, glycoengineered monoclonal antibody that targets a unique epitopefully-integrated, commercial stage biopharmaceutical company focused on the CD20 antigen foundacquisition, development and commercialization of novel treatments for B cell mediated diseases, our key corporate objectives include:
● | Successfully commercializing BRIUMVI in the U.S. for relapsing forms of multiple sclerosis; |
● | Building upon the BRIUMVI approval to evaluate other uses for BRIUMVI in additional MS indications and/or other autoimmune diseases; |
● | Continuing to expand our pipeline with mechanisms of importance to B-cell mediated diseases; |
● | Evaluating potential strategic collaborations to maximize the value of our programs and B-cell directed platform; and |
● | Maintaining our “patient first” culture as we grow our business. |
Our Approach and Platform
Our approach to drug development is centered on developing therapies for B-cell mediated diseases. Our process begins by identifying validated targets against B-cell mediated diseases, and then searching for and, ideally, acquiring what we believe to be “best-in-class” compounds with complementary mechanisms against these targets.
Our approach is enabled by our clinical development platform which includes an internal team with a deep understanding of B-cell mediated diseases and Belgium whichsignificant experience successfully obtaining FDA approval for innovative treatments for these complex diseases.
AUTOIMMUNE DISEASE OVERVIEW
An autoimmune disease occurs when the body’s immune system attacks and destroys healthy body tissue by mistake. There are currently more than 80 types of autoimmune disorders that have been retained by LFB Biotechnologies (“LFB”),identified. Some of these diseases may result from inappropriate production of antibodies from the B-cells. These antibodies cannot discriminate “self” from “non-self,” and South Koreainadvertently mount a disabling immune response against normal organs. Some of these diseases may not be antibody mediated but may still result from aberrant activity of B-cells. Examples of common and Southeast Asiavery debilitating autoimmune disorders for which were licensed by us to Ildong Pharmaceutical Co. Ltd (“Ildong”) in November 2012.
The Company’s current focus is generally used in combination with other anti-cancer agents where it demonstrates maximum activity as opposed to single agent usage. As a result, subsequent clinical development for TG-1101 has focused on combination therapy. Currently, our priority combination trials for TG-1101 are:
Multiple Sclerosis (MS) and in an investigator initiated Phase 1 study for the treatment of acute neuromyelitis optica (NMO) relapses, with additional autoimmune related indications planned to be studied. On August 1, 2017, we announced we had reached an agreement with the U.S. Food and Drug Administration (FDA) regarding a Special Protocol Assessment (SPA) on the design of two global Phase 3 clinical trials for TG-1101, referred to as the ULTIMATE I and ULTIMATE II Phase 3 clinical trials, both of which are currently open to enrollment.
RMS is currently performed by a contract manufacturer based in the US and our partner, LFB Biotechnologies.
| TG-1101 plus Ibrutinib | Ibrutinib | P-value | |
| Treated Population (n) | n=59 | n=58 | |
| Overall Response Rate (ORR) | 78% | 45% | P<0.001 |
| Complete Response (CR) | 7% | 0% | NS |
| MRD-Negative | 19% (n=53) * | 2% (n=53) * | P<0.01 |
OUR PRODUCTS
We currently license worldwide development and commercial rights, subject to certain limited geographical restrictions, for all of our products under development. The following table summarizes the current status for our lead drug candidates as of February 2024.
| Clinical Drug Candidate: (molecular target) | Initial Target Disease | Stage of Development (trial name) | ||
Ublituximab (anti-CD20 mAb) | Relapsing Forms of Multiple Sclerosis (RMS) | APPROVED | ||
TG-1701 (BTK inhibitor) | B-cell disorders | Phase 1 trial | ||
TG-1801 (anti-CD47/CD19 bispecific mAb) | B-cell disorders | Phase 1 trial | ||
| Azer-cel | Auto-immune disorders | Phase 1 (pending) |
BRIUMVI (ublituximab-xiiy) Overview
BRIUMVI is the first and only anti-CD20 monoclonal antibody approved for the treatment of RMS, to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults, that can be administered in a twice a year one-hour infusion following the starting dose.
Late-Stage Clinical Assistant Professor at the UniversityDevelopment of Texas Medical BranchUblituximab-xiiy
ULTIMATE I & II Trials Evaluating Single Agent Ublituximab in Round Rock, TX. The primary objective of the study is to determine the optimal dosing regimen for TG-1101 with a focus on accelerating infusion times. In addition to monitoring for safety and tolerability at each dosing cohort, B-cell depletion and established MS efficacy endpoints will also be evaluated.
In December 2020, we announced positive topline results from the ULTIMATE I & II trials. Both studies met their primary endpoint of significantly reducing ARR over a 96-week period (p<0.005 in each study) with ublituximab-xiiy demonstrating an ARR of <0.10 in each of the studies. Relative reductions of approximately 60% and 50% in ARR over teriflunomide were observed in ULTIMATE I & II, respectively. Key secondary magnetic resonance imaging (MRI) endpoints were also met.
On August 22, 2022, the full results from the ULTIMATE I & II trials were published in the New England Journal of Medicine.
ENHANCE Phase 3b Trial: On October 11, 2023, we presented the first data from the ENHANCE Phase 3b trial evaluating BRIUMVI in patients with RMS who switch from another anti-CD20 therapy to BRIUMVI. The presentation occurred at the 2023 European Committee for Treatment and Research in Multiple Sclerosis Annual Meeting. In this study, patients with low levels of B-cells as pre-specified in the protocol are eligible to proceed directly to a full dose of BRIUMVI 450mg without receiving a 150 mg loading dose. As of the presentation, 13 patients switched from Ocrevus to BRIUMVI 450mg as a 2-hour infusion with no infusion related reactions reported and no unexpected side effects. An additional 2 patients switched from Ocrevus to BRIUMVI 450mg as a 1-hour infusion again with no infusion related reactions reported and no unexpected side effects. The study has continued to enroll patients at 450mg as a 1-hour infusion and additional data is ongoing and will enroll approximately 440 subjects, randomized in a 1:1 ratio, with approximately 880 patientsexpected to be enrolled across both trials.
U.S. Commercialization of BRIUMVI (ublituximab-xiiy)
On December 28, 2022, we announced the FDA approval of BRIUMVI (ublituximab-xiiy) for the combinationtreatment of TG-1101RMS, to include clinically isolated syndrome, relapsing-remitting disease, and TGR-1202
Ex-U.S. Commercialization of BRIUMVI
On June 1, 2023, we announced that the FDA hasEC granted orphan drug designation covering the combinationapproval of TG-1101 and TGR-1202BRIUMVI for the treatment of adult patients with CLLRMS who have active disease defined by clinical or imaging features. With this approval, the centralized marketing authorization is valid in all EU member states, Iceland, Norway and DLBCL.
On August 1, 2023, we announced an agreement with Neuraxpharm, a leading European specialty pharmaceutical company focused on the treatment of CNS disorders, for the Ex-US commercialization of BRIUMVI. Under the terms of the commercialization agreement, we received an upfront payment of $140 million, and are eligible to receive an additional $12.5 million upon launch in the first EU country and up to an additional $492.5 million in milestone-based payments on achievement of certain launch and commercial milestones. The phosphoinositide-3-kinases (“PI3Ks”) are a family of enzymes involvedtotal deal is valued at up to $645 million in various cellular functions, including cell proliferationupfront and survival, cell differentiation, intracellular trafficking,milestone payments. In addition, we will receive tiered double-digit royalties on net product sales up to 30%. In exchange, Neuraxpharm will have the exclusive right to commercialize BRIUMVI in certain territories outside the United States, Canada and immunity. There are four isoforms of PI3K (alpha, beta, delta, and gamma), ofMexico, the commercialization rights for which the delta (d) isoform is strongly expressed in cells of hematopoietic origin, and often implicated in B-cell related lymphomas.
On November 1, 2023, we announced that TGR-1202 hadwe also received orphan drug designationapproval by the MHRA for the treatment of CLL.
On February 26, 2024, we announced the commercial launch of Blood,BRIUMVI in the JournalEuropean Union (EU) by Neuraxpharm, with BRIUMVI made available for commercial sale in Germany, with additional EU markets expected to follow.
TG-1701 (BTK inhibitor) Overview
TG-1701 is a novel, orally available and covalently-bound Bruton’s tyrosine kinase (BTK) inhibitor that exhibits strong selectivity to BTK in in vitro kinase screening.
B-cell receptor (BCR) signaling is crucial for normal B-cell development and supports the survival and growth of B-cells.
We are currently evaluating TG-1701 in a Phase 1, multi-center, dose-escalation clinical trial in patients with B-cell malignancies. Data from this trial was last presented at the 2021 American Society of Hematology. The publication presents preclinical data describing the synergy of TGR-1202 with the proteasome inhibitor carfilzomibHematology (ASH) annual meeting.
TG-1801 (anti-CD47/anti-CD19 bispecific monoclonal antibody) Overview
TG-1801 is a potentially first-in-class, bispecific CD47 and the unique effects of the combination to silence c-Myc in various preclinical lymphoma and myeloma models. In addition, the manuscript forCD19 antibody. It is the first time reports on TGR-1202's unique complimentary mechanismtherapy to target both CD19, a B-cell specific marker widely expressed across B-cell malignancies, and CD47, the "don’t eat me" signal used by both healthy and tumor cells to evade macrophage mediated phagocytosis.
In the first quarter of inhibiting the protein kinase casein kinase-1 (CK1) epsilon, which may contribute to the silencing2019, we commenced a Phase 1 first-in-human, dose-escalation study of c-Myc and explain TGR-1202's clinical activityTG-1801 in aggressive lymphoma, including Diffuse Largepatients with B-cell Lymphoma (DLBCL).
In additionthe first half of 2021, we commenced a second Phase 1 study of TG-1801 in the U.S. to TG-1701, the global license agreement covers TG-1702 (SHR-1266), another BTK inhibitor in pre-clinical development.
Azercabtagene Zapreleucel (azer-cel)
Azer-cel is an essential component ofallogeneic (off-the-shelf) CD19 CAR T cell therapy program for autoimmune diseases and all other non-oncology indications. Made from donor-derived T cells modified using a proprietary ARCUS genome editing technology, azer-cel recognizes the well characterized B-cell receptor signaling pathways that regulate the survival, activation, proliferation,surface protein CD19, an important and differentiation of B lymphocytes. Targeting BTK with small molecule inhibitors has been demonstrated to be an effective treatment option forvalidated target in several B-cell lymphomascancers and autoimmune diseases.
INTELLECTUAL PROPERTY AND PATENTS
General
Our goal is to obtain, maintain and enforce patent protection for our products, formulations, processes, methods and other proprietary technologies, preserve our trade secrets, and operate without infringing on the proprietary rights of other parties, both in the United States and in other countries. Our policy is to actively seek to obtain, where appropriate, the broadest intellectual property protection possible for our product candidates, proprietary information and proprietary technology through a combination of contractual arrangements and patents, both in the U.S. and elsewhere in the world.
We also depend upon the skills, knowledge and experience of our scientific and technical personnel, as well as that of our advisors, consultants and other contractors. This knowledge, trade secrets, proprietary information and experience we call “know-how.” To help protect our proprietary know-how, which is not patentable, and for inventions for which patents may be difficult to enforce, we rely on trade secret protection and confidentiality agreements to protect our interests. To this end, we require all employees, consultants, advisorsseek to protect our proprietary technology and other contractors to enterprocesses, in part, by entering into confidentiality agreements which prohibitwith our collaborators, scientific advisors, employees and consultants, and invention assignment agreements with our employees and consultants. There can be no assurance, however, that we can prevent unauthorized disclosure or use of our trade secrets, know-how and proprietary information despite the disclosureexistence of confidential information and, where applicable, require disclosure and assignment to us of the ideas, developments, discoveries and inventions important to our business.
Patents and other proprietary rights are crucial to the development of our business. We will be able to protect our proprietary technologies from unauthorized use by third parties only to the extent that our proprietary rights are covered by valid and enforceable patents, supported by regulatory exclusivity or are effectively maintained as trade secrets. We have a number of issued patents and pending patent applications related to our compounds and other technology, but we cannot guarantee the scope of protection of the issued patents, or that such patents will survive a validity or enforceability challenge, or that any of the pending patent applications will issue as patents.
Generally, patent applications in the U.S. are maintained in secrecy for a period of 18 months or more. Since publication of discoveries in the scientific or patent literature often laglags behind actual discoveries, we are not certain that we were the first to make the inventions covered by each of our issued patents and pending patent applications or that we were the first to file those patent applications.applications covering such inventions. The patent positions of biotechnology and pharmaceutical companies are highly uncertain and involve complex legal and factual questions. Therefore, we cannot predict the breadth of claims allowed in biotechnology and pharmaceutical patents, or their enforceability. To date, there has been no consistent policy regarding the breadth of claims allowed in biotechnology patents. Therefore, we cannot predict the breadth of claims that may be ultimately allowed from our pending patent applications, cannot predict whether the claims in our issued patents will be invalidated or modified through the district courts, Patent Trial and Appeal Board (PTAB) proceedings, or reexamination proceedings at the United States Patent and Trademark Office (USPTO), and thus cannot predict the enforceability of the claims in our issued patents or the claims that may ultimately issue from our pending patent applications. Third parties or competitors may challenge or circumvent our patents or patent applications, if issued. If our competitors prepare and file patent applications in the U.S. that claim technology also claimed by us in a pending patent application or issued patent, we may have to participate in interference proceedings declared by the U.S. Patent and Trademark Office to determine priority of invention, which could result in substantial cost, even if the eventual outcome is favorable to us. Because of the extensive time required for development, testing and regulatory review of a potential product, it is possible that before we commercialize any of our products, any related patent may expire or remain in existence for only a short period following commercialization, thus reducing any advantage of the patent. However, the life of a patent covering a product that has been subject to regulatory approval may have the ability to be extended through the patent restoration program, although any such extension could still be minimal.
Moreover, physicians may prescribe such a competitive identical product for indications other than the one for which the product has been approved, or off-label indications, that are covered by the applicable patents. Although such off-label prescriptions may directly infringe or contribute to or induce infringement of method of use patents, such infringement is difficult to prevent or prosecute.
U.S. Patent Term Restoration and Marketing Exclusivity
Depending upon the timing, duration and specifics of any FDA approval of our drug candidates, some of our U.S. patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, commonly referred to as the Hatch-Waxman Act. The Hatch-Waxman Act permits restoration of the term of certain types of patents for up to five years as compensation for patent term lost during the FDA regulatory review process. However, patent term restoration cannot extend the remaining term of a patent beyond a total of 14 years from the product’s approval date. The patent term restoration period is generally one-half the time between the effective date of an Investigational New Drug (IND) application and the submission date of a New Drug Application (NDA) or BLA plus the time between the submission date of an NDA or BLA and the approval of that application. The calculation is subject to several subtractions for any portion of the regulatory review process that occurred before the date the patent was issued and any portion during which the FDA determined a lack of due diligence. Only one patent applicable to an approved drug is eligible for the extension and the application for the extension must be submitted prior to the expiration of the patent, and within 60 days of a product’s approval. The USPTO, in consultation with the FDA, reviews and approves the application for any patent term extension. Moreover, a patent can only be extended once, and thus, if a single patent is applicable to multiple products, it can only be extended based on one product. Following the approval of BRIUMVI in the U.S., we have applied for patent term extensions for certain of our issued U.S. patents covering our product and/or their methods of use. Similar provisions are available in Europe and certain other foreign jurisdictions to extend the term of a patent that covers an approved drug and have been filed for in certain European Patent (EP) countries.
Also, under the Hatch-Waxman Act, drugs that are new chemical entities (NCEs) are eligible for a five-year period of marketing exclusivity in the United States. During the exclusivity period, the FDA may not accept for review an abbreviated new drug application (ANDA) or a 505(b)(2) NDA submitted by another company for another drug based on the same active moiety, regardless of whether the drug is intended for the same indication as the original innovator drug or for another indication, where the applicant does not own or have a legal right of reference to all the data required for approval. However, an application may be submitted after four years if it contains a certification of patent invalidity or non-infringement to one of the patents listed with the FDA by the innovator NDA holder. The Hatch-Waxman Act also provides three years of marketing exclusivity for a drug product that contains an active moiety that has been previously approved, if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant are deemed by the FDA to be essential to the approval of the application, for example new indications, dosages or strengths of an existing drug. This three-year exclusivity covers only the modification for which the drug received approval on the basis of the new clinical investigations. During this period, FDA will not approve an application filed by a third party for the protected conditions of use that relies on any of the data from the new clinical investigations that was submitted by the innovator company. Five-year and three-year exclusivity will not delay the submission or approval of a full NDA that does not rely on the innovator company’s data.
The Biologics Price Competition and Innovation Act of 2009 (BPCIA) created an abbreviated pathway for companies to bring biologic drugs to market that are biosimilar to previously approved branded reference products by relying on clinical studies that were performed by the reference product sponsor. The BPCIA also created a 12-year period of data exclusivity for innovator biologics, whereby the FDA cannot approve a biological license application (BLA) for a biosimilar product relying on data for a specific reference product until 12 years after the reference product is first licensed. BLA supplements are not eligible for any additional exclusivity. The objectives of the BPCIA are conceptually similar to those of the Hatch-Waxman Act described above. The implementation of an abbreviated approval pathway for biosimilar products is under the direction of the FDA. Since the enactment of the BPCIA, the FDA has issued guidance on biosimilars, addressing scientific, quality and procedural issues relevant to an abbreviated application for a biosimilar product. As of December 2022, the FDA had approved 40 biosimilar products.
Pediatric exclusivity, if granted, adds six months to existing exclusivity periods and patent terms. This six-month exclusivity, which runs from the end of other exclusivity protection or patent term, may be granted based on the voluntary completion of a pediatric trial in accordance with an FDA-issued “Written Request” for such a trial.
We, or those companies from which we have licensed our drug candidates, file patent applications directed to our drug candidates in an effort to establish intellectual property positions regarding these new chemical entities as well as uses of these new chemical entities in the treatment of diseases. We also file patent applications directed to novel combinations of our drugs together and with drugs developed by others. The intellectual property portfolios for our most advanced drug candidates as of February 2024 are summarized below. Each of these portfolios contains one or more pending patent applications covering our products and product candidates and uses and combinations thereof. For those patents, prosecution is in progress. Prosecution is a lengthy process, during which the scope of the claims initially submitted for examination by the USPTO is often significantly narrowed by the time they issue, if they issue at all. This may be the case with respect to our pending patent applications referred to below.
BRIUMVI (ublituximab-xiiy)
Pursuant to our license for TG-1101 (ublituximab)ublituximab with LFB Biotechnologies, GTC Biotherapeutics, and LFB/GTC LLC, we have the exclusive commercial rights to a series of patents and patent applications in the U.S. and in multiple countries around the world, as well as a non-exclusive license to additional background patent rights. These patents and patent protectionsapplications include composition of matter patents relating to the structure and mechanism of action for TG-1101ublituximab, as well as method of use patents which cover use of TG-1101ublituximab in combination with various agents and for various therapeutic indications.
Our earliest in time patent families relate to compositions of matter patent for TG-1101ublituximab, which has been issued in the United StatesU.S., Europe and Europe, which affordsother jurisdictions, including Australia, Canada, China, Japan, Korea and India. The expected expiration for the composition of matter patent protection untilis 2029 in the USU.S. and 2025 in Europe and other non-U.S. jurisdictions, exclusive of patent term extensions.
Our most recently filed patent family relates to compositions of matter comprising ublituximab, methods of manufacturing those compositions and methods for treating multiple sclerosis using those compositions. This family includes three issued U.S. patents and pedningone recently allowed U.S. application. We also have patent applications outsidepending in this family in the USU.S., Argentina, the EU and Taiwan. The Patent Cooperation Treaty application , from which include claims directedfurther national phase applications may be filed, is also pending. Patents issuing from this family may first begin to expire as early as 2042.
In the compositionU.S., the Biologics Price Competition and Innovation Act provides that BRIUMVI is eligible for 12 years of matter and methodsmarket exclusivity from the date of treatment with TG-1101 in various settings.
TG-1701 (BTK inhibitor)
Pursuant to our license for TGR-1202agreement with Rhizen,Jiangsu Hengrui Medicine Co. (Hengrui), we have the exclusive commercial rights to a series of patent applications in the U.S. and abroad. The patent applications include compositiontreatment of matter patents relating to the structure, mechanism of action, and formulation for TGR-1202 as well as method of use patents which cover use of TGR-1202 in combination with various agents and for various therapeutic indications. Our composition of matter patent for TGR-1202 has been issued in the United States and Europe, which affords patent protection until 2033, exclusive of patent term extensions. We also have a method of use patent on the combination of TGR-1202 and TG-1101 which has been issued in the United States and is pending in other territories globally. All other patent applications currently filed for TG-1202 are currently pending. Because the dates for any potential regulatory approval are currently unknown we cannot predict the expected expiration date, and it is possible that the life of these patents following regulatory approval could be minimal.
TG-1801 (anti-CD47/anti-CD19 bispecific antibody)
Pursuant to our Global Collaborationjoint venture and license option agreement with Checkpoint,Novimmune SA (Novimmune), we maintain an exclusive option, exercisable at specific times during development, to license the intellectual property includescommercial rights to a series of global patent applications and patents, and the non-exclusive right to certain technology patent applications. Patents directed to a bispecific antibody have issued patents in a number of countries,Australia, China, Europe, Japan, and Russia and are pending in other jurisdictions including the United States and Europe, as well as pending patent applications in several countries elsewhere. The PD-L1 segment of the portfolio includes patent applications pending in the United States, Australia, Canada, Europe, Israel and Korea.U.S. Any patents maturing from these pending applications will expire no sooner than October 2033. The GITR segment of the portfolio includes an International Application No. PCT/US2015/054010, filed in October 2015. Any national stage applications, which are pursued off of this international application (including one in the United States Patent and Trademark Office), would expire no earlier than October 2035.
Azer-Cel (allogeneic CD19 CAR T)
Pursuant to our BTK Agreementlicense agreement with Jiangsu, Precision, we have an exclusive license to develop and commercialize Precision’s azer-cel for the exclusive commercialtreatment of autoimmune and other non-oncology diseases and conditions as well as a non-exclusive license to manufacture azer-cel. The license agreement includes non-exclusive rights to a series of patents and patent family which coversapplications in the U.S. and in multiple countries around the world, as well as non-exclusive rights to additional background patent rights. These patents and patent applications include composition of matter and proposed methodspatents relating to azer-cel, as well as method of use for various therapeutic indications. All patent applications currently filed for the BTK program are currently pending. Because the date for any potential regulatory approval is currently unknown we cannot predict the expected expiration date,patents which cover use of azer-cel.
Limitations on Patent Rights and it is possible that the life of these patents following regulatory approval could be minimal
The patent rights that we own or have licensed relating to our product candidates are limited in ways that may affect our ability to exclude third parties from competing against us if we obtain regulatory approval to market these product candidates. See “Item 1A – Risk Factors -- Risks Related to the Company’sCompany’s Intellectual Property.”
Proof of direct infringement by a competitor for method of use patents can prove difficult because the competitors making and marketing a product typically do not engage in the patented use. Additionally, proof that a competitor contributes to or induces infringement of a patented method of use by another can also prove difficult because an off-label use of a product could prohibit a finding of contributory infringement, and inducement of infringement requires proof of intent by the competitor.
LICENSING AGREEMENTS AND COLLABORATIONS
We have formed strategic alliances with a number of companies for the manufacture and commercialization of our products. Our current key strategic alliances are discussed below.
BRIUMVI (ublituximab-xiiy)
LFB Biotechnologies S.A.S, GTC Biotherapeutics, LFB/GTC LLC.
In January 2012, we entered into an exclusive license agreement with LFB Biotechnologies, GTC Biotherapeutics and LFB/GTC LLC, all wholly-owned subsidiaries of LFB Group, relating to the development of TG-1101.ublituximab (the LFB License Agreement). Under the license agreement,terms of the LFB License Agreement, we have acquired the exclusive worldwide rights (exclusive of France/Belgium) for the development and commercialization of TG-1101 (ublituximab). To date,ublituximab. As of December 31, 2022, we have made no paymentsincurred expenses of approximately $25.0 million related to milestones in accordance with the terms of the LFB Group andLicense Agreement, $12.0 million of which was incurred in December of 2022 related to a milestone associated with receiving approval of BRIUMVI by the FDA. LFB Group is eligible to receive future payments of up to an aggregate of approximately $31.0$6.0 million, upon our successful achievement of certain clinical development, regulatory and sales milestones, in addition to royalty payments on net sales of TG-1101ublituximab at a royalty rate that escalates from mid-single digits toin the high-single digits. The license will terminate on a country by countrycountry-by-country basis upon the expiration of the last licensed patent right or 15 years after the first commercial sale of a product in such country, unless the agreement is earlier terminated (i) by LFB if the Company challenges any of the licensed patent rights, (ii) by either party due to a breach of the agreement, or (iii) by either party in the event of the insolvency of the other party.
Ildong Pharmaceutical Co. Ltd.
In November 2012, we entered into an exclusive (within the territory) sublicense agreement with Ildong relating to the development and commercialization of TG-1101ublituximab in South Korea and Southeast Asia. Under the terms of the sublicense agreement, Ildong has been granted a royalty bearing, exclusive right, including the right to grant sublicenses, to develop and commercialize TG-1101ublituximab in South Korea, Taiwan, Singapore, Indonesia, Malaysia, Thailand, Philippines, Vietnam, and Myanmar. To date, we have received $2 million in the form of an upfront payment from Ildong and are eligible to receive sales basedsales-based milestone payments up to an aggregate of $5 million and royalty payments on net sales of TG-1101ublituximab at a royalty rate that escalates from mid-teens to high-teens upon approval in South Korea and/or Southeast Asia. The license will terminate on a country by country basis upon the expiration of the last licensed patent right or 15 years after the first commercial sale of a product in such country, unless the agreement is earlier terminated (i) by Ildong if the Company challenges any of the licensed patent rights, (ii) by either party due to a breach of the agreement, or (iii) by either party in the event of the insolvency of the other party.
Neuraxpharm
In September 2014,August 2023, we exercised our option to license the global rights to TGR-1202, thereby enteringentered into an exclusive licensing agreement (the “TGR-1202 License”) with Rhizen Pharmaceuticals, S A (“Rhizen”)Neuraxpharm, for the development andex-U.S. commercialization of TGR-1202. Prior to this, we had been jointly developing TGR-1202 in a 50:50 joint venture with Rhizen.
TG-1701 (BTK inhibitor)
In January 2018, we entered into a global exclusive license agreement with Jiangsu Hengrui, Medicine Co., or Jiangsu, to acquire worldwide intellectual property rights,, excluding Asia but including Japan, and for the research, development, manufacturing, and commercialization of products containing or comprising of any of Jiangsu’sHengrui’s Bruton’s Tyrosine Kinase inhibitors containing the compounds of either TG-1701 (SHR-1459TG 1701 (SHR1459 or EBI-1459)EBI1459) or TG-1702 (SHR-1266TG1702 (SHR1266 or EBI-1266)EBI1266). Pursuant to the agreement, we paid Jiangsu an upfront fee of $1.0 million in our common stock. JiangsuHengrui is eligible to receive milestone payments totaling approximately $350 million upon and subject to the achievement of certain milestones. Various provisions allow for payments in conjunction with the agreement to be made in cash or our common stock, while others limit the form of payment. In July 2020, we paid Hengrui $2.0 million as part of a milestone in accordance with the license agreement. Royalty payments in the low double digits are due on net sales of licensed products and revenue from sublicenses. Additionally, before we can license, sell, develop, or commercialize ublituximab (TG-1101) within China, we must notify Jiangsu, giving Jiangsu the right of first offer.
The term of the agreement expires after the expiration of the last royalty term to expire with respect to any of the patent rights under the agreement. We or JiangsuHengrui may terminate the agreement upon notice to the other upon breach without remedy or upon insolvency. In addition, either party may terminate the agreement upon a material breach, after providing the other party with adequate notice and allowing 45 days to cure.
TG-1801 (anti-CD47/anti-CD19 bispecific antibody)
In June 2018, we entered into a Joint Venture and License Option Agreement with Novimmune to collaborate on the development and commercialization of Novimmune’s novel first-in-class anti-CD47/anti-CD19 bispecific antibody known as TG 1801 (previously NI 1701). The companies will jointly develop the product on a worldwide basis, focusing on indications in the area of hematologic B-cell malignancies. We serve as the primary responsible party for the development, manufacturing and commercialization of the product. Milestone payments will be paid based on early clinical development, and the Company will be responsible for the costs of clinical development of the product through the end of the Phase 2 clinical trials, after which the Company and Novimmune will be jointly responsible for all development and commercialization costs. The Company and Novimmune will each maintain an exclusive option, exercisable at specific times during development, for the Company to license the rights to TG 1801, in which case Novimmune is eligible to receive additional milestone payments totaling approximately $185 million as well as tiered royalties on net sales in the high single to low double digits upon and subject to the achievement of certain milestones.
Azer-Cel(allogeneic CD19 CAR T)
In January 2024, we, through our wholly-owned subsidiary, TG Cell Therapy, Inc., entered into a global exclusive license agreement with Precision to develop and commercialize azer-cel for autoimmune diseases and all other non-oncology indications. Pursuant to such license Agreement, the Company made an upfront payment to Precision of $7.5 million, consisting of (i) $5.25 million in cash and (ii) $2.25 million as an equity investment. The Company will make an additional deferred payment of $2.5 million to Precision as an equity investment to Precision within 12 months at a pre-specified premium. Upon achievement of certain near-term clinical or time-based milestones, the Company will make a further $7.5 million payment to Precision, a portion of which will also be an equity investment in Precision’s common stock at a pre-specified premium. Precision will be eligible to receive up to $288 million in additional milestone payments based on the achievement of certain clinical, regulatory and commercial milestones. In addition, the Company is obligated to pay Precision high-single-digit to low-double-digit royalties on net sales of the licensed product on a country-by-country basis until the latest to occur of patent expiration, loss of regulatory exclusivity or a period of ten years following the first commercial sale of the licensed product in such country. The Company has also agreed to make certain payments to Precision’s licensors during the term of our license agreement with Precision.
UKONIQ (umbralisib)
In September 2014, we exercised our option to license the global rights to umbralisib, thereby entering into an exclusive licensing agreement (the Umbralisib License) with Rhizen Pharmaceuticals, S A (Rhizen) for the development and commercialization of umbralisib. Rhizen is eligible to receive approval and sales-based milestone payments in the aggregate of approximately $175 million. Additionally, Rhizen receives tiered royalties that escalate from high single digits to low double digits on any net sales of umbralisib. The license will terminate on a country-by-country basis upon the expiration of the last licensed patent right or any other exclusivity right in such country, unless the agreement is earlier terminated (i) by us for any reason, or (ii) by either party due to a breach of the agreement.
Cosibelimab
In March 2015, we entered into a global collaboration (the Collaboration Agreement) with Checkpoint Therapeutics, Inc. (Checkpoint) for the development and commercialization of Checkpoint’s anti-PD-L1 and anti-GITR antibody research programs in the field of hematological malignancies with an option to acquire rights in autoimmune diseases. In September 2023, we terminated this agreement and have no remaining obligations or commitments under the Collaboration Agreement.
COMPETITION
Competition in the pharmaceutical and biotechnology industries is intense. Our competitors include pharmaceutical companies and biotechnology companies, as well as universities and public and private research institutions. In addition, companies that are active in different but related fields represent substantial competition for us. Many of our competitors have significantly greater capital resources, larger research and development staffs and facilities and greater experience in drug development, regulation, manufacturing and marketing than we do. These organizations also compete with us to recruit qualified personnel, attract partners for joint ventures or other collaborations, and license technologies that are competitive with ours. To compete successfully in this industry, we must identify novel and unique drugs or methods of treatment and then complete the development of those drugs as treatments in advance of our competitors.
The drugs that we are attempting to develop will have to compete with existing therapies. In addition, a large number of companies are pursuing the development of pharmaceuticals that target the same diseases and conditions that we are targeting. Other companies have products or drug candidates in various stages of pre-clinical or clinical development to treat diseases for which we are also seeking to discover and develop drug candidates. Some of these potential competing drugs are further advanced in development than our drug candidates and may be commercialized earlier.
For BRIUMVI, there are a number of pharmaceutical companies are developing antibodies targeting CD20, CD19,established therapies with which we will compete:
● | We expect BRIUMVI will primarily compete against other iv CD20-targeted agents, while the group of CD20-targeted agents will also compete broadly against a number of already approved MS therapies. Currently, there is one other approved intravenously delivered anti-CD20 monoclonal antibody ocrelizumab (Roche Holdings AG). In addition, while we believe not directly competitive, there is also a subcutaneous anti-CD20 monoclonal antibody approved for MS, ofatumumab (Novartis AG). |
TG-1701, TG-1801 and other B-cell associated targets, chimeric antigen receptor T-cell (CAR-T) immunotherapy, and other B-cell ablative therapy which,azer-cel, if approved would potentially compete with TG-1101 both in oncology settings as well as in autoimmune disorders. Earlier this year,will also face competition from drugs on the Roche Group’s anti-CD20 antibody ocrelizumab was approved for the treatment of MS. Genmabmarket and GSK’s (ofatumumab) is also under clinical development for patients with MS. New developments, including the development of other pharmaceutical technologies and methods of treating disease, occur in the pharmaceutical and life sciences industries at a rapid pace.
Additional information can be found under Item “1A - Risk Factors – Other Risks Related to Our Business” within this report.
We have limited experience in manufacturing products for clinical or commercial purposes. We currently do not have any manufacturing capabilities.capabilities of our own. We have established a contract manufacturing relationshipsrelationship for the commercial supply of TG-1101 as part of our license agreementBRIUMVI with LFB Biotechnologies and also with a U.S. based contract manufacturer. We have also established contract manufacturing relationships for the supply of TGR-1202 as part of our licensing agreement with Rhizen.Samsung Biologics. As with any supply program, obtaining pre-clinical and clinical materials of sufficient quality and quantity to meet the requirements of the market demand for BRIUMVI and our ublituximab development programs cannot be guaranteed and we cannot ensure that we will be successful in this endeavor. In addition, we anticipate the need for the current scale of production for each of our products to be significantly expanded as we enter later stages of development. There can be no assurance given that such scale-up will be successful in providing pharmaceutical product that is of sufficient quantity, or of a quality that is consistent with our previously established specifications, or that meets the requirements set by regulatory agencies under which we may seek approval of our product candidates.
To the extent possible and commercially practicable, we would seekplan to engage adevelop back-up supplierstrategies for eachraw materials, manufacturing and testing services for our commercial products. Given the long lead times and cost of our product candidates. Until such time,establishing additional commercial manufacturing sites we expect that we will rely on a single contract manufacturermanufacturers to produce each of our product candidatescommercial products under current Good Manufacturing Practice, or cGMP, regulations.regulations for many years. Our third-party manufacturerscommercial manufacturing partners have a limited number of facilities in which our product candidates can be produced and will have limited experience in manufacturing our product candidates in quantities sufficient for commercialization. Our third-party manufacturers will have other clients and may have other priorities that could affect their ability to perform the work satisfactorily and/or on a timely basis. Both of these occurrences would be beyond our control.
We expect to similarly rely on contract manufacturing relationships for any products that we may in-license or acquire in the future. However, there can be no assurance that we will be able to successfully contract with such manufacturers on terms acceptable to us, or at all.
Contract manufacturers are subject to ongoing periodic and unannounced inspections by the FDA, the Drug Enforcement Administration if applicable, and corresponding state agencies to ensure strict compliance with cGMP and other state and federal regulations. Our contractors outside of the United States faceWhere manufactured products are globally registered, similar challengesregulatory inspection burdens are applicable from the numerous localeach and regional agenciesevery marketed territory. If our manufacturing partners are inspected and authorized bodies. We do not have control over third-party manufacturers’ compliance with these regulations and standards, other than through contractual obligations. If they are deemed out of compliance with cGMPs, product recalls could result, inventory could be destroyed, production could be stopped, and supplies could be delayed or otherwise disrupted.
If we need to change manufacturers after commercialization, the FDA and corresponding foreign regulatory agencies mustmay need to approve these new manufacturers in advance, which will involve testing, regulatory submissions, and additional inspections to ensure compliance with FDA regulations and standards and may require significant lead times and delay. Furthermore, switching manufacturers may be difficult because the number of potential manufacturers is limited. It may be difficult or impossible for us to find a replacement manufacturer quickly or on terms acceptable to us, or at all.
GOVERNMENT AND INDUSTRY REGULATION
Numerous governmental authorities, principally the FDA and corresponding state and foreign regulatory agencies, impose substantial regulations upon the clinical development, manufacture and marketing of our drugproduct candidates, as well as our ongoing research and development activities. We, along with our third-party contractors, will be required to navigate the various pre- and post-approval requirements of the governing regulatory agencies of the jurisdictions in which we wish to conduct clinical studies or market our product candidates. None of our drugproduct candidates, have beenexcept BRIUMVI, are approved for sale in any market in which we have marketing rights. Before marketing in the U.S., any drug that we develop must undergo rigorous pre-clinical testing and clinical trials and an extensive regulatory review and approval process implemented by the FDA under the FDCA.Federal Food, Drug, and Cosmetic Act (FDCA) and, in the case of biologics, the Public Health Service Act. The FDA regulates, among other things, the pre-clinical and clinical testing, safety, efficacy, approval, manufacturing, quality control and assurance, record keeping, pharmacovigilance and adverse event reporting, packaging, labeling, storage, advertising, promotion, import and export, sale and distribution of biopharmaceutical products. The process of obtaining regulatory approvals and the subsequent compliance with applicable federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources.
Product Development and Applications for Marketing Authorization
The regulatory review and approval process is lengthy, expensive, and uncertain. We are required to submit extensive pre-clinical and clinical data and supporting information to the FDA for each indication or use to establish a drug candidate’s safety and efficacy before we can secure FDA approval to market or sell a product in the U.S. The approval process takes many years, requires the expenditure of substantial resources, and may involve ongoing requirements for post-marketing studies or surveillance. Before commencing clinical trials in humans, we must submit an IND to the FDA containing, among other things, pre-clinical data, chemistry, manufacturing and control information, and an investigative plan. Our submission of an IND may not result in FDA authorization to commence a clinical trial.
For purposes of clinical development evaluation, and marketing of new therapies intended to treat persons with seriouspursue NDA or life-threatening conditions for which there is an unmet medical need under its fast track drug development programs. A sponsor can apply for fast track designation at the time of submission of an IND, or at any time prior to receiving marketingBLA approval, of the new drug application, or NDA. To receive Fast Track designation, an applicant must demonstrate:
● | Phase 1: The drug is administered to a small group of humans, either healthy volunteers or patients, to test for safety, dosage tolerance, absorption, metabolism, excretion, and clinical pharmacology. |
● | Phase 2: Studies are conducted on more patients to assess the product's efficacy, to ascertain dose tolerance and the optimal dose range, and to gather additional data relating to safety and potential adverse events. |
● | Phase 3: Studies establish safety and efficacy in an expanded patient population. |
● | Phase 4: The FDA may require Phase 4 post-marketing studies to find out more about the drug’s long-term risks, benefits, and optimal use, or to test the drug in different populations. |
Clinical testing must meet requirements for institutional review board oversight, informed consent and good clinical practices, and must be conducted pursuant to an IND, unless exempted.
The length of time necessary to complete clinical trials varies significantly and may be difficult to predict. Clinical results are frequently susceptible to varying interpretations that may delay, limit or prevent regulatory approvals. Additional factors that can cause delay or termination of our clinical trials, or that may increase the costs of these trials, include:
● | slow patient enrollment due to the nature of the clinical trial plan, the proximity of patients to clinical sites, the eligibility criteria for participation in the study or other factors; |
● | inadequately trained or insufficient personnel at the study site to assist in overseeing and monitoring clinical trials or delays in approvals from a study site’s review board; |
● | longer treatment time required to demonstrate efficacy or determine the appropriate product dose; |
● | insufficient supply of the drug candidates; |
● | adverse medical events or side effects in treated patients; and |
● | ineffectiveness of the drug candidates. |
In December 2022, with the passage of Food and Drug Omnibus Reform Act, Congress required sponsors to develop and submit a diversity action plan (DAP) for each Phase 3 clinical trial or any other “pivotal study” of a new drug or biological product. These plans are meant to encourage the enrollment of more diverse patient populations in late-stage clinical trials of FDA-regulated products. Specifically, DAPs must include the sponsor’s goals for enrollment, the underlying rationale for those goals and an explanation of how the sponsor intends to meet them. In addition to these requirements, the legislation directs the FDA to issue new guidance on diversity action plans.
For clinical trials that are intended to form the basis of a new drug or biologics license application for approval, sponsors of drugs may apply for an SPAa Special Protocol Assessment (SPA) from the FDA. The SPA process is a procedureFDA, by which the FDA provides official evaluation and written guidance on the design and size of proposed protocols that are intended to formprotocols. While obtaining an SPA provides some assurance the basisdesign of a trial should be sufficient for a new drug application. However,approval, the final marketing approval depends on the results of efficacy, the adverse event profile and an evaluation of the benefit/risk of treatment demonstrated in the Phase 3 trial. The SPA agreement may only be changed through a written agreement between the sponsor and the FDA, or if the FDA becomes aware of a substantial scientific issue essential to product safety or efficacy.
The FDA may permit expedited development, evaluation, and marketing of new therapies intended to treat persons with serious or life-threatening conditions for which there is an unmet medical need under its expedited drug development programs. A sponsor can apply for Fast Track designation at the time of submission of an IND, or at any time prior to receiving marketing approval of the new drug application, or NDA. To receive Fast Track designation, an applicant must demonstrate:
● | that the drug is intended to treat a serious or life-threatening condition; and |
● | that nonclinical or clinical data demonstrate the potential to address an unmet medical need. |
The FDA approvalmust respond to marketa request for Fast Track designation within 60 calendar days of receipt of the request. Over the course of drug development, a product wein a Fast Track development program must demonstratecontinue to meet the criteria for Fast Track designation. Sponsors of products in Fast Track drug development programs must be in regular contact with the reviewing division of the FDA to ensure that the product is safeevidence necessary to support marketing approval will be developed and effective for its intended use by submittingpresented in a format conducive to the FDAan efficient review. Sponsors of products in Fast Track drug development programs are also permitted to submit portions of an NDA or BLA containingto the pre-clinical and clinical data that have been accumulated, together with chemistry and manufacturing and controls specifications and information, and proposed labeling, among other things. The FDA may refuse to accept an NDA/BLA for filing if certain content criteria are not met and, even after accepting an NDA/BLA,on a rolling basis where the FDA may often require additional information, includingconsider reviewing portions of a marketing application before the sponsor submits the complete application.
In addition, sponsors may also apply to the FDA for Breakthrough Therapy Designation (BTD). The procedures and requirements for BTD are similar to those required for Fast Track such that the Breakthrough Therapy Designation is intended to expedite the development and review of a potential new drug for serious or life-threatening diseases, however, with BTD, there is a further requirement that the sponsor present “preliminary clinical data, beforeevidence” which “indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development.” The designation of a drug as a Breakthrough Therapy was enacted as part of the 2012 Food and Drug Administration Safety and Innovation Act.
Sponsors of drugs granted Fast Track or breakthrough therapy designation also may seek approval under the FDA’s accelerated approval regulations. Under this authority, the FDA may grant marketing approval for a new drug product on the basis of marketingadequate and well-controlled clinical trials establishing that the drug product has an effect on a product.
It is also becoming more common for the FDA to request a Risk Evaluation and Mitigation Strategy, or REMS, as part of aan NDA/BLA. The REMS plan contains post-market obligations of the sponsor to train prescribing physicians, monitor off-label drug use, and conduct sufficient Phase 4 follow-up studies and registries to ensure the continued safe use of the drug.
The NDA and BLA review process also generally includes a pre-approval inspection, or PAI, to assess the approval process, the FDA must inspectmanufacturing facilities and approve each manufacturing facility.relevant processes and data for compliance, and readiness for commercial manufacture in accordance with cGMPs. Among the conditions of approval is the requirement that a manufacturer’s quality controlsystems and manufacturing procedures conform to cGMP. ManufacturersEven when product approval is received, manufacturers must expend significant time, money and effort to ensure continued compliance, and the FDA conducts periodic surveillance inspections to certifymonitor the manufacturing process and drug quality and evaluate whether the manufacturers are in compliance. It may be difficult for our manufacturers or us to comply with the applicable cGMP, as interpreted by the FDA, and other FDA regulatory requirements. If we, or our contract manufacturers, fail to comply, then the FDA may not allow us to market products that have been affected by the failure.
Post-Approval Requirements
Any products for which the product is safe and effective, as demonstrated through clinical studies. Further, a product may be marketed only in those dosage forms and for those indications approved in the NDA/BLA. Certain changes to an approved NDA/BLA, including, with certain exceptions, any significant changes to labeling, requirewe receive FDA approval of a supplemental application before the drug may be marketed as changed. Any products that we manufacture or distribute pursuant to FDA approvals are subject to continuing monitoring and regulation by the FDA and other federal and state regulators on a wide range of matters, including, compliance with cGMPamong other things cGMPs and theproduct quality, pharmacovigilance and reporting of adverse experiencesevents, product distribution requirements, fulfilling post-marketing or confirmatory study or REMS commitments, and complying with the drugs. The nature of marketing claims that the FDA will permit us to make in the labelingpromotion and advertising of our products will generally be limited to those specified in FDA approved labeling, and the advertising of our products will be subject to comprehensive monitoring and regulation by the FDA. Drugs whose review was accelerated may carry additional restrictions on marketing activities, including the requirement that all promotional materials are pre-submitted to the FDA. Claims exceeding those contained in approved labeling will constitute a violation of the FDCA.requirements. Violations of the FDCA or other post-approval regulatory requirements at any time during the product development process, approval process, or marketing and sale following approval may result in agency enforcement actions, including withdrawal of approval, recall, seizure of products, warning letters, injunctions, fines and/or civil or criminal penalties. Any agency enforcement action could have a material adverse effect on our business.
The FDA promotion and advertising requirements applicable to marketed products include, among other things, standards for direct-to-consumer advertising, restrictions against promoting products for uses or in patient populations that are not either described in the product’s approved indications and uses or otherwise consistent with the FDA-approved product labeling, limitations on industry-sponsored scientific and educational activities, rules regarding communication of health care economic information regarding biopharmaceutical products to payors and formularies, and requirements for promotional activities involving the internet. Drugs whose review was accelerated may carry additional requirements on marketing activities, including the requirement that all promotional materials are pre-submitted to the FDA.
After product approval, quality control and manufacturing procedures must continue to conform to applicable manufacturing requirements. FDA regulations require among other things, quality control and quality assurance as well as the corresponding maintenance of records and documentation and the obligation to investigate and correct any deviations from cGMPs. Manufacturers and other entities involved in the manufacture and distribution of approved products are required to register their establishments and list their products with the FDA and certain state agencies. Manufacturers and their third-party contractors may be subject to periodic unannounced inspections by the FDA and certain state agencies for assessment of compliance with cGMPs and other applicable laws. Accordingly, manufacturers must continue to expend time, money, and effort in the areas of production and quality control to maintain quality control and manufacturing compliance. Discovery of problems with a product after approval may result in restrictions on a product, including, among other things, withdrawal of approval, recall or withdrawal of the product from the market. In addition, changes to the manufacturing process are strictly regulated, and depending on the significance of the change, may require prior FDA approval or notification before being implemented. Other types of changes to the approved product, such as adding new indications and claims to the product labeling, are also subject to further FDA review and approval.
Marketed products must meet the requirements of the Drug Supply Chain Security Act, or DSCSA, which regulates the commercial distribution of prescription drug products at the federal level. The DSCSA sets certain standards for federal or state registration, requires tracing of products through the pharmaceutical distribution supply chain, and imposes other requirements on entities in the supply chain, including manufacturers and repackagers, wholesale distributors, third-party logistics providers, and dispensers. The DSCSA requirements, development of standards, and the system for product tracing have been and will continue to be phased in per the DSCSA implementation timeline established by the FDA.
In addition, the post-marketing discovery of previously unknown problems with a product or the failure to comply with applicable FDA requirements can have negative consequences, including adverse publicity, judicial or administrative enforcement, warning letters from the FDA, mandated corrective advertising or communications with doctors, and civil or criminal penalties, among others. Newly discovered or developed safety or effectiveness data may require changes to a product’s approved labeling, including the addition of new warnings and contraindications, and may require the implementation of other risk management measures.
From time to time, legislation is drafted, introduced and passed in Congress that could significantly change the statutory provisions governing the approval, manufacturing and marketing of products regulated by the FDA. In addition to new legislation, FDA regulations, guidance documents, and policies are often revised or reinterpreted by the agency in ways that may significantly affect our business. It is impossible to predict whether further legislative or FDA regulation or policy changes will be enacted or implemented and what the impact of such changes, if any, may be.
Should we wish to market our products outside the U.S., we must receive marketing authorization from the appropriate foreign regulatory authorities. The requirements governing the conduct of clinical trials, marketing authorization, pricing and reimbursement vary widely from country to country. Importantly, the level of evidence of efficacy and safety necessary to apply for marketing authorization for a drug candidate differs from country to country. In particular, clinical trial endpoints, and the level of clinical evidence that may support, for example, an accelerated approval filing with the FDA, may be insufficient to file for marketing applications outside of the U.S. At present, companies are typically required to apply for foreign marketing authorizations at a national level. However, within the European Union, centralized registration procedures are available to companies wishing to market a product in more than oneacross the European Union member state.states. Typically, if the regulatory authority is satisfied that a company has presented adequate evidence of safety, quality and efficacy, then the regulatory authority will grant a marketing authorization. This foreign regulatory approval process, however, involves risks similar or identical to the risks associated with FDA approval discussed above, and therefore we cannot guarantee that we will be able to obtain the appropriate marketing authorization for any product in any particular country.
Failure to comply with applicable federal, state and foreign laws and regulations would likely have a material adverse effect on our business. In addition, federal, state and foreign laws and regulations regarding the manufacture and sale of new drugs are subject to future changes. We cannot predict the likelihood, nature, effect or extent of adverse governmental regulation that might arise from future legislative or administrative action, either in the U.S. or abroad.
Coverage and Reimbursement
Sales of our drugs will depend, in part, on the extent to which our drugs will be covered by third-party payors, such as government health programs, commercial insurance and managed healthcare organizations. These third-party payors are increasingly reducing reimbursements for medical drugs and services. In addition, the containment of healthcare costs has become a priority of foreign and U.S. federal and state governments, and the prices of drugs have been a focus in this effort. The U.S. government, state legislatures and foreign governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on reimbursement, importation, and requirements for substitution of generic drugs. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit our net revenue and results. Decreases in third-party reimbursement for our drug candidates, if approved, or a decision by a third-party payor to not cover our drug candidates could reduce physician usage of such drugs and have a material adverse effect on our sales, results of operations and financial condition.
In the U.S., the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010, or collectively the Affordable Care Act, enacted in March 2010, has had a significant impact on the health care industry. The Affordable Care Act expanded coverage for the uninsured while at the same time containing overall healthcare costs. With regard to pharmaceutical products, the Affordable Care Act, among other things, created a new average manufacturer price definition under the Medicaid Drug Rebate Program for drugs that are inhaled, infused, instilled, implanted or injected and not generally dispensed through the retail channel, increased the minimum Medicaid rebates owed by manufacturers under the Medicaid Drug Rebate Program and extended the rebate program to individuals enrolled in Medicaid managed care organizations, established annual fees and taxes on manufacturers of certain branded prescription drugs, and a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period (subsequent legislation increased this to 70% effective as of January 1, 2019), as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D.
Since the enactment of the Affordable Care Act, certain provisions of the Affordable Care Act have been subject to judicial challenges as well as efforts to repeal or replace them or to alter their interpretation or implementation. For example, the Tax Cuts and Jobs Act enacted on December 22, 2017, eliminated the shared responsibility payment for individuals who fail to maintain minimum essential coverage under section 5000A of the Internal Revenue Code of 1986, commonly referred to as the individual mandate, effective January 1, 2019. Although litigation and legislation over the Affordable Care Act are likely to continue, with unpredictable and uncertain results, we expect that the Biden administration may seek to expand and strengthen the Affordable Care Act.
On August 16, 2022, President Biden signed into law the Inflation Reduction Act of 2022 (the Act), which, among other provisions, included several measures intended to lower the cost of prescription drugs and related healthcare reforms. Specifically, the Act authorizes and directs the Department of Health and Human Services (the DHHS) to set drug price caps for certain high-cost Medicare Part B and Part D qualified drugs, with the initial list of drugs selected on August 29, 2023, and the first year of maximum price applicability to begin in 2026. The Act further authorizes the DHHS to penalize pharmaceutical manufacturers that increase the price of certain Medicare Part B and Part D drugs faster than the rate of inflation. Finally, the Act creates significant changes to the Medicare Part D benefit design by capping Part D beneficiaries’ annual out-of-pocket spending at $2,000 beginning in 2025. We cannot be sure whether additional or related legislation or rulemaking will be issued or enacted, or what impact, if any, such changes will have on the profitability of any of our drug candidates, if approved for commercial use, in the future.
At the state level, individual states are increasingly aggressive in passing legislation and implementing regulations designed to control prescription drug pricing, including price and marketing cost disclosure and transparency measures, and, in some cases, authorizing importation of prescription drugs from other countries. In addition, regional health care authorities and individual hospitals are increasingly using bidding procedures to determine what pharmaceutical products and which suppliers will be included in their prescription drug and other health care programs. These measures could reduce the ultimate demand for our products or put pressure on our product pricing. We expect that additional state healthcare reform measures will be adopted in the future, which could limit the amounts that state governments will pay for healthcare products and services and result in additional pricing pressures.
In addition, in some foreign countries, the proposed pricing for a prescription drug must be approved before the drug may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the United Kingdom and many European Union member states have robust health technology assessment processes to determine pricing and reimbursement for pharmaceuticals through their national health insurance system. Many European Union members states also include either direct or indirect price referencing, or other price control mechanisms, in determining the price of a pharmaceutical in their market. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical drugs will allow favorable reimbursement and pricing arrangements for any of our products. Historically, drugs launched in the European Union do not follow price structures of the U.S. and generally tend to be significantly lower.
Other U.S. Healthcare Laws
We may also be subject to healthcare regulation and enforcement by the federal government and the states and foreign governments where we may market our product candidates, if approved. These laws include, without limitation: state and federal anti-kickback, fraud and abuse, false claims, privacy and security laws; laws governing interactions with healthcare professionals and related transparency requirements (such as the federal Sunshine Act and a range of state biopharmaceutical marketing and transparency laws); and requirements for manufacturers to report certain calculated product prices to the government or provide certain discounts or rebates to government authorities or private entities, often as a condition of reimbursement under government healthcare programs. The compliance and enforcement landscape is informed by government enforcement precedent and settlement history, Advisory Opinions, and Special Fraud Alerts. The risks we face and our approach to compliance may evolve over time in light of these types of developments. The potential safe harbors available for, example, relative to the Anti-Kickback Statute, are subject to change through legislative and regulatory action, and we may decide to adjust our business practices or be subject to heightened scrutiny as a result.
The federal Anti-Kickback Statute prohibits, among other things, any person from knowingly and willfully offering, soliciting, receiving or paying remuneration, directly or indirectly, to induce either the referral of an individual, for an item or service or the purchasing or ordering of a good or service, for which payment may be made under federal healthcare programs such as the Medicare and Medicaid programs. The government has enforced the Anti-Kickback Statute to reach large settlements with healthcare companies based on research, consulting and other financial arrangements with physicians that the government alleged were not based on the provision of bona fide services and were intended as an inducement or reward. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. In addition, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal False Claims Act. The majority of states also have anti-kickback laws, which establish similar prohibitions and in some cases may apply to items or services reimbursed by any third-party payor, including commercial insurers.
In addition, the civil False Claims Act prohibits, among other things, knowingly presenting or causing the presentation of a false, fictitious or fraudulent claim for payment to the U.S. government. Actions under the False Claims Act may be brought by the Attorney General or as a qui tam action by a private individual in the name of the government. Violations of the False Claims Act can result in very significant monetary penalties and treble damages. The federal government is using the False Claims Act, and the accompanying threat of significant liability, in its investigation and prosecution of pharmaceutical and biotechnology companies throughout the U.S., for example, in connection with the promotion of products for unapproved uses and other sales and marketing practices. The government has obtained multi-million and multi-billion dollar settlements under the False Claims Act in addition to individual criminal convictions under applicable criminal statutes. Given the significant size of actual and potential settlements, it is expected that the government will continue to devote substantial resources to investigating healthcare providers’ and manufacturers’ compliance with applicable fraud and abuse laws.
The federal Health Insurance Portability and Accountability Act of 1996, (HIPAA), also created new federal criminal statutes that prohibit among other actions, knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third-party payors, knowingly and willfully embezzling or stealing from a healthcare benefit program, willfully obstructing a criminal investigation of a healthcare offense, and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
There has also been a recent trend of increased federal and state regulation of payments made to physicians and other healthcare providers. The Affordable Care Act, among other things, imposes reporting requirements on drug manufacturers for payments made by them to physicians and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members. Failure to submit required information may result in civil monetary penalties of up to an aggregate of $150,000 per year (or up to an aggregate of $1 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately and completely reported in an annual submission. Drug manufacturers are required to submit annual reports to the Centers for Medicare & Medicaid Services, which publicly posts the data on its website. Effective January 1, 2022, these reporting obligations extend to include transfers of value made to certain non-physician providers such as physician assistants and nurse practitioners. Certain states also mandate implementation of compliance programs, impose restrictions on drug manufacturer marketing practices and/or require the tracking and reporting of gifts, compensation and other remuneration to physicians.
We may also be subject to data privacy and security regulation by both the federal government and the states in which we conduct our business. HIPAA, as amended by the Health Information Technology and Clinical Health Act, (HITECH), and their respective implementing regulations, including the final omnibus rule published on January 25, 2013, imposes specified requirements relating to the privacy, security and transmission of individually identifiable health information. Among other things, HITECH makes HIPAA’s privacy and security standards directly applicable to “business associates,” defined as independent contractors or agents of covered entities that create, receive, maintain or transmit protected health information in connection with providing a service for or on behalf of a covered entity. HITECH also increased the civil and criminal penalties that may be imposed against covered entities, business associates and possibly other persons, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorney’s fees and costs associated with pursuing federal civil actions. In addition, according to the U.S. Federal Trade Commission, (FTC), failing to take appropriate steps to keep consumers' personal information secure constitutes unfair acts or practices in or affecting commerce in violation of Section 5(a) of the Federal Trade Commission Act. The FTC expects a company's data security measures to be reasonable and appropriate in light of the sensitivity and volume of consumer information it holds, the size and complexity of its business, and the cost of available tools to improve security and reduce vulnerabilities. Medical data is considered sensitive data that merits stronger safeguards. The FTC's guidance for appropriately securing consumers' personal information is similar to what is required under HIPAA.
In addition, we may be subject to state law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers, and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways, thus complicating compliance efforts. For example, the California Consumer Protection Act, (CCPA), which went into effect on January 1, 2020, established a privacy framework for covered businesses by creating an expanded definition of personal information, data privacy rights for consumers in California, and a potentially severe statutory damages framework for violations of the CCPA and for businesses that fail to implement reasonable security procedures and practices to prevent data breaches. The CCPA was recently amended by the California Privacy Rights Act (CPRA), expanding certain consumer rights such as the right to know. It remains unclear what, if any, additional modifications will be made to these laws by the California legislature or how these laws will be interpreted and enforced. The potential effects of the CCPA and CPRA are significant and may cause us to incur substantial costs and expenses to comply.
Rest of the World Healthcare Regulation
For other countries outside of the U.S. and the European Union, the requirements governing the conduct of clinical trials, drug licensing, sales and marketing, pricing and reimbursement vary from country to country. If we fail to comply with applicable foreign regulatory requirements, we may be subject to, among other things, fines, suspension or withdrawal of regulatory approvals, product recalls, seizure of products, operating restrictions and criminal prosecution.
European Union member states, the United Kingdom, Switzerland, and other foreign jurisdictions have adopted data protection laws and regulations, which impose significant compliance obligations. In the European Union and the United Kingdom, the collection and use of personal data, including clinical trial data, is governed by the provisions of the General Data Protection Regulation, or GDPR. The GDPR, together with national legislation, regulations and guidelines of the European Union member states and the United Kingdom governing the processing of personal data, impose strict obligations and restrictions on the ability to collect, analyze and transfer personal data, including health data from clinical trials and adverse event reporting. In particular, these obligations and restrictions concern the consent of the individuals to whom the personal data relates, the information provided to the individuals, the transfer of personal data out of the European Union or the United Kingdom, security breach notifications, security and confidentiality of the personal data and imposition of substantial potential fines for breaches of the data protection obligations. Compliance with the GDPR is a rigorous and time-intensive process that may increase the cost of doing business to ensure full compliance. Furthermore, European data protection authorities may interpret the GDPR and national laws differently and impose additional requirements, which add to the complexity of processing personal data in or from the European Union or United Kingdom.
Human Capital
As of March 1, 2018,February 26, 2024, we had 75 full and part-time264 full-time employees. None of our employees are represented by a collective bargaining agreement, and we have never experienced a work stoppage.
We considerbelieve that our relationsfuture success largely depends upon our continued ability to attract and retain a diverse workforce of highly skilled and dedicated employees. We pride ourselves on being an equal opportunity employer and strictly prohibit unlawful discrimination based on color, religion, gender, sexual orientation, gender identity/expression, national origin/ancestry, age, disability, marital and veteran status.
We expect to continue to grow our organization to support the commercialization of BRIUMVI and to enhance our overall development capabilities for current or future products under development. As part of that process, we will continue to evaluate the business needs and market opportunities, balancing in-house expertise and core competencies with our employeesoutsourced capacity.
Drug development and commercialization requires deep expertise across a broad array of disciplines. Pharmaceutical companies of all sizes compete for a limited number of qualified applicants to be good.fill specialized positions. To attract qualified candidates, the Company offers an attractive total rewards package, consisting of base salary, cash bonus, a comprehensive benefit package, equity compensation, and 401(k) plan. Bonus opportunities and equity compensation increase as a percentage of total compensation based on level of responsibility, and actual bonus awards are based on performance.
You should carefully consider the following risksrisk factors and uncertainties.the other information contained elsewhere in this Annual Report before making an investment in our securities. If any of the following occurs,risks occur, our business, financial condition or operating results could be materially harmed. An investment in our securities is speculative in nature, involves a high degree of risk, and should not be made by an investor who cannot bear the economic risk of its investment for an indefinite period of time and who cannot afford the loss of its entire investment. You should carefully considerThe risks described below are not the following risk factorsonly ones that our business faces. Additional risks not currently known to us or that we currently deem to be immaterial may adversely impact our business in the future.
Risks Related to Commercialization
If we obtain U.S. Food and Drug Administration (FDA) or European Medicines Agency (EMA) approval for a product candidate and do not achieve broad market acceptance among physicians, patients, healthcare payors, and the medical community, the revenues that we generate from product sales will be limited.
We currently have one marketed product, BRIUMVI, which received approval from the FDA on December 28, 2022, for the treatment of relapsing forms of multiple sclerosis (RMS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults. Additionally, BRIUMVI received approval from the European Commission (EC) on June 1, 2023, and later in 2023, from the Medicines and Healthcare products Regulatory Agency (MHRA) for the treatment of adult patients with RMS who have active disease defined by clinical or imaging features in the EU and UK, respectively.
While we have initiated the commercial launch of BRIUMVI in the U.S., we have limited experience as a commercial company, and our ability to successfully overcome the risks associated with commercializing drugs in the biopharmaceutical industry, including the risk that our products do not achieve an adequate level of acceptance, remains uncertain. BRIUMVI, as well as other drugs that we may bring to the market in the future, may not gain market acceptance by physicians, patients, third-party payors and others in the healthcare community. As a result, we may not generate significant revenues or meet our revenue projections or guidance and may not become profitable. The degree of market acceptance of BRIUMVI, as well as any future product candidates for which we may receive marketing approval, will depend on a number of factors, including:
● | the timing of our receipt of marketing approvals, the terms of such approvals, and the countries in which such approvals are obtained; |
● | the efficacy, safety and tolerability as demonstrated in clinical trials and as compared to alternative treatments; |
● | the timing of market introduction of BRIUMVI and any of our product candidates, as well as competitive products; |
● | the indications for which our products are approved, and other aspects of the approved labeling for such products; |
● | acceptance by physicians, advanced practitioners, major operators of neurology clinics, and patients of our products as safe, tolerable and effective treatments; |
● | the potential and perceived advantages or disadvantages of our products compared to alternative treatments; |
● | our ability to offer our products for sale at competitive prices; |
● | the availability of adequate reimbursement by third-party payors and government authorities; |
● | the extent of patient cost-sharing obligations, including copays and deductibles; |
● | changes in regulatory requirements by government authorities for our products; |
● | relative convenience and ease of administration; |
● | the prevalence and severity of side effects and adverse events; |
● | the willingness of the target patient population to try new therapies and of physicians to prescribe these therapies; |
● | the effectiveness of our sales and marketing efforts, as well as those of any current or future partners; |
● | protecting our rights in our intellectual property portfolio; |
● | our ability to maintain a reliable supply of our products that meets market demand; and |
● | favorable or unfavorable publicity relating to our products or relating to the Company. |
In addition, global health concerns such as the COVID-19 pandemic could impact commercialization of BRIUMVI. Patients and healthcare providers have raised concerns that immunosuppressive products like anti-CD20 antibodies and other B-cell targeted agents may increase the risk of acquiring viruses such as COVID-19 or lead to more severe complications or outcomes upon infection, including death. These or other similar concerns may impact the commercial potential for BRIUMVI and other immunosuppressive products that we have in development.
If BRIUMVI, or any future product candidates for which we receive regulatory approval, do not achieve an adequate level of acceptance by physicians, hospitals, healthcare payors and patients, we may not generate sufficient revenue from these products and we may not become or remain profitable, which would have a material adverse effect on our business.
We may be subject to limitations on the indicated uses or requirements to fulfill certain post-marketing requirements to the satisfaction of regulatory authorities or may be unable to maintain marketing approval for BRIUMVI or future products that we may bring to market.
Regulatory approvals for our product or any of our product candidates may be subject to conditions and limitations on the approved indicated uses for which the product may be marketed or contain requirements for potentially costly post-marketing testing, including Phase 4 clinical trials, and surveillance to monitor the safety and efficacy of the approved product candidate. For example, with respect to the FDA’s approval of BRIUMVI for RMS, the approval is subject to certain post-marketing requirements and commitments, including long-term safety studies, as well as studies to evaluate the effects of BRIUMVI in pregnant women and pediatric populations, among others. Similar post-approval studies are required by other regulatory authorities outside of the U.S., including but not limited to, the EMA in the EU and the MHRA in the United Kingdom (UK). These studies are highly specialized in their design and conduct and are associated with considerable expenses, and based on the outcome, could result in further labeling restrictions that could impair or restrict the way in which we are able to market BRIUMVI, or negatively impact its overall clinical profile.
In addition, with respect to BRIUMVI and any product candidate that the FDA or a comparable foreign regulatory authority approves, the manufacturing processes, testing, labeling, packaging, distribution, import, export, adverse event reporting, storage, advertising, promotion and recordkeeping for the product will be subject to extensive and ongoing regulatory requirements. These requirements include submissions of safety and other post-marketing information contained elsewhereand reports, registration, as well as continued compliance with current Good Manufacturing Practices (cGMPs), with Good Clinical Practices (GCPs), for any clinical trials that we conduct post-approval, and with Good Laboratory Practices (GLPs), for any nonclinical studies. Later discovery of previously unknown problems with a product or with our third-party manufacturers or manufacturing processes, or failure to comply with regulatory requirements, may result in, this Annual Reportamong other things, restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market, mandatory safety labeling changes or product recalls, suspension or revocation of product approvals, product seizure or detention, refusal to permit the import or export of products, and injunctions or the imposition of civil or criminal penalties, all of which would adversely affect our business, prospects and ability to achieve or sustain profitability.
BRIUMVI, and any of our product candidates for which we in the future obtain approval, may, after approval, be found to cause undesirable side effects that could result in significant negative consequences following commercialization.
As BRIUMVI or any future approved products are used more widely or for a longer duration after being brought to market, data may emerge from clinical studies, including confirmatory or other post-marketing studies, or from adverse event reporting, that may affect the commercial potential of our products. For example, as additional patients are exposed for longer durations to a product in the commercial and clinical settings, it is unknown whether greater frequency and/or severity of adverse events are likely to occur or whether an acceptable safety and tolerability profile will continue to be demonstrated. If we or others identify unexpected side effects caused by BRIUMVI or other products or product candidates within the RMS space following introduction into the market, a number of potentially significant negative consequences could result, including:
● | regulatory authorities may withdraw approval or limit the approved indications for use of such products; |
● | regulatory authorities may require the addition of new or different labeling statements, including warnings or boxed warnings, precautions, or contraindications that could diminish the usage of the product or otherwise limit the commercial success of the affected product; |
● | we may be required to change the way such drug candidates are distributed or administered, or to conduct additional clinical trials; |
● | regulatory authorities may require a Risk Evaluation and Mitigation Strategy (REMS), a plan to mitigate risks, which could include a Medication Guide, physician communication plans, or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools; |
● | we may be subject to regulatory investigations and government enforcement actions; |
● | we may decide to remove such drug candidates from the marketplace; |
● | we may not be able to enter into collaboration agreements on acceptable terms and execute on our business model; |
● | we could be sued and held liable for injury caused to individuals exposed to or taking our products; and |
● | our reputation may suffer. |
Any one or a combination of these events could prevent us from maintaining regulatory approval and achieving or maintaining market acceptance of the affected product or could substantially increase the costs and expenses of commercializing the affected product, which in turn could significantly impact our ability to successfully commercialize our drug candidates and generate revenues.
The incidence and prevalence for target patient populations of BRIUMVI and our product candidates, including TG-1701 and TG-1801 in B-cell disorders and azer-cel in non-oncology indications, have not been established with precision. If the market opportunities for BRIUMVI and our product candidates are smaller than we estimate or if any approval that we obtain is based on a narrower definition of the patient population, our revenue and ability to achieve profitability will be adversely affected.
The precise incidence and/or prevalence of RMS are unknown. Our projections for BRIUMVI in RMS are based on estimates and our current knowledge and understanding of the disease. These estimates are typically based on one-on-one and group interactions with target physicians and other sources available at the time we make the estimates, including the scientific literature, healthcare utilization databases and market research. Although we believe our estimates are reasonable, many factors may limit their accuracy. For example, the sources we use to make the estimates may prove to be incorrect. Further, new studies may change the estimated incidence or prevalence of these diseases and the number of patients may turn out to be lower than expected.
The total addressable market opportunity for BRIUMVI and our product candidates, if approved, ultimately depends upon, among other things, the approved prescribing information, acceptance by the medical community, patient access, and drug pricing and reimbursement. The number of patients in major markets, including the number of addressable patients in those markets, may turn out to be lower than expected, patients may not be otherwise amenable to treatment with our drugs, new patients may become increasingly difficult to identify or gain access to, patients and physicians may choose to utilize competitive products or reimbursement may be unfavorable, all of which would adversely affect our results of operations and our business.
We face substantial competition, which may result in others commercializing drugs before making anor more successfully than we do resulting in the reduction or elimination of our commercial opportunity.
We operate in a highly competitive segment of the biotechnology and biopharmaceutical market. We face competition from numerous sources, including commercial pharmaceutical and biotechnology enterprises, academic institutions, government agencies, and private and public research institutions. Many of our competitors have significantly greater financial, product development, manufacturing and commercialization resources. Large pharmaceutical companies have extensive experience commercializing products and may have significant existing relationships with customers and more resources available to them to promote their products. Many are active in the same diseases that we are, including within the neurological and immunological fields, some in direct competition with us. We may also compete with these organizations to recruit commercial and other key personnel. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies.
Our commercial opportunity could be reduced or eliminated if our competitors develop and commercialize drugs that are more effective, have fewer or less severe side effects, are more convenient or are priced or contracted differently than any drugs that we or our collaborators may develop. Our competitors also may obtain FDA or other regulatory approval for their drugs more rapidly than we may obtain approval for ours, which could result in our competitors establishing a strong market position before we or our collaborators are able to enter the market. In a competitive environment, a company’s communications may also be subject to heightened scrutiny from regulators and competitors, under laws, regulations, and guidance about promotional communications (advertising and promotional labeling) and non-promotional communications (e.g., certain educational and scientific exchange); and with regard to potential competitor actions under federal law (the Lanham Act) and congruous state law, which protect businesses against the unfair competition of misleading advertising or labeling.
The key competitive factors affecting the success of all of our drug candidates, if approved, are likely to be their efficacy, safety, convenience, price, the level of generic or biosimilar competition and the availability of reimbursement from government and other third-party payors.
New developments, including the development of other pharmaceutical technologies and methods of treating disease, occur in the pharmaceutical and life sciences industries at a rapid pace. These developments may render our product or product candidates obsolete or noncompetitive. Compared to us, many of our potential competitors have substantially greater:
● | research and development resources, including personnel and technology; |
● | regulatory experience; |
● | pharmaceutical development, clinical trial and pharmaceutical commercialization experience; |
● | experience and expertise in exploitation of intellectual property rights; and |
● | capital resources. |
We will also face competition from these third parties in recruiting and retaining qualified personnel, establishing clinical trial sites, patient registration for clinical trials, and in identifying and in-licensing new products and product candidates.
BRIUMVI, as well as any products that we are able to commercialize in the future, may become subject to unfavorable pricing regulations or third-party payor coverage and reimbursement policies, which would harm our business.
The regulations that govern regulatory approvals, pricing and reimbursement for new drugs vary widely from country to country. Current and future legislation may significantly change the approval requirements in ways that could involve additional costs and cause delays in obtaining approvals. Some countries require approval of the sale price of a drug before it can be marketed. In many countries, the pricing review period begins after marketing approval is granted. In some markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain marketing approval for a product in a particular country, but then be subject to price regulations that delay our commercial launch of the drug candidate, possibly for lengthy time periods, and negatively impact the revenues we are able to generate from the sale of the drug candidate in that country. Adverse pricing limitations may hinder our ability to recoup our investment in one or more products, even if more of our securities.product candidates obtain marketing approval. Eligibility for reimbursement does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Interim reimbursement levels for new drugs, if applicable, may also be insufficient to cover our costs and may not be made permanent. On April 27, 2023, we received a product-specific J-Code for BRIUMVI (J2329), which became effective July 1, 2023 and is expected to help reduce reluctance by physicians to prescribe BRIUMVI based on reimbursement concerns. However, some third-party payors may nevertheless still require documented proof that patients meet certain eligibility criteria in order to be reimbursed for BRIUMVI.
Our ability to commercialize any product successfully also will depend in part on the extent to which coverage and reimbursement for our products and related treatments will be available from government authorities, private health insurers and other organizations. Government authorities and third-party payors, such as private health insurers and health maintenance organizations, decide which medications they will pay for and establish reimbursement and co-payment levels. A primary trend in the U.S. healthcare industry and elsewhere is cost containment. Government authorities and third-party payors have attempted to control costs by restricting coverage and limiting the amount of reimbursement for particular drugs. Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for drugs, examining the cost effectiveness of drugs in addition to their safety and efficacy. Third-party commercial payors often rely upon Medicare coverage policy and payment limitations in setting their own reimbursement policies. Payors may restrict coverage of some products by using formularies under which only selected drugs are covered, variable co-payments that make drugs that are not preferred by the payor more expensive for patients, and utilization management controls, such as requirements for prior authorization or failure first on another type of treatment. Payors may target higher-priced drugs for imposition of these obstacles to coverage, and consequently our products may be subject to payor-driven restrictions. Additionally, in countries where patients have access to insurance, as in the U.S., insurance co-payment amounts or other benefit limits may represent a barrier to obtaining or continuing use of our products that receive regulatory approval. If we are unable to obtain or maintain coverage, or coverage is reduced in one or more countries, our product sales may be lower than anticipated and our financial condition could be harmed.
Net prices for drugs may be reduced by mandatory discounts or rebates required by government healthcare programs or private payors and by any future relaxation of laws that presently restrict imports of drugs from countries where they may be sold at lower prices. In the United States, for example, we must offer discounted pricing or rebates on purchases of pharmaceutical products under various federal and state healthcare programs, such as the Medicaid Drug Rebate Program, the 340B drug pricing program and the Medicare Part D Program. We must also report specific prices to government agencies under healthcare programs, such as the Medicaid Drug Rebate Program and Medicare Part B. The calculations necessary to determine the prices reported are complex and the failure to report prices accurately may expose us to penalties.
If we are unable to expand our commercialization operations, we may not be successful in commercializing BRIUMVI or any product candidate, if and when such product candidates are approved, and we may not be able to generate revenue.
Commercialization of pharmaceutical products is an extremely complex and highly capital and resource-intensive process. Even for established companies with existing infrastructure and significantly greater resources than we have, challenges have occurred.
We have made and continue to make significant investments in our commercial organization and infrastructure. We built processes and systems to support the commercialization of BRIUMVI following its commercial launch on January 26, 2023. There are risks involved with establishing our own commercialization capabilities. For example, if we are unable to recruit and retain adequate numbers of effective personnel to support the ongoing commercialization of BRIUMVI, we may not be successful in marketing and selling the product.
Additional factors that may inhibit our efforts to commercialize BRIUMVI and our other product candidates on our own, or through partnership, and generate product revenues include:
● | the costs and time associated with the initial and ongoing training of commercialization personnel on the applicable disease states, products, competitors, and legal and regulatory compliance matters; |
● | the inability of commercialization personnel to obtain access to physicians or to effectively promote or provide education about BRIUMVI and any future approved products; |
● | the lack of complementary drugs to be offered by the Company, which may put us at a competitive disadvantage relative to companies with more extensive product lines; |
● | decisions by third-party payors to deny reimbursement of or delay coverage decisions regarding BRIUMVI or following approval of any product candidates; |
● | our inability to maintain a healthcare compliance program including effective mechanisms for compliance monitoring; |
● | our inability to establish and maintain commercial partnerships outside the U.S.; | |
● | our inability, or the inability of a third party with whom we have partnered, to maintain the necessary regulatory approvals required to operate in markets outside of the U.S.; |
● | the timing of product availability for commercial sale following approval and continued product supply; and |
● | unforeseen costs and expenses associated with creating a commercialization organization. |
In addition, we have entered into a commercialization agreement, and may enter into additional agreements in the future, that facilitate commercialization of BRIUMVI and/or future products that receive approval in markets outside the U.S. through partnerships. However, there are also risks with entering into these types of arrangements with third parties to perform sales, marketing and distribution services. For example, we may not be able to enter into such arrangements on terms that are favorable to us. Our drug revenues or the profitability of these drug revenues to us are likely to be lower than if we were to market and sell any products or product candidates that we develop ourselves. In addition, we likely will have little control over such third parties, and any of them may fail to devote the necessary resources and attention to sell and market our product or product candidates effectively. If we do not establish sales and marketing capabilities successfully, either on our own or in collaboration with third parties, we will not be successful in commercializing our drug candidates. Further, our business, results of operations, financial condition and prospects will be materially adversely affected.
We believe there is potential market opportunity for BRIUMVI outside of the U.S., including in the EU. We have entered into a commercialization agreement for the sale of BRIUMVI in certain territories outside the U.S., Canada and Mexico, the commercialization rights for which had been previously retained by TG, thus excluding certain Asian countries subject to previously existing partnerships, and we also may enter into certain collaboration and/or commercialization agreements with third parties in the future to facilitate market expansion. To the extent we do expand into other markets outside of the U.S. in which we are responsible for building and maintaining a commercial infrastructure, we expect to incur significant expenses in establishing an infrastructure to commercialize our drug products. Depending on the expenses incurred, it could have a negative impact on our cash resources.
Product liability lawsuits against us could cause us to incur substantial liabilities and could limit commercialization of any drug candidates that we may develop.
We face an inherent risk of product liability exposure related to the testing of our product candidates in human clinical trials, and an even greater risk in connection with the commercialization of BRIUMVI and any other products for which we may receive marketing authorization in the future. If we cannot successfully defend ourselves against claims that BRIUMVI or any of our product candidates caused injuries, we could incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
● | decreased demand for any products that we may commercialize; |
● | injury to our reputation and significant negative media attention; |
● | withdrawal of clinical trial participants; |
● | significant costs to defend the related litigation, including the risk that any individuals who may face such related litigation may in turn seek to recover from us; |
● | substantial monetary awards to trial participants or patients; |
● | loss of revenue; and |
● | the inability to commercialize any products or product candidates that we may develop. |
Although we maintain product liability insurance coverage, it may not be adequate to cover all liabilities that we may incur. Insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise.
Risks Related to Our BusinessFinancial Position and Need for Additional Capital
We have incurred significant operating losses since our inception, and we may incur losses in the future.
Biopharmaceutical drug development is a highly speculative undertaking and involves a substantial degree of risk. We commenced operations in January 2012. To date, our operations have been limited primarily to organizing and staffing our company, business planning, raising capital, developing our technology, identifying potential drug candidates, undertaking pre-clinical studies and clinical trials, commercializing UKONIQ (withdrawn from sale) and launching and commercializing BRIUMVI. We are transitioning from a company with a research and development focus and commercialization capabilities in oncology to a company capable of supporting commercial activities in neurology and immunology in the U.S. and outside the U.S. This transition involves a wide variety of risks, and we may not be successful in such transition.
Since inception, we have focused our efforts and financial resources on clinical trials, manufacturing of our product and product candidates and preparing to support a commercial product. To date, we have financed our operations primarily through public offerings of our common stock and debt financing. Since inception, we have incurred significant operating losses. Substantially all our operating losses have resulted from costs incurred in connection with our research and development programs and from selling, general and administrative costs associated with our operations, including our commercialization activities. We expect to continue to incur significant expenses and operating losses for the foreseeable future. Our prior losses, combined with expected future losses, have had, and will continue to have an adverse effect on our stockholders’ deficit and working capital. BRIUMVI is currently our only marketed product. We expect to continue to incur significant research and development expenses, and we expect to continue to incur significant commercialization and outsourced-manufacturing expenses as we commercialize BRIUMVI. Because of the numerous risks and uncertainties associated with developing pharmaceuticals, we are unable to predict the extent of any future losses or when we will become profitable, if at all. Even if we do become profitable, we may not be able to sustain or increase our profitability on a quarterly or annual basis. Our ability to become profitable depends upon our ability to generate substantial revenue.
To become and remain profitable, we must succeed in developing (or in-licensing) and commercializing our products or product candidates that generate significant revenue. It is uncertain when and if we will generate any significant revenue from the sale of our product or any product candidates, if approved, in the future. Furthermore, no assurance can be given that we will meet revenue projections or guidance with respect to BRIUMVI or our product candidates, if approved. To obtain significant and sustained revenues and meet our revenue projections or guidance, we must succeed, either alone or with others, in (i) obtaining and maintaining regulatory approval for our product and product candidates; and (ii) manufacturing and marketing our product and product candidates. Our ability to generate sustained revenue depends on a number of factors, including, but not limited to, our ability to:
● | successfully complete clinical trials that meet their clinical endpoints; |
● | initiate and successfully complete all safety, pharmacokinetic, biodistribution, and non-clinical studies required to obtain U.S. and foreign marketing approval for our product and product candidates; |
● | obtain approval from the FDA and foreign equivalents to market and sell our product and product candidates, and maintain FDA and EMA approvals of BRIUMVI for RMS; |
● | establish and maintain commercial manufacturing capabilities with third parties that are satisfactory to the regulatory authorities, cost effective, and that are capable of providing commercial supply of our product and product candidates; |
● | expand on our commercialization infrastructure to commercialize BRIUMVI, and/or entering into collaborations with third parties; and |
● | achieve market acceptance of BRIUMVI and any other products for which we may receive regulatory approval in the medical community and with third-party payors. |
If we are unable to generate significant and sustained revenues, we will not become profitable and we will be unable to continue our operations without continued funding.
While we do not expect to need to raise additional capital, we may need to do so. If we are unable to raise capital, if needed, we may be required to delay, limit, reduce or eliminate some of our drug development programs or commercialization efforts.
The development of pharmaceuticals is capital-intensive. We are also continuing to generate additional clinical data for BRIUMVI to support and potentially expand commercial adoption, including assessing long-term tolerability in an Open-Label Extension of the Phase 3 ULTIMATE I and II trials and Phase 4 clinical studies necessary to satisfy post-approval commitments for regulatory authorities or those undertaken voluntarily by the Company to evaluate the use of BRIUMVI in alternate settings or with alternate methods of administration. Moreover, now that we have launched BRIUMVI, we will need to expend substantial resources on maintaining approvals and continuing commercialization, manufacturing and distribution over the foreseeable future. Additionally, we expect to commence a trial evaluating azer-cel in autoimmune disease in 2024. We are also currently advancing our early-stage drug candidates, TG-1701 and TG-1801 in ongoing Phase 1 studies to identify tolerable and efficacious doses.
The amount and timing of our future funding requirements will depend on many factors, including, but not limited to, the following:
● | the success of the commercialization of BRIUMVI and any other products for which we receive regulatory approval; |
● | the costs and timing of clinical and commercial manufacturing supply arrangements for each product and product candidate; |
● | the costs of expanding our sales, distribution, and other commercialization capabilities; |
● | the costs and timing of regulatory approvals; |
● | the progress of our clinical trials, including expenses to support the trials and milestone payments that may become payable under our license agreements; |
● | our ability to establish and maintain strategic collaborations, including licensing and other arrangements; |
● | the costs involved in enforcing or defending patent claims or other intellectual property rights; and |
● | the extent to which we in-license or invest in other indications or product candidates. |
As a result, significant additional funding may be required. Additional sources of financing to continue our operations in the future might not be available on favorable terms, if at all. If we do not succeed in raising additional funds on acceptable terms, we could be forced to discontinue product development, reduce or forego commercialization efforts that are required for successful commercialization of BRIUMVI or any of our product candidates and otherwise forego attractive business opportunities. Any additional sources of financing may involve the issuance of our equity securities, which would have a dilutive effect to stockholders. Currently, other than BRIUMVI, our products are investigational and have not been approved by the FDA or any foreign regulatory authority for sale. For the foreseeable future, we will have to fund all our operations and capital expenditures from sales of BRIUMVI, cash on hand and amounts raised in future offerings or financings. Accordingly, our prospects must be considered in light of the uncertainties, risks, expenses and difficulties frequently encountered by companies in the early stages of commercial operations and the competitive environment in which we operate.
Raising additional capital may cause dilution to our stockholders, restrict our operations or require us to relinquish rights to our technologies or drug candidates and occupy valuable management time and resources.
Until such time, if ever, as we can generate substantial revenues, we expect to finance our cash needs through a combination of public and private equity offerings, debt financings, collaborations, strategic alliances, licensing agreements or other arrangements. We do not have any committed external source of funds, other than funds already borrowed under the loan and security agreement that we entered into with Hercules in February 2019, amended and restated in December 2021 and amended on March 31, 2023 (see Note 7 to our consolidated financial statements for more information). To the extent that we raise additional capital through the sale of common stock or securities convertible or exchangeable into common stock, the ownership interest of our stockholders will be diluted, and the terms of these securities may include liquidation or other preferences that materially adversely affect the rights of our common stockholders. We may also seek funds through collaborations, strategic alliances or licensing arrangements with third parties at a time that is not desirable to us and we may be required to relinquish valuable rights to some intellectual property, future revenue streams, research programs or products and product candidates or to grant licenses on terms that may not be favorable to us, any of which may have a material adverse effect on our business, operating results and prospects. Debt financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures, or declaring dividends. We cannot guarantee that future financing will be available in sufficient amounts or on terms acceptable to us, if at all, which could limit our ability to expand our business operations and could harm our overall business prospects.
Additionally, fundraising efforts may divert our management from their day-to-day activities, which may adversely affect our ability to develop and commercialize our drug candidates. Dislocations in the financial markets have generally made equity and debt financing more difficult to obtain and may have a material adverse effect on our ability to meet our fundraising needs. Moreover, the issuance of additional securities, whether equity or debt, by us, or the possibility of such issuance, may cause the market price of our shares to decline.
Due to limited resources, we may fail to capitalize on programs or product candidates that may present a greater commercial opportunity or for which there is a greater likelihood of success.
Because we have limited resources, we may forego or delay pursuit of opportunities with certain programs or product candidates or for indications that later prove to have greater commercial potential. Our estimates regarding the potential market for a product candidate could be inaccurate, and our spending on current and future research and development programs may not yield any commercially viable products. If we do not accurately evaluate the commercial potential for a particular product candidate, we may relinquish valuable rights to that product candidate through strategic collaboration, licensing, sale or other arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such product candidate. We may focus our efforts and resources on potential product candidates or other potential programs that ultimately prove to be unsuccessful. Alternatively, we may allocate internal resources to a product candidate in a therapeutic area in which it would have been more advantageous to enter into a partnering arrangement.
There can be no assurance that we will ever be able to identify additional therapeutic opportunities for our product candidates or to develop suitable potential product candidates through internal research programs, which could materially adversely affect our future growth and prospects. If any of the aforementioned events occur, we may be forced to abandon or delay our development efforts with respect to a particular product candidate or fail to develop a potentially successful product candidate, which could have a material adverse effect on our business, financial condition, results of operations and prospects.
Our level of indebtedness and debt service obligations could adversely affect our financial condition and may make it more difficult for us to fund our operations.
In February 2019, we entered into a Loan and Security Agreement, with Hercules Capital, Inc., a Maryland corporation (Hercules), and on December 30, 2021 (the Amendment Closing Date), the Company entered into an Amended and Restated Loan and Security Agreement (the Amended Loan Agreement) with Hercules. Under the Amended Loan Agreement, Hercules increased the aggregate principal amount of the loan, available at the Company’s option, from $60.0 million to $200.0 million. On March 31, 2023 (the First Amendment Effective Date), the Company entered into a First Amendment to the Amended Loan Agreement (the First Amendment) with Hercules. An advance of $25.0 million was drawn at the First Amendment Effective Date (see Note 7 to our consolidated financial statements for more information). We have the option to request additional loan advances in an aggregate principal amount of up to $85.0 million under the First Amendment.
All obligations under the Amended Loan Agreement, as amended, are secured by substantially all our existing property and assets, excluding intellectual property. This indebtedness may create additional financing risk for us, particularly if our business or prevailing financial market conditions are not conducive to paying off or refinancing its outstanding debt obligations at maturity. This indebtedness could also have important negative consequences, including:
● | we will need to repay the indebtedness by making payments of interest and principal, which will reduce the amount of money available to finance our operations, our research and development efforts and other general corporate activities; and |
● | our failure to comply with the restrictive covenants in the Amended Loan Agreement, as amended, could result in an event of default that, if not cured or waived, would accelerate our obligation to repay this indebtedness, and Hercules could seek to enforce its security interest in the assets securing such indebtedness. |
To the extent additional debt is added to our current debt levels, the risks described above could increase.
We may not have cash available in an amount sufficient to enable us to make interest or principal payments on our indebtedness when due.
Failure to satisfy our current and future debt obligations under the Amended Loan Agreement, as amended,, or the breach of any of its covenants, subject to specified cure periods with respect to certain breaches, could result in an event of default and, as a result, Hercules could accelerate all the amounts due. In the event of an acceleration of amounts due under the Amended Loan Agreement, as amended, as a result of an event of default, we may not have enough available cash or be able to raise additional funds through equity or debt financings to repay such indebtedness at the time of such acceleration. In that case, we may be required to delay, limit, reduce or terminate our product candidate development or commercialization efforts or grant to others rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves. Hercules could also exercise its rights as collateral agent to take possession and dispose of the collateral securing the term loan for its benefit, which collateral includes substantially all our property other than intellectual property. Our business, financial condition and results of operations could be materially adversely affected as a result of any of these events.
The Amended Loan Agreement, as amended, imposes operating and other restrictions on the Company. Such restrictions will affect, and in many respects limit or prohibit, our ability and the ability of any future subsidiary to, among other things:
● | dispose of certain assets; |
● | change its lines of business; |
● | engage in mergers, acquisitions or consolidations; |
● | incur additional indebtedness; |
● | create liens on assets; |
● | pay dividends and make contributions or repurchase our capital stock; and |
● | engage in certain transactions with affiliates. |
The breach of any of these restrictive covenants could have a material adverse effect on our business and prospects.
Our cash and cash equivalents could be adversely affected if the financial institutions in which we hold our cash and cash equivalents fail.
On March 10, 2023, the Federal Deposit Insurance Corporation (FDIC) announced that Silicon Valley Bank had been closed by the California Department of Financial Protection and Innovation, and on March 12, 2023, Signature Bank was closed by the New York State Department of Financial Services, and the FDIC was named receiver. Although we did not maintain any bank accounts with Silicon Valley Bank or Signature Bank, we regularly maintain cash balances at third-party financial institutions in excess of the FDIC insurance limit. Any failure of a depository institution to return any of our deposits, or any other adverse conditions in the financial or credit markets affecting depository institutions, could impact access to our invested cash or cash equivalents and could adversely impact our operating liquidity and financial performance.
Risks Related to Drug Development and Regulatory Approval
If we are unable to obtain and maintain regulatory approval for our product and product candidates and ultimately cannot successfully commercialize our product or product candidates, or experience significant delays in doing so, our business will be materially harmed.
Our ability to generate revenues from product sales will depend largely on the successful commercialization of BRIUMVI. Each of our product candidates will require additional non-clinical or clinical development, regulatory approval, and sufficient clinical and commercial supply. The success of our development programs and achievement of regulatory approval of our product candidates will depend on several factors, including, among others, the following:
● | successful completion of our clinical programs with positive results that support a finding of effectiveness and an acceptable safety profile of our product candidates in the intended populations within the timeframes we have projected; |
● | Investigational New Drugs (INDs) and clinical trial applications (CTAs), being cleared/approved such that our product candidates can commence clinical trials; |
● | successful initiation and completion of preclinical studies and successful initiation of, enrollment in, and completion of clinical trials; |
● | sufficiency of our financial and other resources to complete the necessary preclinical studies and clinical trials; |
● | receipt of regulatory approvals from applicable regulatory authorities for our product candidates; |
● | establishing commercially viable arrangements with third-party manufacturers for clinical supply and commercial manufacturing; and |
● | obtaining and maintaining patent and trade secret protection or regulatory exclusivity for our product candidates. |
If we do not achieve one or more of these factors in a timely manner or at all, we could experience significant delays in our clinical programs and regulatory submission timelines and may not be able to obtain regulatory approval for our product candidates.
Because results of preclinical studies and early clinical trials are not necessarily predictive of future results, any product candidate we advance may not have favorable results in later clinical trials or receive regulatory approval. Moreover, interim, “top-line,” and preliminary data from our clinical trials that we announce or publish may change, or the perceived product profile may be negatively impacted, as more patient data or additional endpoints (including efficacy and safety) are analyzed.
Pharmaceutical development has inherent risks. The outcome of preclinical development testing and early clinical trials may not be predictive of the outcome of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses, and many companies have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval. Once a product candidate has displayed sufficient preclinical data to warrant clinical investigation, we will be required to demonstrate, through adequate and well-controlled clinical trials, that our product candidates are effective with a favorable benefit-risk profile for use in populations for their target indications before we can seek regulatory approvals for their commercial sale. Many drug candidates fail in the early stages of clinical development for safety and tolerability issues or for insufficient clinical activity, despite promising pre-clinical results. Accordingly, no assurance can be made that a safe and efficacious dose can be found for these compounds or that they will ever enter into advanced clinical trials alone or in combination with other product candidates. Moreover, success in early clinical trials does not mean that later clinical trials will be successful because product candidates in later-stage clinical trials may fail to demonstrate sufficient safety or efficacy despite having progressed through initial clinical testing. Companies frequently experience significant setbacks in advanced clinical trials, even after earlier clinical trials have shown promising results. There is an extremely high rate of failure of pharmaceutical candidates proceeding through clinical trials.
Individually reported outcomes of patients treated in clinical trials may not be representative of the entire population of treated patients in such studies. In addition, larger scale Phase 3 studies, which are often conducted internationally, are inherently subject to increased operational risks compared to earlier stage studies, including the risk that the results could vary on a region to region or country to country basis, which could materially adversely affect the outcome of the study or the opinion of the validity of the study results by applicable regulatory agencies.
From time to time, we may publicly disclose top-line or preliminary data from our clinical trials, which is based on a preliminary analysis of available data, and the results and related findings and conclusions are subject to change following a more comprehensive review of the data related to the particular study or trial. We also make assumptions, estimations, calculations and conclusions as part of our analyses of such data, and we may not have received or had the opportunity to fully and carefully evaluate all data from the particular study or trial, including all endpoints and safety data. As a result, top-line or preliminary results that we report may differ from future results of the same studies, or different conclusions or considerations may qualify such results once additional data have been received and fully evaluated. Top-line or preliminary data also remain subject to audit and verification procedures that may result in the final data being materially different from the topline, interim, or preliminary data we previously published. When providing top-line results, we may disclose the primary endpoint of a study before all secondary endpoints have been fully analyzed. A positive primary endpoint does not translate to all, or any, secondary endpoints being met. As a result, top-line and preliminary data should be viewed with caution until the final data are available, including data from the full safety analysis and the final analysis of all endpoints.
Further, from time to time, we may also disclose interim data from our preclinical studies and clinical trials. Interim data from clinical trials that we may complete are subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment continues and more patient data become available. For example, time-to-event based endpoints such as duration of response (DOR) and progression-free survival (PFS), and continuously observed data such as annualized relapse rate (ARR) have the potential to change with longer follow-up. In addition, as patients continue on therapy, there can be no assurance given that the final safety data from studies, once fully analyzed, will be consistent with prior safety data presented, will be differentiated from other similar agents in the same class, will support continued development, or will be favorable enough to support regulatory approvals for the indications studied. Further, others, including regulatory agencies, may not accept or agree with our assumptions, estimates, calculations, conclusions or analyses or may interpret or weigh the importance of data differently, which could impact the value of the particular program, the approvability or commercialization of the particular product candidate or product and our company in general. The information we choose to publicly disclose regarding a particular study or clinical trial is based on what is typically extensive information, and regulators or others may not agree with what we determine is material or otherwise appropriate information to include in our disclosure. If the interim, top-line or preliminary data that we report differ from final results, or if others, including regulatory authorities, disagree with the conclusions we have reached, our ability to obtain approval for, or successfully commercialize, our product or product candidates may be harmed, which could harm our business, operating results, prospects or financial condition.
Many of the results reported in our early clinical trials rely on local investigator-assessed efficacy outcomes which may be subject to greater variability or subjectivity than results assessed in a blinded, independent, centrally reviewed manner, often required of later phase, adequate and well-controlled registration-directed clinical trials. If the results from our registration-directed trials are different from the results found in the earlier studies, we may need to terminate or revise our clinical development plan, which could extend the time for conducting our development program and could have a material adverse effect on our business.
Clinical drug development involves a lengthy and expensive process, with an uncertain outcome. We may incur additional costs or experience delays in completing, or ultimately be unable to complete, the development and commercialization of our product candidates.
Before obtaining marketing approval from regulatory authorities for the sale of any product candidate, we must complete pre-clinical studies and then conduct extensive clinical trials to demonstrate the safety and efficacy of our product candidates in humans. Clinical testing is expensive, is difficult to design and implement, can take many years to complete and is uncertain as to outcome. It is impossible to predict when or if our product candidates will prove effective and safe in humans, will receive regulatory approval or will have a differentiated safety and tolerability profile. A failure of one or more clinical trials can occur at any stage of testing. Accordingly, our ongoing trials and future clinical trials may not be successful. Even if our clinical trials produce positive results, there can be no guarantee that the positive outcomes will be replicated in future studies either within the same indication as previously evaluated or in alternate indications and settings.
Successful completion of our clinical trials is a prerequisite to submitting a New Drug Application (NDA) or a Biologics License Application (BLA) to the FDA and a Marketing Authorization Application (MAA) to the EMA for each product candidate and, consequently, the ultimate approval and commercial marketing of our product candidates. We do not know whether any of our ongoing or future clinical trials for our product candidates will be completed on schedule, if at all.
Whether or not and how quickly we complete clinical trials depends in part upon the rate at which we are able to engage clinical research/trial sites and, thereafter, the rate of enrollment of patients, and the rate at which we collect, clean, lock and analyze the clinical trial database. Patient enrollment is a function of many factors, including the size of the patient population, the proximity of patients to clinical sites, the eligibility criteria for the study, the existence of competitive clinical trials, and whether existing or new drugs are approved for the indication we are studying. We are aware that other companies are currently conducting or planning clinical trials that seek to enroll patients with the same diseases that we are studying. We may experience unforeseen events, such as the COVID-19 pandemic, that could delay or prevent our ability to complete current clinical trials, initiate new trials, receive marketing approval or commercialize our product candidates, including:
● | the FDA or other regulatory authorities may require us to submit additional data or impose other requirements before permitting us to initiate a clinical trial; |
● | the FDA or other regulatory authorities or institutional review boards (IRBs) or ethics committees (ECs) may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site or in a country; we may experience delays in reaching, or fail to reach, agreement on acceptable terms with prospective trial sites and prospective clinical research organizations (CROs), the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
● | clinical trials of our drug candidates may produce negative or inconclusive results, and we may decide, or regulatory authorities may require us, to conduct additional pre-clinical studies or clinical trials or we may decide to abandon drug development programs; |
● | the number of patients required for clinical trials of our drug candidates may be larger than we anticipate, and enrollment in these clinical trials may be slower than we anticipate or participants may drop out of these clinical trials or fail to return for post-treatment follow-up at a higher rate than we anticipate; |
● | our third-party contractors, including our clinical trial sites, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all, or may deviate from the clinical trial protocol or drop out of the trial, which may require that we add new clinical trial sites or investigators; |
● | we may elect to or regulatory authorities or IRBs or ECs may require that we or our investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements or a finding that the participants are being exposed to unacceptable health risks; |
● | the cost of clinical trials of our product candidates may be greater than we anticipate; |
● | the supply or quality of our product candidates or other materials necessary to conduct clinical trials of our product candidates may be insufficient or inadequate, including, without limitation, as a result of disruptions to our supply chains caused by global health crises, such as the COVID-19 pandemic, international conflicts such as the Russian invasion of Ukraine or the Israel-Hamas war, economic instability, or natural disasters; |
● | regulatory authorities may revise the requirements applicable to our product candidates, or such requirements may not be as we anticipate; and |
● | our product candidates may have undesirable side effects or other unexpected characteristics, causing us or our investigators, regulatory authorities, IRBs or ECs to suspend or terminate the trials, or reports may arise from pre-clinical or clinical testing of other therapies in the same or a similar class that raise safety or efficacy concerns about our product candidates. |
We also could encounter delays if a clinical trial is suspended or terminated by us, by the IRBs of the institutions in which such trials are being conducted, by the Data and Safety Monitoring Board (DSMB) for such trial or by the FDA or other regulatory authorities. Such regulatory authorities may impose a suspension or termination due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA or other regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a drug, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial. In addition to the FDA, the DSMB for our clinical trials may recommend modification to the study design or closure of the study entirely based on the DSMB’s interpretation of the benefit-risk of the study. While we develop charters that guide the nature of the DSMB meetings, their analysis and interpretation of study data occurs independently from us and is wholly within their control. Even if the DSMB finds no safety concerns and recommends no modifications to the ongoing study, this does not mean the safety profile reported in the study may support a marketing approval or commercial acceptance if marketing approval is granted. Many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory approval of our product candidates.
Negative or inconclusive results from the clinical trials we conduct, unanticipated adverse medical events, or changes in regulatory policy could cause us to have to delay, repeat or terminate the clinical trials. If we are required to repeat or conduct additional clinical trials or other testing of our drug candidates beyond those that we currently contemplate, if we are unable to successfully complete clinical trials of our drug candidates or other testing, if the results of these trials or tests are not positive or are only modestly positive or if there are safety concerns, we may:
● | be delayed in obtaining marketing approval for our product candidates; |
● | not obtain marketing approval at all; |
● | obtain marketing approval in some countries and not others; |
● | obtain approval for indications or patient populations that are not as broad as intended or desired; |
● | be subject to post-marketing requirements or post-marketing commitments; |
● | be subject to increased pricing pressure; or |
● | have the drug removed from the market after obtaining marketing approval. |
In addition, changes in regulatory policy could cause us to have to repeat or conduct additional clinical trials or change our clinical development strategy. For example, in December 2022, with the passage of Food and Drug Omnibus Reform Act, Congress required sponsors to develop and submit a diversity action plan for each Phase 3 clinical trial or any other “pivotal study” of a new drug or biological product. These plans are meant to encourage the enrollment of more diverse patient populations in late-stage clinical trials of FDA-regulated products. If we are not able to adhere to these new requirements, our ability to conduct clinical trials may be delayed or halted. Our drug development costs will also increase if we experience delays in testing or regulatory approvals. Certain clinical trials are designed to continue until a pre-determined number of events have occurred in the patients enrolled. Trials such as this are subject to delays stemming from patient withdrawal and from lower-than-expected event rates. Significant clinical trial delays could also shorten any periods during which we may have the exclusive right to commercialize our product candidates or allow our competitors to bring products to market before we do and impair our ability to successfully commercialize our product candidates. Any delays in our pre-clinical or future clinical development programs may harm our business, financial condition and prospects significantly. We may also incur additional costs if enrollment is increased.
In addition, principal investigators for our clinical trials may serve as scientific advisors or consultants to us from time to time and receive compensation in connection with such services. If these relationships and any related compensation result in perceived or actual conflicts of interest, the integrity of the data generated at the applicable clinical trial site or the FDA’s acceptance of such data, may be jeopardized.
Biologics carry unique risks and uncertainties, which could have a negative impact on our business.
The successful development, manufacturing and sale of biologics is a long, expensive and uncertain process. There are unique risks and uncertainties with biologics. For example, access to and supply of necessary biological materials, such as cell lines, may be limited, and governmental regulations restrict access to and regulate the transport and use of such materials. In addition, the development, manufacturing and sale of biologics is subject to regulations that are often more complex and extensive than the regulations applicable to other pharmaceutical products. Manufacturing biologics, especially in large quantities, is often complex and may require the use of innovative technologies. Such manufacturing also requires facilities specifically designed and validated for this purpose and sophisticated quality assurance and quality control procedures. Biologics are also frequently costly to manufacture. Failure to successfully, develop, manufacture and sell BRIUMVI could adversely affect our business.
Our product or product candidates may cause undesirable side effects that could delay or prevent their regulatory approval or impact their availability and commercial potential after approval.
Unexpected or undesirable adverse events caused by BRIUMVI or any of our product candidates that we take into clinical trials could cause either a DSMB or regulatory authorities to interrupt, delay, modify or suspend clinical trials and could result in a more restrictive label or the delay or denial of regulatory approval by the FDA or other regulatory authorities. Even if a product candidate has obtained marketing approval, undesirable side effects may inhibit market acceptance of the approved product due to its tolerability versus other therapies. This could prevent us from commercializing the affected product candidate and generating revenues from its sale.
As is the case with all drugs, it is likely that there will be side effects associated with the use of our drug candidates. Results of our trials could reveal a higher than expected and unacceptable severity and prevalence of side effects. In such an event, our trials could be suspended or terminated and the FDA or comparable foreign regulatory authorities could order us to discontinue an ongoing trial or deny approval of our drug candidates for any or all targeted indications. The drug-related side effects could also affect patient recruitment or the ability of enrolled patients to complete the trial or result in potential product liability claims. In addition, data may emerge, from confirmatory or other post-marketing studies, or from pharmacovigilance reporting, as products are used more widely, or for a longer duration, after approval that may affect the commercial potential of our products. Any of these occurrences may harm our business, financial condition and prospects significantly.
Many compounds that initially showed promise in early-stage testing have later been found to cause side effects that prevented further development of the compound. Further, early clinical trials by their nature utilize a small sample of the potential patient population. With a limited number of patients and limited duration of exposure, rare and serious side effects of our drug candidates may only be uncovered when a significantly larger number of patients are exposed to the drug candidate in Phase 3 or registration-directed trials or when the drug candidate is on the market. If any of our product candidates cause unacceptable adverse events in clinical trials, we may not be able to obtain marketing approval and generate revenues from its sale, or even if approved for sale may lack differentiation from competitive products, which could have a material adverse impact on our business and operations. Further, clinical trials by their nature utilize a sample of the potential patient population. With a limited number of patients, rare and severe side effects of BRIUMVI or our other product candidates may only be uncovered with a significantly larger number of patients exposed to the product.
Any products or product candidates we may advance through clinical development are subject to extensive regulation, which can be costly and time consuming, cause unanticipated delays or prevent the receipt of the required approvals.
The clinical development, manufacturing, labeling, packaging, storage, record-keeping, advertising, promotion, import, export, marketing and distribution, and pharmacovigilance and adverse event reporting of our product or product candidates or any future product candidates are subject to extensive regulation by the FDA in the United States and by comparable regulatory authorities worldwide. In the United States, we are not permitted to market a product candidate until we receive approval of a BLA or NDA from the FDA. The process of obtaining a BLA or NDA approval is expensive, often takes many years, and can vary substantially based upon the type, complexity and novelty of the products involved. In addition, approval policies or regulations may change over time. If we fail to gain approval to commercialize our product candidates from the FDA and other foreign regulatory authorities in the timelines we project or at all, we may be unable to generate the revenues that we may project or generate revenues at levels sufficient to sustain our business.
The FDA and foreign regulatory authorities have complete control over the pharmaceutical product approval process, including substantial discretion to delay, limit or deny approval of a product candidate for many reasons. During the regulatory review process, the FDA or other regulatory authorities may disagree with or not accept our clinical trial design, may have questions about the potential impact of our study design on conclusions that can be drawn from the data, may interpret results differently than we do, may apply the results of our trials in one disease to the review of a regulatory application for a different disease even if the doses and therapeutic areas are distinct, and may change its view on the criteria that must be met for approval. This could happen even for a protocol used to support a trial that is subject to an SPA agreement with the FDA. There is no guarantee that the FDA will not delay, limit or deny approval of our product candidates in the future.
Furthermore, some of our clinical trials may be conducted as open-label studies, meaning that trial participants, investigators, site staff, some employees of our CROs, and our field-level employees (e.g., clinical research associates and monitors), among others, have knowledge of treatment arm assignments on a patient-level, which has the potential to introduce bias into study conduct. Further, even when our clinical trials are double-blind, double-dummy studies, unblinding of treatment arm assignment may occur from time to time, for example, on the occurrence of unexpected safety events which may necessitate understanding of study treatment. While we believe we have put in place adequate firewalls to prevent inappropriate unblinding of study data consistent with standard industry practice for these types of studies, no assurance can be given that issues related to study conduct will not be raised. The FDA may raise issues of safety, study conduct, bias, deviation from the protocol, statistical power, patient completion rates, changes in scientific or medical parameters or internal inconsistencies in the study design or data prior to making its final decision. The FDA may also seek the guidance of an outside advisory committee in evaluating (among other things) clinical data and safety and effectiveness considerations prior to making its final decision. These issues could cause a delay in the FDA’s review, lead the FDA to deny approval, or lead the Company to withdraw a regulatory application.
Other reasons that the FDA or regulatory authorities around the world may delay, limit or deny approval of a product candidate, include:
● | we may be unable to demonstrate to the satisfaction of the FDA or comparable foreign regulatory authorities that a product candidate is tolerable and effective for an indication; |
● | the FDA may not accept clinical data from trials conducted by individual investigators or in countries where the standard of care or the patient population, is potentially different from that of the United States; |
● | the results of clinical trials may not meet the level of statistical significance required by the FDA or comparable foreign regulatory authorities for approval; |
● | we may be unable to demonstrate that a product candidate’s clinical and other benefits outweigh its safety risks; |
● | the FDA or comparable foreign regulatory authorities may disagree with our interpretation of data from preclinical studies and/or clinical trials; |
● | the data collected from clinical trials of our product candidates may not be sufficient to support the submission of a BLA, NDA or other marketing authorization submission to obtain regulatory approval in the United States or elsewhere; |
● | the FDA or comparable foreign regulatory authorities may identify issues related to the manufacturing processes or facilities of third-party manufacturers with which we or our collaborators currently contract for clinical supplies and plan to contract for commercial supplies; during the course of review, the FDA or foreign regulatory authorities may raise issues and request or require additional preclinical, clinical, chemistry, manufacturing, and control (CMC), or other data and information, and the development and provision of these data and information may be time consuming. We may not be able to generate the data within the time period necessary to obtain approval within the established regulatory review timelines, such as by a PDUFA goal date or at all to satisfy the FDA or foreign regulatory authorities; |
● | the approval processes of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval; or |
● | interruptions or delays in the operations of the FDA and foreign regulatory authorities as a result of global health or economic crises, such as the COVID-19 pandemic, international conflict, or national disasters may negatively impact review, inspection, and approval timelines. |
Even if we succeed in obtaining regulatory approval for a product candidate, the FDA may require post-marketing studies, including additional clinical trials such as those necessary to assess drug interactions or activity of a product in specific populations, which may be costly. The outcomes of post-marketing studies may impact product labeling and therefore, there can be no guarantee that the product attributes contained in the initial prescribing information will be maintained as future studies produce data. This includes, without limitation, additional results from studies evaluating drug-drug interactions and patients with certain comorbidities that may restrict the use of an approved product in select populations or introduce dose modifications or contraindicated concomitant medications that have the potential to impact the utility of a product or its perceived product profile among prescribers. Post-marketing studies may also lead to the introduction of new warnings in the product prescribing information. The FDA may require adoption of a REMS program requiring prescriber training or a post-marketing registry or may restrict the marketing and dissemination of our products. Finally, failure to complete a post-marketing commitment by the applicable post-marketing milestone date may lead to withdrawal of the product or indication. Any requirements to conduct post-approval studies or fulfill special post-approval requirements could impact our ability to commercialize our product or product candidates and increase our costs.
A Breakthrough Therapy or Fast Track designation by the FDA may not actually lead to a faster development or regulatory review or approval process.
We may seek Breakthrough Therapy or Fast Track designation for some of our drug candidates. If a drug is intended for the treatment of a serious or life-threatening condition, and the drug demonstrates the potential to address an unmet medical need for this condition, the Sponsor may apply for Fast Track designation or Breakthrough Therapy designation, the latter of which has more significant requirements. The FDA has broad discretion whether or not to grant these designations, so even if we believe a particular drug candidate is eligible for such a designation, we cannot be sure that the FDA would decide to grant it. Even if we receive Breakthrough Therapy or Fast Track designation for a drug candidate, we may not experience a faster development process, review or approval compared to conventional FDA procedures. A drug that receives Fast Track designation is eligible for more frequent interactions with the FDA, priority review if relevant criteria are met, and rolling submission of the BLA or NDA. Even if rolling review is allowed, there is no guarantee that the FDA will have commenced or completed review of the BLA or NDA modules submitted earlier in the rolling review process. Neither Breakthrough Therapy nor Fast Track designation guarantees Priority Review of an NDA or BLA application.
We may seek orphan drug designation for some of our drug candidates. However, we may be unsuccessful in obtaining or may be unable to maintain the benefits associated with orphan drug designation, including the potential for market exclusivity.
Regulatory authorities in some jurisdictions, including the United States, the European Union, and the United Kingdom, may designate drugs for relatively small patient populations as orphan drugs. Under the U.S. Orphan Drug Act, the FDA may designate a drug as an orphan drug if it is a drug intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals annually in the United States, or a patient population greater than 200,000 in the United States where there is no reasonable expectation that the cost of developing the drug will be recovered from sales in the United States. In the United States, orphan drug designation entitles a party to financial incentives, such as opportunities for grant funding towards clinical trial costs, tax advantages, and user-fee waivers. Orphan drug designations are required to be maintained through annual reporting and are subject to re-evaluation. Based on the evolving data and development plans for our product candidates and changing incidence and prevalence rates for our intended indications, there can be no guarantee that we will be able to successfully maintain orphan drug designations that we have for certain of our drug candidates or that we will be successful in obtaining orphan designation for other drug candidates in the future.
Generally, if a product with an orphan drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the product is entitled to a period of marketing exclusivity, which precludes FDA or EMA from approving another marketing application for the same drug or biologic for that time period. Even if we obtain orphan drug exclusivity for a drug, that exclusivity may not effectively protect the designated drug from competition because different drugs can be approved for the same condition. Even after an orphan drug is approved, the FDA can subsequently approve another product that meets the definition of a “same drug” under 21 C.F.R. 316.3 for the same condition if the FDA concludes that the later product is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care. In addition, a designated orphan drug may not receive orphan drug exclusivity if it is approved for a use that is broader than the indication for which it received orphan drug designation. Moreover, orphan drug exclusive marketing rights in the United States may be lost if the FDA exercises its authority to revoke orphan drug designation, which it may do on a variety of grounds, including that the request contained an untrue statement of material fact or omitted material information, or that the drug in fact was not eligible for orphan drug designation. Orphan drug designation neither shortens the development time or regulatory review time of a drug nor gives the drug any advantage in the regulatory review or approval process. While we intend to seek orphan drug designation for our other drug candidates, we may never receive such designations. Even if we receive orphan drug designation for any of our drug candidates, there is no guarantee that we will enjoy the benefits of those designations or obtain orphan drug exclusivity. In addition, the U.S. Orphan Drug Act may be subject to amendments that could reduce the period of marketing exclusivity or change the qualifications for orphan drug designation, which could adversely impact our products or product candidates that have or may be eligible for orphan drug designation.
We are conducting clinical trials and anticipate conducting additional clinical trials for our product and product candidates at sites outside the United States, and the FDA may not accept data from trials conducted in such locations or clinical trial activities in such locations may be impacted by political conditions, including international conflict.
Many of our clinical trials utilize international clinical research sites. We work with what we believe are reputable CROs and clinical research sites in conducting our studies internationally. Nevertheless, there can be heightened challenges to monitoring and oversight of global clinical trials and sponsors are subject to the risk that fraud, misconduct, incompetence, unexpected patient variability and other issues affecting the reliability, quality, and outcome of studies. The geographic variability of the COVID-19 pandemic also introduces increased risk in the conduct of clinical research in certain countries and territories where vaccination rates and available standard of care anti-viral therapy varies significantly. Such problems, if they were to occur, could negatively impact trial results, and depending on the circumstances and scope of concerns could potentially even prevent a trial from being useful or acceptable for regulatory approval. If such events were to occur with respect to any of our trials (and in particular with respect to registration-directed studies), they would have a substantial negative impact on our business.
In addition, our clinical studies with sites outside the United States may be adversely impacted by international conflict. For example, in February 2022, Russia initiated a full-scale military invasion of Ukraine. In one or both countries, as well as neighboring countries that may be impacted by this conflict (e.g. Poland, Slovakia, Belarus, Georgia), we have clinical trial sites for our RMS and/or oncology programs. While no clinical trials are actively enrolling patients in these territories, there are a number of trial subjects in long-term treatment and follow-up. The political and physical conditions in Russia and Ukraine have disrupted our ability to supply investigational drug product to impacted sites; impacted patients’ ability to partake in our clinical trials and our ability to gather data on those patients, including long-term follow-up data; and resulted in suspension of clinical trial activities at impacted sites. Furthermore, the United States and its European allies have imposed significant sanctions against Russia and Belarus, including regional embargoes, full blocking sanctions, and other restrictions targeting major Russian financial institutions. Specifically, such sanctions have included, among other things, a prohibition on doing business with certain Russian companies, officials, and oligarchs; a commitment by certain countries and the European Union to remove selected Russian banks from the Society for Worldwide Interbank Financial Telecommunications (SWIFT) electronic banking network that connects banks globally; and restrictive measures to prevent the Russian Central Bank from undermining the impact of the sanctions. Our ability to conduct clinical trials in Russia, Belarus, Ukraine and elsewhere in the region may also become restricted under applicable sanctions laws. The conflict, as well as government responses, has resulted in global economic instability, which could affect our supply chain and commercialization efforts. While we do not believe this conflict will have a material impact on product development or our overall business, given the rapidly evolving situation and the potential to expand beyond Ukraine and Russia, the full impact of the conflict remains uncertain.
Approval of one of our product candidates in the United States would not assure approval of that candidate in foreign jurisdictions.
We intend to seek additional product approvals in certain countries outside of the United States. The approval procedures for pharmaceuticals vary among countries and obtaining approval in one jurisdiction does not guarantee approval in another jurisdiction. For example, even if the FDA grants approval of a product candidate comparable regulatory authorities in foreign jurisdictions may not approve the same product candidate, or the same indications for use for the product candidate, or may require additional evidence for approval. The time required to obtain approval in other countries might differ from that required to obtain FDA approval. In many countries outside the United States, the product must be approved for reimbursement before it can be marketed. As a general matter, however, the foreign regulatory approval process involves a lengthy and challenging process with risks similar or identical to the risks associated with the FDA approval discussed above. Therefore, we cannot guarantee that we, or future collaborators, will obtain approvals of our product and product candidates in any foreign jurisdiction on a timely basis, if at all. Failure to receive approval in certain foreign markets could significantly impact the full market potential of our product and product candidates and may negatively impact the regulatory process in other countries. Furthermore, if we obtain regulatory approval for a product or product candidate in a foreign jurisdiction, we will be subject to the burden of complying with complex regulatory, legal, and other requirements that could be costly and could subject us to additional risks and uncertainties.
We have product candidates still under development and are also engaging manufacturing partners in commercial manufacturing activities, and as such clinical and commercial manufacturing site additions and process improvements implemented in the production of our product and product candidates may affect their timely delivery or quality.
We have limited experience in manufacturing products for clinical or commercial purposes. We currently do not have any manufacturing capabilities of our own. We have established a contract manufacturing relationship for the commercial supply of BRIUMVI with Samsung Biologics. As with any supply program, obtaining materials of sufficient quality and quantity to meet the requirements of the market demand for BRIUMVI and our development programs cannot be guaranteed and we cannot ensure that we will be successful in these endeavors.
To the extent possible and commercially practicable, we plan to develop back-up strategies for raw materials, manufacturing and testing services for our commercial products. Given the long lead times and cost of establishing additional commercial manufacturing sites we expect that we will rely on single contract manufacturers to produce our commercial products under current Good Manufacturing Practice, or cGMP, regulations for many years. Our commercial manufacturing partners have a limited number of facilities in which our product candidates can be produced and will have limited experience in manufacturing our product candidates in quantities sufficient for commercialization. Our third-party manufacturers will have other clients and may have other priorities that could affect their ability to perform the work satisfactorily and/or on a timely basis. Both of these occurrences would be beyond our control.
We expect to similarly rely on contract manufacturing relationships for our development programs and any products that we may in-license or acquire in the future. However, there can be no assurance that we will be able to successfully contract with such manufacturers on terms acceptable to us, or at all.
Contract manufacturers are subject to ongoing periodic and unannounced inspections by the FDA, the Drug Enforcement Administration, if applicable, and corresponding state agencies to ensure strict compliance with cGMP requirements and other state and federal regulations. Where manufactured products are globally registered, similar regulatory inspection burdens are applicable from each and every marketed territory. If our manufacturing partners are inspected and deemed out of compliance with cGMPs, product recalls could result, inventory could be destroyed, production could be stopped, and supplies could be delayed or otherwise disrupted.
If we need to change manufacturers either before or after commercialization, the FDA and corresponding foreign regulatory agencies may need to approve these new manufacturers in advance, which will involve testing, regulatory submissions, and additional inspections to ensure compliance with FDA and other regulations and standards, and may require significant lead times and delay. Furthermore, switching manufacturers may be difficult because the number of potential manufacturers is limited. It may be difficult or impossible for us to find a replacement manufacturer quickly or on terms acceptable to us, or at all.
Some of our product and product candidates are currently manufactured in relatively small batches for use in pre-clinical and clinical studies. Process improvements implemented to date have changed, and process improvements in the future may change, the activity and/or analytical profile of the product or product candidates, which may affect the safety and efficacy of the products. It is possible that additional and/or different adverse events may appear among patients exposed to drug product manufactured under one process compared to the other, or that adverse events may arise with greater frequency, intensity and duration among patients exposed to drug product manufactured under one process compared to the other.
Further, no assurance can be given that the material manufactured from any future optimized processes, if any, for BRIUMVI or any of our product candidates will perform comparably to the product or product candidates as manufactured to date which could result in an unexpected safety or efficacy outcome as compared to the data published or presented to date. Similarly, following each round of process improvements, if any, for any of our drug candidates, future clinical trial results conducted with the new material will be subject to uncertainty related to the effects, if any, of those additional process improvements that were made.
Risks Related to Governmental Regulation of Pharmaceutical Industry and Legal Compliance Matters
We are subject to new legislation, regulatory proposals and third-party payor initiatives that may increase our costs of compliance and adversely affect our ability to market our products, obtain collaborators and raise capital.
In both the United States and certain foreign countries, there have been a number of legislative and regulatory changes or proposed changes to the healthcare system, many of which have focused on prescription drug pricing and lowering overall healthcare costs, that could impact our ability to sell our products profitably and support future innovation. We expect prescription drug pricing and other healthcare costs to continue to be subject to intense political and social pressures on a global basis.
In the United States, the President, federal and state legislatures, health agencies and third-party payors continue to focus on containing the cost of healthcare and addressing public concern over access and affordability of prescription drugs. The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010 (collectively, the ACA) was enacted in 2010 and made significant changes to the U.S. healthcare system. ACA changes included expanding healthcare coverage through Medicaid expansion and implementation of the individual health insurance mandate; changing coverage and reimbursement of drug products under government healthcare programs; imposing an annual fee on manufacturers of branded drugs; and expanding government enforcement authority. Although the ACA has been the subject of a number of legislative and litigation challenges since it passed, it is expected that the Biden Administration will seek to strengthen and expand the ACA. We cannot predict what effect, if any, further changes to the ACA would have on our business.
Beyond the ACA, there has been increasing legislative, regulatory and enforcement interest with respect to prescription drug pricing practices. Proposals that may garner bipartisan legislative support or become legislation through reconciliation include adding a cap on out-of-pocket spending under Medicare Part D, authorizing Medicare to negotiate certain drugs covered by Medicare Parts D and B directly with manufacturers, and imposing limits on increases in drug prices. In addition, President Biden may take executive action to introduce new drug pricing models and other drug pricing initiatives. The Biden Administration also may propose substantial changes to the U.S. healthcare system, including expanding government-funded health insurance options. We are uncertain of the impact or outcome of potential Executive Orders, rescission of rules and policy statements, or new legislation, especially any relative impact on the healthcare regulatory and policy landscape, or the impact they may have on our business. We expect drug pricing will continue to be a focus of the Biden Administration. At the state level, legislatures have increasingly passed legislation and implemented regulations designed to control pharmaceutical pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing.
There have been several recent U.S. Congressional inquiries and proposed and enacted legislation designed to bring more transparency to drug pricing, reduce the cost of prescription drugs under Medicare, limit price increases, evaluate the relationship between pricing and manufacturer patient programs, and reform government health care program reimbursement methodologies for prescription drugs. For example, the Bipartisan Budget Act of 2018 (the BBA) increased manufacturer point-of-sale discounts off negotiated prices of applicable brand drugs in the Medicare Part D coverage gap from 50% to 70% effective as of January 1, 2019, ultimately increasing the liability for brand drug manufacturers. We expect that health care reform measures that may be adopted in the future, may result in more rigorous coverage criteria, increased manufactured financial liability and additional downward pressure on the price that we may receive for any of our product candidates, if approved. Any reduction in reimbursement from Medicare or other government health care programs may result in a similar reduction in payments from private payors.
There continue to be efforts to lower drug prices through increased competition, with policy proposals seeking to facilitate generic and biosimilar approval and marketing authorization. For example, in 2018, the FDA announced the Biosimilar Action Plan and sought input on how the agency can best facilitate greater availability of biosimilar products, including input on whether changes to an approved biologic (e.g., a new indication) would be protected by the remainder of the statutory 12-year exclusivity period (commonly referred to as umbrella exclusivity). In the event there is a modification to the biologic exclusivity period or other steps taken to facilitate biosimilar or generic approvals, we could experience biosimilar/generic competition of any products for which we receive FDA approval at an earlier time than currently anticipated.
Most recently, on August 16, 2022, President Biden signed into law the Inflation Reduction Act of 2022 (the Act), which, among other provisions, included several measures intended to lower the cost of prescription drugs and related healthcare reforms. Specifically, the Act authorizes and directs the Department of Health and Human Services (DHHS) to set drug price caps for certain high-cost Medicare Part B and Part D qualified drugs, with the initial list of drugs selected on August 29, 2023, and the first year of maximum price applicability to begin in 2026. On October 3, 2023, the Centers for Medicare & Medicaid Services announced that all manufacturers of the initially selected drugs opted to participate. The Act further authorizes the DHHS to penalize pharmaceutical manufacturers that increase the price of certain Medicare Part B and Part D drugs faster than the rate of inflation. Finally, the Act creates significant changes to the Medicare Part D benefit design by capping Part D beneficiaries’ annual out-of-pocket spending at $2,000 beginning in 2025. We cannot be sure whether additional or related legislation or rulemaking will be issued or enacted, or what impact, if any, such changes will have on the profitability of any of our drug candidates, if approved for commercial use, in the future.
At the state level, individual states are experiencing significant economic pressure within their respective Medicaid programs and responding to public concern over the cost of healthcare. States, including California, Florida, Nevada and Maine, among others, have responded to these pressures with a range of legislative enactments and policy proposals designed to control prescription drug prices by, for example, allowing importation of pharmaceutical products from jurisdictions outside the U.S., imposing price controls on state drug purchases, consolidating state drug purchasing to a single purchaser, and imposing transparency measures around prescription drug prices and marketing costs. These measures, which vary by state, could reduce the ultimate demand for our products, if approved, or put pressure on our product pricing.
In addition, other legislative changes have been adopted that could have an adverse effect upon, and could prevent, our products’ or product candidates’ commercial success. More broadly, the Budget Control Act of 2011, as amended, or the Budget Control Act, includes provisions intended to reduce the federal deficit, including reductions in Medicare payments to providers through 2030 (except May 1, 2020 to December 31, 2020). Any significant spending reductions affecting Medicare, Medicaid or other publicly funded or subsidized health programs, or any significant taxes or fees imposed as part of any broader deficit reduction effort or legislative replacement to the Budget Control Act, or otherwise, could have an adverse impact on our anticipated product revenues.
Furthermore, legislative and regulatory proposals have been made to expand post-approval requirements, make changes the Orphan Drug Act and related guidance, reform the 340B Drug Pricing Program, and restrict sales and promotional activities for drugs. With respect to the 340B Drug Pricing Program recent legislative proposals as well as judicial challenges to DHHS’s policies present both opportunities and challenges for drug manufacturers participating in the program. Further, we cannot be sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our product candidates, if any, may be. In addition, increased scrutiny by Congress of the FDA’s approval process may significantly delay or prevent marketing approval, as well as subject us to more stringent product labeling and post-marketing testing and other requirements.
In many international markets, including the European Union, the government regulates prescription drug prices, patient access, and/or reimbursement levels to control the biopharmaceutical budget of their government-sponsored healthcare system. The European Union and some individual countries have announced or implemented measures and may in the future implement new or additional measures, to reduce biopharmaceutical costs to contain the overall level of healthcare expenditures. These measures vary by country and may include, among other things, non-coverage decisions, patient access restrictions, international price referencing, mandatory discounts or rebates, and cross-border sales of prescription drugs. These measures may adversely affect our ability to generate revenues or commercialize our product or product candidates in certain international markets.
There likely will continue to be pressure on prescription drug prices globally and legislative and regulatory proposals, including at the federal and state levels in the U.S., directed at broadening the availability of health care and containing or lowering the cost of health care products and services. We cannot predict the initiatives that may be adopted in the future. The continuing efforts of the government, health insurance companies, managed care organizations and other payors of health care services to contain or reduce costs of health care may adversely affect, among other things:
● | our ability to generate revenues and achieve or maintain profitability; |
● | the demand for any products for which we may obtain regulatory approval; |
● | our ability to set a price that we believe is fair for our products; |
● | the level of taxes that we are required to pay; and |
● | the availability of capital. |
In addition, governments may impose price controls, which may adversely affect our future profitability.
Our relationships with customers and third-party payors are subject to applicable fraud and abuse laws, false claims laws, transparency and disclosure laws, health information and security laws, and other healthcare laws and regulations, which could expose us to criminal sanctions, civil penalties, exclusion from government healthcare programs, contractual damages, reputational harm and diminished profits and future earnings.
With the FDA and EMA approval of BRIUMVI, we are subject to additional extensive healthcare statutory and regulatory requirements and oversight by the federal government and the states and foreign governments in which we conduct our business. Healthcare providers and third-party payors play a primary role in the recommendation and prescription of any drug candidates for which we obtain marketing approval. Our past, current and future relationships, arrangements and interactions with these professionals and entities, as well as with patients and patient advocacy organizations expose us to broadly applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we market, sell and distribute our product and product candidates for which we obtain marketing approval. Restrictions under applicable federal and state healthcare laws and regulations include the following:
● | the federal Anti-Kickback Statute prohibits, among other things, persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under federal and state healthcare programs such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation; |
● | the federal False Claims Act imposes civil penalties, including through civil whistleblower or qui tam actions, against individuals or entities for, among other things, knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government. In addition, the government may assert that a claim including items and services resulting from a violation of the federal Anti-Kickback Statute or the Federal Food, Drug, and Cosmetic Act (FDCA) constitutes a false or fraudulent claim for purposes of the False Claims Act; |
● | the federal Health Insurance Portability and Accountability Act of 1996 (HIPAA) imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program, or knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statement in connection with the delivery of or payment for healthcare benefits, items or services; similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation; |
● | the Physician Payments Sunshine Act under section 6002 of the Affordable Care Act requires manufacturers of drugs, devices, biologics and medical supplies that are reimbursable under Medicare, Medicaid or the Children’s Health Insurance Program to monitor and report certain information related to payments and other transfers of value to and the ownership and investment interests of physicians and certain other healthcare providers as well as teaching hospitals to the federal government for redisclosure to the public; |
● | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009 and its implementing regulations, which also imposes obligations on certain covered entity healthcare providers, health plans, and healthcare clearinghouses as well as their business associates that perform certain services involving the use or disclosure of individually identifiable health information, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
● | a wide range of federal and state consumer protection and unfair competition laws, which broadly regulate marketplace activities and activities that potentially harm consumers including those related to privacy; |
● | the FDCA and its implementing regulations, which among other things, strictly regulate drug product marketing and prohibit manufacturers from promotion and marketing of products prior to approval or for uses inconsistent with the FDA-required labeling; | |
● | federal laws, including the Medicaid Drug Rebate Program, that require pharmaceutical manufacturers to report certain calculated product prices to the government or provide certain discounts or rebates to government authorities or private entities, often as a condition of reimbursement under government healthcare programs; |
● | the Drug Supply Chain Security Act (DSCSA), which imposes obligations on entities in the commercial product supply chain, including manufacturers, to identify and track prescription drugs as they are distributed in the U.S.; and |
● | state law equivalents of some of the above federal laws, such as anti-kickback and false claims laws that may apply to items or services reimbursed by any third-party payor, including commercial insurers, state transparency laws, state laws limiting interactions between pharmaceutical manufacturers and members of the healthcare industry, and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by federal laws, thus complicating compliance efforts. |
As we continue commercialization of BRIUMVI, we are taking steps to provide patient support services to help patients access the product. Our patient support programs are administered in conjunction with a patient support program vendor and other third parties. There has been heightened governmental scrutiny over the scope of patient support programs and the manner in which drug manufacturers and their vendors operate such programs. We cannot ensure that our compliance controls, policies, and procedures will be sufficient to protect against acts of our employees, business partners or vendors that may violate the laws, regulations, or evolving government guidance on patient support programs. A government investigation, regardless of its outcome, could impact our business practices, harm our reputation, divert attention of management, increase our expenses and reduce availability of assistance to patients. If we or our vendors are deemed to fail to comply with relevant laws, regulations or government guidance in the operation of these programs, we could be subject to damages, fines, penalties or other criminal, civil or administrative sanctions or enforcement actions.
Ensuring that our business arrangements with third parties comply with applicable healthcare laws and regulations involves substantial costs. It is possible that governmental authorities will conclude that our business practices do not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. The compliance and enforcement landscape, and related risk, is informed by government enforcement precedent and settlement history, Advisory Opinions, and Special Fraud Alerts. Our approach to compliance may evolve over time in light of these types of developments. Additionally, the potential safe harbors available under the federal Anti-Kickback Statute are subject to change through legislative and regulatory action, and we may decide to adjust our business practices or be subject to heightened scrutiny as a result. If our operations, including activities to be conducted by our sales team, were to be found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, exclusion from government-funded healthcare programs, such as Medicare and Medicaid, qui tam actions brought by individual whistleblowers in the name of the government, and the curtailment or restructuring of our operations.
If we violate applicable data privacy and security laws, we may be subject to penalties, including civil and criminal penalties, damages, fines, reputation harm and the curtailment or restructuring of our operations.
We may be subject to privacy and security laws in the various jurisdictions in which we operate, obtain or store personal information. The legislative and regulatory landscape for privacy and data protection continues to evolve, and there has been an increasing focus on privacy and data protection issues with the potential to affect our business.
Within the United States, various federal and state laws regulate the privacy and security of personal information and
so may affect our business operations. For example, at the federal level, our operations may be affected by the data privacy and security provisions of HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act and its implementing regulations. HIPAA affects the ability of healthcare providers and other entities with which we may interact, including clinical trial sites, to disclose patient health information to us. Under Section 5(a) of the Federal Trade Commission Act (FTCA), the Federal Trade Commission (FTC) expects a company’s data security measures to be reasonable and appropriate in light of the sensitivity and volume of consumer information it holds, the size and complexity of its business, and the cost of available tools to improve security and reduce vulnerabilities. Medical data is considered sensitive data that merits stronger safeguards. States may also impose requirements. For example, the California Consumer Privacy Act (CCPA), went into effect in January 2020 creating data privacy obligations for covered companies and providing privacy rights to California residents, including the right to opt out of certain disclosures of their information. Colorado, Connecticut, Utah, Virginia and Iowa have also enacted data privacy statutes, and both California and Colorado are also undergoing or have undergone rulemaking procedures to finalize regulatory regimes to supplement their privacy statutes.
Numerous other jurisdictions regulate the privacy and security of personally identifiable data. For example, the processing of personal data in the European Economic Area (EEA), is subject to the General Data Protection Regulation (GDPR), which took effect in May 2018. The GDPR increases obligations with respect to clinical trials conducted in the EEA, such as in relation to the provision of fair processing notices, exercising data subject rights and reporting certain data breaches to regulators and affected individuals, as well as how we document our relationships with third parties that process GDPR-covered personal data on our behalf. The GDPR also increases the scrutiny applied to transfers of personal data from the EEA (including from clinical trial sites in the EEA) to countries that are considered by the EC to lack an adequate level of data protection, such as the United States. In July 2020, the Court of Justice of the European Union invalidated the EU-U.S. Privacy Shield framework, one of the mechanisms used to legitimize the transfer of personal data from the EEA to the U.S., which decision may lead to increased scrutiny on data transfers from the EEA to the U.S. generally and increase our costs of compliance with data privacy legislation.
If our operations are found to be in violation of any data privacy and security laws, rules or regulations that apply to us, we may be subject to penalties, including civil and criminal penalties, damages, fines and the curtailment or restructuring of our operations, which could adversely affect our ability to operate our business and our financial results. Although compliance programs can mitigate the risk of investigation and prosecution for violations of these laws, rules or regulations, we cannot be certain that our program will address all areas of potential exposure and the risks in this area cannot be entirely eliminated, particularly because the requirements and government interpretations of the requirements in this space are constantly evolving. Any action against us for violation of these laws, rules or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business, as well as damage our business or reputation. Moreover, achieving and sustaining compliance with applicable federal and state privacy, security, fraud and reporting laws may prove costly.
If we fail to adequately understand and comply with the local laws and customs as we expand into new international markets, these operations may incur losses or otherwise adversely affect our business and results of operations.
We expect to operate a portion of our business in certain countries through subsidiaries or through supply, marketing, and distributor arrangements. In those countries where we have limited experience in operating subsidiaries and in reviewing equity investees, we will be subject to additional risks related to complying with a wide variety of national and local laws, including restrictions on the import and export of certain intermediates, drugs, technologies and multiple and possibly overlapping tax laws. In addition, we may face competition in certain countries from companies that may have more experience with operations in such countries or with international operations generally. We may also face difficulties integrating new facilities in different countries into our existing operations, as well as integrating employees hired in different countries into our existing corporate culture. If we do not effectively manage our operations in these subsidiaries and review equity investees effectively, or if we fail to manage our alliances, we may lose money in these countries, and it may adversely affect our business and results of our operations. In all interactions with foreign regulatory authorities and other government agencies, we are exposed to liability risks under the Foreign Corrupt Practices Act or similar anti-bribery laws.
Any product for which we obtain marketing approval, including BRIUMVI, could be subject to restrictions or withdrawal from the market and we may be subject to penalties if we fail to comply with regulatory requirements or if we experience unanticipated problems with products.
Any regulatory approvals that we receive for our drug candidates may be subject to limitations on the indicated uses for which the drug may be marketed or to conditions of approval that may require potentially costly post-marketing clinical trials or surveillance to monitor safety and efficacy of the drug candidate. In addition, any product for which we obtain marketing approval, along with the manufacturing processes and facilities, post-approval clinical data, labeling, advertising and promotional activities for such product, will be subject to continual requirements of, and review by, the FDA, EMA and comparable regulatory authorities. These requirements include submissions of safety and other post-marketing information and reports, registration requirements, cGMP requirements relating to quality control, quality assurance and corresponding maintenance of records and documents, and requirements regarding promotional interactions with healthcare professionals.
Failure to comply with these regulatory requirements or later discovery of previously unknown problems with products, manufacturers, or manufacturing processes, may result in actions such as:
● | restrictions on product manufacturing, distribution or use; |
● | restrictions on the labeling or marketing of a product; |
● | requirements to conduct post-marketing studies or clinical trials; |
● | warning letters or other advisory actions; |
● | request for withdrawal of the products from the market; |
● | refusal to approve pending applications or supplements to approved applications that we or our subsidiaries submit; |
● | recalls; |
● | suspension or termination of ongoing clinical trials; |
● | fines, restitutions, or disgorgement of profits or revenues; |
● | refusal to permit the import or export of products; |
● | product seizure or detentions; |
● | injunctions or the imposition of civil or criminal penalties; and |
● | adverse publicity. |
Any government investigation of alleged violations of law could require us to expend significant time and resources in response and could generate negative publicity. In addition, the FDA’s or EMA’s regulations, policies or guidance may change and new or additional statutes or government regulations may be enacted that could prevent or delay regulatory approval of our product candidates or further restrict or regulate post-approval activities. We also cannot predict the likelihood, nature, or extent of adverse government regulation that may arise from pending or future legislation or administrative action, either in the United States or abroad.
If we, or our respective suppliers, third-party contractors, clinical investigators or collaborators are slow to adapt, or are unable to adapt, to changes in existing regulatory requirements or adoption of new regulatory requirements or policies, we, our subsidiaries, or our respective collaborators may be subject to the actions listed above, including losing marketing approval for products, resulting in decreased revenue from milestones, product sales or royalties.
If we or any of our contract manufacturers and suppliers fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could seriously harm our business.
Our third-party manufacturers, suppliers, and we are subject to federal, state, and local laws and regulations governing the use, manufacture, storage, handling, release, disposal of, and exposure to, hazardous and regulated materials. Violation of these laws and regulations could lead to substantial fines and penalties. Although we believe that our safety procedures, and those of our third-party manufacturers, for handling and disposing of these materials comply with the standards prescribed by these laws and regulations, we cannot eliminate the risk of accidental contamination or injury from these materials. In the event of an accident, state or federal authorities may curtail our use of these materials and interrupt our business operations. In addition, we could become subject to potentially material liabilities relating to the investigation and cleanup of any contamination, whether currently unknown or caused by future releases.
Risks Related to Our Dependence on Third Parties
We rely on third parties to generate clinical, preclinical and other data necessary to support the regulatory applications needed to conduct clinical trials and submit for marketing approval. We rely on third parties to help conduct our planned clinical trials. If these third parties do not perform their services as required, we may not be able to obtain regulatory approval for or commercialize our product or product candidates when expected or at all.
In order to submit an IND, BLA, or NDA to the FDA and maintain these applications, it is necessary to submit all information on the clinical, non-clinical, chemistry, manufacturing, controls and quality aspects of the product candidate. Clinical trial applications and marketing authorization applications for foreign regulatory bodies have substantially similar requirements. We rely on our third-party contractors and our licensing partners to provide portions of this data. If we are unable to obtain this data, or the data is not sufficient to meet the regulatory requirements, we may experience significant delays in our development programs and commercialization efforts.
Additionally, we use CROs to assist in the conduct of our current clinical trials and expect to use such services for future clinical trials and we rely upon medical institutions, clinical investigators and contract laboratories to conduct our trials in accordance with our clinical protocols and appropriate regulations. Our current and future CROs, investigators and other third parties play a significant role in the conduct of our trials and the subsequent collection and analysis of data from the clinical trials. There is no guarantee that any CROs, investigators and other third parties will devote adequate time and resources to our clinical trials or perform as contractually required. If any third parties upon whom we rely for administration and conduct of our clinical trials fail to meet expected deadlines, fail to adhere to its clinical protocols or otherwise perform in a substandard manner, our clinical trials may be extended, delayed or terminated, and we may not be able to commercialize our product or product candidates. In addition to the third parties identified above, we are also heavily reliant on the conduct of our patients enrolled to our studies by our third-party investigators. We rely on our clinical trial sites and investigators to properly identify and screen eligible candidates for our clinical trials, and for them to ensure participants adhere to our clinical protocol requirements. The majority of our clinical trial conduct occurs in the outpatient setting, where patients are expected to continue to adhere to our study protocol specified requirements. The ability of our enrolled patients to properly identify, document, and report adverse events; take protocol specified study drugs at the correct quantity, time, and setting, as applicable; avoid contraindicated medications; and comply with other protocol specified procedures such as returning to the trial site for scheduled laboratory and disease assessments, is wholly out of our control. Deviations from protocol procedures, such as those identified previously, could materially affect the quality of our clinical trial data, and therefore ultimately affect our ability to develop and commercialize our drug candidates. If any of our clinical trial sites terminates for any reason, we may experience the loss of follow-up information on patients enrolled in our ongoing clinical trials unless we are able to transfer the care of those patients to another qualified clinical trial site. If any of our clinical trial sites is required by the FDA or IRB to close down due to data management or patient management or any other issues, we may lose clinical trial subjects.
Whether conducted through a CRO or through our internal staff, we are solely responsible for ensuring that each of our clinical trials is conducted in accordance with the applicable protocol, legal and regulatory requirements and scientific standards, and our reliance on CROs will not relieve us of our regulatory responsibilities. For any violations of laws and regulations during the conduct of our clinical trials, we could be subject to warning letters or other enforcement actions that may include civil penalties or criminal prosecution. We and our CROs are required to comply with regulations, including GCP guidelines for conducting, monitoring, recording and reporting the results of clinical trials to ensure that the data and results are scientifically credible and accurate, and that the trial patients are adequately informed of the potential risks of participating in clinical trials and their rights are protected. These regulations are enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area and comparable foreign regulatory authorities for any drug candidates in clinical development. The FDA enforces GCP regulations through periodic inspections of clinical trial sponsors, clinical investigators, CROs, institutional review boards, and non-clinical laboratories. If we, our CROs, our investigators or other third parties fail to comply with applicable GCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that, upon inspection, the FDA will determine that our current or future clinical trials comply with GCPs. In addition, our clinical trials must be conducted with drug candidates produced under cGMP regulations. Our failure or the failure of our CROs or CMOs to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process and could also subject us to enforcement action. We also are required to register most ongoing clinical trials and post the results of completed clinical trials on government-sponsored databases, e.g., ClinicalTrials.gov, within certain timeframes. Failure to do so can result in fines, adverse publicity and civil and criminal sanctions.
CROs play an important role in the conduct of our clinical trials, especially outside of the United States. As a result, many important aspects of our development programs, including their conduct and timing, will be outside of our direct control. Our reliance on third parties to conduct current or future clinical trials will also result in less direct control over the management of data developed through clinical trials than would be the case if we were relying entirely upon our own staff. Communicating with outside parties can also be challenging, potentially leading to mistakes as well as difficulties in coordinating activities. Outside parties may:
● | have staffing difficulties; |
● | fail to comply with contractual obligations; |
● | experience regulatory compliance issues; |
● | undergo changes in priorities or become financially distressed; or |
● | form relationships with other entities, some of which may be our competitors. |
These factors may materially adversely affect the willingness or ability of third parties to conduct our clinical trials and may subject us to unexpected cost increases that are beyond our control. If the CROs do not perform clinical trials in a satisfactory manner, breach their obligations to us or fail to comply with regulatory requirements, the development, regulatory approval and commercialization of our drug candidates may be delayed, we may not be able to obtain regulatory approval and commercialize our drug candidates, or our development program may be materially and irreversibly harmed. If we are unable to rely on clinical data collected by our CROs, we could be required to repeat, extend the duration of, or increase the size of any clinical trials we conduct, and this could significantly delay commercialization and require significantly greater expenditures.
If any of our relationships with these third-party CROs terminate, we may not be able to enter into arrangements with alternative CROs. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, any clinical trials such CROs are associated with may be extended, delayed or terminated, and we may not be able to obtain regulatory approval for or successfully commercialize our product or product candidates. As a result, we believe that our financial results and the commercial prospects for our product or product candidates in the subject indication would be harmed, our costs could increase and our ability to generate revenue could be delayed.
We contract with third parties for the manufacture of BRIUMVI for commercial supply, as well as all of our clinical product supply, and we expect to continue to do so. This reliance on third parties increases the risk that we will not have sufficient quantities of our products or product candidates or such quantities at an acceptable cost or quality, which could delay, prevent or impair our development or commercialization efforts.
We do not currently own or operate, nor do we have any plans to establish in the future, any manufacturing facilities. We rely, and expect to continue to rely, on third parties for the manufacture, testing, packaging and labeling of any products that we commercialize and our product candidates for pre-clinical development and clinical testing. For example, we currently rely on Samsung Biologics for clinical and commercial supply of BRIUMVI. In addition, we utilize multiple vendors who provide testing services. Our reliance on third parties increases the risk that we will not have sufficient quantities of our products or product candidates or such quantities at an acceptable cost or quality, which could delay, prevent or impair our development or commercialization efforts.
The facilities used by contract manufacturers to manufacture, test, package, and label our product and product candidates typically undergo periodic inspections by the FDA or a comparable foreign regulatory authority to verify compliance with applicable cGMP regulations. Additional inspections may be conducted after we submit our marketing applications to or receive marketing approval from the FDA or a comparable foreign regulatory authority. Although the FDA and other regulators impose requirements regarding our selection, qualification, oversight, and monitoring of our contract manufacturers and hold us responsible for the ultimate compliance of our products, we do not directly control the manufacturing process of our third-party contract manufacturers and are subject to risks associated with their ability to comply with cGMPs in connection with the manufacture of our products and product candidates. If our contract manufacturers cannot successfully manufacture material that conforms to our specifications and the strict regulatory requirements of the FDA or others and the compliance concerns cannot be resolved, remediated, or otherwise addressed to the FDA’s or others’ satisfaction in a timely manner during the review of any marketing applications that we submit, it may negatively impact our ability to obtain regulatory approval for our drug candidates or obtain approval within projected timelines. We cannot guarantee the ability of our third-party manufacturers to maintain compliance with cGMP regulations, including having adequate quality control, quality assurance and qualified personnel. Further, our failure, or the failure of our third-party manufacturers, to comply with applicable regulations could result in sanctions being imposed on us, including clinical holds, fines, injunctions, civil penalties, delays, suspension or withdrawal of approvals, license revocation, seizures or recalls of products or product candidates, operating restrictions and criminal prosecutions, any of which could significantly and adversely affect our business and supplies of our products or product candidates.
Our reliance on third-party manufacturers entails additional risks, including:
● | reliance on the third party for regulatory compliance and quality assurance; |
● | the possible breach of the manufacturing, supply or quality agreement by the third party; |
● | the possible misappropriation of our proprietary information, including our trade secrets and know-how; and |
● | the possible termination or nonrenewal of the agreement by the third party at a time that is costly or inconvenient for us. |
Moreover, our current long-term supply agreement for BRIUMVI contains certain minimum purchases in what are commonly referred to as a “take or pay” provision, and it is possible that future supply agreements could contain such provisions. To the extent our demand does not meet the minimum supply required amounts, we would be forced to pay more than desired. This could create a situation where we are spending more than required and could impact our on-going operations and entail curtailing other important research and development or commercialization efforts, all of which could have a material adverse effect on the Company. In negotiating our supply agreement for BRIUMVI, there is no guarantee that we have foreseen all eventualities or that our third-party manufacturer will be able to accommodate unforeseen changes in business direction in a timely fashion or at all. Scheduling of manufacturing at our third-party manufacturer is governed by contractual terms that require us to make investments in inventory of materials, with limited shelf-life, in advance of regulatory approval and based on preliminary commercial forecasting, and such inventory may not be used if timelines and supply needs shift.
Our drug candidates and any drugs that we may develop may compete with other drug candidates and approved drugs for access to manufacturing facilities. There are a limited number of manufacturers that operate under cGMP regulations and that might be capable of manufacturing for us. Any third-party manufacturer with which we contract will have other clients, and our relative importance as a customer may adversely impact contractual terms or the performance of services in a satisfactory manner or on a timely basis.
Any performance failure on the part of our existing or future manufacturers could delay clinical development or marketing approval or interrupt commercial distribution. If our current contract manufacturers cannot perform as agreed, we may be required to replace such manufacturers causing additional costs and delays in identifying and qualifying any such replacement. If a new contract manufacturer is not successful in replicating the product or experiences delays, or if regulatory authorities impose unforeseen requirements with respect to product comparability from multiple manufacturing sources, we may experience delays in clinical development or an interruption in our commercial supply. No assurance can be given that any new manufacturer will be successful or that material manufactured by a new manufacturer will perform comparably to product manufactured by the previous manufacturer or that the relevant regulatory agencies will agree with our interpretation of comparability. Any significant delays or gaps in supply of commercial or clinical products may adversely affect our clinical development program, our ability to commercialize any drugs that receive marketing approval on a timely and competitive basis, and our future profit margins.
We also rely on other third parties to store and distribute drug supplies for our clinical trials and for commercial demand for BRIUMVI and expect to continue to do so for any other potential commercial products. Any performance failure on the part of our distributors could delay clinical development or marketing approval of any future product candidates or commercialization of our products, producing additional losses and depriving us of potential product revenue.
The third parties upon whom we rely for the supply of starting materials, intermediates, active pharmaceutical ingredient (API)/drug substance, drug product, and other materials used in our drug candidates are our sole source of supply, and the loss or disruption of any of these suppliers could significantly harm our business.
The starting materials, intermediates, API/drug substance, and drug product used in many of our drug candidates are currently supplied to us from single-source suppliers. Our ability to successfully develop our drug candidates, supply our drug candidates for clinical trials and to ultimately supply our commercial drugs in quantities sufficient to meet the market demand, depends in part on our ability to obtain starting materials, intermediates, API/drug substance, and drug product for these drugs in accordance with regulatory requirements and in sufficient quantities for clinical testing and commercialization. It is expected that many of our manufacturing partners will be sole source suppliers from single site locations for the foreseeable future. Various raw materials, components, and testing services required for our product and product candidates may also be single sourced. We are not certain that our single-source suppliers will be able to supply sufficient quantities of their products or on the timelines necessary to meet our needs, either because of the nature of our agreements with those suppliers, our limited experience with those suppliers, our relative importance as a customer to those suppliers, international political conflicts that may impact trade or the supply chain within a particular region, public health emergencies such as the COVID-19 pandemic or natural disasters that may cause those suppliers to stop work for a period of time or lead to a sudden increase in demand for selected materials resulting in short-term unavailability of such materials. If any of our suppliers ceases operations for any reason or is unable or unwilling to supply starting materials, intermediates, API/drug substance, and drug product in sufficient quantities or on the timelines necessary to meet our needs, it could significantly and adversely affect our business, the supply of our drug products and drug candidates and our financial condition. In addition, if our current or future supply of any of our products or product candidates should fail to meet specifications during its stability program there could be a voluntary or mandatory product recall if the product is approved and, even in the absence of a recall, there could be significant interruption of our supply of drug, which would adversely affect the clinical development and commercialization of the product.
We continually evaluate our supply chains to identify potential risks and needs for additional manufacturers and other suppliers for the production of our products and product candidates. Establishing additional or replacement suppliers for the API/drug substance, drug product, and certain raw materials, if required, may not be accomplished quickly, or at all, and may involve significant expense. If we are able to find a replacement supplier, we would need to evaluate and qualify such replacement supplier and its ability to meet quality and compliance standards. Any change in suppliers or the manufacturing process could require additional regulatory approval and result in operational delays. While we seek to maintain adequate inventory of materials necessary for the production of our products and product candidates, any supply interruption or delay, or our inability to identify alternate sources at acceptable prices in a timely manner could impede, delay, limit or prevent our commercialization and development efforts, which could harm our business, results of operations, financial condition and prospects.
Because we have in-licensed BRIUMVI and our product candidates from third parties, any dispute with or non-performance by our licensors will adversely affect our ability to develop and commercialize the applicable product candidates.
Because we license BRIUMVI and our foundational intellectual propertyproduct candidates from third parties and we expect to continue to in-license additional intellectual property rights,product candidates, if there is any dispute between us and our licensor regarding our rights under a
● | the scope of rights granted under the license agreement and other interpretation-related issues; |
● | the extent to which our technology and processes infringe on intellectual property of the licensor that is not subject to the license agreement; |
● | the sublicensing of patent and other rights under our collaborative development relationships and obligations associated with sublicensing; |
● | our diligence obligations under the license agreement and what activities satisfy those diligence obligations; |
● | the ownership of inventions and know-how resulting from the joint creation or use of intellectual property by our licensors and us and our partners; and |
● | the priority of invention of patented technology. |
In addition, the agreements under which we currently license intellectual property or technologyBRIUMVI and our product candidates from third parties are
If conflicts arise between us and our future collaborators or strategic partners, these parties may act in a manner adverse to us and could limit our ability to implement our strategies.
If conflicts arise between our future corporate or academic collaborators or strategic partners and us, the other party may act in a manner adverse to us and could limit our ability to implement our strategies. Future collaborators or strategic partners, may develop, either alone or with others, products in related fields that are competitive with the products or potential products that are the subject of these collaborations. Competing products, either developed by the collaborators or strategic partners or to which the collaborators or strategic partners have rights, may result in the withdrawal of partner support for any future product candidates. Our current or future collaborators or strategic partners may preclude us from entering into collaborations with their competitors, fail to obtain timely regulatory approvals, terminate their agreements with us prematurely, or fail to devote sufficient resources to the development and commercialization of products. Any of these developments could harm any future product development efforts.
We are dependent upon our relationships with collaboration and commercialization partners to further develop, fund, manufacture and commercialize our drug products and our product candidates. If such relationships are unsuccessful, or if a collaboration or commercialization partner terminates its collaboration or commercialization agreement with us, it could negatively impact our ability to conduct our business and generate net product revenue. Failure by a collaboration or commercialization partner to perform its duties under its collaboration or commercialization agreement with us (e.g. financial reporting or internal control compliance) may negatively affect us.
On July 28, 2023, we entered into a commercialization agreement (the Commercialization Agreement) with Neuraxpharm Pharmaceuticals, S.L. (Neuraxpharm), pursuant to which Neuraxpharm has the right to commercialize BRIUMVI in certain markets outside of the U.S. In addition to the Commercialization Agreement, we may enter into collaboration arrangements with other collaboration and commercialization partners.
We are subject to a number of risks associated with our dependence on our relationships with our collaboration and commercialization partners, including:
● | our collaboration and commercialization partners may terminate their collaboration or commercialization agreements with us for reasons specified in the collaboration or commercialization agreements, including our breach; |
● | the need for us to identify and secure on commercially reasonable terms the services of third parties to perform key activities, including development and commercialization activities, currently performed by our collaboration or commercialization partners in the event that a collaboration or commercialization partner terminates its agreement with us; |
● | adverse decisions by a collaboration or commercialization partner regarding the amount and timing of resource expenditures for the commercialization, distribution, and sale of our drug products; |
● | failure by a collaboration or commercialization partner to perform its duties under its agreement with us (e.g., its failure to comply with regulatory requirements which may disrupt its performance of its obligations under the agreement with us); |
● | failure by a collaboration or commercialization partner to timely deliver accurate and complete financial information to us or to maintain adequate and effective internal control over its financial reporting may negatively affect our ability to meet our financial reporting obligations as required by the SEC; |
● | failure by a collaboration or commercialization partner to timely deliver accurate and complete medical or clinical information to us or to maintain adequate and effective internal control over its pharmacovigilance activities and reporting may negatively affect our ability to meet our reporting obligations as required by the FDA and other regulatory bodies; |
● | collaboration or commercialization partners’ and their affiliates’ development and commercialization of products that compete directly or indirectly with our products or product candidates; |
● | decisions by a collaboration or commercialization partner to prioritize others of its current or future products more highly than our drug products or our product candidates when it performs its duties; |
● | possible disagreements with a collaboration or commercialization partner as to the timing, nature and extent of our development plans or distribution and sales and marketing plans; and |
● | the financial returns to us, if any, under our collaboration agreement with Neuraxpharm depends in large part on the achievement of milestones and generation of product sales, and if Neuraxpharm fails to perform or satisfy its obligations under the collaboration agreements, the development and commercialization of our drug products could be delayed, hindered or may not occur, and our business and prospects could be materially and adversely affected. |
While the Commercialization Agreement contains provisions that allow for dispute resolution, arbitration, and/or termination of the agreement by the Company in the event of a breach by Neuraxpharm, there can be no assurance that the Company and Neuraxpharm will agree on a cure for such a breach, and in the event of termination, there can be no assurance that the Company would be appropriately compensated and/or recover any losses sustained. Due to these factors and other possible disagreements with our collaboration and commercialization partners, we may be delayed or prevented from further developing, manufacturing or commercializing our drug products or our product candidates or we may become involved in litigation or arbitration, which would be time consuming and expensive.
If any collaboration or commercialization partner were to terminate our relationship with it unilaterally, we would need to obtain FDA approvalundertake development, commercialization or distribution or sale activities for our drug products and product candidates solely at our own expense, and/or seek one or more other partners for some or all of any proposed product brand names, and any failure or delay associated with such approval may adversely impact our business.
We may not become or remain profitable.
Our drug development programs and the potential commercialization of our drug candidates or limitwill require substantial additional cash to fund expenses. For some of our drug candidates, we may decide to collaborate with additional pharmaceutical and biotechnology companies for the development and potential commercialization of any approved products. An individualthose drug candidates.
We face significant competition in seeking appropriate collaborators. Whether we reach a definitive agreement for a collaboration will depend, among other things, upon our assessment of the collaborator’s resources and expertise, the terms and conditions of the proposed collaboration, and the proposed collaborator’s evaluation of a number of factors. Those factors may bring a liability claim against us if oneinclude the design or results of our clinical trials, the likelihood of approval by the FDA, EMA or similar regulatory authorities outside the United States, the potential market for the subject product candidate, the costs and complexities of manufacturing and delivering such product candidate to patients, the potential of competing drugs, the existence of uncertainty with respect to our ownership of technology, which can exist if there is a challenge to such ownership without regard to the merits of the challenge, and industry and market conditions generally. The collaborator may also consider alternative product candidates causes, or merely appearstechnologies for similar indications that may be available to have caused, an injury. If we cannot successfully defend our self against product liability claims, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
We may be unablerestricted under our collaboration agreements from entering into future agreements on certain terms with potential collaborators. Collaborations are complex and time-consuming to obtain this product liability insurance on commercially reasonable termsnegotiate and with insurance coverage that will be adequate to satisfy any liability that may arise. On occasion, large judgmentsdocument. In addition, there have been awarded in class action or individual lawsuits relating to marketed pharmaceuticals. A successful product liability claim or series of claims brought against us could cause our stock price to decline and, if judgments exceed our insurance coverage, could decrease our cash and adversely affect our business.
We may not be able to provide datanegotiate additional collaborations on a timely basis, on acceptable terms, or at all. If we are unable to do so, we may have to curtail the development of the product candidate for which we are seeking to collaborate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms or at all. If we do not have sufficient funds, we may not be able to gain acceptancefurther develop our product candidates or bring them to market and generate revenue from their sales.
Risks Relating to Our Intellectual Property
Our success depends upon our ability to obtain and protect our intellectual property and proprietary technologies. If the scope of our patent protection obtained is not sufficiently broad, our competitors could develop and commercialize technology and drugs similar or identical to ours, and our ability to successfully commercialize our technology and drugs may be impaired.
Our commercial success in part depends on obtaining and maintaining patent protection and trade secret protection in the United States and other countries with respect to coverageany product we commercialize, including BRIUMVI, our product candidates, their formulations and reimbursement. If reimbursementuses and the methods we use to manufacture them, as well as successfully defending these patents against third-party challenges. We seek to protect our proprietary and intellectual property position by filing patent applications in the United States and abroad related to our novel technologies and product candidates, and by maintenance of our futuretrade secrets through proper procedures. Because we in-license our products isand product candidates, we also rely on our licensors to protect the patent and other intellectual property rights necessary for commercialization.
We will only be able to protect our technologies from unauthorized use by third parties to the extent that valid and enforceable patents or trade secrets cover them in the market they are being used or developed. The degree of patent protection we require to successfully commercialize our products and product candidates may be unavailable or severely limited in some cases and may not adequately protect our rights or permit us to gain or keep any competitive advantage. We cannot provide any assurances that any of our patents have, or that any of our pending patent applications that mature into issued patents will include, claims with a scope or amount, or if pricingsufficient to protect any of our products. In addition, the laws of foreign countries may not protect our patent rights to the same extent as the patent laws of the United States.
Furthermore, patents have a limited lifespan. In the United States, the natural expiration of a patent is set at unsatisfactory levels, wegenerally twenty years after it is filed. Various extensions may be unableavailable; however, the life of a patent, and the protection it affords, is limited. Given the amount of time required for the development, testing and regulatory review of new drug candidates, patents protecting such candidates might expire before or shortly after such candidates are commercialized. As a result, our patent portfolio may not provide us with adequate and continuing patent protection sufficient to achieveexclude others from commercializing drugs similar or sustain profitability. Additionally, whileidentical to our product or product candidates, including generic versions of such drugs.
Currently, we may seek approval of our productshave several granted patents in combination with eachthe United States and EU, among other therecountries, and several pending patent applications that have not yet been issued or have been issued in certain jurisdictions but not all jurisdictions in which such applications have been filed. There can be no guarantee that weany pending patent applications, nor any patent applications filed in the future will obtain coverage and reimbursement forbe granted in any of our products together,or all jurisdictions in which they were filed, or that all patent claims initially submitted for examination in such reimbursementpatent applications will incentivize the use of our products in combination with each other as opposed to in combination with other agents which may be priced more favorably to the medical community.
These risks and uncertainties include the following:
● | the patent applications that we or our licensors file may not issue as patent; |
● | patents that may be issued or in-licensed may be challenged, invalidated, modified, revoked or circumvented, or otherwise may not provide any competitive advantage; |
● | as of March 16, 2013, the United States converted from a first-to-invent to a first-to-file system. If we do not win the filing race, we will not be entitled to inventive priority; |
● | our competitors, many of whom have substantially greater resources than we do, and many of whom have made significant investments in competing technologies, may seek, or may already have obtained, patents that will limit, interfere with, or eliminate our ability to file new patent applications covering our products, or make, use, and/or sell our products either in the United States or in international markets; |
● | there may be significant pressure on the United States government and other international governmental bodies to limit the scope of patent protection both inside and outside the United States for disease treatments that prove successful as a matter of public policy regarding worldwide health concerns, which could limit our ability to fully monetize our intellectual property rights; and |
● | countries other than the United States may have less restrictive patent laws than those of the United States, allowing foreign competitors to exploit such less restrictive patent laws to make, use, and/or sell competing products in their respective jurisdictions. |
If we are not able to obtain patents that protect our product and product candidates, it could have a material adverse effect on our business.
In addition, the provisionspatent prosecution process is expensive and time-consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. Further, with respect to some of the ACApending patent applications covering our drug candidates, prosecution has yet to commence. Patent prosecution is a lengthy process, during which the scope of importancethe claims initially submitted for examination by the United States Patent and Trademark Office (USPTO) can be significantly narrowed by the time they issue, if at all. It is also possible that we will fail to identify any patentable aspects of our potentialresearch and development output and methodology, and, even if we do, an opportunity to obtain patent protection may have passed. Given the uncertain and time-consuming process of filing patent applications and prosecuting them, it is possible that our product(s) or process(es) originally covered by the scope of our patent applications may change or be modified throughout the patent prosecution process, leaving our product(s) or process(es) without patent protection. Moreover, in some circumstances, we do not have the right to control the preparation, filing and prosecution of patent applications, or to maintain the patents, that cover technology licensed from third parties. Therefore, these patents and applications may not be prosecuted and enforced in a manner consistent with the best interests of our business. If our licensors or we fail to appropriately prosecute and maintain patent protection or trade secret protection for one or more products or product candidates, are:
The patent position of biotechnology and pharmaceutical companies generally is highly uncertain, involves complex legal and factual questions, and has in recent years been the subject of much litigation. In addition, no consistent policy regarding the breadth of claims allowed in pharmaceutical or biotechnology patents has emerged to date in the United States. The patent situation outside the United States is even more uncertain. The patent laws of foreign countries may not protect our patent rights to the same extent as the laws of the United States, and we may fail to seek or obtain patent protection in all major markets. For example, European patent law restricts the patentability of methods of treatment of the human body more than United States patent law does. Our pending and future patent applications may not result in patents being issued which protect our technology or products, in whole or in part, or which effectively prevent others from commercializing competitive technologies and products. Changes in either the patent laws or interpretation of the patent laws in the U.S. and other countries may diminish the value of our patents or narrow the scope of our patent protection. For example, the federal courts of the United States have taken an increasingly dim view of the patent eligibility of certain subject matter, such as naturally occurring nucleic acid sequences, amino acid sequences and certain methods of utilizing same, which include their detection in a biological sample and diagnostic conclusions arising from their detection. Such subject matter, which had long been a staple of the biotechnology and biopharmaceutical industry to protect their discoveries, is now considered, with few exceptions, ineligible in the first instance for protection under the patent laws of the United States. Accordingly, we cannot predict the breadth of claims that may be allowed or enforced in our patents or in those licensed from a thirdparty.
In addition, U.S. patent laws may change, which could prevent or limit us, our subsidiaries, or our licensors from filing patent applications or patent claims to protect products and/or technologies or limit the exclusivity periods that are available to patent holders, as well as affect the validity, enforceability, or scope of issued patents. For example, on September 16, 2011, the Leahy-Smith America Invents Act was signed into law. The Leahy-Smith Act includes a number of significant changes to United States patent law. These include the transition from a first-to-invent system to a first-to-file system and changes to the way issued patents are challenged. The formation of the Patent Trial and Appeal Board now provides a quicker and less expensive process for challenging issued patents.
The patents or patent applications owned or filed by us, or by our licensors or other collaborators, may be affected by third-party pre-issuance submissions of prior art to the USPTO, or by opposition, derivation, reexamination, inter parties review, post-grant review or interference proceedings. The costs of these proceedings could be substantial, and it is possible that our efforts to establish priority of invention would be unsuccessful, resulting in a material adverse effect on our U.S. patent position. An adverse determination in any such submission, patent office trial, proceeding or litigation could reduce the scope of, render unenforceable, or invalidate, our patent rights, allow third parties to commercialize our technology or products and compete directly with us, without payment to us, or result in our inability to manufacture or commercialize products without infringing third-party patent rights. In addition, if the breadth or strength of protection provided by patents and patent applications for our drug candidates is threatened, it could dissuade companies from collaborating with us to license, develop or commercialize current or future products or product candidates.
The issuance of a patent does not foreclose challenges to its inventorship, scope, validity or enforceability. Therefore, our owned and licensed patents may be challenged in the courts or patent offices in the U.S. and abroad. Such challenges may result in loss of exclusivity or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and products, or limit the duration of the patent protection of our technology and products. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such product candidates might expire before or shortly after such product candidates are commercialized. As a result, our owned and licensed patent portfolio may not provide us with enough rights to exclude others from commercializing products similar or identical to ours.
Even if our patent applications issue as patents, and they are unchallenged, our issued patents and pending patent applications, if issued, may not provide us with any meaningful protection or prevent competitors from designing around our patent claims to circumvent our owned or licensed patents by developing similar or alternative technologies or drugs in a non-infringing manner. For example, a third party may develop a competitive drug that provides benefits similar to one or more of our products or product candidates but that has a different composition that falls outside the scope of our patent protection. If the patent protection provided by the patents and patent applications we hold or pursue with respect to our products or product candidates is not sufficiently broad to impede such competition, our ability to successfully commercialize our products or product candidates could be negatively affected, which would harm our business.
In addition, we may in the future be subject to claims by our former employees or consultants asserting an ownership right in our patents or patent applications, as a result of the work they performed on our behalf. Although we have entered into agreements with many of our employees, consultants and advisors and any other third parties who have access to our proprietary know-how, information or technology for the purpose of assigning or granting similar rights to their inventions to us, we cannot be certain that we have executed such agreements with all parties who may have contributed to our intellectual property, nor can we be certain that our agreements with such parties will be upheld in the face of a potential challenge, or that they will not be breached, for which we may not have an adequate remedy. An adverse determination in any such submission or proceeding may result in loss of exclusivity or freedom to operate or in patent claims being narrowed, invalidated or held unenforceable, in whole or in part, which could limit our ability to stop others from using or commercializing similar or identical technology and drugs, without payment to us, or could limit the duration of the patent protection covering our technology and drug candidates. Such challenges may also result in our inability to manufacture or commercialize our products and product candidates without infringing third-party patent rights. In addition, if the breadth or strength of protection provided by our patents and patent applications is threatened, it could dissuade companies from collaborating with us to license, develop or commercialize current or future drug candidates.
Patent protection and other intellectual property protection are crucial to the success of our business and prospects, and there is a substantial risk that such protections will prove inadequate.
Obtaining and maintaining patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
The USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. In addition, periodic maintenance fees on issued patents often must be paid to the USPTO and foreign patent agencies over the lifetime of the patent. While an unintentional lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction.
Non-compliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. If we fail to maintain the patents and patent applications covering our drugs or procedures, we may not be able to stop a competitor from marketing drugs that are the same as or similar to our products or product candidates, which would have a material adverse effect on our business.
If we do not obtain patent term extensions under the Hatch-Waxman Act and similar foreign legislation extending the terms of our licensed patents and any future patents we may own, our business may be materially harmed.
Depending on the timing, duration, and specifics of any FDA regulatory approval for our drug candidates, one or more of our licensed U.S. patents or future U.S. patents that we may license or own may be eligible for limited patent term restoration under the Hatch-Waxman Act. The Hatch-Waxman Act permit a patent term extension of up to five years as compensation for patent term lost during the FDA regulatory review process. A patent term extension cannot extend the remaining term of a patent beyond 14 years from the date of product approval by the FDA, and only one patent covering the approved product may be extended.
The application for a patent term extension is subject to approval by the USPTO, in conjunction with the FDA. We may not be granted an extension because of, for example, failing to apply within applicable deadlines, failing to apply prior to expiration of relevant patents or otherwise failing to satisfy applicable requirements. Moreover, the applicable time period or the scope of the patent protection afforded could be less than what we request. If we are unable to obtain patent term extension or any term of such extension is less than we request, the period during which we will have the right to exclusively market our product will be shortened and our competitors may obtain earlier approval of competing products, and our ability to generate revenues could be materially adversely affected.
We may not be able to enforce our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on drug candidates throughout the world would be prohibitively expensive. Competitors may use our licensed and owned technologies in jurisdictions where we have not licensed or obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories where we may obtain or license patent protection, but where patent enforcement is not as strong as that in the United States. These products may compete with our products in jurisdictions where we do not have any issued or licensed patents and any future patent claims or other intellectual property rights may not be effective or sufficient to prevent them from so competing.
Moreover, our ability to protect and enforce our intellectual property rights may be adversely affected by unforeseen changes in foreign intellectual property laws. Additionally, laws of some countries outside of the United States and Europe do not afford intellectual property protection to the same extent as the laws of the United States and Europe. Many companies have encountered significant problems in protecting and defending intellectual property rights in certain foreign jurisdictions. The legal systems of some countries, including India, China and other developing countries, do not favor the enforcement of patents and other intellectual property rights. This could make it difficult for us to stop the infringement of our patents or the misappropriation of our other intellectual property. For example, many foreign countries have compulsory licensing laws under which a patent owner must grant licenses to third parties. Consequently, we may not be able to prevent third parties from practicing our inventions in certain countries outside the United States and Europe.
Proceedings to enforce our future patent rights, if any, in foreign jurisdictions could result in substantial cost and divert our resources and attention from other aspects of our business. Moreover, such proceedings could put our patents at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate, and the damages or other remedies awarded, if any, may not be meaningful. Furthermore, while we intend to protect our intellectual property rights in major markets for our products, we cannot ensure that we will be able to initiate or maintain profitability;
We may be involved in lawsuits to protect or enforce our patents or the levelpatents of taxesour licensors, which could be expensive, time consuming and unsuccessful.
Competitors may infringe our patents or the patents of our licensors. To counter infringement or unauthorized use, we may be required to file infringement claims, which typically are very expensive, time-consuming and disruptive to our day-to-day business operations. Any claims we assert against accused infringers could provoke these parties to assert counterclaims against us alleging invalidity of our or certain of our subsidiaries’ patents or that we infringe their patents; or provoke those parties to petition the USPTO to institute inter parties review against the asserted patents, which may lead to a finding that all or some of the claims of the asserted patents are invalid. In addition, in an infringement proceeding, a court may decide that a patent of ours or our licensors is not valid or is unenforceable or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation or defense proceedings could put one or more of our pending patents at risk of being invalidated, held unenforceable, or interpreted narrowly.
In patent litigation in the United States, defendant counterclaims challenging the validity, enforceability or scope of asserted patents are commonplace. In addition, third parties may initiate legal proceedings against us to assert such challenges to our intellectual property rights. The outcome of any such proceeding is generally unpredictable. Grounds for a validity challenge could be an alleged failure to meet any of several statutory requirements, including lack of novelty, obviousness or non-enablement. Patents may be unenforceable if someone connected with the prosecution of the patent withheld relevant information from the USPTO or made a misleading statement during prosecution. It is possible that prior art of which we and the patent examiner were unaware during prosecution exists, which could render our patents invalid. Moreover, it is also possible that prior art may exist that we are aware of but do not believe is relevant to our current or future patents, but that could nevertheless be determined to render our patents invalid.
Competing drugs may also be sold in other countries in which our patent coverage might not exist or be as strong as in the United States. If we lose a foreign patent lawsuit, alleging our infringement of a competitor’s patents, we could be prevented from marketing our drugs in one or more foreign countries. Any of these outcomes would have a material adverse effect on our business.
In addition, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. Furthermore, adverse results on United States patents may affect related patents in our global portfolio. The adverse result could also put related pending patent applications at risk of not issuing. Additionally, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of our common stock.
Interference proceedings provoked by third parties or brought by the USPTO may be necessary to determine the priority of inventions with respect to our patents or pending patent applications or those of our collaborators or licensors. An unfavorable outcome could require us to cease using the related technology or to attempt to license rights to it from the prevailing party. The costs of these proceedings could be substantial. As a result, the issuance, scope, validity, enforceability and commercial value of our or any of our respective licensors’ patent rights are highly uncertain. Our business could be harmed if the prevailing party does not offer us a license on commercially reasonable terms. Litigation or interference proceedings may fail and, even if successful, may result in substantial costs and distract our management and other employees. We may not be able to prevent, alone or with our licensors, misappropriation of our trade secrets or confidential information, particularly in countries where the laws may not protect those rights as fully as in the United States.
We may not have sufficient financial or other resources to adequately conduct such litigation or proceedings. Some of our competitors may be able to sustain the costs of such litigation or proceedings more effectively than we can because of their greater financial resources and more mature and developed intellectual property portfolios. Accordingly, despite our efforts, we may not be able to prevent third parties from infringing upon or misappropriating or from successfully challenging our intellectual property rights. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could have a material adverse effect on our ability to compete in the marketplace.
If we or our partners are sued for infringing intellectual property rights of third parties, it will be costly and time consuming, and an unfavorable outcome in that litigation would have a material adverse effect on our business.
Our commercial success depends upon our ability and the ability of our collaborators to develop, manufacture, market and sell our drug candidates and use our proprietary technologies without infringing the proprietary rights and intellectual property of third parties. The biotechnology and pharmaceutical industries are characterized by extensive and frequent litigation regarding patents and other intellectual property rights. We may in the future become party to, or threatened with, adversarial proceedings or litigation regarding intellectual property rights with respect to our drug candidates and technology, including interference proceedings before the USPTO.
Our competitors or other third parties may assert infringement claims against us, alleging that our drugs are covered by their patents. Given the vast number of patents in our field of technology, we cannot be certain that we do not infringe existing patents or that we will not infringe patents that may be granted in the future. Numerous United States and foreign issued patents and pending patent applications, which are owned by third parties, exist in the fields in which we are developing products, some of which may be directed at claims that overlap with the subject matter of our intellectual property. In addition, because patent applications can take many years to issue, there may be currently pending applications, unknown to us, which may later result in issued patents that our product or product candidates or proprietary technologies may infringe. Similarly, there may be issued patents relevant to our product or product candidates of which we are not aware. Publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until 18 months after a first filing, or in some cases not at all. Therefore, we cannot know with certainty whether we or our licensors were the first to make the inventions claimed in patents or pending patent applications that we own or licensed, or that we or our licensors were the first to file for patent protection of such inventions.
We are aware of certain patents that may pose issues for our commercialization of our product and product candidates. If we decide to initiate proceedings to challenge the validity of these patents in the future, we may be unsuccessful, as courts or patent offices in the United States and abroad could uphold the validity of any such patents. If we were to challenge the validity of any issued United States patent in court, we would need to overcome a statutory presumption of validity that attaches to every United States patent. This means that in order to prevail, we would have to present clear and convincing evidence as to the invalidity of the patent’s claims. If we are unable to do so, we may be forced to delay the launch of our product candidates or launch at the risk of litigation for patent infringement, which may have a material adverse effect on our business and results of operations.
If a third-party claims that we or any collaborators of ours infringe their intellectual property rights, we may have to defend litigation or administrative proceedings which may be costly whether we win or lose, and which could result in a substantial diversion of our financial and management resources. If we are found to infringe a third party’s intellectual property rights, we could be required to pay;obtain a license from such third party to continue developing and
No assurance can be given that patents issued to third parties do not exist, have not been filed, or could not be filed or issued, which contain claims covering their products, technology or methods that may impose price controls,encompass all or a portion of our products and methods. Given the number of patents issued and patent applications filed in our technical areas or fields, we believe there is a risk that third parties may allege they have patent rights encompassing our products or methods.
Other products or product candidates that we may in-license or acquire could be subject to similar risks and uncertainties.
We may need to license certain intellectual property from third parties, and such licenses may not be available or may not be available on commercially reasonable terms.
A third party may hold intellectual property, including patent rights that are important or necessary to the development and commercialization of our products. It may be necessary for us to use the patented or proprietary technology of third parties to commercialize our products, in which case we would be required to obtain a license from these third parties, whom may or may not be interested in granting such a license, on commercially reasonable terms, in which case our business could be harmed, possibly materially. For example, we engage extensively with third parties, including academic institutions, to conduct non-clinical and clinical research on our product and product candidates. While we seek to ensure all material transfer and service agreements governing this research provide us with favorable terms covering newly generated intellectual property, a general principle under which much of this research with academic institutions is conducted provides third-party ownership of newly generated intellectual property, with an exclusive option available for us to obtain a license to such intellectual property. Through the conduct of this research, it is possible that valuable intellectual property could be developed by a third party, which we will then need to license in order to better develop or commercialize our products. No assurance can be given that we will be able to successfully negotiate such a license on commercially reasonable terms, or at all. Further, should we fail to successfully negotiate a license to such intellectual property, most institutions are then free to license such intellectual property to any other third party, including potentially direct competitors of ours. Should we fail to adequately secure a license to any newly generated intellectual property, our ability to successfully develop or commercialize our products may be hindered, possibly materially.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position may be harmed.
In addition to the protection afforded by patents, we rely upon unpatented trade secret protection, unpatented know-how and continuing technological innovation to develop and maintain our competitive position. With respect to the building of our proprietary compound library, we consider trade secrets and know-how to be our primary intellectual property. We seek to protect our proprietary technology and processes, in part, by entering into confidentiality agreements with our collaborators, scientific advisors, employees and consultants, and invention assignment agreements with our consultants and employees. We may not be able to prevent the unauthorized disclosure or use of our technical know-how or other trade secrets by the parties to these agreements, however, despite the existence of confidentiality agreements and other contractual restrictions. Monitoring unauthorized uses and disclosures is difficult, and we do not know whether the steps we have taken to protect our proprietary technologies will be effective. If any of the collaborators, scientific advisors, employees and consultants who are parties to these agreements breach or violate the terms of any of these agreements, we may not have adequate remedies for any such breach or violation, and we could lose our trade secrets as a result. Enforcing a claim that a third party illegally obtained and is using our trade secrets, like patent litigation, is expensive and time-consuming, and the outcome is unpredictable. In addition, courts outside the United States are sometimes less willing to protect trade secrets.
Our trade secrets could otherwise become known or be independently discovered by our competitors. Competitors could purchase our drug candidates and attempt to replicate some or all of the competitive advantages we derive from our development efforts, willfully infringe our intellectual property rights, design around our protected technology or develop their own competitive technologies that fall outside of our intellectual property rights. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with us. If our trade secrets are not adequately protected so as to protect our market against competitors’ drugs, our competitive position could be adversely affected, as could our business.
We may be subject to damages resulting from claims that we or our employees have wrongfully used or disclosed alleged trade secrets of our competitors or are in breach of non-competition or non-solicitation agreements with our competitors.
We could in the future be subject to claims that we or our employees have inadvertently or otherwise used or disclosed alleged trade secrets or other proprietary information of former employers or competitors. Although we try to ensure that our employees and consultants do not use the intellectual property, proprietary information, know-how or trade secrets of others in their work for us, we may in the future be subject to claims that we caused an employee to breach the terms of his or her non-competition or non-solicitation agreement, or that we or these individuals have, inadvertently or otherwise, used or disclosed the alleged trade secrets or other proprietary information of a former employer or competitor. Litigation may be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial costs and could be a distraction to management. If our defenses to these claims fail, in addition to requiring us to pay monetary damages, a court could prohibit us from using technologies or features that are essential to our drug candidates, if such technologies or features are found to incorporate or be derived from the trade secrets or other proprietary information of the former employers. An inability to incorporate such technologies or features would have a material adverse effect on our business and may prevent us from successfully commercializing our drug candidates. In addition, we may lose valuable intellectual property rights or personnel as a result of such claims. Moreover, any such litigation or the threat thereof may adversely affect our future profitability.
Risks Related to Our Business Organization and Governance, Strategy, Employees and Growth Management
If we fail to attract and keep key management, commercial, and clinical development personnel, we may be unable to successfully develop or commercialize our product and product candidates.
We are highly dependent on the research and development, commercialization, manufacturing, quality, financial and legal expertise of our senior management team as well as the other principal members of our management. Although we have entered into an employment agreement with our chief executive officer and employment letters with our senior managers, each of our executive officers may terminate their employment with us at any time. We do not maintain key person insurance for any of our executives or other employees. In addition, we rely on consultants and advisors, including scientific and clinical advisors, to assist us in formulating our research and development and commercialization strategy. Our consultants and advisors may be employed by employers other than us and may have commitments under consulting or advisory contracts with other entities that may limit their availability to us. If we are unable to continue to attract and retain high quality personnel, our ability to pursue our growth strategy will be limited.
Recruiting and retaining qualified scientific, clinical, manufacturing and medical affairs, and commercial personnel, particularly in MS, will be critical to our success. The loss of the services of our chief executive officer or other key employees could impede the achievement of our research, development and commercialization objectives and seriously harm our ability to successfully implement our business strategy. Furthermore, replacing key employees may be difficult and may take an extended period of time because of the limited number of individuals in our industry with the breadth of skills and experience required to successfully develop, gain regulatory approval of and commercialize products. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these key personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. If we are not able to attract and retain the necessary personnel to accomplish our business objectives, we may experience constraints that will significantly impede the achievement of our development and commercialization objectives, our ability to raise additional capital, and our ability to implement our business strategy.
We will need to increase the size ofdevelop and expand our organization and the scope of our outside vendor relationships,business, and we may experienceencounter difficulties in managing this growth.
We may attempt to expand our business by acquiring additional businesses or drugs, forming strategic alliances or creating joint ventures with third parties. We may encounter numerous difficulties in developing, manufacturing, and marketing any new products resulting from any such arrangement or transaction that may delay or prevent us from realizing their expected benefits. If we are unable to successfully integrate such acquired businesses with our existing operations and company culture, we may never realize the benefits of such acquisitions or strategic alliances. We cannot assure you that, following any such transaction, we will achieve the expected synergies to justify the transaction.
As of February 26, 2024, we had 264 full-time employees. To manage our anticipated future growth and focus in neurology and immunology, we must continue to implement and improve our managerial, operational and financial systems, and other resources in ordercontinue to managerecruit and fundtrain additional qualified personnel. Also, our operations and clinical trials, continue research and developmentmanagement may need to divert a disproportionate amount of its attention away from its day-to-day activities and commercializedevote a substantial amount of time to managing these activities. Due to our product candidates. Our management and scientific personnel, systems and facilities currently in placelimited resources, we may not be adequateable to supporteffectively manage the expansion and shift of our future growth. Our needoperations or recruit and train additional qualified personnel. This may result in weaknesses in our infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among remaining employees. If our management is unable to effectively manage our operations, growth,transition to a strategy primarily focused on neurology and various projects requires that we:
Additionally, to improve our operational, financial and management controls and reporting systems and procedures; and
Certain anti-takeover provisions in our chartergoverning documents and Delaware law could make a third-party acquisition of us difficult. This could limit the price investors might be willing to pay in the future for our common stock.
Certain provisions in our amended and restated certificate of incorporation and restated bylaws could have the effect of makingmay make it more difficult for a third party to acquire us or of discouragingdiscourage a third party from attempting to acquire or control us. These factors couldus and may limit the price that certain investors might be willing to pay in the future for shares of our common stock. OurFor example, our amended and restated certificate of incorporation allows us to issue preferred stock without the approval of our stockholders. Thestockholders, the issuance of preferred stockwhich could decrease the amount of earnings and assets available for distribution to, the holders of our common stock or could adversely affect the rights and powers, including voting rights, of such holders.our common stockholders. In certain circumstances, such issuance could have the effect of decreasing the market price of our common stock. OurIn addition, our restated bylaws eliminate the right of stockholders to call a special meeting of stockholders, which could make it more difficult for stockholders to effect certain corporate actions. Any of these provisions could also have the effect of delaying or preventing a change in control.
On July 18, 2014, the Board of Directors declared a distribution of one right for each outstanding share of common stock. The rights may have certain anti-takeover effects. The rights will cause substantial dilution to a person or group that attempts to acquire us on terms not approved by the Board of Directors unless the offer is conditioned on a substantial number of rights being acquired. However, the rights should not interfere with any merger, statutory share exchange or other business combination approved by the Board of Directors since the rights may be terminated by us upon resolution of the Board of Directors. Thus, the rights are intended to encourage persons who may seek to acquire control of the Company to initiate such an acquisition through negotiations with the Board of Directors. However, the effect of the rights may be to discourage a third party from making a partial tender offer or otherwise attempting to obtain a substantial equity position in the equity securities of, or seeking to obtain control of, the Company. To the extent any potential acquirers are deterred by the rights, the rights may have the effect of preserving incumbent management in office.
Our ability to utilize our net operating loss carryforwards and certain other tax attributes may be limited.
Under Section 382 of the Internal Revenue Code of 1986, as amended, if a corporation undergoes an ownership change (generally defined as a greater than 50% change (by value) in the ownership of its equity over a three-year period), the corporation’s ability to use its pre-change net operating loss carryforwards and certain other pre-change tax attributes to offset its post-change income may be limited. We may have experienced such ownership changes in the past, and we may experience ownership changes in the future as a result of shifts in our stock ownership, some of which are outside our control. As of December 31, 2023, we had federal net operating loss carryforwards of approximately $1.4 billion, and our ability to utilize those net operating loss carryforwards could be limited by an ownership change as described above, which could result in increased tax liability to us. In addition, pursuant to the Tax Act, we may not use net operating loss carry-forwards to reduce our taxable income in any year by more than 80%, and we may not carry back any net operating losses to prior years. On March 27, 2020, the Coronavirus Aid, Relief, and Economic Security (CARES) Act was signed by President Trump. Certain provisions of the CARES Act alter the rules regarding net-operating losses for such losses arising in 2018, 2019 and 2020. Such losses may be carried back for five years. We cannot assure you, however, of our ability to utilize these favorable offset rules within the applicable time period. These rules apply regardless of the occurrence of an ownership change.
Certain of our executive officers, directors, principal stockholders and their affiliates maintain the ability to exercise significant influence over our company and all matters submitted to stockholders for approval.
Certain of our executive officers, directors and stockholders own more than 5% of our outstanding common stock and, together with their affiliates and related persons, beneficially own a significant percentage of our capital stock. If these stockholders were to choose to act together, they would be able to influence our management and affairs and the outcome of matters submitted to our stockholders for approval, including the election of directors and any sale, merger, consolidation, or sale of all or substantially all of our assets. This concentration of voting power could delay or prevent an acquisition of our company on terms that other stockholders may desire. In addition, this concentration of ownership might adversely affect the market price of our common stock by:
● | delaying, deferring or preventing a change of control of us; |
● | impeding a merger, consolidation, takeover or other business combination involving us; or |
● | discouraging a potential acquirer from making a tender offer or otherwise attempting to obtain control of us. |
Our internal information technology systems, or those of our third-party CROs, CMOs, or other contractors or consultants, may fail or suffer security breaches, which could result in a material disruption of our drug candidates’ development programs and our commercialization of any products for which we receive regulatory approval.
Despite the implementation of security measures, our internal information technology systems and those of our third-party CROs, CMOs, and other contractors and consultants are vulnerable to damage from computer viruses, unauthorized access, cyber-attacks or cyber-intrusions over the Internet, natural disasters, terrorism, war and telecommunication and electrical failures. Although we have been the targets of cyber-attacks and cyber-intrusions, the impact on our operations and financial condition has not been material. We expect such cybersecurity threats to continue and become involvedmore sophisticated, even more so due to the conflict between Russia and Ukraine. A significant cyber-attack or cyber-intrusion could cause our systems to fail, leakage of confidential information, or business interruption, which could result in securities class action litigationa material disruption of our operations, financial loss, or reputational harm. For example, the loss of clinical trial data for our drug candidates could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. We have invested in protections and monitoring practices of our data and information technology systems to reduce these risks and expect to continue do so as our information technology systems increase in magnitude and complexity. However, there can be no assurance that our efforts and investments will prevent breakdowns or breaches in our systems that could divert management’s attentionadversely affect our business.
Unfavorable global economic conditions could adversely affect our business, financial condition or results of operations.
Our results of operations could be adversely affected by general conditions in the global economy and harm our business.
Likewise, the capital and credit markets may be adversely affected by the conflicts between Russia and Ukraine and Israel and Hamas, the possibility of wider European, Middle Eastern or global conflicts, and the global sanctions imposed in response thereto. Other international events such as trade disputes, separatist movements, leadership changes and political and military conflicts could also adversely affect global financial activity and markets and could negatively affect the U.S. economy. These conditions could result in decreased economic activity, heightened risk of cyberattacks and inflation, as well as impact our ability to raise capital. Additionally, the Federal Reserve Board (FRB) and other major central banks have been consistently removing or reducing monetary accommodation, increasing the risk of recession and also potentially negatively impacting asset values and credit spreads that were boosted by extraordinary monetary stimulus. A severe or prolonged economic downturn could result in a variety of risks to our business, including, weakened demand for our drug candidates and our ability to raise additional capital when needed on acceptable terms, if at all. A weak or declining economy could also strain our suppliers, possibly resulting in supply disruption, or cause our customers to delay making payments for our marketed product and services. We cannot anticipate all of the ways in which the foregoing, and the current economic climate and financial market conditions, could adversely impact our business.
Our employees, principal investigators, CROs, CMOs and consultants may engage in misconduct or other improper activities, including non-compliance with regulatory standards and requirements and insider trading, which could have a material adverse effect on our business.
We are exposed to the risk that our employees, principal investigators, CROs, CMOs, and consultants may engage in fraudulent conduct or other illegal activity. Misconduct by these parties could include intentional failures to comply with FDA regulations, provide accurate information to the FDA, comply with manufacturing standards we have established, comply with federal and state healthcare fraud and abuse laws and regulations, report financial information or data accurately or disclose unauthorized activities to us. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, misconduct, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Activities subject to these laws also involve the improper use of information obtained in the course of clinical trials or creating fraudulent data in our pre-clinical studies or clinical trials, which could result in regulatory sanctions and cause serious harm to our reputation. We have adopted a code of ethics applicable to all of our employees and have implemented a compliance program, but it is not always possible to identify and deter misconduct by employees and other third parties, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to comply with these laws or regulations. In addition, we are subject to the risk that a person could allege such fraud or other misconduct, even if none occurred. If any such actions are instituted against us, regardless of the outcome, our reputation and our business may suffer. If we are not successful in defending ourselves or asserting our rights, those actions could lead to imposition of civil, criminal and administrative penalties, damages, monetary fines, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings, and curtailment of our operations, any of which could adversely affect our ability to operate our business.
We may acquire businesses or drugs, or form strategic alliances, in the future, and we may not realize the benefits of such acquisitions.
We may acquire additional businesses or drugs, form strategic alliances or create joint ventures with third parties that we believe will complement or augment our existing business. If we acquire businesses with promising markets or technologies, we may not be able to realize the benefit of acquiring such businesses if we are unable to successfully integrate them with our existing operations and company culture. We may encounter numerous difficulties in developing, manufacturing and marketing any new products resulting from a strategic alliance or acquisition that delay or prevent us from realizing their expected benefits or enhancing our business. We cannot assure you that, following any such acquisition, we will achieve the expected synergies to justify the transaction.
We may be subject to adverse legislative or regulatory tax changes that could negatively impact our financial condition.
The rules dealing with U.S. federal, state and local income taxation are constantly under review by persons involved in the legislative process and by the IRS and the U.S. Treasury Department. Changes to tax laws (which changes may have retroactive application) could adversely affect our stockholders or us. In recent years, many such changes have been made and changes are likely to continue to occur in the future. We cannot predict whether, when, in what form, or with what effective dates, tax laws, regulations and rulings may be enacted, promulgated or decided, which could result in an increase in our, or our stockholders, tax liability or require changes in the manner in which we operate in order to minimize increases in our tax liability.
On December 22, 2017, legislation commonly referred to as the Tax Act was signed into law and is generally effective after December 31, 2017. The Tax Act makes significant changes to the United States federal income tax rules for taxation of individuals and business entities. Most of the changes applicable to individuals are temporary and apply only to taxable years beginning after December 31, 2017 and before January 1, 2026. For corporations, the Tax Act reduces the top corporate income tax rate to 21% and repeals the corporate alternative minimum tax, limits the deduction for net interest expense, limits the deduction for net operating losses and eliminates net operating loss carrybacks, modifies or repeals many business deductions and credits, shifts the United States toward a more territorial tax system, and imposes new taxes to combat erosion of the U.S. federal income tax base. The Tax Act makes numerous other large and small changes to the federal income tax rules that may affect potential investors and may directly or indirectly affect us. We continue to examine the impact this tax reform legislation may have on our business. However, the effect of the Tax Act on us, whether adverse or favorable, is uncertain, and may not become evident for some period of time. This document does not discuss such legislation or the manner in which it might affect us or purchasers of our common stock. Prospective investors are urged to consult with their legal and tax advisors with respect to the Tax Act and any other regulatory or administrative developments and proposals, and their potential effects on them based on their unique circumstances.
General Risks
Risks Related to Our Common Stock and Being a Publicly Traded Company
Our stock price is, and we expect it to remain, volatile, which could limit investors’ ability to sell stock at a profit.
The trading price of our common stock has been and is likely to continue to be highly volatile and subject to wide fluctuations in price in response to various factors, many of which are beyond our control. These factors include, among others:
● | reception and success of BRIUMVI in the U.S. market; |
● | the anticipated launch of BRIUMVI in European markets; |
● | publicity regarding actual or potential clinical results relating to our product or products under development by our competitors or us; |
● | delay or failure in initiating, completing or analyzing nonclinical or clinical trials or the unsatisfactory design or results of these trials; |
● | achievement or rejection of regulatory approvals by us or our competitors; |
● | any delay in our regulatory review for products and product candidates we may develop, and any adverse development or perceived adverse development with respect to the applicable regulatory authority’s review of such filings, including without limitation a change to the projected approval date, scheduling of an advisory committee meeting or issuance of a “refusal to file” letter; |
● | announcements of technological innovations or new commercial products by our competitors or us; |
● | developments concerning proprietary rights, including patents; |
● | developments concerning our collaborations; |
● | regulatory developments in the United States and foreign countries; |
● | economic or other crises and other external factors such as the disruptions in the global economy caused by the COVID-19 pandemic, the conflict between Russia and Ukraine, and the Israel-Hamas war; |
● | period-to-period fluctuations in our revenues and other results of operations; |
● | failure to meet our revenue projections or guidance; |
● | changes in financial estimates by securities analysts; and |
● | sales of our common stock by us. |
We will not be able to control many of these factors, and we believe that period-to-period comparisons of our financial results will not necessarily be indicative of our future performance.
In addition, the stock market in general, and the market for biotechnology companies in particular, has experienced significantextreme price and volume fluctuations that may have affectedbeen unrelated or disproportionate to the market prices for the common stockoperating performance of biotechnology and pharmaceuticalindividual companies. These broad market fluctuationsand industry factors may causeseriously harm the market price of our common stock, regardless of our operating performance. As a result of this volatility, investors may not be able to sell their common stock at or above the price paid for the shares.
We are subject to risks related to corporate social responsibility and reputational matters.
Our reputation and the reputation of our brands, including the perception held by our customers, end-users, business partners, investors, other key stakeholders and the communities in which we do business are influenced by various factors. There is an increased focus from our stakeholders on Environmental, Social, and Governance (ESG) practices and disclosure - and if we fail, or are perceived to have failed, in any number of ESG matters, such as environmental stewardship, inclusion and diversity, workplace conduct and support for local communities, or if we fail, or are perceived to have failed, to effectively respond to changes in legal or regulatory requirements concerning climate change or other sustainability concerns, our reputation or the reputation of our brands may suffer. Such damage to our reputation and the reputation of our brands may negatively impact our business, financial condition and results of operations. In addition, negative or inaccurate postings or comments on social media or networking websites about the Company or our brands could generate adverse publicity that could damage our reputation or the reputation of our brands. If we are unable to effectively manage real or perceived issues, including concerns about product quality, safety, corporate social responsibility or other matters, sentiments toward the Company or our products could be negatively impacted, and our financial results could suffer.
Because we do not anticipate paying any cash dividends on our capital stock in the foreseeable future, capital appreciation, if any, will likely be the sole source of gain for our stockholders.
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the growth and development of our business. However, any future determination relating to the use of our future earnings, if any, will be made at the discretion of the Board of Directors and will depend on a number of factors, including capital requirements, financial conditions, future prospects, contractual restrictions and covenants and other factors that the Board of Directors may deem relevant. In addition, under the Amended Loan Agreement, as amended, with Hercules, we are currently restricted from paying cash dividends, and we expect these restrictions to continue in the future. Furthermore, the terms of any future debt agreements may continue to preclude us from paying dividends. As a result, capital appreciation, if any, of our common stock will be likely the sole source of gain for our stockholders for the foreseeable future.
An active trading market for our common stock may not be sustained, and investors may not be able to resell their shares at or above the price they paid.
Although we have listed our common stock on the Nasdaq Capital Market, an active trading market for our shares may not be sustained. In the absence of an active trading market for our common stock, investors may not be able to sell their common stock at or above the price at which they acquired their shares or at the time that they would like to sell. An inactive trading market may also impair our ability to raise capital to continue to fund operations by selling shares and may impair our ability to acquire other companies or technologies by using our shares as consideration.
If equity research analysts do not publish research or reports about our business or if they publish negative evaluations of or downgrade our common stock, the price of our common stock could decline.
The trading market for our common stock relies in part on the research and reports that equity research analysts publish about us or our business. We do not control these analysts. If one or more of the analysts covering our business downgrade their evaluations of our common stock, the price of our common stock could decline. If one or more of these analysts cease to cover our common stock, we could lose visibility in the market for our common stock, which in turn could cause our common stock price to decline.
We incur significant increased costs as a result of operating as a public company, and our management is required to devote substantial time to compliance initiatives.
As a public company, we incur significant legal, accounting and other expenses under the Sarbanes-Oxley Act of 2002, as well as rules subsequently implemented by the SEC, and the rules of any stock exchange on which we are listed. These rules impose various requirements on public companies, including requiring establishment and maintenance of effective disclosure and financial controls and appropriate corporate governance practices. Our team has devoted and will continue to devote a substantial amount of time to these compliance initiatives. Moreover, these rules and regulations increase our legal and financial compliance costs and make some activities more time-consuming and costly.
The Sarbanes-Oxley Act of 2002 requires, among other things, that we maintain effective internal control over financial reporting and disclosure controls and procedures. As a result, we are required to periodically perform an evaluation of our internal control over financial reporting to allow management to report on the effectiveness of those controls, as required by Section 404 of the Sarbanes-Oxley Act. Additionally, our independent auditors are required to perform a similar evaluation and report on the effectiveness of our internal control over financial reporting. These efforts to comply with Section 404 will require the commitment of significant financial and managerial resources. While we anticipate maintaining the integrity of our internal control over financial reporting and all other aspects of Section 404, we cannot be certain that a material weakness will not be identified when we test the effectiveness of our control systems in the future. If a material weakness is identified, we could be subject to sanctions or investigations by the SEC or other regulatory authorities, which would require additional financial and management resources, costly litigation or a loss of public confidence in our internal control over financial reporting, which could have an adverse effect on the market price of our stock.
Volatility in the price of our common stock may subject us to securities and shareholder derivative litigation, which could cause us to incur substantial costs and divert management’s attention, financial resources and other company assets.
In the past, securities class action and shareholder derivative litigation has often been brought against a company following a declineperiods of volatility in the market price of its securities. This risk is especially relevant for us because biotechnology and biopharmaceuticalpharmaceutical companies have experienced significant stock price volatility in recent years. WePast lawsuits and any future lawsuits to which we may become involved in this type of litigation in the future. Litigation often isa party are subject to inherent uncertainties and will likely be expensive and divertstime-consuming to investigate, defend, and resolve, and will divert our management’s attention and financial and other resources. The outcome of litigation is necessarily uncertain, and we could be forced to expend significant resources in the defense of these and other suits in which we may not prevail. Any litigation to which we are a party may result in an onerous or unfavorable judgment that may not be reversed upon appeal or in payments of substantial monetary damages or fines, or we may decide to settle this or other lawsuits on similarly unfavorable terms, which could adversely affect our business.
Future sales of our common stock, including by us or our directors and executive officers or shares issued upon the exercise of currently outstanding options, could cause our stock price to decline.
A substantial portion of our outstanding common stock can be traded without restriction at any time. In addition, a portion of our outstanding common stock is currently restricted as a result of federal securities laws but can be sold at any time subject to applicable volume limitations. As such, sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, by us or others, could reduce the market price of our common stock or impair our ability to raise adequate capital through the sale of additional equity securities. In addition, we have a significant number of shares that are subject to outstanding options. The exercise of these options and the subsequent sale of the underlying common stock could cause a further decline in our stock price. These sales also might make it difficult for us to sell equity securities in the future at a time and at a price that we deem appropriate. We cannot predict the number, timing or size of future issuances or the effect, if any, that any future issuances may have on the market price for our common stock.
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
Risk Management and Strategy
We have implemented and maintain various information security processes designed to mitigate risks on a case-by-case basis from cybersecurity threats to our critical computer networks, third party-hosted services, communications systems, hardware and software, and our critical data, including intellectual property, confidential information that is proprietary, strategic or competitive in nature, and data related to patients and clinical trials (IT Assets). The potential consequences of a material cybersecurity incident could include reputational damage, litigation with third parties, regulatory criticism or proceedings and increased cybersecurity protection and remediation costs, which in turn could materially adversely affect our results of operations. The Company’s information security program evaluates threats posed by internal and external factors and supports daily operational functions that prevent unauthorized access or compromise.
Depending on the environment, we implement and maintain various technical, physical, and organizational measures, processes, standards and policies designed to manage and mitigate material risks from cybersecurity threats to our IT Assets, including, for example: implementing policies and guidelines governing the individual use and protection of IT Assets by employees, employee training, and leveraging the capability of third-party service providers to support our internal cybersecurity processes. We will continue to monitor proposed cybersecurity disclosure rules from the SEC and alter our procedures accordingly.
Risks from cybersecurity threats have, to date, not materially affected us, our business strategy, results of operations or financial condition. For a description of the risks from cybersecurity threats that may materially affect us and how they may do so, see our risk factors under Part 1. Item 1A. Risk Factors in this Annual Report on Form 10-K, including the risk factor captioned “Our internal information technology systems, or those of our third-party CROs, CMOs, or other contractors or consultants, may fail or suffer security breaches, which could result in a material disruption of our drug candidates’ development programs and our commercialization of any products for which we receive regulatory approval.”
Governance
Our information technology (IT) team leads the Company’s overall cybersecurity efforts and is responsible for the day-to-day management of risks we face, while our Board of Directors/management provides guidance on the oversight of risk management. Our Information Security Incident Response Plan is designed to escalate cybersecurity incidents, depending on the circumstances, to appropriate stakeholders as defined by internal Standard Operating Procedures. As part of such process, the corporate IT Security Team receives aggregate monthly reports from a third-party managed services organization contracted to monitor the TGTX IT environment. Additionally, the Vice President of IT receives regular reports from the corporate IT Security Team concerning the Company’s significant cybersecurity threats and risks and the processes the Company has implemented to address them. Significant events are reported to the Chief Financial Officer.
We maintain corporate and executive office is locatedspace in New York, New York. Our New York facility consists of leased office space at 2 Gansevoort Street, 9th Floor,Morrisville, North Carolina, New York, New York, 10014.and Edison, New Jersey. We are also currently leasing small office spacesspace in Cary, North Carolina and Kingsport, Tennessee to accommodate our clinical operations groups.Boca Raton, Florida. We believe that our existing facilities are adequate to meet our current requirements. We do not own any real property.
We, and our subsidiaries, are not a purported securities class action complaint was filed in New York federal court againstparty to, and our property is not the Company and certainsubject of, its directors, officers or consultants on behalf of all shareholders who purchased or otherwise acquired TG Therapeutics common stock between September 15, 2014 and October 12, 2016 (the “Class Period”). The case was captioned John Lyon v. TG Therapeutics, Michael S. Weiss, Sean A. Power and Robert Niecestro, Case No. 1:17-cv-00112-VM (S.D.N.Y.). The complaint alleged that, throughout the Class Period various statements made by the Company regarding its GENUINE Phase 3 trial were materially false or misleading when made in violation of the Securities Exchange Act of 1934 and Rule 10b-5 promulgated thereunder. On January 24, 2017, a second purported class action complaint was filed in New York federal court against the Company and certain of its directors, officers or consultants on behalf of all shareholders who purchased or otherwise acquired TG Therapeutics common stock between September 15, 2014 and October 12, 2016. The case was captioned Kenneth C. Wyzgoski v. TG Therapeutics, Michael S. Weiss, Sean A. Power and Robert Niecestro, Case No. 1:17-cv-00508-VM (S.D.N.Y.). The claims and allegations in the Wyzgoski complaint were substantially identical to those in the Lyon case. By order dated March 23, 2017, the court consolidated the Lyon and Wyzgoski cases into one action, captioned In re TG Therapeutics Securities Litigation, Case No. 1:17-cv-00112-VM (S.D.N.Y.), appointed lead plaintiffs in the case, and approved lead plaintiffs’ selection of lead counsel. On April 5, 2017 the Court so ordered a stipulation pursuant to which lead plaintiffs voluntarily dismissed the consolidated action in its entirety without prejudice. The Company denies the allegations and claims made in the above-referenced actions and no consideration was given by the Company in connection with lead plaintiffs’ voluntary dismissal of the consolidated action.
ITEM4. MINE SAFETY DISCLOSURES
DISCLOSURES.
None.
ITEM5. MARKET FOR REGISTRANT’SREGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES.
Market Information
Our common stock is listed on the Nasdaq Capital Market and trades under the symbol “TGTX”.
Fiscal Year Ended December 31, 2017 | High | Low |
| Fourth Quarter | $12.30 | $7.35 |
| Third Quarter | $12.70 | $10.00 |
| Second Quarter | $13.85 | $9.90 |
| First Quarter | $14.45 | $4.20 |
Fiscal Year Ended December 31, 2016 | High | Low |
| Fourth Quarter | $9.33 | $4.65 |
| Third Quarter | $7.98 | $5.49 |
| Second Quarter | $10.23 | $5.97 |
| First Quarter | $11.41 | $7.83 |
Holders
The number of record holders of our common stock as of March 1, 2018February 23, 2024 was 271.
Dividends
We have never declared or paid any cash dividends on our common stock and do not anticipate paying any cash dividends in the foreseeable future. Any future determination to pay dividends will be at the discretion of our board of directors.
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information as of December 31, 2017,2023, regarding the securities authorized for issuance under our equity compensation plan,plans, the TG Therapeutics, Inc. Amended and Restated 2012 Incentive Plan (the 2012 Incentive Plan) and the TG Therapeutics, Inc. 2022 Incentive Plan (the 2022 Incentive Plan). There were no additional shares available to be issued under the 2012 Incentive Plan.
Equity Compensation Plan Information
| | Number of | ||||||||||
| | | securities | |||||||||
| | | remaining | |||||||||
| | | available for | |||||||||
| Number of | | future issuance | |||||||||
| securities to be | | under equity | |||||||||
| issued upon | Weighted-average | compensation | |||||||||
| exercise of | exercise price of | plans (excluding | |||||||||
| outstanding | outstanding | securities reflected | |||||||||
Plan Category | options | options | in column 1) | |||||||||
Equity compensation plans approved by security holders | 4,697,029 | $ | 6.98 | 8,751,892 | ||||||||
Equity compensation plans not approved by security holders | — | — | — | |||||||||
Total | 4,697,029 | $ | 6.98 | 8,751,892 | ||||||||
For information about all of our equity compensation plans see Note 56 to our Consolidated Financial Statements included in this report.
COMMON STOCK PERFORMANCE GRAPH

The following graph compares the cumulative total stockholder return on our common stock for the period from December 31, 2011(1)2018 through December 31, 2017,2023, with the cumulative total return over such period on (i) the U.S. Index of The Nasdaq Stock Market and (ii) the Biotechnology Index of The Nasdaq Stock Market. The graph assumes an investment of $100 on December 31, 2011,2018, in our common stock (at the adjusted closing market price) and in each of the indices listed above, and assumes the reinvestment of all dividends. Measurement points are December 31 of each year.
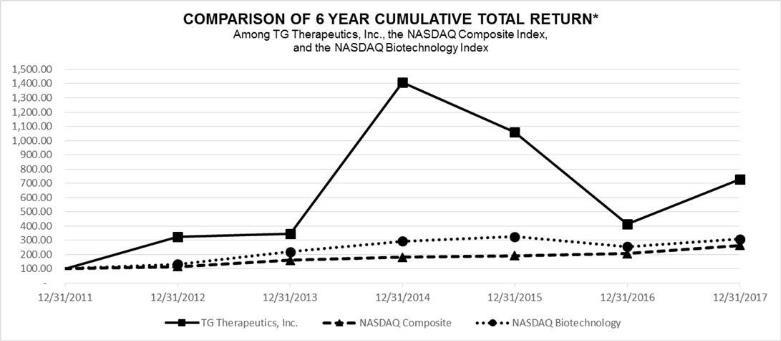
*
ITEM 6. SELECTED FINANCIAL DATAREMOVED AND RESERVED
ITEM7. Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “Item 8. Financial Statements and Supplementary Data.”
Years ended December 31, | |||||
2017 | 2016 | 2015 | 2014 | 2013 | |
License revenue | $152,381 | $152,381 | $152,381 | $152,381 | $152,381 |
| Costs and expenses: | |||||
| Research and development: | |||||
| Noncash stock expense associated with in-licensing agreements | -- | -- | -- | 5,350,094 | -- |
| Noncash compensation | 5,646,716 | 2,742,354 | 4,261,406 | 8,731,566 | 1,041,519 |
Other research and development | 96,886,134 | 66,489,820 | 43,445,817 | 26,004,687 | 12,621,161 |
Total research and development | 102,532,850 | 69,232,174 | 47,707,223 | 40,086,347 | 13,662,680 |
| General and administrative: | |||||
| Noncash compensation | 10,298,568 | 4,767,645 | 11,435,686 | 12,373,726 | 4,161,629 |
Other general and administrative | 6,032,714 | 5,121,690 | 4,189,488 | 3,413,400 | 2,496,461 |
Total general and administrative | 16,331,282 | 9,889,335 | 15,625,174 | 15,787,126 | 6,658,090 |
Impairment of in-process research and development | -- | -- | -- | -- | 2,797,600 |
Total costs and expenses | 118,864,132 | 79,121,509 | 63,332,397 | 55,873,473 | 23,118,370 |
Operating loss | (118,711,751) | (78,969,128) | (63,180,016) | (55,721,092) | (22,965,989) |
| Other (income) expense: | |||||
| Interest income | (294,478) | (323,032) | (174,653) | (55,049) | (30,822) |
Other (income) expense | 58,739 | (393,202) | (56,717) | 115,234 | (2,456,957) |
Total other (income) expense, net | (235,739) | (716,234) | (231,370) | 60,185 | (2,487,779) |
| Net loss | $(118,476,012) | $(78,252,894) | $(62,948,646) | $(55,781,277) | $(20,478,210) |
| Basic and diluted net loss per common share | $(1.91) | $(1.60) | $(1.38) | $(1.64) | $(0.81) |
December 31, | |||||
2017 | 2016 | 2015 | 2014 | 2013 | |
| Cash, cash equivalents, investment securities and interest receivable | $84,825,125 | $44,968,992 | $102,416,894 | $78,861,334 | $45,431,532 |
| Total assets | 97,381,535 | 54,781,547 | 113,473,201 | 86,746,890 | 48,112,390 |
| Accumulated deficit | (354,862,832) | (236,386,820) | (158,133,926) | (95,185,280) | (39,404,003) |
| Total equity | 66,993,055 | 35,867,802 | 101,573,302 | 80,101,884 | 40,054,492 |
The following discussion and analysis contains forward-looking statements about our plans and expectations of what may happen in the future. Forward-looking statements are based on a number of assumptions and estimates that are inherently subject to significant risks and uncertainties, and our results could differ materially from the results anticipated by our forward-looking statements as a result of many known or unknown factors, including, but not limited to, those factors discussed in “Item 1A. Risk“Risk Factors.” See also the “Special Cautionary Notice Regarding Forward-Looking Statements” set forth at the beginning of this report.
You should read the following discussion and analysis in conjunction with “Item 8. Financial Statements and Supplementary Data,” and our consolidated financial statements beginning on page F-1 of this report.
Overview
TG Therapeutics is a fully-integrated, commercial stage, biopharmaceutical company focused on the acquisition, development and commercialization of novel treatments for B-cell malignancies and autoimmune diseases. Currently,In addition to a research pipeline including several investigational medicines, TG has received approval from the Company is developing two therapies targeting hematological malignancies. TG-1101 (ublituximab) is a novel, glycoengineered monoclonal antibody that targets a unique epitope onFDA for BRIUMVI (ublituximab-xiiy) for the CD20 antigen found on mature B-lymphocytes. We are also developing TGR-1202, an orally available PI3K delta inhibitor. The delta isoformtreatment of PI3K is strongly expressed in cells of hematopoietic origin and is believed to be important in the proliferation and survival of B-lymphocytes. Both TG-1101 and TGR-1202 are in clinical development foradult patients with hematologic malignancies. We also have pre-clinical programs seekingRMS, to develop IRAK4 (interleukin-1 receptor-associated kinase 4) inhibitors, BET (Bromodomaininclude clinically isolated syndrome, relapsing-remitting disease, and Extra Terminal) inhibitors, and anti-PD-L1 and anti-GITR antibodies.
On February 5, 2021, we have not receivedannounced that the FDA granted accelerated approval of umbralisib, the Company’s PI3K delta inhibitor, then commercially referred to as UKONIQ, for the treatment of adult patients with relapsed or refractory MZL who have received at least one prior anti-CD20 based regimen and adult patients with relapsed or refractory FL who have received at least three prior lines of systemic therapy. On April 15, 2022, we announced the voluntary withdrawal of UKONIQ from sale for the approved indications. During the year ended December 31, 2023, our only sources of anyproduct revenues were from the sales of BRIUMVI. Product revenues are recorded net of estimates of variable consideration. For further discussion of our drug candidates in any marketrevenue recognition policy, see “Critical Accounting Policies and Significant Judgements and Estimates” below.
Cost of revenue consists primarily of materials and third-party manufacturing costs, as well as freight and royalties owed to our licensing partner for BRIUMVI sales. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, a portion of the manufacturing costs of BRIUMVI units recognized as revenue during the year ended December 31, 2023 were expensed prior to receipt of FDA approval on December 28, 2022, and therefore haveare not generated anyincluded in costs of product sales from our drug candidates.
Our license revenues currently consist of license fees arising from our agreement with Ildong. We recognize upfront license fee revenues ratably over the estimated period in which we will have certain significant ongoing responsibilities under the sublicense agreement, with unamortized amounts recorded as deferred revenue.
The following table sets forth the research and development expenses per project, exclusive of non-cashnoncash compensation expenses, for the periods presented.
(in thousands) | 2023 | 2022 | 2021 | |||||||||
Ublituximab | $ | 50,972 | $ | 59,307 | $ | 112,522 | ||||||
Umbralisib | 5,925 | 38,468 | 63,033 | |||||||||
Early Clinical Pipeline & Pre-Clinical | 6,285 | 14,353 | 22,977 | |||||||||
Total | $ | 63,182 | $ | 112,128 | $ | 198,532 | ||||||
2017 | 2016 | 2015 | |
| TG-1101 | $62,441,133 | $40,839,899 | $29,816,042 |
| TGR-1202 | 31,963,775 | 21,394,427 | 11,671,889 |
Pre-clinical assets / Other | 2,481,226 | 4,255,494 | 1,957,886 |
| Total | $96,886,134 | $66,489,820 | $43,445,817 |
Our selling, general and administrative expenses consist primarily of expenses related to the commercial launch of our products, including salaries and related expenses for our commercialization team and commercial development activities. Other selling, general and administrative expenses consist of executive, finance and other administrative personnel, recruitment expenses, professional fees and other corporate expenses, including investor relations, legal activities and facilities-related expenses such as rent expense and amortization of leasehold interest.
Our results of operations include non-cashnoncash compensation expenses as a result of the grants of restricted stock options and restricted stock.stock options. Compensation expense for awards of optionsrestricted stock and restricted stock options granted to employees and directors represents the fair value of the award recorded over the respective vesting periods of the individual awards. The expense is included in the respective categories of expense in the consolidated statements of operations. We expect to continue to incur significant non-cashnoncash compensation expenses.
We recognize all share-based payments to employees and restricted stock to consultants and other third-parties,non-employee directors (as compensation for service) as noncash compensation expense is determined atin the “measurement date.” The expense is recognized over the vesting period of the award. Until the measurement date is reached, the total amount of compensation expense remains uncertain. We record compensation expenseconsolidated financial statements based on the fair values of such payments. Stock-based compensation expense recognized each period is based on the value of the awardportion of share-based payment awards that is ultimately expected to vest during the period. Forfeitures are estimated at the reporting date. The awards to consultants and other third-parties are then revalued, or the total compensation is recalculated based on the then current fair value, at each subsequent reporting date. This results in a change to the amount previously recorded in respecttime of the equity award grant and additional expense or a reversal of expense may be recordedrevised, if necessary, in subsequent periods based on changes in the assumptions used to calculate fair value, such as changes in market price, until the measurement date is reached and the compensation expense is finalized.
RESULTS OF OPERATIONS
Comparison of the Years Ended December 31, 2017, 20162023 and 2015
| Years Ended December 31, | |||
2017 | 2016 | 2015 | |
License revenue | $152,381 | $152,381 | $152,381 |
| Costs and expenses: | |||
| Research and development: | |||
| Noncash compensation | 5,646,716 | 2,742,354 | 4,261,406 |
Other research and development | 96,886,134 | 66,489,820 | 43,445,817 |
Total research and development | 102,532,850 | 69,232,174 | 47,707,223 |
| General and administrative: | |||
| Noncash compensation | 10,298,568 | 4,767,645 | 11,435,686 |
Other general and administrative | 6,032,714 | 5,121,690 | 4,189,488 |
Total general and administrative | 16,331,282 | 9,889,335 | 15,625,174 |
Total costs and expenses | 118,864,132 | 79,121,509 | 63,332,397 |
| Operating loss | (118,711,751) | (78,969,128) | (63,180,016) |
Other income, net | (235,739) | (716,234) | (231,370) |
Net loss | $(118,476,012) | $(78,252,894) | $(62,948,646) |
The following table summarizes the results of operations for each of the years ended December 31, 20172023 and 2016.2022:
(in thousands) | 2023 | 2022 | ||||||
Product revenue, net | $ | 92,005 | $ | 2,633 | ||||
License, milestone and other revenue | 141,657 | 152 | ||||||
Total Revenue | $ | 233,662 | $ | 2,785 | ||||
Costs and expenses: | ||||||||
Cost of revenue | 14,131 | 265 | ||||||
Research and development: | ||||||||
Noncash compensation | 13,010 | 13,224 | ||||||
Other research and development | 63,182 | 112,128 | ||||||
Total research and development | 76,192 | 125,352 | ||||||
Selling, General and administrative: | ||||||||
Noncash compensation | 24,923 | 5,961 | ||||||
Other selling, general and administrative | 97,783 | 64,046 | ||||||
Total selling, general and administrative | 122,706 | 70,007 | ||||||
Total costs and expenses | 213,029 | 195,624 | ||||||
Interest expense | 12,615 | 10,191 | ||||||
Other income | (5,044 | ) | (4,695 | ) | ||||
Total other expense, net | 7,571 | 5,496 | ||||||
Net income (loss) before taxes | 13,062 | (198,335 | ) | |||||
Income taxes | 390 | |||||||
Net income (loss) | $ | 12,672 | $ | (198,335 | ) | |||
Product Revenue, net. Product revenue, net increased for the year ended December 31, 2023 compared to the comparable period ended December 31, 2022 primarily due to an increase in net product revenues from sales of our sole commercial product, BRIUMVI, which was commercially launched in the U.S. in January 2023, following FDA approval. Product revenue, net for the year ended December 31, 2022, consisted of net product sales of UKONIQ, which was officially withdrawn from the market in May 2022.
License Revenue. License revenue was $140.2 million and $0.2 million for the years ended December 31, 2023 and December 31, 2022, respectively. License revenue for the year ended December 31, 2023 is related topredominantly comprised of recognition of license revenue from the amortization of anone-time $140.0 million non-refundable upfront payment recognized in the third quarter of $2.0 million associated2023 as part of the Commercialization Agreement with our license agreement with Ildong. TheNeuraxpharm (see Note 2 for more information). License revenue for the year ended December 31, 2022 is comprised of recognition of a portion of the upfront payment from Ildong will bethe ublituximab sublicense agreement with Ildong.
Other Revenue. Other revenue was $1.5 million and zero for the year ended December 31, 2023 and December 31, 2022, respectively. Other revenue for the year ended December 31, 2023 is comprised of consideration received for development and regulatory activities performed on behalf of Neuraxpharm in accordance with the Commercialization Agreement.
Cost of Revenue. Cost of revenue for the year ended December 31, 2023 increased compared to the comparable period ended December 31, 2022 due to increased product sales resulting from the commercial launch of BRIUMVI in the U.S. market which began in January 2023 following FDA approval. During the year ended December 31, 2023 the cost of revenue consisted primarily of third-party manufacturing, distribution, overhead costs and royalties on net sales of BRIUMVI owed to our licensing partner. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, a portion of the manufacturing costs of BRIUMVI units recognized as license revenue on a straight-line basisduring the year ended December 31, 2023 were expensed as research and development expenses prior to receipt of FDA approval, and therefore are not reflected in the cost of revenue. We expect the cost of revenue for BRIUMVI to increase in relation to product revenues as we deplete these inventories and we expect to use the remaining pre-commercialization inventory for product sales through Decemberthe first half of 2025 which represents the estimated period over which the Company will have certain ongoing responsibilities under the sublicense agreement.
Noncash Compensation Expense (Research and Development).
Noncash compensation expense (research and development) related to equity incentive grants totaledOther Research and Development Expense. Other research and development expense decreased for the year ended December 31, 2023, by approximately $48.9 million to $63.2 million as compared to the prior year ended December 31, 2022. The decrease in other research and development expense during the year ended December 31, 2023 was primarily attributable to reduced manufacturing expense, a decrease in license milestones and reduced clinical trial related expenses. Prior to the approval of BRIUMVI, manufacturing costs pertaining to BRIUMVI were expensed to research and development expense in the period incurred, and following approval are reflected in inventory.
Noncash Compensation Expense (Selling, General and Administrative). Noncash compensation expense (selling, general and administrative) related to equity incentive grants totaled $24.0 million for the year ended December 31, 2023, as compared to $6.0 million during the comparable period in 2022. The increase in noncash compensation expense was primarily relateddue to milestone-based vesting of restricted stockmilestone-based grants to personnel and an increasea decrease in the measurement date fair value of certain consultant restricted stockforfeitures during the year ended December 31, 2017.
Other ResearchSelling, General and Development Expenses
Interest Expense. Interest expense for the year ended December 31, 2023 was $12.6 million compared to $10.2 million for the comparable period ended December 31, 2022. The $2.4 million increase is mainly due to greater interest expense related to First Amendment to the Amended Loan Agreement
Other Income. Other income increased by $0.3 million to $5.0 million for the year ended December 31, 20162023, as compared to $96.9$4.7 million for the year ended December 31, 2017. The increase in other research and development expenses was due primarily to new and ongoing clinical development programs and related manufacturing costs for TG-1101 and TGR-1202 during the year ended December 31, 2017. We expect our other research and development costs to remain relatively consistent during 2018 as our UNITY-CLL program winds down and our MS Phase 3 program ramps up.
Income Taxes. Income tax increased by $5.5$0.4 million from $4.8to $0.4 million for the year ended December 31, 20162023, as compared to $10.3zero for the year ended December 31, 2022. The $0.4 million increase is due to state tax liabilities incurred during the year ended December 31, 2017. 2023.
Comparison of the Years Ended December 31, 2022 and 2021
The increasefollowing table summarizes the results of operations for the years ended December 31, 2022 and 2021:
(in thousands) | 2022 | 2021 | ||||||
Product revenue, net | $ | 2,633 | $ | 6,537 | ||||
License revenue | 152 | 152 | ||||||
Total Revenue | $ | 2,785 | $ | 6,689 | ||||
Costs and expenses: | ||||||||
Cost of product revenue | 265 | 790 | ||||||
Research and development: | ||||||||
Noncash compensation | 13,224 | 24,047 | ||||||
Other research and development | 112,128 | 198,532 | ||||||
Total research and development | 125,352 | 222,579 | ||||||
General and administrative: | ||||||||
Noncash compensation | 5,961 | 37,227 | ||||||
Other selling, general and administrative | 64,046 | 90,863 | ||||||
Total general and administrative | 70,007 | 128,090 | ||||||
Total costs and expenses | 195,624 | 351,459 | ||||||
Interest expense | 10,191 | 5,638 | ||||||
Other income | (4,695 | ) | (2,307 | ) | ||||
Total other expense, net | 5,496 | 3,331 | ||||||
Net Loss | $ | (198,335 | ) | $ | (348,101 | ) | ||
Revenues. Total revenue for the year ended December 31, 2022 decreased compared to the comparable period ended December 31, 2021 due to a decrease in noncash compensationnet product revenues resulting from the voluntary withdrawal from the U.S. market of our sole commercial product, UKONIQ.
Cost of Product Revenue. Cost of product revenue for the year ended December 31, 2022 decreased compared to the comparable period ended December 31, 2021 due to the stoppage of product sales resulting from the withdrawal from the U.S. market of our sole commercial product UKONIQ. During the year ended December 31, 2022 the cost of product revenue consists primarily of freight and royalties on net sales of UKONIQ owed to our licensing partner. Based on our policy to expense was primarily relatedcosts associated with the manufacture of our products prior to greater compensation expenseregulatory approval, the manufacturing costs of UKONIQ units recognized as revenue during the year ended December 31, 2017 related2022 were expensed as research and development expenses prior to restricted stock granted to executive personnel.
Noncash Compensation Expense (Research and Development).
Noncash compensation expense (research and development) related to equity incentive grants totaledOther Research and Development Expenses
Noncash Compensation Expense (Selling, General and Administrative). Noncash compensation expense (selling, general and administrative) related to equity incentive grants totaled $6.0 million for the year ended December 31, 20152022, as compared to $66.5 million for the year ended December 31, 2016. The increase in other research and development expenses was due primarily to a $1.0 million licensing fee for the Jubilant sub-license agreement, as well as the ongoing clinical development programs and related manufacturing costs for TG-1101 and TGR-1202 during the year ended December 31, 2016. We expect our other research and development costs to increase modestly during 2017 as enrollment of additional patients in our Phase 3 clinical trials increases and we prepare for a commercial launch.
Other Selling, General and Administrative Expenses
Interest Expense. Interest expense for the year ended December 31, 2022 was $10.2 million compared to $5.6 million for the comparable period ended December 31, 2021. The $4.6 million increase is mainly due to greater interest expense related to the Amended Loan Agreement entered into in December 2021.
Other Income.Other income increased by $0.9$2.4 million from $4.2to $4.7 million for the year ended December 31, 20152022, as compared to $5.1$2.3 million for the year ended December 31, 2016. The increase was due primarily to the straight-line rent expense of our new office space, as well as increased personnel and other general and administrative costs. We expect our other general and administrative expenses to increase modestly during 2017.
LIQUIDITY AND CAPITAL RESOURCES
Historically, we have incurred operating losses since our inception; however, the Company experienced a net profit during the twelve months ended December 31, 2023 due to a $140.0 million non-refundable upfront payment recognized as license revenue in the third quarter of 2023 as part of our Commercialization Agreement with Neuraxpharm (see Note 2 for more information). We expect to continue to incur operating losses in the near term and may never become profitable. As of December 31, 2023, we have an accumulated deficit of $1.5 billion.
Our primarymajor sources of cash have been proceeds from the saleprivate placements and public offerings of equity securities, from our loan and security agreements executed with Hercules (see Note 7 for more information), and the upfront payment from the Commercialization Agreement (see Note 2 for more information). Substantially all our Sublicense Agreementoperating losses have resulted from costs incurred in connection with Ildong,our research and warrantdevelopment programs and option exercises. We have not yet commercialized anyfrom selling, general and administrative costs associated with our operations, including our commercialization activities. As of December 31 2023, we had generated $92.0 million in product revenue from sales of BRIUMVI. BRIUMVI first became commercially available in the United States in January of 2023. Even with the commercialization of BRIUMVI and the possible future commercialization of our drug candidates and cannot be sure if we will ever be able to do so. Even if we commercialize one or more of ourother drug candidates, we may not become profitable. Our ability to achieve profitability depends on a number ofour ability to generate revenue and many other factors, including our ability to obtain regulatory approval for our drug candidates, successfully complete any post-approval regulatory obligations and successfully commercialize our drug candidates alone or in partnership.partnership; successfully complete any post-approval regulatory obligations and our ability to maintain or obtain regulatory approval for our drug candidates. We may continue to incur substantial operating losses even ifnow that we begin to generateare generating revenues from our drug candidates.
As of December 31, 2017,2023, we had $84.8$217.5 million in cash and cash equivalents, and investment securities, and interest receivable. Subsequent to the year ended December 31, 2017, we sold a total of approximately 2.9 million shares of common stock under the 2017 At-the-Market Issuance Sales Agreement (the “2017 ATM”) for aggregate net proceeds of approximately $35.3 million.
Discussion of Cash Flows
The following table summarizes our cash flows for the years ended December 31, 2023 and 2022:
(in thousands) | 2023 | 2022 | ||||||
Net cash used in operating activities | $ | (31,413 | ) | $ | (176,170 | ) | ||
Net cash used in investing activities | $ | (50,651 | ) | $ | (20,013 | ) | ||
Net cash provided by (used in) financing activities | $ | 72,705 | $ | (391 | ) | |||
Cash used in operating activities for the year ended December 31, 20172023 was $93.8$31.4 million as compared to $61.6$176.2 million for the year ended December 31, 2016.2022. The increasedecrease in cash used in operating activities was due primarily to increased expenditures associated with our clinical development programs for TG-1101 and TGR-1202.the one-time upfront payment of $140.0 million from Neuraxpharm, as part of the Commercialization Agreement during the year ended December 31, 2023.
For the year ended December 31, 2017,2023, net cash used in investing activities was $8.2$50.7 million as compared to cash provided by investing activities of $26.5$20.0 million for the year ended December 31, 2016.2022. The decreaseincrease in net cash provided byused in investing activities was primarily due to investmentsgreater investment in short-term securities during the year ended December 31, 2017.
For the year ended December 31, 2017,2023, net cash provided by financing activities was $72.7 million as compared to net cash used in financing activities of $133.7$0.4 million related to proceeds from our March 2017 offering and our program under an At-the-Market Issuance Sales Agreement (the “ATM Program”), as well as proceeds from the exercise of warrants. Forfor the year ended December 31, 2016,2022. The increase in net cash provided by financing activities of $5.0 million relatedwas primarily attributable to our program under the ATM Program”), as well asproceeds from debt financings and net proceeds from the exerciseissuance of warrants.
ATM Program
On June 21, 2013,September 5, 2019, we filed an automatic “shelf registration” statement on Form S-3 (the 2019 WKSI Shelf) as a “well-known seasoned issuer” as defined in Rule 405 under the Securities Act, which registered an unlimited and indeterminate amount of debt or equity securities for future issuance and sale. The 2019 WKSI Shelf was declared effective in September 2019. In connection with the 2019 WKSI Shelf, we entered into an At-the-Market Issuance Sales Agreement (the ”2013 ATM”)2020 ATM) with MLVJefferies LLC, Cantor Fitzgerald & Co. LLC (“MLV”) under which we could issue and sellB. Riley Securities, Inc. (each a 2020 Agent and collectively, the 2020 Agents), relating to the sale of shares of our common stock, having aggregate offering proceeds of up to $50.0 million, from time to time through MLV, acting as the sales agent.stock. Under the agreement we would pay MLV a commission rate of up to 3.0% of the gross proceeds from the sale of any shares of common stock sold through MLV.
During the year ended December 31, 2021, we sold a total of 72,000 shares of common stock under the 2021 ATM for aggregate total gross proceeds of approximately $2.5 million at an average selling price of $34.25 per share, resulting in net proceeds of approximately $2.4 million after deducting commissions and other transactions costs.
On September 2, 2022, we filed an automatic “shelf registration” statement on Form S-3 (the 2022 WKSI Shelf) as a “well-known seasoned issuer” as defined in Rule 405 under the Securities Act, which registered an unlimited and indeterminate amount of debt or equity securities for future issuance and sale. The 2022 WKSI Shelf was declared effective in September 2022. In connection with the 2022 WKSI Shelf, we entered into an At-the-Market Issuance Sales Agreement (the 2022 ATM) with Cantor Fitzgerald & Co., FBR Capital Markets & Co., SunTrust Robinson Humphrey, and B. Riley Securities, Inc., Raymond James & Associates, Inc., Ladenburg Thalmann & Co. Inc. and H.C. Wainwright & Co., LLC (each a "2017 Agent"2022 Agent and collectively, the "2017 Agents")2022 Agents), relating to the sale of shares of our common stock. Under the 20172022 ATM, we will pay the 20172022 Agents a commission rate of up to 3.0% of the gross proceeds from the sale of any shares of common stock.
During the year ended December 31, 2017,2023, we sold a total of 4,689,4181,385,700 shares of common stock under the 20172022 ATM for aggregate total gross proceeds of approximately $47.7$47.1 million at an average selling price of $10.18$34.01 per share, resulting in net proceeds of approximately $46.9$46.3 million after deducting commissions and other transactions costs.
The 2022 WKSI Shelf is currently our only active shelf registration statement. We may offer any combination of the securities registered under the 2022 WKSI Shelf from time to time in response to market conditions or other circumstances if we believe such a plan of financing is in the best interests of our stockholders. We may need to file additional shelf registration statements in the future to provide us with the flexibility to raise additional capital to finance our operations as needed.
Debt Financings
On February 28, 2019 (the Closing Date), we entered into a term loan facility of up to $60.0 million (Term Loan) with Hercules Capital, Inc. (Hercules), the proceeds of which were used for research and development programs and for general corporate purposes. The Term Loan is governed by a loan and security agreement, dated February 28, 2019 (the Loan Agreement), which provides for up to four separate advances. The first advance of $30.0 million was drawn on the Closing Date. An additional $30.0 million was available with different milestones and time points that have lapsed.
On December 30, 2021 (the First Amendment Closing Date), the Company entered into an Amended and Restated Loan and Security Agreement (the Amended Loan Agreement) with Hercules Capital, Inc. The Amended Loan Agreement amended the terms of the Loan Agreement to, among other things, (i) increase the aggregate principal amount of the loan, available at the Company’s option, from $60.0 million to $200.0 million (the Amended Term Loan), (ii) issue a first advance of $70.0 million drawn at the First Amendment Closing Date, a portion of which was used to refinance the current outstanding loan balance of approximately $7.8 million and pay for expenses incurred by the Lender in executing the agreements, (iii) change the draw amounts and dates available in Tranche 2 through Tranche 4 including increasing the amount available under Tranche 2 subject to the achievement of performance milestones from $10.0 million to $20.0 million, increasing the amount available under Tranche 3 subject to the achievement of performance milestones from $10.0 million to $45.0 million, and increasing the amount under Tranche 4 subject to the approval of Hercules’ investment committee from $10.0 million to $65.0 million, (iv) extend the maturity date of the facility from the original March 1, 2022 to January 1, 2026, (v) reset and extend the interest only period from April 1, 2021 to February 1, 2025 and extendable to August 1, 2025 subject to the achievement of certain performance milestones, and (vi) modify the cash interest rate to be the greater of either (a) the “prime rate” as reported in The Wall Street Journal plus 2.15%, and (b) 5.40%. The performance milestones are based on achievement of certain U.S. Food and Drug Administration approvals and impact the potential extension of the interest only period, access to future advances under the Loan Agreement and minimum cash levels required under the Amended Loan Agreement.
On March 31, 2023 (the First Amendment Effective Date), the Company entered into a First Amendment to the Amended and Restated Loan and Security Agreement (the First Amendment) with Hercules. The First Amendment amended the terms of the Amended Loan Agreement to, among other things, (i) issue an advance of $25.0 million drawn at the First Amendment Effective Date (the Tranche 3A Advance), (ii) provide for the formal expiration of Tranche 2, (iii) change the draw amounts and dates available under subsequent tranches, including splitting the remaining balance of Tranche 3 into two additional advances in an aggregate principal amount of up to $20.0 million, in increments of $10.0 million (a Tranche 3B Advance and a Tranche 3C Advance), decreasing the amount available under Tranche 4 from $65.0 million to $60.0 million, and adding a Tranche 5 of $25.0 million, subject to the achievement of revenue related performance milestones, (iv) extend the interest only period from February 1, 2025 to August 1, 2025 and (v) modify the cash interest rate to be the greater of either (a) the “prime rate” as reported in The Wall Street Journal plus 1.20%, and (b) 8.95%. In addition to the cash interest rate, the principal balance will accrue paid-in-kind interest at a rate of 2.25%, which amount will be capitalized and added to the outstanding principal balance of the Amended Term Loan and payable at the maturity date of the Amended Loan Agreement, as amended, The Amended Loan Agreement, as amended, contains financial covenants that require the Company to maintain certain levels of unrestricted cash and additional financial covenants related to market capitalization. As of December 31, 2017,2023, we sold an aggregateare in compliance with all financial covenants.
The Amended Loan Agreement, as amended also contains warrant coverage of 2,889,3442.95% of the total amount funded. A warrant (the Warrant) was issued by the Company to Hercules to purchase 115,042 shares of common stock pursuant to the 2017 ATM for total gross proceeds of approximately $35.9 million atwith an average sellingexercise price of $12.42 per share, resulting in$17.95 for the initial amount funded at the Closing Date. The Warrant shall be exercisable for seven years from the date of issuance. Hercules may exercise the Warrant either by (a) cash or check or (b) through a net proceeds of approximately $35.3 million after deducting commissions and other transactions costs.
In addition, the Company is required to pay a final payment fee equal to 5.95% of the aggregate principal amount of the Term Loan Advances (as defined in the Amended Loan Agreement, as amended)
The Company may, at its option, prepay the Amended Term Loan in full or in part, subject to a prepayment penalty equal to (i) 1.5% of the principal amount prepaid if the prepayment occurs prior to the first anniversary of the First Amendment Effective Date, and (ii) 1.0% of the principal amount prepaid if the prepayment occurs on or after the first anniversary of the First Amendment Effective Date.
Leases
In October 2014, we entered into an agreement (the Office Agreement) with Fortress Biotech, Inc. (FBIO) to occupy approximately 45% of the 24,000 square feet of New York City office space leased by FBIO. The Office Agreement requires us to pay our respective share of the average annual rent and other costs of the 15-year lease. We approximate an average annual rental obligation of $1.8 million under the Office Agreement. We began to occupy this offering, includingnew space in April 2016, with rental payments beginning in the overallotment option, werethird quarter of 2016. Also in connection with this lease, we have pledged $1.3 million to secure a line of credit as a security deposit for the Office Agreement, which has been recorded as restricted cash in the accompanying condensed consolidated balance sheets.
Total rental expense was approximately $54$2.2 million, net$2.7 million and $2.2 million for the years ended December 31, 2023, 2022 and 2021, respectively.
Future minimum lease commitments as of underwriting discountsDecember 31, 2023 total, in the aggregate, approximately $15.0 million through December 31, 2032. Our future minimum lease commitments include our office leases in New York, New Jersey and offering expensesNorth Carolina as of approximately $3.6 million.
OFF-BALANCE SHEET ARRANGEMENTS
We have not entered into any transactions with unconsolidated entities whereby we have financial guarantees, subordinated retained interests, derivative instruments or other contingent arrangements that expose us to material continuing risks, contingent liabilities, or any other obligations under a variable interest in an unconsolidated entity that provides us with financing, liquidity, market risk or credit risk support.
Payment due by period | |||||
Total | Less than 1 year | 1-3 years | 3-5 years | More than 5 years | |
| Contractual obligations | |||||
Operating leases | $15,592,733 | $1,081,927 | $2,084,258 | $2,154,566 | $10,271,981 |
| Total | $15,592,733 | $1,081,927 | $2,084,258 | $2,154,566 | $10,271,981 |
CRITICAL ACCOUNTING POLICIES
The discussion and analysis of our financial condition and results of operations isare based upon our consolidated financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amount of assets and liabilities and related disclosure of contingent assets and liabilities at the date of our financial statements and the reported amounts of revenues and expenses during the applicable period. Actual results may differ from these estimates under different assumptions or conditions.
We define critical accounting policies as those that are reflective of significant judgments and uncertainties and which may potentially result in materially different results under different assumptions and conditions. In applying these critical accounting policies, our management uses its judgment to determine the appropriate assumptions to be used in making certain estimates. These estimates are subject to an inherent degree of uncertainty. Our critical accounting policies include the following:
Revenue Recognition
.At contract inception, we assess the goods or services renderedpromised within each contract and assess whether each promised good or service is distinct and determine those that represent the culmination of a separate earnings process and no furtherare performance obligation exists under the contract.obligations. We then recognize milestone payments as revenue upon the achievement of specified milestones only if (1) the milestone payment is non-refundable, (2) substantive effort is involved in achieving the milestone, (3) the amount of the milestonetransaction price that is reasonable in relationallocated to the effort expended orrespective performance obligation when the risk associated with achievementperformance obligation is satisfied.
Product Revenue, Net – The Company recognizes product revenues, net of variable consideration related to certain allowances and accruals, when the customer takes control of the product, which is typically upon delivery to the customer. Product revenue is recorded at the net sales price, or transaction price. The Company records product revenue reserves, which are classified as a reduction in product revenues, to account for the components of variable consideration. Variable consideration includes the following components, which are described below: chargebacks, government rebates, trade discounts and allowances, product returns, and co-payment assistance.
These reserves are based on estimates of the amounts earned or to be claimed on the related sales and are classified as reductions of accounts receivable (if the amount is expected to be settled with a credit against the Company's customer account) or a liability (if the amount is expected to be settled with a cash payment). The Company's estimates of reserves established for variable consideration are calculated based upon a consistent application of the expected value method, which is the sum of probability-weighted amounts in a range of possible consideration amounts. These estimates reflect the Company's current contractual and statutory requirements, specific known market events and trends, industry data, and forecasted customer buying and payment patterns. The amount of variable consideration that is included in the transaction price may be subject to constraint and is included in net product revenues only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will not occur in a future period. Actual amounts of consideration received may ultimately differ from the Company's estimates. If actual results vary, the Company adjusts these estimates, which could have an effect on earnings in the period of adjustment. For a complete discussion of the accounting for product revenue, see Note 1 – Organization and Summary of Significant Accounting Policies in the Notes to Consolidated Financial Statements.
License Revenue - Revenue recognized from license agreements will include royalties on sales, upfront, milestone and (4)other payments, if any, under any current or future licensing agreements, including revenues related to the milestone is at risksupply of our drug candidates or approved drugs to our various licensing partners under these types of contracts. For a complete discussion of the accounting for both parties. If anylicense revenue, see Note 1 – Organization and Summary of these conditions are not met, we deferSignificant Accounting Policies in the milestone payment and recognize it as revenue over the estimated period of performance under the contract.
Stock Compensation
. We have granted stock options and restricted stock to employees, directors and consultants, as well as warrants to other third parties. For employee, director andAccrued Research and Development
● | fees paid to contract research organizations (CROs) in connection with clinical studies; |
● | fees paid to contract manufacturing organizations (CMOs); |
● | fees paid to trial sites in connection with clinical studies; and |
● | fees paid to vendors associated with licenses/milestones. |
We base our expenses related to clinical research organizations, or CROs, and clinical site costs. We analyzestudies on our estimates of the progress of clinical trials, including levels of patient enrollment, invoicesservices received and contracted costs when evaluating the adequacy of the amount expensedefforts expended pursuant to contracts with multiple CROs that conduct and the related prepaid asset and accrued liability. Significant judgments and estimates must be made and used in determining the accrued balance and expense in any accounting period. We review and accrue CRO expenses andmanage clinical trial study expenses basedstudies on work performed and rely upon estimates of those costs applicable to the stage of completion of a study. Accrued CRO costs are subject to revisions as such trials progress to completion. Revisions are charged to expense in the period in which the facts that give rise to the revision become known. With respect to clinical site costs, theour behalf. The financial terms of these agreements are subject to an initial negotiation, and vary from contract to contract.contract and may result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the clinical expense. Payments under some of these contracts may be uneven, and depend on factors such as the achievementsuccessful enrollment of certain events, the successful recruitment of patients and the completion of portionsclinical trial milestones. In accruing certain service fees, we estimate the time period over which services will be performed, enrollment of patients, number of sites activated and the level of effort to be expended in each period. If the actual timing of the clinical trialperformance of services or similar conditions. The objectivethe level of effort varies from our policy isestimate, we adjust the accrual or prepaid accordingly. Although we do not expect our estimates to matchbe materially different from amounts actually incurred, our understanding of the recordingstatus and timing of expenses in our financial statementsservices performed relative to the actual status and timing of services receivedperformed may vary and efforts expended. As such, expense accruals related to clinical site costs are recognized based on our estimate of the degree of completion of the event or events specified in the specific clinical study or trial contract.
RECENTLY ISSUED ACCOUNTING STANDARDS
Management does not affectbelieve that any of the inputs to the valuation technique that the entity uses to value the award, the entity is not required to estimate the value immediately before and after the modification.
ITEM7A. QUANTITATIVE AND QUALITATIVE DISCLOSURE ABOUT MARKET RISK.
The primary objective of our investment activities is to preserve principal while maximizing our income from investments and minimizing our market risk. We currently invest in government and investment-grade corporate debt in accordance with our investment policy, which we may change from time to time. The securities in which we invest have market risk. This means that a change in prevailing interest rates, and/or credit risk, may cause the fair value of the investment to fluctuate. For example, if we hold a security that was issued with a fixed interest rate at the then-prevailing rate and the prevailing interest rate later rises, the fair value of our investment will probably decline. As of December 31, 2017,2023, our portfolio of financial instruments consists of cash equivalents and short-term interest bearinginterest-bearing securities, including government debt and money market funds. The average duration of all of our held-to-maturity investments held as of December 31, 2017,2023, was less than 1224 months. Due to the relativerelatively short-term nature of these financial instruments, we believe there is no material exposure to interest rate risk, and/or credit risk, arising from our portfolio of financial instruments.
Our consolidated financial statements and the notes thereto, included in Part IV, Item 15(a)14(a), part 1, are incorporated by reference into this Item 8.
Not applicable.
Evaluation of Disclosure Controls and Procedures.
As of December 31,Management’s Annual Report on Internal Control over Financial Reporting.
Our management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Rule 13a-15(f) or Rule 15d-15(f) under the Exchange Act). Our management assessed the effectiveness of our internal control over financial reporting as of December 31,The effectiveness of our internal control over financial reporting as of December 31, 20172023 was audited by CohnReznickKPMG LLP, our independent registered public accounting firm, as stated in their report appearing below, which expressed an unqualified opinion on the effectiveness of our internal control over financial reporting as of December 31, 2017.
Changes in Internal Control Over Financial Reporting.
There were no changes in our internal control over financial reporting during the quarter ended December 31,Limitations on the Effectiveness of Controls.
Our management, including our Chief Executive Officer and Chief Financial Officer, does not expect that our disclosure controls and procedures or our internal control over financial reporting will prevent all errors and all fraud. A control system, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, within our Company have been detected.Securities Trading Plans of Directors and Executive Officers
During the three months ended December 31, 2023, none of our directors or executive officers adopted or terminated a Rule 10b5-1 trading arrangement (as defined in Item 408(a)(1)(i) of Regulation S-K) or adopted or terminated a non-Rule 10b5-1 trading arrangement (as defined in Item 408(c) of Regulation S-K) for the purchase or sale of the Company’s securities that was intended to satisfy the affirmative defense conditions of Rule 10b5-1(c).
ITEM10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2024 Annual Meeting of Stockholders.
ITEM11. EXECUTIVE COMPENSATION.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2024 Annual Meeting of Stockholders.
ITEM12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2024 Annual Meeting of Stockholders.
ITEM13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2024 Annual Meeting of Stockholders.
ITEM14. PRINCIPAL ACCOUNTING FEES AND SERVICES.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2024 Annual Meeting of Stockholders.
ITEM15. EXHIBITS and FINANCIAL STATEMENT SCHEDULES.
1. Consolidated Financial Statements
The following consolidated financial statements of TG Therapeutics, Inc. are filed as part of this report.
2. Consolidated Financial Statement Schedules
All schedules are omitted as the information required is inapplicable or the information is presented in the consolidated financial statements or the related notes.
3. Exhibits
Exhibit | |
Number | Exhibit Description |
| |
Amended and Restated Certificate of Incorporation of TG Therapeutics, Inc. dated April 26, 2012 (incorporated by reference to Exhibit 3.1 to the Registrant’s Form 10-Q for the quarter ended June 30, 2012). | |
| |
Certificate of Amendment to Amended and Restated Certificate of Incorporation of TG Therapeutics, Inc. dated June 9, 2014 (incorporated by reference to Exhibit 3.2 to the Registrant’s Form 10-Q for the quarter ended June 30, 2014). | |
Certificate of Amendment to Amended and Restated Certificate of Incorporation of TG Therapeutics, Inc. dated June 16, 2021 (incorporated by reference to Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed on June 21, 2021). | |
Amended and Restated Bylaws of TG Therapeutics, Inc. dated July 18, 2014 (incorporated by reference to Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed on July 21, 2014). | |
| |
Specimen common stock certificate (incorporated by reference to Exhibit 4.1 to the Registrant’s Form 10-K for the year ended December 31, 2011). | |
| |
Stockholder Protection Rights Agreement, dated July 18, 2014 between TG Therapeutics, Inc. and American Stock Transfer & Trust Company, LLC, as Rights Agent (incorporated by reference to Exhibit 4.1 to the Registrant’s Current Report on Form 8-K filed on July 21, 2014). | |
| |
Description of Securities of TG Therapeutics, Inc. (incorporated by reference to Exhibit 4.5 of the Registrant’s Annual Report on Form 10-K for the fiscal year ended December 31, 2020). |
Employment Agreement, effective December 29, 2011, between the Registrant and Michael Weiss (incorporated by reference to Exhibit 10.30 to the Registrant’s Form 10-K for the fiscal year ended December 31, 2011). † | |
| |
Restricted Stock Subscription Agreement, effective December 29, 2011, between the Registrant and Michael Weiss (incorporated by reference to Exhibit 10.31 to the Registrant’s Form 10-K for the fiscal year ended December 31, 2011). † | |
| |
Amendment to Restricted Stock Agreement, dated July 12, 2013, by and between TG Therapeutics, Inc. and Michael S. Weiss (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on July 16, 2013). † | |
| |
Amendment to Restricted Stock Agreements, dated December 31, 2014, by and between TG Therapeutics, Inc. and Michael S. Weiss (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on January 7, 2015). † | |
| |
Employment Agreement, effective December 29, 2011, between the Registrant and Sean Power (incorporated by reference to Exhibit 10.32 to the Registrant’s Form 10-K for the fiscal year ended December 31, 2011). † | |
| |
Restricted Stock Subscription Agreement, effective December 29, 2011 between the Registrant and Sean Power (incorporated by reference to Exhibit 10.33 to the Registrant’s Form 10-K for the fiscal year ended December 31, 2011). † | |
| |
Amendment to Restricted Stock Agreement, dated July 12, 2013, by and between TG Therapeutics, Inc. and Sean A. Power (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on July 16, 2013). † | |
| |
Amendment to Restricted Stock Agreements, dated December 31, 2014, by and between TG Therapeutics, Inc. and Sean A. Power (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on January 7, 2015). † | |
| |
License Agreement dated January 30, 2012, by and among the Registrant, GTC Biotherapeutics, Inc., LFB Biotechnologies S.A.S. and LFB/GTC LLC (incorporated by reference to Exhibit 10.35 to the Registrant’s Form 10-K for the fiscal year ended December 31, 2011). * | |
| |
Sublicense Agreement between TG Therapeutics, Inc. and Ildong Pharmaceutical Co. Ltd., dated November 13, 2012 (incorporated by reference to Exhibit 10.37 to the Registrant’s Form 10-K for the fiscal year ended December 31, 2012). * | |
| |
License Agreement between TG Therapeutics, Inc. and Ligand Pharmaceuticals Incorporated, dated June 23, 2014 (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10-Q for the quarter ended June 30, 2014).* | |
| |
License Agreement between TG Therapeutics, Inc. and Rhizen Pharmaceuticals SA, dated September 22, 2014 (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on January 20, 2015). * | |
| |
Collaboration Agreement between TG Therapeutics, Inc. and Checkpoint Therapeutics, Inc., dated March 3, 2015 (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10-Q for the quarter ended March 31, 2015). * | |
| |
Sublicense Agreement between TG Therapeutics, Inc. and Checkpoint Therapeutics, Inc., dated May 27, 2016, (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10-Q for the quarter ended June 30, 2016). * | |
| |
Amendment to Employment Agreement, effective January 1, 2017, between TG Therapeutics, Inc. and Michael S. Weiss (incorporated by reference to Exhibit 10.18 to the Registrant’s Form 10-K/A for the year ended December 31, 2016). † | |
| |
License Agreement between TG Therapeutics, Inc. and Jiangsu Hengrui Medicine Co., dated January 8, 2018 (incorporated by reference to Exhibit 10.20 to the Registrant’s Form 10-K for the year ended December 31, 2017). * | |
| |
Joint Venture and License Option Agreement by and between TG Therapeutics, Inc. and Novimmune S.A., dated June 18, 2018 (incorporated by reference to Exhibit 10.20 to the Registrant’s Form 10-Q for the quarter ended June 30, 2018). * |
Master Services Agreement between Samsung Biologics Co., Ltd. And TG Therapeutics, Inc., effective February 21, 2018 (incorporated by reference to the Exhibit 10.2 to the Registrant’s Form 10-Q for the quarter ended June 30, 2019). * | |
| |
Loan and Security Agreement, dated February 28, 2019, by and among TG Therapeutics, Inc., TG Biologics, Inc. and Hercules Capital, Inc. (incorporated by reference to the Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on March 5, 2019). | |
| |
Warrant Agreement, dated February 28, 2019, by and between TG Therapeutics, Inc. and Hercules Capital, Inc. (incorporated by reference to the Exhibit 10.3 to the Registrant’s Current Report on Form 8-K filed on March 5, 2019). | |
| |
Warrant Agreement, dated February 28, 2019, by and between TG Therapeutics, Inc. and Hercules Technology III, L.P. (incorporated by reference to the Exhibit 10.4 to the Registrant’s Current Report on Form 8-K filed on March 5, 2019). | |
| |
Amended and Restated Collaboration Agreement by and between TG Therapeutics, Inc. and Checkpoint Therapeutics, Inc., dated June 19, 2019 (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10-Q for the quarter ended June 30, 2019). * | |
| |
Amended and Restated Employment Agreement by and between TG Therapeutics, Inc. and Michael S. Weiss, dated June 18, 2021 (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10 Q for the quarter ended June 30, 2021). † | |
| |
Amended and Restated Loan and Security Agreement, dated December 30, 2021, by and among TG Therapeutics, Inc., TG Biologics, Inc. and Hercules Capital, Inc. (incorporated by reference to Exhibit 10.28 to the Registrant’s Form 10-K for the year ended December 31, 2021). | |
| |
Warrant Agreement, dated December 30, 2021, by and between TG Therapeutics, Inc. and Hercules Capital Inc. (incorporated by reference to Exhibit 10.29 to the Registrant’s Form 10-K for the year ended December 31, 2021). | |
| |
Warrant Agreement, dated December 30, 2021, by and between TG Therapeutics, Inc. and Hercules Private Credit Fund I L.P. (incorporated by reference to Exhibit 10.30 to the Registrant’s Form 10-K for the year ended December 31, 2021). | |
| |
Warrant Agreement, dated December 30, 2021, by and between TG Therapeutics, Inc. and Hercules Private Global Venture Growth Fund I L.P. (incorporated by reference to Exhibit 10.31 to the Registrant’s Form 10-K for the year ended December 31, 2021). | |
| |
TG Therapeutics, Inc. 2022 Incentive Plan (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on June 23, 2022). † | |
| |
| 10.29 | First Amendment to Amended and Restated Loan and Security Agreement, dated March 31, 2023, by and among TG Therapeutics, Inc., TG Biologics, Inc. and Hercules Capital, Inc. (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.30 | Amended and Restated Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Capital Inc. (incorporated by reference to Exhibit 10.2 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.31 | Amended and Restated Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Funding IV, LLC. (incorporated by reference to Exhibit 10.3 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.32 | Amended and Restated Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Private Credit Fund 1 L.P. (incorporated by reference to Exhibit 10.4 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.33 | Amended and Restated Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Private Global Venture Growth Fund I L.P. (incorporated by reference to Exhibit 10.5 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.34 | Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Capital Inc. (incorporated by reference to Exhibit 10.6 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). |
| 10.35 | Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Private Credit Fund 1 L.P. (incorporated by reference to Exhibit 10.7 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.36 | Warrant Agreement, dated March 31, 2023, by and between TG Therapeutics, Inc. and Hercules Private Global Venture Growth Fund I L.P. (incorporated by reference to Exhibit 10.8 to the Registrant’s Form 10-Q for the quarter ended March 31, 2023). * |
| 10.37 | Commercialization Agreement by and between TG Therapeutics, Inc. and Neuraxpharm Pharmaceuticals, S.L., dated as of July 28, 2023 (incorporated by reference to Exhibit 10.1 to the Registrant’s Form 10-Q for the quarter ended June 30, 2023). * |
| 10.38 | License Agreement, dated January 7, 2024, by and between TG Therapeutics, Inc., TG Cell Therapy, Inc., and Precision BioSciences, Inc. # * |
| 19.1 | TG Therapeutics, Inc. Insider Trading Policy # |
Subsidiaries of TG Therapeutics, Inc. # | |
| |
Consent of Independent Registered Public Accounting Firm (KPMG, LLP). # | |
| |
Power of Attorney (included in signature page). | |
| |
Certification of Principal Executive Officer. # | |
| |
Certification of Principal Financial Officer. # | |
| |
Certification of Chief Executive Officer pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. # | |
| |
Certification of Chief Financial Officer pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. # |
| 97.1 | TG Therapeutics, Inc. Clawback Policy # |
101 | The following financial information from TG Therapeutics, Inc.’s Annual Report on Form 10-K for the year ended December 31, 2023, formatted in iXBRL (Inline eXtensible Business Reporting Language): (i) Consolidated Balance Sheets, (ii) Consolidated Statements of Operations, (iii) Consolidated Statements of Stockholders’ Equity, (iv) Consolidated Statements of Cash Flows, (v) the Notes to Consolidated Financial Statements. |
| |
104 | Cover Page Interactive Data File (embedded within the Inline XBRL document). |
# | Filed Herewith. |
† | Indicates management contract or compensatory plan or arrangement. |
* | Certain portions of this exhibit have been omitted pursuant to Item 601(b)(10) of Regulation S-K. |
TG Therapeutics,Inc.
Consolidated Financial Statements
To the Stockholders and Board of Directors and
TG Therapeutics, Inc.:
Opinion on theConsolidated Financial Statements
We have audited the accompanying consolidated balance sheets of TG Therapeutics, Inc.
We also have audited, TG Therapeutics, Inc. (the Company’s)in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company’s internal control over financial reporting as of December 31, 2017,2023, based on criteria established in Internal Control—Control – Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission, (COSO).and our report dated February 29, 2024 expressed an unqualified opinion on the effectiveness of the Company’s internal control over financial reporting.
Basis for Opinion
These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matter
The critical audit matter communicated below is a matter arising from the current period audit of the consolidated financial statements that was communicated or required to be communicated to the audit committee and that: (1) relates to accounts or disclosures that are material to the consolidated financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of a critical audit matter does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing a separate opinion on the critical audit matter or on the accounts or disclosures to which it relates.
Commercialization agreement with Neuraxpharm
As discussed in Note 2 to the consolidated financial statements, the Company entered into a commercialization agreement (the Commercialization Agreement) with Neuraxpharm Pharmaceuticals, S.L. (Neuraxpharm) that granted Neuraxpharm the exclusive right to commercialize BRIUMVI in certain territories. The arrangement also provides Neuraxpharm with the right to make optional purchases of BRIUMVI. The consideration for these optional purchases of BRIUMVI by Neuraxpharm approximates the price that a customer in the territories would be willing to pay for these goods. In 2023, the Company recognized a non-refundable upfront payment of $140.0 million as License Revenue related to the Commercialization Agreement.
We identified the evaluation of the accounting for the supply terms of the Commercialization Agreement with Neuraxpharm as a critical audit matter. Specifically, complex auditor judgment was required to evaluate the Company’s assessment of whether the optional purchases of BRIUMVI granted a material right to Neuraxpharm, due to the complexity of evaluating whether the contractual pricing is commensurate with standalone selling price.
The following are the primary procedures we performed to address this critical audit matter. We evaluated the design and tested the operating effectiveness of an internal control in the Company’s revenue process used to evaluate key terms of contracts with customers, including the evaluation of the standalone selling price of BRIUMVI. We obtained an understanding of the Commercialization Agreement by reading the contracts and conducting meetings with Company personnel responsible for negotiating the contracts. We evaluated management’s accounting conclusions with respect to the supply terms within the Commercialization Agreement. We recalculated the contractual price of the optional purchases and inspected the Company’s analysis of the standalone selling price of BRIUMVI using an expected cost plus a margin approach. We obtained and inspected both external and internal evidence used by the Company in its analysis of the standalone selling price and compared this evidence to available industry information for the relevant territories. We also performed a sensitivity analysis to evaluate the impact that a change in margin would have on the conclusion that the contractual pricing of optional purchases of BRIUMVI is commensurate with standalone selling price.
/s/ KPMG LLP
We have served as the Company’s auditor since 2021.
New York, New York
February 29, 2024
Report of Independent Registered Public Accounting Firm
To the Stockholders and Board of Directors
TG Therapeutics, Inc.:
Opinion on Internal Control Over Financial Reporting
We have audited TG Therapeutics, Inc. and subsidiaries' (the Company) internal control over financial reporting as of December 31, 2023, based on criteria established in Internal Control – Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2017,2023, based on criteria established in Internal Control—Control – Integrated Framework (2013) issued by COSO.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United Stated)States) (PCAOB), the consolidated balance sheets of the Company as of December 31, 2023 and 2022, the related consolidated statements of operations, stockholders’ equity, and cash flows for each of the Companyyears in the three-year period ended December 31, 2023, and the related notes (collectively, the consolidated financial statements), and our report dated March 15, 2018,February 29, 2024 expressed an unqualified opinion.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’sManagement's Annual Report on Internal Control Overover Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audit also included performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control overOver Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ CohnReznickKPMG LLP
New York, New York
February 29, 2024
F-3
Consolidated Balance Sheets as of December31
(in thousands, except share and per share amounts)
| December 31, | December 31, | ||||||
| 2023 | 2022 | ||||||
| | | ||||||
Assets | ||||||||
Current assets: | | | ||||||
Cash and cash equivalents | $ | 92,933 | $ | 102,304 | ||||
Short-term investment securities | 124,575 | 59,374 | ||||||
Accounts receivable, net | 51,093 | — | ||||||
Inventories | 39,823 | — | ||||||
Prepaid research and development | 4,183 | 4,237 | ||||||
Other current assets | 5,336 | 2,359 | ||||||
Total current assets | 317,943 | 168,274 | ||||||
Restricted cash | 1,285 | 1,273 | ||||||
Long-term investment securities | — | 12,404 | ||||||
Right of use assets | 8,050 | 8,888 | ||||||
Leasehold interest, net | 1,415 | 1,627 | ||||||
Equipment, net | 95 | 307 | ||||||
Goodwill | 799 | 799 | ||||||
Total assets | $ | 329,587 | $ | 193,572 | ||||
| ||||||||
Liabilities and stockholders’ equity | ||||||||
Current liabilities: | ||||||||
Accounts payable and accrued expenses | $ | 38,471 | $ | 42,019 | ||||
Other current liabilities | 1,631 | 1,169 | ||||||
Lease liability – current portion | 1,446 | 1,581 | ||||||
Accrued compensation | 12,172 | 8,432 | ||||||
Total current liabilities | 53,720 | 53,201 | ||||||
Deferred revenue | 6,016 | 305 | ||||||
Loan payable | 100,118 | 71,135 | ||||||
Lease liability – non-current | 9,231 | 10,344 | ||||||
Total liabilities | 169,085 | 134,985 | ||||||
Commitments and contingencies | ||||||||
Stockholders’ equity: | ||||||||
Common stock, $0.001 par value per share (175,000,000 shares authorized, 151,465,598 and 146,426,697 shares issued, 151,424,289 and 146,385,388 shares outstanding at December 31, 2023 and December 31, 2022, respectively | 151 | 146 | ||||||
Additional paid-in capital | 1,674,946 | 1,585,708 | ||||||
Treasury stock, at cost, 41,309 shares at December 31, 2023 and December 31, 2022 | (234 | ) | (234 | ) | ||||
Accumulated deficit | (1,514,361 | ) | (1,527,033 | ) | ||||
Total stockholders’ equity | 160,502 | 58,587 | ||||||
Total liabilities and stockholders’ equity | $ | 329,587 | $ | 193,572 | ||||
2017 | 2016 | |
| Assets | ||
| Current assets: | ||
| Cash and cash equivalents | $56,717,847 | $25,031,280 |
| Short-term investment securities | 27,998,810 | 19,853,860 |
| Interest receivable | 108,468 | 83,852 |
| Prepaid research and development | 8,055,486 | 5,678,755 |
| Other current assets | 436,789 | 216,397 |
| Total current assets | 93,317,400 | 50,864,144 |
| Restricted cash | 587,291 | 583,208 |
| Leasehold interest, net | 2,429,434 | 2,042,281 |
| Equipment, net | 248,020 | 328,148 |
| Goodwill | 799,391 | 799,391 |
| Other assets | -- | 164,375 |
| Total assets | $97,381,536 | $54,781,547 |
| Liabilities and stockholders’ equity | ||
| Current liabilities: | ||
| Accounts payable and accrued expenses | $25,877,218 | $15,267,668 |
| Accrued compensation | 1,800,000 | 1,389,516 |
| Current portion of deferred revenue | 152,381 | 152,381 |
| Notes payable | 127,614 | 68,875 |
| Total current liabilities | 27,957,213 | 16,878,440 |
| Deferred rent | 1,364,601 | 816,257 |
Deferred revenue, net of current portion | 1,066,667 | 1,219,048 |
Total liabilities | 30,388,481 | 18,913,745 |
| Commitments and contingencies | ||
| Stockholders’ equity: | ||
| Preferred stock, $0.001 par value per share (10,000,000 shares authorized, none issued and outstanding as of December 31, 2017 and 2016) | -- | -- |
| Common stock, $0.001 par value per share (150,000,000 shares authorized, 73,181,750 and 56,820,422 shares issued, 73,140,441 and 56,779,113 shares outstanding at December 31, 2017 and 2016, respectively) | 73,182 | 56,820 |
| Additional paid-in capital | 422,017,042 | 272,432,139 |
| Treasury stock, at cost, 41,309 shares at December 31, 2017 and 2016 | (234,337) | (234,337) |
Accumulated deficit | (354,862,832) | (236,386,820) |
Total stockholders’ equity | 66,993,055 | 35,867,802 |
Total liabilities and stockholders’ equity | $97,381,536 | $54,781,547 |
The accompanying notes are an integral part of the consolidated financial statements.
Consolidated Statements of Operations for theYears Ended December31
(in thousands, except share and per share amounts)
| 2023 | 2022 | 2021 | |||||||||
Revenue: | ||||||||||||
Product revenue, net | 92,005 | 2,633 | 6,537 | |||||||||
License, milestone and other revenue | $ 141,657 | $ 152 | $ 152 | |||||||||
Total revenue | 233,662 | 2,785 | 6,689 | |||||||||
| ||||||||||||
Costs and expenses: | ||||||||||||
Cost of revenue | 14,131 | 265 | 790 | |||||||||
Research and development: | ||||||||||||
Noncash compensation | 13,010 | 13,224 | 24,047 | |||||||||
Other research and development | 63,182 | 112,128 | 198,532 | |||||||||
Total research and development | 76,192 | 125,352 | 222,579 | |||||||||
| | | | |||||||||
Selling, general and administrative: | | | | |||||||||
Noncash compensation | 24,923 | 5,961 | 37,227 | |||||||||
Other selling, general and administrative | 97,783 | 64,046 | 90,863 | |||||||||
Total selling, general and administrative | 122,706 | 70,007 | 128,090 | |||||||||
| | | | |||||||||
Total costs and expenses | 213,029 | 195,624 | 351,459 | |||||||||
| ||||||||||||
Operating income (loss) | 20,633 | (192,839) | (344,770) | |||||||||
| ||||||||||||
Other expense (income): | ||||||||||||
Interest expense | 12,615 | 10,191 | 5,638 | |||||||||
Other income | (5,044) | (4,695) | (2,307) | |||||||||
Total other expense (income), net | 7,571 | 5,496 | 3,331 | |||||||||
| ||||||||||||
Net income (loss) before taxes | $ 13,062 | $ (198,335) | $ (348,101) | |||||||||
Income taxes | 390 | — | — | |||||||||
Net income (loss) | $ 12,672 | $ (198,335) | $ (348,101) | |||||||||
| ||||||||||||
Net income (loss) per common share: | ||||||||||||
Basic | $ 0.09 | $ (1.46) | $ (2.63) | |||||||||
Diluted | $ 0.09 | $ (1.46) | $ (2.63) | |||||||||
Weighted-average shares outstanding: | ||||||||||||
Basic | 141,955,112 | 135,411,258 | 132,222,753 | |||||||||
Diluted | 148,508,465 | 135,411,258 | 132,222,753 | |||||||||
2017 | 2016 | 2015 | |
License revenue | $152,381 | $152,381 | $152,381 |
| Costs and expenses: | |||
| Research and development: | |||
| Noncash compensation | 5,646,716 | 2,742,354 | 4,261,406 |
Other research and development | 96,886,134 | 66,489,820 | 43,445,817 |
Total research and development | 102,532,850 | 69,232,174 | 47,707,223 |
| General and administrative: | |||
| Noncash compensation | 10,298,568 | 4,767,645 | 11,435,686 |
Other general and administrative | 6,032,714 | 5,121,690 | 4,189,488 |
Total general and administrative | 16,331,282 | 9,889,335 | 15,625,174 |
Total costs and expenses | 118,864,132 | 79,121,509 | 63,332,397 |
Operating loss | (118,711,751) | (78,969,128) | (63,180,016) |
| Other (income) expense: | |||
| Interest income | (294,478) | (323,032) | (174,653) |
Other (income) expense | 58,739 | (393,202) | (56,717) |
Total other income, net | (235,739) | (716,234) | (231,370) |
| Net loss | $(118,476,012) | $(78,252,894) | $(62,948,646) |
| Basic and diluted net loss per common share | $(1.91) | $(1.60) | $(1.38) |
| Weighted average shares used in computing basic and diluted net loss per common share | 62,069,570 | 49,041,354 | 45,646,414 |
The accompanying notes are an integral part of the consolidated financial statements.
Consolidated Statements of Stockholders’Stockholders’ Equity for theYears Ended December31 2017, 2016 and 2015
(in thousands, except share amounts)
Additional | ||||||||||||||||||||||||||||
Common Stock | paid-in | Treasury Stock | Accumulated | |||||||||||||||||||||||||
| Shares | Amount | capital | Shares | Amount | Deficit | Total | |||||||||||||||||||||
Balance at January 1, 2021 | 140,617,606 | 141 | 1,500,040 | 41,309 | (234 | ) | (980,597 | ) | 519,350 | |||||||||||||||||||
Issuance of common stock in connection with exercise of options | 52,694 | * | 216 | — | — | — | 216 | |||||||||||||||||||||
Issuance of restricted stock | 2,738,974 | 2 | (2 | ) | — | — | — | — | ||||||||||||||||||||
Warrants issued with debt financing | — | — | 2,195 | — | — | — | 2,195 | |||||||||||||||||||||
Forfeiture of restricted stock | (189,231 | ) | * | — | — | — | — | — | ||||||||||||||||||||
Offering Costs Paid | — | — | (204 | ) | — | — | — | (204 | ) | |||||||||||||||||||
Issuance of common stock in At-the-Market offerings (net of offering costs of $0.1 million) | 72,000 | * | 2,423 | — | — | — | 2,423 | |||||||||||||||||||||
Compensation in respect of restricted stock granted to employees, directors and consultants | — | — | 61,274 | — | — | — | 61,274 | |||||||||||||||||||||
Net income (loss) | — | — | — | — | — | (348,101 | ) | (348,101 | ) | |||||||||||||||||||
Balance at December 31, 2021 | 143,292,043 | 143 | 1,565,942 | 41,309 | (234 | ) | (1,328,698 | ) | 237,153 | |||||||||||||||||||
Issuance of common stock in connection with exercise of options | 142,409 | * | 584 | — | — | — | 584 | |||||||||||||||||||||
Issuance of restricted stock | 5,179,201 | 5 | (5 | ) | — | — | — | — | ||||||||||||||||||||
Forfeiture of restricted stock | (2,186,956 | ) | (2 | ) | 2 | — | — | — | — | |||||||||||||||||||
Compensation in respect of restricted stock granted to employees, directors and consultants | — | — | 19,185 | — | — | — | 19,185 | |||||||||||||||||||||
Net income (loss) | — | — | — | — | — | (198,335 | ) | (198,335 | ) | |||||||||||||||||||
Balance at December 31, 2022 | 146,426,697 | 146 | 1,585,708 | 41,309 | (234 | ) | (1,527,033 | ) | 58,587 | |||||||||||||||||||
Issuance of common stock in connection with exercise of options | 246,156 | — | 1,534 | — | — | — | 1,534 | |||||||||||||||||||||
Issuance of restricted stock | 3,620,237 | 4 | (4 | ) | — | — | — | — | ||||||||||||||||||||
Warrants issued with debt financing | — | — | 595 | — | — | — | 595 | |||||||||||||||||||||
Forfeiture of restricted stock | (213,192 | ) | — | — | — | — | — | — | ||||||||||||||||||||
Issuance of common stock in At-the-Market offerings (net of offering costs of $0.8 million) | 1,385,700 | 1 | 46,295 | — | — | — | 46,296 | |||||||||||||||||||||
Compensation in respect of restricted stock granted to employees, directors and consultants | — | — | 40,818 | — | — | — | 40,818 | |||||||||||||||||||||
Net income (loss) | — | — | — | — | — | 12,672 | 12,672 | |||||||||||||||||||||
Balance at December 31, 2023 | 151,465,598 | $ | 151 | $ | 1,674,946 | 41,309 | $ | (234 | ) | $ | (1,514,361 | ) | 160,502 | |||||||||||||||
Common Stock | Contingently issuable | Additional Paid-in | Treasury Stock | Accumulated | ||||
Shares | Amount | Shares | Capital | Shares | Amount | Deficit | Total | |
| Balance at January 1, 2015 | 44,974,248 | $44,974 | $6 | $175,476,521 | 41,309 | $(234,337) | $(95,185,280) | $80,101,884 |
| Issuance of common stock in connection with exercise of warrants | 2,946,703 | 2,946 | 1,064,393 | 1,067,339 | ||||
| Issuance of common stock in connection with cashless exercise of warrants | 2,915 | 3 | (3) | -- | ||||
| Issuance of common stock in connection with conversion of notes payable | 522 | 1 | 6,924 | 6,925 | ||||
| Issuance of restricted stock | 1,992,535 | 1,993 | (1,993) | -- | ||||
| Forfeiture of restricted stock | (31,166) | (31) | 31 | -- | ||||
| Issuance of common stock to related party for cash (See Note 9) | 114,855 | 115 | 749,890 | 750,005 | ||||
| Issuance of common stock in At-the-Market offering (net of offering costs of $1,310,591) | 4,094,498 | 4,094 | 66,894,609 | 66,898,703 | ||||
| Compensation in respect of restricted stock granted to employees, directors and consultants | 15,697,092 | 15,697,092 | ||||||
| Net loss | (62,948,646) | (62,948,646) | ||||||
| Balance at December 31, 2015 | 54,095,110 | 54,095 | 6 | 259,887,464 | 41,309 | (234,337) | (158,133,926) | 101,573,302 |
| Issuance of common stock in connection with exercise of warrants | 273,370 | 273 | 617,969 | 618,242 | ||||
| Issuance of common stock in connection with conversion of notes payable | 3,710 | 4 | 33,013 | 33,017 | ||||
| Issuance of restricted stock | 1,924,639 | 1,925 | (1,925) | -- | ||||
| Forfeiture of restricted stock | (46,773) | (47) | 47 | -- | ||||
| Issuance of common stock in At-the-Market offering (net of offering costs of $108,185) | 570,366 | 570 | 4,385,566 | 4,386,136 | ||||
| Compensation in respect of restricted stock granted to employees, directors and consultants | 7,509,999 | 7,509,999 | ||||||
| Adjustment to contingently issuable shares | (6) | 6 | -- | |||||
| Net loss | (78,252,894) | (78,252,894) | ||||||
| Balance at December 31, 2016 | 56,820,422 | 56,820 | -- | 272,432,139 | 41,309 | (234,337) | (236,386,820) | 35,867,802 |
| Issuance of common stock in connection with exercise of warrants | 887,585 | 888 | 2,142,197 | 2,143,085 | ||||
| Issuance of restricted stock | 1,836,511 | 1,837 | (1,837) | -- | ||||
| Forfeiture of restricted stock | (53,875) | (54) | 54 | -- | ||||
| Issuance of common stock in public offering (net of offering costs of $3.6 million) | 5,897,436 | 5,897 | 53,634,115 | 53,640,012 | ||||
| Issuance of common stock in At-the-Market offering (net of offering costs of $1.1 million) | 7,793,671 | 7,794 | 77,865,090 | 77,872,884 | ||||
| Compensation in respect of restricted stock granted to employees, directors and consultants | 15,945,284 | 15,945,284 | ||||||
| Net loss | (118,476,012) | (118,476,012) | ||||||
| Balance at December 31, 2017 | 73,181,750 | $73,182 | $-- | $422,017,042 | 41,309 | $(234,337) | $(354,862,832) | $66,993,055 |
* Amount less than one thousand dollars.
The accompanying notes are an integral part of the consolidated financial statements.
Consolidated Statements of Cash Flows for theYears Ended December31
(in thousands)
| 2023 | 2022 | 2021 | |||||||||
CASH FLOWS FROM OPERATING ACTIVITIES | | | | |||||||||
| | | | |||||||||
Net income (loss) | $ | 12,672 | $ | (198,335 | ) | $ | (348,101 | ) | ||||
Adjustments to reconcile net income (loss) to net cash used in operating activities: | | | | |||||||||
Noncash stock compensation expense | 37,933 | 19,185 | 61,274 | |||||||||
Depreciation and amortization | 211 | 303 | 282 | |||||||||
Amortization of premium (discount) on investment securities | (2,236 | ) | (331 | ) | 517 | |||||||
Amortization of debt issuance costs | 2,378 | 1,844 | 1,080 | |||||||||
Amortization of leasehold interest | 212 | 212 | 212 | |||||||||
Noncash change in lease liability and right of use asset | 1,963 | 2,715 | 1,896 | |||||||||
Change in fair value of notes payable | 113 | (116 | ) | (578 | ) | |||||||
Changes in assets and liabilities: | | | | |||||||||
Increase in inventory | (36,938 | ) | — | — | ||||||||
Decrease (increase) in other current assets | (2,831 | ) | 8,181 | (8,508 | ) | |||||||
Decrease (increase) in accounts receivable | (51,093 | ) | 1,389 | (1,389 | ) | |||||||
(Decrease) increase in accounts payable and accrued expenses | 192 | (11,010 | ) | 15,991 | ||||||||
Decrease in lease liabilities | (2,375 | ) | (2,332 | ) | (2,012 | ) | ||||||
Increase (decrease) in other current liabilities | 2,675 | 2,277 | (16,146 | ) | ||||||||
Increase (decrease) in deferred revenue | 5,711 | (152 | ) | (152 | ) | |||||||
Net cash used in operating activities | (31,413 | ) | (176,170 | ) | (295,634 | ) | ||||||
| ||||||||||||
CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||
Proceeds from maturity of short-term securities | 96,229 | 87,275 | 55,600 | |||||||||
Investment in held-to-maturity securities | (146,880 | ) | (107,274 | ) | (55,531 | ) | ||||||
Purchases of PPE | — | (14 | ) | (401 | ) | |||||||
Net cash used in investing activities | (50,651 | ) | (20,013 | ) | (332 | ) | ||||||
| ||||||||||||
CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||
Payment of loan payable | — | (975 | ) | (30,000 | ) | |||||||
Proceeds from sale of common stock, net | 46,296 | — | 2,219 | |||||||||
Proceeds from exercise of options | 1,534 | 584 | 216 | |||||||||
Proceeds from debt financings | 25,000 | — | 70,000 | |||||||||
Financing costs paid | (125 | ) | — | (1,016 | ) | |||||||
Net cash provided by (used in) financing activities | 72,705 | (391 | ) | 41,419 | ||||||||
| ||||||||||||
NET DECREASE IN CASH, CASH EQUIVALENTS AND RESTRICTED CASH | (9,359 | ) | (196,574 | ) | (254,547 | ) | ||||||
| ||||||||||||
CASH, CASH EQUIVALENTS AND RESTRICTED CASH AT BEGINNING OF PERIOD | 103,577 | 300,151 | 554,698 | |||||||||
| ||||||||||||
CASH, CASH EQUIVALENTS AND RESTRICTED CASH AT END OF PERIOD | $ | 94,218 | $ | 103,577 | $ | 300,151 | ||||||
| ||||||||||||
Reconciliation to amounts on condensed consolidated balance sheets: | ||||||||||||
Cash and cash equivalents | $ | 92,933 | $ | 102,304 | $ | 298,887 | ||||||
Restricted cash | 1,285 | 1,273 | 1,264 | |||||||||
Total cash, cash equivalents and restricted cash | $ | 94,218 | $ | 103,577 | $ | 300,151 | ||||||
| ||||||||||||
Cash paid for: | ||||||||||||
Interest | 8,771 | $ | 5,445 | $ | 3,466 | |||||||
NONCASH TRANSACTIONS | ||||||||||||
Deferred Financing Costs | $ | 1,238 | — | — | ||||||||
Warrants issued with debt financing | $ | 595 | — | — | ||||||||
2017 | 2016 | 2015 | |
| CASH FLOWS FROM OPERATING ACTIVITIES | |||
| Consolidated net loss | $(118,476,012) | $(78,252,894) | $(62,948,646) |
| Adjustments to reconcile consolidated net loss to net cash used in operating activities: | |||
| Gain on sale of long-term securities | -- | (33,042) | -- |
| Noncash stock compensation expense | 15,945,284 | 7,509,999 | 15,697,092 |
| Depreciation and amortization | 82,355 | 62,960 | 15,452 |
| Amortization of premium on investment securities | 61,320 | 459,429 | 536,142 |
| Change in fair value of notes payable and accrued interest | 58,739 | (109,657) | (56,717) |
| Changes in assets and liabilities: | |||
| Increase in restricted cash | (4,083) | (4,065) | (4,131) |
| (Increase) decrease in other current assets | (2,665,222) | 3,564,316 | (3,105,771) |
| Decrease (increase) in leasehold interest | 124,947 | (2,042,281) | -- |
| (Increase) decrease in accrued interest receivable | (24,616) | 102,169 | (100,505) |
| Decrease (increase) in other assets | 161,730 | (4,784) | (41,722) |
| Increase in accounts payable and accrued expenses | 11,020,034 | 6,492,644 | 5,470,915 |
| Increase in deferred rent | 104,343 | 816,257 | -- |
Decrease in deferred revenue | (152,381) | (152,381) | (152,381) |
Net cash used in operating activities | (93,763,562) | (61,591,330) | (44,690,272) |
| CASH FLOWS FROM INVESTING ACTIVITIES | |||
| Purchases of equipment | (2,227) | (343,985) | (42,217) |
| Investment in held-to-maturity securities | (28,006,270) | (15,199,922) | (48,993,652) |
| Proceeds from maturity of short-term securities | 19,800,000 | 29,500,000 | 24,350,000 |
Proceeds from the sale of long-term securities | -- | 12,589,219 | -- |
Net cash (used in) provided by investing activities | (8,208,497) | 26,545,312 | (24,685,869) |
| CASH FLOWS FROM FINANCING ACTIVITIES | |||
| Proceeds from the exercise of warrants | 2,143,085 | 618,242 | 1,067,339 |
| Proceeds from sale of common stock, net | 131,515,541 | 4,411,233 | 67,760,517 |
Deferred financing costs paid | - | (13,506) | (104,170) |
Net cash provided by financing activities | 133,658,626 | 5,015,969 | 68,723,686 |
| NET INCREASE (DECREASE) IN CASH AND CASH EQUIVALENTS | 31,686,567 | (30,030,049) | (652,455) |
Cash and cash equivalents at beginning of year | 25,031,280 | 55,061,329 | 55,713,784 |
| CASH AND CASH EQUIVALENTS AT END OF YEAR | $56,717,847 | $25,031,280 | $55,061,329 |
| NONCASH TRANSACTIONS | |||
Reclassification of deferred financing costs to additional paid-in capital | $(2,645) | $(25,097) | $(111,810) |
| Conversion of convertible notes payable to common stock | -- | $33,017 | $6,924 |
The accompanying notes are an integral part of the consolidated financial statements.
Unless the context requires otherwise, references in this report to “TG,“TG,” “Company,“Company,” “we,“we,” “us”“us” and “our”“our” refer to TG Therapeutics,Inc. and our subsidiaries.
NOTE1 - – ORGANIZATION AND SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
DESCRIPTION OF BUSINESS
TG Therapeutics is a fully-integrated, commercial stage, biopharmaceutical company focused on the acquisition, development and commercialization of novel treatments for B-cell malignanciesdiseases. In addition to a research pipeline including several investigational medicines, TG has received approval from the U.S. Food and autoimmune diseases. Currently, we are developing two therapies targeting hematologic malignancies. TG-1101 (ublituximab) is a novel, glycoengineered monoclonal antibody that targets a unique epitope onDrug Administration (FDA) for BRIUMVI® (ublituximab-xiiy) for the CD20 antigen found on mature B-lymphocytes. We are also developing TGR-1202 (umbralisib), an orally available PI3K delta inhibitor. The delta isoformtreatment of PI3K is strongly expressed in cells of hematopoietic origin and is believed to be important in the proliferation and survival of B-lymphocytes. Both TG-1101 and TGR-1202, or the combination of which is referred to as "U2," are in Phase 3 clinical development foradult patients with hematologic malignancies,relapsing forms of multiple sclerosis (RMS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults, as well as approval by the European Commission (EC) and the Medicines and Healthcare Products Regulatory Agency (MHRA) for BRIUMVI to treat adult patients with TG-1101 alsoRMS who have active disease defined by clinical or imaging features in Phase 3 clinical development for Multiple Sclerosis. Additionally,Europe and the Company has recently brought its anti-PD-L1 monoclonal antibody into Phase 1 development and aims to bring additional pipeline assets into the clinic in the future.
LIQUIDITY AND CAPITAL RESOURCES
Historically, we have incurred operating losses since our inception, andinception; however, the Company experienced a net profit during the twelve months ended December 31, 2023 due to a $140.0 million non-refundable upfront payment recognized as license revenue in the third quarter of 2023 as part of our ex-U.S. commercialization agreement (the Commercialization Agreement) with Neuraxpharm Pharmaceuticals, S.L. (Neuraxpharm) (see Note 2 for more information). We expect to continue to incur operating losses forin the foreseeable futurenear term and may never become profitable. As of December 31, 2017, 2023, we have an accumulated deficit of $354.9 million.
Our major sources of cash have been proceeds from the private placementplacements and public offeringofferings of equity securities.securities, from our loan and security agreements executed with Hercules Capital, Inc. (Hercules) (see Note 7 for more information), and the upfront payment from the Commercialization Agreement (see Note 2 for more information). Substantially all our operating losses have resulted from costs incurred in connection with our research and development programs and from selling, general and administrative costs associated with our operations, including our commercialization activities. As of December 31 2023, we had generated $92.0 million in product revenue from sales of BRIUMVI. BRIUMVI first became commercially available in the United States in January of 2023. We have not yet commercialized anyalso began shipping BRIUMVI to our ex-U.S. licensing partner, Neuraxpharm, in November 2023. Even with the commercialization of BRIUMVI and the possible future commercialization of our drug candidates and cannot be sure if we will ever be able to do so. Even if we commercialize one or more of ourother drug candidates, we may not become profitable. Our ability to achieve profitability depends on our ability to generate revenue and many other factors, including our ability to obtain regulatory approval for our drug candidates; successfully complete any post-approval regulatory obligations; and successfully commercialize our drug candidates alone or in partnership.partnership; successfully complete any post-approval regulatory obligations; and our ability to maintain or obtain regulatory approval for our drug candidates. We may continue to incur substantial operating losses even ifnow that we begin to generateare generating revenues from our drug candidates.
As of December 31, 2017, 2023, we had $84.8$217.5 million in cash and cash equivalents, and investment securities, and interest receivable. The Company believes itssecurities. We anticipate that our cash, cash equivalents, and investment securities and interest receivable on hand as of December 31, 2017 2023, combined with projected revenues associated with the additional capital raisedsale of BRIUMVI in the first quarterU.S. and ex-U.S., will provide sufficient liquidity for more than a twelve-month period from the date of 2018 (see Note 13) will be sufficient to fund the Company’s planned operations into the second quarter of 2019.filing this Annual Report on Form 10-K. The actual amount of cash that we will need to operate is subject to many factors, including, but not limited to, our commercialization efforts for BRIUMVI, preparations for the potential commercialization of our other drug candidates, and the timing, design and conduct of clinical trials for our drug candidates as well as the costs associated with licensing or otherwise acquiring new product candidates. We aremay be dependent upon significant future financing to provide the cash necessary to execute our currentongoing and future operations, including the commercialization of any of our drug candidates.
Our common stock is quoted on the Nasdaq Capital Market and trades under the symbol “TGTX.”
RECENTLY ISSUED ACCOUNTING STANDARDS
Management does not believe that any recently issued, but not yet effective, accounting pronouncements, if currently adopted, would have a material effect on the Company’s financial statements.
USE OF ESTIMATES
The preparation of financial statements in conformity with U.S. generally accepted accounting principles (“GAAP”)(GAAP) requires management to make estimates and judgments that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the applicable reporting period. On an ongoing basis, we evaluate our estimates and judgments, including those related to revenue, accrued clinical trial expenses and stock-based compensation. Actual results could differ from those estimates. Such differences could be material to the financial statements.
CASH AND CASH EQUIVALENTS
We treat liquid investments with original maturities of less than three months when purchased as cash and cash equivalents.
RESTRICTED CASH
We record cash pledged or held in trust as restricted cash. As of December 31, 2017,2023 and 2022, we have approximately $0.6$1.3 million of restricted cash pledged to secure a line of credit as a security deposit for an Office Agreement (see Note 9)7).
INVESTMENT SECURITIES
Investment securities at both December 31, 2017 2023 and 20162022 consist of short-term and long-term government securities. We classify these securities as held-to-maturity. Held-to-maturity securities are those securities in which we have the ability and intent to hold the security until maturity. Held-to-maturity securities are recorded at amortized cost, adjusted for the amortization or accretion of premiums or discounts. Premiums and discounts are amortized or accreted over the life of the related held-to-maturity security as an adjustment to yield using the effective interest method.
A decline in the market value of any investment security below cost that is deemed to be other than temporary, results in a reduction in the carrying amount to fair value. The impairment is charged to operations and a new cost basis for the security is established. Other-than-temporary impairment charges are included in interest and other income (expense), net. Unrealized gains, if determined to be temporary, are included in accumulated other comprehensive income in equity. Dividend and interest income are recognized when earned.
CREDIT RISK
Financial instruments that potentially subject the Company to concentrations of credit risk consist primarily of cash and cash equivalents and short-term investments. The Company maintains its cash and cash equivalents and short-term investments with high-credit quality financial institutions. At times, such amounts may exceed federally-insured limits.
REVENUE RECOGNITION
Pursuant to determine the appropriate revenue recognition. The terms of the license agreement may include payments to us of non-refundable up-front license fees, milestone payments if specified objectives are achieved, and/or royalties on product sales. WeTopic 606, we recognize revenue from upfront payments overto depict the periodtransfer of significant involvement underpromised goods or services to customers in an amount that reflects the related agreements unless the fee isconsideration to which we expect to be entitled in exchange for products deliveredthose goods or services. To achieve this core principle, Topic 606 includes provisions within a five-step model that includes i) identifying the contract with a customer, ii) identifying the performance obligations in the contract, iii) determining the transaction price, iv) allocating the transaction price to the performance obligations, and v) recognizing revenue when, or as, an entity satisfies a performance obligation.
At contract inception, we assess the goods or services renderedpromised within each contract and assess whether each promised good or service is distinct and determine those that represent the culmination of a separate earnings process and no furtherare performance obligation exists under the contract.obligations. We then recognize milestone payments as revenue upon the achievement of specified milestones only if (1) the milestone payment is non-refundable, (2) substantive effort is involved in achieving the milestone, (3) the amount of the milestonetransaction price that is reasonable in relationallocated to the effort expended orrespective performance obligation when the risk associated with achievementperformance obligation is satisfied.
Product Revenue, Net – The Company recognizes product revenues, net of variable consideration related to certain allowances and accruals, when the customer takes control of the product, which is typically upon delivery to the customer. Product revenue is recorded at the net sales price, or transaction price. The Company records product revenue reserves, which are classified as a reduction in product revenues, to account for the components of variable consideration. Variable consideration includes the following components, which are described below: chargebacks, government rebates, trade discounts and allowances, commercial payer rebates, product returns, and co-payment assistance.
These reserves are based on estimates of the amounts earned or to be claimed on the related sales and are classified as reductions of accounts receivable (if the amount is expected to be settled with a credit against the Company's customer account) or a liability (if the amount is expected to be settled with a cash payment). The Company's estimates of reserves established for variable consideration are calculated based upon a consistent application of the expected value method, which is the sum of probability-weighted amounts in a range of possible consideration amounts. These estimates reflect the Company's current contractual and statutory requirements, specific known market events and trends, industry data, and forecasted customer buying and payment patterns. The amount of variable consideration that is included in the transaction price may be subject to constraint and is included in net product revenues only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will not occur in a future period. Actual amounts of consideration received may ultimately differ from the Company's estimates. If actual results vary, the Company adjusts these estimates, which could have an effect on earnings in the period of adjustment.
Chargebacks: Chargebacks for discounts represent the Company’s estimated obligations resulting from contractual commitments to sell product to qualified healthcare providers and government agencies at prices lower than the list prices charged to the customers who directly purchase the product from the Company. The customers charge the Company for the difference between what the customers pay the Company for the product and the customers’ ultimate contractually committed or government required lower selling price to the qualified healthcare providers.
Government Rebates: Government rebates consist of Medicare, Tricare, and Medicaid rebates. These reserves are recorded in the same period the related revenue is recognized. For Medicare, the Company also estimates the number of patients in the prescription drug coverage gap for whom it will owe a rebate under the Medicare Part D program.
Trade Discounts and Allowances: The Company provides its customers with discounts that are explicitly stated in the contracts and are recorded in the period the related product revenue is recognized. In addition, the Company also receives sales order management, inventory management, and data services from its customers in exchange for certain fees.
Commercial Payer Rebates: The Company contracts with various private payer organizations, primarily insurance companies and pharmacy benefit managers, for the payment of rebates with respect to utilization of our product and contracted formulary status. The Company estimates these rebates and records such estimates in the same period the related revenue is recognized, resulting in a reduction of product revenue and the establishment of a current liability.
Product Returns: Consistent with industry practice, the Company generally offers customers a limited right of return for product that has been purchased from the Company. The Company estimates the amount of its product sales that may be returned by its customers and records this estimate in the period the related product revenue is recognized. The Company currently estimates product return liabilities based on data from similar products and other qualitative considerations, such as visibility into the inventory remaining in the distribution channel.
Subject to certain limitations, the Company’s return policy allows for eligible returns of commercial products sold for credit under the following circumstances:
● | receipt of damaged product; |
● | shipment errors that were a result of an error by the Company; |
● | expired product that is returned during the period beginning three months prior to the product’s expiration and ending six months after the expiration date; |
● | product subject to a recall; and |
● | product that the Company, at its sole discretion, has specified can be returned for credit. |
As of December 31, 2023, the Company has not received any returns related to sales of BRIUMVI.
Co-Payment Assistance Programs: Co-payment assistance is provided to qualified patients with commercial insurance, whereby the Company may provide financial assistance to patients with prescription drug co-payments required by the patient's insurance provider. Reserves for co-payment assistance are recorded in the same period the related revenue is recognized.
License Agreements –
The Company generates revenue from license or similar agreements with pharmaceutical companies for the development and commercialization of certain products. Such agreements may include the transfer of intellectual property rights in the form of licenses. Payments made by the customer may include non-refundable upfront fees, payments based upon the achievement of defined milestones, and royalties on sales of products. Licenses of intellectual property: If a license to the Company’s intellectual property is determined to be distinct from the other performance obligations identified in the arrangement, the Company recognizes the transaction price allocated to the license as revenue upon transfer of control of the license. All other promised goods or services in the agreement are evaluated to determine if they are distinct. If they are not distinct, they are combined with other promised goods or services to create a bundle of promised goods or services that is distinct.
Milestone payments: Contingent milestones at contract inception are estimated at the amount which is not probable of a material reversal and included in the transaction price using the most likely amount method. Milestone payments that are not within the Company's control, such as regulatory approvals, are not considered probable of being achieved until those approvals are received and therefore the variable consideration is constrained. The transaction price is then allocated to each performance obligation on a relative stand-alone selling price basis, for which the Company recognizes revenue as or when the performance obligations under the contract are satisfied. At the end of each reporting period, the Company re-evaluates the probability of achieving development or sales-based milestone payments that maynot be subject to a material reversal and, if necessary, adjust the estimate of the overall transaction price. Any such adjustments are recorded on a cumulative catch-up basis, which would affect license and other revenue, as well as earnings, in the period of adjustment.
Sales-based royalties: For arrangements that include sales-based royalties and a license of intellectual property that is deemed to be the predominant item to which the royalties relate, revenue is recognized at the later of when the related sales occur or when the performance obligation to which some or all of the royalties have been allocated has been satisfied (or partially satisfied).
Optional Purchases: The Company’s arrangements may provide the licensee the right to make optional purchases of the licensed product. These optional purchases are accounted for as separate contracts when the licensee determines that it will make such a purchase, unless the option conveys a material right.
Other Revenue
Revenue is also generated from service-based fees recognized for providing regulatory support and development services to customers. Service fee revenue is recognized overtime as the services are transferred to the customer.
DEFERRED PRODUCT REVENUE
When consideration is received, or such consideration is unconditionally due, from a customer prior to the Company completing its performance obligation to the customer under the terms of a contract, a contract liability is recorded as deferred revenue. Deferred revenues expected to be recognized as revenue within the 12 months following the balance sheet date are classified as current liabilities. Deferred revenues not expected to be recognized as revenue within the 12 months following the balance sheet date are classified as long-term liabilities.
ACCOUNTS RECEIVABLE
In general, accounts receivable consists of amounts due from customers, net of customer allowances for cash discounts, product returns and chargebacks. Our contracts with customers have standard payment terms. We analyze accounts that are past due for collectability, and regularly evaluate the creditworthiness of our customers so that we can properly assess and respond to changes in their credit profiles. As of December 31, 2023, we determined an allowance for expected credit losses related to outstanding accounts receivable was currently not required based upon our review of contractual payment terms and individual customer circumstances.
COST OF REVENUE
Cost of revenue consists primarily of third-party manufacturing costs, distribution, overhead and royalties owed to our licensing partner for BRIUMVI sales. Cost of revenue may also include costs related to excess or obsolete inventory adjustment charges, abnormal costs, unabsorbed manufacturing and overhead costs, and manufacturing variances. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, a portion of the costs of producing BRIUMVI sold to date was expensed as research and development prior to FDA approval of BRIUMVI and therefore it is not reflected in the cost of revenue. Our cost of revenue also relates to providing regulatory support & development services to customers.
INVENTORY
Inventories are stated at the lower of cost or estimated net realizable value with cost based on the first-in-first-out method (FIFO). Prior to regulatory approval, we expense costs relating to the production of inventory as research and development expense in the period incurred. Following regulatory approval, costs to manufacture those approved products will be capitalized. Inventory that can be used in either the production of clinical or commercial products is expensed as research and development costs when identified for use in clinical trials.
Prior to the approval of BRIUMVI, all manufacturing and other potential costs related to the commercial launch of BRIUMVI were expensed to research and development expense in the period incurred.
RESEARCH AND DEVELOPMENT COSTS
Generally, research and development costs are expensed as incurred. Nonrefundable advance paymentsResearch and development expenses consist primarily of costs incurred to third-party service providers for goods or services that will be used or renderedthe conduct of research, preclinical and clinical studies, contract manufacturing costs, license milestone fees, personnel costs for futureour research and development activities are deferredemployees, consulting, and amortized over the period that the goods are delivered or theother related services are performed, subject to an assessment of recoverability.expenses. We make estimates of costs incurred in relation to external clinicalrecognize research, organizations, or CROs,preclinical and clinical site costs. We analyze the progress of clinical trials, including levels of patient enrollment, invoices received and contracted costs when evaluating the adequacy of the amount expensed and the related prepaid asset and accrued liability. Significant judgments and estimates must be made and used in determining the accrued balance and expense in any accounting period. We review and accrue CRO expenses and clinical trial study expenses based on workservices performed, pursuant to contracts with third-party research and rely upon estimates of those costs applicable todevelopment organizations that conduct and manage research, preclinical and clinical activities on our behalf. We accrue these expenses based on the progress or stage of completion of a study. Accrued CRO costs are subjectservices and the contracted fees to revisions asbe paid for such trials progress to completion. Revisions are charged to expense inservices. If the period in whichactual timing of the facts that give rise toperformance of services or the revision become known.level of effort varies from the original accrual, we will adjust the accrual accordingly. With respect to clinical sitetrial costs, the financial terms of these agreements are subject to an initial negotiation and vary from contract to contract. Payments under these contracts may be uneven and depend on factors such as the achievement of certain events, the successful recruitment of patients, the completion of portions of the clinical trial or similar conditions. The objective of our policy is to match the recording of expenses in our financial statements to the actual services received and efforts expended. As such, certain expense accruals related to clinical site costs are recognized based on our estimate of the degree of completionperformance of the event or events specified in the specific clinical study or trial contract.
Prepaid research and development in our consolidated balance sheets includes, among other things, costs related to agreements with CROs, certain feescosts to third-party service providers related to development and manufacturing services.services as well as clinical development. These development and manufacturing agreements often require payments in advance of services performed or goods received. Accordingly, as of December 31, 20172023 and 2016,December 31, 2022, we recorded approximately $8.1$4.2 million and $5.7 million, respectively, in prepaid research and development related to such advance agreements.
INCOME TAXES
Income taxes are accounted for under the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to temporary differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases, operating losses and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period that includes the enactment date. If the likelihood of realizing the deferred tax assets or liability is less than “more likely than not,” a valuation allowance is then created.
We, and our subsidiaries, file income tax returns in the U.S. Federalfederal jurisdiction and in various states. We have tax net operating loss carryforwards that are subject to examination for a number of years beyond the year in which they were generated for tax purposes. Since a portion of these net operating loss carryforwards may be utilized in the future, many of these net operating loss carryforwards will remain subject to examination. We recognize interest and penalties related to uncertain income tax positions in income tax expense. Refer to Note 79 for further information foron impact of tax reform.
STOCK-BASED COMPENSATION
The Company measures employee and non-employee stock-based compensation based on the grant date fair value of the stock-based compensation award. The Company grants stock options at exercise prices equal to the fair value of the Company’s common stock on the date of grant, based on observable market prices. The Company uses the Black-Scholes option-pricing model to measure the fair value of stock option awards. We recognize all share-basedstock-based payments to employees and non-employee directors (as compensation for service) as noncash compensation expense in the consolidated financial statements based on the fair values of such payments.statements. Stock-based compensation expense recognized each period is based on the value of the portion of share-basedstock-based payment awards that is ultimately expected to vest during the period. Forfeitures are estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates.
In addition, because some of the options, restricted stock and warrants issued to employees, consultants and other third-partiesthird parties vest upon achievement of certain milestones, the total expense is uncertain. Compensation expense for such awards that vest upon the achievement of milestones is recognized when the achievement of such milestonemilestones becomes probable.
NET LOSSINCOME (LOSS) PER COMMON SHARE
Basic net lossincome (loss) per share of our common sharestock is calculated by dividing net lossincome (loss) applicable to the common sharesstock by the weighted-average number of our common sharesstock outstanding for the period. Diluted net lossincome (loss) per share of common stock includes the effect, if any, from the potential exercise or conversion of securities, such as warrants, stock options, and restricted stock, which would result in the issuance of incremental shares of common stock. The impact of these items is anti-dilutive during periods of net loss. Therefore, basic and diluted net income (loss) per share iswere the same for all periods presented in the consolidated statement of operations, except for the yearended December 31, 2023, as basicthe Company had net loss per common share, sinceincome for that period
The following table summarizes our potentially dilutive securities from stock options, stock warrants and convertible notes would have an antidilutive effect either because the Company incurred a net loss during the period presented or because such potentially dilutive securities were out of the money and the Company realized net income during the period presented. The amounts of potentially dilutive securities excluded from the calculation were 4,835,706, 8,033,779 and 7,064,396 at December 31, 2017, 20162023, 2022 and 2015, respectively. During the years ended December 31, 2017, 2016 and 2015 the Company incurred a net loss, therefore, all of the securities are antidilutive and excluded from the2021:
| December 31, | |||||||||||
| 2023 | 2022 | 2021 | |||||||||
Unvested restricted stock | 8,139,037 | 7,232,254 | 10,532,029 | |||||||||
Options | 4,697,029 | 5,135,685 | 2,467,537 | |||||||||
Warrants | 312,272 | 262,100 | 262,100 | |||||||||
Shares issuable upon note conversion | 20,902 | 20,619 | 18,942 | |||||||||
Total | 13,169,240 | 12,650,658 | 13,280,608 | |||||||||
The computation of basic and diluted lossearnings per share.
December 31, | |||||
| 2017 | 2016 | 2015 | |||
| Unvested restricted stock | 4,820,143 | 7,142,055 | 5,859,914 | ||
| Shares issuable upon note conversion | 15,563 | 14,812 | 17,733 | ||
| Warrants | -- | 876,912 | 1,186,749 | ||
| Total | 4,835,706 | 8,033,779 | 7,064,396 | ||
| Year ended | |||||||||||
| December 31, | |||||||||||
(in thousands, except share and per share data) | 2023 | 2022 | 2021 | |||||||||
Net income (loss) | 12,672 | (198,335 | ) | (348,101 | ) | |||||||
Weighted-average common shares outstanding | 141,955,112 | 135,411,258 | 132,222,753 | |||||||||
Dilutive effect of potential common shares | 6,553,353 | - | - | |||||||||
Weighted-average common shares outstanding assuming dilution | 148,508,465 | 135,411,258 | 132,222,753 | |||||||||
| ||||||||||||
Net income (loss) per share - basic | 0.09 | (1.46 | ) | (2.63 | ) | |||||||
Net income (loss) per share - diluted | 0.09 | (1.46 | ) | (2.63 | ) | |||||||
LONG-LIVED ASSETS AND GOODWILL
Long-lived assets are reviewed for anpotential impairment loss when circumstances indicate that the carrying value of long-lived tangible and intangible assets with finite lives may not be recoverable. Management’s policy in determining whether an impairment indicator exists, a triggering event, exists comprises measurable operating performance criteria as well as qualitative measures. If an analysis is necessitated by the occurrence of a triggering event, we make certain assumptions in determining the impairment amount. If the carrying amount of an asset exceeds its estimated future cash flows, an impairment charge is recognized.
Goodwill results from excess consideration in a business combination over the fair value of identifiable net assets acquired. Goodwill is not amortized but is reviewed for impairment at least annually, or when events arisemore frequently if impairment indicators are present, by first assessing qualitative factors to determine whether it is more likely than not that could indicatethe fair value is less than its carrying amount. If we conclude it is more likely than not that an impairment exists. Wethe fair value is less than the carrying amount, a quantitative test for goodwill impairment using a two-step process. The first stepthat compares the fair value to its carrying value is performed to determine the amount of any impairment.
LEASES
All leases with a lease term greater than 12 months, regardless of lease type classification, are recorded as an obligation on the balance sheet with a corresponding right-of-use asset. Operating leases are reflected as lease liabilities on the commencement date of the reporting unit withlease based on the unit's carrying value, including goodwill. When the carryingpresent value of the reporting unit is greater than fair value,lease payments to be made over the unit’s goodwill may be impaired,lease term. Current operating lease liabilities are reflected in lease liabilities – current portion and noncurrent operating lease liabilities are reflected in lease liabilities – non-current on the second step must be completed to measureconsolidated balance sheet. Right-of-use assets are valued at the amountinitial measurement of the goodwill impairment charge, if any. Inlease liability, plus any initial direct costs or rent prepayments, minus lease incentives and any deferred lease payments. Operating lease right-of-use assets are recorded right of use assets on the second step,consolidated balance sheet and lease cost is recognized on a straight-line basis. Leases with an initial term of 12 months or less are not recorded on the implied fair valuebalance sheet and we recognize lease expense for these leases on a straight-line basis over the term of the reporting unit’s goodwill is compared withlease. In determining whether a contract contains a lease, asset and service agreements are assessed at onset and upon modification for criteria of specifically identified assets, control and economic benefit.
NOTE 2 - REVENUE
As discussed in Note 1, revenues are recognized under guidance within ASC 606. The following table presents our disaggregated revenue for the carrying amountperiods presented (in thousands):
(in thousands) | Year ended December 31, | |||||||||||
| 2023 | 2022 | 2021 | |||||||||
Total product revenue, net | $ | 92,005 | 2,633 | 6,537 | ||||||||
License Revenue | 140,153 | 152 | 152 | |||||||||
Other Revenue | 1,504 | - | - | |||||||||
Total Revenue | $ | 233,662 | $ | 2,785 | $ | 6,689 | ||||||
Product revenue, net
The following tables summarizetable presents our cashdisaggregated revenue by product and cash equivalents at geography for the periods presented:
(in thousands) | Year ended December 31, | ||||||||||
| 2023 | 2022 | 2021 | ||||||||
BRIUMVI | |||||||||||
U.S. | $ | 88,786 | $ | - | $ | - | |||||
International | 3,219 | - | - | ||||||||
Worldwide | $ | 92,005 | $ | - | $ | - | |||||
UKONIQ | |||||||||||
U.S. | $ | - | $ | 2,633 | $ | 6,537 | |||||
International | - | - | - | ||||||||
Worldwide | $ | - | $ | 2,633 | $ | 6,537 | |||||
Total product revenue, net | |||||||||||
U.S. | $ | 88,786 | $ | 2,633 | $ | 6,537 | |||||
International | 3,219 | - | - | ||||||||
Worldwide | $ | 92,005 | $ | 2,633 | $ | 6,537 | |||||
We began shipping BRIUMVI to our U.S. customers in January 2023. We also began shipping BRIUMVI to our ex-U.S. licensing partner, Neuraxpharm, in November 2023. UKONIQ was voluntarily withdrawn from the U.S. market effective May 31, 2022.
During 2023, approximately $9.2 million of gross-to-net accruals entirely related to U.S. sales of BRIUMVI have been recorded as a reduction of accounts receivable, net and within accounts payable and accrued expenses on the condensed consolidated balance sheets.
License Agreements
Neuraxpharm Commercialization Agreement
On July 28, 2023, the Company entered into the Commercialization Agreement with Neuraxpharm. The Company granted Neuraxpharm the exclusive right to commercialize BRIUMVI in certain territories outside the United States, Canada, and Mexico, the commercialization rights for which had been previously retained by the Company, thus excluding certain Asian countries subject to previously existing partnerships (the Territory). In addition, the Company will perform certain development and regulatory activities for Neuraxpharm to support its obligations under the Commercialization Agreement to secure and maintain the regulatory approvals required to sell BRIUMVI in the Territory. As part of the overall arrangement, the Company has agreed to supply BRIUMVI to Neuraxpharm throughout the term of the Commercialization Agreement.
In consideration for entering the Commercialization Agreement, the Company received a non-refundable upfront payment of $140.0 million. The Company will also receive tiered double-digit royalties up to 30% on net product sales in the Territory and is eligible to receive sales-based or other milestone payments totaling up to $505.0 million.
The Company evaluated the Commercialization Agreement under ASC 606 and concluded that Neuraxpharm represents a customer in the transaction. In accordance with this guidance, the Company identified the following commitments under the arrangement: (i) grant the exclusive right to develop, sell, offer to sell and import BRIUMVI in the Territory (the “License”); and (ii) perform certain development and regulatory activities (“Development and Regulatory Activities”).
The License to the Company’s intellectual property represents a distinct performance obligation, therefore, the $140 million non-refundable upfront payment related to this performance obligation was recognized as License Revenue in 2023.
The Development and Regulatory Activities also represent a distinct performance obligation and are satisfied over time because Neuraxpharm simultaneously receives and consumes the benefits provided by the Company’s performance of the services. Therefore, revenue is recognized as the activities are completed by the Company. During 2023 the Company recognized Other Revenue of $1.5 million related to the Development and Regulatory Activities.
The arrangement also provides Neuraxpharm with the right to make optional purchases of BRIUMVI (the “Supply of Licensed Product”). These optional purchases are accounted for as a separate contract when the right to purchase BRIUMVI is exercised. The consideration for optional purchases of BRIUMVI by Neuraxpharm approximates the price that a customer in the Territory would be willing to pay for these goods.
The performance obligation related to the Supply of Licensed Product is satisfied when control of the product passes to Neuraxpharm. The consideration received from Neuraxpharm for the supply of BRIUMVI is recognized by the Company as a component of product revenue, net. As of December 31, 20172023, the Company has an unconditional right to receive $1.9 million in consideration from Neuraxpharm related to the performance obligation to supply BRIUMVI, which is recorded as accounts receivable, net. A portion of the performance obligation to supply BRIUMVI has not yet been satisfied, therefore, as of December 31, 2023, $5.9 million has been recorded as deferred revenue. During 2023 the Company recognized $3.2 million in BRIUMVI product sales, net related to performance obligations that were satisfied during the year ended December 31, 2023. The Company will reevaluate the consideration received, and 2016:performance obligations satisfied at the end of each reporting period. Such reevaluations may result in a change to the amount of product revenue, net, recognized and deferred revenue.
The remaining forms of consideration are variable because they are dependent on the achievement of sales-based or other milestones. The Company evaluated the constraint on variable consideration and concluded that the milestone payments are highly dependent on factors outside of the Company’s control. Therefore, at contract inception, the milestones are not included in the transaction price as it is not probable that a significant reversal of revenue would not occur. Sales-based milestones will be recognized as revenue in the period when the related sales threshold is met. All other milestones will be recognized as revenue immediately in the period the achievement of the underlying milestone is probable. Any consideration related to sales-based royalties will be recognized when the related sales occur. No royalty or milestone revenue was recognized during 2023.
December 31, 2017 | December 31, 2016 | |
| Checking and bank deposits | $55,681,820 | $4,052,333 |
| Money market funds | 1,036,027 | 20,978,947 |
| Total | $56,717,847 | $25,031,280 |
NOTE3 – INVESTMENT SECURITIES
Our investments as of December 31, 2017 2023 and 20162022 are classified as held-to-maturity. Held-to-maturity investments are recorded at amortized cost. During the year ended December 31, 2016, we liquidated our long-term investment securities with a net carrying amount of approximately $12.6 million, realizing a gain of approximately $33,000 on the sale. The decision to sell our long-term securities was made due to market rate conditions on long-term securities coupled with the recognized gain we were able to yield on the sale of the securities.
The following tables summarize our investment securities at December 31, 2017 2023 and 2016:
| December 31, 2023 | |||||||||||||||
Amortized | Gross | Gross | ||||||||||||||
| cost, as | unrealized | unrealized | Estimated | ||||||||||||
(in thousands) | adjusted | holding gains | holding losses | fair value | ||||||||||||
Short-term investments: | | | | | ||||||||||||
Obligations of domestic governmental agencies (maturing between January 2024 and June 2024) (held-to-maturity) | $ | 124,575 | $ | 30 | $ | 53 | $ | 124,552 | ||||||||
Total short-term investment securities | $ | 124,575 | $ | 30 | $ | 53 | $ | 124,552 | ||||||||
December 31, 2022 | ||||||||||||||||
Amortized | Gross | Gross | ||||||||||||||
| cost, as | unrealized | unrealized | Estimated | ||||||||||||
| adjusted | holding gains | holding losses | fair value | ||||||||||||
Short-term investments: | | | | | ||||||||||||
Obligations of domestic governmental agencies (maturing between January 2023 and December 2023) (held-to-maturity) | $ | 59,374 | $ | — | $ | 1,053 | $ | 58,321 | ||||||||
Long-term investments: | ||||||||||||||||
Obligations of domestic governmental agencies (maturing between January 2024 and February 2024) (held-to-maturity) | 12,404 | — | 429 | 11,975 | ||||||||||||
Total short-term and long-term investment securities | $ | 71,778 | $ | — | $ | 1,482 | $ | 70,296 | ||||||||
December 31, 2017 | ||||
Amortized cost, as adjusted | Gross unrealized holding gains | Gross unrealized holding losses | Estimated fair value | |
| Short-term investments: | ||||
Obligations of domestic governmental agencies (maturing between January 2018 and November 2018) (held-to-maturity) | $27,998,810 | $-- | $35,235 | $27,963,575 |
| Total short-term investment securities | $27,998,810 | $-- | $35,235 | $27,963,575 |
December 31, 2016 | ||||
Amortized cost, as adjusted | Gross unrealized holding gains | Gross unrealized holding losses | Estimated fair value | |
| Short-term investments: | ||||
| Obligations of domestic governmental agencies (maturing between February 2017 and September 2017) (held-to-maturity) | $19,853,860 | $3,270 | $2,492 | $19,854,638 |
| Total short-term investment securities | $19,853,860 | $3,270 | $2,492 | $19,854,638 |
NOTE4 –INVENTORY
The following table presents our inventory as of December 31, 2023 (in thousands):
December 31, 2023 | ||
Raw Materials | $ 6,582 | |
Work in Process | 31,243 | |
Finished Goods | 1,999 | |
Total Inventory | $ 39,824 |
Inventory is stated at the lower of cost or net realizable value and consists of raw materials, work-in-process and finished goods. Cost is determined using a standard cost method, which approximates actual cost, and assumes a FIFO flow of goods. At December 31,2023, all our inventory was related to BRIUMVI, which was approved by the FDA on December 28, 2022, at which time we began to capitalize costs to manufacture BRIUMVI. Prior to FDA approval of BRIUMVI, all costs related to the manufacturing of BRIUMVI and related material were charged to research and development expense in the period incurred. No costs related to the manufacturing of BRIUMVI and the related material were incurred between the approval date and year end 2022, therefore, inventory is not included in the December 31, 2022 consolidated balance sheet. Inventory that is used for clinical development purposes is expensed to research and development expense when consumed. For December 30, 2023 we determined that a reserve related to BRIUMVI inventory is not required.
NOTE 45 – FAIR VALUE MEASUREMENTS
We measure certain financial assets and liabilities at fair value on a recurring basis in the financial statements. The fair value hierarchy ranks the quality and reliability of inputs, or assumptions, used in the determination of fair value and requires financial assets and liabilities carried at fair value to be classified and disclosed in one of the following three categories:
● | Level 1 – quoted prices in active markets for identical assets and liabilities; |
● | Level 2 – inputs other than Level 1 quoted prices that are directly or indirectly observable; and |
● | Level 3 – unobservable inputs that are not corroborated by market data. |
At the time of our merger (we were then known as Manhattan Pharmaceuticals, Inc. (“Manhattan”)(Manhattan)) with Ariston Pharmaceuticals, Inc. (“Ariston”)(Ariston) in March 2010, Ariston issued $15.5 million of five-yearfive-year 5% notes payable (the “5% Notes”)5% Notes) in satisfaction of several note payable issuances. The 5% Notes and accrued and unpaid interest thereon are convertible at the option of the holder into common stock at the conversion price of $1,125 per share. Ariston agreed to make quarterly payments on the 5% Notes equal to 50% of the net product cash flow received from the exploitation or commercialization of Ariston’s product candidates, AST-726 and AST-915. We have no obligations under the 5% Notes aside from a) 50% of the net product cash flows from Ariston’s product candidates, if any, payable to noteholders; and b) the conversion feature, discussed above.
The following tables provide the fair value measurements of applicable financial liabilities as of December 31, 2017 2023 and 2016:
Financial liabilities at fair value as of December 31, 2017 | ||||
Level 1 | Level 2 | Level 3 | Total | |
| 5% Notes | $-- | $-- | $127,614 | $127,614 |
| Totals | $-- | $-- | $127,614 | $127,614 |
Financial liabilities at fair value as of December 31, 2016 | ||||
Level 1 | Level 2 | Level 3 | Total | |
| 5% Notes | $-- | $-- | $68,875 | $68,875 |
| Totals | $-- | $-- | $68,875 | $68,875 |
| Financial liabilities at fair value as of December 31, 2023 | |||||||||||||||
(in thousands) | Level 1 | Level 2 | Level 3 | Total | ||||||||||||
| | | | | ||||||||||||
5% Notes | $ | — | $ | — | $ | 357 | $ | 357 | ||||||||
Total | $ | — | $ | — | $ | 357 | $ | 357 | ||||||||
| Financial liabilities at fair value as of December 31, 2022 | |||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | ||||||||||||
| | | | | ||||||||||||
5% Notes | $ | — | $ | — | $ | 243 | $ | 243 | ||||||||
Total | $ | — | $ | — | $ | 243 | $ | 243 | ||||||||
The Level 3 amounts above represent the fair value of the 5% Notes and related accrued interest.
The Company’s financial instruments include cash, cash equivalents consisting of money market funds, accounts receivable, accounts payable and Subsidiaries
We have no Level 1 or Level 2 instruments. Our Level 3 instrument amounts represent the fair value of the 5%Notes to Consolidated Financial Statements
(in thousands) | ||||
Balance at January 1, 2022 | 360 | |||
Interest accrued on face value of 5% Notes | 1,073 | |||
Change in fair value of Level 3 liabilities | (1,190 | ) | ||
Balance at December 31, 2022 | $ | 243 | ||
Interest accrued on face value of 5% Notes | 1,133 | |||
Change in fair value of Level 3 liabilities | (1,019 | ) | ||
Balance at December 31, 2023 | $ | 357 |
The change in the fair value of the Level 3 liabilities is reported in other (income) expense in the accompanying consolidated statements of operations.
NOTE 56 – STOCKHOLDERS’ STOCKHOLDERS’ EQUITY
Preferred Stock
Our amended and restated certificate of incorporation authorizes the issuance of up to 10,000,000 shares of preferred stock, $0.001 par value, with rights senior to those of our common stock, issuable in one or more series. Upon issuance, the Companywe can determine the rights, preferences, privileges and restrictions thereof. These rights, preferences and privileges could include dividend rights, conversion rights, voting rights, terms of redemption, liquidation preferences, sinking fund terms and the number of shares constituting any series or the designation of such series, any or all of which may be greater than the rights of common stock.
Stockholder Rights Plan
On July 18,2014, we adopted a stockholder rights plan. The stockholder rights plan is embodied in the Stockholder Protection Rights Agreement dated as of July 18,2014 (the "Rights Agreement")Rights Agreement), between us and American Stock Transfer & Trust Company, LLC, as rights agent (the "Rights Agent")Rights Agent).
Accordingly, the Board of Directors declared a distribution of one right (a “Right”) for each outstanding share of common stock, to stockholders of record at the close of business on July 28,2014, for each share of common stock issued (including shares distributed from treasury)Treasury) by us thereafter and prior to the Separation Time (as defined in the Rights Agreement), and for certain shares of common stock issued after the Separation Time. Following the Separation Time, each Right entitles the registered holder to purchase from us one one-thousandth (1/1,000)one-thousandth (1/1,000) of a share of Series A Junior Participating Preferred Stock, par value $0.001 per share (the "Preferred Stock")Preferred Stock), at a purchase price of $100.00 (the "Exercise Price")Exercise Price), subject to adjustment. The description and terms of the Rights are set forth in the Rights Agreement. Each one one-thousandthone-thousandth of a share of Preferred Stock has substantially the same rights as one share of common stock. Subject to the terms and conditions of the Rights Agreement, Rights become exercisable ten days after the public announcement that a “Person” has become an “Acquiring Person” (as each such term is defined in the Rights Agreement). Any Rights held by an Acquiring Person are void and may not be exercised.
The Rights Agreement was approved by our Board of Directors on July 18,2014. The Rights will expire at the close of business on its ten year-year anniversary, unless earlier exchanged or terminated by us.
Common Stock
Our amended and restated certificate of incorporation authorizes the issuance of up to 150,000,000175,000,000 shares of $0.001 par value common stock.
On June 21, 2013,September 5, 2019, we filed an automatic “shelf registration” statement on Form S-3 (the 2019 WKSI Shelf) as a “well-known seasoned issuer” as defined in Rule 405 under the Securities Act, which registered an unlimited and indeterminate amount of debt or equity securities for future issuance and sale. The 2019 WKSI Shelf was declared effective in September 2019. In connection with the 2019 WKSI Shelf, we entered into an At-the-Market Issuance Sales Agreement (the "2013 ATM")2020 ATM) with MLVJefferies LLC, Cantor Fitzgerald & Co. LLC ("MLV") under which we could issue and sellB. Riley Securities, Inc. (each a 2020 Agent and collectively, the 2020 Agents), relating to the sale of shares of our common stock, having an aggregate offering price of up to $50.0 million, from time to time through MLV, acting as the sales agent.stock. Under the agreement we would pay MLV a commission rate of up to 3.0% of the gross proceeds from the sale of any shares of common stock sold through MLV.
During the year ended December 31, 2021, we sold a total of 72,000 shares of common stock under the 2021 ATM for aggregate total gross proceeds of approximately $2.5 million at an average selling price of $34.25 per share, resulting in net proceeds of approximately $2.4 million after deducting commissions and other transactions costs.
On September 2, 2022, we filed an automatic “shelf registration” statement on Form S-3 (the 2022 WKSI Shelf) as a “well-known seasoned issuer” as defined in Rule 405 under the Securities Act, which registered an unlimited and indeterminate amount of debt or equity securities for future issuance and sale. The 2022 WKSI Shelf was declared effective in September 2022. In connection with the 2022 WKSI Shelf, we entered into an At-the-Market Issuance Sales Agreement (the 2022 ATM) with Cantor Fitzgerald & Co., FBR Capital Markets & Co., SunTrust Robinson Humphrey, and B. Riley Securities, Inc., Raymond James & Associates, Inc., Ladenburg Thalmann & Co. Inc. and H.C. Wainwright & Co., LLC (each a "2017 Agent"2022 Agent and collectively, the "2017 Agents")2022 Agents), relating to the sale of shares of our common stock. Under the 20172022 ATM, we will pay the 20172022 Agents a commission rate of up to 3.0% of the gross proceeds from the sale of any shares of common stock.
During the year ended December 31, 2017, 2023, we sold a total of 4,689,4181,385,700 shares of common stock under the 20172022 ATM for aggregate total gross proceeds of approximately $47.7$47.1 million at an average selling price of $10.18$34.01 per share, resulting in net proceeds of approximately $46.9$46.3 million after deducting commissions and other transactions costs.
Treasury Stock
As of December 31, 2017 2023 and 2016,2022, 41,309 shares of common stock are being held in Treasury, at a cost of approximately $234,000,$0.2 million, representing the fair market value on the date the shares were surrendered to the Company to satisfy employee tax obligations.
Equity Incentive Plans
The TG Therapeutics, Inc. Amended and Restated 20122022 Incentive Plan (“2012(the 2022 Incentive Plan”)Plan) was approved by stockholders in June 2015.2022 with 17 million shares available to be issued, of which not more than 10 million shares may be issued pursuant to “full-value awards.” Full-value awards include any award other than an option or stock appreciation right and which is settled by the issuance of stock. As of December 31, 20172023, 4,631,204 shares of restricted stock and 2016, no2,272,500 options were outstanding, and up to an additional 504,1288,751,892 shares maywere available to be issued under the 20122022 Incentive Plan.
The TG Therapeutics, Inc. Amended and Restated 2012 Incentive Plan
Total stock-based compensation expense recognition as a resultincluded in the consolidated statements of operations was $37.9 million, $19.2 million and $61.3 million during the modification.years ended December 31, 2023, 2022 and 2021, respectively. The $37.9 million is net of $2.9 million of stock-based compensation expense that was capitalized into inventory during the year ended December 31, 2023.
Stock Options
The estimated fair value of the options granted in the years ended December 31, 2023, 2022 and 2021 was determined utilizing the Black-Scholes option-pricing model at the date of grant. The following table summarizes stock option activity for the years ended December 31, 2017, 20162023, 2022 and 2015:
| Number of shares | Weighted- average exercise price | Weighted- average contractual term | Aggregate intrinsic value | |
(in years) | ||||
| Outstanding at January 1, 2015 | 194 | 971.70 | 3.50 | $-- |
| Granted | -- | -- | ||
| Exercised | -- | -- | ||
| Forfeited | (152) | 463.32 | ||
| Expired | (42) | 2,811.53 | ||
Outstanding at December 31, 2015 | -- | -- | -- | $-- |
| Granted | -- | -- | ||
| Exercised | -- | -- | ||
| Forfeited | -- | -- | -- | |
| Expired | -- | -- | ||
Outstanding at December 31, 2016 | -- | -- | -- | $-- |
| Granted | -- | -- | ||
| Exercised | -- | -- | ||
| Forfeited | -- | -- | ||
| Expired | -- | -- | ||
| Outstanding at December 31, 2017 | -- | $-- | -- | $-- |
| Exercisable at December 31, 2017 | -- | $-- | -- | $-- |
| | | Weighted- | | ||||||||||||
| | | average | | ||||||||||||
| | Weighted- | contractual | | ||||||||||||
| Number of | average | term | Aggregate | ||||||||||||
| shares | exercise price | (in years) | intrinsic value | ||||||||||||
| ||||||||||||||||
Outstanding at January 1, 2021 | 2,526,166 | 6.99 | 8.10 | $ | 115,472,832 | |||||||||||
Granted | — | $ | — | | | |||||||||||
Exercised | (52,694 | ) | 4.10 | | | |||||||||||
Forfeited | (5,935 | ) | 4.10 | | | |||||||||||
Expired | — | — | | | ||||||||||||
Outstanding at December 31, 2021 | 2,467,537 | $ | 7.06 | 6.99 | $ | 29,503,551 | ||||||||||
Granted | 2,975,000 | 7.00 | | | ||||||||||||
Exercised | (142,409 | ) | 4.10 | | | |||||||||||
Forfeited | (164,443 | ) | 7.84 | | | |||||||||||
Expired | — | — | | | ||||||||||||
Outstanding at December 31, 2022 | 5,135,685 | $ | 7.10 | 5.09 | $ | 25,064,799 | ||||||||||
Granted | — | — | | | ||||||||||||
Exercised | (246,156 | ) | 6.08 | | | |||||||||||
Forfeited | (192,500 | ) | 11.30 | | | |||||||||||
Expired | — | — | | | ||||||||||||
Outstanding at December 31, 2023 | 4,697,029 | $ | 6.98 | 4.10 | $ | 47,607,209 | ||||||||||
| | | | | ||||||||||||
Exercisable at December 31, 2023 | 2,133,273 | $ | 6.60 | 4.72 | $ | 22,518,984 | ||||||||||
Total expense associated with stock options was approximately $3.9 million, $3.3 million and $2.9 million during the years ended December 31, 2023, 2022 and 2021, respectively. As of December 31, 2017,2023, there are no unvested option awards and nowas approximately $4.1 million of total unrecognized compensation cost related to unvested time-based stock options, which is expected to be recognized over a weighted-average period of 2.6 years. As of December 31, 2023, the stock options outstanding include options granted to both employees and non-employees which are both time-based and milestone-based. Stock-based compensation for milestone-based options will be recorded if and when a milestone becomes probable. We did not recognize stock-based compensation expense during the year ended December 31, 2023 for these stock options.
The fair value of the Company’s option awards.
| Year Ended | |||||||||||
| December 31, 2023 | December 31, 2022 | December 31, 2021 | |||||||||
Volatility | N/A | 88.37 - 89.67 | % | N/A | ||||||||
Expected term (in years) | N/A | 3.13 - 4.0 | N/A | |||||||||
Risk-free rate | N/A | 2.99 - 3.35 | % | N/A | ||||||||
Expected dividend yield | N/A | — | % | N/A | ||||||||
Restricted Stock
Certain employees, directors and consultants have been awarded restricted stock. The restricted stock vesting consists of milestone and time-based vesting. The following table summarizes restricted share activity for the years ended December 31, 2017, 20162023, 2022 and 2015:
Number of Shares | Weighted Average Grant Date Fair Value | |
| Outstanding at January 1, 2015 | 6,400,001 | 5.86 |
| Granted | 1,992,535 | 12.89 |
| Vested | (1,001,455) | 5.04 |
| Forfeited | (31,166) | 16.76 |
| Outstanding at December 31, 2015 | 7,359,915 | 7.83 |
| Granted | 1,924,639 | 4.99 |
| Vested | (595,726) | 7.38 |
| Forfeited | (46,773) | 10.34 |
| Outstanding at December 31, 2016 | 8,642,055 | $7.20 |
| Granted | 1,836,511 | 6.40 |
| Vested | (4,103,048) | 5.24 |
| Forfeited | (53,875) | 8.47 |
| Outstanding at December 31, 2017 | 6,321,643 | $7.17 |
| | Weighted-average | ||||||
| | grant date fair | ||||||
| Number of shares | value | ||||||
Outstanding at January 1, 2021 | 10,785,034 | 13.38 | ||||||
Granted | 2,738,974 | 39.49 | ||||||
Vested | (1,302,737 | ) | 18.14 | |||||
Forfeited | (189,231 | ) | 21.80 | |||||
Outstanding at December 31, 2021 | 12,032,040 | 18.67 | ||||||
Granted | 5,179,201 | 12.75 | ||||||
Vested | (6,291,999 | ) | 11.28 | |||||
Forfeited | (2,186,956 | ) | 22.44 | |||||
Outstanding at December 31, 2022 | 8,732,286 | 16.12 | ||||||
Granted | 3,620,237 | 13.77 | ||||||
Vested | (2,500,263 | ) | 11.98 | |||||
Forfeited | (213,192 | ) | 12.14 | |||||
Outstanding at December 31, 2023 | 9,639,068 | $ | 17.05 | |||||
Total compensation expense associated with restricted stock grants was $15,945,284, $7,509,999$34.1 million, $15.8 million and $15,697,092$58.4 million during the years ended December 31, 2017, 20162023, 2022 and 2015,2021, respectively. As of December 31, 2017,2023, there was approximately $14.8$27.8 million of total unrecognized compensation expense related to unvested time-based restricted stock, which is expected to be recognized over a weghted-averageweighted-average period of 1.0 year.2.7 years. This amount does not include, as of December 31, 2017, 242,0002023, 2,470,770 shares of restricted stock outstanding which are milestone-based and vest upon certain corporate milestones; and 2,413,917 shares of restricted stock outstanding issued to non-employees. milestones. Milestone-based non-cashnoncash compensation expense will be measured and recorded if and when a milestone becomes probable.
Warrants
The Company’s only outstanding warrants are the warrants issued to Hercules as part of the Loan Agreement, the Amended Loan Agreement and the First Amendment (please refer to Note 7– Loan Payable) to purchase 147,058, 115,042 and 50,172 shares of our common stock with exercise prices of $4.08, $17.95 and $14.70, respectively. See Note 7 for further details. As the warrants could not require cash settlement, the warrants were classified as equity. There will not be any ongoing stock compensation expense volatility associated with these warrants.
NOTE 7– LOAN PAYABLE
On February 28,2019 (the Closing Date), we entered into a term loan facility with Hercules Capital, Inc. (Hercules or Lender), which provided us with the capacity to borrow up to an aggregate principal amount of $60.0 million (Term Loan). The Term Loan is governed by a loan and security agreement, dated February 28,2019 (the Loan Agreement), which provides for non-employee shares is determinedup to four separate advances. The first advance of $30.0 million was drawn on the Closing Date. An additional $30.0 million under the Term Loan was previously available upon the completion of different milestones and time points that have now lapsed.
On December 30, 2021 (the Amended Loan Agreement Closing Date), the Company entered into an Amended and Restated Loan and Security Agreement (the Amended Loan Agreement) with Hercules Capital, Inc. The Amended Loan Agreement amended the terms of the Loan Agreement to, among other things, (i) increase the aggregate principal amount of the loan, available at the “measurement date.” The expense is recognized overCompany’s option, from $60.0 million to $200.0 million (the Amended Term Loan), (ii) issue a first advance of $70.0 million drawn at the vesting periodAmended Loan Agreement Closing Date, a portion of which was used to refinance the current outstanding loan balance of approximately $7.8 million and pay for expenses incurred by the Lender in executing the agreements, (iii) change the draw amounts and dates available in subsequent tranches, (iv) extend the maturity date of the award. Untilfacility from the measurementoriginal March 1, 2022 to January 1, 2026, (v) reset and extend the interest only period from April 1, 2021 to February 1, 2025 and extendable to August 1, 2025 subject to the achievement of certain performance milestones, and (vi) modify the cash interest rate to be the greater of either (a) the “prime rate” as reported in The Wall Street Journal plus 2.15%, and (b) 5.40%. In addition to the cash interest rate, the principal balance accrues paid-in-kind interest at a rate of 3.45%, which amount will be capitalized and added to the outstanding principal balance of the Amended Term Loan and payable at the maturity date is reached,of the totalAmended Loan Agreement.
On March 31, 2023 (the First Amendment Effective Date), the Company entered into a First Amendment to the Amended and Restated Loan and Security Agreement (the First Amendment) with Hercules. The First Amendment amended the terms of the Amended Loan Agreement to, among other things: (i) issue an advance of $25.0 million drawn at the First Amendment Effective Date (the Tranche 3A Advance), (ii) provide for the formal expiration of Tranche 2, (iii) change the draw amounts and dates available under subsequent tranches, including splitting the remaining balance of Tranche 3 into two additional advances in an aggregate principal amount of compensation expense remains uncertain. We record compensation expense basedup to $20.0 million, in increments of $10.0 million (a Tranche 3B Advance and a Tranche 3C Advance), decreasing the amount available under Tranche 4 from $65.0 million to $60.0 million, and adding a Tranche 5 of $25.0 million, subject to the achievement of revenue related performance milestones, (iv) extend the interest only period from February 1, 2025 to August 1, 2025 and (v) modify the cash interest rate to be the greater of either (a) the “prime rate” as reported in The Wall Street Journal plus 1.20%, and (b) 8.95%. In addition to the cash interest rate, the principal balance will accrue paid-in-kind interest at a rate of 2.25%, which amount will be capitalized and added to the outstanding principal balance of the Amended Term Loan and payable at the maturity date of the Amended Loan Agreement, as amended. The Amended Loan agreement, as amended, contains financial covenants that require the Company to maintain certain levels of unrestricted cash and additional financial covenants related to market capitalization. As of December 31, 2023, we are in compliance with all financial covenants.
The First Amendment also contains warrant coverage of 2.95% of each advance amount funded. A warrant (the Warrant) was issued by the Company to Hercules to purchase 115,042 shares of common stock with an exercise price of $17.95 for the initial amount funded at the Closing Date. The Warrant shall be exercisable for seven years from the date of issuance. Hercules may exercise the Warrant either by (a) cash or check or (b) through a net issuance conversion. Additionally, a warrant was issued by the Company to Hercules to purchase 50,172 shares of common stock with an exercise price of $14.70 for the amount funded pertaining to the Tranche 3A Advance (the First Amendment Warrant). The First Amendment Warrant shall be exercisable for seven years from the date of issuance. Hercules may exercise the First Amendment Warrant either by (a) cash or check or (b) through a net issuance conversion
In addition, the Company is required to pay a final payment fee equal to 5.95% of the aggregate principal amount of the Term Loan Advances (as defined in the Amended Loan Agreement, as amended) plus 4.95% of the aggregate principal amount of all other advances.
The Company may, at its option, prepay the Amended Term Loan in full or in part, subject to a prepayment penalty equal to (i) 1.5% of the principal amount prepaid if the prepayment occurs prior to the first anniversary of the First Amendment Effective Date, and (ii) 1.0% of the principal amount prepaid if the prepayment occurs on or after the first anniversary of the First Amendment Effective Date.
The Company evaluated whether the First Amendment represented a debt modification or extinguishment of the Amended Term Loan in accordance with ASC 470-50, Debt – Modifications and Extinguishments. As a result of the modification of terms and no repayment or retirement of the Amended Term Loan, the Amended Term Loan was accounted for by the Company under the modification accounting model. The Company capitalized the facility charge from the First Amendment advance to debt issuance costs and expensed third party fees in the Company’s statement of operations for the year ended December 31, 2023.
The Company estimated the fair value of the award atWarrant using the reporting date.
| The First Amendment | The Amended Loan Agreement | The Loan Agreement | |||||||||
Exercise price | $ | 14.70 | $ | 17.95 | $ | 4.08 | ||||||
Common share price on date of issuance | $ | 15.04 | $ | 19.35 | $ | 6.80 | ||||||
Volatility | 0.88 | % | 184.40 | % | 195.90 | % | ||||||
Risk-free interest rate | 3.6 | % | 1.4 | % | 2.6 | % | ||||||
Expected dividend yield | — | % | — | % | — | % | ||||||
Contractual term (in years) | 7.00 | 7.00 | 7.00 | |||||||||
The following table summarizes warrant activityCompany incurred financing expenses of $2.0 million (including the fair value of the First Amendment Warrant) related to the First Amendment which are recorded as debt issuance costs and as an offset to loan payable on the Company’s consolidated balance sheet The debt issuance costs are being amortized over the term of the debt using the straight-line method, which approximates the effective interest method, and will be included in interest expense in the Company’s consolidated statements of operations. Amortization of debt issuance costs was $2.4 million, $1.8 million and $1.1 million for the years ended December 31, 2017,2023, 2022 and 2021, respectively. At December 31, 2023, the remaining unamortized balance of debt issuance costs was $5.1 million.
The loan payable as of December 31, 2023 and 2022, is as follows:
| December 31, | December 31, | ||||||
(in thousands) | 2023 | 2022 | ||||||
Loan payable | $ | 95,000 | $ | 70,000 | ||||
Add: Accreted Liability of final payment fee | 10,230 | 6,667 | ||||||
| 105,230 | 76,667 | ||||||
Less: unamortized debt issuance costs | (5,112 | ) | (5,532 | ) | ||||
| 100,118 | 71,135 | ||||||
Less: principal payments | — | — | ||||||
Total loan payable | 100,118 | 71,135 | ||||||
Less: current portion | — | — | ||||||
Loan payable non-current | $ | 100,118 | $ | 71,135 | ||||
NOTE 8– LEASES
In October 2014, we entered into an agreement (the Office Agreement) with Fortress Biotech, Inc. (FBIO) to occupy approximately 45% of the 24,000 square feet of New York City office space leased by FBIO. The Office Agreement requires us to pay our respective share of the average annual rent and other costs of the 15-year lease. We approximate an average annual rental obligation of $1.8 million under the Office Agreement. We began to occupy this new space in April 2016, with rental payments beginning in the third quarter of 2016. At January 1, 2019, we recognized a lease liability and 2015:corresponding right-of-use (ROU) asset of $9.5 million and $8.1 million, respectively, based on the present value of the remaining lease payments for all of our leased office spaces, the majority of which is comprised of our New York City office space. The present values of our lease liability and corresponding ROU asset are $10.7 million and $8.1 million, respectively, as of December 31, 2023. Our leases have remaining lease terms of approximately 2 years to 8 years. One lease has a renewal option to extend the lease for an additional term of five years.
Also, in connection with this lease, in October 2014 we pledged $0.6 million to secure a line of credit as a security deposit for the Office Agreement, which has been recorded as restricted cash in the accompanying consolidated balance sheets. Additional collateral of $0.6 million was pledged in April 2018 to increase the letter of credit for the office space.
In October 2019, we finalized a five-year lease for office space in New Jersey (the NJ Lease). We approximate an average annual rental obligation of $0.3 million under the NJ Lease.
Warrants | Weighted- average exercise price | Aggregate intrinsic value | |
| Outstanding at January 1, 2015 | 4,148,228 | 0.94 | $61,792,184 |
| Issued | -- | -- | |
| Exercised | (2,950,115) | 0.36 | |
| Expired | (11,364) | 2.25 | |
| Outstanding at December 31, 2015 | 1,186,749 | 2.37 | $11,341,452 |
| Issued | -- | -- | |
| Exercised | (273,370) | 2.26 | |
| Expired | -- | 2.25 | |
| Outstanding at December 31, 2016 | 913,379 | $2.41 | $1,961,403 |
| Issued | -- | -- | |
| Exercised | (887,585) | 2.41 | |
| Expired | (25,794) | -- | |
| Outstanding at December 31, 2017 | -- | $-- | $-- |
In October 2021, we finalized a five-year lease for office space in North Carolina (the NC Lease). We approximate an average annual rental obligation of $0.2 million under the NC Lease. We took possession of this space in February 2022, with rental payments beginning in April 2022.
Operating lease cost was $2.2 million, $2.7 million and $2.2 million for the years ended December 31, 2023, 2022 and 2021, respectively.
As of December 31, 2023, the weighted-average remaining operating lease term was 5.8 years and the weighted-average discount rate for operating leases was 10.00%. Cash paid for amounts included in the measurement of operating lease liabilities during the year ended December 31, 2023 was $2.4 million.
The following is a summarybalance sheet classification of notes payable:
December 31, 2017 | December 31, 2016 | |||||
Current portion, net | Non-current portion, net | Total | Current portion, net | Non-current portion, net | Total | |
| Convertible 5% Notes Payable | $127,614 | $-- | $127,614 | $68,875 | $-- | $68,875 |
| Totals | $127,614 | $-- | $127,614 | $68,875 | $-- | $68,875 |
| December 31, | December 31, | ||||||
(in thousands) | 2023 | 2022 | ||||||
Liabilities | | | ||||||
Lease liability current portion | $ | 1,446 | $ | 1,581 | ||||
Lease liability non-current | 9,231 | 10,344 | ||||||
Total lease liability | $ | 10,677 | $ | 11,925 | ||||
As of December 31, 2023, the maturities of lease liabilities were as follows:
Operating | ||||
leases | ||||
2024 | $ | 2,388 | ||
2025 | 2,100 | |||
2026 | 2,080 | |||
2027 | 1,913 | |||
2028 | 1,827 | |||
After 2028 | 4,715 | |||
Total lease payments | 15,023 | |||
Less: interest | (4,346 | ) | ||
Present value of lease liabilities(*) | $ | 10,677 | ||
(*) As our leases do not provide an implicit rate, we use our incremental borrowing rate based on the information available at commencement date and accrued and unpaid interest thereon are convertible atconsidering the optionterm of the holder into common stock atlease to determine the conversion pricepresent value of $1,125 per share. lease payments. We have no obligation underused the 5% Notes aside from (a) 50%incremental borrowing rate of the net product cash flows from Ariston’s product candidates, if any, payable10.25% on February 28, 2019, for leases that commenced prior to noteholders; and (b) the conversion feature, discussed above. Interest accrues monthly, is added to principal on an annual basis, every March 8, and is payable at maturity, which was March 8, 2015 (see Note 4 for further details).
NOTE 79 – INCOME TAXES
We account for income taxes under the asset and liability method. Deferred tax assets and liabilities are determined based on differences between the financial reporting and tax basis of assets and liabilities and are measured using the enacted tax rates and laws that will be in effect when the differences are expected to reverse. A valuation allowance is established when necessary to reduce deferred tax assets to the amount expected to be realized. In determining the need for a valuation allowance, management reviews both positive and negative evidence, including current and historical results of operations, future income projections and the overall prospects of our business. Based upon management's assessment of all available evidence, we believe that it is more-likely-than-notmore-likely-than-not that the deferred tax assets will not be realizable, and therefore, a valuation allowance has been established. The valuation allowance for deferred tax assets was approximately $99,713,000$418.3 million and $116,172,000$400.4 million as of December 31, 2017 2023 and 2016,2022, respectively.
The Tax Cuts and Jobs Act (the “Act”) was signed into law. Among other things,of 2017 (TCJA) included changes to the Act reduces our corporate federaltreatment of research and development expenses under IRC Section 174. Formerly, a company could deduct research and development expenses under IRC Section 174 as incurred. Effective for tax rate from 34% to 21% effective January 1, 2018. As a result, weyears beginning after December 31, 2021, research and development expenses under IRC Section 174 are required to re-measure, throughbe capitalized, with an amortization period of 5 years for costs incurred in the U.S. and 15 years for costs incurred in a non-U.S. jurisdiction. The Company incurred approximately $61.8 million of U.S. research and development costs and approximately $13.9 million of non-U.S. research and development costs that were capitalized during the year ended December 31, 2023.
The Inflation Reduction Act of 2022 (IRA) was enacted on August 16, 2022. The IRA provided for a Corporate Alternative Minimum Tax (Corp AMT), applicable to tax years beginning after December 31, 2022. The Corp AMT will impose a 15% tax on companies with adjusted financial statement income tax expense, our deferred tax assets and liabilities usingof over $1 billion for US-based organizations. At this time, it is not anticipated that the enacted rate at which we expect them toCorp AMT will be recovered or settled. The re-measurement of our net deferred tax asset would have resulted in additional income tax expense of $51,767,584; however, with full valuation allowance in place,applicable for the expense is reversed through a corresponding adjustment to the valuation allowance, resulting in no impact on income tax expense.
As of December 31, 2017,2023, we have U.S. net operating loss carryforwards (“NOLs”) of approximately $375,475,000 and$1.4 billion , research and development credit carryforwards (“R(R&D credits”)credits) of approximately $10,491,000.$45.8 million and business interest expense carryforward of $14.5 million. For income tax purposes, these NOLs and R&D credits will expire in various amounts through 2037.2040. NOLs generated after 2017 and the business interest expense carryforwards do not expire. The Tax Reform Act of 1986 contains provisions which limit the ability to utilize net operating loss carryforwards and R&D credit carryforwards in the case of certain events including significant changes in ownership interests. The Exchange Transaction with TG Bio may have resulted in a “change in ownership” as defined by IRC Section 382 of the Internal Revenue Code of 1986, as amended. Additionally, stock issuance activities may have resulted in a “change in ownership” as defined by IRC Section 382 of the Internal Revenue Code of 1986, as amended. Accordingly, a substantial portion of the Company’s NOLs above may be subject to annual limitations in reducing any future year’s taxable income, and a substantial portion of the R&D Credit carryforwards may be subject to annual limitations in reducing any future year’s tax.
The tax effects of temporary differences that give rise to significant portions of the deferred tax assets and deferred tax liabilities at December 31, 2017 2023 and 20162022 are presented below.
2017 | 2016 | |
| Deferred tax assets (liabilities): | ||
| Net operating loss carryforwards | $83,655,879 | $95,329,928 |
| Research and development credit | 10,490,793 | 7,326,715 |
| Noncash compensation | 4,933,807 | 12,915,672 |
| Other | 632,274 | 599,514 |
| Deferred tax asset, excluding valuation allowance | 99,712,753 | 116,171,829 |
| Less valuation allowance | (99,712,753) | (116,171,829) |
| Net deferred tax assets | $-- | $-- |
(in thousands) | 2023 | 2022 | ||||||
Deferred tax assets: | | | ||||||
Net operating loss carryforwards | $ | 316,962 | $ | 303,729 | ||||
Research and development credit | 45,806 | 42,031 | ||||||
Noncash compensation | 12,275 | 10,325 | ||||||
Disallowed interest | 3,328 | 3,882 | ||||||
Capitalized R&D Expenses | 36,613 | 39,411 | ||||||
Other | 3,333 | 985 | ||||||
Deferred tax asset, excluding valuation allowance | 418,317 | 400,363 | ||||||
Less valuation allowance | (418,317 | ) | (400,363 | ) | ||||
Net deferred tax assets | $ | — | $ | — | ||||
There was noapproximately $0.4 million of current or deferred income tax expense for the year ended December 31, 2017.2023. Income tax expense differed from amounts computed by applying the US Federalfederal income tax rate of 34%21% for the years ending December 31, 2023, 2022 and 2021, to pretax lossincome (loss) as follows:
For the year ended December 31, | |||
2017 | 2016 | 2015 | |
| Loss before income taxes, as reported in the consolidated statements of operations | $(118,476,012) | $(78,252,894) | $(62,948,646) |
| Computed “expected” tax benefit | $(40,281,844) | $(26,605,984) | $(21,402,540) |
| Increase (decrease) in income taxes resulting from: | |||
| Expected benefit from state and local taxes | (1,105,708) | (835,072) | (672,306) |
| Research and development credits | (3,697,258) | (2,364,417) | (1,603,364) |
| Other | 1,563,114 | (7,506) | 566,310 |
| Impact of change in state tax rates on deferred taxes | -- | -- | 5,836,819 |
| Stock awards | 8,213,188 | ||
| Effects of federal tax reform rate changes | 51,767,584 | ||
| Change in the balance of the valuation allowance for deferred tax assets | (16,459,076) | 29,812,979 | 17,275,081 |
$-- | $-- | $-- | |
| For the year ended December 31, | |||||||||||
(in thousands) | 2023 | 2022 | 2021 | |||||||||
Loss before income taxes, as reported in the consolidated statements of operations | $ | 13,062 | $ | (198,335 | ) | $ | (348,101 | ) | ||||
| | | | |||||||||
Computed “expected” tax benefit | $ | 2,743 | $ | (41,650 | ) | $ | (73,101 | ) | ||||
| | | | |||||||||
Increase (decrease) in income taxes resulting from: | | | | |||||||||
Expected benefit from state and local taxes | 111 | (7,242 | ) | (3,445 | ) | |||||||
Research and development credits | (3,430 | ) | (6,389 | ) | (8,337 | ) | ||||||
Officer Compensation Limitation | 1,167 | 4,391 | 439 | |||||||||
Other | (179 | ) | 374 | 428 | ||||||||
Stock options | (12,445 | ) | 17,599 | (6,726 | ) | |||||||
Change in state tax rates | (5,531 | ) | - | - | ||||||||
Change in the balance of the valuation allowance for deferred tax assets | 17,954 | 32,917 | 90,742 | |||||||||
| $ | 390 | $ | — | $ | — | ||||||
We file income tax returns in the U.S Federalfederal and various state and local jurisdictions. With certain exceptions, the Company is no longer subject to U.S. Federalfederal and state income tax examinations by tax authorities for years prior to 2014.2020. However, NOLs and tax credits generated from those prior years could still be adjusted upon audit.
The Company would recognize interest and penalties, if any, to uncertain tax position in income tax expense in the statement of operations. There was no accrual for interest and penalties related to uncertain tax positions for 2017.2023. We do not believe that there will be a material change in our unrecognized tax positions over the next twelve months. All of the unrecognized tax benefits, if recognized, would be offset by the valuation allowance.
NOTE 810 – LICENSE AGREEMENTS
BRIUMVI (Ublituximab)
In May 2016, as part of a broader agreement with Jubilant Biosys (“Jubilant”), an India-based biotechnology company, January 2012, we entered into a sub-licensean exclusive license agreement (“JBET Agreement”) with Checkpoint Therapeutics, Inc. (“Checkpoint”) (see Note 9),LFB Biotechnologies, GTC Biotherapeutics and LFB/GTC LLC, all wholly-owned subsidiaries of LFB Group, relating to the development of ublituximab (the LFB License Agreement). Under the terms of the LFB License Agreement, we have acquired the exclusive worldwide rights (exclusive of France/Belgium) for the development and commercialization of Jubilant’s novel BET inhibitor programublituximab. For the period ended December 31, 2023, we have incurred expenses of approximately $31.0 million related to the achievement of certain milestones of the LFB License Agreement. These expenses are included in other research and development expenses in the fieldaccompanying consolidated statements of hematological malignancies.
LFB Group is eligible to receive future payments of the agreement, we paid Checkpoint an up-front licensing feeapproximately $6.0 million, upon our successful achievement of $1.0 million and will make additional payments contingent on certain preclinical, clinical, and regulatory milestones, including commercial milestones totaling upin addition to approximately $177 million and a single-digit royalty payments on net sales. TG will also provide funding to support certain targeted research effortssales of ublituximab at Jubilant.
In lieu of sales milestones and royalties on net sales, Rhizen shall also be eligible to participate in sublicensing revenue, if any, based on a percentage that decreases as a function of the number of patients treated in clinical trials following the exercise of the license option. Rhizen will retain global manufacturing rights to TGR-1202, provided that they are price competitive with alternative manufacturers.
An upfront payment of $2.0 million, which was received in December 2012, net of $0.3 million of income tax withholdings,
We may receive up to an additional $5.0 million in payments upon the achievement of pre-specified milestones. In addition, upon commercialization, Ildong will make royalty payments to us on net sales of TG-1101ublituximab in the sublicense territory.
In July 2023, the Company entered into the Commercialization Agreement with Neuraxpharm. The Company granted Neuraxpharm the exclusive right to commercialize BRIUMVI in certain territories outside the United States, Canada, and Mexico, the commercialization rights for which had been previously retained by the Company, thus, and excluding certain Asian countries subject to previously existing partnerships. Under the terms of the Commercialization Agreement, the Company received a one-time, non-refundable payment of $140.0 million upon contract execution (please refer to Note 2 – RELATED PARTY TRANSACTIONS
TG-1701: BTK
In January 30, 2012,2018, we entered into ana global exclusive license agreement with LFB Biotechnologies, GTC BiotherapeuticsJiangsu Hengrui, to acquire worldwide intellectual property rights, excluding Asia but including Japan, and LFB/GTC LLC, all wholly-owned subsidiariesfor the research, development, manufacturing, and commercialization of LFB Group, relatingproducts containing or comprising of any of Hengrui’s Bruton’s Tyrosine Kinase inhibitors containing the compounds of either TG-1701 (SHR1459 or EBI1459) or TG1702 (SHR1266 or EBI1266). Hengrui is eligible to receive milestone payments totaling approximately $350 million upon and subject to the developmentachievement of ublituximab (the “LFB License Agreement”). In connectioncertain milestones. Various provisions allow for payments in conjunction with the LFB License Agreement, LFB Group was issued 5,000,000 shares of common stock, and a warrantagreement to purchase 2,500,000 shares of common stock at a purchase price of $0.001 per share. In addition, on November 9, 2012, we nominated Dr. Yann Echelard to our Board of Directors as LFB Group’s nominee. LFB Group maintains the right to nominate a board member until such time as LFB Group owns less than 10% of the outstanding common stock.
TG-1801: anti-CD47/anti-CD19
In June 2018, we entered into a Joint Venture and License Option Agreement with Novimmune to collaborate on the development and commercialization of Novimmune’s novel first-in-class anti-CD47/anti-CD19 bispecific antibody known as TG-1801 (previously NI-1701). The companies will jointly develop the product on a worldwide basis, focusing on indications in the area of hematologic B-cell malignancies. We serve as the primary responsible party for the development, manufacturing and commercialization of the product. Milestone payments will be paid based on early clinical development, and the Company will be responsible for the costs of clinical development of the product through the end of the Phase 2 clinical trials, after which the Company and Novimmune will be jointly responsible for all development and commercialization costs. The Company and Novimmune will each maintain an exclusive option, exercisable at specific times during development, for the Company to license the rights to TG-1801, in which case Novimmune is eligible to receive additional milestone payments totaling approximately $185 million as well as tiered royalties on net sales in the high single to low double digits upon and subject to the achievement of certain milestones.
UKONIQ (umbralisib)
On September 22, 2014, we exercised our option to license the global rights to umbralisib, thereby entering into an exclusive licensing agreement (the TGR-1202 License) with Rhizen Pharmaceuticals, SA (Rhizen) for the development and commercialization of umbralisib. As of December 31, 2023, we have incurred approximately $24.0 million related to the achievement of certain milestones of the Umbralisib License.
Under the terms of the LFBTGR 1202 License, Rhizen is eligible to receive approval and sales-based milestone payments in the aggregate of approximately $175 million payable. For the year ended December 31, 2021, we paid Rhizen $12.0 million as part of a primary indication approval milestone for launch of product in the US in accordance with the terms of the Umbralisib License. Additionally, Rhizen receives tiered royalties that escalate from high single digits to low double digits on any net sales of umbralisib. UKONIQ was officialy withdrawn from the market in May 2022 and all commercialization activities were discontinued. As a result of the withdrawal, during the year ended December 31, 2023, the Company recorded zero related to the worldwide royalty due under the Umbralisib License in cost of revenue based on U.S. sales of UKONIQ, and as of December 31, 2023, no royalties were payable under the Umbralisib License. Due to the withdrawal of UKONIQ from the U.S. market and discontinuation of all commercialization activities, we do not expect to incur any additional costs related to this license agreement.
TG-1501: Cosibelimab
In March 2015, we entered into a Global Collaboration Agreement we utilize LFB Group(Collaboration Agreement) with Checkpoint for certainthe development and manufacturing services.commercialization of anti-PD-L1 and anti-GITR antibody research programs in the field of hematological malignancies. The Collaboration Agreement was amended in June 2019 and in March of 2020. We incurred expenses of approximately $2.3$0.1 million $8.1 million and $9.3 million in expenses for such services duringeach of the years ended December 31, 2023, 2022 and 2021, 2017, 2016the majority of which relates to manufacturing expenses, clinical study expenses and 2015, respectively, which have been includedmilestone payments of PD-L1. The relevant expenses are recorded in other research and development expenses in the accompanying consolidated statements of operations. As of December 31, 2017, and 2016, we had zero and approximately $0.4 million, respectively, recorded in accounts payable related to the LFB License Agreement. In conjunction with the development and manufacturing services discussed above, certain agreements between us and LFB Group require payments in advance of services performed or goods delivered. Accordingly, as of December 31, 2017 and 2016, we recorded zero and approximately $1.3 million, respectively, in prepaid research and development for such advance payments.
NOTE11 – RELATED PARTY TRANSACTIONS
In March 2014, we entered into a shared services agreement (the “Opus Shared Services Agreement”) with Opus Point Partners Management, LLC (“Opus”) in which the parties agreed to share a rented facility and costs for certain other services. Michael S. Weiss, our Executive Chairman and CEO, is a Managing Member of Opus. During the years ended December 31, 2017 and 2016, we incurred expenses of zero and approximately $0.3 million, respectively, principally for rent, related to this Opus Shared Services Agreement. As of December 31, 2017 and 2016, we had zero accounts payable related to this Opus Shared Services Agreement. The Opus Shared Services Agreement is no longer in effect as we began occupying new space in April 2016.
In March 2015, we entered into the Collaboration Agreement with Checkpoint, a subsidiary of FBIO, for the development and commercialization of anti-PD-L1 and anti-GITR antibody research programs in the field of hematological malignancies. In May 2016, as part of a broader agreement with Jubilant, an India-based biotechnology company, we entered into the JBET Agreementa sublicense agreement (JBET Agreement) with Checkpoint a subsidiary of FBIO, for the development and commercialization of Jubilant’s novel BET inhibitor program in the field of hematological malignancies. We paid Checkpoint an up-front licensing fee of $1.0 million in July 2016 and incurred expenses of $0.2 million in March 2017 for the first milestone achievementMr. Weiss also serves as partChairman of the JBETBoard of Directors of Checkpoint.
Please refer to Note 8 - Leases for details regarding the Office Agreement recorded in other research and development inwith FBIO, as well as Note 10 - License Agreements for details regarding the accompanying consolidated statement of operations. As of December 31, 2017 and 2016, we had approximately $0.3 million and $0.8 million, respectively, recorded in accounts payable, related mostly to the JBET Agreement. Mr. Weiss is also the Executive Chairman ofCollaboration Agreement with Checkpoint.
NOTE 1012 – COMMITMENTS AND CONTINGENCIES
As of December 31, 2017,2023, we have known contractual obligations,obligations; commitments and contingencies of approximately $15.6$115.4 million related to our short- and long-term liabilities and operating lease obligations.
Payment due by period | |||||
Total | Less than 1 year | 1-3 years | 3-5 years | More than 5 years | |
| Contractual obligations | |||||
| Operating leases | $15,592,733 | $1,081,927 | $2,084,258 | $2,154,566 | $10,271,981 |
| Total | $15,592,733 | $1,081,927 | $2,084,258 | $2,154,566 | $10,271,981 |
Less than | More than | |||||||||||||||||||
Payment due by period (in thousands) | Total | 1 year | 1-3 years | 3-5 years | 5 years | |||||||||||||||
Contractual obligations | | | | | | |||||||||||||||
Operating leases | $ | 15,023 | $ | 2,388 | $ | 4,180 | $ | 3,740 | $ | 4,715 | ||||||||||
Long-term debt | 100,403 | — | 100,403 | — | — | |||||||||||||||
Total | $ | 115,426 | $ | 2,388 | $ | 104,583 | $ | 3,740 | $ | 4,715 | ||||||||||
Leases
See Note 98 - leases for a detailed description of our lease arrangementarrangements in New York.York, New Jersey and North Carolina. Total rental expense was approximately $1.4$2.2 million, $1.6$2.7 million and $0.3$2.2 million for the years ended December 31, 2017, 20162023, 2022 and 2015,2021, respectively.
Future minimum lease commitments as of December 31, 2017,2023, in the aggregate total approximately $15.6$15.0 million through DecemberJuly 31, 2031. The preceding table shows future minimum lease commitments, which include our office leases in New York, New Jersey, and North Carolina and Tennessee, by year as of December 31, 2017.
Loan Payable
See Note 7 – Loan payable for a detail description of our loan agreement.
NOTE 13 – Subsequent Events
Precision Bio
On January 7, 2024, TG Therapeutics,and its wholly-owned subsidiary, TG Cell Therapy, Inc. and Subsidiaries
3 Months Ended | ||||
March 31, 2017 | June 30, 2017 | September 30, 2017 | December 31, 2017 | |
| License revenue | $38,095 | $38,095 | $38,096 | $38,095 |
| Total costs and expenses | 27,704,517 | 28,463,466 | 31,623,323 | 31,072,826 |
| Net loss | $(27,727,509) | $(28,353,084) | $(31,535,652) | $(30,859,767) |
| Basic and diluted net loss per common share | $(0.52) | $(0.45) | $(0.48) | $(0.46) |
3 Months Ended | ||||
March 31, 2016 | June 30, 2016 �� | September 30, 2016 | December 31, 2016 | |
| License revenue | $38,095 | $38,095 | $38,096 | $38,095 |
| Total costs and expenses | 14,030,251 | 16,061,538 | 24,963,567 | 24,066,153 |
| Net loss | $(13,848,662) | $(15,899,062) | $(24,831,027) | $(23,674,143) |
| Basic and diluted net loss per common share | $(0.28) | $(0.33) | $(0.50) | $(0.48) |
Pursuant to the Precision License Agreement, the Company will make an upfront payment to Precision of $7.5 million, consisting of (i) $5.25 million in its entirety without prejudice.cash and (ii) $2.25 million, as an equity investment, for the purchase of 2,920,816 shares of Precision’s common stock at a price of $0.77 per share. Within 12 months of the Precision License Agreement, the Company will make a deferred payment of $2.5 million to Precision, consisting of an equity investment in Precision’s common stock at a 100% premium to the 30-day volume-weighted average price (the 30-day VWAP) prior to purchase. Upon achievement of certain near-term clinical or time-based milestones, the Company will make a $7.5 million payment to Precision, a portion of which will also be an equity investment in Precision’s common stock at a 100% premium to the 30-day VWAP prior to purchase. Precision will be eligible to receive up to $288 million in additional milestone payments based on the achievement of certain clinical, regulatory, and commercial milestones. In addition, the Company is obligated to pay Precision high-single-digit to low-double-digit royalties on net sales of the licensed product on a country-by-country basis until the latest to occur of patent expiration, loss of regulatory exclusivity, and a period of ten years following the first commercial sale of the licensed product in such country. The Company denieshas also agreed to make certain payments to Precision’s licensors during the allegations and claims made in the above-referenced actions and no consideration was given by the Company in connection with lead plaintiffs’ voluntary dismissalterm of the consolidated action.
Ex-U.S. BRIUMVI Launch
On February 26, 2024, TG announced that its ex-US partner, Neuraxpharm launched BRIUMVI in Europe, for the treatment of adults patients with relapsing forms of multiple sclerosis (RMS), who have active disease defined by clinical or imaging features. The launch commenced in Germany, with additional launches throughout Europe to follow. In accordance with the ex-US commercialization agreement, TG will receive a milestone payment of $12.5 million for the first launch of BRIUMVI in a European country.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| TG THERAPEUTICS,INC. | ||
| | | |
Date: | By: | /s/ Michael S. Weiss | |
| | Michael S. Weiss | |
| | Chairman and Chief Executive Officer | |
KNOW ALL MENPERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints each of Michael S. Weiss and Sean A. Power, his true and lawful attorney-in-fact and agent, with full power of substitution and resubstitution, for him and his name, place and stead, in any and all capacities, to sign any or all amendments to this annual report on Form 10-K, and to file the same, with all exhibits thereto and other documents in connection therewith, with the SEC, granting unto said attorney-in-fact and agent, full power and authority to do and perform each and every act and thing requisite and necessary to be done in and about the premises, as fully to all intents and purposes as he might or could do in person, hereby ratifying and confirming all that said attorney-in-fact and agent or any of his substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this Form 10-K has been signed by the following persons on behalf of the Registrant on March 15, 2018,February 29, 2024, and in the capacities indicated:
Signatures | Title | |
/s/ Michael S. Weiss Michael S. Weiss | | Chairman, Chief Executive Officer and President |
| | |
/s/ Sean A. Power Sean A. Power | | Chief Financial Officer, |
| | |
/s/ Laurence N. Charney Laurence N. Charney | | Director |
| | |
/s/ Yann Echelard Yann Echelard | | Director |
| | |
/s/ Kenneth Hoberman Kenneth Hoberman | | Director |
| | |
/s/ Daniel Hume Daniel Hume | | Director |
| | |
/s/ Sagar Lonial | | Director |