●
It may take longer than expected to determine whether or not a treatment is safe and effective.
●
Patients involved in our clinical trials may suffer severe adverse side effects even up to death, whether as a result of treatment with our products, the withholding of such treatment, or other reasons which may not include the effects of our treatment (whether within or outside of our control).
●
We may fail to be able to enroll a sufficient number of patients in our clinical trials.
●
Patients enrolled in our clinical trials may not have the safety or efficacy characteristics necessary to obtain regulatory approval for a particular indication.
●
We may be unable to produce sufficient quantities of product to complete the clinical trials.
●
Even if we are successful in our clinical trials, any required governmental approvals may still not be obtained or, if obtained, may not be maintained.
●
If approval for commercialization is granted, it is possible the authorized use will be more limited than is necessary for commercial success, or that approval may be conditioned on completion of further clinical trials or other activities, which will cause a substantial increase in costs and which we might not succeed in performing or completing.
●
If granted, approval may be withdrawn or limited if problems with our products emerge or are suggested by the data arising from their use or if there is a change in law or regulation.
Any success we may achieve at a given stage of our clinical trials does not guarantee that we will achieve success at any subsequent stage, including without limitation final FDA or other regulatory organizations’ approval.
We may encounter delays or rejections in the regulatory approval process because of additional government regulation resulting from future legislation or administrative action, or from changes in the policies of the FDA or other regulatory bodies during the period of product development, clinical trials, or regulatory review. Failure to comply with applicable regulatory requirements may result in criminal prosecution, civil penalties, recall or seizure of products, total or partial suspension of production, or an injunction preventing certain activity, as well as other regulatory action against our product candidates or us. As a company, we have no experience in successfully obtaining regulatory approval for a drugproduct and thus may be poorly equipped to gauge, and may prove unable to manage, risks relating to obtaining such approval.
Outside the U.S., our ability to market a product is contingent upon receiving clearances from appropriate non-U.S. regulatory authorities. Non-U.S. regulatory approval typically includes all of the risks associated with FDA clearance discussed above as well as geopolitical uncertainties and the additional uncertainties and potential prejudices faced by U.S. pharmaceutical companies conducting business abroad. In certain cases, governmental pricing restrictions and practices can make achieving even limited profitability very difficult.
Even if we complete the clinical trials we discussed with the FDA, there is no guarantee that at the time of submission the FDA will accept our new drug application (“NDA”) based on the trials discussed.
The FDA provided guidance on our proposed VOICE adaptive design trial, but the FDA is not bound by the guidance they give, and can change their position in the future. Any future decision by the FDA will be driven largely by the data generated from the VOICE clinical program. However, the FDA and other regulatory organizations will learn from their total experience in the review of multiple drugs in multiple indications and they will apply the knowledge of broad and diverse experience even if not a perfect match with our product.
As a company, we have never completed a clinical trial and have limited experience in completing regulatory filings and any delays in regulatory filings could materially affect our financial condition.
While members of our team have conducted numerous clinical trials at previous companies, and have launched and marketed innovative pharmaceutical products in the U.S. and internationally, as a company, we have not yet completed any clinical trials of our product candidates, nor have we demonstrated the ability to obtain marketing approvals, manufacture product candidates at a commercial scale, or conduct sales and marketing activities necessary for the successful commercialization of a product. Consequently, we have no historical basis as a company by which one can evaluate or predict reliably our future success or viability.
Additionally, while our team has experience at prior companies with regulatory filings, as a company, we have limited experience with regulatory filings with agencies such as the FDA or EMA. Any delay in our regulatory filings for our product candidates, and any adverse development or perceived adverse development with respect to the applicable regulatory authority’s review of such filings, including, without limitation, the FDA’s issuance of a “refuse to file” letter or a request for additional information, could materially affect our financial condition.
We may seek fast track designation for one or more of our current and future product candidates, but we might not receive such designation, and even if we do, such designation may not actually lead to a faster development or regulatory review or approval process.
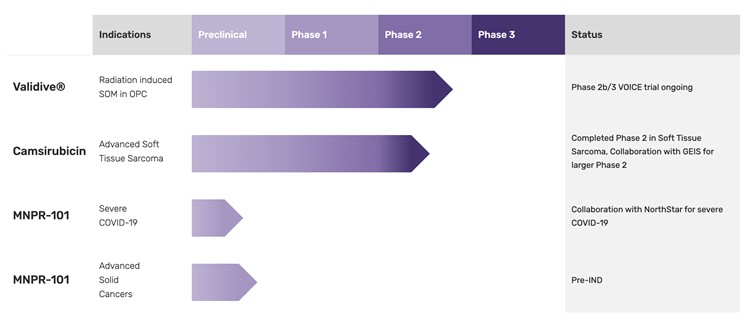
Our lead product candidate, Validive, has been given fast track designation from the FDA. Fast track designation does not ensure that we will receive marketing approval or that approval will be granted within any particular timeframe. We may not experience a faster development, regulatory review or approval process with fast track designation compared to conventional FDA procedures. Additionally, the FDA may withdraw fast track designation, for reasons such as it comes to believe a drug candidate no longer adequately addresses an unmet medical need. Fast track designation alone does not guarantee qualification for the FDA’s priority review procedures. If we seek fast track designation for other product candidates, we may not receive such a designation from the FDA.
We, or any future collaborators, may not be able to obtain and maintain orphan drug exclusivity for our product candidates in the U.S. and Europe.
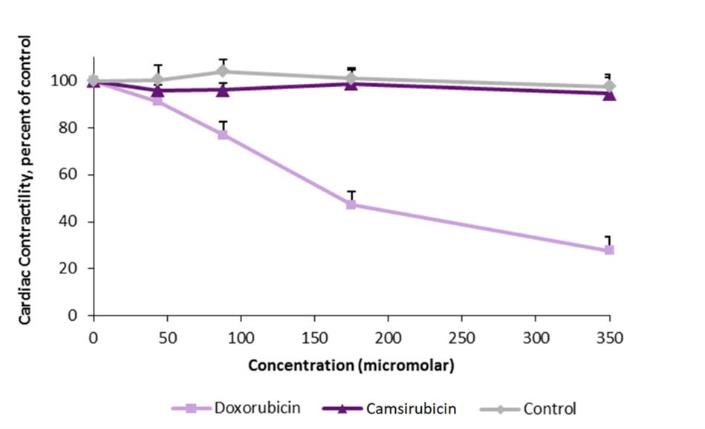
Validive has been granted orphan drug designation for the treatment of SOM in the EU. Camsirubicin has been granted orphan drug designation for the treatment of soft tissue sarcoma in the U.S. and in the EU. We may seek additional orphan drug designations or regulatory incentives for our pipeline product candidates, for other indications or for future product candidates. There can be no assurances that we will be able to obtain such designations.
Even if we obtain orphan drug designation for a product candidate, we may not be able to maintain orphan drug exclusivity for that drug. For example, orphan drug designation may be removed if the prevalence of an indication increases beyond the patient number limit required to maintain designation. Generally, if a drug with an orphan drug designation subsequently receives the first marketing approval for the indication for which it has such designation, the drug is entitled to a period of marketing exclusivity, which precludes the EMA or the FDA from approving another marketing application for the same product in the same indication for that time period. Orphan drug exclusivity may be lost if the FDA or EMA determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the product to meet the needs of patients with the rare disease or condition. Moreover, even after an orphan drug is approved, the FDA can subsequently approve a different drug for the same condition if the FDA concludes that the later drug is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care compared to our product.
The FDA may reevaluate the Orphan Drug Act and its regulations and policies, and similarly the EMA may reevaluate its policies and regulations. We do not know if, when, or how the FDA or EMA may change their orphan drug regulations and policies in the future, and it is uncertain how any changes might affect our business. Depending on what changes the FDA and/or EMA may make to their orphan drug regulations and policies, our business could be adversely impacted.
If serious adverse or undesirable side effects are identified during the development of our product candidates, we may abandon or limit our development or commercialization of such product candidates.
If our product candidates are associated with undesirable side effects or have unexpected characteristics, we may need to abandon their development or limit development to certain uses or subpopulations in which the undesirable side effects or other characteristics are less prevalent, less severe or more acceptable from a risk-benefit perspective.
If we elect or are forced to suspend or terminate any clinical trial with one of our product candidates, the commercial prospects of such product candidate will be harmed, and our ability to generate revenue from such product candidate will be delayed or eliminated. Any of these occurrences may harm our business, financial condition and prospects significantly.
With regard to our lead product candidate, unforeseen side effects from Validive could arise either during clinical development or, if approved, after Validive has been marketed. This could cause regulatory approvals for, or market acceptance of, Validive harder and costlier to obtain.
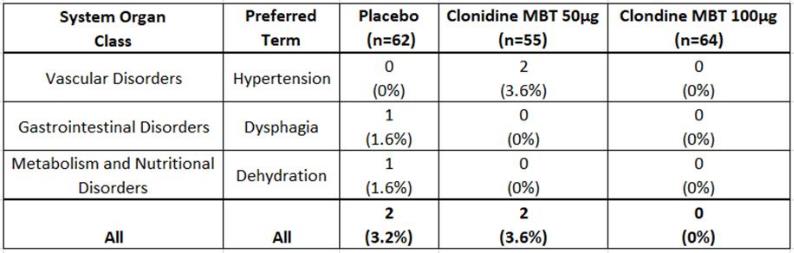
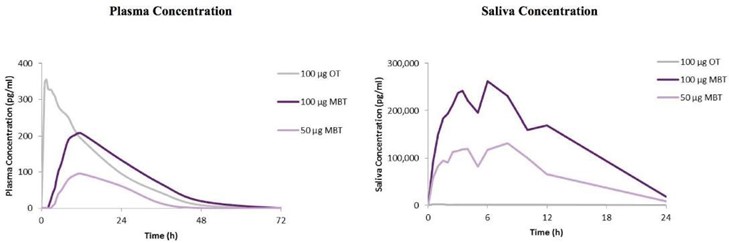
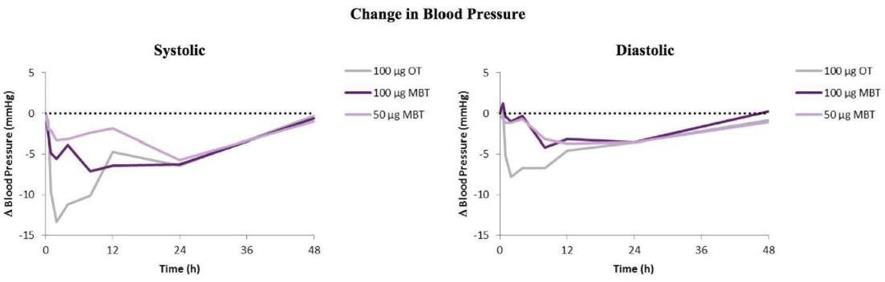
To date, no difference in the frequency of serious adverse events (“SAEs”) has been observed in patients treated with Validive compared to placebo. In the Phase 2 clinical trial, two patients in the placebo group and 2 patients in the Validive 50 µg group experienced SAEs that were assessed as treatment related. No patients in the Validive treated cohorts were discontinued due to study drug. Clonidine, the active ingredient of Validive, has been used for over 50 years as an orally swallowed systemic treatment for high blood pressure. Validive administration leads to very low, but still detectable exposure of clonidine outside the oral cavity. Thus, there is some risk that patients may experience side effects due to this systemic exposure, which could include a reduction in blood pressure, irregular heartbeat, drowsiness or dry mouth.
The results of our current or any future clinical trials may show that the side effects of Validive are unacceptable or intolerable, which could interrupt, delay or halt clinical trials, and result in delay of, or failure to obtain, marketing approval from the FDA or EMA and other regulatory authorities, or result in marketing approval from the FDA or EMA and other regulatory authorities with restrictive label warnings.
If Validive receives marketing approval and we or others later identify undesirable or unacceptable side effects caused by the use of Validive:
● regulatory authorities may withdraw their approval of the product, which would force us to remove Validive from the market;
● regulatory authorities may require the addition of labeling statements, specific warnings, a contraindication, or field alerts to physicians and pharmacies;
● we may be required to change instructions regarding the way the product is administered, conduct additional clinical trials or change the labeling of the product;
● we may be subject to limitations on how we may promote the product;
● sales of the product may decrease significantly;
● we may be subject to litigation or product liability claims; and
● our reputation may suffer.
Any of these events could prevent us or our potential future collaborators from achieving or maintaining market acceptance of Validive and/or could substantially increase commercialization costs and expenses, which in turn could delay or prevent us from generating significant revenues from the sale of Validive.
As with any clinical trial, our VOICE clinical program entails significant risk of not meeting clinical endpoints. If the results of VOICE are not statistically significant, the FDA will likely not approve Validive for marketing which will result in a decrease in our stock price and market value.
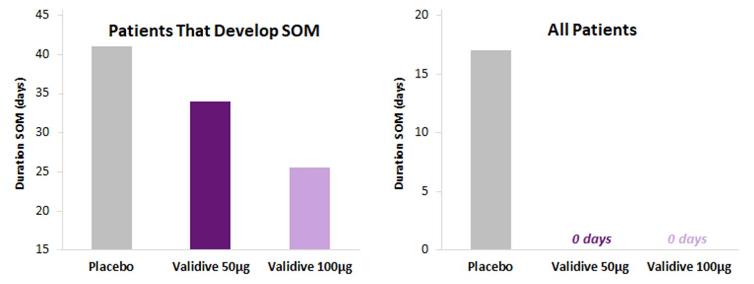
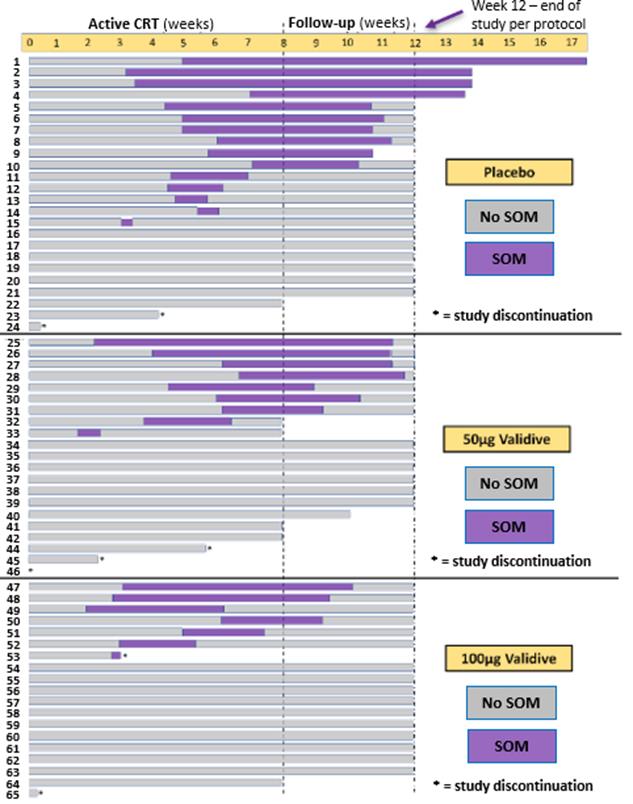
The VOICE clinical program has been designed based on an analysis of the 64 oropharyngeal cancer (“OPC”) patients included in the Phase 2 trial (n= 24 in the placebo group, n= 21 Validive 50 µg group, and n= 19 Validive 100 µg group). While a dose response was observed in the Validive treated OPC cohorts compared to placebo across multiple clinically meaningful endpoints, the ability to establish statistical significance was limited by the relatively small sample size. This increases the risk that the VOICE may not achieve its prospectively defined endpoints. Given the large unmet medical need for the prevention of CRT-induced SOM in OPC patients, we have decided to pursue an adaptive design Phase 2b/3 clinical development strategy in an effort to mitigate this risk. VOICE has a simplified design and includes an interim analysis after the 2b portion that allows for an assessment of the primary (and only) endpoint, incidence of SOM, before proceeding to the Phase 3 portion of the trial. By focusing VOICE on a single endpoint, touch points with patients and sites are minimized. This seamless design will allow us to immediately advance to the Phase 3 portion of the trial if supported by the interim data at the end of the Phase 2b portion of the trial. We may also be required to conduct a smaller second Phase 3 confirmatory clinical trial which may not yield the same results. If our VOICE clinical trial results are not statistically significant, the FDA will likely not approve Validive for marketing, which will result in a decrease in our stock price and market value.
If we experience delays or difficulties in the enrollment of subjects to our clinical trials, our receipt of necessary regulatory approvals could be delayed or prevented, which could materially affect our financial condition.
Identifying, screening and enrolling patients to participate in clinical trials of our product candidates is critical to our success, and we may not be able to identify, recruit, enroll and dose a sufficient number of patients with the required or desired characteristics to complete our clinical trials in a timely manner. The timing of our clinical trials depends on our ability to recruit patients to participate as well as to subsequently dose these patients and complete required follow-up periods. In particular, because our current clinical trials of Validive and camsirubicin are focused on indications with relatively small patient populations, our ability to enroll eligible patients may be limited or may result in slower enrollment than we anticipate.
In addition, we may experience enrollment delays related to increased or unforeseen regulatory, legal and logistical requirements and COVID-19-related issues at certain clinical trial sites. These delays could be caused by reviews by regulatory authorities and contractual discussions with individual clinical trial sites. Any delays in enrolling and/or dosing patients in our current clinical trials could result in increased costs, delays in advancing our product candidates, delays in testing the effectiveness of our product candidates or in termination of the clinical trials altogether.
Patient enrollment may be affected if our competitors have ongoing clinical trials with products for the same indications as our product candidates, and patients who would otherwise be eligible for our clinical trials instead enroll in our competitors’ clinical trials. Patient enrollment may also be affected by other factors, including:
● delays in U.S. or foreign regulatory approval to start the clinical trial;
● coordination with clinical research organizations to enroll and administer the clinical trials;
● coordination and recruitment of collaborators and investigators at individual sites;
● size of the patient population and process for identifying patients;
● design of the clinical trial protocol;
● eligibility and exclusion criteria;
● perceived risks and benefits of the product candidates under study;
● availability of competing commercially available therapies and other competing products’ clinical trials;
● time of year in which the trials are initiated or conducted;
● severity of the diseases under investigation;
● ability to obtain and maintain subject consents;
● ability to enroll and treat patients in a timely manner;
● risk that enrolled subjects will drop out before completion of the trials;
● proximity and availability of clinical trial sites for prospective patients;
● ability to monitor subjects adequately during and after treatment;
● patient referral practices of physicians; and
● potential effects of the COVID-19 pandemic.
Our inability to enroll a sufficient number of patients for clinical trials would result in significant delays and could require us to abandon one or more clinical trials altogether. Enrollment delays in these clinical trials may result in increased development costs for our product candidates, which could materially affect our financial condition.
If we or our licensees, development collaborators, or suppliers are unable to manufacture our products in sufficient quantities or at defined quality specifications, or are unable to obtain regulatory approvals for the manufacturing facility, we may be unable to develop and/or meet demand for our products and lose time to market and potential revenues.
Completion of our clinical trials and commercialization of our product candidates require access to, or development of, facilities to manufacture a sufficient supply of our product candidates. We currently contract with outside sourceswill utilize third parties to manufacture Validive, camsirubicin, and MNPR-101. In order to be able to manufacture sufficient quantities of MNPR-101 to be able to proceed with human clinical trials, Cancer Research UK developed a new cell line under our CTOA. We received notification of termination of CRUK’s work on MNPR-101 under the CTOA on March 21, 2018. There can be no assurance that this new cell line will be successful or that sufficient quantities of MNPR-101 will be able to be manufactured. Since Cancer Research UK has decided to terminate its involvement with MNPR-101, we will need to make othercurrently have manufacturing arrangements for the clinical testing, developmentValidive and manufacture of our drug product candidate. There can be no assurance that such alternative arrangements can be madecamsirubicin. We have not yet secured a manufacturing agreement for MNPR-101 or on terms favorable to us. We inuPRITs.
In the future we may become unable, for various reasons, to rely on our sources for the manufacture of our product candidates, either for clinical trials or, at some future date, for commercial distribution. We may not be successful in identifying additional or replacement third-party manufacturers, or in negotiating acceptable terms with any we do identify. We may face competition for access to these manufacturers’ facilities and may be subject to manufacturing delays if the manufacturers give other clients higher priority than they give to us. Even if we are able to identify an additional or replacement third-party manufacturer, the delays and costs associated with establishing and maintaining a relationship with such manufacturer may have a material adverse effect on us.
Before we can begin to commercially manufacture Validive, MNPR-201,camsirubicin, MNPR-101, or any other product candidate, we must obtain regulatory approval of the manufacturing facility and process. Manufacturing of drugs for clinical and commercial purposes must comply with the FDA's current Good Manufacturing Practices requirements, commonly known as “cGMP”, and applicable non-U.S. regulatory requirements.“cGMP.” The cGMP requirements govern quality control and documentation policies and procedures. Complying with cGMP and non-U.S. regulatory requirements will require that we expend time, money, and effort in production, recordkeeping, and quality control to ensure that the product meets applicable specifications and other requirements. We, or our contracted manufacturing facility, must also pass a pre-approval inspection prior to FDA approval. Failure to pass a pre-approval inspection may significantly delay or prevent FDA approval of our products. If we fail to comply with these requirements, we would be subject to possible regulatory action and may be limited in the jurisdictions in which we are permitted to sell our products and will lose time to market and potential revenues.
It is uncertain whether product liability insurance will be adequate to address product liability claims, or that insurance against such claims will be affordable or available on acceptable terms in the future.
Clinical research involves the testing of new drugs on human volunteers pursuant to a clinical trial protocol. Such testing involves a risk of liability for personal injury to or death of patients due to, among other causes, adverse side effects, improper administration of the new drug, or improper volunteer behavior. Claims may arise from patients, clinical trial volunteers, consumers, physicians, hospitals, companies, institutions, researchers, or others using, selling, or buying our products, as well as from governmental bodies.bodies including a possibility in some states for product liability claims being made based on generic copies of our drugs. In addition, product liability and related risks are likely to increase over time, in particular upon the commercialization or marketing of any products by us or parties with which we enter into development, marketing, or distribution collaborations. Although we are contracting for generalhave obtained product liability insurance in connection with our ongoing business,clinical trials, there can be no assurance that the amount and scope of such insurance coverage will be appropriate and sufficient in the event any claims arise, that we will be able to secure additional coverage should we attempt to do so, or that our insurers would not contest or refuse any attempt by us to collect on such insurance policies. Furthermore, there canRegardless of their merit or eventual outcome, product liability claims may result in:
● withdrawal of clinical trial volunteers;
● decreased demand for our products when approved;
● injury to our reputation and significant, adverse media attention; and
● potentially significant litigation costs, including without limitation, any damages awarded to the plaintiffs if we lose or settle claims.
If the market opportunities for our current and potential future drug candidates are smaller than we believe they are, our ability to generate product revenues will be no assurance that suitable insurance will continueadversely affected and our business may suffer.
Our understanding of the number of people who suffer from SOM resulting from CRT for the treatment of OPC, whom Validive may have the potential to treat, is based upon estimates and on various reports from governments or medical institutions. These estimates or reports may prove to be available on terms acceptableincorrect, and new studies may demonstrate or suggest a lower estimated incidence or prevalence of this condition. The number of patients in the U.S. or elsewhere may turn out to usbe lower than expected, may not be otherwise amenable to Validive treatment, or attreatment-amenable patients may become increasingly difficult to identify and access, all of which would adversely affect our business prospects and financial condition. In particular, the treatable population for Validive may further be reduced if our estimates of addressable populations are erroneous or that, if obtained,sub-populations of patients within the insurance coverage will be appropriate and sufficient to cover any potential claims or liabilities.addressable population do not derive benefit from Validive.
Risks Related to Our Reliance on Third Parties
Corporate, non-profit, and academic collaborators may take actions (including lack of effective actions) to delay, prevent, or undermine the success of our products.
Our operating and financial strategy for the development, clinical testing, manufacture, and commercialization of drug product candidates is heavily dependent on us entering into collaborations with corporations, non-profit organizations, academic institutions, licensors, licensees, and other parties. There can be no assurance that we will be successful in establishing such collaborations. Some of our existingCurrent and future collaborations are and future collaborations may be terminable at the sole discretion of the collaborator. For example, our collaboration with Cancer Research UK on MNPR-101, we recently received notification of termination by CRUK of its involvement with MNPR-101 and we will need to seek alternate arrangements. Replacement collaborations might not be available on attractive terms, or at all. The activities of any collaborator will not be within our direct control and may not be in our power to influence. There can be no assurance that any collaborator will perform its obligations to our satisfaction or at all; that we will derive any revenue, profits, or benefit from such collaborations; or that any collaborator will not compete with us. If any collaboration is not pursued, we may require substantially greater capital to undertake development and commercialization of our proposed products, and may not be able to develop and commercialize such products effectively, if at all. In addition, a lack of development and commercialization collaborations may lead to significant delays in introducing proposed products into certain markets and/or reduced sales of proposed products in such markets. Furthermore, current orand future collaborators may act deliberately or inadvertently in ways detrimental to our interests.
The termination of third-party licenses could adversely affect our rights to important compounds.compounds or technologies.
We have exercised our option to license Validive; as such, Onxeo has the ability to terminate the license if we breach our obligations under the license agreement. A termination of the license agreement might force us to cease developing and/or selling Validive, if it gets to market. We rely on certain rights to MNPR-101 that we have secured through a non-exclusive license agreement with XOMA. XOMA, as licensor, has the ability to terminate the license if we breach our obligations under the license agreement and do not remedy any such breach inwithin a set time after receiving written notice of such breach from XOMA. A termination of the license agreement might force us to cease developing and/or selling MNPR-101, if it gets to market. We have exercised our option to license Validive; as such, Onxeo has the ability to terminate the license if we breach our obligations under the option and license agreement. A termination of the option and license agreement might force us to cease developing and/or selling Validive.
Data provided by collaborators and other parties upon which we rely have not been independently verified and could turn out to be false,inaccurate, misleading, or incomplete.
We rely on third-party vendors, scientists, and collaborators to provide us with significant data and other information related to our projects, clinical trials, and business. We do not independently verify or audit all of such data (including possibly material portions thereof). As a result, such data may be inaccurate, misleading, or incomplete.
In certain cases, we may need to rely on a single supplier for a particular manufacturing material or service, and any interruption in or termination of service by such supplier could delay or disrupt the commercialization of our products.
We rely on third-party suppliers for the materials used to manufacture our compounds. Some of these materials may at times only be available from one supplier. Any interruption in or termination of service by such single source suppliers could result in a delay or disruption in manufacturing until we locate an alternative source of supply. There can be no assurance that we would be successful in locating suchan alternative source of supply or in negotiating acceptable terms with such prospective supplier.
Our Validive manufacturer is in the United Kingdom (“UK”), and it is unknown in the long-term how they will be impacted by Brexit; however, if they are negatively impacted, this could increase our manufacturing costs, delivery schedules, and adversely impact our financial condition.
The UK left the European Union (“EU”) on January 31, 2020, which is commonly referred to as “Brexit.”The full long-term impact of Brexit, however, remains uncertain. Our Validive manufacturer may be negatively affected by interest rate, exchange rate and other market and economic volatility, as well as regulatory and political uncertainty. The tax consequences of the UK’s withdrawal from the EU are uncertain as well. If Brexit has a detrimental effect on our Validive manufacturer, it could, in turn, adversely impact our manufacturing costs and financial condition.
Our contracted camsirubicin manufacturing plant is located outside of the U.S. and may be affected by imposed tariffs and regional geopolitical factors outside of its control, which may affect the supply of camsirubicin active pharmaceutical ingredient. If we need to enlist a new contract manufacturer and it will delay our camsirubicin clinical program with GEIS and may increase our cost in supporting the GEIS Phase 2 clinical trial.
We currently have a single manufacturer of camsirubicin active pharmaceutical ingredient outside of the U.S. If we need to retain another contract manufacturer, it will cause a further delay to our GEIS-sponsored Phase 2 clinical program and may increase our manufacturing costs.
We rely on third parties to conduct our non-clinical studies and our clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may be unable to obtain regulatory approval for or commercialize our current product candidates or any future products, on a timely basis or at all, and our financial condition will be adversely affected.
We do not have the ability to independently conduct non-clinical studies and clinical trials. We rely on medical institutions, clinical investigators, contract laboratories, collaborative partners and other third parties, such as contract research organizations or clinical research organizations, to conduct non-clinical studies and clinical trials on our product candidates. The third parties with whom we contract for execution of our non-clinical studies and clinical trials play a significant role in the conduct of these studies and trials and the subsequent collection and analysis of data. However, these third parties are not our employees, and except for contractual duties and obligations, we have limited ability to control the amount or timing of resources that they devote to our programs.
Although we rely on third parties to conduct our non-clinical studies and clinical trials, we remain responsible for ensuring that each of our non-clinical studies and clinical trials is conducted in accordance with its investigational plan and protocol. Moreover, the FDA, EMA and other foreign regulatory authorities require us to comply with regulations and standards, including some regulations commonly referred to as good clinical practices (“GCPs”), for conducting, monitoring, recording and reporting the results of clinical trials to ensure that the data and results are scientifically credible and accurate, and that the trial subjects are adequately informed of the potential risks of participating in clinical trials.
In addition, the execution of non-clinical studies and clinical trials, and the subsequent compilation and analyses of the data produced, requires coordination among various parties. In order for these functions to be carried out effectively and efficiently, it is imperative that these parties communicate and coordinate with one another. Moreover, these third parties may also have relationships with other commercial entities, some of which may compete with us. Under certain circumstances, these third parties may be able to terminate their agreements with us upon short notice. If the third parties conducting our clinical trials do not perform their contractual duties or obligations, experience work stoppages, do not meet expected deadlines, terminate their agreements with us or need to be replaced, or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical trial protocols or GCPs, or for any other reason, we may need to enter into new arrangements with alternative third parties, which could be difficult, costly or impossible, and our clinical trials may be extended, delayed or terminated or may need to be repeated. If any of the foregoing were to occur, we may not be able to obtain, on a timely basis or at all, regulatory approval for or to commercialize the product candidate being tested in such trials, and as a result, our financial condition will be adversely affected.
Risks Related to Commercialization of Our Product Candidates
We have no experience as a company in commercializing any product. If we fail to obtain commercial expertise, upon product approval by regulatory agencies, our product launch and revenues could be delayed.
As a company, we have never obtained regulatory approval for, or commercialized, any product. Accordingly, we have not yet begun to build out any sales or marketing or distribution capabilities. If we are unable to establish, or contract for, effective sales and marketing and distribution capabilities, or if we are unable to enter into agreements with third parties to commercialize our product candidates on favorable terms or on any reasonable terms at all, we may not be able to effectively generate product revenues once our product candidates are approved for marketing. If we fail to obtain commercial expertise or capabilities, upon drug approval, our product launch and subsequent revenues could be delayed and /or fail to reach their commercial potential.
Our product development efforts are at an early stage. We have not yet undertaken any marketing efforts, and there can be no assurancesassurance that future anticipated market testing and analyses will validate our marketing strategy and therefore westrategy. We may need to modify the products, or willwe may not be successful in either developing or marketing those products.
We As a company, we have not completed the development or clinical trials of any product candidates and, accordingly, have not yet begun to market or generate revenue from the commercialization of any products. CommercializingObtaining approvals of these product candidates will require substantial additional research and development as well as costly clinical trials. There can be no assurance that we will successfully complete development of our product candidates or successfully market them. We may encounter problems and delays relating to research and development, regulatory approval, intellectual property rights of product candidates, or other factors. There can be no assurance that our development programs will be successful, that our products, if successfully developed,product candidates will prove to be safe and effective in or after clinical trials, that the necessary regulatory approvals for any product candidates will be obtained, or, even if obtained, will be as broad as sought or will be maintained for any period thereafter, that patents will issue on our patent applications, that any intellectual property protections we secure will be adequate, or that our collaboration arrangements will not diminish the value of our intellectual property through licensing or other arrangements. Furthermore, there can be no assurance that any product we might market will be received favorably by customers (whether physicians, payers, patients, or both)all three), adequately reimbursed by third partythird-party payers, or that competitive products will not perform better and/or be marketed more successfully. Additionally, there can be no assurances that any future market testing and analyses will validate our marketing strategies. We may need to seek to modify the product labels through additional studies in order to be able to market them successfully.successfully to reach their commercial potential.
If we are unable to establish relationships with licensees or collaborators to carry out sales, marketing, and distribution functions or to create effective marketing, sales, and distribution capabilities, we will be unable to market our products successfully.
Our business strategy may include out-licensing product candidates to or collaborating with larger firms with experience in marketing and selling pharmaceutical products. There can be no assurance that we will successfully be able to establish marketing, sales, or distribution relationships with any third party,third-party, that such relationships, if established, will be successful, or that we will be successful in gaining market acceptance for any products we might develop. To the extent that we enter into any marketing, sales, or distribution arrangements with third parties, our product revenues per unit sold are expected to be lower than if we marketed, sold, and distributed our products directly, and any revenues we receive will depend upon the efforts of such third parties.
If we are unable to establish such third-party marketing and sales relationships, or choose not to do so, we would have to establish in-house marketing and sales capabilities. We have no experience in marketing or selling oncology pharmaceutical products, and currently have no marketing, sales, or distribution infrastructure and no experience developing or managing such infrastructure for an oncology related product. To market any products directly, we would have to establish a marketing, sales, and distribution force that hadhas technical expertise and could support a distribution capability. Competition in the biopharmaceutical industry for technically proficient marketing, sales, and distribution personnel is intense and attracting and retaining such personnel may significantly increase our costs. There can be no assurance that we will be able to establish internal marketing, sales, or distribution capabilities or that these capabilities will be sufficient to meet our needs.
Commercial success of our product candidates will depend on the acceptance of these products by physicians, payers, and patients.
Any product candidate that we may develop may not gain market acceptance among physicians, payers and patients. Market acceptance of and demand for any product that we may develop will depend on many factors, including without limitation:
● Comparative superiority of the efficacy and safety in the treatment of the disease indication compared to alternative treatments;
●
Less incidence, less prevalence and more severity of adverse side effects;
●
potential Potential advantages over alternative treatments;
● Cost effectiveness;
●
cost effectiveness;
●
convenience Convenience and ease of administration;
●
sufficient Sufficient third-party coverage and/or reimbursement;
●
strength Strength of sales, marketing and distribution support; and
●
our Our ability to provide acceptable and compelling evidence of safety and efficacy.
If any product candidate developed by us receives regulatory approval but does not achieve an adequate level of market acceptance by physicians, payers, and patients, we may generate insufficient, little, or no product revenue to earn appropriate returns on the investment of product development costs and may not become profitable.profitable at sufficient product sales volumes to earn sustainable profitability.
Our products may not be accepted for reimbursement or properlyadequately reimbursed by third-party payers.
The successful commercialization of any products we might develop will depend substantially on whether the costs of our products and related treatments are reimbursed at acceptable levels by government authorities, private healthcare insurers, and other third-party payers, such as health maintenance organizations. Reimbursement rates may vary, depending upon the third-party payer, the type of insurance plan, and other similar or dissimilar factors. If our products aredo not subject toachieve adequate reimbursement, physiciansthen the number of physician prescriptions of our products may not prescribe for our products inbe sufficient amounts to make our products profitable.profitable, and to earn a sufficient profit to earn a reasonable return on our investment and a provide a cash flow to finance future investments on the next generation of products and investments in new technological platforms.
Comparative effectiveness research demonstrating benefits inof a competitor’s product could adversely affect the sales of our drug product candidates. If third-party payers do not consider our products to be cost-effective compared to other available therapies, they may not cover our products as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow us to sell our products on a profitable basis.basis sufficient for our Company to remain competitive and thrive.
Adequate third-party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on our investment in the product development.development of that product. In addition, in the U.S. there is a growing emphasis on comparative effectiveness research, both by private payers and by government agencies. To the extent other drugs or therapies are found to be more effective than our products, payers may elect to cover such therapies in lieu of our products and/or reimburse our products at a lower rate.
In addition, emphasis
The effects of economic and political pressure to lower pharmaceutical prices are a major threat to the economic viability of new research-based pharmaceutical products, and any significant decrease in drug prices could materially and adversely affect our prospects.
Emphasis on managed care and government price controls in the U.S. has increased and we expect this will continue to increase the pressure on pharmaceutical pricing. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which we receive regulatory approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
Any development along these lines could materially and adversely affect our prospects. We are unable to predict what political, legislative or regulatory changes relating to the healthcare industry, including without limitation any changes affecting governmental and/or private or third partythird-party coverage and reimbursement, may be enacted in the future, or what effect such legislative or regulatory changes would have on our business. However, if governmental price management does not provide for the very high price of pharmaceutical research, it could create very demanding challenges for our industry and our prospects or require breakthroughs in research productivity, which there can be no assurance of.
If we obtain FDA approval for any of our product candidates, we will be subject to various federal and state fraud and abuse laws; these laws may impact, among other things, our proposed sales, marketing and education programs. Fraud and abuse laws are expected to increase in breadth and in detail, which will likely increase our operating costs and the complexity of our programs to insureensure compliance with such enhanced laws.
If we obtain FDA approval for any of our product candidates and begin commercializing those products in the U.S., our operations may be directly, or indirectly through our customers, distributors, or other business partners, subject to various federal and state fraud and abuse laws, including, without limitation, anti-kickback statutes and false claims statutes which may increase our operating costs. These laws may impact, among other things, our proposed sales, marketing and education programs. In addition, we may be subject to data privacy and security regulation by both the federal government and the states in which we conduct business.
If our operations are found to be in violation of any of the federal and state fraud and abuse laws or any other governmental regulations that apply to us, we may be subject to criminal actions and significant civil monetary penalties, which would adversely affect our ability to operate our business and our results of operations.
If our operations are found to be in violation, even inadvertently, of any of the federal and state fraud and abuse laws, described aboveincluding, without limitation, anti-kickback statutes and false claims statutes or any other governmental regulations that apply to us, we may be subject to penalties, including criminal and significant civil monetary penalties, damages, fines, imprisonment, exclusion from participation in government healthcare programs, and the curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business and our results of operations. To the extent that any of our product candidates are ultimately sold in a foreign country, we may be subject to similar foreign laws and regulations, which may include, for instance, applicable post-marketing requirements, including safety surveillance, anti-fraud and abuse laws, and implementation of corporate compliance programs and reporting of payments or transfers of value to healthcare professionals.
Negotiated prices for our products covered by a Part D prescription drug plan and other government programs will likely be lower than the prices we might otherwise obtain.
Government payment for some of the costs of prescription drugs may increase demand for our products for which we receive marketing approval,approval; however, any negotiated prices for our products covered by a Part D prescription drug plan and other government programs will likely be lower than the prices we might otherwise obtain. We anticipate that the number and type of products that will be subject to federal pricing will increase over time. There may be rules to demand that the government and medical institutions, which are in part supported by government funding, will be granted access to medicines at the same highly favorable prices given to the governmental direct medical care programs.
Risks Related to Our Intellectual Property
If we and our third-party licensors do not obtain and preserve protection for our respective intellectual property rights, our competitors may be able to take advantage of our (and our licensors’) development efforts to develop competing drugs.
Our commercial success will depend in part on obtaining patent protection for any products and other technologies we might develop, and successfully defending any patents we obtain against third-party challenges. We licensehave licensed all intellectual property related to Validive from Onxeo S.A., a French public company. See “Material“Business – License, Development and Collaboration Agreements”. The assignment and transfer of the MNPR-201 (GPX-150)camsirubicin (formerly GPX-150) patent portfolio from TacticGem, LLC (“TacticGem”) to us has been completed. We filed and have been granted in the U.S. and various countries around the world patents for antibodies that target uPAR.uPAR for our MNPR-101 program. We have also been granted in the U.S. and various countries around the world patents to a specific sequence of amino acids on uPAR, to which our MNPR-101 antibody binds. We are currently prosecuting this patent in other countries around the world to further protect MNPR-101. The patent process is subject to numerous risks and uncertainties, and there can be no assurance that we will be successful in obtaining and defending patents. See “Intellectual“Business - Intellectual Property Portfolio”Portfolio and Exclusivity”. These risks and uncertainties include without limitation the following:
●
Patents that may be issued or licensed may be challenged, invalidated, or circumvented; or may not provide any competitive advantage for other reasons.
● Our licensors may terminate or breach our existing or future license agreements, thereby reducing or preventing our ability to exclude competition; termination of such license agreements may also subject us to risk of patent infringement of patents to which we no longer have a license.
●
Our competitors, many of which have substantially greater resources than us and have made significant investments in competing technologies, may seek, or may already have obtained, patents that will limit, interfere with, or eliminate our ability to make, use, and sell our potential products either in the U.S. or in international markets.
●
As a matter of public policy regarding worldwide health concerns, there may be significant pressure on the U.S. government and other international governmental bodies to limit the scope of domestic and international patent protection for cancer treatments that prove successful.
●
Countries other than the U.S. may have less restrictive patent laws than those upheld by the U.S. courts; therefore, non-U.S. competitors could exploit these laws to create, develop, and market competing products.
In addition, the USPTOU.S. Patent and Trademark Office (“USPTO”) and patent offices in other jurisdictions have often required that patent applications concerning pharmaceutical and/or biotechnology-related inventions be limited or narrowed substantially to cover only the specific innovations exemplified in the patent application, thereby limiting their scope of protection against competitive challenges. Thus, even if we or our licensors are able to obtain patents, the scope of the patents may be substantially narrower than anticipated.
If we permit our patents to lapse or expire, we will not be protected and will have less of a competitive advantage. The value of our products may be greatly reduced if this occurs. Our patents expire at different times and are subject to the laws of multiple countries. Some of our patents are currently near expiration and we may pursue patent term extensions for these where appropriate. See “Intellectual“Business - Intellectual Property Portfolio”Portfolio and Exclusivity”.
In addition to patents, we also rely on trade secrets and proprietary know-how. While we take measures to protect this information by entering into confidentiality and invention agreements with our employees, consultants and collaborators, we cannot provide any assurances that these agreements will be fully enforceable and will not be breached, that we will be able to protect ourselves from the harmful effects of disclosure if they are not fully enforceable or are breached, that any remedy for a breach will adequately compensate us, that these agreements will achieve their intended aims, or that our trade secrets will not otherwise become known or be independently discovered by competitors. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, some courts inside and outside the U.S., are less willing or unwilling to protect trade secrets. If any of these events for which we cannot provide assurances occurs, or we otherwise lose protection for our trade secrets were to be lawfully obtained or proprietary know-how,independently developed by a competitor, we would have no right to prevent them from using that technology or information to compete with us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our competitive position would be harmed and the value of this informationthe trade secrets may be greatly reduced.
The patent protection we obtain and preserve for our product candidates may not be sufficient to provide us with any material competitive advantage.
We may be subject to competition despite the existence of intellectual property we license or own. We can give no assurances that our intellectual property claims will be sufficient to prevent third parties from designing around patents we own or license and developing and commercializing competitive products. The existence of competitive products that avoid our intellectual property could materially adversely affect our operating results and financial condition. Furthermore, limitations, or perceived limitations, in our intellectual property may limit the interest of third parties to partner, collaborate or otherwise transact with us, if third parties perceive a higher than acceptable risk to commercialization of our products or future products. When looking at our Validive patents’ ability to block competition, the protection offered by our patents may be, to some extent, more limited than the protection provided by patents claiming the composition of matter of entirely new chemical structures previously unknown. If a competitor were able to successfully design around any method of use and formulation patents we may have now or in the future, it is highly likely that our business and competitive advantage would be adversely affected.
Patent terms may be inadequate to protect our competitive position on our product candidates for an adequate amount of time.
Patents have a limited lifespan. In the U.S., if all maintenance fees are timely paid, the natural expiration of a patent is generally 20 years from its earliest U.S. non-provisional filing date. Various extensions may be available, but the life of a patent, and the protection it affords, is limited. Even if patents covering our product candidates are obtained, once the patent life has expired for a product candidate, we may be open to competition from competitive medications, including generic medications. Given the amount of time required for the development, testing and regulatory review of new product candidates, patents protecting such product candidates might expire before or shortly after such product candidates are commercialized. As a result, our owned and licensed patent portfolio may not provide us with sufficient rights to exclude others from commercializing product candidates similar or identical to ours.
Depending upon the timing, duration and conditions of any FDA marketing approval of our product candidates, one or more of our U.S. patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, referred to as the Hatch-Waxman Amendments, and similar legislation in the European Union. The Hatch-Waxman Amendments permit a patent term extension of up to five years for a patent covering an approved product as compensation for effective patent term lost during product development and the FDA regulatory review process. However, we may not receive an extension if we fail to exercise due diligence during the testing phase or regulatory review process, fail to apply within applicable deadlines, fail to apply prior to expiration of relevant patents or otherwise fail to satisfy applicable requirements. Moreover, the length of the extension could be less than we request. Only one patent per approved product can be extended, the extension cannot extend the total patent term beyond 14 years from approval and only those claims covering the approved drug, a method for using it or a method for manufacturing it may be extended. If we are unable to obtain patent term extension or the term of any such extension is less than we request, the period during which we can enforce our patent rights for the applicable product candidate will be shortened and our competitors may obtain approval to market competing products sooner. As a result, our revenue from applicable products could be reduced. Further, if this occurs, our competitors may take advantage of our investment in development and trials by referencing our clinical and preclinical data and launch their product earlier than might otherwise be the case, and our competitive position, business, financial condition, results of operations, and prospects would be materially harmed.
Intellectual property disputes could require us to spend time and money to address such disputes and could limit our intellectual property rights.
The biopharmaceutical industry has been characterized by extensive litigation regarding patents and other intellectual property rights, and companies have employed intellectual property litigation and USPTO post-grant proceedings to gain a competitive advantage. We may become subject to infringement claims or litigation arising out of patents and pending applications of our competitors, or additional interference proceedings declared by the USPTO to determine the priority and patentability of inventions. The defense and prosecution of intellectual property suits, USPTO proceedings, and related legal and administrative proceedings are costly and time-consuming to pursue, and their outcome is uncertain. Litigation may be necessary to enforce our issued patents, to protect our trade secrets and know-how, or to determine the enforceability, scope, and validity of the proprietary rights of others. An adverse determination in litigation or USPTO post-grant and interference proceedings to which we may become a party could subject us to significant liabilities, require us to obtain licenses from third parties, or restrict or prevent us from selling our products in certain markets. Even if a given patent or intellectual property dispute were settled through licensing or similar arrangements, our costs associated with such arrangements may be substantial and could include the payment by us of large fixed payments and ongoing royalties. Furthermore, the necessary licenses may not be available on satisfactory terms or at all. In addition, evenEven where we have meritorious claims or defenses, the costs of litigation may prevent us from pursuing these claims or defenses and/or may require extensive financial and personnel resources to pursue these claims or defenses. In addition, it is possible there may be defects of form in our current and future patents that could result in our inability to defend the intended claims. Intellectual property disputes arising from the aforementioned factors, or other factors, may materially harm our business.
We may not be able to enforce our intellectual property rights throughout the world.
The laws of some foreign countries do not protect intellectual property rights to the same extent as the laws of the U.S. Companies have encountered significant problems in protecting and defending intellectual property rights in certain foreign jurisdictions. The legal systems of some countries, particularly developing countries, do not favor the enforcement of patents and other intellectual property protection, especially those relating to life sciences. This could make it difficult for us to stop the infringement of our patents or the misappropriation of our other intellectual property rights. For example, many foreign countries have compulsory licensing laws under which a patent owner must grant licenses to third parties. In addition, many countries limit the enforceability of patents against third parties, including government agencies or government contractors. In these countries, patents may provide limited or no benefit.
Proceedings to enforce our patent rights in foreign jurisdictions, whether or not successful, could result in substantial costs and divert our efforts and attention from other aspects of our business. Furthermore, while we intend to protect our intellectual property rights in our expected significant markets, we cannot ensure that we will be able to initiate or maintain similar efforts in all jurisdictions in which we may wish to market Validive or any future products. Accordingly, our efforts to protect our intellectual property rights in such countries may be inadequate. In addition, changes in the law and legal decisions by courts in the U.S. and foreign countries may affect our ability to obtain and enforce adequate intellectual property protection for our products and technology.
Changes to the patent law in the U.S. and other jurisdictions could diminish the value of patents in general, thereby impairing our ability to protect our product candidates.
As is the case with other biopharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involves both technological and legal diligence and complexity. Therefore, obtaining and enforcing biopharmaceutical patents is costly, time consuming and inherently uncertain. In addition, the U.S. has recently enacted and is currently implementing wide ranging patent reform legislation. The U.S. Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents once obtained. Depending on future actions by the U.S. Congress, the federal courts and the USPTO, as well as other jurisdictions around the world, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce our existing patents and patents that we might obtain in the future.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
The USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other provisions during the patent process. There are situations in which noncompliance can result in abandonment or lapse of a patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. In such an event, competitors might be able to enter the market earlier than would otherwise have been the case.
If we fail to comply with our obligations under any license, collaboration or other intellectual property-related agreements, we may be required to pay damages and could lose intellectual property rights that may be necessary for developing, commercializing and protecting our current or future technologies or drug candidates or we could lose certain rights to grant sublicenses.
Any license, collaboration or other intellectual property-related agreements impose, and any future license, collaboration or other intellectual property-related agreements we enter into are likely to impose, various development, commercialization, funding, milestone, royalty, diligence, sublicensing, insurance, patent prosecution and enforcement or other obligations on us. If we breach any of these obligations, or use the intellectual property licensed to us in an unauthorized manner, we may be required to pay damages and the licensor may have the right to terminate the license. In spite of our best efforts, any of our future licensors might conclude that we have materially breached our license agreements and might therefore terminate the license agreements, thereby removing our ability to develop and commercialize products and technologies covered by these license agreements. Any license agreements we enter into may be complex, and certain provisions in such agreements may be susceptible to multiple interpretations. The resolution of any contract interpretation disagreement that may arise could narrow what we believe to be the scope our rights to the relevant intellectual property or technology, or increase what we believe to be our financial or other obligations under the relevant agreement, either of which could have a material adverse effect on our business, financial condition, results of operations, and prospects.
We may seek to obtain licenses from licensors in the future, however, we may be unable to obtain any such licenses at a reasonable cost or on reasonable terms, if at all. In addition, if any of our future licensors terminate any such license agreements, such license termination could result in our inability to develop, manufacture and sell products that are covered by the licensed technology or could enable a competitor to gain access to the licensed technology. Any of these events could have a material adverse effect on our competitive position, business, financial condition, results of operations, and ability to achieve profitability.
Furthermore, we may not have the right to control the preparation, filing, prosecution, maintenance, enforcement and defense of patents and patent applications that we license from third parties. Therefore, we cannot be certain that these patents and patent applications will be prepared, filed, prosecuted, maintained, enforced and defended in a manner consistent with the best interests of our business. If our future licensors fail to prosecute, maintain, enforce and defend patents we may in-license, or lose rights to licensed patents or patent applications, our license rights may be reduced or eliminated. In such circumstances, our right to develop and commercialize any of our products or drug candidates that is the subject of such licensed rights could be materially adversely affected. In certain circumstances, our licensed patent rights are subject to our reimbursing our licensors for their patent prosecution and maintenance costs.
Moreover, our licensors may own or control intellectual property that has not been licensed to us and, as a result, we may be subject to claims, regardless of their merit, that we are infringing, misappropriating or otherwise violating the licensor’s intellectual property rights and the amount of any damages or future royalty obligations that would result, if any such claims were successful, would depend on the technology and intellectual property we use in products that we successfully develop and commercialize, if any. Therefore, even if we successfully develop and commercialize products, due to such obligations, we may be unable to achieve or maintain profitability.
Third parties may initiate legal proceedings alleging that we are infringing, misappropriating or otherwise violating their intellectual property rights, the outcome of which would be uncertain and could have a material adverse impact on the success of our business.
Our commercial success depends, in part, upon our ability or the ability of any of our future collaborators to develop, manufacture, market and sell our current or any future drug candidates and to use our proprietary technologies without infringing, misappropriating or otherwise violating the proprietary and intellectual property rights of third parties. The biotechnology and pharmaceutical industries are characterized by extensive and complex litigation regarding patents and other intellectual property rights.
We or any of our future licensors or strategic partners, may be party to, or be threatened with, adversarial proceedings or litigation regarding intellectual property rights with respect to our current or any potential future drug candidates and technologies, including derivation, reexamination, inter partes review, post-grant review or interference proceedings before the USPTO and similar proceedings in jurisdictions outside of the U.S. such as opposition proceedings. If we or our licensors or strategic partners are unsuccessful in any interference proceedings or other priority or validity disputes (including through any patent oppositions) to which we or they are subject, we may lose valuable intellectual property rights through the loss of one or more patents or our patent claims may be narrowed, invalidated, or held unenforceable. In some instances, we may be required to indemnify our licensors or strategic partners for the costs associated with any such adversarial proceedings or litigation. Third parties may also assert infringement, misappropriation or other claims against us, our licensors or our strategic partners based on existing patents or patents that may be granted in the future, as well as other intellectual property rights, regardless of their merit. There is a risk that third parties may choose to engage in litigation or other adversarial proceedings with us, our licensors or our strategic partners to enforce or otherwise assert their patent rights or other intellectual property rights. Even if we believe such claims are without merit, a court of competent jurisdiction could hold that these third-party patents and other intellectual property rights are valid, enforceable and infringed, which could have a material adverse impact on our ability to utilize our developed technologies or to commercialize our current or any future drug candidates deemed to be infringing. In order to successfully challenge the validity of any such U.S. patent in federal court, we would need to overcome a presumption of validity by presenting clear and convincing evidence of invalidity. There is no assurance that a court of competent jurisdiction, even if presented with evidence we believe to be clear and convincing, would invalidate the claims of any such U.S. patent.
Further, we cannot guarantee that we will be able to successfully settle or otherwise resolve such adversarial proceedings or litigation. If we are unable to successfully settle future claims on terms acceptable to us, we may be required to engage in or to continue costly, unpredictable and time-consuming litigation and may be prevented from or experience substantial delays in marketing our drug candidates. If we or any of our licensors or strategic partners are found to infringe, misappropriate or violate a third-party patent or other intellectual property rights, we could be required to pay damages, including treble damages and attorney’s fees, if we are found to have willfully infringed. In addition, we, or any of our licensors or strategic partners may choose to seek, or be required to seek, a license from a third-party, which may not be available on commercially reasonable terms, if at all. Even if a license can be obtained on commercially reasonable terms, the rights may be non-exclusive, which could give our competitors access to the same technology or intellectual property rights licensed to us, and we could be required to make substantial licensing and royalty payments. We also could be forced, including by court order, to cease utilizing, developing, manufacturing and commercializing our developed technologies or drug candidates deemed to be infringing. We may be forced to redesign current or future technologies or products. Any of the foregoing could have a material adverse effect on our ability to generate revenue or achieve profitability and possibly prevent us from generating revenue sufficient to sustain our operations.
In addition, we or our licensors or strategic partners may find it necessary to pursue claims or to initiate lawsuits to protect or enforce our patent or other intellectual property rights. If we or our licensors or strategic partners were to initiate legal proceedings against a third-party to enforce a patent covering one of our drug candidates or our developed technology, the defendant could counterclaim that such patent is invalid or unenforceable. In patent litigation in the U.S., defendant counterclaims alleging invalidity or unenforceability are commonplace. Grounds for a validity challenge could be an alleged failure to meet any of several statutory requirements, for example, claiming patent-ineligible subject matter, lack of novelty, indefiniteness, lack of written description, non-enablement, anticipation or obviousness. Grounds for an unenforceability assertion could be an allegation that someone connected with prosecution of the patent withheld relevant information from the USPTO or made a misleading statement during prosecution. The outcome of such invalidity and unenforceability claims is unpredictable. With respect to the validity question, for example, we cannot be certain that there is no invalidating prior art of which we or our licensors or strategic partners and the patent examiner were unaware during prosecution. If a defendant were to prevail on a legal assertion of invalidity or unenforceability, we could lose at least part, and perhaps all, of the patent protection for one or more of our drug candidates. The narrowing or loss of our owned and licensed patent claims could limit our ability to stop others from using or commercializing similar or identical technologies and products. All of these events could have a material adverse effect on our business, financial condition, results of operations and prospects. Patent and other intellectual property rights also will not protect our drug candidates and technologies if competitors or third parties design around such drug candidates and technologies without legally infringing, misappropriating or violating our patent or other intellectual property rights.
The cost to us in defending or initiating any litigation or other proceedings relating to our patent or other intellectual property rights, even if resolved in our favor, could be substantial, and any litigation or other proceedings would divert our management’s attention and distract our personnel from their normal responsibilities. Such litigation or proceedings could materially increase our operating losses and reduce the resources available for development activities or any future sales, marketing or distribution activities. We may not have sufficient financial or other resources to conduct such litigation or proceedings adequately. Some of our competitors may be able to more effectively sustain the costs of complex patent litigation because they have substantially greater resources. Uncertainties resulting from the initiation and continuation of patent litigation or other proceedings could delay our research and development efforts and materially limit our ability to continue our operations. Furthermore, because of the substantial amount of discovery required in connection with certain such proceedings, there is a risk that some of our confidential information could be compromised by disclosure. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments and if securities analysts or investors perceive these results to be negative, such announcements could have a material adverse effect on the price of our common stock.
Intellectual property rights of third parties could adversely affect our ability to commercialize our current or future technologies or drug candidates, and we might be required to litigate or obtain licenses from third parties to develop or market our current or future technologies or drug candidates, which may not be available on commercially reasonable terms, or at all.
There are numerous companies that have pending patent applications and issued patents broadly covering immune-therapies generally or covering small molecules directed against the same targets as, or targets similar to, those we are pursuing. Our competitive position may materially suffer if patents issued to third parties or other third-party intellectual property rights cover our current or future technologies, drug candidates or elements thereof, or our manufacture or uses relevant to our development plans. In such cases, we may not be in a position to develop or commercialize current or future technologies or drug candidates unless we successfully pursue litigation to nullify or invalidate the third-party intellectual property rights concerned, or enter into a license agreement with the intellectual property rights holder, if available on commercially reasonable terms. There may be issued patents of which we are not aware, held by third parties that, if found to be valid and enforceable, could be alleged to be infringed by our current or future technologies or drug candidates. There also may be pending patent applications of which we are not aware that may result in issued patents, which could be alleged to be infringed by our current or future technologies or drug candidates. Should such an infringement claim be successfully brought, we may be required to pay substantial damages or be forced to abandon our current or future technologies or drug candidates or to seek a license from any patent holders. No assurances can be given that a license will be available on commercially reasonable terms, if at all.
Third-party intellectual property rights holders may also actively bring infringement, misappropriation or other claims alleging violations of intellectual property rights against us. We cannot guarantee that we will be able to successfully settle or otherwise resolve such claims. If we are unable to successfully settle future claims on terms acceptable to us, we may be required to engage in or to continue costly, unpredictable and time-consuming litigation and may be prevented from, or experience substantial delays in, marketing our drug candidates. If we fail in any such dispute, in addition to being forced to pay damages, we may be temporarily or permanently prohibited from commercializing any of our current or future technologies or drug candidates that are held to be infringing, misappropriating or otherwise violating third-party intellectual property rights. We might, if possible, also be forced to redesign current or future technologies or drug candidates so that we no longer infringe, misappropriate or violate the third-party intellectual property rights. Any of these events, even if we were ultimately to prevail, could require us to divert substantial financial and management resources that we would otherwise be able to devote to our business, which could have a material adverse effect on our financial condition and results of operations.
Risks Related to Our Business Operations and Industry
WeAs a recently established entity, we have a limited operating history as we are a new entity.history.
As of March 1, 2018, To date, we have engaged exclusively in acquiring pharmaceutical drug product candidates, licensing rights to drug product candidates and entering into collaboration agreements with respect to key services or technologies for our drug product development, and have not completed any clinical trials, received any governmental approvals, brought any product to market, manufactured or produced products in clinical or commercial quantities or sold any pharmaceutical products. WeAs a company we have limited experience in negotiating, establishing, and maintaining strategic relationships, conducting clinical trials, and managing the regulatory approval process, all of which will be necessary if we are to be successful. Our lack of experience in these critical areas makes it difficult for a prospective investor to evaluate our abilities and increases the risk that we will fail to successfully execute our strategies.
Furthermore, if our business grows rapidly, our operational, managerial, legal, and financial resources will be strained. Our development will require continued improvement and expansion of our management team and our operational, managerial, legal, and financial systems and controls.
In the normal course of business, we have evaluated and expect to evaluate potential acquisitions and/or licenses of patents, compounds, and technologies that our management believes could complement or expand our business. We have limited history of conducting acquisitions, and negotiating and acquiring licenses. In the event that we identify an acquisition or license candidate we find attractive, there is no assurance that we will be successful in negotiating an agreement to acquire or license, or in financing or profitably exploiting, such patents, compounds, or technologies. Furthermore, such an acquisition or license could divert management time and resources away from other activities that would further our current business development.
If we lose key management leadership, and/or scientific personnel, and if we cannot recruit qualified employees, managers, directors, officers, or other significant personnel, it is highly likely that we maywill experience program delays and increases in compensation costs, and our business will be materially disrupted.
Our future success is highly dependent on the continued service of principal members of our management, leadership, and scientific personnel, who are able to terminate their employment with us at any time and may be able to compete with us. The loss of any of our key management, leadership, or scientific personnel including, in particular, Christopher M. Starr, our Executive Chairman of the Board of Directors (referred to as the “Board”), Chandler D. Robinson, our President and CEO, and Andrew P. Mazar, our Executive Vice President of Research and Development and Chief Scientific Officer, could materially disrupt our business and materially delay or prevent the successful product development and commercialization of our product candidates. We have employment agreements with Dr. Robinson and Dr. Mazar which have no term but are for at-will employment, meaning the executives have the ability to terminate their employment at any time. We do not have an employment agreement with Dr. Starr.
Our future success will also depend on our continuing ability to identify, hire, and retain highly skilled personnel for all areas of the organization. Competition in the biopharmaceutical industry for scientifically and technically qualified personnel is intense, and we may be unsuccessful in identifying, hiring, and retaining qualified personnel. Our continued abilityrequirement to identify, hire, and retain highly skilledcompetent personnel may cause our compensation costs to increase materially.
We incur costs as a result of operating as a stock trading public company, and our management is required to devote substantial time to investor relations, information and communication to the public, and related compliance initiatives and corporate governance practices.
As a stock trading public company, and particularly after we are no longer an emerging growth company, we will incur significant legal, accounting and other expenses that we did not incur as a private company. The Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act, the listing requirements of the Nasdaq Capital Market and other applicable securities rules and regulations impose various requirements on stock trading public companies, including establishment and maintenance of effective disclosure and financial controls and corporate governance practices. Our management and other personnel devote a substantial amount of time to these compliance initiatives. Moreover, these rules and regulations increase our legal and financial compliance costs and make some activities more time-consuming and costly. For example, we expect that these rules and regulations may make it more difficult and more expensive for us to obtain director and officer liability insurance, which in turn could make it more difficult for us to attract and retain qualified members of our Board. However, these rules and regulations are often subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies. This could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to disclosure and governance practices.
Despite ongoing compliance training and periodic education, our employees and consultants may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements, which could result in delays or terminations of our development programs and adversely affect our business.
Although we regularly train our employees on compliance and we are aware of no misconduct or improper activities to date, we are exposed to the risk of employee or consultant fraud or other misconduct. Misconduct by our employees or consultants could include intentional failures to: comply with FDA regulations; provide accurate information to the FDA; comply with manufacturing standards; comply with federal and state healthcare fraud and abuse laws and regulations; report financial information or data accurately or disclose unauthorized activities to us. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Employee and consultant misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter such misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant fines or other sanctions. Such actions could adversely affect our business including delaying or terminating one or more of our development programs.
We are an emerging growth company and we cannot be certain if the reduced disclosure requirements applicable to emerging growth companies will make our common stock less attractive to investors.
We are an emerging growth company. Under the Jumpstart Our Business Startups Act of 2012 (the “JOBS Act”), emerging growth companies can delay adopting new or revised accounting standards until such time as those standards apply to private companies. Therefore,We have irrevocably elected to opt out of this provision and, as a result, we may not be subject to the samewill comply with new or revised accounting standards as otherwhen they are required to be adopted by public companies that are not “emergingemerging growth companies.”
For as long as we continue to be an emerging growth company, we also intend to take advantage of certain other exemptions from various reporting requirements that are applicable to other public companies including, but not limited to, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements, exemptions from the requirements of holding a nonbinding advisory stockholder vote on executive compensation and any golden parachute payments not previously approved, exemption from the requirement of auditor attestation in the assessment of our internal control over financial reporting and exemption from any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements (auditor discussion and analysis). If we do take advantage of these exemptions, the information that we provide stockholders will be different than what is available with respect to other public companies. We cannot predict if investors will find our Common Stockcommon stock less attractive because we will rely on these exemptions. If investors find our Common Stockcommon stock less attractive as a result of our status as an emerging growth company, there may be less liquidity for our Common Stockcommon stock and our stock price may be more volatile.
We will remain an emerging growth company until the earliest of (i)(1) the endlast day of the fiscal year (a) following the fifth anniversary of the completion of our initial public offering, (b) in which we have total annual gross revenue of at least $1.07 billion or (c) in which we are deemed to be a large accelerated filer, which means the market value of our common stock that is held by non-affiliates exceeds $700 million as of the end of the second fiscal quarter, (ii) the end of the fiscal year in which we have total annual gross revenues of $1 billion or more during such fiscal year, (iii)prior June 30th, and (2) the date on which we issuehave issued more than $1$1.0 billion in non-convertible debt in asecurities during the prior three-year period or (iv) the end of the fiscal year following the fifth anniversary of the date of the first sale of our Common Stock pursuant to an effective registration statement filed under the Act.period.
Competition and technological change may make our product candidates obsoleteless competitive or non-competitive.obsolete.
The biopharmaceutical industry is subject to rapid technological change. We have many potential competitors, including major drug and chemical companies, specialized biopharmaceutical firms, and universities and other research institutions. These companies, firms, and other institutions may develop products that are more effective than our product candidates or that would make our product candidates obsoleteless competitive or non-competitive.obsolete. Many of these companies, firms, and other institutions have greater financial resources than us and may be better able to withstand and respond to adverse market conditions within the biopharmaceutical industry, including without limitation the lengthy product development and regulatory approval processprocesses for product candidates.
We face significant competition from other biotechnology and pharmaceutical companies, and our operating results will suffer if we fail to compete effectively.
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. While we believe we have significant competitive advantages with our expertise in small molecules and biologics, and rare disease clinical development, along with a strong intellectual property portfolio, we currently face and will continue to face competition for our drug development programs from companies that target SOM, are developing doxorubicin analogs/replacement, are targeting severe COVID-19 and are targeting uPAR. The competition is likely to come from multiple sources, including larger pharmaceutical companies, biotechnology companies and academia. Accordingly, our competitors may have more resources and be more successful than us in obtaining approval for treatments and achieving widespread market acceptance. For any products that we may ultimately commercialize, not only will we compete with any existing therapies and those therapies currently in development, we will have to compete with new therapies that may become available in the future.
We may engage in strategic transactions that could impact our liquidity, increase our expenses and present significant distractions to our management.
From time to time, we may consider strategic transactions, such as acquisitions of companies, asset purchases, and out-licensing or in-licensing of products, product candidates or technologies. Additional potential transactions that we may consider include a variety of different business arrangements, including spin-offs, strategic partnerships, joint ventures, restructurings, divestitures, business combinations and investments. Any such transaction will require us to incur non-recurring or other charges, may increase our near- and long-term expenditures and may pose significant integration challenges or disrupt our management or business, which could adversely affect our operations and financial results. For example, these transactions may entail numerous operational and financial risks, including:
● exposure to unknown technologies, product candidates, medical conditions and indications, product manufacturing challenges and uncertainties, and other unknown factors of potential high risk;
● disruption of our business and diversion of our management's time and attention in order to develop acquired products, product candidates or technologies;
● incurrence of substantial debt or dilutive issuances of equity securities to pay for acquisitions;
● higher-than-expected acquisition and integration costs;
● write-downs of assets, goodwill or impairment charges;
● increased amortization expenses;
● difficulty and cost in combining the operations and personnel of any acquired businesses with our operations and personnel;
● impairment of relationships with key suppliers or customers of any acquired businesses due to changes in management and ownership; and
● inability to retain key employees of any acquired businesses or for our current business based on changed circumstances.
Accordingly, although there can be no assurance that we will undertake or successfully complete any transactions of the nature described above, any transactions that we do complete may be subject to the foregoing or other risks, and could have a material adverse effect on our business, results of operations, financial condition and prospects.
Our business and operations are vulnerable to computer system failures, cyber-attacks or deficiencies in our cyber-security, which could increase our expenses, divert the attention of our management and key personnel away from our business operations and adversely affect our results of operations.
Despite the implementation of security measures, our internal computer systems, and those of third parties on which we rely, are vulnerable to damage from: computer viruses; malware; natural disasters; terrorism; war; telecommunication and electrical failures; cyber-attacks or cyber-intrusions over the Internet; attachments to emails; persons inside our organization; or persons with access to systems inside our organization. The risk of a security breach or disruption, particularly through cyber-attacks or cyber intrusion, including by computer hackers, foreign governments, and cyber terrorists, has generally increased as the number, intensity and sophistication of attempted attacks and intrusions from around the world have increased. If such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our product development programs. For example, the loss of clinical trial data from completed or ongoing or planned clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach was to result in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur material legal claims and liability, lawsuitsand damage to our reputation, and the further development of our product candidates could be delayed. We could be forced to expend significant resources in response to a cyber security breach, including repairing system damage, increasing cyber security protection costs by deploying additional personnel and protection technologies, paying regulatory fines and resolving legal claims and regulatory actions, all of which would increase our expenses, divert the attention of our management and key personnel away from our business operations and adversely affect our results of operations.
Failure to comply with health and data protection laws and regulations could lead to government enforcement actions (which could include civil or criminal penalties), private litigation or adverse publicity and could negatively affect our operating results and business.
We and our current and any of our future collaborators may be subject to federal, state and foreign data protection laws and regulations (i.e., laws and regulations that address privacy and data security). In the U.S., numerous federal and state laws and regulations, including federal health information privacy laws (e.g., the Health Insurance Portability and Accountability Act (“HIPAA”), as amended by the Health Information Technology for Economic and Clinical Health Act (“HITECH”)), state data breach notification laws, state health information privacy laws and federal and state consumer protection laws (e.g., Section 5 of the Federal Trade Commission Act), that govern the collection, use, disclosure and protection of health-related and other personal information could apply to our operations or the operations of our collaborators. In addition, we may obtain health information from third parties (including research institutions from which we obtain clinical trial data) that are broughtsubject to privacy and security requirements under HIPAA, as amended by HITECH, or other privacy and data security laws. Depending on the facts and circumstances, we could be subject to criminal penalties if we knowingly obtain, use, or disclose individually identifiable health information maintained by a HIPAA-covered entity in a manner that is not authorized or permitted by HIPAA.
International data protection laws, including Regulation 2016/679, known as the General Data Protection Regulation (“GDPR”) may also apply to health-related and other personal information obtained outside of the U.S. The GDPR went into effect on May 25, 2018. The GDPR introduced new data protection requirements in the EU, as well as potential fines for non-compliant companies of up to the greater of €20 million or 4% of annual global revenue. The regulation imposes numerous new requirements for the collection, use, storage and disclosure of personal information, including more stringent requirements relating to consent and the information that must be shared with data subjects about how their personal information is used, the obligation to notify regulators and affected individuals of personal data breaches, extensive new internal privacy governance obligations and obligations to honor expanded rights of individuals in relation to their personal information (e.g., the right to access, correct and delete their data). In addition, the GDPR includes restrictions on cross-border data transfers. The GDPR increased our responsibility and liability in relation to personal data that we process where such processing is subject to the GDPR, and we may be required to put in place additional mechanisms to ensure compliance with the GDPR, including as implemented by individual countries. Further Brexit has created uncertainty with regard to data protection regulation in the United Kingdom. In particular, it is unclear how data transfers to and from the United Kingdom will be regulated.
In addition, California recently enacted the California Consumer Privacy Act (“CCPA”), which creates new individual privacy rights for California consumers (as defined in the law) and places increased privacy and security obligations on entities handling personal data of consumers or households. The CCPA will require covered companies to provide new disclosure to consumers about such companies’ data collection, use and sharing practices, provide such consumers new ways to opt-out of certain sales or transfers of personal information, and provide consumers with additional causes of action. The CCPA went into effect on January 1, 2020, and the California Attorney General may bring enforcement actions for violations beginning July 1, 2020. The CCPA was amended on September 23, 2018, and it remains unclear what, if any, further modifications will be made to this legislation or how it will be interpreted. As currently written, the CCPA may impact our business activities and exemplifies the vulnerability of our business to the evolving regulatory environment related to personal data and protected health information.
Compliance with U.S. and international data protection laws and regulations could require us to take on more onerous obligations in our contracts, restrict our ability to collect, use and disclose data, or in some cases, impact our ability to operate in certain jurisdictions. Failure to comply with U.S. and international data protection laws and regulations could result in government enforcement actions (which could include civil or criminal penalties), private litigation or adverse publicity and could negatively affect our operating results and business.
If we, our contract research organizations ("CROs") or our IT vendors experience security or data privacy breaches or other unauthorized or improper access to, use of, or destruction of personal data, we may face costs, significant liabilities, harm to our brand and business disruption.
In connection with our drug research and development efforts, we or our CROs may collect and use a variety of personal data, such as names, mailing addresses, email addresses, phone numbers and clinical trial information. Although we have extensive measures in place to prevent the sharing and loss of patient data in our clinical trial processes associated with our developed technologies and drug candidates, any failure to prevent or mitigate security breaches or improper access to, use of, or disclosure of our clinical data or patients’ personal data could result in significant liability under state (e.g., state breach notification laws), federal (e.g., HIPAA, as amended by HITECH), and international laws (e.g., the GDPR). Any failure to prevent or mitigate security breaches or improper access to, use of, or disclosure of our clinical data or patients’ personal data may cause a material adverse impact to our reputation, affect our ability to conduct new studies and potentially disrupt our business. We may also rely on third-party IT vendors to host or otherwise process some of our data and that of users, and any failure by such IT vendor to prevent or mitigate security breaches or improper access to or disclosure of such information could have similarly adverse consequences for us. If we are unable to prevent or mitigate the impact of such security or data privacy breaches, we could be exposed to litigation and governmental investigations, which could lead to a potential disruption to our business.
If we do not comply with laws regulating the protection of the environment and health and human safety, our business could be adversely affected.
Our research and development and drug candidates and future commercial manufacturing may involve the use of hazardous materials and various chemicals. We currently do not maintain a research laboratory, but we engage third-party research organizations and manufacturers to conduct our preclinical studies, clinical trials and manufacturing. These third-party laboratories and manufacturers are subject to federal, state and local laws and regulations governing the use, manufacture, storage, handling and disposal of these hazardous materials. We must rely on the third parties’ procedures for storing, handling and disposing of these materials in their facilities to comply with the relevant guidelines of the states in which they operate and the Occupational Safety and Health Administration of the U.S. Department of Labor. Although we believe that their safety procedures for handling and disposing of these materials comply with the standards mandated by applicable regulations, the risk of accidental contamination or injury from these materials cannot be eliminated. If an accident occurs, this could result in significant delays in our development. We are also subject to numerous environmental, health and workplace safety laws and regulations. Although we maintain workers’ compensation insurance to cover us for costs and expenses, we may incur due to injuries to our employees, this insurance may not provide adequate coverage against us, wepotential liabilities. Additional federal, state and local laws and regulations affecting our operations may be adopted in the future. We may incur substantial costs to defend themcomply with, and address any damages awarded, and demand for our products could be reduced as a result of such lawsuits.
The testing and marketing of medical products is subject to an inherent risk of product liability claims. Since we currently are not sponsoring a clinical trial, we do not have product liability insurance coverage, but plan to obtain appropriate coverage when we enroll patients in a Validivesubstantial fines or other clinical trial. Regardless of their merit or eventual outcome, product liability claims may result in:
●
decreased demand for our products;
●
injury to our reputation and significant, adverse media attention;
●
withdrawal of clinical trial volunteers; and
●
potentially significant litigation costs, including without limitation any damages awarded to the plaintiffspenalties if we lose or settle claims.
We use hazardous materials, including radioactive materials, in our business, andviolate, any claims relating to improper handling, storage, or disposal of these materials could materially harm our business.laws or regulations.
Our business involves the use of a broad range of hazardous chemicals and materials, including radioactive materials. Environmental laws impose stringent civil and criminal penalties for improper handling, disposal, and storage of these materials. In addition, in the event of an improper or unauthorized release of, or exposure of individuals to, hazardous materials, we could be subject to civil damages due to personal injury or property damage caused by the release or exposure. A failure to comply with environmental laws could result in fines and the revocation of environmental permits, which could prevent us from conducting our business.
We have limited the liability of and indemnified our directors and officers.
Although our directors and officers are accountable to us and must exercise good faith, good business judgement, and integrity in handling our affairs, our Second Amended and Restated Certificate of Incorporation (the “Certificate of Incorporation”), and indemnification agreements executed by all of our non-employee directors and officers provides that our non-employee directors and officers will be indemnified to the fullest extent permitted under Delaware law. As a result, our stockholders may have fewer rights against our non-employee directors and officers than they would have absent such provisions in our Certificate of Incorporation and indemnification agreements, and a stockholder’s ability to seek and recover damages for a breach of fiduciary duties may be reduced or restricted. Delaware law allows indemnification of our non-employee directors and officer, if our Board Memberthey (a) hashave acted in good faith, in a manner the Board Membernon-employee director or officer reasonably believes to be in or not opposed to our best interests, and (b) with respect to any criminal action or proceeding, if the Board Membernon-employee director or officer had no reasonable cause to believe the conduct was unlawful.
Pursuant to the Certificate of Incorporation and indemnification agreement, each non-employee director and (to the extent approved by our Board) each of our officersofficer who is made a party to a legal proceeding because he or she is or was a Board Membernon-employee director or officer, is indemnified by us from and against any and all liability, except that we may not indemnify a Board Membernon-employee director or officer: (a) for any liability incurred in a proceeding in which such person is adjudged liable to Monopar or is subjected to injunctive relief in favor of Monopar; (b) for acts or omissions that involve intentional misconduct or a knowing violation of law, fraud or gross negligence; (c) for unlawful distributions; (d) for any transaction for which such Board Membernon-employee director or officer received a personal benefit or as otherwise prohibited by or as may be disallowed under Delaware law; or (e) with respect to any dispute or proceeding between us and such Board Membernon-employee director or officer unless such indemnification has been approved by a disinterested majority of the Board Members or by a majority in interest of disinterested stockholders. We are required to pay or reimburse attorney’s fees and expenses of a Board Membernon-employee director or officer seeking indemnification as they are incurred, provided the non-employee director or officer executes an agreement to repay the amount to be paid or reimbursed if there is a final determination by a court of competent jurisdiction that such person is not entitled to indemnification.
Future legislation or executive or private sector actions may increase the difficulty and cost for us to commercialize our products and adversely affect the prices obtained for such products.
There In the U.S., there have been several attempts madeand continue to repealbe a number of legislative initiatives to contain healthcare costs. For example, in March 2010, the Patient Protection and Affordable Care Act (the “PPACA”“ACA”), was enacted, which substantially changed the way healthcare is financed by both governmental and modificationprivate insurers, and partial or complete repealsignificantly impacted the U.S. pharmaceutical industry.
Since its enactment, there have been numerous judicial, administrative, executive, and legislative challenges to certain aspects of the Affordable Care ActACA, and we expect there will be additional challenges and amendments to the ACA in the future is possible. On December 22, 2017,future. Various portions of the Tax CutsACA are currently undergoing legal and Jobs Act became law – one of its provisions repealed what is known as the individual mandate under PPACA which could have the effect of negating such law. Healthcare reform measures that may be adoptedconstitutional challenges in the future may resultUS Supreme Court; the Trump Administration signed various executive orders and other directives that eliminated cost sharing subsidies and various provisions that would impose a fiscal burden on states or a cost, fee, tax, penalty or regulatory burden on individuals, healthcare providers, health insurers, or manufacturers of pharmaceuticals or medical devices; and Congress has introduced several pieces of legislation aimed at significantly revising or repealing the ACA. The US Supreme Court is expected to rule on a legal challenge to the constitutionality of the ACA in more rigorous coverage criteria2021. The American Rescue Plan Act of 2021 which was recently enacted into law includes provisions which further the ACA, including expansion of marketplace subsidies and lower reimbursement,credits to reduce or eliminate premiums in the federal exchange for persons with certain income levels and in additionalproviding subsidies for state exchanges. The implementation of the ACA is ongoing, the law appears likely to continue the downward pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase regulatory burdens and operating costs. Litigation and legislation related to the ACA are likely to continue, with unpredictable and uncertain results. It is unclear whether the ACA will be overturned, repealed, replaced, or further amended. We cannot predict what affect further changes to the ACA would have on our business.
In addition, government price thatreporting and payment regulations are complex and we will be required to continually assess the methods by which we plan to calculate and report any future pricing in accordance with these obligations. Our methodologies for calculations are inherently subjective and may be charged for any ofsubject to review and challenge by various government agencies, which may disagree with our product candidates, if approved.interpretation. If the government disagrees with our reported calculations, we may need to restate the previously reported data and could be subject to additional financial and legal liability.
The Further, the increasing cost of healthcare as a percentage of GDP and the massive and increasing deferred liabilities behind most governmental health carehealthcare programs (such as Medicare and Medicaid)Medicaid and state and local healthcare programs especially for retirement benefits) continue to be an economic challenge which affectsthreatens the overall economic health of the U.S. High cost healthcare products and therapies that are early in their life cycle are attractive targets for parties that believe that the cost of healthcare must be better controlled and significantly reduced. Pharmaceutical prices and healthcare reform hashave been debated and acted upon by legislators for many years. Future legislation or executive or private sector actions related to healthcare reform could materially and adversely affect our business by reducing our ability to generate revenue at prices sufficient to reward for the risks and costs of pharmaceutical development, to raise capital, and to market our products.
Additionally, Executive Orders and policy statements issued by President Trump have increased the uncertainty regarding the timing for the FDA’s interpretation and implementation of requirements under the Federal Food, Drug and Cosmetic Act (“FDCA”). Some of these executive actions may also negatively affect the FDA’s exercise of regulatory oversight and ability to timely review industry submissions and applications in connection with the drug development and approval process. Notably, on April 12, 2017, the Director for the Office of Management and Budget (“OMB”) implemented a long-term plan to reduce the size of the federal workforce. Although the FDA is funded in the near-term, in the future, an under-staffed FDA could result in increasing delays in the FDA’s responsiveness or in its ability to review applications, issue regulations or guidance, or implement or enforce regulatory requirements in a timely fashion or at all. A January 30, 2017 Executive Order also included a budget neutrality provision that requires the total incremental cost of all new regulations in the 2017 fiscal year, including repealed regulations, to be no greater than zero, except in limited circumstances. It is difficult to predict how these requirements will be interpreted and implemented, and the extent to which they will impact the FDA’s ability to continue engaging in its regulatory authorities under the FDCA. If executive or legislative actions impose restrictions on the FDA’s ability to engage in oversight and implementation activities in the normal course, our business may be negatively impacted. On August 18, 2017, the FDA Reauthorization Act of 2017 was signed which, among other things, established user fees for human drug applications which are to be directed toward expediting the drug development process. On December 12, 2017, an amendment to the FDCA was passed to authorize additional emergency uses for medical products during a military emergency. Both of these actions restore increased funding for the FDA. The user fees for human drug applications can result in funding which is variable depending on the work load created by applications that is supported by the user fees. There is no assurance that federal or state health carehealthcare reform will not adversely affect our future business and financial results, and we cannot predict how future federal or state legislative, judicial or administrative changes relating to healthcare reform and third partythird-party payers will affect the pharmaceutical industry in general and our business in particular.
Even if we are able to commercialize any drug candidate, such drug candidate may become subject to unfavorable pricing regulations or third-party coverage and reimbursement policies, which would harm our business.
Our ability to commercialize any products successfully will depend, in part, on the extent to which coverage and adequate reimbursement for these products and related treatments will be available from third-party payors, such as government authorities, private healthcare insurers and health maintenance organizations. Patients who are prescribed medications for the treatment of their conditions generally rely on third-party payors to reimburse all or part of the costs associated with their prescription drugs. Coverage and adequate reimbursement from government healthcare programs, such as Medicare and Medicaid, and private healthcare insurers are critical to new product acceptance. Patients are unlikely to use our future products, if any, unless coverage is provided and reimbursement is adequate to cover a significant portion of the cost.
Cost-containment is a priority in the U.S. healthcare industry and elsewhere. As a result, government authorities and other third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. Third-party payors also may request additional clinical evidence beyond the data required to obtain marketing approval, requiring a company to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost-effectiveness of its products. Commercial third-party payors often rely upon Medicare coverage policy and payment limitations in setting their reimbursement rates, but also have their own methods and approval process apart from Medicare determinations. Therefore, coverage and reimbursement for pharmaceutical products in the U.S. can differ significantly from payor to payor. We cannot be sure that coverage and adequate reimbursement will be available for any product that we commercialize and, if reimbursement is available, that the level of reimbursement will be adequate. Coverage and reimbursement may impact the demand for, or the price of, any drug candidate for which we obtain marketing approval. If coverage and reimbursement are not available or are available only at limited levels, we may not be able to successfully commercialize any drug candidate for which we obtain marketing approval.
Additionally, the regulations that govern regulatory approvals, pricing and reimbursement for new drugs and therapeutic biologics vary widely from country to country. Some countries require approval of the sale price of a drug or therapeutic biologic before it can be marketed. In many countries, the pricing review period begins after marketing approval is granted. In some foreign markets, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. As a result, we might obtain regulatory approval for a product in a particular country, but then be subject to price regulations that delay our commercial launch of the product, possibly for lengthy time periods, and negatively impact the revenues we are able to generate from the sale of the product in that country. Adverse pricing limitations may hinder our ability to recoup our investment in one or more drug candidates, even if our drug candidates obtain regulatory approval.
Politically divided governmental actions and related political actions outside of government can impact the FDA’s role in the timely and effective review of new pharmaceutical products in the U.S. and our business may be adversely impacted.
A relevant example of dysfunctional government was the 35-day government shutdown that ended February 15, 2019 which limited the FDA to activities necessary to address imminent threats to human life and to activities funded by carry-over user fees. Future government shutdowns or other activities which limit the financial resources available to the FDA (and in particular to the Center for Drug Evaluation and Research) will delay the processing of new product drug development submissions, reviews, and approvals and other required regulatory actions. Such delays will adversely impact our business and financial condition.
Effective collaboration with the FDA’s Center for Drug Evaluation and Research (“CDER”) for the approval of drug candidates is a highly demanding process which can result in increased time and expense to gain approvals.
Our lead drug development program, Validive, will be reviewed by CDER. Efficient and professional collaboration with the FDA’s CDER is essential for the timely clinical testing, test evaluations, analysis and approval of our drug candidates. CDER has an outstanding record of drug approvals and substantial funds to operate a highly professional organization, but is also very demanding as to the quality of clinical research and applications for marketing approvals for drug candidates.
Our Company has in-house expertise and experience in the management of drug approvals. Qualified consultants and drug research organizations are also available to aid in our drug approval process; however, there is a meaningful risk that discussions and interactions inherent in the drug approval process and future developments or new improvements will result in delays, added expenses and new scientific/medical requirements which will cause adverse financial results and will likely impact the price of the Company’s stock.
Future tax reform measures may negatively impact our financial position.
Our business may be negatively impacted by tax reform measures. If tax Tax reform measures are passed, thereunpredictable and can be no assurance that we will continue to receive favorable tax treatment related to our patents.change as the U.S. Congress and executive leadership changes. For example, on December 22, 2017, the Tax Cuts and Jobs Act of 2017 was signed into law that significantly revisesrevised the Internal Revenue Code of 1986, as amended. The newly enacted federal income tax law, among other things, contains significant changes to corporate taxation, including reduction of the corporate tax rate from a top marginal rate of 35% to a flat rate of 21%, limitation of the tax deduction for interest expense to 30% of adjusted earnings (except for certain small businesses), limitation of the deduction for net operating losses to 80% of current year taxable income and elimination of net operating loss carrybacks, treatment of proceeds from the sale of “self-created” patents as ordinary income, and modifying or repealing many business deductions and credits (including reducing the business tax credit for certain clinical testing expenses incurred in the testing of orphan drugs from 50% to 25%amended (the “Code”). Notwithstanding the reduction in the corporate income tax rate, the overall impact of the new federal tax law is uncertain and our business and financial condition could be adversely affected. In addition, it is uncertain if and to what extent various states will conform to the newly enacted federal tax law. The impact of this tax reform on holders of our common stock is also uncertain. We urge our stockholders to consult with their legal and tax advisors with respect to this legislation and the potential tax consequences of investing in or holding our common stock. It is difficult to predict what future tax reform measures, if any, could be implemented and the extent to which they will impact our accounting practicesfinancial condition and our business.
Foreign currency exchange rates may adversely affect our consolidated financial statements.
Sales and purchases in currencies other than the U.S. Dollar expose us to fluctuations in foreign currencies relative to the U.S. Dollar and may adversely affect our consolidated financial statements. Increased strength of the U.S. Dollar increases the effective price of our future drug products sold in U.S. Dollars into other countries, which may require us to lower our prices or adversely affect sales to the extent we do not increase local currency prices. Decreased strength of the U.S. Dollar could adversely affect the cost of materials, products and services we purchase overseas. Sales and expenses of our non-U.S. businesses are also translated into U.S. Dollars for reporting purposes and the strengthening or weakening of the U.S. Dollar could result in unfavorable foreign currency translation and transaction effects. In addition, certain of our businesses may in the future invoice customers in a currency other than the business’ functional currency, and movements in the invoiced currency relative to the functional currency could also result in unfavorable foreign currency translation and transaction effects. We also face exchange rate risk from our investments in subsidiaries owned and operated in foreign countries.
Our anticipated operating expenses and capital expenditures over the next year are based upon our management’s estimates of possible future events. Actual amounts and the cost of new conditions could differ materially from those estimated by our management.
Development of pharmaceuticals and cancer drugs is extremely risky and unpredictable. We have estimated operating expenses and capital expenditures over the next year based on certain assumptions. Any change in the assumptions could and will cause the actual results to vary substantially from the anticipated expenses and expenditures and could result in material differences in actual versus forecasted expenses or expenditures. Furthermore, all of the factors are subject to the effect of unforeseeable future events. The estimates of capital expenditures and operating expenses represent forward-looking statements within the meaning of the federal securities laws. Prospective investors are cautioned that any such forward-looking statements are not guarantees of future performance and involve risks and uncertainties. Actual events or results may differ materially from those discussed in the forward-looking statements as a result of various factors, including the risk factors set forth under "Risk Factors"this “Risk Factors” section in this Annual Report on Form 10-K. In view
The financial and operational projections that we may make from time to time are subject to inherent risks.
The projections that we provide herein or our management may provide from time to time (including, but not limited to,our success in raising strategic and substantial financial resources, the cost and timing of our clinical trials, clinical and regulatory timelines, production and supply matters, commercial launch dates, and other financial or operational matters) reflect numerous assumptions made by our management, including assumptions with respect to our specific as well as general business, regulatory, economic, market and financial conditions and other matters, all of which are difficult to predict and many of which are beyond our control. Accordingly, there is a risk that the assumptions made in preparing the projections, or the projections themselves, will prove inaccurate. There may be differences between actual and projected results, and actual results may be materially different from those contained in the projections. The inclusion of the foregoing, investorsprojections in this Annual Report on Form 10-K should not relybe regarded as an indication that our management considered or consider the projections to be a guaranteed prediction of future events, and the projections should not be relied upon as such. See “Cautionary Statement Concerning Forward-Looking Statements.”
Our present and potential future international operations may expose us to business, political, operational, and financial risks associated with doing business outside of the United States.
Our business is subject to risks associated with conducting business internationally. Some of our suppliers and clinical research organizations and clinical trial sites are located outside of the U.S. Furthermore, if we or any future collaborator succeeds in developing any products, we anticipate marketing them in the EU, the United Kingdom and other jurisdictions in addition to the U.S. If approved, we or our collaborator may hire sales representatives and conduct physician and patient association outreach activities outside of the U.S. Doing business internationally involves a number of risks, including but not limited to:
● multiple, conflicting and changing laws and regulations such as privacy regulations, tax laws, export and import restrictions, employment laws, regulatory requirements, and other governmental approvals, permits and licenses which can vary jurisdictions to jurisdiction with different degrees of review and enforcement;
● failure by us to obtain and maintain regulatory approvals for the use of our products in various countries;
● rejection or qualification of foreign clinical trial data by the competent authorities of other countries;
● additional potentially relevant third-party patent and other intellectual property rights that may be necessary to develop and commercialize our products and drug candidates;
● complexities and difficulties in obtaining, maintaining, enforcing and defending our patent and other intellectual property rights;
● difficulties in staffing and managing foreign operations by a small scale organization;
● complexities associated with managing multiple payor reimbursement regimes, government payors or patient self-pay systems;
● limits, as a U.S.-based company, in our ability to penetrate international markets;
● financial risks, such as longer payment cycles, difficulty collecting accounts receivable, the impact of local and regional financial crises on demand and payment for our products and exposure to foreign currency exchange rate fluctuations;
● natural disasters, political and economic instability, including wars, terrorism and political unrest, outbreak of disease, boycotts, curtailment of trade and other business restrictions, implementation of tariffs;
● certain expenses including, among others, expenses for travel, translation and insurance; and
● regulatory and compliance risks that relate to anti-corruption compliance and record-keeping that may fall within the purview of the U.S. Foreign Corrupt Practices Act, its accounting provisions or its anti-bribery provisions or provisions of anti-corruption or anti-bribery laws in other countries.
Any of these estimatesfactors could harm our ongoing international clinical operations and supply chain, as well as any future international expansion and operations and, consequently, our business, financial condition, prospects and results of operations.
We are subject to U.S. and foreign anti-corruption and anti-money laundering laws with respect to our operations and non-compliance with such laws can subject us to criminal or civil liability and harm our business.
We are subject to the U.S. Foreign Corrupt Practices Act of 1977, as amended (“the FCPA”), the U.S. domestic bribery statute contained in making18 U.S.C. § 201, the U.S. Travel Act, the USA PATRIOT Act, and possibly other state and national anti-bribery and anti-money laundering laws in countries in which we conduct activities. Anti-corruption laws are interpreted broadly and prohibit companies and their employees, agents, third-party intermediaries, joint venture partners and collaborators from authorizing, promising, offering or providing, directly or indirectly, improper payments or benefits to recipients in the public or private sector. We interact with officials and employees of government agencies and government-affiliated hospitals, universities and other organizations. In addition, we may engage third-party intermediaries to promote our clinical research activities abroad or to obtain necessary permits, licenses and other regulatory approvals. We can be held liable for the corrupt or other illegal activities of these third-party intermediaries, our employees, representatives, contractors, partners and agents, even if we do not explicitly authorize or have actual knowledge of such activities.
We have a decisionCode of Business Conduct and Ethics which mandates compliance with the FCPA and other anti-corruption laws applicable to investour business throughout the world. However, we cannot assure you that our employees and third-party intermediaries will comply with this code or such anti-corruption laws. Noncompliance with anti-corruption and anti-money laundering laws could subject us to whistleblower complaints, investigations, sanctions, settlements, prosecution, other enforcement actions, disgorgement of profits, significant fines, damages, other civil and criminal penalties or injunctions, suspension or debarment from contracting with certain persons, the loss of export privileges, reputational harm, adverse media coverage and other collateral consequences. If any subpoenas, investigations or other enforcement actions are launched, or governmental or other sanctions are imposed, or if we do not prevail in us.any possible civil or criminal litigation, our business, results of operations and financial condition could be materially harmed. In addition, responding to any action will likely result in a materially significant diversion of management’s attention and resources and significant defense and compliance costs and other professional fees. In certain cases, enforcement authorities may even cause us to appoint an independent compliance monitor which can result in added costs and administrative burdens.
Risks Associated with Our Capitalour Common Stock
We may never provide liquidity to our investors.
No public market exists with respect to any of our securities. There is no assurance that any public offering, merger, combination, sale, or other liquidity event relating to us will ever take place, or that any public offering, merger, combination, sale, or other event that might take place would provide liquidity for our investors or that we will be able to provide liquidity to our investors in any fashion. In the event that we are unable to affect a public offering, merger, combination, sale, or other liquidity event, our investors would likely be unable to sell their interests in us.
Existing and new investors will experience dilution as a result of future sales or issuances of our common stock and future option exercises under our stock option2016 Stock Incentive Plan and any amendments to the plan.
Our Board Members,non-employee directors, employees, and certain of our consultants have been and will be issued equity and/or granted options that vest with the passage of time. Up to a total of 1,600,0003,100,000 shares of our Common Stockcommon stock may be issued as stock options or restricted stock units under the Amended and Restated Monopar Therapeutics Inc. 2016 Stock Incentive Plan, and stock options for the purchase of up to 690,5961,436,640 shares of our common stock have already been granted. See Item 11 - “Stock Option Plan.”granted (1,022,909 stock options are exercisable) and are outstanding along with 154,423 restricted stock units that have been granted to non-employee directors and employees as of March 5, 2021. The issuance of such equity upon vesting of restricted stock units and/or the exercise of such options will dilute both our existing and our new investors. As of March 1, 2018, no5, 2021, 21,346 stock options have been exercised.
Our existing and our new investors will likely also experience substantial dilution resulting from the issuance by us of equity securities in connection with certain transactions, including without limitation, future offering of shares in future fundraising efforts, intellectual property licensing, acquisition, or commercialization arrangements.
Holders of the shares of our Common Stockcommon stock will have no control of our operations or of decisions on major transactions.
Our business and affairs are managed by or under the direction of our Board. Our Stockholdersstockholders are entitled to vote only on actions that require a Stockholderstockholder vote under federal or state law. Stockholder approval requires the consent and approval of holders of a majority or more of our outstanding stock. Shares of stock do not have cumulative voting rights and therefore, holders of a majority of the shares of our outstanding stock will be able to elect all Board Members.members. TacticGem, LLC (“TacticGem”) owns 7,166,667 shares of common stock (77.1%(57%). The limited liability company agreement of TacticGem, LLC provides that the manager will vote its shares of Monopar to elect to the Board of Directors those persons nominated by TacticPharma LLC plus one person nominated by Gem Pharmaceuticals, LLC. Additionally, other than in the elections of directors the limited liability company agreement requires TacticGem to pass through votes (including the vote for the election of directors) to its members in proportion to their membership percentages in TacticGem.TacticGem (57.367% owned by Tactic Pharma and 42.633% owned by Gem). As a result, Tactic Pharma, our initial investor, holds an approximately 46%34% beneficial interest in us and together with Gem’s beneficial ownership of approximately 33%24%, the two entities control a majority of our stock and will be able to elect all Board Membersmembers and control our affairs. Some of our Board Membersmembers and executive officers own and control Tactic Pharma. Although no single person has a controlling interest in Tactic Pharma, acting together, they are able to control Tactic Pharma and a large voting block of Monoparour common stock and together with Gem can elect over a majority of our Board of Directors. See Item 12 - “Security Ownership of Certain Beneficial Owners and Management.”Board.
Our ability to list on Nasdaq in the future will require raising significant additional capital and likely require a public stock transaction; failure to qualify to trade onmeet the continued listing requirements of The Nasdaq will make it more difficult to raise capital.Capital Market could result in a de-listing of our common stock.
We will need If we fail to raise significant funds insatisfy the next 24 months to execute our clinical development plans and we believe that if our stock is trading on Nasdaq’scontinued listing requirements of The Nasdaq Capital Market, itsuch as the corporate governance requirements or the minimum closing bid price requirement, the Nasdaq Stock Market (“Nasdaq”) may take steps to de-list our common stock. Such a de-listing or the announcement of such de-listing will enable better accesshave a negative effect on the price of our common stock and would impair your ability to capital.sell or purchase our common stock when you wish to do so. In the event of a de-listing, we would take actions to restore our compliance with the Nasdaq has listing requirements, but we can provide no assurance that any such action taken by us would allow our common stock to become listed again, stabilize the market price or improve the liquidity of our common stock, prevent our common stock from dropping below the Nasdaq minimum bid price requirement or prevent future non-compliance with the Nasdaq listing requirements.
The stock price of our common stock may be volatile or may decline regardless of our operating performance.
The market prices for inclusionsecurities of securities forbiotechnology and pharmaceutical companies have historically been highly volatile, and the market has from time to time experienced significant price and volume fluctuations that appear to be unrelated to the operating performance of particular companies. Our common stock has only been trading on the Nasdaq Capital Market including stockholders equitysince December 19, 2019 and has experienced significant volatility in market prices through March 5, 2021,ranging from a low of $4 million (market value standard) or $5 million (equity standard),$4.28 to a high of $48.00. Our small public float and relatively low and inconsistent trading volumes exacerbate volatility.
The market value of publicly held shares of $15 million, an operating history of 2 years under the equity standard or a market value of listed securities of $50 million under the market value standard, 1 million publicly held shares, 300 shareholders, three market makers and a $4 bid price or a closing price of $3 (equity standard)our common stock is likely to remain highly volatile and may fluctuate substantially due to many factors, including:
●
announcements concerning the progress and success of our clinical trials, our ability to obtain regulatory approval for and commercialize our product candidates, including any requests we receive from the FDA for additional studies or $2 (market value standard). If we are unable to list on Nasdaq, it could make it harder for us to raise capitaldata that result in both the immediate time frame anddelays in obtaining regulatory approval or launching our product candidates, if approved;
●
unstable market conditions in the long-term. If we are unablepharmaceutical and biotechnology sectors or the economy as a whole;
●
price and volume fluctuations in the overall stock market;
●
the failure of our product candidates, if approved, to raise capital when neededachieve anticipated commercial success;
●
announcements of the clinical success, NDA approval or introduction of new products by us or our direct competitors;
●
announcements of developments concerning product development results or intellectual property rights of others;
●
litigation or public concern about the safety and/or efficacy of our potential or approved products;
●
actual fluctuations in our quarterly or annual operating results, and concerns by investors that such fluctuations may occur in the future we may haveand are indicative of internal problems;
●
deviations in our operating results from the estimates of securities analysts or other analyst comments;
●
additions or departures of key personnel;
●
healthcare reform legislation, including measures directed at controlling the pricing of pharmaceutical products, and third-party coverage and reimbursement policies;
●
announcements or publicity concerning current or future strategic collaborations;
●
discussion of our Company, our stock price or our potential future market value by the financial and scientific press and online investor communities; and
●
market responses to cease or reduce operations.the fluctuating conditions of the COVID-19 pandemic.
We may become involved in securities class action litigation that could divert management’s attention and harm our business.
The stock markets have from time to time experienced significant price and volume fluctuations that have affected the market prices for the common stock of biotechnology and pharmaceutical companies. Our stock price has experienced such fluctuations since our initial public offering. These broad market fluctuations may cause the market price of our stock to advance or decline. In the past, securities class action litigation has often been brought against a company following a decline in the market price of its securities. This risk is especially relevant for us because biotechnology and biopharmaceutical companies have experienced significant stock price volatility in recent years. We may become involved in this type of litigation in the future. Litigation often is expensive and diverts management’s attention and resources, which could adversely affect our business.
Substantial amounts of our outstanding shares may be sold into the market. If there are substantial sales of shares of our common stock, the price of our common stock could decline.
The price of our common stock could decline if there are substantial sales of our common stock, particularly sales by our non-employee directors, executive officers and significant stockholders, or if there is a large number of shares of our common stock available for sale and the market perceives that sales will occur. We have 12,566,929 outstanding shares of our common stock as of March 5, 2021. A majority of our outstanding shares of common stock are currently held by non-employee directors, executive officers and other affiliates and are subject to volume limitations under Rule 144 under the Securities Act of 1933, as amended (Securities Act).
Our largest stockholders have rights, subject to some conditions, to require us to file registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or our stockholders. We have also registered shares of common stock that we have issued and may issue under our employee equity incentive plans. These shares are able to be sold freely in the public market upon issuance, subject to existing internal practices which prohibit sales under certain circumstances. The market price of the shares of our common stock could decline as a result of the sale of a substantial number of our shares of common stock in the public market or the perception in the market that the holders of a large number of shares intend to sell their shares.
Our ability to use our net operating loss carry-forwards and certain other tax attributes may be limited.
Under Section 382 of the Code, if a corporation undergoes an “ownership change” (generally defined as a greater than 50% change, by value, in its equity ownership over a three-year period), the corporation’s ability to use its pre-change net operating loss carry-forwards and other pre-change tax attributes (such as research tax credits) to offset its post-change income may be limited. We believe that additional fundraising efforts in the next three years, may trigger an “ownership change” limitation in the near future. As a result, if we earn net taxable income, our ability to use our pre-change net operating loss carry-forwards to offset U.S. federal taxable income will be subject to limitations, which could result in increased future tax liability to us had we not been subject to such limitations.
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our stock price and trading volume could decline.
The trading market for our common stock will depend in part on the research and reports that securities or industry analysts publish about us or our business. If one or more of the analysts who covers us downgrades our stock or publishes inaccurate or unfavorable research about our business, our stock price may decline. If one or more of these analysts ceases coverage of our Company or fails to publish reports on us regularly, demand for our stock could decrease, which might cause our stock price and trading volume to decline.
We do not intend to pay dividends for the foreseeable future and, as a result, your ability to achieve a return on your investment will depend on appreciation in the price of our common stock.
We have never declared or paid any cash dividends on our capital stock and we do not intend to pay any cash dividends in the foreseeable future. Any determination to pay dividends in the future will be at the discretion of our Board. Accordingly, investors must rely on sales of their common stock after price appreciation, which may never occur, as the only way to realize any future gains as a return on their investments.
There can be no assurance that we will ever provide liquidity to our investors through a sale of our Company.
While acquisitions of pharmaceutical companies like ours are not uncommon, potential investors are cautioned that no assurances can be given that any form of merger, combination, or sale of our Company will take place or that any merger, combination, or sale, even if consummated, would provide liquidity or a profit for our investors. You should not invest in our Company with the expectation that we will be able to sell the business in order to provide liquidity or a profit for our investors.
Delaware law and provisions in our amended and restated bylaws could make a merger, tender offer or proxy contest difficult, thereby depressing the potential trading price of our common stock.
Anti-takeover provisions in our charter documents and under Delaware law could make an acquisition of us difficult, limit attempts by our stockholders to replace or remove our current management or Board and adversely affect our stock price.
Provisions of our amended and restated bylaws may delay or discourage transactions involving an actual or potential change in our control or change in our management, including transactions in which stockholders might otherwise receive a premium for their shares, or transactions that our stockholders might otherwise deem to be in their best interests. Therefore, these provisions could adversely affect the price of our stock. Among other things, our amended and restated bylaws:
● provide that all vacancies on our Board may only be filled by our Board and not by stockholders;
● allow the holders of a plurality of the shares of common stock entitled to vote in any election of directors to elect all of the directors standing for election, if they should so choose; and
● provide that special meetings of our stockholders may be called only by our Board.
In addition, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which generally prohibits a Delaware corporation from engaging in any of a broad range of business combinations with any “interested” stockholder for a period of three years following the date on which the stockholder became an “interested” stockholder.
Item 2.IPtem 2. Propertiesroperties
We lease approximately 1,202 square feet of space in the Village of Wilmette, Illinois for our corporate offices, underoffices. Our original two-year lease ended on December 31, 2019, at which time we agreed to lease the space on a lease which runs through the end of 2019. We lease approximately 160 square feet formonth-to-month basis. In February 2019, also on a month-to-month basis, we leased additional office space at our Seattle, Washington office.corporate headquarters. We believe that we will requirelease additional office space within the next 12 months as we begin to hire additional personnel.
Item 3.ILtem 3. Legalegal Proceedings
We are currently not, and to date have never been, a party to any material legal proceedings.
PART II
Itemtem 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information
There is no established public trading market in our common stock. Our securities are not listed for trading on any national securities exchange nor are bid or asked quotations reported in any over-the-counter quotation service.
Rule 144 Eligibility
As of March 1, 2018, 1,335,079.3 shares of ourOur common stock are eligible for saleis listed under Rule 144.the symbol “MNPR” on the Nasdaq Capital Market.
We cannot estimate the number of shares of our common stock that our existing stockholders will elect to sell under Rule 144.
Holders
As of March 1, 2018,5, 2021, there were 9,291,420.61412,566,929 shares of our common stock outstanding held by 43 holders. In addition, there were nine32 holders of stock options to purchase up to 690,596 shares of our common stock.record and approximately 800 beneficial stockholders.
Dividends
We have never paid cash dividends on any of our capital stock and we currently intend to retain our future earnings, if any, to fund the development and growth of our business. We do not intend to pay cash dividends to holders of our common stock in the foreseeable future.
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information as of December 31, 2017, with respect to shares of our common stock that may be issued under existing equity compensation plans. There are no equity compensation plans that have not been approved by our security holders.
| Number of Securities to be Issued Upon Exercise of Outstanding Options, Warrants and Rights | Weighted Average Exercise Price of Outstanding Options, Warrants and Rights | Number of Securities Remaining Available For Future Issuance under Equity Compensation Plans |
| Equity compensation plans approved by security holders (1) | 658,592 | $0.94 | 941,408 |
(1) The Monopar Therapeutics Inc. 2016 Stock Incentive Plan.
Registration Rights
We are subject to an agreement with TacticGem, (pursuant to the Gem Transaction as discussed later in this document)LLC (“TacticGem”), our largest stockholder, which obligates us to file a Form S-3 or other appropriate form of registration statement covering the resale of any of our Common Stockcommon stock by TacticGem, or its members Gem Pharmaceuticals, LLC, or Tactic Pharma, LLC, upon direction by TacticGem at any time after we have been subject to the reporting requirements of the 1934 Act for at least twelve months (the “Initial Holding Period’).TacticGem. We are required to use our best efforts to have such registration statement declared effective as soon as practical after it is filed. In the event that such registration statement for resale is not approved by the SEC, and TacticGem submits a written request, we are required to prepare and file a registration statement on Form S-1 registering such Common Stockcommon stock for resale and to use our best efforts to have such registration statement declared effective as soon as practical thereafter. Additionally, if we propose to register our common stock for sale for cash, TacticGem and its members have the right to include some of their shares in such registration After registration, pursuant to these rights, these shares will become freely tradable without restriction under the Securities Act other than pursuant to restrictions on affiliates under Rule 144.
Recent Sales of Unregistered Securities.
Set forth below is information regarding shares of common stock issued and options granted by us in the year ended December 31, 2017,
There were no securities issuances that were not registered under the Securities Act. Also included isAct during the consideration, if any, received by us, for such shares and options and information relating to the Securities Act, or rule of the SEC, under which exemption from registration was claimed. No underwriters were involved in the foregoing issuances of securities. Below this description of recent sales of unregistered securities is a description of the exemptions from registration which were applicable to each sale or grant.
(a) On February 20, 2017, we granted stock options for 1,200 shares of our Common Stock to each of Dr. Christopher M. Starr, Dr. Chandler D. Robinson, and Dr. Andrew P. Mazar in exchange for services. Pursuant to the “Conversion” in March 2017, these stock options were each adjusted to be for 84,000 shares. On the same date, we granted a stock option for 336 shares of our Common Stock to Kim R. Tsuchimoto in exchange for services, which was adjusted to be for 23,520 shares pursuant to the Conversion. The exercise price of each of these options was $0.001 per share and the options expire on February 19, 2027.
(b) During March 2017 through June 2017, 340,840.33 shares of Common Stock were sold to accredited investors at a price of $6.00 per share.
(c) During August 2017 through September 2017, 448,834 shares of Common Stock were sold to accredited investors at a price of $6.00 per share.
(d) On September 1, 2017, we granted options for 21,024 shares of Common Stock to Arthur Klausner, and on September 18, 2017, we granted options for 21,024 shares of Common Stock to each of Michael J. Brown and Raymond W. Anderson, in exchange for services as Directors. The exercise price of the options was $6.00 per share and the options expire on August 31, 2027 and September 17, 2027, respectively.
(e) On August 25, 2017, 3,055,394.12 shares of our Common Stock were issued to TacticGem in exchange for the Gem Contributed Assets (including assets and $5 million in cash) as part of the Gem Transaction.
(f) On November 1, 2017, we granted options for 40,000 shares of Common Stock to Kirsten Anderson in exchange for services. The exercise price of the options was $6.00 per share and the options expire on October 31, 2027.
(g) On January 1, 2018, we granted options for 32,004 shares of Common Stock to Patrice Rioux in exchange for services. The exercise price of the option was $6.00 per share and the options expire on December 31, 2027.reporting period.
The offers, sales and issuances of the securities described in paragraphs (a), (d), (f), and (g) were deemed to be exempt from registration under the Securities Act in reliance on both Section 4(a)(2) of the Act and Rule 701 in that the transactions were under compensatory benefit plans and contracts relating to compensation as provided under Rule 701. The recipients of such securities were our employees, officers, bona fide consultants and advisors and received the securities under our Plan. Appropriate legends were affixed to the securities issued in these transactions. Each of the recipients of securities in these transactions had adequate access, through employment, business or other relationships, to information about us and had knowledge and experience to make the decision to accept the stock options.
The offers, sales and issuances of the securities described in paragraph (b), (c), and (e) were deemed to be exempt from registration under the Securities Act in reliance on Rule 506(b) of Regulation D in that the issuance of securities to the accredited investors did not involve a public offering. The recipients of securities in each of these transactions acquired the securities for investment only and not with a view to or for sale in connection with any distribution thereof. Each of the recipients of securities in these transactions was an accredited investor under Rule 501 of Regulation D. Form D was filed related to the offer described in paragraph (b) on March 28, 2017; and Form D was filed related to the offer described in paragraph (c) on August 23, 2017.
Item 7.Management's Discussion and Analysis of Financial Condition and Results of Operations.
You should read the following discussion and analysis of our financial condition and results of operations together with our financial statements and related notes appearing at the end of this Annual Report on Form 10-K. Some of the information contained in this discussion and analysis or set forth elsewhere in this Annual Report on Form 10-K, including information with respect to our plans and strategy for our business and related financing activities, includes forward-looking statements that involve risks and uncertainties. You should read the "Risk Factors" section of this Annual Report on Form 10-K, Item 1A, for a discussion of important factors that could cause actual results to differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Overview
Our mission is
We are a clinical stage biopharmaceutical company primarily focused on developing proprietary therapeutics designed to develop innovative drugs and drug combinations toextend life or improve clinical outcomesquality of life for cancer patients. We are building a drug development pipeline through the licensing orand acquisition of oncology therapeutics in late preclinical and clinical development stages. We leverage our scientific and clinical experience to help reduce the risk of and accelerate the clinical development of our drug product candidates.
In December 2019, we completed our initial public offering (including the exercise of the over-allotment by the underwriters) by selling 1,277,778 shares of our common stock at a public offering price of $8.00 per share. Net proceeds were approximately $9.4 million, after deducting underwriting discounts and accrued, unpaid offering expenses. Our common stock began trading on the Nasdaq Capital Market on December 19, 2019.
In January 2020, we entered into a Capital on DemandTM Sales Agreement with JonesTrading Institutional Services, LLC (“JonesTrading”), as sales agent, pursuant to which we offered and sold (at our discretion), from time to time, through or to JonesTrading shares of our common stock, having an aggregate offering price of up to $19.7 million. Pursuant to this agreement, through December 31, 2020, we have sold 860,677 shares of our common stock at an average gross price of $9.79 per share for net proceeds of $8,175,290, after fees and commissions of $253,036. From January 1, 2021 through February 11, 2021, we sold an additional 1,104,047 shares of our common stock at an average gross price of $10.20 per share for net proceeds of $10,925,311, after fees and commissions of $338,153.
In June 2020, we entered into a 50/50 collaboration development agreement with NorthStar Medical Radioisotopes, LLC (“NorthStar”) to develop potential Radio-Immuno-Therapeutics (“RITs”) to treat severe COVID-19 (patients with SARS-CoV-2 infection). NorthStar is a commercial producer and supplier of medical radioisotopes. This collaboration combines NorthStar’s expertise in the innovative production, supply, and distribution of important medical radioisotopes with our expertise in therapeutic drug development and our pre-IND stage humanized urokinase plasminogen activator receptor (“uPAR”) targeted monoclonal antibody known as MNPR-101, along with a proprietary portfolio of related monoclonal antibodies that target uPAR or its ligand uPA. uPAR seems to be selectively expressed on aberrantly activated immune cells. In response to coronavirus infection, these rogue immune cells produce pro-inflammatory cytokines that can cause runaway inflammation throughout the body, commonly referred to as a cytokine storm. It is this systemic hyper-inflammatory state that is thought to be largely responsible for the severe lung injury and multiple organ damage that contributes to poor outcomes and death in patients with severe COVID-19.
In this collaboration, we have coupled MNPR-101 to therapeutic radioisotopes supplied by NorthStar. The resulting conjugates are designed to be a highly selective agents that have the potential to kill aberrantly activated cytokine-producing immune cells. By eradicating these cells with a uPAR-targeted RIT (“uPRIT”), the goal is to spare healthy cells while quickly reducing the cytokine storm and its harmful systemic effects. Through March 5, 2021, we have incurred immaterial amounts of expenses related to the NorthStar collaboration, while partnering with several key companies and institutions to further the collaboration’s development efforts. These collaborators include: IsoTherapeutics Group, LLC, which generated the uPRIT candidates; Aragen Bioscience Inc., which screened the uPRIT candidates through preclinical biochemical testing; and Texas Lung Injury Institute / University of Texas Health Science Center at Tyler, which plans to perform preclinical testing and, if successful, clinical testing.
In August 2020, we announced a plan to develop a test to potentially triage COVID-19 patients into those likely versus unlikely to progress to severe respiratory failure. The test would use our proprietary monoclonal antibody, ATN-658, to detect soluble urokinase plasminogen activator receptor (“suPAR”) in COVID-19 patient plasma. A suPAR test for COVID-19 patients, if successful, could identify those at high risk for severe respiratory failure, facilitating earlier therapeutic interventions and/or allowing for the staging of patients to an optimal treatment based on their disease characteristics.
In November 2020, we announced a series of recently issued patents for our Phase 2b/3 clinical-stage lead product candidate, Validive (clonidine HCl mucobuccal tablet). These patents, including U.S. Patent No. 10,675,271, provide claims covering “Clonidine and/or clonidine derivatives for use in the prevention and/or treatment of adverse side effects of chemotherapy”. These patents expand the potential use of Validive in cancer patients, beyond the earlier allowed claims for the prevention of oral mucositis in patients receiving CRT. Specifically, they provide protection for the potential ability of Validive to prevent or treat common chemotherapy-associated side effects such as asthenia and fatigue and would provide protection should we determine in the future to conduct additional Validive development activities related to adverse side effects of chemotherapy beyond oropharyngeal cancer.
In December 2020, we announced the issuance of a U.S. patent (US 10,450,340) covering compositions of matter (2-pyrrilino camsirubicin) for a novel family of camsirubicin analogs. This patent, which expands the Company’s camsirubicin intellectual property portfolio, is expected to expire in 2038 not including any patent term extensions. The patent broadens our camsirubicin portfolio and creates a pipeline that has been designed to retain the potentially favorable non-cardiotoxic chemical backbone of camsirubicin and the potent broad-spectrum antitumor activity of doxorubicin. Further, preclinical evidence suggests that this new family of 2-pyrrilino camsirubicin analogs could be active in doxorubicin-resistant tumor cells which may enable use in cancer types beyond those possible with camsirubicin.
In February 2021, we announced the first patient dosed in our Phase 2b/3 VOICE trial of Validive® for the prevention of CRT-induced severe oral mucositis in patients with oropharyngeal cancer (“VOICE”).
Given the COVID-19 pandemic and its effects on clinical trials, we have adjusted our clinical development plans accordingly to fit what is feasible in the current environment. We have simplified the design of the previously planned Phase 3 clinical trial for our lead product candidate, Validive, to a seamless design Phase 2b/3 clinical trial (our VOICE trial) that will allow us to minimize touch points with patients and sites. This seamless design will allow us to immediately advance to the Phase 3 portion of the trial if supported by the interim data at the late preclinical through advancedend of the Phase 2b portion of the trial. To complete the VOICE clinical development stage.program, including, if required, completing a smaller second Phase 3 confirmatory clinical trial, we will require additional funding in the millions or tens of millions of dollars (depending on if we have consummated a collaboration or partnership or neither for Validive), which we are planning to pursue within the next 12 months.
Along with our VOICE trial, we continue to prioritize supporting the camsirubicin Phase 2 clinical trial for which we signed a collaboration agreement in June 2019 with Grupo Español de Investigación en Sarcomas (“GEIS”), discussed in further detail below. We believe we have funds sufficient to obtain topline results from the run-in portion of the trial.
In February 2021, we also announced the publication of a peer-reviewed study in the European Journal of Cancer which shows the potential utility of MNPR-101 conjugates as uPAR imaging agents to improve surgical outcomes in bladder cancer and for surveillance post-resection. This publication builds on previous studies using conjugates of MNPR-101 and its mouse analog, ATN-658, for the optical imaging of oral and colon cancer.
Our Product Pipeline
Our Product Candidates
Validive (clonidine mucobuccal tablet; clonidine MBT)
Validive is beinga mucobuccal tablet (MBT) formulation of clonidine. The MBT formulation was developed to enhance the oral mucosal drug delivery and significantly increase the salivary concentrations of the active ingredient while minimizing systemic absorption. The Validive tablet is tasteless and self-administered once daily by affixing it to the outside of the patient’s upper gum where it dissolves slowly over the period of several hours, resulting in the extended release of clonidine into the oral cavity and oropharynx, the site of SOM following chemoradiation treatment (“CRT”) for OPC. Validive therapy is designed to begin on the treatmentfirst day of radiation-induced SOM.CRT and continue daily through the last day of CRT.
SOM is a frequent major adversepainful and debilitating inflammation and ulceration of the mucous membranes lining the oral cavity and oropharynx in response to chemoradiation therapy. Patients receiving CRT to treat their OPC often develop SOM, which remains one of the most common and devastating side effect foreffects of treatment in this indication. We believe Validive has the potential to address several critical elements that affect SOM patients, with headincluding:
Reduction in the incidence of SOM. SOM can increase the risk of acute and neck cancer whochronic comorbidities, including dysphagia, trismus and lung complications, which are treated by radiation treatment. SOM causes intense oral painoften irreversible and limits a patient’s abilitylead to eat and drink, which causes additional treatment complications. Many affected patients requireincreased hospitalization and the SOM symptoms can force patients to stop cancer treatments early, which reduces the success of treatments. Validive is designed to deliver the active ingredient, clonidine, to the at-risk oropharyngeal mucosa. Clonidine reduces the production of cytokines, the molecules that cause ulcerations and pain in patients that develop SOM. Preclinical studies andneed for additional interventions. In a Phase 2 clinical trial, havethe OPC patient cohort treated with Validive 100 µg demonstrated thata reduction in the absolute incidence of SOM compared to placebo of 26.3% (incidence rate of 65.2% in placebo, 45.0% in Validive has the potential for reducing the frequency50 µg group, 38.9% in Validive 100 µg group). A reduced incidence of developing SOM in additionOPC patients may lower the risk of acute and chronic comorbidities and improve quality of life.
Delay in the time to improving its symptoms,onset of SOM. SOM can cause cancer treatment delay and/or discontinuation, which may impact overall survival outcomes. In the Phase 2 clinical trial, OPC patients had a time to onset of SOM of 37 days in the placebo cohort; 45-day time to onset of SOM in the Validive 50 µg cohort; and median was not reached in the Validive 100 µg group as comparedfewer than half of the patients developed SOM. Prolonging time to onset of SOM may lead to fewer missed CRT treatments, resulting in improved overall survival outcomes.
Decrease in the duration of SOM. Longer duration of SOM leads to a placebo. Onhigher risk of the need for parenteral nutrition and lower quality of life. SOM patients experience difficulty or inability to drink and/or eat, and difficulty in swallowing often results in malnourishment and feeding tube intervention. The Phase 2 clinical trial data demonstrated a 15.5-day reduction (by 37.8%) in the duration of SOM for patients treated with Validive 100 µg (41 day median duration with placebo, 34 days with the Validive 50 µg group, and 25.5 days for the Validive 100 µg group) in patients that developed SOM. Median duration across all patients, inclusive of both those that did and did not develop SOM, was 17 days in the placebo group and 0 days in each of the Validive 50 and 100 µg groups. Reduced duration of SOM may result in lower risk of malnourishment and feeding tube intervention, and fewer treatment terminations/delays.
In September 8, 2017, we exercised our exclusivean option to license Validive from Onxeo S.A., the company that had developed Validive through its Phase 2 clinical trial. In this completed Phase 2 clinical trial, Validive demonstrated clinically meaningful and dose-dependent efficacy signals within the 64-patient OPC population randomized to placebo. Additionally, patients in orderthe Validive cohorts in the Phase 2 clinical trial demonstrated a safety profile similar to advancethat of placebo. While not designed by us, Onxeo’s promising preclinical studies and Phase 2 clinical trial have informed the developmentdesign and conduct of what we believe will be an effective Phase 2b/3 (VOICE) clinical trial.
SOM typically arises in the immune tissue at the back of the tongue and throat, which comprise the oropharynx, and consists of acute severe tissue damage and pain that prevents patients from swallowing, eating and drinking. Validive stimulates the alpha-2 adrenergic receptor (alpha-2AR) on macrophages (white blood cells present in the immune tissues of the oropharynx) suppressing pro-inflammatory cytokine expression. Validive exerts its effects locally in the oral cavity and oropharynx over a prolonged period of time through its unique MBT formulation. Patients who develop SOM are also at increased risk of developing late-onset toxicities, including trismus (jaw, neck, and throat spasms), dysphagia, and lung complications, which are often irreversible and lead to increased hospitalization and the need for further interventions sometimes years after completion of CRT. We believe that a reduction in the incidence and duration of SOM by Validive will have the potential to reduce treatment discontinuation and/or treatment delays potentially leading to improved survival outcomes, and reducing or eliminating long-term morbidities resulting from CRT.
The OPC target population for Validive is the most rapidly growing segment of head and neck cancer (“HNC”) patients, estimated to exceed 40,000 new cases annually of OPC in the U.S alone. The growth in OPC is driven by the increasing prevalence of oral human papilloma virus (“HPV”) infections in the U.S. and around the world. Despite the availability of a pediatric/adolescent HPV vaccine, the rate of OPC incidence in adults is not anticipated to be materially reduced for decades due to low adoption of the vaccine to date. As a result, the incidence of HPV-driven OPC is projected to increase for many years to come and will continue to support a clinical need for Validive for the prevention of CRT-induced SOM in patients with OPC since CRT is the standard of care treatment, and we do not anticipate this changing for years to come.
A pre-Phase 3 meeting with the near-term goal of commencingFDA was held, and based on the meeting discussion a Phase 3 development program. If successful, thisclinical protocol and accompanying statistical analysis plan (“SAP”) was submitted to the FDA for review and comments. We have also received protocol assistance and advice on our Phase 3 protocol and SAP from the European Medicines Agency Committee on Human Medicinal Products (EMA/CHMP/SAWP). Based on comments and guidance provided by FDA and EMA, and our analysis of the current COVID-19 pandemic and its effects on clinical trials, we have modified our original adaptive design Phase 3 clinical trial to be a seamless Phase 2b/3 (VOICE) clinical trial to better fit the current clinical research environment. The primary endpoint, absolute incidence of SOM, remains the same, but the overall design of the trial has been simplified and the touch points with the healthcare system have been minimized. We have now initiated clinical trial sites and commenced dosing in the Phase 2b portion of our VOICE trial. We anticipate the interim (completion of Phase 2b portion of the VOICE trial) will be reached in the first quarter of 2022, and the Phase 3 enrollment will be completed in the fourth quarter of 2022. Initiating the Phase 3 portion of the VOICE trial will be subject to the interim (Phase 2b) results. We will need to raise additional funding or find a suitable pharmaceutical partner to complete the VOICE clinical program may allow us to applyincluding, if required, completing a smaller second Phase 3 confirmatory clinical trial. Validive has been granted fast track designation in the U.S., orphan drug designation in the EU, and has global intellectual property patent protection through mid-2029 not accounting for marketing approval. See “Material Agreements” and “Strategy.”possible extensions.
Camsirubicin (5-imino-13-deoxydoxorubicin; formerly MNPR-201, GPX-150)
In August 2017, we acquired MNPR-201 (GPX-150; 5-imino-13-deoxydoxorubicin), Camsirubicin is a proprietary doxorubicin analog of doxorubicin that is selective for topoisomerase II-alpha. Doxorubicin is widely used to treat adult and pediatric solid and blood (hematologic) cancers, including soft tissue sarcomas, breast, gastric, ovarian and bladder cancers, leukemias and lymphomas. Despite clinical studies demonstrating the anti-cancer benefit of higher cumulative doses of doxorubicin, the clinical efficacy of doxorubicin has historically been limited by the risk of patients developing irreversible, potentially life-threatening cardiotoxicity. For example, several clinical studies completed in the 1990s demonstrated that concurrent doxorubicin (60 mg/m topoisomerase-II-alpha from TacticGem. MNPR-2012, 8 cycles) and paclitaxel gave a 94% overall response rate in patients with metastatic breast cancer but led to 18% of these patients developing congestive heart failure. Reduction of doxorubicin to 4-6 cycles of treatment decreased the incidence of congestive heart failure, but also reduced response rates to 45-55%. In a clinical study looking at dose response, sarcoma patients on the high dose (75 mg/m2) doxorubicin had a response rate of 37% compared to just 18% in the low dose (45 mg/m2) doxorubicin group. With the cumulative dose restriction on doxorubicin, the median progression free survival for ASTS patients is approximately 6 months, with median overall survival of 12-15 months. There is a significant unmet opportunity to develop a replacement for doxorubicin that can be dosed higher and for longer.
Camsirubicin has been engineered specifically to retain the anticancer activity of doxorubicin while minimizing the toxic effects on the heart. Similar to doxorubicin, the antitumor effects of camsirubicin are mediated through the stabilization of the topoisomerase II complex after a DNA strand break and DNA intercalation leading to tumor cell apoptosis (cell death). Inhibiting the topoisomerase II-alpha isoform is desired for the anti-cancer effect, while inhibiting the topoisomerase II-beta isoform has been demonstrated to mediate, at least in part, the cardiotoxicity associated with doxorubicin. Camsirubicin is more selective than doxorubicin for inhibiting topoisomerase II-alpha versus topoisomerase II-beta. This selectivity may at least partly explain the minimal cardiotoxicity that has been observed for camsirubicin in preclinical and clinical studies to date. We believe these attributes provide a strong rationale to develop camsirubicin without restriction on cumulative dose, in a broad spectrum of cancer types.
A Phase 2 clinical trial for camsirubicin has been completed in patients with advanced (e.g. unresectable or metastatic) soft tissue sarcoma (“ASTS”). Median progression free survival for ASTS patients is approximately 6 months and average life expectancy for these patients is 12-15 months. In this study, 52.6% of patients evaluable for tumor progression demonstrated clinical benefit (partial response or stable disease), which was proportional to dose and consistently observed at higher cumulative doses of camsirubicin (>1000 mg/m2). Camsirubicin was very well tolerated in this study and underscored the ability to potentially administer camsirubicin without restriction of cumulative dose in patients with ASTS. Although doxorubicin has been the standard of care treatment for over 40 years for patients with ASTS, doxorubicin is limited to a lifetime cumulative dose maximum of 450 mg/m2. This means that even if a patient is responding, they are pulled off of doxorubicin treatment once this cumulative dose has been reached. Thus, there is a significant unmet opportunity to develop a replacement for doxorubicin that retains anti-cancer activity while reducing or eliminating the risk for irreversible heart damage.
Based on encouraging clinical results to date, we plan to continue the development of camsirubicin as first-line treatment in patients with ASTS, where the current first-line treatment is doxorubicin. The aim is to administer camsirubicin without restricting cumulative dose, thereby potentially improving efficacy beyond that of doxorubicin by continuing to treat patients who are responding on treatment. In June 2019, we entered into a clinical collaboration with GEIS. GEIS will lead a multi-country, randomized, open-label Phase 2 clinical trial evaluating camsirubicin head-to-head against doxorubicin in patients with ASTS. GEIS is an internationally renowned non-profit organization focused on the research, development and management of clinical trials for sarcoma that has worked with many of the leading biotech and global pharmaceutical companies. Enrollment of the trial is currently anticipated to begin in the second quarter of 2021, and to include approximately 170 ASTS patients, an interim analysis, and take around two years to enroll. The trial will begin with a dose escalation (“run-in”) prior to the randomization portion of the trial. The primary endpoint of the trial will be progression-free survival, with secondary endpoints including overall survival, response rate and incidence of treatment-emergent adverse events. Camsirubicin has been granted orphan drug designation for the treatment of soft tissue sarcoma in the U.S. and EU.
MNPR-101 (formerly huATN-658)
MNPR-101 is a novel, preclinical stage drug product candidate designedcandidate. It is a first-in-class humanized monoclonal antibody to reduce tumor growth by targetingthe urokinase plasminogen activator receptor (“uPAR”), a specific receptor, uPAR, which is present in a range of tumor types, including pancreatic and ovarian tumors.well-credentialed cancer therapeutic target. uPAR is a protein receptor that resides on the cell surface and is overexpressed in many deadly cancers, but has little to no expression in healthy tissue; several Phase 1 imaging studies in human advanced cancer patients show that uPAR is detected selectively in the tumor.
In normal cells, uPAR is transiently expressed as part of a highly regulated process required for the breakdown of the extracellular matrix during normal cell repair process in non-cancerous cells;tissue remodeling. In cancer, however, in cancerous cellsuPAR is constitutively overexpressed by the tumor hijackscell, and the uPAR to helpextracellular matrix degrading function is hijacked by the tumor growto support tissue invasion, metastasis, and spread. Preclinicalangiogenesis. uPAR expression is important to tumor cell survival, and uPAR expression increases in high grade and metastatic disease.
MNPR-101 has demonstrated significant antitumor activity in numerous preclinical models have shown that MNPR-101 is effective at reducingof tumor growth, both used aloneas a monotherapy and in combination with existing therapies.In May 2015,other therapeutics and is being advanced toward an IND. Based on the selective expression of uPAR in numerous tumor types, we anticipate MNPR-101 will be well-tolerated and amenable to a variety of combination treatment approaches in the clinic.
uPRIT as a Potential Therapeutic for Severe COVID-19
MNPR-101 is also being developed for the treatment of severe COVID-19 and other respiratory diseases. We have entered into a Clinical Trialcollaboration development agreement with NorthStar to develop potential uPRITs to treat severe COVID-19. This collaboration combines NorthStar’s expertise in the innovative production, supply, and Option Agreementdistribution of important medical radioisotopes with Cancer Research UKour expertise in therapeutic drug development. NorthStar and we have coupled MNPR-101 with respecta therapeutic radioisotope. uPAR seems to our drug product candidate MNPR-101 (formerly huATN-658)be selectively expressed on aberrantly activated immune cells. In response to coronavirus infection, these rogue immune cells produce pro-inflammatory cytokines that can cause runaway inflammation throughout the body, commonly referred to as a “cytokine storm.” It is this systemic hyper-inflammatory state that is thought to be largely responsible for the severe lung injury and further multiple organ damage that contributes to poor outcomes and death in patients with severe COVID-19.
In collaboration with NorthStar, we have filed a provisional patent application entitled “Precision Radioimmunotherapeutic Targeting of the Urokinase Plasminogen Activator Receptor (uPAR) for Treatment of Severe COVID-19 Disease” with the U.S. Patent and Trademark Office (“USPTO”). PursuantThis application covers novel compositions and uses of cytotoxic radioisotopes attached to this agreement Cancer Research UK conducted preclinical work, improvedantibodies that bind to uPAR, thereby creating precision targeted radiotherapeutics, also known as uPRITs, for the manufacturing,treatment of severe COVID-19 and planned to conductother respiratory diseases. Advanced COVID-19 patients frequently develop severe, life-threatening, pulmonary inflammation as a Phase 1a/1b clinical trial in cancer patients. As partresult of a portfolio reprioritization review, on March 21, 2018 Cancer Research UK notified us it was closingviral induced cytokine storm. The development of this cytokine storm is associated with a high rate of mortality in severe COVID-19 patients, even when oxygen support and mechanical ventilation are utilized. uPRITs have been designed with the goal of selectively eradicating the aberrantly activated immune cells responsible for causing cytokine storm and its project relatedharmful systemic effects. The co-inventors of the provisional patent application are James Harvey, Chief Scientific Officer of NorthStar, and Andrew P. Mazar, our Chief Scientific Officer. We have also entered into collaborations with: IsoTherapeutics Group, LLC, which generated the uPRIT candidates; Aragen Bioscience Inc., which screened the uPRIT candidates through preclinical biochemical testing; and Texas Lung Injury Institute / University of Texas Health Science Center at Tyler, which plans to MNPR-101perform preclinical testing and, would work to make arrangements to formally terminate the agreement. We are currently reviewing potential alternative collaboration opportunities for MNPR-101 and continue to maintain the program’s intellectual property portfolio.if successful, clinical testing.
OverATN-658 as a Potential Diagnostic for Severe COVID-19
A prototype enzyme-linked immunosorbent assay (“ELISA”) for measuring blood suPAR levels using the next three years,non-humanized version of MNPR-101 (ATN-658) has been developed, and we planare in discussions with several parties to executefurther develop and commercialize a suPAR-based test in COVID-19 patients.
The use of suPAR for triaging COVID-19 patients is supported by a growing body of recent studies. Rovina et al. 2020 showed that patients with elevated levels of suPAR at the time of hospital admission are 17 times more likely to develop severe respiratory failure (p=.0000000012); Arnold et al. 2020 showed suPAR to have the best performance in predicting outcome (such as intensive care unit admission and death) of all the biomarkers examined; and Eugen-Olsen et al. 2020 showed that low levels of suPAR are predictive of mild outcome in COVID-19 patients.
MNPR-101 as a Potential Imaging Agent
Using MNPR-101, a multimodal imaging probe was developed and tested in vivo in human bladder cancer models. A publication in the European Journal of Cancer (Baart et al. 2021) reported that high expression of uPAR in bladder cancer is localized at the tumor periphery, suggesting that using a fluorescent-conjugated MNPR-101 probe might allow surgeons to better visualize the borders of the tumor, potentially resulting in more complete tumor resection and thereby minimizing relapse. Similar approaches have been utilized successfully in the resection of other tumor types, such as breast cancer.
Bladder cancer is often treated with transurethral resection to remove cancerous tissue; however, recurrence can occur in up to 78% of patients within 5 years. Up to 40% of recurrent cases develop muscle invasive disease, which has a poor prognosis and requires complete removal of the bladder. Many patients with muscle-invasive bladder cancer go on to develop and succumb to metastatic disease.
Our Strategy
Our management team has extensive experience in developing therapeutics through regulatory approval and commercialization. In aggregate, companies they co-founded have achieved four drug approvals in the U.S. and the EU, successfully sold an asset developed by management which is currently in Phase 3 clinical trials, and completed the sale of a biopharmaceutical company for over $800 million in cash. Understanding the preclinical, clinical, regulatory and commercial development processes and hurdles are key factors in successful drug development and the expertise demonstrated by our management team across all of these areas increases the probability of success in advancing the product candidates in our product pipeline. Our strategic goal is to acquire, develop and commercialize promising oncology product candidates that address important unmet medical needs of cancer patients. The six key elements of our strategy to achieve this goal are to:
●
Leverage data generated from the Phase 2 Validive clinical trial to position us effectively for a successful VOICE clinical program for Validive continuefor SOM in OPC. In the Phase 2 clinical trial the absolute incidence of SOM in OPC patients was reduced by 26.3%, the time to onset was delayed, and the duration of disease in patients that developed SOM was decreased by 15.5 days in the Validive 100 µg cohort versus placebo. In addition to the data from the Phase 2 clinical trial, we believe the guidance from our key opinion leaders (“KOLs”) as well as from the FDA and EMA, and our own internal clinical trial design expertise, position us well for an effective VOICE clinical trial program.
●
Obtain FDA approval of Validive and maximize the commercial potential of Validive in the U.S. and the EU, seeking partnerships outside these markets. If the VOICE clinical program of Validive is successful and FDA approval is obtained, we currently intend to commercialize Validive in the U.S. and the EU ourselves, which may include establishing our own specialty sales force and seeking partnerships outside of these territories for regulatory approval and drug sales and distribution.
●
Advance the clinical development of MNPR-201, pursue collaboration opportunitiescamsirubicin, by pursuing clinical indications where doxorubicin has demonstrated efficacy. ASTS will be the first indication, which will allow camsirubicin to go head-to-head against doxorubicin, the current first-line treatment. In this indication, camsirubicin previously demonstrated clinical benefit (stable disease or partial response) in 52.6% of patients evaluable for tumor progression in a single-arm Phase 2 study. Clinical benefit was proportional to dose and consistently observed at higher cumulative doses of camsirubicin (>1000 mg/m2). Camsirubicin was very well tolerated in this Phase 2 study and underscored the ability to potentially administer camsirubicin without restriction as to cumulative dose (doxorubicin is limited to 450 mg/m2 cumulative dose due to heart toxicity).
●
Continue the development of MNPR-101 and related molecules as a therapeutic, a diagnostic and imaging agents. We plan to continue the development of MNPR-101 for initial clinical development, raise additional capital to funddiagnostic and therapeutic use in severe COVID-19 and in cancer.
●
Expand our drug development programs, acquirepipeline through advancing current assets, in-license and acquisition of oncology product candidates. The 2-pyrrilino camsirubicin analogs represent proprietary compositions of matter that retain the non-cardiotoxic backbone of camsirubicin but may have features in terms of antitumor activity and mechanism that distinguish this family of compounds from camsirubicin. We plan to continue the expansion of our drug development pipeline through acquiring or in-licensein-licensing additional drugoncology product candidates, particularly those that leverage existing scientific and promote publicclinical data that helps reduce the risks of the next steps in clinical development.
●
Utilize the expertise and biotech investor awarenessprior experience of us.our team in the areas of asset acquisition, drug development and commercialization to establish ourselves as a leading biopharmaceutical company. Our senior executive team has relevant experience in biopharmaceutical in-licensing and acquisitions as well as developing product candidates through approval and commercialization. In aggregate, our team has co-founded BioMarin Pharmaceutical (Nasdaq: BMRN), Raptor Pharmaceuticals ($800 million sale to Horizon Pharma), and Tactic Pharma, LLC (“Tactic Pharma”) (sale of lead asset, choline tetrathiomolybdate, which was ultimately acquired by Alexion in June 2018 for $764 million; Alexion is currently in the process of being acquired by AstraZeneca).
DevelopingRisks Associated with our Business
Our business is subject to numerous risks and uncertainties, including those highlighted in “Item 1A - Risk Factors”. These risks include, among others, the following:
●
We are a new drug and conducting clinical trials for one or more disease indications involves substantial costs and resources. Our operating andstage biopharmaceutical company with a history of financial strategylosses. We expect to continue to incur significant losses for the foreseeable future and may never achieve or maintain profitability, which could result in a decline in the market value of our common stock.
●
Funds raised to-date are not sufficient to complete the VOICE clinical program, including, if required, completing a smaller second Phase 3 confirmatory clinical trial, to support further development clinical testing, manufactureof camsirubicin beyond Phase 2, or to support continued development of MNPR-101 and commercialization of drug product candidates is heavily dependent on our entering into collaborations with corporations, non-profits, scientific institutions, licensors, licensees and other parties, which enables us to utilize their financial and other resources to assist in drug development. Additionally,related compounds. If we will needare unable to raise significantenough funds in the next 12–2412 months to executefrom the sale of our clinical development of Validive and potential approval and commercialization plans. We believe that we will have better access to capital as a public reporting company and if a trading market develops for our stock. This would increase corporate visibility, provide increased liquidity for our stockholders, and create a market value for our pipeline of oncology drug product candidates. Therefore, we became a public reporting company under the Securities Exchange Act of 1934 (the “34 Act”) through the filing of a Form 10 registration statement with the SEC. We are working with investment bankers and market makers, with the intention of listing on Nasdaq as soon as we are able to meet the shareholder number, capitalization and other requirements for such a listing, which will likely require a public offering of ourcommon stock or other public stock transaction. See “Risk Factors – Our abilityfinancing efforts, we may have to list on Nasdaq in the future will require raising significant additional capital and likely requireconsider strategic options such as out-licensing Validive or other product candidates, entering into a public stock transaction; failure to qualify to trade on Nasdaq will make itclinical partnership, or terminating one or more difficult to raise capital.”programs. There can be no assurance that we can find a suitable partner on satisfactory terms.
●
We have a limited operating history, no revenues from operations, and are dependent upon raising capital to continue our drug development programs.
●
We do not have and may never have any approved products on the market. Our business is highly dependent upon receiving approvals from various U.S. and international governmental agencies and will be successfulseverely harmed if we are not granted approval to manufacture and sell our product candidates.
●
Our clinical trials may not yield sufficiently conclusive results for regulatory agencies to approve the use of our products.
●
If we experience delays or difficulties in includingthe enrollment of subjects in clinical trials, our receipt of necessary regulatory approvals will be delayed or prevented, which will materially delay our program schedules and adversely affect our financial condition.
●
We rely on third parties to conduct our manufacturing, non-clinical studies, and our clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines or performance goals, the initiation or conduct of our clinical trials may be delayed and we may be unable to obtain regulatory approval for, or commercialize our, current product candidates or any future products, and our financial condition will be adversely affected.
●
We face significant competition from other biotechnology and pharmaceutical companies, and our operating results will suffer if we fail to compete effectively. Competition and technological change may make our product candidates obsolete or non-competitive.
●
The termination of third-party licenses will adversely affect our rights to important compounds or technologies.
●
If we and our third-party licensors do not obtain and preserve protection for our respective intellectual property rights, our competitors may be able to take advantage of our development efforts to develop competing drugs.
●
If we lose key management leadership, and/or scientific personnel, and if we cannot recruit qualified employees or other significant personnel, we may experience program delays and increased compensation costs, and our business will be materially disrupted.
●
The COVID-19 pandemic could have a substantial negative impact on our business, financial condition, operating results, stock for tradingprice and ability raise additional funds.
Implications of Being an Emerging Growth Company
We qualify as an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012 (“JOBS Act”). An emerging growth company may take advantage of specified reduced reporting burdens that are otherwise applicable generally to public companies. These provisions include, but are not limited to:
●
inclusion of only two years, as compared to three years, of audited financial statements in addition to any required unaudited interim financial statements with correspondingly reduced “Management’s discussion and analysis of financial condition and results of operations” disclosures;
●
an exemption from the auditor attestation requirement in the assessment of our internal control over financial reporting pursuant to the Sarbanes-Oxley Act of 2002 (“Sarbanes-Oxley Act”);
●
an exemption from compliance with any new requirements adopted by the Public Company Accounting Oversight Board (“PCAOB”) requiring mandatory audit firm rotation;
●
reduced disclosure about executive compensation arrangements; and
●
an exemption from the requirement to seek non-binding advisory votes on Nasdaqexecutive compensation or golden parachute arrangements.
We may take advantage of these provisions until we are no longer an emerging growth company. We will remain an emerging growth company until the earliest of (1) the last day of the year (a) following the fifth anniversary of the completion of our initial public offering, (b) in which we have total annual gross revenue of at least $1.07 billion or (c) in which we are deemed to be a large accelerated filer, which means the market value of our common stock that is held by non-affiliates exceeds $700 million as of the prior June 30th, and (2) the date on which we have issued more than $1.0 billion in non-convertible debt during the prior three-year period.
We have elected to take advantage of certain of the reduced disclosure obligations in this Annual Report on Form 10-K, and may elect to take advantage of other reduced reporting requirements in future filings. As a result, the information that we provide to our stockholders may be reduced and /or less detailed than what you might find from other public reporting companies.
The JOBS Act permits an emerging growth company such as us to take advantage of an extended transition period to comply with new or revised accounting standards applicable to public companies until those standards would otherwise apply to private companies. We have irrevocably elected to opt out of this provision and, as a result, we will comply with new or revised accounting standards when they are required to be adopted by public companies that are not emerging growth companies. In addition, we are also a “smaller reporting company” as defined in Rule 12b-2 of the Exchange Act and have elected to take advantage of certain of the scaled disclosure requirements available to smaller reporting companies such as avoiding the extensive narrative disclosure required of other reporting companies, particularly in the description of executive compensation.
Corporate Information
We were formed as a Delaware limited liability company in December 2014, with the name Monopar Therapeutics, LLC. In December 2015, we converted to a Delaware C corporation. Our principal executive offices are located at 1000 Skokie Blvd, Suite 350, Wilmette, IL 60091. Our telephone number is (847) 388-0349. Our corporate website is located at www.monopartx.com. Any information contained in, or that a market will developcan be accessed through our website, is not incorporated by reference in this Annual Report on Form 10-K.
Trademark notice
We have registered trademarks with the U.S. Patent and Trademark Office (“USPTO”), for our stock. See Item 1A - “Risk Factors – Risks Related to Our Financial Conditionthe following trademarks: “Validive”, “Baxefyn”, “Vidarys”, “Cotilix”, “Arvita” and Capital Requirements”,“Clonidol”. All other trademarks, service marks and “Risks Related to Our Business Operationstrade names in this Annual Report on Form 10-K are the property of their respective owners. We have omitted the ® and Industry.”™ designations, as applicable, for the trademarks used herein.
Revenues
We are an emerging growth company, have no approved drugs and have not generated any revenues.
Conversion of Preferred Stock to Common Stock
In March 2017, holders of a majority in interest of our Series A Preferred Stock and holders of a majority in interest of our Series Z Preferred Stock voted to adopt the Second Amended and Restated Certificate of Incorporation of the Company (the “Certificate of Incorporation”). When the Certificate of Incorporation took effect, each share of Series A Preferred Stock was automatically converted into 84 shares of common stock of the Company (a 1.2 for 1 conversion to Common Stock concurrent with a 70 for 1 stock split) and each share of Series Z Preferred Stock was automatically converted into 70 shares of common stock of the Company (a 1 for 1 conversion to common stock concurrent with a 70 for 1 stock split) and Series A Preferred Stock and Series Z Preferred Stock were eliminated (the “Conversion”). 100,000 shares of Series Z Preferred Stock were converted into 7,000,000 shares of common stock and 15,894 shares of Series A Preferred Stock were converted into 1,335,079.284 shares of common stock. All references in this “Management’s Discussion and Analysis of Financial Conditions and Results of Operations” to common stock authorized, issued and outstanding and common stock options take into account the stock split that occurred as part of the Conversion.
Critical Accounting Policies and Use of Estimates
While our significant accounting policies are described in more detail in Note 2 of our financial statements included elsewhere in this Annual Report on Form 10-K, we believe the following accounting policies to be critical to the judgments and estimates used in the preparation of our financial statements.
Use of Estimates
The preparation of financial statements in conformity with GAAP requires our management to make estimates and assumptions that affect the reported amounts of assets and liabilities, disclosure of contingent assets and liabilities, and reported amounts of revenues and expenses in the financial statements and accompanying notes. Actual results could differ from those estimates.
Going Concern Assessment
We adopted Accounting Standards Updates (“ASU”) 2014-15, Disclosure of Uncertainties about an Entity’s Ability to Continue as a Going Concern, which the Financial Accounting Standards Board (“FASB”) issued to provide guidance on determining when and how reporting companies must disclose going-concern uncertainties in their financial statements. The ASU requires management to perform interim and annual assessments of an entity’s ability to continue as a going concern within one year of the date of issuance of the entity’s financial statements (or within one year after the date on which the financial statements are available to be issued, when applicable). Further, a company must provide certain disclosures if there is “substantial doubt about the entity’s ability to continue as a going concern.” In February 2018, we analyzed our minimum cash requirements through March 2019 and have determined that, based upon our current available cash, we have no substantial doubt about our ability to continue as a going concern. See Item 1A - “Risk Factors” – our anticipated operating expenses over the next year are based upon our management’s estimates of possible future events. Actual operating expenses could differ materially from those projected by our management.
Revenue
We are an emerging growth company, have no approved drugs and have not generated any revenues. See “Overview – Revenues”. To date, we have engaged in acquiring pharmaceutical drug product candidates, licensing rights to drug product candidates, entering into collaboration agreements for testing and clinical development of our drug product candidates and providing the infrastructure to support the clinical development of our drug product candidates. We do not anticipate commercial revenues from operations until we complete testing and development of one of our drug product candidates and obtain marketing approval or we sell, enter into a collaborative marketing arrangement, or out-license one of our drug product candidates to another party. See “Liquidity and Capital Resources”.
Recently Issued and Adopted Accounting Pronouncements
A description of recently issued accounting pronouncements that may potentially impact our financial position and consolidated results of operations is disclosed in Note 2 to our consolidated financial statements appearing elsewhere in this Annual Report on Form 10-K.
Critical Accounting Policies and Use of Estimates
While our significant accounting policies are described in more detail in Note 2 of our consolidated financial statements included elsewhere in this Annual Report on Form 10-K, we believe the following accounting policies to be critical to the judgments and estimates used in the preparation of our consolidated financial statements.
Stock-Based Compensation
We account for stock-based compensation arrangements with employees, non-employee directors and consultants using a fair value method, which requires the recognition of compensation expense for costs related to all stock-based awards, including stock option grants and restricted stock units (“RSUs”). The fair value method requires us to estimate the fair value of stock-based payment awards on the date of grant using an option pricing model or the closing stock price on the date of grant in the case of RSUs.
Stock-based compensation costs for stock awards granted to our employees and non-employee directors are based on the fair value of the underlying instruments calculated using the Black-Scholes option-pricing model on the date of grant for stock options and using the closing stock price on the date of grant for RSUs and recognized as expense on a straight-line basis over the requisite service period, which is the vesting period. Determining the appropriate fair value model and related assumptions requires judgment, including selecting methods for estimating the Company’s future stock price volatility, forfeiture rates and expected term. The expected volatility rates are estimated based on the actual volatility of comparable public companies over recent historical periods of the same length as the expected term. We generally selected these companies based on reasonably comparable characteristics, including market capitalization, risk profiles, stage of corporate development and with historical share price information sufficient to meet the expected term of the stock-based awards. The expected term for stock options granted during the years ended December 31, 2020 and 2019 was estimated using the simplified method. Forfeitures are estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. We have not paid dividends and do not anticipate paying a cash dividend in future vesting periods and, accordingly, use an expected dividend yield of zero. The risk-free interest rate is based on the rate of U.S. Treasury securities with maturities consistent with the estimated expected term of the awards. Prior to January 1, 2019, the measurement of consultant stock-based compensation was subject to periodic adjustments as the underlying equity instruments vest. Since January 1, 2019, consultant stock-based compensation is valued on the grant date and is recognized as an expense straight-line over the period during which services are rendered.
Results of Operations
Comparison of the Years Ended December 31, 2020 and December 31, 2019
The following table summarizes the results of our operations for the years ended December 31, 2020 and 2019:
| | | |
| (in thousands) | | | |
| Research and development expenses | $4,065 | $1,969 | $ 2,096
|
| General and administrative expenses | 2,444 | 2,355 | |
| Total operating expenses | 6,509 | 4,324 | |
| Operating loss | (6,509) | (4,324) | (2,185) |
| Other income from PPP loan forgiveness | 122 | | 122 |
| Interest income | 82 | 99 | |
| Net loss | $(6,305) | $(4,225) | |
Research and Development Expenses
Research and developmentDevelopment (“R&D”) costs are expensed as incurred. Major componentsexpenses for the year ended December 31, 2020 were approximately $4,065,000, compared to approximately $1,969,000 for the year ended December 31, 2019. This represents an increase of researchapproximately $2,096,000 primarily attributed to increases in expenses of $1,144,000 for the planning of the GEIS camsirubicin Phase 2 clinical trial including manufacturing, $48,000 for increases in Validive clinical trial planning and development expenses includemanufacturing costs, $924,000 for annual R&D personnel salary increases, annual (non-cash) equity grants and salaries and benefits of three new R&D staff, fees paidpersonnel and a higher allocation of the CEO's salary and benefits to consultants andR&D expenses due to the entities that conduct certain development activities on our behalf and materials and supplies.
We accrue and expense the costs forstart-up of clinical trial activities, performedpartially offset by third parties based upon estimates$20,000 for net decreases other R&D expenses.
General and Administrative Expenses
General and administrative (“G&A”) expenses for the year ended December 31, 2020 were approximately $2,444,000, compared to approximately $2,355,000 for the year ended December 31, 2019. This represents an increase of approximately $89,000 primarily attributed to $430,000 for net increases in stock-based compensation for annual (non-cash) equity grants and increases in annual G&A personnel salary and benefits, $202,000 for increases in fees related to public company compliance, including Nasdaq, legal and audit fees, $32,000 for increases in Delaware franchise tax and Australian income tax, and $16,000 for net increases in general costs of operations, partially offset by $475,000 in CEO's salary and benefits allocated from G&A expenses to R&D expenses, and $116,000 for decreases in stock-based compensation for non-employee directors (non-cash).
Other Income from PPP Loan Forgiveness
Other income from PPP loan forgiveness of approximately $122,000 represents the percentagePPP loan granted by the Small Business Administration (“SBA”) in May 2020, which repayment was forgiven by the SBA in December 2020.
Interest Income
Interest income for the year ended December 31, 2020 decreased by approximately $17,000 versus the year ended December 31, 2019 due to a significant decrease in bank interest rates partially offset by an increase in bank balances resulting from our initial public offering in December 2019 and funds raised in our Capital on DemandTM Sales Agreement with JonesTrading during 2020.
Liquidity and Capital Resources
Sources of work completed overLiquidity
We have incurred losses and cumulative negative cash flows from operations since our inception in December 2014 resulting in an accumulated deficit of approximately $32.2 million as of December 31, 2020. We anticipate that we will continue to incur losses for the life of the individual study in accordance with agreements established with contract research organizations and clinical trial sites.foreseeable future. We determine the estimates through discussions with internal clinical personnel and external service providers as to progress or stage of completion of trials or services and the agreed upon fee to be paid for such services. Costs of setting up clinical trial sites for participation in the trials are expensed immediately asexpect that our research and development expenses. Clinical trial site costsand general and administrative expenses will increase to enable the execution of our strategic plan. As a result, we anticipate that we will seek to raise additional capital in 2021 to fund our future operations. We will seek to obtain needed capital through a combination of equity offerings, debt financings, strategic collaborations and grant funding. To date, we have funded our operations through net proceeds from the initial public offering of our common stock and net proceeds from sales under our Capital on DemandTM Sales Agreement, private placements of our preferred and common stock, and the net receipt of funds related to patient enrollment are accruedthe acquisition of camsirubicin as patients are entered intodiscussed in our Annual Report on Form 10-K for the trial.year ended December 31, 2019 under Item 7 Management's Discussion and Analysis of Financial Condition and Results of Operations, Liquidity and Resources, filed with the SEC on March 27, 2020. We anticipate that the currently available funds as of March 5, 2021, will fund our planned operations at least through March 31, 2022.
We invest our cash equivalents in a money market account.
Cash Flows
The following table provides information regarding our cash flows for the years ended December 31, 2020 and 2019.
| | |
|
| (in thousands) | | | |
| Net cash used in operating activities | $(4,662) | $(3,018) | $ (1,644)
|
| Net cash provided by financing activities | 8,182 | 9,347 | (1,165)
|
| Effect of exchange rates on cash and cash equivalents | 3 | (8) | |
| Net increase in cash and cash equivalents | $3,523 | $6,321 | |
During the previous two fiscal years ended December 31, 2020 and 2019, we had net cash inflows of approximately $3,523,000 and $6,321,000, respectively, a decrease of approximately $2,798,000, due primarily to higher net cash used in operating activities in 2020 and less cash raised in 2020 compared to 2019.
Cash Flow Used in Operating Activities
The increase to cash flow used in operating activities during the year ended December 31, 2020 compared to the year ended December 31, 2019 of approximately $1,644,000 was primarily a result of increased R&D and G&A cash operating expenses.
Cash Flow Used in Investing Activities
There was no cash flow provided by or used in investing activities for the years ended December 31, 2020 and 2019.
Cash Flow Provided by Financing Activities
The decrease in cash flow provided by financing activities during the year ended December 31, 2020 compared to the year ended December 31, 2019 of approximately ($1,165,000) was due to net proceeds from the initial public offering of our common stock and the exercise of stock options offset by deferred offering costs during the year ended December 31, 2019 being higher than the net sales of our common stock under our Capital on DemandTM Sales Agreement with JonesTrading and the receipt of the forgiven PPP loan during the year ended December 31, 2020.
Future Funding Requirements
To date, we have not generated any revenue from product sales. We do not know when, or if, we will generate any revenue from product sales. We do not expect to generate any revenue from product sales unless and until we obtain regulatory approval of and commercialize any of our current or future drug product candidates or we out-license or sell a drug product candidate to another party. At the same time, we expect our expenses to increase in connection with our ongoing development activities, particularly as we continue the research, development, future preclinical studies and clinical trials in progress.
The successful development of, and seek regulatory approval for, our current and future drug product pipeline is highly uncertain. We cannot reasonably estimate the nature, timing or costs of the efforts that will be necessary to complete the remainder of the developmentcandidates. If we obtain regulatory approval of any of our current or future drug product candidates, we will need substantial additional funding for commercialization requirements and our continuing drug product development operations.
As a company, we have not completed development through marketing approvals of any therapeutic products. We expect to continue to incur significant increases in expenses and increasing operating losses for the foreseeable future. We anticipate that our expenses will increase substantially as we:
● advance the clinical development and execute the regulatory strategy for Validive;
● continue the clinical development and execute the regulatory strategy for camsirubicin;
● continue the preclinical activities and potentially enter clinical development of MNPR-101 (and related compounds) for severe COVID-19 and/or other indications;
● acquire and/or license additional pipeline drug product candidates and pursue the period, iffuture preclinical and/or clinical development of such drug product candidates;
● seek regulatory approvals for any inof our current and future drug product candidates that successfully complete registration clinical trials;
● establish or purchase the services of a sales, marketing and distribution infrastructure to commercialize any products for which material net cash inflows fromwe may obtain marketing approval;
● develop our manufacturing/quality capabilities or establish a reliable, high quality supply chain sufficient to support our clinical requirements and to provide sufficient capacity to launch and grow the sales of any product for which we obtain marketing approval; and
● add or contract for required operational, financial and management information systems and capabilities and other specialized expert personnel to support our drug product candidatescandidate development and planned commercialization efforts.
We anticipate that the funds available as of March 5, 2021, will fund our operations at least through March 2022. We have based this estimate on assumptions that may commence. This is dueprove to be wrong, and we could use our available capital resources sooner than we currently expect. Because of the numerous risks and uncertainties associated with developingthe development and commercialization of our drug product candidates, and the extent to which we enter into collaborations with third parties to participate in the development and commercialization of our drug product candidates, we are unable to accurately estimate with high reliability the amounts and timing required for increased capital outlays and operating expenditures associated with our current and anticipated drug product candidate development programs. Our future capital requirements will depend on many factors, including:
● the progress of regulatory interactions and clinical development of Validive;
● the progress of clinical development and regulatory outcomes of camsirubicin;
● the progress of preclinical and clinical development of MNPR-101 (and related compounds) including through our collaboration with NorthStar;
●
receiving less funding than we require;
●
slower than expected progress in developing Validive, MNPR-201, MNPR-101 or the number and characteristics of other drug product candidates;
●
higher than expected costs to produce our the scope, progress, timing, cost and results of research, preclinical development and clinical trials of current and future drug product candidates;
● the costs, timing and outcomes of seeking and obtaining FDA and international regulatory approvals;
●
higher than expected costs for preclinical testing of our future and current acquired and/or in-licensed programs;