
As filed with the Securities and Exchange Commission on January 5,18, 2006
Registration No. 333-128827
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
AMENDMENT NO. 23 TO
FORM S-1
REGISTRATION STATEMENT
UNDER
THE SECURITIES ACT OF 1933
ACORDA THERAPEUTICS, INC.
(Exact Name of Registrant as Specified in its Charter)
| Delaware | 2836 | 13-3831168 | ||
| (State or Other Jurisdiction of Incorporation or Organization) | (Primary Standard Industrial Classification Code Number) | (I.R.S. Employer Identification Number) |
15 Skyline Drive
Hawthorne, New York 10532
(914) 347-4300
(Address, Including Zip Code, and Telephone Number,
Including Area Code, of Registrant's Principal Executive Offices)
Ron Cohen
Chief Executive Officer
15 Skyline Drive
Hawthorne, New York 10532
(914) 347-4300
(Name, Address, Including Zip Code, and Telephone Number,
Including Area Code, of Agent For Service)
Copy To:
| Ellen B. Corenswet Covington & Burling 1330 Avenue of the Americas New York, New York 10019 (212) 841-1000 | Danielle Carbone Shearman & Sterling LLP 599 Lexington Avenue New York, New York 10022 (212) 848-4000 |
Approximate date of commencement of proposed sale to the public: As soon as practicable after the effective date of this Registration Statement.
If the securities being registered on this form are being offered on a delayed or continuous basis pursuant to Rule 415 under the Securities Act of 1933, check the following box. o
If this form is filed to register additional securities for an offering pursuant to Rule 462(b) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. o
If this form is a post-effective amendment filed pursuant to Rule 462(c) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. o
If this form is a post-effective amendment filed pursuant to Rule 462(d) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. o
If delivery of the prospectus is expected to be made pursuant to Rule 434 under the Securities Act, please check the following box. o
The registrant hereby amends this registration statement on such date or dates as may be necessary to delay its effective date until the registrant shall file a further amendment which specifically states that this registration statement shall thereafter become effective in accordance with Section 8(a) of the Securities Act of 1933, or until this registration statement shall become effective on such date as the Securities and Exchange Commission, acting pursuant to said Section 8(a), may determine.
The information in this prospectus is not complete and may be changed. We may not sell these securities until the registration statement filed with the Securities and Exchange Commission is effective. This prospectus is not an offer to sell these securities and is not soliciting offers to buy these securities in any state where the offer or sale is not permitted.
SUBJECT TO COMPLETION, DATED JANUARY 5,18, 2006
Prospectus
Shares
Common Stock
Acorda Therapeutics, Inc. is offering shares of common stock. This is our initial public offering, and no public market currently exists for our shares. We anticipate that the initial public offering price will be between $ and $ per share. After the offering, the market price for our shares may be outside this range.
We will apply to list our common stock on the Nasdaq National Market under the symbol "ACOR."
Investing in our common stock involves a high degree of risk. See "Risk Factors" beginning on page 9.
| | Per Share | Total | ||||
|---|---|---|---|---|---|---|
| Offering price | $ | $ | ||||
| Discounts and commissions to underwriters | $ | $ | ||||
Offering proceeds to Acorda Therapeutics, Inc., before expenses | $ | $ | ||||
Neither the Securities and Exchange Commission nor any state securities commission has approved or disapproved these securities or determined if this prospectus is accurate or complete. Any representation to the contrary is a criminal offense.
We have granted the underwriters the right to purchase up to additional shares of common stock to cover any over-allotments. The underwriters can exercise this right at any time within 30 days after the offering. The underwriters expect to deliver the shares on or about , 2006.
Banc of America Securities LLC
| Lazard Capital Markets |
| Piper Jaffray |
| SG Cowen & Co. |
, 2006
You should rely only on the information contained in this prospectus. We have not, and the underwriters have not, authorized anyone to provide you with different information. We are not making offers to sell or seeking offers to buy these securities in any jurisdiction where the offer or sale is not permitted. You should assume that the information contained in this prospectus is accurate as of the date on the front of this prospectus only. Our business, financial condition, results of operations and prospects may have changed since that date.
| | Page | |
|---|---|---|
| Summary | 1 | |
| Risk Factors | 9 | |
| Forward-Looking Statements | 25 | |
| Use of Proceeds | 26 | |
| Dividend Policy | 26 | |
| Capitalization | 27 | |
| Dilution | 29 | |
| Selected Consolidated Financial Data | 31 | |
| Management's Discussion and Analysis of Financial Condition and Results of Operations | 34 | |
| Business | 58 | |
| Management | 92 | |
| Summary Compensation Table | ||
| Certain Relationships and Related Transactions | ||
| Principal Stockholders | ||
| Description of Capital Stock | ||
| Shares Eligible for Future Sale | ||
| Certain United States Federal Income and Estate Tax Consequences to Non-U.S. Holders | ||
| Underwriting | ||
| Legal Matters | ||
| Experts | ||
| Where You Can Find Additional Information |
i
This summary highlights information contained elsewhere in this prospectus. You should read the entire prospectus carefully before making an investment decision.
We are a commercial-stage biopharmaceutical company dedicated to the identification, development and commercialization of novel therapies that improve neurological function in people with multiple sclerosis, or MS, spinal cord injury, or SCI, multiple sclerosis, or MS, and other disorders of the central nervous system, or CNS. Our marketed product, Zanaflex Capsules, is FDA-approved for the management of spasticity. Our lead product candidate, Fampridine-SR, is in a Phase 3 clinical trial for the improvement of walking ability in people with MS. Our preclinical programs also target MS and SCI, as well as other CNS disorders, including stroke and traumatic brain injury.
Approximately 650,000 people in the United States suffer from MS or SCI and the combined annual cost of treatment for these conditions exceeds $13 billion. It is estimated that a total of approximately 10 million people live with the long-term consequences of traumatic brain injury and stroke.
Our goal is to continue to grow as a fully-integrated biopharmaceutical company by commercializing pharmaceutical products, developing our product candidates and advancing our preclinical programs for these large and underserved markets. We plan to accomplish this through our sales and marketing infrastructure, our extensive scientific and medical network, our partnerships and our clinical and management experience.
Zanaflex
Our products, Zanaflex Capsules and Zanaflex tablets, are FDA-approved for the management of spasticity, a symptom of conditions such as MS and SCI that is commonly characterized by stiffness and rigidity, restriction of movement and painful muscle spasms. Zanaflex Capsules and Zanaflex tablets contain tizanidine hydrochloride, or tizanidine, one of the two leading treatments currently used for the management of spasticity. We acquired Zanaflex Capsules and Zanaflex tablets from a wholly-owned subsidiary of Elan Corporation, plc, or Elan, in July 2004. This strategic acquisition provided us with the opportunity to build a commercial infrastructure, develop sales and marketing expertise and create a foundation for future product launches, in addition to generating product revenue.
In April 2005, we launched Zanaflex Capsules, a new capsule formulation of tizanidine. This product is protected by an issued U.S. patent. Zanaflex tablets lost compound patent protection in 2002 and both products now compete with 11 generic versions of tizanidine tablets.
We believe that Zanaflex Capsules offer important benefits over Zanaflex tablets and generic tizanidine tablets. When taken with food, Zanaflex Capsules have a different blood absorption profile, referred to as pharmacokinetic profile, than Zanaflex tablets and generic tizanidine tablets, generally resulting in a lower level and more gradual rise of peak levels of tizanidine in a patient's blood. As a result of this different pharmacokinetic profile, Zanaflex tablets and generic tizanidine tablets are not therapeutically equivalent, or AB-rated, with Zanaflex Capsules. Therefore, under state pharmacy laws, prescriptions written for Zanaflex Capsules may not properly be filled by the pharmacist with Zanaflex tablets or generic tizanidine tablets. Zanaflex Capsules are also available in a higher dose, which gives patients and prescribers an additional choice in dosing and an opportunity to reduce the number of pills a person must take daily. In addition, people who have difficulty swallowing may find Zanaflex Capsules easier to take.
To support our commercialization of Zanaflex Capsules, we have established a sales and marketing infrastructure consisting of our internal specialty sales force, a contract sales force and a pharmaceutical telesales group. Our internal specialty sales force currently consists of 14 sales professionals who call on neurologists and other prescribers specializing in treating patients with conditions that involve spasticity. Members of this sales force also call on managed care organizations, pharmacists and wholesale drug distribution customers. We plan to expand our specialty sales force to approximately 30 sales professionals in the first quarter of 2006. Our contract sales force is provided by Cardinal Health PTS, LLC, or Cardinal Health, and consists of approximately 160 sales representatives who market Zanaflex Capsules to primary care physicians.physicians, on a non-exclusive basis. We also have a contract with Access Worldwide Communications to provide a small, dedicated sales force of pharmaceutical telesales professionals to contact primary care physicians, specialty physicians and pharmacists. Our current sales and marketing infrastructure enables us to reach virtually all high-volume prescribers of Zanaflex tablets and generic tizanidine. We believe that these prescribers are also potential high-volume prescribers for our lead product candidate, Fampridine-SR, if approved.
Fampridine-SR
Fampridine-SR is currently in a Phase 3 clinical trial for the improvement of walking ability in people with MS. The trial is being conducted pursuant to a Special Protocol Assessment, or SPA, with the FDA. The FDA has agreed that, if successful, this trial could qualify as one of the pivotal efficacy studies required for drug approval. Fampridine-SR is a small molecule drug contained in a sustained release oral tablet form. Laboratory studies have shown that fampridine, the active molecule in Fampridine-SR, improves impulse conduction in nerve fibers in which the insulating outer layer, called the myelin sheath, has been damaged. This damage may be caused by the body's own immune system, in the case of MS, or by physical trauma, in the case of SCI.
More than 800 people have been treated with Fampridine-SR in over 25 clinical trials, including nine clinical trials in MS and 11 clinical trials in SCI. In six Phase 2 clinical trials, treatment with Fampridine-SR has been associated with a variety of neurological benefits in people with MS or SCI. In our most recently completed Phase 2 clinical trial, there was a trend toward improvement in the primary endpoint of walking speed and, when analyzed using the same methodology that the FDA has now agreed to in the SPA for our Phase 3 clinical trial, these results would have beenare statistically significant. We expect the recruitment period for the current Phase 3 clinical trial, which began in June 2005, to require approximately six to eight months.end in February 2006. The treatment period is 14 weeks and the subjects are involved in trial procedures for approximately five months. We expect to be able to evaluate data from this clinical trial in the third quarter of 2006.
We believe Fampridine-SR is the first potential therapy in late-stage clinical development for MS that seeks to improve the function of damaged nerve fibers, rather than only treating the symptoms of MS or slowing the progression of disease. To our knowledge, there are no current drug therapies that improve walking ability in people with MS. We plan to commercialize Fampridine-SR, if approved, ourselves in the United States, and possibly Canada, and with partners in various markets throughout the rest of the world.
Preclinical programs
We have three preclinical programs focused on novel approaches to repair damaged components of the CNS:
We believe that all of our preclinical therapies have the potential to address conditions for which no effective treatment currently exists. In addition to applicability in MS, SCI and various other CNS disorders, we believe that our preclinical programs also may have applicability in such fields as orthopedics, cardiology, oncology and ophthalmology.
Our strategy is to continue to grow as a fully-integrated biopharmaceutical company focused on the identification, development and commercialization of a range of nervous system therapeutics. We are using our scientific and clinical expertise in MS and SCI as strategic points of access to additional CNS markets, including stroke and traumatic brain injury. Key aspects of our strategy are to:
We have established an advisory team and network of well-recognized scientists, clinicians and opinion leaders in the fields of MS and SCI. Depending on their expertise, these advisors provide assistance in trial design, conduct clinical trials, keep us apprised of the latest scientific advances and help us identify and evaluate business development opportunities. In addition, we have recruited over 35 MS centers and 80 SCI rehabilitation centers in the United States and Canada to conduct our clinical trials. Our clinical management team has extensive experience in the areas of MS and SCI and works closely with this network.
Risks Associated with our Business
Our business is subject to numerous risks, as more fully described in the section entitled "Risk Factors" immediately following this prospectus summary. We may be unable, for many reasons, including those that are beyond our control, to implement our current business strategy. Those reasons
could include failure to successfully promote Zanaflex Capsules and any other future marketed products; delays in obtaining, or a failure to obtain, regulatory approval for our product candidates; and failure to maintain and to protect our proprietary intellectual property assets, among others. The information about our preclinical and clinical trials may be useful to you in evaluating our company's current stage of development and our near-term and long-term prospects; however, you should note that of the large number of drugs in development only a small percentage successfully complete the FDA regulatory approval process and are commercialized.
We have a limited operating history and, as of September 30, 2005, had an accumulated deficit of approximately $198.5 million. We expect to incur losses for at least the next several years. We had net losses of $26.0 million and $44.7 million for the nine months ended September 30, 2005 and for the year ended December 31, 2004, respectively. We are unable to predict the extent of future losses or when we will become profitable, if at all. Even if we succeed in promoting Zanaflex Capsules and developing and commercializing one or more of our product candidates, we may never generate sufficient sales revenue to achieve and sustain profitability.
We were incorporated in 1995 as a Delaware corporation. Our principal executive offices are located at 15 Skyline Drive, Hawthorne, New York 10532. Our telephone number is (914) 347-4300. Our website iswww.acorda.com. The information on our website is not part of this prospectus.
"Acorda Therapeutics" is a registered trademark that we own and "Zanaflex" is a registered trademark that we exclusively license. We have pending U.S. trademark applications for our logo and "Zanaflex Capsules." Other trademarks, trade names and service marks used in this prospectus are the property of their respective owners.
| Common stock offered | shares | |
Common stock outstanding after this offering | shares | |
Use of proceeds | We intend to use the net proceeds of this offering for sales and marketing activities, clinical and preclinical development programs and for general corporate purposes. See "Use of Proceeds." | |
Proposed Nasdaq National Market symbol | ACOR | |
Risk factors | See "Risk Factors" and the other information included in this prospectus for a discussion of factors you should carefully consider before deciding to invest in shares of our common stock. |
The number of shares of common stock to be outstanding after this offering is based on the number of shares outstanding as of September 30, 2005 and reflects or assumesexcludes the following:
Unless we specifically state otherwise, all information in this prospectus, including the number of shares of common stock to be outstanding after this offering:
In the table above, the number of shares of common stock outstanding after this offering excludes, as of September 30, 2005:
SUMMARY CONSOLIDATED FINANCIAL DATA
The following table presents a summary of our historical financial information. You should read this information in conjunction with our consolidated financial statements and related notes and the information under "Selected Consolidated Financial Data" and "Management's Discussion and Analysis of Financial Condition and Results of Operations" included elsewhere in this prospectus. We changed our fiscal year end from June 30 to December 31, beginning with the six months ended December 31, 2003.
Pro forma amounts in the following table reflect the conversion of our outstanding convertible and mandatorily redeemable convertible preferred stock into 13,338,279 shares of common stock upon completionon the closing of this offering, assuming that shares of our preferred stock were outstanding for the entire periods presented.
| | | | | | | Nine Months Ended September 30, | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | | | Six Months Ended December 31, | | |||||||||||||||||||
| | Year Ended June 30, | Year Ended December 31, | ||||||||||||||||||||||
| | 2004 | 2005 | ||||||||||||||||||||||
| | 2001 | 2002 | 2003 | 2003 | 2004 | (unaudited) | ||||||||||||||||||
| | ||||||||||||||||||||||||
| | (in thousands, except per share data) | |||||||||||||||||||||||
| Statement of Operations Data: | ||||||||||||||||||||||||
| Gross sales—Zanaflex | $ | — | $ | — | $ | — | $ | — | $ | — | $ | — | $ | 3,239 | ||||||||||
| Less: discounts and allowances | — | — | — | — | (4,417 | ) | (144 | ) | (992 | ) | ||||||||||||||
| Net sales | — | — | — | — | (4,417 | ) | (144 | ) | 2,247 | |||||||||||||||
| Grant revenue | 462 | 132 | 474 | 382 | 479 | 445 | 184 | |||||||||||||||||
| Total net revenue | 462 | 132 | 474 | 382 | (3,938 | ) | (301 | ) | 2,431 | |||||||||||||||
| Less: cost of sales | — | — | — | — | (885 | ) | (363 | ) | (2,274 | ) | ||||||||||||||
| Gross profit | 462 | 132 | 474 | 382 | (4,823 | ) | (62 | ) | 157 | |||||||||||||||
Operating expenses: | ||||||||||||||||||||||||
| Research and development | 6,142 | 11,147 | 17,527 | 16,743 | 21,999 | 18,621 | 9,652 | |||||||||||||||||
| Research and development—related party | 2,223 | 4,687 | 2,265 | 3,343 | — | — | — | |||||||||||||||||
| Sales and marketing | — | — | — | — | 4,662 | 2,793 | 9,657 | |||||||||||||||||
| General and administrative | 3,489 | 6,636 | 6,388 | 17,069 | 13,283 | 11,034 | 6,339 | |||||||||||||||||
| Total operating expenses | 11,854 | 22,470 | 26,180 | 37,155 | 39,944 | 32,448 | 25,648 | |||||||||||||||||
| Operating loss | (11,392 | ) | (22,338 | ) | (25,706 | ) | (36,773 | ) | (44,767 | ) | (32,510 | ) | (25,491 | ) | ||||||||||
Other income (expense): | ||||||||||||||||||||||||
| Interest and amortization of debt discount expense | — | — | (78 | ) | (38 | ) | (385 | ) | (297 | ) | (824 | ) | ||||||||||||
| Interest and amortization of debt discount expense—related party | (443 | ) | (408 | ) | (369 | ) | (184 | ) | — | — | — | |||||||||||||
| Interest income | 1,824 | 984 | 393 | 276 | 409 | 329 | 347 | |||||||||||||||||
| Other income | — | — | 26 | 7 | 2 | 2 | 1 | |||||||||||||||||
| Total other income (expense) | 1,381 | 576 | (28 | ) | 61 | 26 | 34 | (476 | ) | |||||||||||||||
| Minority interest—related party | 699 | 580 | — | — | — | — | — | |||||||||||||||||
| Cumulative effect of change in accounting principle | — | — | — | — | — | — | 3 | |||||||||||||||||
| Net loss | (9,313 | ) | (21,181 | ) | (25,734 | ) | (36,712 | ) | (44,741 | ) | (32,476 | ) | (25,964 | ) | ||||||||||
Beneficial conversion feature, accretion of issuance costs, preferred dividends, and fair value of warrants issued to convertible preferred stockholders | (36 | ) | (55 | ) | (24,320 | ) | (11,985 | ) | (24,746 | ) | (18,496 | ) | (18,636 | ) | ||||||||||
| Net loss allocable to common stockholders | $ | (9,349 | ) | $ | (21,236 | ) | $ | (50,054 | ) | $ | (48,697 | ) | $ | (69,487 | ) | $ | (50,972 | ) | $ | (44,600 | ) | |||
| Net loss per share allocable to common stockholders—basic & diluted | $ | (50.81 | ) | $ | (111.90 | ) | $ | (261.38 | ) | $ | (252.87 | ) | $ | (351.76 | ) | $ | (259.22 | ) | $ | (221.17 | ) | |||
| | | | | | | Nine Months Ended September 30, | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | | | Six Months Ended December 31, | | ||||||||||||
| | Year Ended June 30, | Year Ended December 31, | |||||||||||||||
| | 2004 | 2005 | |||||||||||||||
| | 2001 | 2002 | 2003 | 2003 | 2004 | (unaudited) | |||||||||||
| | |||||||||||||||||
| Pro forma net loss per share allocable to common stockholders—basic & diluted (unaudited) | $ | (9.63 | ) | $ | (1.92 | ) | |||||||||||
| Weighted average shares of common stock outstanding used in computing net loss per share allocable to common stockholders—basic & diluted | 184 | 190 | 191 | 193 | 198 | 197 | 202 | ||||||||||
| Weighted average shares of common stock outstanding used in computing pro forma net loss per share allocable to common stockholders—basic & diluted (unaudited) | 13,536 | 13,547 | |||||||||||||||
The following table sets forth our cash, cash equivalents and short-term investments and capitalization as of September 30, 2005:
| | As of September 30, 2005 | As of September 30, 2005 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Actual (unaudited) | Pro Forma (unaudited) | Pro Forma As Adjusted (unaudited) | Actual (unaudited) | Pro Forma (unaudited) | Pro Forma As Adjusted (unaudited) | |||||||||||
| | (in thousands) | (in thousands) | |||||||||||||||
| Balance Sheet Data: | |||||||||||||||||
| Cash and cash equivalents | $ | 3,581 | $ | 14,879 | $ | 3,581 | $ | 14,879 | |||||||||
| Restricted cash | 261 | 261 | 261 | 261 | |||||||||||||
| Short-term investments | 5,160 | 5,160 | 5,160 | 5,160 | |||||||||||||
| Working capital | (12,203 | ) | (10,506 | ) | (12,203 | ) | (14,207 | ) | |||||||||
| Capitalized transaction costs—PRF transaction | — | 500 | |||||||||||||||
| Total assets | 25,543 | 37,342 | 25,543 | 37,842 | |||||||||||||
| Deferred product revenue—Zanaflex Capsules | 4,960 | 4,960 | 4,960 | 4,960 | |||||||||||||
| Deferred product revenue—Zanaflex tablets | 10,686 | 10,686 | 10,686 | 10,686 | |||||||||||||
| Current portion of notes payable | 2,347 | 1,150 | 2,347 | 1,150 | |||||||||||||
| Revenue interest liability—PRF transaction | — | 11,299 | — | 14,600 | |||||||||||||
| Put/call option liability—PRF transaction | — | 400 | |||||||||||||||
| Long-term portion of notes payable | 3,534 | 1,731 | 3,534 | 1,731 | |||||||||||||
| Long-term convertible notes payable—principal amount plus accrued interest, less unamortized debt discount—related party | 8,695 | 8,695 | 8,695 | 8,695 | |||||||||||||
| Mandatorily redeemable preferred stock | 85,000 | — | 85,000 | — | |||||||||||||
| Total stockholders' (deficit) | (101,669 | ) | (16,869 | ) | (101,669 | ) | (16,869 | ) | |||||||||
An investment in our common stock involves a high degree of risk. You should consider carefully the following risk factors and the other information contained in this prospectus before you decide to purchase our common stock. Additional risks that are not currently known or foreseeable to us may materialize at a future date. The trading price of our common stock could decline if any of these risks or uncertainties occur and you might lose all or part of your investment.
Risks Related To Our Business
We have a history of operating losses and we expect to continue to incur losses and may never be profitable.
As of September 30, 2005, we had an accumulated deficit of approximately $198.5 million. We had net losses of $26.0 million and $44.7 million for the nine months ended September 30, 2005, and the year ended December 31, 2004, respectively. We have had operating losses since inception as a result of our significant clinical development, research and development, general and administrative, sales and marketing and business development expenses. We expect to incur losses for at least the next several years as we expand our sales and marketing capabilities and continue our clinical trials and research and development activities.
Our prospects for achieving profitability will depend primarily on how successful we are in executing our business plan to:
If we are not successful in executing our business plan, we may never achieve or may not sustain profitability.
We will be substantially dependent on sales of one product, Zanaflex Capsules, to generate revenue for the foreseeable future.
We currently derive substantially all of our revenue from the sale of Zanaflex Capsules and Zanaflex tablets, which are our only FDA-approved products. Although we currently distribute Zanaflex tablets, our marketing efforts are focused on Zanaflex Capsules and we do not, and do not intend to, actively promote Zanaflex tablets. As a result, prescriptions for Zanaflex tablets have declined and we expect that they will continue to decline. Our goal is to convert sales of Zanaflex tablets and generic tizanidine tablets to sales of Zanaflex Capsules. We believe that sales of Zanaflex Capsules will constitute a significant portion of our total revenue for the foreseeable future. If we are unable to convert tablet sales to capsule sales or are otherwise unable to increase our revenue from the sale of this product, our business, financial condition and results of operations could be adversely affected.
If we are unable to successfully differentiate Zanaflex Capsules from both Zanaflex tablets and generic tizanidine tablets we may not be able to increase sales of Zanaflex Capsules.
There are currently 11 generic versions of tizanidine tablets on the market and they are significantly cheaper than either Zanaflex Capsules or Zanaflex tablets. In 2004, these generic versions of tizanidine tablets constituted 95% of tizanidine sales in the United States. Although Zanaflex Capsules have a different pharmacokinetic profile when taken with food and are available in a higher dose than Zanaflex tablets and their generic equivalents, we may be unsuccessful in convincing prescribers, patients and third-party payors that these differences justify the higher price of Zanaflex Capsules. Prescribers may prescribe generic tizanidine tablets instead of Zanaflex Capsules, and third-party payors may establish unfavorable reimbursement policies for Zanaflex Capsules or otherwise seek
to encourage patients and prescribers to use generic tizanidine tablets instead of Zanaflex Capsules. In
addition, although the FDA has determined that neither Zanaflex tablets nor generic tizanidine tablets are therapeutically equivalent, or "AB-rated," to Zanaflex Capsules, it is possible that pharmacists may improperly fill prescriptions with generic tizanidine tablets or may seek to influence patients or physicians to change prescriptions from Zanaflex Capsules to generic tizanidine tablets. If we are unable to successfully differentiate Zanaflex Capsules from Zanaflex tablets and generic tizanidine tablets in the minds of prescribers, pharmacists, patients and third-party payors, our ability to generate meaningful revenue from this product will be adversely affected.
Our company has limited sales and marketing experience and we may not be successful in building an effective sales and marketing organization to market Zanaflex Capsules to specialty physicians.
As a company, we have limited sales and marketing experience, having only launched Zanaflex Capsules in April 2005. In order to successfully commercialize Zanaflex Capsules or any other products that we may bring to market, we will need to have adequate sales, marketing and distribution capabilities. OurAlthough we plan to expand our internal specialty sales force of 14 persons to approximately 30 persons in the first quarter of 2006, we may need to be significantly expandedfurther expand that sales force in the future. We may not be able to attract and train skilled sales and marketing personnel, in a timely manner or at all, or integrate and manage a growing sales and marketing organization.
Returns of Zanaflex tablets may adversely affect our results of operations.
Prior to the launch of generic tizanidine tablets in June 2002, wholesalers established larger than normal inventories of Zanaflex tablets. These inventories had expiration dates that extended to June 2005. Our return policy is to accept returns for six months before and 12 months after the product's expiration date. According to our Zanaflex asset purchase agreement with Elan, we are responsible for all returns of Zanaflex tablets after January 17, 2005. Zanaflex tablets sold by Elan can be returned to us through June 2006. In the year ended December 31, 2004, we took a $4.1 million charge to establish a reserve for expected returns of Zanaflex tablets sold by Elan. This charge is an estimate. If returns for products not sold by us are higher than we have estimated, we will have to record additional charges, which will adversely affect our results of operations.
Our product candidates must undergo rigorous clinical testing, the results of which are uncertain and could substantially delay or prevent us from bringing them to market.
Before we can obtain regulatory approval for a product candidate, we must undertake extensive clinical testing in humans to demonstrate safety and efficacy to the satisfaction of the FDA and other regulatory agencies. Clinical trials of new product candidates sufficient to obtain regulatory marketing approval are expensive and take years to complete, and the outcome of such trials is uncertain.
Clinical development of any product candidate that we determine to take into clinical trials may be curtailed, redirected, delayed or eliminated at any time for some or all of the following reasons:
A delay in or termination of any of our clinical development programs could have an adverse effect on our business.
If our Phase 3 clinical trials of Fampridine-SR are unsuccessful, or if we are unable to obtain regulatory approval for this product candidate or any approval is unduly limited in scope, our business prospects will be adversely affected.
In June 2005, we initiated a Phase 3 clinical trial for Fampridine-SR for the improvement of walking ability in patients with MS. In April 2004, we released results from a Phase 2 clinical trial designed to assess the relative safety and efficacy of varying doses of Fampridine-SR in MS. Our results did not reach statistical significance for the primary endpoint in this trial. Although we have designed the current Phase 3 clinical trial to address the difficulties we encountered in interpreting the patient data from the earlier trial, we cannot be sure that the results from our current clinical trial will be statistically significant.
To achieve the primary endpoint in our current Phase 3 clinical trial for MS, we need to show statistical improvement in the walking speed of the patients in the trial and that this improvement is both sustained and clinically meaningful to these patients. If we fail to achieve the primary endpoint in this clinical trial or the results are ambiguous, we will have to determine whether to re-design our MS trial and protocols and continue with additional testing, or cease development activities in this area. Redesigning the program could be extremely costly and time-consuming. Even if we are able to achieve the primary endpoint, we will need positive results from at least one other clinical trial to support the filing of a new drug application, or NDA, with the FDA. We cannot predict how long the second trial, or any additional trial that might be required by the FDA, will take or what the cost will be.
Our Phase 3 clinical trial for Fampridine-SR in MS is being conducted pursuant to a special protocol assessment, or SPA, with the FDA and the FDA has agreed that, if successful, this trial could qualify as one of the pivotal trials needed to support regulatory approval. This SPA may not be changed by either us or the FDA. However, if the FDA determines that a substantial scientific issue essential to determining the safety or efficacy of Fampridine-SR is identified after the trial began, the FDA may alter its conclusion on the adequacy of the protocol. In addition, even if the SPA remains in place and the trial meets its primary endpoint, the FDA could determine that the overall balance of risks and benefits for Fampridine-SR is not adequate to support approval, or only justifies approval for a narrow set of uses or approval with restricted distribution or other burdensome post-approval requirements and limitations. If the FDA denies approval of Fampridine-SR in MS, FDA approval is substantially delayed, approval is granted on a narrow basis or with restricted distribution or other burdensome post-approval requirements, or if the Fampridine-SR program is terminated, our business prospects will be adversely affected.
In March 2004, we completed two Phase 3 clinical trials of Fampridine-SR in SCI in which our results failed to reach their primary endpoints. We expect to resume development of Fampridine-SR for SCI after we have completed further development of the drug for MS. We cannot predict whether future clinical trials of Fampridine-SR in SCI will achieve their primary endpoints, how long these clinical trials will take or how much they will cost.
Our other drug development programs are in early stages of development and may never be commercialized.
All of our development programs other than Fampridine-SR are in the preclinical phase. Our future success depends, in part, on our ability to select promising product candidates, complete preclinical development of these product candidates and advance them to clinical trials. These product candidates will require significant development, preclinical studies and clinical trials, regulatory clearances and substantial additional investment before they can be commercialized.
Our preclinical programs may not lead to commercially viable products for several reasons. For example, we may fail to identify promising product candidates, our product candidates may fail to be safe and effective in preclinical tests or clinical trials, or we may have inadequate financial or other resources to pursue discovery and development efforts for new product candidates. In addition, because we have limited resources, we are focusing on product candidates that we believe are the most promising. As a result, we may delay or forego pursuit of opportunities with other product candidates. From time to time, we may establish and announce certain development goals for our product candidates and programs; however, given the complex nature of the drug discovery and development process, it is difficult to predict accurately if and when we will achieve these goals. If we are unsuccessful in advancing our preclinical programs into clinical testing or in obtaining regulatory approval, our long-term business prospects will be harmed.
The pharmaceutical industry is subject to stringent regulation and failure to obtain regulatory approval will prevent commercialization of our product candidates.
Our research, development, preclinical and clinical trial activities, as well as the manufacture and marketing of any products that we may successfully develop, are subject to an extensive regulatory approval process by the FDA and other regulatory agencies abroad. The process of obtaining required regulatory approvals for drugs is lengthy, expensive and uncertain, and any regulatory approvals may contain limitations on the indicated usage of a drug, distribution restrictions or may be conditioned on burdensome post-approval study or other requirements, including the requirement that we institute and follow a special risk management plan to monitor and manage potential safety issues, all of which may eliminate or reduce the drug's market potential. Post-market evaluation of a product could result in marketing restrictions or withdrawal from the market.
The results of preclinical and Phase 1 and Phase 2 clinical studies are not necessarily indicative of whether a product will demonstrate safety and efficacy in larger patient populations, as evaluated in Phase 3 clinical trials. Additional adverse events that could impact commercial success, or even continued regulatory approval, might emerge with more extensive post-approval patient use. Of the large number of drugs in development, only a small percentage result in the submission of an NDA to the FDA and even fewer are approved for commercialization.
In order to conduct clinical trials to obtain FDA approval to commercialize any product candidate, an IND application must first be submitted to the FDA and must become effective before clinical trials may begin. Subsequently, an NDA must be submitted to the FDA, including the results of adequate and well-controlled clinical trials demonstrating, among other things, that the product candidate is safe and effective for use in humans for each target indication. In addition, the manufacturing facilities used to produce the products must comply with current good manufacturing practices and must pass a pre-approval FDA inspection. Extensive submissions of preclinical and clinical trial data are required to demonstrate the safety, efficacy, potency and purity for each intended use. The FDA may refuse to accept our regulatory submissions for filing if they are incomplete.
Clinical trials are subject to oversight by institutional review boards and the FDA to ensure compliance with the FDA's good clinical practice requirements, as well as other requirements for the protection of clinical trial participants. We depend, in part, on third-party laboratories and medical institutions to conduct preclinical studies and clinical trials for our products and other third-party organizations to perform data collection and analysis, all of which must maintain both good laboratory
and good clinical practices required by regulators. If any such standards are not complied with in our clinical trials, the resulting data from the clinical trial may not be usable or we, an institutional review board or the FDA may suspend or terminate such trial, which would severely delay our development and possibly end the development of such product candidate. We also depend upon third party manufacturers of our products to qualify for FDA approval and to comply with good manufacturing practices required by regulators. We cannot be certain that our present or future manufacturers and suppliers will comply with current good manufacturing practices. The failure to comply with good
manufacturing practices may result in the termination of clinical studies, restrictions in the sale of, or withdrawal of the products from the market. Compliance by third parties with these standards and practices is outside of our direct control.
In addition, we are subject to regulation under other state and federal laws, including requirements regarding occupational safety, laboratory practices, environmental protection and hazardous substance control, and may be subject to other local, state, federal and foreign regulations. We cannot predict the impact of such regulations on us, although it could impose significant restrictions on our business and additional expenses to comply with these regulations.
Our products and product candidates may not gain market acceptance among physicians, patients and the medical community, thereby limiting our potential to generate revenue.
Market acceptance of our products and product candidates will depend on the benefits of our products in terms of safety, efficacy, convenience, ease of administration and cost effectiveness and our ability to demonstrate these benefits to physicians and patients. We believe market acceptance also depends on the pricing of our products and the reimbursement policies of government and third-party payors, as well as on the effectiveness of our sales and marketing activities. Physicians may not prescribe our products, and patients may determine, for any reason, that our products are not useful to them. For example, physicians may not believe that the benefits of Zanaflex Capsules outweigh their higher cost in relation to Zanaflex tablets or generic tizanidine tablets. The failure of any of our products or product candidates, once approved, to achieve market acceptance would limit our ability to generate revenue and would adversely affect our results of operations.
Our potential products may not be commercially viable if we fail to obtain an adequate level of reimbursement for these products by Medicaid, Medicare or other third-party payors.
Our commercial success will depend in part on third-party payors, such as government health administrative authorities, including Medicaid and Medicare, private health insurers and other such organizations, agreeing to reimburse patients for the cost of our products. Significant uncertainty exists as to the reimbursement status of newly-approved healthcare products. Our business would be materially adversely affected if the Medicaid program, Medicare program or other third-party payors were to deny reimbursement for our products or provide reimbursement only on unfavorable terms. Our business could also be adversely affected if the Medicaid program, Medicare program or other reimbursing bodies or payors limit the indications for which our products will be reimbursed to a smaller set of indications than we believe is appropriate.
Third-party payors frequently require that drug companies negotiate agreements with them that provide discounts or rebates from list prices. At present we do not have any such agreements with private third-party payors and only a small number of such agreements with government payors. If sales of Zanaflex Capsules increase we may need to offer larger discounts or discounts to a greater number of third-party payors to maintain acceptable reimbursement levels. If we were required to negotiate such agreements, there is no guarantee that we would be able to negotiate them at price levels that are profitable to us, or at all. If we are unsuccessful in maintaining reimbursement for our products at acceptable levels, our business will be adversely affected. In addition, if our competitors reduce the prices of their products, or otherwise demonstrate that they are better or more cost effective than our products,
this may result in a greater level of reimbursement for their products relative to our products, which would reduce our sales and adversely affect our results of operations.
We may experience pressure to lower prices on our approved products due to new and/or proposed federal legislation.
Federal legislation enacted in December 2003 added an outpatient prescription drug benefit to Medicare, effective January 2006. In the interim, Congress has established a discount drug card program for Medicare beneficiaries. Both benefits will be provided primarily through private entities,
which will attempt to negotiate price concessions from pharmaceutical manufacturers. These negotiations may increase pressure to lower prescription drug prices. While the new law specifically prohibits the U.S. government from interfering in price negotiations between manufacturers and Medicare drug plan sponsors, some members of Congress are pursuing legislation that would permit the U.S. government to use its enormous purchasing power to demand discounts from pharmaceutical companies, thereby creating de facto price controls on prescription drugs. In addition, the new law contains triggers for Congressional consideration of cost containment measures for Medicare in the event Medicare cost increases exceed a certain level. These cost containment measures could include limitations on prescription drug prices. This Medicare prescription drug coverage legislation, as well as additional healthcare legislation that may be enacted at a future date, could reduce our sales and adversely affect our results of operations.
If our competitors develop and market products that are more effective, safer or more convenient than our approved products, or obtain marketing approval before we obtain approval of future products, our commercial opportunity will be reduced or eliminated.
Competition in the pharmaceutical and biotechnology industries is intense and is expected to increase. Composition of matter patents on tizanidine, the active ingredient in Zanaflex Capsules and Zanaflex tablets, expired in 2002. There are currently 11 generic versions of tizanidine tablets on the market. To the extent that we are not able to differentiate Zanaflex Capsules from Zanaflex tablets and generic tizanidine tablets and/or pharmacists improperly substitute generic tizanidine tablets when filling prescriptions for Zanaflex Capsules, we may be unable to convert a meaningful amount of sales of Zanaflex tablets and generic tizanidine tablets to Zanaflex Capsules and our ability to generate revenue from this product will be adversely affected. Although no other FDA-approved capsule formulation of tizanidine exists, another company could develop a capsule or other formulation of tizanidine that competes with Zanaflex Capsules.
Many biotechnology and pharmaceutical companies, as well as academic laboratories, are involved in research and/or product development for various neurological diseases, including MS and SCI. We are aware of a company developing a sodium/potassium channel blocker and a second company developing an immediate release form of fampridine, both of which may compete with Fampridine-SR, if approved. In certain circumstances, pharmacists are not prohibited from formulating certain drug compounds to fill prescriptions on an individual patient basis. We are aware that at present compounded fampridine is used by some people with MS or SCI and it is possible that some people will want to continue to use compounded formulations even if Fampridine-SR is approved. Several companies are engaged in developing products that include novel immune system approaches and cell transplant approaches to remyelination for the treatment of people with MS. These programs are in early stages of development and may compete in the future with Fampridine-SR or our preclinical candidates.
Our competitors may succeed in developing products that are more effective, safer or more convenient than our products or the ones we have under development or that render our approved or proposed products or technologies noncompetitive or obsolete. In addition, our competitors may achieve product commercialization before we do. If any of our competitors develops a product that is more effective, safer or more convenient for patients, or is able to obtain FDA approval for
commercialization before we do, we may not be able to achieve market acceptance for our products, which would adversely affect our ability to generate revenues and recover the substantial development costs we have incurred and will continue to incur.
Our products may be subject to competition from lower-priced versions of such products and competing products imported into the United States from Canada, Mexico and other countries where there are government price controls or other market dynamics that make the products lower priced.
Our operations could be curtailed if we are unable to obtain any necessary additional financing on favorable terms or at all.
On September 30, 2005, on a pro forma as-adjusted basis after giving effect to this offering and our entry into our revenue interest assignment arrangement with PRF, we would have had approximately $ million in cash, cash equivalents and short-term investments. Although we anticipate this will be sufficient to fund our operations for approximately the next 24 months, we have several product candidates in various stages of development, and all will require significant further investment to develop, test and obtain regulatory approval prior to commercialization. We will likely need to seek additional equity or debt financing or strategic collaborations to continue our product development activities, and could require substantial funding to commercialize any products that we successfully develop. We may also require additional financing to support and expand our commercialization of Zanaflex Capsules. We do not currently have any funding commitments or arrangements with third parties to provide funding. We may not be able to raise additional capital on favorable terms or at all.
To the extent that we are able to raise additional capital through the sale of equity securities, the issuance of those securities would result in dilution to our stockholders. Holders of such new equity securities may also have rights, preference or privileges that are senior to yours. If additional capital is raised through the incurrence of indebtedness, we may become subject to various restrictions and covenants that could limit our ability to respond to market conditions, provide for unanticipated capital investments or take advantage of business opportunities. To the extent funding is raised through collaborations or intellectual property-based financings, we may be required to give up some or all of the rights and related intellectual property to one or more of our products, product candidates or preclinical programs. If we are unable to obtain sufficient financing on favorable terms when and if needed, we may be required to reduce, defer or discontinue one or more of our product development programs or devote fewer resources to marketing Zanaflex Capsules.
Under our financing arrangement with PRF, upon the occurrence of certain events, PRF may require us to repurchase the right to receive revenues that we assigned to it or may foreclose on certain assets that secure our obligations to PRF. Any exercise by PRF of its right to cause us to repurchase the assigned right or any foreclosure by PRF could adversely affect our results of operations and our financial condition.
On December 23, 2005, we entered into a Revenue Interests Assignment Agreementrevenue interests assignment agreement with PRF pursuant to which we assigned to PRF the right to receive a portion of our net revenues from Zanaflex Capsules, Zanaflex tablets and any future Zanaflex products. To secure our obligations to PRF, we also granted PRF a security interest in substantially all of our assets related to Zanaflex.
Under our arrangement with PRF, upon the occurrence of certain events, including if we experience a change of control, undergo certain bankruptcy events, transfer any of our interests in Zanaflex (other than pursuant to a license agreement, development, commercialization, co-promotion, collaboration, partnering or similar agreement), transfer all or substantially all of our assets, or breach certain of the covenants, representations or warranties under the Revenue Interests Assignment Agreement,revenue interests assignment agreement, PRF may (i) require us to repurchase the rights we assigned to it at the "put/call price" in effect on the date such right is exercised or (ii) foreclose on the Zanaflex assets that secure our obligations to PRF. Except in the case of certain bankruptcy events, if PRF exercises its right to cause us to repurchase the rights we assigned to it, PRF may not foreclose unless we fail to pay the put/call price as required. The put/call price on a given date is the greater of (i) 150% of all payments made by
PRF to us as of such date, less all payments received by PRF from us as of such date, and (ii) an amount that would generate an internal rate of return to PRF of 25% on all payments made by PRF to us as of such date, taking into account the amount and timing of all payments received by PRF from us as of such date.
If PRF were to exercise its right to cause us to repurchase the right we assigned to it, we cannot assure you that we would have sufficient funds available to pay the put/call price in effect at that time. Even if we have sufficient funds available, we may have to use funds that we planned to use for other purposes and our results of operations and financial condition could be adversely affected. If PRF were to foreclose on the Zanaflex assets that secure our obligations to PRF, our results of operations and
financial condition could also be adversely affected. Because PRF's right to cause us to repurchase the rights we assigned to it is triggered by, among other things, a change in control, transfer of any of our interests in Zanaflex (other than pursuant to a license agreement, development, commercialization, co-promotion, collaboration, partnering or similar agreement) or transfer of all or substantially all of our assets, the existence of that right could discourage us or a potential acquirer from entering into a business transaction that would result in the occurrence of any of those events.
The loss of our key management and scientific personnel may hinder our ability to execute our business plan.
Our success depends on the continuing contributions of our management team and scientific personnel, and maintaining relationships with our scientific and medical network and the network of centers in the United States and Canada that conducts our clinical trials. We are highly dependent on the services of Dr. Ron Cohen, our President and Chief Executive Officer, as well as the other principal members of our management and scientific staff. Our success depends in large part upon our ability to attract and retain highly qualified personnel. We face intense competition in our hiring efforts with other pharmaceutical and biotechnology companies, as well as universities and nonprofit research organizations, and we may have to pay higher salaries to attract and retain qualified personnel. With the exception of Dr. Ron Cohen, we do not maintain "key man" life insurance policies on the lives of our officers, directors or employees. The loss of one or more of our key employees, or our inability to attract additional qualified personnel, could substantially impair our ability to implement our business plan.
We face an inherent risk of liability in the event that the use or misuse of our products results in personal injury or death.
If the use or misuse of Zanaflex Capsules or any other FDA-approved products we may sell in the future harms people, we may be subject to costly and damaging product liability claims brought against us by consumers, healthcare providers, pharmaceutical companies, third-party payors or others. The use of our product candidates in clinical trials could also expose us to product liability claims. We currently maintain a product liability insurance policy that includes coverage of our clinical trials. This insurance policy has a $10 million per claim limit and the aggregate amount of claims under the policy is also capped at $10 million. We cannot predict all of the possible harms or side effects that may result from the use of our products or the testing of product candidates and, therefore, the amount of insurance coverage we currently have may not be adequate to cover all liabilities or defense costs we might incur. A product liability claim or series of claims brought against us could give rise to a substantial liability that could exceed our resources. Even if claims are not successful, the costs of defending such claims and potential adverse publicity could be harmful to our business.
We are subject to various federal and state laws regulating the marketing of Zanaflex Capsules and, if we do not comply with these regulations, we could face substantial penalties.
Our sales, promotion and other activities related to Zanaflex Capsules, or any of our other products under development following their regulatory approval, are subject to regulatory and law enforcement authorities in addition to the FDA, including the Federal Trade Commission, the
Department of Justice, and state and local governments. We are subject to various federal and state laws pertaining to health care "fraud and abuse," including both federal and state anti-kickback laws. Anti-kickback laws make it illegal for a prescription drug manufacturer to solicit, offer, receive or pay any remuneration as an inducement for the referral of business, including the use, recommendation, purchase or prescription of a particular drug. The federal government has published regulations that identify "safe harbors" or exemptions for certain payment arrangements that do not violate the anti-kickback statutes. Although we seek to comply with these statutes, it is possible that our practices, or those of our contract sales force, might be challenged under anti-kickback or similar laws. Violations of fraud and abuse laws may be punishable by civil or criminal sanctions, including fines and civil monetary penalties, and future exclusion from participation in government healthcare programs.
We may be subject to penalties if we fail to comply with post-approval legal and regulatory requirements and our products could be subject to restrictions or withdrawal from the market.
Any product for which we currently have or may obtain marketing approval, along with the associated manufacturing processes, any post-approval clinical data that we might be required to collect and the advertising and promotional activities for the product, are subject to continual recordkeeping and reporting requirements, review and periodic inspections by the FDA and other regulatory bodies. Regulatory approval of a product may be subject to limitations on the indicated uses for which the product may be marketed or to other restrictive conditions of approval that limit our ability to promote, sell or distribute a product. Furthermore, any approval may contain requirements for costly post-marketing testing and surveillance to monitor the safety or efficacy of the product.
We have an outstanding commitment with the FDA, inherited from Elan, to evaluate Zanaflex Capsules for pediatric use by December 2005February 2007, in accordance with the requirements of the Pediatric Research Equity Act. We intendAct, or PREA. The NDA for Zanaflex Capsules was approved with a plan to discuss this matter withaddress the FDA and seek a deferral or waiverrequirements of the requirementPREA through a pediatric pharmacokinetic study. We have submitted a proposed design for this pharmacokinetic study to conduct pediatric studies. Without a waiver,the FDA. Depending on the FDA's response to our submission or the outcome of this study, we willmay be required to conduct a pediatric study of Zanaflex Capsulesadditional studies. These studies could be more extensive and incurmore costly than the related costs of this clinical trial.currently-planned study.
Our advertising and promotion are subject to stringent FDA rules and oversight. In particular, the claims in our promotional materials and activities must be consistent with the FDA approvals for our products, and must be appropriately substantiated and fairly balanced with information on the safety risks and limitations of the products. Any free samples we distribute to physicians must be carefully monitored and controlled, and must otherwise comply with the requirements of the Prescription Drug Marketing Act, as amended, and FDA regulations. We must continually review adverse event information that we receive concerning our drugs and make expedited and periodic adverse event reports to the FDA and other regulatory authorities.
In addition, the research, manufacturing, distribution, sale and promotion of drug and biological products are potentially subject to regulation by various federal, state and local authorities in addition to the FDA, including the Centers for Medicare and Medicaid Services, other divisions of the U.S. Department of Health and Human Services, the U.S. Department of Justice and individual U.S. Attorney offices within the Department of Justice, and state and local governments. For example, sales, marketing and scientific/educational grant programs must comply with the anti-kickback and fraud and abuse provisions of the Social Security Act, as amended, the False Claims Act, as amended, the privacy provisions of the Health Insurance Portability and Accountability Act and similar state laws. Pricing and rebate programs must comply with the Medicaid rebate requirements of the Omnibus Budget Reconciliation Act of 1990, as amended, and the Veterans Health Care Act of 1992, as amended. If products are made available to authorized users of the Federal Supply Schedule of the General Services Administration, additional laws and requirements apply. All of these activities are also potentially subject to federal and state consumer protection and unfair competition laws.
We may be slow to adapt, or we may not be able to adapt, to changes in existing regulatory requirements or adoption of new legal or regulatory requirements or policies. Later discovery of
previously unknown problems with our products, manufacturing processes, or failure to comply with regulatory requirements, may result in:
In addition, the FDA or another regulatory agency may conduct periodic unannounced inspections. If they determine that we are not in compliance with applicable requirements, they may issue a notice of inspectional observations. If the observations are significant, we may have to devote significant resources to respond and undertake appropriate corrective and preventive actions, which could adversely affect our business prospects. For example, the FDA recently completed an inspection relating to our adverse event and product complaint handling and reporting for Zanaflex. The FDA has informed us that there are several observations that they will be including in a Form 483, Inspectional Observations. We have completed or expect to complete shortly all necessary corrective actions. The cost of the corrective actions is not expected to be material.
State pharmaceutical marketing compliance and reporting requirements may expose us to regulatory and legal action by state governments or other government authorities.
In recent years, several states, including California, Vermont, Maine, Minnesota, New Mexico and West Virginia, have enacted legislation requiring pharmaceutical companies to establish marketing compliance programs and file periodic reports with the state on sales, marketing, pricing and other activities. For example, California has enacted a statute requiring pharmaceutical companies to adopt a comprehensive compliance program that is in accordance with the Office of Inspector General of the Department of Health and Human ServicesCompliance Program Guidance for Pharmaceutical Manufacturers. This compliance program must include policies for compliance with the Pharmaceutical Research and Manufacturers of AmericaCode on Interactions with Healthcare Professionals, as well as a specific annual dollar limit on gifts or other items given to individual healthcare professionals in California. The law requires posting policies on a company's public web site along with an annual declaration of compliance.
Vermont, Maine, Minnesota, New Mexico, and West Virginia have also enacted statutes of varying scope that impose reporting and disclosure requirements upon pharmaceutical companies pertaining to drug pricing and payments and costs associated with pharmaceutical marketing, advertising and promotional activities, as well as restrictions upon the types of gifts that may be provided to healthcare practitioners. Similar legislation is being considered in other states. Many of these requirements are new and uncertain and the penalties for failure to comply with these requirements are unclear. We are not aware of any companies against which fines or penalties have been assessed under these state reporting and disclosure laws to date. We are currently in the process of developing a formal compliance infrastructure and standard operating procedures to comply with such laws. Unless we are in full compliance with these laws, we could face enforcement action and fines and other penalties, and could receive adverse publicity.
If we seek to market our products in foreign jurisdictions, we will need to obtain regulatory approval in these jurisdictions.
In order to market our products in the European Union and many other foreign jurisdictions, we must obtain separate regulatory approvals and comply with numerous and varying regulatory requirements. Approval procedures vary among countries and can involve additional clinical testing. The time required to obtain approval may differ from that required to obtain FDA approval. Should we decide to market our products abroad, we may fail to obtain foreign regulatory approvals on a timely basis, if at all. Approval by the FDA does not ensure approval by regulatory authorities in other countries, and approval by one foreign regulatory authority does not ensure approval by regulatory authorities in other foreign countries or by the FDA. We may not be able to file for, and may not receive, necessary regulatory approvals to commercialize our products in any foreign market, which could adversely affect our business prospects.
If we use biological and hazardous materials in a manner that causes injury, we may be liable for damages.
Our research and development activities involve the controlled use of potentially harmful biological materials, hazardous materials and chemicals that are subject to federal, state and local laws and regulations governing their use, storage, handling and disposal. These materials include ketamine, buprinex,buprenophine, sodium peantabarbitol,pentobarbital, ether, acetonitrile, hexanes, chloroform, xylene, dehydrated alcohol, xylene petroleum, ether methanol, ethyl alcohol, acetonitrile UV, hexanes, chloroform, alcohol-propyl, alcohol isopropylisopropanol and ether formaldehyde solution 37%.formaldehyde. We cannot completely eliminate the risk of accidental contamination or injury from the use, storage, handling or disposal of these materials. If we fail to comply with environmental regulations, we could be subject to criminal sanctions and/or substantial liability for any damages that result, and any substantial liability could exceed our resources. We currently maintain a general liability insurance policy that has a $2 million per claim limit and also caps aggregate claims at $2 million. In addition, we have an umbrella insurance policy that covers up to $9 million of liability in excess of the general liability policy's $2 million limit. This amount of insurance coverage may not be adequate to cover all liabilities or defense costs we might incur. In addition, the cost of compliance with environmental and health and safety regulations may be substantial.
Risks Related to Our Dependence on Third Parties
We currently have no manufacturing capabilities and are substantially dependent upon Elan, Novartis and other third party suppliers to manufacture Zanaflex Capsules, Zanaflex tablets and Fampridine-SR.
We do not own or operate, and currently do not plan to own or operate, manufacturing facilities for production of Zanaflex Capsules, Zanaflex tablets or Fampridine-SR. We rely and expect to continue to rely on third parties for the production of our products and clinical trial materials.
We rely on a single manufacturer, Elan, for the supply of Zanaflex Capsules. Zanaflex Capsules are manufactured using Elan's proprietary SODAS (spheroidal oral drug absorption system) multiparticulate drug delivery technology. Elan is obligated, in the event of a failure to supply Zanaflex Capsules, to use commercially reasonable efforts to assist us in either producing Zanaflex Capsules ourselves or in transferring production of Zanaflex Capsules to a third-party manufacturer, provided that such third-party manufacturer is not a technological competitor of Elan. In the event production is transferred to a third party, the FDA may require us to demonstrate through bioequivalence studies and laboratory testing that the product made by the new supplier is equivalent to the current Zanaflex Capsules before we could distribute products from that supplier. The process of transferring the technology and qualifying the new supplier could take a year or more.
Under our supply agreement with Elan, we provide Elan with monthly written 18-month forecasts and with annual written two-year forecasts of our supply requirements for Zanaflex Capsules. In each of the five months following the submission of our written 18-month forecast we are obligated to purchase the quantity specified in the forecast, even if our actual requirements are greater or less. Elan is not obligated to supply us with quantities in excess of our forecasted amounts, although it has agreed to use commercially reasonable efforts to do so. Because we have a limited history of selling Zanaflex Capsules, our forecasts of our supply requirements may be inaccurate. As a result, we may have an excess or insufficient supply of Zanaflex Capsules.
The Elan facility located in Gainesville, Georgia, which is responsible for bottling Zanaflex Capsules, has been operating under a court-ordered consent decree and injunction since 2001, which were imposed following adverse FDA inspections and FDA allegations that the facility was failing to comply with current good manufacturing requirements. These prior issues were not related to the manufacture of our products. If, however, Elan fails to comply with the requirements of the consent decree and injunction, it could be held in contempt and the facility could be shut down and the manufacturing of our products halted or interrupted.
We currently rely on Novartis for our supply of Zanaflex tablets and tizanidine, the active pharmaceutical ingredient, or API, in both Zanaflex Capsules and Zanaflex tablets. Under a supply
agreement we assumed from Elan, Novartis is responsible for manufacturing Zanaflex tablets and
tizanidine for us through February 2007. This includes the tizanidine that Elan uses to manufacture Zanaflex Capsules for us. Novartis currently produces tizanidine, but has arranged with another party to formulate Zanaflex tablets. We have arranged for another company, Sharp Corporation, ("Sharp"), to package and bottle Zanaflex tablets. Novartis has informed us that it intends to discontinue production of tizanidine by the end of 2005.the first quarter of 2006. It is our understanding that Novartis is currently in the process of qualifying an alternativetransferring the methods of manufacturing tizanidine manufacturer.to Rohner, a manufacturer in Pratteln, Switzerland. We have established relationshipsalso identified an alternate source for tizanidine in collaboration with the companies that currently formulate, bottle and package the tablets, however, weElan but do not have a relationshipan agreement with anthat alternative manufacturer of tizanidine.source or any other alternate manufacturer. By the expiration of our contract with Novartis in 2007, we will need to have established a direct relationship with an alternative supplier of tizanidine.tizanidine for Zanaflex tablets if we want them to continue to be manufactured.
We also rely exclusively on Elan to supply us with our requirements for Fampridine-SR. Elan relies on a third-party manufacturer to supply fampridine, the API in Fampridine-SR. Under our supply agreement with Elan, we are obligated to purchase at least 75% of our yearly supply of Fampridine-SR from Elan, and we are required to make compensatory payments if we do not purchase 100% of our requirements from Elan, subject to certain exceptions. We and Elan have agreed that we may purchase up to 25% of our annual requirements from Patheon, Inc., a mutually agreed-upon and qualified second manufacturing source, without compensatory payment.
Our dependence on others to manufacture our marketed products and clinical trial materials may adversely affect our ability to develop and commercialize our products on a timely and competitive basis.
If third-party contract research organizations do not perform in an acceptable and timely manner, our preclinical testing or clinical trials could be delayed or unsuccessful.
We do not have the ability to conduct all aspects of our preclinical testing or clinical trials ourselves. We rely and will continue to rely on clinical investigators, third-party contract research organizations and consultants to perform some or all of the functions associated with preclinical testing or clinical trials. The failure of any of these vendors to perform in an acceptable and timely manner in the future, including in accordance with any applicable regulatory requirements, such as good clinical and laboratory practices, or preclinical testing or clinical trial protocols, could cause a delay or otherwise adversely affect on our preclinical testing or clinical trials and ultimately on the timely advancement of our development programs.
We rely on a third party to provide the sales representatives to market Zanaflex Capsules to primary care physicians.
We recently entered into a contract with Cardinal Health pursuant to which it provides us with approximately 160 sales representatives who market Zanaflex Capsules to primary care physicians. These sales representatives are not our employees and we do not have control over their performance or compliance with applicable laws. Their failure to increase prescriptions for Zanaflex Capsules from the targeted primary care physicians would negatively impact our sales growth, and their failure to comply with applicable laws could subject us to liability.
Risks Related to Our Intellectual Property
If we cannot protect our intellectual property, our ability to develop and commercialize our products will be severely limited.
Our success will depend in part on our and our licensors' ability to obtain, maintain and enforce patent protection for the technologies, compounds and products, if any, resulting from our licenses and development programs. Without protection for the intellectual property we use, other companies could offer substantially identical products for sale without incurring the sizable discovery, development and
licensing costs that we have incurred. Our ability to recover these expenditures and realize profits upon the sale of products could be diminished.
We have in-licensed or are the assignee of more than 25 U.S. patents, more than 60 foreign patents and over 65 patent applications pending in the United States or abroad for our own technologies and for technologies from our in-licensed programs. The process of obtaining patents can be time consuming and expensive with no certainty of success. Even if we spend the necessary time and money, a patent may not issue or it may not have sufficient scope or strength to protect the technology it was intended to protect or to provide us with any commercial advantage. We may never be certain that we were the first to develop the technology or that we were the first to file a patent application for the particular technology because U.S. patent applications are confidential until they are published, and publications in the scientific or patent literature lag behind actual discoveries. The degree of future protection for our proprietary rights will remain uncertain if our pending patent applications are not approved for any reason or if we are unable to develop additional proprietary technologies that are patentable. Furthermore, third parties may independently develop similar or alternative technologies, duplicate some or all of our technologies, design around our patented technologies or challenge our issued patents or the patents of our licensors.
We may initiate actions to protect our intellectual property and in any litigation in which our patents or our licensors' patents are asserted, a court may determine that the patents are invalid or unenforceable. Even if the validity or enforceability of these patents is upheld by a court, a court may not prevent alleged infringement on the grounds that such activity is not covered by the patent claims. In addition, effective intellectual property enforcement may be unavailable or limited in some foreign countries. Any litigation, whether to enforce our rights to use our or our licensors' patents or to defend against allegations that we infringe third party rights, would be costly, time consuming, and may distract management from other important tasks.
As is commonplace in the biotechnology and pharmaceutical industry, we employ individuals who were previously employed at other biotechnology or pharmaceutical companies, including our competitors or potential competitors. To the extent our employees are involved in research areas that are similar to those areas in which they were involved at their former employers, we may be subject to claims that such employees and/or we have inadvertently or otherwise used or disclosed the alleged trade secrets or other proprietary information of the former employers. Litigation may be necessary to defend against such claims, which could result in substantial costs and be a distraction to management and which could have an adverse effect on us, even if we are successful in defending such claims.
We also rely in our business on trade secrets, know-how and other proprietary information. We seek to protect this information, in part, through the use of confidentiality agreements with employees, consultants, advisors and others. Nonetheless, those agreements may not provide adequate protection for our trade secrets, know-how or other proprietary information and prevent their unauthorized use or disclosure. To the extent that consultants, key employees or other third parties apply technological information independently developed by them or by others to our proposed products, disputes may arise as to the proprietary rights to such information which may not be resolved in our favor. The risk that other parties may breach confidentiality agreements or that our trade secrets become known or independently discovered by competitors, could adversely affect us by enabling our competitors, who may have greater experience and financial resources, to copy or use our trade secrets and other proprietary information in the advancement of their products, methods or technologies. Policing unauthorized use of our or our licensors' intellectual property is difficult, expensive and time-consuming, and we may be unable to determine the extent of any unauthorized use. Adequate remedies may not exist in the event of unauthorized use or disclosure.
If third parties successfully claim that we infringed their patents or proprietary rights, our ability to continue to develop and successfully commercialize our product candidates could be delayed.
Third parties may claim that we or our licensors or suppliers are infringing their patents or are misappropriating their proprietary information. In the event of a successful claim against us or our
licensors or suppliers for infringement of the patents or proprietary rights of others relating to any of our marketed products or product candidates, we may be required to:
In addition, from time to time, we become aware of third parties who have, or claim to have, intellectual property rights covering matters such as methods for doing business, conducting research, diagnosing diseases or prescribing medications that are alleged to be broadly applicable across sectors of the industry, and we may receive assertions that these rights apply to us. The existence of such intellectual property rights could present a risk to our business.
A license required under any patents or proprietary rights held by a third party may not be available to us, or may not be available on acceptable terms. If we or our licensors or suppliers are sued for infringement we could encounter substantial delays in, or be prohibited from developing, manufacturing and commercializing our product candidates and advancing our preclinical programs.
We are dependent on our license agreements and if we fail to meet our obligations under these license agreements, or our agreements are terminated for any reason, we may lose our rights to our in-licensed patents and technologies.
We are dependent on licenses for intellectual property related to Zanaflex, Fampridine-SR and all of our preclinical programs. Our failure to meet any of our obligations under these license agreements could result in the loss of our rights to this intellectual property. If we lose our rights under any of these license agreements, we may be unable to commercialize a product that uses licensed intellectual property.
We could lose our rights to Fampridine-SR under our license agreement with Elan in countries in which we have a license, including the United States, if we fail to file regulatory approvals within a commercially reasonable time after completion and receipt of positive data from all preclinical and clinical studies required for the related NDA, or any NDA-equivalent. We could also lose our rights under our license agreement with Elan if we fail to launch a product in such countries, within 180 days of NDA or equivalent approval. Elan could also terminate our license agreement if we fail to make payments due under the license agreement. If we lose our rights to Fampridine-SR our prospects for generating revenue and recovering our substantial investment in the development of this product would be materially harmed.
Risks Relating To The Offering
There is no existing market for our common stock. An active trading market may not develop and you may not be able to resell your shares at or above the initial offering price.
Prior to this offering, there has been no public market for our common stock. We cannot predict the extent to which trading will lead to the development of an active and liquid trading market in our common stock. The initial public offering price of our common stock was determined by negotiations between the representatives of the underwriters and us and may not be indicative of future market
prices. The market price for our common stock may decline below the initial offering price. Our stock price could fluctuate significantly due to a number of factors, including:
Many of these factors are beyond our control. In addition, the stock markets in general, and the Nasdaq National Market and the market for biopharmaceutical companies in particular, have experienced extreme price and volume fluctuations recently. These fluctuations often have been unrelated or disproportionate to the operating performance of these companies. These broad market and industry factors may adversely affect the market price of our common stock, regardless of our actual operating performance.
As a new investor, you will experience immediate and substantial dilution in the net tangible book value of your investment and may experience further dilution in the future.
The initial public offering price for this offering is substantially higher than the pro forma net tangible book value per share of our outstanding common stock. Investors purchasing shares of our common stock in this offering will pay more for their shares than the amount paid by existing stockholders who acquired shares prior to this offering. Accordingly, if you purchase common stock in this offering, you will incur immediate dilution in pro forma net tangible book value of approximately $ per share. If the holders of outstanding options or warrants exercise these options or warrants, you will incur further dilution. Investors purchasing shares of our common stock in this offering will contribute approximately % of the total amount we have raised since our inception, but will own only approximately % of our total common stock immediately following the completion of this offering.
Future sales of our common stock could cause our stock price to decline.
Sales of substantial amounts of our common stock in the public market after this offering, or the possibility of those sales or other distributions, could put downward pressure on the market price of our common stock. After the consummation of this offering, our current stockholders will be subject to a 180-day lock up on the sale of their shares. After the lock-up expires, based on the number of shares outstanding as of December 31, 2005, 19,698,104 shares of common stock will be eligible for sale subject to Rule 144, Rule 144(k) or Rule 701. The remaining 913,155 shares held by existing stockholders will be eligible for sale from time to time in the future under Rule 144, Rule 144(k) or Rule 701 and holders of 13,338,279 shares of our common stock will have rights to cause us to file a registration statement on their behalf and to include their shares in registration statements that we may file on our behalf or on behalf of other stockholders. By exercising their registration rights and selling a large number of shares, these holders could cause the price of our common stock to decline.
If our officers, directors and largest stockholders choose to act together, they may be able to control the outcome of a stockholder vote.
After this offering, our officers, directors and holders of 5% or more of our outstanding common stock will beneficially own approximately % of our common stock. Moreover, a majority of our directors are principals or representatives of entities that own substantial amounts of our common stock. As a result, these stockholders, acting together, will be able to significantly influence all matters requiring approval by our stockholders, including the election of directors and the approval or mergers or other business combination transactions. The interests of this group of stockholders may not always
coincide with the interests of other stockholders, and they may act in a manner that advances their best interests and not necessarily those of other stockholders.
Certain provisions of Delaware law, our certificate of incorporation and our by-laws may delay or prevent an acquisition of us that stockholders may consider favorable or may prevent efforts by our stockholders to change our directors or our management, which could decrease the value of your shares.
Following this offering, our certificate of incorporation and by-laws will contain provisions that could make it more difficult for a third party to acquire us, and may have the effect of preventing or hindering any attempt by our stockholders to replace our current directors or officers. These provisions include:
As a Delaware corporation, we are also subject to certain anti-takeover provisions of Delaware law. Under Delaware law, a corporation may not engage in a business combination with any holder of 15% or more of its capital stock unless the holders has held the stock for three years or, among other things, the board of directors has approved the transaction. Our board of directors could rely on Delaware law to prevent or delay an acquisition of us, which could have the effect of reducing your ability to receive a premium on your common stock.
Because we do not intend to pay dividends, you will benefit from an investment in our common stock only if it appreciates in value.
We have not paid cash dividends on any of our classes of capital stock to date, and we currently intend to retain our future earnings, if any, to fund the development and growth of our business. As a result, we do not expect to pay any cash dividends in the foreseeable future. The success of your investment in our common stock will depend entirely upon any future appreciation. There is no guarantee that our common stock will appreciate in value after the offering or even maintain the price at which you purchased your shares.
This prospectus, including the sections entitled "Summary," "Risk Factors," "Management's Discussion and Analysis of Financial Condition and Results of Operations," and "Business," contains forward-looking statements. These statements relate to future events or to our future financial performance, and involve known and unknown risks, uncertainties and other factors that may cause our actual results, levels of activity, performance, or achievements to be materially different from any future results, levels of activity, performance or achievements expressed or implied by these forward-looking statements. In some cases, you can identify forward-looking statements by the use of words such as "may," "could," "expect," "intend," "plan," "seek," "anticipate," "believe," "estimate," "predict," "potential," "continue," or the negative of these terms or other comparable terminology. You should not place undue reliance on forward-looking statements, since they involve known and unknown risks, uncertainties and other factors which are, in some cases, beyond our control and which could materially affect actual results, levels of activity, performance or achievements. Factors that may cause actual results to differ materially from current expectations, which we describe in more detail elsewhere in this prospectus under the heading "Risk Factors," include, but are not limited to:
If one or more of these or other risks or uncertainties materialize, or if our underlying assumptions prove to be incorrect, actual results may vary significantly from what we projected. Any forward-looking statement you read in this prospectus reflects our current views with respect to future events and is subject to these and other risks, uncertainties and assumptions relating to our operations, results of operations, growth strategy and liquidity. We assume no obligation to publicly update or revise these forward-looking statements for any reason, or to update the reasons actual results could differ materially from those anticipated in these forward-looking statements, even if new information becomes available in the future.
The safe harbor for forward-looking statements contained in the Securities Litigation Reform Act of 1995 protects companies from liability for their forward looking statements if they comply with the requirements of the Act. The Act does not provide this protection for initial public offerings.
We estimate that we will receive approximately $ million in net proceeds from the sale of our common stock in this offering, or approximately $ million if the underwriters exercise their over-allotment option in full, based on an assumed initial public offering price of $ per share (the midpoint of the estimated price range shown on the cover of this prospectus) after deducting the estimated underwriting discounts and commissions and estimated offering expenses payable by us.
We intend to use the proceeds of this offering as follows:
Under our revenue interest assignment arrangement with PRF, if this offering results in our having a total market capitalization in excess of $150.0 million, we will have the option, for 180 days, to repurchase PRF's rights at the "put/call price" in effect on the date such right is exercised. The put/call price on a given date is the greater of (i) 150% of the payments made by PRF to us as of such date, less all payments received by PRF from us as of such date, and (ii) an amount that would generate an internal rate of return to PRF of 25% of all payments made by PRF to us as of such date, taking into account the amount and timing of all payments received by PRF from us as of such date. We do not currently intend to exercise this option if it becomes exercisable, but we may reevaluate whether we would exercise the option during the 180-day period. If we do exercise any such option, we would use a portion of the proceeds from this offering to make the repayment. Unless earlier terminated, the revenue interest assignment arrangement will expire on December 31, 2015. We entered into our revenue interest assignment arrangement with PRF in order to provide additional immediate funding to support the commercialization of Zanaflex Capsules. All funds from the PRF transaction must be used for the commercialization and other activities and obligations related specifically to our Zanaflex operations. We currently intend to use $3 million of the PRF proceeds to pay a Zanaflex Capsules sales-based milestone due to Elan on March 31, 2006.
We expect that the proceeds of this offering will allow us to complete our current Fampridine-SR Phase 3 clinical trial. The amount and timing of our actual expenditures on sales and marketing and our research and development programs will depend on numerous factors, including the progress of our research and development activities, the progress of our clinical trials and regulatory approval process, the number and breadth of our product development programs, our success in marketing Zanaflex Capsules, and any in-licensing and acquisition activities. Our research programs are in an early stage of development and it is difficult to predict what advances, if any, we will make in our research activities using the proceeds of this offering. Accordingly, we will retain broad discretion in the allocation and use of the proceeds of this offering. Currently we have no specific plans or commitments related to any acquisitions or licenses.
Pending application of the net proceeds, we intend to invest them in short-term, investment-grade, interest-bearing instruments.
We have never declared or paid any cash dividends on our common stock. We currently intend to retain our future earnings, if any, to finance the further development and expansion of our business and do not intend to pay cash dividends for the foreseeable future. Any future determination to pay dividends will be at the discretion of our board of directors and will depend on our financial condition, results of operations, capital requirements, restrictions contained in current or future financing instruments and other factors our board of directors deems relevant.
The following table sets forth our cash, cash equivalents and short-term investments and capitalization as of September 30, 2005:
| | | As of September 30, 2005 | | As of September 30, 2005 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | Actual (unaudited) | Pro Forma (unaudited) | Pro Forma As Adjusted (unaudited) | | Actual (unaudited) | Pro Forma (unaudited) | Pro Forma As Adjusted (unaudited) | ||||||||||||
| | | (in thousands) | | (in thousands) | ||||||||||||||||
| Cash, cash equivalents and short-term investments | Cash, cash equivalents and short-term investments | $ | 8,741 | $ | 20,039 | $ | Cash, cash equivalents and short-term investments | $ | 8,741 | $ | 20,039 | $ | ||||||||
| Current portion of notes payable | Current portion of notes payable | 2,347 | 1,150 | |||||||||||||||||
| Revenue interest liability—PRF transaction | Revenue interest liability—PRF transaction | — | 14,600 | |||||||||||||||||
| Put/call option liability—PRF transaction | Put/call option liability—PRF transaction | — | 400 | |||||||||||||||||
| Long-term portion of notes payable | Long-term portion of notes payable | 3,534 | 1,731 | Long-term portion of notes payable | 3,534 | 1,731 | ||||||||||||||
| Long-term convertible notes payable—principal amount plus accrued interest, less unamortized debt discount—Related party | Long-term convertible notes payable—principal amount plus accrued interest, less unamortized debt discount—Related party | 8,695 | 8,695 | Long-term convertible notes payable—principal amount plus accrued interest, less unamortized debt discount—Related party | 8,695 | 8,695 | ||||||||||||||
| Mandatorily Redeemable Convertible Preferred Stock, $.001 par value: 7,472,612 shares of Series E convertible preferred stock authorized, issued and outstanding at September 30, 2005; 10,204,047 shares of Series I convertible preferred stock authorized, issued and outstanding at September 30, 2005; 112,790,246 shares of Series J convertible preferred stock authorized, 112,790,233 shares issued and outstanding at September 30, 2005; 1,533,330 shares of Series K convertible preferred stock authorized, 1,533,327 shares issued and outstanding at September 30, 2005; 0 shares issued and outstanding on a pro forma and pro forma as adjusted basis | 85,000 | — | ||||||||||||||||||
| Mandatorily Redeemable Convertible Preferred Stock, $.001 par value: 7,472,612 shares of Series E convertible preferred stock authorized, issued and outstanding at September 30, 2005; 10,204,047 shares of Series I convertible preferred stock authorized, issued and outstanding at September 30, 2005; 112,790,246 shares of Series J convertible preferred stock authorized, 112,790,233 shares issued and outstanding at September 30, 2005; 1,573,330 shares of Series K convertible preferred stock authorized, 1,533,327 shares issued and outstanding at September 30, 2005; 0 shares issued and outstanding on a pro forma and pro forma as adjusted basis | Mandatorily Redeemable Convertible Preferred Stock, $.001 par value: 7,472,612 shares of Series E convertible preferred stock authorized, issued and outstanding at September 30, 2005; 10,204,047 shares of Series I convertible preferred stock authorized, issued and outstanding at September 30, 2005; 112,790,246 shares of Series J convertible preferred stock authorized, 112,790,233 shares issued and outstanding at September 30, 2005; 1,573,330 shares of Series K convertible preferred stock authorized, 1,533,327 shares issued and outstanding at September 30, 2005; 0 shares issued and outstanding on a pro forma and pro forma as adjusted basis | 85,000 | — | |||||||||||||||||
| Stockholders' equity (deficit): | Stockholders' equity (deficit): | Stockholders' equity (deficit): | ||||||||||||||||||
| Non-redeemable Convertible Preferred Stock, $.001 par value: 1,306,068 shares of Series A convertible preferred stock; 900,000 shares of Series B convertible preferred stock; 333,333 shares of Series C convertible preferred stock; 0 shares of Series D preferred stock; 2,300,000 shares of Series F convertible preferred stock; 0 shares of Series G preferred stock; 1,575,229 shares of Series H convertible preferred stock; 0 shares issued and outstanding on a pro forma and pro forma as adjusted basis | 6 | — | Non-redeemable Convertible Preferred Stock, $.001 par value: 1,306,068 shares of Series A convertible preferred stock; 900,000 shares of Series B convertible preferred stock; 333,333 shares of Series C convertible preferred stock; 0 shares of Series D preferred stock; 2,300,000 shares of Series F convertible preferred stock; 0 shares of Series G preferred stock; 1,575,229 shares of Series H convertible preferred stock; 0 shares issued and outstanding on a pro forma and pro forma as adjusted basis | 6 | — | |||||||||||||||
| Common stock, $.001 par value; 260,000,000 shares authorized at September 30, 2005 and 80,000,000 shares authorized on a pro forma and on a pro forma as adjusted basis; 208,766 shares issued and outstanding at September 30, 2005, issued and outstanding on a pro forma basis and on a pro forma as adjusted basis, respectively | — | 13 | Common stock, $.001 par value; 200,000,000 shares authorized at September 30, 2005 and 80,000,000 shares authorized on a pro forma and on a pro forma as adjusted basis; 208,766 shares issued and outstanding at September 30, 2005, issued and outstanding on a pro forma basis and on a pro forma as adjusted basis, respectively | — | 13 | |||||||||||||||
| Additional paid-in capital | Additional paid-in capital | 96,808 | 181,801 | Additional paid-in capital | 96,806 | 181,801 | ||||||||||||||
| Accumulated deficit | Accumulated deficit | (198,475 | ) | (198,677 | ) | Accumulated deficit | (198,475 | ) | (198,677 | ) | ||||||||||
| Other comprehensive loss | Other comprehensive loss | (6 | ) | (6 | ) | Other comprehensive loss | (6 | ) | (6 | ) | ||||||||||
| Total stockholders' (deficit) | Total stockholders' (deficit) | (101,669 | ) | (16,869 | ) | Total stockholders' (deficit) | (101,669 | ) | (16,869 | ) | ||||||||||
| Total capitalization | Total capitalization | $ | (4,438 | ) | $ | (6,444 | ) | Total capitalization | $ | (2,093 | ) | $ | 9,707 | $ | ||||||
The table above excludes, as of September 30, 2005:
Our net tangible book deficit attributable to common stockholdersvalue as of September 30, 2005 was approximately $123.0$(123.0) million, or approximately $(9.08)$ per share based on 13,547,022 shares of common stock outstanding as of September 30, 2005, calculated after giving effect to the automatic conversion of all of our outstanding convertible preferred stock and mandatorily redeemable convertible preferred stock into 13,338,279 shares of common stock upon the closing of this offering. Net tangible book deficit per share represents our total tangible assets reduced by our total liabilities, mandatorily redeemable convertible preferred stock, deferred offering costs and the liquidation value of our convertible preferred stock and divided by the number of shares of common stock outstanding. Dilution per share to new investors represents the difference between the amount per share that you pay in this offering and the pro forma as adjusted net tangible book value per share immediately after this offering.
Our pro forma as adjusted net tangible book value as of September 30, 2005, would have been approximately $ million, or approximately $ per share, after giving effect to:
Net tangible book value per share represents our total tangible assets reduced by usour total liabilities, mandatorily redeemable convertible preferred stock, deferred offering costs and the liquidation value of our convertible preferred stock and divided by the number of shares of common stock outstanding. Dilution per share to new investors represents the difference between the amount per share that you pay for our common stock in this offering and the pro forma as adjusted net tangible book value per share of our common stock immediately after this offering.
Our pro forma as adjusted net tangible book value as of September 30, 2005, would have been approximately $ million, or approximately $ per share, after giving further effect to our sale of shares in this offering, assuming an initial public offering price of $ per share (the midpoint of the estimated price range shown on the cover of this prospectus), after deducting underwriting discounts and commissions and estimated offering expenses; and
expenses. This represents an immediate increase in net tangible book value of $ per share to existing stockholders and an immediate decrease in net tangible book value per share of $ to you. The following table illustrates the dilution.
| Assumed initial public offering price per share | $ | ||||||
$ | |||||||
Pro forma as adjusted increase in net tangible book value per share attributable to | $ | ||||||
Pro forma as adjusted net tangible book value per share after this offering | |||||||
| Dilution per share to new investors | $ | ||||||
If the underwriters exercise their over-allotment option in full, the pro forma net tangible book value per share after the offering would be $ per share, the increase in net tangible book value per share to existing stockholders would be $ per share and the dilution to new investors would be $ per share.
The following table sets forth, as of September 30, 2005, on a pro forma as adjusted basis, (i) the difference between existing stockholders and new investors with respect to thetotal number of shares of common stock purchased from us, after giving effect to this offering and the reverse stock split and automatic conversion of our outstanding preferred stock described above,
(ii) the total consideration paid to us, and (iii) the average price per share paid.paid by the existing stockholders and by new investors purchasing shares in this offering.
| | Shares Purchased | Total Consideration | | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Average Price Per Share | |||||||||||
| | Number | % | Amount | % | ||||||||
| Existing stockholders | 13,547,022 | % | $ | % | $ | |||||||
| New investors(1) | ||||||||||||
| Total | 100.0% | $ | 100.0% | |||||||||
The table above assumes no exercise of stock options or warrants outstanding as of September 30, 2005. At September 30, 2005, there were 1,816,518 shares of common stock issuable upon exercise of outstanding stock options and warrants at a weighted average exercise price of $5.13 per share. To the extent that outstanding options or warrants are exercised in the future, there will be further dilution to new investors. To the extent all of such outstanding options and warrants had been exercised as of September 30, 2005, pro forma as adjusted net tangible book value per share after this offering would be $ and total dilution per share to new investors would be $ .
The issuance of additional common stock will result in further dilution to new investors.
If the underwriters' over-allotment option is exercised in full, the number of shares of our common stock held by existing stockholders will be reduced to % of the aggregate number of shares of our common stock outstanding after this offering, and the number of shares of common stock held by new investors will be increased to or % of the aggregate number of shares of common stock outstanding after this offering.
SELECTED CONSOLIDATED FINANCIAL DATA
The selected consolidated statement of operations data for the fiscal years ended June 30, 2001, 2002 and 2003, six month period ended December 31, 2003, and the year ended December 31, 2004 and the selected consolidated balance sheet data presented below as of June 30, 2001, 2002 and 2003, and December 31, 2003 and 2004, set forth below are derived from, and are qualified by reference to, our consolidated financial statements other than the pro forma financial information, which have been audited by KPMG LLP, our Independent Registered Public Accounting Firm, and that are included elsewhere in this prospectus for the years ended June 30, 2002 and 2003, six months ended December 31, 2003 and year ended 2004.
We changed our fiscal year end from June 30 to December 31, effective for the six months ended December 31, 2003. The selected consolidated statement of operations data presented below for the nine months ended September 30, 2004 and 2005, and selected consolidated balance sheet data presented below as of September 30, 2005, have been derived from our unaudited consolidated financial statements included elsewhere in this prospectus. The unaudited consolidated financial information include, in the opinion of management, all adjustments, consisting of normal and recurring adjustments, that management considers necessary for a fair presentation, in all material respects, of its consolidated results for those periods. Our historical results are not necessarily indicative of the results to be expected in the future periods and the results for the nine months ended September 30, 2005, should not be considered indicative of results expected for the full year.
This data should be read in conjunction with our "Management's Discussion and Analysis of Financial Condition and Results of Operations" and our Consolidated Financial Statements and the related notes included elsewhere in this prospectus.
Pro forma per share amounts in the following table reflect the conversion of our outstanding convertible and mandatorily redeemable convertible preferred stock into 13,338,279 shares of common stock upon completionon the closing of this offering, assuming that shares of our preferred stock were outstanding for the entire periods presented. Pro forma balance sheet data amounts in the following table reflect the conversion of our outstanding convertible and mandatorily redeemable convertible preferred stock, as well as our entry into a revenue interest assignment arrangement with PRF on December 23, 2005, including (i) our receipt at signing of a payment in the amount of $15.0 million, (ii) our use of approximately $3.0 million of that payment to repay a portion of the amount we owe to GE Capital and approximately $700,000 of that payment to pay fees and expenses related to the transaction, including expenses incurred by PRF, and (iii) our recognition of a short-termrevenue interest liability of approximately $11.3 million.$14.6 million, (iv) our recognition of a put/call option liability of approximately $400,000, and (v) our capitalization of approximately $500,000 in fees and expenses related to the transaction.
| | | | | | | Nine Months Ended September 30, | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | | | Six Months Ended December 31, | | |||||||||||||||||||
| | Year Ended June 30, | Year Ended December 31, | ||||||||||||||||||||||
| | 2004 | 2005 | ||||||||||||||||||||||
| | 2001 | 2002 | 2003 | 2003 | 2004 | (unaudited) | ||||||||||||||||||
| | ||||||||||||||||||||||||
| | (in thousands, except per share data) | |||||||||||||||||||||||
| Statement of Operations Data: | ||||||||||||||||||||||||
| Gross sales—Zanaflex | $ | — | $ | — | $ | — | $ | — | $ | — | $ | — | $ | 3,239 | ||||||||||
| Less: discounts and allowances | — | — | — | — | (4,417 | ) | (144 | ) | (992 | ) | ||||||||||||||
| Net sales | — | — | — | — | (4,417 | ) | (144 | ) | 2,247 | |||||||||||||||
| Grant revenue | 462 | 132 | 474 | 382 | 479 | 445 | 184 | |||||||||||||||||
| Total net revenue | 462 | 132 | 474 | 382 | (3,938 | ) | (301 | ) | 2,431 | |||||||||||||||
| Less: cost of sales | — | — | — | — | (885 | ) | (363 | ) | (2,274 | ) | ||||||||||||||
| Gross profit | 462 | 132 | 474 | 382 | (4,823 | ) | (62 | ) | 157 | |||||||||||||||
Operating expenses: | ||||||||||||||||||||||||
| Research and development | 6,142 | 11,147 | 17,527 | 16,743 | 21,999 | 18,621 | 9,652 | |||||||||||||||||
| Research and development—related party | 2,223 | 4,687 | 2,265 | 3,343 | — | — | — | |||||||||||||||||
| Sales and marketing | — | — | — | — | 4,662 | 2,793 | 9,657 | |||||||||||||||||
| General and administrative | 3,489 | 6,636 | 6,388 | 17,069 | 13,283 | 11,034 | 6,339 | |||||||||||||||||
| Total operating expenses | 11,854 | 22,470 | 26,180 | 37,155 | 39,944 | 32,448 | 25,648 | |||||||||||||||||
| Operating loss | (11,392 | ) | (22,338 | ) | (25,706 | ) | (36,773 | ) | (44,767 | ) | (32,510 | ) | (25,491 | ) | ||||||||||
Other income (expense): | ||||||||||||||||||||||||
| Interest and amortization of debt discount expense | — | — | (78 | ) | (38 | ) | (385 | ) | (297 | ) | (824 | ) | ||||||||||||
| Interest and amortization of debt discount expense—related party | (443 | ) | (408 | ) | (369 | ) | (184 | ) | — | — | — | |||||||||||||
| Interest income | 1,824 | 984 | 393 | 276 | 409 | 329 | 347 | |||||||||||||||||
| Other income | — | — | 26 | 7 | 2 | 2 | 1 | |||||||||||||||||
| Total other income (expense) | 1,381 | 576 | (28 | ) | 61 | 26 | 34 | (476 | ) | |||||||||||||||
| Minority interest—related party | 699 | 580 | — | — | — | — | — | |||||||||||||||||
| Cumulative effect of change in accounting principle | — | — | — | — | — | — | 3 | |||||||||||||||||
| Net loss | (9,313 | ) | (21,181 | ) | (25,734 | ) | (36,712 | ) | (44,741 | ) | (32,476 | ) | (25,964 | ) | ||||||||||
Beneficial conversion feature, accretion of issuance costs, preferred dividends, and fair value of warrants issued to convertible preferred stockholders | (36 | ) | (55 | ) | (24,320 | ) | (11,985 | ) | (24,746 | ) | (18,496 | ) | (18,636 | ) | ||||||||||
| Net loss allocable to common stockholders | $ | (9,349 | ) | $ | (21,236 | ) | $ | (50,054 | ) | $ | (48,697 | ) | $ | (69,487 | ) | $ | (50,972 | ) | $ | (44,600 | ) | |||
| Net loss per share allocable to common stockholders—basic & diluted | $ | (50.81 | ) | $ | (111.90 | ) | $ | (261.38 | ) | $ | (252.87 | ) | $ | (351.76 | ) | $ | (259.22 | ) | $ | (221.17 | ) | |||
| | | | | | | Nine Months Ended September 30, | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | | | Six Months Ended December 31, | | ||||||||||||
| | Year Ended June 30, | Year Ended December 31, | |||||||||||||||
| | 2004 | 2005 | |||||||||||||||
| | 2001 | 2002 | 2003 | 2003 | 2004 | (unaudited) | |||||||||||
| | |||||||||||||||||
| Pro forma net loss per share allocable to common stockholders—basic & diluted (unaudited)(1) | $ | (9.63 | ) | $ | (1.92 | ) | |||||||||||
| Weighted average shares of common stock outstanding used in computing net loss per share allocable to common stockholders—basic & diluted | 184 | 190 | 191 | 193 | 198 | 197 | 202 | ||||||||||
| Weighted average shares of common stock outstanding used in computing pro forma net loss per share allocable to common stockholders—basic & diluted (unaudited)(1)(2) | 13,536 | 13,547 | |||||||||||||||
| | As of June 30, | As of December 31, | As of September 30, | Pro Forma As of September 30, | As of June 30, | As of December 31, | As of September 30, | Pro Forma As of September 30, | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | 2001 | 2002 | 2003 | 2003 | 2004 | 2005 | 2005 | 2001 | 2002 | 2003 | 2003 | 2004 | 2005 | 2005 | ||||||||||||||||||||||||||||||
| | (in thousands) | (unaudited) | (in thousands) | (unaudited) | ||||||||||||||||||||||||||||||||||||||||
| Consolidated Balance Sheet Data: | ||||||||||||||||||||||||||||||||||||||||||||
| Cash and cash equivalents | $ | 48,083 | $ | 27,012 | $ | 48,319 | $ | 8,965 | $ | 11,729 | $ | 3,581 | $ | 14,879 | $ | 48,083 | $ | 27,012 | $ | 48,319 | $ | 8,965 | $ | 11,729 | $ | 3,581 | $ | 14,879 | ||||||||||||||||
| Restricted cash | 243 | 250 | 253 | 254 | 257 | 261 | 261 | 243 | 250 | 253 | 254 | 257 | 261 | 261 | ||||||||||||||||||||||||||||||
| Short-term investments | — | 2,836 | 12,250 | 32,250 | 9,397 | 5,160 | 5,160 | — | 2,836 | 12,250 | 32,250 | 9,397 | 5,160 | 5,160 | ||||||||||||||||||||||||||||||
| Capitalized transaction costs—PRF transaction | — | — | — | — | — | — | 500 | |||||||||||||||||||||||||||||||||||||
| Working capital | 46,115 | 27,097 | 58,975 | 35,375 | 9,067 | (12,203 | ) | (10,506 | ) | 46,115 | 27,097 | 58,975 | 35,375 | 9,067 | (12,203 | ) | (14,207 | ) | ||||||||||||||||||||||||||
| Total assets | 50,349 | 33,597 | 64,807 | 45,960 | 30,982 | 25,543 | 37,342 | 50,349 | 33,597 | 64,807 | 45,960 | 30,982 | 25,543 | 37,842 | ||||||||||||||||||||||||||||||
| Deferred grant revenue | — | — | 95 | 48 | — | — | — | — | — | 95 | 48 | — | — | — | ||||||||||||||||||||||||||||||
| Deferred product revenue—Zanaflex Capsules | — | — | — | — | — | 4,960 | 4,960 | — | — | — | — | — | 4,960 | 4,960 | ||||||||||||||||||||||||||||||
| Deferred product revenue—Zanaflex tablets | — | — | — | — | 6,668 | 10,686 | 10,686 | — | — | — | — | 6,668 | 10,686 | 10,686 | ||||||||||||||||||||||||||||||
| Current portion of notes payable | — | — | 310 | 324 | 302 | 2,347 | 1,150 | — | — | 310 | 324 | 302 | 2,347 | 1,150 | ||||||||||||||||||||||||||||||
| Non-current portion of notes payable | — | — | 612 | 447 | 145 | 3,534 | 1,731 | — | — | 612 | 447 | 145 | 3,534 | 1,731 | ||||||||||||||||||||||||||||||
| Revenue interest liability | — | — | — | — | — | — | 11,299 | |||||||||||||||||||||||||||||||||||||
| Revenue interest liability—PRF transaction | — | — | — | — | — | — | 14,600 | |||||||||||||||||||||||||||||||||||||
| Put/call option liability—PRF transaction | — | — | — | — | — | — | 400 | |||||||||||||||||||||||||||||||||||||
| Long-term convertible notes payable—related party | 7,131 | 7,538 | 7,907 | 8,091 | 8,422 | 8,695 | 8,695 | 7,131 | 7,538 | 7,907 | 8,091 | 8,422 | 8,695 | 8,695 | ||||||||||||||||||||||||||||||
| Mandatorily redeemable preferred stock | 59,604 | 59,659 | 18,187 | 30,171 | 66,364 | 85,000 | — | 59,604 | 59,659 | 18,187 | 30,171 | 66,364 | 85,000 | — | ||||||||||||||||||||||||||||||
| Total stockholders' (deficit) | (19,041 | ) | (36,910 | ) | 35,328 | (130 | ) | (60,571 | ) | (101,669 | ) | (16,869 | ) | (19,041 | ) | (36,910 | ) | 35,328 | (130 | ) | (60,571 | ) | (101,669 | ) | (16,869 | ) | ||||||||||||||||||
MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL
CONDITION AND RESULTS OF OPERATIONS
The following discussion and analysis of our consolidated financial condition and results of operations should be read in conjunction with our audited consolidated financial statements and related notes included in this prospectus. This discussion and analysis contains forward-looking statements that are subject to risks, uncertainties and other factors, including, but not limited to, those discussed under "Risk Factors" and elsewhere in this prospectus, that could cause our actual results, performance, prospects or opportunities to differ materially from those expressed in, or implied by, these forward-looking statements. See "Forward-Looking Statements."
Background
Since we commenced operations in 1995, we have devoted substantially all of our resources to the identification, development and commercialization of novel therapies that improve neurological function in people with MS, SCI and other disorders of the CNS. Our marketed drug, Zanaflex Capsules, is FDA-approved for the management of spasticity. Our lead product candidate, Fampridine-SR, is in a Phase 3 clinical trial for the improvement of walking ability in people with MS. Our preclinical programs also target MS and SCI, as well as other CNS disorders, including stroke and traumatic brain injury.
From 1995 until mid-2004, we were engaged almost exclusively in the in-licensing of compounds and the preclinical and clinical development of these compounds. We licensed the rights to Fampridine-SR from Elan for the treatment of SCI in 1997. In 1998, we formed a joint venture, MS Research & Development Corporation, or MSRD, with Elan International Services, Ltd., or EIS, a subsidiary of Elan, to develop Fampridine-SR for the treatment of MS under an exclusive worldwide license from Elan.
In September 2003, we entered into a termination and assignment agreement with Elan, EIS and MSRD, pursuant to which MSRD assigned to us its assets, including the license from Elan for Fampridine-SR for MS. We paid MSRD approximately $11.5 million for all of the assets and assumed all of the liabilities of MSRD, and MSRD distributed to us approximately $9.5 million as our pro rata portion of the purchase price. From the time of establishment of MSRD until the sale of MSRD's assets to us, Elan was considered to be a related party under generally accepted accounting principles. In conjunction with the termination and assignment, we entered into an amended license agreement with Elan that granted us exclusive worldwide rights to Fampridine-SR in return for the payment of royalties and milestones. In addition, we entered into a supply agreement under which Elan provides Fampridine-SR based upon an agreed upon price schedule.
In September 2003, we entered into a collaboration agreement with Teva Pharmaceutical Industries Ltd., or Teva, to jointly develop and promote in the United States products containing valrocemide, pursuant to which we made an initial payment to Teva of $2.1 million. We and Teva amicably terminated this collaboration agreement in June 2005 and in connection with the termination we paid Teva approximately $3.1 million. We and Teva have no further obligations to each other under this collaboration agreement.
We have expended a significant portion of our funds on a number of clinical trials for Fampridine-SR, our most advanced product candidate, including two Phase 3 clinical trials of Fampridine-SR in SCI and a Phase 2 clinical trial in MS, the results of which were announced in March 2004. An earlier Phase 2 clinical trial in MS was completed in 2001. In mid-2004, we decided to put our clinical trials of Fampridine-SR in SCI on hold, and refocused our efforts on our ongoing Fampridine-SR in MS program, leading to our current Phase 3 clinical trial of Fampridine-SR for improvement of walking ability in people with MS. We may resume our clinical development of Fampridine-SR for SCI following completion of our MS clinical program, or sooner.
In July 2004, we acquired all of Elan's research, development, distribution, sales and marketing rights to Zanaflex Capsules and Zanaflex tablets in the United States. These products are FDA-approved for the management of spasticity. We made an upfront payment to Elan of $2.0 million and are obligated to pay royalties on sales and to make milestone payments upon achievement of specified sales levels. To date, we have achieved two milestones, the first triggering a payment of $1.5 million, 50% of which was paid in the first quarter of 2005 and 50% of which is due in the first quarter of 2006. The second milestone of $3.0 million is due in the first quarter ofon March 31, 2006. As part of our Zanaflex acquisition, we entered into a long-term supply agreement with Elan under which Elan provides us with Zanaflex Capsules. Elan also assigned us its rights under an agreement with Novartis for the supply of tizanidine and Zanaflex tablets.
Our marketing efforts are focused on Zanaflex Capsules, which we launched in April 2005. Zanaflex tablets lost compound patent protection in 2002 and both Zanaflex Capsules and Zanaflex tablets compete with 11 generic tizanidine products. Although we currently distribute Zanaflex tablets, we do not, and do not intend to, actively promote Zanaflex tablets. As a result, prescriptions for Zanaflex tablets have declined and we expect that they will continue to decline. Our goal is to convert as many sales of Zanaflex tablets and generic tizanidine tablets to sales of Zanaflex Capsules as possible. We believe that sales of Zanaflex Capsules will constitute a significant portion of our total revenue for the foreseeable future.
In late 2004, we began establishing our own specialty sales force in the United States, which consisted of 14 sales professionals as of September 30, 2005. This sales force targets neurologists and other prescribers who specialize in treating people with conditions that involve spasticity. Members of this sales force also call on managed care organizations, pharmacists and distribution customers. We plan to expand our specialty sales force to approximately 30 sales professionals in the first quarter of 2006. We have also entered into an agreement with Cardinal Health, under which, since August 2005, they have provided approximately 160 sales representatives to market Zanaflex Capsules, on a non-exclusive basis, to primary care physicians in the United States. We have retained Access Worldwide Communications to provide a small, dedicated sales force of pharmaceutical telesales professionals to contact primary care, specialty physicians and pharmacists. We expect to expand this sales and marketing infrastructure in the future, as appropriate.
In February 2004, we changed our fiscal year end from June 30 to December 31, effective for the six months ended December 31, 2003.
In December 2005, we entered into a Revenue Interests Assignment Agreementrevenue interests assignment agreement with PRF pursuant to which we assigned PRF the right to receive a portion of our net revenues (as defined in the agreement) from Zanaflex Capsules, Zanaflex tablets and any future Zanaflex products. The agreement covers all Zanaflex net revenues generated from October 1, 2005 through and including December 31, 2015, unless the agreement is terminated earlier. In consideration for the assignment, PRF paid us $15.0 million at signing. We used approximately $3.0 million of that payment to repay a portion of the amount we owe to GE Capital, $200,000 of that payment for expenses associated with such repayment and $500,000 of that payment to reimburse PRF for expenses it incurred in the transaction. Under our agreement with PRF, we are required to use the remainder of the amount we received at signing and any other amounts we receive under the agreement to support commercialization, sales, marketing, clinical and regulatory activities and other financial obligations related specifically and solely to our Zanaflex operations. At our election, PRF is also required to pay us (i) an additional $5.0 million if our Zanaflex net revenues in 2005 equal or exceed $11.0 million and our Zanaflex net revenues in the first six months of 2006 equal or exceed $16.0 million, and (ii) an additional $5.0 million if our Zanaflex net revenues in 2006 equal or exceed $33.5 million. If we meet these milestones and decide to borrow these additional funds, we would be required to pay PRF $5.0 million on December 1, 2009 in the case of the first additional payment and $5.0 million on December 1, 2010 in the case of the second additional payment. For more information regarding our agreement with PRF, see "—Liquidity and Capital Resources—Financing Arrangements."
Product Revenue and Returns
Ongoing Zanaflex Capsule and Tablet Sales
Product revenue consists of sales of Zanaflex Capsules and Zanaflex tablets. Under SFAS 48,Revenue Recognition When the Right of Return Exists, we are not permitted to recognize revenue until we can reasonably estimate the likely return rate for our products. Since we have only limited sales history with Zanaflex Capsules and due to generic competition and customer conversion from Zanaflex tablets to Zanaflex Capsules, we cannot reasonably determine a return rate. As a result, we account for sales of these products using a deferred revenue recognition model. At a future point in time, which could be in a number of years, when we are able to reasonably estimate product returns we will begin to recognize revenue based on shipments of product to our wholesale drug distributors.
Under our deferred revenue model, we do not recognize revenue upon shipment of product to our wholesale drug distributors. Instead, we record deferred revenue at gross invoice sales price, and classify the cost basis of the inventory held by the wholesaler as a component of inventory. We recognize revenue when prescriptions are filled to end-users because once prescriptions are filled the product cannot be returned. We use monthly prescription data that we purchase from NDC Health, a leading provider of healthcare data, to determine the amount of revenue to be recognized. When we receive the prescription data, we use the number of units of product prescribed to record gross sales. We then reduce deferred revenue and record cost of goods sold. We began receiving end-user prescription data in March 2005 which enabled us to begin recognizing revenue from Zanaflex tablet sales. We began marketing Zanaflex Capsules in April 2005 and began receiving prescription data and recognizing revenue in the same month. Through September 30, 2005, we have recognized $2.1 million in revenue from Zanaflex tablets and $1.1 million from Zanaflex Capsules.
Under our Revenue Interests Assignment Agreementrevenue interests assignment agreement with PRF, PRF is entitled to a portion of our net revenues from Zanaflex Capsules, Zanaflex tablets and any future Zanaflex products. The agreement covers all Zanaflex net revenues generated from October 1, 2005 through and including December 31, 2015, unless the agreement terminates earlier. Under the agreement, PRF is entitled to the following portion of Zanaflex net revenues:
Notwithstanding the foregoing, once PRF has received and retained payments under the agreement that are at least twice the aggregate amount PRF has paid us under the agreement, PRF will only be entitled to 1% of Zanaflex net revenues.
We accept returns of products for six months prior to and 12 months after their expiration date. Returns of products sold by us are charged directly against deferred revenue, reducing the amount of deferred revenue that we may recognize.
Sale of Zanaflex Tablet Inventory Acquired From Elan
When we acquired Zanaflex from Elan, we also acquired Elan's inventory of Zanaflex tablets. This inventory included partial lots with expiration dating of less than 12 months and full lots with expiration dating greater than 12 months. We have deferred recognition of any revenue from sales of the partial lot inventory until the return period for the product expires in June 2006, and will recognize revenue
then only to the extent that deferred revenues exceed returns. We cannot use prescription data to recognize revenue associated with the partial lot inventory acquired from Elan because we cannot determine whether the prescription was filled with product that Elan sold prior to our acquisition of Zanaflex or with product we sold.
All Zanaflex tablet partial lot inventory that we acquired from Elan has either been sold or is no longer being sold by us. As a result, after the return period expires in June 2006, there will no longer be deferred revenue associated with the Zanaflex tablet partial lot inventory acquired from Elan.
In July 2005 we began to recognize revenue from the full lots based on prescriptions filled for Zanaflex tablets. All of the Zanaflex tablet inventory sold by Elan prior to our acquisition reached expiration in June 2005, therefore any prescriptions filled for Zanaflex tablets subsequent to June 2005 must be from the full inventory lots acquired by and sold by us.
We are uncertain about the amount of returns that we may receive on these products, for a number of reasons including our limited historical returns experience. Returns of Zanaflex tablet inventory acquired from Elan and sold by us are charged against deferred revenue, reducing the amount of deferred revenue that we may recognize.
Returns of Zanaflex Tablets sold by Elan
As part of the acquisition of Zanaflex, we agreed to accept returns of Zanaflex tablets that were returned subsequent to January 17, 2005, including returns of product that was originally sold by Elan. Product returns prior to January 17, 2005, were the responsibility of Elan. We have recorded a charge of $4.1 million in the year ended December 31, 2004, for the estimated returns of Zanaflex tablets sold by Elan. To the extent that returns exceed the estimated charge, we will be required to record further charges. The return period for Zanaflex tablets sold by Elan ends in June 2006, after which time we do not anticipate any further charges resulting from Zanaflex tablets sold by Elan.
Discounts and Allowances
Discounts and allowances consist of estimated reserves for cash discounts, rebates and chargebacks. At the time product is shipped to wholesalers an allowance is recorded for these discounts and allowances. Allowances are established on a product-by-product basis. These allowances are established by management as its best estimate based on each product's historical experience adjusted to reflect known changes in the factors that impact such reserves. Reserves for chargebacks, rebates and discounts are established based on the contractual terms with customers, analysis of historical levels of discounts, chargebacks and rebates, communications with customers and the levels of inventory remaining in the distribution channel as well as expectations about the market for each product and anticipated introduction of competitive products.
Grant Revenue
Grant revenue is recognized when the related research expenses are incurred and our performance obligations under the terms of the respective contract are satisfied. To the extent expended, grant revenue related to purchase of equipment is deferred and amortized over the shorter of its useful life or the life of the related contract.
Cost of Sales
Cost of sales consists of cost of inventory, royalty expense and milestone amortization of intangible assets associated with the Zanaflex acquisition, packaging costs, freight and required inventory stability testing costs. Our inventory costs, royalty obligations and milestone obligations are set forth in the agreements entered into in connection with our Zanaflex acquisition. The Company does not expect
any payments it makes to PRF in connection with the revenue interests assignment transaction entered into in December 2005 to constitute royalty expense or otherwise affect the Company's cost of sales or other operating expenses. See "—Liquidity and Capital Resources—Financing Arrangements."
Research and Development Expenses
Research and development expenses consist primarily of salaries and related expenses for personnel, fees paid to professional service providers in conjunction with independently monitoring our clinical trials and acquiring and evaluating data from our clinical trials, costs of contract manufacturing services, costs of materials used in clinical trials and research and development, depreciation of capital resources used to develop our products, costs of facilities and the legal costs of pursuing patent protection of our intellectual property. We expense research and development costs as incurred. We expect our research and development expenses to increase as we continue to develop our product candidates and preclinical programs.
The following table summarizes our research and development expenses for the fiscal years ended June 30, 2001, 2002, 2003, the six months ended December 31, 2003, the year ended December 31, 2004 and the nine months ended September 30, 2005. Included in this table are our external research and development costs, consisting largely of clinical trial and research services provided by outside laboratories and vendors recognized in connection with each product candidate currently in clinical development and all preclinical programs as a group. Many of our internal research and development costs, including personnel costs, related benefits and stock-based compensation, are not attributable to any individual project because we use these resources across several development projects. Compensation expense for option grants is classified between clinical development and preclinical research and development based on employee job function.
| | | | | | | Nine Months Ended September 30, | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Year Ended June 30, | Six Months Ended December 31, 2003 | | ||||||||||||||||||
| | Year Ended December 31, 2004 | ||||||||||||||||||||
| | 2001 | 2002 | 2003 | 2004 | 2005 | ||||||||||||||||
| | | | | | | (unaudited) | |||||||||||||||
| | (in thousands) | ||||||||||||||||||||
| Clinical development: | |||||||||||||||||||||
| Contract expense—SCI | $ | 1,557 | $ | 3,359 | $ | 5,777 | $ | 4,266 | $ | 5,853 | $ | 5,630 | $ | 30 | |||||||
| Contract expense—MS | 649 | 908 | 1,613 | 2,116 | 2,850 | 2,205 | 2,296 | ||||||||||||||
| Other contract expense | — | — | 1,015 | 1,388 | 4,945 | 4,292 | 3,729 | ||||||||||||||
| Operating expense | 695 | 1,518 | 2,356 | 1,789 | 2,652 | 2,108 | 951 | ||||||||||||||
| Licensing expense—Teva | — | — | — | 2,000 | — | — | — | ||||||||||||||
| Total clinical development | 2,901 | 5,785 | 10,761 | 11,559 | 16,300 | 14,235 | 7,006 | ||||||||||||||
| Preclinical research & development: | |||||||||||||||||||||
| Research contracts | 586 | 617 | 271 | 412 | 628 | 469 | 68 | ||||||||||||||
| Contract expense | — | 213 | 1,441 | 216 | 113 | 47 | 62 | ||||||||||||||
| Operating expense | 2,655 | 4,531 | 5,054 | 4,556 | 4,958 | 3,870 | 2,516 | ||||||||||||||
| Total preclinical research & development | 3,241 | 5,361 | 6,766 | 5,184 | 5,699 | 4,386 | 2,646 | ||||||||||||||
| Total research & development | 6,142 | 11,146 | 17,527 | 16,743 | 21,999 | 18,621 | 9,652 | ||||||||||||||
| Research & development—related party expense | 2,223 | 4,687 | 2,265 | 3,343 | — | — | — | ||||||||||||||
| Total | $ | 8,365 | $ | 15,833 | $ | 19,792 | $ | 20,086 | $ | 21,999 | $ | 18,621 | $ | 9,652 | |||||||
Research and Development—Related Party
In cooperation with Elan, we have conducted a series of clinical trials during the past eight years evaluating Fampridine-SR. Elan was considered to be a related party during the period from April,
1998 when MSRD, our jointly-owned venture with Elan to develop Fampridine-SR in MS, was formed until September 2003, when Elan's interest in MSRD was sold to us (see Note 11 to our consolidated financial statements included in this prospectus). Related party research and development or sales and marketing expenses have been included as a separate line item in our financial statements for this period and in the table above. These expenses consisted of the contracted development and supply of our lead product candidate, Fampridine-SR, license fees and expenses associated with our acquisition of Elan's interest in MSRD.
Sales and Marketing Expenses
Sales and marketing expenses includes the costs of salaries for our sales and marketing personnel and the cost of our advertising, promotion and education programs. Sales and marketing expenses include the cost of our contract sales force provided by Cardinal Health and our contract pharmaceutical telesales services provided by Access Worldwide.
General and Administrative Expenses
General and administrative expenses consist primarily of salaries and other related costs for personnel serving executive, finance, business development, legal, information technology and human resource functions. Other costs include facility costs not otherwise included in research and development or sales and marketing expense and professional fees for legal and accounting services. We expect that our general and administrative expenses will increase as we add personnel and become subject to the reporting obligations applicable to public companies.
Stock-Based Compensation
We have accounted for options and restricted stock granted to employees and directors in accordance with SFAS No. 123,Accounting for Stock-Based Compensation, and related interpretations. As such, compensation expense is recorded on stock option and restricted stock grants based on the fair value of the restricted stock and options granted, which is estimated on the date of grant using an option-pricing model and it is recognized on a straight-line basis over the vesting period. Compensation expense for options and restricted stock granted to employees amounted to $643,000, $1.3 million, $1.6 million, $13.2 million, $9.0 million, and $3.5 million for the years ended June 30, 2001, 2002 and 2003, the six months ended December 31, 2003, the year ended December 31, 2004 and the nine months ended September 30, 2005. Compensation expense for options and restricted stock granted to employees are classified between research and development and general and administrative expense based on employee job function.
We have accounted for stock options granted to non-employees on a fair-value basis in accordance with SFAS No. 123,Accounting for Stock-Based Compensation, Emerging Issues Task Force ("EITF") Issue No. 96-18,Accounting for Equity Instruments That Are Issued to Other Than Employees for Acquiring, or in Conjunction with Selling, Goods or Services, and FASB Interpretations No. 28,Accounting for Stock Appreciation Rights and Other Variable Stock Option or Award Plans an Interpretation of APB Opinion No. 15 and 25. As a result, the non-cash charge to operations for non-employee options with vesting or other performance criteria is affected each reporting period by changes in the fair value of our common stock. Compensation expense for options granted to non-employees amounted to $94,000, $75,000, ($7,000), $8,000, $15,000 and $47,000 for the years ended June 30, 2001, 2002 and 2003, the six months ended December 31, 2003, the year ended December 31, 2004 and the nine months ended September 30, 2005, respectively. The amount of compensation expense to be recorded in the future for options granted to non-employees is subject to change each reporting period based upon changes in the fair value of our common stock, estimated volatility and risk free interest rate until the non-employee completes performance under the option agreement.
We may record additional deferred stock-based compensation if we grant additional options or change the terms of the options granted to our employees.
Beneficial Conversion Feature
In May 2003, we completed a private placement of 112,790,233 shares of Series J convertible preferred stock for an aggregate purchase price of approximately $55.3 million. As a result of this financing, our Series A through Series I preferred stockholders' original conversion prices were reduced due to anti-dilution adjustments, which resulted in a beneficial conversion of $80.7 million in accordance with EITF No. 98-5,Accounting for Convertible Securities with Beneficial Conversion Features or Contingently Adjustable Conversion Ratios and EITF No. 00-27,Application of Issue No. 98-5 to Certain Convertible Instruments. The beneficial conversion of $20.9 million was recorded as an immediate charge to additional paid-in capital, relating to our Series A, Series B, Series C, Series F and Series H convertible preferred stock, which are not mandatorily redeemable and may be converted to common stock at any time at the option of the holders. The remaining beneficial conversion of $59.9 million, relating to our Series E and Series I convertible preferred stock, which are mandatorily redeemable at any time on or after June 30, 2008, is being accreted ratably over the mandatory redemption period. Such accretion amounted to $1.7 million, $5.8 million, $11.6 million and $8.7 million for the year ended June 30, 2003, the six months ended December 31, 2003, the year ended December 31, 2004, and the nine months ended September 30, 2005, respectively, and is charged to additional paid-in capital.
The issuance of Series J mandatorily redeemable convertible preferred stock resulted in a beneficial conversion amounting to $40.0 million in accordance with EITF No. 98-5. The beneficial conversion is calculated based on the estimated fair value of our common stock price per share at the date of issuance of Series J preferred stock of approximately $10.14 per share of common stock, which was calculated based on the estimated projected midpoint of the range of our initial public offering price per common share, which was planned in the fourth calendar quarter of 2003, and the stock price appreciation in comparable public companies from May 2003 to August 2003. The beneficial conversion feature is being accreted ratably over the mandatory redemption period, with a charge to additional paid-in capital of $1.1 million, $3.9 million, $7.8 million and $5.8 million for the year ended June 30, 2003, the six months ended December 31, 2003, the year ended December 31, 2004, and the nine months ended September 30, 2005, respectively.
The unamortized portion of the beneficial conversion at September 30, 2005 was $53.3 million. Upon the closing of this offering, we will recognize a one time non-cash charge to additional paid in capital, reflecting the unamortized portion of the beneficial conversion feature as a result of the automatic conversion of all outstanding convertible preferred stock and mandatorily redeemable convertible preferred stock to common stock upon completion of this offering.
Other Income (Expense)
Interest income consists of interest earned on our cash, cash equivalents and short-term investments. Interest expense consists of interest expense on our GE Capital notes. Interest expense-related party consists of amortization of debt discount and accrued interest on our $7.5 million aggregate principal amount of EIS convertible notes, outstanding as of September 30, 2005. Other income consists primarily of unrealized gains from our investment securities. In future periods, we expect to recognize higher levels of interest expense in connection with the revenue interests assignment arrangement we entered into with PRF in December 2005. In addition, we expect to recognize a net liability associated with the fair value of PRF's put option and our call option under the revenue interests assignment arrangement. This liability will be revalued on a quarterly basis to reflect any changes in the fair value and we will recognize a gain or loss based on that revaluation. See "—Liquidity and Capital Resources—Financing Arrangements."
Results of Operations
Nine Months Ended September 30, 2005 Compared to Nine Months Ended September 30, 2004
Product Sales
We recognized revenue from the sale of Zanaflex Capsules and Zanaflex tablets of $3.2 million for the nine months ended September 30, 2005, as compared to $0 for the nine months ended September 30, 2004. We recognize product sales using a deferred revenue recognition model meaning that product sales are recorded as deferred revenue when shipped to the wholesaler and only recognized as revenue when end-user prescriptions of the product are filled. Product sales in the nine months ended September 30, 2005, consist of Zanaflex tablet sales beginning in March 2005, which is
when we began receiving prescription data for tablets containing a code clearly identifying these prescriptions as having been filled with product we sold, and Zanaflex Capsules prescription data beginning after our launch of the product in April 2005.
Deferred revenue from Zanaflex Capsules was $5.0 million as of September 30, 2005, as compared to $0 as of September 30, 2004. The increase in deferred revenue of Zanaflex Capsules was a result of our launch of the product in April 2005. We expect deferred revenue from Zanaflex Capsules to increase in the future as our sales and marketing efforts ramp up, and prescription data continues to lag wholesaler orders made in anticipation of demand.
Deferred revenue from Zanaflex tablets was $10.7 million as of September 30, 2005, an increase of $4.0 million since December 31, 2004, as compared to $2.8 million as of September 30, 2004. The increase in deferred revenue of Zanaflex tablets was a result of continued sales of the product and the fact that we are not recognizing any of the deferred revenue from Zanaflex tablet inventory acquired from Elan that had an expiration date of less than twelve months at the date of acquisition until after the return period expires in June 2006. With respect to the $10.7 million of deferred revenue at September 30, 2005, approximately $2.5 million relates to product that we acquired from Elan that had an expiration date of less than 12 months at the time we sold it during 2004. We believe there is a high likelihood that this product will be returned, which would result in our inability to recognize revenue related to these sales. We expect deferred revenue from Zanaflex tablets to decline over time as we attempt to convert Zanaflex tablet sales to Zanaflex Capsules sales.
Discounts and Allowances
We recorded discounts and allowances of $992,000 for the nine months ended September 30, 2005 as compared to $144,000 for the nine months ended September 30, 2004. Discounts and allowances are recorded when Zanaflex Capsules and Zanaflex tablets are shipped to wholesalers. We began shipping Zanaflex tablets after our acquisition from Elan in July 2004 and Zanaflex Capsules in April 2005. Discounts and allowances for the nine months ended September 30, 2005 consisted of $683,000 in cash discounts and $308,000 in reserves for chargebacks and rebates. Discounts and allowances for the nine months ended September 30, 2004, consisted of $55,000 in cash discounts and $89,000 for chargebacks and rebates. As part of our April 2005 launch of Zanaflex Capsules, in April, May and September 2005 we extended a 6% promotional cash discount over and above the standard 2% discount provided to drug wholesalers and a 4% rebate on products resold by the wholesalers to pharmacies, hospitals and other third parties. We expect cash discounts to decrease in future periods as a percentage of sales.
Grant Revenue
Grant revenue for the nine months ended September 30, 2005 was $184,000 compared to $445,000 for the nine months ended September 30, 2004. Grant revenue is recognized when the related research expenses are incurred and our performance obligations under the terms of the respective contract are satisfied.
Cost of Sales
We recorded cost of sales of $2.3 million for the nine months ended September 30, 2005 as compared to $363,000 for the nine months ended September 30, 2004. Cost of sales for the nine
months ended September 30, 2005, consisted of $1.2 million in royalty fees, $249,000 in milestone amortization of intangible assets, $561,000 in inventory costs and $275,000 in costs related to packaging, freight, and stability testing. Cost of sales for the nine months ended September 30, 2004, consisted of $261,000 in royalty fees, $37,000 in milestone amortization of intangible assets and $65,000 in inventory costs. We began incurring cost of sales upon the acquisition of Zanaflex in July 2004.
Research and Development
Research and development expenses for the nine months ended September 30, 2005, were $9.7 million as compared to $18.6 million for the nine months ended September 30, 2004, a decrease of approximately $8.9 million, or 47.8%. The decrease in research and development expenses was primarily attributable to completion of two Phase 3 clinical trials of Fampridine-SR in SCI, and one Phase 2 clinical trial of Fampridine-SR in MS, during the first quarter of 2004. The SCI clinical development program expense decreased from $5.6 million for the nine months ended September 30, 2004 to $30,000 for the nine months ended September 30, 2005, due to our decision to put the program on hold. The MS clinical development program expense increased from $2.2 million for the nine months ended September 30, 2004 to $2.3 million for the nine months ended September 30, 2005, an increase of 4.5%. We expect that expenses associated with our MS clinical development program will increase as we continue our Phase 3 clinical trial.
Other contract expenses decreased to $3.8 million in the nine months ended September 30, 2005, from $4.3 million in the nine months ended September 30, 2004, a decrease of 11.6%. This decrease is primarily due to a $3.1 million decrease in expenses for the manufacture of clinical supplies from the period ended September 30, 2004, offset by a $2.2 million increase in expenses related to the valrocemide collaboration, primarily due to expenses of $3.1 million related to the termination of that collaboration in the nine months ended September 30, 2005.
Operating expenses for clinical development and preclinical research and development decreased to $3.3 million in the nine months ended September 30, 2005, from $6.0 million in the nine months ended September 30, 2004, a decrease of $2.5 million, or 41.7%. This decrease was a result of a $1.1 million decrease in preclinical salaries and benefits due to a staff reduction in early 2005. These expenses also include non-cash stock-based compensation expense of $465,000 for the nine months ended September 30, 2005, and $1.4 million for the nine months ended September 30, 2004.
Sales and Marketing
Sales and marketing expenses for the nine months ended September 30, 2005, were $9.7 million compared to $2.8 million for the nine months ended September 30, 2004, an increase of approximately $6.9 million or 246.4%. This increase was primarily attributable to $3.3 million for marketing and distribution and sales administration expense related to the launch of Zanaflex Capsules and the distribution of Zanaflex tablets and $3.0 million in salaries and benefits related to our Zanaflex Capsules specialty sales force.
General and Administrative
General and administrative expenses for the nine months ended September 30, 2005, were $6.3 million compared to $11.0 million for the nine months ended September 30, 2004, a decrease of approximately $4.7 million, or 42.7%. Total general and administrative expenses include non-cash stock based compensation expense of $2.0 million for the nine months ended September 30, 2005, as compared to $5.3 million for the nine months ended September 30, 2004, primarily attributable to the repricing in the first quarter of 2004 of options granted prior to 2004. In addition, the nine months ended September 30, 2004, included approximately $1.2 million in outside NDA preparation services related to our Phase 3 trials of Fampridine-SR in SCI.
Other Income (Expense)
Other income (expense) decreased to a loss of $476,000 for the nine months ended September 30, 2005, from a gain of $34,000 in the nine months ended September 30, 2004, a decrease of $510,000.
Interest expense increased by $527,000 primarily related to a $6.0 million secured term loan with GE Capital entered into in January 2005. The increase in interest expense was offset by an increase in interest income of $18,000 during the nine months ended September 30, 2005.
Beneficial Conversion Feature, Accretion of Issuance Costs, Preferred Dividends and Fair Value of Warrants Issued to Convertible Preferred Stockholders
Charges related to preferred stock remained relatively flat at $18.6 million for the nine months ended September 30, 2005, and $18.5 million for the nine months ended September 30, 2004. These charges primarily comprised accretion of issuance costs on Series E, Series I and Series J mandatorily redeemable convertible preferred stock, accrual of preferred dividend of on Series J and Series K mandatorily redeemable convertible preferred stock, accretion of beneficial conversion feature on Series A through Series I preferred stock for reset in conversion price and accretion of beneficial conversion feature on Series J preferred stock (see Notes 3, 8 and 11 to our consolidated financial statements included in this prospectus).
Year Ended December 31, 2004 Compared to Twelve Months Ended December 31, 2003(1)
| | Twelve Months Ended December 31, 2003 | Year Ended December 31, 2004 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| | (unaudited) | | |||||||
| | (in thousands) | ||||||||
| Gross sales—Zanaflex | $ | — | $ | — | |||||
| Less: discounts and allowances | — | (4,417 | ) | ||||||
| Net sales | — | (4,417 | ) | ||||||
| Grant revenue | 764 | 479 | |||||||
| Total net revenue | 764 | (3,938 | ) | ||||||
| Less: cost of sales | — | (885 | ) | ||||||
| Gross profit | 764 | (4,823 | ) | ||||||
| Operating expenses: | |||||||||
| Research and development | 26,228 | 21,999 | |||||||
| Research and development—related party | 4,016 | — | |||||||
| Sales and marketing | — | 4,662 | |||||||
| General and administrative | 21,220 | 13,283 | |||||||
| Total operating expenses | 51,464 | 39,944 | |||||||
| Operating loss | (50,700 | ) | (44,767 | ) | |||||
| Other income (expense): | |||||||||
| Interest and amortization of debt discount expense | (82 | ) | (385 | ) | |||||
| Interest and amortization of debt discount expense—related party | (445 | ) | — | ||||||
| Interest income | 417 | 409 | |||||||
| Other income | 30 | 2 | |||||||
| Total other income (expense) | (80 | ) | 26 | ||||||
| Net loss | (50,780 | ) | (44,741 | ) | |||||
| Beneficial conversion feature, accretion of issuance costs, preferred dividends, and fair value of warrants issued to convertible preferred stockholders | (36,277 | ) | (24,746 | ) | |||||
| Net loss allocable to common stockholders | $ | (87,057 | ) | $ | (69,487 | ) | |||
Product Sales
We did not record product sales from the sale of either Zanaflex Capsules or Zanaflex tablets in the year ended December 31, 2004, or the twelve months ended December 31, 2003.
We did not record deferred revenue from Zanaflex Capsules in either period, as the product was not launched until April 2005. Deferred revenue from Zanaflex tablets was $6.7 million as of December 31, 2004, as compared to $0 as of December 31, 2003. With respect to the $6.7 million of deferred revenue at December 31, 2004, approximately $3.6 million related to product that we acquired from Elan that had an expiration date of less than 12 months at the time we sold it during 2004. We believe there is a high likelihood that this product will be returned, which would result in our inability to recognize revenue related to these sales.
Discounts and Allowances
We recorded discounts and allowances of $4.4 million for the year ended December 31, 2004, as compared to $0 for the twelve months ended December 31, 2003. Discounts and allowances for the year ended December 31, 2004, consisted of $128,000 in cash discounts and $207,000 for chargebacks and rebates. Additionally, in the year ended December 31, 2004, we took a $4.1 million charge to establish a reserve for expected returns of Zanaflex tablets sold by Elan prior to our acquisition of Zanaflex. As part of the acquisition of Zanaflex, we agreed to accept any returns of Zanaflex tablets that were returned subsequent to January 17, 2005, including returns of product that was originally sold by Elan.
Grant Revenue
Grant revenue for the year ended December 31, 2004, was $479,000 compared to $764,000 for the twelve months ended December 31, 2003. Grant revenue is recognized when the related research expenses are incurred and our performance obligations under the terms of the respective contract are satisfied.
Cost of Sales
We recorded cost of sales of $885,000 for the year ended December 31, 2004 as compared with $0 for the twelve months ended December 31, 2003. Cost of sales for the year ended December 31, 2004, consisted of $519,000 in royalty fees, $114,000 in milestone amortization of intangible assets and $252,000 in inventory costs related to the sale of Zanaflex tablets. For the twelve months ended December 31, 2003, we had no product sales and, as a result, no cost of sales.
Research and Development
Research and development expense for the year ended December 31, 2004, was $22.0 million, as compared to $26.2 million for the twelve months ended December 31, 2003, a decrease of approximately $4.2 million, or 16.0%. Contributing to this decrease was completion of two Phase 3 clinical trials of Fampridine-SR in SCI, and one Phase 2 clinical trial of Fampridine-SR in MS, during the first quarter of 2004. The SCI clinical development program expense decreased to $5.9 million for the year ended December 31, 2004, as compared to $7.2 million for the twelve months ended December 31, 2003, a decrease of $1.3 million, or 18.1%. The MS clinical development program expense decreased to $2.9 million for the year ended December 31, 2004, as compared to $3.3 million for the twelve months ended December 31, 2003, a decrease of $400,000, or 12.1%. We expect that expenses associated with our MS clinical development program will increase as we continue our Phase 3 clinical trial. Our licensing expense decreased to $0 for the year ended December 31, 2004, as compared to $2.0 million for the twelve months ended December 31, 2003. This expense was attributable to an initial payment to Teva for our collaboration agreement for valrocemide.
Other contract expenses increased to $5.0 million for the year ended December 31, 2004, as compared to $1.9 million for the twelve months ended December 31, 2003, an increase of $3.1 million, or 163.2%. This increase is primarily the result of the inclusion of costs related to the drug development and supply of Fampridine-SR in other contract expenses for the year ended December 31, 2004. Prior to the termination of the joint venture with Elan in September 2003, this cost was included in Research and development—related party expense. Also contributing to this increase was a cost of $914,000 relating to a terminated development program.
Operating expense for clinical development and preclinical research and development decreased to $7.6 million for the year ended December 31, 2004, as compared to $11.2 million for the twelve months ended December 31, 2003, a decrease of $3.6 million, or 32.1%. This decrease was partly attributable to a decline in non-cash stock-based compensation expense to $1.8 million for the year ended December 31, 2004, as compared to $3.0 million for the twelve months ended December 31, 2003. The decrease was also attributable to other expenses in the twelve months ended December 31, 2003, which included $508,000 of NDA expense and a $452,000 bonus accrual. In addition, research and development lab expense for the year ended December 31, 2004 was $277,000, as compared to $557,000 for the twelve months ended December 31, 2003, a decrease of $280,000.
Research and development—related party expenses for the year ended December 31, 2004, were $0, as compared to $4.0 million for the twelve months ended December 31, 2003. This decrease was attributable to the termination of our MSRD joint venture with Elan in September 2003, after which all MSRD-related research and development expenses were included in clinical development expenses. Research and development—related party expenses for the twelve months ended December 31, 2003 also included $2.0 million related to termination of the joint venture and $2.0 million in drug development and supply cost.
Sales and Marketing
Sales and marketing expense was $4.7 million for the year ended December 31, 2004, as compared to $0 for the twelve months ended December 31, 2003. This increase was attributable to the beginning of our commercial efforts after our acquisition of the Zanaflex products in July 2004 and included $2.1 million in expense for marketing, distribution, and sales administration, $1.2 million in salaries and benefits, approximately $765,000 in non-cash stock-based compensation expense, and approximately $600,000 in additional sales and marketing overhead expenses.
General and Administrative
General and administrative expense decreased to $13.3 million for the year ended December 31, 2004, from $21.2 million for the twelve months ended December 31, 2003, a decrease of approximately $7.9 million, or 37.3%. This decrease was partly attributable to a decrease in non-cash stock based compensation expense to $6.5 million for the year ended December 31, 2004, as compared to $11.8 million for the twelve months ended December 31, 2003, a decrease of approximately $5.3 million, or 44.9%. In addition, for the twelve months ended December 31, 2003, we had an additional $1.4 million in financing-related expenses as compared to the year ended December 31, 2004.
Other Income (Expense)
Other income (expense) increased to a gain of $26,000 for the year ended December 31, 2004, compared to a loss of $80,000 for the twelve months ended December 31, 2003, an increase of $106,000. Interest expense decreased by $142,000 due to a decrease in interest expense on our EIS convertible promissory notes, offset by an increase in interest expense from our GE Capital notes, and a decrease of $8,000 in interest income for the year ended December 31, 2004, as compared to the twelve months ended December 31, 2003.
Beneficial Conversion Feature Accretion of Issuance Costs, Preferred Dividends and Fair Value of Warrants Issued to Convertible Preferred Stockholders
Charges related to preferred stock decreased to $24.8 million for the year ended December 31, 2004, from $36.3 million for the twelve months ended December 31, 2003. For the year ended December 31, 2004, charges were primarily comprised of beneficial conversion charges of $19.5 million on Series E, Series I and Series J convertible preferred stock, accretion of issuance costs of $106,000, and preferred dividends of $5.2 million (see Notes 3 and 8 to our consolidated financial statements in this prospectus). For the twelve months ended December 31, 2003, charges were primarily comprised of beneficial conversion charges of $33.9 million on Series A, B, C, F and H convertible preferred stock, and Series E, I and J mandatorily redeemable convertible preferred stock, accretion of issuance costs of $86,000, and preferred dividends of $2.8 million (see Notes 3, 8 and 11 to our consolidated financial statements in this prospectus).
Year Ended June 30, 2003 Compared to Year Ended June 30, 2002
Grant Revenue
Grant revenue for the year ended June 30, 2003, was $474,000 compared to $132,000 for the year ended June 30, 2002. For the year ended June 30, 2003, we deferred approximately $95,000 in grant revenue since it related to funding for the purchase of equipment.
Research and Development
Research and development expense for the year ended June 30, 2003, was $17.5 million, as compared to $11.1 million for the year ended June 30, 2002, an increase of approximately $6.4 million, or 57.7%. The increase was primarily attributable to acceleration in patient enrollment for both the Phase 2 clinical trial of Fampridine-SR in MS, as well as two Phase 3 clinical trials of Fampridine-SR in SCI. The SCI study expenses increased to $5.8 million for the year ended June 30, 2003, as compared to $3.4 million for the year ended June 30, 2002, an increase of $2.4 million, or 70.6%. The MS study expense increased to $1.6 million for the year ended June 30, 2003, as compared to $900,000 for the year ended June 30, 2002.
Operating and other contract expense for clinical development and preclinical research and development increased to $8.4 million for the year ended June 30, 2003, as compared to $6.0 million for the year ended June 30, 2002, an increase of $2.4 million, or 40.0%. These expenses include a non-cash stock-based compensation expense of $478,000 for the year ended June 30, 2003, as compared to $455,000 for the year ended June 30, 2002. This increase is also attributable to increased staffing and support required for the new clinical trials.
Research and development-related party expenses were $2.3 million for the year ended June 30, 2003, as compared to $4.7 million for the year ended June 30, 2002, a decrease of $2.4 million, or 51.1%. This decrease in expense was due to reduced development activities by Elan related to Fampridine-SR during the year ended June 30, 2003.
General and Administrative
General and administrative expense of $6.4 million remained relatively flat for the year ended June 30, 2003, as compared to $6.6 million for the year ended June 30, 2002. The decrease in general and administrative expense was primarily due to management's decision to defer spending for market research and medical communications during the year ended June 30, 2003. General and administrative expenses also include non-cash stock based compensation expense of $1.1 million for the year ended June 30, 2003, as compared to $950,000 for the year ended June 30, 2002, an increase of approximately $150,000, or 15.8%.
Other Income (Expense)
Other income (expense) decreased to a loss of $28,000 for the year ended June 30, 2003, compared to a gain of $576,000 for the year ended June 30, 2002, a decrease of $604,000. This decrease was primarily attributable to a decrease in interest income of $591,000 due to lower average cash balances and lower interest earned on cash balances during the year ended June 30, 2003.
Minority Interest
Minority interest decreased to $0 for the year ended June 30, 2003, compared to $580,000 for the year ended June 30, 2002. Elan's previous ownership interest in MSRD, a joint venture that was owned approximately 83% by Acorda and approximately 17% by Elan and another minority stockholder, was reflected as minority interest in our consolidated financial statements. In the year ended June 30, 2003, Elan ceased funding its share of the joint venture's expenses, and therefore there is no minority interest for the year ended June 30, 2003. The assets of this joint venture were transferred to us as of September 2003.
Beneficial conversion feature, accretion of issuance costs, preferred dividends and fair value of warrants issued to convertible preferred stockholders
Charges related to preferred stock increased to $24.3 million for the year ended June 30, 2003, as compared to $55,000 for the year ended June 30, 2002. For the year ended June 30, 2003, charges were primarily comprised of accretion of issuance costs of $66,000 on Series E, Series I and Series J mandatorily redeemable convertible preferred stock, accrual of preferred dividend of $630,000 on Series J mandatorily redeemable convertible preferred stock, accretion of beneficial conversion feature of $23.6 million on Series A through Series J preferred stock for reset in conversion price and accretion of beneficial conversion feature of $1.1 million on Series J preferred stock (see Notes 3, 8 and 11 to our consolidated financial statements included in this prospectus). For the year ended June 30, 2002, charges were primarily comprised of accretion of issuance costs on Series E and Series I mandatorily redeemable convertible preferred stock (see Note 3 and 8 to our consolidated financial statements included in this prospectus).
Liquidity and Capital Resources
We have incurred annual operating losses since inception, and, as of September 30, 2005, we had an accumulated deficit of approximately $198.5 million. We have financed our operations primarily through private placements of our securities, and, to a lesser extent, from loans, government grants and, more recently, our financing arrangement with PRF.
Financing Arrangements
From our inception through September 30, 2005, we raised aggregate net proceeds of $147.9 million through private placements of equity securities. In January 1997, EIS loaned us an aggregate of $7.5 million pursuant to two convertible promissory notes to partly fund our research and development activities, all of which was outstanding as of June 30, 2005. In August and September 2002, we financed certain of our fixed assets through two financing agreements with General Electric Capital Corporation, or GE Capital, in the aggregate amount of approximately $1.2 million, of which $194,000 was outstanding as of September 30, 2005. In January 2005, we entered into a $6.0 million senior secured term loan, which is collateralized by all of our personal property and fixtures, other than the property that secures our revenue interests assignment arrangement with PRF.
On December 23, 2005, we entered into a Revenue Interests Assignment Agreementrevenue interests assignment agreement with PRF, a dedicated healthcare investment fund, pursuant to which we assigned to PRF the right to a portion of our net revenues (as defined in the agreement) from Zanaflex Capsules, Zanaflex tablets and any
future Zanaflex products. To secure our obligations to PRF, we also granted PRF a security interest in substantially all of our assets related to Zanaflex. Our agreement with PRF covers all Zanaflex net revenues generated from October 1, 2005 through and including December 31, 2015, unless the agreement terminates earlier. Under the agreement, PRF is entitled to the following portion of Zanaflex net revenues:
Notwithstanding the foregoing, once PRF has received and retained payments under the agreement that are at least twice the aggregate amount PRF has paid us under the agreement, PRF will only be entitled to 1% of Zanaflex net revenues. In connection with the transaction, we recognizedexpect to record a short-termliability, referred to as the revenue interest liability, of approximately $11.3 million.$14.6 million in accordance with EITF 88-18,Sales of Future Revenues. We will also impute interest expense associated with this liability using the effective interest rate method and will record a corresponding accrued interest liability. The effective interest rate is calculated based on the rate that would enable the debt to be repaid in full over the life of the arrangement. The interest rate on this liability may vary during the term of the agreement depending on a number of factors, including the level of Zanaflex sales. We currently estimate that the imputed interest rate associated with this liability will be approximately 8.9%. Payments made to PRF as a result of Zanaflex sales levels will reduce the accrued interest liability and the principal amount of the revenue interest liability.
In consideration for our assignment of the right to receive a portion of Zanaflex net revenues, PRF paid us $15.0 million at signing of the agreement. We used approximately $3.0 million of the signing payment to repay a portion of the amount we owe to GE Capital, approximately $400,000$200,000 of the signing payment for fees and expenses associated with such repayment and $500,000 of the signing payment to reimburse PRF for expenses it estimated it incurred in the transaction. If $500,000 exceeds the actual amount of expenses PRF incurred in the transaction, PRF is required to pay us the excess within 90 days of the signing date. Under our agreement with PRF, we are required to use the remainder of the amount we received at signing and any other amounts we receive under the agreement to support commercialization, sales, marketing, clinical and regulatory activities and other financial obligations related specifically and solely to our Zanaflex operations. We may not use any proceeds from our agreement with PRF to support any of our other products unless such use is ancillary to the support of commercialization of Zanaflex.
At our election, PRF is also required to pay us (i) an additional $5.0 million if our Zanaflex net revenues in 2005 equal or exceed $11.0 million and our Zanaflex net revenues in the first six months of 2006 equal or exceed $16.0 million, and (ii) an additional $5.0 million if our Zanaflex net revenues in 2006 equal or exceed $33.5 million. If we meet these milestones and decide to borrow these additional funds, we would be required to pay PRF $5.0 million on December 1, 2009 in the case of the first additional payment and $5.0 million on December 1, 2010 in the case of the second additional payment.
Upon the occurrence of certain events, including if we experience a change of control, undergo certain bankruptcy events, transfer any of our interests in Zanaflex (other than pursuant to a license agreement, development, commercialization, co-promotion, collaboration, partnering or similar agreement), transfer all or substantially all of our assets, or breach certain of the covenants, representations or warranties we make under the agreement, PRF may (i) require us to repurchase the rights we sold them at the "put/call price" in effect on the date such right is exercised or (ii) foreclose on the Zanaflex assets that secure our
obligations to PRF. Except in the case of certain bankruptcy events, if PRF exercises its right, which we refer to as PRF's put option, to cause us to repurchase the rights we assigned to it, PRF may not foreclose unless we fail to pay the put/call price as required. If we experience a change of control or complete an initial public offering of shares of our common stock that results in our having a total market capitalization in excess of $150.0 million, we have the right, which we refer to as our call option, to repurchase the rights we sold to PRF at the "put/call price" in effect on the date such right is exercised. If our call option becomes exercisable as a result of this offering, we will have a period of 180 days during which to exercise the option. We do not currently intend to exercise our call option if it becomes exercisable as a result of this offering but we may reevaluate whether we would exercise the option during the 180-day period. If we do exercise our call option, we would use a portion of the proceeds from this offering to make the repayment. See "Use of Proceeds." The put/call price on a given
date is the greater of (i) 150% of all payments made by PRF to us as of such date, less all payments received by PRF from us as of such date, and (ii) an amount that would generate an internal rate of return to PRF of 25% on all payments made by PRF to us as of such date, taking into account the amount and timing of all payments received by PRF from us as of such date. We have determined that PRF's put option and our call option meet the criteria to be considered an embedded derivative and should be accounted for as such. Therefore, we expect to record a net liability of approximately $400,000 related to the put/call option to reflect its estimated fair value as of the date of the agreement, in accordance with SFAS No. 133,Accounting for Derivatives Instruments and Hedging Activities. This liability will be revalued on a quarterly basis to reflect any changes in the fair value and any gain or loss resulting from the revaluation will be recorded in earnings.
During any period during which PRF has the right to receive 15% of Zanaflex net revenues, then 8% of the first $30.0 million in gross product revenues (as defined in the agreement) for Zanaflex we receive in any fiscal year will be distributed to PRF on a daily basis. Following the end of each fiscal quarter, if the aggregate amount actually received by PRF during such quarter exceeds the amount of net revenues PRF was entitled to receive, PRF will remit such excess to us. If the amount of net revenues PRF was entitled to receive during such quarter under the first paragraph above exceeds the aggregate amount actually received by PRF during such quarter, we will remit such excess to PRF.
PRF also has the right to appoint a representative to receive all notices and materials provided to our board of directors and to attend as an observer all meetings of our board of directors, subject to certain exceptions. This right will terminate on the earlier to occur of the fourth anniversary of the completion of an initial public offering of shares of our common stock or termination of the Revenue Interests Assignment Agreement.revenue interests assignment agreement.
Investment Activities
At September 30, 2005, cash and cash equivalents and short-term investments were approximately $8.7 million, as compared to $23.6 million at September 30, 2004. Our cash and cash equivalents consist of highly liquid investments with original maturities of three months or less at date of purchase and consist of time deposits and investments in money market funds with commercial banks and financial institutions and high-quality government and investment grade corporate bonds. Also, we maintain cash balances with financial institutions in excess of insured limits. We do not anticipate any losses with respect to such cash balances. Our short-term investments consist of corporate debt securities with original maturities greater than three months and less than one year. The balance of these investments was $5.2 million as of September 30, 2005, as compared to $18.7 million as of September 30, 2004. As of September 30, 2005, our cash and cash equivalents were $3.6 million, and our short-term investments were $5.2 million, as compared to $4.9 million and $18.7 million respectively, as of September 30, 2004.
Net Cash Used by Operations
Net cash used by operations was $18.1 million, $24.3 million, and $26.9 million for the years ended June 30, 2002 and 2003 and the year ended December 31, 2004, respectively, and $25.8 million and $16.9 million for the nine months ended September 30, 2004 and 2005, respectively. Cash used by
operations for the nine months ended September 30, 2005 was primarily attributable to a net loss of $26.0 million, an increase in prepaid expenses and other current assets of $1.5 million, a decrease in return-related liabilities of $2.1 million and an increase in inventory of $4.5 million attributable to the launch of Zanaflex Capsules. Cash used in operations for the nine months ended September 30, 2005, was offset by stock compensation expense of $3.5 million, an increase in deferred revenue of $9.0 million from Zanaflex sales, and a $2.7 million increase in accounts payable, accrued expenses and other current liabilities. Amounts classified as royalty payable as of December 31, 2004, are included in accounts payable, accrued expenses and other current liabilities as of September 30, 2005, due to their reclassification as a current liability.
Cash used by operations for the nine months ended September 30, 2004, of $25.8 million was primarily due to a net loss of approximately $32.5 million, an increase in accounts receivable of $1.6 million due to the acquisition of Zanaflex and a decrease in accounts payable of $2.4 million due to timing of our payments. The cash used in operations for the nine months ended September 30, 2004,
was offset by stock compensation expense of $7.3 million and an increase in deferred revenue of $2.8 million due to Zanaflex sales.
Cash used by operations for the year ended December 31, 2004, of $26.9 million was due to a net loss of $44.7 million, a $1.9 million increase in accounts receivable from Zanaflex sales and a $3.4 million decrease in accounts payable; accrued expenses and other current liabilities, primarily due to a $1.1 million decrease in bonus accruals. Cash used by operations for the year ended December 31, 2004, was offset by stock compensation expense of $9.1 million, depreciation and amortization expense of $1.2 million; an increase in deferred product revenue of $6.7 million; an increase in returns liability of $4.1 million; amortization of discount on short-term investments of $1.7 million; and an increase in royalty payable of $750,000 for Zanaflex sales.
Cash used by operations for the year ended June 30, 2003, of $24.3 million was due to a net loss of $25.7 million; a reduction in amounts due to Elan of $593,000, primarily due to lower drug development charges; an increase in prepaid expenses and other current assets of $402,000; a $154,000 increase in interest receivable on our short term investments and an increase in other receivables and an increase in grant receivable of $214,000. The cash used in operations for the year ended June 30, 2003 was offset by stock compensation expense of $1.6 million, depreciation and amortization expense of $740,000 and amortization of debt discount relating to our $7.5 million aggregate principal amount convertible notes payable to EIS of $219,000.
Cash used by operations for the year ended June 30, 2002, of $18.1 million was due to a net loss of approximately $21.2 million and minority interest of $580,000. The cash used in operations for the year ended June 30, 2002, was partially offset by stock compensation expenses of $1.4 million; expensing of warrants and beneficial conversion charge of $618,000 on Series C preferred stock issued to Elan, an increase of $580,000 primarily due to increased drug development charges from Elan, depreciation and amortization expense of $417,000, amortization of debt discount relating to our $7.5 million aggregate principal amount of convertible promissory notes payable to EIS of $258,000, increase in accounts payable and accrued expenses and other current liabilities of $224,000 due to higher expenses incurred as research and development projects progress.
Net Cash Used in/Provided by Investing
Net cash provided by investing activities for the nine months ended September 30, 2005, was $3.2 million, primarily due to $4.1 million in net proceeds received from maturities of short-term investments. In addition, we purchased property and equipment of $142,000 in the nine months ended September 30, 2005. Net cash provided by investing activities for the nine months ended September 30, 2005 was offset by $750,000 in purchases of intangible assets relating to the Zanaflex milestone accrual. Net cash provided by investing activities for the nine months ended September 30, 2004, was $10.5 million, primarily due to $12.9 million in net proceeds received from maturities of short-term investments. Net cash provided by investing activities for the nine months ended September 30, 2004,
was offset by $2 million in purchases of intangible assets related to the acquisition of Zanaflex and $463,000 in purchases of property and equipment. We had no material commitments to purchase property and equipment as of September 30, 2005.
Net cash provided by investing activities for the year ended December 31, 2004, was $18.6 million, primarily due to $21.1 million in net proceeds received from maturities of short-term investments. Net cash provided by investing activities for the year ended December 31, 2004, was offset by $2.0 million in purchases of intangible assets related to the acquisition of Zanaflex and $532,000 in purchases of property and equipment.
Net cash used in investing activities for the year ended June 30, 2003 was $10.4 million, primarily due to the net reinvestment of $9.7 million of surplus cash into marketable securities and purchase of property and equipment of $748,000. Net cash used in investing activities for the year ended June 30,
2002 was $5.1 million and was primarily due to purchase of short-term investment of $2.8 million and purchase of purchased property and equipment of $2.2 million in the year ended June 30, 2002. We incurred significant expenses in acquiring property and equipment in the year ended June 30, 2002 as a result of the expansion of our office and laboratory facilities.
Net Cash Used in/Provided by Financing
Net cash provided by financing activities for the nine months ended September 30, 2005, was $5.6 million, primarily due to $5.8 million in proceeds received from the GE Capital senior secured loan and $215,000 in proceeds received from issuance of warrants to GE Capital in conjunction with the issuance of the GE Capital senior secured loan, offset by approximately $429,000 in repayments of notes payable.
Net cash provided by financing activities for the nine months ended September 30, 2004, was $11.2 million, primarily due to proceeds from issuance of preferred stock. In March 2004, we completed a private placement of 1,533,327 shares of Series K mandatorily redeemable convertible preferred stock at $7.50 per share for an aggregate purchase price of approximately $11.5 million. Issuance costs of $55,000 related to this financing were netted against proceeds received. Net cash provided by financing activities for the nine months ended September 30, 2004, was offset by $240,000 in repayments of notes payable to GE Capital.
Net cash provided by financing activities for the year ended December 31, 2004, was $11.1 million, primarily due to proceeds from issuance of the Series K preferred stock. Net cash provided by financing activities for the year ended December 31, 2004, was offset by $324,000 in repayments of notes payable to GE Capital.
Net cash provided by financing activities in the years ended June 30, 2003, and 2002 was $55.9 million and $2.1 million, respectively. The cash provided in the year ended June 30, 2003, was primarily due to proceeds of $55.3 million from the issuance of Series J mandatorily redeemable stock. Issuance costs of $334,000 related to this financing were netted against proceeds received. In the year ended June 30, 2003, also we entered into two financing agreements with GE Capital and received aggregate proceeds in the amount of $1.2 million. In the year ended June 30, 2002, we received proceeds from the issuance of preferred stock of approximately $1.3 million. Proceeds from the issuance of preferred stock primarily consisted of the issuance of 150,000 Series B preferred stock for an aggregate purchase price of $300,000 and 333,333 Series C preferred stock for an aggregate purchase price of $1.0 million to Elan as part of our January 1997 License and Supply Agreement.
Future Capital Needs
Our future capital requirements will depend on a number of factors, including the amount of revenue generated from sales of Zanaflex Capsules, the continued progress of our research and development activities, the timing and outcome of regulatory approvals, the amount and timing of milestone or other payments made under collaborative agreements, the costs involved in preparing, filing, prosecuting, maintaining, defending and enforcing patent claims and other intellectual property
rights and the acquisition of licenses to new products or compounds. We expect to incur losses from operations for at least the next several years as we continue to expand our sales and marketing infrastructure and increase our marketing efforts to support the commercialization of Zanaflex Capsules, continue our clinical development of Fampridine-SR and advance our preclinical programs.
We believe our existing cash and cash equivalents and short-term investment, together with the net proceeds from our financing arrangement with PRF and this offering, will be sufficient to fund our operating expenses, debt repayments and capital equipment requirements for approximately the next 18 months from the date of this prospectus.24 months. To the extent our capital resources are insufficient to meet future operating requirements, we will need to raise additional capital or incur indebtedness to fund
our operations. We may be unable to obtain additional debt or equity financing on acceptable terms, if at all. If adequate funds are not available, we may be required to curtail our sales and marketing efforts, delay, reduce the scope of or eliminate some of our research and development programs or obtain funds through arrangements with collaborative partners or others that may require us to relinquish rights to certain product candidates that we might otherwise seek to develop or commercialize independently.
Contractual Obligations and Commitments
In January 2005, we entered into a $6.0 million senior secured term loan with GE Capital. In December 2005, we used a portion of the initial payment we received under our revenue interest assignment arrangement with PRF to repay approximately $3.0 million of this loan. We are required to pay monthly installments until February 2008, with interest-only payments for the first six months followed by principal and interest payments for the remaining 29 months. Interest is fixed at the rate of 9.93% per annum. The loan is secured by all of our personal property and fixtures, other than the property that secures our financing arrangement with PRF.
In 2002, we entered into two financing agreements with GE Capital for an aggregate amount of approximately $1.2 million, to finance the purchase of certain property and equipment. One note is for $766,781 and bears an annual fixed interest rate of 8.88%. The second note is for $386,731 and bears an annual fixed interest rate of 8.57%. These financing arrangements are secured by certain of our property and equipment and do not include any debt covenants. We are required to pay monthly installments until October 2006. The aggregate principal payments required subsequent to June 30, 2005 are $129,115 in 2005, and $144,654 in 2006.
In January 1997, EIS loaned us an aggregate of $7.5 million pursuant to two convertible promissory notes. One promissory note in the principal amount of $5.0 million bears interest at a rate of 3% which began on the first anniversary of the note. The other promissory note in the amount of $2.5 million is non-interest bearing. The unpaid principal of $5.0 million note is convertible into shares of our Series D preferred stock at a conversion price of $12.50 per share. The $2.5 million promissory note is convertible after January 22, 1999, into either shares of Series B preferred stock at a conversion price of $2.00 per share or into an undesignated series of preferred stock at a conversion price equal to 80% of the most recently completed equity financing, whichever conversion price is greater. If our preferred stock is no longer outstanding, these notes will be convertible into shares of our common stock. Principal and interest are repayable, if not converted, ratably over a seven-year period, beginning one year after we receive regulatory approval for certain products to be developed, subject to limitations related to gross margin on product sales. If we and Elan determine that regulatory approval will not likely occur, the $5.0 million promissory note will automatically convert into the underlying common stock. If our license and supply agreements with Elan are terminated for any other reason, the principal and interest is repayable ratably over 15 years. Both promissory notes restrict our ability to incur indebtedness that is senior to the notes, subject to certain exceptions, including for our revenue interests assignment arrangement with PRF.
Under our Zanaflex purchase agreement with Elan, we are obligated to make milestone payments to Elan of up to $19.5 million based on cumulative gross sales of Zanaflex tablets and Zanaflex Capsules. As of September 30, 2005, we have made or accrued $4.5 million of these milestone
payments in the consolidated financial statements. Under our Zanaflex supply agreement with Elan, we are required to provide to Elan an 18-month rolling forecast at the beginning of each month and a two-year forecast not later than July 1 of each year. We are bound to order one hundred percent of the forecast required quantities for each five month period immediately following each monthly forecast report. At September 30, 2005, the forecast requirement for the five month period following September 30, 2005 amounted to approximately $4.9 million.
Under our Fampridine-SR license agreement with Elan, we are obligated to make milestone payments to Elan of up to $15.0 million over the life of the contract and royalty payments as a
percentage of product sales. In addition, under our various other research, license and collaboration agreements we are obligated to make milestone payments of up to an aggregate of approximately $16.8 million over the life of the contracts.
The following table summarizes our minimum contractual obligations as of December 31, 2004. This table does not reflect contingent milestone or royalty payments that may result in future periods from our collaborations, alliances and/or license agreements. This table should be read in conjunction with the accompanying notes to our consolidated financial statements:
| Twelve Month Period Ending December 31, | Notes Payable(1) | Operating Leases | ||||
|---|---|---|---|---|---|---|
| | (in thousands) | |||||
| 2005 | $ | 1,202 | $ | 642 | ||
| 2006 | 2,462 | 642 | ||||
| 2007 | 2,558 | 642 | ||||
| 2008 | 225 | 53 | ||||
| Total | $ | 6,447 | $ | 1,979 | ||
Under the terms of the employment agreement with our chief executive officer, Ron Cohen, we are obligated to pay severance under certain circumstances. If the employment agreement is terminated by us or by our chief executive officer for reasons other than for cause, we must pay (i) an amount equal to the base salary the chief executive officer would have received during the fifteen month period immediately following the date of termination, plus (ii) bonus equal to last annual bonus received by chief executive officer multiplied by a fraction, the numerator of which shall be the number of days in the calendar year elapsed as of the termination date and the denominator of which shall be 365.
Under the terms of the employment agreements with our Chief Scientific Officer,chief scientific officer, Andrew Blight, our Chief Operating Officer,chief operating officer, Mary Fisher, our Chief Financial Officer,chief financial officer, David Lawrence and our General Counsel,general counsel, Jane Wasman, we are obligated to pay severance under certain circumstances. In the event we terminate our employment agreement with Dr. Blight, Ms. Fisher, Mr. Lawrence or Ms. Wasman without cause, or if one of them voluntarily terminates his or her agreements with good reason, we are obligated to make severance payments equal to nine months base annual salary, in the case of Dr. Blight and Ms. Fisher, and seven months base annual salary, in the case of Mr. Lawrence and Ms. Wasman, as well as COBRA premium payments for the severance period. In such event, all options, stock appreciation rights awards and restricted stock awards that have vested as of the termination date shall remain exercisable for 90 days following such date. All unvested options, stock
appreciation rights awards and stock awards will be cancelled on the date of termination. If Dr. Blight, Ms. Fisher, Mr. Lawrence or Ms. Wasman voluntarily terminates his or her employment without good reason or if we terminate his or her employment without cause within 18 months after a change in control, we are obligated to make severance payments equal to one year's base annual salary, in the case of Dr. Blight and Ms. Fisher, and nine months base annual salary, in the case of Mr. Lawrence and Ms. Wasman, in each case paid in a lump sum within 30 days after termination, as well as COBRA premium payments for the severance period plus a bonus equal to the prior year's bonus pro rated for the number of days worked prior to termination. We are also obligated to pay salary earned but not
paid, vacation and sick leave days that have accrued, and reimbursable business expenses incurred through the date of termination. In such event, not less than 50% of the unvested options, stock appreciation rights and restricted or other stock awards shall become immediately and full vested and shall remain exercisable for 18 months following such date. All options that have vested as of the termination date shall remain exercisable for 90 days following such date. All unvested options, stock appreciation rights awards and stock awards will be cancelled on the date of termination.
Subsequent Events
For a discussion of material events that have taken place subsequent to September 30, 2005, please refer to Note 17 to our consolidated financial statements included in this prospectus.
Quantitative and Qualitative Disclosures about Market Risk
Our financial instruments consist of cash and cash equivalents, short-term investments, grant receivable, notes payable, convertible notes payable and accounts payable. The estimated fair values of all of our financial instruments, excluding convertible notes payable to EIS, approximate their carrying amounts at September 30, 2005. The terms of these notes are disclosed at Note 11 to the consolidated financial statements.
We have cash equivalents and short-term investments at September 30, 2005, which are exposed to the impact of interest rate changes and our interest income fluctuates as our interest rates change. Due to the short-term nature of our investments in money market funds and corporate debt securities, the carrying value of our cash equivalents and short-term investments approximate their fair value at September 30, 2005.
We maintain an investment portfolio in accordance with our investment policy. The primary objectives of our investment policy are to preserve principal, maintain proper liquidity to meet operating needs and maximize yields. Although our investments are subject to credit risk, our investment policy specifies credit quality standards for our investments and limits the amount of credit exposure from any single issue, issuer or type of investment. Our investments are also subject to interest rate risk and will decrease in value if market interest rates increase. However, due to the conservative nature of our investments and relatively short duration, interest rate risk is mitigated. We do not own derivative financial instruments. Accordingly, we do not believe that there is any material market risk exposure with respect to derivative or other financial instruments.
Effects of Inflation
Our most liquid assets are cash, cash equivalents and short-term investments. Because of their liquidity, these assets are not directly affected by inflation. Because we intend to retain and continue to use our equipment, furniture and fixtures and leasehold improvements, we believe that the incremental inflation related to replacement costs of such items will not materially affect our operations. However, the rate of inflation affects our expenses, primarily employee compensation and contract services, which could increase our level of expenses.
Critical Accounting Policies and Estimates
The following discussion of critical accounting policies identifies the accounting policies that require application of management's most difficult, subjective or complex judgments, often as a result
of the need to make estimates about the effect of matters that are inherently uncertain and may change in subsequent periods. It is not intended to be a comprehensive list of all of our significant accounting policies, which are more fully described in Note 2 of the notes to the consolidated financial statements included in this prospectus. In many cases, the accounting treatment of a particular transaction is specifically dictated by generally accepted accounting principles, with no need for management's
judgment in their application. There are also areas in which the selection of an available alternative policy would not produce a materially different result. We have identified the following as our areas of critical accounting policies: sales revenue recognition, research and development, income taxes, and stock-based compensation.
Revenue Recognition
We apply the revenue recognition guidance in SFAS No. 48,Revenue Recognition When the Right of Return Exists, which among other criteria requires that future returns can be reasonably estimated in order to recognize revenue. Under SFAS 48 we are not permitted to recognize revenue until we can reasonably estimate the likely return rate for our products. Since we have only limited sales history with Zanaflex Capsules and due to generic competition and customer conversion from Zanaflex tablets to Zanaflex Capsules, we do not believe we can reasonably determine a return rate. As a result, we account for sales of these products using a deferred revenue recognition model. At a future point in time, which could be in a number of years, when we are able to reasonably estimate product returns we will begin to recognize revenue based on shipments of product to our wholesale drug distributors.
Under our deferred revenue model, we do not recognize revenue upon shipment of product to our wholesale drug distributors. Instead, we record deferred revenue at gross invoice sales price, and classify the cost basis of the inventory shipped as a component of inventory. We recognize revenue when prescriptions are filled to an end-user because once a prescription is filled the product cannot be returned. We use monthly prescription data that we purchase from NDC Health, a leading provider of healthcare data, to determine the amount of revenue to be recognized. We receive this data approximately 45 days after the end of a given month. We estimate prescription sales until the NDC data becomes available, at which time adjustments are made to revenue and cost of sales to account for any differences between our estimates and the actual data. To date such differences have been immaterial. The estimated prescription sales are based on assumed monthly prescription growth rates of 0% for Zanaflex tablets and an amount equal to the prior month's prescription growth rate for Zanaflex Capsules. The method for estimating prescription growth for Zanaflex Capsules will be reevaluated as more prescription data becomes available. When we receive the prescription data, we use the number of units of product prescribed to record gross sales. We then reduce deferred revenue and record cost of goods sold. We began receiving end-user prescription data in March 2005 which enabled us to begin recognizing revenue from Zanaflex tablet sales. We began marketing Zanaflex Capsules in April 2005 and began receiving prescription data and recognizing revenue in the same month.
In addition to the prescription data we receive from NDC Health, we also receive data that we use to monitor ex-wholesalertrends in sales trends.from wholesalers to their customers. We receive this data from an outside vendor on a monthly basis. This data includes bottles shipped from certain wholesalers to their accounts/customers. We also periodically compare our ex-factory shipments to wholesalers to prescription reports to further assess inventory in the distribution channel.channel on a monthly basis. We use the wholesaler sales trend data and the wholesaler vs. prescription comparison to better understand market conditions, but not as a basis for recognizing revenue.
We accept returns of products for six months prior to and 12 months after their expiration date. Returns of products sold by us are charged directly against deferred revenue, reducing the amount of deferred revenue that we may recognize.
Sale of Zanaflex Tablet Inventory Acquired From Elan
When we acquired Zanaflex from Elan, we also acquired Elan's inventory of Zanaflex tablets. This inventory included partial lots with expiration dating of less than 12 months and full lots with expiration dating greater than 12 months. We have deferred recognition of any revenue from sales of the partial lot inventory until the return period for the product expires in June 2006, and will recognize revenue then only to the extent that deferred revenues exceed returns. We cannot use prescription data to recognize revenue associated with the partial lot inventory acquired from Elan because we cannot determine whether the prescription was filled with product that Elan sold prior to our acquisition of Zanaflex or with product we sold.
All Zanaflex tablet partial lot inventory that we acquired from Elan has either been sold or is no longer being sold by us. As a result, after the return period expires in June 2006, there will no longer be deferred revenue associated with the Zanaflex tablet partial lot inventory acquired from Elan.
In July 2005 we began to recognize revenue from the full lots based on prescriptions filled for Zanaflex tablets. All of the Zanaflex tablet inventory sold by Elan prior to our acquisition reached expiration in June 2005, therefore any prescriptions filled for Zanaflex tablets subsequent to June 2005 must be from the full inventory lots acquired by and sold by us.
We are uncertain about the amount of returns that we may receive on these products, for a number of reasons including our limited historical returns experience. Returns of Zanaflex tablet inventory acquired from Elan and sold by us are charged against deferred revenue, reducing the amount of deferred revenue that we may recognize.
At December 31, 2004, and September 30, 2005, we had deferred revenue from Zanaflex tablets of $6.6 million and $10.7 million (unaudited), respectively, of which $3.6 million and $2.5 million (unaudited), respectively, was related to product acquired from Elan that had an expiration date of less than 12 months at the time it was sold during 2004. We believe there is a high likelihood that this product will be returned, which would result in our inability to recognize related revenue.
Returns of Zanaflex Tablets sold by Elan
As part of the acquisition of Zanaflex, we agreed to accept any returns of Zanaflex tablets that were returned subsequent to January 17, 2005, including returns of product that was originally sold by Elan. Product returns prior to January 17, 2005, were the responsibility of Elan. We have recorded a charge of $4.1 million in the year ended December 31, 2004, for the estimated returns of Zanaflex tablets sold by Elan. To the extent that returns exceed the estimated charge, we will be required to record further charges. The return period for Zanaflex tablets sold by Elan ends in June 2006, after which time we do not anticipate any further charges resulting from Zanaflex tablets sold by Elan.
Research and Development
Research and development expenses include the costs associated with our internal research and development activities including, salaries and benefits, occupancy costs, and research and development conducted for us by third parties, such as sponsored university-based research, and clinical trial vendors. In addition, research and development expenses include expenses related to grant revenue and the cost of clinical trial drug supply shipped to our clinical study vendors. We account for our clinical study costs by estimating the total cost to treat a patient in each clinical trial and recognizing this cost as we estimate when the patient receives treatment, beginning when the patient enrolls in the trial. This estimated cost includes payments to the trial site and patient-related costs, including laboratory costs related to the conduct of the trial. Cost per patient varies based on the type of clinical trial, the site of the clinical trial, and the length of the treatment period for each patient. As actual costs become known to us, we adjust our accrual; such changes in estimate may be a material change in our clinical study accrual, which could also materially affect our results of operations.
Income Taxes
As part of the process of preparing our financial statements we are required to estimate our income taxes in each of the jurisdictions in which we operate. We account for income taxes by the liability method. Under this method, deferred income taxes are recognized for tax consequences in future years of differences between the tax bases of assets and liabilities and their financial reporting amounts at each year-end, based on enacted laws and statutory tax rates applicable to the periods in which the differences are expected to affect taxable income. Valuation allowances are provided if, based upon the weight of available evidence, it is more likely than not that some or all of the deferred tax assets will not be realized.
We have not recorded any tax provision or benefit for the years ended June 30, 2002 and 2003 and December 31, 2004 and for the nine months ended September 30, 2005. We have provided a valuation allowance for the full amount of our net deferred tax assets since realization of any future benefit from deductible temporary differences and net operating loss carry-forwards cannot be sufficiently assured at September 30, 2005.
As of September 30, 2005, we had available net operating loss carry-forwards of approximately $63.5 million for federal and state income tax purposes, which are available to offset future federal and state taxable income, if any, and expire between 2009 and 2024 and research and development tax credit carry-forwards of approximately $1.5 million for federal income tax reporting purposes which are available to reduce federal income taxes, if any, through 2018. Since our inception, we have incurred substantial losses and expect to incur substantial and recurring losses in future periods. The Internal Revenue Code of 1986, as amended, the Code, provides for a limitation of the annual use of net operating loss and research and development tax credit carry forwards (following certain ownership changes, as defined by the Code) that could significantly limit our ability to utilize these carry-forwards. We have experienced various ownership changes, as defined by the Code, as a result of past financings. Accordingly, our ability to utilize the aforementioned carry-forwards may be limited. Additionally, because U.S. tax laws limit the time during which these carry forwards may be applied against future taxes we may not be able to take full advantage of these attributes for federal income tax purposes.
Stock-Based Compensation
We account for options and restricted stock granted to employees and directors in accordance with Statement of Financial Accounting Standards ("SFAS") No. 123,Accounting for Stock-Based Compensation, and related interpretations. As such, compensation expense is recorded on stock option grants based on the fair value of the options granted, which is estimated on the date of grant using the Black-Scholes option-pricing model and it is recognized on a straight-line basis over the vesting period. Compensation expense for restricted stock granted is based on the fair value of the restricted stock granted and is recognized on a straight-line basis over the vesting period. We account for stock options granted to non-employees on a fair-value basis in accordance with SFAS No. 123, Emerging Issues Task Force Issue No. 96-18,Accounting for Equity Instruments That Are Issued to Other Than Employees for Acquiring, or in Conjunction with Selling, Goods or Services, and FASB Interpretations No. 28,Accounting for Stock Appreciation Rights and Other Variable Stock Option or Award Plans an Interpretation of APB Opinion No. 15 and 25. As a result, the non-cash charge to operations for non-employee options with vesting or other performance criteria is affected each reporting period by changes in the estimated fair value of our common stock. The two factors which most affect charges or credits to operations related to stock-based compensation are the fair value of the common stock underlying stock options for which stock-based compensation is recorded and the volatility of such fair value. If our estimates of the fair value of these equity instruments change, it would have the effect of changing compensation expenses. Because shares of our common stock have not been publicly traded, we estimate the fair value of our common stock considering, among other factors, the most recent previous sale of convertible preferred stock (pro forma for the 1-for-1.3 reverse split that we intend to effect on or about the date of this prospectus)January 11, 2006). We do not discount the issuance price of our preferred stock in estimating the fair value of our common stock.
Acorda Therapeutics is a commercial-stage biopharmaceutical company dedicated to the identification, development and commercialization of novel therapies that improve neurological function in people with multiple sclerosis, or MS, spinal cord injury, or SCI, multiple sclerosis, or MS, and other disorders of the central nervous system, or CNS. Our marketed drug, Zanaflex Capsules, is FDA-approved for the management of spasticity. Our lead product candidate, Fampridine-SR, is in a Phase 3 clinical trial for the improvement of walking ability in people with MS. Our preclinical programs also target MS and SCI as well as other CNS disorders, including stroke and traumatic brain injury.
Approximately 650,000 people in the United States suffer from MS or SCI and the combined annual cost of treatment for these conditions exceeds $13 billion. In addition, it is estimated that a total of approximately 10 million people live with the long-term consequences of traumatic brain injury and stroke in the United States. Our goal is to continue to grow as a fully-integrated biopharmaceutical company by commercializing therapeutic products, developing our product candidates and advancing our preclinical programs for these large and underserved markets.
Company Highlights
pivotal efficacy studies required for drug approval. We believe Fampridine-SR is the first potential therapy in late-stage clinical development for MS that seeks to improve the function of damaged nerve fibers and would be complementary to existing drugs used to treat MS. To our knowledge, there are no current therapies approved or in development that improve walking ability in people with MS.
Background and Market Opportunity
The Challenge of Nervous System Disorders
The spinal cord and brain together comprise the CNS. The billions of nerve cells that make up the CNS, in conjunction with the nerve bundles that run through all parts of the body, which is calledmake up the peripheral nervous system, transmit the electrical impulses necessary to sustain, regulate and monitor every aspect of human life. The spinal cord serves as the master link between the brain and the body and carries information that regulates movement, sensation and involuntary functions, such as breathing, blood pressure, temperature control, and bladder, bowel and sexual functions.
Nerve impulses travel within and between the brain and spinal cord via long, thin fibers, or axons, that transmit information to other nerve cells through microscopic junctions called synapses. When axons are damaged or lost, they do not normally regenerate, and there is only very limited adaptability, or plasticity, of the surviving axons that allow them to take over the role of damaged or lost axons. The myelin sheath that surrounds axons in the brain and spinal cord provides insulation that facilitates the transmission of nerve impulses. We refer to the axon and its surrounding myelin sheath as a nerve fiber. The myelin sheath is composed of multiple layers of tightly packed cell membrane and is vulnerable to damage in conditions like MS and SCI. Once damaged, it is often not effectively repaired. Although nerve fibers can survive in a demyelinated state, their ability to conduct nerve impulses may be completely lost or severely compromised.
Our Approach to the Market for CNS Disorders
We are focused on identifying, developing and commercializing novel pharmaceutical products that address large and underserved CNS markets. We view MS and SCI as the primary markets for our
products as well as strategic points of access to a broad range of additional neurological conditions for the following reasons:
For people with MS, SCI and similar chronic neurological conditions, even relatively small and incremental improvements in CNS function can produce meaningful benefits in their quality of life.
Spasticity
Spasticity refers to the often painful involuntary tensing, stiffening or contracting of muscles. Spasticity is not a disease but a symptom of other conditions, such as MS, SCI, stroke, traumatic brain injury and cerebral palsy, where portions of the nervous system that control voluntary movement have been damaged. This damage results in the nerve cells in the spinal cord becoming disconnected from controlling centers in the brain and, as a result, transmitting unregulated impulses to the muscles. People who have spasticity may not experience it all the time—it may be triggered by a stimulus, such as pain, pressure sores, cold weather or a urinary tract infection. Up to 75% of people with chronic SCI, and the majority of people with MS, experience some form of spasticity. We Move, a non-profit organization dedicated to movement disorders, estimates that spasticity affects approximately 500,000 people in the United States and over 12 million worldwide.
Current treatments for spasticity are focused on reducing spasm frequency, pain or irritating stimuli that can provoke spasticity. Treatment of spasticity often involves a combination of physical therapy and oral medications. Baclofen and tizanidine, the active ingredient in the Zanaflex products, are the two most frequently prescribed oral medications for spasticity. For more intractable spasticity, treatments sometimes include surgical or chemical destruction of nerve roots in the affected area.
Multiple Sclerosis
The National Multiple Sclerosis Society, or NMSS, currently estimates that 400,000 people in the United States have multiple sclerosis. The NMSS estimates that the medical costs associated with treating MS in the United States were approximately $6.2 billion in 2004. Medications accounted for approximately $3.5 billion of these costs. MS is more prevalent in Caucasians and women and is generally diagnosed between the ages of 20 and 50.
MS is a degenerative CNS disorder in which the immune system attacks and damages the insulating myelin sheath. This damage, which can occur at multiple sites in the CNS, blocks or diminishes conduction of electrical impulses. People with MS may suffer impairments in any number of neurological functions. These impairments vary from individual to individual and over the course of time, depending on which parts of the brain and spinal cord are affected, and often include difficulty walking, spasticity, fatigue, lack of stamina and loss or disturbance of vision. They may also include loss of sensation, loss of bowel and bladder control, sexual dysfunction, depression, neuropathic pain,
muscle paralysis, dizziness, tremors and cognitive difficulties. Individuals vary in the severity of the impairments they suffer on a day-to-day basis, with impairments becoming better or worse depending on the activity of the disease on a given day. An individual with MS may function normally one day and experience one or more symptoms of MS the next.
MS is generally classified by how the disease progresses. The most common classification is relapsing-remitting MS, in which people go through periods during which their disease is relatively stable or in remission, only to experience a recurrence of their disease, known as a relapse, which creates additional damage and loss of function. Approximately 10% of MS cases in the United States. are diagnosed as primary progressive MS, which does not involve distinct attacks but rather a steady worsening of symptoms. Secondary progressive MS involves an initial period of relapsing-remitting disease followed by a steady worsening that is punctuated by more severe flare-ups and partial remissions. Most people with relapsing-remitting disease will eventually convert to secondary progressive disease, though this may not occur for many years.
There are no current treatments that address the weakness and loss of mobility that is a major aspect of the progressive disability experienced by people with MS. Existing treatments are classified as relapse management, disease course management and symptom relief.
Relapse Management. The majority of neurologists treating people with MS use intravenous high-dose corticosteroids for the treatment of sudden and severe relapses. Generally, people experiencing a severe relapse receive a four-day course of steroids on either an in-patient or out-patient basis. This treatment may shorten the time required for recovery from such a relapse.
Disease Course Management. Drugs that modify the immune reactions associated with nerve damage in MS include Avonex, Betaseron, Copaxone and Rebif. These drugs are approved only for the relapsing-remitting form of the disease. Other drugs that suppress the immune system include drugs initially approved to treat cancer, such as Novantrone, which is approved for the treatment of relapsing or secondary progressive MS, and methotrexate. These medications produce a reduction in relapse rate, rather than a halting or reversal of the disease process. They do not restore lost neurological function.
Symptom Relief. Doctors also prescribe a number of drugs to address the secondary disabilities, or symptoms, associated with MS. These include treatments for spasticity, fatigue, bladder and bowel control, depression and pain. Baclofen and tizanidine are the most frequently prescribed drugs for spasticity. Commonly prescribed drugs for other symptoms include Ditropan or Detrol for bladder dysfunction, Provigil for fatigue, fluoxetine for depression, and amitriptyline for pain.
Spinal Cord Injury
According to the National Spinal Cord Injury Statistical Center, approximately 250,000 people in the United States live with the long-term consequences of SCI and approximately 11,000 new spinal cord injuries occur each year, typically in young men. The majority of people with SCI are injured under the age of 30 and live with permanent disability and multiple related medical conditions for more than 40 years after their injury. The National Spinal Cord Injury Database at the University of Alabama estimates that the average lifetime costs directly attributable to SCI for an individual injured at age 25 varies from approximately $600,000 to $2.8 million depending on the severity of the injury.
The spinal cord can be injured by physical trauma that bends the neck or body violently, such as vehicular or diving accidents, or by objects that penetrate or impact the spinal cord, such as a bullet or a knife. The spinal cord can also be injured by loss of blood flow due to damage to major blood vessels or during surgical procedures. When an area of the spinal cord is damaged, motor and sensory function are impaired throughout those parts of the body that are below the level of the injury.
Until recently, SCI was considered an untreatable and incurable condition. Within the last two decades, researchers have shown that the spinal cord is not severed in most people with SCI. Rather, stretching or compression of the cord causes nerve fibers and blood vessels to tear and unleashes a secondary process of bleeding, loss of blood flow and inflammation that causes more tissue damage. The majority of people with spinal cord injury have some axons that survive within or around the site of injury. Because of these surviving axons, approximately 50% of people with SCI have some motor and/or sensory function remaining below the level of the injury and are said to have incomplete SCI. Those with no detectable function below the injury level are said to have complete SCI. Researchers have also shown that many axons that survive trauma are damaged and permanently lose part of their myelin sheath.
In addition to the impact of paralysis on mobility and independence, chronic SCI is often associated with several life-altering conditions that vary depending on the individual and the extent of injury. These include spasticity, as well as persistent pain, loss of control of bowel and bladder functions, loss of sexual function, compromised breathing, loss of sensation, and unstable control of blood pressure, heart rate and body temperature. There is no cure for SCI and no treatment available that is capable of improving neurological function. Methylprednisolone, a high-dose steroid, is currently the standard of care in the United States. Methylprednisolone is a one-time treatment administered to the patient immediately following an injury to prevent secondary tissue damage. There are several treatments for the symptoms of SCI, many of which are the same treatments used to address the symptoms of MS. We believe that novel therapies that offer even an incremental improvement in these conditions would have a meaningful impact on the quality of life for people with SCI.
Other Disorders of the Central Nervous System
Neurological injuries and degenerative diseases of the CNS, including stroke, traumatic brain injury, Parkinson's disease and Alzheimer's disease, are among the most devastating and costly of human ailments. These conditions are most often chronic and historically have been extremely difficult to treat. These disorders, like MS and SCI, involve damage to nerve cells and nerve fibers and would likely benefit from similar approaches to tissue protection and repair. For example, the inflammation process that occurs naturally after many types of tissue injury may damage both injured and healthy CNS cells. As with MS and SCI, these conditions could be treated with interventions that replace nerve cells, stimulate new nerve fiber growth, or increase the adaptability of connections within the nervous system.
Our Strategy
Our strategy is to continue to grow as a fully-integrated biopharmaceutical company focused on the identification, development and commercialization of a range of nervous system therapeutics. We are using our scientific, clinical and commercial expertise in MS and SCI as strategic points of access to additional CNS markets, including stroke and traumatic brain injury. Key aspects of our strategy are:
trials necessary for regulatory approval. We may also pursue subsequent approvals of Fampridine-SR in additional CNS disorders, including SCI.
Our Product Pipeline
| Name | Primary Indication | Status | Marketing Rights | |||
|---|---|---|---|---|---|---|
| Zanaflex Capsules | Spasticity | FDA-approved | U.S. | |||
Zanaflex (tablets) | Spasticity | FDA-approved | U.S. | |||
Fampridine-SR | MS | Phase 3 | Worldwide | |||
Chondroitinase Program | SCI | Preclinical | Worldwide | |||
Neuregulin Program | MS | Preclinical | Worldwide | |||
Remyelinating Antibody Program | MS | Preclinical | Worldwide |
Zanaflex Products
Zanaflex Capsules and Zanaflex tablets are short-acting drugs approved by the FDA for the management of spasticity. We acquired all of Elan's U.S. sales, marketing and distribution rights to Zanaflex Capsules and Zanaflex tablets in July 2004. These products contain tizanidine, one of the two leading treatments for the management of spasticity. Zanaflex tablets were approved by the FDA in 1996 and lost compound patent protection in 2002. There are currently 11 generic versions of tizanidine tablets on the market. However, substantial brand loyalty remains in the prescriber community for the Zanaflex brand. Approximately 90% of all prescriptions for tizanidine are written as "Zanaflex," although most are switched automatically at the pharmacy for a generic tizanidine tablet. Zanaflex Capsules were approved by the FDA in 2002, but were never marketed by Elan. We began marketing Zanaflex Capsules in April 2005.
Clinical trials conducted by Elan demonstrated that Zanaflex Capsules, when taken with food, produce average peak levels of tizanidine in a person's blood that are lower and rise more gradually compared to the peak levels following a similar dose of the tablet form. The FDA recognizes these differences and has determined that Zanaflex tablets and generic tizanidine tablets are not
therapeutically equivalent and are not AB-rated to Zanaflex Capsules. As a result, under state pharmacy laws, prescriptions written for Zanaflex Capsules may not be filled by the pharmacist with Zanaflex tablets or generic tizanidine tablets, although some substitution does take place in practice. Zanaflex Capsules are available in 2 mg, 4 mg and 6 mg doses, while tablet formulations are only available in 2 mg and 4 mg doses. The 6 mg capsule gives patients and physicians an additional dosing choice and an opportunity to reduce the number of pills a patient must take daily. In addition, many patients may find capsules easier to swallow than tablets. In addition, people who have difficulty swallowing may open the capsule and sprinkle it on food. The pharmacokinetic effect of sprinkling contents of the capsule on food, however, is different from when the intact capsule is taken with food.
In 2004, retail sales of Zanaflex tablets and generic equivalents of Zanaflex tablets totaled approximately $300 million in the United States, with Zanaflex tablets accounting for about $15 million of that amount. The vast majority of prescriptions for these products are written by a relatively small group of prescribers. In 2004, over 117,000 physicians wrote one or more prescriptions for generic tizanidine or Zanaflex tablets. However, 78% of all such prescriptions were generated by approximately 9,200 prescribers. We believe that our internal specialty sales force, contract sales force and contract telesales group, will be able to reach virtually all of these high-volume prescribers.
Sales and promotional support for Zanaflex Capsules
To support our commercialization of Zanaflex Capsules, we have established a sales and marketing infrastructure consisting of an internal specialty sales force, a contract sales force and a pharmaceutical telesales group. Our internal specialty sales force currently consists of 14 sales professionals who call on neurologists and other prescribers specializing in treating patients with conditions that involve spasticity. Members of our internal sales force also call on managed care organizations, pharmacists and distribution customers. We plan to expand our specialty sales force to approximately 30 sales professionals in the first quarter of 2006. In addition, Cardinal Health provides us with a contract sales force of approximately 160 sales representatives to market Zanaflex Capsules, on a non-exclusive basis, to primary care physicians who currently prescribe Zanaflex tablets or generic tizanidine tablets. We use a pharmaceutical telesales group to contact primary care physicians, specialty physicians and pharmacists to provide information regarding Zanaflex Capsules or determine their interest in receiving samples of Zanaflex Capsules or a visit from a sales representative.
After the introduction of generic tizanidine tablets in June 2002, Elan discontinued promotional and educational support for Zanaflex tablets. To our knowledge, none of the distributors of generic tizanidine or baclofen, the other leading spasticity treatment, which is also generic, has engaged in any educational programs on the treatment of spasticity. Concurrent with our launch of Zanaflex Capsules in April 2005, we initiated a sampling program as well as a number of educational, promotional and drug safety monitoring programs for prescribers and patients. In addition to our programs for prescribers and patients, we also have a number of programs in place to educate pharmacists about Zanaflex Capsules and the pharmacokinetic differences between tizanidine tablets, including generic tizanidine tablets and Zanaflex tablets, and Zanaflex Capsules.
Since April 2005, we have seen continued growth in monthly prescriptions of Zanaflex Capsules. We believe that this trend will continue as we extend our reach into the population of high-volume prescribers of tizanidine. We are seeking FDA approval of improvements in labeling and we will also explore the potential for new indications.
Pharmacokinetic differences between Zanaflex Capsules and tizanidine tablets
Although tizanidine, the active ingredient in Zanaflex Capsules, Zanaflex tablets and generic tizanidine tablets, is the same, there are some important differences between the capsule and tablet formulations. To establish the differences between Zanaflex Capsules and Zanaflex tablets, Elan conducted a single dose clinical trial with 96 healthy volunteers. That trial demonstrated that Zanaflex Capsules, when taken with food, resulted, on average, in a more gradual rise in tizanidine levels in the blood and a lower peak concentration. By contrast, the trial demonstrated that Zanaflex Capsules taken without food resulted in essentially the same pharmacokinetic effect as the tablet formulation of tizanidine. The results of the trial are illustrated in Figure 1 below.
Figure 1. Average Blood Concentration Over Time
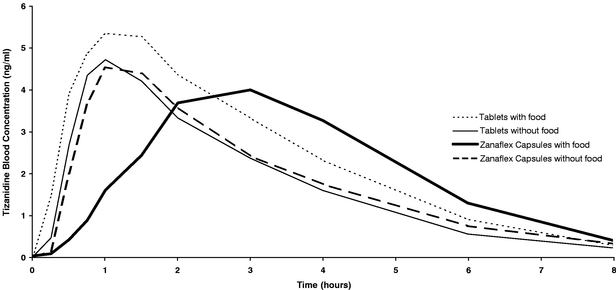
Average blood concentrations of tizanidine in subjects following a single dose of 4 mg Zanaflex tablet or a 4 mg dose of Zanaflex Capsules, taken either with or without food.
As a result of this difference in absorption rate and blood level when taken with food, the FDA has determined that neither Zanaflex tablets nor generic tizanidine tablets are therapeutically equivalent or AB-rated, to Zanaflex Capsules. Therefore, under state pharmacy laws, pharmacists cannot fill prescriptions written for Zanaflex Capsules with Zanaflex tablets or generic tizanidine tablets. The FDA-approved package insert for Zanaflex Capsules contains the following language regarding the differences between the products: "Food has complex effects on tizanidine pharmacokinetics, which differ with different formulations. These pharmacokinetic differences may result in clinically significant differences when (1) switching administration of the tablet between the fed or fasted state, (2) switching administration of the capsule between the fed or fasted state, (3) switching between the tablet and capsule in the fed state, or (4) switching between the intact capsule and sprinkling the contents of the capsule on applesauce. These changes may result in increased adverse events or delayed/more rapid onset of activity, depending on the nature of the switch. For this reason, the prescriber should be thoroughly familiar with the changes in kinetics associated with these different conditions."
The most frequent adverse events associated with the use of tizanidine include dry mouth, drowsiness, fatigue and dizziness. These events are generally mild to moderate and are believed to be dose-related. In one single-dose study where patients were not titrated, two-thirds of patients experienced hypotension. Zanaflex Capsules have a short-acting effect, and patients are advised to take it at the times during the day when they most need relief from spasticity.
Fampridine-SR
Fampridine-SR, our lead product candidate, is currently in a Phase 3 clinical trial for the improvement of walking ability in people with MS pursuant to an SPA issued by the FDA. The FDA has agreed that this trial, if successful, could qualify as one of the pivotal efficacy studies required for drug approval. Fampridine-SR is a small molecule drug contained in a sustained-release tablet form. Laboratory studies have shown that fampridine, the active ingredient in Fampridine-SR, improves impulse conduction in nerve fibers in which the myelin sheath has been damaged. Fampridine is not currently FDA-approved for use in MS or any other indications. We believe that Fampridine-SR could represent a fundamental shift in the treatment of people with MS because it may improve neurological function rather than treating the symptoms or slowing the progression of disease, as current treatments do. We have obtained Orphan Drug designations from the FDA for Fampridine-SR in both MS and incomplete SCI.
In MS, the myelin sheath is damaged by the body's own immune system, causing areas of myelin sheath loss, also known as demyelination. When a nerve fiber is demyelinated after injury, large numbers of the specialized potassium channels on the surface of the axon that are normally hidden or covered by the myelin sheath are exposed and leak potassium ions, causing the nerve fiber to short circuit its electrical impulses. Fampridine blocks these exposed channels, thereby permitting the nerve fiber to transmit impulses again, even in a demyelinated state. Fampridine may also serve to amplify electrical signals at sites of contact or synapses between nerve cells by blocking the same channels in the tips of the nerve fiber, thereby improving the function of surviving tissue in the injured nervous system. Fampridine-SR is a sustained release formulation of fampridine that we believe enables safer and more effective blood levels to be maintained throughout the day, which cannot be easily accomplished with an immediate-release formulation.
We have a worldwide, exclusive license from Elan for all of its rights to, among other things, develop, promote, distribute, use and sell Fampridine-SR in all human clinical indications, and to develop, promote, distribute, use and sell other patented sustained-release formulations of the drug. Elan also manufactures Fampridine-SR for us.
We believe there are compelling reasons to develop Fampridine-SR as a new therapy for improving walking ability in people with MS:
Clinical Trials of Fampridine-SR
We have conducted a series of clinical trials to establish the safety, pharmacokinetics and optimal dosing of Fampridine-SR in MS and SCI, as well as to assess its efficacy. More than 800 people have been treated with Fampridine-SR in over 25 clinical trials, including nine clinical trials in MS and 11 clinical trials in SCI.
Clinical Trials in Multiple Sclerosis
Current Phase 3 Trial. Our current Phase 3 clinical trial, MS-F203, was initiated in June 2005, after we reached agreement with the FDA on the protocol design and received a Special Protocol Assessment from the FDA Division of Neuropharmacological Drug Products. The FDA has agreed that this trial, if successful, could qualify as one of the pivotal efficacy studies required for drug approval.
MS-F203 is a double-blind clinical trial designed to enroll 240 people at up to 35 MS centers in the United States and Canada. Subjects will complete a Timed 25-Foot Walking Test at each visit during the clinical trial. This test involves timing the subject's completion of a 25-foot walk as fast as he or she can do so safely. Such a test is relevant as a measure of the subject's ability to perform tasks that are required in daily life, such as crossing the street in the time period allotted by a traffic light. In addition, subjects will also be asked to fill out a 12-item questionnaire known as the MS Walking Scale or MSWS-12. The MSWS-12 is a subjective measure of the degree to which walking disability impacts the subject's daily life.
Trial results will be analyzed using our proprietary responder analysis, for which we have applied for a patent. A subject will be deemed to be a responder if his or her score on the 25-foot walk was better during the majority of his or her visits in the treatment phase of the trial, than the best visit during the non-treatment phase. The primary endpoint of the trial will be the comparison of the percentage of responders in the Fampridine-SR group to the percentage of responders in the placebo group. To validate the clinical importance of improvements in the timed walk measurements, the MSWS-12 scores of the responders will be compared against those of non-responders. This analysis is designed to ensure that being deemed a responder is clinically meaningful to the subject. In addition, the trial will also test for significant improvement in walking ability in the Fampridine-SR-treated responder group at the last treatment visit versus the placebo group. This analysis is designed to ensure that the improvements seen by responders are maintained over the duration of the trial. As a secondary endpoint, the trial will also measure lower extremity muscle strength, as assessed by the modified British Medical Research Council manual muscle testing procedures, referred to as the Lower Extremity Manual Muscle Test or LEMMT.
The design of our Phase 3 clinical trial was closely modeled on the design of the preceding Phase 2 clinical trial, MS-F202, and builds on our clinical trial experience in measuring improvements in neurological function against the variability in function that is inherent in people with MS. Individuals who suffer from MS vary in the severity of the impairments they experience on a day-to-day basis, depending on the activity of the disease on a given day. As a result, from one clinical trial visit to the next, a subject's walking ability can vary significantly. This variability makes it difficult to distinguish treatment-related changes in walking ability from disease-related changes in walking ability. Our review of MS-F202 data demonstrated that a responder form of analysis helps overcome the effect of the inherent variability of disease activity that people with MS experience.
We expect the recruitment period for the current trial, which began in June 2005, to require approximately six to eight months.end in February 2006. The treatment period is 14 weeks and each subject is involved in trial procedures for approximately five months overall. We currently expect to be able to evaluate data from this clinical trial in the third quarter of 2006, if patient recruitment proceeds as planned.
Phase 2 Clinical Trials. Our most recently completed Phase 2 clinical trial, MS-F202, was designed to compare 10 mg, 15 mg and 20 mg doses of Fampridine-SR taken twice per day and to assess their relative safety and efficacy over a stable treatment period of 12 weeks. The pre-specified primary endpoint of the clinical trial was an improvement in average walking speed using the Timed 25-Foot Walk. The clinical trial was initiated in early 2003 and completed enrollment of 211 subjects in 24 major MS centers in August 2003. The clinical trial was designed to give us a clear indication of optimal dose and the number of subjects that we would need to establish efficacy in a subsequent Phase 3 trial. The overall design of our MS-F202 Phase 2 clinical trial is illustrated in Figure 2 below.
Figure 2. Design of Fampridine-SR MS-F202 Phase 2 clinical trial.

The efficacy results, based on the prospective analysis plan of MS-F202, indicated a trend for improvement from baseline in walking ability (using the Timed 25-Foot Walk test) in the Fampridine-SR-treated subjects, relative to the placebo-treated subjects. Statistical significance was not reached on the primary efficacy analysis, which was defined as the percentage change from baseline in average walking speed during the 12 weeks of stable double-blind treatment. Statistical significance was obtained for the secondary outcome measure of lower extremity muscle strength, as assessed by LEMMT. All three Fampridine-SR dose groups showed greater mean increases from baseline in LEMMT scores relative to the placebo group and the differences were statistically significant for the 10 mg and 15 mg Fampridine-SR groups (p< 0.05). A p-value is a statistical term that indicates the probability that a difference between treatment groups is random. The smaller the p-value, the lower the likelihood that the difference was random. Generally a p-value of less than 0.05 is considered to represent a statistically significant difference.
Our analysis of the data led us to believe that part of the reason that statistical significance was not achieved on the primary endpoint was related to the disease-related variability of walking ability for a subject from visit to visit, together with the fact that not all subjects are expected to respond to the treatment. We believe this variability in walking ability, much of which is contributed by subjects who do not respond, made it difficult to establish the significance of treatment-related improvements using the average walking speed measure that had been prospectively defined as the endpoint of the trial. In order to try to reduce the effect of this variability, we developed an analysis designed to classify subjects as responders only if they demonstrated consistent improvement during the treatment period, when subjects were taking either Fampridine-SR or placebo. Subjects were deemed to be responders if their Timed 25-Foot Walk test results were better during at least three of the four treatment visits than their best score during the non-treatment period. When examined using this form of analysis, all three of the groups receiving Fampridine-SR had a statistically significant increase in the number of responders compared to placebo, as shown in Figure 3.
Figure 3. Responder rates for treatment groups in MS-F202.
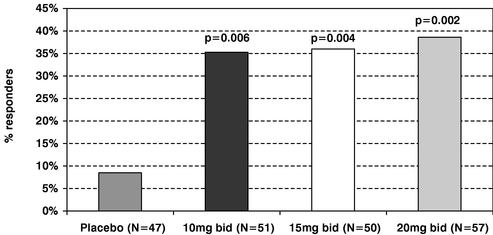
Since the differences in responder rates among the three doses examined were small, more detailed analyses were performed comparing the pooled Fampridine-SR-treated groups against the placebo-treated group. The difference in responder rate between the pooled Fampridine-SR-treated subjects and the placebo-treated subjects was statistically significant (p-value<0.001), as shown below.
| Status | Placebo | Fampridine-SR Pooled | ||
|---|---|---|---|---|
| | (N=47) | (N=158) | ||
Responders | 8.5% | 36.7% | ||
Non-responders | 91.5% | 63.3% |
The responder analysis allows characteristics of the response to be appreciated in more detail. The improvement in walking in responders appeared to be substantial and sustained. The average increase in walking speed of responders was more than 25%, as compared to approximately 2% for non-responders. This was consistent over the 3-month period of treatment and was statistically significant at every visit, as shown in Figure 4.
Figure 4. The average percent change from baseline in walking speed.
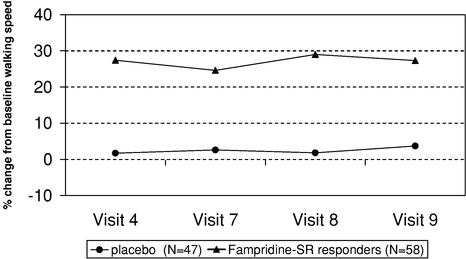
The graph depicts the average change in walking speed during the treatment period for study MS-F202, comparing Fampridine-SR-treated responders to the placebo-treated group. Differences between the groups were statistically significant (p<0.001) at all visits.
In MS-F202, subjects were required to fill out the MSWS-12 questionnaire. When the results of this questionnaire were analyzed for all evaluable subjects, the average improvement, or reduction in score, during the treatment period was greater for responders than for non-responders, in each case including those subjects on placebo, and the difference was statistically significant. We believe this result demonstrates that being a timed-walk responder is clinically meaningful to patients. These results are shown in Figure 5.
Figure 5. Average change in MS Walking Scale Score.
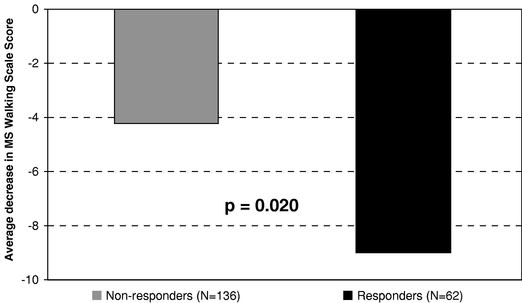
Histogram to show the average change in score for the MS Walking Scale for responders and non-responders between the baseline and stable treatment periods. A reduction in score represents a subject's perception that there has been improvement in the effect of walking disability on activities of daily life.
This analysis of the MS-F202 clinical trial served as the basis for the design of the Phase 3 MS-F203 clinical trial. The results of MS-F202 using this analysis showed that there was a statistically significant increase in the number of people being treated who experienced a consistent increase in walking ability, compared to placebo, and that this improvement was sustained and clinically meaningful to patients. These data also show that the benefit was maintained for the full 14 weeks of treatment. These results are similar whether the pooled Fampridine-SR-treated subjects or just those subjects receiving the current target dose of 10 mg twice a day are compared with the placebo-treated group.
In 2001, we completed a smaller double-blind Phase 2 clinical trial of Fampridine-SR, MS-F201. This clinical trial was designed to determine the optimal dose range of Fampridine-SR and to evaluate possible ways in which to measure the effect of the drug on symptoms of the disease, including motor strength, timed walking and self-reported fatigue. The clinical trial involved a total of 36 MS subjects in four major academic MS research centers. A total of 25 subjects received Fampridine-SR in doses increasing from 10 mg to 40 mg twice per day during seven weeks of treatment and 11 subjects were given placebo during the same period. This treatment period was preceded by a series of baseline evaluations during the course of four weeks to allow the subjects to become adjusted to the clinic visits and allow the various measurements to stabilize. A one-week blinded treatment with placebo tablets preceded the first drug administration to look for potential placebo effects on the various outcome measures.
The clinical trial demonstrated that doses up to 25 mg twice a day were well tolerated and were associated with statistically significant improvements in walking ability and leg muscle strength. All the improvement in strength and walking ability was apparent within these first four weeks of the
treatment, at doses from 10 mg to 25 mg twice a day. The placebo-treated subjects showed some tendency to improve or worsen in walking ability, mostly within 20% of their baseline average. However, the Fampridine-SR-treated group showed a marked tendency for improvement in walking speed, with 9 of 25 subjects improving more than 20% from baseline and two with greater than 50% improvement. These findings were consistent with the results of an earlier, small, crossover study sponsored by Elan, using doses of 17.5 mg twice a day for one week, which was published in the journalNeurology in 1997.
We re-examined the data from the MS-F201 clinical trial using an equivalent responder analysis in which we defined a responder as a subject who showed walking ability on the 25-Foot Walk that was faster in a majority of treatment visits than the fastest speed recorded during the non-treatment period. In MS-F201, this meant that four or more of the seven treatment visits had to show faster walking than the visits during the non-treatment period. We found that the responder rates in this trial were 40% (10 of 25) for the Fampridine-SR-treated subjects and 9.1% (1 of 11) for the placebo-treated subjects. Hence, the response rate by this measurement was similar to that seen in the MS-F202 clinical trial. We did not incorporate the MSWS-12 measure in the MS-F201 clinical trial.
Clinical Trials in Spinal Cord Injury
Recent clinical research using imaging and post-mortem studies has shown that the majority of people with SCI do not have severed spinal cords and maintain some nerve fibers that cross the site of injury. However, these surviving nerve fibers are often damaged and lose their myelin sheath. A series of preclinical studies and clinical trials have indicated that fampridine can potentially improve conduction in nerve fibers injured by spinal cord injury and improve function in people with spinal cord injury.
Phase 3 Clinical Trials. In March 2004, we released results from two Phase 3 double-blind clinical trials of Fampridine-SR in people with SCI. The trials did not reach statistical significance in their primary endpoints, which were reduction of spasticity, as measured by the Ashworth scale, and improvement of patients' Subject Global Impression, or SGI. The Ashworth scale is a validated, 5-point clinician assessment of an individual's spasticity. The SGI is a seven-point scale in which trial participants rate how they feel about the overall effect of the trial drug. In one of the SCI trials, the data showed a positive trend (p=0.069) toward improvement on the Ashworth scale when analyzed across all observations during the double-blind trial treatment period, which was the trial's pre-specified plan of analysis. When analyzed based on the subjects' last observation carried forward, a commonly used method of analysis, the improvement in, or reduction of, Ashworth score in that trial was statistically significant (p=0.006). The drug groups in both trials showed a progressive mean improvement on the Ashworth score during the double-blind treatment period. However, the placebo group in one of the trials showed a more pronounced reduction in Ashworth Score than expected.
The design of these Phase 3 clinical trials was based on a series of earlier Phase 2 clinical trials in which the most consistent finding was a greater reduction in spasticity in Fampridine-SR-treated subjects relative to placebo-treated subjects, as measured by the Ashworth Score. Other benefits observed in the Phase 2 trials were improved motor, bowel, bladder and sexual function. Unlike the design of our Phase 3 clinical trials, our Phase 2 clinical trials did not require a minimum spasticity level for enrollment and the treatment period was from one to four weeks rather than 14 weeks. These changes were made in the Phase 3 trials because the FDA required minimum twelve week duration of treatment for approval of a long-term therapy of this kind and because adequate measurement of benefit required a certain degree of spasticity at baseline.
Based on the entire body of data in clinical trials of fampridine in people with SCI and the new approaches to evaluating response to the drug that we have learned in MS trials, we expect to resume
development of Fampridine-SR for SCI after we have completed further development of the drug for MS.
Safety Profile of Fampridine-SR
To date, Fampridine-SR has been tested in over 800 subjects. The adverse events most commonly experienced in all double blind, placebo-controlled Phase 2 and Phase 3 studies were insomnia, numbness or tingling in the extremities, dizziness and nausea. These events were generally mild to moderate and are believed to have been dose-related. Seizures have also been observed in some prior trials of Fampridine-SR with higher doses of the drug. No seizures have been reported to date in patients with the dose that we have selected for our Phase 3 clinical trial. We are carefully monitoring the potential for seizure as a side effect, including the possibility of interaction with other drugs that are known to lower the threshold for seizure in susceptible subjects. We are also aware that people with MS are reported to have a higher incidence of seizures than the unaffected population. We have excluded from these trials subjects at known risk for seizures because of previous experience or abnormal electroencephalogram indicative of such risk.
As part of our continuing evaluation of safety, we have established extension studies that allow subjects in earlier clinical trials to receive Fampridine-SR on an unblinded, or open-label basis, with their progress followed for at least a year and the potential for continuing treatment until the drug is approved. By their open-label design, these studies will allow us to gain some additional knowledge of the longer term efficacy and safety of the drug, albeit limited by the lack of a placebo control group. These studies are intended primarily to gain sufficient subject experience to satisfy the regulatory guidelines for long-term and overall safety assessments. As of September 2005, approximately 176 subjects from MS-F202 have beenwere enrolled in an extension trial and 37 remain137 remained active in the trial, with approximately 42 subjects who havehad taken the drug for over a year. A new extension study for subjects of the current Phase 3 clinical trial is expected to enroll a majority of the MS-F203 trial subjects, beginning in the fourth quarter of 2005.
Only limited data are yet available from these ongoing safety studies, since no interim analysis of the data is planned, but there have been two incidences of seizures in subjects enrolled in the MS-F202 extension. These seizures occurred in subjects who had been taking the drug at a dose of 15 mg twice a day for six months and five months respectively, before the adverse event. The protocol has now been amended to restrict doses to 10 mg twice a day in order to gather more safety data at the dose that we are examining in the current Phase 3 trial and for which we intend to seek approval. To date, we have had no report of seizure at the 10 mg twice a day dose.
Other Research and Development Programs
Chondroitinase Program
We have developed a program based on the concept of breaking down the matrix of scar tissue that develops as a result of an injury to the CNS. Published research has demonstrated that this scar matrix is partly responsible for limiting the regeneration of nerve fibers in the CNS and restricting their ability to modify existing neural connections, which is the process known as plasticity. This scar matrix may also inhibit repair of the myelin sheath by restricting the movements of the myelinating cells into the area of damage.
Major components of the scar matrix, known as proteoglycans, consist of a combination of protein and sugar molecules. Chondroitin sulfate proteoglycans, or CSPGs, are the specific types of proteoglycans found in the scar matrix. Cell culture studies and a number of animal studies have shown that these CSPGs inhibit the growth of nerve fibers and are likely to be key factors in the failure of the spinal cord or brain to regenerate and repair. Studies also have shown that bacterial enzymes produced
by the body called chondroitinases break down the CSPG molecules, thereby reducing their inhibitory activity.
Four independent laboratories have published animal studies showing that application of chondroitinase results in recovery of function following injuries to various areas of the brain or spinal cord. These functions have included walking, forelimb grasping, sensation, and visual and bladder function. We have produced a recombinant version of naturally-occurring Chondroitinase ABC-I and successfully tested its ability to improve function in an animal model of spinal cord injury. These studies were recently published in the Journal of Neurotrauma. In these studies, rats that sustained a spinal cord injury were treated with either chondroitinase or an ineffective enzyme control and evaluated over 10 weeks of recovery. Animals treated with chondroitinase showed significant improvements both in motor function of the limbs and in bladder function, compared to those treated with the control enzyme.
We are conducting a research program, which has been funded in part by federal and state grants, to develop second generation approaches to overcoming the proteoglycan matrix. These include novel enzyme molecules and alternative approaches to blocking matrix formation. We are now exploring research grants from the NIH and potential partnerships with other companies for completing our preclinical program in chondroitinase. In 2003, we obtained an exclusive worldwide license to certain patents and technology from Cambridge University Technical Services Limited and King's College London related to our chondroitinase program. We are also building our intellectual property position with respect to this technology with patent applications around uses of the known compound and new chemical structures.
Remyelination Programs
Our remyelination programs include two distinct therapeutic approaches to stimulate repair of the damaged myelin sheath in MS, Glial Growth Factor 2, or GGF-2, and remyelinating antibodies. These two approaches address remyelination by different and potentially complementary routes. Both programs require finalizing production of clinical-grade material and completion of preclinical toxicology tests before moving into clinical development. We believe a therapy that could permanently repair myelin sheaths has the potential to restore substantial neurological function to those affected by demyelinating conditions.
Neuregulins/GGF-2
GGF-2 is a member of the neuregulin family of growth factors related to epidermal growth factor. The neuregulins bind to erbB receptors, which translate the growth factor signal to the cell and cause changes in cell growth, protein production and gene expression. The molecule was shown in published studies to stimulate remyelination in animal models of MS and to have a range of other effects in neural protection and repair. In 2002, we obtained from CeNeS an exclusive worldwide license to its neuregulin patents and related technology, including GGF-2. We initially plan to develop GGF-2 for the treatment of MS.
Neuregulins covered in the portfolio from CeNeS have additional potential applications in treatment of heart disease and cancer. Neuregulins and their erbB receptors are essential for cardiac development and have been shown to protect cardiac muscle cells from stressors that model congestive heart failure and myocardial infarction. Additionally, GGF-2 has been shown to protect the heart and brain from the toxicity of commonly used chemotherapeutic agents, such as cisplatin. The neuregulins may also have the potential, when coupled with toxins, to target erbB receptor positive tumors such as those found in certain types of breast cancers.
Remyelinating Antibodies Program
Our remyelinating antibodies program is based on more than 15 years of research performed at Mayo Clinic. Under a license agreement entered into with Mayo Clinic in September 2000, we have exclusive worldwide rights to patents and other intellectual property for these antibodies related to use and treatment of CNS disorders. Studies have demonstrated the ability of this family of antibodies to stimulate repair of the myelin sheath in three different animal models of MS. In particular, these antibodies were found to react with molecules on the surface of the cells that make the myelin sheath and stimulate them in a number of ways, leading to increased remyelination activity. First identified in mice, similar antibodies were subsequently identified in human blood samples by the Mayo team and we have been able to produce a recombinant human antibody that may be suitable for clinical development.
We have also supported preclinical studies at Mayo Clinic to learn more about the ways the antibodies act to stimulate the myelin sheath-forming cells. In 2004, Mayo Clinic received a $2 million grant to develop and manufacture clinical-grade material and progress the program towards clinical development.
Sales and Marketing
We have established three sales channels for marketing Zanaflex Capsules: an internal specialty sales force, a contract sales force and a telemarketing group.
We focus our sales and marketing efforts on physicians and other prescribers who treat spasticity in the United States. Approximately 9,200 physicians generated roughly 78% of the prescriptions for Zanaflex and generic tizanidine tablets in the United States in 2004. Most of these physicians are located at major medical centers. We have existing relationships with the majority of these centers through our Fampridine-SR clinical trial process.
We believe that, in general, people with MS and SCI are knowledgeable about their conditions, actively seek new treatments, and directly influence their prescriber's evaluation of treatment options. We have existing relationships with the major advocacy groups that focus on MS and SCI. We provide regular updates regarding our development programs and we sponsor or support several educational initiatives. We have implemented a comprehensive series of educational and promotional programs to support Zanaflex Capsules. These include educational materials, a peer-to-peer speakers' program, samples, medical information and drug safety monitoring services, as well as a patient assistance program. At the request of the FDA, we have also implemented an educational program to inform
pharmacists, prescribers and patients that Zanaflex tablets or generic tizanidine tablets are not therapeutically equivalent to Zanaflex Capsules and that, as a result, a prescription for Zanaflex Capsules should not be substituted with any tablet formulations at the pharmacy.
We believe that the expertise we are developing through commercializing Zanaflex Capsules will provide a strong foundation for our marketing of Fampridine-SR, if approved, as well as for additional potential treatments in CNS conditions. As a result, we plan to market Fampridine-SR ourselves in the United States and possibly in Canada, if it is approved in both countries. We expect that the sales force for Zanaflex Capsules would also promote Fampridine-SR in the United States since both products would have many of the same prescribers. We do not currently intend to build commercial capabilities outside North America but intend to secure those capabilities through one or more partners.
Similar to other phamaceutical companies, our principal customers are wholesale pharmaceutical distributors. We currently depend on three key customers. For the nine months ended September 30, 2005, Cardinal Health, McKesson Corporation and AmerisourceBergen Corporation accounted for approximately 51.4%, 27.3% and 13.2% of our shipments, respectively.
Scientific and Medical Network
We have an established advisory team and network of well-recognized scientists, clinicians and opinion leaders in the fields of MS and SCI. Depending on their expertise, these advisors provide assistance in trial design, conduct clinical trials, keep us apprised of the latest scientific advances and help us identify and evaluate business development opportunities. A number of the members of this network form our Scientific Advisory Board. The members of our Scientific Advisory Board are highlighted below:
| Name | Affilation | |
|---|---|---|
| Michael S. Beattie, Ph.D. | Brumbaugh Professor and Chair of the Department of Neuroscience, Ohio State University. | |
Jacqueline C. Breshnahan, Ph.D. | Professor of Neuroscience, Ohio State University. | |
Mary B. Bunge, Ph.D. | Professer of Cell Biology and Anatomy, Neurological Surgery and Neurology, University of Miami School of Medicine. | |
Carl W. Cotman, Ph.D. | Professor of Psychobiology and Neurology, University of California, Irvine. | |
James W. Fawcett, Ph.D. | Merck Company Professor of Experimental Neurology, Cambridge University, and Chairman of the MRC Cambridge Centre for Brain Repair. | |
Martin Grumet, Ph.D. | Professor of Cell Biology and Neuroscience, Rutgers University Director, W. M. Keck Center for Collaborative Neuroscience. | |
Eugene Johnson, Jr., Ph.D. | Norman J. Stupp Professor of Neurology, and Professor of Molecular Biology and Pharmacology at Washington University School of Medicine, St. Louis. | |
Mark D. Noble, Ph.D. | Professor of Genetics at the Center for Cancer Biology, University of Rochester Medical Center. | |
Melitta Schachner, Ph.D. | Professor and Director of the Institute for Synthesis of Neural Structures, University of Hamburg, Germany. | |
Jerry Silver, Ph.D. | Professor of Neurosciences, Case Western Reserve University. | |
Patrick A. Tresco, Ph.D. | Professor of Bioengineering, Director Keck Center for Bioengineering, University of Utah. | |
Mark H. Tuszynski, M.D., Ph.D. | Professor of Neurosciences, Director of the Center for Neural Repair, and Attending Neurologist at the University of California, San Diego. | |
Stephen G. Waxman, M.D., Ph.D. | Chairman of the Department of Neurology, Yale University School of Medicine. | |
Wise Young, Ph.D., M.D. | Professor II and Founding Director of the W. M. Keck Center for Collaborative Neuroscience, Rutgers University. |
In addition, we have recruited over 35 MS centers and 80 SCI rehabilitation centers in the United States and Canada to conduct our clinical trials. Our clinical management team has extensive experience in the areas of MS and SCI and works closely with this network.
Collaborations, Alliances and License Agreements
Elan Corporation plc
Zanaflex
In July 2004, we entered into an Asset Purchase Agreement with Elan pursuant to which we acquired all of Elan's research, development, distribution, sales and marketing rights to Zanaflex Capsules and Zanaflex tablets in the United States. The assets acquired include the products' FDA registrations and FDA dossiers, proprietary product know-how, a patent and two related patent applications, certain inventory of Zanaflex tablets and certain product books and records. Elan has granted us a license that allows us to use the Zanaflex trademarks in the United States and has given us the right to buy the Zanaflex trademark for a nominal sum once specified milestone and royalty payments have been made. Elan also granted us an exclusive, perpetual and royalty-free license to certain intellectual property relating to technology contained in Zanaflex Capsules and Zanaflex tablets or used in the manufacture of Zanaflex Capsules, for use in connection with the sale and marketing of Zanaflex Capsules and Zanaflex tablets in the United States. We also acquired the right to develop new indications, formulations, dosage forms, delivery systems and process improvements of Zanaflex. Under the agreement, Elan agreed not to directly or indirectly market, distribute or sell any products containing tizanidine as an active pharmaceutical ingredient in the United States until the later of the end of our obligation to pay royalties to Elan or valid termination of our supply agreement with Elan. In addition, we agreed not to directly or indirectly market, distribute or sell any products containing tizanidine as its active pharmaceutical ingredient in the United Kingdom or Ireland until July 2007.
Our agreement with Elan obligates us to pay a combination of sales-based milestone payments of up to $19.5 million and royalties on future sales of Zanaflex Capsules and Zanaflex tablets. We have made or accrued an aggregate of $3.5 million in payments under this agreement through September 30, 2005. Our obligation to pay royalties to Elan for Zanaflex tablets and Zanaflex Capsules ends on the later of July 2014 or when the last patent included in the acquisition expires. We also agreed to use commercially reasonable efforts to commercialize Zanaflex Capsules.
As part of the acquisition, we assumed certain of Elan's rights and obligations relating to Zanaflex under a license agreement with Novartis, to the extent that these rights and obligations arise subsequent to our acquisition of Zanaflex. Under this agreement we obtained certain rights to market and sell tizanidine products and rights to product improvements developed by Novartis. We are obligated to pay Novartis royalties based on net sales of Zanaflex Capsules and Zanaflex tablets until
the agreement expires in February 2007, after which time we will have a fully paid-up license from Novartis to these rights.
Elan and Novartis manufacture Zanaflex Capsules and tablets for us, respectively. See "—Manufacturing." In December 2005, we entered into a financing arrangement with PRF pursuant to which we assigned PRF the right to receive a portion of our net revenues from Zanaflex Capsules, Zanaflex tablets and any future Zanaflex products. The arrangement covers all Zanaflex net revenues generated from October 1, 2005 through and including December 31, 2015, unless the arrangement is terminated earlier. See "Business—"Management's Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources—Financing Activities."
Fampridine-SR
In January 1997, we licensed from Elan exclusive worldwide rights to Elan's sustained release formulation of fampridine, Fampridine-SR, for the treatment of SCI. In April 1998, we formed MS Research & Development Corporation, or MSRD, with Elan's subsidiary, Elan International Services, Ltd., or EIS, to develop Fampridine-SR for treatment of MS. At that time, MSRD licensed from Elan exclusive worldwide rights to Fampridine-SR for the treatment of MS.
In September 2003, we entered into a termination and assignment agreement with Elan, EIS and MSRD pursuant to which MSRD assigned to us its assets, including the license from Elan for Fampridine-SR for MS. We paid MSRD approximately $11.5 million for all the assets and assumed liabilities of MSRD. MSRD distributed the purchase price to its shareholders according to their equity ownership interest. We received a distribution of approximately $9.5 million as a result of this distribution. We also purchased EIS's shares at par value, and own approximately 88% of MSRD, which now has no assets or liabilities and is inactive.
In September 2003, we entered into an amended and restated license with Elan, which replaced the two prior licenses for Fampridine-SR in oral sustained release dosage form. Under this agreement, Elan granted us exclusive worldwide rights to Fampridine-SR for all indications, including SCI, MS and all other indications. We agreed to pay Elan milestone payments of up to $15.0 million and royalties based on net sales of the product, if approved. We have not made any payments under this agreement through September 30, 2005.
Elan is responsible for completing the chemistry, manufacturing and controls section of our NDA for Fampridine-SR and equivalent regulatory applications outside the United States. Elan is also supplying us with product for our clinical trials under this agreement.
Elan may terminate our license in countries in which we have a license, including the United States, if we fail to file regulatory approvals within a commercially reasonable time after completion and receipt of positive data from all preclinical and clinical studies required for the related NDA or any NDA equivalent. We could also lose our rights under the license agreement if we fail to launch a product in such countries within 180 days of NDA or equivalent approval or if we fail to fulfill our payment obligations under the license agreement. If Elan terminates our license in any applicable country, Elan is entitled to license from us our patent rights and know-how relating to the product and to market the product in the applicable country, subject to royalty payments to us.
We have the right to terminate the Elan license at any time by written notice. In addition, the Elan license may be immediately terminated by either party following an incurable breach of any term or provision by the other party. The Elan license may also be terminated by either party following notice and a cure period with respect to an uncured breach by either party.
Subject to the early termination provisions, the Elan license terminates on a country by country basis on the last to occur of fifteen years from the date of the agreement, the expiration of the last to expire Elan patent or the existence of competition in that country.
Cardinal Health PTS, LLC
In August 2005, we entered into a sales force agreement with Cardinal Health. Under this agreement, approximately 160 of Cardinal Health's sales representatives market Zanaflex Capsules to approximately 4,000 high prescribing primary care physicians identified by us throughout the United States. Although these sales representatives do not exclusively represent Acorda, our agreement with Cardinal Health provides that they will not market any other products during their sales calls related to Zanaflex Capsules. We are responsible for providing training to the Cardinal Health sales representatives regarding the medical and technical aspects of Zanaflex Capsules and on our specific sales strategies and policies. We also provide all samples and promotional materials for use by these sales representatives. Cardinal Health is responsible for general supervision and management of the sales force, including ensuring legal and regulatory compliance, including maintaining procedures relating to the handling of drugs by their sales representatives in compliance with applicable laws and prudent management practices.
We have agreed to pay Cardinal Health service fees based on the achievement of targeted sales levels and to reimburse Cardinal Health for certain costs. The agreement has a term of two years and cannotcan be terminated without cause prior to December 31, 2005.cause.
Rush-Presbyterian St. Luke's Medical Center
In 1990, Elan licensed from Rush-Presbyterian St. Luke's Medical Center, or Rush, know-how relating to fampridine for the treatment of MS. We subsequently licensed this know-how from Elan. In September 2003, we entered into an agreement with Rush and Elan terminating the Rush license to Elan and providing for mutual releases. We also entered into a license agreement with Rush in which Rush granted us an exclusive worldwide license to its know-how relating to fampridine for the treatment of MS. Rush has also assigned to us its Orphan Drug Designation for fampridine for the relief of symptoms of MS.
We agreed to pay Rush a license fee, milestone payments of up to $1.15 million and royalties based on net sales of the product for neurological indications. We have made an aggregate of $200,000 in payments under this agreement through September 30, 2005.
The Rush license may be terminated by either party following an uncured material breach by the other party and notice. The Rush license may also be terminated upon the filing or institution of bankruptcy, reorganization, liquidation or receivership proceedings, or upon an assignment of a substantial portion of the assets for the benefit of creditors by the other party. We also entered into an agreement with Elan relating to the allocation of payments between us and Elan of certain payments to Rush under the Rush license. Subject to the early termination provisions, the Rush license terminates upon expiration of the royalty obligations, which expire fifteen years from the date of the agreement.
Canadian Spinal Research Organization
In August 2003, we entered into an Amended and Restated License Agreement with the Canadian Spinal Research Organization, CSRO. Under this agreement we were granted an exclusive and worldwide license under certain patent assets and know-how of CSRO relating to the use of fampridine in the reduction of chronic pain and spasticity in a spinal cord injured subject.
We are required to pay to CSRO royalties based on a percentage of net sales of any product incorporating the licensed rights, including royalties on the sale of Fampridine-SR for any indication.
We have the right to terminate the CSRO agreement at any time by written notice. In addition, the CSRO agreement may be terminated by either party following an uncured material breach by the other party. The CSRO agreement may also be terminated by either party upon the filing or institution of bankruptcy, reorganization, liquidation or receivership proceedings, or upon an assignment of assets, by the other party. Subject to the early termination provisions, the CSRO agreement will expire upon the termination of all royalty or other payment obligations on a country-by-country basis, which will be
no longer than the earlier of the expiration of the last to expire licensed patent in such country or ten years from the date of the first commercial sale of the product in such country.
Cornell Research Foundation, Inc.
In February 2003, we entered into a license agreement with Cornell Research Foundation, Inc., pursuant to which we were granted an exclusive license under a patent for the use of fampridine in the treatment of anterior horn cell diseases. In consideration for the license, we paid Cornell an upfront license fee and are required to make payments of up to $150,000 to Cornell upon the achievement of certain milestones relating to the successful reissuance or reexamination of the patents licensed to us and, the completion of a clinical trial testing the use of Fampridine-SR in amyotrophic lateral sclerosis. We have made an aggregate of $50,000 in payments under this agreement through September 30, 2005. We are also obligated to pay Cornell an annual royalty on net sales of Fampridine-SR in any and all indications, subject to a minimum annual royalty requirement of $25,000.
Under the Cornell agreement, Cornell is responsible for all patent prosecution and maintenance activities relating to the licensed patent, and we are responsible for paying all fees incurred by Cornell in connection therewith. We have the right under this agreement to enforce any patent rights within the licensed patents against infringement by third parties at our own expense.
We have the right to terminate the Cornell Agreement at any time by written notice. In addition, the Cornell agreement may be terminated by either party following an uncured material breach by the other party. Subject to the early termination provisions, the term of the Cornell agreement will continue until the expiration of the last to expire valid claim under the licensed patent.
Cambridge University Technical Services Limited and King's College London
In December 2003, we entered into a license agreement with Cambridge University Technical Services Limited and King's College London, pursuant to which we were granted an exclusive worldwide license, including the right to sublicense, under a U.S. patent application and its foreign counterpart to develop and commercialize products related to enzymatic methods, including chondroitinase, of treating CNS disorders. We were also granted a non-exclusive worldwide license, including the right to sublicense, under the same U.S. and foreign patent applications to develop and commercialize products related to small molecule inhibitors for use in treating CNS disorders.
In consideration for these licenses, we paid an upfront license fee and are required to make payments of up to $2.15 million upon the achievement of certain milestones. We have made an aggregate of $45,000 in payments under this agreement through September 30, 2005. We are also obligated to pay royalties on net sales and on any sublicense royalties that we receive.
The King's College license may be terminated by any party following an uncured material breach by any other party. The King's College license may also be terminated by any party if any other party ceases to carry on business, is declared by a court of competent jurisdiction to be bankrupt or upon the appointment of a liquidator of that party. Subject to the early termination provisions, the King's College license agreement will continue until the expiration of the last to expire valid claim under the licensed patent applications, at which time the licenses granted under the license agreement will automatically become non-exclusive, worldwide, fully paid-up and irrevocable.
Mayo Foundation for Medical Education and Research
In September 2000, we entered into a license agreement with Mayo Foundation for Education and Research, or Mayo Clinic, pursuant to which we were granted an exclusive worldwide license to its patents and other intellectual property on remyelinating antibodies. Under this agreement, we have the right to develop, make, use and sell the remyelinating antibody products for the prevention, mitigation and treatment of CNS disorders. We have worked closely with one of Mayo Clinic's research groups on developing and patenting this emerging technology in connection with the therapeutic use of these
antibodies, specifically myelination and remyelination in MS and SCI. Mayo Clinic has the right to continue researching the antibodies and, in the event it develops other applications related to the licensed patent, which are outside of the scope of our current license, but are for the treatment of CNS disorders. Mayo Clinic is required to offer rights in these new applications to us before it offers such rights to a third party.
Under the Mayo Clinic agreement, we are obligated to make milestone payments of up to $1.875 million. We also pay royalties based on net sales. We have not made any milestone or royalty payments under this agreement through September 30,December 31, 2005. The Mayo Clinic agreement may be terminated by either party following an uncured material breach by the other party. We may terminate the Mayo Clinic agreement at will upon prior written notice to Mayo. In addition, either party also has the right to terminate upon the insolvency of the other party, the filing of bankruptcy by or against the other party, or the assignment of assets to the benefit of creditors by the other party. Unless otherwise terminated, this license agreement will terminate upon the expiration of the last licensed patent in any such licensed product.
We have also supported preclinical studies at Mayo Clinic to learn more about the ways the antibodies act to stimulate the myelin sheath-forming cells. In 2004, Mayo Clinic received a $2 million grant to develop and manufacture clinical-grade material and progress the program towards clinical development. A subsequent letter agreement between Mayo Clinic and us acknowledges that the work under this grant is being performed subject to and pursuant to the Mayo Clinic agreement.
CeNeS Pharmaceuticals plc
In November 2002, we entered into two license agreements with CeNeS Pharmaceuticals plc. The first agreement relates to an exclusive worldwide sublicense under certain patents, patent applications and know-how to make, have made, use, import, offer for sale and sell protein products composed of GGF-2 and non-protein products developed through the use of material covered by a valid claim in the patents. The license to these patents and the right to sub-license these patents were granted to CeNeS by the Ludwig Institute for Cancer Research.
Our payment obligations to CeNeS include payment of an upfront license fee, royalties based on annual net sales of the product, if any, as well as payments of up to $8.5 million upon achieving certain milestones in connection with the development, testing and regulatory approval of any protein products. We have not made any payments under this agreement through September 30,December 31, 2005. We are obligated to make minimum royalty payments commencing on the third calendar year following the first commercial sale of any licensed product. If we fail to pay any minimum royalty, CeNeS will have the option to convert our license or any sublicense to a non-exclusive license. This agreement with CeNeS is effective until the later of November 12, 2017 or the expiration of the last-to-expire valid claim in the licensed patents. We may terminate this agreement at will upon prior written notice to CeNeS. In addition, this first agreement may be terminated by either party following an uncured material breach by the other party and if this agreement is terminated under that provision, we may retain the exclusive worldwide sublicense granted to us under this agreement, provided that we continue to pay royalties.
The second agreement relates to an exclusive worldwide sublicense to us under certain patents, patent applications and know-how to make and have made, use and have used, sell, offer for sale, have sold and import protein products composed of one or more proteins encoded by the growth factor gene nrg-2 and non-protein products developed through the use of material covered by a valid claim of the patents. The license to this patent and the right to sub-license this patent was granted to CeNeS by the President and Fellows of Harvard College ("Harvard").College.
We have agreed to a timeline to achieve certain milestones relating to the research and development and the clinical testing and filing of regulatory approvals for the products. We are also required to make milestone payments of up to $5.93 million. If we are unable to meet a milestone, CeNeS has agreed to negotiate in good faith with us to agree for a reasonable extension of the time to
achieve the milestone up to one year. We are obligated to pay CeNeS a license fee and royalties based on a percentage of net sales of protein products and non-protein products covered under the agreement. We have not made any payments under this agreement through September 30,December 31, 2005.
This second agreement may be terminated by either party following an unremedied default of a material obligation by the other party. CeNeS may terminate this agreement upon our failure to cure a default in our obligations relating to maintenance of insurance liability or our failure meet certain milestones. Harvard may terminate the underlying Harvard license if CeNeS becomes insolvent, makes an assignment of assets for the benefit of creditors, or has a petition bankruptcy filed for or against it. In that case, Harvard is required, upon our written request, to enter into a direct license with us under the same terms as those set forth in the agreement. We have the right to terminate this agreement upon written notice to CeNeS. The license granted to us pursuant to this agreement continues after the expiration of this agreement and may continue after the termination of this agreement, depending upon the circumstances under which this agreement is terminated.
Subject to early termination provisions, this agreement remains effective until the last patent, patent application or claim included in the licensed patents has expired, been abandoned or been held finally rejected or invalid.
Teva Pharmaceuticals Industries Ltd.
In September 2003, we entered into a collaboration agreement with Teva Pharmaceuticals Industries Ltd. ("Teva"), or Teva, under which we were granted a co-exclusive license with Teva to jointly develop and promote in the United States products containing valrocemide.
We made an initial payment to Teva of $2 million that was charged as research and development expenses for the year ended December 31, 2003, upon execution of the collaboration agreement, and were obligated to make payments to Teva relating to the development of valrocemide.
We and Teva amicably terminated the collaboration agreement as of June 27, 2005 and in connection with the termination we paid Teva approximately $3.1 million. We and Teva have no further obligations to each other under the collaboration agreement.
Manufacturing
Zanaflex
We currently rely on Elan, Novartis and other third parties to supply us with Zanaflex Capsules and Zanaflex tablets. Zanaflex Capsules are manufactured using Elan's proprietary SODAS (spheroidal oral drug absorption system) multiparticulate drug delivery technology. We agreed to provide Elan with monthly written 18-month forecasts, and with annual written two-year forecasts, of our supply requirements for Zanaflex Capsules. In each of the five months following the submission of our 18-month forecast we are obligated to purchase the quantity specified in the forecast, even if our actual requirements are greater or less. Elan is not obligated to supply products in excess of our forecast requirements, but will use commercially reasonable efforts to fulfill any such orders. The initial term of the agreement expires in 2009, with two automatic two-year renewal terms. Either party may terminate the agreement by notifying the other party at least 12 months prior to the expiration of the initial term or any renewal term. In addition, either party may terminate the agreement if the other party commits a material breach that remains uncured. If a failure to supply occurs under the agreement, other than a force majeure event, or if we terminate the supply agreement for cause, Elan must use commercially reasonable efforts to assist us in transferring production of Zanaflex Capsules to us or a third-party manufacturer, provided that such third party is not a technological competitor of Elan. If we need to transfer production, Elan has agreed to grant us a royalty-free, fully paid-up license of its manufacturing know-how and other information and rights related to the production of Zanaflex Capsules, including a license to use its SODAS technology for specified purposes. We have the right to sublicense this know-how to a third party manufacturer, provided that this third party is not a
technological competitor of Elan. In the event of termination of the supply agreement due to a force majeure event that continues for more than three months, Elan has agreed to enter into negotiations with us to preserve the continuity of supply of products, including the possibility of transferring manufacturing of Zanaflex Capsules to us or a third party manufacturer. Elan obtains tizanidine, the active ingredient in Zanaflex Capsules, from Novartis.
We currently rely on Novartis for our supply of Zanaflex tablets. Novartis currently produces tizanidine, but has arranged with another party to formulate tablets. We have arranged with another company, Sharp, to bottle and package Zanaflex tablets. Under a supply agreement we assumed from Elan, Novartis is responsible for manufacturing Zanaflex tablets and tizanidine, the API in both Zanaflex Capsules and Zanaflex tablets, for us through February 2007.
Although Novartis currently produces tizanidine, it has informed us that it intends to discontinue tizanidine production by the end of 2005.the first quarter of 2006. It is our understanding that Novartis is currently in the process of qualifying an alternative tizanidine manufacturer. We have established relationships with the companies that currently formulate, bottle and package the tablets, however, we do not have an agreement with an alternative tizanidine manufacturer. It is the responsibility of each of Novartis and Elan to procure the API required to meet its contractual obligations to supply us with product. We do not anticipate an interruption in API supply. Novartis is currently transferring the methods of manufacturing tizanidine to Rohner, an API manufacturer in Pratteln, Switzerland. We have verified this transfer and plan to audit Rohner's manufacturing site towardstoward the end of the first quarter of 2006, following the commencement of Rohner's manufacture of tizanidine. We have also identified an alternate source for tizanidine in collaboration with Elan. WeHowever, we do not have an agreement with an alternative tizanidine manufacturer, and we do not anticipate entering into a supply agreement for API with either party. AnyElan or Rohner. It is the responsibility of each of Novartis and Elan to procure the API required to meet their contractual obligations under their respective supply agreements with us. We do not anticipate an interruption in API supply, and any cost associated with validating API suppliers would be incurred by Novartis or Elan. The costs of our audit of Rohner or any other supplier are not material and are considered part of our normal course of business. We have arranged with another company, Sharp Corporation, to bottle and package Zanaflex tablets.
Fampridine-SR
In September 2003, we entered into an agreement with Elan for the supply of Fampridine-SR. Under that agreement, we are required to purchase at least 75% of our annual requirements of Fampridine-SR from Elan unless Elan is unable or unwilling to meet our requirements. In addition, the agreement also obligates us to make compensatory payments if we do not purchase 100% of our requirements from Elan.
As permitted by our agreement with Elan, we have designated Patheon, Inc. as a qualified second manufacturing source of Fampridine-SR. In connection with that designation, Elan assisted us in transferring manufacturing technology to Patheon. We and Elan have agreed that we may purchase up to 25% of our annual requirements from Patheon without making compensatory payments to Elan. In addition, Patheon may supply us with Fampridine-SR if Elan is unable or unwilling to meet our requirements.
Preclinical Products
We have established the internal capability to manufacture research quantities of antibody and protein product candidates and have contracted for testing and manufacturing development activities for GGF-2 to be performed by an outside contractor.
Intellectual Property
We have in-licensed, or are the assignee of, over 25 U.S. patents, over 60 foreign patents and over 65 patent applications pending in the United States or abroad. There are five major families of patents in our portfolio.
Zanaflex
As part of our purchase from Elan of the Zanaflex assets, we acquired one issued U.S. patent and two pending U.S. patent applications. Our issued patent is generally directed to certain methods of reducing somnolence and reducing peak plasma concentrations in patients receiving tizanidine therapy. This issued patent expires in 2021. Our two pending U.S. patent applications are directed to
multiparticulate formulations of tizanidine and certain other methods of using tizanidine. The process of seeking patent protection can be time consuming and we cannot assure you that patents will be issued from these pending applications or that, if patents are issued, they will be of sufficient scope to provide meaningful protection of our products.
In addition, we entered into a Supply Agreement with Elan as part of the acquisition, whereby Zanaflex Capsules are manufactured for us by Elan using Elan's proprietary SODAS technology and proprietary information. This proprietary technology is owned by Elan and, in the event Elan ceases to manufacture Zanaflex Capsules, Elan has agreed to grant us a royalty-free, fully paid-up license of its manufacturing know-how and other information and rights related to the production of Zanaflex Capsules, including a license to use its SODAS technology for specified purposes. We have the right to sublicense this know-how to a third party manufacturer, so long as this third party is not a technological competitor of Elan.
Elan has granted us a license that allows us to use the Zanaflex trademark in the United States and gave us the right to buy the Zanaflex trademark for a nominal sum once specified milestone and royalty payments have been made.
Fampridine-SR
We hold an exclusive, worldwide license from CSRO for a U.S. patent and its foreign counterparts for the use of fampridine in the treatment of spasticity and neuropathic pain in chronic SCI. The U.S. patent expires in 2013.
We hold an exclusive, worldwide license from Elan to three U.S. patents, with corresponding issued patents and pending applications in a number of foreign countries, relating to timed delivery formulations of a family of aminopyridine compounds, including fampridine, which also claim methods of administration and treatment for relevant neurological conditions. One of the three U.S. patents expires in 2011 and the other two U.S. patents expire in 2013.
We hold an exclusive license from Cornell University for an issued patent that relates to the use of aminopyridine compositions, including fampridine, for the treatment of diseases of anterior horn cells, including amyotrophic lateral sclerosis, which is also known as Lou Gehrig's disease. This patent expires in 2016.
We also have a pending U.S. patent application and its foreign equivalent directed to methods of using aminopyridines and a pending U.S. patent directed to aminopyridine formulations.
Chondroitinase
We have a license to a U.S. application and its foreign counterpart from King's College, University of Cambridge directed to treatment of CNS damage. We have recently filed a number of U.S. patent applications and their foreign counterparts directed to chondroitinase enzymes and methods of use and preparation. In particular, we have filed seven U.S. applications, with foreign equivalents to four of them, directed to fusion proteins of chondroitinase, chimeric proteins including chondroitinase, deletion mutants, and certain methods relating to chondroitinase.
Neuregulins
We are the exclusive licensee under a license agreement with CeNeS Pharmaceuticals, plc, of a worldwide portfolio of patents and patent applications related to products of neuregulin genes,
including GGF-2. These patents claim the use of particular neuregulins to treat various pathophysiological conditions, particularly stimulating myelinating cells in order to treat demyelinating conditions of the central and peripheral nervous system. These patents also claim a number of additional potential applications of neuregulins, including stimulation of growth in mammalian muscle cells and treating cardiac failure, peripheral neuropathy and nerve injury.
Remyelinating Antibodies
We are the exclusive licensee of a portfolio of patents and patent applications related to a series of remyelinating antibodies discovered in the laboratory of Dr. Moses Rodriguez at the Mayo Clinic in Rochester, Minnesota for the treatment of CNS disorders. One U.S. patent has been issued and foreign counterparts of this patent have also issued in Australia, Mexico, New Zealand and South Korea, as well as in Europe, where patents have been validated in Germany, Spain, France, Great Britain and Italy. Applications are pending elsewhere, including Canada and Japan.
Competition
The market for developing and marketing pharmaceutical products is highly competitive. We are aware of many biotechnology and pharmaceutical companies that are engaged in development and/or marketing of therapeutics for a broad range of CNS conditions. Many of our competitors have substantially greater financial, research and development, human and other resources than we do. Furthermore, many of these companies have significantly more experience than we do in preclinical testing, human clinical trials, regulatory approval procedures and sales and marketing.
Spasticity
Tizanidine, the active pharmaceutical ingredient in Zanaflex Capsules, Zanaflex tablets and generic tizanidine tablets, is one of the two leading FDA-approved treatments for spasticity, a symptom suffered by both MS and SCI patients. Zanaflex tablets were approved by the FDA in 1996 and lost compound patent protection in 2002. Eleven generic manufacturers of tizanidine are distributing their own tablet formulations. Baclofen, which is also available generically, is the other leading drug for the treatment of spasticity. The mechanism of action and associated effects of baclofen are different from those of tizanidine. Due to the different pharmacokinetic profile of Zanaflex Capsules, Zanaflex tablets and generic tizanidine tablets are not AB-rated with Zanaflex Capsules. To our knowledge there are currently no other treatments for spasticity in clinical development.
MS and SCI
Current disease management approaches to MS are classified either as relapse management or disease course management approaches. For relapse management, the majority of neurologists treat sudden and severe relapses with a four-day course of intravenous high-dose corticosteroids. Many of these corticosteroids are available generically. For disease course management, there are a number of FDA-approved MS therapies that seek to modify the immune system. These treatments attempt to reduce the frequency and severity of exacerbations or slow the accumulation of physical disability for people with certain types of MS, though their precise mechanisms of action are not known. These products include Avonex from Biogen-IDEC, Betaseron from Schering AG, Copaxone from Teva and Rebif from Serono.
Several biotechnology and pharmaceutical companies, as well as academic laboratories, are involved in research and/or product development for various neurological diseases, including MS and SCI. We are aware that Aventis is developing a sodium/potassium channel blocker, HP 184, with a potential indication in SCI, MS and other conditions. We believe that HP 184 is in clinical trials for SCI and any resulting product could compete with Fampridine-SR. Neurorecovery Inc. has publicly disclosed that it has an immediate release form of fampridine for peripheral nervous system conditions in Phase 2 trials and any resulting product might compete with Fampridine-SR. In certain
circumstances, pharmacists are not prohibited from formulating certain drug compounds to fill prescriptions on an individual patient basis. We are aware that at present compounded fampridine is used by some people with MS or SCI. Although we expect this use to decrease substantially if Fampridine-SR is approved, it is possible that some people will continue to use this formulation of fampridine. Several companies are engaged in developing products that include novel immune system approaches and cell transplant approaches to remyelination for the treatment of people with MS. These
programs are in early stages of development and may compete with Fampridine-SR or our preclinical candidates in the future.
Our lead product candidate, Fampridine-SR, is the first product to our knowledge that acts to improve neurological function in subjects with MS. We are not aware of other companies in clinical development with products that specifically address walking ability in subjects with MS. As a result of its focus on improving function, we believe that Fampridine-SR may be complementary to both the relapse management and disease course management therapies that are commercially available. Nonetheless, Fampridine-SR will compete for market acceptance with these current treatments because they have been accepted and regularly prescribed to people with MS by physicians.
Government Regulation
FDA Regulation and Product Approval
The FDA and comparable regulatory agencies in state and local jurisdictions and in foreign countries impose substantial requirements upon the preclinical testing, clinical development, manufacture, distribution and marketing of pharmaceutical products. These agencies and other federal, state and local entities regulate research and development activities and the testing, manufacture, quality control, safety, effectiveness, labeling, storage, distribution, record keeping, approval, advertising, sale, promotion, import and export of our products and product candidates.
In the United States, Zanaflex tablets, Zanaflex Capsules, and some of our product candidates are regulated by the FDA as drugs. Other of our product candidates are potentially regulated both as drugs and as biological products. Drugs are subject to the Federal Food, Drug, and Cosmetic Act, as amended, and the regulations of the FDA, as well as to other federal, state, and local statutes and regulations. Biologics are also regulated under the Public Health Service Act, as amended. Violations of regulatory requirements at any stage may result in various adverse consequences, including FDA's and other health authorities' delay in approving or refusal to approve a product. Violations of regulatory requirements also may result in enforcement actions, including withdrawal of approval, labeling restrictions, seizure of products, fines, injunctions and/or civil or criminal penalties.
The process required by the FDA under these laws before our product candidates may be marketed in the United States generally involves the following:
The research, development and approval process requires substantial time, effort, and financial resources and we cannot be certain that any approval will be granted on a timely or commercially viable basis, if at all.
Preclinical studies include laboratory evaluation of the product candidate, its chemistry, formulation and stability, as well as animal studies to assess its potential safety and efficacy. We then submit the results of the preclinical studies, together with manufacturing information, analytical data and any available clinical data or literature to the FDA as part of an IND application, which must
become effective before we may begin human clinical trials. The IND becomes effective 30 days after the FDA acknowledges that the filing is complete, unless the FDA, within the 30-day time period, raises concerns or questions about the conduct of the preclinical trials or the design of the proposed clinical trials as outlined in the IND. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before clinical trials can begin. Further, an independent Institutional Review Board charged with protecting the welfare of human subjects involved in research at each medical center proposing to conduct the clinical trials must review and approve any clinical trial and study subjects must provide informed consent for their participation in the research.
Human clinical trials are typically conducted in three sequential phases which may overlap:
In the case of product candidates for severe or life-threatening diseases such as MS, the initial human testing is often conducted in affected subjects rather than in healthy volunteers. Since these subjects already have the target condition, these clinical trials may provide initial evidence of efficacy traditionally obtained in Phase 2 clinical trials and thus these clinical trials are frequently referred to as Phase 1b clinical trials.
Before proceeding with a study, sponsors may seek a written agreement from the FDA regarding the design, size, and conduct of a clinical trial. This is known as an SPA. Three types of studies are eligible for SPAs: (1) animal carcinogenicity studies, (2) final product stability studies, and (3) clinical studies for pivotal trials whose data will form the primary basis to establish a product's efficacy. Where the FDA agrees to an SPA, the agreement may not be changed by either the sponsor or the FDA except if the sponsor and the FDA agree to a change, or an appropriately senior FDA official determines that a substantial scientific issue essential to determining the safety or effectiveness of the product was identified after the testing began. SPAs thus help establish up front agreement with the FDA about the adequacy of the design of a clinical trial to support a regulatory approval, but the agreement is not binding if new circumstances arise. In addition, even if an SPA remains in place and the trial meets its endpoints with statistical significance, the FDA could determine that the overall balance of risks and benefits for the product candidate is not adequate to support approval, or only justifies approval for a narrow set of uses or approval with restricted distribution or other burdensome post-approval requirements or limitations. There is thus no guarantee that a study will ultimately be adequate to support an approval even if the study is subject to an SPA.
U.S. law requires that studies conducted to support approval for product marketing be "adequate and well controlled." In general, this means that either a placebo or a product already approved for the
treatment of the disease or condition under study must be used as a reference control. Studies must also be conducted in compliance with good clinical practice, or GCP, requirements.
We cannot be certain that we will successfully complete Phase 1, Phase 2 or Phase 3 testing of our product candidates within any specific time period, if at all. Furthermore, the FDA or the Institutional Review Boards or the sponsor may prevent clinical trials from beginning or may place clinical trials on hold or terminate them at any point in this process if, among other reasons, they conclude that study subjects are being exposed to an unacceptable health risk.
In the U.S., the results of product development, preclinical studies and clinical trials must be submitted to the FDA for review and approval prior to marketing and commercial shipment of the product candidate. If the product is regulated as a drug, a New Drug Application, or NDA, must be submitted and approved before commercial marketing may begin. If the product, such as an antibody, is regulated as a biologic, a Biologic License Application, or BLA, must be submitted and approved before commercial marketing may begin. The NDA or BLA must include a substantial amount of data and other information concerning the safety and effectiveness (and, in the case of a biologic, purity and potency) of the compound from laboratory, animal and clinical testing, as well as data and information on manufacturing, product stability, and proposed product labeling.
Each domestic and foreign manufacturing establishment, including any contract manufacturers we may decide to use, must be listed in the NDA or BLA and must be registered with the FDA. The application will generally not be approved until the FDA conducts a manufacturing inspection, approves the applicable manufacturing process for the drug or biological product, and determines that the facility is in compliance with current good manufacturing practice, or cGMP, requirements. If the manufacturing facilities and processes fail to pass the FDA inspection, we will not receive approval to market these products.
Under the Prescription Drug User Fee Act, as amended, the FDA receives fees for reviewing a BLA or NDA and supplements thereto, as well as annual fees for commercial manufacturing establishments and for approved products. These fees can be significant. The NDA or BLA review fee alone can exceed $700,000, although certain limited deferrals, waivers and reductions may be available.
Under applicable laws and FDA regulations, each NDA or BLA submitted for FDA approval is usually reviewed for administrative completeness and reviewability within 45 to 60 days following submission of the application. If deemed complete, the FDA will "file" the NDA or BLA, thereby triggering substantive review of the application. The FDA can refuse to file any NDA or BLA that it deems incomplete or not properly reviewable. If the FDA refuses to file an application, the FDA will retain 25% of the user fee as a penalty. The FDA has established performance goals for the review of NDAs and BLAs—six months for priority applications and 10 months for regular applications. However, the FDA is not legally required to complete its review within these periods and these performance goals may change over time. Moreover, the outcome of the review, even if generally favorable, typically is not an actual approval but an "action letter" that describes additional work that must be done before the application can be approved. The FDA's review of an application may involve review and recommendations by an independent FDA advisory committee.
The FDA may deny an NDA or BLA if the applicable regulatory criteria are not satisfied or may require additional clinical data. Even if such data is submitted, the FDA may ultimately decide that the NDA or BLA does not satisfy the criteria for approval. If the FDA approves a product, it may limit the approved therapeutic uses for the product as described in the product labeling, require that contraindications, warning statements or precautions be included in the product labeling, require that additional studies be conducted following approval as a condition of the approval, impose restrictions and conditions on product distribution, prescribing or dispensing in the form of a risk management plan, or otherwise limit the scope of any approval or post-approval, or limit labeling. Once issued, the FDA may withdraw product approval if compliance with regulatory standards is not maintained or if problems occur after the product reaches the market. In addition, the FDA may require testing and
surveillance programs to monitor the effect of approved products which have been commercialized, and the agency has the power to prevent or limit further marketing of a product based on the results of these post-marketing programs.
Satisfaction of the above FDA requirements or similar requirements of state, local and foreign regulatory agencies typically takes several years or more and the actual time required may vary substantially, based upon the type, complexity and novelty of the pharmaceutical product candidate. Government regulation may delay or prevent marketing of potential products for a considerable period
of time or permanently and impose costly procedures upon our activities. We cannot be certain that the FDA or any other regulatory agency will grant approval for any of our product candidates on a timely basis, or on a commercially viable basis, if at all. Success in preclinical or early stage clinical trials does not assure success in later stage clinical trials. Data obtained from preclinical and clinical activities is not always conclusive and may be susceptible to varying interpretations which could delay, limit or prevent regulatory approval. Even if a product candidate receives regulatory approval, the approval may be significantly limited to specific indications. Further, even after regulatory approval is obtained, later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market. Delays in obtaining, or failures to obtain regulatory approvals would have a material adverse effect on our business. Marketing our product candidates abroad will require similar regulatory approvals and is subject to similar risks. In addition, we cannot predict what adverse governmental regulations may arise from future U.S. or foreign governmental action.
Any products manufactured or distributed by us pursuant to FDA clearances or approvals are subject to pervasive and continuing regulation by the FDA, including record-keeping requirements, reporting of adverse experiences with the drug, other reporting, advertising and promotion restrictions. The FDA's rules for advertising and promotion require in particular that we not promote our products for unapproved uses, and that our promotion be fairly balanced and adequately substantiated. We must also submit appropriate new and supplemental applications and obtain FDA approval for certain changes to the approved product, product labeling or manufacturing process. Drug manufacturers and their subcontractors are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with current Good Manufacturing Practices, which impose certain procedural and documentation requirements upon us and our third-party manufacturers. We cannot be certain that we or our present or future suppliers will be able to comply with the current Good Manufacturing Practices and other FDA regulatory requirements. The FDA also enforces the requirements of the Prescription Drug Marketing Act, or PDMA, which, among other things, imposes various requirements in connection with the distribution of product samples to physicians.
In addition to inspections related to manufacturing, we are subject to periodic unannounced inspections by the FDA and other regulatory bodies related to the other regulatory requirements that apply to drugs manufactured or distributed by us. For example, the FDA may conduct periodic inspections regarding our reporting of adverse events, and the FDA has indicated to the industry that it may be conducting increased inspections related to compliance with the requirements of the PDMA concerning the handling of drug samples. When the FDA conducts an inspection, it will identify any deficiencies it believes exist in the form of a notice of inspectional observations, or Form FDA 483. The observations may be more or less significant. If we receive a notice of inspectional observations, we likely will be required to respond in writing, and may be required to undertake corrective and preventive actions in order to address the FDA's concerns.
We and our product candidates are also subject to a variety of state laws and regulations in those states or localities where they are or will be marketed. Any applicable state or local regulations may hinder our ability to market our product candidates in those states or localities.
The FDA's policies may change and additional government regulations may be enacted which could prevent or delay regulatory approval of our potential products. Moreover, increased attention to the containment of health care costs in the United States and in foreign markets could result in new government regulations which could have a material adverse effect on our business. We cannot predict the likelihood, nature or extent of adverse governmental regulation which might arise from future legislative or administrative action, either in the United States or abroad.
Orphan Drugs
Under the Orphan Drug Act, special incentives exist for sponsors to develop products for rare diseases or conditions, which are defined to include those diseases or conditions that affect fewer than 200,000 people in the U.S. Sponsors may request that FDA grant a drug orphan designation prior to
approval. We have received Orphan Drug designation for Fampridine-SR for the treatment of both MS and incomplete SCI.
Products designated as orphan drugs are eligible for special grant funding for research and development, FDA assistance with the review of clinical trial protocols, potential tax credits for research, reduced filing fees for marketing applications, and a special seven-year period of market exclusivity after marketing approval. Orphan drug exclusivity prevents FDA approval of applications by others for the same drug and the designated orphan disease or condition. FDA may approve a subsequent application from another person if FDA determines that the application is for a different drug or different use, or if FDA determines that the subsequent product is clinically superior, or that the holder of the initial orphan drug approval cannot assure the availability of sufficient quantities of the drug to meet the public's need. In addition, even when a drug has orphan exclusivity, the FDA may approve a competing drug for the same orphan use. The FDA may also approve someone else's application for the same drug that has orphan exclusivity, but for a different use, in which case the competing drug could be prescribed by physicians outside its FDA approval for the orphan use, notwithstanding the existence of orphan exclusivity. A grant of an orphan designation is not a guarantee that a product will be approved. If a sponsor receives orphan drug exclusivity upon approval, there can be no assurance that the exclusivity will prevent another person from receiving approval for the same or a similar drug for the same or other uses.
Generic Drugs, AB Ratings and Pharmacy Substitution
Generic drugs are approved through an abbreviated process, which differs in important ways from the process followed for innovative products. Generally an abbreviated new drug application, or ANDA, is filed with the FDA. The ANDA must seek approval of a drug product that has the same active ingredient(s), dosage form, strength, route of administration, and conditions of use (labeling) as a so-called "reference listed drug" approved under an NDA with full supporting data to establish safety and effectiveness. Only limited exceptions exist to this ANDA sameness requirement, including certain limited variations approved by the FDA through a special suitability petition process. The ANDA also generally contains clinical data to demonstrate that the product covered by the ANDA is absorbed in the body at the same rate and to the same extent as the reference listed drug. This is known as bioequivalence. In addition, the ANDA must contain information regarding the manufacturing processes and facilities that will be used to ensure product quality, and must contain certifications to patents listed with the FDA for the reference listed drug.
Every state has a law permitting or requiring pharmacists to substitute generic equivalents for brand-name prescriptions unless the physician has prohibited substitution. Managed care organizations often urge physicians to prescribe drugs with generic equivalents, and to authorize substitution, as a means of controlling costs. They also may require lower copayments as an incentive to patients to ask for and accept generics.
While the question of substitutability is one of state law, most states look to the FDA to determine whether a generic is substitutable. FDA lists therapeutic equivalence ratings in a publication often referred to as the Orange Book. In general, a generic drug that is listed in the Orange Book as therapeutically equivalent to the branded product will be substitutable under state law and, conversely, a generic drug that is not so listed will not be substitutable. To be considered therapeutically equivalent, a generic drug must first be a pharmaceutical equivalent of the branded drug. This means that the generic has the same active ingredient, dosage form, strength or concentration and route of
administration as the brand-name drug. Tablets and capsules are presently considered different dosage forms that are pharmaceutical alternatives and not substitutable pharmaceutical equivalents.
In addition to being pharmaceutical equivalents, therapeutic equivalents must be bioequivalent to their branded counterparts. Bioequivalence for this purpose is defined in the same manner as for
ANDA approvals, and usually requires a showing of comparable rate and extent of absorption in a small human study.
Solid oral dosage form drug products generally are rated AB in the Orange Book if they are considered therapeutic equivalents. If bioequivalence has been adequately demonstrated, the products will be rated "AB."
Foreign Regulation and Product Approval
Outside the United States, our ability to market a product candidate is contingent upon receiving a marketing authorization from the appropriate regulatory authorities. The requirements governing the conduct of clinical trials, marketing authorization, pricing and reimbursement vary widely from country to country. At present, foreign marketing authorizations are applied for at a national level, although within the European Community, or EC, registration procedures are available to companies wishing to market a product in more than one EC member state. If the regulatory authority is satisfied that adequate evidence of safety, quality and efficacy has been presented, a marketing authorization will be granted. This foreign regulatory approval process involves all of the risks associated with FDA clearance discussed above.
Other Regulations
In the U.S., the research, manufacturing, distribution, sale, and promotion of drug and biological products are potentially subject to regulation by various federal, state and local authorities in addition to the FDA, including the Centers for Medicare and Medicaid Services (formerly the Health Care Financing Administration), other divisions of the U.S. Department of Health and Human Services (e.g., the Office of Inspector General), the U.S. Department of Justice and individual U.S. Attorney offices within the Department of Justice, and state and local governments. For example, sales, marketing and scientific/educational grant programs must comply with the anti-kickback and fraud and abuse provisions of the Social Security Act, as amended, the False Claims Act, also as amended, the privacy provisions of the Health Insurance Portability and Accountability Act, or HIPAA, and similar state laws. Pricing and rebate programs must comply with the Medicaid rebate requirements of the Omnibus Budget Reconciliation Act of 1990, as amended, and the Veterans Health Care Act of 1992, as amended. If products are made available to authorized users of the Federal Supply Schedule of the General Services Administration, additional laws and requirements apply. All of these activities are also potentially subject to federal and state consumer protection and unfair competition laws.
We are also subject to numerous federal, state and local laws relating to such matters as safe working conditions, manufacturing practices, environmental protection, fire hazard control, and disposal of hazardous or potentially hazardous substances. We may incur significant costs to comply with such laws and regulations now or in the future.
Reimbursement and Pricing Controls
In many of the markets where we or our collaborative partners would commercialize a product following regulatory approval, the prices of pharmaceutical products are subject to direct price controls (by law) and to drug reimbursement programs with varying price control mechanisms.
In the United States, there has been an increased focus on drug pricing in recent years. Although there are currently no direct government price controls over private sector purchases in the United States, federal legislation requires pharmaceutical manufacturers to pay prescribed rebates on certain drugs to enable them to be eligible for reimbursement under certain public health care programs such
as Medicaid. Various states have adopted further mechanisms under Medicaid and otherwise that seek to control drug prices, including by disfavoring certain higher priced drugs and by seeking supplemental rebates from manufacturers. Managed care has also become a potent force in the market place that increases downward pressure on the prices of pharmaceutical products. Federal legislation, enacted in
December 2003, has altered the way in which physician-administered drugs covered by Medicare are reimbursed. Under the new reimbursement methodology, physicians are reimbursed based on a product's "average sales price," or ASP. This new reimbursement methodology has generally led to lower reimbursement levels. The new federal legislation also has added an outpatient prescription drug benefit to Medicare, effective January 2006. In the interim, Congress has established a discount drug card program for Medicare beneficiaries. Both benefits will be provided primarily through private entities, which will attempt to negotiate price concessions from pharmaceutical manufacturers.
Public and private health care payors control costs and influence drug pricing through a variety of mechanisms, including through negotiating discounts with the manufacturers and through the use of tiered formularies and other mechanisms that provide preferential access to certain drugs over others within a therapeutic class. Payors also set other criteria to govern the uses of a drug that will be deemed medically appropriate and therefore reimbursed or otherwise covered. In particular, many public and private health care payors limit reimbursement and coverage to the uses of a drug that are either approved by the FDA or that are supported by other appropriate evidence (for example, published medical literature) and appear in a recognized drug compendium. Drug compendia are publications that summarize the available medical evidence for particular drug products and identify which uses of a drug are supported or not supported by the available evidence, whether or not such uses have been approved by the FDA. For example, in the case of Medicare coverage for physician-administered oncology drugs, the Omnibus Budget Reconciliation Act of 1993, or OBRA '93, with certain exceptions, prohibits Medicare carriers from refusing to cover unapproved uses of an FDA-approved drug if the unapproved use is supported by one or more citations in the American Hospital Formulary Service Drug Information, the American Medical Association Drug Evaluations, or the U.S. Pharmacopoeia Drug Information. Another commonly cited compendium, for example under Medicaid, is the DRUGDEX Information System.
Different pricing and reimbursement schemes exist in other countries. For example, in the European Union, governments influence the price of pharmaceutical products through their pricing and reimbursement rules and control of national health care systems that fund a large part of the cost of such products to consumers. The approach taken varies from member state to member state. Some jurisdictions operate positive and/or negative list systems under which products may only be marketed once a reimbursement price has been agreed. Other member states allow companies to fix their own prices for medicines, but monitor and control company profits. The downward pressure on health care costs in general, particularly prescription drugs, has become very intense. As a result, increasingly high barriers are being erected to the entry of new products, as exemplified by the National Institute for Clinical Excellence in the UK which evaluates the data supporting new medicines and passes reimbursement recommendations to the government. In addition, in some countries cross-border imports from low-priced markets (parallel imports) exert a commercial pressure on pricing within a country.
Employees
As of January 3, 2006, we had 67 employees. Of the 67 employees, 24 perform research and development activities, including both preclinical programs and clinical trials, 29 work in sales, marketing, business development and communications and 14 perform general and administrative tasks.
Facilities
Our principal executive offices are located in an approximately 30,000 square foot facility in Hawthorne, NY, which houses offices and laboratory space. The current annual rent for this facility is $642,000. We believe that our facility is currently adequate for our purposes and that it will continue to be so for the foreseeable future. The lease for this facility expires in January 2008.
Legal Proceedings
We are not currently a party to any material legal proceedings.
Executive Officers and Directors
The following table sets forth, as of December 31, 2005,January 11, 2006, information about our executive officers and directors.
| Name | Age | Position(s) | ||
|---|---|---|---|---|
| Ron Cohen, M.D. | 49 | President, Chief Executive Officer and Director | ||
| Andrew R. Blight, Ph.D. | 55 | Chief Scientific Officer | ||
| Mary Fisher | 44 | Chief Operating Officer | ||
| David Lawrence, M.B.A. | 48 | Chief Financial Officer | ||
| Jane Wasman | 49 | Executive Vice President, General Counsel and Secretary | ||
| Standish M. Fleming(2) | 58 | Director | ||
| John Friedman | 52 | Director | ||
| Sandra Panem, Ph.D.(1) | 59 | Director | ||
| Barclay A. Phillips(2) | 43 | Director | ||
| Mark R.E. Pinney, M.B.A., C.F.A., M.S. | 51 | Director | ||
| Lorin J. Randall(2) | 62 | Director | ||
| Steven M. Rauscher(1) | 52 | Director | ||
| Michael Steinmetz, Ph.D.(2) | 58 | Director | ||
| Wise Young, Ph.D., M.D.(1) | Director |
Ron Cohen, M.D.,has served as our President and Chief Executive Officer since he founded Acorda in 1995. Dr. Cohen previously was a principal in the startup of Advanced Tissue Sciences, Inc., a biotechnology company engaged in the growth of human organ tissues for transplantation uses. Dr. Cohen received his B.A. degree with honors in Psychology from Princeton University, and his M.D. from the Columbia College of Physicians & Surgeons. He completed a residency in Internal Medicine at the University of Virginia Medical Center, and is Board Certified in Internal Medicine. Dr. Cohen serves on the Board of Directors of Zymenex A/S, a Danish pharmaceutical company, and on the Emerging Company Section of the Board of the Biotechnology Industry Organization (BIO). He is Chairman Emeritus and a Director of the Board of the New York Biotechnology Association and also serves as on the Scientific Advisory Board of the Daniel Heumann Fund and as a member of the Columbia-Presbyterian Health Sciences Advisory Council.
Andrew R. Blight, Ph.D., has been our Chief Scientific Officer since January 2004 and previously served as our Executive Vice President, Research and Development from 2000 to 2004, and Vice President, Research and Development, from 1998 to 2000. Prior to joining Acorda, Dr. Blight spent approximately six years as Professor and Director of the Neurosurgery Research Laboratory at the University of North Carolina at Chapel Hill. Dr. Blight held prior academic positions at Purdue University and New York University. Dr. Blight is a leader in SCI pathophysiology research and has made several important contributions to the field, particularly on the role of demyelination in SCI. He also pioneered the therapeutic application of 4-AP in SCI animal models and in human clinical trials. Dr. Blight is a member of the editorial board of the Journal of Neurotrauma and has served as a member of the NIH NSDA review committee. He was previously Secretary, Treasurer and Vice President of the National Neurotrauma Society. Dr. Blight received his B.S. in Zoology and his Ph.D. in Zoology/Neurobiology from the University of Bristol, U.K.
Mary Fisher has been our Chief Operating Officer since January 2005 and previously served as our Vice President, Commercial Operations from 2003 through 2004 and Vice President, Marketing
and Strategic Planning from 2000 to 2003. From 1999 to 2000, Ms. Fisher was an independent consultant to various pharmaceutical companies. From 1994 to 1999, Ms. Fisher was Vice President, Strategic Healthcare and Commercial Operations for Cephalon, Inc. In that capacity she was responsible for the company's corporate sales, managed care marketing, pricing, reimbursement, health economics, patient support programs, product planning, commercial manufacturing, distribution and customer service. From 1990 until joining Cephalon, Ms. Fisher was Corporate Communications Manager for Immunex Corporation.
David Lawrence, M.B.A., has been our Chief Financial Officer since January 2005. He previously served as our Vice President, Finance from January 2001 through 2004, and Director, Finance from 1999 to 2001. From 1991 to 1999, Mr. Lawrence held several positions for Tel-Air Communications, Inc. including Vice President and Controller. Prior to Tel-Air, he held financial management positions of Controller and Finance Manager for Southwestern Bell and Metromedia Telecommunications respectively. Mr. Lawrence received his undergraduate degree in Accounting from Roger Williams College, and an M.B.A in Finance from Iona College. Mr. Lawrence is a founding member and currently serves on the Board of Directors as Treasurer of The Brian Ahearn Children's Fund.
Jane Wasman, J.D., has been our Executive Vice President, General Counsel and Corporate Secretary since May 2004. From 1995 to 2004, Ms. Wasman held various leadership positions at Schering-Plough Corporation, including Staff Vice President and Associate General Counsel responsible for legal support for U.S. Pharmaceuticals operations, including sales, marketing and compliance; FDA regulatory matters; global research and development; and, corporate licensing and business development. She served as Staff Vice President, International in 2001 and as Staff Vice President, European Operations—Legal from 1998 to 2000. Previously, Ms. Wasman specialized in litigation at Fried, Frank, Harris, Shriver & Jacobson. She also served as Associate General Counsel to the U.S. Senate Committee on Veteran's Affairs. Ms. Wasman graduated Magna Cum Laude from Princeton University and earned her J.D. from Harvard Law School.
Standish M. Fleming has been a member of our Board of Directors since 2004. He is a 19-year veteran of life sciences venture capital investing. Mr. Fleming co-founded Forward Ventures in 1993. Before establishing Forward Ventures II in 1993, Mr. Fleming served as start-up chairman, president and CEO of GeneSys Therapeutics (now part of Cell Genesys). He has served as founding director and acting president of Triangle Pharmaceuticals (now part of Gilead Sciences, Inc.), CombiChem (now part of Bristol-Myers Squibb) and Corixa and GenQuest (now both part of GlaxoSmithKline). Mr. Fleming was a founding board member of Ciphergen Biosystems and Gryphon Sciences. He is a former president of the Biotechnology Venture Investors Group. Mr. Fleming began his venture career with Ventana Growth Funds in San Diego in 1986. Mr. Fleming earned his B.A. from Amherst College and his M.B.A. from the UCLA Graduate School of Management. Mr. Fleming has served on the boards of 19 venture-backed companies and is also currently a director of Ambit and Sanarus Medical, and a founding director of Arizeke Pharmaceuticals and Nereus Pharmaceuticals.
John Friedman has been a member of our Board of Directors since 2003. Mr. Friedman is the Managing Partner of Easton Hunt Capital Partners, L.P., a private investment firm that he founded in 1999. Since 1991, Mr. Friedman has also been the President of Easton Capital Corp., a private investment firm. He also helped manage Atrium Capital Corporation, an investment firm, from 1991 to 1993. From 1989 to 1991, Mr. Friedman was the founder and Managing General Partner of Security Pacific Capital Investors, a private investment firm. Prior to joining Security Pacific, Mr. Friedman was a Managing Director and Partner at E.M. Warburg, Pincus & Co., Inc., where he was employed from 1981 to 1989. From 1978 to 1980, Mr. Friedman was an attorney with Sullivan & Cromwell LLP and during 1980 he was employed at Shearson Loeb Rhoades. Mr. Friedman received a B.A. in History from Yale
College and a J.D. degree from Yale Law School. Mr. Friedman is a member of the board of directors of Comverse Technology, Inc., a telecommunications equipment company, YM BioSciences, Inc., a
biotechnology company, Renovis, a biotechnology company, Conor Medsystems, Inc., a drug delivery technology company, as well as several private companies. Mr. Friedman is also co-chairman of the President's Council of the Cold Spring Harbor Laboratory.
Sandra Panem, Ph.D., has been a member of our Board of Directors since 1998. She is currently a partner at Cross Atlantic Partners, which she joined in 2000. From 1994 to 1999, Dr. Panem was President of Vector Fund Management, the then asset management affiliate of Vector Securities International. Prior thereto, Dr. Panem served as Vice President and Portfolio Manager for the Oppenheimer Global BioTech Fund, a mutual fund that invested in public and private biotechnology companies. Previously, she was Vice President at Salomon Brothers Venture Capital, a fund focused on early and later-stage life sciences and technology investments. Dr. Panem was also a Science and Public Policy Fellow in economic studies at the Brookings Institution, and an Assistant Professor of Pathology at the University of Chicago. She received a B.S. in biochemistry and Ph.D. in microbiology from the University of Chicago. Dr. Panem currently serves on the boards of directors of Martek Biosciences Corp., Bioject Medical Technologies, Inc., Labcyte, Inc. and Confluent Surgical, Inc.
Barclay A. Phillips has been a member of our Board of Directors since September 2004. Mr. Phillips has been a Managing Director of Vector Fund Management, a venture capital firm focused on investments in the life sciences and healthcare industry, since 1999. From 1991 to 1999, Mr. Phillips served in various roles including Director of Private Placements and Biotechnology Analyst for INVESCO Funds Group, Inc. From 1985 to 1990, Mr. Phillips held positions in sales and trading with Paine Webber, Inc. and Shearson Lehman Hutton, Inc. Over the last twelve years, Mr. Phillips has served on the boards of a number of private companies and currently serves as a Director of CancerVax Corp. Mr. Phillips received a B.A. in economics from the University of Colorado.
Mark R. E. Pinney, M.B.A., C.F.A., M.S., joined our Board of Directors at our founding. He was also our Chief Financial Officer from 2001 to 2004. Since 2004, he has served as Chief Financial Officer and Chief Privacy Officer of Tacoda Systems, Inc. From 2000 to 2001, Mr. Pinney was Chairman of CanDo, Inc., an Internet company that offered product and service solutions to people with disabilities. In 1998, he co-founded and was Chief Executive Officer of LifeWire, Inc., a company developing community-based destination web sites for the disability population. LifeWire merged with CanDo in 2000. Mr. Pinney also co-founded Real Media, Inc., an Internet advertising software and services firm, in 1996. From 1984 to 1988, he was Vice President, Corporate Finance for Merrill Lynch Capital Markets and from 1988 to 1992, he was Vice President, Private Transactions at Dillon Read & Co., Inc. Mr. Pinney also serves on the Advisory Board of United Spinal Association. He received an undergraduate degree in engineering at the University of Exeter, England, an M.B.A. from the University of Chicago Graduate School of Business and a masters degree in engineering from Columbia University. He is a Chartered Financial Analyst.
Lorin J. Randallhas been a member of our Board of Directors since January 2006. Mr. Randall has been Senior Vice President and Chief Financial Officer of Eximias Pharmaceutical Corporation, a development-stage drug development company since 2004. From 2002 to 2004, Mr. Randall served as Senior Vice President and Chief Financial Officer of i-STAT Corporation, a publicly-traded manufacturer of medical diagnostic devices which was acquired by Abbott Laboratories in 2004. From 1995 to 2001, Mr. Randall was Vice President and Chief Financial Officer of CFM Technologies, Inc. a publicly-traded manufacturer of semiconductor manufacturing equipment. Mr. Randall previously served on the board of Quad Systems Corporation, a publicly-traded manufacturer of electronics manufacturing equipment where he served as Chairman of the Audit Committee. Mr. Randall received a B.S. in accounting from The Pennsylvania State University and an M.B.A. from Northeastern University.
Steven M. Rauscher has served on our Board of Directors since 2005. He is President and CEO of Oscient Pharmaceuticals Corporation, a commercial stage biopharmaceutical company. He joined Oscient in 2000 having served as a member of the Board of Directors since 1993. Previously, Mr. Rauscher was CEO of AmericasDoctor, a company providing clinical research services to the pharmaceutical industry. Prior to AmericasDoctor, he held a number of leadership positions at Abbott Laboratories, including Vice President of Corporate Licensing, Vice President of Business Development, International Division and Vice President of Sales, U.S. Pharmaceuticals. Mr. Rauscher received a B.S. from Indiana University and an M.B.A. from the University of Chicago.
Michael Steinmetz, Ph.D., has been a member of our Board of Directors since 1999. Dr. Steinmetz is a Managing Director at Clarus Ventures LLC, a company he co-founded in 2005. From 1999 to June 2005, he was a General Partner of MPM's BioVentures' Funds. Prior to MPM, he held positions at various academic institutions, including the California Institute of Technology and the Basel Institute for Immunology where he was a permanent member. In 1986, he joined Hoffmann-La Roche and held
various leadership positions in R&D, initially in Switzerland and subsequently in the United States where, as Vice President of Preclinical Research and Development, he was responsible for Roche's drug discovery activities in the United States and Roche's global biotechnology efforts. Dr. Steinmetz received a degree in chemistry from the University of Hamburg, Germany and holds a Ph.D. from the University of Munich, Germany. He has done academic research in the areas of Biochemistry, Molecular Biology and Immunology and has published over 130 manuscripts in leading scientific journals.
Wise Young, Ph.D., M.D., has been a member of the board of directors and of our scientific advisory board since the founding of the company in 1995. Dr. Young has been at Rutgers University since 1997, where he serves as Professor and Chair of the Department of Cell Biology and Neuroscience, Professor II and Director of the Neuroscience Center and founderFounding Director of the W.M. Keck Center for Neuroscience. Dr. Young is one of the preeminent scientists in the fields of spinal cord injury and neurotrauma, SCI animal models, and the pharmacological therapy of SCI. He was the Principal Investigator for the Multicenter Animal Spinal Cord Injury Study, funded by the National Institutes of Health; is editor-in-chief ofCurrent Concepts in Critical Care and Trauma; and serves on numerous editorial boards, including those ofExperimental Neurology, Journal of Neurotrauma, Brain Research andStroke. Dr. Young has received the Wakeman Award for Research in Neurosciences, and a Jacob Javits Neuroscience Award from the National Institute of Neurological Disorder and Stroke. He is also a member of the Scientific Advisory Council of the American Paralysis Association and of the National Acute Spinal Cord Injury Study executive committee. Dr. Young received a B.A. in biology and chemistry from Reed College, a Ph.D. in physiology and biophysics from the University of Iowa and an M.D. from Stanford University.
Board Composition
Our board of directors currently has nine members. Upon completion of this offering, our board of directors will consist of nine directors divided into three classes, with each class serving for a term of three years:
At each annual meeting of stockholders, the successors to directors whose terms will then expire will be elected for three-year terms. This classification of the board of directors may have the effect of delaying or preventing changes in control or management. See "Risk Factors—Certain provisions of Delaware law, our certificate of incorporation and our by-laws may delay or prevent an acquisition of us that stockholders may consider favorable or may prevent efforts by our stockholders to change our directors or our management, which could decrease the value of your shares."
We believe that a majority of the members of our Board of Directors will be independent under the current independence requirements of the Nasdaq National Market and the Securities and Exchange Commission, or the SEC. The authorized number of directors may be changed by resolution adopted by a majority of the board of directors.
Board Observation Rights
In connection with our Revenue Interests Assignment Agreementrevenue interests assignment agreement with PRF, we granted PRF the right to appoint a representative to receive all notices and materials provided to our board of directors
and to attend as an observer all meetings of our board of directors, subject to certain exceptions. Mr. Gregory B. Brown, M.D. is the initial representative designated by PRF for such purpose. This right will terminate on the earlier to occur of the fourth anniversary of the completion of an initial public offering of shares of our common stock or termination of our agreement with PRF.
Director Compensation
Our outside directors compensation policy provides that new outside directors on our board receive an initial grant of stock options in the amount of 0.2% of the fully diluted shares of our common stock, or a comparable adjusted number of stock appreciation rights or shares of restricted stock, with a fair market value exercise price and a three-year quarterly vesting schedule commencing on the date of the award, unless they hold at least an equivalent amount of common stock through prior ownership. On an annual basis, at the discretion of the board of directors upon the recommendation of the compensation committee, outside directors can receive stock options in the amount of up to 0.02% of the fully diluted shares of our common stock, or a comparable adjusted number of stock appreciation rights or shares of restricted stock, with a fair market value exercise price and a one-year quarterly vesting schedule. Upon consummation of this offering, this compensation policy will be extended to all of the outside directors on our board of directors. Directors are also reimbursed for reasonable expenses related to their service on our board of directors.
Board Committees
Our board of directors has an audit committee, a compensation committee and a nominations committee.
Audit Committee
Our audit committee consists of Mr. Phillips, Mr. Fleming, Mr. Randall and Dr. Steinmetz. Mr. Phillips serves as chair of our audit committee. Our board of directors has determined that Mr. Fleming qualifiesand Mr. Randall each qualify as an "audit committee financial expert" as that term is defined in Item 401(h) of Regulation S-K of the Securities Act. We believe that the composition of our audit committee meets, and the functioning of our audit committee will comply with, the applicable requirements of the Sarbanes-Oxley Act of 2002, the Nasdaq National Market and SEC rules and regulations.
Our audit committee is responsible for:
We have adopted a written audit committee charter that we will make available on our website.
Compensation Committee
Our compensation committee consists of Dr. Panem, Mr. Rauscher and Dr. Young. Dr. Panem serves as chair of our compensation committee. We believe that the composition of our compensation committee meets, and the functioning of our compensation committee will comply with, the applicable requirements of the Nasdaq National Market and SEC rules and regulations. Our compensation committee is responsible for:
We have adopted a written compensation committee charter that we will make available on our website.
Nominations Committee
Effective upon the closing of this offering, our nominations committee will consist of Mr. Friedman, Dr. Panem and Dr. Steinmetz. Mr. Friedman will serve as chair of the committee. The nominations committee will be responsible for identifying potential candidates to serve on our board. We have approved a written nominations committee charter that also will be effective upon the closing of this offering and that sets forth procedures for the consideration of director nominees and other related matters.
Code of Ethics
Our board of directors has adopted a code of ethics for all directors, officers and employees. We will make this code available on our website upon completion of this offering.
Compensation Committee Interlocks and Insider Participation
The compensation of our executive officers is currently determined by our compensation committee, as described above. None of our executive officers has served as a member of the board of directors or compensation committee of any entity that has one or more executive officers serving as a member of our board of directors or compensation committee.
Dr. Panem is affiliated with Cross Atlantic Partners, which participated in the sale of our Series J preferred stock in a private placement consummated in May 2003. Pursuant to an amended and restated registration rights agreement among us and certain of our stockholders, including entities affiliated with Dr. Panem, the parties to the registration rights agreement have demand and piggy-back registration rights. See "Certain Relationships and Related Transactions."
Executive Compensation
The following summary compensation table sets forth the aggregate compensation awarded to, earned by or paid to the following individuals during the fiscal yearyears ended December 31, 2005:2005 and 2004:
We refer to these individuals as our "named executive officers."
| | | | | Long-Term Compensation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Annual Compensation | Securities Underlying | ||||||||||
| Name and Principal Position | Year | Salary | Bonus(2) | Restricted Stock Award(3) | Options(4) | |||||||
| Ron Cohen, M.D. President and Chief Executive Officer | 2005 | $ | 305,000 | $ | 0 | 260,385 | 51,265 | |||||
| Andrew R. Blight, Ph.D. Chief Scientific Officer | 2005 | $ | 215,000 | $ | 0 | 97,385 | 52,338 | |||||
| Mary Fisher Chief Operating Officer | 2005 | $ | 225,000 | $ | 0 | 157,231 | 132,323 | |||||
| Jane Wasman Executive VP & General Counsel | 2005 | $ | 225,000 | $ | — | 77,615 | 44,769 | |||||
| David Lawrence M.B.A. Chief Financial Officer | 2005 | $ | 180,000 | $ | 0 | 64,231 | 70,109 | |||||
| 835,847 | (1) | 350,804 | ||||||||||
| Long-Term Compensation | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Annual Compensation | Securities Underlying | ||||||||||||||
| Name and Principal Position | Year | Salary | Bonus(1) | Restricted Stock Award(2) | Options(3) | All Other Compensation | |||||||||
| Ron Cohen, M.D. President and Chief Executive Officer | 2005 2004 | $ | 305,000 305,000 | $ | — 120,000 | 260,385 | 51,265 — | — — | |||||||
Andrew R. Blight, Ph.D. Chief Scientific Officer | 2005 2004 | 215,000 210,000 | — 65,450 | 97,385 | 52,338 — | — — | |||||||||
Mary Fisher Chief Operating Officer(4) | 2005 2004 | 225,000 210,000 | — 74,000 | 157,231 | 132,323 — | $ | — 109,087 | ||||||||
Jane Wasman Executive VP & General Counsel(5) | 2005 2004 | 225,000 225,000 | — — | 77,615 | 44,769 — | $ | — 25,000 | ||||||||
David Lawrence M.B.A. Chief Financial Officer(6) | 2005 2004 | 180,000 164,800 | — 64,000 | 64,231 | 70,109 — | — — | |||||||||
Stock Options
Aggregate Exercise of Stock Options and Year-end Option Values
The following table contains information regarding the number of shares of common stock subject to both exercisable and unexercisable stock options, as well as the value of unexercisable in-the-money options as of December 31, 2005 for the named executive officers. There was no public market for our common stock as of December 31, 2005. Accordingly, the value of unexercised in-the-money options as of such date has been calculated by determining the difference between the exercise price per share
and an assumed offering price of $ per share, which is the midpoint of the estimated price range shown on the cover of this prospectus.
| | | | Number of Securities Underlying Unexercised Options at December 31, 2005 | Value of Unexercised In-the-Money Options at December 31, 2005 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Shares Acquired on Exercise | | ||||||||||||
| Name | Value Realized ($) | |||||||||||||
| Exercisable | Unexercisable | Exercisable | Unexercisable | |||||||||||
| Ron Cohen | 0 | 0 | 665,721 | 38,452 | $ | $ | ||||||||
| Andrew Blight | 0 | 0 | 108,205 | 39,255 | ||||||||||
| Mary Fisher | 0 | 0 | 69,965 | 99,245 | ||||||||||
| Jane Wasman | 0 | 0 | 11,193 | 33,576 | ||||||||||
| David Lawrence | 0 | 0 | 46,415 | 52,584 | ||||||||||
The following table sets forth the number of shares underlying options that have been issued to each of the named executive officers in calendar year 2005. No stock appreciation rights have been granted to these individuals. The potential realizable value set forth in the last column of the table is calculated based on the term of the option at the time of grant, which is ten years. This value is based on assumed rates of stock price appreciation of 0%, 5% and 10% compounded annually from the date of grant until their expiration date, assuming a fair market value equal to the mid-point of the estimated price range of an offering, minus the applicable exercise price. These numbers are calculated based on the requirements of the SEC and do not reflect our estimate of future stock price growth. Actual gains, if any, on stock option exercises will depend on future performance of the common stock on the date on which the options are exercised.
| | | | | | | Potential Realizable Value at Assumed Annual Rates of Stock Price Appreciation for Option Term(2) | | | | | | Potential Realizable Value at Assumed Annual Rates of Stock Price Appreciation for Option Term(2) | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Number of Shares Underlying Stock Options Granted in Calendar Year 2005(1) | | | | | Number of Shares Underlying Stock Options Granted in Calendar Year 2005(1) | | | | | |||||||||||||||||||||||
| | Percent of Total Options Granted to Employees in Fiscal Year | | Market Price on Date of Grant ($/share) | | Percent of Total Options Granted to Employees in Fiscal Year | | Market Price on Date of Grant ($/share) | | |||||||||||||||||||||||||
| Name | Exercise Price ($/share) | Expiration Date | Exercise Price ($/share) | Expiration Date | |||||||||||||||||||||||||||||
| 10% | Market Price on Date of Grant ($/share) | Market Price on Date of Grant ($/share) | 10% | ||||||||||||||||||||||||||||||
| Ron Cohen | 51,265 | 8.8% | $ | 8.14 | 1/1/2015 | 51,265 | 8.8% | $ | 8.14 | $ | 1/1/2015 | $ | |||||||||||||||||||||
| Andrew Blight | 52,338 | 9.0% | $ | 8.14 | 1/1/2015 | 52,338 | 9.0% | $ | 8.14 | $ | 1/1/2015 | ||||||||||||||||||||||
| Mary Fisher | 132,323 | 22.7% | $ | 8.14 | 1/1/2015 | 132,323 | 22.7% | $ | 8.14 | $ | 1/1/2015 | ||||||||||||||||||||||
| Jane Wasman | 44,769 | 7.7% | $ | 8.14 | 1/1/2015 | 44,769 | 7.7% | $ | 8.14 | $ | 1/1/2015 | ||||||||||||||||||||||
| David Lawrence | 70,109 | 12.0% | $ | 8.14 | 1/1/2015 | 70,109 | 12.0% | $ | 8.14 | $ | 1/1/2015 | ||||||||||||||||||||||
Stock Incentive Plans
Our board of directors has adopted two equity incentive plans: our 2006 StockEmployee Incentive Plan (the 2006 Plan) and our 1999 Employee Stock Option Plan (the 1999 Plan and, together with the 2006 Plan, the Plans). AAs of January 15, 2006, a total of 3,723,7365,481,334 shares of our common stock will be availablehad been reserved for issuance under the Plans, including 700,5223,000,000 shares remaining eligiblereserved for the grant of awards. Following the effective date ofawards under the 2006 Plan, noPlan. No additional awards will be made under the 1999 Plan.
The 2006 Plan was adopted on January 3, 2006 will becomeand became effective, on the date as of which it is approvedfollowing approval by our stockholders.stockholders, on January 11, 2006. The 1999 Plan was adopted by our board of directors in June 1999. The Plans allow us to issue incentive and nonstatutory stock options, restricted stock awards and stock
appreciation rights for shares of our common stock. The 2006 Plan will terminate ten years after the effective date of the plan.
There are a total of 3,723,736The 3,000,000 shares of common stock that will be availablereserved for issuance under the 2006 Plan (including an amount towill be added under the "evergreen" provision described below on the day the plan is approvedincreased by the shareholders), which includes thenumber of shares issuable upon the exercise of our common stock, if any, that are subject to outstanding awards under the 1999 Plan and a number of shares equalat January 11, 2006, to the remainingextent that such shares reserved for awards under the 1999 Plan.are surrendered before exercise, lapse, are terminated without being exercised or are forfeited after such date.
In addition, the 2006 Plan contains an "evergreen" provision which provides for automatic annual increases to the share reserve under the 2006 Plan on the first day of each fiscal year by a number of shares equal to the lesser of:
Although a similar evergreen provision is contained in our 1999 Plan, this provision has been amended, effective upon the adoption of the 2006 Plan by our board of directors, so as not to increase the reserved shares under the 1999 Plan.
Our compensation committee administers the Plans, selects those persons who are to be granted awards under the 2006 Plan and determines the terms and conditions of those awards. Our directors, key employees, independent contractors, agents and consultants are eligible to receive awards under our Plans, but only employees and officers may receive incentive stock options.
The exercise price per share of the incentive stock options awarded under the Plans must be at least equal to the fair market value of a share of our common stock on the date of grant. The exercise price per share of nonstatutory stock options awarded under the Plans must be equal to the fair market value of a share of our common stock on the date of grant, or such other price that the compensation committee may determine is appropriate. The compensation committee determines the exercise period of the stock options, but in no event will the stock options expire later than ten years from the date of grant. Except as the compensation committee may otherwise determine, upon the voluntary termination or involuntary termination without cause of the option holder, the stock options may be exercised for a period of three months after such termination. In the case of termination of the option holder by reason of retirement or due to disability, the stock options may be exercised at any time to the extent that such stock option was vested, but only within one year of termination in the case of incentive stock options. In the case of termination by death, the option holder's estate, or any person who acquires the stock option by reason of the option holder's death, may exercise the stock option within a period of three years after the option holder's death.
An award under our Plans will become vested only if the vesting conditions set forth in the award agreement, as determined by the compensation committee, are satisfied. The vesting conditions may include performance of services for a specified period, achievement of performance objectives or a combination of the two types of criteria. Performance objectives may be based on financial or operating measures. In granting performance-based awards under the 2006 Plan, which are regulated by Section 162(m) of the Internal Revenue Code, the compensation committee is bound to follow the criteria established under the 2006 Plan.
Under the 2006 Plan, upon a reorganization event, as defined, each outstanding award under the 2006 Plan, with certain exceptions, must either be assumed or an equivalent exercisable or unrestricted award substituted by the successor entity in the reorganization. If an award is assumed and, within 18 months after the reorganization event the recipient's employment is terminated without cause or he or she terminates employment for good reason, the award will become exercisable in full. If the successor entity does not assume outstanding awards at the time of a reorganization event, the compensation committee must provide that either (i) all or some portion of outstanding awards will be accelerated immediately prior to the reorganization event, or (ii) all outstanding awards will terminate upon consummation of the reorganization event and each recipient of an award will receive, in
exchange for the award, a cash
payment equal to the value of the award, or (iii) if our common stock remains publicly traded, the awards will remain in place unchanged.
Under the 1999 Plan, in the event of a tender offer by a person or persons other than us, for all or any part of the outstanding stock which, following consummation of the tender offer would result in the offeror's or offerors' owning, beneficially or of record, an aggregate of more than 25% of our outstanding common stock, or in the event of a change of control as defined, stock options under the 1999 Plan will become immediately exercisable to the extent of the total number of shares subject to the stock options. The compensation committee may authorize payment of cash upon exercise of a stock appreciation right in the event of a tender offer as described above, or a change of control.
In September 2003, we repriced 115,578 stock options issued to employees, which had an exercise price per option of more than $7.64, with a new exercise price of $7.64. In March 2004, we repriced 1,227,648 stock options issued to employees, which had an exercise price per option of more than $2.60, with a new exercise price per option of $2.60. We recognized additional compensation charges for these repricings (see Note 9 to our consolidated financial statements included in this prospectus).
401(k) Plan
Effective September 1, 1999, we adopted a defined contribution 401(k) savings plan covering all of our employees. Participants may elect to defer a percentage of their annual pre-tax compensation to the 401(k) plan, subject to defined limitations. Our board of directors has discretion to match contributions made by our employees. We did not make any matching contributions to the plan in fiscal years 2000, 2001, 2002 or in calendar years 2003 and 2004.
Employment Contracts, Termination of Employment and Change-in-Control Arrangements
We are a party to an employment agreement with Dr. Cohen that governs the terms and conditions of his employment as our President and Chief Executive Officer. The employment agreement provides for a base annual salary of $280,000, subject to annual increases and bonuses at the discretion of the board of directors. His current salary is $305,000. Dr. Cohen is eligible to receive annual performance-based stock options to purchase common stock in an amount determined by the board of directors based on Dr. Cohen's individual performance and the achievement of our goals and objectives. Dr. Cohen's employment agreement would have expired in January 2004, but is subject to automatic successive one-year renewal periods unless either Dr. Cohen or we give the other written notice at least 60 days prior to the expiration date that Dr. Cohen or we do not intend to renew the contract. Dr. Cohen's employment agreement has been renewed effective January 20052006 for a one-year period. In the event we terminate the agreement with Dr. Cohen without cause, or if Dr. Cohen voluntarily terminates the agreement with good reason, we are obligated to make severance payments equal to one year's base annual salary and COBRA premium payments for the severance period plus a bonus equal to his prior year's bonus pro rated for the number of days worked prior to termination. In such event, all of Dr. Cohen's options will become immediately exercisable and will remain exercisable for 48 months following termination. If Dr. Cohen's employment terminates for death or disability, we are obligated to pay his base salary for three months and COBRA premiums for the COBRA coverage period and 65% of his outstanding options will become immediately vested and remain exercisable for 48 months following such termination. In the event of a change in control, the vesting of Dr. Cohen's options will be governed by the terms of our stock option plan and his stock option agreement, but in no event will less than 65% of Dr. Cohen's then unvested stock options become immediately vested and exercisable. If Dr. Cohen voluntarily terminates his employment without good reason following a change in control, he is entitled to receive the same severance and bonus package described above, however, only 65% of his outstanding options will become immediately vested and remain exercisable for 48 months following termination. Following his termination of employment, Dr. Cohen will remain subject to confidentiality, non-competition and non-solicitation covenants for one year in the case of non-competition and non-solicitation and five years in the case of confidentiality.
On September 26, 2004, we entered into an amendment to Dr. Cohen's employment agreement to increase the amount of severance to which he would be entitled in the event of a termination of his employment by us without cause or by Dr. Cohen with good reason from one year to 15 months and to make such severance, together with his prorated bonus, payable in one lump sum within 30 days after such termination.
We are party to an employment agreement with Dr. Blight that governs the terms and conditions of his employment as our Chief Scientific Officer. The employment agreement provides for a base annual salary of $215,000, subject to annual review by Dr. Cohen and by the compensation committee of the Board of Directors. His current salary is $215,000.
We are party to an employment agreement with Ms. Fisher that governs the terms and conditions of her employment as our Chief Operating Officer. The employment agreement provides for a base annual salary of $225,000, subject to annual review by Dr. Cohen and by the compensation committee of the Board of Directors. Her current salary is $225,000.
We are party to an employment agreement with Mr. Lawrence that governs the terms and conditions of his employment as our Chief Financial Officer. The employment agreement provides for a base annual salary of $180,000, subject to annual review by Dr. Cohen and by the compensation committee of the Board of Directors. His current salary is $180,000.
We are party to an employment agreement with Ms. Wasman that governs the terms and conditions of her employment as our Executive Vice President, General Counsel and Corporate Secretary. The employment agreement provides for a base annual salary of $225,000, subject to annual review by Dr. Cohen and by the compensation committee of the Board of Directors. Her current salary is $225,000.
Pursuant to their employment agreements, Dr. Blight, Ms. Fisher, Mr. Lawrence and Ms. Wasman are eligible to receive an annual bonus and to receive annual performance-based stock options to purchase common stock, stock appreciation rights awards and/or restricted stock awards of common stock in an amount to be recommended by the compensation committee and approved by the board of directors based on their respective performances and upon the achievement of our goals and objectives. Each of their employment agreements expires on December 19, 2006 but is subject to extension by the mutual agreement of both parties.
In the event we terminate our employment agreement with Dr. Blight, Ms. Fisher, Mr. Lawrence or Ms. Wasman without cause, or if one of them voluntarily terminates his or her agreements with good reason, we are obligated to make severance payments equal to nine months base annual salary, in the case of Dr. Blight and Ms. Fisher, and seven months base annual salary, in the case of Mr. Lawrence and Ms. Wasman, as well as COBRA premium payments for the severance period. In such event, all options, stock appreciation rights awards and restricted stock awards that have vested as of the termination date shall remain exercisable for 90 days following such date. All unvested options, stock appreciation rights awards and stock awards will be cancelled on the date of termination. If Dr. Blight, Ms. Fisher, Mr. Lawrence or Ms. Wasman voluntarily terminates his or her employment without good reason or if we terminate his or her employment without cause within 18 months after a change in control, we are obligated to make severance payments equal to one year's base annual salary, in the case of Dr. Blight and Ms. Fisher, and nine months base annual salary, in the case of Mr. Lawrence and Ms. Wasman, in each case paid in a lump sum within 30 days after termination, as well as COBRA premium payments for the severance period plus a bonus equal to a prior year's bonus pro rated for the number of days worked prior to termination. We are also obligated to pay salary earned but not paid, vacation and sick leave days that have accrued, and reimbursable business expenses incurred through the date of termination. In such event, not less than 50% of the unvested options, stock appreciation rights and restricted or other stock awards shall become immediately and full vested and shall remain exercisable for 18 months following such date. All options that have vested
as of the termination date shall remain exercisable for 90 days following such date. All unvested options, stock appreciation rights awards and stock awards will be cancelled on the date of termination.
Indemnification of Directors and Executive Officers and Limitation on Liability
Our certificate of incorporation currently provides and, upon the closing of this offering, our amended and restated certificate of incorporation will provide, that we shall indemnify our directors and officers to the fullest extent permitted by Delaware law. Upon the closing of this offering, our amended and restated certificate of incorporation will also provide that, with respect to proceedings initiated by our officers and directors, we are only required to indemnify these persons if the proceeding was authorized by our board of directors. Our amended bylaws permit us, by action of our board of directors, to indemnify our other employees and agents to the same extent as we are required to indemnify our officers and directors.
In addition, our certificate of incorporation provides, and upon the closing of this offering our amended and restated certificate of incorporation will provide, that our directors will not be personally liable to us or our stockholders for monetary damages for any breach of fiduciary duty as a director, except for liability:
There is no pending litigation or proceeding involving any of our directors or officers for which indemnification is being sought, nor are we aware of any pending or threatened litigation that may result in claims for indemnification by any director or officer.
CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS
Sale of Securities
In March 2001, we consummated a private placement of 10,204,047 shares of Series I preferred stock for an aggregate purchase price of approximately $39,694,000. Except for Michael Steinmetz, Standish Fleming and Barclay Phillips, who are affiliated with MPM/BB Bioventure, Forward Ventures and Vector Fund Management, respectively, none of our executive officers or directors purchased any shares of the Series I preferred stock.
The following table sets forth, with respect to the Series I preferred stock transaction, the purchase price per share, the aggregate shares purchased and the total investment for MPM/BB Bioventure Group, Forward Ventures and Vector Fund Management:
| Investor | Purchase Price per Share of Series I Preferred | Aggregate Shares of Series I Preferred Purchased | Total Investment in Series I Preferred | |||
|---|---|---|---|---|---|---|
| MPM/BB Bioventure Group | $3.89 | 639,359 | $2,487,107 | |||
| Forward Ventures | $3.89 | 1,542,417 | $6,000,002 | |||
| Vector Fund Management | $3.89 | 398,547 | $1,550,348 |
In May 2003, we consummated a private placement of 112,790,233 shares of Series J preferred stock for an aggregate purchase price of approximately $55,267,000. Except for Michael Steinmetz, John Friedman, Sandra Panem, Standish Fleming and Barclay Phillips, who are affiliated with MPM/BB Bioventure Group, Easton Hunt Capital Partners, Cross Atlantic Partners, Forward Ventures and Vector Fund Management, respectively, none of our executive officers or directors purchased any shares of the Series J preferred stock.
The following table sets forth, with respect to the Series J preferred stock transaction, the purchase price per share, the aggregate shares purchased and the total investment for each of MPM/BB Bioventure Group, Easton Hunt Capital Partners, Cross Atlantic Partners, Forward Ventures and Vector Fund Management:
| Investor | Purchase Price per Share of Series J Preferred | Aggregate Shares of Series J Preferred Purchased | Total Investment in Series J Preferred | |||||
|---|---|---|---|---|---|---|---|---|
| MPM/BB Bioventure group | $ | 0.49 | 15,306,121 | $ | 7,500,000 | |||
| Easton Hunt Capital Partners | $ | 0.49 | 11,224,490 | $ | 5,500,000 | |||
| Cross Atlantic Partners | $ | 0.49 | 8,506,256 | $ | 4,168,065 | |||
| Forward Ventures | $ | 0.49 | 8,163,264 | $ | 4,000,000 | |||
| Vector Fund Management | $ | 0.49 | 2,040,816 | $ | 1,000,000 | |||
In March 2004, we consummated a private placement of 1,533,330 shares of Series K preferred stock for an aggregate purchase price of approximately $11,499,958. Except for John Friedman and Sandra Panem, who are affiliated with Easton Hunt Capital Partners and Cross Atlantic Partners, respectively, none of our executive officers or directors purchased any shares of the Series K preferred stock.
The following table sets forth, with respect to the Series K preferred stock transaction, the purchase price per share, the aggregate shares purchased and the total investment for each of Easton Hunt Capital Partners, Easton Hunt New York and Cross Atlantic Partners:
| Investor | Purchase Price per Share of Series K Preferred | Aggregate Shares of Series K Preferred Purchased | Total Investment in Series K Preferred | |||||
|---|---|---|---|---|---|---|---|---|
| Easton Hunt Capital Partners | $ | 7.50 | 100,000 | $ | 750,000 | |||
| Easton Hunt New York | $ | 7.50 | 100,000 | $ | 750,000 | |||
| Cross Atlantic Partners | $ | 7.50 | 55,574 | $ | 416,805 | |||
Board Representation and Registration Rights
Pursuant to an amended and restated registration rights agreement dated as of March 3, 2004, the holders of our Series I Preferred, Series J Preferred and Series K preferred stock have demand and piggy-back registration rights. Pursuant to the terms of this agreement, holders of at least 30% of outstanding "registrable securities" have the right to initiate a demand registration, subject to our ability to delay registration under certain circumstances.
In addition, if we propose to register any of our securities under the Securities Act, including in this offering, certain of our other stockholders are entitled to notice of the registration and to include their registrable shares in the offering. If the managing underwriter determines that marketing factors require a limitation on the number of shares to be underwritten, the managing underwriters may limit or exclude from such underwriting the registrable securities and other securities of these stockholders. If we are so advised by the managing underwriter, then all securities other than registrable securities shall first be excluded from the registration. In no event, however, will the amount of stockholders' securities to be included in the offering be reduced below 30% of the total securities in the offering. We are required to bear substantially all costs incurred in these registrations, other than underwriting discounts and commissions.
Pursuant to the lock-up agreements with the underwriters, holders of greater than 70% of the "registrable securities" under our registration rights agreement have waived their rights to demand registration and participation in this offering under the registration rights agreement until the later of October 30, 2006 or expiration of the lock-up agreements.
AgreementsAgreement with Former Director
In November, 2004, we entered into an agreement with Mark Pinney, under which we agreed to extend the last date by which Mr. Pinney is entitled to exercise vested stock options previously granted to him to 90 days after he is no longer a director or consultant to us. In addition, he will be entitled to retain certain shares of restricted stock if the vesting requirements for these shares are met within the extended time period. On September 26, 2005, Mr. Pinney was issued 5,000 shares of restricted stock for services rendered as a member of our board of directors from November 1, 2004 through December 31, 2005. Mr. Pinney's shares of restricted stock are otherwise subject to the vesting in the manner described in footnote 3 to the Summary Compensation Table found on page 92.
Agreements with Elan
In September 2003, we entered into the following agreements with Elan, which holds more than 5% of our outstanding common stock:Elan:
Fampridine-SR. We Fampridine-SR and under which we are obligated under the license to make milestone and royalty payments to Elan.
In July 2004, we entered into the following agreements with Elan, which holds more than 5% of our outstanding common stock:Elan:
For a more detailed description of these agreements with Elan see "Business—Collaborations and License Agreements".
Until December 23, 2005, Elan held more than 5% of our outstanding common stock. On December 23, 2005, Elan transferred to funds affiliated with Saints Capital 900,000 shares of our Series B convertible preferred stock, 333,333 shares of our Series C convertible preferred stock, 2,300,000 shares of our Series F convertible preferred stock, a warrant to purchase 100,000 shares of our Series B convertible preferred stock, a $2,500,000 convertible promissory note convertible into shares of our Series B convertible stock or an undesignated series and a $5,000,000 convertible promissory note convertible into shares of our Series D convertible preferred stock.
The following table contains information as of December 31, 2005 about the beneficial ownership of our common stock before and after the consummation of this offering for:
Unless otherwise indicated, the address for each person or entity named below is c/o Acorda Therapeutics, Inc., 15 Skyline Drive, Hawthorne, New York 10532.
Beneficial ownership is determined on the basis of the rules and regulations of the Securities and Exchange Commission. In computing the number of shares beneficially owned by a person and the percentage ownership of that person, shares of common stock subject to options held by that person that are currently exercisable or exercisable within 60 days of the date hereof are deemed outstanding. Such shares, however, are not deemed outstanding for the purposes of computing the percentage ownership of any other person. For the purpose of calculating the amounts set forth in the following table, all outstanding shares of preferred stock have been deemed to have been converted into shares of common stock, which conversion will occur upon the closing of this offering. Except as indicated in the footnotes to the following table or pursuant to applicable community property laws, each stockholder named in the table has sole voting and investment power with respect to the shares set forth opposite such stockholder's name. The percentage of beneficial ownership is based on 13,547,022 shares of common stock outstanding, on an as converted basis, on December 31, 2005.
| | | | Percentage of Common Stock Outstanding | | | Percentage of Common Stock Outstanding | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beneficial Owner | Beneficial Owner | Number of Shares(1) | Before Offering | After Offering(2) | Beneficial Owner | Number of Shares(1) | Before Offering | After Offering(2) | ||||||||
| Five Percent Stockholders: | Five Percent Stockholders: | Five Percent Stockholders: | ||||||||||||||
| MPM/BB Bioventure group(3) | 1,640,137 | 12.1 | % | % | MPM/BB Bioventure group(3) | 1,640,137 | 12.1 | % | % | |||||||
| Elan group(4) | 997,775 | 7.4 | Saints Capital(4) | 965,170 | 7.1 | |||||||||||
| Forward Ventures group(5) | 873,890 | 6.5 | Forward Ventures group(5) | 873,890 | 6.5 | |||||||||||
| Easton Hunt(6) | 873,364 | 6.4 | Easton Hunt(6) | 873,364 | 6.4 | |||||||||||
| Cross Atlantic Partners(7) | 705,388 | 5.2 | Cross Atlantic Partners(7) | 705,388 | 5.2 | |||||||||||
| TVM Life Sciences(8) | 705,388 | 5.2 | TVM Life Sciences(8) | 705,388 | 5.2 | |||||||||||
| MDS/Neuroscience Partners Healthcare(9) | 674,295 | 5.0 | MDS/Neuroscience Partners Healthcare(9) | 674,295 | 5.0 | |||||||||||
| Directors and Executive Officers: | Directors and Executive Officers: | Directors and Executive Officers: | ||||||||||||||
| Ron Cohen, M.D.(10) | 887,229 | 6.5 | Ron Cohen, M.D.(10) | 887,229 | 6.5 | |||||||||||
| Andrew R. Blight, Ph.D.(11) | 152,411 | 1.1 | Andrew R. Blight, Ph.D.(11) | 152,411 | 1.1 | |||||||||||
| Mary Fisher(12) | 138,749 | 1.0 | Mary Fisher(12) | 138,749 | 1.0 | |||||||||||
| David Lawrence, M.B.A.(13) | 74,514 | * | David Lawrence, M.B.A.(13) | 74,514 | * | |||||||||||
| Jane Wasman, J.D.(14) | 45,147 | * | Jane Wasman, J.D.(14) | 45,147 | * | |||||||||||
| John Friedman(15) | 873,364 | 6.4 | John Friedman(15) | 873,364 | 6.4 | |||||||||||
| Sandra Panem, Ph.D.(16) | 711,102 | 5.2 | Sandra Panem, Ph.D.(16) | 711,102 | 5.2 | |||||||||||
| Michael Steinmetz, Ph.D.(17) | 1,640,137 | 12.1 | Michael Steinmetz, Ph.D.(17) | 1,640,137 | 12.1 | |||||||||||
| Wise Young, Ph.D., M.D.(18) | 22,434 | * | Wise Young, Ph.D., M.D.(18) | 22,434 | * | |||||||||||
| Standish Fleming(19) | 873,890 | 6.5 | Standish Fleming(19) | 873,890 | 6.5 | |||||||||||
| Mark Pinney, M.B.A., C.F.A.(20) | 174,497 | 1.3 | Mark Pinney, M.B.A., C.F.A.(20) | 174,497 | 1.3 | |||||||||||
| Barclay Phillips(21) | 543,803 | 4.0 | Barclay Phillips(21) | 543,803 | 4.0 | |||||||||||
| Steven Rauscher(22) | 8,173 | * | Steven Rauscher(22) | 8,173 | * | |||||||||||
| All directors and executive officers as a group (13 persons)(23) | 6,145,450 | 45.4 | % | % | ||||||||||||
| Lorin J. Randall | — | — | ||||||||||||||
| All directors and executive officers as a group (14 persons)(23) | All directors and executive officers as a group (14 persons)(23) | 6,145,450 | 45.4 | % | % | |||||||||||
Dr. Panem is a partner of Cross Atlantic Partners and exercises investment and voting power over these shares. Dr. Panem disclaims beneficial ownership of these shares.
The following is a description of the material terms of our amended and restated certificate of incorporation and bylaws as each is anticipated to be in effect immediately following the closing of this offering and the filing of our amended and restated certificate of incorporation. We refer you to our amended and restated certificate of incorporation and bylaws, copies of which will be filed as exhibits to the registration statement of which this prospectus forms a part.
Authorized Capitalization
On September 18, 2005, our Board of Directors approved a 1-for-1.3 reverse stock split, which will become effective prior to the effective date of this registration statement.we effected on January 11, 2006. All references to common stock, common shares outstanding, average number of common shares outstanding, per share amounts, options and warrants and Elan notes payable in this registration statement have been restated to reflect the 1-for-1.3 common stock reverse split on a retroactive basis.
As of September 30, 2005, our authorized capital stock consisted of (i) 260,000,000 shares of common stock, with a par value of $0.001 per share, of which 208,743 shares were issued and outstanding, and (ii) 141,754,865 shares of preferred stock, with a par value of $0.001 per share, of which 106,472,984 shares are issued and outstanding. Immediately following the closing of this offering and the filing of our amended and restated certificate of incorporation, our authorized capital stock will consist of 80,000,000 shares of common stock, with a par value of $0.001 per share and 20,000,000 shares of preferred stock, with a par value of $0.001 per share. As of the consummation of this offering, all of the outstanding shares of preferred stock will automatically convert into 13,338,279 shares of common stock. After giving effect to this conversion, we expect there to be shares of common stock issued and outstanding (or shares of common stock if the underwriter exercises its over-allotment option in full), and no shares of preferred stock issued and outstanding.
Common Stock
Voting Rights
Holders of common stock are entitled to one vote per share on all matters submitted for action by the stockholders. The holders of common stock do not have cumulative voting rights in the election of directors. Accordingly, the holders of more than 50% of the shares of common stock can, if they choose to do so, elect all the directors. In such event, the holders of the remaining shares of common stock will not be able to elect any directors.
Dividend Rights
Holders of common stock are entitled to receive ratably dividends if, as and when dividends are declared from time to time by our board of directors out of funds legally available for that purpose, after payment of dividends required to be paid on outstanding preferred stock, if any. Our secured term loan imposes restrictions on our ability to declare dividends on our common stock.
Liquidation Rights
Upon our liquidation, dissolution or winding up, any business combination or a sale or disposition of all or substantially all of our assets, the holders of common stock are entitled to receive ratably the assets available for distribution to the stockholders after payment of liabilities and accumulated and unpaid dividends and liquidation preferences on outstanding preferred stock, if any.
Other Matters
Holders of common stock have no preemptive rights and are not subject to further calls or assessment by us. There are no redemption or sinking fund provisions applicable to our common stock. All outstanding shares of our common stock, including the shares of common stock offered in this offering, are fully paid and non-assessable.
Preferred Stock
Our amended and restated certificate of incorporation authorizes our board of directors to establish one or more series of up to 20,000,000 shares of preferred stock. Unless required by law or by any stock exchange on which our common stock is listed, the authorized shares of preferred stock will be available for issuance without further action by our stockholders. Our board of directors is able to determine, with respect to any series of preferred stock, the terms and rights of that series including:
Restricted Stock
As of December 31, 2005, we had 755,083 shares of restricted stock outstanding.
Warrants
As of December 31, 2005, we had outstanding warrants to purchase 50,200 shares of common stock at a weighted average exercise price of $16.54 per share.
Stock Options
As of December 31, 2005, 1,767,904 shares of common stock are issuable upon the exercise of outstanding stock options to purchase our common stock. AfterOn the effective date of the registration statement, of which this offering,prospectus is a part, we intend to file a registration statement on Form S-8 to register the shares of common stock reserved for issuance upon exercise of outstanding options.options under both our 1999 Plan and our 2006 Plan. The registration statement is expected to be filed and become
effective approximately six months after the closing of this offering. Accordingly, shares registered under the
registration statement will be available for sale in the open market without restriction, except with respect to Rule 144 volume limitations that apply to our affiliates.
Convertible Promissory Notes
In January 1997, EIS loaned us an aggregate of $7.5 million pursuant to two promissory notes that are convertible into 278,339 shares of our common stock. On December 23, 2005, Elan transferred these promissory notes to funds affiliated with Saints Capital.
Registration Rights
Pursuant to an amended and restated registration rights agreement between us and certain of our stockholders dated as of March 3, 2004, holders of an aggregate of 13,338,279 shares of our common stock have demand and piggy-back registration rights. The demand rights may be exercised by holders of 30% of the registrable securities at any time after completion of this offering. Additionally, if at any time we propose to register our common stock under the Securities Act for our own account or the account of any of our stockholders or both, the stockholders party to the registration rights agreement are entitled to notice of the registration and to include registrable shares in the offering, provided that the underwriters of that offering do not limit the number of shares included in the registration. In no event, however, will the amount of stockholders' securities to be included in the offering be reduced below 30% of the total securities in the offering. We are required to bear substantially all costs incurred in these registrations, other than underwriting discounts and commissions. The registration rights described above could result in substantial future expenses for us and adversely affect any future equity offering. Pursuant to the lock-up agreements with the underwriters, holders of greater than 70% of the "registrable securities" under our registration rights agreement have waived their rights to demand registration and participation in this offering under the registration rights agreement until the later of October 30, 2006 and expiration of the lock-up agreements. In addition, holders of the requisite amount of registrable securities have waived their rights to registration through the completion of this offering.
Authorized but Unissued Capital Stock
The Delaware General Corporation Law does not require stockholder approval for any issuance of authorized shares. These additional shares may be used for a variety of corporate purposes, including future public offerings, to raise additional capital or to facilitate acquisitions.
One of the effects of the existence of unissued and unreserved common stock or preferred stock may be to enable our board of directors to issue shares to persons friendly to current management, which issuance could render more difficult or discourage an attempt to obtain control of our company by means of a merger, tender offer, proxy contest or otherwise, and thereby protect the continuity of our management and possibly deprive the stockholders of opportunities to sell their shares of common stock at prices higher than prevailing market prices.
Delaware Anti-Takeover Statute
We are subject to Section 203 of the Delaware General Corporation Law. Subject to specific exceptions, Section 203 prohibits a publicly held Delaware corporation from engaging in a "business combination" with an "interested stockholder" for a period of three years after the date of the transaction in which the person became an interested stockholder, unless:
"Business combinations" include mergers, asset sales and other transactions resulting in a financial benefit to the "interested stockholder." Subject to various exceptions, an "interested stockholder" is a person who, together with his or her affiliates and associates, owns, or within three years did own, 15% or more of the corporation's outstanding voting stock. These restrictions could prohibit or delay the accomplishment of mergers or other takeover or change in control attempts with respect to us and, therefore, may discourage attempts to acquire us.
Transfer Agent and Registrar
Registrar and Transfer Company is the transfer agent and registrar for our common stock.
Listing
We will apply to list our common stock on The Nasdaq National Market, subject to official notice of issuance, under the symbol "ACOR."
SHARES ELIGIBLE FOR FUTURE SALE
Prior to this offering, there has been no market for our common stock. Upon completion of this offering, we will have outstanding an aggregate of million shares of common stock, and if the underwriters exercise their over-allotment option in full, we will have outstanding an aggregate of million shares of common stock. All of the shares sold in this offering will be freely tradable without restriction or further registration under the Securities Act, except that any shares purchased in the offering by our affiliates, as that term is defined in Rule 144 of the Securities Act, may generally only be sold in compliance with the limitations of Rule 144 described below. The remaining 913,155 millionAfter the offering, all 20,611,259 shares of our outstanding common stock outstanding will be "restricted securities," as that term is defined under Rule 144 and Rule 701 under the Securities Act. Restricted securities may be sold in the public market only if registered or if they qualify for an exemption from registration under Rule 144 or 144(k) under the Securities Act, which are summarized below.
Sales of substantial amounts of our common stock in the public market could put downward pressure on the market price of our common stock. We cannot estimate the number of shares of common stock that may be sold by third parties in the future because such sales will depend on market prices, the circumstances of sellers and other factors.
Rule 144
In general, under Rule 144 as currently in effect, beginning 90 days after the date of this prospectus, a person or persons whose shares are aggregated, who has beneficially owned restricted shares for at least one year, including persons who may be deemed to be our "affiliates," would be entitled to sell within any three-month period a number of shares that does not exceed the greater of:
Sales under Rule 144 are also subject to manner of sale provisions and notice requirements and to the availability of current public information about us.
Rule 144(k)
In addition, under Rule 144(k), a person who is not and has not been our affiliate at any time during the 90 days preceding a sale and at least two years have elapsed since the shares were acquired from us or any affiliate of ours, is entitled to sell those shares immediately after the consummation of this offering without regard to the manner of sale, public information, volume limitation or notice requirements of Rule 144.
Rule 701
Generally, an employee, officer, director or consultant who purchased shares of our common stock before the effective date of the registration statement of which this prospectus is a part, or who holds options as of that date, pursuant to a written compensatory plan or contract, may rely on the resale provisions of Rule 701 under the Securities Act. Under Rule 701, these persons who are not our affiliates may generally sell their eligible securities, commencing 90 days after the effective date of the registration statement of which this prospectus is a part, without having to comply with the public information, holding period, volume limitation or notice provisions of Rule 144.
Sale of Restricted Shares
Based on the number of shares outstanding as of December 31, 2005, 20,611,259 shares of our common stock will become eligible for sale pursuant to Rule 144 or Rule 701 without registration approximately as follows, assuming conversion of our preferred stock upon consummation of this offering and no exercise of outstanding options and warrants, and assuming no shares are released from the lock-up agreements described below prior to 180 days after the date of this prospectus:
Rules 144, 144(k) and Rule 701 do not supersede the contractual obligations of our security holders set forth in the lock-up agreements described below.
Lock-up Agreements
We, our directors and executive officers and substantially all of our stockholders and option holders have entered into lock-up agreements with the underwriters. Under these agreements, subject to exceptions, we may not issue any new shares of common stock, and those holders of stock and options may not, directly or indirectly, sell, offer, contract or grant any option to sell, pledge, transfer or otherwise dispose of or hedge any common securities convertible into or exchangeable for shares of common stock, or publicly announce the intention to do any of the foregoing, without the prior written consent of Banc of America Securities LLC, for a period of 180 days from the date of this prospectus related to this offering, subject to a potential extension of up to an additional 34 days under certain circumstances. This consent may be given at any time without public notice. In addition, during this period, we have also agreed not to file any registration statement for any shares of our common stock without the prior written consent of Banc of America Securities LLC. Pursuant to the lock-up agreements holders of greater than 70% of the "registrable securities" under our registration rights agreement have also agreed not to make any demand for, or exercise any right to registration of any shares of common stock or any securities convertible into or exercisable or exchangeable for common stock, without the prior written consent of Banc of America Securities LLC.
Registration Rights
Following the completion of this offering, holders of an aggregate of 13,338,279 shares of our common stock will be entitled to certain rights with respect to the registration of their shares under the Securities Act. See "Description of Capital Stock—Registration Rights." Registration of their shares under the Securities Act would result in these shares becoming freely tradable without restriction under the Securities Act immediately upon the effectiveness of the registration.
CERTAIN UNITED STATES FEDERAL INCOME AND ESTATE TAX CONSEQUENCES TO NON-U.S. HOLDERS
The following discussion is a summary of certain U.S. federal income and estate tax consequences of the purchase, ownership and disposition of our common stock as of the date hereof. Except where noted, this summary deals only with common stock that is held as a capital asset by a non-U.S. holder.
A "non-U.S. holder" means a beneficial owner of our common stock (other than a partnership) that is not, for U.S. federal income tax purposes, any of the following:
This summary is based upon provisions of the Code and regulations, rulings and judicial decisions as of the date hereof. Those authorities may be changed, perhaps retroactively, so as to result in U.S. federal income and estate tax consequences different from those summarized below. This summary does not address all aspects of U.S. federal income and estate taxes and does not deal with foreign, state, local or other tax considerations that may be relevant to non-U.S. holders in light of their personal circumstances. In addition, it does not represent a description of the U.S. federal income and estate tax consequences applicable to you if you are subject to special treatment under the U.S. federal income tax laws (including if you are a U.S. expatriate, "controlled foreign corporation," "passive foreign investment company," corporation that accumulates earnings to avoid U.S. federal income tax, a tax exempttax-exempt organization, a bank, an insurance company, a dealer in securities, a person that holds our common stock as part of a "straddle," "hedge," "conversion transaction," or other integrated transaction, a pass throughpass-through entity or an investor in a pass-through entity). We cannot assure you that a change in law will not alter significantly the tax considerations that we describe in this summary.
If a partnership holds our common stock, the tax treatment of a partner will generally depend upon the status of the partner and the activities of the partnership. If you are a partner of a partnership holding our common stock, you should consult your tax advisors. In this summary, "partnership" includes any entity treated as a partnership and "partner" includes any person treated as a partner for U.S. federal income tax purposes.
If you are considering the purchase of our common stock, you should consult your own tax advisors concerning the particular U.S. federal income and estate tax consequences to you of the ownership of our common stock, as well as the consequences to you arising under the laws of any other taxing jurisdiction.
Dividends
We do not currently anticipate paying dividends on our common stock. See "Dividend Policy" above. If we were to pay dividends in the future, dividends paid to a non-U.S. holder of our common stock generally will be subject to withholding of U.S. federal income tax at a 30% rate or such lower rate as may be specified by an applicable income tax treaty. However, dividends that are effectively connected with the conduct of a trade or business by the non-U.S. holder within the United States (and, where a tax treaty applies, are attributable to a U.S. permanent establishment of the non-U.S.
holder) are not subject to the withholding tax, provided certain certification and disclosure requirements are satisfied. Instead, such dividends are subject to U.S. federal income tax on a net income basis in the same manner as if the non-U.S. holder were a U.S. person as defined under the Code. Any such effectively connected dividends received by a foreign corporation may be subject to an additional "branch profits tax" at a 30% rate or such lower rate as may be specified by an applicable income tax treaty.
A non-U.S. holder of our common stock who wishes to claim the benefit of an applicable treaty rate for dividends will be required to complete Internal Revenue Service Form W-8BEN (or other applicable form) and certify under penalty of perjury that such holder is eligible for benefits under the applicable treaty. Special certification and other requirements apply to certain non-U.S. holders that are pass-through entities rather than corporations or individuals. In addition, Treasury regulations provide special procedures for payments of dividends through certain intermediaries.
A non-U.S. holder of our common stock eligible for a reduced rate of U.S. withholding tax pursuant to an income tax treaty may obtain a refund of any excess amounts withheld by filing an appropriate claim for refund with the Internal Revenue Service.
Gain on Disposition of Common Stock
Any gain realized on the disposition of our common stock generally will not be subject to U.S. federal income tax unless:
An individual non-U.S. holder described in the first bullet point immediately above will be subject to tax on the net gain derived from the sale under regular graduated U.S. federal income tax rates. An individual non-U.S. holder described in the second bullet point immediately above will be subject to a flat 30% tax on the gain derived from the sale, which may be offset by U.S. source capital losses, even though the individual is not considered a resident of the United States. If a non-U.S. holder that is a foreign corporation falls under the first bullet point immediately above, it will be subject to tax on its net gain in the same manner as if it were a U.S. person as defined under the Code and, in addition, may be subject to the branch profits tax equal to 30% of its effectively connected earnings and profits or at such lower rate as may be specified by an applicable income tax treaty.
We believe we are not and do not anticipate becoming a USRPHC for U.S. federal income tax purposes, however no assurances can be provided that we will not be a USRPHC in the future.
U.S. Federal Estate Tax
Common stock owned or treated as owned by an individual who is not a citizen or resident of the United States, as specifically defined for U.S. estate tax purposes, at the time of death will be included in such holder's gross estate for U.S. federal estate tax purposes, and may be subject to U.S. federal estate tax unless an applicable estate tax treaty provides otherwise.
Information Reporting and Backup Withholding
We must report annually to the Internal Revenue Service and to each non-U.S. holder the amount of dividends paid to such holder and the tax withheld with respect to such dividends, regardless of whether withholding was required. Copies of the information returns reporting such dividends and withholding may also be made available to the tax authorities in the country in which the non-U.S. holder resides under the provisions of an applicable income tax treaty.
A non-U.S. holder will be subject to backup withholding for dividends paid to such holder unless such holder certifies under penalty of perjury that it is a non-U.S. holder (and the payor does not have actual knowledge or reason to know that such holder is a U.S. person as defined under the Code), or such holder otherwise establishes an exemption.
Information reporting and, depending on the circumstances, backup withholding will apply to the proceeds of a sale of our common stock within the United States or conducted through certain U.S.-related financial intermediaries, unless the beneficial owner certifies under penalty of perjury that it is a non-U.S. holder (and the payor does not have actual knowledge or reason to know that the beneficial owner is a U.S. person as defined under the Code) or such owner otherwise establishes an exemption. Certain shareholders, including all corporations, are exempt from the backup withholding rules.
Backup withholding is not an additional tax. Any amounts withheld under the backup withholding rules may be allowed as a refund or a credit against a non-U.S. holder's U.S. federal income tax liability provided the required information is furnished to the Internal Revenue Service.
We are offering the shares of common stock described in this prospectus through a number of underwriters. Banc of America Securities LLC, Lazard Capital Markets LLC, Piper Jaffray & Co. and SG Cowen & Co., LLC, are the representatives of the underwriters. We have entered into a firm commitment underwriting agreement with the representatives. Subject to the terms and conditions of the underwriting agreement, we have agreed to sell to the underwriters, and each underwriter has agreed to purchase, the number of shares of common stock listed next to its name in the following table:
| Underwriter | Number of Shares | |
|---|---|---|
| Banc of America Securities LLC | ||
| Lazard Capital Markets LLC | ||
| Piper Jaffray & Co. | ||
| SG Cowen & Co., LLC | ||
| Total | ||
The underwriting agreement is subject to a number of terms and conditions and provides that the underwriters must buy all of the shares if they buy any of them. The underwriters will sell the shares to the public when and if the underwriters buy the shares from us.
The underwriters initially will offer the shares to the public at the price specified on the cover page of this prospectus. The underwriters may allow a concession of not more than $ per share to selected dealers. The underwriters may also allow, and those dealers may reallow, a concession of not more than $ per share to some other dealers. If all the shares are not sold at the public offering price, the underwriters may change the public offering price and the other selling terms. Our common stock is offered subject to a number of conditions, including:
Over-Allotment Options. We have granted the underwriters an over-allotment option to buy up to additional shares of our common stock at the same price per share as they are paying for the shares shown in the table below. These additional shares would cover sales of shares by the underwriters that exceed the total number of shares shown in the table above. The underwriters may exercise this option at any time within 30 days after the date of this prospectus. To the extent that the underwriters exercise this option, each underwriter will purchase additional shares from us in approximately the same proportion as it purchased the shares shown in the table above. If purchased, the additional shares will be sold by the underwriters on the same terms as those on which the other shares are sold.
Discount and Commissions. The following table shows the per share and total underwriting discounts and commissions to be paid to the underwriters by us. These amounts are shown assuming no exercise and full exercise of the underwriters' option to purchase additional shares.
We estimate that the expenses of the offering to be paid by us, not including the underwriting discounts and commissions, will be approximately $ .
| | Paid by Us | |||||
|---|---|---|---|---|---|---|
| | No Exercise | Full Exercise | ||||
| Per share | $ | $ | ||||
| Total | $ | $ | ||||
Listing. We will apply to have our common stock included for quotation on the NASDAQ National Market under the symbol "ACOR."
Stabilization. In connection with this offering, the underwriters may engage in activities that stabilize, maintain or otherwise affect the price of our common stock, including:
Stabilizing transactions consist of bids or purchases made for the purpose of preventing or retarding a decline in the market price of our common stock while this offering is in progress. Stabilizing transactions may include making short sales of our common stock, which involves the sale by the underwriters of a greater number of shares of common stock than they are required to purchase in this offering, and purchasing shares of common stock from us or in the open market to cover positions created by short sales. Short sales may be "covered" shorts, which are short positions in an amount not greater than the underwriters' over-allotment option referred to above, or may be "naked" shorts, which are short positions in excess of that amount. Syndicate covering transactions involve purchases of our common stock in the open market after the distribution has been completed in order to cover syndicate short positions.
The underwriters may close out any covered short position either by exercising their over-allotment option, in whole or in part, or by purchasing shares in the open market. In making this determination, the underwriters will consider, among other things, the price of shares available for purchase in the open market compared to the price at which the underwriters may purchase shares pursuant to the over-allotment option.
A naked short position is more likely to be created if the underwriters are concerned that there may be downward pressure on the price of the common stock in the open market that could adversely affect investors who purchased in this offering. To the extent that the underwriters create a naked short position, they will purchase shares in the open market to cover the position.
The representatives also may impose a penalty bid on underwriters and dealers participating in the offering. This means that the representatives may reclaim from any syndicate members or other dealers participating in the offering the underwriting discounts on shares sold by them and purchased by the representatives in stabilizing or short covering transactions.
These activities may have the effect of raising or maintaining the market price of our common stock or preventing or retarding a decline in the market price of our common stock. As a result of these activities, the price of our common stock may be higher than the price that otherwise might exist in the open market. If the underwriters commence these activities, they may discontinue them at any
time. The underwriters may carry out these transactions on the Nasdaq National Market, in the over-the-counter market or otherwise.
The underwriters have informed us that they do not expect to make sales to accounts over which they exercise discretionary authority in excess of 5% of the shares of common stock being offered.
IPO Pricing. Prior to this offering, there has been no public market for our common stock. The initial public offering price will be negotiated between us and the representatives of the underwriters. Among the factors to be considered in these negotiations are:
Lock-up Agreement. We, our executive officers and directors and substantially all of our stockholders have entered into or will, prior to the completion of this offering, enter into lock-up agreements with the underwriters. Under these agreements, subject to exceptions, we may not issue any new shares of common stock, and those holders of stock and options may not, directly or indirectly, sell, offer, contract or grant any option to sell, pledge, transfer or otherwise dispose of or hedge any common securities convertible into or exchangeable for shares of common stock, or publicly announce the intention to do any of the foregoing, without the prior written consent of Banc of America Securities LLC for a period of 180 days from the date of this prospectus related to this offering, subject to a potential extension of up to an additional 34 days under certain circumstances. This consent may be given at any time without public notice. In addition, during this period, we have also agreed not to file any registration statement for any shares of our common stock, other than a registration statement covering shares issued under our incentive compensation plans, without the prior written consent of Banc of America Securities LLC. Pursuant to the lock-up agreements holders of greater than 70% of the "registrable securities" under our registration rights agreement have also agreed not to make any demand for, or exercise any right to registration of any shares of common stock or any securities convertible into or exercisable or exchangeable for common stock, without the prior written consent of Banc of America Securities LLC.
Indemnification. We will indemnify the underwriters against some liabilities, including liabilities under the Securities Act. If we are unable to provide this indemnification, we will contribute to payments the underwriters may be required to make in respect of those liabilities.
The underwriters and their affiliates have provided, and may in the future provide, various investment banking, commercial banking and other financial services for us.
Compliance with Non-U.S. Laws and Regulations
Each underwriter intends to comply with all applicable laws and regulations in each jurisdiction in which it acquires, offers, sells or delivers shares of our common stock or has in its possession or distributes the prospectus.
European Economic Area
In relation to each Member State of the European Economic Area which has implemented the Prospectus Directive (each, a Relevant Member State), with effect from and including the date on which the Prospectus Directive is implemented in that Relevant Member State (the Relevant Implementation Date) an offer of shares to the public may not be made in that Relevant Member State prior to the publication of a prospectus in relation to shares which has been approved by the competent authority in that Relevant Member State or, where appropriate, approved in another Relevant Member State and notified to the competent authority in that Relevant Member State, all in accordance with the Prospectus Directive, except that it may, with effect from and including the Relevant Implementation Date, make an offer of shares to the public in that Relevant Member State at any time:
For the purposes of this provision, the expression an "offer of shares to the public" in relation to any shares in any Relevant Member State means the communication in any form and by any means of sufficient information on the terms of the offer and the shares to be offered so as to enable an investor to decide to purchase or subscribe the shares, as the same may be varied in that Member State by any measure implementing the Prospectus Directive in that Member State and the expression Prospectus Directive means Directive 2003/71/EC and includes any relevant implementing measure in each Relevant Member State.
France
No prospectus (including any amendment, supplement or replacement thereto) has been prepared in connection with the offering of the shares that has been approved by theAutorité des marchés financiers or by the competent authority of another State that is a contracting party to the Agreement on the European Economic Area and notified to theAutorité des marchés financiers; no shares have been offered or sold and will be offered or sold, directly or indirectly, to the public in France except to permitted investors ("Permitted Investors") consisting of persons licensed to provide the investment service of portfolio management for the account of third parties, qualified investors (investisseurs qualifiés) acting for their own account and/or corporate investors meeting one of the four criteria provided in Article 1 of Decree No 2004-1019 of September 28, 2004 and belonging to a limited circle of investors (cercle restreint d'investisseurs) acting for their own account, with "qualified investors" and "limited circle of investors" having the meaning ascribed to them in Article L. 411-2 of the FrenchCode Monétaire et Financier and applicable regulations thereunder; none of the prospectus supplement, the accompanying prospectus, or any other materials related to the offering or information contained therein relating to the shares has been released, issued or distributed to the public in France except to Permitted Investors; and the direct or indirect resale to the public in France of any shares acquired by
any Permitted Investors may be made only as provided by articles L. 412-1 and L. 621-8 of the FrenchCode Monétaire et Financier and applicable regulations thereunder.
United Kingdom
Each underwriter acknowledges and agrees that:
This document is only being distributed to and is only directed at (i) persons who are outside the United Kingdom or (ii) to investment professionals falling within Article 19(5) of the Financial Services and Markets Act 2000 (Financial Promotion) Order 2005 (the "Order") or (iii) high net worth entities, and other persons to whom it may lawfully be communicated, falling within Article 49(2)(a) to (d) of the Order (all such persons together being referred to as "relevant persons"). The shares are only available to, and any invitation, offer or agreement to subscribe, purchase or otherwise acquire such shares will be engaged in only with, relevant persons. Any person who is not a relevant person should not act or rely on this document or any of its contents.
Italy
Each underwriter acknowledges and agrees that the offering of the shares has not been cleared by the Italian Securities Exchange Commission (Commissione Nazionale per le Società e la Borsa, the "CONSOB") pursuant to Italian securities legislation and, accordingly, acknowledges and agrees that the shares may not and will not be offered, sold or delivered, nor may or will copies of the prospectus or any other documents relating to the shares or the prospectus be distributed in Italy other than to professional investors (investitori professionali), as defined in Article 31, paragraph 2 of CONSOB Regulation No. 11522 of July 1, 1998, as amended ("Regulation No. 11522") or pursuant to another exemption from the requirements of Articles 94 and seq. of Legislative Decree No. 58 of February 24, 1998 (the "Italian Finance Law") and CONSOB Regulation No. 11971 of May 14, 1999 ("Regulation No. 11971").
Each underwriter acknowledges and agrees that any offer, sale or delivery of the shares or distribution of copies of the prospectus or any other document relating to the shares or the prospectus in Italy may and will be effected in accordance with all Italian securities, tax, exchange control and other applicable laws and regulations, and, in particular, will be:
(the "Italian Banking Law"), Legislative Decree No. 58 of February 24, 1998, as amended, CONSOB Regulation No. 11522 of July 1, 1998, and any other applicable laws and regulations;
Any investor purchasing the shares in this offering is solely responsible for ensuring that any offer or resale of the shares it purchased in this offering occurs in compliance with applicable laws and regulations.
This prospectus and the information contained herein are intended only for the use of its recipient and are not to be distributed to any third party resident or located in Italy for any reason. No person resident or located in Italy other than the original recipients of this document may rely on it or its content.
In addition to the above (which shall continue to apply to the extent not inconsistent with the implementing measures of the Prospectus Directive in Italy), after the implementation of the Prospectus Directive in Italy, the restrictions, acknowledgments and agreements set out under the heading "European Economic Area" above shall apply to Italy.
The validity of the issuance of the shares of common stock offered hereby will be passed upon for us by Covington & Burling, New York, New York. Shearman & Sterling LLP, New York, New York, will pass upon certain legal matters in connection with this offering for the underwriters.
Our consolidated financial statements as of December 31, 2004 and 2003 and for the year ended December 31, 2004, the six month period ended December 31, 2003, and years ended June 30, 2003 and 2002 have been included herein and in the registration statement in reliance upon the report of KPMG LLP, independent registered public accounting firm, appearing elsewhere herein, and upon the authority of said firm as experts in accounting and auditing.
The statements of net revenues and direct expenses for the period from January 1, 2004 through July 21, 2004 and the year ended December 31, 2003 of the Zanaflex Product Line of Elan Corporation, plc have been included herein in reliance upon the report of KPMG, independent public accounting firm, appearing elsewhere herein, and upon the authority of said firm as experts in accounting and auditing.
WHERE YOU CAN FIND ADDITIONAL INFORMATION
We have filed with the SEC a registration statement on Form S-1 under the Securities Act with respect to the common stock offered by this prospectus. This prospectus, which is a part of the registration statement, does not include all of the information included in the registration statement. For further information with respect to us and our common stock, reference is made to the registration statement.
We are not currently subject to the informational requirements of the Securities Exchange Act of 1934, or the Exchange Act. As a result of this offering, we will become subject to the informational requirements of the Exchange Act, and, in accordance therewith, will file reports and other information with the SEC. The registration statement, such reports and other information can be inspected and copied at the Public Reference Room of the SEC located at 100 F Street, N.E., Washington D.C. 20549. Copies of such materials, including copies of all or any portion of the registration statement, can be obtained from the Public Reference Room of the SEC at prescribed rates. You can call the SEC at 1-800-SEC-0330 to obtain information on the operation of the Public Reference Room. Such materials may also be accessed electronically by means of the SEC's home page on the Internet (www.sec.gov).
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
| | PAGE | ||
|---|---|---|---|
| Consolidated Financial | |||
| Report of Independent Registered Public Accounting Firm | F-2 | ||
| Consolidated Balance Sheets | F-3 | ||
| Consolidated Statements of Operations | F-5 | ||
| Consolidated Statements of Stockholders' (Deficit) | F-6 | ||
| Consolidated Statements of Cash Flows | F-11 | ||
| Notes to Consolidated Financial Statements | F-12 | ||
| Statements of Net Revenues and Direct Expenses of Zanaflex Product Line of Elan Corporation, plc: | |||
| Report of Independent Public Accounting Firm | F-47 | ||
| Statements of Net Revenues and Direct Expenses | F-48 | ||
| Notes to Financial Statements | F-49 | ||
| Unaudited Pro Forma Combined Statement of Operations: | |||
| Introduction to Unaudited Pro Forma Combined Statement of Operations | F-52 | ||
| Unaudited Pro Forma Combined Statement of Operations | F-53 | ||
| Notes to Unaudited Pro Forma Combined Statement of Operations | F-54 | ||
THE ACCOMPANYING FINANCIAL STATEMENTS INCLUDE THE EFFECTS OF A REVERSE STOCK SPLIT OF THE COMPANY'S COMMON STOCK APPROVED BY THE COMPANY'S BOARD OF DIRECTORS WHICH WILL BECOME EFFECTIVE PRIOR TO THE EFFECTIVE DATE OF THE FORM S-1 REGISTRATION STATEMENT FILED IN CONNECTION WITH THE COMPANY'S INITIAL PUBLIC OFFERING. THE ABOVE OPINION IS THE FORM WHICH WILL BE SIGNED BY KPMG LLP UPON CONSUMMATION OF THE REVERSE STOCK SPLIT, WHICH IS DESCRIBED IN NOTE (16) OF THE NOTES TO THE FINANCIAL STATEMENTS, AND ASSUMING THAT, FROM OCTOBER 3, 2005 TO THE DATE OF SUCH REVERSE STOCK SPLIT, NO OTHER EVENTS HAVE OCCURRED THAT WOULD AFFECT THE ACCOMPANYING FINANCIAL STATEMENTS AND NOTES THERETO, EXCEPT AS DISCLOSED IN NOTES TO THE FINANCIAL STATEMENTS.
October 3, 2005
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Stockholders
Acorda Therapeutics, Inc.:
We have audited the accompanying consolidated balance sheets of Acorda Therapeutics, Inc. and subsidiary (the Company) as of December 31, 2004 and 2003, and the related consolidated statements of operations, stockholders' (deficit), and cash flows for the year ended December 31, 2004, the six-month period ended December 31, 2003, and years ended June 30, 2003 and 2002. These consolidated financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of December 31, 2004 and 2003, and the results of their operations and their cash flows for the year ended December 31, 2004, the six-month period ended December 31, 2003, and years ended June 30, 2003 and 2002, in conformity with U.S. generally accepted accounting principles.
| /s/ KPMG LLP |
Short Hills, New Jersey
October 3, 2005, except for note 16
(as to the effects of a reverse stock splitsplit)
which is as of January , 2006)11, 2006
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Balance Sheets
| | | December 31, | | | December 31, | | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | September 30, 2005 | | September 30, 2005 | ||||||||||||||||||||
| | | 2003 | 2004 | | 2003 | 2004 | ||||||||||||||||||
| | | | | (unaudited) | | | | (unaudited) | ||||||||||||||||
| Assets | Assets | Assets | ||||||||||||||||||||||
| Current assets: | Current assets: | Current assets: | ||||||||||||||||||||||
| Cash and cash equivalents | $ | 8,965,173 | $ | 11,729,112 | $ | 3,580,613 | Cash and cash equivalents | $ | 8,965,173 | $ | 11,729,112 | $ | 3,580,613 | |||||||||||
| Restricted cash | 254,078 | 256,568 | 261,037 | Restricted cash | 254,078 | 256,568 | 261,037 | |||||||||||||||||
| Short-term investments | 32,250,263 | 9,396,677 | 5,160,275 | Short-term investments | 32,250,263 | 9,396,677 | 5,160,275 | |||||||||||||||||
| Trade accounts receivable, net | — | 1,922,838 | 729,811 | Trade accounts receivable, net | — | 1,922,838 | 729,811 | |||||||||||||||||
| Grant receivable | 171,181 | 141,815 | 90,530 | Grant receivable | 171,181 | 141,815 | 90,530 | |||||||||||||||||
| Prepaid expenses | 920,084 | 827,891 | 1,460,959 | Prepaid expenses | 920,084 | 827,891 | 1,460,959 | |||||||||||||||||
| Finished goods inventory held by the Company | — | 192,452 | 3,852,435 | Finished goods inventory held by the Company | — | 192,452 | 3,852,435 | |||||||||||||||||
| Finished goods inventory held by others | — | 230,748 | 1,101,183 | Finished goods inventory held by others | — | 230,748 | 1,101,183 | |||||||||||||||||
| Other current assets | 194,962 | 241,251 | 1,154,966 | Other current assets | 194,962 | 241,251 | 1,154,966 | |||||||||||||||||
| Total current assets | 42,755,741 | 24,939,352 | 17,391,809 | Total current assets | 42,755,741 | 24,939,352 | 17,391,809 | |||||||||||||||||
| Property and equipment, net of accumulated depreciation | Property and equipment, net of accumulated depreciation | 3,093,154 | 2,547,014 | 1,905,063 | Property and equipment, net of accumulated depreciation | 3,093,154 | 2,547,014 | 1,905,063 | ||||||||||||||||
| Intangible Assets, net of accumulated amortization | Intangible Assets, net of accumulated amortization | — | 3,386,050 | 6,137,023 | Intangible Assets, net of accumulated amortization | — | 3,386,050 | 6,137,023 | ||||||||||||||||
| Other assets | Other assets | 111,516 | 109,234 | 109,235 | Other assets | 111,516 | 109,234 | 109,235 | ||||||||||||||||
| Total assets | $ | 45,960,411 | $ | 30,981,650 | $ | 25,543,130 | Total assets | $ | 45,960,411 | $ | 30,981,650 | $ | 25,543,130 | |||||||||||
| Liabilities, Mandatorily Redeemable Convertible Preferred Stock and Stockholders' (Deficit) | Liabilities, Mandatorily Redeemable Convertible Preferred Stock and Stockholders' (Deficit) | Liabilities, Mandatorily Redeemable Convertible Preferred Stock and Stockholders' (Deficit) | ||||||||||||||||||||||
| Current liabilities: | Current liabilities: | Current liabilities: | ||||||||||||||||||||||
| Accounts payable | $ | 2,354,131 | $ | 1,929,394 | 1,810,123 | Accounts payable | $ | 2,354,131 | $ | 1,929,394 | 1,810,123 | |||||||||||||
| Accounts payable to related party | 305,088 | — | — | Accounts payable to related party | 305,088 | — | — | |||||||||||||||||
| Accrued expenses and other current liabilities | 4,349,828 | 2,890,218 | 7,825,869 | Accrued expenses and other current liabilities | 4,349,828 | 2,890,218 | 7,825,869 | |||||||||||||||||
| Accrued product returns | — | 4,081,910 | 1,966,343 | Accrued product returns | — | 4,081,910 | 1,966,343 | |||||||||||||||||
| Deferred grant revenue | 48,043 | — | — | Deferred grant revenue | 48,043 | — | — | |||||||||||||||||
| Deferred product revenue—Zanaflex tablets | — | 6,668,491 | 10,685,860 | Deferred product revenue—Zanaflex tablets | — | 6,668,491 | 10,685,860 | |||||||||||||||||
| Deferred product revenue—Zanaflex Capsules | — | — | 4,959,993 | Deferred product revenue—Zanaflex Capsules | — | — | 4,959,993 | |||||||||||||||||
| Current portion of notes payable | 323,971 | 301,938 | 2,346,985 | Current portion of notes payable | 323,971 | 301,938 | 2,346,985 | |||||||||||||||||
| Total current liabilities | 7,381,061 | 15,871,951 | 29,595,173 | Total current liabilities | 7,381,061 | 15,871,951 | 29,595,173 | |||||||||||||||||
| Long-term portion of notes payable | Long-term portion of notes payable | 446,592 | 144,654 | 3,533,601 | Long-term portion of notes payable | 446,592 | 144,654 | 3,533,601 | ||||||||||||||||
| Other long-term liabilities | Other long-term liabilities | — | 750,000 | — | Other long-term liabilities | — | 750,000 | — | ||||||||||||||||
| Warrant liability | Warrant liability | — | — | 388,135 | Warrant liability | — | — | 388,135 | ||||||||||||||||
| Long-term convertible notes payable—principal amount, plus accrued interest less unamortized debt discount of $329,374, $175,312 and $82,818 as of December 31, 2003 and 2004 and September 30, 2005 (unaudited) respectively | Long-term convertible notes payable—principal amount, plus accrued interest less unamortized debt discount of $329,374, $175,312 and $82,818 as of December 31, 2003 and 2004 and September 30, 2005 (unaudited) respectively | 8,091,412 | 8,421,996 | 8,694,877 | Long-term convertible notes payable—principal amount, plus accrued interest less unamortized debt discount of $329,374, $175,312 and $82,818 as of December 31, 2003 and 2004 and September 30, 2005 (unaudited) respectively | 8,091,412 | 8,421,996 | 8,694,877 | ||||||||||||||||
| Mandatorily Redeemable Convertible Preferred Stock: | Mandatorily Redeemable Convertible Preferred Stock: | Mandatorily Redeemable Convertible Preferred Stock: | ||||||||||||||||||||||
| Series E convertible preferred stock—$0.001 par value. Authorized, issued, and outstanding 7,472,612 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $20,176,052 as of December 31, 2004) | 2,449,656 | 6,396,021 | 9,347,741 | Series E convertible preferred stock—$0.001 par value. Authorized, issued, and outstanding 7,472,612 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $20,176,052 as of December 31, 2004) | 2,449,656 | 6,396,021 | 9,347,741 | |||||||||||||||||
| Series I convertible preferred stock—$0.001 par value. Authorized, issued and outstanding, 10,204,047 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $39,693,743 as of December 31, 2004) | 4,897,447 | 12,644,040 | 18,438,141 | Series I convertible preferred stock—$0.001 par value. Authorized, issued and outstanding, 10,204,047 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $39,693,743 as of December 31, 2004) | 4,897,447 | 12,644,040 | 18,438,141 | |||||||||||||||||
| Series J convertible preferred stock—$0.001 par value. Authorized, 112,790,246 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued, and outstanding 112,790,233 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $64,109,973 as of December 31, 2004) | 22,824,094 | 35,100,482 | 44,291,812 | Series J convertible preferred stock—$0.001 par value. Authorized, 112,790,233 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued, and outstanding 112,790,233 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $64,109,973 as of December 31, 2004) | 22,824,094 | 35,100,482 | 44,291,812 | |||||||||||||||||
| Series K convertible preferred stock—$0.001 par value. Authorized, 1,533,330 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 1,533,327 shares at December 31, 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $12,720,513 at December 31, 2004) | — | 12,223,211 | 12,922,497 | Series K convertible preferred stock—$0.001 par value. Authorized, 1,573,330 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 1,533,327 shares at December 31, 2004 and September 30, 2005 (unaudited) (Redemption and liquidation value of $12,720,513 at December 31, 2004) | — | 12,223,211 | 12,922,497 | |||||||||||||||||
| Commitments and contingencies | Commitments and contingencies | Commitments and contingencies | ||||||||||||||||||||||
| Stockholders' (deficit): | Stockholders' (deficit): | Stockholders' (deficit): | ||||||||||||||||||||||
| Series A convertible preferred stock, $0.001 par value. Authorized 1,646,068 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 1,306,068 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $1,306,068 as of December 31, 2004) | 1,306 | 1,306 | 1,306 | Series A convertible preferred stock, $0.001 par value. Authorized 1,646,068 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 1,306,068 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $1,306,068 as of December 31, 2004) | 1,306 | 1,306 | 1,306 | |||||||||||||||||
| Series B convertible preferred stock, $0.001 par value. Authorized 2,250,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 900,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $1,800,000 as of December 31, 2004) | 900 | 900 | 900 | Series B convertible preferred stock, $0.001 par value. Authorized 2,250,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 900,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $1,800,000 as of December 31, 2004) | 900 | 900 | 900 | |||||||||||||||||
| Series C convertible preferred stock, $0.001 par value. Authorized, issued, and outstanding 333,333 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $999,999 as of December 31, 2004) | 333 | 333 | 333 | Series C convertible preferred stock, $0.001 par value. Authorized, issued, and outstanding 333,333 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $999,999 as of December 31, 2004) | 333 | 333 | 333 | |||||||||||||||||
| Series D convertible preferred stock, $0.001 par value. Authorized 400,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding—none | — | — | — | Series D convertible preferred stock, $0.001 par value. Authorized 400,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding—none | — | — | — | |||||||||||||||||
| Series F convertible preferred stock, $0.001 par value. Authorized, issued, and outstanding 2,300,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $11,999,100 as of December 31, 2004) | 2,300 | 2,300 | 2,300 | Series F convertible preferred stock, $0.001 par value. Authorized, issued, and outstanding 2,300,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $11,999,100 as of December 31, 2004) | 2,300 | 2,300 | 2,300 | |||||||||||||||||
| Series G convertible preferred stock, $0.001 par value. Authorized 1,250,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding—none | — | — | — | Series G convertible preferred stock, $0.001 par value. Authorized 1,250,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding—none | — | — | — | |||||||||||||||||
| Series H convertible preferred stock, $0.001 par value. Authorized, issued, and outstanding 1,575,229 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $5,119,494 as of December 31, 2004) | 1,575 | 1,575 | 1,575 | Series H convertible preferred stock, $0.001 par value. Authorized, issued, and outstanding 1,575,229 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited) (liquidation value of $5,119,494 as of December 31, 2004) | 1,575 | 1,575 | 1,575 | |||||||||||||||||
| Common stock, $0.001 par value. Authorized 260,000,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 195,209, 197,569 and 208,743 shares as of December 31, 2003 and 2004 and September 30, 2005 (unaudited), respectively | 195 | 198 | 209 | Common stock, $0.001 par value. Authorized 200,000,000 shares at December 31, 2003 and 2004 and September 30, 2005 (unaudited); issued and outstanding 195,209, 197,569 and 208,743 shares as of December 31, 2003 and 2004 and September 30, 2005 (unaudited), respectively | 195 | 198 | 209 | |||||||||||||||||
| Additional paid-in capital | Additional paid-in capital | 127,631,942 | 111,957,403 | 96,806,331 | Additional paid-in capital | 127,631,942 | 111,957,403 | 96,806,331 | ||||||||||||||||
| Accumulated deficit | Accumulated deficit | (127,770,920 | ) | (172,511,684 | ) | (198,475,470 | ) | Accumulated deficit | (127,770,920 | ) | (172,511,684 | ) | (198,475,470 | ) | ||||||||||
| Other comprehensive income (loss) | Other comprehensive income (loss) | 2,518 | (23,036 | ) | (6,331 | ) | Other comprehensive income (loss) | 2,518 | (23,036 | ) | (6,331 | ) | ||||||||||||
| Total stockholders' (deficit) | (129,851 | ) | (60,570,705 | ) | (101,668,847 | ) | Total stockholders' (deficit) | (129,851 | ) | (60,570,705 | ) | (101,668,847 | ) | |||||||||||
| Total liabilities, mandatorily redeemable convertible preferred stock and stockholders' (deficit) | $ | 45,960,411 | $ | 30,981,650 | $ | 25,543,130 | Total liabilities, mandatorily redeemable convertible preferred stock and stockholders' (deficit) | $ | 45,960,411 | $ | 30,981,650 | $ | 25,543,130 | |||||||||||
See accompanying Notes to Consolidated Financial Statements
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Operations
| | | | | | Nine-month period ended September 30, | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Year ended June 30, | | | ||||||||||||||||||
| | Six-month period ended December 31, 2003 | Year ended December 31, 2004 | |||||||||||||||||||
| | 2002 | 2003 | 2004 | 2005 | |||||||||||||||||
| | | | | | (unaudited) | (unaudited) | |||||||||||||||
| Gross sales—Zanaflex | $ | — | $ | — | $ | — | $ | — | $ | — | $ | 3,239,091 | |||||||||
| Less: discounts and allowances | — | — | — | (4,416,691 | ) | (144,338 | ) | (991,560 | ) | ||||||||||||
| Net sales | — | — | — | (4,416,691 | ) | (144,338 | ) | 2,247,531 | |||||||||||||
| Grant revenue | 131,592 | 473,588 | 382,094 | 479,495 | 444,920 | 184,195 | |||||||||||||||
| Total net revenue | 131,592 | 473,588 | 382,094 | (3,937,196 | ) | 300,582 | 2,431,726 | ||||||||||||||
| Less: cost of sales | — | — | — | (885,450 | ) | (362,695 | ) | (2,273,970 | ) | ||||||||||||
| Gross profit | 131,592 | 473,588 | 382,094 | (4,822,646 | ) | (62,113 | ) | 157,756 | |||||||||||||
Operating expenses: | |||||||||||||||||||||
| Research and development | 11,146,415 | 17,526,656 | 16,743,098 | 21,999,091 | 18,620,938 | 9,652,543 | |||||||||||||||
| Research and development—related party | 4,686,671 | 2,265,233 | 3,343,681 | — | — | — | |||||||||||||||
| Sales and marketing | — | — | — | 4,661,643 | 2,792,962 | 9,657,233 | |||||||||||||||
| General and administrative | 6,636,306 | 6,387,999 | 17,068,746 | 13,283,506 | 11,033,820 | 6,338,716 | |||||||||||||||
| Total operating expenses | 22,469,392 | 26,179,888 | 37,155,525 | 39,944,240 | 32,447,720 | 25,648,492 | |||||||||||||||
| Operating loss | (22,337,800 | ) | (25,706,300 | ) | (36,773,431 | ) | (44,766,886 | ) | (32,509,833 | ) | (25,490,736 | ) | |||||||||
| Other income (expense): | |||||||||||||||||||||
| Interest and amortization of debt discount expense | — | (77,712 | ) | (37,646 | ) | (385,419 | ) | (297,419 | ) | (824,196 | ) | ||||||||||
| Interest and amortization of debt discount expense—related party | (407,686 | ) | (368,935 | ) | (184,226 | ) | — | — | — | ||||||||||||
| Interest income | 983,876 | 392,742 | 276,334 | 409,118 | 329,263 | 347,352 | |||||||||||||||
| Other income | — | 25,903 | 6,998 | 2,423 | 2,423 | 989 | |||||||||||||||
| Total other income (expense) | 576,190 | (28,002 | ) | 61,460 | 26,122 | 34,267 | (475,855 | ) | |||||||||||||
| Minority interest—related party | 580,467 | — | — | — | — | — | |||||||||||||||
| Cumulative effect of change in accounting principle | — | — | — | — | — | 2,805 | |||||||||||||||
| Net loss | (21,181,143 | ) | (25,734,302 | ) | (36,711,971 | ) | (44,740,764 | ) | (32,475,566 | ) | (25,963,786 | ) | |||||||||
| Beneficial conversion feature, accretion of issuance costs, preferred dividends, and fair value of warrants issued to convertible preferred stockholders | (54,973 | ) | (24,320,031 | ) | (11,984,669 | ) | (24,746,337 | ) | (18,496,128 | ) | (18,636,443 | ) | |||||||||
| Net loss allocable to common stockholders | $ | (21,236,116 | ) | $ | (50,054,333 | ) | $ | (48,696,640 | ) | $ | (69,487,101 | ) | $ | (50,971,694 | ) | $ | (44,600,229 | ) | |||
| Net loss per share allocable to common stockholders—basic and diluted | $(111.90 | ) | $(261.38 | ) | $(252.87 | ) | $(351.76 | ) | $(259.22 | ) | $(221.17 | ) | |||||||||
| Weighted average common shares outstanding used in computing net loss per share allocable to common stockholders—basic and diluted | 189,786 | 191,497 | 192,573 | 197,541 | 196,636 | 201,656 | |||||||||||||||
See accompanying Notes to Consolidated Financial Statements
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Changes in Stockholders' (Deficit)
| | Stockholders' (deficit) | | | | | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series A convertible preferred stock | Series B convertible preferred stock | Series C convertible preferred stock | Series F convertible preferred stock | Series H convertible preferred stock | | | | | | | ||||||||||||||||||||||||||||||||
| | Common Stock | | | | | ||||||||||||||||||||||||||||||||||||||
| | | | Accumulated Comprehensive Income (Loss) | | |||||||||||||||||||||||||||||||||||||||
| | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Additional paid-in capital | Accumulated Deficit | Total stockholders' (deficit) | ||||||||||||||||||||||||||||
| Balance at June 30, 2001 | 1,255,000 | $ | 1,255 | 750,000 | $ | 750 | — | $ | — | 2,300,000 | $ | 2,300 | 1,575,229 | $ | 1,575 | 188,120 | $ | 188 | $ | 25,096,201 | $ | (44,143,504 | ) | $ | — | $ | (19,041,235 | ) | |||||||||||||||
| Issuance of Series A convertible preferred stock in May 2002, $1.00 per share | 51,068 | 51 | — | — | — | — | — | — | — | — | — | — | 22,749 | — | — | 22,800 | |||||||||||||||||||||||||||
| Issuance of Series B convertible preferred stock in January 2002, $2.00 per share | — | — | 150,000 | 150 | — | — | — | — | — | — | — | — | 299,850 | — | — | 300,000 | |||||||||||||||||||||||||||
| Issuance of Series C convertible preferred stock in February 2002, $3.00 per share | — | — | — | — | 333,333 | 333 | — | — | — | — | — | — | 999,666 | — | — | 999,999 | |||||||||||||||||||||||||||
| Issuance of common stock in September and October 2001 and February 2002, $4.68 per share | — | — | — | — | — | — | — | — | — | — | 3,381 | 4 | 20,615 | — | — | 20,619 | |||||||||||||||||||||||||||
| Research and development expense for issuance of stock options to nonemployees | — | — | — | — | — | — | — | — | — | — | — | — | 74,624 | — | — | 74,624 | |||||||||||||||||||||||||||
| Compensation expense for issuance of stock options to employees | — | — | — | — | — | — | — | — | — | — | — | — | 1,331,911 | — | — | 1,331,911 | |||||||||||||||||||||||||||
| Accretion of issuance costs related to Series F mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (27,337 | ) | — | — | (27,337 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series I mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (27,636 | ) | — | — | (27,636 | ) | |||||||||||||||||||||||||
| Research and development expense for issuance of warrants and Series C preferred stock on obtaining Phase II clinical trial approval | — | — | — | — | — | — | — | — | — | — | — | — | 617,666 | — | — | 617,666 | |||||||||||||||||||||||||||
| Net loss | — | — | — | — | — | — | — | — | — | — | — | — | — | (21,181,143 | ) | — | (21,181,143 | ) | |||||||||||||||||||||||||
| Balance at June 30, 2002 | 1,306,068 | $ | 1,306 | 900,000 | $ | 900 | 333,333 | $ | 333 | 2,300,000 | $ | 2,300 | 1,575,229 | $ | 1,575 | 191,501 | $ | 192 | $ | 28,408,309 | $ | (65,324,647 | ) | $ | - | $ | (36,909,732 | ) | |||||||||||||||
See accompanying Notes to Consolidated Financial Statements.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Changes in Stockholders' (Deficit) (continued)
| | Stockholders' (deficit) | | | | | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series A convertible preferred stock | Series B convertible preferred stock | Series C convertible preferred stock | Series F convertible preferred stock | Series H convertible preferred stock | | | | | | | ||||||||||||||||||||||||||||||||
| | Common Stock | | | | | ||||||||||||||||||||||||||||||||||||||
| | | | Accumulated Comprehensive Income (Loss) | | |||||||||||||||||||||||||||||||||||||||
| | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Additional paid-in capital | Accumulated Deficit | Total stockholders' (deficit) | ||||||||||||||||||||||||||||
| Research and development expense for issuance of stock options to nonemployees | — | — | — | — | — | — | — | — | — | — | — | — | (6,539 | ) | — | — | (6,539 | ) | |||||||||||||||||||||||||
| Compensation expense for issuance of stock options to employees | — | — | — | — | — | — | — | — | — | — | — | — | 1,580,054 | — | — | 1,580,054 | |||||||||||||||||||||||||||
| Accretion of issuance costs related to Series E, I and J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (27,337 | ) | — | — | (27,337 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series I mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (27,636 | ) | — | — | (27,636 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (10,990 | ) | — | — | (10,990 | ) | |||||||||||||||||||||||||
| Accrual of preferred dividends of Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (629,895 | ) | — | — | (629,895 | ) | |||||||||||||||||||||||||
| Beneficial conversion feature for reduction in conversion price | — | — | — | — | — | — | — | — | — | — | — | — | 80,730,286 | — | — | 80,730,286 | |||||||||||||||||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price, Series A, B, C, F and H | — | — | — | — | — | — | — | — | — | — | — | — | (20,860,491 | ) | — | — | (20,860,491 | ) | |||||||||||||||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price, Series E and I | — | — | — | — | — | — | — | — | — | — | — | — | (1,656,854 | ) | — | — | (1,656,854 | ) | |||||||||||||||||||||||||
| Issuance of preferred stock with beneficial conversion feature, Series J | — | — | — | — | — | — | — | — | — | — | — | — | 39,994,812 | — | — | 39,994,812 | |||||||||||||||||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature, Series J | — | — | — | — | — | — | — | — | — | — | — | — | (1,106,828 | ) | — | — | (1,106,828 | ) | |||||||||||||||||||||||||
| Comprehensive loss -Unrealized loss on investment securities | — | — | — | — | — | — | — | — | — | — | — | — | — | — | (6,078 | ) | (6,078 | ) | |||||||||||||||||||||||||
| Net loss | — | — | — | — | — | — | — | — | — | — | — | — | — | (25,734,302 | ) | — | (25,734,302 | ) | |||||||||||||||||||||||||
| Total Comprehensive loss | (25,740,380 | ) | |||||||||||||||||||||||||||||||||||||||||
| Balance at June 30, 2003 | 1,306,068 | $ | 1,306 | 900,000 | $ | 900 | 333,333 | $ | 333 | 2,300,000 | $ | 2,300 | 1,575,229 | $ | 1,575 | 191,501 | $ | 192 | $ | 126,386,891 | $ | (91,058,949 | ) | $ | (6,078 | ) | $ | 35,328,470 | |||||||||||||||
See accompanying Notes to Consolidated Financial Statements.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Changes in Stockholders' (Deficit) (continued)
| | Stockholders' (deficit) | | | | | |||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series A convertible preferred stock | Series B convertible preferred stock | Series C convertible preferred stock | Series F convertible preferred stock | Series H convertible preferred stock | | | | | | | |||||||||||||||||||||||||||||||
| | Common Stock | | | | | |||||||||||||||||||||||||||||||||||||
| | | | Accumulated Comprehensive Income (Loss) | | ||||||||||||||||||||||||||||||||||||||
| | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Additional paid-in capital | Accumulated Deficit | Total stockholders' (deficit) | |||||||||||||||||||||||||||
| Research and development expense for issuance of stock options to nonemployees | — | — | — | — | — | — | — | — | — | — | — | — | 8,488 | — | — | 8,488 | ||||||||||||||||||||||||||
| Compensation expense for issuance of stock options to employees | — | — | — | — | — | — | — | — | — | — | — | — | 13,198,080 | — | — | 13,198,080 | ||||||||||||||||||||||||||
| Exercise of stock options | — | — | — | — | — | — | — | — | — | — | 3,687 | 3 | 23,232 | — | — | 23,235 | ||||||||||||||||||||||||||
| Accretion of issuance costs related to Series E, I and mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (8,188 | ) | — | — | (8,188 | ) | ||||||||||||||||||||||||
| Accretion of issuance costs related to Series I mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (7,434 | ) | — | — | (7,434 | ) | ||||||||||||||||||||||||
| Accretion of issuance costs related to Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (32,323 | ) | — | — | (32,323 | ) | ||||||||||||||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price, Series E and I | — | — | — | — | — | — | — | — | — | — | — | — | (5,830,852 | ) | — | — | (5,830,852 | ) | ||||||||||||||||||||||||
| Accrual of preferred dividends on Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (2,210,688 | ) | — | — | (2,210,688 | ) | ||||||||||||||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature, Series J | — | — | — | — | — | — | — | — | — | — | — | — | (3,895,184 | ) | — | — | (3,895,184 | ) | ||||||||||||||||||||||||
| Fractional share reimbursement liability due to reverse stock split | — | — | — | — | — | — | — | — | — | — | — | — | (80 | ) | — | — | (80 | ) | ||||||||||||||||||||||||
| Comprehensive loss | ||||||||||||||||||||||||||||||||||||||||||
| Unrealized gain on investment securities | — | — | — | — | — | — | — | — | — | — | — | — | — | — | 8,596 | 8,596 | ||||||||||||||||||||||||||
| Net loss | — | — | — | — | — | — | — | — | — | — | — | — | — | (36,711,971 | ) | — | (36,711,971 | ) | ||||||||||||||||||||||||
| Total Comprehensive loss | (36,703,375 | ) | ||||||||||||||||||||||||||||||||||||||||
| Balance at December 31, 2003 | 1,306,068 | $ | 1,306 | 900,000 | $ | 900 | 333,333 | $ | 333 | 2,300,000 | $ | 2,300 | 1,575,229 | $ | 1,575 | 195,188 | $ | 195 | $ | 127,631,942 | $ | (127,770,920 | ) | $ | 2,518 | $(129,851 | ) | |||||||||||||||
See accompanying Notes to Consolidated Financial Statements.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Changes in Stockholders' (Deficit) (continued)
| | Stockholders' (deficit) | | | | | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series A convertible preferred stock | Series B convertible preferred stock | Series C convertible preferred stock | Series F convertible preferred stock | Series H convertible preferred stock | | | | | | | ||||||||||||||||||||||||||||||||
| | Common Stock | | | | | ||||||||||||||||||||||||||||||||||||||
| | | | Accumulated Comprehensive Income (Loss) | Total stockholders' equity (deficit) | |||||||||||||||||||||||||||||||||||||||
| | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Additional paid-in capital | Accumulated Deficit | |||||||||||||||||||||||||||||
| Research and development expense for issuance of stock options to nonemployees | — | — | — | — | — | — | — | — | — | — | — | — | 15,458 | — | — | 15,458 | |||||||||||||||||||||||||||
| Compensation expense for issuance of stock options to employees | — | — | — | — | — | — | — | — | — | — | — | — | 6,812,795 | — | — | 6,812,795 | |||||||||||||||||||||||||||
| Compensation expense for issuance of restricted stock to employees | — | — | — | — | — | — | — | — | — | — | — | — | 2,235,263 | — | — | 2,235,263 | |||||||||||||||||||||||||||
| Exercise of stock options | — | — | — | — | — | — | — | — | — | — | 2,360 | 3 | 8,282 | — | — | 8,285 | |||||||||||||||||||||||||||
| Accretion of issuance costs related to Series E, I, J and K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (16,376 | ) | — | — | (16,376 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series I mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (14,869 | ) | — | — | (14,869 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (64,646 | ) | — | — | (64,646 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (10,332 | ) | — | — | (10,332 | ) | |||||||||||||||||||||||||
| Accrual of preferred dividends of Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (4,421,377 | ) | — | — | (4,421,377 | ) | |||||||||||||||||||||||||
| Accrual of preferred dividends of Series K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (766,664 | ) | — | — | (766,664 | ) | |||||||||||||||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price, Series E and I | — | — | — | — | — | — | — | — | — | — | — | — | (11,661,705 | ) | — | — | (11,661,705 | ) | |||||||||||||||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature, Series J | — | — | — | — | — | — | — | — | — | — | — | — | (7,790,368 | ) | — | — | (7,790,368 | ) | |||||||||||||||||||||||||
| Comprehensive loss | |||||||||||||||||||||||||||||||||||||||||||
| Unrealized loss on investment securities | — | — | — | — | — | — | — | — | — | — | — | — | — | — | (25,554 | ) | (25,554 | ) | |||||||||||||||||||||||||
| Net loss | — | — | — | — | — | — | — | — | — | — | — | — | — | (44,740,764 | ) | — | (44,740,764 | ) | |||||||||||||||||||||||||
| Total Comprehensive loss | (44,766,318 | ) | |||||||||||||||||||||||||||||||||||||||||
| Balance at December 31, 2004 | 1,306,068 | $ | 1,306 | 900,000 | $ | 900 | 333,333 | $ | 333 | 2,300,000 | $ | 2,300 | 1,575,229 | $ | 1,575 | 197,548 | $ | 198 | $ | 111,957,403 | $ | (172,511,684 | ) | $ | (23,036 | ) | $ | (60,570,705 | ) | ||||||||||||||
See accompanying Notes to Consolidated Financial Statements.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Changes in Stockholders' (Deficit) (continued)
| | Stockholders' (deficit) | | | | | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series A convertible preferred stock | Series B convertible preferred stock | Series C convertible preferred stock | Series F convertible preferred stock | Series H convertible preferred stock | | | | | | | ||||||||||||||||||||||||||||||||
| | Common Stock | | | | | ||||||||||||||||||||||||||||||||||||||
| | | | Accumulated Comprehensive Income (Loss) | | |||||||||||||||||||||||||||||||||||||||
| (Unaudited) | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Number of shares | Par value | Additional paid-in capital | Accumulated Deficit | Total stockholders' (deficit) | ||||||||||||||||||||||||||||
| Research and development expense for issuance of stock options to nonemployees | — | — | — | — | — | — | — | — | — | — | — | — | 47,246 | — | — | 47,246 | |||||||||||||||||||||||||||
| Compensation expense for issuance of stock options to employees | — | — | — | — | — | — | — | — | — | — | — | — | 1,991,827 | — | — | 1,991,827 | |||||||||||||||||||||||||||
| Compensation expense for issuance of restricted stock to employees | — | — | — | — | — | — | — | — | — | — | — | — | 1,425,861 | — | — | 1,425,861 | |||||||||||||||||||||||||||
| Exercise of stock options | — | — | — | — | — | 11,195 | 15 | 20,433 | — | — | 20,448 | ||||||||||||||||||||||||||||||||
| One for one point three reverse stock split | — | — | — | — | — | — | — | — | — | — | — | (4 | ) | 4 | — | — | — | ||||||||||||||||||||||||||
| Accretion of issuance costs related to Series E, I, J and K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (12,282 | ) | — | — | (12,282 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series I mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (11,152 | ) | — | — | (11,152 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (48,485 | ) | — | — | (48,485 | ) | |||||||||||||||||||||||||
| Accretion of issuance costs related to Series K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (9,300 | ) | — | — | (9,300 | ) | |||||||||||||||||||||||||
| Accrual of preferred dividends of Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (3,316,033 | ) | — | — | (3,316,033 | ) | |||||||||||||||||||||||||
| Accrual of preferred dividends of Series K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | — | — | — | — | — | (689,997 | ) | — | — | (689,997 | ) | |||||||||||||||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price, Series E and I | — | — | — | — | — | — | — | — | — | — | — | — | (8,722,382 | ) | — | — | (8,722,382 | ) | |||||||||||||||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature, Series J | — | — | — | — | — | — | — | — | — | — | — | — | (5,826,812 | ) | — | — | (5,826,812 | ) | |||||||||||||||||||||||||
| Comprehensive loss | |||||||||||||||||||||||||||||||||||||||||||
| Unrealized gain on investment securities | — | — | — | — | — | — | — | — | — | — | — | — | — | — | 16,705 | 16,705 | |||||||||||||||||||||||||||
| Net loss | — | — | — | — | — | — | — | — | — | — | — | — | — | (25,963,786 | ) | — | (25,963,786 | ) | |||||||||||||||||||||||||
| Total Comprehensive loss | (25,947,081 | ) | |||||||||||||||||||||||||||||||||||||||||
| Balance at September 30, 2005 (unaudited) | 1,306,068 | $ | 1,306 | 900,000 | $ | 900 | 333,333 | $ | 333 | 2,300,000 | $ | 2,300 | 1,575,229 | $ | 1,575 | 208,743 | $ | 209 | $ | 96,806,331 | $ | (198,475,470 | ) | $ | (6,331 | ) | $ | (101,668,847 | ) | ||||||||||||||
See accompanying Notes to Consolidated Financial Statements.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Consolidated Statements of Cash Flows
| | | Year ended June 30, | Six months ended December 31, | Year ended December 31, | Nine months ended September 30, | | Year ended June 30, | Six months ended December 31, | Year ended December 31, | Nine months ended September 30, | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | | 2002 | 2003 | 2003 | 2004 | 2004 | 2005 | | 2002 | 2003 | 2003 | 2004 | 2004 | 2005 | ||||||||||||||||||||||||||||||||
| | | | | | | (unaudited) | (unaudited) | | | | | | (unaudited) | (unaudited) | ||||||||||||||||||||||||||||||||
| Cash flows from operating activities: | Cash flows from operating activities: | Cash flows from operating activities: | ||||||||||||||||||||||||||||||||||||||||||||
| Net loss | $ | (21,181,143 | ) | $ | (25,734,302 | ) | $ | (36,711,971 | ) | $ | (44,740,764 | ) | $ | (32,475,566 | ) | $ | (25,963,786 | ) | Net loss | $ | (21,181,143 | ) | $ | (25,734,302 | ) | $ | (36,711,971 | ) | $ | (44,740,764 | ) | $ | (32,475,566 | ) | $ | (25,963,786 | ) | |||||||||
| Adjustments to reconcile net loss to net cash used in operating activities: | Adjustments to reconcile net loss to net cash used in operating activities: | |||||||||||||||||||||||||||||||||||||||||||||
| Stock compensation expense | 1,406,535 | 1,573,514 | 13,206,567 | 9,063,517 | 7,307,146 | 3,464,928 | Stock compensation expense | 1,406,535 | 1,573,514 | 13,206,567 | 9,063,517 | 7,307,146 | 3,464,928 | |||||||||||||||||||||||||||||||||
| Expensing of warrants and beneficial conversion | 617,666 | — | — | — | — | — | Expensing of warrants and beneficial conversion | 617,666 | — | — | — | — | — | |||||||||||||||||||||||||||||||||
| Amortization of note discount | 257,686 | 218,935 | 88,440 | 154,062 | 116,244 | 92,495 | Amortization of note discount | 257,686 | 218,935 | 88,440 | 154,062 | 116,244 | 92,495 | |||||||||||||||||||||||||||||||||
| Amortization of discount on short-term investments | — | 264,519 | 160,735 | 1,723,827 | 563,108 | 193,930 | Amortization of discount on short-term investments | — | 264,519 | 160,735 | 1,723,827 | 563,108 | 193,930 | |||||||||||||||||||||||||||||||||
| Accretion of note payable | — | — | — | — | — | 251,373 | Accretion of note payable | — | — | — | — | — | 251,373 | |||||||||||||||||||||||||||||||||
| Depreciation and amortization expense | 417,479 | 740,201 | 445,260 | 1,191,860 | 886,862 | 1,033,130 | Depreciation and amortization expense | 417,479 | 740,201 | 445,260 | 1,191,860 | 886,862 | 1,033,130 | |||||||||||||||||||||||||||||||||
| Minority interest—Related party | (580,467 | ) | — | — | — | — | — | Minority interest—Related party | (580,467 | ) | — | — | — | — | — | |||||||||||||||||||||||||||||||
| Changes in assets and liabilities: | Changes in assets and liabilities: | |||||||||||||||||||||||||||||||||||||||||||||
| Increase in accounts receivable | — | — | — | (1,922,838 | ) | (1,576,380 | ) | 1,193,027 | Increase in accounts receivable | — | — | — | (1,922,838 | ) | (1,576,380 | ) | 1,193,027 | |||||||||||||||||||||||||||||
| Decrease (increase) in grant receivables | 50,993 | (213,886 | ) | 190,426 | 29,366 | (11,493 | ) | 51,285 | Decrease (increase) in grant receivables | 50,993 | (213,886 | ) | 190,426 | 29,366 | (11,493 | ) | 51,285 | |||||||||||||||||||||||||||||
| Decrease (increase) in prepaid expenses and other current assets | 84,917 | (401,706 | ) | (551,888 | ) | 45,904 | 1,313 | (1,546,783 | ) | Decrease (increase) in prepaid expenses and other current assets | 84,917 | (401,706 | ) | (551,888 | ) | 45,904 | 1,313 | (1,546,783 | ) | |||||||||||||||||||||||||||
| Increase in inventory held by the Company | — | — | — | (192,452 | ) | (610,672 | ) | (3,659,983 | ) | Increase in inventory held by the Company | — | — | — | (192,452 | ) | (610,672 | ) | (3,659,983 | ) | |||||||||||||||||||||||||||
| Increase in inventory held by others | — | — | — | (230,748 | ) | — | (870,435 | ) | Increase in inventory held by others | — | — | — | (230,748 | ) | — | (870,435 | ) | |||||||||||||||||||||||||||||
| Decrease in other assets | 23,639 | 28,300 | — | 2,282 | 2,281 | — | Decrease in other assets | 23,639 | 28,300 | — | 2,282 | 2,281 | — | |||||||||||||||||||||||||||||||||
| Increase (decrease) in accounts payable, accrued expenses, other current liabilities | 223,984 | (200,072 | ) | 4,624,205 | (3,384,347 | ) | (2,425,393 | ) | 2,746,766 | Increase (decrease) in accounts payable, accrued expenses, other current liabilities | 223,984 | (200,072 | ) | 4,624,205 | (3,384,347 | ) | (2,425,393 | ) | 2,746,766 | |||||||||||||||||||||||||||
| Increase (decrease) in returns liability | — | — | — | 4,081,910 | — | (2,115,567 | ) | Increase (decrease) in returns liability | — | — | — | 4,081,910 | — | (2,115,567 | ) | |||||||||||||||||||||||||||||||
| Increase (decrease) in amounts due to related party | 579,983 | (592,901 | ) | 113,946 | (128,566 | ) | (305,088 | ) | — | Increase (decrease) in amounts due to related party | 579,983 | (592,901 | ) | 113,946 | (128,566 | ) | (305,088 | ) | — | |||||||||||||||||||||||||||
| Increase (decrease) in deferred grant revenue | — | 95,462 | (47,419 | ) | (48,043 | ) | (38,502 | ) | — | Increase (decrease) in deferred grant revenue | — | 95,462 | (47,419 | ) | (48,043 | ) | (38,502 | ) | — | |||||||||||||||||||||||||||
| Increase in deferred product revenue—tablets | — | — | — | 6,668,491 | 2,764,881 | 4,959,993 | Increase in deferred product revenue—tablets | — | — | — | 6,668,491 | 2,764,881 | 4,959,993 | |||||||||||||||||||||||||||||||||
| Increase in deferred product revenue—capsules | — | — | — | — | — | 4,017,369 | Increase in deferred product revenue—capsules | — | — | — | — | — | 4,017,369 | |||||||||||||||||||||||||||||||||
| Increase (decrease) in royalty payable | — | — | — | 750,000 | — | (750,000 | ) | Increase (decrease) in royalty payable | — | — | — | 750,000 | — | (750,000 | ) | |||||||||||||||||||||||||||||||
| Restricted cash | (6,015 | ) | (3,495 | ) | (1,081 | ) | (2,490 | ) | (1,754 | ) | (4,470 | ) | Restricted cash | (6,015 | ) | (3,495 | ) | (1,081 | ) | (2,490 | ) | (1,754 | ) | (4,470 | ) | |||||||||||||||||||||
| Net cash used in operating activities | (18,104,743 | ) | (24,225,431 | ) | (18,482,780 | ) | (26,939,029 | ) | (25,803,013 | ) | (16,906,728 | ) | Net cash used in operating activities | (18,104,743 | ) | (24,225,431 | ) | (18,482,780 | ) | (26,939,029 | ) | (25,803,013 | ) | (16,906,728 | ) | |||||||||||||||||||||
| Cash flows from investing activities: | Cash flows from investing activities: | Cash flows from investing activities: | ||||||||||||||||||||||||||||||||||||||||||||
| Purchases of property and equipment | (2,230,916 | ) | (747,981 | ) | (590,666 | ) | (531,770 | ) | (462,822 | ) | (142,154 | ) | Purchases of property and equipment | (2,230,916 | ) | (747,981 | ) | (590,666 | ) | (531,770 | ) | (462,822 | ) | (142,154 | ) | |||||||||||||||||||||
| Purchases of intangible assets | — | — | — | (2,000,000 | ) | (2,000,000 | ) | (750,000 | ) | Purchases of intangible assets | — | — | — | (2,000,000 | ) | (2,000,000 | ) | (750,000 | ) | |||||||||||||||||||||||||||
| Purchases of short-term investments | (2,835,526 | ) | (18,940,520 | ) | (39,763,681 | ) | (19,179,583 | ) | (19,179,583 | ) | (11,520,820 | ) | Purchases of short-term investments | (2,835,526 | ) | (18,940,520 | ) | (39,763,681 | ) | (19,179,583 | ) | (19,179,583 | ) | (11,520,820 | ) | |||||||||||||||||||||
| Proceeds from maturities of short-term investments | — | 9,255,000 | 19,611,727 | 40,283,788 | 32,188,787 | 15,580,000 | Proceeds from maturities of short-term investments | — | 9,255,000 | 19,611,727 | 40,283,788 | 32,118,787 | 15,580,000 | |||||||||||||||||||||||||||||||||
| Net cash (used in) provided by investing activities | (5,066,442 | ) | (10,433,501 | ) | (20,742,620 | ) | 18,572,435 | 10,546,382 | 3,167,026 | Net cash (used in) provided by investing activities | (5,066,442 | ) | (10,433,501 | ) | (20,742,620 | ) | 18,572,435 | 10,476,382 | 3,167,026 | |||||||||||||||||||||||||||
| Cash flows from financing activities: | Cash flows from financing activities: | Cash flows from financing activities: | ||||||||||||||||||||||||||||||||||||||||||||
| Proceeds from issuance of preferred stock, net of issuance costs | 1,322,799 | 54,933,001 | — | 11,446,219 | 11,446,219 | — | Proceeds from issuance of preferred stock, net of issuance costs | 1,322,799 | 54,933,001 | — | 11,446,219 | 11,446,219 | — | |||||||||||||||||||||||||||||||||
| Funding received from minority owner | 757,566 | 110,374 | — | — | — | — | Funding received from minority owner | 757,566 | 110,374 | — | — | — | — | |||||||||||||||||||||||||||||||||
| Proceeds from issuance of common stock | 20,619 | — | 23,235 | 8,285 | 8,285 | 20,448 | Proceeds from issuance of common stock | 20,619 | — | 23,235 | 8,285 | 8,285 | 20,448 | |||||||||||||||||||||||||||||||||
| Proceeds from issuance of notes payable | — | 1,163,511 | — | — | — | 5,785,215 | Proceeds from issuance of notes payable | — | 1,163,511 | — | — | — | 5,785,215 | |||||||||||||||||||||||||||||||||
| Proceeds from issuance of warrants | — | — | — | — | — | 214,785 | Proceeds from issuance of warrants | — | — | — | — | — | 214,785 | |||||||||||||||||||||||||||||||||
| Repayments of notes payable | — | (241,191 | ) | (151,757 | ) | (323,971 | ) | (240,327 | ) | (429,245 | ) | Repayments of notes payable | — | (241,191 | ) | (151,757 | ) | (323,971 | ) | (240,327 | ) | (429,245 | ) | |||||||||||||||||||||||
| Reverse stock split fractional share liability | — | — | (80 | ) | — | — | — | Reverse stock split fractional share liability | — | — | (80 | ) | — | — | — | |||||||||||||||||||||||||||||||
| Net cash provided by (used in) financing activities | 2,100,984 | 55,965,695 | (128,602 | ) | 11,130,533 | 11,214,177 | 5,591,203 | Net cash provided by (used in) financing activities | 2,100,984 | 55,965,695 | (128,602 | ) | 11,130,533 | 11,214,177 | 5,591,203 | |||||||||||||||||||||||||||||||
| Net increase (decrease) in cash and cash equivalents | (21,070,201 | ) | 21,306,763 | (39,354,002 | ) | 2,763,939 | (4,112,454 | ) | (8,148,499 | ) | Net increase (decrease) in cash and cash equivalents | (21,070,201 | ) | 21,306,763 | (39,354,002 | ) | 2,763,939 | (4,112,454 | ) | (8,148,499 | ) | |||||||||||||||||||||||||
Cash and cash equivalents at beginning of period | Cash and cash equivalents at beginning of period | 48,082,613 | 27,012,412 | 48,319,175 | 8,965,173 | 8,965,173 | 11,729,112 | Cash and cash equivalents at beginning of period | 48,082,613 | 27,012,412 | 48,319,175 | 8,965,173 | 8,965,173 | 11,729,112 | ||||||||||||||||||||||||||||||||
| Cash and cash equivalents at end of period | Cash and cash equivalents at end of period | $ | 27,012,412 | $ | 48,319,175 | $ | 8,965,173 | $ | 11,729,112 | $ | 4,852,719 | 3,580,613 | Cash and cash equivalents at end of period | $ | 27,012,412 | $ | 48,319,175 | $ | 8,965,173 | $ | 11,729,112 | $ | 4,852,719 | $ | 3,580,613 | |||||||||||||||||||||
Supplemental disclosure: | Supplemental disclosure: | Supplemental disclosure: | ||||||||||||||||||||||||||||||||||||||||||||
| Cash paid for interest | Cash paid for interest | — | 77,293 | 37,646 | 54,835 | 43,777 | 374,535 | Cash paid for interest | $ | — | $ | 77,293 | $ | 37,646 | $ | 54,835 | $ | 43,777 | $ | 374,535 | ||||||||||||||||||||||||||
Non-cash charges related to convertible preferred stock: | Non-cash charges related to convertible preferred stock: | Non-cash charges related to convertible preferred stock: | ||||||||||||||||||||||||||||||||||||||||||||
| Beneficial conversion feature | — | 23,624,173 | 9,726,036 | 19,452,073 | 14,564,279 | 14,549,194 | Beneficial conversion feature | — | 23,624,173 | 9,726,036 | 19,452,073 | 14,564,279 | 14,549,194 | |||||||||||||||||||||||||||||||||
| Accretion of issuance costs | 54,973 | 65,963 | 47,945 | 106,223 | 79,151 | 81,219 | Accretion of issuance costs | 54,973 | 65,963 | 47,945 | 106,223 | 79,151 | 81,219 | |||||||||||||||||||||||||||||||||
| Preferred dividend | — | 629,895 | 2,210,688 | 5,188,041 | 3,852,697 | 4,006,030 | Preferred dividend | — | 629,895 | 2,210,688 | 5,188,041 | 3,852,697 | 4,006,030 | |||||||||||||||||||||||||||||||||
Non-cash investing activities: | Non-cash investing activities: | |||||||||||||||||||||||||||||||||||||||||||||
| Accrual for milestone payments | — | — | — | 1,500,000 | — | 2,250,000 | Accrued Zanaflex milestone payments | — | — | — | 1,500,000 | — | 2,250,000 | |||||||||||||||||||||||||||||||||
See accompanying Notes to Consolidated Financial Statements.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Notes to Consolidated Financial Statements
(1) Organization and Business Activities
Acorda Therapeutics, Inc. ("Acorda" or the "Company") was incorporated in Delaware on March 17, 1995. The Company is a commercial stage biopharmaceutical company dedicated to the identification, development and commercialization of novel therapies that improve neurological function in people with multiple sclerosis, spinal cord injury and other disorders of the central nervous system. Prior to the fiscal year ended December 31, 2004, the Company was a development stage enterprise.
On February 24, 2004, the Board of Directors of Acorda adopted a resolution to change the Company's fiscal year end from June 30 to December 31, effective for the six-month period ended December 31, 2003. For the six-month period ended December 31, 2002 (unaudited) grant revenue and gross profit were $25,494, net loss was $7,215,511, beneficial conversion feature accretion of issuance costs was $27,487 and the net loss applicable to common stockholders was $7,188,024.
The Company acquired all of Elan Corporation plc's ("Elan") U.S. sales, marketing and distribution rights to Zanaflex Capsules and Zanaflex tablets in July 2004. These products are approved for the management of spasticity. Zanaflex tablets were approved by the FDA in 1996 and lost patent protection in 2002. There are currently 11 generic versions of Zanaflex tablets on the market. Zanaflex Capsules were approved by the FDA in 2002, but were never marketed by Elan. The Company began marketing Zanaflex Capsules in April 2005. The Company made an initial payment to Elan of $2 million and is obligated to make royalty payments as well as additional contingent payments upon achieving certain cumulative sales milestones.
The Company is devoting substantially all of its efforts to promoting sales of Zanaflex Capsules, conducting clinical trials, pursuing regulatory approval for products under development, and engaging in preclinical development. The Company has begun to generate product revenues but has not achieved profitable operations or positive cash flows from operations. There is no assurance that profitable operations, if ever achieved, could be sustained on a continuing basis. The Company's accumulated deficit since inception through September 30, 2005 was $198.5 million (unaudited) and the Company expects to continue to incur losses for the foreseeable future. Further, the Company's future operations are dependent on the success of the Company in commercializing Zanaflex Capsules, completing the clinical development of Fampridine-SR in MS and obtaining regulatory approval and market acceptance of this product candidate and advancing its preclinical programs.
The Company plans to finance its operations through a combination of issuance of equity securities, revenues from Zanaflex Capsules, loans and, to a lesser extent, grants. There are no assurances that the Company will be successful in obtaining an adequate level of financing needed to fund its development and commercialization efforts. The Company believes that its current financial resources and sources of liquidity should be adequate to fund operations at least through January 1, 2006 based on the Company's current projected spending levels.
(2) Summary of Significant Accounting Policies
Unaudited Interim Financial Information
The accompanying consolidated balance sheet as of September 30, 2005, the consolidated statements of operations and cash flow for the nine months ended September 30, 2004 and 2005, and the statement of Stockholders' (deficit) for the nine months ended September 30, 2005 are unaudited. The unaudited interim financial statements have been prepared in accordance with U.S. generally accepted accounting principles. In the opinion of the Company's management, the unaudited interim
financial statements have been prepared on the same basis as the audited financial statements and include all adjustments consisting of normal recurring adjustments and accruals necessary for the fair presentation of the Company's financial position, results of operations and its cash flows for the nine months ended September 30, 2004 and 2005. The results for the nine months ended September 30, 2005 are not necessarily indicative of the results to be expected for the year ended December 31, 2005.
Principles of Consolidation
The accompanying consolidated financial statements are prepared in accordance with accounting principles generally accepted in the United States of America and include the results of operations of the Company and its majority owned subsidiary (see Notes 7 and 11). All intercompany accounts and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of the consolidated financial statements requires management of the Company to make a number of estimates and assumptions relating to the reported amount of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the period. Significant items subject to such estimates and assumptions include research and development (clinical trial accrual), beneficial conversion charges, stock warrants and option accounting, which are all dependent on the fair value of the Company's equity security. In addition, the Company recognizes revenue based on estimated prescriptions filled. The Company adjusts its inventory value based on an estimate of inventory that may expire. Actual results could differ from those estimates.
Cash and Cash Equivalents
The Company considers all highly liquid debt instruments with original maturities of three months or less to be cash equivalents. All cash and cash equivalents are held in United States financial institutions and money market funds, which are unrestricted as to withdrawal or use. To date, the Company has not experienced any losses on its cash and cash equivalents. The carrying amount of cash and cash equivalents approximates its fair value due to its short-term and liquid nature.
Restricted Cash
Restricted cash represents a certificate of deposit placed by the Company with a bank for issuance of a letter of credit to the Company's lessor for office space.
Short-Term Investments
Short-term investments consist of corporate debt securities with original maturities greater than three months. In accordance with Statement of Financial Accounting Standards ("SFAS") No. 115 ("SFAS 115"),Accounting for Certain Investments in Debt and Equity Securities, the Company classifies its short-term investments as available-for-sale. Available-for-sale securities are recorded at fair value of the investments based on quoted market prices. The Company considers all of these investments to be available-for-sale.
Unrealized holding gains and losses on available-for-sale securities, which are determined to be temporary, are excluded from earnings and are reported as a separate component of other comprehensive income (loss).
Premiums and discounts on investments are amortized over the life of the related available-for-sale security as an adjustment to yield using the effective- interest method. Dividend and interest income are recognized when earned. Realized gains and losses are determined on the average cost method. Amortized premiums and discounts, dividend and interest income and realized gains and losses are included in interest income.
Inventory
Inventory is stated at the lower of cost or market value and includes amounts for both Zanaflex tablet and Zanaflex capsule inventories. All inventories consist of finished goods. Cost is determined using the first-in, first-out method (FIFO) for all inventories. The Company adjusts its inventory value based on an estimate of inventory that may expire.
Property and Equipment
Property and equipment are stated at cost, net of accumulated depreciation. Depreciation is computed on the straight-line basis over the estimated useful lives of the assets, which range from three to seven years. Leasehold improvements are recorded at cost, less accumulated amortization, which is computed on the straight-line basis over the shorter of the useful lives of the asset or the remaining lease term. Expenditures for maintenance and repairs are charged to expense as incurred.
Intangible Assets
The Company has recorded intangible assets related to its Zanaflex acquisition. These intangible assets are amortized on a straight line basis over the period in which the Company expects to receive economic benefit and are reviewed for impairment when facts and circumstances indicate that the carrying value of the asset may not be recoverable. The determination of the expected life will be dependent upon the use and underlying characteristics of the intangible asset. In the Company's evaluation of the intangible assets, it considers the term of the underlying patent life and the expected life of the product line. If the carrying value is not recoverable, impairment is measured as the amount by which the carrying value exceeds its estimated fair value. Fair value is generally estimated based on either appraised value or other valuation techniques.
Impairment of Long-Lived Assets
In accordance with the Financial Accounting Standards Board ("FASB") SFAS No. 144,Accounting for the Impairment or Disposal of Long-Lived Assets, the Company continually evaluates whether events or circumstances have occurred that indicate that the estimated remaining useful life of its long-lived assets may warrant revision or that the carrying value of these assets may be impaired. The Company evaluates the realizability of its long-lived assets based on profitability and cash flow expectations for the related asset. Any write-downs are treated as permanent reductions in the carrying amount of the assets. Based on this evaluation, the Company believes that, as of each of the balance sheet dates presented, none of the Company's long-lived assets was impaired.
Warrants
In January 2005, the Company issued warrants that provide the holder with the right to purchase $300,000 (unaudited) worth of shares of preferred stock in the Company's next qualifying equity round or 40,000 shares of Series K mandatorily redeemable preferred stock if no such round is completed
prior to December 31, 2005. Beginning July 1, 2005, these warrants are subject to FASB Staff Position No. 150-5 ("FSP 150-5"), which addresses whether freestanding warrants and other similar instruments on shares that are either puttable or mandatorily redeemable would be subject to the requirements of FASB Statement No. 150,Accounting for Certain Financial Instruments with Characteristics of both Liabilities and Equity, regardless of the timing of the redemption feature or the redemption price. Upon adoption of FSP 150-5 on July 1, 2005, the Company reclassified the warrants from additional paid in capital to a liability based on its fair value on July 1, 2005. The warrant will be marked to market each reporting period thereafter with the change in fair value recorded to earnings. The adoption of this statement resulted in gain from a net effect of change in accounting principle of $2,805, as a result of the change in fair value of the warrant from January 2005 to July 1, 2005.
In November 2005, the Company modified the terms of this warrant to provide the holder with the right to purchase $300,000 (unaudited) worth of (i) shares of preferred stock in the Company's next Qualifying Equity Round or, (ii) to the extent the Company has consummated an IPO on or before February 28, 2006, shares of Common Stock at the lower of (A) the per share price of the Common Stock sold in the IPO and (B) $7.50 per share, or (iii) to the extent the Company has not consummated either a qualifying equity round or an IPO on or before February 28, 2006, then Series K mandatorily redeemable preferred stock at $7.50 per share.
Patent Costs
Patent application and maintenance costs are expensed as incurred.
Research and Development
Research and development expenses include the clinical development costs associated with the Company's product candidates and research and development costs associated with the Company's preclinical programs. These expenses include internal research and developments costs and the costs of research and development conducted on behalf of the Company by third parties, including sponsored university-based research agreements, and clinical study vendors. All research and development costs are expensed as incurred. Costs incurred in obtaining technology licenses are charged immediately to research and development expense if the technology licensed has not reached technological feasibility and has no alternative future uses.
Accounting for Income Taxes
Income taxes are accounted for under the asset and liability method with deferred tax assets and liabilities recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax basis. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be reversed or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period that includes the enactment date. Deferred tax assets are reduced by a valuation allowance for the amounts of any tax benefits which, more likely than not, will not be realized.
Revenue Recognition
The Company applies the revenue recognition guidance in SFAS No. 48,Revenue Recognition When the Right of Return Exists, which amongst other criteria requires that future returns can be reasonably
estimated in order to recognize revenue. The amount of future tablet returns is uncertain due to generic competition and customer conversion to Zanaflex Capsules. Zanaflex Capsules are a new product with no historical return data. Due to the uncertainty of returns for both products, the Company is accounting for these product shipments using a deferred revenue recognition model. Under the deferred revenue model, the Company does not recognize revenue upon product shipment. For these product shipments, the Company invoices the wholesaler, records deferred revenue at gross invoice sales price, and classifies the cost basis of the product held by the wholesaler as a component of inventory. The Company recognizes revenue when prescribed to the end-user, on a first-in first-out (FIFO) basis. The Company's revenue to be recognized is based on (1) the estimated prescription demand-based on pharmacy sales for its products, and (2) the Company's analysis of third-party information, including third-party market research data, (3) the Company's internal product sales information and (4) wholesaler inventory levels and re-order information.data. The Company's estimates are subject to the inherent limitations of estimates that rely on third-party data, as certain third-party information was itself in the form of estimates, and reflect other limitations. The Company's sales and revenue recognition reflects the Company's estimates of actual product prescribed to the end-user.
When the Company acquired Zanaflex from Elan, it also acquired Elan's inventory of Zanaflex tablets, which included both partial lots with expiration dating of less than 12 months and full lots with expiration dating greater than 12 months. The Zanaflex tablet inventory the Company acquired from Elan was labeled with a code identifying the inventory as Elan's.
For partial tablet lots acquired, the Company has deferred recognition of revenue until the product return period expires in June 2006, since it is unable to determine whether the prescriptions filled for Zanaflex tablet with Elan's code relate to product sold by Elan or sold by the Company. After the product return period expires in June 2006, the Company will recognize revenue only to the extent of unreturned product.
With regards to the full tablet lots acquired, the Company began recognizing revenue in July 2005 for prescriptions filled for Zanaflex tablets with Elan's code. All of the Zanaflex tablet inventory sold by Elan prior to the acquisition reached its expiration date in June 2005, therefore any prescriptions filled for Zanaflex tablets subsequent to June 2005 can only be from the full inventory lots acquired by the Company and sold by the Company.
Inventory manufactured after the Company's acquisition of Zanaflex is labeled with a code that enables it to identify the inventory as the Company's. These codes are contained on end-user prescription data that the Company uses to recognize revenue.
The Company began receiving end-user prescription data containing its code, which enabled it to begin recognizing revenue from Zanaflex tablet sales in March 2005. The Company began marketing Zanaflex Capsules in April 2005 and began recognizing revenue in the same month.
At December 31, 2004 and September 30, 2005 the Company had deferred revenue from Zanaflex tablets of $6.7 million and $10.7 million (unaudited), respectively, of which $3.6 million and $2.5 million (unaudited), respectively, was related to product acquired from Elan that had an expiration date of less than 12 months at the time the Company sold it during 2004. The Company believes there is a high likelihood that this product will be returned which would result in its inability to recognize related revenue. If such product is returned the deferred revenue liability upon a return would offset the associated receivable or any credit we may issue if the wholesaler previously paid the invoice.
The Company's net revenues represent total revenues less allowances for customer credits, including estimated discounts, rebates, and chargebacks. Product shipping and handling costs are
included in cost of sales. These reserves are recorded in accordance with Emerging Issues Task Force (EITF) Issue No. 01-9,Accounting for Consideration Given by a Vendor to a Customer, which states that cash consideration given by a vendor to a customer is presumed to be a reduction of the selling prices of the vendor's products or services and, therefore, should be characterized as a reduction of revenue when recognized in the vendor's income statement. At the time product is shipped to wholesalers, an adjustment is recorded for estimated chargebacks, rebates, and discounts. These reserves are established by management as its best estimate based on available information and is adjusted to reflect known changes in the factors that impact such reserves. Reserves for chargebacks, rebates and discounts are established based on the contractual terms with customers, analysis of historical levels of discounts, chargebacks and rebates, communications with customers and the levels of inventory remaining in the distribution channel, as well as expectations about the market for each product and anticipated introduction of competitive products. In addition, the Company records a charge to cost of goods sold for the cost basis of the estimated product returns the Company believes may ultimately be realized at the time of product shipment to wholesalers. The Company has recognized this charge at the date of shipment since it is probable that it will receive a level of returned products; upon the return of such product it will be unable to resell the product considering its expiration dating; and it can reasonably estimate a range of returns. This charge represents the cost basis for the low end of the range of the Company's estimated returns.
As part of the acquisition of Zanaflex, the Company agreed to accept any returns of Zanaflex tablets that were returned subsequent to January 17, 2005, including returns of product that was originally sold by Elan. Product returns prior to that date were the responsibility of Elan. The Company has recorded a charge to discounts and allowances of $4.1 million in 2004 for the estimated liability for product originally sold by Elan that will ultimately be returned to the Company for a refund under its returned product policy of Zanaflex tablets sold by Elan. This obligation to accept returns for product sold by Elan expires in June 2006.
Revenue Recognition—Grants
Revenue related to research and development grants is recognized when the related research expenses are incurred and the Company's specific performance obligations under the terms of the respective contract are satisfied. To the extent expended, grant funding related to purchases of equipment is deferred and amortized over the shorter of the equipment's useful life or the life of the related contract. Revenue recognized in the accompanying consolidated financial statements is not subject to repayment. Payments, if any, received in advance of performance under the contract are deferred and recognized as revenue when earned.
Planned Initial Public Offering Costs
The Company originally deferred the planned initial public offering costs incurred in 2003 in accordance with SEC Staff Accounting Bulletin ("SAB") Topic 5A, Expenses of Offering. In December 2003, the Company deferred its plan for an initial public offering. As a result, the related costs of approximately $1.3 million were expensed and included in the Company's consolidated statements of operations for the six month period ended December 31, 2003.
Concentration of Risk
Financial instruments that potentially subject the Company to concentrations of credit risk consist principally of investments in cash and cash equivalents, restricted cash, accounts receivable and debt securities. The Company maintains cash and cash equivalents, restricted cash and debt securities with approved financial institutions. The Company is exposed to credit risks in the event of default by the financial institutions or issuers of investments in excess of FDIC insured limits. The Company performs periodic evaluations of the relative credit standing of these financial institutions and limits the amount of credit exposure with any institution.
The Company is substantially dependent upon Elan for several activities related to the development and commercialization of Fampridine-SR. The Company will rely on Elan to complete the chemistry, manufacturing and controls section of the New Drug Application ("NDA") for Fampridine-SR in multiple sclerosis. If Elan fails to provide these parts of the NDA in a complete and timely manner the Company could incur delays in filing of its NDA for Fampridine-SR in multiple sclerosis.
The Company relies on a single manufacturer, Elan, for the supply of Zanaflex Capsules and on another single manufacturer, Novartis, for the supply of tizanadine.tizanadine, the active pharmaceutical ingredient, or API, in Zanaflex Capsules. If either Elan or Novartis experiences any disruption in their operations, a delay or interruption in the supply of the Company's products could result until the affected supplier cures the problem or the Company locates an alternative source of supply. The Company may not be able to enter into alternative supply arrangements on terms that are commercially favorable, if at all. Any new supplier would also be required to qualify under applicable regulatory requirements. The Company could experience substantial delays before it is able to qualify any new supplier and transfer the required manufacturing technology to that supplier. Novartis has informed usthe Company that they intendit intends to discontinue tizanidine production by the end of 2005. We havethe first quarter of 2006. The Company has established relationships with the companiescompany that currently formulateformulates the tablets and the company that bottles and package Zanaflex tablets,tablets; however, we dothe Company does not have an agreement with an alternative manufacturer of tizanidine. It is the responsibility of each of Novartis and Elan to procure the API required to meet its contractual obligations to supply the Company with product. The Company does not anticipate an interruption in API supply. Novartis is currently transferring the methods of manufacturing tizanidine to Rohner, an API manufacturer in Pratteln, Switzerland. The Company has verified this transfer and plans to audit Rohner's manufacturing site towards the end of first quarter 2006, following the commencement of Rohner's manufacture of tizanidine. The Company has also identified an alternate source for tizanidine in collaboration with Elan. The Company does not anticipate entering into a supply agreement for API with either party. Any cost associated with validating API suppliers would be incurred by Novartis or Elan. The costs of the Company's audit of Rohner or any other supplier are not material and are considered part of its normal course of business.
The Company has agreed to purchase at least 75% of its Fampridine-SR product requirements from Elan, and must make compensatory payments if it does not purchase 100% of its requirements from Elan. The Company and Elan have agreed that the Company may purchase up to 25% of its annual Fampridine-SR requirements from Patheon, Inc., a qualified manufacturing source of Fampridine-SR, without making compensatory payments to Elan. In addition, the Company does not have direct contractual relationships with the suppliers of fampridine, the active pharmaceutical ingredient in Fampridine-SR, referred to as API. Currently, the Company is relying on Elan's contracts
with third parties to supply API. If Elan or an alternative manufacturer is unable to obtain API from these suppliers for any reason, a new supplier would have to be identified by the Company. Although
there are other potential sources of API available, any new supplier would be required to qualify under applicable regulatory requirements. Any delays in obtaining API to manufacture Fampridine-SR could delay the clinical trials of Fampridine-SR.
Similar to other pharmaceutical companies, the Company's principal customers are wholesale pharmaceutical distributors. The Company periodically assesses the financial strength of these customers and establishes allowances for anticipated losses, if necessary. To date, such losses have been minimal.
| | % of total trade accounts receivable | |||||
|---|---|---|---|---|---|---|
| | As of December 31, 2004 | As of September 30, 2005 | ||||
| | | (unaudited) | ||||
| Major customers: | ||||||
| Cardinal | 27 | % | 11 | % | ||
| McKesson | 52 | 60 | ||||
| Amerisource | 13 | 11 | ||||
| Total | 92 | % | 82 | % | ||
Allowance for Doubtful Accounts
A portion of the Company's accounts receivable may not be collected due principally to customer disputes and sales returns. The Company provides reserves for these situations based on the evaluation of the aging of its trade receivable portfolio and an analysis of high-risk customers. The Company has not recognized an allowance as of December 31, 2004 or September 30, 2005 (unaudited) as management believes all outstanding accounts receivable are fully collectible.
Fair Value of Financial Instruments
The fair value of a financial instrument represents the amount at which the instrument could be exchanged in a current transaction between willing parties, other than in a forced sale or liquidation. Significant differences can arise between the fair value and carrying amounts of financial instruments that are recognized at historical cost amounts.
The following methods are used to estimate the Company's financial instruments:
It is not practical for the Company to estimate the fair value of the convertible notes payable to Elan due to the specific provisions of these notes including the uncertainty of the timing of repayment which is dependent upon regulatory approval of certain products. The terms of these notes are disclosed at Note 11.
Earnings per Share
Net loss per share is computed in accordance with SFAS No. 128,Earnings Per Share, by dividing the net loss allocable to common stockholders by the weighted average number of shares of common stock outstanding. The Company has certain options, warrants, convertible preferred stock and mandatorily redeemable convertible preferred stock (see Notes 3 and 8), which have not been used in the calculation of diluted net loss per share because to do so would be anti-dilutive. Anti- dilutive shares totaled 24,091,289 as of June 30, 2002, 136,881,522 as of June 30, 2003 and December 31, 2003, and 138,414,849 as of December 31, 2004 and September 30, 2005 (unaudited). As such, the numerator and the denominator used in computing both basic and diluted net loss per share allocable to common stockholders for each year are equal. The Company has reflected the beneficial conversion feature for Series E, Series I and Series J, accretion of issuance costs for Series E, Series I, Series J and Series K, and preferred dividend for Series J and Series K in the net loss allocable to common stockholders as set forth below.
| | Beneficial conversion feature | Accretion of issuance costs | Preferred dividend | ||||||
|---|---|---|---|---|---|---|---|---|---|
| For the year ended December 31, 2004 | $ | 19,452,073 | $ | 106,223 | $ | 5,188,041 | |||
| For the six month period ended December 31, 2003 | 9,726,036 | 47,945 | 2,210,688 | ||||||
| For the year ended June 30, 2003 | 23,624,173 | 65,963 | 629,895 | ||||||
| For the year ended June 30, 2002 | — | 54,973 | — | ||||||
For the nine month period ended September 30, 2005 (unaudited) | 14,549,194 | 81,219 | 4,006,030 | ||||||
| For the nine month period ended September 30, 2004 (unaudited) | 14,564,279 | 79,151 | 3,852,697 | ||||||
Stock-Based Compensation
The Company has various stock-based employee and non-employee compensation plans, which are described more fully in Note 9. The Company accounts for options and restricted stock granted to employees and directors in accordance with the fair value method of SFAS No. 123,Accounting for Stock-Based Compensation ("SFAS No. 123"), as amended by SFAS No. 148,Accounting for Stock-Based Compensation Transition and Disclosure an amendment of FASB Statement No. 123 and related interpretations. As such, compensation expense is recorded on stock option and restricted stock grants based on the fair value of the options or restricted stock granted, which is estimated on the date of grant using the Black-Scholes option-pricing model for stock options granted, and is recognized on a straight-line basis over the vesting period. The Company accounts for stock options granted to non-employees on a fair-value basis in accordance with EITF No. 96-18,Accounting for Equity Instruments That Are Issued to Other Than Employees for Acquiring, or in Conjunction with Selling, Goods or Services, and FASB Interpretation No. 28,Accounting for Stock Appreciation Rights and Other Variable Stock Option or Award Plans an Interpretation of APB Opinion No. 15 and 25. As a result, the non-cash charge to operations for non-employee options with vesting or other performance criteria is affected each reporting period by changes in the estimated fair value of the Company's common stock. The two factors which most affect charges or credits to operations related to stock-based compensation are the fair value of the common stock underlying stock options for which stock-based compensation is
recorded and the volatility of such fair value. If the Company's estimates of the fair value of these equity instruments changes, it would have the effect of changing compensation expense. Because shares of the Company's common stock have not been publicly traded, the Company generally estimates the fair value of its common stock based on the most recent previous sale of convertible preferred stock (convertible on a one-for-one basis into common stock). The Company does not discount the issuance price of its preferred stock in estimating the fair value of its common stock.
Segment Information
The Company is managed and operated as one business. The entire business is managed by a single management team that reports to the chief executive officer. The Company does not operate separate lines of business with respect to any of its product candidates. Accordingly, the Company does not prepare discrete financial information with respect to separate product candidates or by location and does not have separately reportable segments as defined by SFAS No. 131,Disclosures about Segments of an Enterprise and Related Information.
Comprehensive Income (Loss)
SFAS No. 130,Reporting Comprehensive Income ("SFAS No. 130") establishes standards for the reporting and display of comprehensive income (loss) and its components in a full set of financial statements. SFAS No. 130 requires that unrealized gains (losses) from the Company's investment securities be included in other comprehensive income (loss).
Recent Accounting Pronouncements
In December 2004, the FASB issued SFAS No. 123R. This statement is a revision of FASB Statement No. 123,Accounting for Stock-Based Compensation. This statement supersedes APB Opinion No. 25,Accounting for Stock Issued to Employees, and its related implementation guidance. This statement establishes standards for the accounting for transactions in which an entity exchanges its equity instruments for goods or services. It also addresses transactions in which an entity incurs liabilities in exchange for goods or services that are based on the fair value of the entity's equity instruments or that may be settled by the issuance of those equity instruments. The full impact of adoption of SFAS 123R cannot be predicted at this time because it will depend on levels of share-based payments granted in the future. However, had the Company adopted SFAS 123R in prior periods, management believes the impact of that standard would have approximated the impact of SFAS 123.
(3) Beneficial Conversion Feature
In May 2003, the Company completed a private placement of 112,790,233 shares of Series J mandatorily redeemable convertible preferred stock at $0.49 per share for an aggregate purchase price of approximately $55,267,000. The terms of the preferred stock are more fully described in Note 8.
As part of this financing, the original conversion price of the Series A through Series I preferred stock was reduced as a result of anti-dilution adjustments, which resulted in a beneficial conversion amounting to $80,730,286 in accordance with EITF No. 98-5,Accounting for Convertible Securities with Beneficial Conversion Features or Contingently Adjustable Conversion Ratios and EITF No. 00-27,Application of Issue No. 98-5 to Certain Convertible Instruments. The beneficial conversion charge of $20,860,491 relating to Series A, Series B, Series C, Series F and Series H convertible preferred stock, which are not mandatorily redeemable and may be converted at any time at the option of the holders to common stock, has been recorded as an immediate charge to additional paid-in capital. The remaining beneficial conversion amount of $59,869,795 related to Series E and Series I convertible preferred stock, which are mandatorily redeemable at any time on or after June 30, 2008, is being accreted ratably over the mandatory redemption period. Such accretion amounted to $1,656,854, $5,830,852, $11,661,705 and $8,722,382 (unaudited) for the year ended June 30, 2003, the six month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005, respectively, and is charged to additional paid-in capital.
In addition, the issuance of Series J mandatorily redeemable convertible preferred stock resulted in a beneficial conversion amounting to $39,994,812 in accordance with EITF No. 98-5. The beneficial conversion is calculated based on the estimated fair value of the Company's common stock price per share at the date of issuance of Series J preferred stock of approximately $10.14 per share of common stock, which was calculated based on the estimated projected midpoint of the range of the Company's initial public offering price per common share, which was planned in the fourth calendar quarter of 2003, and the stock price appreciation in comparable public companies from May 2003 to August 2003. The beneficial conversion feature is being accreted ratably over the mandatory redemption period, with a charge to additional paid-in capital of $1,106,828, $3,895,184, $7,790,368 and $5,826,812 (unaudited) for the year ended June 30, 2003, the six month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005 (unaudited), respectively.
(4) Short-Term Investments
The Company has accounted for its investments in accordance with SFAS No. 115,Accounting for Certain Investments in Debt and Equity Securities, and determined that all of its short-term investments are classified as available-for-sale. Available-for-sale securities are carried at fair value with interest on these securities included in interest income. Available-for-sale securities consisted of the following:
| | Amortized Cost | Gross unrealized gains | Gross unrealized losses | Estimated fair value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Corporate debt securities | |||||||||||||
| As of December 31, 2003 | $ | 32,247,745 | $ | 25,690 | $ | (23,172 | ) | $ | 32,250,263 | ||||
| As of December 31, 2004 | 9,419,713 | — | (23,036 | ) | 9,396,677 | ||||||||
| As of September 30, 2005 (unaudited) | 5,166,606 | — | (6,331 | ) | 5,160,275 | ||||||||
The contractual maturities of available-for-sale debt securities at December 31, 2004 and September 30, 2005 are within one year.
Investments are considered impaired when a decline in fair value is determined to be other-than-temporary. The Company employs a systematic methodology that considers available evidence in evaluating potential impairment of its investments in accordance with EITF Issue No. 03-1,The
Meaning of Other-Than-Temporary Impairment and Its Application to Certain Investments ("EITF 03-01"). In the event that the cost of an investment exceeds its fair value, the Company evaluates, among other factors, the duration and extent to which the fair value is less than cost; the financial health of and business outlook for the investment or investee; and the Company's intent and ability to hold the investment. The Company has determined that there were no other-than-temporary declines in the fair values of its short term investments as of December 31, 2004.
The following table shows the gross unrealized losses and fair value of the Company's available-for-sale securities with unrealized losses that are not deemed to be other-than-temporarily impaired, aggregated by investment category and length of time that individual securities have been in a continuous unrealized loss position, at December 31, 2004 (in thousands):
| | Less than 12 months | 12 Months or Greater | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Description of Securities | Fair value | Unrealized loss | Fair value | Unrealized loss | |||||||||
| Corporate debt securities(1) | $ | 9,397 | $ | (23 | ) | $ | — | $ | — | ||||
| Total | $ | 9,397 | $ | (23 | ) | $ | — | $ | — | ||||
Short-term investments with original maturity of three months or less have been classified as cash and cash equivalents, and amounted to $7,551,356, $7,878,024 and $2,277,746 (unaudited) as of December 31, 2003, December 31, 2004 and September 30, 2005, respectively.
(5) Property and Equipment
Property and equipment consisted of the following:
| | December 31, 2003 | December 31, 2004 | September 30, 2005 | Estimated useful lives | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| | | | (unaudited) | | |||||||
| Laboratory equipment | $ | 2,068,502 | $ | 2,113,093 | $ | 2,099,396 | 5 years | ||||
| Furniture and fixtures | 535,200 | 537,473 | 514,181 | 5 years | |||||||
| Computer equipment | 585,244 | 759,949 | 680,008 | 3 years | |||||||
| Leasehold improvements | 1,727,813 | 2,023,033 | 2,052,309 | 5 to 7 years | |||||||
| 4,916,759 | 5,433,548 | 5,345,894 | |||||||||
| Less accumulated depreciation | 1,823,605 | 2,886,534 | 3,440,831 | ||||||||
| $ | 3,093,154 | $ | 2,547,014 | $ | 1,905,063 | ||||||
Depreciation and amortization expense on property and equipment was $417,479 and $740,201 for the fiscal year ended June 30, 2002 and 2003, $445,260 for the six-month period ended December 31, 2003, $1,077,910 for the year ended December 31, 2004 and $788,572 (unaudited) for the nine-month period ended September 30, 2005.
(6) Accrued Expenses and Other Current Liabilities
Accrued expense and other current liabilities consisted of the following:
| | December 31, 2003 | December 31, 2004 | September 30, 2005 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| | | | (unaudited) | ||||||
| Bonus payable | $ | 1,106,698 | $ | — | $ | 514,002 | |||
| Milestone payable to Elan | — | 750,000 | 3,750,000 | ||||||
| Royalties payable | — | 519,531 | 223,493 | ||||||
| Accrued research and development expenses | 2,649,368 | 825,166 | 859,812 | ||||||
| Return credits payable to customers | — | — | 1,278,801 | ||||||
| Other accrued expenses | 593,762 | 795,521 | 1,199,761 | ||||||
| $ | 4,349,828 | $ | 2,890,218 | $ | 7,825,869 | ||||
Accrued research and development expenses include amounts relating to the clinical trials as well as preclinical operating costs. Other accrued expenses include legal and business development accruals, payroll liabilities, vacation and commission accruals and other operating expense accruals.
(7) Notes Payable
In 2003, the Company entered into two financing agreements with General Electric Capital Corporation in the aggregate amount of $1,153,511, bearing annual fixed interest rates of 8.57% and 8.88%, to finance the purchase of certain property and equipment. Borrowings are secured by a security interest in certain property and equipment of the Company and the agreements do not include any debt covenants. The Company is required to pay monthly installments until October 2006. The aggregate principal payments required subsequent to December 31, 2004 are: $301,938 in 2005, and $144,654 in 2006. The related interest payments required subsequent to December 31, 2004 are: $26,001 in 2005, and $5,109 in 2006.
In 2005 (unaudited), the Company entered into a $6 million senior secured term loan with General Electric Capital Corporation ("GE"), that bears an annual fixed interest rate of 9.93%. The Company is required to pay monthly installments until February 2008, with interest-only payments for the first six months followed by principal and interest payments for the remaining 29 months. The loan is secured by all of the Company's personal property and fixtures owned at closing or subsequently acquired. The aggregate principal payments required subsequent to December 31, 2004 are: $899,887 in 2005, $2,317,217 in 2006, $2,558,084 in 2007 and $224,813 in 2008. The related interest payments required subsequent to December 31, 2004 are: $283,130 in 2005, $402,862 in 2006, $161,995 in 2007 and $1,860 in 2008. See Note 8.
For long-term convertible notes payable to related party see Note 11.
(8) Mandatorily Redeemable Convertible Preferred Stock and Convertible Preferred Stock
The board of directors of the Company has authorized 141,754,865 shares of convertible preferred stock, designated as Series A, B, C, D, E, F, G, H, I, J and K preferred stock (Series A, Series B, Series C, Series D, Series E, Series F, Series G, Series H, Series I, Series J and Series K; collectively, the Preferred Stock). Series E, Series I, Series J and Series K are mandatorily redeemable convertible preferred stock (Redeemable Preferred Stock). Upon an initial public offering, the preferred stock will automatically convert into common stock.
The terms of the Preferred Stock are as follows:
(a) Dividends
The Preferred Stock (except Series J and Series K) is entitled to noncumulative dividends prior to and in preference to dividends declared or paid on the common stock, at the rate of $0.10 per share per annum for Series A through Series H and at the rate of $0.39 per share per annum for Series I when and if declared by the board of directors. Dividends on Series J and Series K are cumulative and accrue on each share of Series J Preferred Stock and Series K Preferred Stock commencing on the date of issuance, whether or not earned or declared at the rate of $0.0392 per share per annum for Series J and at the rate of $0.60 per share per annum for Series K, based on the original issue price of Series J Preferred Stock and Series K Preferred Stock, prior and in preference to any declaration or payment of any dividend on any other Series of Preferred Stock holders (Series A through Series I). Series J and Series K dividends are payable when declared by the Board of Directors or upon liquidation, as defined or upon redemption, provided, however, that the amount of any dividend payable shall not exceed the original issue price of such series of preferred stock. Accrued dividends for Series J and K were $6.6 million and $761,000 as of December 31, 2004 and $9.9 million and $1.5 million (unaudited) as of September 30, 2005, respectively.
(b) Liquidation
The preferred stockholders have liquidation preferences over common stockholders based on the series of Preferred Stock held. In the event of liquidation, dissolution, or winding up of the Company, each holder of shares of Series J Preferred Stock and Series K Preferred Stock is entitled to be paid in preference to common stockholders and any other Series of Preferred Stock holders (Series A through Series I) an amount equal to the original issue price per share of $0.49 for Series J and $7.50 for Series K, plus all accrued or declared but unpaid dividends. After payment has been made to Series J and Series K Preferred Stock, the Series I, Series E-1, Series E-2, Series F and Series H shall be entitled to receive out of the available assets, on a pro rata basis, an amount per share of $3.89, $1.31, $1.07, $1.09 and $1.36, respectively, plus all declared but unpaid dividends on each such share issued. After payment of the above mentioned preferential amounts the holders of Series E, Series F and Series H Preferred Stock shall be entitled to be paid out of the remaining available assets an amount per share equal to $0.26, $0.21 and $0.27, respectively, plus all declared but unpaid dividends. After payment of the above mentioned preferential amounts, the holders of Series A through Series H Preferred Stock shall be entitled to be paid out of remaining available assets an amount per share up to and including such amounts paid in accordance with as mentioned above, equal to $1.00, $2.00, $3.00, $12.50, $3.13, $5.22, the greater of $2.00 and 80% of the closing price per share of the Institutional Financing, as defined, most recently completed by the Company prior to the issuance of the Series G Preferred Stock and $3.25, respectively.
(c) Conversion
The Preferred Stock will be automatically converted into common stock upon an initial public offering of the Company's common stock or upon either the approval by written consent of the holders of a majority of the then outstanding shares of Series A, Series B, Series C, Series D, Series E, Series F, Series G, Series H and Series I voting together as a single class and upon approval by written consent of the holders of a majority of the then outstanding shares of Series J and Series K.
| Preferred stock | Shares outstanding at December 31, 2004 | Conversion Price | Shares of Common Stock | ||||
|---|---|---|---|---|---|---|---|
| Series A | 1,306,068 | $ | 9.06 | 144,074 | |||
| Series B | 900,000 | 11.86 | 151,820 | ||||
| Series C | 333,333 | 14.64 | 68,339 | ||||
| Series D | — | 11.86 | — | ||||
| Series E | 7,472,612 | 13.81 | 1,461,363 | ||||
| Series F | 2,300,000 | 13.81 | 449,803 | ||||
| Series G | — | (1 | ) | — | |||
| Series H | 1,575,229 | 15.34 | 333,827 | ||||
| Series I | 10,204,047 | 17.11 | 2,319,457 | ||||
| Series J | 112,790,233 | 7.64 | 7,230,118 | ||||
| Series K | 1,533,327 | 9.75 | 1,179,478 | ||||
In the event the convertible promissory notes payable to Elan are converted into common stock, the per share conversion price on the Series I and Series J preferred stock would be adjusted to $16.37 and $7.12, respectively. Other than in an initial public offering or certain other specified instances, in the event the Company issues common stock (or securities convertible into common stock) at an effective common stock issuance price of less than a specified amount the conversion price on all preferred stock will be reduced based on anti-dilution provisions.
(d) Redemption
Holders of Series E, Series I, Series J and Series K Preferred Stock may at any time on or after June 30, 2008, require the Company to redeem all or any portion of such holders' redeemable preferred stock at a redemption price, as specified below, provided, however, that no holder of redeemable preferred stock may so require such redemption unless and until (i) the holders of not less than a majority of the redeemable preferred stock then issued and outstanding make such election and (ii) the holders of a majority of the Series J and Series K preferred stock then issued and outstanding make such election prior to September 30, 2008 (these terms collectively, the Redemption Date). The redemption price for each share of redeemable preferred stock shall be the original issue price plus accrued but unpaid dividends. One half of such aggregate redemption price for all redeemable preferred stock shall be payable in cash on the Redemption Date, as defined and the second half of such aggregate redemption price shall be payable in cash on the first anniversary of the Redemption Date, as defined.
(e) Voting
Each holder of outstanding Preferred Stock (other than Series F) shall be entitled to the number of votes equal to the number of shares of common stock into which the shares of Preferred Stock so held could be converted. The holders of Series F Preferred Stock shall have no voting rights except as required by Delaware General Corporation Law. The board of directors consists of nine directors: (i) two directors elected by the holders of Series A, Series E and Series H Preferred Stock, voting as a single class; (ii) one director elected by Series I Preferred Stock; (iii) two directors elected by Series J Preferred Stock; (iv) one director elected by holders of common stock; and (v) three directors elected by the holders of common stock and Preferred Stock, voting as a single class. The Company's certificate of incorporation includes provisions which restrict the Company from certain actions without the approval of a defined percentage of the preferred stockholders.
Convertible Preferred Stock
Series A
In May 1995, the Company issued 610,000 shares of Series A, at a per share price of $1.00, for aggregate proceeds of $610,000, and granted each purchaser a warrant to purchase one additional share of Series A for every ten Series A shares purchased, at an exercise price of $1.00 per share. The Company estimated the fair value of warrants at approximately $44,971. The fair value was determined by the Black-Scholes valuation method, using a risk free interest rate of 6.5%, the warrants' contractual life of seven years, an annual volatility of 73% and no expected dividends. Such amount was credited to additional paid-in capital and charged immediately to additional paid-in capital, as the warrants were exercisable at any time at the option of the holder. Each warrant was exercised for one share of Series A. During fiscal 2002, 22,800 of these warrants were exercised on a cash basis and 28,268 were exercised in a cashless exercise resulting in total proceeds of $22,800. The remaining 9,932 of these warrants were not exercised and have expired.
In fiscal 1996 and 1997, the Company issued 450,000 and 195,000 shares of Series A, at a per share price of $1.00, for aggregate proceeds of $450,000 and $195,000, respectively. In August 1996 and January 1997, the Company granted 340,000 warrants to purchase shares of Series A at an exercise price of $1.00. These warrants expired in August 2003 and January 2004, respectively. None of these warrants were exercised. The Company estimated the fair value of warrants at approximately $254,110. Such value was determined by the Black-Scholes valuation method, using a risk free interest rate of 6.5%, the warrant's contractual life of seven years, an annual volatility of 75% and no expected dividends. Such amount was credited to additional paid-in capital and charged immediately to additional paid-in capital as the warrants were exercisable at any time at the option of the holder.
Series B
In January 1997, the Company issued 750,000 shares of Series B, at a per share price of $2.00, for aggregate proceeds of $1,500,000. In January 2002, the Company issued 150,000 shares of Series B, at a per share price of $2.00, for aggregate proceeds of $300,000 (see Note 11).
As of September 30, 2005 (unaudited), 100,000 Series B warrants were outstanding with an exercise price per share of $2.00. The warrants to acquire Series B Preferred Stock enable the holder to acquire 21,929 shares of common stock.
Series C
In February 2002, the Company issued to Elan and affiliates 333,333 shares of Series C, at a per share price of $3.00, for aggregate proceeds of $999,999.
Series F
In April 1998, the Company issued to Elan 2,300,000 shares of Series F, at a per share price of approximately $5.22, for aggregate proceeds of approximately $12 million. Also, in April 1998, the Company entered into a joint venture agreement with Elan. The $12 million proceeds from the sale of the shares of Series F was then transferred to MS Research and Development Corp. ("MSRD"), a joint venture company of which the Company owned approximately 80% and Elan owned 20%. To purchase its approximate 20% interest, Elan invested an additional $3 million into MSRD. The combined $15 million was subsequently used to license research and development technology from Elan to develop Elan's proprietary oral sustained release formulation of fampridine for the treatment of multiple sclerosis. For the years ended June 30, 2002 and 2003 and for six-month period ended December 31, 2003, MSRD incurred approximately $2.9 million, $3.2 million and $3.3 million, respectively, in research and development expenses, which is included as research and development expense in the accompanying statements of operations, of which the Company funded 80% and Elan funded 20% until June 30, 2002, in accordance with the terms of the original development agreement. Elan's ownership interest in MSRD is reflected as minority interest in the accompanying statement of operations. The minority interest share of the MSRD losses were being funded by Elan, and through June 30, 2002 the Company received $1,279,361 as a reimbursement of this funding. In fiscal 2003, Elan ceased funding its approximately 20% share of the operating expenses of MSRD and the Company ceased recognizing the related minority interest benefit resulting in an increase in the Company's ownership interest to 83% pursuant to the original agreement (see Note 11 for discussion on license and research agreement.) In September 2003, the Company entered into a termination and assignment agreement with Elan, EIS and MSRD, pursuant to which MSRD assigned to the Company its assets, including the license from Elan for Fampridine-SR for MS. The Company paid MSRD approximately $11.5 million for all of the assets and assumed all of the liabilities of MSRD, and MSRD distributed to the Company approximately $9.5 million as pro rata portion of the purchase price. From the time of establishment of MSRD until the sale of MSRD's assets to the Company, Elan was considered to be a related party under generally accepted accounting principles.
Series H
In August 1999, the Company completed a private placement of 1,575,229 shares of Series H at $3.25 per share, resulting in net proceeds to the Company of $5,119,494 after payment of legal and certain other fees.
Mandatorily Redeemable Convertible Preferred Stock
The following convertible preferred stock are based on the redemption rights and conversion option as discussed above under terms of the Preferred Stock.
Series E
In July and November 1998, the Company issued 7,472,612 shares of Series E, that are mandatorily redeemable at $2.70 per share for an aggregate purchase price of approximately
$20,176,000. The Company incurred issuance costs of $209,270. Such costs are netted against the proceeds of the Series E, and are being amortized over the mandatory redemption period.
Series I
In March 2001, the Company issued 10,204,047 shares of Series I that are mandatorily redeemable at $3.89 per share for an aggregate purchase price of approximately $39,694,000. The Company incurred issuance costs of $138,179. Such costs are netted against the proceeds of the Series I, and are being amortized over the mandatory redemption period.
Series J
In May 2003, the Company issued 112,790,233 shares of Series J that are mandatorily redeemable at $0.49 per share for an aggregate purchase price of approximately $55,267,000. The Company incurred issuance costs of $334,219. Such costs are netted against the proceeds of the Series J, and are being amortized over the mandatory redemption period.
In September 2003, the Company obtained approval by the written consent from the holders of Series J preferred stock voting together as a single class and the holders of the Preferred Stock, voting separately as a single class on an as if converted basis for a reduction in the price per share of common stock offered to the public in an initial public offering which would trigger automatic conversion of the preferred stock into common stock from an offering price of not less than $14.76 per share to an offering price of not less than $12.00 per share.
Series K
In March 2004, the Company issued 1,533,327 shares of Series K which are mandatorily redeemable at $7.50 per share for an aggregate purchase price of $11,499,943. The Company incurred issuance costs of $53,728. Such costs are netted against the proceeds of the Series K, and will be amortized over the mandatory redemption period.
In January 2005, the Company granted warrants to purchase $300,000 (unaudited) worth of shares of Preferred Stock in the Company's next qualifying equity round, or Series K if no such round is issued prior to December 31, 2005. The number of Series K shares to be received upon exercise is 40,000 at the Series K issue price of $7.50 per share, which converts to 30,769 common shares. The Company estimated the fair value of warrants at approximately $214,785. Such value was determined by the Black-Scholes valuation method, using a risk free interest rate of 3.5%, the warrant's contractual life of ten years, an annual volatility of 90% and no expected dividends. These warrants were issued to GE in conjunction with the $6 million senior secured term loan (see Note 7). The discount of the note related to the warrants is being accreted over the life of the notes and resulted in a $78,023 (unaudited) charge to interest expense for the nine-month period ended September 30, 2005.
The changes in mandatorily redeemable convertible preferred stock are as follows:
| | Mandatorily Redeemable Convertible Preferred Stock (in thousands) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series E | Series I | Series J | Series K | ||||||||||||||
| | Number of Shares | Amount | Number of Shares | Amount | Number of Shares | Amount | Number of Shares | Amount | ||||||||||
| Balance at June 30, 2001 | 7,473 | $ | 20,040 | 10,204 | $ | 39,564 | — | — | — | — | ||||||||
| Accretion of issuance costs | — | 27 | — | 28 | — | — | — | — | ||||||||||
| Balance at June 30, 2002 | 7,473 | 20,067 | 10,204 | 39,592 | — | — | — | — | ||||||||||
| Issuance of Series J mandatorily redeemable convertible preferred stock | — | — | — | — | 112,790 | 54,933 | — | — | ||||||||||
| Accretion of issuance costs | — | 27 | — | 28 | — | 11 | — | — | ||||||||||
| Accrual of preferred dividend on Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | 630 | — | — | ||||||||||
| Beneficial conversion feature for reduction in conversion price | — | (20,176 | ) | — | (39,694 | ) | — | — | — | — | ||||||||
| Beneficial conversion feature on issuance | — | — | — | — | — | (39,995 | ) | — | — | |||||||||
| Deemed dividends on preferred stock for reduction in conversion price | — | 558 | — | 1,098 | — | — | — | — | ||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature | — | — | — | — | — | 1,107 | — | — | ||||||||||
| | Mandatorily Redeemable Convertible Preferred Stock (in thousands) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Series E | Series I | Series J | Series K | ||||||||||||||||
| | Number of Shares | Amount | Number of Shares | Amount | Number of Shares | Amount | Number of Shares | Amount | ||||||||||||
| Balance at June 30, 2003 | 7,473 | $ | 476 | 10,204 | $ | 1,024 | 112,790 | $ | 16,686 | — | — | |||||||||
| Accretion of issuance costs | — | 8 | — | 7 | — | 32 | — | — | ||||||||||||
| Accrual of preferred dividend on Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | 2,211 | — | — | ||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price | — | 1,965 | — | 3,866 | — | — | — | — | ||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature | — | — | — | — | — | 3,895 | — | — | ||||||||||||
| Balance at December 31, 2003 | 7,473 | $ | 2,450 | 10,204 | $ | 4,897 | 112,790 | $ | 22,824 | — | — | |||||||||
| Issuance of Series K mandatorily redeemable convertible preferred stock | 1,533 | $ | 11,446 | |||||||||||||||||
| Accretion of issuance costs | — | 16 | — | 15 | — | 65 | — | 10 | ||||||||||||
| Accrual of preferred dividend on Series K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | 767 | ||||||||||||
| Accrual of preferred dividend on Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | 4,421 | — | — | ||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price | — | 3,930 | — | 7,732 | — | — | — | — | ||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature | — | — | — | — | — | 7,790 | — | — | ||||||||||||
| Balance at December 31, 2004 | 7,473 | $ | 6,396 | 10,204 | $ | 12,644 | 112,790 | $ | 35,100 | 1,533 | $ | 12,223 | ||||||||
| Accretion of issuance costs | — | 12 | — | 11 | — | 48 | — | 9 | ||||||||||||
| Accrual of preferred dividend on Series K mandatorily redeemable convertible preferred stock | — | — | — | — | — | — | — | 690 | ||||||||||||
| Accrual of preferred dividend on Series J mandatorily redeemable convertible preferred stock | — | — | — | — | — | 3,316 | — | — | ||||||||||||
| Deemed dividends on preferred stock for reduction in conversion price | — | 2,939 | — | 5,783 | — | — | — | — | ||||||||||||
| Deemed dividends on preferred stock for issuance of preferred stock with beneficial conversion feature | — | — | — | — | — | 5,827 | — | — | ||||||||||||
| Balance at September 30, 2005 (unaudited) | 7,473 | $ | 9,347 | 10,204 | $ | 18,438 | 112,790 | $ | 44,291 | 1,533 | $ | 12,922 | ||||||||
(9) Common Stock Options, Warrants and Restricted Stock
Upon inception of the Company in March 1995, the founders, directors, and certain employees purchased 166,827 shares of restricted common stock at a per share price of $0.16.
On June 18, 1999, the Company's board of directors approved the adoption of the Acorda Therapeutics, Inc. 1999 Employee Stock Option Plan (the "Plan"). All employees of the Company are eligible to participate in the Plan, including executive officers, as well as directors, independent contractors, and agents of the Company. The Plan is administered by the Compensation Committee of the board of directors, which selects the individuals to be granted options and stock appreciation rights, determines the time or times at which options and stock appreciation rights shall be granted under the Plan, determines the number of shares to be granted subject to any option or stock appreciation right under the Plan and the duration of each option and stock appreciation right, and makes any other determinations necessary, advisable, and/or appropriate to administer the Plan. Under the Plan, each option granted expires no later than the tenth anniversary of the date of its grant. Options vest over a four year period on a quarterly basis commencing with the date of award. Compensation expense is calculated using a Black-Scholes calculation with the expense being recognized over the vesting period. No option may be granted pursuant to the Plan more than ten years after the date on which the Plan was adopted by the board of directors and any option granted under the Plan shall, by its terms, not be exercisable more than ten years after the date of grant. In March 2004, the number of shares authorized for issuance under the Plan was increased from 1,275,641 shares to 2,451,088 shares. In
September 2005, the number of shares authorized for issuance under the Plan was increased from 2,451,088 to 3,186,856.
The effects of applying SFAS No. 123 in a particular year, may not be representative of the effects on reported net income or loss for future years. The fair value of each option granted is estimated on the date of grant using an option-pricing model with the following weighted average assumptions:
| | Year ended June 30, | | | | | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| | Six-month period ended December 31, 2003 | | Nine-month period ended September 30, 2004 | Nine-month period ended September 30, 2005 | ||||||||||
| | Year ended December 31, 2004 | |||||||||||||
| | 2002 | 2003 | ||||||||||||
| | | | | | (unaudited) | (unaudited) | ||||||||
| Employees and directors: | ||||||||||||||
| Estimated volatility | 97.7 | % | 94.0 | % | 89.8 | % | 90.0 | % | 88.42 | % | 78.4 | % | ||
| Expected life in years | 5 | 5 | 5 | 5 | 5 | 5 | ||||||||
| Risk free interest rate | 4.41 | % | 3.04 | % | 3.28 | % | 3.41 | % | 2.78 | % | 4.1 | % | ||
| Dividend yield | — | — | — | — | — | — | ||||||||
The Company estimated volatility for purposes of computing compensation expense on its employee and non-employee options using the volatility of public companies that the Company considered comparable. The expected life used to estimate the fair value of non-employee options is equal to the contractual life of the option granted, which is 10 years.
The weighted average fair value per share of options granted to employees for the years ended June 30, 2002 and 2003, the six month period ended December 31, 2003, the year ended December 31, 2004 and the nine month period ended September 30, 2005 amounted to approximately $51.95, $52.73, $16.22, $6.95, and $5.41 (unaudited) respectively. The weighted average fair value per share of options granted to non-employees for the six month period ended December 31, 2003 amounted to approximately $7.64. No options were granted to non-employees for the years ended June 30, 2002, and 2003, and December 31, 2004, and the nine month period ended September 30, 2005 (unaudited).
Common stock option and warrant activity from June 30, 2001 to September 30, 2005 is as follows (this table does not include warrants to acquire Series B and Series K Preferred stock, which are discussed in Note 8):
| | Shares | Exercise Price per share | ||
|---|---|---|---|---|
| Balance at June 30, 2001 | 147,532 | |||
| Granted | 43,631 | $23.40 - $31.20 | ||
| Forfeited | (3,050 | ) | 5.46 - 23.40 | |
| Exercised | (3,381 | ) | 5.46 - 23.40 | |
| Balance at June 30, 2002 | 184,732 | |||
| Granted | 11,170 | 12.48 - 31.20 | ||
| Forfeited | (4,588 | ) | 5.46 - 31.20 | |
| Balance at June 30, 2003 | 191,314 | |||
| Granted (original price $7.64, repriced to $2.60) | 1,112,082 | 2.60 | ||
| Forfeited | (14,114 | ) | 7.64 - 31.20 | |
| Exercised | (3,687 | ) | 1.56 - 12.48 | |
| Balance at December 31, 2003 | 1,285,595 | |||
| Granted | 67,488 | 2.60 - 9.75 | ||
| Forfeited | (61,588 | ) | 2.60 - 7.64 | |
| Exercised | (2,360 | ) | 1.56 - 7.64 | |
| Balance at December 31, 2004 | 1,289,135 | |||
| Granted | 615,798 | 8.14 | ||
| Forfeited | (124,737 | ) | 2.60 | |
| Exercised | (11,195 | ) | 2.60 | |
| Balance at September 30, 2005 (unaudited) | 1,769,001 | |||
Options available to grant at December 31, 2004 were 70,570.
Options and Warrants outstanding | Options and Warrants exercisable | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Range of exercise prices | Outstanding as of December 31, 2004 | Weighted average remaining contractual life | Weighted average exercise price | Exercisable as of December 31, 2004 | Weighted average exercise price | |||||||
| $.16 - $3.12 | 42,628 | 1.67 | $ | 1.52 | 42,628 | $ | 1.52 | |||||
| $2.60 | 1,177,815 | 8.40 | 2.60 | 1,102,774 | 2.60 | |||||||
| $9.75 - $12.48 | 64,619 | 9.69 | 9.80 | 5,072 | 10.44 | |||||||
| $23.40 | 4,071 | 6.69 | 23.40 | 3,451 | 23.40 | |||||||
| 1,289,135 | 8.24 | 2.99 | 1,153,926 | 2.66 | ||||||||
This table represents the equity instruments issued since January 1, 2004 through September 30, 2005.
| Transaction Date | Options Granted | Restricted Shares Granted | Fair Market Value at Grant Date | Exercise Price Per Share | Intrinsic Value | Recipient | Compensation Expense Recognized Thru September 2005 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jan-04(1) | 1,912 | — | $ | 7.64 | $ | 2.60 | $ | 9,636 | Employees | $ | 5,796 | |||||||
| Mar-04 | 17,192 | — | 9.75 | 9.75 | — | Employees | 40,618 | |||||||||||
| Mar-04 | — | 1,134,423 | 9.75 | n/a | — | Employees | 3,581,830 | |||||||||||
| Aug-04 | 3,769 | — | 9.75 | 9.75 | — | Employees | 3,129 | |||||||||||
| Aug-04 | — | 5,077 | 9.75 | n/a | — | Employees | 2,149 | |||||||||||
| Nov-04 | 44,615 | — | 9.75 | 9.75 | — | Employees | 67,462 | |||||||||||
| Total 2004 | 67,488 | 1,139,500 | ||||||||||||||||
| Jan-05 (unaudited) | 34,615 | — | 9.75 | Employees | 41,021 | |||||||||||||
| Aug-05 (unaudited) | 548,484 | — | 8.14 | Employees | 720,092 | |||||||||||||
| Aug-05 (unaudited) | 32,699 | — | 8.14 | Director | 46,458 | |||||||||||||
| Sep-05 (unaudited) | — | 7,692 | n/a | Directors | 77,140 | |||||||||||||
| Total 2005 (unaudited) | 615,798 | 7,692 | ||||||||||||||||
In January 2005, the Company issued warrants that provide the holder with the right to purchase $300,000 (unaudited) worth of shares of preferred stock in the Company's next qualifying equity round or 40,000 shares of Series K mandatorily redeemable preferred stock if no such round is issued prior to December 31, 2005. In November 2005, the Company modified the terms of this warrant to provide the holder with the right to purchase $300,000 worth of shares of preferred stock in the Company's next qualifying equity round or; to the extent the Company has consummated an IPO on or before February 28, 2006, shares of Common Stock at the lower of (A) the per share price of the Common Stock sold in the IPO and (B) $9.75 per share or; to the extent the Company has not consummated either a qualifying equity round or an IPO on or before February 28, 2006, then $9.75 per share.
In September 2003, the Company re-priced 118,142 stock options issued to employees, which had an exercise price per option of more than $7.64, with a new exercise price per share of $7.64. As a result of this repricing, the Company has recognized an additional compensation charge based on the estimated fair value of the repriced options of $575,563, of which $449,585, $92,054 and $15,737 (unaudited) was recognized during the six-month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005, respectively, with the balance to be recognized over the remaining respective vesting periods of the repriced options. Such compensation expense was calculated based on the estimated fair value based upon the Black-Scholes model of the repriced options compared to the value of the options immediately prior to the date of the repricing based on the original terms.
In September 2003, the Company granted 1,062,081 stock options, that had been authorized for issuance under the Plan in May 2003, to employees under the Plan at an exercise price of $7.64 per share, which was below the estimated fair value of the Company's common stock at the date of grant. Compensation expense of approximately $11.0 million, attributable to the fair value of the options granted, was recognized for the six-month period ended December 31, 2003 as certain of the options issued to employees vested immediately and the balance of $6.1 million will be recognized over the remaining respective vesting periods of the options. Such compensation expense was calculated based on the estimated projected midpoint of the range of the Company's initial public offering price per common share, which
was planned in the fourth calendar quarter of 2003, and the stock price appreciation in comparable public companies from May 2003 to August 2003 (the estimated fair value of the Company's common stock on the date of grant.) In December 2003, the Company deferred its plan for an initial public offering.
In October 2003, the Company granted 38,462 stock options to its chief executive officer and 9,615 stock options to its executive director-marketing and commercialization at exercise prices of $7.64 per share, which was below the estimated fair value of the Company's common stock at the date of grant. Compensation expense of approximately $425,000 attributable to the fair value of the options granted was recognized for the six-month period ended December 31, 2003, as certain of the options issued to employees vested immediately and the balance of $355,000 will be recognized over the remaining respective vesting periods of the options.
In March 2004, the Company repriced 1,250,853 stock options issued to employees, which had an exercise price per share of more than $2.60, with a new exercise price per share of $2.60. Most of these options were originally issued in September 2003. As a result of this repricing, the Company has recognized an additional compensation charge of $2,200,330, of which $1,869,872 and $89,198 was recognized during the year ended December 31, 2004 and the nine-month period ended September 30, 2005 (unaudited), respectively, with the balance to be recognized over the remaining respective vesting periods of the repriced options. Such compensation expense was calculated based on the estimated fair value of the repriced options compared to the value of the options immediately prior to the date of the repricing based on the original terms.
In March 2004, the Company granted 1,134,423 restricted shares and 17,192 stock options to employees under the Plan. The stock options were issued with an exercise price of $9.75 per share which was the fair value of the Company's common stock at the date of grant. The restricted shares were granted for no cash consideration. The option grants are exercisable based on a four-year quarterly vesting schedule, commencing with the date of award March 9, 2004. The restricted stock awards are subject to vesting over a four-year period as follows: the first installment will vest on the last to occur of (a) the expiration of the lock-up period following our initial public offering, and (b) the third day after public announcement of data regarding either the primary outcome measure of our Fampridine-SR Phase 3 trial in MS or suspension or termination of the trial, whichever comes first, and (c) in the case of Ron Cohen, June 30, 2007; except that if the vesting date under (a) or (b) or (c) would occur during a "blackout" period under our insider trading policy, the vesting date will be the first day following termination of the blackout period. The first vested installment under each restricted stock award will be calculated as the total number of shares covered by the award multiplied by a fraction, the numerator of which is the number of months from the vesting commencement date to the date on which the first installment of restricted shares vest, or the "initial vesting date," and the denominator is 48. All remaining restricted shares will vest in equal quarterly installments, measured from the vesting commencement date, except that for any partial quarter in which the initial vesting date occurs, the unvested portion of shares remaining for that quarter will vest at the end of such quarter. As a result of these grants, the total compensation charge is approximately $11,177,540, of which compensation expense of $2,256,103 and $1,366,345 (unaudited) was recognized during the year ended December 31, 2004 and the nine months ended September 30, 2005, with the balance to be recognized over the remaining respective vesting periods of the options and restricted shares. The Company recognized compensation expense ratably over four years.
In August and November 2004, the Company granted 48,384 options to employees under the plan. The stock options were issued with an exercise price of $9.75 per share. The options will vest over a four-year vesting schedule. As a result of these grants the total compensation charge is $325,109 of which $14,053 and $56,538 (unaudited) was recognized during the year ended December 31, 2004 and the nine months ended September 30, 2005.
In January 2005, the Company granted 34,615 options to employees under the plan. The stock options were issued with an exercise price of $9.75 per share. The options will vest over a four-year vesting schedule. As a result of these grants the total compensation charge is $228,495 (unaudited) of which $41,021 (unaudited) was recognized during the nine months ended September 30, 2005.
In August 2005, the Company granted 548,484 and 32,699 stock options to employees and non-employees, respectively, under the Plan. The stock options were issued with an exercise price of $8.14 per share. 87,624 and 6,122 of the employee and non-employee grants, respectively, vested immediately upon the grant date of the award. The balance will be vested based on a four-year quarterly vesting schedule for employee grants and a three-year quarterly vesting schedule for non-employee grants. $4,538,220 (unaudited), of which compensation expense of $766,550 (unaudited) was recognized during the nine months ended September 30, 2005, with the balance to be recognized over the remaining respective vesting periods of the options.
In August 2005, the Company granted 7,692 restricted shares to non-employees. 5,769 of these grants vested immediately upon the date of award of August 3, 2005, and the balance will be vested based on a one-year quarterly vesting schedule, contingent upon certain restrictions defined in the restricted stock agreement. As a result of these grants, the total compensation charge is approximately $84,612 (unaudited), of which compensation expense of $77,140 (unaudited) was recognized through September 30, 2005, with the balance to be recognized over the remaining respective vesting periods of the restricted shares. As of December 31, 2004 and September 30, 2005 1,127,808 and 756,620 (unaudited) restricted shares remain outstanding.
Compensation expense for options and restricted stock granted to employees amounted to $1,331,911, $1,580,054, $13,198,079, $9,049,858 and $3,417,684 (unaudited) for the years ended June 30, 2002 and 2003, the six-month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005, respectively. Compensation expense for options and restricted stock granted to employees are classified between research and development and general and administrative expense based on employee job function.
Options granted to non-employees vest immediately or over a one to four year period based upon future service requirements. Compensation expense for options granted to non-employees amounted to $74,624, ($6,539), $8,488, $15,458 and $47,246 (unaudited) for the years ended June 30, 2002 and 2003, the six-month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005, respectively. The amount of compensation expense to be recorded in the future for options granted to non-employees is subject to change each reporting period based upon changes in the estimated fair value of the Company's common stock, estimated volatility and risk free interest rate until the non-employee completed performance under the option agreement. As of December 31, 2004 and September 30, 2005, respectively, 1,756 and 27,619 (unaudited) options subject to this treatment remain unvested.
With the exception of options to purchase 1,912 shares of common stock made in January 2004, the Company granted all of its 2004 common stock options and warrants at an exercise price of $9.75, which was equal to the price of its March 2004 financing transaction of Series K Preferred Stock. Although the preferred shares have certain preferential rights such as liquidation preferences, convertibility features, dividend rights and anti-dilution protections that would result in differences between the fair value of its preferred and common stock, the Company estimated the fair value of its common stock at $9.75 per share during 2004 and recorded compensation expense based on the $9.75 fair market value.
(10) Income Taxes
The Company had available net operating loss carry-forwards ("NOL") of approximately $131,843,113 and $154,641,684 as of December 31, 2004 and September 30, 2005 (unaudited), for federal and state income tax purposes, which are available to offset future federal and state taxable income, if any, and expire between 2010 and 2025. The Company also has research and development tax credit carryforwards of approximately $1,254,000 and $1,515,641 as of December 31, 2004 and September 30, 2005 (unaudited), for federal income tax reporting purposes that are available to reduce federal income taxes, if any, and expire in future years beginning in 2018.
The tax effect of temporary differences that give rise to significant portions of the deferred tax assets and deferred tax liabilities as of December 31, 2003 and 2004 and September 30, 2005, are presented below:
| | December 31, 2003 | December 31, 2004 | September 30, 2005 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| | | | (unaudited) | |||||||
| Net operating loss carryforwards | $ | 39,167,783 | $ | 54,055,676 | $ | 63,403,090 | ||||
| Research and development tax credit | 783,500 | 1,254,426 | 1,515,641 | |||||||
| Property and equipment | (298,728 | ) | 110,266 | 219,207 | ||||||
| Intellectual property | 5,398,333 | 5,310,070 | 4,970,111 | |||||||
| Stock options and warrants | 5,413,596 | 9,130,376 | 11,360,515 | |||||||
| Other temporary differences | 43,302 | 124,141 | 136,465 | |||||||
| 59,507,786 | 69,984,955 | 81,605,030 | ||||||||
| Less valuation allowance | (59,507,786 | ) | (69,984,955 | ) | (81,605,030 | ) | ||||
| Net deferred tax assets | $ | — | $ | — | $ | — | ||||
Changes in the valuation allowance for the six-month period ended December 31, 2003, for the year ended December 31, 2004, and for the nine-month period ended September 30, 2005 (unaudited) amounted to approximately $11,580,075, $19,477,170 and $11,620,075, respectively. Since inception, the Company has incurred substantial losses and expects to incur substantial losses in future periods. The Tax Reform Act of 1986 (the "Act") provides for a limitation of the annual use of NOL and research and development tax credit carryforwards (following certain ownership changes, as defined by the Act) that could significantly limit the Company's ability to utilize these carryforwards. The Company has experienced various ownership changes, as a result of past financings. Accordingly, the Company's
ability to utilize the aforementioned carryforwards may be limited. Additionally, because U.S. tax laws limit the time during which these carryforwards may be applied against future taxes, the Company may not be able to take full advantage of these attributes for federal income tax purposes. Because of the above mentioned factors, the Company has not recognized its net deferred tax assets as of and for all periods presented. Accordingly, the Company has provided a full valuation allowance against its net deferred tax assets and no tax benefit has been recognized relative to its pretax losses.
(11) License and Research Agreements
Elan
In January 1997, the Company entered into several agreements with Elan, including a License and Supply Agreement to develop Elan's, sustained-release formulation of Fampridine-SR for treatment of spinal cord injury. In return for this exclusive license granted by Elan, the Company paid a license fee of $5 million which was expensed in fiscal 1997. The term of the agreement is equal to the greater of 20 years or the duration of relevant Fampridine-SR patent rights. Any mutually agreed to research conducted by Elan will be paid by the Company at cost plus 45%. The Company will be responsible for all clinical trials and regulatory approvals. Elan will have the right to manufacture, subject to certain exceptions, products for the Company upon regulatory approval at specified prices as a percentage of net selling price. In the event Elan does not manufacture the products, it is entitled to a royalty as a stated percentage of the products' net selling price.
Series B and C Preferred Stock Purchase
Concurrent with the License and Supply Agreement, the Company entered into a Preferred Stock, Convertible Note and Warrant Purchase Agreement (the "Agreement") with Elan. Under this Agreement, Elan purchased 750,000 shares of the Company's Series B at a per share price of $2.00 and also agreed to purchase 333,333 shares of the Company's Series C at a per share price of $3.00 within 30 days of the completion of Phase 2 clinical trials relating to products to be developed under the License and Supply Agreement. Concurrent with the purchase of Series B, the Company issued to Elan a warrant to purchase an additional 150,000 shares of Series B at a per share exercise price of $2.00 for a period of five years. The Company estimated the fair value of warrants at approximately $198,031. Such value was determined by the Black-Scholes valuation method, using a risk free interest rate of 6.4%, the warrant's contractual life of five years, an annual volatility of 75% and no expected dividends. Such amount was credited to additional paid-in capital and charged immediately to additional paid-in capital as the Series B was convertible at any time at the option of the holder.
Phase 2 clinical trials relating to products to be developed under the License and Supply Agreement were completed in February 2002 and Elan purchased 333,333 shares of Series C at a per share price of $3.00 resulting in total proceeds of $999,999. Elan also exercised its Series B warrant and the Company issued 150,000 shares of Series B at a per share price of $2.00 resulting in total proceeds of $300,000. The Company also issued an additional five-year warrant to purchase 100,000 shares of Series B at a per share exercise price of $2.00 for a period of five years from the date of issuance on January 4, 2002. The Company estimated the fair value of the five-year warrant to purchase 100,000 shares of Series B at approximately $321,000. Such value was determined by the Black-Scholes valuation method, using a risk free interest rate of 4.3%, the warrant's contractual life of five years, an annual volatility of 102% and no expected dividends. Such amount was credited to additional paid-in
capital and charged immediately to research and development expenses as these warrants were issued in connection with the Company completing Phase 2 clinical trials. In addition, the Company recognized $296,666 as a beneficial conversion feature on issuance of Series C convertible preferred stock and charged this amount to research and development expenses as these shares were issued upon the Company completing Phase II clinical trials pursuant to a previous arrangement.
Convertible Note
Under the Agreement, Elan also loaned to the Company an aggregate of $7.5 million pursuant to two convertible promissory notes. One promissory note in the amount of $5.0 million bears interest at a rate of 3% beginning on the first anniversary of the issuance of the note. The unpaid principal is convertible into shares of the Company's Series D at a conversion price of $12.50 per share. Principal and interest are repayable, if not converted, ratably over a seven-year period beginning one year after the Company receives certain regulatory approval for the products to be developed, subject to limitations related to gross margin on product sales. If it is determined by both parties that regulatory approval will not likely occur, all principal and interest will not be repayable and the note will be cancellable after a defined notice period, if not earlier converted. If the License and Supply Agreement is otherwise terminated, the principal and interest is repayable ratably over 15 years. Both promissory notes restrict our ability to incur indebtedness that is senior to the notes, subject to certain exceptions, including for our revenue interests assignment arrangement with PRF (See Note 17).
The second promissory note in the amount of $2.5 million is non-interest bearing. This promissory note is convertible after January 22, 1999 into either shares of Series B at a conversion price of $2.00 per share or into an undesignated series (currently authorized as Series D) of Preferred Stock at a conversion price equal to 80% of the-then most recently completed equity financing, whichever conversion price is greater. This promissory note is repayable by the Company, if not converted by Elan, ratably over a seven-year period beginning one year after the Company receives certain regulatory approval for the products to be developed. If it is determined by both parties that regulatory approval will not likely occur or if the License and Supply Agreement is otherwise terminated, the note is repayable ratably over 15 years from the date of determination. Interest on these convertible promissory notes has been imputed using 9% on 50% of the $5 million note and 8% on the $2.5 million note. In case of the $5 million note, the Company did not impute interest on 50% of the $5 million note based on the provision in the License and Supply Agreement that provided for a recovery of up to $2.5 million of the license fee paid, which was dependent upon regulatory approval of the product. If regulatory approval of the product is received, the convertible note would be repayable and the Company would have been entitled to recovery of up to $2.5 million based on the aforementioned provision. If the parties determine that regulatory approval will not likely occur, the note will not be repayable and the Company would not receive recovery of up to $2.5 million of the license fee. The $2,173,127 difference between the $7.5 million principal amount of the notes and the discounted balance is being accreted to interest expense over the estimated term of the notes. Elan was considered to be a related party based on its ownership interest in the Company, significant license agreements entered into and involvement with research and development activities of the Company. In addition, Elan had a right to appoint a representative on the board of directors from January 22, 1997 through May 8, 2003. Elan ceased to be a related party in September 2003 upon termination of the jointly owned corporation as described below. The aggregate amount of the $7.5 million convertible notes payable are convertible into 278,339 shares of common stock.
In April 1998, the Company entered into an agreement with Elan to develop Elan's proprietary oral sustained release formulation of fampridine for the treatment of multiple sclerosis. Upon approval of an NDA for the product by the FDA in the United States, the Company is obligated to pay Elan $2.5 million. In addition, the Company is obligated to pay an additional $2.5 million to Elan, upon the earlier occurrence of the following: (a) first anniversary from the date of approval of NDA approval in the United States, or (b) upon approval of the product by a regulatory authority in Japan, the United Kingdom, Germany, France or Italy. Also, in April 1998, the Company formed MS Research & Development Corporation ("MSRD,") with Elan and one of its affiliates to develop Fampridine-SR for treatment of multiple sclerosis. At that time, MSRD licensed from Elan exclusive worldwide rights to Fampridine-SR for the treatment of multiple sclerosis.
Termination and Assignment Agreement. In September 2003, the Company entered into a termination and assignment agreement with Elan, Elan's affiliate, and MSRD pursuant to which MSRD (83% owned by Acorda immediately prior to entering into the agreement) assigned to the Company its assets, including the license from Elan for Fampridine-SR for treatment of multiple sclerosis. The Company paid MSRD approximately $11.5 million for all the assets and liabilities of MSRD. MSRD distributed the purchase price to its shareholders according to their equity ownership interest. The Company has received a distribution of approximately $9.5 million as a result of this distribution and the remaining distribution of $2 million was expensed in September 30, 2003 as acquired in-process research and development and classified under Research and Development-related party. The Company also purchased Elan's affiliate shares at par value and now owns approximately 88% of MSRD, which now has no assets or liabilities and is inactive.
Amended and Restated License. In September 2003, the Company entered into an amended and restated license with Elan, which replaced the two prior licenses for Fampridine-SR. Under this agreement, Elan granted the Company exclusive worldwide rights to Fampridine-SR, as well as Elan's formulation for any other mono- or di-aminopyridines, for all indications, including spinal cord injury and multiple sclerosis. The Company agreed to pay Elan milestone payments and royalties based on net sales of the product if and when approved.
Elan may terminate the Company's license in the United States, the major European markets or Japan if the Company does not file to obtain regulatory approval or launch the product after regulatory approval in the applicable country within specified periods. If Elan terminates the Company's license in any applicable country, Elan is entitled to license from the Company patents rights and know-how relating to the product and to market the product in the applicable country, subject to royalty payments.
Elan is responsible for completing the chemistry, manufacturing and controls section of the NDA for Fampridine-SR and equivalent regulatory applications outside the United States. Elan is also responsible for supplying the product for clinical trials under this agreement.
Subject to early termination provisions, the Elan license terminates on a country by country basis on the latter to occur of fifteen years from the date of the agreement, the expiration of the last to expire Elan patent or the existence of competition in that country.
Supply Agreement. In September 2003, the Company entered into a supply agreement with Elan relating to the manufacture and supply of Fampridine-SR by Elan. The Company agreed to purchase at least 75% of its annual requirements of product from Elan, unless Elan is unable or unwilling to meet
its requirements, for a purchase price based on a specified percentage of net sales. In those circumstances, where the Company elects to purchase less than 100% of its requirements from Elan, the Company agreed to make certain compensatory payments to Elan. Elan agreed to assist the Company in qualifying a second manufacturer to manufacture and supply the Company with Fampridine-SR subject to its obligations to Elan.
Securities Amendment Agreement. In September 2003, the Company entered into a securities amendment agreement with Elan to modify certain provisions in some existing agreements between Elan and the Company. These included:
Teva Collaboration Agreement. In September 2003, the Company entered into a collaboration agreement with Teva Pharmaceuticals Industries Ltd. ("Teva") under which the Company was granted a co-exclusive license with Teva to jointly develop and promote in the United States products containing valrocemide.
The Company made an initial payment to Teva of $2.0 million that was charged as research and development expenses for the year ended December 31, 2003, upon execution of the collaboration agreement, and was obligated to make payments to Teva relating to the development of valrocemide.
The Company and Teva amicably terminated the Collaboration Agreement as of June 27, 2005, and in connection with the termination the Company paid Teva approximately $3.1 million. The Company and Teva have no further obligations to each other under the Collaboration Agreement.
(12) Employee Benefit Plan
Effective September 1, 1999, the Company adopted a defined contribution 401(k) savings plan (the "401(k) plan") covering all employees of the Company. Participants may elect to defer a percentage of their annual pretax compensation to the 401(k) plan, subject to defined limitations. No contributions were made by the Company for the years ended June 30, 2002 and 2003, the six-month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005, respectively.
(13) Commitments and Contingencies
During 1998, the Company entered into a lease agreement for its facility. During November 2000 and May 2001, the Company entered into amendments of the lease for its facility. Under the amendments, the Company increased the total leased space and extended the lease term for its original
leased space. Future minimum commitments under all non-cancelable leases required subsequent to December 31, 2004 are as follows:
| 2005 | $ | 641,808 | |
| 2006 | 641,808 | ||
| 2007 | 641,808 | ||
| 2008 | 53,484 | ||
| $ | 1,978,908 | ||
Rent expense under these operating leases during the years ended June 30, 2002 and 2003, the six-month period ended December 31, 2003, the year ended December 31, 2004 and the nine-month period ended September 30, 2005 was $468,309, $652,339, $334,348, $670,413 and $501,395 (unaudited) respectively.
Under the terms of the employment agreement with the Company's chief executive officer, the Company is obligated to pay severance under certain circumstances. If the employment agreement is terminated by the Company or by the Company's chief executive officer for reasons other than for cause, the Company must pay (i) an amount equal to the base salary the chief executive officer would have received during the fifteen month period immediately following the date of termination, plus (ii) bonus equal to last annual bonus received by chief executive officer multiplied by a fraction, the numerator of which shall be the number of days in the calendar year elapsed as of the termination date and the denominator of which shall be 365.
The Company is not a party to any material legal proceedings. It is the Company's policy to accrue for amounts related to legal matters if it is probable that a liability has been incurred and the amount is reasonably estimable.
(14) Product Returns
As part of the terms of the Zanaflex asset purchase agreement, any product returned within six months of acquisition date was the obligation of Elan. Beginning in January 2005, such returns became a liability of the Company. Through September 30, 2005, the Company has accepted $4.0 million (unaudited) in total product returns, of which $2.1 million (unaudited) was for product not sold by the Company. As the Company will accept product returned up to twelve months subsequent to its expiration date, the Company expects to continue to receive returns of Zanaflex tablets sold by Elan through June 2006. The Company has recorded a changecharge to cost of salesdiscounts and allowances of $4.1 million in the year ending December 31, 2004 to record an estimated liability for these returns, of which $1,966,343 (unaudited) remains as of September 30, 2005.
As part of the Zanaflex acquisition, the Company purchased certain tablet from Elan that expires within one year. The majority of this product was sold by the Company during July 2004 though March 2005. The Company has deferred revenue for this product due to the uncertainty of future returns. Included in deferred product revenue-tablets is $3.7 million and $2.5 million (unaudited) as of December 31, 2004 and September 30, 2005, respectively related to the sale of short dated product. The Company recorded a charge of $177,000 during 2004 to write-off the cost of the short dated product.
(15) Zanaflex Asset Purchase Agreement
The Company acquired all of Elan's U.S. sales, marketing and distribution rights to Zanaflex Capsules and Zanaflex tablets in July 2004 for $2.0 million plus $675,000 for finished goods inventory. The Company is also responsible for up to $19.5 million in future contingent milestone payments based on cumulative gross sales of Zanaflex tablets and Zanaflex Capsules. These products are approved for the management of spasticity. Zanaflex tablets were approved by the FDA in 1996 and lost patent protection in 2002. There are currently 11 generic versions of Zanaflex tablets on the market. Zanaflex Capsules were approved by the FDA in 2002, but were never marketed by Elan. The Company began marketing Zanaflex Capsules in April 2005.
The Company is responsible for royalty payments to Elan and Novartis, based upon Net Sales of Zanaflex Capsules and tablets beginning on the closing date.
In connection with this transaction, the Company acquired the rights to the tradename "Zanaflex®", one issued U.S. patent and two patent applications related to Zanaflex Capsules, and the remaining tablet inventory on hand with Elan. Additionally, the Company assumed Elan's existing contract with Novartis to manufacture Zanaflex tablets and entered into a separate contract with Elan to manufacture Zanaflex Capsules. The Company separately launched Zanaflex Capsules in April 2005. The Company did not acquire any receivables, employees, facilities or fixed assets. The Company has allocated, on a relative fair value basis, the initial consideration paid to Elan to the assets acquired, principally the Zanaflex tradename $200,000 and the capsulation patent $1.8 million. The Company has allocated $150,000 and $1,350,000 of the first milestone payment owed to the tradename and patent, respectively, upon achievement of that milestone's criteria in October 2004, and has allocated $300,000 (unaudited) and $2,700,000 (unaudited) of the second milestone payment owed to the tradename and patent, respectively, upon achievement of that milestone's criteria in September 2005. There is no expected residual value of these intangible assets. As future milestone payments are made to Elan, such amounts will be allocated, on a relative fair value basis, to the assets acquired. The Company will amortize the allocated fair value of the tradename and patent over their estimated economic benefit to be achieved of approximately 2.5 years and 17 years, respectively.
Intangible Assets consisted of the following:
| | December 31, 2004 | September 30, 2005 | Estimated useful lives | |||||
|---|---|---|---|---|---|---|---|---|
| | | (unaudited) | | |||||
| Zanaflex patent | $ | 3,150,000 | $ | 5,850,000 | 17 years | |||
| Zanaflex tradename | 350,000 | 650,000 | 2.5 years | |||||
| 3,500,000 | 6,500,000 | |||||||
| Less accumulated amortization | 113,950 | 362,977 | ||||||
| $ | 3,386,050 | $ | 6,137,023 | |||||
The Company recorded $114,000 and $249,000 (unaudited) in amortization expense related to these intangible assets in the year ending December 31, 2004 and the nine-month period ending September 30, 2005, respectively.
Estimated future amortization expense for these intangible assets subsequent to December 31, 2004 is as follows:
| 2005 | $ | 433,789 | |
| 2006 | 739,047 | ||
| 2007 | 349,489 | ||
| 2008 | 349,489 | ||
| $ | 1,871,814 | ||
(16) Reverse Stock Split
On September 18, 2005, the Company's Board of Directors approved a 1-for-1.3 reverse stock split, which will becomebecame effective prior to the effective date of the Form S-1 registration statement filed in connection with the Company's initial public offering.on January 11, 2006. All references to common stock, common shares outstanding, average number of common shares outstanding, per share amounts, options and warrants and Elan notes payable in these financial statements and notes to financial statements have been restated to reflect the one-for-one point three common stock reverse split on a retroactive basis.
(17) Subsequent Events (unaudited)
On December 23, 2005, the Company entered into an agreement with an affiliate of Paul Royalty Fund, or PRF, under which the Company received $15.0 million in cash. In exchange the Company has assigned PRF revenue interests in Zanaflex Capsules, Zanaflex tablets and any future Zanaflex products. The agreement covers all Zanaflex net revenues (as defined in the agreement) generated from October 1, 2005 through and including December 31, 2015, unless the agreement terminates earlier. Under the agreement, PRF is entitled to the following portion of Zanaflex net revenues:
Notwithstanding the foregoing, once PRF has received and retained payments under the agreement that are at least twice the aggregate amount PRF has paid usthe Company under the agreement, PRF will only be entitled to 1% of Zanaflex net revenues. If PRF is entitled to 15% of net revenues as described above, the Company will remit 8% of cash payments received from wholesalers to PRF on a daily basis, with a quarterly reconciliation and settlement.
The Company also has the option to receive two additional payments:
If the Company meets these milestones and decides to borrow these additional funds, they would be required to repay PRF $5.0 million on December 1, 2009 in the case of the first additional payment and $5.0 million on December 1, 2010 in the case of the second additional payment.
Under the terms of the agreement the Company used $3.0 million of the $15.0 million in proceeds to partially repay its $6 million senior secured term loan with GE (see Note 7). The Company also incurred approximately $200,000 of expenses associated with the repayment of the GE term loan and approximately $500,000 of other transaction-related expenses that will be capitalized and amortized over the life of the arrangement. Under the terms of the prepayment GE relinquished its rights to the Company's personal property owned at closing or subsequently acquired that relates to the interests in Zanaflex acquired by PRF. This payment changed the aggregate principal payments to GE required subsequent to December 31, 2004 to: $3,858,654 in 2005; $890,521 in 2006; $1,062,180 in 2007; and $187,645
$187,645 in 2008. The related interest payments required subsequent to December 31, 2004 are: $524,687 in 2005; $163,196 in 2006; $76,683 in 2007; and $2,332 in 2008.
In connection with the transaction, the Company expects to record a liability, referred to as the revenue interest liability, of approximately $14.6 million in accordance with EITF 88-18,Sales of Future Revenues.The Company will impute interest expense associated with this liability using the effective interest rate method and will record a corresponding accrued interest liability. The effective interest rate is calculated based on the rate that would enable the debt to be repaid in full over the life of the arrangement. The interest rate on this liability may vary during the term of the agreement depending on a number of factors, including the level of Zanaflex sales. The Company currently estimates that the imputed interest rate associated with this liability will be approximately 8.9%. Payments made to PRF as a result of Zanaflex sales levels will reduce the accrued interest liability and the principal amount of the revenue interest liability.
The Company also has the option to receive two additional payments from PRF under the revenue interest assignment agreement, which essentially take the form of additional borrowings:
If the Company meets these milestones and decides to borrow these additional funds, it would be required to repay PRF $5.0 million on December 1, 2009 in the case of the first additional payment and $5.0 million on December 1, 2010 in the case of the second additional payment.
The agreement also contains put and call options whereby the Company may repurchase the revenue interest either at its option or can be required by PRF to repurchase the option of the Company or the option of PRF,revenue interest, contingent upon certain events. If the Company experiences a change of control, undergoes certain bankruptcy events, transfers any of their interests in Zanaflex (other than pursuant to a license agreement, development, commercialization, co-promotion, collaboration, partnering or similar agreement), transfers all or substantially all of theirits assets, or breaches certain of the covenants, representations or warranties made under the agreement, PRF canhas the right, which we refer to as PRF's put option, to require the Company to repurchase the rights sold to PRF at the "put/call price" in effect on the date such right is exercised. If the Company experiences a change of control or completes an initial public offering of shares of theirits common stock that results in the Company having a total market capitalization in excess of $150.0 million, they haveit has the right, which we refer to as the Company's call option, to repurchase the rights sold to PRF at the "put/call price" in effect on the date such right is exercised. If the Company's call option becomes exercisable as a result of this offering, the Company will have a period of 180 days during which to exercise the option. The Company does not currently intend to exercise its call option if it becomes exercisable as a result of this offering but may reevaluate whether it would exercise the option during the 180-day period. The put/call price on a given date is the greater of (i) 150% of all payments made by PRF as of such date, less all payments received by PRF as of such date, and (ii) an amount that would generate an internal rate of return to PRF of 25% on all payments made by PRF as of such date, taking into account the amount and timing of all payments received by PRF as of such date. The Company has determined that PRF's put option and the Company's call option meet the criteria to be considered an embedded derivative and should be accounted for as such. Therefore, the Company expects to record a net liability of approximately $400,000 related to the put/call option to reflect its estimated fair value as of the date of the agreement, in accordance with SFAS No. 133,Accounting for Derivatives Instruments and Hedging Activities. This liability will be revalued on a quarterly basis to reflect any changes in the fair value and any gain or loss resulting from the revaluation will be recorded in earnings.
Report of Independent Public Accounting Firm
The Board of Directors
Elan Corporation, plc:
We have audited the accompanying statements of net revenues and direct expenses for the period from January 1, 2004 through July 21, 2004, and the year ended December 31, 2003 of the Zanaflex Product Line of Elan Corporation, plc. These financial statements are the responsibility of Elan Corporation, plc's management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of Elan Corporation, plc's internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
The accompanying statements were prepared for the purpose of complying with the rules and regulations of the Securities and Exchange Commission and for inclusion in the Form S-1 of Acorda Therapeutics, Inc., as described in Note 2. The presentation is not intended to be a complete presentation of the Zanaflex results of operations.
In our opinion, the financial statements referred to above present fairly, in all material respects, the Zanaflex Product Line's net revenues and direct expenses for the period from January 1, 2004 through July 21, 2004 and the year ended December 31, 2003, in conformity with U.S. generally accepted accounting principles.
/s/ KPMG
KPMG
Dublin, Ireland
January 18, 2006
ZANAFLEX PRODUCT LINE
(A Product of the Elan Group)
Statements of Net Revenues and Direct Expenses
For the period from January 1, 2004 through July 21, 2004
and the year ended December 31, 2003
(In US $000)
| | Period from January 1, 2004 through July 21, 2004 | Year Ended December 31, 2003 | |||||
|---|---|---|---|---|---|---|---|
| Net product revenue (note 4) | $ | 5,656 | $ | 4,121 | |||
| Cost of product sold (note 2) | 1,265 | 891 | |||||
| Gross profit | 4,391 | 3,230 | |||||
| Research and development expenses | 572 | 609 | |||||
| Excess of net product revenue over direct expenses | $ | 3,819 | $ | 2,621 | |||
See accompanying notes to financial statements.
ZANAFLEX PRODUCT LINE
(A Product of the Elan Group)
Notes to Financial Statements
(1) Description of Business
Elan licensed Zanaflex (tizanidine hydrochloride) Product Line (Zanaflex or the Product) for the U.S. market from Novartis Pharma A.G. and subsequently launched the tablet formulation in 1997. It was approved by the FDA as a short-acting drug for the management of spasticity. In June 2002, Eon Laboratories received FDA approval to market a generic version of tizanidine tablets. A number of other generic applications for tizanidine tablets have since received approval from the FDA. Elan has experienced a significant decline in the sales and profitability of the Zanaflex brand, which it believes is attributable to the availability of generic alternatives to Zanaflex. The Zanaflex brand is sold primarily to drug wholesalers in the U.S.
In the third quarter of 2002, Elan received FDA approval of an alternative capsule formulation of tizanidine which was not marketed until the product was acquired by Acorda Therapeutics.
Pursuant to an Asset Purchase Agreement, dated as of July 21, 2004 (the Asset Purchase Agreement), Elan Pharmaceuticals, Inc., and certain wholly owned subsidiaries of Elan (collectively, the Elan Group) agreed to sell to Acorda Therapeutics their rights to the Zanaflex product, along with certain related assets and agreements.
(2) Basis of Presentation
The statements of net revenues and direct expenses of the Zanaflex Product Line have been prepared in accordance with accounting principles generally accepted in the United States of America. These statements were prepared for the purpose of complying with the rules and regulations of the Securities and Exchange Commission. The net revenues and direct expenses have been derived from the historical accounting records of the Company. Historically, financial statements have not been prepared for the Zanaflex Product Line as the Company did not maintain the Zanaflex Product Line as a separate business unit. The statements of net revenues and direct expenses set forth the revenues, net and direct expenses attributable to the Zanaflex Product Line and do not purport to reflect all the costs, expenses, and resultant operating earnings and cash flows that would have been incurred had the Zanaflex Product Line been operated as a stand-alone, separate company. Net revenues include gross sales less product-specific sales returns, cash discounts, government and commercial rebates, and customer chargebacks. Direct expenses consist principally of cost of sales and research and development expenses. The statements do not include general administrative expenses or general corporate overhead such as corporate management, legal services, administration of insurance, treasury, payroll administration, corporate income tax, administration and benefit management, nor does it include any interest income and expense, as such items are not directly associated with Zanaflex Product Line.
Costs of product sold include the purchase price of the inventories, distribution costs for the respective product, and royalty payments to third-parties which are based on percentage or unit basis of gross product sales in accordance with the respective royalty agreements. The amounts of royalties were $581,409 and $445,431 for the period from January 1, 2004 through July 21, 2004 and for the year ended December 31, 2003, respectively.
Since the product was not promoted in 2003 and 2004, there were minimal selling and marketing expenses associated with the Zanaflex Product Line. Certain research and development expenses are specifically identifiable and others, although direct expenses, require allocation to the Zanaflex Product Line since certain individuals performed research services on multiple product lines. These allocations
are made based on the percentage of time worked on the Zanaflex Product Line by individuals in research and development, and include salaries and professional fees.
(3) Summary of Significant Accounting Policies
(a) Revenue Recognition
Revenues from the sale of the Product are recognized when title passes, net of applicable discounts and allowances.
(b) Use of Estimates
The preparation of financial statements in conformity with U.S. generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying disclosures. Actual results could differ from these estimates. As discussed in note 2, the financial statements include allocations and estimates that are not necessarily indicative of the costs and expenses that would have resulted if the Zanaflex Product Line had been operated as a separate entity.
(c) Rebates and Chargebacks, Cash Discounts, and Sales Returns
Revenue is recorded net of provision, made at the time of sale for rebates, chargebacks and cash discounts, as described below. The Elan Group entered into contracts with certain managed care organizations to provide access to the Zanaflex Product through formularies. Based on the managed care organization's market share performance and utilization of the Zanaflex Product, the organization receives managed care rebates from the Elan Group. In addition, the Elan Group is bound under certain laws and regulations to provide product at a discounted rate to Medicaid recipients. Medicaid rebates are paid to each state in the United States based on claims filed by pharmacies that provide the Zanaflex Product to Medicaid recipients at the reduced rate. Managed care and Medicaid rebates are charged to the Zanaflex Product, determined by estimating the actual usage of the Zanaflex Product by Medicaid recipients and managed care participants covered by the contracted prices.
Chargebacks are amounts credited to wholesalers to reimburse the wholesaler for sales to third parties at reduced prices based on contracts the Elan Group negotiates. Chargebacks are recorded based on the historical experience.
The Elan Group offers a cash discount to customers if invoices are paid within a certain time period.
In addition, sales returns are charged to the Zanaflex Product based upon estimates derived from the Elan Group's historical experience updated for changes in fact and circumstances, as appropriate.
(4) Net Product Revenues
Returns, chargebacks, and discounts and rebates charged to gross product revenues are as follows (in US $000):
| | Period from January 1, 2004 through July 21, 2004 | Year Ended December 31, 2003 | ||||||
|---|---|---|---|---|---|---|---|---|
| Zanaflex: | ||||||||
| Gross product revenues | $ | 8,979 | $ | 6,879 | ||||
| Returns | 1,777 | 1,500 | ||||||
| Customer chargebacks | 1,153 | 719 | ||||||
| Discounts and rebates | 393 | 539 | ||||||
| Net product revenues | $ | 5,656 | $ | 4,121 | ||||
(5) Corporate Services
The Elan Group performed certain corporate functions for the Zanaflex Product Line for the period from January 1, 2004 through July 21, 2004 and the year ended December 31, 2003, including, but not limited to, corporate management, certain legal services, administration of insurance, treasury, payroll administration, corporate income tax administration, employee compensation and benefit management, and administration. The costs of these corporate services are not included in costs of goods sold, as the Elan Group does not allocate such costs by product.
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Introduction to Unaudited Pro Forma Combined Statement of Operations
On July 21, 2004, Acorda Therapeutics, Inc (the "Company") acquired the U.S. sales, marketing and distribution rights to Zanaflex Capsules and Zanaflex tablets (the "Zanaflex Product Line") from Elan Pharmaceuticals, Inc., a wholly owned subsidiary of Elan Corporation, plc (with its consolidated subsidiaries, "Elan") pursuant to an Asset Purchase Agreement. The assets acquired included the U.S. Food and Drug Administration registration for each product, a patent and two related patent applications and existing Zanaflex tablet inventory. The acquisition did not include physical facilities, an employee base, working capital accounts, customer base, production techniques or a market distribution system. The Company made an upfront payment to Elan of $2.0 million plus $675,000 for finished goods inventory. The Company is also responsible for up to $19.5 million in future contingent milestone payments based on cumulative gross sales of Zanaflex tablets and Zanaflex Capsules. These products are approved for the management of spasticity. Zanaflex tablets were approved by the FDA in 1996 and lost patent protection in 2002. There are currently 11 generic versions of Zanaflex tablets on the market. Zanaflex Capsules were approved by the FDA in 2002, but were never marketed by Elan. The Company began marketing Zanaflex Capsules in April 2005. The Company is responsible for royalty payments to Elan and Novartis, based upon Net Sales of Zanaflex Capsules and Zanaflex tablets beginning on the closing date.
In connection with this transaction, the Company acquired the rights to the tradename "Zanaflex", one issued U.S. patent and two patent applications related to Zanaflex Capsules, and the remaining Zanaflex tablet inventory on hand with Elan. Additionally, the Company assumed Elan's existing contract with Novartis to manufacture Zanaflex tablets and entered into a separate contract with Elan to manufacture Zanaflex Capsules. The Company separately launched Zanaflex Capsules in April 2005.
The accompanying unaudited pro forma statement of operations for the year ended December 31, 2004 combines the historical consolidated statement of operations of the Company for the year ended December 31, 2004 with the statements of net revenues and direct expenses of the Zanaflex Product Line of Elan for the period January 1, 2004 through July 21, 2004 included elsewhere in this registration statement to give effect to our acquisition of the Zanaflex Product Line as if the acquisition had occurred on January 1, 2004. The Company made pro forma adjustments to its historical consolidated consolidated statement of operations information to give effect to events that are (i) directly attributable to the acquisition, (ii) expected to have a continuing impact on the combined results, and (iii) factually supportable.
It is impracticable to prepare complete financial statements in accordance with Rules 3-01 and 3-02 of Regulation S-X relating to the assets acquired, as Elan did not account for the Zanaflex Product Line as a separate entity and cannot objectively allocate certain expenses to the assets. The statements of net revenues and direct expenses for the Zanaflex Product Line of Elan included elsewhere in this registration statement include certain allocations that Elan's management believes are reasonable; however, these allocations are not necessarily indicative of costs that would have been incurred related to the Zanaflex Product Line on a stand-alone basis. For instance, tax expense and interest income have not been included in the accompanying statements of net revenues and direct expenses, as they are not specifically identifiable to the Zanaflex Product Line.
The unaudited pro forma combined statement of operations is not necessarily indicative of the results that would have occurred had our acquisition of the Zanaflex Product Line occurred on January 1, 2004 and should not be construed as being representative of future operating results. The unaudited financial information should be read in conjunction with:
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Unaudited Pro Forma Combined Statement of Operations
For the Year Ended December 31, 2004
| | Acorda | Zanaflex Product Line | Pro forma adjustments | Notes | Pro forma Acorda | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gross sales—Zanaflex | $ | — | $ | 8,979 | $ | (25 | ) | A | $ | 8,954 | |||||||
| Less: Discounts and allowances | (4,417 | ) | (3,323 | ) | (7,740 | ) | |||||||||||
| Net sales | (4,417 | ) | 5,656 | (25 | ) | 1,214 | |||||||||||
| Grant revenue | 479 | — | 479 | ||||||||||||||
| Total net revenue | (3,938 | ) | 5,656 | (25 | ) | 1,693 | |||||||||||
| Less: Cost of sales | (885 | ) | (1,265 | ) | (324 | ) | A, B, C | (2,474 | ) | ||||||||
| Gross profit | (4,823 | ) | 4,391 | (349 | ) | (781 | ) | ||||||||||
Operating expenses: | |||||||||||||||||
| Research and development | 21,999 | 572 | 22,571 | ||||||||||||||
| Sales and Marketing | 4,662 | 4,662 | |||||||||||||||
| General and administrative | 13,283 | 13,283 | |||||||||||||||
| Total operating expenses | 39,944 | 572 | — | 40,516 | |||||||||||||
| Operating loss | (44,767 | ) | 3,819 | (349 | ) | (41,297 | ) | ||||||||||
| Other income (expense): | |||||||||||||||||
Interest and amortization of debt discount expense | (385 | ) | (385 | ) | |||||||||||||
| Interest income | 409 | (55 | ) | D | 354 | ||||||||||||
| Other income | 2 | 2 | |||||||||||||||
| Total other income (expense) | 26 | — | (55 | ) | (29 | ) | |||||||||||
| Net loss | (44,741 | ) | 3,819 | (404 | ) | (41,326 | ) | ||||||||||
| Beneficial conversion feature, accretion of issuance costs, preferred dividends, and fair value of warrants issued to convertible preferred stockholders | (24,746 | ) | (24,746 | ) | |||||||||||||
| Net loss allocable to common stockholders | $ | (69,487 | ) | $ | 3,819 | $ | (404 | ) | $ | (66,072 | ) | ||||||
ACORDA THERAPEUTICS, INC. AND SUBSIDIARY
Notes to Unaudited Pro Forma Combined Statement of Operations
(1) Adjustments to Unaudited Pro Forma Combined Statement of Operations
(2) Intangible Assets
The Company has allocated, on a relative fair value basis, the initial consideration paid to Elan to the assets acquired, principally the Zanaflex tradename $200,000 and the capsulation patent $1.8 million. The Company has allocated $150,000 and $1,350,000 of the first milestone payment owed to the tradename and patent, respectively, upon achievement of that milestone's criteria in October 2004. There is no expected residual value of these intangible assets. As future milestone payments are made to Elan, such amounts will be allocated, on a relative fair value basis, to the assets acquired. The Company will amortize the allocated fair value of the tradename and patent over their estimated period of economic benefit, of approximately 2.5 years and 17 years, respectively.
The pro forma amounts below give effect to the acquisition of the Zanaflex Product Line as if the transaction had occurred on January 1, 2004. The pro forma effects below reflect the achievement of the sales milestones based on cumulative sales from January 1, 2004. This results in additional pro forma expense of approximately $158,000. The pro forma effects include:
Intangible Assets consisted of the following:
| | Historical December 31, 2004 | Useful lives | Pro forma December 31, 2004 | Useful lives | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Zanaflex Capsules patent | $ | 3,150,000 | 17 years | $ | 5,850,000 | 18 years | ||||
| Zanaflex tradename | 350,000 | 2.5 years | 650,000 | 3 years | ||||||
| 3,600,000 | 6,500,000 | |||||||||
Less accumulated amortization | 113,950 | 271,835 | ||||||||
| $ | 3,386,050 | $ | 6,228,165 | |||||||
Shares
Common Stock
Prospectus
, 2006
Banc of America Securities LLC
Lazard Capital Markets
Piper Jaffray
SG Cowen & Co.
Until , 2006, all dealers that buy, sell or trade the common stock may be required to deliver a prospectus, regardless of whether they are participating in this offering. This is in addition to the dealers' obligation to deliver a prospectus when acting as underwriters and with respect to their unsold allotments or subscriptions.
Part II
INFORMATION NOT REQUIRED IN PROSPECTUS
ITEM 13. OTHER EXPENSES OF ISSUANCE AND DISTRIBUTION
The following table sets forth our estimated costs and expenses (other than underwriting discounts) payable in connection with this offering.
| SEC Registration Fee | SEC Registration Fee | $ | 10,152.00 | SEC Registration Fee | $ | 10,152.00 | ||
| NASD Filing Fee | NASD Filing Fee | $ | 9,125.00 | NASD Filing Fee | 9,125.00 | |||
| Nasdaq National Market Listing Fee | Nasdaq National Market Listing Fee | 5,000.00 | ||||||
| Printing and Engraving Expenses | Printing and Engraving Expenses | * | Printing and Engraving Expenses | * | ||||
| Legal Fees and Expenses | Legal Fees and Expenses | * | Legal Fees and Expenses | * | ||||
| Accounting Fees and Expenses | Accounting Fees and Expenses | * | Accounting Fees and Expenses | * | ||||
| Blue Sky Qualification Fees and Expenses | * | |||||||
| NASD-related Legal Fees and Expenses | NASD-related Legal Fees and Expenses | * | ||||||
| Transfer Agent and Registrar Fees and Expenses | Transfer Agent and Registrar Fees and Expenses | * | Transfer Agent and Registrar Fees and Expenses | * | ||||
| Miscellaneous | Miscellaneous | * | Miscellaneous | * | ||||
| Total | $ | * | Total | $ | * | |||
ITEM 14. INDEMNIFICATION OF DIRECTORS AND OFFICERS
Acorda Therapeutics, Inc., or the Registrant, is a Delaware corporation. Section 145 of the Delaware General Corporation Law, or the DGCL, grants each corporation organized thereunder the power to "indemnify any person who is or was a director, officer, employee or agent of a corporation or enterprise, against expenses, attorneys' fees, judgments, fines and amounts paid in settlement actually and reasonably incurred by him in connection with any threatened, pending or completed action, suit or proceeding, whether civil, criminal, administrative or investigative, other than an action by or in the right of the corporation, by reason of being or having been in any such capacity if he acted in good faith in a manner reasonably believed to be in or not opposed to the best interests of the corporation, and, with respect to any criminal action or proceeding, had no reasonable cause to believe his conduct was unlawful."
Section 102(b)(7) of the DGCL enables a corporation in its certificate of incorporation or an amendment thereto to eliminate or limit the personal liability of a director to the corporation or its stockholders for monetary damages for violations or the directors' fiduciary duty of care, except (i) for any breach of the director's duty of loyalty to the corporation or its stockholders, (ii) for acts or omissions not in good faith or which involve intentional misconduct or a knowing violation of law, (iii) pursuant to Section l74 of the DGCL (providing for liability of directors for unlawful payment of dividends or unlawful stock purchases or redemptions) or (iv) for any transaction from which a director derived an improper personal benefit.
Article Six of the Registrant's Amended and Restated Certificate of Incorporation (filed as Exhibit 3.1) provides that except as otherwise provided by the DGCL, no director of the Registrant shall be personally liable to the Registrant or its stockholders for monetary damages for breach of fiduciary duty as a director.
Article Six of the Registrant's Amended and Restated Certificate of Incorporation and Article Six of the Registrant's Amended Bylaws provide that, to the fullest extent permitted by the DGCL, the Registrant shall indemnify any current or former director or officer of the Registrant and may, at the discretion of the Board of Directors, indemnify any current or former employee or agent of the Registrant against all expenses (including attorneys' fees) judgments, fines and amounts paid in
II-1
settlement actually and reasonably incurred in connection with any threatened, pending or completed
II-1
action, suit or proceeding, whether civil, criminal, administrative or investigative, by reason of the fact that he or she is or was a director or officer of the Registrant, or is or was serving as a director, officer, employee or agent of another corporation, partnership, joint venture, trust or other enterprise.
Article Six of the Registrant's Amended and Restated Certificate of Incorporation also provides that the Registrant shall advance expenses incurred by a director or officer of the Registrant in defending any civil, criminal, administrative or investigative such action, suit or proceeding in advance of the final disposition of such action, suit or proceeding upon receipt of an undertaking by or on behalf of such director or officer to repay such advances if it shall ultimately be determined that he is not entitled to be indemnified by the Registrant as authorized by the Registrant's By-laws. In addition, upon the closing of this offering, our amended and restated certificate of incorporation (filed as exhibit 3.2) will provide that if a claim under the Registrant's By-laws is not paid in full by the Registrant within thirty days after a written claim has been received by the Registrant, the claimant may at any time thereafter bring suit against the Registrant to recover the unpaid amount of the claim, and if successful in whole or in part on the merits or otherwise in establishing his or her right to indemnification or to the advancement of expenses, the claimant shall be paid also the expense of prosecuting such claim.
ITEM 15. RECENT SALES OF UNREGISTERED SECURITIES
Within the past three years, the Registrant has issued securities in the following transactions, each of which was exempt from the registration requirements of the Securities Act of 1933, as amended, as transactions by an issuer not involving any public offering thereunder. All of the below-referenced securities are deemed restricted securities for the purpose of the Securities Act.
In May 2003, we consummated a private placement of 112,790,233 shares of our Series J Convertible Preferred Stock to a group of accredited investors at a purchase price of $0.49 per share for aggregate consideration of approximately $55,267,000.
In March 2004, we consummated a private placement of 1,533,330 shares of our Series K Convertible Preferred Stock to a group of accredited investors at a purchase price of $7.50 per share for aggregate consideration of approximately $11,499,958.
Stock Options
In the fourth quarter of 2002, we issued options to purchase 2,218 shares of our common stock with a fair market value price of $2.60 to a number of our employees.
In the first quarter of 2003, we issued options to purchase 5,465 shares of our common stock with a fair market value price of $2.60 to a number of our employees. We also issued 1,282 options to purchase our common stock with a fair market value price of $2.60 to a non-employee director.
In the second quarter of 2003, we issued options to purchase 288 shares of our common stock with a fair market value price of $2.60 to a number of our employees.
In the third quarter of 2003, we issued options to purchase 1,062,081 shares of our common stock with a fair market value price of $2.60 to a number of our employees.
In the fourth quarter of 2003, we issued options to purchase 48,077 shares of our common stock with a fair market value price of $2.60 to a number of our employees. We also issued 1,924 options to purchase our common stock with a fair market value price of $2.60 to a number of non-employees.
In the first quarter of 2004, we issued options to purchase 17,192 shares of our common stock with a fair market value price of $9.75 to a number of our employees. We also issued 1,912 options to purchase our common stock with a fair market value price of $7.64 to a number of employees.
II-2
In the third quarter of 2004, we issued options to purchase 3,769 shares of our common stock with a fair market value price of $9.75 to a number of our employees.
In the fourth quarter of 2004, we issued options to purchase 44,615 shares of our common stock with a fair market value price of $9.75 to a number of our employees.
In the first quarter of 2005, we issued options to purchase 34,615 shares of our common stock with a exercise price of $8.14 to a number of our employees.
In the third quarter of 2005, we issued options to purchase 548,484 shares of our common stock with a exercise price of $8.14 to a number of our employees. We also issued 32,699 options to purchase our common stock with a exercise price of $8.14 to a non-employee director.
In the fourth quarter of 2005, we issued options to purchase 3,461 shares of our common stock with an exercise price of $8.14 to a number of our employees.
Restricted Shares
On March 9, 2004, and August 6, 2004, we issued 1,134,393 and 5,077 restricted shares, respectively, to a number of our employees.
On August 3, 2005, we issued 7,692 restricted shares to two of our non-employee directors.
Warrants
On January 28, 2005, in connection with entering into our senior secured term loan with GE Capital, we issued to GE Capital a warrant to purchase up to $300,000 worth of shares of our preferred stock (or, if we have consummated our initial public offering, shares of our common stock) in an amount and at a price to be determined pursuant to the terms thereof.
ITEM 16. EXHIBITS AND FINANCIAL STATEMENT SCHEDULES
(a) Exhibit Index
A list of exhibits filed with this registration statement on Form S-1 is set forth on the Exhibit Index and is incorporated in this Item 16(a) by reference.
(b) Financial Statement Schedules
None
ITEM 17. UNDERTAKINGS
Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of the registrant pursuant to the foregoing provisions, or otherwise, the registrants have been advised that in the opinion of the SEC such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by the registrant of expenses incurred or paid by a director, officer or controlling person of the registrant in the successful defense of any action, suit or proceeding) is asserted by such director, officer or controlling person in connection with the securities being registered, the registrant will, unless in the opinion of its counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
II-3
(1) The undersigned registrant hereby undertakes to provide to the underwriter at the closing specified in the underwriting agreements, certificates in such denominations and registered in such names as required by the underwriter to permit prompt delivery to each purchaser.
(2) The undersigned registrant hereby undertakes that:
(a) For purposes of determining any liability under the Securities Act, the information omitted from the form of prospectus filed as part of this registration statement in reliance upon Rule 430A and contained in a form of prospectus filed by the registrant pursuant to Rule 424(b)(1) or (4) or 497(h) under the Securities Act shall be deemed to be part of this registration statement as of the time it was declared effective.
(b) For purposes of determining any liability under the Securities Act, each post-effective amendment that contains a form of prospectus shall be deemed to be a new registration statement relating to the securities offering therein, and the offering of such securities at that time shall be deemed to be the initial bona fide offering thereof.
II-4
Pursuant to the requirements of the Securities Act, the Registrant has duly caused this Amendment to Registration Statement to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of New York, State of New York, on January 5,18, 2006
| By: | /s/ RON COHEN Ron Cohen, President and Chief Executive Officer |
Pursuant to the requirements of the Securities Act of 1933, as amended, this Amendment to Registration Statement has been signed by the following persons in the capacities and on the dates indicated:
| Signature | Title | Date | ||||
|---|---|---|---|---|---|---|
| /s/ RON COHEN Ron Cohen, M.D. | President, Chief Executive Officer and Director (Principal Executive Officer) | January | ||||
/s/ DAVID LAWRENCE David Lawrence, M.B.A. | Chief Financial Officer (Principal Financial Officer and Principal Accounting Officer) | January | ||||
* Standish M. Fleming, M.B.A. | Director | January | ||||
* John H. Friedman, J.D. | Director | January | ||||
* Sandra Panem, Ph.D. | Director | January | ||||
* Barclay A. Phillips | Director | January | ||||
* Mark R.E. Pinney, M.B.A., C.F.A., M.Sc. | Director | January | ||||
* | Director | January | ||||
II-5
* Steven M. Rauscher, M.B.A. | Director | January 18, 2006 | ||||
* Michael Steinmetz, Ph.D. | Director | January | ||||
* Wise Young, Ph.D., M.D. | Director | January | ||||
*By: | /s/ RON COHEN Ron Cohen Attorney-in-fact |
II-6
| Exhibit No. | Description | |
|---|---|---|
1.1 | ** | Form of Underwriting Agreement |
3.1 | * | Amended and Restated Certificate of Incorporation |
3.2 | * | Amended Bylaws |
3.3 | * | Form of Post-IPO Amended and Restated Certificate of Incorporation |
3.4 | * | Form of Post-IPO Amended Bylaws |
3.5 | Amendment No. 1 to Amended and Restated Certificate of Incorporation | |
3.6 | Amendment No. 2 to Amended and Restated Certificate of Incorporation | |
4.1 | * | Specimen Stock Certificate |
4.2 | * | Warrant to purchase 100,000 shares of Series B Preferred Stock, $2.00 par value per share, dated February 4, 2002, issued by the Registrant to Elan International Services, Ltd. |
4.3 | * | Warrant to purchase 40,000 shares of common stock, $0.10 par value per share, dated May 1, 1996, issued by the Registrant to Mark Noble and Margo Meyer |
4.4 | * | Warrant to purchase $300,000 worth of Warrant Shares, dated January 28, 2005, issued by the Registrant to General Electric Capital Corporation |
5.1 | ** | Opinion of Covington & Burling |
10.1 | * | Acorda Therapeutics 1999 Employee Stock Option Plan |
10.2 | * | Amendment to 1999 Employee Stock Option Plan |
10.3 | * | Amendment No. 2 to 1999 Employee Stock Option Plan |
10.4 | * | Acorda Therapeutics 2006 Employee Incentive Plan |
10.5 | Acorda Therapeutics 2006 Employee Incentive Plan, as amended as of January 13, 2005 | |
10.6 | * | Sixth Amended and Restated Registration Rights Agreement, dated March 3, 2004, by and among the Registrant and certain stockholders named therein |
* | Employment Agreement, dated August 11, 2002, by and between the Registrant and Ron Cohen | |
* | Amendment to August 11, 2002 Employment Agreement, dated September 26, 2005, by and between the Registrant and Ron Cohen | |
* | Letter Agreement, dated November 30, 2004, by and between the Registrant and Mark Pinney | |
* | Employment Agreement, dated as of December 19, 2005, by and between the Registrant and Andrew R. Blight | |
* | Employment Agreement, dated as of December 19, 2005, by and between the Registrant and Mary Fisher | |
* | Employment Agreement, dated as of December 19, 2005, by and between the Registrant and David Lawrence | |
* | Employment Agreement, dated as of December 19, 2005, by and between the Registrant and Jane Wasman | |
†* | Amended and Restated License Agreement, dated September 26, 2003, by and between the Registrant and Elan Corporation, plc. | |
†* | Supply Agreement, dated September 26, 2003, by and between the Registrant and Elan Corporation, plc. | |
†* | License Agreement, dated September 26, 2003, by and between the Registrant and Rush-Presbyterian-St. Luke's Medical Center | |
* | Side Agreement, dated September 26, 2003, by and among the Registrant, Rush-Presbyterian-St. Luke's Medical Center, and Elan Corporation, plc. | |
†* | Payment Agreement, dated September 26, 2003, by and among the Registrant, Rush-Presbyterian-St. Luke's Medical Center, and Elan Corporation, plc. | |
†* | Amendment No. 1 to the Payment Agreement, dated as of October 27, 2003, by and between the Registrant and Elan Corporation, plc. | |
†* | Amended and Restated License Agreement, dated August 1, 2003, by and between the Registrant and Canadian Spinal Research Organization | |
†* | License Agreement, dated February 3, 2003, by and between the Registrant and Cornell Research Foundation, Inc. | |
10.22 | †* | License Agreement, dated November 12, 2002, by and between the Registrant and CeNeS Pharmaceuticals, plc |
10.23 | †* | License Agreement, dated November 12, 2002, by and between the Registrant and CeNeS Pharmaceuticals, plc |
10.24 | †* | License Agreement, dated September 8, 2000, by and between the Registrant and Mayo Foundation for Medical Education and Research |
†* | Side Letter Agreement, dated June 21, 2005, by and between the Registrant and Mayo Foundation for Medical Education and Research | |
†* | Asset Purchase Agreement, dated as of July 21, 2004, by and between the Registrant and Elan Pharmaceuticals, Inc. | |
†* | Zanaflex Supply Agreement, dated as of July 21, 2004, by and between the Registrant and Elan Pharma International Limited | |
†* | Assignment and Assumption Agreement, dated as of July 21, 2004, by and among the Registrant, Elan Pharmaceuticals, Inc., and Novartis Pharma AG | |
†* | License Agreement, dated April 17, 1991, by and between Sandoz Pharma, now Novartis Pharma AG and Athena Neurosciences, Inc., now Elan Pharmaceuticals, Inc. | |
* | Patent Assignment Agreement, dated as of July 21, 2004, by and between the Registrant and Elan Pharmaceuticals, Inc. | |
* | Trademark License Agreement, dated as of July 21, 2004, by and between the Registrant and Elan Pharmaceuticals, Inc. | |
†* | Agreement Relating to Additional Trademark, dated as of July 2005, by and between the Registrant and Elan Pharmaceuticals, Inc. | |
* | Domain Name Assignment Agreement, dated as of July 21, 2004, by and between the Registrant and Elan Pharmaceuticals, Inc. | |
* | Bill of Sale and Assignment and Assumption Agreement, dated as of July 21, 2004, by and between the Registrant and Elan Pharmaceuticals, Inc. | |
* | Limited Recourse Convertible Promissory Note issued to Elan International Services, Ltd. | |
* | Full Recourse Convertible Promissory Note issued to Elan International Services, Ltd. | |
Note Modification and Amendment, dated as of December 23, 2005, by and between the Registrant and Elan Pharma International Limited | ||
* | Securities Amendment Agreement, dated September 26, 2003, by and among the Registrant, Elan Corporation plc and Elan International Services, Ltd. | |
†* | Syndicated Sales Force Agreement, dated as of August 1, 2005, between the Registrant and Cardinal Health PTS, LLC | |
†* | License Agreement, dated as of December 19, 2003, by and among the Registrant, Cambridge University Technical Services Limited, and King's College London | |
* | Promissory Note issued to General Electric Capital Corporation | |
* | Revenue Interests Assignment Agreement, dated as of December 23, 2005, between the Registrant and King George Holdings Luxembourg IIA S.à.r.l., an affiliate of Paul Royalty Fund II, L.P. | |
21.1 | * | List of Subsidiaries of the Registrant |
23.1 | Consent of KPMG LLP, Independent Registered Public Accounting Firm | |
23.2 | Consent of KPMG Independent Public Accounting Firm | |
23.3 | ** | Consent of Covington & Burling (included in Exhibit 5.1) |
24.1 | * | Power of Attorney |
24.2 | Power of Attorney of Lorin J. Randall |