UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 6-K
REPORT OF FOREIGN PRIVATE ISSUER
PURSUANT TO RULE 13a-16 OR 15d-16
UNDER THE SECURITIES EXCHANGE ACT OF 1934
For the month of November, 2018
Commission File Number
Kazia Therapeutics Limited
(Translation of registrant’s name into English)
Three International Towers Level 24 300 Barangaroo Avenue Sydney NSW 2000
(Address of principal executive office)
Indicate by check mark whether the registrant files or will file annual reports under cover of Form 20-F or Form 40-F.
Form 20-F ☑ Form 40-F ☐
Indicate by check mark if the registrant is submitting the Form 6-K in paper as permitted by Regulation S-T Rule 101(b)(1): ☐
Note: Regulation S-T Rule 101(b)(1) only permits the submission in paper of a Form 6-K if submitted solely to provide an attached annual report to security holders.
Indicate by check mark if the registrant is submitting the Form 6-K in paper as permitted by Regulation S-T Rule 101(b)(7): ☐
Note: Regulation S-T Rule 101(b)(7) only permits the submission in paper of a Form 6-K if submitted to furnish a report or other document that the registrant foreign private issuer must furnish and make public under the laws of the jurisdiction in which the registrant is incorporated, domiciled or legally organized (the registrant’s “home country”), or under the rules of the home country exchange on which the registrant’s securities are traded, as long as the report or other document is not a press release, is not required to be and has not been distributed to the registrant’s security holders, and, if discussing a material event, has already been the subject of a Form 6-K submission or other Commission filing on EDGAR.
Indicate by check mark if the registrant by furnishing the information contained in this form is also thereby furnishing the information to the Commission pursuant to Rule 12g3-2(b) under the Securities Exchange Act of 1934. Yes ☐ No ☑
If “yes” is marked, indicate below the file number assigned to the registrant in connection with Rule 12g3-2(b)
SIGNATURE
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
Kazia Therapeutics Limited(Registrant)
Kate Hill
Kate Hill
Company Secretary
Date 14 November 2018

ASX RELEASE
14 November 2018
KAZIA PRESENTATION TO SNO
Sydney, 14 November 2018 – Kazia Therapeutics Limited (ASX: KZA; NASDAQ: KZIA), an Australian oncology-focused biotechnology company, is pleased to provide a copy of the poster which is to be presented at the Society of Neuro-Oncology in New Orleans on Friday 16 November.
[ENDS]
About Kazia Therapeutics Limited
Kazia Therapeutics Limited (ASX: KZA, NASDAQ: KZIA) is an innovative oncology-focused biotechnology company, based in Sydney, Australia. Our pipeline includes two clinical-stage drug development candidates, and we are working to develop therapies across a range of oncology indications.
Our lead program is GDC-0084, a small molecule inhibitor of the PI3K / AKT / mTOR pathway, which is being developed to treat glioblastoma multiforme, the most common and most aggressive form of primary brain cancer. Licensed from Genentech in late 2016, GDC-0084 is due to enter a phase II clinical trial early in 2018. Initial data is expected in early calendar 2019, and the study is expected to complete in 2021.
TRX-E-002-1 (Cantrixil), is a third-generation benzopyran molecule with activity against cancer stem cells, and is being developed to treat ovarian cancer. TRX-E-002-1 is currently undergoing a phase I clinical trial in Australia and the United States. Initial data is expected in the first half of calendar 2018.
Board of Directors
Mr Iain RossChairman,Non-Executive Director
Mr Bryce CarmineNon-Executive Director
Mr Steven CoffeyNon-Executive Director
Dr James GarnerChief Executive Officer, Managing Director
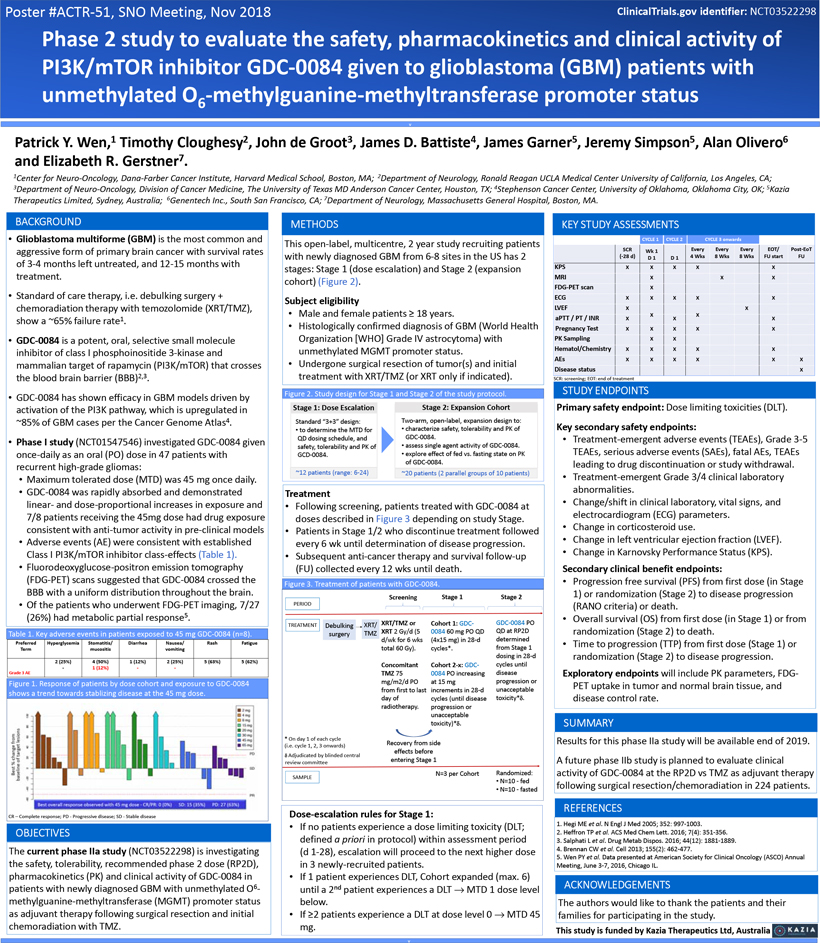
Poster#ACTR-51, SNO Meeting, Nov 2018 ClinicalTrials.gov identifier: NCT03522298 Phase 2 study to evaluate the safety, pharmacokinetics and clinical activity of PI3K/mTOR inhibitorGDC-0084 given to glioblastoma (GBM) patients with unmethylatedO6-methylguanine-methyltransferase promoter status v Patrick Y. Wen,1 Timothy Cloughesy2, John de Groot3, James D. Battiste4, James Garner5, Jeremy Simpson5, Alan Olivero6 and Elizabeth R. Gerstner7. 1Center for Neuro-Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA; 2Department of Neurology, Ronald Reagan UCLA Medical Center University of California, Los Angeles, CA; 3Department of Neuro-Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX; 4Stephenson Cancer Center, University of Oklahoma, Oklahoma City, OK; 5Kazia Therapeutics Limited, Sydney, Australia; 6Genentech Inc., South San Francisco, CA; 7Department of Neurology, Massachusetts General Hospital, Boston, MA. BACKGROUND Glioblastoma multiforme (GBM) is the most common and aggressive form of primary brain cancer with survival rates of3-4 months left untreated, and12-15 months with treatment. Standard of care therapy, i.e. debulking surgery + chemoradiation therapy with temozolomide (XRT/TMZ), show a ~65% failure rate1.GDC-0084 is a potent, oral, selective small molecule inhibitor of class I phosphoinositide3-kinase and mammalian target of rapamycin (PI3K/mTOR) that crosses the blood brain barrier (BBB)2,3.GDC-0084 has shown efficacy in GBM models driven by activation of the PI3K pathway, which is upregulated in ~85% of GBM cases per the Cancer Genome Atlas4. Phase I study (NCT01547546) investigatedGDC-0084 given once-daily as an oral (PO) dose in 47 patients with recurrent high-grade gliomas: Maximum tolerated dose (MTD) was 45 mg once daily.GDC-0084 was rapidly absorbed and demonstrated linear- and dose-proportional increases in exposure and 7/8 patients receiving the 45mg dose had drug exposure consistent with anti-tumor activity inpre-clinical models Adverse events (AE) were consistent with established Class I PI3K/mTOR inhibitor class-effects (Table 1). Fluorodeoxyglucose-positron emission tomography(FDG-PET) scans suggested thatGDC-0084 crossed the BBB with a uniform distribution throughout the brain. Of the patients who underwentFDG-PET imaging, 7/27 (26%) had metabolic partial response5. Table 1. Key adverse events in patients exposed to 45 mgGDC-0084 (n=8). Preferred Hyperglycemia Stomatitis/ Diarrhea Nausea/ Rash Fatigue Term mucositis vomiting 2 (25%) 4 (50%) 1 (12%) 2 (25%) 5 (63%) 5 (62%)—1 (12%) — Grade 3 AE Figure 1. Response of patients by dose cohort and exposure toGDC-0084 shows a trend towards stablizing disease at the 45 mg dose. CR – Complete response; PD—Progressive disease; SD—Stable disease OBJECTIVES The current phase IIa study (NCT03522298) is investigating the safety, tolerability, recommended phase 2 dose (RP2D), pharmacokinetics (PK) and clinical activity ofGDC-0084 in patients with newly diagnosed GBM with unmethylatedO6-methylguanine-methyltransferase (MGMT) promoter status as adjuvant therapy following surgical resection and initial chemoradiation with TMZ. METHODS This open-label, multicentre, 2 year study recruiting patients with newly diagnosed GBM from6-8 sites in the US has 2 stages: Stage 1 (dose escalation) and Stage 2 (expansion cohort) (Figure 2). Subject eligibility Male and female patients³ 18 years. Histologically confirmed diagnosis of GBM (World Health Organization [WHO] Grade IV astrocytoma) with unmethylated MGMT promoter status. Undergone surgical resection of tumor(s) and initial treatment with XRT/TMZ (or XRT only if indicated). Figure 2. Study design for Stage 1 and Stage 2 of the study protocol. Stage 1: Dose Escalation Standard “3+3” design: to determine the MTD for QD dosing schedule, and safety, tolerability and PK ofGCD-0084. ~12 patients (range:6-24) Stage 2: Expansion CohortTwo-arm, open-label, expansion design to: characterize safety, tolerability and PK ofGDC-0084. assess single agent activity ofGDC-0084. explore effect of fed vs. fasting state on PK ofGDC-0084. ~20 patients (2 parallel groups of 10 patients) Treatment Following screening, patients treated withGDC-0084 at doses described in Figure 3 depending on study Stage. Patients in Stage 1/2 who discontinue treatment followed every 6 wk until determination of disease progression. Subsequent anti-cancer therapy and survivalfollow-up (FU) collected every 12 wks until death. Figure 3. Treatment of patients withGDC-0084. Screening Stage 1 Stage 2 PERIOD XRT/TMZ or Cohort 1:GDC-GDC-0084 PO TREATMENT Debulking XRT/ TMZ XRT 2 Gy/d (5 0084 60 mg PO QD QD at RP2D surgery determined d/wk for 6 wks (4x15 mg) in28-d total 60 Gy). cycles*. from Stage 1 dosing in28-d Concomitant Cohort2-x:GDC- cycles until TMZ 75 0084 PO increasing disease mg/m2/d PO at 15 mg progression or from first to last increments in28-d unacceptable day of cycles (until disease toxicity* radiotherapy. progression or unacceptable toxicity)* * On day 1 of each cycle Recovery from side (i.e. cycle 1, 2, 3 onwards) effects before Adjudicated by blinded central review committee entering Stage 1 N=3 per Cohort Randomized: SAMPLE N=10—fed N=10—fasted Dose-escalation rules for Stage 1: If no patients experience a dose limiting toxicity (DLT; defined a priori in protocol) within assessment period (d1-28), escalation will proceed to the next higher dose in 3 newly-recruited patients. If 1 patient experiences DLT, Cohort expanded (max. 6) until a 2nd patient experiences a DLT MTD 1 dose level below. If³2 patients experience a DLT at dose level 0 MTD 45 mg. KEY STUDY ASSESSMENTS CYCLE 1CYCLE 2CYCLE 3 onwards SCRWk1EveryEveryEveryEOT/Post-EoT(-28 d)D 1D 14 Wks8 Wks8 WksFU startFU KPSXXXXX MRIXXXFDG-PET scanX ECGXXXXX LVEFXX aPTT / PT / INRXXXXX Pregnancy TestXXXXX PK SamplingXX Hematol/ChemistryXXXXX AEsXXXXXX Disease statusX SCR: screening; EOT: end of treatment STUDY ENDPOINTS Primary safety endpoint: Dose limiting toxicities (DLT). Key secondary safety endpoints: Treatment-emergent adverse events (TEAEs), Grade3-5 TEAEs, serious adverse events (SAEs), fatal AEs, TEAEs leading to drug discontinuation or study withdrawal. Treatment-emergent Grade 3/4 clinical laboratory abnormalities. Change/shift in clinical laboratory, vital signs, and electrocardiogram (ECG) parameters. Change in corticosteroid use. Change in left ventricular ejection fraction (LVEF). Change in Karnovsky Performance Status (KPS). Secondary clinical benefit endpoints: Progression free survival (PFS) from first dose (in Stage 1) or randomization (Stage 2) to disease progression (RANO criteria) or death. Overall survival (OS) from first dose (in Stage 1) or from randomization (Stage 2) to death. Time to progression (TTP) from first dose (Stage 1) or randomization (Stage 2) to disease progression. Exploratory endpoints will include PK parameters,FDG-PET uptake in tumor and normal brain tissue, and disease control rate. SUMMARY Results for this phase IIa study will be available end of 2019. A future phase IIb study is planned to evaluate clinical activity ofGDC-0084 at the RP2D vs TMZ as adjuvant therapy following surgical resection/chemoradiation in 224 patients. REFERENCES 1. Hegi ME et al. N Engl J Med 2005; 352:997-1003. 2. Heffron TP et al. ACS Med Chem Lett. 2016; 7(4):351-356. 3. Salphati L et al. Drug Metab Dispos. 2016; 44(12): 1881-1889. 4. Brennan CW et al. Cell 2013; 155(2):462-477. 5. Wen PY et al. Data presented at American Society for Clinical Oncology (ASCO) Annual Meeting, June3-7, 2016, Chicago IL. ACKNOWLEDGEMENTS The authors would like to thank the patients and their families for participating in the study. This study is funded by Kazia Therapeutics Ltd, Australia