|
Exhibit 99.2 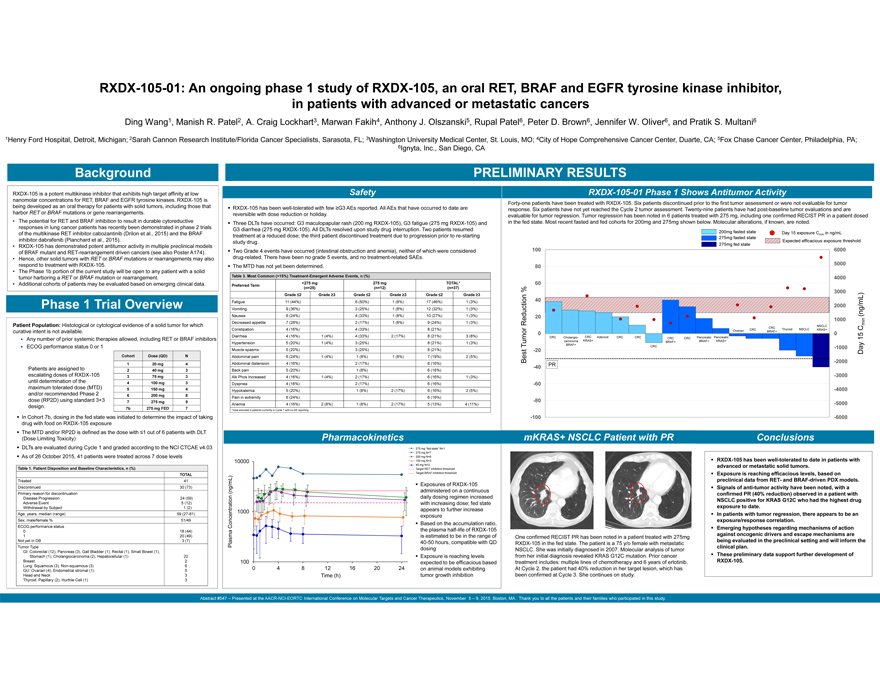
|
RXDX-105-01: An ongoing phase 1 study of RXDX-105, an oral RET, BRAF and EGFR tyrosine kinase inhibitor, in patients with advanced or metastatic cancers
Ding Wang1, Manish R. Patel2, A. Craig Lockhart3, Marwan Fakih4, Anthony J. Olszanski5, Rupal Patel6, Peter D. Brown6, Jennifer W. Oliver6, and Pratik S. Multani6
1Henry Ford Hospital, Detroit, Michigan; 2Sarah Cannon Research Institute/Florida Cancer Specialists, Sarasota, FL; 3Washington University Medical Center, St. Louis, MO; 4City of Hope Comprehensive Cancer Center, Duarte, CA; 5Fox Chase Cancer Center, Philadelphia, PA; 6Ignyta, Inc., San Diego, CA
PRELIMINARY RESULTS
Background
RXDX-105 is a potent multikinase inhibitor that exhibits high target affinity at low nanomolar concentrations for RET, BRAF and EGFR tyrosine kinases. RXDX-105 is being developed as an oral therapy for patients with solid tumors, including those that harbor RET or BRAF mutations or gene rearrangements.
• The potential for RET and BRAF inhibition to result in durable cytoreductive responses in lung cancer patients has recently been demonstrated in phase 2 trials of the multikinase RET inhibitor cabozantinib (Drilon et al., 2015) and the BRAF inhibitor dabrafenib (Planchard et al., 2015).
• RXDX-105 has demonstrated potent antitumor activity in multiple preclinical models of BRAF mutant and RET-rearrangement driven cancers (see also Poster A174).
• Hence, other solid tumors with RET or BRAF mutations or rearrangements may also respond to treatment with RXDX-105.
• The Phase 1b portion of the current study will be open to any patient with a solid tumor harboring a RET or BRAF mutation or rearrangement.
• Additional cohorts of patients may be evaluated based on emerging clinical data.
1 Trial Overview
Patient Population: Histological or cytological evidence of a solid tumor for which curative intent is not available.
? Any number of prior systemic therapies allowed, including RET or BRAF inhibitors
? ECOG performance status 0 or 1
Cohort Dose (QD) N
1 20 mg 4
Patients are assigned to 2 40 mg 3
escalating doses of RXDX-105 3 75 mg 3
until determination of the 4 100 mg 3
maximum tolerated dose (MTD) 5 150 mg 4
and/or recommended Phase 2 6 200 mg 8
dose (RP2D) using standard 3+3 7 275 mg 9
design. 7b 275 mg FED 7
In Cohort 7b, dosing in the fed state was initiated to determine the impact of taking drug with food on RXDX-105 exposure ? The MTD and/or RP2D is defined as the dose with d1 out of 6 patients with DLT
(Dose Limiting Toxicity)
DLTs are evaluated during Cycle 1 and graded according to the NCI CTCAE v4.03? As of 26 October 2015, 41 patients were treated across 7 dose levels
Table 1. Patient Disposition and Baseline Characteristics, n (%)
TOTAL
Treated 41
Discontinued 30 (73)
Primary reason for discontinuation
Disease Progression 24 (59)
Adverse Event 5 (12)
Withdrawal by Subject 1 (2)
Age, years, median (range) 59 (27-81)
Sex, male/female % 51/49
ECOG performance status
0 18 (44)
1 20 (49)
Not yet in DB 3 (7)
Tumor Type
GI: Colorectal (12), Pancreas (3), Gall Bladder (1), Rectal (1), Small Bowel (1),
Stomach (1), Cholangiocarcinoma (2), Hepatocellular (1) 22
Breast 2
Lung: Squamous (3), Non-squamous (3) 6
GU: Ovarian (4), Endometrial stromal (1) 5
Head and Neck 3
Thyroid: Papillary (2), Hurthle Cell (1) 3
Safety
RXDX-105 has been well-tolerated with few eG3 AEs reported. All AEs that have occurred to date are
reversible with dose reduction or holiday.
Three DLTs have occurred: G3 maculopapular rash (200 mg RXDX-105), G3 fatigue (275 mg RXDX-105) and
G3 diarrhea (275 mg RXDX-105). All DLTs resolved upon study drug interruption. Two patients resumed
treatment at a reduced dose; the third patient discontinued treatment due to progression prior to re-starting
study drug.
Two Grade 4 events have occurred (intestinal obstruction and anemia), neither of which were considered
drug-related. There have been no grade 5 events, and no treatment-related SAEs.
? The MTD has not yet been determined.
Table 3. Most Common (>15%) Treatment-Emergent Adverse Events, n (%)
<275 mg 275 mg TOTAL*
Preferred Term (n=25) (n=12) (n=37)
Grade =2 Grade =3 Grade =2 Grade =3 Grade =2 Grade =3
Fatigue 11 (44%) 6 (50%) 1 (8%) 17 (46%) 1 (3%)
Vomiting 9 (36%) 3 (25%) 1 (8%) 12 (32%) 1 (3%)
Nausea 6 (24%) 4 (33%) 1 (8%) 10 (27%) 1 (3%)
Decreased appetite 7 (28%) 2 (17%) 1 (8%) 9 (24%) 1 (3%)
Constipation 4 (16%) 4 (33%) 8 (21%)
Diarrhea 4 (16%) 1 (4%) 4 (33%) 2 (17%) 8 (21%) 3 (8%)
Hypertension 5 (20%) 1 (4%) 3 (25%) 8 (21%) 1 (3%)
Muscle spasms 5 (20%) 3 (25%) 8 (21%)
Abdominal pain 6 (24%) 1 (4%) 1 (8%) 1 (8%) 7 (19%) 2 (5%)
Abdominal distension 4 (16%) 2 (17%) 6 (16%)
Back pain 5 (20%) 1 (8%) 6 (16%)
Alk Phos Increased 4 (16%) 1 (4%) 2 (17%) 6 (16%) 1 (3%)
Dyspnea 4 (16%) 2 (17%) 6 (16%)
Hypokalemia 5 (20%) 1 (8%) 2 (17%) 6 (16%) 2 (5%)
Pain in extremity 6 (24%) 6 (16%)
Anemia 4 (16%) 2 (8%) 1 (8%) 2 (17%) 5 (13%) 4 (11%)
a total excluded 4 patients currently in Cycle 1 with no AE reporting
Pharmacokinetics
275 mg “fed state” N=1
275 mg N=7
200 mg N=6
10000 100 mg N=3
40 mg N=3
Target RET inhibition threshold
Target BRAF inhibition threshold
? Exposures of RXDX-105
(ng/mL) administered on a continuous
daily dosing regimen increased
with increasing dose; fed state
1000 appears to further increase
exposure
Concentration ? Based on the accumulation ratio,
the plasma half-life of RXDX-105
is estimated to be in the range of
Plasma 40-50 hours, compatible with QD
dosing
Exposure is reaching levels
100 expected to be efficacious based
0 4 8 12 16 20 24 on animal models exhibiting
Time (h) tumor growth inhibition
Forty-one patients have been treated with RXDX-105. Six patients discontinued prior to the first tumor assessment or were not evaluable for tumor response. Six patients have not yet reached the Cycle 2 tumor assessment. Twenty-nine patients have had post-baseline tumor evaluations and are evaluable for tumor regression. Tumor regression has been noted in 6 patients treated with 275 mg, including one confirmed RECIST PR in a patient dosed in the fed state. Most recent fasted and fed cohorts for 200mg and 275mg shown below. Molecular alterations, if known, are noted.
200mg fasted state Day 15 exposure Cmin in ng/mL
275mg fasted state
Expected efficacious exposure threshold
275mg fed state
100 6000
80 5000
4000
60
% 3000
40
2000
20
Reduction 1000 (ng/mL) min
CRC NSCLC C
Ovarian CRC Thyroid NSCLC KRAS+
0 BRAF+ 0
CRC Cholangio- CRC Adenoid CRC CRC CRC CRC Pancreatic Pancreatic 15
Tumor carcinoma KRAS+ BRAF+ BRAF+ KRAS+
-20 BRAF+ CRC -1000 Day
Best -2000
-40 PR
-3000
-60
-4000
-80 -5000
-100 -6000
mKRAS+ NSCLC Patient with PR
One confirmed RECIST PR has been noted in a patient treated with 275mg RXDX-105 in the fed state. The patient is a 75 y/o female with metastatic NSCLC. She was initially diagnosed in 2007. Molecular analysis of tumor from her initial diagnosis revealed KRAS G12C mutation. Prior cancer treatment includes: multiple lines of chemotherapy and 6 years of erlotinib. At Cycle 2, the patient had 40% reduction in her target lesion, which has been confirmed at Cycle 3. She continues on study.
• RXDX-105 has been well-tolerated to date in patients with advanced or metastatic solid tumors.
• Exposure is reaching efficacious levels, based on preclinical data from RET- and BRAF-driven PDX models.
• Signals of anti-tumor activity have been noted, with a confirmed PR (40% reduction) observed in a patient with NSCLC positive for KRAS G12C who had the highest drug exposure to date.
• In patients with tumor regression, there appears to be an exposure/response correlation.
• Emerging hypotheses regarding mechanisms of action against oncogenic drivers and escape mechanisms are being evaluated in the preclinical setting and will inform the clinical plan.
• These preliminary data support further development of RXDX-105.
Conclusions
• RXDX-105 has been well-tolerated to date in patients with advanced or metastatic solid tumors.
• Exposure is reaching efficacious levels, based on preclinical data from RET- and BRAF-driven PDX models.
• Signals of anti-tumor activity have been noted, with a confirmed PR (40% reduction) observed in a patient with NSCLC positive for KRAS G12C who had the highest drug exposure to date.
• In patients with tumor regression, there appears to be an exposure/response correlation.
• Emerging hypotheses regarding mechanisms of action against oncogenic drivers and escape mechanisms are being evaluated in the preclinical setting and will inform the clinical plan.
• These preliminary data support further development of RXDX-105.