Exhibit 99.2

JP Morgan 2021 APPENDIX

Research and development portfolio of designed molecules: brain, lung, GI and eye 2 Molecular Design Biology Medicinal Chemistry DMPK Development and Commercial Symptomatic nOH (Neurogenic orthostatic hypotension) Asthma Lung Transplant Rejection IPF (idiopathic pulmonary fibrosis) COPD (chronic obstructive pulmonary disorder) — APPROVED COVID - 19 CD (Crohn’s disease) UC (ulcerative colitis) Celiac Disease DME (diabetic macular edema) DMPK, drug metabolism and pharmacokinetics; GI, gastrointestinal.

YUPELRI ® (revefenacin) inhalation solution First and only once - daily, nebulized maintenance medicine for COPD

YUPELRI ® launch metrics Majority of YUPELRI ® volume flows through durable medical equipment channel (approximately 3 - month lag in data capture); remaining volume flows thro ugh hospitals, retail and long - term care pharmacies. Wholesale acquisition cost (WAC): $1,066 per month (or ~$35 per day). 1. Launch through October 2, 2020. 2. TBPH estimate derived from int egrating multiple data sources. 3. For patients with supplemental insurance; approximately 20% of patients may be responsible for co - pay and/or supplemental insurance. Source: www.CMS.gov. 4 191 wins (equates to 363 accounts) 78% of formulary accounts ordering 100% medical support requests fulfilled <30 days FORMULARY 1 Field force continues hybrid approach to customer interactions (live and virtual) ~50,000 patients 2 prescribed (through Q3 2020) PATIENT 100% Medicare Part B 3 74% of commercial payer lives covered (comprises ~8% of the YUPELRI ® business) ACCESS 65% 35% TBPH VTRS Strong customer acceptance and market uptake ‣ Theravance Biopharma’s implied 35% share of Net Sales during Q3 2020 was $13M ‣ Increased market share and achieved quarter - over - quarter Net Sales growth of 22%
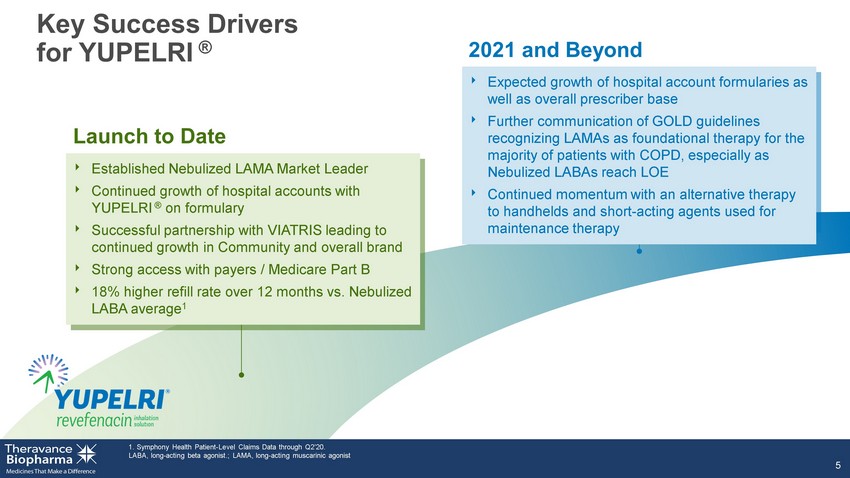
LAMA, long - acting muscarinic agonist; LABA, long - acting beta agonist. 5 Launch to Date 2021 and Beyond Key Success Drivers for YUPELRI ® ‣ Established Nebulized LAMA Market Leader ‣ Continued growth of hospital accounts with YUPELRI on formulary ‣ Successful partnership with VIATRIS leading to continued growth in Community and overall brand ‣ Strong access with payers / Medicare Part B ‣ 18% higher refill rate over 12 months vs Nebulized LABA average ‣ Expected growth of hospital account formularies as well as overall prescriber base ‣ Further communication of GOLD guidelines recognizing LAMAs as foundational therapy for majority of patients with COPD, especially as Nebulized LABAs reach LOE ‣ Momentum with switches from handhelds and short - acting agents used for maintenance therapy
Ampreloxetine (TD - 9855) Once - daily norepinephrine reuptake inhibitor to treat symptomatic neurogenic orthostatic hypotension

Untreated nOH NE Release at Neurovascular Junction Systolic Blood Pressure Designed to reduce symptoms of nOH by prolonging the effect of endogenous norepinephrine 1. Palma JA, Kaufmann H. Mov Disord Clin Pract 2017;4:298 - 308. NE, norepinephrine; NET, norepinephrine transporters. 7 Vasodilation Blood pressure Vasoconstriction Blood pressure Syncope Normal x Increased standing blood pressure x Increased brain perfusion x Reduce symptoms of symptomatic nOH 1 NE A XON TERMINAL D ENDRITE + Ampreloxetine Ampreloxetine Reduction in syncope Normal

Decentralized trials move activities from the clinic to home ‣ Site - centric operating model ‣ Burden on site resources ‣ Patient burden Source: Theravance Biopharma Clinical Operations. 8 Global clinical trials are being decentralized along a continuum Traditional Trial Operations Decentralized Trial ‣ Patient - centric model ‣ Leverage technology for remote visits, monitoring and data collection ‣ Established home health and distribution channels

nOH is included in medical treatment guidelines for PD and MSA patients; once diagnosed, patients get on drug treatment quickly A concentrated group of neurologists and cardiologists treat patients with nOH; ‘at risk’ patients already identified and managed by specialty institutions TBPH ’s infrastructure capable of commercializing ampreloxetine in the US with limited and targeted additions to current resources Physicians report high urgency to treat snOH due to the high impact on patients’ QoL, high risk of injury from falls and caregiver burden Meaningful value proposition will drive patient access; Ampreloxetine has the potential to improve the durability of treatment effect and thereby reduce costly events associated with nOH Strong message from Parkinson’s and MSA advocacy groups that patients need new therapies to better manage nOH Ampreloxetine: has the potential to transform Theravance Biopharma into an independent commercial biopharma snOH , symptomatic neurogenic orthostatic hypotension 9 Established disease, targeted market Established nOH treatment paradigm Specialist networks in place Manageable opportunity A strong value proposition An urgency to treat Understanding of current access barriers Established patient advocacy

Izencitinib (TD - 1473) (JNJ - 8398) Oral gut - selective pan - JAK inhibitor to treat inflammatory bowel diseases
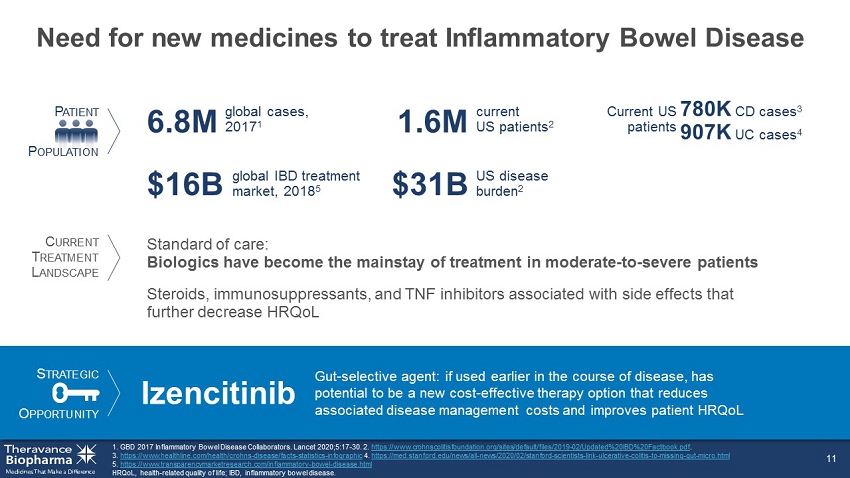
Need for new medicines to treat Inflammatory Bowel Disease 11 HRQoL, health - related quality of life; IBD, inflammatory bowel disease. 1. GBD 2017 Inflammatory Bowel Disease Collaborators. Lancet 2020;5:17 - 30. 2. https://www.crohnscolitisfoundation.org/sites/default/files/2019 - 02/Updated%20IBD%20Factbook.pdf . 3. https://www.healthline.com/health/crohns - disease/facts - statistics - infographic 4. https://med.stanford.edu/news/all - news/2020/02/stanford - scientists - link - ulcerative - colitis - to - missing - gut - micro.html 5. https://www.transparencymarketresearch.com/inflammatory - bowel - disease.html P ATIENT P OPULATION US disease burden 2 $31B Standard of care: Biologics have become the mainstay of treatment in moderate - to - severe patients global cases, 2017 1 6.8M global IBD treatment market, 2018 5 $16B Current US patients Steroids, immunosuppressants, and TNF inhibitors associated with side effects that further decrease HRQoL S TRATEGIC O PPORTUNITY Izencitinib Gut - selective agent: if used earlier in the course of disease, has potential to be a new cost - effective therapy option that reduces associated disease management costs and improves patient HRQoL current US patients 2 1.6M C URRENT T REATMENT L ANDSCAPE 780K CD cases 3 907K UC cases 4

STAT - induced Inflammation α N UCLEUS STAT P STAT P STAT P STAT P STAT JAK β γ JAK JAK inhibitor JAK - STAT pathway: orchestrating signaling of multiple pro - inflammatory cytokines Clark JD, et al. J Med Chem 2014; 57:5023 - 5038. EPO, erythropoietin; GM - CSF, granulocyte - macrophage colony - stimulating factor; TPO, thrombopoietin; Tyk , tyrosine kinase. 12 γ c cytokines (IL - 2, IL - 4, IL - 7, IL - 9, IL - 15, IL - 21) Type 1 IFNs, IL - 10 family IL - 6, IL - 11, IL - 13, IL - 27, IL - 31, IL - 35 IFN γ IL - 12, IL - 23 EPO, TPO GM - CSF, IL - 3, IL - 5 α JAK1 β γ JAK3 α JAK1 β γ Tyk2 α JAK1 β γ JAK2 Tyk2 α JAK1 β γ JAK2 α JAK2 β γ Tyk2 α JAK2 β γ JAK2
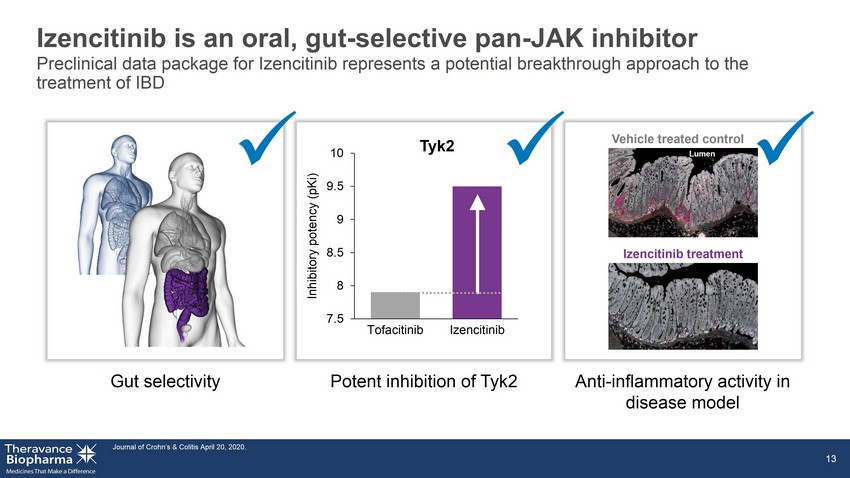
Izencitinib is an oral, gut - selective pan - JAK inhibitor Journal of Crohn’s & Colitis April 20, 2020. 13 Gut selectivity Potent inhibition of Tyk2 Anti - inflammatory activity in disease model x x Lumen Vehicle treated control Izencitinib treatment x 7.5 8 8.5 9 9.5 10 Tofacitinib Izencitinib Inhibitory potency (pKi) Tyk2 Preclinical data package for Izencitinib represents a potential breakthrough approach to the treatment of IBD

Systemic exposures low; tissue concentrations at or above JAK inhibition levels *Tofacitinib concentrations extracted from J Pharmacol Exp Ther 348:165 – 173, January 2014. BID, twice daily; IC 50 , concentration to produce 50% maximal inhibition; PK, pharmacokinetics. 14 Tofacitinib 10 mg BID* Izencitinib 20 mg Izencitinib 80 mg Izencitinib 270 mg Colonic Tissue Concentrations of Izencitinib Izencitinib Dose 1 10 100 1000 10,000 20 mg 80 mg 270 mg Range of JAK IC 50 values Izencitinib Total Concentration (nM) Plasma Concentrations in UC Patients Time (h) 100 200 300 0 0 1 2 3 4 Plasma Concentration (nM)

TD - 0903 Program Nebulized lung - selective pan - JAK inhibitor to treat: ► Acute hyperinflammation of the lung in COVID - 19 ► Chronic inflammation for the prevention of lung transplant rejection

Leveraging respiratory expertise for potential acute treatment in response to a global pandemic 1. https://coronavirus.jhu.edu/map.html, number as of 12/22. 2. IHME. 3. https://www.fda.gov/drugs/coronavirus - covid - 19 - drugs/coronavirus - treatment - acceleration - program - ctap#dashboard 1. 4. https://www.fda.gov/emergency - preparedness - and - response/mcm - legal - regulatory - and - policy - framework/emergency - use - authorization#ot hercurrenteuas 2. 5. https://www.fda.gov/media/136832/download#:~:text=This%20EUA%20authorizes%20the%20use,and%20who%20are%20at%20high 6. https://www.statista.com/statistics/1106306/coronavirus - clinical - trials - worldwide/ According to ClinicalTrials.gov, there are 4,266 studies currently registered which are investigating the coronavirus disease (COVID - 19). This statistic shows th e total number of results from a search of "covid - 19" on ClinicalTrials.gov database, as of December 22, 2020, by region. 16 US patients 1 >22M patients become hospitalized 2 ~2.4% 2 vaccines available via Emergency Use Authorization 3,4 1 approved treatment; 8 available via Emergency Use Authorization 3,4 370 active trials in US 5 4,266 studies registered worldwide 6 S TRATEGIC O PPORTUNITY TD - 0903 Inhaled lung - specific therapeutic: potential to be used in combination with other treatment modalities (e.g., antivirals) to provide additional therapeutic benefit with reduced risk of systemic immunosuppressive issues that may occur with systemic anti - inflammatories P ATIENT P OPULATION C URRENT US T REATMENT L ANDSCAPE patients worldwide 1 >88M
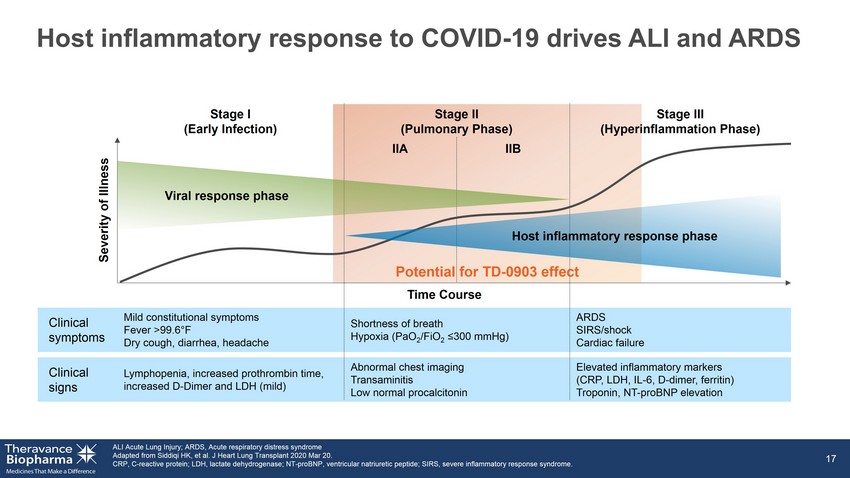
Potential for TD - 0903 effect Host inflammatory response to COVID - 19 drives ALI and ARDS ALI Acute Lung Injury; ARDS, Acute respiratory distress syndrome Adapted from Siddiqi HK, et al. J Heart Lung Transplant 2020 Mar 20. CRP, C - reactive protein; LDH, lactate dehydrogenase; NT - proBNP, ventricular natriuretic peptide; SIRS, severe inflammatory respo nse syndrome. 17 Clinical symptoms Clinical signs Mild constitutional symptoms Fever >99.6 ° F Dry cough, diarrhea, headache Shortness of breath Hypoxia (PaO 2 /FiO 2 ≤300 mmHg) Lymphopenia, increased prothrombin time, increased D - Dimer and LDH (mild) Abnormal chest imaging Transaminitis Low normal procalcitonin ARDS SIRS/shock Cardiac failure Elevated inflammatory markers (CRP, LDH, IL - 6, D - dimer, ferritin) Troponin, NT - proBNP elevation Time Course IIA IIB Severity of Illness Stage I (Early Infection) Stage II (Pulmonary Phase) Stage III (Hyperinflammation Phase) Viral response phase Host inflammatory response phase
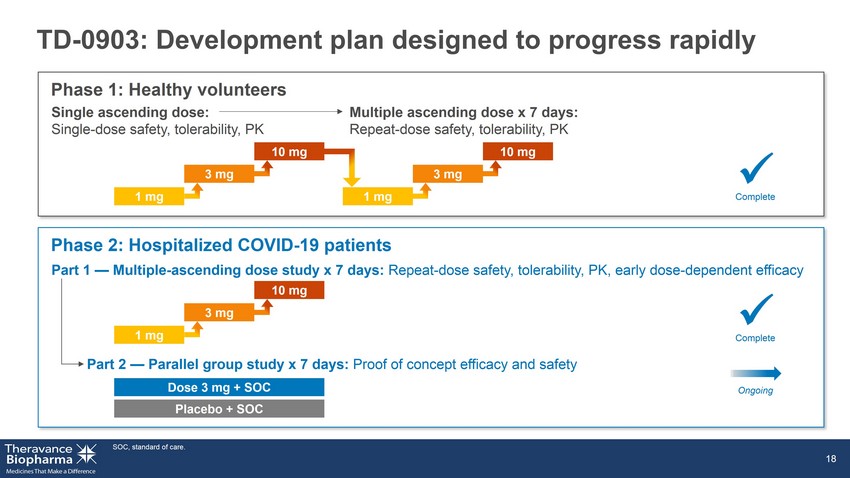
TD - 0903: Development plan designed to progress rapidly SOC, standard of care. 18 Phase 2: Hospitalized COVID - 19 patients Dose 3 mg + SOC Placebo + SOC Phase 1: Healthy volunteers Single ascending dose: Single - dose safety, tolerability, PK Multiple ascending dose x 7 days: Repeat - dose safety, tolerability, PK Part 1 — Multiple - ascending dose study x 7 days: Repeat - dose safety, tolerability, PK, early dose - dependent efficacy Part 2 — Parallel group study x 7 days: Proof of concept efficacy and safety 1 mg 3 mg 10 mg 1 mg 3 mg 10 mg 1 mg 3 mg 10 mg x Complete x Complete Ongoing
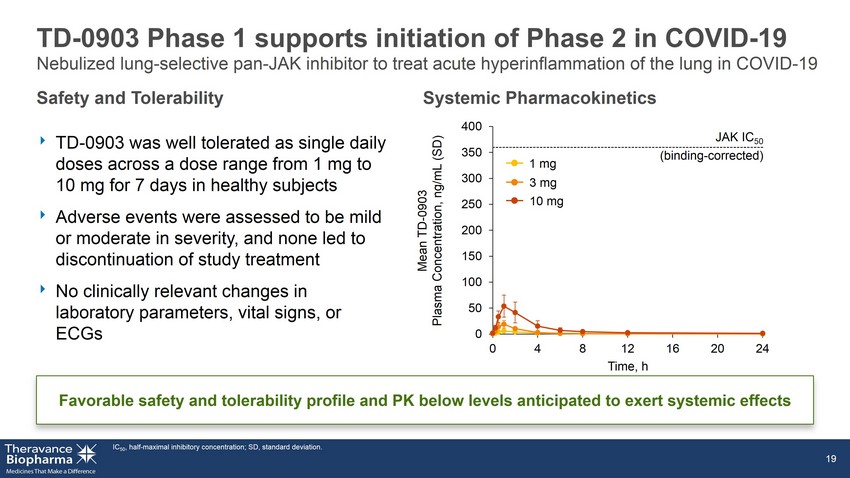
TD - 0903 Phase 1 supports initiation of Phase 2 in COVID - 19 ‣ TD - 0903 was well tolerated as single daily doses across a dose range from 1 mg to 10 mg for 7 days in healthy subjects ‣ Adverse events were assessed to be mild or moderate in severity, and none led to discontinuation of study treatment ‣ No clinically relevant changes in laboratory parameters, vital signs, or ECGs IC 50 , half - maximal inhibitory concentration; SD, standard deviation. 19 Favorable safety and tolerability profile and PK below levels anticipated to exert systemic effects Safety and Tolerability Systemic Pharmacokinetics 0 50 100 150 200 250 300 350 400 0 4 8 12 16 20 24 3 mg 1 mg 10 mg JAK IC 50 (binding - corrected) Mean TD - 0903 Plasma Concentration, ng/mL (SD) Time, h Nebulized lung - selective pan - JAK inhibitor to treat acute hyperinflammation of the lung in COVID - 19

S TRATEGIC O PPORTUNITY First - in - disease opportunity for the prevention of lung transplant rejection ‣ Calcineurin inhibitors (tacrolimus) ‣ Anti - proliferative agents (MMF) 1. http://www.transplant - observatory.org/data - charts - and - tables/ . 2. United Network for Organ Sharing (UNOS), https://unos.org/data/transplant - trends. 3. Chambers DC et al, JHLT 2018; 37(10): 1169 - 1183. 4. JHEOR. 2015. CA Jones https://pdfs.semanticscholar.org/108c/5cb16aaab19fa 9e9a1ccba64ae5869336f26.pdf CAGR, compound annual growth rate; IPF, idiopathic pulmonary fibrosis; CF, cystic fibrosis; CLAD, chronic lung allograft dysf unc tion; mAb, monoclonal antibody; MMF, mycophenolate mofetil. 20 lung transplants per year in US 2 2,714 TD - 0903 Potential first approved therapy specifically to prevent acute lung transplant rejection and development of CLAD Use following lung transplantation could potentially improve patient morbidity and mortality risk, and reduce need for re - transplantation Lung transplants have the poorest prognosis of all solid organ transplants COPD, IPF, and CF top 3 diagnoses driving need for lung transplantation CAGR since 1988 2 15% mortality at 6 years post transplant 3 ~50% No FDA - approved therapies to prevent lung transplant rejection or CLAD Current standard of care: triple immunosuppression therapy medical/productivity costs (2015 – 2025) 4 $3.5B P ATIENT P OPULATION C URRENT T REATMENT L ANDSCAPE lung transplants worldwide, 2019 1 6,240 ‣ Corticosteroids ‣ IL - 2 mAb induction therapy (basiliximab)

Month 6 0 5 10 15 20 F i r s t B P A R R a t e ( % ) Pan - JAK inhibitors can prevent transplant rejections ‣ JAK inhibition was superior to cyclosporine in prevention of acute and chronic rejections ‣ Serious infections increased with systemic JAK inhibitors including CMV 1. Vincenti F, et al. Am J Transplant 2015;15:1644 - 53. *p<0.001 vs CsA . BPAR, biopsy - proven acute rejection; CMV, cytomegalovirus; IF/TA, Interstitial Fibrosis/Tabular Atrophy; SE, standard error; TWC2, time - weighted 2 - h post - dose concentrations . 21 Chronic Rejection Tofacitinib is superior to CsA in efficacy measures Acute Rejection Increased infection risk with tofacitinib over CsA CsA Tofacitinib 50 40 30 20 10 0 Month 12 * IF/TA % 24 5 53 25 0 20 40 60 Tofacitinib CsA CMV disease Serious infection 12 - month Kaplan - Meier estimates, % (SE) Noninferiority trial of tofacitinib vs cyclosporine ( CsA ) in kidney transplant recipients 1

TD - 8236 Potential first inhaled JAKi for asthma
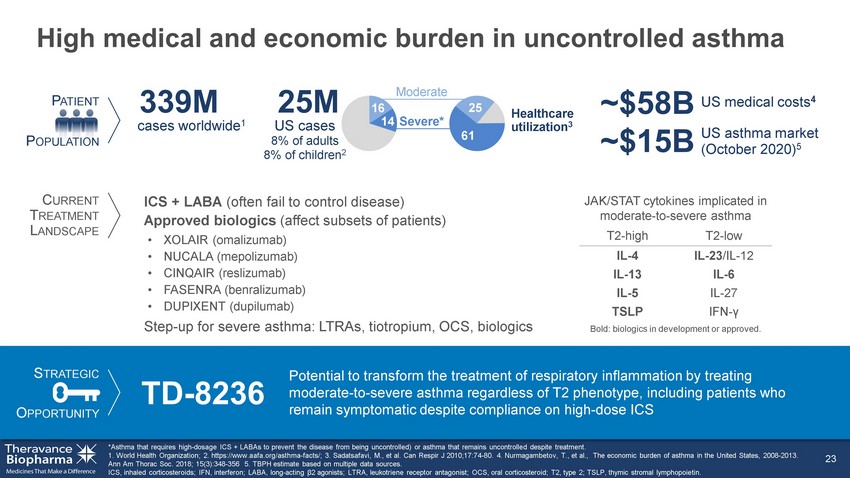
High medical and economic burden in uncontrolled asthma *Asthma that requires high - dosage ICS + LABAs to prevent the disease from being uncontrolled) or asthma that remains uncontrolle d despite treatment. World Health Organization; 2. https://www.aafa.org/asthma - facts/; 3. Sadatsafavi, M., et al. Can Respir J 2010;17:74 - 80. 4. Nurmagambetov , T., et al., The economic burden of asthma in the United States, 2008 - 2013. Ann Am Thorac Soc. 2018; 15(3):348 - 356 5. ICS, inhaled corticosteroids; IFN, interferon; LABA, long - acting β2 agonists; LTRA, leukotriene receptor antagonist; OCS, oral corticosteroid; T2, type 2; TSLP, thymic stromal lymphopoietin. 23 16 14 Severe* Moderate US asthma market (May 2020) 5 61 25 US cases 8% of adults 8% of children 2 Healthcare utilization 3 25M ~$15B P ATIENT P OPULATION C URRENT T REATMENT L ANDSCAPE S TRATEGIC O PPORTUNITY TD - 8236 Potential to transform the treatment of respiratory inflammation by treating moderate - to - severe asthma regardless of T2 phenotype, including patients who remain symptomatic despite compliance on high - dose ICS ICS + LABA (often fail to control disease) Approved biologics (affect subsets of patients) US medical costs 4 ~$58B T2 - high T2 - low IL - 4 IL - 23 /IL - 12 IL - 13 IL - 6 IL - 5 IL - 27 TSLP IFN - γ Bold: biologics in development or approved. JAK/STAT cytokines implicated in moderate - to - severe asthma • XOLAIR (omalizumab) • NUCALA (mepolizumab) • CINQAIR (reslizumab) • FASENRA (benralizumab) • DUPIXENT (dupilumab) Step - up for severe asthma: LTRAs, tiotropium, OCS, biologics cases worldwide 1 339M

TD - 8236: Phase 1 clinical trial design FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; MAD, multiple - ascending dose; MoA , Mechanism of Action; PK, pharmacokinetic; PD, pharmacodynamic; pSTAT , phosphorylated signal transducer and activator of transcription; SAD, single - ascending dose. 24 Parts A & B completed September 2019; Part C enrollment completed — data reported in Q4 2020 Part B: MAD (Mild asthmatics) Part A: SAD (Healthy volunteers) Safety, PK Safety, PK, PD ( FeNO ) All cohorts: N=6 active/2 Placebo 4500 µg 500 µg 1500 µg 150 µg 50 µg 4000 µg 1 2 3 4 5 6 7 D 150 µg 500 µg 1500 µg 1 2 3 4 5 6 7 D 1 2 3 4 5 6 7 D 1 2 3 4 5 6 7 D Part C: MoA Biomarkers (Moderate - to - severe asthmatics + ICS) N=16 active/8 placebo 1 2 3 4 5 6 7 D 1500 µg ‣ Goal: build confidence in compound, MoA and dose in early - development ‣ Endpoints: FeNO; pSTAT1 and pSTAT6 in bronchoalveolar lavage fluid; cytokines; epithelial gene expression T2 - dominant, n=8 Non - T2 - dominant, n=8 x x

TD - 8236: Positive Phase 1 trial in healthy subjects and patients with mild and moderate - to - severe asthma ‣ Biomarkers of JAK target engagement (pSTAT1 and pSTAT6) significantly reduced in lungs of T2 high and T2 low moderate/severe asthmatics on top of inhaled corticosteroids ‣ Ongoing analysis of effect of TD - 8236 on additional biomarkers including cytokines and gene expression ICS, inhaled corticosteroids; PK, pharmacokinetic; PD, pharmacodynamic; FeNO , fractional exhaled nitric oxide 25 Phase 1 Profile Healthy Volunteer Single Dose (Part A) Mild Asthma Multiple Dose (Part B) Moderate - to - Severe Asthma [+ ICS] Multiple Dose (Part C) Generally well tolerated x x x Minimal systemic exposure x x x PK and PD profile consistent with once - daily dosing x x x Biologic activity in lungs of patients with asthma x ↓ FeNO x ↓ FeNO, pSTAT1, pSTAT6

-50 -40 -30 -20 -10 0 10 20 30 40 -0.4 -0.2 0.0 0.2 0.4 Favors Placebo Favors TD - 8236 Favors TD - 8236 Favors Placebo No impact of TD - 8236 on the Late Asthmatic Response (LAR) ‣ TD - 8236 was generally well tolerated as a single - daily dose administered for 14 consecutive days 26 Primary Endpoint: Weighted Mean Area Under the Curve, 3 – 8 h. LS, least - squares; CI, confidence interval. % Change in FeNO Late Asthmatic Response Difference from Placebo, Liters (LS Means ± 95% CI) Difference from Placebo, % (LS Means ± 95% CI) 1500 µg 150 µg Day 14 Day 14 Day 7 - 0.01 n=22 - 0.04 n=20 4.28 n=22 - 20.16 n=24 - 3.72 n=22 - 26.87 n=23 Significant reductions in inflammation marker ( FeNO ) and favorable safety and tolerability

-50 -40 -30 -20 -10 0 10 20 30 40 TD - 8236 FeNO reductions consistent across Phase 1 and 2 ‣ FeNO reductions observed in moderate - to - severe asthmatics taking inhaled corticosteroids ICS, inhaled corticosteroids; LAC, lung allergen challenge; LS, least - squares; CI, confidence interval. 27 Phase 1 (Part B) Mild Asthmatics Phase 2 (LAC) Mild Asthmatics Phase 1 (Part C) Moderate – Severe Asthmatics + ICS Difference from Placebo (%) (LS Means ± 95% CI) 1500 µg 150 µg Day 7 Day 7 Day 14 Day 7 - 7.65 n=6 - 24.90 n=6 4.28 n=22 - 20.16 n=24 - 3.72 n=22 - 26.87 n=23 - 22.80 n=8 Favors Placebo Favors TD - 8236

TD - 5202 Organ - gut selective irreversible JAK3 inhibitor to treat inflammatory intestinal diseases

Celiac disease has no current treatments and serious health consequences 29 1. http://www.drschaer - institute.com/us/celiac - disease/epidemiology - 1033.html 2. 1% prevalence in US, BeyondCeliac.org. 3. 2018 US population 327M Census.gov. 4. Reunala T, et al. Dermatitis Herpetiformis: A Common Extraintestinal Manifestation of Coeliac Disease. Nutrients 2018;10(5). pii : E602 5. Guandalini et al. Direct Costs in Patients with Celiac Disease in the USA: A Retrospective Claims Analysis. Digestive Diseases Sciences 20 16; 61(10):2823 - 30 6. Theravance Market Research. S TRATEGIC O PPORTUNITY P ATIENT P OPULATION US patients 2,3 3.3M No approved treatment Only available intervention is strict life - long gluten - free diet 30% of diagnosed patients are poorly controlled despite best dietary efforts 6 TD - 5202 Organ - gut selective irreversible JAK3 inhibitor: potential to deliver significant value for both patients and payers increase in US over past 50 y 4 4 – 4.5x Global prevalence 1 1% higher healthcare costs than controls 5 >2x C URRENT T REATMENT L ANDSCAPE Celiac Normal

JAK3 - dependent cytokines play central role in pathogenesis of celiac disease ‣ Proof - of - relevance from recent positive Phase 2 data with systemic JAK3 inhibitor in alopecia areata, another T - cell mediated disease ‣ Localized JAK3 inhibition has the potential to avoid systemic immunosuppression (genetic JAK3 deficiency leads to severe immunodeficiency) Figure adapted from Jabri B and Sollid L. J Immunol 2017;198:3005 - 14. IE - CTL, intraepithelial cytotoxic lymphocyte; IEL, intraepithelial lymphocyte. 30 IL - 2, IL - 4, IL - 7, IL - 9, IL - 15, IL - 21 I MMUNE C ELL CD Pathogenesis α N UCLEUS STAT P STAT P STAT P STAT P STAT JAK1 β γ JAK3 P P P Gluten peptides G LUTEN - S PECIFIC T H 1 CELLS I NTESTINAL E PITHELIUM L AMINA P ROPIA I NTESTINAL L UMEN IFNγ IL - 2 IL - 21 IEL IE - CTL IL - 15

TD - 5202 First - in - human overall results summary ‣ No serious or severe AEs were reported ‣ All treatment - emergent AEs in TD - 5202 - treated subjects were mild in severity AE, adverse event; C max,ss , maximal steady - state concentration; NK, natural killer. 31 TD - 5202: generally well - tolerated (single dose ≤2000 mg, multiple doses ≤1000 mg BID) for 10 consecutive days in healthy subjects ‣ Systemic exposures were dose proportional from 100 to 1000 mg BID ‣ Low steady - state systemic exposures: mean C max,ss ~11 - fold below the protein - adjusted JAK IC 50 at the highest tested dose (1000 mg BID), consistent with a gut - selective approach ‣ No clinically significant changes from baseline in vital signs and ECG assessments ‣ No clinically significant changes in chemistry or hematology parameters – No changes in NK cell count
Inhaled ALK5i Potential best - in - disease therapy for the treatment of idiopathic pulmonary fibrosis (IPF)

Limited treatment options 2 currently approved therapies, with modest efficacy and poor tolerability S TRATEGIC O PPORTUNITY P ATIENT P OPULATION Inhaled ALK5i Potential first - in - class inhaled ALK5 inhibitor anti - fibrotic agent for IPF Despite treatment with the current SoC, IPF patients continue to experience disease progression and exacerbation C URRENT T REATMENT L ANDSCAPE Idiopathic pulmonary fibrosis (IPF) remains a fatal chronic lung disease with limited treatment options 1. Raghu G, et al. Lancet Resp. 2014: 2(7):566 - 572. 2. Raghu G, et al. Eur Respir J . 2016: 48(1):179 - 186. 3. National Heart Lung and Blood Institute (NIH), Public Domain, https://commons.wikimedia.org/w/index.php?curid=29590103. S oc, Standard of Care. US prevalence; currently orphan disease 1,2 140,000 Lungs with IPF 3 33 Profound dyspnea, unrelenting cough, impairment of activities of daily living Mortality with IPF remains high
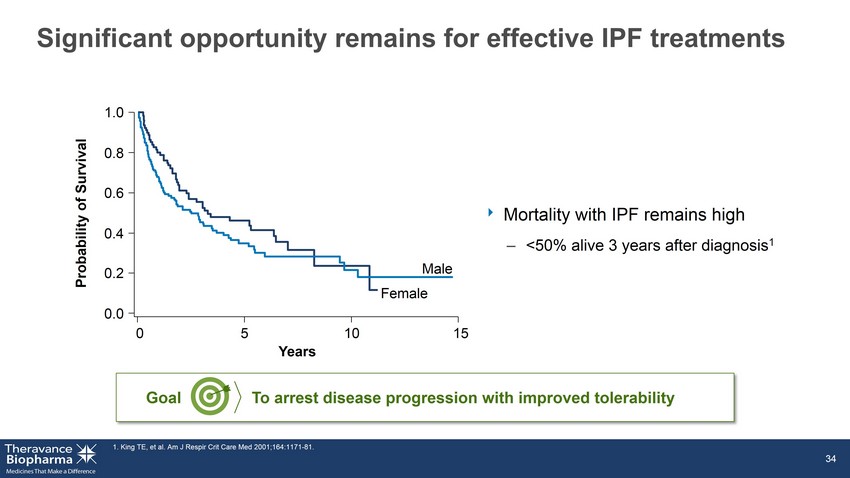
Significant opportunity remains for effective IPF treatments ‣ Mortality with IPF remains high – <50% alive 3 years after diagnosis 1 1. King TE, et al. Am J Respir Crit Care Med 2001;164:1171 - 81. 34 1.0 0.8 0.6 0.4 0.2 0.0 0 5 10 15 Years Probability of Survival Male Female To arrest disease progression with improved tolerability Goal

TGFβ, transforming growth factor β. 35 S CARRING TISSUES Collagen deposition Stimuli Genetic susceptibility Repetitive injury AEC damage TGF β A LVEOLAR E PITHELIAL C ELLS (AEC) T YPE 2 T YPE 1 Normal M YOFIBROBLASTS Fibrogenesis, proliferation Targeting the TGFβ pathway A core signaling pathway that drives fibrosis

a SMA , a - smooth muscle actin; ERK, extracellular signal - regulated kinase; JNK, c - Jun N - terminal kinase; PI3K, phosphatidylinositol - 4,5 - b isphosphate 3 - kinase; Smad2/3, mothers against decapentaplegic homolog 2/3; TGFR (ALK5), TGFβ receptor. Adapted from: Neuzillet C, et al. Oncotarget 2013;5:78 – 94. 36 F IBROBLASTS M YOFIBROBLASTS Fibroblast to Myofibroblast Transition (FMT) Increased extracellular matrix Increased a SMA Increased migration ERK Smad2/3 PI3K p38 JNK Rho IPF progression P P ALK5i Activation: Multiple an integrins Proteases Thrombospondin Free Radicals TGFR2 Latent TGFβ TGFR1 (ALK5) Selectively targeting the TGFβ pathway through ALK5 inhibition Inhibiting a core signaling pathway that drives fibrosis regardless of activation mechanism

ALK5 inhibition directly interrupts FMT 1 in IPF FTM, fibroblast to myofibroblast transition 37 Reference Standard ALK5i Log [M] % inhibition of α SMA - 9 - 8 - 7 - 6 - 5 0 50 100 150 FMT a SMA expressed a SMA reduced Negative control ALK5i treated

Current treatment options have no effect on FMT at clinically relevant concentrations FTM, fibroblast to myofibroblast transition; C max , maximal concentration; IC 50 , half maximal inhibitory concentration. 1. https://www.tga.gov.au/sites/default/files/auspar - nintedanib - esilate - 160208.pdf . 2. Ogura T, et al. Eur Respir J. 2015;45:1382 - 92. 38 -10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 Pirfenidone Nintedanib Log [M] Nintedanib IC 50 Pirfenidone IC 50 Clinical C max Unbound 1,2

Wound repair Bone healing Cardiovascular homeostasis Tumor suppression Endocrine function Lung selectivity avoids unwanted systemic side effects Modified from: Akhurst RJ, Hata A. Nat Rev Drug Discov 2012;11:790 - 811. TGFβ, transforming growth factor β. 39 Maintaining key systemic regulatory roles of TGFβ Inhaled ALK5i Minimizing systemic inhibition of a cytokine essential for homeostasis

Ocular JAKi Potential best - in - disease, pan - JAK inhibitor with long - acting ocular anti - inflammatory activity

Diabetic macular edema causes blindness in diabetics 41 1. © 2016 DR/Decision Resources, LLC. All rights reserved. Reproduction, distribution, transmission or publication is prohibit ed. Reprinted with permission. 2. Romero - Aroca, World J Diabetes 2011;2(6): 98 - 104. 3. Lee et al Curr Med Res Opin 2008;24:1549 - 59. Images from Angiogenesis Foundation, www.scienceofdme.org . DME, Diabetic macular edema; VEGFi , vascular endothelial growth factor inhibitor. Vision with DME Normal vision US prevalence 1 2.7 million #1 Anti - VEGF treatments Most patients have suboptimal response S TRATEGIC O PPORTUNITY P ATIENT P OPULATION Ocular JAKi C URRENT T REATMENT L ANDSCAPE Potential to offer an alternative treatment for DME patients who are not optimally responding to treatment with VEGFi 140% higher direct and indirect healthcare costs in patients with DME vs diabetics without ocular disease 3 cause of blindness in diabetes 2 1st Intraocular steroids Side effects limit utility 2nd Nonpharmacological treatments (e.g. laser coagulation) limited efficacy and significant adverse events
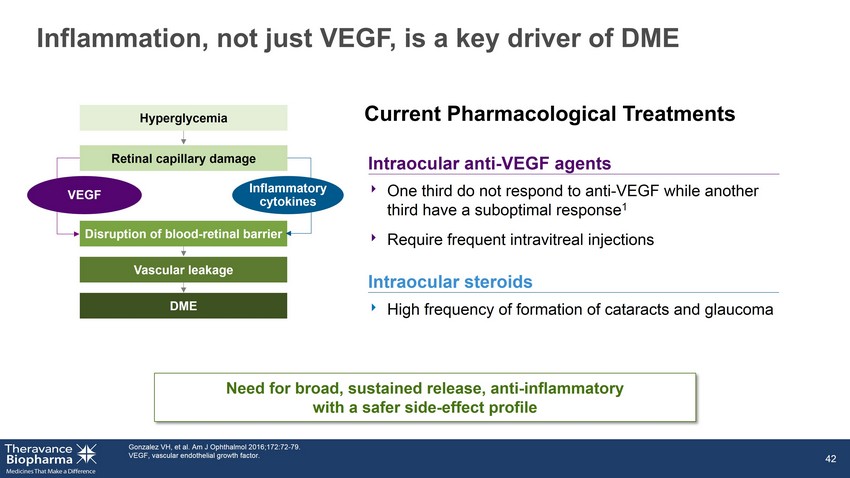
Inflammation, not just VEGF, is a key driver of DME Intraocular anti - VEGF agents 42 1. Gonzalez VH, et al. Am J Ophthalmol 2016;172:72 - 79. 2. VEGF, vascular endothelial growth factor. Current Pharmacological Treatments Intraocular steroids Hyperglycemia Disruption of blood - retinal barrier Vascular leakage DME VEGF Retinal capillary damage Inflammatory cytokines Need for broad, sustained release, anti - inflammatory with a safer side - effect profile ‣ High frequency of formation of cataracts and glaucoma ‣ One third do not respond to anti - VEGF while another third have a suboptimal response 1 ‣ Require frequent intravitreal injections

0.00 0.25 0.50 0.75 1.00 1.25 VEGF IL-6 IP-10 MCP-1 Unmet need for an anti - inflammatory drug: opportunity for eye - selective JAK inhibition Adapted from Sohn HJ, et. al. Am J Ophthalmol 2011; 152:686 - 694. 43 Effect of anti - VEGF Effect of Steroids 0.00 0.25 0.50 0.75 1.00 1.25 VEGF IL-6 IP-10 MCP-1 Untreated Treated Normalized Protein Level

Ocular pan - JAK inhibition has the potential to address key disease pathways in DME 44 TD - EyeJAKi inhibits key DME inflammatory pathways: JAK2 JAK1 IL - 6 Tyk2 JAK1 Interferons MCP - 1 IP - 10 TD - EyeJAKi ‣ IL - 6 and interferon signaling pathways in human primary cells ‣ IL - 6 induced pSTAT3 and interferon - induced IP - 10 in the back of the eye in vivo

0 1 2 3 0.000001 0.00001 0.0001 0.001 0.01 0.1 1 10 100 1000 Time (months) C o m p o u n d c o n c e n t r a t i o n ( g / m L o r g / g ) A pan - JAK inhibitor designed for eye selectivity with projected dosing interval of at least three months 45 Single intravitreal injection of TD - Eye JAKi in Rabbits Vitreous humor (depot) Retina Plasma α STAT P STAT P STAT JAK β γ JAK N UCLEUS P STAT P STAT JAKi
About YUPELRI ® (revefenacin) inhalation solution YUPELRI ® (revefenacin) inhalation solution is a once - daily nebulized LAMA approved for the maintenance treatment of COPD in the US . Market research by Theravance Biopharma indicates approximately 9 % of the treated COPD patients in the US use nebulizers for ongoing maintenance therapy . 1 LAMAs are a cornerstone of maintenance therapy for COPD and YUPELRI ® is positioned as the first once - daily single - agent bronchodilator product for COPD patients who require, or prefer, nebulized therapy . YUPELRI ® ’s stability in both metered dose inhaler and dry powder device formulations suggest that this LAMA could also serve as a foundation for novel handheld combination products . 1. TBPH market research (N=160 physicians); refers to US COPD patients. 46

YUPELRI ® (revefenacin) inhalation solution YUPELRI ® inhalation solution is indicated for the maintenance treatment of patients with chronic obstructive pulmonary disease (COPD) . Important Safety Information (US) YUPELRI is contraindicated in patients with hypersensitivity to revefenacin or any component of this product . YUPELRI should not be initiated in patients during acutely deteriorating or potentially life - threatening episodes of COPD, or for the relief of acute symptoms, i . e . , as rescue therapy for the treatment of acute episodes of bronchospasm . Acute symptoms should be treated with an inhaled short - acting beta 2 - agonist . As with other inhaled medicines, YUPELRI can produce paradoxical bronchospasm that may be life - threatening . If paradoxical bronchospasm occurs following dosing with YUPELRI, it should be treated immediately with an inhaled, short - acting bronchodilator . YUPELRI should be discontinued immediately and alternative therapy should be instituted . YUPELRI should be used with caution in patients with narrow - angle glaucoma . Patients should be instructed to immediately consult their healthcare provider if they develop any signs and symptoms of acute narrow - angle glaucoma, including eye pain or discomfort, blurred vision, visual halos or colored images in association with red eyes from conjunctival congestion and corneal edema . Worsening of urinary retention may occur . Use with caution in patients with prostatic hyperplasia or bladder - neck obstruction and instruct patients to contact a healthcare provider immediately if symptoms occur . Immediate hypersensitivity reactions may occur after administration of YUPELRI . If a reaction occurs, YUPELRI should be stopped at once and alternative treatments considered . The most common adverse reactions occurring in clinical trials at an incidence greater than or equal to 2 % in the YUPELRI group, and higher than placebo, included cough, nasopharyngitis, upper respiratory infection, headache and back pain . Coadministration of anticholinergic medicines or OATP 1 B 1 and OATP 1 B 3 inhibitors with YUPELRI is not recommended . YUPELRI is not recommended in patients with any degree of hepatic impairment . OATP, organic anion transporting polypeptide. 47