Exhibit 99.1

Apitegromab Positioned to be the Potential Next Transformative Therapy for Patients Suffering with SMA KOL Event and Panel DiscussionJune 15, 2021

Disclaimers Various statements in this presentation concerning the future expectations, plans and prospects of Scholar Rock, Inc. (“Scholar Rock”), including without limitation, Scholar Rock’s expectations regarding its strategy, its product candidate selection and development timing, including timing for the initiation of and reporting results from its clinical trials for its product candidates, its disease indication selection and timing for such selection, the ability of apitegromab (SRK-015) to affect the treatment of patients suffering from Spinal Muscular Atrophy (SMA) either as a monotherapy or in conjunction with the current standard of care, and the ability of SRK-181 to affect the treatment of cancer patients in a manner consistent with preclinical data constitute forward-looking statements for the purposes of the safe harbor provisions under The Private Securities Litigation Reform Act of 1995. The use of words such as “may,” “might,” “will,” “should,” “expect,” “plan,” “anticipate,” “believe,” “estimate,” “target,” “project,” “intend,” “future,” “potential,” or “continue,” and other similar expressions are intended to identify such forward-looking statements. Actual results may differ materially from those indicated by these forward-looking statements as a result of various important factors, including, without limitation, preclinical and clinical data, including the 12-month top-line results from the Phase 2 trial of apitegromab, are not predictive of, are inconsistent with, or more favorable than, data generated from future clinical trials of the same product candidate, including the planned Phase 3 trial of apitegromab in SMA, Scholar Rock’s ability to provide the financial support, resources and expertise necessary to identify and develop product candidates on the expected timeline, information provided or decisions made by regulatory authorities differ from the company’s expectations, competition from third parties that are developing products for similar uses, Scholar Rock’s ability to identify and develop multiple product candidates on the expected timeline, the impacts of the COVID-19 pandemic, Scholar Rock’s ability to obtain, maintain and protect its intellectual property, Scholar Rock’s dependence on third parties for development and manufacture of product candidates including to supply any clinical trials, and Scholar Rock’s ability to manage expenses and to obtain additional funding when needed to support its business activities and establish and maintain strategic business alliances and new business initiatives as well as those risks more fully discussed in the section entitled "Risk Factors" in the Quarterly Report on Form 10-Q for the quarter ended March 31, 2021, which is on file with the Securities and Exchange Commission, as well as discussions of potential risks, uncertainties, and other important factors in Scholar Rock’s subsequent filings with the Securities and Exchange Commission. Any forward-looking statements represent Scholar Rock’s views only as of today and should not be relied upon as representing its views as of any subsequent date. Scholar Rock explicitly disclaims any obligation to update any forward-looking statements unless required by law.© Scholar Rock, Inc. All rights reserved. June 2021.

Agenda 3 Opening Remarks and Spinal Muscular Atrophy Treatment Landscape Tony KingsleyPresident & CEO Apitegromab TOPAZ Phase 2 Proof-of-Concept Trial ResultsApitegromab Phase 3 Trial Design Considerations Yung Chyung M.D.CMO Moderated byYung Chyung, M.D. Panel Discussion with TOPAZ Trial Investigators:Thomas Crawford, M.D. - Johns Hopkins MedicineBasil Darras, M.D. – Boston Children’s Hospital & Harvard Medical School Jill Jarecki, Ph.D.CSO of Cure SMA Unmet Medical Needs of Individuals with SMA

Apitegromab Shows Transformative Potential in Patients with Type 2 and 3 SMA Spinal Muscular Atrophy (SMA) remains a devastating and debilitating disease despite the utilization of SMN upregulatorsMulti-pronged approach may be needed in treating SMA; muscle-directed therapy may further improve motor functionApitegromab showed transformative potential in patients with Type 2/3 SMA thru the TOPAZ Phase 2 trialExciting potential path forward for apitegromabin a rational, targeted, and efficient Phase 3 trial 4 Apitegromab is an investigational product candidate that is currently being evaluated in a clinical development program for the treatment of SMA. Apitegromab has not been approved by the U.S. Food and Drug Administration (FDA), the European Commission, or any other health or regulatory authority. The safety and effectiveness of this molecule have not been established.

5 Spinal Muscular Atrophy Overview Significant, progressive motor functionimpairment; many lose ambulation Infantile onset; unable to sit upindependently Severe, progressive disabilities and unable to walk independently Type 114% Type 251% Type 335% Global disease with 30,000-35,000affected in U.S. and Europe alone TOPAZ* 12-month results showed transformative potential in non-ambulatory Type 2 and 3 patients Represents ~2/3 of overall patient population Motor neuron impairment and loss due to SMN genetic deficiency, leading to muscle atrophy and weakness *TOPAZ Phase 2 trial evaluated patients with Type 2 and 3 SMA (did not include Type 1)Lallyet al, OrphanetJournal of Rare Diseases, 2017

6 Potential to Pioneer a New Treatment Era: Opportunity forMuscle-Directed Therapy to Complement SMN Upregulators Phase 3Trial Design Indication MarketPenetration Non-ambulatory Type 2/32-12 years of agePrimary endpoint: Mean change from baseline in HFMSE at 15 months >11,000* patients treated WW$2+ billion in revenues (LTM) ~1,200*** patients treated WW~$1.1 billion in revenues (LTM) ~3,000** patients treated WW~CHF135 million in revenues (LTM) Type 1, 2, and 3 SMA in pediatricand adult patients Type 1, 2, 3 SMA in patients 2 months of age and older SMA in patients less than 2 years ofage Non-ambulatory Type 2/32-25 years of agePrimary endpoint: Mean change from baseline in MFM-32 at 12 months Infantile-onset Type 1<6 months of agePrimary endpoints: Ability to sit independently and event-free survival *As of 1Q21 financial update on 4/22/21; includes patients treated worldwide in post-marketing setting, expanded access program, and clinical trials.**As of 1Q21 financial update on 4/21/21; includes patients treated worldwide between clinical trials, commercial, and compassionate use program.***As of 1Q21 financial update on 4/27/21; commercially, via managed access programs and in clinical trials HFMSE = Hammersmith Functional Motor Scale Expanded; MFM-32 = Motor Function Measure – 32 items Patients continue to experience major functional impairments despite utilization of SMN upregulators

Apitegromab: Muscle-Directed Therapy Aimed at Complementing SMN Upregulators 7 Myostatin is a negative regulatorof skeletal muscle growthApitegromab is a fully human, mAb that specifically binds to proforms of myostatin and inhibits myostatin activation Apitegromab is a muscle-directed approach aimed at improving motor function Adapted from images courtesy of the SMA Foundation Apitegromab SMN upregulators prevent further degeneration of motor neurons...but do not directly address muscle atrophy Motor neurondegeneration Muscle fiber atrophy

Cure SMA Jill Jarecki, PhDCSO June 15, 2021

Cure SMA We fund groundbreaking research and provide families thesupport they need for today.Annual budget of $15M$85 Million in research funding 36 Chapters in the US9,000 affected individuals in membership database300 newly diagnosed contacts annuallyNewly diagnosed care and info packetsInfo on clinical trial recruitment4,000 families obtain services annuallyAnnual conference, with 2500 attendees

The Evolving Landscape in SMA The FDA-approval of 3 new therapies has revolutionized and dramatically changed the natural history of SMAEarly identification and treatment dramatically alter long-termoutcomes, most strikingly presymptomaticallySymptomatic treatment providing improvements through increases,stabilization, and slowingMany unmet needs remain when addressing the complexities of SMAUnmet need is higher in older patients compared to younger patients.
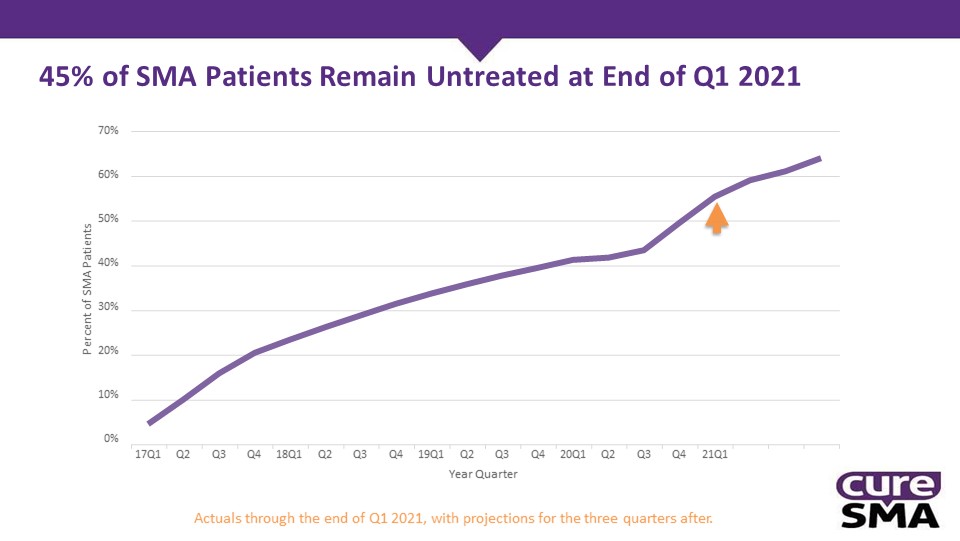
45% of SMA Patients Remain Untreated at End of Q1 2021 Percent of SMA Patients 70%60%50%40%30%20%10%0%17Q1 Q2 Q3 Q4 18Q1 Q2 Q3 Q4 19Q1 Q2 Q3 Q4 20Q1 Q2 Q3 Q4 21Q1Year QuarterActuals through the end of Q1 2021, with projections for the three quarters after.

Almost Half of Those with SMA Type I Currently Sit without Support 12.90 % 21.90 % 35.37 % 37.66 % 44.64 % 87.10% 78.08% 64.63% 62.30% 55.36% 100%90%80%70%60%50%40%30%20%10%0% 2017 (n=93) 2019 (n=147) 2020 (n=231) 2021 (n=56) 2018 (n=146)Sit without Support Cannot sit without support

Can Stand With or Without Support Currently among SMA Type II 10.94% 11.44% 17.05% 18.36% 89.06% 88.56% 82.95% 81.64% 100%90%80%70%60%50%40%30%20%10%0% 2017(n=265) 2018(n=271) 2019(n=258) 2020(n=414) Can stand (with or without) support Cannot stand (with or without) support2017 & 2018: Question was what is your maximum current motor function. Assumed able to stand with or without support if any of the following choices were picked: walk alone, walk with assist, cruise along furniture, stand without support, or stand with support;2019 & 2020: Respondents were asked to answer yes or no if affected child could currently can stand with assistance or stand alone.

What Comes Next - SMA is Not Cured Yet Need More Impact for older ages and stage of SMADifferent for symptomatic vs NBS patientsSlow to Stop to Reverse Reverse – Restore Function -FutureStop Progression – Prevent SymptomsSlower Progression -ImprovementNatural History - Untreated

Unmet Needs that Future Therapies will Address – From Adults in the 2020 Community Update Survey 75% 75% 81%80% 71% 29% 89% 89% 81%82%80% 39% 31% 94%94%98% 90% 15% 94% 94% 94% 100%90%80%70%60%50%40%30%20%10%0% Reducing Fatigue Improving breathing function Improving swallowing Gaining muscle strength Achieving new motor function Improving Improving communication activities of daily through speech living and/or technology Type I Type II Type III

NeuroprotectionNeural transmissionRegenerative targetsMuscle enhancementApitegromab - Scholar RockGenetic modifiersCombinations of above with SMNenhancer Therapeutic Strategies – SMN Independent

Thank You!

Cure SMA Jill Jarecki, PhDCSO June 15, 2021

Apitegromab Showed Transformative Potential in SMA Phase 2 Trial Yung Chyung, M.D.Chief Medical Officer

TOPAZ: Evolving Understanding of Apitegromab’sTransformative Potential in Type 2 and Type 3 SMA June 2021Additional Analyses April 202112-month top-line October 20206-month interim Showed Initial Proof-of-Concept Interim data showed the therapeutic potential of apitegromab in Type 2 and 3 SMA as add-on therapy to background nusinersenHFMSE increases in patients who had already received on average ~2 years of background nusinersen therapyMeaningful HFMSE gains over 6-month time frame Further Support for Efficacy Signal Largest HFMSE increases in non-ambulatory Type 2 and 3 patients; represents ~2/3 of SMA prevalenceDurability of effect with continued improvement in a subset of patientsSupports advancing to a Phase 3 trialAnticipated focus on patients with non- ambulatory Type 2 and 3 2021 √ √ √ Additional exploratory analyses to be presented at future medical congresses… Further Support TherapeuticPotential and Phase 3 Plans Additional insights from exploratory analyses offer deeper understanding of apitegromab’s potential profile:Age of patientsDuration of prior background therapySecondary efficacy endpoint (WHO Motor Milestones) 20

21 TOPAZ Top-Line Data Showed Apitegromab’sTransformative Potential in Patients with Type 2/3 SMA ✔ Apitegromab treatment (as add-on to background nusinersen) led to improvements inHFMSE in both non-ambulatory cohorts * Pooled cohorts of non-ambulatory patients treated with apitegromab 20 mg/kg and 2 mg/kg**Non-ambulatory patients who initiated background nusinersen at a young age of <5 years and treated with apitegromab 20 mg/kg dose At 12 months Mean HFMSE increase ≥1-point increase ≥3-point increase Initiated background nusinersen age <5** +7.1 points 88% (7/8) of patients 63% (5/8) of patients Initiated background nusinersen age ≥5 +0.6 points 64% (9/14) of patients 29% (4/14) of patients ✔ Majority of non-ambulatory patients observed a clinical improvement in HFMSE* 20151050-5-10 HFMSE change from baseline

Evaluating range of exploratory analyses to better understand the therapeutic responseInitial findings from non-ambulatory cohorts:HFMSE improvements observed across age range with relatively larger gains from earlier treatmentDuration of prior nusinersen treatment not correlated with HFMSE increaseProvides further support that improvements may be attributable to apitegromabPatients were already in chronic maintenance phase of nusinersen at enrollmentAchievement by some patients of WHO motor milestones (additional high bar efficacy endpoint) further shows apitegromab’s potentialTotal of 7 patients gained new WHO motor milestones across both non-ambulatory cohorts1 patient* gained 3 milestones (hands & knees crawling, standing with assistance, walking with assistance)1 patient** gained 2 new milestones (hands & knees crawling, standing with assistance)Phase 3 trial in patients with non-ambulatory Type 2 and 3 anticipated to initiate by end of 2021*initiated nusinersen age <5, apitegromab 20 mg/kg 22**initiated nusinersen age ≥5 Additional TOPAZ Analyses Further SupportApitegromab’s Potential to Improve Motor Function
23 Expectations for Patients on BackgroundSMN Upregulator Therapy Yung Chyung, M.D. Chief Medical Officer

Patients with Type 2 and 3 SMA Continue to Experience MajorFunctional Deficits Despite Improvement from Nusinersen 24 Darras, B., et.al. Nusinersen in later-onset spinal muscular atrophy. Neurology. May 2019; 92 (21) e2492-e2506.This third-party information is provided for background only and is not intended to convey or imply a comparison to the TOPAZ clinical trial results. 3.9-point increase in HFMSE from nusinersen 0Mean improvement in HFMSE experienced by patients withnon-ambulatory Type 2/3 SMA in nusinersen Phase 3 CHERISH trial 20 40 HFMSE Score at Month 15 80Total Possible HFMSE Scoreof 6660 SMN upregulator treated patients continue to experience major functional deficits…

†Mercuri E, et.al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N Engl J Med. 2018;378:625-635.This third-party information is provided for background only and is not intended to convey or imply a comparison to the TOPAZ clinical trial results. CHERISH Trial in Non-Ambulatory Type 2/3 SMA† Majority of patients treated with nusinersen after the age of 5 did not observe an improvement Nusinersen Does Not Increase HFMSE on Average inChildren Who Initiate Treatment After the Age of 5 Years 25

Plateauing of HFMSE Increases Observed After First 15Months of Nusinersen Treatment in Type 2 and 3 SMA 26 “Longer-term treatment with nusinersen: results in later-onset spinal muscular atrophy from the SHINE study” P.257, World Muscle Society Congress 2020This third-party information is provided for background only and is not intended to convey or imply a comparison to the TOPAZ clinical trial results. Most nusinersen-treated patients in CHERISH were <5 years of age at therapy initiation Mean (+ SE) Change in HFMSE Total Score From Baseline 1 92 169 253 350 450 690 930Analysis Visit, days 1170 1410 1650 876543210-1-2-3-4 Nusinersen observed plateauing of improvement during chronic maintenance phase… <1-point increase in HFMSE afterfirst year of treatment +3.9-points +4.6-points Unmet Need for Motor Function Gains Initial treatmentCHERISH Chronic maintenance phaseSHINE
27 Review of Positive TOPAZ Top-Line Results Yung Chyung, M.D. Chief Medical Officer

Apitegromab Phase 2 Trial Design 28 Patients with Type 2 and 3 SMA Ambulatory Type 3 patients (ages 5-21)Apitegromab 20 mg/kg IV Q4W monotherapy or withchronic nusinersen maintenance Key objectives: RHS and safety at 12 months Non-ambulatory Type 2 patients (ages ≥2) on chronicmaintenance nusinersen (initiated <5 years of age)Apitegromab 2 mg/kg and 20 mg/kg IV Q4W + nusinersen Key objectives: HFMSE and safety at 12 months Non-ambulatory Type 2/3 patients (ages 5-21) on chronicmaintenance nusinersen (initiated ≥5 years of age)Apitegromab 20 mg/kg IV Q4W + nusinersen Key objectives: HFMSE and safety at 12 months Patients on background SMN therapy were in chronic maintenance phase of nusinersen(~5 mean maintenance doses at baseline) *Excludes one patient from Cohort 1 that discontinued from the trial All 57* patients who completed the 12-month trial elected to opt into the extension period

Baseline CharacteristicsNusinersen-treated patients well into chronic maintenance phase 29 Non-Ambulatory,Ages ≥2 and initiated nusinersen <5 years Non-Ambulatory,Ages 5-21 Ambulatory,Ages 5-21 20 mg/kg+nusinersen 2 mg/kg+nusinersen Pooled 20 mg/kg+nusinersen 20 mg/kg monotherapy 20 mg/kg+nusinersen Pooled N 10 10 20 15 11 12 23 Mean age at baseline (min, max) 3.8 (2, 6) 4.1 (2, 6) 4.0 (2, 6) 11.7 (8, 19) 12.1 (7, 19) 13.1 (7, 21) 12.6 (7, 21) Mean RHS score (min, max) 47.6 (26, 63) 51.3 (43, 62) 49.6 (26, 63) Mean HFMSE score (min, max) 23.5 (14, 42) 26.1 (12, 44) 24.8 (12, 44) 22.7 (13, 39) Mean # of nusinersen maintenance doses (min, max) 5.4 (3, 8) 5.5 (2, 9) 5.5 (2, 9) 5.1 (2, 9) N/A 5.6 (2, 8) N/A SMN2 Gene Copy* (#, %) 2 1 (10%) 1 (10%) 2 (10%) 1 (9%) 0 (0%) 1 (4%) 3 8 (80%) 8 (80%) 16 (80%) 11 (73%) 4 (36%) 9 (75%) 13 (57%) 4 0 (0%) 1 (10%) 1 (5%) 2 (13%) 4 (36%) 1 (8%) 5 (22%) Discontinuation(s) 0 0 0 0 0 1** 1** *Data not available for all patients**Patient who discontinued study for reasons unrelated to study drug HFMSE=Hammersmith Functional Motor Scale Expanded; RHS=Revised Hammersmith Scale Data on file. Scholar Rock, Inc. Cambridge, MA

Patients Enrolled in TOPAZ Already in Chronic MaintenancePhase of Nusinersen Treatment 30 *Reflects non-ambulatory cohorts in TOPAZ**The HFMSE time course plot for background nusinersen effect is hypothetical and intended for illustrative purposes only. The data presented here do not reflect any cross-trial comparisons. TOPAZ was not a placebo-controlled trial, it is not possible to draw direct conclusions in relation to background nusinersen effects alone. Time** Initial treatment phase of nusinersen Chronic maintenance phase ofnusinersen�� HFMSE TOPAZ patients in chronic maintenance phase of nusinersen therapy~2 years at enrollment~3 years at 12-month efficacy timepointTOPAZ baseline meanHFMSE score*: 22.7-26.1 CONCEPTUAL

Non-Ambulatory Type 2 Cohort:Initiated nusinersen age <5 31 Apitegromab (20 mg/kg) + nusinersen n=8 Mean change from baseline in HFMSE(95% CI) +7.1(1.8, 12.5) # (%) patients achieving: ≥1-pt increase in HFMSE 7/8 (88%) ≥3-pt increase in HFMSE 5/8 (63%) ≥5-pt increase in HFMSE 5/8 (63%) Baseline characteristics: mean (min, max) n=10 Age 3.8 (2, 6) HFMSE score 23.5 (14, 42) # of nusinersen maintenance doses 5.4 (3, 8) Sizable increases in HFMSE observed in patients already treated with chronic maintenance nusinersen88% (7/8) improved63% (5/8) with ≥5-point increase38% (3/8) with >10-point increaseContinuous and durable improvements observed through 12-months of treatment Data on file. Scholar Rock, Inc. Cambridge, MA

Non-Ambulatory Type 2/3 Cohort:Initiated nusinersen age ≥5 Apitegromab (20 mg/kg) + nusinersen Per Protocol Population* (n=13) Intent-to-Treat Population (n=14) Mean change from baseline in HFMSE (95% CI) +1.2(-0.5, 2.9) +0.6(-1.4, 2.7) # (%) patients achieving: ≥1-pt increase in HFMSE 9/13 (69%) 9/14 (64%) ≥3-pt increase in HFMSE 4/13 (31%) 4/14 (29%) ≥5-pt increase in HFMSE 2/13 (15%) 2/14 (14%) Baseline characteristics: mean (min, max) n=15 Age 11.7 (8, 19) HFMSE score 22.7 (13, 39) # of nusinersen maintenance doses 5.1 (2, 9) 32 Majority of patients improved in HFMSE (despite initiating background nusinersen age ≥5)~2/3 with ≥1-point increase~30% with ≥3-point increaseDurability of effect observedthrough 12-months of treatment *Patient had concomitant exposure to an acetylcholinesterase inhibitor, which was not permitted per the TOPAZ trial protocolData on file. Scholar Rock, Inc. Cambridge, MA

TOPAZ Results SuppPhase 3 Trial ort Evaluation of Apitegromab in Treatment-emergent adverse events (TEAEs) Apitegromab 2 mg/kg (n=10) Apitegromab 20 mg/kg (n=48) Total (n=58) Any TEAE 9 (90.0%) 44 (91.7%) 53 (91.4%) Any Serious TEAE 1 (10.0%) 4 (8.3%) 5 (8.6%) Any TEAE leading to study drug discontinuation 0 (0.0%) 1 (2.1%) 1 (1.7%) Any Grade 3 (severe) or higher TEAE 0 (0.0%) 3 (6.2%) 3 (5.2%) 33 Treatment-emergent adverse events (TEAEs) are defined as AEs that start after the first dose of study drug or start prior to the administration of study drug and worsen in severity/grade or relationship to investigational medication after the administrat ion of study drug.*TEAE rates are across all patients in TOPAZ trialData on file. Scholar Rock, Inc. Cambridge, MA Five most frequently reported TEAEs*: Headache (24%), pyrexia (22%), upper respiratory tract infection (22%), cough (22%), and nasopharyngitis (21%).SAEs, Grade 3 AEs and AE leading to early study discontinuation were all assessed by investigators as unrelated to study drugAnti-drug antibodies (ADA) were present at low titers following apitegromab treatment in 3 out of 58 enrolled patients. No apparent impact on drug exposure was observed and was not associated with any hypersensitivity reactions.Incidence and severity of AEs were consistent with the underlying patient population and background therapy

Serious and Severe Treatment-Emergent Adverse Events(TEAEs) 34 Treatment-emergent adverse events (TEAEs) are defined as AEs that start after the first dose of study drug or start prior to the administration of study drug and worsen in severity/grade or relationship to investigational medication after the administration of study drug. Data on file. Scholar Rock, Inc. Cambridge, MA Serious TEAEs; All Assessed by Trial Investigators as Unrelated to Apitegromab 2 mg/kg:Cohort 3: 1 patient hospitalized due to adenoidal and tonsillar hypertrophy and scheduled adenotonsillectomy (Grade 2).Resolved without sequelae.20 mg/kg:Cohort 1: 2 patients with gait inability considered a significant disability (both Grade 3). Events remain ongoing.Cohort 1: 1 patient hospitalized with post lumbar puncture syndrome (Grade 2). Resolved without sequelae.Cohort 1: 1 patient hospitalized due to viral upper respiratory infection (Grade 2/prior history). Resolved without sequelae. Other Severe TEAE; Assessed by Trial Investigator as Unrelated to Apitegromab Cohort 1: 1 patient presented with post lumbar puncture syndrome (non-serious Grade 3). Resolved without sequelae. Study Discontinuation; Assessed by Trial Investigator as Unrelated to Apitegromab Cohort 1: 1 patient withdrew consent after ~2 months in the trial. Grade 2 leg muscle fatigue (developed prior to enrollment).

35 Additional Exploratory Analyses Further Support Apitegromab’s Potential Additive Benefit on Top of Nusinersen Yung Chyung, M.D.Chief Medical Officer

HFMSE Improvements Observed Across Age Range of Non-AmbulatoryPatients with Relatively Larger Gains from Earlier Treatment *Pooled cohorts of non-ambulatory patients treated with apitegromab 20 mg/kg and 2 mg/kg; excludes 4 patients who each missed 3 doses of apitegromab due to COVID-19-related site access restrictions and were not included in the primary (intent-to-treat) analysis.Data on file. Scholar Rock, Inc. Cambridge, MA HFMSE change from baseline Youngest(2 years) Oldest(19 years) Age of patient at baseline in TOPAZ 36

Increases in HFMSE Not Correlated with Duration of PriorNusinersen Treatment Change in HFMSE Not Correlated With Number ofNusinersen Maintenance Doses(post-hoc analysis of TOPAZ non-ambulatory patients) Further data suggesting increases inHFMSE may be attributable to apitegromab No correlation between duration of priornusinersen treatment and change in HFMSEPatients in TOPAZ were already in chronicmaintenance phase of nusinersen (mean of~2 years at enrollment) Data on file. Scholar Rock, Inc. Cambridge, MA -10 -5 0 5 10 15 20 HFMSE change from baseline 2(~10 months) 9(~3 years) # of maintenance nusinersen doses5(~2 years) 37

Clinical Outcome Measures: Progressive Levels of Difficultyin Measuring Gross Motor Functions 38 WHO Motor Milestones – Different and MoreChallenging Tests of Self-Sufficient Locomotion 6 gross motor skills considered to be universal* Sitting without support – head erect for at least 10seconds; no use of arms or hands to balanceHands and knees crawling – at least 3 movements in a row and stomach does not touch supporting surfaceStanding with assistance – upright on both feet for at least 10 seconds without leaning on any objectWalking with assistance – takes at least 5 steps holding astable objectStanding alone – at least 10 seconds with no contact withperson or objectWalking alone – takes at least 5 steps independently HFMSE - Validated Regulatory EndpointUsed in SMA Trials 33 distinct measures of an individual’s abilityto perform various activitiesTotal achievable score of 66Quality and execution of each movement is ranked on a scale of 0, 1, 2 0 - cannot perform the task1 – can perform task but with adaptation2 – can perform task Examples of HFMSE tasks: Raising hand(s) to head in sittingLifting head from proneRolls prone to supineHigh kneeling to half kneelAscending/descending 4 stairs For complete descriptions of the 6 WHO motor development milestones, please refer to https://cdn.who.int/media/docs/default -source/child- growth/child-growth-standards/indicators/motor-development-milestones/assessment-of-gross-motor-development-in-the-who- multicentre-growth-reference-study.pdf?sfvrsn=81277ea7_0
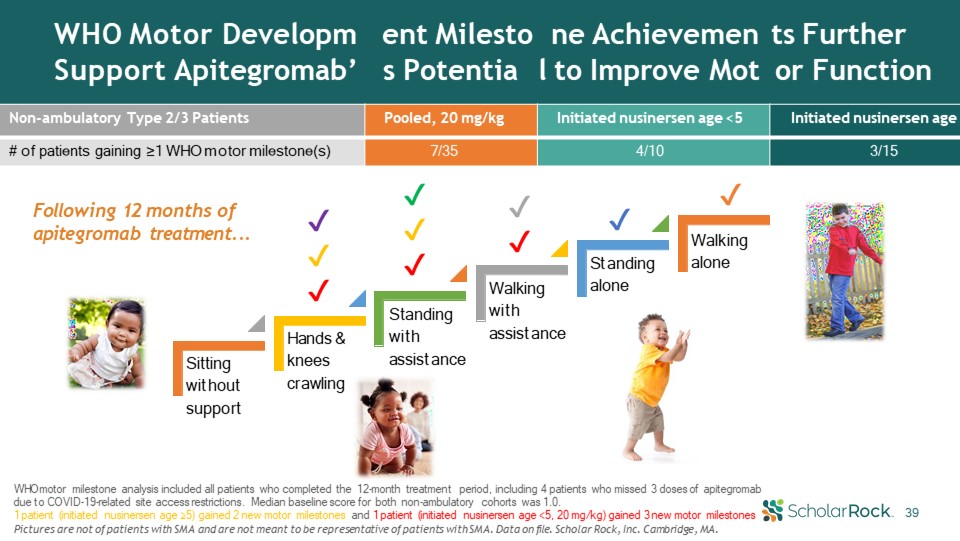
WHO Motor DevelopmSupport Apitegromab’ ent Milestos Potentia ne Achievemenl to Improve Mot ts Furtheror Function Non-ambulatory Type 2/3 Patients Pooled, 20 mg/kg Initiated nusinersen age <5 Initiated nusinersen age ≥5 # of patients gaining ≥1 WHO motor milestone(s) 7/35 4/10 3/15 39 WHO motor milestone analysis included all patients who completed the 12-month treatment period, including 4 patients who missed 3 doses of apitegromab due to COVID-19-related site access restrictions. Median baseline score for both non-ambulatory cohorts was 1.0.1 patient (initiated nusinersen age ≥5) gained 2 new motor milestones and 1 patient (initiated nusinersen age <5, 20 mg/kg) gained 3 new motor milestonesPictures are not of patients with SMA and are not meant to be representative of patients with SMA. Data on file. Scholar Rock, Inc. Cambridge, MA. Sitting without support Hands & knees crawling Standing with assistance Walking with assistance Standing alone Walkingalone ✔✔ ✔✔✔ ✔✔✔ ✔ ✔ Following 12 months ofapitegromab treatment...
Apitegromab to Advanceto Phase 3 Trial in Patients with Non-Ambulatory Type 2/3 SMA Yung Chyung, M.D.Chief Medical Officer

41 Initial Development Strategy Focuses on Non- Ambulatory Patients on Background SMN Upregulators Global disease with30,000-35,000 affected inU.S. and Europe alone A Ambulatory patients Smaller population but high unmet need as benefits of SMN regulators not well-establishedTOPAZ suggests potential clinical benefit in a subset of patients C Type 1 patients, including those treated with gene therapyHighest incidence population and growing prevalence due toSMN upregulator treatmentTOPAZ showed benefits of early treatment suggestingpotential in Type 1 patients B Type 114% Type 251% Type 335% Apitegromab in non-ambulatory Type 2 and 3 with background SMN upregulatorsRepresents 2/3 of overall patientsMany patients already treated with or areeligible for SMN upregulator therapyImprovements in motor function on top of SMN upregulators observed in TOPAZ Anticipated Focus of Phase 3 Trial

42 Preliminary Thoughts on Apitegromab Phase 3 Trial Design Design Subjects Key Objectives Timeline Non-ambulatory Type 2 and Type 3 SMAPediatric population in chronic maintenance phase of SMN therapy HFMSESafety Aim to initiate by end of 2021 Randomized, double-blind, placebo-controlled12-month treatment periodApitegromab IV Q4W as add-on to nusinersen or risdiplamTOPAZ data support investigation of up to 20 mg/kg Apitegromab recently received Fast Track (FDA) and PRIME (EMA)designations, recognizing unmet medical needs in SMA Phase 3 trial design subject to regulator interactions and feedback
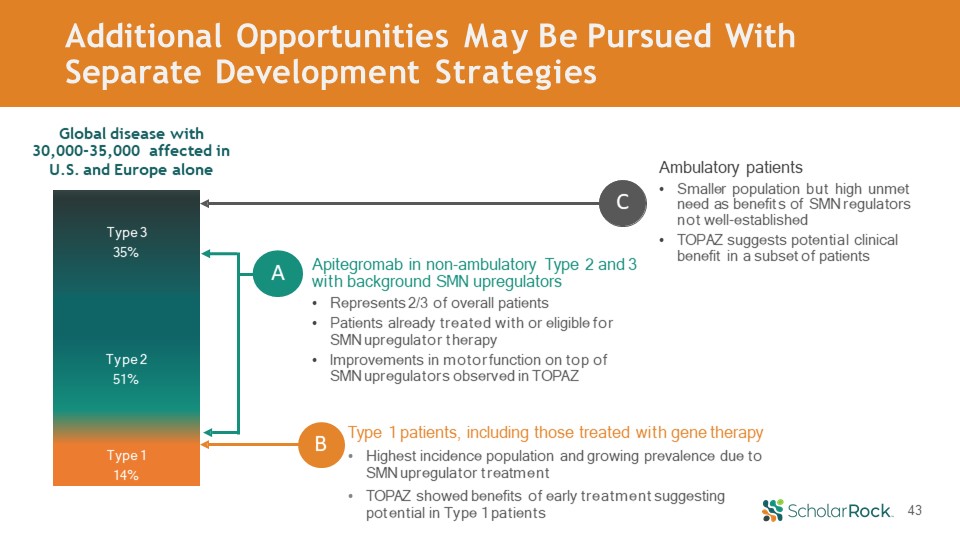
43 Additional Opportunities May Be Pursued With Separate Development Strategies Global disease with30,000-35,000 affected inU.S. and Europe alone A Ambulatory patients Smaller population but high unmet need as benefits of SMN regulators not well-establishedTOPAZ suggests potential clinical benefit in a subset of patients C Type 1 patients, including those treated with gene therapyHighest incidence population and growing prevalence due toSMN upregulator treatmentTOPAZ showed benefits of early treatment suggestingpotential in Type 1 patients B Type 114% Type 251% Type 335% Apitegromab in non-ambulatory Type 2 and 3 with background SMN upregulatorsRepresents 2/3 of overall patientsPatients already treated with or eligible forSMN upregulator therapyImprovements in motor function on top of SMN upregulators observed in TOPAZ

Panel Discussion onApitegromab’s Therapeutic Potential in SMA Thomas Crawford, M.D.Johns Hopkins Medicine Basil Darras, M.D.Boston Children’s HospitalHarvard Medical School

Esteemed Panelists: TOPAZ Trial Investigators Member of the Department of Neurology at Johns Hopkins since 1987.Practice involves general child neurology with a principal interest in caring for children with neuromuscular, neuromotor, and ataxic disorders.On the Medical and Scientific Advisory Boards of Families of Spinal Muscular Atrophy, and theMedical Advisory Committee for the MuscularDystrophy Association. Thomas Crawford, MDCo-Director, MDA Clinic and Professorof Neurology and Pediatrics, Johns Hopkins MedicineLead TOPAZ Principal Investigator Chief of the division of clinical neurology in the Department of Neurology at Boston Children’s Hospital.Director of Neuromuscular Center and SpinalMuscular Atrophy program.Special focus is in the care of children with neuromuscular conditions originating from inherited or acquired conditions of the motor unit. Basil Darras, MDAssociate Neurologist-in-Chief, Boston Children’s Hospital and Professor of Neurology, Harvard Medical SchoolTOPAZ Trial Investigator 45

Thank You for Participating! Pictures of individuals with SMA courtesy of Cure SMA 46

Appendix

Majority of Ambulatory Patients Maintained or Improved inRHS Score from Baseline 48 Apitegromab 20 mg/kg monotherapy Apitegromab 20 mg/kg + nusinersen Mean change from baseline in RHS (95% CI) -0.4 (-3.9, 3.1) -0.3 (-2.0, 1.4) # (%) patients achieving: ≥0-pt increase in RHS 6/11 (55%) 7/12 (58%) ≥1-pt increase in RHS 4/11 (36%) 5/12 (42%) ≥3-pt increase in RHS 3/11 (27%) 2/12 (17%) Baseline characteristics: mean (min, max) n=11 n=12 Age 12.1 (7, 19) 13.1 (7, 21) HFMSE score 47.6 (26, 63) 51.3 (43, 62) # of nusinersen maintenance doses n/a 5.6 (2, 8) Majority maintained or improved57% (13/23) with ≥0-point increase39% (9/23) with ≥1-point increaseUp to 8-point increase observedResults contrast with declines typically observed with natural history of ambulatory patients Data on file. Scholar Rock, Inc. Cambridge, MA

Non-Ambulatory Type 2 Cohort (Age ≥2 years):Dose Response Observed in PD and Efficacy Data Mean (±SEM) change from baseline 20 mg/kg dose numerically offered greater HFMSE increasesthan 2 mg/kg dose across all timepointsDurability of effect observed through 12-months of treatment Greater target engagement and efficacy observed with 20 mg/kg Both 2 mg/kg and 20 mg/kg doses yielded high levels oftarget engagement (>100-fold increase from baseline)20 mg/kg offered relatively higher magnitude of targetengagement 1 10 100 1000 0 28 56 84 112 140 168 196 224 252 280 308 336 364Time (days) Mean (±SD) Latent Myostatin Concentration (ng/mL) TOPAZ Cohort 3 (2 TO Apitegromab achieved robust target engagement10000 Sizable increases in HFMSE achieved by patients on chronic maintenance nusinersen Data on file. Scholar Rock, Inc. Cambridge, MA 49
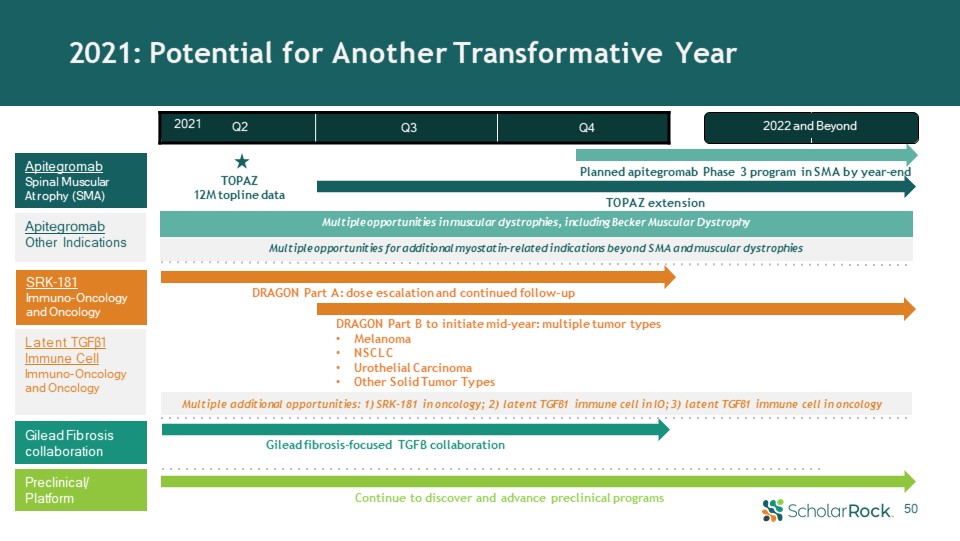
50 Gilead fibrosis-focused TGFβ collaboration DRAGON Part A: dose escalation and continued follow-up Apitegromab Spinal Muscular Atrophy (SMA) SRK-181Immuno-Oncology and Oncology Preclinical/ Platform TOPAZ12M topline data Planned apitegromab Phase 3 program in SMA by year-end 2021: Potential for Another Transformative Year TOPAZ extension Continue to discover and advance preclinical programs Multiple opportunities for additional myostatin-related indications beyond SMA and muscular dystrophies Multiple additional opportunities: 1) SRK-181 in oncology; 2) latent TGFβ1 immune cell in IO; 3) latent TGFβ1 immune cell in oncology Gilead Fibrosis collaboration 2022 and Beyond 2021 Q2 Q3 Q4 Latent TGFβ1 Immune Cell Immuno-Oncology and Oncology DRAGON Part B to initiate mid-year: multiple tumor typesMelanomaNSCLCUrothelial CarcinomaOther Solid Tumor Types ApitegromabOther Indications Multiple opportunities in muscular dystrophies, including Becker Muscular Dystrophy