UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
_________________________________________________________________________________________________________________________________
FORM 10-K | | | | | |
| ☒ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934. |
For the fiscal year ended December 31, 2024. | | | | | |
| ☐ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934. |
For the transition period from to .
Commission file number: 001-38900
_______________________________________________________________________________________________________________________________________
THE PENNANT GROUP, INC.
(Exact Name of Registrant as Specified in Its Charter) | | | | | |
| Delaware | 83-3349931 |
| (State or Other Jurisdiction of | (I.R.S. Employer |
| Incorporation or Organization) | Identification No.) |
1675 East Riverside Drive, Suite 150, Eagle, ID 83616
(Address of Principal Executive Offices and Zip Code)
(208) 506-6100
(Registrant’s Telephone Number, Including Area Code)
__________________________________________________________________________________________________________________________________________________
Securities registered pursuant to Section 12(b) of the Exchange Act:
| | | | | | | | |
| Title of each class | Trading Symbol(s) | Name of each exchange on which registered |
| Common Stock, par value $0.001 per share | PNTG | Nasdaq Global Select Market |
Securities registered pursuant to Section 12(g) of the Exchange Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. ☒Yes ☐No
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. ☐ Yes ☒ No
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. ☒ Yes ☐ No
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). ☒ Yes ☐ No
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act: | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Large accelerated filer | ☐ | Accelerated filer | ☒ | Non-accelerated filer | ☐ | Smaller reporting company | ☐ | Emerging growth company | ☐ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☒
If securities are registered pursuant to Section 12(b) of the Exchange Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). ☐
Indicate by a check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). ☐ Yes ☒ No
As of February 24, 2025, 34,429,989 shares of the registrant’s common stock were outstanding. The aggregate market value of the shares of common stock held by non-affiliates of the registrant on the last business day of the registrant's most recently completed second fiscal quarter (June 30, 2024) was approximately $669,703,000 based upon the closing price of the common stock on such date. For purposes of this calculation, the registrant has excluded the market value of all common stock beneficially owned by all executive officers and directors of the registrant.
Note on Incorporation by Reference
Part III of this Form 10-K incorporates information by reference from the Registrant's definitive proxy statement on Schedule 14A for the Registrant's 2025 Annual Meeting of Stockholders to be filed within 120 days after the close of the fiscal year covered by this annual report.
THE PENNANT GROUP, INC.
ANNUAL REPORT ON FORM 10-K
FOR THE FISCAL YEAR ENDED DECEMBER 31, 2024
TABLE OF CONTENTS | | | | | | | | | | | | |
| | | Part I. | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | Part II. | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | Part III. | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | Part IV. | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | |
| | | |
| | | |
| | | |
| | | |
| | | | |
| | | | |
| | | |
Cautionary Note Regarding Forward-Looking Statements
Our reports, filings and other public announcements, including this Annual Report on Form 10-K may from time to time contain statements that do not directly or exclusively relate to historical facts. Such statements are “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, and typically include, but are not limited to, our expected future financial position, results of operations, cash flows, financing plans, business strategy, budgets, capital expenditures, competitive positions, growth opportunities and plans and objectives of management. Forward-looking statements can often be identified by words such as “anticipate,” “expect,” “intend,” “plan,” “predict,” “believe,” “seek,” “estimate,” “may,” “will,” “should,” “would,” “could,” “potential,” “continue,” “ongoing,” similar expressions, and variations or negatives of these words. These statements are subject to the safe harbors created under the Securities Act of 1933, as amended (the “Securities Act”), and the Securities Exchange Act of 1934, as amended (the “Exchange Act”). These statements are not guarantees of future performance and are subject to risks, uncertainties and assumptions that are difficult to predict. Therefore, our actual results could differ materially and adversely from those expressed in any forward-looking statements as a result of various factors, some of which are listed in Part I, Item 1A., Risk Factors, of this Annual Report on Form 10-K for the year ended December 31, 2024. Accordingly, you should not rely upon forward-looking statements as predictions of future events. These forward-looking statements speak only as of the date of this Annual Report, and are based on our current expectations, estimates and projections about our industry and business, management's beliefs, and certain assumptions made by us, all of which are subject to change. We undertake no obligation to revise or update publicly any forward-looking statement for any reason, except as otherwise required by law.
As used in this Annual Report on Form 10-K, the words, “Pennant,” “Company,” “we,” “our” and “us” refer to The Pennant Group, Inc. and its consolidated subsidiaries. All of our independent operating subsidiaries, and the Service Center (defined below) are operated by separate, wholly-owned, independent subsidiaries that have their own management, employees and assets. References herein to the consolidated “Company” and “its” assets and activities, as well as the use of the terms “we,” “us,” “our” and similar terms in this Annual Report are not meant to imply, nor should they be construed as meaning, that The Pennant Group, Inc. has direct operating assets, employees or revenue, or that any of the subsidiaries are operated by The Pennant Group, Inc.
The Pennant Group, Inc. is a holding company with no direct operating assets, employees or revenues. In addition, certain of our wholly-owned independent subsidiaries, collectively referred to as the “Service Center,” provide centralized accounting, payroll, human resources, information technology, legal, risk management, compliance oversight and other services to the other independent operating subsidiaries through contractual relationships with such subsidiaries.
The address of our headquarters is 1675 East Riverside Drive, Suite 150, Eagle, ID 83616, and our telephone number is (208) 506-6100. Our corporate website is located at www.pennantgroup.com. The information contained in, or that can be accessed through, our website does not constitute a part of this Annual Report on form 10-K.
Part I.
Item 1. Business
Overview
The Pennant Group, Inc. is a leading provider of high-quality healthcare services to patients or residents of all ages, including the growing senior population, in the United States. Through our innovative operating model and unique core values, we strive to be the provider of choice in the communities we serve.
As of December 31, 2024, we operate multiple lines of business, including home health, hospice and senior living, throughout Arizona, California, Colorado, Idaho, Montana, Nevada, Oklahoma, Oregon, Texas, Utah, Washington, Wisconsin and Wyoming. We also provide home health and hospice operational support through a management service agreement in Connecticut. We provide home health and hospice services through 123 agencies, and senior living services at 57 communities with 3,960 total units in our assisted living, independent living and memory care business. We derive revenue from a diversified blend of payors including Medicare and Medicaid programs, private pay patients and residents, and managed care payors.
We believe our key differentiators are our (1) ability to recruit, train, and develop talented local leaders at each of our operations; (2) innovative operating model that empowers those leaders to make decisions that meet the needs of patients and residents, employees, referral sources and the communities they serve with the support of our service center; (3) disciplined growth strategy; and (4) ability to achieve quality care outcomes in cost effective settings. In our experience, healthcare is a local endeavor, largely dependent upon personal and professional relationships, community reputation and an ability to adapt to the changing needs of patients, residents, partners and communities. As our operational leaders build strong relationships with key partners in their local communities, they are empowered to make informed and critical operational decisions that produce quality care outcomes and more effectively meet the needs of our patients and residents.
We believe our home health and hospice businesses achieve quality outcomes—as measured by multiple industry and value-based metrics (such as hospital readmission rates)—in cost-effective settings. We believe our senior living business is able to offer our residents a safe and tailored quality-of-life at an affordable cost, thus appealing to a broad population. With our platform of diversified service offerings, we believe that we are well-positioned to take advantage of favorable demographic shifts as well as industry trends that reward providers offering quality care in lower cost settings.
Our Innovative Operating Model
Our innovative operating model is the foundation of our superior performance and success. Our operating model is founded on two core principles: (1) healthcare is a local business where providers are most successful when key operational decision-making meets local community needs and occurs close to patients or residents and employees, and (2) peer accountability from operational and resource partners is more effective at driving excellent clinical and financial results than traditional hierarchical or “top-down” accountability structures.
Our model is innovative because each operation functions under the direction of local clinical and operational leaders, each of whom is empowered to make decisions based on the unique needs of the patients or residents, partners and communities they serve. This is in contrast to typical models where control and key decision-making is centralized at the corporate level. Moreover, we utilize a “cluster model,” where every operation is part of a defined “cluster,” which is a group of geographically proximate operations working together to allow leaders to communicate and provide support and accountability to each other. Clusters create incentives for leaders to share best practices and real-time data and benchmark clinical and financial performance with their cluster partners. We believe this locally-driven data-sharing and peer accountability model is unique among healthcare and senior living providers and has proven effective in improving clinical care, enhancing patient and resident satisfaction and promoting operational efficiencies. This “cluster” operating model is the same model used by local leaders prior to our spin-off from The Ensign Group, Inc. in 2019 (further discussed below under Company History) and is key to the success of our future operations.
Our organizational structure empowers our highly dedicated leaders and staff at the local level to make key decisions and creates a sense of ownership over operational and clinical results and the overall employee experience. Each operation’s leader and their staff are encouraged to make their operations the “provider of choice” in the communities they serve. To accomplish this goal, our leaders work closely with their clinical staff and our expert resources to identify unique patient and resident needs and priorities in their communities and to create superior service offerings tailored to those needs and priorities. We believe that our localized approach to program development and care leads prospective patients or residents and referral sources to choose or recommend our operations.
Similarly, our emphasis on empowering local decision-makers encourages leaders to strive to become the “employer of choice” in the communities they serve. One of our core values is the principle that the best patient care is provided by employees who experience significant work satisfaction because they are valued as individuals. Our leaders work hard to embody this core value to attract, train, and retain outstanding clinical staff by creating a work environment that fosters critical thinking, measurement, and relevance. Our local teams are motivated and empowered to quickly and proactively meet the needs of those they serve, without waiting for permission to act or being bound to a “one-size-fits-all” corporate strategy. In many markets, we attribute census growth and excellent clinical and financial outcomes to a healthy organizational culture built on these principles. With strong employee satisfaction across the organization, we believe we can continue to attract and retain the best talent in our industries.
Lastly, while our teams are local, they are also supported by cutting-edge systems and our “Service Center”, which is staffed with teams of subject-matter experts who advise regarding their respective fields of expertise, including information technology, compliance oversight, human resources, accounting, payroll, legal, risk management, and other services. The partnership and peer accountability that exists between our local leaders and Service Center resources allows each operation to improve while benefiting from the technical expertise, systems and accountability provided by our Service Center.
Partner of Choice in Local Healthcare Communities
We view healthcare services primarily as a local business, driven by personal relationships, reputation and the ability to identify and address unmet community needs. We believe our success is largely driven by our ability to build strong relationships with key stakeholders within the local healthcare communities, leveraging our reputation for providing superior care.
We believe we are a partner of choice to payors, providers, patients, residents and employees in the healthcare communities we serve. As a partner, we focus on improving care outcomes and the quality of life of our patients and residents in their home. Our local leadership approach facilitates the development of strong professional relationships within communities, which allows us to better understand and meet the needs of our partners. We believe our emphasis on working closely with other providers, payors, residents and patients yields unique, customized solutions and programs that meet local market needs and improve clinical outcomes, which in turn accelerates revenue growth and profitability.
We are a trusted partner to, and work closely with, payors and acute and post-acute providers to deliver innovative healthcare solutions in lower cost settings. In the markets we serve, we have initiated joint venture partnerships, developed formal and informal preferred provider relationships with key referral sources, and implemented transitional care programs that result in better coordination within the care continuum. These solutions have produced significant benefits to patients, residents, payors, and other providers, including reduced hospital readmission rates, appropriate transitions within the care continuum, overall cost savings, increased patient satisfaction and improved quality outcomes. In addition, positive, repeated interactions and data sharing result in strong local relationships and encourage referrals from our acute and post-acute care partners. As we continue to strengthen these formal and informal relationships and expand our referral base, we believe we will continue to drive revenue growth and operational results.
Company History
The Pennant Group, Inc. was incorporated as a Delaware corporation on January 24, 2019, for the purpose of holding the home health and hospice agencies and substantially all of the senior living businesses of The Ensign Group, Inc. (“Ensign”), which was formed in 1999 with the goal of establishing a new level of quality care within the skilled nursing industry. On October 1, 2019, Ensign completed the separation of Pennant (the “Spin-Off”). We believe that, through our innovative operating model, we can foster a new level of patient care and professional competence at our independent operating subsidiaries and set new industry standards for quality home health and hospice and senior living services.
Our independent operating subsidiaries are organized into industry-specific portfolio companies, which we believe has enabled us to maintain a local, field-driven organizational structure, to attract qualified leaders and expert resources, and to effectively identify, acquire, and improve operations. Each of our portfolio companies has its own leader. These experienced and proven leaders are generally taken from the ranks of our operational leaders to serve as resources to independent operating subsidiaries within their own portfolio companies and have the primary responsibility for recruiting qualified talent, finding potential acquisition targets, and identifying other strategic and organic growth opportunities. We believe this decentralized organizational structure will continue to improve the quality of our recruiting and facilitate successful acquisitions.
We have two reportable segments: (1) home health and hospice services, which includes our home health, hospice, home care, and geriatric primary and palliative care businesses; and (2) senior living services, which includes our assisted living, independent living and memory care services. We also report an “all other” category that includes general and administrative expense. Our reporting segments are business units that offer different services and are managed separately to provide greater visibility into those operations. For more information about our operating segments, as well as financial information, see “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and Note 6, Business Segments, to the Consolidated Financial Statements.
Services
Home Health and Hospice. As of December 31, 2024, we provided home health and hospice services through 123 agencies. We also provide home health and hospice operational support through a management service agreement in Connecticut. Our home health services consist of providing a combination of clinical services including nursing, speech, occupational and physical therapy, medical social work and home health aide services within a patient's home. Home health is often a cost-effective solution for patients and can also increase their quality of life by allowing them to receive excellent clinical services in the comfort and convenience of each patient’s home. Our hospice services focus on the physical, spiritual and psychosocial needs of terminally ill patients and their families and consist primarily of clinical care, education and counseling. Our home care services include the provision of case management services, personal care services, and assistance with the activities of daily living. Our geriatric primary and palliative care services include physician and nurse practitioner services provided in the home, facility, or other appropriate setting. We generated approximately 64.7%, 66.9% and 67.7% of our home health and hospice segment revenue from Medicare during the years ended December 31, 2024, 2023 and 2022, respectively.
Senior Living. As of December 31, 2024, we provided assisted living, independent living and memory care services in 57 communities with 3,960 total available units. Our senior living operations provide a variety of services tailored to our residents’ needs, including residential accommodations, activities, meals, housekeeping and assistance in the activities of daily living to seniors who are independent or who require some support, but not at the level of clinical care provided in a skilled nursing facility. We generate revenue in these communities primarily from private pay sources, with a portion earned from Medicaid or other state-specific programs. We derived approximately 69.4%, 68.8% and 71.3% of our senior living revenue from private pay sources during the years ended December 31, 2024, 2023 and 2022, respectively.
Our Growth Strategy
We believe that the following strategies are primarily responsible for our growth to date and will continue to drive the growth of our business:
Grow Talent Base and Develop Future Leaders. We view ourselves as a leadership company. Our growth strategy is focused on expanding our talent base and recruiting and developing future leaders. A key component of our organizational culture is our belief that strong local leadership is a primary ingredient to operational success. We use a multi-faceted strategy to identify and recruit proven business leaders from various industries and backgrounds. To develop these leaders, we have a rigorous “CEO-in-Training Program” that includes significant in-person instruction on leadership, clinical and operational topics, as well as extensive on-the-ground training and active learning with key leaders from across the organization. After placement in a local operation, our leaders continue to receive training and regular feedback and support from operational, clinical and Service Center peers. We also have similar programs for our new and emerging clinical leaders. We believe our model of empowering local leaders and providing them a platform of support, including expert resources and industry-leading systems, will continue to attract and retain highly talented and entrepreneurial leaders.
Focus on Organic Growth. We believe that we have a significant opportunity to drive organic growth within our current portfolio, including recently acquired operations. As we improve clinical outcomes, quality of care and operational results at each of our existing and newly acquired operations, we believe we will become a provider of choice in the communities we serve, which leads to census growth. Through this census growth, and as we continue to expand our service areas and offerings, we believe we will continue to translate revenue growth into bottom line success with rigorous adherence to our core operating principles. By effectively using data systems and analytics and embracing a culture of transparency and accountability, we expect to see our local leaders steadily improving operational results. We believe our unique operating model will continue to cultivate steady and consistent organic growth in the future.
Pursue Disciplined Acquisition Strategy. The disciplined acquisition and integration of strategic and underperforming operations is a key element of our past success and is integral to our future growth plans. Historically, we have successfully transitioned both turnaround and stable target businesses, transforming them into top-quality operations preferred by referral
sources and community partners. We plan to continue to take advantage of the fragmented home health, hospice and senior living industries by being proactive yet disciplined in acquiring strategic and underperforming operations with high upside potential within both existing and new geographic markets. With experienced leaders in place at the local level and demonstrated success in improving operating conditions at acquired businesses, we believe we are well positioned to continue expanding our footprint through strategic and opportunistic acquisitions.
Leverage Our Operational Capabilities to Expand Partnerships. Our local leadership approach enables us to adapt to and efficiently meet the needs of our partners in the communities we serve. Our clinical and data analytics capabilities foster solutions and allow us to optimize clinical outcomes. We use this data to communicate with key partners in an effort to reduce overall cost of care and drive improved clinical outcomes. We also operate joint ventures with leading health systems, which allows us to expand our partnership in the space, and we may undertake additional joint ventures in the future. We will continue to expand formal and informal partnerships across the healthcare continuum by strategically investing in programs and data analytics that help us and our partners improve care transitions, achieve better outcomes and reduce costs.
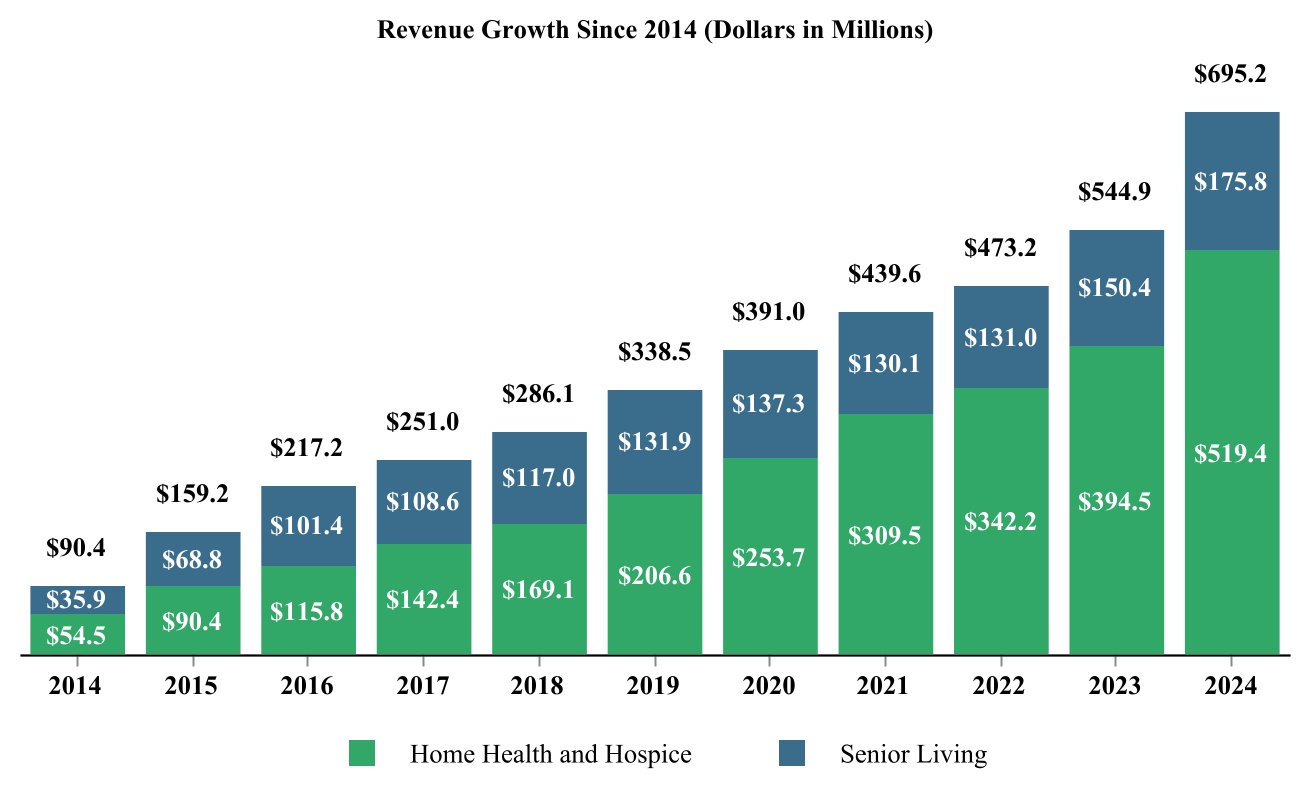
Growth and Acquisition History
Much of our historical growth can be attributed to our expertise in acquiring strategic and underperforming operations and transforming them into market leaders in clinical quality, staff competency and financial performance. Our local leaders are trained to identify these opportunities for long-term organic growth as we strive to become the provider of choice in our local communities. Accordingly, we plan to continue to drive organic growth and acquire additional operations in existing and new markets in a disciplined manner.
From 2014 to 2024, we grew our home health and hospice services and senior living services revenue by 669.0% or a compounded annual growth rate of 22.6%.
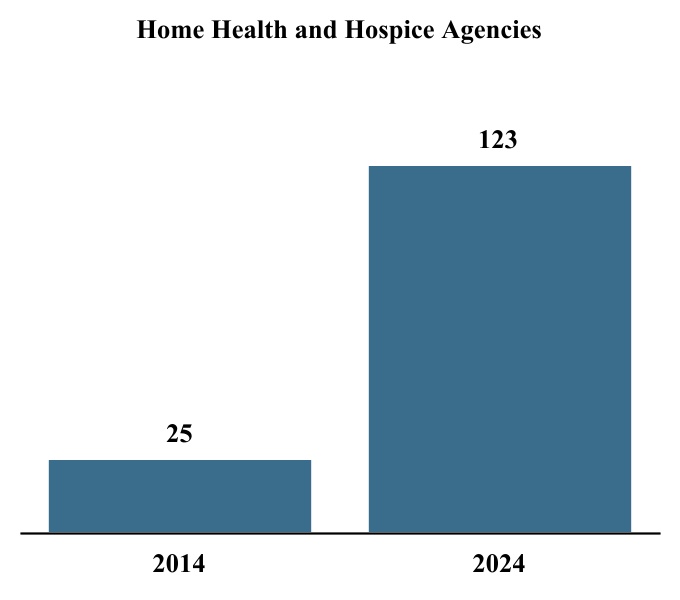
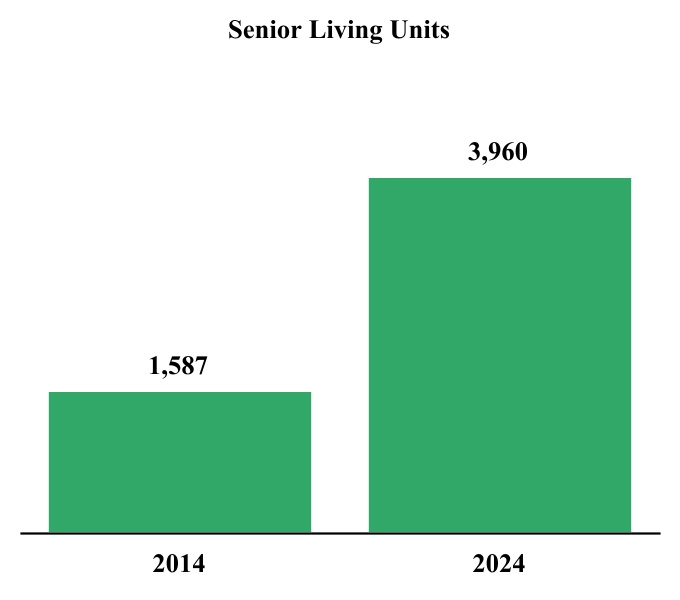
From December 31, 2014 to December 31, 2024, we grew the number of our home health and hospice agencies and senior living units by 392.0% and 149.5%, respectively.
Agency and Unit Growth Since 2014
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| 2014 | | 2015 | | 2016 | | 2017 | | 2018 | | 2019 | | 2020 | | 2021 | | 2022 | | 2023 | | 2024 |
| Home health and hospice agencies | 25 | | | 32 | | | 39 | | | 46 | | | 54 | | | 63 | | | 76 | | | 88 | | | 95 | | | 111 | | | 123 | |
Senior living communities(a) | 15 | | | 36 | | | 36 | | | 43 | | | 50 | | | 52 | | | 54 | | | 54 | | | 49 | | | 51 | | | 57 | |
Senior living units(a) | 1,587 | | | 3,184 | | | 3,184 | | | 3,434 | | | 3,820 | | | 3,963 | | | 4,127 | | | 4,127 | | | 3,500 | | | 3,588 | | | 3,960 | |
| Total number of home health, hospice, and senior living operations | 40 | | | 68 | | | 75 | | | 89 | | | 104 | | | 115 | | | 130 | | | 142 | | | 144 | | | 162 | | | 180 | |
| | | | | | | | |
| (a) | | During January 2022, affiliates of the Company entered into certain operations transfer agreements with affiliates of Ensign, providing for the transfer of the operations of five senior living communities. |
We aim to continue to grow our revenue and earnings by expanding our existing operations and acquiring additional operations in existing and new markets.
Industry Trends
The healthcare sector is one of the largest and fastest-growing sectors of the U.S. economy. According to the Centers for Medicare and Medicaid Services (“CMS”), national healthcare spending increased from 8.9% of U.S. GDP, or $253 billion, in 1980 to an estimated 17.6% of GDP, or $4.8 trillion, in 2023. CMS projects national healthcare spending will grow by an average of 5.6% annually from 2023 through 2032, accounting for approximately 19.7% of U.S. GDP, or approximately $7.7 trillion, in 2032.
The home health and hospice segment is growing within the overall healthcare landscape in the United States. According to Grandview Research, Inc., the home health market is expected to grow at a compounded annual growth rate (“CAGR”) of 8.0% from 2024 to 2030. The hospice industry is estimated at approximately $37.9 billion and is projected to grow at an estimated CAGR of 8.1% from 2024 to 2030. The senior living market is expected to expand at an estimated CAGR of 4.2% between 2024 to 2030. We believe that the industries in which we operate will continue to benefit from several macroeconomic and regulatory trends highlighted below:
Increased Demand Driven by Aging Populations. As seniors account for an increasing percentage of the total U.S. population, we believe demand for home health and hospice will continue to increase and demand for senior living services will improve. According to the U.S. Census Bureau in 2023, between 2022 and 2060, the number of individuals over 65 years old is projected to be one of the fastest growing segments of the United States population, growing from 17% to 24%. The Bureau
identified the year 2030 as the year all baby boomers will be more than 65 years of age. The Bureau expects the over-65 population segment to increase nearly 54% to 89 million by 2060 (from 2022) as compared to the total U.S. population which is projected to increase by 9.3% over that same time period. Furthermore, the generation currently retiring has access to fewer post-retirement benefits and accumulated less savings than in the past, creating demand for more affordable senior housing and in-home care options. As a high-quality provider in lower cost settings, we believe we are well-positioned to benefit from this trend.
Shift of Patient Care to Lower Cost Alternatives. The growth of the senior population in the U.S. continues to increase healthcare costs, often at a rate faster than the available funding from government-sponsored healthcare programs. In response, government payors have adopted measures that encourage the treatment of patients in their homes and other cost-effective settings where the staffing requirements and associated costs are often significantly lower than the alternatives. With our emphasis on the home health, hospice and senior living industries, which are among the lowest cost settings within the post-acute care continuum, we expect this shift to continue to drive our growth.
Transition to Value-Based Payment Models. In response to rising healthcare spending, certain markets’ commercial, government and other payors are shifting away from fee-for-service payment models toward value-based models, including risk-based payment models that tie financial incentives to quality, efficiency and coordination of care. We believe that payors will continue to emphasize reimbursement models driven by value and that our clinical outcomes combined with our services in cost effective settings will be increasingly rewarded. Many of our home health agencies already receive value-based payments, and we are well-positioned to capitalize on this trend as it unfolds across the markets we serve. Please see further discussion of value-based payment models below under Government Regulation.
Significant Acquisition and Consolidation Opportunities. The home health, hospice and senior living industries are highly fragmented markets with thousands of small and regional providers and only a handful of large national players. There were over 11,300 Medicare-certified home health agencies operating in 2022, with the top ten largest operators accounting for approximately 26.6% of the market. There are approximately 6,000 hospice agencies in the U.S. with the top ten largest operators accounting for about 19.1% of the total market share. As with the home health and hospice industries, there is significant fragmentation in the senior housing industry, with the top 25 operators owning approximately 28% of the licensed beds within the US. We believe that our strategy of acquiring strategic and underperforming operations in these highly fragmented markets will be an instrumental to our future growth.
Changing Regulatory Framework. Regulations and reimbursement change frequently in our industries. Our model is designed to successfully navigate these regulatory and reimbursement changes. For example, effective January 1, 2020, CMS enacted additional changes to the Medicare home health prospective payment system (“HH PPS”) with the implementation of the Patient Driven Groupings Model (“PDGM”). As discussed in greater detail below under Government Regulation, and adjusted in subsequent calendar years’ payment rules, this reimbursement structure involved case mix calculation methodology refinements, changes to low-utilization payment adjustment (“LUPA”) thresholds, the elimination of therapy thresholds, a change to the unit of payment from a 60-day episode to a 30-day period of care, and reduction in fiscal year 2020 and full elimination in fiscal year 2021 of requests for anticipated payments (“RAPs”), which were no longer available by January 1, 2022. In fiscal year 2022, CMS replaced the RAP process with the home health Notice of Admission (“NOA”), which requires a single NOA filing that will cover continuous 30-day periods of care until the patient is discharged. We believe our unique operating model has allowed us to effectively transition to PDGM as local operations and clinical leaders, supported by our expert resources, have adapted to the new reimbursement environment.
Payor Sources
We derive revenue primarily from Medicare and Medicaid programs, managed care and private insurance, and private and other payors.
Medicare. Medicare is a federal program that provides healthcare benefits to individuals who are 65 years of age or older or are disabled. The Medicare home health benefit is available both for patients who need care following discharge from an inpatient facility and patients who suffer from chronic conditions that require ongoing but intermittent care. The Medicare hospice benefit is also available to Medicare-eligible patients with terminal illnesses, certified by a physician, where life expectancy is six months or less.
Medicaid. Medicaid is a program financed by state funds and matching federal funds administered by state agencies or managed care organizations on their behalf. Medicaid programs generally provide health benefits for qualifying individuals and may supplement Medicare benefits for the disabled and for persons aged 65 and older meeting financial eligibility
requirements. Medicaid reimbursement formulas are established by each state with the approval of the federal government in accordance with federal guidelines.
Medicaid reimbursement varies from state to state and is based upon a number of different methodologies, including cost-based, prospective payment, case mixed adjusted payments, and negotiated rates. Rates are subject to a state’s annual budgetary requirements and funding, statutory and regulatory changes and interpretations and rulings by individual state agencies and State Plan Amendments approved by CMS.
Managed Care and Private Insurance. Managed care patients consist of individuals who are insured by certain third-party entities, or who are Medicare beneficiaries who have assigned their Medicare benefits to a managed care organization plan. Another type of insurance, long-term care insurance, is also becoming more widely available to consumers and is not expected to contribute significantly to industry revenues in the near term.
Private and Other Payors. Private and other payors consist primarily of individuals, family members or other third parties who directly pay for the services we provide.
The following table sets forth our total revenue by payor source as a percent of revenue generated by each of our reportable segments and as a percentage of total revenue for the year ended December 31, 2024:
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, 2024 |
| | Home Health and Hospice Services | | | | |
| | Home Health Services | | Hospice Services | | Senior Living Services | | Total Revenue |
| Medicare | | 45.8 | % | | 86.6 | % | | — | % | | 48.3 | % |
| Medicaid | | 4.3 | | | 10.8 | | | 30.6 | | | 13.2 | |
| Subtotal | | 50.1 | | | 97.4 | | | 30.6 | | | 61.5 | |
| Managed care | | 31.5 | | | 2.0 | | | — | | | 13.3 | |
Private and other(a) | | 18.4 | | | 0.6 | | | 69.4 | | | 25.2 | |
| Total revenue | | 100.0 | % | | 100.0 | % | | 100.0 | % | | 100.0 | % |
| | | | | | | | |
| (a) | | Private and other payors in the Company’s home health services includes revenue from all payors generated in the Company’s home care operations and management services agreement. |
Reimbursement for Specific Services
Historically, adjustments to reimbursement under Medicare and Medicaid have had a significant effect on our revenue and results of operations. Recently enacted, pending and proposed legislation and administrative rulemaking at the federal and state levels could have similar effects on our business. Efforts to impose reduced reimbursement rates, greater discounts, cost sequestrations in federal spending bills passed by Congress, and more stringent cost controls by government and other payors are expected to continue for the foreseeable future and could adversely affect our business, financial condition and results of operations. Additionally, any delay or default by the federal or state governments in making Medicare and/or Medicaid reimbursement payments could materially and adversely affect our business, financial condition and results of operations.
Reimbursement for Home Health Services. Our home health business derives substantially all of its revenue from Medicare, managed care, and private pay sources, which may vary in the markets we serve. Our home health services generally consist of providing some combination of the services of registered nurses, speech, occupational and physical therapists, medical social workers and certified home health aides. Home health is often a cost-effective solution for patients and can also increase their quality of life and allow them to receive quality medical care in the comfort and convenience of a familiar setting.
Reimbursement for Hospice Services. Hospice revenues are primarily derived from Medicare. We receive one of four predetermined rate categories based on four different levels of care provided: routine home care, continuous home care, inpatient respite care and general inpatient care. This payment structure is designed to include all of the services needed to manage a beneficiary’s care, consisting primarily of clinical care, education and counseling. These rates are subject to annual adjustments based on inflation and geographic wage considerations.
Reimbursement for Senior Living Services. Assisted living, independent living and memory care community revenue is primarily derived from private pay residents at rates we establish based upon the services we provide and market conditions
in the area of operation. In addition, Medicaid or other state-specific programs in some states where we operate supplement payments for board and care services provided in assisted living and memory care communities.
Competition
The post-acute care industry is highly competitive, and we expect that the industry will become increasingly competitive in the future. The industry is highly fragmented and characterized by numerous local and regional providers, in addition to large national providers that have achieved geographic diversity and economies of scale. Some of our independent operating subsidiaries also compete with skilled nursing facilities, inpatient rehabilitation facilities and long-term acute care hospitals. Competitiveness may vary significantly from location to location, depending upon factors such as the number of competing operations, availability of services, expertise of staff, and the physical appearance and amenities of senior living communities. We believe that the primary competitive factors in the post-acute care industry are:
•ability to attract and to retain qualified leaders and caregivers;
•reputation and achievements of quality healthcare outcomes and patient and resident satisfaction;
•attractiveness and location of senior living communities and other physical assets;
•the expertise and commitment of operational leaders and employees; and
•private equity, payors, and other firms with greater financial resources and/or lower costs of capital with similar asset acquisition objectives.
We seek to compete effectively in each market by establishing a reputation within the local community as the “provider of choice.” This means that the operation leaders are generally free to discern and address the unique needs and priorities of healthcare professionals, customers and other stakeholders in the local community or market, and then create superior service offerings that are calculated to encourage prospective customers and referral sources to choose or recommend the operation.
Increased competition could limit our ability to attract and retain patients and residents, maintain or increase rates of reimbursement or to expand our business. Some of our competitors have greater financial and other resources than we have, may have greater brand recognition and may be more established in their respective communities than we are. Competing companies may also offer newer or more recently renovated communities or different programs or services than we offer and may, therefore, attract individuals who are currently patients of our operations, potential residents of our senior living communities, or who are otherwise receiving our healthcare services. Other competitors may have lower expenses or other competitive advantages than we do and, therefore, provide services at lower prices than we offer.
There are few barriers to entry in the home health and hospice business in jurisdictions that do not require certificates of need or permits of approval. Our primary competition in these jurisdictions comes from local privately and publicly owned providers and hospital-owned healthcare providers. We compete based on the availability of personnel, the quality of services, expertise of visiting staff, and, in certain instances, on the price of our services. In addition, we compete with a number of non-profit organizations that finance acquisitions and capital expenditures on a tax-exempt basis and charity-funded programs that may have strong ties to their local medical communities and receive charitable contributions that are unavailable to us.
Our senior living services also compete with local, regional and national companies. The primary competitive factors in these businesses include reputation, attractiveness and location of physical assets, cost of services, quality of clinical services, responsiveness to patient or resident needs, location and the ability to provide support in other areas such as third-party reimbursement, information management and patient recordkeeping. The market for acquiring and/or operating senior living communities is highly competitive, and some of our present and potential senior living competitors have, or may obtain, greater financial resources than us and may have a lower cost of capital.
Our Competitive Strengths
We believe that we are well positioned to benefit from the ongoing regulatory, reimbursement and demographic changes within the home health, hospice and senior living industries. We believe that we will achieve clinical, financial and cultural success as a direct result of the following key competitive strengths:
Innovative Operating Model. We believe healthcare should be operated primarily as a local business. Our innovative operating model, described in Part 1, Item 1 - “Our Innovative Operating Model”, is one of our key competitive strengths.
Effective Talent Recruitment, Development and Retention. We believe we have an advantage and are successful in attracting, developing, and retaining outstanding business and clinical leaders to lead our independent operating subsidiaries. Our unique operating model, which emphasizes local decision making and team building, supported by our platform of expert resources and best-in-class systems, attracts a highly talented and entrepreneurial group of leaders. Our operational leaders are committed to ongoing training and participate in regular leadership development and educational programs. We believe that our commitment to professional development strengthens the quality of our operational leaders and staff and will continue to differentiate us from our competitors.
Proven Track Record of Successful Acquisitions. We adhere to a disciplined acquisition strategy focused on sourcing and selectively acquiring operations within our target markets. Local leaders are heavily involved in the acquisition process and are recognized and rewarded as these acquired operations become the provider of choice in the communities they serve. Through our innovative operating model and disciplined approach to strategic growth, we have completed and successfully transitioned dozens of value-add operations. Our expertise in acquiring and transforming strategic and underperforming operations allows us to consider a broad range of potential acquisition targets and will be a key element of our future success.
Superior Clinical Outcomes and Quality Care. We will continue to succeed by delivering high quality home health, hospice and senior living services. Using the CMS five-star quality rating criteria, our home health agencies achieved an average of 4.1 out of 5 stars across all agencies for the for the year ended December 31, 2024, compared to the industry average of 3.0 stars (see Government Regulation below for further discussion on the five-star quality rating system). Our locally driven, patient-centered approach to clinical care allows us to meet the unique needs of our patients, resulting in improved clinical outcomes, including reduced hospital readmission rates. These improved outcomes are driven by both our talented local clinicians and our data-driven analytical approach to patient care and risk stratification. We believe that our achievement of high-quality clinical outcomes positions us as a solution for patients, residents and referral sources, leading to census growth and improved profitability.
Diversified Portfolio by Payor and Services. As of December 31, 2024, we operated 123 home health and hospice agencies and 57 senior living communities across 13 states. Because of this diversified portfolio, our blended payor mix was 48.3% Medicare, 13.2% Medicaid, 13.3% managed care and 25.2% private pay and other for the year ended December 31, 2024. Our balanced payor mix can provide greater business stability through economic cycles and mitigates volatility arising from government-driven reimbursement changes. For the year ended December 31, 2024, we generated 74.7% of our revenue from home health and hospice services and 25.3% of our revenue from senior living services. Our diversified service portfolio allows us to opportunistically execute on our acquisition strategy as valuations fluctuate over industry cycles.
Human Capital
The operation of our home health and hospice operations and senior living communities requires a large number of highly skilled healthcare professionals and support staff. As of December 31, 2024, we had approximately 7,000 employees who were employed by our independent operating subsidiaries or our Service Center.
Our ability to attract and retain future leaders is critical to our ongoing success. Therefore, we are dedicated to continuously recruiting and developing a diverse group of capable leaders. As described in Part 1, Item 1., Grow Talent Base and Develop Future Leaders, our CEO-in-Training and Clinical Operations Leadership Training programs provide significant in-person instruction and extensive training with key leaders from across the organization to empower local leaders.
For the year ended December 31, 2024, 67.7% of our total expenses were payroll related. Periodically, market forces, which vary by region, require that we increase wages in excess of general inflation or increases in reimbursement rates we receive. We believe that we staff appropriately, focusing primarily on the acuity level and day-to-day needs of our patients and residents. We seek to manage our labor costs by improving staff retention, improving operating efficiencies, maintaining competitive wage rates and benefits and reducing reliance on overtime compensation and temporary nursing agency services.
The healthcare industry as a whole has been experiencing shortages of qualified professional clinical staff. We believe that our ability to attract and retain qualified professional clinical staff stems from our ability to offer attractive wage and benefits packages, a high level of employee training, a culture that provides incentives for individual efforts and a quality work environment.
Government Regulation
General. The laws and statutes affecting the regulatory landscape of the home health, hospice and senior living industries continue to expand. We expect that these changes will continue. In addition to this changing regulatory environment,
federal, state and local officials are increasingly focusing their efforts on the enforcement of these laws. In order to operate our businesses, we must comply with federal, state and local laws relating to, among other things, licensure, delivery and adequacy of medical care, distribution of pharmaceuticals, equipment, personnel, operating policies, fire prevention, immigration, employment, rate-setting, billing and reimbursement, building codes and environmental protection. Additionally, we must also adhere to federal and state anti-fraud and abuse laws, such as anti-kickback statutes and, physician referral laws, as well as safety and health standards set by the Occupational Safety and Health Administration (“OSHA”). Changes in laws or regulations, or new interpretations of existing laws may have an adverse impact on our methods and costs of doing business.
Our independent operating subsidiaries are also subject to various regulations and licensing requirements promulgated by state and local health and social service agencies and other regulatory authorities. Requirements vary from state to state, and these requirements can affect, among other things, personnel education and training, patient and personnel records, services, staffing levels, monitoring of patient wellness, patient furnishings, housekeeping services, dietary requirements, emergency plans and procedures, certification and licensing of staff prior to beginning employment, and patient rights. These laws and regulations could limit our ability to expand into new markets and to expand our services and facilities in existing markets.
Recent Updates. On July 30, 2024, CMS issued the 2025 Hospice Payment Rate Update Final Rule (the “Hospice Payment Final Rule”). The Hospice Payment Final Rule’s payment update percentage is 2.9%, which is an estimated increase of $790 million in payments from fiscal year 2024. The payment update percentage is based on a 3.4% market basket percentage increase, which is reduced by a 0.5% productivity adjustment. Hospices that fail to meet quality reporting requirements under the Hospice Quality Reporting Program (“HQRP”) will receive a 4% reduction to the annual hospice payment update percentage increase for that year, resulting in a total decrease of 1.1% to those non-compliant hospices’ payments and more than negating the payment update percentage for fiscal year 2025. The Hospice Payment Final Rule also adds two new process measures to HQRP: timely reassessment of pain impact, and timely reassessment of non-pain symptom impact, which are both expected to begin in fiscal year 2028. In addition, the Hospice Payment Final Rule updates the statutory aggregate cap that limits the overall payments per patient that may be made to a hospice annually. The hospice cap amount for the 2025 fiscal year is $34,465.34, increased from the 2024 fiscal year cap of $33,494.01. The Hospice Payment Final Rule also includes clarifying revisions to the hospice conditions of participation; updates statistical area delineations; and makes changes to the Consumer Assessment of Healthcare Providers and Systems (“CAHPS”) Hospice Survey.
On November 1, 2024, CMS issued the 2025 Home Health Prospective Payment System Final Rule (the “Home Health Payment Final Rule”). The Home Health Payment Final Rule’s payment update percentage for calendar year 2025 is 2.7%, an estimated increase of $445 million from calendar year 2024, which is reduced by an estimated 1.8% behavioral adjustment, along with a 0.4% estimated reduction for fixed dollar losses, resulting in an aggregate net increase of 0.5%, or $85 million, for the calendar year 2025 payment rate compared to calendar year 2024. The Home Health Payment Final Rule also recalibrates PDGM case-mix weights, finalizes an update to the home health wage index, updates home health conditions of participation to require patient acceptance policies, and establishes or updates certain LUPA add-on factors.
In June 2024, CMS announced a Period of Enhanced Oversight for newly enrolled hospices in Arizona, California, Nevada, and Texas. The program includes hospices that are newly enrolled, or that undergo a change of ownership, or reactivating after being in a deactivated status after July 13, 2023. Such hospices are subject to enhanced oversight for up to one year and may undergo medical review by CMS contractors to deter fraud, waste and abuse of Medicare funds. This period of enhanced oversight may last up to one year.
On April 22, 2024, CMS published the Ensuring Access to Medicaid Services Final Rule (the “Access Rule”), which creates and, over the course of five years, implements new obligations for providers of home- and community-based services (“HCBS”), including non-skilled personal care services in the home. The Access Rule requires that, beginning in 2030, states must implement data collection and monitoring systems to ensure that, subject to exceptions, Medicaid-funded HCBS providers spend at least 80% of their Medicaid HCBS reimbursement on compensation for direct care workers, as opposed to administrative overhead or profits. The Access Rule further requires states to establish a grievance system for addressing services provided in the fee-for-service context, publish fee-for-service payment rates paid by Medicaid, publish the average hourly rate paid to HCBS care providers, and develop hardship exemptions and separate requirements for small providers, with these requirements to be implemented within one to three years from the Access Rule taking effect. We anticipate potential changes to the Access Rule, or offsetting Medicaid rate increases, before the Access Rule’s ultimate implementation in six years.
Medicare. All providers are subject to compliance with various federal, state and local statutes and regulations in the U.S. and receive periodic inspection by state licensing agencies to review standards of medical care, equipment and safety.
Conditions of Participation. Our home health and hospice operations must comply with regulations promulgated by the United States Department of Health and Human Services (“HHS”) and CMS in order to participate
in the Medicare program and receive Medicare payments. Among other things, these conditions of participation (the “CoPs”), relate to the type of operation, its personnel and its standards of medical care, as well as its compliance with state and local laws and regulations.
Home Health Quality Reporting Requirements. The CoPs require home health agencies to submit quality reporting data through Outcome and Assessment Information Set (“OASIS”) assessments within 30 days of completing the assessment of the Medicare and Medicaid beneficiary as a condition of payment and for quality measurement purposes. If the OASIS assessment is not found in CMS’s quality system upon receipt of a final claim for a home health episode and the receipt date of the claim is more than 30 days after the assessment completion date, CMS will deny the claim. Home health agencies that do not submit quality measure data to CMS incur a 4% reduction in their annual home health payment update. Under this CoP, all home health agencies are required to timely submit both a Start of Care or Resumption of Care OASIS assessment and a Transfer or Discharge OASIS assessment for a minimum of 90% of all episodes.
In addition, CMS requires that all Medicare certified home health and hospice agencies participate in CAHPS surveys. CAHPS surveys are designed to produce comparable data on the perspective of patients and their caregivers that allows meaningful and objective comparisons between agencies. Home health and hospice agencies that do not submit the required data incur a 4% reduction in their annual base rate payment update.
Home Health Star Rating. As a consumer tool for selecting a home health provider, CMS has used a five-star rating model to rate home health agencies since 2015. This Quality of Patient Care Star Rating is a summary measure of a home health agency’s performance based upon how well it provides patient care. CMS uses seven measurements indicating quality to determine its quality of patient care rating, including how often the agency initiated care in a timely manner, how often patients demonstrated improvements in ambulation, bed transferring, bathing, oral medication administration, less shortness of breath, and decreased need for acute care hospitalization. According to CMS, a 3-star rating means the agency provides good quality of care, as a 3-star rating applies to most home health agencies. According to the January 2025 quarterly refresh of CMS Home Health Compare star rating criteria, our home health agencies have achieved an average of 4.1 out of 5 stars across all agencies compared to the industry average of 3.0 stars.
Home Health Reimbursement Under PDGM. To qualify for home health services, Medicare CoPs require that beneficiaries (1) be homebound (meaning that the beneficiary is unable to leave their home without a considerable and taxing effort); (2) require intermittent skilled nursing, physical therapy, or speech therapy services; (3) have a face to face encounter that (a) has occurred no more than 90 days prior to the start of care or within 30 days after the start of care, (b) was related to the primary reason the patient requires home health services, and (c) was performed by a physician or allowed non-physician provider; and (4) receive treatment under a plan of care established and periodically reviewed by a physician.
Under PDGM, Medicare provides agencies with payments for each 30-day payment period provided to beneficiaries. There is no limit to the number of periods of care a beneficiary who remains eligible for the home health benefit can receive. The reimbursement rate is determined by a set of factors intended to account for the cost of providing care to each patient. Payments may be adjusted for certain variables including, but not limited to the number of visits provided, patient transfers, and other factors.
Home Health Value Based Purchasing (“HHVBP”). After introducing HHVBP models in select states from 2016 to 2021, CMS expanded HHVBP to all fifty states beginning on January 1, 2022. Fiscal Year (“FY”) 2022 was the pre-implementation year wherein CMS provided Home Health Agencies (“HHAs”) with resources and training, which allowed HHAs time to prepare and learn about the expectations and requirements of the expanded HHVBP Model without risk to payments. FY 2023 (beginning on January 1, 2023) was the first full performance year for the expanded HHVBP Model. FY 2024 was the second year for the expanded HHVBP model, based on FY 2022 for its baseline, and HHA performance for the FY 2024 applicable measure set determines payment adjustments applicable to FY 2026 Medicare fee-for-service claims by HHAs. FY 2025 is the first year when payment will be adjusted determined on FY 2023 performance. Payment adjustments could be as much as 5% in 2025 based on data obtained in FY 2023 and CMS could increase the payment adjustment percentage in future years.
Review Choice Demonstration for Home Health Services. The Review Choice Demonstration for Home Health Services (“RCD”) is mandatory for our HHAs in Texas and allows them to select from three initial options for payment review:
•Pre-claim review
•Post-payment review
•Minimal post-payment review with a 25% payment reduction
After a 6-month period, HHAs demonstrating compliance with Medicare rules through pre-claim review or post-payment review will have additional choices, including relief from most reviews except for a review of a small sample of claims. (To be eligible, HHAs must meet a 90% target full provisional affirmation rate based on a minimum 10 requests or claims submitted.) This program is designed to reduce the number of Medicare appeals, improve provider compliance with Medicare program requirements, should not delay care to Medicare beneficiaries, and does not alter or reduce the Medicare home health benefit.
Hospice Special Focus Program. In 2024, CMS implemented a Hospice Special Focus Program (“HSFP”). Under this program, 50 hospices will be selected annually for inclusion in the HSFP based on certain quality and survey data. Hospices in the HSFP will be surveyed at least semiannually every 6 months for a period of 18 months. To successfully exit the HSFP, a hospice must have two surveys within 18 months with no uncorrected condition-level deficiencies, and no pending complaint investigations triaged at the immediate jeopardy or condition-level and must otherwise be substantially compliant with all applicable requirements.
Hospice Reimbursement and Cap Amounts. Payments are based on daily rates for each day a beneficiary is enrolled in the hospice benefit and are subject to two annual caps. Rates are set based on specific levels of care, are adjusted by a wage index to reflect healthcare labor costs across the country and are established annually through federal legislation. The following are the four levels of care provided under the hospice benefit:
•Routine Home Care (“RHC”). Care that is not classified under any of the other levels of care, such as the work of nurses, social workers or home health aides.
•General Inpatient Care. Pain control or acute or chronic symptom management that cannot be managed in a setting other than an inpatient Medicare-certified facility, such as a hospital, skilled nursing facility or hospice inpatient facility.
•Continuous Home Care. Care for patients experiencing a medical crisis that requires nursing services to achieve palliation and symptom control, if the agency provides a minimum of eight hours of care within a 24-hour period.
•Inpatient Respite Care. Short-term, inpatient care to give temporary relief to the caregiver who regularly provides care to the patient.
CMS has established a two-tiered payment system for RHC. Hospices are reimbursed at a higher rate for RHC services provided from days of service one through 60 and then a lower rate for all subsequent days of service. CMS also provided for a Service Intensity Add-On, which increases payments for certain RHC services provided by registered nurses and social workers to hospice patients during the final seven days of life.
Medicare payments are subject to two fixed annual caps, which are assessed on a provider-number basis and are broken into an inpatient cap amount and an overall payment cap. These cap amounts are calculated and published by the applicable Medicare fiscal intermediary on an annual basis covering the fiscal year, measured as the period from October 1 through September 30. The inpatient cap limits hospice care provided on an inpatient basis. This cap limits the number of days that are paid at the higher inpatient care rate to 20.0% of the total number of days of hospice care that are provided to all Medicare beneficiaries served by a provider. The daily rate for all days exceeding the cap is the standard RHC daily rate, and the provider must reimburse Medicare for any payments received exceeding that amount. The Medicare fiscal intermediary calculates the overall payment cap at the end of each hospice cap period to determine the maximum allowable payments to a hospice provider during the period. We estimate our potential cap exposure by using available information to compare our actual reimbursement for all hospice services provided during the period to the number of beneficiaries we served multiplied by the statutory per beneficiary cap amount. If payments received by any one of our hospice provider numbers exceeds either of these caps, we are required to reimburse Medicare for payments received in excess of the cap amounts. The hospice cap amount for the 2024 fiscal year was $33,494.01. The hospice cap amount for the 2025 fiscal year is $34,465.34, which is a 2.9% increase over the 2024 fiscal year hospice cap.
Improving Medicare Post-Acute Care Transformation Act of 2014 (“IMPACT Act”). The IMPACT Act requires the submission of standardized assessment data for quality improvement, payment and discharge planning purposes across the spectrum of post-acute care providers (“PACs”), including home health agencies. Failure to report such data when required subjects a PAC to a 2% reduction in market basket prices then in effect.
Hospice Quality Reporting Requirements. HQRP, mandated by the Patient Protection and Affordable Care Act, requires hospice agencies to submit required quality data for inclusion on the public facing Hospice Compare website hosted by CMS. Hospices that fail to meet quality reporting requirements receive a 4.0% reduction to the annual market basket update for the next fiscal year.
Licensure and Certificates of Need (“CON”). Home health, hospice and most senior living communities operate under licenses granted by the health authorities of their respective states. Some states require healthcare providers (including home health, hospice and most senior living providers) to obtain prior state approval for the purchase, construction or expansion of healthcare operations, or changes in services. Certain states, including a number in which we operate, carefully restrict new entrants into the market based on demographic and/or demonstrative usage of additional providers. These states limit the entry of new providers or services and the expansion of existing providers or services in their markets through a CON process, which is periodically evaluated and updated as required by applicable state law. For those states that require a CON, we must also complete a separate application process establishing a location and must receive required approvals. Washington and Montana are the only CON states in which we operate home health or hospice agencies.
Patient Protection and Affordable Care Act (“ACA”). Various healthcare reform provisions became law upon enactment of the ACA in 2010. The reforms contained in the ACA have affected our independent operating subsidiaries in some manner and are directed in large part at increased quality and cost reductions. These reforms include modifications to the conditions of qualification for payment, bundling of payments to cover both acute and post-acute care and the imposition of enrollment limitations on new providers. In 2022 and 2023, HHS engaged in rulemaking under Section 1557 of the ACA that would expand the influence and authority of existing civil rights laws, and prohibitions against discrimination on the bases of race, national origin, sex (or sex stereotype), gender identity or expression, disability, or age, within the healthcare context. On April 27, 2024, HHS finalized and published a final rule containing revised regulations that implemented Section 1557 of the ACA and its anti-discrimination provisions, which contains staggered implementation dates that began taking effect on July 5, 2024. Presidential and congressional elections may result in significant changes in legislation, regulation, and implementation of Medicare, Medicaid, and government policy, along with potential changes to tax rates and other tax treatment of our operations. We continually monitor these developments so we can respond to the changing regulatory environment impacting our business. These rules could be amended by the current administration.
Civil Rights. On January 25, 2024, the HHS Office for Civil Rights (“OCR”) issued guidance to healthcare providers, services, and facilities emphasizing the importance of non-discriminatory visitation policies consistent with CMS regulations and the U.S. National Strategy to Counter Antisemitism, highlighting the prohibition of discrimination based on religion or other protected characteristics during public health emergencies. This guidance also addresses instances of non-compliance, such as unequal treatment based on religious beliefs or dietary restrictions, and outlines the support OCR provides to ensure compliance, encouraging affected individuals to file complaints for potential enforcement actions. This guidance could be amended by the current administration.
Civil and Criminal Fraud and Abuse Laws and Enforcement. Various complex federal and state laws exist which govern a wide array of referrals, relationships and arrangements, and prohibit fraud by healthcare providers. Governmental agencies are devoting increasing attention and resources to such anti-fraud efforts. In connection with our involvement with federal healthcare reimbursement programs, the government or those acting on its behalf may bring an action under the False Claims Act (“FCA”), alleging that a healthcare provider has defrauded the government by submitting a claim for items or services not rendered as claimed, which may include coding errors, billing for services not provided, and submitting false or erroneous cost reports. The FCA is a frequent topic of analysis for the United States Supreme Court. As a result, interpretations of the FCA’s meaning periodically change, and the FCA has been, and may be in the future, amended by Congress as a result of United States Supreme Court decisions. Civil monetary penalties (“CMPs”) under the FCA and other authorities, including the Civil Monetary Penalties Law, 42 U.S.C. § 1320a-7a, are substantial and are adjusted annually for inflation. Under the qui tam or “whistleblower” provisions of the FCA, a private individual with knowledge of fraud may bring a claim on behalf of the federal government and receive a percentage of the federal government’s recovery. Due to these whistleblower incentives, lawsuits have become more frequent. Many states also have a false claim prohibition that mirrors or tracks the federal FCA. Federal law also provides that the Office of the Inspector General for HHS (“OIG”) has the authority to exclude individuals and entities from federally funded healthcare programs on a number of grounds, including, but not limited to, certain types of criminal offenses, licensure revocations or suspensions, and exclusion from state or other federal healthcare programs. In addition, CMS can recover overpayments from healthcare providers up to five years following the year in which payment was made.
We may also face adverse consequences if we violate federal law related to certain Medicare physician referrals. Section 1877 of the Social Security Act, commonly known as the “Stark Law,” provides that a physician may not refer a
Medicare or Medicaid patient for a “designated health service” to an entity with which the physician or an immediate family member has a financial relationship unless the financial arrangement meets an exception under the Stark Law or its regulations. Any funds collected for an item or service resulting from a referral that violates the Stark Law must be repaid to Medicare or Medicaid, any other third-party payor, and the patient. In addition, CMPs, which are adjusted for annual inflation, treble damages, and Medicare exclusion may be imposed for presenting or causing to be presented, a claim for a service rendered in violation of the Stark Law. Many states have enacted healthcare provider referral laws that go beyond physician self-referrals or apply to a greater range of services than just the designated health services under the Stark Law.
Monitoring Compliance in our Operations. As a healthcare provider, we have a compliance program to help us comply with various requirements of federal, state and private healthcare programs. Our compliance program includes, among other things, (1) policies and procedures modeled after applicable laws, regulations, government manuals and industry practices and customs that govern the clinical, reimbursement and operational aspects of our subsidiaries; (2) training about our compliance process for the employees of our independent operating subsidiaries, our directors and officers; (3) training about Medicare and Medicaid laws, fraud and abuse prevention, clinical standards and practices, and claim submission and reimbursement policies and procedures for appropriate employees; and (4) internal controls that monitor, for example, the accuracy of claims, reimbursement submissions, cost reports and source documents, provision of patient care, services, and supplies as required by applicable standards and laws, accuracy of clinical assessment and treatment documentation, and implementation of judicial and regulatory requirements (e.g., background checks, licensing and training). The results of our compliance program are regularly reported to the board of directors.
Additionally, government agencies and other authorities periodically inspect our operations to assess our compliance with various standards, rules and regulations. The robust regulatory and enforcement environment continues to impact healthcare providers, especially in connection with responses to any alleged noncompliance identified in periodic surveys and other inspections by government authorities. Unannounced surveys or inspections generally occur at least annually at our independent operating subsidiaries and may also follow a government agency's receipt of a complaint about an operation. We are also subject to regulatory reviews relating to Medicare services, billings and potential overpayments resulting from the Recovery Audit Contractors, Zone Program Integrity Contractors, Program Safeguard Contractors, Unified Program Integrity Contractors, Supplemental Medical Review Contractors and Medicaid Integrity Contributors programs in which third party firms engaged by CMS conduct extensive reviews of claims data and medical and other records to identify potential improper payments under the Medicare programs. We must pass these inspections to maintain our licensure under state law, to obtain or maintain certification under the Medicare and Medicaid programs, to continue participation in the Veterans Administration (“VA”) program at some operations, and/or to comply with our provider contracts with managed care clients at many operations. From time to time, we, like others in the healthcare industry, may receive notices from federal and state regulatory agencies alleging that we failed to substantially comply with applicable standards, rules or regulations. These notices may require us to take corrective action, may impose CMPs for noncompliance, and may threaten or impose other sanctions and operating restrictions, up through and including the loss of licensure and termination of, or exclusion from, important payor relationships. If our operations fail to comply with these directives or otherwise fail to comply substantially with licensure and certification laws, rules and regulations, we could lose our certification as a Medicare or Medicaid provider, lose our state licenses to operate and be subject to fines and penalties.
Healthcare operations in our industries with otherwise acceptable regulatory histories are generally given an opportunity to correct deficiencies and continue their participation in the Medicare and Medicaid programs by a certain date, usually within nine months, although where denial of payment or similar remedies are asserted, such interim remedies go into effect much sooner. Operations with poor regulatory histories continue to be classified by CMS as poor performing operations notwithstanding any intervening change in ownership, unless the new owner obtains a new Medicare provider agreement instead of assuming the operation's existing agreement. However, new owners (including us, historically) nearly always assume the existing Medicare provider agreement due to the difficulty and time delays generally associated with obtaining new Medicare certifications, especially in previously certified locations with sub-par operating histories. Accordingly, operations that have poor regulatory histories before we acquire them may be more likely to have sanctions imposed upon them by CMS or state regulators.
Regulations Regarding Patient Record Confidentiality. We are also subject to laws and regulations enacted to protect the confidentiality of patient health information. For example, HHS has issued rules pursuant to Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) as amended by the Health Information Technology for Economic and Clinical Health (“HITECH”) Act, which relate to the privacy of certain patient information and provide patients with the right of access to their health information. These rules govern our use and disclosure of protected health information. We have established policies and procedures to comply with HIPAA privacy, security and breach notification requirements at our facilities and operations subject to HIPAA. We maintain a company-wide HIPAA compliance plan, which we believe complies with the HIPAA regulations. The HIPAA regulations have and will continue to impose significant costs on our facilities in order to
comply with these standards. Our operations are also subject to any federal or state privacy-related laws that are more restrictive than the privacy regulations issued under HIPAA. These laws vary and could impose additional penalties for privacy and security breaches. In December 2024, HHS issued a notice of proposed rulemaking proposing several changes to HIPAA’s security rule, including, among other things, requiring written procedures to respond to security incidents, annual security compliance audits, encryption of PHI, and use of multi-factor authentication. These requirements could change before the proposed rule is finalized.
Climate Laws. In 2023, California enacted SB 253 and SB 261, which require new climate disclosures from companies doing business in California. SB 253 requires companies with annual revenues of $1 billion or more to disclose their greenhouse gas emissions. SB 261 requires companies with annual revenues of $500 million or more to disclose their climate-related risks and the measures they use to reduce and adapt to those risks. These reports are first due from companies in 2026. Additional details regarding the application and requirements of these laws will be included in future regulations.
Antitrust Laws. We are also subject to federal and state antitrust laws. Enforcement of the antitrust laws against healthcare providers is common, and antitrust liability may arise in a wide variety of circumstances, including third party contracting, physician relations, joint venture, merger, affiliation and acquisition activities. In some respects, the application of federal and state antitrust laws to healthcare is still evolving, and enforcement activity by federal and state agencies appears to be increasing. At various times, healthcare providers and insurance and managed care organizations may be subject to an investigation by a governmental agency charged with the enforcement of antitrust laws or may be subject to administrative or judicial action by a federal or state agency or a private party. Violators of the antitrust laws could be subject to criminal and civil enforcement by federal and state agencies, as well as by private litigants.
Regulations Specific to Senior Living Communities. Senior living services revenue is primarily derived from private pay residents at rates we establish based upon the needs of the resident, the amount of services we provide the resident, and market rate environment in the area of operation. In addition, Medicaid or other state-specific programs may supplement payments for board and care services provided in senior living communities. A majority of states provide, or are approved to provide, Medicaid payments for personal care and medical services to some residents in licensed senior living communities under waivers granted by or under Medicaid state plans approved by CMS. State Medicaid programs control costs for assisted living and other home- and community-based services by various means such as restrictive financial and functional eligibility standards, enrollment limits and waiting lists. States that administer Medicaid programs for services in senior living communities are responsible for monitoring the services at, and physical conditions of, the participating communities. As a result of the growth of assisted living in recent years, states have adopted licensing standards applicable to assisted living communities. Most state licensing standards apply to assisted living communities regardless of whether they accept Medicaid funding.
Our senior living segment is subject to a variety of federal, state and local environmental laws and regulations. As a senior living services provider, we face regulatory requirements in areas of air and water quality control, medical and low-level radioactive waste management and disposal, asbestos management, response to mold and lead-based paint in our facilities and employee safety.
As an operator of our communities, we also may be required to investigate and remediate hazardous substances that are located on and/or under the property, including any such substances that may have migrated off, or may have been discharged or transported from the property. Part of our operations involves the handling, use, storage, transportation, disposal and discharge of medical, biological, infectious, toxic, flammable and other hazardous materials, wastes, pollutants or contaminants. In addition, we are sometimes unable to determine with certainty whether prior uses of our communities and properties or surrounding properties may have produced continuing environmental contamination or noncompliance, particularly where the timing or cost of making such determinations is not deemed cost-effective. These activities, as well as the possible presence of such materials in, on and under our properties, may result in damage to individuals, property or the environment; may interrupt operations or increase costs; may result in legal liability, damages, injunctions or fines; may result in investigations, administrative proceedings, penalties or other governmental agency actions. Associated costs may not be covered by insurance.
Available Information
We are subject to the reporting requirements under the Securities Exchange Act of 1934, as amended (the “Exchange Act”). Consequently, we are required to file reports and information with the Securities and Exchange Commission (“SEC”), including reports on the following forms: annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act. These reports and other information concerning our company may be accessed through the SEC’s website at http://www.sec.gov.
You may also find on our website at www.pennantgroup.com electronic copies of our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act. Such filings are placed on our website as soon as reasonably possible after they are filed with the SEC. All such filings are available free of charge. Information contained in our website is not deemed to be a part of this Annual Report on Form 10-K.
Item 1A. Risk Factors -
Based on the information currently known to us, we believe that the following information identifies material risk factors affecting our company. However, the risks and uncertainties we face are not limited to those described below. Additional risks and uncertainties may also adversely affect our business. If any of the following risks and uncertainties develops into actual events, these events could have a material adverse effect on our business, financial condition or results of operations. In such case, the trading price of our common stock could decline.
Risks Related to Our Business and Industry
Our revenue could be impacted by federal changes to reimbursement and other aspects of Medicare. We derived 48.3% of our revenue from the Medicare program for the year ended December 31, 2024, which is typical. In addition, other payors may use published Medicare rates as a basis for reimbursements. The Medicare program and its reimbursement rates, caps, deductibles and rules are subject to frequent change for a variety of reasons, which is discussed in Item 1., Government Regulation. Budget pressures also frequently lead the federal government to reduce or limit reimbursement rates under Medicare, and to adjust when or how those reductions or limitations are implemented, including sometimes doing so retroactively. Additionally, Medicare payments can be delayed or denied (including retroactively) due to determinations that certain costs, services or providers are not covered. Accordingly, if Medicare reimbursement rates are reduced or fail to increase as quickly as our costs, if we do not realize an adequate percentage of billed Medicare charges, or if there are changes in the way these programs pay for services or what services or providers are covered, our business and results of operations would be adversely affected. CMS has also introduced in the past, and will likely introduce in the future, new payment models, such as value-based arrangements or payment models that look to numerous factors in order to issue full payment, in markets in which we operate. Those models may depend on the formation of preferred provider relationships among payors and providers. Our operations may not successfully implement or adapt to these changes and our operations could be materially impacted.
Reductions in Medicaid reimbursement rates or changes in the rules governing the Medicaid program could have a material, adverse effect on our revenues, financial condition and results of operations. We derived 13.2% of our revenue from Medicaid programs for the year ended December 31, 2024, which is typical. Any budget reductions or funding restrictions, discontinuance or reduction of federal matching, change in payment methodology or delays in states in which we operate could adversely affect our net patient service revenue and profitability. Like Medicare payments, Medicaid payments can be delayed due to budgetary constraints of the state or state agencies responsible for making such payments, and Medicaid payments may be declined (including retroactively) due to determinations that certain costs, services or providers are not covered by the state Medicaid agency or its intermediary organizations. Additionally, in many states where we operate Medicaid benefits are administered through Medicaid Managed Care Organizations (“MCOs”), which are operated by private insurance companies. These MCOs may apply different, stricter standards for reimbursement and prior authorization of our services, which may further adversely affect our ability to be paid for our services. We can expect continuing cost containment pressures on Medicaid outlays, whether administered directly by a state program or through an MCO, for our services.
Reforms to the U.S. healthcare system continue to impose new requirements upon us and may lower our reimbursements. Healthcare reform is a key political and legislative focal point. We cannot predict what effect legislative or regulatory changes (including, for instance, proposals for Medicare-for-All or public option insurers operated by one or more individual states), will have on our business, including the demand for our services or the amount of reimbursement available for those services. The consequences of elections are not yet fully known for this industry, and our industry may be affected by presidential and congressional election outcomes. It is possible new laws may lower reimbursement or increase the cost of doing business and adversely affect our business.
We are subject to various government reviews, audits and investigations that could adversely affect our business, including an obligation to refund amounts previously paid to us, potential criminal charges, the imposition of fines, and/or the loss of our right to participate in Medicare and Medicaid programs. As discussed in greater detail in Item 1., Government Regulation, as a result of our participation in the Medicaid and Medicare programs, we are frequently subject to various governmental reviews, audits and investigations to verify our compliance with these programs. In addition to routine audits, in its November 2023 Final Rule, CMS finalized a provisional period of enhanced oversight, including prepayment medical reviews, for all
hospice providers that are newly enrolled or undergo a change of ownership, which expanded in June 2024 to include reactivated hospice providers in states where we operate. Private pay sources also reserve the right to conduct audits. Disagreements about billing and reimbursement are common in our industry due in part to the subjectivity inherent in patient diagnosis and care, record keeping, claims processing and other aspects of the patient service and reimbursement processes. An adverse review, audit or investigation could result in (1) an obligation to refund amounts previously paid to us by payors in amounts that could vastly exceed the revenue derived from claims actually reviewed in the audit, and could be material to our business; (2) state or federal agencies imposing fines, penalties and other sanctions on us; (3) suspension of Medicare or Medicaid payments (4) loss of our right to participate in the Medicare or Medicaid programs or one or more private payor networks; (5) an increase in private litigation against us; and (6) damage to our reputation with potential residents, referral sources, and others in various markets.
In cases where claim and documentation review by any CMS contractor results in repeated poor performance, an operation can be subjected to protracted oversight. Sustained failure to demonstrate improvement towards meeting all claim filing and documentation requirements could ultimately lead to Medicare decertification. Additionally, both federal and state government agencies have heightened and coordinated civil and criminal enforcement efforts as part of numerous ongoing investigations of healthcare companies. The focuses of these investigations include among other things: cost reporting and billing practices; quality of care; financial relationships with referral sources; and medical necessity of services provided. If any of our affiliated operations is decertified, loses its license(s), or is subject to criminal charges or civil claims, administrative sanctions or penalties, our revenue, financial condition or results of operations would be adversely affected. We or some of the key personnel of our independent operating subsidiaries could also be temporarily or permanently excluded from future participation in state and federal healthcare reimbursement programs such as Medicaid and Medicare. In addition, the report of such issues at any of our affiliated operations could harm our reputation for quality care and could cause us to be in default under some of our agreements, including agreements governing outstanding indebtedness. Responding to audits, litigation or enforcement efforts diverts material time, resources and attention, and could have a materially detrimental impact on our results of operations during and after any such investigation or proceedings, regardless of whether we prevail.
If we do not operate in compliance with the extensive laws and regulations to which we are subject, or if these laws and regulations change, we could be required to make significant expenditures or change our operations to bring our operations into compliance. We, like other companies in the healthcare industry, are required to comply with extensive and complex laws and regulations at the federal, state and local government levels as discussed in greater detail in Item 1., Government Regulation. These laws and regulations are subject to frequent and unpredictable change. If we fail to comply with these applicable laws and regulations, we could suffer civil or criminal penalties and other detrimental consequences, including denial of reimbursement, imposition of fines, temporary suspension of admission of new patients, suspension or decertification from the Medicaid and Medicare programs, restrictions on our ability to acquire new operations or expand or operate existing operations, the loss of our licenses to operate and the loss of our ability to participate in federal and state reimbursement programs. These laws and regulations are complex, and we do not always have the benefit of significant regulatory or judicial interpretation of these laws and regulations. Changing interpretations or enforcement of these laws and regulations could subject our current or past practices to allegations of impropriety or illegality or could require us to change our operations, equipment, personnel, services, capital expenditure programs and operating expenses.
Public and government calls for increased survey and enforcement efforts toward our industries could result in increased scrutiny and potential sanctions or costly remedies. Government authorities have increased the scope or number of inspections or surveys and the severity of consequent citations for alleged failure to comply with regulatory requirements. As discussed in Item 1., Government Regulation, from time to time in the ordinary course of business, we receive deficiency reports from state and federal regulatory bodies resulting from such inspections or surveys. Although most inspection deficiencies are resolved through an agreed-upon plan of corrective action, the reviewing agency typically has the authority to take further action against a licensed or certified operation, which could result in the imposition of fines and penalties, reports to the national practitioner data bank, imposition of a provisional or conditional license, suspension or revocation of a license, suspension of new admission or bed holds, loss of certification as a provider under state or federal healthcare programs or termination of the operations’ payment relationships with those programs, or imposition of other sanctions, including criminal penalties. Furthermore, in some states, citations issued against one operation can affect other operations in the state, particularly where there is any element of common or affiliated ownership. Revocation of a license or decertification at a given operation could therefore impair our ability to obtain new licenses or to renew existing licenses at other operations, which may also trigger defaults or cross-defaults under our leases and our credit arrangements, or adversely affect our ability to operate in the future. If state or federal regulators were to determine, formally or otherwise, that one operation’s regulatory history ought to impact another of our existing or prospective businesses, this could also increase costs, result in additional fines or penalties, result in increased scrutiny by state and federal survey agencies, and impact our expansion plans as well as our ongoing operations. In addition, from time to time, we may opt to voluntarily stop accepting new patients pending completion of a new state survey, to
avoid straining staff and other resources while retraining staff, upgrading operating systems or making other operational improvements, all of which can impact our financial results.
Future cost containment initiatives undertaken by payors may limit our future revenue and profitability. Our managed care revenue and profitability may be affected by continuing efforts of third-party payors to maintain or reduce costs of healthcare by lowering payment rates, narrowing the scope of covered services and network providers, increasing case management review of services and negotiating pricing. In addition, sustained unfavorable economic conditions may affect the number of patients enrolled in managed care programs and the profitability of managed care companies, which could result in reduced revenue due to reduced reimbursement for our services. There can be no assurance that third-party payors will make timely payments for our services, not seek recoupment of payments on grounds that may or may not be valid, or that we will continue to maintain our current payor or revenue mix. We are continuing our efforts to develop our private pay sources of revenue. Any changes in payment levels from current or future third-party payors could have a material adverse effect on our business, financial condition, results of operations and cash flows. In addition, enrollment in Medicare Advantage programs continues to grow nationwide, and an increasing proportion of Medicare and Medicaid funds are managed by MCOs that also act as third-party payors who may seek to reduce reimbursement as described above.
Any economic downturn, deepening of an economic downturn, continued deficit spending by the Federal Government or state budget pressures may result in a reduction in payments and covered services. Adverse economic developments in the United States could lead to a reduction in Federal Government expenditures, including government-funded programs in which we participate, such as Medicare and Medicaid. In addition, if at any time the Federal Government is not able to meet its debt payments due to Congress failing to appropriate funds for the payment of these obligations, the Federal Government may stop or delay making payments on its obligations, including funding for government programs in which we participate, such as Medicare and Medicaid. Failure of the government to make payments under these programs could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Further, any failure by the United States Congress to complete the federal budget process and fund government operations may result in a Federal Government shutdown, potentially causing us to incur substantial costs without reimbursement under the Medicare program, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. As an example, the failure of the 2011 Joint Select Committee to meet its Deficit Reduction goal resulted in an automatic reduction in Medicare home health and hospice payments of 2% beginning April 1, 2013 (“sequestration” - suspended from May 1, 2020 through March 31, 2022; further extended by the Infrastructure Investment and Jobs Act of 2023, the Consolidated Appropriations Act of 2023, and the Consolidated Appropriations Act of 2024; the continuing resolution for further spending passed in the American Relief Act of 2025 (“ARA”) did waive the 4% pay-as-you-go sequestration, but the ARA did not halt reductions found in Medicare payment rules that took effect for fiscal year 2025, including those reductions that exceeded 2%). In addition, the Federal Reserve has increased interest rates repeatedly and significantly in recent quarters and may further increase or decrease interest rates in future quarters, impacting our cost of capital, our operating costs, and the economy as a whole.
Increased competition for, or a shortage of, nurses and other skilled personnel could increase our staffing and labor costs and negatively impact our operations. Our success depends upon our ability to retain and attract nurses, certified nurse assistants, social workers and speech, physical and occupational therapists, as well as skilled personnel who are responsible for the day-to-day operations of each of our affiliated operations. If we fail to attract and retain qualified and skilled personnel, or if the associated costs to do so increase, our independent operating subsidiaries’ ability to conduct their business operations effectively could be harmed. Staffing challenges increased during the pandemic and have persisted due to health care worker burnout, COVID-19 exposures, vaccine mandates, and wage inflation, increasing the competition for qualified staff and cost of retaining personnel, and continue to affect our operations. There can be no assurance that we will be able to attract and retain key personnel going forward.
We depend on our management team and local leaders, and the loss of their services could harm our business. We believe that our success depends in part on the continued services of our executive management and local leadership teams. The loss of, or failure to recruit, such key personnel could have a material adverse effect on our business and could adversely affect our strategic relationships and impede our ability to execute our business strategies. The market for qualified individuals is highly competitive and finding and recruiting suitable replacements for our leaders may be difficult, time-consuming and costly.
Our hospice independent operating subsidiaries are subject to annual Medicare caps calculated by Medicare. With respect to our hospice independent operating subsidiaries, overall payments made by Medicare for each Medicare beneficiary are subject to caps calculated by Medicare, as discussed in greater detail in Item 1., Government Regulation. If payments received by any one of our hospice provider numbers exceeds the caps for the beneficiary, we are required to reimburse Medicare for payments received in excess of the caps, which could have a material adverse effect on our business. Additionally, the annual increase in
Medicare beneficiary caps may not keep pace with the rate of inflation or increased operating costs as it applies to the costs of caring for such patients, potentially resulting in our hospice independent operating subsidiaries treating these patients at a loss.
Security breaches and other cyber-security incidents could subject us to significant liability. Data breaches and leaks, which represent a material risk to our business, are reported to have occurred with greater frequency and severity in 2024 than in prior years. Our business depends on the proper functioning and availability of our computer systems and networks. Our security measures designed to protect our information systems, data and patient health information and disaster recovery plan may not prevent damage, interruption, or breach of our information systems and operations. In addition, hardware, software or applications we use may contain defects in design or manufacture or other problems that could unexpectedly compromise the security of our information systems. Unauthorized parties may attempt to gain access to our systems or operations, or those of third parties with whom we do business, through fraud or other forms of deceiving our employees or contractors. In addition, costs and potential problems and interruptions associated with the implementation of new or upgraded systems and technology or with maintenance or support of existing systems also could disrupt or reduce the efficiency of our operations. If a cyber-security attack or other unauthorized attempt to access our systems, such as a ransomware attack, were to be successful, the incident could result in the theft, destruction, loss, misappropriation or release of confidential information or intellectual property, and could cause delays or disruptions that may materially impact our ability to provide various healthcare services. Any successful cyber-security attack or other unauthorized attempt to access our systems or operations also could result in negative publicity which could damage our reputation or brand with our patients, referral sources, payors or other third parties and could subject us to substantial regulatory, civil or criminal penalties, fines, investigations and enforcement actions, including under HIPAA and other federal and state privacy laws, including, for example, the California Consumer Privacy Act and Nevada Privacy Law, which includes a private right of action that may expose us to private litigation regarding our privacy practices and significant damages awards or settlements in civil litigation.
State efforts to regulate or deregulate the healthcare services industry or the construction or expansion of the number of home health, hospice or senior living operations could impair our ability to expand or result in increased competition. As discussed in greater detail in Item 1., Government Regulation, our ability to acquire or establish new home health, hospice or senior living operations or expand or provide new services at existing operations would be adversely affected if we are unable to obtain the necessary approvals, if there are changes in the standards applicable to those approvals, new laws or changes in applicable laws governing CON requirements (or increasing the circumstances where a CON is needed), or if we experience delays and increased expenses associated with obtaining those approvals. We may not be able to obtain licensure, CON approval, Medicare or Medicaid certification, Attorney General approval or other necessary approvals for future expansion projects. In recent years, states including, but not limited to, California and Oregon have introduced additional regulatory reviews and other barriers to health care transactions. Conversely, and specific to the highly competitive senior living industry, the elimination or reduction of state regulations that limit the construction, expansion or renovation of new or existing communities could result in increased competition to us. In general, regulatory and other barriers to entry in the senior living industry are not prohibitive. Over the last several years, there has been a significant increase in the construction of new senior living communities, including in the markets where we provide services. This has resulted in increased competition in many of our markets. Such new competition may limit our ability to attract new residents, raise rents or otherwise expand our senior living business, which could have a material adverse effect on our revenues, results of operations and cash flow.
Changes in federal and state employment-related laws and regulations could increase our cost of doing business. Our independent operating subsidiaries are subject to a variety of federal and state employment-related laws and regulations, including, but not limited to, the U.S. Fair Labor Standards Act which governs such matters as minimum wages, overtime and other working conditions, the Americans with Disabilities Act (the “ADA”) and similar state laws that provide civil rights protections to individuals with disabilities in the context of employment, public accommodations and other areas, the National Labor Relations Act, regulations of the Equal Employment Opportunity Commission, regulations of the Office of Civil Rights, regulations of state Attorneys General, family leave mandates and a variety of similar laws. Because labor represents a large portion of our operating costs, changes in federal and state employment-related laws and regulations could increase our cost of doing business. We also may be subject to employee-related claims such as wrongful discharge, discrimination or violation of equal employment law. Employment claims, such as wage and hour claims, frequently are the subject of class action lawsuits in many states in which our independent affiliates operate, including, for example, California.
Required regulatory approvals could delay or prohibit transfers of our healthcare operations, which could result in periods in which we are unable to receive reimbursement for such properties. Our independent operating subsidiaries must be licensed under applicable state law and, depending upon the type of operation, certified or approved as providers under the Medicare and/or Medicaid programs. In the process of acquiring or transferring operating assets, our operations must receive change of ownership approvals from state licensing agencies, Medicare and Medicaid, and third-party payors. If there are any delays in receiving regulatory approvals from the applicable federal, state or local government agencies, or from independent accreditation authorities that may be required by federal, state or local government agencies, or the inability to receive such
approvals, such delays could result in delayed or lost reimbursement related to periods of service prior to the receipt of such approvals. By way of example, in 2022 California passed Assembly Bill 2673 which prohibits issuance of new hospice licenses and limits transfer of existing licenses, and other states where we operate may introduce similar legislation in the future. In 2024, CMS implemented a rule prohibiting hospice ownership from being transferred more than once in a 36-month period.
Compliance with federal and state fair housing, fire, safety and other regulations may require us to make unanticipated expenditures, which could be costly to us. We must incur the expense of complying with the federal Fair Housing Act and similar state laws, and applicable fire and safety regulations, building codes and other land use regulations and food licensing or certification requirements as they may be adopted by governmental agencies and bodies from time to time and the expense may be substantial. Changes to these laws may require us to close operations, limit occupancy, or make other costly changes.
Our revenue, financial condition and results of operations could be negatively impacted by any changes in the acuity mix of patients in our affiliated operations as well as payor mix and payment methodologies. Our revenue is determined in part by the acuity of home health and hospice patients and senior living residents. Changes in the acuity level of patients we attract, as well as our payor mix among Medicare, Medicaid, managed care organizations and private payors, may significantly affect our profitability because we generally receive higher reimbursement rates for high acuity patients and because the payors reimburse us at different rates. For the year ended December 31, 2024, 61.5% of our revenue was provided by government payors that reimburse us at predetermined rates, which is typical. If we fail to maintain our proportion of high acuity patients or if there is any significant increase in the percentage of the patients of our independent operating subsidiaries for whom we receive Medicaid reimbursement, our results of operations may be adversely affected. Among other initiatives, these payors attempt to control healthcare costs by contracting with healthcare providers to obtain services on a discounted basis. We believe that this trend will continue and may limit reimbursements for healthcare services. If insurers or managed care companies from whom we receive substantial payments were to reduce the amounts they pay for services, we may lose patients if we choose not to renew our contracts with these insurers at lower rates.
We are subject to litigation that could result in significant legal costs and large settlement amounts or damage awards. Our business involves a significant risk of liability given the age and health of the patients and residents of our independent operating subsidiaries and the services we provide. The frequency and severity of litigation in the healthcare industry has increased, due in part to large verdicts and punitive damage awards. Claims are filed based upon a wide variety of assertions and theories, including deficiencies in conditions of participation under certain state and federal healthcare programs and wage and hour class actions. Plaintiffs’ attorneys have become increasingly aggressive in their pursuit of claims against healthcare providers, including home health, hospice and senior living providers, employing a wide variety of advertising and solicitation activities to generate more claims. Additionally, California, through its passage of AB 35, has increased the non-economic (i.e., pain and suffering) damages that may be recovered by attorneys on claims of professional negligence or malpractice in healthcare cases filed in California, and may embolden plaintiff’s attorneys to be more aggressive in their pursuit of facilities operated by our independent operating subsidiaries and the services provided through them. Since California’s passage of AB 35, Iowa and Nevada have enacted similar laws that increase the non-economic damages that may serve as the basis for the recovery for attorney’s fees in those states, which may stimulate additional litigation in those states and could have an adverse material effect on our financial performance. The defense of lawsuits may result in significant legal costs, regardless of the outcome. Further, such litigation against us or our independent operating subsidiaries may result in increased liability insurance premiums and/or a decline in available insurance coverage levels, which could materially and adversely affect our business, financial condition and results of operations.
Instances of noncompliance can decrease our revenue. As discussed under Item 1., Monitoring Compliance in our Operations, we have internal compliance policies and procedures, including ongoing monitoring and controls, pursuant to which we have identified, and may in the future identify, deficiencies in the assessment of and recordkeeping for patients and residents. We must accrue liabilities for claim costs and interest and repay any amounts due in normal course. Failure to refund overpayments within required time frames (as described in greater detail under Item 1., Government Regulation) could result in FCA liability and other penalties, fines, or sanctions. If future investigations ultimately result in findings of significant billing and reimbursement noncompliance, which require us to record significant additional provisions or remit payments, our business, financial condition and results of operations could be materially and adversely affected.
We may be unable to complete future acquisitions at attractive prices or at all, which may adversely affect our revenue growth. To date, our revenue growth has been significantly accelerated by our acquisition of new operations. Subject to general market conditions and the availability of essential resources and leadership within our company, we continue to seek home health, hospice and senior living acquisition opportunities that are consistent with our geographic, financial and operating objectives. We face competition for the acquisition of operations and businesses and expect this competition to increase. Based upon factors such as our ability to identify suitable acquisition candidates, the purchase price of the operations, prevailing market conditions, the availability of leadership to manage new operations and our own willingness to take on new operations,
the rate at which we have historically acquired home health, hospice and senior living operations has fluctuated and we anticipate similar fluctuation in the future. Further, acquisitions may require financing, which may not be available to us or may be available to us only on terms that are not favorable. If funds are raised through the issuance of additional equity securities, the percentage ownership of our stockholders would be diluted, and any newly issued equity securities may have rights, preferences or privileges senior to those of our common stock. We may acquire operations that prove to be non-strategic or less desirable, and we may consider disposing of such operations or exchanging them for operations which are more desirable.
We may not be able to successfully integrate acquired operations, and we may not achieve the benefits we expect from our acquisitions. We may not be able to successfully or efficiently integrate new acquisitions with our existing independent operating subsidiaries, culture and systems. We also may determine that renovations of acquired operations and changes in staff and operating management personnel are necessary to successfully integrate those acquisitions into our existing operations. We may not be able to recover the costs incurred to reposition or renovate newly independent operating subsidiaries. The financial benefits we expect to realize from many of our acquisitions are largely dependent upon our ability to improve clinical performance, overcome regulatory deficiencies, rehabilitate or improve the reputation of the operations in the community, increase and maintain census, control costs, and in some cases change the patient acuity mix. Growth also places significant demands on our leaders and operational, financial and management information systems. If we are unable to accomplish any of these objectives at the independent operating subsidiaries we acquire, we will not realize the anticipated benefits and we may experience lower than anticipated profits, or even losses.
In undertaking acquisitions, we may be impacted by costs, liabilities and regulatory issues that may adversely affect our operations. In undertaking acquisitions, we also may be adversely impacted by unforeseen liabilities attributable to the prior providers who operated the acquired operations, against whom we may have little or no recourse. Many operations we have historically acquired were underperforming prior to the acquisition. Even where operations have been improved, we still may face post-acquisition regulatory issues related to pre-acquisition events. These may include, without limitation, payment recoupment related to our predecessors’ prior noncompliance, the imposition of fines, penalties, operational restrictions or special regulatory status. Further, we may incur post-acquisition compliance risk due to the difficulty or impossibility of immediately or quickly bringing non-compliant operations into full compliance. Diligence materials pertaining to acquisition targets, especially the underperforming operations that often represent the greatest opportunity for return, are often inadequate, inaccurate or impossible to obtain, sometimes requiring us to make acquisition decisions with incomplete information. Operations that we have acquired or may acquire in the future may generate unexpectedly low returns, may cause us to incur substantial losses (including sanctions, fines, penalties, and other liabilities that state and federal authorities may seek to impose upon us under various theories of successor liability despite our efforts to prevent such liabilities during our transactions), may require unexpected levels of management time, expenditures or other resources, or may otherwise not meet a risk profile that our investors find acceptable. We also incur regulatory risk in acquiring certain operations due to the licensing, certification and other regulatory requirements affecting our right to operate the acquired operations, which are frequently obtained post-closing. If we were denied licensure or certification for any reason, we might not realize the expected benefits of the acquisition and would likely incur unanticipated costs and other challenges which could cause our business to suffer.
If our referral sources fail to view us as an attractive provider, or if our referral sources otherwise refer fewer patients or residents, our patient or resident base may decrease. We rely on appropriate referrals from physicians, hospitals and other healthcare providers in the communities we serve to attract appropriate residents and patients to our affiliated operations. Our referral sources are not obligated to refer business to us and may refer business to other healthcare providers. If we lose, or fail to maintain, existing relationships with our referral resources, fail to develop new relationships, or if we are perceived by our referral sources as not providing high quality patient care, our independent subsidiaries’ respective censuses could decline and our patient mix could change. In addition, if any of our referral sources have a reduction in patients whom they can refer due to a decrease in their business, our census could decline and patient mix could change.
If we do not achieve and maintain competitive quality of care ratings from CMS and private organizations engaged in similar monitoring activities, our business may be negatively affected. Providing quality patient care is the cornerstone of our business. We believe that referral sources, residents and patients select us in large part because of our reputation for delivering quality care. If we should fail to attain our goals regarding acute care hospitalization readmission rates and other quality metrics, we expect our ability to generate referrals would be adversely impacted, which could have a material adverse effect upon our business, financial condition, results of operations and cash flows. In addition, our home health payment rates could be reduced, as described in Item 1., Government Regulation - Home Health Value Based Purchasing (HHVBP); further, our star ratings measured by CMS on a five-star basis may decrease, resulting in lower estimation by potential residents and patients and reducing the likelihood of having those potential residents and patients use our services, as described in Item 1.,
Our Competitive Strengths - Superior Clinical Outcomes and Quality Care.
If we are unable to obtain insurance, or if insurance becomes more costly for us to obtain, our business may be adversely affected. It may become more difficult and costly for us to obtain coverage for patient care liabilities and other risks, including property and casualty insurance. Our claims history, asset mix, or other factors may adversely affect our ability to obtain insurance at favorable rates. Recent legislation in Nevada that prohibits the reduction of funds available to pay claims based on the costs of defending claims or litigation may result in higher premiums for our operations within that state. Similarly, recent legislation in California and Nevada increasing the amounts of non-economic damages recoverable in actions based on professional negligence against healthcare providers may also result in higher premiums for our operations within those states and limit the options for available coverage. Our insurance carriers may require us to pay substantially higher premiums for the same or reduced coverage for insurance, including workers compensation, property and casualty, automobile, employment practices liability, directors and officers liability, employee healthcare insurance benefits, and general and professional liability coverages. Further, many claims and other risks we face are not insurable. Climate change and the proliferation of natural disasters may increase the cost of coverage or make coverage impossible to obtain.
We retain certain risks related to our insurance coverage. Under our insurance policies, we bear the risk of loss up to specified deductible limits, which may be substantial if there is a surge in the volume of claims subject to the deductible. We recognize obligations associated with these costs in the period in which a claim is incurred, including with respect to both reported claims and claims incurred but not reported. These costs generally are estimated based on our historical claims experience. Projections of self-insured retention losses are estimates that are subject to significant variability, and as a result, our actual losses and expenses may be more or less than recorded liabilities.
Our self-insurance programs may expose us to significant and unexpected costs and losses. Our general liability and workers compensation insurance policies include self-insured retentions under which we are responsible to pay for a portion of each claim. We establish insurance loss reserves based on an estimation process that use information obtained from both company-specific and industry data. The estimation process requires us to continually monitor and evaluate the life cycle of claims. Using data obtained from this monitoring and our assumptions about emerging trends, we, along with an independent actuary, develop information about the size of ultimate claims based on historical experience and other available industry information. The most significant assumptions used in the estimation process include determining the trend in costs, the expected cost of claims incurred but not reported and the expected costs to settle or pay damages with respect to unpaid claims. It is possible, however, that the actual liabilities may exceed our estimates of loss. We may also experience an unexpectedly large number of successful claims or claims that result in costs or liability significantly exceeding our projections. For these and other reasons, our self-insurance reserves could prove to be inadequate, resulting in liabilities exceeding our available insurance and self-insurance reserves. If a successful claim is made against us and it is not covered by our insurance or exceeds the insurance policy limits, our business may be negatively and materially impacted. Further, because our self-insured retentions under our general and professional liability and workers’ compensation program apply on a per claim basis, there is no limit to the maximum number of claims or the total amount for which we could be responsible during any policy period. We also self-insure our employee health benefits. With respect to our health benefits self-insurance, our reserves and premiums are computed based on a mix of company-specific and general industry data. Even with a combination of limited company-specific loss data and general industry data, our loss reserves are based on actuarial estimates that may not correlate to actual loss experience in the future. Therefore, our reserves may prove to be insufficient, and we may be exposed to significant and unexpected losses.
The unionization of our workers may adversely affect our revenue and profitability. To date, with the exception of one joint venture, where certain employees had elected to unionize prior to our acquisition, our employees have chosen not to unionize. Throughout 2023 and 2024, however, there has been a nationwide trend of increasing union activity, including strikes in the healthcare industry and in states, such as California, in which we operate. Increasing trends of service workers successfully organizing to unionize their workplaces may increase the likelihood of our employees seeking to unionize their activities at one or more additional locations controlled by our independent operating subsidiaries. If union activity among our employees increases, our cost of doing business could increase, our operations could experience disruption, and affected operations may no longer be economical to continue operating. Further, labor disputes and unionization efforts, among our own employees or among the employees of our referral partners, payors, vendors, joint venture partners, acquisition targets, or other parties, could lead to work stoppages, slowdown, strikes, lockouts, and increased costs, which could materially and adversely impact our operations.
Because we lease most of our affiliated senior living communities, we could experience risks associated with leased property, including risks relating to lease termination, lease extensions and special charges, which could adversely affect our business, financial position or results of operations. As of December 31, 2024, we leased all of our senior living communities, except for three. We also leased all of our administrative offices. Most of our leases are triple-net leases, which means that, in addition to rent, we are required to pay for the costs related to the property (including property taxes, insurance, and maintenance and repair costs), the cost of which tend to increase year-over year and may adversely affect us with future increases and operating expense reconciliations due for prior years. Under certain master leases, a breach at a single community
could subject one or more of the other communities covered by the same master lease to the same default risk. Failure to comply with provider requirements is a default under several of the leases and master lease agreements. In addition, lease defaults could trigger cross-default provisions in our outstanding debt arrangements and other leases. With an indivisible lease, it is difficult to restructure the composition of the portfolio or economic terms of the lease without the consent of the landlord.
A housing downturn could decrease demand for assisted living services. Seniors often use the proceeds of home sales to fund their admission to assisted living communities. A downturn in the housing markets, such as the slowdown in activity that was ongoing in 2023 and 2024 as a result of higher-than-normal mortgage interest rates, could adversely affect seniors’ ability to afford our resident fees and entrance fees. If national or local housing markets enter a persistent decline in prices or transaction activity, our occupancy rates, revenues, results of operations and cash flow could be negatively impacted.
Failure to generate sufficient cash flow to cover required payments or meet operating covenants under our long-term debt and operating leases could result in defaults under such agreements and cross-defaults under other debt or operating lease arrangements, which could harm our independent operating subsidiaries and cause us to lose operations or experience foreclosures. We have significant future operating lease obligations. We intend to continue financing operations through long-term operating leases, mortgage financing and other types of financing, including borrowings under future credit facilities we may obtain. We may not generate sufficient cash flow from operations to cover required interest, principal and lease payments. If we are unable to generate sufficient cash flow from operations in the future to service our debt or to make lease payments on our operating leases, we may be required, among other things, to seek additional financing in the debt or equity markets, refinance or restructure all or a portion of our indebtedness, sell selected assets, reduce or delay planned capital expenditures or delay or abandon desirable acquisitions. Such measures might not be sufficient to enable us to service our debt or to make lease payments on our operating leases. The failure to make required payments on our debt or operating leases or the delay or abandonment of our planned growth strategy could adversely affect our future ability to generate revenue and sustain profitability and subject us to foreclosure. In addition, any such financing, refinancing or sale of assets might not be available on terms that are economically favorable to us, or at all. Our financing arrangements contain restrictions, covenants and events of default that, among other things, could limit our ability to respond to market conditions, provide for capital investment needs or take advantage of business opportunities by restricting our ability to incur or guarantee additional indebtedness or requiring us to offer to repurchase such indebtedness in the event of a change of control or a change of control triggering event; pay dividends or make distributions; make investments or acquisitions; sell, transfer or otherwise dispose of certain assets; create liens; consolidate or merge; enter into transactions with affiliates; and prepay and repurchase or redeem certain indebtedness.
The condition of the financial markets, including volatility and deterioration in the capital and credit markets, could limit the availability of debt and equity financing sources to fund the capital and liquidity requirements of our business, as well as negatively impact or impair the value of our future portfolio of cash, cash equivalents and investments. Credit markets are cyclical. Volatility in financial and credit markets may reduce the availability of certain types of debt financing and restrict the availability of credit. Further, we anticipate that our future cash, cash equivalents and investments may be held in a variety of interest-bearing instruments. As a result of the uncertain domestic and global political, credit and financial market conditions, investments in these types of instruments pose risks arising from liquidity and credit concerns.
Inflation may negatively impact profitability. The annual inflation rate in recent years has impacted our operations, placing upward pricing pressure on all things from wages to supplies to energy costs. Inflation is expected to ease in 2025 but may continue to affect the Company’s profit in providing services. We have historically derived a substantial portion of our revenue from the Medicare program. We also derive revenue from state Medicaid and similar reimbursement programs. Payments under these programs generally provide for reimbursement levels that are adjusted for inflation annually. These inflation-based increases may not continue in the future, such as in the case of Medicare payments subject to reduction under sequestration required by prior legislation. Even if these reimbursement rate increases continued, such adjustments may not reflect the actual increase in our costs for providing healthcare services. Labor and supply expenses make up a substantial portion of our cost of services. Those expenses are subject to increase in periods of rising inflation and when labor shortages occur in the marketplace. Inflation has led, and may continue to lead, to increased interest rates, which have and could continue to increase our cost of capital, impair consumers’ ability to purchase our services, or otherwise harm us financially.
Changes to immigration law or enforcement could adversely affect our results from operations. Changes to immigration laws and policies, or increased enforcement of existing laws and regulations, could impact our employees or the labor pool from which we hire future employees. Such changes could reduce the number of eligible workers and increase wage costs, including for skilled workers who may work or receive professional training in the United States under various visa programs, making it more difficult or impossible for us to staff our operations.
Extreme weather, natural disasters, or other catastrophic events could adversely affect our results from operations. We operate and are subject to long term leases in areas particularly susceptible to damage or losses caused by catastrophic or extreme weather and other natural events, including fires, snow, rain or ice storms, windstorms, tornadoes, hurricanes, earthquakes, landslides or mudslides, flooding and other severe weather. Many of our services require our employees to travel to patients’ homes by car. Adverse weather events could impair our ability to provide services and could cause substantial damages or losses to our communities or operations, which may not be covered by insurance. These events may also indirectly affect our business by increasing the cost of (or making unavailable) insurance on terms we find acceptable. Changes in regulations relating to climate change could require us to change the way we provide services and could result in increased costs without a corresponding increase in revenue.
Delays in reimbursement may cause liquidity problems. If we experience problems with our billing information systems or if payment issues arise with Medicare, Medicaid or other payors, we may encounter delays in our payment cycle or delays in submitting required cost reports. From time to time, we have experienced such delays as a result of government payors instituting planned reimbursement delays for budget balancing purposes or as a result of prepayment reviews. Some states in which we operate experience or have experienced budget deficits or could have a budget deficit in the future, which may delay reimbursement in a manner that would adversely affect our liquidity. In addition, from time to time, procedural issues require us to resubmit claims before payment is remitted, which contributes to aged receivables. Unanticipated delays in receiving reimbursement from state programs due to changes in their policies or billing or audit procedures may adversely impact our liquidity and working capital. Failure to timely submit required cost reports may result in financial penalties.
Compliance with the regulations of the Department of Housing and Urban Development (“HUD”) may require us to make unanticipated expenditures which could increase our costs. Seventeen of our affiliated senior living communities are currently subject to regulatory agreements with HUD that give the Commissioner of HUD broad authority to have us replaced as the operator of those communities in the event that the Commissioner determines there are operational deficiencies at such communities under HUD regulations. Compliance with HUD’s requirements can often be difficult because these requirements are not always consistent with the requirements of other federal and state agencies and, in some instances, may require us to make additional capital expenditures to meet HUD’s heightened requirements. Appealing a failed inspection can be costly and time-consuming and, if we do not successfully remediate the failed inspection, we could be precluded from obtaining HUD financing in the future or we may encounter limitations or prohibitions on our operation of HUD-insured communities.
Failure to comply with existing environmental laws could result in increased expenditures, litigation and potential loss to our business and in our asset value. Our independent operating subsidiaries are subject to regulations under various federal, state and local environmental laws, primarily those relating to the handling, storage, transportation, treatment and disposal of medical waste; the identification and warning of the presence of asbestos-containing materials in buildings, as well as the encapsulation or removal of such materials; and the presence of other substances in the environment. The presence of such materials may be unknown and could result in remediation costs, fines, damages and other material harm to our business.
We are a holding company with no operations and rely upon our independent operating subsidiaries to provide us with the funds necessary to meet our financial obligations. We are a holding company with no direct operating assets, employees or revenues. Each of our affiliated operations is operated through a separate, independent subsidiary, which has its own management, employees and assets. Our principal assets are the equity interests we directly or indirectly hold in our independent operating subsidiaries. As a result, we are dependent upon distributions from our subsidiaries to generate the funds necessary to meet our financial obligations. Our subsidiaries are legally distinct from us and have no obligation to make funds available to us. The ability of our subsidiaries to make distributions to us will depend substantially on their respective operating results and will be subject to restrictions under, among other things, the laws of their jurisdiction of organization, which may limit the amount of funds available for distribution to investors or stockholders, agreements of those subsidiaries, the terms of our financing arrangements and the terms of any future financing arrangements of our subsidiaries.
Two of our directors continue to serve as a director on the Ensign board of directors, and ownership of shares of Ensign common stock or equity awards of Ensign by our directors and executive officers may create conflicts of interest or the appearance of conflicts of interest. Two of our directors continue to serve on the Ensign board of directors and a portion of our executive officers and non-employee directors own shares of Ensign common stock. This could create, or appear to create, potential conflicts of interest when our or Ensign’s management or directors face decisions that could have different implications for us and Ensign, including our existing long term leases, any commercial agreements entered into in the future between us and Ensign and the allocation of such directors’ time between us and Ensign.
Risks Related to Ownership of Our Common Stock
Anti-takeover provisions in our organizational documents and Delaware law might discourage or delay acquisition attempts for us that you might consider favorable. Our amended and restated certificate of incorporation and amended and restated bylaws may make the merger or acquisition of our company more difficult without the approval of our board of directors. Among other things, these provisions: allow us to authorize the issuance of undesignated preferred stock, the terms of which may be established and the shares of which may be issued without stockholder approval, and which may include super voting, special approval, dividend, or other rights or preferences superior to the rights of the holders of common stock; establish advance notice requirements for nominations for elections to our board or for proposing matters that can be acted upon by stockholders at stockholder meetings; create a classified board of directors whose members serve staggered three-year terms; and limit the ability of our stockholders to call and bring business before special meetings. Further, as a Delaware corporation, we are also subject to provisions of Delaware law, which may impair a takeover attempt that our stockholders may find beneficial. These provisions could discourage, delay or prevent a transaction involving a change in control of our company, including actions that our stockholders may deem advantageous, or negatively affect the trading price of our common stock. These provisions could also discourage proxy contests and make it more difficult for our stockholders to elect directors of their choosing and to cause us to take other corporate actions desired.
Item 1B. Unresolved Staff Comments
None.
Item 1C. Cybersecurity
We leverage information technology to enable our teams to share best practices, stay informed, adapt to challenges and opportunities promptly, improve the quality of care, mitigate risks, and enhance both clinical outcomes and financial performance. Additionally, we have invested in specialized healthcare technology systems to support our nursing and support staff. Our software and technology in each operation allows our clinical staff to monitor and deliver patient care and record patient information more efficiently, but the use of information systems also introduces cybersecurity risks, including system disruption, security breaches, ransomware, theft, espionage, and inadvertent release of information.
Risk Management and Strategy
Risk Management
We assess and identify security risks to the organization by:
•Conducting regular risk assessments to determine the likelihood and magnitude of an attack from unauthorized access, use, disclosure, disruption, modification, or destruction of information systems and related information processes, stored, or transmitted;
•Performing annual security assessments and producing security assessment reports for review by Information Technology (“IT”) senior leadership, including the service center's Chief Information Officer (“CIO”) and Chief Information Security Officer (“CISO”);
•Regularly assessing security controls for effectiveness, proper functioning, and satisfactory results; and
•Continuously monitoring and addressing vulnerabilities.
Monitoring
We have established a monitoring strategy and program, which includes:
•Active, automated threat detection and screening;
•Clearly defined security metrics to be monitored;
•Regular security control assessments;
•Regular communication about security issues with the executive team and board of directors;
•Monitoring information systems to detect attacks and indicators of potential attacks or compromises;
•Identifying unauthorized use of information system resources; and
•Deploying monitoring systems and agents strategically within the information system environment.
Data Protection
We have implemented policies and programs to secure sensitive data. These include:
•Data security policies for the Company and its subsidiaries;
•Frequent security training;
•Establishing controls over network devices, actively tracking, monitoring, and evaluating them for new, missing, or updated software needed to strengthen security, patch known vulnerabilities, or stabilize software or operating system issues;
•Protecting sensitive data through encryption techniques; and
•Utilizing systems with backup and recoverability principles, such as periodic data backups and safeguards in case of a disaster.
Incident Management
Our cybersecurity incident management plan includes the following five-step process:
1.The service center's CIO and CISO lead the Information Security (“IS”) team in developing, documenting, reviewing, and testing security and incident management procedures;
2.The IS team works with the executive team to identify, assess, verify, and classify incidents to determine affected stakeholders and appropriate parties for contact;
3.In the event of a security incident, the service center's CIO and CISO are responsible for launching an Incident Response Team (“IRT”) if necessary and notifying the executive team, who will contact the board of directors and the Audit Committee to validate the response;
4.The IRT, in consultation with outside experts if needed, is responsible for initial containment, analysis, incident containment, incident eradication, and recovery. The IS team also coordinates with our legal and compliance teams as needed; and
5.After each significant incident, analyses are conducted to improve prevention and make incident response processes more efficient and effective.
We have not experienced a material cybersecurity breach as an organization in the past five years. Moreover, cybersecurity threats have not materially affected our business strategy, results of operations, or financial condition. While we have implemented processes and procedures to address and mitigate cybersecurity threats, there can be no assurances that such an incident will not occur despite our efforts, as described in Item 1A. Risk Factors.
Governance
Our Audit Committee receives quarterly reports on our information security and cyber fraud prevention programs from the service center's CIO and CISO, each of whom has over 15 years of experience in IT, including various leadership roles at other large corporations. Directors Scott E. Lamb, Gregory K. Morris M.D., and John G. Nackel, Ph.D. provide key oversight on cybersecurity matters. Our executive team is also regularly briefed on any significant security risks during monthly leadership meetings.
The IS team, established by the service center's CIO and CISO, has dedicated cybersecurity staff focusing on security monitoring, vulnerability management, incident response, risk assessments, employee training, security engineering, and management of cybersecurity policies, standards, and regulatory compliance. The Company implements security standards that include SOC 1 and SOC 2 compliance. We align with a Cyber Security Framework and take a risk-based approach during control assessment and implementation, following the National Institute of Standards and Technology (“NIST”) framework. We are committed to protecting our data, systems, and network and continually invest in enhancements to mitigate or reduce the impact of cybersecurity threats. We conduct periodic tests to maintain readiness and resiliency while regularly reviewing policies to protect data security. External companies or agencies may provide consulting, guidance, assistance, or support in response to a cybersecurity incident. Employees receive regular training, at least annually, on cybersecurity threats and best practices to maintain information security.
Item 2. Properties
Service Center
We lease office space to accommodate our Service Center. Our primary Service Center is located in Eagle, Idaho. The leased property consists of approximately 16,794 square feet of office space and the lease term expires March 31, 2025. We also have leased office space for service centers in Midvale, Utah and Farmington, Connecticut.
Home Health and Hospice Agencies and Senior Living Communities
As of December 31, 2024, we operated 123 home health, hospice and home care agencies in Arizona, California, Colorado, Idaho, Montana, Nevada, Oklahoma, Oregon, Texas, Utah, Washington, Wisconsin and Wyoming. Office space is leased within geographies served by our agencies.
As of December 31, 2024, we operated 57 affiliated senior living communities in Arizona, California, Idaho, Nevada, Texas, Utah, and Wisconsin with 3,960 Senior Living units. We lease 54 of our communities through long-term, triple-net lease arrangements, and own the remaining 3 properties.
The following table provides summary information regarding the locations of our home health and hospice agencies and our senior living communities and operational units as of December 31, 2024:
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| State | | Home Health Agencies | | Hospice Agencies | | Senior Living Communities | | Senior Living Units |
| Arizona | | 7 | | | 13 | | | 5 | | | 840 | |
| California | | 9 | | | 12 | | | 7 | | | 629 | |
| Colorado | | 9 | | | 2 | | | — | | | — | |
| Idaho | | 6 | | | 5 | | | 3 | | | 232 | |
| Montana | | 1 | | | 1 | | | — | | | — | |
| Nevada | | 1 | | | 2 | | | 4 | | | 385 | |
| Oklahoma | | 2 | | | 2 | | | — | | | — | |
| Oregon | | 2 | | | 1 | | | — | | | — | |
| Texas | | 6 | | | 10 | | | 12 | | | 709 | |
| Utah | | 8 | | | 5 | | | 2 | | | 188 | |
| Washington | | 10 | | | 4 | | | — | | | — | |
| Wisconsin | | 2 | | | 1 | | | 24 | | | 977 | |
| Wyoming | | 1 | | | 1 | | | — | | | — | |
| Total | | 64 | | | 59 | | | 57 | | | 3,960 | |
Item 3. Legal Proceedings
We are involved in various claims and lawsuits arising in the ordinary course of business, none of which, in the opinion of management, is expected to have a material adverse effect on our results of operations or financial condition. However, the results of such matters cannot be predicted with certainty, and we cannot assure you that the ultimate resolution of any legal or administrative proceeding or dispute will not have a material adverse effect on our business, financial condition, results of operations and cash flows. See Note 16, Commitments and Contingencies, to the Consolidated Financial Statements for a description of claims and legal actions arising in the ordinary course of our business.
Item 4. Mine Safety Disclosures
None.
Part II.
Item 5. Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information
Our Common stock trades under the symbol “PNTG” on the NASDAQ Global Select Market. As of February 24, 2025, there are approximately 71 holders of record of our stock.
Dividend Policy
We do not intend to pay dividends on our common stock for the foreseeable future. Instead, we anticipate that all of our future earnings will be retained to support our operations and to finance the growth and development of our business.
Issuer Repurchases of Equity Securities
The Company did not repurchase any shares in 2024, nor did it approve any share repurchase program.
Stock Performance Graph
The following Stock Performance Graph and related information shall not be deemed “soliciting material” or “filed” with the SEC, nor should such information be incorporated by reference into any future filings under the Securities Act or the Exchange Act except to the extent that we specifically incorporate it by reference in such filing.
The graph below compares the cumulative total stockholder return on our common stock, $0.001 par value per share, during the period from January 1, 2020, through December 31, 2024, with the cumulative total return on the NASDAQ composite index and an industry peer group over the same period (assuming the investment of $100 in our common stock, the NASDAQ composite index and the industry peer group on January 1, 2020 and the reinvestment of dividends). The peer group we selected is comprised of: Amedysis, Inc. (“AMED”), Addus Homecare Corporation (“ADUS”), Chemed Corporation (“CHE”), Encompass Health Corporation (“EHC”), Sonida Senior Living Inc., formerly known as Capital Senior Living Corporation (“SNDA”), and Brookdale Senior Living, Inc. (“BKD”). The cumulative total stockholder return on the following graph is historical and is not necessarily indicative of future stock price performance. No cash dividends have been paid on our common stock.
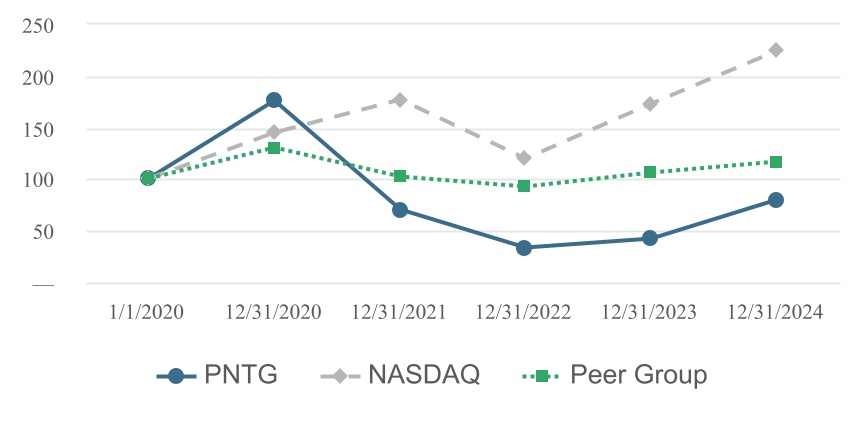
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | 1/1/2020 | | 12/2020 | | 12/2021 | | 12/2022 | | 12/2023 | | 12/2024 |
| PNTG | | $ | 100.0 | | | $ | 175.6 | | | $ | 69.8 | | | $ | 33.2 | | | $ | 42.1 | | | $ | 80.1 | |
| NASDAQ | | 100.0 | | | 144.9 | | | 177.1 | | | 119.5 | | | 172.8 | | | 223.9 | |
| Peer Group | | 100.0 | | | 130.3 | | | 102.6 | | | 92.3 | | | 105.8 | | | 116.6 | |
Item 6. [Reserved]
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion should be read in conjunction with the consolidated financial statements and accompanying notes, which appear elsewhere in this Annual Report. This discussion contains forward-looking statements that involve risks and uncertainties. Our actual results could differ materially from those anticipated in these forward-looking statements as a result of various factors, including those discussed below and elsewhere in this Annual Report. See Item 1A., Risk Factors and Cautionary Note Regarding Forward-Looking Statements.
Overview
We are a leading provider of high-quality healthcare services to patients and residents of all ages, including the growing senior population, in the United States. We strive to be the provider of choice in the communities we serve through our innovative operating model. We operate in multiple lines of businesses including home health, hospice and senior living services across Arizona, California, Colorado, Idaho, Montana, Nevada, Oklahoma, Oregon, Texas, Utah, Washington, Wisconsin and Wyoming. We also provide home health and hospice operational support through a management service agreement in Connecticut. As of December 31, 2024, our home health and hospice business provided home health, hospice and
home care services from 123 agencies operating across 13 states, and our senior living business operated 57 senior living communities throughout seven states.
The following table summarizes our affiliated home health and hospice agencies and senior living communities as of:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | |
| 2014 | | 2015 | | 2016 | | 2017 | | 2018 | | 2019 | | 2020 | | 2021 | | 2022 | | 2023 | | 2024 |
| Home health and hospice agencies | 25 | | | 32 | | | 39 | | | 46 | | | 54 | | | 63 | | | 76 | | | 88 | | 95 | | | 111 | | | 123 | |
| Senior living communities | 15 | | | 36 | | | 36 | | | 43 | | | 50 | | | 52 | | | 54 | | | 54 | | 49 | | | 51 | | | 57 | |
| Senior living units | 1,587 | | | 3,184 | | | 3,184 | | | 3,434 | | | 3,820 | | | 3,963 | | | 4,127 | | | 4,127 | | | 3,500 | | | 3,588 | | | 3,960 | |
| Total number of home health, hospice, and senior living operations | 40 | | 68 | | | 75 | | | 89 | | | 104 | | | 115 | | | 130 | | | 142 | | | 144 | | | 162 | | | 180 | |
Recent Activities
Acquisitions. During 2024, we expanded our operations with the addition of eight home health agencies, three hospice agencies, and six senior living communities. A subsidiary of the Company entered into a separate purchase agreements with the prior operator of each acquired operation as part of each transaction.
Trends
We have experienced stable senior living occupancy through the year ended December 31, 2024. Although we saw steady improvements in occupancy throughout 2023 as a result of renewed consideration of senior living communities as the negative impacts of the global pandemic subsided, and stable occupancy during 2024, the highly competitive environment for senior living residents and inflationary factors will continue to impact our occupancy levels in our senior living communities.
When we acquire turnaround or start-up operations, we expect that our combined metrics may be impacted. We expect these metrics to vary from period to period based upon the maturity of the operations within our portfolio. We have generally experienced lower occupancy rates and higher costs at our senior living communities and lower census and higher costs at our home health and hospice agencies for recently acquired operations; as a result, we generally anticipate lower and/or fluctuating consolidated and segment margins during years of acquisition growth.
Segments
We have two reportable segments: (1) home health and hospice services, which includes our home health, hospice, home care, and geriatric primary and palliative care businesses; and (2) senior living services, which includes our assisted living, independent living and memory care services. Our Chief Executive Officer, who is our Chief Operating Decision Maker (“CODM”), reviews financial information at the operating segment level using segment adjusted EBITDAR from operations. We also report an “all other” category that includes general and administrative expense from our Service Center.
Key Performance Indicators
We manage the fiscal aspects of our business by monitoring key performance indicators that affect our financial performance. These indicators and their definitions include the following:
Home Health and Hospice Services
•Total home health admissions. The total admissions of home health patients, including new acquisitions, new admissions and readmissions.
•Total Medicare home health admissions. Total admissions of home health patients, who are receiving care under Medicare reimbursement programs, including new acquisitions, new admissions and readmissions.
•Average Medicare revenue per completed 60-day home health episode. The average amount of revenue for each completed 60-day home health episode generated from patients who are receiving care under Medicare reimbursement programs.
•Total hospice admissions. Total admissions of hospice patients, including new acquisitions, new admissions and recertifications.
•Average hospice daily census. The average number of patients who are receiving hospice care during any measurement period divided by the number of days during such measurement period.
•Hospice Medicare revenue per day. The average daily Medicare revenue recorded during any measurement period for services provided to hospice patients.
The following table summarizes our overall home health and hospice services statistics for the periods indicated:
| | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 |
| Home health services: | | | |
| Total home health admissions | 59,741 | | | 43,508 | |
| Total Medicare home health admissions | 24,598 | | | 19,389 | |
Average Medicare revenue per completed 60-day home health episode(a) | $ | 3,677 | | | $ | 3,468 | |
| Hospice services: | | | |
| Total hospice admissions | 12,208 | | | 9,746 | |
| Average hospice daily census | 3,268 | | | 2,607 | |
| Hospice Medicare revenue per day | $ | 183 | | | $ | 185 | |
| | | | | | | | |
| (a) | | The year to date average for Medicare revenue per 60-day completed episode includes post period claim adjustments for prior periods. |
Senior Living Services
•Occupancy. The ratio of actual number of days our units are occupied during any measurement period to the number of units available for occupancy during such measurement period.
•Average monthly revenue per occupied unit. The revenue for senior living services during any measurement period divided by actual occupied senior living units for such measurement period divided by the number of months for such measurement period.
The following table summarizes our senior living statistics for the periods indicated:
| | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 |
| Occupancy | 78.8 | % | | 78.5 | % |
| Average monthly revenue per occupied unit | $ | 4,811 | | | $ | 4,443 | |
Revenue Sources
Home Health and Hospice Services
Home Health. We derive the majority of our home health revenue from Medicare and managed care. The Medicare payment is adjusted for differences between estimated and actual payment amounts, an inability to obtain appropriate billing documentation or authorizations acceptable to the payor and other reasons unrelated to credit risk. Net service revenue is recognized in accordance with PDGM methodology. Under PDGM, Medicare provides agencies with payments for each 30-day period of care provided to beneficiaries. If a beneficiary is still eligible for care after the end of the first 30-day payment period, a second 30-day payment period can begin. There are no limits to the number of periods of care a beneficiary who remains eligible for the home health benefit can receive. While payment for each 30-day period of care is adjusted to reflect the beneficiary’s health condition and needs, a special outlier provision exists to ensure appropriate payment for those beneficiaries that have the most expensive care needs. The PDGM payment under the Medicare program is also adjusted for certain variables including, but not limited to: (a) a low utilization payment adjustment if the number of visits is below an established threshold that varies based on the diagnosis of a beneficiary; (b) a partial payment if the patient transferred to another provider or the Company received a patient from another provider before completing the period of care; (c) adjustment to the admission source
of claim if it is determined that the patient had a qualifying stay in a post-acute care setting within 14 days prior to the start of a 30-day payment period; (d) the timing of the 30-day payment period provided to a patient in relation to the admission date, regardless of whether the same home health provider provided care for the entire series of episodes; (e) changes to the acuity of the patient during the previous 30-day period of care; (f) changes in the base payments established by the Medicare program; (g) adjustments to the base payments for case mix and geographic wages; and (h) recoveries of overpayments.
Hospice. We derive the majority of our hospice business revenue from Medicare reimbursement. The estimated payment rates are calculated as daily rates for each of the levels of care we deliver. Rates are set based on specific levels of care, are adjusted by a wage index to reflect healthcare labor costs across the country and are established annually through federal legislation. The following are the four levels of care provided under the hospice benefit:
•Routine Home Care (RHC). Care that is not classified under any of the other levels of care, such as the work of nurses, social workers or home health aides.
•General Inpatient Care. Pain control or acute or chronic symptom management that cannot be managed in a setting other than an inpatient Medicare-certified facility, such as a hospital, skilled nursing facility or hospice inpatient facility.
•Continuous Home Care. Care for patients experiencing a medical crisis that requires nursing services to achieve palliation and symptom control, if the agency provides a minimum of eight hours of care within a 24-hour period.
•Inpatient Respite Care. Short-term, inpatient care to give temporary relief to the caregiver who regularly provides care to the patient.
CMS has established a two-tiered payment system for RHC. Hospices are reimbursed at a higher rate for RHC services provided from days of service 1 through 60 and a lower rate for all subsequent days of service. CMS also provided for a Service Intensity Add-On, which increases payments for certain RHC services provided by registered nurses and social workers to hospice patients during the final seven days of life.
Medicare reimbursement is adjusted for an inability to obtain appropriate billing documentation or authorizations acceptable to the payor and other reasons unrelated to credit risk. Additionally, as Medicare hospice revenue is subject to an inpatient cap limit and an overall payment cap, we monitor our provider numbers and based upon empirical experience estimate amounts due back to Medicare to the extent that the cap has been exceeded.
Senior Living Services. Within our senior living operations, we generate revenue primarily from private pay sources, with a portion earned from Medicaid or other state-specific programs.
Primary Components of Expense
Cost of Services (excluding rent, general and administrative expense and depreciation and amortization). Our cost of services represents the costs of operating our independent operating subsidiaries, which primarily consists of employee wages and related benefits, share-based compensation, supplies, purchased services, and ancillary expenses such as the cost of pharmacy and therapy services provided to patients or residents. Cost of services also includes the cost of general and professional liability insurance and other general cost of services specifically attributable to our operations.
Rent—Cost of Services. Rent—cost of services consists solely of base minimum rent amounts payable under lease agreements to our landlords. Our subsidiaries lease and operate but do not own the underlying real estate at our operations, and these amounts do not include taxes, insurance, impounds, capital reserves or other charges payable under the applicable lease agreements, which are included in cost of services and general and administrative expense.
General and Administrative Expense. General and administrative expense consists primarily of payroll and related benefits and travel expenses for our Service Center personnel in providing training and other operational support. General and administrative expense also includes professional fees (such as accounting and legal fees), costs relating to our information systems, share-based compensation and rent for our Service Center offices.
Depreciation and Amortization. Property and equipment are initially recorded at their historical cost. Depreciation is computed using the straight-line method over the estimated useful lives of the depreciable assets (ranging from one to 40 years). Leasehold improvements are amortized on a straight-line basis over the shorter of their estimated useful lives or the remaining lease term.
Critical Accounting Policies and Estimates
Our discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles (“GAAP”). The preparation of these financial statements and related disclosures requires us to make judgments, estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting periods. On an ongoing basis we review our judgments and estimates, including but not limited to those related to self-insurance reserves, revenue, and intangible assets and goodwill. We base our estimates and judgments upon our historical experience, knowledge of current conditions and our belief of what could occur in the future considering available information, including assumptions that we believe to be reasonable under the circumstances. By their nature, these estimates and judgments are subject to an inherent degree of uncertainty, and actual results could differ materially from the amounts reported. While we believe that our estimates, assumptions, and judgments are reasonable, they are based on information available when the estimate was made. Refer to Note 2, Basis of Presentation and Summary of Significant Accounting Policies, within the Consolidated Financial Statements for further information on our critical accounting estimates and policies, which are as follows:
•Self-insurance reserves - The Company is self-insured for general and professional liability, workers’ compensation, automobile, and its employee health plans while maintaining stop-loss coverage with third-party insurers to limit its total liability exposure. The valuation methods and assumptions used in estimating costs up to retention amounts to settle open claims of insureds and an estimate of the cost of insured claims up to retention amounts that have been incurred but not reported;
•Revenue recognition - The amounts owed by private pay individuals for services and estimate of variable considerations to arrive at the transaction price, including methods and assumptions, used to determine settlements with Medicare and Medicaid adjustments due to audits and reviews; and
•Acquisition accounting and goodwill - The assumptions used to allocate the purchase price paid for assets acquired and liabilities assumed in connection with our acquisitions, and the review of goodwill for impairment at the Company’s annual impairment test date or upon the occurrence of a triggering event.
Recent Accounting Pronouncements
Information concerning recently issued accounting pronouncements which are not yet effective is included in Note 2, Basis of Presentation and Summary of Significant Accounting Policies in the Consolidated Financial Statements.
Results of Operations
The following table sets forth details of our expenses and earnings as a percentage of total revenue for the periods indicated:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| | | | | |
| | | | | |
| | | | | |
| Total revenue | 100.0 | % | | 100.0 | % | | 100.0 | % |
| Expense: | | | | | |
| Cost of services | 80.3 | | | 80.4 | | | 79.6 | |
| Rent—cost of services | 6.2 | | | 7.3 | | | 8.0 | |
| General and administrative expense | 7.2 | | | 6.7 | | | 7.2 | |
| Depreciation and amortization | 0.9 | | | 0.9 | | | 1.0 | |
| (Gain) loss on asset dispositions and impairment, net | (0.1) | | | — | | | 1.5 | |
| Total expenses | 94.5 | | | 95.3 | | | 97.3 | |
| Income from operations | 5.5 | | | 4.7 | | | 2.7 | |
| Other expense, net: | | | | | |
| Other income | — | | | 0.1 | | | — | |
| Interest expense, net | (1.0) | | | (1.2) | | | (0.8) | |
| Other expense, net | (1.0) | | | (1.1) | | | (0.8) | |
| Income before provision for income taxes | 4.5 | | | 3.6 | | | 1.9 | |
| Provision for income taxes | 1.0 | | | 1.0 | | | 0.4 | |
| Net income | 3.5 | | | 2.6 | | | 1.5 | |
| Less: net income attributable to noncontrolling interest | 0.3 | | | 0.1 | | | 0.1 | |
| Net income attributable to Pennant | 3.2 | % | | 2.5 | % | | 1.4 | % |
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| (In thousands) |
| Consolidated GAAP Financial Measures: | | | | | |
| Total revenue | $ | 695,240 | | | $ | 544,891 | | | $ | 473,241 | |
| Total expenses | 657,124 | | | 519,722 | | | 460,502 | |
| Income from operations | $ | 38,116 | | | $ | 25,169 | | | $ | 12,739 | |
The following table presents certain financial information regarding our reportable segments. General and administrative expenses are not allocated to the reportable segments:
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Home Health and Hospice Services | | Senior Living Services | | All Other | | Total |
| Year Ended December 31, 2024 | | | | | | | | |
| Segment Revenue | | $ | 515,344 | | | $ | 174,767 | | | $ | 5,129 | | | $ | 695,240 | |
| Segment Cost of Services | | 427,635 | | | 123,107 | | | | | |
| Segment Adjusted EBITDAR from Operations | | $ | 87,709 | | | $ | 51,660 | | | | | $ | 139,369 | |
| Year Ended December 31, 2023 | | | | | | | | |
| Segment Revenue | | $ | 385,652 | | | $ | 148,198 | | | $ | 11,041 | | | $ | 544,891 | |
| Segment Cost of Services | | 320,046 | | | 102,904 | | | | | |
| Segment Adjusted EBITDAR from Operations | | $ | 65,606 | | | $ | 45,294 | | | | | $ | 110,900 | |
| Year Ended December 31, 2022 | | | | | | | | |
| Segment Revenue | | $ | 337,371 | | | $ | 126,758 | | | $ | 9,112 | | | $ | 473,241 | |
| Segment Cost of Services | | 275,544 | | | 89,195 | | | | | |
| Segment Adjusted EBITDAR from Operations | | $ | 61,827 | | | $ | 37,563 | | | | | $ | 99,390 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
The table below provides a reconciliation of Segment Adjusted EBITDAR from Operations above to income from operations:
| | | | | | | | | | | | | | | | | |
| 2024 | | 2023 | | 2022 |
Segment Adjusted EBITDAR from Operations(a) | $ | 139,369 | | | $ | 110,900 | | | $ | 99,390 | |
| Less: Unallocated corporate expenses | 43,587 | | | 31,704 | | | 31,435 | |
| Less: Depreciation and amortization | 6,119 | | | 5,130 | | | 4,900 | |
| Rent—cost of services | 43,029 | | | 39,759 | | | 38,018 | |
| Other income | 207 | | | 339 | | | (31) | |
| Adjustments to Segment EBITDAR from Operations: | | | | | |
Less: Costs at start-up operations (b) | 137 | | | 102 | | | 1,435 | |
Share-based compensation expense(c) | 8,242 | | | 5,565 | | | 3,363 | |
Acquisition related costs and credit allowances(d) | 1,278 | | | 476 | | | 731 | |
| | | | | |
Costs associated with transitioning operations(e) | (570) | | | 612 | | | 6,103 | |
Unusual, non-recurring or redundant charges(f) | 1,004 | | | 2,575 | | | 1,297 | |
| Add: Net income attributable to noncontrolling interest | 1,780 | | | 531 | | | 600 | |
| Income from operations | $ | 38,116 | | | $ | 25,169 | | | $ | 12,739 | |
| | | | | |
| | | | | | | | |
| (a) | | Segment Adjusted EBITDAR from Operations is net income attributable to the Company's reportable segments excluding interest expense, provision for income taxes, depreciation and amortization expense, rent, unallocated corporate and administrative expenses, and, in order to view the operations performance on a comparable basis from period to period, certain adjustments including: (1) costs at start-up operations, (2) share-based compensation expense, (3) acquisition related costs and credit allowances, (4) costs associated with transitioning operations, (5) unusual, non-recurring or redundant charges, and (6) net income (loss) attributable to noncontrolling interest. General and administrative expenses are not allocated to the reportable segments, and are included as “All Other”, accordingly the segment earnings measure reported is before allocation of corporate general and administrative expenses. The Company's segment measures may be different from the calculation methods used by other companies and, therefore, comparability may be limited. |
| (b) | | Represents results related to start-up operations. This amount excludes rent and depreciation and amortization expense related to such operations. |
| (c) | | Share-based compensation expense and related payroll taxes incurred, including the impact of the modification of certain restricted stock units described below in Note 12, Options and Awards, to the Consolidated Financial Statements. Share-based compensation expense and related payroll taxes are included in cost of services and general and administrative expense. |
| (d) | | Non-capitalizable costs associated with acquisitions and credit allowances for amounts in dispute with the prior owners of certain acquired operations. |
| | |
| | |
| | |
| | |
| (e) | | During the year ended December 31, 2023, an affiliate of the Company placed its memory care units into transition and is converting the facility into an assisted living community. We received insurance proceeds related to the property in 2024 which were recorded as a gain on asset disposition on the consolidated statements of income. The amounts reported exclude rent and depreciation and amortization expense related to such operations and include legal settlement costs associated with one of the entities transitioned to Ensign.
During January 2022, affiliates of the Company entered into Transfer Agreements with affiliates of Ensign, providing for the transfer of the operations of certain senior living communities (the “Transaction”) from affiliates of the Company to affiliates of Ensign. The closing of the Transaction was completed in two phases with the transfer of two operations on March 1, 2022 and the remainder transferred on April 1, 2022. The amount above represents the net impact on revenue and cost of service attributable to all of the transferred entities. The amounts reported exclude rent and depreciation and amortization expense related to such operations. |
| (f) | | Represents unusual or non-recurring charges for legal services, implementation costs, integration costs, and consulting fees in general and administrative and cost of services expenses. The amounts reported for the year ended December 31, 2022 include certain costs identified as redundant or non-recurring incurred by the Company for services provided by Ensign under the Transition Services Agreement, and were included in general and administrative expense. |
Performance and Valuation Measures:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| (In thousands) |
| Consolidated Non-GAAP Financial Measures: | | | | | |
| Performance Metrics | | | | | |
| Consolidated EBITDA | $ | 42,662 | | | $ | 30,107 | | | $ | 17,008 | |
| Consolidated Adjusted EBITDA | $ | 53,286 | | | $ | 40,716 | | | $ | 31,545 | |
| Valuation Metric | | | | | |
| Consolidated Adjusted EBITDAR | $ | 95,782 | | | | | |
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| (In thousands) |
Segment Non-GAAP Measures:(a) | | | | | |
| Segment Adjusted EBITDA from Operations | | | | | |
| Home health and hospice services | $ | 80,660 | | | $ | 60,128 | | | $ | 56,977 | |
| Senior living services | $ | 16,213 | | | $ | 12,293 | | | $ | 6,003 | |
| | | | | | | | |
| (a) | | General and administrative expenses are not allocated to any segment for purposes of determining segment profit or loss. |
The table below reconciles Consolidated Net Income to Consolidated EBITDA, Consolidated Adjusted EBITDA and Consolidated Adjusted EBITDAR for the periods presented:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| (In thousands) |
| Consolidated Net income | $ | 24,339 | | | $ | 13,910 | | | $ | 7,243 | |
| Less: Net income attributable to noncontrolling interest | 1,780 | | | 531 | | | 600 | |
| Add: Provision for income taxes | 7,028 | | | 5,674 | | | 1,649 | |
| Net interest expense | 6,956 | | | 5,924 | | | 3,816 | |
| Depreciation and amortization | 6,119 | | | 5,130 | | | 4,900 | |
| Consolidated EBITDA | 42,662 | | | 30,107 | | | 17,008 | |
| Adjustments to Consolidated EBITDA | | | | | |
Add: Costs at start-up operations(a) | 137 | | | 102 | | | 1,435 | |
Share-based compensation expense(b) | 8,242 | | | 5,565 | | | 3,363 | |
Acquisition related costs and credit allowances(c) | 1,278 | | | 476 | | | 731 | |
| | | | | |
| | | | | |
| | | | | |
| | | | | |
Activities associated with transitioning operations(d) | (570) | | | 612 | | | 6,103 | |
Unusual or non-recurring charges(e) | 1,004 | | | 2,575 | | | 1,297 | |
| Rent related to items (a) and (e) above | 533 | | | 1,279 | | | 1,608 | |
| Consolidated Adjusted EBITDA | 53,286 | | | 40,716 | | | 31,545 | |
| Rent—cost of services | 43,029 | | | 39,759 | | | 38,018 | |
| Rent related to items (a) and (e) above | (533) | | | (1,279) | | | (1,608) | |
| Adjusted rent—cost of services | 42,496 | | | 38,480 | | | 36,410 | |
| Consolidated Adjusted EBITDAR | $ | 95,782 | | | | | |
| | | | | | | | |
| (a) | | Represents results related to start-up operations. This amount excludes rent and depreciation and amortization expense related to such operations. |
| (b) | | Share-based compensation expense and related payroll taxes incurred, including the impact of the modification of certain restricted stock units described below in Note 12, Options and Awards, to the Consolidated Financial Statements. Share-based compensation expense and related payroll taxes are included in cost of services and general and administrative expense. |
| (c) | | Non-capitalizable costs associated with acquisitions and credit allowances for amounts in dispute with the prior owners of certain acquired operations. |
| | |
| | |
| | |
| | |
| (d) | | During the year ended December 31, 2023, an affiliate of the Company placed its memory care units into transition and is converting the facility into an assisted living community. We received insurance proceeds related to the property in 2024 which were recorded as a gain on asset disposition on the consolidated statements of income. The amounts reported exclude rent and depreciation and amortization expense related to such operations and include legal settlement costs associated with one of the entities transitioned to Ensign.
During January 2022, affiliates of the Company entered into Transfer Agreements with affiliates of Ensign, providing for the transfer of the operations of certain senior living communities (the “Transaction”) from affiliates of the Company to affiliates of Ensign. The closing of the Transaction was completed in two phases with the transfer of two operations on March 1, 2022 and the remainder transferred on April 1, 2022. The amount above represents the net impact on revenue and cost of service attributable to all of the transferred entities. The amounts reported exclude rent and depreciation and amortization expense related to such operations. |
| (e) | | Represents unusual or non-recurring charges for legal services, implementation costs, integration costs, and consulting fees in general and administrative and cost of services expenses. The amounts reported for the year ended December 31, 2022 include certain costs identified as redundant or non-recurring incurred by the Company for services provided by Ensign under the Transition Services Agreement, and were included in general and administrative expense. |
The table below reconciles Segment Adjusted EBITDAR from Operations to Segment Adjusted EBITDA from Operations for the periods presented:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| Home Health and Hospice | | Senior Living |
| 2024 | | 2023 | | 2022 | | 2024 | | 2023 | | 2022 |
| (In thousands) |
| Segment Adjusted EBITDAR from Operations | $ | 87,709 | | | $ | 65,606 | | | $ | 61,827 | | | $ | 51,660 | | | $ | 45,294 | | | $ | 37,563 | |
| Less: Rent—cost of services | 7,189 | | | 5,791 | | | 5,060 | | | 35,840 | | | 33,967 | | | 32,958 | |
| Rent related to start-up and transitioning operations | (140) | | | (313) | | | (210) | | | (393) | | | (966) | | | (1,398) | |
| Segment Adjusted EBITDA from Operations | $ | 80,660 | | | $ | 60,128 | | | $ | 56,977 | | | $ | 16,213 | | | $ | 12,293 | | | $ | 6,003 | |
The following discussion includes references to certain performance and valuation measures, which are non-GAAP financial measures, including Consolidated EBITDA, Consolidated Adjusted EBITDA, Segment Adjusted EBITDA from Operations, and Consolidated Adjusted EBITDAR (collectively, “Non-GAAP Financial Measures”). Non-GAAP Financial Measures are used in addition to, and in conjunction with, results presented in accordance with GAAP and should not be relied upon to the exclusion of GAAP financial measures. Non-GAAP Financial Measures reflect an additional way of viewing aspects of our operations and company that, when viewed with our GAAP results and the accompanying reconciliations to corresponding GAAP financial measures, we believe can provide a more comprehensive understanding of factors and trends affecting our business.
We believe these Non-GAAP Financial Measures are useful to investors and other external users of our financial statements regarding our results of operations because:
•they are widely used by investors and analysts in our industry as a supplemental measure to evaluate the overall performance of companies in our industry without regard to items such as interest expense, rent expense and depreciation and amortization, which can vary substantially from company to company depending on the book value of assets, the length of the lease to which the asset applies, the method by which assets were acquired, and differences in capital structures;
•they help investors evaluate and compare the results of our operations from period to period by removing the impact of our asset base and capital structure from our operating results; and
•Consolidated Adjusted EBITDAR is used by investors and analysts in our industry to value the companies in our industry without regard to capital structures.
We use Non-GAAP Financial Measures:
•as measurements of our operating performance to assist us in comparing our operating performance on a consistent basis from period to period;
•to allocate resources to enhance the financial performance of our business;
•to assess the value of a potential acquisition;
•to assess the value of a transformed operation’s performance;
•to evaluate the effectiveness of our operational strategies; and
•to compare our operating performance to that of our competitors.
We typically use Non-GAAP Financial Measures to compare the operating performance of each operation from period to period. We find that Non-GAAP Financial Measures are useful for this purpose because they do not include such costs as interest expense, income taxes, depreciation and amortization expense, which may vary from period-to-period depending upon various factors, including the method used to finance operations, the date of acquisition of a community or business, and the tax law of the state in which a business unit operates.
Non-GAAP Financial Measures have no standardized meaning defined by GAAP. Therefore, our Non-GAAP Financial Measures have limitations as analytical tools, and they should not be considered in isolation, or as a substitute for analysis of our results as reported in accordance with GAAP. Some of these limitations are:
•they do not reflect our current or future cash requirements for capital expenditures or contractual commitments;
•they do not reflect changes in, or cash requirements for, our working capital needs;
•they do not reflect the net interest expense, or the cash requirements necessary to service interest or principal payments, on our debt;
•in the case of Consolidated Adjusted EBITDAR, it does not reflect rent expenses, which are normal and recurring operating expenses that are necessary to operate our leased operations;
•they do not reflect any income tax payments we may be required to make;
•although depreciation and amortization are non-cash charges, the assets being depreciated and amortized will often have to be replaced in the future, and these non-cash charges do not reflect any cash requirements for such replacements; and
•other companies in our industry may calculate the same Non-GAAP Financial Measures differently than we do, which may limit their usefulness as comparative measures.
We compensate for these limitations by using Non-GAAP Financial Measures only to supplement net income on a basis prepared in accordance with GAAP in order to provide a more complete understanding of the factors and trends affecting our business.
We strongly encourage investors to review our Consolidated Financial Statements, included in this report in their entirety and to not rely on any single financial measure. Because these Non-GAAP Financial Measures are not standardized, it may not be possible to compare these financial measures with other companies’ Non-GAAP financial measures having the same or similar names. These Non-GAAP Financial Measures should not be considered a substitute for, nor superior to, financial results and measures determined or calculated in accordance with GAAP. We strongly urge you to review the reconciliation of income from operations to the Non-GAAP Financial Measures in the table presented above, along with our Consolidated Financial Statements and related notes included elsewhere in this report.
We believe the following Non-GAAP Financial Measures are useful to investors as key operating performance measures and valuation measures:
Performance Measures:
Consolidated EBITDA
We believe Consolidated EBITDA is useful to investors in evaluating our operating performance because it helps investors evaluate and compare the results of our operations from period to period by removing the impact of our asset base (depreciation and amortization expense) from our operating results.
We calculate Consolidated EBITDA as net income, adjusted for net income (loss) attributable to noncontrolling interest, before (a) interest expense (b) provision for income taxes and (c) depreciation and amortization.
Consolidated Adjusted EBITDA
We adjust Consolidated EBITDA when evaluating our performance because we believe that the exclusion of certain additional items described below provides useful supplemental information to investors regarding our ongoing operating performance. We believe that the presentation of Consolidated Adjusted EBITDA, when considered with Consolidated EBITDA and GAAP net income, is beneficial to an investor’s complete understanding of our operating performance.
We calculate Consolidated Adjusted EBITDA by adjusting Consolidated EBITDA to exclude the effects of non-core business items, which for the reported periods includes, to the extent applicable:
•costs at start-up operations;
•share-based compensation expense;
•acquisition related costs and credit allowances;
•costs associated with transitioning operations; and
•unusual or non-recurring charges.
Segment Adjusted EBITDA from Operations
We calculate Segment Adjusted EBITDA from Operations by adjusting Segment Adjusted EBITDAR from Operations to include rent-cost of services. We believe that the inclusion of rent-cost of services provides useful supplemental information to investors regarding our ongoing operating performance for each segment.
Valuation Measure:
Consolidated Adjusted EBITDAR
We use Consolidated Adjusted EBITDAR as one measure in determining the value of prospective acquisitions. It is also a measure commonly used by us, research analysts and investors to compare the enterprise value of different companies in the healthcare industry, without regard to differences in capital structures. Additionally, we believe the use of Consolidated Adjusted EBITDAR allows us, research analysts and investors, to compare operational results of companies without regard to operating or financed leases. A significant portion of financed lease expenditures are recorded in interest, whereas operating lease expenditures are recorded in rent expense.
This measure is not displayed as a performance measure as it excludes rent expense, which is a normal and recurring operating expense and, as such, does not reflect our cash requirements for leasing commitments. Our presentation of Consolidated Adjusted EBITDAR should not be construed as a financial performance measure.
The adjustments made and previously described in the computation of Consolidated Adjusted EBITDA are also made when computing Consolidated Adjusted EBITDAR. We calculate Consolidated Adjusted EBITDAR by excluding rent-cost of services and rent related to start up operations from Consolidated Adjusted EBITDA.
Year Ended December 31, 2024 Compared to the Year Ended December 31, 2023
Revenue
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 |
| Revenue Dollars | | Revenue Percentage | | Revenue Dollars | | Revenue Percentage |
| (In thousands) |
| Home health and hospice services | | | | | | | |
| Home health | $ | 239,539 | | | 34.5 | % | | $ | 175,044 | | | 32.1 | % |
| Hospice | 240,102 | | | 34.5 | | | 194,627 | | | 35.7 | |
Home care and other(a) | 39,843 | | | 5.7 | | | 24,793 | | | 4.6 | |
| Total home health and hospice services | 519,484 | | | 74.7 | | | 394,464 | | | 72.4 | |
| Senior living services | 175,756 | | | 25.3 | | | 150,427 | | | 27.6 | |
| Total revenue | $ | 695,240 | | | 100.0 | % | | $ | 544,891 | | | 100.0 | % |
| | | | | | | | |
| (a) | | Home care and other revenue is included with home health revenue in other disclosures in this report. |
Our consolidated revenue increased $150.3 million, or 27.6%, driven by the net organic growth of existing operations across all segments of $59.2 million or 10.9% as well as increased revenue from acquired operations of $91.1 million, or 16.7%, during the year ended December 31, 2024.
Home Health and Hospice Services
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2024 | | 2023 | | Change | | % Change |
| (In thousands) | | |
| Home health and hospice revenue | | | | | | | |
| Home health services | $ | 239,539 | | | $ | 175,044 | | | $ | 64,495 | | | 36.8 | % |
| Hospice services | 240,102 | | | 194,627 | | | 45,475 | | | 23.4 | |
| Home care and other | 39,843 | | | 24,793 | | | 15,050 | | | 60.7 | |
| Total home health and hospice revenue | $ | 519,484 | | | $ | 394,464 | | | $ | 125,020 | | | 31.7 | % |
| | | | | | | |
| Year Ended December 31, | | | | |
| 2024 | | 2023 | | Change | | % Change |
| Home health services: | | | | | | | |
| Total home health admissions | 59,741 | | | 43,508 | | | 16,233 | | | 37.3 | % |
| Total Medicare home health admissions | 24,598 | | | 19,389 | | | 5,209 | | | 26.9 | |
Average Medicare revenue per 60-day completed episode(a) | $ | 3,677 | | | $ | 3,468 | | | $ | 209 | | | 6.0 | |
| Hospice services: | | | | | | | |
| Total hospice admissions | 12,208 | | | 9,746 | | | 2,462 | | | 25.3 | |
| Average daily census | 3,268 | | | 2,607 | | | 661 | | | 25.4 | |
| Hospice Medicare revenue per day | $ | 183 | | | $ | 185 | | | $ | (2) | | | (1.1) | |
| Number of home health and hospice agencies at period end | 123 | | | 111 | | | 12 | | | 10.8 | % |
| | | | | | | | |
| (a) | | The year to date average for Medicare revenue per 60-day completed episode includes post period claim adjustments for prior periods. |
Home health and hospice revenue increased $125.0 million, or 31.7%. Revenue grew due to an increase in almost all key performance indicators including an increase in total home health admissions of 37.3%, an increase in Medicare home health admissions of 26.9%, an increase in average Medicare revenue per 60-day completed episode of 6.0%, an increase of 25.3% in total hospice admissions, and an increase of 25.4% in hospice average daily census, while Hospice Medicare revenue per day decreased by 1.1%. The improvement in these metrics resulted in net organic revenue growth of $46.4 million for the year ended December 31, 2024. Growth was also driven by the acquisition of eleven home health and hospice operations during the year ended December 31, 2024, and the acquisition of thirteen home health, home care, and hospice operations during the year ended December 31, 2023, resulting in an increase in revenue of $78.6 million, or 19.9% overall.
Senior Living Services
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2024 | | 2023 | | Change | | % Change |
| Revenue (in thousands) | $ | 175,756 | | | $ | 150,427 | | | $ | 25,329 | | | 16.8 | % |
| Number of communities at period end | 57 | | | 51 | | | 6 | | | 11.8 | |
| Occupancy | 78.8 | % | | 78.5 | % | | 0.3 | % | | |
| Average monthly revenue per occupied unit | $ | 4,811 | | | $ | 4,443 | | | $ | 368 | | | 8.3 | % |
Senior living revenue increased $25.3 million, or 16.8%, for the year ended December 31, 2024 when compared to the same period in the prior year primarily due to a 8.3% increase in average monthly revenue per occupied unit and a 0.3% increase in occupancy rate. Growth in revenue was also driven by the acquisition of six senior living communities during the year ended December 31, 2024, and the acquisition of two senior living communities during the year ended December 31, 2023, resulting in an increase of $12.5 million, or 8.3% overall.
Cost of Services
The following table sets forth total cost of services by each of our reportable segments for the periods indicated:
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2024 | | 2023 | | Change | | % Change |
| (In thousands) | | |
| Home Health and Hospice | $ | 433,474 | | | $ | 331,844 | | | $ | 101,630 | | | 30.6 | % |
| Senior Living | 124,975 | | | 106,252 | | | 18,723 | | | 17.6 | |
| Total cost of services | $ | 558,449 | | | $ | 438,096 | | | $ | 120,353 | | | 27.5 | % |
Consolidated cost of services increased $120.4 million, or 27.5%, for the year ended December 31, 2024 when compared to the year ended December 31, 2023. The increase in the amount of cost of services was driven primarily by volume of services provided and increased wages and benefits. Cost of services as a percentage of revenue decreased by 10 basis points from 80.4% to 80.3% over the same time period.
Home Health and Hospice Services
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2024 | | 2023 | | Change | | % Change |
| (In thousands) | | | | |
| Cost of service | $ | 433,474 | | | $ | 331,844 | | | $ | 101,630 | | | 30.6 | % |
| Cost of services as a percentage of revenue | 83.4 | % | | 84.1 | % | | (0.7) | % | | |
Cost of services related to our Home Health and Hospice services segment increased $101.6 million, or 30.6%, primarily due to increased volume of services from the growth in admissions and average daily census as well as increased wages and benefits. Cost of services as a percentage of revenue for the year ended December 31, 2024 decreased by 70 basis points compared to the year ended December 31, 2023 primarily due to increased efficiency in our operations.
Senior Living Services
| | | | | | | | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2024 | | 2023 | | Change | | % Change |
| (In thousands) | | | | |
| Cost of service | $ | 124,975 | | | $ | 106,252 | | | $ | 18,723 | | | 17.6 | % |
| Cost of services as a percentage of revenue | 71.1 | % | | 70.6 | % | | 0.5 | % | | |
Cost of services related to our Senior Living services segment increased $18.7 million, or 17.6%, during the year ended December 31, 2024 in response to higher occupancy, acquisitions and wage rate increases. As a percentage of revenue, costs of service increased by 50 basis points during the year ended December 31, 2024 when compared to the year ended December 31, 2023 primarily due to increased wages and benefits.
Rent—Cost of Services. Rent increased 8.2% from $39.8 million to $43.0 million for the year ended December 31, 2024 compared to the year ended December 31, 2023, primarily as a result of the newly acquired senior living communities. As a percentage of revenue, rent—cost of services decreased 110 basis points when compared to the year ended December 31, 2023 due to improved overall sales leverage and performance.
General and Administrative Expense. General and administrative expense increased $13.5 million, or 36.9%, from $36.7 million to $50.2 million for the year ended December 31, 2024 when compared to the year ended December 31, 2023. The increase in general and administrative expense was primarily due to an increase of $12.5 million in wages and benefits for the year ended December 31, 2024 when compared to the year ended December 31, 2023.
Depreciation and Amortization. Depreciation and amortization expense stayed flat as a percentage of total revenue.
(Gain) loss on Asset Dispositions and Impairment, Net. (Gain) loss on asset dispositions and impairment, net is a gain of $0.7 million for the year ended December 31, 2024 compared to a loss of $0.1 million for the year ended December 31, 2023 primarily due to insurance proceeds related to one of our senior living communities.
Provision for Income Taxes. Our effective tax rate for the year ended December 31, 2024 was 22.4% of earnings before income taxes compared with an effective tax rate of 29.0% for the year ended December 31, 2023. The decrease in the effective tax rate is primarily due to a change in deductible equity compensation expenses. See Note 14, Income Taxes, to the Consolidated Financial Statements included elsewhere in this report filed on Form 10-K for further discussion.
Comparison of Prior Year Information
For a comparison of our results of operations of the fiscal year ended December 31, 2023 as compared to the year ended December 31, 2022 refer to Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations on Form 10-K filed with the SEC on February 28, 2024.
Liquidity and Capital Resources
Our primary sources of liquidity are cash generated through operating activities and borrowings under our revolving credit facility.
Revolving Credit Facility
On July 31, 2024, Pennant amended and restated its existing credit agreement (as amended, the “Amended Credit Agreement”), which provides for an increased revolving credit facility with a syndicate of banks with a borrowing capacity of $250.0 million (the “Amended Revolving Credit Facility”). The Amended Revolving Credit Facility is not subject to interim amortization and the Company will not be required to repay any loans under the Amended Revolving Credit Facility prior to maturity in 2029. The Company is permitted to prepay all or any portion of the loans under the Amended Revolving Credit Facility prior to maturity without premium or penalty, subject to reimbursement of any SOFR breakage costs of the lenders.
The Amended Credit Agreement contains customary covenants that, among other things, restrict, subject to certain exceptions, the ability of the Company and its independent operating subsidiaries to grant liens on their assets, incur indebtedness, sell assets, make investments, engage in acquisitions, mergers or consolidations, amend certain material agreements and pay certain dividends and other restricted payments. Financial covenants require compliance with certain levels of leverage ratios that impact the amount of interest. As of December 31, 2024, the Company was compliant with all such financial covenants.
On October 2, 2024, the Company closed the public offering (the “Offering”) of 4,025 shares of its common stock, $0.001 par value per share (“common stock”). The net proceeds to the Company from the offering, after underwriting discounts, commissions, and expenses, was approximately $118.1 million. The majority of the proceeds were subsequently used to pay the outstanding balance on our Amended Revolving Credit Facility.
As of December 31, 2024 we had $24.2 million of cash and $245.8 million of available borrowing capacity on our Amended Revolving Credit Facility.
We believe that our existing cash, cash generated through operations, and access to available borrowing capacity under our Amended Credit Agreement, will be sufficient to provide adequate liquidity for the next twelve months for both our operating activities and opportunities for acquisition growth.
The following table presents selected data from our statement of cash flows for the periods presented:
| | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 |
| (In thousands) |
| Net cash provided by operating activities | $ | 39,298 | | | $ | 33,090 | |
| Net cash used in investing activities | (70,684) | | | (30,222) | |
| Net cash provided by financing activities | 49,573 | | | 1,112 | |
| Net change in cash | 18,187 | | | 3,980 | |
| Cash at beginning of year | 6,059 | | | 2,079 | |
| Cash at end of year | $ | 24,246 | | | $ | 6,059 | |
Year Ended December 31, 2024 Compared to the Year Ended December 31, 2023
Our net cash flow from operating activities for the year ended December 31, 2024 increased by $6.2 million when compared to the year ended December 31, 2023. The primary drivers of this difference was a $10.4 million increase in net income, offset by a $2.5 million net decrease in cash flows from the change in operating assets and liabilities and a net decrease of $1.7 million in non-cash expenses.
Our net cash used in investing activities for the year ended December 31, 2024 increased by $40.5 million compared to the year ended December 31, 2023, primarily driven by a $40.4 million increase in business acquisitions, asset acquisitions, and escrow deposits during the year ended December 31, 2024 compared to the year ended December 31, 2023.
Our net cash provided by financing activities increased by $48.5 million for the year ended December 31, 2024 when compared to the year ended December 31, 2023 primarily due to an issuance of equity through a secondary offering totaling $118.1 million offset by a net repayment of debt totaling $65.0 million and payments for deferred financing costs of $3.9 million during the year ended December 31, 2024.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk. We are exposed to risks associated with market changes in interest rates. On July 31, 2024, Pennant entered into the Amended Credit Agreement, which provides for a revolving credit facility with a syndicate of banks with a borrowing capacity of $250.0 million. A 1.0% interest rate change would cause interest expense to remain constant based upon our outstanding long-term debt as of December 31, 2024. We manage our exposure to this market risk by monitoring available financing alternatives.
Item 8. Financial Statements and Supplementary Data
The consolidated financial statements and accompanying notes listed in Part IV, Item 15(a)(1) of this Annual Report on Form 10-K are included elsewhere in this report.
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
Under the supervision and with the participation of our management, including the Chief Executive Officer and Chief Financial Officer, we have evaluated the effectiveness of our disclosure controls and procedures (as such term is defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the “Exchange Act”)), as of the end of the period covered by this Annual Report. Based on that evaluation, the Chief Executive Officer and Chief Financial Officer have concluded that these disclosure controls and procedures were effective to provide reasonable assurance that information we are required to disclose in reports that we file or submit under the Exchange Act is recorded, processed, summarized, and
reported within the time periods specified in SEC rules and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure.
Management’s Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Rule 13a-15(f) promulgated under the Exchange Act. Internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management, with the participation of our Chief Executive Officer and our Chief Financial Officer, evaluated the effectiveness of our internal control over financial reporting using the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission in Internal Control - Integrated Framework (2013). As a result of this assessment, management concluded that, as of December 31, 2024, our internal control over financial reporting was effective in providing reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles.
Our independent registered public accounting firm, Deloitte & Touche LLP, has audited the consolidated financial statements included in this Annual Report on Form 10-K and, as part of their audit, has issued an audit report, included herein, on the effectiveness of our internal control over financial reporting. Their report is set forth below.
Changes in Internal Control over Financial Reporting
During the fiscal quarter ended December 31, 2024, there were no material changes in our internal control over financial reporting that occurred during our most recent fiscal quarter that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and the Board of Directors of The Pennant Group, Inc.
Opinion on Internal Control over Financial Reporting
We have audited the internal control over financial reporting of The Pennant Group, Inc. and subsidiaries (the “Company”) as of December 31, 2024, based on criteria established in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2024, based on criteria established in Internal Control — Integrated Framework (2013) issued by COSO.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the consolidated financial statements as of and for the year ended December 31, 2024, of the Company and our report dated February 27, 2025, expressed an unqualified opinion on those financial statements.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in Management's report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ DELOITTE & TOUCHE LLP
Boise, ID
February 27, 2025
Item 9B. Other Information
Rule 10b5-1 Plan Election
JoAnne Stringfield, Director, entered into a Rule 10b5-1 trading arrangement on November 11, 2024. Ms. Stringfield’s 10b5-1 Plan provides for the sale of 7,750 shares of the Company’s common stock on predetermined dates from April 21, 2025 to January 20, 2026.
These Rule 10b5-1 trading arrangements were entered into during open trading windows and are intended to satisfy the affirmative defense conditions of Rule 10b5-1(c) under the Securities Exchange Act of 1934, as amended, and the Company's policies regarding transactions in Company securities.
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections
None.
Part III.
Item 10. Directors, Executive Officers and Corporate Governance
The information required by this Item is hereby incorporated by reference to our definitive proxy statement on Form 14A for the 2025 Annual Meeting of Stockholders.
Item 11. Executive Compensation
The information required by this Item is hereby incorporated by reference to our definitive proxy statement on Form 14A for the 2025 Annual Meeting of Stockholders.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required by this Item is hereby incorporated by reference to our definitive proxy statement on Form 14A for the 2025 Annual Meeting of Stockholders.
Item 13. Certain Relationships and Related Transactions and Director Independence
The information required by this Item is hereby incorporated by reference to our definitive proxy statement on Form 14A for the 2025 Annual Meeting of Stockholders.
Item 14. Principal Accountant Fees and Services
The information required by this Item is hereby incorporated by reference to our definitive proxy statement on Form 14A for the 2025 Annual Meeting of Stockholders.
Part IV.
Item 15. Exhibits and Financial Statement Schedules
The following documents are filed as a part of this report:
(a)(1) Financial Statements:
The following Consolidated Financial Statements of the Company are included in Part II, Item 8 of this Annual Report on Form 10-K.
•Report of Independent Registered Public Accounting Firm
•Consolidated Balance Sheets as of December 31, 2024 and 2023
•Consolidated Statements of Income for the Years Ended December 31, 2024, 2023 and 2022
•Consolidated Statements of Changes in Stockholders' Equity for the Years Ended December 31, 2024, 2023 and 2022
•Consolidated Statements of Cash Flows for the Years Ended December 31, 2024, 2023 and 2022
•Notes to the Consolidated Financial Statements
(a)(2) Financial Statement Schedules:
There are no financial schedules included in this Report as they are either not applicable or included in the financial statements.
(a) (3) Exhibits: The following exhibits are filed with this Report or incorporated by reference:
Exhibits
| | | | | |
| Exhibit No. | Exhibit Description |
| Master Separation Agreement, dated as of October 1, 2019, by and between The Ensign Group, Inc. and The Pennant Group, Inc. (incorporated by reference to Exhibit 2.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| Form of Operations Transfer Agreement, dated as of January 27, 2022, entered into by affiliates of the Company and affiliates of Ensign (incorporated by reference to Exhibit 2.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on January 27, 2022). |
| Amended and Restated Certificate of Incorporation of The Pennant Group, Inc., effective as of September 27, 2019 (incorporated by reference to Exhibit 3.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| Second Amended and Restated Bylaws of The Pennant Group, Inc., effective as of February 21, 2022 (incorporated by reference to Exhibit 3.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC February 22, 2022). |
| Description of Securities of The Pennant Group, Inc. (incorporated by reference to Exhibit 4.1 to The Pennant Group, Inc.’s Annual Report on Form 10-K (File No. 001-389000) filed with the SEC on March 4, 2020). |
| Form of Indenture (incorporated by reference to Exhibit 4.4 to The Pennant Group, Inc.’s Registration Statement on Form S-3 (File No. 333-281302) filed with the SEC August 6, 2024 ). |
| Transition Services Agreement, dated as of October 1, 2019, by and between The Ensign Group, Inc. and The Pennant Group, Inc. (incorporated by reference to Exhibit 10.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| Tax Matters Agreement, dated as of October 1, 2019, by and between The Ensign Group, Inc. and The Pennant Group, Inc. (incorporated by reference to Exhibit 10.2 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| Employee Matters Agreement, dated as of October 1, 2019, by and between The Ensign Group, Inc. and The Pennant Group, Inc. (incorporated by reference to Exhibit 10.3 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| | | | | |
| Form of Lease Agreement by and among subsidiaries of The Ensign Group, Inc. and subsidiaries of The Pennant Group, Inc. (incorporated by reference to Exhibit 10.4 to The Pennant Group, Inc.’s Amendment No. 2 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on August 19, 2019). |
| The Pennant Group, Inc. 2019 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.12 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| Form of Options Granted Under The Pennant Group, Inc. 2019 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.6 to The Pennant Group, Inc.’s Amendment No. 2 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on August 19, 2019). |
| Form of RSUs Granted Under The Pennant Group, Inc. 2019 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.7 to The Pennant Group, Inc.’s Amendment No. 2 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on August 19, 2019). |
| Form of RS Granted Under The Pennant Group, Inc. 2019 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.8 to The Pennant Group, Inc.’s Amendment No. 2 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on August 19, 2019). |
| The Pennant Group, Inc. 2019 Long Term Incentive Plan (incorporated by reference to Exhibit 10.11 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on October 3, 2019). |
| Form of LTIP RS Granted Under The Pennant Group, Inc. 2019 Long Term Incentive Plan (incorporated by reference to Exhibit 10.10 to The Pennant Group, Inc.’s Amendment No. 2 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on August 19, 2019). |
| Form of Indemnification Agreement to be entered into between The Pennant Group, Inc. and each of its directors and executive officers (incorporated by reference to Exhibit 10.11 to The Pennant Group, Inc.’s Amendment No. 2 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on August 19, 2019). |
| Credit Agreement, dated February 23, 2021, by and among the Company and certain of its subsidiaries, the lenders named therein, and Truist Bank (successor by merger to SunTrust Bank), as administrative agent for the lenders (incorporated by reference to Exhibit 10.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on February 24, 2021). |
| Cornerstone Healthcare, Inc. 2016 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.13 to The Pennant Group, Inc.’s Amendment No. 3 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on September 3, 2019). |
| The Ensign Group, Inc. 2017 Omnibus Incentive Plan (incorporated by reference to Exhibit 10.14 to The Pennant Group, Inc.’s Amendment No. 3 to the Registration Statement on Form 10 (File No. 001-38900) filed with the SEC on September 3, 2019). |
| Consulting Agreement, dated July 25, 2022, by and between The Pennant Group, Inc. and Daniel H. Walker (incorporated by reference to Exhibit 10.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on July 29, 2022). |
| Amendment to Restricted Stock Unit Agreement, dated July 25, 2022, by and between The Pennant Group, Inc. and Daniel H. Walker (incorporated by reference to Exhibit 10.2 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on July 29, 2022). |
| Credit Agreement, dated June 12, 2023, by and among the Company and certain of its subsidiaries, the lenders named therein, and Truist Bank (successor by merger to SunTrust Bank), as administrative agent for the lenders (incorporated by reference to Exhibit 10.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC on June 12, 2023). |
| Amended and Restated Credit Agreement, dated as of July 31, 2024, by and among The Pennant Group, Inc. and Truist Bank, as administrative agent, and the lenders party thereto (incorporated by reference to Exhibit 10.1 to The Pennant Group, Inc.’s Current Report on Form 8-K (File No. 001-38900) filed with the SEC August 1, 2024 ). |
| Statement of Company Policy Regarding Insider Trading |
| Subsidiaries of The Pennant Group, Inc. |
| Consent of Deloitte & Touche LLP. |
| |
| Certification of Chief Executive Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. |
| Certification of Chief Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. |
| | | | | |
| Certification of Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. |
| Certification of Chief Financial Officer pursuant 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. |
| Clawback Policy of The Pennant Group, Inc. |
| 101.INS* | Instance Document - the instance document does not appear in the Interactive Data File because its XBRL tags are embedded within the Inline XBRL document. |
| 101.SCH* | Inline XBRL Taxonomy Extension Schema Document. |
| 101.CAL* | Inline XBRL Taxonomy Extension Calculation Linkbase Document. |
| 101.DEF* | Inline XBRL Taxonomy Extension Definition Linkbase Document. |
| 101.LAB* | Inline XBRL Taxonomy Extension Label Linkbase Document. |
| 101.PRE* | Inline XBRL Taxonomy Extension Presentation Linkbase Document. |
| 104* | Cover Page Interactive Data File – the cover page XBRL tags are embedded within the Inline XBRL document. |
| * Filed with this report.
** Furnished with this report.
+ Exhibit constitutes a management contract or compensatory plan or agreement.
# Schedules omitted pursuant to Item 601(b)(2) of Regulation S-K. The Pennant Group Inc. agrees to furnish a supplemental copy of any omitted schedule to the SEC upon request. |
Item 16. Form 10-K Summary
Not applicable.
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
| | | | | | | | |
| | The Pennant Group, Inc. |
| | |
| Dated: February 27, 2025 | BY: | /s/ LYNETTE B. WALBOM |
| | | Lynette B. Walbom |
| | | Chief Financial Officer (Principal Financial Officer, Principal Accounting Officer and Duly Authorized Officer) |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant in the capacities and on the dates indicated.
| | | | | | | | | | | | | | |
| Signature | | Title | | Date |
| | | | |
| /s/ BRENT J. GUERISOLI | | Chief Executive Officer (Principal Executive Officer) | | February 27, 2025 |
| Brent J. Guerisoli | | | | |
| | | | |
| /s/ LYNETTE B. WALBOM | | Chief Financial Officer (Principal Financial Officer, Principal Accounting Officer and Duly Authorized Officer) | | February 27, 2025 |
| Lynette B. Walbom | | | | |
| | | | |
| /s/ BARRY M. SMITH | | Chairman | | February 27, 2025 |
| Barry M. Smith | | | | |
| | | | |
| /s/ CHRISTOPER R. CHRISTENSEN | | Director | | February 27, 2025 |
| Christopher R. Christensen | | | | |
| | | | |
| /s/ JOHN G. NACKEL, Ph.D. | | Director | | February 27, 2025 |
| John G. Nackel, Ph.D. | | | | |
| | | | |
| /s/ STEPHEN M. R. COVEY | | Director | | February 27, 2025 |
| Stephen M. R. Covey | | | | |
| | | | |
| /s/ JOANNE STRINGFIELD | | Director | | February 27, 2025 |
| JoAnne Stringfield | | | | |
| | | | |
| /s/ SCOTT E. LAMB | | Director | | February 27, 2025 |
| Scott E. Lamb | | | | |
| | | | |
| /s/ GREGORY K. MORRIS M.D. | | Director | | February 27, 2025 |
| Gregory K. Morris M.D. | | | | |
| | | | |
THE PENNANT GROUP, INC.
INDEX TO THE CONSOLIDATED FINANCIAL STATEMENTS
AND FINANCIAL STATEMENT SCHEDULE
| | | | | |
| |
| Consolidated Financial Statements: | |
| |
| |
| |
| |
| |
| |
| |
| |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and the Board of Directors of The Pennant Group, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of The Pennant Group, Inc. and subsidiaries (the "Company") as of December 31, 2024 and 2023, the related consolidated statements of income, stockholders' equity, and cash flows, for each of the three years in the period ended December 31, 2024, and the related notes (collectively referred to as the "financial statements"). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2024 and 2023, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2024, in conformity with accounting principles generally accepted in the United States of America.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company's internal control over financial reporting as of December 31, 2024, based on criteria established in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated February 27, 2025, expressed an unqualified opinion on the Company's internal control over financial reporting.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company's financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matter
The critical audit matter communicated below is a matter arising from the current-period audit of the financial statements that was communicated or required to be communicated to the audit committee and that (1) relates to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing a separate opinion on the critical audit matter or on the accounts or disclosures to which it relates.
Self-Insurance Reserve — Refer to Note 2 and Note 16 to the financial statements
Critical Audit Matter Description
The Company is self-insured for general and professional liability, workers’ compensation, automobile, and its employee health plans while maintaining stop-loss coverage with third-party insurers to limit its total liability exposure. The self-insurance reserves are undiscounted. Self-insurance reserves consist of the projected settlement value of reported and unreported claims. The projected settlement values are estimated based on the Company’s historical claim experience, supplemented with industry experience, as necessary and are established using actuarial methods followed in the insurance industry.
We identified the evaluation of the Company’s self-insurance reserves for general and professional liability and workers’ compensation as a critical audit matter because estimating projected settlement value of reported and unreported claims involves significant estimation by management. This required a high degree of auditor judgment and an increased extent of effort, including the need to involve our actuarial specialists, when performing audit procedures to evaluate whether self-insurance reserves were appropriately recorded as of December 31, 2024.
How the Critical Audit Matter Was Addressed in the Audit
Our audit procedures related to the self-insurance reserves for general and professional liability and workers’ compensation included the following among others:
•We tested the effectiveness of controls related to self-insurance reserves for general and professional liability and workers’ compensation, including management’s controls over the review of the historical claim data and the projection of the settlement value of the reported and unreported claims.
•We evaluated the methods and assumptions used by management to estimate the self-insurance reserves for general and professional liability and workers’ compensation by:
◦Reading the Company’s insurance policies and compared the coverage and terms to the assumptions used by management.
◦Testing the underlying data that served as the basis for the actuarial analysis, including historical claims, to test that the inputs to the actuarial estimate were accurate and complete.
◦Comparing management's change in ultimate loss to the differential between expected development and actuals incurred during the current year to identify potential bias in the determination of the insurance reserves.
•With the assistance of our actuarial specialists, we developed independent estimates of self-insurance reserves for general and professional liability and workers’ compensation and compared our estimates to management’s estimates.
/s/ DELOITTE & TOUCHE LLP
Boise, ID
February 27, 2025
We have served as the Company's auditor since 2019.
THE PENNANT GROUP, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except par value)
| | | | | | | | | | | |
| December 31, 2024 | | December 31, 2023 |
| Assets | | | |
| Current assets: | | | |
| Cash | $ | 24,246 | | | $ | 6,059 | |
| Accounts receivable—less allowance for doubtful accounts of $232 and $259 at December 31, 2024 and 2023, respectively | 81,302 | | | 61,116 | |
| Prepaid expenses and other current assets | 17,308 | | | 12,902 | |
| Total current assets | 122,856 | | | 80,077 | |
| Property and equipment, net | 43,296 | | | 28,598 | |
| Right-of-use assets | 270,586 | | | 262,923 | |
| | | |
| Restricted and other assets | 17,477 | | | 9,337 | |
| Goodwill | 129,124 | | | 91,014 | |
| Other indefinite-lived intangibles | 96,182 | | | 67,742 | |
| Total assets | $ | 679,521 | | | $ | 539,691 | |
| Liabilities and equity | | | |
| Current liabilities: | | | |
| Accounts payable | $ | 18,737 | | | $ | 10,841 | |
| Accrued wages and related liabilities | 43,106 | | | 28,256 | |
| Lease liabilities—current | 19,671 | | | 17,122 | |
| Other accrued liabilities | 20,186 | | | 15,330 | |
| Total current liabilities | 101,700 | | | 71,549 | |
| Long-term lease liabilities—less current portion | 253,420 | | | 248,596 | |
| Deferred tax liabilities, net | 1,861 | | | 1,855 | |
| Other long-term liabilities | 10,575 | | | 8,262 | |
| Long-term debt, net | — | | | 63,914 | |
| Total liabilities | 367,556 | | | 394,176 | |
| Commitments and contingencies (Note 16) | | | |
| Equity: | | | |
| Common stock, $0.001 par value; 100,000 shares authorized; 34,670 and 34,373 shares issued and outstanding at December 31, 2024, respectively, and 30,297 and 29,948 shares issued and outstanding at December 31, 2023, respectively | 35 | | | 29 | |
| Additional paid-in capital | 236,091 | | | 105,712 | |
| Retained earnings | 57,222 | | | 34,663 | |
| Treasury stock, at cost, 3 shares at December 31, 2024 and 2023 | (65) | | | (65) | |
| Total The Pennant Group, Inc. stockholders' equity | 293,283 | | | 140,339 | |
| Noncontrolling interest | 18,682 | | | 5,176 | |
| Total equity | 311,965 | | | 145,515 | |
| Total liabilities and equity | $ | 679,521 | | | $ | 539,691 | |
See accompanying notes to the consolidated financial statements.
THE PENNANT GROUP, INC.
CONSOLIDATED STATEMENTS OF INCOME
(In thousands, except for per-share amounts)
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| | | |
| Revenue | $ | 695,240 | | | $ | 544,891 | | | $ | 473,241 | |
| | | | | |
| Expense: | | | | | |
| Cost of services | 558,449 | | | 438,096 | | | 376,638 | |
| Rent—cost of services | 43,029 | | | 39,759 | | | 38,018 | |
| General and administrative expense | 50,209 | | | 36,667 | | | 33,981 | |
| Depreciation and amortization | 6,119 | | | 5,130 | | | 4,900 | |
| (Gain) loss on asset dispositions and impairment, net | (682) | | | 70 | | | 6,965 | |
| Total expenses | 657,124 | | | 519,722 | | | 460,502 | |
| Income from operations | 38,116 | | | 25,169 | | | 12,739 | |
| Other income (expense), net: | | | | | |
| Other income (expense) | 207 | | | 339 | | | (31) | |
| Interest expense, net | (6,956) | | | (5,924) | | | (3,816) | |
| Other expense, net | (6,749) | | | (5,585) | | | (3,847) | |
| Income before provision for income taxes | 31,367 | | | 19,584 | | | 8,892 | |
| Provision for income taxes | 7,028 | | | 5,674 | | | 1,649 | |
| Net income | 24,339 | | | 13,910 | | | 7,243 | |
| Less: net income attributable to noncontrolling interest | 1,780 | | | 531 | | | 600 | |
| Net income and other comprehensive income attributable to The Pennant Group, Inc. | $ | 22,559 | | | $ | 13,379 | | | $ | 6,643 | |
| Earnings per share: | | | | | |
| Basic | $ | 0.72 | | | $ | 0.45 | | | $ | 0.23 | |
| Diluted | $ | 0.70 | | | $ | 0.44 | | | $ | 0.22 | |
| Weighted average common shares outstanding: | | | | | |
| Basic | 31,191 | | | 29,863 | | | 29,064 | |
| Diluted | 32,000 | | | 30,193 | | | 30,159 | |
See accompanying notes to the consolidated financial statements.
THE PENNANT GROUP, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
(In thousands) | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Common Stock | | Additional Paid-In Capital | | Retained Earnings | | Treasury Stock | | | | Non-controlling Interest | | Total Equity |
| Shares | | Amount | | | | Shares | | Amount | | | | |
| | | | | | | | | | | | | | | | | |
| Balance at December 31, 2021 | 28,826 | | | $ | 28 | | | $ | 95,595 | | | $ | 14,641 | | | 3 | | | $ | (65) | | | | | $ | 4,045 | | | $ | 114,244 | |
| Net income attributable to The Pennant Group, Inc. | — | | | — | | | — | | | 6,643 | | | — | | | — | | | | | — | | | 6,643 | |
| Net income attributable to Non-controlling interests | — | | | — | | | — | | | — | | | — | | | — | | | | | 600 | | | 600 | |
| Share-based compensation | — | | | — | | | 3,086 | | | — | | | — | | | — | | | | | — | | | 3,086 | |
| Net issuance of common stock due to share based compensation | 125 | | | 1 | | | 1,083 | | | — | | | — | | | — | | | | | — | | | 1,084 | |
| Net issuance of restricted stock | 1,198 | | | — | | | — | | | — | | | — | | | — | | | | | — | | | — | |
| Balance at December 31, 2022 | 30,149 | | | 29 | | | 99,764 | | | 21,284 | | | 3 | | | (65) | | | | | 4,645 | | | 125,657 | |
| Net income attributable to The Pennant Group, Inc. | — | | | — | | | — | | | 13,379 | | | — | | | — | | | | | — | | | 13,379 | |
| Net income attributable to Non-controlling interests | — | | | — | | | — | | | — | | | — | | | — | | | | | 531 | | | 531 | |
| Share-based compensation | — | | | — | | | 5,369 | | | — | | | — | | | — | | | | | — | | | 5,369 | |
| Net issuance of common stock due to share based compensation | 89 | | | — | | | 579 | | | — | | | — | | | — | | | | | — | | | 579 | |
| Net issuance of restricted stock | 59 | | | — | | | — | | | — | | | — | | | — | | | | | — | | | — | |
| Balance at December 31, 2023 | 30,297 | | | 29 | | | 105,712 | | | 34,663 | | | 3 | | | (65) | | | | | 5,176 | | | 145,515 | |
| Net income attributable to The Pennant Group, Inc. | — | | | — | | | — | | | 22,559 | | | — | | | — | | | | | — | | | 22,559 | |
| Noncontrolling interests assumed related to acquisitions | — | | | — | | | — | | | — | | | — | | | — | | | | | 11,726 | | | 11,726 | |
| Equity adjustments related to acquisitions | — | | | — | | | 3,602 | | | — | | | — | | | — | | | | | — | | | 3,602 | |
| Net income attributable to Non-controlling interests | — | | | — | | | — | | | — | | | — | | | — | | | | | 1,780 | | | 1,780 | |
| Share-based compensation | — | | | — | | | 7,781 | | | — | | | — | | | — | | | | | — | | | 7,781 | |
| Net issuance of common stock due to share based compensation | 254 | | | 2 | | | 851 | | | — | | | — | | | — | | | | | — | | | 853 | |
| Net issuance of restricted stock | 94 | | | — | | | — | | | — | | | — | | | — | | | | | — | | | — | |
| Issuance of equity through secondary offering | 4,025 | | | $ | 4 | | | $ | 118,145 | | | $ | — | | | — | | | $ | — | | | | | $ | — | | | $ | 118,149 | |
| Balance at December 31, 2024 | 34,670 | | | $ | 35 | | | $ | 236,091 | | | $ | 57,222 | | | 3 | | | $ | (65) | | | | | $ | 18,682 | | | $ | 311,965 | |
See accompanying notes to the consolidated financial statements.
THE PENNANT GROUP, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands) | | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Cash flows from operating activities: | | | | | |
| Net income | $ | 24,339 | | | $ | 13,910 | | | $ | 7,243 | |
| Adjustments to reconcile net income to net cash provided by operating activities: | | | | | |
| Depreciation and amortization | 6,119 | | | 5,130 | | | 4,900 | |
| Amortization and write-off of deferred financing fees | 1,096 | | | 521 | | | 520 | |
| Provision for doubtful accounts | 903 | | | 646 | | | 881 | |
| Share-based compensation | 7,781 | | | 5,369 | | | 3,086 | |
| Deferred income taxes | (1,187) | | | 4,004 | | | 1,700 | |
| (Gain) loss on asset dispositions and impairment | (682) | | | 70 | | | 218 | |
| Change in operating assets and liabilities, net of effects of business acquisitions: | | | | | |
| Accounts receivable | (21,088) | | | (7,350) | | | (361) | |
| Prepaid expenses and other assets | (5,604) | | | 7,770 | | | (7,426) | |
| Operating lease obligations | (349) | | | (12) | | | (67) | |
| Accounts payable | 8,052 | | | (1,845) | | | 2,368 | |
| Accrued wages and related liabilities | 14,504 | | | 4,972 | | | (197) | |
| Other accrued liabilities | 4,497 | | | (814) | | | 1,856 | |
| Advance payments | — | | | — | | | (6,211) | |
| | | | | |
| Other long-term liabilities | 917 | | | 719 | | | 534 | |
| Net cash provided by operating activities | 39,298 | | | 33,090 | | | 9,044 | |
| Cash flows from investing activities: | | | | | |
| Purchase of property and equipment | (8,992) | | | (8,105) | | | (14,170) | |
| Cash payments for business acquisitions | (48,416) | | | (21,376) | | | (10,130) | |
| Cash payments for asset acquisitions | (11,380) | | | (211) | | | — | |
| | | | | |
| | | | | |
| Escrow deposits | (2,344) | | | (201) | | | (49) | |
| Other investing activities | 448 | | | (329) | | | 110 | |
| Net cash used in investing activities | (70,684) | | | (30,222) | | | (24,239) | |
| Cash flows from financing activities: | | | | | |
| Proceeds from secondary offering, net of expenses | 118,149 | | | — | | | — | |
| | | | | |
| | | | | |
| | | | | |
| | | | | |
| Proceeds from revolver agreement | 309,500 | | | 182,000 | | | 129,500 | |
| Payments on revolver agreement | (374,500) | | | (181,500) | | | (118,500) | |
| | | | | |
| Payments for deferred financing costs | (3,915) | | | — | | | — | |
| Net issuance of common stock due to share based compensation | 853 | | | 579 | | | 1,084 | |
| Other financing activities | (514) | | | 33 | | | — | |
| Net cash provided by financing activities | 49,573 | | | 1,112 | | | 12,084 | |
| Net increase (decrease) in cash | 18,187 | | | 3,980 | | | (3,111) | |
| Cash beginning of period | 6,059 | | | 2,079 | | | 5,190 | |
| Cash end of period | $ | 24,246 | | | $ | 6,059 | | | $ | 2,079 | |
See accompanying notes to the consolidated financial statements.
THE PENNANT GROUP, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS - (Continued)
(In Thousands) | | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Supplemental disclosures of cash flow information: | | | | | |
| Cash paid during the period for: | | | | | |
| Interest | $ | 6,521 | | | $ | 5,012 | | | $ | 3,027 | |
| Income taxes | $ | 7,351 | | | $ | 841 | | | $ | 99 | |
| Operating lease liabilities | $ | 39,503 | | | $ | 36,653 | | | $ | 35,994 | |
| Right-of-use assets obtained in exchange for new operating lease obligations | $ | 25,267 | | | $ | 12,826 | | | $ | 12,645 | |
| Finance lease assets obtained in exchange for new finance lease obligations | $ | 506 | | | $ | 633 | | | $ | — | |
| Non-cash adjustment to right-of-use assets and lease liabilities from lease modifications | $ | 260 | | | $ | 5,195 | | | $ | 6,270 | |
| Non-cash adjustment to right-of-use assets and lease liabilities from lease terminations and assignments | $ | — | | | $ | — | | | $ | (43,136) | |
| Non-cash investing activity: | | | | | |
| Capital expenditures in accounts payable and other accrued liabilities | $ | 1,333 | | | $ | 319 | | | $ | 1,280 | |
See accompanying notes to the consolidated financial statements.
THE PENNANT GROUP INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
(Dollars in thousands, except per share data and operational senior living units)
1. DESCRIPTION OF BUSINESS
The Pennant Group, Inc. (herein referred to as “Pennant,” the “Company,” “it,” or “its”), is a holding company with no direct operating assets, employees or revenue. The Company, through its independent operating subsidiaries, provides healthcare services across the post-acute care continuum. As of December 31, 2024, the Company’s subsidiaries operated 123 home health, hospice and home care agencies and 57 senior living communities located in Arizona, California, Colorado, Idaho, Montana, Nevada, Oklahoma, Oregon, Texas, Utah, Washington, Wisconsin and Wyoming. We also provide home health and hospice operational support through a management service agreement in Connecticut.
Certain of the Company’s subsidiaries, collectively referred to as the Service Center, provide accounting, payroll, human resources, information technology, legal, risk management, and other services to the operations through contractual relationships.
Each of the Company’s affiliated operations are operated by separate, independent subsidiaries that have their own management, employees and assets. References herein to the consolidated “Company” and “its” assets and activities are not meant to imply, nor should they be construed as meaning, that Pennant has direct operating assets, employees or revenue, or that any of the subsidiaries, are operated by Pennant.
2. BASIS OF PRESENTATION AND SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Basis of Presentation - The accompanying consolidated financial statements of the Company (the “Financial Statements”) reflect the Company’s financial position for the years ended December 31, 2024 and 2023, and the Company’s results of operations and cash flows for the years ended December 31, 2024, 2023 and 2022 and have been prepared in accordance with accounting principles generally accepted in the United States (“GAAP”) and pursuant to the regulations of the Securities and Exchange Commission (“SEC”). The Company presents noncontrolling interests within the equity section of its consolidated balance sheets and the amount of consolidated net income (loss) that is attributable to The Pennant Group, Inc. and the noncontrolling interest in its consolidated statements of income.
All intercompany transactions and balances between the various legal entities comprising the Company have been eliminated in consolidation. The consolidated statements of income reflect income that is attributable to the Company and the noncontrolling interest.
The Company consists of various limited liability companies and corporations established to operate home health, hospice, home care, and senior living operations. The Financial Statements include the accounts of all entities controlled by the Company through its ownership of a majority voting interest. Revenue was derived from transactional information specific to the Company’s services provided.
Reclassifications - Certain amounts in the prior financial statements have been reclassified to conform to the presentation of the current period financial statements.
Estimates and Assumptions - The preparation of the Financial Statements in conformity with GAAP requires management to make certain estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the Financial Statements and the reported amounts of revenue and expenses during the reporting periods. The most significant estimates in the Financial Statements relate to self-insurance reserves, revenue recognition, and intangible assets and goodwill. Actual results could differ from those estimates.
Revenue Recognition - Revenues are recognized when services are provided to the patients at the amount that reflects the consideration to which the Company expects to be entitled from patients and third-party payors, including Medicaid, Medicare and insurers (private and Medicare replacement plans), in exchange for providing patient care. Revenue recognized from healthcare services are adjusted for estimates of variable consideration to arrive at the transaction price. The Company determines the transaction price based on contractually agreed-upon amounts or rate, adjusted for estimates of variable consideration. The Company uses the expected value method in determining the variable component that should be used to arrive at the transaction price, using contractual agreements and historical reimbursement experience within each payor type. The amount of variable consideration which is included in the transaction price may be constrained and is included in the net revenue only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
not occur in a future period. If actual amounts of consideration ultimately received differ from the Company’s estimates, the Company adjusts these estimates, which would effect net service revenue in the period such variances become known.
As the Company’s contracts have an original duration of one year or less, the Company uses the practical expedient applicable to its contracts and does not consider the time value of money. Further, because of the short duration of these contracts, the Company has not disclosed the transaction price for the remaining performance obligations as of the end of each reporting period or when the Company expects to recognize this revenue. In addition, the Company has applied the practical expedient provided by Accounting Standard Codification (“ASC”) Topic 340, Other Assets and Deferred Costs, and all incremental customer contract acquisition costs are expensed as they are incurred because the amortization period would have been one year or less. See Note 5, Revenue and Accounts Receivable.
CARES Act - The Coronavirus Aid, Relief, and Economic Security Act (the “CARES Act”) was enacted on March 27, 2020 in the United States. The CARES Act allowed for deferred payment of the employer-paid portion of social security taxes through the end of 2020, with 50% due on December 31, 2021 and the remainder due on December 31, 2022. The Company deferred approximately $7,836 of employer-paid portion of social security tax, all of which was repaid as of December 31, 2022. The CARES Act also expanded the Centers for Medicare & Medicaid Services’ (“CMS”) ability to provide accelerated/advance payments intended to increase the cash flow of healthcare providers and suppliers impacted by COVID-19. During 2020, the Company applied for and received $27,997 in funds under the Accelerated and Advance Payment (“AAP”) Program, all of which was recouped as of June 23, 2022.
Cash - Cash consists of bank deposits and therefore approximates fair value. The Company places its cash with high credit quality financial institutions.
Accounts Receivable and Allowance for Doubtful Accounts - Accounts receivable consist primarily of amounts due from Medicare and Medicaid programs, other government programs, healthcare systems, managed care health plans and private payor sources, net of estimates for variable consideration. The allowance for doubtful accounts is the Company’s best estimate of current expected credit losses in the accounts receivable balance.
Property and Equipment - Property and equipment are initially recorded at their historical cost. Depreciation is computed using the straight-line method over the estimated useful lives of the depreciable assets (ranging from one to 40 years). Leasehold improvements are amortized on a straight-line basis over the shorter of their estimated useful lives or the remaining lease term. Repairs and maintenance are expensed as incurred.
Impairment of Long-Lived Assets - The Company reviews the carrying value of long-lived assets that are held and used in the independent operating subsidiaries for impairment on an annual basis or whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability of these assets is determined based upon expected undiscounted future net cash flows from the operating subsidiary to which the assets relate, utilizing management’s best estimate, appropriate assumptions, and projections at the time. If the carrying value is determined to be unrecoverable from future operating cash flows, the asset is deemed impaired and an impairment loss would be recognized to the extent the carrying value exceeded the estimated fair value of the asset. The Company estimates the fair value of assets on a non-recurring basis and the inputs used to determine the fair value of the long-lived assets are considered Level 3 measurements due to their subjective nature. There were no long-lived asset impairments during the years ended December 31, 2024 and 2023. Management evaluated its long-lived assets and the Company identified $218 in long-lived asset impairments related to six senior living communities for the year ended December 31, 2022.
Intangible Assets and Goodwill - The Company’s indefinite-lived intangible assets consist of trade names and Medicare and Medicaid licenses. The Company tests indefinite-lived intangible assets for impairment on an annual basis or more frequently if events or changes in circumstances indicate that the carrying amount of the intangible asset may not be recoverable.
Goodwill represents the excess of the purchase price over the fair value of identifiable net assets acquired in business combinations. The Company reviews goodwill for impairment annually on the first day of the fourth quarter and also if events or changes in circumstances indicate the occurrence of a triggering event. The Company assesses qualitative factors to determine whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount. If the Company determines it is more likely than not that the fair value of a reporting unit is less than its carrying amount, then it is required to perform a quantitative impairment test by comparing the fair value with the carrying amount of the reporting unit. If
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
the carrying amount of a reporting unit exceeds its fair value, then the Company records an impairment of goodwill equal to the amount that the carrying amount of a reporting unit exceeds its fair value.
As of December 31, 2024, we evaluated potential triggering events that might be indicators that our goodwill and indefinite-lived intangible assets were impaired. As a result of our evaluation, no goodwill or indefinite-lived intangible asset impairments were recorded during the years ended December 31, 2024, 2023 and 2022. See further discussion at Note 9, Goodwill and Intangible Assets.
Self-Insurance Reserve - The Company retains risk for a substantial portion of potential claims for general and professional liability and workers’ compensation. The Company recognizes obligations associated with these costs, up to specified deductible limits in the period in which a claim is incurred, including with respect to both reported claims and claims incurred but not reported. The Company evaluates the adequacy of the self-insurance reserves in conjunction with an independent actuarial assessment. As of December 31, 2024, the general and professional liability insurance has a retention limit of $250 per claim with a $500 corridor as an additional out-of-pocket retention we must satisfy for claims within the policy year before the carrier will reimburse losses. The workers’ compensation insurance has a retention limit of $250 per claim, except for policies held in Texas, Washington, and Wyoming, which are subject to state insurance and possess their own limits.
These costs have generally been estimated based on historical data of our claims experience. Such estimates, and the resulting reserves, are reviewed and updated by us on a quarterly basis.
The following table presents details of the Company's insurance program, including general and professional liability and workers’ compensation, and amounts accrued for the periods indicated in other accrued liabilities and other long-term liabilities in our accompanying consolidated balance sheets. The amounts accrued are undiscounted and established using actuarial methods followed in the insurance industry based on claims filed and an estimate of claims incurred but not reported. The amounts accrued below represent the total estimated liability for individual claims that are less than our noted insurance coverage amounts, which includes outstanding claims and claims incurred but not reported. The amounts are reported gross of reinsurance receivable of $3,613 and $2,045 included in restricted and other assets for the years ended December 31, 2024 and 2023, respectively, and $205 and $237 included in prepaid expenses and other current assets for the years ended December 31, 2024 and 2023, respectively.
| | | | | | | | | | | |
| As of December 31, |
| 2024 | | 2023 |
| Type of Insurance | | | |
| General and professional liability | $ | 5,343 | | | $ | 4,078 | |
| Workers’ compensation | 5,441 | | | 4,892 | |
| Total estimated liability | 10,784 | | | 8,970 | |
| Less: long-term portion, included in other long-term liabilities | (7,739) | | | (6,509) | |
| Current portion of estimated liability, included in other accrued liabilities | $ | 3,045 | | | $ | 2,461 | |
Beginning on January 1, 2022, the Company transitioned its employee health plans to a self-insurance model. Prior to that date, the Company did not retain risk related to its employee health plans. The Company self-funds medical, including prescription drugs, dental healthcare, and vision benefits for its employees. The Company is fully liable for all financial and legal aspects of these benefit plans. To protect itself against loss exposure associated with this policy, the Company has purchased individual stop-loss insurance coverage that insures individual claims that exceed $350 for each covered person for fiscal year 2024 and $325 for each covered person for fiscal year 2023. As of December 31, 2024 and 2023, our medical benefits liability was $2,650 and $1,931, respectively, recorded as a component of accrued wages and related liabilities and other accrued liabilities.
Fair Value of Financial Instruments - The Company’s financial instruments consist principally of cash, accounts receivable, accounts payable, accrued liabilities, and debt. The Company believes all of the financial instruments’ recorded values approximate fair values because of their nature or respective short durations. The Company determines fair value measurements based on a three-tier hierarchy that prioritizes the inputs used to measure fair value. These tiers include: Level 1, defined as observable inputs such as quoted market prices in active markets; Level 2, defined as inputs other than quoted prices
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
included within Level 1 that are observable for the asset or liability, either directly or indirectly; and Level 3, defined as unobservable inputs for which little or no market data exists, therefore requiring an entity to develop its own assumptions.
Income Taxes - Deferred tax assets and liabilities are established for temporary differences between the financial reporting basis and the tax basis of the Company’s assets and liabilities at tax rates in effect when such temporary differences are expected to reverse. The Company generally expects to fully utilize its deferred tax assets; however, when necessary, the Company records a valuation allowance to reduce its net deferred tax assets to the amount that is more likely than not to be realized.
In determining the need for a valuation allowance or the need for and magnitude of liabilities for uncertain tax positions, the Company makes certain estimates and assumptions. These estimates and assumptions are based on, among other things, knowledge of operations, markets, historical trends and likely future changes and, when appropriate, the opinions of advisors with knowledge and expertise in certain fields. Due to certain risks associated with the Company’s estimates and assumptions, actual results could differ.
Common Stock - Each share of common stock, $0.001 par value per share (“common stock”) has the right to one vote. On October 2, 2024, the Company closed the public offering (the “Offering”) of 4,025 shares of its common stock. The net proceeds to the Company from the offering, after underwriting discounts, commissions, and expenses, was approximately $118,145. The majority of the proceeds were subsequently used to pay the then outstanding balance on our Amended Revolving Credit Facility.
Noncontrolling Interest - The noncontrolling interest in a subsidiary is initially recognized at estimated fair value on the acquisition date and is presented within total equity in the Company's consolidated balance sheets. The Company presents the noncontrolling interest and the amount of consolidated net income and other comprehensive income attributable to The Pennant Group, Inc. in its consolidated statements of income. Net income per share is calculated based on net income attributable to The Pennant Group, Inc.'s stockholders. The carrying amount of the noncontrolling interest is adjusted based on an allocation of subsidiary earnings based on ownership interest.
Share-Based Compensation - The Company measures and recognizes compensation expense for all share-based payment awards, including employee stock options and restricted stock, made to employees and Pennant’s directors based on estimated fair values, ratably over the requisite service period of the award. The Company accounts for forfeitures as they occur. The total amount of share-based compensation was $7,781, $5,369, and $3,086 for the years ended December 31, 2024, 2023 and 2022, respectively, of which $3,927, $2,250 and $647, respectively, was recorded in general and administrative expense, with the difference being recorded in cost of services. For further discussion see Note 12, Options and Awards.
State Relief Funding - The Company receives state relief funding through programs from various states, including healthcare relief funding under the American Rescue Plan Act (“ARPA”), and other state specific relief programs. The funding generally incorporates specific use requirements primarily for direct patient care including labor-related expenses that are attributable to the COVID-19 pandemic or are associated with providing patient care.
These funds are recognized as a reduction of cost of services when related expenses are incurred. As of December 31, 2024 and 2023, the Company had $705 and $780 in unapplied state relief funds, respectively. The unapplied state relief funds received are recorded in other accrued liabilities on the consolidated balance sheets. As of December 31, 2024 and 2023, the Company recognized state relief funding totaling $3,331 and $4,654, respectively, which the Company recognized as a reduction of cost of services.
Recent Accounting Pronouncements - Except for rules and interpretive releases of the Securities and Exchange Commission (SEC) under authority of federal securities laws and a limited number of grandfathered standards, the FASB ASC is the sole source of authoritative GAAP literature recognized by the FASB and applicable to the Company. For any new pronouncements announced, the Company considers whether the new pronouncements could alter previous generally accepted accounting principles and determines whether any new or modified principles will have a material impact on the Company's reported financial position or operations in the near term. The applicability of any standard is subject to the formal review of the Company's financial management and certain standards are under consideration.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
Recent Accounting Standards Adopted by the Company - In November 2023, the FASB issued ASU 2023-07, “Segment Reporting (Topic 280): Improvements to Reportable Segment Disclosures”, which requires the Company to expand the breadth and frequency of segment disclosures to include additional information about significant segment expenses, the chief operating decision maker and other items, and also require the annual disclosures on an interim basis. This guidance is effective for annual periods beginning after December 15, 2023. The Company adopted the requirements of this ASU in Note 6, Business Segments.
Recently Issued Accounting Pronouncements Not Yet Adopted - In October 2023, the FASB issued ASU 2023-06 “Codification Amendments in Response to the SEC’s Disclosure Update and Simplification Initiative,” which amends U.S. GAAP to include 14 disclosure requirements that are currently required under SEC Regulation S-X or Regulation S-K. Each amendment will be effective on the date on which the SEC removes the related disclosure requirement from SEC Regulation S-X or Regulation S-K. The adoption is not expected to have a material impact on the Company’s Financial Statements as these requirements were previously incorporated under the SEC Regulations.
In December 2023, the FASB issued ASU 2023-09, “Income Taxes (Topic 740): Improvements to Income Tax Disclosures”, which requires the Company to disclose disaggregated jurisdictional and categorical information for the tax rate reconciliation, income taxes paid and other income tax related amounts. This guidance is effective for annual periods beginning after December 15, 2024, which will be the Company's fiscal year 2025, with early adoption permitted. The Company is currently evaluating the impact of this ASU on its Consolidated Financial Statements.
In November 2024, the FASB issued ASU 2024-03 “Disaggregation of Income Statement Expenses,” which requires the Company to disaggregate key expense categories such as employee compensation, depreciation and intangible asset amortization within its financial statements. This guidance is effective for annual periods beginning after December 15, 2026, which will be the Company’s fiscal year 2027, and interim periods within the Company’s fiscal year 2028, with early adoption permitted. The Company is currently evaluating the impact of this ASU on its Consolidated Financial Statements.
3. TRANSACTIONS WITH ENSIGN
On October 1, 2019, The Ensign Group, Inc. (“Ensign”) completed the separation of Pennant (the “Spin-Off”). Pennant and Ensign continue to partner in the provision of services along the healthcare continuum.
The Company has incurred costs of $959, $1,035, and $1,561 for the years ended December 31, 2024, 2023 and 2022, respectively, that related primarily to shared services at proximate operations.
Expenses related to room and board charges at Ensign skilled nursing facilities for hospice patients were $5,529, $4,583, and $3,211 for the years ended December 31, 2024, 2023 and 2022, respectively.
The Company’s independent operating subsidiaries leased 32 of its senior living communities from subsidiaries of Ensign under two master lease arrangements as of December 31, 2024. See further discussion below at Note 13, Leases.
On January 27, 2022, affiliates of the Company entered into certain operations transfer agreements (collectively, the “Transfer Agreements”) with affiliates of Ensign, providing for the transfer of the operations of five senior living communities (the “Transaction”). The Transfer Agreements required one of the transferors to place $6,500 in escrow to cover post-closing capital expenditures and operating losses related to one of the communities, and such escrow was funded by an initial payment by the transferor at closing followed by eight equal monthly installments. The Company recorded the amount in loss on asset dispositions and impairment, net during 2022. The Transaction closed in April 2022.
4. COMPUTATION OF NET INCOME PER COMMON SHARE
Basic net income per share is computed by dividing net income attributable to stockholders of the Company by the weighted average number of outstanding common shares for the period. The computation of diluted net income per share is similar to the computation of basic net income per share except that the denominator is increased to include the number of additional common shares that would have been outstanding if the dilutive potential common shares had been issued.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
The following table sets forth the computation of basic and diluted net income per share for the periods presented:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| | 2024 | | 2023 | | 2022 |
| Numerator: | | | | | |
| Net income | $ | 24,339 | | | $ | 13,910 | | | $ | 7,243 | |
| Less: net income attributable to noncontrolling interest | 1,780 | | | 531 | | | 600 | |
| Net income attributable to The Pennant Group, Inc. | $ | 22,559 | | | $ | 13,379 | | | $ | 6,643 | |
| | | | | |
| Denominator: | | | | | |
| Weighted average shares outstanding for basic net income per share | 31,191 | | | 29,863 | | | 29,064 | |
Plus: incremental shares from assumed conversion(a) | 809 | | | 330 | | | 1,095 | |
| Adjusted weighted average common shares outstanding for diluted income per share | 32,000 | | | 30,193 | | | 30,159 | |
| | | | | |
| Earnings Per Share: | | | | | |
| Basic net income per common share | $ | 0.72 | | | $ | 0.45 | | | $ | 0.23 | |
| Diluted net income per common share | $ | 0.70 | | | $ | 0.44 | | | $ | 0.22 | |
| | | | | | | | |
| (a) | | The calculation of dilutive shares outstanding excludes out-of-the-money stock options (i.e., such options’ exercise prices were greater than the average market price of our common shares for the period) because their inclusion would have been antidilutive. Options outstanding which are anti-dilutive and therefore not factored into the weighted average common shares amount above were 1,271, 2,363, and 1,860 for the years ended December 31, 2024, 2023 and 2022, respectively. |
| | |
5. REVENUE AND ACCOUNTS RECEIVABLE
Revenue is recognized when services are provided to the patients at the amount that reflects the consideration to which the Company expects to be entitled from patients and third-party payors, including Medicaid, Medicare and managed care programs (Commercial, Medicare Advantage and Managed Medicaid plans). The healthcare services in home health and hospice patient contracts include routine services in exchange for a contractual agreed-upon amount or rate. Routine services are treated as a single performance obligation satisfied over time as services are rendered. As such, patient care services represent a bundle of services that are not capable of being distinct within the context of the contract. Additionally, there may be ancillary services which are not included in the rates for routine services, but instead are treated as separate performance obligations satisfied at a point in time, if and when those services are rendered.
Revenue recognized from healthcare services are adjusted for estimates of variable consideration to arrive at the transaction price. The Company determines the transaction price based on contractually agreed-upon amounts or rate, adjusted for estimates of variable consideration. The Company uses the expected value method in determining the variable component that should be used to arrive at the transaction price, using contractual agreements and historical reimbursement experience within each payor type. The amount of variable consideration which is included in the transaction price may be constrained and is included in the net revenue only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will not occur in a future period. If actual amounts of consideration ultimately received differ from the Company’s estimates, the Company adjusts these estimates, which would affect net service revenue in the period such variances become known.
The Company records revenue from Medicare, Medicaid and managed care programs as services are performed at their expected net realizable amounts under these programs. The Company’s revenue from governmental and managed care programs is subject to audit and retroactive adjustment by governmental and third-party agencies. Consistent with healthcare industry accounting practices, any changes to these governmental revenue estimates are recorded in the period the change or adjustment becomes known based on final settlement.
Disaggregation of Revenue
The Company disaggregates revenue from contracts with its patients or residents by reportable operating segments and payors. The Company has determined that disaggregating revenue into these categories achieves the disclosure objectives to
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
depict how the nature, amount, timing and uncertainty of revenue and cash flows are affected by economic factors. A reconciliation of disaggregated revenue to segment revenue as well as revenue by payor is provided below.
The Company’s service specific revenue recognition policies are as follows:
Home Health Revenue
Medicare Revenue
Net service revenue is recognized in accordance with the Patient Driven Groupings Model (“PDGM”). Under PDGM, Medicare provides agencies with payments for each 30-day payment period provided to beneficiaries. If a beneficiary is still eligible for care after the end of the first 30-day payment period, a second 30-day payment period can begin. There are no limits to the number of periods of care a beneficiary who remains eligible for the home health benefit can receive. While payment for each 30-day payment period is adjusted to reflect the beneficiary’s health condition and needs, a special outlier provision exists to ensure appropriate payment for those beneficiaries that have the most expensive care needs. The payment under the Medicare program is also adjusted for certain variables including, but not limited to: (a) a low utilization payment adjustment if the number of visits is below an established threshold that varies based on the diagnosis of a beneficiary; (b) a partial payment if the patient transferred to another provider or the Company received a patient from another provider before completing the period of care; (c) adjustment to the admission source of claim if it is determined that the patient had a qualifying stay in a post-acute care setting within 14 days prior to the start of a 30-day payment period; (d) the timing of the 30-day payment period provided to a patient in relation to the admission date, regardless of whether the same home health provider provided care for the entire series of episodes; (e) changes to the acuity of the patient during the previous 30-day payment period; (f) changes in the base payments established by the Medicare program; (g) adjustments to the base payments for case mix and geographic wages; and (h) recoveries of overpayments.
The Company adjusts Medicare revenue on completed episodes to reflect differences between estimated and actual payment amounts, an inability to obtain appropriate billing documentation and other reasons unrelated to credit risk. Therefore, the Company believes that its reported net service revenue and patient accounts receivable will be the net amounts to be realized from Medicare for services rendered.
In addition to revenue recognized on completed episodes and periods, the Company also recognizes a portion of revenue associated with episodes and periods in progress. Episodes in progress are 30-day payment periods that begin during the reporting period but were not completed as of the end of the period. As such, the Company estimates revenue and recognizes it on a daily basis. The primary factors underlying this estimate are the number of episodes in progress at the end of the reporting period, expected Medicare revenue per period of care or episode of care and the Company’s estimate of the average percentage complete based on the scheduled end of period and end of episode dates.
Non-Medicare Revenue
Episodic Based Revenue - The Company recognizes revenue in a similar manner as it recognizes Medicare revenue for episodic-based rates that are paid by other insurance carriers, including Medicare Advantage programs; however, these rates can vary based upon the negotiated terms.
Non-episodic Based Revenue - Revenue is recognized on an accrual basis based upon the date of service at amounts equal to its established or estimated per visit rates, as applicable.
Management Services Revenue - The Company recognizes revenue earned from its management service agreements as the services are provided. Fees charges are based upon the contractual terms of each agreement.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
Hospice Revenue
Revenue is recognized on an accrual basis based upon the date of service at amounts equal to the estimated payment rates. The estimated payment rates are calculated as daily rates for each of the levels of care the Company delivers. Revenue is adjusted for an inability to obtain appropriate billing documentation or authorizations acceptable to Medicare and other reasons unrelated to credit risk. Additionally, as Medicare hospice revenue is subject to an inpatient cap and an overall payment cap, the Company monitors its provider numbers and estimates amounts due back to Medicare if a cap has been exceeded. The Company regularly evaluates and records these adjustments as a reduction to revenue and an increase to other accrued liabilities.
Senior Living Revenue
The Company has elected the lessor practical expedient within ASC Topic 842, Leases, and therefore recognizes, measures, presents, and discloses the revenue for services rendered under the Company’s senior living residency agreements based upon the predominant component, either the lease or non-lease component, of the contracts. The Company has determined that the services included under the Company’s senior living residency agreements each have the same timing and pattern of transfer. The Company recognizes revenue under ASC Topic 606, Revenue from Contracts with Customers, for its senior residency agreements, for which it has determined that the non-lease components of such residency agreements are the predominant component of each such contract.
The Company’s senior living revenue consists of fees for basic housing and assisted living care. Accordingly, we record revenue when services are rendered on the date services are provided at amounts billable to individual residents. Residency agreements are generally for a term of 30 days, with resident fees billed monthly in advance. For residents under reimbursement arrangements with Medicaid, revenue is recorded based on contractually agreed-upon amounts or rates on a per resident, daily basis or as services are rendered.
Revenue by payor for the years ended December 31, 2024, 2023 and 2022, is summarized in the following tables:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, 2024 |
| | Home Health and Hospice Services | | | | | | |
| | Home Health Services | | Hospice Services | | Senior Living Services | | Total Revenue | | Revenue % |
| Medicare | | $ | 127,891 | | | $ | 207,971 | | | $ | — | | | $ | 335,862 | | | 48.3 | % |
| Medicaid | | 12,037 | | | 25,904 | | | 53,763 | | | 91,704 | | | 13.2 | |
| Subtotal | | 139,928 | | | 233,875 | | | 53,763 | | | 427,566 | | | 61.5 | |
| Managed care | | 87,981 | | | 4,716 | | | — | | | 92,697 | | | 13.3 | |
Private and other(a) | | 51,473 | | | 1,511 | | | 121,993 | | | 174,977 | | | 25.2 | |
| Total revenue | | $ | 279,382 | | | $ | 240,102 | | | $ | 175,756 | | | $ | 695,240 | | | 100.0 | % |
| | | | | | | | |
| (a) | | Private and other payors in the Company’s home health services includes revenue from all payors generated in the Company’s home care operations and management services agreement. |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, 2023 |
| | Home Health and Hospice Services | | | | | | |
| | Home Health Services | | Hospice Services | | Senior Living Services | | Total Revenue | | Revenue % |
| Medicare | | $ | 96,035 | | | $ | 167,775 | | | $ | — | | | $ | 263,810 | | | 48.4 | % |
| Medicaid | | 9,625 | | | 20,738 | | | 46,974 | | | 77,337 | | | 14.2 | |
| Subtotal | | 105,660 | | | 188,513 | | | 46,974 | | | 341,147 | | | 62.6 | |
| Managed care | | 68,260 | | | 5,488 | | | — | | | 73,748 | | | 13.5 | |
Private and other(a) | | 25,917 | | | 626 | | | 103,453 | | | 129,996 | | | 23.9 | |
| Total revenue | | $ | 199,837 | | | $ | 194,627 | | | $ | 150,427 | | | $ | 544,891 | | | 100.0 | % |
| | | | | | | | |
| (a) | | Private and other payors in the Company’s home health services includes revenue from all payors generated in the Company’s home care operations. |
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, 2022 |
| | Home Health and Hospice Services | | | | | | |
| | Home Health Services | | Hospice Services | | Senior Living Services | | Total Revenue | | Revenue % |
| Medicare | | $ | 91,415 | | | $ | 140,338 | | | $ | — | | | $ | 231,753 | | | 49.0 | % |
| Medicaid | | 9,749 | | | 15,568 | | | 37,617 | | | 62,934 | | | 13.3 | |
| Subtotal | | 101,164 | | | 155,906 | | | 37,617 | | | 294,687 | | | 62.3 | |
| Managed care | | 57,824 | | | 4,277 | | | — | | | 62,101 | | | 13.1 | |
Private and other(a) | | 22,741 | | | 337 | | | 93,375 | | | 116,453 | | | 24.6 | |
| Total revenue | | $ | 181,729 | | | $ | 160,520 | | | $ | 130,992 | | | $ | 473,241 | | | 100.0 | % |
| | | | | | | | |
| (a) | | Private and other payors in the Company’s home health services includes revenue from all payors generated in the Company’s home care operations. |
Balance Sheet Impact
Included in the Company’s consolidated balance sheets are contract assets, comprised of billed accounts receivable and unbilled receivables, which are the result of the timing of revenue recognition, billings and cash collections, as well as, contract liabilities, which primarily represent payments the Company receives in advance of services provided.
Accounts receivable as of December 31, 2024 and December 31, 2023 is summarized in the following table:
| | | | | | | | | | | |
| December 31, 2024 | | December 31, 2023 |
| Medicare | $ | 46,677 | | | $ | 35,665 | |
| Medicaid | 13,382 | | | 11,578 | |
| Managed care | 14,220 | | | 11,752 | |
| Private and other | 7,255 | | | 2,380 | |
| Accounts receivable, gross | 81,534 | | | 61,375 | |
| Less: allowance for doubtful accounts | (232) | | | (259) | |
| Accounts receivable, net | $ | 81,302 | | | $ | 61,116 | |
The following table summarizes the activity for our allowance for doubtful accounts for the years ended December 31, 2024, 2023 and 2022:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Balance at beginning of period | $ | 259 | | | $ | 592 | | | $ | 902 | |
| Additions to bad debt expense | 903 | | | 646 | | | 881 | |
| Write-offs of uncollectible accounts | (930) | | | (979) | | | (1,191) | |
| Balance at end of period | $ | 232 | | | $ | 259 | | | $ | 592 | |
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
Concentrations- Credit Risk
Credit Risk - The Company has significant accounts receivable balances, the collectability of which is dependent on the availability of funds from certain governmental programs, primarily Medicare and Medicaid. These receivables represent the only significant concentration of credit risk for the Company. The Company does not believe there are significant credit risks associated with these governmental programs. The Company believes that an appropriate allowance has been recorded for the possibility of these receivables proving uncollectible, and continually monitors and adjusts these allowances as necessary. The Company’s gross receivables from the Medicare and Medicaid programs accounted for approximately 73.7% and 77.0% of its total gross accounts receivable as of December 31, 2024 and December 31, 2023, respectively. Revenue from reimbursement under the Medicare and Medicaid programs accounted for 61.5%, 62.6%, and 62.3% of the Company's revenue for the years ended December 31, 2024, 2023 and 2022, respectively.
6. BUSINESS SEGMENTS
The Company classifies its operations into the following reportable operating segments: (1) home health and hospice services, which includes the Company’s home health, hospice, home care, and geriatric primary and palliative care businesses; and (2) senior living services, which includes the operation of assisted living, independent living and memory care communities. The reporting segments are business units that offer different services and are managed separately to provide greater visibility into those operations. The Company’s Chief Executive Officer, who is the Company’s Chief Operating Decision Maker (“CODM”), reviews financial information at the operating segment level.
As of December 31, 2024, the Company provided services through 123 affiliated home health, hospice and home care agencies, and 57 affiliated senior living operations. The Company evaluates performance and allocates capital resources to each segment based on an operating model that is designed to maximize the quality of care provided and profitability. The Company’s Service Center provides various services to all lines of business. The CODM does not review assets by segment and therefore assets and capital expenditure by segment are not disclosed below.
The CODM uses Segment Adjusted EBITDAR from Operations as the primary measure of profit and loss for the Company's reportable segments and to compare the performance of its operations with those of its competitors. The CODM monitors these results and provides guidance to the segment leadership to allocate enterprise-wide resources. Segment Adjusted EBITDAR from Operations is net income attributable to the Company's reportable segments excluding interest expense, provision for income taxes, depreciation and amortization expense, rent, unallocated corporate and administrative expenses, and, in order to view the operations performance on a comparable basis from period to period, certain adjustments including: (1) costs at start-up operations, (2) share-based compensation expense, (3) acquisition related costs and credit allowances, (4) costs associated with transitioning operations, (5) unusual, non-recurring or redundant charges, and (6) net income (loss) attributable to noncontrolling interest. “All Other” consists of revenues generated at operating locations not included in the segment financial information reviewed by the CODM. Revenue included in the “All Other” category is insignificant individually, and therefore do not constitute a reportable segment. General and administrative expenses are not allocated to the reportable segments, and are included as “Unallocated corporate expenses”, accordingly the segment earnings measure reported is before allocation of corporate general and administrative expenses. The Company's segment measures may be different from the calculation methods used by other companies and, therefore, comparability may be limited.
The following table presents certain financial information regarding the Company’s reportable segments, provided that general and administrative expenses are not allocated to the reportable segments.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Home Health and Hospice Services | | Senior Living Services | | All Other | | Total |
| Year Ended December 31, 2024 | | | | | | | | |
| Segment Revenue | | $ | 515,344 | | | $ | 174,767 | | | $ | 5,129 | | | $ | 695,240 | |
| Segment Cost of Services | | 427,635 | | | 123,107 | | | | | |
| Segment Adjusted EBITDAR from Operations | | $ | 87,709 | | | $ | 51,660 | | | | | $ | 139,369 | |
| Year Ended December 31, 2023 | | | | | | | | |
| Segment Revenue | | $ | 385,652 | | | $ | 148,198 | | | $ | 11,041 | | | $ | 544,891 | |
| Segment Cost of Services | | 320,046 | | | 102,904 | | | | | |
| Segment Adjusted EBITDAR from Operations | | $ | 65,606 | | | $ | 45,294 | | | | | $ | 110,900 | |
| Year Ended December 31, 2022 | | | | | | | | |
| Segment Revenue | | $ | 337,371 | | | $ | 126,758 | | | $ | 9,112 | | | $ | 473,241 | |
| Segment Cost of Services | | 275,544 | | | 89,195 | | | | | |
| Segment Adjusted EBITDAR from Operations | | $ | 61,827 | | | $ | 37,563 | | | | | $ | 99,390 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | | | | | | | | | | |
| 2024 | | 2023 | | 2022 |
| Segment Adjusted EBITDAR from Operations | $ | 139,369 | | | $ | 110,900 | | | $ | 99,390 | |
| Less: Unallocated corporate expenses | 43,587 | | | 31,704 | | | 31,435 | |
| Less: Depreciation and amortization | 6,119 | | | 5,130 | | | 4,900 | |
| Rent—cost of services | 43,029 | | | 39,759 | | | 38,018 | |
| Other income | 207 | | | 339 | | | (31) | |
| Adjustments to Segment EBITDAR from Operations: | | | | | |
Less: Costs at start-up operations (a) | 137 | | | 102 | | | 1,435 | |
Share-based compensation expense(b) | 8,242 | | | 5,565 | | | 3,363 | |
Acquisition related costs and credit allowances(c) | 1,278 | | | 476 | | | 731 | |
| | | | | |
Costs associated with transitioning operations(d) | (570) | | | 612 | | | 6,103 | |
Unusual, non-recurring or redundant charges(e) | 1,004 | | | 2,575 | | | 1,297 | |
| Add: Net income attributable to noncontrolling interest | 1,780 | | | 531 | | | 600 | |
| Income from operations | $ | 38,116 | | | $ | 25,169 | | | $ | 12,739 | |
| | | | | |
| | | | | | | | |
| (a) | | Represents results related to start-up operations. This amount excludes rent and depreciation and amortization expense related to such operations. |
| (b) | | Share-based compensation expense and related payroll taxes incurred, including the impact of the modification of certain restricted stock units described below in Note 12, Options and Awards, to the Consolidated Financial Statements. Share-based compensation expense and related payroll taxes are included in cost of services and general and administrative expense. |
| (c) | | Non-capitalizable costs associated with acquisitions and credit allowances for amounts in dispute with the prior owners of certain acquired operations. |
| | |
| | |
| | |
| (e) | | During the year ended December 31, 2023, an affiliate of the Company placed its memory care units into transition and is converting the facility into an assisted living community. We received insurance proceeds related to the property in 2024 which were recorded as a gain on asset disposition on the consolidated statements of income. The amounts reported exclude rent and depreciation and amortization expense related to such operations and include legal settlement costs associated with one of the entities transitioned to Ensign.
During January 2022, affiliates of the Company entered into Transfer Agreements with affiliates of Ensign, providing for the transfer of the operations of certain senior living communities (the “Transaction”) from affiliates of the Company to affiliates of Ensign. The closing of the Transaction was completed in two phases with the transfer of two operations on March 1, 2022 and the remainder transferred on April 1, 2022. The amount above represents the net impact on revenue and cost of service attributable to all of the transferred entities. The amounts reported exclude rent and depreciation and amortization expense related to such operations. |
| (f) | | Represents unusual or non-recurring charges for legal services, implementation costs, integration costs, and consulting fees in general and administrative and cost of services expenses. The amounts reported for the year ended December 31, 2022 include certain costs identified as redundant or non-recurring incurred by the Company for services provided by Ensign under the Transition Services Agreement, and were included in general and administrative expense. |
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
| | | | | | | | | | | | | | | | | |
| Adjusted segment depreciation expense | | Home Health and Hospice Services | | Senior Living Services | |
| Year Ended December 31, 2024 | | $ | 870 | | | $ | 4,107 | | |
| Year Ended December 31, 2023 | | $ | 1,208 | | | $ | 3,452 | | |
| Year Ended December 31, 2022 | | $ | 1,407 | | | $ | 2,662 | | |
7. ACQUISITIONS
The Company’s acquisition focus is to purchase or lease operations that are complementary to the Company’s current businesses, accretive to the Company’s business or otherwise advance the Company’s strategy. The results of all the Company’s independent operating subsidiaries are included in the Financial Statements subsequent to the date of acquisition. Acquisitions are accounted for using the acquisition method of accounting.
2024 Acquisitions
During the year ended December 31, 2024, the Company expanded its operations with the addition of eight home health agencies, three hospice agencies, and six senior living communities. The Company also acquired the real estate of two of the six acquired senior living communities. The aggregate purchase price of the real estate of the two senior living communities acquired was $10,380, which consisted primarily of land and buildings and were accounted for as asset acquisitions. In connection with the remaining senior living communities acquired, the Company entered into new long-term “triple-net” leases. A subsidiary of the Company entered into a separate operations transfer agreement with the prior operator of each acquired operation as part of each transaction. These new communities included 386 operational senior living units to be operated by the Company's independent operating subsidiaries.
On January 1, 2024, the Company announced it closed on a joint venture for a home health agency with John Muir Health (“Muir”), a leading nonprofit integrated health system serving communities throughout the east bay region of San Francisco, California. The transaction combines certain assets and the operations of Muir’s home health business with the assets and operations of a local Pennant-affiliated home health agency. The joint venture is majority-owned and managed by an independent operating subsidiary of the Company and provides home health services to patients throughout the San Francisco east bay region. The Company contributed certain assets of a local Pennant-affiliated home health agency to the joint venture and paid Muir $11,680 for a 60% controlling ownership interest in the joint venture.
The fair value of assets for the joint venture acquired was mostly concentrated in goodwill and intangible assets and as such, this transaction was classified as a business combination in accordance with ASC Topic 805, Business Combinations (“ASC 805”). The fair value of assets acquired for the business combination was $28,200, which consisted of goodwill of $15,500, indefinite-lived intangible assets of $8,600 related to a Medicare and Medicaid license, and tradenames of $4,100. Through its contributions of assets to the joint venture, Muir retained a non-controlling ownership interest which resulted in the Company recording a 40% noncontrolling interest with a fair value of $11,726, a deferred tax liability of $1,193, and an adjustment to additional paid-in capital of $3,601. The Company anticipates that the total goodwill recognized will be partially deductible for tax purposes. The Muir acquisition contributed $28,614 in revenue and operating income of $5,163 during the year ended December 31, 2024.
On May 16, 2024, the Company acquired one home health agency and one hospice agency. On July 1, 2024, one acquisition of a provider service agency was completed. These transactions were classified as a business combination in accordance with ASC 805. The aggregate purchase price for the business combinations was $5,350, which consisted of goodwill of $2,310 and indefinite-lived intangible assets of $3,040 related to Medicare and Medicaid licenses. The Company anticipates that the total goodwill recognized will be fully deductible for tax purposes. The acquisitions contributed $4,982 in revenue and operating income of $954 during the year ended December 31, 2024.
On August 1, 2024, the Company completed the first part of its planned acquisition of certain Signature Group, LLC operations. Through the completed acquisition, the Company acquired four home health agencies and one hospice agency. The transaction was classified as business combination in accordance with ASC 805. The aggregate purchase price for the business combinations was $32,000, including acquired liabilities, which consisted of goodwill of $20,300, indefinite-lived intangible assets of $9,000 related to Medicare and Medicaid licenses, and tradenames of $2,700. The Company anticipates that the total goodwill recognized will be fully deductible for tax purposes. The Company completed an additional acquisition transaction with Signature Group, LLC that closed on January 1, 2025, and is described in “Subsequent Events” below. The Company
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
anticipates that the total goodwill recognized will be fully deductible for tax purposes. The Signature Group, LLC acquisition contributed $9,787 in revenue and operating income of $2,190 during the year ended December 31, 2024.
The Company acquired one hospice and two home health Medicare licenses through asset acquisitions. The fair value of the assets acquired in these transactions primarily consisted of indefinite-lived intangibles of $1,000.
There were no material acquisition costs that were incurred related to the business combinations during the year ended December 31, 2024.
2023 Acquisitions
During the year ended December 31, 2023, the Company expanded its operations with the addition of three home health agencies, eight hospice agencies, two home care agencies, and two senior living communities. In connection with the addition of the two senior living communities, the Company entered into a new long-term “triple-net” lease. A subsidiary of the Company entered into a separate operations transfer agreement with the prior operator of each acquired operation as part of each transaction.
The fair value of assets for two home health agencies, eight hospice agencies, and two home care agencies acquired were mostly concentrated in goodwill and indefinite-lived intangible assets and as such, these transactions were classified as business combinations in accordance with ASC 805. The purchase price for the business combinations was $21,376, which primarily consisted of goodwill of $11,517, indefinite-lived intangible assets of $8,914 related to Medicare and Medicaid licenses, and equipment, other assets and accounts receivable of $1,026, less assumed liabilities of $81. The acquisitions contributed $10,549 in revenue and operating income of $280 during the year ended December 31, 2023.
One home health agency acquired a Medicare license and was considered an asset acquisition. The fair value of the home health license acquired was $211 and was recorded in other indefinite-lived intangibles.
There were no material acquisition costs that were expensed related to the business combinations during the year ended December 31, 2023.
2022 Acquisitions
During the year ended December 31, 2022, the Company expanded its operations with the addition of three home health agencies, four hospice agencies, and one senior living community. In connection with the addition of the senior living community, the Company entered into a new long-term “triple-net” lease. A subsidiary of the Company entered into a separate operations transfer agreement with the prior operator of each acquired operation as part of each transaction.
The aggregate purchase price for the home health and hospice acquisitions was $10,130. The goodwill was primarily attributable to indefinite-lived intangible assets that do not qualify for separate recognition, and to synergies the Company expects to achieve related to the acquisition, which was allocated to the Company's operating segments which are its reporting units. Total goodwill recognized was fully deductible for tax purposes. There were no material acquisition costs that were expensed related to the business combination during the year ended December 31, 2022.
The fair value of assets for home health and hospice acquisitions was mostly concentrated in goodwill and as such, these transactions were classified as business combinations in accordance with ASC 805. The table below presents the
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
allocation of the purchase price for the operations acquired in acquisitions during the years ended December 31, 2024, 2023 and 2022 as noted above:
| | | | | | | | | | | | | | | | | |
| December 31, |
| 2024 | | 2023 | | 2022 |
| Property and equipment, net | $ | 10,380 | | | $ | 34 | | | $ | 188 | |
| Goodwill | 38,110 | | | 11,517 | | | 5,232 | |
| Other indefinite-lived intangible assets | 28,440 | | | 8,914 | | | 4,897 | |
| | | | | |
| Other assets | 23 | | | 992 | | | — | |
| Liabilities assumed | (1,830) | | | (81) | | | (187) | |
| Total acquisitions | $ | 75,123 | | | $ | 21,376 | | | $ | 10,130 | |
Less: noncontrolling interest(a) | (11,726) | | | — | | | — | |
| Less: additional paid in capital | (3,601) | | | — | | | — | |
| | | | | |
| Total cash paid for acquisitions | $ | 59,796 | | | $ | 21,376 | | | $ | 10,130 | |
| | | | | | | | |
| (a) | | Consists of the of noncontrolling interest related to John Muir Health contribution of assets to the joint venture. |
| | |
Subsequent Events
On January 1, 2025, the Company closed the second part of its planned acquisition of certain Signature Group, LLC operations. The purchase price was $48,480 paid through a combination of cash on hand and available credit on our revolving credit facility. Through the completed acquisition, the Company acquired five home health agencies and four hospice agencies located in Oregon.
On February 1, 2025, the Company closed on the acquisition of three senior living communities. These new communities included 188 operational senior living units to be operated by the Company's independent operating subsidiaries. In connection with each of the senior living communities, the Company entered into a new long-term “triple-net” lease. A subsidiary of the Company entered into a separate operations transfer agreement with the prior operator of each acquired operation as part of the transaction.
8. PROPERTY AND EQUIPMENT, NET
Property and equipment, net consist of the following:
| | | | | | | | | | | |
| December 31, |
| 2024 | | 2023 |
| Land | $ | 5,632 | | | $ | 96 | |
| Building | 8,778 | | | 1,890 | |
| Leasehold improvements | 21,879 | | | 21,204 | |
| Equipment | 31,200 | | | 27,984 | |
| Construction in progress | 2,715 | | | 1,263 | |
| Furniture and fixtures | 1,541 | | | 1,238 | |
| Total property and equipment | 71,745 | | | 53,675 | |
| Less: accumulated depreciation | (28,449) | | | (25,077) | |
| Property and equipment, net | $ | 43,296 | | | $ | 28,598 | |
Depreciation expense was $6,119, $5,120 and $4,856 for the years ended December 31, 2024, 2023 and 2022, respectively.
9. GOODWILL AND INTANGIBLE ASSETS
The Company tests goodwill annually and also if events or changes in circumstances indicate the occurrence of a
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
triggering event which might indicate there may be impairment. The Company performs its goodwill impairment analysis for each reporting unit that constitutes a component for which (1) discrete financial information is available and (2) segment management regularly reviews the operating results of that component, in accordance with the provisions of ASC Topic 350, Intangibles-Goodwill and Other.
The Company reviews goodwill for impairment by initially considering qualitative factors to determine whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount as a basis for determining whether it is necessary to perform a quantitative analysis. If it is determined that it is more likely than not that the fair value of a reporting unit is less than its carrying amount, a quantitative analysis is performed to identify goodwill impairment. If it is determined that it is not more likely than not that the fair value of the reporting unit is less than its carrying amount, it is unnecessary to perform a quantitative analysis. The Company may elect to bypass the qualitative assessment and proceed directly to performing a quantitative analysis. An impairment loss is recognized for the amount that the carrying amount of the reporting unit, including goodwill, exceeds its fair value, limited to the total amount of goodwill allocated to that reporting unit. The Company did not identify any impairment charges during the years ended December 31, 2024, 2023 and 2022.
The following table represents activity in goodwill by segment:
| | | | | | | | | | | | | | | | | |
| Home Health and Hospice Services | | Senior Living Services | | Total |
| December 31, 2022 | $ | 75,855 | | | $ | 3,642 | | | $ | 79,497 | |
| Additions | 11,517 | | | — | | | 11,517 | |
| | | | | |
| December 31, 2023 | 87,372 | | | 3,642 | | | 91,014 | |
| Additions | 38,110 | | | — | | | 38,110 | |
| | | | | |
| December 31, 2024 | $ | 125,482 | | | $ | 3,642 | | | $ | 129,124 | |
Other indefinite-lived intangible assets consist of the following:
| | | | | | | | | | | |
| December 31, |
| 2024 | | 2023 |
| Trade names | $ | 8,465 | | | $ | 1,385 | |
| Medicare and Medicaid licenses | 87,717 | | | 66,357 | |
| Total other indefinite-lived intangibles | $ | 96,182 | | | $ | 67,742 | |
10. OTHER ACCRUED LIABILITIES
Other accrued liabilities consist of the following:
| | | | | | | | | | | | | | |
| | December 31, 2024 | | December 31, 2023 |
| Refunds payable | | $ | 1,382 | | | $ | 1,566 | |
| Deferred revenue | | 2,284 | | | 1,658 | |
| Resident deposits | | 1,399 | | | 2,367 | |
| | | | |
| Property taxes | | 1,028 | | | 1,255 | |
| Deferred state relief funds | | 705 | | | 780 | |
| Accrued self-insurance liabilities | | 5,396 | | | 4,392 | |
| Hospice CAP liabilities | | 4,007 | | | 661 | |
| Software license payable | | 1,170 | | | — | |
| Other | | 2,815 | | | 2,651 | |
| Other accrued liabilities | | $ | 20,186 | | | $ | 15,330 | |
Refunds payable includes payables related to overpayments, duplicate payments and credit balances from various payor sources. Deferred revenue occurs when the Company receives payments in advance of services provided. Resident
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
deposits include refundable deposits to residents and a small portion consists of non-refundable deposits recognized into revenue over a period of time. Deferred state relief funds are relief funds the Company has received from various states that will offset against future related expenses.
11. DEBT
Long-term debt, net consists of the following:
| | | | | | | | | | | |
| December 31, |
| 2024 | | 2023 |
Revolving credit facility(a) | $ | — | | | $ | 65,000 | |
Less: unamortized debt issuance costs(b) | — | | | (1,086) | |
| Long-term debt, net | $ | — | | | $ | 63,914 | |
| | | | | | | | |
| (a) | | On October 4, 2024, the Company used the proceeds from the Offering of common stock to pay in full the outstanding balance on our Amended Revolving Credit Facility. |
| (b) | | Amortization expense for debt issuance costs, including expense of $428 related to the July 31, 2024 refinancing of our Revolving Credit Facility, was $1,096, $521, and $520 for the years ended December 31, 2024, 2023 and 2022, respectively, and is recorded in interest expense, net on the consolidated statements of income. For year ended December 31, 2024, the outstanding debt issuance costs of $3,906 are recorded in Restricted and other assets. |
On February 23, 2021, Pennant entered into an amendment to its existing credit agreement (as amended, the “Credit Agreement”), which provided for an increased revolving credit facility with a syndicate of banks with a borrowing capacity of $150,000 (the “Revolving Credit Facility”). On June 12, 2023, Pennant entered into a second amendment to the Credit Agreement that modified the reference rate from LIBOR to Standard Overnight Financing Rate (“SOFR”). The interest rates applicable to loans under the Revolving Credit Facility were, at the Company’s election, either (i) Adjusted Term SOFR (as defined in the Credit Agreement) plus a margin ranging from 2.25% to 3.25% per annum or (ii) Base Rate plus a margin ranging from 1.25% to 2.25% per annum, in each case, based on the ratio of Consolidated Total Net Debt to Consolidated EBITDA (each, as defined in the Credit Agreement). In addition, Pennant paid a commitment fee on the undrawn portion of the commitments under the Revolving Credit Facility which ranged from 0.35% to 0.50% per annum, depending on the Consolidated Total Net Debt to Consolidated EBITDA ratio of the Company and its subsidiaries.
On July 31, 2024, Pennant entered into an Amended and Restated Credit Agreement (the Credit Agreement, as amended and restated, the “Amended Credit Agreement”), which provides for a revolving credit facility (the Revolving Credit Facility, as upsized, the “Amended Revolving Credit Facility”) with a syndicate of banks with a borrowing capacity of $250,000. In conjunction with the amendment, the Company incurred additional debt issuance costs of $3,915 and wrote off previously deferred unamortized debt issuance costs of $428. After the effectiveness of the Amended Credit Agreement, the interest rates applicable to loans under the Amended Revolving Credit Facility are, at the Company’s election, either (i) Term SOFR (as defined in the Amended Credit Agreement) plus a margin ranging from 1.75% to 2.75% per annum or (ii) Base Rate plus a margin ranging from 0.75% to 1.75% per annum, in each case based on the ratio of Consolidated Total Net Debt to Consolidated EBITDA (each, as defined in the Amended Credit Agreement). In addition, Pennant pays a commitment fee on the undrawn portion of the commitments under the Amended Revolving Credit Facility that ranges from 0.25% to 0.45% per annum, depending on the Consolidated Total Net Debt to Consolidated EBITDA ratio of the Company and its subsidiaries. The Company is not required to repay any loans under the Amended Credit Agreement prior to maturity in July 2029. On October 4, 2024, the Company used the proceeds from the Offering of common stock to pay in full the outstanding balance on our Amended Revolving Credit Facility. As of December 31, 2024, the Company’s weighted average interest rate on its outstanding debt was 0.0%. As of December 31, 2024, the Company had available borrowing on the Revolving Credit Facility of $245,814, which is net of outstanding letters of credit of $4,186.
The fair value of the Amended Revolving Credit Facility approximates carrying value, due to the short-term nature and variable interest rates. The fair value of this debt is categorized within Level 2 of the fair value hierarchy based on the observable market borrowing rates.
The Amended Credit Agreement is guaranteed, jointly and severally, by certain of the Company’s independent operating subsidiaries, and is secured by a pledge of stock of the Company's material independent operating subsidiaries as well as a first lien on substantially all of each material operating subsidiary's personal property. The Amended Credit Agreement contains customary covenants that, among other things, restrict, subject to certain exceptions, the ability of the Company and its independent operating subsidiaries to grant liens on their assets, incur indebtedness, sell assets, make investments, engage in
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
acquisitions, mergers or consolidations, amend certain material agreements and pay certain dividends and other restricted payments. Financial covenants require compliance with certain levels of leverage ratios that impact the amount of interest. As of December 31, 2024 and 2023, the Company was compliant with all such financial covenants.
12. OPTIONS AND AWARDS
Outstanding options and restricted stock awards of the Company were granted under the 2019 Omnibus Incentive Plan and Long-Term Incentive Plan (the “LTIP”), (together referred to as the “Pennant Plans”).
Under the Pennant Plans, stock-based payment awards, including employee stock options, restricted stock awards (“RSA”), and restricted stock units (“RSU” and together with RSA, “Restricted Stock”) are issued based on estimated fair value. The following disclosures represent share-based compensation expense relating to employees of the Company’s subsidiaries and non-employee directors who have awards under the Pennant Plans.
Share-Based Compensation
The following disclosures represent share-based compensation expense relating to the Pennant Plans, including awards to employees of the Company’s subsidiaries.
Total share-based compensation expense for all of the Pennant Plans for the years ended December 31, 2024, 2023 and 2022 were as follows:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Share-based compensation expense related to stock options | $ | 4,944 | | | $ | 3,945 | | | $ | 3,266 | |
| Share-based compensation expense related to Restricted Stock | 561 | | | 712 | | | (467) | |
| Share-based compensation expense related to Restricted Stock to non-employee directors | 2,276 | | | 712 | | | 287 | |
| Total share-based compensation | $ | 7,781 | | | $ | 5,369 | | | $ | 3,086 | |
In future periods, the Company estimates it will recognize the following share-based compensation expense for unvested stock options and unvested Restricted Stock. Total unrecognized share-based compensation as of December 31, 2024 was as follows:
| | | | | | | | | | | |
| Unrecognized Share-Based Compensation Expense | | Weighted Average Recognition Period (in years) |
| Unvested stock options | $ | 14,734 | | | 3.6 |
| Unvested Restricted Stock | 2,203 | | | 3.3 |
| Total unrecognized share-based compensation expense | $ | 16,937 | | | |
On July 25, 2022 the Company modified certain outstanding RSUs granted to the former chief executive officer of the Company in connection with the Spin-Off. All the RSUs had an original vesting date of October 1, 2022. The modification resulted in the forfeiture of 250 outstanding RSUs and accelerated the vesting on the remaining 943 RSUs from October 1, 2022 to July 31, 2022. The modification of the award resulted in a net reduction of share-based compensation expense related to the awards of $3,812 recorded in general and administrative expense during 2022. There were no modifications of awards during 2024 and 2023.
Stock Options
Under the Pennant Plans, options granted to employees of the subsidiaries of Pennant generally vest over five years at 20% per year on the anniversary of the grant date. Options expire ten years after the date of grant.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
The Company uses the Black-Scholes option-pricing model to determine the grant date fair value which is used to recognize the value of share-based compensation expense for share-based payment awards under the Pennant Plans. Determining the appropriate fair-value model and calculating the fair value of share-based awards at the grant date requires considerable judgment, including estimating stock price volatility and expected option life. The Company develops estimates based on historical data and market information, which can change significantly over time.
The fair value of each option is estimated on the grant date using a Black-Scholes option-pricing model with the following weighted average assumptions for stock options granted:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Grant Year | | Options Granted | | Risk-Free Interest Rate | | Expected Life(a) | | Expected Volatility(b) | | Dividend Yield | | Weighted Average Fair Value of Options |
| 2024 | | 850 | | | 4.3 | % | | 6.5 | | 42.6 | % | | — | % | | $ | 10.88 | |
| 2023 | | 924 | | | 4.2 | % | | 6.5 | | 41.8 | % | | — | % | | $ | 6.59 | |
| 2022 | | 448 | | | 2.7 | % | | 6.5 | | 39.8 | % | | — | % | | $ | 6.35 | |
| | | | | | | | | | | | |
| | | | | | | | | | | | |
| | | | | | | | |
| (a) | | Under the midpoint method, the expected option life is the midpoint between the contractual option life and the average vesting period for the options being granted. This resulted in an expected option life of 6.5 years for the options granted. |
| (b) | | Because the Company’s equity shares have been traded for a relatively short period of time, expected volatility assumption was based on the volatility of related industry stocks. |
The following table represents the employee stock option activity during the year ended December 31, 2024:
| | | | | | | | | | | | | | | | | | | | | | | |
| Number of Options Outstanding | | Weighted Average Exercise Price | | Number of Options Vested | | Weighted Average Exercise Price of Options Vested |
| | | | | | | |
| | | | | | | |
| | | | | | | |
| | | | | | | |
| December 31, 2023 | 2,924 | | | $ | 18.79 | | | 1,190 | | | $ | 19.14 | |
| Granted | 850 | | | $ | 22.03 | | | | | |
| Exercised | (254) | | | $ | 9.82 | | | | | |
| Forfeited | (128) | | | $ | 20.04 | | | | | |
| Expired | (61) | | | $ | 30.71 | | | | | |
| December 31, 2024 | 3,331 | | | $ | 20.01 | | | 1,367 | | | $ | 20.67 | |
The aggregate intrinsic value of options outstanding, vested, unvested and exercised as of and for the year ended December 31, 2024 is as follows:
| | | | | |
| Options | December 31, 2024 |
| Outstanding | $ | 28,471 | |
| Vested | 12,103 | |
| Unvested | 16,368 | |
| Exercised | 3,500 | |
The intrinsic value is calculated as the difference between the market value of the underlying common stock and the exercise price of the options. There were 1,964 unvested and outstanding options at December 31, 2024. The weighted average contractual life for options outstanding, vested and expected to vest at December 31, 2024 was 7.23 years.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
Restricted Stock
Under the Pennant Plans, the Company granted Restricted Stock to Pennant employees, Ensign employees, and to non-employee directors. All awards generally vest between three to five years. A summary of the status of Pennant’s non-vested Restricted Stock, and changes during the year ended December 31, 2024, is presented below:
| | | | | | | | | | | |
| Non-Vested Restricted Awards | | Weighted Average Grant Date Fair Value |
| December 31, 2023 | 265 | | | $ | 14.27 | |
| Granted | 114 | | | 26.04 | |
| Vested | (206) | | | 19.12 | |
| Forfeited | (21) | | | 16.26 | |
| December 31, 2024 | 152 | | | $ | 16.27 | |
13. LEASES
The Company’s independent operating subsidiaries lease senior living communities under non-cancelable operating leases, most of which have initial lease terms ranging from 15 to 25 years. The Company’s independent operating subsidiaries also lease the administrative offices of home health and hospice agencies and the service centers which generally range from one to seven years. Most of these leases contain renewal options, most involve rent increases and none contain purchase options. The lease term excludes lease renewals because the renewal rents are not at a bargain, there are no economic penalties for the Company to renew the lease, and it is not reasonably certain that the Company will exercise the extension options. The Company elected the accounting policy practical expedients in ASC 842 to: (i) combine associated lease and non-lease components into a single lease component; and (ii) exclude recording short-term leases as right-of-use assets and liabilities on the consolidated balance sheets. Non-lease components, which are not significant overall, are combined with lease components. The Company has an insignificant amount of finance lease right of use assets included in Restricted and other assets and finance lease liabilities included in Other accrued liabilities and Other long-term liabilities on our consolidated balance sheets. Amortization and interest expense was $214 and $35, respectively for the year ended December 31, 2024. As of December 31, 2024, the weighted average remaining lease term and the weighted average discount rate was 3.4 years and 6.9% for finance leases, respectively.
As of December 31, 2024, the Company’s independent operating subsidiaries leased 32 senior living communities from subsidiaries of Ensign (“Ensign Leases”) under two master lease arrangements. The existing leases with subsidiaries of Ensign are for initial terms of between 14 to 20 years. The total amount of rent expense included in rent - cost of services paid to subsidiaries of Ensign was $14,018, $13,567, and $13,595, for the years ended December 31, 2024, 2023 and 2022, respectively. In addition to rent, each of the operating companies are required to pay the following: (1) all impositions and taxes levied on or with respect to the leased properties (other than taxes on the income of the lessor); (2) all utilities and other services necessary or appropriate for the leased properties and the business conducted on the leased properties; (3) all insurance required in connection with the leased properties and the business conducted on the leased properties; (4) all community maintenance and repair costs; and (5) all fees in connection with any licenses or authorizations necessary or appropriate for the leased properties and the business conducted on the leased properties.
Fourteen of the Company’s affiliated senior living communities, excluding the communities that are operated under the Ensign Leases (as defined herein), are operated under three separate master lease arrangements. Under these master leases, a breach at a single community could subject one or more of the other communities covered by the same master lease to the same default risk. Failure to comply with Medicare and Medicaid provider requirements is a default under several of the Company’s leases and master leases. With an indivisible lease, it is difficult to restructure the composition of the portfolio or economic terms of the master lease without the consent of the landlord.
As further described in Note 3, Transactions with Ensign, on January 27, 2022, affiliates of the Company entered into Transfer Agreements with affiliates of Ensign, providing for the transfer of the operations of five senior living communities. The closing of the Transaction was completed in two phases with the transfer of two operations on March 1, 2022 and the remainder transferred on April 1, 2022. As a result of the lease terminations, the Company reduced both the right of use assets and the lease liabilities by $42,506. Four of the terminated leases were part of a master lease agreement. As a result of the transferred leases being removed from the master lease arrangement, the remaining lease components under the master lease
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
arrangement were modified which resulted in a net increase to the lease liability and ROU asset balance of $6,161 for the year ended December 31, 2022.
The components of operating lease cost, are as follows:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Operating lease costs: | | | | | |
| Facility rent—cost of services | $ | 35,840 | | | $ | 33,992 | | | $ | 32,958 | |
| Office rent—cost of services | 7,189 | | | 5,767 | | | 5,060 | |
Rent—cost of services(a) | $ | 43,029 | | | $ | 39,759 | | | $ | 38,018 | |
| | | | | |
| General and administrative expense | $ | 451 | | | $ | 385 | | | $ | 370 | |
Variable lease cost(b) | $ | 8,688 | | | $ | 7,369 | | | $ | 6,281 | |
| | | | | | | | |
| (a) | | Includes short-term lease cost, which is immaterial |
| (b) | | Represents variable lease cost for operating leases including property taxes, insurance, common area maintenance, and consumer price index increases. Costs of $5,348, $4,891, and $4,451 are recorded in cost of services and $3,340, $2,478, and $1,830 are included in rent-cost of services for the years ended December 31, 2024, 2023 and 2022. |
The following table shows the lease maturity analysis for all leases as of December 31, 2024:
| | | | | |
| Year | Operating Leases |
| 2025 | $ | 40,349 | |
| 2026 | 38,522 | |
| 2027 | 37,452 | |
| 2028 | 36,473 | |
| 2029 | 35,340 | |
| Thereafter | 235,690 | |
| Total lease payments | 423,826 | |
| Less: present value adjustments | (150,735) | |
| Present value of total lease liabilities | 273,091 | |
| Less: current lease liabilities | (19,671) | |
| Long-term operating lease liabilities | $ | 253,420 | |
At lease commencement, lease liabilities are based on the net present value of the remaining lease payments over the remaining lease term. In determining the present value of lease payments, the Company used its incremental borrowing rate based on the information available at each lease’s commencement date to determine each lease's liability. As of December 31, 2024, the weighted average remaining lease term and the weighted average discount rate was 11.8 years and 8.0% for operating leases, respectively.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
14. INCOME TAXES
The provision for income tax expense for the years ended December 31, 2024, 2023 and 2022 is summarized as follows:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Current: | | | | | |
| Federal | $ | 6,449 | | | $ | 1,178 | | | $ | (193) | |
| State | 1,766 | | | 492 | | | 146 | |
| Total current | 8,215 | | | 1,670 | | | (47) | |
| Deferred: | | | | | |
| Federal | (998) | | | 3,217 | | | 1,334 | |
| State | (189) | | | 787 | | | 362 | |
| Total deferred | (1,187) | | | 4,004 | | | 1,696 | |
| | | | | |
| Total provision for income taxes | $ | 7,028 | | | $ | 5,674 | | | $ | 1,649 | |
A reconciliation of the federal statutory tax rate to the effective tax rate for income from continuing operations for the years ended December 31, 2024, 2023 and 2022, respectively, is comprised as follows:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Income tax expense at statutory rate | 21.0 | % | | 21.0 | % | | 21.0 | % |
| State income taxes - net of federal benefit | 4.2 | | | 5.3 | | | 4.7 | |
| Non-deductible meals and entertainment | 0.5 | | | 0.8 | | | 0.6 | |
| | | | | |
Section 162(m) limitation(a) | 3.1 | | | 3.0 | | | (5.5) | |
| | | | | |
| Other non-deductible expenses | — | | | 0.2 | | | 0.2 | |
| | | | | |
| Tax credits | (0.3) | | | (0.2) | | | — | |
Stock based compensation(b) | (4.6) | | | — | | | (0.8) | |
| Noncontrolling interest | (1.4) | | | (0.7) | | | (1.7) | |
| Other adjustments | (0.1) | | | (0.4) | | | — | |
| Total income tax expense at effective rate | 22.4 | % | | 29.0 | % | | 18.5 | % |
| | | | | | | | |
| (a) | | During the year ended December 31, 2023, approximately $2,078 of the share-based compensation expense related to restricted stock that originally resulted in a deferred tax asset was written off. |
| (b) | | During the year ended December 31, 2024, employees exercised stock options representing approximately 254 shares. Although the Company had slightly higher option expirations in the year ended December 31, 2024, the tax deductions from the significantly increased option exercises resulted in a significant tax benefit. During the year ended December 31, 2023, employees exercised stock options representing approximately 89 shares. The Company had decreased exercises and increased expirations of stock options in the year ended December 31, 2023 and coupled with an increase in book income has caused the effect of this on the effective tax rate to be minimal. During the year ended December 31, 2022, employees exercised stock options representing approximately 125 shares. |
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
The Company’s deferred tax assets and liabilities for the years ended December 31, 2024 and 2023 are summarized below.
| | | | | | | | | | | |
| Year Ended December 31, |
| | 2024 | | 2023 |
| Deferred tax assets (liabilities): | | | |
| Accrued compensation | $ | 11,196 | | | $ | 8,472 | |
| Allowance for doubtful accounts | 1,690 | | | 960 | |
| State taxes | 128 | | | 64 | |
| | | |
| Lease liabilities | 70,706 | | | 69,029 | |
| Insurance | 1,839 | | | 1,769 | |
| Other | 1,276 | | | 756 | |
| Total deferred tax assets | 86,835 | | | 81,050 | |
| | | |
| | | |
| Depreciation and amortization | (16,010) | | | (13,714) | |
| Prepaid expenses | (902) | | | (786) | |
| Right-of-use assets | (69,813) | | | (68,105) | |
| | | |
| Other | (1,971) | | | (300) | |
| Total deferred tax liabilities | (88,696) | | | (82,905) | |
| Net deferred tax liabilities | $ | (1,861) | | | $ | (1,855) | |
During the year ended December 31, 2023, the Company fully utilized all of its federal and state net operating loss carryforwards from the year ended December 31, 2022.
A reconciliation of the beginning and ending amount of unrecognized tax benefits is as follows:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, |
| 2024 | | 2023 | | 2022 |
| Balance at January 1 | $ | — | | | $ | — | | | $ | 65 | |
| Additions for tax positions of prior years | — | | | — | | | — | |
| | | | | |
| Reductions for tax positions related to the current year | — | | | — | | | (65) | |
| Balance at December 31 | $ | — | | | $ | — | | | $ | — | |
None of the unrecognized tax benefits net of their state benefits would affect the Company’s effective tax rate for the years ended December 31, 2024, 2023 and 2022. The Company classifies interest and/or penalties on income tax liabilities or refunds as additional income tax expense or income. Such amounts are not material.
As of December 31, 2024, the Company is no longer subject to federal tax examinations for the fiscal years prior to 2021, and in most states, is no longer subject to state income tax examinations for fiscal years before 2020. The lapsing of the statutes of limitation for the years ended December 31, 2020 and December 31, 2019 had no impact on the Company’s unrecognized tax benefits.
15. DEFINED CONTRIBUTION PLAN
The Company has a 401(k) defined contribution plan (the “401(k) Plan”), whereby eligible employees may contribute up to 90% of their annual basic earnings, subject to applicable annual Internal Revenue Code limits. Additionally, the 401(k) Plan provides for discretionary matching contributions (as defined in the 401(k) Plan) by the Company. The Company expensed matching contributions to the 401(k) Plan of $1,219, $866, and $627 during the years ended December 31, 2024, 2023 and 2022, respectively.
During fiscal year 2021, the Company implemented a non-qualified deferred compensation plan (the “DCP”) for executives, other highly compensated employees, independent contractors and non-employee directors which went into effect
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
on June 1, 2021, effective for compensation to be paid in 2022 and thereafter. The independent contractors and non-employee directors are otherwise ineligible for participation in the Company's 401(k) plan. The DCP allows participants to defer the receipt of a portion of their base compensation, and further allows certain participants to defer up to 80% of their base salary and bonus compensation or director fees. At the participant’s election, payments can be deferred until a specific date at least one year after the year of deferral or until termination of engagement with the Company and can be paid in a lump sum or in up to ten annual installments. Separate deferral elections can be made for each year, and in limited circumstances, existing payment elections may be changed. The amounts deferred are credited with earnings and losses based upon the actual performance of the deemed investments selected by the participant. The rate of return for each participant varies depending on the specific investment elections made by the participant. Additionally, the plan deposits the employee deferrals into a rabbi trust and the funds are generally invested in individual variable life insurance contracts owned by the Company that are specifically designed to informally fund savings plans of this nature. The Company paid for related administrative costs, which were immaterial during the fiscal years presented.
As of December 31, 2024 and 2023, the Company’s deferred compensation liabilities were $2,170 and $1,108, respectively, in other long-term liabilities on the consolidated balance sheets. The cash surrender value of the individual variable life insurance contracts is based on investment funds that shadow the investment allocations specified by participants in the DCP. As of December 31, 2024 and 2023, the cash surrender value of the company owned life insurance (“COLI”) policies were $2,182 and $1,123, respectively, and were included as a component of restricted and other assets on the consolidated balance sheets. There are no outstanding loan amounts offset against the cash surrender value of the COLI policies. The losses recorded for the change in cash surrender value were immaterial for each period presented.
16. COMMITMENTS AND CONTINGENCIES
Regulatory Matters - The Company provides services in complex and highly regulated industries. The Company’s compliance with applicable U.S. federal, state and local laws and regulations governing these industries may be subject to governmental review and adverse findings may result in significant regulatory action, which could include sanctions, damages, fines, penalties (many of which may not be covered by insurance), and even exclusion from government programs. The Company is a party to various regulatory and other governmental audits and investigations in the ordinary course of business and cannot predict the ultimate outcome of any federal or state regulatory survey, audit or investigation. While governmental audits and investigations are the subject of administrative appeals, the appeals process, even if successful, may take several years to resolve and penalties subject to appeal may remain in place during such appeals. The Department of Justice, CMS, or other federal and state enforcement and regulatory agencies may conduct additional investigations related to the Company's businesses. The Company believes that it is presently in compliance in all material respects with all applicable laws and regulations.
Cost-Containment Measures - Government and third-party payors have instituted cost-containment measures designed to limit payments made to providers of healthcare services, may propose future cost-containment measures, and there can be no assurance that future measures designed to limit payments made to providers will not adversely affect the Company.
Indemnities - From time to time, the Company enters into certain types of contracts that contingently require the Company to indemnify parties against third-party claims. These contracts primarily include (i) certain real estate leases, under which the Company may be required to indemnify property owners or prior operators for post-transfer environmental or other liabilities and other claims arising from the Company’s use of the applicable premises, (ii) operations transfer agreements, in which the Company agrees to indemnify past operators of agencies and communities the Company acquires against certain liabilities arising from the transfer of the operation and/or the operation thereof after the transfer, (iii) certain Ensign lending agreements, and (iv) certain agreements with management, directors and employees, under which the subsidiaries of the Company may be required to indemnify such persons for liabilities arising out of their employment relationships. The terms of such obligations vary by contract, and, in most instances, a specific or maximum dollar amount is not explicitly stated therein. Generally, amounts under these contracts cannot be reasonably estimated until a specific claim is asserted. Consequently, because no claims have been asserted, no liabilities have been recorded for these obligations on the Company’s consolidated balance sheets for any of the periods presented.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
Litigation - The Company’s businesses involve a significant risk of liability given the age and health of the patients and residents served by its independent operating subsidiaries. The Company, its operating companies, and others in the industry may be subject to a number of claims and lawsuits, including professional liability claims, alleging that services provided have resulted in personal injury, elder abuse, wrongful death or other related claims. Healthcare litigation (including class action litigation) is common and is filed based upon a wide variety of claims and theories, and the Company is routinely subjected to these claims in the ordinary course of business, including potential claims related to patient care and treatment, and professional negligence. The Company may also face employment related claims, including wage and hour class actions, which are frequent in our industries. If there were a significant increase in the number of these claims or an increase in amounts owing should plaintiffs be successful in their prosecution of these claims, this could materially adversely affect the Company’s business, financial condition, results of operations and cash flows. In addition, the defense of these lawsuits may result in significant legal costs, regardless of the outcome, and may result in large settlement amounts or damage awards.
In addition to the potential lawsuits and claims described above, the Company is also subject to potential lawsuits under the False Claims Act (the “FCA”) and comparable state laws alleging submission of fraudulent claims for services to any healthcare program (such as Medicare) or payor. A violation may provide the basis for exclusion from federally funded healthcare programs. Such exclusions could have a correlative negative impact on the Company’s financial performance. Some states, including California, Arizona and Texas, have enacted similar whistleblower and false claims laws and regulations. In addition, the Deficit Reduction Act of 2005 created incentives for states to enact anti-fraud legislation modeled on the FCA, for which 18 states have qualified, including California and Texas, where we conduct business. As such, the Company could face increased scrutiny, potential liability and legal expenses and costs based on claims under state false claims acts in markets in which it conducts business.
Under the Fraud Enforcement and Recovery Act (“FERA”) and its associated rules, healthcare providers face significant penalties for the knowing retention of government overpayments, even if no false claim was involved. Providers have an obligation to proactively exercise “reasonable diligence” to identify overpayments and return those overpayments to CMS within 60 days of “identification” or the date any corresponding cost report is due, whichever is later. Retention of overpayments beyond this period may create liability under the FCA. In addition, FERA protects whistleblowers (including employees, contractors, and agents) from retaliation.
The Company cannot predict or provide any assurance as to the possible outcome of any litigation. If any litigation were to proceed, and the Company and its operating companies are subjected to, alleged to be liable for, or agree to a settlement of, claims or obligations under federal Medicare statutes, the FCA, or similar state and federal statutes and related regulations, the Company’s business, financial condition and results of operations and cash flows could be materially and adversely affected. Among other things, any settlement or litigation could involve the payment of substantial sums to settle any alleged civil violations and may also include the assumption of specific procedural and financial obligations by the Company or its independent operating subsidiaries going forward under a corporate integrity agreement and/or other arrangement with the government. The Company establishes reserves to cover the anticipated costs of such litigation, including legal fees and expected settlements, based on the Company’s historical litigation experience, current developments, and other factors.
Medicare Revenue Recoupments - The Company is subject to probe reviews relating to Medicare services, billings and potential overpayments by Unified Program Integrity Contractors (“UPIC”), Recovery Audit Contractors (“RAC”), Zone Program Integrity Contractors (“ZPIC”), Program Safeguard Contractors (“PSC”), Supplemental Medical Review Contractors (“SMRC”) and Medicaid Integrity Contributors (“MIC”) programs, (each of the foregoing collectively referred to as “Reviews.”)
As of December 31, 2024, 13 of the Company’s independent operating subsidiaries had Reviews scheduled, on appeal or in dispute resolution process, both pre- and post-payment. If an operation fails an initial or subsequent Review, the operation could then be subject to extended Review, suspension of payment, or extrapolation of the identified error rate to all billing in the same time period. The Company, from time to time, receives record requests in Reviews which have resulted in claim denials on paid claims. The Company has appealed substantially all denials arising from these Reviews using the applicable appeals process. As of December 31, 2024, and through the filing of this Annual Report on Form 10-K, the Company’s independent operating subsidiaries have responded to the Reviews that are currently ongoing, on appeal or in dispute resolution process. The Company cannot predict the ultimate outcome of any regulatory and other governmental Reviews. While such reviews are the subject of administrative appeals, the appeals process, even if successful, may take several years to resolve. The costs to respond to and defend such Reviews may be significant and an adverse determination in such reviews may subject the Company to sanctions, damages, extrapolation of damage findings, additional recoupments, fines, other penalties (some of which may not be covered by insurance), and termination from Medicare programs which may, either individually or in the aggregate, have a material adverse effect on the Company's business and financial condition.
THE PENNANT GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS - (Continued)
From June 2021 to May 2022, one hospice provider number was subject to a Medicare payment suspension imposed by a UPIC. The total amount suspended was $5,105, which represents all Medicare payments due to the provider number during the suspension. As of December 31, 2024, the total amount due from the government payor impacted by the suspension was $246 and was recorded in long-term other assets.
In May 2022, the Company received communication that the Medicare payment suspension, for the above-referenced hospice provider number, was terminated and the UPIC’s review was complete. The UPIC reviewed 107 patient records covering a 10-month period to determine whether, in its view, a Medicare overpayment was made. Based on the results of the review, the UPIC initially alleged sampled and extrapolated overpayments of $5,105, and withheld that amount through continued recoupment of Medicare payments. The Company is pursuing its appeal rights through the administrative appeals process, including contesting the methodology used by the UPIC to perform statistical extrapolation. To date the Company has been successful in appealing the majority of the previously denied claims. The Company received the refund of previously withheld amounts totaling $1,610 and $3,249 during the years ended December 31, 2024 and 2023, respectively. The Company continues to work through the appeals process for the remaining denied claims of $246 and expects to be successful in those appeals. Based on the information currently available to the Company, the Company cannot predict the timing or the ultimate outcome of this review including refunds to be received.
Insurance - The Company retains risk for a substantial portion of potential claims for general and professional liability, workers’ compensation and automobile liability. The Company recognizes obligations associated with these costs, up to specified deductible limits in the period in which a claim is incurred, including with respect to both reported claims and claims incurred but not reported. The general and professional liability insurance has a retention limit of $250 per claim with a $500 corridor as an additional out-of-pocket retention the Company must satisfy for claims within the policy year before the carrier will reimburse losses. The workers’ compensation insurance has a retention limit of $250 per claim, except for policies held in Texas, Washington and Wyoming which are subject to state insurance and possess their own limits.
Effective January 1, 2022, the Company is self-insured for claims related to employee health, dental and vision care. To protect itself against loss exposure, the Company has purchased individual stop-loss insurance coverage that insures individual health claims that exceed $350 for each covered person for fiscal year 2024, and $325 for each covered person for fiscal year 2023.