UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d)
of the Securities Exchange Act of 1934
Date of Report (Date of earliest event reported): August 30, 2022
SANGAMO THERAPEUTICS, INC.
(Exact name of registrant as specified in its charter)
| | | | | | | | | | | | | | |
| | | | |
| Delaware | | 000-30171 | | 68-0359556 |
(State or other jurisdiction of
incorporation) | | (Commission
File Number) | | (IRS Employer
ID Number) |
7000 Marina Blvd., Brisbane, California 94005
(Address of principal executive offices) (Zip Code)
(510) 970-6000
(Registrant’s telephone number, including area code)
Not Applicable
(Former Name or Former Address, if Changed Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| | | | | |
| ☐ | Written communications pursuant to Rule 425 under the Securities Act (17 CFR 230.425) |
| | | | | |
| ☐ | Soliciting material pursuant to Rule 14a-12 under the Exchange Act (17 CFR 240.14a-12) |
| | | | | |
| ☐ | Pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act (17 CFR 240.14d-2(b)) |
| | | | | |
| ☐ | Pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b) of the Act: | | | | | | | | | | | | | | |
| | | | |
| Title of each class | | Trading Symbol(s) | | Name of each exchange on which registered |
| Common Stock, $0.01 par value per share | | SGMO | | Nasdaq Global Select Market |
Indicate by check mark whether the registrant is an emerging growth company as defined in Rule 405 of the Securities Act of 1933 (§ 230.405 of this chapter) or Rule 12b-2 of the Securities Exchange Act of 1934 (§ 240.12b-2 of this chapter).
Emerging growth company ☐
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Item 8.01 Other Events.
Update Regarding Isaralgagene Civaparvovec (Fabry Disease)
On August 30, 2022, Sangamo Therapeutics, Inc. (the “Company” or “Sangamo”) announced updated preliminary clinical data from the Phase 1/2 STAAR study evaluating isaralgagene civaparvovec, or ST-920, a wholly owned gene therapy product candidate for the treatment of Fabry disease, in advance of its presentation at the Society for the Study of Inborn Errors of Metabolism (SSIEM) Annual Meeting on August 31, 2022. A summary of the data is below.
Summary of Updated Preliminary Results from the Phase 1/2 STAAR Study of Isaralgagene Civaparvovec
•STAAR is an ongoing Phase 1/2 multicenter, open-label, dose-ranging clinical study designed to assess the safety and tolerability of a single infusion of isaralgagene civaparvovec in Fabry disease patients over 18 years of age. Patients are infused intravenously with a single dose of ST-920 and then are followed for 52 weeks. A separate long-term follow-up study is underway to monitor the patients treated in this study for up to five years following treatment. The study design provides for at least two patients to be dosed in each dose cohort before dose escalation, and also allows potential expansion in each cohort. Patients who are on stable enzyme replacement therapy, or ERT, may withdraw from ERT after treatment in a controlled and monitored fashion at the discretion of the patient and the investigator.
•The dose escalation phase includes males with classic Fabry disease. During the dose expansion phase, female patients and patients with Fabry-associated cardiac or renal disease may also be enrolled. The study’s primary endpoint is incidence of treatment-emergent adverse events. Additional safety evaluations include routine hematology, chemistry and liver tests; vital signs; electrocardiogram; echocardiogram; serial alpha-fetoprotein testing and magnetic resonance imaging, or MRI, of liver to monitor for potential formation of any liver mass. Secondary endpoints include change from baseline at specific time points over the one-year study period in alpha-galactosidase A, or α-Gal A, activity, globotriaosylceramide, or Gb3, and lyso-Gb3 levels in plasma; frequency of ERT infusion; changes in renal function, cardiac function and left ventricular mass, measured by cardiac MRI and rAAV2/6 vector clearance. Key exploratory endpoints include quality of life, Fabry symptoms and neuropathic pain scores; and immune response to AAV6 capsid and α-Gal A.
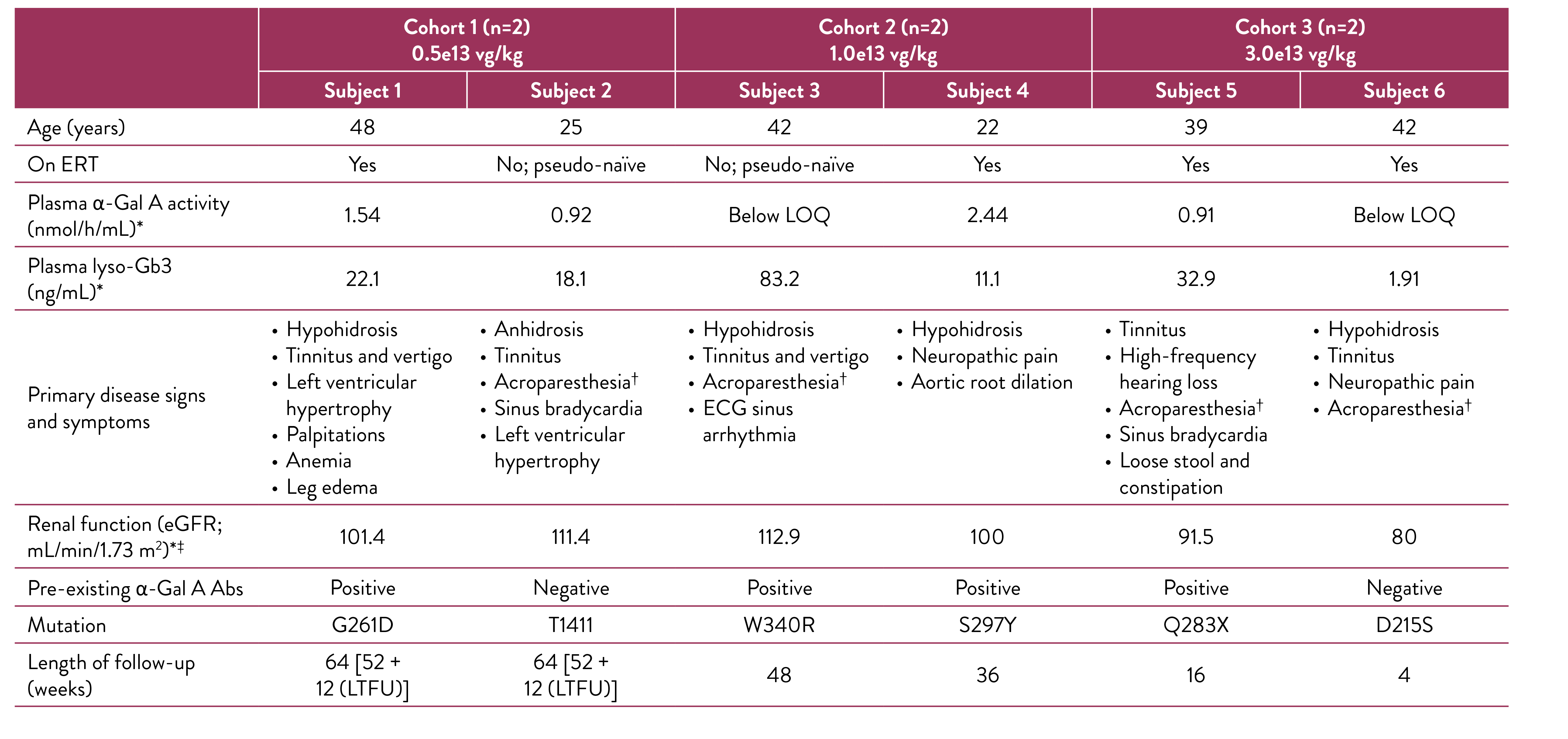
•As of the February 14, 2022 cutoff date, six patients, ranging in age from 22 to 48 years, were treated with isaralgagene civaparvovec. Baseline characteristics of these six patients are shown in the figure below. Two patients were treated in Cohort 1 at the dose of 0.5e13 vg/kg, two patients were dosed in Cohort 2 at the dose of 1e13 vg/kg and two patients were dosed in Cohort 3 at the dose of 3e13 vg/kg. As of the cutoff date, the first treated patients had been followed for at least 15 months and the most recently treated patient had been followed for two weeks.
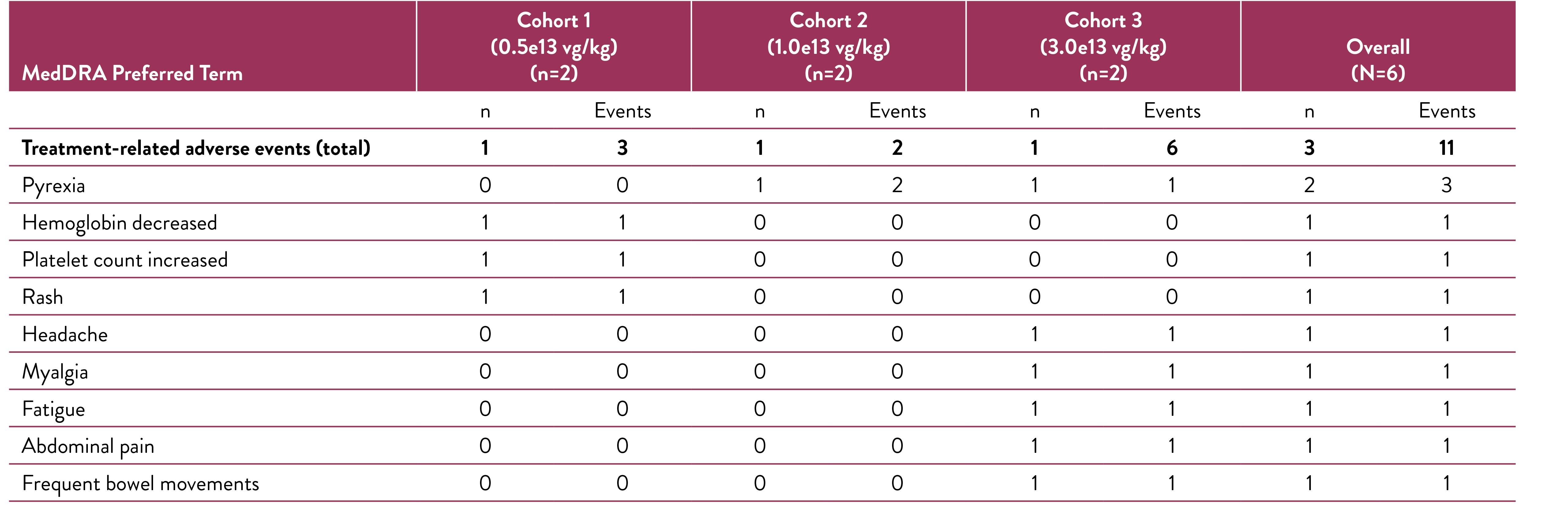
•As of the February 14, 2022 cutoff date, isaralgagene civaparvovec continued to be generally well tolerated across the three dose cohorts in the six treated patients. A summary of the treatment-related adverse events reported as of the cutoff date is shown in the figure below. One patient each in Cohorts 1, 2 and 3 exhibited treatment-related adverse events for a total of eleven events, which were all graded as mild (Grade 1). No treatment-related serious adverse events were reported. Prophylactic steroids were not required per the study protocol and, as of the cutoff date, no patients had exhibited liver enzyme elevations necessitating steroid treatment, and no prophylactic steroids had been used.
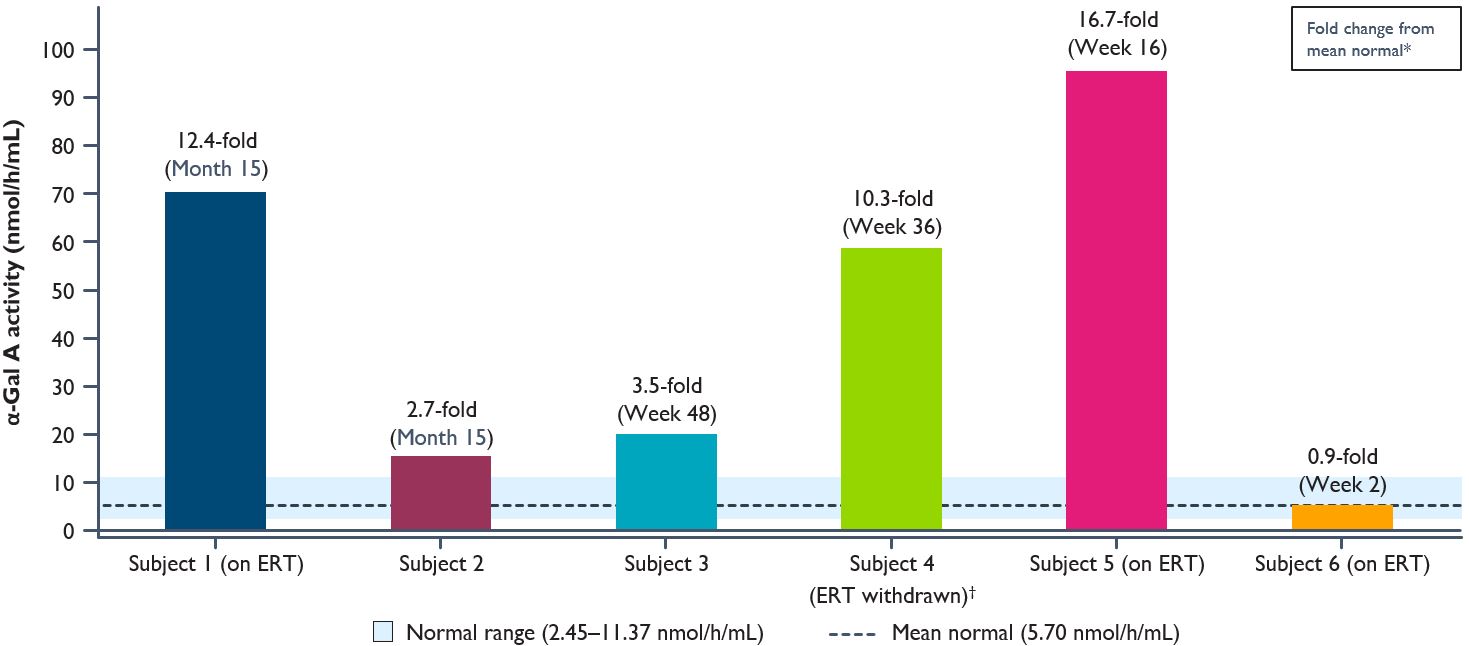
•Results of plasma a-Gal A activity as of the cutoff date for the six treated patients are shown in the figure below and described in further detail below. The five longest treated patients continued to exhibit elevated α-Gal A activity, sustained up to 15 months as of the last date of measurement. The sixth patient exhibited elevated α-Gal A activity to within normal range at two weeks post dosing.
◦Cohort 1, Patient 1 [on ERT at the cutoff date]: α-Gal A activity measured at ERT trough was 12.4-fold above mean normal at Month 15.
◦Cohort 1, Patient 2 [not on ERT]: α-Gal A activity was 2.7-fold above mean normal at Month 15.
◦Cohort 2, Patient 1 [not on ERT]: α-Gal A activity was 3.5-fold above mean normal at Week 48.
◦Cohort 2, Patient 2 [began the study on ERT and was subsequently withdrawn from ERT at week 24]: α-Gal A activity was 10.3-fold above mean normal at Week 36. This represents a sustained α-Gal A expression compared with the 10-fold above mean normal levels previously exhibited as of November 9, 2021, with α-Gal A expression one week post ERT withdrawal.
◦Cohort 3, Patient 1 [on ERT at the cutoff date]: α-Gal A activity measured at ERT trough was 16.7-fold above mean normal at Week 16.
◦Cohort 3, Patient 2 [on ERT at the cutoff date]: α-Gal A activity measured at ERT trough increased to within normal range at Week 2.
•As of the February 14, 2022 cutoff date, withdrawal from ERT had been completed for the second patient in Cohort 2. This patient sustained elevated α-Gal A plasma activity at 12 weeks following withdrawal with moderate increase in lyso-Gb3 levels as of the cutoff date. This patient continues to remain off ERT to date.
•The first patient in Cohort 2 with a significant elevation in plasma lyso-Gb3 levels pre-treatment showed a reduction of approximately 40% from baseline levels of lyso-Gb3 within ten weeks after dosing, which was maintained through Week 48. Of the other five treated patients with lower baseline levels of lyso-Gb3, four patients maintained steady levels through the cutoff date and the second patient in Cohort 2 who was withdrawn from ERT demonstrated a moderate increase in lyso-Gb3 levels since the withdrawal of ERT.
•Several of the patients reported subjective improvements in quality-of-life measures as of the cutoff date. Three patients have reported improvements in their symptoms, including improvements in anhidrosis (inability to sweat) or hypohydrosis (reduced ability to sweat), a primary and common Fabry disease symptom. No progression of Fabry cardiomyopathy was observed in those patients who presented with signs of cardiomyopathy on cardiac MRI at baseline.
•Since the cutoff date, an additional five patients have been dosed in the Phase 1/2 STAAR study, resulting in a total of eleven patients dosed to date – one additional patient in Cohort 3, two patients in Cohort 4 at the 5e13vg/kg dose level and the first two patients in the expansion phase at the 5e13vg/kg dose level. There are multiple additional patients in screening, including both male and female candidates. Out of the five treated patients in the dose escalation phase who began the STAAR study on ERT, since the cutoff date an additional four have been withdrawn from ERT, completing ERT withdrawal for all patients in this dose escalation phase of the study. Sangamo expects to provide additional results from the STAAR study in the second half of 2022.
Baseline Patient Characteristics
*The time point immediately preceding ST-920 administration was presented as the baseline value.
†Burning, tingling, or numbness in the extremities.
‡eGFR was calculated using the CKD-EPI.
α-Gal A, alpha galactosidase A; Ab, antibody; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; ECG, electrocardiogram; eGFR, estimated glomerular filtration rate; LOQ, limit of quantitation; LTFU, long-term follow-up; lyso-Gb3, globotriaosylsphingosine; vg/kg, vector genomes per kilogram of body weight.
Treatment Related Adverse Events
MedDRA, Medical Dictionary for Regulatory Activities; vg/kg, vector genomes per kilogram of body weight.
Plasma α-Gal A Activity at Cutoff Date
Biomarker results were evaluated from the 6 subjects in dose cohorts 1, 2, 3 (0.5e13 vg/kg, 1.0e13 vg/kg, 3.0e13 vg/kg) as of the cutoff date of February 14, 2022.
*Fold change was calculated at last measured time point. α-Gal A activity was measured using a 3-hour reaction time and is presented in nmol/h/mL. For Subjects 1, 4-6, sampling was at ERT trough.
Normal range and mean were determined based on healthy male individuals.
†Subject was withdrawn from ERT at week 24.
α-Gal A, alpha galactosidase A; ERT, enzyme replacement therapy; LTFU, long-term follow-up.
Forward-Looking Statements
This Current Report on Form 8-K contains forward-looking statements regarding Sangamo's current expectations. These forward-looking statements include, without limitation: the therapeutic potential of isaralgagene civaparvovec; the Phase 1/2 STAAR study design and Sangamo’s expectations and plans related thereto, including the potential to include additional male and female patients in the study; and other statements that are not historical fact. These statements are not guarantees of future performance and are subject to certain risks and uncertainties that are difficult to predict. Sangamo’s actual results may differ materially and adversely from those expressed in these forward-looking statements. Factors that could cause actual results to differ include, but are not limited to, risks and uncertainties related to: the evolving COVID-19 pandemic and its impact on the global business environment, healthcare systems and the business and operations of Sangamo, including the enrollment of patients in and operation of clinical trials; the research and development process; the uncertain timing and unpredictable nature of clinical trial results, including the risk that the therapeutic effects observed in the updated preliminary clinical data from the Phase 1/2 STAAR study will not be durable in patients and that final clinical trial data from the study will not validate the safety and efficacy of isaralgagene civaparvovec; the unpredictable regulatory approval process for product candidates across multiple regulatory authorities; Sangamo’s lack of resources to fully develop, obtain regulatory approval for and commercialize its product candidates, including isaralgagene civaparvovec; the potential for technological developments that obviate technologies used by Sangamo in isaralgagene civaparvovec; Sangamo’s lack of resources to fully develop, obtain regulatory approval for and commercialize its product candidates; and other risks and uncertainties described in Sangamo’s filings with the U.S. Securities and Exchange Commission, including its Annual Report on Form 10-K for the year ended December 31, 2021, as supplemented by Sangamo’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2022. The information contained in this Current Report on Form 8-K is as of August 30, 2022, and Sangamo undertakes no duty to update forward-looking statements contained in this Current Report on Form 8-K except as required by applicable laws.
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| | | | | | | | | | | | | | | | | | | | |
| | | | | | |
| | | | SANGAMO THERAPEUTICS, INC. |
| | | |
| Dated: August 30, 2022 | | | | By: | | /s/ SCOTT B. WILLOUGHBY |
| | | | Name: | | Scott B. Willoughby |
| | | | Title: | | Senior Vice President, General Counsel and Corporate Secretary |