Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10/A
(Amendment No. 4)
CymaBay Therapeutics, Inc.
(Exact name of Registrant as specified in its charter)
| Delaware | 94-3103561 | |
| (State or Other Jurisdiction of Incorporation or Organization) | (I.R.S. Employer Identification No.) |
3876 Bay Center Place
Hayward, California 94545
(Address of principal executive offices) (Zip Code)
Registrant’s telephone number, including area code: (510) 293-8800
Securities registered pursuant to Section 12(b) of the Act: None
Securities registered pursuant to Section 12(g) of the Act:
Common Stock, $0.0001 Par Value Per Share
(Title of class)
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer”, “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer | ¨ | Accelerated filer | ¨ | |||
| Non-accelerated filer | ¨ (Do not check if a smaller reporting company) | Smaller reporting company | x | |||
We are an “emerging growth company” as defined under the federal securities laws. For implications of our status as an emerging growth company, please see “Business” in Item 1, “Risk Factors” in Item 1A and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” in Item 2 of this registration statement.
Table of Contents
CymaBay Therapeutics, Inc.
FORM 10
INFORMATION REQUIRED IN REGISTRATION STATEMENT
ITEM 1 | 3 | |||||
ITEM 1A. | 37 | |||||
ITEM 2. | 61 | |||||
ITEM 3. | 71 | |||||
ITEM 4. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT | 71 | ||||
ITEM 5. | 74 | |||||
ITEM 6. | 78 | |||||
ITEM 7. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE | 85 | ||||
ITEM 8. | 87 | |||||
ITEM 9. | MARKET PRICE OF AND DIVIDENDS ON THE REGISTRANT’S COMMON EQUITY AND RELATED STOCKHOLDER MATTERS | 87 | ||||
ITEM 10. | 88 | |||||
ITEM 11. | 89 | |||||
ITEM 12. | INDEMNIFICATION OF DIRECTORS AND OFFICERS | 94 | ||||
ITEM 13. | 95 | |||||
ITEM 14. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE | 95 | ||||
ITEM 15. | 96 | |||||
2
Table of Contents
DISCLOSURE REGARDING FORWARD LOOKING STATEMENTS
This Form 10 contains forward-looking statements regarding future events and our future results that are based on current expectations, estimates, forecasts, and projections about the industries in which we operate and the beliefs and assumptions of our management. Words such as “expects,” “will,” “anticipates,” “targets,” “goals,” “projects,” “intends,” “plans,” “believes,” “seeks,” “estimates,” “potential,” “should,” “could,” variations of such words, and similar expressions are intended to identify forward-looking statements. In addition, any statements which refer to projections of our future financial performance, our anticipated growth and trends in our business, and other characterizations of future events or circumstances, are forward-looking statements, including, but not limited to: statements regarding the steps, timing and costs of our development programs; the availability of additional financing and access to capital; the formation of a trading market for our common stock; discussions and approvals of regulatory agencies; and the period of time for which we will be able to fund our operations. These forward-looking statements are based on management’s beliefs and assumptions and on information currently available to our management and involve significant elements of subjective judgment and analysis. Readers are cautioned that these forward-looking statements are only predictions and are subject to risks, uncertainties, and assumptions that are difficult to predict, including, but not limited to, the ability to obtain substantial additional funding, obtain and maintain all necessary patents or licenses, demonstrate the safety and efficacy of product candidates at each stage of development, meet applicable regulatory standards and receive required regulatory approvals, meet obligations and required milestones under agreements, manufacture and distribute any product candidates or products that we may develop in commercial quantities at reasonable costs, compete successfully against other products and market products in a profitable manner. Therefore, actual results may differ materially and adversely from those expressed in any forward-looking statements. Readers are directed to the risks and uncertainties identified below, under “Item 1A. Risk Factors” and elsewhere herein, for additional factors that may cause actual results to be different from those expressed in these forward-looking statements. Any forward-looking statement speaks only as of the date on which it is made, and except as required by law, we undertake no obligation to revise or update publicly any forward-looking statements for any reason.
For convenience in this Form 10, “CymaBay,” “we,” “us,” and “our” refer to CymaBay Therapeutics, Inc. and its subsidiaries taken as a whole. The word trademark “CymaBay” is registered on the Principal Register of the United States Patent and Trademark Office. This document also contains trademarks and trade names of other companies, and those trademarks and trade names are the property of their respective owners. We do not intend our use or display of other companies’ trademarks or trade names to imply a relationship with, or endorsement or sponsorship of us by, any other companies or products.
| ITEM 1. | BUSINESS. |
CymaBay Overview
CymaBay Therapeutics Inc., formerly Metabolex, Inc., is focused on developing therapies to treat metabolic diseases. Arhalofenate, our lead product candidate, is being developed for the treatment of gout. Arhalofenate has demonstrated two therapeutic actions: the prevention of painful attacks of gout in joints (flares) and the lowering of serum uric acid (sUA) by promoting excretion of uric acid by the kidney. In addition, arhalofenate provides physicians with what they identified in a recent survey (TreatmentTrends®: Gout U.S. August 2011) as the most important attributes when selecting a gout therapy: no serious safety issues, well tolerated, minimize frequency of flares and use in patients with a broad range of comorbidities, (other diseases that individual patients have in addition to gout).
CymaBay has completed three Phase 2 studies of arhalofenate in gout patients in which it demonstrated a consistent pattern of reduction of flare incidence and duration and lowering of serum uric acid (sUA). Arhalofenate has established a safety profile in toxicology studies in animals and in clinical studies involving nearly 1,000 patients exposed to arhalofenate. One additional Phase 2b clinical study of 12 weeks duration is planned to confirm the safety and efficacy of a higher dose prior to initiating Phase 3 studies. Due to its safety profile and ability to both reduce flares and lower sUA, we believe that arhalofenate has a differentiated profile
3
Table of Contents
that is attractive for use in a large population, with significant advantages over marketed and emerging agents which have limitations in their efficacy, tolerability, and use in patients with common comorbidities. CymaBay is poised to follow arhalofenate with two additional clinical stage product candidates, one in diabetes and one that has potential utility in high unmet need (no existing or limited therapies) and/or orphan diseases (rare diseases).
CymaBay has had net losses of $11.1 million, $23.9 million and $17.1 million for the six months ended June 30, 2013, and the twelve months ended December 31, 2012 and 2011, respectively. Our cash balance as of June 30, 2013, was $3.6 million. Our average monthly cash usage for the six months ending June 30, 2013, was $0.7 million. On September 30, 2013, we sold shares of our common stock and warrants to purchase shares of our common stock in a private placement for aggregate gross proceeds of $26.8 million, and raised an additional $5.0 million in venture debt financing pursuant to a $10.0 million loan agreement which we entered into simultaneously with the private placement on September 30, 2013, resulting in aggregate net proceeds to CymaBay of $28.9 million after deducting placement agent fees and estimated offering expenses. At the same time we issued shares of our common stock in cancellation of approximately $16.9 million of debt owed to the holder of that debt. On October 31, 2013, we sold additional shares of our common stock and warrants to purchase shares of our common stock, which sales are also part of the private placement, for aggregate net proceeds of $2.8 million after deducting placement agent fees and estimated offering expenses. We refer to the private placement, the venture debt financing and the issuance of our common stock in cancellation of the $16.9 million of debt as the 2013 financing. After giving effect to the 2013 financing, we believe that our existing cash will allow us to continue operation through the third quarter of 2015. As set forth in the notes to our financial statements, our auditors expressed substantial doubt as to our ability to continue as a going concern if we are unable to raise additional capital, without giving effect to the 2013 financing.
Concurrent with the portion of the 2013 financing that closed on September 30, 2013, we engaged in a 1-for-79.5 reverse split of our preferred stock and common stock, which we refer to as the reverse stock split, and all of the shares of our outstanding preferred stock converted to common stock. The discussion in this Form 10 gives retroactive effect to the reverse stock split for all periods presented. The conversion of the preferred stock is also reflected in this Form 10, except where specifically stated to the contrary.
Implications of Being an “Emerging Growth Company”
We qualify as an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012, or the JOBS Act. As an “emerging growth company,” we may take advantage of specified reduced disclosure and other requirements that are otherwise applicable generally to public companies. These provisions include:
| • | only two years of audited financial statements in addition to any required unaudited interim financial statements with correspondingly reduced “Management’s Discussion and Analysis of Financial Condition and Results of Operations” disclosure; |
| • | reduced disclosure about our executive compensation arrangements; |
| • | no requirement that we solicit non-binding advisory votes on executive compensation or golden parachute arrangements; and |
| • | exemption from the auditor attestation requirement in the assessment of our internal control over financial reporting. |
CymaBay intends to take advantage of the reduced disclosure obligations. Section 107 of the JOBS Act also provides that an emerging growth company can take advantage of the extended transition period provided in the Securities Act of 1933 as amended, or the Securities Act, for complying with new or revised accounting standards. In other words, an emerging growth company can elect to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. CymaBay has elected to avail itself of this exemption to take advantage of the extended transition period for complying with new or revised accounting standards.
4
Table of Contents
CymaBay could remain an emerging growth company for up to five years, or until the earliest of (i) the last day of the first fiscal year in which CymaBay’s annual gross revenues exceed $1 billion, (ii) the date that CymaBay becomes a “large accelerated filer” as defined in Rule 12b-2 under the Securities Exchange Act of 1934, as amended, or the Exchange Act, which would occur if the market value of CymaBay’s common stock that are held by non-affiliates exceeds $700 million as of the last business day of CymaBay’s most recently completed second fiscal quarter, (iii) the date on which CymaBay has issued more than $1 billion in non-convertible debt during the preceding three-year period and (iv) the last day of the fiscal year following the fifth anniversary of the date of the first sale of our common equity securities pursuant to an effective registration statement under the Securities Act. At this time CymaBay expects to remain an “emerging growth company” for the foreseeable future.
CymaBay also will qualify as a “smaller reporting company” and thus have the advantage of not being required to provide the same level of disclosure as larger public companies.
CymaBay Strategy
Our goal is to become a leading biopharmaceutical company focused on developing and commercializing proprietary new medicines for metabolic diseases. Key elements of our strategy are to:
| �� | develop arhalofenate as a treatment for gout, including through a near-term Phase 2b study; |
| • | obtain U.S. Food and Drug Administration (FDA) approval for arhalofenate as a treatment for gout; |
| • | pursue partnerships to broadly commercialize arhalofenate; |
| • | develop our other product candidates subject to availability of resources; and |
| • | strengthen our patent portfolio and other means of protecting exclusivity. |
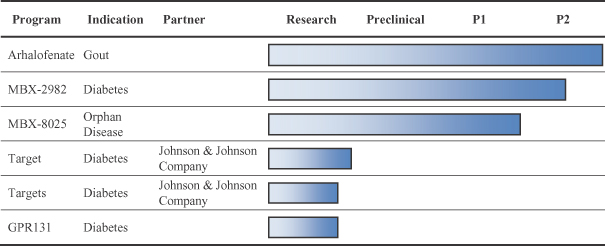
CymaBay Pipeline Overview
Our pipeline includes three unpartnered clinical stage programs and a number of partnered and unpartnered preclinical programs. Across this portfolio, a total of 21 clinical studies, including nine Phase 2 studies, have been completed. An investigational new drug application (IND) has been filed with the FDA for each clinical stage program. An IND for arhalofenate in gout was filed in April 2011. An IND for MBX-2982 in diabetes was filed in January 2008. The IND for MBX-8025 was filed by Johnson & Johnson Pharmaceutical Research & Development in July 2005 and transferred to CymaBay in March 2007.
5
Table of Contents
Arhalofenate—Gout
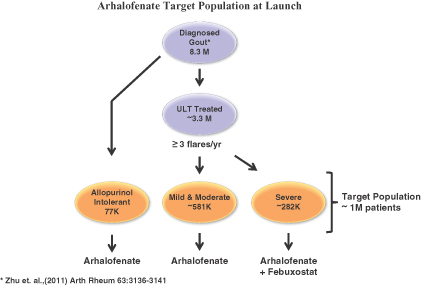
Gouty arthritis, or simply gout, is the most common form of inflammatory arthritis in men and affects more than 8 million people in the United States (U.S.) (Zhu et. al., 2011 Arth Rheum 63:3136-3141). The hallmark symptom of gout is a flare, characterized by debilitating pain, along with tenderness and inflammation of affected joints. Gout has a significant impact on patients’ quality of life and health care utilization. Patients experiencing gout flares miss an average of 4.6 more days of work per year than those without gout. Gout flares also result in increased health care utilization with approximately 35% of moderate and 50% of severe gout patients who experience a flare having at least one acute care visit per year.
Gout flares are recurring and excruciatingly painful episodes of joint inflammation that are triggered by the presence of monosodium urate (MSU) crystals. MSU crystals are formed when the concentration of uric acid in tissues exceeds its solubility limit, approximately 6.8 milligrams per deciliter (mg/dL). Elevated levels of circulating uric acid, or hyperuricemia, most commonly results from the under excretion of uric acid in the kidney. This is caused by its reabsorption from urine and transport back to the blood by specialized urate transporters/exchangers in the proximal renal tubule. Long term accumulation of MSU crystals in the body leads to the progression of gout with an increase in the frequency of flares, the involvement of multiple joints, the formation of visible masses of MSU crystals (tophi) and the debilitation that results from deformation of joints.
Many scientific surveys (Fuldeore, et. al., 2011 BMC Nephrology 12:36-44; Riedel, et. al, 2004 J Clin Rheumatol 10:308-314; Stamp, et. al. 2013 Rheumatology 52:34-44; Wu, et. al., 2012 Am J Therapeutics 19:e157-e166) and large clinical studies in gout (Rilonacept Briefing Package FDA Advisory Committee Meeting May 8, 2012; Febuxostat Briefing Package FDA Advisory Committee Meeting November 24, 2008) indicate that gout patients have a high incidence of cardiovascular and metabolic comorbidities, such as hypertension (50% or more), coronary artery disease (>35%), chronic kidney disease (~40%), and diabetes (~20%). Managing patients with these comorbidities is challenging because many of them are contraindicated in the medication currently used to treat gout. Examples include corticosteroids which can cause hypertension and worsening of dysglycemia and non-steroidal anti-inflammatory drugs (NSAIDs) which have renal toxicity.
Market Opportunity
Unmet Needs in the Treatment of Gout
Of the 8 million patients with gout in the U.S., we estimate that over 3 million are on urate lowering therapy (ULT) and of these patients on ULTs, about 1 million will continue to experience 3 or more flares per year, with significant impact to patient quality of life and the health care system. According to a 2012 study (Wu, et. al., 2012 Comorbidity Burden, Healthcare Resource Utilization, and Costs in Chronic Gout Patients Refractory to Conventional Urate Lowering Therapy Am J Therapeutics 19:e157-e166), patients having 3 or more flares per year typically incur $10,000 more in annual health care costs than patients without gout. In order to halt the progression of the disease and provide long term reduction in flares, MSU crystals must be eliminated from the body. Therefore, the two major goals of gout treatment are to prevent flares and lower sUA to below 6 mg/dL in order to dissolve MSU crystals from tissue. The most important limitation in achieving these goals is that all existing ULTs paradoxically cause an increase in flares upon initiation of treatment, leading many patients to discontinue or avoid therapy. Non-adherence to therapy is a significant problem. In one long term study, only about 40% of allopurinol patients reached the goal of sUA < 6 mg/dL (Febuxostat Briefing Package FDA Advisory Committee Meeting November 24, 2008). Failure to get to goal results in progression of the disease and continued flaring.
6
Table of Contents
Limitations of Current Therapies
Allopurinol and febuxostat (marketed by Takeda Pharmaceutical Company Limited as Uloric®), the most common drugs prescribed to lower sUA, substantially increase flares for up to 6 – 12 months following initiation of treatment (see figure from Takeda’s Phase 3 Febuxostat Versus Allopurinol Control Trial in Subjects with Gout (FACT) study below). The ULT-initiated flare phenomenon is common to all ULTs and leads to increased health care utilization and high patient discontinuation with progression of disease.
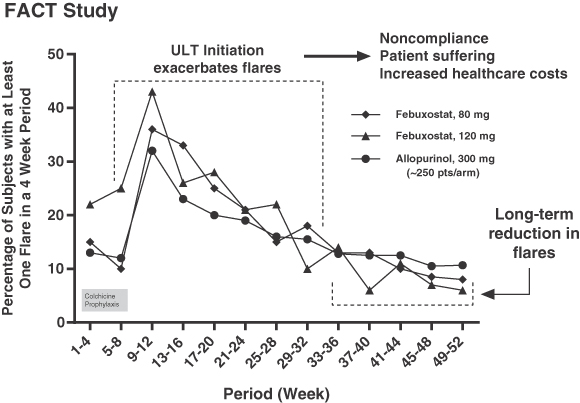
Becker, et. al., 2005 N Engl J Med. 353(23):2450-61.
To address the increase in flare rate associated with initiation of ULT therapy, anti-inflammatory drugs such as colchicine and NSAIDs are co-prescribed with ULTs. However, use of these agents carries a risk for causing adverse effects. Some known adverse effects of colchicine include diarrhea, nausea, vomiting, destruction of skeletal muscle, neuromuscular toxicity, and decreased blood cell production. Chronic use of NSAIDs, which only provide symptom relief, is associated with increased risk of renal toxicity, gastrointestinal (GI) bleeding and cardiovascular events. Similarly, steroids are linked to hypertension and a worsening of blood glucose, which is problematic for diabetics and patients with hypertension and/or heart disease, respectively. Given the prevalence of cardiovascular and metabolic comorbidities in gout patients, the use of these agents can be problematic in a significant number of gout patients.
Anti-Flare Competition
The largest selling branded gout drug in the U.S. is Colcrys® (branded colchicine), prescribed for the prevention and treatment of gout flares. Despite the availability of low cost generic NSAIDs and steroids, Takeda reported U.S. sales of $496 million for Colcrys in 2012 (Takeda Pharmaceutical Company Presentation, May 9, 2013) highlighting the importance of preventing and treating gout flares effectively. While colchicine has been shown to reduce the percentage of patients experiencing flares by 57% (Borstad, et. al., 2004 J Rheumatol 31:2429-2432), it carries significant limitations in terms of safety and tolerability.
7
Table of Contents
Emerging therapies for treating gout flares include the interleukin-1 beta (IL-1ß) neutralizing therapies rilonacept (Arcalyst®) and canakinumab (Ilaris®). These biologics, agents produced by biological rather than chemical processes, have demonstrated in well controlled clinical trials that this class can reduce ULT-initiated flares by up to ~80% (Rilonacept Briefing Package FDA Advisory Committee Meeting May 8, 2012). These agents have validated the blockade of IL-1ß as an approach to flare control. However, only Ilaris is approved for flares and it is administered by injection, has a high cost, and carries a warning for increased risk of serious infections. Ilaris is specifically indicated for the symptomatic treatment of adult patients with frequent gouty arthritis attacks (at least 3 attacks in the previous 12 months) for whom NSAIDs and colchicine are contraindicated, are not tolerated, or do not provide an adequate response, and for whom repeated courses of corticosteroids are not appropriate.
Serum Uric Acid Lowering Competition
Xanthine oxidase (XO) inhibitors (allopurinol and febuxostat) dominate the ULT market with generic allopurinol up to 300 mg accounting for about 90% of ULT prescriptions in the U.S. (Sarawate, et. al., 2006 Mayo Clin Proc 81:925-934). Allopurinol may potentially lead to undertreatment because of the occurrence of skin rash and a rare but serious hypersensitivity reaction which can be fatal. In addition, it must be used with caution in renally impaired patients (a common comorbidity in gout) and is recommended to undergo dose escalation. Febuxostat, approved by the Food and Drug Administration (FDA) in 2009 and marketed in the U.S. as Uloric, is the first new treatment approved for gout in more than 40 years. We estimate that its market penetration was 6.2% in 2012. Its wholesale price is approximately $7 per tablet compared to less than $1 per tablet for generic allopurinol.
Lesinurad is a drug in Phase 3 development, which was recently acquired by AstraZeneca PLC in its purchase of Ardea Biosciences, Inc. for $1.26 billion. Like arhalofenate, it lowers sUA by promoting the excretion of uric acid by the kidney. Lesinurad, like all other ULTs, increases flares upon initiation of treatment, whereas arhalofenate is expected to reduce flares. Lesinurad is being studied as an add-on treatment to allopurinol patients not reaching target sUA levels, as an add-on to febuxostat in tophaceous gout patients and as monotherapy (given as a single drug) for patients who are intolerant to XO inhibitors. The reported percentage of patients that achieve sUA < 6 mg/dL for the combination of lesinurad and allopurinol at 44 weeks was 78% (Ardea Study 203 Safety Extension 2012 Ann Rheum Dis 71(Suppl3):439) which is similar to the 74% reported for febuxostat at 80 mg in the FACT trial which was one of a similar duration and with a similar patient population.
While medically important, the case for sUA lowering alone is not sufficient to ensure success in the market because hyperuricemia is asymptomatic and patients usually seek treatment for their flares. This is evident by the modest sales of Uloric, which in spite of greater sUA reduction compared to the most common dose of generic allopurinol, has only generated about $216 million in 2012 sales (Takeda Pharmaceutical Company Presentation May 9, 2013). Lesinurad (in development by AstraZeneca), a novel uricosuric drug (a substance that increases the excretion of uric acid into the urine) intended to add to allopurinol in order to provide additional sUA lowering, has sUA lowering comparable to 80 mg Uloric.
Arhalofenate Addresses the Unmet Needs in Gout
CymaBay believes that a significant opportunity exists for arhalofenate as a result of its combined anti-flare and sUA lowering profile for the treatment of gout. It addresses key unmet needs by preventing flares and achieving sUA target goals as monotherapy. In patients who need additional sUA lowering, it can be combined with other ULTs to significantly reduce sUA without the induction of flares seen with all other ULTs.
CymaBay has undertaken an analysis of the gout market expected at the time of arhalofenate’s launch. Arhalofenate has dual pharmacology, whereas all of the gout drugs discussed above are limited to one of either anti-flare or sUA lowering. Given arhalofenate reduces and prevents flares while also lowering sUA, we believe it will be the preferred alternative for the approximately 1 million patients who flare 3 or more times per year despite being on ULT. The poor compliance of patients treated with existing ULTs also leads to more than
8
Table of Contents
1 million discontinuations and restarts of therapy every year. The cycling of patients on and off ULTs offers opportunities for physicians to prescribe arhalofenate for its many advantages over other therapies.
As a monotherapy, we believe arhalofenate will be a single, safe, easy-to-use replacement for the combination of allopurinol and Colcrys, which is the current standard of care.
For those patients needing additional sUA reduction, our clinical trial data have demonstrated that arhalofenate can be combined with febuxostat to provide large (~60%) reductions in sUA, but without the large increases in the incidence of flares seen with all other ULTs.
Arhalofenate Overview
Scientific Rationale
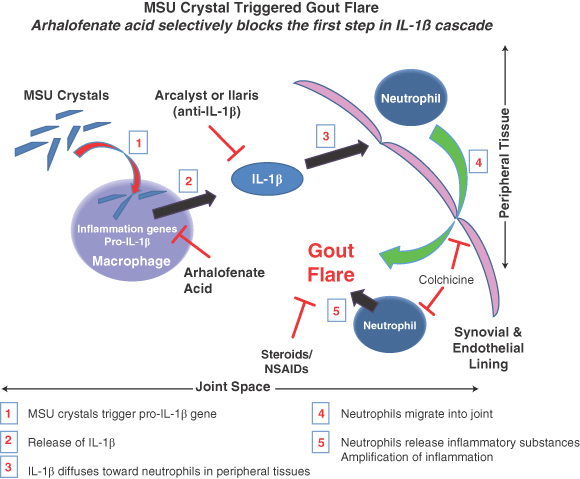
Arhalofenate is a prodrug which upon absorption is converted to its active form, arhalofenate acid. Arhalofenate acid’s dual actions are to block the MSU crystal-stimulated production of IL-1ß by macrophages (white blood cells that play an important role in the body’s defense against pathogens and foreign matter) in joints and to inhibit uric acid reabsorption by urate transporters in the kidney.
Anti-Inflammatory Activity
A simplified model of gouty inflammation which reflects many of the important features of the IL-1ß mediated inflammatory cascade, a sequence of biochemical events that produces inflammatory proteins, caused by MSU crystals is depicted below. Arhalofenate (through arhalofenate acid) is unique among available anti-inflammatory drugs because it prevents the initiation of the inflammatory cascade and acts upstream from other therapies. The anti-inflammatory action comes from a unique trans-repression (a type of inhibition) of peroxisome proliferator-activated receptor-gamma (PPARg) which blocks the production of IL-1ß and other inflammatory proteins by macrophages that produce a flare. Neutralization of IL-1ß has been shown in clinical trials to reduce flares by about 70%. Because arhalofenate acid acts upstream of colchicine, it may be able to replace colchicine.
9
Table of Contents
The anti-inflammatory mechanism of arhalofenate acid has been elucidated in preclinical models. In experiments with isolated macrophages, arhalofenate acid is able to suppress MSU crystal-stimulated release of IL-1ß protein by blocking expression of the precursor pro-IL-1ß gene. Importantly, this activity is seen at concentrations that are achieved in humans.
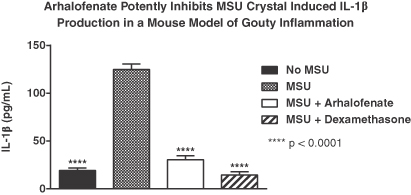
In vivo confirmation of this effect was seen in a mouse model of gouty inflammation. Injecting MSU crystals into mice produces many of the molecular and cellular steps involved in a gout flare. As shown below, administration of arhalofenate at doses that produce clinically relevant exposures was able to suppress the release of IL-1ß in response to MSU crystals to a degree similar to that of dexamethasone, a potent anti-inflammatory steroid drug. Importantly, it also suppresses other important inflammatory mediators that colchicine does not.
10
Table of Contents
This suggests arhalofenate could be superior to colchicine in being able to suppress additional inflammatory pathways caused by MSU crystals.
Uric Acid Lowering Activity
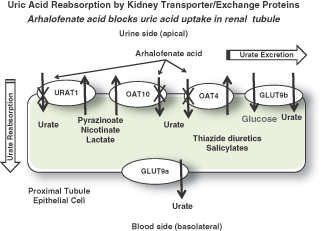
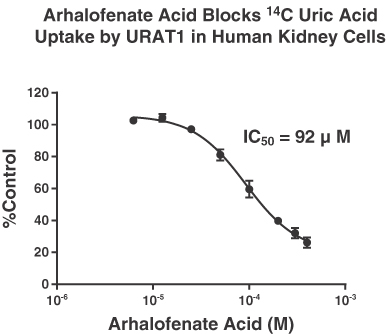
Uric acid is an anionic, or negatively charged, molecule that is removed from the body by filtration through the kidney into urine. For about 80-90% of patients, hyperuricemia is a result of under excretion of uric acid due to its reabsorption by organic anion transporters (OAT) in the proximal renal tubule. As depicted in the figure below, arhalofenate acid blocks 14C-uric acid uptake in an embryonic kidney cell line that expresses human urate transporter 1 (URAT1), one of the predominant renal transporters of urate. The inhibition is pharmacologically relevant because it occurs at concentrations that are less than those seen in human urine in clinical trials. Arhalofenate acid was shown to inhibit uric acid uptake by URAT1, OAT4 and OAT10, three of the transporters that play a critical role in uric acid reabsorption. The pattern of attenuation of uric acid transport is similar to that of other uricosuric drugs such as lesinurad. This mechanism is consistent with the clinical pharmacology in which arhalofenate was shown to dose-dependently increase urate clearance into urine in gout patients.
11
Table of Contents
The available preclinical evidence provides an explanation for the dual mode-of-action observed for arhalofenate in treating gout patients. CymaBay has completed three clinical studies in gout patients which have shown that arhalofenate has the potential for both decreasing the incidence, severity and duration of gout flares, including those that often occur upon initiation of ULT, and reducing sUA. This profile would seem well suited to the treatment of gout.
CymaBay has completed a robust nonclinical program for arhalofenate, including genotoxicity, chronic repeat dose toxicology in rats and monkeys, safety pharmacology, reproductive toxicology and 2-year rodent carcinogenicity studies. The results of these studies have all been submitted to the FDA.
CymaBay has developed a manufacturing process for arhalofenate and ~200 kg of drug substance is available to initiate the Phase 3 program. Tablets for the Phase 2b study have already been manufactured. Both the drug substance and tablet manufacturing processes will be scaled up to support the registration and commercial chemistry, manufacturing and controls program.
Clinical Studies with Arhalofenate
The Gout Development Program
Arhalofenate has been studied in three Phase 2 gout clinical trials including a monotherapy study, febuxostat combination study and an allopurinol combination study.
Monotherapy Study
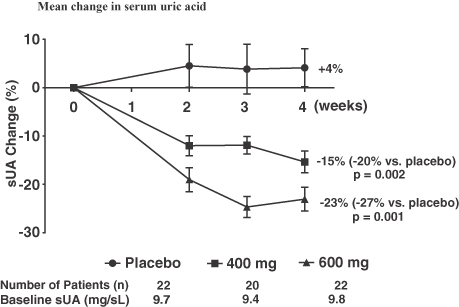
The monotherapy study was a randomized, double-blind, placebo-controlled study evaluating the safety and efficacy of arhalofenate for the treatment of hyperuricemia in patients with gout. Arhalofenate was given daily at doses of 400 mg and 600 mg for four weeks. A total of 64 patients completed the treatment phase: 22 received placebo, 20 received arhalofenate 400 mg, and 22 received arhalofenate 600 mg. All randomized patients also received colchicine 0.6 mg daily as flare prophylaxis, a preventive treatment for flares. Compared to placebo, patients treated with arhalofenate demonstrated dose-dependent reductions in gout flare and sUA, as shown
12
Table of Contents
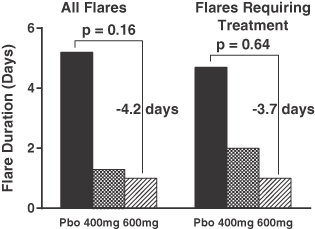
below. The proportion of patients reporting at least one flare during the treatment phase was 23% (5 of 22), 20% (4 of 20), and 5% (1 of 22) in the placebo, 400 mg, and 600 mg groups, respectively. In addition to flare frequency, both severity and duration of flare were less in arhalofenate-treated patients.

13
Table of Contents
Overall, adverse events (AEs) were similar among the placebo and arhalofenate-treated groups. There were no severe or serious AEs, discontinuations due to AEs, or deaths during the study. Overall, the types and frequencies of AEs were similar among patients receiving placebo or arhalofenate 400 mg or 600 mg and there were no clinically meaningful differences observed in safety laboratory test results.
Febuxostat Combination Study
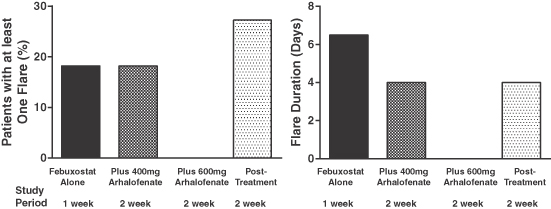
In the febuxostat combination study, arhalofenate up to 600 mg daily was added to febuxostat 80 mg in an open-label, in-patient study to determine the efficacy, safety, and tolerability of arhalofenate in combination with 80 mg febuxostat once daily. A total of 11 patients were dosed with 80 mg febuxostat during Week 1, 80 mg febuxostat plus 400 mg arhalofenate during Weeks 2-3 and 80 mg febuxostat plus 600 mg arhalofenate during Weeks 4-5. All patients also received 0.6 mg colchicine daily as prophylaxis for gout flare.
The proportion of these patients reporting at least one flare was 18% (2 of 11 patients) during Week 1 (febuxostat 80 mg) and 18% (2 of 11 patients) during Weeks 2-3 (febuxostat 80 mg plus arhalofenate 400 mg), respectively. No patient reported the initiation of a flare during Weeks 4-5 (febuxostat 80 mg plus arhalofenate 600 mg). The proportion of patients reporting at least one flare in the two-week follow-up period was 27% (3 of 11 patients).
14
Table of Contents
Mean sUA reductions were -48% at Day 8 (febuxostat 80 mg), -54% at Day 22 (febuxostat 80 mg plus arhalofenate 400 mg), and -60% at Day 36 (febuxostat 80 mg plus arhalofenate 600 mg). Historically, one week of dosing with febuxostat 80 mg has been shown to give the full effect of sUA reduction, and the mean reductions in this study at Day 8 are consistent with other reported study results. The proportion of patients who achieved various sUA target levels during treatment is shown below. Patients with advanced gout have large stores of MSU crystals in the body, and driving sUA levels to lower values (eg, < 4 mg/dL) has been shown with other ULTs to accelerate clinical benefits such as the reduction of tophi (masses of MSU crystals).

No patients experienced severe or serious AEs or deaths, and there were no discontinuations because of AEs. No clinically meaningful differences were observed among the study treatments in safety laboratory test results.
Allopurinol Combination Study
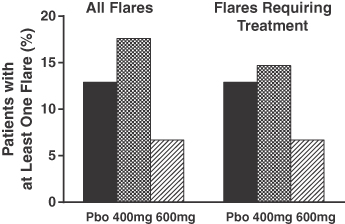
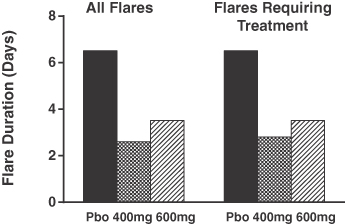
This study was a randomized, double-blind, placebo-controlled clinical trial designed to evaluate the efficacy, safety and tolerability of arhalofenate 400 mg and 600 mg when given in combination with allopurinol 300 mg and also to evaluate the effect of arhalofenate on the pharmacokinetics (PK, drug levels in the blood) of allopurinol and oxypurinol, the product of metabolism, or active metabolite, of allopurinol that forms in the body after ingestion of allopurinol. Arhalofenate (or placebo) was given once daily at doses of 400 mg and 600 mg, in addition to allopurinol 300 mg, for four weeks to patients who had failed to reach the sUA target of <6 mg/dL with allopurinol 300 mg. All randomized patients also received colchicine 0.6 mg daily as flare prophylaxis. A reduction in gout flares was observed in the arhalofenate plus allopurinol groups compared to the allopurinol only group. The proportion of patients in a pre-specified per protocol population reporting at least one flare during the 4-week treatment phase was 13% (4 of 31) in the allopurinol 300 mg only group, 18% (6 of 34) in the allopurinol 300 mg plus arhalofenate 400 mg group, and 7% (2 of 32) in the allopurinol 300 mg plus arhalofenate 600 mg group. The mean duration of flares was longer in the allopurinol plus placebo group (6.5 days) than in either the allopurinol plus 400 mg arhalofenate group (2.6 days) or the allopurinol plus 600 mg arhalofenate group (3.5 days).
There was no statistically significant difference in sUA reduction in the arhalofenate plus allopurinol groups compared to the allopurinol only group. In the per protocol population, the proportion of patients who reached a sUA target of <6 mg/dL at the end of the treatment phase was 35.5%, 52.9%, and 43.3% in the allopurinol plus placebo group, the allopurinol plus 400 mg arhalofenate group, and the allopurinol plus 600 mg arhalofenate group, respectively. The modest additional sUA reduction observed in the arhalofenate plus allopurinol groups in this study is attributable to an interaction in which arhalofenate reduces the concentration of oxypurinol, the active metabolite of allopurinol. Specifically, arhalofenate promotes the excretion of uric acid as well as
15
Table of Contents
oxypurinol given both are typically reabsorbed into the blood stream through the same renal transporters arhalofenate is responsible for blocking.
No severe or serious AEs were reported. Two patients discontinued from the study due to moderate AEs. Overall, the types and frequencies of AEs were similar among the treatment groups and there were no clinically meaningful differences observed among the study treatments in safety laboratory test results.
Prior Clinical Experience with Arhalofenate
Prior to the Phase 2 trials in gout described above, eight Phase 1 studies and four Phase 2 studies in type 2 diabetes mellitus (T2DM) were conducted with arhalofenate. In these studies a total of 873 subjects were studied. Daily treatment with arhalofenate up to 600 mg for up to 24 weeks in T2DM patients was found to be safe and well tolerated.
In these T2DM studies, daily treatment with arhalofenate up to 600 mg for up to 24 weeks in T2DM patients also showed improvements in glucose parameters (hemoglobin A1c [HbA1c] and fasting plasma glucose), as well as a lowering of serum triglycerides in patients with elevated levels at baseline. Arhalofenate was found to be safe and well tolerated with no meaningful treatment group differences in laboratory safety values and AEs including special interest AEs (edema, weight gain, and upper GI AEs), discontinuation due to AEs, serious AEs, and death. There were no reports of urinary tract stones in any of these studies.
16
Table of Contents
A pooled analysis of sUA data from these diabetes studies showed statistically significant dose dependent reductions from baseline in mean sUA with arhalofenate: +2% in the placebo group (n=252), -11% in the 200 mg group (n=125), -20% in the 400 mg group (n=174), and -27% in the 600 mg group (n=159); p<0.0001 for each active group vs. placebo comparison. A p-value is a statistical measure of the probability that the difference in two values could have occurred by chance. The smaller the p-value the greater the confidence that the results are significant. For example, in the preceding studies, there is less than a 0.01% probability that the difference between two values is due to chance and, conversely there is a 99.99% probability that the observed difference was not due to chance. Similar sUA reduction was observed in patients with mild to moderate renal impairment and without additional worsening of renal function. Comparable sUA reduction was also achieved with arhalofenate in patients on concomitant low-dose aspirin (up to 325 mg daily) and on diuretics (blood pressure lowering agents).
Conclusions of Arhalofenate’s Clinical Experience
Arhalofenate has been studied in a total of 15 clinical trials with nearly a thousand subjects. These include Phase 1 studies of safety, tolerability and PK, Phase 2 studies of blood glucose effects in diabetics, and Phase 2 studies of sUA and flare effects in gout patients. Arhalofenate has had a consistent pattern of good safety and tolerability. Despite having differing objectives across these studies, arhalofenate demonstrated comparable dose-dependent reductions in sUA.
In addition to its primary characteristics for reduction of flare incidence and duration and in sUA lowering, arhalofenate also has additional features which are important in the gout population. It has shown an ability to lower triglycerides in subsets of patients with elevated serum triglycerides and to improve blood glucose parameters in diabetics, which are common comorbidities in gout patients. In an exploratory analysis, it retained its ability to lower sUA in patients with impaired renal function, another highly prevalent comorbidity in gout patients. In addition, arhalofenate gave comparable reductions in sUA whether or not patients were on low dose aspirin or thiazide diuretic (first-line therapy for uncomplicated hypertension) therapies, these latter agents being known to exacerbate hyperuricemia and to sometimes trigger flares when their treatment is initiated.
In the treatment of over a hundred patients with hyperuricemia and a diagnosis of gout, arhalofenate was safe and well tolerated and produced a consistent reduction in flare incidence and duration and in lowering sUA whether administered alone or in combination with allopurinol 300 mg or febuxostat 80 mg. The time-course of reductions in sUA was gradual and favorable for those of a drug intended to treat gout in which rapid fluctuations in sUA levels are inadvisable. It was shown as a single agent to dose-dependently increase urate excretion and fractional urate clearance, establishing that its sUA mechanism is uricosuria (i.e., it is a uricosuric).
Future Clinical Development of Arhalofenate for Treatment of Gout
Planned Phase 2b Study
The goal of our planned Phase 2b study will be to investigate the full potential benefit of arhalofenate monotherapy with regard to flare prevention and sUA lowering in a more robust, longer trial. Importantly, we intend to investigate the benefits of two doses of arhalofenate monotherapy, including a higher dose than we studied in previous gout studies, without colchicine. The study includes the most common dose of allopurinol (300 mg) with and without colchicine for flare prophylaxis in order to assess treatment effects for sUA and flares against standard of care.
This randomized, double-blind, placebo-controlled Phase 2b study is designed to evaluate the efficacy of each of two dose levels of arhalofenate for the prevention of flares, without concomitant use of colchicine, and the reduction of sUA in approximately 225 gout patients with hyperuricemia and a history of frequent flares. Arhalofenate 600 mg and 800 mg will be administered once daily for up to 12 weeks. Allopurinol 300 mg once daily will also be included as an active control treatment.
In the multiple ascending dose study of healthy volunteers, a sUA reduction of 33% was observed from baseline following 8 days of arhalofenate 800 mg daily. A similar level of sUA lowering is expected in gout
17
Table of Contents
patients and would be comparable to the most commonly used dosages of marketed ULTs (e.g. allopurinol 300 mg or febuxostat 40 mg).
Based on seven completed Phase 2 studies, including three studies in gout patients with arhalofenate up to 600 mg daily for up to 24 weeks, it is expected that a 12-week study in gout patients with arhalofenate 600 mg and 800 mg should be safe and well tolerated.
The Phase 2b study is designed to be conducted to a research standard that would support the consideration of this trial, if positive, as a registration study. If this Phase 2b study is successful, an appropriate Phase 3 dose of arhalofenate will be selected based on efficacy, safety, and tolerability, and Phase 3 pivotal studies, similar in design and endpoints, will be initiated.
Phase 3 Gout Program
The details (design, size, duration, etc.) of the Phase 3 program will be the subject of discussion at an End-of-Phase 2 meeting with the FDA, and will be designed to support an indication for both arhalofenate monotherapy and combination treatment with febuxostat.
In order to support this indication, and the broad use of arhalofenate to both prevent flares and reduce sUA, the Phase 3 clinical program is currently planned to include two pivotal gout studies: one arhalofenate monotherapy study, and one study of arhalofenate in combination with febuxostat. These will both be randomized, double-blind studies, with appropriate controls and statistical power. The program will also include a single arm, open label safety study to accumulate additional longer term safety data needed for the New Drug Application (at least 100 patients dosed for 1 year). A small number of Phase 1 studies, including necessary drug-drug interaction studies, or special population studies, will also be conducted during Phase 3.
MBX-8025
MBX-8025 has potential therapeutic application for disorders linked to deficits in lipid storage, handling and utilization, many of which result in metabolic disorders. To date, it has been in development as a first-in-class treatment that effectively addresses all three lipid disorders associated with mixed dyslipidemia (abnormal lipid levels in the blood) as well as a majority of the cardiovascular risk factors that define metabolic syndrome. The future development program will focus on high unmet need indications in dyslipidemia as well as in high unmet need specialty and orphan diseases.
Scientific Rationale/Nonclinical Overview
MBX-8025 is a selective agonist (a substance that stimulates a response by binding to a receptor) for the peroxisome proliferator-activated receptor delta (PPARd), a nuclear receptor that regulates genes involved in lipid storage and transport (particularly in fatty acid oxidation) and insulin signaling and sensitivity. In preclinical studies in rodents, dogs and primates, MBX-8025 demonstrated a variety of beneficial effects on the lipid profile and other metabolic parameters. MBX-8025 treatment increased peripheral oxidation of fatty acids leading to reduced levels of triglycerides (TGs) and low-density lipoprotein (LDL), while raising high-density lipoprotein (HDL). MBX-8025 inhibited fat mass accumulation, resulting in attenuation of body weight gain in rodent models of obesity.
Three-month toxicology studies in rodents (alone and in combination with atorvastatin, the generic name of the cholesterol lowering drug Lipitor®) and in monkeys have been completed. In addition, the 2-year carcinogenicity studies in mice and rats have been completed. Johnson & Johnson Pharmaceutical Research & Development filed an IND for this compound with the FDA in July 2005 and subsequently transferred the application to CymaBay in March 2007.
The multiple beneficial actions of MBX-8025 support continued clinical development.
18
Table of Contents
Clinical Studies with MBX-8025
Five Phase 1 clinical studies and one Phase 2 clinical study with MBX-8025 have been completed. The 8-week Phase 2 study investigated MBX-8025 at doses of 50 or 100 mg/day in moderately obese patients with mixed dyslipidemia. The study demonstrated that treatment with MBX-8025 led to significant reductions in total LDL (~20%) and selective depletion of the small dense atherogenic (promotion of arterial plaque formation) LDL particles, resulting in an exceptional improvement in the LDL particle size profile. It also decreased TGs (~30%) and raised HDL (~12%). This unique combination of effects significantly decreased the atherogenic risk of patients’ lipid profile. When administered in combination with atorvastatin (Lipitor®), MBX-8025 provided a comprehensive improvement in all lipid and cardiovascular risk parameters without side effects seen in other combination lipid therapies. The beneficial effects demonstrated in the Phase 2 study have been published in the peer-reviewed journals Atherosclerosis and Journal of Clinical Endocrinology & Metabolism.
In addition, MBX-8025 addressed other aspects of metabolic syndrome, including improvements in insulin sensitivity and trends toward decreased waist circumference and body fat. Over half of the patients that entered the Phase 2 study meeting the criteria for metabolic syndrome no longer met the criteria at the end of the study. MBX-8025 demonstrated potent anti-inflammatory activity resulting in 43-72% reductions of high-sensitivity C-reactive protein. MBX-8025 also improved surrogate markers of liver health, suggesting the possibility that it may reduce abnormal fat accumulation in the liver. All of these effects provide potential benefits to patients in multiple high unmet need diseases.
Next Steps in Development
The pharmacological action of MBX-8025 has been established in the setting of mixed dyslipidemia, but because this indication does have other therapies available, its greatest benefit to patients is likely to be in orphan or other high unmet need indications. CymaBay is actively engaged in a selection process that involves using the scientific literature together with scientific experts and regulatory authorities to prioritize among the therapeutic opportunities that have a rational connection to PPARd’s role in human health and disease.
MBX-2982
Type 2 diabetes is a chronic debilitating disease characterized by a progressive loss of the normal control of glucose levels in the blood and other tissues. The normal handling by the body of sugar, fat and protein in the diet becomes deranged in diabetics through the loss of the ability by the body to appropriately regulate the secretion and action of key hormones such as insulin and glucagon. Chronic exposure of diabetics to elevated glucose levels (hyperglycemia) leads to loss of sensitivity of tissues to the action of insulin and to the eventual destruction of pancreatic islets, the body’s source of insulin. It also results over time in microvessel disease, a broad term in which the deterioration of the structure and function of peripheral vasculature results in diminished delivery of blood, oxygen and nutrients to tissue. The ultimate consequences of microvessel disease include increased risk for the deterioration of kidney function, for the possibility of infection and limb amputation, for the deterioration of peripheral nerves in limb extremities leading to chronic pain and loss of feeling with a heightened risk of unintended self-injury, and for the loss of function in the retina with diminished visual acuity including blindness. Another important consequence of chronic hyperglycemia is the strong association with increased cardiovascular and cerebrovascular disease including hypertension and atherosclerosis, which are associated with untoward consequences that include angina, myocardial infarction, heart failure, and stroke. An assessment by the U.S. CDC (2011 National Diabetes Fact Sheet) reported that heart disease (68%) and stroke (15%) are commonly listed on diabetes-related death certificates among people 65 or older.
According to the International Diabetes Federation (IDF), approximately 371 million people, over 8% of the world’s population, had diabetes in 2012. In North America, IDF estimated that 10.5% of the adult population (38 million) have diabetes of which 29% are undiagnosed. The American Diabetes Association (ADA) concluded that in 2011 there were 79 million Americans with pre-diabetic state of impaired glucose tolerance. Cost
19
Table of Contents
estimates (IDF, 2012) are that the 24 million diabetics in the U.S. spend on average $8,478 while the ADA states that 12% of national pharmacy costs are for drugs and diabetic supplies.
There are several established and emerging classes of drug therapies for diabetes. In the end stage of the disease, patients become dependent on various forms of injectable insulin to manage their blood glucose. A major goal of the development of oral anti–diabetic drugs is to regulate glucose without the risk for hypoglycemia (potentially life threatening) and/or cause an increase in other cardiovascular risk factors such as weight gain or hypertension. Diabetes is managed with a combination of diet, exercise and other lifestyle changes, and when glucose is inadequately controlled, metformin (generic) is the most-common first-line therapy. Other common oral anti-diabetics include the insulin sensitizer pioglitizone and dipeptidyl peptidase-4 inhibitors that include sitagliptin. Older drugs such as sulfonylureas are still widely used, but less so in developed countries due to their increased risk for hypoglycemia and the lack of durability in response for many patients. It is quite common for patients to take more than one class of drugs in order to get to the goal of reducing HbA1c, an integrated laboratory marker of blood glucose levels, to below 7%.
Canagliflozin is the first of a new class of drugs called the inhibitors of the sodium glucose co-transporter 2 (SGLT2). This drug promotes excretion of glucose into urine by preventing its reabsorption in the kidney thereby lowering blood glucose. It has a secondary benefit of providing weight loss.
Over the last decade, injectable drugs have emerged as competing drugs with significant benefits in glucose control as well as effects on weight loss and the potential to protect the pancreas from the damage wrought by the progression of diabetes. These drugs are primarily analogs of the natural hormone glucagon-like 1 peptide (GLP-1), and include exenatide, liraglitide and lixisenatide among others. These drugs are given by subcutaneous injection once or twice daily. Their action is to provide glucose-regulated insulin secretion with weight loss and the potential to preserve function of pancreatic islets. New members of this class with once weekly to once monthly dose schedules have been approved or are in late stage development. In spite of the variety of drugs available for the treatment of diabetes, the medications used to manage diabetes have not led to optimal control of hyperglycemia and many are associated with dose-limiting side effects. MBX-2982 is an oral, G-protein coupled receptor (GPR119) agonist being evaluated as a novel therapeutic agent for patients with T2DM, with a dual mechanism including direct effects and indirect effects mediated by gastrointestinal hormones known as incretins on glucose-dependent insulin secretion, as well as potentially beneficial effects on islet health.
GPR119 is expressed in pancreatic islet cells and gastrointestinal hormone secreting cells (enteroendocrine cells). Activation of GPR119 in pancreatic ß-islets either by natural (endogenous) substances or by drugs developed to interact with it (GPR119 agonists) results in direct stimulation of glucose-dependent insulin secretion in vitro. Activation of GPR119 in intestinal enteroendocrine cells either by endogenous substances or by GPR119 agonists results in stimulation of glucagon-like peptide 1 (GLP-1) and gastrointestinal inhibitory peptide release, and subsequent enhanced glucose-dependent insulin secretion and suppression of glucagon, leading to improved acute glucose tolerance, both in vitro and in vivo. MBX-2982 was synthesized and screened as a GPR119 agonist, and is capable of activating endogenous GPR119 in a cell line over-expressing the receptor. MBX-2982 has been shown to increase glucose-dependent insulin secretion in both in vitro and in animal models. MBX-2982 also increases incretin hormone levels in animals, which may contribute to its glucose lowering effects.
Nonclinical studies show that MBX-2982 has desirable effects on blood glucose levels, and this effect is additive to the effect of the dipeptidyl peptidase-4 (DPP-4) inhibitor, sitagliptin. Based on these results, there may be an important role for MBX-2982 as a novel therapeutic agent in the treatment of T2DM, alone or in combination with other anti-diabetic agents, including the DPP-4 inhibitors. Presently, there are no other agents approved in the U.S. within this pharmacologic class for the treatment of T2DM.
Extensive preclinical toxicological (up to 6 months in rats and dogs) have been completed, and PK profiling of MBX-2982 has shown low potential for safety risk. We filed an IND for MBX-2982 with the FDA in January 2008.
20
Table of Contents
Clinical Studies with MBX-2982
Four Phase 1 clinical studies and one Phase 2 clinical study with MBX-2982 have been completed and the safety and PK review showed no safety or tolerability concerns with MBX-2982 administered in escalating doses (25, 100, and 300 mg/day) tested for up to 4 weeks of dosing. A four-week study in type 2 diabetics can be summarized as follows:
| • | MBX-2982 generally lowered mean weighted glucose and post-meal glucose during an extended mixed-meal tolerance test (MMTT), although not always to a statistically significant degree and not to the extent of sitagliptin. The effect at the 300 mg dose may have been mitigated by the inclusion of a very small number of patients who experienced extreme worsening of glucose to the degree of being statistical outliers. Decreases in fasting glucose were generally not observed with MBX-2982. |
| • | Four weeks of treatment with MBX-2982 tended to increase insulin, active GLP-1, and total GLP-1 during an extended MMTT. Decreases in glucagon were not as consistently observed. Changes in active GLP-1 were not as robust as those observed with sitagliptin. Four weeks of treatment with MBX-2982 also tended to increase fasting insulin and c-peptide, and decrease fasting triglycerides. |
| • | Overall, the data suggest that MBX-2982 may decrease glucose, potentially through effects on GLP-1, glucagon, and insulin. Changes in HbA1c are difficult to assess over a 4-week treatment period, but trended in the downward direction. Glucose-lowering effects and mechanism of action will need to be explored more robustly in longer duration trials of MBX-2982. |
| • | The PK results observed in this study are similar to those seen in the completed Phase 1 study that used the same formulation, demonstrating dose-dependent increases in drug exposure and a profile supporting once daily oral dosing. |
| • | MBX-2982 at doses of 25, 100, and 300 mg was safe and well tolerated. |
Based on these results, further testing with MBX-2982 in combination with sitagliptin and/or metformin for the treatment of diabetes is warranted.
Future Clinical Development of MBX-2982: Summary and Conclusions
A proof-of-concept study has been designed to determine the effects of MBX-2982 on fasting and post-challenge blood glucose in patients with T2DM either as dual therapy in combination with either metformin or sitagliptin, or as triple therapy in combination with metformin and sitagliptin. Secondary goals would be to determine the effects of MBX-2982 on islet beta-cell function as assessed using a MMTT and a graded glucose infusion, and to determine the effects of MBX-2982 on circulating levels of GLP-1.
The study design is a double-blind, randomized, placebo-controlled, parallel group study enrolling approximately 75 patients in order to ensure 64 completers for the 14-day treatment period. Subjects will be type 2 diabetics treated with medical nutritional therapy alone for > 2 weeks, and either treatment naïve or washed off of metformin or sulfonylurea. Other criteria are typical for diabetics in a study of this type. Successful achievement of study goals would position the drug for a Phase 2b study, followed by a Phase 3 program.
CymaBay does not anticipate conducting this study until a suitable partner is found to contribute funding or resources for the project, or until sometime in the future when the goals and capital needs of arhalofenate are fully met.
Preclinical Programs
The most advanced preclinical program is one developing agonists of the GPR131 receptor, also known as TGR5 or the bile acid receptor. GPR131 agonists have utility in the treatment of T2DM by acting as an oral therapy that causes GLP-1 secretion with clinical features that mimic those of the injectable drug liraglutide (Victoza®). In preclinical models it causes potent release of GLP-1 that is amplified by co-treatment with
21
Table of Contents
sitagliptin. It has the potential to stimulate fat-restricted energy metabolism. Among its features supported by its scientific rationale are the potential for anti-inflammatory activity with insulin sensitization effects, and robust glucose control with no hypoglycemia, favorable weight effects, and improvement in beta cell function.
CymaBay has discovered three novel chemical series from which it has prepared more than 750 compounds with leads possessing good pharmaceutical properties. Two patent applications are pending. The compounds have demonstrated robust in vivo GLP-1 secretion and glucose lowering activities. The next step in the lead optimization phase is to improve their metabolic stability and other key drug-like features, as well as to document their effects in combination with sitagliptin (or other DPP-4 inhibitors).
CymaBay is seeking a partner to assume further development of the lead chemical series leading to the identification of a clinical candidate in order to establish proof-of-pharmacology in humans.
License Agreements and Intellectual Property
General
CymaBay actively seeks to obtain, where appropriate, patent protection and regulatory exclusivity for the proprietary technology that it considers important to its business, including compounds, compositions and formulations, their methods of use and processes for their manufacture both in the United States and other countries. CymaBay also relies on trade secrets, know-how, continuing technological innovation and in-licensing to develop and maintain its proprietary position. Our success depends in part on our ability to obtain, maintain and enforce proprietary protection for our product candidates, technology and know–how, to operate without infringing the proprietary rights of others, and to exclude others from infringing our proprietary rights. However, patent protection may not afford CymaBay complete protection against competitors who seek to circumvent CymaBay’s patents.
CymaBay also depends upon the skills, knowledge, experience and know-how of its management, research and development personnel, as well as that of its advisors, consultants and other contractors. To help protect its proprietary know-how, which is not patentable, and for inventions for which patents may be difficult to enforce, CymaBay currently relies and will in the future rely on trade secret protection and confidentiality agreements to protect its interests. To this end, CymaBay requires all of its employees, consultants, advisors and other contractors to enter into confidentiality agreements that prohibit the disclosure of confidential information and, where applicable, require disclosure and assignment to it of the ideas, developments, discoveries and inventions important to its business.
Collaborations and Licensing Agreements
CymaBay has entered into various arrangements with licensors and licensees. The current collaborations are summarized below.
Ortho: In August 2006, CymaBay entered into a strategic alliance with Ortho-McNeil, Inc., a Johnson & Johnson Company. As part of the alliance, Janssen Pharmaceutical NV, an affiliate of Ortho-McNeil, granted to CymaBay an exclusive worldwide, royalty-bearing license to MBX-8025 and certain other PPARd compounds (the “PPARd Products”) with the right to grant sublicenses to third parties to make, use and sell such PPARd Products. Under the terms of the agreement, CymaBay has full control and responsibility over the research, development and registration of any PPARd Products and is required to use diligent efforts to conduct all such activities. Janssen has the sole responsibility for the preparation, filing, prosecution, maintenance of, and defense of the patents with respect to, the PPARd Products. Janssen has a right of first negotiation under the agreement to license a particular PPARd Product from CymaBay in the event that CymaBay elects to seek a third party corporate partner for the research, development, promotion, and/or commercialization of such PPARd Products. Under the terms of the agreement Janssen is entitled to receive up to an 8% royalty on sales of PPARd Products. Under the terms of the agreement, if CymaBay does not expend more than a de minimus amount of effort and resources on the research and/or development of at least one PPARd product, such action would constitute a
22
Table of Contents
default under the agreement. In addition, if CymaBay fails to make any payment called for under the agreement, discloses any non-exempt confidential information related to the agreement, or fails to use diligent efforts to promote, market and sell any PPARd product under the agreement, such action would constitute a default under the agreement. In the event of such default, or upon CymaBay’s termination of the agreement, CymaBay shall grant Janssen a worldwide, exclusive, irrevocable license under the agreement in all information that is controlled, developed or acquired by CymaBay which relate to a PPARd compound or PPARd product and in all patents that are filed during the term of the agreement with a priority date after the effective date of the agreement and relate to a PPARd compound or PPARd product.
In June 2010, CymaBay entered into two development and license agreements with Ortho-McNeil-Janssen Pharmaceuticals, Inc. (OMJPI) to further develop and discover undisclosed metabolic disease target agonists for the treatment of T2DM and other disorders and received a one-time nonrefundable technology access fee related to the agreements. CymaBay is also eligible to receive up to $330 million in contingent payments if certain development and commercial events are achieved as well as royalties on worldwide product sales. No such payments have been made to date. Under the terms of the agreements, OMJPI has full control and responsibility over the research, development and registration of any products developed and/or discovered from the metabolic disease targets and is required to use diligent efforts to conduct all such activities. A joint steering committee with equal representation from each party will oversee the development of products. Following June 2012, all decisions of the joint steering committee will be made by OMJPI. CymaBay has the sole responsibility, for the preparation, filing, prosecution, maintenance of, and defense of the CymaBay patents with respect to, metabolic disease target agonists. Under the terms of the agreements, if CymaBay discloses any non-exempt confidential information related to the agreements, such action would constitute a default under the agreements. In addition, if CymaBay breaches any of its representations or warranties under the agreements, such action would constitute a default. In the event of a default, the agreements do not provide that CymaBay will lose any of its rights to the intellectual property developed under the agreement.
DiaTex: On June 30, 1998, we entered into a License and Development Agreement with DiaTex, Inc. Under the agreement, DiaTex granted us an exclusive license to develop and commercialize therapeutic products containing halofenate its enantiomers (mirror images, including arhalofenate), derivatives, and analogs (the licensed products) for the treatment of diseases. Under terms of the agreement, DiaTex will work cooperatively and assist us in conducting a program for the research and development of halofenate and its enantiomers including the right to sublicense, to use and to practice all patents controlled by DiaTex that claim halofenate and its enantiomers, and all information, data, know-how, trade secrets, inventions, developments, results, techniques and materials, whether or not patentable, that are necessary or useful towards such commercialization. Under the agreement, we are obligated to use diligent efforts to conduct preclinical and clinical testing of halofenate and its enantiomers in order to determine its efficacy for use in the treatment or prevention of human diseases or conditions. On April 15, 1999 the agreement was amended by the parties to allow DiaTex to transfer to us their interest in an IND application that they filed with the FDA. The amendment also provided for DiaTex to indemnify us against any and all losses resulting or arising from any third party claims, actions or proceedings under the IND application, any negligent or wrongful acts or omissions of DiaTex in connection with the IND application, and any misrepresentations by DiaTex relating to the license agreement. Under the amendment, we will provide the same indemnifications to DiaTex with respect to any third party claims, actions, or proceedings in connection with negligent or wrongful conduct of clinical trials relating to the license agreement, provided the claims are not related to negligent or wrongful acts or omissions committed by DiaTex.
The license agreement contains a $2,000 per month license fee as well as a requirement to make additional payments for development achievements and royalty payments on any sales of licensed products. DiaTex is entitled to up to $0.8 million for the future development of arhalofenate, as well as a 2% royalty payment on any sales of products containing arhalofenate. A $50,000 milestone payment was made in May 2005 but no other milestone or royalty payments have been made since then. The agreement will expire upon the expiration of the last of DiaTex’s patents related to the license granted, or, if later, the expiration of all payment obligations under the agreement. The agreement may also terminate upon a material breach by DiaTex or us, if written notice of
23
Table of Contents
such breach is delivered to the breaching party, and the breaching party has not (i) cured the breach or (ii) initiated good faith efforts to cure the breach within a specified time period. Under the terms of the agreement, if we fail to use diligent efforts to conduct preclinical and clinical testing of halofenate and its enantiomers to determine its efficacy for use in the treatment or prevention of human diseases or conditions, fail to make any payment called for under the agreement, or disclose non-exempt confidential information under the agreement, such action would constitute a material breach under the agreement. In addition, if we fail to execute all instruments and assignments or fail to take any action to effect joint ownership of any enantiomer patent with DiaTex, such action would constitute a material breach under the agreement. We may terminate the agreement at any time if we determine we are no longer interested in DiaTex’s license grant, provided we provide sufficient written notice within a specified time period.
Intellectual Property
CymaBay owns a total of 37 United States patents, 124 foreign patents, as well as 17 United States patent applications and 178 foreign and Patent Cooperation Treaty applications which are counterparts to certain United States patents and patent applications. In addition, we license from third parties a total of 3 United States patents and 1 United States patent application, 60 foreign patents and 9 foreign and Patent Cooperation Treaty applications which are counterparts to certain United States patents and patent applications. These patents and patent applications include claims covering various aspects of our product pipeline and research and development strategies, including: arhalofenate crystal forms, methods of use both alone and in combination with other drugs and methods of manufacture, certain PPAR delta agonists, their compositions and uses, certain GPR119 agonist compositions and uses and undisclosed metabolic disease target agonist compositions and uses.
Patent and trade secret protection is critical to our business. Our success will depend in large part on our ability to obtain, maintain, defend and enforce patents and other intellectual property to extend the life of patents covering our product candidates, to preserve trade secrets and proprietary know-how, and to operate without infringing the patents and proprietary rights of third parties we actively seek patent protection in the U.S.
Arhalofenate
The patent portfolio on arhalofenate (MBX-102) includes 13 issued U.S. and 107 foreign patents and 8 pending U.S. and 38 foreign patent applications covering crystal forms of the chemical compound, methods of treating hyperuricemia, methods of treating and preventing flares and other methods of using the compound, and methods of manufacture. Patent term expiration 2019-2028.
MBX-2982
The patent portfolio on MBX-2982 and second generation compounds includes 5 issued U.S. and 5 foreign patents and 6 pending U.S. and 44 foreign patent applications covering chemical compositions, crystal forms of the chemical compound, methods of treating diabetes, methods of treating diabetes in combination with other drugs, formulation and methods of manufacture. Patent term expiration 2027-2031.
MBX-8025
The patent portfolio on MBX-8025 and second generation compounds includes 3 issued U.S. and 60 foreign patents and 2 pending U.S. and 19 foreign patent applications covering chemical compositions, salt forms of the chemical compound and methods of treating dyslipidemia. Patent term expiration 2024-2026.
Manufacturing
CymaBay does not currently own or operate manufacturing facilities for the production or testing of arhalofenate or other product candidates that it develops, nor does it have plans to develop its own manufacturing operations in the foreseeable future. CymaBay presently depends on third party contract manufacturers to obtain
24
Table of Contents
all of its required raw materials, Active Pharmaceutical Ingredients (APIs) and finished products for its clinical studies for arhalofenate. CymaBay has executed manufacturing agreements for its API and tablet supplies of arhalofenate with established manufacturing firms which are responsible for sourcing and obtaining the raw materials necessary for the finished products. The raw materials necessary to manufacture the API for arhalofenate, MBX-8025 and MBX-2982 are available from more than one source and CymaBay has also executed manufacturing agreements for the APIs and products for MBX-8025 and MBX-2982.
Siegfried AG
On April 30, 2012, CymaBay entered into a Development and Clinical Manufacture Agreement with Siegfried AG for the manufacturing of the API necessary for the tablet form of arhalofenate. Under the agreement, CymaBay shall deliver or Siegfried shall obtain the raw materials necessary for the API. CymaBay owns the rights, title and interest to the deliverables and intellectual property covering the deliverables generated under the agreement and under certain circumstances. Siegfried shall grant a non-exclusive license to CymaBay to use Siegfried intellectual property to exploit any product or service based or derived from the deliverables under the agreement. Both Siegfried and CymaBay have agreed to indemnify the other party with respect to losses due to the breach of a covenant or obligation under the agreement or the gross negligence, recklessness or intentional misconduct of the other party. CymaBay may terminate the agreement at anytime with written notice and Siegfried may terminate the agreement in the event CymaBay discontinues its activities related to the development or commercialization of the API for arhalofenate. In addition, either party may terminate the agreement at any time for material breach under the agreement or in the case of insolvency of the other party.
Patheon Inc.
On June 5, 2012, CymaBay entered into a Development and Clinical Manufacture Agreement with Patheon Inc. for the manufacturing of the tablet form of arhalofenate. Under the agreement, CymaBay shall deliver the API or Patheon shall obtain the API from a qualified vendor. CymaBay owns the rights, title and interest to the deliverables and intellectual property generated by Patheon in connection with the performance of the services for CymaBay under the agreement. Both Patheon and CymaBay have agreed to indemnify the other party with respect to losses due to the breach of a covenant or obligation under the agreement or the gross negligence, recklessness or intentional misconduct of the other party. CymaBay may terminate the agreement at anytime with written notice provided however that CymaBay terminates the agreement within certain times in advance of the start date of certain services. In addition, either party may terminate the agreement at any time for material breach under the agreement.
Metrics Inc.
On October 31, 2006, CymaBay entered into a Standard Development Agreement with Metrics, Inc. Under the agreement, Metrics will provide CymaBay with pharmaceutical development, formulation and analytical services in consideration of which CymaBay will provide appropriate compensation as outlined in the agreement. CymaBay owns the rights, title and interest to the intellectual property relating to all pharmaceutical products developed or manufactured for CymaBay by Metrics, as well as any active pharmaceutical ingredient provided to Metrics by CymaBay. CymaBay has agreed to indemnify Metrics against third party claims that involve the breach by CymaBay of any of its obligations, warranties or representations under the agreement, and Metrics has agreed to indemnify CymaBay against third party claims that involve (i) the negligence, gross negligence, or intentional misconduct on the part of Metrics, (ii) a failure by Metrics to comply with the law in their performance of the agreement, or (iii) a breach of Metrics’ obligations, covenants, representations, or warranties under the agreement. Either party may terminate the agreement at any time with advance written notice.
Research & Development Costs
Research and development costs for the six months ended June 30, 2013 and 2012, and years ended December 31, 2012 and 2011 were $2.5 million, $5.3 million, $9.3 million and $14.4 million, respectively.
25
Table of Contents
Government Regulation and Product Approval
Government authorities in the United States, at the federal, state and local level, and other countries extensively regulate, among other things, the research, development, testing, manufacture, quality control, approval, labeling, packaging, storage, record-keeping, promotion, advertising, distribution, post-approval monitoring and reporting, marketing and export and import of products such as those CymaBay is developing. The pharmaceutical drug product candidates that CymaBay develops must be approved by the Food and Drug Administration (FDA) before they may be legally marketed in the United States.
United States Pharmaceutical Product Development Process
In the United States, the FDA regulates pharmaceutical products under the Federal Food, Drug and Cosmetic Act, and implementing regulations. Pharmaceutical products are also subject to other federal, state and local statutes and regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable United States requirements at any time during the product development process, approval process or after approval, may subject an applicant to administrative or judicial sanctions. FDA sanctions could include refusal to approve pending applications, withdrawal of an approval, a clinical hold, warning letters, product recalls, product seizures, total or partial suspension of production or distribution injunctions, fines, refusals of government contracts, restitution, disgorgement or civil or criminal penalties. Any agency or judicial enforcement action could have a material adverse effect on CymaBay. The process required by the FDA before a non-biological pharmaceutical product may be marketed in the United States generally involves the following:
| • | Completion of preclinical laboratory tests, animal studies and formulation studies according to Good Laboratory Practices (GLP) or other applicable regulations; |
| • | Submission to the FDA of an Investigational New Drug application (IND), which must become effective before human clinical studies may begin; |
| • | Performance of adequate and well-controlled human clinical studies according to the FDA’s current Good Clinical Practices (GCP), to establish the safety and efficacy of the proposed pharmaceutical product for its intended use; |
| • | Submission to the FDA of a New Drug Application (NDA) for a new pharmaceutical product; |
| • | Satisfactory completion of an FDA inspection of the manufacturing facility or facilities where the pharmaceutical product is produced to assess compliance with the FDA’s current Good Manufacturing Practice standards (cGMP), to assure that the facilities, methods and controls are adequate to preserve the pharmaceutical product’s identity, strength, quality and purity; |
| • | Potential FDA audit of the preclinical and clinical study sites that generated the data in support of the NDA; and |
| • | FDA review and approval of the NDA. |
The lengthy process of seeking required approvals and the continuing need for compliance with applicable statutes and regulations require the expenditure of substantial resources and approvals are inherently uncertain.
Before testing any compounds with potential therapeutic value in humans, the pharmaceutical product candidate enters the preclinical testing stage. Preclinical tests include laboratory evaluations of product chemistry, toxicity and formulation, as well as animal studies to assess the potential safety and activity of the pharmaceutical product candidate. These early proof-of-principle studies are done using sound scientific procedures and thorough documentation. The conduct of the single and repeat dose toxicology and toxicokinetic studies in animals must comply with federal regulations and requirements including Good Laboratory Practices. The sponsor must submit the results of the preclinical tests, together with manufacturing information, analytical data, any available clinical data or literature and a proposed clinical protocol, to the FDA as part of the IND. The
26
Table of Contents
IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA has concerns and notifies the sponsor. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical study can begin. If resolution cannot be reached within the 30-day review period, either the FDA places the IND on clinical hold or the sponsor withdraws the application. The FDA may also impose clinical holds on a pharmaceutical product candidate at any time before or during clinical studies due to safety concerns or non-compliance. Accordingly, CymaBay cannot be sure that submission of an IND will result in the FDA allowing clinical studies to begin, or that, once begun, issues will not arise that suspend or terminate such clinical study.
During the development of a new drug, sponsors are given opportunities to meet with the FDA at certain points. These points may be prior to submission of an IND, at the end of Phase 2, and before an NDA is submitted. Meetings at other times may be requested. These meetings can provide an opportunity for the sponsor to share information about the data gathered to date, for the FDA to provide advice, and for the sponsor and FDA to reach agreement on the next phase of development. Sponsors typically use the End-of-Phase 2 meeting to discuss their Phase 2 clinical results and present their plans for the pivotal Phase 3 clinical trial that they believe will support approval of the new drug. If this type of discussion occurred, a sponsor may be able to request a Special Protocol Assessment, or SPA, the purpose of which is to reach agreement with the FDA on the design of the Phase 3 clinical trial protocol design and analysis that will form the primary basis of an efficacy claim.
According to FDA guidance for industry on the SPA process, a sponsor which meets the prerequisites may make a specific request for a SPA and provide information regarding the design and size of the proposed clinical trial. The FDA is supposed to evaluate the protocol within 45 days of the request to assess whether the proposed trial is adequate, and that evaluation may result in discussions and a request for additional information. A SPA request must be made before the proposed trial begins, and all open issues must be resolved before the trial begins. If a written agreement is reached, it will be documented and made part of the record. The agreement will be binding on the FDA and may not be changed by the sponsor or the FDA after the trial begins except with the written agreement of the sponsor and the FDA or if the FDA determines that a substantial scientific issue essential to determining the safety or efficacy of the drug was identified after the testing began.
Clinical studies involve the administration of the pharmaceutical product candidate to healthy volunteers or patients under the supervision of qualified investigators, generally physicians not employed by or under the clinical study sponsor’s control. Clinical studies are conducted under protocols detailing, among other things, the objectives of the clinical study, dosing procedures, subject selection and exclusion criteria, how the results will be analyzed and presented and the parameters to be used to monitor subject safety. Each protocol must be submitted to the FDA as part of the IND. Clinical studies must be conducted in accordance with GCP. Further, each clinical study must be reviewed and approved by an independent institutional review board (IRB) at, or servicing, each institution at which the clinical study will be conducted. An IRB is charged with protecting the welfare and rights of study participants and considers such items as whether the risks to individuals participating in the clinical studies are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the informed consent form that must be provided to each clinical study subject or his or her legal representative and must monitor the clinical study until completed.
Human clinical studies are typically conducted in three sequential phases that may overlap or be combined:
| • | Phase 1. The pharmaceutical product is initially introduced into healthy human subjects and tested for safety, dosage tolerance, absorption, metabolism, distribution and excretion. |
| • | Phase 2. The pharmaceutical product is evaluated in a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases, to determine dosage tolerance, optimal dosage and dosing schedule and to identify patient populations with specific characteristics where the pharmaceutical product may be more effective. |
| • | Phase 3. Clinical studies are undertaken to further evaluate dosage, clinical efficacy and safety in an expanded patient population at geographically dispersed clinical study sites. These clinical studies are intended to establish the overall risk/benefit ratio of the product and provide an adequate basis for product labeling. The studies must be well-controlled and usually include a control arm for |
27
Table of Contents
comparison. One or two Phase 3 studies are required by the FDA for an NDA approval, depending on the disease severity and other available treatment options. |
| • | Post-approval studies, or Phase 4 clinical studies, may be conducted after initial marketing approval. These studies are used to gain additional experience from the treatment of patients in the intended therapeutic indication. |
| • | Progress reports detailing the results of the clinical studies must be submitted at least annually to the FDA and written IND safety reports must be submitted to the FDA and the investigators for serious and unexpected adverse events or any finding from tests in laboratory animals that suggests a significant risk for human subjects. Phase 1, Phase 2 and Phase 3 clinical studies may not be completed successfully within any specified period, if at all. The FDA or the sponsor or its data safety monitoring board may suspend a clinical study at any time on various grounds, including a finding that the research subjects or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical study at its institution if the clinical study is not being conducted in accordance with the IRB’s requirements or if the pharmaceutical product has been associated with unexpected serious harm to patients. |
Concurrent with clinical studies, companies usually complete additional animal studies and must also develop additional information about the chemistry and physical characteristics of the pharmaceutical product as well as finalize a process for manufacturing the product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the pharmaceutical product candidate and, among other things, must develop methods for testing the identity, strength, quality and purity of the final pharmaceutical product. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the pharmaceutical product candidate does not undergo unacceptable deterioration over its shelf life.
United States Review and Approval Processes
The results of product development, preclinical studies and clinical studies, along with descriptions of the manufacturing process, analytical tests conducted on the chemistry of the pharmaceutical product, proposed labeling and other relevant information are submitted to the FDA as part of an NDA requesting approval to market the product. The submission of an NDA is subject to the payment of substantial user fees; a waiver of such fees may be obtained under certain limited circumstances.
In addition, under the Pediatric Research Equity Act (PREA), an NDA or supplement to an NDA must contain data to assess the safety and effectiveness of the pharmaceutical product for the claimed indications in all relevant pediatric subpopulations and to support dosing and administration for each pediatric subpopulation for which the product is safe and effective. The FDA may grant deferrals for submission of data or full or partial waivers. Unless otherwise required by regulation, PREA does not apply to any pharmaceutical product for an indication for which orphan designation has been granted.
The FDA reviews all NDAs submitted before it accepts them for filing and may request additional information rather than accepting an NDA for filing. Once the submission is accepted for filing, the FDA begins an in-depth review of the NDA. Under the goals and policies agreed to by the FDA under the Prescription Drug User Fee Act (PDUFA), the FDA has 10 months in which to complete its initial review of a standard NDA and respond to the applicant, and six months for a priority NDA. The FDA does not always meet its PDUFA goal dates for standard and priority NDAs. The review process and the PDUFA goal date may be extended by three months if the FDA requests or if the NDA sponsor otherwise provides additional information or clarification regarding information already provided in the submission within the last three months before the PDUFA goal date.
After the NDA submission is accepted for filing, the FDA reviews the NDA application to determine, among other things, whether the proposed product is safe and effective for its intended use, and whether the product is being manufactured in accordance with cGMP to assure and preserve the product’s identity, strength, quality and purity. The FDA may refer applications for novel pharmaceutical products or pharmaceutical products which
28
Table of Contents
present difficult questions of safety or efficacy to an advisory committee, typically a panel that includes clinicians and other experts, for review, evaluation and a recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers such recommendations carefully when making decisions. During the pharmaceutical product approval process, the FDA also will determine whether a risk evaluation and mitigation strategy (REMS) is necessary to assure the safe use of the pharmaceutical product. If the FDA concludes that a REMS is needed, the sponsor of the NDA must submit a proposed REMS; the FDA will not approve the NDA without a REMS, if required.
Before approving an NDA, the FDA will inspect the facilities at which the product is manufactured. The FDA will not approve the product unless it determines that the manufacturing processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required specifications. Additionally, before approving an NDA, the FDA will typically inspect one or more clinical sites as well as the site where the pharmaceutical product is manufactured to assure compliance with GCP and cGMP. If the FDA determines the application, manufacturing process or manufacturing facilities are not acceptable, it will outline the deficiencies in the submission and often will request additional testing or information. In addition, the FDA will require the review and approval of product labeling.
The NDA review and approval process is lengthy and difficult and the FDA may refuse to approve an NDA if the applicable regulatory criteria are not satisfied or may require additional clinical data or other data and information. Even if such data and information is submitted, the FDA may ultimately decide that the NDA does not satisfy the criteria for approval. Data obtained from clinical studies are not always conclusive and the FDA may interpret data differently than CymaBay interprets the same data. The FDA will issue a complete response letter if the agency decides not to approve the NDA. The complete response letter usually describes all of the specific deficiencies in the NDA identified by the FDA. The deficiencies identified may be minor, for example, requiring labeling changes, or major, for example, requiring additional clinical studies. Additionally, the complete response letter may include recommended actions that the applicant might take to place the application in a condition for approval. If a complete response letter is issued, the applicant may either resubmit the NDA, addressing all of the deficiencies identified in the letter, or withdraw the application.
If a product receives regulatory approval, the approval may be significantly limited to specific diseases and dosages or the indications for use may otherwise be limited, which could restrict the commercial value of the product. Further, the FDA may require that certain contraindications, warnings or precautions be included in the product labeling. In addition, the FDA may require Phase 4 testing which involves clinical studies designed to further assess pharmaceutical product safety and effectiveness and may require testing and surveillance programs to monitor the safety of approved products that have been commercialized.
Expedited Development and Review Programs
The FDA has a Fast Track program that is intended to expedite or facilitate the process for reviewing new pharmaceutical products that meet certain criteria. Specifically, new pharmaceutical products are eligible for Fast Track designation if they are intended to treat a serious or life-threatening condition and demonstrate the potential to address unmet medical needs for the condition. Fast Track designation applies to the combination of the product and the specific indication for which it is being studied. Unique to a Fast Track product, the FDA may consider for review sections of the NDA on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the NDA, if the FDA agrees to accept sections of the NDA and determines that the schedule is acceptable and if the sponsor pays any required user fees upon submission of the first section of the NDA.
Any product submitted to the FDA for market, including a Fast Track program, may also be eligible for other types of FDA programs intended to expedite development and review, such as priority review and accelerated approval. Any product is eligible for priority review if it has the potential to provide safe and effective therapy where no satisfactory alternative therapy exists or a significant improvement in the treatment, diagnosis or prevention of a disease compared to marketed products. The FDA will attempt to direct additional
29
Table of Contents
resources to the evaluation of an application for a new pharmaceutical product designated for priority review in an effort to facilitate the review. Additionally, a product may be eligible for accelerated approval. Pharmaceutical products studied for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may receive accelerated approval, which means that the products may be approved on the basis of adequate and well-controlled clinical studies establishing that the product has an effect on a surrogate endpoint that is reasonably likely to predict a clinical benefit, or on the basis of an effect on a clinical endpoint other than survival or irreversible morbidity. As a condition of approval, the FDA may require that a sponsor of a pharmaceutical product receiving accelerated approval perform adequate and well-controlled post-marketing clinical studies. In addition, the FDA currently requires as a condition for accelerated approval pre-approval of promotional materials, which could adversely impact the timing of the commercial launch of the product. Fast Track designation, priority review and accelerated approval do not change the standards for approval but may expedite the development or approval process.
Post-Approval Requirements
Any pharmaceutical products for which CymaBay receives FDA approvals are subject to continuing regulation by the FDA, including, among other things, record-keeping requirements, reporting of adverse experiences with the product, providing the FDA with updated safety and efficacy information, product sampling and distribution requirements, complying with certain electronic records and signature requirements and complying with FDA promotion and advertising requirements, which include, among others, standards for direct-to-consumer advertising, prohibitions on promoting pharmaceutical products for uses or in patient populations that are not described in the pharmaceutical product’s approved labeling (known as “off-label use”), industry-sponsored scientific and educational activities and promotional activities involving the internet. Failure to comply with FDA requirements can have negative consequences, including adverse publicity, enforcement letters from the FDA, actions by the United States Department of Justice and/or United States Department of Health and Human Services Office of Inspector General, mandated corrective advertising or communications with doctors, and civil or criminal penalties. Although physicians may prescribe legally available pharmaceutical products for off-label uses, manufacturers may not directly or indirectly market or promote such off-label uses.
CymaBay relies, and expects to continue to rely, on third parties for the production of clinical and commercial quantities of CymaBay’s products. Manufacturers of CymaBay’s products are required to comply with applicable FDA manufacturing requirements contained in the FDA’s cGMP regulations. cGMP regulations require, among other things, quality control and quality assurance, as well as the corresponding maintenance of records and documentation. Pharmaceutical product manufacturers and other entities involved in the manufacture and distribution of approved pharmaceutical products are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMP and other laws. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain cGMP compliance. Discovery of problems with a product after approval may result in restrictions on a product, manufacturer or holder of an approved NDA, including withdrawal of the product from the market. In addition, changes to the manufacturing process generally require prior FDA approval before being implemented and other types of changes to the approved product, such as adding new indications and additional labeling claims, are also subject to further FDA review and approval.
The FDA also may require post-marketing testing, known as Phase 4 testing, risk minimization action plans and surveillance to monitor the effects of an approved product or place conditions on an approval that could restrict the distribution or use of the product.
U.S. Foreign Corrupt Practices Act
The U.S. Foreign Corrupt Practices Act, or FCPA, prohibits certain individuals and entities, including CymaBay, from promising, paying, offering to pay, or authorizing the payment of anything of value to any foreign government official, directly or indirectly, to obtain or retain business or an improper advantage. The
30
Table of Contents
U.S. Department of Justice and the U.S. Securities and Exchange Commission, or SEC, have increased their enforcement efforts with respect to the FCPA. Violations of the FCPA may result in large civil and criminal penalties and could result in an adverse effect on a company’s reputation, operations, and financial condition. A company may also face collateral consequences such as debarment and the loss of export privileges.
Federal and state fraud and abuse laws
In addition to FDA restrictions on marketing of pharmaceutical products, several other types of state and federal laws have been applied to restrict certain business practices in the biopharmaceutical industry in recent years. These laws include anti-kickback statutes and false claims statutes. The federal Anti-Kickback Statute prohibits, among other things, knowingly and willfully offering, paying, soliciting, or receiving remuneration to induce or in return for purchasing, leasing, ordering, or arranging for the purchase, lease, or order of any healthcare item or service reimbursable under Medicare, Medicaid, or other federally financed healthcare programs. The term “remuneration” has been broadly interpreted to include anything of value, including for example, gifts, discounts, the furnishing of supplies or equipment, credit arrangements, payments of cash, waivers of payment, ownership interests and providing anything at less than its fair market value. The Anti-Kickback Statute has been interpreted to apply to arrangements between pharmaceutical manufacturers on one hand and prescribers, purchasers, and formulary managers on the other. Although there are a number of statutory exemptions and regulatory safe harbors protecting certain common activities from prosecution, the exemptions and safe harbors are drawn narrowly, and CymaBay’s practices may not in all cases meet all of the criteria for statutory exemptions or safe harbor protection. Practices that involve remuneration that may be alleged to be intended to induce prescribing, purchases, or recommendations may be subject to scrutiny if they do not qualify for an exemption or safe harbor. Several courts have interpreted the statute’s intent requirement to mean that if any one purpose of an arrangement involving remuneration is to induce referrals of federal healthcare covered business, the statute has been violated. The reach of the Anti-Kickback Statute was also broadened by the Patient Protection and Affordable Health Care Act, as amended by the Health Care and Education Affordability Reconciliation Act, or collectively the PPACA, which, among other things, amends the intent requirement of the federal Anti-Kickback Statute. Pursuant to the statutory amendment, a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it in order to have committed a violation. In addition, the PPACA provides that the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the civil False Claims Act (discussed below) or the civil monetary penalties statute, which imposes penalties against any person who is determined to have presented or caused to be presented a claim to a federal health program that the person knows or should know is for an item or service that was not provided as claimed or is false or fraudulent.
The federal False Claims Act prohibits any person from knowingly presenting, or causing to be presented, a false claim for payment to the federal government. Recently, several pharmaceutical and other healthcare companies have been prosecuted under these laws for allegedly providing free product to customers with the expectation that the customers would bill federal programs for the product. Other companies have been prosecuted for causing false claims to be submitted because of the companies’ marketing of the product for unapproved, and thus non-reimbursable, uses. Many states also have statutes or regulations similar to the federal Anti-Kickback Statute and False Claims Act, which state laws apply to items and services reimbursed under Medicaid and other state programs, or, in several states, apply regardless of the payer. Also, the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, created new federal criminal statutes that prohibit knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private third-party payers and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Because of the breadth of these laws and the narrowness of the federal Anti-Kickback Statute’s safe harbors, it is possible that some of our business activities could be subject to challenge under one or more of such laws. Such a challenge could have a material adverse effect on our business, financial condition and results of operations. If CymaBay obtains FDA approval for any of our product candidates and begin commercializing those products in the United States, CymaBay’s operations may be
31
Table of Contents
directly, or indirectly through our customers, distributors, or other business partners, subject to various federal and state fraud and abuse laws, including, without limitation, anti-kickback statutes and false claims statutes. These laws may impact, among other things, our proposed sales, marketing and education programs. In addition, we may be subject to data privacy and security regulation by both the federal government and the states in which we conduct our business. HIPAA, as amended by the Health Information Technology and Clinical Health Act, or HITECH, and its implementing regulations, imposes certain requirements relating to the privacy, security and transmission of individually identifiable health information. Among other things, HITECH makes HIPAA’s privacy and security standards directly applicable to “business associates”—independent contractors or agents of covered entities that receive or obtain protected health information in connection with providing a service on behalf of a covered entity. HITECH also increased the civil and criminal penalties that may be imposed against covered entities, business associates and possibly other persons, and gave state attorneys general new authority to file civil actions for damages or injunctions in federal courts to enforce the federal HIPAA laws and seek attorney’s fees and costs associated with pursuing federal civil actions. In addition, state laws govern the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts.
If CymaBay’s operations are found to be in violation of any of the federal and state laws described above or any other governmental regulations that apply to CymaBay, CymaBay may be subject to penalties, including criminal and significant civil monetary penalties, damages, fines, imprisonment, exclusion from participation in government healthcare programs, and the curtailment or restructuring of CymaBay’s operations, any of which could adversely affect CymaBay’s ability to operate its business and CymaBay’s results of operations. To the extent that any of CymaBay’s product candidates are ultimately sold in a foreign country, we may be subject to similar foreign laws and regulations, which may include, for instance, applicable post-marketing requirements, including safety surveillance, anti-fraud and abuse laws, and implementation of corporate compliance programs and reporting of payments or transfers of value to healthcare professionals.
In the United States and foreign jurisdictions, there have been a number of legislative and regulatory changes to the healthcare system that could affect our future results of operations. In particular, there have been and continue to be a number of initiatives at the United States federal and state levels that seek to reduce healthcare costs. The Medicare Prescription Drug, Improvement, and Modernization Act of 2003, or the MMA, imposed new requirements for the distribution and pricing of prescription drugs for Medicare beneficiaries. Under Part D, Medicare beneficiaries may enroll in prescription drug plans offered by private entities which will provide coverage of outpatient prescription drugs. Part D plans include both stand-alone prescription drug benefit plans and prescription drug coverage as a supplement to Medicare Advantage plans. Unlike Medicare Part A and B, Part D coverage is not standardized. Part D prescription drug plan sponsors are not required to pay for all covered Part D drugs, and each drug plan can develop its own drug formulary that identifies which drugs it will cover and at what tier or level. However, Part D prescription drug formularies must include drugs within each therapeutic category and class of covered Part D drugs, though not necessarily all the drugs in each category or class. Any formulary used by a Part D prescription drug plan must be developed and reviewed by a pharmacy and therapeutic committee. Government payment for some of the costs of prescription drugs may increase demand for CymaBay’s products for which CymaBay receives marketing approval. However, any negotiated prices for CymaBay’s products covered by a Part D prescription drug plan will likely be lower than the prices CymaBay might otherwise obtain. Moreover, while the MMA applies only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own payment rates. Any reduction in payment that results from Medicare Part D may result in a similar reduction in payments from non-governmental payors.
The American Recovery and Reinvestment Act of 2009 provides funding for the federal government to compare the effectiveness of different treatments for the same illness. A plan for the research will be developed by the Department of Health and Human Services, the Agency for Healthcare Research and Quality and the National Institutes for Health, and periodic reports on the status of the research and related expenditures will be made to Congress. Although the results of the comparative effectiveness studies are not intended to mandate coverage
32
Table of Contents
policies for public or private payors, it is not clear what effect, if any, the research will have on the sales of any product, if any such product or the condition that it is intended to treat is the subject of a study. It is also possible that comparative effectiveness research demonstrating benefits in a competitor’s product could adversely affect the sales of our product candidates. If third-party payors do not consider CymaBay’s products to be cost-effective compared to other available therapies, they may not cover our products as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow CymaBay to sell its products on a profitable basis.
In March 2010 the PPACA was enacted, which includes measures to significantly change the way healthcare is financed by both governmental and private insurers. Among the provisions of the PPACA of importance to the pharmaceutical and biotechnology industry are the following:
| • | an annual, nondeductible fee on any entity that manufactures or imports certain branded prescription drugs and biologic agents, apportioned among these entities according to their market share in certain government healthcare programs, that began in 2011; |
| • | an increase in the rebates a manufacturer must pay under the Medicaid Drug Rebate Program to 23.1% and 13% of the average manufacturer price for branded and generic drugs, respectively; |
| • | a new Medicare Part D coverage gap discount program, in which manufacturers must agree to offer 50% point-of-sale discounts to negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D; |
| • | extension of manufacturers’ Medicaid rebate liability to covered drugs dispensed to individuals who are enrolled in Medicaid managed care organizations; |
| • | expansion of eligibility criteria for Medicaid programs by, among other things, allowing states to offer Medicaid coverage to additional individuals and by adding new mandatory eligibility categories for certain individuals with income at or below 133% of the Federal Poverty Level beginning in 2014, thereby potentially increasing manufacturers’ Medicaid rebate liability; |
| • | expansion of the entities eligible for discounts under the Public Health Service pharmaceutical pricing program; |
| • | new requirements under the federal Open Payments program, created under Section 6002 of the PPACA and its implementing regulations, that manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) report annually to the U.S. Department of Health and Human Services, or HHS, information related to “payments or other transfers of value” made or distributed to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, and that applicable manufacturers and applicable group purchasing organizations report annually to HHS ownership and investment interests held by physicians (as defined above) and their immediate family members, with data collection required beginning August 1, 2013 and reporting to the Centers for Medicare & Medicaid Services, or CMS, required by March 31, 2014 and by the 90th day of each subsequent calendar year; |
| • | a requirement to annually report drug samples that manufacturers and distributors provide to physicians, effective April 1, 2012; |
| • | expansion of health care fraud and abuse laws, including the False Claims Act and the Anti-Kickback Statute, new government investigative powers, and enhanced penalties for noncompliance; |
| • | a licensure framework for follow-on biologic products; |
| • | a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research; |
| • | creation of the Independent Payment Advisory Board which, beginning in 2014, will have authority to recommend certain changes to the Medicare program that could result in reduced payments for prescription drugs and those recommendations could have the effect of law even if Congress does not act on the recommendations; and |
33
Table of Contents
| • | establishment of a Center for Medicare Innovation at CMS to test innovative payment and service delivery models to lower Medicare and Medicaid spending, potentially including prescription drug spending that began on January 1, 2011. |
In addition, other legislative changes have been proposed and adopted since the PPACA was enacted. In August 2011, the president signed into law the Budget Control Act of 2011, which, among other things, created the Joint Select Committee on Deficit Reduction, or joint committee, to recommend proposals in spending reductions to Congress. The joint committee did not achieve its targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, triggering automatic reductions to several government programs. These reductions include aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, starting in 2013. In January 2013, the president signed into law the American Taxpayer Relief Act of 2012, which, among other things, reduced Medicare payments to several providers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. These new laws may result in additional reductions in Medicare and other healthcare funding, which could have a material adverse effect on our financial operations.
Patent Term Restoration and Marketing Exclusivity
Depending upon the timing, duration and specifics of the FDA approval of the use of CymaBay’s pharmaceutical product candidates, some of CymaBay’s products to be licensed under United States patents may be eligible for limited patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984, commonly referred to as the Hatch-Waxman Amendments. The Hatch-Waxman Amendments permits a patent restoration term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, patent term restoration cannot extend the remaining term of a patent beyond a total of 14 years from the product’s approval date. The patent term restoration period is generally one-half the time between the effective date of an IND and the submission date of an NDA plus the time between the submission date of an NDA and the approval of that application. Only one patent applicable to an approved pharmaceutical product is eligible for the extension and the application for the extension must be submitted prior to the expiration of the patent. The United States Patent and Trademark Office, in consultation with the FDA, reviews and approves the application for any patent term extension or restoration. In the future, CymaBay may intend to apply for restoration of patent term for one of its currently owned or licensed patents to add patent life beyond its current expiration date, depending upon the expected length of the clinical studies and other factors involved in the filing of the relevant NDA.
Market exclusivity provisions under the U.S. Food, Drug, and Cosmetic Act can also delay the submission or the approval of certain applications of other companies seeking to reference another company’s NDA. Currently seven years of reference product exclusivity are available to pharmaceutical products designated as Orphan Drugs, during which the FDA may not approve generic products relying upon the reference product’s data. Pediatric exclusivity is another type of regulatory market exclusivity in the United States. Pediatric exclusivity, if granted, adds six months to existing exclusivity periods and patent terms. This six-month exclusivity, which runs from the end of other exclusivity protection or patent term, may be granted based on the voluntary completion of a pediatric clinical study in accordance with an FDA-issued “Written Request” for such a clinical study.
Pharmaceutical Coverage, Pricing and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any pharmaceutical product candidates for which CymaBay obtains regulatory approval. In the United States and markets in other countries, sales of any products for which CymaBay receives regulatory approval for commercial sale will depend in part upon the availability of reimbursement from third-party payors. Third-party payors include government payors such as Medicare and Medicaid, managed care providers, private health insurers and other organizations. The process for determining whether a payor will provide coverage for a pharmaceutical product may be separate from the process for setting the price or reimbursement rate that the payor will pay for the pharmaceutical product. Third-party payors may limit coverage to specific pharmaceutical products on an approved list, or formulary, which might not include all of the FDA-approved pharmaceutical products for a particular indication.
34
Table of Contents
Third-party payors are increasingly challenging the price and examining the medical necessity and cost-effectiveness of medical products and services, in addition to their safety and efficacy. CymaBay may need to conduct expensive pharmaco-economic studies in order to demonstrate the medical necessity and cost-effectiveness of its products, in addition to the costs required to obtain the FDA approvals. CymaBay’s pharmaceutical product candidates may not be considered medically necessary or cost-effective. A payor’s decision to provide coverage for a pharmaceutical product does not imply that an adequate reimbursement rate will be approved. Adequate third-party reimbursement may not be available to enable CymaBay to maintain price levels sufficient to realize an appropriate return on CymaBay’s investment in product development. In addition, in the United States there is a growing emphasis on comparative effectiveness research, both by private payors and by government agencies. To the extent other drugs or therapies are found to be more effective than CymaBay’s products, payors may elect to cover such therapies in lieu of CymaBay’s products and/or reimburse CymaBay’s products at a lower rate.
In 2003, the United States government enacted legislation providing a partial prescription drug benefit for Medicare recipients, which became effective at the beginning of 2006. Government payment for some of the costs of prescription drugs may increase demand for any products for which CymaBay receives marketing approval. However, to obtain payments under this program, CymaBay would be required to sell products to Medicare recipients through prescription drug plans operating pursuant to this legislation. As part of their participation in the Medicare prescription drug program, these plans negotiate discounted prices for prescription drugs and will likely do so for CymaBay’s products. Federal, state and local governments in the United States continue to consider legislation to limit the growth of health care costs, including the cost of prescription drugs. Future legislation and regulations could limit payments for pharmaceuticals such as the drug candidates that CymaBay is developing.
Different pricing and reimbursement schemes exist in other countries. In the European Community, governments influence the price of pharmaceutical products through their pricing and reimbursement rules and control of national health care systems that fund a large part of the cost of those products to consumers. Some jurisdictions operate positive and negative list systems under which products may only be marketed once a reimbursement price has been agreed upon. To obtain reimbursement or pricing approval, some of these countries may require the completion of clinical studies that compare the cost-effectiveness of a particular pharmaceutical product candidate to currently available therapies. Other member states allow companies to fix their own prices for medicines, but monitor and control company profits. The downward pressure on health care costs in general, particularly prescription drugs, has become very intense. As a result, increasingly high barriers are being erected to the entry of new products. In addition, in some countries, cross-border imports from low-priced markets exert a commercial pressure on pricing within a country.
The marketability of any pharmaceutical product candidates for which CymaBay receives regulatory approval for commercial sale may suffer if the government and third-party payors fail to provide adequate coverage and reimbursement. In addition, emphasis on managed care in the United States has increased and CymaBay expects this will continue to increase the pressure on pharmaceutical pricing. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which CymaBay receives regulatory approval, less favorable coverage policies and reimbursement rates may be implemented in the future.
International Regulation
In addition to regulations in the United States, there are a variety of foreign regulations governing clinical studies and commercial sales and distribution of CymaBay’s future product candidates. Whether or not FDA approval is obtained for a product, approval of a product must be obtained by the comparable regulatory authorities of foreign countries before clinical studies or marketing of the product can commence in those countries. The approval process varies from country to country, and the time may be longer or shorter than that required for FDA approval. The requirements governing the conduct of clinical studies, product licensing, pricing and reimbursement vary greatly from country to country. In addition, certain regulatory authorities in select
35
Table of Contents
countries may require CymaBay to repeat previously conducted preclinical and/or clinical studies under specific criteria for approval in their respective country which may delay and/or greatly increase the cost of approval in certain markets targeted for approval by CymaBay.
Under European Union regulatory systems, marketing applications for pharmaceutical products must be submitted under a centralized procedure to the European Medicines Agency (“EMA”). The centralized procedure provides for the grant of a single marketing authorization that is valid for all European Union member states. The EMA also has designations for Orphan Drugs which, if applicable, can provide for faster review, lower fees and more access to advice during drug development. While the marketing authorization in the European Union is centralized, the system for clinical studies (application, review and requirements) is handled by each individual country. Approval to run a clinical study in one country does not guarantee approval in any other country.
The pharmaceutical industry in Canada is regulated by Health Canada. A New Drug Submission (NOS) is the equivalent of a United States NDA and must be filed to obtain approval to market a pharmaceutical product in Canada. Marketing regulations and reimbursement are subject to national and provincial laws.
In Japan, applications for approval to manufacture and market new drugs must be approved by the Ministry of Health, Labor and Welfare. Nonclinical and clinical studies must meet the requirements of Japanese laws. Results from clinical studies conducted outside of Japan must be supplemented with at least a bridging clinical study conducted in Japan.
In addition to regulations in Europe, Canada, Japan and the United States, there are a variety of foreign regulations governing clinical studies, commercial distribution and reimbursement of future product candidates which CymaBay may be subject to as it pursues regulatory approval and commercialization of arhalofenate or any future product candidates internationally.
Corporate Information
CymaBay Therapeutics, Inc., formerly Metabolex, Inc., was incorporated under the laws of the State of Delaware on October 5, 1988, originally under the name Transtech Corporation. Our executive offices are located at 3876 Bay Center Place, Hayward, California 94545. The telephone number at our executive office is (510) 293-8800. Our corporate website address is www.cymabay.com. We do not incorporate the information contained on, or accessible through, our website into this Form 10, and you should not consider it part of this Form 10.
Employees
As of August 1, 2013, CymaBay has twelve full-time employees, seven of whom hold Ph.D.s and one of whom holds a Masters degree in relevant areas of expertise, and three consultants.
36
Table of Contents
| ITEM 1A. | RISK FACTORS. |
An investment in our common stock involves a high degree of risk. A prospective investor should carefully consider the following information about these risks, together with the other information appearing elsewhere in this Form 10, before deciding to invest in our common stock. The occurrence of any of the following risks could have a material adverse effect on CymaBay’s business, financial condition, results of operations and future prospects. In these circumstances, the value of our common stock could decline, and the investor may lose all or part of the money paid to acquire our common stock.
Risks Related to Our Financial Condition and Capital Requirements
If we fail to obtain additional financing, we could be forced to delay, reduce or eliminate our product development programs, seek corporate partners for the development of our product development programs or relinquish or license on unfavorable terms, our rights to technologies or product candidates.
As of June 30, 2013, we had net cash on hand of approximately $3.6 million. On September 30, 2013, we raised aggregate net proceeds of approximately $28.9 million and issued common stock in cancellation of $16.9 million of debt owed to the holder of that debt in the 2013 financing, and on October 31, 2013, we raised an additional aggregate net proceeds of $2.8 million in the 2013 financing. After giving effect to the 2013 financing, we believe that our existing cash will allow us to continue operation through the third quarter of 2015. As set forth in the notes to our financial statements, our auditors expressed substantial doubt as to our ability to continue as a going concern if we are unable to raise additional capital without giving effect to the 2013 financing. Our monthly spending levels vary based on new and ongoing development and corporate activities.
Developing pharmaceutical products, including conducting preclinical studies and clinical trials, is a time-consuming, expensive and uncertain process that takes years to complete. We expect our research and development expenses to substantially increase in connection with our ongoing activities, particularly as we advance development of our lead clinical product candidate, arhalofenate, for the prevention of gout flares and the treatment of hyperuricemia in patients with gout.
In the event CymaBay does not successfully raise sufficient funds in financing(s), its product development activities, particularly related to the development of arhalofenate, will necessarily be curtailed commensurate with the magnitude of the shortfall or may cease altogether. To the extent that the costs of the planned Phase 2b study of arhalofenate in patients with gout exceed current estimates and CymaBay is unable to raise sufficient additional capital to cover such additional costs, CymaBay will need to reduce operating expenses, enter into a collaboration or other similar arrangement with respect to development and/or commercialization rights to arhalofenate, outlicense intellectual property rights to arhalofenate, sell assets or effect a combination of the above. No assurance can be given that CymaBay will be able to effect any of such transactions on acceptable terms, if at all. Failure to progress the development of arhalofenate will have a negative effect on CymaBay’s business, future prospects and ability to obtain further financing on acceptable terms (if at all).
Beyond the plan of operations outlined above, CymaBay’s future funding requirements and sources will depend on many factors, including but not limited to the following:
| • | the rate of progress and cost of its clinical studies, including in particular the Phase 3 studies of arhalofenate; |
| • | the need for additional or expanded clinical studies; |
| • | the rate of progress and cost of its Chemistry, Manufacturing and Control registration and validation program; |
| • | the timing, economic and other terms of any licensing, collaboration or other similar arrangement into which CymaBay may enter; |
37
Table of Contents
| • | the costs and timing of seeking and obtaining FDA and other regulatory approvals; |
| • | the extent of CymaBay’s other development activities; |
| • | the costs of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights; and |
| • | the effect of competing products and market developments. |
If we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we will be prevented from pursuing development and commercialization efforts, which will have a material adverse effect on our business, operating results and prospects and on our ability to develop our product candidates.
We have incurred significant losses since our inception. We anticipate that we will continue to incur significant losses for the foreseeable future, and we may never achieve or maintain profitability.
We are a biopharmaceutical company focused primarily on developing our lead product candidate, arhalofenate. We have incurred significant net losses in each year since our inception, including net losses of approximately $11.3 million and $4.5 million for the fiscal years ended 2012 and 2011, respectively. As of June 30, 2013, we had an accumulated deficit of $340.6 million.
To date, we have financed our operations primarily through the sale of equity securities, licensing fees, issuance of debt and collaborations with third parties. We have devoted most of our financial resources to research and development, including our preclinical development activities and clinical trials. We have not completed development of any product candidates. We expect to continue to incur significant and increasing losses and negative cash flows for the foreseeable future. The size of our losses will depend, in part, on the rate of future expenditures and our ability to generate revenues. In particular, we expect to incur substantial and increased expenses as we:
| • | continue the development of our lead product candidate, arhalofenate, for the prevention of flares and treatment of hyperuricemia in patients with gout; |
| • | seek to obtain regulatory approvals for arhalofenate; |
| • | prepare for the potential commercialization of arhalofenate; |
| • | scale up manufacturing capabilities to commercialize arhalofenate for any indications for which we receive regulatory approval; |
| • | begin outsourcing of the commercial manufacturing of arhalofenate for any indications for which we receive regulatory approval; |
| • | establish an infrastructure for the sales, marketing and distribution of arhalofenate for any indications for which we receive regulatory approval; |
| • | expand our research and development activities and advance our clinical programs; |
| • | maintain, expand and protect our intellectual property portfolio; |
| • | continue our research and development efforts and seek to discover additional product candidates; and |
| • | add operational, financial and management information systems and personnel, including personnel to support our product development and commercialization efforts and operations as a public company. |
CymaBay does not anticipate that it will generate revenue from the sale of products for the foreseeable future. CymaBay’s ability to become profitable depends upon its ability to generate significant continuing revenues.
In the absence of additional sources of capital, which may not be available to CymaBay on acceptable terms, or at all, the development of arhalofenate or future product candidates may be reduced in scope, delayed or
38
Table of Contents
terminated. If CymaBay’s product candidates or those of its collaborators fail in clinical studies or do not gain regulatory approval, or if its future products, if any, do not achieve market acceptance, CymaBay may never become profitable.
Even if we do achieve profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis. Our failure to become and remain profitable would depress the value of our company and could impair our ability to raise capital, expand our business, diversify our product offerings or continue our operations.
Our ability to generate future revenues from product sales is uncertain and depends upon our ability to successfully develop, obtain regulatory approval for, and commercialize our product candidates.
Our ability to generate revenue and achieve profitability depends on our ability, alone or with collaborators, to successfully complete the development, obtain the necessary regulatory approvals and commercialize our product candidates. We do not anticipate generating revenues from sales of our product candidates for the foreseeable future, if ever. Our ability to generate future revenues from product sales depends heavily on our success in:
| • | obtaining favorable results for and advancing the development of arhalofenate, including successfully initiating and completing our Phase 2b and Phase 3 clinical development; |
| • | obtaining United States (U.S.) and foreign regulatory approvals for arhalofenate; |
| • | launching and commercializing arhalofenate, either on our own or with a partner, including building a sales force and collaborating with third parties; |
| • | achieving broad market acceptance of arhalofenate in the medical community and by third-party payors and patients; and |
| • | generating a pipeline of product candidates. |
Conducting preclinical testing and clinical trials is a time-consuming, expensive and uncertain process that takes years to complete, and we may never generate the necessary data required to obtain regulatory approval and achieve product sales. Our anticipated development costs would likely increase if we do not obtain favorable results or if development of our product candidates is delayed. In particular, we would likely incur higher costs than we currently anticipate if development of our product candidates is delayed because we are required by the U.S. FDA to perform studies or trials in addition to those that we currently anticipate. Because of the numerous risks and uncertainties associated with pharmaceutical product development, we are unable to predict the timing or amount of any increase in our anticipated development costs.
In addition, our product candidates, if approved, may not achieve commercial success. Our commercial revenues, if any, will be derived from sales of products that we do not expect to be commercially available for several years, if at all. Even if one or more of our product candidates is approved for commercial sale, we anticipate incurring significant costs in connection with commercialization. As a result, we cannot assure you that we will be able to generate revenues from sales of any approved product candidates, or that we will achieve or maintain profitability even if we do generate sales.
Raising additional capital may cause dilution to our existing stockholders, restrict our operations or require us to relinquish rights to our technologies or product candidates.
Until such time, if ever, as we can generate substantial product revenues, we expect to finance our cash needs through a combination of equity offerings, debt financings, collaborations, strategic alliances, licensing arrangements and other marketing and distribution arrangements. We do not have any committed external source of funds.
39
Table of Contents
In order to raise additional funds to support our operations, we may sell additional equity or debt securities, enter into collaborations, strategic alliances, or licensing arrangements or other marketing or distribution arrangements. To the extent that we raise additional capital through the sale of equity or convertible debt securities, your ownership interest will be diluted, and the terms of these securities may include liquidation or other preferences that adversely affect your rights as a stockholder. Debt financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions, such as incurring additional debt, making capital expenditures, and declaring dividends, and will impose limitations on our ability to acquire, sell or license intellectual property rights and other operating restrictions that could adversely impact our ability to conduct our business.
If we raise additional funds through collaborations, strategic alliances, or licensing arrangements or other marketing or distribution arrangements with third parties, we may have to relinquish valuable rights to our technologies, future revenue streams, research programs or product candidates, or grant licenses on terms that may not be favorable to us. If we are unable to expand our operations or otherwise capitalize on our business opportunities, our business, financial condition and results of operations could be materially adversely affected and we may not be able to meet our debt service obligations. If we are unable to raise additional funds through equity or debt financings when needed, we may be required to delay, limit, reduce or terminate our product development or commercialization efforts, or grant others rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves.
We are an emerging growth company and we cannot be certain if the reduced disclosure requirements applicable to emerging growth companies will make our common stock less attractive to investors.
We are an emerging growth company. Under the Jumpstart Our Business Startups Act of 2012, or the JOBS Act, emerging growth companies can delay adopting new or revised accounting standards until such time as those standards apply to private companies. We plan to avail ourselves of this exemption from new or revised accounting standards and, therefore, we may not be subject to the same new or revised accounting standards as other public companies that are not “emerging growth companies.”
For as long as we continue to be an emerging growth company, we also intend to take advantage of certain other exemptions from various reporting requirements that are applicable to other public companies including, but not limited to, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements, exemptions from the requirements of holding a nonbinding advisory stockholder vote on executive compensation and any golden parachute payments not previously approved, exemption from the requirement of auditor attestation in the assessment of our internal control over financial reporting and exemption from any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements (auditor discussion and analysis). If we do, the information that we provide stockholders may be different than what is available with respect to other public companies. We cannot predict if investors will find our common stock less attractive because we will rely on these exemptions. If investors find our common stock less attractive as a result of our status as an emerging growth company, there may be less liquidity for our common stock and our stock price may be more volatile.
We will remain an emerging growth company until the earliest of (i) the end of the fiscal year in which the market value of our common stock that is held by non-affiliates exceeds $700 million as of the end of the second fiscal quarter, (ii) the end of the fiscal year in which we have total annual gross revenues of $1 billion or more during such fiscal year, (iii) the date on which we issue more than $1 billion in non-convertible debt in a three-year period or (iv) the end of the fiscal year following the fifth anniversary of the date of the first sale of our common stock pursuant to an effective registration statement filed under the Securities Act.
40
Table of Contents
Risks Related to Clinical Development and Regulatory Approval
We depend on the success of our lead product candidate, arhalofenate, which is still under clinical development, and may not obtain regulatory approval or be successfully commercialized.
We have not marketed, distributed or sold any products. The success of our business depends upon our ability to develop and commercialize our lead product candidate, arhalofenate, which has completed seven Phase 1 and seven Phase 2 clinical trials, including three Phase 2 studies in gout. We plan to conduct a Phase 2b clinical trial for arhalofenate in preventing flares and reducing serum uric acid in gout patients prior to initiation of a Phase 3 program. There is no guarantee that our clinical trials will be completed or, if completed, will be successful. The success of arhalofenate will depend on several factors, including the following:
| • | successful enrollment and completion of clinical trials; |
| • | receipt of marketing approvals from the FDA and regulatory authorities outside the U.S. for our product candidate; |
| • | establishing commercial manufacturing capabilities by making arrangements with third-party manufacturers; |
| • | launching commercial sales of the product, whether alone or in collaboration with others; |
| • | acceptance of the product by patients, the medical community and third-party payors; |
| • | effectively competing with other therapies; |
| • | a continued acceptable safety profile of the product following approval; and |
| • | obtaining, maintaining, enforcing and defending intellectual property rights and claims. |
If we do not achieve one or more of these factors in a timely manner or at all, we could experience significant delays or an inability to successfully commercialize arhalofenate, which would materially harm our business.
We have never obtained regulatory approval for a drug and we may be unable to obtain, or may be delayed in obtaining, regulatory approval for arhalofenate.
We have never obtained regulatory approval for a drug. In the U.S. it is possible that the FDA may refuse to accept our New Drug Application (NDA) for substantive review or may conclude after review of our data that our application is insufficient to obtain regulatory approval of arhalofenate. If the FDA does not accept or approve our NDA, it may require that we conduct additional clinical, nonclinical or manufacturing validation studies and submit that data before it will reconsider our application. Depending on the extent of these or any other FDA required studies, approval of any NDA or application that we submit may be delayed by several years, or may require us to expend more resources than we have available. It is also possible that additional studies, if performed and completed, may not be considered sufficient by the FDA to approve our NDA.
We currently do not know when we might commence our Phase 3 study of arhalofenate or achieve FDA approval of arhalofenate. We currently do not have the capital necessary to conduct or complete our Phase 3 study of arhalofenate and we may not be able to raise sufficient funds necessary to conduct this study. We believe that our existing cash will be sufficient to enable us to complete our Phase 2b study, which we anticipate completing the second quarter of 2015, and will allow us to continue operation through the third quarter of 2015. We currently believe that we will need to raise additional capital to continue our operations beyond the third quarter of 2015.
Any delay in obtaining, or an inability to obtain, regulatory approvals would prevent us from commercializing arhalofenate, generating revenues and achieving and sustaining profitability. If any of these outcomes occur, we may be forced to abandon our development efforts for arhalofenate, which would have a material adverse effect on our business and could potentially cause us to cease operations.
41
Table of Contents
We depend on the successful completion of clinical trials for our product candidates, including arhalofenate. The positive clinical results obtained for our product candidates in prior clinical studies may not be repeated in future clinical studies.
Before obtaining regulatory approval for the sale of our product candidates, including arhalofenate, we must conduct additional clinical trials to demonstrate the safety and efficacy of our product candidates in humans. Clinical testing is expensive, difficult to design and implement, can take many years to complete and is uncertain as to outcome. A failure of one or more of our clinical trials can occur at any stage of testing. The outcome of preclinical testing and early clinical trials may not be predictive of the success of later clinical trials, and interim results of a clinical trial do not necessarily predict final results. Moreover, preclinical and clinical data are often susceptible to varying interpretations and analyses, and many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have nonetheless failed to obtain marketing approval for their products.
We have completed three Phase 2 clinical studies of arhalofenate in gout. In addition, six clinical studies with MBX-8025 and five clinical studies with MBX-2982 have been completed. However, we have never conducted a Phase 3 clinical trial. The positive results we have seen to date in our Phase 2 clinical trials of arhalofenate for gout do not ensure that later clinical trials will demonstrate similar results. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy characteristics despite having progressed satisfactorily through preclinical studies and initial clinical testing. A number of companies in the pharmaceutical and biotechnology industries, including those with greater resources and experience, have suffered significant setbacks in Phase 3 clinical development, even after seeing promising results in earlier clinical trials.
We may experience a number of unforeseen events during clinical trials for our product candidates, including arhalofenate, that could delay or prevent the commencement and/or completion of our clinical trials, including the following:
| • | regulators or institutional review boards may not authorize us or our investigators to commence a clinical trial or conduct a clinical trial at a prospective trial site; |
| • | the clinical study protocol may require one or more amendments delaying study completion; |
| • | clinical trials of our product candidates may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical trials or abandon product development programs; |
| • | the number of subjects required for clinical trials of our product candidates may be larger than we anticipate, enrollment in these clinical trials may be insufficient or slower than we anticipate or subjects may drop out of these clinical trials at a higher rate than we anticipate; |
| • | clinical investigators or study subjects fail to comply with clinical study protocols; |
| • | trial conduct and data analysis errors may occur, including, but not limited to, data entry and/or labeling errors; |
| • | our third-party contractors may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
| • | we might have to suspend or terminate clinical trials of our product candidates for various reasons, including a finding that the subjects are being exposed to unacceptable health risks; |
| • | regulators or institutional review boards may require that we or our investigators suspend or terminate clinical research for various reasons, including noncompliance with regulatory requirements; |
| • | the cost of clinical trials of our product candidates may be greater than we anticipate; |
42
Table of Contents
| • | the supply or quality of our clinical trial materials or other materials necessary to conduct clinical trials of our product candidates may be insufficient or inadequate; and |
| • | our product candidates may have undesirable side effects or other unexpected characteristics, causing us or our investigators to suspend or terminate the trials. |
We expect our research and development expenses to increase in connection with our ongoing activities, particularly if we commence a Phase 3 clinical trial with arhalofenate and undertake additional clinical trials of our other product candidates MBX-8025 and MBX-2982. Before we commence a Phase 3 clinical trial for arhalofenate, we will need to raise substantial additional capital. We also will need to raise substantial additional capital in the future to complete the development and commercialization of MBX-8025 and MBX-2982, for which we currently have no planned clinical trials. Because successful development of our product candidates is uncertain, we are unable to estimate the actual funds required to complete research and development and commercialize our products under development.
Negative or inconclusive results of our future clinical trials of arhalofenate, or any other clinical trial we conduct, could cause the FDA to require that we repeat or conduct additional clinical studies. Despite the results reported in earlier clinical trials for arhalofenate, we do not know whether any clinical trials we may conduct will demonstrate adequate efficacy and safety to result in regulatory approval to market our product candidates, including arhalofenate. If later stage clinical trials do not produce favorable results, our ability to obtain regulatory approval for our product candidates, including arhalofenate, may be adversely impacted.
We have never conducted a clinical trial of arhalofenate as a monotherapy for the treatment of gout flares. If arhalofenate does not demonstrate efficacy in the treatment of such flares in our planned Phase 2b clinical trial, our ability to successfully commercialize arhalofenate may be adversely affected.
We have not previously conducted a clinical trial of arhalofenate for the purpose of measuring its effect on flare reduction and control without the use of colchicine. We plan to conduct a Phase 2b clinical trial to investigate the potential benefit of arhalofenate monotherapy with regard to flare prevention and serum uric acid (sUA) lowering. In addition, our Phase 2b study will investigate the benefits of two doses of arhalofenate monotherapy, including a higher dose than we studied in previous gout studies, without colchicine. If we do not obtain favorable efficacy and safety results in the Phase 2b trial, our ability to successfully market arhalofenate could be adversely affected.
Delays in clinical trials are common and have many causes, and any delay could result in increased costs to us and jeopardize or delay our ability to obtain regulatory approval and commence product sales.
Clinical testing is expensive, difficult to design and implement, can take many years to complete, and is uncertain as to outcome. We may experience delays in clinical trials at any stage of development and testing of our product candidates. Our planned clinical trials may not begin on time, have an effective design, enroll a sufficient number of subjects, or be completed on schedule, if at all.
Events which may result in delays or unsuccessful completion of clinical trials, including our future clinical trials for arhalofenate, include the following:
| • | inability to raise funding necessary to initiate or continue a trial; |
| • | delays in obtaining regulatory approval to commence a trial; |
| • | delays in reaching agreement with the FDA on final trial design; |
| • | imposition of a clinical hold following an inspection of our clinical trial operations or trial sites by the FDA or other regulatory authorities; |
43
Table of Contents
| • | delays in reaching agreement on acceptable terms with prospective contract research organizations (CROs) and clinical trial sites; |
| • | delays in obtaining required institutional review board (IRB) approval at each site; |
| • | delays in recruiting suitable patients to participate in a trial; |
| • | delays in having subjects complete participation in a trial or return for post-treatment follow-up; |
| • | delays caused by subjects dropping out of a trial due to side effects or otherwise; |
| • | delays caused by clinical sites dropping out of a trial; |
| • | time required to add new clinical sites; and |
| • | delays by our contract manufacturers to produce and deliver sufficient supply of clinical trial materials. |
If initiation or completion of any of our clinical trials for our product candidates, including arhalofenate, are delayed for any of the above reasons, our development costs may increase, the approval process could be delayed, any periods during which we may have the exclusive right to commercialize our product candidates may be reduced and our competitors may bring products to market before us. Any of these events could impair our ability to generate revenues from product sales and impair our ability to generate regulatory and commercialization milestones and royalties, all of which could have a material adverse effect on our business.
Our product candidates may cause adverse effects or have other properties that could delay or prevent their regulatory approval or limit the scope of any approved label or market acceptance.
Arhalofenate has been studied in a total of 15 clinical trials with nearly a thousand subjects. The emergence of adverse events (AEs) caused by arhalofenate in future studies could cause us, other reviewing entities, clinical study sites or regulatory authorities to interrupt, delay or halt clinical studies and could result in the denial of regulatory approval. There is also a risk that our other product candidates may induce AEs, many of which may be unknown at this time. If an unacceptable frequency and/or severity of AEs are reported in our clinical trials for our product candidates, our ability to obtain regulatory approval for product candidates, including arhalofenate, may be negatively impacted.
Furthermore, if any of our approved products cause serious or unexpected side effects after receiving market approval, a number of potentially significant negative consequences could result, including the following:
| • | regulatory authorities may withdraw their approval of the product or impose restrictions on its distribution in a form of a modified risk evaluation and mitigation strategy; |
| • | regulatory authorities may require the addition of labeling statements, such as warnings or contraindications that could diminish the usage of the product or otherwise limit the commercial success of the affected product; |
| • | we may be required to change the way the product is administered or to conduct additional clinical studies; |
| • | we may choose to discontinue sale of the product; |
| • | we could be sued and held liable for harm caused to patients; and |
| • | our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the affected product candidate and could substantially increase the costs of commercializing our product candidates.
44
Table of Contents
If any product candidate that CymaBay successfully develops does not achieve broad market acceptance among physicians, patients, health care payors and the medical community, the revenues that it generates from its sales will be limited.
Even if arhalofenate or any other product candidates receive regulatory approval, the products may not gain market acceptance among physicians, patients, health care payors and the medical community. Coverage and reimbursement of CymaBay’s product candidates by third-party payors, including government payors, generally is also necessary for commercial success. The degree of market acceptance of any of CymaBay’s approved products will depend upon a number of factors, including:
| • | the efficacy and safety, as demonstrated in clinical studies; |
| • | the risk/benefit profile of CymaBay’s products such as arhalofenate; |
| • | the prevalence and severity of any side effects; |
| • | the clinical indications for which the product is approved; |
| • | acceptance of the product by physicians, other health care providers and patients as a safe and effective treatment; |
| • | the potential and perceived advantages of product candidates over alternative treatments; |
| • | the safety of product candidates seen in a broader patient group, including its use outside the approved indications; |
| • | the cost of treatment in relation to alternative treatments; |
| • | the timing of market introduction of competitive products; |
| • | the availability of adequate reimbursement and pricing by third parties and government authorities; |
| • | relative convenience and ease of administration; and |
| • | the effectiveness of CymaBay’s or its partners’ sales, marketing and distribution efforts. |
If any product candidate is approved but does not achieve an adequate level of acceptance by physicians, hospitals, health care payors and patients, CymaBay may not generate sufficient revenue from these products and CymaBay may not become or remain profitable.
Potential conflicts of interest arising from relationships and any related compensation with respect to clinical studies could adversely affect the process.
Principal investigators for CymaBay’s clinical studies may serve as scientific advisors or consultants to CymaBay from time to time and receive cash compensation in connection with such services. If these relationships and any related compensation result in perceived or actual conflicts of interest, the integrity of the data generated at the applicable clinical study site may be questioned or jeopardized.
CymaBay may be subject to costly claims related to its clinical studies and may not be able to obtain adequate insurance.
Because CymaBay conducts clinical studies in humans, CymaBay faces the risk that the use of arhalofenate or future product candidates, will result in adverse side effects. CymaBay cannot predict the possible harms or side effects that may result from its clinical studies. Although CymaBay has clinical study liability insurance, CymaBay’s insurance may be insufficient to cover any such events. There is also a risk that CymaBay may not be able to continue to obtain clinical study coverage on acceptable terms. In addition, CymaBay may not have sufficient resources to pay for any liabilities resulting from a claim excluded from, or beyond the limit of, CymaBay’s insurance coverage. There is also a risk that third parties that CymaBay has agreed to indemnify could incur liability. Any litigation arising from its clinical studies, even if CymaBay is ultimately successful, would consume substantial amounts of CymaBay’s financial and managerial resources and may create adverse publicity.
45
Table of Contents
After the completion of our clinical trials, we cannot predict whether or when we will obtain regulatory approval to commercialize arhalofenate and we cannot, therefore, predict the timing of any future revenue from arhalofenate. Regulatory approval of an NDA is not guaranteed, and the approval process is expensive, uncertain and lengthy.
We cannot commercialize our product candidates, including arhalofenate until the appropriate regulatory authorities, such as the FDA, have reviewed and approved the product candidate. The regulatory agencies may not complete their review processes in a timely manner, or we may not be able to obtain regulatory approval for arhalofenate. Additional delays may result if arhalofenate is brought before an FDA advisory committee, which could recommend restrictions on approval or recommend non-approval of the product candidate. In addition, we may experience delays or rejections based upon additional government regulation from future legislation or administrative action, or changes in regulatory agency policy during the period of product development, clinical studies and the review process. As a result, we cannot predict when, if at all, we will receive any future revenue from commercialization of any of our product candidates, including arhalofenate. The FDA has substantial discretion in the drug approval process, including the ability to delay, limit or deny approval of a product candidate for many reasons, including the following:
| • | CymaBay may be unable to demonstrate to the satisfaction of regulatory authorities that a product candidate is safe and effective for any indication; |
| • | regulatory authorities may not find the data from nonclinical studies and clinical studies sufficient or may differ in the interpretation of the data; |
| • | regulatory authorities may require additional nonclinical or clinical studies; |
| • | the FDA or foreign regulatory authority might not approve CymaBay’s third party manufacturers’ processes or facilities for clinical or commercial product; |
| • | the FDA or foreign regulatory authority may change its approval policies or adopt new regulations; |
| • | the FDA or foreign regulatory authorities may disagree with the design or implementation of CymaBay’s clinical studies; |
| • | the FDA or foreign regulatory authority may not accept clinical data from studies that are conducted in countries where the standard of care is potentially different from that in the U.S.; |
| • | the results of clinical studies may not meet the level of statistical significance required by the FDA or foreign regulatory authorities for approval; |
| • | CymaBay may be unable to demonstrate that a product candidate’s clinical and other benefits outweigh its safety risks; and |
| • | the data collection from clinical studies of CymaBay’s product candidates may not be sufficient to support the submission of a NDA or other submission or to obtain regulatory approval in the U.S. or elsewhere. |
In addition, events raising questions about the safety of certain marketed pharmaceuticals may result in increased caution by the FDA and other regulatory authorities in reviewing new pharmaceuticals based on safety, efficacy or other regulatory considerations and may result in significant delays in obtaining regulatory approvals.
Even if we obtain regulatory approval for arhalofenate and our other product candidates, we will still face extensive regulatory requirements and our products may face future development and regulatory difficulties.
Even if we obtain regulatory approval in the U.S., the FDA may still impose significant restrictions on the indicated uses or marketing of our product candidates, including arhalofenate, or impose ongoing requirements for potentially costly post-approval studies or post-market surveillance. For example, the labeling ultimately approved for our product candidates, including arhalofenate, may include restrictions on use due to the specific patient population and manner of use in which the drug was evaluated and the safety and efficacy data obtained in those evaluations.
46
Table of Contents
Arhalofenate and our other product candidates will also be subject to additional ongoing FDA requirements governing the labeling, packaging, storage, distribution, safety surveillance, advertising, promotion, record-keeping and reporting of safety and other post-market information. The holder of an approved NDA is obligated to monitor and report AEs and any failure of a product to meet the specifications in the NDA. The holder of an approved NDA must also submit new or supplemental applications and obtain FDA approval for certain changes to the approved product, product labeling or manufacturing process. Advertising and promotional materials must comply with FDA rules and are subject to FDA review, in addition to other potentially applicable federal and state laws. Furthermore, promotional materials must be approved by the FDA prior to use for any drug receiving accelerated approval, the pathway we are pursuing for arhalofenate in the U.S.
In addition, manufacturers of drug products and their facilities are subject to payment of user fees and continual review and periodic inspections by the FDA and other regulatory authorities for compliance with current Good Manufacturing Practices (cGMP), and adherence to commitments made in the NDA. If we, or a regulatory agency, discover previously unknown problems with a product, such as quality issues or AEs of unanticipated severity or frequency, or problems with the facility where the product is manufactured, a regulatory agency may impose restrictions relative to that product or the manufacturing facility, including requiring recall or withdrawal of the product from the market or suspension of manufacturing.
If we, or our third party contractors, fail to comply with applicable regulatory requirements following approval of our product candidate, a regulatory agency may:
| • | issue an untitled or warning letter asserting violation of the law; |
| • | seek an injunction or impose civil or criminal penalties or monetary fines; |
| • | suspend or withdraw regulatory approval; |
| • | suspend any ongoing clinical trials; |
| • | refuse to approve a pending NDA or supplements to an NDA; or |
| • | recall and/or seize product. |
Any government investigation of alleged violations of law could require us to expend significant time and resources in response and could generate negative publicity. The occurrence of any event or penalty described above may inhibit our ability to commercialize arhalofenate and our other product candidates and inhibit our ability to generate revenues.
Even if we obtain FDA approval for arhalofenate or any of our other products in the U.S., we may never obtain approval for or commercialize arhalofenate or any of our other products outside of the U.S., which would limit our ability to realize their full market potential.
In order to market any products outside of the U.S., we must establish and comply with numerous and varying regulatory requirements on a country-by-country basis regarding safety and efficacy. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions. In addition, clinical trials conducted in one country may not be accepted by regulatory authorities in other countries, and regulatory approval in one country does not guarantee regulatory approval in any other country. Approval processes vary among countries and can involve additional product testing and validation and additional administrative review periods. Seeking foreign regulatory approval could result in difficulties and costs for us and require additional preclinical studies or clinical trials which could be costly and time consuming. Regulatory requirements can vary widely from country to country and could delay or prevent the introduction of our products in those countries. We do not have any product candidates approved for sale in any jurisdiction, including international markets, and we do not have experience in obtaining regulatory approval in international markets. If we fail to comply with regulatory requirements in international markets or to obtain and maintain required approvals, or if regulatory approvals in international markets are delayed, our target market will be reduced and our ability to realize the full market potential of our products will be unrealized.
47
Table of Contents
Our relationships with customers and payors will be subject to applicable anti-kickback, fraud and abuse and other health care laws and regulations, which could expose us to criminal sanctions, civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Health care providers, physicians and others play a primary role in the recommendation and prescription of any products for which we obtain marketing approval. Our future arrangements with third-party payors and customers may expose us to broadly applicable fraud and abuse and other health care laws and regulations that may constrain the business or financial arrangements and relationships through which we market, sell and distribute our products for which we obtain marketing approval. Restrictions under applicable federal and state health care laws and regulations, include the following:
| • | the federal health care anti-kickback statute prohibits, among other things, persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under federal health care programs such as Medicare and Medicaid; |
| • | the federal False Claims Act imposes criminal and civil penalties, including civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| • | the federal Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act, imposes criminal and civil liability for executing a scheme to defraud any health care benefit program and also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
| • | the federal false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statement in connection with the delivery of or payment for health care benefits, items or services; |
| • | the federal transparency requirements under the Health Care and Education Reconciliation Act of 2010 (Health Care Reform Law) require manufacturers of drugs, devices, biologics and medical supplies to report to the Department of Health and Human Services information related to physician payments and other transfers of value and physician ownership and investment interests; and |
| • | analogous state laws and regulations, such as state anti-kickback and false claims laws, may apply to sales or marketing arrangements and claims involving health care items or services reimbursed by non-governmental third-party payors, including private insurers, and some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government in addition to requiring manufacturers to report information related to payments to physicians and other health care providers or marketing expenditures. |
Efforts to ensure that our business arrangements with third parties will comply with applicable health care laws and regulations will involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other health care laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, exclusion from government funded health care programs, such as Medicare and Medicaid, and the curtailment or restructuring of our operations. If any of the physicians or other providers or entities with whom we expect to do business are found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded health care programs.
48
Table of Contents
Recently enacted and future legislation may increase the difficulty and cost for us to obtain marketing approval of and commercialize our product candidates and affect the prices we may obtain.
In the U.S. and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the health care system that could prevent or delay marketing approval of our product candidates, restrict or regulate post-approval activities and affect our ability to profitably sell any products for which we obtain marketing approval.
In the U.S., the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (Medicare Modernization Act) changed the way Medicare covers and pays for pharmaceutical products. The legislation expanded Medicare coverage for drug purchases by the elderly and introduced a new reimbursement methodology based on average sales prices for physician administered drugs. In addition, this legislation provided authority for limiting the number of drugs that will be covered in any therapeutic class. Cost reduction initiatives and other provisions of this legislation could decrease the coverage and price that we receive for any approved products. While the Medicare Modernization Act applies only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates. Therefore, any reduction in reimbursement that results from the Medicare Modernization Act may result in a similar reduction in payments from private payors.
More recently, in March 2010, the Health Care Reform Law was enacted to broaden access to health insurance, reduce or constrain the growth of health care spending, enhance remedies against fraud and abuse, add new transparency requirements for health care and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms. The Health Care Reform Law revises the definition of “average manufacturer price” for reporting purposes, which could increase the amount of Medicaid drug rebates to states. Further, the new law imposes a significant annual fee on companies that manufacture or import branded prescription drug products. New provisions affecting compliance have also been enacted, which may affect our business practices with health care practitioners. We will not know the full effects of the Health Care Reform Law until applicable federal and state agencies issue regulations or guidance under the new law. Although it is too early to determine the effect of the Health Care Reform Law, the new law appears likely to continue the pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase our regulatory burdens and operating costs.
Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We are not sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the marketing approvals of our product candidates, if any, may be.
Risks Related to Our Reliance on Third Parties
We rely on third-party manufacturers to produce our preclinical and clinical drug supplies, and we intend to rely on third parties to produce commercial supplies of any approved product candidates.
We do not own or operate, and we do not expect to own or operate, facilities for product manufacturing, storage and distribution, or testing. In the past we have relied on third-party manufacturers for supply of our preclinical and clinical drug supplies. We expect that in the future we will continue to rely on such manufacturers for drug supplies that will be used in clinical trials of our product candidates, including arhalofenate, and for commercialization of any of our product candidates that receive regulatory approval.
The facilities used by our contract manufacturers to manufacture the product candidates must be approved by the FDA pursuant to inspections that will be conducted only after we submit an NDA to the FDA, if at all. We do not control the manufacturing process of our product candidates and are completely dependent on our contract
49
Table of Contents
manufacturing partners for compliance with the FDA’s requirements for manufacture of finished pharmaceutical products. If our contract manufacturers cannot successfully manufacture material that conforms to our specifications and the FDA’s strict regulatory requirements of safety, purity and potency, we will not be able to secure and/or maintain FDA approval for our product candidates. In addition, we have no direct control over the ability of the contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. If our contract manufacturers cannot meet FDA standards, we may need to find alternative manufacturing facilities, which would significantly impact our ability to develop, obtain regulatory approval for or market our product candidates. No assurance can be given that our manufacturers can continue to make clinical and commercial supplies of arhalofenate, or future product candidates, at an appropriate scale and cost to make it commercially feasible.
In addition, we do not have the capability to package and distribute finished products to pharmacies and other customers. Prior to commercial launch, we will enter into agreements with one or more pharmaceutical product packager/distributor to ensure proper supply chain management once we are authorized to make commercial sales of our product candidates. If we receive marketing approval from the FDA, we intend to sell pharmaceutical product packaged and distributed by such suppliers. Although we have entered into agreements with our current contract manufacturers and packager/distributor for clinical trial material, we may be unable to maintain an agreement on commercially reasonable terms, which could have a material adverse impact upon our business.
We rely on limited sources of supply for the drug substance for our lead product candidate, arhalofenate, and any disruption in the chain of supply may cause delay in developing and commercializing arhalofenate.
We are currently transferring the drug substance manufacturing process to our selected contractor that will produce the supplies needed to meet clinical development, registration and forecasted commercial demand. It is our expectation that only one supplier of drug substance and one supplier of drug product will be qualified by the FDA. If supply from an approved vendor is interrupted, there could be a significant disruption in commercial supply of arhalofenate. An alternative vendor would need to be qualified through an NDA supplement which would be expensive and could result in further delay. The FDA or other regulatory agencies outside of the U.S. may also require additional studies if a new drug substance or drug product supplier is relied upon for commercial production. These factors could cause the delay of clinical trials, regulatory submissions, required approvals or commercialization of arhalofenate, and cause us to incur additional costs. Furthermore, if our suppliers fail to deliver the required commercial quantities of active pharmaceutical ingredient on a timely basis and at commercially reasonable prices, and we are unable to secure one or more replacement suppliers capable of production at a substantially equivalent cost, our supply chain for arhalofenate may be delayed, which could inhibit our ability to generate revenues.
Manufacturing issues may arise that could increase product and regulatory approval costs or delay commercialization of arhalofenate.
We are modifying the drug substance production process for arhalofenate at the selected commercial manufacturer to cost effectively remove impurities. As the modified process is scaled up it may reveal previously unknown impurities which could require resolution in order to proceed with our planned clinical trials and obtain regulatory approval for the commercial marketing of arhalofenate. In the future, we may identify impurities, which could result in increased scrutiny by the regulatory agencies, delays in the clinical program and regulatory approval for arhalofenate, increases in our operating expenses, or failure to obtain or maintain approval for arhalofenate.
Our reliance on third-party manufacturers entails risks, including the following:
| • | the inability to meet our product specifications and quality requirements consistently; |
| • | a delay or inability to procure or expand sufficient manufacturing capacity; |
| • | manufacturing and product quality issues related to scale-up of manufacturing; |
50
Table of Contents
| • | costs and validation of new equipment and facilities required for scale-up; |
| • | a failure to comply with cGMP and similar foreign standards; |
| • | the inability to negotiate manufacturing agreements with third parties under commercially reasonable terms; |
| • | termination or nonrenewal of manufacturing agreements with third parties in a manner or at a time that is costly or damaging to us; |
| • | the reliance on a limited number of sources, and in some cases, single sources for key materials, such that if we are unable to secure a sufficient supply of these key materials, we will be unable to manufacture and sell our product candidates in a timely fashion, in sufficient quantities or under acceptable terms; |
| • | the lack of qualified backup suppliers for those materials that are currently purchased from a sole or single source supplier; |
| • | operations of our third-party manufacturers or suppliers could be disrupted by conditions unrelated to our business or operations, including the bankruptcy of the manufacturer or supplier; |
| • | carrier disruptions or increased costs that are beyond our control; and |
| • | the failure to deliver our products under specified storage conditions and in a timely manner. |
Any of these events could lead to clinical study delays, failure to obtain regulatory approval or impact our ability to successfully commercialize our products. Some of these events could be the basis for FDA or other regulatory authorities’ action, including injunction, recall, seizure, or total or partial suspension of production.
We rely on third parties to conduct, supervise and monitor our clinical studies, and if those third parties perform in an unsatisfactory manner, it may harm our business.
We rely on contract service providers (CSPs) including clinical research organizations, clinical trial sites, central laboratories and other service providers to ensure the proper and timely conduct of our clinical trials. While we have agreements governing their activities, we have limited influence over their actual performance. We have relied and plan to continue to rely upon CSPs to monitor and manage data for our ongoing clinical programs for arhalofenate and our other product candidates, as well as the execution of nonclinical studies. We control only certain aspects of our CSPs’ activities. Nevertheless, we are responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards and our reliance on the CSPs does not relieve us of our regulatory responsibilities.
We and our CSPs are required to comply with the FDA’s guidance, which follows the International Conference on Harmonization Good Clinical Practice (ICH GCP), which are regulations and guidelines enforced by the FDA for all of our product candidates in clinical development. The FDA enforces the ICH GCP through periodic inspections of trial sponsors, principal investigators and clinical trial sites. If we or our CSPs fail to comply with the ICH GCP, the clinical data generated in our clinical trials may be deemed unreliable and the FDA may require us to perform additional clinical trials before approving our marketing applications. For example, upon inspection, the FDA may determine that our Phase 3 clinical trial for arhalofenate, does not comply with the ICH GCP. In addition, our Phase 3 clinical trials for arhalofenate will require a sufficiently large number of test subjects to evaluate the safety and effectiveness of arhalofenate. Accordingly, if our CSPs fail to comply with these regulations or fail to recruit a sufficient number of subjects, we may be required to repeat these Phase 3 clinical trials, which would delay the regulatory approval process.
Our CSPs are not our employees, and we cannot control whether or not they devote sufficient time and resources to our ongoing clinical and nonclinical programs. These CSPs may also have relationships with other entities, including our competitors, for whom they may also be conducting clinical studies, or other drug
51
Table of Contents
development activities which could harm our competitive position. We face the risk of potential unauthorized disclosure or misappropriation of our intellectual property by CSPs, which may reduce our trade secret protection and allow our potential competitors to access and exploit our proprietary technology. If our CSPs do not successfully carry out their contractual duties or obligations, fail to meet expected deadlines, or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols or regulatory requirements or for any other reasons, our clinical trials may be extended, delayed or terminated, and we may not be able to obtain regulatory approval for, or successfully commercialize arhalofenate or our other product candidates. As a result, our financial results and the commercial prospects for arhalofenate and any other product candidates that we develop would be harmed, our costs could increase, and our ability to generate revenues could be delayed.
Risks Related to Commercialization of Our Product Candidates
The commercial success of arhalofenate and our other product candidates will depend upon the acceptance of these products by the medical community, including physicians, patients and health care payors.
If any of our product candidates, including arhalofenate, receive marketing approval, they may nonetheless not gain sufficient market acceptance by physicians, patients, health care payors and others in the medical community. If these products do not achieve an adequate level of acceptance, we may not generate significant product revenues and we may not become profitable. The degree of market acceptance of any of our product candidates, including arhalofenate, will depend on a number of factors, including the following:
| • | demonstration of clinical safety and efficacy in our clinical trials; |
| • | the risk/benefit profile of our products such as arhalofenate; |
| • | the relative convenience, ease of administration and acceptance by physicians, patients and health care payors; |
| • | the prevalence and severity of any side effects; |
| • | the safety of product candidates seen in a broader patient group, including its use outside the approved indications; |
| • | limitations or warnings contained in the FDA and other regulatory authorities approved label for the relevant product candidate; |
| • | acceptance of the product by physicians, other health care providers and patients as a safe and effective treatment; |
| • | the potential and perceived advantages of product candidates over alternative treatments; |
| • | the timing of market introduction of competitive products; |
| • | pricing and cost-effectiveness; |
| • | the effectiveness of our or any future collaborators’ sales and marketing strategies; |
| • | our ability to obtain formulary approval; |
| • | our ability to obtain and maintain sufficient third-party coverage or reimbursement, which may vary from country to country; and |
| • | the effectiveness of our or any future collaborators’ sales, marketing and distribution efforts. |
If any of our product candidates, including arhalofenate, is approved but does not achieve an adequate level of acceptance by physicians, patients and health care payors, we may not generate sufficient revenue and we may not become or remain profitable.
52
Table of Contents
If we are unable to establish sales and marketing capabilities or enter into agreements with third parties to market and sell our product candidates, we may be unable to generate any revenue.
We currently do not have an organization for the sales, marketing and distribution of pharmaceutical products and the cost of establishing and maintaining such an organization may exceed the cost-effectiveness of doing so. In order to market any products that may be approved, including arhalofenate, we must build our sales, marketing, managerial and other non-technical capabilities or make arrangements with third parties to perform these services. We may enter into strategic partnerships with third parties to commercialize our product candidates, including arhalofenate.
If we are unable to build our own sales force or negotiate a strategic partnership for the commercialization of arhalofenate, we may be forced to delay the potential commercialization of arhalofenate, or reduce the scope of our sales or marketing activities for arhalofenate. If we elect to increase our expenditures to fund commercialization activities ourselves, we will need to obtain additional capital, which may not be available to us on acceptable terms, or at all. If we do not have sufficient funds, we will not be able to bring arhalofenate to market or generate product revenue.
If we are unable to establish adequate sales, marketing and distribution capabilities, whether independently or with third parties, we may not be able to generate sufficient product revenue and may not become profitable. We will be competing with companies that currently have extensive and well-funded marketing and sales operations. Without an internal team or the support of a third party to perform marketing and sales functions, we may be unable to compete successfully against these more established companies.
In addition, there are risks involved with both establishing our own sales and marketing capabilities and entering into arrangements with third parties to perform these services. For example, recruiting and training a sales force is expensive and time-consuming and could delay any product launch. If the commercial launch of a product candidate for which we recruit a sales force and establish marketing capabilities is delayed or does not occur for any reason, we would have prematurely or unnecessarily incurred these commercialization expenses. This may be costly, and our investment would be lost if we cannot retain or reposition our sales and marketing personnel.
If we obtain approval to commercialize any products outside of the U.S., a variety of risks associated with international operations could materially adversely affect our business.
If our product candidates are approved for commercialization, we intend to enter into agreements with third parties to market those product candidates outside the U.S., including for arhalofenate. We expect that we will be subject to additional risks related to international operations, including the following:
| • | different regulatory requirements for drug approvals in foreign countries; |
| • | reduced protection for intellectual property rights; |
| • | unexpected changes in tariffs, trade barriers and regulatory requirements; |
| • | economic weakness, including inflation, or political instability in particular foreign economies and markets; |
| • | compliance with tax, employment, immigration and labor laws for employees living or traveling abroad; |
| • | foreign taxes, including withholding of payroll taxes; |
| • | foreign currency fluctuations, which could result in increased operating expenses and reduced revenues, and other obligations incident to doing business in another country; |
| • | workforce uncertainty in countries where labor unrest is more common than in the U.S.; |
53
Table of Contents
| • | production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad; and |
| • | business interruptions resulting from geopolitical actions, including war and terrorism, pandemics, or natural disasters including earthquakes, typhoons, volcanic eruptions, floods and fires. |
We have no prior experience in these areas. In addition, there are complex regulatory, tax, labor and other legal requirements imposed by both the European Union and many of the individual countries in Europe with which we will need to comply. Many U.S.-based biopharmaceutical companies have found the process of marketing their own products in Europe to be very challenging.
If our competitors develop and market products that are more effective, safer or less expensive than arhalofenate, our commercial opportunities will be negatively impacted.
The life sciences industry is highly competitive, and we face significant competition from other pharmaceutical, biopharmaceutical and biotechnology companies and possibly from academic institutions, government agencies and private and public research institutions that are researching, developing and marketing products designed to address the treatment of gout. Our competitors may have significantly greater financial, manufacturing, marketing and drug development resources. Large pharmaceutical companies, in particular, have extensive experience in the clinical testing of, obtaining regulatory approvals for, and marketing of, drugs. New developments, including the development of other pharmaceutical technologies and methods of treating disease, occur in the pharmaceutical and life sciences industries at a rapid pace.
These developments may render our product candidates obsolete or noncompetitive. Compared to us, potential competitors may have substantially greater:
| • | research and development resources, including personnel and technology; |
| • | regulatory experience; |
| • | experience in pharmaceutical development and commercialization; |
| • | ability to negotiate competitive pricing and reimbursement with third-party payors; |
| • | experience and expertise in exploitation of intellectual property rights; and |
| • | capital resources. |
As a result of these factors, our competitors may obtain regulatory approval of their products more rapidly than we do or may obtain patent protection or other intellectual property rights that limit our ability to develop or commercialize our product candidates. The competitors may also develop products that are more effective, better tolerated, more useful and less costly than our products and they may also be more successful in manufacturing and marketing their products.
Formulary approval and reimbursement may not be available for arhalofenate and our other product candidates, which could make it difficult for us to sell our products profitably.
Obtaining formulary approval can be an expensive and time consuming process. We cannot be certain if and when we will obtain formulary approval to allow us to promote our product candidates, including arhalofenate, into our target markets. Failure to obtain timely formulary approval will limit our commercial success.
Furthermore, market acceptance and sales of arhalofenate, or any other product candidates that we develop, will depend in part on the extent to which reimbursement for these products and related treatments will be available from government health administration authorities, private health insurers and other organizations. Government authorities and third-party payors, such as private health insurers and health maintenance
54
Table of Contents
organizations, decide which medications they will pay for and establish reimbursement levels. A prevailing trend in the U.S. health care industry and elsewhere is cost containment. Government authorities and these third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. Increasingly, third-party payors are requiring that companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. We cannot be sure that reimbursement will be available for any product that we commercialize and, if reimbursement is available, what the level of reimbursement will be. Reimbursement may impact the demand for, or the price of, any product for which we obtain marketing approval. We cannot be sure that reimbursement will be available for arhalofenate, or any other product candidates. Also, reimbursement amounts may reduce the demand for, or the price of, our products. If reimbursement is not available, or is available only to limited levels, we may not be able to successfully commercialize arhalofenate, or any other product candidates that we develop.
There have been a number of legislative and regulatory proposals to change the health care system in the U.S. and in some foreign jurisdictions that could affect our ability to sell any future products profitably. These legislative and regulatory changes may negatively impact the reimbursement for any future products, following approval. The availability of generic treatments may also substantially reduce the likelihood of reimbursement for any future products, including arhalofenate. The application of user fees to generic drug products will likely expedite the approval of additional generic drug treatments. We expect to experience pricing pressures in connection with the sale of arhalofenate and any other product candidate that we develop, due to the trend toward managed health care, the increasing influence of health maintenance organizations and additional legislative changes.
In addition, there may be significant delays in obtaining reimbursement for approved products, and coverage may be more limited than the purposes for which the product is approved by the FDA or health authorities in other countries. Moreover, eligibility for reimbursement does not imply that any product will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Interim payments for new products, if applicable, may also not be sufficient to cover our costs and may not be made permanent. Payment rates may vary according to the use of the product and the clinical setting in which it is used, may be based on payments allowed for lower cost products that are already reimbursed, and may be incorporated into existing payments for other services. Net prices for products may be reduced by mandatory discounts or rebates required by government health care programs or private payors and by any future relaxation of laws that presently restrict imports of products from countries where they may be sold at lower prices than in the U.S. Third-party payors often rely upon Medicare coverage policy and payment limitations in setting their own reimbursement policies.
If we are unable to promptly obtain coverage and profitable payment rates from both government funded and private payors for any of our product candidates, including arhalofenate, it could have a material adverse effect on our operating results, our ability to raise capital needed to commercialize products and our overall financial condition.
Even if we receive regulatory approval for arhalofenate, we will be subject to ongoing FDA and other regulatory obligations and continued regulatory review, which may result in significant additional expense and limit our ability to commercialize arhalofenate.
Any regulatory approvals that we or potential collaboration partners receive for arhalofenate or future product candidates, may also be subject to limitations on the indicated uses for which the product may be marketed or contain requirements for potentially costly post-marketing studies. In addition, even if approved, the labeling, packaging, adverse event reporting, storage, advertising, promotion and recordkeeping for any product will be subject to extensive and ongoing regulatory requirements. The subsequent discovery of previously unknown problems with a product, including AEs of unanticipated severity or frequency, may result in restrictions on the marketing of the product, and could include withdrawal of the product from the market.
55
Table of Contents
Regulatory policies may change and additional government regulations may be enacted that could prevent or delay regulatory approval of our product candidates. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the U.S. or abroad. If we are not able to maintain regulatory compliance, we might not be permitted to market arhalofenate or future products, if any, and we may not achieve or sustain profitability.
If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of our product candidates.
We face an inherent risk of product liability exposure related to the testing of our product candidates in human clinical studies, and will face an even greater risk if we sell our product candidates commercially. An individual may bring a liability claim against us if one of our product candidates causes, or merely appears to have caused, an injury. If we cannot successfully defend ourselves against product liability claims, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in the following:
| • | decreased demand for our product candidates; |
| • | impairment to our business reputation; |
| • | withdrawal of clinical study participants; |
| • | distraction of management’s attention from our primary business; |
| • | substantial monetary awards to patients or other claimants; |
| • | the inability to commercialize our product candidates; and |
| • | loss of revenues. |
We do carry product liability insurance for our clinical studies. Further, we intend to expand our insurance coverage to include the sale of commercial products if marketing approval is obtained for any of our product candidates. However, we may be unable to obtain this product liability insurance on commercially reasonable terms and with insurance coverage that will be adequate to satisfy any liability that may arise. On occasion, large judgments have been awarded in class action or individual lawsuits relating to marketed pharmaceuticals. A successful product liability claim or series of claims brought against us could cause our stock price to decline and, if judgments exceed our insurance coverage, could decrease our cash and adversely affect our business.
We may expend our limited resources to pursue a particular product candidate or indication and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success.
The success of our business depends primarily upon our ability to identify, develop and commercialize product candidates. Because we have limited financial and managerial resources, we focus on product candidates for specific indications. As a result, we may forego or delay pursuit of opportunities with other product candidates or other indications that later prove to have greater commercial potential. We may focus our efforts and resources on product candidates that ultimately prove to be unsuccessful.
If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through collaboration, licensing or other royalty arrangements in cases in which it would have been advantageous for us to retain sole development and commercialization rights.
56
Table of Contents
Risks Related to Our Intellectual Property
If we are unable to obtain or protect intellectual property rights related to our products and product candidates, we may not be able to compete effectively in our market.
We rely upon a combination of patents, trade secret protection and confidentiality agreements to protect the intellectual property related to our products and product candidates. The strength of patents in the biotechnology and pharmaceutical field involves complex legal and scientific questions and can be uncertain. The patent applications that we own or in-license may fail to result in issued patents with claims that cover the products in the U.S. or in other countries. If this were to occur, early generic competition could be expected against arhalofenate and other product candidates in development. There is no assurance that all of the potentially relevant prior art relating to our patents and patent applications has been found, which can invalidate a patent or prevent a patent from issuing based on a pending patent application. Even if patents do successfully issue, third parties may challenge their validity, enforceability, scope or ownership, which may result in such patents, or our rights to such patents, being narrowed or invalidated. Furthermore, even if they are unchallenged, our patents and patent applications may not adequately protect our intellectual property or prevent others from designing around our claims. If the patent applications we hold or license with respect to arhalofenate fail to issue or if their breadth or strength of protection is threatened, it could dissuade companies from collaborating with us and threaten our ability to commercialize our products. We cannot offer any assurances about which, if any, patents will issue or whether any issued patents will be found invalid or unenforceable, will be challenged by third parties or will adequately protect our products and product candidates. Further, if we encounter delays in development or regulatory approvals, the period of time during which we could market arhalofenate under patent protection could be reduced. Since patent applications in the U.S. and most other countries are confidential for a period of time after filing, and some remain so until issued, we cannot be certain that we or our licensors were the first to file any patent application related to arhalofenate or our other product candidates. Furthermore, if third parties have filed such patent applications, an interference proceeding in the U.S. can be provoked by a third party or instituted by us to determine who was the first to invent any of the subject matter covered by the patent claims of our applications. An unfavorable outcome could require us to cease using the related technology or to attempt to license it from the prevailing party, which may not be available on commercially reasonable terms or at all.
In addition to the protection afforded by patents, we rely on trade secret protection and confidentiality agreements to protect proprietary know-how that is not patentable, processes for which patents are difficult to enforce and other elements of our drug discovery and development processes that involve proprietary know-how, information or technology that is not covered by patents. Although we expect all of our employees to assign their inventions to us, and all of our employees, consultants, advisors and any third parties who have access to our proprietary know-how, information or technology to enter into confidentiality agreements, we cannot provide any assurances that all such agreements have been duly executed, that such agreements provide adequate protection and will not be breached, that our trade secrets and other confidential proprietary information will not otherwise be disclosed or that competitors will not otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. If we are unable to prevent material disclosure of the non-patented intellectual property related to our technologies to third parties, and there is no guarantee that we will have any such enforceable trade secret protection, we may not be able to establish or maintain a competitive advantage in our market, which could materially adversely affect our business, results of operations and financial condition.
Further, the laws of some foreign countries do not protect patents and other proprietary rights to the same extent or in the same manner as the laws of the U.S. As a result, we may encounter significant problems in protecting and defending our intellectual property abroad. We may also fail to pursue or obtain patents and other intellectual property protection relating to our products and product candidates in all foreign countries.
57
Table of Contents
Third-party claims of intellectual property infringement may prevent or delay our development and commercialization efforts or otherwise affect our business.
Our commercial success depends in part on our avoiding infringement and other violations of the patents and proprietary rights of third parties. There is a substantial amount of litigation, both within and outside the U.S., involving patent and other intellectual property rights in the biotechnology and pharmaceutical industries, including patent infringement lawsuits, interferences, oppositions and inter party re-examination proceedings before the U.S. Patent and Trademark Office (U.S. PTO) and its foreign counterparts. Numerous U.S. and foreign issued patents and pending patent applications, which are owned by third parties, exist in the fields in which we and our collaborators are developing product candidates. As the biotechnology and pharmaceutical industries expand and more patents are issued, and as we gain greater visibility and market exposure as a public company, the risk increases that our product candidates or other business activities may be subject to claims of infringement of the patent and other proprietary rights of third parties.
Third parties may assert that we are employing their proprietary technology without authorization. There may be third-party patents or patent applications with claims to materials, formulations, methods of manufacture or methods for treatment related to the use or manufacture of arhalofenate and/or our other product candidates. Because patent applications can take many years to issue, there may be currently pending patent applications which may later result in issued patents that our product candidates may infringe. In addition, third parties may obtain patents in the future and claim that use of our technologies infringes upon these patents. If any third-party patents were held by a court of competent jurisdiction to cover the manufacturing process of any of our product candidates, any molecules formed during the manufacturing process or any final product itself, the holders of any such patents may be able to block our ability to commercialize such product candidate unless we obtained a license under the applicable patents, or until such patents expire. Similarly, if any third-party patent were held by a court of competent jurisdiction to cover aspects of our formulations, processes for manufacture or methods of use, including combination therapy, the holders of any such patent may be able to block our ability to develop and commercialize the applicable product candidate unless we obtained a license or until such patent expires. In either case, such a license may not be available on commercially reasonable terms or at all. In addition, we may be subject to claims that we are infringing other intellectual property rights, such as trademarks or copyrights, or misappropriating the trade secrets of others, and to the extent that our employees, consultants or contractors use intellectual property or proprietary information owned by others in their work for us, disputes may arise as to the rights in related or resulting know-how and inventions.
Parties making claims against us may obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our product candidates. Defense of these claims, regardless of their merit, would involve substantial litigation expense and would be a substantial diversion of employee resources from our business. In the event of a successful infringement or other intellectual property claim against us, we may have to pay substantial damages, including treble damages and attorneys’ fees for willful infringement, obtain one or more licenses from third parties, pay royalties or redesign our affected products, which may be impossible or require substantial time and monetary expenditure. We cannot predict whether any such license would be available at all or whether it would be available on commercially reasonable terms. Furthermore, even in the absence of litigation, we may need to obtain licenses from third parties to advance our research or allow commercialization of our product candidates, and we have done so from time to time. We may fail to obtain any of these licenses at a reasonable cost or on reasonable terms, if at all. In that event, we would be unable to further develop and commercialize one or more of our product candidates, which could harm our business significantly. We cannot provide any assurances that third-party patents do not exist which might be enforced against our products or product candidates, resulting in either an injunction prohibiting our sales, or, with respect to our sales, an obligation on our part to pay royalties and/or other forms of compensation to third parties.
58
Table of Contents
We license certain key intellectual property from third parties, and the loss of our license rights could have a materially adverse effect on our business.
We are a party to a number of technology licenses that are important to our business and expect to enter into additional licenses in the future. For example, we rely on an exclusive license to certain patents, proprietary technology and know-how from DiaTex, which include arhalofenate. During the term of the exclusive license with DiaTex we may perform research and development of compounds and products for the treatment of human disease based on the patents, proprietary technology and know-how from DiaTex. If we fail to comply with our obligations under our agreement with DiaTex, including our obligations to pay royalty payments during the development and commercialization of arhalofenate, or our other license agreements, or if we are subject to a bankruptcy, the licensor may have the right to terminate the license, in which event we would not be able to develop or market products covered by the license, including in the case of the DiaTex license, arhalofenate, which would have a materially adverse effect on our business.
We may be involved in lawsuits to protect or enforce our patents, the patents of our licensors or our other intellectual property rights, which could be expensive, time consuming and unsuccessful.
Competitors may infringe or otherwise violate our patents, the patents of our licensors or our other intellectual property rights. To counter infringement or unauthorized use, we may be required to file legal claims, which can be expensive and time-consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours or our licensors is not valid or is unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation or defense proceedings could put one or more of our patents at risk of being invalidated or interpreted narrowly and could put our patent applications at risk of not issuing. The initiation of a claim against a third party may also cause the third party to bring counter-claims against us.
We may not be able to prevent, alone or with our licensors, misappropriation of our intellectual property rights, particularly in countries where the laws may not protect those rights as fully as in the U.S. Our business could be harmed if in a litigation if the prevailing party does not offer us a license on commercially reasonable terms. Any litigation or other proceedings to enforce our intellectual property rights may fail, and even if successful, may result in substantial costs and distract our management and other employees.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. There could also be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock.
Obtaining and maintaining our patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
Periodic maintenance fees on any issued patent are due to be paid to the U.S. PTO and foreign patent agencies in several stages over the lifetime of the patent. The U.S. PTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. While an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Non-compliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. If we or our licensors that control the prosecution and maintenance of our licensed patents fail to maintain the patents and patent applications covering our product candidates, we may lose our rights and our competitors might be able to enter the market, which would have a material adverse effect on our business.
59
Table of Contents
Risks Related to Our Business Operations and Industry
Our future success depends on our ability to retain key executives and to attract, retain and motivate qualified personnel.
We are highly dependent on principal members of our executive team listed under “Management.” While we have entered into employment agreements or offer letters with each of our executive officers, any of them could leave our employment at any time, as all of our employees are “at will” employees. We do not maintain “key person” insurance for any of our executives or other employees. Recruiting and retaining other qualified employees for our business, including scientific and technical personnel, will also be critical to our success. There is currently a shortage of skilled executives in our industry, which is likely to continue. We also experience competition from universities and research institutions for the hiring of scientific and clinical personnel. As a result, competition for skilled personnel is intense and the turnover rate can be high. We may not be able to attract and retain personnel on acceptable terms given the competition among numerous pharmaceutical and biotechnology companies for similar personnel. In addition, failure of any of our clinical studies may make it more challenging to recruit and retain qualified personnel. If we are unable to successfully recruit key employees or replace the loss of services of any executive or key employee, it may adversely affect the progress of our research, development and commercialization objectives.
In addition, we rely on consultants and advisors, including scientific and clinical advisors, to assist us in formulating our research and development and commercialization strategy. Our consultants and advisors may be employed by employers other than us and may have commitments under consulting or advisory contracts with other entities that may limit their availability to us, which could also adversely affect the progress of our research, development and commercialization objectives.
We will need to expand our organization, and we may experience difficulties in managing this growth, which could disrupt our operations.
As of August 1, 2013, we had 12 full-time employees and three consultants. As our company matures, we expect to expand our employee base to increase our managerial, clinical, scientific and engineering, operational, sales, and marketing teams. Future growth would impose significant additional responsibilities on our management, including the need to identify, recruit, maintain, motivate and integrate additional employees, consultants and contractors. Also, our management may need to divert a disproportionate amount of its attention away from our day-to-day activities and devote a substantial amount of time to managing these growth activities. We may not be able to effectively manage the expansion of our operations, which may result in weaknesses in our infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among remaining employees. Our expected growth could require significant capital expenditures and may divert financial resources from other projects, such as the development of product candidates. If our management is unable to effectively manage our growth, our expenses may increase more than expected, our ability to generate and/or grow revenues could be reduced, and we may not be able to implement our business strategy. Our future financial performance and our ability to commercialize arhalofenate and our other product candidates and compete effectively will depend, in part, on our ability to effectively manage any future growth.
60
Table of Contents
ITEM 2. FINANCIAL INFORMATION.
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
Forward-Looking Statements
Some of the statements under in this “Management’s Discussion and Analysis of Financial Condition and Results of Operations” are forward-looking statements. These forward-looking statements are based on management’s beliefs and assumptions and on information currently available to our management and involve significant elements of subjective judgment and analysis. Words such as “expects,” “will,” “anticipates,” “targets,” “goals,” “projects,” “intends,” “plans,” “believes,” “seeks,” “estimates,” “potential,” “should,” “could,” variations of such words, and similar expressions are intended to identify forward-looking statements. Our actual results and the timing of events may differ significantly from the results discussed in the forward-looking statements. Factors that might cause such a difference include those discussed under the caption “Disclosure Regarding Forward Looking Statements” at the beginning of this Form 10, and in “Item 1A. Risk Factors” and elsewhere in this Form 10. These and many other factors could affect our future financial and operating results. We undertake no obligation to update any forward-looking statement to reflect events after the date of this Form 10.
Overview
CymaBay Therapeutics is a clinical-stage biopharmaceutical company that is focused on the development and commercialization of proprietary new medicines for the treatment of metabolic diseases. Arhalofenate, CymaBay’s lead product candidate, has completed three Phase 2 studies for the treatment of gout. Arhalofenate possesses two therapeutic actions: in gout patients it is intended to prevent painful attacks in joints while promoting excretion of uric acid by the kidney. CymaBay intends to initiate a Phase 2b study for arhalofenate in 225 patients. CymaBay is also developing a pipeline of product candidates for the treatment of diabetes and dyslipidemia.
We are an emerging growth company. Under the JOBS Act emerging growth companies can delay adopting new or revised accounting standards until such time of those standards apply to private companies. We plan to avail ourselves of this exemption from new or revised accounting standards, and therefore, we may not be subject to the same new or revised accounting standards as other public companies that are not “emerging growth companies.”
Reverse Stock Split and Conversion of Preferred Stock
On September 30, 2013, we effected a 1-for-79.5 reverse split of our preferred stock and common stock, which we refer to as the reverse stock split, all of the shares of our outstanding preferred stock converted to common stock, we sold shares of our common stock and warrants to purchase shares of our common stock in a private placement for aggregate gross proceeds of $26.8 million, and raised an additional $5.0 million in venture debt financing pursuant to a $10.0 million loan agreement which we entered into simultaneously with the private placement, resulting in aggregate net proceeds to CymaBay of $28.9 million after deducting placement agent fees and estimated offering expenses. At the same time we issued shares of our common stock in cancellation of approximately $16.9 million of debt owed to the holder of that debt. On October 31, 2013, we sold additional shares of our common stock and warrants to purchase shares of our common stock, which sales are also part of the private placement, for aggregate net proceeds to CymaBay of $2.8 million after deducting placement agent fees and estimated offering expenses. We refer to the private placement, the venture debt financing and the issuance of our common stock in cancellation of the $16.9 million of debt as the 2013 financing. The discussion in this “Management’s Discussion and Analysis of Financial Conditions and Results of Operations” gives retroactive effect to the reverse stock split that occurred on September 30, 2013.
Critical Accounting Policies and Use of Estimates
Our management’s discussion and analysis of our financial condition and results of operations is based on our financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements, as well as the reported revenues and expenses during the reporting periods. We
61
Table of Contents
base our estimates on historical experience and on various other factors that we believe to be materially reasonable under the circumstances and review our estimates on an ongoing basis. Actual results may materially differ from these estimates under different assumptions or conditions.
While our significant accounting policies are described in more detail in Note 2 of our financial statements included in this Form 10, we believe the following accounting policies to be critical to the judgments and estimates used in the preparation of our financial statements.
Revenue Recognition
Our contract revenues are generated primarily through research and development collaboration agreements, which may include nonrefundable, non-creditable upfront fees, funding for research and development efforts, and milestone or other contingent payments for achievements with regards to our licensed products. We have not materially modified any previous collaboration agreements or entered into any new agreements in 2012, nor have we received any milestone payments in 2012. Therefore, all collaboration agreements have been accounted for in accordance with the accounting guidance applicable to such arrangements prior to the adoption of Accounting Standards Update (ASU) 2009-13, Multiple-Deliverable Revenue Arrangements, and ASU 2010-17, Revenue Recognition – Milestone Method.
We recognize revenue when pervasive evidence of an arrangement exists, transfer of technology has been completed, services are performed or products have been delivered, the fee is fixed and determinable, and collection is reasonably assured.
Upfront payments for licensing our intellectual property to date have not been separable from the activity of providing research and development services because the license has not been assessed to have stand-alone value separate from the research and development services provided. Such upfront payments are recorded as deferred revenue in the balance sheet and are recognized as contract revenue over the contractual or estimated substantive performance period, which is consistent with the term of the research and development obligations contained in the research and development collaboration agreement.
Payments resulting from our research and development efforts under license agreements are recognized as the activities are performed.
Substantive, at-risk milestone payments are recognized as revenue when the milestone is achieved and collectability is reasonably assured. When contingent payments are not for substantive and at-risk milestones, revenue is recognized over the estimated remaining term of the related service period or, if there are no continuing performance obligations under the arrangement, upon receipt provided that collection is reasonably assured and other revenue recognition criteria have been satisfied.
Research and Development Expenses
As part of the process of preparing our financial statements, we are required to estimate our accrued research and development expenses. This process involves reviewing contracts, reviewing the terms of our license agreements, communicating with our applicable personnel to identify services that have been performed on our behalf and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of actual cost. The majority of our service providers invoice us monthly in arrears for services performed. We make estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy of our estimates with the service providers and make adjustments if necessary. Examples of estimated accrued research and development expenses include fees to:
| • | contract research organizations and other service providers in connection with clinical studies; |
| • | contract manufacturers in connection with the production of clinical trial materials; and |
| • | vendors in connection with preclinical development activities. |
62
Table of Contents
We base our expenses related to clinical studies on our estimates of the services received and efforts expended pursuant to contracts with multiple research institutions and contract research organizations that conduct and manage clinical studies on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may result in uneven payment flows and expense recognition. Payments under some of these contracts depend on factors such as the successful enrollment of patients and the completion of clinical trial milestones. In accruing service fees, we estimate the time period over which services will be performed and the level of effort to be expended in each period. If the actual timing of the performance of services or the level of effort varies from our estimate, we adjust the accrual accordingly. Our understanding of the status and timing of services performed relative to the actual status and timing of services performed may vary and may result in our reporting changes in estimates in any particular period. Adjustments to prior period estimates have not been material for the years ended December 31, 2011 and 2012, and for the six months ended June 30, 2013 and 2012.
Stock-Based Compensation
We expense stock-based compensation to employees over the requisite service period based on the estimated grant-date fair value-based measurement of the awards and considering estimated forfeiture rates. For stock-based compensation awards to non-employees, we re-measure the fair value-based measurement of the non-employee awards at each reporting period prior to vesting and finally at the vesting date of the award. Changes in the estimated fair value-based measurement of these non-employee awards are recognized as compensation expense in the period of change.
Determining the appropriate fair value-based measurement of stock-based awards requires the use of subjective assumptions. In the absence of a public trading market for our common stock, we conducted periodic assessments of the valuation of our common stock. These valuations were performed concurrently with the achievement of significant milestones, with major financing transactions or when prior valuations became stale under Section 409A of the Internal Revenue Code. The determination of the fair value-based measurement of options using an option-pricing model is affected by our estimated common stock fair value as well as assumptions regarding a number of other subjective variables. These other variables include the expected term of the options, our expected stock price volatility over the expected term of the options, stock option exercise and cancellation behaviors, risk-free interest rates, and expected dividends, which are estimated as follows:
| • | Fair Value of our Common Stock: Because our stock is not publicly traded, we must estimate its fair value, as discussed in “Common Stock Valuations” below. |
| • | Expected Term: We do not believe we are able to rely on our historical exercise and post-vesting termination activity to provide accurate data for estimating the expected term for use in determining the fair value-based measurement of our options. Therefore, we have opted to use the “simplified method” for estimating the expected term of options. |
| • | Volatility: As we do not have a trading history for our common stock, the expected stock price volatility for our common stock was estimated by taking an average weighted historic price volatility for industry peers based on daily price observations over a period equivalent to the expected term of the stock option grants. Industry peers consist of several public companies in the biopharmaceutical industry similar in size, stage of life cycle and financial leverage. We did not rely on implied volatilities of traded options in our industry peers’ common stock because the volume of activity was relatively low. We intend to continue to consistently apply this process using the same or similar public companies until a sufficient amount of historical information regarding the volatility of our own common stock share price becomes available, or unless circumstances change such that the identified companies are no longer similar to us, in which case, more suitable companies whose share prices are publicly available would be utilized in the calculation. |
| • | Risk-free Rate: The risk-free interest rate is based on the yields of U.S. Treasury securities with maturities similar to the expected term of the options for each option group. |
63
Table of Contents
| • | Dividend Yield: We have never declared or paid any cash dividends and do not presently plan to pay cash dividends in the foreseeable future. Consequently, we used an expected dividend yield of zero. |
The estimation of the number of stock awards that will ultimately vest requires judgment, and to the extent actual results or updated estimates differ from our current estimates, such amounts will be recorded as a cumulative adjustment in the period in which estimates are revised. Forfeitures are estimated such that we only recognize expense for those shares expected to vest, and adjustments are made if actual forfeitures differ from those estimates.
For the years ended December 31, 2012 and 2011, stock-based compensation expense was $0.1 million, and $0.8 million, respectively. For the six month periods ended June 30, 2013 and 2012 stock-based compensation expense was $34,000 and $42,000, respectively. As of June 30, 2013 and December 31, 2012, we had $37,000 and $91,000 of total unrecognized compensation expense, net of related forfeiture estimates, which we expect to recognize over a weighted-average period of approximately 2.2 years and 2.8 years, respectively.
If any of the assumptions used in a Black-Scholes model changes significantly, stock-based compensation for future awards may differ materially compared with the awards granted previously.
Common Stock Valuations
The fair value of the common stock underlying our stock options and restricted stock was determined by our board of directors, which intended all options granted to be exercisable at a price per share not less than the per share fair value of our common stock underlying those options on the date of grant. All stock awards previously granted or to be granted in the future were or are expected to be granted at the grant date fair value of the award. The valuations of our common stock were determined in accordance with the guidelines outlined in the American Institute of Certified Public Accountants Practice Aid, Valuation of Privately-Held-Company Equity Securities Issued as Compensation. Valuation analysis of our common stock was performed on our behalf by third party valuation specialists. The methodology used by the third party valuation specialists to determine the fair value of our common stock included estimating the fair value of the enterprise, subtracting the fair value of debt from this enterprise value, and then allocating this value using the Option Pricing Method to all of the equity interests. The assumptions used in the valuation model to determine the fair value of our common stock as of the date of each option and restricted stock award, are based on numerous objective and subjective factors combined with management judgment including the following:
| • | progress of research and development activities; |
| • | our operating and financial performance; |
| • | market conditions; |
| • | developmental milestones achieved; |
| • | sales of our convertible preferred stock in arms-length transactions; |
| • | business risks; and |
| • | management and board of director experience. |
We have granted stock options during the period from January 1, 2011, through June 30, 2013, as summarized below:
Date of Issuance | Number of Shares Subject to Options Granted | Exercise Price per Share | Fair Value Estimate per Common Share | Estimated Total Fair Value-Based Measurement of Options Granted (In thousands) | ||||||||||||
January 25, 2012 | 15,094 | $ | 4.77 | $ | 3.97 | $ | 58 | |||||||||
Management and our board of directors performed valuation analyses with the assistance of independent valuation specialists to determine the then current fair value of our common stock. To facilitate these valuation analyses, we developed projections of our future revenues and operating expenses. Key assumptions reflected in
64
Table of Contents
the income approach calculations included the anticipated timing of a potential liquidity event, the estimated volatility of our common stock, and the discount for lack of marketability of our common stock. These income approach assumptions are set forth below for each of the valuations performed as of December 31, 2012 and 2011:
| December 31, | ||||||||
| 2011 | 2012 | |||||||
Common Stock Value per Share | $ | 4.77 | $ | 0.80 | ||||
Time to Liquidity (in years) | 1.5 | 2.0 | ||||||
Volatility | 92.7 | % | 94.7 | % | ||||
Risk-Free Interest Rate | 0.20 | % | 0.30 | % | ||||
Marketability Discount Rate | 42.8 | % | 49.2 | % | ||||
For grants of stock awards made on dates for which there was no valuation performed by an independent valuation specialist, our board of directors determined the fair value of our common stock on the date of grant based upon the immediately preceding valuation and other pertinent information available to it at the time of grant.
Results of Operations
General
To date, we have not generated any net income from operations. Since our date of incorporation through June 30, 2013, we have an accumulated deficit of $340.6 million, primarily as a result of expenditures for research and development and general and administrative expenses. While we may in the future generate revenue from a variety of sources, including license fees and milestone payments in connection with strategic partnerships, our product candidates are at a mid-level stage of development and may never be successfully developed or commercialized. Accordingly, we expect to continue to incur substantial losses from operations for the foreseeable future and there can be no assurance that we will ever generate sufficient revenue to achieve and sustain profitability.
Contract Revenue
Our recent revenue comprises primarily collaboration agreement-related revenue. Collaboration agreement-related revenue has included license fees, payments for research and development services and milestone and other contingent payments. For the six months ended June 30, 2013 there were no collaboration revenues.
65
Table of Contents
Research & Development Expenses
Conducting research and development is central to our business model. For the years ended December 31, 2012 and 2011, and the six months ended June 30, 2013 and 2012, research and development expenses were $9.3 million, $14.4 million, $2.5 million, and $5.3 million, respectively. Research and development expenses are detailed in the table below:
| (In thousands) | ||||||||||||||||
| Six months ended June 30, | Year ended December 31, | |||||||||||||||
| 2013 | 2012 | 2012 | 2011 | |||||||||||||
(unaudited) | ||||||||||||||||
MBX-102 Clinical and Non-Clinical | $ | 20 | $ | 10 | $ | 39 | $ | 123 | ||||||||
MBX-102 Gout – Three Phase 2 Randomized Studies | 560 | 2,395 | 3,741 | 5,774 | ||||||||||||
MBX-8025 | — | 4 | 21 | 48 | ||||||||||||
MBX-2982 | 25 | 70 | 118 | 394 | ||||||||||||
Other Projects | 1 | — | — | 202 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total Project Costs | 606 | 2,479 | 3,919 | 6,541 | ||||||||||||
Internal Research and Development Costs | 1,853 | 2,799 | 5,361 | 7,850 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total Research and Development | $ | 2,459 | $ | 5,279 | $ | 9,280 | $ | 14,391 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Our external research and development costs consist primarily of:
| • | expenses incurred under agreements with contract research organizations, investigative sites and consultants that conduct our clinical trials and a substantial portion of our preclinical activities; |
| • | the cost of acquiring and manufacturing clinical trial and other materials; and |
| • | other costs associated with development activities, including additional studies |
Internal research and development costs consist primarily of salaries and related fringe benefits costs for our employees (such as workers compensation and health insurance premiums), stock-based compensation charges, travel costs, lab supplies and overhead expenses. Internal costs generally benefit multiple projects and are not separately tracked per project.
We expect to continue to incur substantial expenses related to our development activities for the foreseeable future as we continue product development and initiate our next clinical study for arhalofenate. Since product candidates in later stages of clinical development generally have higher development costs than those in earlier stages of clinical development, primarily due to the increased size and duration of later stage clinical trials, we expect that our research and development expenses will increase in the future. In addition, if our product development efforts are successful, we expect to incur substantial costs to prepare for potential Phase 3 clinical trials and activities.
General and Administrative Expenses
General and administrative expenses consist principally of personnel-related costs, professional fees for legal, consulting, audit services, rent and other general operating expenses not otherwise included in research and development. For the years ended December 31, 2012 and 2011, and the six months ended June 30, 2013 and 2012, general and administrative expenses were $4.2 million, $4.7 million, $2.1 million, and $2.4 million, respectively. We anticipate general and administrative expenses will increase in future periods, reflecting an expanding infrastructure and increased professional fees associated with being a public reporting company under the Exchange Act.
66
Table of Contents
Comparison of Six Months Ended June 30, 2013 and 2012
| For the Six Months Ended June 30, | ||||||||||||
| 2013 | 2012 | Variance | ||||||||||
| (unaudited) | ||||||||||||
($ in thousands) | ||||||||||||
Contract revenue | $ | — | $ | 125 | $ | (125 | ) | |||||
Operating expenses: | ||||||||||||
Research and development | 2,459 | 5,279 | (2,820 | ) | ||||||||
General and administrative | 2,097 | 2,418 | (321 | ) | ||||||||
|
|
|
|
|
| |||||||
Loss from operations | (4,556 | ) | (7,572 | ) | 3,016 | |||||||
Interest income (expense), net | (419 | ) | (383 | ) | (37 | ) | ||||||
Other income (expense), net | 124 | 2 | 122 | |||||||||
|
|
|
|
|
| |||||||
Net loss from operations | $ | (4,851 | ) | $ | (7,953 | ) | $ | 3,101 | ||||
|
|
|
|
|
| |||||||
Contract revenue as of June 30, 2012, was related to specific research and development funding with Takeda San Francisco, Inc. (“Takeda”). The decrease in contract revenue from the six months ended June 30, 2012, to the six months ended June 30, 2013, was due to the termination of the agreement effective March 31, 2013.
Research and development expenses decreased $2.8 million, from $5.3 million to $2.5 million for the six months ended June 30, 2012 and 2013, respectively. The reduction in costs primarily arose due to the completion of several clinical trials in early 2012 and reduction in labor costs due to the voluntary attrition of eight people from June 30, 2012 to June 30, 2013.
General and administrative expenses decreased $0.3 million from $2.4 million for the six months ended June 30, 2012, to $2.1 million for the six months ended June 30, 2013. The decrease in general and administrative expenses was primarily due to a reduction of $0.3 million in labor costs from the voluntary attrition of four people and a reduction in travel and entertainment costs of $0.1 million due to cost cutting measures. This was offset by an increase of $0.1 million in professional costs primarily associated with an increase in audit fees due to reviews associated with filing of our Form-10 with the SEC.
Interest income (expense), net, decreased by approximately $37,000 for the six months ended June 30, 2013 compared to June 30, 2012 due to the recognition of interest expense being calculated on the principal debt balance and increasing cumulative interest due.
Comparison of Years Ended December 31, 2012 and 2011
| For the Year Ended December 31, | ||||||||||||
| ($ in thousands) | 2012 | 2011 | Variance | |||||||||
Contract revenue | $ | 3,050 | $ | 15,147 | $ | (12,097 | ) | |||||
Operating expenses: | ||||||||||||
Research and development | 9,280 | 14,391 | (5,111 | ) | ||||||||
General and administrative | 4,208 | 4,654 | (446 | ) | ||||||||
|
|
|
|
|
| |||||||
Loss from operations | (10,438 | ) | (3,898 | ) | (6,540 | ) | ||||||
Interest income (expense), net | (819 | ) | (627 | ) | (192 | ) | ||||||
Other income (expense), net | 2 | 28 | (26 | ) | ||||||||
|
|
|
|
|
| |||||||
Net loss | $ | (11,255 | ) | $ | (4,497 | ) | $ | (6,758 | ) | |||
|
|
|
|
|
| |||||||
67
Table of Contents
Contract revenue in each period related to our arrangement with Takeda for an annual license fee and research and development services totaled $0.2 million and $0.1 million for the years ended December 31, 2011 and 2012, respectively. We recognized approximately $2.9 million in contract revenue in 2012, which was received as a final payment of contract revenue associated with termination of a collaboration agreement with Sanofi-Aventis. Contract revenue decreased by $12.1 million from the year ended December 31, 2011, to the year ended December 31, 2012. This decrease was primarily attributable to the termination of the collaboration agreement with Sanofi-Aventis.
Research and development expenses decreased by $5.1 million from the year ended December 31, 2011, to the year ended December 31, 2012. This decrease was attributable to a decrease in clinical trial cost of $2.6 million in 2012 and decreases in consulting and personnel related expenses, including salaries, travel and supplies of $1.4 million. Stock compensation expense, depreciation and overhead allocations totaling $0.7 million accounts for the remainder of the decrease. The decrease in clinical trial costs is primarily related to the completion of three small Phase 2 clinical trials. The decrease in personnel related expenses was primarily attributed to a reduction of six employees in our research and development organization which also impacted stock compensation expense.
General and administrative expenses decreased $0.4 million from the year ended December 31, 2011, to the year ended December 31, 2012. This decrease is primarily attributable to a decrease in personnel related expenses, including stock compensation, and facility and office costs, and bank service charges of $0.7 million. This was partially offset by an increase in travel related to obtaining financing and professional costs of $0.4 million.
Interest expense increased $0.1 million in 2012 from $0.7 million for the year ended December 31, 2011, due to interest expense being calculated on the principal balance and an increasing cumulative interest balance due. Also in 2012, the interest rate on the convertible debt was increased by 0.5% due to several amendments in which the maturity dates of the note were extended to March 31, 2013 and then August 1, 2013. Also as a result of these amendments, a conversion option which increased the convertible debt by $70,000 was recognized in 2012. Sixty thousand of the conversion option was amortized to interest expense as of December 31, 2012. Interest income was $22,000 for the year ended December 31, 2012 and $78,000 for the year ended December 31, 2011. The decrease was attributable to reduced yields from lower investment balances in our portfolio which consisted primarily of government securities and money market funds.
Income Taxes
As of December 31, 2012, we had federal and state net operating loss carryforwards of approximately $156.0 million to offset future federal income taxes which will expire beginning in 2024 through 2032 and the state income taxes which will expire beginning in 2014 through 2032. Current federal and state tax laws include substantial restrictions on the utilization of net operating losses and tax credits in the event of an ownership change. Even if the carryforwards are available, they may be subject to annual limitations, lack of future taxable income, or future ownership changes that could result in the expiration of the carryforwards before they are utilized. At December 31, 2012, we recorded a 100% valuation allowance against our deferred assets of approximately $1.7 million as our management believes it is uncertain that they will be fully realized. If we determine in the future that we will be able to realize all or a portion of our net operating loss carryforwards, an adjustment to our net operating loss carryforwards would increase net income in the period in which we make such a determination.
Liquidity and Capital Resources
To date, we have funded our operations through the sale of equity securities, licensing fees, issuance of debt and collaborations with third parties. At June 30, 2013, we had cash and cash equivalents of $3.6 million. As stated above under “Reverse Stock Split and Conversion of Preferred Stock,” on September 30, 2013, we raised
68
Table of Contents
aggregate net proceeds of $28.9 million and issued common stock in cancellation of $16.9 million of debt owed to the holder of that debt in the 2013 financing, and on October 31, 2013, we raised an additional aggregate net proceeds of $2.8 million in the 2013 financing.
In addition, on September 30, 2013, we entered into a term loan facility with Silicon Valley Bank and Oxford Finance LLC, collectively referred to as the lenders, for an aggregate amount of $10 million, $5 million of which was made available to us as of September 30, 2013, and the remaining $5 million, which we refer to as the second tranche, of which shall be made available to us upon the achievement of positive data and successful completion of all primary endpoints for either the 600mg or 800mg dose of arhalofenate in our planned Phase 2b study (the “second draw milestone”). The second tranche shall be available to us until the earlier of June 30, 2015, or the occurrence and continuation of an event of default (as described in the term loan facility). Each tranche matures 48 months following the funding date of such tranche. The proceeds of the term loan facility may be used for general corporate purposes.
The first tranche loans under the term loan facility bear interest at a rate equal 8.75% per annum. Loans under the second tranche will bear interest at a rate fixed at the time of borrowing equal to the greater of (i) 8.75% per annum and (ii) the sum of the Wall Street Journal prime rate plus 4.25% per annum. We were also required to pay a facility fee of 1.00% on the term loan facility commitment.
We are permitted to make voluntary prepayments of the term loans with a prepayment fee equal to 3% of the term loans prepaid. On each tranche, we are required to make 12 monthly interest only payments after the funding date followed by a repayment schedule equal to 36 equal monthly payments of the outstanding principal of the outstanding term loans of each tranche. After the 36-month amortization period of each tranche, the remaining balance of such tranche and a final payment equal to 6.50% of the original principal amount of the applicable tranche are payable on the maturity date of such tranche. We are required to make mandatory prepayments of the outstanding term loans upon the acceleration by the lenders of such loans following the occurrence of an event of default, along with a payment of the final payment, the prepayment fee and any all other obligations (each as defined or described under the term loan facility) that are due and payable at the time of the prepayment.
Our obligations under the term loan facility are secured, subject to customary permitted liens and other agreed upon exceptions, (1) by a first priority pledge of all of the equity interests of each of our direct and indirect subsidiaries, and (2) a perfected first priority interest in all of our tangible and intangible assets, including all of our intellectual property.
The term loan facility contains customary representations and warranties and customary affirmative and negative covenants applicable to us and our subsidiaries, including, among other things, restrictions on dispositions, changes in business, management, ownership or business locations, mergers or acquisitions, indebtedness, encumbrances, distributions, investments, transactions with affiliates and subordinated debt. Until the occurrence of the second draw milestone, the term loan facility contains financial covenants that require us to maintain a certain cash liquidity. The term loan facility also contains performance covenants that require that (a) by no later than June 30, 2014, shares of our common stock must be publicly traded on NASDAQ; (b) within one hundred twenty (120) days of us becoming eligible to file a registration statement with the United States Securities and Exchange Commission on Form S-3, we must have access to an At The Market facility; and (c) by no later than March 31, 2015, the lenders must have received evidence of the occurrence of the second draw milestone; provided that our failure to comply with these performance covenants shall not be an event of default under the term loan facility so long as we deposit an amount equal to 100% of the aggregate outstanding term loans in a segregated, blocked deposit account at Silicon Valley Bank.
The term loan facility also includes customary events of default, including but not limited to the nonpayment of principal or interest, violations of covenants, material adverse change, attachment, levy, restraint on business, cross-defaults on our or any our subsidiary’s material indebtedness, bankruptcy, material judgments and misrepresentations. Upon an event of default, the lenders may, among other things, accelerate the loans and foreclose on the collateral.
69
Table of Contents
The following table summarizes our equity funding sources from inception through to November 1, 2013:
Series | Year | Number of Shares | Gross Proceeds | |||||||
| ($ millions) | ||||||||||
A-1 Convertible Preferred Stock, net | 1990 - 2001 | 12,734 | $ | 73.2 | ||||||
B-1 Convertible Preferred Stock, net | 2003 - 2008 | 373,223 | 85.9 | |||||||
C-1 Convertible Preferred Stock, net | 2006 | 27,345 | 9.9 | |||||||
D-1 Convertible Preferred Stock, net | 2007 | 136,948 | 28.7 | |||||||
E-1 Convertible Preferred Stock, net | 2009 - 2010 | 39,265 | 9.1 | |||||||
E-3 Convertible Preferred Stock, net | 2010 | 71,543 | 26.1 | |||||||
Common Stock and Warrants, net1 | 2013 | | 6,655,972 (and warrants to | | 30.2 | |||||
|
|
|
| |||||||
TOTAL | | 7,317,030 (and warrants to purchase | | $ | 263.1 | |||||
|
|
|
| |||||||
| 1 | Includes shares of common stock issued in cancellation of approximately $16.9 million of debt and warrants issued to the venture debt lenders and to the placement agent in the 2013 financing. |
Cash Flows for the Six Months Ended June 30, 2013 and 2012 and the Years Ended December 31, 2012 and 2011
Operating Activities
Cash used in operating activities decreased $3.2 million for the six months ended June 30, 2013, compared to the six months ended June 30, 2012, primarily due to a $3.1 million decrease in net loss. Cash used in operating activities decreased $6.6 million for the year ended December 31, 2012 as compared to the year ended December 31, 2011 primarily due to an increase in the net loss of $6.8 million and a decrease in recognized deferred revenue of $14.7 million.
Investing Activities
Cash used in and provided by investing activities for the six months ended June 30, 2013 and 2012, and the years ended December 31, 2012 and 2011 decreased by $7.4 million and $8.2 million, respectively, primarily due to decreases in purchases of marketable securities and proceeds from maturities of marketable securities.
Financing Activities
Cash used in financing activities decreased $0.2 million for the twelve months ended December 31, 2012, compared to the twelve months ended December 31, 2011, primarily due to principal payments on equipment loans.
Management believes that cash and cash equivalents as of November 1, 2013, including the funds raised in the 2013 financing, are sufficient to sustain the operations of the company through the third quarter of 2015. We expect to incur substantial expenditures in the foreseeable future for the development and potential commercialization of our product candidates. We will continue to require additional financing to develop our products and fund operating losses. We will seek funds through equity financings, collaborative or other arrangements with corporate sources, or through other sources of financing, including a public offering. Adequate additional funding may not be available to us on acceptable terms or at all. Our failure to raise capital as and when needed could have a negative impact on our financial condition and our ability to pursue our business strategies. If adequate funds are not available to us, we may be required to close our business.
70
Table of Contents
Contractual Obligations and Commitments
We have lease obligations consisting of an operating lease for our operating facility that commenced in July 2010 and expires April 2014, for approximately 41,600 square feet in Hayward, CA.
Preferred stockholders were entitled to receive cumulative dividends of $92.1 million as of June 30, 2013, when and as declared by the board of directors but only out of funds that are legally available. All such dividends would accrue automatically on a daily basis and all accrued and unpaid dividends shall be fully paid prior to payment of any other dividend on shares of the company’s common stock. As of June 30, 2013, no dividends had been declared by the board. On September 30, 2013, all shares of the company’s preferred stock converted to common stock without the payment of dividends.
Off-Balance Sheet Arrangements
We do not currently have, nor have we ever had, any relationships with unconsolidated entities or financial partnerships, such as entities often referred to as structured finance or special purpose entities, established for the purpose of facilitating off-balance sheet arrangements or other contractually narrow or limited purposes. In addition, we do not engage in trading activities involving non-exchange traded contracts.
| ITEM 3. | PROPERTIES. |
CymaBay leases its corporate office located in Hayward, California, under a lease that expires in April 2014, with an option to renew for a two-year term. CymaBay believes that its existing facilities are adequate to meet its current requirements.
| ITEM 4. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT. |
Beneficial Ownership of Common Stock
The following table sets forth information regarding the beneficial ownership of CymaBay common stock as of November 1, 2013, after giving effect to the reverse stock split and the 2013 financing, by (1) each of our directors and named executive officers, (2) each person that beneficially owns more than 5% of CymaBay common stock and (3) all of our executive officers and directors as a group. Unless otherwise indicated, the address for each of the beneficial owners in the table below is c/o CymaBay Therapeutics, Inc., 3876 Bay Center Place, Hayward, California 94545.
| Name of Beneficial Owner (1) | Amount Nature of Beneficial Ownership | Percentage of Class | ||||||
Harold Van Wart (2) | 240,865 | 2.48 | % | |||||
Charles McWherter (3) | 71,181 | * | % | |||||
Bonnie Charpentier (4) | 4,690 | * | % | |||||
Robert Martin (5) | 4,401 | * | % | |||||
Patrick J. O’Mara III (6) | 4,880 | * | % | |||||
Diana Petty (7) | 2,898 | * | % | |||||
Lou Lange (8) | 31,422 | * | % | |||||
Carl Goldfischer M.D. (9) | 53,199 | * | % | |||||
Hari Kumar Ph.D. (10) | 6,470 | * | % | |||||
Edward E. Penhoet Ph.D. (11) | 6,470 | * | % | |||||
Kurt von Emster (12) | 27,078 | * | % | |||||
Entities Associated With Alta BioPharma (13) | 1,123,600 | 11.79 | % | |||||
Entities Associated With Deerfield Funds (14) | 593,206 | 6.22 | % | |||||
Johnson & Johnson Development Corporation (15) | 860,266 | 9.09 | % | |||||
Entities Associated With Versant Venture Capital (16) | 1,123,600 | 11.79 | % | |||||
Pictet Biotech (17) | 491,384 | 5.18 | % | |||||
D&O as Group (18) | 453,554 | 4.73 | % | |||||
71
Table of Contents
| * | Less than 1%. |
| (1) | Beneficial ownership is calculated based on 9,455,064 shares of common stock issued and outstanding as of November 1, 2013. The number of shares beneficially owned by a person also includes shares of common stock underlying options or warrants held by that person that are currently exercisable or exercisable within 60 days of November 1, 2013. The shares issuable pursuant to the exercise of those options or warrants are deemed outstanding for computing the percentage ownership of the person holding those options and warrants but are not deemed outstanding for the purposes of computing the percentage ownership of any other person. Unless otherwise indicated, the persons and entities named in the table have sole voting and sole investment power with respect to the shares set forth opposite that person’s name, subject to community property laws, where applicable. |
| (2) | Includes shares issuable upon options to acquire 240,407 shares of common stock exercisable within 60 days of November 1, 2013. |
| (3) | Includes shares issuable upon options to acquire 71,181 shares of common stock exercisable within 60 days of November 1, 2013. |
| (4) | Includes shares issuable upon options to acquire 4,690 shares of common stock exercisable within 60 days of November 1, 2013. |
| (5) | Includes shares issuable upon options to acquire 4,401 shares of common stock exercisable within 60 days of November 1, 2013. |
| (6) | Includes shares issuable upon options to acquire 4,858 shares of common stock exercisable within 60 days of November 1, 2013. |
| (7) | Includes shares issuable upon options to acquire 2,898 shares of common stock exercisable within 60 days of November 1, 2013. |
| (8) | Includes shares issuable upon options to acquire 29,976 shares of common stock exercisable within 60 days of November 1, 2013. |
| (9) | Includes 41 shares of common stock held by Bay City Capital LLC, 43,824 shares of common stock held by The Bay City Capital Fund II, L.P. and 2,864 shares of common stock held by The Bay City Capital Fund II Co-Investment Fund, L.P (collectively the “Bay City Capital Funds”), and shares issuable upon options to acquire 6,470 shares of common stock exercisable within 60 days of November 1, 2013. Carl Goldfischer is a managing director of Bay City Capital Funds, and has voting and investment control over the shares owned by the Bay City Capital Funds. Mr. Goldfischer disclaims beneficial ownership of the shares owned by the Bay City Capital Funds, except to the extent of his pecuniary interest therein. |
| (10) | Includes shares issuable upon options to acquire 6,470 shares of common stock exercisable within 60 days of November 1, 2013. |
| (11) | Includes shares issuable upon options to acquire 6,470 shares of common stock exercisable within 60 days of November 1, 2013. |
| (12) | Consists of 17,326 shares held by The Konrad Hans von Emster III and Elizabeth F. von Emster Revocable Trust dated January 18, 2005, shares issuable upon exercise of warrants to acquire 2,000 shares of common stock and shares issuable upon options to acquire 7,752 shares of common stock exercisable within 60 days of November 1, 2013. |
| (13) | Consists of 64,501 shares of common stock and warrants exercisable for 4,613 shares of common stock held by Alta BioPharma Partners III GmbH & Co. Beteiligungs KG, 960,433 shares of common stock and warrants exercisable for 68,693 shares of common stock held by Alta BioPharma Partners III, L.P., and 23,668 shares of common stock and warrants exercisable for 1,692 shares of common stock held by Alta Embarcadero BioPharma Partners III, LLC. Farah Champsi, Edward Penhoet and Edward Hurwitz (collectively known as “the Principals”) are directors of Alta BioPharma Management III, LLC (which is the general partner of Alta BioPharma Partners III, L.P. and the managing limited partner of Alta BioPharma Partners III GmbH & Co. Beteiligungs KG), and managers of Alta Embarcadero BioPharma Partners III, LLC. Voting and investment decisions for the funds are made by a majority vote of the Principals. The Principals disclaim beneficial ownership of all such shares held by the foregoing funds, except to the extent of their proportionate pecuniary interests therein. Alta Partners III, Inc. provides investment advisory services to several venture capital funds including, Alta BioPharma Partners III, L.P., Alta BioPharma Partners III GmbH & Co. Beteiligungs KG and Alta Embarcadero BioPharma Partners III, LLC. Alta Partners III, Inc. is a venture capital firm with an office |
72
Table of Contents
| in San Francisco. Alta Partners III, Inc. is a California Corporation. Alta BioPharma Partners III, L.P. is a Delaware Limited Partnership. Alta BioPharma Partners III GmbH & Co. Beteiligungs KG is a German Limited Partnership, and Alta Embarcadero BioPharma Partners III, LLC is a California Limited Liability Company. The address of the Alta BioPharma entities is: One Embarcadero Center, Suite 3700, San Francisco, CA 94111. |
| (14) | Consists of 255,071 shares of common stock and warrants exercisable for 35,920 shares of common stock held by Deerfield Special Situations International Master Fund, L.P., and 258,135 shares of common stock and warrants exercisable for 44,080 shares of common stock held by Deerfield Special Situations Fund, LP (collectively, the “Deerfield Funds”). Deerfield MGMT, L.P. (“Deerfield MGMT”) is the general partner, and Deerfield Management Company, L.P. (“Deerfield Management”) is the investment advisor, of the Deerfield Funds, James E. Flynn, president of the general partners of Deerfield MGMT and Deerfield Management, holds voting and dispositive power over the shares held by the Deerfield Funds. The address of the Deerfield Funds is 780 Third Avenue 37th Floor, New York, NY 10017. |
| (15) | Consists of 850,266 shares of common stock and warrants exercisable for 10,000 shares of common stock held by the Johnson & Johnson Development Corporation. Linda M. Vogel, Manager, Operations of Johnson & Johnson Development Corporation (“JJDC”) exercises voting and dispositive power over the shares held by JJDC. The address of JJDC is: 410 George St., New Brunswick, NJ 08901. |
| (16) | Consists of 19,358 shares of common stock and warrants exercisable for 1,384 shares of common stock held by Versant Affiliates Fund II-A, L.P., 9,116 shares of common stock and warrants exercisable for 652 shares of common stock held by Versant Side Fund II, L.P., and 1,020,127 shares of common stock and warrants exercisable for 72,963 shares of common stock held by Versant Venture Capital II, L.P. Versant Ventures II, LLC, the general partner of Versant Venture Capital II, L.P., Versant Side Fund II, L.P. and Versant Affiliates Fund II-A (collectively, the “Versant Funds”), has the authority to vote for or dispose of the CymaBay stock held by the Versant Funds. The managing directors of the general partners are Brian Atwood, Sam Colella, Ross Jaffe, Bill Link, Barbara Lubash, Don Milder, Rebecca Robertson, Charles Warden and Brad Bolzon, who share voting and signing authority with respect to the general partner. The address of The Versant Funds is: 3000 Sand Hill Rd., Building 4, Suite 210, Menlo Park, CA 94025. |
| (17) | Consists of 458,585 shares of common stock and warrants exercisable for 32,799 shares of common stock held by Pictet Biotech (“Pictet Biotech”). Michael Sjostrom, Chief Investment Officer of Pictet Biotech exercises voting and dispositive power over the shares held by Pictet Biotech. The address of Pictet Biotech is: 7 Rue du Marché, 1204 Geneva, Switzerland. |
| (18) | Consists of shares held by each executive officer and director including the shares described in footnotes 2 through 12 above. |
73
Table of Contents
ITEM 5. DIRECTORS AND EXECUTIVE OFFICERS.
The following table sets forth information regarding CymaBay’s executive officers, directors, key employees and consultants, as of November 1, 2013.
Management Team
Name | Age | Position Held With CymaBay | ||
| Executive Officers | ||||
Harold Van Wart, Ph.D. Sujal Shah | 66 40 | President, Chief Executive Officer & Director Acting Chief Financial Officer | ||
| Mary Jean Stempien, MS, MD, FACP | 61 | Interim Chief Medical Officer | ||
| Charles A. McWherter, Ph.D. | 58 | Senior Vice President, Research and Preclinical Development | ||
| Bonnie A. Charpentier, Ph.D. | 61 | Vice President, Regulatory and Quality | ||
| Robert L. Martin, Ph.D. | 51 | Vice President, Nonclinical Development and Project Management | ||
| Patrick J. O’Mara | 52 | Vice President, Business Development | ||
| Diana Petty | 62 | Vice President, Human Resources and Administration | ||
| Directors | ||||
| Louis G. Lange, M.D., Ph.D. | 65 | Chairman of the Board | ||
| Carl Goldfischer, M.D. | 55 | Director | ||
| Hari Kumar, Ph.D. | 57 | Director | ||
| Edward E. Penhoet, Ph.D. | 72 | Director | ||
| Harold Van Wart, Ph.D. | 65 | Director | ||
| Kurt von Emster, CFA | 46 | Director | ||
Biographical Information
Executive Officers
Harold E. Van Wart, Ph.D. has served as CymaBay’s Chief Executive Officer since 2003, a member of its board of directors since January 2003, and President since April 2001. He served as Chief Operating Officer from December 2002 to January 2003 and Senior Vice President, Research and Development from October 2000 to December 2002. From 1999 to 2000, Dr. Van Wart was vice president and therapy head for arthritis and fibrotic diseases at Roche Biosciences, a biopharmaceutical company. From 1992 to 1999, he was vice president and director of the institute of biochemistry and cell biology at Syntex Corporation, a biopharmaceutical company acquired by Roche Biosciences in 1994. From 1978 to 1992, Dr. Van Wart served on the faculty of Florida State University. Dr. Van Wart holds a Ph.D. from Cornell University and a B.A. from SUNY Binghamton. He currently serves on the Emerging Companies and Health Section Governing Boards of the Biotechnology Industry Organization (BIO), as well as on its board of directors.
Sujal Shah has served as our acting Chief Financial Officer since June 27, 2012. From 2010 to 2012 Mr. Shah served as Director, Health Care Investment Banking Group for Citigroup. From 2004 to 2010 Mr. Shah served as Vice President, Health Care Investment Banking Group for Credit-Suisse. Mr. Shah received an MBA from Carnegie Mellon University – Tepper School of Business in 2004 and a MS from Northwestern University in Biomedical Engineering in 1997.
Charles A. McWherter, Ph.D. has served as our Senior Vice President, Research and Preclinical Development since July 2007. From 2003 to 2007, he served as Vice President and head of the cardiovascular therapeutics areas of Pfizer Inc., a biopharmaceutical company. From 2001 to 2003, Dr. McWherter served as Vice President of Drug Discovery at Sugen, Inc., a biopharmaceutical company acquired by Pfizer Inc. in 2003. Dr. McWherter obtained his Ph.D. from Cornell University.
74
Table of Contents
Bonnie A. Charpentier, Ph.D. joined CymaBay in 2007 as Vice President of Regulatory Affairs, and became Vice President of Regulatory and Quality later that year. She previously was Vice President of Regulatory and Quality at Genitope Corp. from 2001 to 2006. From 1995 to 2001, Dr. Charpentier held regulatory positions at Roche Global Development, a division of F. Hoffman-La Roche Ltd., including serving as Vice President and Regulatory Site Head in Palo Alto, CA. From 1991 to 1995 she held regulatory positions of increasing responsibility at Syntex Corporation. Dr. Charpentier obtained her Ph.D. in Biology from the University of Houston. She currently serves on the Board of Directors of the American Chemical Society.
Mary Jean Stempien, M.S., M.D., F.A.C.P. has served as our acting Chief Medical Officer since June 23, 2012. Dr. Stempien has over 16 years of drug development experience obtained at Syntex Corp, Roche Pharmaceuticals, Tularik, Inc. and Cerimon Pharmaceuticals. At Tularik and Cerimon, she was Vice President, Clinical Development, with responsibility for clinical development projects in several therapeutic areas (oncology, autoimmune disorders, inflammation, pain). Her development work at Roche and Syntex contributed to marketing approvals of two antiviral agents, ganciclovir (Cytovene®) and valganciclovir (Valcyte®), as well as the transplant rejection agent mycophenolate mofetil (CellCept®). She has been directly involved in five successful NDAs (or sNDAs) and 4 successful FDA Advisory Committee hearings. Dr. Stempien has a B.S. in Pharmacy from University of Connecticut, an M.S. in Pharmaceutical Chemistry from UCSF, and an M.D. from University of Massachusetts. Dr. Stempien is board-certified in Internal Medicine, and is a Fellow of the American College of Physicians.
Robert L. Martin, Ph.D. has served as our Vice President of Nonclinical Development and Project Management since 2008. Dr. Martin served as our Sr. Director of Preclinical Development and Project Management from 2006 to 2008 and our Director of Preclinical Development and Project Management from 2004 to 2006. From 1994 to 2004, Dr. Martin served in various positions with Roche Palo Alto, a division of F. Hoffman-La Roche Ltd. Dr. Martin obtained his Ph.D. in Biochemistry from the University of California, Davis.
Patrick J. O’Mara joined CymaBay in 1991 and has served CymaBay in a variety of operational and business development positions. He became Vice President for Business Development in August 2006. Before joining CymaBay, Mr. O’Mara worked at Thymax Corporation and Thomas Research Corp. Mr. O’Mara received a B.A. in Biochemistry from the University of California, Berkeley.
Diana Petty joined CymaBay as Vice President of Human Resources and Administration in September 2006. Prior to joining CymaBay, Ms. Petty managed her own human resources consulting firm for 15 years in the biotech and high tech industries. Earlier in her career, she held leadership positions in Human Resources at 3M Corporation’s Life Science Division and at SmithKline Corporation. Ms. Petty obtained a M.S. in Human Resources Development from Villanova University.
Directors
Louis G. Lange, M.D., Ph.D. has been a member of our Board of Directors since November 2003 and has been chairman of the board since October 2009. Dr. Lange was elected to the Board of Directors due to his significant drug development experience and leadership roles held in various companies and academic institutions. Dr. Lange has 22 years experience in academic medicine at Harvard and Washington University, where he served as Chief of Cardiology and Professor of Medicine at Jewish Hospital from 1985-1992 and was one of the first academicians in molecular cardiology. He founded CV Therapeutics based on this broad field and as Chairman, CEO and Chief Scientific Officer, led the IPO in 1996 and the overall pipeline development and the initiatives for U.S. FDA and European EMEA approval for Ranexa®, a first-in-class late sodium channel blocker and the first anti-anginal drug class approved in 30 years in the U.S. He also led the approval of Lexiscan®, a first-in-class adenosine A2a receptor agonist for use in myocardial perfusion imaging studies. Dr. Lange oversaw the commercial success of CV Therapeutics and its sale to Gilead in 2009 for $1.4 billion dollars. As a member of the Board of Trustees at the University of Rochester since 1998 and as Chair of the Health Affairs committee that oversaw all of the medical operations for five years, Dr. Lange has been part of the leadership team for
75
Table of Contents
strategic re-invigoration of the medical center with construction of two research buildings and recruitment of over 100 faculty members. As a member of BIO Board of Directors (the trade organization of biotech companies) from 1999 to 2009, Dr. Lange led the largest committee of member companies for two years and was picked as one of two biotech executives to attend the ceremonies at the White House for the signing of the Bioterrorism bill in 2004. Dr. Lange has been a General Partner at Asset Management since 2009; remains a senior advisor to Gilead and serves on numerous other public and private Boards in both the non-profit and for-profit arena.
Carl Goldfischer, M.D. has been a member of our Board of Directors since August 2003. Dr. Goldfischer was elected to the Board of Directors as a result of Bay City Capital’s investment in the company and his in-depth knowledge of the pharmaceutical industry. Dr. Goldfischer is an investment partner and managing director of Bay City Capital, serving as a member of the board of directors and executive committee, and has been with the firm since December 2000. His background includes extensive public and private investment and transaction work, as well as clinical trial development knowledge. Prior to joining Bay City Capital, Dr. Goldfischer was chief financial officer of ImClone Systems. Previously, he was a research analyst with the Reliance Insurance Company, helping to establish its portfolio and presence in the health care investment community. Dr. Goldfischer is a member of the board of directors for BrainCells, EnteroMedics and Epizyme. Dr. Goldfischer received an M.D. with honors in scientific research from Albert Einstein College of Medicine and a B.A. from Sarah Lawrence College.
Hari Kumar, Ph.D. has been a member of our Board of Directors since September 2012. Dr. Kumar was elected to the Board of Directors as a result his in depth knowledge and experience in the pharmaceutical industry. Dr. Kumar has over 25 years of pharmaceutical experience. Dr. Kumar spent a number of years at Hoffmann La Roche starting in basic research, moving to sales and marketing, lifecycle management and finally to business development. During the period 1996 through 1999, Dr. Kumar moved to Eisai Ltd, as their European Marketing Director before returning to Roche in 1999. He moved to Amira Pharmaceuticals, Inc in 2007 as Chief Business Officer and after Amira’s acquisition in 2011, became Chief Executive Officer of Panmira Pharmaceuticals LLC. In his time, Dr. Kumar has overseen the launch of the immunosuppressive, CellCept®, the Alzheimer’s drug, Aricept® and gastric ulcer drug, Aciphex®. He was also involved in guiding cross functional teams at Roche for the Transplantation franchise which resulted in the growth of the products in the franchise to achieve billion dollar sales. In his role as lead in-licensing person for inflammation at Roche, he identified and partnered valuable products that have enhanced Roche’s portfolio. He was instrumental in partnerships with Isotechnika, Biotie, Biocryst and Actellion. Experience in almost all aspects of the pharmaceutical industry has given Dr. Kumar a unique understanding on what makes a successful drug. At Amira, Dr. Kumar led the process that resulted in the acquisition by Bristol Myers Squibb in 2011. He then led the spin out company, Panmira Pharmaceuticals LLC. In July 2013, he was appointed Chief Executive Officer and Board Director of Adheron Therapeutics, Inc. Having trained as an immunologist at University College London where he completed his Ph.D. under the supervision of Prof N.A. Mitchison, Dr. Kumar completed a postdoctoral fellowship at Tufts New England Medical Center in Boston and another fellowship at the Marie Curie Cancer Research Centre in UK.
Edward E. Penhoet, Ph.D. has been a member of our Board of Directors since November 2004. Dr. Penhoet was elected to the Board of Directors as a result of Alta Partner’s investment in the company and his in depth knowledge and experience in the pharmaceutical industry. Dr. Penhoet joined Alta in 2000 as a Director and has been full time at Alta since 2008. He currently serves on the board of directors of Immune Design and Scynexis. A co-founder of Chiron, Dr. Penhoet served as Chiron’s President and Chief Executive Officer from its formation in 1981 until April 1998. He served as Vice-Chair of the governing board of the Independent Citizens Oversight Committee for the California Institute of Regenerative Medicine (CIRM) from 2005 to 2010, and served as the President of the Gordon and Betty Moore Foundation from 2004 to 2008. Dr. Penhoet was recently appointed to President Obama’s Council of Advisors on Science and Technology (PCAST). PCAST is an advisory group comprised of 20 of the nation’s leading scientists and engineers who directly advise the President and the Executive Office of the President. PCAST makes policy recommendations in the many areas where
76
Table of Contents
understanding of science, technology, and innovation is key to strengthening our economy and forming policy that works for the American people. For 10 years prior to founding Chiron, Dr. Penhoet was a faculty member of the Biochemistry Department of the University of California, Berkeley. Dr. Penhoet is the immediate past Dean of the School of Public Health at the University of California, Berkeley. He is a member of both the Institute of Medicine of the National Academies and the American Academy of Arts and Sciences. He has co-authored more than 50 scientific articles and papers.
Harold E. Van Wart, Ph.D. has served as CymaBay’s Chief Executive Officer since 2003, a member of its board of directors since January 2003, and President since April 2001. Dr. Van Wart was elected to the Board of Directors as a result of his appointment to Chief Executive Officer. He served as Chief Operating Officer from December 2002 to January 2003 and Senior Vice President, Research and Development from October 2000 to December 2002. From 1999 to 2000, Dr. Van Wart was vice president and therapy head for arthritis and fibrotic diseases at Roche Biosciences, a biopharmaceutical company. From 1992 to 1999, he was vice president and director of the institute of biochemistry and cell biology at Syntex Corporation, a biopharmaceutical company acquired by Roche Biosciences in 1994. From 1978 to 1992, Dr. Van Wart served on the faculty of Florida State University. Dr. Van Wart holds a Ph.D. from Cornell University and a B.A. from SUNY Binghamton. He currently serves on the Emerging Companies and Health Section Governing Boards of BIO, as well as on its board of directors.
Kurt von Emster, CFA has been a member of our Board of Directors since April 2009. Dr. von Emster was elected to the Board of Directors as a result of MPM BioEquities Master Fund LP’s investment in the company and his in depth knowledge of the pharmaceutical industry. Mr. von Emster is a co-founder and Managing Partner of venBio. He has been an institutional biotechnology and health care analyst and portfolio manager for 22 years. He is a member of the board of directors of Cytos AG, a former member of the board of Facet Biotech Corporation (sold to Abbott Laboratories in 2010) and Somaxon Pharmaceuticals (sold to Pernix Therapeutics in 2013), and a former board observer of Acceleron Pharma. Mr. von Emster’s investment career started in 1989 at Franklin Templeton where he founded and managed several health and biotechnology funds in the 1990s, each achieving a 5-star Morningstar ranking. In 2000, he was managing over $2B in biotech and health care funds for Franklin Templeton. In 2001, Mr. von Emster became a General Partner at MPM Capital, a leading biotechnology private equity firm, and launched the MPM BioEquities Fund, a cross over public and private biotechnology hedge fund. He was the portfolio manager of this fund from inception in 2001 until his departure in 2009. He also co-founded the MPM Biogen Idec Strategic Fund during his tenure at MPM. Mr. von Emster is based in venBio’s San Francisco office.
77
Table of Contents
ITEM 6. EXECUTIVE COMPENSATION.
Summary Compensation Table
The following table shows information regarding the compensation earned during the fiscal year ending December 31, 2012, by (i) our Chief Executive Officer, (ii) our Senior Vice President, Research and Pre-clinical Development, (iii) our Chief Medical Officer and (iv) our Vice President, Regulatory and Quality, each of whom were serving as executive officers in 2012. The officers listed below are collectively referred to as the “Named Executive Officers” in this Form 10.
Name | Fiscal Year | Salary | Option/Stock Awards (1) | All Other Compensation | Total | |||||||||||||||
Harold Van Wart, Ph.D. | 2012 | $ | 411,830 | $ | 26,353 | $ | 12,430 | (2) | $ | 450,613 | ||||||||||
President and Chief Executive Officer | ||||||||||||||||||||
Charles A. McWherter | 2012 | $ | 327,309 | $ | 11,400 | $ | 13,755 | (2) | $ | 352,464 | ||||||||||
Senior Vice President, Research and | ||||||||||||||||||||
Raymond Urbanski | 2012 | $ | 151,574 | $ | 20,278 | $ | 193,555 | (2)(3) | $ | 365,407 | ||||||||||
Chief Medical Officer | ||||||||||||||||||||
Bonnie Charpentier, Ph.D. | 2012 | 270,097 | $ | 3,969 | $ | 19,462 | (2) | $ | 293,528 | |||||||||||
Vice President, Regulatory and Quality | ||||||||||||||||||||
| (1) | The aggregate fair value of the equity compensation paid to our Named Executive Officers for the year ended December 31, 2012. The aggregate fair value is computed in accordance with FASB ASC Topic 718. See Note 11 to our consolidated financial statements contained in this report regarding assumptions underlying valuation of equity awards. Options in the table above were granted from the 2003 Equity Incentive Plan and vest and are exercisable in equal monthly installments over forty-eight (48) months from the grant date and are fully vested within four years from the grant date subject to the optionee’s continued employment or service with CymaBay. The options generally have a maximum term of 10 years, subject to earlier termination in certain situations related to cessation of employment or service. |
| (2) | Represents health insurance, group term life insurance, accidental death and dismemberment insurance, and disability insurance premiums paid by the company. |
| (3) | Represents $8,705 in health insurance, group term life insurance, accidental death and dismemberment insurance, and disability insurance premiums paid by the company and $184,850 in payments made to Dr. Urbanski in connection with his separation from the company in June, 2012 pursuant to a separation agreement. |
78
Table of Contents
Outstanding Equity Awards at Fiscal Year-End
The following table presents the outstanding equity awards held by each of the Named Executive Officers as of December 31, 2012. The share numbers below give retroactive effect to the reverse stock split that occurred on September 30, 2013. Stock options were granted pursuant to our 2003 Equity Incentive Plan (the “Plan”).
| Option Awards |
| |||||||||||||||
| Name | Number of Securities Underlying Unexercised Options (#) Exercisable | Number of Securities Underlying Unexercised Options (#) Unexercisable | Option Exercise Price ($) | Option Expiration Date | ||||||||||||
Harold Van Wart, Ph.D. | 9,745 | 0 | 30.21 | 1/11/2014 | ||||||||||||
|
| 358 6,213 1,258 1,494 5,536 4,730 1,009 |
|
| 0 0 0 0 0 1,245 3,394 |
(1) (2) |
| 30.21 30.21 62.80 39.75 39.75 15.90 4.77 |
|
| 1/11/2014 01/06/2015 11/17/2015 6/4/2018 6/4/2018 1/9/2020 1/24/2022 |
| |||||
Charles A. McWherter, Ph.D. | 5,660 | 0 | 39.75 | 6/4/2018 | ||||||||||||
|
| 1,494 577 |
|
| 393 1,939 | (1) (2) |
| 15.90 4.77 |
|
| 1/9/2020 1/24/2022 |
| |||||
Raymond Urbanski, M.D. | 8,176 | 8,176 | (3) | 12.72 | 10/04/2021 | |||||||||||
Bonnie Charpentier, Ph.D. | 1,258 | 0 | 39.75 | 3/25/2018 | ||||||||||||
| 245 | 0 | 39.75 | 6/4/2018 | |||||||||||||
| 2,019 | 0 | 39.75 | 6/4/2018 | |||||||||||||
| 665 | 175 | (2) | 15.90 | 10/14/2019 | ||||||||||||
| 159 | 533 | (2) | 4.77 | 1/24/2022 | ||||||||||||
| (1) | These options were granted from the 2003 Equity Incentive Plan. The option vests in equal monthly installments of over forty-eight (48) months, provided however, that initially, the vesting did not commence until achievement of a milestone, such that upon achievement of such milestone, the number of shares that would have vested under the option equal to the number of months between the date of grant and the date of achievement of the milestone vested and thereafter 1/48 of the shares underlying the option vest monthly thereafter subject to the optionee’s continued employment or service with CymaBay. The options generally have a maximum term of 10 years, subject to earlier termination in certain situations related to cessation of employment or service. |
| (2) | These options were granted from the 2003 Equity Incentive Plan and vest and are exercisable in equal monthly installments over forty-eight (48) months from the grant date and are fully vested within four years from the grant date subject to the optionee’s continued employment or service with CymaBay. The options generally have a maximum term of 10 years, subject to earlier termination in certain situations related to cessation of employment or service. |
| (3) | The option was granted from the 2003 Equity Incentive Plan and 25% of the shares underlying the option vest on the one-year anniversary of the date of grant and the remainder vest in equal monthly installments over the following thirty-six (36) months and are fully vested within four years from the grant date subject to the optionee’s continued employment or service with CymaBay. The options generally have a maximum term of 10 years, subject to earlier termination in certain situations related to cessation of employment or service. |
79
Table of Contents
Employment Contracts and Termination of Employment and Change of Control Arrangements
Chief Executive Officer
CymaBay entered into an employment letter agreement with Dr. Harold Van Wart as our President and Chief Executive Officer on March 1, 2004. The agreement letter was amended on October 10, 2007 in order to address the requirement of Section 409A of the Internal Revenue Code. Dr. Van Wart’s employment agreement will continue until terminated by him or by the company. Dr. Van Wart serves as Chief Executive Officer of the company.
Base Salary, Bonus, Benefits: Dr. Van Wart received an annual base salary of $411,830 in FY 2012. In addition, Dr. Van Wart is eligible to earn an annual cash performance bonus, based upon achievement of annual performance goals and objectives set by the Board of Directors each, year, with a target bonus of 35% of his base salary. In addition, Dr. Van Wart is entitled to participate in any employee benefit plans that the company may from time to time have in effect for its employees. Dr. Van Wart is also eligible to participate in an individual disability income protection plan. The company reimbursed Dr. Van Wart for reasonable business expenses incurred in the discharge of duties in accordance with the general practices and policies of the company and subject to the company’s annual expense budget.
Termination: Pursuant to the terms of the employment agreement, Dr. Van Wart entered into an at-will employment relationship with the company. Either Dr. Van Wart or the company may terminate the employment relationship at any time, with or without Cause and with or without advance notice. The company may give Dr. Van Wart twelve (12) months of his base salary in effect as of his termination date. In addition, Dr. Van Wart is eligible to receive his potential annual discretionary bonus amount as if all performance targets established have been satisfied, pro-rated for the number of months elapsed in the year in which his employment terminates. Base salary and bonus severance will be paid in equal installments during the twelve (12) month period following the termination date. Additionally, Dr. Van Wart is eligible to continue coverage of group health benefits under COBRA. The company will pay premiums for COBRA coverage for up to 12 months following the termination date, provided that Dr. Van Wart does not attain full-time employment within this period. Upon termination, the vesting of Dr. Van Wart’s stock options shall be accelerated such that the options are fully vested and exercisable upon the termination date and such stock options shall be exercisable for the remainder of their original term, without regard to termination of employment.
Termination for Cause: If Dr. Van Wart’s employment is terminated for cause, he will receive only the portion of his base salary that has been earned and is then payable, but has not yet been paid.
Change in Control: For the purpose of Dr. Van Wart’s employee agreement, “Change in Control” means an event or a series of related events (collectively, a “Transaction”) wherein the stockholders of the company immediately before the Transaction do not retain direct or indirect beneficial ownership of more than fifty percent (50%) of the total combined voting power of the outstanding securities of the company or, in the case of a Transaction described as the sale, exchange or transfer of all or substantially all of the assets of the company, the corporation or other business entity to which the assets of the company were transferred. At the close of a Change in Control, Dr. Van Wart’s outstanding stock options shall become vested and exercisable with respect to fifty percent (50%) of his then-unvested shares of the company’s common stock. In addition, within twelve (12) months following a Change in Control, if the company terminates Dr. Van Wart’s employment without cause or, if he were to resign for good reason, the remaining unvested portion of all of his stock options shall have accelerated vesting such that all options are fully vested and exercisable as of the date of the Change in Control Termination.
Sr. VP of Research and Preclinical Development
CymaBay entered into an employment letter agreement with Dr. Charles A. McWherter on June 5, 2007. The agreement letter was amended on October 10, 2007 in order to address the requirement of Section 409A of
80
Table of Contents
the Internal Revenue Code. Dr. McWherter’s employment agreement will continue until terminated by him or by the company. Dr. McWherter will serve as VP of Research and Preclinical Development of the company.
Base Salary, Bonus, Benefits: Dr. McWherter received an annual base salary of $327,309 in FY 2012. In addition, Dr. McWherter is eligible to earn an annual cash performance bonus, based upon achievement of annual performance goals and objectives set by the Chief Executive Officer each, year, with a target bonus of 25% of his base salary. In addition, Dr. McWherter is entitled to participate in any employee benefit plans that the company may from time to time have in effect for its employees. Dr. McWherter is also eligible to participate in an individual disability income protection plan. The company will reimburse Dr. McWherter for reasonable business expenses incurred in the discharge of duties in accordance with the general practices and policies of the company and subject to the company’s annual expense budget.
Termination: Pursuant to the terms of the employment agreement, Dr. McWherter entered into an at-will employment relationship with the company. Either Dr. McWherter or the company may terminate the employment relationship at any time, with or without Cause and with or without advance notice. The company may give Dr. McWherter twelve (12) months of his base salary in effect as of his termination date. In addition, Dr. McWherter is eligible to receive his potential annual discretionary bonus amount as if all performance targets have been satisfied, pro-rated for the number of months elapsed in the year in which his employment terminates. Base salary and bonus severance will be paid in equal installments during the twelve (12) month period following the termination date. Additionally, Dr. McWherter is eligible to continue coverage of group health benefits under COBRA. The company will pay premiums for COBRA coverage for up to 12 months following the termination date, provided that Dr. McWherter does not attain full-time employment within this period.
Termination for Cause: If Dr. McWherter’s employment is terminated for cause, he will receive only the portion of his base salary that has been earned and is then payable, but has not yet been paid.
Change in Control: For the purpose of Dr. McWherter’s employee agreement, “Change in Control” means an event or a series of related events (collectively, a “Transaction”) wherein the stockholders of the company immediately before the Transaction do not retain direct or indirect beneficial ownership of more than fifty percent (50%) of the total combined voting power of the outstanding securities of the company or, in the case of a Transaction described as the sale, exchange or transfer of all or substantially all of the assets of the company, the corporation or other business entity to which the assets of the company were transferred. At the close of a Change in Control, Dr. McWherter’s outstanding stock options shall become vested and exercisable with respect to fifty percent (50%) of his then-unvested shares of the company’s common stock. In addition, within twelve (12) months following a Change in Control, if the company terminates Dr. McWherter’s employment or, if he resigns his employment, the remaining unvested portion of his stock options shall have accelerated vesting such that all options are fully vested and exercisable as of the date of the Change in Control Termination.
Chief Medical Officer
CymaBay entered into an employment letter agreement with Dr. Raymond Urbanski on October 3, 2011.
Base Salary, Bonus, Benefits: During the term of his 2012 employment, Dr. Urbanski received a base salary of $151,574. In addition, Dr. Urbanski was eligible to earn an annual cash performance bonus, based upon achievement of annual performance goals and objectives set by the Chief Executive Officer each year, with a target bonus of 25% of his base salary. Dr. Urbanski did not receive a bonus payment upon terminating his employment relationship. In addition, Dr. Urbanski was entitled to participate in any employee benefit plans that the company may from time to time have in effect for its employees. Dr. Urbanski was also eligible to participate in an individual disability income protection plan. Dr. Urbanski resigned from CymaBay in June 2012.
Termination: Pursuant to the terms of the employment agreement, Dr. Urbanski entered into an at-will employment relationship with the company pursuant to which Dr. Urbanski was eligible to receive twelve
81
Table of Contents
(12) months of his base salary in effect as of his termination date. In addition, Dr. Urbanski was eligible to receive his potential annual discretionary bonus amount as if all performance targets had been satisfied, pro-rated for the number of months elapsed in the year in which his employment terminated. Pursuant to his employment agreement, base salary and bonus severance were to be paid in equal installments during the twelve (12) month period following his termination date.
Vice President, Regulatory and Quality
CymaBay entered into an employment relationship with Dr. Charpentier on May 1, 2007.
Base Salary, Bonus, Benefits: Dr. Charpentier received an annual base salary of $270,097 in FY 2012. In addition, Dr. Charpentier is eligible to earn an annual case performance bonus, based upon achievement of annual performance goals and objectives set by the Chief Executive Officer each year, with a target bonus of 25% of her base salary. In addition, Dr. Charpentier is entitled to participate in any employee benefit plans that the company may from time to time have in effect for its employees. Dr. Charpentier is also eligible to participate in an individual disability income protection plan. The company will reimburse Dr. Charpentier for reasonable business expenses incurred in the discharge of duties in accordance with the general practices and policies of the company and subject to the company’s annual expense budget.
Termination: Dr. Charpentier entered into an at-will employment relationship with the company. Either Dr. Charpentier or the company may terminate the employment relationship at any time, with or without Cause and with or without advance notice.
Termination for Cause: If Dr. Charpentier’s employment is terminated for cause, she will receive only the portion of her base salary that has been earned and is then payable, but has not yet been paid.
Stock Options
In August 2003, the company’s stockholders approved the 2003 Equity Incentive Plan (2003 Plan), under which shares of common stock are reserved for the granting of options, stock bonuses, and restricted stock awards by the company. These awards may be granted to employees, members of the Board of Directors, and consultants to the company. The 2003 Plan terminated in accordance with its terms on July 31, 2013 and replaced the 1993 Stock Option Plan, which had similar terms.
The 2003 Plan permits the company to (i) grant incentive stock options to directors and employees at not less than 100% of the fair value of common stock on the date of grant; (ii) grant nonqualified options to employees, directors, and consultants at not less than 85% of fair value; (iii) award stock bonuses; and (iv) grant rights to acquire restricted stock at not less than 85% of fair value. Options generally vest over a four- or five-year period and have a term of ten years. Options granted to 10% stockholders have a maximum term of five years and require an exercise price equal to at least 110% of the fair value on the date of grant. The exercise price of all options granted to date has been at least equal to the fair value of common stock on the date of grant. Restricted stock units granted in 2007 vested over a four- or five-year period, subject to certain performance conditions, and terminated on August 19, 2012.
On September 25, 2013, our stockholders approved the 2013 Equity Incentive Plan, or 2013 Plan, under which shares of our common stock are reserved for issuance pursuant to stock awards, including, but not limited to, incentive stock options, nonstatutory stock options, stock appreciation rights, restricted stock awards, restricted stock unit awards, performance stock awards, and performance cash awards. We have reserved an aggregate of 577,294 shares under the plan for issuance pursuant to stock awards, including shares which may be returned to the share reserve under options outstanding as of September 25, 2013, under the 2003 Plan. In addition, the share reserve will automatically increase on January 1st of each year, for a period of not more than ten years, commencing on January 1, 2014, in an amount equal to 5% of the total number of shares of capital stock outstanding on December 31st of the preceding calendar year, unless the Board determines otherwise prior
82
Table of Contents
to December 31st of such calendar year. As of November 1, 2013, we had issued options exercisable for an aggregate of 321,574 shares of our common stock under the 2013 Plan.
In the past, our Board of Directors has determined the fair market value of our common stock based upon inputs including valuation reports prepared by third party valuation firms. Generally, our stock options granted to new hires have vested as 25% of the total number of option shares granted on the first anniversary of the award and in equal monthly installments over the ensuring 36 months, whereas subsequent grants to employees generally vest in equal monthly installments over 48 months. We have offered our Executive Officers the opportunity to purchase the unvested shares subject to their options, with the company retaining a right to repurchase from the employee any shares that remain unvested if the employee’s services with us terminate prior to the date on which the options are fully vested.
Director Compensation
The following table shows for the fiscal year ended December 31, 2012, certain information with respect to the compensation of all non-employee directors of CymaBay:
Name | Fees Earned or Paid in Cash | Option Awards (1) (2) | Total ($) | |||||||||
Louis G. Lange, M.D., Ph.D. | $ | 0 | $ | 11,215 | $ | 11,215 | ||||||
Eric Converse (3) | $ | 0 | $ | 0 | $ | 0 | ||||||
Anthony B. Evnin, Ph.D. (4) | $ | 0 | $ | 0 | $ | 0 | ||||||
Carl Goldfischer, M.D. | $ | 0 | $ | 0 | $ | 0 | ||||||
Bradley Bolzon, Ph.D. (5) | $ | 0 | $ | 0 | $ | 0 | ||||||
Hari Kumar, Ph.D. | $ | 0 | $ | 0 | $ | 0 | ||||||
Edward E. Penhoet, Ph.D. | $ | 0 | $ | 0 | $ | 0 | ||||||
Kurt von Emster, CFA | $ | 0 | $ | 3,042 | $ | 3,042 | ||||||
Robert Zerbe, M.D. (6) | $ | 0 | $ | 2,579 | $ | 2,579 | ||||||
| (1) | These amounts are not cash compensation, but rather the aggregate fair value of the equity compensation paid to our Named Executive Officers during the fiscal year. The aggregate fair value is computed in accordance with FASB ASC Topic 718. See Note 11 to our consolidated financial statements contained in this report regarding assumptions underlying valuation of equity awards. |
| (2) | Assumptions made in the valuation of stock options granted are discussed in Note 11 to CymaBay’s 2012 Consolidated Financial Statements. Reflects the aggregate grant date fair value computed in accordance with ASC 718. Each director received only one option grant award in 2012, the fair market value of which is reflected in the table. |
| (3) | Mr. Converse resigned from the Board of Directors effective September 24, 2013. |
| (4) | Dr. Evnin resigned from the Board of Directors effective September 26, 2013. |
| (5) | Dr. Bolzon resigned from the Board of Directors effective September 19, 2012. |
| (6) | Dr. Zerbe resigned from the Board of Directors effective December 12, 2012. |
83
Table of Contents
At December 31, 2012, the following non-employee directors held options to purchase the following number of shares (the share numbers give retroactive effect to the reverse stock split that occurred on September 30, 2013):
| Name | Options | |||
Louis G. Lange, M.D., Ph.D. | 1,258 | |||
| 456 | ||||
| 3,145 | ||||
| 123 | ||||
Eric Converse (1) | 0 | |||
Anthony B. Evnin, Ph.D. (2) | 0 | |||
Carl Goldfischer, M.D. | 0 | |||
Bradley Bolzon, Ph.D. (3) | 0 | |||
Edward E. Penhoet, Ph.D. | 0 | |||
Hari Kumar, Ph.D. | 0 | |||
Kurt von Emster, CFA | 943 | |||
| 943 | ||||
Robert Zerbe, M.D. (4) | 943 | |||
| 943 | ||||
| (1) | Mr. Converse resigned from the Board of Directors effective September 24, 2013. |
| (2) | Dr. Evnin resigned from the Board of Directors effective September 26, 2013. |
| (3) | Dr. Bolzon resigned from the Board of Directors effective September 19, 2012. |
| (4) | Dr. Zerbe resigned from the Board of Directors effective December 12, 2012. |
84
Table of Contents
| ITEM 7. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE. |
Related Party Transactions
There have been no transactions since January 1, 2011, to which we have been a party, in which the amount involved exceeded or will exceed $120,000, and in which any of our directors, executive officers or beneficial owners of more than 5% of our preferred stock or common stock, or an affiliate or immediate family member thereof, had or will have a direct or indirect material interest, other than compensation, termination and change-in-control arrangements, which are described under “Executive Compensation” and under “2013 Financing” below.
2013 Financing
On September 30, 2013, CymaBay issued: (a) 374,999 shares of its common stock and warrants exercisable for 74,998 shares of its common stock to entities affiliated with Alta BioPharma for an aggregate purchase price of $1,874,995 (Ed Penhoet is a director of CymaBay and is affiliated with the Alta BioPharama entities); (b) 10,000 shares of its common stock and warrants exercisable for 2,000 shares of its common stock to The Konrad Hans von Emster III and Elizabeth F. von Emster Revocable Trust dated January 18, 2005 (the “von Emster Trust”) for an aggregate purchase price of $50,000 (Kurt von Emster is a director of CymaBay and affiliated with the von Emster Trust); (c) 50,000 shares of its common stock and warrants exercisable for 10,000 shares of its common stock to JJDC for an aggregate purchase price of $250,000 and 624,944 shares of its common stock to JJDC in cancellation of approximately $16.9 million of debt; (d) 400,000 shares of its common stock and warrants exercisable for 80,000 shares of its common stock to entities affiliated with the Deerfield Funds for an aggregate purchase price of $2,000,000; (e) 163,998 shares of its common stock and warrants exercisable for 32,799 shares of its commons stock to Pictet Biotech for an aggregate purchase price of $819,990; and (f) 374,999, shares of its common stock and warrants exercisable for 74,999 shares of its common stock to entities affiliated with Versant Venture Capital for an aggregate purchase price of $1,874,995.
Indemnification Agreements
We have entered into indemnification agreements with certain of our officers and directors. The form of agreement provides that we will indemnify our directors against any and all expenses incurred by that director because of his or her status as one of our directors to the fullest extent permitted by Delaware law, our amended and restated certificate of incorporation and our amended and restated bylaws (except under certain circumstances including on account of such officer’s or director’s breach of a duty to CymaBay as determined by a final judgment or in a proceeding initiated by such person without board approval). In addition, the form agreement provides that, to the fullest extent permitted by Delaware law, we will pay for all expenses incurred by our directors, in connection with a legal proceeding.
Director Independence
CymaBay’s business and affairs are organized under the direction of its board of directors, which currently consists of six members. The company considers each director, other than Dr. Van Wart, to be an independent director using the standards under the rules of the Nasdaq Stock Market. The primary responsibilities of the board of directors are to provide oversight, strategic guidance, counseling and direction to the company’s management. Each director shall hold office until a successor is elected and qualified or until the director resigns or is removed. Any director may be removed, with cause, by the holders of a majority of shares then entitled to vote at a meeting for the election of directors. Vacancies occurring on the board of directors will be filled by the vote of a majority of the remaining directors and may be removed, without cause, by the holders of sixty-six and two-thirds percent (66 2/3%) of the shares then entitled to vote at a meeting for the election of directors. The board of directors may, by resolution passed by a majority of the whole board of directors, designate one or more committees, each committee to consist of one or more of the directors of the corporation. In 2012, the non-executive members of the company’s board of directors did not receive compensation.
85
Table of Contents
On November 1, 2013, the Compensation Committee of the Board granted options to purchase shares of the Company’s common stock under our 2013 Plan to the following officers and directors: (a) an option to purchase 207,724 shares of our common stock, at an exercise price of $5.00 per share, to Harold Van Wart who is our Chief Executive Officer and a director, (b) an option to purchase 62,430 shares of our common stock, at an exercise price of $5.00 per share, to Charles McWherter, our Senior Vice President, Research and Pre-Clinical Development, and (c) an option to purchase 25,653 shares of our common stock, at an exercise price of $5.00 per share, to Louis G. Lange, our Chairman of the Board.
The board of directors at CymaBay currently has three 3 committees:
Compensation Committee:
Louis G. Lange, M.D., Ph.D.–Chairman
Carl Goldfischer, M.D.
Edward E. Penhoet, Ph.D.
Audit Committee:
Carl Goldfischer, M.D.—Chairman
Hari Kumar, Ph.D.
Nominating and Corporate Governance Committee:
Kurt von Emster, CFA – Chairman
Hari Kumar, Ph.D.
86
Table of Contents
| ITEM 8. | LEGAL PROCEEDINGS. |
CymaBay is not a party, nor is any of its property subject to any legal proceedings.
| ITEM 9. | MARKET PRICE OF AND DIVIDENDS ON THE REGISTRANT’S COMMON EQUITY AND RELATED STOCKHOLDER MATTERS. |
Market information
There is currently no established public trading market for our common stock.
Rule 144
Shares of our common stock that are restricted securities will be eligible for resale in compliance with Rule 144 of the Securities Act, subject to the requirements described below. “Restricted securities,” as defined under Rule 144, were issued and sold by us in reliance on exemptions from the registration requirements of the Securities Act. These shares may be sold in the public market only if registered or if they qualify for an exemption from registration, such as Rule 144. Below is a summary of the requirements for sales of our common stock pursuant to Rule 144, after the effectiveness of this registration statement. Beginning 90 days after the effectiveness of this registration statement, a person who is our affiliate or who was our affiliate at any time during the preceding six months and who has beneficially owned restricted securities for at least six months, will generally be entitled to sell within any three month period a number of shares that does not exceed one percent of the number of shares in the same class of securities. Sales under Rule 144 by our affiliates are also subject to manner of sale provisions and notice requirements and to the availability of current public information about us. Persons who may be deemed to be our affiliates generally include individuals or entities that control, or are controlled by, or are under common control with, us and may include our directors and officers, as well as our significant stockholders. For a person who has not been deemed to have been one of our affiliates at any time during the 90 days preceding a sale, sales of our shares of common stock held longer than six months, but less than one year, will be subject only to the current public information requirement and can be sold under Rule 144 beginning 90 days after the effectiveness of this registration statement without restriction. A person who is not deemed to have been one of our affiliates at any time during the 90 days preceding a sale, and who has beneficially owned the shares proposed to be sold for at least one year, is entitled to sell his or her shares without complying with the manner of sale, public information, volume limitation or notice provisions of Rule 144. We cannot estimate the number of shares of our common stock that our existing stockholders will elect to sell under Rule 144.
Rule 701
Rule 701 under the Securities Act permits sales of shares issued in reliance on Rule 701 by CymaBay to its officers, directors, employees and certain consultants. Rule 701 is only available to an issuer of securities, such as CymaBay, and does not cover resales of securities by any person. Shares issued by CymaBay in reliance upon Rule 701 may be sold by the holder pursuant to Rule 144 and, 90 days after the effective date of this registration statement, (1) in the case of non-affiliates, without compliance with the holding period and public information requirements of Rule 144, and (2) in the case of affiliates, without compliance with the holding period requirement of Rule 144.
Holders
As of November 1, 2013, there were 9,455,064 shares of our common stock outstanding, which were held by approximately 576 record holders.
87
Table of Contents
Dividends
We have not paid, nor do we currently intend to pay, any dividends on our common stock. On September 30, 2013, we entered into credit facility in any amount up to $10,000,000 and pursuant to the terms of such credit facility, we are not permitted to pay any dividends on our capital stock (other than dividends payable solely in capital stock) without the prior written consent of the lenders under the credit facility.
Equity Compensation Plan Information
The following table provides information as of December 31, 2012, with respect to shares of our common stock that may be issued under existing equity compensation plans (the share numbers give retroactive effect to the reverse stock split that occurred on September 30, 2013).
Plan Category | Number of Securities to be Issued Upon Exercise of Outstanding Options, Warrants and Rights | Weighted Average Exercise Price of Outstanding Options, Warrants and Rights | Number of Securities Remaining Available For Future Issuance under Equity Compensation Plans | |||||||||
Equity compensation plans approved by security holders (1) | 103,760 | $ | 34.18 | 36,707 | ||||||||
| 1. | Consists of our 2003 stock plan. |
| ITEM 10. | RECENT SALES OF UNREGISTERED SECURITIES. |
CymaBay has completed sales of the following unregistered securities since July 10, 2010 (the share numbers give retroactive effect to the reverse stock split that occurred on September 30, 2013, except where specifically indicated to the contrary):
| (1) | On December 17, 2010, CymaBay issued 71,543 shares of Series E-3 Preferred Stock to Johnson and Johnson Development Company (“JJDC”) pursuant to the conversion of certain outstanding promissory notes in the principal amount of $14,000,000, and accrued interest, at a conversion price of $232.93 per share of Series E-3 Preferred Stock and issued 37,119 shares of Series E-1 Preferred Stock pursuant to the conversion of certain outstanding promissory notes in the principal amount of $8,072,202 at a conversion price of $232.93 per share. CymaBay relied on Regulation D and Section 4(2) under the Securities Act of 1933, as amended. |
| (2) | On April 6, 2012, CymaBay issued 36 shares of common stock (on a pre-reverse stock split basis) to George Daley pursuant to the exercise of outstanding warrants for an aggregate purchase price of $13.68 in reliance on Regulation D and Section 4(2) under the Securities Act of 1933. |
| (3) | From July 10, 2010 to September 16, 2013, CymaBay issued an aggregate of 97 shares of common stock to four (4) of its employees upon the exercise of employee stock options for an aggregate purchase price of $671.16, in reliance on Rule 701 under the Securities Act. In addition, from July 10, 2010 to November 1, 2013, CymaBay issued options to purchase an aggregate of 347,203 shares of common stock to 38 of its employees and directors at a weighted average exercise price of $5.25, in reliance on Section 4(2) and Rule 701 under the Securities Act. |
| (4) | On September 30, 2013, CymaBay issued an aggregate of 5,366,728 shares of common stock, and warrants to purchase 1,073,338 shares of common stock, to approximately 260 investors. The shares and warrants were issued to the investors in reliance on Rule 506 of Regulation D, in that all of the investors represented that they were “accredited investors” as that term is defined in Regulation D. The shares and related warrants were sold for an aggregate offering price of $26,833,640. National Securities Corporation, or NSC, acted as placement agent with respect to 3,483,597 shares and related warrants issued in the transaction, and |
88
Table of Contents
| received an aggregate placement agent commission of $1.8 million in cash and warrants to purchase 348,360 shares of common stock at an exercise price of $5.75 per share. The warrants issued to NSC in reliance on Rule 506 of Regulation D, in that NSC represented it was an “accredited investor” as that term is defined in Regulation D. |
| (5) | On September 30, 2013, CymaBay issued an aggregate of 2,793,281 shares of common stock to the 118 holders of its preferred stock upon conversion of the preferred stock to common stock. The shares were issued to these investors in reliance on Section 3(a)(9) of the Securities Act of 1933, as amended. |
| (6) | On September 30, 2013, CymaBay issued an aggregate of 624,944 shares of common stock to Johnson & Johnson Development Corporation, or JJDC and entered into an amendment to the Development and License Agreement, dated June 15, 2010, with Janssen Pharmaceuticals, Inc. (formerly known as Ortho-McNeil, Inc.) an affiliate of JJDC, pursuant to which CymaBay agreed to forego certain milestone payments and modify future contingent royalty payments as consideration for the cancellation of $13.7 million in aggregate principal and $3.2 million in aggregate accrued interest of our debt. The shares were issued in reliance on Rule 506 of Regulation D, in that JJDC represented it was an “accredited investor” as that term is defined in Regulation D. |
| (7) | On September 30, 2013, CymaBay issued warrants to purchase an aggregate of 121,739 shares of common stock to Silicon Valley Bank, or SVB, and Oxford Finance LLC, or Oxford, as partial consideration for SVB and Oxford entering into a $10,000,000 credit facility with CymaBay. The shares were issued in reliance on Rule 506 of Regulation D, in that each of SVB and Oxford represented each was an “accredited investor” as that term is defined in Regulation D. |
| (8) | On October 31, 2013, CymaBay issued an aggregate of 664,300 shares of common stock, and warrants to purchase 132,860 shares of common stock, to approximately 73 investors. The shares and warrants were issued to the investors in reliance on Rule 506 of Regulation D, in that all of the investors represented that they were “accredited investors” as that term is defined in Regulation D. The shares and related warrants were sold for an aggregate offering price of $3,321,500. NSC acted as placement agent with respect to these shares and related warrants issued in the transaction, and received an aggregate placement agent commission of $459,545 in cash and warrants to purchase 66,430 shares of common stock at an exercise price of $5.75 per share. The warrants issued to NSC in reliance on Rule 506 of Regulation D, in that NSC represented it was an “accredited investor” as that term is defined in Regulation D. |
| ITEM 11. | DESCRIPTION OF REGISTRANT’S SECURITIES TO BE REGISTERED. |
The following description of CymaBay’s capital stock does not purport to be complete and is subject in all respects to applicable Delaware law and to the provisions of CymaBay’s certificate of incorporation, and bylaws, copies of which have been filed as exhibits to the Registration Statement.
We are registering on this registration statement only our common stock, the terms of which are described below.
Common Stock
Outstanding Shares. CymaBay’s certificate of incorporation provides that an aggregate of 100,000,000 shares of CymaBay common stock, par value $0.0001 per share, are authorized for issuance. As of November 1, 2013, 9,455,064 shares of common stock and the following options and warrants to purchase common stock were issued and outstanding:
| • | 411,130 shares of CymaBay’s common stock issuable upon the exercise of stock options outstanding at a weighted average exercise price of $11.57 per share. |
| • | 1,742,727 shares of CymaBay’s common stock issuable upon the exercise of warrants outstanding at a weighted average exercise price of $5.70 per share. |
89
Table of Contents
The following is a summary of the material rights of CymaBay’s common stock as set forth in its certificate of incorporation and bylaws.
Voting Rights. Each holder of common stock is entitled to one vote for each share of common stock held on all matters submitted to a vote of the stockholders, including the election of directors. The certificate of incorporation and by-laws do not provide for cumulative voting rights in connection with election of directors unless, at the time of such election, CymaBay is subject to Section 2115(b) of the California General Corporation Law. The affirmative vote of holders of 66 2/3% of the voting power of all of the then-outstanding shares of capital stock, voting as a single class, will be required to amend certain provisions of our amended and restated certificate of incorporation, including provisions relating to amending our amended and restated bylaws, and removal of directors.
Dividends. Subject to preferences that may be applicable to any then outstanding preferred stock, the holders of outstanding shares of common stock may receive dividends, if any, as may be declared from time to time by the Board of Directors out of legally available funds. CymaBay has never issued a dividend on shares of its common stock and has no intention to do so in the future.
Liquidation. In the event of liquidation, dissolution or winding up of CymaBay, the assets legally available for distribution shall be distributed ratably to the holders of shares of common stock and preferred stock, subject to the satisfaction of any liquidation preference granted to the holders of any outstanding shares of preferred stock.
Rights and Preferences. Holders of common stock have no preemptive, conversion or subscription rights, and there are no redemption or sinking fund provisions applicable to the common stock. The rights, preferences and privileges of the holders of common stock are subject to, and may be adversely affected by, the rights of the holders of shares of any series of preferred stock that CymaBay may designate and issue in the future.
Fully Paid and Nonassessable. All outstanding shares of common stock are fully paid and nonassessable.
Warrants
In connection with the 2013 financing, and as described in Recent Sales of Unregistered Securities, CymaBay issued warrants exercisable for 1,206,198 shares of our common stock to purchasers in the 2013 financing (the “Financing Warrants”). The Financing Warrants are exercisable for a period of five (5) years from September 30, 2013, at an exercise price of $5.75 per share. The exercise prices for such Financing Warrants may be adjusted in the event of any recapitalization, reclassification, exchange, or subdivision of our outstanding shares of Common Stock. In the event CymaBay was to declare and pay a dividend or other distribution on the shares of its common stock, then the holder of the Financing Warrants, shall be entitled to receive such dividends or distributions to the same extent as if the holder had exercised the Financing Warrant and held common stock. In the event of an acquisition or change (a “Major Transaction”) of control of CymaBay, the proceeds payable to the holder of a Financing Warrant shall be determined as more completely described in the Financing Warrants using the Black-Scholes Option Pricing Model as set forth in Schedule 1 of the Financing Warrants. Furthermore, the Company may be subject to liquidated damages in the event of certain “Events of Failure” as described in the Financing Warrants, including failure to deliver shares upon exercise of the Financing Warrants, failure to remove a restrictive legend from a Financing Warrant or the underlying shares, or failure to affect a transfer of a Financing Warrant. The Company may be subject to liquidated damages in connection with any Event of Failure in the form of cash payments or issuance of shares of common stock in connection with any such Event of Failure, each as determined by the Black-Scholes Option Pricing Model. The Company may be subject to additional liquidated damages in the event of certain “Events of Default” as described in the Financing Warrants, including Events of Failure that are not cured within the requisite periods or in the event the Company fails to provide for appropriate payments to the holders of Financing Warrants in connection with a Major Transaction. The Company may be subject to liquidated damages or early mandatory termination of the Financing Warrant in
90
Table of Contents
connection with any Event of Default in the form of cash payments or issuance of shares of common stock in full satisfaction of the Financing Warrants, each as determined by the Black-Scholes Option Pricing Model. CymaBay further issued warrants exercisable for 414,790 shares of its common stock to NSC in its capacity as placement agent in the 2013 financing under the same terms and conditions as the Financing Warrants.
On September 30, 2013, CymaBay issued warrants to purchase an aggregate of 121,739 shares of common stock to SVB and Oxford, as partial consideration for SVB and Oxford entering into a $10,000,000 credit facility with CymaBay (the “Bank Warrants”). The Bank Warrants are exercisable for a period of ten (10) years from September 30, 2013, at an exercise price of $5.00 per share. The exercise prices for such Bank Warrants may be adjusted in the event of any recapitalization, reclassification, exchange, or subdivision of our outstanding shares of Common Stock. In the event CymaBay was to declare and pay a dividend or other distribution on the shares of its common stock, then upon exercise of the Bank Warrants, the holder shall be entitled to receive, without additional cost to the holder, the total number and kind of securities and property which the holder would have received had holder owned the shares of record as of the date the dividend or distribution occurred. In the event of any merger or acquisition of CymaBay, the holder of any Bank Warrant is obligated to exercise the Bank Warrant prior to the consummation of such merger or acquisition and the Bank Warrant shall expire immediately prior to the consummation of such merger or acquisition, unless the consideration to be paid to the holders of the Company’s common stock is something other than cash or marketable securities, in which case any successor entity to CymaBay shall be obligated to assume the Bank Warrants.
Preferred Stock
CymaBay’s board of directors is authorized, subject to limitations prescribed by Delaware law, to issue up to 10,000,000 shares of preferred stock in one or more series, to establish from time to time the number of shares to be included in each series and to fix the designation, powers, preferences and rights of the shares of each series and any of its qualifications, limitations or restrictions. CymaBay’s board of directors can also increase or decrease the number of shares of any series, but not below the number of shares of that series then outstanding, without any further vote or action by the company’s stockholders. CymaBay’s board of directors may authorize the issuance of preferred stock with voting or conversion rights that could adversely affect the voting power or other rights of the holders of the common stock. The issuance of preferred stock, while providing flexibility in connection with possible acquisitions and other corporate purposes, could, among other things, have the effect of delaying, deferring, discouraging or preventing a change in control of CymaBay and may adversely affect the market price of CymaBay’s common stock and the voting and other rights of the holders of common stock.
Registration Rights
Holders of 9,226,095 shares of CymaBay’s common stock, and holders of warrants to purchase 1,206,198 shares of CymaBay’s common stock, have the right to require CymaBay to register with the SEC the shares of common stock and the shares of common stock issuable upon exercise of such warrants so that those shares of common stock may be publicly resold, or to include those shares in any registration statement CymaBay files.
Resale Registration Statement. Pursuant to CymaBay’s Registration Rights Agreement, dated September 30, 2013, entered into in connection with the 2013 financing (the “Registration Agreement”), CymaBay is obligated to file resale registration statements with the SEC to register the Shares, Warrant Shares and Conversion Shares (each as defined in the Registration Agreement) within the time frames permitted under the Registration Agreement. Currently, CymaBay anticipates filing the first of its resale registration statements no later than December 2, 2013 (the “Initial Registration Statement”). CymaBay is required to cause the Initial Registration Statement be to be made effective no later than December 30, 2013, unless CymaBay receives comments to the Initial Registration Statement from the SEC in which case the deadline for causing such Initial Registration Statement to go effective shall be extended until January 29, 2014. Thereafter, CymaBay shall be obligated, as promptly as practicable, to cause any Shares, Warrant Shares or Conversion Shares that were not
91
Table of Contents
registered under the Initial Registration Statement to register the maximum allowable number of such shares as permitted by the SEC under any remaining registration statements to cause all of the shares registrable under the Registration Agreement to be registered for resale. In the event CymaBay fails to timely file the Initial Registration Statement or any remaining registration statement or fails to keep such registration statement effective during the period required for such registration statement, then CymaBay shall pay to each holder of such affected registrable securities liquidated damages in an amount in cash equal to 1.5% of the aggregate purchase price paid by such holder for such registrable securities required to be included in such registration statement, provided that the amount of such liquidated damages paid to each holder may not exceed more than 25% of the aggregate purchase price paid by such holder for such registrable securities. On October 30, 2013, the Company entered into Amendment No. 1 to the Registration Rights Agreement to permit the Company to join institutional investors to the Registration Rights Agreement, provided such parties enter into a purchase agreement with the Company on or before November 22, 2013.
“Piggyback” Registration Rights. If CymaBay registers any securities for public sale (other than any registration statement relating to any employee benefit plan, any corporate reorganization or stock issued upon conversion of debt securities), holders of registrable securities under the Registration Agreement shall have the right to include their shares in the registration statement. The underwriters of any underwritten offering will have the right to limit the number of shares having registration rights to be included in the registration statement.
Expenses of Registration. CymaBay will pay all expenses relating to all registrations and piggyback registrations provided for under the terms of the Registration Agreement.
Termination of Registration Rights. All registration rights described above shall terminate and be of no further force and effect at such time that all holders can sell their registrable securities under Rule 144 (1) without limitations as to volume of sales, method of sale requirements or notice requirements and (2) without the requirement for the Company to be in compliance with the current public information requirement under Rule 144(c)(1).
Anti-Takeover Provisions
Our amended and restated certificate of incorporation and amended and restated bylaws, include a number of provisions that may deter or impede hostile takeovers or changes of control or management. These provisions include:
Issuance of undesignated preferred stock. Our board of directors has the authority, without further action by the stockholders, to issue up to 10,000,000 shares of undesignated preferred stock with rights and preferences, including voting rights, designated from time to time by our board of directors. The existence of authorized but unissued shares of preferred stock enables our board of directors to make it more difficult or to discourage an attempt to obtain control of us by means of a merger, tender offer, proxy contest or otherwise.
Board of directors vacancies. Our amended and restated certificate of incorporation and amended and restated bylaws authorize only our board of directors to fill vacant directorships. In addition, the number of directors constituting our board of directors may be set only by resolution adopted by a majority vote of our entire board of directors. These provisions prevent a stockholder from increasing the size of our board of directors and gaining control of our board of directors by filling the resulting vacancies with its own nominees.
Stockholder action; special meetings of stockholders. Our amended and restated certificate of incorporation provides that our stockholders may not take action by written consent, but may only take action at annual or special meetings of our stockholders. Stockholders will not be permitted to cumulate their votes for the election of directors unless required by applicable law. Our amended and restated certificate of incorporation further provides that only the chairman of our board of directors, chief executive officer or a majority of our board of directors may call special meetings of our stockholders.
92
Table of Contents
Advance notice requirements for stockholder proposals and director nominations. Our amended and restated bylaws provide advance notice procedures for stockholders seeking to bring business before our annual meeting of stockholders, or to nominate candidates for election as directors at our annual meeting of stockholders. Our amended and restated bylaws also specify certain requirements as to the form and content of a stockholder’s notice. These provisions may make it more difficult for our stockholders to bring matters before our annual meeting of stockholders or to nominate directors at annual meetings of stockholders.
CymaBay designed these provisions to enhance the likelihood of continued stability in the composition of our board of directors and its policies, to discourage certain types of transactions that may involve an actual or threatened acquisition of us, and to reduce our vulnerability to an unsolicited acquisition proposal. We also designed these provisions to discourage certain tactics that may be used in proxy fights. However, these provisions could have the effect of discouraging others from making tender offers for our shares and, as a consequence, they may also reduce fluctuations in the market price of our shares that could result from actual or rumored takeover attempts.
Section 203 of the Delaware General Corporation Law
We are subject to Section 203 of the DGCL, which prohibits a Delaware corporation from engaging in a business combination with any interested stockholder for a period of three years following the date the person became an interested stockholder, with the following exceptions:
| • | before such date, the board of directors of the corporation approved either the business combination or the transaction that resulted in the stockholder becoming an interested holder; |
| • | upon completion of the transaction that resulted in the stockholder becoming an interested stockholder, the interested stockholder owned at least 85% of the voting stock of the corporation outstanding at the time the transaction began, excluding for purposes of determining the voting stock outstanding (but not the outstanding voting stock owned by the interested stockholder) those shares owned (a) by persons who are directors and also officers and (b) pursuant to employee stock plans in which employee participants do not have the right to determine confidentially whether shares held subject to the plan will be tendered in a tender or exchange offer; and |
| • | on or after such date, the business combination is approved by the board of directors and authorized at an annual or special meeting of the stockholders, and not by written consent, by the affirmative vote of at least 66 2/3% of the outstanding voting stock that is not owned by the interested stockholder. |
| • | In general, Section 203 of the DGCL defines business combination to include the following: |
| • | any merger or consolidation involving the corporation and the interested stockholder; |
| • | any sale, transfer, pledge or other disposition of 10% or more of the assets of the corporation involving the interested stockholder; |
| • | subject to certain exceptions, any transaction that results in the issuance or transfer by the corporation of any stock of the corporation to the interested stockholder; |
| • | any transaction involving the corporation that has the effect of increasing the proportionate share of the stock or any class or series of the corporation beneficially owned by the interested stockholder; and |
| • | the receipt by the interested stockholder of the benefit of any loans, advances, guarantees, pledges or other financial benefits by or through the corporation. |
In general, Section 203 of the DGCL defines an “interested stockholder” as an entity or person who, together with the entity’s or person’s affiliates and associates, beneficially owns, or is an affiliate of the corporation and within three years prior to the time of determination of interested stockholder status did own, 15% or more of the outstanding voting stock of the corporation. A Delaware corporation may “opt out” of these provisions with an express provision in its certificate of incorporation. We have not opted out of these provisions, which may as a result, discourage or prevent mergers or other takeover or change of control attempts of us.
93
Table of Contents
Transfer Agent and Registrar
Our transfer agent and registrar for our common stock is American Stock Transfer & Trust Company, LLC.
| ITEM 12. | INDEMNIFICATION OF DIRECTORS AND OFFICERS. |
Section 145 of the Delaware General Corporation Law authorizes a court to award, or a corporation’s board of directors to grant indemnity to directors and officers under certain circumstances and subject to certain limitations. The terms of Section 145 of the Delaware General Corporation Law are sufficiently broad to permit indemnification under certain circumstances for liabilities, including reimbursement of expenses incurred, arising under the Securities Act.
As permitted by the Delaware General Corporation Law, CymaBay’s certificate of incorporation contains provisions that eliminate the personal liability of its directors for monetary damages for any breach of fiduciary duties as a director, except liability for the following:
| • | any breach of the director’s duty of loyalty to CymaBay or its stockholders; |
| • | acts or omissions not in good faith or that involve intentional misconduct or a knowing violation of law; |
| • | under Section 174 of the Delaware General Corporation Law (regarding unlawful dividends and stock purchases); or |
| • | any transaction from which the director derived an improper personal benefit. |
As permitted by the Delaware General Corporation Law, CymaBay’s amended and restated bylaws provide that:
| • | CymaBay is required to indemnify its directors and executive officers to the fullest extent permitted by the Delaware General Corporation Law, subject to very limited exceptions; |
| • | CymaBay may indemnify its other employees and agents as set forth in the Delaware General Corporation Law; |
| • | CymaBay is required to advance expenses, as incurred, to its directors and executive officers in connection with a legal proceeding to the fullest extent permitted by the Delaware General Corporation Law, subject to very limited exceptions; and |
| • | the rights conferred in the bylaws are not exclusive. |
CymaBay has entered, and intends to continue to enter, into separate indemnification agreements with its directors and executive officers to provide these directors and executive officers additional contractual assurances regarding the scope of the indemnification set forth in CymaBay’s certificate of incorporation and restated bylaws and to provide additional procedural protections. At present, there is no pending litigation or proceeding involving a director or executive officer of CymaBay regarding which indemnification is sought. The indemnification provisions in CymaBay’s restated certificate of incorporation, restated bylaws and the indemnification agreements entered into or to be entered into between CymaBay and each of its directors and executive officers may be sufficiently broad to permit indemnification of CymaBay’s directors and executive officers for liabilities arising under the Securities Act. Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of CymaBay pursuant to the foregoing provisions, or otherwise, CymaBay has been advised that in the opinion of the Securities and Exchange Commission such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable.
CymaBay currently carries liability insurance for its directors and officers.
94
Table of Contents
| ITEM 13. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA. |
The information required by this item may be found beginning on page F-1 of this Form 10 following the signature page of this Form 10.
| ITEM 14. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE. |
None.
95
Table of Contents
| ITEM 15. | FINANCIAL STATEMENTS AND EXHIBITS. |
| (a) | Financial Statements filed as part of this registration statement: |
| Page | ||||
| F-2 | ||||
Balance Sheets as of December 31, 2012 and 2011 (audited) and June 30, 2013 (unaudited) | F-3 | |||
| F-4 | ||||
| F-5 | ||||
| F-6 | ||||
| F-7 | ||||
| (b) | Exhibits. |
See the Exhibit Index which follows the signature page and financial pages of this Form 10, which is incorporated by reference here.
96
Table of Contents
SIGNATURES
Pursuant to the requirements of Section 12 of the Securities Exchange Act of 1934, the registrant has duly caused this registration statement to be signed on its behalf by the undersigned, thereunto duly authorized.
| CymaBay Therapeutics, Inc. | ||||||
| Date: November 22, 2013 | By: | /s/ Harold Van Wart | ||||
| Harold Van Wart, Ph.D. | ||||||
| President and Chief Executive Officer | ||||||
97
Table of Contents
CymaBay Therapeutics, Inc.
Financial Statements
Index to Financial Statements Table of Contents
| F-2 | ||||
Balance Sheets as of December 31, 2012 and 2011 (audited) and June 30, 2013 (unaudited) | F-3 | |||
| F-4 | ||||
| F-5 | ||||
| F-6 | ||||
| F-7 |
F-1
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders
CymaBay Therapeutics, Inc.
We have audited the accompanying balance sheets of CymaBay Therapeutics, Inc., formerly known as Metabolex, Inc., as of December 31, 2012 and 2011, and the related statements of operations and comprehensive loss, convertible preferred stock and stockholders’ deficit, and cash flows for each of the two years in the period ended December 31, 2012. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. We were not engaged to perform an audit of the Company’s internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of CymaBay Therapeutics, Inc. at December 31, 2012 and 2011, and the results of its operations and its cash flows for each of the two years in the period ended December 31, 2012 in conformity with U.S. generally accepted accounting principles.
The accompanying financial statements have been prepared assuming that the Company will continue as a going concern. As discussed in Note 1 to the financial statements, the Company has recurring losses from operations and has a net capital deficiency that raise substantial doubt about its ability to continue as a going concern. Management’s plans in regard to these matters are also described in Note 1. The financial statements do not include any adjustments that might result from the outcome of this uncertainty.
/s/ Ernst & Young LLP | ||
Redwood City, CA
June 17, 2013
Except for Note 15, as to which the date is August 9, 2013, and except for the retroactive effect of the 1-for-79.5 reverse stock split as described in Note 2, as to which the date is October 11, 2013
F-2
Table of Contents
CymaBay Therapeutics, Inc.
(In thousands, except share and per share amounts)
| December 31, | June 30, | |||||||||||
| 2012 | 2011 | 2013 (unaudited) | ||||||||||
Assets | ||||||||||||
Current assets: | ||||||||||||
Cash and cash equivalents | $ | 7,726 | $ | 8,021 | $ | 3,556 | ||||||
Marketable securities | — | 11,012 | — | |||||||||
Contract receivables | 108 | 124 | — | |||||||||
Accrued interest receivable | 9 | 100 | — | |||||||||
Prepaid expenses | 147 | 234 | 26 | |||||||||
|
|
|
|
|
| |||||||
Total current assets | 7,990 | 19,491 | 3,582 | |||||||||
Property and equipment, net | 84 | 203 | 19 | |||||||||
Other assets | 42 | 93 | 114 | |||||||||
|
|
|
|
|
| |||||||
Total assets | $ | 8,116 | $ | 19,787 | $ | 3,715 | ||||||
|
|
|
|
|
| |||||||
Liabilities and redeemable convertible preferred stock and stockholders’ deficit | ||||||||||||
Current liabilities: | ||||||||||||
Accounts payable | $ | 657 | $ | 1,608 | $ | 698 | ||||||
Accrued liabilities | 894 | 1,185 | 891 | |||||||||
Convertible notes | 13,737 | — | 13,747 | |||||||||
Accrued interest payable | 2,566 | — | 2,979 | |||||||||
Equipment loans | — | 12 | — | |||||||||
|
|
|
|
|
| |||||||
Total current liabilities | 17,854 | 2,805 | 18,315 | |||||||||
Convertible notes | — | 13,747 | — | |||||||||
Accrued interest payable | — | 1,785 | — | |||||||||
Deferred rent | 132 | 214 | 86 | |||||||||
|
|
|
|
|
| |||||||
Total Liabilities | 17,986 | 18,551 | 18,401 | |||||||||
Commitments and contingencies (Note 8) | ||||||||||||
Redeemable convertible preferred stock, $0.0001 par value: 55,258,608 shares authorized; 661,059 shares issued and outstanding; aggregate liquidation preference of $263,003, $256,750 and $244,107 as of June 30, 2013, December 31, 2012 and 2011, respectively | 318,697 | 306,053 | 324,950 | |||||||||
Stockholders’ deficit: | ||||||||||||
Common stock, $0.0001 par value: 74,000,000 shares authorized; 5,870, 5,792 and 5,773 shares issued and outstanding as of June 30, 2013, December 31, 2012 and 2011, respectively | — | — | — | |||||||||
Additional paid-in capital | 913 | 762 | 948 | |||||||||
Accumulated other comprehensive income (loss) | — | 2 | — | |||||||||
Accumulated deficit | (329,480 | ) | (305,581 | ) | (340,584 | ) | ||||||
|
|
|
|
|
| |||||||
Total stockholders’ deficit | (328,567 | ) | (304,817 | ) | (339,636 | ) | ||||||
|
|
|
|
|
| |||||||
Total liabilities and redeemable convertible preferred stock and stockholders’ deficit | $ | 8,116 | $ | 19,787 | $ | 3,715 | ||||||
|
|
|
|
|
| |||||||
See accompanying notes.
F-3
Table of Contents
CymaBay Therapeutics, Inc.
Statements of Operations and Comprehensive Loss
(In Thousands, except share and per share information)
| Years Ended December 31, | Six Months Ended June 30, | |||||||||||||||
| 2012 | 2011 | 2013 | 2012 | |||||||||||||
| (Unaudited) | ||||||||||||||||
Contract revenue | $ | 3,050 | $ | 15,147 | — | 125 | ||||||||||
Operating expenses: | ||||||||||||||||
Research and development | 9,280 | 14,391 | 2,459 | 5,279 | ||||||||||||
General and administrative | 4,208 | 4,654 | 2,097 | 2,418 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total operating expenses | 13,488 | 19,045 | 4,556 | 7,697 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss from operations | (10,438 | ) | (3,898 | ) | (4,556 | ) | (7,572 | ) | ||||||||
Other income (expense): | ||||||||||||||||
Interest income | 22 | 78 | 2 | 17 | ||||||||||||
Interest expense | (841 | ) | (705 | ) | (421 | ) | (400 | ) | ||||||||
Other income, net | 2 | 28 | 124 | 2 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss | (11,255 | ) | (4,497 | ) | (4,851 | ) | (7,953 | ) | ||||||||
Accretion to redemption value of redeemable convertible preferred stock | (12,644 | ) | (12,609 | ) | (6,253 | ) | (6,245 | ) | ||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss attributable to stockholders | (23,899 | ) | (17,106 | ) | (11,104 | ) | (14,198 | ) | ||||||||
Other comprehensive loss/income: | ||||||||||||||||
Unrealized (losses) gains on marketable securities | (2 | ) | 14 | — | (2 | ) | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Other comprehensive (loss) income | (2 | ) | 14 | — | (2 | ) | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Comprehensive loss | $ | (11,257 | ) | $ | (4,483 | ) | $ | (4,851 | ) | $ | (7,955 | ) | ||||
|
|
|
|
|
|
|
| |||||||||
Basic and diluted net loss per common share | $ | (4,128.71 | ) | $ | (2,963.11 | ) | $ | (1,902.45 | ) | $ | (2,457.86 | ) | ||||
|
|
|
|
|
|
|
| |||||||||
Weighted average common shares outstanding used to calculate basic and diluted net loss per common share | 5,788 | 5,773 | 5,833 | 5,777 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
See accompanying notes.
F-4
Table of Contents
CymaBay Therapeutics, Inc.
Statements of Convertible Preferred Stock and Stockholders’ Deficit
(In Thousands, except share and per share information)
| Redeemable Convertible Preferred Stock | Common Stock | Additional Paid-in Capital | Accumulated Other Comprehensive Income (Loss) | Accumulated Deficit | Total Stockholders’ Equity (Deficit) | |||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||||
Balances as of December 31, 2010 | 661,059 | $ | 293,444 | 5,773 | $ | — | $ | — | $ | (12 | ) | $ | (288,475 | ) | $ | (288,487 | ) | |||||||||||||||
Non-employee stock-based compensation expense | — | — | — | — | 5 | — | — | 5 | ||||||||||||||||||||||||
Employee and director stock-based compensation expense | — | — | — | — | 757 | — | — | 757 | ||||||||||||||||||||||||
Accretion to redemption value of redeembable convertible preferred stock | — | 12,609 | — | — | — | — | (12,609 | ) | (12,609 | ) | ||||||||||||||||||||||
Net loss | — | — | — | — | — | — | (4,497 | ) | (4,497 | ) | ||||||||||||||||||||||
Net unrealized loss on marketable securities | — | — | — | — | — | 14 | — | 14 | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||
Balances as of December 31, 2011 | 661,059 | $ | 306,053 | 5,773 | $ | — | $ | 762 | $ | 2 | $ | (305,581 | ) | $ | (304,817 | ) | ||||||||||||||||
Discount conversion feature associated with convertible notes | — | — | — | — | 70 | — | — | 70 | ||||||||||||||||||||||||
Issuance of common stock upon exercise of options | — | — | 19 | — | — | — | — | — | ||||||||||||||||||||||||
Non-employee stock-based compensation expense | — | — | 0 | — | 1 | — | — | 1 | ||||||||||||||||||||||||
Employee and director stock-based compensation expense | — | — | — | — | 80 | — | — | 80 | ||||||||||||||||||||||||
Accretion to redemption value of redeembable convertible preferred stock | — | 12,644 | — | — | — | — | (12,644 | ) | (12,644 | ) | ||||||||||||||||||||||
Net loss | — | — | — | — | — | — | (11,255 | ) | (11,255 | ) | ||||||||||||||||||||||
Net unrealized gain on marketable securities | — | — | — | — | — | (2 | ) | — | (2 | ) | ||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||
Balances as of December 31, 2012 | 661,059 | $ | 318,697 | 5,792 | $ | — | $ | 913 | $ | — | $ | (329,480 | ) | $ | (328,567 | ) | ||||||||||||||||
Issuance of common stock upon exercise of options | — | — | 78 | — | — | — | — | — | ||||||||||||||||||||||||
Non-employee stock-based compensation expense | — | — | — | — | 1 | — | — | 1 | ||||||||||||||||||||||||
Employee and director stock-based compensation expense | — | — | — | — | 34 | — | — | 34 | ||||||||||||||||||||||||
Accretion to redemption value of redeembable convertible preferred stock | — | 6,253 | — | — | — | — | (6,253 | ) | (6,253 | ) | ||||||||||||||||||||||
Net loss | — | — | — | — | — | — | (4,851 | ) | (4,851 | ) | ||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||
Balances as of June 30, 2013 (unaudited) | 661,059 | $ | 324,950 | 5,870 | $ | — | $ | 948 | $ | — | $ | (340,584 | ) | $ | (339,636 | ) | ||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||
See accompanying notes.
F-5
Table of Contents
CymaBay Therapeutics, Inc.
(In Thousands)
| Year Ended December 31, | Six Months Ended June 30, | |||||||||||||||
| 2012 | 2011 | 2013 | 2012 | |||||||||||||
| (unaudited) | ||||||||||||||||
Operating activities | ||||||||||||||||
Net loss | $ | (11,255 | ) | $ | (4,497 | ) | $ | (4,851 | ) | $ | (7,953 | ) | ||||
Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||||||||||
Depreciation and amortization | 119 | 210 | 41 | 62 | ||||||||||||
Amortization of notes payable conversion option | 10 | (40 | ) | |||||||||||||
Non-employee stock-based compensation expense | 1 | 6 | — | 1 | ||||||||||||
Employee and director stock-based compensation expense | 80 | 757 | 34 | 42 | ||||||||||||
Non-cash interest associated with discount accretion | 60 | — | — | — | ||||||||||||
Change in fair value of warrant liability | — | — | — | 69 | ||||||||||||
Gain on sale of property and equipment | — | — | (126 | ) | — | |||||||||||
Changes in assets and liabilities: | ||||||||||||||||
Contract receivables | 16 | 267 | 108 | (15 | ) | |||||||||||
Accrued interest receivable | 91 | 250 | 9 | 63 | ||||||||||||
Prepaid expenses | 87 | 12 | 121 | 76 | ||||||||||||
Other assets | 51 | 110 | (72 | ) | 51 | |||||||||||
Accounts payable | (951 | ) | (557 | ) | 41 | (669 | ) | |||||||||
Accrued liabilities | (291 | ) | (520 | ) | (3 | ) | 470 | |||||||||
Accrued interest payable | 781 | 693 | 413 | 370 | ||||||||||||
Deferred rent | (82 | ) | 69 | (46 | ) | (36 | ) | |||||||||
Deferred revenue | — | (14,725 | ) | — | 25 | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Net cash used in operating activities | (11,293 | ) | (17,925 | ) | (4,320 | ) | (7,484 | ) | ||||||||
Investing activities | ||||||||||||||||
Purchases of property and equipment | — | (37 | ) | 150 | — | |||||||||||
Purchases of marketable securities | (2,881 | ) | (21,714 | ) | — | (2,887 | ) | |||||||||
Proceeds from maturities of marketable securities | 13,891 | 40,985 | — | 10,441 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Net cash provided by investing activities | 11,010 | 19,234 | 150 | 7,554 | ||||||||||||
Financing activities | ||||||||||||||||
Principal payments on equipment loans | (12 | ) | (200 | ) | — | (12 | ) | |||||||||
|
|
|
|
|
|
|
| |||||||||
Net cash used in financing activities | (12 | ) | (200 | ) | — | (12 | ) | |||||||||
|
|
|
|
|
|
|
| |||||||||
Net (decrease)/increase in cash and cash equivalents | (295 | ) | 1,109 | (4,170 | ) | 58 | ||||||||||
Cash and cash equivalents at beginning of year | 8,021 | 6,912 | 7,726 | 8,021 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Cash and cash equivalents at end of year | $ | 7,726 | $ | 8,021 | $ | 3,556 | $ | 8,079 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Supplemental disclosure of cash flow information | ||||||||||||||||
Interest paid | $ | — | $ | 10 | — | — | ||||||||||
|
|
|
|
|
|
|
| |||||||||
See accompanying notes.
F-6
Table of Contents
1. Organization and Description of Business
CymaBay Therapeutics, Inc., formerly Metabolex, Inc. (the Company) is a biopharmaceutical company focused on the discovery and development of proprietary new medicines for the treatment of gout and metabolic diseases. The Company was incorporated in Delaware in October 1988 as Transtech Corporation.
Since inception, the Company has funded its operations primarily through the sale of convertible preferred stock, receipts from the exercise of related warrants to purchase preferred stock, the issuance of convertible notes, and up-front fees, milestones, and research and development funding received under collaboration agreements. The primary uses of funds to date have been for research, pre-clinical and clinical development, drug manufacturing, license payments, business development and administration, and spending on capital items.
Need to Raise Additional Capital
The accompanying financial statements for the years ended December 31, 2012 and 2011, have been prepared on a going concern basis, which contemplates the realization of assets and the settlement of liabilities and commitments in the normal course of business for the foreseeable future. The Company has incurred net losses from operations since its inception and has an accumulated deficit of $329.5 million at December 31, 2012. The Company recorded net losses of $11.3 million and $4.5 million for the years ended December 31, 2012 and 2011, respectively. The Company also recorded negative cash flows from operating activities during 2012 and 2011 of $11.3 million and $17.9 million, respectively. To date, none of the Company’s product candidates have been approved for marketing and sale, and the Company has not recorded any product sales. Management expects operating losses to continue for the next several years. The Company’s ability to achieve profitability is dependent primarily on its ability to successfully develop, acquire or in-license additional product candidates, continue clinical trials for product candidates currently in clinical development, obtain regulatory approvals, and support commercialization activities for partnered product candidates. Products developed by the Company will require approval of the U.S. Food and Drug Administration (FDA) or a foreign regulatory authority prior to commercial sale. The regulatory approval process is expensive, time-consuming, and uncertain, and any denial or delay of approval could have a material adverse effect on the Company. Even if approved, the Company’s products may not achieve market acceptance and will face competition from both generic and branded pharmaceutical products. As of December 31, 2012, the Company had cash and cash equivalents of $7.7 million and a working capital deficit of $9.9 million. The Company will require additional financial resources to fund its ongoing operations, which management plans to raise primarily through equity and/or debt financings and/or collaboration activities. Such funding may not be available to the Company on acceptable terms, or at all. The Company has recurring losses from operations and has a net capital deficiency that raises substantial doubt about its ability to continue as a going concern if additional financial resources are not obtained. The accompanying financial statements do not include any adjustments relating to the recoverability of the carrying amounts of recorded assets or the amount of liabilities that might result from the outcome of uncertainties.
2. Summary of Significant Accounting Policies
Basis of Presentation and Use of Estimates
The financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (U.S. GAAP), which requires management to make estimates and assumptions that affect the amounts and disclosures reported in the financial statements and accompanying notes. Management bases its estimates on historical experience and on assumptions believed to be reasonable under the circumstances. The estimation process often may yield a range of potentially reasonable estimates of the ultimate future outcomes, and management must select an amount that falls within that range of reasonable estimates. Actual results could differ materially from those estimates. The Company believes significant judgment is involved in determining revenue recognition and in estimating stock-based compensation, accrued liabilities, and equity instrument valuations.
F-7
Table of Contents
Reverse Stock Split
On September 30, 2013, the Company filed amended and restated certificates of incorporation under which the Company’s preferred stock and common stock was reverse split on a 1-for-79.5 basis. The accompanying financial statements and notes to the financial statements, other than with respect to the authorized number of shares, give retroactive effect to the reverse split for all periods presented.
Unaudited Interim Financial Information
The accompanying balance sheet as of June 30, 2013, the statements of operations and comprehensive loss and cash flows for the six months ended June 30, 2013 and 2012, and the statements of convertible preferred stock and stockholder’s deficit for the six months ended June 30, 2013, are unaudited. The financial data and other information disclosed in these notes to the financial statements related to June 30, 2013, and the six months period ended June 30, 2012, are also unaudited. The unaudited interim financial statements have been prepared on the same basis as the annual financial statements and, in the opinion of management, reflect all adjustments, which include only normal recurring adjustments, necessary to state fairly the Company’s financial position as of June 30, 2012, and the results of its operations and cash flows for the six months ended June 30, 2013, and 2012. The results for the six months ended June 30, 2013, are not necessarily indicative of results to be expected for the year ending December 31, 2013, or for any other interim period or for any future year.
Concentration of Credit Risk
Cash, cash equivalents, and marketable securities consist of financial instruments that potentially subject the Company to a concentration of credit risk to the extent of the fair value recorded in the balance sheet. The Company invests cash that is not required for immediate operating needs primarily in highly liquid instruments that bear minimal risk. The Company has established guidelines relating to the quality, diversification, and maturities of securities to enable the Company to manage its credit risk.
Fair Value of Financial Instruments
The Company’s financial instruments consist of cash and cash equivalents, short-term marketable securities, accounts payable, accrued expenses, and convertible notes. Fair value estimates of these instruments are made at a specific point in time, based on relevant market information. These estimates may be subjective in nature and involve uncertainties and matters of significant judgment and therefore cannot be determined with precision. The carrying amounts of cash and cash equivalents, and accrued liabilities are generally considered to be representative of their respective fair values because of the short-term nature of those instruments.
Fair value is defined as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants at the measurement date. Assets and liabilities that are measured at fair value are reported using a three-level fair value hierarchy that prioritizes the inputs used to measure fair value. This hierarchy maximizes the use of observable inputs and maximizes the use of unobservable inputs and is as follows:
Level 1—Quoted prices in active markets for identical assets or liabilities that the Company has the ability to access at the measurement date.
Level 2—Inputs other than quoted prices in active markets that are observable for the asset or liability, either directly or indirectly.
Level 3—Inputs that are unobservable for the asset or liability.
The carrying amounts of financial instruments such as cash and cash equivalents, short-term marketable securities, accounts payable, convertible notes, and accrued expenses approximate the related fair values due to the short-term maturities of these instruments. Marketable securities consist of available-for-sale securities that are reported at fair value, with the related unrealized gains and losses included in accumulated other comprehensive income (loss), a component of stockholders’ deficit. The Company values cash equivalents and marketable securities using quoted market prices or alternative pricing sources and models utilizing observable
F-8
Table of Contents
market inputs and, as such, classifies cash equivalents and marketable securities within Level 1 or Level 2. As of June 30, 2013, December 31, 2012 and 2011, the Company had no assets or liabilities measured at fair value on a recurring basis within the Level 3 hierarchy.
Cash, Cash Equivalents, and Marketable Securities
The Company considers all highly liquid investments with a remaining maturity of 90 days or less at the time of purchase to be cash equivalents. Cash and cash equivalents consist of deposits with commercial banks in checking, interest-bearing, and demand money market accounts. The Company invests excess cash in marketable securities with high credit ratings. These securities consist primarily of U.S. Treasury or agency obligations and corporate debt and are classified as “available-for-sale.” Management may liquidate any of these investments in order to meet the Company’s liquidity needs in the next year. Accordingly, any investments with contractual maturities greater than one year from the balance sheet date are classified as short-term in the balance sheet.
Realized gains and losses from the sale of marketable securities, if any, are calculated using the specific-identification method. Realized gains and losses and declines in value judged to be other-than-temporary are included in interest income or expense in the statements of operations. Unrealized holding gains and losses are reported in accumulated other comprehensive loss, in the balance sheet. To date, the Company has not recorded any impairment charges on its marketable securities related to other-than-temporary declines in market value. In determining whether a decline in market value is other-than-temporary, various factors are considered, including the cause, duration of time and severity of the impairment, any adverse changes in the investees’ financial condition, and the Company’s intent and ability to hold the security for a period of time sufficient to allow for an anticipated recovery in market value.
Property and Equipment
Property and equipment is stated at cost, less accumulated depreciation and amortization. Depreciation and amortization is calculated using the straight-line method, and the cost is amortized over the estimated useful lives of the respective assets, generally three to seven years. Leasehold improvements are amortized over the shorter of the useful lives or the non-cancelable term of the related lease. Maintenance and repair costs are charged as expense in the statements of operations and comprehensive loss as incurred.
Impairment of Long-Lived Assets
The Company reviews long-lived assets for impairment whenever events or changes in business circumstances indicate that the carrying amount of the assets may not be fully recoverable. An impairment loss is recognized if the estimated undiscounted future cash flow expected to result from the use and eventual disposition of an asset is less than the carrying amount. While the Company’s current and historical operating losses and cash flows are indicators of impairment, the Company believes the future cash flows to be received support the carrying value of its long-lived assets. Accordingly, the Company has not recognized any impairment losses as of June 30, 2013, December 31, 2012 and 2011.
Deferred Rent
The Company records its costs under facility operating lease agreements as rent expense. Rent expense is recognized on a straight-line basis over the non-cancelable term of the operating lease. The difference between the actual amounts paid and amounts recorded as rent expense is recorded to deferred rent in the balance sheet.
Revenue Recognition
The Company recognizes revenue when (i) persuasive evidence of an arrangement exists, (ii) delivery has occurred or services have been rendered, (iii) the price is fixed and determinable, and (iv) collectability is reasonably assured. Payments received in advance of work performed are recorded as deferred revenue and recognized when earned. All revenue recognized to date under the collaboration agreements has been nonrefundable.
F-9
Table of Contents
Contract revenue from two strategic partners accounted for 95% and 5%, respectively, of total contract revenue in 2011. In 2012, 100% of contract revenue was from one strategic partner. There was no contract revenue for the six months ended June 30, 2013.
Multiple Element Arrangements
The Company evaluates revenue from agreements that have multiple elements to determine whether the components of the arrangement represent separate units of accounting. Management considers whether components of an arrangement represent separate units of accounting based upon whether certain criteria are met, including whether the delivered element has stand-alone value to the customer. To date, all of the Company’s collaboration agreements have been assessed to have one unit of accounting. Up-front and license fees received for a combined unit of accounting have been deferred and recognized ratably over the projected performance period. Non-refundable fees where the Company has no continuing performance obligations have been recognized as revenue when collection is reasonably assured and all other revenue recognition criteria have been met.
Milestones and Contingent Payments
Contingent consideration received from the achievement of a substantive milestone will be recognized in its entirety in the period in which the milestone is achieved. A milestone is defined as an event having all of the following characteristics: (i) there is substantive uncertainty at the date the arrangement is entered into that the event will be achieved, (ii) the event can only be achieved based in whole or in part on either the company’s performance or a specific outcome resulting from the company’s performance and (iii) if achieved, the event would result in additional payments being due to the company.
The Company’s future research and development and license agreements may provide for success fees or payments to be paid to the Company upon the achievement of certain development milestones. Given the challenges inherent in developing biologic products, there may be substantial uncertainty as to whether any such milestones would be achieved at the time the agreements are executed. In addition, the Company will evaluate whether the development milestones meet all of the conditions to be considered substantive. The conditions include: (1) the consideration is commensurate with either of the following: (a) the Company’s performance to achieve the milestone or (b) the enhancement of the value of the delivered item or items as a result of a specific outcome resulting from the Company’s performance to achieve the milestone; (2) the consideration relates solely to past performance; and (3) the consideration is reasonable relative to all of the deliverables and payment terms within the arrangement. If the Company considers the development milestones to be substantive, revenue related to such future milestone payments will be recognized as the Company achieves each milestone. Research and Development Funding Internal and external research and development costs reimbursed in connection with research and development funding or collaboration agreements are recognized as revenue in the same period as the costs are incurred, and are presented on a gross basis because the Company acts as a principal, has the discretion to choose suppliers, bears credit risk, and performs part of the services.
Research and Development Expenses
Research and development expenses consist of costs incurred in identifying, developing, and testing product candidates. These expenses consist primarily of costs for research and development personnel, including related stock-based compensation; contract research organizations and other third parties that assist in managing, monitoring, and analyzing clinical trials; investigator and site fees; laboratory services; consultants; contract manufacturing services; non-clinical studies, including materials; and allocated expenses, such as depreciation of assets, and facilities and information technology that support research and development activities. Research and development costs are expensed as incurred, including expenses that may or may not be reimbursed under research and development funding arrangements. Research and development expenses under collaboration agreements approximate the revenue recognized under such agreements.
F-10
Table of Contents
The expenses related to clinical trials are based upon estimates of the services received and efforts expended pursuant to contracts with multiple research institutions and clinical research organizations that conduct and manage clinical trials on behalf of the Company. Expenses related to clinical trials are accrued based upon the level of activity incurred under each contract as indicated by such factors as progress made against specified milestones or targets in each period, patient enrollment levels, and other trial activities. Payments made to third parties under these clinical trial arrangements in advance of the receipt of the related services are recorded as prepaid assets, depending on the terms of the agreement, until the services are rendered.
Stock-Based Compensation
Employee and director stock-based compensation is measured at the grant date, based on the fair-value-based measurements of the stock awards, and the portion that is ultimately expected to vest is recognized as an expense over the related vesting periods, net of estimated forfeitures. The Company calculates the fair-value-based measurements of options using the Black-Scholes valuation model and the single-option approach and recognizes expense using the straight-line attribution method.
Equity awards granted to non-employees have been accounted for using the Black-Scholes valuation model to determine the fair value-based measurements of such instruments. The fair value-based measurements of options and warrants granted to non-employees are re-measured over the related vesting period and amortized to expense as earned.
Income Taxes
The Company utilizes the liability method of accounting for income taxes. Under this method, deferred tax assets and liabilities are determined based on differences between the financial reporting and the tax bases of assets and liabilities and are measured using enacted tax rates and laws that will be in effect when the differences are expected to reverse. A valuation allowance is recorded when it is more likely than not that all or part of a deferred tax asset will not be realized.
The Company follows the accounting guidance for uncertainty in income taxes. The guidance prescribes a recognition threshold and measurement attribute criteria for the financial recognition and measurement of tax positions taken or expected to be taken in a tax return. For those benefits to be recognized, a tax position must be more likely than not to be sustained upon examination based on the technical merits of the position. Due to the Company’s ongoing operating losses since inception, the Company has not recorded reserves for uncertain tax positions as of December 31, 2012 and 2011.
The Company recognizes the financial statement effects of a tax position when it is more likely than not, based on the technical merits, that the position will be sustained upon examination. The Company records interest related to income taxes, if any, as interest, and any penalties would be recorded as other expense in the statements of operations and comprehensive loss. There was no interest or penalties related to income taxes recorded during the years ended December 31, 2012 and 2011.
Comprehensive Loss
Comprehensive loss includes net loss and net unrealized gains and losses on marketable securities, which are presented in a single continuous statement. Comprehensive loss is disclosed in the statements of convertible preferred stock and stockholders’ deficit, and is stated net of related tax effects, if any.
Net Loss Per Common Share
Basic net loss per share of common stock is based on the weighted average number of shares of common stock outstanding during the period. Diluted net loss per share of common stock is based on the weighted average number of shares outstanding during the period, adjusted to include the assumed conversion of certain stock options, and warrants for common stock.
F-11
Table of Contents
Potentially dilutive securities are excluded from the calculation of loss per share if their inclusion is anti-dilutive. The following table shows the total outstanding securities considered anti-dilutive and therefore excluded from the computation of diluted net loss per share (in thousands):
Six months ended June 30, | Year ended December 31, | |||||||||||||||
| (unaudited) | ||||||||||||||||
| 2013 | 2012 | 2012 | 2011 | |||||||||||||
Common stock options | 97 | 111 | 104 | 122 | ||||||||||||
Warrants for common stock | — | 30 | 28 | 30 | ||||||||||||
For the six and twelve months ended June 30, 2013 and 2012 and December 31, 2012 and 2011, all outstanding securities were considered anti-dilutive, and therefore the calculation of basic and diluted net loss per share was the same.
Recent Accounting Pronouncements
In June 2011, the Financial Accounting Standards Board (the FASB) issued Accounting Standards Update (ASU) No. 2011-05, Presentation of Comprehensive Income. This ASU gives an entity the option to present the total of comprehensive income, the components of net income, and the components of other comprehensive income either in a single continuous statement of comprehensive income or in two separate but consecutive statements. This guidance is effective on a retrospective basis in the Company’s financial statements for the year ending December 31, 2012. The Company adopted this pronouncement and elected to present a single continuous statement of comprehensive income. The retrospective application had only a presentation impact on the Company’s financial statements for the twelve months ended December 31, 2012.
In May 2011, the FASB issued ASU No. 2011-04, Amendments to Achieve Common Fair Value Measurement and Disclosure Requirements in U.S. GAAP and IFRSs. This ASU is the result of joint efforts by the FASB and International Accounting Standards Board to develop a single, converged fair value framework. While this ASU is largely consistent with existing fair value measurement principles in U.S. GAAP, it expands the existing disclosure requirements for fair value measurements in Accounting Standards Codification (ASC) Topic 820, Fair Value Measurement, and makes other amendments. Many of these amendments were made to eliminate unnecessary wording differences between U.S. GAAP and International Financial Reporting Standards, which could change how fair value measurement guidance in ASC 820 is applied. This guidance was effective on a prospective basis for the Company on January 1, 2012. The prospective application had only a disclosure impact on the Company’s financial statements for the year ended December 31, 2012.
3. Marketable Securities
There were no unrealized losses or gains and the amortized cost and estimated fair value was $0 as of June 30, 2013 and December 31, 2012. Marketable available-for-sale securities as of December 31, 2011 consist of the following (in thousands):
| Amortized Cost | Gross Unrealized Gains | Gross Unrealized Losses | Estimated Fair Value | |||||||||||||
As of December 31, 2011: | ||||||||||||||||
Obligations of U.S. government agencies | $ | 4,495 | $ | 1 | $ | — | $ | 4,496 | ||||||||
Corporate debt securities | 6,516 | — | — | 6,516 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
| $ | 11,011 | $ | 1 | $ | — | $ | 11,012 | |||||||||
|
|
|
|
|
|
|
| |||||||||
As of December 31, 2011, all marketable securities had contractual maturities of less than one year. Realized gains and losses were immaterial for the years ended December 31, 2012 and 2011 and the six months ended June 30, 2013 and 2012.
F-12
Table of Contents
4. Certain Balance Sheet Items
Property and equipment consists of the following (in thousands):
| December 31, | June 30, | |||||||||||
| 2012 | 2011 | 2013 (unaudited) | ||||||||||
Laboratory equipment | $ | 3,778 | $ | 3,778 | $ | 3,405 | ||||||
Office and computer equipment | 983 | 983 | 982 | |||||||||
Purchased software | 166 | 166 | 166 | |||||||||
Furniture and fixtures | 174 | 174 | 174 | |||||||||
Leasehold improvements | 2,534 | 2,534 | 2,534 | |||||||||
|
|
|
|
|
| |||||||
Total | 7,635 | 7,635 | 7,261 | |||||||||
Less accumulated depreciation and amortization | (7,551 | ) | (7,432 | ) | (7,242 | ) | ||||||
|
|
|
|
|
| |||||||
Property and equipment, net | $ | 84 | $ | 203 | 19 | |||||||
|
|
|
|
|
| |||||||
Property and equipment includes assets financed through equipment loans, which were fully paid in January 2012. Property and equipment and accumulated depreciation related to assets financed by equipment loans was $1.1 million as of December 31, 2011.
Accrued liabilities consist of the following (in thousands):
| December 31, | June 30, | |||||||||||
| 2012 | 2011 | 2013 (unaudited) | ||||||||||
Accrued compensation | $ | 291 | $ | 362 | $ | 250 | ||||||
Accrued pre-clinical and clinical trial expenses | 304 | 496 | 178 | |||||||||
Accrued professional fees | 285 | 292 | 434 | |||||||||
Other accruals | 14 | 35 | 29 | |||||||||
|
|
|
|
|
| |||||||
Total accrued liabilities | $ | 894 | $ | 1,185 | $ | 891 | ||||||
|
|
|
|
|
| |||||||
5. Collaboration Agreements
Sanofi-Aventis Deutschland GMBH
In June 2010, the Company entered into a development and license agreement effective July 21, 2010, with Sanofi-Aventis Deutschland GMBH (Sanofi-Aventis), whereby Sanofi-Aventis received an exclusive worldwide license for the research, development, manufacture and commercialization of small molecules that modulate the G-protein coupled receptor 119 (GPR119). The agreement includes rights to MBX-2982, a potent selective orally active GPR119 agonist discovered by the Company. Upon the effective date of this agreement, the Company received a one-time nonrefundable up-front license payment of $25.0 million. The Company was eligible to receive milestones if certain development and commercial events were achieved, as well as royalties on worldwide product sales, if any. The one-time nonrefundable up-front license payment was being recognized as revenue ratably over the period that the Company expected to complete certain research and development activities that represent the Company’s substantive performance obligations under the agreement. Of this up-front license fee, $11.0 million was recognized as contract revenue in 2011 and none was recognized in 2012.
On June 15, 2011, the arrangement was terminated by Sanofi-Aventis. Following termination, the Company retained rights to the current programs under this agreement and may continue to develop the programs and commercialize any products resulting from the programs, or the Company may elect to cease progressing the programs and/or seek other partners for further development and commercialization of the programs.
In 2012, the Company recognized a final payment from Sanofi-Aventis of $2.9 million as contract revenue.
F-13
Table of Contents
Takeda San Francisco, Inc.
In March 2010, the Company entered into a research collaboration agreement with Takeda San Francisco, Inc. (TSF), a wholly owned subsidiary of Takeda Pharmaceutical Company Limited. The Company collaborated with TSF on the evaluation and validation of protein targets for the development of biological products. In March 2010, the Company received $1.5 million, representing $0.9 million of one-time nonrefundable technology access fees and $0.6 million of specified research and development funding for the research term of the collaboration. The technology access fee and the research and development funding were deferred and were being recognized ratably over the funded research term, which was scheduled from March 2010 to August 2011. The Company recognized $0.7 million and $0.8 million as contract revenue in 2011 and 2010, respectively, under this arrangement. Approximately $0.1 was recognized as specific research and development funding under this agreement in the year ended December 31, 2012. Takeda terminated this agreement on March 16, 2013 with no further payments being made as of June 30, 2013.
Pfizer, Inc.
In December 1998, the Company entered into a collaboration agreement in the area of insulin secretion target discovery with the Parke-Davis division of Warner-Lambert Company, since acquired by Pfizer Inc., to identify genes involved in diabetes and to develop therapeutic compounds from the research. The collaboration agreement provided for an initial five-year funded research term, which was subsequently extended an additional year until December 2004. The Company received payments for research and development costs for the funded research term and is entitled to receive payments for specified drug development achievements. If products resulting from the collaboration are eventually marketed and sold, the Company will also receive royalties on sales of such products. No amounts were received under this agreement in the six months ended June 30, 2013 and the years ended December 31, 2012 and, 2011.
The Company was also eligible to receive contingent payments if certain development and commercial events were achieved as well as royalties on worldwide product sales, if any. The $7.5 million one-time nonrefundable technology access fee was recognized as revenue in 2010, as the Company had no substantive performance obligations under this arrangement. No amounts were received under this agreement in the six months ended June 30, 2013 and for the years ended December 31, 2012 and 2011.
6. License Agreements
In June 1998, the Company entered into a license agreement with DiaTex, Inc. (DiaTex) relating to products containing halofenate, its enantiomers, derivatives, and analogs (the licensed products). The license agreement provides that DiaTex and the Company are joint owners of all of the patents and patent applications covering the licensed products and methods of producing or using such compounds, as well as certain other know-how (the covered IP). As part of the license agreement, the Company received an exclusive worldwide license, including as to DiaTex, to use the covered IP to develop and commercialize the licensed products. The Company also retained the right to sub-license the covered IP. The license agreement contains a $2,000 per month license fee as well as a requirement to make additional payments for development achievements and royalty payments on any sales of licensed products. Pursuant to the license agreement, all of the Company’s patents and patent applications related to MBX-102, its use, and production are jointly owned with DiaTex. DiaTex is entitled to up to $0.8 million for the future development of MBX-102, as well as royalty payments on any sales of products containing MBX-102. No development payments were made in the years ended December 31, 2012 and, 2011 or the six months ended June 30, 2013 and no royalties have been paid to date.
7. Debt
On June 20, 2006 the Company entered into a equity and loan facility with the Johnson and Johnson Development Corporation (“JJDC”) pursuant to which the Company could drawn down up to an aggregate of $30 million in loans in the form of convertible preferred stock promissory notes. In March and September 2008, the Company issued notes in the aggregate amount of $3.5 million and $10.5 million, respectively. The notes
F-14
Table of Contents
were due on March 17 and September 17, 2011, including interest that accrued at 7.57% per annum. In December 2010, the aggregate principal amount and all accrued interest under the notes issued in March and September 2008 were converted into the Company’s Series E-3 convertible preferred stock (Series E-3 Preferred) at 232.93 per share.
In February and July 2009, the Company issued notes in the aggregate amount of $7.0 million and $6.7 million, respectively, which represented the remaining amount available to the Company, in accordance with the terms of the equity and loan facility with JJDC. The notes were due in February 2012 and July 2012, including interest that accrued at 4.42% per annum and 4.960% per annum, respectively. In January 2012, the Company amended the maturity dates of the outstanding $7.0 million and $6.7 million convertible promissory notes to extend the maturity date to March 1, 2013 (see Note 15 for additional extension), and interest rates were increased to 4.919% and 5.46% per annum, respectively. In addition, the conversion price of the notes to convert into shares of the Company’s Series C-1 Preferred Stock was decreased from $438.84 per share to $292.56 per share. All of these notes were further amended in March 2013, to extend the maturity date on the notes to August 1, 2013, and to make the notes subordinate to repayment of the Company’s severance obligations to all employees until January 1, 2014. On July 31, 2013, the maturity date was extended to December 31, 2013. For the years ended December 31, 2012 and 2011, the Company recognized $0.7 million and $0.7 million, respectively, of interest expense related to the convertible promissory notes. For the six months ended June 30, 2013 and 2012, the Company recognized $0.2 million and $0.2 million, respectively, of interest expense related to the convertible promissory note. There are no financial covenants associated with the notes.
Equipment Loans
In February 2007, the Company entered into an equipment loan and security agreement with General Electric Capital Corporation (GECC) under which GECC provided loans to the Company totaling $1.1 million in 2007, each with a term of four years, at fixed rates of interest between 9.78% and 9.91%. GECC has been granted a security interest in all equipment financed by the loans. There are no financial covenants associated with the agreement. As part of finalizing the loan agreement, the Company made a one-time deposit to GECC in the amount of $0.2 million. In 2011, $0.1 million of the deposit was returned to the Company, and the remaining outstanding deposit balance was returned upon full repayment of the principal balance in January 2012.
8. Commitments and Contingencies
Operating Lease Commitments
The Company leases office and laboratory space in a single building in Hayward, California. The facility lease, as amended on July 15, 2010, has a term of four years, unless terminated earlier by the Company, and expires on April 30, 2014. Rent expense was $0.5 million for the years ended December 31, 2012 and 2011 and $0.2 million for each of the six months ended June 30, 2013 and 2012.
Future minimum lease payments under this amended agreement are as follows (in thousands):
| Lease Payments | ||||
Year ending December 31: | ||||
2013 | $ | 422 | ||
2014 | 143 | |||
|
| |||
Total future minimum payments | $ | 565 | ||
|
| |||
Indemnification
In the normal course of business, the Company enters into contracts and agreements that contain a variety of representations and warranties and provide for general indemnification, including indemnification associated
F-15
Table of Contents
with product liability or infringement of intellectual property rights. The Company’s exposure under these agreements is unknown because it involves future claims that may be made against the Company that may be, but have not yet been, made. To date, the Company has not paid any claims or been required to defend any action related to these indemnification obligations, and no amounts have been accrued in the accompanying balance sheets related to these indemnification obligations.
The Company has agreed to indemnify its executive officers and directors for losses and costs incurred in connection with certain events or occurrences, including advancing money to cover certain costs, subject to certain limitations. The maximum potential amount of future payments the Company could be required to make under this indemnification is unlimited; however, the Company maintains insurance policies that may limit its exposure and may enable it to recover a portion of any future amounts paid. Assuming the applicability of coverage, the willingness of the insurer to assume coverage, and subject to certain retention, loss limits, and other policy provisions, the Company believes the fair value of these indemnification obligations is not material. Accordingly, the Company has not recognized any liabilities relating to these obligations as of December 31, 2012 and 2011. No assurances can be given that the covering insurers will not attempt to dispute the validity, applicability, or amount of coverage without expensive litigation against these insurers, in which case the Company may incur substantial liabilities as a result of these indemnification obligations.
9. Redeemable Convertible Preferred Stock
The Company has the following series of outstanding convertible preferred stock (collectively, the Preferred Stock): Series A-1 Preferred, Series B-1 Preferred, Series C-1 Preferred, Series D-1 Preferred, Series E-1 Preferred and Series E-3 Preferred. Series E-1 Preferred and Series E-3 Preferred are collectively referred to as the Series E Preferred. The Preferred Stock was initially recorded at its original purchase price, which represented fair value on the date of issuance, net of issuance costs, if any. The original purchase price per share of Series A-1 Preferred, Series B-1 Preferred, Series C-1 Preferred, Series D-1 Preferred, and Series E Preferred is equal to $232.93, $232.93, $365.70, $232.94, and $232.93 per share, respectively. The preferred stock balances are recorded at the original fair value and the accreted dividends based on the per share terms at issuance of Series A-1 Preferred, Series B-1 Preferred, Series C-1 Preferred, Series D-1 Preferred, and Series E Preferred, which are equal to $18.64, $18.64, $29.26, $18.64, and $18.64 per share per annum, respectively.
The shares of Series B-1 Preferred, Series D-1 Preferred, and Series E Preferred are redeemable upon the request of the holders of at least 66 2/3% of outstanding shares of Series B-1 Preferred, voting as a separate class, and 51% of outstanding shares of Series D-1 Preferred and Series E Preferred, voting together as a separate class. In this event, the Company would be required to redeem the shares in three equal annual installments, beginning in September 2021, at the applicable original purchase price per share. All shares of Preferred Stock are redeemable in the event of a change of control at their liquidation preferences.
As all Preferred Stock is redeemable either at the option of the holder or upon an event outside the control of the Company (i.e., a change in control), the related amounts have been presented outside of stockholders’ equity (deficit). In August and December 2003, the Company completed two closings of a private placement of Series B-1 Preferred, in which the Company issued a total of 136,520 shares at a price of $232.93 per share for gross proceeds of $31.8 million. In November and December 2004, the Company completed two further closings of Series B-1 Preferred, in which the Company issued a total of 188,894 shares at a price of $232.93 per share for gross proceeds of $44.0 million. The Series B-1 Preferred investors in these two final closings also purchased warrants for 29,245 shares of common stock at an exercise price of $30.21 per share, with an exercise period of five years from the date of purchase, for $1.51 cents per share of common stock covered by the warrants. In November 2009, the exercise period of these warrants was extended to December 31, 2011. In December 2012, the Company’s Board of Directors reduced the number of shares exercisable under these warrant by 45% of the original shares and approved the extension of the exercise period until April 1, 2013 (Note 10). As of December 31, 2012, warrants to purchase 13,160 shares of common stock were outstanding.
F-16
Table of Contents
In August 2006, the Company issued 27,345 shares of Series C-1 Preferred to JJDC at a price of $365.70 per share, for gross proceeds of $10.0 million (Note 5).
In April 2007, the Company issued 137,592 shares of Series D-1 Preferred at a price of $232.94 per share, for gross proceeds of $32.0 million. In connection with the issuance, the Series D-1 Preferred investors also purchased warrants for an aggregate of 20,639 shares of common stock at an exercise price of $22.13 per share, with an exercise period of five years from the date of purchase, for $0.79 cents per share of common stock covered by the warrants.
In August 2008, the Company repurchased 646, 1,610 and 472 shares of Series A-1 Preferred, Series B-1 Preferred and Series D-1 Preferred, respectively, and a warrant for 71 shares of common stock, for an aggregate purchase price of $82,000. The Company allocated the purchase price among the preferred shares and warrant based upon their respective fair values.
In November 2009, the Company issued 1,288 shares of Series E-1 Preferred upon the conversion of debt issued under a loan agreement. In June and December 2010, the Company issued 859 and 37,119 shares of Series E-1 Preferred, respectively, upon conversion of debt issued under a loan agreement.
In December 2010, the Company issued 71,543 shares of Series E-3 Preferred upon conversion of the JJDC convertible notes that were due in 2011 (Note 7).
As of June 30, 2013 (unaudited), convertible preferred stock balances were as follows (in thousands, except share amounts):
| Shares Authorized | Shares Issued and Outstanding | Aggregate Liquidation Preference | Carrying Value | |||||||||||||
Series A-1 | 12,734 | 12,734 | $ | 5,305 | $ | 75,572 | ||||||||||
Series B-1 | 373,223 | 373,223 | 149,998 | 148,857 | ||||||||||||
Series C-1 | 75,472 | 27,345 | 15,519 | 15,471 | ||||||||||||
Series D-1 | 136,948 | 136,949 | 47,785 | 44,536 | ||||||||||||
Series E-1 | 40,252 | 39,265 | 20,183 | 11,037 | ||||||||||||
Series E-3 | 93,082 | 71,543 | 24,213 | 29,477 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 731,711 | 661,059 | $ | 263,003 | $ | 324,950 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
As of December 31, 2012, convertible preferred stock balances were as follows (in thousands, except share amounts):
| Shares Authorized | Shares Issued and Outstanding | Aggregate Liquidation Preference | Carrying Value | |||||||||||||
Series A-1 | 12,734 | 12,734 | $ | 5,187 | $ | 75,454 | ||||||||||
Series B-1 | 373,223 | 373,223 | 146,549 | 145,408 | ||||||||||||
Series C-1 | 75,472 | 27,345 | 15,122 | 15,074 | ||||||||||||
Series D-1 | 136,948 | 136,949 | 46,520 | 43,271 | ||||||||||||
Series E-1 | 40,252 | 39,265 | 19,820 | 10,674 | ||||||||||||
Series E-3 | 93,082 | 71,543 | 23,552 | 28,816 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 731,711 | 661,059 | $ | 256,750 | $ | 318,697 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
F-17
Table of Contents
As of December 31, 2011, convertible preferred stock balances were as follows (in thousands, except share amounts):
| Shares Authorized | Shares Issued and Outstanding | Aggregate Liquidation Preference | Carrying Value | |||||||||||||
Series A-1 | 12,734 | 12,734 | $ | 4,949 | $ | 75,216 | ||||||||||
Series B-1 | 373,223 | 373,223 | 139,575 | 138,434 | ||||||||||||
Series C-1 | 75,472 | 27,345 | 14,320 | 14,272 | ||||||||||||
Series D-1 | 136,948 | 136,949 | 43,961 | 40,712 | ||||||||||||
Series E-1 | 40,252 | 39,265 | 19,086 | 9,940 | ||||||||||||
Series E-3 | 93,082 | 71,543 | 22,216 | 27,479 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 731,711 | 661,059 | $ | 244,107 | $ | 306,053 | ||||||||||
|
|
|
|
|
|
|
| |||||||||
The significant rights, privileges, and preferences of the Preferred Stock are as follows:
Election of Directors
The holders of Series B-1 Preferred are entitled to elect five members of the Company’s Board of Directors, the holders of Series D-1 Preferred are entitled to elect one member of the Company’s Board of Directors, and the holders of common stock are entitled to elect one member of the Company’s Board of Directors, subject to certain restrictions. All remaining members of the Company’s Board of Directors are elected by all of the stockholders voting on an as-if-converted basis.
Voting Rights
Preferred Stock carries voting rights equal to the number of shares of common stock into which it can be converted. Additionally, certain corporate actions may be exercised upon the approval of holders of 66 2/3% of the outstanding shares of Series B-1 Preferred and Series C-1 Preferred, voting together as a single class, and 51% of the outstanding shares of Series D-1 Preferred and Series E Preferred, voting together as a single class.
Dividends
All dividends are payable when and if declared by the Company’s Board of Directors. The holders of Series E Preferred are entitled to cumulative dividends in preference to the holders of Series A-1 Preferred, Series B-1 Preferred, Series C-1 Preferred, Series D-1 Preferred, and common stock. The holders of Series D-1 Preferred are entitled to cumulative dividends in preference to the holders of Series A-1 Preferred, Series B-1 Preferred, Series C-1 Preferred, and common stock. The holders of Series B-1 Preferred and Series C-1 Preferred are entitled to cumulative dividends in preference to the holders of Series A-1 Preferred and common stock. The holders of Series A-1 Preferred are entitled to cumulative dividends in preference to the holders of common stock. The dividend rate is $18.64, $18.64, $29.26, $18.64, and $18.64 per annum for each outstanding share of Series E Preferred, Series D-1 Preferred, Series C-1 Preferred, Series B-1 Preferred, and Series A-1 Preferred, respectively. Additionally, if dividends are paid to any holder of common stock, the holders of Preferred Stock will receive a dividend of a per share amount (on an as-if-converted to common stock basis) equal to the amount paid to the holders of common stock.
No dividends were declared as of December 31, 2012 and 2011. The aggregate cumulative dividends as of June 30, 2013, were $3.4 million ($47.28 per share), $1.9 million ($48.14 per share), $15.9 million ($116.00 per share), $5.6 million ($201.83 per share), $63.1 million ($168.96 per share), and $2.3 million ($183.64 per share) for Series E-3 Preferred, Series E-1 Preferred, Series D-1 Preferred, Series C-1 Preferred, Series B-1 Preferred, and Series A-1 Preferred, respectively. The aggregate cumulative dividends as of December 31, 2012, were $2.7 million ($38.04 per share), 1.5 million ($38.90 per share), $14.6 million ($106.75
F-18
Table of Contents
per share), $5.1 million ($187.32 per share), $59.6 million ($159.72 per share), and $2.2 million ($174.40 per share) for Series E-3 Preferred, Series E-1 Preferred, Series D-1 Preferred, Series C-1 Preferred, Series B-1 Preferred, and Series A-1 Preferred, respectively.
Liquidation Preference
In the event of a liquidation, dissolution, winding up, or change in control of the Company, the liquidation preference of each stockholder class is to be paid in the following order, from available funds: first to the holders of Series E-1 Preferred and Series E-3 Preferred, second to the holders of Series D-1 Preferred, third to the holders of Series B-1 Preferred and Series C-1 Preferred, and fourth to the holders of Series A-1 Preferred. After payment of the Preferred Stock liquidation preferences, the remaining assets of the Company are to be distributed ratably to all holders of common stock and Preferred Stock on an as-if-converted basis. The liquidation preference of Series E-1 Preferred, Series E-3 Preferred, Series D-1 Preferred, Series C-1 Preferred, Series B-1 Preferred, and Series A-1 Preferred is equal to $465.87, $290.97, $232.94, $365.70, $232.93, and $232.93 per share, respectively, plus any cumulative unpaid dividends. If there are insufficient funds available to satisfy each liquidation preference in its entirety, the holders of Preferred Stock are to be paid a pro rata amount based on their liquidation preference.
Conversion Rights
Each share of Preferred Stock is convertible at any time, at the option of the holder, into shares of the Company’s common stock at the applicable conversion rate. The conversion rate for each of the series of Preferred Stock is currently 1:1, except for the Series D-1 Preferred, which has a conversion rate of 1.365:1. With respect to the Series E Preferred, Series D-1 Preferred, Series B-1 Preferred, and Series A-1 Preferred, if the Company issues common stock or securities convertible into or exercisable for shares of common stock at a price less than the respective original purchase price per share, the conversion rate of such stock shall be adjusted to the lowest price per share paid in such issuance. The conversion rate for Preferred Stock will not be adjusted for common stock issuances on the exercise of options or warrants issued to employees, directors, or consultants of the Company and in certain other circumstances.
Each share of Preferred Stock automatically converts into common stock upon the approval of holders of 66 2/3% of the outstanding shares of Series B-1 Preferred, voting as a separate class, and 51% of the outstanding shares of Series D-1 Preferred and Series E Preferred, voting together as a separate class, or upon the closing of an underwritten public offering of the Company’s common stock pursuant to an effective registration statement under the Securities Act of 1933, as amended, at a per share price of at least $8.00, and raising aggregate gross proceeds of at least $30.0 million. In connection with the next sale and issuance of capital stock of the Company, with aggregate proceeds to the Company of not less than $1,000,000, each holder of the Company’s preferred stock that participates in such financing for between 1% and up to 99% of such holders “Pro Rata Share” (as defined in the Company’s certificate of incorporation) shall have each shares of preferred stock represented by such participation amount convertible into four shares of common stock and the balance of any shares of preferred stock convertible at the applicable conversion rate as defined in the certificate of incorporation. Any holder that participates in such financing for between 100% and 300% of such holder’s Pro Rata Share (the “Participation Multiple”) shall have each shares of preferred stock convert into shares of common stock by multiplying the product of (y) the aggregate number of shares of preferred stock held by such holder multiplied by the applicable Participation Multiple and (z) four (4).
Upon any conversion, any declared and unpaid dividends shall be paid to the holders of Preferred Stock in cash, or to the extent sufficient funds are not legally available, in common stock at the common stock’s fair market value.
Rights of First Refusal
Pursuant to the Company’s By-laws and a Right of First Refusal and Co-Sale Agreement, the Company has the right to purchase any outstanding common stock that is available or offered for sale prior to an initial public
F-19
Table of Contents
offering. Additionally, if certain holders of the Company’s common stock and/or holders of the Company’s Series E Preferred, Series D-1 Preferred, Series C-1 Preferred, or Series B-1 Preferred wish to sell any of their stock, they are required to offer the stock for sale under the same terms and conditions first to the Company and then to the holders of the Company’s Series E Preferred, Series D-1 Preferred, Series C-1 Preferred, and Series B-1 Preferred. Certain holders of Preferred Stock have the right to participate in future financings of the Company, subject to their pro rata share, assuming full conversion and exercise of outstanding warrants or options held by them. The right expires upon the earlier of an initial public offering or a change in control of the Company.
10. Common Stock
The Company was authorized to issue 74,000,000 shares of common stock for the audited periods December 31, 2012 and 2011. In November 2009, the Company’s Board of Directors approved the extension of the time period in which the holders of warrants to purchase 29,245 shares of common stock are able to exercise their warrants that were issued in connection with the issuance of Series B-1 Preferred. The exercise periods of the warrants that originally ended in November 2009 were extended to December 31, 2010. The value of the exercise period extension of $0.1 million was recorded to accumulated deficit and was determined using the Black-Scholes valuation model, with the following inputs used to determine the value of the modification: fair value of the Company’s common stock of $15.90 per share, expected life of the modified warrants of 1.10 years, risk-free interest rate of 0.41%, and expected common stock price volatility of 97%.
In December 2010, the Company’s Board of Directors modified the warrants to purchase common stock that were issued in connection with the issuance of Series B-1 Preferred. The number of shares exercisable under the warrants issued with the issuance of the Series B-1 Preferred was reduced by 50% to 14,623, and the exercise period was extended to December 31, 2012. In December 2012, the Company’s Board of Directors again modified the warrants to purchase common stock that were issued in connection with the issuance of Series B-1 Preferred. The number of shares exercisable under the warrants issued with the issuance of the Series B-1 Preferred was reduced by 45% of the original shares to 13,163, and the exercise period was extended to April 1, 2013. The extension of the agreement did not make a material change in value.
In December 2010, the Company’s Board of Directors modified the warrants to purchase common stock that were issued in connection with the issuance of Series D-1 Preferred. The exercise period of the warrants issued in connection with the Series D-1 Preferred issuance was extended to April 13, 2013. The charge related to the modifications to these warrants of $0.1 million was recorded to accumulated deficit and was determined using the Black-Scholes valuation model, with the following inputs used to determine the charge related to the modification: fair value of the Company’s common stock of $15.90 per share, expected life of the modified warrants of one to two years, risk-free interest rate of 0.50%, and expected common stock price volatility of 83%.
As of June 30, 2013 and December 31, 2012, the Company had reserved shares of authorized but unissued common stock as follows:
| Shares Reserved June 30, 2013 (unaudited) | Shares Reserved December 31, 2012 | |||||||
Conversion of convertible preferred stock | 661,059 | 661,059 | ||||||
Outstanding common stock warrants | — | 28,208 | ||||||
Equity incentive plans | 140,414 | 140,474 | ||||||
|
|
|
| |||||
Total reserved shares of common stock | 801,472 | 829,740 | ||||||
|
|
|
| |||||
In addition to the above reserved shares, the Company has reserved stock for issuance upon conversion of the outstanding convertible notes (Note 7).
F-20
Table of Contents
11. Stock Plans and Stock-Based Compensation
Stock Plans
In August 2003, the Company’s stockholders approved the 2003 Equity Incentive Plan (2003 Plan), under which shares of common stock are reserved for the granting of options, stock bonuses, and restricted stock awards by the Company. These awards may be granted to employees, members of the Board of Directors, and consultants to the Company. The 2003 Plan has a term of ten years and replaced the 1993 Stock Option Plan, which had similar terms. The 2003 Plan permits the Company to (i) grant incentive stock options to directors and employees at not less than 100% of the fair value of common stock on the date of grant; (ii) grant nonqualified options to employees, directors, and consultants at not less than 85% of fair value; (iii) award stock bonuses; and (iv) grant rights to acquire restricted stock at not less than 85% of fair value. Options generally vest over a four- or five-year period and have a term of ten years. Options granted to 10% stockholders have a maximum term of five years and require an exercise price equal to at least 110% of the fair value on the date of grant. The exercise price of all options granted to date has been at least equal to the fair value of common stock on the date of grant. Restricted stock units granted in 2007 vested over a four- or five-year period, subject to certain performance conditions, and terminated on August 19, 2012.
Stock Plan Activity
In March 2008, the Company’s Board of Directors approved an exchange offer program (the Exchange Offer) under which current employees, directors, and scientific advisory board members could elect to exchange all of their unexercised stock options with an exercise price of greater than $127.20 and cancel all of their restricted stock units in exchange for new stock options for the same number of shares as the unexercised stock options being exchanged. The newly granted options would be issued under the 2003 Plan and have an exercise price equal to the fair value of the Company’s common stock on the date of grant, and a term of ten years. New options replacing vested canceled options would be fully vested upon grant and new options replacing unvested canceled options would vest over a three-year period. In June 2008, under this program, unexercised options for 46,130 shares and 7,552 restricted stock units were canceled and exchanged for 46,130 new options at an exercise price of $39.75 per share. For stock options granted under the Exchange Offer, the Company will recognize the remaining unamortized expense related to the original options as of the exchange date of $5.2 million over the vesting period of the new awards. The incremental expense resulting from the Exchange Offer of $0.5 million will also be recognized over the same period. In the years ended December 31, 2012 and 2011, the Company recognized $0.0 million and $0.8 million, respectively, of noncash stock-based compensation expense related to the new awards, including a portion of the unamortized expense related to the original options as of the exchange date.
As of June 30, 2013, December 31, 2012 and 2011, 42,940, 36,707 shares and 18,494 shares were available for grant under the 2003 Plan.
F-21
Table of Contents
The following table summarizes stock option activity:
| Shares Subject to Outstanding Options | Weighted- Average Exercise Price of Options | Weighted- Average Remaining Contractual Term (Years) | Aggregate Intrinsic Value (In Thousands) | |||||||||||||
Outstanding as of December 31, 2011 | 121,983 | $ | 35.77 | 4.58 | $ | 3 | ||||||||||
Vested and expected to vest as of December 31, 2011 | 121,224 | $ | 35.77 | 4.55 | $ | 3 | ||||||||||
|
| |||||||||||||||
Exercisable as of December 31, 2011 | 100,526 | $ | 39.75 | 3.87 | $ | 2 | ||||||||||
Options granted | 15,094 | 4.77 | ||||||||||||||
Options exercised | (19 | ) | 15.90 | |||||||||||||
Options forfeited | (11,139 | ) | 14.31 | |||||||||||||
Options expired | (22,159 | ) | 33.39 | |||||||||||||
|
| |||||||||||||||
Outstanding as of December 31, 2012 | 103,760 | $ | 34.19 | 4.43 | $ | 0 | ||||||||||
|
| |||||||||||||||
Vested and expected to vest as of December 31, 2012 | 103,288 | $ | 34.19 | 4.41 | $ | 0 | ||||||||||
|
| |||||||||||||||
Exercisable as of December 31, 2012 | 87,849 | $ | 38.96 | 3.84 | $ | 0 | ||||||||||
|
| |||||||||||||||
Options granted | — | |||||||||||||||
Options exercised | (78 | ) | 4.77 | |||||||||||||
Options forfeited | (1,656 | ) | 10.34 | |||||||||||||
Options expired | (4,577 | ) | 31.01 | |||||||||||||
|
| |||||||||||||||
Outstanding as of June 30, 2013 | 97,449 | 34.98 | 4.21 | $ | 0 | |||||||||||
|
| |||||||||||||||
Vested and expected to vest as of June 30, 2013 | 97,049 | 34.98 | 4.20 | $ | 0 | |||||||||||
|
| |||||||||||||||
Exercisable as of June 30, 2013 (unaudited) | 87,982 | 38.16 | 3.68 | $ | 0 | |||||||||||
|
| |||||||||||||||
The following table summarizes information about stock options outstanding as of December 31, 2012:
| Options Outstanding | Options Exercisable | |||||||||||
Exercise Price | Number of Shares | Weighted- Average Remaining Contractual Term (Years) | Number of Shares | |||||||||
$4.77 | 14,446 | 8.47 | 3,355 | |||||||||
$9.54 | 943 | 6.42 | 865 | |||||||||
$15.90 | 20,328 | 6.02 | 15,622 | |||||||||
$23.85 | 893 | 6.14 | 857 | |||||||||
$30.21 | 32,103 | 1.35 | 32,103 | |||||||||
$39.75 | 29,218 | 4.81 | 29,218 | |||||||||
$54.86 | 189 | 2.43 | 189 | |||||||||
$62.81 | 2,138 | 2.58 | 2,138 | |||||||||
$238.50 | 3,501 | 3.70 | 3,501 | |||||||||
|
|
|
|
|
| |||||||
| 103,759 | 4.43 | 87,848 | ||||||||||
|
|
|
|
|
| |||||||
F-22
Table of Contents
No restricted stock units were granted in the six months ended June 30, 2013 or the years ended December 31, 2012 and 2011. No restricted stock units vested in the six months ended June 30, 2013 or the years ended December 31, 2012 and 2011. As of June 30, 2013, December 31, 2012 and 2011, there were 0 and 9 restricted stock units outstanding, respectively, with a weighted-average grant date fair value of $238.50 per share and a weighted-average remaining contractual term of 0.00 and 0.64 years, respectively. No expense has been recorded to date related to the Company’s restricted stock units, as no restricted stock units have vested. Vesting of the restricted stock units is contingent upon either an initial public offering of the Company’s common stock or a change in control.
Grant Date Fair Value
The following table presents the weighted-average assumptions the Company used with the Black-Scholes valuation model to derive the grant date fair value-based measurements of employee and director stock options and the resulting estimated weighted-average grant date fair-value-based measurements per share:
| Year Ended December 31, | Six Months Ended June 30, | |||||||||||||||
| 2012 | 2011 | 2013 | 2012 | |||||||||||||
| (unaudited) | ||||||||||||||||
Weighted-average assumptions: | ||||||||||||||||
Expected term | 6.25 yrs | 6.25 yrs | 6.25 yrs | 6.25 yrs | ||||||||||||
Expected volatility | 100 | % | 100 | % | 94 | % | 102 | % | ||||||||
Risk-free interest rate | 1.01 | % | 1.27 | % | 1.45 | % | 0.95 | % | ||||||||
Expected dividend yield | 0 | % | 0 | % | 0 | % | 0 | % | ||||||||
Weighted-average grant date fair value-based measurement per share | $ | 3.97 | $ | 11.13 | $ | 3.97 | $ | 3.97 | ||||||||
Expected Term
The Company does not believe it can place reliance on its historical exercise and post-vesting termination activity to provide accurate data for estimating the expected term. Therefore, for stock option grants made during the six months ended June 30, 2013 and years ended December 31, 2012 and 2011, the Company has opted to use the simplified method for estimating the expected term.
Expected Volatility
As the Company does not have any trading history for its common stock, the expected stock price volatility for the Company’s common stock was estimated by considering the volatility rates of publicly traded peer entities within the life sciences industry.
Risk-Free Interest Rate
The risk-free interest rate assumption was based on U.S. Treasury instruments with constant maturities whose term was consistent with the expected term of stock options granted by the Company.
Expected Dividend Yield
The Company has never declared or paid cash dividends and does not plan to pay cash dividends in the foreseeable future. Consequently, the Company uses an expected dividend yield of zero.
Common Stock Fair Value
The Company’s Board of Directors has historically determined the fair value of the Company’s common stock for the purpose of pricing the Company’s equity awards to employees, directors, and consultants. As there
F-23
Table of Contents
has been no public market for the Company’s common stock, the Company’s Board of Directors, in making such fair value determinations, considered a number of factors, including the price at which Preferred Stock was issued to outside investors in arm’s-length transactions, the rights, preferences, and privileges of the Preferred Stock relative to the common stock, important developments relating to advancement of the Company’s technology and clinical programs, the Company’s stage of development and business strategy, the likelihood of achieving a liquidity event for the shares of common stock, such as an initial public offering or sale of the Company, prevailing market conditions, and the market prices of various publicly held life sciences companies. Additionally, the Board of Directors considered contemporaneous valuations provided by third-party valuation specialists.
Forfeitures
The Company estimates forfeitures at the time of grant and revises these estimates in subsequent periods if actual forfeitures differ from those estimates. Changes in forfeiture estimates impact compensation in the period in which the change occurs.
The total intrinsic value of options exercised in the six months ended June 30, 2013 and years ended December 31, 2012 and 2011, was $0, $0 and $3,000, respectively.
Vested and Unvested Awards
The total fair value of options vested in the six months ended June 30, 2013 and years ended December 31, 2012 and 2011, was $0.0 million, $0.1 million and $0.1 million, respectively.
As of June 30, 2013 and December 31, 2012, the total compensation expense related to unvested employee stock options to be recognized in future periods, excluding estimated forfeitures, was less than $100,000 and $0.2 million, respectively. The weighted-average periods over which this compensation expense is expected to be recognized are 1.4 years and 2.0 years as of June 30, 2013 and December 31, 2012, respectively. The weighted-average period over which compensation expense related to these restricted stock units is expected to be recognized is not determinable, as vesting is contingent upon future events.
Stock-Based Compensation Expense
Employee and Director Expense
Employee and director stock-based compensation expense recorded was as follows (in thousands):
| Year Ended December 31 | Six Months Ended June 30, | |||||||||||||||
| 2012 | 2011 | 2013 | 2012 | |||||||||||||
| (unaudited) | ||||||||||||||||
Research and development | $ | 26 | $ | 380 | $ | 11 | $ | 13 | ||||||||
General and administrative | 54 | 377 | 23 | 29 | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | $ | 80 | $ | 757 | $ | 34 | $ | 42 | ||||||||
|
|
|
|
|
|
|
| |||||||||
In January 2004, the Company’s Board of Directors canceled outstanding employee options under the 1993 Stock Option Plan and replaced them with new options to purchase 1,230 shares of common stock under the 2003 Plan at an exercise price of $30.21 per share. These replacement options were fully vested on the grant date and are exercisable for ten years, or 18 months after an initial public offering, if earlier. All replacement options are being accounted for as variable from the date of issuance to the date the options are exercised, forfeited or expire. During the six months ended June 30, 2013 and years ended December 31, 2012 and 2011, as a result of decreases in the fair market value of its common stock, the Company did not record any compensation expense related to these options.
F-24
Table of Contents
Non-Employee Expense
The Company has issued options to purchase shares of common stock to members of its Scientific Advisory Board (SAB) and certain consultants. The stock options have various exercise prices, a term of ten years, and vest over periods up to sixty months. In 2011, the Company did not grant any options to its SAB members or consultants. In 2012 the Company granted options to purchase 3,145 to its SAB members and consultants. As of December 31, 2012, options to purchase 3,432 shares of common stock remained unvested, and compensation related to these stock options is subject to periodic adjustment as the shares vest. The Company recorded $1,000 (unaudited), $1,000 and $6,000 of expense in the six months ended June 30, 2013 and years ended December 31, 2012 and 2011, respectively, related to these awards.
The Company has not recognized, and does not expect to recognize in the near future, any tax benefit related to employee stock-based compensation costs.
12. 401(k) Plan
The Company provides a qualified 401(k) savings plan for its employees. All employees are eligible to participate, provided they meet the requirements of the plan. While the Company may elect to match employee contributions, no such matching contributions have been made through June 30, 2013, December 31, 2012 and 2011.
13. Income Taxes
No provision for U.S. income taxes exists due to tax losses incurred in all periods presented. Deferred income taxes reflect the tax effects of net operating loss and tax credit carryforwards and the net temporary differences between the carrying amounts of assets and liabilities for financial reporting and the amounts used for income tax purposes. Significant components of the Company’s deferred tax assets are as follows (in thousands):
| December 31 | ||||||||
| 2012 | 2011 | |||||||
Deferred tax assets: | ||||||||
Federal and state net operating loss carryforwards | $ | 62,745 | $ | 57,901 | ||||
Capitalized research and development | 22,490 | 22,541 | ||||||
Federal and state tax credit carryforwards | 6,153 | 6,059 | ||||||
Other | 1,200 | 1,390 | ||||||
|
|
|
| |||||
Total deferred tax assets | 92,588 | 87,891 | ||||||
Valuation allowance | (92,588 | ) | (87,891 | ) | ||||
|
|
|
| |||||
Net deferred tax assets | $ | — | $ | — | ||||
|
|
|
| |||||
Realization of the net deferred tax assets is dependent upon future taxable income, if any, the amount and timing of which is uncertain. Based on available objective evidence, management believes it more likely than not that the Company’s deferred tax assets are not realizable. Accordingly, the net deferred tax assets have been fully offset by a valuation allowance. The net valuation allowance increased by $4.5 million and $2.0 million during the years ended December 31, 2012 and 2011, respectively.
As of December 31, 2012, we had federal and state net operating loss carryforwards of approximately $156.0 million to offset future federal income taxes which will expire beginning in 2024 through 2032 and the state income taxes which will expire beginning in 2014 through 2032. Current federal and state tax laws include substantial restrictions on the utilization of net operating losses and tax credits in the event of an ownership change. Even if the carryforwards are available, they may be subject to annual limitations, lack of future taxable income, or future ownership changes that could result in the expiration of the carryforwards before they are utilized. If we determine in the future that we will be able to realize all or a portion of our net operating loss carryforwards, an adjustment to our net operating loss carryforwards would increase net income in the period in which we make such a determination.
F-25
Table of Contents
Utilization of the net operating loss and tax credits carryforwards may be subject to a substantial annual limitation due to the ownership change limitations provided by the Internal Revenue Code of 1986, as amended, and similar state provisions. The annual limitation may result in the expiration of net operating loss and tax credit carryforwards before utilization.
The following table summarizes activity related to the Company’s gross unrecognized tax benefits (in thousands):
| Total | ||||
Balance as of December 31, 2010 | $ | 1,543 | ||
Increases related to 2011 tax positions | 168 | |||
|
| |||
Balance as of December 31, 2011 | 1,711 | |||
Increases related to 2012 tax positions | 36 | |||
|
| |||
Balance as of December 31, 2012 | $ | 1,747 | ||
|
| |||
The unrecognized tax benefits, if recognized, would not have an impact on the Company’s effective tax rate. The Company does not expect a significant change to its unrecognized tax benefits over the next twelve months. The unrecognized tax benefits may increase or change during the next year for items that arise in the ordinary course of business.
The Company files income tax returns in the U.S. federal and California jurisdiction and is not currently under examination by federal, state, or local taxing authorities for any open tax years. The tax years 1998 through 2012 remain open to examination by the major taxing authorities.
14. Related-Party Transactions
The Company paid a former member of its Board of Directors, who is also a member of its Scientific and Clinical Advisory Boards, a total of $60,000 per year in the years ended December 31, 2012 and 2011, respectively, and $30,000 for the six months ended June 30, 2013, in monthly cash retainers. The Company also issued options to purchase shares of common stock to this individual in his capacity as a member of its Scientific Advisory Board (Note 11).
15. Subsequent Events
Contingent Severance Obligation
In January 2013, the Company Board of Directors approved a lump-sum severance benefit to employees in the event of the Company’s cessation of operations due to bankruptcy. The severance benefit had not been used previously and is due to expire on January 1, 2014. It contained no service requirement and because it was not considered to be company policy, it was not communicated to all employees.
Convertible Notes – JJDC
On March 18, 2013, the Company’s equity and loan facility agreement with JJDC was amended. Under the terms of the amendment, the maturity dates of the convertible notes outstanding were extended to August 1, 2013, and the payment of the note is to rank junior in priority for up to an aggregate of $1.1 million in payments to the Company’s officers and employees in connection with severance obligations. On July 31, 2013, the Company and JJDC entered into a further amendment to the loan facility to extend the maturity date of the convertible notes outstanding until December 31, 2013. In connection with the 2013 financing, described below, the Company issued an aggregate of 624,944 shares of common stock to JJDC as partial consideration for the cancellation of the aggregate principal amount and all accrued interest under the equity and loan facility agreements.
F-26
Table of Contents
Preferred Stock – KBC Equity
On August 7, 2013, the Company purchased back from various KBC Equity Funds 30,050 shares of Series B-1 Preferred Stock, 6,257 shares of Series D-1 Preferred Stock and 3,297 shares of Series E-1 Preferred Stock for $3,000.
2013 Financing
On September 30, 2013, we sold shares of our common stock and warrants to purchase shares of our common stock in a private placement for aggregate gross proceeds of $26.8 million, and raised an additional $5.0 million in venture debt financing pursuant to a $10.0 million loan agreement which we entered into simultaneously with the private placement, resulting in aggregate net proceeds to CymaBay of $28.9 million after deducting placement agent fees and estimated offering expenses. At the same time we issued shares of our common stock in cancellation of approximately $16.9 million of debt owed to the holder of that debt. On October 31, 2013, we sold additional shares of our common stock and warrants to purchase shares of our common stock, which sales are also part of the private placement, for aggregate net proceeds to CymaBay of $2.8 million after deducting placement agent fees and estimated offering expenses. We refer to the private placement, the venture debt financing and the issuance of our common stock in cancellation of the $16.9 million of debt as the 2013 financing. Concurrent with the portion of the 2013 financing that closed on September 30, 2013, all preferred stock converted to common stock.
Sale of Fixed Assets
In the third quarter of 2013, CymaBay sold or disposed of all of their machinery and equipment and a portion of their computers and furniture and fixtures which resulted in a gain on sale of assets of $0.4 million.
F-27
Table of Contents
INDEX TO EXHIBITS
Exhibit No. | Description of Document | |
| 3.1††† | Amended and Restated Certificate of Incorporation. | |
| 3.2††† | Amended and Restated By-Laws. | |
| 4.1 | Reference is made to Exhibits 3.1 and 3.2 | |
| 4.2††† | Form of Registration Rights Agreement | |
| 4.3††† | Form of 2013 Financing Warrant | |
| 10.1*† | 2003 Equity Incentive Plan | |
| 10.2*† | Form of 2003 Equity Incentive Plan Stock Option Agreement | |
| 10.3*† | Form of 2003 Equity Incentive Plan Early Exercise Stock Option Agreement | |
| 10.4††† | Form of CymaBay Indemnity Agreement | |
| 10.5††† | Loan and Security Agreement, dated September 30, 2013, by and among CymaBay Therapeutics, Inc., Silicon Valley Bank and Oxford Finance LLC | |
| 10.6† | Lease, dated February 18, 1992, by and among Transplantation Technology, Inc., Metabolex, Inc. and Spieker-Singleton #87 | |
| 10.7† | Amendment No. 1 to Lease, dated October 8, 1996, between Metabolex, Inc. and Spieker Properties, L.P. | |
| 10.8† | Amendment No. 2 to Lease, dated November 20, 1996, by and among Transplantation Technology, Inc., Metabolex, Inc. and Spieker Properties, L.P. | |
| 10.9† | Amendment No. 3 to Lease, dated May 27, 1998, between Metabolex, Inc. and Spieker Properties, L.P. | |
| 10.10† | Amendment No. 4 to Lease, dated May 29, 2003, between Metabolex, Inc. and EOP-Industrial Portfolio, L.L.C. | |
| 10.11† | Amendment No. 5 to Lease, dated February 15, 2005, between Metabolex, Inc. and RREEF America REIT II, Corp. LLL | |
| 10.12† | Amendment No. 6 to Lease, dated September 29, 2006, between Metabolex, Inc. and RREEF America REIT II, Corp. LLL | |
| 10.13† | Amendment No. 7 to Lease, dated July 15, 2010, between Metabolex, Inc. and Northern California Industrial Portfolio, Inc. | |
| 10.14#± | Development and Clinical Manufacture Agreement, dated June 5, 2012, between Metabolex, Inc. and Patheon Inc. | |
| 10.15#± | Standard Development Agreement, dated October 31, 2006, between Metabolex, Inc. and Metrics, Inc. | |
| 10.16#± | License and Development Agreement, dated June 30, 1998, between Metabolex, Inc. and DiaTex, Inc. | |
| 10.17#± | First Amendment to License and Development Agreement, dated April 15, 1999, between Metabolex, Inc. and DiaTex, Inc. | |
| 10.18#± | Development and Clinical Manufacture Agreement, dated April 30, 2012, between Metabolex, Inc. and Siegfried AG | |
| 10.19†† | Form of Metabolex, Inc. Indemnity Agreement | |
Table of Contents
Exhibit No. | Description of Document | |
| 10.20*†† | Offer Letter, dated September 8, 2000, as amended, between Metabolex, Inc. and Harold Van Wart | |
| 10.21*†† | Offer Letter, dated June 5, 2007, as amended, between Metabolex, Inc. and Charles A. McWherter | |
| 10.22*†† | Consulting Agreement, dated June 27, 2012, as amended, between Metabolex, Inc. and SNPLive, LLC | |
| 10.23*††† | Offer Letter, dated October 3, 2011, between Metabolex, Inc. and Raymond Urbanski | |
| 10.24*††† | Resignation Agreement, dated June 25, 2012, between Metabolex, Inc. and Raymond W. Urbanski | |
| 10.25*††† | 2013 Equity Incentive Plan | |
| 10.26*††† | Form of Option Grant Notice and Option Agreement under the 2013 Equity Incentive Plan | |
| * | Indicates management contract or compensatory plan. |
| † | Previously filed as the like numbered exhibits to our Registration Statement on Form 10, filed with the SEC on August 12, 2013. |
| †† | Previously filed as the like numbered exhibits to our Amendment No. 1 to Registration Statement on Form 10, filed with the SEC on September 19, 2013. |
| ††† | Previously filed as the like numbered exhibits to our Amendment No. 2 to Registration Statement on Form 10, filed with the SEC on October 17, 2013. |
| ± | Previously filed as the like numbered exhibits to our Amendment No. 3 to Registration Statement on Form 10, filed with the SEC on November 8, 2013. |
| # | Portions of this exhibit have been omitted pursuant to a request for confidential treatment, which portions were omitted and filed separately with the Securities and Exchange Commission. |