Table of Contents
8. OPERATIONS PHASE REQUIREMENTS................................................8-14
8.1 General Scope of Work....................................................................................8-14
8.1.1 Administration and Contract Management..................................................8-14
8.1.2 Covered Services........................................................................................8-16
8.1.3 Access to Care............................................................................................8-19
8.1.4 Provider Network.........................................................................................8-23
8.1.5 Member Services.........................................................................................8-31
8.1.6 Marketing and Prohibited Practices.............................................................8-38
8.1.7 Quality Assessment and Performance Improvement..................................8-38
8.1.8 Utilization Management...............................................................................8-41
8.1.9 Early Childhood Intervention (ECI)..............................................................8-42
8.1.10 Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) - Specific Requirements..................................................................8-43
8.1.11 Coordination with Texas Department of Family and Protective Services..8-43
8.1.12 Services for People with Special Health Care Needs................................8-44
8.1.13 Service Management for Certain Populations...........................................8-47
8.1.14 Disease Management (DM).......................................................................8-47
8.1.15 Behavioral Health (BH) Network and Services..........................................8-48
8.1.16 Financial Requirements for Covered Services..........................................8-51
8.1.17 Accounting and Financial Reporting Requirements..................................8-51
8.1.18 Management Information System Requirements......................................8-56
8.1.19 Fraud and Abuse.......................................................................................8-61
8.1.20 Reporting Requirements............................................................................8-62
8.2 Additional Medicaid HMO Scope of Work......................................................8-66
8.2.1 Continuity of Care and Out-of-Network Providers.......................................8-66
8.2.2 Provisions Related to Covered Services for Medicaid Members.................8-67
8.2.3 Medicaid Significant Traditional Providers...................................................8-77
8.2.4 Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs)...................................................................................................................8-77
8.2.5 Provider Complaints and Appeals...............................................................8-78
8.2.6 Member Rights and Responsibilities...........................................................8-79
8.2.7 Medicaid Member Complaint and Appeal System.......................................8-79
8.2.8 Additional Medicaid Behavioral Health Provisions......................................8-87
8.2.9 Third Party Liability and Recovery..............................................................8-90
8.2.10 Coordination With Public Health Entities...................................................8-90
8.2.11 Coordination with Other State Health and Human Services (HHS) Programs...................................................................................................................8-91
8.2.12 Advance Directives....................................................................................8-92
8.3 Additional STAR+PLUS Scope of Work.........................................................8-93
8.3.1 Covered Community-Based Long-Term Care Services..............................8-93
8.3.2 Service Coordination...................................................................................8-95
8.3.3 STAR+PLUS Assessment Instruments.......................................................8-99
8.3.4 1915(c) Nursing Facility Waiver Service Eligibility.....................................8-100
8.3.5 Consumer Directed Services Options.......................................................8-101
8.3.6 Community Based Long-term Care Service Providers..............................8-103
8.4 Additional CHIP Scope of Work....................................................................8-104
8.4.1 CHIP Provider Network.............................................................................8-104
8.4.2 CHIP Provider Complaint and Appeals.....................................................8-105
8.4.3 CHIP Member Complaint and Appeal Process.........................................8-105
8.4.4 Dental Coverage for CHIP Members.........................................................8-105
8.4.5 Third Party Liability and Recovery.............................................................8-105
8.4.6 Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs).................................................................................................................8-106
8.5 Additional CHIP Perinatal Scope of Work....................................................8-106
8.5.1 CHIP Perinatal Provider Network..............................................................8-106
8.5.2 CHIP Perinatal Program Provider Complaint and Appeals.......................8-106
8.5.3 CHIP Perinatal Program Member Complaint and Appeal Process...........8-106
8.5.4 Dental Coverage for CHIP Perinate Newborn Members...........................8-107
8.5.5 Third Party Liability and Recovery.............................................................8-107
8.5.6 Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs).................................................................................................................8-107
| 8. OPERATIONS PHASE REQUIREMENTS |
This Section is designed to provide HMOs with sufficient information to understand the HMOs' responsibilities. This Section describes scope of work requirements for the Operations Phase of the Contract.
Section 8.1 includes the general scope of work that applies to the STAR, STAR+PLUS, CHIP, and CHIP Perinatal HMO Programs.
Section 8.2 includes the additional Medicaid scope of work that applies only to the STAR and STAR+PLUS HMOs.
Section 8.3 includes the additional scope of work that applies only to STAR+PLUS HMOs.
Section 8.4 includes the additional scope of work that applies only to CHIP HMOs.
Section 8.5 includes the additional scope of work that applies only to CHIP Perinatal HMOs.
The Section does not include detailed information on the STAR, STAR+PLUS, CHIP, and CHIP Perinatal HMO Program requirements, such as the time frame and format for all reporting requirements. HHSC has included this information in the Uniform Managed Care Contract Terms and Conditions (Attachment A) and the Uniform Managed Care Manual. HHSC reserves the right to modify these documents as it deems necessary using the procedures set forth in the Uniform Managed Care Contract Terms and Conditions.
| 8.1 General Scope of Work |
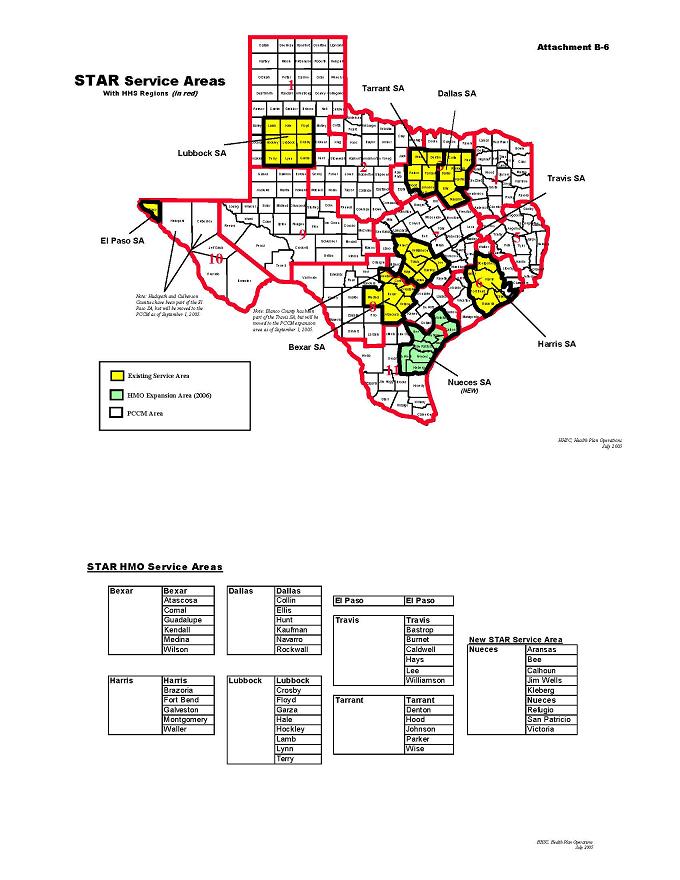
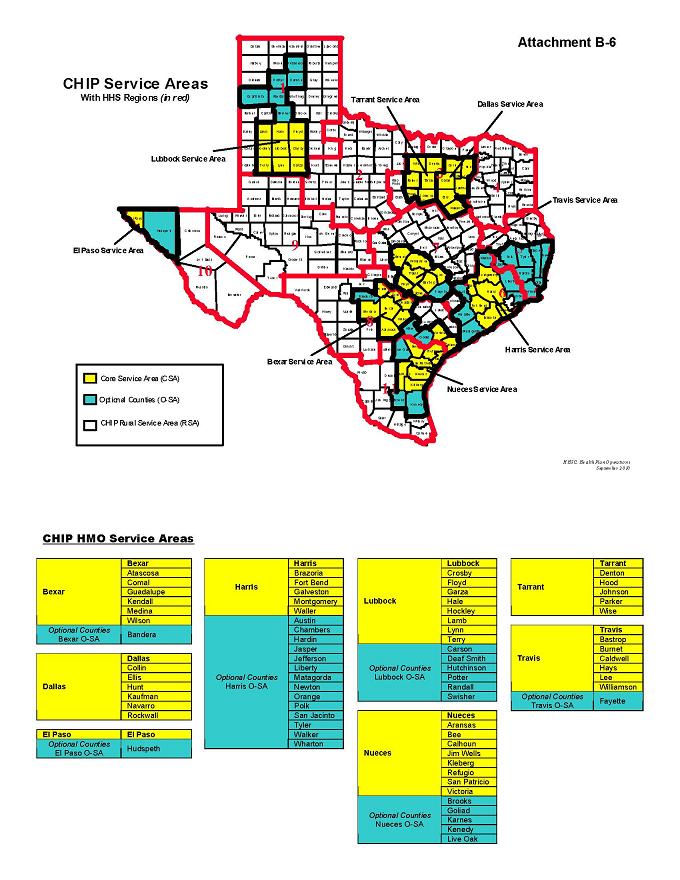
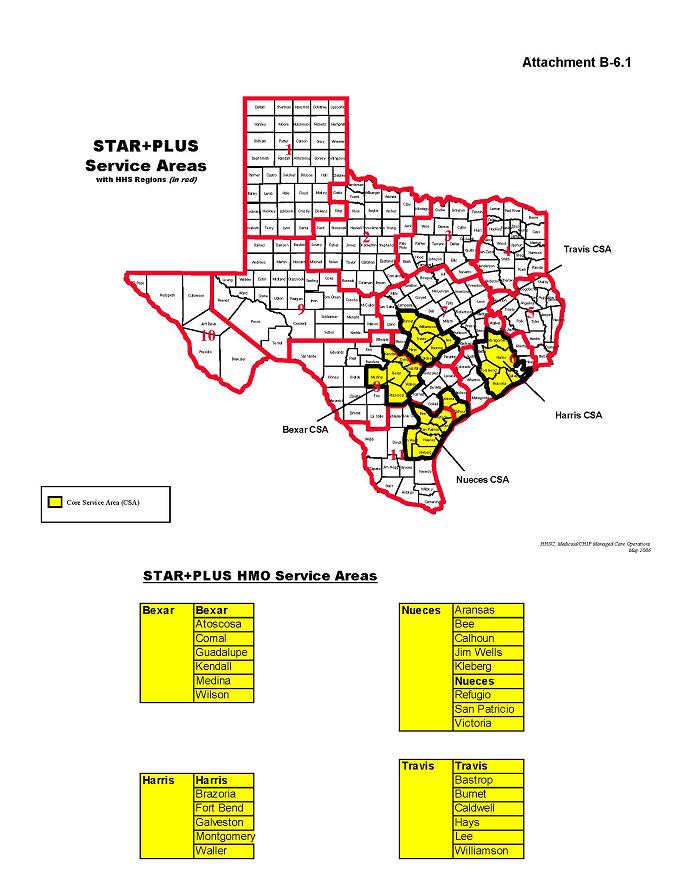
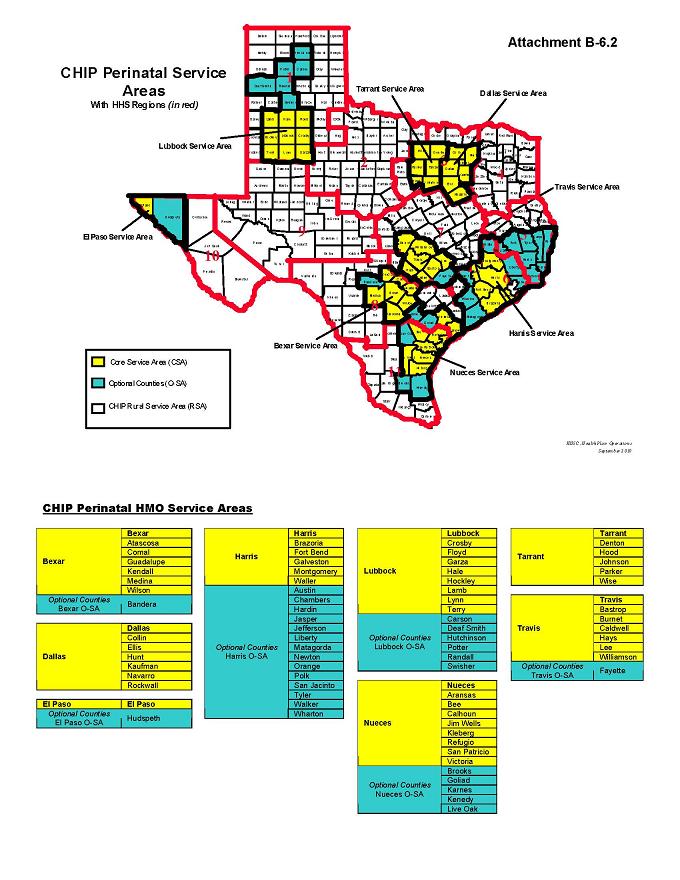
In each HMO Program Service Area, HHSC will select HMOs for each HMO Program to provide health care services to Members. The HMO must be licensed by the Texas Department of Insurance (TDI) as an HMO or an ANHC in all zip codes in the respective Service Area(s).
Coverage for benefits will be available to enrolled Members effective on the Operational Start Date. The Operational Start Date is September 1, 2006 for STAR and CHIP HMOs, January 1, 2007 for CHIP Perinatal HMOs, and February 1, 2007 for the STAR+PLUS HMOs.
8.1.1 Administration and Contract Management
The HMO must comply, to the satisfaction of HHSC, with (1) all provisions set forth in this Contract, and (2) all applicable provisions of state and federal laws, rules, regulations, and waivers.
8.1.1.1 Performance Evaluation
The HMO must identify and propose to HHSC, in writing, no later than May 1st of each State Fiscal Year (SFY) after the Operational Start Date, annual HMO Performance Improvement Goals for the next fiscal year, as well as measures and time frames for demonstrating that such goals are being met. Performance Improvement Goals must be based on HHSC priorities and identified opportunities for improvement (see Attachment B-4, Performance Improvement Goals). The Parties will negotiate such Performance Improvement Goals, the measures that will be used to assess goal achievement, and the time frames for completion, which will be incorporated into the Contract. If HHSC and the HMO cannot agree on the Performance Imp rovement Goals, measures, or time frames, HHSC will set the goals, measures, or time frames.
For State Fiscal Year 2011, HHSC has established overarching goals for each Program. These overarching goals are as follows:
Goal 1 (STAR and STAR+PLUS) Improve treatment for Ambulatory Care Sensitive Conditions (ACSC) through reduction of inpatient admissions. (CHIP) Improve treatment for ACSC through reduction of inpatient admissions and/or emergency department visits. (CHIP Perinatal) Improve prenatal care received by CHIP Perinate members.
Goal 2 (STAR and STAR+PLUS) Improve treatment for ACSC through reduction of emergency department visits. (CHIP) Increase access to needed care and specialized services, including behavioral health treatment and counseling.
Note: The HMO is required to propose customized sub-goals specific to the HMO’s Programs for all overarching goals. The sub-goals must be approved by HHSC as part of the negotiation process.
The specific percentages of expected achievement for each sub-goal will be negotiated by HHSC and the HMO before the Operational Start Date.
For STAR+PLUS HMOs, HHSC will negotiate and implement Performance Improvement Goals for the first full fiscal year following the STAR+PLUS Operational Start Date. One standard STAR+PLUS goal will relate to Consumer-Directed Services. STAR+PLUS improvement goals for SFY2008 will be included in Attachment B-4.1.
For CHIP Perinatal HMOs, HHSC will negotiate and implement Performance Improvement Goals for the first full State Fiscal Year following the CHIP Perinatal Operational Start Date.
The HMO must participate in semi-annual Contract Status Meetings (CSMs) with HHSC for the primary purpose of reviewing progress toward the achievement of annual Performance Improvement Goals and Contract requirements. HHSC may request additional CSMs, as it deems necessary to address areas of noncompliance. HHSC will provide the HMO with reasonable advance notice of additional CSMs, generally at least five (5) business days.
The HMO must provide to HHSC, no later than 14 business days prior to each semi-annual CSM, one electronic copy of a written update, detailing and documenting the HMO’s progress toward meeting the annual Performance Improvement Goals or other areas of noncompliance.
HHSC will track HMO performance on Performance Improvement Goals. It will also track other key facets of HMO performance through the use of a Performance Indicator Dashboard (see HHSC’s Uniform Managed Care Manual). HHSC will compile the Performance Indicator Dashboard based on HMO submissions, data from the External Quality Review Organization (EQRO), and other data available to HHSC. HHSC will share the Performance Indicator Dashboard with the HMO on a quarterly basis.
8.1.1.2 Additional Readiness Reviews and Monitoring Efforts
During the Operations Phase, HHSC may conduct desk and/or onsite reviews as part of its normal Contract monitoring efforts. Additionally, an HMO that chooses to make a change to any operational system or undergo any major transition may be subject to an additional Readiness Review(s). HHSC will determine whether the proposed changes will require a desk review and/or an onsite review. The HMO is responsible for all reasonable travel costs incurred by HHSC or its authorized agent for onsite reviews conducted as part of Readiness Review or HHSC’s normal Contract monitoring efforts. For purposes of this section, “reasonable travel costs” include airfare, lodging, meals, car rental and fuel, taxi, mileage, parking and other incidental travel expenses incurred by HHSC or its authorized agent in connection with the onsite revie ws. This provision does not limit HHSC’s ability to collect other costs as damages in accordance with Attachment A, Section 12.02(e), “Damages.”
Refer to Attachment B-1, Section 7 and Attachment B-1, Section 8.1.18 for additional information regarding HMO Readiness Reviews. Refer to Attachment A, Section 4.08(c) for information regarding Readiness Reviews of the HMO’s Material Subcontractors.
8.1.2 Covered Services
The HMO is responsible for authorizing, arranging, coordinating, and providing Covered Services in accordance with the requirements of the Contract. The HMO must provide Medically Necessary Covered Services to all Members beginning on the Member’s date of enrollment regardless of pre-existing conditions, prior diagnosis and/or receipt of any prior health care services. STAR+PLUS HMOs must also provide Functionally Necessary Community Long-term Care Services to all Members beginning on the Member’s date of enrollment regardless of pre-existing conditions, prior diagnosis and/or receipt of any prior health care services. The HMO must not impose any pre-existing condition limitations or exclusions or require Evidence of Insurability to provide coverage to any Member.
The HMO must provide full coverage for Medically Necessary Covered Services to all Members and, for STAR+PLUS Members, Functionally Necessary Community Long-term Care Services, without regard to the Member’s:
| | 1. previous coverage, if any, or the reason for termination of such coverage; |
| | 3. confinement in a health care facility; or |
Please Note:
(STAR HMOs): A Member cannot change from one STAR HMO to another STAR HMO during an inpatient hospital stay. The STAR HMO responsible for the hospital charges for STAR Members at the start of an Inpatient Stay remains responsible for hospital charges until the time of discharge or until such time that there is a loss of Medicaid eligibility. STAR HMOs are responsible for professional charges during every month for which the HMO receives a full capitation for a Member.
(STAR+PLUS HMOs): A Member cannot change from one STAR+PLUS HMO to another STAR+PLUS HMO during an inpatient hospital stay. The STAR+PLUS HMO is responsible for authorization and management of the inpatient hospital stay until the time of discharge, or until such time that there is a loss of Medicaid eligibility. STAR+PLUS HMOs are responsible for professional charges during every month for which the HMO receives a full capitation for a Member.
A Member cannot change from one STAR+PLUS HMO to another STAR+PLUS HMO during a nursing facility stay.
(CHIP HMOs): If a CHIP Member’s Effective Date of Coverage occurs while the CHIP Member is confined in a hospital, HMO is responsible for the CHIP Member’s costs of Covered Services beginning on the Effective Date of Coverage. If a CHIP Member is disenrolled while the CHIP Member is confined in a hospital, HMO’s responsibility for the CHIP Member’s costs of Covered Services terminates on the Date of Disenrollment.
(CHIP Perinatal HMOs): If a CHIP Perinate’s Effective Date of Coverage occurs while the CHIP Perinate is confined in a Hospital, HMO is responsible for the CHIP Perinate’s costs of Covered Services beginning on the Effective Date of Coverage. If a CHIP Perinate is disenrolled while the CHIP Perinate is confined in a Hospital, HMO’s responsibility for the CHIP Perinate’s costs of Covered Services terminates on the Date of Disenrollment.
The HMO must not practice discriminatory selection, or encourage segregation among the total group of eligible Members by excluding, seeking to exclude, or otherwise discriminating against any group or class of individuals.
Covered Services for all Medicaid HMO Members are listed in Attachments B-2 and B-2.1 of the Contract (STAR and STAR+PLUS Covered Services). As noted in Attachments B-2 and B-2.1, all Medicaid HMOs must provide Covered Services described in the most recent Texas Medicaid Provider Procedures Manual (Provider Procedures Manual and in all Texas Medicaid Bulletins, which update the Texas Provider Procedures Manual except for those services identified in Section 8.2.2.8 as non-capitated services. A description of CHIP Covered Services and exclusions is provided inAttachment B-2 of the Contract. A description of CHIP Perinatal Program Covered Services and exclusions is provided in Attachment B-2.2 of the Contract. Covered Services are subject to change due to changes in federal and state law, changes in Medicaid, CHIP or CHIP Perinatal Program policy, and changes in medical practice, clinical protocols, or technology.
8.1.2.1 Value-added Services
HMOs may propose additional services for coverage. These are referred to as “Value-added Services.” Value-added Services may be actual Health Care Services, benefits, or positive incentives that HHSC determines will promote healthy lifestyles and improved health outcomes among Members. Value-added Services that promote healthy lifestyles should target specific weight loss, smoking cessation, or other programs approved by HHSC. Temporary phones, cell phones, additional transportation benefits, and extra home health services may be Value-added Services, if approved by HHSC. Best practice approaches to delivering Covered Services are not considered Value-added Services.
If offered, Value-added Services must be offered to all mandatory STAR, and CHIP and CHIP Perinatal HMO Members within the applicable HMO Program and Service Area. For STAR+PLUS Acute Care services, the HMO may distinguish between the Dual Eligible and non-Dual Eligible populations. Value-added Services do not need to be consistent across more than one HMO Program or across more than one Service Area. Value-added Services that are approved by HHSC during the contracting process will be included in the Contract’s scope of services.
The HMO must provide Value-added Services at no additional cost to HHSC. The HMO must not pass on the cost of the Value-added Services to Providers. The HMO must specify the conditions and parameters regarding the delivery of the Value-added Services in the HMO’s Marketing Materials and Member Handbook, and must clearly describe any limitations or conditions specific to the Value-added Services.
Transition Phase. During the Transition Phase, HHSC will offer a one-time opportunity for the HMO to propose two additional Value-added Services to its list of current, approved Value-added Services. (See Attachment B-3, Value-Added Services). HHSC will establish the requirements and the timeframes for submitting the two additional proposed Value-added Services.
During this HHSC-designated opportunity, the HMO may propose either to add new Value-added Services or to enhance its current, approved Value-added Services. The HMO may propose two additional Value-added Services per HMO Program, and the services do not have to be the same for each HMO Program. HHSC will review the proposed additional services and, if appropriate, will approve the additional Value-added Services, which will be effective on the Operational Start Date. The HMO’s Contract will be amended to reflect the additional, approved Value-added Services.
The HMO does not have to add Value-added Services during the HHSC-designated opportunity, but this will be the only time during the Transition Phase for the HMO to add Value-added Services. At no time during the Transition Phase will the HMO be allowed to delete, limit or restrict any of its current, approved Value-added Services.
Operations Phase. During the Operations Phase, Value-added Services can be added or removed only by written amendment of the Contract. HMOs will be given the opportunity to add or enhance Value-added Services twice per State Fiscal Year, with changes to be effective September 1 and March 1. HMOs will also be given the opportunity to delete or reduce Value-added Services once per State Fiscal Year, with changes to be effective September 1. HHSC may
allow additional modifications to Value-added Services if Covered Services are amended by HHSC during a State Fiscal Year. This approach allows HHSC to coordinate biannual revisions to HHSC’s HMO Comparison Charts for Members. A HMO’s request to add, enhance, delete, or reduce a Value-added Service must be submitted to HHSC by April 1 of each year to be effective September 1 for the following contract period. A second request to add or enhance Value-added Services must be submitted to HHSC by October 1 each year to be effective March 1. (For STAR and CHIP, see Attachment B-3, Value-Added Services. For STAR+PLUS, see Attachment B-3.1, STAR+PLUS Value-Added Services. For CHIP Perinatal, see Attachment B-3.2, CHIP Perinatal Value-Added Services.)
A HMO’s request to add a Value-added Service must:
| | a. Define and describe the proposed Value-added Service; |
| | b. Specify the Service Areas and HMO Programs for the proposed Value-added Service; |
| | c. Identify the category or group of mandatory Members eligible to receive the Value-added Service if it is a type of service that is not appropriate for all mandatory Members; |
| | d. Note any limits or restrictions that apply to the Value-added Service; |
| | e. Identify the Providers responsible for providing the Value-added Service; |
| | f. Describe how the HMO will identify the Value-added Service in administrative (Encounter) data; |
| | g. Propose how and when the HMO will notify Providers and mandatory Members about the availability of such Value-added Service; |
| | h. Describe how a Member may obtain or access the Value-added Service; and |
| | i. Include a statement that the HMO will provide such Value-added Service for at least 12 months from the September 1 effective date. |
A HMO cannot include a Value-added Service in any material distributed to mandatory Members or prospective mandatory Members until the Parties have amended the Contract to include that Value-added Service. If a Value-added Service is deleted by amendment, the HMO must notify each mandatory Member that the service is no longer available through the HMO. The HMO must also revise all materials distributed to prospective mandatory Members to reflect the change in Value-added Services.
8.1.2.2 Case-by-Case Added Services
Except as provided below, the HMO may offer additional benefits that are outside the scope of services to individual Members on a case-by-case basis, based on Medical Necessity, cost-effectiveness, the wishes of the Member/Member’s family, the potential for improved health status of the Member, and for STAR+PLUS Members based on functional necessity.
Section 8.1.2.2, Case-by-Case Added Services, does not apply to the CHIP Perinatal Program.
8.1.3 Access to Care
All Covered Services must be available to Members on a timely basis in accordance with medically appropriate guidelines, and consistent with generally accepted practice parameters, requirements in this Contract. The HMO must comply with the access requirements as established by the Texas Department of Insurance (TDI) for all HMOs doing business in Texas, except as otherwise required by this Contract. Medicaid HMOs must be responsive to the possibility of increased Members due to the phase-out of the PCCM model in Service Areas where adequate HMO coverage exists.
The HMO must provide coverage for Emergency Services to Members 24 hours a day and 7 days a week, without regard to prior authorization or the Emergency Service provider’s contractual relationship with the HMO. The HMO’s policy and procedures, Covered Services, claims adjudication methodology, and reimbursement performance for Emergency Services must comply with all applicable state and federal laws and regulations, whether the provider is in-network or Out-of-Network. A HMO is not responsible for payment for unauthorized non-emergency services provided to a Member by Out-of-Network providers.
The HMO must also have an emergency and crisis Behavioral Health Services Hotline available 24 hours a day, 7 days a week, toll-free throughout the Service Area. The Behavioral Health Services Hotline must meet the requirements described in Section 8.1.15. For Medicaid Members, a HMO must provide coverage for Emergency Services in compliance with 42 C.F.R. §438.114, and as described in more detail in Section 8.2.2.1. The HMO may arrange Emergency Services and crisis Behavioral Health Services through mobile crisis teams.
For CHIP Members, Emergency Services, including emergency Behavioral Health Services, must be provided in accordance with the Texas Insurance Code and TDI regulations.
For the CHIP Perinatal Program, refer to Attachment B-2.2 for description of emergency services for CHIP Perinates and CHIP Perinate Newborns.
For the STAR, STAR+PLUS, and CHIP Programs, and for CHIP Perinate Newborns, HMO must require, and make best efforts to ensure, that PCPs are accessible to Members 24 hours a day, 7 days a week and that its Network Primary Care Providers (PCPs) have after-hours telephone availability that is consistent with, Section 8.1.4. CHIP Perinatal HMOs are not required to establish PCP Networks for CHIP Perinates.
The HMO must provide that if Medically Necessary Covered Services are not available through Network physicians or other Providers, the HMO must, upon the request of a Network physician or other Provider, within the time appropriate to the circumstances relating to the delivery of the services and the condition of the patient, but in no event to exceed five business days after receipt of reasonably requested documentation, allow a referral to a non-network physician or provider. The HMO must fully reimburse the non-network provider in accordance with the Out-of-Network methodology for Medicaid as defined by HHSC, and for CHIP, at the usual and customary rate defined by TDI in 28 T.A.C. Section 11.506.
The Member will not be responsible for any payment for Medically Necessary Covered Services, including Functionally Necessary Covered Services, other than:
| | (1) HHSC-specified co-payments for CHIP Members, where applicable; and |
| | (2) STAR+PLUS Members who qualify for 1915(c) Nursing Facility Waiver services and enter a 24-hour setting will be required to pay the provider of care room and board costs and any income in excess of the personal needs allowance, as established by HHSC. If the HMO provides Members who do not qualify for the 1915(c) Nursing Facility Waiver services in a 24-hour setting as an alternative to nursing facility or hospitalization, the Member will be required to pay the provider of care room and board costs and any income in excess of the personal needs allowance, as established by HHSC. |
8.1.3.1 Waiting Times for Appointments
Through its Provider Network composition and management, the HMO must ensure that appointments for the following types of Covered Services are provided within the time frames specified below. In all cases below, “day” is defined as a calendar day.
| | 1. Emergency Services must be provided upon Member presentation at the service delivery site, including at non-network and out-of-area facilities; |
| | 2. Urgent care, including urgent specialty care, must be provided within 24 hours of request. |
| | 3. Routine primary care must be provided within 14 days of request; |
| | 4. Initial outpatient behavioral health visits must be provided within 14 days of request; |
| | 5. Routine specialty care referrals must be provided within 30 days of request; |
| | 6. Pre-natal care must be provided within 14 days of request, except for high-risk pregnancies or new Members in the third trimester, for whom an appointment must be offered within five days, or immediately, if an emergency exists; |
| | 7. Preventive health services for adults must be offered to a Member within 90 days of request; and |
| | 8. Preventive health services for children, including well-child checkups should be offered to CHIP Members in accordance with the American Academy of Pediatrics (AAP) periodicity schedule. Medicaid HMOs should utilize the Texas Health Steps periodicity schedule. For a New Members under age 21, overdue or upcoming well-child checkups, including Texas Health Steps medical checkups, should be offered as soon as practicable, but in no case later than 14 days of enrollment for newborns, and no later than 90 days of enrollment for all other eligible child Members. Effective September 1, 2010, the Texas Health Steps annual medical checkup for an Existing Member age 36 months and older is due on the child’s birthday. The annual medical checkup is considered timely if it occurs no later than 364 calendar days after the child’s birthday. For pur poses of this requirement, the terms “New Member” and “Existing Member” are defined in Chapter 12.4 of the Uniform Managed Care Manual. |
8.1.3.2 Access to Network Providers
The HMO’s Network shall have within its Network, PCPs in sufficient numbers, and with sufficient capacity, to provide timely access to regular and preventive pediatric care and Texas Health Steps services to all child Members in accordance with the waiting times for appointments in Section 8.1.3.1.
PCP Access: At a minimum, the HMO must ensure that all Members have access to an age-appropriate PCP in the Provider Network with an Open Panel within 30 miles of the Member’s residence. For the purposes of assessing compliance with this requirement, an internist who
provides primary care to adults only is not considered an age-appropriate PCP choice for a Member under age 21, and a pediatrician is not considered an age-appropriate choice for a Member age 21 and over. Note: This provision does not apply to CHIP Perinates, but it does apply to CHIP Perinate Newborns.
OB/GYN Access and CHIP Perinatal Program Provider Access: STAR, STAR+PLUS and CHIP Program Network: at a minimum, STAR, STAR+PLUS and CHIP HMOs must ensure that all female Members have access to an OB/GYN in the Provider Network within 75 miles of the Member’s residence. (If the OB/GYN is acting as the Member’s PCP, the HMO must follow the access requirements for the PCP.) The HMO must allow female Members to select an OB/GYN within its Provider Network. A female Member who selects an OB/GYN must be allowed direct access to the OB/GYN’s health care services without a referral from the Member’s PCP or a prior authorization. A pregnant Member with 12 weeks or less remaining before the expected delivery date must be allowed to remain under the Member’s curr ent OB/GYN care though the Member’s post-partum checkup, even if the OB/GYN provider is, or becomes, Out-of-Network.
CHIP Perinatal Program Network: At a minimum, CHIP Perinatal HMOs must ensure that CHIP Perinates have access to a Provider of perinate services within 75 miles of the Member’s residence if the Member resides in an urban area and within 125 miles of the Member’s residence if the Member resides in a rural area.
Outpatient Behavioral Health Service Provider Access: At a minimum, the HMO must ensure that all Members except CHIP Perinates have access to an outpatient Behavioral Health Service Provider in the Network within 75 miles of the Member’s residence. Outpatient Behavioral Health Service Providers must include Masters and Doctorate-level trained practitioners practicing independently or at community mental health centers, other clinics or at outpatient hospital departments. A Qualified Mental Health Provider – Community Services (QMHP-CS), is defined by the Texas Department of State Health Services (DSHS) in Title 25 T.A.C., Part I, Chapter 412, Subchapter G, Division 1, §412.303(48). QMHP-CSs shall be providers working through a DSHS-contracted Local Mental Health Auth ority or a separate DSHS-contracted entity. QMHP-CSs shall be supervised by a licensed mental health professional or physician and provide services in accordance with DSHS standards. Those services include individual and group skills training (which can be components of interventions such as day treatment and in-home services), patient and family education, and crisis services.
Other Specialist Physician Access: At a minimum, the HMO must ensure that all Members except CHIP Perinates have access to a Network specialist physician within 75 miles of the Member’s residence for common medical specialties. For adult Members, common medical specialties shall include general surgery, cardiology, orthopedics, urology, and ophthalmology. For child Members, common medical specialties shall include orthopedics and otolaryngology. In addition, all Members must be allowed to: 1) select an in-network opthalmologist or therapeutic optometrist to provide eye Health Care Services, other than surgery, and 2) have access without a PCP referral to eye Health Care Services from a Network specialist who is an ophthalmologist or therapeutic optometrist for non-surgical serv ices.
Hospital Access: The HMO must ensure that all Members have access to an Acute Care hospital in the Provider Network within 30 miles of the Member’s residence. For HMOs participating in
the CHIP Perinatal Program, exceptions to this access standard may be requested on a case-by-case basis and must have HHSC approval.
All other Covered Services, except for services provided in the Member’s residence: At a minimum, the HMO must ensure that all Members have access to at least one Network Provider for each of the remaining Covered Services described in Attachment B-2, within 75 miles of the Member’s residence. This access requirement includes, but is not limited to, specialists, specialty hospitals, psychiatric hospitals, diagnostic and therapeutic services, and single or limited service health care physicians or Providers, as applicable to the HMO Program.
The HMO is not precluded from making arrangements with physicians or providers outside the HMO’s Service Area for Members to receive a higher level of skill or specialty than the level available within the Service Area, including but not limited to, treatment of cancer, burns, and cardiac diseases. HHSC may consider exceptions to the above access-related requirements when an HMO has established, through utilization data provided to HHSC, that a normal pattern for securing health care services within an area does not meet these standards, or when an HMO is providing care of a higher skill level or specialty than the level which is available within the Service Area such as, but not limited to, treatment of cancer, burns, and cardiac diseases.
8.1.3.3 Monitoring Access
The HMO is required to systematically and regularly verify that Covered Services furnished by Network Providers are available and accessible to Members in compliance with the standards described in Sections 8.1.3.1 and 8.1.3.2, and for Covered Services furnished by PCPs, the standards described in Section 8.1.4.2.
The HMO must enforce access and other Network standards required by the Contract and take appropriate action with Providers whose performance is determined by the HMO to be out of compliance.
8.1.4 Provider Network
The HMO must enter into written contracts with properly credentialed Providers as described in this Section. The Provider contracts must comply with the Uniform Managed Care Manual’s requirements.
The HMO must maintain a Provider Network sufficient to provide all Members with access to the full range of Covered Services required under the Contract. The HMO must ensure its Providers and subcontractors meet all current and future state and federal eligibility criteria, reporting requirements, and any other applicable rules and/or regulations related to the Contract.
The Provider Network must be responsive to the linguistic, cultural, and other unique needs of any minority, elderly, or disabled individuals, or other special population in the Service Areas and HMO Programs served by the HMO, including the capacity to communicate with Members in languages other than English, when necessary, as well as with those who are deaf or hearing impaired.
The HMO must seek to obtain the participation in its Provider Network of qualified providers currently serving the Medicaid and CHIP Members in the HMO’s proposed Service Area(s). Medicaid HMOs utilizing Out-of-Network providers to render services to their Members must not exceed the utilization standards established in 1 T.A.C. §353.4. HHSC may modify this requirement for Medicaid HMOs that demonstrate good cause for noncompliance, as set forth in §353.4(e)(3).
NOTE: The following Provider descriptions do not require STAR+PLUS HMOs to contract with Hospital providers for Inpatient Stay services. STAR+PLUS HMOs are required, however, to contract with Hospitals for Outpatient Hospital Services , and with Hospital Providers for Inpatient Behavioral Health Services resulting from a behavioral health primary diagnosis.
All Providers: All Providers must be licensed in the State of Texas to provide the Covered Services for which the HMO is contracting with the Provider, and not be under sanction or exclusion from the Medicaid program. All Acute Care Providers serving Medicaid Members must be enrolled as Medicaid providers and have a Texas Provider Identification Number (TPIN). Long-term Care Providers are not required to have a TPIN but must have a LTC Provider number. Providers must also have a National Provider Identifier (NPI) in accordance with the timelines established in 45 C.F.R. Part 162, Subpart D (for most Providers, the NPI must be in place by May 23, 2007.)
Inpatient hospital and medical services: The HMO must ensure that Acute Care hospitals and specialty hospitals are available and accessible 24 hours per day, seven days per week, within the HMO’s Network to provide Covered Services to Members throughout the Service Area.
Children’s Hospitals/hospitals with specialized pediatric services: The HMO must ensure Members access to hospitals designated as Children’s Hospitals by Medicare and hospitals with specialized pediatric services, such as teaching hospitals and hospitals with designated children’s wings, so that these services are available and accessible 24 hours per day, seven days per week, to provide Covered Services to Members throughout the Service Area. The HMO must make Out-of-Network reimbursement arrangements with a designated Children’s Hospital and/or hospital with specialized pediatric services in proximity to the Member’s residence, and such arrangements must be in writing, if the HMO does not include such hospitals in its Provider Network. Provider Directo ries, Member materials, and Marketing materials must clearly distinguish between hospitals designated as Children’s Hospitals and hospitals that have designated children’s units.
Trauma: The HMO must ensure Members access to Texas Department of State Health Services (TDSHS) designated Level I and Level II trauma centers within the State or hospitals meeting the equivalent level of trauma care in the HMO’s Service Area, or in close proximity to such Service Area. The HMO must make Out-of-Network reimbursement arrangements with the DSHS-designated Level I and Level II trauma centers or hospitals meeting equivalent levels of trauma care, and such arrangements must be in writing, if the HMO does not include such a trauma center in its Provider Network.
Transplant centers: The HMO must ensure Member access to HHSC-designated transplant centers or centers meeting equivalent levels of care. A list of HHSC-designated transplant centers can be found in the Procurement Library in Attachment H. The HMO must make Out-of-Network
reimbursement arrangements with a designated transplant center or center meeting equivalent levels of care in proximity to the Member’s residence, and such arrangements must be in writing, if the HMO does not include such a center in its Provider Network.
Hemophilia centers: The HMO must ensure Member access to hemophilia centers supported by the Centers for Disease Control (CDC). A list of these hemophilia centers can be found at http://www.cdc.gov/ncbddd/hbd/htc_list.htm. The HMO must make Out-of-Network reimbursement arrangements with a CDC-supported hemophilia center, and such arrangements must be in writing, if the HMO does not include such a center in its Provider Network.
Physician services: The HMO must ensure that Primary Care Providers are available and accessible 24 hours per day, seven days per week, within the Provider Network. The HMO must contract with a sufficient number of participating physicians and specialists within each Service Area to comply with the access requirements throughout Section 8.1.3 and meet the needs of Members for all Covered Services.
The HMO must ensure that an adequate number of participating physicians have admitting privileges at one or more participating Acute Care hospitals in the Provider Network to ensure that necessary admissions are made. In no case may there be less than one in-network PCP with admitting privileges available and accessible 24 hours per day, seven days per week for each Acute Care hospital in the Provider Network.
The HMO must ensure that an adequate number of participating specialty physicians have admitting privileges at one or more participating hospitals in the HMO’s Provider Network to ensure necessary admissions are made. The HMO shall require that all physicians who admit to hospitals maintain hospital access for their patients through appropriate call coverage.
Laboratory services: The HMO must ensure that in-network reference laboratory services must be of sufficient size and scope to meet the non-emergency and emergency needs of the enrolled population and the access requirements in Section 8.1.3. Reference laboratory specimen procurement services must facilitate the provision of clinical diagnostic services for physicians, Providers and Members through the use of convenient reference satellite labs in each Service Area, strategically located specimen collection areas in each Service Area, and the use of a courier system under the management of the reference lab. For Medicaid Members, Texas Health Steps requires that laboratory specimens obtained as part of a Texas Health Steps medic al checkup visit must be sent to the TDSHS Laboratory.
Diagnostic imaging: The HMO must ensure that diagnostic imaging services are available and accessible to all Members in each Service Area in accordance with the access standards in Section 8.1.3. The HMO must ensure that diagnostic imaging procedures that require the injection or ingestion of radiopaque chemicals are performed only under the direction of physicians qualified to perform those procedures.
Home health services: The HMO must have a contract(s) with a home health Provider so that all Members living within the HMO’s Service Area will have access to at least one such Provider for home health Covered Services. (These services are provided as part of the Acute Care Covered Services, not the Community Long-term Care Services.)
Community Long-term Care services: STAR+PLUS HMOs must have contracts with Community Long-term Care service Providers, so that all Members living within the Contractor’s Service Area will have access to Medically Necessary and Functionally Necessary Covered Services.
8.1.4.1 Provider Contract Requirements
The HMO is prohibited from requiring a provider or provider group to enter into an exclusive contracting arrangement with the HMO as a condition for participation in its Provider Network.
The HMO’s contract with health care Providers must be in writing, must be in compliance with applicable federal and state laws and regulations, and must include minimum requirements specified in the Uniform Managed Care Contract Terms and Conditions (Attachment A) and HHSC’s Uniform Managed Care Manual.
The HMO must submit model Provider contracts to HHSC for review during Readiness Review. HHSC retains the right to reject or require changes to any model Provider contract that does not comply with HMO Program requirements or the HHSC-HMO Contract.
8.1.4.2 Primary Care Providers
The HMO’s PCP Network may include Providers from any of the following practice areas: General Practice; Family Practice; Internal Medicine; Pediatrics; Obstetrics/Gynecology (OB/GYN); Advanced Practice Nurses (APNs) and Physician Assistants (PAs) (when APNs and PAs are practicing under the supervision of a physician specializing in Family Practice, Internal Medicine, Pediatrics or Obstetrics/Gynecology who also qualifies as a PCP under this contract); Federally Qualified Health Centers (FQHCs), Rural Health Clinics (RHCs), and similar community clinics; and specialist physicians who are willing to provide a Medical Home to selected Members with special needs and conditions. Section 533.005(a)(13), Government Code, requires the HMO to use Advanced Practice Nurses practicing under the supervision of a physician as PCPs in its Provider Network for STAR and STAR+PLUS.
CHIP Perinatal HMOs are not required to develop PCP Networks for CHIP Perinates. CHIP Perinatal HMOs may use the same PCP Network for CHIP Members and CHIP Perinatal Newborns.
An internist or other Provider who provides primary care to adults only is not considered an age-appropriate PCP choice for a Member under age 21. An internist or other Provider who provides primary care to adults and children may be a PCP for children if:
| | 1. the Provider assumes all HMO PCP responsibilities for such Members in a specific age group under age 21, |
| | 2. the Provider has a history of practicing as a PCP for the specified age group as evidenced by the Provider’s primary care practice including an established patient population under age 20 and within the specified age range, and |
| | 3. the Provider has admitting privileges to a local hospital that includes admissions to pediatric units. |
A pediatrician is not considered an age-appropriate choice for a Member age 21 and over.
The PCP for a Member with disabilities, Special Health Care Needs, or Chronic or Complex Conditions may be a specialist physician who agrees to provide PCP services to the Member. The specialty physician must agree to perform all PCP duties required in the Contract and PCP duties must be within the scope of the specialist’s license. Any interested person may initiate the request through the HMO for a specialist to serve as a PCP for a Member with disabilities, Special Health Care Needs, or Chronic or Complex Conditions. The HMO shall handle such requests in accordance with 28 T.A.C. Part 1, Chapter 11, Subchapter J.
PCPs who provide Covered Services for STAR, CHIP, and CHIP Perinatal Newborns must either have admitting privileges at a Hospital that is part of the HMO’s Provider Network or make referral arrangements with a Provider who has admitting privileges to a Network Hospital. STAR+PLUS PCPs must either have admitting privileges at a Medicaid Hospital or make referral arrangements with a Provider who has admitting privileges to a Medicaid Hospital.
The HMO must require, through contract provisions, that PCPs are accessible to Members 24 hours a day, 7 days a week. The HMO is encouraged to include in its Network sites that offer primary care services during evening and weekend hours. The following are acceptable and unacceptable telephone arrangements for contacting PCPs after their normal business hours.
Acceptable after-hours coverage:
| | 1. The office telephone is answered after-hours by an answering service, which meets language requirements of the Major Population Groups and which can contact the PCP or another designated medical practitioner. All calls answered by an answering service must be returned within 30 minutes; |
| | 2. The office telephone is answered after normal business hours by a recording in the language of each of the Major Population Groups served, directing the patient to call another number to reach the PCP or another provider designated by the PCP. Someone must be available to answer the designated provider’s telephone. Another recording is not acceptable; and |
| | 3. The office telephone is transferred after office hours to another location where someone will answer the telephone and be able to contact the PCP or another designated medical practitioner, who can return the call within 30 minutes. |
Unacceptable after-hours coverage:
| | 1. The office telephone is only answered during office hours; |
| | 2. The office telephone is answered after-hours by a recording that tells patients to leave a message; |
| | 3. The office telephone is answered after-hours by a recording that directs patients to go to an Emergency Room for any services needed; and |
| | 4. Returning after-hours calls outside of 30 minutes. |
The CHIP HMOs must require PCPs, through contract provisions or Provider Manual, to provide children under the age of 21 with preventive services in accordance with the AAP recommendations for CHIP Members and CHIP Perinate Newborns. Medicaid HMOs must
require PCPs, through contract provisions or Provider Manual, to provide children under the age of 21 with preventive services in accordance with the Texas Health Steps periodicity schedule. The HMO must require PCPs, through contract provisions or Provider Manual, to provide adults with preventive services in accordance with the U.S. Preventive Services Task Force requirements. The HMO must make best efforts to ensure that PCPs follow these periodicity requirements for children and adult Members. Best efforts must include, but not be limited to, Provider education, Provider profiling, monitoring, and feedback activities.
The HMO must require PCPs, through contract provisions or Provider Manual, to assess the medical needs of Members for referral to specialty care providers and provide referrals as needed. PCPs must coordinate Members’ care with specialty care providers after referral. The HMO must make best efforts to ensure that PCPs assess Member needs for referrals and make such referrals. Best efforts must include, but not be limited to, Provider education activities and review of Provider referral patterns.
8.1.4.3 PCP Notification
The HMO must furnish each PCP with a current list of enrolled Members enrolled or assigned to that Provider no later than five (5) working days after the HMO receives the Enrollment File from the HHSC Administrative Services Contractor each month. The HMO may offer and provide such enrollment information in alternative formats, such as through access to a secure Internet site, when such format is acceptable to the PCP.
8.1.4.4 Provider Credentialing and Re-credentialing
The HMO must review, approve and periodically recertify the credentials of all participating physician Providers and all other licensed Providers who participate in the HMO’s Provider Network. The HMO may subcontract with another entity to which it delegates such credentialing activities if such delegated credentialing is maintained in accordance with the National Committee for Quality Assurance (NCQA) delegated credentialing requirements and any comparable requirements defined by HHSC.
At a minimum, the scope and structure of a HMO’s credentialing and re-credentialing processes must be consistent with recognized HMO industry standards such as those provided by NCQA and relevant state and federal regulations including 28 T.A.C. §§11.1902, relating to provider credentialing and notice, and as an additional requirement for Medicaid HMOs, 42 C.F.R. §438.12 and 42 C.F.R. §438.214(b). The initial credentialing process, including application and verification of information, must be completed before the effective date of the initial contract with the physician or Provider. The re-credentialing process must occur at least every three years.
The HMO may not discriminate for the participation, reimbursement, or indemnification of any provider who is acting within the scope of his or her license or certification under applicable State law, solely on the basis of that license or certification. Additionally, if the HMO declines to include individual or groups of providers in its Network, it must give the affected providers written notice of the reasons for its decision.
The re-credentialing process must take into consideration Provider performance data including, but not be limited to, Member Complaints and Appeals, quality of care, and utilization management.
HMOs must comply with the requirements of Texas Insurance Code Chapter 1452, Subchapter C, regarding expedited credentialing and payment of physicians who have joined medical groups that are already contracted with the HMO.
8.1.4.5 Board Certification Status
The HMO must maintain a policy with respect to Board Certification for PCPs and specialty physicians that encourage participation of board certified PCPs and specialty physicians in the Provider Network. The HMO must make information on the percentage of Board-certified PCPs in the Provider Network and the percentage of Board-certified specialty physicians, by specialty, available to HHSC upon request.
8.1.4.6 Provider Manual, Materials and Training
The HMO must prepare and issue a Provider Manual(s), including any necessary specialty manuals (e.g., behavioral health) to all existing Network Providers. For newly contracted Providers, the HMO must issue copies of the Provider Manual(s) within five (5) working days from inclusion of the Provider into the Network. The Provider Manual must contain sections relating to special requirements of the HMO Program(s) and the enrolled populations in compliance with the requirements of this Contract.
HHSC or its designee must approve the Provider Manual, and any substantive revisions to the Provider Manual, prior to publication and distribution to Providers. The Provider Manual must contain the critical elements defined in the Uniform Managed Care Manual. HHSC’s initial review of the Provider Manual is part of the Operational Readiness Review described in Attachment B-1, Section 7.
The HMO must provide training to all Providers and their staff regarding the requirements of the Contract and special needs of Members. The HMO’s Medicaid, CHIP and/or CHIP Perinatal Program training must be completed within 30 days of placing a newly contracted Provider on active status. The HMO must provide on-going training to new and existing Providers as required by the HMO or HHSC to comply with the Contract. The HMO must maintain and make available upon request enrollment or attendance rosters dated and signed by each attendee or other written evidence of training of each Provider and their staff.
The HMO must establish ongoing Provider training that includes, but is not limited to, the following issues:
| | 1. Covered Services and the Provider’s responsibilities for providing and/or coordinating such services. Special emphasis must be placed on areas that vary from commercial coverage rules (e.g., Early Intervention services, therapies and DME/Medical Supplies); and for Medicaid, making referrals and coordination with Non-capitated Services; |
| | 2. Relevant requirements of the Contract; |
| | 3. The HMO’s quality assurance and performance improvement program and the Provider’s role in such a program; and |
| | 4. The HMO’s policies and procedures, especially regarding in-network and Out-of-Network referrals. |
Provider Materials produced by the HMO, relating to Medicaid Managed Care, the CHIP Program, and/or the CHIP Perinatal Program must be in compliance with State and Federal laws and requirements of the HHSC Uniform Managed Care Contract Terms and Conditions. HMO must make available any provider materials to HHSC upon request.
8.1.4.7 Provider Hotline
The HMO must operate a toll-free telephone line for Provider inquiries from 8 a.m. to 5 p.m. local time for the Service Area, Monday through Friday, except for State-approved holidays. The Provider Hotline must be staffed with personnel who are knowledgeable about Covered Services and each applicable HMO Program, and for Medicaid, about Non-capitated Services.
The HMO must ensure that after regular business hours the line is answered by an automated system with the capability to provide callers with operating hours information and instructions on how to verify enrollment for a Member with an Urgent Condition or an Emergency Medical Condition. The HMO must have a process in place to handle after-hours inquiries from Providers seeking to verify enrollment for a Member with an Urgent Condition or an Emergency Medical Condition, provided, however, that the HMO and its Providers must not require such verification prior to providing Emergency Services.
The HMO must ensure that the Provider Hotline meets the following minimum performance requirements for all HMO Programs and Service Areas:
| | 1. 99% of calls are answered by the fourth ring or an automated call pick-up system is used; |
| | 2. no more than one percent of incoming calls receive a busy signal; |
| | 3. the average hold time is 2 minutes or less; and |
| | 4. the call abandonment rate is 7% or less. |
The HMO must conduct ongoing call quality assurance to ensure these standards are met. The Provider Hotline may serve multiple HMO Programs if Hotline staff is knowledgeable about all of the HMO’s Programs. The Provider Hotline may serve multiple Service Areas if the Hotline staff is knowledgeable about all such Service Areas, including the Provider Network in such Service Areas.
The HMO must monitor its performance regarding Provider Hotline standards and submit performance reports summarizing call center performance for the Hotline as indicated in Section
8.1.20. If the HMO subcontracts with a Behavioral Health Organization (BHO) that is responsible for Provider Hotline functions related to Behavioral Health Services, the BHO’s Provider Hotline must meet the requirements in Section 8.1.4.7.
If HHSC determines that it is necessary to conduct onsite monitoring of the HMO’s Provider Hotline functions, the HMO is responsible for all reasonable costs incurred by HHSC or its authorized agent(s) relating to such monitoring.
8.1.4.8 Provider Reimbursement
The HMO must make payment for all Medically Necessary Covered Services provided to all Members for whom the HMO is paid a capitation. A STAR+PLUS HMO must also make payment for all Functionally Necessary Covered Services provided to all Members for whom the HMO is paid a capitation. The HMO must ensure that claims payment is timely and accurate as described in Section 8.1.18.5. The HMO must require tax identification numbers from all participating Providers. The HMO is required to do back-up withholding from all payments to Providers who fail to give tax identification numbers or who give incorrect numbers.
8.1.4.9 Termination of Provider Contracts
Unless prohibited or limited by applicable law, at least 15 days prior to the effective date of the HMO’s termination of contract of any participating Provider the HMO must notify the HHSC Administrative Services Contractor and notify affected current Members in writing. Affected Members include all Members in a PCP’s panel and all Members who have been receiving ongoing care from the terminated Provider, where ongoing care is defined as two or more visits for home-based or office-based care in the past 12 months.
For the CHIP and CHIP Perinatal Programs, the HMO’s process for terminating Provider contracts must comply with the Texas Insurance Code and TDI regulations.
8.1.5 Member Services
The HMO must maintain a Member Services Department to assist Members and Members’ family members or guardians in obtaining Covered Services for Members. The HMO must maintain employment standards and requirements (e.g., education, training, and experience) for Member Services Department staff and provide a sufficient number of staff for the Member Services Department to meet the requirements of this Section, including Member Hotline response times, and Linguistic Access capabilities, see 8.1.5.6 Member Hotline Requirements.
8.1.5.1 Member Materials
The HMO must design, print and distribute Member identification (ID) cards and a Member Handbook to Members. Within five business days following the receipt of an Enrollment File from the HHSC Administrative Services Contractor, the HMO must mail a Member’s ID card and Member Handbook to the Case Head or Account Name for each new Member. When the Case Head or Account Name is on behalf of two or more new Members, the HMO is only required to send one Member Handbook. The HMO is responsible for mailing materials only to those Members for whom valid address data are contained in the Enrollment File.
The HMO must design, print and distribute a Provider Directory to the HHSC Administrative Services Contractor as described in Section 8.1.5.4.
Member materials must be at or below a 6th grade reading level as measured by the appropriate score on the Flesch reading ease test. Member materials must be available in English, Spanish, and the languages of other Major Population Groups making up 10% or more of the managed
care eligible population in the HMO’s Service Area, as specified by HHSC. HHSC will provide the HMO with reasonable notice when the enrolled population reaches 10% within the HMO’s Service Area. All Member materials must be available in a format accessible to the visually impaired, which may include large print, Braille, and audiotapes.
The HMO must submit member materials to HHSC for approval prior to use or mailing. HHSC will identify any required changes to the Member materials within 15 business days. If HHSC has not responded to the Contractor by the fifteenth day, the Contractor may proceed to use the submitted materials. HHSC reserves the right to require discontinuation of any Member materials that violate the terms of the Uniform Managed Care Terms and Conditions, including but not limited to “Marketing Policies and Procedures” as described in the Uniform Managed Care Manual.
8.1.5.2 Member Identification (ID) Card
All Member ID cards must, at a minimum, include the following information:
2. the Member’s Medicaid, CHIP or CHIP Perinatal Program number;
| | 3. the effective date of the PCP assignment (excluding CHIP Perinates); |
| | 4. the PCP’s name, address (optional for all products), and telephone number (excluding CHIP Perinates); |
| | 6. the 24-hour, seven (7) day a week toll-free Member services telephone number and BH Hotline number operated by the HMO; and |
| | 7. any other critical elements identified in the Uniform Managed Care Manual. |
The HMO must reissue the Member ID card if a Member reports a lost card, there is a Member name change, if the Member requests a new PCP, or for any other reason that results in a change to the information disclosed on the ID card. CHIP Perinatal HMOs must issue Member ID cards to both CHIP Perinates and CHIP Perinate Newborns.
8.1.5.3 Member Handbook
HHSC must approve the Member Handbook, and any substantive revisions, prior to publication and distribution. As described in Attachment B-1, Section 7, the HMO must develop and submit to HHSC the draft Member Handbook for approval during the Readiness Review and must submit a final Member Handbook incorporating changes required by HHSC prior to the Operational Start Date.
The Member Handbook for each applicable HMO Program must, at a minimum, meet the Member materials requirements specified by Section 8.1.5.1 above and must include critical elements in the Uniform Managed Care Manual. CHIP Perinatal HMOs must issue Member Handbooks to both CHIP Perinates and CHIP Perinate Newborns. The Member Handbook for CHIP Perinate Newborns may be the same as that used for CHIP.
The HMO must produce a revised Member Handbook, or an insert informing Members of changes to Covered Services upon HHSC notification and at least 30 days prior to the effective
date of such change in Covered Services. In addition to modifying the Member materials for new Members, the HMO must notify all existing Members of the Covered Services change during the time frame specified in this subsection.
8.1.5.4 Provider Directory
The Provider Directory for each applicable HMO Program, and any substantive revisions, must be approved by HHSC prior to publication and distribution. The HMO is responsible for submitting draft Provider directory updates to HHSC for prior review and approval if changes other than PCP information or clerical corrections are incorporated into the Provider Directory.
As described in Attachment B-1, Section 7, during the Readiness Review, the HMO must develop and submit to HHSC the draft Provider Directory template for approval and must submit a final Provider Directory incorporating changes required by HHSC prior to the Operational Start Date. Such draft and final Provider Directories must be submitted according to the deadlines established in Attachment B-1, Section 7.
The Provider Directory for each applicable HMO Program must, at a minimum, meet the Member Materials requirements specified by Section 8.1.5.1 above and must include critical elements in the Uniform Managed Care Manual. The Provider Directory must include only Network Providers credentialed by the HMO in accordance with Section 8.1.4.4. If the HMO contracts with limited Provider Networks, the Provider Directory must comply with the requirements of 28 T.A.C. §11.1600(b)(11), relating to the disclosure and notice of limited Provider Networks.
CHIP Perinatal HMOs must develop Provider Directories for both CHIP Perinates and CHIP Perinate Newborns. The Provider Directory for CHIP Perinate Newborns may be the same as that used for the CHIP Program.
The HMO must update the Provider Directory on a quarterly basis. The HMO must make such update available to existing Members on request, and must provide such update to the HHSC Administrative Services Contractor at the beginning of each state fiscal quarter. HHSC will consult with the HMOs and the HHSC Administrative Services Contractors to discuss methods for reducing the HMO’s administrative costs of producing new Provider Directories, including considering submission of new Provider Directories on a semi-annual rather than a quarterly basis if a HMO has not made major changes in its Provider Network, as determined by HHSC. HHSC will establish weight limits for the Provider Directories. Weight limits may vary by Service Area. HHSC will require HMOs that exceed the weight limits to compensate HHSC for postage fees in excess of the weight limits.
The HMO must send the most recent Provider Directory, including any updates, to Members upon request. The HMO must, at least annually, include written and verbal offers of such Provider Directory in its Member outreach and education materials.
8.1.5.5 Internet Website
The HMO must develop and maintain, consistent with HHSC standards and Section 843.2015 of the Texas Insurance Code and other applicable state laws, a website to provide general information about the HMO’s Program(s), its Provider Network, its customer services, and its Complaints and Appeals process. The HMO may develop a page within its existing website to meet the requirements of this section. The HMO must maintain a Provider Directory for its HMO Program on the MCO’s website. The HMO must ensure that Members have access to the most current and accurate information concerning the HMO’s Network Provider participation. To comply with this requirement, at least twice per month the HMO must update provider information in either: (1) its online Provider Directory, or (2) its online Provider search functionality, if applicab le. The online Provider Directory or online Provider search functionality must designate Providers with open versus closed panels. The online Provider Directory or online Provider search functionality must also identify Providers that provide Long-Term Services and Supports (LTSS). All HMOs must list Home Health Ancillary providers on their websites, with an indicator for Pediatric services if provided. The HMO’s website must comply with the Marketing Policies and Procedures for each applicable HHSC HMO Program.
The website’s HMO Program content must be:
| | 1. Written in Major Population Group languages (which under this contract include only English and Spanish); |
| | 2. Culturally appropriate; |
| | 3. Written for understanding at the 6th grade reading level; and |
| | 4. Be geared to the health needs of the enrolled HMO Program population. |
To minimize download and “wait times,” the website must avoid tools or techniques that require significant memory or disk resources or require special intervention on the customer side to install plug-ins or additional software. Use of proprietary items that would require a specific browser are not allowed. HHSC strongly encourages the use of tools that take advantage of efficient data access methods and reduce the load on the server or bandwidth.
8.1.5.6 Member Hotline
The HMO must operate a toll-free hotline that Members can call 24 hours a day, seven (7) days a week. The Member Hotline must be staffed with personnel who are knowledgeable about its HMO Program(s) and Covered Services, between the hours of 8:00 a.m. to 5:00 p.m. local time for the Service Area, Monday through Friday, excluding state-approved holidays.
The HMO must ensure that after hours, on weekends, and on holidays the Member Services Hotline is answered by an automated system with the capability to provide callers with operating hours and instructions on what to do in cases of emergency. All recordings must be in English and in Spanish. A voice mailbox must be available after hours for callers to leave messages. The HMO’s Member Services representatives must return member calls received by the automated system on the next working day.
If the Member Hotline does not have a voice-activated menu system, the HMO must have a menu system that will accommodate Members who cannot access the system through other physical means, such as pushing a button.
The HMO must ensure that its Member Service representatives treat all callers with dignity and respect the callers’ need for privacy. At a minimum, the HMO’s Member Service representatives must be:
| | 1. Knowledgeable about Covered Services; |
| | 2. Able to answer non-technical questions pertaining to the role of the PCP, as applicable; |
| | 3. Able to answer non-clinical questions pertaining to referrals or the process for receiving authorization for procedures or services; |
| | 4. Able to give information about Providers in a particular area; |
| | 5. Knowledgeable about Fraud, Abuse, and Waste and the requirements to report any conduct that, if substantiated, may constitute Fraud, Abuse, or Waste in the HMO Program; |
| | 6. Trained regarding Cultural Competency; |
| | 7. Trained regarding the process used to confirm the status of persons with Special Health Care Needs; |
| | 8. For Medicaid members, able to answer non-clinical questions pertaining to accessing Non-capitated Services. |
| | 9. For Medicaid Members, trained regarding: a) the emergency prescription process and what steps to take to immediately address problems when pharmacies do not provide a 72-hour supply of emergency medicines; and b) DME processes for obtaining services and how to address common problems. |
| | 10. For CHIP Members, able to give correct cost-sharing information relating to premiums, co-pays or deductibles, as applicable. (Cost-sharing does not apply to CHIP Perinates or CHIP Perinate Newborns.) |
Hotline services must meet Cultural Competency requirements and must appropriately handle calls from non-English speaking (and particularly, Spanish-speaking) callers, as well as calls from individuals who are deaf or hard-of-hearing. To meet these requirements, the HMO must employ bilingual Spanish-speaking Member Services representatives and must secure the services of other contractors as necessary to meet these requirements.
The HMO must process all incoming Member correspondence and telephone inquiries in a timely and responsive manner. The HMO cannot impose maximum call duration limits but must allow calls to be of sufficient length to ensure adequate information is provided to the Member. The HMO must ensure that the toll-free Member Hotline meets the following minimum performance requirements for all HMO Programs and Service Areas:
| | 1. 99% of calls are answered by the fourth ring or an automated call pick-up system; |
| | 2. no more than one percent (1%) of incoming calls receive a busy signal; |
| | 3. at least 80% of calls must be answered by toll-free line staff within 30 seconds measured from the time the call is placed in queue after selecting an option; |
| | 4. the call abandonment rate is 7% or less; and |
| | 5. the average hold time is 2 minutes or less. |
The HMO must conduct ongoing quality assurance to ensure these standards are met.
The Member Services Hotline may serve multiple HMO Programs if Hotline staff is knowledgeable about all of the HMO’s Medicaid and/or CHIP Programs. The Member Services Hotline may serve multiple Service Areas if the Hotline staff is knowledgeable about all such Service Areas, including the Provider Network in each Service Area.
The HMO must monitor its performance regarding HHSC Member Hotline standards and submit performance reports summarizing call center performance for the Member Hotline as indicated in Section 8.1.20 and the Uniform Managed Care Manual.
If HHSC determines that it is necessary to conduct onsite monitoring of the HMO’s Member Hotline functions, the HMO is responsible for all reasonable costs incurred by HHSC or its authorized agent(s) relating to such monitoring.
HMO is encouraged to train staff at its 24-hour nurse hotline about: a) emergency prescription process and what steps to take to immediately address Medicaid Members’ problems when pharmacies do not provide a 72-hour supply of emergency medicines; and b) DME processes for obtaining services and how to address common problems. The 24-hour nurse hotline will attempt to respond immediately to problems concerning emergency medicines by means at its disposal, including explaining the rules to Medicaid Members so that they understand their rights and, if need be, by offering to contact the pharmacy that is refusing to fill the prescription to explain the 72-hour supply policy and DME processes.
8.1.5.7 Member Education
The HMO must, at a minimum, develop and implement health education initiatives that educate Members about:
| | 1. How the HMO system operates, including the role of the PCP; |
| | 2. Covered Services, limitations and any Value-added Services offered by the HMO; |
| | 3. The value of screening and preventive care, and |
| | 4. How to obtain Covered Services, including: |
| | b. Accessing OB/GYN and specialty care; |
| | c. Behavioral Health Services; |
| | d. Disease Management programs; |
| | e. Service Coordination, treatment for pregnant women, Members with Special Health Care Needs, including Children with Special Health Care Needs; and other special populations; |
| | f. Early Childhood Intervention (ECI) Services; |
| | g. Screening and preventive services, including well-child care (Texas Health Steps medical checkups for Medicaid Members); |
| | h. For CHIP Members, Member co-payments |
| | j. Identification and health education related to Obesity; and |
| | k. Obtaining 72 hour supplies of emergency prescriptions from pharmacies enrolled with HHSC as Medicaid providers. |
The HMO must provide a range of health promotion and wellness information and activities for Members in formats that meet the needs of all Members. The HMO must propose, implement, and assess innovative Member education strategies for wellness care and immunization, as well as general health promotion and prevention. The HMO must conduct wellness promotion
programs to improve the health status of its Members. The HMO may cooperatively conduct health education classes for all enrolled Members with one or more HMOs also contracting with HHSC in the Service Area. The HMO must work with its Providers to integrate health education, wellness and prevention training into the care of each Member.
The HMO also must provide condition and disease-specific information and educational materials to Members, including information on its Service Management and Disease Management programs described in Section 8.1.13 and Section 8.1. Condition- and disease-specific information must be oriented to various groups within the managed care eligible population, such as children, the elderly, persons with disabilities and non-English speaking Members, as appropriate to the HMO’s Medicaid, CHIP and/or CHIP Perinatal Program(s).
8.1.5.8 Cultural Competency Plan
The HMO must have a comprehensive written Cultural Competency Plan describing how the HMO will ensure culturally competent services, and provide Linguistic Access and Disability-related Access. The Cultural Competency Plan must describe how the individuals and systems within the HMO will effectively provide services to people of all cultures, races, ethnic backgrounds, and religions as well as those with disabilities in a manner that recognizes, values, affirms, and respects the worth of the individuals and protects and preserves the dignity of each. The HMO must submit the Cultural Competency Plan to HHSC for Readiness Review. Modifications and amendments to the plan must be submitted to HHSC no later than 30 days prior to implementation. The Plan must also be made available to the HMO’s Network of Providers.
8.1.5.9 Member Complaint and Appeal Process
The HMO must develop, implement and maintain a system for tracking, resolving, and reporting Member Complaints regarding its services, processes, procedures, and staff. The HMO must ensure that Member Complaints are resolved within 30 calendar days after receipt. The HMO is subject to remedies, including liquidated damages, if at least 98 percent of Member Complaints are not resolved within 30 days of receipt of the Complaint by the HMO. Please see the Uniform Managed Care Contract Terms & Conditions and Attachment B-5, Deliverables/Liquidated Damages Matrix.
The HMO must develop, implement and maintain a system for tracking, resolving, and reporting Member Appeals regarding the denial or limited authorization of a requested service, including the type or level of service and the denial, in whole or in part, of payment for service. Within this process, the HMO must respond fully and completely to each Appeal and establish a tracking mechanism to document the status and final disposition of each Appeal.
The HMO must ensure that Member Appeals are resolved within 30 calendar days, unless the HMO can document that the Member requested an extension or the HMO shows there is a need for additional information and the delay is in the Member's interest. The HMO is subject to liquidated damages if at least 98 percent of Member Appeals are not resolved within 30 days of receipt of the Appeal by the HMO. Please see the Uniform Managed Care Contract Terms & Conditions and Attachment B-5, Deliverables/Liquidated Damages Matrix.
Medicaid HMOs must follow the Member Complaint and Appeal Process described in Section 8.2.6. CHIP and CHIP Perinatal HMOs must comply with the CHIP Complaint and Appeal Process described in Sections 8.4.2 and 8.5.2, respectively.
8.1.6 Marketing and Prohibited Practices
The HMO and its Subcontractors must adhere to the Marketing Policies and Procedures as set forth by HHSC in the Contract, and the HHSC Uniform Managed Care Manual.
8.1.7 Quality Assessment and Performance Improvement
The HMO must provide for the delivery of quality care with the primary goal of improving the health status of Members and, where the Member’s condition is not amenable to improvement, maintain the Member’s current health status by implementing measures to prevent any further decline in condition or deterioration of health status. The HMO must work in collaboration with Providers to actively improve the quality of care provided to Members, consistent with the Quality Improvement Goals and all other requirements of the Contract. The HMO must provide mechanisms for Members and Providers to offer input into the HMO’s quality improvement activities.
8.1.7.1 QAPI Program Overview
The HMO must develop, maintain, and operate a quality assessment and performance improvement (QAPI) Program consistent with the Contract, and TDI requirements, including 28 T.A.C. §11.1901(a)(5) and §11.1902. Medicaid HMOs must also meet the requirements of 42 C.F.R. §438.240.
The HMO must have on file with HHSC an approved plan describing its QAPI Program, including how the HMO will accomplish the activities required by this section. The HMO must submit a QAPI Program Annual Summary in a format and timeframe specified by HHSC or its designee. The HMO must keep participating physicians and other Network Providers informed about the QAPI Program and related activities. The HMO must include in Provider contracts a requirement securing cooperation with the QAPI.
The HMO must approach all clinical and non-clinical aspects of quality assessment and performance improvement based on principles of Continuous Quality Improvement (CQI)/Total Quality Management (TQM) and must:
| | 1. Evaluate performance using objective quality indicators; |
| | 2. Foster data-driven decision-making; |
| | 3. Recognize that opportunities for improvement are unlimited; |
| | 4. Solicit Member and Provider input on performance and QAPI activities; |
| | 5. Support continuous ongoing measurement of clinical and non-clinical effectiveness and Member satisfaction; |
| | 6. Support programmatic improvements of clinical and non-clinical processes based on findings from on-going measurements; and |
| | 7. Support re-measurement of effectiveness and Member satisfaction, and continued development and implementation of improvement interventions as appropriate. |
8.1.7.2 QAPI Program Structure
The HMO must maintain a well-defined QAPI structure that includes a planned systematic approach to improving clinical and non-clinical processes and outcomes. The HMO must designate a senior executive responsible for the QAPI Program and the Medical Director must have substantial involvement in QAPI Program activities. At a minimum, the HMO must ensure that the QAPI Program structure:
| | 1. Is organization-wide, with clear lines of accountability within the organization; |
| | 2. Includes a set of functions, roles, and responsibilities for the oversight of QAPI activities that are clearly defined and assigned to appropriate individuals, including physicians, other clinicians, and non-clinicians; |
| | 3. Includes annual objectives and/or goals for planned projects or activities including clinical and non-clinical programs or initiatives and measurement activities; and |
| | 4. Evaluates the effectiveness of clinical and non-clinical initiatives. |
8.1.7.3 Clinical Indicators
The HMO must engage in the collection of clinical indicator data. The HMO must use such clinical indicator data in the development, assessment, and modification of its QAPI Program.
8.1.7.4 QAPI Program Subcontracting
If the HMO subcontracts any of the essential functions or reporting requirements contained within the QAPI Program to another entity, the HMO must maintain a file of the subcontractors. The file must be available for review by HHSC or its designee upon request.
8.1.7.5 Behavioral Health Integration into QAPI Program
If the HMO provides Behavioral Health Services within the Covered Services as defined in Attachments B-2, B-2.1, and B-2.2, it must integrate behavioral health into its QAPI Program and include a systematic and on-going process for monitoring, evaluating, and improving the quality and appropriateness of Behavioral Health Services provided to Members. The HMO must collect data, and monitor and evaluate for improvements to physical health outcomes resulting from behavioral health integration into the Member’s overall care.
8.1.7.6 Clinical Practice Guidelines
The HMO must adopt not less than two evidence-based clinical practice guidelines for each applicable HMO Program. Such practice guidelines must be based on valid and reliable clinical evidence, consider the needs of the HMO’s Members, be adopted in consultation with contracting health care professionals, and be reviewed and updated periodically, as appropriate. The HMO must develop practice guidelines based on the health needs and opportunities for improvement identified as part of the QAPI Program.
The HMO may coordinate the development of clinical practice guidelines with other HHSC HMOs to avoid providers in a Service Area receiving conflicting practice guidelines from different HMOs.
The HMO must disseminate the practice guidelines to all affected Providers and, upon request, to Members and potential Members.
The HMO must take steps to encourage adoption of the guidelines, and to measure compliance with the guidelines, until such point that 90% or more of the Providers are consistently in compliance, based on HMO measurement findings. The HMO must employ substantive Provider motivational incentive strategies, such as financial and non-financial incentives, to improve Provider compliance with clinical practice guidelines. The HMO’s decisions regarding utilization management, Member education, coverage of services, and other areas included in the practice guidelines must be consistent with the HMO’s clinical practice guidelines.
8.1.7.7 Provider Profiling
The HMO must conduct PCP and other Provider profiling activities at least annually. As part of its QAPI Program, the HMO must describe the methodology it uses to identify which and how many Providers to profile and to identify measures to use for profiling such Providers.
Provider profiling activities must include, but not be limited to:
1. Developing PCP and Provider-specific reports that include a multi-dimensional assessment of a PCP or Provider’s performance using clinical, administrative, and Member satisfaction indicators of care that are accurate, measurable, and relevant to the enrolled population;
| 2. Establishing PCP, Provider, group, Service Area or regional Benchmarks for areas profiled, where applicable, including STAR, STAR+PLUS, CHIP and CHIP Perinatal Program-specific Benchmarks, where appropriate; and |
| 3. Providing feedback to individual PCPs and Providers regarding the results of their performance and the overall performance of the Provider Network. |
8.1.7.8 Network Management
The HMO must:
| | 1. Use the results of its Provider profiling activities to identify areas of improvement for individual PCPs and Providers, and/or groups of Providers; |
| | 2. Establish Provider-specific quality improvement goals for priority areas in which a Provider or Providers do not meet established HMO standards or improvement goals; |
| | 3. Develop and implement incentives, which may include financial and non-financial incentives, to motivate Providers to improve performance on profiled measures; and |
| | 4. At least annually, measure and report to HHSC on the Provider Network and individual Providers’ progress, or lack of progress, towards such improvement goals. |
8.1.7.9 Collaboration with the EQRO
The HMO will collaborate with HHSC’s external quality review organization (EQRO) to develop studies, surveys, or other analytical approaches that will be carried out by the EQRO. The purpose of the studies, surveys, or other analytical approaches is to assess the quality of care and service provided to Members and to identify opportunities for HMO improvement. To facilitate this process, the HMO will supply claims data to the EQRO in a format identified by HHSC in consultation with HMOs, and will supply medical records for focused clinical reviews conducted by the EQRO. The HMO must also work collaboratively with HHSC and the EQRO to annually measure selected HEDIS measures that require chart reviews. During the first year of operations, HHSC anticipates that the selected measures will include, at a minimum, well-child visits and im munizations, appropriate use of asthma medications, measures related to Members with diabetes, and control of high blood pressure.
8.1.8 Utilization Management
The HMO must have a written utilization management (UM) program description, which includes, at a minimum:
| | 1. Procedures to evaluate the need for Medically Necessary Covered Services; |
| | 2. The clinical review criteria used, the information sources, the process used to review and approve the provision of Covered Services; |
| | 3. The method for periodically reviewing and amending the UM clinical review criteria; and |
| | 4. The staff position functionally responsible for the day-to-day management of the UM function. |
The HMO must make best efforts to obtain all necessary information, including pertinent clinical information, and consult with the treating physician as appropriate in making UM determinations.
The HMO must issue coverage determinations, including adverse determinations, according to the following timelines:
| | • Within three (3) business days after receipt of the request for authorization of services; |
| | • Within one (1) business day for concurrent hospitalization decisions; and |
| | • Within one (1) hour for post-stabilization or life-threatening conditions, except that for Emergency Medical Conditions and Emergency Behavioral Health Conditions, the HMO must not require prior authorization. |
The HMO’s UM Program must include written policies and procedures to ensure:
| | 1. Consistent application of review criteria that are compatible with Members’ needs and situations; |
| | 2. Determinations to deny or limit services are made by physicians under the direction of the Medical Director; |
| | 3. Appropriate personnel are available to respond to utilization review inquiries 8:00 a.m. to 5:00 p.m., Monday through Friday, with a telephone system capable of accepting utilization review inquiries after normal business hours. The HMO must respond to calls within one business day; |
| | 4. Confidentiality of clinical information; and |
| | 5. Quality is not adversely impacted by financial and reimbursement-related processes and decisions. |
For HMOs with preauthorization or concurrent review programs, qualified medical professionals must supervise preauthorization and concurrent review decisions.
The HMO UM Program must include polices and procedures to:
| 1. Routinely assess the effectiveness and the efficiency of the UM Program; |
| 2. Evaluate the appropriate use of medical technologies, including medical procedures, drugs and devices; |
| 3. target areas of suspected inappropriate service utilization; |
| 4. Detect over- and under-utilization; |
| 5. Routinely generate Provider profiles regarding utilization patterns and compliance with utilization review criteria and policies; |
| 6. Compare Member and Provider utilization with norms for comparable individuals; |
| 7. Routinely monitor inpatient admissions, emergency room use, ancillary, and out-of-area services; |
8. Ensure that when Members are receiving Behavioral Health Services from the local mental health authority that the HMO is using the same UM guidelines as those prescribed for use by Local Mental Health Authorities by MHMR which are published at: http://www.mhmr.state.tx.us/centraloffice/behavioralhealthservices/RDMClinGuide.html; and
9. Refer suspected cases of provider or Member Fraud, Abuse, or Waste to the Office of Inspector General (OIG) as required by Section 8.1.19.
8.1.9 Early Childhood Intervention (ECI)
The HMO must ensure that Network Providers are educated regarding their responsibility under federal laws (e.g., 20 U.S.C. §1435 (a)(5); 34 C.F.R. §303.321(d)) to identify and refer any Member age three (3) or under suspected of having a developmental disability or delay, or who is at risk of delay, to the designated ECI program for screening and assessment within two (2) working days from the day the Provider identifies the Member. The HMO must use written educational materials developed or approved by the Department of Assistive and Rehabilitative Services – Division for Early Childhood Intervention Services for these “child find” activities. Eligibility for ECI services will be determined by the local ECI program using the criteria contained in 40 T.A.C. §108.25.
The HMO must contract with qualified ECI Providers to provide ECI services to Members under age three who have been determined eligible for ECI services. The HMO must permit Members to self refer to local ECI Service Providers without requiring a referral from the Member’s PCP. The HMO’s policies and procedures, including its Provider Manual, must include written policies and procedures for allowing such self-referral to ECI providers.
The HMO must coordinate and cooperate with local ECI programs in the development and implementation of the Individual Family Service Plan (IFSP), including on-going case management and other non-capitated services required by the Member’s IFSP. The IFSP is an agreement developed by the interdisciplinary team that consists of the ECI Case Manager/Service Coordinator, the Member/family, and other professionals who participated in the Member’s evaluation or are providing direct services to the Member, and may include the Member’s Primary Care Physician (PCP) with parental consent. The IFSP identifies the Member’s present level of development based on assessment, describes the services to be provided to the child to meet the needs of the child and the family, and identifies the person or persons responsible for each se rvice required by the plan. The IFSP shall be transmitted by the ECI Provider to the HMO and the PCP with parental consent to enhance coordination of the plan of care. The IFSP may be included in the Member’s medical record.
Cooperation with the ECI program includes covering medical diagnostic procedures and providing medical records required to perform developmental assessments and developing the IFSP within the 45-day timeline established in federal rule (34 C.F.R. §303.342(a)). The HMO must require compliance with these requirements through Provider contract provisions. The HMO must not withhold authorization for the provision of such medical diagnostic procedures. The HMO must promptly provide to the ECI program, relevant medical records available to the HMO.
The interdisciplinary team will determine Medical Necessity for health and Behavioral Health Services as approved by the Member’s PCP. The HMO must require, through contract provisions, that all Medically Necessary health and Behavioral Health Services contained in the Member’s IFSP are provided to the Member in the amount, duration, scope and service setting established by the IFSP. The HMO must allow services to be provided by a non-network provider if a Network Provider is not available to provide the services in the amount, duration, scope and service setting as required by the IFSP. The HMO cannot modify the plan of care or alter the amount, duration, scope, or service setting required by the Member’s IFSP. The HMO cannot create unnecessary barriers for the Member to obtain IFSP services, including requiring prior a uthorization for the ECI assessment or establishing insufficient authorization periods for prior authorized services.
8.1.10 Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) - Specific Requirements
The HMO must, by contract, require its Providers to coordinate with the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) to provide medical information necessary for WIC eligibility determinations, such as height, weight, hematocrit or hemoglobin. The HMO must make referrals to WIC for Members potentially eligible for WIC. The HMO may use the nutrition education provided by WIC to satisfy certain health education requirements of the Contract.
8.1.11 Coordination with Texas Department of Family and Protective Services
The HMO must cooperate and coordinate with the Texas Department of Family and Protective Services (TDFPS) (formerly the Department of Protective and Regulatory Services) for the care of a child who is receiving services from or has been placed in the conservatorship of TDFPS.
The HMO must comply with all provisions related to Covered Services, including Behavioral Health Services, in the following documents:
| | • A court order (Order) entered by a Court of Continuing Jurisdiction placing a child under the protective custody of TDFPS. |
| | • A TDFPS Service Plan entered by a Court of Continuing Jurisdiction placing a child under the protective custody of TDFPS. |
| | • A TDFPS Service Plan voluntarily entered into by the parents or person having legal custody of a Member and TDFPS. |
The HMO cannot deny, reduce, or controvert the Medical Necessity of any health or Behavioral Health Services included in an Order. The HMO may participate in the preparation of the medical and behavioral care plan prior to TDFPS submitting the health care plan to the Court. Any modification or termination of court-ordered services must be presented and approved by the court having jurisdiction over the matter.
A Member or the parent or guardian whose rights are subject to an Order or Service Plan cannot use the HMO’s Complaint or Appeal processes, or the HHSC Fair Hearing process to Appeal the necessity of the Covered Services.
The HMO must include information in its Provider Manuals and training materials regarding:
| | 1. Providing medical records to TDFPS; |
| | 2. Scheduling medical and Behavioral Health Services appointments within 14 days unless requested earlier by TDFPS; and |
| | 3. Recognition of abuse and neglect, and appropriate referral to TDFPS. |
The HMO must continue to provide all Covered Services to a Member receiving services from, or in the protective custody of, TDFPS until the Member has been;(1) disenrolled from the HMO due to loss of Medicaid managed care eligibility; or (2) enrolled in HHSC’s managed care program for children in foster care, once the program is implemented.
8.1.12 Services for People with Special Health Care Needs
This section applies to STAR, STAR+PLUS, and CHIP HMOs. It applies to CHIP Perinatal HMOs with respect to their Perinate Newborn Members only.
8.1.12.1 Identification
The HMO must develop and maintain a system and procedures for identifying Members with Special Health Care Needs (MSHCN), including people with disabilities or chronic or complex
medical and behavioral health conditions and Children with Special Health Care Needs (CSHCN)1.
The HMO must contact Members pre-screened by the HHSC Administrative Services Contractor as MSHCN to determine whether they meet the HMO’s MSHCN assessment criteria, and to determine whether the Member requires special services described in this section. The HMO must provide information to the HHSC Administrative Services Contractor that identifies Members who the HMO has assessed to be MSHCN, including any Members pre-screened by the HHSC Administrative Services Contractor and confirmed by the HMO as a MSHCN. The information must be provided, in a format and on a timeline to be specified by HHSC in the Uniform Managed Care Manual, and updated with newly identified MSHCN by the 10th day of each month. In the event that a MSHCN changes HMOs, the HMO must provide the receiving co ntractor information concerning the results of the HMO’s identification and assessment of that Member’s needs, to prevent duplication of those activities.
8.1.12.2 Access to Care and Service Management
Once identified, the HMO must have effective systems to ensure the provision of Covered Services to meet the special preventive, primary Acute Care, and specialty health care needs appropriate for treatment of the individual Member’s condition(s). All STAR+PLUS Members are considered to be MSHCN.
The HMO must provide access to identified PCPs and specialty care Providers with experience serving MSHCN. Such Providers must be board-qualified or board-eligible in their specialty. The HMO may request exceptions from HHSC for approval of traditional providers who are not board-qualified or board-eligible but who otherwise meet the HMO’s credentialing requirements.
For services to CSHCN, the HMO must have Network PCPs and specialty care Providers that have demonstrated experience with CSHCN in pediatric specialty centers such as children’s hospitals, teaching hospitals, and tertiary care centers.
The HMO is responsible for working with MSHCN, their families and legal guardians if applicable, and their health care providers to develop a seamless package of care in which primary, Acute Care, and specialty service needs are met through a Service Plan that is understandable to the Member, or, when applicable, the Member’s legal guardian.
The HMO is responsible for providing Service Management to develop a Service Plan and ensure MSHCN, including CSHCN, have access to treatment by a multidisciplinary team when the Member’s PCP determines the treatment is Medically Necessary, or to avoid separate and fragmented evaluations and service plans. The team must include both physician and non-
______________________
1 CSHCN is a term often used to refer to a services program for children with special health care needs administered by DSHS, and described in 25 TAC, Part 1, Section 38.1. Although children served through this program may also be served by Medicaid or CHIP, the reference to “CSHCN” in this Contract does not refer to children served through this program.
__________________________
physician providers determined to be necessary by the Member’s PCP for the comprehensive treatment of the Member. The team must:
| | 1. Participate in hospital discharge planning; |
| | 2. Participate in pre-admission hospital planning for non-emergency hospitalizations; |
| | 3. Develop specialty care and support service recommendations to be incorporated into the Service Plan; and |
| | 4. Provide information to the Member, or when applicable, the Member’s legal guardian concerning the specialty care recommendations. |
MSHCN, their families, or their health providers may request Service Management from the HMO. The HMO must make an assessment of whether Service Management is needed and furnish Service Management when appropriate. The HMO may also recommend to a MSHCN, or to a CSHCN’s family, that Service Management be furnished if the HMO determines that Service Management would benefit the Member.
The HMO must provide information and education in its Member Handbook and Provider Manual about the care and treatment available in the HMO’s plan for Members with Special Health Care Needs, including the availability of Service Management.
The HMO must have a mechanism in place to allow Members with Special Health Care Needs to have direct access to a specialist as appropriate for the Member’s condition and identified needs, such as a standing referral to a specialty physician. The HMO must also provide MSHCN with access to non-primary care physician specialists as PCPs, as required by 28 T.A.C. §11.900 and Section 8.1.
The HMO must implement a systematic process to coordinate Non-capitated Services, and enlist the involvement of community organizations that may not be providing Covered Services but are otherwise important to the health and wellbeing of Members. The HMO also must make a best effort to establish relationships with State and local programs and community organizations, such as those listed below, in order to make referrals for MSHCN and other Members who need community services:
| | • Community Resource Coordination Groups (CRCGs); |
| | • Early Childhood Intervention (ECI) Program; |
| | • Local school districts (Special Education); |
| | • Health and Human Services Commission’s Medical Transportation Program (MTP); |
| | • Texas Department of Assistive and Rehabilitative Services (DARS) Blind Children’s Vocational Discovery and Development Program; |
| | • Texas Department of State Health (DSHS) services, including community mental health programs, and Title V Maternal and Child Health and Children with Special Health Care Needs (CSHCN) Programs; |
| | • Other state and local agencies and programs such as food stamps, and the Women, Infants, and Children’s (WIC) Program; |
| | • Civic and religious organizations and consumer and advocacy groups, such as United Cerebral Palsy, which also work on behalf of the MSHCN population. |
8.1.13 Service Management for Certain Populations
The HMO must have service management programs and procedures for the following populations, as applicable to the HMO’s Medicaid and/or CHIP Program(s) (See CHIP Perinatal Program Covered Services, Attachment B-2.2, for the applicability of these services to the CHIP Perinatal Program):
| | 1. High-cost catastrophic cases; |
| | 2. Women with high-risk pregnancies (STAR and STAR+PLUS Programs only); |
| | 3. Individuals with mental illness and co-occurring substance abuse; and |
| | 4. FWC (STAR and STAR+PLUS Programs only). |
8.1.14 Disease Management (DM)
The HMO must provide, or arrange to have provided to Members, comprehensive disease management services consistent with state statutes and regulations. Such DM services must be part of person-based approach to DM and holistically address the needs of persons with multiple chronic conditions. The HMO must develop and implement DM services that relate to chronic conditions that are prevalent in HMO Program Members. HMOs must have DM Programs that address chronic conditions identified in HHSC’sUniform Managed Care Manual. HHSC will not identify individual Members with chronic conditions. The HMO must implement policies and procedures to ensure that Members that require DM services are identified and enrolled in a program to provide such DM services. The HMO must develop and mainta in screening and evaluation procedures for the early detection, prevention, treatment, or referral of participants at risk for or diagnosed with the chronic conditions identified in the Uniform Managed Care Manual. The HMO must ensure that all Members identified for DM are enrolled into a DM Program with the opportunity to opt out of these services within 30 days while still maintaining access to all other Covered Services.
For all new Members not previously enrolled in the HMO and who require DM services, the HMO must evaluate and ensure continuity of care with any previous DM services in accordance with the requirements in the Uniform Managed Care Manual.
The DM Program(s) must include:
| | 1. Patient self-management education; |
| | 3. Evidence-based models and minimum standards of care; |
| | 4. Standardized protocols and participation criteria; |
| | 5. Physician-directed or physician-supervised care; |
| | 6. Implementation of interventions that address the continuum of care; |
| | 7. Mechanisms to modify or change interventions that are not proven effective; and |
| | 8. Mechanisms to monitor the impact of the DM Program over time, including both the clinical and the financial impact. |
The HMO must maintain a system to track and monitor all DM participants for clinical, utilization, and cost measures.
The HMO must provide designated staff to implement and maintain DM Programs and to assist participating Members in accessing DM services. The HMO must educate Members and Providers about the HMO’s DM Programs and activities. Additional requirements related to the HMO’s Disease Management Programs and activities are found in the HHSC Uniform Managed Care Manual.
8.1.14.1 DM Services and Participating Providers
At a minimum, the HMO must:
| | 1. Implement a system for Providers to request specific DM interventions; |
| | 2. Give Providers information, including differences between recommended prevention and treatment and actual care received by Members enrolled in a DM Program, and information concerning such Members’ adherence to a service plan; and |
| | 3. For Members enrolled in a DM Program, provide reports on changes in a Member’s health status to their PCP. |
8.1.14.2 HMO DM Evaluation
HHSC or its EQRO will evaluate the HMO’s DM Program.
8.1.15 Behavioral Health (BH) Network and Services
The requirements in this sub-section pertain to all HMOs except: (1) the STAR HMOs in the Dallas CSA, whose Members receive Behavioral Health Services through the NorthSTAR Program, and (2) the CHIP Perinatal Program HMOs with respect to their Perinate Members.
The HMO must provide, or arrange to have provided, to Members all Medically Necessary Behavioral Health (BH) Services as described in Attachments B-2, B-2.1, and B-2.2. All BH Services must be provided in conformance with the access standards included in Section 8.1.3. For Medicaid HMOs, BH Services are described in more detail in the Texas Medicaid Provider Procedures Manual and the Texas Medicaid Bulletins. When assessing Members for BH Services, the HMO and its Network Behavioral Health Service Providers must use the DSM-IV multi-axial classification. HHSC may require use of other assessment instrument/outcome measu res in addition to the DSM-IV. Providers must document DSM-IV and assessment/outcome information in the Member’s medical record.
8.1.15.1 BH Provider Network
The HMO must maintain a Behavioral Health Services Provider Network that includes psychiatrists, psychologists, and other Behavioral Health Service Providers. The Provider Network must include Behavioral Health Service Providers with experience serving special populations among the HMO Program(s)’ enrolled population, including, as applicable, children and adolescents, persons with disabilities, the elderly, and cultural or linguistic minorities, to ensure accessibility and availability of qualified Providers to all Members in the Service Area.
8.1.15.2 Member Education and Self-referral for Behavioral Health Services
The HMO must maintain a Member education process to help Members know where and how to obtain Behavioral Health Services.
The HMO must permit Members to self refer to any in-network Behavioral Health Services Provider without a referral from the Member’s PCP. The HMOs’ policies and procedures, including its Provider Manual, must include written policies and procedures for allowing such self- referral to BH services.
The HMO must permit Members to participate in the selection of the appropriate behavioral health individual practitioner(s) who will serve them and must provide the Member with information on accessible in-network Providers with relevant experience.
8.1.15.3 Behavioral Health Services Hotline
This Section includes Hotline functions pertaining to Members. Requirements for Provider Hotlines are found in Section 8.1.4.7. The HMO must have an emergency and crisis Behavioral Health Services Hotline staffed by trained personnel 24 hours a day, 7 days a week, toll-free throughout the Service Area. Crisis hotline staff must include or have access to qualified Behavioral Health Services professionals to assess behavioral health emergencies. Emergency and crisis Behavioral Health Services may be arranged through mobile crisis teams. It is not acceptable for an emergency intake line to be answered by an answering machine.
The HMO must operate a toll-free hotline as described in Section 8.1.5.6 to handle Behavioral Health-related calls. The HMO may operate one hotline to handle emergency and crisis calls and routine Member calls. The HMO cannot impose maximum call duration limits and must allow calls to be of sufficient length to ensure adequate information is provided to the Member. Hotline services must meet Cultural Competency requirements and provide linguistic access to all Members, including the interpretive services required for effective communication.
The Behavioral Health Services Hotline may serve multiple HMO Programs if the Hotline staff is knowledgeable about all of the HMO Programs. The Behavioral Health Services Hotline may serve multiple Service Areas if the Hotline staff is knowledgeable about all such Service Areas, including the Behavioral Health Provider Network in each Service Area. The HMO must ensure that the toll-free Behavioral Health Services Hotline meets the following minimum performance requirements for all HMO Programs and Service Areas:
| | 1. 99% of calls are answered by the fourth ring or an automated call pick-up system; |
| | 2. no incoming calls receive a busy signal; |
| | 3. at least 80% of calls must be answered by toll-free line staff within 30 seconds measured from the time the call is placed in queue after selecting an option; |
| | 4. the call abandonment rate is 7% or less; and |
| | 5. the average hold time is 2 minutes or less. |
The HMO must conduct on-going quality assurance to ensure these standards are met.
The HMO must monitor the HMO’s performance against the Behavioral Health Services Hotline standards and submit performance reports summarizing call center performance as indicated in Section 8.1.20 and the Uniform Managed Care Manual.
If HHSC determines that it is necessary to conduct onsite monitoring of the HMO’s Behavioral Health Services Hotline functions, the HMO is responsible for all reasonable costs incurred by HHSC or its authorized agent(s) relating to such monitoring.
8.1.15.4 Coordination between the BH Provider and the PCP
The HMO must require, through contract provisions, that PCPs have screening and evaluation procedures for the detection and treatment of, or referral for, any known or suspected behavioral health problems and disorders. PCPs may provide any clinically appropriate Behavioral Health Services within the scope of their practice.
The HMO must provide training to network PCPs on how to screen for and identify behavioral health disorders, the HMO’s referral process for Behavioral Health Services and clinical coordination requirements for such services. The HMO must include training on coordination and quality of care such as behavioral health screening techniques for PCPs and new models of behavioral health interventions.
The HMO shall develop and disseminate policies regarding clinical coordination between Behavioral Health Service Providers and PCPs. The HMO must require that Behavioral Health Service Providers refer Members with known or suspected and untreated physical health problems or disorders to their PCP for examination and treatment, with the Member’s or the Member’s legal guardian’s consent. Behavioral Health Providers may only provide physical health care services if they are licensed to do so. This requirement must be specified in all Provider Manuals.
The HMO must require that behavioral health Providers send initial and quarterly (or more frequently if clinically indicated) summary reports of a Members’ behavioral health status to the PCP, with the Member’s or the Member’s legal guardian’s consent. This requirement must be specified in all Provider Manuals.
8.1.15.5 Follow-up after Hospitalization for Behavioral Health Services
The HMO must require, through Provider contract provisions, that all Members receiving inpatient psychiatric services are scheduled for outpatient follow-up and/or continuing treatment prior to discharge. The outpatient treatment must occur within seven (7) days from the date of discharge. The HMO must ensure that Behavioral Health Service Providers contact Members who have missed appointments within 24 hours to reschedule appointments.
8.1.15.6 Chemical Dependency
The HMO must comply with 28 T.A.C. §3.8001 et seq., regarding utilization review for Chemical Dependency Treatment. Chemical Dependency Treatment must conform to the standards set forth in 28 T.A.C. Part 1, Chapter 3, Subchapter HH.
8.1.15.7 Court-Ordered Services
“Court-Ordered Commitment” means a commitment of a Member to a psychiatric facility for treatment that is ordered by a court of law pursuant to the Texas Health and Safety Code, Title VII, Subtitle C.
The HMO must provide inpatient psychiatric services to Members under the age of 21, up to the annual limit, who have been ordered to receive the services by a court of competent jurisdiction under the provisions of Chapters 573 and 574 of the Texas Health and Safety Code, relating to Court-Ordered Commitments to psychiatric facilities. The HMO is not obligated to cover placements as a condition of probation, authorized by the Texas Family Code.
The HMO cannot deny, reduce or controvert the Medical Necessity of inpatient psychiatric services provided pursuant to a Court-ordered Commitment for Members under age 21. Any modification or termination of services must be presented to the court with jurisdiction over the matter for determination.
A Member who has been ordered to receive treatment under the provisions of Chapter 573 or 574 of the Texas Health and Safety Code can only Appeal the commitment through the court system.
8.1.15.8 Local Mental Health Authority (LMHA)
The HMO must coordinate with the Local Mental Health Authority (LMHA) and state psychiatric facility regarding admission and discharge planning, treatment objectives and projected length of stay for Members committed by a court of law to the state psychiatric facility.
Medicaid HMOs are required to comply with additional Behavioral Health Services requirements relating to coordination with the LMHA and care for special populations. These Medicaid HMO requirements are described in Section 8.2.8.
8.1.16 Financial Requirements for Covered Services
The HMO must pay for or reimburse Providers for all Medically Necessary Covered Services provided to all Members. The HMO is not liable for cost incurred in connection with health care rendered prior to the date of the Member’s Effective Date of Coverage in that HMO. A Member may receive collateral health benefits under a different type of insurance such as workers compensation or personal injury protection under an automobile policy. If a Member is entitled to coverage for specific services payable under another insurance plan and the HMO paid for such Covered Services, the HMO may obtain reimbursement from the responsible insurance entity not to exceed 100% of the value of Covered Services paid.
8.1.17 Accounting and Financial Reporting Requirements
The HMO’s accounting records and supporting information related to all aspects of the Contract must be accumulated in accordance with Federal Acquisition Regulations (“FAR”), Generally Accepted Accounting Principles (GAAP), and the cost principles contained in the Cost Principles
Document in the Uniform Managed Care Manual. The State will not recognize or pay services that cannot be properly substantiated by the HMO and verified by HHSC.
The HMO must:
| | 1. Maintain accounting records for each applicable HMO Program separate and apart from other corporate accounting records; |
| | 2. Maintain records for all claims payments, refunds and adjustment payments to providers, capitation payments, interest income and payments for administrative services or functions and must maintain separate records for medical and administrative fees, charges, and payments; |
| | 3. Maintain an accounting system that provides an audit trail containing sufficient financial documentation to allow for the reconciliation of billings, reports, and financial statements with all general ledger accounts; and |
| | 4. Within 60 days after Contract execution, submit an accounting policy manual that includes all proposed policies and procedures the HMO will follow during the duration of the Contract. Substantive modifications to the accounting policy manual must be approved by HHSC. |
The HMO agrees to pay for all reasonable costs incurred by HHSC to perform an examination, review or audit of the HMO’s books pertaining to the Contract.
8.1.17.1 General Access to Accounting Records
The HMO must provide authorized representatives of the Texas and federal government full access to all financial and accounting records related to the performance of the Contract.
The HMO must:
| | 1. Cooperate with the State and federal governments in their evaluation, inspection, audit, and/or review of accounting records and any necessary supporting information; |
| | 2. Permit authorized representatives of the State and federal governments full access, during normal business hours, to the accounting records that the State and the Federal government determine are relevant to the Contract. Such access is guaranteed at all times during the performance and retention period of the Contract, and will include both announced and unannounced inspections, on-site audits, and the review, analysis, and reproduction of reports produced by the HMO; |
| | 3. Make copies of any accounting records or supporting documentation relevant to the Contract, including Network Provider agreements, available to HHSC or its agents within seven (7) Business Days, or as otherwise specified by HHSC, of receiving a written request from HHSC for specified records or information. If such documentation is not made available as requested, the HMO agrees to reimburse HHSC for all costs, including, but not limited to, transportation, lodging, and subsistence for all State and federal representatives, or their agents, to carry out their inspection, audit, review, analysis, and reproduction functions at the location(s) of such accounting records; and |
| | 4. Pay any and all additional costs incurred by the State and federal government that are the result of the HMO’s failure to provide the requested accounting records or financial |
| | information within ten (10) business days of receiving a written request from the State or federal government. |
8.1.17.2 Financial Reporting Requirements
HHSC will require the HMO to provide financial reports by HMO Program and by Service Area to support Contract monitoring as well as State and Federal reporting requirements. HHSC will consult with HMOs regarding the format and frequency of such reporting. All financial information and reports that are not Member-specific are property of HHSC and will be public record. Any deliverable or report in Section 8.1.17.2 without a specified due date is due quarterly on the last day of the month. Where the due date states 30 days, the HMO is to provide the deliverable by the last day of the month following the end of the reporting period. Where the due date states 45 days, the HMO is to provide the deliverable by the 15th day of the second month following the end of the reporting period.
CHIP Perinatal Program data must be reported, and the data will be integrated into existing CHIP Program financial reports. Except for the Financial Statistical Report, no separate CHIP Perinatal Program reports are required. For all other CHIP financial reports, where appropriate, HHSC will designate specific attributes within the CHIP Program financial reports that the CHIP Perinatal HMOs must complete to allow HHSC to extract financial data particular to the CHIP Perinatal Program.
HHSC’s Uniform Managed Care Manual will govern the timing, format and content for the following reports.
(a) Audited Financial Statement –The HMO must provide the annual audited financial statement, for each year covered under the Contract, no later than June 30. The HMO must provide the most recent annual financial statements, as required by the Texas Department of Insurance for each year covered under the Contract, no later than March 1.
(b) Affiliate Report – The HMO must submit an Affiliate Report to HHSC if this information has changed since the last report submission. The report must contain the following:
| | 1. A list of all Affiliates, and |
| | 2. For HHSC’s prior review and approval, a schedule of all transactions with Affiliates that, under the provisions of the Contract, will be allowable as expenses in the FSR Report for services provided to the HMO by the Affiliate. Those should include financial terms, a detailed description of the services to be provided, and an estimated amount that will be incurred by the HMO for such services during the Contract Period. |
(c) BSP Report - The Medicaid HMOs must submit a monthly Bariatric Supplemental Payment (BSP) Report that includes the data elements specified in the Uniform Managed Care Manual. The BSP Report must include only bariatric surgeries that meet all of the following requirements:
| | • unduplicated reports of bariatric surgeries; |
| | • bariatric surgeries that the HMO has paid under the group of procedure codes defined as allowable for bariatric reimbursement, as designated in the “Texas Medicaid Providers Procedures Manual”, including the Texas Medicaid Bulletins; and |
| | • bariatric surgeries that were performed no earlier than 210 days prior to the date HHSC receives the Report, or that were included in the Report within thirty days from the date of discharge from the hospital for the stay related to the bariatric surgery, whichever is later. If a medical service provider does not submit a claim to the HMO by the deadline described herein, the HMO may request and exception to include the claim in the BSP report. HHSC may, at its sole discretion, grant or deny the request. |
(d) Employee Bonus and/or Incentive Payment Plan – If a HMO intends to include Employee Bonus or Incentive Payments as allowable administrative expenses, the HMO must furnish a written Employee Bonus and/or Incentive Payments Plan to HHSC so it may determine whether such payments are allowable administrative expenses in accordance with Cost Principles Document in the Uniform Managed Care Manual. The written plan must include a description of the HMO’s criteria for establishing bonus and/or incentive payments, the methodology to calculate bonus and/or incentive payments, and the timing of bonus and/or incentive payments. The Bonus and/or Incentive Payment Plan and description must be submitted to HHSC for approval no later than 30 days after the Effective Date of the Contract and any Contract renewal. If the HMO substantively revises the Employee Bonus and/or Incentive Payment Plan, the HMO must submit the revised plan to HHSC for prior review and approval.
(e) Claims Lag Report - The HMO must submit Claims Lag Report as a Contract year-to-date report. The report must be submitted quarterly by the last day of the month following the reporting period. The report must be submitted to HHSC in a format specified by HHSC. The report format is contained in the Uniform Managed Care Manual Chapter 5, Section 5.6.2. The report must disclose the amount of incurred claims each month and the amount paid each month.
(f) DSP Report - The HMO must submit a monthly Delivery Supplemental Payment (DSP) Report that includes the data elements specified by HHSC in the format specified by HHSC. HHSC will consult with contracted HMOs prior to revising the DSP Report data elements and requirements. The DSP Report must include only unduplicated deliveries and only deliveries for which the HMO has made a payment, to either a hospital or other provider.
(g) Financial Disclosure Report - The HMO must file:
| | 1. a Financial Disclosure Report prior to the start of Operations; |
| | 2. an updated Financial Disclosure Report no later than 30 days after the end of each Contract Year; and |
| | 3. a “change notification” abbreviated version of the report, no later than 30 days after any of the following events: |
| | a. entering into, renewing, modifying, or terminating a relationship with an affiliated party; |
| | b. after any change in control, ownership, or affiliations; or, |
| | c. after any material change in, or need for addition to, the information previously disclosed. |
The Financial Disclosure Report will include, at a minimum, a listing of the HMO’s control, ownership, and any affiliations, and information regarding Affiliate transactions. This report will replace, and be in lieu of, the former “Section 1318 Financial Disclosure Report” and the “Form CMS 1513,” and will disclose the same information, plus other information as may be required by HHSC and/or CMS Program Integrity requirements. Minor quarterly adjustments in stock holdings for publicly-traded corporations are excluded from the reporting requirements. The reporting format will be included in the Uniform Managed Care Manual. Until the reporting format is included in the Uniform Managed Care Manual, the HMO will continue to report the information described herein on CMS 1513 form.
(h) FSR Reports – The HMO must file quarterly and annual Financial-Statistical Reports (FSR) in the format and timeframe specified by HHSC. HHSC will include FSR format and directions in the Uniform Managed Care Manual. The HMO must incorporate financial and statistical data of delegated networks (e.g., IPAs, ANHCs, Limited Provider Networks), if any, in its FSR Reports. Administrative expenses reported in the FSRs must be reported in accordance with the Cost Principles Document in the Uniform Managed Care Manual. Quarterly FSR reports are due no later than 30 days after the end of the quarter and must provide information for the current quarter and year-to-date infor mation through the current quarter. The first annual FSR report must reflect expenses incurred through the 90th day after the end of the fiscal year. The first annual report must be filed on or before the 120th day after the end of each fiscal year. Subsequent annual reports must reflect data completed through the 334th day after the end of each fiscal year and must be filed on or before the 365th day following the end of each fiscal year.
HHSC will post all FSRs on the HHSC website.
CHIP Perinatal HMOs are required to submit separate FSRs for the CHIP Perinatal Program following the instructions outlined above and in the Uniform Managed Care Manual.
(i) HUB Reports – Upon contract award, the HMO must attend a post award meeting in Austin, Texas, at a time specified by HHSC, to discuss the development and submission of a Client Services HUB Subcontracting Plan for inclusion and the HMO’s good faith efforts to notify HUBs of subcontracting opportunities. The HMO must maintain its HUB Subcontracting Plan and submit monthly reports documenting the HMO’s Historically Underutilized Business (HUB) program efforts and accomplishments to the HHSC HUB Office. The report must include a narrative description of the HMO’s program efforts and a financial report reflecting payments made to HUBs. HMOs must use the formats included in HHSC’s Uniform Managed Care Manua l for the HUB monthly reports. The HMO must comply with HHSC’s standard Client Services HUB Subcontracting Plan requirements for all subcontractors.
(j) IBNR Plan - The HMO must furnish a written IBNR Plan to manage incurred-but-not-reported (IBNR) expenses, and a description of the method of insuring against insolvency, including information on all existing or proposed insurance policies. The Plan must include the methodology for estimating IBNR. The plan and description must be submitted to HHSC no later than 60 days after the Effective Date of the Contract. Substantive changes to a HMO’s IBNR plan and description must be submitted to HHSC no later than 30 days before the HMO implements changes to the IBNR plan.
(k) Medicaid Disproportionate Share Hospital (DSH) Reports – Medicaid HMOs must file preliminary and final Medicaid DSH reports, required by HHSC to identify and reimburse hospitals that qualify for Medicaid DSH funds. The preliminary and final DSH reports must include the data elements and be submitted in the form and format specified by HHSC in the Uniform Managed Care Manual. The preliminary DSH reports are due on or before March 1 of the year following the federal fiscal reporting year. The final DSH reports are due no later than April 1 of the year following the federal fiscal reporting year. This reporting requirement does not apply to CHIP or CHIP Perinatal Program HMOs.
(l) Out-of-Network Utilization Reports – The HMO must file quarterly Out-of Network Utilization Reports in the format and timeframe specified by HHSC. HHSC will include the report format and directions in the Uniform Managed Care Manual. Quarterly reports are due 30 days after the end of each quarter.
(m)TDI Examination Report - The HMO must furnish a copy of any TDI Examination Report, including the financial, market conduct, target exam, quality of care components, and corrective action plans and responses, no later than 10 days after receipt of the final report from TDI.
(n) TDI Filings – The HMO must submit annual figures for controlled risk-based capital, as well as its quarterly financial statements, both as required by TDI.
(o) Registration Statement (also known as the “Form B”) - If the HMO is a part of an insurance holding company system, the HMO must submit to HHSC a complete registration statement, also known as Form B, and all amendments to this form, and any other information filed by such insurer with the insurance regulatory authority of its domiciliary jurisdiction.
(p) Third Party Recovery (TPR) Reports - The HMO must file TPR Reports in accordance with the format developed by HHSC in the Uniform Managed Care Manual. HHSC will require the HMO to submit TPR reports no more often than quarterly. TPR reports must include total dollars recovered from third party payers for each HMO Program for services to the HMO’s Members, and the total dollars recovered through coordination of benefits, subrogation, and worker’s compensation.
8.1.18 Management Information System Requirements
The HMO must maintain a Management Information System (MIS) that supports all functions of the HMO’s processes and procedures for the flow and use of HMO data. The HMO must have hardware, software, and a network and communications system with the capability and capacity to handle and operate all MIS subsystems for the following operational and administrative areas:
| | 1. Enrollment/Eligibility Subsystem; |
| | 3. Encounter/Claims Processing Subsystem; |
| | 5. Utilization/Quality Improvement Subsystem; |
| | 7. Interface Subsystem; and |
| | 8. TPR Subsystem, as applicable to each HMO Program. |
The MIS must enable the HMO to meet the Contract requirements, including all applicable state and federal laws, rules, and regulations. The MIS must have the capacity and capability to capture and utilize various data elements required for HMO administration.
HHSC will provide the HMO with pharmacy data on the HMO’s Members on a weekly basis through the HHSC Vendor Drug Program, or should these services be outsourced, through the Pharmacy Benefit Manager. HHSC will provide a sample format of pharmacy data to contract awardees.
The HMO must have a system that can be adapted to changes in Business Practices/Policies within the timeframes negotiated by the Parties. The HMO is expected to cover the cost of such systems modifications over the life of the Contract.
The HMO is required to participate in the HHSC Systems Work Group.
The HMO must provide HHSC prior written notice of major systems changes and implementations, no later than 180 days prior to the planned change or implementation, including any changes relating to Material Subcontractors, in accordance with the requirements of this Contract and the Uniform Managed Care Terms and Conditions. HHSC retains the right to modify or waive the notification requirement contingent upon the nature of the request from the HMO.
The HMO must provide HHSC any updates to the HMO’s organizational chart relating to MIS and the description of MIS responsibilities at least 30 days prior to the effective date of the change. The HMO must provide HHSC official points of contact for MIS issues on an on-going basis.
HHSC, or its agent, may conduct a Systems Readiness Review to validate the HMO’s ability to meet the MIS requirements as described in Attachment B-1, Section 7. The System Readiness Review may include a desk review and/or an onsite review and must be conducted for the following events:
| | 1. A new plan is brought into the HMO Program; |
| | 2. An existing plan begins business in a new Service Area; |
| | 3. An existing plan changes location; |
| | 4. An existing plan changes its processing system, including changes in Material Subcontractors performing MIS or claims processing functions; and |
| | 5. An existing plan in one or two HHSC HMO Programs is initiating a Contract to participate in any additional HMO Programs. |
If HHSC determines that it is necessary to conduct an onsite review, the HMO is responsible for all reasonable travel costs associated with such onsite reviews. For purposes of this section, “reasonable travel costs” include airfare, lodging, meals, car rental and fuel, taxi, mileage, parking, and other incidental travel expenses incurred by HHSC or its authorized agent in
connection with the onsite reviews. This provision does not limit HHSC’s ability to collect other costs as damages in accordance with Attachment A, Section 12.02(e), “Damages.”
If for any reason, a HMO does not fully meet the MIS requirements, then the HMO must, upon request by HHSC, either correct such deficiency or submit to HHSC a Corrective Action Plan and Risk Mitigation Plan to address such deficiency as requested by HHSC. Immediately upon identifying a deficiency, HHSC may impose remedies and either actual or liquidated damages according to the severity of the deficiency. HHSC may also freeze enrollment into the HMO’s plan for any of its HMO Programs until such deficiency is corrected. Refer to Attachment A, Article 12 and Attachment B-5 for additional information regarding remedies and damages. Refer to Attachment B-1, Section 7 and Attachment B-1, Section 8.1.1.2 for additional information regarding HMO Readiness Reviews. Refer to Attachment A, Section 4.08(c) for information regarding Readiness Reviews of the HMO’s Material Subcontractors.
8.1.18.1 Encounter Data
The HMO must provide complete Encounter Data for all Covered Services, including Value-added Services. Encounter Data must follow the format, and data elements as described in the HIPAA-compliant 837 format. HHSC will specify the method of transmission, the submission schedule, and any other requirements in the Uniform Managed Care Manual. The HMO must submit Encounter Data transmissions monthly, and include all Encounter Data and Encounter Data adjustments processed by the HMO. Encounter Data quality validation must incorporate assessment standards developed jointly by the HMO and HHSC. The HMO must submit complete and accurate encounter data not later than the 30th calendar day after the last day of the month in which the claim was adjudicated. The HMO must make original records available for inspection by HHSC for validation purposes. Encounter Data that do not meet quality standards must be corrected and returned within a time period specified by HHSC.
In addition to providing Encounter Data in the 837 format described above, HMOs may be requested to submit an Encounter Data file to HHSC's EQRO, in the format provided in the Uniform Managed Care Manual. This additional submission requirement is time-limited and may not be required for the entire term of the Contract.
For reporting Encounters and fee-for-service claims to HHSC, the HMO must use the procedure codes, diagnosis codes, and other codes as directed by HHSC. Any exceptions will be considered on a code-by-code basis after HHSC receives written notice from the HMO requesting an exception. The HMO must also use the provider numbers as directed by HHSC for both Encounter and fee-for-service claims submissions, as applicable.
8.1.18.2 HMO Deliverables related to MIS Requirements
At the beginning of each state fiscal year, the HMO must submit the following documents and corresponding checklists for HHSC’s review and approval:
1. Disaster Recovery Plan;*
2. Business Continuity Plan;* and
3. Security Plan
* The Business Continuity Plan and the Disaster Recovery Plan may be combined into one document.
Additionally, at the beginning of each state fiscal year, if the HMO modifies the following documents, it must submit the revised documents and corresponding checklists for HHSC’s review and approval:
| | 2. Risk Management Plan; and |
| | 3. Systems Quality Assurance Plan. |
The HMO must submit plans and checklists to HHSC according to the format and schedule identified in the HHSC Uniform Managed Care Manual. Additionally, if a Systems Readiness Review is triggered by one of the events described in Section 8.1.18, the HMO must submit all of the plans identified in this Section 8.1.18.2 in accordance with an HHSC-approved timeline
The HMO must follow all applicable Joint Interface Plans (JIPs) and all required file submissions for HHSC’s Administrative Services Contractor, External Quality Review Organization (EQRO) and HHSC Medicaid Claims Administrator. The JIPs can be accessed through the Uniform Managed Care Manual.
8.1.18.3 System-wide Functions
The HMO’s MIS system must include key business processing functions and/or features, which must apply across all subsystems as follows:
| | 1. Process electronic data transmission or media to add, delete or modify membership records with accurate begin and end dates; |
| | 2. Track Covered Services received by Members through the system, and accurately and fully maintain those Covered Services as HIPAA-compliant Encounter transactions; |
| | 3. Transmit or transfer Encounter Data transactions on electronic media in the HIPAA format to the contractor designated by HHSC to receive the Encounter Data; |
| | 4. Maintain a history of changes and adjustments and audit trails for current and retroactive data; |
| | 5. Maintain procedures and processes for accumulating, archiving, and restoring data in the event of a system or subsystem failure; |
| | 6. Employ industry standard medical billing taxonomies (procedure codes, diagnosis codes) to describe services delivered and Encounter transactions produced; |
| | 7. Accommodate the coordination of benefits; |
| | 8. Produce standard Explanation of Benefits (EOBs); |
| | 9. Pay financial transactions to Providers in compliance with federal and state laws, rules and regulations; |
| | 10. Ensure that all financial transactions are auditable according to GAAP guidelines. |
| | 11. Relate and extract data elements to produce report formats (provided within the Uniform Managed Care Manual) or otherwise required by HHSC; |
| | 12. Ensure that written process and procedures manuals document and describe all manual and automated system procedures and processes for the MIS; |
| | 13. Maintain and cross-reference all Member-related information with the most current Medicaid, CHIP or CHIP Perinatal Program Provider number; and |
| | 14. Ensure that the MIS is able to integrate pharmacy data from HHSC’s Drug Vendor file (available through the Virtual Private Network (VPN)) into the HMO’s Member data. |
8.1.18.4 Health Insurance Portability and Accountability Act (HIPAA) Compliance
The HMO’s MIS system must comply with applicable certificate of coverage and data specification and reporting requirements promulgated pursuant to the Health Insurance Portability and Accountability Act (HIPAA) of 1996, P.L. 104-191 (August 21, 1996), as amended or modified. The HMO must comply with HIPAA EDI requirements. HMO’s enrollment files must be in the 834 HIPAA-compliant format. Eligibility inquiries must be in the 270/271 format and all claims and remittance transactions in the 837/835 format.
The HMO must provide its Members with a privacy notice as required by HIPAA. The HMO must provide HHSC with a copy of its privacy notice for filing.
8.1.18.5 Claims Processing Requirements
The HMO must process and adjudicate all provider claims for Medically Necessary Covered Services that are filed within the time frames specified in the Uniform Managed Care Manual. The HMO is subject to remedies, including liquidated damages and interest, if the HMO does not process and adjudicate claims within the timeframes listed in the Uniform Managed Care Manual.
The HMO must administer an effective, accurate, and efficient claims payment process in compliance with federal laws and regulations, applicable state laws and rules, the Contract, and the Uniform Managed Care Manual. In addition, a Medicaid HMO must be able to accept and process provider claims in compliance with the Texas Medicaid Provider Procedures Manual and The Texas Medicaid Bulletin.
The HMO must maintain an automated claims processing system that registers the date a claim is received by the MCO, the detail of each claim transaction (or action) at the time the transaction occurs, and has the capability to report each claim transaction by date and type to include interest payments. The claims system must maintain information at the claim and line detail level. The claims system must maintain adequate audit trails and report accurate claims performance measures to HHSC.
The HMO’s claims system must maintain online and archived files. The HMO must keep online automated claims payment history for the most current 18 months. The HMO must retain other financial information and records, including all original claims forms, for the time period established in Attachment A, Section 9.01. All claims data must be easily sorted and produced in formats as requested by HHSC.
The HMO must offer its Providers/Subcontractors the option of submitting and receiving claims information through electronic data interchange (EDI) that allows for automated processing and adjudication of claims. EDI processing must be offered as an alternative to the filing of paper claims. Electronic claims must use HIPAA-compliant electronic formats.
The HMO must make an electronic funds transfer (EFT) payment process (for direct deposit) available to in-network providers when processing claims for Medically Necessary covered STAR+PLUS services.
The HMO may deny a claim submitted by a provider for failure to file in a timely manner as provided for in the Uniform Managed Care Manual. The HMO must not pay any claim submitted by a provider excluded or suspended from the Medicare, Medicaid, CHIP or CHIP Perinatal programs for Fraud, Abuse, or Waste. The HMO must not pay any claim submitted by a Provider that is on payment hold under the authority of HHSC or its authorized agent(s), or who has pending accounts receivable with HHSC.
The HMO is subject to the requirements related to coordination of benefits for secondary payors in the Texas Insurance Code Section 843.349 (e) and (f).
The HMO must notify HHSC of major claim system changes in writing no later than 180 days prior to implementation. The HMO must provide an implementation plan and schedule of proposed changes. HHSC reserves the right to require a desk or on-site readiness review of the changes.
The HMO must inform all Network Providers about the information required to submit a claim at least 30 days prior to the Operational Start Date and as a provision within the HMO/Provider contract. The HMO must make available to Providers claims coding and processing guidelines for the applicable provider type. Providers must receive 90 days notice prior to the HMO’s implementation of changes to claims guidelines.
8.1.18.6 National Correct Coding Initiative
Effective for claims filed on or after October 1, 2010, the HMO must comply with the requirements of Section 6507 of the Patient Protection and Affordable Care Act of 2010 (P.L. 111-148), regarding “Mandatory State Use of National Correct Coding Initiatives,” including all applicable rules, regulations, and methodologies implemented as a result of this initiative.
8.1.19 Fraud and Abuse
A HMO is subject to all state and federal laws and regulations relating to Fraud, Abuse, and Waste in health care and the Medicaid and CHIP programs. The HMO must cooperate and assist HHSC and any state or federal agency charged with the duty of identifying, investigating, sanctioning or prosecuting suspected Fraud, Abuse or Waste. The HMO must provide originals and/or copies of all records and information requested and allow access to premises and provide records to the Inspector General for the Texas Health and Human Services System, HHSC or its authorized agent(s), the Centers for Medicare and Medicaid Services (CMS), the U.S. Department of Health and Human Services (DHHS), Federal Bureau of Investigation, TDI, or other units of state government. The HMO must provide all copies of records free of charge.
The HMO must submit a written Fraud and Abuse compliance plan to the Office of Inspector General at HHSC for approval each year. The plan must be submitted 60 days prior to the start of the State fiscal year. (See Attachment B-1, Section 7 for requirements regarding timeframes for submitting the original plan.) If an HMO has not made any changes to its plan from the previous
year, it may notify the HHSC OIG that: (1) no changes have been made to the previously-approved plan, (2) the plan will remain in place for the upcoming State Fiscal Year. The notification must be signed and certified by an officer or director of the HMO that is responsible for carrying out the Fraud and Abuse compliance plan. Upon receipt of a written request from the HHSC OIG, the HMO must submit the complete Fraud and Abuse compliance plan.
The HMO is subject to and must meet all requirements in Section 531.103 of the Texas Government Code, Title 1 Texas Administrative Code (TAC), Part 15, Chapter 353, Subchapter F, Rule 353.501-353.505, and Title 1 Texas Administrative Code (TAC), Part 15, Chapter 370, Subchapter F, Rule 370.501-370.505.
Additional Requirements for STAR and STAR+PLUS HMOs:
In accordance with Section 1902(a)(68) of the Social Security Act, STAR and STAR+PLUS HMOs that receive or make annual Medicaid payments of at least $5 million must:
| | 1. Establish written policies for all employees, managers, officers, contractors, subcontractors, and agents of the HMO, which provide detailed information about the False Claims Act, administrative remedies for false claims and statements, any state laws pertaining to civil or criminal penalties for false claims, and whistleblower protections under such laws, as described in Section 1902(a)(68)(A). |
| | 2. Include as part of such written policies, detailed provisions regarding the HMO’s policies and procedures for detecting and preventing fraud, waste, and abuse. |
| | 3. Include in any employee handbook a specific discussion of the laws described in Section 1902(a)(68)(A), the rights of employees to be protected as whistleblowers, and the HMO’s policies and procedures for detecting and preventing fraud, waste, and abuse. |
8.1.20 Reporting Requirements
The HMO must provide and must require its subcontractors to provide:
| | 1. All information required under the Contract, including but not limited to, the reporting requirements or other information related to the performance of its responsibilities hereunder as reasonably requested by the HHSC; and |
| | 2. Any information in its possession sufficient to permit HHSC to comply with the Federal Balanced Budget Act of 1997 or other Federal or state laws, rules, and regulations. All information must be provided in accordance with the timelines, definitions, formats and instructions as specified by HHSC. Where practicable, HHSC may consult with HMOs to establish time frames and formats reasonably acceptable to both parties. |
Any deliverable or report in Section 8.1.20 without a specified due date is due quarterly on the last day of the month following the end of the reporting period. Where the due date states 30 days, the HMO is to provide the deliverable by the last day of the month following the end of the reporting period. Where the due date states 45 days, the HMO is to provide the deliverable by the 15th day of the second month following the end of the reporting period.
The HMO’s Chief Executive and Chief Financial Officers, or persons in equivalent positions, must certify that financial data, Encounter Data and other measurement data has been reviewed by the HMO and is true and accurate to the best of their knowledge after reasonable inquiry.
8.1.20.1 HEDIS and Other Statistical Performance Measures
The HMO must provide to HHSC or its designee all information necessary to analyze the HMO’s provision of quality care to Members using measures to be determined by HHSC in consultation with the HMO. Such measures must be consistent with HEDIS or other externally based measures or measurement sets, and involve collection of information beyond that present in Encounter Data. The Performance Indicator Dashboard, found in the Uniform Managed Care Manual provides additional information on the role of the HMO and the EQRO in the collection and calculation of HEDIS, CAHPS, and other performance measures.
8.1.20.2 Reports
The HMO must provide the following reports, in addition to the Financial Reports described in Section 8.1.17 and those reporting requirements listed elsewhere in the Contract. The HHSC Uniform Managed Care Manual will include a list of all required reports, and a description of the format, content, file layout and submission deadlines for each report.
For the following reports, CHIP Perinatal Program data will be integrated into existing CHIP Program reports. Generally, no separate CHIP Perinatal Program reports are required. Where appropriate, HHSC will designate specific attributes within the CHIP Program reports that the CHIP Perinatal HMOs must complete to allow HHSC to extract data particular to the CHIP Perinatal Program.
| | (a) Claims Summary Report - The HMO must submit quarterly Claims Summary Reports to HHSC by HMO Program, Service Area and claim type by the 30th day following the end of the reporting period unless otherwise specified. Claim Types include facility and/or professional services for Acute Care, Behavioral Health, Vision, and Long Term Services and Supports. Within each claim type, claims data must be reported separately on the UB and CMS 1500 claim forms. The format for the Claims Summary Report is contained in Chapter 5, Section 5.6.1 of the Uniform Managed Care Manual. |
| | (b) QAPI Program Annual Summary Report - The HMO must submit a QAPI Program Annual Summary in a format and timeframe as specified in the Uniform Managed Care Manual. |
| | (c) Fraudulent Practices Report - Utilizing the HHSC-Office of Inspector General (OIG) fraud referral form, the HMO’s assigned officer or director must report and refer all possible acts of waste, abuse or fraud to the HHSC-OIG within 30 working days of receiving the reports of possible acts of waste, abuse or fraud from the HMO’s Special Investigative Unit (SIU). The report and referral must include: an investigative report identifying the allegation, statutes/regulations violated or considered, and the results of the investigation; copies of program rules and regulations violated for the time period in question; the estimated overpayment identified; a summary of the interviews conducted; the encounter data submitted by the provider for the time period in question; and all supporting documentation obtained as |
| | the result of the investigation. This requirement applies to all reports of possible acts of waste, abuse and fraud. |
Additional reports required by the Office of the Inspector General relating to waste, abuse or fraud are listed in the HHSC Uniform Managed Care Manual.
| | (d) Provider Termination Report: (CHIP (including integrated CHIP Perinatal Program data), STAR, and STAR+PLUS) - MCO must submit a quarterly report that identifies any providers who cease to participate in MCO's provider network, either voluntarily or involuntarily. The report must be submitted to HHSC in the format specified by HHSC, no later than 30 days after the end of the reporting period. |
| | (e) PCP Network & Capacity Report: (CHIP only (including integrated CHIP Perinatal Program data)) - For the CHIP Program, MCO must submit a quarterly report listing all unduplicated PCPs in the MCO's Provider Network. For the CHIP Perinatal Program, the Perinatal Newborns are assigned PCPs that are part of the CHIP PCP Network. The report must be submitted to HHSC in the format specified by HHSC, no later than 30 days after the end of the reporting quarter. |
| | (f) Summary Report of Member Complaints and Appeals - The HMO must submit quarterly Member Complaints and Appeals reports. The HMO must include in its reports Complaints and Appeals submitted to its subcontracted risk groups (e.g., IPAs) and any other subcontractor that provides Member services. The HMO must submit the Complaint and Appeals reports electronically on or before 45 days following the end of the state fiscal quarter, using the format specified by HHSC in the HHSC Uniform Managed Care Manual, Chapter 5.4.2. |
HHSC may direct the CHIP Perinatal HMOs to provide segregated Member Complaints and Appeals reports on an as-needed basis.
| | (g) Summary Report of Provider Complaints - The HMO must submit Provider complaints reports on a quarterly basis. The HMO must include in its reports complaints submitted by providers to its subcontracted risk groups (e.g., IPAs) and any other subcontractor that provides Provider services. The complaint reports must be submitted electronically on or before 45 days following the end of the state fiscal quarter, using the format specified by HHSC in the HHSC Uniform Managed Care Manual, Chapter 5.4.2. |
HHSC may direct the CHIP Perinatal HMOs to provide segregated Provider Complaints and Appeals reports on an as-needed basis.
| | (h) Hotline Reports - The HMO must submit, on a quarterly basis, a status report for the Member Hotline, the Behavioral Health Services Hotline, and the Provider Hotline in comparison with the performance standards set out in Sections 8.1.5.6, 8.1.15.3, and 8.1.4.7. The HMO shall submit such reports using a format to be prescribed by HHSC in consultation with the HMOs. |
If the HMO is not meeting a hotline performance standard, HHSC may require the HMO to submit monthly hotline performance reports and implement corrective actions until the hotline performance standards are met. If a HMO has a single hotline serving multiple
Service Areas, multiple HMO Programs, or multiple hotline functions, (i.e. Member, Provider, Behavioral Health Services hotlines), HHSC may request on an annual basis that the HMO submit certain hotline response information by HMO Program, by Service Area, and by hotline function, as applicable to the HMO. HHSC may also request this type of hotline information if a HMO is not meeting a hotline performance standard.
| | (i) Audit Reports – The HMO must comply with the Uniform Managed Care Manual’s requirements regarding notification and/or submission of audit reports. |
| | (j) Medicaid Managed Care Texas Health Steps Medical Checkups Reports – Medicaid HMOs must submit reports identifying the number of New Members and Existing Members receiving Texas Health Steps medical checkups. |
Medicaid HMOs must also document and report those Members refusing to obtain the medical checkups. The documentation must include the reason the Member refused the checkup or the reason the checkup was not received.
The definitions, timeframe, format, and details of the reports are contained and described in the Uniform Managed Care Manual, Chapters 12.4, 12.5, 12.6, and 12.13.
| | (k) Children of Migrant Farm Workers Annual Report (FWC Annual Report) Beginning in SFY 2008, Medicaid HMOs must submit an annual report, in the timeframe and format described in the Uniform Managed Care Manual, about the identification of and delivery of services to children of migrant farm workers (FWC). The report will include a description and results of the each of the following: |
| | (1) the HMO’s efforts to identify as many community and statewide groups that work with FWC as possible within each of its Service Areas; |
| | (2) the HMO’s efforts to coordinate and cooperate with as many of such groups as possible; and |
| | (3) the HMO’s efforts to encourage the community groups to assist in the identification of FWC. |
The HMO will maintain accurate, current lists of all identified FWC Members.
| | (l) Frew Quarterly Monitoring Report |
Each calendar year quarter, HHSC prepares a report for the court that addresses the status of the Consent Decree paragraphs of the Frew vs. Suehs lawsuit. Medicaid HMOs must prepare responses to questions posed by HHSC on the Frew Quarterly Monitoring Report template.
The timeframe, format, and details of the report are set forth in the Uniform Managed Care Manual.
| | (m) Frew Health Care Provider Training Report |
Per the Frew vs. Suehs' “Corrective Action Order: Health Care Provider Training,” HHSC must compile a summary of the training health care providers receive throughout the year for
the October Quarterly Monitoring Report for the court. Medicaid HMOs must report to HHSC health care provider training conducted throughout the year to be included in this report.
The timeframe, format, and details of the report are contained and described in the Uniform Managed Care Manual.
| | (n) Frew Provider Recognition Report |
Per the Frew vs. Suehs’ “Corrective Action Order: Health Care Provider Training,” HHSC must recognize Medicaid enrolled healthcare providers who complete Frew and/or Texas Health Steps (THSteps) training. Medicaid HMOs must collect and track provider training recognition information for all Frew and/or THSteps trainings conducted and report the names of those Medicaid enrolled healthcare providers who consent to being recognized to HHSC quarterly.
The timeframe, format, and details of the report are contained and described in the Uniform Managed Care Manual.
8.2 Additional Medicaid HMO Scope of Work
The following provisions apply to any HMO participating in the STAR or STAR+PLUS HMO Program.
8.2.1 Continuity of Care and Out-of-Network Providers
The HMO must ensure that the care of newly enrolled Members is not disrupted or interrupted. The HMO must take special care to provide continuity in the care of newly enrolled Members whose health or behavioral health condition has been treated by specialty care providers or whose health could be placed in jeopardy if Medically Necessary Covered Services are disrupted or interrupted. See Section 8.1.14 Disease Management for specific requirements for new Members transferring to the HMO’s DM Program.
The HMO must allow pregnant Members with 12 weeks or less remaining before the expected delivery date to remain under the care of the Member’s current OB/GYN through the Member’s postpartum checkup, even if the provider is Out-of-Network. If a Member wants to change her OB/GYN to one who is in the Network, she must be allowed to do so if the Provider to whom she wishes to transfer agrees to accept her in the last trimester of pregnancy.
The HMO must pay a Member’s existing Out-of-Network providers for Medically Necessary Covered Services until the Member’s records, clinical information and care can be transferred to a Network Provider, or until such time as the Member is no longer enrolled in that HMO, whichever is shorter. Payment to Out-of-Network providers must be made within the time period required for Network Providers. The HMO must comply with out-of-network provider reimbursement rules as adopted by HHSC.
This Article does not extend the obligation of the HMO to reimburse the Member’s existing Out-of-Network providers for on-going care for:
| | 1. More than 90 days after a Member enrolls in the HMO’s Program, or |
| | 2. For more than nine (9) months in the case of a Member who, at the time of enrollment in the HMO, has been diagnosed with and receiving treatment for a terminal illness and remains enrolled in the HMO. |
The HMO’s obligation to reimburse the Member’s existing Out-of-Network provider for services provided to a pregnant Member with 12 weeks or less remaining before the expected delivery date extends through delivery of the child, immediate postpartum care, and the follow-up checkup within the first six weeks of delivery.
The HMO must provide or pay Out-of-Network providers who provide Medically Necessary Covered Services to Members who move out of the Service Area through the end of the period for which capitation has been paid for the Member.
The HMO must provide Members with timely and adequate access to Out-of-Network services for as long as those services are necessary and covered benefits not available within the network, in accordance with 42 C.F.R. §438.206(b)(4). The HMO will not be obligated to provide a Member with access to Out-of-Network services if such services become available from a Network Provider.
The HMO must ensure that each Member has access to a second opinion regarding the use of any Medically Necessary Covered Service. A Member must be allowed access to a second opinion from a Network Provider or Out-of-Network provider if a Network Provider is not available, at no cost to the Member, in accordance with 42 C.F.R. §438.206(b)(3).
8.2.2 Provisions Related to Covered Services for Medicaid Members
8.2.2.1 Emergency Services
HMO policy and procedures, Covered Services, claims adjudication methodology, and reimbursement performance for Emergency Services must comply with all applicable state and federal laws, rules, and regulations including 42 C.F.R. §438.114, whether the provider is in-network or Out-of-Network. HMO policies and procedures must be consistent with the prudent layperson definition of an Emergency Medical Condition and the claims adjudication processes required under the Contract and 42 C.F.R. §438.114.
The HMO must pay for the professional, facility, and ancillary services that are Medically Necessary to perform the medical screening examination and stabilization of a Member presenting with an Emergency Medical Condition or an Emergency Behavioral Health Condition to the hospital emergency department, 24 hours a day, 7 days a week, rendered by either the HMO's Network or Out-of-Network providers.
The HMO cannot require prior authorization as a condition for payment for an Emergency Medical Condition, an Emergency Behavioral Health Condition, or labor and delivery. The HMO
cannot limit what constitutes an Emergency Medical Condition on the basis of lists of diagnoses or symptoms. The HMO cannot refuse to cover Emergency Services based on the emergency room provider, hospital, or fiscal agent not notifying the Member’s PCP or the HMO of the Member’s screening and treatment within 10 calendar days of presentation for Emergency Services. The HMO may not hold the Member who has an Emergency Medical Condition liable for payment of subsequent screening and treatment needed to diagnose the specific condition or stabilize the patient. The HMO must accept the emergency physician or provider’s determination of when the Member is sufficiently stabilized for transfer or discharge.
A medical screening examination needed to diagnose an Emergency Medical Condition must be provided in a hospital based emergency department that meets the requirements of the Emergency Medical Treatment and Active Labor Act (EMTALA) (42 C.F.R. §§489.20, 489.24 and 438.114(b)&(c)). The HMO must pay for the emergency medical screening examination, as required by 42 U.S.C. §1395dd. The HMO must reimburse for both the physician's services and the hospital's Emergency Services, including the emergency room and its ancillary services.
When the medical screening examination determines that an Emergency Medical Condition exists, the HMO must pay for Emergency Services performed to stabilize the Member. The emergency physician must document these services in the Member's medical record. The HMO must reimburse for both the physician's and hospital's emergency stabilization services including the emergency room and its ancillary services.
The HMO must cover and pay for Post-Stabilization Care Services in the amount, duration, and scope necessary to comply with 42 C.F.R. §438.114(b)&(e) and 42 C.F.R. §422.113(c)(iii). The HMO is financially responsible for post-stabilization care services obtained within or outside the Network that are not pre-approved by a Provider or other HMO representative, but administered to maintain, improve, or resolve the Member’s stabilized condition if:
| | 1. The HMO does not respond to a request for pre-approval within 1 hour; |
| | 2. The HMO cannot be contacted; or |
| | 3. The HMO representative and the treating physician cannot reach an agreement concerning the Member’s care and a Network physician is not available for consultation. In this situation, the HMO must give the treating physician the opportunity to consult with a Network physician and the treating physician may continue with care of the patient until an HMO physician is reached. The HMO’s financial responsibility ends as follows: the HMO physician with privileges at the treating hospital assumes responsibility for the Member’s care; the HMO physician assumes responsibility for the Member’s care through transfer; the HMO representative and the treating physician reach an agreement concerning the Member’s care; or the Member is discharged. |
8.2.2.2 Family Planning - Specific Requirements
The HMO must require, through Provider contract provisions, that Members requesting contraceptive services or family planning services are also provided counseling and education about the family planning and family planning services available to Members. The HMO must develop outreach programs to increase community support for family planning and encourage Members to use available family planning services.
The HMO must ensure that Members have the right to choose any Medicaid participating family planning provider, whether the provider chosen by the Member is in or outside the Provider Network. The HMO must provide Members access to information about available providers of family planning services and the Member’s right to choose any Medicaid family planning provider. The HMO must provide access to confidential family planning services.
The HMO must provide, at minimum, the full scope of services available under the Texas Medicaid program for family planning services. The HMO will reimburse family planning agencies the Medicaid fee-for service amounts for family planning services, including Medically Necessary medications, contraceptives, and supplies not covered by the Vendor Drug Program and will reimburse Out-of-Network family planning providers in accordance with HHSC’s administrative rules. The HMO cannot require prior authorization for family planning services whether rendered by a Network or Out-of-Network provider.
The HMO must provide medically approved methods of contraception to Members, provided that the methods of contraception are Covered Services. Contraceptive methods must be accompanied by verbal and written instructions on their correct use. The HMO must establish mechanisms to ensure all medically approved methods of contraception are made available to the Member, either directly or by referral to a subcontractor.
The HMO must develop, implement, monitor, and maintain standards, policies and procedures for providing information regarding family planning to Providers and Members, specifically regarding State and federal laws governing Member confidentiality (including minors). Providers and family planning agencies cannot require parental consent for minors to receive family planning services. The HMO must require, through contractual provisions, that subcontractors have mechanisms in place to ensure Member’s (including minor’s) confidentiality for family planning services.
8.2.2.3 Texas Health Steps (EPSDT)
The HMO must develop effective methods to ensure that children under the age of 21 receive Texas Health Steps services when due and according to the recommendations established by the Texas Health Steps periodicity schedule for children. The HMO must arrange for Texas Health Steps services for all eligible Members except when a Member knowingly and voluntarily declines or refuses services after receiving sufficient information to make an informed decision.
For New Members under age 21, overdue or upcoming Texas Health Steps medical checkups should be offered as soon as practicable, but in no case later than 14 days of enrollment for newborns, and no later than 90 days of enrollment for all other eligible child Members. Effective September 1, 2010, the Texas Health Steps annual medical checkup for an Existing Member age 36 months and older is due on the child’s birthday. The annual medical checkup is considered timely if it occurs no later than 364 calendar days after the child’s birthday. For purposes of this requirement, the terms “New Member” and “Existing Member” are defined in Chapter 12.4 of the Uniform Managed Care Manual.
The HMO must ensure that Members are provided information and educational materials about the services available through the Texas Health Steps Program, and how and when they may obtain the services. The information should tell the Member how they can obtain dental benefits,
transportation services through the Medical Transportation Program, and advocacy assistance from the HMO. The HMO will encourage Medicaid-enrolled pharmacies to also become Medicaid-enrolled durable medical equipment (DME) providers.
The HMO must provide appropriate training to all Network Providers and Provider staff in the Providers’ area of practice regarding the scope of benefits available and the Texas Health Steps Program. Training must include:
| | 1. Texas Health Steps benefits, |
| | 2. The periodicity schedule for Texas Health Steps medical checkups and immunizations, |
| | 3. The required elements of Texas Health Steps medical checkups, |
| | 4. Providing or arranging for all required lab screening tests (including lead screening), and Comprehensive Care Program (CCP) services available under the Texas Health Steps program to Members under age 21 years. |
HMO must also educate and train Providers regarding the requirements imposed on HHSC and contracting HMOs under the Consent Decree and Corrective Action Orders entered in Frew v. Suehs, et. al., Civil Action No. 3:93CV65, in the United States District Court for the Eastern District of Texas, Paris Division. Providers should be educated and trained to treat each Texas Health Steps visit as an opportunity for a comprehensive assessment of the Member.
The HMO must provide outreach to Members to ensure they receive prompt services and are effectively informed about available Texas Health Steps services. Each month, the HMO must retrieve from the HHSC Administrative Services Contractor Bulletin Board System a list of Members who are due and overdue Texas Health Steps services. Using these lists and its own internally generated list, the HMO will contact such Members to obtain the service as soon as possible. The HMO outreach staff must coordinate with Texas Health Steps outreach unit to ensure that Members have access to the Medical Transportation Program, and that any coordination with other agencies is maintained.
The HMO must cooperate and coordinate with the State, outreach programs and Texas Health Steps regional program staff and agents to ensure prompt delivery of services to children of migrant farm workers and other migrant populations who may transition into and out of the HMO’s Program more rapidly and/or unpredictably than the general population.
The HMO must have mechanisms in place to ensure that all newborn Members have an initial newborn checkup before discharge from the hospital and in accordance with the Texas Health Steps periodicity schedule. The HMO must require Providers to send all Texas Health Steps newborn screens to the DSHS Laboratory Services Section or to a laboratory approved by the department under Section 33.016 of the Health and Safety Code. Providers must include detailed identifying information for all screened newborn Members and the Member’s mother to allow DSHS to link the screens performed at the hospital with screens performed at the newborn follow up Texas Health Steps medical checkup.
All laboratory specimens collected as a required component of a Texas Health Steps checkup (see Texas Medicaid Provider Procedures Manual for age-specific requirements) must be submitted to the DSHS Laboratory Services Section or to a laboratory approved by the department under
Section 33.016 of the Health and Safety Code for analysis. The HMO must educate Providers about Texas Health Steps Program requirements for submitting laboratory tests to the DSHS Laboratory Services Section.
The HMO must make an effort to coordinate and cooperate with existing community and school-based health and education programs that offer services to school-aged children in a location that is both familiar and convenient to the Members. The HMO must make a good faith effort to comply with Head Start’s requirement that Members participating in Head Start receive their Texas Health Steps checkup no later than 45 days after enrolling into either program.
The HMO must educate Providers on the Immunization Standard Requirements set forth in Chapter 161, Health and Safety Code; the standards in the Advisory Committee on Immunization Practices (ACIP) Immunization Schedule; the AAP Periodicity Schedule for CHIP Members; and the Texas Health Steps Periodicity Schedule for Medicaid Members. The HMO shall educate Providers that Medicaid Members under age 21 must be immunized during the Texas Health Steps checkup according to the ACIP routine immunization schedule. The HMO shall also educate Providers that the screening provider is responsible for administration of the immunization and should not refer children to Local Health Departments to receive immunizations.
The HMO must educate Providers about, and require Providers to comply with, the requirements of Chapter 161, Health and Safety Code, relating to the Texas Immunization Registry (ImmTrac), to include parental consent on the Vaccine Information Statement.
The HMO must require all Texas Health Steps Providers to submit claims for services paid (either on a capitated or fee-for service basis) on the CMS 1500 claim form and use the HIPAA compliant code set required by HHSC.
Encounter Data will be validated by chart review of a random sample of Texas Health Steps eligible enrollees against monthly Encounter Data reported by the HMO. HHSC or its designee will conduct chart reviews to validate that all screens are performed when due and as reported, and that reported data is accurate and timely. Substantial deviation between reported and charted Encounter Data could result in the HMO and/or Network Providers being investigated for potential Fraud, Abuse, or Waste without notice to the HMO or the Provider.
8.2.2.3.1 Oral Evaluation and Fluoride Varnish
The HMO must educate Providers on the availability of the Oral Evaluation and Fluoride Varnish (OEVS) Medicaid benefit that can be rendered and billed by certified Texas Health Steps providers when performed on the same day as the Texas Health Steps medical checkup. The Provider education must include information about how to assist a Member with referral to a dentist to establish a dental home.
8.2.2.4 Perinatal Services
The HMO’s perinatal health care services must ensure appropriate care is provided to women and infant Members of the HMO from the preconception period through the infant’s first year of life. The HMO’s perinatal health care system must comply with the requirements of the Texas Health and Safety Code, Chapter 32 (the Maternal and Infant Health Improvement Act) and administrative rules codified at 25 T.A.C. Chapter 37, Subchapter M.
The HMO must have a perinatal health care system in place that, at a minimum, provides the following services:
| | 1. Pregnancy planning and perinatal health promotion and education for reproductive- age women; |
| | 2. Perinatal risk assessment of non-pregnant women, pregnant and postpartum women, and infants up to one year of age; |
| | 3. Access to appropriate levels of care based on risk assessment, including emergency care; |
| | 4. Transfer and care of pregnant women, newborns, and infants to tertiary care facilities when necessary; |
| | 5. Availability and accessibility of OB/GYNs, anesthesiologists, and neonatologists capable of dealing with complicated perinatal problems; and |
| | 6. Availability and accessibility of appropriate outpatient and inpatient facilities capable of dealing with complicated perinatal problems. |
The HMO must have a process to expedite scheduling a prenatal appointment for an obstetrical exam for a TP40 Member no later than two weeks after receiving the daily Enrollment File verifying the Member’s enrollment into the HMO.
The HMO must have procedures in place to contact and assist a pregnant/delivering Member in selecting a PCP for her baby either before the birth or as soon as the baby is born.
The HMO must provide inpatient care and professional services relating to labor and delivery for its pregnant/delivering Members, and neonatal care for its newborn Members at the time of delivery and for up to 48 hours following an uncomplicated vaginal delivery and 96 hours following an uncomplicated Caesarian delivery.
The HMO must Adjudicate provider claims for services provided to a newborn Member in accordance with HHSC’s claims processing requirements using the proxy ID number or State-issued Medicaid ID number. The HMO cannot deny claims based on a provider’s non-use of State-issued Medicaid ID number for a newborn Member. The HMO must accept provider claims for newborn services based on mother’s name and/or Medicaid ID number with accommodations for multiple births, as specified by the HMO.
The HMO must notify providers involved in the care of pregnant/delivering women and newborns (including Out-of-Network providers and hospitals) of the HMO’s prior authorization requirements. The HMO cannot require a prior authorization for services provided to a pregnant/delivering Member or newborn Member for a medical condition that requires Emergency Services, regardless of when the emergency condition arises.
8.2.2.5 Sexually Transmitted Diseases (STDs) and Human Immunodeficiency Virus (HIV)
The HMO must provide STD services that include STD/HIV prevention, screening, counseling, diagnosis, and treatment. The HMO is responsible for implementing procedures to ensure that Members have prompt access to appropriate services for STDs, including HIV. The HMO must allow Members access to STD services and HIV diagnosis services without prior authorization or referral by a PCP.
The HMO must comply with Texas Family Code Section 32.003, relating to consent to treatment by a child. The HMO must provide all Covered Services required to form the basis for a diagnosis by the Provider as well as the STD/HIV treatment plan.
The HMO must make education available to Providers and Members on the prevention, detection and effective treatment of STDs, including HIV.
The HMO must require Providers to report all confirmed cases of STDs, including HIV, to the local or regional health authority according to 25 T.A.C. §§97.131 - 97.134, using the required forms and procedures for reporting STDs. The HMO must require the Providers to coordinate with the HHSC regional health authority to ensure that Members with confirmed cases of syphilis, chancroid, gonorrhea, chlamydia and HIV receive risk reduction and partner elicitation/notification counseling.
The HMO must have established procedures to make Member records available to public health agencies with authority to conduct disease investigation, receive confidential Member information, and provide follow up activities.
The HMO must require that Providers have procedures in place to protect the confidentiality of Members provided STD/HIV services. These procedures must include, but are not limited to, the manner in which medical records are to be safeguarded, how employees are to protect medical information, and under what conditions information can be shared. The HMO must inform and require its Providers who provide STD/HIV services to comply with all state laws relating to communicable disease reporting requirements. The HMO must implement policies and procedures to monitor Provider compliance with confidentiality requirements.
The HMO must have policies and procedures in place regarding obtaining informed consent and counseling Members provided STD/HIV services.
8.2.2.6 Tuberculosis (TB)
The HMO must provide Members and Providers with education on the prevention, detection and effective treatment of tuberculosis (TB). The HMO must establish mechanisms to ensure all procedures required to screen at-risk Members and to form the basis for a diagnosis and proper prophylaxis and management of TB are available to all Members, except services referenced in Section 8.2.2.8 as Non-Capitated Services. The HMO must develop policies and procedures to ensure that Members who may be or are at risk for exposure to TB are screened for TB. An at-risk Member means a person who is susceptible to TB because of the association with certain risk factors, behaviors, drug resistance, or environmental conditions. The HMO must consult with the local TB control program to ensure that all services and treatments are in compliance with the guidelines recommended by the American Thoracic Society (ATS), the Centers for Disease Control and Prevention (CDC), and DSHS policies and standards.
The HMO must implement policies and procedures requiring Providers to report all confirmed or suspected cases of TB to the local TB control program within one working day of identification, using the most recent DSHS forms and procedures for reporting TB. The HMO must provide access to Member medical records to DSHS and the local TB control program for all confirmed and suspected TB cases upon request.
The HMO must coordinate with the local TB control program to ensure that all Members with confirmed or suspected TB have a contact investigation and receive Directly Observed Therapy (DOT). The HMO must require, through contract provisions, that Providers report to DSHS or the local TB control program any Member who is non-compliant, drug resistant, or who is or may be posing a public health threat. The HMO must cooperate with the local TB control program in enforcing the control measures and quarantine procedures contained in Chapter 81 of the Texas Health and Safety Code.
The HMO must have a mechanism for coordinating a post-discharge plan for follow-up DOT with the local TB program. The HMO must coordinate with the DSHS South Texas Hospital and Texas Center for Infectious Disease for voluntary and court-ordered admission, discharge plans, treatment objectives and projected length of stay for Members with multi-drug resistant TB.
8.2.2.7 Objection to Provide Certain Services
In accordance with 42 C.F.R. §438.102, the HMO may file an objection to providing, reimbursing for, or providing coverage of, a counseling or referral service for a Covered Service based on moral or religious grounds. The HMO must work with HHSC to develop a work plan to complete the necessary tasks and determine an appropriate date for implementation of the requested changes to the requirements related to Covered Services. The work plan will include timeframes for completing the necessary Contract and waiver amendments, adjustments to Capitation Rates, identification of the HMO and enrollment materials needing revision, and notifications to Members.
In order to meet the requirements of this section, the HMO must notify HHSC of grounds for and provide detail concerning its moral or religious objections and the specific services covered under the objection, no less than 120 days prior to the proposed effective date of the policy change.
8.2.2.8 Medicaid Non-capitated Services
The following Texas Medicaid programs and services have been excluded from HMO Covered Services. Medicaid Members are eligible to receive these Non-capitated Services on a Fee-for-Service basis from Texas Medicaid providers. HMOs should refer to relevant chapters in the Provider Procedures Manual and the Texas Medicaid Bulletins for more information.
| | 1. Texas Health Steps dental (including orthodontia); |
| | 2. Early Childhood Intervention (ECI) case management/service coordination; |
| | 3. DSHS targeted case management; |
| | 4. DSHS mental health rehabilitation; |
| | 5. DSHS case management for Children and Pregnant Women; |
| | 6. Texas School Health and Related Services (SHARS); |
| | 7. Department of Assistive and Rehabilitative Services Blind Children’s Vocational Discovery and Development Program; |
| | 8. Tuberculosis services provided by DSHS-approved providers (directly observed therapy and contact investigation); |
| | 9. Vendor Drug Program (out-of-office drugs); |
| | 10. Health and Human Services Commission’s Medical Transportation; |
| | 11. DADS hospice services (all Members are disenrolled from their health plan upon enrollment into hospice except STAR+PLUS members); |
| | 12. Audiology services and hearing aids for children (under age 21) (hearing screening services are provided through the Texas Health Steps Program and are capitated). |
| | 13. For STAR+PLUS, Inpatient Stays are Non-capitated (with the exception of inpatient mental health services, which are capitated). |
| | 14. For STAR, Personal Care Services for persons under age 21 are Non-capitated Services. |
| | 15. For STAR+PLUS, nursing facility services are Non-capitated Services; and |
| | 16. For Members who are enrolled in STAR or STAR+PLUS during and Inpatient Stay under one of the exceptions identified in Attachment A, Section 5.05(a)(2), Hospital facility charges associated with the Inpatient Stay are Non-Capitated Services under the circumstances described in Attachment A, Section 5.05(a)(2).. |
8.2.2.9 Referrals for Non-capitated Services
Although Medicaid HMOs are not responsible for paying or reimbursing for Non-capitated Services, HMOs are responsible for educating Members about the availability of Non-capitated Services, and for providing appropriate referrals for Members to obtain or access these services. The HMO is responsible for informing Providers that bills for all Non-capitated Services must be submitted to HHSC’s Claims Administrator for reimbursement.
8.2.2.10 Cooperation with Immunization Registry
The HMO must work with HHSC and health care providers to improve the immunization rate of Medicaid clients and the reporting of immunization information for inclusion in the Texas Immunization Registry, called “ImmTrac.”
8.2.2.11 Case Management for Children and Pregnant Women
The HMO must educate Members and Providers on the services available through Case Management for Children and Pregnant Women (CPW) as described on the program’s website at http://www.dshs.state.tx.us/caseman/default.shtm. An HMO may provide information about CPW’s website and basic information about CPW services in order to meet this requirement. CPW information and materials must be included in the HMO’s Provider Manual, Member Handbook and Provider orientations. The information and materials must also inform Providers that the disclosure of medical records or information between Providers, HMO’s and CPW case managers does not require a medical release form from the Member.
The HMO must coordinate services with CPW regarding a Member’s health care needs that are identified by CPW and referred to the HMO. Upon receipt of a referral or assessment from a CPW case manager, the HMO’s designated staff are required to review the assessment and determine, based on the HMO’s policies, the appropriate level of health care and services. The HMO’s staff must also coordinate with the Member’s family, Member’s Primary Care Provider (PCP), in and Out-of-Network Providers, agencies, and the HMO’s utilization management staff to ensure that the health care and services identified are properly referred, authorized, scheduled and provided within a timely manner.
The HMO must ensure that access to medically necessary health care needed by the Member is available within the standards established by HHSC for respective care. HMOs are not required to arrange or provide for any covered or non-covered services identified in the CPW assessment. The decision whether to authorize these services is made by the HMO. Within five (5) business days of identifying any non-covered health care services or other services that the Member may need, the HMO’s staff must report to the CPW case manager which items/services will not be performed by the HMO. Additionally, within ten (10) business days after all of the authorized services have been provided, the HMO’s staff must follow-up with CPW case manager to report the provision of services. The HMO’s staff must ensure that all services provided to a Member by an HMO Provider are reported to the Member’s PCP.
The CPW program requires its contracted case managers to coordinate with the HMO and the HMO’s PCPs. The HMO should report problems regarding CPW referrals, assessments or coordination activities to HHSC for follow-up with CPW program staff.
8.2.2.12 Children of Migrant Farmworkers (FWC)
The HMO must cooperate and coordinate with the State, outreach programs, and Texas Health Steps regional program staff and agents to ensure prompt delivery of services, in accordance with the timeframes in this Contract, to FWC Members and other migrant populations who may transition into and out of the HMO more rapidly and/or unpredictably than the general population.
The HMO must provide accelerated services to FWC Members. For purposes of this section, “accelerated services” are services that are provided to a child of a migrant farm worker prior to their leaving Texas to work in other states. Accelerated services include the provision of preventive Health Care Services that will be due during the time the FWC Member is out of Texas. The need for accelerated services must be determined on a case-by-case and according to the FWC Member’s age, periodicity schedule and health care needs.
The HMO must develop a plan annually for the process it will use to identify FWC and for the methods that will be used to provide accelerated services and submit an annual certification that the HMO will comply with the plan. The plan for FY2008 must be submitted for HHSC approval no later than December 1, 2007 and implemented by February 1, 2008. The plan must include at a minimum:
| | • Identification of community and statewide groups that work with FWC Members within the HMO’s Service Areas; |
| | • Participation of the community groups in assisting with the identification of FWC Members; |
| | • Appropriate aggressive efforts to reach each identified FWC to provide timely medical checkups and follow up care if needed; |
| | • Methods to maintain accurate, current lists of all identified FWC Members; |
| | • Methods that the HMO and its Subcontractors will implement to maintain the confidentiality of information about the identity of FWC; and |
| | • Methods to provide accelerated services to FWC. |
8.2.3 Medicaid Significant Traditional Providers
In the first three (3) years of a Medicaid HMO Program operating in a Service Area, the HMO must seek participation in its Network from all Medicaid Significant Traditional Providers (STPs) defined by HHSC in the applicable Service Area for the applicable HMO Program. For STAR HMOs, the Medicaid STP requirements only apply in the Nueces Service Area. For STAR+PLUS HMOs, the Medicaid STP requirements apply to all Service Areas, except Harris County within the Harris Service Area.
Medicaid STPs are defined as PCPs and, for STAR+PLUS, Community-based Long Term Care providers in a county, that, when listed by provider type by county in descending order by unduplicated number of clients, served the top 80% of unduplicated clients. Hospitals receiving Disproportionate Share Hospital (DSH) funds are also considered STPs in the Service Area in which they are located. Note that STAR+PLUS HMOs are not required to contract with Hospitals for Inpatient Stays, but are required to contract with Hospitals for Outpatient Hospital Services. The HHSC website includes a list of Medicaid STPs by Service Area.
Because the STP lists were produced in FY2005, HHSC has developed an updated list for Long Term Care Providers. The list will be provided to HMOs and posted on HHSC’s website.
The STP requirement will be in place for three years after the program has been implemented. During that time, providers who believe they meet the STP requirements may contact HHSC request HHSC’s consideration for STP status. STAR+PLUS HMOs will be notified when Providers are added to the list of STPs for a Service Area.
The HMO must give STPs the opportunity to participate in its Network for at least three (3) years commencing on the implementation date of Medicaid managed care in the Service Area. However, the STP provider must:
| | 1. Agree to accept the HMO’s Provider reimbursement rate for the provider type; and |
| | 2. Meet the standard credentialing requirements of the HMO, provided that lack of board certification or accreditation by the Joint Commission on Accreditation of Health Care Organizations (JCAHO) is not the sole grounds for exclusion from the Provider Network. |
8.2.4 Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs)
The HMO must make reasonable efforts to include FQHCs and RHCs (freestanding and hospital-based) in its Provider Network. The HMO must reimburse FQHCs, RHCs, and Municipal Health Department’s public clinics for Health Care Services provided outside of regular business hours, as defined by HHSC in rules, including weekend days or holidays, at a rate that is equal to the allowable rate for those services as determined under Section 32.028, Human Resources Code, if the Member does not have a referral from their PCP. Depending on the date of the claim, FQHCs or RHCs may receive a cost settlement from HHSC and must agree to accept initial payments from the HMO in an amount that is equal to or greater than the HMO’s payment terms for other Providers providing the same or similar services.
| | 1. Prior to September 1, 2007: For claims accruing prior to September 1, 2007, cost settlements apply to all Service Areas except the Nueces Service Area and the STAR+PLUS Service Areas. The HMOs serving the Nueces Service Area and the STAR+PLUS Service Areas must pay the full encounter rates to the FQHCs and RHCs for claims accruing before September 1, 2007. |
| | 2. September 1, 2007 to September 1, 2008: For claims accruing on or after September 1, 2007 but prior to September 1, 2008, HMOs are not required to pay full encounter rates to the FQHCs and RHCs. Therefore, HHSC cost settlements for FQHC’s will continue to apply to all STAR and STAR+PLUS Service Areas for this period of time. |
| | 3. On or after September 1, 2008: HMOs are required to pay the full encounter rates to RHCs for claims accruing on or after September 1, 2008; therefore, HHSC cost settlements will not apply to RHCs for this period of time. However, HMOs are not required to pay the full encounter rates to FQHCs for claims accruing on or after September 1, 2008; therefore, HHSC cost settlements will apply to FQHCs for this period of time. |
The HMO must submit monthly FQHC and RHC encounter and payment reports to all contracted FQHCs and RHCs, and FQHCs and RHCs with which there have been encounters, not later than 21 days from the end of the month for which the report is submitted. The format will be developed by HHSC and provided in the Uniform Managed Care Manual. The FQHC and RHC must validate the encounter and payment information contained in the report(s). The HMO and the FQHC/RHC must both sign the report(s) after each party agrees that it accurately reflects encounters and payments for the month reported. The HMO must submit the signed FQHC and RHC encounter and payment reports to HHSC not later than 45 days from the end of the reported month. Encounter and payment reports will not be necessary for
| | 1. the Nueces Service Area and the STAR+PLUS Service Areas for claims accruing before September 1, 2007, since the HMOs in those Areas will pay the full encounter rates to the FQHCs and RHCs for this period of time; and |
| | 2. for claims paid to RHCs on or after September 1, 2008, because the HMOs will pay full encounter rates to RHCs for this period of time. |
8.2.5 Provider Complaints and Appeals
8.2.5.1 Provider Complaints
Medicaid HMOs must develop, implement, and maintain a system for tracking and resolving all Medicaid Provider complaints. Within this process, the HMO must respond fully and completely to each complaint and establish a tracking mechanism to document the status and final disposition of each Provider complaint. The HMO must resolve Provider Complaints within 30 days from the date the Complaint is received. HHSC may, in its reasonable discretion, grant a written extension if the HMO demonstrates good cause.
HMOs must also resolve Provider Complaints received by HHSC no later than the due date indicated on HHSC’s notification form. HHSC will generally provide HMOs ten (10) Business Days to resolve such Complaints. If an HMO cannot resolve a Complaint by the due date indicated on the notification form, it may submit a request to extend the deadline. HHSC may, in its reasonable discretion, grant a written extension if the HMO demonstrates good cause.
Unless HHSC has granted a written extension as described above, the HMO is subject to remedies, including liquidated damages if Provider Complaints are not resolved by the timeframes indicated herein.
8.2.5.2 Appeal of Provider Claims
Medicaid HMOs must develop, implement, and maintain a system for tracking and resolving all Medicaid Provider appeals related to claims payment. Within this process, the HMO must respond fully and completely to each Medicaid Provider’s claims payment appeal and establish a tracking mechanism to document the status and final disposition of each Medicaid Provider’s claims payment appeal.
Medicaid HMOs must contract with physicians who are not Network Providers to resolve claims disputes related to denial on the basis of medical necessity that remain unresolved subsequent to a Provider appeal. The determination of the physician resolving the dispute must be binding on the HMO and the Provider. The physician resolving the dispute must hold the same specialty or a related specialty as the appealing Provider. HHSC reserves the right to amend this process to include an independent review process established by HHSC for final determination on these disputes.
8.2.6 Member Rights and Responsibilities
In accordance with 42 C.F.R. §438.100, all Medicaid HMOs must maintain written policies and procedures for informing Members of their rights and responsibilities, and must notify their Members of their right to request a copy of these rights and responsibilities. The Member Handbook must include notification of Member rights and responsibilities.
8.2.7 Medicaid Member Complaint and Appeal System
The HMO must develop, implement, and maintain a Member Complaint and Appeal system that complies with the requirements in applicable federal and state laws and regulations, including 42 C.F.R. §431.200, 42 C.F.R. Part 438, Subpart F, “Grievance System,” and the provisions of 1 T.A.C. Chapter 357 relating to Medicaid managed care organizations.
The Complaint and Appeal system must include a Complaint process, an Appeal process, and access to HHSC’s Fair Hearing System. The procedures must be the same for all Members and must be reviewed and approved in writing by HHSC or its designee. Modifications and amendments to the Member Complaint and Appeal system must be submitted for HHSC’s approval at least 30 days prior to the implementation.
8.2.7.1 Member Complaint Process
The HMO must have written policies and procedures for receiving, tracking, responding to, reviewing, reporting and resolving Complaints by Members or their authorized representatives. For purposes of this Section 8.2.7, an “authorized representative” is any person or entity acting on behalf of the Member and with the Member’s written consent. A Provider may be an authorized representative.
HMOs also must resolve Member Complaints received by HHSC no later than the due date indicated on HHSC’s notification form. HHSC will provide HMOs up to ten (10) Business Days to resolve such Complaints, depending on the severity and/or urgency of the Complaint. HHSC may, in its reasonable discretion, grant a written extension if the HMO demonstrates good cause.
Unless the HHSC has granted a written extension as described above, the HMO is subject to remedies, including liquidated damages if Member Complaints are not resolved by the timeframes indicated herein.
The HMO must resolve Complaints within 30 days from the date the Complaint is received. The HMO is subject to remedies, including liquidated damages, if at least 98 percent of Member Complaints are not resolved within 30 days of receipt of the Complaint by the HMO. Please see the Uniform Managed Care Contract Terms & Conditions and Attachment B-5, Deliverables/Liquidated Damages Matrix. The Complaint procedure must be the same for all Members under the Contract. The Member or Member’s authorized representative may file a Complaint either orally or in writing. The HMO must also inform Members how to file a Complaint directly with HHSC, once the Member has exhausted the HMO’s complaint process.
The HMO must designate an officer of the HMO who has primary responsibility for ensuring that Complaints are resolved in compliance with written policy and within the required timeframe. For purposes of Section 8.2.7.2, an “officer” of the HMO means a president, vice president, secretary, treasurer, or chairperson of the board for a corporation, the sole proprietor, the managing general partner of a partnership, or a person having similar executive authority in the organization.
The HMO must have a routine process to detect patterns of Complaints. Management, supervisory, and quality improvement staff must be involved in developing policy and procedure improvements to address the Complaints.
The HMO’s Complaint procedures must be provided to Members in writing and through oral interpretive services. A written description of the HMO’s Complaint procedures must be available in prevalent non-English languages for Major Population Groups identified by HHSC, at no more than a 6th grade reading level.
The HMO must include a written description of the Complaint process in the Member Handbook. The HMO must maintain and publish in the Member Handbook, at least one local and one toll-free telephone number with TeleTypewriter/Telecommunications Device for the Deaf (TTY/TDD) and interpreter capabilities for making Complaints.
The HMO’s process must require that every Complaint received in person, by telephone, or in writing must be acknowledged and recorded in a written record and logged with the following details:
| | 2. Identification of the individual filing the Complaint; |
| | 3. Identification of the individual recording the Complaint; |
| | 4. Nature of the Complaint; |
| | 5. Disposition of the Complaint (i.e., how the HMO resolved the Complaint); |
| | 6. Corrective action required; and |
The HMO is prohibited from discriminating or taking punitive action against a Member or his or her representative for making a Complaint.
If the Member makes a request for disenrollment, the HMO must give the Member information on the disenrollment process and direct the Member to the HHSC Administrative Services Contractor. If the request for disenrollment includes a Complaint by the Member, the Complaint will be processed separately from the disenrollment request, through the Complaint process.
The HMO will cooperate with the HHSC’s Administrative Services Contractor and HHSC or its designee to resolve all Member Complaints. Such cooperation may include, but is not limited to, providing information or assistance to internal Complaint committees.
The HMO must provide designated Member Advocates to assist Members in understanding and using the HMO’s Complaint system as described in Section 8.2.7.9. The HMO’s Member Advocates must assist Members in writing or filing a Complaint and monitoring the Complaint through the HMO’s Complaint process until the issue is resolved.
8.2.7.2 Medicaid Standard Member Appeal Process
The HMO must develop, implement and maintain an Appeal procedure that complies with state and federal laws and regulations, including 42 C.F.R.§ 431.200 and 42 C.F.R. Part 438, Subpart F, “Grievance System.” An Appeal is a disagreement with an HMO Action as defined in HHSC’s Uniform Contract Terms and Conditions. The Appeal procedure must be the same for all Members. When a Member or his or her authorized representative expresses orally or in writing any dissatisfaction or disagreement with an Action, the HMO must regard the expression of dissatisfaction as a request to Appeal an Action.
A Member must file a request for an Appeal with the HMO within 30 days from receipt of the notice of the Action. The HMO is subject to remedies, including liquidated damages, if at least 98 percent of Member Appeals are not resolved within 30 days of receipt of the Appeal by the HMO. Please see the Uniform Managed Care Contract Terms & Conditions and Attachment B-5, Deliverables/Liquidated Damages Matrix. To ensure continuation of currently authorized services, however, the Member must file the Appeal on or before the later of 10 days following the HMO’s mailing of the notice of the Action, or the intended effective date of the proposed Action. The HMO must designate an officer who has primary responsibility for ensuring that Appeals are resolved in compliance with written policy and within the 30-day time limit.
The provisions of Chapter 4201, Texas Insurance Code, relating to a Member’s right to Appeal an Adverse Determination made by the HMO or a utilization review agent to an independent review organization, do not apply to a Medicaid recipient. Chapter 4201 is pre-empted by federal Fair Hearings requirements.
The HMO must have policies and procedures in place outlining the Medical Director’s role in an Appeal of an Action. The Medical Director must have a significant role in monitoring, investigating and hearing Appeals. In accordance with 42 C.F.R.§ 438.406, the HMO’s policies and procedures must require that individuals who make decisions on Appeals are not involved in any previous level of review or decision-making, and are health care professionals who have the appropriate clinical expertise in treating the Member’s condition or disease.
The HMO must provide designated Member Advocates, as described in Section 8.2.7.9, to assist Members in understanding and using the Appeal process. The HMO’s Member Advocates must assist Members in writing or filing an Appeal and monitoring the Appeal through the HMO’s Appeal process until the issue is resolved.
The HMO must have a routine process to detect patterns of Appeals. Management, supervisory, and quality improvement staff must be involved in developing policy and procedure improvements to address the Appeals.
The HMO’s Appeal procedures must be provided to Members in writing and through oral interpretive services. A written description of the Appeal procedures must be available in prevalent non-English languages identified by HHSC, at no more than a 6th grade reading level. The HMO must include a written description of the Appeals process in the Member Handbook. The HMO must maintain and publish in the Member Handbook at least one local and one toll-free telephone number with TTY/TDD and interpreter capabilities for requesting an Appeal of an Action.
The HMO’s process must require that every oral Appeal received must be confirmed by a written, signed Appeal by the Member or his or her representative, unless the Member or his or her representative requests an expedited resolution. All Appeals must be recorded in a written record and logged with the following details:
| | 2) Effective date of the Action; |
| | 3) Date the Member or his or her representative requested the Appeal; |
| | 4) Date the Appeal was followed up in writing; |
| | 5) Identification of the individual filing; |
| | 6) Nature of the Appeal; and |
| | 7) Disposition of the Appeal, and notice of disposition to Member. |
The HMO must send a letter to the Member within five (5) business days acknowledging receipt of the Appeal request. Except for the resolution of an Expedited Appeal as provided in Section 8.2.7.3, the HMO must complete the entire standard Appeal process within 30 calendar days after receipt of the initial written or oral request for Appeal. The timeframe for a standard Appeal may be extended up to 14 calendar days if the Member or his or her representative requests an extension; or the HMO shows that there is a need for additional information and how the delay is
in the Member’s interest. If the timeframe is extended, the HMO must give the Member written notice of the reason for delay if the Member had not requested the delay. The HMO must designate an officer who has primary responsibility for ensuring that Appeals are resolved within these timeframes and in accordance with the HMO’s written policies.
During the Appeal process, the HMO must provide the Member a reasonable opportunity to present evidence and any allegations of fact or law in person as well as in writing. The HMO must inform the Member of the time available for providing this information and that, in the case of an expedited resolution, limited time will be available.
The HMO must provide the Member and his or her representative opportunity, before and during the Appeal process, to examine the Member’s case file, including medical records and any other documents considered during the Appeal process. The HMO must include, as parties to the Appeal, the Member and his or her representative or the legal representative of a deceased Member’s estate.
In accordance with 42 C.F.R.§ 438.420, the HMO must continue the Member’s benefits currently being received by the Member, including the benefit that is the subject of the Appeal, if all of the following criteria are met:
| | 1. The Member or his or her representative files the Appeal timely as defined in this Contract: |
| | 2. The Appeal involves the termination, suspension, or reduction of a previously authorized course of treatment; |
| | 3. The services were ordered by an authorized provider; |
| | 4. The original period covered by the original authorization has not expired; and |
| | 5. The Member requests an extension of the benefits. |
If, at the Member’s request, the HMO continues or reinstates the Member’s benefits while the Appeal is pending, the benefits must be continued until one of the following occurs:
1. The Member withdraws the Appeal;
2. Ten (10) days pass after the HMO mails the notice resolving the Appeal against the Member, unless the Member, within the 10-day timeframe, has requested a Fair Hearing with continuation of benefits until a Fair Hearing decision can be reached; or
3. A state Fair Hearing officer issues a hearing decision adverse to the Member or the time period or service limits of a previously authorized service has been met.
In accordance with 42 C.F.R.§ 438.420(d), if the final resolution of the Appeal is adverse to the Member and upholds the HMO’s Action, then to the extent that the services were furnished to comply with the Contract, the HMO may recover such costs from the Member.
If the HMO or State Fair Hearing Officer reverses a decision to deny, limit, or delay services that were not furnished while the Appeal was pending, the HMO must authorize or provide the disputed services promptly and as expeditiously as the Member’s health condition requires.
If the HMO or State Fair Hearing Officer reverses a decision to deny authorization of services and the Member received the disputed services while the Appeal was pending, the HMO is responsible for the payment of services.
The HMO is prohibited from discriminating or taking punitive action against a Member or his or her representative for making an Appeal.
8.2.7.3 Expedited Medicaid HMO Appeals
In accordance with 42 C.F.R. §438.410, the HMO must establish and maintain an expedited review process for Appeals, when the HMO determines (for a request from a Member) or the provider indicates (in making the request on the Member’s behalf or supporting the Member’s request) that taking the time for a standard resolution could seriously jeopardize the Member’s life or health. The HMO must follow all Appeal requirements for standard Member Appeals as set forth in Section 8.2.7.2), except where differences are specifically noted. The HMO must accept oral or written requests for Expedited Appeals.
Members must exhaust the HMO’s Expedited Appeal process before making a request for an expedited Fair Hearing. After the HMO receives the request for an Expedited Appeal, it must hear an approved request for a Member to have an Expedited Appeal and notify the Member of the outcome of the Expedited Appeal within 3 business days, except that the HMO must complete investigation and resolution of an Appeal relating to an ongoing emergency or denial of continued hospitalization: (1) in accordance with the medical or dental immediacy of the case; and (2) not later than one (1) business day after receiving the Member’s request for Expedited Appeal is received.
Except for an Appeal relating to an ongoing emergency or denial of continued hospitalization, the timeframe for notifying the Member of the outcome of the Expedited Appeal may be extended up to 14 calendar days if the Member requests an extension or the HMO shows (to the satisfaction of HHSC, upon HHSC’s request) that there is a need for additional information and how the delay is in the Member’s interest. If the timeframe is extended, the HMO must give the Member written notice of the reason for delay if the Member had not requested the delay.
If the decision is adverse to the Member, the HMO must follow the procedures relating to the notice in Section 8.2.7.5. The HMO is responsible for notifying the Member of his or her right to access an expedited Fair Hearing from HHSC. The HMO will be responsible for providing documentation to the State and the Member, indicating how the decision was made, prior to HHSC’s expedited Fair Hearing.
The HMO is prohibited from discriminating or taking punitive action against a Member or his or her representative for requesting an Expedited Appeal. The HMO must ensure that punitive action is neither taken against a provider who requests an expedited resolution or supports a Member’s request.
If the HMO denies a request for expedited resolution of an Appeal, it must:
| | (1) Transfer the Appeal to the timeframe for standard resolution, and |
| | (2) Make a reasonable effort to give the Member prompt oral notice of the denial, and follow up within two (2) calendar days with a written notice. |
8.2.7.4 Access to Fair Hearing for Medicaid Members
The HMO must inform Members that they have the right to access the Fair Hearing process at any time during the Appeal system provided by the HMO. In the case of an expedited Fair Hearing process, the HMO must inform the Member that he or she must first exhaust the HMO’s internal Expedited Appeal process prior to filing an Expedited Fair Hearing. The HMO must notify Members that they may be represented by an authorized representative in the Fair Hearing process.
If a Member requests a Fair Hearing, the HMO will complete the request for Fair Hearing, and submit the form via facsimile to the appropriate Fair Hearings office, within five (5) calendar days of the Member's request for a Fair Hearing.
Within five (5) calendar days of notification that the Fair Hearing is set, the HMO will prepare an evidence packet for submission to the HHSC Fair Hearings staff and send a copy of the packet to the Member. The evidence packet must comply with HHSC’s Fair Hearings requirements.
8.2.7.5 Notices of Action and Disposition of Appeals for Medicaid Members
The HMO must notify the Member, in accordance with 1 T.A.C. Chapter 357, whenever the HMO takes an Action. The notice must, at a minimum, include any information required by 1 T.A.C. Chapter 357 that relates to a managed care organization’s notice of Action and any information required by 42 C.F.R. §438.404 as directed by HHSC, including but not limited to:
1. The dates, types and amount of service requested;
| | 2. The Action the HMO has taken or intends to take; |
| | 3. The reasons for the Action (If the Action taken is based upon a determination that the requested service is not medically necessary, the HMO must provide an explanation of the medical basis for the decision, application of policy or accepted standards of medical practice to the individuals medical circumstances, in it’s notice to the member.); |
| | 4. The Member’s right to access the HMO’s Appeal process. |
| | 5. The procedures by which the Member may Appeal the HMO’s Action; |
| | 6. The circumstances under which expedited resolution is available and how to request it; |
| | 7. The circumstances under which a Member may continue to receive benefits pending resolution of the Appeal, how to request that benefits be continued, and the circumstances under which the Member may be required to pay the costs of these services; |
| | 8. The date the Action will be taken; |
| | 9. A reference to the HMO policies and procedures supporting the HMO’s Action; |
| | 10. An address where written requests may be sent and a toll-free number that the Member can call to request the assistance of a Member representative, file an Appeal, or request a Fair Hearing; |
| | 11. An explanation that Members may represent themselves, or be represented by a provider, a friend, a relative, legal counsel or another spokesperson; |
| | 12. A statement that if the Member wants a Fair Hearing on the Action, the Member must make the request for a Fair Hearing within 90 days of the date on the notice or the right to request a hearing is waived; |
| | 13. A statement explaining that the HMO must make its decision within 30 days from the date the Appeal is received by the HMO, or 3 business days in the case of an Expedited Appeal; and |
| | 14. A statement explaining that the hearing officer must make a final decision within 90 days from the date a Fair Hearing is requested. |
8.2.7.6 Timeframe for Notice of Action
In accordance with 42 C.F.R.§ 438.404(c), the HMO must mail a notice of Action within the following timeframes:
| | 1. For termination, suspension, or reduction of previously authorized Medicaid-covered services, within the timeframes specified in 42 C.F.R.§§ 431.211, 431.213, and 431.214; |
| | 2. For denial of payment, at the time of any Action affecting the claim; |
| | 3. For standard service authorization decisions that deny or limit services, within the timeframe specified in 42 C.F.R.§ 438.210(d)(1); |
| | 4. If the HMO extends the timeframe in accordance with 42 C.F.R. §438.210(d)(1), it must: |
| | 5. give the Member written notice of the reason for the decision to extend the timeframe and inform the Member of the right to file an Appeal if he or she disagrees with that decision; and |
| | 6. issue and carry out its determination as expeditiously as the Member’s health condition requires and no later than the date the extension expires; |
| | 7. For service authorization decisions not reached within the timeframes specified in 42 C.F.R.§ 438.210(d) (which constitutes a denial and is thus an adverse Action), on the date that the timeframes expire; and |
| | 8. For expedited service authorization decisions, within the timeframes specified in 42 C.F.R. 438.210(d). |
8.2.7.7 Notice of Disposition of Appeal
In accordance with 42 C.F.R.§ 438.408(e), the HMO must provide written notice of disposition of all Appeals including Expedited Appeals. The written resolution notice must include the results and date of the Appeal resolution. For decisions not wholly in the Member’s favor, the notice must contain:
| | 1. The right to request a Fair Hearing; |
| | 2. How to request a Fair Hearing; |
| | 3. The circumstances under which the Member may continue to receive benefits pending a Fair Hearing; |
| | 4. How to request the continuation of benefits; |
| | 5. If the HMO’s Action is upheld in a Fair Hearing, the Member may be liable for the cost of any services furnished to the Member while the Appeal is pending; and |
| | 6. Any other information required by 1 T.A.C. Chapter 357 that relates to a managed care organization’s notice of disposition of an Appeal. |
8.2.7.8 Timeframe for Notice of Resolution of Appeals
In accordance with 42 C.F.R.§ 438.408, the HMO must provide written notice of resolution of Appeals, including Expedited Appeals, as expeditiously as the Member’s health condition requires, but the notice must not exceed the timelines as provided in this Section for Standard or Expedited Appeals. For expedited resolution of Appeals, the HMO must make reasonable efforts to give the Member prompt oral notice of resolution of the Appeal, and follow up with a written notice within the timeframes set forth in this Section for Expedited Appeals. If the HMO denies a request for expedited resolution of an Appeal, the HMO must transfer the Appeal to the timeframe for standard resolution as provided in this Section, and make reasonable efforts to give the Member prompt oral notice of the denial, and follow up within two calendar days wit h a written notice.
8.2.7.9 Medicaid Member Advocates
The HMO must provide Member Advocates to assist Members. Member Advocates must be physically located within the Service Area unless an exception is approved by HHSC. Member Advocates must inform Members of the following:
| | 1. Their rights and responsibilities, |
| | 2. The Complaint process, |
| | 4. Covered Services available to them, including preventive services, and |
| | 5. Non-capitated Services available to them. |
Member Advocates must assist Members in writing Complaints and are responsible for monitoring the Complaint through the HMO’s Complaint process.
Member Advocates are responsible for making recommendations to management on any changes needed to improve either the care provided or the way care is delivered. Member Advocates are also responsible for helping or referring Members to community resources available to meet Member needs that are not available from the HMO as Medicaid Covered Services.
8.2.8 Additional Medicaid Behavioral Health Provisions
8.2.8.1 Local Mental Health Authority (LMHA)
Assessment to determine eligibility for rehabilitative and targeted DSHS case management services is a function of the LMHA. Covered Services must be provided to Members with severe and persistent mental illness (SPMI) and severe emotional disturbance (SED), when Medically Necessary, whether or not they are also receiving targeted case management or rehabilitation services through the LMHA.
The HMO must enter into written agreements with all LMHAs in the Service Area that describe the process(es) that the HMO and LMHAs will use to coordinate services for Medicaid Members with SPMI or SED. The agreements will:
1. Describe the Behavioral Health Services indicated in detail in the Provider Procedures Manual and in the Texas Medicaid Bulletin, include the amount, duration, and scope of basic and Value-added Services, and the HMO’s responsibility to provide these services; |
| 2. Describe criteria, protocols, procedures and instrumentation for referral of Medicaid Members from and to the HMO and the LMHA; |
| 3. Describe processes and procedures for referring Members with SPMI or SED to the LMHA for assessment and determination of eligibility for rehabilitation or targeted case management services; |
| 4. Describe how the LMHA and the HMO will coordinate providing Behavioral Health Services to Members with SPMI or SED; |
| 5. Establish clinical consultation procedures between the HMO and LMHA including consultation to effect referrals and on-going consultation regarding the Member’s progress; |
| 6. Establish procedures to authorize release and exchange of clinical treatment records; |
| 7. Establish procedures for coordination of assessment, intake/triage, utilization review/utilization management and care for persons with SPMI or SED; |
| 8. Establish procedures for coordination of inpatient psychiatric services (including Court- ordered Commitment of Members under 21) in state psychiatric facilities within the LMHA’s catchment area; |
| 9. Establish procedures for coordination of emergency and urgent services to Members; |
| 10. Establish procedures for coordination of care and transition of care for new Members who are receiving treatment through the LMHA; and |
11. Establish that when Members are receiving Behavioral Health Services from the Local Mental Health Authority that the HMO is using the same UM guidelines as those prescribed for use by local mental health authorities by DSHS which are published at: http://www.mhmr.state.tx.us/centraloffice/behavioralhealthservices/RDMClinGuide.html.
The HMO must offer licensed practitioners of the healing arts (defined in 25 T.A.C., Part 2, Chapter 419, Subchapter L), who are part of the Member’s treatment team for rehabilitation services, the opportunity to participate in the HMO’s Network. The practitioner must agree to accept the HMO’s Provider reimbursement rate, meet the credentialing requirements, and comply with all the terms and conditions of the HMO’s standard Provider contract.
HMOs must allow Members receiving rehabilitation services to choose the licensed practitioners of the healing arts who are currently a part of the Member’s treatment team for rehabilitation services to provide Covered Services. If the Member chooses to receive these services from licensed practitioners of the healing arts who are part of the Member’s rehabilitation services treatment team but are not part of the HMO’s Network, the HMO must reimburse the Local Mental Health Authority through Out-of-Network reimbursement arrangements.
Nothing in this section diminishes the potential for the Local Mental Health Authority to seek best value for rehabilitative services by providing these services under arrangement, where possible, as specified is 25 T.A.C. §419.455.
8.2.8.2 Substance Abuse Benefit
Substance Abuse and Dependency Treatment Services
The requirements in this subsection apply to STAR+PLUS HMOs in all Service Areas and to STAR HMOs in all Service Areas except the Dallas Service Area. Members in the Dallas Service Area receive Behavioral Health Services through the NorthSTAR Program.
Benefits related to the treatment of substance use disorder must be available to Medicaid Members by the later of September 1, 2010, or the effective date(s) noted in the Medicaid State Plan, 1915(b) STAR+PLUS waiver and 1915(b) STAR waiver for “Mental Health and Substance Use Disorder Treatment Services.” Substance use disorder includes substance abuse and dependence as defined by the current Diagnostic and Statistical Manual of Mental Disorders (DSM).
Providers
Providers for this benefit include: hospitals, chemical dependency treatment facilities licensed by the Department of State Health Services, and practitioners of the healing arts.
Medicaid HMOs must include Significant Traditional Providers (STPs) of these benefits in its Network, and provide STPs with expedited credentialing. Medicaid HMOs must enter into provider agreements with any willing Significant Traditional Provider (STP) of these benefits that meets the Medicaid enrollment requirements, HMO credentialing requirements and agrees to the HMO’s contract terms and rates. For purposes of this section, STPs are providers who meet the Medicaid enrollment requirements and have a contract with the Department of State Health Services (DSHS) to receive funding for treatment under the Federal Substance Abuse Prevention and Treatment block grant.
Medicaid HMOs must maintain a provider education process to inform substance abuse treatment Providers in the HMO’s Network on how to refer Members for treatment.
Service Coordination
Medicaid HMOs shall ensure service coordination is provided to Members with a substance use disorder. Medicaid HMOs must work with providers, facilities, and Members to coordinate care for Members with a substance use disorder and to ensure Members have access to the full continuum of Covered Services (including without limitation assessment, detoxification, residential treatment, outpatient services, and medication therapy) as medically necessary and appropriate. Medicaid HMOs must also coordinate services with the DSHS, DFPS, and their designees for Members requiring Non-Capitated Services. Non-Capitated Services includes, without limitation, services that are not available for coverage under the Contract, State Plan or Waiver that are available under the Federal Substance Abuse and Prevention and Treatment block grant when provided by a DSHS-funded provider or covered by the DFPS under direct contract with a treatment provider. Medicaid HMOs must work with DSHS, DFPS, and providers to ensure payment for Covered Services is available to Out-of-Network Providers who also provide related Non-capitated Services when the Covered Services are not available through Network Providers.
Member Education and Self-Referral for Substance Abuse Treatment Services
Medicaid HMOs must maintain a Member education process (including hotlines, manuals, policies and other Member Materials) to inform Members of the availability of and access to substance abuse treatment services, including information on self-referral.
8.2.9 Third Party Liability and Recovery
Medicaid HMOs are responsible for establishing a plan and process for recovering costs for services that should have been paid through a third party in accordance with State and Federal law and regulations. To recognize this requirement, capitation payments to the HMOs are reduced by the projected amount of TPR that the HMO is expected to recover.
The HMOs must provide required reports as stated in Section 8.1.17.2, Financial Reporting Requirements.
After 120-days from the date of adjudication on any claim, encounter, or other Medicaid related payment by the HMO subject to Third Party Recovery, HHSC may attempt recovery independent of any HMO action. HHSC will retain, in full, all funds received as a result of the state initiated recovery or subrogation action.
HMOs shall provide a Member quarterly file, which contains the following information if available to the HMO: the Member name, address, claim submission address, group number, employer's mailing address, social security number, and date of birth for each subscriber or policyholder and each dependent of the subscriber or policyholder covered by the insurer. The file shall be used for the purpose of matching the Texas Medicaid eligibility file against the HMO Member file to identify Medicaid clients enrolled in the HMO, which may not be known the Medicaid Program.
8.2.10 Coordination With Public Health Entities
8.2.10.1 Reimbursed Arrangements with Public Health Entities
The HMO must make a good faith effort to enter into a subcontract for Covered Services with Public Health Entities. Possible Covered Services that could be provided by Public Health Entities include, but are not limited to, the following services:
| | 1. Sexually Transmitted Diseases (STDs) services; |
| | 2. Confidential HIV testing; |
| | 4. Tuberculosis (TB) care; |
| | 5. Family Planning services; |
| | 6. Texas Health Steps medical checkups, and |
These subcontracts must be available for review by HHSC or its designated agent(s) on the same basis as all other subcontracts. If the HMO is unable to enter into a contract with Public Health Entities, the HMO must document efforts to contract with Public Health Entities, and make such documentation available to HHSC upon request.
HMO Contracts with Public Health Entities must specify the scope of responsibilities of both parties, the methodology and agreements regarding billing and reimbursements, reporting responsibilities, Member and Provider educational responsibilities, and the methodology and agreements regarding sharing of confidential medical record information between the Public Health Entity and the HMO or PCP.
The HMO must:
| | 1. Identify care managers who will be available to assist public health providers and PCPs in efficiently referring Members to the public health providers, specialists, and health-related service providers either within or outside the HMO’s Network; and |
| | 2. Inform Members that confidential healthcare information will be provided to the PCP, and educate Members on how to better utilize their PCPs, public health providers, emergency departments, specialists, and health-related service providers. |
8.2.10.2 Non-Reimbursed Arrangements with Local Public Health Entities
The HMO must coordinate with Public Health Entities in each Service Area regarding the provision of essential public health care services. In addition to the requirements listed above in Section 8.2.2, or otherwise required under state law or this contract, the HMO must meet the following requirements:
| | 1. Report to public health entities regarding communicable diseases and/or diseases that are preventable by immunization as defined by state law; |
| | 2. Notify the local Public Health Entity, as defined by state law, of communicable disease outbreaks involving Members; |
| | 3. Educate Members and Providers regarding WIC services available to Members; and |
| | 4. Coordinate with local public health entities that have a child lead program, or with DSHS regional staff when the local public health entity does not have a child lead program, for follow-up of suspected or confirmed cases of childhood lead exposure. |
8.2.11 Coordination with Other State Health and Human Services (HHS) Programs
The HMO must coordinate with other state HHS Programs in each Service Area regarding the provision of essential public health care services. In addition to the requirements listed above in Section 8.2.2. or otherwise required under state law or this contract, the HMO must meet the following requirements:
| | 1. Require Providers to use the DSHS Bureau of Laboratories for specimens obtained as part of a Texas Health Steps medical checkup, including Texas Health Steps newborn screens, lead testing, and hemoglobin/hematocrit tests; |
| | 2. Notify Providers of the availability of vaccines through the Texas Vaccines for Children Program; |
| | 3. Work with HHSC and Providers to improve the reporting of immunizations to the statewide ImmTrac Registry; |
| | 4. Educate Providers and Members about the Department of State Health Services (DSHS) Case Management for Children and Pregnant Women (CPW) services available; |
| | 5. Coordinate services with CPW specifically in regard to an HMO Member’s health care needs that are identified by CPW and referred to the HMO; |
| | 6. Participate, to the extent practicable, in the community-based coalitions with the Medicaid-funded case management programs in the Department of Assistive and Rehabilitative Services (DARS), the Department of Aging and Disability Services (DADS), and DSHS; |
| | 7. Cooperate with activities required of state and local public health authorities necessary to conduct the annual population and community based needs assessment; |
| | 8. Report all blood lead results, coordinate and follow-up of suspected or confirmed cases of childhood lead exposure with the Childhood Lead Poisoning Prevention Program in DSHS; and |
| | 9. Coordinate with Texas Health Steps. |
8.2.12 Advance Directives
Federal and state law require HMOs and providers to maintain written policies and procedures for informing all adult Members 18 years of age and older about their rights to refuse, withhold or withdraw medical treatment and mental health treatment through advance directives (see Social Security Act §1902(a)(57) and §1903(m)(1)(A)). The HMO’s policies and procedures must include written notification to Members and comply with provisions contained in 42 C.F.R. § 489, Subpart I, relating to advance directives for all hospitals, critical access hospitals, skilled nursing facilities, home health agencies, providers of home health care, providers of personal care services and hospices, as well as the following state laws and rules:
| | 1. A Member’s right to self-determination in making health care decisions; |
| | 2. The Advance Directives Act, Chapter 166, Texas Health and Safety Code, which includes: |
| | a. A Member’s right to execute an advance written directive to physicians and family or surrogates, or to make a non-written directive to administer, withhold or withdraw life-sustaining treatment in the event of a terminal or irreversible condition; |
| | b. A Member’s right to make written and non-written out-of-hospital do-not-resuscitate (DNR) orders; |
| | c. A Member’s right to execute a Medical Power of Attorney to appoint an agent to make health care decisions on the Member’s behalf if the Member becomes incompetent; and |
| | 3. The Declaration for Mental Health Treatment, Chapter 137, Texas Civil Practice and Remedies Code, which includes: a Member’s right to execute a Declaration for Mental Health Treatment in a document making a declaration of preferences or instructions regarding mental health treatment. |
The HMO must maintain written policies for implementing a Member’s advance directive. Those policies must include a clear and precise statement of limitation if the HMO or a Provider cannot or will not implement a Member’s advance directive.
The HMO cannot require a Member to execute or issue an advance directive as a condition of receiving health care services. The HMO cannot discriminate against a Member based on whether or not the Member has executed or issued an advance directive.
The HMO’s policies and procedures must require the HMO and subcontractors to comply with the requirements of state and federal law relating to advance directives. The HMO must provide education and training to employees and Members on issues concerning advance directives.
All materials provided to Members regarding advance directives must be written at a 7th - 8th grade reading comprehension level, except where a provision is required by state or federal law and the provision cannot be reduced or modified to a 7th - 8th grade reading level because it is a reference to the law or is required to be included “as written” in the state or federal law.
The HMO must notify Members of any changes in state or federal laws relating to advance directives within 90 days from the effective date of the change, unless the law or regulation contains a specific time requirement for notification.
8.3 Additional STAR+PLUS Scope of Work
8.3.1 Covered Community-Based Long-Term Care Services
The HMO must ensure that STAR+PLUS Members needing Community Long-term Care Services are identified and that services are referred and authorized in a timely manner. The HMO must ensure that Providers of Community Long-term Care Services are licensed to deliver the service they provide. The inclusion of Community Long-term Care Services in a managed care model presents challenges, opportunities and responsibilities.
Community Long-term Care Services may be necessary as a preventative service to avoid more expensive hospitalizations, emergency room visits, or institutionalization. Community Long-term Care Services should also be made available to Members to assure maintenance of the highest level of functioning possible in the least restrictive setting. A Member’s need for Community Long-term Care Services to assist with the activities of daily living must be considered as important as needs related to a medical condition. HMOs must provide Functionally Necessary Covered Services to Community Long-term Care Service Members.
8.3.1.1 Community Based Long-Term Care Services Available to All Members
The HMO shall enter into written contracts with Providers of Personal Assistance Services and Day Activity and Health Services (DAHS) to make them available to all STAR+PLUS Members. These Providers must at a minimum, meet all of the following state licensure and certification requirements for providing the services in Attachment B-2.1, Covered Services.
| Community Long-Term Care Services Available to All Members |
| Service | Licensure and Certification Requirements |
| Personal Attendant Services | The Provider must be licensed by the Texas Department of Human Services as a Home and Community Support Services Agency. The level of licensure required depends on the type of service delivered. NOTE: For primary home care and client managed attendant care, the agency may have only the Personal Assistance Services level of licensure. |
Community Long-Term Care Services Available to All Members Service Licensure and Certification Requirements
| Day Activity and Health Services (DAHS) | The Provider must be licensed by the Texas Department of Human Services, Long Term Care Regulatory Division, as an adult day care provider. To provide DAHS, the Provider must provide the range of services required for DAHS. |
8.3.1.2 1915(c) Nursing Facility Waiver Services Available to Members Who Qualify for 1915 (c) Nursing Facility Waiver Services
The 1915(c) Nursing Facility Waiver provides Community Long-term Care Services to Medicaid Eligibles who are elderly and to adults with disabilities as a cost-effective alternative to living in a nursing facility. These Members must be age 21 or older, be a Medicaid recipient or be otherwise financially eligible for waiver services. To be eligible for 1915(c) Nursing Facility Waiver Services, a Member must meet income and resource requirements for Medicaid nursing facility care, and receive a determination from HHSC on the medical necessity of the nursing facility care. The HMO must make available to STAR+PLUS Members who meet the eligibility requirements the array of services allowable through HHSC’s CMS-appro ved 1915(c) Nursing Facility Waiver (see Appendix B-2.1, STAR+PLUS Covered Services).
| Community Long-Term Care Services Under the 1915(c) Nursing Facility Waiver |
| Service | Licensure and Certification Requirements |
| Personal Attendant Services | The Provider must be licensed by the Texas Department of Human Services as a Home and Community Support Services Agency. The level of licensure required depends on the type of service delivered. For Primary Home Care and Client Managed Attendant Care, the agency may have only the Personal Assistance Services level of licensure. |
| Assisted Living | The Provider must be licensed by the Texas Department of Aging and Disability Services, Long Term Care Regulatory Division. The type of licensure determines what services may be provided. |
| Emergency Response Service Provider | Texas Department of Aging and Disability Services (DADS) Standards for Emergency Response Services at 40 T.A.C. §52.201(a), and be licensed by the Texas Board of Private Investigators and Private Security Agencies, unless exempt from licensure. |
| Adult Foster Home | TDSHS Provider standards for Adult Foster Care and TDSHS Rules at 40 T.A.C. §48.6032. Four bed homes also licensed under TDSHS Rules at 40 T.A.C. §481.8906. DFPS licensure in accordance with 24-hour Care Licensing requirements found in T.A.C., Title 40, Part 19, Chapter 720. |
Home Delivered Meals | T.A.C., Title 40, Part 1, Chapter 55. |
Community Long-Term Care Services Under the 1915(c) Nursing Facility Waiver Service Licensure and Certification Requirements
Physical Therapy | Licensed Physical Therapist through the Texas Board of Physical Therapy Examiners, Chapter 453. |
Occupational Therapy | Licensed Occupational Therapist through the Texas Board of Occupational Therapy Examiners, Chapter 454. |
| Speech Therapy | Licensed Speech Therapist Through the Department of State Health Services. |
| Consumer Directed Services | Home and Community Support Services Agency (HCSSA) |
| Transition Assistance Services | No licensure or certification requirements. |
| Minor Home Modification | No licensure or certification requirements. |
| Adaptive Aids and Medicaid Equipment | No licensure or certification requirements. |
| Medical supplies | No licensure or certification requirements. |
8.3.2 Service Coordination
The HMO must furnish a Service Coordinator to all STAR+PLUS Members who request one. The HMO should also furnish a Service Coordinator to a STAR+PLUS Member when the HMO determines one is required through an assessment of the Member’s health and support needs. The HMO must ensure that each STAR+PLUS Member has a qualified PCP who is responsible for overall clinical direction and, in conjunction with the Service Coordinator, serves as a central point of integration and coordination of Covered Services, including primary, Acute Care, long-term care and Behavioral Health Services.
The Service Coordinator must work as a team with the PCP, and coordinate all STAR+PLUS Covered Services and any applicable Non-capitated Services with the PCP. This requirement applies whether or not the PCP is in the HMO’s Network, as some STAR+PLUS Members dually eligible for Medicare may have a PCP that is not in the HMO’s Provider Network. In order to integrate the Member’s Acute Care and primary care, and stay abreast of the Member’s needs and condition, the Service Coordinator must also actively involve and coordinate with the Member’s primary and specialty care providers, including Behavioral Health Service providers, and providers of Non-capitated Services.
STAR+PLUS Members dually eligible for Medicare will receive most prescription drug services through Medicare rather than Medicaid. The Texas Vendor Drug Program will pay for a limited number of medications not covered by Medicare.
The HMO must identify and train Members or their families to coordinate their own care, to the extent of the Member’s or the family’s capability and willingness to coordinate care.
8.3.2.1 Service Coordinators
The HMO must employ as Service Coordinators persons experienced in meeting the needs of vulnerable populations who have Chronic or Complex Conditions. Such Service Coordinators are Key HMO Personnel as described in Attachment A, HHSC’s Uniform Managed Care Contract Terms and Conditions, Section 4.02, and must meet the requirements set forth in Section 4.04.1 of HHSC’s Uniform Managed Care Contract Terms and Conditions.
8.3.2.2 Referral to Community Organizations
The HMO must provide information about and referral to community organizations that may not be providing STAR+PLUS Covered Services, but are otherwise important to the health and well being of Members. These organizations include, but are not limited to:
| | 1. State/federal agencies (e.g., those agencies with jurisdiction over aging, public health, substance abuse, mental health/retardation, rehabilitation, developmental disabilities, income support, nutritional assistance, family support agencies, etc.); |
| | 2. social service agencies (e.g., Area Agencies on Aging, residential support agencies, independent living centers, supported employment agencies, etc.); |
| | 3. city and county agencies (e.g., welfare departments, housing programs, etc.); |
| | 4. civic and religious organizations; and |
| | 5. consumer groups, advocates, and councils (e.g., legal aid offices, consumer/family support groups, permanency planning, etc.). |
8.3.2.3 Discharge Planning
The HMO must have a protocol for quickly assessing the needs of Members discharged from a Hospital or other care or treatment facility.
The HMO’s Service Coordinator must work with the Member’s PCP, the hospital discharge planner(s), the attending physician, the Member, and the Member’s family to assess and plan for the Member’s discharge. When long-term care is needed, the HMO must ensure that the Member’s discharge plan includes arrangements for receiving community-based care whenever possible. The HMO must ensure that the Member, the Member’s family, and the Member’s PCP are all well informed of all service options available to meet the Member’s needs in the community.
8.3.2.4 Transition Plan for New STAR+PLUS Members
The HMO must provide a transition plan for Members enrolled in the STAR+PLUS Program. HHSC, and/or the previous STAR+PLUS HMO contractor, will provide the HMO with detailed Care Plans, names of current providers, etc., for newly enrolled Members already receiving long-term care services at the time of enrollment. The HMO must ensure that current providers are paid for Medically Necessary Covered Services that are delivered in accordance with the Member’s existing treatment/long-term care services plan after the Member has become enrolled in the HMO and until the transition plan is developed.
The transition planning process must include, but is not limited to, the following:
| | 1. review of existing DADS long-term care services plans; |
| | 2. preparation of a transition plan that ensures continuous care under the Member’s existing Care Plan during the transfer into the HMO’s Network while the HMO conducts an appropriate assessment and development of a new plan, if needed; |
| | 3. if durable medical equipment or supplies had been ordered prior to enrollment but have not been received by the time of enrollment, coordination and follow-through to ensure that the Member receives the necessary supportive equipment and supplies without undue delay; and |
| | 4. payment to the existing provider of service under the existing authorization until the HMO has completed the assessment and service plans and issued new authorizations. |
The HMO must review any existing care plan and develop a transition plan within 30 days of receiving the Member’s enrollment. The transition plan will remain in place until the HMO contacts the Member and coordinates modifications to the Member’s current treatment/long-term care services plan. The HMO must ensure that the existing services continue and that there are no breaks in services. For initial implementation of the STAR+PLUS program in a Service Area, the HMO must complete this process within 90-days of the Member’s enrollment.
The HMO must ensure that the Member is involved in the assessment process and fully informed about options, is included in the development of the care plan, and is in agreement with the plan when completed.
8.3.2.5 Centralized Medical Record and Confidentiality
The Service Coordinator shall be responsible for maintaining a centralized record related to Member contacts, assessments and service authorizations. The HMO shall ensure that the organization of and documentation included in the centralized Member record meets all applicable professional standards ensuring confidentiality of Member records, referrals, and documentation of information.
The HMO must have a systematic process for generating or receiving referrals and sharing confidential medical, treatment, and planning information across providers.
8.3.2.6 Nursing Facilities
Nursing facility care, although a part of the care continuum, presents a challenge for managed care. Because of the process for becoming eligible for Medicaid assistance in a nursing facility, there is frequently a significant time gap between entry into the nursing home and determination of Medicaid eligibility. During this gap from entry to Medicaid eligibility, the resident has “nested” in the facility and many of the community supports are no longer available. To require participation of all nursing facility residents would result in the HMO maintaining a Member in the nursing facility without many options for managing their health. For this reason, persons who qualify for Medicaid as a result of nursing facility residency are not enrolled in STAR+PLUS.
The STAR+PLUS HMO must participate in the Promoting Independence initiative for such individuals. Promoting Independence (PI) is a philosophy that aged and disabled individuals
remain in the most integrated setting to receive long-term care services. PI is Texas' response to the U.S. Supreme Court ruling in Olmstead v. L.C. that requires states to provide community-based services for persons with disabilities who would otherwise be entitled to institutional services, when:
| | • the state's treatment professionals determine that such placement is appropriate; |
| | • the affected persons do not oppose such treatment; and |
| | • the placement can be reasonably accommodated, taking into account the resources available to the state and the needs of others who are receiving state supported disability services. |
In accordance with legislative direction, the HMO must designate a point of contact to receive referrals for nursing facility residents who may potentially be able to return to the community through the use of 1915(c) Nursing Facility Waiver services. To be eligible for this option, an individual must reside in a nursing facility until a written plan of care for safely moving the resident back into a community setting has been developed and approved.
A STAR+PLUS Member who enters a nursing facility will remain a STAR+PLUS Member for a total of four months. The nursing facility will bill the state directly for covered nursing facility services delivered while the Member is in the nursing facility. See Section 8.3.2.7 for further information.
The HMO is responsible for the Member at the time of nursing facility entry and must utilize the Service Coordinator staff to complete an assessment of the Member within 30 days of entry in the nursing facility, and develop a plan of care to transition the Member back into the community if possible. If at this initial review, return to the community is possible, the Service Coordinator will work with the resident and family to return the Member to the community using 1915(c) Waiver Services.
If the initial review does not support a return to the community, the Service Coordinator will conduct a second assessment 90 days after the initial assessment to determine any changes in the individual’s condition or circumstances that would allow a return to the community. The Service Coordinator will develop and implement the transition plan.
The HMO will provide these services as part of the Promoting Independence initiative. The HMO must maintain the documentation of the assessments completed and make them available for state review at any time.
It is possible that the STAR+PLUS HMO will be unaware of the Member’s entry into a nursing facility. It is the responsibility of the nursing facility to review the Member’s Medicaid card upon entry into the facility and notify the HMO. The nursing facility is also required to notify HHSC of the entry of a new resident.
8.3.2.7 HMO Four-Month Liability for Nursing Facility Care
A STAR+PLUS Member who enters a nursing facility will remain a STAR+PLUS Member for a total of four months. The four months do not have to be consecutive. Upon completion of four
months of nursing facility care, the individual will be disenrolled from the STAR+PLUS Program and the Medicaid Fee-for-Service program will provide Medicaid benefits. A STAR+PLUS Member may not change HMOs while in a nursing facility.
Tracking the four months of liability is done through a counter system. The four-month counter starts with the earlier of: (1) the date of the Medicaid admission to the nursing facility, or (2) on the 21st day of a Medicare stay, if applicable. A partial month counts as a full month. In other words, the month in which the Medicaid admission occurs or the month on which the 21st day of the Medicare stay occurs, is counted as one of the four months.
The HMO will not be liable for the cost of care provided in a nursing facility. For Medicaid-only Members, the cost of all other Covered Services will be included in the capitation payment analysis. The HMO will not maintain nursing facilities in its Provider Network, and will not reimburse the nursing facilities for Covered Services provided in such facilities. Nursing facilities will use the traditional Fee-for-Service (FFS) system of billing HHSC rather than billing the HMO.
8.3.3 STAR+PLUS Assessment Instruments
The HMO must have and use functional assessment instruments to identify Members with significant health problems, Members requiring immediate attention, and Members who need or are at risk of needing long-term care services. The HMO, a subcontractor, or a Provider may complete assessment instruments, but the HMO remains responsible for the data recorded.
HMOs must use the DADS Form 2060, as amended or modified, to assess a Member’s need for Functionally Necessary Personal Attendant Services. The HMO may adapt the form to reflect the HMO’s name or distribution instructions, but the elements must be the same and instructions for completion must be followed without amendment.
The DADS Form 2060 must be completed if a need for or a change in Personal Attendant Services is warranted at the initial contact, at the annual reassessment, and anytime a Member requests the services or requests a change in services. The DADS Form 2060 must also be completed at any time the HMO determines the Member requires the services or requires a change in the Personal Attendant Services that are authorized.
HMOs must use the Texas Medicaid Personal Care Assessment Form (PCAF Form) in lieu of the DADS Form 2060 for children under the age of 21 when assessing the Member’s need for Functional Necessary Personal Attendant Services. HMOs may adapt the PCAF Form to reflect the HMO’s name or distribution instructions, but the elements must be the same and instructions for completion must be followed without amendment. Reassessments using the PCAF Form must be completed every twelve months and as requested by the Member’s parent or other legal guardian. The PCAF Form must also be completed at any time the HMO determines the Member may require a change in the number of authorized Personal Attendant Service hours.
For Members and applicants seeking or needing the 1915(c) Nursing Facility Waiver services, the HMOs must use the Community Medical Necessity and Level of Care Assessment Instrument, as amended or modified, to assess Members and to supply current medical information for Medical Necessity determinations. The HMO must also complete the Individual Service Plan (ISP), Form 3671 for each Member receiving 1915(c) Nursing Facility Waiver Services. The ISP is established for a one-year period. After the initial ISP is established, the ISP must be completed on an annual basis and the end date or expiration date does not change. Both of these forms (Community Medical Necessity and Level of Care Assessment Instrument and Form 3671) must be completed annually at reass essment. The HMO is responsible for tracking the end dates of the ISP to ensure all Member reassessment activities have been completed and posted on the LTC online portal prior to the expiration date of the ISP. Note that the HMO cannot submit its initial Community Medical Necessity and Level of Care Assessment Instrument cannot be submitted earlier than 120 days prior to the expiration date of the ISP. An Initial Community Medical Necessity and Level of Care determination will expire 120 days after it is approved by the HHSC Claims Administrator. The HMO cannot submit a renewal of the Community Medical Necessity and Level of Care Assessment Instrument earlier than 90 days prior to the expiration date of the ISP. Such renewal will expire 90 days after it is approved by the HHSC Claims Administrator.
8.3.4 1915(c) Nursing Facility Waiver Service Eligibility
Recipients of 1915(c) Nursing Facility Waiver services must meet nursing facility criteria for participation in the waiver and must have a plan of care at initial determination of eligibility in which the plan’s annualized cost is equal to or less than 200% of the annualized cost of care if the individual were to enter a nursing facility. If the HMO determines that the recipient’s cost of care will exceed the 200% limit, the HMO will submit to Health Plan Operations a request to consider the use of State General Revenue Funds to cover costs over the 200% allowance, as per HHSC’s policy and procedures related to use of general revenue for 1915(c) Nursing Facility Waiver participants. If HHSC approves the use of general revenue funds, the HMO will be allowed to provide waiver services as per the Individual Service Plan, an d non-waiver services (services in excess of the 200% allowance) utilizing State General Revenue Funds. Non-waiver services are not Medicaid Allowable Expenses, and may not be reported as such on the FSRs. The HMO will submit reports documenting expenses for non-waiver services in accordance with the requirements of the Uniform Managed Care Manual. HHSC will reimburse the HMO for such expenses in accordance with the procedures set forth in the Uniform Managed Care Manual.
8.3.4.1 For Members
The HMO must notify HHSC when it initiates 1915(c) Nursing Facility Waiver eligibility testing on a STAR+PLUS Member. The HMO must apply risk criteria, complete the Community Medical Necessity and Level of Care Assessment Instrument for Medical Necessity determination, complete the assessment documentation, and prepare a 1915(c) Nursing Facility Waiver Individual Service Plan (ISP) for each Member requesting 1915(c) Nursing Facility Waiver services and for Members the HMO has identified as needing 1915(c) Nursing Facility Waiver services. The HMO must provide HHSC the results of the assessment activities within 45 days of initiating the assessment process.
HHSC will notify the Member and the HMO of the eligibility determination, which will be based on the information provided by the HMO. If the STAR+PLUS Member is eligible for 1915(c) Nursing Facility Waiver services, HHSC will notify the Member of the effective date of eligibility. If the Member is not eligible for 1915(c) Nursing Facility Waiver services, HHSC will provide the Member information on right to Appeal the Adverse Determination. Regardless of the 1915(c) Nursing Facility Waiver eligibility determination, HHSC will send a copy of the Member notice to the HMO.
8.3.4.2 For Medical Assistance Only (MAO) Non-Member Applicants
Non-Member persons who are not eligible for Medicaid in the community may apply for participation in the 1915(c) Nursing Facility Waiver program under the financial and functional eligibility requirements for MAO. HHSC will inform the applicant that services are provided through an HMO and allow the applicant to select the HMO. HHSC will authorize the selected HMO to initiate pre-enrollment assessment services required under the 1915(c) Nursing Facility Waiver for the non-member. The HMO must complete Community Medical Necessity and Level of Care Assessment Instrument for Medical Necessity determination, complete the assessment documentation, and prepare a 1915(c) Nursing Facility Waiver service plan for each applicant referred by HHSC. The initial home visit with the applicant must occur within 14 days of the receipt of the referral. The HMO must provide HHSC the results of the assessment activities within 45 days of the receipt of the referral.
HHSC will notify the applicant and the HMO of the results of its eligibility determination. If the applicant is eligible, HHSC will notify the applicant and the HMO will be notified of the effective date of eligibility, which will be the first day of the month following the determination of eligibility. The HMO must initiate the Individual Service Plan (ISP) on the date of enrollment.
If the applicant is not eligible, the HHSC notice will provide information on the applicant’s right to Appeal the Adverse Determination. HHSC will also send notice to the HMO if the applicant is not eligible for 1915(c) Nursing Facility Waiver services.
8.3.4.3 Annual Reassessment
Prior to the end date of the annual ISP, the HMO must initiate an annual reassessment to determine and validate continued eligibility for 1915(c) Nursing Facility Waiver services for each Member receiving such services. The HMO will be expected to complete the same activities for each annual reassessment as required for the initial eligibility determination.
8.3.5 Consumer Directed Services Options
There are three options available to STAR+PLUS Members desiring the delivery of Personal Attendant Services (PAS) and/or In-Home or Out-of-Home Respite: 1) Self-Directed; 2) Agency Model, Self-Directed; and 3) Agency Model. The HMO must provide information concerning the three options to all Members: (1) who meet the functional requirements for Primary Home Care Services in the 1915(b) Waiver and the requirements for PAS in the STAR+PLUS 1915(c) Waiver (the functional criteria for these services are described in the Form 2060), and (2) who are eligible for In-Home or Out-of-Home Respite Services. In addition to providing information concerning the three options, the HMO must provide Member orientation in the option selected by the Member. The HMO must provide the information to any STAR+PLUS Member receiving PAS and/or In-Home or Out-of-H ome Respite:
| | • at annual reassessment or annual contact with the STAR+PLUS Member; |
| | • at any time when a STAR+PLUS Member receiving PAS requests the information; and |
| | • in the Member Handbook. |
The HMO must contract with providers who are able to offer PAS and/or In-Home or Out-of-Home Respite and must also educate/train the HMO Network Providers regarding the three PAS options. To participate as a PAS Network Provider, the Provider must have a contract with DADS for the delivery of PAS and/or In-Home or Out-of-Home Respite. The HMO must assure compliance with the Texas Administrative Code in Title 40, Part 1, Chapter 41, Sections 41.101, 41.103, and 41.105. The HMO must include the requirements in the Provider Manual and in the STAR+PLUS Provider training.
8.3.5.1 Self-Directed Model
In the Self-Directed Model, the Member or the Member’s legal guardian is the employer of record and retains control over the hiring, management, and termination of an individual providing Personal Attendant Services and/or In-Home or Out-of Home Respite. The Member is responsible for assuring that the employee meets the requirements for Personal Attendant Services and/or In-Home or Out-of Home Respite, including the criminal history check. The Member uses a Home and Community Support Services (HCSS) agency to handle the employer-related administrative functions such as payroll, substitute (back-up), and filing tax-related reports of Personal Attendant Services and/or In-Home or Out-of Home Respite.
8.3.5.2 Agency Model, Self-Directed
In the Agency Model, Self-Directed, the Member or the Member’s legal guardian chooses a Home and Community Support Services (HCSS) agency in the HMO Provider Network who is the employer of record. In this model, the Member selects the personal attendant from the HCSS agency’s personal attendant employees. The personal attendant’s schedule is set up based on the Member input, and the Member manages the Personal Attendant Services and/or In-Home or Out-of Home Respite. The Member retains the right to supervise and train the personal attendant. The Member may request a different personal attendant and the HCSS agency would be expected to honor the request. The HCSS agency establishes the payment rate, benefits, and provides all administrative functions such as payroll, substitute (back-up), and filing tax-related reports of personal attendant services and/or In-Home or Out-of Home Respite.
8.3.5.3 Agency Model
In the Agency Model, the Member chooses a Home and Community Support Services (HCSS) agency to hire, manage, and terminate the individual providing Personal Attendant Services and/or In-Home or Out-of Home Respite. The HCSS agency is selected by the Member from the HCSS agencies in the HMO Provider Network. The Service Coordinator and Member develop the schedule and send it to the HCSS agency. The Member retains the right to supervise and train the personal attendant. The Member may request a different personal attendant and the HCSS agency would be expected to honor the request. The HCSS agency establishes the payment rate, benefits, and provides all administrative functions such as payroll, substitute (back-up), and filing tax-related reports of personal attendant services and/or In-Home or Out-of Home Respite.
8.3.6 Community Based Long-term Care Service Providers
8.3.6.1 Training
The HMO must comply with Section 8.1.4.6 regarding Provider Manual and Provider training specific to the STAR+PLUS Program. The HMO must train all Community Long-term Care Service Providers regarding the requirements of the Contract and special needs of STAR+PLUS Members. The HMO must establish ongoing STAR+PLUS Provider training addressing the following issues at a minimum:
| | 1. Covered Services and the Provider’s responsibilities for providing such services to STAR+PLUS Members and billing the HMO for such services. The HMO must place special emphasis on Community Long-term Care Services and STAR+PLUS requirements, policies, and procedures that vary from Medicaid Fee-for-Service and commercial coverage rules, including payment policies and procedures. |
| | 2. Inpatient Stay hospital services and the authorization and billing of such services for STAR+PLUS Members. |
| | 3. Relevant requirements of the STAR+PLUS Contract, including the role of the Service Coordinator; |
| | 4. Processes for making referrals and coordinating Non-capitated Services; |
| | 5. The HMO’s quality assurance and performance improvement program and the Provider’s role in such programs; and |
| | 6. The HMO’s STAR+PLUS policies and procedures, including those relating to Network and Out-of-Network referrals. |
8.3.6.2 LTC Provider Billing
Long-term care providers are not required to utilize the billing systems that most medical facilities use on a regular basis. For this reason, the HMO must make accommodations to the claims processing system for such providers to allow for a smooth transition from traditional Medicaid to Managed Care Medicaid.
HHSC will meet with HMOs to develop a standardized method long-term care billing. All STAR+PLUS HMOs will be required to utilize the standardized method, which will be incorporated into the HHSC Uniform Managed Care Manual.
8.3.6.3 Rate Enhancement Payments for Agencies Providing Attendant Care
All HMOs participating in the STAR+PLUS program must allow their Long-term Support Services (LTSS) Providers to participate in the STAR+PLUS Attendant Care Enhancement Program.
Attachment B-7, STAR+PLUS Attendant Care Enhanced Payment Methodology explains the methodology that the STAR+PLUS HMO will use to implement and pay the enhanced payments, including a description of the timing of the payments, in accordance with the requirements in the Uniform Managed Care Manual and the intent of the 2000-01 General Appropriations Act (Rider 27, House Bill 1, 76th Legislature, Regular Session, 1999) and T.A.C. Title 1, Part 15, Chapter 355.
8.3.6.4 Payment for 1915(c) Nursing Facility Waiver Services for Non-Members
Disenrolled Members: Occasionally, the Social Security Administration will place SSI recipients on hold for a short period of time, usually due failure to provide timely updates required for the continuation of SSI benefits. During this period, the recipients will not appear to be eligible for Medicaid or 1915(c) Nursing Facility Waiver services. Often the Social Security Administration reinstates these Medicaid Eligibles retroactively without a break in Medicaid coverage. To deal with this situation, for at least thirty (30) days after disenrollment, the HMO will continue to authorize and pay for 1915(c) Nursing Facility Waiver services for disenrolled STAR+PLUS Members who appear to lose eligibility due to an administrative problem related to SSI. If at the end of the thirty (30) d ays, the Medicaid Eligible’s 1915(c) Nursing Facility Waiver eligibility is reinstated, the Medicaid Eligible will be manually enrolled into the STAR+PLUS HMO back to the date of disenrollment and the retroactive adjustment system will properly reimburse the HMO. If after thirty (30) days, the former STAR+PLUS Member continues to be ineligible for Medicaid, the individual will not be retroactively enrolled, and the HMO will bill HHSC for 1915(c) Nursing Facility Waiver services rendered during this time.
8.3.6.5 STAR+PLUS Handbook
The STAR+PLUS Handbook will contain HHSC-approved policies and procedures related to the STAR+PLUS Program, including policies and procedures relating to the 1915(b) and 1915(c) STAR+PLUS Waivers. The STAR+PLUS Handbook will include additional requirements regarding the STAR+PLUS Program and guidance for the HMOs, the STAR+PLUS Support Units at DADS, and HHSC staff for administrating and managing STAR+PLUS Program operations. The STAR+PLUS Handbook, once approved by HHSC, is incorporated by reference into this Contract.
| 8.4 Additional CHIP Scope of Work |
The following provisions only apply to HMOs participating in CHIP.
8.4.1 CHIP Provider Network
In each Service Area, the HMO must seek to obtain the participation in its Provider Network of CHIP Significant Traditional Providers (STPs), defined by HHSC as PCP Providers currently serving the CHIP population and DSH hospitals. The Procurement Library includes CHIP STPs by Service Area.
The HMO must give STPs the opportunity to participate in its Network if the STPs:
| | 1. Agree to accept the HMO’s Provider reimbursement rate for the provider type; and |
| | 2. Meet the standard credentialing requirements of the HMO, provided that lack of board certification or accreditation by the Joint Commission on Accreditation of Health Care Organizations (JCAHO) is not the sole grounds for exclusion from the Provider Network. |
8.4.2 CHIP Provider Complaint and Appeals
CHIP Provider Complaints and Appeals are subject to disposition consistent with the Texas Insurance Code and any applicable TDI regulations. The HMO must resolve Provider Complaints within 30 days from the date the Complaint is received.
8.4.3 CHIP Member Complaint and Appeal Process
CHIP Member Complaints and Appeals are subject to disposition consistent with the Texas Insurance Code and any applicable TDI regulations. HHSC will require the HMO to resolve Complaints and Appeals (that are not elevated to TDI) within 30 days from the date the Complaint or Appeal is received. The HMO is subject to remedies, including liquidated damages, if at least 98 percent of Member Complaints or Member Appeals are not resolved within 30 days of receipt of the Complaint or Appeal by the HMO. Please see the Uniform Managed Care Contract Terms & Conditions and Attachment B-5, Deliverables/Liquidated Damages Matrix. Any person, including those dissatisfied with a HMO’s resolution of a Complaint or Appeal, may report an alleged violation to TDI.
8.4.4 Dental Coverage for CHIP Members
The HMO is not responsible for reimbursing dental providers for preventive and therapeutic dental services obtained by CHIP Members. However, medical and/or hospital charges, such as anesthesia, that are necessary in order for CHIP Members to access standard therapeutic dental services, are Covered Services for CHIP Members. The HMO must provide access to facilities and physician services that are necessary to support the dentist who is providing dental services to a CHIP Member under general anesthesia or intravenous (IV) sedation.
The HMO must inform Network facilities, anesthesiologists, and PCPs what authorization procedures are required, and how Providers are to be reimbursed for the preoperative evaluations by the PCP and/or anesthesiologist and for the facility services. For dental-related medical Emergency Services, the HMO must reimburse in-network and Out-of-Network providers in accordance with federal and state laws, rules, and regulations.
8.4.5 Third Party Liability and Recovery
CHIP HMOs are authorized to engage in Third Party Recovery (TPR) actions for claims resulting from the care and/or treatment of CHIP Members. CHIP HMOs are responsible for establishing a plan and process for recovering costs for services that should have been paid through a third party in accordance with applicable State and Federal laws and regulations, including State insurance laws and regulations. HHSC may reduce capitation payments to CHIP HMOs by the projected amount of TPR that the HMOs are expected to recover.
CHIP HMOs must provide required reports as stated in Section 8.1.17.2, Financial Reporting Requirements.
After 120-days from the date of service on any claim, encounter, or other CHIP related payment by the HMO subject to TPR, HHSC may attempt recovery independent of any HMO action.
HHSC will retain, in full, all funds received as a result of the state initiated recovery or subrogation action.
CHIP HMOs shall provide a Member quarterly file, which contains the following information if available to the HMO: the Member name, address, claim submission address, group number, employer's mailing address, social security number, and date of birth for each subscriber or policyholder and each dependent of the subscriber or policyholder covered by the insurer. The file shall be used for the purpose of matching the Texas CHIP eligibility file against the HMO Member file to identify CHIP Members enrolled in the HMO who may have TPR information not known to the CHIP Program.
8.4.6 Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs)
On or after October 1, 2009: CHIP HMOs are required to pay the full encounter rates as determined by HHSC to FQHCs and RHCs for dates of services occurring on or after October 1, 2009.
8.5 Additional CHIP Perinatal Scope of Work
The following provisions only apply to HMOs participating in CHIP Perinatal Program.
8.5.1 CHIP Perinatal Provider Network
In each Service Area, the CHIP Perinatal HMO must seek to obtain the participation of Providers for CHIP Perinate Members. CHIP Perinatal HMOs are encouraged to obtain the participation of Obstetricians/Gynecologists (OB/GYNs), Family Practice Physicians with experience in prenatal care, or other qualified health care Providers as CHIP Perinate Providers.
See Sections 8.1.3.2, Access to Network Providers, and 8.1.4.2, Primary Care Providers, regarding distinctions in the provider networks for CHIP Perinates and CHIP Perinate Newborns.
8.5.2 CHIP Perinatal Program Provider Complaint and Appeals
CHIP Perinatal Program Provider Complaints and Appeals are subject to disposition consistent with the Texas Insurance Code and any applicable TDI regulations. The HMO must resolve Provider Complaints within 30 days from the date the Complaint is received.
8.5.3 CHIP Perinatal Program Member Complaint and Appeal Process
CHIP Perinatal Program Member Complaints and Appeals are subject to disposition consistent with the Texas Insurance Code and any applicable TDI regulations. HHSC will require the HMO to resolve Complaints and Appeals (that are not elevated to TDI) within 30 days from the date the Complaint or Appeal is received. Any person, including those dissatisfied with a HMO’s resolution of a Complaint or Appeal, may report an alleged violation to TDI.
8.5.4 Dental Coverage for CHIP Perinate Newborn Members
The HMO is not responsible for reimbursing dental providers for preventive and therapeutic dental services obtained by CHIP Perinate Newborn Members. However, medical and/or hospital charges, such as anesthesia, that are necessary in order for CHIP Perinate Newborn Members to access standard therapeutic dental services, are Covered Services for CHIP Perinate Newborn Members. The HMO must provide access to facilities and physician services that are necessary to support the dentist who is providing dental services to a CHIP Perinate Newborn Member under general anesthesia or intravenous (IV) sedation.
The HMO must inform Network facilities, anesthesiologists, and PCPs what authorization procedures are required, and how Providers are to be reimbursed for the preoperative evaluations by the PCP and/or anesthesiologist and for the facility services. For dental-related medical Emergency Services, the HMO must reimburse Network and Out-of-Network Providers in accordance with federal and state laws, rules, and regulations.
8.5.5 Third Party Liability and Recovery
CHIP Perinatal HMOs are authorized to engage in Third Party Recovery (TPR) actions for claims resulting from the care and/or treatment of CHIP Perinatal Program Members. CHIP Perinatal HMOs are responsible for establishing a plan and process for recovering costs for services that should have been paid through a third party in accordance with applicable State and Federal laws and regulations, including State insurance laws and regulations. HHSC may reduce capitation payments to the CHIP Perinatal HMOs by the projected amount of TPR that the HMOs are expected to recover.
CHIP Perinatal HMOs must provide required reports as stated in Section 8.1.17.2, Financial Reporting Requirements.
After 120-days from the date of service on any claim, encounter, or other CHIP Perinatal Program-related payment by the HMO subject to TPR, HHSC may attempt recovery independent of any HMO action. HHSC will retain, in full, all funds received as a result of the state initiated recovery or subrogation action.
CHIP Perinatal HMOs shall provide a Member quarterly file, which contains the following information if available to the HMO: the Member name, address, claim submission address, group number, employer's mailing address, social security number, and date of birth for each subscriber or policyholder and each dependent of the subscriber or policyholder covered by the insurer. The file shall be used for the purpose of matching the Texas CHIP Perinatal Program eligibility file against the HMO Member file to identify CHIP Perinatal Program Members enrolled in the HMO who may have TPL information not known to the CHIP Perinatal Program.
8.5.6 Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs)
On or after October 1, 2009: CHIP Perinatal HMOs are required to pay the full encounter rates as determined by HHSC to FQHCs and RHCs for dates of services occurring on or after October 1, 2009.