Exhibit 99.1
| Telavancin • A novel rapidly bactericidal lipoglycopeptide • Unique multifunctional mechanism of action – inhibition of bacterial cell wall synthesis – depolarization of the bacterial membrane • Active against clinically relevant Gram-positive pathogens including strains resistant to other Gram-positive agents • At least as efficacious as vancomycin in patients with complicated skin and soft tissue infections caused by MRSA • Exceptional intracellular and extracellular activity • Good penetration into pulmonary fluids and alveolar macrophages |

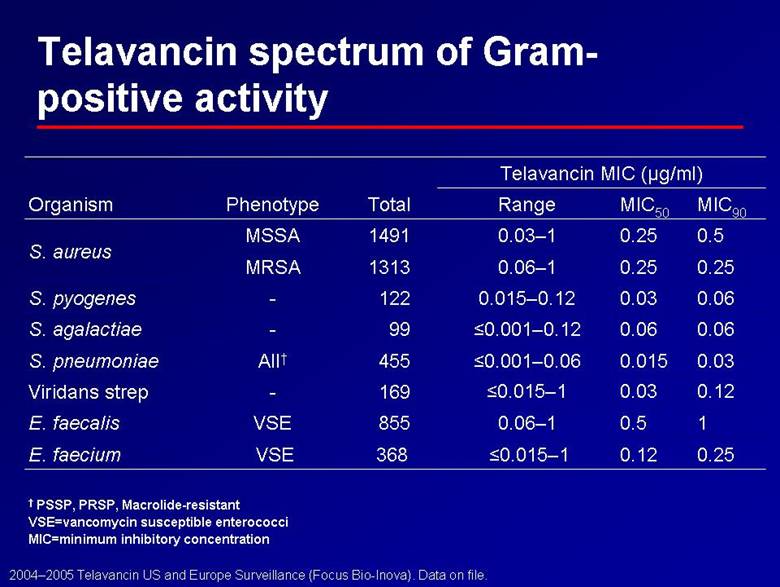
| Telavancin spectrum of Gram-positive activity 0.12 0.03 <0.015–1 169 - Viridans strep 0.03 0.015 <0.001–0.06 455 All† S. pneumoniae 0.06 0.06 <0.001–0.12 99 - S. agalactiae 0.06 0.03 0.015–0.12 122 - S. pyogenes 1 0.5 0.06–1 855 VSE E. faecalis 0.25 0.12 <0.015–1 368 VSE E. faecium 0.25 0.25 0.06–1 1313 MRSA 0.5 0.25 0.03–1 1491 MSSA S. aureus MIC90 MIC50 Range Total Phenotype Organism Telavancin MIC (µg/ml) † PSSP, PRSP, Macrolide-resistant VSE=vancomycin susceptible enterococci MIC=minimum inhibitory concentration 2004–2005 Telavancin US and Europe Surveillance (Focus Bio-Inova). Data on file. |
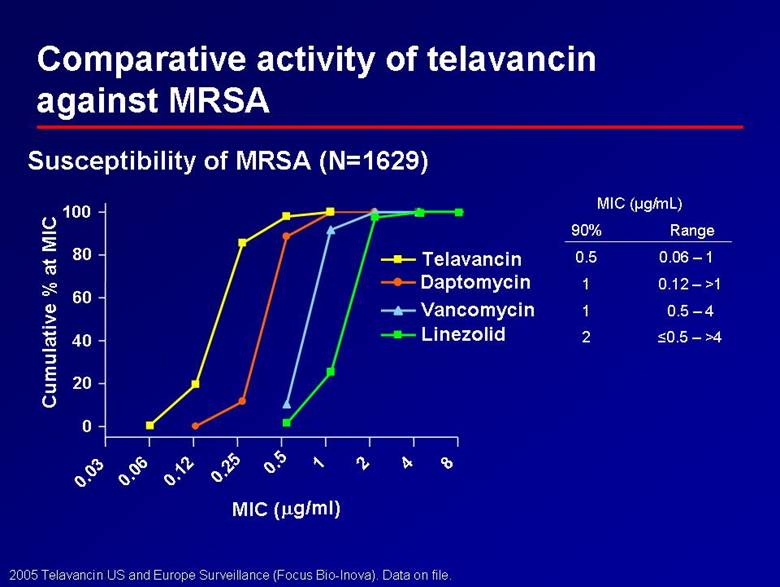
| Comparative activity of telavancin against MRSA Daptomycin Susceptibility of MRSA (N=1629) <0.5 – >4 2 0.5 – 4 1 0.12 – >1 1 0.06 – 1 0.5 Range 90% MIC (µg/mL) 0.03 0.06 0.12 0.25 0.5 1 2 4 8 0 20 40 60 80 100 Telavancin Vancomycin Linezolid MIC (µg/ml) Cumulative % at MIC 2005 Telavancin US and Europe Surveillance (Focus Bio-Inova). Data on file. |
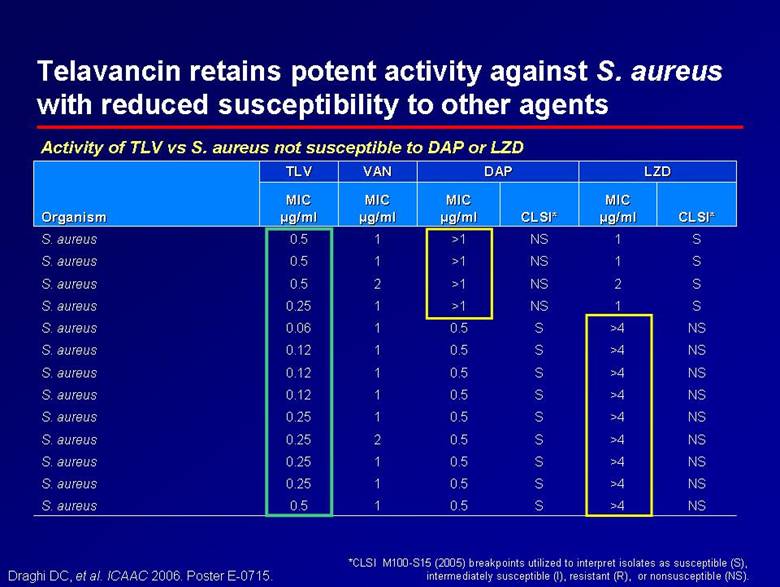
| Telavancin retains potent activity against S. aureus with reduced susceptibility to other agents 1 1 1 2 1 1 1 1 1 1 2 1 1 MIC MIC µg/ml µg/ml VAN VAN NS >4 S 0.5 0.12 S. aureus NS >4 S 0.5 0.12 S. aureus NS >4 S 0.5 0.12 S. aureus NS >4 S 0.5 0.06 S. aureus S 1 NS >1 0.25 S. aureus S 2 NS >1 0.5 S. aureus S 1 NS >1 0.5 S. aureus >4 >4 >4 >4 >4 1 MIC MIC µg/ml µg/ml LZD LZD NS NS NS NS NS S CLSI* CLSI* S S S S S NS CLSI* CLSI* 0.5 0.5 0.5 0.5 0.5 >1 MIC MIC µg/ml µg/ml DAP DAP 0.5 0.25 0.25 0.25 0.25 0.5 MIC MIC µg/ml µg/ml TLV TLV S. aureus S. aureus S. aureus S. aureus S. aureus S. aureus Organism Organism Draghi DC, et al. ICAAC 2006. Poster E-0715. Activity of TLV vs S. aureus not susceptible to DAP or LZD *CLSI M100-S15 (2005) breakpoints utilized to interpret isolates as susceptible (S), intermediately susceptible (I), resistant (R), or nonsusceptible (NS). |
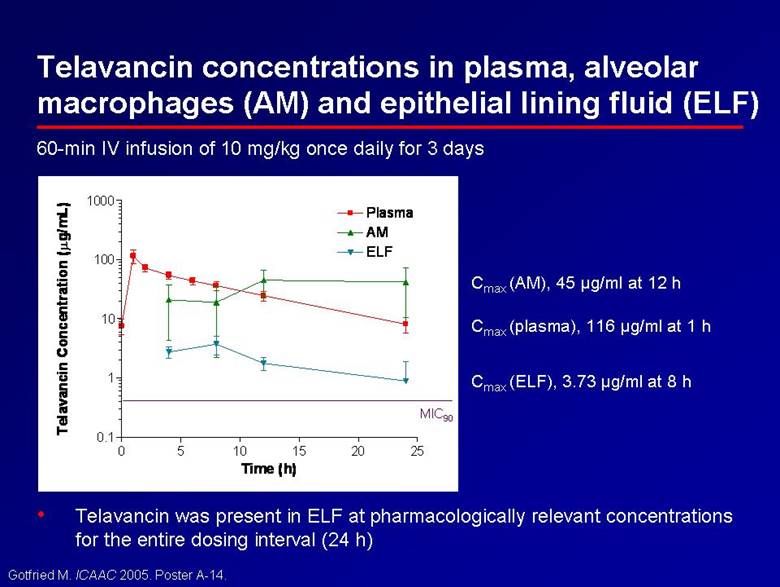
| 60-min IV infusion of 10 mg/kg once daily for 3 days • Telavancin was present in ELF at pharmacologically relevant concentrations for the entire dosing interval (24 h) Telavancin concentrations in plasma, alveolar macrophages (AM) and epithelial lining fluid (ELF) 0 5 10 15 20 25 0.1 1 10 100 1000 Plasma AM ELF Time (h) Telavancin Concentration (µg/mL) MIC90 Cmax (ELF), 3.73 µg/ml at 8 h Cmax (plasma), 116 µg/ml at 1 h Cmax (AM), 45 µg/ml at 12 h Gotfried M. ICAAC 2005. Poster A-14. |
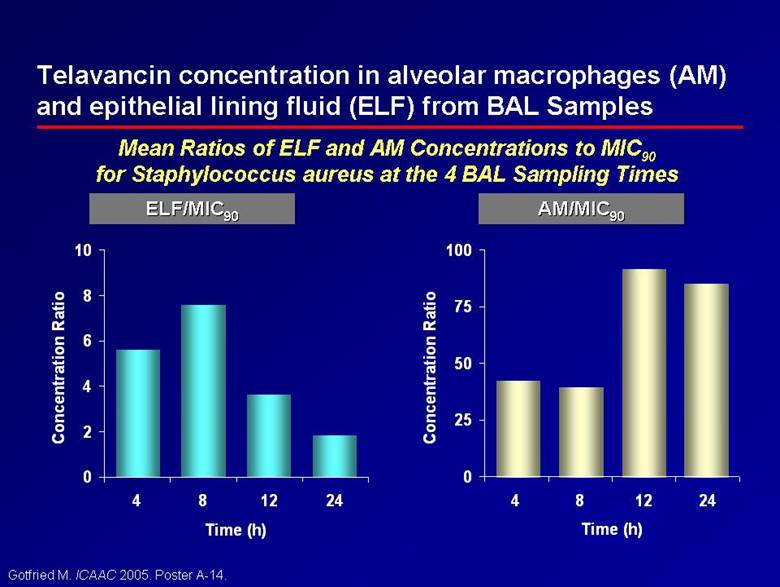
| Telavancin concentration in alveolar macrophages (AM) and epithelial lining fluid (ELF) from BAL Samples Gotfried M. ICAAC 2005. Poster A-14. Mean Ratios of ELF and AM Concentrations to MIC90 for Staphylococcus aureus at the 4 BAL Sampling Times ELF/MIC ELF/MIC90 90 AM/MIC AM/MIC90 90 0 25 50 75 100 4 8 12 24 Time (h) Concentration Ratio 0 2 4 6 8 10 4 8 12 24 Time (h) Concentration Ratio |
| Telavancin clinical programme • Indications studied: cSSTI and HAP – Two large, methodologically identical, double-blind, multicentre, multinational, randomised, active controlled studies to evaluate the efficacy and safety of telavancin in each indication • Large patient populations – No upper age limit – Included moderate and severe renal impairment in contrast to other registrational programs excluding renal impairment • Focus on MRSA – Community- and hospital-acquired MRSA – Largest registrational trial experience of MRSA infections to date |
| Corey R, et al. IDSA 2006. Poster LB-17. ATLAS phase 3 cSSTI: conclusions • Telavancin was shown to be as effective as vancomycin for the treatment of cSSTI • The telavancin safety profile was compatible with treatment of serious Gram-positive infections due to resistant bacteria • These data support the efficacy and safety of once-daily telavancin in the treatment of Gram-positive cSSTI |
| The ATTAIN programme: ATTAIN 1 & 2 • Two large, methodologically identical, double-blind, multicentre, multinational, randomised, active controlled studies to evaluate the efficacy and safety of telavancin versus vancomycin for treatment of hospital-acquired pneumonia due to Gram-positive bacteria • Primary endpoint – non-inferiority in clinical cure at test-of-cure (TOC) visit in the all-treated (AT) and clinically evaluable (CE) populations • Study population – 1503 patients treated in 38 countries – 464 with MRSA identified at baseline culture |
| Key patient inclusion and exclusion criteria Inclusion: • Male and female patients > 18 years old • Clinical signs and symptoms of pneumonia acquired after > 48 hours of hospitalisation OR acquired < 7 days after discharge from > 3 days of hospitalisation • Diagnosis of pneumonia by chest radiograph < 48 hours prior to randomisation • Respiratory or sputum specimens for Gram-staining and culture available • Patients with renal impairment, including patients on hemodialysis were not excluded Exclusion: • > 24 hours potentially effective antibiotic therapy – known infection with MSSA or S. pneumoniae AND required concomitant therapy for Gram-positives > 24 hours active against either of these • Respiratory specimen with only Gram-negative bacteria on Gram stain or culture • Legionella pneumophilia pneumonia, meningitis, infectious endocarditis or osteomyelitis • Neutropenia |
| Treatment regimen • Randomisation (1:1) to – Telavancin 10 mg/kg IV q24h – Vancomycin 1 g IV q12h ¦ dosing optimisation allowed per individual site guidelines ¦ switching to antistaphylococcal penicillin allowed for MSSA infections • Study treatment for 7–21 days ¦ concomitant aztreonam and/or metronidazole permitted for patients with confirmed or suspected polymicrobial infections ¦ piperacillin-tazobactam or imipenem may be administered for Gram-negative coverage only if aztreonam is not appropriate due to resistance issues • Follow-up for test-of-cure 7–14 days after end of study treatment |
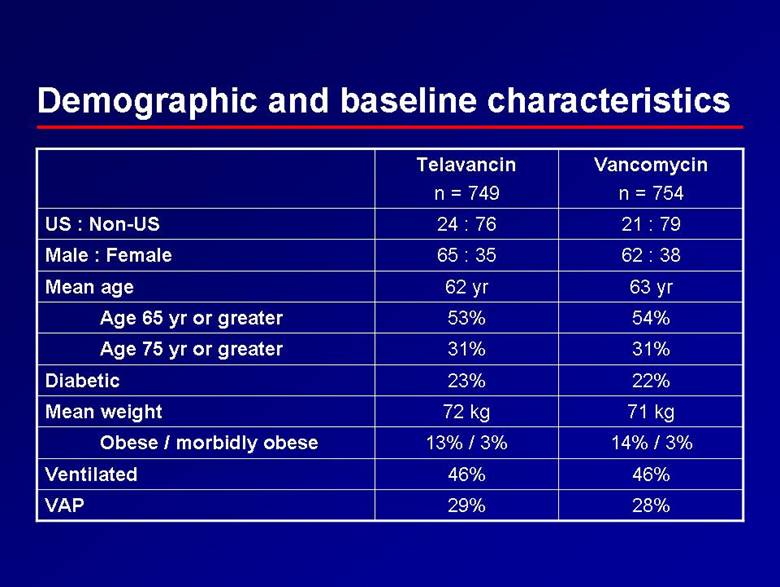
| Demographic and baseline characteristics 28% 29% VAP 46% 46% Ventilated 14% / 3% 13% / 3% Obese / morbidly obese 71 kg 72 kg Mean weight 22% 23% Diabetic 31% 31% Age 75 yr or greater 54% 53% Age 65 yr or greater 63 yr 62 yr Mean age 62 : 38 65 : 35 Male : Female 21 : 79 24 : 76 US : Non-US Vancomycin n = 754 Telavancin n = 749 |
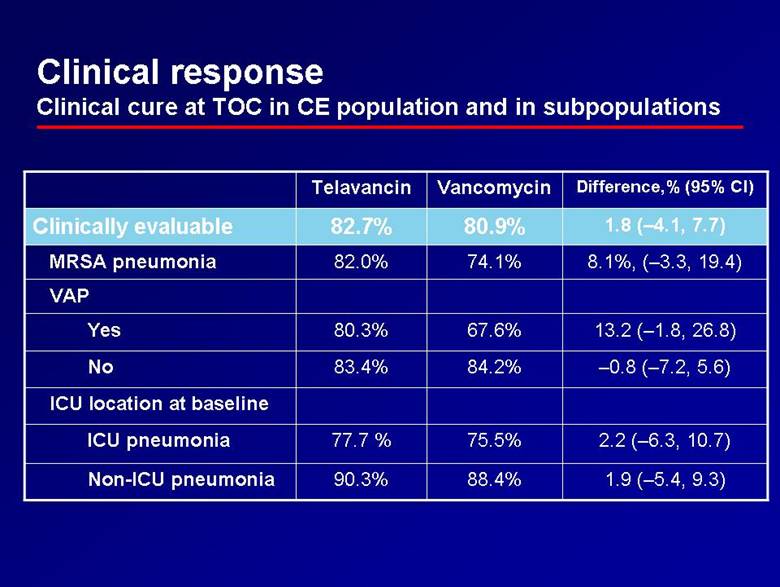
| Clinical response Clinical cure at TOC in CE population and in subpopulations VAP 1.8 (–4.1, 7.7) 80.9% 82.7% Clinically evaluable 88.4% 75.5% 84.2% 67.6% 74.1% Vancomycin 1.9 (–5.4, 9.3) 90.3% Non-ICU pneumonia 13.2 (–1.8, 26.8) 80.3% Yes –0.8 (–7.2, 5.6) 83.4% No 2.2 (–6.3, 10.7) 77.7 % ICU pneumonia ICU location at baseline 8.1%, (–3.3, 19.4) 82.0% MRSA pneumonia Difference,% (95% CI) Telavancin |
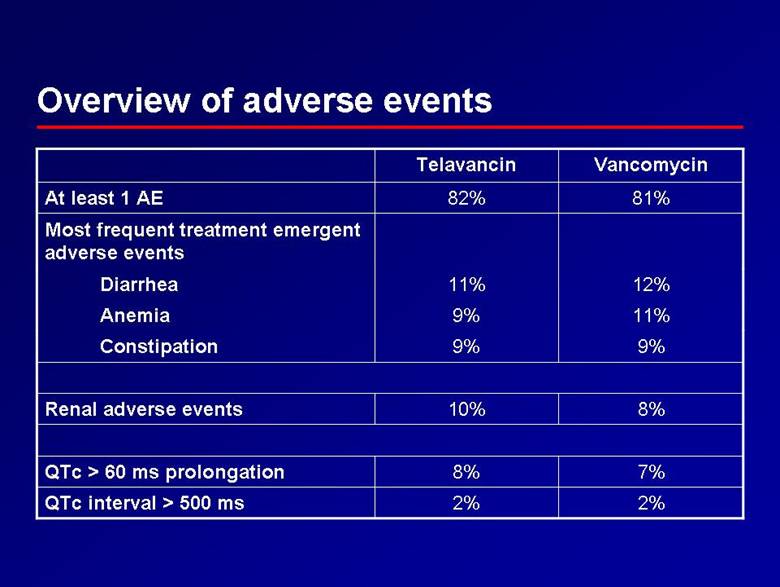
| Overview of adverse events 8% 10% Renal adverse events 7% 8% QTc > 60 ms prolongation 2% 2% QTc interval > 500 ms 9% 9% Constipation 11% 9% Anemia 12% 11% Diarrhea Most frequent treatment emergent adverse events 81% 82% At least 1 AE Vancomycin Telavancin |
| Conclusions Telavancin in HAP Phase 3 programme • Study met primary endpoint – non-inferiority attained in AT and CE populations in both studies, 95% CIs well within 10% margin • Numerical trends favouring telavancin in subpopulations of patients with severe disease – VAP, MRSA • Safety profile compatible with treatment of serious Gram-positive infections |