Exhibit 99.2
POSTER NO. PS272
Ethnic sensitivity assessment of fluticasone furoate (FF)/vilanterol (VI) in asthma patients in Japan and Korea: a pre-specified subgroup analysis
Gross AS(1), Goldfrad C(2), Hozawa S(3), James M(4), Clifton CS(1), Sugiyama Y(5), Jacques L(6)
(1)Clinical Pharmacology Modelling & Simulation, GlaxoSmithKline, Sydney, Australia; (2)Quantitative Sciences Division, GlaxoSmithKline, Uxbridge, UK; (3)Hiroshima Allergy and Respiratory Clinic, Hiroshima, Japan; (4)Medical Affairs, GlaxoSmithKline K.K., Tokyo, Japan; (5)Medicines Development Respiratory, GlaxoSmithKline K.K., Tokyo, Japan; (6)Respiratory Medicines Discovery and Development, GlaxoSmithKline, Uxbridge, UK
INTRODUCTION
· Inhaled corticosteroid (ICS)/long-acting beta2-agonist (LABA) combinations are recommended by Japanese(1) and global asthma guidelines(2) for asthma patients uncontrolled on ICS alone.
· FF/VI is a once-daily ICS/LABA combination therapy delivered via the ELLIPTATM dry powder inhaler, which is effective for 24h.
· Responses to pharmacotherapy can vary across ethnic groups(3),(4) including in Japanese patients.
OBJECTIVES
· To establish whether doses of FF/VI recommended from multinational studies are relevant to asthma patients in Japan.
· To compare the efficacy, safety, PK and PD data for FF/VI in patients from Japan and/or Korea with data from patients not from Japan or Korea
· Patients from Korea were included due to similarities in a range of intrinsic and extrinsic ethnic factors between the populations of Japan and Korea.(5)–(7)
METHODS
· A pre-specified subgroup analysis of multicentre, randomised, double-blind, parallel-group international studies that included asthma patients from Japan and/or Korea.
· Inclusion criteria: >12 years of age, pre-bronchodilator % predicted forced expiratory volume in one second (FEV1) of 40–90%, FEV1 reversibility of >12% and >200mL.
· Efficacy results were pooled from three Phase III studies, ranging from 12 to 76 weeks duration, that included patients from Japan (GSK study numbers: HZA106827; HZA106829; HZA106837).
· Change from baseline in trough FEV1 after 12 weeks with once-daily FF/VI 100/25mcg, once-daily FF 100mcg or placebo was analysed across two studies (HZA106827; HZA106837) and data for once-daily FF/VI 200/25mcg, once-daily FF 200mcg and twice-daily fluticasone propionate (FP) 500mcg were from one study (HZA106829).
· Safety data were pooled from the three studies noted above and an additional three placebo-controlled Phase IIb studies, ranging from 28 days to 8 weeks duration, that included patients from Korea (B2C109575; FFA109685; FFA109687).
· PK data were estimated based on a post-hoc analysis of population PK data for FF(8) and of study DB111207 data for VI(9); PD data, including 24h urinary cortisol excretion, were assessed.
RESULTS
Table 1. Demographic and baseline characteristics
Demographic and baseline characteristics (Efficacy population)
|
| Japan |
| Not-Japan |
| Overall |
|
|
| N=148 |
| N=3066 |
| N=3214 |
|
Age(1) (years) |
| 47.5 (14.66) |
| 41.9 (16.63) |
| 42.2 (16.59) |
|
Male (%) |
| 38 |
| 36 |
| 36 |
|
Weight(1) (kg) |
| 62.5 (13.63) |
| 76.2 (19.29) |
| 75.5 (19.28) |
|
Height(1) (cm) |
| 160.7 (8.05) |
| 165.7 (9.98) |
| 165.5 (9.96) |
|
FEV1(1) (L) |
| 1.933(2) (0.5481) |
| 2.231(3) (0.6469) |
| 2.218(4) (0.6456) |
|
% Predicted FEV1(1) |
| 74.7(2) (11.13) |
| 70.6(3) (11.18) |
| 70.8(4) (11.21) |
|
Demographic characteristics (Safety population)
|
|
|
| Not- |
|
|
|
|
| Japan+Korea |
| Japan+Korea |
| Overall |
|
|
| N=194 |
| N=4037 |
| N=4231 |
|
Age(1) (years) |
| 46.1 (15.00) |
| 41.3 (16.47) |
| 41.5 (16.44) |
|
Male (%) |
| 40 |
| 37 |
| 37 |
|
Weight(1) (kg) |
| 63.5 (13.37) |
| 76.1(5) (19.68) |
| 75.5(6) (19.61) |
|
Height(1) (cm) |
| 161.6 (8.46) |
| 165.7 (10.21) |
| 165.5 (10.17) |
|
(1)Mean (SD); (2)n=147; (3)n=3059; (4)n=3206; (5)n=4036; (6)n=4230
Efficacy
· Efficacy data were compared between patients (N=3214) from Japan and ‘Not-Japan’; 85% (N=2739) completed the studies.
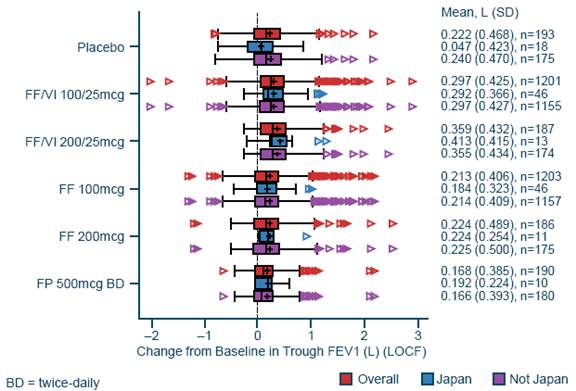
· Improvements in trough FEV1 were reported in all populations for FF/VI 100/25mcg and FF 100mcg versus placebo and for FF/VI 100/25mcg versus FF 100mcg (Table 2)
· There was no evidence of a statistically significant difference in treatment effect between patients from Japan and Not-Japan (p=0.403).
· Changes from baseline in FEV1 were similar with FF/VI 200/25mcg and FF 200mcg in patients from Japan and the overall population (Figure 1)
· Improvements were greater than with twice-daily FP 500mcg.
Table 2. Comparison of change from baseline in trough FEV1 at Week 12 between treatment arms (Efficacy population)
|
|
|
| FF/VI |
| FF |
|
|
|
|
| 100/25mcg |
| 100mcg |
|
|
|
|
|
|
|
|
|
|
| N |
| 1201 |
| 1203 |
|
|
|
|
| 0.181 |
| 0.105 |
|
|
| Difference vs. placebo(1) |
| (0.111, 0.252) |
| (0.034, 0.175) |
|
|
|
|
| p<0.001 |
| p=0.003 |
|
Overall |
|
|
|
|
|
|
|
|
|
|
| 0. 077 |
| — |
|
|
| Difference vs. FF 100mcg |
| (0.045, 0.108) |
|
| |
|
|
|
| p<0.001 |
|
| |
|
|
|
|
|
|
|
|
|
| n |
| 46 |
| 46 |
|
|
|
|
| 0.323 |
| 0.216 |
|
Japan |
| Difference vs. placebo(2) |
| (0.104, 0.542) |
| (–0.003, 0.436) |
|
|
|
|
|
|
|
|
|
|
| Difference vs. FF 100mcg |
| 0.107 |
| — |
|
|
|
|
| (–0.056, 0.270) |
|
| |
|
|
|
|
|
|
|
|
|
| n |
| 1155 |
| 1157 |
|
Not-Japan |
| Difference vs. placebo(3) |
| 0.168 |
| 0.093 |
|
|
|
|
| (0.095, 0.241) |
| (0.020, 0.166) |
|
|
|
|
|
|
|
|
|
|
| Difference vs. FF 100mcg |
| 0.075 |
| — |
|
|
|
|
| (0.043, 0.108) |
|
|
|
Least squares mean change (95% confidence interval). Studies included: HZA106827, HZA106837. Data were analysed using a Last Observation Carried Forward Analysis of Covariance model, with terms for baseline FEV1, region, gender, age, treatment group, study & region by treatment interaction. 1n=193; 2n=18, 3n=175
Figure 1. Box plot of change from baseline in trough FEV1 at Week 12 by geographic region (Efficacy population)
Safety
· Safety data were compared between patients (N=4231) from Japan/Korea and Not-Japan/Korea; N=3584 (85%) completed the studies.
· In all active treatment groups, a greater proportion of patients from Japan/Korea versus Not-Japan/Korea reported on-treatment adverse events; this trend was also observed in the placebo group, suggesting that this is not related to FF or VI (Table 3).
Table 3. Summary of on-treatment adverse events and serious adverse events (Safety population)
|
|
|
| FF/VI |
| FF/VI |
| FF |
| FF |
|
| Placebo |
| 100/25mcg |
| 200/25 mcg |
| 100mcg |
| 200mcg |
All on-treatment adverse events |
|
|
|
|
|
|
|
|
|
|
Japan+Korea |
| 12/29 (41) |
| 37/47 (79)(1) |
| 9/14 (64)(1) |
| 38/55 (69) |
| 16/22 (73) |
Not-Japan/Korea |
| 87/375 (23) |
| 658/1163 (57) |
| 83/183 (45) |
| 744/1375 (54) |
| 134/386 (36) |
Overall |
| 99/404 (25) |
| 695/1210 (57) |
| 92/197 (47) |
| 782/1430 (55) |
| 150/390 (38) |
On-treatment non-fatal serious adverse events |
|
|
|
|
|
|
|
|
|
|
Japan+Korea |
| 0/29 (0) |
| 1/47 (2)(1) |
| 0/14 (0)(1) |
| 1/55 (2) |
| 0/22 (0) |
Overall |
| 0/404 (0) |
| 40/1210 (3) |
| 6/197 (3) |
| 30/1430 (2) |
| 1/390 (<1) |
On-treatment fatal adverse events |
|
|
|
|
|
|
|
|
|
|
Japan+Korea |
| 0/29 (0) |
| 0/47 (0)(1) |
| 0/14 (0)(1) |
| 0/55 (0) |
| 0/22 (0) |
Overall |
| 0/404 (0) |
| 1/1210(2) (<1) |
| 0/197 (0) |
| 1/1430 (<1) |
| 0/390 (0) |
Data presented as number of patients with an adverse event/number of patients in population group (%);
(1)Only subjects from Japan;
(2)One additional subject (South East Asian) died during follow-up
Safety (cont’d)
· Serious adverse events reported for patients from Japan+Korea (1 FF/VI 100/25mcg, 1 FF 100mcg: both subarachnoid haemorrhage) were not considered drug related.
PK/PD
· Estimated FF AUC(0-24) and VI Cmax were higher in Japanese versus White/Caucasian patients (Table 4).
PK/PD (cont’d)
· No clinically relevant effects on cortisol concentrations (Figure 2) or heart rate were observed.
· The PK profile of FF at clinical doses (<200mcg) did not differ when administered simultaneously with VI 25mcg compared with FF alone for either Japanese or White/Caucasian patients.
Table 4. Model predicted PK parameters
Race |
| Treatment |
| N |
| C max (pg/mL) |
| AUC (0-24) (pg.h/mL) |
Model predicted FF PK parameters |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| 18.0 |
| 348.6 |
|
| FF/VI 100/25mcg |
| 14 |
| [11.8, 26.1] |
| [214.7, 510.8] |
|
|
|
|
|
| 19.9 |
| 304.6 |
Japanese |
| FF 100mcg |
| 15 |
| [13.2, 27.8] |
| [240.4, 382.6] |
|
|
|
|
|
| 42.4 |
| 605.1 |
|
| FF/VI 200/25mcg |
| 13 |
| [28.2, 59.7] |
| [489.2, 871.8] |
|
|
|
|
|
| 34.6 |
| 581.9 |
|
| FF 200mcg |
| 8 |
| [24.2, 49.8] |
| [374.1, 855.1] |
|
|
|
|
|
|
|
|
|
|
| FF/VI 100/25mcg; |
|
|
| 15.2 |
| 232.2 |
White / |
| FF 100mcg |
| 492 |
| [14.9, 15.6] |
| [226.0, 238.5] |
Caucasian |
| FF/VI 200/25mcg; |
|
|
| 30.0 |
| 471.6 |
|
| FF 200mcg |
| 471 |
| [29.1, 30.8] |
| [459.0, 484.1] |
|
|
|
|
|
|
|
|
|
Model predicted VI PK parameters |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| 113.3 |
| 139.1 |
|
| FF/VI 100/25mcg |
| 14 |
| [38.7, 243.7] |
| [117.2, 159.0] |
Japanese |
|
|
|
|
| 144.9 |
| 146.1 |
|
| FF/VI 200/25mcg |
| 13 |
| [63.4, 236.1] |
| [119.4, 168.0] |
|
|
|
|
|
|
|
|
|
White / |
| FF/VI 100/25mcg; |
|
|
| 42.2 |
| 165.7 |
Caucasian |
| FF/VI 200/25mcg |
| 660 |
| [39.7, 44.9] |
| [160.2, 171.4] |
Geometric mean (95% confidence interval); FF data from post-hoc analysis of population PK data(8); VI data from post-hoc analysis of study DB111207(9)
Figure 2. Ratio of 24h urinary cortisol excretion to baseline at the end of treatment (Urinary cortisol population(1))
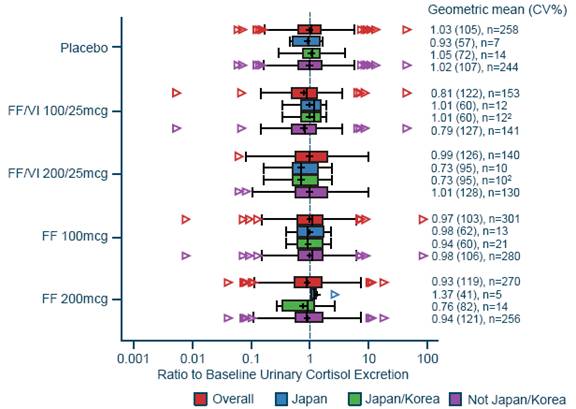
(1)Urinary cortisol population: subset of patients from Safety population, that were not considered to have confounding factors, and for whom urine samples were available;
(2)Only subjects from Japan
CONCLUSIONS
· The efficacy and safety profile of FF/VI is similar in asthma patients from Japan+Korea and Not-Japan+Korea.
· The FF/VI clinical doses recommended based on global studies are also suitable for asthma patients in Japan.
REFERENCES
(1) Ohta K, et al. Allergol Int. 2011;60:115–45.
(2) Global Initiative for Asthma. Global Burden of Asthma. Available at: http://www.ginasthma.org/ local/uploads/files/GINABurdenReport_1.pdf. Last accessed: 10 Sept 2013.
(3) Bjornsson TD, et al. J Clin Pharmacol 2003;43:943–67.
(4) Huang SM, et al. Clin Pharmacol Ther 2008;84:287–94.
(5) Jin HJ, et al. PLoS ONE 2009;4:1–10.
(6) HUGO Pan-Asian SNP Consortium, et al. Science 2009;326:1541–45.
(7) Chowbay B, et al. Drug Metab Rev 2005;37:327–78.
(8) GSK data on file.
(9) Nakahara N, et al. Int J Clin Pharmacol Ther 2013;51:660–72
ACKNOWLEDEGMENTS
· The presenting author, Yutaro Sugiyama, is employed by GlaxoSmithKline.
· The authors acknowledge the contributions of the following employees of GlaxoSmithKline: Dr Romina Nand, Dr Carol Lee and Dr Ann Allen.
· These studies were funded by GlaxoSmithKline (GSK study codes HZA106827 (cllinicaltrial.gov registration number: NCT01165138); HZA106829 (NCT01134042); HZA106837 (NCT01086384); B2C109575 (NCT00600171); FFA109685 (NCT00603278); FFA109687 (NCT00603382); DB111207 (NCT00964249).
· Editorial support (in the form of writing assistance, assembling tables and figures, collating author comments, grammatical editing and referencing) was provided by Laura Maguire, MChem, at Gardiner-Caldwell Communications (Macclesfield, UK) and was funded by GlaxoSmithKline.

ELLIPTATM is a trade mark of the GlaxoSmithKline group of companies
Presented at the 18th Congress of the Asian Pacific Society of Respirology, Yokohama, Japan, 11–14 November 2013