Exhibit 99.2

NASDAQ: MRNS @MarinusPharma Corporate Overview 2020
©2020 Marinus Pharmaceuticals. All Rights Reserved I Safe Harbor Statement 2 To the extent that statements contained in this presentation are not descriptions of historical facts regarding Marinus, they ar e forward - looking statements reflecting the current beliefs and expectations of management made pursuant to the safe harbor provisions of the Private Securities Liti gat ion Reform Act of 1995. Words such as “may”, “will”, “expect”, “anticipate”, “estimate”, “intend”, “believe”, and similar expressions (as well as other words or ex pressions referencing future events, conditions or circumstances) are intended to identify forward - looking statements. Examples of forward - looking statements contai ned in this presentation include, among others, statements regarding our clinical development plans for ganaxolone; expected dosing in our clinical trials; the cl inical development schedule and milestones; our expected timing to begin and complete enrollment in our clinical trials; the expected trial design, target pa tie nt population and endpoints for our clinical trials; interpretation of scientific basis for ganaxolone use; timing for availability and release of data, includin g t he expected release of topline data from our Phase 3 trial in status epilepticus (SE) in the 1H 2022; and from the proof of concept study in PCDH19 in the first half of 2 021 , and from the Phase 2 tuberous sclerosis complex (TSC) trial in mid 2021; the potential safety and efficacy and therapeutical potential of ganaxolone; timing and expe cta tion regarding submissions of regulatory applications, including our expectation to submit an NDA for ganaxolone in CDD in mid - 2021 and an MAA by end Q3 2021; expectations regarding commercial launch of ganaxolone in CDD in 1H 2022; expectations regarding our agreement with BARDA; expectations regarding th e p otential market opportunities for our product candidates, including oral ganaxolone; potential commercial alliances; and our expectations regarding the eff ect of the COVID - 19 pandemic on our business and clinical development plans. Forward - looking statements in this presentation involve substantial risks and uncertain ties that could cause our clinical development programs, future results, performance or achievements to differ significantly from those expressed or implied by the forward - looking statements. Such risks and uncertainties include, among others, uncertainties and delays relating to the design, enrollment, completion, and r esu lts of clinical trials; interpretation of results of clinical trials; unanticipated costs and expenses; early clinical trials may not be indicative of the results in l ate r clinical trials; clinical trial results may not support regulatory approval or further development in a specified indication or at all; actions or advice of the FDA or other re gulatory agencies may affect the design, initiation, timing, continuation and/or progress of clinical trials or result in the need for additional clinical trials; our ab ility to obtain and maintain regulatory approval for our product candidate; our ability to obtain and maintain patent protection for our product candidates; delays, interruptions or failures in the manufacture and supply of our product candidate; our ability to raise additional capital; the effect of the COVID - 19 pandemic on our business, the medi cal community and the global economy; and the availability or potential availability of alternative products or treatments for conditions targeted by us that could af fect the availability or commercial potential of our product candidate. Marinus undertakes no obligation to update or revise any forward - looking statements. For a further descri ption of the risks and uncertainties that could cause actual results to differ from those expressed in these forward - looking statements, as well as risks relating to the business of the Company in general, see filings Marinus has made with the Securities and Exchange Commission. You may access these documents for free by visiting E DGAR on the SEC web site at www.sec.gov .
©2020 Marinus Pharmaceuticals. All Rights Reserved I Ganaxolone (GNX) Targets Synaptic & Extrasynaptic GABA A Receptors 3 Ganaxolone a positive allosteric GABA A receptor modulator with a well - defined MOA designed to treat patients suffering from epilepsy and neuropsychiatric disorders. GNX is designed to modulate both synaptic and extrasynaptic GABA A receptors to calm over - excited neurons Clinical development focused on status epilepticus and rare genetic epilepsies that have few or no treatment options Multiple dose formulations IV and oral – to meet the needs of adult and pediatric patients in acute and chronic care settings Extensive safety record in more than 1,600 patients both pediatric and adult, at therapeutically relevant dose levels for up to two years GNX is a synthetic analog of allopregnanolone

©2020 Marinus Pharmaceuticals. All Rights Reserved I Evaluation of IV and Oral Opportunities Building Upon Status Epilepticus (SE) Maximizing Value for Orphan Epilepsies • Expand clinical opportunities from refractory status epilepticus (RSE) to broader SE market • Initiate commercial plan • Create a global development strategy • Develop pharmacoeconomic value proposition • Complete BARDA activities • Continue CDKL5 deficiency disorder (CDD) and tuberous sclerosis complex (TSC) clinical development • Consider expansion opportunities based on scientific rationale • Further develop commercial roadmap, including scientific and clinical differentiation Leveraging GNX Molecule • Explore opportunities to improve bioavailability and PK • Prioritize clinical trials based on unmet need, improved product profile • New therapeutic indications driven by scientific rationale Marinus Corporate Strategy Corporate Strategy 4
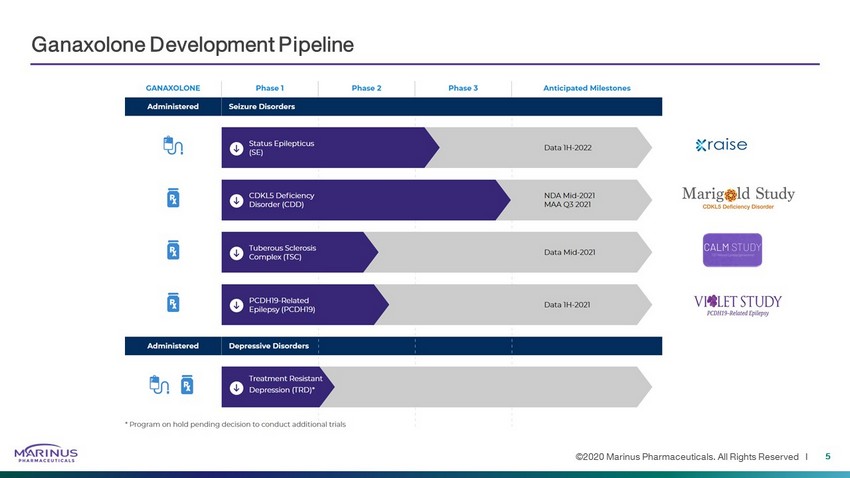
©2020 Marinus Pharmaceuticals. All Rights Reserved I Ganaxolone Development Pipeline 5
Status Epilepticus Indication
©2020 Marinus Pharmaceuticals. All Rights Reserved I Status Epilepticus (SE): Definition and Epidemiology Background • Continuous seizures lasting >5 min • Heterogenous patient population with various etiologies, including glioblastoma, vascular disease, encephalitis, drug or alcohol withdrawal or overdose • Pre - existing epilepsy in less than half of SE cases • Prolonged seizure activity can result in permanent neuronal damage and contribute to high morbidity and mortality • SE becomes more treatment refractory as it progresses 7 SE is the second most common neurologic emergency in the U.S. 1 1. Anaethesia and Intensive Care Medicine, February 02, 2018 , Update on the management of status epilepticus
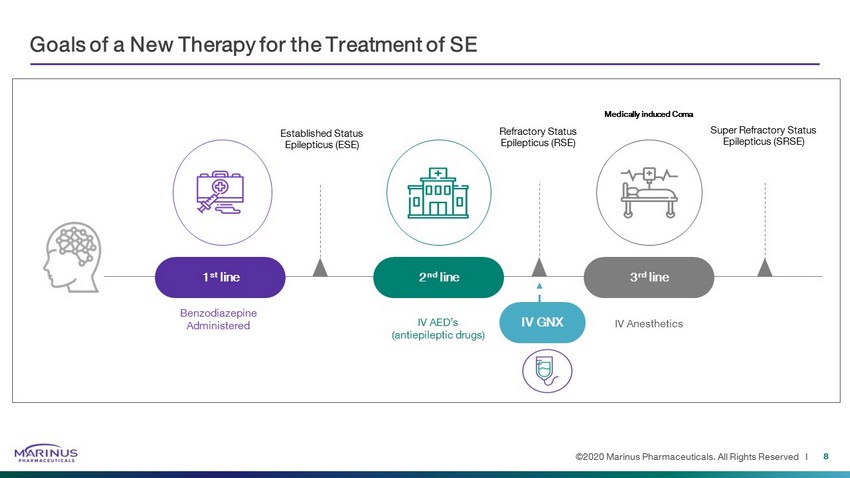
©2020 Marinus Pharmaceuticals. All Rights Reserved I Goals of a New Therapy for the Treatment of SE 8 Benzodiazepine Administered Medically induced Coma Established Status Epilepticus (ESE) 1 st line 2 nd line IV AED’s (antiepileptic drugs) 3 rd line IV Anesthetics Super Refractory Status Epilepticus (SRSE) Refractory Status Epilepticus (RSE) IV GNX
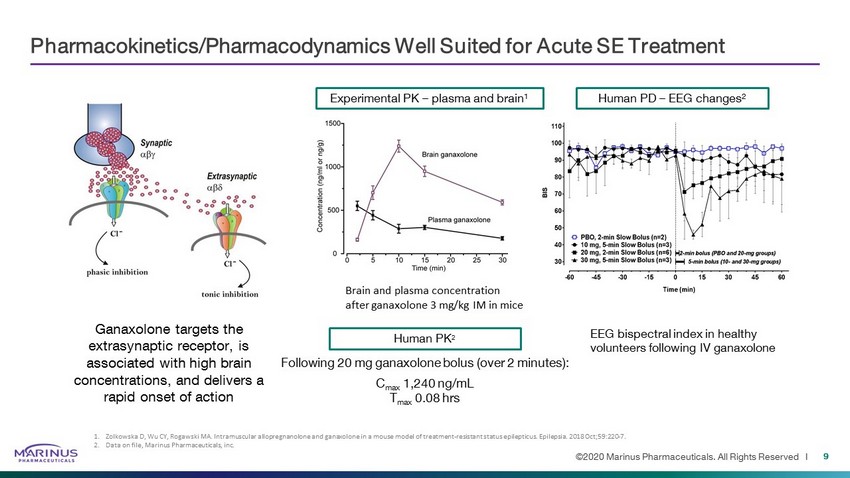
©2020 Marinus Pharmaceuticals. All Rights Reserved I Pharmacokinetics/Pharmacodynamics Well Suited for Acute SE Treatment Experimental PK – plasma and brain 1 Brain and plasma concentration after ganaxolone 3 mg/kg IM in mice Human PD – EEG changes 2 EEG bispectral index in healthy volunteers following IV ganaxolone 1. Zolkowska D, Wu CY, Rogawski MA. Intramuscular allopregnanolone and ganaxolone in a mouse model of treatment-resistant status ep ilepticus. Epilepsia. 2018 Oct;59:220 - 7. 2. Data on file, Marinus Pharmaceuticals, inc. Human PK 2 Following 20 mg ganaxolone bolus (over 2 minutes): C max 1,240 ng/mL T max 0.08 hrs Ganaxolone targets the extrasynaptic receptor, is associated with high brain concentrations, and delivers a rapid onset of action 9

©2020 Marinus Pharmaceuticals. All Rights Reserved I Treatment Period Loading Dose Maintenance Taper Phase 2 SE Trial Design 10 Diagnosis of convulsive or non - convulsive SE Failed at least one 2 nd line IV AED but had not progressed to 3 rd line IV anesthetics Bolus plus continuous infusion 2 - 4 day infusion 18 - hour taper Screening Post - treatment Follow - up 24 hour Weeks 2, 3, 4 SE Patients Cohort Dose of GNX/day N Low 500mg/day 5 Medium 650mg/day 4 High 713mg/day 8 Evaluate IV ganaxolone in refractory SE patients Goals of a new treatment Rapid cessation Maintenance of seizure control Prevent progression to IV anesthetics Limitations of current treatments 1st line Benzodiazepines ineffective in 45% - 50%; limited by cardiovascular and respiratory side effects 2nd line Ineffective in over 50% of established SE; further decreased response in refractory SE 3rd line IV Anesthetics: high morbidity, mortality ~35%; increased duration of hospitalization and costs of care Endpoints Primary: Percent of patients who did not require escalation of treatment with IV anesthetic within the first 24 hours after ganaxolone initiation Secondary: Additional efficacy, safety and tolerability
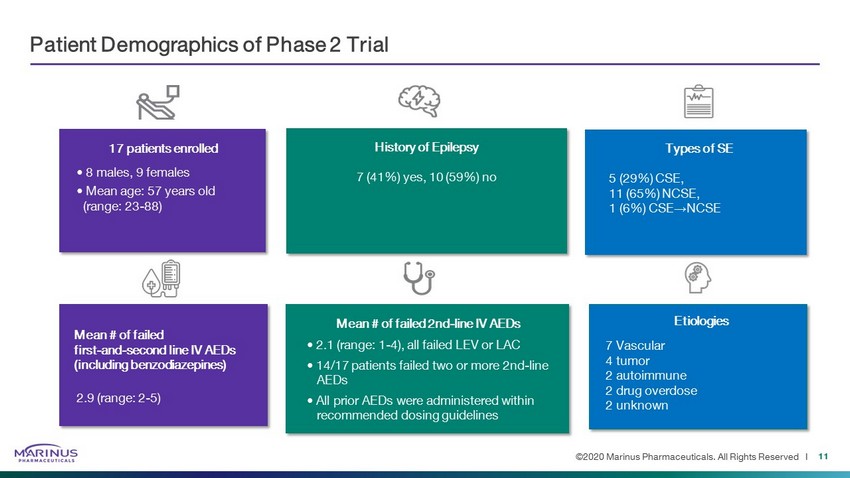
©2020 Marinus Pharmaceuticals. All Rights Reserved I Patient Demographics of Phase 2 Trial 11 • 8 males, 9 females • Mean age: 57 years old (range: 23 - 88) 5 (29%) CSE, 11 (65%) NCSE, 1 (6%) CSE → NCSE 7 (41%) yes, 10 (59%) no 17 patients enrolled Types of SE History of Epilepsy Mean # of failed 2nd - line IV AEDs • 2.1 (range: 1 - 4), all failed LEV or LAC • 14/17 patients failed two or more 2nd - line AEDs • All prior AEDs were administered within recommended dosing guidelines Mean # of failed first - and - second line IV AEDs (including benzodiazepines) 2.9 (range: 2 - 5) 7 Vascular 4 tumor 2 autoimmune 2 drug overdose 2 unknown Etiologies
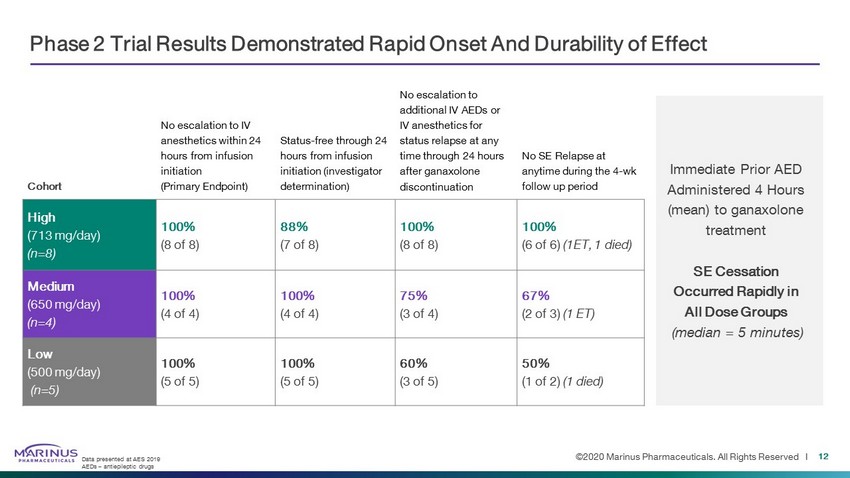
©2020 Marinus Pharmaceuticals. All Rights Reserved I Phase 2 Trial Results Demonstrated Rapid Onset And Durability of Effect Cohort No escalation to IV anesthetics within 24 hours from infusion initiation (Primary Endpoint) Status - free through 24 hours from infusion initiation (investigator determination) No escalation to additional IV AEDs or IV anesthetics for status relapse at any time through 24 hours after ganaxolone discontinuation No SE Relapse at anytime during the 4 - wk follow up period High (713 mg/day) (n=8) 100% (8 of 8) 88% (7 of 8) 100% (8 of 8) 100% (6 of 6) (1ET, 1 died) Medium (650 mg/day) (n=4) 100% (4 of 4) 100% (4 of 4) 75% (3 of 4) 67% (2 of 3) (1 ET) Low (500 mg/day) (n=5) 100% (5 of 5) 100% (5 of 5) 60% (3 of 5) 50% (1 of 2) (1 died) Immediate Prior AED Administered 4 Hours (mean) to ganaxolone treatment SE Cessation Occurred Rapidly in All Dose Groups (median = 5 minutes) Data presented at AES 2019 AEDs – antiepileptic drugs 12
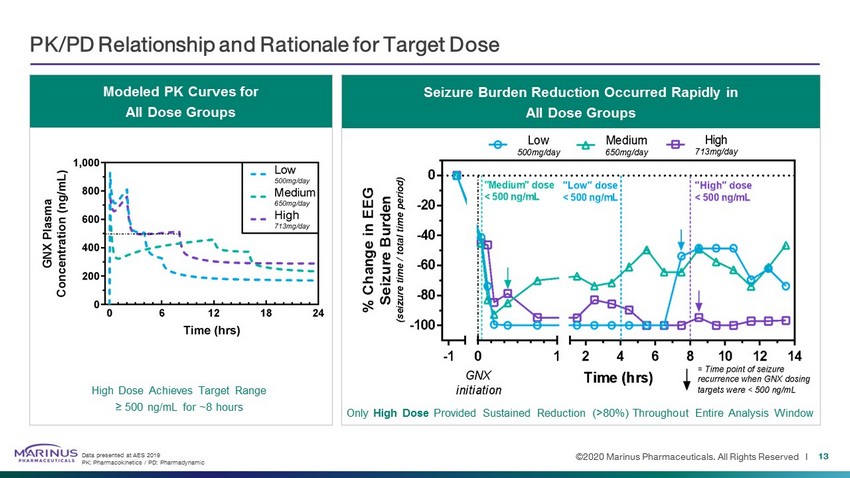
©2020 Marinus Pharmaceuticals. All Rights Reserved I PK/PD Relationship and Rationale for Target Dose 13 Seizure Burden Reduction Occurred Rapidly in All Dose Groups Modeled PK Curves for All Dose Groups High Dose Achieves Target Range ≥ 500 ng/mL for ~8 hours Only High Dose Provided Sustained Reduction (>80%) Throughout Entire Analysis Window Data presented at AES 2019 PK: Pharmacokinetics / PD: Pharmadynamic

©2020 Marinus Pharmaceuticals. All Rights Reserved I IV Ganaxolone Safety Summary 14 Intubation: 9 patients were not intubated upon enrollment. Of these, 6 remained intubation - free during the entire ganaxolone treatment perio d Data presented at AES 2019 AE: adverse event / SAE: serious adverse event 10 SAEs in 6 patients (also included in AEs) 2 related in 2 patients • 2 severe sedation 8 non - related in 4 patients • 1 Death due to withdrawal of life support - 1 Respiratory depression • 1 Bowel perforation (fatal) • 1 Sepsis (fatal) • 1 Fall - 1 Loss of consciousness - 1 Pneumothorax - 1 Multiple fracture 13 related in 7 patients • 6 mild (2 hypotension, 2 somnolence, 1 urinary retention, 1 hypercarbia) • 5 moderate (4 somnolence; 1 hypercarbia) • 2 severe (2 sedation) 37 not - related in 12 patients • 20 mild • 8 moderate (2 pain; 2 pneumonia, 2 dysphagia, • 1 delirium, 1 hypertension) • 9 severe (respiratory depression, death due to withdrawal of support, sepsis, embolic stroke, perforated bowel, fall, loss of consciousness, multiple fractures, pneumothorax) 50 AEs in 16 patients
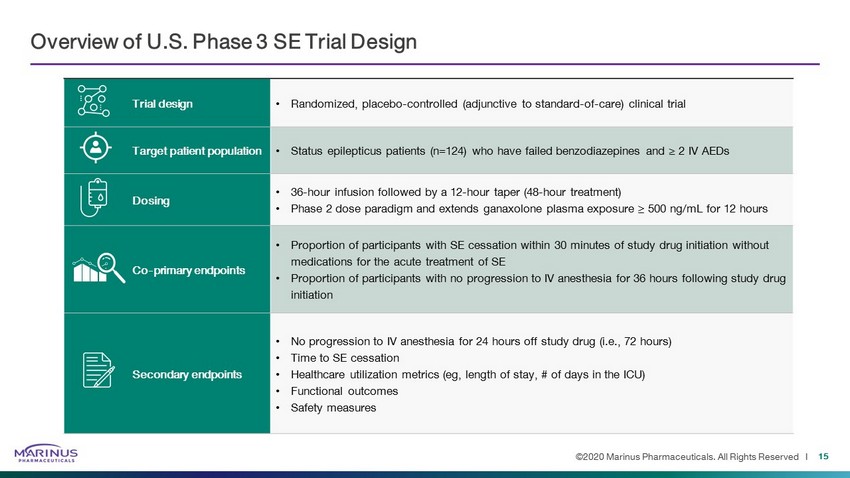
©2020 Marinus Pharmaceuticals. All Rights Reserved I Overview of U.S. Phase 3 SE Trial Design Trial design • Randomized, placebo - controlled (adjunctive to standard - of - care) clinical trial Target patient population • Status epilepticus patients (n=124) who have failed benzodiazepines and ≥ 2 IV AEDs Dosing • 36 - hour infusion followed by a 12 - hour taper (48 - hour treatment) • Phase 2 dose paradigm and extends ganaxolone plasma exposure ≥ 500 ng/mL for 12 hours Co - primary endpoints • Proportion of participants with SE cessation within 30 minutes of study drug initiation without medications for the acute treatment of SE • Proportion of participants with no progression to IV anesthesia for 36 hours following study drug initiation Secondary endpoints • No progression to IV anesthesia for 24 hours off study drug (i.e., 72 hours) • Time to SE cessation • Healthcare utilization metrics ( eg , length of stay, # of days in the ICU) • Functional outcomes • Safety measures 15
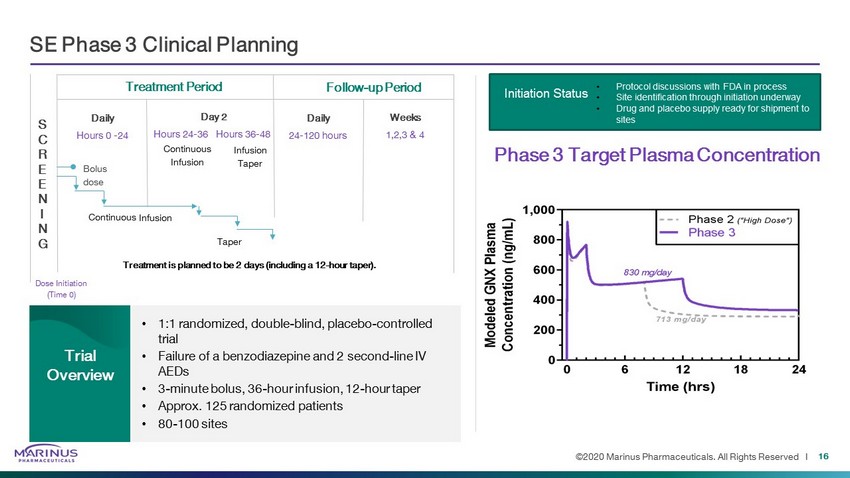
©2020 Marinus Pharmaceuticals. All Rights Reserved I SE Phase 3 Clinical Planning 16 • 1:1 randomized, double - blind, placebo - controlled trial • Failure of a benzodiazepine and 2 second - line IV AEDs • 3 - minute bolus, 36 - hour infusion, 12 - hour taper • Approx. 125 randomized patients • 80 - 100 sites Trial Overview S C R E E N I N G Dose Initiation (Time 0) Treatment Period Follow - up Period Weeks 1,2,3 & 4 Daily 24 - 120 hours Day 2 Hours 24 - 36 Hours 36 - 48 Daily Hours 0 - 24 Bolus dose Continuous Infusion Taper Treatment is planned to be 2 days (including a 12 - hour taper). Phase 3 Target Plasma Concentration Continuous Infusion Infusion Taper • Protocol discussions with FDA in process • Site identification through initiation underway • Drug and placebo supply ready for shipment to sites Initiation Status

©2020 Marinus Pharmaceuticals. All Rights Reserved I RAISE Trial Sites Standard of Care Progression to IV Anesthesia • Surveyed PI’s at selected RAISE Trail sites to learn more about their standard of care natural history progression to IV anesthesia following the failure of one versus more than one 2 nd - line IV AEDs 17 Trial population Of those that escalate to 3 rd - line IV anesthesia, they do so in ~2.5 hours following failure of the second 2 nd - line IV AED Clear unmet medical need in patients that fail two or more 2 nd line IV AEDs Guides site selection and approximates placebo response for escalation to IV anesthesia co - primary Patients with non - convulsive status epilepticus (NCSE) median 1 2 0 20 40 60 80 100 # of failed 2 nd -line IV AEDs % o f P a t i e n t s P r o g r e s s i n g t o 3 r d - l i n e I V a n e s t h e t i c s median + 95% CI
©2020 Marinus Pharmaceuticals. All Rights Reserved I BARDA Contract – Refractory Status Epilepticus 18 Key Contract Parameters • BARDA to contribute $21 million in base contract to support the Phase 3 clinical trial in RSE and preclinical studies of ganaxolone in nerve agent exposure animal models. • BARDA may contribute up to an additional $30 million in support of manufacturing, supply chain, clinical, regulatory and toxicology activities based on favorable clinical and pre - clinical outcomes. • Total contract value = $84 million; $51 million BARDA / $33 million Marinus - if all options are undertaken. • On successful development, BARDA and Marinus may negotiate for a supply of ganaxolone for a potential response to nerve gas exposure threats.
©2020 Marinus Pharmaceuticals. All Rights Reserved I Quantifying the Significant Clinical and Economic Burden of SE The Phase 3 trial of ganaxolone in refractory SE aims to demonstrate rapid onset of action capable of preventing escalation to IV anesthetics. Treatment with IV anesthetics has been reported to lead to increased length of hospital admission and risk of infections, new disability, and death. 1 - 3 There’s a potential pharmacoeconomic opportunity to quantify cost of care and characterize clinical outcomes based on treatment progression to IV anesthetics. 1 Sutter R et al. 2014 Neurology 2 Hawkes MA et al. 2019 Crit. Care Med. 3 Marchi NA et al. 2015 Crit. Care Med. $ $ Understanding the spectrum of clinical and economic burden based on disease severity will help support treatment value 19
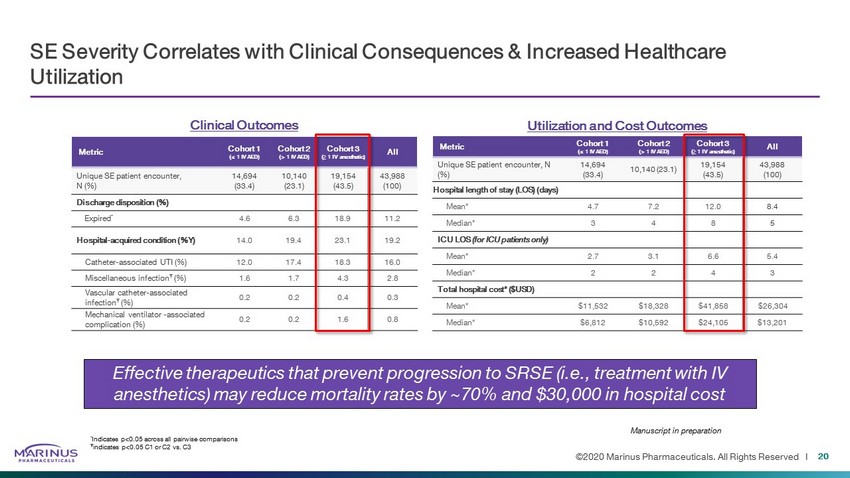
©2020 Marinus Pharmaceuticals. All Rights Reserved I SE Severity Correlates with Clinical Consequences & Increased Healthcare Utilization Utilization and Cost Outcomes Metric Cohort 1 (≤ 1 IV AED) Cohort 2 (> 1 IV AED) Cohort 3 ( ≥ 1 IV anesthetic) All Unique SE patient encounter, N (%) 14,694 (33.4) 10,140 (23.1) 19,154 (43.5) 43,988 (100) Hospital length of stay (LOS) (days) Mean* 4.7 7.2 12.0 8.4 Median* 3 4 8 5 ICU LOS (for ICU patients only) Mean* 2.7 3.1 6.6 5.4 Median* 2 2 4 3 Total hospital cost* ($USD) Mean* $11,532 $18,328 $41,858 $26,304 Median* $6,812 $10,592 $24,105 $13,201 Clinical Outcomes Metric Cohort 1 (≤ 1 IV AED) Cohort 2 (> 1 IV AED) Cohort 3 ( ≥ 1 IV anesthetic) All Unique SE patient encounter, N (%) 14,694 (33.4) 10,140 (23.1) 19,154 (43.5) 43,988 (100) Discharge disposition (%) Expired * 4.6 6.3 18.9 11.2 Hospital - acquired condition (%Y) 14.0 19.4 23.1 19.2 Catheter - associated UTI (%) 12.0 17.4 18.3 16.0 Miscellaneous infection Ŧ (%) 1.6 1.7 4.3 2.8 Vascular catheter - associated infection Ŧ (%) 0.2 0.2 0.4 0.3 Mechanical ventilator - associated complication (%) 0.2 0.2 1.6 0.8 * Indicates p<0.05 across all pairwise comparisons Ŧ indicates p<0.05 C1 or C2 vs. C3 Effective therapeutics that prevent progression to SRSE (i.e., treatment with IV anesthetics) may reduce mortality rates by ~70% and $30,000 in hospital cost Manuscript in preparation 20
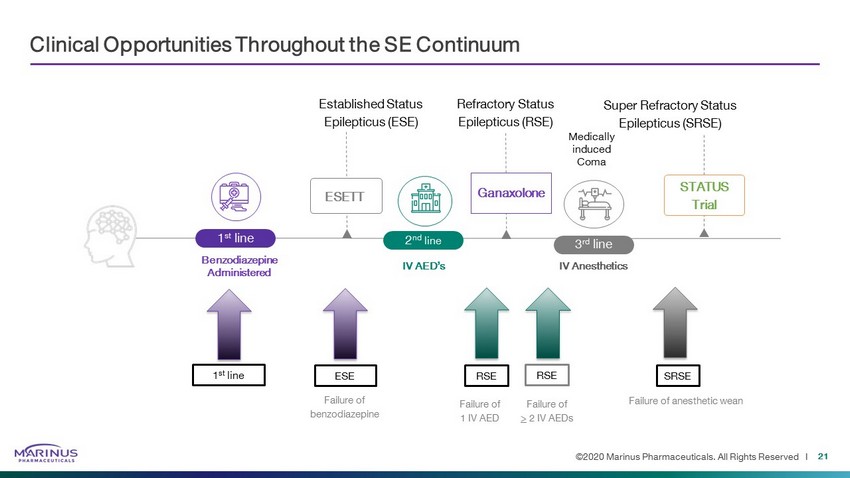
©2020 Marinus Pharmaceuticals. All Rights Reserved I Clinical Opportunities Throughout the SE Continuum Benzodiazepine Administered Medically induced Coma Established Status Epilepticus (ESE) 1 st line 2 nd line IV AED’s 3 rd line IV Anesthetics Super Refractory Status Epilepticus (SRSE) Refractory Status Epilepticus (RSE) ESETT Ganaxolone STATUS Trial ESE 1 st line SRSE RSE RSE Failure of benzodiazepine Failure of > 2 IV AEDs Failure of 1 IV AED Failure of anesthetic wean 21
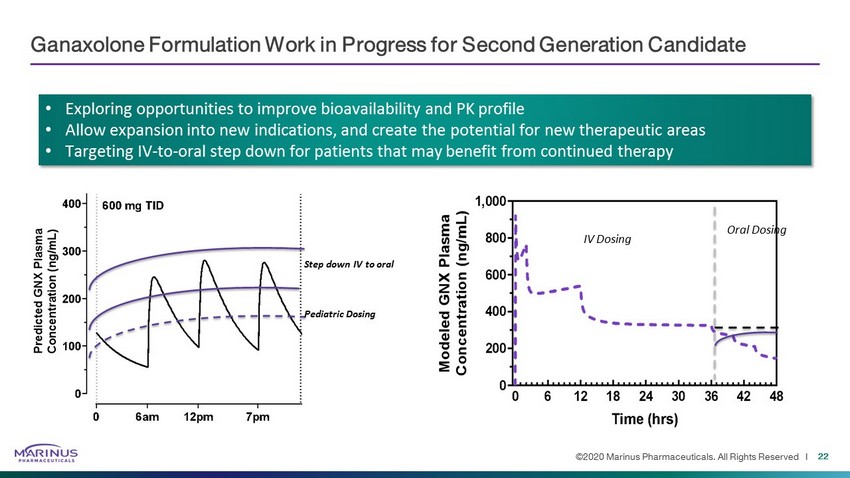
©2020 Marinus Pharmaceuticals. All Rights Reserved I Ganaxolone Formulation Work in Progress for Second Generation Candidate Step down IV to oral Pediatric Dosing IV Dosing Oral Dosing • Exploring opportunities to improve bioavailability and PK profile • Allow expansion into new indications, and create the potential for new therapeutic areas • Targeting IV - to - oral step down for patients that may benefit from continued therapy 22
Genetic Epilepsy Franchise

CDKL5 Deficiency Disorder
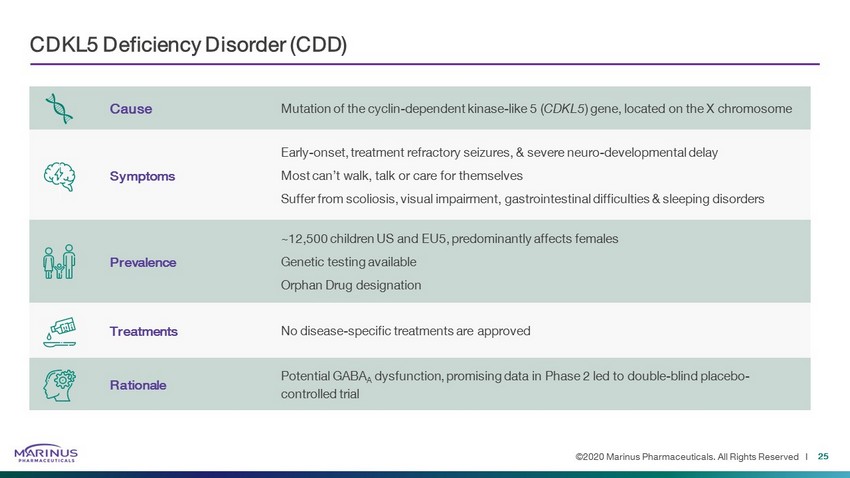
©2020 Marinus Pharmaceuticals. All Rights Reserved I Cause Mutation of the cyclin - dependent kinase - like 5 ( CDKL5 ) gene, located on the X chromosome Symptoms Early - onset, treatment refractory seizures, & severe neuro - developmental delay Most can’t walk, talk or care for themselves Suffer from scoliosis, visual impairment, gastrointestinal difficulties & sleeping disorders Prevalence ~12,500 children US and EU5, predominantly affects females Genetic testing available Orphan Drug designation Treatments No disease - specific treatments are approved Rationale Potential GABA A dysfunction, promising data in Phase 2 led to double - blind placebo - controlled trial CDKL5 Deficiency Disorder (CDD) 25
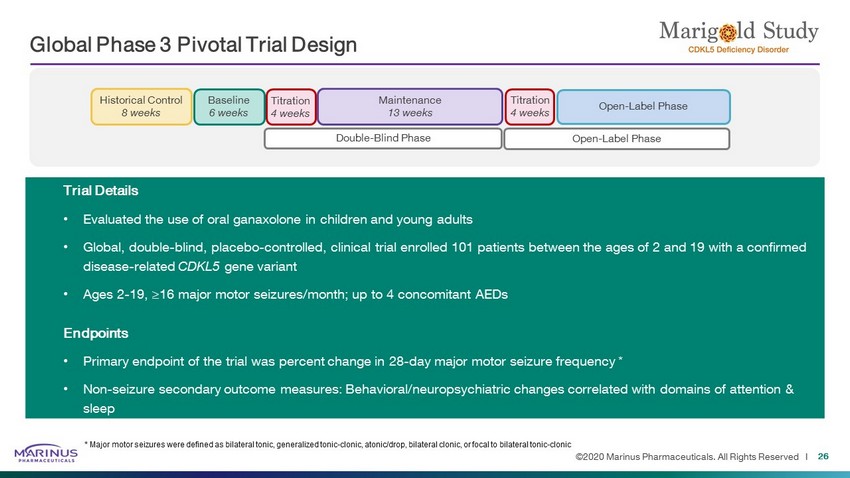
©2020 Marinus Pharmaceuticals. All Rights Reserved I Global Phase 3 Pivotal Trial Design 26 Baseline 6 weeks Historical Control 8 weeks Double - Blind Phase Open - Label Phase Maintenance 13 weeks Titration 4 weeks Titration 4 weeks Open - Label Phase Trial Details • Evaluated the use of oral ganaxolone in children and young adults • Global, double - blind, placebo - controlled, clinical trial enrolled 101 patients between the ages of 2 and 19 with a confirmed disease - related CDKL5 gene variant • Ages 2 - 19, ≥16 major motor seizures/month; up to 4 concomitant AEDs Endpoints • Primary endpoint of the trial was percent change in 28 - day major motor seizure frequency * • Non - seizure secondary outcome measures: Behavioral/neuropsychiatric changes correlated with domains of attention & sleep * Major motor seizures were defined as bilateral tonic, generalized tonic - clonic , atonic/drop, bilateral clonic , or focal to bilateral tonic - clonic
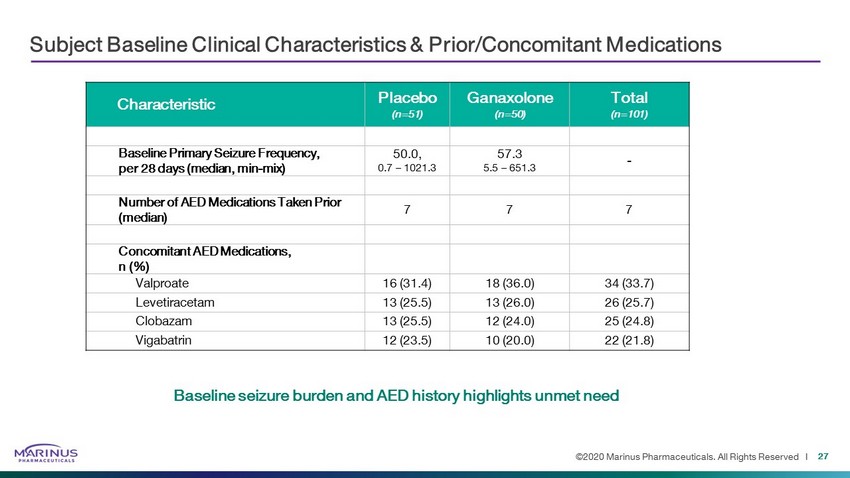
©2020 Marinus Pharmaceuticals. All Rights Reserved I Subject Baseline Clinical Characteristics & Prior/Concomitant Medications 27 Characteristic Placebo (n=51) Ganaxolone (n=50) Total (n=101) Baseline Primary Seizure Frequency, per 28 days (median, min - mix ) 50.0, 0.7 – 1021.3 57.3 5.5 – 651.3 - Number of AED Medications Taken Prior (median) 7 7 7 Concomitant AED Medications, n (%) Valproate 16 (31.4) 18 (36.0) 34 (33.7) Levetiracetam 13 (25.5) 13 (26.0) 26 (25.7) Clobazam 13 (25.5) 12 (24.0) 25 (24.8) Vigabatrin 12 (23.5) 10 (20.0) 22 (21.8) Baseline seizure burden and AED history highlights unmet need
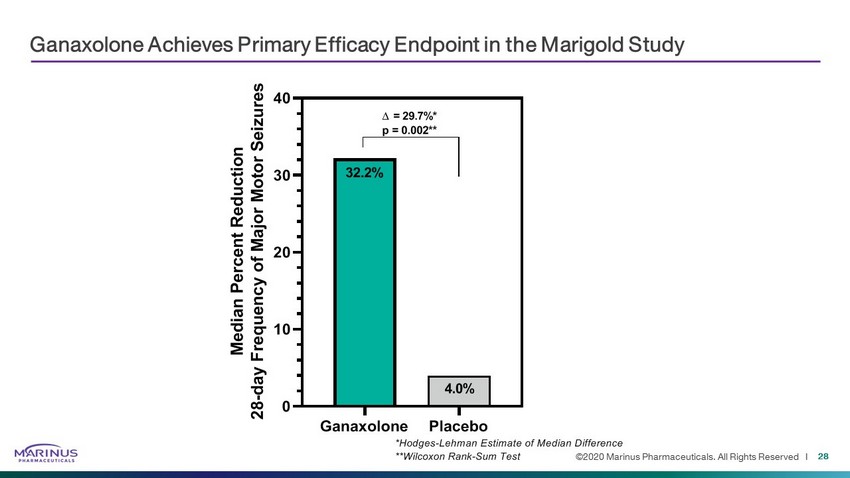
©2020 Marinus Pharmaceuticals. All Rights Reserved I Ganaxolone Achieves Primary Efficacy Endpoint in the Marigold Study 28 Ganaxolone Placebo 0 10 20 30 40 M e d i a n P e r c e n t R e d u c t i o n 2 8 - d a y F r e q u e n c y o f M a j o r M o t o r S e i z u r e s 32.2% 4.0% = 29.7%* p = 0.002** *Hodges-Lehman Estimate of Median Difference **Wilcoxon Rank-Sum Test
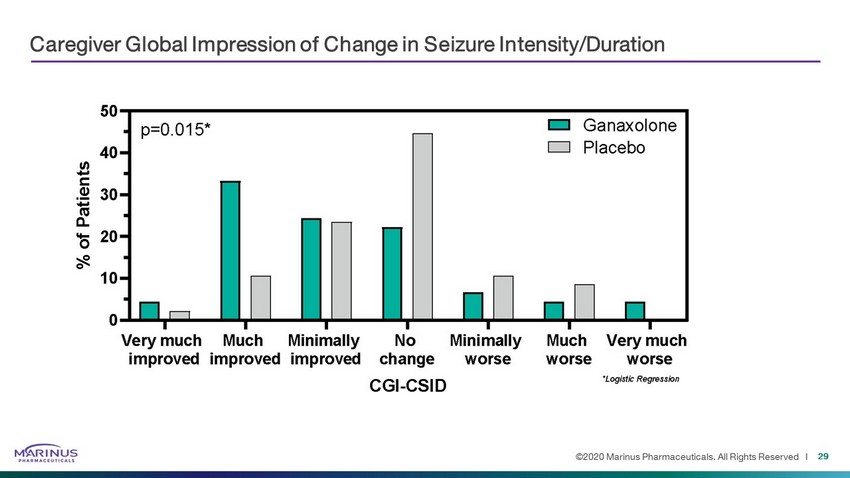
©2020 Marinus Pharmaceuticals. All Rights Reserved I Caregiver Global Impression of Change in Seizure Intensity/Duration 29
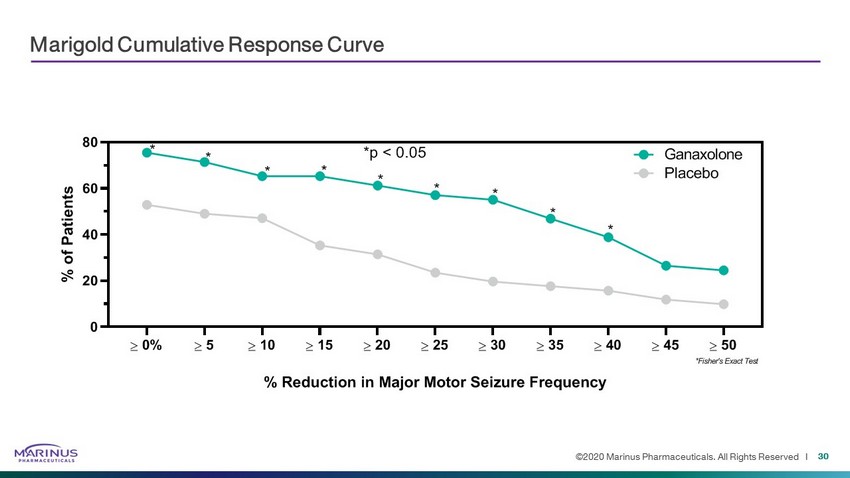
©2020 Marinus Pharmaceuticals. All Rights Reserved I Marigold Cumulative Response Curve 30 0% 5 10 15 20 25 30 35 40 45 50 0 20 40 60 80 % Reduction in Major Motor Seizure Frequency % o f P a t i e n t s Ganaxolone Placebo * * * * * * * * * *p < 0.05 *Fisher's Exact Test
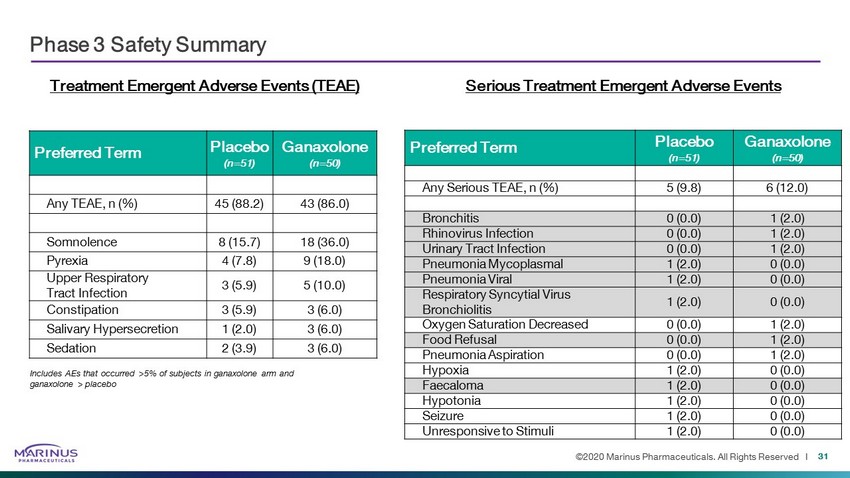
©2020 Marinus Pharmaceuticals. All Rights Reserved I Phase 3 Safety Summary 31 Treatment Emergent Adverse Events (TEAE) Preferred Term Placebo (n=51) Ganaxolone (n=50) Any TEAE, n (%) 45 (88.2) 43 (86.0) Somnolence 8 (15.7) 18 (36.0) Pyrexia 4 (7.8) 9 (18.0) Upper Respiratory Tract Infection 3 (5.9) 5 (10.0) Constipation 3 (5.9) 3 (6.0) Salivary Hypersecretion 1 (2.0) 3 (6.0) Sedation 2 (3.9) 3 (6.0) Includes AEs that occurred >5% of subjects in ganaxolone arm and ganaxolone > placebo Preferred Term Placebo (n=51) Ganaxolone (n=50) Any Serious TEAE, n (%) 5 (9.8) 6 (12.0) Bronchitis 0 (0.0) 1 (2.0) Rhinovirus Infection 0 (0.0) 1 (2.0) Urinary Tract Infection 0 (0.0) 1 (2.0) Pneumonia Mycoplasmal 1 (2.0) 0 (0.0) Pneumonia Viral 1 (2.0) 0 (0.0) Respiratory Syncytial Virus Bronchiolitis 1 (2.0) 0 (0.0) Oxygen Saturation Decreased 0 (0.0) 1 (2.0) Food Refusal 0 (0.0) 1 (2.0) Pneumonia Aspiration 0 (0.0) 1 (2.0) Hypoxia 1 (2.0) 0 (0.0) Faecaloma 1 (2.0) 0 (0.0) Hypotonia 1 (2.0) 0 (0.0) Seizure 1 (2.0) 0 (0.0) Unresponsive to Stimuli 1 (2.0) 0 (0.0) Serious Treatment Emergent Adverse Events
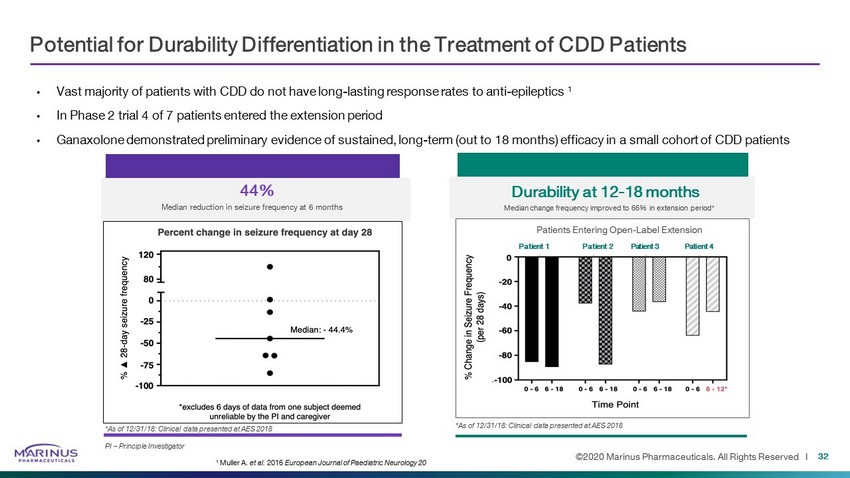
©2020 Marinus Pharmaceuticals. All Rights Reserved I Potential for Durability Differentiation in the Treatment of CDD Patients • Vast majority of patients with CDD do not have long - lasting response rates to anti - epileptics 1 • In Phase 2 trial 4 of 7 patients entered the extension period • Ganaxolone demonstrated preliminary evidence of sustained, long - term (out to 18 months) efficacy in a small cohort of CDD patien ts 32 *As of 12/31/18: Clinical data presented at AES 2018 PI – Principle Investigator 44% Median reduction in seizure frequency at 6 months Durability at 12 - 18 months Median change frequency improved to 66% in extension period* Patients Entering Open - Label Extension Patient 1 Patient 2 Patient 3 Patient 4 1 Muller A. et al. 2016 European Journal of Paediatric Neurology 20 *As of 12/31/18: Clinical data presented at AES 2018
©2020 Marinus Pharmaceuticals. All Rights Reserved I Commercialization Preparedness Executing research with Payers and Physicians around TPP / Value Proposition Identifying organizational needs for field resources, systems and processes Developing plans to scale up Advocacy, Scientific Affairs and Commercial teams Readying supply chain to support packaging and scale up needs to commercialize Potential for operational leverage across indications within concentrated rare epilepsy care model 33 TPP – Target Product Profile
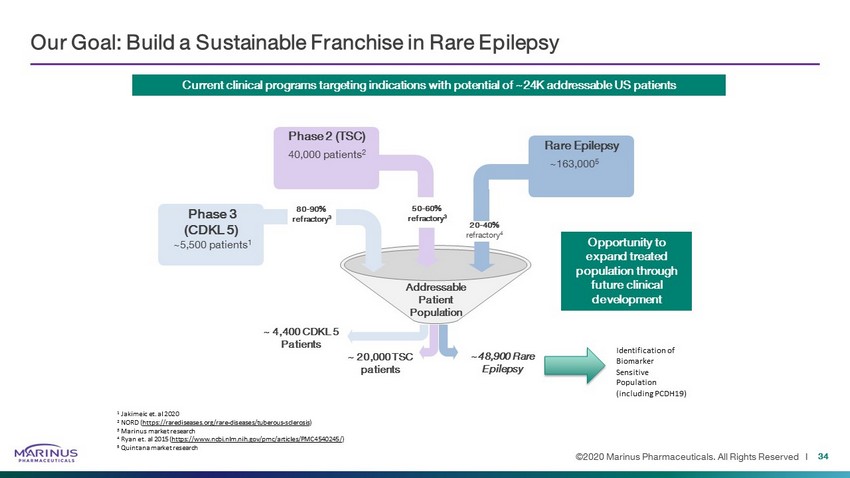
©2020 Marinus Pharmaceuticals. All Rights Reserved I ~48,900 Rare Epilepsy ~ 4,400 CDKL 5 Patients ~ 20,000 TSC patients Addressable Patient Population 20 - 40% refractory 4 Phase 2 (TSC) 40,000 patients 2 50 - 60% refractory 3 Phase 3 (CDKL 5) ~5,500 patients 1 80 - 90% refractory 3 ~163,000 5 Rare Epilepsy Current clinical programs targeting indications with potential of ~24K addressable US patients Our Goal: Build a Sustainable Franchise in Rare Epilepsy Opportunity to expand treated population through future clinical development Identification of Biomarker Sensitive Population (including PCDH19) 1 Jakimeic et. al 2020 2 NORD ( https://rarediseases.org/rare - diseases/tuberous - sclerosis ) 3 Marinus market research 4 Ryan et. al 2015 ( https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4540245/ ) 5 Quintana market research 34
Tuberous Sclerosis Complex
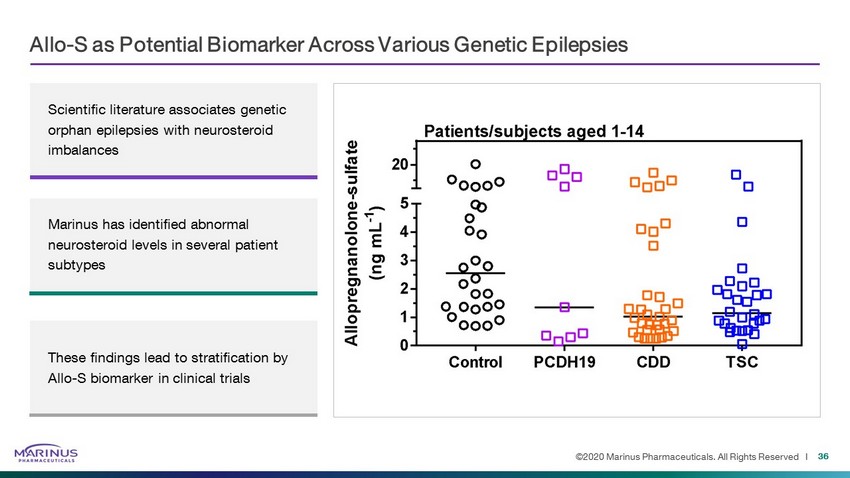
©2020 Marinus Pharmaceuticals. All Rights Reserved I Allo - S as Potential Biomarker Across Various Genetic Epilepsies 36 Scientific literature associates genetic orphan epilepsies with neurosteroid imbalances Marinus has identified abnormal neurosteroid levels in several patient subtypes These findings lead to stratification by Allo - S biomarker in clinical trials
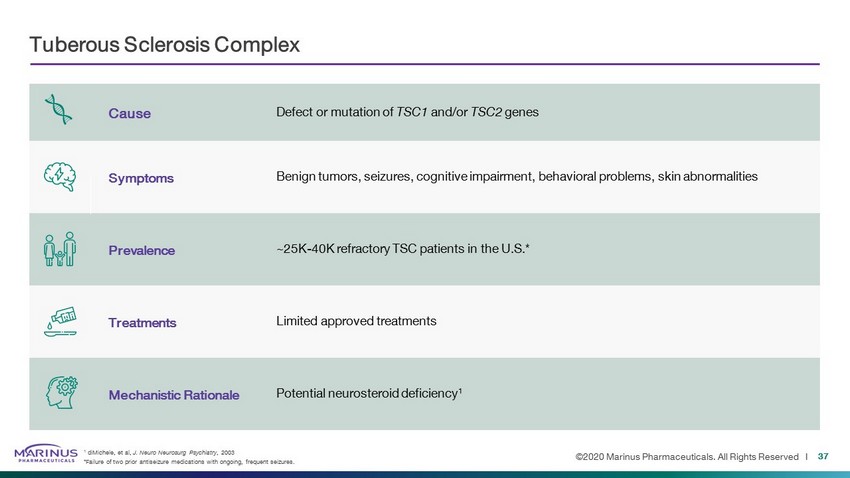
©2020 Marinus Pharmaceuticals. All Rights Reserved I Cause Defect or mutation of TSC1 and/or TSC2 genes Symptoms Benign tumors, seizures, cognitive impairment, behavioral problems, skin abnormalities Prevalence ~25K - 40K refractory TSC patients in the U.S.* Treatments Limited approved treatments Mechanistic Rationale Potential neurosteroid deficiency 1 Tuberous Sclerosis Complex 37 1 diMichele, et al, J. Neuro Neurosurg Psychiatry , 2003 *Failure of two prior antiseizure medications with ongoing, frequent seizures.
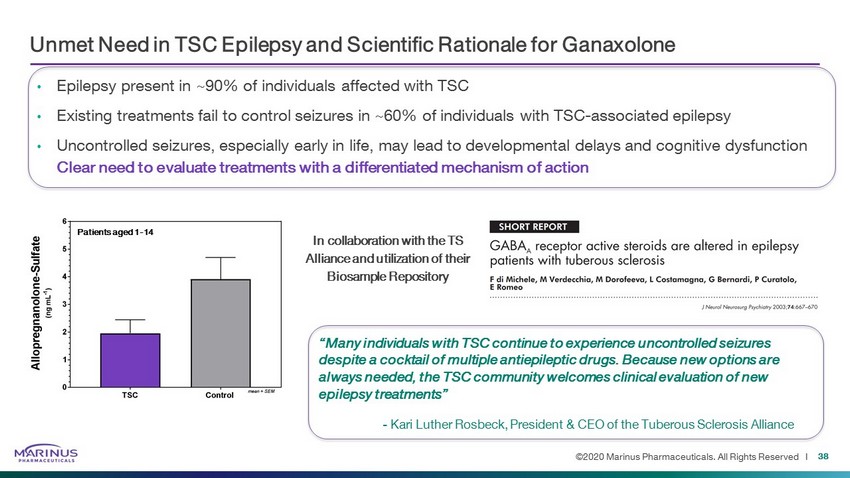
©2020 Marinus Pharmaceuticals. All Rights Reserved I Unmet Need in TSC Epilepsy and Scientific Rationale for Ganaxolone • Epilepsy present in ~90% of individuals affected with TSC • Existing treatments fail to control seizures in ~60% of individuals with TSC - associated epilepsy • Uncontrolled seizures, especially early in life, may lead to developmental delays and cognitive dysfunction 38 Clear need to evaluate treatments with a differentiated mechanism of action In collaboration with the TS Alliance and utilization of their Biosample Repository Patients aged 1 - 14 “Many individuals with TSC continue to experience uncontrolled seizures despite a cocktail of multiple antiepileptic drugs. Because new options are always needed, the TSC community welcomes clinical evaluation of new epilepsy treatments” - Kari Luther Rosbeck, President & CEO of the Tuberous Sclerosis Alliance
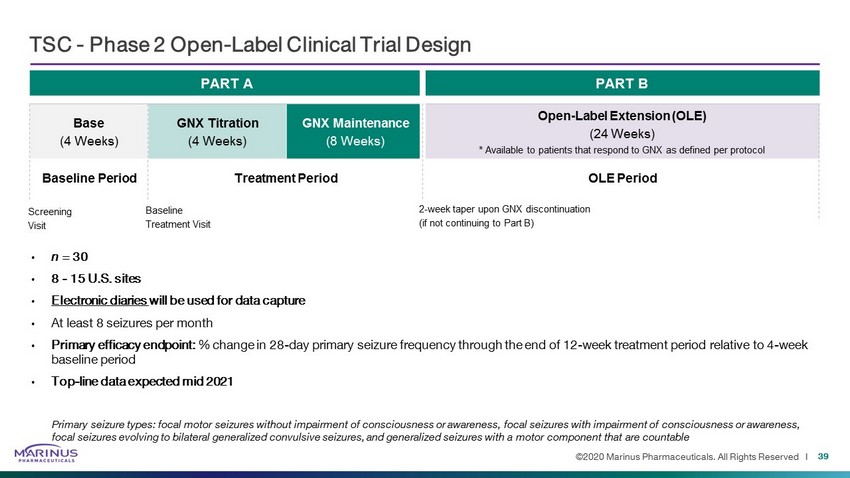
©2020 Marinus Pharmaceuticals. All Rights Reserved I PART A PART B Base (4 Weeks) GNX Titration (4 Weeks) GNX Maintenance (8 Weeks) Open - Label Extension (OLE) (24 Weeks) * Available to patients that respond to GNX as defined per protocol TSC - Phase 2 Open - Label Clinical Trial Design • n = 30 • 8 - 15 U.S. sites • Electronic diaries will be used for data capture • At least 8 seizures per month • Primary efficacy endpoint: % change in 28 - day primary seizure frequency through the end of 12 - week treatment period relative to 4 - week baseline period • Top - line data expected mid 2021 Primary seizure types: focal motor seizures without impairment of consciousness or awareness, focal seizures with impairment of consciousness or awareness, focal seizures evolving to bilateral generalized convulsive seizures, and generalized seizures with a motor component that ar e c ountable 39 Baseline Period Treatment Period OLE Period Screening Visit Baseline Treatment Visit 2 - week taper upon GNX discontinuation (if not continuing to Part B)

PCDH19 Related Epilepsy
©2020 Marinus Pharmaceuticals. All Rights Reserved I Cause Inherited mutation of protocadherin 19 ( PCDH19 ) gene. Located on X chromosome Symptoms Early - onset seizures, cognitive and sensory impairment, and psychiatric and behavioral disorders. Seizures last from days to weeks; sensitive to fever Prevalence Affects ~10K children US and EU Predominantly females Genetic testing becoming more readily available Orphan Drug designation Treatments No disease - specific treatments are approved Mechanistic Rationale Associated with low levels of allopregnanolone 1 and potential GABA ergic dysfunction PCDH19 - Related Epilepsy 41 1 Gecz, et.al, Human Molecular Genetics, 2015
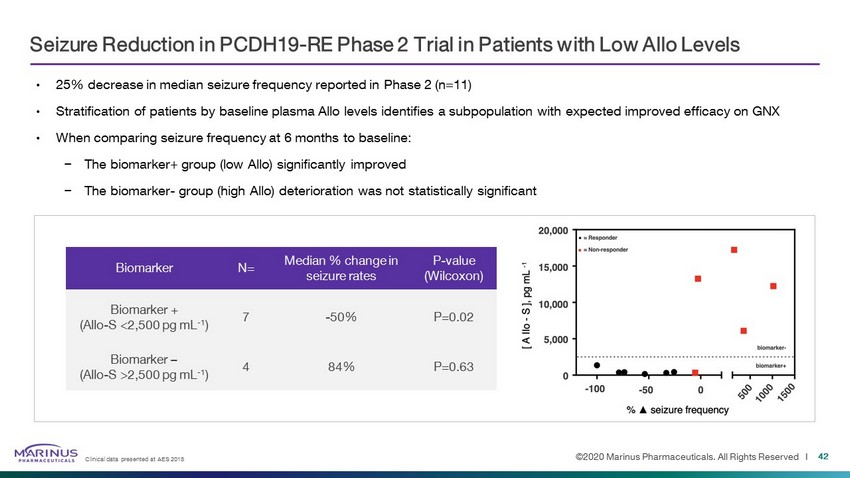
©2020 Marinus Pharmaceuticals. All Rights Reserved I Seizure Reduction in PCDH19 - RE Phase 2 Trial in Patients with Low Allo Levels • 25% decrease in median seizure frequency reported in Phase 2 (n=11) • Stratification of patients by baseline plasma Allo levels identifies a subpopulation with expected improved efficacy on GNX • When comparing seizure frequency at 6 months to baseline: − The biomarker+ group (low Allo) significantly improved − The biomarker - group (high Allo) deterioration was not statistically significant Biomarker N= Median % change in seizure rates P - value (Wilcoxon) Biomarker + (Allo - S <2,500 pg mL - 1 ) 7 - 50% P=0.02 Biomarker – (Allo - S >2,500 pg mL - 1 ) 4 84% P=0.63 42 Clinical data presented at AES 2018
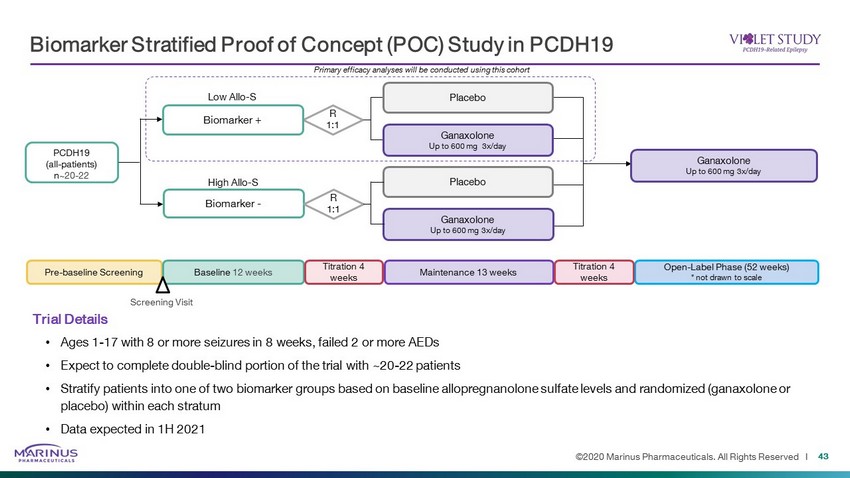
©2020 Marinus Pharmaceuticals. All Rights Reserved I Biomarker Stratified Proof of Concept (POC) Study in PCDH19 43 Trial Details • Ages 1 - 17 with 8 or more seizures in 8 weeks, failed 2 or more AEDs • Expect to complete double - blind portion of the trial with ~20 - 22 patients • Stratify patients into one of two biomarker groups based on baseline allopregnanolone sulfate levels and randomized (ganaxolo ne or placebo) within each stratum • Data expected in 1H 2021 R 1:1 PCDH19 (all - patients) n ~20 - 22 Biomarker + Low Allo - S Primary efficacy analyses will be conducted using this cohort Biomarker - High Allo - S R 1:1 Ganaxolone Up to 600 mg 3x/day Placebo Ganaxolone Up to 600 mg 3x/day Placebo Ganaxolone Up to 600 mg 3x/day Pre - baseline Screening Maintenance 13 weeks Baseline 12 weeks Titration 4 weeks Open - Label Phase (52 weeks) * not drawn to scale Titration 4 weeks Screening Visit

Intellectual Property
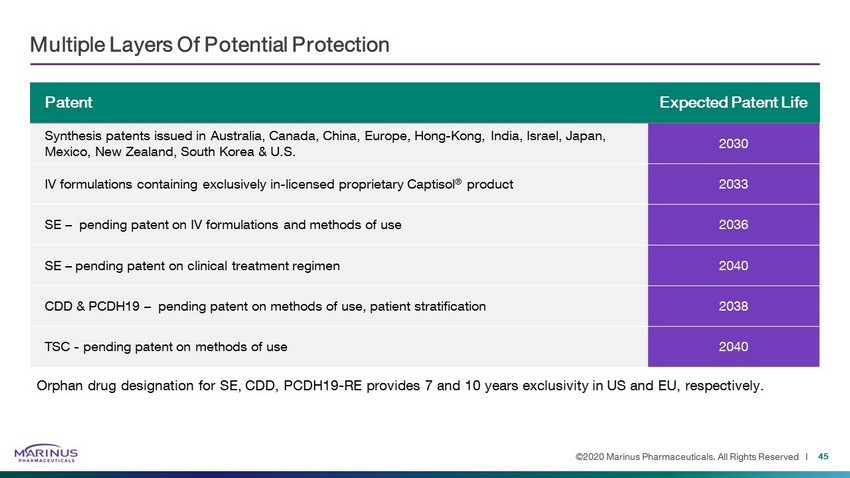
©2020 Marinus Pharmaceuticals. All Rights Reserved I Patent Expected Patent Life Synthesis patents issued in Australia, Canada, China, Europe, Hong - Kong, India, Israel, Japan, Mexico, New Zealand, South Korea & U.S. 2030 IV formulations containing exclusively in - licensed proprietary Captisol ® product 2033 SE – pending patent on IV formulations and methods of use 2036 SE – pending patent on clinical treatment regimen 2040 CDD & PCDH19 – pending patent on methods of use, patient stratification 2038 TSC - pending patent on methods of use 2040 Multiple Layers Of Potential Protection 45 Orphan drug designation for SE, CDD, PCDH19 - RE provides 7 and 10 years exclusivity in US and EU, respectively.

Thank You
©2020 Marinus Pharmaceuticals. All Rights Reserved I Appendix 47
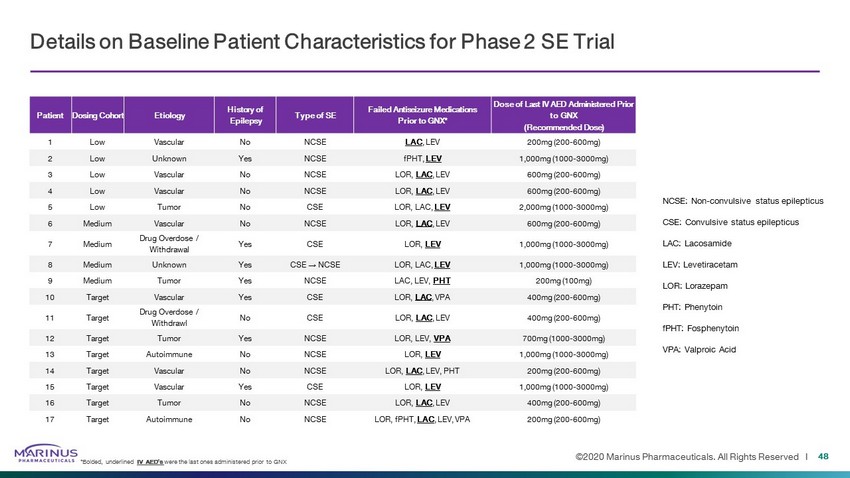
©2020 Marinus Pharmaceuticals. All Rights Reserved I 48 NCSE: Non - convulsive status epilepticus CSE: Convulsive status epilepticus LAC: Lacosamide LEV: Levetiracetam LOR: Lorazepam PHT: Phenytoin fPHT: Fosphenytoin VPA: Valproic Acid Details on Baseline Patient Characteristics for Phase 2 SE Trial *Bolded, underlined IV AED’s were the last ones administered prior to GNX Patient Dosing Cohort Etiology History of Epilepsy Type of SE Failed Antiseizure Medications Prior to GNX* Dose of Last IV AED Administered Prior to GNX (Recommended Dose) 1 Low Vascular No NCSE LAC , LEV 200mg (200 - 600mg) 2 Low Unknown Yes NCSE fPHT, LEV 1,000mg (1000 - 3000mg) 3 Low Vascular No NCSE LOR, LAC , LEV 600mg (200 - 600mg) 4 Low Vascular No NCSE LOR, LAC , LEV 600mg (200 - 600mg) 5 Low Tumor No CSE LOR, LAC, LEV 2,000mg (1000 - 3000mg) 6 Medium Vascular No NCSE LOR, LAC , LEV 600mg (200 - 600mg) 7 Medium Drug Overdose / Withdrawal Yes CSE LOR, LEV 1,000mg (1000 - 3000mg) 8 Medium Unknown Yes CSE → NCSE LOR, LAC, LEV 1,000mg (1000 - 3000mg) 9 Medium Tumor Yes NCSE LAC, LEV, PHT 200mg (100mg) 10 Target Vascular Yes CSE LOR, LAC , VPA 400mg (200 - 600mg) 11 Target Drug Overdose / Withdrawl No CSE LOR, LAC , LEV 400mg (200 - 600mg) 12 Target Tumor Yes NCSE LOR, LEV, VPA 700mg (1000 - 3000mg) 13 Target Autoimmune No NCSE LOR, LEV 1,000mg (1000 - 3000mg) 14 Target Vascular No NCSE LOR, LAC , LEV, PHT 200mg (200 - 600mg) 15 Target Vascular Yes CSE LOR, LEV 1,000mg (1000 - 3000mg) 16 Target Tumor No NCSE LOR, LAC , LEV 400mg (200 - 600mg) 17 Target Autoimmune No NCSE LOR, fPHT, LAC , LEV, VPA 200mg (200 - 600mg)
©2020 Marinus Pharmaceuticals. All Rights Reserved I 49 HEOR Opportunities to Expand Potential Value Proposition of Ganaxolone in SE Quantify total cost of care in SE patients following hospital discharge • Many patients were discharged to long - term care or skilled nursing facilities and correlated with more severe SE Effective treatment options aimed at limiting the progression of SE severity may lead to favorable discharge settings and reduce post - hospital costs Quantify total cost of care of an inpatient episode of SE in patients that transfer between hospitals • 13% of patients with an SE diagnosis code were excluded due to being transferred into or out of a Premier hospital (i.e., incomplete SE episode details and cost) • These patients are likely high - acuity cases in need of specialized care and may result in: − Increased duration in SE − Increased length of hospital stay and overall healthcare utilization Effective treatment of SE at the initial site of care has the potential to dramatically improve outcomes and reduce costs HEOR - Health economics and outcome research
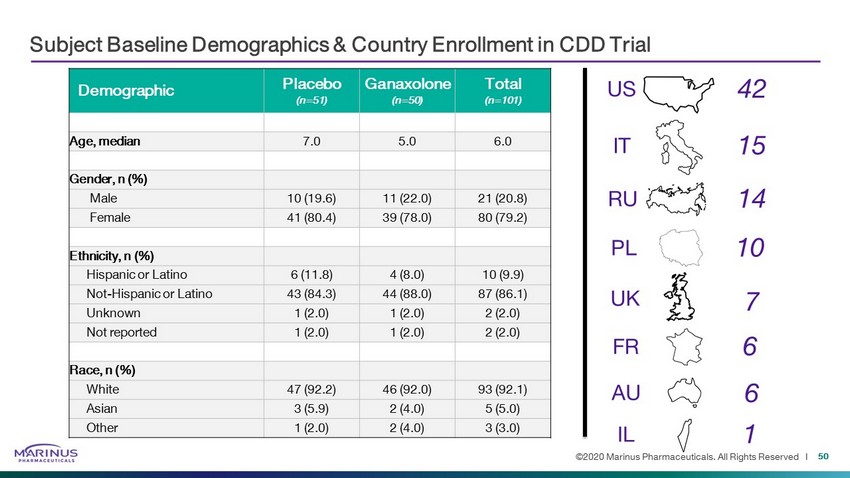
©2020 Marinus Pharmaceuticals. All Rights Reserved I Subject Baseline Demographics & Country Enrollment in CDD Trial 50 Demographic Placebo (n=51) Ganaxolone (n=50) Total (n=101) Age, median 7.0 5.0 6.0 Gender, n (%) Male 10 (19.6) 11 (22.0) 21 (20.8) Female 41 (80.4) 39 (78.0) 80 (79.2) Ethnicity, n (%) Hispanic or Latino 6 (11.8) 4 (8.0) 10 (9.9) Not - Hispanic or Latino 43 (84.3) 44 (88.0) 87 (86.1) Unknown 1 (2.0) 1 (2.0) 2 (2.0) Not reported 1 (2.0) 1 (2.0) 2 (2.0) Race, n (%) White 47 (92.2) 46 (92.0) 93 (92.1) Asian 3 (5.9) 2 (4.0) 5 (5.0) Other 1 (2.0) 2 (4.0) 3 (3.0) US IT RU UK PL FR AU IL 42 15 14 10 7 6 6 1
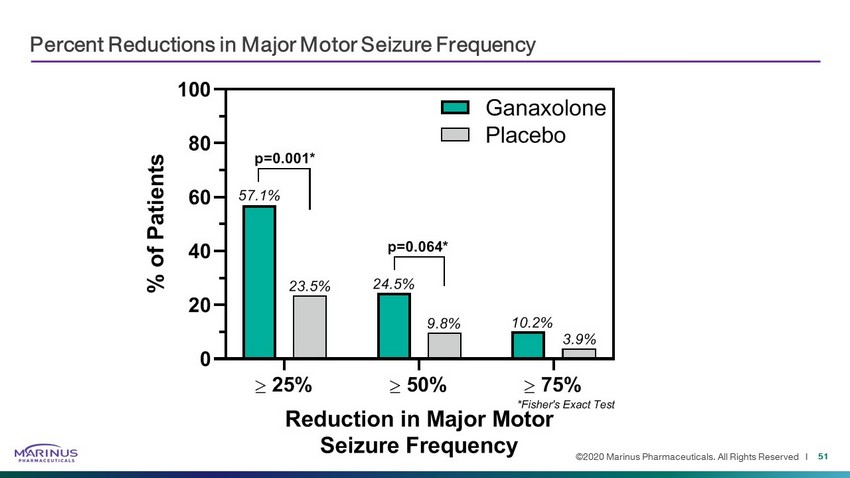
©2020 Marinus Pharmaceuticals. All Rights Reserved I Percent Reductions in Major Motor Seizure Frequency 51 25% 50% 75% 0 20 40 60 80 100 Reduction in Major Motor Seizure Frequency % o f P a t i e n t s Ganaxolone Placebo 57.1% 23.5% 24.5% 9.8% 10.2% 3.9% p=0.064* *Fisher's Exact Test p=0.001*