UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
| þ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2013
or
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number: 001-35337
WebMD Health Corp.
(Exact name of registrant as specified in its charter)
| | |
| Delaware | | 20-2783228 |
| (State of incorporation) | | (I.R.S. Employer Identification No.) |
| |
| 111 Eighth Avenue | | 10011 |
New York, New York (Address of principal executive office) | | (Zip code) |
(212) 624-3700
(Registrant’s telephone number including area code)
Securities registered pursuant to Section 12(b) of the Act:
| | |
| |
Title of Each Class | | Name of Each Exchange on Which Registered |
| |
| Common Stock, par value $0.01 per share | | The Nasdaq Stock Market LLC (Global Select Market) |
Securities registered pursuant to Section 12(g) of the Act:Not Applicable
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes þ No ¨
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No þ
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes þ No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes þ No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference into Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| | | | | | |
| Large accelerated filer þ | | Accelerated filer ¨ | | Non-accelerated filer ¨ | | Smaller reporting company ¨ |
| | (Do not check if a smaller reporting company) |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act.) Yes ¨ No þ
As of June 28, 2013, the aggregate market value of the registrant’s Common Stock held by non-affiliates of the registrant was approximately $1,034,260,000 (based on the closing price of the Common Stock of $29.37 per share on that date, as reported on the Nasdaq Global Select Market).
As of February 24, 2014, there were 40,718,375 shares of Common Stock outstanding (including unvested shares of restricted Common Stock).
DOCUMENTS INCORPORATED BY REFERENCE
Certain information in the registrant’s definitive proxy statement to be filed with the Commission relating to the registrant’s 2014 Annual Meeting of Stockholders is incorporated by reference into Part III.
TABLE OF CONTENTS
WebMD®, Medscape®, CME Circle®, Medpulse®, eMedicine®, MedicineNet®, theheart.org®, RxList® and Select Quality Care® are among the trademarks of WebMD Health Corp. or its subsidiaries.
i
FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K contains both historical and forward-looking statements. All statements other than statements of historical fact are, or may be, forward-looking statements. For example, statements concerning projections, predictions, expectations, estimates or forecasts and statements that describe our objectives, future performance, plans or goals are, or may be, forward-looking statements. These forward-looking statements reflect management’s current expectations concerning future results and events and can generally be identified by the use of expressions such as “may,” “will,” “should,” “could,” “would,” “likely,” “predict,” “potential,” “continue,” “future,” “estimate,” “believe,” “expect,” “anticipate,” “intend,” “plan,” “foresee,” and other similar words or phrases, as well as statements in the future tense.
Forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause our actual results, performance or achievements to be different from any future results, performance and achievements expressed or implied by these statements. The following important risks and uncertainties could affect our future results, causing those results to differ materially from those expressed in our forward-looking statements:
| | • | | failure to achieve sufficient levels of usage of our public and private portals and mobile platforms; |
| | • | | failure to attract sufficient consumers and healthcare professionals to our public portals and mobile platforms, including as a result of existing and new competitors for those audiences; |
| | • | | competition for advertisers and sponsors for our public portals and mobile platforms; |
| | • | | reductions in promotional and educational spending by pharmaceutical and biotechnology companies, whether resulting from the number and timing of regulatory approvals of new products or indications, from the number and timing of regulatory approvals of generic products that compete with existing brand name products or from other factors affecting the relevant markets; |
| | • | | the inability to successfully deploy new or updated applications or services for our public portals, mobile platforms and private portals or, if deployed, the failure to create new or enhanced revenue streams from those applications or services; |
| | • | | failure to preserve and enhance the “WebMD” and “Medscape” brands and our other brands; |
| | • | | the inability to provide health coaching and condition management services that meet the needs of clients and potential clients of our private portals or the failure to do so with sufficient efficiency to make those services profitable for us; |
| | • | | the inability to attract and retain qualified personnel; |
| | • | | adverse economic conditions and disruptions in the capital markets; |
| | • | | adverse changes in general business or regulatory conditions affecting the healthcare, information technology and Internet industries; and |
| | • | | the Risk Factors described in Item 1A of this Annual Report. |
These factors are not necessarily all of the important factors that could cause actual results to differ materially from those expressed in any of our forward-looking statements. Other factors, including unknown or unpredictable ones, also could have material adverse effects on our future results.
The forward-looking statements included in this Annual Report on Form 10-K are made only as of the date of this Annual Report. Except as required by law or regulation, we do not undertake any obligation to update any forward-looking statements to reflect subsequent events or circumstances.
ii
DEFINITIONS OF CERTAIN MEASURES
In this Annual Report, we provide information regarding usage ofThe WebMD Health Networkthat we have determined using internal technology that identifies and monitors usage by individual computers, smartphones, tablets and other electronic devices used to access the Internet (which we refer to, collectively, as electronic devices). As used in this Annual Report:
| | • | | A “unique user” or “unique visitor” during any calendar month is an individual electronic device, using a specific Web browser, that accesses a page inThe WebMD Health Networkduring the course of such calendar month, as determined by our tracking technology. Accordingly, with respect to such calendar month, once an individual electronic device, using a specific Web browser, accesses a page inThe WebMD Health Network, that electronic device will generally be included in the total number of unique users or visitors for that month. Similarly, with respect to any calendar month, an individual electronic device using a specific Web browser accessing a specific public portal, Website or mobile property inThe WebMD Health Network (which we refer to as a “WebMD Destination”) may be counted only once as a single unique user or visitor regardless of the number of times it accesses that WebMD Destination or the number of individuals who may use it. However, if an electronic device using a specific Web browser accesses more than one WebMD Destination withinThe WebMD Health Networkduring a calendar month, it will be counted once for each such WebMD Destination. An electronic device that accesses a WebMD Destination using more than one Web browser will be counted as if it were a separate device for each browser used. In addition, if an electronic device blocks our tracking technology, it will be counted as a unique user or visitor in a particular month each time it visits a WebMD Destination. An electronic device that does not access any WebMD Destination during a particular calendar month is not included in the total number of unique users or visitors for that calendar month, even if such electronic device has, in the past, accessed one or more WebMD Destinations. |
| | • | | A “page view” is a page that is viewed on an electronic device. The number of “page views” inThe WebMD Health Networkis not limited by its number of unique users or visitors. Accordingly, each unique user or visitor may generate multiple page views. |
| | • | | With respect to any given time period, “aggregate page views” are the total number of “page views” during such time period onThe WebMD Health Networkas a whole. |
Third party services that measure Internet usage apply their own methodologies to do so and, accordingly, may provide different usage statistics than those reported by our internal tracking technology.
OurWebMD Health Services private portals are provided to employers and health plans for use by their employees and members. These private portals are not part ofThe WebMD Health Network,do not involve advertising or sponsorship by third parties, and their users and page views are not included in measurements ofThe WebMD Health Network’straffic volume.
REFERENCES TO OUR WEBSITES
The contents of the Websites inThe WebMD Health Network and our other Websites referred to in this Annual Report are not incorporated into this filing. In addition, references to URLs for our Websites are intended to be inactive textual references only.
iii
PART I
INTRODUCTION
Overview of Our Services
We are a leading provider of health information services to consumers, physicians and other healthcare professionals, employers and health plans through our public and private online portals, mobile platforms and health-focused publications. We engage consumers, physicians and other healthcare professionals across a multi-screen experience, allowing us to empower and enable health decisions anytime and anywhere.
The WebMD Health Network — Our Public Portals. Our network of public portals for consumers and healthcare professionals, includes:www.WebMD.com (which we sometimes refer to asWebMD Health), our primary public portal for consumers and related mobile-optimized sites and mobile apps;www.Medscape.com, our primary public portal for physicians and other healthcare professionals and related mobile-optimized sites and mobile apps; and other sites through which we provide our branded health and wellness content, tools and services.
| | • | | Our Websites and mobile applications for consumers help them take an active role in managing their health by providing objective health and wellness information and access to decision-support tools and other services. We also provide content relating to lifestyle and healthy living, including healthy beauty, diet and food, exercise and fitness, and family and pregnancy. Our content offerings for consumers include news articles and features, special reports, interactive guides, originally produced videos, self-assessment questionnaires, expert led Q&As, community discussions, and reference resources. Our mobile applications for consumers, which include theWebMD App, theWebMD Pregnancy App, theWebMD Baby App, theWebMD Pain Coach App, theWebMD Allergy App and theWebMD Magazine App, had been downloaded a total of more than 22 million times through the end of 2013. |
| | • | | Our Websites and mobile applications for healthcare professionals help them improve their clinical knowledge and practice of medicine. We make it easier for physicians and other healthcare professionals to access clinical reference sources, to stay abreast of the latest clinical information, to learn about new treatment options, to earn continuing medical education (or CME) and continuing education (or CE) credit, and to communicate with peers.Medscape’s original content includes daily medical news, conference coverage and expert commentary and columns by authors from widely respected clinical and academic institutions. Medscape also provide access to full-text journal articles, reference materials and other medical content. ThroughMedscape Education (www.medscape.org),we offer a wide selection of free online CME and CE activities designed to educate healthcare professionals about important diagnostic and therapeutic issues. OurMedscape App for physicians and other healthcare professionals provides formulary information, medical calculators, drug, disease and condition references, and a drug interaction checker. |
In 2013,The WebMD Health Network reached an average of approximately 138 million monthly unique visitors and delivered approximately 11.55 billion page views during the year, increases of 25% and 14% over the prior year, respectively. Traffic to our online portals for physicians and other healthcare professionals averaged approximately 5.5 million physician sessions per month during 2013, an increase of approximately 7% over the prior year. For additional information regarding traffic toThe WebMD Health Network, see “Management’s Discussion and Analysis of Financial Condition and Results of Operations — Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Traffic Trends” in Item 7 below.
We do not charge any usage, membership or download fees for access to our public portals or mobile applications. Our public portals generate revenue primarily through the sale of various types of advertising and sponsorship products to its clients, which include: pharmaceutical, biotechnology and medical device companies; hospitals, clinics and other healthcare services companies; health insurance providers; consumer products companies whose products or services relate to health, wellness, diet, fitness, lifestyle, safety and illness
1
prevention; and various other businesses, organizations and governmental entities. Advertisers and sponsors use our services to reach, educate and inform target audiences of consumers, physicians and other healthcare professionals. We also generate revenue through the sale of advertising inWebMD Magazine, a consumer publication that we distribute free of charge to physician office waiting rooms and make available online and through an iPad app. In addition, we generate revenue from the sale of certain information and data products.
WebMD Health Services — Our Private Portals. For more than a decade, we have helped employers and health plans improve the health of their employee and plan participant populations and reduce healthcare costs. We offer a cloud-based population health management platform, including an online personal health record application, to private and governmental employers and health plans for use by their employees and plan participants. OurWebMD Health Services solutions include a comprehensive set of decision-support and transparency tools that help their employees and plan participants understand the financial implications of their benefits options and make more informed benefits-related purchase decisions and also provide access to information and services that can help them factor quality and cost into decisions about care and treatment options. We also offer telephonic, online and onsite health coaching and targeted condition management programs that help employees and plan participants make healthier lifestyle choices and achieve their wellness goals.
We host ourWebMD Health Services platform for our clients. Our flexible architecture allows us to tie in with the client’s existing programs and intranet sites. We provide a secure, personalized user experience that integrates individual participant data and plan-specific data from our employer or health plan clients with our decision-support tools and other resources. Our online services are typically accessed through a client’s Website or intranet and are presented to each employee or plan participant as a personal home page, with direct access to relevant content, tools and other resources specific to the individual’s eligibility, coverage and health profile.
We generate revenue from subscriptions to ourWebMD Health Services platform by employers and health plans, either directly or through distribution relationships with employee benefits outsourcing companies, employee benefits consultants and other companies that assist employers in purchasing or managing employee benefits. In addition, we offer our health coaching and condition management services on a per participant basis. OurWebMD Health Services private portals do not display or generate revenue from advertising or sponsorship.
Our Goals andInitiatives. We are pursuing, and intend to continue to identify, new business opportunities where our consumer and physician audiences and our resources can be leveraged to develop additional services. One of our goals is to establish WebMD as a place where consumers store, access and manage their health information in a trusted environment. Examples of business initiatives we are working on include the following:
| | • | | We are in the early stages of developing the capabilities to positionWebMD andMedscape as a hub for a set of services that will facilitate information exchange and digital communication between healthcare providers and their patients. As an initial step, our flagshipWebMD App for iPhone® will support a new “Patient Instructions” feature available to healthcare professionals in ourMedscape App.Medscape Patient Instructions allows physicians and other medical professionals to securely send education and instructions on conditions, procedures and drugs to their patients. Patients can securely and conveniently read the instructions and information on theWebMD App for iPhone®, as well as on the WebMD consumer portal and the related mobile-optimized site. In addition, in late 2013, we acquired a start-up technology company called Avado to accelerate our connectivity efforts. We are working to integrate key aspects of Avado’s technology into our platform. We expect that Avado’s cloud-based patient relationship management platform will serve as a key building block for a suite of services connecting patients to their physicians and other healthcare providers. |
| | • | | A forthcoming version of theWebMD App will leverage the 2net™ Platform from Qualcomm Life, Inc., a subsidiary of Qualcomm Incorporated, to enable health-conscious consumers to access and manage biometric data from devices such as glucometers, wireless scales, and wearable devices directly from theWebMD App, and wrap that data within a health improvement program health data.TheWebMD App will use the biometric data to tailor content, provide personalized insights, and to set and measure progress against goals. WebMD and Qualcomm Life also plan to introduce, later in 2014, a new online storefront where consumers will be able to purchase a variety of biometric devices from the industry’s leading providers. |
2
We may pursue initiatives to create new or enhanced revenue streams or, alternatively, to increase audience engagement even when we have not identified any potential related revenue stream.
Corporate Information
WebMD Health Corp. is a Delaware corporation that was incorporated on May 3, 2005 under the name WebMD Health Holdings, Inc. Our principal executive offices are located at 111 Eighth Avenue, New York, New York 10011 and our telephone number is (212) 624-3700. We completed the initial public offering of our Class A Common Stock on September 28, 2005. Prior to that time, WebMD was a wholly-owned subsidiary of HLTH Corporation (which we refer to as HLTH). Upon completion of our merger with HLTH in October 2009 and the resulting cancellation of our Class B Common Stock (all of which had been owned by HLTH), our Class A Common Stock began being referred to simply as Common Stock. Our Common Stock trades on the NASDAQ Global Select Market under the symbol “WBMD.”
Available Information
We make available free of charge atwww.wbmd.com(in the “Investor Relations” section) copies of materials we file with, or furnish to, the Securities and Exchange Commission, or SEC, including our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and amendments to those reports, as soon as reasonably practicable after we electronically file such materials with, or furnish them to, the SEC.
3
THE WebMD HEALTH NETWORK —OUR PUBLIC PORTALS
Overview of The WebMD Health Network
The WebMD Health Network delivers content through a multi-screen platform that engages users regardless of whether they are on a personal computer, a smartphone or a tablet. Our consumer portals and mobile applications help consumers take an active role in managing their health by providing objective health and wellness information. Our content offerings for consumers include access to news articles and features and decision-support tools that help them make better informed decisions about treatment options, health risks and healthcare providers. Our Websites and mobile application for physicians and other healthcare professionals help them improve their clinical knowledge and practice of medicine. Our content offerings for these professionals, which include daily medical news, conference coverage, expert commentary and columns and CME activities, are written by authors from widely respected clinical and academic institutions and edited and managed by our in-house editorial staff. For information regarding traffic toThe WebMD Health Network, see “Management’s Discussion and Analysis of Financial Condition and Results of Operations — Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Traffic Trends” in Item 7 below.
The following provides a summary of the Websites included inThe WebMD Health Network:
| | |
Consumer Sites | | Description |
| |
www.webmd.com | | WebMD Health, our flagship consumer portal. |
www.medicinenet.com | | A health information site for consumers offering content that is written and edited by practicing physicians, including an online medical dictionary with thousands of medical terms. |
www.rxlist.com | | An online drug directory, which provides comprehensive descriptions of pharmaceutical products (including chemical names, brand names, molecular structure, clinical pharmacology, directions and dosage, side effects, drug interactions and precautions). |
www.emedicinehealth.com | | A health information site for consumers offering articles written and edited by physicians for consumers, including first aid and emergency information that is also accessible atfirstaid.webmd.com. |
| |
| Professional Sites | | |
www.medscape.com | | Medscape, our flagship portal for physicians and other healthcare professionals, is organized by medical specialty, with each supported specialty having its own customized home page.Medscape content includes: • News Content — including coverage of breaking medical news, expert perspectives and columns, medical conference coverage, business of medicine content, slideshows, special reports and access to full-text journal articles. • Reference Content — including comprehensive clinical overviews of diseases and conditions, procedures and drugs. During 2013, we merged ourtheheart.org site into ourMedscape Cardiology offering onmedscape.com. |
www.medscape.org | | Medscape Education, the Website through which Medscape, LLC distributes online CME and CE to physicians and other healthcare professionals. |
4
We also provide related mobile applications, which are included inThe WebMD Health Network. Our mobile applications for consumers, which include theWebMD App, theWebMD Pregnancy App, theWebMD Baby App, theWebMD Pain Coach App, theWebMD Allergy App and theWebMD Magazine App, had been downloaded a total of more than 22 million times through the end of 2013.OurMedscape App for physicians and other healthcare professionals provides formulary information, medical calculators, drug, disease and condition references, and a drug interaction checker. We also provide access to our content through versions of our Websites tailored for viewing through mobile browsers. For a discussion of our efforts to increase revenue from our mobile services, see “Management’s Discussion and Analysis of Financial Condition and Results of Operations — Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Efforts to Increase Advertising and Sponsorship Revenue from Mobile” in Item 7 below.
The WebMD Health Network also includes our international sites: the co-branded Boots WebMD health information site for United Kingdom consumers atwww.WebMD.boots.com; and Medscape France (www.medscape.fr) and Medscape Germany (www.medscape.de), our physician portals in those two countries.
Consumer Services
Introduction. The Internet has fundamentally changed the way consumers obtain information, enabling them to have immediate access to searchable information and dynamic interactive content. Healthcare consumers increasingly seek to educate themselves online about their health-related issues, motivated in part by the larger share of healthcare costs they are being asked to bear due to changes in the benefit designs being offered by health plans and employers. Our goal is to provide consumers with an objective and trusted source of information and online tools that helps them play an active role in managing their health. We also provide content relating to lifestyle and healthy living, including healthy beauty, diet and food, exercise and fitness, and family and pregnancy.
In the past several years, video and multimedia applications have become an important part of what users expect from Internet sites. In addition, consumers are increasingly using the Internet to access social media as a means to communicate and exchange information, including information regarding health and wellness. Consumers are also increasingly using mobile devices and tablets to access online content and tools. Mobile, while not yet a meaningful source of revenue for us, could be an important area of growth for the future. We have invested and intend to continue to invest in software and systems that allow us to meet the demands of our users and sponsors, including customized content management and publishing technology to deliver interactive content, multimedia programming and personalized health applications that engage our users. In addition, we continue to focus on delivering a multi-screen platform that extends the user experience onto mobile devices and tablets.
Overview of Content and Service Offerings. WebMD Healthand the other consumer portals inThe WebMD Health Network provide our users with information, tools and applications in a variety of content formats. These content offerings include access to news articles and features, special reports, interactive guides, originally produced videos, self-assessment questionnaires, expert led Q&As, community discussions, and reference resources. By becoming a registered WebMD member, consumers can participate in our online communities and can opt-in to receive e-newsletters from WebMD on a variety of health-related topics or on specific conditions. There are no membership fees, usage charges or download charges for our consumer portals or mobile applications.
Our in-house staff, which includes professional writers, editors, designers, board-certified physicians and other healthcare professionals, creates content forThe WebMD Health Network. Our in-house staff is supplemented by medical advisors and authors from widely respected academic and clinical institutions. The news stories and other original content and reporting presented inThe WebMD Health Network are based on our editors’ selections of the most important and relevant public health events occurring on any given day, obtained from an array of credible sources, including peer-reviewed medical journals, medical conferences, federal or state government actions and materials derived from interviews with medical experts. We offer searchable access to the full content of our Websites, including licensed content and reference-based content.
5
Key Features of WebMD Health. WebMD Healthincludes the following key features:
| | |
Feature | | Description |
WebMD News Center | | Health news articles that are written by journalists and reviewed by our professional staff. Content focuses on “news you can use” and the article topics reflect national news stories of interest in the popular media that day with original perspective from health and medical experts. |
WebMD Editorial Features | | Comprehensive content focusing on major health, wellness and lifestyle issues that are in the news or otherwise contemporary, with emphasis on health trends and national health issues. |
WebMD Health and Wellness Centers | | WebMD Health and Wellness Centers are centralized locations for content and services for bothWebMD Healtheditorial offerings and sponsor offerings focusing on topics related to health, wellness and lifestyle. Each Center features expert and medically reviewed information enabling the user to easily locate the top articles, news, videos, community features and health or wellness assessments for each topic. We also provide users an alphabetical listing of all Health and Wellness Centers and other collections of articles, organized by specific health conditions and concerns, known as Health A-Z. |
WebMD Health Guides and Wellness Guides | | Anchored within our Health and Wellness Centers, our Health Guides and Wellness Guides are designed to guide users through their individual health journey. The most current symptom, diagnosis, treatment and care information related to a particular disease or condition topic can be found in our Health Guides. Our Wellness Guides cover a broad range of topics, including nutrition, fitness, pregnancy and parenting. These guides were created by our editorial staff of professional health writers in collaboration with our proprietary physician network. |
WebMD Answers | | WebMD Answers provides a trusted environment for consumers to ask health-related questions and receive information from physicians and other experts, as well as from other consumers. WebMD Answers also gives users the ability to “follow” topics, people, organizations, and trending questions. Consumers can stay informed on the latest information relevant to their interests either via email messaging or by signing into WebMD and accessing a personalized WebMD Answers experience. |
WebMD Video | | Originally produced multi-media content served on our custom video player. Includes health-related video of real patient stories and expert interviews, among other things, and includes narration, graphics and links to additional content on a given health |
6
| | |
Feature | | Description |
| | topic. Sponsors are able to stream promotional messages within the video feature itself and within the surrounding viewing area. Videos are also included in our Health and Wellness Centers. |
Slideshows | | Our slideshows are designed to educate users on specific conditions and other health and healthy living topics in an engaging, visually rich format. |
General Medical Information | | Our medical library allows consumers to research information relating to diseases and common health conditions by providing searchable access and easy-to-read content, including: |
| | — self-care articles |
| | — drug and supplement references from leading publications, including First Data Bank® |
| | — clinical trials and research study information |
| | — a patient’s guide to medical tests |
| | — interactive, illustrated presentations that visually explain common health conditions and diseases |
| | — a medical dictionary |
| | — doctors’ views on important health topics. |
For a description of the access we provide to health information from the U.S. Food and Drug Administration, see “— Content-Sharing and Other Relationships” below.
Decision-Support Services and Other Online Tools. Our decision-support services and other online tools help consumers make better-informed decisions about treatment options, health risks and healthcare providers, and assist consumers in their management and monitoring, on an ongoing basis, of personal health goals, specific conditions and treatment regimens.
| | |
Feature | | Description |
WebMD Health Checks and Evaluators | | Clinical, algorithm-based self assessments for health conditions and wellness topics, including a personalized risk score based on the user’s individual self-reported characteristics (e.g., gender, age, behavioral risks, heredity), along with customized recommendations for further education, potential treatment options and a summary report to share with the user’s physician or healthcare professional. |
WebMD Symptom Checker | | An interactive graphic interface with advanced clinical decision-support rules that allows users to identify potential conditions associated with their physical symptoms, gender and age. |
WebMD Healthcare Reform Center | | A comprehensive consumer guide to healthcare reform, educating consumers on the Affordable Care Act and helping them navigate the changes in health insurance and evaluate their coverage options. For consumers nationwide, this site is intended to serve as a valuable resource for understanding how health insurance works and how changes in coverage availability and affordability affect them. |
7
| | |
Feature | | Description |
WebMD Food & Fitness Planner | | Our Food & Fitness Planner is an online journaling service focusing on diet, food and fitness, designed to help users attain their personal health, weight loss and weight management goals. Our Food & Fitness Planner helps users make more informed food, beverage and nutrition choices. |
WebMD Recipe Finder | | Our Recipe Finder allows users to search our collection of recipes from WebMD,Eating Well magazine and other sources to help make healthy meal choices. Recipes can be searched and filtered by nutritional criteria. |
First Aid & Emergencies | | Directs users to educational and treatment information that may be useful in the event of certain medical emergencies. Also included in this resource is a First Aid A-Z glossary of terms. |
Health and Wellness Tests & Tools | | Provides access to interactive calculators and quizzes to assess or demonstrate health topics, including a target heart rate calculator, body mass index calculator, pregnancy due date calculator and ovulation calendar. |
Drugs & Treatments | | Users can search for information about prescription and over-the-counter medications by brand or generic name, or by condition. |
WebMD Physician Directory | | Enables users to find a physician based on the physician or practice name, specialty, zip code and distance. |
Mobile. We provide access to our consumer content and tools throughWebMD Mobile, a version of our WebMD.com site tailored for viewing through mobile browsers atwww.m.webmd.com. In addition, we offer the following mobile applications for consumers, which had been downloaded a total of more than 22 million times through the end of 2013:
| | • | | OurWebMD App, which is available for Android™, iPhone®, iPad® and Kindle Fire®, provides mobile access to certain WebMD content and tools, including Symptom Checker, First Aid, and Pill Identifier applications, as well as other health information. The mobile-optimized content also covers health and beauty, diet, parenting and children’s health, and sex and relationships.WebMD App users can choose from and save information tailored to their specific interests and can select topics to populate tips, fun facts, articles, videos and quizzes relevant to their healthy-living goals. TheWebMD App also connects with the Patient Instructions feature in theMedscape App for healthcare professionals, which allows physicians to securely send education and instructions on thousands of conditions, procedures and drugs to their patients, as described under “Introduction — Overview of Our Services — Our Goals and Initiatives” above. A forthcoming version of theWebMD App for iPhone® will enable consumers to upload biometric data and receive personalized content and actionable insights to help make informed health and wellness decisions. |
| | • | | OurWebMD Magazine App, which is available for iPad®, provides a tablet-optimized reading experience forWebMD Magazine, offering links to relevant articles, videos, blogs and slideshows on WebMD.com. |
| | • | | OurWebMD Baby App, which is available for Android™ and iPhone®, gives new parents access to content created exclusively for the app, personalized for a baby’s specific age.WebMD Baby helps keep parents informed with easily accessible baby health and wellness information that they can trust. A personal growth chart for baby/toddler is also integrated into the app, allowing information to be easily added right from the pediatrician’s office.WebMD Baby received the 2012 Medical Marketing & Media Gold Award for Best Mobile App for Consumers. |
8
| | • | | OurWebMD Pregnancy App, which is available for iPhone®, combines trusted medical information and fun, shareable content to help expecting mothers celebrate the milestones along their pregnancy journey and empower them to make healthy decisions.WebMD Pregnancydelivers timely physician-reviewed content based on the baby’s expected delivery date, including checklists, questions to ask the doctor, and multimedia information. |
| | • | | OurWebMD Pain Coach App, which is available for Android™ and iPhone®, is a mobile companion to coach people living with chronic pain through daily health and wellness choices so that they can better manage their pain while living a healthy life. It offers users a personalized experience by delivering daily physician-reviewed tips about managing their specific conditions to their mobile device, including those suffering from chronic back pain, neck pain, nerve pain, fibromyalgia, migraine, osteoarthritis, and rheumatoid arthritis. With the app, WebMD helps users take control of their lifestyle choices by enabling them to easily review their pain patterns so they can understand triggers, set goals and share progress with their physician. |
| | • | | OurWebMD Allergy App, which is available for Android™ and iPhone®, empowers users to take control of their allergies. TheWebMD Allergy App provides allergy sufferers with personalized location-based allergy condition forecasts in combination with WebMD’s trusted information and insights. TheWebMD Allergy App is further personalized with optional mobile push notifications that warn when allergen levels are high, enabling app users to proactively manage their allergy conditions. |
Social Networking. The WebMD Community, our social networking initiative, gives consumers the ability to connect with health experts and with other WebMD members to exchange information, experiences and support. Members are empowered to create their own communities and to exchange information with other users. Users can also access content and experts through WebMD’s social media offerings on Facebook, Twitter, and Pinterest.
International. We plan to pursue opportunities to expand the reach of our brands outside the United States. In certain markets outside the United States, we expect to accomplish this through partnerships or joint ventures with other companies having expertise in the specific country or region, while in other such markets we expect to rely primarily on our own internal resources. In October 2009, we launched a new health information Website in the United Kingdom with Boots UK, the United Kingdom’s leading pharmacy-led health and beauty retailer. The co-branded Boots WebMD site atwww.WebMD.boots.com features daily health and wellness news, condition and healthy living centers, interactive health tools, WebMD’s symptom checker, specialized health search, health videos and interactive slide shows. However, because of restrictions on consumer advertising by pharmaceutical and medical device companies that apply in many countries, we expect to focus our efforts outside the United States primarily on expanding our offerings for physicians and other healthcare professionals, rather than consumer offerings. For additional information, see “– Professional Services – International” below.
WebMD Magazine
WebMD Magazine is delivered free of charge to physicians in the United States for use in their office waiting rooms and reaches consumers right before they meet with their physicians. This allows sponsors to extend their advertising reach and to deliver their message when consumers are actively engaged in the healthcare process, and allows us to extend the WebMD brand into offline channels. We publish eight issues per year and had a rate base, in 2013, of approximately 1.4 million copies of each issue. We estimate that more than eight million people are reading each issue ofWebMD Magazine.
The editorial format ofWebMD Magazineis specifically designed for the physician’s waiting room. Its editorial features and highly interactive format of assessments, quizzes and questions are designed to inform consumers about important health and wellness topics. We also publish a digital edition ofWebMD Magazine online and, as described under “— Mobile” above,WebMD Magazine is available as a free interactive application for the iPad®. We also produce certain specialized editions ofWebMD Magazine, including one for college campuses.
9
Professional Services
Introduction. The Internet has become a primary source of information for physicians and other healthcare professionals, and is growing relative to other sources, such as conferences, meetings and offline journals. Our Websites for healthcare professionals includeMedscape andMedscape Education.During 2013, we merged ourtheheart.org site into ourMedscape Cardiology offering. We also provide a version of each of these Websites that is tailored for viewing through mobile browsers. OurMedscapeApp is a free mobile application for physicians that provides access to articles and other resources fromMedscape and CME fromMedscape Education.
There are no membership fees and no usage charges for our professional sites or ourMedscapeApp. However, users must register to access the full array of content and features. We generate revenue from our professional services by selling advertising and sponsorship programs primarily to companies that desire to reach physicians and other healthcare professionals. We also generate revenue through educational grants.
Medscape. Medscape (www.medscape.com), our flagship portal for physicians and other healthcare professionals, is organized by medical specialty, with each supported specialty having its own customized content.Medscape also includes areas for nurses, pharmacists, medical students, and members interested in medical policy and business of medicine topics. Registration by users enables us to deliver medical content targeted to their specialty and areas of interest, based on information they provide in their registration profiles. The registration process also enables professional members to choose a home page tailored to their medical specialty or interests.Medscape members receive e-mail newsletters, tailored to their specialty and other areas of interest they select, that highlight new information and resources onMedscape.Medscape content includes:
| | • | | News Content. Medscape provides timely coverage of medical news, including insightful perspectives from leading medical experts in both video and written formats.Medscape news content is written by our in-house team of professional journalists and editors, faculty from widely respected academic and clinical institutions, and seasoned professional writers.Medscape news content is edited and managed by our editorial staff. The content is produced in various formats, including: in-depth interviews with experts on topics related to the current and future practice of medicine; news alerts on critical clinical issues such as breaking drug information, including pharmaceutical recalls and product advisories; coverage of healthcare policy and politics, including analysis of the Affordable Care Act and its impact on clinical practice; and coverage of key professional meetings and conferences from around the world. Medscape’s news content also includes widely read Business of Medicine coverage on complex practice management, compensation, legal, and ethical issues. TheMedscape editorial team also creates recurring features such as clinical cases, slideshows, and special reports.Medscape also provides access to wire service news stories and to licensed full-text journal articles. For a description of the access thatMedscape News provides to information from the U.S. Food and Drug Administration and The Centers for Disease Control and Prevention, see “— Content-Sharing and Other Relationships” below. |
| | • | | Reference Content. Medscape provides original content prepared for Medscape by physician and pharmacist authors and reviewers from leading medical centers, in the following categories: |
| | — | | Disease and Condition Articles. Evidence-based and physician-reviewed disease and condition articles are organized to answer clinical questions, as well as to provide in-depth information in support of diagnosis, treatment, and other clinical decision-making. Most of these articles are illustrated with clinical photos and radiographic images. |
| | — | | Drug Reference. A drug reference database, with more than 2,200 monographs, for researching prescribing and safety information on brand-name, generic and over-the counter (OTC) drugs, including herbals and supplements. |
| | — | | Drug Interaction Checker. A drug interaction checker that identifies more than 100,000 interactions for drugs, herbals and/or supplements, with detailed information from minor to contraindicated interactions. |
10
| | — | | Clinical Procedure Articles. More than 800 clinical procedure articles provide detailed instructions, and include videos and images to help clinicians with new techniques or to improve their skills in procedures they have previously performed. |
| | — | | Image Collections. Image collections are visually engaging presentations of both common and uncommon diseases, case presentations, and current controversies in medicine. They are presented in a slideshow format and are designed to challenge and expand physicians’ knowledge of clinically important topics. |
OurMedscape App is a free mobile application, available on Android™, Blackberry®, iPhone®, iPad®, and Kindle Fire®, for physicians and other healthcare professionals that provides registered users with access toMedscape news content and reference content, including: articles and other resources; the drug reference database and drug interaction checker; clinical reference, treatment and procedure guides; and physician, pharmacy and hospital directories. OurMedscape App also provides access to CME programs fromMedscape Education(described below). In addition, ourMedscape App gives users offline access to reference content, treatment guides and the drug interaction checker.
Continuing Medical Education (CME). Medscape Education (www.medscape.org) is the primary Website through which our ACCME-accredited CME provider, Medscape, LLC, distributes online CME and CE to physicians and other healthcare professionals. The ACCME (the Accreditation Council for Continuing Medical Education) accredits and oversees providers of CME credit, as described under “Government Regulation, Industry Standards and Related Matters — Regulation and Accreditation of Continuing Medical Education” below. Medscape is also accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation and as a provider of continuing pharmacy education by the Accreditation Council for Pharmacy Education.
Medscape Educationoffers a wide selection of free online CME and CE activities designed to educate healthcare professionals about important diagnostic and therapeutic issues,including both original CME and CE activities that it develops as well as activities developed and accredited by third parties.Medscape Educationeducational activities are supported by independent educational grants provided by pharmaceutical and medical device companies, as well as foundations and government agencies. In addition, in order to provide broad and timely coverage of areas of interest to healthcare professionals,Medscape Education offers numerous CME and CE activities for which it does not receive grants or other outside support.
International. We are pursuing opportunities to expand the reach of theMedscape brand outside the United States. In addition to visits to Medscape from physicians and health care professionals outside the United States, we have begun providing medical news, expert perspective, and online continuing medical education in the local language directly to healthcare professionals in France (www.medscape.fr) and Germany (www.medscape.de). In doing this, our in-house journalists and editors in these countries rely on their own expertise and on the expertise ofMedscape as a whole in delivering relevant medical information to healthcare professionals
Advertising and Sponsorship
We believe thatThe WebMD Health Networkoffers an efficient means for advertisers and sponsors to reach a large audience of health-involved consumers, clinically active physicians and other healthcare professionals or to target specific groups of consumers, physicians and other healthcare professionals based on their interests or specialties with placements in relevant locations onThe WebMD Health Network or in our e-newsletters. The following are some of the types of placements and programs we offer to advertisers and sponsors:
| | • | | Media Solutions. These are traditional online advertising solutions, such as banners, used to reach health-involved consumers and physicians and other healthcare professionals. In addition, customers can select targeted media packages, including condition-specific or specialty-specific e-newsletters, keyword searches and educational programs. |
| | • | | Sponsored Solutions. These are customized collections of articles, topics, and decision-support tools and applications, sponsored by clients and distributed withinThe WebMD Health Network. |
11
The pricing for our advertising and sponsorship services varies from contract to contract based on numerous factors, including the specific services to be provided, the content areas on our Websites where advertisements or sponsored content are to be displayed, the nature of any exclusivity provided, the total size of the commitment by the sponsor, and other factors. We also sell advertising on a CPM (cost per thousand impressions) basis, where an advertiser can purchase a set amount of impressions on that basis. An “impression” is a single instance of an ad appearing on a Web page. However, our services for advertisers and sponsors are generally more complex and have more complex pricing than simple cost per thousand impressions pricing.
We have been investing in improved data analytics capabilities to enhance our ability to demonstrate to advertisers and sponsors how promotional strategies implemented through WebMD impact physician and consumer behaviors and preferences. Enhanced analytic capabilities also support WebMD’s internal development of user engagement strategies and new messaging and education services.
Sales and Marketing
Our sales, marketing and account management personnel work with pharmaceutical, medical device, biotechnology and consumer products companies and their agencies to place their advertisements and other sponsored products onThe WebMD Health Network and inWebMD Magazine. These individuals work closely with clients and potential clients and their agencies to develop innovative ways to bring their companies and their products and services to the attention of specific groups of consumers and healthcare professionals, and to create channels of communication with these audiences.
Content-Sharing and Other Relationships
FDA. We are working with the U.S. Food and Drug Administration (or FDA) to expand consumer access to timely and reliable health information from the FDA, and to increase the FDA’s reach to physicians and healthcare professionals.
Consumers. For consumers:
| | • | | The collaboration includes an online consumer health information resource on WebMD.com (www.webmd.com/fda), through which consumers can access information on the safety of FDA-regulated products, including food, medicine and cosmetics, as well as learn how to report problems involving the safety of these products directly to the FDA. There are also content and multimedia tools on specific topics, such as allergies and asthma, children’s health, diabetes, heart health, and vitamins and supplements. |
| | • | | FDA information is also located within WebMD’s homepage, WebMD Health News, WebMD Health Search, RSS feeds, and targeted WebMD Newsletters and Special Reports, and also included inWebMD Magazine. |
| | • | | WebMD also provides FDA public health alerts to all WebMD registered users and site visitors that request them. The cross-linked joint resource also features the FDA’s Consumer Updates — timely and easy-to-read articles that are also posted on the FDA’s main consumer Web page (www.fda.gov/consumer). |
This joint effort provides health-minded consumers with access to the FDA as a source of timely health information focusing on daily issues such as food safety and the safe use of prescription drugs, over-the-counter medications, and cosmetics.
Healthcare Professionals. For healthcare professionals:
| | • | | Content from the Medscape/FDA collaboration is available on various specialty homepages onMedscape.com and also housed in a dedicated area atMedscape.com/FDA. These materials cover a wide range of topics of interest to healthcare professionals and focus on the FDA’s role in protecting public health through ensuring the safety and quality of medical products. |
| | • | | Medscape and the FDA collaborate on important educational initiatives focusing on safety, risk management and other public health issues, such as the appropriate training of clinical investigators. |
12
CDC. The Centers for Disease Control and Prevention (CDC), part of the United States Department of Health and Human Services, is collaborating withMedscape News on a series of CDC Expert Commentaries, available athttp://www.medscape.com/cdc. In this series, experts from the CDC offer video commentaries on current topics important to our audience of physicians, nurses, pharmacists and other healthcare professionals. The CDC and Medscape have also collaborated on exclusive Q&As with CDC leadership on breaking news topics, slideshows and special reports presenting clinical guidance on infection control and prevention, emerging infectious diseases, important disease outbreaks, and other topics central to public health. Medscape and the CDC also work in collaboration on various educational activities for healthcare professionals on various topics, including: Prevention of Healthcare Associated Infections; Influenza Vaccine Safety; Safe Injection Practices; and Antibiotic Stewardship. In addition, for the past four years, Medscape has been the CME partner of the CDC JournalEmerging Infectious Diseases.
State Health Authorities. Medscape issues alerts to physicians and other healthcare professionals on behalf of governmental health authorities in 17 states.
Boots UK. In October 2009, we launched a new health information Website in the United Kingdom with Boots UK, the United Kingdom’s leading pharmacy-led health and beauty retailer. The co-branded Boots WebMD site atwww.WebMD.boots.com features daily health and wellness news, condition and healthy living centers, interactive health tools, WebMD’s symptom checker, specialized health search, health videos and interactive slideshows. Boots supported the launch with a national marketing and consumer education effort to its large UK customer base to promote the new site, through in-store marketing, in its health and beauty magazines, on its heavily trafficked e-commerce site and to its large base of loyalty program members. In addition, Boots UK has engaged its thousands of pharmacists to create awareness of the site and its offerings during their frequent patient interactions.
WEBMD HEALTH SERVICES —OUR PRIVATE PORTALS
Introduction
In response to increasing healthcare costs, employers and health plans have been changing benefit plan designs to increase deductibles, co-payments and other out-of-pocket costs and taking other steps to motivate employees and plan participants to use healthcare in a cost-effective manner. In connection with shifting greater responsibility for healthcare costs to employees and plan participants, employers and health plans are making available more health and benefits information and decision-support applications to help their employees and plan participants make informed decisions about treatment options, health risks and healthcare providers. The goal is to encourage individuals to take a more active role in managing their healthcare by providing relevant information, including data related to healthcare costs and quality. Since lifestyle choices, including choices regarding nutrition, exercise and tobacco use, are key drivers of health and can dramatically impact risks for acquiring chronic, costly health conditions, employers and health plans are also interested in reducing demand for healthcare services by focusing on health and wellness initiatives for their employees and plan participants.
For more than a decade, we have helped employers and health plans improve the health of their employee and plan participant populations and reduce healthcare costs. We offer a cloud-based population health management platform, including an online personal health record application, to private and governmental employers and health plans for use by their employees and plan participants (we generally refer to the individuals given access to our services by their employers and health plans as “participants” below). OurWebMD Health Services solutions include a comprehensive set of decision-support and transparency tools that help their employees and plan participants understand the financial implications of their benefits options and make more informed benefits-related purchase decisions and also provide access to information and services that can help them factor quality and cost into decisions about care and treatment options. We provide a secure, personalized user experience that integrates individual participant data and plan-specific data from our employer or health plan clients with our decision-support tools and other resources. Our online services are typically accessed through a client’s Website or intranet and are presented to each employee or plan participant as a personal home page, with direct access to relevant content, tools and other resources specific to the individual’s eligibility, coverage and health profile. We also offer telephonic, online and onsite health coaching and targeted condition management programs that help employees and plan participants make healthier lifestyle choices and achieve their wellness goals.
13
We generate revenue from subscriptions to ourWebMD Health Services platform by employers and health plans, either directly or through distribution relationships with employee benefits outsourcing companies, employee benefits consultants and other companies that assist employers in purchasing or managing employee benefits. In addition, we offer our health coaching and condition management services on a per participant basis. OurWebMD Health Services private portals do not display or generate revenue from advertising or sponsorship.
Our Online Platform
OurWebMD Health Services cloud-based platform provides a personalized user experience by integrating: individual user data (including personal health information); plan-specific data from clients; and WebMD content, decision-support technology and personal communication services. We host ourWebMD Health Services platform for our clients. Our flexible architecture allows us to tie in with the client’s existing programs and intranet sites.
Our platform has been designed to integrate complex data from multiple sources, including health and pharmacy claims, electronic medical records, lab results, and biometric data. A health profile drives personalized messaging to the individual, including recommendations for educational resources and online tools. The health profile relies upon the integrated data, as well as our proprietary health risk assessment (HRA) completed by the participant, which identifies modifiable risk factors and health conditions. Health trackers allow individuals to graphically track health measurements over time.
Our WebMD Health RecordSM helps participants gather, store, manage and share their essential health data. The WebMD Health Record provides a secure personal health record for self-reported and professionally sourced health data. Medical and pharmacy claims data as well as lab and biometric results can be automatically imported into individuals’ health records. In addition, the WebMD Health Record allows individual users to authorize access by healthcare providers, which can encourage better communication and coordination of care. We also provide the capability to upload, track, and share data from mobile devices and home medical devices.
We provide communications services and incentive program services to support program launches, to increase completion rates of the health risk assessments, and to drive ongoing utilization of our tools and services by our clients’ participants. With the rewards platform, we assist clients to motivate their participants through wellness incentive programs that encourage and reward use of the services we provide and specific health behaviors. Our flexible rewards platform enables clients to design and manage custom rewards programs based on participation, activity or outcomes. Rewards fulfillment may include premium reductions, gift cards, electronic funds transfer into HSA accounts, rewards debit cards or check rewards. Our messaging platform enables targeted email communication campaigns that inform and motivate participants to change their behaviors and improve health status. Messages can be targeted based on health profile characteristics, demographics, or site usage, and they can be designed to raise awareness of specific resources and programs or to motivate lifestyle changes. We also provide print newsletters as an additional channel to motivate utilization by individuals and their dependents. To enable our communications and incentive program services, we have developed several proprietary tools, including the WebMD Engagement IndexSM and the WebMD Engagement HubSM. The Engagement Index measures engagement across a variety of dimensions and helps guide communication strategy and optimization initiatives. The Engagement Hub serves as an online resource center and collaboration hub for onsite wellness coordinators and program administrators.
Our Health Coaching and Condition Management Services
Telephonic, online, or onsite health coaching can be integrated with our online platform. Our health coaches work one-on-one with participants to motivate them to improve their own health status by managing modifiable risk factors that lead to health conditions, by pursuing health-conscious lifestyles, by actively seeking health and wellness knowledge and by understanding the impact of lifestyle decisions. In addition, a health coach can refer participants to employer or plan sponsored health programs or recommend appropriate online or offline health resources to help them meet their wellness goals. We also offer tobacco cessation and weight management specialty coaching programs to address the health risks specifically associated with smoking and obesity.
We tailor WebMD Lifestyle FirstSM coaching programs to the goals of our clients by offering different levels of coaching intensity and allowing targeting of various risk factor profiles for coaching eligibility.
14
Individuals are notified about their eligibility to participate in telephonic health coaching under programs selected by their employer or health plan. Our health coaching services, together with our online services, not only can help high-risk individuals identify important risk factors and change unhealthy behaviors, but also can help moderate-risk individuals to lower their risks and those who are healthy to stay that way. In addition to telephonic coaching, we offer the following related services:
| | • | | Online Coaching. WebMD Digital Health AssistantSM online, self-directed health coaching programs focus on exercise, nutrition, smoking cessation, weight management, emotional health and stress management. These programs let individuals set and track wellness goals, learn more about their behaviors and risks and follow self-paced personal action plans to improve their health. Each program includes comprehensive education modules and interactive goal setting and experience tracking. |
| | • | | Onsite Services. We offer three types of onsite services to our employer clients: onsite wellness coordinators help to augment in-house staff; onsite health coaches that extend the telephonic coaching model to an onsite, in-person model (often delivered within an onsite clinic); and turnkey biometric screening and health fair solutions through a combination of third-party vendors and our own services. |
WebMD Lifestyle FirstSM coaching programs also extend to cover condition management. These condition management programs are designed to give individuals access to a wide range of online and offline resources to provide long-term support and motivation and help them make better decisions to manage their health, including ongoing, intensive one-on-one coaching by condition specialists, along with progress tracking tools and personalized messaging and rewards programs. We offer Condition Management Programs for five conditions: coronary artery disease, congestive heart failure, diabetes, chronic obstructive pulmonary disease and asthma.
We also offer tools and services that enable our clients to integrate programs from third parties, including their disease management vendors, into the programs and portal solutions we offer. Users are referred to third-party services through our health risk assessment process, and those services can be promoted throughout the online or coaching experiences that we deliver.
Our Decision Support and Transparency Tools
We offer clients a comprehensive set of decision support and transparency tools to help their participants understand the financial implications of their benefits options, make more informed benefits-related purchase decisions, and to provide access to information and services that can help them factor quality and cost into decisions about care and treatment options. These tools include:
| | • | | WebMD Health ConciergeSM is a decision-support application designed to help participants make more informed healthcare decisions. Health Concierge provides access to information on conditions, treatments, and drugs. Participants are able to search for specific health-related terms and are presented with an integrated set of personalized results based on their gender, location, age, benefit plan and financial balances. Integrated results include out-of-pocket cost estimates, medication information, news and alerts from WebMD and government sources, questions to ask their doctor, treatment options to consider, and health education. |
| | • | | WebMD Coverage AdvisorSM allows participants to compare costs across available health plan options based on personalized information regarding coverage alternatives, using cost-modeling and projection utilities that take into consideration the individual’s gender, geographic location, family composition, eligibility status, and projected utilization. Coverage Advisor dynamically displays benefit plan features, co-pays, pharmacy coverage, and provider coverage, and can also help participants determine appropriate contributions to flexible spending accounts (FSAs), health savings accounts (HSAs), and health reimbursement accounts (HRAs). |
| | • | | WebMD Provider Selection AdvisorSM is a provider directory tool that enables participants to search by provider name, location, clinical specialty, plan participation, and gender. It displays information in an intuitive side-by-side comparison chart and also has optional features allowing clients to include their own cost, quality, and provider information. |
15
| | • | | WebMD Hospital AdvisorSM is a quality outcomes and cost comparison tool that allows individuals to evaluate hospitals based upon particular procedures, diagnoses, and locations. The quality comparisons are based on evidence-based measures, such as volume of patients treated for particular illnesses or procedures, mortality rates, unfavorable outcomes for specific problems, and average length of hospital stay. Hospital Advisor can be integrated with Provider Selection Advisor and can optionally include data to facilitate comparisons of outpatient facilities, procedures, and tests, as well as their corresponding costs and service volumes. |
| | • | | WebMD Medication AdvisorSM provides out-of-pocket and total medication costs for branded and generic therapies, presented alongside one another to facilitate straightforward comparisons. Using Medication Advisor, participants can determine less expensive alternatives based upon their drug benefit plan and formulary. |
Sales and Marketing
We market ourWebMD Health Services cloud-based platform and health coaching and condition management services to private and governmental employers and health plans through a dedicated sales, marketing and account management team. Our services are also distributed through relationships with employee benefits outsourcing companies, employee benefits consultants and other companies that assist employers in purchasing or managing employee benefits. A typical contract provides for a multi-year term. The pricing of these contracts is generally based on several factors, including the complexity involved in integrating our online platform for the client, the number of wellness and decision support tools and other services being provided, the degree of customization of the services involved and the anticipated number of participants covered by such contract.
TECHNOLOGICAL INFRASTRUCTURE
Our services are delivered through Websites and mobile platforms designed to address the healthcare information needs of our users with easy-to-use interfaces and navigation capabilities. We use customized content management and publishing technology to develop, edit, publish, manage, and organize our content. We use ad-serving technology to store, manage and serve online advertisements. We also use specialized software for delivering personalized content through our private portals and, for registered members, through our public Websites and related mobile applications. We have invested and intend to continue to invest in software and systems that allow us to meet the demands of our users and sponsors and the clients of our private portals. For additional information, see “– Introduction – Overview of Our Services – Our Goals and Initiatives” above.
Continued development of our technological infrastructure is critical to our success. Our development teams work closely with marketing and account management employees to create content management capabilities, interactive tools and other applications. The goal of our current and planned investments is to further develop our content and technology platform serving various end-users, including consumers and physicians, and to create innovative services that provide value for healthcare advertisers and sponsors forThe WebMD Health Network and for the employer and payer customers of our private portals.
USER PRIVACY AND TRUST
We have adopted internal policies and practices relating to, among other things, content standards and user privacy, designed to foster our relationships with our users. In addition, we participate in the following external, independent verification programs:
| | • | | URAC. We have been awarded e-Health accreditation from URAC, an independent accrediting body that has reviewed and approved the WebMD.com site and ourWebMD Health Services platform for compliance with its quality and ethics standards. We are currently in the process of seeking renewal of our accreditation, which expires on July 1, 2014, for an additional two-year period. |
| | • | | TRUSTe. WebMD.com, MedicineNet.com, RxList.com, and eMedicineHealth.com, our mobile site and our mobile Applications are licensees of the TRUSTe Privacy Seal and ourWebMD Health Services |
16
| | platform is a recipient of the TRUSTe EU Safe Harbor programs. TRUSTe is an independent, non-profit organization whose goal is to build users’ trust and confidence in the Internet. |
| | • | | Health on the Net Foundation. Our WebMD.com, eMedicine.com, eMedicineHealth.com, and MedicineNet.com sites and theWebMD Health Services platform comply with the principles of the HON Code of Conduct established by the Health on the Net Foundation. |
| | • | | Children’s Advertising Review Unit (CARU). Ourfit WebMD site complies with the standards set forth by CARU. CARU is the children’s arm of the advertising industry’s self-regulation program and evaluates child-directed advertising and promotional material in all media to advance truthfulness, accuracy and consistency with itsSelf-Regulatory Guidelines for Children’s Advertising and relevant laws. |
| | • | | Digital Advertising Alliance (About Ads). WebMD.com, MedicineNet.com, RxList.com, and eMedicineHealth.com are licensees of the Digital Advertising Alliance’sAd Choicesprogram. The Digital Advertising Alliance is a self-regulatory body that develops industry best practices and effective self-regulatory solutions for consumer choice in online behavioral advertising. |
| | • | | U.S. Department of Commerce. OurWebMD Health Services platform is self-certified to the U.S. Department of Commerce in conjunction with the TRUSTe E.U. and Swiss Safe Harbor Certification program for compliance with the E.U. and Swiss Safe Harbor Frameworks. |
We have won numerous awards for our Websites and for specific articles. Some of the awards we have received in the past two years include the Webby Award in the Health Category as well as the Webby People’s Voice Award in the Health Category, the prestigious Society of Professional Journalists Award for deadline reporting, the Weidenbaum Center Award for Evidence-Based Journalism, and a Gold Award from Medical Marketing and Media (MM&M) for Best Mobile App for Consumers (WebMD Baby App).
Privacy Policies
We understand how important the privacy of personal information is to our users. Our Privacy Policies are posted on our Websites and inform users regarding the information we collect about them and about their use of our portals and our services. Our Privacy Policies also explain the choices users have about how their personal information is used and how we protect that information.
Policies Regarding Advertisements, Sponsorships and Promotions
All advertisements, sponsorships and promotions that appear on our Websites are subject to our Advertising Policies and/or our Sponsor Policy. We do not accept advertising that, in our opinion, is not factually accurate or is not in good taste. WebMD makes a clear distinction between the news stories, articles and other content that we create or license and the promotional information that comes from our sponsors. While content from a sponsor is subject to our Advertising Policy, it is not subject to our Editorial Policy. The sponsor is responsible for the accuracy and objectivity of its content and it is not reviewed by our Editorial Department for accuracy, objectivity or balance. Sponsors may also provide funding directly to WebMD without the sponsor having any control over the content.
Editorial Policies
General. We are dedicated to providing quality health and wellness information and to upholding the integrity of our editorial process. The goal of our Editorial Policies is to make WebMD an objective, practical and relevant content source for health and medical information. Our original content is reviewed by physician reviewers and by our editors for accuracy, objectivity, appropriateness of medical language, and proper characterization of findings. We uphold traditional journalistic principles in reviewing and corroborating information from other sources.
Licensed Content. When WebMD licenses health and wellness content from third parties for publication on our site, our editors review the third party’s editorial policies and procedures for consistency with the WebMD Editorial Policies. Our physician reviewers and other editorial staff review a representative sample of the content to ensure that the third party follows the editorial policy and procedures reviewed by WebMD.
17
COMPETITION
The markets we participate in are intensely competitive, continually evolving and, in some cases, are subject to rapid change. Some of our competitors have greater financial, technical, marketing and other resources than we do, and some are better known than we are. We cannot provide assurance that we will be able to compete successfully against these organizations.
Public Portals
Overview. Our public portals and mobile applications face competition from numerous other companies, both in attracting users and in generating revenue from advertisers and sponsors, and we expect that additional competitors will continue to enter the markets we participate in. Our advertisers and sponsors have numerous alternatives to choose from, including traditional media, Internet search engines, social media Internet sites, and general interest consumer sites, as well as the alternative of communicating through their own Websites or other channels that they manage in-house or through their advertising agencies. Such competition may result in smaller customer commitments or pressure to reduce prices, both of which could reduce our revenues and profit margins. Competitors for the attention of consumers and healthcare professionals also include public sector, non-profit and other Websites that provide healthcare information without advertising or sponsorships from third parties.
Consumer Portals. Our consumer portals and mobile applications compete with online services, Websites and mobile applications that provide health, wellness and lifestyle information for consumers. These competitors include:
| | • | | general purpose consumer Websites or search engines that offer specialized health, wellness and lifestyle sub-channels or functions, such as yahoo.com, msn.com, AOL.com, Google and Bing; |
| | • | | other high traffic Websites that include healthcare-related and non-healthcare-related content and services, including social media Websites, such as Facebook and Google+; and |
| | • | | Websites and mobile applications that provide information and tools relating to specific diseases and conditions or other specific types of health, wellness and lifestyle content, such as Demand Media and Everyday Health as well as online communities, social media sites and blogs focused on these matters. |
Competitors to our consumer portals also include advertising networks that aggregate traffic from multiple Websites, including advertising.com (which is owned by AOL), Tribal Fusion, Undertone Networks and AdBlade. Other competitors to our consumer portals include publishers and distributors of traditional offline media, including television, radio, books, newspapers and magazines targeted to consumers.
Professional Portals. Competitors to our professional portals and mobile applications include Epocrates, Inc. (which is part of athenahealth, Inc.), Clinical Care Options, MedPage Today (which is owned by Everyday Health), QuantiaMD, Sermo (which is operated by WorldOne) and UpToDate Inc. (which is owned by Wolters Kluwer Health). Other competitors to our professional portals include:
| | • | | print journals and other specialized media targeted to healthcare professionals, many of which have established or may establish their own Websites or partner with other Websites; |
| | • | | offline medical conferences, CME programs and symposia; |
| | • | | vendors of e-detailing services, such as Physicians Interactive, and our clients’ own in-house detailing efforts; and |
| | • | | vendors of healthcare information and related services distributed through other means, including direct sales, mail and fax messaging. |
Private Portals
OurWebMD Health Services private portals and coaching services compete, directly or indirectly, with various types of services provided by many different types of companies, including:
| | • | | similar services offered by health plans and their affiliates, such as Aetna, Humana, Kaiser Permanente and United Healthcare; |
18
| | • | | services offered by health management and disease management vendors, such as Mayo Foundation for Medical Education and Research, Wellness + Prevention, Inc. (which was formerly known as HealthMedia), Healthways, Health Dialog (which is owned by Bupa) and Alere (a division of Inverness Medical Innovations); and |
| | • | | services of other providers of online personal health records, health and benefits decision-support tools and related applications and platforms, such as, Castlight Health, Change Healthcare, Dossia, Epic Systems, HealthSparq, Microsoft, and a variety of other companies. |
GOVERNMENT REGULATION, INDUSTRY STANDARDS AND RELATED MATTERS
Introduction
Healthcare Regulation. The healthcare industry is highly regulated and is subject to changing political, regulatory and other influences. Most of our revenue is derived either directly from the healthcare industry or from other sources that are subject to healthcare laws and related regulations and could be affected by changes in those laws and regulations. This section of our Annual Report contains a description of healthcare laws and regulations applicable to us, either directly or through their effect on our healthcare industry customers, as well as healthcare industry standards that serve a self-regulatory function, and certain related matters. Changes in those laws, regulations and standards may create unexpected liabilities for us, may cause us to incur additional costs and may restrict our operations.
Many healthcare laws are complex, and their application to specific products, services, and business arrangements may not be clear. In particular, many existing healthcare laws and regulations, when enacted, did not anticipate the healthcare information services that we provide. However, these laws, regulations and industry standards may nonetheless be applied to our products, services, and business arrangements. We cannot provide assurance that we will be able to accurately anticipate the application of these laws, regulations and industry standards to our operations. Our failure to accurately anticipate the application of these laws and regulations to our operations, or other failure to comply, could create liability for us, result in adverse publicity and negatively affect our business. Even in areas where we are not subject to healthcare regulation directly, we may become involved in governmental actions or investigations through our relationships with customers that are regulated, and participation in such actions or investigations, even if we are not a party and not the subject of an investigation, may cause us to incur significant expenses.
Other Applicable Regulation. This section of our Annual Report also contains a description of other laws and regulations, including general consumer protection laws and Internet-related laws that may affect our operations. Laws and regulations have been adopted, and may be adopted in the future, that address Internet-related issues, including online content, privacy, online marketing, unsolicited commercial email, taxation, pricing, and quality of products and services. Some of these laws and regulations, particularly those that relate specifically to the Internet, were adopted relatively recently, and their scope and application may still be subject to uncertainties. Interpretations of these laws, as well as any new or revised laws or regulations, could decrease demand for our services, increase our cost of doing business, or otherwise cause our business to suffer.
Regulation of Drug and Medical Device Advertising and Promotion
The FDA and the Federal Trade Commission, or FTC, regulate the form, content and dissemination of labeling, advertising and promotional materials prepared by, or for, pharmaceutical or medical device companies. The FTC regulates over-the-counter drug advertising and, in some cases, medical device advertising. Based on FDA requirements, regulated companies must limit advertising and promotional materials to discussions of FDA-approved uses and claims. In limited circumstances, regulated companies may disseminate certain non-promotional scientific information or disease-state information.
Information on our Websites that promotes the use of pharmaceutical products or medical devices is subject to FDA and FTC requirements and enforcement actions, and information regarding other products and services is subject to FTC requirements. If either agency finds that information on our Websites violates regulations or guidance, it may take regulatory or judicial action against us or the advertiser or sponsor of that information.
19
State attorneys general may also take similar action based on their state’s consumer protection statutes. Areas of our Websites that could be the primary focus of regulators include pages and programs that discuss use of a regulated product or that the regulators believe may lack editorial independence from the influence of sponsoring pharmaceutical or device companies. Television broadcast advertisements that we may provide may also be subject to FTC and FDA regulation, depending on the content. The agencies place the principal burden of compliance with advertising and promotional regulations on advertisers and sponsors to make truthful, substantiated claims.
The Federal Food, Drug, and Cosmetic Act, or FDC Act, and its implementing regulations require that prescription drugs be approved by the FDA prior to marketing. It is a violation to market, advertise or otherwise commercialize such products prior to approval. The FDA allows for preapproval exchange of scientific information, provided it is non-promotional in nature and does not draw conclusions regarding the ultimate safety or effectiveness of the unapproved drug. The FDA also refrains from regulating certain disease state materials so long as those materials do not make a representation or suggestion about a drug or device. Upon approval or clearance, the FDA’s regulatory authority extends to the labeling and advertising of prescription drugs and medical devices. Such products may be promoted and advertised only for uses reviewed and approved by the FDA. Labeling and advertising can be neither false nor misleading and must present all material information, including risk information, in a clear, conspicuous and neutral manner. There are also requirements for certain information (the “prescribing information” or “package insert” for promotional labeling and the “brief summary” for advertising) to be part of labeling and advertising. Labeling and advertising that violate these legal standards are subject to enforcement.
The FDA also regulates the safety, effectiveness, and labeling of over-the-counter (OTC) drugs either through specific product approvals or through regulations that define approved claims for specific categories of products. The FTC regulates the advertising of OTC drugs under the section of the Federal Trade Commission Act that prohibits unfair or deceptive trade practices. The FDA and FTC regulatory framework requires that OTC drugs be formulated and labeled in accordance with FDA approvals or regulations and promoted in a manner that is truthful, adequately substantiated, and consistent with the labeled uses. OTC drugs that do not meet these requirements are subject to FDA or FTC enforcement action depending on the nature of the violation. In addition, state attorneys general may bring enforcement actions for alleged unfair or deceptive advertising.
There are several administrative, civil and criminal sanctions available to the FDA for violations of the FDC Act or FDA regulations as they relate to labeling and advertising. Administrative sanctions include a written request that violative advertising or promotion cease and/or that corrective action be taken, such as requiring a company to provide to healthcare providers and/or consumers information to correct misinformation previously conveyed. More serious civil sanctions include seizures, injunctions, fines and consent decrees. Any of these enforcement measures could prevent a company from introducing or maintaining its product in the marketplace. Criminal penalties for severe violations can result in a prison term and/or substantial fines. State attorneys general have similar investigative tools and sanctions available to them.
In the last 15 years, the FDA has gradually relaxed its formerly restrictive policies on DTC advertising of prescription drugs, allowing companies to advertise prescription drugs to consumers in any medium, provided that they satisfy FDA requirements. Should the FDA change its DTC policies, it could be more difficult for us to obtain ad and sponsorship revenue.
In response to a Congressional directive, the FDA has issued several guidance documents regarding the use of the Internet to promote FDA-regulated medical products. The FDA issued a 2011 guidance addressing the use of social media by consumers, which was limited to guidance regarding drug and device firms’ responses to public unsolicited requests for information made on Websites. In January 2014, the FDA issued a draft guidance clarifying rules regarding drug promotion through interactive social media tools. Neither draft guidance directly affects a core part of our current business, but, to the extent that they affect social media aspects of our Websites, they may trigger obligations for our customers. We also do not know how our customers might change their business practices in light of the January 2014 guidance. We cannot predict what effect any such changes will have on our business.
There are also advertising restrictions that apply outside of the United States. Our European Websites belonging toThe WebMD Health Network must comply with the national laws of the respective countries whose
20
physicians they address. Under these European laws, there are several restrictions regarding advertising of drugs or medical devices. There are, in particular, broad prohibitions on the advertising of prescription or reimbursed drugs to the general public, the use of indirect or disguised marketing, and the offering and providing of gifts or benefits with promotional purpose that are not of only minor value. If the relevant European national competent authorities find that any of our products and services, or any information on our Websites or in our mobile applications, violate applicable regulations, they may take regulatory or judicial action against us and/or the advertisers or sponsors of that information. Moreover, our competitors, or even competitors of advertisers and sponsors, may take actions against us and/or advertisers or sponsors of the information.
Regulation and Accreditation of Continuing Medical Education
Activities and information provided in the context of an independent medical or scientific educational program, often referred to as continuing medical education, or CME, usually are treated as non-promotional and fall outside the FDA’s jurisdiction. The FDA does, however, evaluate CME activities to determine whether they are independent of the promotional influence of the activities’ supporters. To determine whether a CME provider’s activities are sufficiently independent, the FDA looks at a number of factors related to the planning, content, speakers and audience selection of such activities. To the extent that the FDA concludes that such activities are not independent, such content must fully comply with the FDA’s requirements and restrictions regarding promotional activities.
Medscape, LLC distributes online CME to physicians and other healthcare professionals and is accredited by the Accreditation Council for Continuing Medical Education (ACCME), which oversees providers of CME credit.Medscape Education (www.medscape.org) is the Website through which Medscape, LLC distributes online CME. If any CME activity that Medscape, LLC certifies for CME credit is considered promotional, Medscape, LLC may face regulatory action or the loss of accreditation by the ACCME. Supporters of CME activities may also face regulatory action, potentially leading to termination of support.
Medscape, LLC’s current ACCME accreditation expires in 2016. In order for Medscape, LLC to renew its accreditation, it will be required to demonstrate to the ACCME that it continues to meet ACCME requirements. If Medscape, LLC fails to maintain its status as an accredited ACCME provider (whether at the time of such renewal or at an earlier time as a result of a failure to comply with existing or additional ACCME standards), it will not be permitted to accredit CME activities for physicians and other healthcare professionals. Instead, Medscape, LLC would be required to use third parties to provide such CME-related accreditation services. That, in turn, could discourage potential supporters from engaging Medscape, LLC to develop CME or education-related activities, which could have a material adverse effect on our business.
Medscape, LLC’s CME activities are planned and implemented in accordance with the Essential Areas and Elements and the Policies of the ACCME and other applicable accreditation standards. The ACCME’s standards for commercial support of CME are intended to ensure, among other things, that CME activities of ACCME-accredited providers, such as Medscape, LLC, are independent of “commercial interests,” which are defined as entities that produce, market, re-sell or distribute health care goods and services, excluding certain organizations. “Commercial interests,” and entities owned or controlled by “commercial interests,” are ineligible for accreditation by the ACCME. The standards also provide that accredited CME providers may not place their CME content on Websites owned or controlled by a “commercial interest.” In addition, accredited CME providers may not ask “commercial interests” for speaker or topic suggestions, and are also prohibited from asking “commercial interests” to review CME content prior to delivery. Further, there are limitations and requirements for CME providers using employees of a commercial interest as planners or speakers at CME events.
From time to time, the ACCME revises its standards for commercial support of CME. As a result of certain past ACCME revisions, we adjusted our corporate structure and made changes to our management and operations intended to allow Medscape, LLC to provide CME activities that are developed independently from those programs developed by its sister companies, which may not be independent of “commercial interests.” We believe that these changes allow Medscape, LLC to satisfy the applicable standards.
Recently, the ACCME and other organizations have been discussing ways to assure that commercial interests do not bias CME activities. The ACCME has published several proposals since 2008, including
21
proposals to reduce communications between commercial interests and CME providers and to create special designations for CME activities that are not funded by commercial interests. The ACCME also suggested creating an independent CME funding entity to build a firewall between commercial interests and CME activities. The ACCME has not adopted these proposals but has revised its policies. It is possible that adoption of additional proposals could significantly affect Medscape, LLC’s business model.
Educational activities directed at physicians, including CME, have been subject to increased governmental scrutiny to ensure that sponsors do not influence or control the content of the activities. The Department of Justice continues to examine CME sponsorship by manufacturers and companies have developed and implemented internal controls and procedures that promote adherence to applicable regulations and requirements. In implementing these controls and procedures, supporters of CME may interpret the regulations and requirements differently and may implement varying procedures or requirements. These controls and procedures:
| | • | | may discourage pharmaceutical companies from providing grants for independent educational activities; |
| | • | | may slow their internal approval for such grants; |
| | • | | may reduce the volume of sponsored educational programs that Medscape, LLC produces to levels that are lower than in the past, thereby reducing revenue; and |
| | • | | may require Medscape, LLC to make changes to how it offers or provides educational programs, including CME. |
Future changes to laws, regulations or accreditation standards, or to the internal compliance programs of supporters or potential supporters, may further discourage, significantly limit, or prohibit supporters or potential supporters from engaging in educational activities with Medscape, LLC, or may require Medscape, LLC to make further changes in the way it offers or provides educational activities.
CME regulations also apply in other countries. For example, under German law, certain CME programs must be approved by the State Medical Chamber. Additionally, German CME-related services must be free of commercial/business interests and the provider of CME services must be compliant with German laws and regulations. In France, a similar new regulatory framework which restricts the organization of CME activities has been completed. These or similar restrictions in other countries may restrict our ability to carry out activities related to CME programs and/or refer to drugs or medical devices in such CME programs. Moreover, if we are not able to demonstrate compliance with these regulations, applicable approvals may not be obtained from competent authorities, which may impact our ability to provide CME-related services and which could have an adverse effect on our business.
Federal False Claims Act
The Federal False Claims Act imposes liability on any person or entity who, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment by a Federal healthcare program. The whistleblower (or “qui tam”) provisions of the Federal False Claims Act allow a private individual to bring actions on behalf of the Federal government alleging that the defendant has submitted a false claim to the federal government and to share in any monetary recovery. After the filing of aqui tamsuit, the Federal government must determine whether it will intervene and control the case and, if it does not, the private individual may pursue the claim. In addition, various states and European countries have enacted false claim laws analogous to the Federal False Claims Act, and many of these laws apply where a claim is submitted to any third-party payor and not merely a Federal healthcare program. When an entity is determined to have violated the Federal False Claims Act, it may be required to pay up to three times the actual damages sustained by the government, plus civil penalties. Federal False Claims Act cases have been brought against drug manufacturers, and resulted in significant monetary settlements and the imposition of federally-supervised corporate integrity agreements in circumstances that include allegations that company-sponsored CME was unlawful off-label promotion. It is not clear whether there is a basis for the application of the Federal False Claims Act to the types of services that WebMD provides. However, plaintiffs have in the past, and may in the future, seek to name us as defendants in these types of cases. Any action against us for violation of these laws could cause us to incur significant legal expenses and may adversely affect our ability to operate our business.
22
HIPAA Privacy Standards and Security Standards
The Privacy Standards and Security Standards under the Health Insurance Portability and Accountability Act of 1996 (referred to as HIPAA), as amended by the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, establish a set of national privacy and security standards for the protection of individually identifiable health information by health plans, healthcare clearinghouses and healthcare providers (referred to as “covered entities”) and their “business associates,” which are persons or entities that perform certain services for or on behalf of a covered entity that involve the use or disclosure of protected health information. In connection with the sale by HLTH of its Emdeon Business Services business (or EBS), EBS agreed to license, through February 2018, certain de-identified data to HLTH for use in the development and commercialization of certain information products and services that use clinical data. We are currently using the data received under this license in our information services products. As a “business associate” of covered entities we are subject to HIPAA with regard to certain aspects of our business, such as managing employee or plan member health information for employers or health plans.
With respect to ourWebMD Health Services private portals and coaching services, HITECH creates obligations for us to report any unauthorized use or disclosure of protected health information, known as a breach, to our covered entity customers. The 2013 final HITECH rule modifies the breach reporting standard in a manner that will likely make more data security incidents qualify as reportable breaches. In addition, HITECH and its implementing regulations impose similar data breach notification requirements on vendors of personal health records that require us to notify affected individuals and the FTC in the event of a data breach involving the unsecured personal information of users of our public portal services.
Violations of HIPAA may result in civil and criminal penalties. HITECH increased civil penalty amounts for violations of HIPAA and significantly strengthens enforcement by requiring the U.S. Department of Health and Human Services (HHS) to conduct periodic audits to confirm compliance and authorizing state attorneys general to bring civil actions seeking either injunctions or damages in response to violations of HIPAA Privacy Standards and Security Standards that threaten the privacy of state residents. These new Privacy and Security provisions will require us to incur additional costs and may restrict our business operations. These new provisions, as modified by the 2013 final HITECH rule, may be subject to interpretation by various courts and other governmental authorities, thus creating potentially complex compliance issues for us and our customers and strategic partners.
Genetic Information Nondiscrimination Act (GINA)
The Genetic Information Nondiscrimination Act (referred to as GINA), enacted in May 2008, does not apply directly to WebMD, although it does apply to ourWebMD Health Services private portal customers, including both employers and group health plans. GINA was enacted to prevent discrimination by group health plans, health insurance issuers and employers on the basis of genetic information. OurWebMD Health Services health risk assessment (HRA) is typically offered to employees by their employer or group health plan as a voluntary component of a wellness program. The U.S. Departments of Labor, HHS and Treasury published Interim Final Rules implementing portions of Title I of GINA in October 2009, which generally apply to group health plans and health insurance issuers for plan years that began on or after December 7, 2009. The Interim Final Rules prohibit health plans from requesting, requiring or purchasing genetic information prior to or in connection with enrollment, or at any time for underwriting purposes, and state that “underwriting purposes” includes any incentive or disincentive (such as decreasing or increasing premiums) for completing an HRA. “Genetic information” is defined broadly to include information about an individual’s family medical history. The agencies have not finalized the regulations to date. However, in September 2010, the Department of Labor provided additional guidance in the form of frequently asked questions stating that, while a plan may not require an individual to complete an HRA that requests family medical history in order to receive a wellness program reward, it may use genetic information to make a determination regarding payment, or regarding the medical appropriateness of a treatment or service. HHS also issued a final rule implementing section 105 of GINA in January 2013. The final rule specifically provides that genetic information is a type of health information that is covered by HIPAA’s Privacy Standards and Security Standards, and specifically prohibits it from being used or disclosed for underwriting purposes (including any incentive or disincentive for completing an HRA).
23
Title II of GINA prohibits employment discrimination based on genetic information as well as the request or purchase of genetic information of employees or their family members with limited exceptions. The Equal Employment Opportunity Commission issued final rules implementing Title II in November 2010, effective in 2011. The final rules specify that genetic information may be collected in an HRA that is part of a wellness program only if participation in the collection of such information is voluntary, and indicate that the agency will consider participation voluntary if the employer neither requires participation nor penalizes employees who do not participate.
While each customer is responsible for ensuring that the wellness and benefit selections it offers are compliant with GINA, WebMD may face challenges as a result of varying interpretations of the law by our customers and by the multiple enforcing agencies and uncertainties over the final form of certain of the rules. Our customers’ interpretations of the law have required us to modify ourWebMD Health Services HRA product and we could experience increases in operational costs or decreases in demand for our products.
State legislation, such as recent legislation in California prohibiting any form of discrimination by businesses based on genetic information, including in housing, public accommodation, and the provision of emergency services, could have additional implications for service we provide in those states.
Other Restrictions Regarding Confidentiality, Privacy and Security of Health Information
In addition to HIPAA, numerous other state and federal laws, including those described in “— Consumer Protection Regulation” below, govern the collection, dissemination, use, access to, confidentiality and security of patient health and prescriber information. In addition, Congress and some states are considering new laws and regulations that further protect the privacy and security of medical records or medical information. In some cases, more protective state privacy and security laws are not preempted by the HIPAA Privacy and Security Standards and may be subject to interpretation by various courts and other governmental authorities, thus creating potentially complex compliance issues for us and our customers and strategic partners.
These laws at a state or federal level, or new interpretations of these laws, could create liability for us, could impose additional operational requirements on our business, could affect the manner in which we use and transmit patient information and could increase our cost of doing business. Claims of violations of privacy rights or contractual breaches, even if we are not found liable, could be expensive and time-consuming to defend and could result in adverse publicity that could harm our business.
Anti-Corruption Laws
The United States and other countries have adopted anti-corruption laws that generally prohibit directly or indirectly giving, offering or promising inducements to public officials to elicit an improper commercial advantage. Under applicable U.S., German, and most European law, this prohibition has been interpreted to apply to doctors and other medical professionals who work in state-run hospitals and state-run healthcare systems outside the United States. Some of these laws also prohibit directly or indirectly giving, offering or promising (and, in some cases, accepting or soliciting) inducements to (or from) private parties to elicit (or grant) an improper commercial advantage. In recent years, the U.S. government brought enforcement actions that resulted in significant monetary penalties against several companies operating in the global healthcare industry for violations ofanti-corruption laws resulting from illegal payments made to non-U.S. medical professionals.
As our business expands outside the United States, we (and others acting on our behalf) increasingly interact with non-U.S. doctors and other medical professionals, at least some of whom work in state-run hospitals or healthcare systems. Such interactions inherently increase the risk of violating applicable anti-corruption laws. While we believe that we have appropriate compliance policies and procedures in place to mitigate such risk, our personnel and others acting on our behalf might engage in conduct that violates such laws, for which we might be held responsible. Under such circumstances, we could be subject to civil and/or criminal penalties and other consequences that could have a material adverse effect on our business, financial condition and results of operations. In addition, our brand and reputation, our sales activities and the price of our Common Stock and other securities could be adversely affected if we were to become the target of any resulting negative publicity.
24
Anti-Kickback Laws
There are federal and state laws that govern patient referrals, physician financial relationships and inducements to healthcare providers and patients. The federal healthcare program anti-kickback law prohibits any person or entity from offering, paying, soliciting or receiving anything of value, directly or indirectly, for the referral of patients covered by Medicare, Medicaid and other federal healthcare programs or the leasing, purchasing, ordering or arranging for or recommending the lease, purchase or order of any item, good, facility or service covered by these programs. Many states and European countries also have similar anti-kickback laws that are not necessarily limited to items or services for which payment is made by a government healthcare program. These laws are applicable to manufacturers and distributors and, therefore, may restrict how we and some of our customers market products to healthcare providers, including e-details. Also, in 2002, the Office of the Inspector General (or OIG) of the United States Department of HHS, the federal government agency primarily responsible for interpreting the federal anti-kickback law, issued an advisory opinion that concluded that the sale of advertising and sponsorships to healthcare providers and vendors by Web-based information services implicates the federal anti-kickback law. However, the advisory opinion suggests that enforcement action will not result if the fees paid represent fair market value for the advertising/sponsorship arrangements, the fees do not vary based on the volume or value of business generated by the advertising and the advertising/sponsorship relationships are clearly identified as such to users so as not to imply an endorsement of the providers or vendors. We carefully review our practices with regulatory experts in an effort to ensure that we comply with all applicable laws. However, the laws in this area are both broad and vague, and it is often difficult or impossible to determine precisely how the laws will be applied, particularly to new services. Penalties for violating the federalanti-kickback law include imprisonment, fines and exclusion from participating, directly or indirectly, in Medicare, Medicaid and other federal healthcare programs. Any determination by a state, federal, or foreign regulatory agency that any of our practices violate any of these laws could subject us to civil or criminal penalties and require us to change or terminate some portions of our business and could have an adverse effect on our business. Even an unsuccessful challenge by regulatory authorities of our practices could cause us adverse publicity and be costly for us to respond to.
International Regulation
We are pursuing opportunities to expand the reach of our brands outside the United States. In certain markets outside the United States, we expect to accomplish this through partnerships or joint ventures with other companies having expertise in the specific country or region, while in other such markets we expect to rely primarily on our own internal resources. We intend to structure our participation in markets outside the United States in compliance with the laws and regulations that apply to such participation. However, as in the United States, the healthcare industry is highly regulated in many other jurisdictions and we may not be able to accurately anticipate the applicability of healthcare laws and regulations to our participation in such markets.
Many European countries have adopted laws and regulations similar to the U.S. laws and regulations described elsewhere in this section of the Annual Report. These include, for example, regulations like theanti-kickback laws, false claim laws, medical professional regulations, genetic privacy and nondiscrimination regulations, restrictions regarding advertising and promotion of drugs and medical devices, sunshine regulations and CME regulations. These European laws and regulations may impose additional operational requirements or restrictions on our business, and increase our cost of doing business. For example, we have implemented certain Website access restrictions that are intended to limit the display of advertising of drugs and medical devices if required by local law, so that such advertising will be seen only by appropriate healthcare professionals. If the applicable regulatory authorities find our access restrictions to be inadequate, they may require us to establish stricter access restrictions. Moreover, such authorities and/or our competitors or even competitors of our advertisers and sponsors may take action against us and/or our advertisers or sponsors if they believe that we have violated the applicable laws.
In addition, many countries and governmental bodies have, or are developing, laws that may apply to online health information services of the types we provide, or to Internet sites generally, including laws regarding the collection, use, storage and dissemination of personal information or patient data. To the extent our operations are located within their jurisdiction or are directed at individuals within their jurisdiction, these laws may apply to us. In addition, those governments may attempt to apply such laws extraterritorially or through treaties or other
25
arrangements with U.S. governmental entities. To the extent we fail to accurately anticipate the application or interpretation of these laws, we could be subject to liability and adverse publicity, which could negatively affect our business. In Europe, the current national implementations of the existing general data protection Directive 95/46/EC and of the e-Privacy Directive 2002/58/EC provide for criminal and administrative sanctions in case of violations, even though criminal sanctions are very rarely imposed. For example, France and Germany provide for administrative fines of up to 300,000 Euros (approximately 360,000 USD) in case of illegal collection or processing of personal identifiable information. Under the new draft General Data Protection Regulation on data protection proposed by the European Commission in January 2012, as modified by the European Parliament in October 2013, fines of up to 100,000,000 Euros (approximately 120,000,000 USD) or up to 5% of the global sales of the infringer could be imposed.
Many European countries have established cost reduction measures within their health systems or are intending to do so. This is intended to reduce the spending of the mainly publicly funded health systems in Europe. For example, Germany already established a new risk benefit drug assessment that adversely affects the prices of newly introduced medicinal products. Thus, it is possible that our advertisers and sponsors will face cost reduction measures and reduce their expenditures or postpone expenditure decisions, including expenditures for our services, which could have material adverse effects on our business.
Consumer Protection Regulation
General. Advertising and promotional activities presented to visitors on our Websites are subject to federal and state consumer protection laws that regulate unfair and deceptive practices. We are also subject to various other federal and state consumer protection laws, including the specific ones described later in this section.
The FTC and many state attorneys general are applying federal and state consumer protection laws to advertising activities and to require that the online collection, use and dissemination of data, including personal information, and the presentation of Website content, comply with certain standards for notice, choice, security and access. Courts may also adopt these developing standards. In many cases, the specific limitations imposed by these standards are subject to interpretation by courts and other governmental authorities. We believe that we are in compliance with the consumer protection standards that apply to our Websites, but a determination by a state or federal agency or court that any of our practices do not meet these standards could result in liability and adversely affect our business. New interpretations of these standards could also require us to incur additional costs and restrict our business operations. In addition, claims that we are violating any such standards could, even if we are not found liable, be expensive and time-consuming to defend and could result in adverse publicity that could harm our business.
In February 2009, the FTC published Self Regulatory Principles for Online Behavioral Advertising to address consumer privacy issues that may arise from so-called “behavioral advertising” (i.e., the tracking of online activities) and to encourage industry self-regulation. These principles serve as guidelines to industry. In addition, there is a possibility, supported by certain public statements, that the FTC may revise or eliminate the principles in favor of a more restrictive approach for companies that utilize behavioral advertising. There is also a possibility of legislation, regulations and increased enforcement activities, relating to behavioral advertising. To the extent that our existing practices are inconsistent with any revised principles, new rules, new legislation and/or future enforcement activities, our business may become subject to restrictions that could reduce our revenues or increase our cost of doing business.
In October 2009, the FTC adopted revised Guides Concerning the Use of Endorsements and Testimonials in Advertising. These Guides, which were last updated in 1980, became effective December 1, 2009. In addition to revising certain provisions regarding disclosures relating to endorsements and testimonials, the FTC clarified the Guides’ applicability to online and social media forums. In 2013, the FTC also revised guidance applicable to online advertising known as the Dot Com Disclosures, which was originally released in 2000. The revised Guides, the revised Dot Com Disclosures, and a 2013 FTC workshop on “native advertising” (i.e., blending advertising content with other content) may be an indication that the FTC may apply increased scrutiny to the use of endorsements, testimonials, and other advertising content online and through traditional media. To the extent we rely on endorsements or testimonials, we will review any relevant relationships for compliance with the Guides and we will otherwise endeavor to follow legal standards applicable to advertising.
26
In December 2010, following a series of workshops, the FTC issued a preliminary staff report containing a proposed framework for businesses and policymakers for online consumer privacy issues and, in March 2012, the FTC issued a final report setting forth its current views on best practices, to protect the privacy of consumers, to be implemented by companies that collect and use consumer data. Also in March 2012, the White House released a Privacy White Paper that outlined the Obama Administration’s proposal for a new American privacy framework based on a Consumer Bill of Privacy Rights and which called for the development ofindustry-specific voluntary, enforceable privacy codes of conduct through a collaborative multi-stakeholder process. Both the FTC and the White House called for Congress to develop baseline privacy legislation and the FTC also called on industry to accelerate the pace of self-regulation. The FTC is also holding a seminar in 2014 regarding privacy issues associated with “consumer generated and controlled health data,” which may be relevant to services we offer.
Both the FTC’s staff report and the White House’s Privacy White Paper, and the FTC’s workshop on consumer generated and controlled health data, reflect a continuing governmental interest in, and assessment of, online privacy issues. How these issues are ultimately resolved, whether through self-regulatory programs, legislation and regulation or some combination and the specifics of any such regimes, may significantly impact our operations.
In Europe, Directive 2009/136/EC of the European Parliament and of the Council requires the user’s full information and consent prior to the installation and use of any so-called “cookie” on a user’s computer. This Directive has been implemented differently, in various member states of the European Union, and national requirements to remain compliant with the respective laws may vary. Nevertheless, the provisions of this directive, whether effectively implemented in national laws, are now applicable in all the member states of the European Union and enforcement actions are now being considered by local data protection authorities. In addition, the new draft General Data Protection Regulation mentioned above revises the currently applicable data protection framework. The potential resulting new framework sets out additional requirements for users’ consent for offline and online marketing. If enacted, this instrument will further strengthen the already very densely regulated area of Internet privacy in Europe. In addition, this revised European legislation, if adopted, would increase the likelihood of the applicability of European law to entities established outside the European Union but processing data of European data subjects.
European healthcare advertising laws stipulate several restrictions on advertising of drugs and medical devices to the public. In particular, in several countries, the advertising of prescription drugs to the general public is not allowed. Thus, these European countries require access restrictions for Websites that contain such advertisements, which are only allowed to be addressed to healthcare professionals. Accordingly, Websites inThe WebMD Health Network that are addressed to physicians in specific European countries (such as the Medscape Germany or France Websites) must be accessible only to healthcare professionals by an appropriate access check. If the applicable European competent authority does not acknowledge the respective Website to have appropriate access controls, the authority may require us to establish stricter access controls or ultimately may take action against us.
Data Protection Regulation. With the recent increase in publicity regarding data breaches resulting in improper dissemination of consumer information, many states have passed laws regulating the actions that a business must take if it experiences a data breach, such as prompt disclosure to affected customers. Generally, these laws are limited to electronic data and make some exemptions for smaller breaches. Congress has also been considering similar federal legislation relating to data breaches. The FTC has also brought enforcement actions and prosecuted some data breach cases as unfair and/or deceptive acts or practices under the FTC Act. In addition to data breach notification laws, some states have enacted statutes and rules requiring businesses to reasonably protect certain types of personal information they hold or to otherwise comply with certain specified data security requirements for personal information. These laws may apply directly to our business or indirectly by contract when we provide services to other companies. We intend to continue to comprehensively protect all consumer data and to comply with all applicable laws regarding the protection of this data.
CAN-SPAM Act. On January 1, 2004, the Controlling the Assault of Non-Solicited Pornography and Marketing Act of 2003, or the CAN-SPAM Act, became effective. The CAN-SPAM Act regulates commercial emails, provides a right on the part of the recipient to request the sender to stop sending messages, and
27
establishes penalties for the sending of email messages that are intended to deceive the recipient as to source or content. Under the CAN-SPAM Act, senders of commercial emails (and other persons who initiate those emails) are required to make sure that those emails do not contain false or misleading transmission information. Commercial emails are required to include a valid return email address and other subject heading information so that the sender and the Internet location from which the message has been sent are accurately identified. Recipients must be furnished with an electronic method of informing the sender of the recipient’s decision to not receive further commercial emails. In addition, the email must include a postal address of the sender and notice that the email is an advertisement. We are following the CAN-SPAM requirements in the e-newsletters that WebMD’s public portals distribute to members and some of our other email communications, and believe that our email practices comply with the requirements of the CAN-SPAM Act, even though we believe that FTC regulations issued in May 2008 confirmed our existing understanding that these email newsletter communications are not generally commercial emails. Many states have also enacted anti-spam laws. The CAN-SPAM Act preempts many of these statutes. To the extent that these laws are not preempted, we believe that our email practices are designed to comply with these laws.
COPPA. The Children’s Online Privacy Protection Act, or COPPA, applies to operators of commercial Websites and online services directed to U.S. children under the age of 13 that collect personal information from children, and to operators of general audience sites with actual knowledge that they are collecting information from U.S. children under the age of 13. Except for ourfit.WebMD.com site, our sites are not directed at children and our general audience site,WebMD Health, states that no one under the applicable age is entitled to use the site. In addition,WebMD Health employs a kick-out procedure whereby users identifying themselves as being under the age of 13 during the registration process are not allowed to register for the site’s member only services, such as message boards and live chat events. Ourfit.WebMD.com site is designed to comply with the provisions of COPPA. The FTC issued a revised COPPA rule in late 2012. We do not anticipate ourfit.WebMD.com site or other sites not being in compliance with the revised rule.
FACTA. In an effort to reduce the risk of identity theft from the improper disposal of consumer information, Congress passed the Fair and Accurate Credit Transactions Act (or FACTA), which requires businesses to take reasonable measures to prevent unauthorized access to such information. FACTA’s disposal standards are flexible and allow businesses discretion in determining what measures are reasonable based upon the sensitivity of the information, the costs and benefits of different disposal methods and relevant changes in technology. We believe that we are in compliance with FACTA.
Telemarketing. The Telemarketing and Consumer Fraud Abuse Prevention Act (TCFAPA) and the Telephone Consumer Protection Act (TCPA) are laws that govern telemarketing and other calling activities. Both the FTC (via the Telephone Sales Rule) and the FCC have enacted rules under these statutes that implement the national do not call registry and which also apply to a broad range of other telephone calling activities including as relevant to text message marketing and autodialed calls to cell phones. States also have their own telemarketing laws governing an array of telephone calling activities. We believe that we are in compliance with the TCFAPA, the TCPA, and state telemarketing laws.
Regulation of Wellness Incentive Programs
Certain provisions of HIPAA (commonly referred to as the HIPAA nondiscrimination provisions) generally prohibit group health plans from charging similarly situated individuals different premiums or contributions or imposing different deductible, co-payment, or other cost-sharing requirements based on a “health factor.” Such differentials are, however, acceptable under the HIPAA nondiscrimination provisions if the differentials are applied through “wellness programs.” The Department of Labor, in coordination with the Departments of the Treasury and HHS, has issued regulations (finalized in 2013) that define “wellness programs” for purposes of the HIPAA nondiscrimination provisions, establishing specific requirements for wellness programs that reward participants who satisfy a standard related to a health factor (referred to as “health-contingent wellness programs”) and for other types of wellness programs. These requirements for health-contingent wellness programs include (1) limiting the amount of the wellness program’s rewards, which the Affordable Care Act generally increased to 30% (50% for programs designed to prevent or reduce tobacco use) of the cost of coverage, (2) the wellness program being reasonably designed to promote good health and prevent disease,
28
(3) giving those eligible to participate in the wellness program the opportunity to qualify for the reward at least once a year, (4) providing a reward that is available to all similarly situated individuals, and (5) requiring disclosure of reasonable alternative standards that must be available under the wellness program.
Although HIPAA and its regulations state that certain excepted benefits, including supplemental benefits, are not subject to the wellness program rules, it does not define the term “similar supplemental coverage.” On December 7, 2007, the Department of Labor, in coordination with the Departments of the Treasury and HHS, released Field Assistance Bulletin No. 2007-04 (FAB 2007-04) in response to the development of questionable health and wellness programs that were marketed as “similar supplemental coverage.” FAB 2007-04 clarifies the rules for supplemental programs and provides that supplemental benefits under a wellness program cannot discriminate on the basis of a health factor. With these new requirements in place, wellness programs that require individuals to meet certain health factors can no longer be considered supplemental and thus have to comply with HIPAA wellness program regulations described in the immediately preceding paragraph. According to FAB 2007- 04, programs that do not meet these requirements may be subject to enforcement actions. HHS provided parallel guidance in Program Memorandum 08-01 (May 2008).
The Americans with Disabilities Act (ADA) prohibits discrimination on the basis of an employee’s disability or perceived disability. Among other things, it limits employers from inquiring about the disabilities of employees unless the questions are job-related and consistent with business necessity. The ADA also limits the circumstances in which an employer may require physical examinations or answers to medical inquiries. However, the ADA allows employers to conduct voluntary medical examinations and activities, including voluntary medical histories, as part of a voluntary wellness program. A wellness program is “voluntary” if the employer neither requires participation nor penalizes employees who do not participate. Records acquired as part of a wellness program must be kept confidential and may not be used for a discriminatory purpose. Many states and localities provide similar protections to employees.
The Genetic Information Nondiscrimination Act restricts the collection or use of genetic information for underwriting purposes, and treats the offering of incentives or disincentives for completing an HRA or participating in a wellness program as underwriting. See “— Genetic Information Nondiscrimination Act (GINA)” above.
We provide services related to wellness programs in connection with ourWebMD Health Services private portals and coaching services. See “WebMD Health Services — Our Private Portals” above. We believe that we are in compliance with the laws and regulations applicable to these services, to the extent they apply to us.
Medical Professional Regulation
The practice of most healthcare professions requires licensing under applicable state law, as well as under applicable national law of most of the European countries. In addition, the laws in some states and European countries prohibit business entities from practicing medicine, which is generally referred to as the prohibition against the corporate practice of medicine. We do not believe that we engage in the practice of medicine, and we have attempted to structure our Websites, strategic relationships and other operations to avoid violating these state licensing and professional practice laws. We do not believe that we provide professional medical advice, diagnosis or treatment. We employ and contract with physicians who provide only health information to consumers, and we have no intention to provide medical care or advice. A state or other enforcement authority, however, may determine that some portion of our business violates these laws and may seek to have us discontinue those portions or subject us to penalties or licensure requirements. Any determination that we are a healthcare provider and acted improperly as a healthcare provider may result in liability to us.
Healthcare Reform
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010 (which we refer to as the Affordable Care Act), was signed into law in March 2010. The Affordable Care Act makes extensive changes to the system of healthcare insurance and benefits in the U.S. In general, the Affordable Care Act seeks to reduce healthcare costs and decrease the number of uninsured legal U.S. residents by, among other things, requiring individuals to carry, and certain employers to offer, health insurance or be subject to penalties. The Affordable Care Act also imposes new regulations on health insurers,
29
including guaranteed coverage requirements, prohibitions on certain annual and all lifetime limits on amounts paid on behalf of or to plan members, increased restrictions on rescinding coverage, establishment of minimum medical loss ratio requirements, a requirement to cover certain preventive services on a first dollar basis, the establishment of state insurance exchanges and essential benefit packages, and greater limitations on how health insurers price certain of their products. The Affordable Care Act also contains provisions that will affect the revenues and profits of pharmaceutical and medical device companies, including new taxes on certain sales of their products.
Many of the provisions of the Affordable Care Act that expand insurance coverage did not become effective until 2014, and some will not become effective until later, and many provisions will require additional regulations and interpretive guidance to be issued before they will be fully implemented. Some provisions do not apply to health plans that were in place when the Affordable Care Act was enacted and have not been substantially changed since. It is difficult to foresee how individuals and businesses will respond to the choices available to them under the Affordable Care Act. Furthermore, the Affordable Care Act will result in future state legislative and regulatory changes, which we are unable to predict at this time, in order for states to comply with certain provisions of the Affordable Care Act and to participate in grants and other incentive opportunities. In addition, Congress has considered various proposals to repeal some or all of the Affordable Care Act.
While we do not currently anticipate any significant adverse effects on WebMD as a direct result of application of the Affordable Care Act to our business or on our company in its capacity as an employer, we are unable to predict what the indirect impacts of the Affordable Care Act will be on WebMD’s business through its effects on other healthcare industry participants, including pharmaceutical and medical device companies that are advertisers and sponsors of our public portals and employers and health plans that are clients of our private portals. Healthcare industry participants may respond to the Affordable Care Act or to uncertainties created by the Affordable Care Act by reducing their expenditures or postponing expenditure decisions, including expenditures for our services, which could have a material adverse effect on our business.
However, we believe that certain aspects of the Affordable Care Act and future implementing regulations that seek to reduce healthcare costs may create opportunities for WebMD, including with respect to our personal health record applications and health and benefits decision-support tools and, more generally, with respect to our capabilities in providing health and wellness information and education. For example, the Affordable Care Act encourages use of wellness programs through grants to small employers to establish such programs, permission for employers to offer larger rewards than under prior law, in the form of waivers of cost-sharing, premium discounts, or additional benefits, to employees for participating in these programs and meeting certain standards, and the inclusion of wellness services and chronic disease management among the essential health benefits that certain plans are required to provide. In addition, in connection with the implementation of the Affordable Care Act, we have launched a new channel on WebMD.com that provides information and decision-support tools to help consumers understand their options and choose an appropriate health plan based on their needs. However, we cannot yet determine the scope of the other opportunities that the Affordable Care Act may create or what competition we may face in our efforts to pursue such opportunities.
30
OTHER INFORMATION
Employees
As of December 31, 2013, we had approximately 1,600 employees.
Intellectual Property
We use trademarks, trade names and service marks for our products and services, including those listed below the Table of Contents of this Annual Report. We also use other registered and unregistered trademarks and service marks for our products and services. In addition, we have registered domain names, including “webmd.com” and “medscape.com” and the other domain names listed in this Annual Report. If we are unable to protect our marks and domain names adequately, that could have a material adverse effect on our business and hurt us in establishing and maintaining our brands.
We rely upon a combination of patent, trade secret, copyright and trademark laws, license agreements, confidentiality procedures, employee and client nondisclosure agreements and technical measures to protect intellectual property used in our businesses. We also rely on a variety of intellectual property rights licensed from third parties, including Internet server software, databases and healthcare content used on our Websites. These third-party licenses may not continue to be available to us on commercially reasonable terms. Our loss of or inability to maintain or obtain upgrades to any of these licenses could significantly harm us. In addition, because we license content from third parties, we may be exposed to copyright infringement actions if those parties are subject to claims regarding the origin and ownership of that content.
Seasonality
For a discussion of seasonality affecting our business, see “Management’s Discussion and Analysis of Financial Condition and Results of Operations — Seasonality” in Item 7 below.
Other
To the extent required by Item 1 of Form 10-K, the information contained in Item 7 of this Annual Report is hereby incorporated by reference in this Item 1.
31
This section describes circumstances or events that could have a negative effect on our financial results or operations or that could change, for the worse, existing trends in some or all of our businesses. The occurrence of one or more of the circumstances or events described below could have a material adverse effect on our financial condition, results of operations and cash flows or on the trading prices of our Common Stock and Convertible Notes or of securities that we may issue in the future. The risks and uncertainties described in this Annual Report are not the only ones facing us. Additional risks and uncertainties that are not currently known to us, or that we currently believe are immaterial, may also adversely affect our business and operations.
Risks Related to Our Operations and the Healthcare Content We Provide
If we are unable to provide content and services that attract users to The WebMD Health Network on a consistent basis, our advertising and sponsorship revenue could be reduced
Users ofThe WebMD Health Networkhave numerous other online and offline sources of healthcare information and related services. Our ability to compete for user traffic on our public portals depends upon our ability to make available a variety of health, wellness and medical content, decision-support applications and other services that meet the needs of a variety of types of users, including consumers, physicians and other healthcare professionals, with a variety of reasons for seeking information. Our ability to do so depends, in turn, on:
| | • | | our ability to hire and retain qualified authors, journalists and independent writers; |
| | • | | our ability to license quality content from third parties; and |
| | • | | our ability to monitor and respond to increases and decreases in user interest in specific topics. |
If consumers and healthcare professionals do not perceive our content, applications and tools to be useful, reliable and trustworthy, we may not be able to attract or retain users or otherwise maintain or increase the frequency and duration of their engagement with our health information services. We cannot assure you that we will be able to continue to develop or acquire needed content, applications and tools at a reasonable cost. In addition, since consumer users of our public portals may be attracted toThe WebMD Health Network as a result of a specific condition or for a specific purpose, it is difficult for us to predict the rate at which they will return to our public portals. Because we generate revenue by, among other things, selling sponsorships of specific pages, sections or events onThe WebMD Health Network, a decline in user traffic levels or a reduction in the number of pages viewed by users could cause our revenue to decrease and could have a material adverse effect on our results of operations.
A significant portion of the traffic to The WebMD Health Network is directed to us through algorithmic search results on Internet search engines and, if we are listed less prominently in search result listings, our business and operating results could be harmed
A significant portion of the traffic toThe WebMD Health Network is directed to us through the algorithmic search results on Internet search engines such as Google. Algorithms are developed and used by search engine providers to determine the listings, and the order of such listings, displayed in response to specific searches. Accordingly, in addition to providing quality content and tools, we seek to design our Websites to deliver the content and tools in ways that will cause them to rank well in algorithmic search engine results, which makes it more likely that search engine users will visit our Websites. This is commonly referred to as search engine optimization, or SEO. However, there can be no assurance that our SEO efforts will succeed in improving the ranking of our content or, even if they do result in such improvement, that the improved ranking will result in increased numbers of users and page views for our Websites. In addition, search engines frequently change the criteria that determine site rankings in their search results and our SEO efforts will not be successful if we do not respond to those changes appropriately and on a timely basis. One factor that we believe significantly reduced traffic, in the first half of 2013, to some of the consumer sites inThe WebMD Health Network (other than WebMD.com, our flagship site) was changes in Google’s algorithms and other processes that lowered the
32
ranking of those sites in Google search results during that period. Although we saw a reversal of this trend beginning in the third quarter of 2013, we cannot be certain whether the improvement will continue or, if it does, how long it can be maintained. Search engine providers may also prioritize search results generated by certain types of queries, including health-related queries, based on criteria they select or may otherwise intermediate in the search results generated, which could, in some circumstances, reduce the ranking that would otherwise be provided to our Websites and increase the ranking of other sites. If we are unable to respond effectively to changes made by search engine providers in their algorithms and other processes, a substantial decrease in traffic toThe WebMD Health Network could occur, which could cause our revenue to decrease and have a material adverse effect on our results of operations.
Increasingly, individuals are using mobile devices to access online content and services and, if we fail to capture a significant share of this portion of the market for online health information services or fail to generate revenue from it, our business could be adversely affected
The number of people who access online content and services through smartphones, tablets and other mobile devices has increased dramatically in the past few years, including the number of physicians and other healthcare professionals who do so. Accordingly, the portion of our page views from mobile devices has increased rapidly and is expected to continue to increase. In addition, for each of the first three quarters of 2013, we experienced a year-over-year decline in page views from personal computers (or PCs) as the usage from mobile devices has increased. It is difficult to predict the problems we may encounter in developing and maintaining competitive mobile services and we may need to devote significant resources to their creation, maintenance and support.
We do not currently generate meaningful revenue from our mobile health information services on smartphones, and our ability to do so successfully is unproven. Even if demand for our mobile platforms and applications exists and we achieve a significant share of the usage of mobile health information services on smartphones, we cannot assure you that we will be able to achieve significant revenue or profits from these services. Although monetization of tablet page views is generally similar to monetization of PC page views, the monetization of smartphone page views will require different strategies and techniques because of the smaller screen size. We are in the early stages of developing and testing those strategies and techniques and, accordingly, cannot provide assurance that our efforts to monetize smartphone page views will be successful or, even if they begin to produce some positive results, how long that would last in light of changing preferences of users and of advertisers and sponsors, ongoing technological changes and changes in applicable laws, regulations and other standards. If users access our services through smartphones as a substitute for access through personal computers and tablets, and if we are unable to successfully implement monetization strategies for smartphone traffic, our revenue and financial results may be negatively affected.
We face significant competition for our healthcare information products and services
The markets for healthcare information products and services are intensely competitive, continually evolving and, in some cases, subject to rapid change.
| | • | | The WebMD Health Network faces competition from numerous other companies, both in attracting users and in generating revenue from advertisers and sponsors. We compete for users with Websites and mobile applications that provide health-related information, including both commercial ones and not-for-profit ones. We compete for advertisers and sponsors with: health-related Websites and mobile applications; general interest consumer Websites that offer specialized health sub-channels or functions; other high-traffic Websites that include both healthcare-related and non-healthcare-related content and services, including social media Websites; search engines that provide specialized health search; and advertising networks that aggregate traffic from multiple sites.The WebMD Health Network also faces competition from traditional media and offline publications and information services. |
| | • | | OurWebMD Health Services private portals and coaching services compete with: providers of healthcare decision-support tools and online health management applications, including personal health records; wellness and disease management vendors; and health information services and health management offerings of healthcare benefits companies and their affiliates. |
33
Many of our competitors have greater financial, technical, product development, marketing and other resources than we do. These organizations may be better known than we are and have more customers or users than we do. We cannot provide assurance that we will be able to compete successfully against these organizations. In addition, we expect that competitors will continue to enter these markets. The competition we face for our services may result in fewer or smaller customer commitments or pressure to reduce prices, which could reduce our profit margins.
Developing and implementing new and updated features and services for our public and private portals and our mobile applications may be more difficult than expected, may take longer and cost more than expected, and may not result in sufficient increases in revenue to justify the costs
Attracting and retaining users of our public portals and our mobile applications and clients for our private portals requires us to continue to improve the technology underlying those portals and applications and to continue to develop new and updated features and services for those portals and applications. If we are unable to do so on a timely basis or if we are unable to implement new features and services without disruption to our existing ones, we may lose potential users and clients.
We rely on a combination of internal development, strategic relationships, licensing and acquisitions to develop our portals, mobile applications and related features and services. Our development and/or implementation of new technologies, features and services may cost more than expected, may take longer than originally expected, may require more testing than originally anticipated and may require the acquisition of additional personnel and other resources. There can be no assurance that the revenue opportunities from any new or updated technologies, applications, features or services will justify the amounts spent.
Failure to effectively identify, assess and pursue new business initiatives could adversely affect our company and its prospects
We are working to broaden our portfolio of services and taking steps to diversify our client base and revenue streams. Some of the business initiatives we are working on have challenges that are different than those associated with our existing products and services and could strain our financial, operational and management resources. Furthermore, there can be no assurance that the potential revenue streams from any investments that we may make in pursuing new business opportunities will justify the amounts spent. Failure to effectively identify, assess and pursue new business initiatives may adversely affect our company and its prospects.
Failure to enhance the analytic capabilities we use to demonstrate the value of our services to advertisers and sponsors could adversely affect our ability to market our services
We are working to enhance the analytic capabilities we use to demonstrate to advertisers and sponsors how promotional strategies implemented throughThe WebMD Health Network impact physician and consumer behaviors and preferences. Our ability to demonstrate the value of advertising and sponsorship onThe WebMD Health Network will depend, in part, on the accuracy of our analytics and measurement capabilities, on our ability to develop reporting tools using the capabilities and our ability to further improve such capabilities and tools. If we are unable to enhance our analytic capabilities, it could adversely affect our ability to market our services and we may lose business to competitors even if our advertising and sponsorship services are superior to theirs.
Restrictions on our ability to access or use various forms and sources of data could adversely impact our business
We are increasingly using data analytics based on information that we collect regarding usage of our public portals, as well as other third party sources of data. Our use of data regarding users of our public portals is governed by the privacy policies posted on those sites and is designed to comply with applicable laws and regulations, including HIPAA, as is our use of any third-party data. In addition, we sell certain information products on a standalone basis utilizing de-identified data that we license from a third-party source. Changes to our ability to access or use data could adversely affect our ability to implement improved analytics or to offer information products on a standalone basis. Accordingly, our business could be adversely impacted if, for any reason (including, but not limited to, changes in applicable laws and regulations) the data we use becomes
34
unavailable or the conditions on its availability are not commercially reasonable or are inconsistent with our planned usage. In addition, the quality of our data analytics depends on the reliability of the information that we are able to obtain. If the information we use contains errors or is otherwise unreliable, analyses we create and actions we take based on those analyses could be wrong, which could hurt our reputation and business.
Failure to maintain and enhance the “WebMD” and “Medscape” brands could have a material adverse effect on our business
We believe that the “WebMD” and “Medscape” brand identities that we have developed have contributed to the success of our business and have helped us achieve recognition as a trusted source of health and wellness information and tools for consumers and of online content for physicians and other healthcare professionals. We also believe that maintaining and enhancing those brands is important to expanding the user base for our public portals and to our relationships with sponsors and advertisers. The “WebMD” brand is also important to our ability to gain additional employer and healthcare payer clients for our private portals. We have expended considerable resources on establishing and enhancing the “WebMD” and “Medscape” brands and our other brands, and we have developed policies and procedures designed to preserve and enhance our brands, including editorial procedures designed to provide quality control of the information we publish. We expect to continue to devote resources and efforts to maintain and enhance our brands. However, we may not be able to successfully maintain or enhance our brands, and events outside of our control may have a negative effect on our brands. If we are unable to maintain or enhance our brands, and do so in a cost-effective manner, our business could be adversely affected.
We have a limited operating history
We have a limited operating history and participate in relatively new markets. These markets, and our business, have undergone significant changes during their short history and can be expected to continue to change. Many companies with business plans based on providing healthcare information and related services through the Internet have failed to be profitable and some have filed for bankruptcy or ceased operations. Even if demand from users exists, we cannot assure you that our business will be profitable.
Our failure to attract and retain qualified executives and employees may have a material adverse effect on our business
Our business depends largely on the skills, experience and performance of key members of our management team and other key employees. We also depend, in part, on our ability to attract and retain qualified writers and editors, software developers and other technical personnel and sales and marketing personnel. Competition for qualified personnel in the healthcare information services and Internet industries is intense. We cannot assure you that we will be able to hire or retain a sufficient number of qualified personnel to meet our requirements, or that we will be able to do so at costs that are acceptable to us. Failure to do so may have an adverse effect on our business.
Our advertising and sponsorship revenue may vary significantly from quarter to quarter and its amount and timing may be subject to factors beyond our control, including regulatory changes
Our advertising and sponsorship revenue may vary significantly from quarter to quarter due to a number of factors, many of which are not within our control, and some of which may be difficult to forecast accurately, including potential effects on demand for our services as a result of regulatory changes affecting advertising and promotion of drugs and medical devices and general economic conditions. The majority of our advertising and sponsorship programs are for terms of approximately four to twelve months. We have relatively few longer term advertising and sponsorship programs. We cannot assure you that our current advertisers and sponsors will continue to use our services beyond the terms of their existing contracts or that they will enter into any additional contracts.
The time between the date of initial contact with a potential advertiser or sponsor regarding a specific program and the execution of a contract with the advertiser or sponsor for that program, as well as the additional time period before our services are delivered, may be longer than expected, especially for medium-sized and larger contracts, and may be subject to delays over which we have little or no control, including as a result of
35
budgetary constraints of the advertiser or sponsor or their need for internal approvals, including internal approvals relating to compliance with the laws and regulations applicable to the marketing of healthcare products. We have experienced, from time to time, a lengthening of this internal review process by pharmaceutical and biotechnology companies, which has resulted in delays in contracting as well as delays in recognizing expected revenue under executed contracts and which may continue to cause such delays. Other factors that could affect the timing of contracting for specific programs with advertisers and sponsors, or receipt of revenue under such contracts, include:
| | • | | the timing of Food and Drug Administration (FDA) approval for new products or for new approved uses for existing products; |
| | • | | the timing of FDA approval of generic products that compete with existing brand name products and any increase in the number or significance of such approvals; |
| | • | | the timing of withdrawals of products from the market; |
| | • | | consolidation of companies in the pharmaceutical and biotechnology industries; |
| | • | | the timing of rollouts of new or enhanced services on our public portals; |
| | • | | seasonal factors relating to the prevalence of specific health conditions and other seasonal factors that may affect the timing of promotional campaigns for specific products; and |
| | • | | the scheduling of conferences for physicians and other healthcare professionals. |
Some of our pharmaceutical company customers have experienced patent expirations for certain of their products in the past several years and some are expected to experience patent expirations over the next several years. In the pharmaceutical industry, patent expirations allow for competition from lower-priced generic versions of the patented drugs and generally result in the termination of marketing efforts for the drug. In 2012, we believe that patent expirations led to, and could in the future lead to, overall reductions in marketing, selling and educational expenditures by some of these pharmaceutical companies across their entire product portfolios.
We may be unsuccessful in our efforts to generate advertising and sponsorship revenue from consumer products companies
Much of our advertising and sponsorship revenue has, in the past, come from pharmaceutical, biotechnology and medical device companies. We also seek to generate advertising and sponsorship revenue from consumer products companies that are interested in communicating health-related or safety-related information about their products to our audience. However, while many consumer products companies are increasing the portion of their promotional spending used on the Internet, we cannot assure you that these advertisers and sponsors will find our consumer Websites to be as effective for promoting their products and services as competing channels, which include traditional media, Internet search engines, social media Internet sites, general interest consumer sites, and numerous other alternatives. Competition for this business may also result in smaller customer commitments or pressure to reduce prices, both of which could reduce our profit margins even if we are able to generate revenue.
In addition, revenues from consumer products companies are more likely to reflect general economic conditions, and to be reduced to a greater extent during economic downturns, than revenues from pharmaceutical, biotechnology and medical device companies. Accordingly, revenues from this portion of our business may be subject to significant quarter-to-quarter variations and we may be unsuccessful in our efforts to develop it further.
Lengthy sales and implementation cycles for our WebMD Health Services private online portals make it difficult to forecast our revenues from these applications and may have an adverse impact on our business
The period from our initial contact with a potential client for a private online portal and entry into a contract for a subscription to our solution by the client is difficult to predict. In the past, this period has generally ranged from six to twelve months, but in some cases has been longer. Potential contracts may be subject to delays or cancellations due to a client’s internal procedures for approving large expenditures and other factors beyond our control, including the effect of general economic conditions on the willingness of potential clients to subscribe to ourWebMD Health Services solution. The time it takes to implement a private online portal is also difficult to predict and has lasted as long as six months from contract execution to the commencement of live operation.
36
Implementation may be subject to delays based on the availability of the internal resources of the client that are needed and other factors outside of our control. As a result, we have limited ability to forecast the timing of revenue from new clients. This, in turn, makes it more difficult to forecast our financial performance for future periods. In addition, some of our client contracts may permit termination, by the client, prior to the end of the stated contract term, which can also make it more difficult to forecast our future financial performance.
During the contracting cycle and the implementation period, we may expend substantial time, effort and money preparing contract proposals, negotiating contracts and implementing our population health management platform without receiving any related revenue. In addition, many of the expenses related to providing our platform are relatively fixed in the short term, including personnel costs and technology and infrastructure costs. If our private portal services revenue is lower than expected, we may not be able to reduce related short-term spending in response. Any shortfall in such revenue would have a direct impact on our results of operations.
Our ability to renew existing agreements with employers and health plans will depend, in part, on our ability to continue to increase usage of our private portal services by their employees and plan members
In a healthcare market where a greater share of the responsibility for healthcare costs and decision-making has been shifting to consumers, use of information technology (including personal health records) to assist consumers in making informed decisions about healthcare has also increased. We believe that through ourWebMD Health Servicesprivate online portals, including our personal health record application, we are well positioned to play a role in this environment. However, our strategy depends, in part, on increasing usage of our services by our employer and health plan clients’ employees and plan participants and being able to demonstrate a sufficient return on investment and other benefits for our clients from those services. Increasing usage of our private portal services requires us to continue to develop new and updated applications, features and services. In addition, we face competition in the area of healthcare decision-support tools and online health management applications and health information services. Many of our competitors have greater financial, technical, product development, marketing and other resources than we do, and may be better known than we are. We cannot provide assurance that we will be able to meet our development and implementation goals or that we will be able to compete successfully against other vendors offering competitive services and, if we are unable to do so, we may experience static or diminished usage for our private portal services and possible non-renewals of our customer agreements.
We are beginning to provide condition management services to clients of our WebMD Health Services private portals, which will involve additional risks and challenges and which may not be profitable
We are beginning to provide condition management services to clients of ourWebMD Health Services private portals and plan to expand that portion of our business. Our initial offerings include programs targeting individuals struggling with obesity, diabetes, coronary artery disease and congestive heart failure. Our condition management programs include ongoing, intensive one-on-one coaching by condition specialists, along with targeted online resources and progress tracking tools. Providing condition management services involves new risks and challenges for us, including: the need to obtain and retain necessary licenses, permits and regulatory clearances and approvals related to these services; difficulty in quantifying the costs savings and other benefits for our clients from these services; and difficulty in differentiating our condition management services from those of competitors, some of whom may be able to provide such services at a lower cost. We cannot predict the demand among our existing private portals clients and other potential clients for our condition management services and cannot provide assurance that the revenue opportunities from providing these services will justify the costs involved in developing the required capabilities and delivering the services to clients.
Contractual relationships with governmental customers may impose special burdens on us and provide special benefits to those customers, including the right to change or terminate the contract in response to budgetary constraints or policy changes
A portion of our revenues come from customers that are governmental agencies or vendors to such agencies. Government contracts and subcontracts may be subject to some or all of the following:
| | • | | termination when appropriated funding for the current fiscal year is exhausted or becomes unavailable; |
37
| | • | | termination for the governmental customer’s convenience, subject to a negotiated settlement for costs incurred and profit on work completed, along with the right to place contracts out for bid before the full contract term, as well as the right to make unilateral changes in contract requirements, subject to negotiated price adjustments; |
| | • | | “most-favored” pricing disclosure requirements that are designed to ensure that the government can negotiate and receive pricing akin to that offered commercially and requirements to submit proprietary cost or pricing data to ensure that government contract pricing is fair and reasonable; |
| | • | | commercial customer price tracking requirements that require contractors to monitor pricing offered to a specified class of customers and to extend price reductions offered to that class of customers to the government; |
| | • | | reporting and compliance requirements related to, among other things: equal employment opportunity, affirmative action for veterans and for workers with disabilities, and accessibility for the disabled; |
| | • | | broader audit rights than we would usually grant to non-governmental customers; and |
| | • | | specialized remedies for breach and default or failure to meet service level commitments, including setoff rights, retroactive price adjustments, and civil or criminal fraud penalties, as well as mandatory administrative dispute resolution procedures instead of state contract law remedies. |
In addition, certain violations of federal law may subject government contractors to having their contracts terminated and, under certain circumstances, suspension and/or debarment from future government contracts.
Expansion to markets outside the United States will subject us to additional risks
One element of our growth strategy is to seek to expand our online services to markets outside the United States. In certain markets outside the United States, we expect to accomplish this through partnerships or joint ventures with other companies having expertise in the specific country or region, while in other such markets we expect to rely primarily on our own internal resources. For example, in certain markets outside of the United States, we are providing some of our online services in the local language directly to healthcare professionals. The provision of online services in foreign languages presents additional challenges. Our company has only recently begun this activity and, therefore, has limited experience in this area. Our participation in international markets is subject to certain other risks beyond those applicable to our operations in the United States, such as:
| | • | | challenges caused by cultural differences; |
| | • | | difficulties in staffing and managing operations from a distance; |
| | • | | uncertainty regarding liability for services and content; |
| | • | | burdens of complying with a wide variety of legal, regulatory and market requirements; |
| | • | | variability of economic and political conditions, including the extent of the impact of adverse economic conditions in markets outside the United States; |
| | • | | tariffs or other trade barriers; |
| | • | | fluctuations in currency exchange rates; |
| | • | | potentially adverse tax consequences, including restrictions on repatriation of earnings; and |
| | • | | difficulties in protecting intellectual property. |
Furthermore, outside the United States, we face competition from locally-based companies that have experience doing business in their home countries or regions and familiarity with local business practices, customs and laws and, as a result, generally do not face, or are better positioned to face, the risks described above.
38
Risks Related to the Internet and Our Technological Infrastructure
Any service interruption or failure in the systems that we use to provide online services could harm our business
Our online services are designed to operate 24 hours a day, seven days a week, without interruption. However, we have experienced and expect that we will in the future experience interruptions and delays in services and availability from time to time. We rely on internal systems as well as third-party vendors, including data center providers, bandwidth providers and mobile carriers, to provide our online services. We may not maintain redundant systems or facilities for some of these services. In the event of a catastrophic event with respect to one or more of these systems or facilities, we may experience an extended period of system unavailability, which could negatively impact our relationship with users. In addition, system failures may result in loss of data, including user registration data, business intelligence data, content, and other data critical to the operation of our online services, which could cause significant harm to our business and our reputation.
To operate without interruption or loss of data, both we and our service providers must guard against:
| | • | | damage from fire, power loss and other natural disasters; |
| | • | | communications failures; |
| | • | | software and hardware errors, failures and crashes; |
| | • | | security breaches, computer viruses, distributed denial-of-service (DDOS) attacks and similar disruptive problems; and |
| | • | | other potential service interruptions. |
Any disruption in the network access or co-location services provided by third-party providers to us or any failure by these third-party providers or our own systems to handle current or higher volume of use could significantly harm our business. We exercise little control over these third-party vendors, which increases our vulnerability to problems with services they provide.
Any errors, failures, interruptions or delays experienced in connection with these third-party technologies and information services or our own systems could negatively impact our relationships with users and adversely affect our brand and our business and could expose us to liabilities to third parties. Although we maintain insurance for our business, the coverage under our policies may not be adequate to compensate us for all losses that may occur. In addition, we cannot provide assurance that we will continue to be able to obtain adequate insurance coverage at an acceptable cost.
Implementation of additions to or changes in hardware and software platforms used to deliver our online services may result in performance problems and may not provide the additional functionality that was expected
From time to time, we implement additions to or changes in the hardware and software platforms we use for providing our online services. During and after the implementation of additions or changes, a platform may not perform as expected, which could result in interruptions in operations, an increase in response time or an inability to track performance metrics. In addition, in connection with integrating acquired businesses, we may move their operations to our hardware and software platforms or make other changes, any of which could result in interruptions in those operations. Any significant interruption in our ability to operate any of our online services could have an adverse effect on our relationships with users and clients and, as a result, on our financial results. We rely on a combination of purchasing, licensing, internal development, and acquisitions to develop our hardware and software platforms. Our implementation of additions to or changes in these platforms may cost more than originally expected, may take longer than originally expected, and may require more testing than originally anticipated. In addition, we cannot provide assurance that additions to or changes in these platforms will provide the additional functionality and other benefits that were originally expected.
39
If the systems we use to provide online portals experience security breaches or are otherwise perceived to be insecure, our business could suffer
We retain and transmit confidential information, including personal health records, in the processing centers and other facilities we use to provide online services. It is critical that these facilities and infrastructure remain secure and be perceived by the marketplace as secure. A security breach could damage our reputation or result in liability. We may be required to expend significant capital and other resources to protect against security breaches and hackers or to alleviate problems caused by breaches. Despite the implementation of security measures, this infrastructure or other systems that we interface with, including the Internet and related systems, may be vulnerable to physical break-ins, hackers, improper employee or contractor access, computer viruses, programming errors, denial-of-service attacks or other attacks by third parties or similar disruptive problems. Any compromise of our security, whether as a result of our own systems or the systems that they interface with, could reduce demand for our services and could subject us to legal claims from our clients and users, including for breach of contract or breach of warranty.
Our online services are dependent on the development and maintenance of the Internet infrastructure
Our ability to deliver our online services is dependent on the development and maintenance of the infrastructure of the Internet by third parties. The Internet has experienced a variety of outages and other delays as a result of damages to portions of its infrastructure, and it could face outages and delays in the future. The Internet has also experienced, and is likely to continue to experience, significant growth in the number of users and the amount of traffic. If the Internet continues to experience increased usage, the Internet infrastructure may be unable to support the demands placed on it. In addition, the reliability and performance of the Internet may be harmed by increased usage or by denial-of-service attacks. Any resulting interruptions in our services or increases in response time could, if significant, result in a loss of potential or existing users of and advertisers and sponsors on our Websites and, if sustained or repeated, could reduce the attractiveness of our services.
Customers who utilize our online services depend on Internet service providers and other Website operators for access to our Websites. All of these providers have experienced significant outages in the past and could experience outages, delays and other difficulties in the future due to system failures unrelated to our systems. Any such outages or other failures on their part could reduce traffic to our Websites.
Third parties may challenge the enforceability of our online agreements
The law governing the validity and enforceability of online agreements and other electronic transactions is evolving. We could be subject to claims by third parties that the online terms and conditions for use of our Websites, including disclaimers or limitations of liability, are unenforceable. A finding by a court that these terms and conditions or other online agreements are invalid could harm our business.
We could be subject to breach of warranty or other claims by clients of our online portals if the software and systems we use to provide them contain errors or experience failures
Errors in the software and systems we use could cause serious problems for clients of our online portals. We may fail to meet contractual performance standards or client expectations. Clients of our online portals may seek compensation from us or may seek to terminate their agreements with us, withhold payments due to us, seek refunds from us of part or all of the fees charged under those agreements or initiate litigation or other dispute resolution procedures. In addition, we could face breach of warranty or other claims by clients or additional development costs. Our software and systems are inherently complex and, despite testing and quality control, we cannot be certain that they will perform as planned.
We attempt to limit, by contract, our liability to our clients for damages arising from our negligence, errors or mistakes. However, contractual limitations on liability may not be enforceable in certain circumstances or may otherwise not provide sufficient protection to us from liability for damages. We maintain liability insurance coverage, including coverage for errors and omissions. However, it is possible that claims could exceed the amount of our applicable insurance coverage, if any, or that this coverage may not continue to be available on acceptable terms or in sufficient amounts. Even if these claims do not result in liability to us, investigating and
40
defending against them would be expensive and time consuming and could divert management’s attention away from our operations. In addition, negative publicity caused by these events may delay or hinder market acceptance of our services, including unrelated services.
Risks Related to the Healthcare Industry, Healthcare Regulation and Internet Regulation
Developments in the healthcare industry could adversely affect our business
Most of our revenue is derived from the healthcare industry and could be affected by changes affecting healthcare spending. We are particularly dependent on pharmaceutical, biotechnology and medical device companies for our advertising and sponsorship revenue. General reductions in expenditures by healthcare industry participants could result from, among other things:
| | • | | government regulation or private initiatives that affect the manner in which healthcare providers interact with patients, payers or other healthcare industry participants, including changes in pricing or means of delivery of healthcare products and services; |
| | • | | consolidation of healthcare industry participants; |
| | • | | reductions in governmental funding for healthcare; and |
| | • | | adverse changes in business or economic conditions affecting healthcare payers or providers, pharmaceutical, biotechnology or medical device companies or other healthcare industry participants. |
Federal and state legislatures and agencies periodically consider reforming aspects of the United States healthcare system. Significant federal healthcare reform legislation was enacted in March 2010, as discussed in the next risk factor. Additionally, in Europe, the national health care systems may be reformed from time to time.
Even if general expenditures by industry participants remain the same or increase, developments in the healthcare industry may result in reduced spending in some or all of the specific market segments that we serve or are planning to serve. For example, use of our products and services could be affected by:
| | • | | changes in the design of health insurance plans; |
| | • | | the timing of FDA, or European or other national regulatory authority, approvals of generic products that compete with existing brand name products and any increase in the number or significance of such approvals or of withdrawals of brand name products from the market; |
| | • | | the timing of FDA, or European or other national regulatory authority, approvals for new products or few new approved uses for existing products and any decrease in the number or significance of new drugs or medical devices coming to market or new approved uses for existing such products; and |
| | • | | decreases in marketing expenditures by pharmaceutical or medical device companies, including as a result of governmental regulation or private initiatives that discourage or prohibit advertising, sponsorship or educational activities by pharmaceutical or medical device companies or that discourage or prohibit their use of online services for some or all such activities. |
In addition, our customers’ expectations regarding pending or potential industry developments may also affect their budgeting processes and spending plans with respect to products and services of the types we provide.
The healthcare industry has changed significantly in recent years, and we expect that significant changes will continue to occur. However, the timing and impact of developments in the healthcare industry are difficult to predict. We cannot assure you that the markets for our products and services will continue to exist at current levels or that we will have adequate technical, financial and marketing resources to react to changes in those markets.
41
The Affordable Care Act could adversely affect our healthcare industry customers and clients, causing them to reduce expenditures, including expenditures for our services
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010 (which we refer to as the Affordable Care Act), was signed into law in March 2010. The Affordable Care Act makes extensive changes to the system of healthcare insurance and benefits in the U.S. In general, the Affordable Care Act seeks to reduce healthcare costs and decrease the number of uninsured legal U.S. residents by, among other things, requiring individuals to carry, and certain employers to offer, health insurance or be subject to penalties. The Affordable Care Act also imposes new regulations on health insurers, including guaranteed coverage requirements, prohibitions on certain annual and all lifetime limits on amounts paid on behalf of or to plan members, increased restrictions on rescinding coverage, establishment of minimum medical loss ratio requirements, a requirement to cover certain preventive services on a first dollar basis, the establishment of state insurance exchanges and essential benefit packages, and greater limitations on how health insurers price certain of their products. The Affordable Care Act also contains provisions that will affect the revenues and profits of pharmaceutical and medical device companies, including new taxes on certain sales of their products.
Many of the provisions of the Affordable Care Act that expand insurance coverage did not become effective until 2014, and some will not become effective until later, and many provisions will require additional regulations and interpretive guidance to be issued before they will be fully implemented. Some provisions do not apply to health plans that were in place when the Affordable Care Act was enacted and have not been substantially changed since. It is difficult to foresee how individuals and businesses will respond to the choices available to them under the Affordable Care Act. Furthermore, the Affordable Care Act will result in future state legislative and regulatory changes, which we are unable to predict at this time, in order for states to comply with certain provisions of the Affordable Care Act and to participate in grants and other incentive opportunities. In addition, Congress has considered various proposals to repeal some or all of the Affordable Care Act. Accordingly, while we do not currently anticipate any significant adverse effects on WebMD as a direct result of application of the Affordable Care Act to our business or on our company in its capacity as an employer, we are unable to predict what the indirect impacts of the Affordable Care Act will be on WebMD’s business through its effects on other healthcare industry participants, including pharmaceutical and medical device companies that are advertisers and sponsors of our public portals and employers and health plans that are clients of ourWebMD Health Servicesprivate portals. Healthcare industry participants may respond to the Affordable Care Act or to uncertainties created by the Affordable Care Act by reducing their expenditures or postponing expenditure decisions, including expenditures for our services, which could have a material adverse effect on our business.
Government regulation of healthcare creates risks and challenges with respect to our compliance efforts and our business strategies
The healthcare industry is highly regulated and is subject to changing political, legislative, regulatory and other influences. Existing and new laws and regulations affecting the healthcare industry could create unexpected liabilities for us, could cause us to incur additional costs and could restrict our operations. Many healthcare laws are complex, and their application to specific products, services, and business arrangements may not be clear. In particular, many existing healthcare laws and regulations, when enacted, did not anticipate the healthcare information services that we provide. However, these laws and regulations may nonetheless be applied to our products, services, and business arrangements. Our failure to accurately anticipate the application of these laws and regulations, or other failure to comply, could create liability for us, result in adverse publicity and negatively affect our business. Even in areas where we are not subject to healthcare regulation directly, we may become involved in governmental actions or investigations through our relationships with customers that are regulated, and participation in such actions or investigations, even if we are not a party and not the subject of an investigation, may cause us to incur significant expenses. Some of the risks we face from healthcare regulation are as follows:
| | • | | Regulation of Drug and Medical Device Advertising and Promotion. The WebMD Health Networkprovides services involving advertising and promotion of prescription and over-the-counter drugs and medical devices and claims of nutritional supplements. If the FDA or the Federal Trade Commission |
42
| | (FTC) finds that any of our products and services or any information onThe WebMD Health Network, in our mobile applications, or inWebMD Magazineviolates applicable regulations and guidance documents, they may take regulatory or judicial action against us and/or the advertiser or sponsor of that information. State attorneys general may take similar action based on their state’s consumer protection statutes. Any increase or change in regulation of drug or medical device advertising and promotion could make it more difficult for us to contract for sponsorships and advertising. In January 2014, the FDA issued a draft guidance clarifying the application of the FDA’s promotional regulations to certain content on social media Websites. We cannot predict how our customers or others in the industry might implement the FDA’s guidance in the future or how its implementation might affect our business. Recent private industry initiatives have resulted in voluntary restrictions, which advertisers and sponsors have agreed to follow. Advertising restrictions apply not only to our business in the United States but also to our operations in Europe. Our European Websites belonging toThe WebMD Health Network must comply with the national laws of the respective countries whose physicians they address. Under these European laws, there are several restrictions regarding advertising of drugs or medical devices. There are, in particular, broad prohibitions on the advertising of prescription or reimbursed drugs to the general public, the use of indirect or disguised marketing, and the offering and providing of gifts or benefits with promotional purpose which are not only of minor value. If the relevant European national competent authorities find that any of our products and services, or any information on our Websites or in our mobile applications, violated applicable regulations, they may take regulatory or judicial action against us and/or the advertisers or sponsors of that information. Moreover, our competitors, or even competitors of advertisers and sponsors, may take actions against us and/or advertisers or sponsors of the information. Our advertising and sponsorship revenue could be materially reduced by additional restrictions on the advertising of prescription drugs and medical devices to consumers, whether imposed by law or regulation or required under policies adopted by industry members. |
| | • | | Anti-Kickback Laws. There are federal and state laws that govern patient referrals, physician financial relationships and inducements to healthcare providers and patients. The federal healthcare program anti-kickback law prohibits any person or entity from offering, paying, soliciting or receiving anything of value, directly or indirectly, for the referral of patients covered by Medicare, Medicaid and other federal healthcare programs or the leasing, purchasing, ordering or arranging for or recommending the lease, purchase or order of any item, good, facility or service covered by these programs. Many states and European countries also have similar anti-kickback laws that are not necessarily limited to items or services for which payment is made by a government healthcare program. These laws are applicable to manufacturers and distributors and, therefore, may restrict how we and some of our customers market products to healthcare providers, including e-details. Any determination by a state, federal, or foreign regulatory agency that any of our practices violate any of these laws could subject us to civil or criminal penalties and require us to change or terminate some portions of our business and could have an adverse effect on our business. Even an unsuccessful challenge by regulatory authorities to our practices could result in adverse publicity and be costly for us to respond to. |
| | • | | False Claims Laws. The Federal False Claims Act imposes liability on any person or entity who, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment by a Federal healthcare program. In addition, various states and European countries have enacted false claim laws analogous to the Federal False Claims Act, and many of these laws apply where a claim is submitted to any third-party payor and not merely a federal healthcare program. When an entity is determined to have violated the Federal False Claims Act, it may be required to pay up to three times the actual damages sustained by the government plus civil penalties. In recent years an increasing number of Federal False Claims Act cases have been brought against drug manufacturers and resulted in significant monetary settlements and imposition of federally supervised corporate integrity agreements in circumstances that include allegations that company-sponsored CME was unlawful off-label promotion. Any action against us for violation of these laws could cause us to incur significant legal expenses and may adversely affect our ability to operate our business. Similarly, False Claims Act actions and resulting corporate integrity agreements involving our customers may influence their willingness to continue to use our services. |
43
| | • | | Medical Professional Regulation. The practice of most healthcare professions requires licensing under applicable state law, as well as under applicable national law of most of the European countries. In addition, the laws in some states and European countries prohibit business entities from practicing medicine. If a state or other enforcement authority determines that some portion of our business violates these laws, they may seek to have us discontinue those portions or subject us to penalties or licensure requirements. Any determination that we are a healthcare provider and have acted improperly as a healthcare provider may result in liability to us. |
| | • | | GINA. The Genetic Information Nondiscrimination Act (GINA) prohibits discrimination based on genetic information in employment and in health insurance coverage. The law applies to our private portal customers, including both employers and group health plans. WebMD’s Health Risk Assessment (or HRA), HealthQuotient, is typically offered to employees as a voluntary component of their employer-sponsored wellness program. Title I of GINA can have significant implications for wellness programs offered by group health plans in that it prohibits the collection of genetic information, which includes an individual’s family medical history, prior to or in connection with enrollment or for underwriting purposes. Underwriting purposes include providing incentives or rewards for completion of an HRA that requests genetic information. Title II of GINA prohibits employment discrimination based on genetic information, as well as the request or purchase of genetic information of employees or their family members with limited exceptions, including a limited exception for voluntary wellness programs. WebMD may face challenges as a result of varying interpretations of the law by our customers and by the multiple enforcing agencies including the U.S. Departments of Health and Human Services (HHS), Labor and Treasury and the Equal Employment Opportunity Commission. Interpretations of the law have required us to modify the HealthQuotient product, and we could experience increases in operational costs or decreases in demand for our products. State legislation, such as recent legislation in California prohibiting any form of discrimination by businesses based on genetic information, including in housing, public accommodation, and the provision of emergency services, could have additional implications for service we provide in those states. Similar restrictions may also apply in European countries. |
In September 2013, the FDA issued final guidance regarding mobile medical applications. The FDA intends to regulate only those mobile applications that meet the agency’s definition of “device” and could pose a risk to patients’ safety if they fail to work as intended. The FDA intends to exercise enforcement discretion with respect to certain lower risk mobile applications that meet the device definition. Mobile applications that do not meet the device definition are beyond the FDA’s jurisdiction, and therefore, not subject to the agency’s oversight. We believe that none of our existing online services and mobile applications are subject to regulation as a medical device under applicable FDA regulations. We are required to determine whether FDA regulations would apply to any of our applications and the FDA could disagree with the determination we have made. It is also possible that products or services that we may offer in the future could subject us to such regulation or that current rules could change or be interpreted to apply to some of our existing online services or mobile applications. Complying with such regulations could be burdensome and expensive and could delay our introduction of new services or applications.
We may be subject to claims brought against us as a result of content we provide
Consumers access health-related information through our online services, including information regarding particular medical conditions and possible adverse reactions or side effects from medications. Physicians and other healthcare professionals use our services to access clinical reference sources, commentary from leading medical experts, medical news, and coverage of professional meetings and conferences. If our content, or content we obtain from third parties, contains inaccuracies, it is possible that physicians, consumers, employees, health plan members or others may sue us for various causes of action. Although our Websites and mobile applications contain terms and conditions, including disclaimers of liability, that are intended to reduce or eliminate our liability, the law governing the validity and enforceability of online agreements and other electronic transactions is evolving. We could be subject to claims by third parties that our online agreements with consumers and physicians that provide the terms and conditions for use of our public or private portals or mobile applications are unenforceable. A finding by a court that these agreements are invalid and that we are subject to liability could harm our business and require costly changes to our business.
44
We have editorial procedures in place to provide quality control of the information that we publish or provide. However, we cannot assure you that our editorial and other quality control procedures will be sufficient to ensure that there are no errors or omissions in particular content. Even if potential claims do not result in liability to us, investigating and defending against these claims could be expensive and time-consuming and could divert management’s attention away from our operations. In addition, our business is based on establishing the reputation of our portals as trustworthy and dependable sources of healthcare information. Allegations of impropriety or inaccuracy, even if unfounded, could harm our reputation and business.
Government regulation of the Internet could adversely affect our business
The Internet and its associated technologies are subject to government regulation. However, whether and how existing laws and regulations in various jurisdictions, including privacy and consumer protection laws, apply to the Internet is still uncertain. Our failure, or the failure of our business partners or third-party service providers, to accurately anticipate the application of these laws and regulations to our products and services and the manner in which we deliver them, or any other failure to comply with such laws and regulations, could create liability for us, result in adverse publicity and negatively affect our business. In addition, new laws and regulations, or new interpretations of existing laws and regulations, may be adopted with respect to the Internet and online services, including in areas such as user privacy, confidentiality, consumer protection, marketing, pricing, content, copyrights and patents, and characteristics and quality of products and services. We cannot predict how these laws or regulations will affect our business.
In Europe, the respective healthcare advertising laws stipulate several restrictions on advertising of drugs and medical devices to the public. In particular, in several countries, the advertising of prescription drugs to the general public is not allowed. Thus, these European countries require access restrictions for Websites that contain such advertisements, which are only allowed to be addressed to healthcare professionals. This means these Websites ofThe WebMD Health Network that are addressed to physicians in specific European countries (such as the Medscape Germany or France Websites) must be accessible only to healthcare professionals by an appropriate access check. If the respective European competent authority does not acknowledge the respective Website to have appropriate access controls, the authority may require us and/or our European entity to establish stricter access controls or ultimately may take action against us and/or our European entity.
Internet and mobile user privacy, personal data security and the use of consumer information to track online activities are major issues both in the United States and abroad. For example, in February 2009, the FTC published Self-Regulatory Principles to govern the tracking of consumers’ activities online in order to deliver advertising targeted to the interests of individual consumers (sometimes referred to as behavioral advertising). These principles serve as guidelines to the industry. In December 2010, following a series of workshops, the FTC issued a preliminary staff report containing a proposed framework for businesses and policymakers for online consumer privacy issues and, in March 2012, the FTC issued a final report setting forth its current views on best practices, to protect the privacy of consumers, to be implemented by companies that collect and use consumer data. Also in March 2012, the White House released a Privacy White Paper that outlined the Obama Administration’s proposal for a new American privacy framework based on a Consumer Bill of Privacy Rights and which called for the development of industry-specific voluntary, enforceable privacy codes of conduct through a collaborative multi-stakeholder process. Both the FTC and the White House called for Congress to develop baseline privacy legislation and the FTC also called on industry to accelerate the pace of self-regulation. In addition, earlier in 2013, the FTC issued a staff report regarding mobile privacy disclosures that included recommendations for privacy disclosures for mobile applications, and the California Attorney General also issued mobile application privacy guidelines. The FTC and state attorneys general continue to pay close attention to Internet privacy issues and the FTC in 2014 plans to hold a seminar focusing on privacy issues associated with “consumer generated and controlled health data,” which may be relevant to services we offer. The FTC and state attorneys general have otherwise been active in investigating and entering into consent decrees under their current unfair or deceptive trade practices authority with companies because of their online privacy and data security practices. There is a possibility of legislation, regulation and increased enforcement activities relating to privacy and behavioral advertising. For example, the FTC issued revised Children’s Online Privacy Protection Act (COPPA) rules in late 2012 that broaden the scope of the regulations, and amended Federal Communications Commission (FCC) rules under the Telephone Consumer Protection Act (TCPA) relating to certain forms of
45
telemarketing and telephone calls, including text messages, took effect in October 2013. The TCPA’s private right of action and statutory damages has made it increasingly popular for class action litigation, and litigation or liability under the TCPA could adversely affect our business. In addition, some bills have been introduced in Congress, and more are expected, that, if passed, could impose substantial new regulations on online behavioral advertising activities. In addition, changes in industry practice (whether on their own or when combined with regulatory changes) could adversely impact our ability to deliver advertisements based on online behavior. For example, it is possible that at some point in the future, it will be a common Internet practice for Websites to honor “Do Not Track” settings in Internet browsers that are turned on by default. Whether through industry practice or in combination with government regulation, such a development could limit our ability to serve advertisements to consumers based on online behavior on third party sites or on our sites, which could adversely affect our revenue.
In Europe, Directive 2009/136/EC of the European Parliament and of the Council requires the user’s full information and consent prior to the installation and use of any so-called “cookie” on a user’s computer. This Directive has been implemented differently, if at all, in member states of the European Union and national requirements to remain compliant with the respective law may vary. Nevertheless, the provisions of this directive, whether effectively implemented in national laws, are now applicable in all the member states of the European Union and enforcement actions are now being considered by local data protection authorities. In addition, in January 2012, the European Commission published a draft General Data Protection Regulation on data protection for the revision of the currently applicable data protection framework. The potential resulting new framework sets out additional requirements for users’ consent for offline and online marketing. If enacted, this instrument will further strengthen the already very densely regulated area of Internet privacy in Europe. In addition, this revised European legislation, if adopted, would increase the likelihood of applicability of European law to entities established outside the European Union but processing data of European data subjects.
We have privacy policies posted on our Websites that we believe comply with existing applicable laws requiring notice to users about our information collection, use and disclosure practices. We also notify users about our information collection, use and disclosure practices relating to data we receive through offline means such as paper health risk assessments. Moreover, we take steps to reasonably protect certain sensitive personal information we hold. We cannot assure you that the privacy policies and other statements we provide to users of our products and services, or our practices, will be found sufficient to protect us from liability or adverse publicity in this area. A determination by a state or federal agency or court, or European data protection authority or competent court, that any of our practices do not meet applicable standards, or the implementation of new standards or requirements, could adversely affect our business.
Failure to comply with laws relating to privacy and security of personal information, including personal health information, could result in liability to us and concerns about privacy-related issues could damage our reputation and our business
Privacy and security of personal information stored or transmitted electronically, including personal health information, is a major issue in the United States and abroad. While we strive to comply with all applicable privacy and security laws and regulations, as well as our own posted privacy policies, legal standards for privacy including, but not limited to, “unfairness” and “deception” as enforced by the FTC and state attorneys general continue to evolve and any failure or perceived failure to comply may result in proceedings or actions against us by government entities or others, or could cause us to lose users and customers, which could have a material adverse effect on our business. There has been an increase in the number of private privacy-related lawsuits filed against companies recently. In addition, we are unable to predict what additional legislation or regulation in the area of privacy of personal information, including personal health information, could be enacted and what effect that could have on our operations and business. Concerns about our practices with regard to the collection, use, disclosure, or security of personal information or other privacy-related matters, even if unfounded and even if we are in compliance with applicable laws, could damage our reputation and harm our business.
The Privacy Standards and Security Standards under the Health Insurance Portability and Accountability Act of 1996 (or HIPAA), as amended by the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009, establish a set of national privacy and security standards for the protection of individually identifiable health information by health plans, healthcare clearinghouses and healthcare providers
46
(referred to as “covered entities”) and their “business associates,” which are persons or entities that perform certain services for, or on behalf of, a covered entity that involve the use or disclosure of protected health information. Certain portions of our business, such as those managing employee or plan member health information for employers or health plans, are subject to HIPAA as business associates of covered entities. In addition to imposing privacy and security requirements, HIPAA also creates obligations for us to report any unauthorized use or disclosure of protected health information, known as a breach, to our covered entity customers. The 2013 final HITECH rule modifies the breach reporting standard in a manner that will likely make more data security incidents qualify as reportable breaches. In addition, HITECH and its implementing regulations impose similar data breach notification requirements on vendors of personal health records that require us to notify affected individuals and the FTC in the event of a data breach involving the unsecured personal information of users of our public portal services. Violations of HIPAA may result in civil and criminal penalties and could damage our reputation and harm our business. HITECH increased civil penalty amounts for violations of HIPAA and significantly strengthens enforcement by requiring the HHS to conduct periodic audits to confirm compliance and authorizing state attorneys general to bring civil actions seeking either injunctions or damages in response to violations of HIPAA Privacy Standards and Security Standards that threaten the privacy of state residents. We cannot assure you that we will adequately address the risks created by these amended HIPAA Privacy Standards and Security Standards. In addition, we are unable to predict what changes to these Standards might be made in the future or how those changes, or other changes in applicable laws and regulations, could affect our business.
In Europe, the current national implementations of the existing general data protection Directive 95/46/EC and of the e-Privacy Directive 2002/58/EC provide for criminal and administrative sanctions in case of violations, even though criminal sanctions are very rarely imposed. For example, France and Germany provide for administrative fines of up to 300,000 Euros (approximately 360,000 USD) in case of illegal collection or processing of personal identifiable information. Under the new draft General Data Protection Regulation on data protection proposed by the European Commission in January 2012, as modified by the European Parliament in October 2013, fines of up to 100,000,000 Euros (approximately 120,000,000 USD) or up to 5% of the global turnover of the infringer could be imposed.
Failure to maintain CME accreditation could adversely affect Medscape, LLC’s ability to provide online CME offerings
Medscape, LLC’s continuing medical education (or CME) activities are planned and implemented in accordance with the current Essential Areas and Elements and the Policies of the Accreditation Council for Continuing Medical Education (or ACCME), which oversees providers of CME credit, and other applicable accreditation standards. ACCME’s standards for commercial support of CME are intended to assure, among other things, that CME activities of ACCME-accredited providers, such as Medscape, LLC, are independent of “commercial interests,” which are defined as entities that produce, market, re-sell or distribute healthcare goods and services, excluding certain organizations. “Commercial interests,” and entities owned or controlled by “commercial interests,” are ineligible for accreditation by the ACCME.
From time to time, the ACCME revises its standards for commercial support of CME. As a result of certain past ACCME revisions, we adjusted our corporate structure and made changes to our management and operations intended to allow Medscape, LLC to provide CME activities that are developed independently from programs developed by its sister companies, which may not be independent of “commercial interests.” We believe that these changes allow Medscape, LLC to satisfy the applicable standards.
Medscape, LLC’s current ACCME accreditation expires in 2016. In order for Medscape, LLC to renew its accreditation, it will be required to demonstrate to the ACCME that it continues to meet ACCME requirements. If Medscape, LLC fails to maintain its status as an accredited ACCME provider (whether at the time of such renewal or at an earlier time as a result of a failure to comply with existing or additional ACCME standards), it will not be permitted to accredit CME activities for physicians and other healthcare professionals. Instead, Medscape, LLC would be required to use third parties to provide such CME-related services. That, in turn, could discourage potential supporters from engaging Medscape, LLC to develop CME or education-related activities, which could have a material adverse effect on our business.
47
CME regulations also apply in other countries. For example, under German law, certain CME programs must be approved by the State Medical Chamber. Additionally, German CME-related services must be free of commercial/business interests and the provider of CME services must be compliant with German laws and regulations. In France, a similar new regulatory framework that restricts the organization of CME activities has been completed. These or similar restrictions in other countries may restrict our ability to carry out activities related to CME programs and/or refer to drugs or medical devices in such CME programs. Moreover, if we are not able to demonstrate compliance with these regulations, applicable approvals may not be obtained from governmental authorities, which may impact our ability to provide CME-related services and which could have an adverse effect on our business.
Government regulation and industry initiatives could adversely affect the volume of sponsored online CME programs implemented through our Websites or require changes to how Medscape, LLC offers CME
CME activities may be subject to government oversight or regulation by Congress, the FDA, HHS, and state regulatory agencies. Medscape, LLC and/or the sponsors of the CME activities that Medscape, LLC accredits may be subject to enforcement actions if any of these CME activities are deemed improperly promotional, potentially leading to the termination of sponsorships. Medscape, LLC and/or the sponsors of the CME activities that Medscape, LLC accredits also could be affected by industry initiatives regarding funding for CME.
During the past several years, educational activities, including CME, directed at physicians have been subject to increased governmental scrutiny to ensure that sponsors do not influence or control the content of the activities. The Department of Justice continues to examine CME sponsorship by manufacturers. In response, pharmaceutical and medical device companies have developed and implemented internal controls and procedures that promote adherence to applicable regulations and requirements. In implementing these controls and procedures, supporters of CME may interpret the regulations and requirements differently and may implement varying procedures or requirements. These controls and procedures:
| | • | | may discourage pharmaceutical companies from providing grants for independent educational activities; |
| | • | | may slow their internal approval for such grants; |
| | • | | may reduce the volume of sponsored educational programs that Medscape, LLC produces to levels that are lower than in the past, thereby reducing revenue; and |
| | • | | may require Medscape, LLC to make changes to how it offers or provides educational programs, including CME. |
In June 2011, the American Medical Association’s House of Delegates approved a report entitled “Financial Relationships with Industry in Continuing Medical Education” that largely adopts the CME ethical principles already espoused by other industry and accreditation organizations, including ACCME, PhRMA, and AdvaMed. Although the report recognizes that industry support of CME may help make CME more accessible and affordable, the report proposes that CME should, when possible, be provided without commercial support and without the participation of individuals who have financial interest in the educational subject matter. It is possible that the recommendations contained in this report, or other voluntary industry guidelines, could negatively influence the availability of commercial support for Medscape CME programs and/or physician participation in Medscape CME programs funded by commercial support.
Future changes to laws, regulations or accreditation standards, or to the internal compliance programs of supporters or potential supporters, may further discourage, significantly limit, or prohibit supporters or potential supporters from engaging in educational activities with Medscape, LLC, or may require Medscape, LLC to make further changes in the way it offers or provides educational activities.
Failure to comply with applicable anti-corruption laws could subject us to penalties and other adverse consequences
The United States and other countries have adopted anti-corruption laws that generally prohibit directly or indirectly giving, offering or promising inducements to public officials to elicit an improper commercial advantage. Under applicable U.S., German, and most European law, this prohibition has been interpreted to apply
48
to doctors and other medical professionals who work in state-run hospitals and state-run healthcare systems. Some of these laws also prohibit directly or indirectly giving, offering or promising (and, in some cases, accepting or soliciting) inducements to (or from) private parties to elicit (or grant) an improper commercial advantage. In recent years, the U.S. Government has brought enforcement actions that led to significant monetary penalties against several companies operating in the global healthcare industry for violations of anti-corruption laws resulting from illegal payments made to non-U.S. medical professionals.
As our business expands outside the United States, we (and others acting on our behalf) increasingly interact with non-U.S. doctors and other medical professionals, at least some of whom work in state-run hospitals or healthcare systems. Such interactions inherently increase the risk of violating applicable anti-corruption laws. While we believe that we have appropriate compliance policies and procedures in place to mitigate such risk, our personnel and others acting on our behalf could engage in conduct that violates such laws, for which we could be held responsible. Under such circumstances, we could be subject to civil and/or criminal penalties and other consequences that could have a material adverse effect on our business, financial condition and results of operations. In addition, our brand and reputation, our sales activities and the price of our Common Stock and other securities could be adversely affected if we were to become the target of any resulting negative publicity.
Other Risks Applicable to Our Company and to Ownership of Our Securities
Provisions in our organizational documents and Delaware law may inhibit a takeover, which could adversely affect the value of our Common Stock
Our Restated Certificate of Incorporation and Bylaws, as well as Delaware corporate law, contain provisions that could delay or prevent a change of control or changes in our management and board of directors that holders of our Common Stock might consider favorable and may prevent them from receiving a takeover premium for their shares. These provisions include, for example, our classified board structure and the authorization of our board of directors to issue up to 50 million shares of preferred stock without a stockholder vote. In addition, our Restated Certificate of Incorporation provides that stockholders may not act by written consent and may not call special meetings. These provisions apply even if an offer to purchase our company may be considered beneficial by some of our stockholders. If a change of control or change in management is delayed or prevented, the market price of our Common Stock could decline.
If certain transactions occur with respect to our capital stock, limitations may be imposed on our ability to utilize net operating loss carryforwards and tax credits to reduce our income taxes
WebMD has substantial accumulated net operating loss (NOL) carryforwards and tax credits available to offset taxable income in future tax periods. If certain transactions occur with respect to WebMD’s capital stock (including issuances, redemptions, recapitalizations, exercises of options, conversions of convertible debt, purchases or sales by 5%-or-greater shareholders and similar transactions) that result in a cumulative change of more than 50% of the ownership of capital stock over a three-year period (as determined under rules prescribed by Section 382 of the U.S. Internal Revenue Code and applicable Treasury regulations), an annual limitation would be imposed with respect to the ability to utilize WebMD’s NOL carryforwards and federal tax credits that existed at the time of the ownership change.
In November 2008, HLTH repurchased shares of its Common Stock in a tender offer. The tender offer resulted in a cumulative change of more than 50% of the ownership of HLTH’s capital, as determined under rules prescribed by Section 382 of the Code and applicable Treasury regulations. As a result of this ownership change, there is an annual limitation imposed on the amount of the NOL carryforwards and federal tax credits existing at the time of the ownership change that we may use to offset income in each tax year following the ownership change.
On April 3, 2012, WebMD completed a tender offer through which we repurchased 5,769,230 shares of WebMD Common Stock at a price of $26.00 per share (the “2012 Tender Offer”). On September 10, 2013, WebMD completed a tender offer through which we repurchased 5,000,000 shares of WebMD Common Stock at
49
a price of $34.00 per share (the “2013 Tender Offer”). Completion of the 2012 Tender Offer and the 2013 Tender Offer may increase the possibility of another ownership change and corresponding annual limitation, which could decrease the existing annual limitation and would apply to all NOL carryforwards and tax credits generated prior to this potential new ownership change.
We may not be successful in protecting our intellectual property and proprietary rights
Our intellectual property and proprietary rights are important to our businesses. The steps that we take to protect our intellectual property, proprietary information and trade secrets may prove to be inadequate and, whether or not adequate, may be expensive. We rely on a combination of trade secret, patent and other intellectual property laws and confidentiality procedures and non-disclosure contractual provisions to protect our intellectual property. We cannot assure you that we will be able to detect potential or actual misappropriation or infringement of our intellectual property, proprietary information or trade secrets. Even if we detect misappropriation or infringement by a third party, we cannot assure you that we will be able to enforce our rights at a reasonable cost, or at all. In addition, our rights to intellectual property, proprietary information and trade secrets may not prevent independent third-party development and commercialization of competing products or services.
Third parties may claim that we are infringing their intellectual property, and we could suffer significant litigation or licensing expenses or be prevented from providing certain services, which may harm our business
We have been, and may continue to be, subject to claims that we are misappropriating or infringing intellectual property or other proprietary rights of others. These claims, even if not meritorious, may be expensive to defend and divert management’s attention from our operations. If we become liable to third parties for infringing these rights, we could be required to pay a substantial damage award and to develop non-infringing technology, obtain a license or cease selling the products or services that use or contain the infringing intellectual property. We may be unable to develop non-infringing products or services or obtain a license on commercially reasonable terms, or at all. We may also be required to indemnify our customers if they become subject to third-party claims relating to intellectual property that we license or otherwise provide to them, which could be costly.
Acquisitions, business combinations and other transactions may be difficult to complete and, if completed, may have negative consequences for our business and our security holders
WebMD has been built, in part, through acquisitions. We intend to continue to seek to acquire or to engage in business combinations with companies engaged in complementary businesses. In addition, we may enter into joint ventures, strategic alliances or similar arrangements with third parties. These transactions may result in changes in the nature and scope of our operations and changes in our financial condition. Our success in completing these types of transactions will depend on, among other things, our ability to locate suitable candidates and negotiate mutually acceptable terms with them, and to obtain adequate financing. Significant competition for these opportunities exists, which may increase the cost of and decrease the opportunities for these types of transactions. Financing for these transactions may come from several sources, including:
| | • | | cash and cash equivalents on hand and marketable securities; |
| | • | | proceeds from the incurrence of indebtedness; and |
| | • | | proceeds from the issuance of common stock, preferred stock, convertible debt or of other securities. |
The issuance of additional equity or debt securities could:
| | • | | cause substantial dilution of the percentage ownership of our stockholders at the time of the issuance; |
| | • | | cause substantial dilution of our earnings per share; |
| | • | | subject us to the risks associated with increased leverage, including a reduction in our ability to obtain financing or an increase in the cost of any financing we obtain; |
50
| | • | | subject us to restrictive covenants that could limit our flexibility in conducting future business activities; and |
| | • | | adversely affect the prevailing market price for our outstanding securities. |
We do not intend to seek security holder approval for any such acquisition or security issuance unless required by applicable law, regulation or the terms of then-existing securities.
Our business will suffer if we fail to successfully integrate acquired businesses and technologies or to assess the risks in particular transactions
We have in the past acquired, and may in the future acquire, businesses, technologies, services, product lines and other assets. The successful integration of the acquired businesses and assets into our operations, on a cost-effective basis, can be critical to our future performance. The amount and timing of the expected benefits of any acquisition, including potential synergies between our company and the acquired business, are subject to significant risks and uncertainties. These risks and uncertainties include, but are not limited to, those relating to:
| | • | | our ability to maintain relationships with the customers of the acquired business; |
| | • | | our ability to retain or replace key personnel of the acquired business; |
| | • | | potential conflicts in sponsor or advertising relationships or in relationships with strategic partners; |
| | • | | our ability to coordinate organizations that are geographically diverse and may have different business cultures; and |
| | • | | compliance with regulatory requirements. |
We cannot guarantee that any acquired businesses will be successfully integrated with our operations in a timely or cost-effective manner, or at all. Failure to successfully integrate acquired businesses or to achieve anticipated operating synergies, revenue enhancements or cost savings could have a material adverse effect on our business, financial condition and results of operations.
Although our management attempts to evaluate the risks inherent in each transaction and to value acquisition candidates appropriately, we cannot assure you that we will properly ascertain all such risks or that acquired businesses and assets will perform as we expect or enhance the value of our company as a whole. In addition, acquired companies or businesses may have larger than expected liabilities that are not covered by the indemnification, if any, that we are able to obtain from the sellers.
We may not be able to raise additional funds when needed for our business or to exploit opportunities
Our future liquidity and capital requirements will depend upon numerous factors, including the success of our service offerings, market developments, and repurchases of our Common Stock. We may need to raise additional funds to support expansion, develop new or enhanced applications and services, respond to competitive pressures, acquire complementary businesses or technologies or take advantage of unanticipated opportunities. If required, we may raise such additional funds through public or private debt or equity financing, strategic relationships or other arrangements. There can be no assurance that such financing will be available on acceptable terms, if at all, or that such financing will not be dilutive to our stockholders.
| Item 1B. | Unresolved Staff Comments |
None.
We believe that our company’s offices and other facilities are, in general, in good operating condition and adequate for our current operations and that additional leased space in appropriate locations can be obtained on acceptable terms if needed.
51
We lease approximately 100,000 square feet of office space in New York City for our corporate headquarters and certain of our operations under a lease for which the original term expires in December 2015 and, at our option, can be extended to December 2020. We also lease additional office space in New York City and lease office space and operational facilities in: Elmwood Park, New Jersey; Atlanta, Georgia; Montreal, Canada; Chicago, Illinois; Ashburn, Virginia; Indianapolis, Indiana; Portland, Oregon; San Clemente and San Diego, California; Redmond, Washington; and Paris, France.
The information relating to legal proceedings contained in Note 7 to the Consolidated Financial Statements included in this Annual Report is incorporated herein by this reference.
| Item 4. | Mine Safety Disclosures |
Not applicable.
52
PART II
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Market Information
We completed the initial public offering of our Class A Common Stock on September 28, 2005. Our Class A Common Stock began trading on the Nasdaq National Market under the symbol “WBMD” on September 29, 2005. Upon completion of our merger with HLTH Corporation in October 2009 and the resulting cancellation of our Class B Common Stock (all of which had been owned by HLTH), our Class A Common Stock began being referred to simply as Common Stock. Our Common Stock now trades on the Nasdaq Global Select Market. The high and low prices of our Common Stock for each quarterly period during the last two fiscal years are as follows:
| | | | | | | | |
| | | High | | | Low | |
2012 | | | | | | | | |
First quarter | | $ | 40.24 | | | $ | 24.51 | |
Second quarter | | | 25.71 | | | | 20.18 | |
Third quarter | | | 20.99 | | | | 13.52 | |
Fourth quarter | | | 16.82 | | | | 13.13 | |
2013 | | | | | | | | |
First quarter | | $ | 24.85 | | | $ | 14.74 | |
Second quarter | | | 31.63 | | | | 22.23 | |
Third quarter | | | 35.28 | | | | 26.07 | |
Fourth quarter | | | 40.86 | | | | 28.14 | |
The market price of our Common Stock has fluctuated in the past and is likely to fluctuate in the future. Changes in the market price of our Common Stock may result from, among other things:
| | • | | quarter-to-quarter variations in operating results; |
| | • | | operating results being different from our previously announced guidance or from analysts’ estimates or opinions; |
| | • | | changes in analysts’ or financial commentators’ earnings estimates, ratings or opinions; |
| | • | | changes in financial guidance or other forward-looking information; |
| | • | | new products, services or pricing policies introduced by us or our competitors; |
| | • | | acquisitions by us or our competitors; |
| | • | | developments in existing customer relationships; |
| | • | | actual or perceived changes in our business strategy; |
| | • | | developments in new or pending litigation and claims; |
| | • | | sales of large amounts of our Common Stock; |
| | • | | changes in general business or regulatory conditions affecting the healthcare, information technology or Internet industries; |
| | • | | changes in general economic conditions; and |
| | • | | fluctuations in the securities markets in general. |
In addition, the market prices of our Common Stock and of the stock of other Internet-related companies have experienced large fluctuations, sometimes quite rapidly. These fluctuations often may be unrelated to or disproportionate to operating performance.
53
Holders
On February 24, 2014, there were approximately 1,470 holders of record of our Common Stock. Because many of these shares are held by brokers and other institutions on behalf of stockholders, we are unable to determine the total number of stockholders represented by these record holders, but we believe there are more than 20,000 holders of our Common Stock.
Dividends
We have never declared or paid any cash dividends on our Common Stock, and we do not anticipate paying cash dividends in the foreseeable future.
Repurchases of Equity Securities During the Fourth Quarter of 2013
The following table provides information about purchases by WebMD during the three months ended December 31, 2013 of equity securities that are registered by us pursuant to Section 12 of the Exchange Act:
Issuer Purchases of Equity Securities
| | | | | | | | | | | | | | | | |
Period | | Total
Number of
Shares
Purchased(1) | | | Average Price
Paid per Share | | | Total Number of
Shares Purchased as
Part of Publicly
Announced Plans or
Programs(2) | | | Approximate
Dollar Value of
Shares that May Yet
Be Purchased Under
the Plans or
Programs(2) | |
10/01/13 – 10/31/13 | | | 5,544,374 | (3) | | $ | 32.09 | | | | 15,750 | | | $ | 53,185,205 | |
11/01/13 – 11/30/13 | | | 865,373 | | | $ | 35.33 | | | | 839,301 | | | $ | 23,504,647 | |
12/01/13 – 12/31/13 | | | 101,719 | | | $ | 36.77 | | | | 99,130 | | | $ | 19,864,016 | |
| | | | | | | | | | | | | | | | |
Total | | | 6,511,466 | | | $ | 32.59 | | | | 954,181 | | | | | |
| | | | | | | | | | | | | | | | |
| (1) | Includes the following number of shares withheld from WebMD Restricted Common Stock that vested during the respective periods in order to satisfy withholding tax requirements related to the vesting of the awards: 1,191 in October; 26,072 in November; and 2,589 in December. The value of these shares was determined based on the closing price of WebMD Common Stock on the date of vesting. |
| (2) | In August 2011, a stock repurchase program (the “Program”) was established through which WebMD was authorized to use up to $75,000,000 to purchase shares of WebMD Common Stock. During October 2011, WebMD’s Board of Directors authorized a $75,000,000 increase to the Program. In February 2014 (after the period covered in this table), WebMD’s Board authorized a $50,000,000 increase to the Program. For additional information, see Note 10 to the Consolidated Financial Statements included in this Annual Report. |
| (3) | In October 2013, WebMD repurchased 5,527,433 shares of WebMD Common Stock that were beneficially owned by Carl C. Icahn and certain of his affiliates at a price of $32.08 per share. For additional information, see Note 10 to the Consolidated Financial Statements included in this Annual Report. |
54
Performance Graph
The following graph compares the cumulative total stockholder return on WebMD Common Stock with the comparable cumulative return of the NASDAQ Composite Index and the Research Data Group (RDG) Internet Composite Index over the period of time covered in the graph. The graph assumes that $100 was invested in WebMD Common Stock and in each index on December 31, 2008. The stock price performance on the following graph is not necessarily indicative of future stock price performance.
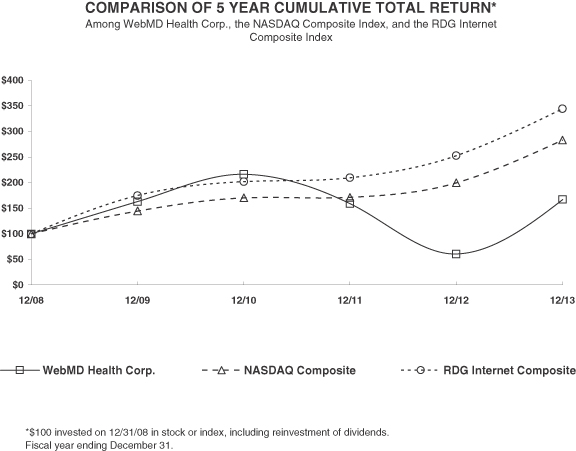
55
| Item 6. | Selected Financial Data |
The following selected consolidated financial data should be read in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and with the Consolidated Financial Statements and notes thereto, which are included elsewhere in this Annual Report.
| | | | | | | | | | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | | | 2010 | | | 2009(1) | |
| | | (In thousands, except per share data) | |
Consolidated Statements of Operations Data: | | | | | | | | | | | | | | | | | | | | |
Revenue | | $ | 515,293 | | | $ | 469,866 | | | $ | 558,775 | | | $ | 534,519 | | | $ | 438,536 | |
Cost of operations | | | 209,740 | | | | 216,361 | | | | 201,677 | | | | 187,831 | | | | 165,753 | |
Sales and marketing | | | 127,997 | | | | 127,659 | | | | 124,326 | | | | 120,874 | | | | 112,101 | |
General and administrative | | | 93,220 | | | | 97,618 | | | | 91,271 | | | | 85,496 | | | | 89,620 | |
Depreciation and amortization | | | 26,606 | | | | 28,399 | | | | 26,801 | | | | 27,578 | | | | 28,185 | |
Interest income | | | 76 | | | | 86 | | | | 112 | | | | 3,949 | | | | 9,149 | |
Interest expense | | | 22,826 | | | | 23,334 | | | | 20,645 | | | | 11,453 | | | | 23,515 | |
Loss (gain) on convertible notes | | | 4,871 | | | | — | | | | — | | | | 23,332 | | | | (10,120 | ) |
Gain (loss) on investments | | | — | | | | 8,074 | | | | 18,516 | | | | (9,517 | ) | | | — | |
Restructuring | | | — | | | | 7,579 | | | | — | | | | — | | | | — | |
Transaction, severance and other expense | | | 1,353 | | | | 2,297 | | | | 2,328 | | | | 72 | | | | 12,435 | |
| | | | | | | | | | | | | | | | | | | | |
Income (loss) from continuing operations before income tax provision (benefit) | | | 28,756 | | | | (25,221 | ) | | | 110,355 | | | | 72,315 | | | | 26,196 | |
Income tax provision (benefit) | | | 13,640 | | | | (2,134 | ) | | | 46,167 | | | | 20,043 | | | | (45,491 | ) |
| | | | | | | | | | | | | | | | | | | | |
Consolidated income (loss) from continuing operations | | | 15,116 | | | | (23,087 | ) | | | 64,188 | | | | 52,272 | | | | 71,687 | |
Consolidated income from discontinued operations, net of tax | | | — | | | | 2,743 | | | | 10,388 | | | | 1,800 | | | | 49,354 | |
| | | | | | | | | | | | | | | | | | | | |
Consolidated net income (loss) inclusive of noncontrolling interest | | | 15,116 | | | | (20,344 | ) | | | 74,576 | | | | 54,072 | | | | 121,041 | |
Income attributable to noncontrolling interest | | | — | | | | — | | | | — | | | | — | | | | (3,705 | ) |
| | | | | | | | | | | | | | | | | | | | |
Net income (loss) attributable to Company stockholders | | $ | 15,116 | | | $ | (20,344 | ) | | $ | 74,576 | | | $ | 54,072 | | | $ | 117,336 | |
| | | | | | | | | | | | | | | | | | | | |
Amounts attributable to Company stockholders: | | | | | | | | | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 15,116 | | | $ | (23,087 | ) | | $ | 64,188 | | | $ | 52,272 | | | $ | 67,018 | |
Income from discontinued operations | | | — | | | | 2,743 | | | | 10,388 | | | | 1,800 | | | | 50,318 | |
| | | | | | | | | | | | | | | | | | | | |
Net income (loss) attributable to Company stockholders | | $ | 15,116 | | | $ | (20,344 | ) | | $ | 74,576 | | | $ | 54,072 | | | $ | 117,336 | |
| | | | | | | | | | | | | | | | | | | | |
Basic income (loss) per common share: | | | | | | | | | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 0.32 | | | $ | (0.45 | ) | | $ | 1.11 | | | $ | 0.93 | | | $ | 1.40 | |
Income from discontinued operations | | | — | | | | 0.05 | | | | 0.18 | | | | 0.04 | | | | 1.05 | |
| | | | | | | | | | | | | | | | | | | | |
Net income (loss) attributable to Company stockholders | | $ | 0.32 | | | $ | (0.40 | ) | | $ | 1.29 | | | $ | 0.97 | | | $ | 2.45 | |
| | | | | | | | | | | | | | | | | | | | |
Diluted income (loss) per common share: | | | | | | | | | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 0.31 | | | $ | (0.45 | ) | | $ | 1.08 | | | $ | 0.85 | | | $ | 1.21 | |
Income from discontinued operations | | | — | | | | 0.05 | | | | 0.17 | | | | 0.03 | | | | 0.86 | |
| | | | | | | | | | | | | | | | | | | | |
Net income (loss) attributable to Company stockholders | | $ | 0.31 | | | $ | (0.40 | ) | | $ | 1.25 | | | $ | 0.88 | | | $ | 2.07 | |
| | | | | | | | | | | | | | | | | | | | |
Weighted-average shares outstanding used in computing per share amounts: | | | | | | | | | | | | | | | | | | | | |
Basic | | | 46,830 | | | | 50,862 | | | | 57,356 | | | | 55,328 | | | | 47,400 | |
| | | | | | | | | | | | | | | | | | | | |
Diluted | | | 48,398 | | | | 50,862 | | | | 59,124 | | | | 62,228 | | | | 57,740 | |
| | | | | | | | | | | | | | | | | | | | |
56
| | | | | | | | | | | | | | | | | | | | |
| | | As of December 31, | |
| | | 2013 | | | 2012 | | | 2011 | | | 2010 | | | 2009(1) | |
| | | (In thousands) | |
Consolidated Balance Sheet Data: | | | | | | | | | | | | | | | | | | | | |
Cash, cash equivalents and investments | | $ | 824,880 | | | $ | 991,835 | | | $ | 1,121,217 | | | $ | 400,501 | | | $ | 808,144 | |
Working capital (excluding assets and liabilities of discontinued operations) | | | 817,088 | | | | 966,235 | | | | 1,132,431 | | | | 420,353 | | | | 159,539 | |
Total assets | | | 1,325,628 | | | | 1,490,625 | | | | 1,641,025 | | | | 942,202 | | | | 1,288,548 | |
Convertible notes, net of discount | | | 952,232 | | | | 800,000 | | | | 800,000 | | | | — | | | | 227,659 | |
Stockholders’ equity | | | 190,900 | | | | 509,989 | | | | 674,436 | | | | 752,895 | | | | 564,768 | |
| (1) | On October 23, 2009, WebMD Health Corp. (“WebMD”) completed a merger (the “Merger”) with HLTH Corporation (“HLTH”), with WebMD continuing as the surviving company. Prior to the Merger, HLTH owned more than 80% of WebMD’s outstanding capital stock. In the Merger, each share of HLTH Common Stock was converted into 0.4444 shares (the “Exchange Ratio”) of WebMD Common Stock. The accounting treatment for the Merger resulted in HLTH being treated as the acquiring entity of the WebMD non-controlling interest. Accordingly, the pre-acquisition consolidated financial statements of HLTH became the historical financial statements of WebMD following the completion of the Merger. The following adjustments have been made to the portion of the year ended December 31, 2009 prior to the completion of the Merger on October 23, 2009: (a) the weighted-average shares outstanding used in computing income per common share have been adjusted by multiplying the historical weighted-average shares outstanding for HLTH by the Exchange Ratio and (b) basic and diluted income per common share have been recalculated to reflect the adjusted weighted-average shares outstanding for the periods presented. |
In addition, in the Consolidated Statements of Operations included in this Item 6, “Net income (loss) attributable to Company stockholders” reflects an adjustment for the noncontrolling stockholders’ share of the net income of WebMD until completion of the Merger.
57
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
This Item 7 contains forward-looking statements that involve risks and uncertainties. Please see “Forward-Looking Statements” on page ii of this Annual Report for a discussion of the uncertainties, risks and assumptions associated with these statements. The results of operations for the periods reflected herein are not necessarily indicative of results that may be expected for future periods, and our actual results may differ materially from those discussed in our forward-looking statements as a result of various factors, including, but not limited to, those listed under “Risk Factors” in Item 1A of this Annual Report and those included elsewhere in this Annual Report. In this Item 7, dollar amounts (other than per share amounts) are stated in thousands, unless otherwise noted.
Overview
Management’s discussion and analysis of financial condition and results of operations, or MD&A, is provided as a supplement to the Consolidated Financial Statements and notes thereto included elsewhere in this Annual Report and is intended to provide an understanding of our results of operations, financial condition and changes in our results of operations and financial condition. Our MD&A is organized as follows:
| | • | | Introduction. This section provides: a general description of our company and its business; background information on certain trends, transactions and other developments affecting our company; and a discussion of how seasonal factors may impact the timing of our revenue. |
| | • | | Critical Accounting Estimates and Policies. This section discusses those accounting policies that are considered important to the evaluation and reporting of our financial condition and results of operations, and whose application requires us to exercise subjective and often complex judgments in making estimates and assumptions. In addition, all of our significant accounting policies, including our critical accounting policies, are summarized in Note 2 to the Consolidated Financial Statements included in this Annual Report. |
| | • | | Results of Operations and Supplemental Financial and Operating Information. These sections provide our analysis and outlook for the significant line items on our statements of operations, as well as other information that we deem meaningful to understand our results of operations on a consolidated basis. |
| | • | | Liquidity and Capital Resources. This section provides an analysis of our liquidity and cash flows, as well as a discussion of our commitments that existed as of December 31, 2013. |
| | • | | Recent Accounting Pronouncements. This section provides a summary of the most recent authoritative accounting standards and guidance that have either been recently adopted by our company or may be adopted in the future. |
Introduction
Our Company. WebMD Health Corp. is a Delaware corporation that was incorporated on May 3, 2005. We completed an initial public offering on September 28, 2005. Our Common Stock trades under the symbol “WBMD” on the Nasdaq Global Select Market.
Our Business. We are a leading provider of health information services to consumers, physicians and other healthcare professionals, employers and health plans through our public and private online portals, mobile platforms and health-focused publications.The WebMD Health Network includes:www.WebMD.com, our primary public portal for consumers and related mobile-optimized sites and mobile apps;www.Medscape.com, our primary public portal for physicians and other healthcare professionals and related mobile services; and other sites through which we provide our branded health and wellness content, tools and services. Our services for consumers enable them to obtain information on health and wellness topics or on a particular disease or condition, to assess their personal health status, to use online trackers, tools and quizzes, to locate physicians, to receive periodic e-mailed newsletters and alerts on topics of individual interest, and to participate in online communities with peers and experts. Our services for physicians and healthcare professionals make it easier for them to access clinical reference sources, stay abreast of the latest clinical information, learn about new treatment
58
options, earn continuing medical education (which we refer to as CME) credit and communicate with peers. We do not charge any usage, membership or download fees for access to our public portals or mobile platforms. We generate revenue from our public portals and mobile platforms primarily through the sale of various types of advertising and sponsorship programs to our clients, which include: pharmaceutical, biotechnology and medical device companies; hospitals, clinics and other healthcare services companies; health insurance providers; consumer products companies whose products or services relate to health, wellness, diet, fitness, lifestyle, safety and illness prevention; and various other businesses, organizations and governmental entities. Advertisers and sponsors use our services to reach, educate and inform target audiences of consumers, physicians and other healthcare professionals. We also generate revenue from advertising sold inWebMD Magazine, a consumer magazine distributed to physician office waiting rooms. In addition, we generate revenue from the sale of certain information products.
Our private portals are a cloud-based population health management platform, hosted by WebMD and provided to private and governmental employers and health plans for use by their employees and plan participants. We market these private portals and related services under theWebMD Health Services brand. TheWebMD Health Services platform enables employers and health plans to provide their employees and plan participants with access to personalized health and benefit information, including an online personal health record application. OurWebMD Health Services solutions include a comprehensive set of decision support and transparency tools that help their employees and plan participants understand the financial implications of their benefits options and make more informed benefits-related purchase decisions and also provide access to information and services that can help them factor quality and cost into decisions about care and treatment options. We also provide telephonic, online and onsite health coaching and targeted condition management programs for use by our private portals clients’ employees and plan participants to help them make healthier lifestyle choices and achieve their wellness goals. We generate revenue from subscriptions to ourWebMD Health Services platform by employers and health plans, either directly or through its distributors. In addition, we offer our health coaching services and our condition management programs on a per participant basis.
Background Information on Certain Trends and Developments Affecting Our Business. Key trends and developments affecting the use of healthcare information services of the types we provide or are developing and our ability to generate revenue from those services include the following:
| | • | | Use of the Internet by Consumers and Physicians. The Internet has emerged as a major communications medium and has fundamentally changed many sectors of the economy, including the marketing and sales of financial services, travel, and entertainment, among others. The Internet is also changing the healthcare industry and has transformed how consumers and physicians find and utilize healthcare information. |
| | — | | Healthcare consumers increasingly seek to educate themselves online about their healthcare-related issues, motivated by the desire to become better informed patients and to become more engaged healthcare consumers because of the larger share of healthcare costs they are being asked to bear due to changes in the benefit designs being offered by health plans and employers. The Internet has fundamentally changed the way consumers obtain health and wellness information, enabling them to have immediate access to searchable information and dynamic interactive content to check symptoms, understand diseases, find providers and evaluate treatment options. |
| | — | | The Internet has become a primary source of information for physicians and other healthcare professionals seeking to improve clinical practice and to interact with their peers. The Internet has also become one of the primary means for physicians and other healthcare professionals to obtain CME and CE. |
| | • | | Online Marketing and Education Spending for Healthcare Products. Pharmaceutical, biotechnology and medical device companies spend large amounts each year marketing their products and educating consumers and physicians about them; however, only a small portion is currently spent on online services. We believe that these companies, which comprise the majority of the advertisers and sponsors of our public portals, are aware of the effectiveness of the Internet relative to traditional media in providing health, clinical and product-related information to consumers and physicians. In addition, in an effort to improve operating efficiencies, some pharmaceutical companies have been reducing their field sales |
59
| | forces in the past several years. However, notwithstanding our general expectation for increased future demand, we cannot predict the extent or the pace of any shift by pharmaceutical, biotechnology and medical device companies of their marketing expenditures to online services. Furthermore, our advertising and sponsorship revenue may vary significantly from quarter to quarter due to a number of other factors, many of which are outside our control, including general economic and regulatory conditions and the following: |
| | — | | The majority of our advertising and sponsorship contracts are for terms of approximately four to twelve months. We have relatively few longer term advertising and sponsorship contracts. |
| | — | | The time between the date of initial contact with a potential advertiser or sponsor regarding a specific program and the execution of a contract with the advertiser or sponsor for that program, as well as the additional time period before our services are delivered, may be longer than expected, especially for medium-sized and larger contracts, and may be subject to delays over which we have little or no control, including as a result of budgetary constraints of the advertiser or sponsor or their need for internal approvals, including internal approvals relating to compliance with the laws and regulations applicable to the marketing of healthcare products. We have experienced, from time to time, a lengthening of this internal review process by pharmaceutical and biotechnology companies, which has resulted in delays in contracting, as well as delays in recognizing expected revenue under executed contracts and which may continue to cause such delays. |
Other factors that may affect the timing of contracting for specific programs with advertisers and sponsors, or receipt of revenue under such contracts, include: the timing of Food and Drug Administration (“FDA”) approval for new products or for new approved uses for existing products; the timing of FDA approval of generic products that compete with existing brand name products and any increase in the number or significance of such approvals or of withdrawals of products from the market; consolidation of companies in the pharmaceutical and biotechnology industries; the timing of roll-outs of new or enhanced services on our public portals; seasonal factors relating to the prevalence of specific health conditions and other seasonal factors that may affect the timing of promotional campaigns for specific products; and the scheduling of conferences for physicians and other healthcare professionals.
| | • | | Other Factors Affecting the Demand for Our Advertising and Sponsorship Services. Some of our pharmaceutical company customers have experienced patent expirations for certain of their products in the past several years and some are expected to experience patent expirations over the next several years. In the pharmaceutical industry, patent expirations allow for competition from lower-priced generic versions of the patented drugs and generally result in the termination of marketing efforts for the drug. We believe that patent expirations led to significant overall reductions in marketing, selling and educational expenditures by some pharmaceutical companies in 2012 across their entire product portfolios. Amounts budgeted for online advertising increased for some of our biopharmaceutical customers in 2013, although we cannot predict if that will continue. |
In addition to pharmaceutical, biotechnology and medical device companies, our public portals advertisers and sponsors include consumer products companies, particularly for products and services that relate to health, wellness, diet, fitness, lifestyle, safety and illness prevention. Revenues from consumer products companies are more likely to reflect general economic conditions, and to be reduced to a greater extent during economic downturns, than revenues from pharmaceutical, biotechnology and medical device companies. Accordingly, revenues from these customers may be subject to significant quarter-to-quarter
60
variations. Our advertising and sponsorship services are subject to competition from numerous alternatives, including other Internet sites that focus on health-related content, Internet search engines, social media Internet sites, general interest consumer sites and traditional media. Such competition may result in smaller customer commitments or pressure to reduce prices, both of which could reduce our revenues and profit margins. In response to changes in the preferences of our advertisers and sponsors, particularly our pharmaceutical company clients, we modified our sales and product approach to offer services that can be executed more quickly and we have simplified our products and pricing. We believe this has allowed our clients to better compare our services, and the value they provide, to other digital alternatives. We have also been investing in more robust data and analytics capabilities to provide our customers with new value measurements and insights through proprietary analytics tools.
| | • | | Traffic Trends. In 2013,The WebMD Health Network reached an average of approximately 138 million monthly unique visitors and delivered approximately 11.55 billion page views during the year, increases of 25% and 14% over the prior year, respectively. Traffic toThe WebMD Health Network was an average of approximately 156 million unique users per month and total traffic of 3.17 billion page views during the fourth quarter of 2013, increases of 33% and 23%, respectively, over the prior year period. Traffic to our online portals for physicians and other healthcare professionals averaged approximately 5.5 million physician sessions per month in 2013, an increase of approximately 7% over the prior year, and averaged approximately 5.7 million physician sessions per month during the fourth quarter of 2013, an increase of approximately 5% over the prior year period. |
During the fourth quarter of 2013, approximately 33% of our page views came from a U.S. personal computer, approximately 31% came from a U.S. smartphone; approximately 8% came from a U.S. tablet device; and approximately 28% came from non-U.S. sources. Our U.S. PC page view traffic was approximately the same in the fourth quarter of 2013 as in the prior year period, in contrast to the declines that we experienced in the first three quarters of 2013, as compared to the respective prior year periods. Combined U.S. PC and tablet page view traffic toThe WebMD Health Network was up approximately 6% in the fourth quarter of 2013, as compared to the prior year period, which represented an improvement from the declines that we experienced in the first three quarters of 2013, as compared to the respective prior year periods. Tablets provide a similar user experience to PCs and we are able to monetize them similarly, so we believe that combined page views from PCs and tablets is a useful metric. One factor that significantly reduced traffic, in the first half of 2013, to some of the consumer sites inThe WebMD Health Network (other than WebMD.com, our flagship site) was changes in Google’s algorithms and other processes that lowered the ranking of those sites in Google search results. Starting in July 2013, we began to see a reversal of that trend, with improvement continuing through the rest of the year. We intend to continue our efforts to increase our page views by providing quality content and tools, as well as by designing our Websites to deliver that content and tools in ways that will cause them to rank well in algorithmic search engine results (which is commonly referred to as search engine optimization or SEO). However, we cannot be certain that our SEO efforts will result in continued improvement or, if they do, how long that will be maintained.
Consumers and healthcare professionals are increasingly using smartphones, tablets and other mobile devices to access the Internet, with physicians increasingly using mobile devices during treatment at the point of care. Accordingly, the portion of our page views from mobile devices has increased rapidly in the past several years as usage has increased on mobile devices. As discussed under “— Efforts to Increase Advertising and Sponsorship Revenue from Mobile” below, we are beginning to see some demand for advertising on smartphones, but the amount of revenue achieved in the fourth quarter of 2013 was not meaningful. We expect to have more than enough PC and tablet page view inventory onThe WebMD Health Network to meet the expected demand from advertisers and sponsors for our services for 2014 and view mobile as an opportunity for incremental revenue. However, if users access our services through smartphones as a substitute for access through personal computers and tablets, or if our page views from personal computers decline for other reasons, and if we are unable to successfully implement monetization strategies for smartphone traffic, our financial results could be negatively affected.
61
| | • | | Efforts to Increase Advertising and Sponsorship Revenue from Mobile. We remain focused on delivering a multi-screen platform that engages users on their personal computers, tablet devices and smartphones. Since we are able to monetize tablet page views similarly to PC page views, our mobile monetization efforts are focused on monetizing page views from smartphones and references to “mobile” and “mobile monetization” below are to smartphones and the page views they generate. |
As we broaden our mobile offerings for consumers and physicians, we are also expanding our mobile sponsorship products for advertisers. Mobile, while not yet a meaningful source of revenue for us, could be an important area of growth for the future and we view mobile monetization as an opportunity for incremental revenue. We are beginning to experience demand from customers for mobile advertising and to include mobile components in many of the program configurations that we offer to advertisers and sponsors. However, we are unable to predict when or to what extent such demand will increase. We are also seeing certain differences in such demand among our offerings:
| | — | | With respect to our mobile offerings for physicians, we are seeing some sales traction with advertisers for our mobile product set. |
| | — | | We are also beginning to experience demand for mobile advertising and sponsorship with respect to our consumer offerings. We expect that our mobile offerings for consumers will be adopted by our consumer products customers sooner than biopharmaceutical customers as consumer products companies do not have the issues regarding medical and regulatory review that biopharmaceutical companies have. Advertisements for biopharmaceutical products are subject to various regulatory requirements, including requirements to include certain specified information, that are more challenging to meet on the smaller smartphone screen size. We are, however, developing strategies to assist our biopharmaceutical customers in navigating the regulatory environment as it relates to consumer advertising on mobile. |
The portion of our page views from smartphones has increased rapidly in the past several years. Accordingly, if we are unable to successfully implement monetization strategies for our mobile services, our business and prospects could be adversely affected.
| | • | | Use of Population Health Management Services. In a healthcare market where a greater share of the responsibility for healthcare costs and decision-making has been shifting to consumers, use of information technology to assist consumers in making informed decisions about healthcare has also increased. We believe that, through ourWebMD Health Servicesprivate portals and related coaching services, we are well positioned to play a role in this environment. For more than a decade, ourcloud-based population health management services have helped employers and health plans improve the health of their employee and plan participant populations and reduce healthcare costs. Our services help employees and plan participants make more informed health and benefit decisions, positively change health behaviors, manage health conditions and lead healthier lives. At the beginning of 2014, we launched ourWebMD Health Services platform for the Blue Cross Blue Shield Federal Employee Program (or FEP). With this program, over 5 million FEP members now have access to a broad range of ourWebMD Health Services solutions, including our online personal health record application, as well as to our health coaching services and to around-the-clock access to nurses by phone, secure message, or chat. Our strategy depends, in part, on increasing usage of our services by our employer and health plan clients’ employees and plan participants and being able to demonstrate a sufficient return on investment and other benefits for our clients from those services. Increasing such usage requires us to continue to develop new and updated applications, features and services. In addition, we face competition for our online population health management applications and related coaching services. Many of our competitors have greater financial, technical, product development, marketing and other resources than we do, and may be better known than we are. |
| | • | | International. The WebMD Health Network includes the following international sites: the co-brandedBoots WebMD health information site for United Kingdom consumers atwww.WebMD.boots.com; andMedscape France(www.medscape.fr) andMedscape Germany (www.medscape.de), our physician portals in those two countries. We also seek to monetize traffic toMedscape from physicians outside the United |
62
| | States. We plan to continue to pursue opportunities to expand the reach of our brands outside the United States. In certain markets outside the United States, we expect to accomplish this through partnerships or joint ventures with other companies having expertise in the specific country or region, while in other such markets we expect to rely primarily on our own internal resources. |
| | • | | Healthcare Reform Legislation. The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act of 2010 (which we refer to as the Affordable Care Act), was signed into law in March 2010. The Affordable Care Act makes extensive changes to the system of healthcare insurance and benefits in the United States. In general, the Affordable Care Act seeks to reduce healthcare costs and decrease the number of uninsured legal United States residents by, among other things, requiring individuals to carry, and certain employers to offer, health insurance or be subject to penalties. The Affordable Care Act also imposes new regulations on health insurers, including guaranteed coverage requirements, prohibitions on certain annual and all lifetime limits on amounts paid on behalf of or to plan members, increased restrictions on rescinding coverage, establishment of minimum medical loss ratio requirements, a requirement to cover certain preventive services on a first dollar basis, the establishment of state insurance exchanges and essential benefit packages, and greater limitations on how health insurers price certain of their products. The Affordable Care Act also contains provisions that will affect the revenues and profits of pharmaceutical and medical device companies, including new taxes on certain sales of their products. Many of the provisions of the Affordable Care Act that expand insurance coverage did not become effective until 2014 and some will not become effective until later, and many provisions will require additional regulations and interpretive guidance to be issued before they will be fully implemented. Some provisions do not apply to health plans that were in place when the Affordable Care Act was enacted and have not been substantially changed since. It is difficult to foresee how individuals and businesses will respond to the choices available to them under the Affordable Care Act. Furthermore, the Affordable Care Act will result in future state legislative and regulatory changes, which we are unable to predict at this time, in order for states to comply with certain provisions of the Affordable Care Act and to participate in grants and other incentive opportunities. In addition, Congress has considered various proposals to repeal some or all of the Affordable Care Act. |
While we do not currently anticipate any significant adverse effects on WebMD as a direct result of the application of the Affordable Care Act to our business or on our company in its capacity as an employer, we are unable to predict what the indirect impacts of the Affordable Care Act will be on WebMD’s business through its effects on other healthcare industry participants, including pharmaceutical and medical device companies that are advertisers and sponsors of our public portals and employers and health plans that are clients of our private portals. Healthcare industry participants may respond to the Affordable Care Act or to uncertainties created by the Affordable Care Act by reducing their expenditures or postponing expenditure decisions, including expenditures for our services, which could have a material adverse effect on our business. However, we believe that certain aspects of the Affordable Care Act and future implementing regulations that seek to reduce healthcare costs may create opportunities for WebMD, including with respect to our personal health record applications and health and benefits decision-support tools and, more generally, with respect to our capabilities in providing health and wellness information and education. For example, the Affordable Care Act encourages use of wellness programs through grants to small employers to establish such programs, permission for employers to offer larger rewards than under prior law, in the form of waivers of cost-sharing, premium discounts, or additional benefits, to employees for participating in these programs and meeting certain standards, and the inclusion of wellness services and chronic disease management among the essential health benefits that certain plans are required to provide. In addition, in connection with the implementation of the Affordable Care Act, we have launched a new channel on WebMD.com that provides information and decision-support tools to help consumers understand their options and choose an appropriate health plan based on their needs. However, we cannot yet determine the scope of the other opportunities that the Affordable Care Act may create or what competition we may face in our efforts to pursue such opportunities.
| | • | | Other Initiatives. We are pursuing, and intend to continue to identify, new business opportunities where our consumer and physician audiences and our resources can be leveraged to develop additional products |
63
| | and services. One of our goals is to establish WebMD as a place where consumers store, access and manage their health information in a trusted environment. Examples of initiatives we are working on include the following: |
| | — | | We are in the early stages of developing the capabilities to positionWebMD andMedscape as a hub for a set of services that will facilitate information exchange and digital communication between healthcare providers and their patients. As an initial step, our flagshipWebMD App for iPhone® will support a new “Patient Instructions” feature available to healthcare professionals in ourMedscape App.Medscape Patient Instructions allows physicians and other medical professionals to securely send education and instructions on conditions, procedures and drugs to their patients. Patients can securely and conveniently read the instructions and information on theWebMD App for iPhone®, as well as on the WebMD consumer portal and the related mobile-optimized site. In addition, in late 2013, we acquired a start-up technology company called Avado to accelerate our connectivity efforts. We are working to integrate key aspects of Avado’s technology into our platform. We expect that Avado’s cloud-based patient relationship management platform will serve as a key building block for a suite of services connecting patients to their physicians and other healthcare providers. |
| | — | | A forthcoming version of theWebMD App will leverage the 2net™ Platform from Qualcomm Life, Inc., a subsidiary of Qualcomm Incorporated, to enable health-conscious consumers to access and manage biometric data from devices such as glucometers, wireless scales, and wearable devices directly from theWebMD App, and wrap that data within a health improvement program health data.TheWebMD App will use the biometric data to tailor content, provide personalized insights, and to set and measure progress against goals. WebMD and Qualcomm Life also plan to introduce, later in 2014, a new online storefront where consumers will be able to purchase a variety of biometric devices from the industry’s leading providers. |
We may pursue initiatives to create new or enhanced revenue streams or, alternatively, to increase audience engagement even when we have not identified any potential related revenue stream. New business initiatives present risks and challenges that may be different than the ones we have faced in the past. In addition, later events may alter the risks that were evaluated at the time decisions are made on specific initiatives. Failure to effectively identify and assess new business initiatives and to successfully implement them may adversely affect our company and its prospects.
The healthcare industry in the United States and relationships among healthcare payers, providers and consumers are very complicated. In addition, the Internet and the market for online and mobile services are relatively new and still evolving. Accordingly, there can be no assurance that the trends identified above will continue or that the expected benefits to our business from our responses to those trends will be achieved. In addition, the market for healthcare information services is highly competitive and not only are our existing competitors seeking to benefit from these same trends, but the trends may also attract additional competitors.
Background Information on Certain Significant Developments and Transactions
Tender Offers. On April 3, 2012, we completed a tender offer (which we refer to as the 2012 Tender Offer) for our Common Stock and repurchased 5,769,230 shares at a price of $26.00 per share for a total cost of $150,759, which includes $759 of costs directly attributable to the purchase. The 2012 Tender Offer represented an opportunity for WebMD to return capital to stockholders who elected to tender their shares of WebMD Common Stock, while stockholders who chose not to participate in the 2012 Tender Offer automatically increased their relative percentage interest in our company at no additional cost to them.
On September 10, 2013, we completed a tender offer (which we refer to as the 2013 Tender Offer) for our Common Stock and repurchased 5,000,000 shares at a price of $34.00 per share for a total cost of $170,516, which includes $516 of costs directly attributable to the purchase. The 2013 Tender Offer represented an opportunity for WebMD to return capital to stockholders who elected to tender their shares of WebMD Common Stock, while stockholders who chose not to participate in the 2013 Tender Offer automatically increased their relative percentage interest in our company at no additional cost to them.
64
Stock Repurchases. During 2011, we repurchased 2,883,798 shares at an aggregate cost of $91,263 through our stock repurchase program. Certain stock repurchases made outside of our stock repurchase program during 2011 are described under “— Convertible Notes” below.
During 2012, we repurchased 1,320,846 shares at an aggregate cost of $26,900 through our stock repurchase program.
During 2013, we repurchased 1,266,962 shares at an aggregate cost of $42,309 through our stock repurchase program. On October 18, 2013, we entered into an agreement to repurchase 5,527,433 shares of our Common Stock from Carl C. Icahn and certain of his affiliates, at a purchase price of $32.08 per share (the NASDAQ Official Closing Price of our Common Stock on October 18, 2013) at an aggregate cost of $177,420, which includes $100 of costs directly attributable to the purchase. The repurchase was completed on October 21, 2013. This repurchase was made outside of our stock repurchase program. As of December 31, 2013, $19,864 remained available for repurchases under the program. In February 2014, our Board of Directors authorized a $50,000 increase to the program.
Convertible Notes. On January 11, 2011, we issued $400,000 aggregate principal amount of 2.50% Convertible Notes due 2018 (which we refer to as the 2.50% Notes) in a private offering. Unless previously converted, the 2.50% Notes will mature on January 31, 2018. Net proceeds from the sale of the 2.50% Notes were approximately $387,345, after deducting the related offering expenses, of which approximately $100,000 was used by us to repurchase 1,920,490 shares of WebMD Common Stock at a price of $52.07 per share, the last reported sale price of WebMD Common Stock on January 5, 2011, which repurchase settled on January 11, 2011. Interest on the 2.50% Notes is payable semi-annually on January 31 and July 31 of each year, commencing July 31, 2011. Under the terms of the 2.50% Notes, as adjusted in April 2012 following completion of the 2012 Tender Offer and in September 2013 following completion of the 2013 Tender Offer, holders may surrender their 2.50% Notes for conversion into WebMD Common Stock at a conversion rate of 15.4764 shares of WebMD Common Stock per thousand dollars principal amount of the 2.50% Notes. This is equivalent to a conversion price of approximately $64.61 per share of Common Stock. In the aggregate, the 2.50% Notes were convertible into 6,190,560 shares of Common Stock as of December 31, 2013.
On March 14, 2011, we issued $400,000 aggregate principal amount of 2.25% Convertible Notes due 2016 (which we refer to as the 2.25% Notes) in a private offering. Unless previously converted, the 2.25% Notes will mature on March 31, 2016. Net proceeds from the sale of the 2.25% Notes were approximately $387,400, after deducting the related offering expenses, of which approximately $50,000 was used to repurchase 868,507 shares of WebMD Common Stock at a price of $57.57 per share, the last reported sale price of WebMD Common Stock on March 8, 2011, which repurchase settled on March 14, 2011. Interest on the 2.25% Notes is payable semi-annually on March 31 and September 30 of each year, commencing September 30, 2011. Under the terms of the 2.25% Notes, as adjusted in April 2012 following completion of the 2012 Tender Offer and in September 2013 following completion of the 2013 Tender Offer, holders may surrender their 2.25% Notes for conversion into WebMD Common Stock at a conversion rate of 13.8884 shares of Common Stock per thousand dollars principal amount of the 2.25% Notes. This is equivalent to a conversion price of approximately $72.00 per share of Common Stock. In the aggregate, the 2.25% Notes were convertible into 3,503,099 shares of Common Stock as of December 31, 2013, at which time the remaining outstanding principal amount was $252,232. During 2013, we repurchased a total of $147,768 principal amount of our 2.25% Notes for $150,354 in cash. We recognized a pre-tax loss of $4,871 related to these repurchases, which is reflected within “Loss on convertible notes” in our Consolidated Statement of Operations. The loss includes the expensing of the remaining deferred issuance costs outstanding related to the repurchased 2.25% Notes.
On November 26, 2013, we issued $300,000 aggregate principal amount of 1.50% Convertible Notes due 2020 (which we refer to as the 1.50% Notes) in a private offering. Unless previously converted, the 1.50% Notes will mature on December 1, 2020. Net proceeds from the sale of the 1.50% Notes were approximately $291,823, after deducting the related offering expenses. Interest on the 1.50% Notes is payable semi-annually on June 1 and December 1 of each year, commencing June 1, 2014. Under the terms of the 1.50% Notes, holders may surrender their 1.50% Notes for conversion into WebMD Common Stock at a conversion rate of 18.9362 shares of Common Stock per thousand dollars principal amount of the 1.50% Notes. This is equivalent to a conversion
65
price of approximately $52.81 per share of Common Stock. In the aggregate, the 1.50% Notes were convertible into 5,680,860 shares of Common Stock as of December 31, 2013.
Restructuring. On December 11, 2012, we announced a plan to streamline our operations, simplify our organizational structure, reduce costs and better focus our resources. These actions included a workforce reduction of approximately 250 positions, or roughly 14% of our employees at that time, and have resulted in a reduction in our operating expenditures. We recorded a restructuring charge of $7,579 during the three months ended December 31, 2012 related to severance and other employee benefits that were provided to terminated employees.
Voluntary Surrender of Certain Option Grants. On February 23, 2012, our directors and certain officers voluntarily surrendered certain grants of non-qualified options to purchase WebMD Common Stock made to them, one of which was made in 2007, some in 2010 and some in 2011 and all of which were out-of-the-money at the time of surrender. None of these individuals received any consideration or promise of consideration in exchange for the surrender of these stock options. These options were originally granted under our 2005 Long-Term Incentive Plan (which we refer to as the 2005 Plan), and therefore, upon their surrender, the shares underlying these options were returned to the 2005 Plan and became available for grant under such plan. These surrenders of stock options were intended to allow WebMD to use the shares that became available under the 2005 Plan to attract new employees and to motivate and retain current key employees. During the three months ended March 31, 2012, we recorded pre-tax stock-based compensation expense of $8,076 related to the voluntary surrender of these options, which represented the remaining unrecognized stock-based compensation amounts for such grants.
Auction Rate Securities. Effective April 20, 2010, we entered into an agreement pursuant to which we sold our holdings of auction rate securities (which we refer to as ARS), for an aggregate of $286,399. Under the terms of the agreement, we retained an option (which we refer to as the ARS Option), for a period of two years from the date of the agreement: (a) to repurchase from the purchaser the same principal amount of any or all of the various series of ARS sold, at the agreed upon purchase prices received on April 20, 2010; and (b) to receive from the purchaser additional proceeds upon certain redemptions of the various series of ARS sold. We received cash proceeds of $9,269 and recorded a pre-tax gain of $8,074 related to the ARS Option during the three months ended March 31, 2012. As of March 31, 2012, we no longer had any remaining positions related to the ARS Option and will receive no further cash proceeds.
Seasonality
The timing of our revenue is affected by seasonal factors. Our public portal advertising and sponsorship revenue is seasonal, primarily due to the annual spending patterns of the advertising and sponsorship clients of our public portals. This portion of our revenue is usually the lowest in the first quarter of each calendar year, and generally increases during each consecutive quarter throughout the year. The timing of revenue in relation to our expenses, many of which do not vary directly with revenue, has an impact on cost of operations, sales and marketing, and general and administrative expenses as a percentage of revenue in each calendar quarter.
Critical Accounting Estimates and Policies
Critical Accounting Estimates
Our MD&A is based upon our Consolidated Financial Statements and Notes to Consolidated Financial Statements, which were prepared in conformity with U.S. generally accepted accounting principles. The preparation of the Consolidated Financial Statements requires us to make estimates and assumptions that affect the amounts reported in the Consolidated Financial Statements and accompanying notes. We base our estimates on historical experience, current business factors, and various other assumptions that we believe are necessary to consider to form a basis for making judgments about the carrying values of assets and liabilities, the recorded amounts of revenue and expenses and the disclosure of contingent assets and liabilities. We are subject to uncertainties such as the impact of future events, economic and political factors, and changes in our business environment; therefore, actual results could differ from these estimates. Accordingly, the accounting estimates used in the preparation of our financial statements will change as new events occur, as more experience is acquired, as additional information is obtained and as our operating environment changes. Changes in estimates
66
are made when circumstances warrant. Such changes in estimates and refinements in estimation methodologies are reflected in reported results of operations; if material, the effects of changes in estimates are disclosed in the Notes to our Consolidated Financial Statements.
We evaluate our estimates on an ongoing basis, including those related to revenue recognition, the allowance for doubtful accounts, the carrying value of long-lived assets (including goodwill and indefinite-lived intangible assets), the amortization period of long-lived assets (excluding goodwill and indefinite-lived intangible assets), the carrying value, capitalization and amortization of software and Website development costs, the carrying value of investments, the provision for income taxes and related deferred tax accounts, certain accrued expenses, contingencies, litigation and related legal accruals and the value attributed to employee stock options and other stock-based awards.
Critical Accounting Policies
We believe the following reflects our critical accounting policies and our more significant judgments and estimates used in the preparation of our Consolidated Financial Statements:
| | • | | Revenue Recognition. Revenue from advertising is recognized as advertisements are delivered or as publications are distributed. Revenue from sponsorship arrangements, content syndication and distribution arrangements, information services and subscriptions to our healthcare management tools and private portals as well as related health coaching services are recognized ratably over the term of the applicable agreement. Revenue from the sponsorship of CME is recognized over the period that we substantially complete our contractual deliverables as determined by the applicable agreements. |
Contracts that contain multiple deliverables are subject to Accounting Standards Update No. 2009-13 Multiple-Deliverable Revenue Arrangements (“ASU 2009-13”). ASU 2009-13 requires the allocation of revenue to each deliverable of multiple-deliverable revenue arrangements, based on the relative selling price of each deliverable. It also defines the level of evidence of selling price required to separate deliverables and allows a company to make its best estimate of the selling price of deliverables when more objective evidence of selling price is not available.
Pursuant to the guidance of ASU 2009-13, when a sales arrangement contains multiple deliverables, we allocate revenue to each deliverable based on relative selling price. The selling price for a deliverable is based on vendor-specific objective evidence (“VSOE”) if available, third-party evidence (“TPE”) if VSOE is not available, or best estimate of selling price if neither VSOE nor TPE is available. We then recognize revenue on each deliverable in accordance with our revenue recognition policies over the period that delivery occurs. VSOE of selling price is based on the price charged when the deliverable is sold separately. In determining VSOE, we require that a substantial majority of the selling prices fall within a reasonable range based on historical pricing trends for specific products and services. TPE is based on competitor prices of similar deliverables when sold separately. We are generally not able to determine TPE of selling price as we are unable to reliably determine what competitors’ selling prices are for comparable services, combined with the fact that our services often contain unique features and customizations such that comparable services do not exist. The determination of best estimate of selling price is a judgmental process that considers multiple factors including, but not limited to, recent selling prices and related discounting practices for each service, market conditions, customer classes, sales channels and other factors.
| | • | | Long-Lived Assets. Our long-lived assets consist of property and equipment, goodwill and other intangible assets. Goodwill and other intangible assets arise from the acquisitions we have made. The amount assigned to intangible assets is subjective and based on fair value using exit price and market participant view, such as discounted cash flow and replacement cost models. Our long-lived assets, excluding goodwill and indefinite-lived intangible assets, are amortized over their estimated useful lives, which we determine based on the consideration of several factors including the period of time the asset is expected to remain in service. We evaluate the carrying value and remaining useful lives of long-lived assets, excluding goodwill and indefinite-lived intangible assets, whenever indicators of impairment are |
67
| | present. We evaluate the carrying value of goodwill and indefinite-lived intangible assets annually, or whenever indicators of impairment are present. We test goodwill for impairment at the reporting unit level only when, after completing a qualitative analysis, it is determined that it is more likely than not that the fair value of the reporting unit is less than its carrying value. Long-lived assets held for sale are reported at the lower of cost or fair value less cost to sell. There was no impairment of goodwill or indefinite-lived intangible assets in 2013, 2012 or 2011. |
| | • | | Stock-Based Compensation. Stock-based compensation expense for all share-based payment awards granted is determined based on the grant-date fair value. The grant date fair value for stock options is estimated using the Black-Scholes Option Pricing Model. We recognize these compensation costs net of an estimated forfeiture rate on a straight-line basis over the requisite service period of the award, which is generally the vesting term of the share-based payment awards. As of December 31, 2013, there was approximately $69,400 of unrecognized stock-based compensation expense (net of estimated forfeitures) related to unvested stock options and restricted stock awards held by employees, which is expected to be recognized over a weighted-average period of approximately 3.0 years, related to our stock-based compensation plans. |
| | • | | Deferred Taxes. Our deferred tax assets are comprised primarily of net operating loss carryforwards and federal tax credits. These net operating loss carryforwards and federal tax credits may be used to offset taxable income in future periods, reducing the amount of taxes we might otherwise be required to pay. A significant portion of our net deferred tax assets, including the portion related to excess tax benefits of stock-based awards, are reserved for by a valuation allowance as required by relevant accounting literature. The remaining portion of our net deferred tax assets are no longer reserved for by a valuation allowance. Management determines the need for a valuation allowance by assessing the probability of realizing deferred tax assets, taking into consideration factors including historical operating results, expectations of future earnings and taxable income. Management will continue to evaluate the need for a valuation allowance in the future. |
| | • | | Tax Contingencies. Our tax contingencies are recorded to address potential exposures involving tax positions we have taken that could be challenged by tax authorities. These potential exposures result from applications of various statutes, rules, regulations and interpretations. Our estimates of tax contingencies reflect assumptions and judgments about potential actions by taxing jurisdictions. We believe that these assumptions and judgments are reasonable. However, our accruals may change in the future due to new developments in each matter and the ultimate resolution of these matters may be greater or less than the amount that we have accrued. Consistent with our historical financial reporting, we have elected to reflect interest and penalties related to uncertain tax positions as part of the income tax provision (benefit). |
68
Results of Operations
The following table sets forth our consolidated statements of operations data and expresses that data as a percentage of revenue for the periods presented:
| | | | | | | | | | | | | | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
| | | $ | | | %(a) | | | $ | | | %(a) | | | $ | | | %(a) | |
Revenue | | $ | 515,293 | | | | 100.0 | | | $ | 469,866 | | | | 100.0 | | | $ | 558,775 | | | | 100.0 | |
Cost of operations | | | 209,740 | | | | 40.7 | | | | 216,361 | | | | 46.0 | | | | 201,677 | | | | 36.1 | |
Sales and marketing | | | 127,997 | | | | 24.8 | | | | 127,659 | | | | 27.2 | | | | 124,326 | | | | 22.2 | |
General and administrative | | | 93,220 | | | | 18.1 | | | | 97,618 | | | | 20.8 | | | | 91,271 | | | | 16.3 | |
Depreciation and amortization | | | 26,606 | | | | 5.2 | | | | 28,399 | | | | 6.0 | | | | 26,801 | | | | 4.8 | |
Interest income | | | 76 | | | | — | | | | 86 | | | | — | | | | 112 | | | | — | |
Interest expense | | | 22,826 | | | | 4.4 | | | | 23,334 | | | | 5.0 | | | | 20,645 | | | | 3.7 | |
Loss on convertible notes | | | 4,871 | | | | 0.9 | | | | — | | | | — | | | | — | | | | — | |
Gain on investments | | | — | | | | — | | | | 8,074 | | | | 1.7 | | | | 18,516 | | | | 3.3 | |
Restructuring | | | — | | | | — | | | | 7,579 | | | | 1.6 | | | | — | | | | — | |
Other expense | | | 1,353 | | | | 0.3 | | | | 2,297 | | | | 0.5 | | | | 2,328 | | | | 0.4 | |
| | | | | | | | | | | | | | | | | | | | | | | | |
Income (loss) from continuing operations before income tax provision (benefit) | | | 28,756 | | | | 5.6 | | | | (25,221 | ) | | | (5.4 | ) | | | 110,355 | | | | 19.7 | |
Income tax provision (benefit) | | | 13,640 | | | | 2.6 | | | | (2,134 | ) | | | (0.5 | ) | | | 46,167 | | | | 8.3 | |
| | | | | | | | | | | | | | | | | | | | | | | | |
Income (loss) from continuing operations | | | 15,116 | | | | 2.9 | | | | (23,087 | ) | | | (4.9 | ) | | | 64,188 | | | | 11.5 | |
Income from discontinued operations, net of tax | | | — | | | | — | | | | 2,743 | | | | 0.6 | | | | 10,388 | | | | 1.9 | |
| | | | | | | | | | | | | | | | | | | | | | | | |
Net income (loss) | | $ | 15,116 | | | | 2.9 | | | $ | (20,344 | ) | | | (4.3 | ) | | $ | 74,576 | | | | 13.3 | |
| | | | | | | | | | | | | | | | | | | | | | | | |
| (a) | Amounts may not add due to rounding. |
Revenue from our public portal advertising and sponsorship is derived from the sale of online advertising and sponsorship products, online CME services, information and data services and other print services (including advertisements inWebMD Magazine). Revenue from our private portal services is derived from subscriptions to our cloud-based population health management platform by private and governmental employers, healthcare payers and others, and from related services including health and condition management programs and personalized health coaching services. Our customers include pharmaceutical, biotechnology, medical device and consumer products companies, as well as employers and health plans.
Cost of operations consists of salaries and related expenses, and non-cash stock-based compensation expense related to providing and distributing services and products we provide to customers and costs associated with the operation and maintenance of our public and private portals. Cost of operations also consists of editorial and production costs, Website operations costs, non-capitalized Website development costs, costs we pay to our distribution partners, costs associated with our health and condition management programs and personalized health coaching services, and costs related to the production and distribution of our publications, including costs related to creating and licensing content, telecommunications, leased properties and printing and distribution.
Sales and marketing expense consists primarily of salaries and related expenses, and non-cash stock-based compensation for account executives, account management and marketing personnel, as well as costs and expenses for marketing programs, and fees for professional marketing and advertising services.
General and administrative expense consists primarily of salaries and related expenses and non-cash stock-based compensation expense for administrative, finance, legal, information technology, human resources and executive personnel. Also included in general and administrative expense are costs of general insurance and professional services expenses.
69
Our discussions throughout this MD&A make references to certain non-cash expenses. Our principal non-cash expenses are related to the awards of all share-based payments to employees and non-employee directors, such as grants of employee stock options and restricted stock. Non-cash stock-based compensation expense is reflected in the same expense captions as the related salary cost of the respective employee.
The following table is a summary of our non-cash expenses included in the respective statements of operations captions.
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Stock-based compensation expense included in: | | | | | | | | | | | | |
Cost of operations | | $ | 6,762 | | | $ | 8,160 | | | $ | 7,707 | |
Sales and marketing | | | 8,395 | | | | 8,201 | | | | 9,079 | |
General and administrative | | | 23,393 | | | | 28,560 | | | | 22,951 | |
| | | | | | | | | | | | |
Total stock-based compensation expense | | $ | 38,550 | | | $ | 44,921 | | | $ | 39,737 | |
| | | | | | | | | | | | |
2013 and 2012
The following discussion is a comparison of our results of operations for the year ended December 31, 2013 to the year ended December 31, 2012.
Revenue. Our total revenue increased 9.7% to $515,293 in 2013 from $469,866 in 2012. The increase was due to an increase of $41,843 of advertising and sponsorship revenue from our public portals and an increase of $3,584 of revenue from our private portals. The increase in revenue related primarily to an increase in advertising of certain of our customers, particularly our biopharmaceutical and consumer products companies. For a more detailed discussion, see “— Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Other Factors Affecting the Demand for Our Advertising and Sponsorship Services.” A more detailed discussion regarding changes in revenue is included below under “—Supplemental Financial and Operating Information.”
Cost of Operations. Cost of operations was $209,740 in 2013, compared to $216,361 in 2012. Our cost of operations represented 40.7% of revenue in 2013, compared to 46.0% of revenue in 2012. Included in cost of operations were non-cash expenses related to stock-based compensation of $6,762 in 2013, compared to $8,160 in 2012.
Cost of operations, excluding the non-cash stock-based compensation expense discussed above, was $202,978, or 39.4% of revenue in 2013, compared to $208,201, or 44.3% of revenue in 2012. The decrease in absolute dollars and as a percentage of revenue in 2013, compared to 2012, was due to our ability to deliver the 9.7% revenue increase with a reduced cost structure resulting from the restructuring actions taken in December 2012.
Sales and Marketing. Sales and marketing expense was $127,997 in 2013, compared to $127,659 in 2012. Our sales and marketing expense represented 24.8% of revenue in 2013, compared to 27.2% in 2012. Included in sales and marketing expense were non-cash expenses related to stock-based compensation of $8,395 in 2013, compared to $8,201 in 2012.
Sales and marketing expense, excluding the non-cash expenses discussed above, was $119,602, or 23.2% of revenue, in 2013, compared to $119,458, or 25.4% of revenue, in 2012. The decrease as a percentage of revenue, excluding the non-cash expenses discussed above, for 2013 compared to 2012, was primarily due to the increase in our revenue of 9.7% without a commensurate increase in our sales and marketing expenses as certain of these expenses are fixed in nature and as a result of the reduced cost structure resulting from the restructuring actions taken in December 2012.
General and Administrative. General and administrative expense was $93,220 in 2013, compared to $97,618 in 2012. Our general and administrative expenses represented 18.1% of revenue in 2013, compared to
70
20.8% of revenue in 2012. Included in general and administrative expense was non-cash stock-based compensation expense of $23,393 in 2013, compared to $28,560 in 2012. The decrease in non-cash stock-based compensation expense for 2013, compared to 2012, was primarily due to the voluntary surrender of stock options by certain of our officers and directors and the related acceleration of the unrecognized stock-based compensation expense associated with those options during 2012 of $8,076 and the lack of a comparable expense in 2013.
General and administrative expense, excluding the non-cash stock-based compensation expense discussed above, was $69,827, or 13.6% of revenue, in 2013, compared to $69,058, or 14.7% of revenue in 2012. The decrease in general and administrative expense as a percentage of revenue, excluding the non-cash expenses discussed above, for 2013 compared to 2012, was primarily due to the increase in our revenue of 9.7% without a commensurate increase in our general and administrative expenses as many of these expenses are fixed in nature and as a result of the reduced cost structure resulting from the restructuring actions taken in December 2012.
Depreciation and Amortization. Depreciation and amortization expense was $26,606, or 5.2% of revenue in 2013, compared to $28,399, or 6.0% of revenue in 2012. This decrease was primarily due to the acceleration, in 2012, of the remaining amortization expense of $1,267 associated with certain trade names that have been retired from use.
Interest Income. Interest income was $76 in 2013, which was relatively consistent when compared to $86 in 2012.
Interest Expense. Interest expense was $22,826 in 2013 compared to $23,334 in 2012. This decrease was primarily due to the repurchase of $147,768 principal amount of our 2.25% Notes during 2013. Interest expense in 2013 and 2012 included non-cash interest expense of $4,192 and $4,326, respectively, related to the amortization of the debt issuance costs for the convertible debt outstanding during those periods.
Loss on Convertible Notes. During 2013, we recorded a loss on convertible notes of $4,871 related to the repurchase of $147,768 principal amount of our 2.25% Notes. See “— Introduction — Background Information on Certain Significant Developments and Transactions — Convertible Notes” for additional information.
Gain on Investments. During 2012, our gain on investments of $8,074 related to amounts we received through our ARS Option.
Restructuring. During 2012, we recorded a restructuring charge of $7,579 related to severance and other employee benefits that were provided to the terminated employees due to the reduction in our workforce as a result of the plan we announced, on December 11, 2012, to streamline our operations, simplify our organizational structure, reduce costs and better focus our resources.
Other Expense. Other expense of $1,353 during 2013 includes cash severance and related expenses due to the May 2013 departure of a Chief Executive Officer of the Company. Other expense of $2,297 during 2012 includes cash severance and related expenses due to the January 2012 departure of a Chief Executive Officer of the Company, and the related search and recruitment of his replacement during that period.
Income Tax Provision (Benefit). The income tax provision of $13,640 in 2013 related to pre-tax income of $28,756, compared to the income tax benefit of $2,134 in 2012 which related to a pre-tax loss of $25,221. The income tax benefit during 2012 included a non-cash income tax expense of $4,724 related to an increase in our valuation allowance for certain research and development tax credits for which scheduled expiration prior to utilization is more likely than not.
Income from Discontinued Operations, Net of Tax. Income from discontinued operations, net of tax, was $2,743 in 2012. During 2012, we recognized an after-tax gain of $2,235 related to the receipt of approximately $3,600 from the United States Department of Justice in relation to the investigation by the United States Attorney for the District of South Carolina (which we refer to as the Investigation). These funds represented the reimbursement to us related to recoveries by the United States Department of Justice from former employees of a subsidiary who pleaded guilty to the matters involved in the Investigation. None of the former employees who pleaded guilty were employees to whom we provided indemnification in connection with the Investigation.
71
Additionally, during 2012, income from discontinued operations includes a net state tax refund of $508 that we received in connection with the finalization of a state tax appeal related to the September 2006 sale of Emdeon Practice Services, Inc. (which we refer to as EPS) to Sage Software, Inc. (which we refer to as the EPS Sale). The income tax provision included within discontinued operations was $555 during 2012.
2012 and 2011
The following discussion is a comparison of our results of operations for the year ended December 31, 2012 to the year ended December 31, 2011.
Revenue. Our total revenue decreased 15.9% to $469,866 in 2012 from $558,775 in 2011. The decrease was due to a decrease of $85,986 of advertising and sponsorship revenue from our public portals and a decrease of $2,923 of revenue from our private portals. We believe that the overall decrease in revenue related primarily to a more cautious business outlook by many of our customers, resulting in a lower volume of advertising and sponsorship programs. For background information, see “— Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Other Factors Affecting the Demand for Our Advertising and Sponsorship Services.” A more detailed discussion regarding changes in revenue is included below under “— Supplemental Financial and Operating Information.”
Cost of Operations. Cost of operations was $216,361 in 2012, compared to $201,677 in 2011. Our cost of operations represented 46.0% of revenue in 2012, compared to 36.1% of revenue in 2011. Included in cost of operations were non-cash expenses related to stock-based compensation of $8,160 in 2012, compared to $7,707 in 2011.
Cost of operations, excluding the non-cash stock-based compensation expense discussed above, was $208,201, or 44.3% of revenue in 2012, compared to $193,970, or 34.7% of revenue in 2011. The increase in absolute dollars in 2012, compared to 2011, was primarily attributable to an increase of approximately $18,600 associated with the operations and maintenance of our network, including efforts to drive and support the increased traffic to our Websites, expenses related to the development of new content and the development of tools and features designed to increase the engagement of visitors to our Websites, and costs associated with the creation and delivery of our advertising and sponsorship programs. The increase in these expenses was partially offset by a decrease of $4,400 of distribution expense related to the phase out of our affiliate partner sites and other distribution partners. The increase as a percentage of revenue, excluding the non-cash expenses discussed above, was due to the decrease in our revenue of 15.9%, combined with the increase in our cost of operations as certain of these expenses are fixed in nature and do not vary directly with revenue.
Sales and Marketing. Sales and marketing expense was $127,659 in 2012, compared to $124,326 in 2011. Our sales and marketing expense represented 27.2% of revenue in 2012, compared to 22.2% in 2011. Included in sales and marketing expense were non-cash expenses related to stock-based compensation of $8,201 in 2012, compared to $9,079 in 2011.
Sales and marketing expense, excluding the non-cash expenses discussed above, was $119,458, or 25.4% of revenue, in 2012, compared to $115,247, or 20.6% of revenue, in 2011. The increase in absolute dollars in 2012 compared to 2011 was primarily attributable to an increase in certain compensation related costs and certain marketing expenses incurred in 2012 compared to the prior year. The increase as a percentage of revenue, excluding the non-cash expenses discussed above, for 2012 compared to 2011 was primarily due to the decrease in our revenue of 15.9% without a commensurate decrease in our sales and marketing expenses as certain of these expenses are fixed in nature.
General and Administrative. General and administrative expense was $97,618 in 2012, compared to $91,271 in 2011. Our general and administrative expenses represented 20.8% of revenue in 2012, compared to 16.3% of revenue in 2011. Included in general and administrative expense was non-cash stock-based compensation expense of $28,560 in 2012, compared to $22,951 in 2011. The increase in non-cash stock-based compensation expense for 2012, compared to 2011, was primarily due to the voluntary surrender of stock options by certain of our officers and directors and the related acceleration of the unrecognized stock-based compensation expense associated with those options during 2012 of $8,076.
72
General and administrative expense, excluding the non-cash stock-based compensation expense discussed above, was $69,058, or 14.7% of revenue, in 2012, compared to $68,320, or 12.2% of revenue in 2011. The increase in general and administrative expense as a percentage of revenue, excluding the non-cash expenses discussed above, for 2012 compared to 2011, was primarily due to the decrease in our revenue of 15.9% without a commensurate decrease in our general and administrative expenses as many of these expenses are fixed in nature.
Depreciation and Amortization. Depreciation and amortization expense was $28,399, or 6.0% of revenue in 2012, compared to $26,801, or 4.8% of revenue in 2011. This increase was primarily due to the acceleration of the remaining amortization expense of $1,267 associated with certain trade names that have been retired from use.
Interest Income. Interest income was $86 in 2012, which was relatively consistent when compared to $112 in 2011.
Interest Expense. Interest expense was $23,334 in 2012, compared to $20,645 in 2011. Interest expense in 2012 and 2011 included non-cash interest expense of $4,326 and $3,758, respectively, related to the amortization of the debt issuance costs for the convertible debt outstanding during those periods. The increase in interest expense is a result of the 2.50% Notes and the 2.25% Notes being outstanding for the full 2012 year, while only being outstanding for a portion of the 2011 period.
Gain on Investments. During 2012 and 2011, our gain on investments of $8,074 and $18,516, respectively, related to amounts we received through our ARS Option.
Restructuring. During 2012, we recorded a restructuring charge of $7,579 related to severance and other employee benefits that were provided to the terminated employees due to the reduction in our workforce as a result of the plan we announced, on December 11, 2012, to streamline our operations, simplify our organizational structure, reduce costs and better focus our resources.
Other Expense. Other expense during 2012 includes cash severance and related expenses due to the January 2012 departure of a Chief Executive Officer of the Company, and the related search and recruitment of his replacement during that period. For 2011, other expense consists primarily of transaction expenses of $2,275 that we incurred related to legal fees and other expenses in connection with the process conducted by our Board of Directors to explore strategic alternatives for our company.
Income Tax Provision (Benefit). The income tax benefit of $2,134 in 2012 related to a pre-tax loss of $25,221, compared to an income tax provision of $46,167 in 2011 which related to pre-tax income of $110,355. The income tax benefit during 2012 included a non-cash income tax expense of $4,724 related to an increase in our valuation allowance for certain research and development tax credits for which scheduled expiration prior to utilization is more likely than not.
Income from Discontinued Operations, Net of Tax. Income from discontinued operations, net of tax, was $2,743 in 2012, compared to $10,388 in 2011. During 2012, we recognized an after-tax gain of $2,235 related to the receipt of approximately $3,600 from the United States Department of Justice in relation to the Investigation. These funds represented the reimbursement to us related to recoveries by the United States Department of Justice from former employees of a subsidiary who pleaded guilty to the matters involved in the Investigation. None of the former employees who pleaded guilty were employees to whom we provided indemnification in connection with the Investigation. Additionally, during 2012, income from discontinued operations includes a net state tax refund of $508 that we received in connection with the finalization of a state tax appeal related to the September 2006 EPS Sale. Income from discontinued operations during 2011 consisted of adjustments to our indemnity obligations related to the Investigation and the SEC and the related insurance coverage litigation, as well as income of $2,994 related to an adjustment of the tax indemnification liability of our former Porex business as a result of the completion of an audit for one of the related matters. The income tax provision included within discontinued operations was $555 and $4,812 during 2012 and 2011, respectively.
73
Supplemental Financial and Operating Information
The following table and the discussion that follows presents information for groups of revenue based on similar services we provide, as well as information related to a non-GAAP performance measure that we use to monitor the performance of our business and which we refer to as “Earnings before interest, taxes, non-cash and other items” or “Adjusted EBITDA.” Due to the fact that Adjusted EBITDA is a non-GAAP measure, we have also included a reconciliation from Adjusted EBITDA to net income (loss).
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Revenue | | | | | | | | | | | | |
Public portal advertising and sponsorship | | $ | 433,182 | | | $ | 391,339 | | | $ | 477,325 | |
Private portal services | | | 82,111 | | | | 78,527 | | | | 81,450 | |
| | | | | | | | | | | | |
| | $ | 515,293 | | | $ | 469,866 | | | $ | 558,775 | |
| | | | | | | | | | | | |
Earnings before interest, taxes, non-cash and other items (Adjusted EBITDA) | | $ | 122,886 | | | $ | 73,149 | | | $ | 181,238 | |
Interest, taxes, non-cash and other items | | | | | | | | | | | | |
Interest income | | | 76 | | | | 86 | | | | 112 | |
Interest expense | | | (22,826 | ) | | | (23,334 | ) | | | (20,645 | ) |
Income tax (provision) benefit | | | (13,640 | ) | | | 2,134 | | | | (46,167 | ) |
Depreciation and amortization | | | (26,606 | ) | | | (28,399 | ) | | | (26,801 | ) |
Non-cash stock-based compensation | | | (38,550 | ) | | | (44,921 | ) | | | (39,737 | ) |
Loss on convertible notes | | | (4,871 | ) | | | — | | | | — | |
Gain on investments | | | — | | | | 8,074 | | | | 18,516 | |
Restructuring | | | — | | | | (7,579 | ) | | | — | |
Other expense | | | (1,353 | ) | | | (2,297 | ) | | | (2,328 | ) |
| | | | | | | | | | | | |
Income (loss) from continuing operations | | | 15,116 | | | | (23,087 | ) | | | 64,188 | |
Income from discontinued operations, net of tax | | | — | | | | 2,743 | | | | 10,388 | |
| | | | | | | | | | | | |
Net income (loss) | | $ | 15,116 | | | $ | (20,344 | ) | | $ | 74,576 | |
| | | | | | | | | | | | |
2013 and 2012
The following discussion is a comparison of the results of operations for our two groups of revenue and our Adjusted EBITDA for the year ended December 31, 2013 to the year ended December 31, 2012.
Public Portal Advertising and Sponsorship. Public portal advertising and sponsorship revenue was $433,182 in 2013, an increase of $41,843, or 10.7%, from 2012. The increase in revenue was attributable to an increase in advertising of certain of our customers, particularly our biopharmaceutical and consumer products companies. For a more detailed discussion, see “— Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Other Factors Affecting the Demand for Our Advertising and Sponsorship Services.” Although there were changes made to simplify our pricing structure in early 2013, any actual changes to prices did not have a significant impact on the increase in revenue during 2013.
Private Portal Services. Private portal services revenue was $82,111 in 2013, an increase of $3,584, or 4.6%, from 2012. In general, the pricing of our private portal services was not a significant source of the revenue increase. The number of clients using our private portal platform at December 31, 2013 was 110, compared to 118 clients using our private portal platform at December 31, 2012.
Adjusted EBITDA. Adjusted EBITDA increased to $122,886 in 2013 compared to $73,149 in 2012. As a percentage of revenue, Adjusted EBITDA was 23.8% of revenue in 2013, compared to 15.6% in 2012. This increase as a percentage of revenue was primarily due to higher revenue in 2013. Many of our expenses are fixed in nature and do not vary directly with revenue, and accordingly, our Adjusted EBITDA as a percentage of
74
revenue will fluctuate primarily as a result of changes in our revenue. Additionally, the increase in Adjusted EBITDA in 2013 compared to 2012 was partially attributable to the restructuring that took place in December 2012 which reduced our operating expenses in 2013 compared to 2012. See “— Introduction — Background Information on Certain Significant Developments and Transactions — Restructuring” for additional information.
2012 and 2011
The following discussion is a comparison of the results of operations for our two groups of revenue and our Adjusted EBITDA for the year ended December 31, 2012 to the year ended December 31, 2011.
Public Portal Advertising and Sponsorship. Public portal advertising and sponsorship revenue was $391,339 in 2012, a decrease of $85,986, or 18.0%, from 2011. We believe that this decrease related primarily to a more cautious business outlook by many of our customers, resulting in a lower volume of advertising and sponsorship programs. In general, the pricing of our advertising and sponsorship programs was not a significant source of the revenue decrease. For background information, see “— Introduction — Background Information on Certain Trends and Developments Affecting Our Business — Other Factors Affecting the Demand for Our Advertising and Sponsorship Services.”
Private Portal Services. Private portal services revenue was $78,527 in 2012, a decrease of $2,923, or 3.6%, from 2011. The decline in revenue during 2012 was primarily due to the full year impact of customers lost during 2011 and 2012 and a reduction in the level of services purchased by some of our customers. In general, the pricing of our private portal services was not a significant source of the revenue decrease. The number of clients using our private portal platform at December 31, 2012 was 118, compared to 124 clients using our private portal platform at December 31, 2011.
Adjusted EBITDA. Adjusted EBITDA decreased to $73,149 in 2012 compared to $181,238 in 2011. As a percentage of revenue, Adjusted EBITDA was 15.6% of revenue in 2012, compared to 32.4% in 2011. This decrease as a percentage of revenue was primarily due to lower revenue in 2012. Many of our expenses are fixed in nature and do not vary directly with revenue, and accordingly, our Adjusted EBITDA as a percentage of revenue will fluctuate primarily as a result of changes in our revenue.
* * * *
Explanatory Note Regarding Adjusted EBITDA. Adjusted EBITDA is a non-GAAP financial measure and should be viewed as supplemental to, and not as an alternative for, “income (loss) from continuing operations” or “net income (loss)” calculated in accordance with GAAP. Our management uses Adjusted EBITDA as an additional measure of performance for purposes of business decision-making, including developing budgets, managing expenditures, and evaluating potential acquisitions or divestitures. Period-to-period comparisons of Adjusted EBITDA help our management identify additional trends in financial results that may not be shown solely by period-to-period comparisons of income (loss) from continuing operations or net income (loss). We believe that the presentation of Adjusted EBITDA is useful to investors in their analysis of our results for reasons similar to the reasons why our management finds it useful and because it helps facilitate investor understanding of decisions made by our management in light of the performance metrics used in making those decisions. In addition, we believe that providing Adjusted EBITDA, together with a reconciliation of Adjusted EBITDA to income (loss) from continuing operations or to net income (loss), helps investors make comparisons between us and other companies that may have different capital structures, different effective income tax rates and tax attributes, different capitalized asset values and/or different forms of employee compensation. Please see the “Explanation of Non-GAAP Financial Information” filed as Exhibit 99.1 to this Annual Report for additional background information regarding our use of Adjusted EBITDA. Exhibit 99.1 is incorporated in this MD&A by reference.
Liquidity and Capital Resources
Cash Flows
As of December 31, 2013, we had $824,880 of cash and cash equivalents and working capital of $815,582. Our cash and cash equivalents and working capital are affected by the timing of each period end in relation to
75
items such as payments received from customers, payments made to vendors, the timing of interest payments related to our convertible debt and internal payroll and billing cycles, as well as the seasonality within our business. Accordingly, our working capital, and its impact on cash flow from operations, can fluctuate materially from period to period.
Cash provided by operating activities in 2013 was $86,094, which related to net income of $15,116, adjusted for a loss on convertible notes of $4,871, a non-cash income tax provision of $13,070 related to deferred income taxes, and other non-cash expenses of $69,348, which include depreciation and amortization expense, non-cash interest expense and non-cash stock-based compensation expense. Additionally, changes in operating assets and liabilities decreased operating cash flow by $16,311, primarily due to an increase in accounts receivable of $17,610 and a decrease in deferred revenue of $7,028, which was offset by an increase in accrued expenses and other long-term liabilities of $8,061 and a decrease in prepaid expenses and other assets of $266.
Cash provided by operating activities from our continuing operations in 2012 was $70,822, which related to a net loss of $20,344, adjusted for income from discontinued operations of $2,743, the gain on investments of $8,074, the non-cash income tax benefit of $2,337 related to deferred income taxes, and other non-cash expenses of $77,646, which include depreciation and amortization expense, non-cash interest expense and non-cash stock-based compensation expense. Additionally, changes in operating assets and liabilities increased operating cash flow by $26,674, primarily due to cash provided by a decrease in accounts receivable of $14,713, an increase in accrued expenses and other long-term liabilities of $9,429, and an increase in deferred revenue of $4,121, which was offset by an increase in prepaid expenses and other assets of $1,589.
Cash used in investing activities was $20,960 in 2013, compared $25,902 in 2012. We used $22,341 in connection with purchases of property and equipment in 2013, compared to $35,171 of property and equipment purchases is 2012. The higher level of purchases of property and equipment in 2012 primarily related to the planned leasehold improvements for our private portal locations as well as planned end-of-life replacement of servers and disk storage for our public portal data centers. Additionally, during 2013 we received $1,381 from the sale of property and equipment, and during 2012 we received $9,269 related to our ARS Option.
Cash used in financing activities was $232,089 in 2013, compared to $178,626 in 2012. We used cash of $390,814 in 2013 and $177,090 in 2012 to repurchase shares of our Common Stock through tender offers, our authorized repurchase program and other repurchases. We also used cash of $150,354 in 2013 to repurchase a portion of our 2.25% Notes. During 2013, these uses of cash were offset by net cash proceeds of $291,823 from the issuance of our 1.50% Notes. During 2013 and 2012, we received cash proceeds of $29,724 and $827, respectively, related to the exercise of stock options, and used cash of $12,526 and $2,740, respectively, for withholding taxes due on stock-based awards. Also included in cash flows from financing activities in 2013 and 2012, were excess tax benefits on stock-based awards of $58 and $377, respectively.
Included in our consolidated statements of cash flows for 2012, is cash provided by discontinued operations of $4,324 which includes the receipt of $3,565 from the United States Department of Justice in relation to the Investigation. These funds represented the reimbursement to us related to recoveries by the United States Department of Justice from former employees of a subsidiary who pleaded guilty to the matters involved in the Investigation. Also included in cash provided by discontinued operations for 2012 is $759 related to the cash received in connection with the finalization of a state tax appeal related to the EPS Sale.
76
Contractual Obligations and Commitments
The following table summarizes our principal commitments as of December 31, 2013 for future specified contractual obligations, as well as the estimated timing of the cash payments associated with these obligations. Management’s estimates of the timing of future cash flows are largely based on historical experience, and accordingly, actual timing of cash flows may vary from these estimates.
| | | | | | | | | | | | | | | | | | | | |
| | | Total | | | Less Than
1 Year | | | 2-3 Years | | | 4-5 Years | | | More Than
5 Years | |
Leases(a) | | $ | 64,187 | | | $ | 11,110 | | | $ | 17,946 | | | $ | 14,555 | | | $ | 20,576 | |
2.25% Convertible Notes due 2016(b) | | $ | 265,001 | | | $ | 5,675 | | | $ | 259,326 | | | $ | — | | | $ | — | |
2.50% Convertible Notes due 2018(b) | | $ | 440,833 | | | $ | 10,000 | | | $ | 20,000 | | | $ | 410,833 | | | $ | — | |
1.50% Convertible Notes due 2020(b) | | $ | 331,125 | | | $ | 4,500 | | | $ | 9,000 | | | $ | 9,000 | | | $ | 308,625 | |
| (a) | The lease amounts are net of sublease income |
| (b) | Amounts include contractual interest payments |
The above table excludes $13,889 of uncertain tax positions, including interest and penalties, as we are unable to reasonably estimate the timing of the settlement of these items. See Note 11, “Income Taxes” located in the Notes to Consolidated Financial Statements included elsewhere in this Annual Report.
Outlook on Future Liquidity
As of December 31, 2013, we had $825 million of cash and cash equivalents.
Potential future uses of cash include repurchases of our Common Stock and our anticipated 2014 capital expenditure requirements. Our capital expenditure requirements during 2014, which we estimate to be approximately $25 million to $30 million, relate to improvements that will be deployed across our public and private portal Websites in order to enable us to service future growth in unique users and page views, as well as to create new sponsorship areas for our customers, and to improve the systems used to provide our private portal applications.
Based on our plans and expectations, we believe that our available cash resources and future cash flow from operations will provide sufficient cash resources to meet the cash commitments of our convertible notes and to fund our currently anticipated working capital and capital expenditure requirements, for at least the next twenty-four months. Our future liquidity and capital requirements will depend upon numerous factors, including retention of customers at current volume and revenue levels, implementation of new or updated application and service offerings, competing technological and market developments and potential future acquisitions. In addition, our ability to generate cash flow is subject to numerous factors beyond our control, including general economic, regulatory and other matters affecting us and our customers. We plan to continue to enhance our online services and to continue to invest in acquisitions, strategic relationships, facilities and technological infrastructure and product development. We intend to grow each of our existing businesses and enter into complementary ones through both internal investments and acquisitions. We may need to raise additional funds to support expansion, develop new or enhanced applications and services, respond to competitive pressures, acquire complementary businesses or technologies or take advantage of unanticipated opportunities. If required, we may raise such additional funds through public or private debt or equity financing, strategic relationships or other arrangements. We cannot assure that such financing will be available on acceptable terms, if at all, or that such financing will not be dilutive to our stockholders. Future indebtedness may impose various restrictions and covenants on us that could limit our ability to respond to market conditions, to provide for unanticipated capital investments or to take advantage of business opportunities.
Off-Balance Sheet Arrangements
We have no material off-balance sheet arrangements.
77
Recent Accounting Pronouncements
Accounting Pronouncement Adopted During 2013
In July 2012, the Financial Accounting Standards Board (the “FASB”) issued an update to the existing guidance for impairment testing of indefinite-lived intangible assets, other than goodwill, similar to previously issued guidance for impairment testing of goodwill. The update simplifies how a company tests indefinite-lived intangible assets for impairment by allowing both public and nonpublic entities an option to first assess qualitative factors to determine whether the existence of events or circumstances leads to a determination that it is more likely than not that the fair value of an indefinite-lived intangible asset is impaired. If an entity elects to perform a qualitative assessment and determines that an impairment is more likely than not, the entity is then required to perform the existing two-step quantitative impairment test, otherwise no further analysis is required. An entity may also elect not to perform the qualitative assessment and proceed directly to the two-step quantitative impairment test. The amendment was effective for annual and interim impairment tests performed for fiscal years beginning after September 15, 2012, which for us was the first quarter of 2013. The adoption of this amendment did not have an impact on our financial condition, results of operations or cash flows.
Accounting Pronouncements to be Adopted in the Future
In July 2013, the FASB issued an update to existing guidance on the financial presentation of unrecognized tax benefits. The update provides that a liability related to an unrecognized tax benefit would be presented as a reduction of a deferred tax asset for a net operating loss carryforward, a similar tax loss or a tax credit carryforward if such settlement is required or expected in the event the uncertain tax position is disallowed. This update is effective for fiscal years, and interim periods within those years, beginning after December 15, 2013, which for us will be the first quarter of 2014. The adoption of this update is expected to have no impact on our financial condition, results of operations or cash flows.
| Item 7A. | Quantitative and Qualitative Disclosures about Market Risk |
Interest Rate Sensitivity
The primary objective of our investment activities is to preserve principal and maintain adequate liquidity.
The value of our cash and money market investments, which were approximately $825 million at December 31, 2013, are not subject to changes in interest rates.
The 2.50% Notes, 2.25% Notes and 1.50% Notes have fixed interest rates; therefore, changes in interest rates will not impact our results of operations or financial position.
Exchange Rate Sensitivity
Currently, substantially all of our sales and expenses are denominated in United States dollars; therefore, changes in exchange rates will not have a material impact on our results of operations or financial position.
| Item 8. | Financial Statements and Supplementary Data |
Financial Statements
Our financial statements required by this item are contained on pages F-1 through F-37 of this Annual Report on Form 10-K. See Item 15(a)(1) for a listing of financial statements provided.
| Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
None.
78
| Item 9A. | Controls and Procedures |
As required by Exchange Act Rule 13a-15(b), WebMD management, including the Chief Executive Officer and Chief Financial Officer, conducted an evaluation of the effectiveness of WebMD’s disclosure controls and procedures, as defined in Exchange Act Rule 13a-15(e), as of December 31, 2013. Based on that evaluation, the Chief Executive Officer and Chief Financial Officer concluded that WebMD’s disclosure controls and procedures were effective as of December 31, 2013.
In connection with the evaluation required by Exchange Act Rule 13a-15(d), WebMD management, including the Chief Executive Officer and Chief Financial Officer, concluded that there were no changes in WebMD’s internal control over financial reporting, as defined in Exchange Act Rule 13a-15(f), during the fourth quarter of 2013 that have materially affected, or are reasonably likely to materially affect, WebMD’s internal control over financial reporting.
| Item 9B. | Other Information |
None.
79
PART III
Information required by Items 10, 11, 12, 13 and 14 of Part III is omitted from this Annual Report and will be filed in a definitive proxy statement or by an amendment to this Annual Report not later than 120 days after the end of the fiscal year covered by this Annual Report.
| Item 10. | Directors, Executive Officers and Corporate Governance |
We will provide information that is responsive to this Item 10 in our definitive proxy statement or in an amendment to this Annual Report not later than 120 days after the end of the fiscal year covered by this Annual Report, in either case under the captions “Directors and Executive Officers” and “Corporate Governance” and possibly elsewhere therein. That information is incorporated in this Item 10 by reference.
| Item 11. | Executive Compensation |
We will provide information that is responsive to this Item 11 in our definitive proxy statement or in an amendment to this Annual Report not later than 120 days after the end of the fiscal year covered by this Annual Report, in either case under the caption “Executive Compensation,” and possibly elsewhere therein. That information is incorporated in this Item 11 by reference.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
We will provide information that is responsive to this Item 12 in our definitive proxy statement or in an amendment to this Annual Report not later than 120 days after the end of the fiscal year covered by this Annual Report, in either case under the caption “Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters,” and possibly elsewhere therein. That information is incorporated in this Item 12 by reference.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence |
We will provide information that is responsive to this Item 13 in our definitive proxy statement or in an amendment to this Annual Report not later than 120 days after the end of the fiscal year covered by this Annual Report, in either case under the caption “Certain Relationships and Related Transactions,” and possibly elsewhere therein. That information is incorporated in this Item 13 by reference.
| Item 14. | Principal Accountant Fees and Services |
We will provide information that is responsive to this Item 14 in our definitive proxy statement or in an amendment to this Annual Report not later than 120 days after the end of the fiscal year covered by this Annual Report, in either case under the caption “Services and Fees of Ernst & Young,” and possibly elsewhere therein. That information is incorporated in this Item 14 by reference.
80
PART IV
| Item 15. | Exhibits and Financial Statement Schedule |
(a)(1)-(2) Financial Statements and Schedule
The financial statements and schedule listed in the accompanying Index to Consolidated Financial Statements and Supplemental Data on page F-1 are filed as part of this Report.
(a)(3) Exhibits
See “Index to Exhibits” beginning on page E-1, which is incorporated by reference herein. The Index to Exhibits lists all exhibits filed with this Report and identifies which of those exhibits are management contracts and compensation plans.
81
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this Annual Report to be signed on its behalf by the undersigned, thereunto duly authorized, on the 3rd day of March, 2014.
| | |
| WEBMD HEALTH CORP. |
| |
| By: | | /S/ PETER ANEVSKI |
| | Peter Anevski Executive Vice President and Chief Financial Officer |
Pursuant to the requirements of the Securities Exchange Act of 1934, this Annual Report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| | | | |
Signature | | Capacity | | Date |
| | |
/S/ DAVID J. SCHLANGER David J. Schlanger | | Chief Executive Officer (principal executive officer) | | March 3, 2014 |
| | |
/S/ PETER ANEVSKI Peter Anevski | | Chief Financial Officer (principal financial and accounting officer) | | March 3, 2014 |
| | |
/S/ MARK J. ADLER, M.D. Mark J. Adler, M.D. | | Director | | March 3, 2014 |
| | |
/S/ KEVIN M. CAMERON Kevin M. Cameron | | Director | | March 3, 2014 |
| | |
/S/ NEIL F. DIMICK Neil F. Dimick | | Director | | March 3, 2014 |
| | |
/S/ JEROME C. KELLER Jerome C. Keller | | Director | | March 3, 2014 |
| | |
/S/ JAMES V. MANNING James V. Manning | | Director | | March 3, 2014 |
| | |
/S/ HERMAN SARKOWSKY Herman Sarkowsky | | Director | | March 3, 2014 |
| | |
/S/ JOSEPH E. SMITH Joseph E. Smith | | Director | | March 3, 2014 |
| | |
/S/ STANLEY S. TROTMAN, JR. Stanley S. Trotman, Jr. | | Director | | March 3, 2014 |
| | |
/S/ MARTIN J. WYGOD Martin J. Wygod | | Director | | March 3, 2014 |
82
WEBMD HEALTH CORP.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS AND SUPPLEMENTAL DATA
All other schedules not listed above have been omitted as not applicable or because the required information is included in the Consolidated Financial Statements or in the notes thereto. Columns omitted from the schedule filed have been omitted because the information is not applicable.
F-1
REPORT OF MANAGEMENT ON INTERNAL CONTROL OVER FINANCIAL REPORTING
Management of WebMD Health Corp. is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is defined in Rules 13a-15(f) and15d-15(f) promulgated under the Securities Exchange Act of 1934 (the Exchange Act) as a process designed by, or under the supervision of, a company’s principal executive and principal financial officers and effected by its board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Internal control over financial reporting includes those policies and procedures that:
| | • | | pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; |
| | • | | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and |
| | • | | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements. |
Internal control over financial reporting includes the controls themselves, monitoring and internal auditing practices and actions taken to correct deficiencies as identified.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
WebMD management assessed the effectiveness of WebMD’s internal control over financial reporting as of December 31, 2013. In making this assessment, WebMD management used the criteria set forth inInternal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (1992 framework). Based on that assessment and those criteria, WebMD management concluded that WebMD maintained effective internal control over financial reporting as of December 31, 2013.
Ernst & Young LLP, the independent registered public accounting firm that audited and reported on the Company’s financial statements as of December 31, 2013 and 2012 and for each of the three years in the period ended December 31, 2013, has audited the Company’s internal control over financial reporting as of December 31, 2013, as stated in their report which appears on page F-3.
March 3, 2014
F-2
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Shareholders of WebMD Health Corp.
We have audited WebMD Health Corp.’s internal control over financial reporting as of December 31, 2013, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (1992 framework) (the COSO criteria). WebMD Health Corp.’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Report of Management on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, WebMD Health Corp. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2013, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of WebMD Health Corp. as of December 31, 2013 and 2012, and the related consolidated statements of operations, equity and cash flows for each of the three years in the period ended December 31, 2013 of WebMD Health Corp. and our report dated March 3, 2014 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
New York, New York
March 3, 2014
F-3
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Stockholders of WebMD Health Corp.
We have audited the accompanying consolidated balance sheets of WebMD Health Corp. as of December 31, 2013 and 2012, and the related consolidated statements of operations, equity, and cash flows for each of the three years in the period ended December 31, 2013. Our audits also included the financial statement schedule listed in the Index at Item 15(a). These financial statements and schedule are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements and schedule based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of WebMD Health Corp. at December 31, 2013 and 2012, and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2013, in conformity with U.S. generally accepted accounting principles. Also, in our opinion, the related financial statement schedule, when considered in relation to the basic financial statements taken as a whole, presents fairly in all material respects the information set forth therein.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), WebMD Health Corp.’s internal control over financial reporting as of December 31, 2013, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (1992 framework) and our report dated March 3, 2014 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
New York, New York
March 3, 2014
F-4
WEBMD HEALTH CORP.
CONSOLIDATED BALANCE SHEETS
(In thousands, except share and per share data)
| | | | | | | | |
| | | December 31, | |
| | | 2013 | | | 2012 | |
ASSETS | | | | | | | | |
Current assets: | | | | | | | | |
Cash and cash equivalents | | $ | 824,880 | | | $ | 991,835 | |
Accounts receivable, net of allowance for doubtful accounts of $793 at December 31, 2013 and $1,304 at December 31, 2012 | | | 124,232 | | | | 106,622 | |
Prepaid expenses and other current assets | | | 13,243 | | | | 13,882 | |
Deferred tax assets | | | 13,620 | | | | 10,328 | |
| | | | | | | | |
Total current assets | | | 975,975 | | | | 1,122,667 | |
Property and equipment, net | | | 64,884 | | | | 66,604 | |
Goodwill | | | 202,980 | | | | 202,104 | |
Intangible assets, net | | | 13,834 | | | | 16,105 | |
Deferred tax assets | | | 38,802 | | | | 56,039 | |
Other assets | | | 29,153 | | | | 27,106 | |
| | | | | | | | |
TOTAL ASSETS | | $ | 1,325,628 | | | $ | 1,490,625 | |
| | | | | | | | |
LIABILITIES AND STOCKHOLDERS’ EQUITY | | | | | | | | |
Current liabilities: | | | | | | | | |
Accrued expenses | | $ | 73,739 | | | $ | 64,256 | |
Deferred revenue | | | 85,148 | | | | 92,176 | |
Liabilities of discontinued operations | | | 1,506 | | | | 1,506 | |
| | | | | | | | |
Total current liabilities | | | 160,393 | | | | 157,938 | |
2.25% convertible notes due 2016 | | | 252,232 | | | | 400,000 | |
2.50% convertible notes due 2018 | | | 400,000 | | | | 400,000 | |
1.50% convertible notes due 2020 | | | 300,000 | | | | — | |
Other long-term liabilities | | | 22,103 | | | | 22,698 | |
Commitments and contingencies | | | | | | | | |
Stockholders’ equity: | | | | | | | | |
Preferred stock, 50,000,000 shares authorized; no shares issued and outstanding | | | — | | | | — | |
Common stock, $0.01 par value per share, 650,000,000 shares authorized; 57,437,992 shares issued at December 31, 2013 and 62,437,992 shares issued at December 31, 2012 | | | 574 | | | | 624 | |
Additional paid-in capital | | | 9,273,712 | | | | 9,489,099 | |
Treasury stock, at cost; 18,281,498 shares at December 31, 2013 and 13,425,144 shares at December 31, 2012 | | | (572,221 | ) | | | (453,453 | ) |
Accumulated deficit | | | (8,511,165 | ) | | | (8,526,281 | ) |
| | | | | | | | |
Stockholders’ equity | | | 190,900 | | | | 509,989 | |
| | | | | | | | |
TOTAL LIABILITIES AND STOCKHOLDERS’ EQUITY | | $ | 1,325,628 | | | $ | 1,490,625 | |
| | | | | | | | |
See accompanying notes.
F-5
WEBMD HEALTH CORP.
CONSOLIDATED STATEMENTS OF OPERATIONS
(In thousands, except per share data)
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Revenue | | $ | 515,293 | | | $ | 469,866 | | | $ | 558,775 | |
Cost of operations | | | 209,740 | | | | 216,361 | | | | 201,677 | |
Sales and marketing | | | 127,997 | | | | 127,659 | | | | 124,326 | |
General and administrative | | | 93,220 | | | | 97,618 | | | | 91,271 | |
Depreciation and amortization | | | 26,606 | | | | 28,399 | | | | 26,801 | |
Interest income | | | 76 | | | | 86 | | | | 112 | |
Interest expense | | | 22,826 | | | | 23,334 | | | | 20,645 | |
Loss on convertible notes | | | 4,871 | | | | — | | | | — | |
Gain on investments | | | — | | | | 8,074 | | | | 18,516 | |
Restructuring | | | — | | | | 7,579 | | | | — | |
Other expense | | | 1,353 | | | | 2,297 | | | | 2,328 | |
| | | | | | | | | | | | |
Income (loss) from continuing operations before income tax provision (benefit) | | | 28,756 | | | | (25,221 | ) | | | 110,355 | |
Income tax provision (benefit) | | | 13,640 | | | | (2,134 | ) | | | 46,167 | |
| | | | | | | | | | | | |
Income (loss) from continuing operations | | | 15,116 | | | | (23,087 | ) | | | 64,188 | |
Income from discontinued operations, net of a tax provision of $555 and $4,812 in 2012 and 2011 | | | — | | | | 2,743 | | | | 10,388 | |
| | | | | | | | | | | | |
Net income (loss) | | $ | 15,116 | | | $ | (20,344 | ) | | $ | 74,576 | |
| | | | | | | | | | | | |
Basic income (loss) per common share: | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 0.32 | | | $ | (0.45 | ) | | $ | 1.11 | |
Income from discontinued operations | | | — | | | | 0.05 | | | | 0.18 | |
| | | | | | | | | | | | |
Net income (loss) | | $ | 0.32 | | | $ | (0.40 | ) | | $ | 1.29 | |
| | | | | | | | | | | | |
Diluted income (loss) per common share: | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 0.31 | | | $ | (0.45 | ) | | $ | 1.08 | |
Income from discontinued operations | | | — | | | | 0.05 | | | | 0.17 | |
| | | | | | | | | | | | |
Net income (loss) | | $ | 0.31 | | | $ | (0.40 | ) | | $ | 1.25 | |
| | | | | | | | | | | | |
Weighted-average shares outstanding used in computing per share amounts: | | | | | | | | | | | | |
Basic | | | 46,830 | | | | 50,862 | | | | 57,356 | |
| | | | | | | | | | | | |
Diluted | | | 48,398 | | | | 50,862 | | | | 59,124 | |
| | | | | | | | | | | | |
See accompanying notes.
F-6
WEBMD HEALTH CORP.
CONSOLIDATED STATEMENTS OF EQUITY
(In thousands, except share data)
| | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | Stockholders’ Equity | |
| | | Common Stock | | | Additional
Paid-In
Capital | | | Treasury Stock | | | Accumulated
Deficit | | | Total
Stockholders’
Equity | |
| | | Shares | | | Amount | | | | Shares | | | Amount | | | |
Balances at December 31, 2010 | | | 62,401,272 | | | $ | 624 | | | $ | 9,462,373 | | | | 2,485,391 | | | $ | (129,589 | ) | | $ | (8,580,513 | ) | | $ | 752,895 | |
Net income | | | — | | | | — | | | | — | | | | — | | | | — | | | | 74,576 | | | | 74,576 | |
Issuance of stock for option exercises and other issuances | | | 8,983 | | | | — | | | | (57,570 | ) | | | (1,472,747 | ) | | | 76,790 | | | | — | | | | 19,220 | |
Tax benefit realized from issuances of common stock | | | — | | | | — | | | | 30,198 | | | | — | | | | — | | | | — | | | | 30,198 | |
Stock-based compensation expense | | | — | | | | — | | | | 39,392 | | | | — | | | | — | | | | — | | | | 39,392 | |
Purchases of treasury stock | | | — | | | | — | | | | — | | | | 5,672,795 | | | | (241,263 | ) | | | — | | | | (241,263 | ) |
Other | | | — | | | | — | | | | (582 | ) | | | — | | | | — | | | | — | | | | (582 | ) |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Balances at December 31, 2011 | | | 62,410,255 | | | | 624 | | | | 9,473,811 | | | | 6,685,439 | | | | (294,062 | ) | | | (8,505,937 | ) | | | 674,436 | |
Net loss | | | — | | | | — | | | | — | | | | — | | | | — | | | | (20,344 | ) | | | (20,344 | ) |
Issuance of stock for option exercises and other issuances | | | 27,737 | | | | — | | | | (19,807 | ) | | | (350,371 | ) | | | 18,268 | | | | — | | | | (1,539 | ) |
Tax benefit realized from issuances of common stock | | | — | | | | — | | | | 377 | | | | — | | | | — | | | | — | | | | 377 | |
Stock-based compensation expense | | | — | | | | — | | | | 44,571 | | | | — | | | | — | | | | — | | | | 44,571 | |
Repurchase of shares through tender offers | | | — | | | | — | | | | — | | | | 5,769,230 | | | | (150,759 | ) | | | — | | | | (150,759 | ) |
Purchases of treasury stock | | | — | | | | — | | | | — | | | | 1,320,846 | | | | (26,900 | ) | | | — | | | | (26,900 | ) |
Tax deficiency from issuances of common stock | | | — | | | | — | | | | (9,853 | ) | | | — | | | | — | | | | — | | | | (9,853 | ) |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Balances at December 31, 2012 | | | 62,437,992 | | | | 624 | | | | 9,489,099 | | | | 13,425,144 | | | | (453,453 | ) | | | (8,526,281 | ) | | | 509,989 | |
Net income | | | — | | | | — | | | | — | | | | — | | | | — | | | | 15,116 | | | | 15,116 | |
Issuance of stock for option exercises and other issuances | | | — | | | | — | | | | (83,165 | ) | | | (1,938,041 | ) | | | 100,961 | | | | — | | | | 17,796 | |
Tax benefit realized from issuances of common stock | | | — | | | | — | | | | 58 | | | | — | | | | — | | | | — | | | | 58 | |
Stock-based compensation expense | | | — | | | | — | | | | 38,186 | | | | — | | | | — | | | | — | | | | 38,186 | |
Repurchase of shares through tender offers | | | (5,000,000 | ) | | | (50 | ) | | | (170,466 | ) | | | — | | | | — | | | | — | | | | (170,516 | ) |
Purchases of treasury stock | | | — | | | | — | | | | — | | | | 6,794,395 | | | | (219,729 | ) | | | — | | | | (219,729 | ) |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Balances at December 31, 2013 | | | 57,437,992 | | | $ | 574 | | | $ | 9,273,712 | | | | 18,281,498 | | | $ | (572,221 | ) | | $ | (8,511,165 | ) | | $ | 190,900 | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | |
See accompanying notes.
F-7
WEBMD HEALTH CORP.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Cash flows from operating activities: | | | | | | | | | | | | |
Net income (loss) | | $ | 15,116 | | | $ | (20,344 | ) | | $ | 74,576 | |
Adjustments to reconcile net income (loss) to net cash provided by operating activities: | | | | | | | | | | | | |
Income from discontinued operations, net of tax | | | — | | | | (2,743 | ) | | | (10,388 | ) |
Depreciation and amortization | | | 26,606 | | | | 28,399 | | | | 26,801 | |
Non-cash interest, net | | | 4,192 | | | | 4,326 | | | | 3,758 | |
Non-cash stock-based compensation | | | 38,550 | | | | 44,921 | | | | 39,737 | |
Deferred income taxes | | | 13,070 | | | | (2,337 | ) | | | 13,696 | |
Loss on convertible notes | | | 4,871 | | | | — | | | | — | |
Gain on investments | | | — | | | | (8,074 | ) | | | (18,516 | ) |
Changes in operating assets and liabilities: | | | | | | | | | | | | |
Accounts receivable | | | (17,610 | ) | | | 14,713 | | | | 13,113 | |
Prepaid expenses and other, net | | | 266 | | | | (1,589 | ) | | | 1,416 | |
Accrued expenses and other long-term liabilities | | | 8,061 | | | | 9,429 | | | | 2,511 | |
Deferred revenue | | | (7,028 | ) | | | 4,121 | | | | (8,988 | ) |
| | | | | | | | | | | | |
Net cash provided by continuing operations | | | 86,094 | | | | 70,822 | | | | 137,716 | |
Net cash provided by (used in) discontinued operations | | | — | | | | 4,324 | | | | (440 | ) |
| | | | | | | | | | | | |
Net cash provided by operating activities | | | 86,094 | | | | 75,146 | | | | 137,276 | |
Cash flows from investing activities: | | | | | | | | | | | | |
Proceeds received from ARS option | | | — | | | | 9,269 | | | | 21,566 | |
Purchases of property and equipment | | | (22,341 | ) | | | (35,171 | ) | | | (20,911 | ) |
Proceeds from sale of property and equipment | | | 1,381 | | | | — | | | | — | |
| | | | | | | | | | | | |
Net cash (used in) provided by investing activities | | | (20,960 | ) | | | (25,902 | ) | | | 655 | |
Cash flows from financing activities: | | | | | | | | | | | | |
Proceeds from exercise of stock options | | | 29,724 | | | | 827 | | | | 28,339 | |
Cash used for withholding taxes due on stock-based awards | | | (12,526 | ) | | | (2,740 | ) | | | (9,234 | ) |
Net proceeds from issuance of convertible notes | | | 291,823 | | | | — | | | | 774,745 | |
Repurchase of convertible notes | | | (150,354 | ) | | | — | | | | — | |
Repurchase of shares through tender offers | | | (170,516 | ) | | | (150,759 | ) | | | — | |
Purchases of treasury stock | | | (220,298 | ) | | | (26,331 | ) | | | (241,263 | ) |
Excess tax benefit on stock-based awards | | | 58 | | | | 377 | | | | 30,198 | |
| | | | | | | | | | | | |
Net cash (used in) provided by financing activities | | | (232,089 | ) | | | (178,626 | ) | | | 582,785 | |
| | | | | | | | | | | | |
Net (decrease) increase in cash and cash equivalents | | | (166,955 | ) | | | (129,382 | ) | | | 720,716 | |
Cash and cash equivalents at beginning of period | | | 991,835 | | | | 1,121,217 | | | | 400,501 | |
| | | | | | | | | | | | |
Cash and cash equivalents at end of period | | $ | 824,880 | | | $ | 991,835 | | | $ | 1,121,217 | |
| | | | | | | | | | | | |
See accompanying notes.
F-8
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
(In thousands, except share and per share data)
1. Background and Basis of Presentation
Background
WebMD Health Corp. (the “Company” or “WebMD”) is a Delaware corporation that was incorporated on May 3, 2005. The Company completed an initial public offering on September 28, 2005. The Company’s Common Stock trades under the symbol “WBMD” on the Nasdaq Global Select Market. From the completion of the initial public offering through the completion of the Company’s merger with HLTH Corporation (“HLTH”) on October 23, 2009 (the “Merger”), the Company was more than 80% owned by HLTH. On October 23, 2009, the Merger was completed, with HLTH merging into WebMD and WebMD continuing as the surviving corporation.
The Company provides health information services to consumers, physicians and other healthcare professionals, private and governmental employers and health plans through its public and private online portals, mobile platforms and health-focused publications.The WebMD Health Network includes:www.WebMD.com, the Company’s primary public portal for consumers and related mobile services;www.Medscape.com, the Company’s primary public portal for physicians and other healthcare professionals and related mobile services; and other sites through which the Company provides branded content. The Company’s services for consumers enable them to obtain information on health and wellness topics or on a particular disease or condition, to assess their personal health status, to use online trackers, tools and quizzes, to locate physicians, to receive periodic e-mailed newsletters and alerts on topics of individual interest, and to participate in online communities with peers and experts. The Company’s services for physicians and healthcare professionals make it easier for them to access clinical reference sources, stay abreast of the latest clinical information, learn about new treatment options, earn continuing medical education (“CME”) credit and communicate with peers. The Company does not charge any usage, membership or download fees for access to its public portals or mobile platforms. The Company generates revenue from its public portals and mobile platforms primarily through the sale of various types of advertising and sponsorship programs to its clients, which include: pharmaceutical, biotechnology and medical device companies; hospitals, clinics and other healthcare services companies; health insurance providers; consumer products companies whose products or services relate to health, wellness, diet, fitness, lifestyle, safety and illness prevention; and various other businesses, organizations and governmental entities. Advertisers and sponsors use the Company’s services to reach, educate and inform target audiences of consumers, physicians and other healthcare professionals. The Company also generates revenue from advertising sold inWebMD Magazine, a consumer magazine distributed to physician office waiting rooms. In addition, the Company generates revenue from the sale of certain information products. The Company’s private portals are a cloud-based population health management platform, hosted by the Company and provided to private and governmental employers and health plans for use by their employees and plan participants. The Company markets these private portals and related services under theWebMD Health Services brand. TheWebMD Health Services platform enables employers and health plans to provide their employees and plan participants with access to personalized health and benefit information and decision-support tools that help them to make more informed benefit, treatment and provider decisions and motivate them to make healthier lifestyle choices. The Company also provides telephonic, online and onsite health coaching and targeted condition management programs for use by its private portals clients’ employees and plan participants to help them achieve their wellness goals. The Company generates revenue from subscriptions to itsWebMD Health Services platform by employers and health plans, either directly or through its distributors. WebMD offers its health coaching services and its condition management programs on a per-participant basis.
Basis of Presentation
The accompanying Consolidated Financial Statements include the consolidated accounts of the Company and its majority-owned subsidiaries and have been prepared in United States dollars, and in accordance with
F-9
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
U.S. generally accepted accounting principles (“GAAP”). The results of operations for companies acquired or disposed of are included in the Consolidated Financial Statements from the effective date of acquisition or up to the date of disposal. All material intercompany balances and transactions have been eliminated in consolidation.
2. Summary of Significant Accounting Policies
Accounting Estimates
The preparation of financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the amounts reported in the Consolidated Financial Statements and accompanying notes. The Company bases its estimates on historical experience, current business factors, and various other assumptions that the Company believes are necessary to consider to form a basis for making judgments about the carrying values of assets and liabilities, the recorded amounts of revenue and expenses, and the disclosure of contingent assets and liabilities. The Company is subject to uncertainties such as the impact of future events, economic and political factors, and changes in the Company’s business environment; therefore, actual results could differ from these estimates. Accordingly, the accounting estimates used in the preparation of the Company’s financial statements will change as new events occur, as more experience is acquired, as additional information is obtained and as the Company’s operating environment changes. Changes in estimates are made when circumstances warrant. Such changes in estimates and refinements in estimation methodologies are reflected in reported results of operations; if material, the effects of changes in estimates are disclosed in the notes to the Consolidated Financial Statements. Significant estimates and assumptions by management affect the allowance for doubtful accounts, the carrying value of long-lived assets (including goodwill and intangible assets), the amortization period of long-lived assets (excluding goodwill and indefinite-lived intangible assets), the carrying value, capitalization and amortization of software and Website development costs, the carrying value of investments, the provision for income taxes and related deferred tax accounts, certain accrued liabilities, revenue recognition, contingencies, litigation and related legal accruals and the value attributed to employee stock options and other stock-based awards.
Seasonality
The timing of the Company’s revenue is affected by seasonal factors. The Company’s public portal advertising and sponsorship revenue is seasonal, primarily due to the annual spending patterns of the advertising and sponsorship clients of the Company’s public portals. This portion of the Company’s revenue is usually the lowest in the first quarter of each calendar year, and generally increases during each consecutive quarter throughout the year. The timing of revenue in relation to the Company’s expenses, many of which do not vary directly with revenue, has an impact on cost of operations, sales and marketing, and general and administrative expenses as a percentage of revenue in each calendar quarter.
Cash and Cash Equivalents
All highly liquid investments with an original maturity from the date of purchase of three months or less are considered to be cash equivalents. These investments are stated at cost, which approximates market. The Company’s cash and cash equivalents are generally invested in various money market accounts.
Fair Value
The carrying amount of cash and cash equivalents, accounts receivable, accrued expenses and deferred revenue is deemed to approximate fair value due to the immediate or short-term maturity of these financial instruments. See Note 12 for further information on the fair value of the Company’s investments.
F-10
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Allowance for Doubtful Accounts
The allowance for doubtful accounts receivable reflects the Company’s best estimate of losses inherent in the Company’s receivable portfolio determined on the basis of historical experience, specific allowances for known troubled accounts and other currently available evidence.
Long-Lived Assets
Property and Equipment
Property and equipment are stated at cost, net of accumulated depreciation. Depreciation is computed using the straight-line method over the estimated useful lives of the related assets. The useful lives are generally as follows:
| | |
Computer equipment | | 3 to 5 years |
Office equipment, furniture and fixtures | | 4 to 7 years |
Software | | 3 to 5 years |
Building and improvements | | Up to 40 years |
Website development costs | | 3 years |
Leasehold improvements | | Shorter of useful life or lease term |
Expenditures for maintenance, repair and renewals of minor items are charged to expense as incurred. Major improvements are capitalized.
Goodwill and Intangible Assets
Goodwill and intangible assets result from business combinations accounted for under the acquisition method. Goodwill and other intangible assets with indefinite lives are not amortized and are subjected to impairment review by applying fair value based tests. Intangible assets with definite lives are amortized on a straight-line basis over the individually estimated useful lives of the related assets as follows:
| | |
Content | | 3 to 5 years |
Customer relationships | | 5 to 12 years |
Acquired technology and patents | | 3 years |
Trade names | | Up to 10 years |
Recoverability
The Company reviews the carrying value of goodwill and indefinite-lived intangible assets annually and whenever indicators of impairment are present. The Company tests goodwill for impairment at the reporting unit level only when, after completing a qualitative analysis, it is determined that it is more likely than not that the fair value of the reporting unit is less than its carrying value. Fair value is determined using an income approach valuation. A reporting unit is defined as an operating segment or one level below an operating segment.
Long-lived assets used in operations are reviewed for impairment whenever events or changes in circumstances indicate that carrying amounts may not be recoverable. For long-lived assets to be held and used, the Company recognizes an impairment loss only if its carrying amount is not recoverable through its undiscounted cash flows and measures the impairment loss based on the difference between the carrying amount and the fair value. Long-lived assets held for sale are reported at the lower of cost or fair value less costs to sell.
F-11
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Based on the Company’s analysis, there was no impairment of goodwill and indefinite-lived intangible assets of any of the Company’s continuing operations during the years ended December 31, 2013, 2012 and 2011.
Internal Use Software
Software development costs that are incurred in the preliminary project stage are expensed as incurred. Once certain criteria have been met, direct costs incurred in developing or obtaining computer software are capitalized. The Company capitalized $9,085 and $5,471 during the years ended December 31, 2013 and 2012, respectively. Capitalized internal use software development costs are included in property and equipment in the accompanying consolidated balance sheets. Training and data conversion costs are expensed as incurred. Capitalized software costs are depreciated over a three-year period. Depreciation expense related to internal use software was $5,070, $6,223 and $6,224 for the years ended December 31, 2013, 2012 and 2011, respectively.
Website Development Costs
Costs related to the planning and post implementation phases of WebMD’s Website development efforts, as well as minor enhancements and maintenance, are expensed as incurred. Direct costs incurred in the development phase are capitalized. The Company capitalized $7,428 and $6,787 during the years ended December 31, 2013 and 2012, respectively. These capitalized costs are included in property and equipment in the accompanying consolidated balance sheets and are depreciated over a three-year period. Depreciation expense related to Website development costs was $5,696, $4,998 and $5,230 during the years ended December 31, 2013, 2012 and 2011, respectively.
Restricted Cash
The Company’s restricted cash primarily relates to collateral for letters of credit obtained to support the Company’s operations. Total restricted cash was $1,730 as of both December 31, 2013 and 2012 and is included in other assets in the accompanying consolidated balance sheets.
Deferred Charges
Other assets includes costs associated with the issuance of the Company’s convertible notes that are amortized to interest expense in the accompanying consolidated statements of operations, using the effective interest method over the period from issuance through the earliest date on which holders can demand redemption. During the year ended December 31, 2011, the Company capitalized issuance costs of $12,655 and $12,595, related to the issuance of its 2.50% Convertible Notes due 2018 (the “2.50% Notes”) and its 2.25% Convertible Notes due 2016 (the “2.25% Notes”), respectively. Additionally, during the year ended December 31, 2013, the Company capitalized $8,177 of issuance costs in connection with the 2013 issuance of its 1.50% Convertible Notes due 2020 (the “1.50% Notes”). The aggregate amortization of these issuance costs, which is included within interest expense in the accompanying statements of operations, was $4,192, $4,326 and $3,758 for the years ended December 31, 2013, 2012 and 2011, respectively. During the year ended December 31, 2013, the Company wrote off issuance costs of $2,285 in connection with the repurchase of a portion of its 2.25% Notes. As of December 31, 2013 and 2012, there were $18,866 and $17,166, respectively, of unamortized issuance costs included in other assets within the accompanying consolidated balance sheets.
Deferred Revenue
Deferred revenue consists of invoices sent to customers or payments received from customers, in advance of revenue recognition and is recognized as the revenue recognition criteria are met. Deferred revenue is influenced
F-12
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
by several factors, including the timing of invoices to our customers and the timing of payments received from our customers in relation to the timing of the revenue recognition for the related customer contract. Deferred revenue at each balance sheet date is expected to be recognized during the succeeding twelve month period and is therefore classified as a current liability within the accompanying balance sheets.
Leases
The Company recognizes rent expense on a straight-line basis, including predetermined fixed escalations, over the initial lease term including reasonably assured renewal periods, net of lease incentives, from the time that the Company controls the leased property. Leasehold improvements made at the inception of the lease are amortized over the shorter of the useful life of the asset or the lease term. Lease incentives are recorded as a deferred credit and recognized as a reduction to rent expense on a straight-line basis over the lease term as described above.
Presentation of Segment Information
The Company generates its revenue through its public and private portals. Discrete financial information related to a measure of profit or loss for these two revenue streams is not available as they leverage many common expenses, and the Company does not separately allocate these common expenses in assessing the performance of its business. Accordingly, the Company views its business as one reportable operating segment.
The following table presents the revenues recognized related to the Company’s public portals and private portals:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Public portal advertising and sponsorship | | $ | 433,182 | | | $ | 391,339 | | | $ | 477,325 | |
Private portal services | | | 82,111 | | | | 78,527 | | | | 81,450 | |
| | | | | | | | | | | | |
| | $ | 515,293 | | | $ | 469,866 | | | $ | 558,775 | |
| | | | | | | | | | | | |
The Company’s revenue is principally generated in the United States. An adverse change in economic conditions in the United States could negatively affect the Company’s revenue and results of operations. The Company recorded revenue from foreign customers of $31,340, $24,206 and $14,679 during the years ended December 31, 2013, 2012 and 2011, respectively.
Sales, Use and Value Added Tax
The Company excludes sales, use and value added tax from revenue in the accompanying consolidated statements of operations.
Advertising Costs
Advertising costs are generally expensed as incurred and totaled $5,174, $2,798 and $3,405 in 2013, 2012 and 2011, respectively.
Foreign Currency
The functional currency of the Company’s foreign operations is the U.S. dollar. Fluctuations in foreign dollar monetary assets and liabilities result in gains or losses which are credited or charged to income. Foreign currency transactional gains or losses are also credited or charged to income.
F-13
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Concentration of Credit Risk
None of the Company’s customers individually accounted for more than 10% of the Company’s revenue in 2013, 2012 or 2011 or more than 10% of the Company’s accounts receivable as of December 31, 2013 or 2012.
Loss Contingencies
The Company accounts for loss contingencies in accordance with FASB ASC No. 450, “Contingencies.” Under ASC No. 450, accruals for loss contingencies are recorded when both (i) the information available indicates that it is probable that a liability has been incurred and (ii) the amount of the loss can be reasonably estimated. The Company records adjustments to these accruals to reflect the status of negotiations, settlements, advice of counsel and other information and events related to an individual matter.
Income Taxes
Deferred income taxes are recognized for the future tax consequence of differences between the tax and financial reporting basis of assets and liabilities at each reporting period. A valuation allowance is established to reduce deferred tax assets to the amount expected to be realized.
Tax contingencies are recorded to address potential exposure involving tax positions the Company has taken that could be challenged by tax authorities. These potential exposures result from applications of various statutes, rules, regulations and interpretations. The Company’s estimates of tax contingencies contain assumptions and judgments about potential actions by taxing jurisdictions. The Company reflects interest and penalties related to uncertain tax positions as part of the income tax provision (benefit) in the accompanying consolidated statements of operations.
Accounting for Stock-Based Compensation
Stock-based compensation expense for all share-based payment awards granted is determined based on the grant-date fair value. The grant-date fair value for stock options is estimated using the Black-Scholes Option Pricing Model. The Company recognizes these compensation costs net of an estimated forfeiture rate on a straight-line basis over the requisite service period of the award, which is generally the vesting term of the share-based payment awards.
Revenue Recognition
Revenue from advertising is recognized as advertisements are delivered or as publications are distributed. Revenue from sponsorship arrangements, content syndication and distribution arrangements, information services and subscriptions to healthcare management tools and private portals as well as related health coaching services are recognized ratably over the term of the applicable agreement. Revenue from the sponsorship of CME is recognized over the period the Company substantially completes its contractual deliverables as determined by the applicable agreements.
Contracts that contain multiple deliverables are subject to Accounting Standards Update No. 2009-13 Multiple-Deliverable Revenue Arrangements (“ASU 2009-13”). ASU 2009-13 requires the allocation of revenue to each deliverable of multiple-deliverable revenue arrangements, based on the relative selling price of each deliverable. It also defines the level of evidence of selling price required to separate deliverables and allows a company to make its best estimate of the selling price of deliverables when more objective evidence of selling price is not available.
F-14
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Pursuant to the guidance of ASU 2009-13, when a sales arrangement contains multiple deliverables, the Company allocates revenue to each deliverable based on relative selling price. The selling price for a deliverable is based on vendor-specific objective evidence (“VSOE”) if available, third-party evidence (“TPE”) if VSOE is not available, or best estimate of selling price if neither VSOE nor TPE is available. The Company then recognizes revenue on each deliverable in accordance with its revenue recognition policies over the period that delivery occurs. VSOE of selling price is based on the price charged when the deliverable is sold separately. In determining VSOE, the Company requires that a substantial majority of the selling prices fall within a reasonable range based on historical pricing trends for specific products and services. TPE is based on competitor prices of similar deliverables when sold separately. The Company is not able to determine TPE of selling price as it is unable to reliably determine what competitors’ selling prices are for comparable services, combined with the fact that its services often contain unique features and customizations such that comparable services do not exist. The determination of best estimate of selling price is a judgmental process that considers multiple factors including, but not limited to, recent selling prices and related discounting practices for each service, market conditions, customer classes, sales channels and other factors.
Net Income (Loss) Per Common Share
Basic income (loss) per common share has been computed using the weighted-average number of shares of Common Stock outstanding during the period, adjusted to give effect to participating non-vested restricted stock during the periods it was outstanding. Diluted income (loss) per common share has been computed using the weighted-average number of shares of Common Stock outstanding during the periods, increased to give effect to potentially dilutive securities and assumes that any dilutive convertible notes were converted, only in the periods in which such effect is dilutive (shares in thousands):
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Numerator: | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 15,116 | | | $ | (23,087 | ) | | $ | 64,188 | |
Effect of participating non-vested restricted stock | | | — | | | | — | | | | (436 | ) |
| | | | | | | | | | | | |
Income (loss) from continuing operations — Basic and Diluted | | $ | 15,116 | | | $ | (23,087 | ) | | $ | 63,752 | |
| | | | | | | | | | | | |
Income from discontinued operations, net of tax | | $ | — | | | $ | 2,743 | | | $ | 10,388 | |
Effect of participating non-vested restricted stock | | | — | | | | — | | | | (71 | ) |
| | | | | | | | | | | | |
Income from discontinued operations, net of tax — Basic and Diluted | | $ | — | | | $ | 2,743 | | | $ | 10,317 | |
| | | | | | | | | | | | |
Denominator: | | | | | | | | | | | | |
Weighted-average shares — Basic | | | 46,830 | | | | 50,862 | | | | 57,356 | |
Stock options and restricted stock | | | 1,568 | | | | — | | | | 1,768 | |
| | | | | | | | | | | | |
Adjusted weighted-average shares after assumed conversions —Diluted | | | 48,398 | | | | 50,862 | | | | 59,124 | |
| | | | | | | | | | | | |
Basic income (loss) per common share: | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 0.32 | | | $ | (0.45 | ) | | $ | 1.11 | |
Income from discontinued operations | | | — | | | | 0.05 | | | | 0.18 | |
| | | | | | | | | | | | |
Net income (loss) | | $ | 0.32 | | | $ | (0.40 | ) | | $ | 1.29 | |
| | | | | | | | | | | | |
Diluted income (loss) per common share: | | | | | | | | | | | | |
Income (loss) from continuing operations | | $ | 0.31 | | | $ | (0.45 | ) | | $ | 1.08 | |
Income from discontinued operations | | | — | | | | 0.05 | | | | 0.17 | |
| | | | | | | | | | | | |
Net income (loss) | | $ | 0.31 | | | $ | (0.40 | ) | | $ | 1.25 | |
| | | | | | | | | | | | |
F-15
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
The Company has excluded its convertible notes, as well as certain outstanding stock options and restricted stock, from the calculation of diluted income (loss) per common share during the periods in which such securities were anti-dilutive. The following table presents the total weighted-average number of potentially dilutive common shares that were excluded from the computation of diluted income (loss) per common share during the periods presented (shares in thousands):
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Options and restricted stock | | | 5,744 | | | | 12,291 | | | | 3,420 | |
1.50% Notes | | | 556 | | | | — | | | | — | |
2.50% Notes | | | 6,148 | | | | 6,108 | | | | 5,881 | |
2.25% Notes | | | 5,020 | | | | 5,482 | | | | 4,343 | |
| | | | | | | | | | | | |
| | | 17,468 | | | | 23,881 | | | | 13,644 | |
| | | | | | | | | | | | |
Discontinued Operations
The operating results of a business unit are reported as discontinued if its operations and cash flows can be clearly distinguished from the rest of the business, the operations have been sold or will be sold within a year, there will be no continuing involvement in the operation after the disposal date and certain other criteria are met. Significant judgments are involved in determining whether a business component meets the criteria for discontinued operation reporting and the period in which these criteria are met.
Reclassifications
Certain reclassifications have been made to the prior period financial statements to conform with the current period presentation.
Recent Accounting Pronouncements
Accounting Pronouncement Adopted During 2013
In July 2012, the Financial Accounting Standards Board (the “FASB”) issued an update to the existing guidance for impairment testing of indefinite-lived intangible assets, other than goodwill, similar to previously issued guidance for impairment testing of goodwill. The update simplifies how a company tests indefinite-lived intangible assets for impairment by allowing both public and nonpublic entities an option to first assess qualitative factors to determine whether the existence of events or circumstances leads to a determination that it is more likely than not that the fair value of an indefinite-lived intangible asset is impaired. If an entity elects to perform a qualitative assessment and determines that an impairment is more likely than not, the entity is then required to perform the existing two-step quantitative impairment test, otherwise no further analysis is required. An entity may also elect not to perform the qualitative assessment and proceed directly to the two-step quantitative impairment test. The amendment is effective for annual and interim impairment tests performed for fiscal years beginning after September 15, 2012, which for the Company was the first quarter of 2013. The adoption of this amendment did not have an impact on the Company’s financial condition, results of operations or cash flows.
Accounting Pronouncements to be Adopted in the Future
In July 2013, the FASB issued an update to existing guidance on the financial presentation of unrecognized tax benefits. The update provides that a liability related to an unrecognized tax benefit would be presented as a
F-16
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
reduction of a deferred tax asset for a net operating loss carryforward, a similar tax loss or a tax credit carryforward if such settlement is required or expected in the event the uncertain tax position is disallowed. This update is effective for fiscal years, and interim periods within those years, beginning after December 15, 2013, which for the Company will be the first quarter of 2014. The adoption of this update is expected to have no impact on the Company’s financial condition, results of operations or cash flows.
3. Discontinued Operations
EPS
On September 14, 2006, the Company completed the sale of Emdeon Practice Services, Inc. (together with its subsidiaries, “EPS”) to Sage Software, Inc., an indirect wholly owned subsidiary of The Sage Group plc (the “EPS Sale”). The Company had certain indemnity obligations to advance amounts for reasonable defense costs for initially ten, and later four, former officers and directors of EPS (the “EPS Indemnification Obligations”) who were indicted in connection with an investigation by the United States Attorney for the District of South Carolina (the “Investigation”) that began in 2003. The Investigation related principally to issues of financial accounting improprieties relating to Medical Manager Corporation, a predecessor of HLTH (by its merger into HLTH in September 2000), and more specifically, HLTH’s former Medical Manager Health Systems, Inc. subsidiary. Medical Manager Health Systems was a predecessor to EPS. On December 15, 2005, the United States Attorney announced the indictments of the ten former officers and employees of Medical Manager Health Systems. The indictment initially charged the defendants with conspiracy to commit mail, wire and securities fraud, a violation of Title 18, United States Code, Section 371 and conspiracy to commit money laundering, a violation of Title 18, United States Code, Section 1956(h), but the second count was dismissed in 2009. One of the defendants passed away in 2008 and was dismissed from the indictment. Four of the defendants were dismissed from the case and two defendants were severed from the case and their cases were transferred to Tampa, Florida. In addition, one of the defendants entered into a Deferred Prosecution Agreement with the United States pursuant to which all charges were dismissed against him on July 26, 2010. The trial of two of the former officers of Medical Manager Health Systems began on January 19, 2010 and, on March 1, 2010, both men were found guilty by the jury; however, the Court set the verdict aside on May 27, 2010 and entered a judgment of acquittal. The government entered a notice of appeal with respect to the Court’s order. At that time, two other former officers of EPS were awaiting trial in Tampa, Florida, which was scheduled to begin on October 4, 2010; however, on July 9, 2010 the Court in Tampa placed the case against those defendants on hold pending resolution of the appeal of the South Carolina ruling. On June 8, 2011, upon the motion of the government, the United States Court of Appeals for the Fourth Circuit dismissed the government’s appeal of the District Court’s rulings, thereby ending the government’s case against the two defendants in South Carolina. On July 8, 2011, upon the motion of the government, the United States District Court for the Middle District of Florida granted a motion to dismiss the government’s case against the remaining two defendants in Florida.
In connection with the EPS Sale, the Company agreed to retain the responsibility for the EPS Indemnification Obligations. During the years ended December 31, 2007 through 2009, the Company recorded pre-tax charges aggregating $116,792, representing the Company’s estimate, and adjustments to its estimate of probable costs with respect to its indemnification obligation which included the defense costs to be incurred during the trial and pre-trial periods. As a result of the June 8, 2011 and July 8, 2011 decisions discussed above, it is the Company’s understanding that the Investigation has concluded. As a result, the Company reversed the remaining accrual with respect to its EPS Indemnification Obligations of $7,206 through income from discontinued operations during the year ended December 31, 2011.
Included within liabilities of discontinued operations related to this matter was $5,000 as of December 31, 2010, which represented certain reimbursements received from the Company’s insurance carriers between
F-17
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
July 31, 2008 and December 31, 2010 under certain directors and officers liability insurance policies (the “Policies”) for expenses that the Company had incurred and expected to continue to incur for the EPS Indemnification Obligations. The Company had previously deferred recognizing these insurance reimbursements within the consolidated statement of operations because of the possibility they might have to be repaid to the insurance carriers under the terms of the applicable Policies. However, as a result of the June 8, 2011 and July 8, 2011 dismissals described above, the Company believes that the insurance carriers do not have the ability to recover this amount and accordingly, the Company reversed this accrual through income from discontinued operations during the year ended December 31, 2011.
During the year ended December 31, 2012, the Company recognized an after-tax gain of $2,235 related to the receipt of approximately $3,600 in relation to the Investigation described above. These funds represented a reimbursement to the Company related to recoveries by the United States Department of Justice from former employees of EPS who pleaded guilty to the matters described above. None of the former employees who pleaded guilty were employees to whom the Company provided indemnification in connection with the Investigation.
Also included in income from discontinued operations during the year ended December 31, 2012 is a gain of $508 related to a state tax refund that the Company received in connection with the finalization of a state tax appeal related to the EPS Sale.
Porex
On October 19, 2009, the Company completed the sale of its Porex business. In connection with the sale of Porex, the Company agreed to indemnify Porex for certain tax matters, which were estimated by the Company to be approximately $4,800. During the year ended December 31, 2011, as a result of the completion of a tax audit for one of the related matters under such indemnification, the Company reduced its indemnification liability by $2,994, and accordingly, this amount is reflected within income from discontinued operations during the year ended December 31, 2011. Additionally, the Company paid $287 related to the completion of this tax audit during the year ended December 31, 2011. The remaining estimate of the Company’s tax indemnification liability related to Porex is $1,506 and is included within liabilities of discontinued operations within the accompanying balance sheets as of December 31, 2013 and 2012.
4. Convertible Notes
1.50% Convertible Notes due 2020
On November 26, 2013, the Company issued $300,000 aggregate principal amount of its 1.50% Notes in a private offering. Unless previously converted, the 1.50% Notes will mature on December 1, 2020. Net proceeds from the sale of the 1.50% Notes were approximately $291,823, after deducting the related offering expenses. Interest on the 1.50% Notes is payable semi-annually on June 1 and December 1 of each year, commencing June 1, 2014. Under the terms of the 1.50% Notes, holders may surrender their 1.50% Notes for conversion into the Company’s Common Stock at an initial conversion rate of 18.9362 shares of Common Stock per thousand dollars principal amount of the 1.50% Notes. This is equivalent to an initial conversion price of approximately $52.81 per share of Common Stock. In the aggregate, the 1.50% Notes are convertible into 5,680,860 shares of the Company’s Common Stock. The conversion rate may be adjusted under certain circumstances.
Under the terms of the 1.50% Notes, if the Company undergoes certain change of control or other fundamental change transactions prior to the maturity date of the 1.50% Notes, holders of the 1.50% Notes will have the right, at their option, to require the Company to repurchase some or all of their 1.50% Notes at a
F-18
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
repurchase price equal to 100% of the principal amount of the 1.50% Notes being repurchased, plus accrued and unpaid interest to, but excluding, the repurchase date. However, the repurchase option will not apply in the case of certain change of control or other fundamental change transactions in which the Company is acquired by a public company, and (a) not less than 90% of the consideration received or to be received by holders of WebMD Common Stock, excluding cash payments for fractional shares, consists of acquirer common stock and (b) as a result of the transaction, the 1.50% Notes become convertible into the same consideration.
2.50% Convertible Notes due 2018
On January 11, 2011, the Company issued $400,000 aggregate principal amount of its 2.50% Notes in a private offering. Unless previously converted, the 2.50% Notes will mature on January 31, 2018. Net proceeds from the sale of the 2.50% Notes were approximately $387,345, after deducting the related offering expenses, of which approximately $100,000 was used to repurchase 1,920,490 shares of the Company’s Common Stock at a price of $52.07 per share, the last reported sale price of the Company’s Common Stock on January 5, 2011, which repurchase settled on January 11, 2011. Interest on the 2.50% Notes is payable semi-annually on January 31 and July 31 of each year, commencing July 31, 2011. Under the terms of the 2.50% Notes, holders were able to surrender their 2.50% Notes for conversion into the Company’s Common Stock at an initial conversion rate of 15.1220 shares of Common Stock per thousand dollars principal amount of the 2.50% Notes. This was equivalent to an initial conversion price of approximately $66.13 per share of Common Stock. In the aggregate, the 2.50% Notes were convertible into 6,048,800 shares of the Company’s Common Stock.
Effective April 4, 2012, after giving effect to an adjustment resulting from a tender offer for the Company’s Common Stock that the Company completed on April 3, 2012 (see Note 10 for additional discussion), the conversion rate was adjusted to 15.3223 shares of Common Stock per thousand dollars principal amount of the 2.50% Notes. This was equivalent to an adjusted conversion price of approximately $65.26 per share of Common Stock. In the aggregate, the 2.50% Notes were convertible into 6,128,920 shares of Common Stock following the April 4, 2012 adjustment. Effective September 11, 2013, after giving effect to an adjustment resulting from a tender offer for the Company’s Common Stock that the Company completed on September 10, 2013 (see Note 10 for additional discussion), the conversion rate was adjusted to 15.4764 shares of Common Stock per thousand dollars principal amount of the 2.50% Notes. This is equivalent to an adjusted conversion price of approximately $64.61 per share of Common Stock. In the aggregate, the 2.50% Notes are convertible into 6,190,560 shares of Common Stock following the September 11, 2013 adjustment.
Under the terms of the 2.50% Notes, if the Company undergoes certain change of control transactions prior to the maturity date of the 2.50% Notes, holders of the 2.50% Notes will have the right, at their option, to require the Company to repurchase some or all of their 2.50% Notes at a repurchase price equal to 100% of the principal amount of the 2.50% Notes being repurchased, plus accrued and unpaid interest to, but excluding, the repurchase date. At the Company’s option, and to the extent permitted by the applicable rules of the Nasdaq Global Select Market (or the applicable rules of such other exchange on which the Company’s Common Stock may be listed), instead of paying the repurchase price in cash, the Company may pay the repurchase price in shares of its Common Stock or a combination of cash and shares of its Common Stock. However, in the case of certain change of control transactions in which the Company is acquired by a public company, the Company may elect to provide for conversion of the 2.50% Notes into acquirer common stock, in which case the repurchase option would not apply.
2.25% Convertible Notes due 2016
On March 14, 2011, the Company issued $400,000 aggregate principal amount of its 2.25% Notes in a private offering. Unless previously converted, the 2.25% Notes will mature on March 31, 2016. Net proceeds
F-19
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
from the sale of the 2.25% Notes were approximately $387,400, after deducting the related offering expenses, of which approximately $50,000 was used to repurchase 868,507 shares of the Company’s Common Stock at a price of $57.57 per share, the last reported sale price of the Company’s Common Stock on March 8, 2011, which repurchase settled on March 14, 2011. Interest on the 2.25% Notes is payable semi-annually on March 31 and September 30 of each year, commencing September 30, 2011. Under the terms of the 2.25% Notes, holders were able to surrender their 2.25% Notes for conversion into the Company’s Common Stock at an initial conversion rate of 13.5704 shares of Common Stock per thousand dollars principal amount of the 2.25% Notes. This was equivalent to an initial conversion price of approximately $73.69 per share of Common Stock. In the aggregate, the 2.25% Notes were convertible into 5,428,160 shares of the Company’s Common Stock.
Effective April 4, 2012, after giving effect to an adjustment resulting from a tender offer for the Company’s Common Stock that the Company completed on April 3, 2012 (see Note 10 for additional discussion), the conversion rate was adjusted to 13.7502 shares of Common Stock per thousand dollars principal amount of the 2.25% Notes. This was equivalent to an adjusted conversion price of approximately $72.73 per share of Common Stock. In the aggregate, the 2.25% Notes are convertible into 5,500,080 shares of Common Stock following the April 4, 2012 adjustment. Effective September 11, 2013, after giving effect to an adjustment resulting from a tender offer for the Company’s Common Stock that the Company completed on September 10, 2013 (see Note 10 for additional discussion), the conversion rate was adjusted to 13.8884 shares of Common Stock per thousand dollars principal amount of the 2.25% Notes. This is equivalent to an adjusted conversion price of approximately $72.00 per share of Common Stock. In the aggregate, the 2.25% Notes were convertible into 5,555,360 shares of Common Stock following the September 11, 2013 adjustment.
During the year ended December 31, 2013, the Company repurchased $100,000 principal amount of its 2.25% Notes for $101,750 in cash in a privately negotiated transaction. Also during the year ended December 31, 2013, the Company repurchased $47,768 principal amount of its 2.25% Notes for $48,604 in cash in the open market. The Company recognized a pre-tax loss of $4,871 in 2013 related to these repurchases, which is reflected within loss on convertible notes in the accompanying consolidated statement of operations. The loss includes the expensing of the remaining deferred issuance costs outstanding related to the repurchased notes. As of December 31, 2013, the remaining principal amount of the 2.25% Notes outstanding was $252,232, which, in the aggregate, is convertible into 3,503,099 shares of Common Stock.
Under the terms of the 2.25% Notes, if the Company undergoes certain change of control transactions prior to the maturity date of the 2.25% Notes, holders of the 2.25% Notes will have the right, at their option, to require the Company to repurchase some or all of their 2.25% Notes at a repurchase price equal to 100% of the principal amount of the 2.25% Notes being repurchased, plus accrued and unpaid interest to, but excluding, the repurchase date. At the Company’s option, and to the extent permitted by the applicable rules of the Nasdaq Global Select Market (or the applicable rules of such other exchange on which the Company’s Common Stock may be listed), instead of paying the repurchase price in cash, the Company may pay the repurchase price in shares of its Common Stock or a combination of cash and shares of its Common Stock. However, in the case of certain change of control transactions in which the Company is acquired by a public company, the Company may elect to provide for conversion of the 2.25% Notes into acquirer common stock, in which case the repurchase option would not apply.
F-20
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
5. Long-Lived Assets
Property and Equipment
Property and equipment consist of the following:
| | | | | | | | |
| | | December 31, | |
| | | 2013 | | | 2012 | |
Software | | $ | 54,972 | | | $ | 45,981 | |
Computer equipment | | | 56,399 | | | | 51,028 | |
Web site development costs | | | 52,383 | | | | 44,940 | |
Leasehold improvements | | | 40,828 | | | | 39,315 | |
Office equipment, furniture and fixtures | | | 14,677 | | | | 14,273 | |
Land and buildings | | | 291 | | | | 1,812 | |
| | | | | | | | |
| | | 219,550 | | | | 197,349 | |
Less: accumulated depreciation | | | (154,666 | ) | | | (130,745 | ) |
| | | | | | | | |
Property and equipment, net | | $ | 64,884 | | | $ | 66,604 | |
| | | | | | | | |
Depreciation expense was $24,335, $24,505 and $24,174 in 2013, 2012 and 2011, respectively.
Goodwill and Intangible Assets
The balance of goodwill was $202,980 and $202,104 as of December 31, 2013 and 2012, respectively. Intangible assets consist of the following:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | December 31, 2013 | | | December 31, 2012 | |
| | | Gross
Carrying
Amount | | | Accumulated
Amortization | | | Net | | | Weighted
Average
Remaining
Useful Life(a) | | | Gross
Carrying
Amount | | | Accumulated
Amortization | | | Net | | | Weighted
Average
Remaining
Useful Life(a) | |
Content | | $ | 15,954 | | | $ | (15,954 | ) | | $ | — | | | | — | | | $ | 15,954 | | | $ | (15,954 | ) | | $ | — | | | | — | |
Customer relationships | | | 34,057 | | | | (25,035 | ) | | | 9,022 | | | | 4.5 | | | | 34,057 | | | | (22,943 | ) | | | 11,114 | | | | 5.5 | |
Technology and patents | | | 14,700 | | | | (14,700 | ) | | | — | | | | — | | | | 14,700 | | | | (14,700 | ) | | | — | | | | — | |
Trade names-definite lives | | | 2,530 | | | | (2,182 | ) | | | 348 | | | | 2.0 | | | | 2,530 | | | | (2,003 | ) | | | 527 | | | | 3.0 | |
Trade names-indefinite lives | | | 4,464 | | | | — | | | | 4,464 | | | | n/a | | | | 4,464 | | | | — | | | | 4,464 | | | | n/a | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Total | | $ | 71,705 | | | $ | (57,871 | ) | | $ | 13,834 | | | | | | | $ | 71,705 | | | $ | (55,600 | ) | | $ | 16,105 | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| (a) | The calculation of the weighted average remaining useful life is based on the net book value and the remaining amortization period of each respective intangible asset. |
Amortization expense was $2,271, $3,894 and $2,627 in 2013, 2012 and 2011, respectively. Future amortization expense for intangible assets is estimated to be:
| | | | |
Year Ending December 31: | | | | |
2014 | | $ | 2,271 | |
2015 | | $ | 2,261 | |
2016 | | $ | 2,059 | |
2017 | | $ | 1,513 | |
2018 | | $ | 1,266 | |
F-21
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
6. Accrued Expenses
Accrued expenses consist of the following:
| | | | | | | | |
| | | December 31, | |
| | | 2013 | | | 2012 | |
Accrued compensation | | $ | 39,346 | | | $ | 31,220 | |
Accrued restructuring | | | 146 | | | | 7,534 | |
Accrued outside services | | | 7,805 | | | | 5,373 | |
Accrued marketing and distribution | | | 5,638 | | | | 3,814 | |
Accrued interest | | | 6,010 | | | | 6,417 | |
Other accrued liabilities | | | 14,794 | | | | 9,898 | |
| | | | | | | | |
| | $ | 73,739 | | | $ | 64,256 | |
| | | | | | | | |
7. Commitments and Contingencies
Legal Proceedings
National Jewish Health v. WebMD Health Services Group, Inc. and WebMD Health Corp.
On October 25, 2012, National Jewish Health, a Colorado non-profit corporation, filed a complaint against the Company in United States District Court for the District of Colorado alleging copyright infringement, misappropriation of trade secrets, tortious interference with prospective business relations, and breach of contract. The allegations relate to a condition management program of the Company’s private portals. The complaint seeks injunctive relief, as well as damages of $8,000 to $10,000. The Court issued a Scheduling Order on February 11, 2013 and the parties completed fact discovery on August 9, 2013, although the Plaintiff has filed a motion seeking to extend the discovery period that is being opposed by the Company. The Court appointed a Special Master to decide the motion and a hearing before the Special Master was held in February 2014. A decision is pending. Each party has also filed a motion for partial summary judgment. Plaintiff is seeking partial summary judgment on the issue of breach of contract, alleging that the Company breached a non-disclosure agreement; and the Company is seeking summary judgment on the issue of damages, alleging that Plaintiff has introduced no evidence that it has suffered any damages as a result of any of the claims that it has alleged against the Company. The briefing of each motion is in process. The Company believes the Plaintiff’s claims are without merit and intends to vigorously defend against them. The Company is unable to predict the outcome of this action or to reasonably estimate the possible loss or range of loss, if any, arising from the claims asserted therein.
MyMedicalRecords, Inc. v. WebMD Health Corp. and WebMD Health Services Corp.
On February 13, 2013, MyMedicalRecords, Inc. filed an action against the Company in the United States District Court in the Central District of California. The complaint alleged that the personal health record tool sold by WebMD Health Services Group, Inc. infringes U.S. Patent No. 8,301,466 issued on October 30, 2012. The complaint sought injunctive relief, as well as damages in unspecified amounts. Pursuant to an agreement between the parties, MyMedicalRecords dismissed the complaint without prejudice in order to enable the parties to try to resolve the matter without the timing constraints of the litigation. The parties were unable to resolve the matter and, on October 2, 2013, MyMedicalRecords filed a new complaint against the Company alleging infringement of U.S. Patent No. 8,301,466 as well as U.S. Patent No. 8,498,883 issued on July 30, 2013. Plaintiff is seeking unspecified damages and an injunction with respect to certain products offered by the Company. The Company has filed an answer. The Court has consolidated Plaintiffs claim against the Company with its claims against several other companies. The Court has scheduled the claims construction hearing for August 18, 2014 and has
F-22
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
suspended fact discovery prior to such hearing except for discovery related solely to the issue of claim construction. The Company believes that the Plaintiff’s claims are without merit. The Company is unable to predict the outcome of this action or to reasonably estimate the possible loss or range of loss, if any, arising from the claims asserted therein.
Coverage Dispute with Stop Loss Carrier for Health Benefit Plan
The Company sponsors and maintains a self-insured group health and prescription benefit plan (the “Health Plan”) for its eligible employees and their dependents. The Company purchases stop loss insurance coverage on an annual basis to reimburse the Company for claims that exceed certain individual and/or aggregate claim amounts under the Health Plan. On May 7, 2013, the Company was advised that the former stop loss carrier for the Health Plan, Everest Reinsurance Company (“Everest”), was attempting to deny payment for certain medical claims under the Health Plan that were pending under the 2012 stop loss policy, and to recover certain payments that had already been made under the 2011 and 2012 stop loss policies. These claims were incurred in 2011 and 2012 and had previously been approved by Horizon Blue Cross and Blue Shield of New Jersey, the third party claims administrator for the Health Plan appointed by the Company. The maximum amount of claims in dispute by Everest is approximately $4,900, of which approximately $1,965 remains unpaid by Everest. On June 27, 2013, the Company filed an action in the Supreme Court, State of New York (“New York Action”), seeking payment from Everest of the $1,965 in outstanding claims. On August 14, 2013, Everest filed an action in the Superior Court, State of New Jersey (“New Jersey Action”), against the Company, the claims administrator and the Company’s insurance broker seeking recovery of approximately $2,935 paid by Everest under the stop loss policies and seeking a declaration that the remaining $1,965 is not payable by Everest. On August 15, 2013, Everest filed a motion in the New York Action seeking to dismiss the complaint filed by the Company on forum non conveniens grounds. On October 3, 2013, the New York Action court granted the Company’s motion for a temporary restraining order and stayed the New Jersey Action pending adjudication of Everest’s motion to dismiss the New York Action and the Company’s cross motion to dismiss the New Jersey Action. A preliminary injunction hearing was held on November 7, 2013 in the New York Action, following which, the New York Action court issued orders: (i) denying Everest’s motion to dismiss (or, in the alternative, for a stay of) the New York Action; and (ii) granting the Company’s motion enjoining Everest from prosecuting the New Jersey Action pending a stipulation of the parties or further order of the court. Everest answered the New York Action complaint on or about December 9, 2013, including the assertion of counterclaims similar in content and substance to its allegations in the New Jersey Action. Everest then voluntarily dismissed the New Jersey Action on or about December 10, 2013. The parties to the New York Action are currently proceeding with discovery. The Company believes the $1,965 outstanding from Everest will be recoverable. Additionally, the Company believes that the $2,935 previously paid by Everest will not be repayable by the Company. Accordingly, no provision has been recorded in the accompanying financial statements related to this matter.
Other Legal Proceedings
In the normal course of business, the Company and its subsidiaries are involved in various claims and legal proceedings. While the ultimate resolution of these matters has yet to be determined, the Company does not believe that their outcomes will have a material adverse effect on the Company’s consolidated financial position, results of operations or liquidity.
Leases
The Company leases its offices and other facilities under operating lease agreements that expire at various dates through 2023. Total rent expense for all operating leases was approximately $8,805, $8,573 and $8,104 in 2013, 2012 and 2011, respectively. Included in other long-term liabilities as of December 31, 2013 and 2012 were $12,279 and $13,545, respectively, related to lease incentives and the difference between rent expense and the rental amount payable for leases with fixed escalations.
F-23
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Future minimum lease commitments under non-cancelable lease agreements at December 31, 2013 were as follows:
| | | | |
Years Ending December 31, | | | | |
2014 | | $ | 11,110 | |
2015 | | | 10,766 | |
2016 | | | 7,180 | |
2017 | | | 7,278 | |
2018 | | | 7,277 | |
Thereafter | | | 20,576 | |
| | | | |
Total minimum lease payments | | $ | 64,187 | |
| | | | |
Other Contingencies
The Company provides certain indemnification provisions within its customer agreements to protect the other party from any liabilities or damages resulting from a claim of misappropriation or infringement by third parties relating to its products and services. The Company has not incurred a liability relating to any of these indemnification provisions in the past and management believes that the likelihood of any future payment relating to these provisions is unlikely. Therefore, the Company has not recorded a liability during any period for these indemnification provisions.
8. Stock-Based Compensation
The Company has various stock-based compensation plans (collectively, the “Plans”) that provide for the grant of stock options, restricted stock awards, and other awards based on WebMD Common Stock.
The 2005 Long-Term Incentive Plan (as amended, the “2005 Plan”) is the only existing plan under which future grants can be made. The maximum number of shares of the Company’s Common Stock that may be subject to awards under the 2005 Plan was 21,575,000 as of December 31, 2013, subject to adjustment in accordance with the terms of the 2005 Plan. The Company had an aggregate of 604,732 shares of Common Stock available for future grants under the 2005 Plan at December 31, 2013.
Equity awards granted to a former Chief Executive Officer of the Company in 2012 were made outside of the 2005 Plan and were approved by the Compensation Committee of the Company’s Board of Directors, in reliance on the NASDAQ Global Select Market exception to shareholder approval for equity grants to new hires.
F-24
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Stock Options
Generally, options under the Plans vest and become exercisable ratably over periods ranging from two to five years based on their individual grant dates, subject to continued employment on the applicable vesting dates, and generally expire within ten years from the date of grant. Options are granted at prices not less than the fair market value of the Company’s Common Stock on the date of grant. The following table summarizes stock option activity for the Plans:
| | | | | | | | | | | | | | | | |
| | | Shares | | | Weighted
Average Exercise
Price Per Share | | | Weighted
Average
Remaining
Contractual
Life (In Years) | | | Aggregate
Intrinsic Value(1) | |
Outstanding at January 1, 2011 | | | 10,227,755 | | | $ | 30.79 | | | | | | | | | |
Granted | | | 3,267,150 | | | | 36.02 | | | | | | | | | |
Exercised | | | (1,530,318 | ) | | | 26.91 | | | | | | | | | |
Cancelled | | | (910,206 | ) | | | 35.81 | | | | | | | | | |
| | | | | | | | | | | | | | | | |
Outstanding at December 31, 2011 | | | 11,054,381 | | | | 32.46 | | | | | | | | | |
Granted | | | 4,888,600 | | | | 18.42 | | | | | | | | | |
Exercised | | | (195,377 | ) | | | 22.80 | | | | | | | | | |
Cancelled | | | (2,446,916 | ) | | | 38.96 | | | | | | | | | |
| | | | | | | | | | | | | | | | |
Outstanding at December 31, 2012 | | | 13,300,688 | | | | 26.24 | | | | | | | | | |
Granted | | | 2,844,500 | | | | 33.64 | | | | | | | | | |
Exercised | | | (2,695,600 | ) | | | 20.90 | | | | | | | | | |
Cancelled | | | (2,020,309 | ) | | | 27.50 | | | | | | | | | |
| | | | | | | | | | | | | | | | |
Outstanding at December 31, 2013 | | | 11,429,279 | | | $ | 29.12 | | | | 7.0 | | | $ | 129,763 | |
| | | | | | | | | | | | | | | | |
Vested and exercisable at the end of the period | | | 5,407,188 | | | $ | 29.37 | | | | 5.4 | | | $ | 63,415 | |
| | | | | | | | | | | | | | | | |
| (1) | The aggregate intrinsic value is based on the market price of the Company’s Common Stock on December 31, 2013, which was $39.50, less the applicable exercise price of the underlying option. This aggregate intrinsic value represents the amount that would have been realized if all the option holders had exercised their options on December 31, 2013. |
The following table summarizes information with respect to options outstanding and options exercisable at December 31, 2013:
| | | | | | | | | | | | | | | | | | | | |
| | | Outstanding | | | Exercisable | |
Exercise Prices | | Shares | | | Weighted
Average Exercise
Price Per Share | | | Weighted
Average
Remaining
Contractual
Life (In Years) | | | Shares | | | Weighted
Average
Exercise Price
Per Share | |
$13.15 | | | 1,561,000 | | | $ | 13.15 | | | | 8.7 | | | | 576,000 | | | $ | 13.15 | |
$13.37-$22.22 | | | 888,749 | | | | 18.57 | | | | 6.4 | | | | 498,149 | | | | 20.01 | |
$22.40-$23.59 | | | 968,911 | | | | 22.66 | | | | 6.0 | | | | 180,036 | | | | 22.88 | |
$23.61 | | | 1,196,140 | | | | 23.61 | | | | 4.9 | | | | 1,196,140 | | | | 23.61 | |
$23.66-$29.27 | | | 953,086 | | | | 27.02 | | | | 5.3 | | | | 612,360 | | | | 26.83 | |
$29.44-$30.00 | | | 1,144,395 | | | | 29.73 | | | | 7.6 | | | | 529,595 | | | | 29.71 | |
$30.03-$33.97 | | | 1,240,071 | | | | 32.57 | | | | 8.2 | | | | 347,621 | | | | 31.68 | |
$34.07-$38.60 | | | 871,713 | | | | 36.63 | | | | 7.5 | | | | 374,738 | | | | 37.24 | |
$38.65-$39.77 | | | 1,322,075 | | | | 39.09 | | | | 9.7 | | | | 67,600 | | | | 39.23 | |
$40.02-$49.95 | | | 900,985 | | | | 45.67 | | | | 4.5 | | | | 752,196 | | | | 45.54 | |
$50.12-$92.61 | | | 382,154 | | | | 54.10 | | | | 5.9 | | | | 272,753 | | | | 54.44 | |
| | | | | | | | | | | | | | | | | | | | |
| | | 11,429,279 | | | $ | 29.12 | | | | 7.0 | | | | 5,407,188 | | | $ | 29.37 | |
| | | | | | | | | | | | | | | | | | | | |
F-25
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
The fair value of each option granted is estimated on the date of grant using the Black-Scholes option pricing model considering the weighted-average assumptions noted in the following table. Expected volatility is based on implied volatility from traded options of the Company’s Common Stock combined with historical volatility of the Company’s Common Stock. The expected term represents the period of time that options are expected to be outstanding following their grant date, and was determined using historical exercise data combined with assumptions for future exercise activity. The risk-free rate is based on the U.S. Treasury yield curve for periods equal to the expected term of the options on the grant date.
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Expected dividend yield | | | 0.0 | % | | | 0.0 | % | | | 0.0 | % |
Expected volatility | | | 0.43-0.48 | | | | 0.42-0.46 | | | | 0.30-0.42 | |
Risk-free interest rate | | | 0.55%-1.62 | % | | | 0.52%-1.04 | % | | | 0.67%-2.33 | % |
Expected term (years) | | | 4.5-5.1 | | | | 4.4-5.1 | | | | 4.4-5.1 | |
Weighted-average fair value of options granted during the period | | $ | 13.95 | | | $ | 6.96 | | | $ | 11.75 | |
On February 23, 2012, the Company’s directors and certain officers voluntarily surrendered a total of 960,600 non-qualified stock options with a weighted-average exercise price of $46.85 per share. None of these individuals received any consideration or promise of consideration in exchange for the surrender of these stock options. These options were originally granted under the 2005 Plan, and therefore, upon their surrender, the shares underlying these options were returned to the 2005 Plan and became available for grant under such plan. During the year ended December 31, 2012, the Company expensed the remaining unrecognized stock-based compensation expense of $8,076 related to these stock options.
Restricted Stock Awards
The Company’s Restricted Stock consists of shares of the Company’s Common Stock which have been awarded to employees with restrictions that cause them to be subject to substantial risk of forfeiture and restrict their sale or other transfer by the employee until they vest. Generally, the Company’s Restricted Stock awards vest ratably over periods ranging from three to five years from their individual award dates subject to continued employment on the applicable vesting dates. The following table summarizes the activity of the Company’s Restricted Stock:
| | | | | | | | | | | | | | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
| | | Shares | | | Weighted
Average Grant
Date Fair Value | | | Shares | | | Weighted
Average Grant
Date Fair Value | | | Shares | | | Weighted
Average Grant
Date Fair Value | |
Balance at beginning of the year | | | 932,386 | | | $ | 31.69 | | | | 1,205,333 | | | $ | 36.18 | | | | 1,106,751 | | | $ | 33.13 | |
Granted | | | 812,000 | | | | 32.65 | | | | 339,800 | | | | 20.64 | | | | 570,367 | | | | 38.73 | |
Vested | | | (401,825 | ) | | | 32.57 | | | | (413,372 | ) | | | 33.92 | | | | (385,285 | ) | | | 31.24 | |
Forfeited | | | (157,600 | ) | | | 24.02 | | | | (199,375 | ) | | | 35.53 | | | | (86,500 | ) | | | 35.95 | |
| | | | | | | | | | | | | | | | | | | | | | | | |
Balance at the end of the year | | | 1,184,961 | | | $ | 33.07 | | | | 932,386 | | | $ | 31.69 | | | | 1,205,333 | | | $ | 36.18 | |
| | | | | | | | | | | | | | | | | | | | | | | | |
Proceeds received from the exercise of options to purchase shares of the Company’s Common Stock were $29,724, $827 and $28,339 for the years ended December 31, 2013, 2012 and 2011, respectively. Additionally, in connection with the exercise of certain stock options and the vesting of restricted stock, the Company made
F-26
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
payments of $12,526, $2,740 and $9,234 during the years ended December 31, 2013, 2012 and 2011, respectively, related to employee statutory withholding taxes that were satisfied by withholding shares of Common Stock of equal value from the respective employees. The proceeds and payments described above are reflected within cash flows from financing activities within the accompanying consolidated statements of cash flows.
The intrinsic value related to stock options that were exercised, combined with the fair value of shares of restricted stock that vested, aggregated $45,882, $9,076 and $54,069 for the years ended December 31, 2013, 2012 and 2011, respectively.
Other
Each year the Company issues shares of its Common Stock to WebMD non-employee directors with a value equal to their annual board and committee retainers. The Company recorded $364, $350 and $345 of stock-based compensation expense for the years ended December 31, 2013, 2012 and 2011, respectively, in connection with these issuances.
Summary of Stock-Based Compensation Expense
The following table summarizes the components and classification of stock-based compensation expense:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Stock options | | $ | 24,483 | | | $ | 31,593 | | | $ | 25,752 | |
Restricted stock | | | 13,703 | | | | 12,978 | | | | 13,640 | |
Other | | | 364 | | | | 350 | | | | 345 | |
| | | | | | | | | | | | |
Total stock-based compensation expense | | $ | 38,550 | | | $ | 44,921 | | | $ | 39,737 | |
| | | | | | | | | | | | |
Included in: | | | | | | | | | | | | |
Cost of operations | | $ | 6,762 | | | $ | 8,160 | | | $ | 7,707 | |
Sales and marketing | | | 8,395 | | | | 8,201 | | | | 9,079 | |
General and administrative | | | 23,393 | | | | 28,560 | | | | 22,951 | |
| | | | | | | | | | | | |
Total stock-based compensation expense | | $ | 38,550 | | | $ | 44,921 | | | $ | 39,737 | |
| | | | | | | | | | | | |
As of December 31, 2013, approximately $69,400 of unrecognized stock-based compensation expense related to unvested awards (net of estimated forfeitures) is expected to be recognized over a weighted-average period of approximately 3.0 years, related to the Plans.
Tax benefits attributable to stock-based compensation represented 39% of stock-based compensation expense during each of the years ended December 31, 2013, 2012 and 2011.
9. Retirement Plans
The Company maintains certain defined contribution retirement plans covering substantially all of its employees, which provide for matching and discretionary contributions. The Company has recorded expenses related to these plans of $3,903, $4,205 and $3,876 for 2013, 2012 and 2011, respectively, related to these matching and discretionary contributions.
F-27
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
10. Equity
Treasury Stock
Repurchased shares are recorded under the cost method and are reflected as treasury stock in the accompanying consolidated balance sheets, unless the shares are cancelled and retired.
Tender Offers
On September 10, 2013, the Company completed a tender offer (the “2013 Tender Offer”) through which it repurchased 5,000,000 shares of its Common Stock at a price of $34.00 per share for total consideration of $170,516, which includes $516 of costs directly attributable to the purchase. The shares repurchased through the 2013 Tender Offer were cancelled and retired.
On April 3, 2012, the Company completed a tender offer (the “2012 Tender Offer”) through which it repurchased 5,769,230 shares of its Common Stock at a price of $26.00 per share for total consideration of $150,759, which includes $759 of costs directly attributable to the purchase. The shares repurchased through the 2012 Tender Offer are reflected as treasury stock in the accompanying consolidated balance sheets.
Stock Repurchase Program
On December 4, 2008, the Board of Directors established a stock repurchase program (the “2008 Program”), at which time the Company was authorized to use up to $30,000, which was subsequently increased by $15,331 in July 2011, to purchase shares of WebMD Common Stock, from time to time, in the open market, through block trades or in private transactions, depending on market conditions and other factors. In August 2011, the Board of Directors terminated the 2008 Program and established a new stock repurchase program (the “2011 Program” and, collectively with the 2008 Program, the “Programs”) through which the Company was authorized to use up to $75,000 to purchase shares of WebMD Common Stock. In October 2011, the Company’s Board of Directors authorized a $75,000 increase to the 2011 Program. During 2011, the Company repurchased 2,883,798 shares at an aggregate cost of $91,263 under the Programs. During 2012, the Company repurchased 1,320,846 shares at an aggregate cost of $26,900 under the 2011 Program. During 2013, the Company repurchased 1,266,962 shares at an aggregate cost of $42,309 under the 2011 Program. The Company paid cash of $569 in 2013 related to the repurchase of 39,857 shares in 2012, that settled in 2013. As of December 31, 2013, $19,864 remained available for repurchases under the 2011 Program. In February 2014, the Company’s Board of Directors authorized a $50,000 increase to the 2011 Program.
Other Repurchase Activity
On October 21, 2013, the Company repurchased 5,527,433 shares of its Common Stock that were beneficially owned by Carl C. Icahn and certain of his affiliates, at a purchase price of $32.08 per share, the NASDAQ official closing price of WebMD Common Stock on October 18, 2013. The total purchase price was $177,420, which includes $100 of costs directly attributable to the purchase. This share repurchase was not made under the Programs.
On January 5, 2011, the Company used $100,000 of the proceeds from the issuance and sale of the 2.50% Notes to repurchase 1,920,490 shares of the Company’s Common Stock at a price of $52.07 per share. Additionally, on March 8, 2011, the Company used $50,000 of the proceeds from the issuance and sale of the 2.25% Notes to repurchase 868,507 shares of the Company’s Common Stock at a price of $57.57 per share. See Note 4 for further discussion of the Company’s 2.50% Notes and 2.25% Notes. Neither of these share repurchases was made under the Programs.
F-28
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
Shareholder Rights Agreement
The Board of Directors of the Company adopted, and the Company entered into, a Stockholder Rights Agreement, dated as of November 2, 2011 (the “Rights Agreement”), by and between the Company and American Stock Transfer & Trust Company, LLC, as Rights Agent. Pursuant to the terms of the Rights Agreement, which had a one-year term until amended (as described below), one preferred stock purchase right (a “Right”) was attached to each outstanding share of the Company’s Common Stock held by holders of record as of the close of business on November 14, 2011. The Company issued one Right with each new share of Common Stock issued after that date until the Rights expired. The Rights initially traded with and were inseparable from the Company’s Common Stock and were not evidenced by separate certificates unless they became exercisable. The Rights would, if they had become exercisable, have caused substantial dilution to a person or group that attempted to acquire the Company on terms not approved by the Company’s Board of Directors. However, the Rights would not have interfered with a merger or other business combination approved by the Company’s Board of Directors. Until amended (as described below), each Right entitled its holder to purchase from the Company one one-thousandth of a share (a “Unit”) of Series A Junior Preferred Stock, par value $0.01 per share (the “Preferred Stock”), at an exercise price of $153.00 per Unit, subject to adjustment in accordance with the terms of the Rights Agreement, once the Rights become exercisable. On October 18, 2012, the Board of Directors of the Company adopted, and the Company entered into, an Amendment to Rights Agreement (the “First Amendment”). The First Amendment: extended the expiration date of the Rights Agreement from October 31, 2012 to October 31, 2014; provided that equity compensation awards to directors would not be included in determining whether a stockholder became an “Acquiring Person” under the Rights Agreement; and decreased the purchase price payable by holders of Rights upon exercise of such Rights from $153.00 per Unit to $66.29 per Unit. On August 1, 2013 the Company entered into a Second Amendment to the Rights Agreement (the “Second Amendment”). Pursuant to the Second Amendment, the final expiration date of the Rights Agreement occurred on August 1, 2013, which terminated the Rights Agreement and caused the Rights issued to WebMD stockholders pursuant to the Rights Agreement to expire at the close of business on that date.
F-29
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
11. Income Taxes
Deferred income taxes reflect the net tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Significant components of the Company’s deferred tax assets (liabilities) were as follows:
| | | | | | | | |
| | | December 31, | |
| | | 2013 | | | 2012 | |
Deferred tax assets: | | | | | | | | |
Federal net operating loss carryforwards | | $ | 105,323 | | | $ | 105,264 | |
State net operating loss carryforwards | | | 39,098 | | | | 40,929 | |
Capital losses | | | 6,016 | | | | 6,048 | |
Federal tax credits | | | 55,976 | | | | 55,870 | |
Accrued expenses | | | 16,748 | | | | 24,523 | |
Stock-based compensation | | | 26,946 | | | | 27,394 | |
Intangible assets | | | 4,596 | | | | 6,074 | |
Other | | | 3,932 | | | | 4,076 | |
| | | | | | | | |
Total deferred tax assets | | | 258,635 | | | | 270,178 | |
Valuation allowance | | | (174,592 | ) | | | (176,403 | ) |
| | | | | | | | |
Net deferred tax assets | | | 84,043 | | | | 93,775 | |
| | | | | | | | |
Deferred tax liabilities: | | | | | | | | |
Property and equipment | | | (3,976 | ) | | | (2,680 | ) |
Goodwill and indefinite-lived intangible asset | | | (27,645 | ) | | | (24,728 | ) |
| | | | | | | | |
Total deferred tax liabilities | | | (31,621 | ) | | | (27,408 | ) |
| | | | | | | | |
Net deferred tax assets | | $ | 52,422 | | | $ | 66,367 | |
| | | | | | | | |
| |
| | | December 31, | |
| | | 2013 | | | 2012 | |
Current deferred tax assets, net: | | | | | | | | |
Current deferred tax assets, net of deferred tax liabilities | | $ | 41,921 | | | $ | 29,732 | |
Valuation allowance | | | (28,301 | ) | | | (19,404 | ) |
| | | | | | | | |
Current deferred tax assets, net | | | 13,620 | | | | 10,328 | |
| | | | | | | | |
Non-current deferred tax assets, net: | | | | | | | | |
Non-current deferred tax assets, net of deferred tax liabilities | | | 185,093 | | | | 213,038 | |
Valuation allowance | | | (146,291 | ) | | | (156,999 | ) |
| | | | | | | | |
Non-current deferred tax assets, net | | | 38,802 | | | | 56,039 | |
| | | | | | | | |
Net deferred tax assets | | $ | 52,422 | | | $ | 66,367 | |
| | | | | | | | |
F-30
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
The income tax provision (benefit) was as follows:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Current: | | | | | | | | | | | | |
Federal | | $ | (73 | ) | | $ | (583 | ) | | $ | 373 | |
State | | | 502 | | | | 295 | | | | 3,165 | |
Foreign | | | 141 | | | | 190 | | | | 145 | |
| | | | | | | | | | | | |
Current income tax provision (benefit) | | | 570 | | | | (98 | ) | | | 3,683 | |
| | | |
Deferred: | | | | | | | | | | | | |
Federal | | | 10,683 | | | | (325 | ) | | | 9,454 | |
State | | | 2,387 | | | | (2,012 | ) | | | 4,242 | |
| | | | | | | | | | | | |
Deferred income tax provision (benefit) | | | 13,070 | | | | (2,337 | ) | | | 13,696 | |
Reversal of valuation allowance applied to additional paid-in capital | | | — | | | | 301 | | | | 28,788 | |
| | | | | | | | | | | | |
Total income tax provision (benefit) | | $ | 13,640 | | | $ | (2,134 | ) | | $ | 46,167 | |
| | | | | | | | | | | | |
The reconciliation between the federal statutory rate and the effective income tax rate is as follows:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
United States federal statutory rate | | | 35.0 | % | | | (35.0 | )% | | | 35.0 | % |
State income taxes (net of federal benefit) | | | 12.5 | | | | (0.3 | ) | | | 5.2 | |
Valuation allowance | | | (6.4 | ) | | | 18.4 | | | | (0.5 | ) |
Non-deductible officer compensation | | | 3.6 | | | | 8.7 | | | | 1.8 | |
Other | | | 2.7 | | | | (0.3 | ) | | | 0.3 | |
| | | | | | | | | | | | |
Effective income tax rate | | | 47.4 | % | | | (8.5 | )% | | | 41.8 | % |
| | | | | | | | | | | | |
During 2013, the Company reversed $1,351 of its deferred tax asset and related valuation allowance through the tax provision as a result of the expiration of state net operating loss carryforwards. During 2012 and 2011, the Company reversed $301 and $28,788, respectively, of its valuation allowance through additional paid-in capital as a result of the utilization of net operating loss carryforwards generated by excess tax benefits of stock-based awards. In 2012, the Company also reversed $801 of its deferred tax asset and related valuation allowance through additional paid-in capital as a result of the expiration of state net operating loss carryforwards generated by excess tax benefits of stock-based awards, and increased its valuation allowance by $4,724 through the tax provision for certain research and development tax credits for which scheduled expiration prior to utilization is more likely than not. The valuation allowance for deferred tax assets decreased by $1,811 in 2013 and increased by $3,571 in 2012.
At December 31, 2013, the Company had net operating loss carryforwards for federal income tax purposes of approximately $701,000, which expire in 2017 through 2033, capital losses of $14,845, which expire in 2017, and federal tax credits of $64,689, which excludes the impact of any unrecognized tax benefits, of which $43,904 expire in 2017 through 2027 and $20,785 can be carried forward indefinitely.
The Company uses the “with-and-without” approach in determining the order in which tax attributes are utilized. Using the “with-and-without” approach, the Company will only recognize a tax benefit from stock-based awards in additional paid-in capital if an incremental tax benefit is realized after all other net operating loss carryforwards currently available to the Company have been utilized, but prior to the utilization of other tax attributes.
F-31
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
The net operating loss carryforwards for federal income tax purposes of approximately $701,000 include approximately $289,000 of excess tax benefits related to share-based payments that are presented on a tax effected basis within the deferred tax assets. Since this amount was recorded through additional paid-in capital, the related valuation allowance on these net operating loss carryforwards will be reversed through additional paid-in capital when these excess tax benefits are realized. Also included in these net operating loss carryforwards are excess tax benefits related to share-based payments of approximately $400,000 that are not recognized as a deferred tax asset as the amounts would not have resulted in a reduction in current taxes payable if all other net operating loss carryforwards currently available to the Company were utilized. The benefit of these deductions will be recognized through additional paid-in capital at the time the tax deduction results in a reduction of current taxes payable.
The tender offer completed on November 25, 2008 resulted in a cumulative change of more than 50% of the ownership of the Company’s capital, as determined under rules prescribed by the U.S. Internal Revenue Code and applicable Treasury regulations. As a result of the ownership change, there is an annual limitation imposed on the Company’s net operating loss carryforwards and federal tax credits. In addition, the Company experienced another cumulative change on February 25, 2011. Despite this second ownership change, the Company’s net operating loss carryforwards and federal tax credits continue to be limited by the November 25, 2008 annual limitation.
As of December 31, 2013 and 2012, the Company had unrecognized income tax benefits of $13,889 and $14,230, respectively, which if recognized, would result in $9,164 and $9,505, respectively, being reflected as a component of the income tax provision (benefit). Included in the unrecognized income tax benefits as of December 31, 2013 and 2012 are accrued interest and penalties of $497 and $281, respectively. If recognized, these benefits would be reflected as a component of the income tax provision (benefit).
The following table summarizes the activity of unrecognized tax benefits, excluding accrued interest and penalties, for the years ended December 31, 2013, 2012 and 2011:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Balance at the beginning of the year | | $ | 13,949 | | | $ | 12,069 | | | $ | 12,869 | |
Increases related to prior year tax positions | | | — | | | | 757 | | | | — | |
Increases related to current year tax positions | | | — | | | | 1,707 | | | | — | |
Decreases related to prior year tax positions | | | (532 | ) | | | — | | | | (545 | ) |
Expiration of the statute of limitations for the assessment of taxes | | | (25 | ) | | | (584 | ) | | | (255 | ) |
| | | | | | | | | | | | |
Balance at the end of the year | | $ | 13,392 | | | $ | 13,949 | | | $ | 12,069 | |
| | | | | | | | | | | | |
Although the Company files U.S. federal and various state and other tax returns, the major taxing jurisdiction is the U.S. The Company is currently under audit in a number of state and local taxing jurisdictions and will have statutes of limitations with respect to certain tax returns expiring within the next twelve months. As a result, it is reasonably possible that there may be a reduction in the unrecognized income tax benefits, prior to any annual increase, in the range of $100 to $200 within the next twelve months. With the exception of adjusting net operating loss carryforwards that may be utilized, the Company is no longer subject to federal income tax examinations for tax years before 2010 and for state and local income tax examinations for tax years before 2005.
F-32
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
12. Fair Value of Financial Instruments
The Company accounts for certain assets and liabilities at fair value, which is defined as the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date. Additionally, the Company uses valuation techniques that maximize the use of observable inputs and minimize the use of unobservable inputs. These inputs are prioritized below:
| | Level 1: | Observable inputs such as quoted market prices in active markets for identical assets or liabilities. |
| | Level 2: | Observable market-based inputs or unobservable inputs that are corroborated by market data. |
| | Level 3: | Unobservable inputs for which there is little or no market data, which require the use of the reporting entity’s own assumptions. |
The Company did not have any Level 2 assets during the years ended December 31, 2013, 2012 and 2011, and only had one Level 3 asset which is discussed in more detail below. The following table sets forth the Company’s Level 1 financial assets that were measured and recorded at fair value on a recurring basis as of December 31, 2013 and 2012:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | Fair Value
Estimate Using: | | | December 31, 2013 | | | December 31, 2012 | |
| | | | Amortized
Cost Basis | | | Fair Value | | | Gross
Unrealized
Gains | | | Amortized
Cost Basis | | | Fair Value | | | Gross
Unrealized
Gains | |
Cash and cash equivalents | | | Level 1 | | | $ | 824,880 | | | $ | 824,880 | | | $ | — | | | $ | 991,835 | | | $ | 991,835 | | | $ | — | |
Through April 20, 2010, the Company held investments in student loan backed auction rate securities (“ARS”). Effective April 20, 2010, the Company entered into an agreement pursuant to which the Company sold all of its holdings of ARS. Under the terms of the agreement, the Company retained an option (the “ARS Option”), for a period of two years from the date of the agreement: (a) to repurchase from the purchaser the same principal amount of any or all of the various series of ARS sold, at the agreed upon purchase prices received on April 20, 2010; and (b) to receive additional proceeds from the purchaser upon certain redemptions of the various series of ARS sold. The ARS Option was classified as a Level 3 asset as its valuation required substantial judgment. The historical redemption activity of the specific ARS underlying the ARS Option was the most significant assumption used to determine an estimated value of the ARS Option. The Company was required to reassess the value of the ARS Option at each reporting period and changes in value were recorded within the statement of operations. As of March 31, 2012, the Company no longer had any remaining positions related to the ARS Option. The following table reconciles the beginning and ending balances of the ARS Option during the years ended December 31, 2012 and 2011:
| | | | | | | | |
| | | Years Ended December 31, | |
| | | 2012 | | | 2011 | |
Fair value as of the beginning of the period | | $ | 1,195 | | | $ | 4,245 | |
Cash proceeds received | | | (9,269 | ) | | | (21,566 | ) |
Gain included in earnings | | | 8,074 | | | | 18,516 | |
| | | | | | | | |
Fair value as of the end of the period | | $ | — | | | $ | 1,195 | |
| | | | | | | | |
The Company also holds an investment in a privately held company which is carried at cost, and not subject to fair value measurements. However, if events or circumstances indicate that its carrying amount may not be recoverable, it would be reviewed for impairment. The Company made this investment on November 19, 2008 by
F-33
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
acquiring Series D preferred stock. The total amount of this investment is $6,471, which includes $470 of acquisition costs. Since the Company does not have the ability to exercise significant influence over this company, the investment is accounted for under the cost method and it is included in other assets on the accompanying balance sheets as of December 31, 2013 and 2012.
For disclosure purposes, the Company is required to measure the outstanding value of its debt on a recurring basis. The following table presents the carrying value and estimated fair value (based on Level 1 market price data) of the Company’s convertible notes that were carried at historical cost as of December 31, 2013 and 2012:
| | | | | | | | | | | | | | | | |
| | | December 31, 2013 | | | December 31, 2012 | |
| | | Carrying
Amount | | | Fair Value | | | Carrying
Amount | | | Fair Value | |
2.25% Notes | | $ | 252,232 | | | $ | 252,863 | | | $ | 400,000 | | | $ | 374,000 | |
2.50% Notes | | | 400,000 | | | | 394,400 | | | | 400,000 | | | | 351,000 | |
1.50% Notes | | | 300,000 | | | | 294,852 | | | | — | | | | — | |
13. Restructuring
In December 2012, the Company announced a plan to streamline its operations, simplify its organizational structure, reduce costs and better focus its resources, which resulted in a reduction of the Company’s workforce. In connection with this reduction in workforce, the Company recorded a restructuring charge of $7,579 during the three months ended December 31, 2012 related to severance and other employee benefits that were provided to the terminated employees. The remaining accrual related to this charge was $146 and $7,534 as of December 31, 2013 and 2012, respectively, and is reflected within accrued expenses in the accompanying consolidated balance sheets. The reduction in this accrual during 2013 was the result of payments of the severance and related employee benefits.
14. Other expense
Other expense consists of the following items:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Severance and recruitment expenses(a) | | $ | 1,353 | | | $ | 2,297 | | | $ | — | |
Transaction expenses(b) | | | — | | | | — | | | | 2,275 | |
Legal expense(c) | | | — | | | | — | | | | 53 | |
| | | | | | | | | | | | |
Other expense | | $ | 1,353 | | | $ | 2,297 | | | $ | 2,328 | |
| | | | | | | | | | | | |
| (a) | For 2013, amount represents cash and related expenses due to the May 2013 departure of a Chief Executive Officer of the Company. For 2012, amount represents severance and related expenses due to the January 2012 departure of a Chief Executive Officer of the Company, and the related search and recruitment of his replacement during that period. |
| (b) | Represents transaction expenses, primarily consisting of legal fees related to the process conducted by the Board of Directors to explore strategic alternatives for the Company. |
| (c) | Represents the costs and expenses incurred by the Company related to the investigation by the United States Attorney for the District of South Carolina and the SEC and the related Coverage Litigation. |
F-34
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
15. Related Party Transactions
Fidelity Employer Services Company LLC
Fidelity Employer Services Company LLC (“FESCO”) is a distributor of the Company’s private portals, integrating the private portals product into the human resources administration and benefit administration services that FESCO provides to its employer clients. FESCO is an affiliate of FMR LLC, which reported beneficial ownership of shares that represented 14.4% of the Company’s outstanding Common Stock as of December 31, 2010. As of, and subsequent to, December 31, 2011, FMR’s beneficial ownership of the Company’s Common Stock has been less than 5% of the shares outstanding and, accordingly, FESCO was no longer deemed to be a related party. The Company recorded revenue of $5,237 for the year ended December 31, 2011 related to the FESCO relationship. Affiliates of FMR LLC have also provided services to the Company in connection with the Company’s 401(k) plan and stock-based compensation plans.
16. Supplemental Disclosures of Cash Flow Information
Supplemental information related to the consolidated statements of cash flows is summarized below:
| | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2013 | | | 2012 | | | 2011 | |
Supplemental Disclosure of Cash Flow Information: | | | | | | | | | | | | |
Interest paid | | $ | 19,038 | | | $ | 19,000 | | | $ | 10,456 | |
| | | | | | | | | | | | |
Taxes paid, net(a) | | $ | 274 | | | $ | 785 | | | $ | 1,042 | |
| | | | | | | | | | | | |
| (a) | As the Company generally files its tax returns on a consolidated basis, taxes paid, net of refunds, includes all taxes paid by the Company, including those of the Company’s discontinued operations. |
F-35
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
17. Quarterly Financial Data (Unaudited)
The following table summarizes the quarterly financial data for 2013 and 2012. The per common share calculations for each of the quarters are based on the weighted-average number of common shares for each period; therefore, the sum of the quarters may not necessarily be equal to the full year per common share amount.
| | | | | | | | | | | | | | | | |
| | | 2013 | |
| | | First
Quarter | | | Second
Quarter | | | Third
Quarter | | | Fourth
Quarter | |
Revenue | | $ | 112,762 | | | $ | 125,317 | | | $ | 130,937 | | | $ | 146,277 | |
Cost of operations | | | 46,943 | | | | 51,596 | | | | 53,438 | | | | 57,763 | |
Sales and marketing | | | 30,933 | | | | 31,422 | | | | 32,561 | | | | 33,081 | |
General and administrative | | | 23,534 | | | | 24,282 | | | | 22,689 | | | | 22,715 | |
Depreciation and amortization | | | 6,853 | | | | 6,635 | | | | 6,552 | | | | 6,566 | |
Interest income | | | 21 | | | | 17 | | | | 16 | | | | 22 | |
Interest expense | | | 5,832 | | | | 5,832 | | | | 5,833 | | | | 5,329 | |
Loss on convertible notes | | | — | | | | — | | | | 3,296 | | | | 1,575 | |
Other expense | | | — | | | | 1,353 | | | | — | | | | — | |
| | | | | | | | | | | | | | | | |
(Loss) income before income tax provision | | | (1,312 | ) | | | 4,214 | | | | 6,584 | | | | 19,270 | |
Income tax provision | | | 226 | | | | 1,603 | | | | 3,353 | | | | 8,458 | |
| | | | | | | | | | | | | | | | |
Net (loss) income | | $ | (1,538 | ) | | $ | 2,611 | | | $ | 3,231 | | | $ | 10,812 | |
| | | | | | | | | | | | | | | | |
Net (loss) income per common share — Basic | | $ | (0.03 | ) | | $ | 0.05 | | | $ | 0.07 | | | $ | 0.27 | |
| | | | | | | | | | | | | | | | |
Net (loss) income per common share — Diluted | | $ | (0.03 | ) | | $ | 0.05 | | | $ | 0.06 | | | $ | 0.25 | |
| | | | | | | | | | | | | | | | |
| | | | |
Net (Loss) Income per Common Share: | | | | | | | | | | | | | | | | |
| | | | |
Numerator: | | | | | | | | | | | | | | | | |
Net (loss) income — Basic | | $ | (1,538 | ) | | $ | 2,611 | | | $ | 3,231 | | | $ | 10,812 | |
Interest expense on 1.50% Notes, net of tax | | | — | | | | — | | | | — | | | | 326 | |
| | | | | | | | | | | | | | | | |
Net (loss) income — Diluted | | $ | (1,538 | ) | | $ | 2,611 | | | $ | 3,231 | | | $ | 11,138 | |
| | | | | | | | | | | | | | | | |
| | | | |
Denominator: | | | | | | | | | | | | | | | | |
Weighted-average shares — Basic | | | 49,007 | | | | 49,315 | | | | 48,540 | | | | 40,457 | |
Stock options and restricted stock | | | — | | | | 1,610 | | | | 2,054 | | | | 2,192 | |
1.50% Notes | | | — | | | | — | | | | — | | | | 2,223 | |
| | | | | | | | | | | | | | | | |
Adjusted weighted-average shares after assumed conversions — Diluted | | | 49,007 | | | | 50,925 | | | | 50,594 | | | | 44,872 | |
| | | | | | | | | | | | | | | | |
F-36
WEBMD HEALTH CORP.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS — (Continued)
| | | | | | | | | | | | | | | | |
| | | 2012 | |
| | | First
Quarter | | | Second
Quarter | | | Third
Quarter | | | Fourth
Quarter | |
Revenue | | $ | 106,947 | | | $ | 112,668 | | | $ | 117,513 | | | $ | 132,738 | |
Cost of operations | | | 53,471 | | | | 54,243 | | | | 53,295 | | | | 55,352 | |
Sales and marketing | | | 30,103 | | | | 31,822 | | | | 33,136 | | | | 32,598 | |
General and administrative | | | 29,022 | | | | 21,746 | | | | 23,083 | | | | 23,767 | |
Depreciation and amortization | | | 6,930 | | | | 6,713 | | | | 6,508 | | | | 8,248 | |
Interest income | | | 11 | | | | 34 | | | | 19 | | | | 22 | |
Interest expense | | | 5,836 | | | | 5,832 | | | | 5,832 | | | | 5,834 | |
Gain on investments | | | 8,074 | | | | — | | | | — | | | | — | |
Restructuring | | | — | | | | — | | | | — | | | | 7,579 | |
Other expense | | | 1,200 | | | | 1,097 | | | | — | | | | — | |
| | | | | | | | | | | | | | | | |
Loss from continuing operations before income tax (benefit) provision | | | (11,530 | ) | | | (8,751 | ) | | | (4,322 | ) | | | (618 | ) |
Income tax (benefit) provision | | | (3,753 | ) | | | (2,649 | ) | | | (1,202 | ) | | | 5,470 | |
| | | | | | | | | | | | | | | | |
Loss from continuing operations | | | (7,777 | ) | | | (6,102 | ) | | | (3,120 | ) | | | (6,088 | ) |
Income from discontinued operations, net of tax | | | — | | | | 508 | | | | 2,235 | | | | — | |
| | | | | | | | | | | | | | | | |
Net loss | | $ | (7,777 | ) | | $ | (5,594 | ) | | $ | (885 | ) | | $ | (6,088 | ) |
| | | | | | | | | | | | | | | | |
Basic (loss) income per common share: | | | | | | | | | | | | | | | | |
Loss from continuing operations | | $ | (0.14 | ) | | $ | (0.12 | ) | | $ | (0.06 | ) | | $ | (0.12 | ) |
Income from discontinued operations | | | — | | | | 0.01 | | | | 0.04 | | | | — | |
| | | | | | | | | | | | | | | | |
Net loss | �� | $ | (0.14 | ) | | $ | (0.11 | ) | | $ | (0.02 | ) | | $ | (0.12 | ) |
| | | | | | | | | | | | | | | | |
Diluted (loss) income per common share: | | | | | | | | | | | | | | | | |
Loss from continuing operations | | $ | (0.14 | ) | | $ | (0.12 | ) | | $ | (0.06 | ) | | $ | (0.12 | ) |
Income from discontinued operations | | | — | | | | 0.01 | | | | 0.04 | | | | — | |
| | | | | | | | | | | | | | | | |
Net loss | | $ | (0.14 | ) | | $ | (0.11 | ) | | $ | (0.02 | ) | | $ | (0.12 | ) |
| | | | | | | | | | | | | | | | |
| | | | |
Net (Loss) Income per Common Share: | | | | | | | | | | | | | | | | |
| | | | |
Numerator: | | | | | | | | | | | | | | | | |
Loss from continuing operations — Basic and Diluted | | $ | (7,777 | ) | | $ | (6,102 | ) | | $ | (3,120 | ) | | $ | (6,088 | ) |
| | | | | | | | | | | | | | | | |
Income from discontinued operations, net of tax — Basic and Diluted | | $ | — | | | $ | 508 | | | $ | 2,235 | | | $ | — | |
| | | | | | | | | | | | | | | | |
| | | | |
Denominator: | | | | | | | | | | | | | | | | |
Weighted-average shares — Basic and Diluted | | | 55,769 | | | | 49,615 | | | | 49,021 | | | | 49,041 | |
| | | | | | | | | | | | | | | | |
F-37
Schedule II. Valuation and Qualifying Accounts
| | | | | | | | | | | | | | | | | | | | |
| | | Years Ended December 31, 2013, 2012 and 2011 | |
| | | Balance at
Beginning
of Year | | | Charged to
Costs and
Expenses | | | Write-offs | | | Other | | | Balance at
End of Year | |
| | | (in thousands) | |
December 31, 2013 | | | | | | | | | | | | | | | | | | | | |
Allowance for Doubtful Accounts | | $ | 1,304 | | | $ | 283 | | | $ | (794 | ) | | $ | — | | | $ | 793 | |
Valuation Allowance for Deferred Tax Assets | | | 176,403 | | | | (1,831 | ) | | | — | | | | 20 | | | | 174,592 | |
December 31, 2012 | | | | | | | | | | | | | | | | | | | | |
Allowance for Doubtful Accounts | | | 1,129 | | | | 511 | | | | (336 | ) | | | — | | | | 1,304 | |
Valuation Allowance for Deferred Tax Assets | | | 172,832 | | | | 4,650 | | | | — | | | | (1,079 | )(a) | | | 176,403 | |
December 31, 2011 | | | | | | | | | | | | | | | | | | | | |
Allowance for Doubtful Accounts | | | 1,493 | | | | 595 | | | | (959 | ) | | | — | | | | 1,129 | |
Valuation Allowance for Deferred Tax Assets | | | 202,189 | | | | (569 | ) | | | — | | | | (28,788 | )(a) | | | 172,832 | |
| (a) | Primarily represents the valuation allowance released as a result of the utilization, and in 2012, the utilization and expiration, of net operating loss carryforwards generated by excess tax benefits of stock-based awards. |
S-1
INDEX TO EXHIBITS
| | |
Exhibit No. | | Description |
| |
| 2.1* | | Stock Purchase Agreement, dated as of August 8, 2006, between HLTH Corporation (“HLTH”) and Sage Software, Inc. (incorporated by reference to Exhibit 2.1 to HLTH’s Current Report on Form 8-K filed on August 11, 2006)(1) |
| |
| 2.2* | | Stock Purchase Agreement, dated as of September 17, 2009, among SNTC Holding, Inc., Aurora Equity Partners III L.P. and Aurora Overseas Equity Partners III, L.P. (incorporated by reference to Exhibit 2.1 to HLTH’s Current Report on Form 8-K filed on September 22, 2009)(1) |
| |
| 2.3* | | Purchase and Release Agreement, dated as of April 20, 2010, between WebMD Health Corp. and Citigroup Global Markets Inc. (incorporated by reference to Exhibit 2.1 to the Registrant’s Current Report on Form 8-K filed on April 26, 2010) |
| |
| 3.1 | | Restated Certificate of Incorporation of the Registrant (incorporated by reference to Exhibit 3.1 to the Registrant’s Registration Statement on Form S-8 filed on October 23, 2009(Reg. No. 333-162651)) |
| |
| 3.2 | | Amended and Restated By-laws of the Registrant (incorporated by reference to Exhibit 3.2 to the Registrant’s Registration Statement on Form S-8 filed on October 23, 2009(Reg. No. 333-162651)) |
| |
| 4.1 | | Specimen Common Stock Certificate (incorporated by reference to Exhibit 4.1 in Amendment No. 1, filed on August 11, 2009, to the Registrant’s Registration Statement on Form S-4 (Reg. No. 333-160530)) |
| |
| 4.2 | | Indenture, dated as of January 11, 2011, between the Registrant and The Bank of New York Mellon Trust Company, N.A. (incorporated by reference to Exhibit 4.1 to Amendment No. 1, filed on January 14, 2011, to the Registrant’s Current Report on Form 8-K filed on January 11, 2011) |
| |
| 4.3 | | Form of 2.50% Convertible Note Due 2018 (included in Exhibit 4.2) |
| |
| 4.4 | | Indenture, dated as of March 14, 2011, between the Registrant and The Bank of New York Mellon Trust Company, N.A. (incorporated by reference to Exhibit 4.1 to Amendment No. 1, filed on March 15, 2011, to the Registrant’s Current Report on Form 8-K filed on March 14, 2011) |
| |
| 4.5 | | Form of 2.25% Convertible Note Due 2016 (included in Exhibit 4.4) |
| |
| 4.6 | | Indenture, dated as of November 26, 2013, between the Registrant and The Bank of New York Mellon Trust Company, N.A. (incorporated by reference to Exhibit 4.1 to Amendment No. 1, filed on November 27, 2013, to the Registrant’s Current Report on Form 8-K filed on November 26, 2013) |
| |
| 4.7 | | Form of 1.50% Convertible Note Due 2020 (included in Exhibit 4.6) |
| |
| 4.8 | | Rights Agreement, dated as of November 2, 2011, between the Registrant and American Stock Transfer & Trust Company, LLC (incorporated by reference to Exhibit 4.1 to the Registrant’s Registration Statement on Form 8-A filed on November 3, 2011) |
| |
| 4.9 | | Amendment to Rights Agreement, dated as of October 18, 2012, between the Registrant and American Stock Transfer & Trust Company, LLC, as Rights Agent (incorporated by reference to Exhibit 4.1 to the Registrant’s Current Report on Form 8-K filed on October 19, 2012) |
| |
| 4.10 | | Second Amendment to Rights Agreement, dated as of August 1, 2013 (incorporated by reference to Exhibit 4.3 to Amendment No. 2, filed on August 2, 2013, to the Registrant’s Registration Statement on Form 8-A) |
| |
| 10.1 | | Form of Indemnification Agreement between HLTH and each of its directors and executive officers (incorporated by reference to Exhibit 10.1 to HLTH’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2002)(1) |
E-1
| | |
Exhibit No. | | Description |
| |
| 10.2 | | Form of Indemnification Agreement between the Registrant and its directors and executive officers (incorporated by reference to Exhibit 10.9 to the Registrant’s Registration Statement on Form S-1 (No. 333-124832) (which we refer to as the “IPO Registration Statement”)) |
| |
| 10.3 | | Form of Letter Agreement between the Registrant and Certain Non-Employee Directors (incorporated by reference to Exhibit 10.3 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2012 (the “2012 Form 10-K”) |
| |
| 10.4** | | WebMD Health Corp. Long-Term Incentive Plan for Employees of Subimo, LLC (incorporated by reference to Exhibit 10.2 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2006)(1) |
| |
| 10.5** | | Amended and Restated Employment Agreement, dated as of August 3, 2005 between HLTH and Martin J. Wygod (incorporated by reference to Exhibit 10.1 to HLTH’s Current Report onForm 8-K filed on August 5, 2005)(1) |
| |
| 10.6** | | Letter Agreement, dated as of February 1, 2006, between HLTH and Martin J. Wygod (incorporated by reference to Exhibit 10.3 to HLTH’s Current Report on Form 8-K filed on February 2, 2006)(1) |
| |
| 10.7** | | Employment Agreement, dated September 23, 2004, between HLTH and Kevin Cameron (incorporated by reference to Exhibit 10.1 to HLTH’s Current Report on Form 8-K filed September 28, 2004)(1) |
| |
| 10.8** | | Letter Agreement, dated as of February 1, 2006, between HLTH and Kevin M. Cameron (incorporated by reference to Exhibit 10.2 to HLTH’s Current Report on Form 8-K filed on February 2, 2006)(1) |
| |
| 10.9** | | Employment Agreement, dated as of April 28, 2005, between WebMD, Inc. and Wayne T. Gattinella (incorporated by reference to Exhibit 99.1 to HLTH’s Current Report on Form 8-K filed on May 3, 2005)(1) |
| |
| 10.10** | | Form of Amendment to HLTH’s Equity Compensation Plans and Stock Option Agreements (incorporated by reference to Exhibit 10.1 to the Quarterly Report on Form 10-Q filed by HLTH on November 9, 2006)(1) |
| |
| 10.11** | | 2001 Employee Non-Qualified Stock Option Plan of HLTH, as amended (incorporated by reference to Exhibit 10.46 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2001, as amended by Amendment No. 1 on Form 10-K/A)(1) |
| |
| 10.12** | | Amended and Restated 1996 Stock Plan of HLTH (incorporated by reference to Exhibit 10.8 to HLTH’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2006)(1) |
| |
| 10.13** | | Amended and Restated 2000 Long-Term Incentive Plan of HLTH (incorporated by reference to Annex E to HLTH’s Proxy Statement for its 2006 Annual Meeting filed on August 14, 2006)(1) |
| |
| 10.14** | | 1991 Director Stock Option Plan of Synetic, Inc. (incorporated by reference to Exhibit 4.2 to Synetic, Inc.’s Registration Statement on Form S-8 (No. 333-46640) filed on March 24, 1992) |
| |
| 10.15** | | Amended and Restated 1991 Special Non-Qualified Stock Option Plan of Synetic, Inc. (incorporated by reference to Exhibit 4.3 to Synetic, Inc.’s Registration Statement on Form S-8 (No. 333-36041) filed September 19, 1997) |
| |
| 10.16** | | 1996 Class C Stock Option Plan of Synetic, Inc. (incorporated by reference to Exhibit 4.1 to Synetic, Inc.’s Registration Statement on Form S-8 (No. 333-36041) filed on September 19, 1997) |
| |
| 10.17** | | CareInsite, Inc. 1999 Director Stock Option Plan (incorporated by reference to Annex H to the Proxy Statement/Prospectus, filed on August 7, 2000, and included in HLTH’s Registration Statement on Form S-4 (No. 333-39592)) |
E-2
| | |
Exhibit No. | | Description |
| |
| 10.18** | | WebMD Health Corp. Amended and Restated 2005 Long-Term Incentive Plan, as amended effective October 31, 2013 (the “2005 LTIP”) (incorporated by reference to Exhibit 4.1 to the Registrant’s Registration Statement on Form S-8 (No. 333-192157) filed on November 7, 2013) |
| |
| 10.19** | | Amended and Restated Employment Agreement, dated as of July 14, 2005, between WebMD Health Corp. and Anthony Vuolo (incorporated by reference to Exhibit 99.2 to HLTH’s Current Report on Form 8-K, as amended, filed on July 19, 2005)(1) |
| |
| 10.20** | | Form of Restricted Stock Agreement with Employees (incorporated by reference to Exhibit 4.2 to the Registrant’s Registration Statement on Form S-8 filed on October 23, 2009 (Reg. No. 333-162653)) |
| |
| 10.21** | | Form of Restricted Stock Agreement with Non-Employee Directors (incorporated by reference to Exhibit 10.49 to the IPO Registration Statement) |
| |
| 10.22** | | Form of Non-Qualified Stock Option Agreement with Employees (incorporated by reference to Exhibit 4.3 to the Registrant’s Registration Statement on Form S-8 filed on October 23, 2009 (Reg. No. 333-162653)) |
| |
| 10.23** | | Form of Non-Qualified Stock Option Agreement with Non-Employee Directors (incorporated by reference to Exhibit 10.51 to the IPO Registration Statement) |
| |
| 10.24** | | Employment Agreement between WebMD Health Holdings, Inc. and Douglas W. Wamsley (incorporated by reference to Exhibit 10.15 to the IPO Registration Statement) |
| |
| 10.25** | | Employment Agreement between WebMD Health Holdings, Inc. and Steven Zatz, M.D. (incorporated by reference to Exhibit 10.17 to the IPO Registration Statement) |
| |
| 10.26 | | Agreement of Lease, dated as of June 30, 2004, between III Chelsea Commerce LP and WebMD, Inc. (incorporated by reference to Exhibit 10.45 to the IPO Registration Statement) |
| |
| 10.27 | | First Amendment to the Lease Agreement, dated as of December 21, 2004, between III Chelsea Commerce LP and WebMD, Inc. (incorporated by reference to Exhibit 10.46 to the IPO Registration Statement) |
| |
| 10.28** | | Form of Restricted Stock Agreement between HLTH and Employees for Grants Under HLTH’s 2000 Long-Term Incentive Plan (incorporated by reference to Exhibit 10.57 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2005)(1) |
| |
| 10.29** | | Form of Non-Qualified Stock Option Agreement between HLTH and Employees for Grants Under HLTH’s 2000 Long-Term Incentive Plan (incorporated by reference to Exhibit 10.58 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2005)(1) |
| |
| 10.30** | | Form of Non-Qualified Stock Option Agreement between HLTH and Employees for Grants Under HLTH’s 1996 Stock Plan (incorporated by reference to Exhibit 10.59 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2005)(1) |
| |
| 10.31** | | Amendment No. 2, dated as of December 1, 2008, between HLTH and Martin J. Wygod (incorporated by reference to Exhibit 10.1 to HLTH’s Current Report on Form 8-K filed on December 5, 2008)(1) |
| |
| 10.32** | | Letter Agreement, dated December 29, 2008, between HLTH and Martin J. Wygod (incorporated by reference to Exhibit 10.52 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2008)(1) |
| |
| 10.33** | | Amendment to Employment Agreement, dated as of December 16, 2008, between HLTH and Kevin M. Cameron (incorporated by reference to Exhibit 10.53 to HLTH’s Annual Report on Form 10-K for the year ended December 31, 2008)(1) |
E-3
| | |
Exhibit No. | | Description |
| |
| 10.34** | | Letter Amendment, dated as of December 10, 2008, between the Registrant and Wayne T. Gattinella (incorporated by reference to Exhibit 10.53 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2008 (the “2008 Form 10-K”))(2) |
| |
| 10.35** | | Letter Amendment, dated as of July 9, 2009, among HLTH Corporation, WebMD Health Corp. and Martin J. Wygod (incorporated by reference to Exhibit 10.1 to the Current Report onForm 8-K filed by the Registrant on July 14, 2009) |
| |
| 10.36** | | WebMD, LLC Supplemental Bonus Program Trust Agreement (incorporated by reference to Exhibit 10.48 to Amendment No. 1, filed on April 29, 2008, to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2007)(2) |
| |
| 10.37** | | Amendment No. 1, dated as of March 30, 2009, to the WebMD Supplemental Bonus Program Trust Agreement (incorporated by reference to Exhibit 10.58 to Amendment No. 1, filed on April 30, 2009, to the 2008 Form 10-K) |
| |
| 10.38** | | Letter Agreement, dated as of October 1, 2007, between the Registrant and William Pence (incorporated by reference to Exhibit 10.59 to Amendment No. 1, filed on April 30, 2009, to the 2008 Form 10-K) |
| |
| 10.39** | | Letter Amendment, dated as of December 10, 2008, between the Registrant and William Pence (incorporated by reference to Exhibit 10.60 to Amendment No. 1, filed on April 30, 2009, to the 2008 Form 10-K) |
| |
| 10.40** | | Amendment, dated as of December 10, 2008 to Amended and Restated Employment Agreement between the Registrant and Anthony Vuolo (incorporated by reference to Exhibit 10.55 to the 2008 Form 10-K) |
| |
| 10.41** | | Letter Agreement, dated as of February 19, 2009, between HLTH and Anthony Vuolo (incorporated by reference to Exhibit 10.57 to the 2008 Form 10-K) |
| |
| 10.42** | | Restricted Stock Agreement, dated November 3, 2009, between the Registrant and Anthony Vuolo (incorporated by reference to Exhibit 10.71 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2009 (the “2009 Form 10-K”)) |
| |
| 10.43** | | Letter Amendment, dated as of November 3, 2009, between the Registrant and Kevin M. Cameron (incorporated by reference to Exhibit 10.72 to the 2009 Form 10-K) |
| |
| 10.44** | | Letter Amendment, dated as of December 14, 2008, between the Registrant and Steven Zatz, M.D. (incorporated by reference to Exhibit 10.74 to Amendment No. 1, filed April 30, 2010, to the 2009 Form 10-K) |
| |
| 10.45** | | Letter Agreement, dated as of June 28, 2010, between the Registrant and Wayne Gattinella (incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2010) |
| |
| 10.46** | | Letter Agreement, dated as of June 28, 2010, between the Registrant and Kevin Cameron (incorporated by reference to Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2010) |
| |
| 10.47** | | Letter Agreement, dated as of June 28, 2010, between the Registrant and Anthony Vuolo (incorporated by reference to Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2010) |
| |
| 10.48** | | Letter Amendment, dated as of February 11, 2011, between the Registrant and William Pence (incorporated by reference to Exhibit 10.56 to Amendment No. 1, filed May 2, 2011, to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2010) |
E-4
| | |
Exhibit No. | | Description |
| |
| 10.49** | | Letter Amendment, dated as of July 23, 2011, between the Registrant and Steven Zatz, M.D. (incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.50** | | Letter Amendment, dated as of July 23, 2011, between the Registrant and William Pence (incorporated by reference to Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.51** | | Letter Agreement, dated as of September 25, 2011, between the Registrant and Wayne Gattinella (incorporated by reference to Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.52** | | Letter Agreement, dated as of September 25, 2011, between the Registrant and Anthony Vuolo (incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.53** | | Letter Agreement, dated as of September 25, 2011, between the Registrant and Kevin Cameron (incorporated by reference to Exhibit 10.5 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.54** | | Letter Agreement, dated as of September 25, 2011, between the Registrant and Martin J. Wygod (incorporated by reference to Exhibit 10.6 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.55** | | Letter Amendment, dated as of September 21, 2011, between the Registrant and Martin J. Wygod (incorporated by reference to Exhibit 10.7 to the Registrant’s Quarterly Report on Form 10-Q filed on November 9, 2011) |
| |
| 10.56** | | Letter Agreement, dated as of January 19, 2012, between the Registrant and Wayne T. Gattinella (incorporated by reference to Exhibit 10.60 to the Registrant’s Annual Report on Form 10-K filed on February 29, 2012) |
| |
| 10.57** | | Form of Agreement to Forfeit Non-Qualified Options, dated as of February 23, 2012, between the Registrant and Each of its Non-Employee Directors (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on February 29, 2012) |
| |
| 10.58** | | Form of Agreement to Forfeit Non-Qualified Options, dated as of February 23, 2012, between the Registrant and Certain Employees (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on February 29, 2012) |
| |
| 10.59** | | Employment Agreement, dated as of May 29, 2012, between the Registrant and Cavan M. Redmond (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on June 1, 2012, as amended on June 6, 2012) |
| |
| 10.60** | �� | Form of Non-Qualified Stock Option Agreement between the Registrant and Cavan M. Redmond (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on June 1, 2012, as amended on June 6, 2012) |
| |
| 10.61** | | Form of Restricted Stock Agreement between the Registrant and Cavan M. Redmond (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on June 1, 2012, as amended on June 6, 2012) |
| |
| 10.62** | | Amended and Restated Employment Agreement, dated as of May 16, 2012, between the Registrant and William Pence (incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2012) |
| |
| 10.63 | | Director Appointment Agreement, dated as of June 8, 2012, by and among the Registrant and the Icahn Group (incorporated by reference to Exhibit 1 to Amendment No. 6, filed on June 11, 2012, to the Icahn Group’s Schedule 13-D relating to the Common Stock of the Registrant) |
E-5
| | |
Exhibit No. | | Description |
| |
| 10.64 | | Director Appointment Agreement, dated as of October 17, 2012, by and among the Registrant and Kensico Capital Management Corp. and the investment funds it advises (incorporated by reference to Exhibit 99.1 to the Registrant’s Current Report on Form 8-K filed on October 17, 2012) |
| |
| 10.65 | | Amendment, dated as of May 7, 2013, to the Director Appointment Agreement, dated as of June 8, 2012, by and among the Registrant and the Icahn Group (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on May 7, 2013) |
| |
| 10.66 | | Amendment, dated as of May 7, 2013, to the Director Appointment Agreement, dated as of October 17, 2012, by and among the Registrant and Kensico Capital Management Corp. and the investment funds it advises (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on May 7, 2013) |
| |
| 10.67 | | Stock Purchase Agreement, dated October 18, 2013, by and among the Registrant and the Icahn Group (incorporated by reference to Exhibit 1 to Amendment No. 10, filed on October 21, 2013, to the Icahn Group’s Schedule 13-D relating to the Common Stock of the Registrant) |
| |
| 10.68** | | Letter Agreement, dated as of November 14, 2012, between the Registrant and Steven Zatz, M.D. (incorporated by reference to Exhibit 10.70 to the 2012 Form 10-K) |
| |
| 10.69** | | Letter Agreement, dated as of November 14, 2012, between the Registrant and Douglas Wamsley (incorporated by reference to Exhibit 10.71 to the 2012 Form 10-K) |
| |
| 10.70** | | Letter Agreement, dated as of November 14, 2012, between the Registrant and William Pence (incorporated by reference to Exhibit 10.72 to the 2012 Form 10-K) |
| |
| 10.71** | | Letter Amendment, dated as of March 5, 2013, between the Registrant and William Pence (incorporated by reference to Exhibit 10.73 to Amendment No. 1, filed April 30, 2013, to the 2012 Form 10-K) |
| |
| 10.72** | | Letter Amendment, dated as of March 5, 2013, between the Registrant and Steven Zatz, M.D. (incorporated by reference to Exhibit 10.74 to Amendment No. 1, filed April 30, 2013, to the 2012 Form 10-K) |
| |
| 10.73** | | Letter Amendment, dated as of May 7, 2013, between the Registrant and David Schlanger (incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2013) |
| |
| 10.74** | | Letter Amendment, dated as of May 7, 2013, between the Registrant and Peter Anevski (incorporated by reference to Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2013) |
| |
| 10.75** | | Letter Amendment, dated as of May 7, 2013, between the Registrant and Cavan M. Redmond (incorporated by reference to Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2013) |
| |
| 10.76** | | Letter Amendment, dated as of May 8, 2013, between the Registrant and Martin J. Wygod (incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2013) |
| |
| 10.77** | | Letter Amendment, dated as of May 7, 2013, between the Registrant and Anthony Vuolo (incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on August 9, 2013) |
| |
| 10.78** | | Amendment, dated as of August 11, 2013, to the Employment Agreement between the Registrant and David J. Schlanger (incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on August 15, 2013) |
E-6
| | |
Exhibit No. | | Description |
| |
| 10.79** | | Amendment, dated as of August 11, 2013, to the Employment Agreement between the Registrant and Steven L. Zatz, M.D. (incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on August 15, 2013) |
| |
| 10.80** | | Amendment No. 2, dated as of January 9, 2012, to the WebMD Supplemental Bonus Program Trust Agreement |
| |
| 10.81** | | Amendment No. 3, dated as of February 25, 2013, to the WebMD Supplemental Bonus Program Trust Agreement |
| |
| 14.1 | | Code of Business Conduct (incorporated by reference to Exhibit 14.1 to the Registrant’s Current Report on Form 8-K filed on February 25, 2014) |
| |
| 21.1 | | Subsidiaries of the Registrant |
| |
| 23.1 | | Consent of Ernst & Young LLP, Independent Registered Public Accounting Firm |
| |
| 31.1 | | Rule 13a-14(a)/15d-14(a) Certification of Chief Executive Officer of the Registrant |
| |
| 31.2 | | Rule 13a-14(a)/15d-14(a) Certification of Chief Financial Officer of the Registrant |
| |
| 32.1 | | Section 1350 Certification of Chief Executive Officer of the Registrant |
| |
| 32.2 | | Section 1350 Certification of Chief Financial Officer of the Registrant |
| |
| 99.1 | | Explanation of Non-GAAP Measures |
| |
| 99.2 | | Audit Committee Charter (incorporated by reference to Exhibit 99.2 to the 2012 Form 10-K) |
| |
| 99.3 | | Compensation Committee Charter |
| |
| 99.4 | | Nominating & Governance Committee Charter |
| |
| 101.INS | | XBRL Instance Document |
| |
| 101.SCH | | XBRL Taxonomy Extension Schema Document |
| |
| 101.CAL | | XBRL Taxonomy Extension Calculation Linkbase Document |
| |
| 101.DEF | | XBRL Taxonomy Extension Definition Linkbase Document |
| |
| 101.LAB | | XBRL Taxonomy Extension Label Linkbase Document |
| |
| 101.PRE | | XBRL Taxonomy Extension Presentation Linkbase Document |
| * | With respect to the agreements filed as Exhibits 2.1 to 2.3, certain of the exhibits and the schedules to that agreement have been omitted pursuant to Item 601(b)(2) of Regulation S-K. The Registrant will furnish copies of any of the exhibits and schedules to the Securities and Exchange Commission upon request. |
| ** | Agreement relates to executive compensation. |
| (1) | This Exhibit is filed under Commission File No. 000-24975. |
| (2) | This Exhibit is filed under Commission File No. 000-51547. |
E-7