Exhibit 99.1
|

February 13, 2012
BGMEDICINE
|
Forward-Looking Statements
This presentation contains forward-looking statements regarding future events or the future financial performance of the BG Medicine, Inc. These statements involve risks, uncertainties and assumptions and are based on the current estimates and assumptions of the BG Medicine management as of the date of this presentation. Actual events or results may differ materially and adversely from these expectations. Given these uncertainties, you should not rely on these forward-looking statements.
We refer you to the documents that BG Medicine files from time to time with the Securities and Exchange Commission, specifically, BG Medicine’s annual report on Form 10-K, its quarterly reports on Form 10-Q, and its current reports on Form 8-K. These documents identify important risk factors that could cause the actual results to differ materially and adversely from those contained in BG Medicine’s projections or forward-looking statements.
All statements contained in this presentation are made only as of the date of this presentation and BG Medicine does not undertake any obligation to publicly update any forward-looking statements.
BGMEDICINE
|
BG Medicine overview
2000: founded on the concept that one cannot predict biology so one has to measure it (mass spectrometry-based systems biology discovery company)
2005: began transition to developing proprietary diagnostics
2006: began HRP Initiative and development of CardioSCORETM (ex-AMIPredict)
2007: in-licensed rights to galectin-3
Nov 2010: received FDA 510k clearance for galectin-3 test
Dec 2011: CardioSCORE FDA submission
BGMEDICINE
2
|
BG Medicine business model
Content diagnostic company developing and commercializing novel biomarkers
Innovative, hardware-independent, low capex needs
Focus on cardiovascular market
Addressing today’s largest unmet medical needs
Galectin-3 – redefining heart failure
CardioSCORE – potential paradigm shift in the identification of people at risk for near term heart attack or stroke
Leveraging world-class partnerships
Robust, proprietary biomarker discovery platform
BGMEDICINE
3
|

BGMEDICINE
CardioSCORE vision:
biological signature for
improved CVD risk prediction
|
Today……
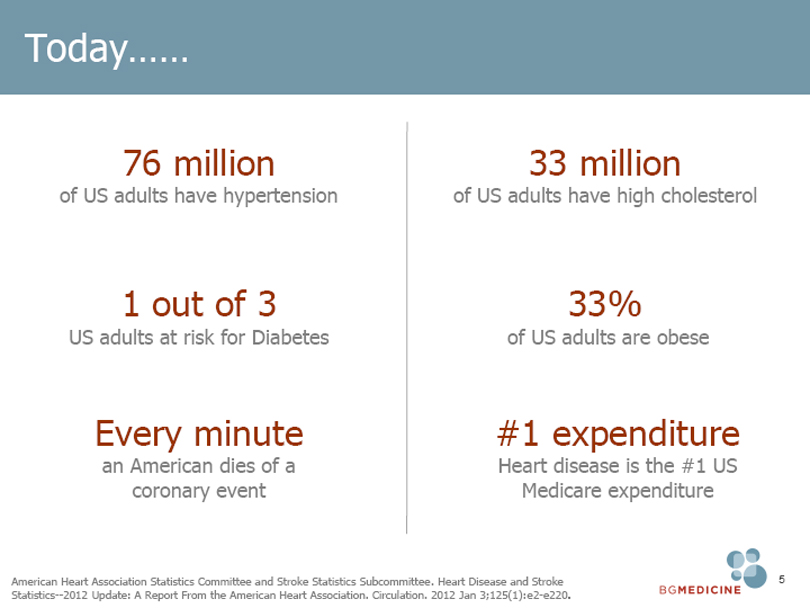
76 million
of US adults have hypertension
1 out of 3
US adults at risk for Diabetes
Every minute
an American dies of a coronary event
33 million
of US adults have high cholesterol
33%
of US adults are obese
#1 expenditure
Heart disease is the #1 US
Medicare expenditure
American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics—2012 Update: A Report From the American Heart Association. Circulation. 2012 Jan 3;125(1):e2-e220.
BGMEDICINE
5
|
Today……
…But…
>70%
of cardiovascular events occur
in individuals who are low or
medium risk based on
Framingham Risk Score
Murphy TP, Dhangana R, et al. Performance of current guidelines for coronary heart disease prevention:
optimal use of the Framingham-based risk assessment. Atherosclerosis. 2011 Jun;216(2):452-7.
BGMEDICINE
6
|
Aram V. Chobanian, MD Dr. Chobanian is a world – renowned cardiologist, a professor of medicine and pharmacology and a John I. Sandson Distinguished Professor of Health Sciences.
Previously served as President of Boston University, Medical Campus Provost, Dean of Boston University School of Medicine and Director of the Whitaker Cardiovascular Institute.
Honored as the recipient of the first Bristol- Meyers Squibb Lifetime Achievement Award in Hypertension, The Modern Medicine Award for Distinguished Achievement, the Award of Merit of the American Heart Association (AHA), The Fries Award of the National High Blood Pressure Program and the Lifetime Achievement Award of the Massachusetts Medical Society.
Chaired several scientific committees including the NHLBI Task Force on Research and Hypertension, FDA Cardiorenal Advisory Committee and the Council for High Blood Pressure Research for the AHA.
Dr. Chobanian has been on numerous editorial boards including the New England Journal of Medicine, Hypertension, the Journal of Hypertension, Blood Pressure, Hypertension Research, the Journal of Vascular Biology, Heart Disease and Post graduate Medicine. Authored or co-authored more than 250 scientific articles and two books.
Dr. Chobanian received his Bachelor of Arts degree from Brown University and a Doctor of Medicine from Harvard Medical School.
BGMEDICINE
7
|
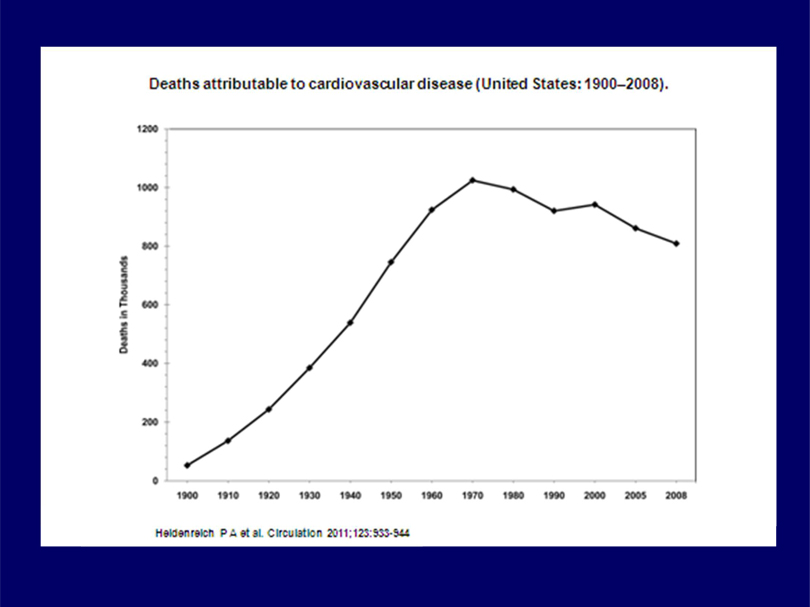
Deaths attributable to cardiovascular disease (United States: 1900-2008).
1200
1000
800
600
400
200
0 1900 1910 1920 1930 1940
1950
1960
1970
1980
1990
2000
2005
2008
Deaths in Thousands
Heldenreich P A et al. Circulation 2011:123:933-944
|
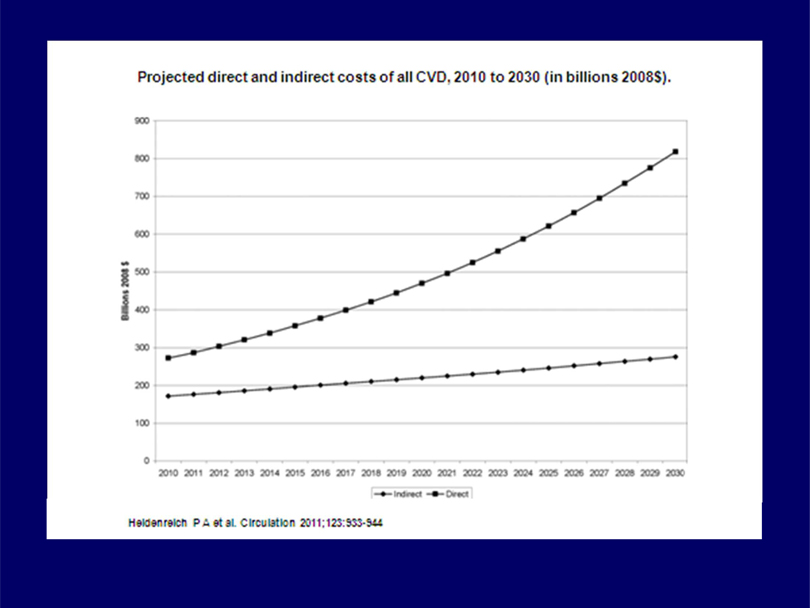
Projected direct and indirect costs of all CVD, 2010 to 2030 (in billions 2008$).
900
800
700
600
500
400
300
200
100
0
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
Billions 2008$
Indirect Direct
Heidenreich PA et al. Circulation 2011;123:933-944
|
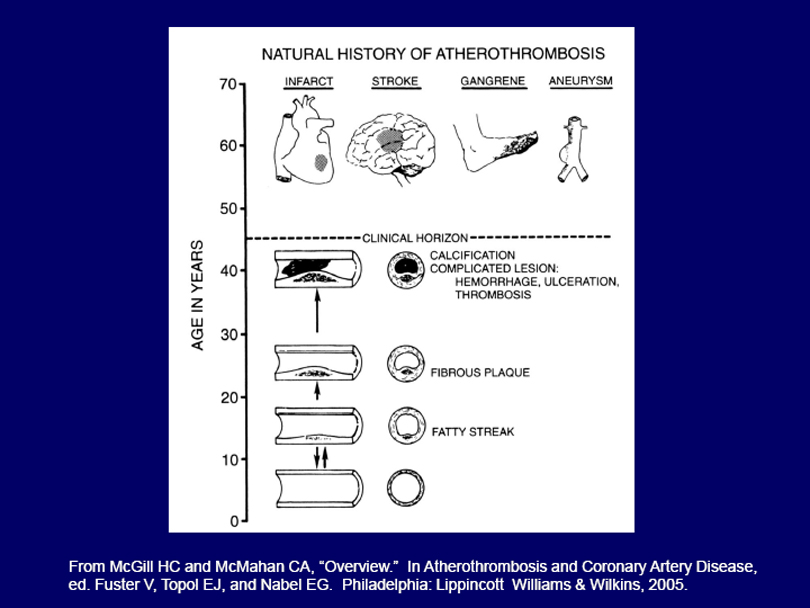
NATURAL HISTORY OF ATHEROTHROMBOSIS
INFARCT STROKE GANGRENE ANEURYSM
AGE IN YEARS
70
60
50
40
30
20
10
0
CLINICAL HORIZON
CALCIFICATION
COMPLICATED LESION:
HEMORRHAGE,
ULCERATION,
THROMBOSIS
FIBROUS PLAQUE
FATTY STREAK
From McGill HC and McMahan CA, “Overview.” In Atherothrombosis and Coronary Artery Disease,
ed. Fuster V, Topol EJ, and Nabel EG. Philadelphia: Lippincott Williams & Wilkins, 2005.
|
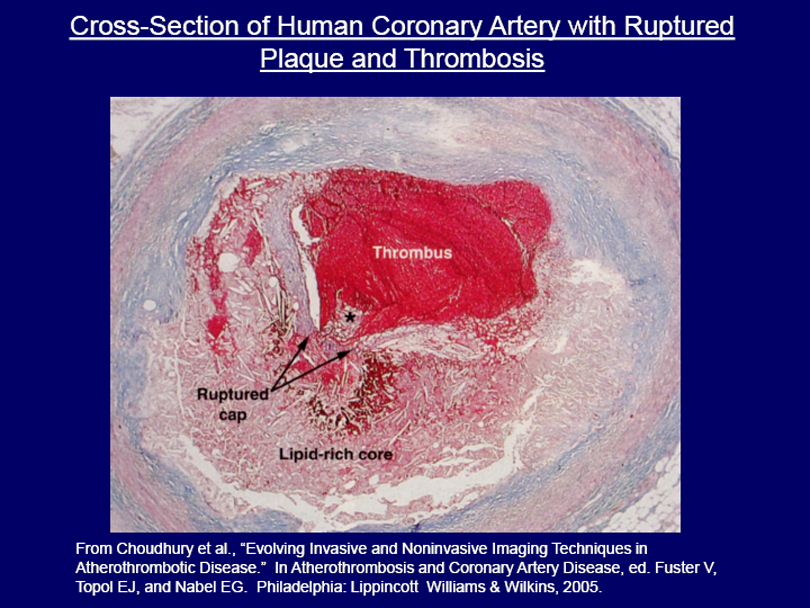
Cross-Section of Human Coronary Artery with Ruptured Plaque and Thrombosis
From Choudhury et al., “Evolving Invasive and Noninvasive Imaging Techniques in
Atherothrombotic Disease.” In Atherothrombosis and Coronary Artery Disease, ed. Fuster V,
Topol EJ, and Nabel EG. Philadelphia: Lippincott Williams & Wilkins, 2005.
|
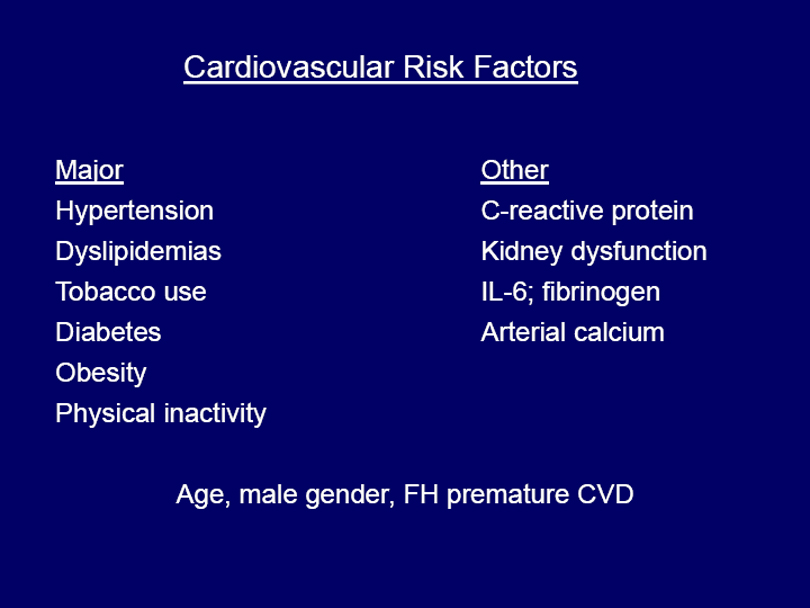
Cardiovascular Risk Factors
Major
Hypertension Dyslipidemias Tobacco use Diabetes Obesity Physical inactivity
Other
C-reactive protein Kidney dysfunction IL-6; fibrinogen Arterial calcium
Age, male gender, FH premature CVD
|
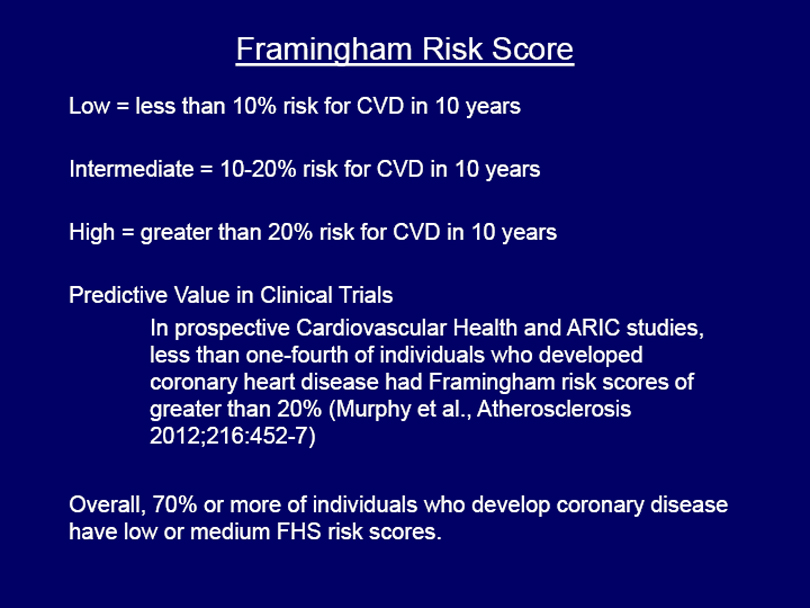
Framingham Risk Score
Low = less than 10% risk for CVD in 10 years Intermediate = 10-20% risk for CVD in 10 years High = greater than 20% risk for CVD in 10 years
Predictive Value in Clinical Trials
In prospective Cardiovascular Health and ARIC studies, less than one-fourth of individuals who developed coronary heart disease had Framingham risk scores of greater than 20% (Murphy et al., Atherosclerosis 2012;216:452-7)
Overall, 70% or more of individuals who develop coronary disease have low or medium FHS risk scores.
|
Coronary Calcium Score to Predict Cardiovascular Risk
Potential Advantages
Calcium deposits in atherosclerotic plaques High score correlates with risk
May improve risk prediction when combined with FHS score
Disadvantages
Cost ($200-400 average)
Radiation exposure (equivalent to 33 chest X-rays)
Insufficient data as yet on value for making clinical decisions
|
BG Medicine VISION
Out of
100
individuals experiencing a cardiovascular event
BGMEDICINE
15
|
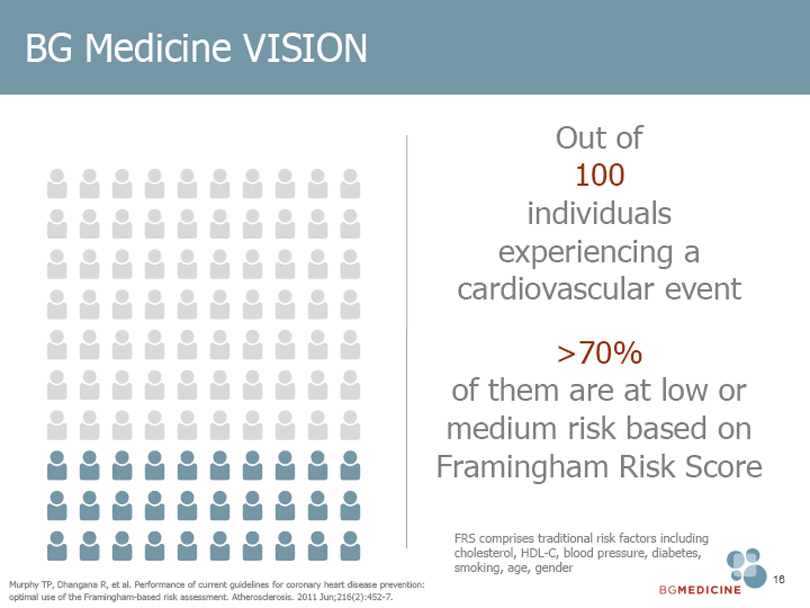
BG Medicine VISION
Out of 100
individuals
experiencing a
cardiovascular event
>70% of them are at low or
medium risk based on
Framingham Risk Score
FRS comprises traditional risk factors including
cholesterol, HDL-C, blood pressure, diabetes,
smoking, age, gender
Murphy TP, Dhangana R, et al. Performance of current guidelines for coronary heart disease prevention:
optimal use of the Framingham-based risk assessment. Atherosclerosis. 2011 Jun;216(2):452-7.
BGMEDICINE 16
|
BG Medicine VISION
To dramatically improve
the risk prediction beyond
traditional risk factor
assessment, with a test
performed on a standard
blood sample
BGMEDICINE 17
|
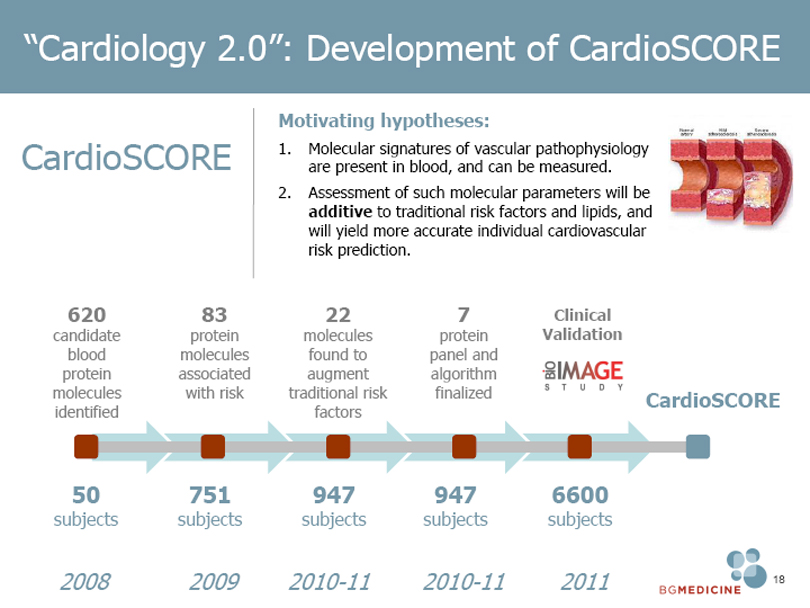
“Cardiology 2.0”: Development of CardioSCORE
CardioSCORE
Motivating hypotheses:
1. Molecular signatures of vascular pathophysiology
are present in blood, and can be measured.
2. Assessment of such molecular parameters will be
additive to traditional risk factors and lipids, and
will yield more accurate individual cardiovascular
risk prediction.
620
candidate
blood
protein
molecules
identified
83
protein
molecules
associated
with risk
22
molecules found to
augment
traditional risk
factors
7
protein
panel and
algorithm
finalized
Clinical Validation
CardioSCORE
50
subjects
751
subjects
947
subjects
947
subjects
6600
subjects
2008
2009
2010-11
2010-11
2011
BGMEDICINE 18
|
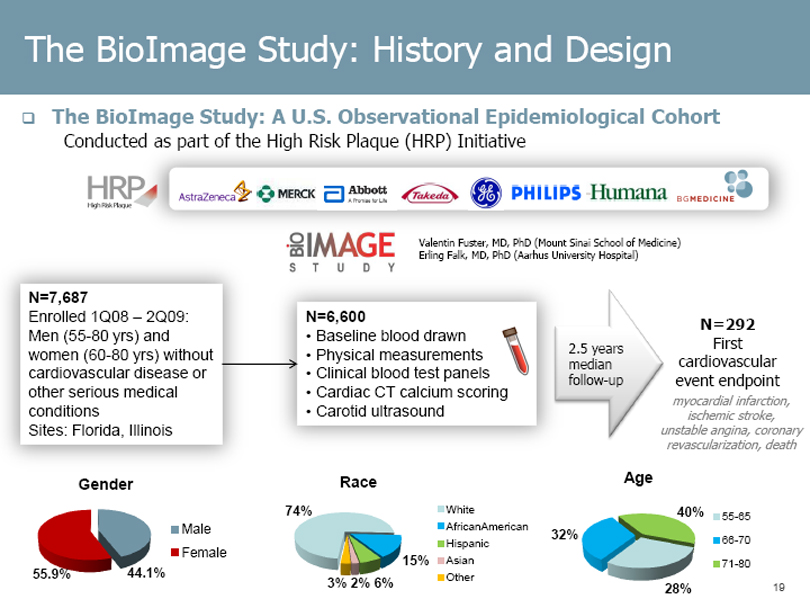
The BioImage Study: History and Design
The BioImage Study: A U.S. Observational Epidemiological Cohort
Conducted as part of the High Risk Plaque (HRP) Initiative
Valentin Fuster, MD, PhD (Mount Sinai School of Medicine)
Erling Falk, MD, PhD (Aarhus University Hospital)
N=7,687
Enrolled 1Q08 – 2Q09:
Men (55-80 yrs) and women (60-80 yrs) without cardiovascular disease or other serious medical conditions Sites: Florida, Illinois
N=6,600
•Baseline blood drawn •Physical measurements •Clinical blood test panels •Cardiac CT calcium scoring •Carotid ultrasound
2.5 years median follow-up
N=292
First cardiovascular event endpoint
myocardial infarction, ischemic stroke, unstable angina, coronary revascularization, death
Gender
55.9%
44.1%
Male Female
Race
74%
15%
3% 2% 6%
White
AfricanAmerican Hispanic Asian Other
Age
32%
40%
28%
55-65 66-70 71-80
19
|
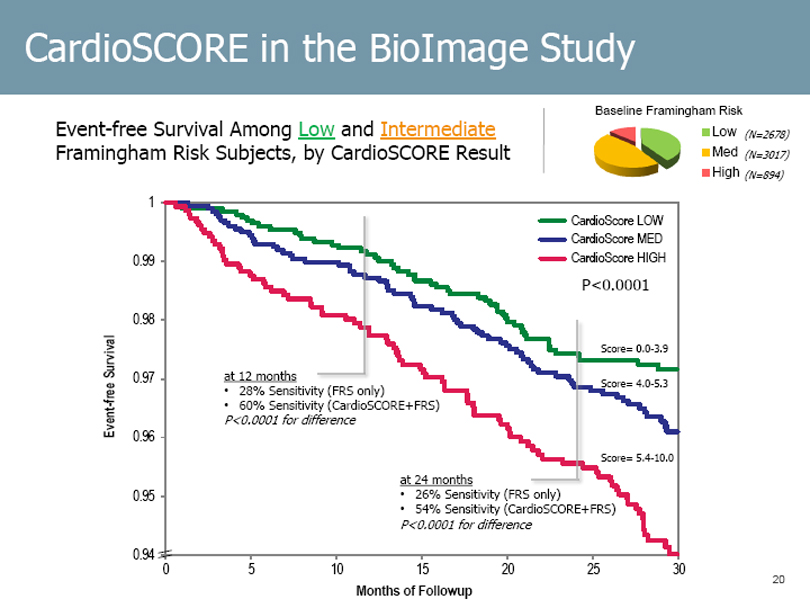
CardioSCORE in the BioImage Study
Event-free Survival Among Low and Intermediate Framingham Risk Subjects, by CardioSCORE Result
Baseline Framingham Risk
Low (N=2678) Med (N=3017) High (N=894)
Event-free Survival
1 0.99 0.98 0.97 0.96 0.95 0.94
CardioScore LOW CardioScore MED CardioScore HIGH
P<0.0001
at 12 months
• 28% Sensitivity (FRS only)
• 60% Sensitivity (CardioSCORE+FRS)
P<0.0001 for difference
Score= 0.0-3.9
Score= 4.0-5.3
Score= 5.4-10.0
at 24 months
• 26% Sensitivity (FRS only)
• 54% Sensitivity (CardioSCORE+FRS)
P<0.0001 for difference
5 10 15 20 25 30
Months of Followup
20
|
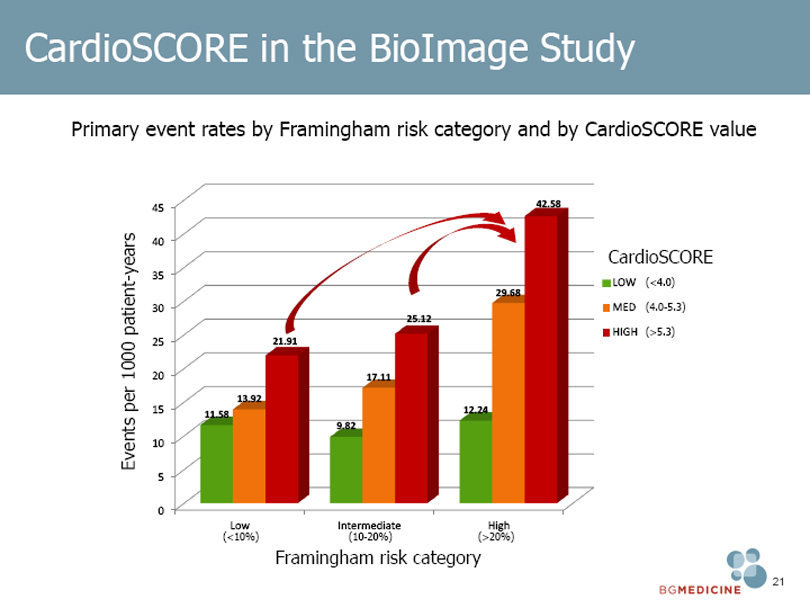
CardioSCORE in the BioImage Study
Primary event rates by Framingham risk category and by CardioSCORE value
Events per 1000 patient-years
45 40 35 30 25 20 15 10 5 0
11.58
13.92
21.91
9.82
17.11
25.12
12.24
29.68
42.58
CardioSCORE
LOW (<4.0)
MED (4.0-5.3)
HIGH (>5.3)
Low Intermediate High
(<10%) (10-20%) (>20%)
Framingham risk category
BGMEDICINE 21
|
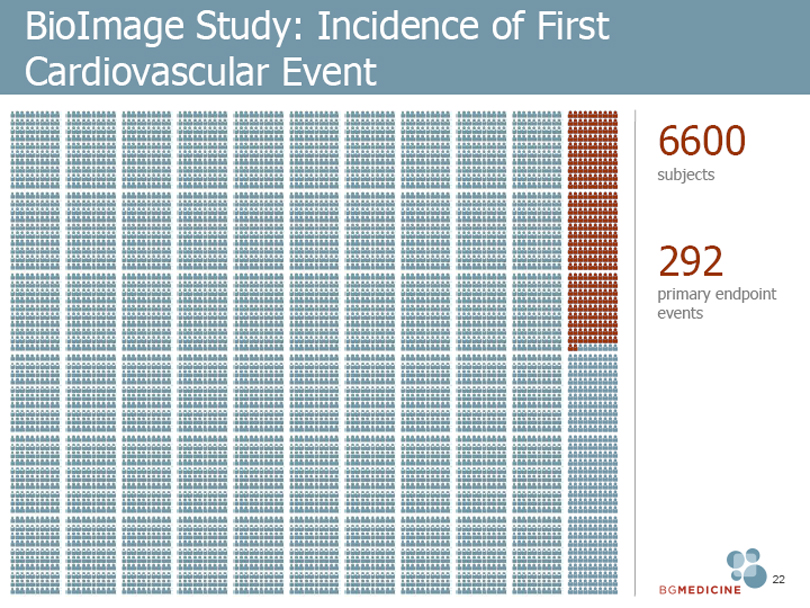
BioImage Study: Incidence of First Cardiovascular Event
6600
subjects
292
primary endpoint events
BGMEDICINE 22
|
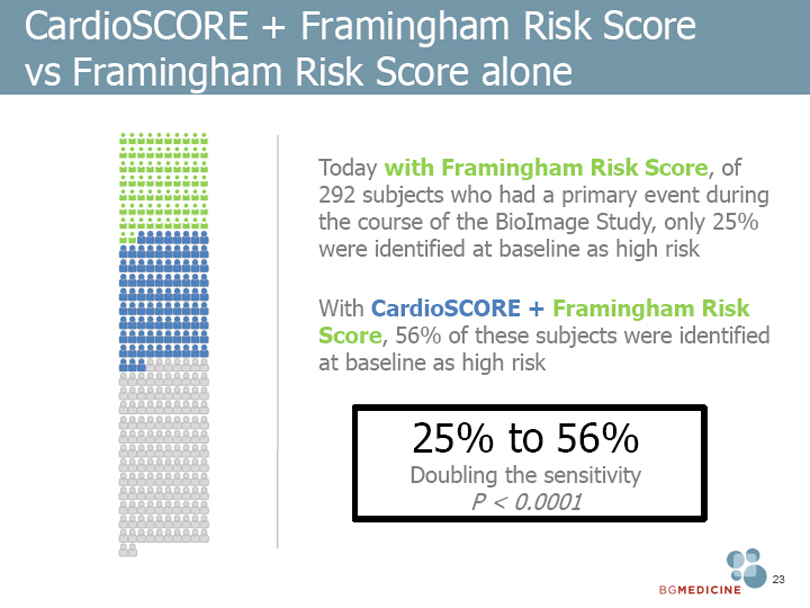
CardioSCORE + Framingham Risk Score vs Framingham Risk Score alone
Today with Framingham Risk Score, of 292 subjects who had a primary event during the course of the BioImage Study, only 25% were identified at baseline as high risk
With CardioSCORE + Framingham Risk Score, 56% of these subjects were identified at baseline as high risk
25% to 56%
Doubling the sensitivity
P < 0.0001
BGMEDICINE 23
|
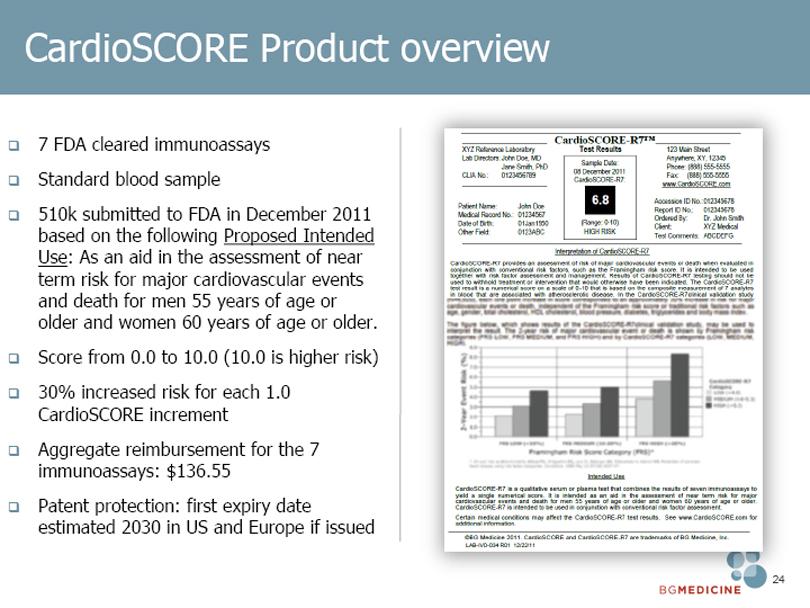
CardioSCORE Product overview
7 FDA cleared immunoassays
Standard blood sample
510k submitted to FDA in December 2011
based on the following Proposed Intended
Use: As an aid in the assessment of near
term risk for major cardiovascular events
and death for men 55 years of age or
older and women 60 years of age or older.
Score from 0.0 to 10.0 (10.0 is higher risk)
30% increased risk for each 1.0
CardioSCORE increment
Aggregate reimbursement for the 7
immunoassays: $136.55
Patent protection: first expiry date
estimated 2030 in US and Europe if issued
BGMEDICINE 24
|
Potential market opportunity for CardioSCORE
Total Cholesterol Test market world wide
>800M tests per year
TriMark Publications “Cardiac Marker Diagnostic Testing Markets,” March 2011
BGMEDICINE 25
|

Galectin-3:
Redefining Heart Failure
BGMEDICINE
|
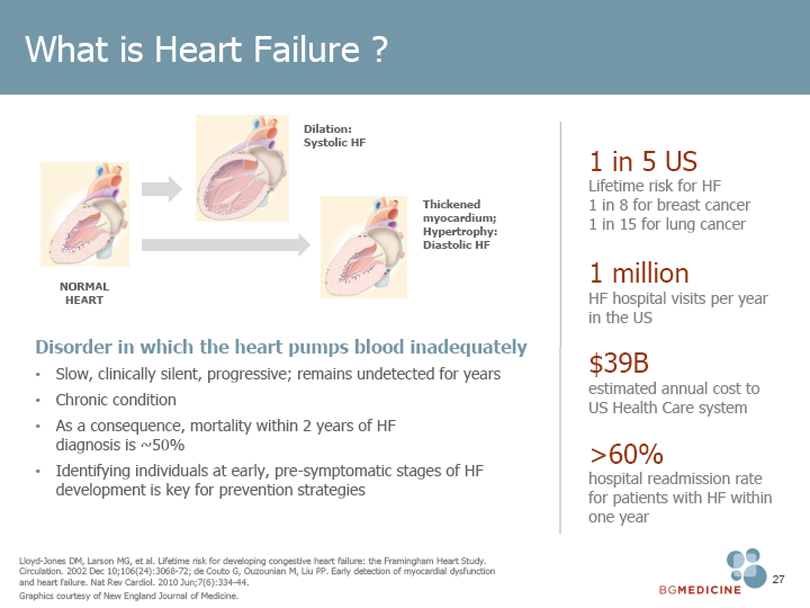
What is Heart Failure ?
NORMAL HEART
Dilation: Systolic HF
Thickened myocardium; Hypertrophy: Diastolic HF
Disorder in which the heart pumps blood inadequately
• Slow, clinically silent, progressive; remains undetected for years
• Chronic condition
• As a consequence, mortality within 2 years of HF diagnosis is ~50%
• Identifying individuals at early, pre-symptomatic stages of HF development is key for prevention strategies
1 in 5 US
Lifetime risk for HF 1 in 8 for breast cancer
1 in 15 for lung cancer
1 million
HF hospital visits per year in the US
$39B
estimated annual cost to US Health Care system
>60%
hospital readmission rate for patients with HF within one year
Lloyd-Jones DM, Larson MG, et al. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002 Dec 10;106(24):3068-72; de Couto G, Ouzounian M, Liu PP. Early detection of myocardial dysfunction and heart failure. Nat Rev Cardiol. 2010 Jun;7(6):334-44.
Graphics courtesy of New England Journal of Medicine.
BGMEDICINE 27
|
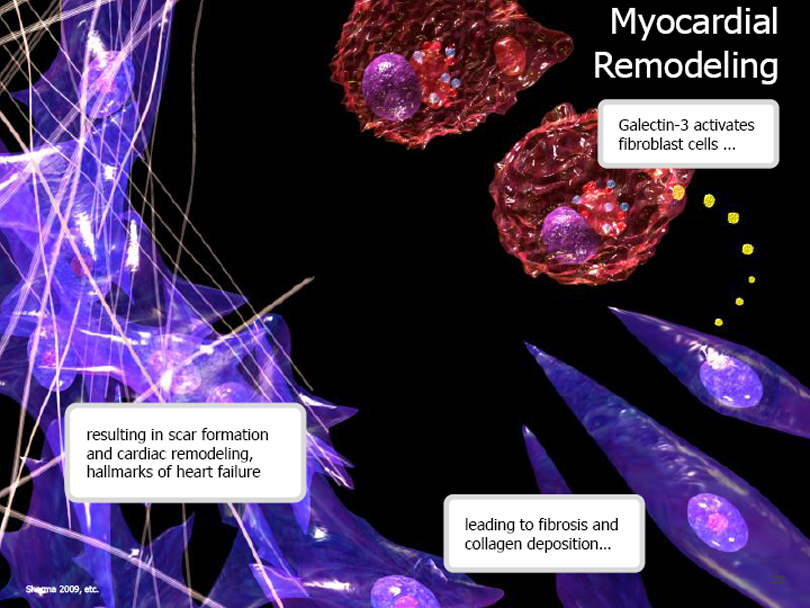
Myocardial
Remodeling
Galectin-3 activates fibroblast cells …
resulting in scar formation and cardiac remodeling, hallmarks of heart failure
leading to fibrosis and collagen deposition …
Sharma 2009, etc.
|
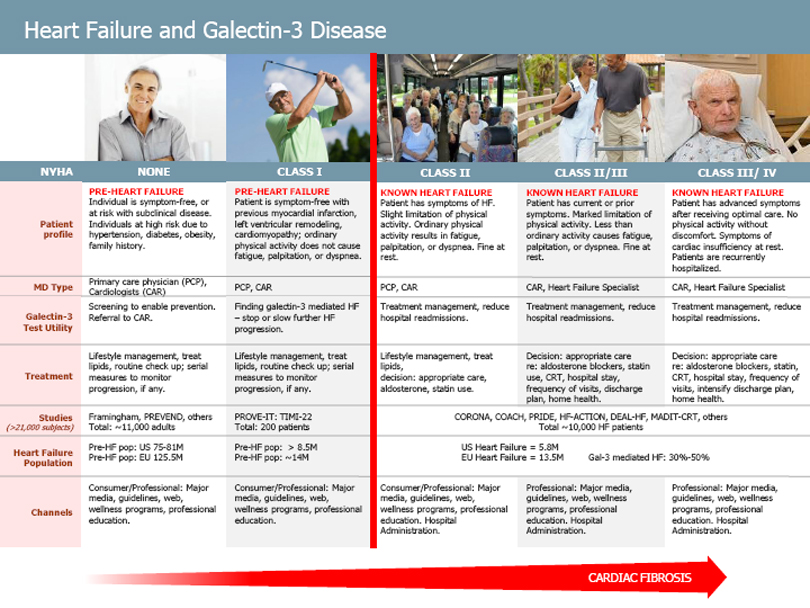
Heart Failure and Galectin-3 Disease
NYHA
Patient profile
MD Type
Galectin-3 Test Utility
Treatment
Studies
(>21,000 subjects)
Heart Failure Population
Channels
NONE
PRE-HEART FAILURE
Individual is symptom-free, or at risk with subclinical disease. Individuals at high risk due to hypertension, diabetes, obesity, family history.
Primary care physician (PCP), Cardiologists (CAR) Screening to enable prevention. Referral to CAR.
Lifestyle management, treat lipids, routine check up; serial measures to monitor progression, if any.
Framingham, PREVEND, others Total: ~11,000 adults Pre-HF pop: US 75-81M Pre-HF pop: EU 125.5M
Consumer/Professional: Major media, guidelines, web, wellness programs, professional education.
CLASS I
PRE-HEART FAILURE
Patient is symptom-free with previous myocardial infarction, left ventricular remodeling, cardiomyopathy; ordinary physical activity does not cause fatigue, palpitation, or dyspnea.
PCP, CAR
Finding galectin-3 mediated HF – stop or slow further HF progression.
Lifestyle management, treat lipids, routine check up; serial measures to monitor progression, if any.
PROVE-IT: TIMI-22 Total: 200 patients
Pre-HF pop: > 8.5M
Pre-HF pop: ~14M
Consumer/Professional: Major media, guidelines, web, wellness programs, professional education.
CLASS II
KNOWN HEART FAILURE
Patient has symptoms of HF. Slight limitation of physical activity. Ordinary physical activity results in fatigue, palpitation, or dyspnea. Fine at rest.
PCP, CAR
Treatment management, reduce hospital readmissions.
Lifestyle management, treat lipids, decision: appropriate care, aldosterone, statin use.
Consumer/Professional: Major media, guidelines, web, wellness programs, professional education. Hospital Administration.
CLASS II/III
KNOWN HEART FAILURE
Patient has current or prior symptoms. Marked limitation of physical activity. Less than ordinary activity causes fatigue, palpitation, or dyspnea. Fine at rest.
CAR, Heart Failure Specialist Treatment management, reduce hospital readmissions.
Decision: appropriate care re: aldosterone blockers, statin use, CRT, hospital stay, frequency of visits, discharge plan, home health.
CORONA, COACH, PRIDE, HF-ACTION, DEAL-HF, MADIT-CRT, others Total ~10,000 HF patients
US Heart Failure = 5.8M
EU Heart Failure = 13.5M
Gal-3 mediated HF: 30%-50%
Professional: Major media, guidelines, web, wellness programs, professional education. Hospital Administration.
CLASS III/ IV
KNOWN HEART FAILURE
Patient has advanced symptoms after receiving optimal care. No physical activity without discomfort. Symptoms of cardiac insufficiency at rest. Patients are recurrently hospitalized.
CAR, Heart Failure Specialist Treatment management, reduce hospital readmissions.
Decision: appropriate care re: aldosterone blockers, statin, CRT, hospital stay, frequency of visits, intensify discharge plan, home health.
Professional: Major media, guidelines, web, wellness programs, professional education. Hospital Administration.
CARDIAC FIBROSIS
|
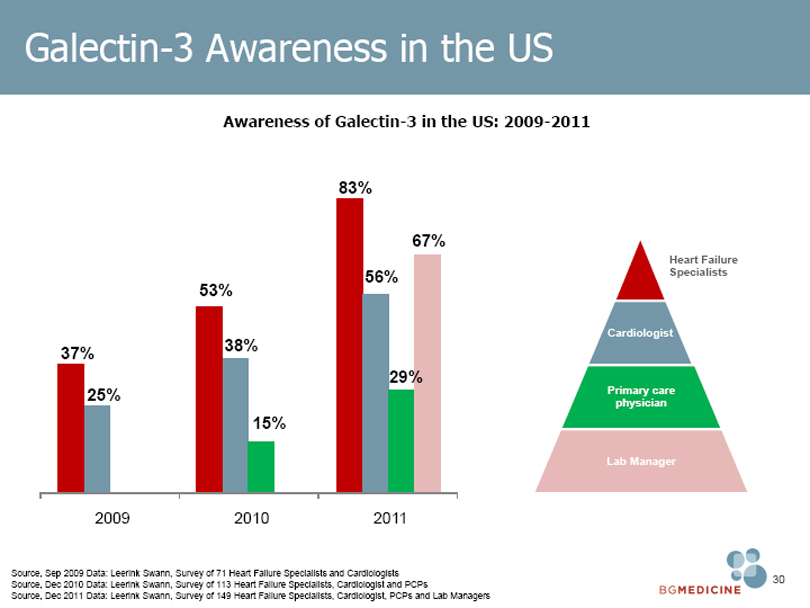
Galectin-3 Awareness in the US
Awareness of Galectin-3 in the US: 2009-2011
83%
67%
56% 53%
38% 37%
29% 25% 15%
2009 2010 2011
Heart Failure Specialists
Cardiologist
Primary care physician
Lab Manager
Source, Sep 2009 Data: Leerink Swann, Survey of 71 Heart Failure Specialists and Cardiologists
Source, Dec 2010 Data: Leerink Swann, Survey of 113 Heart Failure Specialists, Cardiologist and PCPs
Source, Dec 2011 Data: Leerink Swann, Survey of 149 Heart Failure Specialists, Cardiologist, PCPs and Lab Managers
BGMEDICINE 30
|
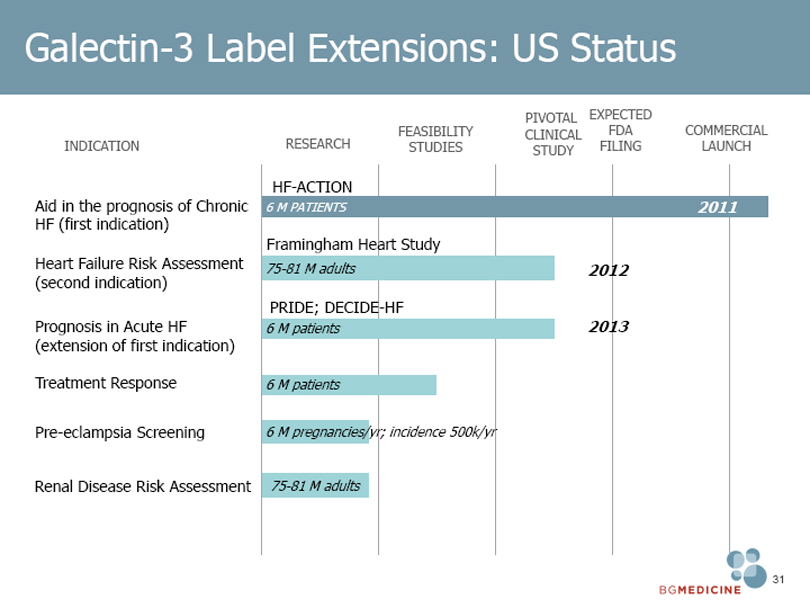
Galectin-3 Label Extensions: US Status
PIVOTAL EXPECTED
FEASIBILITY CLINICAL FDA COMMERCIAL
INDICATION RESEARCH STUDIES STUDY FILING LAUNCH
HF-ACTION
Aid in the prognosis of Chronic 6 M PATIENTS 2011
HF (first indication)
Framingham Heart Study
Heart Failure Risk Assessment 75-81 M adults 2012
(second indication)
PRIDE; DECIDE-HF
Prognosis in Acute HF 6 M patients 2013
(extension of first indication)
Treatment Response 6 M patients
Pre-eclampsia Screening 6 M pregnancies/yr; incidence 500k/yr
Renal Disease Risk Assessment 75-81 M adults
BGMEDICINE 31
|
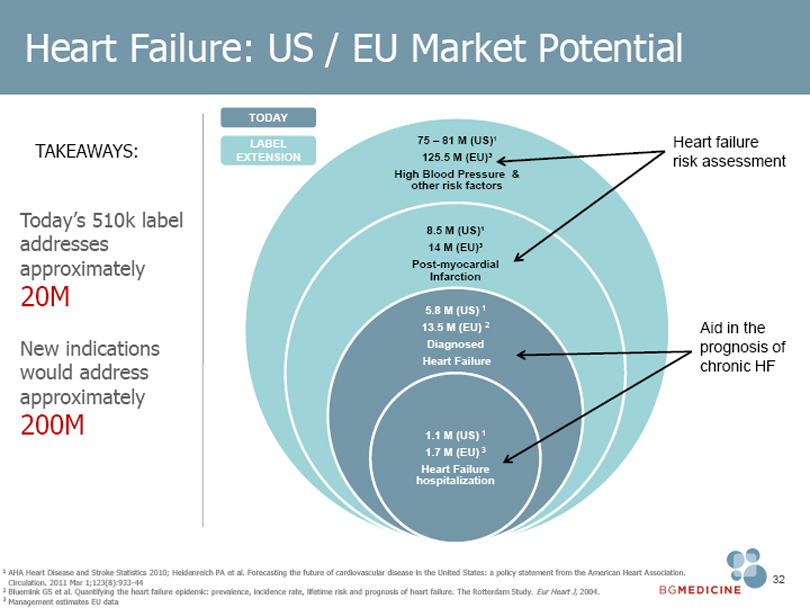
Heart Failure: US / EU Market Potential
TAKEAWAYS:
Today’s addresses approximately
20M
New indications would address approximately
200M
TODAY
LABEL EXTENSION
75 – 81 M (US)1
125.5 M (EU)3
High Blood Pressure &
other risk factors
8.5 M (US)1
14 M (EU)3
Post-myocardial
Infarction
5.8 M (US) 1
13.5 M (EU) 2
Diagnosed
Heart Failure
1.1 M (US) 1
1.7 M (EU) 3
Heart Failure
hospitalization
Heart failure risk assessment
Aid in the prognosis of chronic HF
1 AHA Heart Disease and Stroke Statistics 2010; Heidenreich PA et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011 Mar 1;123(8):933-44
2 Bluemink GS et al. Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure. The Rotterdam Study. Eur Heart J, 2004.
3 Management estimates EU data
BGMEDICINE 32
|
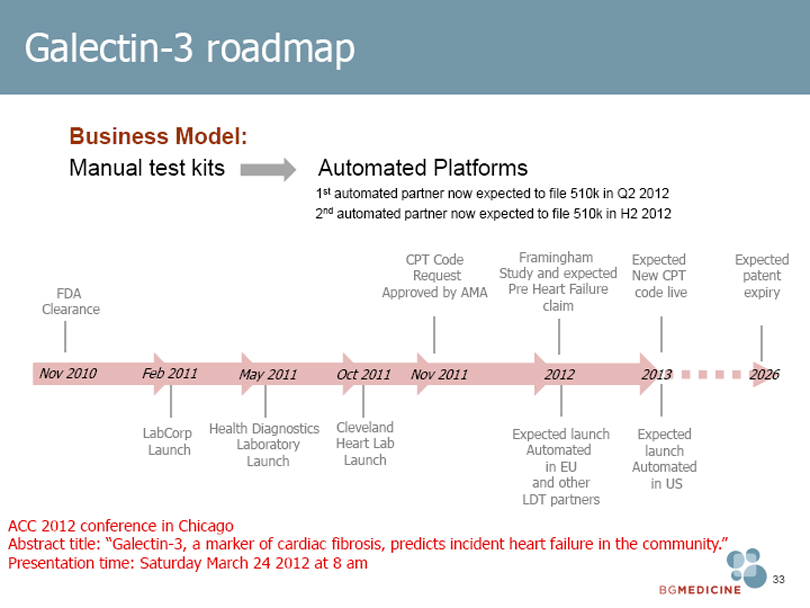
Galectin-3 roadmap
Business Model:
Manual test kits
Automated Platforms
1st automated partner now expected to file 510k in Q2 2012 2nd automated partner now expected to file 510k in H2 2012
CPT Code Framingham Expected Expected Request Study and expected New CPT patent FDA Approved by AMA Pre Heart Failure code live expiry Clearance claim
Nov 2010 Feb 2011 May 2011 Oct 2011 Nov 2011 2012 2013 2026
LabCorp Health Diagnostics Cleveland
Expected launch Expected Launch Laboratory Heart Lab Automated launch Launch Launch in EU Automated and other in US
LDT partners
ACC 2012 conference in Chicago
Abstract title: “Galectin-3, a marker of cardiac fibrosis, predicts incident heart failure in the community.”
Presentation time: Saturday March 24 2012 at 8 am
BGMEDICINE 33
|
BG Medicine: on the move to transform cardiology disease management
Goals for 2012:
BG Medicine evolves into a commercial company
Galectin-3’s launch on automated platform
CardioSCORE 510k cleared by FDA
CardioSCORE: double the sensitivity of the current standard-of-care diagnostic tools
Vast commercial opportunity ahead of us:
Galectin-3 IP protected until 2026, issued in US and pending ROW
CardioSCORE IP protected until 2030, subject to issuance
BGMEDICINE 34