| Item 2. | Management’s Discussion and Analysis of Financial Condition and Results of Operation |
This management’s discussion and analysis (“MD&A”) is presented in order to provide the reader with an overview of the financial results and changes to our consolidated balance sheet at September 30, 2024. This MD&A also explains the material variations in our results of operations for the three and the six months ended September 30, 2024 and 2023, consolidated balance sheets as of September 30, 2024 and March 31, 2024, and cash flows for the six months ended September 30, 2024 and 2023.
Market data, and certain industry data and forecasts included in this MD&A were obtained from internal Company surveys and market research conducted by third parties hired by us, publicly available information, reports of governmental agencies and industry publications, and independent third-party surveys. We have relied upon industry publications as our primary sources for third-party industry data and forecasts. Industry surveys, publications and forecasts generally state that the information they contain has been obtained from sources believed to be reliable, but that the accuracy and completeness of that information are not guaranteed. We have not independently verified any of the data from third-party sources or the underlying economic assumptions they have made. Similarly, internal surveys, industry forecasts and market research, which we believe to be reliable based upon our management’s or contracted third parties’ knowledge of our industry, have not been independently verified. Our estimates involve risks and uncertainties, including assumptions that may prove not to be accurate, and these estimates and certain industry data are subject to change based on various factors, including those discussed in this quarterly report and in our most recently filed Annual Report on Form 10-K, filed with the Securities and Exchange Commission (the “SEC”) on June 21, 2024 (the “Annual Report”). This MD&A contains forward-looking information. You should review our Special Note Regarding Forward-Looking Statements presented at the beginning of this quarterly report.
This MD&A should be read in conjunction with our unaudited condensed consolidated interim financial statements for the three and the six months ended September 30, 2024 and 2023 included elsewhere in this quarterly report. Our unaudited condensed consolidated financial statements were prepared in accordance with U.S. GAAP.
All amounts appearing in this MD&A for the period-by-period discussions are in thousands of U.S. dollars, except share and per share amounts or unless otherwise indicated.
Business Overview
We are focused on developing and commercializing products for rare and orphan diseases that have the potential to improve clinical outcomes by using our novel drug delivery technologies. We seek to apply new proprietary formulations to approved and marketed pharmaceutical compounds to achieve enhanced efficacy, faster onset of action, reduced side effects, more convenient drug delivery and increased patient compliance; all of which could result in improved patient outcomes. The active pharmaceutical ingredients used in the drug candidates under development by Grace Therapeutics may be already approved in a target indication or could be repurposed for use in new indications.
The existing well understood efficacy and safety profiles of these marketed compounds provide the opportunity for us to utilize the Section 505(b)(2) regulatory pathway under the Federal Food, Drug and Cosmetic Act (“FDCA”) for the development of our reformulated versions of these drugs, and therefore may provide a potentially shorter path to regulatory approval. Under Section 505(b)(2), if sufficient support of a product’s safety and efficacy either through previous U.S. Food and Drug Administration (“FDA”) experience or sufficiently within the existing and accepted scientific literature, can be established, it may eliminate the need to conduct some of the pre-clinical studies and clinical trials that new drug candidates might otherwise require.
Our therapeutic pipeline consists of three unique clinical-stage drug candidates supported by an intellectual property portfolio of more than 40 granted and pending patents in various jurisdictions worldwide. These drug candidates aim to improve clinical outcomes in the treatment of rare and orphan diseases by applying proprietary formulation and drug delivery technologies to existing pharmaceutical compounds to achieve improvements over the current standard of care, or to provide treatment for diseases with no currently approved therapies.
We believe that rare disorders represent an attractive area for drug development, and there remains an opportunity for us to utilize already approved drugs that have established safety profiles and clinical experience to potentially address significant unmet medical needs. A key advantage of pursuing therapies for rare disorders is the potential to receive orphan drug designation (“ODD”) from the FDA. Our three drug candidates have received ODD status, provided certain conditions are met at new drug application (“NDA”) approval. ODD provides for seven years of marketing exclusivity in the United States post-launch, provided certain conditions are met, and the potential for faster regulatory review. ODD status can also result in tax credits of up to 50% of clinical development costs conducted in the United States upon marketing approval and a waiver of the NDA fees, which we estimate can translate into savings of approximately $3.2 million for our lead drug candidate, GTx-104. Developing drugs for rare diseases can often allow for clinical trials that are more manageably scaled and may require a smaller, more targeted commercial infrastructure.
The specific diseases targeted for drug development by us are well understood, although the patient populations suffering from such diseases may remain poorly served by available therapies or, in some cases, approved therapies do not yet exist. We aim to effectively treat debilitating symptoms that result from these underlying diseases.
Our management team possesses significant experience in drug formulation and drug delivery research and development, clinical and pharmaceutical development and manufacturing, regulatory affairs, and business development, as well as being well-versed in late-stage drug development and commercialization. Importantly, our team is comprised of industry professionals with deep expertise and knowledge, including a world-renowned practicing neurosurgeon-scientist and respected authority in aSAH, as well as product development, chemistry, manufacturing and controls (CMC”), planning, implementation, management, and execution of global Phase 2 and Phase 3 trials for GTx-104, and drug commercialization.
| • | GTx-104 is a clinical-stage, novel, injectable formulation of nimodipine being developed for intravenous (“IV”) infusion in aneurysmal subarachnoid hemorrhage (“aSAH”) patients to address significant unmet medical needs. The unique nanoparticle technology of GTx-104 facilitates aqueous formulation of insoluble nimodipine for a standard peripheral IV infusion. GTx-104 provides a convenient IV delivery of nimodipine in the intensive care unit eliminating the need for nasogastric tube administration in unconscious or dysphagic patients. IV delivery of GTx-104 also has the potential to lower food effects, drug-to-drug interactions, and eliminate potential dosing errors. Further, GTx-104 has the potential to better manage hypotension in aSAH patients. |
| • | GTx-102 is an oral-mucosal betamethasone spray for the treatment of Ataxia Telangiectasia (“A-T”), a complex orphan pediatric genetic neurodegenerative disorder usually diagnosed in young children, for which no FDA approved treatment currently exists. |
| • | GTx-101 is a topical bio adhesive film-forming bupivacaine spray for Postherpetic Neuralgia (“PHN”), which can be persistent and often causes debilitating pain following infection by the shingles virus. We believe that GTx-101 could be administered to patients with PHN to treat pain associated with the disease. |
In May 2023, we announced the strategic decision to prioritize development of GTx-104 with a goal to advance the product candidate to commercialization, while conserving resources as much as possible to complete development efficiently. We estimate that the deferral of GTx-102 and GTx-101 clinical development could be at least three years given the timeline to complete the development and potential commercial launch of GTx-104. Further development of GTx-102 and GTx-101 will occur at such time as we obtain additional funding or enter into strategic partnerships for license or sale with third parties.
GTx-104
About aneurysmal Subarachnoid Hemorrhage (aSAH)
aSAH is bleeding over the surface of the brain in the subarachnoid space between the brain and the skull, which contains blood vessels that supply the brain. A primary cause of such bleeding is rupture of an aneurysm. The result is a relatively uncommon type of stroke (aSAH) that accounts for about 5% of all strokes and has an incidence of six per 100,000 person years.
Nimodipine Overview
Nimodipine was granted FDA approval in 1988 and is the only approved drug that has been clinically shown to improve neurological outcomes in aSAH patients. It is only available in the United States as a generic oral capsule and as a branded oral liquid solution called NYMALIZE™, which is manufactured and sold by Arbor Pharmaceuticals (acquired in September 2021 by Azurity Pharmaceuticals). Nimodipine has poor water solubility and high permeability characteristics because of its high lipophilicity. Additionally, orally administered nimodipine has dose-limiting side-effects such as hypotension, poor absorption and low bioavailability resulting from high first-pass metabolism, and a narrow administration window as food effects lower bioavailability significantly. Due to these issues, blood levels of orally administered nimodipine can be highly variable, making it difficult to manage blood pressure in aSAH patients. Nimodipine capsules are also difficult to administer, particularly to unconscious patients or those with impaired ability to swallow. Concomitant use with CYP3A inhibitors is contraindicated (NIMODIPINE Capsule PI).
NIMOTOP™ is an injectable form of nimodipine that is manufactured by Bayer Healthcare. It is approved in Europe and in other regulated markets (but not in the United States). It has limited utility for aSAH patients because of its high organic solvent content, namely 23.7% ethanol and 17% polyethylene glycol 400 (NIMOTOP SmPC).
| • | GTx-104 is a clinical-stage, novel, injectable of nimodipine for IV infusion in aSAH patients. It uses surfactant micelles as the drug carrier to solubilize nimodipine. This unique nimodipine aqueous formulation is composed of a nimodipine base, an effective amount of polysorbate 80, a non-ionic hydrophilic surfactant, and a pharmaceutically acceptable carrier for injection. GTx-104 is supplied as an aqueous concentrate that upon dilution with saline, dextrose, or lactated ringer, is a ready-to-use infusion solution, which is stable and clear. |
Key potential benefits of GTx-104 include:
| • | Novel nanoparticle technology facilitates aqueous formulation of insoluble nimodipine for a safe, standard peripheral IV infusion |
| • | Better control of blood pressure and improved management of hypotension |
| • | Eliminates food effects that impact the absorption of the oral form of nimodipine |
| • | Lower inter and intra-subject variability as compared to oral nimodipine |
GTx-104 could provide a more convenient mode of administration as compared to generic nimodipine capsules or NYMALIZE™. GTx-104 is administered as an IV infusion compared to oral administration via a nasogastric tube in unconscious patients every four hours for both nimodipine capsules and NYMALIZE™. Therefore, GTx-104 could make a major contribution to patient care by potentially reducing the dosing associated nursing burden. More convenient, continuous, and consistent dosing may also reduce the risk of medication errors. In addition, as depicted in the charts below, the GTx-140-002 PK study conducted by us has shown that GTx-104 has the potential to provide improved bioavailability and show reduced inter- and intra-subject variability compared to oral nimodipine, which is hypothesized to limit the risk of hypotension and to better achieve desired therapeutic concentration. Following the capsule administration, the variability was observed higher as compared to IV infusion administration (nimodipine exposure variability at steady state observed 37.5% following oral capsule administration versus 15.5%, following GTx-104 IV infusion). Because of its IV formulation, we also expect GTx-104 to reduce certain drug-drug interactions and food effects.
Despite the positive impact it has on recovery, physicians often must discontinue their patients from oral nimodipine, primarily as a result of hypotensive episodes that cannot be controlled by titrating the oral form of drug. Such discontinuation could potentially be avoided by administering GTx-104, which because of its IV administration, may reduce the complexity associated with the need for careful attention to the timing of nimodipine administration at least one hour before or two hours after a meal. Also, unconscious patients will likely receive more consistent concentrations of nimodipine when delivered via the IV route as compared to oral gavage or a nasogastric tube. More consistent dosing is expected to result in a reduction of vasospasm and better, more consistent management of hypotension. As summarized in the table below, we also anticipate reduced use of rescue therapies, such as vasopressors, and expensive hospital resources, such as the angiography suite, are possible by more effectively managing blood pressure with GTx-104. Reduced incidences of vasospasm could result in shorter length of stay and better outcomes.

GTx-104 Market Opportunity
Approximately 50,000 patients in the United States are affected by aSAH per year, based on market research. Outside of the United States, annual cases of aSAH are estimated at approximately 60,000 in the European Union, and approximately 150,000 in China.
In contrast to more common types of ischemic stroke in elderly individuals, aSAH often occurs at a relatively young age, with approximately half the affected patients younger than 60 years old. Approximately 10% to 15% of aSAH patients die before reaching the hospital, and those who survive the initial hours post hemorrhage are admitted or transferred to tertiary care centers with high risk of complications, including rebleeding and delayed cerebral ischemia (“DCI”). Systemic manifestations affecting cardiovascular, pulmonary, and renal function are common and often complicate management of DCI.
We estimate that total addressable market for aSAH is approximately $300 million in the U.S. There are an estimated 150,000 aSAH patients each year in China and approximately 55,000 patients in the European Union. The unmet needs in the treatment of aSAH and the potential of GTx-104 to address the limitations of the current standard of care were the subject of a Key Opinion Leader (“KOL”) event we hosted on October 4, 2023 and will be discussed further at our KOL event planned for November 2024. In an independent market research survey we conducted of hospital administrators, critical and neuro intensive care physicians at institutions with Comprehensive or Advanced Stroke Center certification who are involved in purchasing decisions for their institutions/units, respondents reported 80% likelihood of adopting an IV formulation of nimodipine (GTx-104), assuming 100% bioavailability, better safety, no food effects, effective hypotension management, potential hospital value and patient value.
GTx-104 Phase 1 PK Trial
In September 2021, we initiated our pivotal PK bridging trial to evaluate the relative bioavailability of GTx-104 compared to currently marketed oral nimodipine capsules in approximately 50 healthy subjects. The PK trial was the next required step in our proposed 505(b)(2) regulatory pathway for GTx-104.
Final results from this pivotal PK trial were reported in May 2022, and showed that the bioavailability of GTx-104 compared favorably with the oral formulation of nimodipine in all subjects, and no serious adverse events were observed for GTx-104.
All endpoints indicated that statistically there was no difference in exposures between GTx-104 and oral nimodipine over the defined time periods for both maximum exposure and total exposure. Plasma concentrations obtained following IV administration showed significantly less variability between subjects as compared to oral administration of capsules, since IV administration is not as sensitive to some of the physiological processes that affect oral administration, such as taking the drug with and without meals, variable gastrointestinal transit time, variable drug uptake from the gastrointestinal tract into the systemic circulation, and variable hepatic blood flow and hepatic first pass metabolism. Previous studies have shown these processes significantly affect the oral bioavailability of nimodipine, and therefore cause oral administration to be prone to larger inter- and intra-subject variability.
The bioavailability of oral nimodipine capsules observed was only approximately 8% compared to 100% for GTx-104. Consequently, about one-twelfth the amount of nimodipine is delivered with GTx-104 to achieve the same blood levels as with the oral capsules. This data is presented in the chart below.
No serious adverse events and no adverse events leading to withdrawal were reported during the trial.
GTx-104 has been administered in over 150 healthy volunteers and was well tolerated with significantly lower inter- and intra-subject pharmacokinetic (“PK”) variability compared to oral nimodipine.
GTx-104 Pivotal Phase 3 STRIVE-ON Randomized Safety Trial
In April 2023, we received a Type C written meeting response and clarifying feedback from the FDA on our proposed pivotal Phase 3 safety trial for GTx-104. The FDA provided additional comments on our development plan that, pending submission of the final clinical protocol and FDA approval, would allow us to proceed with a pivotal Phase 3 safety clinical trial in aSAH patients. On July 5, 2023, we announced the alignment with the FDA on our GTx-104 pivotal Phase 3 safety clinical trial protocol.
The FDA concurred with the suitability of the 505(b)(2) regulatory pathway with the selected Reference Listed Drug NIMOTOP oral capsules (“NDA 018869”), and that our GTx-104-002 PK trial may have met the criteria for a scientific bridge.
The design of our Phase 3 safety clinical trial, which we have titled STRIVE-ON (Safety, Tolerability, Randomized, IV and Oral Nimodipine; the STRIVE-ON trial–NCT05995405), is a prospective, open-label, randomized (1:1 ratio), parallel group trial of GTx-104 compared with oral nimodipine, in patients hospitalized for aSAH. Key trial design features include:
| • | Approximately 100 patients will be enrolled at an estimated 25 hospitals in the U.S. |
| • | The primary endpoint is safety and will be measured as comparative adverse events, including hypotension, between the two groups. |
| • | GTx-104 will be administered as a continuous IV infusion of 0.15 mg/hour, and a 30-minute IV bolus of 4 mg every 4 hours. Oral nimodipine will be administered as 60 mg (two 30 mg capsules) every 4 hours. |
| • | Both groups will receive their assigned GTx-104 or oral nimodipine for up to 21 consecutive days and will be evaluated from commencement of patient treatment through a 90-day follow-up period. |
On October 23, 2023, we enrolled our first patient in the STRIVE-ON trial, and on September 25, 2024, we announced the completion of enrollment. We anticipate a data readout from the STRIVE-ON trial in first calendar quarter 2025, and plan to submit an NDA to the FDA in the first half of calendar year 2025. If approved, GTx-104 has the potential to address significant challenges with oral nimodipine administration and may transform the standard of care for patients with aSAH.
GTx-102 Overview
GTx-102 is a novel, concentrated oral-mucosal spray of betamethasone intended to improve neurological symptoms of A-T for which there are currently no FDA-approved therapies. GTx-102 is a stable, concentrated oral spray formulation comprised of the gluco-corticosteroid betamethasone that, together with other excipients can be sprayed conveniently over the tongue of the A-T patient and is rapidly absorbed.
About Ataxia Telangiectasia
A-T is a rare genetic progressive autosomal recessive neurodegenerative disorder that affects children, with the hallmark symptoms of cerebellar ataxia and other motor dysfunction, and dilated blood vessels (telangiectasia) that occur in the sclera of the eyes. A-T is caused by mutations in the ataxia telangiectasia gene, which is responsible for modulating cellular response to stress, including breaks in the double strands of DNA.
Children with A-T begin to experience balance and coordination problems when they begin to walk (toddler age), and ultimately become wheelchair-bound in their second decade of life. In pre-adolescence (between ages 5 and 8), patients experience oculomotor apraxia, dysarthria, and dysphagia. They also often develop compromised immune systems and are at increased risk of developing respiratory tract infections and cancer (typically lymphomas and leukemia).
A-T is diagnosed through a combination of clinical assessment (especially neurologic and oculomotor deficits), laboratory analysis, and genetic testing. There is no known treatment to slow disease progression, and treatments that are used are strictly aimed at controlling the symptoms (e.g., physical, occupational or speech therapy for neurologic issues), or conditions secondary to the disease (e.g., antibiotics for lung infections, chemotherapy for cancer, etc.). There are no FDA-approved therapeutic options currently available. Patients typically die by age 25 from complications of lung disease or cancer. According to a third-party report we commissioned, A-T affects approximately 4,300 patients per year in the United States and has a potential total addressable market of $150 million, based on the number of treatable patients in the United States.
GTx-102 - Research & Development and Clinical Trials to Date
We have licensed the data from the multicenter, double-blinded, randomized, placebo-controlled crossover trial from Azienda Ospedaliera Universitaria Senese, Siena, Italy, where Dr. Zannolli et. al. studied the effect of oral liquid solution of betamethasone to reduce ataxia symptoms in patients with A-T. This oral liquid solution is not marketed in the United States, and therefore is not available for clinical use. Currently, betamethasone is only available in the United States as an injectable or as a topical cream. This license gives us the right to reference the trial’s data in our NDA filing. On November 12, 2015, we submitted the data from the Zannolli trial to the FDA’s Division of Neurology at a pre-Investigational New Drug (“IND”) meeting and received guidance from the agency on the regulatory requirements to seek approval.
In a multicenter, double-blind, randomized, placebo-controlled crossover trial conducted in Italy, Dr. Zannolli et al. studied the effect of an oral liquid solution of betamethasone on the reduction of ataxia symptoms in 13 children (between ages 2 to 8 years) with A-T. The primary outcome measure was the reduction in ataxia symptoms as assessed by the International Cooperative Ataxia Rating Scale (“ICARS”).
In the trial, oral liquid betamethasone reduced the ICARS total score by a median of 13 points in the intent-to-treat population and 16 points in the per-protocol population (the median percent decreases of ataxia symptoms of 28% and 31%, respectively). Adverse events in the trial were minimal, with no compulsory withdrawals and only minor side effects that did not require medical intervention. Clinical trial results in A-T patients administered oral betamethasone indicated that betamethasone significantly reduced ICARS total score relative to placebo (P = 0.01). The median ICARS change score (change in score with betamethasone minus change in score with placebo) was -13 points (95% confidence interval for the difference in medians was -19 to -5.5 points).
Based on the Zannolli data, we believe that our GTx-102 concentrated oral spray has the potential to provide clinical benefits in decreasing A-T symptoms, including assessments of posture and gait disturbance and kinetic, speech and oculomotor functions. In addition, GTx-102 may ease drug administration for patients experiencing A-T given its application of 1-3x/day of 140µL of concentrated betamethasone liquid sprayed onto the tongue using a more convenient metered dose delivery system, as these A-T patients typically have difficulty swallowing.
GTx-102 PK Data to Date:
GTx-102 administered as a concentrated oral spray achieves similar blood levels at only 1/70th the volume of an oral solution of betamethasone. This more convenient mode of administration will be important for A-T patients who have difficulties swallowing large volumes of liquids.
We initiated a PK bridging trial of GTx-102 as compared to the oral liquid solution of betamethasone used in the Zannolli trial and against the injectable form of betamethasone that is approved in the U.S. in the third calendar quarter of 2022. The primary objectives of the PK bridging trial were to evaluate the bioavailability, pharmacokinetics, and safety of GTx-102. In December 2022, we reported that the topline results of this trial met all primary outcome measures.
Results showed that GTx-102 betamethasone blood concentrations were highly predictable and consistent based on AUC (the area under the concentration time curve up to 72 hours post-dose, extrapolated to infinity) and Cmax (the maximum concentration occurring between 0 hour to 72 hours after trial drug administration), indicating good linearity and dose-proportionality. GTx-102 betamethasone blood concentrations were within the same range of exposure as IM betamethasone, based on AUC. This IM formulation will serve as a bridge for GTx-102 in the context of the proposed 505(b)(2) regulatory pathway. GTx-102 betamethasone blood concentrations were also within the same range of exposure as Oral Solution (“OS”), based on AUC. This OS formulation was used by Zannolli and may serve as a clinical comparator for further clinical development. Furthermore, statistically there was no significant difference (p>0.05) between GTx-102 administered at a fast rate (each spray immediately following the preceding one) vs. a slow rate (1 spray/minute), as indicated by Cmax and AUC. We believe this result is important because being able to use the fast or the slow rate of administration may provide greater flexibility for patients and caregivers. The Cmax of GTx-102 was within the same range of exposure as the OS, but the Cmax for the IM formulation was lower than both GTx-102 and the OS, as well as what has been reported previously for the IM in industry publications. It is important to note that achieving bioequivalence with the IM was not an objective of this trial, nor was it expected. Finally, of the 48 healthy adult subjects, no serious adverse events were reported, and the most frequent drug-related adverse effect was mild headache (4 cases).
The further clinical development of GTx-102 has been deprioritized in favor of our focus on development of GTx-104. However, we plan to collaborate with clinical experts to design the Phase 3 safety and efficacy protocol for GTx-102 and gain alignment with the FDA on the development path forward. Further clinical development work will be contingent on additional funding for GTx-102 or the signing of a strategic partnership. It is also possible that we may license or sell our GTx-102 drug candidate.
GTx-101 Overview
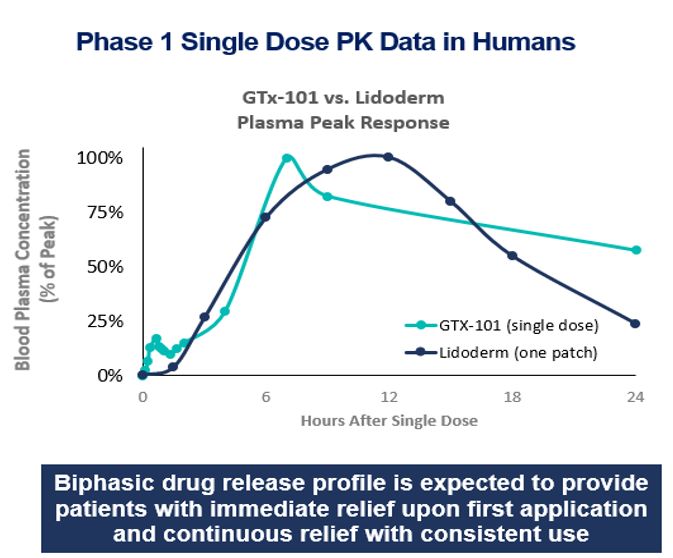
GTx-101 is a non-narcotic, topical bio-adhesive film-forming bupivacaine spray designed to ease the symptoms of patients suffering with postherpetic neuralgia (“PHN”). GTx-101 is administered via a metered-dose of bupivacaine spray and forms a thin bio-adhesive topical film on the surface of the patient’s skin, which enables a touch-free, non-greasy application. It also comes in convenient, portable 30 ml plastic bottles. Unlike oral gabapentin and lidocaine patches which are used for the treatment of PHN, we believe that the biphasic delivery mechanism of GTx-101 has the potential for rapid onset of action and continuous pain relief for up to eight hours. No skin sensitivity was reported in a Phase 1 trial.
About Postherpetic Neuralgia (PHN)
PHN is neuropathic pain due to damage caused by the varicella zoster virus (“VZV”). Infection with VZV causes two distinct clinical conditions. Primary VZV infection causes varicella (i.e., chickenpox), a contagious rash illness that typically occurs among young children. Secondary VZV can reactivate clinically, decades after initial infection, to cause herpes zoster (“HZ”), otherwise known as shingles. Acute HZ arises when dormant virus particles, persisting within an affected sensory ganglion from the earlier, primary infection with VZV become reactivated when cellular immunity to varicella decreases. Viral particles replicate and may spread to the dorsal root, into the dorsal horn of the spinal cord, and through peripheral sensory nerve fibers down to the level of the skin. Viral particles also may circulate in the blood. This reactivation is accompanied by inflammation of the skin, immune response, hemorrhage, and destruction of peripheral and central neurons and their fibers. Following such neural degeneration, distinct types of pathophysiological mechanisms involving both the central and peripheral nervous systems may give rise to the severe nerve pain associated with PHN.
While the rash associated with HZ typically heals within two to four weeks, the pain may persist for months or even years, and this PHN manifestation is the most common and debilitating complication of HZ. There is currently no consensus definition for PHN, but it has been suggested by the Centers for Disease Control and Prevention (“CDC”) that PHN is best defined as pain lasting at least three months after resolution of the rash.
PHN is associated with significant loss of function and reduced quality of life, particularly in the elderly. It has a detrimental effect on all aspects of a patient’s quality of life. The nature of PHN pain varies from mild to severe, constant, intermittent, or triggered by trivial stimuli. Approximately half of patients with PHN describe their pain as “horrible” or “excruciating,” ranging in duration from a few minutes to constant on a daily or almost daily basis. The pain can disrupt sleep, mood, work, and activities of daily living, adversely impacting the quality of life and leading to social withdrawal and depression. PHN is the foremost cause of intractable, debilitating pain in the elderly, and has been cited as the leading cause of suicide in chronic pain patients over the age of 70.
Current treatment of PHN most often consists of oral gabapentin (first line) and prescription lidocaine patches or antidepressants (second line), and refractory cases may be prescribed opioids to address persistent pain. Gabapentin and opioid abuse have continued to proliferate, and lidocaine patches are suboptimal for many reasons. An independent third-party market research firm we commissioned interviewed more than 250 physicians who regularly treat PHN patients and found that approximately 40% of patients using lidocaine patches experience insufficient pain relief. Lidocaine patches are difficult to use, fall off, and look unsightly with possible skin sensitivity and irritation. Additionally, lidocaine patches can only be used for 12 hours and then need to be removed for 12 hours before being reapplied. Prescription lidocaine patches are only approved for PHN, and the market is currently made up of both branded and generic offerings. It is estimated that PHN affects approximately 120,000 patients per year in the United States. According to a third-party report, the total addressable market for GTx-101 could be as large as $2.5 billion, consisting of approximately $200 million for PHN pain and $2.3 billion for non-PHN pain indications.
GTx-101 Research & Development History and Clinical Trials Completed to Date
To date, we have conducted four Phase I trials in healthy volunteers to assess the PK, safety, and tolerability of GTx-101 and to determine the plasma levels of bupivacaine HCl administered as a single dose in various concentrations between 30 mg (three sprays) and 2100 mg (twenty sprays).
These trials confirmed that bupivacaine delivered as a topical spray (GTx-101) is well absorbed through the skin, as demonstrated in the graph below, while very little is absorbed systemically.
In all four trials, the administration of GTx-101 to healthy volunteers was safe and well tolerated. In addition, no evidence of skin irritation was observed at the application site following the spray administrations. The data below is from two separate trials of GTx-101 and the Lidoderm patch superimposed on each other.
GTx-101 activities:
The data from the single dose Phase 1 clinical trial for GTx-101 was submitted to the FDA’s Division of Anesthesiology and feedback was received at a pre-IND meeting that informed the design of pre-clinical toxicology studies and a clinical and regulatory pathway to approval under section 505(b)(2). We completed a minipig skin sensitivity study in the second calendar quarter of 2022, and we initiated a single dose PK trial in healthy human volunteers in July 2022. Topline results from this single dose PK trial were reported in December 2022, and the results met all primary outcome measures.
The median Tmax (the time of maximum concentration between 0 hour and 240 hours after study drug administration) of bupivacaine in plasma following GTx-101 single-dose topical applications ranged between 18 to 24 hours depending on dose, while the median Tmax following the subcutaneous injection of 10 mg of bupivacaine was only 23 minutes. This result suggests that bupivacaine delivered by GTx-101 remains in the skin for a long period of time, potentially inducing prolonged analgesic effects in the sprayed area. The exposure to bupivacaine based on Cmax (the maximum concentration occurring at Tmax between 0 hour and 240 hours after study drug administration) and AUC (the area under the concentration time curve, extrapolated to infinity) following GTx-101 topical application as a single-dose increased with increasing dose.
The systemic exposure to bupivacaine following a 200mg dose of GTx-101 was approximately 29-fold less than a single subcutaneous dose of 10mg of bupivacaine based on Cmax and approximately 6-fold less than a single subcutaneous dose of 10mg of bupivacaine based on AUC. We predict these lower blood levels will correspond to an increased safety margin for GTx-101 with regards to toxicity risk. Mean half-life (“T half”) following GTx-101 single-dose topical applications ranged between 24 to 37 hours depending on dose, suggesting a slow elimination and potentially long duration of effect, while mean Tmax following the subcutaneous injection of 10 mg of bupivacaine was only 8 hours.
There were only two adverse events judged as related to the study drug by the investigator for each of GTx-101 and the bupivacaine subcutaneous injection. Following GTx-101 topical application: headache (1 event = 3%) and numbness (1 event = 3%) at the sprayed area following bupivacaine subcutaneous injection: dizziness (1 event = 8%) and nausea (1 event = 8%).
The further development of GTx-101 has been deprioritized in favor of our focus on development of GTx-104. Pending additional funding for GTx-101 or the signing of a strategic partnership, we plan to follow this successful PK trial with the next step of the clinical development plan including a multiple ascending dose trial. Results from these non-clinical studies and clinical trials are required before the initiation of our Phase 2 program in PHN patients. It is also possible that we may license or sell our GTx-101 drug candidate.
Overall Commercialization Strategy
We have worldwide commercialization rights for all our pipeline drug candidates and plan to maximize the value of each of our drug candidates over time. Currently, we have prioritized the development of GTx-104 over that of GTx-102 and GTx-101. If we receive regulatory approval for GTx-104 in the US, we may look to out-license its commercialization or consider self-commercialization including outsourcing sales to ensure efficient commercial management and maximize market penetration and financial returns. We may further seek commercial partnerships to fully exploit the market potential of GTx-104 in territories outside the US. It is possible that we out-license or sell GTx-102 and/or GTx-101 for the US and/or global markets.
Recent Developments
Completion of Patient Enrollment in Phase 3 STRIVE-ON Safety Trial of GTx-104
As noted above, on September 25, 2024, we announced the completion of enrollment in our Phrase 3 STRIVE-ON trial for GTx-104. We anticipate a data readout from the STRIVE-ON trial in first calendar quarter 2025 and plan to submit an NDA to the FDA in the first half of calendar year 2025.
Continuance and Domestication
We are a Delaware corporation that, as further described below, previously existed under the laws of the Province of Québec, Canada (“Acasti Québec”), before changing our jurisdiction on October 1, 2024, to the Province of British Columbia, Canada (“Acasti British Columbia”). On October 7, 2024, we changed our jurisdiction to the State of Delaware (“Acasti Delaware”).
On October 1, 2024, we changed our jurisdiction of incorporation from the Province of Québec in Canada to the Province of British Columbia in Canada pursuant to a “continuance” effected in accordance with Chapter XII of the Business Corporations Act (Québec) (the “Continuance”). Subsequently on October 7, 2024, we changed our jurisdiction of incorporation from the Province of British Columbia in Canada to the State of Delaware in the United States of America pursuant to a “continuance” effected in accordance with Section 308 of the Business Corporations Act (British Columbia) and a “domestication” (the “Domestication”) under Section 388 of the General Corporation Law of the State of Delaware (the “DGCL”). Both the Continuance and the Domestication were approved by our shareholders at our Annual and Special Meeting of Shareholders held on September 30, 2024.
Prior to the Continuance and Domestication, our Class A common shares, without par value per share were listed on The Nasdaq Stock Market LLC (“Nasdaq”) under symbol “ACST.” Upon the effectiveness of the Continuance, each of our common shares at the time of the Continuance remained issued and outstanding as a common share, without par value per share, of Acasti British Columbia. Upon effectiveness of the Domestication, each of our outstanding common shares at the time of the Domestication automatically became one outstanding share of common stock, par value $0.0001 per share, of Acasti Delaware. Our common stock continues to be listed for trading on Nasdaq.
Corporate Name Change
Effective October 28, 2024, we changed our corporate name to Grace Therapeutics, Inc. and our common stock commenced trading under the trading symbol “GRCE” on Nasdaq.
Basis of Presentation of the Financial Statements
Our unaudited condensed consolidated financial statements, which include the accounts of our wholly owned subsidiaries, have been prepared in accordance with U.S. GAAP and the rules and regulations of the SEC related to quarterly reports filed on Form 10-Q. All intercompany transactions and balances are eliminated on consolidation.
Our assets as of September 30, 2024, include cash, cash equivalents, and short-term investments totaling $15.2 million and intangible assets and goodwill totaling $49.3 million. Our current liabilities total $2.7 million as of September 30, 2024 and are comprised primarily of amounts due to or accrued for creditors. The Company believes its cash runway will be sufficient to fund the Company’s operations into the second calendar quarter of 2026.
Results of Operations for the three and the six months ended September 30, 2024 and 2023
| | | Three months ended | | | Six months ended | |
| | | September 30, 2024 | | | September 30, 2023 | | | Increase (Decrease) | | | September 30, 2024 | | | September 30, 2023 | | | Increase (Decrease) | |
| | |
| $ | | |
| $ | | |
| $ | | |
| $ | | |
| $ | | |
| $ | |
| Operating expenses | | | | | | | | | | | | | | | | | | | | | | | | |
| Research and development expenses, net of government assistance | | | 2,976 | | | | 460 | | | | 2,516 | | | | 5,684 | | | | 1,555 | | | | 4,129 | |
| General and administrative expenses | | | 1,855 | | | | 1,632 | | | | 223 | | | | 4,109 | | | | 3,506 | | | | 603 | |
| Restructuring costs | | | — | | | | — | | | | — | | | | — | | | | 1,485 | | | | (1,485 | ) |
| Loss from operating activities | | | (4,831 | ) | | | (2,092 | ) | | | 2,739 | | | | (9,793 | ) | | | (6,546 | ) | | | 3,247 | |
| | | | | | | | | | | | | | | | | | | | | | | | | |
Foreign exchange gain (loss)
| | | 13 | | | | (13 | ) | | | 26 | | | | 5 | | | | (5 | ) | | | 10 | |
| Change in fair value of derivative warrant liabilities | | | 362 | | | | (1,826 | ) | | | 2,188 | | | | 1,756 | | | | (1,826 | ) | | | 3,582 | |
Interest and other income, net | | | 172 | | | | 212 | | | | (40 | ) | | | 407 | | | | 346 | | | | 61 | |
| Income tax benefit | | | 852 | | | | 446 | | | | 406 | | | | 1,576 | | | | 735 | | | | 841 | |
| Net loss | | | (3,432 | ) | | | (3,273 | ) | | | 159 | | | | (6,049 | ) | | | (7,296 | ) | | | (1,247 | ) |
The net loss of $3.4 million, or $0.30 per share, for the three months ended September 30, 2024, increased by $159 from the net loss of $3.3 million, or $0.43 per share, for the three months ended September 30, 2023. The increase in net loss was primarily due to an increase in research and development expenses of $2.5 million and general and administrative expenses of $223, offset in part by a $2.2 million difference in the change in the fair value of derivative warrant liabilities and a $0.4 million increase in our income tax benefit.
The net loss of $6.0 million, or $0.53 per share, for the six months ended September 30, 2024, decreased by $1.3 million from the net loss of $7.3 million, or $0.97 per share, for the six months ended September 30, 2023. The decrease in net loss was primarily due to a $3.6 million difference in the change in fair value of derivative warrant liabilities, an $841 increase in our income tax benefit, and a $1.5 million decrease in restructuring costs, partly offset by a $4.1 million increase in research and development expenses and a $603 increase in general and administrative expenses.
Research and development expenses, net of government assistance
Research and development expenses consist primarily of:
| • | fees paid to external service providers such as CROs and CMOs related to clinical trials, including contractual obligations for clinical development, clinical sites, manufacturing and scale-up, and formulation of clinical drug supplies; |
| • | fees paid to contract service providers related to drug discovery efforts including chemistry and biology services; and |
| • | salaries and related expenses for research and development personnel, including expenses related to stock options. |
We record research and development expenses as incurred.
Our research and development during the three and the six months ended September 30, 2024 and 2023 was focused primarily on our clinical development program for our GTx-104 drug candidate.
The following table summarizes our research and development expenses:
Research and development
expenses | | | | | | | | | | | | | | | | | | |
| | | Three months ended | | | Six months ended | |
| | | September 30, 2024 | | | September 30, 2023 | | | Increase (Decrease) | | | September 30, 2024 | | | September 30, 2023 | | | Increase (Decrease) | |
| | |
| $ | | |
| $ | | |
| $ | | |
| $ | | |
| $ | | |
| $ | |
Total third-party research and development expenses1 | | | 2,716 | | | | 152 | | | | 2,564 | | | | 5,150 | | | | 965 | | | | 4,185 | |
| Government grants & tax credits | | | — | | | | 4 | | | | (4 | ) | | | — | | | | 55 | | | | (55 | ) |
| Salaries and benefits | | | 200 | | | | 209 | | | | (9 | ) | | | 408 | | | | 435 | | | | (27 | ) |
| Research and development expense before stock-based compensation and depreciation | | | 2,916 | | | | 365 | | | | 2,551 | | | | 5,558 | | | | 1,455 | | | | 4,103 | |
| Stock-based compensation | | | 60 | | | | 83 | | | | (23 | ) | | | 126 | | | | 83 | | | | 43 | |
| Depreciation and loss on disposal of equipment | | | — | | | | 12 | | | | (12 | ) | | | — | | | | 17 | | | | (17 | ) |
| Total | | | 2,976 | | | | 460 | | | | 2,516 | | | | 5,684 | | | | 1,555 | | | | 4,129 | |
1 Total third-party research and development expenses are calculated before salaries and benefits, depreciation, write-off of equipment and stock-based compensation.
Total research and development expenses for the three and the six months ended September 30, 2024 were $3.0 million and $5.7 million, respectively, compared to $460 and $1.5 million for the three months and the six months ended September 30, 2023, respectively. This increase of $2.5 million and $4.1 million for the three and the six months period then ended, respectively, was primarily due to the increase in research activities for the GTx-104 pivotal Phase 3 safety clinical trial.
There were no government grants and tax credits for the three and the six months ended September 30, 2024, compared to $4 and $55 for the three months and the six months ended September 30, 2023, respectively. The changes within government grants and tax credits were due to adjustments of provisions regarding the estimated realizability of credits receivable after assessments and correspondence from tax authorities.
Stock-based compensation of $60 for the three months ended September 30, 2024, decreased by $23 compared to $83 for the three months ended September 30, 2023. Stock-based compensation of $126 for the six months ended September 30, 2024, increased by $43 compared to $83 for the six months ended September 30, 2023. The decrease for the three months ended and the increase for the six months ended, was primarily due to the timing of the issuance of new grants.
General and administrative expenses
General and administrative expenses consist primarily of salaries and related benefits, including stock-based compensation, related to our executive, finance, legal, and support functions, including professional fees for auditing, tax, consulting, rent and utilities and insurance.
General and administrative expenses | | | | | | | | | | | | | | | | | | |
| | | Three months ended | | | Six months ended | |
| | | September 30, 2024 | | | September 30, 2023 | | | Increase (Decrease) | | | September 30, 2024 | | | September 30, 2023 | | | Increase (Decrease) | |
| | |
| $ | | |
| $ | | |
| $ | | |
| $ | | |
| $ | | |
| $ | |
| Salaries and benefits | | | 490 | | | | 228 | | | | 262 | | | | 885 | | | | 585 | | | | 300 | |
| Professional fees | | | 977 | | | | 864 | | | | 113 | | | | 2,431 | | | | 1,829 | | | | 602 | |
| Other | | | 244 | | | | 340 | | | | (96 | ) | | | 476 | | | | 813 | | | | (337 | ) |
General and administrative expense before stock-based compensation and depreciation1 | | | 1,711 | | | | 1,432 | | | | 279 | | | | 3,792 | | | | 3,227 | | | | 565 | |
| Stock-based compensation | | | 142 | | | | 199 | | | | (57 | ) | | | 314 | | | | 275 | | | | 39 | |
| Depreciation | | | 2 | | | | 1 | | | | 1 | | | | 3 | | | | 4 | | | | (1 | ) |
| Total | | | 1,855 | | | | 1,632 | | | | 223 | | | | 4,109 | | | | 3,506 | | | | 603 | |
1 General and administrative sub-total expenses are calculated before stock-based compensation and depreciation.
General and administrative expenses were $1.9 million and $4.1 million for the three and the six months ended September 30, 2024, respectively, an increase of $223 and $603, respectively, from $1.6 million and $3.5 million for the three and the six months ended September 30, 2023, respectively. The increase was primarily a result of increased legal, tax, accounting, audit and other professional fees primarily related to the Continuance and the Domestication, increased salaries and benefits due to merit increases and hiring of new employee, offset by a decrease in other expenses due primarily to adjustments for claims for Canadian goods and services tax and decrease in miscellaneous expenses as a result of restructuring. Stock-based compensation of $142 and $314 for the three and the six months ended September 30, 2024, respectively, decreased by $57 and increased by $39, respectively, compared to $199 and $275 for the three and the six months ended September 30, 2023, respectively. The decrease in three months ended and the increase in the six months ended was primarily due to the timing of the issuance of new grants.
Restructuring Costs
On May 8, 2023, we announced our decision to terminate a substantial amount of our workforce as part of a plan intended to align our organizational and management cost structure to prioritize resources to GTx-104, thereby reducing losses to improve cash flow and extend available cash resources. We incurred $1.5 million of related costs primarily consisting of employee severance costs. There were no restructuring costs during the three and the six months ended September 30, 2024.
Change in fair value of derivative warrant liabilities
For the three months ended September 30, 2024, the decrease in the fair value of derivative warrant liabilities of $362 was a mark-to-market adjustment to the derivative warrant liabilities and primarily due to a decrease in volatility, offset by an increase in our stock price. For the three months ended September 30, 2023, the increase in the fair value of derivative warrant liabilities of $1.8 million was a mark-to-market adjustment to the derivative warrant liabilities primarily due to an increase in our stock price.
For the six months ended September 30, 2024, the decrease in the fair value of derivative warrant liabilities of $1.8 million was a mark-to-market adjustment to the derivative warrant liabilities primarily due to a decrease in our stock price. The increase in the fair value of derivative warrant liabilities of $1.8 million for the six months ended September 30, 2023, was a mark-to-market adjustment to the derivative warrant liabilities primarily attributable to an increase in our stock price.
Interest and other income, net
For the three months ended September 30, 2024, interest and other income was $172, a decrease by $40 compared to $212 for the three months ended September 30, 2023, primarily due to withdrawals of short-term investments upon their maturity used to fund operations, as well as a decrease in interest rates.
For the six months ended September 30, 2024, interest and other income was $407, an increase of $61 compared to $346 for the six months ended September 30, 2023, primarily due to the increase in interest earned on average daily balances of cash and cash equivalents.
Income tax benefit
For the three and the six months ended September 30, 2024, income tax benefit was $852 and $1.6 million, respectively, an increase of $406 and $841, respectively, from $446 and $735 for the three and the six months ended September 30, 2023, respectively, due to net losses recognized by our U.S. subsidiary, which are deemed recoverable to the Company and can be taken as a benefit over time.
Liquidity and Capital Resources
Cash flows and financial condition for the six months ended September 30, 2024 and 2023
Summary
As of September 30, 2024, cash and cash equivalents were $15.1 million, a net decrease of $7.9 million compared to cash and cash equivalents of $23.0 million at March 31, 2024. We believe our existing cash and cash equivalents will be sufficient to fund our operations into the second calendar quarter of 2026.
We will require additional capital to fund our daily operating needs beyond that time. We do not expect to generate revenue from product sales unless and until we successfully complete drug development and obtain regulatory approval, which we expect will take several years and is subject to significant uncertainty. To date, we have financed our operations primarily through public offerings and private placements of our Common Shares, warrants and convertible debt and the proceeds from research tax credits. Until such time that we can generate significant revenue from drug product sales, if ever, we will require additional financing, which is expected to be sourced from a combination of public or private equity or debt financing or other non-dilutive sources, which may include fees, milestone payments and royalties from collaborations with third parties. Arrangements with collaborators or others may require us to relinquish certain rights related to our technologies or drug product candidates. Adequate additional financing may not be available to us on acceptable terms, or at all. Our inability to raise capital as and when needed could have a negative impact on our financial condition and our ability to pursue our business strategy. We plan to raise additional capital in order to maintain adequate liquidity. Negative results from studies or trials, if any, or depressed prices of our Common Shares could impact our ability to raise additional financing. Raising additional equity capital is subject to market conditions that are not within our control. If we are unable to raise additional funds, we may not be able to realize our assets and discharge our liabilities in the normal course of business.
Net cash (used in) operating activities
Net cash used in operating activities for the six months ended September 30, 2024 was $7.8 million, compared to $8.4 million for the six months ended September 30, 2023, a decrease of $0.6 million. The reduction in net cash used in operating activities during the second quarter of 2025 was primarily due to a $4.2 million increase in research and development activities for our GTx-104 pivotal Phase 3 STRIVE-ON trial protocol, a $0.6 million increase in general and administrative expenses for legal, tax, accounting and other professional fees related to the Continuance and Domestication, and a $0.3 million increase in salaries and other benefits, offset by $3.0 million in change in trade and other payables and a $1.5 million decrease in restructuring costs.
Net cash (used in) provided by investing activities
Net cash used in investing activities for the six months ended September 30, 2024, was from our purchase of short-term investments of $15. Net cash provided by investing activities for the six months ended September 30, 2023, was from the proceeds from the sale of equipment of $110.
Net cash provided by financing activities
There were no financing activities for the six months ended September 30, 2024. Net cash provided by financing activities for the six months ended September 30, 2023, was primarily attributable to the $7.3 million net proceeds received from the September 2023 private placement offering of our securities.
Private Placement
On September 24, 2023, we entered into a securities purchase agreement (the “Purchase Agreement”) with certain institutional and accredited investors in connection with a private placement offering of our securities (the “Offering”). Pursuant to the Purchase Agreement, we sold 1,951,371 Common Shares, at a purchase price of $1.848 per Common Share and pre-funded warrants (the “Pre-funded Warrants”) to purchase up to 2,106,853 Common Shares at a purchase price equal to the purchase price per Common Share less $0.0001. Each Pre-funded Warrant is exercisable for one Common Share at an exercise price of $0.0001 per Common Share, was immediately exercisable, and will expire once exercised in full. Pursuant to the Purchase Agreement, we also issued to such institutional and accredited investors common warrants (the “Common Warrants”) to purchase Common Shares, exercisable for an aggregate of 2,536,391 Common Shares. Under the terms of the Purchase Agreement, for each Common Share and each Pre-funded Warrant issued in the Offering, an accompanying five-eighths (0.625) of a Common Warrant was issued to the purchaser thereof. Each whole Common Warrant is exercisable for one Common Share at an exercise price of $3.003 per Common Share, was immediately exercisable, and will expire on the earlier of (i) the 60th day after the date of the acceptance by the FDA of an NDA for our product candidate GTx-104 or (ii) five years from the date of issuance. The Offering closed on September 25, 2023. The net proceeds to us from the Offering were approximately $7.3 million, after deducting fees and expenses.
Contractual Obligations and Commitments
Our contractual obligations and commitments include trade payables, CMO and CRO agreements, and the raw krill oil supply agreement, as described below.
Research and development contracts and contract research organizations agreements
We utilize CMOs for the development and production of clinical materials, and CROs to perform services related to our clinical trials. Pursuant to the agreements with CMOs and CROs, we have either the right to terminate the agreements without penalties or under certain penalty conditions. At September 30, 2024, the Company has $398 commitment to CMOs and $3.9 million of commitments to CROs for the next twelve months.
Raw krill oil supply contract
On October 25, 2019, we entered into a supply agreement with Aker BioMarine Antarctic AS. (“AKBM”) to purchase raw krill oil product for a committed volume of commercial starting material for CaPre, one of our former drug candidates, for a total fixed value of $3.1 million based on the value of krill oil at that time. As of March 31, 2022, the remaining balance of commitment amounted to $2.8 million. During the second calendar quarter of 2022, AKBM informed us that AKBM believed it had satisfied the terms of the supply agreement as to their obligation to deliver the remaining balance of raw krill oil product, and that we were therefore required to accept the remaining product commitment. We disagreed with AKBM’s position and believed that AKBM was not entitled to further payment under the supply agreement. Accordingly, no liability was recorded by us. The dispute remained unresolved as of both March 31, 2023 and 2022. On October 18, 2023, we entered into an agreement with AKBM to settle any and all potential claims regarding amounts due under the supply agreement (the “Settlement Agreement”). Pursuant to the terms of the Settlement Agreement, in exchange for a release and waiver of claims arising out of the supply agreement by AKBM and any of AKBM’s affiliates, we agreed to the following: (a) AKBM retained ownership of all raw krill oil product, including amounts previously delivered to us; (b) AKBM acquired and took ownership of all of our production equipment related to the production of CaPre; (c) AKBM acquired and took ownership of all of our data from research, clinical trials and pre-clinical studies with respect to CaPre; and (d) AKBM acquired and took ownership over all of our rights, title and interest in and to all intellectual property rights, including all patents and trademarks, related to CaPre owned by us. Further, AKBM acknowledged that the CaPre assets were transferred on an “as is” basis, and in connection therewith we disclaimed all representations and warranties in connection with the CaPre assets, including any representations with respect to performance or sufficiency. The value of the raw krill oil previously delivered to us, the production equipment, and the intellectual property rights related to CaPre were fully impaired in prior reporting periods and had a carrying value of nil as of March 31, 2023. For the three and the six months ended September 30, 2024, there was nil and $193, respectively, in expenses recorded by the Company in relation to shipping cost to transport the Company’s production equipment related to the production of CaPre.
We evaluate contingencies on an ongoing basis and establish loss provisions for matters in which losses are probable and the amount of the loss can be reasonably estimated.
Use of Estimates and Measurement of Uncertainty
The preparation of these unaudited condensed consolidated financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, income, and expenses. Actual results may differ from these estimates.
Estimates are based on management’s best knowledge of current events and actions that management may undertake in the future. Estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognized in the period in which the estimates are revised and in any future periods affected.
Estimates and assumptions include the measurement of stock-based compensation, derivative warrant liabilities, accruals for research and development contracts and contract organization agreements, and valuation of intangibles and goodwill. Estimates and assumptions are also involved in determining which research and development expenses qualify for research and development tax credits and in what amounts. The Company recognizes the tax credits once it has reasonable assurance that they will be realized.
Critical Accounting Policies
During the six months ended September 30, 2024, there were no material changes to our critical accounting policies from those described in our Annual Report for the year ended March 31, 2024.
Recent Accounting Pronouncements
We have considered recent accounting pronouncements and concluded that they are either not applicable to our business or that the effect is not expected to be material to our consolidated financial statements as a result of future adoption.
| Item 3. | Quantitative and Qualitative Disclosures About Market Risk |
A smaller reporting company is not required to provide the information required by this Item.
| Item 4. | Controls and Procedures |
Disclosure Controls and Procedures
As of the end of the period covered by this quarterly report, our management, with the participation of our Chief Executive Officer and Principal Financial Officer, has performed an evaluation of the effectiveness of our disclosure controls and procedures within the meaning of Rules 13a-15(e) and 15d-15(e) of the Exchange Act. Based upon this evaluation, our management has concluded that, as of September 30, 2024, our existing disclosure controls and procedures were effective. It should be noted that while our Chief Executive Officer and Principal Financial Officer believe that our disclosure controls and procedures provide a reasonable level of assurance that they are effective, they do not expect the disclosure controls and procedures to be capable of preventing all errors and fraud. A control system, no matter how well conceived or operated, can provide only reasonable, but not absolute, assurance that the objectives of the control system are met.
Changes in Internal Control over Financial Reporting
No changes were made to our internal controls over financial reporting that occurred during the quarter ended September 30, 2024, that have materially affected, or are reasonably likely to materially affect, our internal controls over financial reporting.
PART II. OTHER INFORMATION
In the ordinary course of business, we are at times subject to various legal proceedings and disputes. We assess our liabilities and contingencies in connection with outstanding legal proceedings utilizing the latest information available. Where it is probable that we will incur a loss and the amount of the loss can be reasonably estimated, we record a liability in our unaudited condensed consolidated financial statements. These legal reserves may be increased or decreased to reflect any relevant developments on a quarterly basis. Where a loss is not probable or the amount of loss is not estimable, we do not accrue legal reserves. While the outcome of legal proceedings is inherently uncertain, based on information currently available and available insurance coverage, our management believes that it has established appropriate legal reserves. Any incremental liabilities arising from pending legal proceedings are not expected to have a material adverse effect on our financial position, results of operations, or cash flows. However, it is possible that the ultimate resolution of these matters, if unfavorable, may be material to our financial position, results of operations, or cash flows. We are not currently a party to any legal proceedings that, in the opinion of management, are likely to have a material adverse effect on our business.
There have been no material changes from the risk factors disclosed in our Annual Report.
| Item 2. | Unregistered Sales of Equity Securities and Use of Proceeds |
| Item 3. | Defaults upon Senior Securities |
| Item 4. | Mine Safety Disclosures |
During the three months ended September 30, 2024, no director or officer of the Company adopted or terminated a Rule 10b5-1 trading arrangement or non-Rule 10b5-1 trading arrangement, as each term is defined in Item 408(a) of Regulation S-K.
| | Certificate of Incorporation of Grace Therapeutics, Inc. (incorporated by referenced to Exhibit 3.1 on the Current Report on Form 8-K filed with the Commission on October 7, 2024) |
| | | |
| | Certificate of Amendment to the Certificate of Incorporation of Grace Therapeutics, Inc. (incorporated by referenced to Exhibit 3.1 on the Current Report on Form 8-K filed with the Commission on October 28, 2024) |
| | | |
| | Bylaws of Grace Therapeutics, Inc. (incorporated by reference to Exhibit 3.2 on the Current Report on Form 8-K filed with the Commission on October 28, 2024) |
| | | |
| | Letter Agreement by and between Prashant Kohli and the Company, dated August 12, 2024 (incorporated by reference to Exhibit 10.1 on the Current Report on Form 8-K filed with the Commission on August 16, 2024) |
| | | |
| | Acasti Pharma Inc. 2024 Equity Incentive Plan (incorporated by reference to Exhibit 10.1 on the Current Report on Form 8-K filed with the Commission on September 30, 2024) |
| | | |
| | Form of Indemnification Agreement between Acasti Pharma Inc. and its directors and officers (incorporated by reference to Exhibit 10.1 to the Company’s Registration Statement on Form S-4 filed with the Commission on June 27, 2024) |
| | | |
| | Certification of Chief Executive Officer pursuant to Rule 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934 |
| | |
| | Certification of Principal Financial Officer pursuant to Rule 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934 |
| | |
| | Certification of the Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
| | |
| | Certification of the Principal Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 |
| | | |
| 101.INS | | Inline XBRL Instance Document – the instance document does not appear in the Interactive Data File because its XBRL tags are embedded within the Inline XBRL document |
| 101.SCH | | Inline XBRL Taxonomy Extension Schema With Embedded Linkbase Documents |
| 104 | | Cover Page Interactive Data File (formatted as Inline XBRL and contained in Exhibit 101) |
* Filed or furnished herewith
† Indicates a management contract or compensatory plan.
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| |
| | |
| | |
| | | |
| | | |
| | | |
| | | Title: Chief Executive Officer (Principal Executive Officer) |
| | | |
| | | |
| | | |
| | | Title: Principal Financial Officer (Principal Financial Officer) |