Table of Contents
As filed with the Securities and Exchange Commission on June 23, 2021
Registration No. 333-
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM S-1
REGISTRATION STATEMENT
UNDER
THE SECURITIES ACT OF 1933
SIGHT SCIENCES, INC.
(Exact name of registrant as specified in its charter)
| Delaware | 3841 | 80-0625749 | ||
(State or other jurisdiction of incorporation or organization) | (Primary Standard Industrial Classification Code Number) | (I.R.S. Employer Identification No.) |
4040 Campbell Ave, Suite 100
Menlo Park CA 94025
877-266-1144
(Address, including zip code, and telephone number, including area code, of registrant’s principal executive offices)
Paul Badawi
President and Chief Executive Officer
4040 Campbell Ave, Suite 100
Menlo Park CA 94025
877-266-1144
(Name, address, including zip code, and telephone number, including area code, of agent for service)
Copies to:
Peter N. Handrinos Wesley C. Holmes Latham & Watkins LLP 200 Clarendon Street Boston, MA 02116 (617) 948-6000 | Alan F. Denenberg Stephen Salmon Davis Polk & Wardwell LLP 1600 El Camino Real Menlo Park, CA 94025 (650) 752-2000 |
Approximate date of commencement of proposed sale to the public: As soon as practicable after the effective date of this Registration Statement.
If any of the securities being registered on this Form are to be offered on a delayed or continuous basis pursuant to Rule 415 under the Securities Act of 1933, check the following box. ☐
If this Form is filed to register additional securities for an offering pursuant to Rule 462(b) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
If this Form is a post-effective amendment filed pursuant to Rule 462(c) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
If this Form is a post-effective amendment filed pursuant to Rule 462(d) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ☐ | Accelerated filer | ☐ | |||
| Non-accelerated filer | ☒ | Smaller reporting company | ☒ | |||
| Emerging growth company | ☒ | |||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 7(a)(2)(B) of the Securities Act. ☐
CALCULATION OF REGISTRATION FEE
| ||||
Title of Each Class of Securities To Be Registered | Proposed Maximum Aggregate Offering Price (1) | Amount of Registration Fee (2) | ||
Common Stock, $0.001 par value per share | $100,000,000 | $10,910 | ||
| ||||
| (1) | Estimated solely for the purpose of calculating the registration fee pursuant to Rule 457(o) under the Securities Act of 1933, as amended. Includes the aggregate offering price of additional shares that the underwriters have the option to purchase. |
| (2) | Calculated pursuant to Rule 457(o) based on an estimate of the proposed maximum aggregate offering price. |
The Registrant hereby amends this Registration Statement on such date or dates as may be necessary to delay its effective date until the Registrant shall file a further amendment which specifically states that this Registration Statement shall thereafter become effective in accordance with Section 8(a) of the Securities Act of 1933 or until the Registration Statement shall become effective on such date as the Commission, acting pursuant to said Section 8(a), may determine.
Table of Contents
The information in this prospectus is not complete and may be changed. We may not sell these securities until the registration statement filed with the Securities and Exchange Commission is effective. This prospectus is not an offer to sell these securities and it is not soliciting an offer to buy these securities in any state where the offer or sale is not permitted.
Subject to Completion, dated June 23, 2021
PRELIMINARY PROSPECTUS
Shares

Common Stock
This is Sight Sciences, Inc.’s initial public offering. We are offering shares of our common stock. Prior to this offering, there has been no public market for our common stock. We estimate that the initial public offering price of our common stock will be between $ and $ per share. We have applied to list our common stock on The Nasdaq Global Market under the symbol “SGHT.”
We are an “emerging growth company” and “smaller reporting company” under the federal securities laws and, as such, are subject to reduced public company disclosure standards. See “Prospectus Summary—Implications of Being an Emerging Growth Company and a Smaller Reporting Company.”
Investing in our common stock involves risks. See ‘‘Risk Factors’’ beginning on page 17 of this prospectus.
| Per Share | Total | |||||||
Initial public offering price | $ | $ | ||||||
Underwriting discounts and commissions paid by us(1) | $ | $ | ||||||
Proceeds to us (before expenses) | $ | $ | ||||||
| (1) | We refer you to “Underwriters” beginning on page 207 for additional information regarding underwriting compensation. |
We have granted the underwriters an option to purchase up to additional shares of common stock for a period of 30 days after the date of this prospectus.
Neither the Securities and Exchange Commission nor any state securities commission has approved or disapproved of these securities or determined if this prospectus is truthful or complete. Any representation to the contrary is a criminal offense.
The underwriters expect to deliver the shares against payment to purchasers on or about , 2021 through the book-entry facilities of the Depository Trust Company.
| Morgan Stanley | BofA Securities | |||
| Citigroup | Piper Sandler |
The date of this prospectus is , 2021.
Table of Contents

The Power of Sight
SIGHT SCIENCES
Table of Contents
SIGHT SCIENCES OMNI® Surgical System TearCare® System
Table of Contents
| Page | ||||
| 1 | ||||
| 17 | ||||
| 85 | ||||
| 87 | ||||
| 88 | ||||
| 89 | ||||
| 90 | ||||
| 92 | ||||
| 95 | ||||
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS | 97 | |||
| 120 | ||||
| 185 | ||||
| 191 | ||||
| 201 | ||||
| 204 | ||||
| 207 | ||||
| 212 | ||||
MATERIAL U.S. FEDERAL INCOME TAX CONSEQUENCES TO NON-U.S. HOLDERS | 215 | |||
| 219 | ||||
| 228 | ||||
| 228 | ||||
| 228 | ||||
| F-1 | ||||
Neither we nor the underwriters have authorized anyone to provide any information or to make any representations other than those contained in this prospectus or in any free writing prospectuses prepared by or on behalf of us or to which we have referred you. We take no responsibility for, and can provide no assurance as to the reliability of, any other information that others may give you. This prospectus is an offer to sell only the shares of common stock offered hereby, but only under circumstances and in jurisdictions where it is lawful to do so. The information contained in this prospectus or in any applicable free writing prospectus related thereto is current only as of its date, regardless of its time of delivery or any sale of shares of our common stock. Our business, financial condition, results of operations and prospects may have changed since that date.
We have proprietary rights to trademarks, trade names and service marks appearing in this prospectus that are important to our business. Solely for convenience, the trademarks, trade names and service marks may appear in this prospectus without the ® and TM symbols, but any such references are not intended to indicate, in any way, that we forgo or will not assert, to the fullest extent under applicable law, our rights or the rights of the applicable licensors to these trademarks, trade names and service marks. All trademarks, trade names and service marks appearing in this prospectus are the property of their respective owners. We do not intend our use or display of other parties’ trademarks, trade names or service marks to imply, and such use or display should not be construed to imply, a relationship with, or endorsement or sponsorship of us by, these other parties.
Neither we nor the underwriters have done anything that would permit this offering or possession or distribution of this prospectus in any jurisdiction where action for that purpose is required, other than in the United States. Persons outside the United States who come into possession of this prospectus must inform themselves about, and observe any restrictions relating to, the offering of the shares of common stock and the distribution of this prospectus outside the United States.
i
Table of Contents
Until , 2021, (the 25th day after the date of this prospectus), all dealers that buy, sell or trade shares of our common stock, whether or not participating in this offering, may be required to deliver a prospectus. This is in addition to the dealers’ obligation to deliver a prospectus when acting as underwriters and with respect to their unsold allotments or subscriptions.
ii
Table of Contents
This summary highlights selected information contained elsewhere in this prospectus and is qualified in its entirety by the more detailed information included elsewhere in this prospectus. This summary does not contain all of the information you should consider before investing in our common stock.
You should carefully read this entire prospectus, including the information under the sections titled “Risk Factors,” “Special Note Regarding Forward-Looking Statements” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our financial statements and related notes thereto included elsewhere in this prospectus, before making an investment decision. Unless the context requires otherwise, references in this prospectus to “Sight Sciences,” the “Company,” “we,” “us” and “our” refer to Sight Sciences, Inc.
Overview
Our mission is to transform ophthalmology and optometry through the development and commercialization of proprietary devices that target the underlying causes of the world’s most prevalent eye diseases. We are passionate about improving patients’ lives. Our business philosophy is grounded in the following principles: comprehensively understanding disease physiology; developing products that are intended to restore natural physiological functionality to diseased eyes; developing and marketing products that achieve superior effectiveness versus current treatment paradigms while minimizing complications or side effects; providing intuitive, patient friendly solutions to ophthalmologists and optometrists (together, eyecare professionals or ECPs); and delivering compelling economic value to all stakeholders, including patients, providers and third-party payors such as Medicare and commercial insurers. Our objective is to develop and market products for use in new treatment paradigms and to create an interventional mindset in eyecare whereby our products may be used in procedures which supplant conventional outdated approaches. We believe current eyecare treatment models rely heavily on prescription medications, symptom relief, or either flawed or highly invasive, later-stage procedural interventions and fail to adequately address the true underlying cause of disease.
Our currently marketed products, the OMNI Surgical System, or OMNI, and the TearCare System, or TearCare, target two of the world’s most prevalent and underserved eye diseases, glaucoma and dry eye disease, or DED, respectively. Glaucoma, a group of chronic, often asymptomatic, diseases that damage the optic nerve, is the world’s leading cause of irreversible blindness. Primary open-angle glaucoma, or POAG, is the most prevalent form of glaucoma. Dry eye complaints are the most common reason for a patient visit to an eye doctor and DED symptoms have a significant impact on the quality of life and productivity of patients. If left untreated, DED can be extremely painful, leading to permanent cornea damage and vision impairment. We estimate the annual addressable U.S. market opportunities for OMNI and TearCare are approximately $6 billion and approximately $10 billion, respectively, while 2020 U.S. manufacturer revenues in the surgical glaucoma and DED markets were approximately $350 million and $2.4 billion, respectively, demonstrating that currently available solutions have not addressed a large part of the market need.
OMNI is a handheld, single-use, therapeutic device that allows ophthalmic surgeons to reduce intraocular pressure, or IOP, in adult glaucoma patients with a safe, ab interno, minimally invasive glaucoma surgery, or MIGS. We believe OMNI delivers the highest level of effectiveness of any available MIGS product, as it is the only device which provides access to 360 degrees and all three primary points of resistance of an eye’s diseased conventional outflow pathway through a single clear corneal microincision. We believe our recently expanded indication for use of OMNI is among the most comprehensive in MIGS. The FDA has authorized the use of OMNI for reducing IOP in all adult POAG patients both by itself on a standalone basis, which we refer to as Standalone procedures, or in combination with cataract procedures, which we refer to as Combination Cataract procedures. We believe OMNI is the first custom-designed ab interno MIGS device that was cleared by the FDA to be used in ab
1
Table of Contents
interno MIGS procedures for lowering IOP in both Combination Cataract and Standalone cases for all adults with POAG based upon the review of ab interno Combination Cataract and Standalone clinical data. Several competing MIGS devices, including the current market leaders, have only been authorized by the FDA for use in Combination Cataract procedures for adult patients with Mild-to-Moderate severity. We sell OMNI to facilities where ophthalmic surgeons perform outpatient procedures, mainly ambulatory surgery centers, or ASCs, and hospital outpatient departments, or HOPDs. Our Surgical Glaucoma segment, which includes OMNI, represented 94% of our total revenues for the year ended December 31, 2020 and for the three months ended March 31, 2021.
In March 2021, OMNI was cleared by the FDA for an expanded indication for use based upon the review of clinical data from ROMEO, our recently completed U.S. multi-center clinical study of OMNI in Combination Cataract and Standalone procedures. In ROMEO, we observed that Standalone OMNI patients with preoperative IOP greater than 18 mmHg experienced a mean IOP reduction of 28% (from 21.8 mmHg to 15.6 mmHg) and a mean reduction in hypotensive medication usage of 35% (from 1.71 medications to 1.17 medications) 12 months after treatment. In Combination Cataract patients with preoperative IOP greater than 18 mmHg, we observed a mean IOP reduction of 31% (from 21.9 mmHg to 15.1 mmHg) and a mean reduction in hypotensive medication usage of 45% (from 2.04 medications to 1.13 medications) 12 months after treatment. The Standalone procedure market, which we estimate represents greater than 85% of the addressable U.S. POAG market, is significantly underpenetrated relative to the Combination Cataract market. The development and penetration of the Standalone market is a key element of our growth strategy and we believe that OMNI has the degree of effectiveness and consistency of clinical outcomes to establish a more proactive, interventional treatment paradigm. We believe our recently expanded indication for use of OMNI will help us effectively develop the Standalone market and capitalize on the potential of the Combination Cataract market.
TearCare is a technologically sophisticated system which utilizes a wearable, open-eye design to apply localized heat to eyelids in an anatomically customized way. We believe TearCare has a compelling physiological profile to address obstructions from meibomian gland dysfunction, or MGD, which is the primary cause of evaporative DED, a disease characterized by low quality tears that evaporate prematurely. In OLYMPIA, our large randomized control trial, or RCT, TearCare was associated with statistically significant clinical improvements in all assessed signs and symptoms of DED. This included tear break up time, or TBUT, and meibomian gland secretion score, or MGSS, objective measurements of DED that were the trial’s primary endpoints, as well as patient-reported symptoms surveys including Eye Dryness Score, or EDS, Ocular Surface Disease Index, or OSDI, and Symptom Assessment in Dry Eye, or SANDE, at all time periods measured (both two weeks and four weeks post-treatment). Further, TearCare had a statistically significantly higher proportion of subjects improving by at least one OSDI category than did the group receiving a single treatment using a version of the first device FDA-cleared for the application of localized heat and pressure therapy in adult patients with chronic cystic conditions of the eyelids, including MGD. We sell TearCare to optometry and ophthalmology practices through a targeted commercial approach. Our initial strategic focus for TearCare is on improving patient access, as we believe that MGD is one of the most prevalent diseases in all of medicine that lacks any meaningful reimbursement coverage by Medicare and private payors. Our long-term plan is to maximize patient access to TearCare and further develop the MGD procedures market. This plan leverages a rigorous trial program designed to demonstrate the clinical benefits of TearCare treatments and a comprehensive effort to educate patients, providers and third-party payors regarding the benefits of TearCare treatments. Our Dry Eye segment, which includes TearCare, represented 6% of our total revenues for the year ended December 31, 2020 and for the three months ended March 31, 2021.
We are deeply committed to continuing to conduct clinical studies to evaluate the safety and effectiveness of our products, and we believe the results of our clinical studies will be critical to our continued growth. We are currently conducting robust clinical trial programs in both glaucoma and DED, with 11 ongoing or planned studies, including several head-to-head RCTs against market leading products. We also support investigator- initiated trial, or IIT, programs, of which eight are completed and two are currently in progress. We are focused
2
Table of Contents
on continuous innovation and seek regular input from our network of expert employees (including several ophthalmologists on staff), advisors and customers to rapidly iterate our pre- and post-commercial product designs with the aim of better satisfying the needs of our customers and their patients, and increasing adoption and utilization of our solutions. Their input has helped guide the intuitive design of our products and our hands-on instructional programs that allow ECPs to use OMNI and TearCare with confidence. Between January 2019 and April 2021, we shipped over 50,000 units of OMNI and over 10,000 single-use SmartLid units to customers. During this period, we are aware of nine events that were reported to the FDA in accordance with 21 CFR §803 as 30-day Medical Device Reports (MDRs), representing less than 0.015% of units shipped.
We have experienced significant growth and market adoption since commercially launching OMNI in February 2018 and initiating controlled commercial sales of TearCare in April 2019. We generated revenue of $7.5 million, $23.3 million, and $27.6 million for the years ended December 31, 2018, 2019, and 2020, respectively, and $6.5 million and $8.6 million for the three months ended March 31, 2020 and 2021, respectively. Gross margin was 68.9%, 72.0%, and 66.7% for the years ended December 31, 2018, 2019, and 2020, respectively, and 67.3% and 73.4% for the three months ended March 31, 2020 and 2021, respectively. We also incurred net losses of $14.3 million, $25.9 million, and $34.7 million for the years ended December 31, 2018, 2019, and 2020, respectively, and $9.2 million and $12.2 million for the three months ended March 31, 2020 and 2021, respectively.
Market Opportunity
Advancements in treatment effectiveness across a number of prominent eye diseases has been limited in recent years due to a lack of significant innovation. We believe that we are favorably positioned with each of our products to transform treatment paradigms and, over time, to broadly improve the quality of patient care throughout ophthalmology and optometry.
Primary Open-Angle Glaucoma
Glaucoma, a group of chronic, often asymptomatic, diseases that damage the optic nerve, is the world’s leading cause of irreversible blindness. Glaucoma does not have a cure and is a progressive disease; if left untreated or insufficiently treated, glaucoma can lead to irreversible disability and blindness. In patients with POAG, aqueous humor builds up in the anterior chamber of the eye and the resultant tension can interfere with the blood supply to the optic nerve in the back of the eye, resulting in optic nerve cell death and irreversible vision loss. Decades of research have demonstrated that the fluid buildup primarily results from malfunctions in the eye’s main drainage system, which is known as the conventional aqueous outflow pathway.
In 2020, 102 million people worldwide were estimated to suffer from glaucoma. POAG is the most prevalent form of glaucoma and in 2020 affected over 60 million people worldwide and 4.1 million people in the United States, of whom 3.4 million were diagnosed. We estimate the current annual addressable U.S. market opportunity for OMNI is approximately $6 billion, while 2020 U.S. manufacturer revenues in the surgical glaucoma market were approximately $350 million, demonstrating that currently available surgical solutions have not addressed a large part of the market need. In the U.S., currently marketed trabecular bypass stents are effectively precluded from participating in over 85% of this addressable market because they are only authorized for use in Combination Cataract procedures in patients with Mild-to-Moderate severity and we estimate that less than 15% of the diagnosed POAG population in the U.S. will require cataract surgery in a given year.
3
Table of Contents
Dry Eye Disease
DED refers to a group of disorders caused by either poor quality tears, known as evaporative DED, or inadequate tear production, known as aqueous deficient DED. There are an estimated 739 million people globally and 38 million people in the U.S. who suffer from DED. DED is the most common reason for a patient visit to an eye doctor, yet of the 38 million people with DED in the U.S., only 17 million have been diagnosed with DED. If left untreated, DED can be extremely painful and lead to permanent cornea damage and vision impairment. Studies have shown that evaporative DED resulting from MGD is associated with approximately 86% of all DED cases. Meibum is an oily secretion that forms the protective outer layer of healthy tears and prevents premature tear evaporation. For patients with MGD, meibum hardens within the meibomian glands, which are located in the eyelids, causing obstructions that prevent it from flowing freely onto the tear film. We estimate that the addressable U.S. market for MGD treatment is approximately $10 billion per year, as compared to MGD procedures representing less than $100 million of U.S. manufacturer revenues in 2020, demonstrating that currently available MGD procedures have not addressed a large part of the market need.
Current Alternatives and Limitations
A variety of pharmaceutical and procedure-based treatment alternatives exist for POAG and DED but there is no cure for either disease. Because many of the current alternatives focus on treating symptoms rather than the underlying causes of the disease, they offer suboptimal effectiveness and durability.
Primary Open-Angle Glaucoma
The current treatment paradigm for POAG includes less invasive options, such as prescription eyedrops and laser treatments for Mild and Moderate cases, and more invasive conventional surgical procedures for more severe cases. Each of these treatment modalities addresses just a single aspect of the disease at a specific point in the progression of the disease state. As a complex and progressive disease, there is no “one size fits all” treatment for POAG. Physicians have historically used a combination of treatments because no single treatment could adequately slow disease progression to a manageable level over the long term. Further, due to the progressive nature of the disease, any intervention can become ineffective as the disease state matures.
| • | Prescription eyedrops seek to increase aqueous outflow or reduce aqueous production. Prescription eyedrops are the most common first line therapy used to treat ocular hypertension, or OHT, and Mild glaucoma and often continue to be utilized as part of the treatment for Moderate and Advanced/Severe patients. The effectiveness of prescription eyedrops can be limited by patient behavior and compliance, providing inconsistent protection from glaucoma progression for many who face adherence challenges. If a single prescription medication fails to control IOP, additional medications may be prescribed. Although this step may contribute incremental effectiveness, adding medications can further complicate the treatment regimen, potentially hindering patient compliance, and exacerbate side effects. Studies have demonstrated that chronic use of glaucoma medication contributes to ocular surface disease, an inflammation of the ocular surface that is not only irritating and painful, further contributing to poor adherence, but can also contribute to greater risk of surgical failure should traditional glaucoma surgery, such as trabeculectomy, be required. |
| • | Sustained pharmaceutical delivery through an intraocular implant is a newer method of drug administration. While intracameral sustained delivery mitigates issues relating to patient medication adherence, it could introduce new challenges associated with the risks of leaving an intracameral implant in the eye over several months or years, or the procedural complexity and risks associated with implanting objects in the eye and potentially removing them. Only one intraocular drug delivery implant to treat glaucoma has been authorized for use by the FDA, and it is currently limited to a single six month treatment per eye without retreatment. |
4
Table of Contents
| • | Selective laser trabeculoplasty, or SLT, offers a non-invasive, energy-based solution and short recovery times, with effectiveness similar to certain eyedrops, but with a waning treatment effect at less than one year for up to half of patients. The effectiveness of continued laser therapy after a second treatment is not known at this time. |
| • | MIGS stents, particularly trabecular bypass stents, have steadily grown in usage among surgeons performing Combination Cataract procedures because the devices are efficient to implant, involve minimal complications and provide incremental effectiveness over cataract surgery itself. From 2012 to 2020, the estimated number of trabecular bypass stent procedures in the U.S. grew at a compounded annual growth rate, or CAGR, of 55%, including over 20% from 2018 to 2019. However, the |
| FDA has only authorized trabecular bypass stents for use in Combination Cataract procedures for Mild-to-Moderate cases, limiting their authorized use to less than 15% of all U.S. POAG patients. |
| • | Conventional invasive surgeries include trabeculectomy (also called filtering surgery) and tube shunt implantation, which are bleb-forming procedures, and have each been in use for several decades. Blebs are blister-like reservoirs surgically created on the outside of the eye intended to serve as permanent, artificial drainage channels. Conventional surgery techniques are multi-step invasive procedures and are most typically utilized for maximal reductions in IOP to prevent visual field loss in Advanced/Severe disease when medications, lasers or MIGS treatment of the conventional outflow pathway have failed. Despite their success at reducing IOP, serious complications or even surgical failure are not uncommon. These conventional surgeries are considered a last line of defense for Advanced/Severe stage patients because they create a physiologically artificial pathway that can be difficult to control, carry a life-long risk of complications (e.g., hypotony, blebitis, bleb failure), and typically require longer recovery periods. |
Dry Eye Disease
Although MGD is the primary root cause of DED, we believe it is relatively new to eyecare research and product development. In contrast, we believe aqueous deficiency, which is a less prominent root cause of DED, has historically dominated the medical community’s mindset regarding DED and has been synonymous with the disease. This has contributed to the current DED treatment market being characterized by an abundance of over-the-counter, or OTC, artificial tears and lubricating eyedrops, and prescription DED eyedrops. Given the relatively recent focus on and understanding of MGD, MGD procedures for DED have had limited commercial traction and represent a significant but underdeveloped market opportunity.
| • | Eyedrops for DED include OTC artificial tears and lubricating eyedrops, which are palliative, as well as prescription eyedrops, which aim to alleviate inflammation and/or increase aqueous layer tear production. Although several DED prescription eyedrops have achieved commercial and clinical success, we believe they are limited in their ability to treat the substantial majority of DED sufferers. None of the prescription DED eyedrops are indicated to treat MGD, the primary underlying cause of evaporative DED, which is associated with 86% of DED cases. Furthermore, patient non-compliance, the high rate of side effects, and high out-of-pocket costs further limit the ability of prescription eyedrops to treat DED effectively and with maximal patient access. |
| • | MGD procedures represented less than $100 million of U.S. manufacturer revenues in 2020. In general, available devices for the treatment of MGD can be difficult for providers to administer, which places significant oversight demands on the physician, may be uncomfortable for patients and/or have limited effectiveness. These devices may also require high upfront capital equipment purchases for providers, which lowers the overall economic value proposition to eyecare stakeholders. |
5
Table of Contents
Our Solutions
The OMNI Surgical System and the TearCare System are interventional ophthalmology devices. The past, current and ongoing development of OMNI and TearCare follows our internal product development approach, which is governed by four fundamental requirements that we believe are critical to delivering the most effective, safe and consistent clinical outcomes for patients with eye disease:
| • | Comprehensive Understanding of Disease Physiology. We review and analyze all available clinical data, science and literature that is relevant to a disease to achieve a sound understanding of its underlying cause(s), which guides the development of any of our products. |
| • | Treatment of Underlying Causes. Healthy eyes are self-regulating marvels of evolution, biomechanics, chemistry and physiology. We believe that restoring the natural functionality of diseased eyes by comprehensively treating underlying cause(s) of disease provides the optimal combination of effectiveness and safety. |
| • | Intuitive Design. Our products are designed to transform complex, impractical or invasive treatment approaches into intuitive, minimally invasive, user-friendly procedures. Our product development goals are focused on delivering a preferred “go to” treatment of choice to ophthalmologists and optometrists. |
| • | Patient Access. We seek to maximize the availability and accessibility of our products for as many patients as possible. We believe that our devices have the potential to offer differentiated clinical, experiential and economic value to all eyecare stakeholders. For conditions where patients lack optimal treatment access due to insurance coverage limitations or difficult patient-pay economics, we plan to demonstrate the value proposition of our solutions through rigorous clinical trial data and real-world results to improve access. |
OMNI Surgical System
Commercially launched in February 2018, OMNI is a handheld, single-use, therapeutic device used by ophthalmic surgeons to reduce IOP in adult glaucoma patients. Each OMNI Surgical System consists of 29 separate precision-engineered parts that have been optimized for intuitive use, performance and effectiveness. OMNI facilitates the sequential completion of two well-established, historically invasive glaucoma procedures, canaloplasty and trabeculotomy, with an efficient, minimally invasive approach using just a single, bloodless and sutureless clear corneal microincision. Conventional canaloplasty and trabeculotomy procedures have been used to effectively treat glaucoma for decades but involve invasive approaches that are difficult to perform, traumatize the eye, have higher risk of intraoperative and post-operative complications and require longer patient recovery times. OMNI transforms these two distinct, historically invasive ab externo glaucoma procedures into a single, sequential, ab interno MIGS procedure. MIGS procedures leverage a one to two millimeter clear corneal incision for intraocular access similar to cataract surgery and have a strong demonstrated safety profile, characterized by minimal trauma to the eye and quick patient recovery times. We believe that OMNI is the only MIGS device currently on the market that both provides access to 360 degrees of the diseased conventional outflow pathway and addresses all three primary points of resistance in the conventional outflow pathway (trabecular meshwork, Schlemm’s canal, and the distal collector channels) through a single clear corneal incision.
We have received 510(k) clearance from the FDA and a CE Mark to market OMNI in the U.S. and the EU, respectively. OMNI is indicated for canaloplasty followed by trabeculotomy to reduce IOP in adult patients with POAG in the U.S. and with open-angle glaucoma, or OAG, in the EU. We believe that OMNI is the only device that is authorized by the FDA as an ab interno procedure to: reduce IOP in adult patients with POAG across the spectrum of disease severity; be used in Mild-to-Moderate Combination Cataract or Standalone procedures; access 360 degrees of the diseased conventional outflow pathway through a single clear corneal incision; and
6
Table of Contents
facilitate two consecutive procedures, canaloplasty and trabeculotomy, to comprehensively treat all three primary points of resistance in the conventional outflow pathway in a single operating room visit. The procedure enabled by OMNI, canaloplasty followed by trabeculotomy, is covered and reimbursed by all Medicare Administrative Contractors, or MACs, and numerous private insurers, covering an estimated 67% of U.S. POAG sufferers.
Published data from ROMEO and several single surgeon datasets show a remarkable consistency in IOP reduction following treatment with OMNI. Almost all patients across these groups (98 of 103, 95%) had an IOP decrease following treatment with OMNI, and three out of four (77 of 103, 75%) had at least a 20% decrease. Patients in these studies also experienced reductions in the use of glaucoma medication following their OMNI procedures, a benefit not observed in the “medication washout” trabecular bypass stent trials designed to isolate and thereby maximize IOP reduction in a non-real world manner. We believe OMNI also has a compelling safety profile. Between January 2019 and April 2021, we shipped over 50,000 OMNI devices to customers and we are aware of only eight MDRs submitted to the FDA that were “possibly” related to the device. None of these events were unexpected as possibilities for this type of glaucoma surgery.
We believe the consistent therapeutic outcomes OMNI delivers are important for patients and surgeons alike. For patients, we believe the anxiety that may accompany the need for ocular surgery can be tempered with the knowledge that there is a high likelihood of success. For surgeons, consistent outcomes simplify the treatment choice and the decision to perform a procedure. We believe this is especially important for Standalone MIGS procedures which must deliver a very high consistency of efficacy and a very high degree of effectiveness to not only justify the procedure, but also provide surgeons with enough confidence to recommend Standalone surgery to their patients and take them to the operating room for a singular reason. We believe delivering consistently effective results will be crucial to unlocking the Standalone market, as well as capitalizing on the full potential of the Combination Cataract market, which we believe is currently capturing less than one-third of its potential procedure volume in the U.S.
TearCare System
TearCare is our newest marketed product, comprised of a re-usable hardware controller, the SmartHub, and a breakthrough wearable, software-controlled eyelid technology, the SmartLids. TearCare serves as an elegant, compact, portable, intuitive solution that enables the application of localized heat to the eyelids in an anatomically customized way. We believe TearCare presents a compelling physiological profile to potentially address DED due to MGD. Applied adhesively and non-invasively to the outside of the eyelids, single-use SmartLids deliver a precise therapeutic level of heat into the meibomian glands. Engineering SmartLids to remain comfortably adhered to virtually all shapes and sizes of eyelids while allowing freedom to blink and delivering precise therapeutic heat is one of our most significant design accomplishments. This heating process is intended to melt obstructions in the glands and restore the production and release of healthy, clear liquid meibum, which forms the outer protective layer of tears and helps prevent premature tear evaporation. Additionally, the proprietary, highly conformant, open-eye design of TearCare allows patients to blink naturally throughout the thermal portion of the procedure, which facilitates movement of melted meibum and also provides a comfortable treatment experience. TearCare can be utilized by an ECP in a straightforward in-office procedure and accommodated during the course of a routine patient visit. In our OLYMPIA RCT, we observed that a single use of TearCare was associated with statistically significant clinical improvements in all signs and symptoms of DED assessed, including TBUT and MGSS, objective measurements of DED that were the trial’s primary endpoints, as well as patient-reported symptoms surveys, including EDS, OSDI and SANDE, at both two and four weeks following treatment in subjects with MGD.
We believe TearCare’s design, with the SmartLids applied externally to the eyelids allowing the precise heat delivery to be managed by our software-controlled SmartHub, reduces the risk of adverse events arising from using TearCare. We have shipped over 10,000 single-use SmartLid units to customers through April 2021 and
7
Table of Contents
are aware of only a single MDR reported to the FDA for which the root cause has not been determined and may possibly be related to the device.
We began selling TearCare in a controlled product launch in April 2019. The initial phase of launch was successful in garnering valuable feedback from our customers and the broader DED community as well as demonstrating the existing market demand for an effective MGD solution. Our goals with the development of TearCare are to fully transform the current, outdated treatment paradigm, which relies primarily on OTC and prescription eyedrops, and establish our clinically proven eyelid procedure as the standard of care for the millions of patients suffering from evaporative DED caused by MGD. We are executing our long-term plan to maximize patient access to TearCare and further develop the MGD procedures market by leveraging a rigorous clinical trial program designed to demonstrate the safety, effectiveness and durability of TearCare treatments, and a comprehensive effort to educate patients, providers and third-party payors regarding the benefits of TearCare treatments.
We currently market TearCare as a Class II, 510(k)-exempt powered heating pad. In November 2020, we submitted a 510(k) premarket notification seeking an expanded indication for use for TearCare. The FDA requested several safety tests and modifications which we believe would have required additional time to complete beyond the designated review process. We voluntarily withdrew the submission in May 2021 to allow us to comply with the FDA requests in a comprehensive manner. We are currently conducting these follow-up safety tests and modifications, and we intend to resubmit the 510(k) premarket notification for an expanded indication for use in the second half of 2021.
Our Success Factors
We believe the following factors will drive the future success and growth of our company:
| • | Large market opportunities in eyecare with flawed treatment paradigms; |
| • | Continual development of innovative technologies; |
| • | Consistent delivery of exceptional customer experience; |
| • | Prioritization of clinical excellence and market education; |
| • | Focus on strong economics and value creation for all eyecare stakeholders; and |
| • | Scale culture built on community, passion, courage and perseverance. |
Our Growth Strategy
Our mission is to transform ophthalmology and optometry with proprietary solutions that target the underlying causes of the world’s most prevalent eye diseases. We believe the following elements of our growth strategy will advance our mission and contribute to our future growth:
| • | Establish OMNI as the standard of care for interventional glaucoma treatment; |
| • | Develop the MGD treatment market through a clinically-driven, patient access-led strategy for TearCare; |
| • | Drive adoption and utilization of our products by leveraging additional clinical studies and market education; |
| • | Deepen and broaden our commercial organization; |
| • | Expand into international markets; and |
| • | Continuously innovate premium product offerings throughout eyecare. |
8
Table of Contents
Summary of Risk Factors
Our business is subject to a number of risks and uncertainties of which you should be aware before making an investment decision. You should consider all of the information set forth in this prospectus and, in particular, the specific factors set forth under “Risk Factors” in deciding whether to invest in our common stock. These risks include, without limitation, the following:
| • | We have incurred significant losses since inception and expect to incur significant additional losses for the foreseeable future which may make it difficult to evaluate the success of our business to date and to assess the prospects for our future viability; |
| • | Our business is highly dependent on the success of two current commercial products, and in particular OMNI. The development of TearCare for expanded indications depends upon positive clinical data, and the safety and efficacy of our products are not yet supported by long-term clinical data, which could delay or prevent clearance by regulatory authorities or limit sales if cleared, certified or approved; |
| • | Even if this offering is successful, we may need additional funding in order to finance our planned operations. The inability to raise funds on acceptable terms, if at all, when needed, may force us to delay, reduce or eliminate our product development programs and commercialization efforts; |
| • | The COVID-19 pandemic has impacted, and likely will continue to impact, our operations and financial results and may materially and adversely affect our business and financial results in the future; |
| • | We are subject to extensive and costly government regulation on federal, state and foreign levels and we may not receive, or may be delayed in receiving, the necessary regulatory clearances, certifications or approvals for our future products or modifications to our current products; |
| • | We may incur significant liability if it is determined that we are not complying with federal, state or foreign regulatory requirements, such as if it is determined that we are promoting off-label uses of our products; |
| • | Changes in public health insurance coverage and reimbursement rates may affect the adoption of our products and our future revenue; |
| • | Developments by competitors may render our products or technologies obsolete or noncompetitive and the development of new products, technologies, procedures, medications or other therapies could replace or reduce the importance of our products; |
| • | We rely on third parties for the manufacture and supply of OMNI and TearCare; |
| • | We depend on a limited number of single source suppliers for some of the components, accessories and materials used in OMNI and TearCare and any shortfall in the supply chain may cause our business to materially suffer; |
| • | If we are unable to obtain, protect, maintain, enforce and adequately protect our intellectual property rights with respect to our technology and current and future products, or if the scope of the patent protection obtained is not sufficiently broad, our competitors could develop and commercialize technology and products similar or identical to ours, and our ability to successfully develop and commercialize our technology and current and future products may be adversely affected; and |
| • | If we lose key management or scientific personnel, cannot recruit qualified employees, directors, officers or other significant personnel or experience increases in our compensation costs, our business may materially suffer. |
9
Table of Contents
Implications of Being an Emerging Growth Company and a Smaller Reporting Company
We are an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012, as amended, or the JOBS Act. As such, we may take advantage of certain exemptions from various reporting requirements that are otherwise applicable to public companies. These exemptions include, but are not limited to:
| • | The option to present only two years of audited financial statements and only two years of related management’s discussion and analysis of financial condition and results of operations in this prospectus; |
| • | Not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act of 2002, as amended; |
| • | Not being required to submit certain executive compensation matters to stockholder advisory votes, such as “say-on-pay,” “say-on-frequency,” and “say-on-golden parachutes;” |
| • | Not being required to disclose certain executive compensation-related items such as the correlation between executive compensation and performance and comparisons of the chief executive officer’s compensation to median employee compensation; and |
| • | An exemption from compliance with the requirements of the Public Company Accounting Oversight Board regarding the communication of critical audit matters in the auditor’s report on the financial statements. |
We may take advantage of these provisions until the last day of our fiscal year following the fifth anniversary of the completion of this offering. However, if prior to the end of such five-year period, (i) our annual gross revenue exceeds $1.07 billion, (ii) we issue more than $1.0 billion of non-convertible debt in the previous three-year period or (iii) we become a “large accelerated filer” (as defined in Rule 12b-2 under the Securities Exchange Act of 1934, as amended, or the Exchange Act), we will cease to be an emerging growth company prior to the end of such five-year period. We will be deemed to be a “large accelerated filer” at such time that we (a) have an aggregate worldwide market value of common equity securities held by non-affiliates of $700.0 million or more as of the last business day of our most recently completed second fiscal quarter, (b) have been required to file annual and quarterly reports under the Exchange Act, for a period of at least 12 months and (c) have filed at least one annual report pursuant to the Exchange Act.
We have elected to take advantage of certain of the reduced disclosure obligations in the registration statement of which this prospectus is a part and may elect to take advantage of other reduced reporting requirements in future filings. As a result, the information that we provide to our stockholders may be different than you might receive from other public reporting companies in which you hold equity interests.
In addition, the JOBS Act provides that an emerging growth company can take advantage of an extended transition period for complying with new or revised accounting standards. We have elected not to “opt out” of the exemption for the delayed adoption of certain accounting standards, and, therefore, we will adopt new or revised accounting standards at the time private companies adopt the new or revised accounting standard and will do so until such time that we either (i) irrevocably elect to “opt out” of such extended transition period or (ii) no longer qualify as an emerging growth company. We may choose to early adopt any new or revised accounting standards whenever such early adoption is permitted for private companies.
We are also a “smaller reporting company” as defined under the Securities Act and Exchange Act. We may continue to be a smaller reporting company so long as either (i) the market value of shares of our common stock held by non-affiliates is less than $250 million or (ii) our annual revenue was less than $100 million during the most recently completed fiscal year and the market value of shares of our common stock held by non-affiliates is less than $700 million. If we are a smaller reporting company at the time we cease to be an emerging growth
10
Table of Contents
company, we may continue to rely on exemptions from certain disclosure requirements that are available to smaller reporting companies. Specifically, as a smaller reporting company, we may choose to present only the two most recent fiscal years of audited financial statements in our Annual Report on Form 10-K and have reduced disclosure obligations regarding executive compensation, and, similar to emerging growth companies, if we are a smaller reporting company under the requirements of (ii) above, we would not be required to obtain an attestation report on internal control over financial reporting issued by our independent registered public accounting firm.
Corporate Information
We were incorporated under the laws of the state of Delaware in February 2010 under the name Sight Sciences, Inc. Our principal executive offices are located at 4040 Campbell Ave, Suite 100, Menlo Park, CA 94025 and our telephone number is (877) 266-1144. Our website address is www.sightsciences.com. The information contained in, or accessible through, our website is not incorporated by reference into this prospectus, and you should not consider information on our website to be part of this prospectus. We have included our website address in this prospectus solely as an inactive textual reference.
11
Table of Contents
The Offering
Common stock offered by us | shares. |
Underwriters’ option to purchase additional shares | We have granted the underwriters a 30-day option to purchase up to additional shares of our common stock at the public offering price, less estimated underwriting discounts and commissions. |
Common stock to be outstanding after this offering | shares (or shares if the underwriters exercise their option to purchase additional shares in full). |
Use of proceeds | We estimate that the net proceeds from this offering will be approximately $ million (or approximately $ million if the underwriters exercise in full their option to purchase additional shares of common stock), at an assumed public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and the estimated offering expenses payable by us. We anticipate that we will use the net proceeds of this offering to fund ongoing and future clinical trials for OMNI and TearCare, to support the marketing and sales efforts for our products, for research and development and for working capital and general corporate purposes. See “Use of Proceeds” beginning on page 86 for additional information. |
Reserved Share Program | At our request, the underwriters have reserved for sale, at the initial public offering price, up to 5% of the shares offered by this prospectus for sale to certain individuals associated with us through a reserved share program. If these persons purchase reserved shares, this will reduce the number of shares available for sale to the general public. Any reserved shares that are not so purchased will be offered by the underwriters to the general public on the same terms as the other shares offered by this prospectus. See “Underwriters—Reserved Share Program.” |
Risk factors | You should carefully read the “Risk Factors” beginning on page 15 and the other information included in this prospectus for a discussion of factors you should consider carefully before deciding to invest in our common stock. |
Proposed Nasdaq Global Market symbol | “SGHT” |
The number of shares of our common stock to be outstanding after this offering is based on shares of our common stock outstanding as of , 2021 and excludes:
| • | shares of our common stock issuable upon the exercise of stock options outstanding under our 2011 Stock Incentive Plan, or our Existing Plan, as of , 2021, at a weighted-average exercise price of $ per share; |
12
Table of Contents
| • | additional shares of our common stock reserved for future issuance under our 2021 Incentive Award Plan, referred to as our 2021 Plan, which will become effective in connection with this offering, as well as any automatic increases in the number of shares of our common stock reserved for future issuance under our 2021 Plan; |
| • | shares of our common stock that will become available for future issuance under our 2021 Employee Stock Purchase Plan, or the 2021 ESPP, which will become effective in connection with this offering, as well as any automatic increases in the number of shares of our common stock reserved for future issuance under our 2021 ESPP; and |
| • | shares of common stock issuable upon the exercise of warrants outstanding as of , 2021, at a weighted average exercise price of $ per share, which warrants shall not expire upon the closing of this offering if not exercised. |
Unless otherwise indicated, this prospectus reflects and assumes the following:
| • | A -for- stock split of our common stock, which will become effective prior to the effectiveness of the registration statement of which this prospectus forms a part; |
| • | The automatic conversion of all outstanding shares of our Series A, Series B, Series C, Series D, Series E and Series F redeemable convertible preferred stock into an aggregate of shares of our common stock upon the closing of this offering; |
| • | The automatic conversion of outstanding warrants to purchase shares of our redeemable convertible preferred stock into warrants to purchase shares of our common stock; |
| • | No exercise of outstanding options or warrants after , 2021; |
| • | No exercise by the underwriters of their option to purchase additional shares of our common stock; and |
| • | The filing and effectiveness of our restated certificate of incorporation and the adoption of our amended and restated bylaws, each of which will occur upon the closing of this offering. |
13
Table of Contents
Summary Financial and Other Data
The following tables set forth our summary consolidated financial data as of, and for the periods ended on, the dates indicated. We have derived the consolidated statements of operations and comprehensive loss data for the years ended December 31, 2018, 2019 and 2020 from our audited consolidated financial statements included elsewhere in this prospectus. We have derived the consolidated statements of operations and comprehensive loss data for the three months ended March 31, 2020 and 2021 and the consolidated balance sheet data as of March 31, 2021 from our unaudited condensed consolidated financial statements included elsewhere in this prospectus. We have prepared the unaudited condensed consolidated financial information set forth below on the same basis as our audited consolidated financial statements and have included all adjustments, consisting only of normal recurring adjustments, that we consider necessary for a fair presentation of our financial position and results of operations as of the applicable dates and for the applicable periods. Our historical results are not necessarily indicative of the results that should be expected for any future period. You should read the following summary financial and other data set forth below together with the more detailed information contained in “Selected Financial Data,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our financial statements and the related notes included elsewhere in this prospectus.
| Year Ended December 31, | Three Months Ended March 31, | |||||||||||||||||||
| 2018 | 2019 | 2020 | 2020 | 2021 | ||||||||||||||||
| (in thousands, except share data) | ||||||||||||||||||||
Consolidated Statement of Operations and Comprehensive Loss Data | ||||||||||||||||||||
Revenue | $ | 7,530 | $ | 23,348 | $ | 27,640 | $ | 6,496 | $ | 8,635 | ||||||||||
Cost of goods sold(1) | 2,338 | 6,544 | 9,209 | 2,128 | 2,301 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Gross profit | 5,192 | 16,804 | 18,431 | 4,368 | 6,334 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Operating expenses: | ||||||||||||||||||||
Research and development(1) | 5,426 | 8,124 | 8,874 | 2,400 | 3,440 | |||||||||||||||
Selling, general and administrative(1) | 14,063 | 32,719 | 41,745 | 10,678 | 14,550 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Total operating expenses | 19,489 | 40,843 | 50,619 | 13,078 | 17,990 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Loss from operations | (14,297 | ) | (24,039 | ) | (32,188 | ) | (8,710 | ) | (11,656 | ) | ||||||||||
Interest income | 1 | 174 | 30 | 27 | — | |||||||||||||||
Interest expense | — | (1,961 | ) | (2,403 | ) | (552 | ) | (1,084 | ) | |||||||||||
Other income (expense), net | — | (35 | ) | (71 | ) | 91 | 552 | |||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Loss before income tax | (14,296 | ) | (25,861 | ) | (34,632 | ) | (9,144 | ) | (12,188 | ) | ||||||||||
Provision (benefit) for income tax | (6 | ) | 8 | 61 | 31 | 52 | ||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Net loss and comprehensive loss | $ | (14,290 | ) | $ | (25,869 | ) | $ | (34,693 | ) | $ | (9,175 | ) | $ | (12,240 | ) | |||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Net loss per share outstanding attributable to common stockholders, basic and diluted(2) | $ | (3.10 | ) | $ | (5.51 | ) | $ | (7.41 | ) | $ | (1.94 | ) | $ | (2.57 | ) | |||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Weighted-average common shares outstanding used in computing net loss per share attributable to common stockholders, basic and diluted(2) | 4,611,325 | 4,693,534 | 4,678,109 | 4,724,693 | 4,758,635 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Pro forma net loss per share outstanding, basic and diluted (unaudited) (2) | ||||||||||||||||||||
|
|
|
| |||||||||||||||||
Pro forma weighted-average common shares outstanding used in computing net loss per share attributable to common stockholders, basic and diluted (unaudited) (2) | ||||||||||||||||||||
|
|
|
| |||||||||||||||||
14
Table of Contents
| (1) | Includes stock-based compensation as follows: |
| Year Ended December 31, | Three Months Ended March 31, | |||||||||||||||||||
| 2018 | 2019 | 2020 | 2020 | 2021 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
Cost of goods sold | $ | 2 | $ | 3 | $ | 20 | $ | 1 | $ | 7 | ||||||||||
Research and development | 22 | 42 | 84 | 9 | 37 | |||||||||||||||
Selling, general and administrative | 28 | 73 | 393 | 51 | 233 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Total stock-based compensation expense | $ | 52 | $ | 118 | $ | 497 | $ | 61 | 277 | |||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
| (2) | See the statements of operations and Note 13 to our consolidated financial statements and Note 12 to our unaudited condensed consolidated financial statements included elsewhere in this prospectus for an explanation of the method used to compute the historical net loss per share and pro forma net loss per share and the number of shares used in the computation of the per share amounts for the years ended December 31, 2018, 2019 and 2020 and three months ended March 31, 2021. |
| As of March 31, 2021 | ||||||||||||
| Consolidated Balance Sheet Data | Actual | Pro Forma(2) | Pro Forma As Adjusted(3) | |||||||||
| (in thousands) | ||||||||||||
Cash and cash equivalents | $ | 48,327 | $ | $ | ||||||||
Working capital(1) | 48,239 | |||||||||||
Total assets | 60,533 | |||||||||||
Long-term debt | 32,124 | |||||||||||
Redeemable convertible preferred stock | 117,331 | |||||||||||
Additional paid-in capital | 1,475 | |||||||||||
Accumulated deficit | (102,281 | ) | ||||||||||
Total stockholders’ deficit | (100,801 | ) | ||||||||||
| (1) | Working capital is defined as total current assets less total current liabilities. |
| (2) | The pro forma consolidated balance sheet data gives effect to (i) the automatic conversion of all of our outstanding shares of redeemable convertible preferred stock into shares of our common stock, which will occur upon the closing of this offering, (ii) the automatic conversion of outstanding warrants to purchase shares of our redeemable convertible preferred stock into warrants to purchase shares of our common stock, and the related reclassification of redeemable convertible preferred stock warrant liability to additional paid in capital and (iii) the filing and effectiveness of our amended and restated certificate of incorporation upon the closing of this offering. |
| (3) | The pro forma as consolidated adjusted balance sheet data gives further effect to the issuance and sale by us of shares of our common stock in this offering at the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, after deducting the estimated underwriting discounts and commissions and estimated offering expenses payable by us. |
The pro forma as adjusted consolidated balance sheet data is illustrative only and will change based on the actual initial public offering price and other terms of this offering determined at pricing. Each $1.00 increase (decrease) in the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) each of our pro forma as adjusted cash and cash equivalents, working capital, total assets, additional paid-in capital and total stockholders’ (deficit) equity by $ million, assuming the number of shares of common stock offered by us, as set forth on the cover page of this prospectus, remains the same, and after deducting the estimated underwriting discounts and commissions and estimated offering expenses payable by us. Similarly, each increase (decrease) of 1.0 million shares in the number of shares of common stock offered
15
Table of Contents
by us would increase (decrease) each of our pro forma as adjusted cash and cash equivalents, working capital, total assets, additional paid-in capital, and total stockholders’ (deficit) equity by approximately $ million, assuming the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, remains the same, and after deducting the estimated underwriting discounts and commissions and estimated offering expenses payable by us.
16
Table of Contents
Investing in our common stock involves a high degree of risk. You should carefully consider the risks and uncertainties described below, together with all of the other information in this prospectus, including the section titled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our financial statements and the accompanying notes thereto included elsewhere in this prospectus, before investing in our common stock. Many of the risks and uncertainties are, and will be, exacerbated by the COVID-19 pandemic and any worsening of the global business and economic environment as a result. The risks and uncertainties described below are not the only ones we face. Additional risk and uncertainties that we are unaware of or that we deem immaterial may also become important factors that adversely affect our business. The realization of any of these risks and uncertainties could have a material adverse effect on our reputation, business, financial condition, results of operations, growth and future prospects, as well as our ability to accomplish our strategic objectives. In that event, the market price of our common stock could decline and you could lose part or all of your investment.
Risks Related to Our Business
We are an early-stage company with a history of significant losses, we expect to incur losses in the future and we may not be able to achieve or sustain profitability.
We have incurred annual net losses since our formation in 2010. For the years ended December 31, 2018, 2019 and 2020, we had net losses of $14.3 million, $25.9 million and $34.7 million, respectively, and for the three months ended March 31, 2020 and 2021 we had net losses of $9.2 million and $12.2 million, respectively. As of March 31, 2021, we had an accumulated deficit of $102.3 million. To date, we have financed our operations primarily through equity and debt financings and from sales of our products, the OMNI Surgical System, or OMNI, a device that enables canaloplasty followed by trabeculotomy for the reduction of intraocular pressure in adult patients with primary open-angle glaucoma, or POAG, and our TearCare System, or TearCare, to apply localized heat where the medical community recommends the application of warm compress to the eyelids, as well as predicates to OMNI. The losses and accumulated deficit have primarily been due to the substantial investments we have made to develop our products, costs related to our sales and marketing efforts, general research and development expenses, including costs related to clinical trials and regulatory initiatives to obtain marketing clearance, and infrastructure improvements.
In addition, as a public company, we will incur significant legal, accounting and other expenses that we did not incur as a private company. Accordingly, we expect to continue to incur losses for the foreseeable future and we cannot assure you that we will ever achieve profitability or that, if we do become profitable, we will sustain profitability. Our failure to achieve and sustain profitability in the future would make it more difficult to finance our business and accomplish our strategic objectives, which would have a material adverse effect on our business, financial condition and results of operations. In addition, failure of our products to significantly penetrate our target markets would negatively affect our business, financial condition and results of operations.
Our revenue has been primarily generated from the sales of our products and is expected to continue to be so generated for the near future, and we are therefore highly dependent on the success of those products, and particularly on OMNI. We have limited commercial sales experience regarding our products, which makes it difficult to evaluate our current business, predict our future prospects and forecast our financial performance and growth.
We began selling VISCO360 and TRAB360, commercial predicate devices to OMNI, in 2015 and TearCare in 2019 and therefore do not have a long history operating as a commercial company. Currently, we are highly dependent on the success of OMNI and TearCare. To date, our revenue has primarily been derived, and we expect it to continue to be substantially derived in the near future, from sales of our Surgical Glaucoma and Dry Eye products. We are particularly dependent on the success of OMNI, which accounted for 94% of our total
17
Table of Contents
revenues for the year ended December 31, 2020. Because we devote substantially all of our resources to these products and rely on them as our sole source of revenue, any factors that negatively impact our products, and particularly OMNI, or result in a decrease in sales, could have a material adverse effect on our business, financial condition and results of operations.
Over the next several years, we expect to continue to devote a substantial amount of resources to expand our commercialization efforts, drive increased adoption of our products and continue to develop new and improved products. Our limited commercialization experience and limited number of FDA-cleared products make it difficult to evaluate our current business and predict our future prospects. These factors also make it difficult for us to forecast our future financial performance and growth, and such forecasts are subject to a number of uncertainties, including our ability to successfully complete preclinical studies and clinical trials and obtain FDA pre-market clearance for our current products and for future planned products or changes to existing products.
Ophthalmologist and optometrist (together, eyecare professionals or ECPs) awareness of, and experience with, our products is currently limited. As a result, our products have limited product and brand recognition within the ophthalmic industry. The novelty of our products, together with our limited commercialization experience, makes it difficult to evaluate our current business and predict our future prospects. A number of factors, including some outside of our control, may contribute to fluctuations in our financial results, including:
| • | ECP and patient demand for our products; |
| • | Our ability to obtain and maintain reimbursement coverage for procedures in which our products are used; |
| • | Changes in reimbursement rates by government or commercial payors; |
| • | The results of our clinical trials or investigations; |
| • | Positive or negative media coverage, or public, patient and/or physician perception, of our products or competing products and treatments; |
| • | Any safety or effectiveness concerns that arise regarding our products for either their currently authorized uses or the uses for which we are developing our products; |
| • | The effectiveness of our marketing and sales efforts, including our ability to have a sufficient number of qualified sales representatives to sell our products; |
| • | Unanticipated delays in product development or product launches; |
| • | Our ability to raise additional capital on acceptable terms, or at all, if needed to support the commercialization of our products; |
| • | Our ability to achieve and maintain compliance with all regulatory requirements applicable to our products; |
| • | Our ability to obtain, maintain, protect and enforce our intellectual property rights; |
| • | The ability of patients to access elective procedures at facilities that utilize our products because of the novel strain of coronavirus disease, COVID-19, and related government restrictions; |
| • | Our third-party manufacturers’ ability to supply our products in a timely manner, in accordance with our specifications, and in compliance with applicable regulatory requirements; and |
| • | Introduction of new products or alternative treatments that compete with our products. |
It is therefore difficult to predict our future financial performance and growth, and such forecasts are inherently limited and subject to a number of uncertainties. If our assumptions regarding the risks and uncertainties we face, which we use to plan our business, are incorrect or change due to circumstances in our business or our markets, or if we do not address these risks successfully, our operating and financial results could differ materially from our expectations and our business could suffer.
18
Table of Contents
Our business is dependent upon the broad adoption of our products by ECPs and patients.
Our future growth and profitability largely depend on our ability to increase ECP and patient awareness of our products and on the willingness of ECPs and patients to adopt our products. ECPs may not adopt our products unless they are able to determine, based on experience, clinical data, medical society recommendations and other analyses, that our products are clinically differentiated from, or otherwise preferable to, available alternatives. Even if we are able to raise awareness among ECPs, they may be slow to change their medical treatment practices and may be hesitant to select our products for a variety of reasons, including:
| • | Lack of experience with our products and concerns that we are relatively new to market; |
| • | Perceived liability risk generally associated with the use of new products and treatment options; |
| • | Lack, or perceived lack, of sufficient clinical evidence, including long-term data, supporting clinical benefits or the cost-effectiveness of our products over existing treatments; |
| • | The failure of key opinion leaders to provide recommendations regarding our products, or to assure physicians, patients and healthcare payors of the benefits of our products as an attractive alternative to other treatment options; |
| • | Perceptions that our products are unproven; |
| • | Long-standing relationships with companies, distributors and salespeople that sell competing products; |
| • | Our inability to strengthen and maintain relationships with ECPs and other industry professionals and organizations; |
| • | Lack of availability of adequate third-party payor coverage or reimbursement; |
| • | Competitive response and negative selling efforts from providers of alternative treatments; |
| • | Challenges of integrating TearCare into established ophthalmologic and optometric practices; and |
| • | Perceptions regarding the time commitment and skill development that may be required to gain familiarity and proficiency with our products. |
To effectively market and sell our products, we will need to continue to educate the medical community about the safety, efficacy, necessity and efficiency of our products and about the patient populations that would potentially benefit from the use of our products. We focus our sales, marketing and education efforts primarily on our target ECP providers, ambulatory surgery centers, hospital outpatient departments and potential patient populations. However, we cannot assure you that we will achieve broad education or market acceptance. For example, if first-line ECPs or primary care physicians that serve as the early point of contact for patients are not made aware of our OMNI products, they may not refer patients to ECPs who utilize our products, and those patients may be treated with alternative procedures or treatments. In addition, some physicians may choose to utilize our products on only a subset of their total patient population or may not adopt our products at all. If we are not able to effectively demonstrate that our products are beneficial for a broad range of patients, adoption of our products will be limited and may not occur as rapidly as we anticipate or at all, which would have a material adverse effect on our business, financial condition and results of operations. Further, if we are unable to obtain or maintain favorable third-party reimbursement coverage of procedures in which our OMNI product is used, or if we are unable to obtain favorable reimbursement for procedures in which TearCare is used, adoption of our products by ECPs and patients will suffer. We cannot assure you that our products will achieve broad market acceptance among payors, physicians and patients. Any failure of our products to satisfy demand or to achieve meaningful market acceptance and penetration will harm our future prospects and have a material adverse effect on our business, financial condition and results of operations.
Adoption of OMNI and TearCare depends upon appropriate physician training, practice and patient selection.
The success of our products depends in part on the skill of the ECPs utilizing and administering products to treat patients and on their adherence to our stated patient selection criteria and the proper techniques that we
19
Table of Contents
provide in training sessions. We train ECPs on the correct use of OMNI. However, ECPs rely on their previous medical training and experience when performing ophthalmic surgical procedures and may deviate from the techniques we provide in training sessions. Furthermore, we cannot guarantee that all such ECPs who use OMNI will have the necessary skills or experience to safely and effectively perform these procedures. Similarly, though we train ECPs to ensure correct use of TearCare, including placement of TearCare SmartLids on patients’ eyelids, we cannot guarantee that all such ECPs will have the necessary skills or experience to safely and effectively use these devices.
We do not control which physicians utilize these medical devices in their treatments or how much training they receive, and physicians who have not completed our training sessions may nonetheless attempt to use OMNI as part of an ophthalmic surgical procedure or use TearCare to apply localized heat. In addition, a perception by physicians that OMNI or TearCare are difficult to use may negatively impact adoption by ECPs. If ECPs utilize these devices in a manner that is inconsistent with our labeled indications or with components that are not part of our products, such as viscoelastic fluid that is incompatible with OMNI or without adhering to or completing our training sessions, the patient outcomes may be negative. This could negatively impact the perception of patient benefits and safety associated with OMNI and TearCare and limit adoption of our devices, which would have a material adverse effect on our business, financial condition and results of operations.
Development of TearCare for expanded indications depends upon positive clinical data, and the safety and efficacy of our products for the intended uses for which we intend to seek clearance, certification or approval are not yet supported by long-term clinical data, which could delay or prevent clearance by the FDA (or other foreign authorities) or limit sales if cleared, certified or approved and our products might therefore prove to be less safe or effective than initially thought.
We are developing TearCare for expanded indications for which we intend to seek clearance by the FDA in the future.
We are conducting and intend to continue conducting additional clinical trials or investigations to develop our devices for expanded indications. Historical clinical results, including interim results, are not necessarily predictive of future clinical results, and we cannot assure you that the results reported in these studies will be consistent with, or better than, currently available clinical data. Moreover, the outcomes and updates resulting from these studies, including interim results, may be compared to the results of other products and treatments for POAG or MGD, and if the comparisons are not favorable, it may limit the ability to obtain clearance, certification or approval of the devices for the expanded indications for which we intend to seek clearance, certification or approval, as well as adoption of our products for their current authorized uses. In addition, our competitors and other third parties may also conduct clinical trials or investigations of our products without our participation. Unfavorable or inconsistent clinical data from existing or future clinical trials or investigations conducted by us, our competitors or other third parties, the interpretation of our clinical data or findings of new or more frequent adverse events, could subject us to mandatory or voluntary product recalls, suspension or withdrawal of FDA or other clearance, certification or approval, significant legal liability or harm to our business reputation and could have a material adverse effect on our business, financial condition and results of operations.
Our products will be adopted and compete, in part, based on long-term data regarding patient outcomes and the risk of our products relative to other treatment options. The long-term clinical outcomes of the use of OMNI for its cleared uses are not known and, due to the novelty of our products, there is no long-term data regarding patient outcomes beyond our clinical trials or investigations. The results of short-term clinical experience of our products do not necessarily predict long-term clinical outcomes. We believe that ECPs will compare the rates of long-term clinical outcomes for procedures using our products for their authorized uses against alternative procedures and treatment options. If the long-term data does not meet ECPs’ expectations, or if the long-term data indicates that our products are not as safe or effective as other treatment options or as current short-term data would suggest, physicians may recommend alternative treatments for their patients and our products may not become widely adopted, which will negatively affect our business, financial condition and results of operations.
20
Table of Contents
The safety and efficacy of some of our products is not yet supported by long-term clinical data, which could limit sales, and our products might therefore prove to be less safe or effective than initially thought.
The products that we market in the United States are regulated as medical devices by the FDA. OMNI has received premarket clearance under Section 510(k) of the Federal Food, Drug, and Cosmetic Act, or the FDCA. In the 510(k) clearance process, before a device may be marketed the FDA must determine that a proposed device is “substantially equivalent” to a legally-marketed “predicate” device, which includes a device that has been previously cleared through the 510(k) process, a device that was legally marketed prior to May 28, 1976 (preamendments device), a device that was originally on the U.S. market pursuant to an approved PMA application and later down-classified, or a 510(k)-exempt device. This process is typically shorter and generally requires the submission of less supporting documentation than the FDA’s PMA process and does not always require long-term clinical studies. TearCare is currently marketed as a 510(k)-exempt device, and did not undergo premarket clearance prior to marketing. In November 2020, we submitted a 510(k) premarket notification seeking an expanded indication for use for TearCare. The FDA requested several safety tests and modifications which we believe would have required additional time to complete beyond the designated review process. We voluntarily withdrew this submission in May 2021 to allow us to comply with the FDA requests in a comprehensive manner. We intend to resubmit the application for an expanded indication for use in the second half of 2021.
In the European Economic Area, or EEA, manufacturers of medical devices are required by the Medical Devices Directive to collect post-marketing clinical data in relation to their CE marked medical devices. Post-market surveillance includes the conduct of post-market clinical follow-up studies permitting manufacturers to gather information concerning quality, safety or performance of medical devices after they have been placed on the market in the EU. All information collected as part of the post-market surveillance process must be reviewed, investigated and analyzed on a regular basis in order to determine whether trending conclusions can be made concerning the safety or performance of the medical device and decisions must be taken in relation to the continued marketing of medical devices currently on the market. We expect to incur ongoing costs to comply with these post-market clinical obligations in EEA markets for so long as we continue to market and sell products in those markets.
We are conducting and intend to continue conducting additional clinical trials, including clinical trials to develop TearCare for an expanded indication. In addition, our competitors and other third parties may also conduct clinical trials of our products without our participation. If future patient studies or clinical testing do not support our belief that our products are advantageous for their intended uses, market acceptance of our products could fail to increase or could decrease and our business could be harmed. Moreover, if future results and experience by us, our competitors or other third parties, indicate that our products cause unexpected or serious complications or other unforeseen negative effects, we could be subject to mandatory or voluntary product recalls, suspension or withdrawal of FDA or other governmental clearance or approval or CE Certificates of Conformity, significant legal liability or harm to our business reputation, which could have a material adverse effect on our business, financial condition and results of operations.
We believe that ECPs will compare the rates of long-term clinical outcomes for procedures using our products for their authorized uses against alternative procedures and treatment options. If we choose to, or are required to, conduct additional studies, such studies or experience could reduce the rate of coverage and reimbursement by both public and private third-party payors for procedures that are performed with our products, slow market adoption of our products by ECPs, significantly reduce our ability to achieve expected revenues and prevent us from being profitable.
We have limited experience in training on, and marketing and selling, our products and we may provide inadequate training, fail to increase our sales and marketing capabilities or fail to develop broad brand awareness in a cost-effective manner.
We have limited experience marketing and selling our products. In the United States, we currently rely on our direct sales force and, in certain targeted geographic regions or customer verticals, independent sales
21
Table of Contents
representatives and distributors, and any failure to maintain and grow our sales force could harm our business. In Europe, we currently rely on a combination of direct sales personnel and independent distributors to sell our products, and we intend to grow our international sales through a combination of direct and distributor sales. If we are unable to identify and retain productive direct sales representatives and distributors in the international territories and jurisdictions that we have targeted for commercial expansion, we may not be able to achieve projected revenue goals and our business could suffer. Our sales representatives are trained and possess product specific sales expertise, which we believe is critical in driving the awareness and adoption of our products. The members of our U.S. sales force are at-will employees. The loss of these personnel to competitors, or otherwise, could materially harm our business. If we are unable to retain our direct sales force personnel or replace them with individuals of equivalent expertise and qualifications, or if we are unable to successfully instill such expertise in replacement personnel, our business, financial condition and results of operations could be materially harmed.
In order to generate future growth, we plan to continue to significantly expand and leverage our commercial infrastructure to increase our customer base and increase adoption by existing customers to drive our growth. Identifying and recruiting qualified sales and marketing professionals and training them on our products, on applicable federal and state laws and regulations and on our internal policies and procedures requires significant time, expense and attention. It can take several months or more before a sales representative or distributor representative is fully trained and productive. Our direct sales force may subject us to higher fixed costs than those of companies with competing products or treatments that rely more heavily on independent third parties, placing us at a competitive disadvantage. Our business may be harmed if our efforts to expand and train our sales force and distribution chain do not generate a corresponding increase in product sales and revenue, and our higher fixed costs may slow our ability to reduce costs in the face of a sudden decline in demand for our products. Any failure to hire, develop and retain effective sales personnel, to identify and train distributors and independent sales representatives in targeted international territories, to achieve desired productivity levels in a reasonable period of time or timely reduce fixed costs, could have a material adverse effect on our business, financial condition and results of operations.
Our ability to increase our customer base and achieve broader market acceptance of our products will depend, to a significant extent, on our ability to expand our sales and marketing and educational efforts. We plan to dedicate significant resources to our sales and marketing initiatives, and educational programs through leading medical publications and at large industry and scientific meetings, both directly and through key opinion leaders. Our business may be harmed if these efforts and expenditures do not generate a corresponding increase in revenue. In addition, we believe that developing and maintaining broad awareness of our brand in a cost-effective manner is critical to achieving broad acceptance of our products and reaching new ECPs and patients. Brand promotion activities may not impact ECP or patient awareness or increase revenue, and even if they do, any increase in revenue may not offset the costs and expenses we incur in building our brand. If we fail to successfully promote, maintain and protect our brand, we may fail to attract or retain the market acceptance necessary to realize a sufficient return on our brand building efforts, or to achieve the level of brand awareness that is an important factor for the broad adoption of our products.
Our products are designed to be used in a limited number of procedures, and there is a limited total addressable market for our products. The sizes of the potential and actual markets for our current products have not been established with precision and may be smaller than we estimate.
We currently market our OMNI device for use in the U.S. and select European geographies for canaloplasty followed by trabeculotomy to reduce intraocular pressure in adult patients with POAG. POAG is the most prevalent form of glaucoma and affects 4.1 million people in the United States and over 60 million people worldwide. We currently market TearCare as a Class II, 510(k)-exempt powered heating pad for the delivery of localized heat where the current medical community recommends application of a warm compress. We intend to seek FDA clearance of TearCare for an expanded indication for use in the second half of 2021. There are an estimated 739 million people globally and 38 million people in the U.S. who suffer from DED. DED is the most
22
Table of Contents
common reason for a patient visit to an eye doctor, yet of the 38 million people with DED in the U.S., only 17 million have been diagnosed with DED. Studies have shown that evaporative DED resulting from MGD is associated with approximately 86% of all DED cases.
The total addressable markets for our products are subject to change and, even assuming TearCare is cleared for an expanded indication, its use may be further limited by FDA restrictions or more narrowly defined indications, any of which could have a material adverse effect on our business, financial condition and results of operations.
Further, our estimates of the total addressable markets for our products are based on a number of internal and third-party estimates, including, without limitation, the number of patients with POAG and, if TearCare is cleared for such use, MGD, and the assumed prices at which we can sell our products in markets that have not yet been fully established. While we believe our assumptions and the data underlying our estimates are reasonable, these assumptions and estimates may not be correct and the conditions supporting our assumptions or estimates may change at any time, thereby reducing the predictive accuracy of these underlying factors. As a result, our estimates of the annual total addressable market for our current products may prove to be incorrect. If the actual number of patients who would benefit from our products or the price at which we can sell our products is smaller than we have estimated, it may impair our sales growth and negatively affect our business, financial condition and results of operations.
Our operations and financial results have been, and will continue to be, adversely impacted by the COVID-19 pandemic in the United States and the rest of the world.
In December 2019, a novel strain of coronavirus, SARS-CoV-2, was identified in Wuhan, China. Since then, SARS-CoV-2, and the resulting disease, COVID-19, has spread worldwide. In response to the COVID-19 pandemic, numerous state and local jurisdictions have imposed, and others in the future may impose, “shelter-in-place” orders, quarantines, executive orders and similar government orders and restrictions for their residents. Such orders or restrictions have resulted in work stoppages, slowdowns and delays, travel restrictions and cancellation of events. Disruptions or potential disruptions to our business from COVID-19 or a future pandemic could include the inability of our component suppliers and manufacturers to produce our products, components, or accessories on a timely basis, or at all; disruptions in our logistics and distribution providers to deliver our products to customers on a timely basis, or at all; inventory shortages or obsolescence; diversion of or limitations on employee resources that would otherwise be focused on the operations of our business; delays in growing or reductions in our sales organization, including through delays in hiring, lay-offs, furloughs or other losses of sales representatives; limitations on the ability of our sales representatives and distributors to reach potential customers and reduced opportunities for market education; business adjustments or disruptions of certain third parties, including suppliers and customers; and additional government requirements or other incremental mitigation efforts that may further impact our or our suppliers’ capacity to manufacture our products. For example, as a result of restrictions related to the COVID-19 pandemic our sales representatives have been curtailed in their ability to conduct in-person meetings and demonstrations, and our market education and training efforts have been limited. We may also experience delays in initiating or completing any clinical trials or investigations that we intend to conduct or are conducting, and we do not know whether our clinical trials or investigations will begin on time, need to be redesigned, enroll patients on time, or be completed on schedule, or at all.
We experienced a significant decrease in our revenues for both of our products in the second quarter of 2020 as compared to the first quarter of 2020. As elective eye care procedures in many facilities that utilize OMNI and TearCare were temporarily suspended by governmental authorities, many patients avoided visiting ECPs, and, even in areas that allowed elective procedures, ECPs and healthcare facilities in general severely cut back on the scheduling and performance of such procedures. We felt the decrease in demand due to COVID-19 most significantly in the latter part of the quarter ended March 31, 2020 and the first half of the quarter ended June 30, 2020. Beginning in June 2020, we began to see an increase in the number of procedures using our products. In
23
Table of Contents
the first quarter of 2021, our customers experienced a significant number of procedure cancellations which we believe was largely driven by patients postponing procedures until their COVID-19 vaccinations were completed as opposed to any restrictions imposed on elective procedures.
The extent to which the COVID-19 pandemic impacts our business will depend on future developments, which are highly uncertain and cannot be predicted, including new information which may emerge concerning the severity and spread of COVID-19, any new variants of the virus, the nature, extent and effectiveness of containment and treatment measures, the extent and duration of the effect on the economy and how quickly and to what extent normal economic and operating conditions can resume.
While the potential economic impact brought by and the duration of any pandemic, epidemic or outbreak of an infectious disease, including COVID-19, may be difficult to assess or predict, the COVID-19 pandemic has resulted in, and may continue to result in, significant disruption of global financial markets, reducing our ability to access capital, which could in the future negatively affect our liquidity. In addition, a recession or market correction resulting from the spread of an infectious disease, including COVID-19, could materially affect our business. Such economic recession could have a material adverse effect on our long-term business as hospitals and surgical centers curtail and reduce capital and overall spending. In addition, the current economic downturn is resulting in significant job losses and reductions in disposable income and if patients are unable to obtain or maintain health insurance policies, this may significantly impact their ability to pay for the procedures utilizing our products, further negatively impacting our business, financial condition and results of operations. To the extent the COVID-19 pandemic adversely affects our business and financial results, it may also have the effect of heightening many of the other risks described in this “Risk Factors” section.
We may not be able to maintain adequate levels of third-party coverage and reimbursement for procedures in which OMNI is used, and third parties may rescind or modify their coverage or delay payments related to OMNI. We may not be able to secure any, or adequate levels of, third-party coverage and reimbursement for procedures in which TearCare is used, and even if third parties provide coverage they may rescind or modify their coverage or delay payments related to TearCare.
We derive revenue from sales of OMNI to physicians, ambulatory surgery centers and hospital outpatient departments, which typically bill all or a portion of the costs and fees associated with our products to various third-party payors, including Medicare, Medicaid, private commercial insurance companies, health maintenance organizations and other healthcare-related organizations, and then bill patients for any applicable deductibles or co-payments. As a result, access to adequate coverage and reimbursement for procedures in which OMNI is used by third-party payors is essential to its acceptance and adoption by patients and ECPs.
We also derive revenue from sales of TearCare to ECPs and eye care clinics, which also bill all or a portion of the costs and fees associated with treatments and products to patients or, on a limited basis, to third-party payors. We believe that access to adequate coverage and reimbursement for procedures in which TearCare is used by third-party payors is important to the broad acceptance and adoption of TearCare. Currently, however, no payors have formal policies establishing coverage for the procedures in which TearCare is used. We are pursuing a comprehensive long-term market development and patient access plan for TearCare and focusing our efforts on partnering with key strategic accounts to pursue prior authorization approvals and reimbursement claims for procedures in which TearCare is used, but there is no guarantee that we will be successful. If patients are not willing to pay for procedures in which TearCare is used, or if third-party payors continue to refuse to provide coverage and reimbursement or provide insufficient levels of coverage and reimbursement, it could have a negative impact on ECPs’ adoption of TearCare and sales of TearCare.
Coverage and reimbursement by governmental and third-party payors may depend upon a number of factors, including the determination that the product or service and its use or administration for a particular patient is:
| • | A covered benefit; |
24
Table of Contents
| • | Safe, effective and medically necessary; |
| • | Appropriate for the specific patient; |
| • | Supported by clinical data; |
| • | Supported by guidelines established by the relevant professional societies; |
| • | Cost-effective; and |
| • | Neither experimental nor investigational. |
Third-party payors, whether foreign or domestic, or governmental or commercial, are developing increasingly sophisticated methods of controlling healthcare costs. In addition, no uniform policy of coverage and reimbursement for procedures using our products exists among third-party payors. Therefore, coverage and reimbursement for procedures using our products can differ significantly from payor to payor. Obtaining and maintaining coverage and reimbursement can be a time-consuming process that could require us to provide supporting scientific, clinical and cost-effectiveness data for the use of our products. We may not be able to provide data sufficient to satisfy governmental and third-party payors that procedures using our products should be covered and reimbursed.
In the United States, the American Medical Association, or AMA, generally assigns specific billing codes for procedures under a coding system known as Current Procedure Terminology, or CPT, which surgeons use to bill third-party payors and receive reimbursement. Once a permanent (Category I) CPT code is established for a service, the Centers for Medicare & Medicaid Services, or CMS, establishes payment levels under Medicare, while other payors may establish rates and coverage rules independently. Canaloplasty followed by trabeculotomy procedures using OMNI are typically billed using the Category I CPT code 66174, which describes canaloplasty. Coding for ophthalmic surgical procedures is complex, and changes to the codes used to report services performed with our products may result in significant changes in reimbursement, which could negatively impact our revenue.
The AMA maintains a subset of temporary (Category III) CPT codes used for new and emerging technologies. For example, TearCare was assigned a Category III CPT code effective beginning January 1, 2020. Coverage for Category III CPT codes is often limited. Medicare does not generally establish national payment rates for Category III CPT codes on the Medicare Physician Fee Schedule, or MPFS. As a result, individual Medicare contractors and private payors may establish their own payment rates for services described by Category III CPT codes, which payment rates may be materially below the final reimbursement rates that we are currently targeting, or may determine not to reimburse services described by Category III CPT codes.
Payors also continually review new and existing technologies for possible coverage and can deny or reverse coverage for new or existing products and procedures. There can be no assurance that third-party payor policies provide coverage, or will continue to provide coverage, for procedures in which OMNI is used. If coverage policies change such that Medicare no longer covers procedures in which our products are used, there would be a material adverse effect on our business, financial condition and results of operations. For example, Medicare Administrative Contractors could issue local coverage determinations that could restrict the patients eligible for treatment with our products or that are otherwise unfavorable to our business. If we are not successful in reversing any proposed non-coverage policies, or if third-party payors that currently cover or reimburse procedures in which our products are used reverse or limit their coverage in the future, or if other third-party payors issue similar policies, this could have a material adverse effect on our business.
Further, we believe that future coverage and reimbursement may be subject to increased restrictions, such as additional prior authorization requirements, both in the United States and in international markets. Third-party coverage and reimbursement for procedures using our products or any of our products in development for which we may receive regulatory clearance, certification or approval may not be available or adequate in either the
25
Table of Contents
United States or international markets. Further, other devices or treatments that compete with our products may be more widely covered or subject to different co-pay policies and requirements, which could impact demand for our products. If hospital, surgical center, ECP and/or patient demand for our products is adversely affected by third-party reimbursement policies and decisions, it could have a material adverse effect on our business, financial condition and results of operations.
The market for our products is highly competitive. Our competitors may have longer operating histories, more established products and greater resources than we do, and may be able to develop or market treatments that are safer, more effective or gain greater acceptance in the marketplace than our products.
The medical device industry is highly competitive, subject to rapid change and significantly affected by the introduction of new products and technologies and the other activities of industry participants. We compete, or plan to compete, with medical device and pharmaceutical companies that develop and commercialize products for eye conditions, including Glaukos, Ivantis, AbbVie/Allergan, Novartis, Alcon, and Johnson & Johnson. These companies, or other entrants into the market, may have or develop competing technologies, other products that are in or that enter clinical trials, new devices or additional indications for existing devices that could demonstrate better safety, effectiveness, clinical results, lower costs or greater ECP and market acceptance than our products.
We compete, or may compete in the future, against other companies which have longer, more established operating histories and significantly greater financial, technical, marketing, sales, distribution and other resources, which may prevent us from achieving significant market penetration or improved operating results. These companies may enjoy several competitive advantages, including:
| • | Established treatment patterns pursuant to which prescription medications, traditional glaucoma surgery or more conventional MIGS devices are generally first-line therapies for the treatment of POAG and eye drops or warm-compresses are first-line therapies for the treatment of MGD; |
| • | Established relationships with ECPs who are familiar with their products and procedures for the treatment of POAG or MGD; |
| • | Established relationships with key stakeholders, including hospital outpatient departments, ambulatory surgery centers, optometrists and ophthalmologists, general practitioners and administrators; |
| • | Greater financial and human capital resources; |
| • | Significantly greater name recognition; |
| • | Additional lines of products, and the ability to offer rebates or bundle products to offer greater discounts or incentives to gain a competitive advantage; and |
| • | Established sales, marketing and worldwide distribution networks. |
One of the major hurdles to adoption of our products will be overcoming established treatment patterns, which will require educating ECPs and supportive clinical data. However, because of the size of the market opportunity for devices used in procedures to address POAG and MGD, we believe current and potential future competitors will dedicate significant resources to aggressively promote their products or develop new products or treatments, such as Glaukos’ iStent infinite. Further, new treatment options may be developed that could compete more effectively with our products due to the prevalence of POAG and MGD, and the research and technological progress that exist within the market.
We rely on third parties to manufacture and supply OMNI and TearCare, and we may encounter delays or incur additional costs when we add new manufacturers and suppliers for our products.
Our business strategy depends on our ability to manufacture our current and future products in sufficient quantities and on a timely basis to meet customer demand, while adhering to product quality standards,
26
Table of Contents
complying with regulatory quality system requirements and managing manufacturing costs. We do not have any internal manufacturing capabilities or infrastructure. OMNI is currently being produced and assembled by Second Source Medical LLC and Peter’s Technology (Suzhou) CO LTD., or Peter’s, a subsidiary of Peter’s Co., Ltd., a Taiwan-based manufacturer. We intend to fully transition OMNI production to Peter’s and an additional high-volume contract manufacturer with domestic U.S. production facilities by the end of the third quarter of 2021. The Peter’s Supply Agreement governs the assembly and supply of OMNI, pursuant to which Peter’s purchases components from our approved suppliers for assembly and we make purchases on a purchase order basis. We may encounter delays or incur additional costs in connection with the transition to a new contract manufacturer with domestic U.S. production facilities for OMNI production. For the production of TearCare, we currently have supply arrangements with separate U.S. medical device manufacturers for the production of each of TearCare’s SmartLids and TearCare’s SmartHubs. These companies manufacture, assemble, inspect, test, package and ship OMNI and TearCare and related accessories.
While our existing manufacturers have generally met our demand requirements on a timely basis in the past, their ability and willingness to continue to do so going forward may be limited for several reasons, including if any of our manufacturers’ facilities suffer damage or a force majeure event, our relative importance as a customer to each manufacturer or their inability to provide assembly services to manufacture our products, which may be affected by the COVID-19 pandemic. An interruption in our commercial operations could occur if we encounter delays or difficulties in securing these manufactured products if we cannot obtain an acceptable substitute.
The process of identifying alternative manufacturing facilities for any other reason could be time-consuming and expensive, may result in interruptions in our operations and product delivery, and could affect the performance specifications of our products. If we are required to change any of our contract manufacturers, we will be required to verify that the new manufacturer maintains facilities, procedures and operations that comply with our quality and applicable regulatory requirements, which could further impede our ability to manufacture our products in a timely manner. We cannot assure you that we will be able to identify and engage alternative contract manufacturers on similar terms or without delay. Furthermore, our contract manufacturers could require us to move to a different production facility. The occurrence of any of these events could harm our ability to meet the demand for our products in a timely and cost-effective manner, which could have a material adverse effect on our business, financial condition and results of operations.
We are also subject to numerous other risks relating to our reliance on third parties, including:
| • | Inability to renew or extend contracts and arrangements with such third parties or renew any such contracts or arrangements on terms that are favorable to us; |
| • | Interruption of supply resulting from modifications to, or discontinuation of, a third-party’s operations; |
| • | Delays in shipments resulting from uncorrected defects, reliability issues or a third-party’s failure to manufacture and supply components, accessories and materials that consistently meet our agreed specifications and quality requirements; |
| • | Inability to obtain adequate supply or services in a timely manner or on commercially reasonable terms; |
| • | Difficulty identifying and qualifying, and obtaining new regulatory approvals, for alternative suppliers for our products and product components in a timely manner; |
| • | Inability to design or modify production processes to enable us to produce future products efficiently or implement changes in current products in response to design or regulatory requirements; |
| • | Inability to comply with applicable provisions of the FDA’s Quality System Regulation, or QSR, or other applicable laws or regulations enforced by the FDA, state and foreign regulatory authorities; |
| • | Inability to ensure the quality of products and components manufactured by third parties; |
27
Table of Contents
| • | Failure to timely increase production capacity or volumes to meet demand; |
| • | Production delays related to the evaluation and testing of products and components from alternative third parties and corresponding regulatory qualifications; |
| • | An outbreak of disease or similar public health threat, such as the COVID-19 pandemic, particularly as it may impact our supply chain; |
| • | Long lead time for the production of certain components of our products; |
| • | Price fluctuations due to a lack of long-term supply arrangements with certain of our suppliers; |
| • | Risk of delays or interruption stemming from trade wars; and |
| • | General delays in delivery by our suppliers. |
These risks are likely to be exacerbated by our limited experience with our current products and manufacturing processes. As demand for our products increases, we will have to invest additional resources to manage the manufacturing process. If we fail to secure increased production capacity efficiently, we may not be able to fill customer orders on a timely basis, our sales may not increase in line with our expectations and our operating margins could fluctuate or decline. In addition, although some future products may share product features, components, sub-assemblies and materials with our existing products, the manufacture of these products may require modification of the current production processes or unique production processes, the identification of new suppliers for specific components, sub-assemblies and materials or the development of new manufacturing technologies. It may not be possible for our current third-party manufacturers to produce these products at a cost or in quantities sufficient to make these products commercially viable or to maintain current operating margins, all of which could have a material adverse effect on our business, financial condition and results of operations.
We depend on a limited number of single source suppliers.
We rely on a limited number of third-party manufacturers, many of which are single source suppliers, for a portion of the components, accessories and materials that we utilize in our products. These items are critical and, for certain items, there are relatively few or no readily available alternative sources of supply. These single source suppliers may be unwilling or unable to supply these items reliably and at the levels we anticipate or that are required by the market. Additionally, although we require our suppliers and providers to supply us with components and services that meet our specifications and other applicable legal and regulatory requirements in our agreements and contracts, and appropriate inspections, testing or other acceptance activities are performed to ensure the components meet our requirements, there is a risk that these third parties will not always act consistent with our best interests, and may not always supply components or provide services that meet our requirements or in a timely manner.
While our suppliers have generally met our demand requirements on a timely basis in the past, we cannot guarantee that suppliers will in the future be able to meet our demand, either because of acts of nature, global pandemics, such as the COVID-19 pandemic, the nature of our agreements with those suppliers or our relative importance to them as a customer, and our suppliers may decide in the future to discontinue or reduce the level of business they conduct with us. We may also fail to obtain additional suppliers for any of the components used in our products. If we are unable to meet our demand requirements on a timely basis, we may not have a sufficient number of our products available for delivery to support ECPs that utilize our products as part of their treatment. Any shortfall in the supply of products may result in lower adoption and usage rates of our products and have a material adverse effect on our business, financial condition and results of operations.
The failure of third parties to meet their contractual, regulatory, and other obligations could adversely affect our business.
We rely on suppliers, vendors, outsourcing partners, consultants, alliance partners and other third parties to help research, develop, manufacture, commercialize and distribute our products and manage certain parts of our
28
Table of Contents
business. Using these third parties poses a number of risks, such as: (i) they may not perform to our standards or legal requirements; (ii) they may not produce reliable results; (iii) they may not perform in a timely manner; (iv) they may not maintain confidentiality of our proprietary information; (v) disputes may arise with respect to ownership of rights to technology developed with our partners; and (vi) disagreements could cause delays in, or termination of, the research, development or commercialization of our products or result in litigation or arbitration. Moreover, some third parties are located in markets subject to political and social risk, corruption, infrastructure problems and natural disasters, in addition to country-specific privacy and data security risk given current legal and regulatory environments. Failure of third parties to meet their contractual, regulatory, and other obligations may materially adversely affect our business.
The failure of OMNI or TearCare to meet patient expectations or the occurrence of adverse events from use of OMNI or TearCare could limit their adoption and impair our financial performance.
Our future success depends in part upon patients having an experience with our products that meets their expectations in order to increase ECPs’ demand for our products as a result of positive feedback, social media and word-of-mouth. Patients may be dissatisfied if their expectations of the procedures performed by ECPs using our products, among other things, are not met. Despite what we believe to be the strong safety profile of our products for their intended uses, patients may experience adverse events following canaloplasty or trabeculotomy with OMNI, including, but not limited to, hyphema, mild anterior chamber inflammation and spikes in intraocular pressure. Similarly, patients may experience adverse events following application of localized heat with TearCare, including discomfort, pain or erythema of the eyelids.
If experiences with OMNI or TearCare do not meet the expectations of patients, or if patients experience adverse events, it could discourage the patient and treating physician from referring our products to others. Dissatisfied patients may express negative opinions through social media or other public forums. Any failure to meet patient expectations and any resulting negative publicity could harm our reputation and future sales and therefore adversely affect our business, financial condition and results of operations.
Our results of operations could be materially harmed if we are unable to accurately forecast customer demand for our products and manage our inventory.
We seek to maintain sufficient levels of inventory in order to protect ourselves from supply interruptions, but keep limited components, sub-assemblies, materials and finished products on hand. To ensure adequate inventory supply and manage our operations with our third-party suppliers, we forecast anticipated materials requirements and demand for our products in order to predict inventory needs and then place orders with our suppliers based on these predictions. Our ability to accurately forecast demand for our products could be negatively affected by many factors, including our limited historical commercial experience, rapid growth, failure to accurately manage our expansion strategy, product introductions by competitors, an increase or decrease in customer demand for our products, our failure to accurately forecast customer acceptance and adoption of new products, unanticipated changes in general market conditions or regulatory matters and weakening of economic conditions or consumer confidence in future economic conditions.
Inventory levels in excess of customer demand may result in a portion of our inventory becoming obsolete or expiring, as well as inventory write-downs or write-offs, which would negatively impact our gross margins and impair the strength of our brand. Conversely, if we underestimate customer demand for our products or our own requirements for components, sub-assemblies and materials, our third-party suppliers may not be able to deliver components, sub-assemblies and materials to meet our requirements, which could result in inadequate inventory levels or interruptions, delays or cancellations of deliveries to our customers, any of which would damage our reputation, customer relationships and business. In addition, several components, sub-assemblies and materials incorporated into our products require lengthy order lead times, and additional supplies or materials or additional manufacturing capacity may not be available when required on terms that are acceptable to us, or at all, and our third-party suppliers may not be able to allocate sufficient capacity in order to meet our increased
29
Table of Contents
requirements, any of which could have an adverse effect on our ability to meet customer demand for our products and our business, financial condition and results of operations.
Our quarterly and annual results may fluctuate significantly and may not fully reflect the underlying performance of our business.
Our quarterly and annual results of operations, including our revenue, may vary significantly in the future, and period-to-period comparisons of our operating results may not be meaningful. Accordingly, the results of any one quarter or period should not be relied upon as an indication of future performance or of the results for the year in which such quarter or period occurs. Our quarterly and annual financial results may fluctuate as a result of a variety of factors, many of which are outside our control and, as a result, may not fully reflect the underlying performance of our business. Fluctuations in quarterly and annual results may decrease the value of our common stock or result in volatility of our common stock after this offering. Because our quarterly results may fluctuate, period-to-period comparisons may not be the best indication of the underlying results of our business and should only be relied upon as one factor in determining how our business is performing. These fluctuations may occur due to a variety of factors, many of which are outside of our control, including, but not limited to:
| • | The level of demand for our products which may vary significantly; |
| • | Results of clinical trials or investigations involving the use of our products; |
| • | Regulatory decisions or announcements, including product recalls; |
| • | Data and results relating to our products that are presented in journal publications; |
| • | Expenditures that we may incur to acquire, develop or commercialize additional products and technologies; |
| • | Sales and marketing efforts and expenses; |
| • | Pricing pressures; |
| • | The rate at which we grow our sales force and the speed at which newly hired salespeople become effective; |
| • | Changes in the productivity of our sales force; |
| • | Our ability to expand the geographic reach of our sales force; |
| • | The degree of competition in our industry and any change in the competitive landscape of our industry, including consolidation among our competitors or future partners; |
| • | Changes in coverage and reimbursement policies with respect to our procedures in which our products are used, and potential future products that compete with our products; |
| • | Positive or negative coverage in the media or clinical publications of our products or products of our competitors or our industry; |
| • | The timing of customer orders or medical procedures using our products and the number of available selling days in any quarterly period, which can be impacted by holidays, the mix of products sold and the geographic mix of where products are sold; |
| • | The timing and cost of, and level of investment in, research, development, licenses, regulatory approval, commercialization activities, acquisitions and other strategic transactions, or other significant events relating to our products, which may change from time to time; |
| • | The cost of manufacturing our products, which may vary depending on the quantity of production and the terms of our agreements with third-party suppliers; and |
| • | Future accounting pronouncements or changes in our accounting policies. |
30
Table of Contents
Our long-term growth depends on our ability to enhance our products, expand our indications and develop and commercialize additional products in a timely manner. If we fail to identify, acquire and develop other products, we may be unable to grow our business.
The markets for our products are highly competitive, dynamic, and marked by rapid and substantial technological development and product innovation. New entrants or existing competitors could attempt to develop products that compete directly with ours. Demand for our products and future related products could be diminished by equivalent or superior products and technologies offered by competitors. If we are unable to innovate successfully, our products could become obsolete and our revenue would decline as our customers purchase our competitors’ products. Developing and improving products is expensive and time-consuming and could divert management’s attention away from our existing products. The success of any new product offering or product enhancements to our solutions will depend on several factors, including our ability to:
| • | Maintaining strong relationships with ECPs; |
| • | Assemble sufficient resources to acquire or discover additional products; |
| • | Properly identify and anticipate physician and patient needs; |
| • | Develop and introduce new products and product enhancements in a timely manner; |
| • | Avoid infringing upon, misappropriating or otherwise violating the intellectual property rights of third parties; |
| • | Demonstrate, if required, the safety and efficacy of new products with data from preclinical studies and clinical trials or investigations; |
| • | Obtain the necessary regulatory clearances, certifications or approvals for expanded indications, new products or product modifications; |
| • | Comply with the requirements of FDA and similar foreign regulatory authorities regarding the marketing of new devices or modified products; |
| • | Produce new products in commercial quantities at an acceptable cost; |
| • | Provide adequate training to potential users of our products; |
| • | Receive adequate coding, coverage and reimbursement for procedures performed with our products; and |
| • | Develop an effective and dedicated sales and marketing team. |
If we are unable to develop or improve products, applications or features due to constraints, such as insufficient cash resources, high employee turnover, inability to hire personnel with sufficient technical skills or a lack of other research and development resources, we may not be able to maintain our competitive position compared to other companies. Furthermore, many of our competitors devote a considerably greater amount of funds to their research and development programs than we do, and those that do not may be acquired by larger companies that could allocate greater resources to research and development programs. Our failure or inability to devote adequate research and development resources or compete effectively with the research and development programs of our competitors could harm our business.
In addition, we may choose to focus our efforts and resources on potential products or indications that ultimately prove to be unsuccessful, or to license or purchase a marketed product that does not meet our financial expectations. As a result, we may fail to capitalize on viable commercial products or profitable market opportunities, be required to forego or delay pursuit of opportunities with other potential products or other diseases that may later prove to have greater commercial potential, or relinquish valuable rights to such potential products through collaboration, licensing or other royalty arrangements in cases in which it would have been advantageous for us to retain sole development and commercialization rights, which could adversely impact our business, financial condition and results of operations.
31
Table of Contents
Changes in public health insurance coverage and government reimbursement rates for our products could affect the adoption of our products and our future revenue.
The federal government is considering ways to change, and has changed, the manner in which healthcare services are paid for in the U.S. Individual states may also enact legislation that impacts Medicaid payments to hospitals, surgical centers and physicians. In addition, CMS establishes Medicare payment levels for hospitals, surgical centers and physicians on an annual basis, which can increase or decrease payment to such entities, including for procedures involving our products. Internationally, medical reimbursement systems vary significantly from country to country, with some countries limiting medical centers’ spending through fixed budgets, regardless of levels of patient treatment, and other countries requiring application for, and approval of, government or third-party reimbursement. Even if we succeed in bringing our products to market in additional foreign countries, uncertainties regarding future healthcare policy, legislation and regulation, as well as private market practices, could affect our ability to sell our products in commercially acceptable quantities at acceptable prices.
Cost-containment efforts of our customers, purchasing groups and governmental organizations could have a material adverse effect on our sales and results of operations. Consolidation in the healthcare industry or group purchasing organizations could lead to demands for price concessions, which may affect our ability to sell our products at prices necessary to support our current business strategies.
In an effort to reduce costs, many clinics and hospitals in the United States, including some of our customers, are members of Group Purchasing Organizations, or GPOs, and Integrated Delivery Networks, or IDNs. GPOs and IDNs negotiate pricing arrangements with medical device companies and distributors and then offer these negotiated prices to affiliated hospitals and other members. GPOs and IDNs typically award contracts on a category-by-category basis through a competitive bidding process. Bids are generally solicited from multiple providers with the intention of driving down pricing or reducing the number of vendors. Due to the highly competitive nature of the GPO and IDN contracting processes, we may not be able to obtain new, or maintain existing, contract positions with major GPOs and IDNs. Furthermore, the increasing leverage of organized buying groups may reduce market prices for our products, thereby reducing our revenue and margins.
While having a contract with a GPO or IDN for a given product category can facilitate sales to members of that GPO or IDN, such contract positions can offer no assurance that any level of sales will be achieved, as sales are typically made pursuant to individual purchase orders. Even when a provider is the sole contracted supplier of a GPO or IDN for a certain product category, members of the GPO or IDN are generally free to purchase from other suppliers. Furthermore, GPO and IDN contracts typically are terminable without cause by the GPO or IDN upon 60 to 90 days’ notice. Accordingly, the members of such groups may choose to purchase alternative products due to the price or quality offered by other companies, which could result in a decline in our sales volumes and revenue.
Healthcare costs have risen significantly over the past decade, which has resulted in or led to numerous cost reform initiatives by legislators, regulators and third-party payors. Cost reform has triggered a consolidation trend in the healthcare industry to aggregate purchasing power, which may create more requests for pricing concessions in the future. Additionally, GPOs, IDNs and large single accounts may continue to use their market power to consolidate purchasing decisions for hospitals. We expect that market demand, government regulation, third-party coverage and reimbursement policies and societal pressures will continue to change the healthcare industry worldwide, resulting in further business consolidations and alliances among our customers, which may exert further downward pressure on the prices of our products. Such downward pressure on the prices of our products may affect our results of operations and our ability to support our current business strategies.
We may not be able to achieve or maintain satisfactory pricing and margins for our products.
Medical device companies have a history of price competition, and we can give no assurance that we will be able to achieve satisfactory prices for our products or maintain prices at the levels we have historically achieved.
32
Table of Contents
Any decline in the amount that payors reimburse our customers for procedures that use OMNI or in the amount that customers are willing to pay or that payors reimburse for procedures that use TearCare in the future, could make it difficult for customers to continue using, or to adopt, our products and could create additional pricing pressure for us. If we are forced to lower the price we charge for our products or add more components to our products, our gross margins will decrease, which will adversely affect our ability to invest in and grow our business. If we are unable to maintain our prices, or if our costs increase and we are unable to offset such increase with an increase in our prices, our margins could erode. We are, and will continue to be, subject to significant pricing pressure, which could negatively affect our business, financial condition and results of operations.
We may be unable to manage the anticipated growth of our business.
In order to grow, we need to expand our commercial team, and general and administrative infrastructure. In addition to the need to scale our organization, future growth will impose significant added responsibilities on management, including the need to identify, recruit, train and integrate additional employees. Rapid expansion in personnel could mean that less experienced people market and sell our products, which could result in inefficiencies and unanticipated costs, reduced quality and disruptions to our operations. In addition, rapid and significant growth may strain our administrative and operational infrastructure. Our ability to manage our business and growth will require us to continue to improve our operational, financial and management controls, reporting systems and procedures. For example, we currently rely on a combination of direct sales personnel and independent distributors to sell our products in Europe, and we intend to grow our international sales through a combination of direct and distributor sales. If we are unable to manage our growth effectively, it may be difficult for us to execute our business strategy and our business could be harmed.
As demand for our current products or any of our future products increases, we will need to continue to expand customer service, billing and systems processes and enhance our internal quality assurance program. We cannot assure you that any increases in scale, related improvements and quality assurance will be successfully implemented or that appropriate personnel will be available to facilitate the growth of our business. Failure to implement necessary procedures, transition to new processes or hire the necessary personnel could result in higher costs of processing data or inability to meet increased demand.
Performance issues, service interruptions or price increases by our shipping carriers and distributors could negatively affect our business, financial condition and results of operations and harm our reputation and the relationship between us and the ECPs we work with.
Expedited, reliable shipping is essential to our operations. We rely heavily on providers of transport services for reliable and secure point-to-point transport of our products to our customers and for tracking of these shipments. Should a carrier encounter delivery performance issues such as loss, damage or destruction of any systems, it would be costly to replace such systems in a timely manner and such occurrences may damage our reputation and lead to decreased demand for our solutions and increased cost and expense to our business. In addition, any significant increase in shipping rates could adversely affect our operating margins and results of operations. Similarly, strikes, severe weather, natural disasters or other service interruptions affecting delivery services we use would adversely affect our ability to process orders for our products on a timely basis. These factors could negatively affect our business, financial condition and results of operations and harm our reputation and the relationship between us and the ECPs we work with.
Our products may become obsolete in the future.
The medical device industry is characterized by rapid and significant change. There can be no assurance that other companies will not succeed in developing or marketing devices or products that are more effective than our products or that would render our products obsolete or noncompetitive. Additionally, new surgical procedures, medications and other therapies could be developed that replace or reduce the importance of our products.
33
Table of Contents
Accordingly, our success will depend in part on our ability to respond quickly to medical and other changes through the development and introduction of new products. Product development involves a high degree of risk, and there can be no assurance that our new product development efforts will result in any commercially successful products.
We bear the risk of potential warranty claims on our products.
We provide limited warranties regarding our products, including warranties pertaining to freedom from defects and conformance to specifications. We are generally obligated under our sales contracts to repair, replace or credit or refund the purchase price of defective products. As a result, we bear the risk of potential warranty claims on our products. In the event that we attempt to recover some or all of the expenses associated with a warranty claim against us from our suppliers or vendors, we may not be successful in claiming recovery under any warranty or indemnity provided to us by such suppliers or vendors and any recovery from such vendor or supplier may not be adequate. In addition, warranty claims brought by our customers related to third-party components may arise after our ability to bring corresponding warranty claims against such suppliers expires, which could result in costs to us.
We may enter into collaborations, in-licensing arrangements, joint ventures, strategic alliances or partnerships with third parties that may not result in the development of commercially viable products or product improvements or the generation of significant future revenues.
We may enter into collaborations, in-licensing arrangements, joint ventures, strategic alliances, partnerships or other arrangements to develop new products or product improvements and to pursue new markets. Proposing, negotiating and implementing collaborations, in-licensing arrangements, joint ventures, strategic alliances or partnerships may be a lengthy and complex process. Other companies, including those with substantially greater financial, marketing, sales, technology or other business resources, may compete with us for these opportunities or arrangements. We may not identify, secure, or complete any such transactions or arrangements in a timely manner, on a cost-effective basis, on acceptable terms or at all. We have limited institutional knowledge and experience with respect to these business development activities, and we may also not realize the anticipated benefits of any such transaction or arrangement. In particular, these collaborations may not result in the development of products that achieve commercial success or viable product improvements or result in significant revenues and could be terminated prior to developing any products.
Additionally, we may not be in a position to exercise sole decision-making authority regarding the transaction or arrangement, which could create the potential risk of creating impasses on decisions, and our future collaborators may have economic or business interests or goals that are, or that may become, inconsistent with our business interests or goals. It is possible that conflicts may arise with our collaborators, such as conflicts concerning the achievement of performance milestones, or the interpretation of significant terms under any agreement, such as those related to financial obligations or the ownership or control of intellectual property developed during the collaboration. If any conflicts arise with any future collaborators, they may act in their self-interest, which may be adverse to our best interest, and they may breach their obligations to us. In addition, we may have limited control over the amount and timing of resources that any future collaborators devote to our or their future products.
Disputes between us and any collaborators we may have in the future may result in litigation or arbitration which would increase our expenses and divert the attention of our management. These arrangements may consume management time and resources to establish and maintain. Further, these transactions and arrangements will be contractual in nature and will generally be terminable under the terms of the applicable agreements and, in such event, we may not continue to have rights to the products relating to such transaction or arrangement or may need to purchase such rights at a premium. Any termination of collaborations we enter into in the future, or any delay in entering into collaborations related to our products, could delay the development and commercialization of our products and reduce their competitiveness if they reach the market, which could have a material adverse effect on our business, financial condition and results of operations.
34
Table of Contents
If we enter into in-bound intellectual property license agreements, we may not be able to fully protect the licensed intellectual property rights or maintain those licenses. Future licensors could retain the right to prosecute and defend the intellectual property rights licensed to us, in which case we would depend on the ability of our licensors to obtain, maintain and enforce intellectual property protection for the licensed intellectual property. These licensors may determine not to pursue litigation against other companies or may pursue such litigation less aggressively than we would. Further, entering into such license agreements could impose various diligence, commercialization, royalty or other obligations on us. Future licensors may allege that we have breached our license agreement with them, and accordingly seek to terminate our license and/or seek damages arising out of the alleged breach, which could adversely affect our competitive business position and harm our business prospects.
Our insurance policies are expensive and protect us only from some business risks, which leaves us exposed to significant uninsured liabilities.
We do not carry insurance for all categories of risk that our business may encounter. Although we carry product liability insurance in the United States, we can give no assurance that such coverage will be available or adequate to satisfy any claims. Product liability insurance is expensive, subject to significant deductibles and exclusions, and may not be available on acceptable terms, if at all. If we are unable to obtain or maintain insurance at an acceptable cost or on acceptable terms with adequate coverage or otherwise protect against potential product liability claims, we could be exposed to significant liabilities. A product liability claim, recall or other claim with respect to uninsured liabilities or for amounts in excess of insured liabilities could have a material adverse effect on our business, financial condition and results of operations. Defending a suit, regardless of its merit or eventual outcome, could be costly, could divert management’s attention from our business and might result in adverse publicity, which could result in reduced acceptance of our products in the market, product recalls or market withdrawals.
We also expect that operating as a public company will make it more difficult and more expensive for us to obtain director and officer liability insurance, and we may be required to accept reduced policy limits and coverage or incur substantially higher costs to obtain the same or similar coverage. As a result, it may be more difficult for us to attract and retain qualified people to serve on our board of directors, our board committees or as executive officers. We do not know, however, if we will be able to maintain existing insurance with adequate levels of coverage. Any significant uninsured liability may require us to pay substantial amounts, which would negatively affect our business, financial condition and results of operations.
We depend on our senior management team and the loss of one or more key employees or an inability to attract and retain highly skilled employees will negatively affect our business, financial condition and results of operations.
Our success depends largely on the continued services of key members of our executive management team and others in key management positions. For example, the services of Paul Badawi, our Chief Executive Officer, Jesse Selnick, our Chief Financial Officer, Shawn O’Neil, our Chief Commercial Officer, and Sam Park, our Chief Operating Officer, are essential to driving adoption of our products, executing on our corporate strategy and ensuring the continued operations and integrity of financial reporting within our company. In addition, the services of our sales professionals are critical to driving the growth in sales of our products. Any of our employees may terminate their employment with us at any time. We currently maintain a key person life insurance policy on Mr. Badawi. If we lose one or more key employees, we may experience difficulties in competing effectively, developing our technologies and implementing our business strategy, which in turn would negatively affect our business.
In addition, our research and development programs, clinical and quality operations and sales efforts depend on our ability to attract and retain highly skilled engineers and sales professionals, as well as experienced regulatory, quality and clinical professionals. We may not be able to attract or retain qualified professionals in
35
Table of Contents
the future due to the competition for qualified personnel. We have from time to time experienced, and we expect to continue to experience, difficulty in hiring and retaining employees with appropriate qualifications. Many of the companies with which we compete for experienced personnel have greater resources than we do. If we hire employees from competitors or other companies, their former employers may attempt to assert that these employees or we have breached legal obligations, resulting in a diversion of our time and resources and, potentially, damages.
In addition, job candidates and existing employees often consider the value of the stock awards they receive in connection with their employment. If the perceived benefits of our stock awards decline, either because of unfavorable fluctuations or declines in our stock price or for other reasons, it may harm our ability to recruit and retain highly skilled employees. Many of our employees have become or will soon become vested in a substantial amount of our common stock or a number of common stock options. Our employees may be more likely to leave us if the shares they own have significantly appreciated in value relative to the original purchase prices of the shares, or if the exercise prices of the options that they hold are significantly below the market price of our common stock, particularly after the expiration of the lock-up agreements described herein. Our future success also depends on our ability to continue to attract and retain additional executive officers and other key employees. If we fail to attract new personnel or fail to retain and motivate our current personnel, it will negatively affect our business, financial condition and results of operations.
The use, misuse or off-label use of our products may result in injuries that lead to product liability suits, which could be expensive, divert management’s attention and harm our reputation and business. We may not be able to maintain adequate product liability insurance.
Our products are cleared or authorized by the FDA to be marketed for certain specific intended uses. If physicians elect to use our products in manners outside of the intended uses that have been cleared or authorized by the FDA, then such off-label use of our products may result in outcomes and adverse events that are sight threatening, necessitate medical or surgical intervention to preclude permanent impairment of vision, or result in a permanent impairment of vision, potentially leading to product liability claims. However, we cannot prevent a physician from using our products for off-label applications or using components or products that are not our products when performing procedures with our products. There may be increased risk of injury to patients if physicians attempt to use our devices off-label. In addition, we cannot guarantee that physicians are trained by us or their peers prior to utilizing our products. Complications resulting from the use of our products off-label or use by physicians who have not been trained appropriately, or at all, may not effectively treat the applicable conditions and may expose us to product liability claims or litigation by our customers or their patients and may harm our reputation.
In addition, if our products are defectively designed, manufactured or labeled, contain defective components or are misused, we may become subject to costly litigation initiated by hospitals, surgical centers, ECPs or patients. Product liability claims are especially prevalent in the medical device industry and could harm our reputation, divert management’s attention from our core business, attract negative publicity, be expensive to defend and may result in sizable damage awards against us. Although we maintain product liability insurance, we may not have sufficient insurance coverage for future product liability claims. We are not able to obtain insurance in amounts or scope sufficient to provide us with adequate coverage against all potential liabilities. Any product liability claims brought against us, with or without merit, could increase our product liability insurance rates or prevent us from securing continuing coverage, harm our reputation, significantly increase our expenses, and reduce product sales. Product liability claims could cause us to incur significant legal fees and deductibles and claims in excess of our insurance coverage would be paid out of cash reserves, harming our financial condition and operating results.
36
Table of Contents
We may need additional funding beyond the net proceeds of this offering to finance our planned operations, and may not be able to raise capital on acceptable terms, if at all, which could force us to delay, reduce or eliminate our product development programs and commercialization efforts.
Since inception, we have incurred significant net losses and expect to continue to incur net losses for the foreseeable future. Since our inception, our operations have been financed primarily by net proceeds from the sale of our convertible preferred stock in private placements, indebtedness and, to a lesser extent, product revenue from sales of our products. As of March 31, 2021, we had $48.3 million in cash and cash equivalents, and an accumulated deficit of $102.3 million. Based on our current planned operations, we expect that our cash and cash equivalents and additional borrowings available under our credit facility will enable us to fund our operations for at least the next twelve months. We have based these estimates on assumptions that may prove to be wrong, and we could utilize our available capital resources sooner than we expect.
We expect to continue to invest in clinical trials or investigations that are designed to provide clinical evidence of the safety and efficacy of our products, the growth of our sales and marketing organization, and research and development of product improvements and future products. Moreover, we expect to incur additional expenses associated with operating as a public company, including legal, accounting, insurance, exchange listing and SEC compliance, investor relations and other expenses. Because of these and other factors, we expect to continue to incur net losses and negative cash flows from operations for the foreseeable future. Our future funding requirements will depend on many factors, including:
| • | The degree and rate of market acceptance of our products and procedures; |
| • | Whether we acquire third-party companies, products or technologies; |
| • | Repayment of debt; |
| • | The scope and timing of investment in our sales force and expansion of our commercial organization; |
| • | The impact on our business from the ongoing COVID-19 pandemic, or any other pandemic, epidemic or outbreak of an infectious disease; |
| • | The scope, rate of progress and cost of our current or future clinical trials or investigations and registries; |
| • | The cost of our research and development activities; |
| • | The cost and timing of additional regulatory clearances, certifications or approvals; |
| • | The costs associated with any product recall that may occur; |
| • | The costs of attaining, defending, protecting and enforcing our intellectual property rights; |
| • | The terms and timing of any other collaborative, licensing and other arrangements that we may establish; |
| • | The emergence of competing technologies or other adverse market developments; and |
| • | The rate at which we expand internationally. |
We may seek to raise additional capital through equity offerings or debt financings and such additional financing may not be available to us on acceptable terms, or at all. In addition, any additional equity or debt financing that we raise may contain terms that are not favorable to us or our stockholders. For example, if we raise funds by issuing equity or equity-linked securities, the issuance of such securities could result in dilution to our stockholders. Any equity securities issued may also provide for rights, preferences or privileges senior to those of holders of our common stock. In addition, the issuance of additional equity securities by us, or the possibility of such issuance, may cause the market price of our common stock to decline, and the price per share at which we sell additional shares of our common stock, or securities convertible into or exercisable or exchangeable for shares of our common stock, in future transactions may be higher or lower than the price per share paid by investors in this offering.
37
Table of Contents
In addition, the terms of debt securities issued or borrowings could impose significant restrictions on our operations including restrictive covenants, such as limitations on our ability to incur additional debt or issue additional equity, limitations on our ability to pay dividends, limitations on our ability to acquire or license intellectual property rights, and other operating restrictions that could adversely affect our ability to conduct our business. In the event that we enter into collaborations or licensing arrangements to raise capital, we may be required to accept unfavorable terms, such as relinquishment or licensing of certain technologies or products that we otherwise would seek to develop or commercialize ourselves, or reserve for future potential arrangements when we might otherwise be able to achieve more favorable terms. In addition, we may be forced to work with a partner on one or more of our products or market development programs, which could lower the economic value of those programs to us.
If we are unable to obtain adequate financing on terms satisfactory to us when we require it, we may terminate or delay the development of one or more of our products, delay clinical trials or investigations necessary to market our products, or delay establishment of sales and marketing capabilities or other activities necessary to commercialize our products. If this were to occur, our ability to grow and support our business and to respond to market challenges could be significantly limited, which could have a material adverse effect on our business, financial condition and results of operations.
We have a significant amount of debt, which may affect our ability to operate our business and secure additional financing in the future.
In November 2020, we entered into a new loan and security agreement with MidCap Financial Services, which provides for a term loan facility and revolving line of credit, or the 2020 MidCap Credit Facility. The 2020 MidCap Credit Facility consists of a term loan of up to $35.0 million, or the 2020 Term Loan, which has a stated floating interest rate equal to reserve-adjusted LIBOR plus 7.00%, and a revolving line of credit of $5 million, or the 2020 Revolver, with a stated floating interest rate equal to reserve-adjusted LIBOR plus 4.50%, a 0.5% unused line fee and a 0.5% collateral management fee. As of December 31, 2020 and March 31, 2021, we had an aggregate of approximately $35.0 million in principal borrowings outstanding under the 2020 MidCap Credit Facility, excluding debt discounts. We must make interest payments under the 2020 MidCap Credit Facility, which has diverted and will continue to divert resources from other activities. We incurred an aggregate interest expense of $1.9 million and $2.4 million in the years ended December 31, 2019 and December 31, 2020, respectively, and $1.1 million and $0.6 million in the three months ended March 31, 2020 and March 31, 2021.
Our obligations under the 2020 MidCap Credit Facility are collateralized by a security interest in substantially all of our assets, and we are subject to customary financial and operating covenants limiting our ability to, among other things, relocate or dispose of assets, undergo a change in control, merge or consolidate, enter into certain transactions with affiliates, make acquisitions, incur debt, pay dividends, grant liens, store certain amounts of inventory or equipment with third parties and make investments, in each case subject to certain exceptions. We are also subject to minimum trailing revenue targets that are evaluated on a monthly basis. The covenants related to the 2020 MidCap Credit Facility, as well as any future financing agreements into which we may enter, may restrict our ability to finance our operations and engage in, expand or otherwise pursue our business activities and strategies.
While we have not previously breached and are not currently in breach of these or any other covenants contained in the 2020 MidCap Credit Facility, there can be no guarantee that we will not breach these covenants in the future. Our ability to comply with these covenants may be affected by events beyond our control, and future breaches of any of these covenants could result in a default under the 2020 MidCap Credit Facility. If not waived, future defaults could cause all of the outstanding indebtedness under the 2020 MidCap Credit Facility to become immediately due and payable and terminate commitments to extend further credit and foreclose on the collateral granted to it to collateralize such indebtedness. If we do not have or are unable to generate sufficient cash available to repay our debt obligations when they become due and payable, either upon maturity or in the event of a default, our assets could be foreclosed upon and we may not be able to obtain additional debt or equity
38
Table of Contents
financing on favorable terms, if at all, which may negatively impact our ability to operate and continue our business as a going concern.
In order to service this indebtedness and any additional indebtedness we may incur in the future, we need to generate cash from our operating activities. Our ability to generate cash is subject, in part, to our ability to successfully execute our business strategy, as well as general economic, financial, competitive, regulatory and other factors beyond our control. We cannot assure you that our business will be able to generate sufficient cash flow from operations or that future borrowings or other financings will be available to us in an amount sufficient to enable us to service our indebtedness and fund our other liquidity needs. To the extent we are required to use cash from operations or the proceeds of any future financing to service our indebtedness instead of funding working capital, capital expenditures or other general corporate purposes, we will be less able to plan for, or react to, changes in our business, industry and in the economy generally. This may place us at a competitive disadvantage compared to our competitors that have less indebtedness or greater financial resources to service their debt.
Uncertainty relating to the LIBOR calculation process and potential phasing out of LIBOR after 2021 may adversely affect the market value of our current or future debt obligations.
The London Inter-bank Offered Rate, or LIBOR, and certain other interest “benchmarks” may be subject to regulatory guidance and/or reform that could cause interest rates under our current or future debt agreements to perform differently than in the past or cause other unanticipated consequences. The United Kingdom’s Financial Conduct Authority, which regulates LIBOR, has announced that it intends to stop encouraging or requiring banks to submit LIBOR rates after 2021, and it is unclear if LIBOR will cease to exist or if new methods of calculating LIBOR will evolve. If LIBOR ceases to exist or if the methods of calculating LIBOR change from their current form, there may be adverse impacts on the financial markets generally and interest rates on borrowings under our 2020 Term Loan and 2020 Revolver may be adversely affected.
We may acquire other companies or technologies, which could fail to result in a commercial product or net sales, divert our management’s attention, result in additional dilution to our stockholders and otherwise disrupt our business and adversely affect our results of operations.
Although we currently have no agreements or commitments to complete any such transactions and are not involved in negotiations to do so, we may in the future seek to acquire or invest in businesses, applications or technologies that we believe could complement or expand our portfolio, enhance our technical capabilities or otherwise offer growth opportunities. However, we cannot assure you that we would be able to successfully complete any acquisition we choose to pursue, or that we would be able to successfully integrate any acquired business, product or technology in a cost-effective and non-disruptive manner. The pursuit of potential
acquisitions may divert the attention of management and cause us to incur various costs and expenses in identifying, investigating and pursuing suitable acquisitions, whether or not they are consummated. We may not be able to identify desirable acquisition targets or be successful in entering into an agreement with any particular target or obtain the expected benefits of any acquisition or investment.
To date, the growth of our operations has been largely organic, and we have limited experience in acquiring other businesses or technologies. Furthermore, the anticipated benefit of any strategic alliance, joint venture or acquisition may not materialize, or such strategic alliance, joint venture or acquisition may be prohibited. In November 2020, we amended our credit facilities and entered into the 2020 Term Loan and 2020 Revolver. The 2020 Term Loan and the 2020 Revolver restrict our ability to pursue certain mergers, acquisitions, amalgamations or consolidations that we may believe to be in our best interest.
We may not be able to successfully integrate any acquired personnel, operations and technologies, or effectively manage the combined business following an acquisition. Acquisitions could also result in dilutive issuances of equity securities, the use of our available cash, or the incurrence of debt, which could harm our
39
Table of Contents
operating results. In addition, if an acquired business fails to meet our expectations, our business, financial condition and results of operations may be negatively affected. Additional risks we may face in connection with acquisitions include:
| • | Diversion of management time and focus from operating our business to addressing acquisition integration challenges; |
| • | Coordination of research and development and sales and marketing functions; |
| • | Integration of product and service offerings; |
| • | Retention of key employees from the acquired company; |
| • | Changes in relationships with strategic partners as a result of product acquisitions or strategic positioning resulting from the acquisition; |
| • | Cultural challenges associated with integrating employees from the acquired company into our organization; |
| • | Integration of the acquired company’s accounting, management information, human resources and other administrative systems; |
| • | The need to implement or improve controls, procedures, and policies at a business that prior to the acquisition may have lacked sufficiently effective controls, procedures and policies; |
| • | Financial reporting, revenue recognition or other financial or control deficiencies of the acquired company that we don’t adequately address and that cause our reported results to be incorrect; |
| • | Liability for activities of the acquired company before the acquisition, including intellectual property infringement claims, misappropriation or other violation, violations of laws, commercial disputes, tax liabilities and other known and unknown liabilities; |
| • | Unanticipated write-offs or charges; and |
| • | Litigation or other claims in connection with the acquired company, including claims from terminated employees, customers, former stockholders or other third parties. |
Our failure to address these risks or other problems encountered in connection with acquisitions and investments could cause us to fail to realize the anticipated benefits of these acquisitions or investments, cause us to incur unanticipated liabilities, and harm our business generally.
Taxing authorities may successfully assert that we should have collected or in the future should collect sales and use, gross receipts, value added or similar taxes and may successfully impose additional obligations on us.
One or more jurisdictions may seek to impose additional tax collection obligations on us, including for past sales. A successful assertion by a state, country, or other jurisdiction that we should have been or should be collecting additional sales, use, or other taxes on our services could, among other things, result in substantial tax liabilities for past sales, create significant administrative burdens for us, discourage users from purchasing our products, or otherwise harm our business, results of operations and financial condition.
Our ability to utilize our net operating loss carryforwards, disallowed interest expense carryforwards and research and development carryforwards may be limited.
As of December 31, 2020, we had U.S. federal and state net operating loss carryforwards, or NOLs, of $85.3 million and $83.5 million, respectively, and U.S. federal and state research and development credit carryforwards of $0.8 million and $0.9 million, respectively. In general, under Sections 382 and 383 of the Internal Revenue Code of 1986, as amended, or the Code, a corporation that undergoes an “ownership change,” generally defined as a greater than 50 percentage point change by value in its equity ownership over a rolling
40
Table of Contents
three-year period, is subject to limitations on its ability to utilize its pre-change net operating losses, or NOLs, and its research and development credit carryforwards to offset future taxable income. Our existing NOLs and research and development credit carryforwards could be subject to limitation under Sections 382 and 383 of the Code if we have undergone, or undergo in the future, any ownership changes for purposes of these provisions. If our NOLs and research and development credit carryforwards are subject to these limitations, we may not be able to utilize a material portion of the NOLs and research and development credit carryforwards, even if we attain profitability. In addition, our ability to deduct net interest expense may be limited if we have insufficient taxable income for the year during which the interest is incurred, and any carryovers of such disallowed interest would be subject to the limitation rules similar to those applicable to NOLs and other attributes.
In addition, the tax benefit of NOLs, temporary differences and credit carryforwards are required to be recorded as an asset to the extent that we assess that realization is more likely than not. We believe that recognition of the deferred tax asset arising from these future tax benefits is not likely to be realized and, accordingly, have provided a valuation allowance of $14.4 million and $24.5 million for the years ended December 31, 2019 and 2020, respectively.
The impact of the Tax Cuts and Jobs Act and the CARES Act on our financial results is not entirely clear and could differ materially from the financial statements provided herein.
On December 22, 2017, the United States enacted the Tax Cuts and Jobs Act, or the TCJA, that significantly reformed the Code. The TCJA, among other things, contained significant changes to corporate taxation, including reduction of the corporate tax rate from a top marginal rate of 35% to a flat rate of 21%; limitation of the tax deduction for interest expense; limitation (as modified by the CARES Act as discussed below) of the deduction for NOLs and elimination of NOL carrybacks, in each case, for losses arising in taxable years beginning after December 31, 2017 (though any such tax losses may be carried forward indefinitely); and modifying or repealing many business deductions and credits.
On March 27, 2020, President Trump signed the Coronavirus Aid, Relief, and Economic Security Act (the CARES Act), aimed at helping American workers and businesses impacted by the COVID-19 pandemic. The CARES Act, among other things, temporarily removes the current-law taxable income limitation established under the Tax Cuts and Jobs Act of 2017, and permits NOL carryovers and carrybacks to offset 100% of taxable income for taxable years beginning before 2021. In addition, the CARES Act allows NOLs incurred in 2018, 2019 and 2020 to be carried back to each of the five preceding taxable years. The NOL provisions of the CARES Act are not expected to result in a cash benefit to the Company nor did they impact our NOL balance upon enactment.
The financial statements contained herein reflect the effects of the TCJA and the CARES Act based on current guidance. However, there remain uncertainties and ambiguities in the application of certain provisions of the TCJA and the CARES Act, and, as a result, we made certain judgments and assumptions in the interpretation thereof. The U.S. Treasury Department and the Internal Revenue Service may issue further guidance on how the provisions of the TCJA and the CARES Act will be applied or otherwise administered that differs from our current interpretation. In addition, the TCJA and the CARES Act could be subject to potential amendments and technical corrections, any of which could materially lessen or increase certain adverse impacts of the legislation on us.
41
Table of Contents
The planned international expansion of our business will expose us to market, regulatory, political, operational, financial and economic risks associated with doing business outside of the United States.
We intend to increase our international presence, including securing additional regulatory approvals in targeted countries outside the United States. This strategy may include establishing and maintaining physician outreach and education capabilities outside of the United States and expanding our relationships with international payors. Doing business internationally involves a number of risks, including:
| • | Difficulties in staffing and managing our international operations; |
| • | Multiple, conflicting and changing laws and regulations such as tax laws, privacy laws, export and import restrictions, employment laws, regulatory requirements and other governmental approvals, permits and licenses; |
| • | Reduced or varied protection for intellectual property rights in some countries; |
| • | Obtaining regulatory clearance, certification or approval where required for our products in various countries; |
| • | Requirements to maintain data and the processing of that data on servers located within such countries; |
| • | Complexities associated with managing multiple payor reimbursement regimes, government payors or patient self-pay systems; |
| • | Limits on our ability to penetrate international markets if we are required to manufacture our products locally; |
| • | Financial risks, such as longer payment cycles, difficulty collecting accounts receivable, foreign tax laws and complexities of foreign value-added tax systems, the effect of local and regional financial pressures on demand and payment for our products and exposure to foreign currency exchange rate fluctuations; |
| • | Restrictions on the site-of-service for use of our products and the economics related thereto for physicians, providers and payors; |
| • | Changes in foreign currency exchange rates and costs associated with hedging against such changes; |
| • | Natural disasters, political and economic instability, including wars, terrorism, political unrest, outbreak of disease, boycotts, curtailment of trade and other market restrictions; and |
| • | Regulatory and compliance risks that relate to maintaining accurate information and control over activities subject to regulation under the United States Foreign Corrupt Practices Act of 1977, or FCPA, U.K. Bribery Act of 2010 and comparable laws and regulations in other countries. |
Any of these factors could significantly harm our future international expansion and operations and, consequently, have a material adverse effect on our business, financial condition and results of operations.
We could be adversely affected by violations of the FCPA and similar worldwide anti-bribery laws and any investigation, and the outcome of any investigation, by government agencies of possible violations by us of the FCPA could have a material adverse effect on our business.
The FCPA and similar worldwide anti-bribery laws prohibit companies and their intermediaries from corruptly providing any benefits to government officials for the purpose of obtaining or retaining business. The U.S. Departments of Justice, Commerce, State and Treasury and other federal agencies and authorities have a broad range of civil and criminal penalties they may seek to impose against corporations and individuals for violations of economic sanctions laws, export control laws, the FCPA, and other federal statutes and regulations, including those established by the Office of Foreign Assets Control, or OFAC. In addition, the U.K. Bribery Act of 2010, or the Bribery Act, prohibits both domestic and international bribery, as well as bribery across both
42
Table of Contents
private and public sectors. An organization that fails to prevent bribery by anyone associated with the organization can be charged under the Bribery Act unless the organization can establish the defense of having implemented adequate procedures to prevent bribery. Under these laws and regulations, as well as other anti-corruption laws, anti-money laundering laws, export control laws, customs laws, sanctions laws and other laws governing our operations, various government agencies may require export licenses, may seek to impose modifications to business practices, including cessation of business activities in sanctioned countries or with sanctioned persons or entities and modifications to compliance programs, which may increase compliance costs, and may subject us to fines, penalties and other sanctions.
We have commenced commercial sales of OMNI in certain European countries through a combination of direct sales personnel and independent distributors, and we are also in the process of conducting an EU-based clinical investigation. Further, a portion of our business with respect to our manufacturing is conducted outside of the United States. We expect our international activities to increase in the future. Though we maintain policies, internal controls and other measures reasonably designed to promote compliance with applicable anticorruption and anti-bribery laws and regulations, and certain safeguards designed to ensure compliance with U.S. trade control laws, our employees or agents may nevertheless engage in improper conduct for which we might be held responsible. Any violations of these anti-corruption or trade controls laws, or even allegations of such violations, can lead to an investigation and/or enforcement action, which could disrupt our operations, involve significant management distraction, and lead to significant costs and expenses, including legal fees. If we, or our employees or agents acting on our behalf, are found to have engaged in practices that violate these laws and regulations, we could suffer severe fines and penalties, profit disgorgement, injunctions on future conduct, securities litigation, bans on transacting government business, delisting from securities exchanges and other consequences that may have a material adverse effect on our business, financial condition and results of operations. In addition, our reputation, our net sales or our stock price could be adversely affected if we become the subject of any negative publicity related to actual or potential violations of anti-corruption, anti-bribery or trade control laws and regulations.
Changes in government trade policies, including the imposition of tariffs and export restrictions, could have a negative impact on our manufacturing process, which may materially and adversely affect our sales and results of operations.
Certain public officials, including members of the current U.S. Congress, have made public statements indicating the possibility of significant changes in U.S. trade policy and have taken certain actions that may impact U.S. trade policy, including imposing new or increased tariffs on certain goods imported into the United States during the Trump administration. For example, the United States and China have imposed a number of tariffs and other restrictions on items imported or exported between the United States and China, and have proposed to impose a number of additional tariffs. We cannot predict what actions may ultimately be taken with respect to tariffs or trade relations between the United States and China or other countries, what products may be subject to such actions, or what actions may be taken by the other countries in retaliation.
Since certain of our critical product and product component manufacturers are located outside the United States, such changes, if adopted, could have a negative impact on our business and make our products more expensive and less competitive in domestic markets. Furthermore, changes in U.S. trade policy could trigger retaliatory actions by affected countries, which could impose restrictions on our ability to do business in or with affected countries or prohibit, reduce or discourage purchases of our products by foreign customers. Changes in, and responses to, U.S. trade policy could reduce the competitiveness of our products and cause our sales to decline, which could materially and adversely impact our business, financial condition and results of operations.
The United Kingdom’s withdrawal from the European Union may have a negative effect on global economic conditions, financial markets and our business.
Following a national referendum and enactment of legislation by the government of the United Kingdom, the United Kingdom formally withdrew from the European Union and ratified a trade and cooperation agreement
43
Table of Contents
governing its future relationship with the European Union. The agreement, which is being applied provisionally from January 1, 2021 until it is ratified by the European Parliament and the Council of the European Union, addresses trade, economic arrangements, law enforcement, judicial cooperation and a governance framework including procedures for dispute resolution, among other things. Because the agreement merely sets forth a framework in many respects and will require complex additional bilateral negotiations between the United Kingdom and the European Union as both parties continue to work on the rules for implementation, significant political and economic uncertainty remains about how the precise terms of the relationship between the parties will differ from the terms before withdrawal.
Following the end of the “Brexit” Transition Period, from January 1, 2021 onwards, the Medicines and Healthcare Products Regulatory Agency, or the MHRA, will be responsible for the UK medical device market. The new regulations will require medical devices to be registered with the MHRA (but manufacturers will be given a grace period of four to 12 months to comply with the new registration process). Manufacturers based outside the UK will need to appoint a UK Responsible Person to register devices with the MHRA in line with the grace periods. By July 1, 2023, in the UK (England, Scotland, and Wales), all medical devices will require a UKCA (UK Conformity Assessed) mark but CE marks issued by EU Notified Bodies will remain valid until this period. However, UKCA marking alone will not be recognized in the EU. The rules for placing medical devices on the Northern Ireland market will differ from those in the UK. These modifications may have an effect on the way we conduct our business.
These developments, or the perception that any related developments could occur, have had and may continue to have a material adverse effect on global economic conditions and financial markets, and could significantly reduce global market liquidity and restrict the ability of key market participants to operate in certain financial markets. Asset valuations, currency exchange rates and credit ratings have been and may continue to be subject to increased market volatility. Lack of clarity about future United Kingdom laws and regulations as the United Kingdom determines which European Union laws to replace or replicate could depress economic activity and investment in healthcare technology products.
The withdrawal has also given rise to calls for the governments of other EU member states to consider withdrawal. These developments, or the perception that any of them could occur, have had and may continue to have a material adverse effect on global economic conditions and the stability of global financial markets, and may significantly reduce global market liquidity and restrict the ability of key market participants to operate in certain financial markets. Any of these factors could depress economic activity and restrict our access to capital, which could have a material adverse effect on our business, financial condition and results of operations and reduce the price of our common stock. Any of these factors could have a material adverse effect on our business, financial condition and results of operations.
Security breaches, loss of data and other disruptions could compromise sensitive information related to our business or our customer’s patients, or prevent us from accessing critical information and expose us to liability, which could adversely affect our business and our reputation.
In the ordinary course of our business, we may become exposed to, or collect and store, sensitive data, including procedure-based information and legally-protected health information, credit card, and other financial information, insurance information, and other potentially personally identifiable information. We also store sensitive intellectual property and other proprietary business information. We are taking measures to implement policies and procedures designed to ensure compliance with applicable data security and privacy-related laws and regulations and protect sensitive information from unauthorized access or disclosure. However, our information technology, or IT, and infrastructure, and that of our third-party billing and collections provider and other technology partners and providers, may be vulnerable to cyber-attacks by hackers or viruses or breaches due to employee error, malfeasance or other disruptions. We rely extensively on IT systems, networks and services, including internet sites, data hosting and processing facilities and tools, physical security systems and other hardware, software and technical applications and platforms, some of which are managed, hosted, provided
44
Table of Contents
and/or used by third parties or their vendors, to assist in conducting our business. A significant breakdown, invasion, corruption, destruction or interruption of critical information technology systems or infrastructure, by our workforce, others with authorized access to our systems or unauthorized persons could negatively impact operations. The ever-increasing use and evolution of technology, including cloud-based computing, creates opportunities for the unintentional dissemination or intentional destruction of confidential information stored in our or our third-party providers’ systems, portable media or storage devices. For example, companies have experienced an increase in phishing and social engineering attacks from third parties in connection with the COVID-19 pandemic. We could also experience a business interruption, theft of confidential information or reputational damage from industrial espionage attacks, malware or other cyber-attacks, which may compromise our system infrastructure or lead to data leakage, either internally or at our third-party providers. Although the aggregate impact on our operations and financial condition has not been material to date, we have been the target of events of this nature and expect them to continue as cybersecurity threats have been rapidly evolving in sophistication and becoming more prevalent in the industry. We are investing in protections and monitoring practices of our data and IT to reduce these risks and continue to monitor our systems on an ongoing basis for any current or potential threats. There can be no assurance, however, that our efforts will prevent breakdowns or breaches to our or our third-party providers’ databases or systems, and such breakdowns or breaches could adversely affect our business, financial condition and reputation. We also intend to mitigate the risks related to these risks by purchasing cybersecurity insurance. However, such insurance, if purchased, will not necessarily cover all costs and impacts related to these risks.
Risks Related to Our Intellectual Property
Our success will depend on our, and any of our future licensors’, ability to obtain, maintain and protect our intellectual property rights.
Our commercial success will depend in part on our, and any of our future licensors’, success in obtaining and maintaining issued patents, trademarks and other intellectual property rights in the United States and elsewhere and protecting our proprietary technology. If we, or any of our future licensors, do not adequately protect our intellectual property and proprietary technology, competitors may be able to use our technologies or the goodwill we have acquired in the marketplace and erode or negate any competitive advantage we may have, which could harm our business and ability to achieve profitability.
We rely on a combination of contractual provisions, confidentiality procedures and patent, copyright, trademark, trade secret and other intellectual property laws to protect the proprietary aspects of our products, brands, technologies and data. These legal measures afford only limited protection, and competitors or others may gain access to or use our intellectual property and proprietary information. Our success will depend, in part, on preserving our trade secrets, maintaining the security of our data and know-how and obtaining and maintaining other intellectual property rights. We may not be able to obtain or maintain intellectual property or other proprietary rights necessary to our business or in a form that provides us with a competitive advantage.
In addition, despite our efforts to enter into confidentiality agreements with our employees, consultants, suppliers, clients and other vendors who have access to information that we regard as proprietary, our trade secrets, data, know-how and other proprietary information and technology could be subject to unauthorized access, use, misappropriation, or disclosure to unauthorized parties, and could otherwise become known or be independently discovered by third parties. Our intellectual property, including trademarks, could be challenged, invalidated, infringed, misappropriated, violated and circumvented by third parties, and our trademarks could also be diluted, declared generic or found to be infringing on other marks. If any of the foregoing occurs, we could be forced to re-brand our products, resulting in loss of brand recognition and requiring us to devote resources to advertising and marketing new brands and causing us to suffer other competitive harm. Third parties may also adopt trademarks similar to ours, which could harm our brand identity and lead to market confusion.
Failure to obtain and maintain intellectual property rights necessary to our business and failure to protect, monitor and control the use of our intellectual property rights could negatively impact our ability to compete and
45
Table of Contents
cause us to incur significant expenses. The intellectual property laws and other statutory and contractual arrangements in the United States and other jurisdictions we depend upon may not provide sufficient protection in the future to prevent the infringement, use, violation or misappropriation of our patents, trademarks, data, technology and other intellectual property and services, and may not provide an adequate remedy if our intellectual property rights are infringed, misappropriated or otherwise violated.
Our business relies, in part, on our ability to obtain, maintain, expand, enforce, and defend the scope of our intellectual property portfolio or other proprietary rights, including making any payments required in connection with the licensing, filing, defense and enforcement of any patents or other intellectual property rights. The process of applying for and obtaining a patent is expensive, time consuming and complex, and we may not be able to prepare, file, prosecute, maintain, enforce or license all necessary or desirable patent applications and patents at a reasonable cost, in a timely manner, or in all jurisdictions where protection may be commercially advantageous, or we may not be able to protect our proprietary rights at all. It is also possible that we may fail to identify patentable aspects of inventions made in the course of development and commercialization activities before it is too late to obtain patent protection on them. Although we enter into non-disclosure and confidentiality agreements with parties who have access to patentable aspects of our research and development output, such as our employees, corporate collaborators, outside scientific collaborators, suppliers, consultants, advisors and other third parties, any of these parties may breach the agreements and disclose such output before a patent application is filed, thereby jeopardizing our ability to seek patent protection. Furthermore, publications of discoveries in the scientific literature often lag behind the actual discoveries, and patent applications in the United States and other jurisdictions are typically not published until 18 months after filing, or in some cases not at all. Therefore, we cannot be certain that we were the first to make the inventions claimed in any of our patents or pending patent applications, or that we were the first to file for patent protection of such inventions. Moreover, depending on the terms of any future in-licenses to which we may become a party, we may not have the right to control the preparation, filing and prosecution of patent applications, or to maintain the patents, covering technology in-licensed from third parties. Therefore, these patents and patent applications may not be prosecuted, maintained, and/or enforced in a manner consistent with the best interests of our business. Despite our efforts to protect our proprietary rights, unauthorized parties may be able to obtain and use information that we regard as proprietary. Additionally, if there are material defects in the form, preparation or prosecution of our patents or patent applications, such patents or applications may be invalid and unenforceable. Any of these outcomes could impair our ability to prevent competition from third parties, which may have an adverse impact on our business.
The patent positions of medical device companies may involve complex legal and factual questions and have been the subject of much litigation in recent years, and therefore, the scope, validity and enforceability of any patent claims that we have or may obtain cannot be predicted with certainty. We cannot offer any assurances about which of our patent applications will issue, the breadth of any resulting patent or whether any of the issued patents will be found to be infringed, invalid or unenforceable or will be threatened or challenged by third parties. The coverage claimed in a patent application can be significantly reduced before the patent is issued, and its scope can be reinterpreted after issuance. We cannot offer any assurances that the breadth of our granted patents will be sufficient to stop a competitor from developing and commercializing a product in a non-infringing manner that would be competitive with one or more of our products, or otherwise provide us with any competitive advantage. Furthermore, any successful challenge to these patents or any other patents owned by or licensed to us after patent issuance could deprive us of rights necessary for our commercial success.
Patents have a limited lifespan. In the United States, the natural expiration of a utility patent is generally 20 years. Further, if we encounter delays in any future regulatory approvals, the period of time during which we could market a product under patent protection could be reduced, and, given the amount of time required for the development, testing and regulatory review of planned or future products, patents protecting such products might expire before or shortly after such products are commercialized. As a result, our intellectual property may not provide us with sufficient rights to exclude others from commercializing products similar or identical to ours.
Though an issued patent is presumed valid and enforceable, its issuance is not conclusive as to its validity or its enforceability and it may not provide us with adequate proprietary protection or competitive advantages
46
Table of Contents
against competitors with similar products. Patents, if issued, may be challenged, deemed unenforceable, invalidated, narrowed or circumvented. Proceedings challenging our patents or patent applications could result in either loss of the patent, or denial of the patent application or loss or reduction in the scope of one or more of the claims of the patent or patent application. Any successful challenge to our patents and patent applications could deprive us of exclusive rights necessary for our commercial success. In addition, defending such challenges in such proceedings may be costly. Thus, any patents that we may own may not provide the anticipated level of, or any, protection against competitors. Furthermore, an adverse decision may result in a third party receiving a patent right sought by us, which in turn could affect our ability to commercialize our products. Competitors could purchase our products and attempt to replicate or reverse engineer some or all of the competitive advantages we derive from our development efforts, willfully infringe, misappropriate or otherwise violate our intellectual property rights, design around our patents, or develop and obtain patent protection for more effective technologies, designs or methods. We may be unable to prevent the unauthorized disclosure or use of our technical knowledge or trade secrets by consultants, suppliers, vendors, former employees and current employees. Further, the laws of some foreign countries do not protect our proprietary rights to the same extent as the laws of the United States, and we may encounter significant problems in protecting our proprietary rights in these countries.
In addition, proceedings to enforce or defend our patents could put our patents at risk of being invalidated, held unenforceable or interpreted narrowly. Such proceedings could also provoke third parties to assert claims against us, including that some or all of the claims in one or more of our patents are invalid or otherwise unenforceable. If any of our patents covering our products are invalidated, found unenforceable or interpreted narrowly, or if a court found that valid, enforceable patents held by third parties covered one or more of our products, our competitive position could be harmed or we could be required to incur significant expenses to enforce or defend our rights.
Some of our patents and patent applications may in the future be co-owned with third parties. If we are unable to obtain an exclusive license to any such third-party co-owners’ interest in such patents or patent applications, such co-owners may be able to license their rights to other third parties, including our competitors, and our competitors could market competing products and technology. In addition, we may need the cooperation of any such co-owners of our patents in order to enforce such patents against third parties, and such cooperation may not be provided to us.
The degree of future protection for our proprietary rights is uncertain, and we cannot ensure that:
| • | Any of our patents, or any of our pending patent applications, if issued, will include claims having a scope sufficient to protect our products; |
| • | Any of our pending patent applications will issue as patents; |
| • | We will be able to successfully commercialize our products on a substantial scale, if approved, before our relevant patents we may have expire; |
| • | We were the first to make the inventions covered by each of our patents and pending patent applications; |
| • | We were the first to file patent applications for these inventions; |
| • | Others will not develop similar or alternative technologies that do not infringe our patents; |
| • | Any of our challenged patents will be found to ultimately be valid and enforceable; |
| • | Any patents issued to us will provide a basis for an exclusive market for our commercially viable products, will provide us with any competitive advantages or will not be challenged by third parties; |
| • | We will develop additional proprietary technologies or products that are separately patentable; or |
| • | Our commercial activities or products will not infringe upon the patents of others. |
47
Table of Contents
Even if we are able to obtain patent protection, such patent protection may be of insufficient scope to achieve our business objectives. Issued patents may be challenged, narrowed, invalidated or circumvented. Decisions by courts and governmental patent agencies may introduce uncertainty in the enforceability or scope of patents owned by or that are in the future licensed to us. Furthermore, the issuance of a patent does not give us the right to practice the patented invention. Third parties may have blocking patents that could prevent us from marketing our own products and practicing our own technology. Alternatively, third parties may seek approval to market their own products similar to or otherwise competitive with our products. In these circumstances, we may need to defend and/or assert our patents, including by filing lawsuits alleging patent infringement. In any of these types of proceedings, a court or agency with jurisdiction may find our patents invalid, unenforceable or not infringed; competitors may then be able to market products and use manufacturing and analytical processes that are substantially similar to ours. Even if we have valid and enforceable patents, these patents still may not provide protection against competing products or processes sufficient to achieve our business objectives.
In addition, the U.S. federal government retains certain rights in inventions produced with its financial assistance under the Bayh-Dole Act. The federal government retains a “nonexclusive, nontransferable, irrevocable, paid-up license” for its own benefit. The Bayh-Dole Act also provides federal agencies with “march-in rights.” March-in rights allow the government, in specified circumstances, to require the patent owner or successors in title to the patent to grant a “nonexclusive, partially exclusive, or exclusive license” to a “responsible applicant or applicants.” If the patent owner refuses to do so, the government may grant the license to itself. We cannot be sure that if we acquired intellectual property in the future it will be free from government rights or regulations pursuant to the Bayh-Dole Act. If, in the future, we own, co-own or license in technology which is critical to our business that is developed in whole or in part with federal funds subject to the Bayh-Dole Act, our ability to enforce or otherwise exploit patents covering such technology may be adversely affected. Any of the foregoing could have a material adverse effect on our business, financial condition and results of operations.
Obtaining and maintaining patent protection depends on compliance with various procedural, document submission, fee payment and other requirements imposed by governmental patent agencies, and our patent protection could be reduced or eliminated for non-compliance with these requirements.
The U.S. Patent and Trademark Office, or USPTO, and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. In addition, periodic maintenance fees, renewal fees, annuity fees and various other government fees on issued patents often must be paid to the USPTO and foreign patent agencies over the lifetime of the patent and/or applications and any patent rights we may obtain in the future. While an unintentional lapse of a patent or patent application can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Non-compliance events that could result in abandonment or lapse of a patent or patent application include, but are not limited to, failure to respond to official actions within prescribed time limits, non-payment of fees and failure to properly legalize and submit formal documents. If we fail to maintain the patents and patent applications covering our products, we may not be able to stop a competitor from marketing products that are the same as or similar to our products, which would have a material adverse effect on our business, financial condition and results of operations.
We may be unsuccessful in licensing or acquiring intellectual property from third parties that may be required to develop and commercialize our current and/or future products.
A third party may hold intellectual property rights, including patent rights that are important or necessary to the development and commercialization of our current and/or future products. It may be necessary for us to use the patented or proprietary technology of third parties to commercialize our current and/or future products, in which case we would be required to acquire or obtain a license to such intellectual property from these third
48
Table of Contents
parties, and we may be unable to do so on commercially reasonable terms or at all. The licensing or acquisition of third-party intellectual property rights is a competitive area, and several more established companies may pursue strategies to license or acquire third-party intellectual property rights that we may consider attractive or necessary. These established companies may have a competitive advantage over us due to their size, capital resources and greater clinical development and commercialization capabilities. In addition, companies that perceive us to be a competitor may be unwilling to assign or license rights to us. We also may be unable to license or acquire third-party intellectual property rights on terms that would allow us to make an appropriate return on our investment or at all. If we are unable to successfully obtain rights to required third-party intellectual property rights, we may not be able to develop, manufacture or market a product or future product, which could have a material adverse effect on our business, financial condition and results of operations.
Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect our existing and future products, and could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our patents or our future patents.
Our ability to obtain patents and the breadth of any patents obtained is uncertain in part because, to date, some legal principles remain unresolved, and there has not been a consistent policy regarding the breadth or interpretation of claims allowed in patents in the United States and other countries. Furthermore, changes in either patent laws or interpretations of patent laws in the United States and other countries may diminish the value of our intellectual property or narrow the scope of our patent protection.
Patent reform legislation may pass in the future that could lead to additional uncertainties and increased costs surrounding the prosecution, enforcement and defense of our patents and applications. Furthermore, the U.S. Supreme Court and the U.S. Court of Appeals for the Federal Circuit have made, and will likely continue to make, changes in how the patent laws of the United States are interpreted. The United States Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents, once obtained. Depending on actions by the United States Congress, the federal courts and the USPTO, the laws and regulations governing patents could change in unpredictable ways that would weaken our ability to obtain new patents or to enforce patents that we own or that we might obtain or license in the future. An inability to obtain, enforce, and defend patents covering our proprietary technologies would materially and adversely affect our business prospects and financial condition.
Similarly, foreign courts have made, and will likely continue to make, changes in how the patent laws in their respective jurisdictions are interpreted. Changes in patent laws and regulations in other countries or jurisdictions, changes in the governmental bodies that enforce them, or changes in how the relevant governmental authority enforces patent laws or regulations may weaken our ability to obtain new patents or to enforce patents that we own or may obtain in the future. Further, the laws of some foreign countries do not protect proprietary rights to the same extent or in the same manner as the laws of the United States. As a result, we may encounter significant problems in protecting and defending our intellectual property both in the United States and abroad. For example, if the issuance in a given country of a patent covering an invention is not followed by the issuance in other countries of patents covering the same invention, or if any judicial interpretation of the validity, enforceability or scope of the claims or the written description or enablement in a patent issued in one country is not similar to the interpretation given to the corresponding patent issued in other countries, our ability to protect our intellectual property in those countries may be limited. Changes in either patent laws or in interpretations of patent laws in the United States and other countries may materially diminish the value of our intellectual property or narrow the scope of our patent protection. We cannot predict future changes in the interpretation of patent laws or changes to patent laws that might be enacted into law by U.S. and foreign legislative bodies. Those changes may materially affect our patents or patent applications and our ability to obtain additional patent protection in the future. Any of the foregoing could have a material adverse effect on our business, financial condition and results of operations.
49
Table of Contents
We may become a party to intellectual property litigation or administrative proceedings that could be costly, time-consuming, unsuccessful, and could interfere with our ability to sell and market our products.
Our commercial success depends, in part, upon our ability and the ability of future collaborators, if any, to develop, manufacture, market and sell our products and use our proprietary technologies without infringing, misappropriating or otherwise violating the proprietary rights and intellectual property of third parties. The medical device industry has been characterized by extensive litigation regarding patents, trademarks, trade secrets, and other intellectual property rights, and companies in the industry have used intellectual property litigation to gain a competitive advantage.
Third parties may initiate legal proceedings alleging that we are infringing, misappropriating or otherwise violating their intellectual property rights, the outcome of which would be uncertain and could have a negative impact on the success of our business. It is possible that U.S. and foreign patents and pending patent applications controlled by third parties may be alleged to cover our products, or that we may be accused of misappropriating third parties’ trade secrets or infringing third parties’ trademarks. We may in the future become party to, or be threatened with, adversarial proceedings or litigation regarding intellectual property rights with respect to our products and technology, including interference proceedings, post grant review and inter partes review before the USPTO or equivalent foreign regulatory authority. Third parties may assert infringement claims against us based on existing patents or patents that may be granted in the future, regardless of their merit. Because patent applications can take many years to issue and because publication schedules for pending applications vary by jurisdiction, there may be applications now pending of which we are unaware and which may result in issued patents, which our current or future products infringe. Also, because the claims of published patent applications can change between publication and patent grant, there may be published patent applications that may ultimately issue with claims that we infringe. There is a risk that third parties may choose to engage in litigation with us to enforce or to otherwise assert their patent rights against us. Even if we believe such claims are without merit, a court of competent jurisdiction could hold that these third-party patents are valid, enforceable and infringed, which could have a negative impact on the commercial success of our current and any future products. In order to successfully challenge the validity of any such U.S. patent in federal court, we would need to overcome a presumption of validity. As this burden is a high one requiring us to present clear and convincing evidence as to the invalidity of any such U.S. patent claim, there is no assurance that a court of competent jurisdiction would invalidate the claims of any such U.S. patent. We will have similar burdens to overcome in foreign courts in order to successfully challenge a third-party claim of patent infringement.
If we are found to infringe, misappropriate or otherwise violate a third party’s valid and enforceable intellectual property rights, we could be required to obtain a license from such third party to continue developing, manufacturing and marketing our products and technology. However, we may not be able to obtain any required license on commercially reasonable terms or at all. Even if we were able to obtain a license, it could be non-exclusive, thereby giving our competitors and other third parties access to the same technologies licensed to us, and it could require us to make substantial licensing and royalty payments. We could be forced, including by court order, to cease developing, manufacturing and commercializing the infringing technology or product. In addition, we could be found liable for monetary damages, including treble damages and attorneys’ fees, if we are found to have willfully infringed a patent or other intellectual property right. A finding of infringement could prevent us from manufacturing and commercializing our products or force us to cease some or all of our business operations, which could materially harm our business. Claims that we have misappropriated the confidential information or trade secrets of third parties could have a similar negative impact on our business, financial condition, results of operations and prospects.
Additionally, our products include components that we purchase from vendors, and may include design components that are outside of our direct control. Our competitors, many of which have substantially greater resources and have made substantial investments in patent portfolios, trade secrets, trademarks, and competing technologies, may have applied for or obtained, or may in the future apply for or obtain, patents or trademarks that will prevent, limit or otherwise interfere with our ability to make, use, sell and/or export our products or to
50
Table of Contents
use our technologies or product names. As the number of competitors in our market grows and the number of patents issued in this area increases, the possibility of patent infringement claims against us may increase. Moreover, individuals and groups that are non-practicing entities, commonly referred to as “patent trolls,” purchase patents and other intellectual property assets for the purpose of making claims of infringement in order to extract settlements. From time to time, we may receive threatening letters, notices or “invitations to license,” or may be the subject of claims that our products and business operations infringe, misappropriate or otherwise violate the intellectual property rights of others. The defense of these matters can be time consuming, costly to defend in litigation, divert management’s attention and resources, damage our reputation and brand and cause us to incur significant expenses or make substantial payments. In addition, vendors from whom we purchase hardware or software may not indemnify us in the event that such hardware or software is accused of infringing a third-party’s patent or trademark or of misappropriating a third-party’s trade secret.
We cannot be certain that we were the first to file any patent application related to our products, in part because patent applications are confidential for a period of time after filing. Competitors may also contest our patents, if issued, by demonstrating that the claimed invention was not original, was not novel or was obvious. In litigation, a competitor could claim that our patents are not valid for a number of reasons. If a court agrees, we would lose our rights to those challenged patents.
In addition, we may in the future be subject to claims by our former employees or consultants asserting an ownership right in our patents, patent applications or other intellectual property, as a result of the work they performed on our behalf. Although we generally require all of our employees and consultants and any other partners or collaborators who have access to our proprietary know-how, information or technology to assign or grant similar rights to their inventions to us, we cannot be certain that we have executed such agreements with all parties who may have contributed to our intellectual property, nor can we be certain that our agreements with such parties will be upheld in the face of a potential challenge, or that they will not be breached, for which we may not have an adequate remedy.
Any lawsuits relating to intellectual property rights could subject us to significant liability for damages and invalidate our intellectual property or proprietary rights. Any potential intellectual property litigation also could force us to do one or more of the following:
| • | Stop making, selling or using products or technologies that allegedly infringe, misappropriate or otherwise violate the asserted intellectual property; |
| • | Lose the opportunity to license our intellectual property to others or to collect royalty payments based upon successful protection and assertion of our intellectual property rights against others; |
| • | Incur significant legal expenses; |
| • | Pay substantial damages or royalties to the party whose intellectual property rights we may be found to be infringing, misappropriating or otherwise violating; |
| • | Pay the attorney’s fees and costs of litigation to the party whose intellectual property rights we may be found to be infringing, misappropriating or otherwise violating; |
| • | Redesign those products or technologies that contain the allegedly infringing intellectual property, which could be costly, disruptive and infeasible; and |
| • | Attempt to obtain a license to the relevant intellectual property from third parties, which may not be available on reasonable terms or at all, or from third parties who may attempt to license rights that they do not have. |
In addition, if we are found to willfully infringe third-party patents or trademarks or to have misappropriated trade secrets, we could be required to pay treble damages in addition to other penalties. Although patent, trademark, trade secret, and other intellectual property disputes in the medical device area have often been settled through licensing or similar arrangements, costs associated with such arrangements may be substantial and could include ongoing royalties.
51
Table of Contents
Any litigation or claim against us, even those without merit and even those where we prevail, may cause us to incur substantial costs, and could place a significant strain on our financial resources, divert the attention of management from our core business and harm our reputation. Such litigation or proceedings could substantially increase our operating losses and reduce the resources available for development activities or any future sales, marketing or distribution activities. We may not have sufficient financial or other resources to conduct such litigation or proceedings adequately. Some of our competitors may be able to sustain the costs of litigation or administrative proceedings more effectively than we can because of greater financial resources and more mature and developed intellectual property portfolios. We could encounter delays in product introductions while we attempt to develop alternative methods or products. If we fail to obtain any required licenses or make any necessary changes to our products or technologies, we may have to withdraw existing products from the market or may be unable to commercialize one or more of our products.
If third parties assert infringement, misappropriation or other claims against our customers, these claims may require us to initiate or defend protracted and costly litigation on behalf of our customers, regardless of the merits of these claims. If any of these claims succeed or settle, we may be forced to pay damages or settlement payments on behalf of our customers or may be required to obtain licenses for the products they use. If we cannot obtain all necessary licenses on commercially reasonable terms, our customers may be forced to stop using our products.
Similarly, interference or derivation proceedings provoked by third parties or brought by the USPTO may be necessary to determine priority with respect to our patents or patent applications. An unfavorable outcome could require us to cease using the related technology or force us to take a license under the patent rights of the prevailing party, if available. Furthermore, our business could be harmed if the prevailing party does not offer us a license on commercially reasonable terms. We may also become involved in other proceedings, such as reexamination, inter partes review, derivation or opposition proceedings before the USPTO or other jurisdictional body relating to our intellectual property rights or the intellectual property rights of others. Our defense of any litigation or interference proceedings may fail and, even if successful, may result in substantial costs and distract our management and other employees. Adverse determinations in a judicial or administrative proceeding or failure to obtain necessary licenses could prevent us from manufacturing our products or using product names, which would have a significant adverse impact on our business, financial condition and results of operations.
Additionally, competitors or other third parties may currently, or in the future, infringe, misappropriate or otherwise violate our issued patents or other intellectual property, and we may file lawsuits or initiate other proceedings to protect or enforce our patents or other intellectual property rights, which could be expensive, time consuming and unsuccessful. In certain circumstances it may not be practicable or cost-effective for us to enforce our intellectual property rights fully, particularly in certain developing countries or where the initiation of a claim might harm our business relationships. We may also be hindered or prevented from enforcing our rights with respect to a government entity or instrumentality because of the doctrine of sovereign immunity. Our ability to enforce our patent or other intellectual property rights depends on our ability to detect infringement. It may be difficult to detect infringers who do not advertise the components or methods that are used in connection with their products and services. Moreover, it may be difficult or impossible to obtain evidence of infringement in a competitor’s or potential competitor’s product or service.
If we initiate legal proceedings against a third party to enforce a patent covering one of our products, the defendant could counterclaim that the patent covering our product is invalid and/or unenforceable. In patent litigation in the United States, counterclaims alleging invalidity and/or unenforceability are common, and there are numerous grounds upon which a third party can assert invalidity or unenforceability of a patent. Any claims we assert against perceived infringers could also provoke these parties to assert counterclaims against us alleging that we infringe, misappropriate or otherwise violate their intellectual property. In a patent or other intellectual property infringement proceeding, a court may decide that a patent or other intellectual property of ours is invalid or unenforceable, in whole or in part, construe the patent’s claims or other intellectual property narrowly or
52
Table of Contents
refuse to stop the other party from using the technology at issue on the grounds that our patents or other intellectual property do not cover the technology in question. Furthermore, even if our patents or other intellectual property are found to be valid and infringed, a court may refuse to grant injunctive relief against the infringer and instead grant us monetary damages and/or ongoing royalties. Such monetary compensation may be insufficient to adequately offset the damage to our business caused by the infringer’s competition in the market. An adverse result in any litigation or administrative proceeding could put one or more of our patents or other intellectual property at risk of being invalidated or interpreted narrowly, which could adversely affect our competitive business position, financial condition and results of operations. Moreover, even if we are successful in any litigation, we may incur significant expense in connection with such proceedings, and the amount of any monetary damages may be inadequate to compensate us for damage as a result of the infringement and the proceedings.
Third parties may also raise similar claims before administrative bodies in the United States or abroad, even outside the context of litigation. Such mechanisms include re-examination, post grant review, inter partes review and equivalent proceedings in foreign jurisdictions (for example, opposition proceedings). Such proceedings could result in revocation of or amendment to our patents in such a way that they no longer cover our products. The outcome following legal assertions of invalidity and unenforceability is unpredictable. With respect to the validity question, for example, we cannot be certain that there is no invalidating prior art, of which we, our patent counsel, and the patent examiner were unaware during prosecution. If a defendant were to prevail on a legal assertion of invalidity and/or unenforceability, we may lose some, and perhaps all, of the patent protection on our products.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. There could also be public announcements of the results of hearings, motions, or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock. Any of the foregoing may cause us to incur substantial costs, and could place a significant strain on our financial resources, divert the attention of management from our core business and harm our reputation.
If we are unable to protect the confidentiality of our other proprietary information, our business and competitive position may be harmed.
In addition to patent protection, we also rely on other proprietary rights, including protection of trade secrets, know-how, and/or other proprietary information that is not patentable or that we elect not to patent. However, trade secrets can be difficult to protect and some courts are less willing or unwilling to protect trade secrets. To maintain the confidentiality of our trade secrets and proprietary information, we rely heavily on confidentiality provisions that we have in contracts with our employees, consultants, collaborators and others upon the commencement of their relationship with us. We cannot guarantee that we have entered into such agreements with each party that may have or have had access to our trade secrets or proprietary technology and processes. Although we generally require all of our employees, consultants, advisors and any third parties who have access to our proprietary know-how, information, or technology to enter into confidentiality agreements, we cannot provide any assurances that all such agreements have been duly executed. We may not be able to prevent the unauthorized disclosure or use of our technical knowledge or other trade secrets by such third parties, despite the existence generally of these confidentiality restrictions. These contracts may not provide meaningful protection for our trade secrets, know-how, or other proprietary information in the event the unwanted use is outside the scope of the provisions of the contracts or in the event of any unauthorized use, misappropriation, or disclosure of such trade secrets, know-how, or other proprietary information. There can be no assurance that such third parties will not breach their agreements with us, that we will have adequate remedies for any breach, or that our trade secrets will not otherwise become known or independently developed by competitors. If any of our trade secrets were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent them, or those to whom they communicate it, from using that technology or information to compete with
53
Table of Contents
us. If any of our trade secrets were to be disclosed to or independently developed by a competitor, our competitive position would be harmed.
Despite the protections we do place on our intellectual property or other proprietary rights, monitoring unauthorized use and disclosure of our intellectual property is difficult, and we do not know whether the steps we have taken to protect our intellectual property or other proprietary rights will be adequate. In addition, the laws of many foreign countries will not protect our intellectual property or other proprietary rights to the same extent as the laws of the United States. Consequently, we may be unable to prevent our proprietary technology from being exploited abroad, which could affect our ability to expand to international markets or require costly efforts to protect our technology. To the extent our intellectual property or other proprietary information protection is incomplete, we are exposed to a greater risk of direct competition. A third party could, without authorization, copy or otherwise obtain and use our products or technology, or develop similar technology. Our competitors may independently develop knowledge, methods and know-how equivalent to our trade secrets. Our competitors could also purchase our products and attempt to replicate some or all of the competitive advantages we derive from our development efforts or design around our protected technology. Our failure to secure, protect and enforce our intellectual property rights could substantially harm the value of our products, brand and business. The theft or unauthorized use or publication of our trade secrets and other confidential business information could reduce the differentiation of our products and harm our business, the value of our investment in development or business acquisitions could be reduced and third parties might make claims against us related to losses of their confidential or proprietary information. Any of the foregoing could materially and adversely affect our business, financial condition and results of operations.
Costly and time consuming litigation could be necessary to enforce and determine the scope of our trade secret rights and related confidentiality and nondisclosure provisions. Further, it is possible that others will independently develop the same or similar technology or products or otherwise obtain access to our unpatented technology, and in such cases we could not assert any trade secret rights against such parties. If we fail to obtain or maintain trade secret protection, or if our competitors obtain our trade secrets or independently develop technology or products similar to ours or competing technologies or products, our competitive market position could be materially and adversely affected. In addition, some courts are less willing or unwilling to protect trade secrets and agreement terms that address non-competition are difficult to enforce in many jurisdictions and might not be enforceable in certain cases.
We also seek to preserve the integrity and confidentiality of our data and other confidential information by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these security measures and systems, agreements or security measures may be breached and detecting the disclosure or misappropriation of confidential information and enforcing a claim that a party illegally disclosed or misappropriated confidential information is difficult, expensive and time-consuming, and the outcome is unpredictable. Further, we may not be able to obtain adequate remedies for any breach. Also, if the steps taken to maintain our trade secrets we may have are deemed inadequate, we may have insufficient recourse against third parties for misappropriating the trade secret. In addition, others may independently develop our trade secrets and proprietary information.
We may enjoy only limited geographical protection with respect to certain patents and we may not be able to protect our intellectual property rights throughout the world.
A company may attempt to commercialize competing products utilizing our proprietary technology, design, trademarks or tradenames in foreign countries where we do not have any patents or patent applications, trademarks, and/or other forms of intellectual property and where legal recourse may be limited. This may have a significant commercial impact on our foreign business operations.
Filing, prosecuting and defending patents or trademarks on our current and future products in all countries throughout the world would be prohibitively expensive. The requirements for patentability and trademark
54
Table of Contents
protection may differ in certain countries, particularly developing countries. The laws of some foreign countries do not protect intellectual property rights to the same extent as laws in the United States. Consequently, we may not be able to prevent third parties from utilizing our inventions and trademarks in all countries outside the United States. Competitors may use our technologies or trademarks in jurisdictions where we have not obtained patent or trademark protection to develop or market their own products and further, may export otherwise infringing products to territories where we have patent and trademark protection, but enforcement on infringing activities is inadequate. These products or trademarks may compete with our products or trademarks, and our patents, trademarks or other intellectual property rights may not be effective or sufficient to prevent them from competing.
In addition, we may decide to abandon national and regional patent applications before they are granted. The examination of each national or regional patent application is an independent proceeding. As a result, patent applications in the same family may issue as patents in some jurisdictions, such as in the United States, but may issue as patents with claims of different scope or may even be refused in other jurisdictions. It is also quite common that depending on the country, the scope of patent protection may vary for the same product or technology. For example, certain jurisdictions do not allow for patent protection with respect to method of treatment.
While we seek to protect our intellectual property rights in our expected significant markets, we cannot ensure that we will be able to initiate or maintain similar efforts in all jurisdictions in which we may wish to market our products. Accordingly, our efforts to protect our intellectual property rights in such countries may be inadequate, which may have an adverse effect on our ability to successfully commercialize our products in all of our expected significant foreign markets. If we encounter difficulties in protecting, or are otherwise precluded from effectively protecting, the intellectual property rights important for our business in such jurisdictions, the value of these rights may be diminished, and we may face additional competition from others in those jurisdictions.
The laws of some jurisdictions do not protect intellectual property rights to the same extent as the laws or rules and regulations in the United States and many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents, trademarks and other intellectual property protection, which could make it difficult for us to stop the infringement of our patents and trademarks or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent and trademarks rights in foreign jurisdictions, whether or not successful, could result in substantial costs and divert our efforts and attention from other aspects of our business, could put our patents and trademarks in those jurisdictions, as well as elsewhere at risk of being invalidated or interpreted narrowly and our patent applications at risk of not issuing as patents, and could provoke third parties to assert claims against us. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded, if any, may not be commercially meaningful. Certain countries in Europe and certain developing countries, including India and China, have compulsory licensing laws under which a patent owner may be compelled to grant licenses to third parties. In those countries, we may have limited remedies if our patents are infringed or if we are compelled to grant a license to our patents to a third party, which could materially diminish the value of those patents. This could limit our potential revenue opportunities and our competitive position may be impaired. In addition, some countries limit the enforceability of patents against government agencies or government contractors. In those countries, the patent owner may have limited remedies, which could materially diminish the value of such patents. Accordingly, our efforts to enforce our intellectual property rights around the world may be inadequate to obtain a significant commercial advantage from the intellectual property that we own or license. Finally, our ability to protect and enforce our intellectual property rights may be adversely affected by unforeseen changes in foreign intellectual property laws.
55
Table of Contents
We may be subject to claims that we or our employees have misappropriated the intellectual property of a third party, including trade secrets or know-how, or are in breach of non-competition or non-solicitation agreements with our competitors.
We may be subject to claims that our employees, consultants, or independent contractors have wrongfully used or disclosed confidential information of third parties. Many of our employees and consultants were previously employed at or engaged by other medical device, biotechnology or pharmaceutical companies, including our competitors or potential competitors. Some of these employees, consultants and contractors may have executed proprietary rights, non-disclosure and non-competition agreements in connection with such previous employment. Although we try to ensure that our employees and consultants do not use the intellectual property, proprietary information, know-how or trade secrets of others in their work for us, we may be subject to claims that we or these individuals have, inadvertently or otherwise, misappropriated the intellectual property or disclosed the alleged trade secrets or other proprietary information of these former employers or competitors or other third parties. In addition, we may be subject to claims that we are infringing, misappropriating or otherwise violating other intellectual property rights, such as trademarks or copyrights. To the extent that our employees, consultants or contractors use intellectual property or proprietary information owned by others in their work for us, disputes may arise as to the rights in related or resulting know-how and inventions. Litigation may be necessary to defend against these claims. There is no guarantee of success in defending these claims, and even if we are successful, litigation could result in substantial cost and be a distraction to our management and other employees.
We may be subject to claims challenging the inventorship or ownership of our patents and other intellectual property.
We may also be subject to claims that former employees, collaborators, or other third parties have an ownership interest in our current or future patents, patent applications, or other intellectual property, including as an inventor or co-inventor. We may be subject to ownership or inventorship disputes in the future arising, for example, from conflicting obligations of consultants, contractors or others who are involved in developing our products. Although it is our policy to require our employees and contractors who may be involved in the conception or development of intellectual property to execute agreements assigning such intellectual property to us, we may be unsuccessful in executing such an agreement with each party who, in fact, conceives or develops intellectual property that we regard as our own, and we cannot be certain that our agreements with such parties will be upheld in the face of a potential challenge, or that they will not be breached, for which we may not have an adequate remedy. The assignment of intellectual property rights may not be self-executing or the assignment agreements may be breached, and litigation may be necessary to defend against these and other claims challenging inventorship or ownership. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights, such as exclusive ownership of, or right to use, valuable intellectual property, and other owners may be able to license their rights to other third parties, including our competitors. Such an outcome could have a material adverse effect on our business. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Additionally, we may be subject to claims from third parties challenging our ownership interest in intellectual property we regard as our own, based on claims that our employees or consultants have breached an obligation to assign inventions to another employer, to a former employer, or to another person or entity. Litigation may be necessary to defend against any other claims, and it may be necessary or we may desire to enter into a license to settle any such claim; however, there can be no assurance that we would be able to obtain a license on commercially reasonable terms, if at all. If our defense to those claims fails, in addition to paying monetary damages, a court could prohibit us from using technologies or features that are essential to our products, if such technologies or features are found to incorporate or be derived from the trade secrets or other proprietary information of the former employers. An inability to incorporate technologies or features that are important or essential to our products could have a material adverse effect on our business, financial condition
56
Table of Contents
and results of operations, and may prevent us from selling our products. In addition, we may lose valuable intellectual property rights or personnel. Even if we are successful in defending against these claims, litigation could result in substantial costs and could be a distraction to management. Any litigation or the threat thereof may adversely affect our ability to hire employees or contract with independent sales representatives. A loss of key personnel or their work product could hamper or prevent our ability to commercialize our products, which could have an adverse effect on our business, financial condition and results of operations.
If our trademarks and tradenames are not adequately protected, then we may not be able to build name recognition in our markets and our business may be adversely affected.
We use our trademarks, service marks, tradenames and brand names to distinguish our products from the products of our competitors, and have registered or applied to register these trademarks. Our trademarks or trade names may be challenged, infringed, circumvented, declared generic or determined to be violating or infringing on other marks. We cannot assure you that our trademark applications will be approved for registration. During trademark registration proceedings, we may receive rejections. Although we are given an opportunity to respond to those rejections, we may be unable to overcome such rejections. In addition, in proceedings before the USPTO and comparable agencies in many foreign jurisdictions, third parties are given an opportunity to oppose pending trademark applications and to seek to cancel trademark registrations. Opposition or cancellation proceedings may be filed against our trademark filings in these agencies, and such filings may not survive such proceedings. Our competitors may also infringe or otherwise violate our trademarks and we may not have adequate resources to enforce our trademarks, which may have a material adverse effect on our business. While we may be able to continue the use of our trademarks in the event registration is not available, particularly in the United States, where trademark rights are acquired based on use and not registration, third parties may be able to enjoin the continued use of our trademarks if such parties are able to successfully claim infringement in court. In the event that our trademarks are successfully challenged, we could be forced to rebrand our products, which could result in loss of brand recognition and could require us to devote resources towards advertising and marketing new brands. At times, competitors may adopt trade names or trademarks similar to ours, thereby impeding our ability to build brand identity and possibly leading to market confusion. Certain of our current or future trademarks may become so well known by the public that their use becomes generic and they lose trademark protection. Over the long term, if we are unable to establish name recognition based on our trademarks and trade names, then we may not be able to compete effectively and our business, financial condition and results of operations may be adversely affected.
We have become aware of a third party’s use of and pending U.S. application for the TEARCLEAR trademark in connection with ophthalmic pharmaceuticals, which we believe may be an infringement of our TEARCARE trademark. We are currently considering taking action against this third-party, which may include filing a complaint for trademark infringement in federal court.
Intellectual property rights do not necessarily address all potential threats.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations and may not adequately protect our business or permit us to maintain our competitive advantage. For example:
| • | We, or current or future collaborators, might not have been the first to make the inventions covered by the issued patent or pending patent application that we license or may own in the future; |
| • | We, or current or future collaborators, might not have been the first to file patent applications covering certain of our or their inventions; |
| • | Others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing, misappropriating or otherwise violating our intellectual property rights; |
57
Table of Contents
| • | It is possible that our pending patent applications or those that we may own in the future will not lead to issued patents; |
| • | Issued patents that we hold rights to may be held invalid or unenforceable, including as a result of legal challenges by our competitors; |
| • | Our competitors might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive products for sale in our major commercial markets; |
| • | We may not develop additional proprietary technologies that are patentable; |
| • | The patents of others may harm our business; and |
| • | We may choose not to file a patent in order to maintain certain trade secrets or know-how, and a third party may subsequently file a patent covering such intellectual property. |
Should any of these events occur, they could have a material adverse effect on our business, financial condition, results of operations and prospects.
Risks Related to Government Regulation
Our products and operations are subject to extensive government regulation and oversight in the United States and elsewhere.
Our products are regulated as medical devices by the FDA. We and our products are subject to extensive regulation in the United States and elsewhere, including by state agencies, the FDA and the FDA’s foreign counterparts. The FDA and foreign regulatory agencies regulate, among other things, with respect to medical devices: design, development, manufacturing and release; laboratory, preclinical and clinical testing; labeling, packaging, content and language of instructions for use and storage; product safety and efficacy; establishment registration and device listing; marketing, sales and distribution; pre-market clearance and approval; service operations; record keeping procedures; advertising and promotion; recalls and field safety corrective actions; post-market surveillance, including reporting of deaths or serious injuries and malfunctions that, if they were to recur, could lead to death or serious injury; post-market studies; and product import and export.
The regulations to which we are subject are complex, burdensome to understand and apply and have tended to become more stringent over time. Regulatory changes could result in restrictions on our ability to carry on or expand our operations, higher than anticipated costs or lower than anticipated sales. The FDA enforces these regulatory requirements through, among other means, periodic (unannounced) inspections and periodic reviews of public marketing and promotion materials. We do not know whether we will be found compliant in connection with any future FDA or foreign inspections or reviews. Failure to comply with applicable regulations could jeopardize our ability to sell our products and result in enforcement actions such as: warning letters; untitled letters; fines; injunctions; civil penalties; termination of distribution; recalls or seizures of products; delays in the introduction of products into the market; total or partial suspension of production; refusal to grant future clearances or approvals; withdrawals or suspensions of current approvals, resulting in prohibitions on sales of our products; and in the most serious cases, criminal penalties.
We may not receive, or may be delayed in receiving, the necessary clearances, certifications or approvals for our future products or modifications to our current products, and failure to timely obtain necessary clearances, certifications or approvals for our future products or modifications to our current products would adversely affect our ability to grow our business.
In the U.S., before we can market a new medical device, or a new use of, new claim for or significant modification to an existing product, we must first receive either clearance under Section 510(k) of the FDCA or approval of a pre-market approval application, or PMA, from the FDA, unless an exemption applies. In the
58
Table of Contents
510(k) clearance process, before a device may be marketed, the FDA must determine that a proposed device is “substantially equivalent” to a legally-marketed “predicate” device, which includes a device that has been previously cleared through the 510(k) process, a device that was legally marketed prior to May 28, 1976 (pre-amendments device), a device that was originally on the U.S. market pursuant to an approved PMA and later down-classified, or a 510(k)-exempt device. To be “substantially equivalent,” the proposed device must have the same intended use as the predicate device, and either have the same technological characteristics as the predicate device or have different technological characteristics and not raise different questions of safety or effectiveness than the predicate device. Clinical data are sometimes required to support substantial equivalence. In the process of obtaining PMA approval, the FDA must determine that a proposed device is safe and effective for its intended use based, in part, on extensive data, including, but not limited to, technical, preclinical, clinical trial, manufacturing and labeling data. The PMA process is typically required for devices that are deemed to pose the greatest risk, such as life-sustaining, life-supporting or implantable devices.
Modifications to products that are approved through a PMA application generally require FDA approval. Similarly, certain modifications made to products cleared through a 510(k) may require a new 510(k) clearance. Both the PMA approval and the 510(k) clearance process can be expensive, lengthy and uncertain. The FDA’s 510(k) clearance process usually takes from three to 12 months, but can last longer. The process of obtaining a PMA is much more costly and uncertain than the 510(k) clearance process and generally takes from one to three years, or even longer, from the time the application is submitted to the FDA. Despite the time, effort and cost, a device may not be approved or cleared by the FDA. Any delay or failure to obtain necessary regulatory clearances or approvals could harm our business. Furthermore, even if we are granted regulatory clearances or approvals, they may include significant limitations on the indicated uses for the device, which may limit the market for the device.
In the U.S., we have obtained clearance from the FDA of OMNI through the 510(k) clearance process. We also market TearCare as a 510(k)-exempt device and intend to submit a 510(k) premarket notification seeking an expanded label for the device in the future. Any further modification to these products or their intended uses may require us to submit a new 510(k) premarket notification and obtain clearance, or submit a PMA and obtain FDA approval prior to implementing the change. Specifically, any modification to a 510(k)-cleared device that could significantly affect its safety or effectiveness, or that would constitute a major change in its intended use, design or manufacture, requires a new 510(k) clearance or, possibly, approval of a PMA. The FDA requires every manufacturer to make this determination in the first instance, but the FDA may review any manufacturer’s decision. The FDA may not agree with our decisions regarding whether new clearances or approvals are necessary. We have made modifications to 510(k)-cleared products in the past and have determined based on our review of the applicable FDA regulations and guidance that in certain instances new 510(k) clearances or PMA approvals were not required. We may make modifications or add additional features in the future that we believe do not require a new 510(k) clearance or approval of a PMA. If the FDA disagrees with our determination and requires us to submit new 510(k) notifications or PMA applications for modifications to our products for which we have concluded that new clearances or approvals are unnecessary, we may be required to cease marketing or to recall the modified product until we obtain clearance or approval, and we may be subject to significant regulatory fines or penalties. If the FDA requires us to go through a lengthier, more rigorous examination for future products or modifications to existing products than we had expected, product introductions or modifications could be delayed or canceled, which could adversely affect our ability to grow our business.
The FDA can delay, limit or deny clearance or approval of a device for many reasons, including:
| • | Our inability to demonstrate to the satisfaction of the FDA that our products are safe or effective for their intended uses; |
| • | The disagreement of the FDA with the design or conduct of our clinical trials or the interpretation of data from preclinical studies or clinical trials; |
| • | Serious and unexpected adverse device effects experienced by participants in our clinical trials; |
59
Table of Contents
| • | The data from our preclinical studies and clinical trials may be insufficient to support clearance or approval, where required; |
| • | Our inability to demonstrate that the clinical and other benefits of the device outweigh the risks; |
| • | The manufacturing process or facilities we use may not meet applicable requirements; and |
| • | The potential for approval policies or regulations of the FDA to change significantly in a manner rendering our clinical data or regulatory filings insufficient for clearance or approval. |
In order to sell our products in member states of the EU, our products must comply with the essential requirements of the EU Medical Devices Directive (Council Directive 93/42/EEC). Compliance with these requirements is a prerequisite to be able to affix the CE mark to our products, without which they cannot be sold or marketed in the EU. To demonstrate compliance with the essential requirements we must undergo a conformity assessment procedure, which varies according to the type of medical device and its (risk) classification. Except for low-risk medical devices (Class I non-sterile, non-measuring devices), where the manufacturer can issue an EC Declaration of Conformity based on a self-assessment of the conformity of its products with the essential requirements of the EU Medical Devices Directive, a conformity assessment procedure requires the intervention of an organization accredited or designated by a member state of the EU to conduct conformity assessments, or a Notified Body. Depending on the relevant conformity assessment procedure, the Notified Body would typically audit and examine the technical file and the quality system for the manufacture, design and final inspection of our devices. The Notified Body issues a certificate of conformity following successful completion of a conformity assessment procedure conducted in relation to the medical device and its manufacturer and their conformity with the essential requirements. This certificate entitles the manufacturer to affix the CE mark to its medical devices after having prepared and signed a related EC Declaration of Conformity.
As a general rule, demonstration of conformity of medical devices and their manufacturers with the essential requirements must be based, among other things, on the evaluation of clinical data supporting the safety and performance of the products during normal conditions of use. Specifically, a manufacturer must demonstrate that the device achieves its intended performance during normal conditions of use, that the known and foreseeable risks, and any adverse events, are minimized and acceptable when weighed against the benefits of its intended performance, and that any claims made about the performance and safety of the device are supported by suitable evidence. If we fail to remain in compliance with applicable European laws and directives and corresponding EU member state laws, we would be unable to continue to affix the CE mark to our products, which would prevent us from selling them within the EU.
The aforementioned EU rules are generally applicable in the European Economic Area, or EEA, which consists of the 27 EU member states plus Norway, Liechtenstein and Iceland. Non-compliance with the above requirements would also prevent us from selling our products in these three countries.
Following the end of the “Brexit” Transition Period, from January 1, 2021 onwards, the MHRA will be responsible for the UK medical device market. The new regulations will require medical devices to be registered with the MHRA (but manufacturers will be given a grace period of four to 12 months to comply with the new registration process). Manufacturers based outside the UK will need to appoint a UK Responsible Person to register devices with the MHRA in line with the grace periods. By July 1, 2023, in the UK (England, Scotland, and Wales), all medical devices will require a UKCA (UK Conformity Assessed) mark but CE marks issued by EU Notified Bodies will remain valid until this time. However, UKCA marking alone will not be recognized in the EU. The rules for placing medical devices on the Northern Ireland market will differ from those in the UK. Compliance with this legislation is a prerequisite to be able to affix the UKCA mark to our products, without which they cannot be sold or marketed in the UK.
60
Table of Contents
We may incur significant liability if it is determined that we are promoting off-label uses of our products in violation of federal and state regulations in the United States or elsewhere.
The FDA and other regulatory authorities strictly regulate the promotional claims that may be made about medical devices. In particular, the FDA requires that medical devices be labeled, advertised and promoted only in accordance with their approved or cleared indications for use (or, in the case of products which are exempt from premarket review, in accordance with the regulations pertaining to such premarket clearance-exempt product classification). Similar limitations are imposed through certain national and international requirements outside of the U.S.
We currently market TearCare as a Class II, 510(k)-exempt powered heating pad. We intend to seek FDA clearance of TearCare for an expanded indication for use in the second half of 2021. However, the FDA may determine that the clinical data we have provided or will provide is insufficient to support this indication and therefore not grant or delay clearance. For example, in January 2021, the FDA requested that we provide additional information in connection with such submission, and we are currently in the process of collecting and analyzing the requested additional data. Further, the FDA may disagree with our belief that our existing indication is broad enough to include the delivery of localized heat where the current medical community recommends application of a warm compress, such as MGD, DED, and blepharitis, in which case the FDA could assert that we are marketing the product in a manner that causes the product not to be exempt from premarket clearance.
The FDA does not generally regulate the behavior of physicians in their choice of treatments. While physicians may choose to use medical devices for uses that are not described in the product’s labeling and for uses that differ from those authorized by the FDA, our promotional materials, promotional activities and training methods must comply with applicable FDA regulations and other applicable federal, state and foreign laws and regulations, including the prohibition on the promotion of off-label uses of our products.
If the FDA or equivalent foreign authorities determine that our labeling, promotional materials or other communications (including communications by our employees or other agents) constitute promotion of an off-label use, they could request or require that we modify our promotional materials or subject us to regulatory or enforcement actions, including the issuance of a warning letter or untitled letter, suspension or withdrawal of a product from the market, or requiring a recall or institution of fines, which could result in the disgorgement of money, operating restrictions, injunctions, civil fines and criminal penalties. It is also possible that other federal, state or foreign enforcement authorities might take action if they consider our promotional or training materials to constitute promotion of an off-label use, which could result in significant fines or penalties, such as laws prohibiting false or fraudulent claims for payment of government funds, such as the U.S. federal False Claims Act. In that event, our reputation could be damaged and adoption of our products could be impaired.
Notwithstanding the regulatory restrictions on off-label promotion, the FDA and other regulatory authorities allow medical device companies to engage in truthful, non-misleading and non-promotional scientific exchange concerning their products. If the FDA or other regulatory or enforcement authorities determine that our communications regarding our marketed products are not in compliance with the relevant regulatory requirements and that we have improperly promoted off-label uses, we may be subject to significant liability, including civil, criminal and administrative penalties.
Failure to comply with post-marketing regulatory requirements could subject us to enforcement actions, including substantial penalties, and might require us to recall or withdraw a product from the market.
Even though we have obtained FDA clearance for OMNI and currently market TearCare in the U.S. pursuant to a 510(k) exemption, we are subject to ongoing and pervasive regulatory requirements governing, among other things, the manufacture, marketing, advertising, medical device reporting, sale, promotion, import, export, registration, and listing of devices. For example, we must submit periodic reports to the FDA as a condition of 510(k) clearance. These reports include information about failures and certain adverse events
61
Table of Contents
associated with the device after its clearance. Failure to submit such reports, or failure to submit the reports in a timely manner, could result in enforcement action by the FDA. Following its review of the periodic reports, the FDA might ask for additional information or initiate further investigation. In addition, we must maintain an active registration of our facilities and listing of our products in order to legally market them in the United States. If the FDA were to disagree with our product listing or otherwise take issue with our registration and listing compliance, it could result in delisting of our products or other enforcement action resulting in potential inability to market our products. For example, in October 2020, the FDA communicated to us that TearCare may not be eligible for an exemption from 510(k) clearance. In response to that communication, among other things, we submitted a 510(k) premarket notification seeking clearance for TearCare in November 2020. The FDA requested several safety tests and modifications to this submission which we believe would have required additional time to complete beyond the designated review process. We voluntarily withdrew this submission in May 2021 to allow us to comply with the FDA’s requests in a comprehensive manner. We intend to resubmit the 510(k) premarket notification for an expanded indication for use in the second half of 2021.
The regulations to which we are subject are complex and have become more stringent over time. Regulatory changes could result in restrictions on our ability to continue or expand our operations, higher than anticipated costs, or lower than anticipated sales. Even after we have obtained the proper regulatory clearance to market a device, we have ongoing responsibilities under FDA regulations and applicable foreign laws and regulations. The FDA, state and foreign regulatory authorities have broad enforcement powers. Our failure to comply with applicable regulatory requirements could result in enforcement action by the FDA, state or foreign regulatory authorities, which may include any of the following sanctions:
| • | Untitled letters, warning letters or adverse publicity; |
| • | Fines, injunctions, consent decrees and civil penalties; |
| • | Recalls, termination of distribution, administrative detention, or seizure of our products; |
| • | Customer notifications or repair, replacement or refunds; |
| • | Operating restrictions or partial suspension or total shutdown of production; |
| • | Delays in or refusal to grant our requests for future clearances or approvals or foreign clearance, certification or approval of new products, new intended uses, or modifications to existing products; |
| • | Withdrawals or suspensions of 510(k) clearances, or requirements for new 510(k) clearances, resulting in prohibitions on sales of our products pending such further clearance; |
| • | FDA refusal to issue certificates to foreign governments needed to export products for sale in other countries; and |
| • | Criminal prosecution. |
Any of these sanctions could result in higher than anticipated costs or lower than anticipated sales and have a material adverse effect on our reputation, business, financial condition and results of operations. In addition, the FDA may change its clearance policies, adopt additional regulations or revise existing regulations, or take other actions, which may prevent or delay clearance or approval of our future products under development or impact our ability to modify our currently cleared or 510(k)-exempt products on a timely basis. Such policy or regulatory changes could impose additional requirements upon us that could delay our ability to obtain new clearances or approvals, increase the costs of compliance or restrict our ability to maintain our clearances of our current products.
Our products must be manufactured in accordance with federal, state and foreign regulations, and we could be forced to recall our devices or terminate production if we fail to comply with these regulations.
The methods used in, and the facilities used for, the manufacture of our products must comply with the FDA’s QSR and the European Union Medical Devices Directive (Council Directive 93/42/EEC), both of which
62
Table of Contents
are complex regulatory schemes that cover the procedures and documentation of the design, testing, production, process controls, quality assurance, labeling, packaging, handling, storage, distribution, installation, servicing and shipping of medical devices. Furthermore, we are required to maintain, and to verify that our suppliers maintain, facilities, procedures and operations that comply with our quality standards and applicable regulatory requirements. The FDA enforces the QSR through periodic announced or unannounced inspections of medical device manufacturing facilities, which may include the facilities of subcontractors. Our products are also subject to similar state regulations, various laws and regulations of foreign countries governing manufacturing and a requirement for adherence to industry standards of the International Standards Organization, or ISO, in connection with our medical device operations outside of the United States. Failure to comply with applicable FDA requirements or later discovery of previously unknown problems with our products or manufacturing processes could result in, among other things: warning letters or untitled letters; fines, injunctions or civil penalties; suspension or withdrawal of clearances or approvals; seizures or recalls of our products; total or partial suspension of production or distribution; administrative or judicially imposed sanctions; the FDA’s refusal to grant pending or future clearances or approvals for our products; clinical holds; refusal to permit the import or export of our products; and criminal prosecution of us, our suppliers, or our employees.
We have received ISO 13485:2016 certification for our quality management system. ISO certification generally includes recertification audits every third year, scheduled annual surveillance audits and periodic unannounced audits.
We can provide no assurance that we will be found to remain in compliance with the QSR or ISO standards upon a regulator’s review. If the FDA or other regulator, inspects any of our manufacturers’ facilities and discovers compliance problems, we may have to cease manufacturing and product distribution until we can take the appropriate remedial steps to correct the audit findings. Any of the actions noted above could significantly and negatively affect supply of our products. Taking corrective action may be expensive, time-consuming and a distraction for management. If any of these events occurs, our reputation could be harmed, we could be exposed to product liability claims and we could lose customers and experience reduced sales and increased costs.
Our products may cause or contribute to adverse medical events or be subject to failures or malfunctions that we are required to report to the FDA (or similar foreign authorities), and if we fail to do so, we would be subject to sanctions that could negatively affect our reputation, business, financial condition and results of operations. The discovery of serious safety issues with our products, or a recall of our products either voluntarily or at the direction of the FDA or another governmental authority, could have a negative impact on us.
We are subject to the FDA’s medical device reporting regulations and similar foreign regulations, which require us to report to the FDA (and other foreign regulatory authorities) when we receive or become aware of information that reasonably suggests that one or more of our products may have caused or contributed to a death or serious injury or malfunctioned in a way that, if the malfunction were to recur, it could cause or contribute to a death or serious injury. The timing of our obligation to report is based on the date we become aware of the adverse event as well as on the nature of the event. We may fail to report adverse events of which we become aware within the prescribed timeframe. We may also fail to recognize that we have become aware of a reportable adverse event, especially if it is not reported to us as an adverse event or if it is an adverse event that is unexpected or removed in time from the use of the product. If we fail to comply with our reporting obligations, the FDA or its foreign counterparts could take action, including warning letters, untitled letters, administrative actions, criminal prosecution, imposition of civil monetary penalties, revocation of device clearance or approval, seizure of our products or delay in clearance or approval of future products, which could have a negative impact on us.
The FDA and foreign regulatory bodies have the authority to require the recall of commercialized products in the event of material deficiencies or defects in design or manufacture of a product or in the event that a product poses an unacceptable risk to health. The FDA’s authority to require a recall must be based on a finding
63
Table of Contents
that there is reasonable probability that the device could cause serious injury or death. We may also choose to voluntarily recall a product if any material deficiency is found. A government-mandated or voluntary recall by us could occur as a result of an unacceptable risk to health, component failures, malfunctions, manufacturing defects, labeling or design deficiencies, packaging defects or other deficiencies or failures to comply with applicable regulations. Product defects or other errors may occur in the future.
If we initiate a correction or removal for our products to reduce a risk to health posed by them or to remedy a violation of law that may present a risk to health, we would be required to submit a report to the FDA and may be required to submit similar notifications to other regulatory authorities. This report could lead to increased scrutiny by the FDA, other foreign regulatory agencies and our customers regarding the quality and safety of our products. Furthermore, the submission of these reports, to the extent made publicly available in accordance with FDA regulations, could be used by competitors against us or otherwise publicized and cause physicians to delay or cancel product orders, which will harm our reputation.
If we assess a potential quality issue or complaint as not requiring either a field action or regulatory notification, regulators may review documentation of that decision during a subsequent audit. If regulators disagree with our decision, or take issue with either our investigation process or the resulting documentation, regulatory agencies may impose sanctions and we may be subject to regulatory enforcement actions, including warning letters, all of which will negatively affect our business, financial condition and results of operations.
Depending on the corrective action we take to redress a product’s deficiencies or defects, the FDA or FDA’s foreign counterparts may require, or we may decide, that we will need to obtain new clearances, certifications or approvals for the device before we may market or distribute the corrected device. Seeking such clearances, certifications or approvals may delay our ability to replace the recalled devices in a timely manner. Moreover, if we do not adequately address problems associated with our devices, we may face additional regulatory enforcement action, including FDA warning letters, product seizure, injunctions, administrative penalties or civil or criminal fines.
Companies are required to maintain certain records of recalls and corrections, even if they are not reportable to the FDA. We may initiate voluntary withdrawals or corrections for our products in the future that we determine do not require notification of the FDA. If the FDA disagrees with our determinations, it could require us to report those actions as recalls, and we may be subject to enforcement action. A future recall announcement could harm our reputation with customers, potentially lead to product liability claims against us and negatively affect our sales. Any corrective action, whether voluntary or involuntary, as well as defending ourselves in a lawsuit, will require the dedication of our time and capital, distract management from operating our business and will negatively affect our reputation, business, financial condition and results of operations.
If we do not obtain and maintain applicable regulatory registrations, clearances, certifications or approvals for our products, we will be unable to market and sell our products outside of the U.S.
We intend to expand our sales operations outside of the U.S. Sales of our products outside of the U.S. are subject to foreign regulatory requirements that vary widely from country to country. In addition, the FDA regulates exports of medical devices from the U.S. While the regulations of some countries may not impose barriers to marketing and selling our products or only require notification, others require that we obtain the clearance or approval of a specified regulatory body. Complying with foreign regulatory requirements, including obtaining registrations, clearances, certifications or approvals, can be expensive and time-consuming, and we may not receive regulatory clearances, certifications or approvals in each country in which we plan to market our products or we may be unable to do so on a timely basis. The time required to obtain registrations, clearances, certifications or approvals, if required by other countries, may be longer than that required for FDA clearance or approval, and requirements for such registrations, clearances, certifications or approvals may significantly differ from FDA requirements. If we modify our products, we may need to apply for regulatory clearances or approvals before we are permitted to sell the modified product.
64
Table of Contents
In addition, we may not continue to meet the quality and safety standards required to maintain the authorizations that we have received. If we are unable to maintain our authorizations in a particular country, we will no longer be able to sell the applicable product in that country.
Regulatory clearance or approval by the FDA does not ensure registration, clearance, certification or approval by regulatory authorities in other countries, and registration, clearance, certification or approval by one or more foreign regulatory authorities does not ensure registration, clearance, certification or approval by regulatory authorities in other foreign countries or by the FDA. However, a failure or delay in obtaining registration or regulatory clearance, certification or approval in one country may have a negative effect on the regulatory process in others.
The clinical trial or investigation process is lengthy and expensive with uncertain outcomes. Results of earlier studies may not be predictive of future clinical trial or investigation results, or the safety or efficacy profile for such products for such uses. Further, we may incur significant fines, penalties and other liabilities if it is determined that we are failing or have failed to comply with applicable regulatory requirements for the conduct of our clinical trials.
Clinical testing is difficult to design and implement, can take many years, can be expensive and carries uncertain outcomes. The results of preclinical studies and clinical trials and investigations of our products conducted to date and ongoing or future studies, trials and investigations of our current, planned or future products may not be predictive of the results of later clinical trials or investigations, and interim results of a clinical trial or investigation do not necessarily predict final results. Our interpretation of data and results from our clinical trials or investigations does not ensure that we will achieve similar results in future clinical trials or investigations. In addition, preclinical and clinical data are often susceptible to various interpretations and analyses, and many companies that have believed their products performed satisfactorily in preclinical studies and earlier clinical trials or investigations have nonetheless failed to produce strong results in later clinical trials or investigations. Products in later stages of clinical trials or investigations may fail to show the desired safety and efficacy despite having progressed through nonclinical studies and earlier clinical trials or investigations. We incur substantial expense for, and devote significant time to, clinical trials or investigations but cannot be certain that such trials will yield positive results relating to our products. Failure can occur at any stage of clinical testing. Our clinical trials or investigations may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical and non-clinical testing in addition to those we have planned.
The initiation and completion of any of our clinical trials may be prevented, delayed, or halted for numerous reasons. We may experience delays in our ongoing clinical trials for a number of reasons, which could adversely affect the costs, timing or successful completion of our clinical trials, including related to the following:
| • | We may be required to submit an Investigational Device Exemption, or IDE, application to the FDA, which must become effective prior to commencing certain human clinical trials of medical devices, and the FDA may reject our IDE application and notify us that we may not begin clinical trials; |
| • | Regulators and other comparable foreign regulatory authorities may disagree as to the design or conduct of our clinical trials or investigations; |
| • | Regulators and/or institutional review boards, or IRBs, or other reviewing bodies may not authorize us or our investigators to commence a clinical trial or investigation, or to conduct or continue a clinical trial or investigation at a prospective or specific trial site; |
| • | We may not reach agreement on acceptable terms with prospective contract research organizations, or CROs, and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
| • | Clinical trials or investigations may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical trials or investigations or abandon product development programs; |
65
Table of Contents
| • | The number of subjects or patients required for clinical trials may be larger than we anticipate, enrollment in these clinical trials or investigations may be insufficient or slower than we anticipate, and the number of clinical trials or investigations being conducted at any given time may be high and result in fewer available patients for any given clinical trial, or patients may drop out of these clinical trials or investigations at a higher rate than we anticipate; |
| • | Our third-party contractors, including those manufacturing products or conducting clinical trials or investigations on our behalf, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all; |
| • | We might have to suspend or terminate clinical trials or investigations for various reasons, including difficulties in patient enrollment or a finding that the subjects are being exposed to unacceptable health risks; |
| • | We may have to amend clinical trial or investigation protocols or conduct additional studies to reflect changes in regulatory requirements or guidance, which we may be required to submit to an IRB or other reviewing bodies and/or regulatory authorities for re-examination; |
| • | Regulators, IRBs or other reviewing bodies, or other parties may require or recommend that we or our investigators suspend or terminate clinical research for various reasons, including safety signals or noncompliance with regulatory requirements; |
| • | The cost of clinical trials or investigations may be greater than we anticipate; |
| • | Clinical sites may not adhere to our clinical protocol or may drop out of a clinical trial or investigation; |
| • | We may be unable to recruit a sufficient number of clinical trial or investigation sites; |
| • | Regulators, IRBs, or other reviewing bodies may fail to approve or subsequently find fault with our manufacturing processes or facilities of third-party manufacturers with which we enter into agreement for clinical and commercial supplies, the supply of devices or other materials necessary to conduct clinical trials or investigations may be insufficient, inadequate or not available at an acceptable cost, or we may experience interruptions in supply; |
| • | Approval policies or regulations of the FDA or applicable foreign regulatory agencies may change in a manner rendering our clinical data insufficient for approval; and |
| • | Our current or future products may have undesirable side effects or other unexpected characteristics. |
In addition, disruptions caused by the COVID-19 pandemic may increase the likelihood that we encounter such difficulties or delays in our planned and ongoing clinical trials or investigations. If COVID-19 continues to spread, we may experience disruptions that could have a material adverse impact on our clinical trial plans and timelines, including:
| • | Delays in receiving authorizations from local regulatory authorities to initiate planned clinical trials or investigations; |
| • | Delays or difficulties in enrolling patients in our clinical trials or investigations; |
| • | Delays or difficulties in clinical site initiation, including difficulties in recruiting clinical site investigators and clinical site staff; |
| • | Delays in clinical sites receiving the supplies and materials needed to conduct our clinical trials, including interruptions in global shipping that may affect the transport of clinical trial materials; |
| • | Changes in local regulations as part of a response to the COVID-19 pandemic which may require us to change the ways in which our clinical trials or investigations are conducted, which may result in unexpected costs, or to discontinue the clinical trials or investigations altogether; |
66
Table of Contents
| • | Diversion of healthcare resources away from the conduct of clinical trials or investigations, including the diversion of hospitals serving as our clinical trial sites and hospital staff supporting the conduct of our clinical trials or investigations; |
| • | Interruption of key clinical trial or investigation activities, such as clinical trial site monitoring, due to limitations on travel imposed or recommended by federal or state governments, employers and others, or interruption of clinical trial subject visits and study procedures, the occurrence of which could affect the integrity of clinical trial data; |
| • | Risk that participants enrolled in our clinical trials or investigations will contract COVID-19 while the clinical trial or investigation is ongoing, which could impact the results of the clinical trial or investigation, including by increasing the number of observed adverse events; |
| • | Delays in necessary interactions with local regulators, ethics committees and other third parties and contractors due to limitations in employee resources or forced furlough of government employees; |
| • | Limitations in employee resources that would otherwise be focused on the conduct of our clinical trials or investigations, including because of sickness of employees or their families or the desire of employees to avoid contact with large groups of people; and |
| • | Refusal of the FDA to accept data from clinical trials or investigations in affected geographies. |
Any of these factors may significantly harm our business, financial condition and prospects. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials or investigations may also ultimately lead to the denial of regulatory approval of our product candidates, which may also significantly harm our business, financial condition and prospects.
Patient enrollment in clinical trials or investigations and completion of patient follow-up depend on many factors, including the size of the patient population, the nature of the trial protocol, the proximity of patients to clinical sites, the eligibility criteria for the clinical trial or investigation, patient compliance, competing clinical trials or investigations and clinicians’ and patients’ perceptions as to the potential advantages of the product being studied in relation to other available therapies, including any new treatments that may be approved for the indications we are investigating. For example, patients may be discouraged from enrolling in our clinical trials or investigations if the trial protocol requires them to undergo extensive post-treatment procedures, monitoring or follow-up to assess the safety and efficacy of a product, or they may be persuaded to participate in contemporaneous clinical trials of a competitor’s product. In addition, patients participating in our clinical trials or investigations may drop out before completion of the trial or experience adverse medical events unrelated to our products. Delays in patient enrollment or failure of patients to continue to participate in a clinical trial or investigation may delay commencement or completion of the clinical trial or investigation, cause an increase in the costs of the clinical trial or investigation and delays, or result in the failure of the clinical trial.
Clinical trials and investigations must be conducted in accordance with the regulations of the FDA and other applicable regulatory authorities’ legal requirements, regulations or guidelines, and are subject to oversight by these governmental agencies and IRBs or other regulatory bodies at the medical institutions where the clinical trials or investigations are conducted. In addition, clinical trials and investigations must be conducted with supplies of our devices produced under QSR requirements and other regulations. Further, clinical trials of medical devices for investigational uses must be conducted in accordance with the FDA’s IDE regulations, which govern investigational device labeling, prohibit promotion of the device for investigational uses, and specify an array of recordkeeping, reporting and monitoring responsibilities of study sponsors and study investigators.
For certain devices which present a “significant risk” to human health, as defined by the FDA, the FDA requires the device sponsor to submit an IDE application to the FDA, which must become effective prior to commencing clinical trials. The FDA’s IDE regulations, among other things, govern investigational device labeling, prohibit promotion of the investigational device, and specify an array of recordkeeping, reporting and
67
Table of Contents
monitoring responsibilities of study sponsors and study investigators. Further, clinical trials of investigational devices which are non-significant risk devices must still comply with applicable regulatory requirements, including abbreviated IDE requirements, such as ensuring that investigators obtain informed consent, and labeling and record-keeping requirements. Regardless of the degree of risk presented by the medical device, clinical studies must be approved by, and conducted under the oversight of, an Institutional Review Board, or IRB, for each clinical site. We have in the past, and may in the future, conduct clinical trials and investigations that do not comply with all applicable regulations of the FDA and other applicable regulatory authorities’ legal requirements, regulations or guidelines. For example, we did not seek an IDE from the FDA for the conduct of the GEMINI trial, but instead submitted a justification to the IRB that OMNI was a non-significant risk device. The non-significant risk justification and informed consent documents for the GEMINI trial both initially described the trial as a post-market trial. Subsequently, we amended the study protocol and obtained informed consent for a revised description of the trial. Even if we conclude that the conduct of any of our clinical trials or investigations comply with the applicable requirements, regulations or guidelines, there can be no guarantee that the FDA or other applicable regulatory authorities will agree with such conclusion. The FDA may conclude that our ongoing or planned clinical studies require the submission and approval of an IDE, which would require us to devote additional resources to ensuring compliance with IDE requirements in the conduct of our clinical programs.
If the FDA determines that we have failed to comply with applicable regulatory requirements for the conduct of our clinical trials and investigations, the FDA may refuse to accept any data generated from such clinical trials and investigations in any future premarket applications, and may take a variety of other compliance or enforcement actions, which may result in, among other things, warning letters, untitled letters, fines, injunctions, consent decrees, civil penalties, unanticipated expenditures, repairs, replacements, refunds, recalls or seizures of products, operating restrictions, total or partial suspension of production, the FDA’s refusal to issue certificates to foreign governments needed to export products for sale in other countries, the FDA’s refusal to grant future premarket clearances or approvals, suspensions of current product clearances or approvals and criminal prosecution.
Furthermore, we may rely on CROs, and clinical trial sites to ensure the proper and timely conduct of our clinical trials or investigations and we may have limited influence over their actual performance. We depend on our collaborators and on medical institutions and CROs to conduct our clinical trials or investigations in compliance with good clinical practice, or GCP, requirements. To the extent our collaborators or the CROs fail to enroll participants for our clinical trials and investigations, fail to conduct the study to GCP standards or are delayed for a significant time in the execution of trials, including achieving full enrollment, we may be affected by increased costs, program delays or both. In addition, clinical trials and investigations that are conducted in countries outside the United States may subject us to further delays and expenses as a result of increased shipment costs, additional regulatory requirements and the engagement of non-U.S. CROs, as well as expose us to risks associated with clinical investigators who are unknown to the FDA, and different standards of diagnosis, screening and medical care.
Even if our future products are cleared or approved in the U.S., commercialization of our products in foreign countries would require clearance, certification or approval by regulatory authorities in those countries. Clearance, certification or approval procedures vary among jurisdictions and can involve requirements and administrative review periods different from, and greater than, those in the U.S., including additional preclinical studies or clinical trials or investigations. Any of these occurrences could have an adverse effect on our business, financial condition and results of operations.
68
Table of Contents
Changes in funding for, or disruptions caused by global health concerns impacting, the FDA and other government agencies could hinder their ability to hire and retain key leadership and other personnel, or otherwise prevent new products and services from being developed, cleared or approved or commercialized in a timely manner, which could negatively impact our business.
The ability of the FDA to review and approve new products can be affected by a variety of factors, including government budget and funding levels, ability to hire and retain key personnel and accept the payment of user fees, statutory, regulatory, and policy changes and other events that may otherwise affect the FDA’s ability to perform routine functions. Average review times at the agency have fluctuated in recent years as a result. In addition, government funding of other government agencies that fund research and development activities is subject to the political process, which is inherently fluid and unpredictable.
Disruptions at the FDA and other agencies may also slow the time necessary for new devices to be reviewed and/or approved or cleared by necessary government agencies, which would adversely affect our business. For example, over the last several years, including for 35 days beginning on December 22, 2018, the U.S. government has shut down several times and certain regulatory agencies, such as the FDA, have had to furlough critical FDA employees and stop critical activities. Separately, in response to the COVID-19 pandemic, on March 10, 2020, the FDA announced its intention to postpone inspections of foreign manufacturing facilities and products, and subsequently, on March 18, 2020, the FDA temporarily postponed routine surveillance inspections of domestic manufacturing facilities. Subsequently, on July 10, 2020 the FDA announced its intention to resume certain on-site inspections of domestic manufacturing facilities subject to a risk-based prioritization system. The FDA intends to use this risk-based assessment system to identify the categories of regulatory activity that can occur within a given geographic area, ranging from mission critical inspections to resumption of all regulatory activities. Other regulatory authorities may adopt similar restrictions or other policy measures in response to the COVID-19 pandemic. If a prolonged government shutdown occurs, or if global health concerns continue to prevent the FDA or other regulatory authorities from conducting business as usual or conducting inspections, reviews or other regulatory activities, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business.
In the European Union, Notified Bodies must be officially designated to certify products and services in accordance with the EU Medical Devices Regulation. Notified Bodies which have applied for designation under the EU Medical Devices Regulation are currently undergoing such designation assessments. Only a few Notified Bodies have been designated so far and the COVID-19 pandemic has significantly slowed down their designation process. Without EU Medical Devices Regulation designation, Notified Bodies may not yet start certifying devices in accordance with the new Regulation. This situation could impact the way we are conducting our business and lead to delays in recertification and compliance with the EU Medical Devices Regulation.
Under normal circumstances, medical devices manufacturers must undergo on-site audits by Notified Bodies in order to maintain their CE-mark certifications per the requirements of the EU Medical Devices Directive. As many CE-mark certifications will become void as part of the transition to the EU Medical Devices Regulation, Notified Bodies also have to start certifying medical devices in accordance with the EU Medical Devices Regulation. As another consequence of the COVID-19 pandemic, on-site Notified Bodies’ audits have not been feasible due to quarantine and travel restrictions and most of them have been postponed. Even though some specific measures have been implemented to determine whether remote audits can be conducted or be supplemented with an on-site audit once travel restrictions are lifted, this situation could significantly impact the ability of Notified Bodies to timely review and process our regulatory submissions, which could have a material adverse effect on our business.
69
Table of Contents
We are subject to certain federal, state and foreign fraud and abuse laws, health information privacy and security laws and transparency laws that could subject us to substantial penalties. Additionally, any challenge to or investigation into our practices under these laws could cause adverse publicity and be costly to respond to, and thus could harm our business.
There are numerous U.S. federal and state, as well as foreign, laws pertaining to healthcare fraud and abuse, including anti-kickback, false claims and physician transparency laws. Our business practices and relationships with providers are subject to scrutiny under these laws. We may also be subject to privacy and security regulation related to patient, customer, employee and other third-party information by both the federal government and the states and foreign jurisdictions in which we conduct our business. The healthcare laws and regulations that may affect our ability to operate include, but are not limited to:
| • | The federal Anti-Kickback Statute, which prohibits, among other things, persons and entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce either the referral of an individual or furnishing or arranging for a good or service, for which payment may be made, in whole or in part, under federal healthcare programs, such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it to have committed a violation. The U.S. government has interpreted this law broadly to apply to the marketing and sales activities of manufacturers. Moreover, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal civil False Claims Act. Violations of the federal Anti-Kickback Statute may result in significant civil monetary penalties, plus up to three times the remuneration involved. Civil penalties for such conduct can further be assessed under the federal False Claims Act. Violations can also result in criminal penalties, including significant criminal fines and imprisonment of up to 10 years. Similarly, violations can result in exclusion from participation in government healthcare programs, including Medicare and Medicaid; |
| • | The federal civil and criminal false claims laws and civil monetary penalties laws, including the federal civil False Claims Act, which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid or other federal healthcare programs that are false or fraudulent. These laws can apply to manufacturers who provide information on coverage, coding, and reimbursement of their products to persons who bill third-party payors. Private individuals can bring False Claims Act “qui tam” actions, on behalf of the government and such individuals, commonly known as “whistleblowers,” may share in amounts paid by the entity to the government in fines or settlement. When an entity is determined to have violated the federal civil False Claims Act, the government may impose significant civil fines and penalties for each false claim, plus treble damages, and exclude the entity from participation in Medicare, Medicaid and other federal healthcare programs; |
| • | The federal Civil Monetary Penalties Law, which prohibits, among other things, offering or transferring remuneration to a federal healthcare beneficiary that a person knows or should know is likely to influence the beneficiary’s decision to order or receive items or services reimbursable by the government from a particular provider or supplier; |
| • | The Health Insurance Portability and Accountability Act of 1996, or HIPAA, which created additional federal criminal statutes that prohibit, among other things, executing a scheme to defraud any healthcare benefit program and making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it to have committed a violation; |
| • | The federal Physician Payments Sunshine Act which requires certain applicable manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, or CHIP, to report annually to the DHHS Centers for Medicare and Medicaid Services, or CMS, information related to payments and other transfers of value to physicians, which is defined broadly to include other healthcare providers and |
70
Table of Contents
teaching hospitals, and applicable manufacturers and group purchasing organizations, to report annually ownership and investment interests held by physicians and their immediate family members. Additionally, on October 25, 2018, President Trump signed into law the “Substance Use-Disorder Prevention that Promoted Opioid Recovery and Treatment for Patients and Communities Act” which in part (under a provision entitled “Fighting the Opioid Epidemic with Sunshine”) extends the reporting and transparency requirements for physicians in the Physician Payments Sunshine Act to physician assistants, nurse practitioners, and other mid-level practitioners (with reporting requirements going into effect in 2022 for payments made in 2021). Applicable manufacturers are required to submit annual reports to CMS. Failure to submit required information may result in significant civil monetary penalties (and additional penalties for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately, and completely reported in an annual submission, and may result in liability under other federal laws or regulations; |
| • | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH Act, and their respective implementing regulations, which impose requirements on certain covered healthcare providers, health plans and healthcare clearinghouses as well as their business associates that perform services for them that involve individually identifiable health information, relating to the privacy, security and transmission of individually identifiable health information without appropriate authorization, including mandatory contractual terms as well as directly applicable privacy and security standards and requirements. Failure to comply with the HIPAA privacy and security standards can result in significant civil monetary penalties, and, in certain circumstances, criminal penalties with fines and/or imprisonment. State attorneys general can also bring a civil action to enjoin a HIPAA violation or to obtain statutory damages on behalf of residents of his or her state; |
| • | The FDCA, which prohibits, among other things, the adulteration or misbranding of drugs, biologics and medical devices; |
| • | Federal and state laws and regulations regarding billing and claims payment applicable to our products and regulatory agencies enforcing those laws and regulations; and |
| • | Analogous state and foreign law equivalents of each of the above federal laws, such as anti-kickback and false claims laws, which may apply to items or services reimbursed by any third-party payor, including commercial insurers or patients; state laws that require device companies to comply with the industry’s voluntary compliance guidelines and the applicable compliance guidance promulgated by the federal government or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; state laws that require device manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; consumer protection and unfair competition laws, which broadly regulate marketplace activities and activities that potentially harm customers, foreign and state laws, including the EU General Data Protection Regulation, or GDPR, governing the privacy and security of personal (including health) information in certain circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts; and state laws related to insurance fraud in the case of claims involving private insurers. |
These laws and regulations, among other things, constrain our business, marketing and other promotional and research activities by limiting the kinds of financial arrangements, including sales programs, we may have with hospitals, ambulatory surgery centers, physicians or other potential purchasers of our products. We have entered into consulting agreements with physicians, including some who have ownership interests in us, which could be viewed as influencing the purchase of or use of our products in procedures they perform. Compensation under some of these arrangements includes the provision of stock or stock options. Due to the breadth of these laws, the narrowness of statutory exceptions and regulatory safe harbors available, and the range of interpretations to which they are subject, it is possible that some of our current or future practices might be challenged under one or more of these laws.
71
Table of Contents
Any action brought against us for violations of these laws or regulations, even if successfully defended, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. We may be subject to private qui tam actions brought by individual whistleblowers on behalf of the federal or state governments, with potential liability under the federal False Claims Act including mandatory treble damages and significant per-claim penalties.
To enforce compliance with the healthcare regulatory laws, certain enforcement bodies have recently increased their scrutiny of interactions between healthcare companies and healthcare providers, which has led to a number of investigations, prosecutions, convictions and settlements in the healthcare industry. Responding to investigations can be time-and resource-consuming and can divert management’s attention from the business. Additionally, as a result of these investigations, healthcare providers and entities may have to agree to additional compliance and reporting requirements as part of a consent decree or corporate integrity agreement. Any such investigation or settlement could increase our costs or otherwise have an adverse effect on our business, financial condition and results of operations. Even an unsuccessful challenge or investigation into our practices could cause adverse publicity, and be costly to respond to.
Our activities, including those relating to providing billing, coding, coverage and reimbursement information about procedures using our products to our customers and the sale and marketing of our products, may be subject to scrutiny under these laws. The growth of our business and sales organization and our expansion outside of the United States may increase the potential of violating these laws or our internal policies and procedures. Any action brought against us for violation of these or other laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. If our operations are found to be in violation of any of the federal, state and foreign laws described above or any other current or future fraud and abuse or other healthcare laws and regulations that apply to us, we may be subject to significant penalties, including significant criminal, civil, and administrative penalties, damages, fines, exclusion from participation in government programs, such as Medicare and Medicaid, imprisonment, contractual damages, reputation harm and disgorgement and we could be required to curtail, restructure or cease our operations. Any of the foregoing consequences will negatively affect our business, financial condition and results of operations.
We are subject to governmental regulations and other legal obligations, particularly related to privacy, data protection and information security, and we are subject to consumer protection laws that regulate our marketing practices and prohibit unfair or deceptive acts or practices. Our actual or perceived failure to comply with such obligations could harm our business. Ensuring compliance with such laws could also impair our efforts to maintain and expand our customer base, and thereby decrease our revenue.
In the conduct of our business, we may at times process personal data, including health-related personal data. The U.S. federal government and various states have adopted or proposed laws, regulations, guidelines and rules for the collection, distribution, use and storage of personal information of individuals. We may also be subject to U.S. federal rules, regulations and guidance concerning data security for medical devices, including guidance from the FDA. According to the Federal Trade Commission, or the FTC, failing to take appropriate steps to keep consumers’ personal information secure constitutes unfair acts or practices in or affecting commerce in violation of Section 5(a) of the Federal Trade Commission Act, 15 U.S.C § 45(a). The FTC expects a company’s data security measures to be reasonable and appropriate in light of the sensitivity and volume of consumer information it holds, the size and complexity of its business, and the cost of available tools to improve security and reduce vulnerabilities. Individually identifiable health information is considered sensitive data that merits stronger safeguards. State privacy and security laws vary from state to state and, in some cases, can impose more restrictive requirements than U.S. federal law.
In addition, certain state and non-U.S. laws, such as the European Union General Data Protection Regulation (2016/679), or GDPR, govern the privacy and security of personal (including health) data in certain circumstances, some of which are more stringent than U.S. federal law and many of which differ from each other
72
Table of Contents
in significant ways and may not have the same effect, thus complicating compliance efforts. The GDPR is directly applicable in each member state and is extended to the EEA. Failure to comply with these laws, where applicable, can result in the imposition of significant civil and/or criminal penalties and private litigation. Where state laws are more protective, we must comply with the stricter provisions. In addition to fines and penalties that may be imposed for failure to comply with state law, some states also provide for private rights of action to individuals for misuse of personal information. For example, California enacted the California Consumer Privacy Act, or CCPA, on June 28, 2018, which went into effect on January 1, 2020. The CCPA creates individual privacy rights for California consumers and increases the privacy and security obligations of entities handling certain personal data. The CCPA provides for civil penalties for violations, as well as a private right of action for data breaches that is expected to increase data breach litigation. The CCPA may increase our compliance costs and potential liability, and many similar laws have been proposed at the federal level and in other states.
In Europe, the GDPR went into effect on May 25, 2018 and introduces strict requirements for processing the personal data of European Union data subjects. Companies that must comply with the GDPR face increased compliance obligations and risk, including more robust regulatory enforcement of data protection requirements and potential fines for noncompliance of up to €20 million or 4% of the annual global revenues of the preceding financial year of the noncompliant company, whichever is greater.
Among other requirements, the GDPR regulates transfers of personal data subject to the GDPR to third countries that have not been found to provide adequate protection to such personal data, including the United States, and the efficacy and longevity of current transfer mechanisms between the EU and the United States remains uncertain. For example, in 2016, the EU and United States agreed to a transfer framework for data transferred from the EU to the United States, called the Privacy Shield, but the Privacy Shield was invalidated in July 2020 by the Court of Justice of the European Union.
Further, from January 1, 2021, companies have to comply with the GDPR and also the United Kingdom General Data Protection Regulation, or the UK GDPR, which, together with the amended UK Data Protection Act 2018, retains the GDPR in UK national law. The UK GDPR mirrors the fines under the GDPR, i.e., fines up to the greater of €20 million (£17.5 million) or 4% of global turnover. The relationship between the United Kingdom and the European Union in relation to certain aspects of data protection law remains unclear, and it is also unclear how United Kingdom data protection laws and regulations will develop in the medium to longer term, and how data transfers to and from the United Kingdom will be regulated in the long term. These changes will lead to additional costs and increase our overall risk exposure. Currently there is a four to six month grace period agreed in the EU and United Kingdom Trade and Cooperation Agreement, ending June 30, 2021 at the latest, whilst the parties discuss an adequacy decision. The European Commission published a draft adequacy decision on February 19, 2021. If adopted, the decision will enable data transfers from EU member states to the United Kingdom for a four-year period, subject to subsequent extensions.
Any actual or perceived failure by us or the third parties with whom we work to comply with privacy or security laws, policies, legal obligations or industry standards, or any security incident that results in the unauthorized release or transfer of personally identifiable information, may result in governmental enforcement actions and investigations including by European Data Protection Authorities and U.S. federal and state regulatory authorities, fines and penalties, litigation and/or adverse publicity, including by consumer advocacy groups, and could cause our customers, their patients and other healthcare professionals to lose trust in us, which could harm our reputation and have a material adverse effect on our business, financial condition and results of operations.
We cannot assure you that any third-party service providers with access to our or our customers’, suppliers’, trial patients’ and employees’ personally identifiable and other sensitive or confidential information in relation to which we are responsible will not breach contractual obligations imposed by us, or that they will not experience data security breaches or attempts thereof, which could have a corresponding effect on our business, including putting us in breach of our obligations under privacy laws and regulations and/or which could in turn adversely
73
Table of Contents
affect our business, results of operations and financial condition. We cannot assure you that our contractual measures and our own privacy and security-related safeguards will protect us from the risks associated with the third-party processing, storage and transmission of such information. Increasing use of social media could also give rise to liability, breaches of data security or reputational damage.
Although we work to comply with applicable laws, regulations and standards, our contractual obligations and other legal obligations, these requirements are evolving and may be modified, interpreted and applied in an inconsistent manner from one jurisdiction to another, and may conflict with one another or other legal obligations with which we must comply. Any failure or perceived failure by us or our employees, representatives, contractors, consultants, CROs, collaborators, or other third parties to comply with such requirements or adequately address privacy and security concerns, even if unfounded, could result in additional cost and liability to us, damage our reputation, and adversely affect our business and results of operations.
Our employees, consultants, and other commercial partners may engage in misconduct or other improper activities, including non-compliance with regulatory standards and requirements.
We are exposed to the risk that our employees, consultants, distributors and other commercial partners and business associates may engage in fraudulent or other illegal activity. Misconduct by these parties could include intentional, reckless or negligent conduct or other unauthorized activities that violate the regulations of the FDA and other regulators (both domestic and foreign), including those laws requiring the reporting of true, complete and accurate information to such regulators, manufacturing standards, healthcare fraud and abuse laws and regulations in the U.S. and internationally or laws that require the true, complete and accurate reporting of financial information or data. In particular, sales, marketing and business arrangements in the healthcare industry, including the sale of medical devices, are subject to extensive laws and regulations intended to prevent fraud, misconduct, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. It is not always possible to identify and deter misconduct by our employees, consultants and other third parties, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to comply with these laws or regulations. If any such actions are instituted against us and we are not successful in defending ourselves or asserting our rights, those actions could result in the imposition of significant fines or other sanctions, including the imposition of civil, criminal and administrative penalties, damages, monetary fines, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings, and curtailment of operations, any of which could adversely affect our business, financial condition and results of operations. Whether or not we are successful in defending against such actions or investigations, we could incur substantial costs, including legal fees and reputational harm, and divert the attention of management in defending ourselves against any of these claims or investigations.
Compliance with environmental laws and regulations could be expensive, and the failure to comply with these laws and regulations could subject us to significant liability.
Our research and development operations involve the use of hazardous substances, such as isopropyl alcohol and various adhesives. We are subject to a variety of federal, state, local and foreign environmental laws and regulations relating to the storage, use, handling, generation, manufacture, treatment, discharge and disposal of, hazardous substances. Our products may also contain hazardous substances, and they are subject to laws and regulations relating to labelling requirements and to their sale, collection, recycling, treatment, storage and disposal. Compliance with these laws and regulations may be expensive and noncompliance could result in substantial fines and penalties. Environmental laws and regulations also impose liability for the remediation of releases of hazardous substances into the environment and for personal injuries resulting from exposure to hazardous substances, and they can give rise to substantial remediation costs and to third-party claims, including for property damage and personal injury. Liability under environmental laws and regulations can be joint and
74
Table of Contents
several and without regard to fault or negligence, and they tend to become more stringent over time, imposing greater compliance costs and increased risks and penalties associated with violations. We cannot assure you that violations of these laws and regulations, or releases of or exposure to hazardous substances, will not occur in the future or have not occurred in the past, including as a result of human error, accidents, equipment failure or other causes. The costs of complying with environmental laws and regulations, and liabilities that may be imposed for violating them, or for remediation obligations or responding to third-party claims, could negatively affect our business, financial condition and results of operations.
Healthcare policy changes, including recently enacted legislation reforming the U.S. healthcare system, could harm our business, financial condition and results of operations.
In the U.S., there have been and continue to be a number of legislative initiatives to contain healthcare costs. Federal and state lawmakers regularly propose and, at times, enact legislation that would result in significant changes to the healthcare system, some of which are intended to contain or reduce the costs of medical products and services. Current and future legislative proposals to further reform healthcare or reduce healthcare costs may limit coverage of or lower reimbursement for the procedures associated with the use of our products. The cost containment measures that payors and providers are instituting and the effect of any healthcare reform initiative implemented in the future could impact our revenue from the sale of our products. The Affordable Care Act, or ACA, made a number of substantial changes in the way healthcare is financed by both governmental and private insurers. Among other ways in which it may affect our business, the ACA:
| • | Imposed a new federal excise tax on the sale of certain medical devices, which was suspended, effective January 1, 2016, and permanently repealed in December 2019; |
| • | Established a new Patient-Centered Outcomes Research Institute to oversee and identify priorities in comparative clinical effectiveness research in an effort to coordinate and develop such research; |
| • | Implemented payment system reforms including a national pilot program on payment bundling to encourage hospitals, physicians and other providers to improve the coordination, quality and efficiency of certain healthcare services through bundled payment models; and |
| • | Expanded the eligibility criteria for Medicaid programs. |
Since its enactment, there have been judicial and Congressional challenges to certain aspects of the ACA, and we expect there will be additional challenges and amendments to the ACA in the future. By way of example, the Tax Cuts and Jobs Act of 2017, or TCJA, was enacted, which, among other things, removes penalties for not complying with the individual mandate to carry health insurance. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas (Texas District Court Judge) ruled that the individual mandate is a critical and inseverable feature of the ACA, and therefore, because it was repealed as part of the TCJA, the remaining provisions of the ACA are invalid as well. On December 18, 2019, the U.S. Court of Appeals for the 5th Circuit upheld the District Court ruling that the individual mandate was unconstitutional and remanded the case back to the District Court to determine whether the remaining provisions of the ACA are invalid as well. On March 2, 2020, the United States Supreme Court granted the petitions for writs of certiorari to review this case, and the Court held oral argument on November 10, 2020. The case is expected to be decided in mid-2021. It is unclear how this decision or other efforts to challenge, repeal or replace the ACA will impact the law and our business. Any expansion in the government’s role in the U.S. healthcare industry may result in decreased profits to us, lower reimbursement by payors for procedures using OMNI, and/or reduced medical procedure volumes, any of which may have a material adverse effect on our business, financial condition or results of operations.
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. The Budget Control Act of 2011, among other things, reduced Medicare payments to providers by 2% per fiscal year, effective on April 1, 2013 and, due to subsequent legislative amendments to the statute, will remain in effect through 2030, with the exception of a temporary suspension from May 1, 2020 through March 31, 2021, unless additional Congressional action is taken. Additionally, the American Taxpayer Relief Act
75
Table of Contents
of 2012, among other things, reduced Medicare payments to several providers, including hospitals, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. The Medicare Access and CHIP Reauthorization Act of 2015, or MACRA, enacted on April 16, 2015, repealed the formula by which Medicare made annual payment adjustments to physicians and replaced the former formula with fixed annual updates and a new system of incentive payments that are based on various performance measures and physicians’ participation in alternative payment models such as accountable care organizations. It is unclear what effect new quality and payment programs, such as MACRA, may have on our business, financial condition, results of operations or cash flows.
We expect additional state and federal healthcare policies and reform measures to be adopted in the future, any of which could limit reimbursement for healthcare products and services or otherwise result in reduced demand for our products or additional pricing pressure and have a material adverse effect on our industry generally and on our customers. We cannot predict what other healthcare programs and regulations will ultimately be implemented at the federal or state level or the effect of any future legislation or regulation in the U.S. may negatively affect our business, financial condition and results of operations. The continuing efforts of the government, insurance companies, managed care organizations and other payors of healthcare services to contain or reduce costs of healthcare may adversely affect:
| • | Our ability to set a price that we believe is fair for our products; |
| • | Our ability to generate revenue and achieve or maintain profitability; and |
| • | The availability of capital. |
Any changes of, or uncertainty with respect to, future coverage or reimbursement rates could affect demand for our products, which in turn could impact our ability to successfully commercialize these devices and could have a material adverse effect on our business, financial condition and results of operations.
Our ability to continue sales of our products in the European Union may be materially impaired if we do not take necessary steps to comply with the certification requirements of the new EU Medical Devices Regulation.
On May 25, 2017, the EU Medical Devices Regulation (Regulation 2017/745) entered into force, which repeals and replaces the EU Medical Devices Directive. Unlike directives, which must be implemented into the national laws of the EU member states, regulations are directly applicable (i.e., without the need for adoption of EU member state laws implementing them) in all EU member states and are intended to eliminate current differences in the regulation of medical devices among EU member states. The Medical Devices Regulation, among other things, is intended to establish a uniform, transparent, predictable and sustainable regulatory framework across the EU for medical devices and ensure a high level of safety and health while supporting innovation.
The Medical Devices Regulation was originally intended to become effective three years after publication, but in April 2020 the transition period was extended by the European Parliament and the Council of the EU by an additional year, until May 26, 2021. Devices lawfully placed on the market pursuant to the EU Medical Devices Directive prior to May 26, 2021 may generally continue to be made available on the market or put into service until May 26, 2025. Once effective, the new regulations will among other things:
| • | Strengthen the rules on placing devices on the market and reinforce surveillance once they are available; |
| • | Establish explicit provisions on manufacturers’ responsibilities for the follow-up of the quality, performance and safety of devices placed on the market; |
| • | Improve the traceability of medical devices throughout the supply chain to the end-user or patient through a unique identification number; |
76
Table of Contents
| • | Set up a central database to provide patients, healthcare professionals and the public with comprehensive information on products available in the EU; and |
| • | Strengthen the rules for the assessment of certain high-risk devices, which may have to undergo an additional check by experts before they are placed on the market. |
These modifications may have an effect on the way we design and manufacture products and conduct our business in the EU and EEA (also including Norway, Liechtenstein and Iceland). For example, as a result of the transition towards the new regime, notified body review times have lengthened, and product introductions or modifications could be delayed or canceled, which could adversely affect our ability to grow our business.
The EU-UK Trade and Cooperation Agreement, or TCA, came into effect on January 1, 2021. The TCA does not specifically refer to medical devices. However, as a result of Brexit, the EU Medical Devices Regulation will not be implemented in the UK, and previous legislation that mirrored the EU Medical Devices Regulation in the UK law has been revoked. The regulatory regime for medical devices in the UK will continue to be based on the requirements derived from current EU legislation, and the UK may choose to retain regulatory flexibility or align with the EU MDR going forward. CE markings will continue to be recognized in the UK, and certificates issued by EU-recognized Notified Bodies will be valid in the UK, until June 30, 2023. For medical devices placed on the UK market after this period, the UK Conformity Assessment (UKCA) marking will be mandatory. In contrast, UKCA marking and certificates issued by UK Notified Bodies will not be recognized on the EU market. The TCA does provide for cooperation and exchange of information in the area of product safety and compliance, including market surveillance, enforcement activities and measures, standardization related activities, exchanges of officials, and coordinated product recalls (or other similar actions). For medical devices that are locally manufactured but use components from other countries, the “rules of origin” criteria will need to be reviewed. Depending on which countries products will be ultimately sold in, manufacturers may start seeking alternative sources for components if this would allow them to benefit from no tariffs. The rules for placing medical devices on the Northern Ireland market will differ from those in the UK. These modifications may have an effect on the way we design and manufacture products and we conduct our business in these countries.
Risks Related to This Offering
Our common stock has never been publicly traded, and we expect that the price of our common stock will fluctuate substantially.
Before this initial public offering, there has been no public market for our common stock. The initial public offering price for our common stock will be determined through negotiations between the underwriters and us and may vary substantially from the market price of our common stock following this offering. An active public trading market may not develop after completion of this offering or, if developed, may not be sustained. The lack of an active market may impair your ability to sell your shares at the time you wish to sell them or at a price that you consider reasonable. An inactive market may also impair our ability to raise capital by selling shares and may impair our ability to acquire other products, technologies or businesses using our shares as consideration. Furthermore, although our common stock has been approved for listing on the , there can be no guarantee that we will continue to satisfy the continued listing standards of the . If we fail to satisfy such exchange’s continued listing standards, we could be de-listed, which would have a negative effect on the price of our common stock.
Following this offering, the market price of our common stock may be highly volatile and may fluctuate or decline substantially as a result of a variety of factors, some of which are beyond our control or are related in complex ways, including:
| • | Changes in analysts’ estimates, investors’ perceptions, recommendations by securities analysts or our failure to achieve analysts’ estimates; |
| • | Quarterly variations in our or our competitors’ results of operations; |
77
Table of Contents
| • | Periodic fluctuations in our revenue, which could be due in part to the way in which we recognize revenue; |
| • | The financial projections we may provide to the public, any changes in these projections or our failure to meet these projections; |
| • | Future sales of our common stock or other securities, by us or our stockholders, as well as the anticipation of lock-up releases or lock-up waivers; |
| • | The trading volume of our common stock; |
| • | General market conditions and other factors unrelated to our operating performance or the operating performance of our competitors; |
| • | Changes in reimbursement by current or potential payors; |
| • | Changes in operating performance and stock market valuations of other technology companies generally, or those in the medical device industry in particular; |
| • | Actual or anticipated changes in regulatory oversight of our products; |
| • | The results of our clinical trials; |
| • | The loss of key personnel, including changes in our board of directors and management; |
| • | Product recalls or other problems associated with our products; |
| • | Legislation or regulation of our market; |
| • | Lawsuits threatened or filed against us, including litigation by current or former employees alleging wrongful termination, sexual harassment, whistleblower or other claims; |
| • | The announcement of new products or product enhancements by us or our competitors; |
| • | Announced or completed acquisitions of businesses or technologies by us or our competitors; |
| • | Announcements related to patents issued to us or our competitors and related litigation; and |
| • | Developments in our industry. |
In addition, the trading prices for common stock of other medical device companies have been highly volatile as a result of the COVID-19 pandemic. The COVID-19 outbreak continues to rapidly evolve. The extent to which the outbreak may impact our business will depend on future developments, which are highly uncertain and cannot be predicted with confidence.
In recent years, the stock markets generally have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of listed companies. Broad market and industry factors may significantly affect the market price of our common stock, regardless of our actual operating performance. These fluctuations may be even more pronounced in the trading market for our common stock shortly following this offering. If the market price of shares of our common stock after this offering does not ever exceed the initial public offering price, you may not realize any return on your investment in us and may lose some or all of your investment.
In addition, in the past, stockholders have instituted securities class action litigation following periods of market volatility. If we were to become involved in securities litigation, it could subject us to substantial costs, divert resources and the attention of management from our business and harm our business, results of operations, financial condition and reputation. These factors may materially and adversely affect the market price of our common stock.
78
Table of Contents
Securities analysts may not publish favorable research or reports about our business or may publish no information at all, which could cause our stock price or trading volume to decline.
Our stock price and trading volume may be heavily influenced by the way analysts and investors interpret our financial information and other disclosures. If securities or industry analysts do not publish research or reports about our business, delay publishing reports about our business, or publish negative reports about our business, regardless of accuracy, our common stock price and trading volume could decline.
If a trading market for our common stock develops, the trading market will be influenced to some extent by the research and reports that industry or financial analysts publish about us and our business. We do not control these analysts. As a newly public company, we may be slow to attract research coverage and the analysts who publish information about our common stock will have had relatively little experience with us or our industry, which could affect their ability to accurately forecast our results and could make it more likely that we fail to meet their estimates. In the event we obtain securities or industry analyst coverage, if any of the analysts who cover us provide inaccurate or unfavorable research or issue an adverse opinion regarding our stock price, our stock price could decline. We may also fail to meet the expectations of these analysts, leading to a reduction in the market price of our common stock. If one or more of these analysts cease coverage of us or fail to publish reports covering us regularly, we could lose visibility in the market, which in turn could cause our stock price or trading volume to decline.
Even if our common stock is actively covered by analysts, we do not have any control over the analysts or the measures that analysts or investors may rely upon to forecast our future results. Over-reliance by analysts or investors on any particular metric to forecast our future results may lead to forecasts that differ significantly from our own.
We are an emerging growth company and a smaller reporting company and we cannot be certain if the reduced disclosure requirements applicable to us will make our common stock less attractive to investors.
We are an “emerging growth company,” as defined in the JOBS Act, and we expect to take advantage of certain exemptions and relief from various reporting requirements that are applicable to other public companies that are not emerging growth companies. In particular, while we are an emerging growth company, we will not be required to comply with the auditor attestation requirements of Section 404(b) of the Sarbanes-Oxley Act of 2002, or the Sarbanes-Oxley Act; we will be exempt from any rules that could be adopted by the Public Company Accounting Oversight Board requiring mandatory audit firm rotations or a supplement to the auditor’s report on financial statements; we will be subject to reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements; and we will not be required to hold nonbinding advisory votes on executive compensation or stockholder approval of any golden parachute payments not previously approved.
In addition, while we are an emerging growth company we can take advantage of an extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to take advantage of this extended transition period and, as a result, our operating results and financial statements may not be comparable to the operating results and financial statements of companies who have adopted the new or revised accounting standards.
We will remain an emerging growth company until the earlier of (1) December 31, 2026, (2) the last day of the fiscal year in which we have total annual gross revenue of at least $1.07 billion, (3) the last day of the fiscal year in which we are deemed to be a large accelerated filer, which requires the market value of our common stock that is held by non-affiliates to exceed $700.0 million as of the prior June 30th, or (4) the date on which we have issued more than $1.0 billion in non-convertible debt during the prior three-year period.
We are also a “smaller reporting company” as defined in the Exchange Act. We may continue to be a smaller reporting company even after we are no longer an emerging growth company. We may take advantage of
79
Table of Contents
certain of the scaled disclosures available to smaller reporting companies and will be able to take advantage of these scaled disclosures for so long as our voting and non-voting common stock held by non-affiliates is less than $250.0 million measured on the last business day of our second fiscal quarter, or our annual revenue is less than $100.0 million during the most recently completed fiscal year and our voting and non-voting common stock held by non-affiliates is less than $700.0 million measured on the last business day of our second fiscal quarter.
Investors may find our common stock less attractive to the extent we rely on the exemptions and relief granted by the JOBS Act. We have elected to take advantage of these exemptions and relief. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may decline or become more volatile.
If you purchase our common stock in this offering, you will incur immediate and substantial dilution in the book value of your shares.
Investors purchasing common stock in this offering will pay a price per share that substantially exceeds the pro forma as adjusted net tangible book value per share. As a result, investors purchasing common stock in this offering will incur immediate dilution of $ per share (or $ per share if the underwriters exercise their option to purchase additional shares in full), based on an initial public offering price of $ per share (the midpoint of the price range set forth on the cover page of this prospectus) and our pro forma as adjusted net tangible book value per share as of , 2021. For more information on the dilution you may suffer as a result of investing in this offering, see the section of this prospectus entitled “Dilution.” If outstanding options or warrants are exercised in the future, you will experience additional dilution.
This dilution is due to the substantially lower price paid by our investors who purchased shares prior to this offering as compared to the price offered to the public in this offering.
A significant portion of our total outstanding shares are restricted from immediate resale but may be sold into the market in the near future. This could cause the market price of our common stock to drop significantly, even if our business is doing well.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell their shares, could result in a decrease in the market price of our common stock. Upon the closing of this offering, we will have shares of common stock outstanding based on the number of shares outstanding as of , 2021. This includes the shares that we are selling in this offering, which may be resold in the public market immediately without restriction, unless purchased by our affiliates. Of the remaining shares, shares are currently restricted as a result of vesting restrictions, securities laws or 180-day lock-up agreements (which may be waived, with or without notice, by Morgan Stanley & Co. LLC and BofA Securities, Inc.) but will be able to be sold after the offering as described in the section of this prospectus entitled “Shares Eligible for Future Sale.” Moreover, after this offering, holders of an aggregate of up to shares of our common stock, including shares of our common stock issuable upon the conversion of the shares of our convertible preferred stock that will be outstanding immediately prior to the consummation of this offering, will have rights, subject to some conditions, to require us to file registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or other stockholders as described in the section of this prospectus entitled “Description of Capital Stock—Registration Rights.”
We also intend to register all shares of common stock that we may issue under our equity compensation plans. Once we register these shares, they can be freely sold in the public market, subject to volume limitations applicable to affiliates and the lock-up agreements described in the section of this prospectus entitled “Underwriters.”
Sales of our common stock as restrictions end or pursuant to registration rights may make it more difficult for us to sell equity securities in the future at a time and at a price that we deem appropriate. These sales also
80
Table of Contents
could cause the price of our common stock to fall and make it more difficult for you to sell shares of our common stock.
Our directors, executive officers and principal stockholders have significant voting power and may take actions that may not be in the best interests of our other stockholders.
After this offering, our executive officers, directors and principal stockholders each holding more than 5% of our common stock will collectively control approximately % of our outstanding common stock (assuming no exercise of the underwriters’ option to purchase additional shares of common stock). As a result, these stockholders, if they act together, will be able to control the management and affairs of our company and most matters requiring stockholder approval, including the election of directors and approval of significant corporate transactions. This concentration of ownership may have the effect of delaying or preventing a change of control and might adversely affect the market price of our common stock. This concentration of ownership may not be in the best interests of our other stockholders.
We may allocate the net proceeds from this offering in ways that you and other stockholders may not approve.
Our management will have broad discretion in the application of the net proceeds from this offering, including for any of the purposes described in the section titled “Use of Proceeds.” Because of the number and variability of factors that will determine our use of the net proceeds from this offering, their ultimate use may vary substantially from their currently intended use. Our management might not apply our net proceeds in ways that ultimately increase the value of your investment, and the failure by our management to apply these funds effectively could harm our business. Pending their use, we may invest the net proceeds from this offering in short- and intermediate-term, interest-bearing obligations, investment-grade instruments, certificates of deposit or direct or guaranteed obligations of the U.S. government. These investments may not yield a favorable return to our stockholders. If we do not invest or apply the net proceeds from this offering in ways that enhance stockholder value, we may fail to achieve expected results, which could cause our stock price to decline.
We will incur significant additional costs as a result of being a public company, and our management will be required to devote substantial time to compliance with our public company responsibilities and corporate governance practices.
Upon completion of this offering, we expect to incur costs associated with corporate governance requirements that will become applicable to us as a public company, including rules and regulations of the SEC, under the Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010, and the Exchange Act, as well as the rules of Nasdaq. These rules and regulations are expected to significantly increase our accounting, legal and financial compliance costs and make some activities more time-consuming. We expect such expenses to further increase after we are no longer an emerging growth company. We also expect these rules and regulations to make it more expensive for us to maintain directors’ and officers’ liability insurance. As a result, it may be more difficult for us to attract and retain qualified persons to serve on our board of directors or as executive officers. Furthermore, these rules and regulations will increase our legal and financial compliance costs and will make some activities more time-consuming and costly. We cannot predict or estimate the amount of additional costs we will incur as a public company or the timing of such costs. Accordingly, increases in costs incurred as a result of becoming a publicly traded company may adversely affect our business, financial condition and results of operations.
We may also be subject to more stringent state law requirements. For example, on September 30, 2018, California signed into law Senate Bill 826, which generally requires public companies with principal executive offices in California to have a minimum number of females on the company’s board of directors. By December 31, 2019, each public company with principal executive offices in California was required to have at least one female on its board of directors. By December 31, 2021, each public company is required to have at least two females on its board of directors if the company has at least five directors, and at least three females on
81
Table of Contents
its board of directors if the company has at least six directors. The new law does not provide a transition period for newly listed companies. We are currently compliant with the requirements, but there are no assurances that we will be compliant in the future. If we fail to comply with this new law, we could be fined by the California Secretary of State, with a $100,000 fine for the first violation and a $300,000 fine for each subsequent violation, and our reputation may be adversely affected. Further, in September 2020, California enacted AB 979 requiring public companies headquartered in California to maintain minimum representation on their boards of directors from members of underrepresented communities as follow: by the end of 2021, at least one director from an underrepresented community, by end of 2022, public company boards with more than four but fewer than nine members will be required to have at least two directors from underrepresented communities, and public company boards with nine or more members will be required to have at least three directors from underrepresented communities. Failure to achieve designated minimum levels in a timely manner exposes such companies to financial penalties and reputational harm. If we are unable to recruit, attract and/or retain qualified members of the board and meet the requirements of the California laws it may expose us to penalties and/or reputational harm.
If we fail to maintain effective internal control over financial reporting and effective disclosure controls and procedures, we may not be able to accurately report our financial results in a timely manner or prevent fraud, which may adversely affect investor confidence in our company.
We are not currently required to comply with the rules of the SEC implementing Section 404 and, therefore, we are not required to make a formal assessment of the effectiveness of our internal control over financial reporting for that purpose. Upon becoming a public company, we will be required to comply with the SEC’s rules implementing Sections 302 and 404 of the Sarbanes-Oxley Act, which require management to certify financial and other information in our quarterly and annual reports and provide an annual management report on the effectiveness of controls over financial reporting. Although we will be required to disclose changes made in our internal controls and procedures on a quarterly basis, we are not required to make our first annual assessment of our internal control over financial reporting pursuant to Section 404 until the year following our first annual report required to be filed with the SEC. As an emerging growth company, our independent registered public accounting firm will not be required to attest to the effectiveness of our internal control over financial reporting pursuant to Section 404 until the later of the year following our first annual report required to be filed with the SEC or the date we are no longer an emerging growth company. At such time, our independent registered public accounting firm may issue a report that is adverse in the event material weaknesses have been identified in our internal control over financial reporting.
To comply with the requirements of being a public company, we will need to undertake actions, such as implementing new internal controls and procedures and hiring additional accounting or internal audit staff. Testing and maintaining internal control can divert our management’s attention from other matters that are important to the operation of our business. In addition, when evaluating our internal control over financial reporting, we may identify material weaknesses that we may not be able to remediate in time to meet the applicable deadline imposed upon us for compliance with the requirements of Section 404. If we identify any material weaknesses in our internal controls over financial reporting or we are unable to comply with the requirements of Section 404 in a timely manner or assert that our internal control over financial reporting is effective, or if our independent registered public accounting firm is unable to express an opinion as to the effectiveness of our internal control over financial reporting once we are no longer an emerging growth company, investors may lose confidence in the accuracy and completeness of our financial reports. As a result, the market price of our common stock could be materially adversely affected.
Material weaknesses in our internal control over financial reporting may cause us to fail to timely and accurately report our financial results or result in a material misstatement of our financial statements.
In connection with the audit of our financial statements for the year ended December 31, 2020, we identified a material weakness in our internal controls due to a lack of sufficient full-time accounting personnel with
82
Table of Contents
requisite experience and deep technical accounting knowledge to (i) identify and resolve complex accounting issues under generally accepted accounting principles in the United States, or GAAP, and (ii) enable appropriate segregation of duties and reviews over the financial reviews over the financial close and reporting process.
We are evaluating and implementing additional internal controls and procedures to remediate this material weakness, however, we cannot assure you that these or other measures will fully remediate the material weakness in a timely manner or prevent future material weaknesses from occurring. As part of our remediation plan to address the material weakness identified above, we are actively working to hire additional accounting employees with specific technical accounting and financial reporting experience necessary for a public company. We will continue to assess the adequacy of our accounting personnel and resources, and will add additional personnel, as well as adjust our resources, as necessary, commensurate with any increase in the size and complexity of our business.
If we identify future material weaknesses in our internal controls over financial reporting or fail to meet the demands that will be placed upon us as a public company, including the requirements of the Sarbanes-Oxley Act, we may be unable to accurately report our financial results or report them within the timeframes required by law or stock exchange regulations. Failure to comply with Section 404 could also potentially subject us to sanctions or investigations by the SEC or other regulatory authorities. If additional material weaknesses exist or are discovered in the future, and we are unable to remediate any such material weaknesses, our reputation, financial condition, and operating results could suffer.
Provisions in our restated certificate of incorporation and restated bylaws and under Delaware law could make an acquisition of our company, which may be beneficial to our stockholders, more difficult and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our restated certificate of incorporation and our restated bylaws, which will become effective upon the closing of this offering may discourage, delay or prevent a merger, acquisition or other change in control of our company that stockholders may consider favorable, including transactions in which you might otherwise receive a premium for your shares. These provisions could also limit the price that investors might be willing to pay in the future for shares of our common stock, thereby depressing the market price of our common stock. In addition, because our board of directors is responsible for appointing the members of our management team, these provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors. Among other things, these provisions include those establishing:
| • | A classified board of directors with three-year staggered terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors; |
| • | No cumulative voting in the election of directors, which limits the ability of minority stockholders to elect director candidates; |
| • | The exclusive right of our board of directors to elect a director to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from filling vacancies on our board of directors; |
| • | The ability of our board of directors to authorize the issuance of shares of preferred stock and to determine the terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquirer; |
| • | The ability of our board of directors to alter our bylaws without obtaining stockholder approval; |
| • | The required approval of the holders of at least two-thirds of the shares entitled to vote at an election of directors to adopt, amend or repeal our bylaws or repeal the provisions of our restated certificate of incorporation regarding the election and removal of directors; |
| • | A prohibition on stockholder action by written consent, which forces stockholder action to be taken at an annual or special meeting of our stockholders; |
83
Table of Contents
| • | The requirement that a special meeting of stockholders may be called only by the chairman of the board of directors, the chief executive officer, the president or the board of directors, which may delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors; and |
| • | Advance notice procedures that stockholders must comply with in order to nominate candidates to our board of directors or to propose matters to be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquirer from conducting a solicitation of proxies to elect the acquirer’s own slate of directors or otherwise attempting to obtain control of us. |
Moreover, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the General Corporation Law of the State of Delaware, which prohibits a person who owns in excess of 15% of our outstanding voting stock from merging or combining with us for a period of three years after the date of the transaction in which the person acquired in excess of 15% of our outstanding voting stock, unless the merger or combination is approved in a prescribed manner.
Our restated certificate of incorporation will designate specific courts as the exclusive forum for certain litigation that may be initiated by our stockholders, which could limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us.
Our restated certificate of incorporation, which will become effective upon the closing of this offering, specifies that, unless we consent in writing to the selection of an alternative forum, the Court of Chancery of the State of Delaware will be the sole and exclusive forum for most legal actions involving claims brought against us by stockholders; provided that, the exclusive forum provision will not apply to suits brought to enforce any liability or duty created by the Securities Act, the Exchange Act, the rules and regulations thereunder or any other claim for which the federal courts have exclusive jurisdiction; and provided further that, if and only if the Court of Chancery of the State of Delaware dismisses any such action for lack of subject matter jurisdiction, such action may be brought in another state or federal court sitting in the State of Delaware. Our restated certificate of incorporation further provides that, unless we consent in writing to the selection of an alternative forum, the federal district courts of the United States of America shall, to the fullest extent permitted by law, be the sole and exclusive forum for the resolution of any complaint asserting a cause of action arising under the Securities Act. Any person or entity purchasing or otherwise acquiring any interest in shares of our capital stock shall be deemed to have notice of and to have consented to the provisions of our restated certificate of incorporation described above.
We believe these provisions benefit us by providing increased consistency in the application of Delaware law by chancellors particularly experienced in resolving corporate disputes and in the application of the Securities Act by federal judges, as applicable, efficient administration of cases on a more expedited schedule relative to other forums and protection against the burdens of multi-forum litigation. However, the provision may have the effect of discouraging lawsuits against our directors, officers, employees and agents as it may limit any stockholder’s ability to bring a claim in a judicial forum that such stockholder finds favorable for disputes with us or our directors, officers, employees or agents. The provision may also have the effect of resulting in increased costs to a stockholder seeking to bring a claim against our directors, officers, employees or agents. The enforceability of similar choice of forum provisions in other companies’ certificates of incorporation has been challenged in legal proceedings, and it is possible that, in connection with any applicable action brought against us, a court could find the choice of forum provisions contained in our restated certificate of incorporation to be inapplicable or unenforceable in such action. If a court were to find the choice of forum provision contained in our restated certificate of incorporation to be inapplicable or unenforceable in an action, we may incur additional costs associated with resolving such action in other jurisdictions, which could adversely affect our business, financial condition or results of operations.
84
Table of Contents
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This prospectus contains forward-looking statements about us and our industry. All statements other than statements of historical facts contained in this prospectus are forward-looking statements, including, but not limited to, statements regarding:
| • | Our plans to develop and commercialize our current or future technology or products; |
| • | The timing or outcome of our ongoing or planned clinical trials for OMNI, TearCare and any future products; |
| • | Business disruptions affecting our clinical trials, operations and financial results, including a public health emergency, such as the ongoing COVID-19 pandemic; |
| • | The timing and our ability to obtain and maintain regulatory approvals for OMNI, TearCare and any future products, and to comply with federal, state and foreign regulatory requirements; |
| • | The timing and our ability to obtain and maintain adequate levels of third-party coverage and reimbursement for OMNI, TearCare and any future products; |
| • | The clinical utility of our products; |
| • | Our commercialization, marketing and manufacturing capabilities and strategy; |
| • | Our expectation about the willingness of ECPs to use OMNI, TearCare and any future products; |
| • | Our expectation about the size of the addressable market for OMNI, TearCare and any future products; |
| • | Our intellectual property position, including the scope of protection we are able to obtain, maintain, protect and enforce for intellectual property rights covering our products and technology; |
| • | Our expected use of proceeds from this offering; |
| • | Our competitive position and the development of and projections relating to our competitors or our industry; |
| • | Our ability to identify, recruit and retain key personnel; |
| • | The impact of laws and regulations; |
| • | Our expectations regarding the time during which we will be an emerging growth company under the JOBS Act and a smaller reporting company under the Securities Act and Exchange Act; |
| • | Our estimates and statements regarding our future revenue, future results of operations and financial position; |
| • | Our business strategy; |
| • | Our research and development costs; |
| • | Our plans and objectives for future operations; and |
| • | The plans and objectives of management. |
These statements involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements. In some cases, you can identify forward-looking statements by terms such as “may,” “will,” “should,” “expect,” “plan,” “anticipate,” “could,” “intend,” “target,” “project,” “contemplate,” “believe,” “estimate,” “predict,” “potential,” “would” or “continue” or the negative of these terms or other similar expressions, although not all forward-looking statements contain these words. The forward-looking statements in this prospectus are only predictions and are
85
Table of Contents
based largely on our current expectations and projections about future events and financial trends that we believe may affect our business, financial condition and results of operations. These forward-looking statements speak only as of the date of this prospectus and are subject to a number of known and unknown risks, uncertainties and assumptions, including those described under the sections in this prospectus entitled “Risk Factors” and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in this prospectus. Because forward-looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified and some of which are beyond our control, you should not rely on these forward-looking statements as predictions of future events. The events and circumstances reflected in our forward-looking statements may not be achieved or occur and actual results could differ materially from those projected in the forward-looking statements. Moreover, we operate in an evolving environment. New risk factors and uncertainties may emerge from time to time, and it is not possible for management to predict all risk factors and uncertainties. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise.
86
Table of Contents
We obtained the market and industry data in this prospectus from our own internal estimates and research as well as from industry and general publications and research, surveys and studies conducted by third parties. Industry publications, studies and surveys generally state that they have been obtained from sources believed to be reliable, although they do not guarantee the accuracy or completeness of such information. While we believe that each of these studies and publications is reliable, we have not independently verified market and industry data from third-party sources. Management’s estimates are derived from publicly available information, their knowledge of our industry and their assumptions based on such information and knowledge, which we believe to be reasonable. While we believe our internal company research as to such matters is reliable and the market definitions are appropriate, neither such research nor these definitions have been verified by any independent source. These data involve a number of assumptions and limitations which are necessarily subject to a high degree of uncertainty and risk due to a variety of factors, including those described in “Risk Factors.” These and other factors could cause our future performance to differ materially from the assumptions and estimates made by the independent parties or us.
87
Table of Contents
We estimate that the net proceeds from this offering will be approximately $ million, assuming an initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. If the underwriters’ option to purchase additional shares from us is exercised in full, we estimate that our net proceeds will be approximately $ million, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
A $1.00 increase (decrease) in the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) the net proceeds to us from this offering by approximately $ million, assuming the number of shares offered by us, as set forth on the cover page of this prospectus, remains the same, and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. Similarly, each increase (decrease) of 1,000,000 shares in the number of shares offered by us would increase (decrease) the net proceeds to us from this offering by approximately $ million, assuming no change in the assumed initial public offering price of $ per share, and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
We anticipate that we will use the net proceeds from this offering, together with our existing cash and cash equivalents, for the following purposes:
| • | Approximately $ million to fund ongoing and future clinical trials for OMNI and TearCare; |
| • | Approximately $ million to support the marketing and sales efforts for our products; |
| • | Approximately $ million for research and development; and |
| • | The remainder for working capital and other general corporate purposes. |
This expected use of the net proceeds from this offering represents our intentions based upon our current plans and business conditions, which could change in the future as our plans and business conditions evolve. We may also use a portion of the net proceeds for acquisitions or strategic investments in complementary businesses, services, products, or technologies, although currently we have no specific agreements, commitments or understandings in this regard. As of the date of this prospectus, we cannot predict with certainty all of the particular uses for the net proceeds to be received upon the closing of this offering or the amounts that we will actually spend on the uses set forth above. Predicting the cost necessary to complete clinical trials can be difficult and we anticipate that we may need additional funds in the future. The amounts and timing of our actual expenditures and the extent of clinical development may vary significantly depending on numerous factors, including the progress of our development efforts and FDA feedback, the status of and results from our ongoing clinical trials or any clinical trials we may commence in the future, as well as the effectiveness of our commercial efforts and any unforeseen cash needs. As a result, our management will retain broad discretion over the allocation of the net proceeds from this offering.
Based on our current planned operations and planned use of the net proceeds from this offering, we expect that our cash and cash equivalents and additional borrowings available under our credit facility will enable us to fund our operations for at least the next twelve months. We have based this estimate on assumptions that may prove to be incorrect, and we could use our available capital resources sooner than we currently expect. We may satisfy our future cash needs through the sale of equity securities, debt financings, working capital lines of credit, corporate collaborations or license agreements, grant funding, interest income earned on invested cash balances or a combination of one or more of these sources.
Pending our use of the net proceeds from this offering, we intend to invest the net proceeds in a variety of capital preservation investments, including short-term and intermediate-term, interest-bearing, investment-grade, securities and government securities.
88
Table of Contents
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all available funds and future earnings, if any, to fund the operation, development and expansion of our business, and we do not anticipate paying any cash dividends in the foreseeable future. Any future determination regarding the declaration and payment of dividends will be at the discretion of our board of directors and will depend on then-existing conditions, including our financial condition, operating results, contractual restrictions, capital requirements, business prospects, and other factors our board of directors may deem relevant. In addition, we have entered into, and in the future may enter into additional, agreements that contain restrictions on payments of cash dividends, including the 2020 Term Loan and 2020 Revolver discussed elsewhere in this prospectus.
89
Table of Contents
The following table sets forth our cash and cash equivalents and capitalization as of , 2021:
| • | On an actual basis; |
| • | On a pro forma basis to give effect to (i) the automatic conversion of all outstanding shares of our redeemable convertible preferred stock into an aggregate of shares of common stock upon the closing of this offering, (ii) the automatic conversion of outstanding warrants to purchase shares of our redeemable convertible preferred stock into warrants to purchase shares of our common stock, and the related reclassification of redeemable convertible preferred stock warrant liability to additional paid in capital and (iii) the filing and effectiveness of our restated certificate of incorporation; and |
| • | On a pro forma as adjusted basis to give further effect to our issuance and sale of shares of common stock in this offering at an assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. |
The pro forma as adjusted information below is illustrative only, and our capitalization following the completion of this offering will be adjusted based on the actual initial public offering price and other terms of this offering determined at pricing. You should read the following table together with our financial statements and the related notes appearing at the end of this prospectus and the “Selected Financial Data,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “Description of Capital Stock” sections of this prospectus.
| As of , 2021 | ||||||||||||
| Actual | Pro Forma | Pro Forma As Adjusted (1) | ||||||||||
| (in thousands, except share data) | ||||||||||||
Cash and cash equivalents | $ | $ | $ | |||||||||
|
|
|
|
|
| |||||||
Convertible preferred stock warrant liability Long-term debt | ||||||||||||
Redeemable convertible preferred stock | ||||||||||||
Stockholders’ deficit: | ||||||||||||
Preferred stock, $0.001 par value; no shares authorized, issued or outstanding, actual; shares authorized and no shares issued or outstanding, pro forma and pro forma as adjusted | ||||||||||||
Common stock, par value $0.001 per share; 21,831,000 shares authorized, shares issued and outstanding, actual; shares authorized, pro forma and pro forma as adjusted; shares issued and outstanding, pro forma; shares issued and outstanding, pro forma as adjusted | ||||||||||||
Additional paid in capital | ||||||||||||
Accumulated deficit | ||||||||||||
|
|
|
|
|
| |||||||
Total stockholders’ (deficit) equity | ||||||||||||
|
|
|
|
|
| |||||||
Total capitalization | $ | $ | $ | |||||||||
|
|
|
|
|
| |||||||
| (1) | A $1.00 increase (decrease) in the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents, total stockholders’ (deficit) equity and total capitalization by approximately $ million, assuming that the number of shares |
90
Table of Contents
| offered by us remains the same and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. Similarly, each increase (decrease) of 1,000,000 shares in the number of shares offered by us at the assumed initial public offering price per share would increase (decrease) the pro forma as adjusted amount of each of cash and cash equivalents, total stockholders’ (deficit) equity and total capitalization by approximately $ , assuming the assumed initial public offering price of $ per share remains the same, and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. |
The information presented in the table above does not include:
| • | shares of our common stock issuable upon the exercise of stock options outstanding under our Existing Plan as of , 2021, at a weighted-average exercise price of $ per share; |
| • | shares of our common stock issuable upon the exercise of stock options granted after , 2021 under the Existing Plan; |
| • | shares of our common stock reserved for future issuance under our 2021 Plan, which will become effective in connection with this offering, as well as any automatic increases in the number of shares of our common stock reserved for future issuance under the 2021 Plan; |
| • | shares of our common stock that will become available for future issuance under our 2021 ESPP, which will become effective in connection with this offering, as well as any automatic increases in the number of shares of our common stock reserved for future issuance under the 2021 ESPP; and |
| • | shares of common stock issuable upon the exercise of warrants outstanding as of , 2021, at a weighted average exercise price of $ per share, which warrants shall not expire upon the closing of this offering if not exercised. |
91
Table of Contents
If you invest in our common stock in this offering, your ownership interest will be diluted immediately to the extent of the difference between the initial public offering price per share of our common stock and the pro forma as adjusted net tangible book value per share of our common stock immediately after this offering.
As of , 2021 we had a historical net tangible book value (deficit) of $ million, or $ per share of common stock. Our historical net tangible book value (deficit) is the amount of our total tangible assets less our total liabilities and the carrying value of our preferred stock, which is not included within stockholders’ equity. Historical net tangible book value (deficit) per share represents historical net tangible book value (deficit) divided by the number of shares of our common stock outstanding as of , 2021.
Our pro forma net tangible book value as of , 2021 was $ million, or $ per share of our common stock. Pro forma net tangible book value represents the amount of our total tangible assets less our total liabilities, after giving effect to the automatic conversion of all shares of our preferred stock outstanding as of , 2021 into an aggregate of shares of common stock upon the closing of this offering. Pro forma net tangible book value per share represents our pro forma net tangible book value divided by the total number of shares outstanding as of , 2021 after giving effect to the pro forma adjustment described above.
After giving further effect to receipt of the net proceeds from our issuance and the sale of shares of common stock in this offering at an assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us, our pro forma as adjusted net tangible book value as of , 2021 would have been approximately $ million, or approximately $ per share. This represents an immediate increase in pro forma as adjusted net tangible book value per share of $ to existing stockholders and immediate dilution in pro forma as adjusted net tangible book value per share of $ to new investors purchasing common stock in this offering. Dilution per share to new investors purchasing common stock in this offering is determined by subtracting the pro forma as adjusted net tangible book value per share after this offering from the assumed initial public offering price per share paid by new investors. The following table illustrates this dilution on a per share basis:
Assumed initial public offering price per share | $ | |||||||
Historical net tangible book value per share as of , 2021 | $ | |||||||
|
| |||||||
Increase (decrease) per share attributable to the pro forma adjustments described above | ||||||||
Pro forma net tangible book value (deficit) per share as of , 2021 | ||||||||
Increase per share attributable to this offering | ||||||||
|
| |||||||
Pro forma as adjusted net tangible book value per share after this offering | $ | |||||||
|
| |||||||
Dilution per share to new investors in this offering | $ | |||||||
|
|
The dilution information described above is illustrative only and will change based on the actual initial public offering price and other terms of this offering determined at pricing. A $1.00 increase (decrease) in the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) our pro forma as adjusted net tangible book value per share after this offering by $ , and dilution to new investors purchasing common stock in this offering by $ , assuming that the number of shares offered by us remains the same and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. Similarly, each increase (decrease) of 1,000,000 shares in the number of shares offered by us would increase (decrease) the total consideration paid by new investors by $ million and, in the case of an increase, would increase the
92
Table of Contents
percentage of total consideration paid by new investors by percentage points and, in the case of a decrease, would decrease the percentage of total consideration paid by new investors by percentage points, assuming no change in the assumed initial public offering price.
The table above assumes no exercise of the underwriters’ option to purchase additional shares in this offering. If the underwriters’ option to purchase additional shares is exercised in full, our pro forma as adjusted net tangible book value per share after this offering would be $ , representing an immediate increase in pro forma as adjusted net tangible book value per share of $ to existing stockholders and immediate dilution in pro forma as adjusted net tangible book value per share of $ to new investors purchasing common stock in this offering, assuming an initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, and after deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us.
The following table summarizes, as of , 2021, on the pro forma as adjusted basis described above, the total number of shares of common stock purchased from us on an as converted to common stock basis, the total consideration paid or to be paid, and the average price per share paid or to be paid by existing stockholders and by new investors purchasing common stock in this offering at an assumed initial public offering price of $ per share, which is the midpoint of the price range set forth on the cover page of this prospectus, before deducting estimated underwriting discounts and commissions and estimated offering expenses payable by us. As the table shows, new investors purchasing common stock in this offering will pay an average price per share substantially higher than our existing stockholders paid.
| Shares Purchased | Total Consideration | Average Price | ||||||||||||||||||
| Number | Percent | Amount | Percent | Per Share | ||||||||||||||||
Existing stockholders | % | $ | % | $ | ||||||||||||||||
New investors | ||||||||||||||||||||
Total | 100.0 | % | 100.0 | % | $ | |||||||||||||||
A $1.00 increase (decrease) in the assumed initial public offering price of $ per share, the midpoint of the price range set forth on the cover page of this prospectus, would increase (decrease) the total consideration paid by new investors by $ and, in the case of an increase, would increase the percentage of total consideration paid by new investors by percentage points and, in the case of a decrease, would decrease the percentage of total consideration paid by new investors by percentage points, assuming that the number of shares offered by us remains the same. Similarly, each increase (decrease) of 1,000,000 shares in the number of shares offered by us at the assumed public offering price would increase (decrease) the total consideration paid by new investors by $ million and, in the case of an increase, would increase the percentage of total consideration paid by new investors by percentage points and, in the case of a decrease, would decrease the percentage of total consideration paid by new investors by percentage points, assuming no change in the assumed initial public offering price.
The table above assumes no exercise of the underwriters’ option to purchase additional shares in this offering. If the underwriters’ option to purchase additional shares is exercised in full, the number of shares of our common stock held by existing stockholders would be reduced to % of the total number of shares of our common stock outstanding after this offering, and the number of shares of common stock held by new investors purchasing common stock in this offering would be increased to % of the total number of shares of our common stock outstanding after this offering.
The information presented in the tables and discussions above is based on the number of shares of our common stock outstanding as of , 2021, and excludes:
| • | shares of common stock issuable upon the exercise of stock options outstanding under our Existing Plan as of , 2021, at a weighted-average exercise price of $ per share; |
93
Table of Contents
| • | shares of common stock issuable upon the exercise of stock options granted after , 2021 under our Existing Plan; |
| • | additional shares of our common stock reserved for future issuance under our 2021 Plan, which will become effective in connection with this offering, as well as any automatic increases in the number of shares of our common stock reserved for future issuance under the 2021 Plan; |
| • | shares of our common stock that will become available for future issuance under our 2021 ESPP, which will become effective in connection with this offering, as well as any automatic increases in the number of shares of our common stock reserved for future issuance under the 2021 ESPP; and |
| • | shares of common stock issuable upon the exercise of warrants outstanding as of , 2021, at a weighted average exercise price of $ per share, which warrants shall not expire upon the closing of this offering if not exercised. |
To the extent that outstanding stock options or warrants are exercised, new stock options or warrants are issued, or we issue additional shares of common stock in the future, there will be further dilution to new investors purchasing common stock in this offering. In addition, we may choose to raise additional capital due to market conditions or strategic considerations, even if we believe we have sufficient funds for our current or future operating plans. If we raise additional capital through the sale of equity or convertible debt securities, the issuance of these securities could result in further dilution to our stockholders.
94
Table of Contents
We derived the selected consolidated statements of operations and comprehensive loss data for the fiscal years ended December 31, 2018, 2019 and 2020 and the consolidated balance sheet data as of December 31, 2019 and 2020 have been derived from our audited consolidated financial statements included elsewhere in this prospectus. The consolidated balance sheet data as of December 31, 2018 have been derived from our audited consolidated financial statements not included in this prospectus. The consolidated statement of operations and comprehensive loss data for the three months ended March 31, 2020 and 2021 and the consolidated balance sheet data as of March 31, 2021 have been derived from our unaudited condensed consolidated financial statements appearing elsewhere in this prospectus and have been prepared on the same basis as the audited consolidated financial statements. Results for the three months ended March 31, 2021 are not necessarily indicative of results to be expected for the full year. The selected consolidated financial data included in this section is not intended to replace the consolidated financial statements and related notes included elsewhere in this prospectus. You should read the selected financial data set forth below in conjunction with our consolidated financial statements, the notes to our financial statements and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” contained elsewhere in this prospectus. Our historical results are not necessarily indicative of our future performance.
| Years Ended December 31, | Three Months Ended March 31, | |||||||||||||||||||
| 2018 | 2019 | 2020 | 2020 | 2021 | ||||||||||||||||
| (in thousands, except share data) | ||||||||||||||||||||
Consolidated Statement of Operations and Comprehensive Loss Data | ||||||||||||||||||||
Revenue | $ | 7,530 | $ | 23,348 | $ | 27,640 | $ | 6,496 | $ | 8,635 | ||||||||||
Cost of goods sold(1) | 2,338 | 6,544 | 9,209 | 2,128 | 2,301 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Gross profit | 5,192 | 16,804 | 18,431 | 4,368 | 6,334 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Operating expenses: | ||||||||||||||||||||
Research and development(1) | 5,426 | 8,124 | 8,874 | 2,400 | 3,440 | |||||||||||||||
Selling, general and administrative(1) | 14,063 | 32,719 | 41,745 | 10,678 | 14,550 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Total operating expenses | 19,489 | 40,843 | 50,619 | 13,078 | 17,990 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Loss from operations | (14,297 | ) | (24,039 | ) | (32,188 | ) | (8,710 | ) | (11,656 | ) | ||||||||||
Interest income | 1 | 174 | 30 | 27 | — | |||||||||||||||
Interest expense | — | (1,961 | ) | (2,403 | ) | (552 | ) | (1,084 | ) | |||||||||||
Other income (expense), net | — | (35 | ) | (71 | ) | 91 | 552 | |||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Loss before income tax | (14,296 | ) | (25,861 | ) | (34,632 | ) | (9,144 | ) | (12,188 | ) | ||||||||||
Provision (benefit) for income tax | (6 | ) | 8 | 61 | 31 | 52 | ||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Net loss and comprehensive loss | $ | (14,290 | ) | $ | (25,869 | ) | $ | (34,693 | ) | $ | (9,175 | ) | $ | (12,240 | ) | |||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Net loss per share outstanding attributable to common stockholders, basic and diluted(2) | $ | (3.10 | ) | $ | (5.51 | ) | $ | (7.41 | ) | $ | (1.94 | ) | $ | (2.57 | ) | |||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Weighted-average common shares outstanding used in computing net loss per share attributable to common stockholders, basic and diluted(2) | 4,611,325 | 4,693,534 | 4,678,109 | 4,724,693 | 4,758,635 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Pro forma net loss per share outstanding, basic and diluted (unaudited) (2) | ||||||||||||||||||||
|
|
|
| |||||||||||||||||
Pro forma weighted-average common shares outstanding used in computing net loss per share attributable to common stockholders, basic and diluted (unaudited) (2) | ||||||||||||||||||||
|
|
|
| |||||||||||||||||
95
Table of Contents
| (1) | Includes stock-based compensation as follows: |
| Years Ended December 31, | Three Months Ended March 31, | |||||||||||||||||||
| 2018 | 2019 | 2020 | 2020 | 2021 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
Cost of goods sold | $ | 2 | $ | 3 | $ | 20 | $ | 1 | $ | 7 | ||||||||||
Research and development | 22 | 42 | 84 | 9 | 37 | |||||||||||||||
Selling, general and administrative | 28 | 73 | 393 | 51 | 233 | |||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
Total stock-based compensation expense | $ | 52 | $ | 118 | $ | 497 | $ | 61 | $ | 277 | ||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||
| (2) | See the statements of operations and Note 13 to our consolidated financial statements and Note 12 to our unaudited condensed consolidated financial statements included elsewhere in this prospectus for an explanation of the method used to compute the historical net loss per share and pro forma net loss per share and the number of shares used in the computation of the per share amounts for the years ended December 31, 2018, 2019 and 2020 and three months ended March 31, 2021. |
| As of December 31, | As of March 31, 2021 | |||||||||||||||
| Consolidated Balance Sheet Data | 2018 | 2019 | 2020 | |||||||||||||
| (in thousands) | ||||||||||||||||
Cash and cash equivalents | $ | 4,242 | $ | 21,237 | $ | 61,511 | $ | 48,327 | ||||||||
Working capital(1) | 4,268 | 20,665 | 61,319 | 48,239 | ||||||||||||
Total assets | 8,094 | 30,741 | 72,806 | 60,533 | ||||||||||||
Long-term debt | — | 12,855 | 31,955 | 32,124 | ||||||||||||
Redeemable convertible preferred stock | 34,153 | 64,256 | 117,331 | 117,331 | ||||||||||||
Additional paid-in capital | 512 | 660 | 1,173 | 1,475 | ||||||||||||
Accumulated deficit | (29,479 | ) | (55,348 | ) | (90,041 | ) | (102,281 | ) | ||||||||
Total stockholders’ deficit | (28,962 | ) | (54,683 | ) | (88,849 | ) | (100,801 | ) | ||||||||
| (1) | Working capital is defined as total current assets less total current liabilities. |
96
Table of Contents
MANAGEMENT’S DISCUSSION AND ANALYSIS OF
FINANCIAL CONDITION AND RESULTS OF OPERATIONS
You should read the following discussion and analysis of our financial condition and results of operations together with the section of this prospectus titled “Selected Financial Data” and our financial statements and the related notes included elsewhere in this prospectus. Some of the information contained in this discussion and analysis or set forth elsewhere in this prospectus, including information with respect to our plans and strategy for our business, includes forward-looking statements that involve risks and uncertainties. As a result of many factors, including those factors set forth in the “Risk Factors” section of this prospectus, our actual results could differ materially from the results described in or implied by these forward-looking statements. You should carefully read the “Risk Factors” to gain an understanding of the important factors that could cause actual results to differ materially from our forward-looking statements. Please also see the section of this prospectus titled “Special Note Regarding Forward-Looking Statements.”
Overview
Our mission is to transform ophthalmology and optometry through the development and commercialization of proprietary devices that target the underlying causes of the world’s most prevalent eye diseases. We are passionate about improving patients’ lives. Our business philosophy is grounded in the following principles: comprehensively understanding disease physiology, developing products that are intended to restore natural physiological functionality to diseased eyes; developing and marketing products that achieve superior effectiveness versus current treatment paradigms while minimizing complications or side effects, providing intuitive, patient friendly solutions to ophthalmologists and optometrists; and delivering compelling economic value to all stakeholders, including patients, providers and third-party payors such as Medicare and commercial insurers. Our objective is to develop and market products for use in new treatment paradigms and to create an interventional mindset in eyecare whereby our products may be used in procedures which supplant conventional outdated approaches. We believe current eyecare treatment models rely heavily on prescription medications, symptom relief, or either flawed or highly invasive, later-stage procedural interventions, and fail to adequately address the true underlying cause of disease. We have focused our initial product development on the treatment of two of the world’s most prevalent and underserved eye diseases, glaucoma and dry eye disease.
We have commercial products in each of our two reportable segments, Surgical Glaucoma and Dry Eye. Our Surgical Glaucoma segment consists of sales of the OMNI Surgical System, or OMNI, and also included sales of VISCO360 and TRAB360, OMNI’s predicate devices, until they were discontinued in the first quarter of 2019. Our Dry Eye segment includes sales of the TearCare System, or TearCare, and related components and accessories. For the year ended December 31, 2020 and for the three months ended March 31, 2021, 94% and 6% of our revenues were derived from our Surgical Glaucoma and Dry Eye segments, respectively. We primarily sell both systems through a highly-involved direct sales model that offers intensive education, training and customer service. We believe this philosophy and model not only enables us to differentiate our products and our overall company from competitors, but also to expand our addressable market by educating ECPs, patients and other stakeholders on our products and evolving treatment paradigms. Outside of the U.S., we have historically sold OMNI primarily through a network of distributors, although we began employing a small direct sales force outside of the United States in April 2021.
We commercially launched OMNI and TearCare in February 2018 and April 2019, respectively. In May 2020, we introduced a new version of the OMNI Surgical System called OMNI Next Gen that incorporated extensive feedback from our physician users and that we believe improved upon the first-generation device. We sell OMNI to facilities where ophthalmic surgeons perform outpatient procedures, mainly ASCs and HOPDs, which are typically reimbursed by Medicare or private payors for procedures using our products. We sell TearCare to optometrist and ophthalmologist practices. Currently, there is no meaningful reimbursement coverage by Medicare or private payors for MGD procedures, including TearCare, and patients typically pay out-of-pocket for TearCare. We are continuing our controlled commercial launch and are focused upon
97
Table of Contents
comprehensive, clinical data-driven long-term market development plan that aims to improve awareness and patient access to TearCare. As of March 31, 2021, we employed over 100 people to execute our commercial strategy in direct sales, marketing, training and professional services. The overall success of our approach to eyecare to date is evidenced by the over 60,000 estimated uses of OMNI and its direct predicates in over 1,000 hospitals and ASCs in the U.S. and Europe, and approximately 10,000 estimated uses of TearCare in nearly 400 eyecare facilities in the U.S. through April 30, 2021.
We have no manufacturing facilities of our own and instead contract with third parties for our production requirements. We believe our suppliers will be able to meet our current and anticipated manufacturing needs across all of our products. We do not currently plan to manufacture our products or any related components ourselves.
Our gross margin in our Surgical Glaucoma segment for the year ended December 31, 2020 and for the three months ended March 31, 2021 was 72.8% and 77.2%, respectively. Beginning with the production of finished goods inventory in February 2021, we are in the process of shifting our primary production of OMNI from a U.S.-based third-party contract manufacturer that has been able to partner closely with us on customization initiatives related to the development of OMNI and its predicate devices, to a network of lower cost, higher volume contract manufacturers in the U.S. and Asia. We believe that these cost optimization initiatives, which we expect to complete in 2021, will enable us to improve gross margins in our Surgical Glaucoma segment. The TearCare System includes the SmartHub component, which is typically only sold in initial purchase orders, and single-use SmartLids which are sold as part of initial purchase orders and through repeat orders as the ECP performs procedures over time. In an effort to build a meaningful TearCare installed base and encourage product trial and adoption by ECPs, our pricing strategy for SmartHubs has not focused on gross profit maximization. As the installed base of TearCare customers grows, we believe SmartLids, which generate higher gross margins than SmartHubs, will increase as a proportion of total Dry Eye segment revenues and gross profit. Given the earlier stage of TearCare’s commercial development and our pricing strategy with respect to SmartHubs, we expect our Dry Eye segment’s gross margins to be lower than our Surgical Glaucoma segment’s gross margins for the near and medium-term. Our gross margin for our Dry Eye segment for the year ended December 31, 2020 and for the three months ended March 31, 2021 was (30.5%) and 10.7%, respectively.
We believe in the importance of continued strategic investment in initiatives that: further demonstrate our products’ clinical effectiveness and safety to potential customers, patients, payors and regulators; enhance our commercial capabilities, including resources dedicated to sales, marketing and education; ensure the broadest possible patient access to the treatment alternatives that our products are cleared to offer, enhance and improve upon our existing product technologies; and allow us to innovate new products, devices or drugs, in glaucoma and DED or in new eye disease areas. As a result, we intend to continue to invest in clinical studies, sales and marketing, education initiatives, market access, and product development. Because of these and other factors, we expect to continue to incur net losses for at least the next several fiscal years. Moreover, we expect to incur additional expenses as a result of operating as a public company, including expenses related to compliance with the rules and regulations of the SEC and those of the Nasdaq Stock Market, additional insurance expenses, investor relations activities and other administrative and professional services. As a result of these and other factors, we may require and seek additional debt and equity financing to fund our operations and planned growth.
To date, our primary sources of capital have been private placements of redeemable convertible preferred stock, debt financing arrangements and revenue from sales of our products. Since inception, we have raised a total of $150.2 million in net proceeds from private placements of redeemable convertible preferred stock and the incurrence of debt. As of March 31, 2021, we had an outstanding term loan balance of $35.0 million (excluding debt discount and amortized debt issuance costs). As of March 31, 2021, we had cash and cash equivalents of $48.3 million and an accumulated deficit of $102.3 million.
During the years ended December 31, 2018, 2019 and 2020, we generated revenue of $7.5 million, $23.3 million, and $27.6 million, respectively, and $6.5 million and $8.6 million for the three months ended
98
Table of Contents
March 31, 2020 and 2021, respectively. Gross margin was 68.9%, 72.0%, and 66.7% for the years ended December 31, 2018, 2019, and 2020, respectively, and 67.3% and 73.4% for the three months ended March 31, 2020 and 2021, respectively. Our net loss was $14.3 million, $25.9 million, and $34.7 million for the years ended December 31, 2018, 2019, and 2020, respectively, and $9.2 million and $12.2 million for the three months ended March 31, 2020 and 2021, respectively. For all periods presented, substantially all of our revenue was generated from customers in the U.S.
Impact of COVID-19
In December 2019, a novel strain of coronavirus, COVID-19, emerged in Wuhan, China. The World Health Organization declared COVID-19 to be a pandemic, spreading across the globe and impacting worldwide economic activity. In 2020, certain U.S. federal, state and local governmental authorities issued stay-at-home orders, proclamations and/or directives, including restrictions on elective procedures and therapies, aimed at minimizing the spread of COVID-19. As such, the global COVID-19 pandemic impacted and is expected to continue to impact demand for our products, which are used in procedures and therapies that are considered elective. Although some of these governmental restrictions have since been lifted or scaled back, recent and future surges of COVID-19 may result in restrictions being re-implemented in response to efforts to reduce the spread of COVID-19. We experienced a significant decrease in our revenues for both of our products in the second quarter of 2020 as compared to the first quarter of 2020. As elective eye care procedures in many facilities that utilize our products were temporarily suspended by governmental authorities, many patients avoided visiting ECPs, and, even in areas that allowed elective procedures, ECPs and healthcare facilities in general substantially reduced or. in some cases halted, the scheduling and performance of such procedures. The decrease in demand for our products due to COVID-19 most significantly impacted our revenues in the latter part of the quarter ended March 31, 2020 and the first half of the quarter ended June 30, 2020. Beginning in June 2020, we began to see an increase in the number of procedures using our products. In the first quarter of 2021, our customers experienced a significant number of procedure cancellations which we believe were largely driven by patients postponing in-office treatments until their COVID-19 vaccinations were completed (as opposed to any restrictions imposed on elective procedures), impacting our revenues. As vaccine availability and the vaccinated population increases across the U.S., we expect the recovery of our end markets to resume in the second quarter of 2021 and throughout the remainder of the year, provided that the lifting of restrictions on elective procedures and therapies continues and such restrictions are not reimposed. As a result, we believe that over the course of 2021, there may be a modest benefit to our revenues as glaucoma and DED patients schedule previously deferred elective procedures, provided that the lifting of restrictions on elective procedures and therapies continues and such restrictions are not reimposed.
We are continuing to closely monitor the global COVID-19 pandemic. In order to operate in a safe manner, we are following the health and safety guidelines of the U.S. Centers for Disease Control and Prevention, Occupational Safety and Health Administration, and local and state public health departments where we operate. The majority of our employees at our headquarters have been asked to work from home, with only limited access given to employees to work in the office when necessary. For roles that require employees to be on-site, such as our R&D and manufacturing technical staff, we are providing protective equipment, practicing social distancing, and enforcing mask wearing and we have increased sanitization standards. In addition, we have created a business continuity plan and incident management team to respond quickly and effectively to COVID-19 related issues in order to offer customers uninterrupted products, services and support while safeguarding the best interests of employees, suppliers and stakeholders. The ultimate impact of the global COVID-19 pandemic on our operations is unknown and will depend on future developments which are highly uncertain and cannot be predicted with confidence, including the duration and severity of the COVID-19 pandemic, the status of health and safety actions taken to contain its spread and any additional preventative and protective actions that governments, or we, may direct, any resurgence of COVID-19 that may occur and how quickly and to what extent economic and operating conditions normalize within the markets in which we operate. The global COVID-19 pandemic could disrupt the operations of our third-party manufacturers and other suppliers. Although we have not experienced disruptions in our supply chain to date, we cannot predict how long the pandemic and measures intended to contain the spread of COVID-19 will continue and what effect COVID-19 and the associated containment measures will have on our suppliers and vendors, in particular for any of our suppliers
99
Table of Contents
and vendors that may not qualify as essential businesses and suffer more significant disruptions to their business operations. We are working closely with our manufacturing partners and suppliers to help ensure we are able to source key components and maintain appropriate inventory levels to meet customer demand.
Factors Affecting our Business and Results of Operations
We believe there are several important factors that have impacted and that will continue to impact our business and results of operations. These factors include, but are limited to:
Product Development
We believe our product development approach is a key differentiator of our team and our company. We are focused on continuous innovation and design and utilize input from our network of expert employees (including several ophthalmologists on staff), advisors and customers to rapidly iterate our pre-and post-commercial product designs with the aim of better satisfying the needs of our customers and their patients, and increasing adoption and utilization of our solutions. Once our products are launched, our customer feedback loop helps us further develop our products. This is particularly evident in the evolution of our OMNI Surgical System, which originated from the combined functionality of two internally developed, commercial predicate devices, each of which had their own multiple commercial iterations. We further refined ergonomics and functionality in OMNI Next Gen, which we launched in May 2020. Our future growth is dependent on our ability to continue innovating and applying our expertise of disease physiology to improve existing products and develop new products.
Market Education and Training on the Benefit of our Products vis-à-vis Existing Treatment Alternatives
One of the key drivers of our success is educating ophthalmologists, optometrists, patients, and third-party payors about the clinical and safety benefits of our products and of the benefits of more proactive, interventional approach to treating glaucoma and DED. We believe the required market education and development is best accomplished through a differentiated, highly involved commercial approach. As such, we devote significant resources to onboarding our sales professionals and to continuously augmenting their knowledge and capabilities. Our sales professionals provide ECPs with the necessary education, training and support to adopt and continue to use our products. We believe that increasing acceptance and usage of our products will require continued investment in our sales force and education efforts to ensure ECPs, patients and third-party payors learn more about our products and appreciate our benefits to their target patient populations.
Maximizing Product Usage by Customers
Demand for our products will be highly dependent on our ability to develop their potential addressable markets and maximize the breadth of patients our products can serve. OMNI is indicated for canaloplasty followed by trabeculotomy to reduce IOP in adult patients with POAG in the U.S. and with OAG, in the EU. We believe that OMNI is the only device that is authorized by the FDA as an ab interno procedure to: reduce IOP in adult patients with POAG across the spectrum of disease severity; be used in Mild-to-Moderate Combination Cataract or Standalone procedures; access 360 degrees of the diseased conventional outflow pathway through a single clear corneal incision; and facilitate two consecutive procedures, canaloplasty and trabeculotomy, to comprehensively treat all three primary points of resistance in the conventional outflow pathway in a single operating room visit. Our ability to establish OMNI as the standard of care for all POAG patients by continuing to grow its adoption and utilization in Combination Cataract procedures and by pioneering the development of the market for interventional Standalone procedures will have a substantial impact on our future growth.
TearCare serves as an elegant, compact, portable, intuitive solution that enables the application of localized heat to the eyelids in an anatomically customized way, and we believe it presents a compelling physiological profile to potentially address MGD. The current DED treatment market primarily consists of an abundance of OTC and prescription eyedrops that seek to lubricate the ocular surface, alleviate inflammation and/or increase
100
Table of Contents
tear production. However, OTC and prescription eyedrops are incapable of clearing obstructions in the meibomian glands and do not address MGD’s eyelid-borne physiology and poor tear quality. MGD is associated with 86% of DED cases and is a leading root cause of evaporative DED, which is characterized by low quality tears that evaporate prematurely. Clinical studies have demonstrated that treating MGD by liquefying and removing clogged meibum is the most effective method to eliminate obstructions and restore the lipid layer of tear film, thereby preventing premature evaporation of tears. TearCare was designed to be administered during the course of a routine office visit to an ECP, which makes it convenient for patients, and allows providers to maintain procedural throughput in their practices. Our ability to improve patient access and market education on TearCare and the benefits of proactive MGD treatment will be key drivers of TearCare’s future growth.
Operational excellence and cost efficiency
We aim to achieve operating and financial milestones with optimal capital efficiency, and focus on our market value relative to invested capital as a key measurement of our performance. Since our inception, we have received net proceeds of $150.2 million from equity and debt financings. With a portion of these net proceeds (our March 31, 2021 cash and equivalents was $48.3 million), we believe we have developed and commercially launched two clinically differentiated products, funded multiple completed and ongoing clinical trials, and built our management team and company infrastructure to support the continued growth of our business. We believe that this level of operational and commercial progress relative to our total capital investment to date compares favorably to medical technology peers. We seek to design products that can achieve attractive long-term gross margins. For example, we have targeted the achievement of significantly higher gross margins as one of our long-term objectives for our Surgical Glaucoma segment. The achievement of this objective will be supported by our shift to high-volume contract manufacturers in 2021.
Components of our Results of Operations
Revenue
We currently derive all of our revenue from the sale of OMNI to ASCs and HOPDs and TearCare to ophthalmology and optometry practices. During each of the years ended December 31, 2018, 2019, 2020 and the first quarter of 2021, the revenues from our Surgical Glaucoma segment, including OMNI and its predicate devices, accounted for over 90% of our total revenues. Substantially all of our revenues for 2018, 2019, 2020 and the first quarter of 2021 were generated from sales within the U.S. Our OMNI customers place orders based on their expected procedure volume and reorder as needed, typically on a biweekly, monthly or bimonthly basis. Our TearCare customers typically purchase a TearCare System which consists of one or more SmartHubs, multiple single-use SmartLids and other accessories. After utilizing their initial inventory, customers will reorder SmartLids as needed. No single customer accounted for 10% or more of our revenue for any of the years ended December 31, 2018, 2019 and 2020 and for the three months ended March 31, 2020 and 2021.
The growth in our revenue from 2018 to 2020 was driven by the demand for elective surgery and treatment utilizing our products. Such demand is often lower during summer months because of ECP vacations and in winter months in certain parts of the world because of fewer business or surgery days due to holidays and adverse weather conditions.
Cost of Goods Sold and Gross Margin
Our products are produced by third-party manufacturers. Our cost of goods sold consists primarily of amounts paid for our products to third-party manufacturers, and our manufacturing overhead costs, which consist primarily of personnel expenses, including salaries, benefits and stock-based compensation, and reserves for excess, obsolete and non-sellable inventory. Cost of goods sold also includes depreciation expenses for production equipment which we provide to our third-party manufacturers and certain direct costs, such as shipping and handling costs.
101
Table of Contents
We calculate gross margin as gross profit divided by revenue. Our gross margin has been and will continue to be affected by a variety of factors, including differences in segment gross margins, changes in average selling prices, product sales mix, production and ordering volumes, manufacturing costs, product yields, and headcount. In the near term, we expect our gross margins to increase as we transition production of OMNI to lower-cost manufacturers and as we expect Surgical Glaucoma revenues will grow as a percentage of our overall revenue mix. In general, we expect our gross margins to increase over the long-term to the extent our production and ordering volumes increase and to the extent we spread the fixed portion of our overhead costs over a larger number of units produced. We intend to use our design, engineering and manufacturing know-how and capabilities to further advance and improve the efficiency of our suppliers’ manufacturing processes, which we believe will reduce costs and increase our gross margins. Our gross margins could fluctuate from quarter to quarter as we transition to new suppliers, introduce new products and adopt new manufacturing processes and technologies.
Research and Development Expenses
Research and development, or R&D, expenses consist primarily of engineering, product development, clinical studies to develop and support our products, including clinical trial design, clinical trial site initiation and study costs, internal and external costs associated with our regulatory compliance and quality assurance functions, medical affairs, cost of products used for clinical trials and other costs associated with products and technologies – either new or enhancements of existing platforms – that are in development. These expenses also include personnel expenses, including salaries, benefits and stock-based compensation, supplies, consulting, prototyping, testing, materials, travel expenses, depreciation expenses for equipment and an allocation of IT and facility overhead expenses. Our R&D expenses as a percentage of revenue may vary over time depending on the level and timing of new product development efforts, as well as clinical development, clinical trial and other related activities. We expect our R&D expenses to increase for the next several years as we continue to invest in our active clinical trial program, develop new products and improve our existing products.
Selling, General and Administrative Expenses
Selling, general and administrative, or SG&A, expenses consist primarily of personnel expenses, including salaries, benefits and stock-based compensation related to selling, marketing and corporate functions, allocation of IT and facility overhead expenses, bad debt expense, finance, legal and human resource costs. Other SG&A expenses include training, travel expenses, promotional activities, marketing initiatives, market research and analysis, conferences and trade shows, professional services fees (including external legal, audit, consulting and tax fees), insurance costs, and general corporate expenses. We expect SG&A expenses to continue to increase in absolute dollars as we expand our infrastructure to both drive and support the anticipated growth in revenue and due to additional legal, accounting, insurance and other expenses associated with being a public company.
Interest Expense
Interest expense consists primarily of interest incurred on our outstanding indebtedness and non-cash interest related to the amortization of debt discount and issuance costs associated with our outstanding loan.
Interest Income
Interest income consists of interest earned on our balances of cash and cash equivalents.
Other Income (Expense), Net
Other income (expense), net primarily consists of gains and losses resulting from the remeasurement of the fair value of our redeemable convertible preferred stock warrant liability at each balance sheet date. We will continue to record adjustments to the estimated fair value of the redeemable convertible preferred stock warrants
102
Table of Contents
until they are exercised. At time of the redeemable convertible preferred stock warrants are exercised, the final fair value of the warrant liability will be reclassified to stockholders’ deficit and we will no longer record any related periodic fair value adjustments.
Results of Operations
Comparison of the Three Months Ended March 31, 2020 and 2021 (dollars in thousands)
| Three Months Ended, | Change | |||||||||||||||
| 2020 | 2021 | $ | % | |||||||||||||
| (unaudited) | ||||||||||||||||
Revenue | ||||||||||||||||
Surgical Glaucoma | $ | 6,100 | $ | 8,139 | $ | 2,039 | 33.4 | % | ||||||||
Percentage of total revenue | 93.9 | % | 94.3 | % | ||||||||||||
Dry Eye | 396 | 496 | 100 | 25.3 | % | |||||||||||
Percentage of total revenue | 6.1 | % | 5.7 | % | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 6,496 | 8,635 | 2,139 | 32.9 | % | |||||||||||
Cost of goods sold | ||||||||||||||||
Surgical Glaucoma | 1,514 | 1,858 | 344 | 22.7 | % | |||||||||||
Dry Eye | 614 | 443 | (171 | ) | (27.9 | )% | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 2,128 | 2,301 | 173 | 8.1 | % | |||||||||||
Gross profit | ||||||||||||||||
Surgical Glaucoma | 4,586 | 6,281 | 1,695 | 37.0 | % | |||||||||||
Dry Eye | (218 | ) | 53 | 271 | (124.3 | )% | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 4,368 | 6,334 | 1,966 | 45.0 | % | |||||||||||
Gross margin | ||||||||||||||||
Surgical Glaucoma | 75.2 | % | 77.2 | % | ||||||||||||
Dry Eye | (55.1 | )% | 10.7 | % | ||||||||||||
|
|
|
| |||||||||||||
Total | 67.3 | % | 73.4 | % | ||||||||||||
Operating expenses | ||||||||||||||||
Research and development | 2,400 | 3,440 | 1,040 | 43.3 | % | |||||||||||
Selling, general and administrative | 10,678 | 14,550 | 3,872 | 36.3 | % | |||||||||||
�� |
|
|
|
|
|
|
| |||||||||
Total operating expenses | 13,078 | 17,990 | 4,912 | 37.6 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss from operations | (8,710 | ) | (11,656 | ) | (2,946 | ) | (33.8 | )% | ||||||||
Interest income | 27 | — | (27 | ) | | — | ||||||||||
Interest expense | (552 | ) | (1,084 | ) | (532 | ) | (96.4 | )% | ||||||||
Other income (expense), net | 91 | 552 | 461 | 506.6 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss before income tax | (9,144 | ) | (12,188 | ) | (3,044 | ) | 33.3 | % | ||||||||
Provision (benefit) for income tax | 31 | 52 | 21 | 67.7 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss and comprehensive loss | $ | (9,175 | ) | $ | (12,240 | ) | $ | (3,065 | ) | 33.4 | % | |||||
|
|
|
|
|
|
|
| |||||||||
Revenue. Revenue in three months ended March 31, 2021 was $8.6 million, an increase of $2.1 million, or 32.9%, from our revenue in the three months ended March 31, 2020. Surgical Glaucoma and Dry Eye sales contributed $2.0 million and $0.1 million, respectively, to such increase from 2020 to 2021. The overall increase in Surgical Glaucoma revenue was primarily attributable to an increase in the number of OMNI units sold due to a higher number of ordering facilities and a higher average amount of units per order. This was partially offset by a modest decrease in our average selling prices. Our Dry Eye revenue growth was the result of an increased amount of SmartLids reordered by our existing customer base. Surgical Glaucoma sales represented 93.9% and 94.3% of our revenue generated in the three months ended March 31, 2020 and 2021, respectively.
103
Table of Contents
Cost of Goods Sold and Gross Profit. The $0.2 million increase in cost of goods sold during the three months ended March 31, 2021 compared to the three months ended March 31, 2020 was attributable to a $0.4 million increase in cost of materials and manufacturing overhead driven by increased production to support our sales growth, which was partially offset by a decrease of $0.2 million in our inventory write-down reserve.
Our total gross profit increased $1.9 million from $4.4 million to $6.3 million during the three months ended March 31, 2021 compared to the three months ended March 31, 2020. Our total gross margin increased from 67.3% to 73.4% between the three months ended March 31, 2020 and 2021 primarily due to a higher volume of OMNI units sold. Gross margin in our Surgical Glaucoma segment increased from 75.2% to 77.2% during the three months ended March 31, 2021 compared to the three months ended March 31, 2020, and in our Dry Eye segment gross margin increased from (55.1)% to 10.7% during the three months ended March 31, 2021 compared to the three months ended March 31, 2020 due, in part, to lower average selling prices in 2020 for both SmartHubs and SmartLids designed to encourage new user adoption.
Research and Development Expenses. The $1.0 million increase in R&D expenses during the three months ended March 31, 2021 compared to the three months ended March 31, 2020 was primarily attributable to $0.3 million increase in personnel expenses as a result of increased headcount, $0.2 million net increase in contract manufacturing, lab supplies and Dry Eye product prototype development expenses, $0.2 million in legal services mainly related to registration of patents and $0.3 million in other services driven by overall increase in business activities.
Selling, General, and Administrative Expenses. The $3.9 million increase in SG&A expenses during the three months ended March 31, 2021 compared to the three months ended March 31, 2020 was primarily due to our continued commercial investment and scaling of operations and corporate headcount to support our growth, which resulted in an increase of $2.5 million in personnel expenses through headcount increases during the year, and a $1.4 million net increase in non-personnel SG&A expenses. Our largest areas of growth in non-personnel SG&A expenses between three months ended March 31, 2020 and 2021 were legal fees related to regulatory matters, particularly related to the March 2021 FDA clearance of OMNI’s expanded Indication for Use.
Interest Expense. The $0.5 million increase in interest expense during the three months ended March 31, 2021 compared to the three months ended March 31, 2020 was attributable to the increase in average debt outstanding due to our debt financing in November 2020.
Interest Income and Other Income (Expense), Net. Interest income did not change significantly during the three months ended March 31, 2021 compared to the three months ended March 31, 2020. The increase in other income (expense), net of $0.5 million, during the three months ended March 31, 2021 compared to the three months ended March 31, 2020 was attributable primarily to the remeasurement of our convertible preferred stock warrants and recognition of the change in fair value.
104
Table of Contents
Comparison of the Years Ended December 31, 2019 and 2020 (dollars in thousands)
| Years Ended, | Change | |||||||||||||||
| 2019 | 2020 | $ | % | |||||||||||||
Revenue | ||||||||||||||||
Surgical Glaucoma | $ | 22,304 | $ | 26,000 | $ | 3,696 | 16.6 | % | ||||||||
Percentage of total revenue | 95.5 | % | 94.1 | % | ||||||||||||
Dry Eye | 1,044 | 1,640 | 596 | 57.1 | % | |||||||||||
Percentage of total revenue | 4.5 | % | 5.9 | % | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 23,348 | 27,640 | 4,292 | 18.4 | % | |||||||||||
Cost of goods sold | ||||||||||||||||
Surgical Glaucoma | 5,132 | 7,069 | 1,937 | 37.7 | % | |||||||||||
Dry Eye | 1,412 | 2,140 | 728 | 51.6 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 6,544 | 9,209 | 2,655 | 40.7 | % | |||||||||||
Gross profit | ||||||||||||||||
Surgical Glaucoma | 17,172 | 18,931 | 1,759 | 10.2 | % | |||||||||||
Dry Eye | (368 | ) | (500 | ) | (132 | ) | 35.9 | % | ||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 16,804 | 18,431 | 1,627 | 9.7 | % | |||||||||||
Gross margin | ||||||||||||||||
Surgical Glaucoma | 77.0 | % | 72.8 | % | ||||||||||||
Dry Eye | (35.2 | )% | (30.5 | )% | ||||||||||||
Total | 72.0 | % | 66.7 | % | ||||||||||||
Operating expenses | ||||||||||||||||
Research and development | 8,124 | 8,874 | 750 | 9.2 | % | |||||||||||
Selling, general and administrative | 32,719 | 41,745 | 9,026 | 27.6 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Total operating expenses | 40,843 | 50,619 | 9,776 | 23.9 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss from operations | (24,039 | ) | (32,188 | ) | (8,149 | ) | 33.9 | % | ||||||||
Interest income | 174 | 30 | (144 | ) | (82.8 | )% | ||||||||||
Interest expense | (1,961 | ) | (2,403 | ) | (442 | ) | 22.5 | % | ||||||||
Other income (expense), net | (35 | ) | (71 | ) | (36 | ) | 102.9 | % | ||||||||
|
|
|
|
|
|
|
| |||||||||
Loss before income tax | (25,861 | ) | (34,632 | ) | (8,771 | ) | 33.9 | % | ||||||||
Provision (benefit) for income tax | 8 | 61 | 53 | 662.5 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss and comprehensive loss | $ | (25,869 | ) | $ | (34,693 | ) | $ | (8,824 | ) | 34.1 | % | |||||
|
|
|
|
|
|
|
| |||||||||
Revenue. Revenue in 2020 was $27.6 million, an increase of $4.3 million, or 18.4%, from our revenue in 2019. Surgical Glaucoma and Dry Eye sales contributed $3.7 million and $0.6 million, respectively, to such increase from 2019 to 2020. The overall increase in revenue was primarily attributable to an increase in the number of OMNI units sold, which resulted in a $3.9 million increase in Surgical Glaucoma revenues, as well as the benefit of a full year of commercial sales of our Dry Eye Segment’s TearCare System, which was launched in April 2019. These increases were partially offset by $0.2 million of revenue decrease from 2019 to 2020 due to the discontinuation of TRAB360 and VISCO360 sales in March 2019. Throughout 2019 and 2020, we expanded our overall commercial team from 31 professionals as of January 1, 2019 to 82 professionals as of December 31, 2020. As a result, we increased the number of surgeons and facilities that have been trained on, and the number of facilities that order, OMNI and TearCare. Revenue for the full year 2020 was negatively impacted by a steep decline in the number of products sold, in particular, during the second quarter of 2020 due primarily to the effects of the global COVID-19 pandemic. As a result, our revenues for the second quarter of 2020 decreased by $2.5 million as compared to the second quarter of 2019. Surgical Glaucoma represented 95.5% and 94.1% of our revenues generated in 2019 and 2020, respectively.
105
Table of Contents
Cost of Goods Sold and Gross Profit. The $2.7 million increase in cost of goods sold from 2019 to 2020 was attributable to a $1.4 million write-down in 2020 of legacy OMNI inventory which is being replaced with OMNI Next Gen units, and a $1.3 million increase in the cost of materials and manufacturing overhead driven by increased production to support our sales growth and as a result of increased headcount.
Our total gross profit increased $1.6 million from $16.8 million to $18.4 million from 2019 to 2020. Our total gross margin declined from 72.0% to 66.7% between 2019 and 2020 primarily due to the legacy OMNI inventory write-down and increased sales in our lower margin Dry Eye segment as a percentage of total sales. Gross margin in our Surgical Glaucoma segment decreased from 77.0% in 2019 to 72.8% in 2020, and in our Dry Eye segment gross margin increased from (35.2)% in 2019 to (30.5)% in 2020. Excluding our OMNI inventory write-down, Surgical Glaucoma gross margins in 2020 would have increased to 78.2% due to a higher volume of units sold covering fixed costs. Our Dry Eye segment had a lower gross margin than our Surgical Glaucoma segment because TearCare is earlier in its commercial cycle than OMNI and SmartHub equipment is priced to encourage new user adoption rather than to maximize gross profit for its one-time, upfront purchase by ECPs. Our Dry Eye segment had a negative gross margin in each of 2019 and 2020, due primarily to $0.1 million and $0.4 million of inventory reserve charges in 2019 and 2020, respectively, and sales unit volumes which were not sufficient to cover $0.6 million and $0.9 million of unabsorbed manufacturing overhead in 2019 and 2020, respectively.
Research and Development Expenses. The $0.8 million increase in R&D expenses from 2019 to 2020 was primarily attributable to costs related to OMNI Next Gen, including an increase of $0.5 million in contract manufacturing for Dry Eye product development, $0.4 million in patent related legal expenses, $0.3 million in facility and information technology related expenses to support business growth and an increase of $0.3 million in personnel expenses primarily as a result of increased headcount, partially offset by a decrease of $0.1 million in travel expenses due in part to the global COVID-19 pandemic, and a decrease of $0.5 million in costs associated with our clinical studies as a result of completion of two clinical trials during the year. We expect our clinical trial costs to increase as we initiate and execute additional clinical trials over the coming years, develop new products and improve our existing products.
Selling, General, and Administrative Expenses. The $9.0 million increase in SG&A expenses from 2019 to 2020 was primarily due to our continued commercial investment and scaling of operations and corporate headcount to support our growth, which resulted in an increase of $7.6 million in personnel expenses through headcount increases during the year, and a $1.4 million net increase in non-personnel SG&A expenses. Our largest areas of growth in non-personnel SG&A expenses between 2019 and 2020 were promotional and advertisement expenses related to OMNI Next Gen launch, facility and information technology related expenses to support business growth, and legal fees related to general and regulatory matters. These increases were partially offset by a decrease in conference, tradeshows, training and travel expenses as a result of the global COVID-19 pandemic.
Interest Expense. The $0.4 million increase in interest expense from 2019 to 2020 was attributable to the debt financing in November 2020.
Interest Income and Other Income (Expense), Net. The $0.1 million decrease in interest income from 2019 to 2020 was primarily due to lower interest on our cash and equivalents in 2020. The increase in other income (expense), net, from 2019 to 2020 was attributable primarily to the remeasurement of our convertible preferred stock warrants and recognition of the change in fair value.
106
Table of Contents
Comparison of the Years Ended December 31, 2018 and 2019 (dollars in thousands)
| Years Ended, | Change | |||||||||||||||
| 2018 | 2019 | $ | % | |||||||||||||
Revenue | ||||||||||||||||
Surgical Glaucoma | $ | 7,530 | $ | 22,304 | $ | 14,774 | 196.2 | % | ||||||||
Percentage of total revenue | 100 | % | 95.5 | % | ||||||||||||
Dry Eye | — | 1,044 | 1,044 | — | ||||||||||||
Percentage of total revenue | — | 4.5 | % | |||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 7,530 | 23,348 | 15,818 | 210.1 | % | |||||||||||
Cost of goods sold | ||||||||||||||||
Surgical Glaucoma | 2,338 | 5,132 | 2,794 | 119.5 | % | |||||||||||
Dry Eye | — | 1,412 | 1,412 | — | ||||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 2,338 | 6,544 | 4,206 | 179.9 | % | |||||||||||
Gross profit | ||||||||||||||||
Surgical Glaucoma | 5,192 | 17,172 | 11,980 | 230.7 | % | |||||||||||
Dry Eye | — | (368 | ) | (368 | ) | — | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Total | 5,192 | 16,804 | 11,612 | 224 | % | |||||||||||
Gross margin | ||||||||||||||||
Surgical Glaucoma | 68.9 | % | 77.0 | % | ||||||||||||
Dry Eye | — | (35.2 | )% | |||||||||||||
|
|
|
| |||||||||||||
Total | 68.9 | % | 72.0 | % | ||||||||||||
Operating expenses | ||||||||||||||||
Research and development | 5,426 | 8,124 | 2,698 | 49.7 | % | |||||||||||
Selling, general and administrative | 14,063 | 32,719 | 18,656 | 132.7 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Total operating expenses | 19,489 | 40,843 | 21,354 | 109.6 | % | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss from operations | (14,297 | ) | (24,039 | ) | (9,742 | ) | 68.1 | % | ||||||||
Interest income | 1 | 174 | 173 | 17,300.0 | % | |||||||||||
Interest expense | — | (1,961 | ) | (1,961 | ) | — | ||||||||||
Other income (expense), net | — | (35 | ) | (35 | ) | — | ||||||||||
|
|
|
|
|
|
|
| |||||||||
Loss before income tax | (14,296 | ) | (25,861 | ) | (11,565 | ) | 80.9 | % | ||||||||
Provision (benefit) for income tax | (6 | ) | 8 | 14 | — | |||||||||||
|
|
|
|
|
|
|
| |||||||||
Net loss and comprehensive loss | $ | (14,290 | ) | $ | (25,869 | ) | (11,579 | ) | 81.0 | % | ||||||
|
|
|
|
|
|
|
| |||||||||
Revenue. Revenue in 2019 was $23.3 million, an increase of $15.8 million, or 210.1%, from our revenue in 2018. Sales from our Surgical Glaucoma and Dry Eye segments contributed $14.8 million and $1.0 million, respectively, to our year-over-year revenue growth in 2019. The growth from 2018 to 2019 reflects the impact of the commercial launch of OMNI in February 2018 and TearCare in April 2019 which was partially offset by a decrease of $2.5 million in revenues as a result of discontinuing the sale of TRAB360 and VISCO360 in March 2019. Over the course of the periods indicated, we trained a significant number of ECPs on our products, increased our sales efforts, including expanding our commercial team from 14 professionals as of January 1, 2018 to 70 professionals as of December 31, 2019, and cultivated adoption and recurring use of our products by key accounts, resulting in the increase in the number of units ordered.
Cost of Goods Sold and Gross Profit. Our cost of goods sold increased $4.2 million from 2018 to 2019 due to a $3.9 million increase in the cost of materials and manufacturing overhead driven by the increase in the number of units sold and the introduction of TearCare, including the associated ramp-up of production capacity in the middle of 2019, by an increase in personnel expenses primarily as a result of increased manufacturing-related headcount, and an increase in reserves for excess, obsolete and non-sellable inventory and shipping and handling expenses.
107
Table of Contents
Our total gross profit increased by $11.6 million from 2018 to 2019, including $12.0 million of Surgical Glaucoma gross profit growth and ($0.4) million of gross profit declines in Dry Eye. Overall, our gross margin increased by 3.1% from 2018 to 2019 primarily due to the impact of the economies of scale in Surgical Glaucoma as the volumes of OMNI products sold continued to increase. The overall increase in our gross margin was partially offset by the introduction in mid-2019 of TearCare in our Dry Eye segment, which had a negative gross margin in 2019. The gross margin in our Surgical Glaucoma segment sales increased from 68.9% in 2018 to 77.0% in 2019, while the gross margin in our Dry Eye segment sales was (35.2)% in 2019.
Research and Development Expenses. The $2.7 million increase in R&D expenses from 2018 to 2019 was primarily attributable to an increase of $1.6 million in costs associated with our clinical studies, an increase of $1.3 million in personnel expenses primarily as a result of increased headcount, and an increase of $0.4 million related to development of the OMNI Next Gen prototype. The increase was offset in part by a $1.0 million decrease in contract manufacturing set up related expenses.
Selling, General and Administrative Expenses. The $18.7 million increase in SG&A expenses from 2018 to 2019 was primarily due to our continued investment in commercial capabilities and in the infrastructure to support our growth, which resulted in an increase of $10.4 million in total personnel expenses, an increase of $2.0 million in travel and entertainment expenses, an increase of $2.4 million in non-labor commercial spend, including promotional activities, conferences and tradeshows and marketing initiatives, an increase of $0.8 million in facility and information technology related expenses, an increase of $1.0 million in sales training and demos, an increase of $0.9 million in consulting services to support business growth and an increase of $0.4 million in legal fees related to general and regulatory matters.
Interest Expense. The $2.0 million increase in interest expense from 2018 to 2019 was primarily attributable to the additional interest expense associated with the $14.0 million of borrowings under the 2019 Term Loan. We did not have any debt prior to entering into the 2019 Term Loan and 2019 Revolver in January 2019.
Interest Income and Other Income (Expense), Net. The $0.2 million increase in interest income from 2018 to 2019 was primarily due to higher average cash balances in 2019, resulting from the proceeds from our 2019 Term Loan and our Series D redeemable convertible preferred stock financing. The $35 thousand increase in other expense, net, from 2018 to 2019 was attributable primarily to the remeasurement of our convertible preferred stock warrants and recognition of the change in fair value.
Cash Flows
The following table summarizes our cash flows for the periods indicated (in thousands):
| Year Ended December 31, | Three Months Ended March 31, | |||||||||||||||||||
| 2018 | 2019 | 2020 | 2020 | 2021 | ||||||||||||||||
| (unaudited) | ||||||||||||||||||||
Net cash used in operating activities | $ | (14,475 | ) | $ | (24,997 | ) | $ | (32,174 | ) | $ | (9,561 | ) | $ | (12,870 | ) | |||||
Net cash used in investing activities | (570 | ) | (672 | ) | (953 | ) | (513 | ) | (104 | ) | ||||||||||
Net cash provided by (used in) financing activities | 12,203 | 42,664 | 73,401 | 30,056 | (210 | ) | ||||||||||||||
Net increase (decrease) in cash | $ | (2,842 | ) | $ | 16,995 | $ | 40,274 | $ | 19,982 | $ | (13,184 | ) | ||||||||
Net Cash Used in Operating Activities.
Net cash used in operating activities for the three months ended March 31, 2021 was $12.9 million, consisting primarily of a net loss of $12.2 million and an increase in net operating assets of $1.1 million, partially offset by non-cash charges of $0.4 million. The $1.1 million increase in our net operating assets was primarily due to a $1.8 million decrease in accrued compensation, a $1.0 million increase in other noncurrent assets, and a $0.3 million increase in accounts receivable, partially offset by a $1.0 million increase in accounts payable, and a
108
Table of Contents
$1.0 million increase in accrued and other liabilities. The non-cash charges primarily related to $0.3 million stock-based compensation, a $0.2 million increase in our provision for excess and obsolete inventories, $0.2 million from the accretion of debt discount and amortization of debt issuance costs, $0.2 million of right of use asset amortization related to our office lease, and $0.1 million of depreciation and amortization, partially offset by change in fair value of redeemable convertible preferred stock warrant of $0.6 million.
Net cash used in operating activities for the three months ended March 31, 2020 was $9.6 million, consisting primarily of a net loss of $9.2 million and an increase in net operating assets of $1.3 million, partially offset by non-cash charges of $0.9 million. The increase in net operating assets was primarily due to a $1.1 million decrease in accrued compensation, $0.3 million decrease in accrued and other liabilities, $0.2 million increase in inventory, and $0.2 million increase in prepaid expenses, partially offset by $0.3 million increase in accounts payable, and $0.2 million decrease in accounts receivable. The non-cash charges primarily consisted of a $0.4 million increase of our provision for excess and obsolete inventories, $0.1 million of depreciation and amortization, $0.1 million accretion of debt discount and amortization of debt issuance costs, $0.1 million provision for doubtful accounts, and $0.1 million from the right of use asset amortization related to our office lease.
Net cash used in operating activities for the year ended December 31, 2020 was $32.2 million, consisting primarily of a net loss of $34.7 million, which included a $2.2 million benefit from the proceeds from our Paycheck Protection Program, or PPP, loan under the Coronavirus Aid, Relief, and Economic Security Act, or CARES Act, and an increase in net operating assets of $0.7 million, partially offset by non-cash charges of $4.0 million. The $0.7 million increase in our operating assets was primarily due to a $1.5 million increase in accounts receivable, a $1.7 million increase in our inventory, and a $0.7 million increase in our prepaid expenses, each to support the continued growth of our operations, partially offset by a $1.9 million increase in accrued compensation and $2.0 million in accrued and other liabilities. The non-cash charges primarily consisted of a $1.4 million provision for excess and obsolete inventories, primarily related to the write-down of legacy first generation OMNI inventory due to the launch of our OMNI Next Gen in 2020, $0.5 million related to stock-based compensation, $0.6 million of right of use asset amortization related to office lease, $0.6 million of accretion of debt discount and amortization of debt issuance costs and $0.6 million in depreciation and amortization.
Net cash used in operating activities for the year ended December 31, 2019 was $25.0 million, consisting primarily of a net loss of $25.9 million and an increase in net operating assets of $0.3 million, partially offset by non-cash charges of $1.2 million. The increase in net operating assets was primarily due to increases in accounts receivable of $2.3 million, inventories of $1.8 million and other noncurrent assets to support the growth of our operations, partially offset by similar growth in our accounts payable, accrued compensation and accrued and other liabilities as we scaled our operations. The non-cash charges primarily consisted of depreciation and amortization of $0.3 million, the accretion of debt discount and amortization of debt issuance costs of $0.5 million, stock-based compensation of $0.1 million and non-cash operating lease expense of $0.1 million.
Net cash used in operating activities for the year ended December 31, 2018 was $14.5 million, consisting primarily of a net loss of $14.3 million and an increase in net operating assets of $0.4 million, partially offset by non-cash charges of $0.2 million. The increase in net operating assets was primarily due to increases in accounts receivable of $1.4 million, prepaid expenses of $0.6 million and inventories of $0.2 million to support the growth of our operations, partially offset by similar increases in our accounts payable of $1.0 million, accrued compensation of $0.5 million and accrued and other liabilities of $0.3 million as we scaled our operations. The non-cash charges primarily consisted of depreciation and amortization and stock-compensation expense.
Net Cash Used in Investing Activities.
Net cash used in investing activities in the three months ended March 31, 2020 and 2021 was $0.5 million and $0.1 million, consisting of purchases of property and equipment.
109
Table of Contents
Net cash used in investing activities in the years ended December 31, 2020, 2019 and 2018 was $0.9 million, $0.7 million and $0.6 million, consisting of purchases of property and equipment.
Net Cash Provided by (Used in) Financing Activities.
Net cash used in financing activities in the three months ended March 31, 2021 of $0.2 million primarily relates to payments of costs related to our initial public offering preparation.
Net cash provided by financing activities in the three months ended March 31, 2020 of $30.1 million was primarily related to proceeds from issuance of Series E redeemable convertible preferred stock of $30.2 million, offset by $0.1 million in related offering costs.
Net cash provided by financing activities in the year ended December 31, 2020 of $73.4 million primarily relates to proceeds from issuance of debt of $20.3 million, proceeds of $53.4 million from the issuance of our Series E redeemable convertible preferred stock and Series F redeemable convertible preferred stock, partially offset by the related offering costs of $0.3 million.
Net cash provided by financing activities in the year ended December 31, 2019 was related to proceeds from issuance of debt of $14.0 million and proceeds from issuance of Series D redeemable convertible preferred stock of $30.7 million, offset by $2.1 million in the related offering costs.
Net cash provided by financing activities in the year ended December 31, 2018 of $12.2 million primarily relates to proceeds from the issuance of Series C redeemable convertible preferred stock during 2018, offset by issuance costs of $0.1 million.
110
Table of Contents
Selected Unaudited Quarterly Financial Information
The following table sets forth certain unaudited quarterly information for the nine quarters presented. The unaudited quarterly information set forth below has been prepared on a basis consistent with our audited annual financial statements included elsewhere in this prospectus and include, in our opinion, all normal recurring adjustments necessary for the fair presentation of the results of operations for the periods presented. Our historical quarterly results are not necessarily indicative of the results that may be expected in the future. The following quarterly financial information should be read in conjunction with our financial statements and related notes thereto included elsewhere in this prospectus. The numbers in the following table that relate to dollars are in thousands.
| Three Months Ended, | ||||||||||||||||||||||||||||||||||||
| March 31, 2019 | June 30, 2019 | September 30, 2019 | December 31, 2019 | March 31, 2020 | June 30, 2020 | September 30, 2020 | December 31, 2020 | March 31, 2021 | ||||||||||||||||||||||||||||
Revenue: | ||||||||||||||||||||||||||||||||||||
Surgical Glaucoma | 3,828 | 5,827 | 5,931 | 6,718 | 6,100 | 3,299 | 7,883 | 8,718 | 8,139 | |||||||||||||||||||||||||||
Percentage of total revenue | 100.0 | % | 97.5 | % | 93.4 | % | 93.4 | % | 93.9 | % | 94.2 | % | 91.1 | % | 97.0 | % | 94.3 | % | ||||||||||||||||||
Dry Eye | — | 147 | 420 | 477 | 396 | 203 | 768 | 273 | 496 | |||||||||||||||||||||||||||
Percentage of total revenue | 0.0 | % | 2.5 | % | 6.6 | % | 6.6 | % | 6.1 | % | 5.8 | % | 8.9 | % | 3.0 | % | 5.7 | % | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Total: | 3,828 | 5,974 | 6,351 | 7,195 | 6,496 | 3,502 | 8,651 | 8,991 | 8,635 | |||||||||||||||||||||||||||
Cost of goods sold: | ||||||||||||||||||||||||||||||||||||
Surgical Glaucoma | 962 | 1,476 | 1,263 | 1,431 | 1,514 | 1,508 | 1,946 | 2,101 | 1,858 | |||||||||||||||||||||||||||
Dry Eye | 7 | 482 | 530 | 393 | 614 | 577 | 674 | 275 | 443 | |||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Total: | 969 | 1,958 | 1,793 | 1,824 | 2,128 | 2,085 | 2,620 | 2,376 | 2,301 | |||||||||||||||||||||||||||
Gross Profit: | ||||||||||||||||||||||||||||||||||||
Surgical Glaucoma | 2,866 | 4,351 | 4,668 | 5,287 | 4,586 | 1,791 | 5,937 | 6,617 | 6,281 | |||||||||||||||||||||||||||
Dry Eye | (7 | ) | (335 | ) | (110 | ) | 84 | (218 | ) | (374 | ) | 94 | (2 | ) | 53 | |||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Total: | 2,859 | 4,016 | 4,558 | 5,371 | 4,368 | 1,417 | 6,031 | 6,615 | 6,334 | |||||||||||||||||||||||||||
Gross Margin: | ||||||||||||||||||||||||||||||||||||
Surgical Glaucoma | 74.9 | % | 74.7 | % | 78.7 | % | 78.7 | % | 75.2 | % | 54.3 | % | 75.3 | % | 75.9 | % | 77.2 | % | ||||||||||||||||||
Dry Eye | -100.0 | % | -228.0 | % | -26.1 | % | 17.6 | % | -55.1 | % | -183.8 | % | 12.2 | % | -0.9 | % | 10.8 | % | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Total: | 74.7 | % | 67.2 | % | 71.8 | % | 74.6 | % | 67.3 | % | 40.4 | % | 69.7 | % | 73.6 | % | 73.3 | % | ||||||||||||||||||
Operating expenses: | ||||||||||||||||||||||||||||||||||||
Research and development | 1,487 | 2,045 | 2,063 | 2,529 | 2,400 | 1,443 | 2,158 | 2,873 | 3,440 | |||||||||||||||||||||||||||
Selling, general and administrative | 5,958 | 8,879 | 8,216 | 9,666 | 10,678 | 7,664 | 11,228 | 12,175 | 14,550 | |||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Total operating expenses: | 7,445 | 10,924 | 10,279 | 12,195 | 13,078 | 9,107 | 13,386 | 15,048 | 17,990 | |||||||||||||||||||||||||||
Loss from operations | (4,586 | ) | (6,908 | ) | (5,721 | ) | (6,824 | ) | (8,710 | ) | (7,690 | ) | (7,355 | ) | (8,433 | ) | (11,656 | ) | ||||||||||||||||||
Interest income | 14 | 20 | 68 | 72 | 27 | 2 | 1 | — | — | |||||||||||||||||||||||||||
Interest expense | (392 | ) | (487 | ) | (535 | ) | (547 | ) | (552 | ) | (549 | ) | (538 | ) | (764 | ) | (1,084 | ) | ||||||||||||||||||
Other income (expense) | (2 | ) | 1 | 1 | (35 | ) | 91 | (73 | ) | (197 | ) | 108 | 552 | |||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Loss before income taxes | (4,966 | ) | (7,374 | ) | (6,187 | ) | (7,334 | ) | (9,144 | ) | (8,310 | ) | (8,089 | ) | (9,089 | ) | (12,188 | ) | ||||||||||||||||||
Provision (benefit) for income taxes | (4 | ) | 3 | — | 9 | 31 | 6 | 8 | 16 | 52 | ||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Net loss and comprehensive loss | (4,962 | ) | (7,377 | ) | (6,187 | ) | (7,343 | ) | (9,175 | ) | (8,316 | ) | (8,097 | ) | (9,105 | ) | (12,240 | ) | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||||||
Liquidity and Capital Resources
Sources of Liquidity
To date, our primary sources of capital have been private placements of redeemable convertible preferred stock, debt financing agreements and revenue from the sale of our products. Since our inception, we have raised an aggregate of approximately $117.3 million in net proceeds from the sale of our redeemable convertible preferred stock and borrowed $32.9 million of net proceeds under our term loans.
111
Table of Contents
As of March 31, 2021, we had cash and cash equivalents of $48.3 million, an accumulated deficit of $102.3 million and $35.0 million outstanding under our term loan agreement (before debt discount) and under our PPP loan. Based on our current planned operations, we expect our cash and cash equivalents and additional borrowings available under the 2020 Term Loan and the 2020 Revolver will enable us to fund our operations for at least the next twelve months.
MidCap Loan Agreements
In January 2019, we entered into a loan and security agreement, or the 2019 MidCap Credit Facility, with MidCap Financial Services, or the Lender, which provided for a term loan facility, or the 2019 Term Loan, and a revolving line of credit, or the 2019 Revolver. The original agreement included a maximum of $25.0 million credit facility consisting of a senior secured 2019 Term Loan of up to $20.0 million and a $5.0 million 2019 Revolver. In November 2020, we entered into a loan and security agreement, or the 2020 MidCap Credit Facility, with the Lender, which replaced the 2019 MidCap Credit Facility, and provided for a term loan facility, or the 2020 Term Loan, and a revolving line of credit, or the 2020 Revolver. The 2020 MidCap Credit Facility includes a maximum of $40.0 million credit facility consisting of a senior secured term loan of up to $35.0 million and a $5.0 million revolver.
2019 Term Loan
The 2019 Term Loan had a four-year term and a stated floating interest rate which equated to reserve-adjusted LIBOR, plus 6.75%. Under certain circumstances, the floating interest rate could have been based on the prime rate instead of LIBOR. The Term Loan was split into three tranches as follows: (i) the Tranche One Loans provided for $12.0 million in term loans, (ii) the Tranche Two Loans provided for up to $2.0 million in term loans, and (iii) the Tranche Three Loans provided for up to $6.0 million in term loans. We borrowed $14.0 million under the Tranche One Loans and Tranche Two Loans. Although the conditions necessary to draw the Tranche Three Loans had been met as of December 31, 2019, we did not draw the Tranche Three Term Loans. The 2019 Term Loan required 18 interest only payments, which began on January 31, 2019, followed by 30 equal monthly installments of principal, plus interest. The interest-only period was extended by an additional six months upon achievement of a milestone defined in the agreement with respect to the Tranche Three Loans.
We incurred $1.5 million of issuance costs in conjunction with the 2019 Term Loan which were netted against the borrowed funds in the balance sheet and were being accreted using the effective interest method as interest expense over the contractual period of four years. The 2019 Term Loan had an effective interest rate of 14.52% per year.
In conjunction with the funding of Tranche One Loans and Tranche Two Loans under the 2019 Term Loan, we issued a 10-year warrant to the Lender to purchase 29,514 shares of our Series C redeemable convertible preferred stock, or the 2019 MidCap Warrants, at an exercise price of $9.4868 per share.
The estimated fair value of the 2019 MidCap Warrants was $0.2 million. The 2019 MidCap Warrants were recorded at the fair value as a debt discount and as a warrant liability. The debt discount was being accreted using the effective interest method as interest expense over the contractual period of four years for the 2019 Term Loan.
The 2019 Term Loan granted us the right to voluntarily prepay the borrowings in full, with a prepayment premium beginning at 3.0% in the first year from tranche funding and declining to 2.0% in the second year from tranche funding, to 1.0% in the third year from tranche funding thereafter. In addition, a final payment fee of 5% of the original Tranche One Loans and Tranche Two Loans amounts borrowed was payable at the end of the term or when the borrowings are repaid in full. The borrowings were collateralized by a security interest in substantially all of our assets.
112
Table of Contents
The 2019 Term Loan terms included making us subject to financial covenants related to minimum trailing net revenue targets that began on January 1, 2019 and were tested on a monthly basis. As of December 31, 2019, we were in compliance with the applicable financial covenants.
2019 Revolver
The 2019 Revolver had a four-year term and had a stated floating interest rate which equated to reserve-adjusted LIBOR, plus 4.25%. Under certain circumstances, the floating interest rate could have been based on the prime rate instead of LIBOR. An unused line fee of 0.5% was payable monthly based on the average unused balance and a collateral management fee of 0.5% was payable monthly based on the outstanding balance of the 2019 Revolver. We could have requested to increase the 2019 Revolver commitment amount to $10.0 million under the terms of the agreement. As of December 31, 2019, $4.0 million was available to be drawn under the 2019 Revolver.
The 2019 Revolver provided for a prepayment premium equal to an amount determined by multiplying the commitment amount by 3.0% in the first year, 2.0% in year 2, and 1.0% thereafter.
The 2019 Revolver had not been drawn upon as of December 31, 2019.
2020 Amendment to MidCap Loan Agreements
In November 2020, we amended the 2019 Term Loan and 2019 Revolver agreements, which resulted in an increase to our term loan borrowing availability, an extension of maturities and non-amortization periods, and changes to a number of other terms and conditions as summarized below.
2020 Term Loan
The amended term loan extended the maturity date to November 1, 2025 and increased the stated floating interest rate to reserve-adjusted LIBOR, plus 7.00%. Outstanding principal amounts of Tranche One Loans and Tranche Two Loans borrowed under the 2019 Term Loan were designated as Tranche One Loans and Tranche Two Loans under the 2020 Term Loan, and the Tranche Three Loans commitment amount was increased to $21.0 million. We drew the entire commitment amount of the Tranche Three Loans in November 2020. The 2020 Term Loan begins to amortize on December 1, 2022, and, if certain conditions are met, the initiation of the amortization period can be extended to December 1, 2023 or December 1, 2024. In addition, the final payment fee was increased to 6.0%. We are subject to financial covenants related to minimum trailing revenue targets that began on November 30, 2020, and are tested on a monthly basis. As of December 31, 2020 and March 31, 2021, the Company was in compliance with the applicable financial covenant.
We incurred $0.7 million of issuance costs in conjunction with the 2020 Term Loan which were netted against the borrowed funds in the balance sheet and are being accreted using the effective interest method as interest expense over the contractual period of five years. The 2020 Term Loan had an effective interest rate of 13.59% per year.
In conjunction with the funding of the 2020 Term Loan, we issued a 10-year warrant to the Lender to purchase 300,000 shares of our Series F redeemable convertible preferred stock at an exercise price of $21.8779 per share, or the 2020 MidCap Warrant, with the estimated fair value of $1.8 million. The 2020 MidCap Warrants were recorded at the fair value as a debt discount and as a warrant liability. The debt discount is being accreted using the effective interest method as interest expense over the contractual period of four years for the 2020 Term Loan.
Other key terms of the 2020 Term Loan remained substantially unchanged compared to those of the 2019 Term Loan.
113
Table of Contents
2020 Revolver
The 2020 Revolver extended maturity date to November 1, 2025 and increased the stated floating interest rate to reserve-adjusted LIBOR plus 4.50%. As of December 30, 2020, $4.8 million was available to be drawn under the 2020 Revolver which remains undrawn upon.
Our obligations under the 2020 Term Loan and the 2020 Revolver are guaranteed by us and our future subsidiaries, subject to exceptions for certain foreign subsidiaries. Our obligations under the agreements are secured by substantially all of our assets, including our material intellectual property. Additionally, we are subject to customary affirmative and negative covenants, including covenants that limit or restrict the ability of us to, among other things, incur indebtedness, grant liens, merge or consolidate, make investments, dispose of assets, make acquisitions, pay dividends or make distributions, repurchase stock and enter into certain transactions with affiliates, in each case subject to certain exceptions.
Other key terms of the 2020 Revolver remained substantially unchanged compared to those of 2019 Revolver.
The 2020 Term Loan and the 2020 Revolver each contain events of default that include, among others, non-payment of principal, interest or fees, breach of covenants, inaccuracy of representations and warranties, cross-defaults and bankruptcy and insolvency events.
Paycheck Protection Program Loan
In May 2020, we received a loan of $2.2 million pursuant to the Paycheck Protection Program, or PPP, under the CARES Act. The Small Business Administration required that PPP loans only be used for eligible payroll costs, business mortgage interest payments, rent or utilities. Per SBA guidelines, we would be eligible to apply for loan forgiveness if we used the loan proceeds for acceptable expenses during the 8-week period after disbursement. We believe we have satisfied all of the terms and conditions of the PPP loan and applied for loan forgiveness in September 2020. The PPP loan was forgiven in June 2021. The Company has elected to recognize this government grant income as a reduction of the related expenses.
In connection with the PPP loan, we executed a promissory note in favor of Bank of America. Because the SBA confirmed full and complete forgiveness of the unpaid balance of the PPP loan and reimbursed Bank of America for the total outstanding balance, principal and interest, our obligations under the PPP loan are deemed fully satisfied and paid in full.
Lease Agreements
Our corporate headquarters are located in Menlo Park, California, where we lease approximately 10,823 square feet of office, research and development, engineering and laboratory space which is currently pursuant to a sublease agreement which was effective as of September 17, 2019 and expires on July 31, 2021. Effective August 1, 2021, we will remain in the same space under a new lease agreement with the direct landlord to that space which will extend through August 31, 2024. We also lease approximately 2,040 square feet of office space, which is primarily used by our commercial leadership team, in Southlake, Texas, pursuant to a lease that commenced on April 30, 2019 and expires on May 15, 2024.
Critical Accounting Policies and Estimates
Our financial statements have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these financial statements requires us to make estimates and assumptions for the reported amounts of assets, liabilities, revenue, expenses and related disclosures. Our estimates are based on our historical experience and on various other factors that we believe are reasonable under the circumstances, the
114
Table of Contents
results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions and any such differences may be material.
While our significant accounting policies are more fully described in Note 2 to our financial statements included elsewhere in this prospectus, we believe the following discussion addresses our most critical accounting policies, which are those that are most important to our financial condition and results of operations and require our most difficult, subjective and complex judgments.
Revenue Recognition
We apply the following five steps in order to determine the appropriate amount of revenue to be recognized as we fulfill our obligations under each of its arrangements:
| • | Identify the contract with a customer, |
| • | Identify the performance obligations in the contract, |
| • | Determine the transaction price, |
| • | Allocate the transaction price to performance obligations in the contract, and |
| • | Recognize revenue as the performance obligations are satisfied. |
Our revenue is generated from the sale of our products from our Surgical Glaucoma product portfolio and our Dry Eye product portfolio to hospitals, medical centers and ECPs in the United States through sales representatives and distributors. Our contracts are in the form of a combination of signed agreements and/or purchase orders. We account for a contract with a customer when there is approval and commitment from both parties, the rights and obligations of the parties are identified, payment terms are identified, the contract has commercial substance, and it is probable that we will collect substantially all of the consideration to which it will be entitled.
Each of our Surgical Glaucoma and Dry Eye products specified in a contract represents a distinct good and is accounted for as a separate performance obligation. Revenue is recognized when control of promised goods is transferred to a customer in amount that reflects the consideration that we expect to receive in exchange for those goods. Control of our products is transferred to our customers at a point in time, either upon shipment or delivery of the product to the customer under our standard terms and conditions. The customer is able to direct the use of, and obtain substantially all of the benefits from, the product at the time the product shipped or is delivered. We consider control to have transferred upon shipment or delivery because we have a present right to payment at that time, the customer has legal title to the asset, we have transferred physical possession of the asset, the customer has accepted the asset, and the customer has significant risks and rewards of ownership of the asset.
Payments for our contracts are typically due within 30 days of transfer of control of our products to its customers. We exclude taxes assessed by governmental authorities on revenue-producing transactions from the measurement of the transaction price.
In the normal course of business, we do not accept product returns, unless the item is defective as manufactured. We establish provisions for estimated returns and warranties. In addition, we do not typically provide customers with the right to a refund.
Our contracts all have an original duration of one year or less. As a practical expedient, we do not consider the time value of money for such contracts. Further, because of the short duration of these contracts, we do not disclose the transaction price for the remaining performance obligations as of the end of each reporting period or when we expect to recognize this revenue.
115
Table of Contents
We expense shipping and handling costs as incurred and include them in the cost of goods sold. In those cases where we bill shipping and handling costs to customers, we will classify the amounts billed as a component of revenue.
As a practical expedient, we recognize the incremental costs of obtaining contracts, such as sales commissions, as an expense when incurred since the amortization period of the asset we otherwise would have recognized is one year or less. Sales commissions are recorded within selling, general, and administrative expenses in the statements of operations.
Inventory
Inventory represents finished goods purchased from a third-party manufacturer and is valued at the lower of cost or net realizable value. Cost is determined using actual costs on a first-in, first-out basis for all inventory. Net realizable value is determined as the estimated selling prices in the ordinary course of business, less reasonably predictable costs of completion, disposal, and transportation. We regularly review inventory quantities in consideration of actual loss experiences, projected future demand, and remaining shelf life to record a provision for excess and obsolete inventory when appropriate. The shelf life of our Surgical Glaucoma inventory averages approximately 24 months and for our Dry Eye inventory varies depending on the component of TearCare, as SmartHubs have no expiration date while SmartLids have a shelf life of 24 months. Our policy is to write down inventory that has become obsolete, inventory that has a cost basis in excess of its expected lower of cost or net realizable value, and inventory in excess of expected requirements. The estimate of excess quantities is judgmental and primarily dependent on our estimates of future demand for the particular product.
Stock-Based Compensation and Fair Value of Common Stock
We measure and record the expense related to stock-based payment awards based on the fair value of those awards as determined on the date of grant. We recognize stock-based compensation expense over the requisite service period of the individual grant, generally equal to the vesting period and use the straight-line method to recognize stock-based compensation, and account for forfeitures as they occur. Prior to our initial public offering, we selected the Black-Scholes-Merton, or Black-Scholes, option-pricing model as the method for determining the estimated fair value for stock options. The Black-Scholes option-pricing model requires the use of highly subjective and complex assumptions, which determine the fair value of share-based awards, including the option’s expected term, expected volatility of the underlying stock, risk-free interest rate and expected dividend yield.
| • | Expected Term: The expected term was calculated using the simplified method. The simplified method is based on the vesting period and the contractual term for each grant or for each vesting tranche for awards with graded vesting. The midpoint of the vesting date and the maximum contractual expiration date is used as the expected term under this method. For awards with multiple vesting tranches, the time from grant until the midpoints for each of the tranches may be averaged to provide an overall expected term. |
| • | Expected Volatility: We used an average historical stock price volatility of a peer group of publicly traded companies to be representative of its expected future stock price volatility, as we did not have any trading history for our common stock. For purposes of identifying these peer companies, we considered the industry, stage of development, size, and financial leverage of potential comparable companies. For each grant, we measured historical volatility over a period equivalent to the expected term. |
| • | Risk-Free Interest Rate: The risk-free interest rate is based on the implied yield currently available on US Treasury zero-coupon issues with remaining terms equivalent to the expected term of a stock award. |
| • | Expected Dividend Yield: We have not paid, and do not anticipate paying, any dividends in the near future. Accordingly, we estimated the dividend yield to be 0%. |
116
Table of Contents
Prior to our initial public offering, the fair value of our common stock was determined by the board of directors with assistance from management and, in part, on input from an independent third-party valuation firm. The board of directors determines the fair value of common stock by considering a number of objective and subjective factors, including valuations of comparable companies, sales of redeemable convertible preferred stock, operating and financial performance, the lack of liquidity of our common stock and the general and industry-specific economic outlook.
Our valuations of our common stock were determined in accordance with the guidelines outlined in the American Institute of Certified Public Accountants Practice Aid, Valuation of Privately-Held-Company Equity Securities Issued as Compensation, or the Practice Aid. The methodology to determine the fair value of our common stock included estimating the fair value of the enterprise using the “backsolve” method, which estimates the fair value of our company by reference to the value and preferences of our last round of financing, as well as our capitalization.
The assumptions used to determine the estimated fair value of our common stock are based on numerous objective and subjective factors, combined with management’s judgment, including external market conditions affecting the pharmaceutical and biotechnology industry and trends within the industry:
| • | Our stage of development; |
| • | The rights, preferences, and privileges of our redeemable convertible preferred stock relative to those of our common stock; |
| • | The prices at which we sold shares of our redeemable convertible preferred stock; |
| • | Our financial condition and operating results, including our levels of available capital resources; |
| • | The progress of our research and development efforts, our stage of development, and business strategy; |
| • | Equity market conditions affecting comparable public companies; and |
| • | General U.S. market conditions and the lack of marketability of our common stock. |
The Practice Aid identifies various available methods for allocating enterprise value across classes and series of capital stock to determine the estimated fair value of common stock at each valuation date. In accordance with the Practice Aid, we considered the following methods:
| • | Income approach. The income approach attempts to value an asset or security by estimating the present value of the future economic benefits it is expected to produce. These benefits can include earnings, cost savings, tax deductions, and disposition proceeds from the asset. An indication of value may be developed in this approach by discounting expected cash flows to their present value at a rate of return that incorporates the risk-free rate for the use of funds, the expected rate of inflation over the asset’s holding period, and the risks associated with realizing the cash flows in the amounts and at the times projected. The discount rate selected is typically based on rates of return available from alternative investments of similar type and quality as of the valuation date. The most commonly employed income approach to valuation is the discounted cash flow analysis. |
| • | Market Approach. The market approach attempts to value an asset or security by examining observable market values for similar assets or securities. Sales and offering prices for comparable assets are adjusted to reflect differences between the asset being valued and the comparable assets, such as, location, time and terms of sale, utility, and physical characteristics. When applied to the valuation of equity, the analysis may include consideration of the financial condition and operating performance of the company being valued relative to those of publicly traded companies or to those of companies acquired in a single transaction, which operate in the same or similar lines of business. |
| • | Cost Approach. The cost approach to valuation is based upon the concept of replacement cost as an indicator of value and the notion that an investor would pay no more for an asset than what it would |
117
Table of Contents
cost to replace the asset with one of equal utility. The cost approach estimates value based upon the estimated cost of replacing or reproducing the asset, less adjustments for physical deterioration and functional obsolescence, if relevant. When applied to an enterprise, a type of cost approach referred to as the Net Asset Method is sometimes employed. This method measures the value of equity as the sum of the values of its assets reduced by the sum of the values of its liabilities. The resulting equity is reflective of a 100% ownership interest in the business. This approach is frequently used in valuing holding companies. |
Based on our early stage of development and other relevant factors, our board of directors considered all three approaches and have chosen to apply both income and market approaches in our analyses. Our board of directors determined these approaches were the most appropriate methods for allocating our enterprise value to determine the estimated fair value of our common stock for valuations performed for periods as of December 31, 2020 or earlier. In determining the estimated fair value of our common stock, our board of directors also considered the fact that our stockholders could not freely trade our common stock in the public markets. Accordingly, we applied discounts to reflect the lack of marketability of our common stock based on the estimated time to liquidity. The estimated fair value of our common stock at each grant date reflected a non-marketability discount partially based on the estimated timing of a future liquidity event.
After the completion of this offering, the fair value of each share of underlying common stock will be determined based on the closing quoted market price of our common stock on the date of grant.
Redeemable Convertible Preferred Stock Warrants
Our redeemable convertible preferred stock warrants require liability classification and accounting as the underlying redeemable convertible preferred stock is considered contingently redeemable and may obligate us to transfer assets to the holders at a future date upon occurrence of a deemed liquidation event. The warrants are recorded at fair value upon issuance and are subject to remeasurement to fair value at each balance sheet date, with any changes in fair value recognized as other expense in the statements of operations. The warrants liability is recorded as other noncurrent liabilities in the balance sheets. We will continue to adjust the warrant liability for changes in fair value until the earlier of the exercise or expiration of the redeemable convertible preferred stock warrants, occurrence of a deemed liquidation event, or conversion of redeemable convertible preferred stock into common stock. At that time, the liability associated with the redeemable convertible preferred stock warrants that are converted into warrants to purchase common stock will be reclassified to additional paid-in capital, while the liability associated with any expired warrants will be recognized as a gain within the statements of operations and comprehensive loss. As a result, the redeemable convertible preferred stock warrant liability will be settled and will no longer be subject to remeasurement.
Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk
The risk associated with fluctuating interest rates is primarily limited to our cash equivalents, which are carried at quoted market prices. Due to the short-term maturities and low risk profile of our cash equivalents, an immediate 100 basis point change in interest rates would not have a material effect on the fair value of our cash equivalents. We do not currently use or plan to use financial derivatives in our investment portfolio. As of March 31, 2021, we had $35.0 million in variable rate debt outstanding. Our 2020 Term Loan bears interest per annum at 7.00% plus LIBOR for such interest period, and our 2020 Revolver bears interest per annum at 4.50% plus LIBOR for such interest period. A hypothetical change in interest rates of 10% would have resulted in a change of $0.2 million in interest expense in 2020.
Foreign Currency Risk
Our business is primarily conducted in U.S. dollars. Any transactions that may be conducted in foreign currencies are not expected to have a material effect on our results of operations, financial position or cash flows.
118
Table of Contents
JOBS Act Accounting Election
The Jumpstart Our Business Startups Act of 2012 (JOBS Act) permits an “emerging growth company” such as us to take advantage of an extended transition period to comply with new or revised accounting standards applicable to public companies. We have elected to use this extended transition period under the JOBS Act. As a result, our financial statements may not be comparable to the financial statements of issuers who are required to comply with the effective dates for new or revised accounting standards that are applicable to public companies, which may make comparison of our financials to those of other public companies more difficult.
Recently Issued Accounting Pronouncements
See Note 2 to our financial statements included elsewhere in this prospectus for new accounting pronouncements not yet adopted as of the date of this prospectus.
119
Table of Contents
Overview
Our mission is to transform ophthalmology and optometry through the development and commercialization of proprietary devices that target the underlying causes of the world’s most prevalent eye diseases. We are passionate about improving patients’ lives. Our business philosophy is grounded in the following principles: comprehensively understanding disease physiology; developing products that are intended to restore natural physiological functionality to diseased eyes; developing and marketing products that achieve superior effectiveness versus current treatment paradigms while minimizing complications or side effects; providing intuitive, patient friendly solutions to ophthalmologists and optometrists (together, eyecare professionals or ECPs), and delivering compelling economic value to all stakeholders, including patients, providers and third-party payors such as Medicare and commercial insurers. Our objective is to develop and market products for use in new treatment paradigms and to create an interventional mindset in eyecare whereby our products may be used in procedures which supplant conventional outdated approaches. We believe current eyecare treatment models rely heavily on prescription medications, symptom relief, or either flawed or highly invasive, later-stage procedural interventions, and often fail to adequately address the true underlying cause of disease.
We have focused our initial product development efforts on the treatment of two of the world’s most prevalent and underserved eye diseases, glaucoma and dry eye disease, or DED. We estimate the annual addressable U.S. market opportunities for the products in our Surgical Glaucoma and Dry Eye segments are approximately $6 billion and approximately $10 billion, respectively, while 2020 U.S. manufacturer revenues in the surgical glaucoma and DED markets were approximately $350 million and $2.4 billion, respectively, demonstrating that currently available solutions have not addressed a large part of the market need.
Glaucoma, a group of chronic, often asymptomatic, diseases that damage the optic nerve, is the world’s leading cause of irreversible blindness. Glaucoma does not have a cure and is a progressive disease; if left untreated or insufficiently treated, glaucoma can lead to irreversible disability and blindness. An estimated 102 million people worldwide suffer from glaucoma. Primary open-angle glaucoma, or POAG, is the most prevalent form of glaucoma and affects over 60 million people worldwide, including 4.1 million people in the United States, of whom an estimated 3.4 million have been diagnosed. One of the greatest risk factors for POAG, and the only risk factor that can be controlled, is elevated intraocular pressure, or IOP. Elevated IOP is often caused by malfunctioning drainage pathways in the eye that provide abnormal resistance to the outflow of aqueous humor, a clear, watery fluid which bathes and nourishes the lens and maintains pressure within the eye.
Figure 1. OMNI Enables New Glaucoma Treatment Paradigm
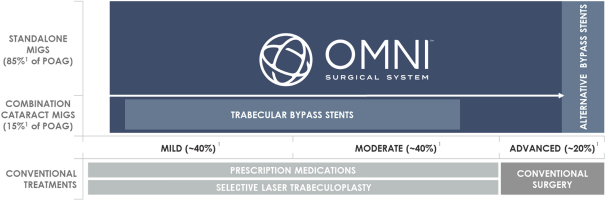
| 1 | Represents % of U.S. POAG patients. |
120
Table of Contents
Our OMNI Surgical System, or OMNI, is a handheld, single use, therapeutic device that allows ophthalmic surgeons to reduce IOP in adult glaucoma patients. OMNI allows the ophthalmic surgeon to sequentially complete two well-established but historically invasive ab externo glaucoma procedures, canaloplasty and trabeculotomy, in an efficient, minimally invasive manner using a single, bloodless and sutureless clear corneal microincision. Conventional canaloplasty and trabeculotomy procedures have been used to effectively treat glaucoma for decades but involve invasive approaches that are difficult to perform, traumatize the eye, have higher risk of intraoperative and post-operative complications and require longer patient recovery times. OMNI allows ophthalmic surgeons to transform these two distinct, historically invasive ab externo glaucoma procedures into a sequential, ab interno minimally invasive glaucoma surgery, or MIGS, procedure. MIGS procedures are performed through a one to two millimeters clear corneal incision similar to those used in cataract surgery for intraocular access and have a strong demonstrated safety profile, characterized by minimal trauma to the eye and quick patient recovery times. The FDA has authorized the use of OMNI for reducing IOP in all adult POAG patients both by itself on a standalone basis, which we refer to as Standalone procedures, or in combination with cataract procedures, which we refer to as Combination Cataract procedures. Several competing MIGS devices, including the current market leaders, have only been authorized by the FDA for use in Combination Cataract procedures for adult patients with Mild-to-Moderate severity. We estimate that over 85% of the U.S. addressable market opportunity for POAG cannot be served with Combination Cataract procedures because less than 15% of POAG patients receive cataract surgery in any given year.
We believe that OMNI delivers the highest level of effectiveness of any available MIGS product, as it is the only device that provides access to 360 degrees of the diseased conventional outflow pathway and can address all three primary points of resistance in the conventional outflow pathway (trabecular meshwork, Schlemm’s canal, and the distal collector channels), through a single clear corneal incision. We believe there is no diagnostic to determine where the resistance lies in the conventional outflow pathway which increases the appeal of OMNI given it is singularly well-suited to address all three primary points of resistance. OMNI’s indication for use, which we believe is among the most comprehensive in MIGS, was cleared by the FDA in March 2021 based upon the review of clinical data from ROMEO, our recently completed U.S. multi-center clinical study of OMNI in Combination Cataract and Standalone procedures. In ROMEO, we observed that Standalone OMNI patients with preoperative IOP greater than 18 mmHg experienced a mean IOP reduction of 28% (from 21.8 mmHg to 15.6 mmHg) and a mean reduction in hypotensive medication usage of 35% (from 1.71 medications to 1.17 medications) 12 months after treatment. In Combination Cataract patients with preoperative IOP greater than 18 mmHg, we observed a mean IOP reduction of 31% (from 21.9 mmHg to 15.1 mmHg) and a mean reduction in hypotensive medication usage of 45% (from 2.04 medications to 1.13 medications) 12 months after treatment. We believe it is noteworthy that our Standalone IOP and medication reduction results are highly comparable to our Combination Cataract results, as it supports our belief that OMNI is the key driver of IOP and medication reduction in both Standalone and Combination Cataract procedures.
Figure 2. Conventional Outflow Pathway – Three Primary Points of Resistance1
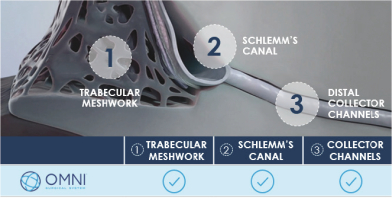
| 1 | Extends 360° around the circumference of the iridocorneal angle where the iris and cornea meet. |
121
Table of Contents
OMNI has received 510(k) clearance from the FDA and a CE Mark to be marketed in the U.S. and the EU, respectively, for canaloplasty (microcatheterization and transluminal viscodilation of Schlemm’s canal) followed by trabeculotomy (cutting of trabecular meshwork) to reduce IOP in adult patients with POAG in the U.S. or with open-angle glaucoma, or OAG, in the EU. We believe OMNI is the first custom-designed, ab interno MIGS device that was cleared by the FDA to lower IOP in both Combination Cataract and Standalone cases for all adults with POAG based upon the review of ab interno Combination Cataract and Standalone clinical data. By comparison, trabecular bypass stents are indicated for use only in Combination Cataract procedures for patients with Mild-to-Moderate severity in the U.S. Other MIGS devices are only authorized for cases with failed prior glaucoma surgery or that are unresponsive to maximum tolerated medical therapy, which are known as Refractory cases, or do not have indications for use that were based on the FDA’s review of accompanying ab interno clinical data. Trabecular bypass stents were the first MIGS implant devices to be authorized by the FDA. We believe the combination of their restricted indication for use and their market leadership position has unnaturally skewed the U.S. MIGS market towards Combination Cataract procedures.
Our goal is to establish OMNI as the standard of care for all POAG patients by continuing to grow its adoption and utilization in the existing Combination Cataract market segment, which we believe remains underpenetrated and estimate is capturing less than one-third of its current potential procedural volume, and by pioneering the development of the Standalone market segment (over 85% of the potential U.S. POAG market). Published data from ROMEO and several single surgeon datasets show a remarkable consistency in IOP reduction following treatment with OMNI. Almost all patients across these groups (98 of 103, 95%) had an IOP decrease following treatment with OMNI, and three out of four (77 of 103, 75%) had at least a 20% decrease. For eyes with preoperative IOP of at least 15 mmHg, we observed lower postoperative IOP in 94 of 96 (98%) cases. Patients in these studies also experienced reductions in the use of glaucoma medication following their OMNI procedures, a benefit not observed in the “medication washout” trabecular bypass stent trials designed to isolate and thereby maximize IOP reduction in a non-real world manner. We believe the consistent therapeutic outcomes OMNI delivers are important for patients and surgeons alike. For patients, we believe the anxiety that may accompany the need for ocular surgery can be tempered with the knowledge that there is a high likelihood of success. For surgeons, consistent outcomes simplify the treatment choice and the decision to perform a procedure. We believe this is especially important for Standalone MIGS procedures which must deliver a very high consistency of efficacy and a very high degree of effectiveness to not only justify the procedure, but also provide surgeons with enough confidence to recommend Standalone surgery to their patients and take them to the operating room for a singular reason. We believe delivering consistently effective results will be crucial to unlocking the Standalone market, as well as capitalizing on the full potential of the Combination Cataract market. An internal field study of our user base has indicated that Standalone procedures in 2020 constituted greater than 20% of our customers’ total OMNI procedures.
After receiving our initial FDA 510(k) clearance for OMNI in late 2017, we began the commercial sale of the device in February 2018. We primarily sell OMNI in the U.S. through our dedicated Surgical Glaucoma sales team, which includes a subset of representatives solely focused on educating existing and potential customers and primary care ECPs on the broad utility and use cases for OMNI and on Standalone treatment alternatives generally. Our commercial strategy for OMNI centers on building confidence and conviction amongst the glaucoma community through continued execution of our clinical trials and publishing their results in peer-reviewed journals. In addition, our highly involved sales and training model serves to promote a world-class surgical experience and identify additional OMNI use cases within its cleared indication, including in additional Standalone procedures and across all addressable POAG severities. The procedure enabled by OMNI, canaloplasty followed by trabeculotomy, is covered and reimbursed by all Medicare Administrative Contractors, or MACs, and numerous private insurers, covering an estimated 67% of U.S. POAG sufferers. Designed for use in well-established clinical procedures, and with advantages that have been observed to promote safe, effective and highly consistent clinical outcomes, we believe that OMNI has the potential to establish a more proactive, interventional paradigm for IOP reduction in POAG. Our Surgical Glaucoma segment, which includes OMNI, represented 94% of our total revenues for the year ended December 31, 2020 and the three months ended March 31, 2021.
122
Table of Contents
The TearCare System, or TearCare, is a technologically sophisticated system which utilizes a wearable, open-eye design to apply localized heat to the eyelids in an anatomically customized way. We believe TearCare has a compelling physiological profile to address obstruction from meibomian gland dysfunction, or MGD, which is the primary cause of evaporative DED, a disease characterized by low quality tears that evaporate prematurely. Dry eye complaints are the most common reason for a patient visit to an eye doctor. There are an estimated 739 million people globally and 38 million people in the U.S. who suffer from DED. DED is the most common reason for a patient visit to an eye doctor, yet of the 38 million people with DED in the U.S., only 17 million have been diagnosed with DED. Dry eye symptoms have a significant impact on the quality of life and productivity of patients suffering from DED. If left untreated, DED can be extremely painful, leading to permanent cornea damage and vision impairment.
Studies have shown that evaporative DED resulting from MGD is associated with approximately 86% of all DED cases. In healthy eyes, there are 25-30 meibomian glands located within each of the upper and lower eyelids. These glands produce and secrete an oily substance called meibum which forms the outer layer of healthy tears, which is also known as the lipid layer. Meibum normally has an olive oil-like consistency and contributes a vital element of the tear film that prevents premature tear evaporation. In patients with MGD, meibum hardens within the glands causing obstructions that can partially or completely block the oily secretions from reaching the tear film. The resulting compromised outer surface of the tear leads to accelerated tear evaporation and DED. Third-party clinical studies have also demonstrated that treating MGD by liquefying and removing clogged meibum is the most effective method of eliminating obstructions and restoring a healthy tear film lipid layer, thereby preventing premature evaporation of tears.
Figure 3. Progression of DED and Ocular Surface Disease
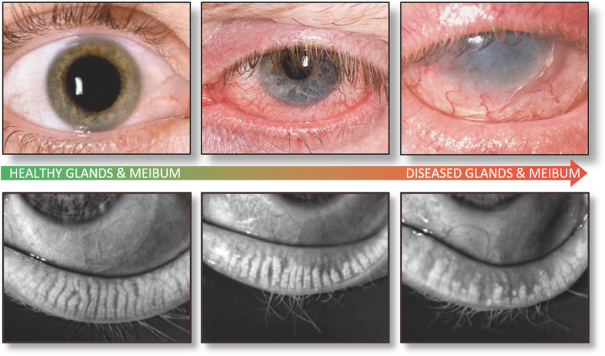
TearCare is designed to enable ECPs to heat and liquefy meibomian gland blockages, followed promptly by manual, comprehensive clearing of these blockages with a separate clearance tool. We developed TearCare to serve as an elegant, compact, portable, and intuitive solution comprised of a re-usable hardware controller, the SmartHub, and a breakthrough, wearable, software-controlled eyelid technology, the SmartLids. Applied adhesively and non-invasively to the outside of the eyelids, single-use SmartLids deliver a precise therapeutic
123
Table of Contents
level of heat into the meibomian glands. Engineering SmartLids to remain comfortably adhered to virtually all shapes and sizes of eyelids while allowing freedom to blink and delivering precise therapeutic heat is one of our most significant design accomplishments. This heating process is intended to melt obstructions in the glands and restore the production and release of healthy, clear meibum onto the tear surface. The proprietary, highly conformant, open-eye design of TearCare allows patients to blink naturally throughout the thermal portion of the procedure, which facilitates movement of melted meibum and also provides a comfortable patient experience. TearCare can be utilized by an ECP in a straightforward in-office procedure and can be accommodated during the course of a routine patient visit. Additionally, TearCare does not require a large capital equipment investment by ECPs, and we believe that it offers an attractive economic value proposition to providers, patients and third-party payors.
In OLYMPIA, our large multi-center, randomized control trial, or RCT, TearCare was associated with statistically significant clinical improvements in all assessed signs and symptoms of DED. This included TBUT and MGSS, objective measurements of DED that were the trial’s primary endpoints, as well as patient-reported symptoms surveys, including EDS, OSDI and SANDE, at all time periods measured (both two weeks and four weeks post-treatment). Further, TearCare had a statistically significantly higher proportion of subjects improving by at least one OSDI category than did the comparator group receiving a single treatment using a version of the first device FDA-cleared for the application of localized heat and pressure therapy in adult patients with chronic cystic conditions of the eyelids, including MGD.
We began selling TearCare in a controlled product launch in mid-2019 to DED-focused ECP practices through a dedicated commercial team. The initial launch phase was successful in garnering valuable feedback from our customers and the broader DED community as well as demonstrating the existing market demand for the product. We believe the MGD market requires additional ECP and patient education, including clinical data to differentiate procedural and product alternatives, and enhanced patient access through the potential advancement of reimbursement coverage. Our goals with the development of TearCare are to fully transform the current outdated treatment paradigm based primarily on over-the-counter, or OTC, and prescription eyedrops which do not address obstruction of the meibomian glands, the primary root cause of MGD, and establish use of TearCare as the standard of care for the millions of patients suffering from evaporative DED caused by MGD. Revenues from our Dry Eye segment, which includes TearCare and related accessories, represented 6% of our total revenues for the year ended December 31, 2020 and the three months ended March 31, 2021.
We currently market TearCare as a Class II, 510-exempt powered heating pad indicated for the application of localized heat where the medical community recommends the application of a warm compress to the eyelids. In November 2020, we submitted a 510(k) premarket notification seeking an expanded indication for use for TearCare. The FDA requested several safety tests and modifications which we believe would have required additional time to complete beyond the designated review process. We voluntarily withdrew this submission in May 2021 to allow us to comply with the FDA’s requests in a comprehensive manner. We are currently conducting these follow-up safety tests and modifications, and we intend to resubmit the 510(k) premarket notification for an expanded indication for use in the second half of 2021.
We focus on continuous innovation and seek regular input from our network of expert employees (including several ophthalmologists on staff), advisors and customers to rapidly iterate our pre- and post-commercial product designs with the aim of better satisfying the needs of our customers and their patients, and increasing adoption and utilization of our solutions. This is particularly evident in the evolution of OMNI, which originated from the combined functionality of two internally developed, commercial predicate devices, each of which went through multiple commercial iterations. We further refined the ergonomics and functionality in OMNI Next Gen, which we launched in May 2020. This dynamic process has also helped guide the intuitive design of our products and our hands-on instructional programs that allow ECPs to use OMNI and TearCare with confidence and with minimal adverse events. Between January 2019 and April 2021, we shipped over 50,000 units of OMNI and over 10,000 single-use SmartLid units to customers. During this period, we became aware of nine events that were reported to the FDA in accordance with 21 CFR §803 as 30-day MDRs, representing less than 0.015% of units shipped.
124
Table of Contents
Our desire and capability to continuously and rapidly innovate our products is a core competency of our company. Our treatment philosophy and approach to product innovation have resulted in a patent portfolio of 27 issued U.S. patents, 34 issued patents outside of the U.S. (including four issued European patents and their national validations), 16 pending U.S. non-provisional patent applications, one pending U.S. provisional patent application, 15 pending foreign patent applications and one pending Patent Cooperation Treaty patent application as of April 30, 2021.
The overall success of our innovative approach to eyecare to date has been confirmed by the over 60,000 estimated uses of OMNI and its direct predicates in over 1,000 hospitals and ambulatory service centers, or ASCs, in the U.S. and EU, and over 10,000 estimated uses of TearCare in over 400 eyecare facilities in the U.S. through April 30, 2021. We have experienced significant growth and market adoption since launching OMNI and are executing a long-term plan for further development of the market for TearCare.
Market Opportunity
We believe there is a significant opportunity to broadly improve existing treatment paradigms throughout ophthalmology and optometry to benefit more patients worldwide. Advancements in treatment effectiveness across a number of prominent eye diseases have been limited in recent years due to a lack of significant innovation. We believe that there are few companies in eyecare that excel in both product development and commercial activities. As a result, conventional treatment algorithms that rely heavily on prescription medications and symptom relief but fail to comprehensively address the true underlying cause of the disease have persisted.
Our objective is to develop products that enable us to open new treatment paradigms and create an interventional mindset in eyecare. We believe that our track record with OMNI and TearCare has demonstrated our ability to leverage our internal capabilities in product development, clinical trial execution, and commercialization to bring viable products to market efficiently and to rapidly refine and innovate them based on real-world input from our customers and advisors. We believe that our products have the potential to transform the treatment paradigms of their respective target diseases. Through continued product and technological innovation, the generation and compilation of differentiated clinical data, and our highly involved and training-intensive user experience programs, we strive to transform and lead two of the most prevalent and most underpenetrated segments of eyecare – POAG and DED.
Primary Open-Angle Glaucoma
Glaucoma, a group of chronic, often asymptomatic, diseases that damage the optic nerve, is the world’s leading cause of irreversible blindness. Glaucoma does not have a cure and is a progressive disease; if left untreated or insufficiently treated, glaucoma can lead to irreversible disability, vision loss and blindness. In 2020, 102 million people worldwide were estimated to suffer from glaucoma. POAG is the most prevalent form of glaucoma and in 2020 affected over 60 million people worldwide and 4.1 million people in the U.S., of whom 3.4 million were diagnosed. Elevated IOP, often caused by malfunctioning drainage pathways in the eye with abnormal resistance to the outflow of aqueous humor, is one of the greatest risk factors for POAG and the only one that can be controlled.
In patients with POAG, increased resistance to aqueous humor outflow causes pressure to build up in the eye and the resultant tension applies stress to and cuts off the blood supply to the optic nerve in the back of the eye, resulting in optic nerve cell death and irreversible vision loss. Decades of research have demonstrated that the fluid buildup primarily results from malfunctions in the eye’s conventional outflow pathway for aqueous humor. If left untreated, glaucoma can damage the optic nerve, resulting in permanent partial or complete loss of vision. The stages of glaucoma are classified based on risk of visual loss on a scale that ranges from ocular hypertension, or OHT, to Mild, to Moderate, then Advanced/Severe, and finally, End-Stage. In the U.S., it is estimated that Mild and Moderate cases each account for approximately 40% of all POAG cases with the
125
Table of Contents
remaining 20% representing Advanced/Severe cases. There is no universally accepted standard for diagnosis of glaucoma severity. OHT, which is characterized by elevated IOP without indications of optic nerve damage or changes in visual field, is a condition that will often progress to glaucoma. While physicians may vary in their diagnostic approach to an individual patient’s stage of glaucoma, Mild and Moderate diagnoses are generally attributed to the abnormal appearance of the optic nerve head (i.e., cupping) with early visual field loss for Moderate cases only, followed by visual abnormalities in both left and right hemispheres of the visual fields for Advanced/Severe cases.
The current treatment paradigm for POAG includes less invasive options such as prescription eyedrops and laser treatments for milder cases and more invasive conventional surgical procedures for more severe cases.
Prescription eyedrops and laser treatments seek to increase aqueous outflow or reduce aqueous production while conventional surgical procedures seek to improve drainage by creating new, artificial, or unnatural outlets for aqueous fluid that bypass the conventional outflow pathway. These conventional surgical procedures involve incisions to the conjunctiva and sclera that can cause significant trauma and scarring to the eye. Safety concerns for conventional surgical procedures are such that they are typically reserved for Severe cases where the risk of vision loss is imminent and outweighs the risk of the invasive procedure itself. Each of these treatment modalities addresses just a single aspect of the disease at a specific point in the progression of the disease state. As a complex progressive disease, there has historically been no “one size fits all” treatment for glaucoma. Physicians have historically used a combination of treatments because no single treatment could adequately slow disease progression to a manageable level over the long term. Further, due to the progressive nature of the disease, data suggest that legacy interventions can become ineffective as the disease state matures. In 2019, worldwide glaucoma prescription medications were estimated to represent over 80% of the nearly $6 billion global glaucoma treatment market. MIGS, glaucoma diagnostic equipment and other surgical devices were estimated to represent 7.0%, 6.3% and 4.8%, respectively.
POAG is the most common type of OAG and is characterized by an open, normal appearing anterior chamber and angle, elevated IOP, typical optic nerve head damage and associated visual field loss, but no other detectable underlying ocular or systemic disease. In healthy eyes, the majority of aqueous fluid drains via the conventional outflow pathway — passing through the trabecular meshwork into Schlemm’s canal and out of the eye through the distal collector channels that connect to the episcleral venous system, with the remainder draining from the alternative uveoscleral or unconventional pathway. We believe treating the conventional outflow pathway with minimally invasive access offers the safest and most effective treatment option for POAG. The ab interno approach involves minimal trauma to the eye, enabling fast healing times with minimal complications, and does not compromise the structural integrity of the eye, thereby allowing episcleral venous pressure, which acts as the body’s natural IOP backstop, to ensure that IOP will not be inadvertently reduced to dangerously low levels (5 mmHg or less), a condition known as hypotony. Other approaches, such as invasive filtering procedures (e.g., trabeculectomy) or suprachoroidal bypass procedures, create artificial drainage channels and are susceptible to serious complications, including hypotony, which can develop when drainage from artificial pathways cannot be adequately controlled. Hypotony can lead to corneal decompensation, accelerated cataract formation, and vision loss.
Recently, MIGS procedures have gained in popularity due to favorable safety profiles, demonstrable effectiveness, and minimal disruption and trauma to ocular tissues. Trabecular bypass stents were the first MIGS implants to come to market in 2012. During a trabecular bypass stent procedure, one or more stents are implanted into the trabecular meshwork through the same type of microincision used to perform cataract surgery. As an implant into the trabecular meshwork, trabecular bypass stents address only one (the diseased trabecular meshwork) of three primary points of potential resistance in the conventional outflow pathway, and have only modest incremental IOP-lowering effectiveness vis-à-vis cataract surgery alone. To date, the FDA has only authorized trabecular bypass stents for use in Combination Cataract surgery for patients with Mild-to-Moderate severity. To attain expanded indications beyond the Mild-to-Moderate Combination Cataract segment in the U.S., we believe trabecular bypass stents will need to demonstrate safety and effectiveness when used alone and without the assistance of the well documented IOP-lowering impact of cataract surgery itself. It is estimated that
126
Table of Contents
there were approximately 205,000 MIGS stent procedures in the U.S. in 2020. In 2019, without COVID-19 related impacts, there were an estimated 220,000 MIGS stent procedures in the U.S.
Alternative bypass stents, another category of implantable MIGS device, have been designed to artificially shunt aqueous humor from the anterior chamber away from the conventional outflow pathway and into the subconjunctival or suprachoroidal spaces in the eye. Alternative bypass stents create a new drainage channel, circumventing the diseased conventional outflow pathway. Currently available alternative bypass stents have only been approved for Refractory cases, such as failed prior surgeries and those unresponsive to maximum tolerated medical therapy, which limits their potential market due to the relatively lower incidence of Refractory cases. Alternative bypass stents that are implanted in a manner that shunts fluid unnaturally have greater safety concerns than MIGS devices that leverage the conventional outflow pathway. In 2018, Alcon’s Cypass stent was withdrawn from the market due to concerns over rates of corneal endothelial cell loss. The FDA classified the event as a Class I recall, which indicates there is a reasonable probability that use of the product will cause serious adverse health consequences or death. The Cypass product has not returned to market.
In surgical glaucoma, each diseased eye requires an independent procedure and, as a result, requires its own surgical device for the treatment. An estimated 4.2 million people in the U.S. suffer from POAG and PEX (pseudoexfoliation glaucoma), of which only 3.5 million have been diagnosed. Of this combined population, 0%-6% are estimated to suffer from PEX, resulting in an estimated 3.4 million people in the U.S. diagnosed with POAG at the 3% PEX midpoint. Applying a ratio of 1.8 assumed eyes with POAG per affected person (or 80% with bilateral POAG) to the estimated 3.4 million people diagnosed with POAG in the U.S. results in a total addressable treatment population of 6.1 million diagnosed eyes with POAG. Based on average selling prices for MIGS devices in 2020, the implied total addressable market opportunity in the U.S. for devices that could effectively treat all diagnosed POAG sufferers is approximately $6 billion. We estimate that currently available trabecular bypass stents are effectively precluded from participating in over 85% of this addressable market given the limitations of their indications for use and the fact that less than 15% of the diagnosed U.S. POAG population has cataract surgery each year based on the estimated 774,000 eyes that had OHT or any type of glaucoma among all of the cataract surgeries performed in 2019. Currently available alternative bypass stents are limited to Refractory cases, which we believe represent a smaller portion of the total U.S. POAG market. The current market for glaucoma surgery devices that can deliver both the effectiveness to substantially reduce IOP and/or IOP-lowering medication utilization, and a best-in-class safety profile, has potential for substantial growth and expansion.
Currently, MIGS devices, which we define as implantable microstents and non-implantable Schlemm’s canal surgery devices that facilitate aqueous drainage and access the eye using an ab interno approach via sutureless corneal microincisions, make up the largest and fastest growing segment of the surgical glaucoma market. The trabecular bypass stent market has projected U.S. and worldwide CAGRs of 27% and 37%, respectively, from 2020 to 2025. The global revenue forecast for canal surgery devices nearly triples from 2020 to 2025, increasing from $77 million in 2020 to $228 million in 2025. MIGS devices accounted for an estimated $342 million of the total estimated $575 million global glaucoma surgical device market in 2020. In 2019, without COVID-related procedural impacts, MIGS devices accounted for $422 million out of the $706 million global glaucoma surgical devices market. Due to the estimated greater than 60% market share held by trabecular bypass stents, however, the U.S. MIGS device market has been unnaturally skewed toward the Combination Cataract Mild-to-Moderate severity segment for which trabecular bypass stents have been authorized. We expect the overall MIGS device market to grow well beyond its current size as surgeons employ more comprehensive and consistently effective non-implantable procedures to treat a broader range of patients. The Combination Cataract market is also expected to exhibit market growth, as we estimate that current Combination Cataract procedure volumes represent less than one-third of their potential in the U.S.
The prevalence of POAG is projected to increase in the U.S. due to aging populations (glaucoma primarily affects people over 60), demographic shifts (POAG has a higher incidence among black and Hispanic populations), and the growth of other medical conditions associated with glaucoma such as diabetes, heart disease and high blood pressure. In addition, glaucoma has been historically underdiagnosed but recent medical
127
Table of Contents
advancements in screening protocols and diagnostic testing combined with growing awareness have contributed to more accurate diagnosis rates. As surgical glaucoma procedures evolve to become more efficient, less invasive and safer while offering increased effectiveness, the potential for these treatments to become the standard of care for POAG patients earlier in the continuum of disease progression continues to increase.
Dry Eye Disease
DED refers to a group of disorders caused by either low quality tears, known as evaporative DED, or inadequate tear production, known as aqueous deficient DED. Studies have shown that dry eye symptoms have a significant impact on patient quality of life and productivity and are the most common reason for a patient visit to an eye doctor. If left untreated, DED can be extremely painful, and lead to permanent cornea damage and vision impairment. Studies have also shown that evaporative DED resulting from meibomian gland dysfunction, or MGD, is associated with approximately 86% of all DED cases.
MGD is a chronic, multifactorial abnormality of the meibomian glands that alters gland morphology and physiology. In healthy eyes, there are 25-30 meibomian glands located within each of the upper and lower eyelids. These glands produce and secrete an oily substance called meibum which forms the outer layer of healthy tears and helps prevent premature tear evaporation. Healthy meibum has the consistency of olive oil and is released with each blink. Alterations in meibum chemistry and gland hyperkeratinization can lead to hyposecretion and ultimately the accumulation and hardening of meibum within the meibomian glands. The resulting gland obstruction, if not treated effectively and efficiently, can cause up-regulation of neighboring glands, gland inflammation, and atrophy of the glands, causing MGD. MGD greatly affects the ocular surface leading to tear film instability, rapid tear evaporation and drying, tear hyperosmolarity and subsequent inflammatory damage of the ocular surface. Clinically, these changes result in symptoms such as visual degradation, blurred vision, ocular fatigue, ocular discomfort and foreign body sensation.
There are an estimated 739 million people globally and 38 million people in the U.S. who suffer from signs and symptoms of DED. Of the 38 million people with DED in the U.S., only 17 million have been diagnosed with DED, of which an estimated 14 million diagnosed sufferers have evaporative DED associated with MGD. MGD prevalence is expected to continue to grow as the population ages and behavioral risk factors like contact lens usage, LASIK surgery, prescription medication usage, and screen viewing time become more common. We estimate that based on current out-of-pocket expenditure levels for DED prescription eyedrops and the estimated size of the MGD patient population, the addressable U.S. market for MGD treatment is approximately $10 billion per year, as compared to MGD procedures representing less than $100 million of U.S. manufacturer revenues in 2020 (in total, U.S. DED treatments represented $2.4 billion of 2020 manufacturer revenues). We believe that evaporative DED caused by MGD is one of the most prevalent diseases in all of medicine that lacks any meaningful reimbursement coverage by Medicare and private payors.
Although MGD is the primary root cause of DED, we believe it is relatively “new” to eyecare research and product development. As a result, despite the enormous population of DED sufferers, the vast majority of eyecare centers have underdeveloped DED treatment practices. We believe this is the direct result of the limited effectiveness of prevailing medications and treatments, and the practically nonexistent reimbursement coverage regimes currently in place among third-party payors for MGD procedures and associated meaningful limitations on patient access. We believe that any devices that have been clinically proven to be safe and effective and authorized by the FDA for use in MGD procedures will have the opportunity to drive ECP and patient adoption and improve patient access. There are approximately 40,000 optometrists and approximately 20,000 general ophthalmologists who regularly see patients with DED at over 40,000 eyecare facilities in the U.S. Only an estimated 5,000 of these facilities, however, have what we consider to be high volume DED practices today. We define “high volume” as facilities that write more than 36 DED prescriptions per month or actively perform in-office DED procedures, such as punctal plug insertion, amniotic membrane grafts or thermal-based MGD procedures. Similar to glaucoma, we believe that improvements in third-party diagnostic capabilities, combined with increasing professional and patient awareness will drive increased diagnosis and treatment of DED. We believe that significant growth of the MGD
128
Table of Contents
procedure market will result from increasing patient access through the potential establishment of broad-based third-party payor coverage, and from greater adoption by ECPs as they accumulate experience in integrating and administering new and improved procedure-based DED solutions in their practices.
Current Alternatives and Limitations
A variety of pharmaceutical and procedure-based treatment alternatives exist for POAG and DED but there is no cure for either disease. Because many of the current alternatives focus on treating symptoms rather than the underlying causes of the disease, they offer suboptimal effectiveness and durability.
Primary Open-Angle Glaucoma
Physicians classify POAG based on risk of visual loss on a scale that ranges from Mild, to Moderate, then Advanced/Severe. General ophthalmologists and optometrists who provide primary eyecare services are typically the first to diagnose and treat POAG. These frontline ECPs typically diagnose OHT or Mild-to-Moderate cases and will refer patients to glaucoma specialists when more advanced treatment is necessary.
Ongoing treatment is complicated by the progressive and chronic nature of POAG. We believe prescription medications and surgical interventions currently offered to treat POAG patients yield suboptimal outcomes due to non-compliance, limited durability of effect, or invasiveness.
Table 1: Treatments for Management of High Intraocular Pressure by Stage of Progression
Stage | Treatment | Notes | ||
| Ocular Hypertension | Topical eyedrops or monitor IOP | Some practitioners prefer to treat with topical eyedrops to reduce the risk of developing glaucoma. | ||
| Mild POAG | Topical eyedrops
Selective Laser Trabeculoplasty (SLT)
Microinvasive glaucoma surgery (MIGS) | Prostaglandin analogs are generally first line due to effectiveness, safety and once-a-day dosing; other classes of medications may be added if needed.
May be a first line alternative to eyedrops where there is risk for poor tolerance or compliance.
Combination Cataract procedures can be employed if cataract surgery is indicated due to minimal added risk with MIGS; trabecular bypass stents are limited to Combination Cataract procedures. Interventional Standalone MIGS procedures such as those using OMNI, are also available. | ||
| Moderate POAG | Sequenced as for Mild, but because there is more advanced disease, threshold for escalating to next steps is reduced.
Bleb-forming procedures (e.g., trabeculectomy, tube-shunts) | Approved Standalone MIGS procedures, such as those using OMNI, may be performed in advance of traditional invasive surgeries or if such surgeries have failed.
Bleb-forming (filtration) surgeries provide maximum IOP-lowering effectiveness but are reserved for cases where drugs and less invasive procedures have failed to halt or sufficiently slow disease progression. Very infrequent usage at this stage. |
129
Table of Contents
Stage | Treatment | Notes | ||
High rate of post-op bleb management/revision; potential risks for sight-threatening adverse events. | ||||
| Advanced/Severe POAG | Bleb-forming procedures | Risk of vision loss high, benefit of maximum IOP-lowering balances surgical risks. Approved Standalone MIGS procedures may be performed after failed conventional surgeries |
Prescription eyedrops are the most common first line therapy used to treat OHT and Mild glaucoma and often continue to be utilized for the treatment of Moderate and Advanced/Severe patients. There are a broad range of prescription medications available to treat glaucoma including prostaglandin analogs, beta blockers, carbonic anhydrase inhibitors and alpha agonists. These medications typically work to either increase the drainage of aqueous fluid through the uveoscleral and conventional pathways (prostaglandin analogs), reduce the production of aqueous fluid (beta blockers, carbonic anhydrase inhibitors) or both (alpha agonists).
The effectiveness of prescription eyedrops for POAG patients is dependent on patient behavior and compliance, providing inconsistent protection from POAG progression for those who have adherence challenges. POAG disproportionately affects an older demographic who may experience several barriers to adhering to medication regimens, including physical limitations that inhibit the self-instillation of eyedrops, forgetfulness, and difficulties following the medication schedule. For example, a systematic review of 29 studies showed that up to 80% of glaucoma patients do not follow their prescribed medication regimen. Further, although multiple eyedrops can add incremental effectiveness to a medication program, they may concurrently complicate the dosing regimen, reduce patient compliance, and exacerbate side effects including damage to the ocular surface.
Studies have demonstrated that chronic use of glaucoma medication contributes to ocular surface disease, an inflammation of the ocular surface, which is irritating and painful (further contributing to poor adherence) and can contribute to greater risk of surgical failure should traditional glaucoma surgery (such as trabeculectomy) be required. It has also been reported that the long-term use of glaucoma medications is associated with increased expression of proinflammatory mediators in the conjunctiva, and that even preservative-free prostaglandin eyedrops have been shown to promote macrophage infiltration in the eyelids with long-term use.
Sustained pharmaceutical delivery through an intraocular implant is another method of drug administration. While intracameral sustained drug delivery mitigates issues relating to patient medication adherence, it could introduce new challenges associated with leaving an intracameral implant in the eye for several months or years, or the procedural complexity and risks associated with implanting objects in the eye and potentially removing them. Durysta, the only intracameral implant for glaucoma that has been approved by the FDA, is a bioabsorbable intracameral implant providing sustained release of a prostaglandin analog (bimatoprost) in a single administration that is designed to elute the drug for a period of four to six months. The FDA has approved Durysta with a label that warns that the drug should be limited to a single implant per eye without retreatment. In the pivotal clinical trials, the IOP reduction associated with Durysta was non-inferior to timolol (beta blocker), with a mean IOP reduction of 5 to 8 mmHg in patients from a mean baseline IOP (washed out) of 24.5 mmHg. Durysta is procedurally appealing because it can be delivered at the slit lamp in an efficient in-office procedure and because it naturally biodegrades and is absorbed by the body over the course of its treatment duration. However, because the implant can freely move around the eye for several months, we believe long-term safety data on the risks of potential complications such as corneal endothelial cell loss resulting from repeated implantations will be key to the long-term viability of this alternative. Another intracameral implant that has not been authorized for use by the FDA is reportedly in Phase II and III clinical trials. This product features a sustained release implant that is surgically implanted and fixed into place within the sclera at the angle where the iris and cornea meet through an ab interno approach similar to MIGS. Unlike Durysta, however, this titanium implant is not biodegradable and requires an initial operating room visit for skilled implantation, as well as potential follow-up ab interno procedures to remove or refill the existing implant or install a new implant at regular intervals.
130
Table of Contents
As POAG progresses to the Moderate stage and beyond, or as medications prove ineffective, there are multiple procedures that can be performed, which range from non-invasive SLT to minimally invasive MIGS to invasive conventional surgery. In an SLT procedure in an ECP’s office, laser energy is applied to the trabecular meshwork tissue in the eye’s conventional outflow pathway which initiates a change in the tissue that results in better drainage of fluid out of the eye. SLT procedures can eventually result in a lowering of IOP. SLT offers a non-invasive, energy-based solution and short recovery times, with effectiveness similar to a prostaglandin analog eyedrop but with a waning treatment effect at less than one year for up to half of patients.
The most common conventional surgical options are bleb-forming procedures, including trabeculectomy (also called filtering surgery) and tube shunt implantation, and each has been in use for several decades. Blebs are permanent blisters on the outside of the eye intended to serve as drainage reservoirs. Conventional surgeries are multi-step invasive procedures, and surgeons only turn to them when they need maximal reductions in IOP to prevent visual field loss or when treatment of the conventional outflow pathway has failed. Unfortunately, despite their success at reducing IOP, serious complications or even surgical failure are not uncommon with conventional surgical procedures. In one prominent study, 34% of the 82 trabeculotomy procedures followed were considered failures after three years. Furthermore, these conventional surgeries are considered as a last line of defense for Advanced/Severe stage patients because the procedures create a physiologically artificial pathway that can be difficult to control, carry a life-long risk of complications (e.g., hypotony, blebitis, bleb failure), and typically require longer recovery periods. Post-operative care can include a regimen of prescription antibiotic and steroid eyedrops to prevent infection and inflammation, wearing protective eye shields when sleeping, avoiding strenuous activities and refraining from driving.
We believe the observed benefits and safety data for the MIGS category generally, and the problems typically associated with topical medications have created a paradigm shift towards earlier surgical intervention. Prior to the introduction of implantable MIGS devices in 2012, there was a significant difference between the relatively low risk and moderate effectiveness of prescription eyedrops and laser procedures and the high risk and high effectiveness of conventional surgical treatments. Trabecular bypass stents have steadily grown in usage among surgeons performing cataract procedures because the devices are relatively straightforward to implant, involve minimal complications and have an established reimbursement pathway. Trabecular bypass stents have demonstrated modest reduction of IOP beyond the IOP-lowering benefits typically seen from Standalone cataract surgery. One RCT found that the trabecular bypass stent plus Combination Cataract cohort had a mean reduction in IOP of 7.0 mmHg versus a mean reduction of 5.4 mmHg at 24 months in the cataract surgery only cohort. The attractive safety profile of MIGS has expanded the intent of MIGS surgery beyond solely IOP lowering goals for patients with elevated IOP to also include medication reduction both in patients with elevated IOP and in patients whose IOP is controlled by medications. The FDA’s authorization of trabecular bypass stents has been limited to Mild-to-Moderate cases in Combination Cataract surgery, thereby restricting the use of procedures with such stents to the less than 15% of diagnosed POAG patients who undergo cataract surgery in a given year.
Based on our field research, we believe that the majority of surgeons who perform Combination Cataract procedures with MIGS stents are primarily specialists whose practices rely on successful cataract procedures. For patients with Mild-to-Moderate POAG, we believe that cataract surgery creates an opportunity for early surgical intervention without adding significant risk to the patient or to the success of the cataract surgery. In many Combination Cataract cases, the incremental effectiveness of a MIGS procedure in reducing IOP is secondary to the success of the cataract procedure, which can immediately and dramatically improve the patient’s vision and is the primary reason for the operating room visit. Given these dynamics and the IOP-lowering impact of cataract surgery by itself, for a Mild Combination Cataract patient, safety and efficiency can be as important as the incremental effectiveness of the trabecular bypass stent procedure. Conversely, MIGS utilization in the Standalone market must be a deterministic, as opposed to an opportunistic, decision. A Standalone procedure is not a mere add-on to a cataract procedure that has already been scheduled, but is the only reason for the operating room visit and must deliver a very high consistency of efficacy and a very high degree of effectiveness to not only justify the procedure, but also provide the surgeon with enough confidence to take the patient to the operating room for a singular reason. Among currently-available MIGS devices, we believe that OMNI is the
131
Table of Contents
only alternative that can deliver consistent, significant IOP reductions in Standalone cases because of its ability to not only address all three primary points of resistance in the conventional outflow pathway through two sequential procedures — canaloplasty and trabeculotomy — and distinct mechanisms of action (high consistency of effectiveness) but also do so in a complete, circumferential, 360-degree fashion (high degree of effectiveness). In contrast to OMNI’s ability to comprehensively address the entire conventional outflow pathway, currently-available trabecular bypass stents were, as their name implies, designed to address only one of the three primary sources of outflow resistance (less expected consistency of effectiveness) and do so over just a single quadrant of the diseased outflow pathway (less expected degree of effectiveness).
Dry Eye Disease
Although MGD is the primary root cause of DED, we believe it is relatively “new” to eyecare research and product development. In contrast, we believe aqueous deficiency, which is a less prominent root cause of DED, has historically dominated the medical community’s mindshare regarding DED and has been synonymous with the disease. This has contributed to the current DED treatment market being characterized by an abundance of OTC artificial tears and lubricating eyedrops, and prescription DED eyedrops. Given the relatively recent focus on and understanding of MGD, MGD procedures for DED have had limited commercial traction and represent a significant but underdeveloped market opportunity.
DED is treated by ophthalmologists and optometrists. OTC eyedrops, which are palliative, and prescription eyedrops, which aim to alleviate inflammation and/or increase aqueous layer tear production, are the predominant current alternatives utilized to treat DED. Both AbbVie’s Restasis and Novartis’ Xiidra DED prescription eyedrops have achieved commercial success, with 2019 global revenues of $1.1 billion and approximately $400 million, respectively. Restasis is believed to partially suppress an immune response that prevents tear production while Xiidra blocks migration of activated T cells to the ocular surface, reducing cytokine release that can cause inflammation. While Restasis and Xiidra have demonstrated the commercial viability of DED solutions, we believe both are limited in their ability to treat the substantial majority of DED sufferers. Neither medication is indicated to treat MGD, the primary underlying cause of evaporative DED, which is associated with 86% of all DED cases. Furthermore, patient non-compliance, the high rate of side effects, and high out-of-pocket costs further limit the ability of prescription eyedrops to treat DED effectively and with maximal patient access.
In contrast, the market for solutions that treat MGD in a targeted manner is highly underdeveloped. MGD procedures represented less than $100 million of U.S. manufacturer revenues in 2020. We are marketing TearCare for its currently-authorized use and, as part of our long term market development plan, intend to seek FDA clearance for an expanded indication for use to more specifically reflect its effectiveness in the treatment of DED due to MGD. In general, currently available devices for the treatment of MGD can be difficult for providers to administer, which places significant time and oversight demands on the ECP and are uncomfortable or ill-fitting for patients. We believe that TearCare uniquely has the required physiological profile to liquefy hardened meibum within the diseased meibomian glands to allow an ECP to remove the underlying obstructions from meibomian glands that cause MGD in a consistently effective manner. Further, we believe lack of patient access to reimbursed MGD procedures has been a major obstacle to widespread adoption and market development. Many competing MGD procedures require high upfront capital equipment purchases for providers, as well as high costs of ongoing consumable supplies, which lowers the overall value proposition to providers, patients and third-party payors.
Our Solutions
We have designed OMNI and TearCare to be interventional ophthalmology devices. We believe that both glaucoma and DED are significantly underserved by current treatment offerings and that there are large market opportunities for effective solutions that restore the natural functionality of diseased eyes.
132
Table of Contents
Our Product Development Approach
The past, current, and ongoing development of OMNI and TearCare follows our internal product development approach, which is governed by four fundamental requirements that we believe are critical to delivering the most effective, safe and consistent clinical outcomes for patients with eye disease.
| • | Comprehensive Understanding of Disease Physiology. We review and analyze all available clinical data, science, and literature that is relevant to a disease to achieve a sound understanding of its underlying cause(s), which guides the development of our products. |
| • | Treatment of Underlying Causes. Healthy eyes are self-regulating marvels of evolution, biomechanics, chemistry and physiology. We believe that restoring the natural functionality of diseased eyes by comprehensively treating underlying cause(s) of disease provides the optimal combination of effectiveness and safety. |
| • | Intuitive Design. Our products are designed to transform complex, impractical or invasive treatment approaches into intuitive, minimally invasive, user-friendly procedures. Our product development goals are focused on delivering a preferred “go to” treatment of choice for ophthalmologists and optometrists. |
| • | Patient Access. We seek to maximize availability and accessibility of our products for as many patients as possible. We believe that our devices have the potential to offer differentiated clinical, experiential and economic value to all eyecare stakeholders. For conditions where patients lack optimal treatment access due to insurance coverage limitations or difficult patient-pay economics, we plan to demonstrate the value proposition of our solutions through data from rigorous clinical trial data and real-world results to improve access. |
We aim and expect to be a clinical leader in every eyecare segment we enter and seek to achieve all four criteria in any of our product development projects. From device ideation to commercialization, we take into consideration the perspectives of patients, providers and third-party payors throughout our product development process. When possible, we seek to streamline our product commercialization process by judiciously designing our products to achieve the most efficient routes for FDA clearance or authorization for each applicable indication and reimbursement coverage by third-party payors.
We also actively seek to protect the intellectual property involving our products, technologies, and methods. As of April 30, 2021, our patent portfolio consisted of 62 issued patents and patent applications for our Surgical Glaucoma segment and 32 issued patents and patent applications for our Dry Eye segment.
133
Table of Contents
OMNI Surgical System
| Figure 4a. Canaloplasty using OMNI | Figure 4b. Trabeculotomy using OMNI |
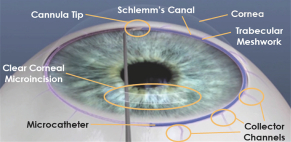 | 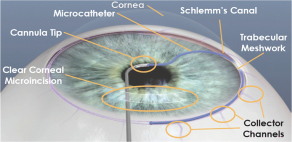 |
OMNI is a handheld, single use, therapeutic device for minimally invasive glaucoma surgery, or MIGS. OMNI is designed to restore the eye’s natural drainage system without compromising the structural integrity of the eye or leaving implants behind post-surgery. We have received 510(k) clearance from the FDA in the U.S. and a CE Mark in the EU to market OMNI. OMNI is indicated for canaloplasty (see Figure 4a; microcatheterization and transluminal viscodilation of Schlemm’s canal) followed by trabeculotomy (see Figure 4b; cutting of trabecular meshwork) to reduce IOP in adult patients with POAG in the U.S. and with OAG in the EU.
In late 2017, OMNI received its initial 510(k) clearance from the FDA for delivery of small amounts of viscoelastic fluid and cutting of the trabecular meshwork during trabeculotomy. In March 2021, OMNI received FDA clearance for its current expanded indication for use, which we believe reflects the capabilities of OMNI to reduce IOP in adult patients with POAG across the spectrum of disease severity in both Combination Cataract and Standalone cases. In connection with this clearance, the FDA reviewed clinical data from our ROMEO multi-center study. We believe that ROMEO represents the first and only ab interno clinical data reviewed by the FDA that has successfully resulted in a Standalone indication in Mild-to-Moderate glaucoma. Together with our clinical trial results, we believe our expanded indication for use will further bolster confidence in the device among current and prospective surgeons, primary care ECPs, patients and third-party payors. We believe that OMNI is the first and only MIGS device that the FDA has indicated for ab interno procedures to lower IOP across all severities of POAG, including Standalone procedures. We further believe that OMNI is also the first and only multi-procedure MIGS device dually indicated for canaloplasty followed by trabeculotomy.
134
Table of Contents
Figure 5. The OMNI Surgical System and Instructions for Use
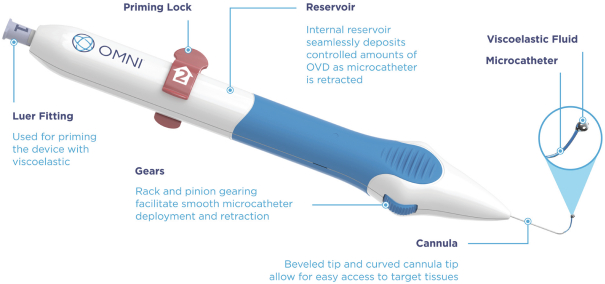
OMNI Instructions for Use:
OMNI includes a stainless-steel cannula, polymeric microcatheter, removable priming lock, internal reservoir and plunger tube, a Luer fitting for direct connection with an OVD cartridge to prime the internal reservoir, and two advancement wheels. A single advancement wheel is located on each side of the handle. This allows OMNI to be used in either eye (OD or OS) and in either hand of the surgeon (left or right), by turning the device 180 degrees along its vertical axis. These wheels are used to advance and retract the microcatheter.
The stainless-steel cannula has a curved shape with a beveled tip for entry through the trabecular meshwork into Schlemm’s canal. To perform the combined and sequential canaloplasty/trabeculotomy procedures, the canaloplasty is performed first, followed by trabeculotomy as explained in further detail below.
Performing Canaloplasty First: the microcatheter is advanced into Schlemm’s canal up to 180 degrees (one hemisphere) by rotating the advancement wheel forward until the wheel stops (about 20 mm). When the device is being used to deliver viscoelastic fluid, retraction of the microcatheter causes the plunger tube to advance into the viscoelastic fluid reservoir thereby automatically dispensing viscoelastic fluid along the length of Schlemm’s canal and collector channels. The microcatheter can be advanced/retracted up to 20 mm per cycle by manually rotating the advancement wheel. The microcatheter can be fully advanced/retracted multiple times, however, viscoelastic fluid can only be dispensed during the first two advancement/retraction cycles in order to dispense viscoelastic fluid along each hemisphere of Schlemm’s canal. Thus, OMNI is designed to be used twice within Schlemm’s canal to deliver a controlled volume of viscoelastic fluid along the first 180 degrees of the canal, followed by a second delivery of viscoelastic fluid along the other 180 degrees. OMNI delivers a total viscoelastic fluid volume of 11 microliters throughout Schlemm’s canal (approximately 5.5 microliters for each of the first two advancement/retraction cycles).
Performing Trabeculotomy Second: the beveled tip of the curved stainless-steel cannula is re-positioned into the same Schlemm’s canal location after finishing canaloplasty. The polymeric microcatheter is re-advanced into Schlemm’s canal up to 180 degrees (one hemisphere) by rotating the advancement wheel forward until the wheel stops (about 20 mm). With the microcatheter resting in the canal, the cannula is removed from the corneal incision and out of the eye causing the microcatheter to cut through the trabecular meshwork. This process can be repeated in the second Schlemm’s hemisphere. |
Surgeons have performed canaloplasty and trabeculotomy to treat glaucoma for decades using conventional, invasive surgical methods. In a canaloplasty procedure, a surgeon advances a specialized microcatheter through the trabecular meshwork then into and around Schlemm’s canal and injects viscoelastic fluid to dilate the drainage canal and points of egress. Canaloplasty primarily addresses distal resistance (i.e., collapsed Schlemm’s canal, blocked collector channel ostia) and has some presumed effects on the inner wall of Schlemm’s canal and the trabecular meshwork due to dilation and stretching. In a trabeculotomy procedure, a surgeon unroofs Schlemm’s canal by cutting the trabecular meshwork to provide aqueous humor with direct access to the drainage points in the conventional outflow pathway. Trabeculotomy addresses proximal resistance (i.e., outflow resistance in the trabecular meshwork and inner wall of Schlemm’s canal). While there exists an abundance of clinical data supporting the effectiveness of canaloplasty and trabeculotomy procedures generally in reducing
135
Table of Contents
IOP, we believe these procedures are difficult to perform, traumatize the eye, have higher risk of intraoperative and post-operative complications and require longer patient recovery times because they were historically performed invasively through an ab externo approach which required deep scleral incisions to access the diseased conventional outflow pathway. During our initial research and development in the glaucoma space, we came to believe that products that could combine the benefits of ab externo circumferential surgery with less invasive clear corneal MIGS access, would have a global impact on POAG by driving mainstream surgeon adoption of intuitive, effective, and interventional surgical procedures to patients across the disease progression spectrum. We believe that the sequential combination of canaloplasty followed by trabeculotomy is uniquely capable of treating all three primary points of resistance in the conventional outflow pathway of the eye as detailed in Figures 6a and 6b below. We believe treating all three primary points of resistance is critical to achieving the consistency and level of effectiveness in reducing IOP and medication requirements necessary to expand the use case for MIGS procedures to the Standalone market and to all disease severities among adult POAG patients.
Figure 6a. Aqueous Humor Outflow through the Conventional Outflow Pathway
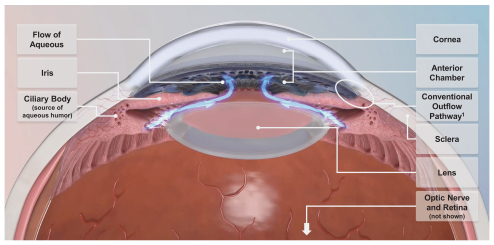
1 Extends 360o around the circumference of the iridocomeal angle where the iris and cornea meet.
Figure 6b. Close Up on the Conventional Outflow Pathway
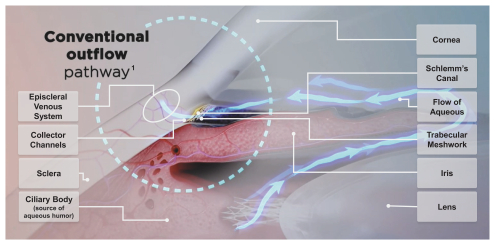
1 Extends 360o around the circumference of the iridocomeal angle where the iris and cornea meet.
136
Table of Contents
OMNI has roots from two handheld predicate devices, the VISCO360 and TRAB360. Both of these devices received CE Marks for the reduction of IOP in patients with POAG in 2016. In the U.S. from 2013 to 2018, VISCO360 and TRAB360 each received FDA clearances to deliver small amounts of viscoelastic fluid during ophthalmic surgery and to cut the trabecular meshwork during trabeculotomy procedures, respectively. After years of extensive development of the predicate devices with our physician advisors and other practicing surgeons across the U.S. and in Europe, we designed OMNI to combine their functionality into a single device. OMNI received its CE Mark in 2015 and its initial FDA 510(k) clearance in December 2017 by demonstrating substantial equivalence to predicate devices. OMNI received 510(k) clearance in March 2021 for its current expanded indication for use.
We have applied our medical expertise, as well as specialized design and engineering capabilities, to create a complex device that is simple in appearance and intuitive to use. Each OMNI device consists of 29 separate precision-engineered parts that have been optimized for performance, effectiveness and usability. After inserting the cannula tip into the corneal microincision and accessing Schlemm’s canal, the surgeon can advance and retract the catheter with a fingertip dial up to 180 degrees. Upon retraction of the catheter, OMNI delivers viscoelastic fluid to complete the viscodilation of Schlemm’s canal. The surgeon can complete a full 360 degree canaloplasty by reinserting the catheter and advancing it in the opposite direction. To perform the trabeculotomy following the canaloplasty, the same microcatheter can be reinserted into Schlemm’s canal and used to deroof the trabecular meshwork in a titratable manner (90, 180, 270 or 360 degrees). OMNI’s versatility and titratable functionality, which we believe are unmatched by other MIGS products currently on the market, enable surgeons to perform sequential comprehensive outflow treatments that they can customize based on an individual patient’s disease severity and eye anatomy in both Combination Cataract and Standalone settings.
We believe that OMNI has the potential to offer the following benefits:
| • | Effectiveness and Safety. We designed OMNI to set the standard for consistently effective IOP reduction in adult POAG patients by focusing on what we believe is a primary underlying cause of the disease: diseased conventional outflow pathway with increased resistance to the drainage of aqueous humor. OMNI facilitates two complementary and sequential procedures, canaloplasty and trabeculotomy, which enable a surgeon to address the three primary points of resistance in the conventional outflow pathway with a single device using a single clear corneal incision during a single outpatient visit. Further, we believe that OMNI fits all of the criteria for a product to have a market leading safety profile: it restores natural functionality to the eyes, involves minimal complications and we are aware of only eight MDRs submitted to the FDA that were “possibly” related to OMNI during that time period. None of these events were unexpected as possibilities for this type of glaucoma surgery. We believe that the effectiveness and safety of OMNI is further demonstrated by the clinical data from our four completed trials and five peer-reviewed publications to date (with several additional publications planned). |
| • | Intuitive Design. The intuitive, ergonomic, single-handed design of OMNI, coupled with surgeon familiarity with the ab interno minimally invasive approach to glaucoma surgery, facilitates physician adoption and utilization. We believe that OMNI’s intuitive design enables a steep learning curve and allows surgeons to become comfortable using OMNI relatively quickly. In May 2020, we introduced a new version of the OMNI Surgical System called OMNI Next Gen that incorporated extensive user and ergonomic feedback from our surgeon team members, advisors, and customers and that we believe improved upon the first-generation device. We designed OMNI Next Gen for improved ergonomics, enhanced canalicular access through modifications of the cannula tip and microcatheter tip, smoother deployment and retraction mechanism for the microcatheter, and increased viscoelastic fluid volume. In the second half of 2020, OMNI Next Gen represented over 90% of our Surgical Glaucoma revenue. |
| • | Versatility. We believe that OMNI’s broad FDA-cleared indication for use and comprehensive titratable 360 degree access to the diseased conventional outflow pathway make it a valuable option for all adult POAG patients in either Standalone or Combination Cataract settings. In practice, our field |
137
Table of Contents
research indicates that surgeons utilize OMNI for cases across the entire POAG disease severity continuum, as well as both on a Standalone basis and in Combination Cataract surgery. We believe that from a device effectiveness and an indication for use standpoint, OMNI should be the MIGS device of choice for IOP reduction in the full range of adult POAG patients and supports transforming physicians’ approach to POAG by bridging the chasm between current first line treatment options, such as eyedrop medications and SLT, and higher risk conventional surgical procedures. |
| • | Market Access. The procedure enabled by OMNI, canaloplasty followed by trabeculotomy, is covered and reimbursed by all MACs and numerous private insurers, covering an estimated 67% of U.S. POAG sufferers. We believe that OMNI enables safe, fast healing and effective ambulatory care procedures that are attractive to all stakeholders, including patients, surgeons, facilities and third-party payors. |
TearCare System
Figure 7. The Open-Eye Design of TearCare’s SmartLids

TearCare has been commercially available since 2019 and is currently marketed as a 510(k)-exempt powered heating pad for the application of localized heat when the current medical community recommends the application of a warm compress to the eyelids. Such applications would include Meibomian Gland Dysfunction, Dry Eye, or Blepharitis. Based on our favorable randomized controlled trial results as well as over 10,000 cases of real-world evidence, we intend to seek clearance of TearCare for an expanded indication for use in the second half of 2021.
In an effort to optimize the treatment of evaporative DED due to MGD, we custom designed TearCare to facilitate what we believe is the optimal method for clearing meibomian gland obstructions based on numerous clinical studies: warming the glands to a minimum of 41 degrees Celsius for 15 minutes to melt congealed meibum followed by manual, clinician customized and performed removal of the liquefied obstructions using forceps to help facilitate restoration of healthy meibum production to naturally fortify the tear’s protective lipid layer. Tear film is a complex, continuously renewed solution that is necessary for maintaining a healthy cornea and optical clarity. Tears consist of three layers: an inner mucous layer that nourishes the cornea and helps stabilize and anchor the tear film; a middle aqueous layer that lubricates the eye, removes particles and prevents infection; and an outer lipid layer, or meibum, that prevents premature evaporation and maintains tear film stability. MGD occurs when meibum accumulates and hardens within the meibomian gland. Over time, the glands can become blocked or clogged, which prevents meibum from reaching the tear, fortifying the outermost tear lipid layer, and protecting the integrity of the tear. As evidenced by our design of TearCare and desired
138
Table of Contents
indication for use, we believe the most effective treatment for DED due to MGD requires the application of consistent therapeutic levels of heat to the meibomian glands for a prescribed period of time followed by a comprehensive clearance of obstructed meibomian glands, thus restoring the eyelid’s natural ability to produce healthy lipid secretions and recovering the integrity of the tear film. We believe that the open-eye design of TearCare allows patients to blink naturally throughout the thermal portion of the procedure. This blinking motion has the potential to facilitate the natural flow of melted meibum which can then be further complemented by an ECP’s manual expression of the previously obstructed glands using forceps.
Figure 8. The TearCare System
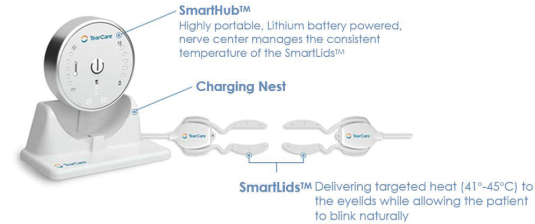
Our TearCare System includes a pair of single-use SmartLids, the first wearable, highly conformant, precision heating device for the eyelids. SmartLids allow for eyes to be open and blink during the thermal portion of the process and are software-controlled, delivering precise heat to the tarsal plates of the eyelids directly overlying the meibomian glands while continuously monitoring temperature and communicating 144 times per second with the SmartHub, a compact, finely calibrated power source and control unit which can make instantaneous adjustments to ensure delivery of the desired amount of heat and therapeutic temperature level. Engineering SmartLids to remain comfortably adhered to virtually all shapes and sizes of eyelids while allowing freedom to blink and delivering precise therapeutic heat is one of our most significant design accomplishments. Following therapeutic heat application by TearCare, ECPs can use commercially available forceps to manually express melted meibum from each gland. ECPs can tailor the amount of pressure applied during expression to specific glands based on a desired full evacuation of the glands, thereby allowing the eyelids to resume the production of healthy, new meibum to coat and protect tears.
According to patient and ECP feedback, treatments using TearCare are comfortable for patients since they can keep their eyes open during the thermal portion of the procedure and have the freedom to blink naturally. Additionally, TearCare was designed to be administered during the course of a routine office visit to an ECP, which makes it convenient for patients, and allows providers to maintain procedural throughput in their practices. We believe that these features of the patient and ECP experience with TearCare procedures offer a stark contrast to other available alternatives which we believe are burdened by ineffective and suboptimal product design, including awkward and uncomfortable patient experiences through closed eye solutions and/or manual solutions that require extremely close patient proximity to the ECP throughout the treatment.
139
Table of Contents
We believe that TearCare has the potential to offer the following benefits:
| • | Compelling Clinical Data. We developed TearCare to address the underlying physiology and root cause of MGD and we believe our clinical data will demonstrate that TearCare treats the signs and symptoms of DED due to MGD. In our OLYMPIA RCT we observed that: |
| • | Use of TearCare in patients with DED was associated with improved symptoms as measured by patient-reported symptoms surveys, such as Ocular Surface Disease Index, or OSDI, and Symptom Assessment in Dry Eye, or SANDE, as well as improved signs, such as tear break up time, or TBUT, and meibomian gland secretion score, or MGSS. TBUT is a measure of the rate of evaporation of the tear film and is an indicator of tear film stability. MGSS is a measure of the quality and quantity of meibum secretion; |
| • | A single TearCare procedure was associated with improvement in each of the signs and symptoms of DED at two and four weeks post-treatment in subjects with MGD, as measured by TBUT, MGSS, corneal and conjunctival staining, and OSDI; and |
| • | The TearCare group had a statistically significantly higher proportion of subjects (72%) improving by at least one OSDI category than the group receiving a competing treatment (59%) |
| • | Minimal MDRs Reported. We believe TearCare’s design, with the SmartLids applied externally to the eyelids allowing the precise heat delivery to be managed by our software-controlled SmartHub, reduces the risk of adverse events arising from using TearCare. We have shipped over 10,000 single-use SmartLid units to customers through April 2021 and have reported to the FDA a single MDR for which the root cause has not been determined and may possibly be related to the device. |
| • | ECP and Patient Experience. We believe our straightforward and intuitive training process helps ECPs and facilities integrate TearCare into their practices quickly. We have already developed the flexibility to train and certify new TearCare customers for the device’s currently-authorized use either in person or remotely via videoconferences, and we believe we could do so for an expanded indication as well. Additionally, TearCare has a compact design, which we believe makes it easy for providers to adopt and implement regardless of their clinic’s physical footprint, as well as providing portability for movement within an office or to other locations for multi-office eyecare practices. TearCare was designed to allow patients to keep their eyes open and blink naturally during the heating process, for a uniquely comfortable treatment experience. |
| • | Versatility. We believe that TearCare has the potential to be a part of the optimal approach for reducing the signs and symptoms of DED due to MGD across all degrees of meibomian gland obstruction and all severities of DED. Our OLYMPIA trial enrolled Moderate and Advanced/Severe dry eye patients and we observed statistically significant clinical improvements in all signs and symptoms of dry eye assessed across both severities of disease, including TBUT and MGSS, objective measurements of DED that were the trial’s primary endpoints, as well as patient-reported symptoms surveys, including EDS, OSDI and SANDE, at both two and four weeks following treatment in subjects with MGD. We believe that TearCare can be used as part of a procedure to restore natural meibomian gland functionality and lead to higher quality tears with a fortified lipid layer. |
| • | Economics. We believe TearCare already provides compelling value for all stakeholders, something that will only increase as its clinical evidence, reimbursement coverage and authorized indications for use each expand. We believe we offer ECPs a thoughtful business model featuring minimal upfront cost, affordable single-use SmartLids, and an efficient patient flow that fits into existing practices and a recurring annual or semiannual procedure cycle. While our initial commercial success has proven that a significant patient-pay market exists for TearCare, we believe that improving access from Medicare and private payors will be the most effective way to meet the needs of the estimated 14 million diagnosed, but underserved, MGD sufferers in the U.S. To that end, we are pursuing a comprehensive long term market development plan that aims to improve patient awareness and insured access to TearCare. |
140
Table of Contents
Our Success Factors
Our mission is to transform eyecare by developing products that address the underlying causes of the world’s most prevalent eye diseases. We design our products to enable ECPs to perform safe and effective interventional procedures that can transform treatment paradigms. We believe the following success factors will drive the growth of our company:
Large market opportunities in eyecare with flawed treatment paradigms. We estimate the total addressable annual market opportunities in the U.S. for OMNI and TearCare are approximately $6 billion and approximately $10 billion, respectively, yet combined 2020 U.S. manufacturer revenues in these markets implied less than 20% total addressable market penetration. We believe the addressable market penetration in Standalone MIGS and in MGD procedures are less than 10% each. We believe that market leading MIGS alternatives do not consistently and comprehensively address the underlying causes of POAG and do not adequately treat a broad enough range of disease sufferers. In POAG, we estimate that over 85% of diagnosed sufferers can only be treated with Standalone procedures because they do not require cataract surgery. Similarly, we believe that the market leading DED products do not address the primary underlying cause of the disease, MGD, while those that do attempt to treat MGD lack user friendly design and do not provide broad patient access. Given the narrow historical product development focus on aqueous deficiency, DED patients are currently limited by a mismatched treatment set (typically prescription or OTC eyedrops) which do not address the root causes of MGD, the predominant underlying cause of the condition. We believe patients suffering from many other eye diseases could also benefit from the transformation of stale treatment practices.
Continual development of innovative technologies. Our ability to transform treatment paradigms in large, underserved eyecare markets will depend on our ability to develop and commercialize products which are differentiated in how they treat underlying diseases, in their safety and effectiveness, in the breadth of their patient access and in their ease of use for the ECP. We believe our product development approach is a key differentiator of our team and our company. We design and iterate our products with continual input from our advisor network, an elite group of ECPs who prioritize efficiency, safety and effectiveness. Once our products are authorized by the FDA and launched, our customer feedback loop helps us further develop our products. This collaborative and iterative process led to the development of our first generation OMNI Surgical System from two predicate devices, as well as our improved OMNI Next Gen which we launched in May 2020, our TearCare System, and new products that are in progress.
Consistent delivery of exceptional customer experience. One of the key drivers of our success will be fully developing the potential addressable markets for POAG and MGD, by maximizing the breadth of patients that our products can serve. We believe developing our target markets requires a consistent, exceptional customer experience, which is best accomplished through a differentiated, highly involved commercial model. Our sales professionals provide ECPs with the necessary education, training and support to adopt and continue to use our products for their authorized uses. We devote significant resources to onboarding our sales professionals and to continuously augmenting their knowledge and capabilities. Our management team and commercial organization are highly experienced in developing primary markets and commercializing disruptive products designed to satisfy unmet patient needs.
Prioritization of clinical excellence and market education. We are deeply committed to a robust clinical trial program and are investing significant resources to generate additional scientific evidence regarding the safety and effectiveness of OMNI and TearCare through numerous clinical studies and the publication of our findings in leading peer-reviewed journals. We believe OMNI is growing rapidly in adoption because of its superior effectiveness and comparable safety compared to alternative MIGS devices and that patients, surgeons and other stakeholders will all benefit from our continued investment in clinical trials and our broader market education initiatives, which include actively engaging in scientific conventions, presenting at conferences, and conducting educational and promotional activities, including peer-to-peer events. We also believe that treatment decisions should be evidence-based and that rigorous clinical studies with high quality data are crucial to achieving and maintaining optimal patient access.
141
Table of Contents
Focus on compelling economics and value creation for all eyecare stakeholders. We focus on developing products to generate substantial benefits for patients, providers and payors. We believe use of our devices will ultimately reduce the all-in cost of treating these diseases for payors. For the sequential procedures using OMNI, surgeons and facilities use the longstanding permanent Category I CPT code for canaloplasty which is broadly covered by Medicare and private payors. TearCare can provide ECP practices with an attractive recurring revenue business model with only a modest initial investment. While there is a viable patient-pay market for TearCare, we believe that improving access to treatments using TearCare through insurance coverage by Medicare and private payors will be the most effective way to reach the largest number of patients. Leveraging the results from our OLYMPIA RCT, we are currently pursuing FDA clearance to expand TearCare’s indication for use and plan to pursue further clearances for more robust indications for use as we build out our library of clinical trial and real-world data regarding the benefits of TearCare treatments. DED is the most common reason for patient visits to an ECP and has major negative effects on patient health and society. One study estimated the overall direct and indirect costs of DED in the U.S. to be $55.4 billion per year.
Scale culture built on community, passion, courage and perseverance. Our organization is designed to be nimble, innovative, adaptive and growth oriented. We have an entrepreneurial and creative foundation that is complemented with an experienced executive team, who provide deep relationships throughout the eyecare community. We share a passion for improving the lives of people suffering from eye diseases and our success has engendered significant esprit-de-corps at all levels of our organization. We believe that our focus on thought leadership, high performance and collaboration, as well as our hiring and recruiting processes, have enabled us to attract and retain a world class team that is prepared to transform eyecare for all stakeholders.
Our Growth Strategy
The fundamental objectives of our growth strategy are to establish robust clinical data to support the development of our target markets and the continued commercialization of our products and to deliver an exceptional customer experience to the ECPs and patients who utilize our products. We believe that our expertise and product innovation process are applicable across many undertreated and prevalent diseases within eyecare. Our current growth strategies include:
| • | Establish OMNI as the standard of care for interventional glaucoma treatment. We believe OMNI has the unique potential to transform the treatment paradigm for IOP reduction in adult POAG patients by greatly expanding the universe of patients who can be treated with MIGS treatment alternatives. We believe OMNI has distinct advantages with respect to effectiveness, safety and its broad indication for use to reduce IOP across all adult POAG patients in both Standalone and Combination Cataract procedures. High-volume cataract surgeons who are familiar with MIGS procedures are our highest priority customer acquisition targets and we have directed our initial commercial efforts towards them. We have successfully gained commercial traction with many of these surgeons. Based on our field research, we believe that after gaining experience using OMNI and confidence in its consistency and effectiveness in familiar Combination Cataract cases, surgeons will often expand the use case for OMNI to include more proactive and interventional POAG cases. We believe many of these cases will involve Mild-to-Moderate Standalone procedures for which we believe OMNI is the only MIGS device authorized by the FDA for lowering IOP via an ab interno approach. An internal field study of our user base has indicated that Standalone procedures constituted greater than 20% of our customers’ total OMNI procedures in 2020. Given these strong initial results, we plan to invest additional resources to execute our interventional POAG market development plan, which includes educating surgeons, facility administrators, primary care ECP referral networks and patients on the clinical benefits of OMNI in both Combination Cataract and Standalone procedures. Our planned clinical studies include head-to-head RCTs versus a leading trabecular bypass stent and a leading prescription OAG medication. |
| • | Develop the MGD treatment market through a patient access-led strategy. We are executing a comprehensive long-term strategy to increase patient access to TearCare beyond its current patient-pay |
142
Table of Contents
market. Our long-term goal is for TearCare procedures to achieve broad reimbursement from private payors and Medicare for effectively treating the signs and symptoms of DED due to MGD. We believe the MGD market is the most underserved in eyecare and that current treatment protocols either fail to directly address MGD’s root cause, require cost-prohibitive capital equipment purchases, lack elegant and user-friendly design, and/or lack the compelling clinical data required to transform treatment paradigms and properly develop the market. Key components of our strategy include: pursuing clearance from the FDA to expand TearCare’s indications for use to treat DED due to MGD; execution of our SAHARA RCT, which will compare treatments using TearCare to the leading prescription eyedrop treatment and assess the durability of TearCare procedures over a 24 month period (SAHARA was designed specifically to provide key clinical data that could support potential reimbursement decisions by third-party payors); developing real-world prior authorization and reimbursement claims evidence to educate payors on the benefits of TearCare for its authorized uses, facilitated by our market access team; and converting our temporary Category III CPT code for TearCare to a permanent Category I CPT code. |
| • | Drive adoption and utilization of our products by leveraging additional clinical trials and market education. We believe our existing clinical data demonstrates the compelling safety and effectiveness of OMNI for its cleared indication, and we plan to continue delivering additional clinical evidence regarding its safety and effectiveness. In our ROMEO study, we observed that use of OMNI was associated with controlled or reduced IOP and reduced medication burden in adult patients. Across several studies, we have observed a consistency of IOP reductions that we believe may appeal to surgeons evaluating the utilization of OMNI in Standalone and Combination Cataract procedures. We intend to dedicate significant resources to further establish definitive clinical studies regarding the use of OMNI for IOP reduction and/or medication reduction in adult patients. We also intend to seek clearance from the FDA for an expanded indication for use for TearCare in the future. We believe the effectiveness and safety data from our OLYMPIA RCT and other ongoing and planned studies and our real-world results could potentially support such a clearance. In our OLYMPIA RCT, we observed that a single use of TearCare was associated with improvement in each of the signs and symptoms of DED assessed, including TBUT and MGSS, objective measurements of DED that were the trial’s primary endpoints, as well as patient-reported symptoms surveys, including EDS, OSDI and SANDE, at both two and four weeks following treatment in subjects with MGD. We have two additional ongoing and planned studies intended to evaluate the safety and effectiveness of TearCare. We believe the results of these studies will support potential clearances for expanded indications for use and our patient access development strategy. |
| • | Deepen and broaden our commercial organization. We plan to continue investing resources to grow our commercial team, both in the U.S. and internationally. In addition to competing in the market for devices used for Combination Cataract MIGS procedures in adult POAG patients, we are investing significant resources in our Standalone market development plan, which includes a team of representatives focused on educating ECPs, ophthalmic surgeons and patients on the broad utility and use cases for OMNI and on Standalone treatment alternatives generally. Through March 31, 2021, we had sold OMNI and its predicate devices to over 1,000 facilities in the U.S. This includes over 600 currently active ordering facilities. There are over 10,000 ophthalmologists focused on performing cataract and glaucoma surgeries in the U.S. and over 3,000 are currently MIGS trained, a figure that is expected to grow as MIGS utilization increases, in part driven by the benefits offered by OMNI. As of March 31, 2021, over 1,000 surgeons have been trained to use OMNI. An internal field study of our user base has indicated that Standalone procedures in 2020 constituted greater than 20% of our customers’ total OMNI procedures — an adoption rate achieved without a focused Standalone marketing campaign. Our targeted and controlled launch of TearCare in the U.S. through a small, dedicated sales team has been successful, providing insights into the large patient-pay market. We plan to grow our commercial organization over time by matching its growth to the achievement of key milestones in our long-term plan to develop our target markets. |
143
Table of Contents
| • | Expand into international markets. We believe there is a substantial market opportunity for clinically effective glaucoma and DED products such as OMNI and TearCare outside of the U.S., or OUS. Over the next several years, we intend to increase our OUS investment. The number of U.S. POAG and DED sufferers represents a small fraction of global sufferers — approximately 6% and 5%, respectively — yet the U.S. represents approximately 60% and approximately 40% of the global glaucoma surgical device and DED treatment markets, respectively. There are currently a number of developed OUS markets with ECPs who have relevant ophthalmologic and optometric experience and existing reimbursement for MIGS devices, particularly in the EU where OMNI has a broad CE Mark to lower IOP for all adult OAG patients. Trabecular bypass stents have established significant markets in Europe and other geographies. We also believe that a number of OUS market fundamentals are attractive with respect to potential OMNI adoption throughout Europe and Asia: |
| • | Surgeons in certain OUS markets choose to intervene at a later stage of eye disease which places increased criticality on highly robust and dependable effectiveness; |
| • | Circumferential canal procedures are widely accepted and adopted in select large OUS markets. For example, ab externo canaloplasty has been very successful in Germany and ab externo circumferential trabeculotomy has been a preferred glaucoma surgery for many years in Japan; and |
| • | Surgeons in certain OUS markets are typically salaried and less specialized than U.S. peers and while procedural efficiency and/or potential case volumes are still significant considerations for these OUS surgeons, clinical effectiveness is of increased relative importance. |
We believe that OUS markets can be extremely compelling for clinically differentiated products. Our OMNI clinical trial program includes head-to-head RCTs against competing treatments in European markets that are designed to address the needs of regulatory bodies and third-party payors in those markets. We believe the results of these trials will help OMNI penetrate and gain adoption in these geographies. We also plan to commercialize TearCare in OUS markets and believe MGD procedures have significant potential. In 2020, we engaged an experienced international commercial leader to develop our European expansion plans and in 2021 we hired this executive as a full-time employee. In Europe, we currently rely on a combination of direct sales personnel (the first of whom were hired in April 2021) and independent distributors to sell our products, and we intend to grow our international sales through a combination of direct and distributor sales.
| • | Continuously innovate premium product offerings throughout eyecare. Over the course of our ten year operating history, we have successfully brought to market multiple iterations of OMNI, its predicate devices and TearCare. Our product development approach, which targets underserved eyecare populations, and our ability to effectively navigate commercialization pathways, has enabled us to launch our products in a highly capital efficient manner, which we believe is distinctive relative to other medical device technology companies and allows us to retain financial flexibility to continue investing in further product enhancements or to explore other avenues of research and development for future pipeline products in eyecare, including drug therapies, sustained release drug delivery platforms and devices. Our internal and external advisor and customer networks provide us with ongoing real-world feedback, which we use to rapidly implement improvements and further develop our products. Our product development roadmap focuses on improving our current products, seeking required FDA authorizations, and disrupting other eyecare categories where stakeholders’ needs remain unmet. We believe our product development capabilities and process provide us with a competitive advantage. |
Clinical Data
We believe that treatment decisions should be evidence-based and hold ourselves to the highest clinical and ethical standards to build and maintain credibility in the medical community. We are deeply committed to conducting studies to evaluate the safety, effectiveness and durability of treatments using our products, and
144
Table of Contents
subjecting the results to the rigorous peer review process for publication in leading journals. Our robust and growing libraries of evidence to support OMNI and TearCare are helping to drive their awareness and adoption, and ultimately advancing patient care in ophthalmology and optometry.
We are currently conducting active and robust clinical trial programs in both POAG and MGD, with two completed studies, 17 papers published in peer-reviewed journals, and an additional eleven ongoing or planned studies that we expect to provide data for future publications. Our completed, ongoing, and planned clinical trials include several head-to-head RCTs against market leading treatments. We also support IIT programs, of which eight are completed and two are currently in progress. We plan to support other IITs in the future.
OMNI Surgical System
OMNI Clinical Program Overview
Building on a solid foundation of completed and ongoing clinical trials, we are investing significant resources to further develop clinical data regarding the use of OMNI. Clinical trial designs for OMNI include both RCTs and retrospective real-world studies, based on our belief that each of these approaches has unique strengths. RCTs provide high-level evidence in a strictly controlled setting minimizing confounding influences and extraneous variability. On the other hand, we believe that retrospective studies provide the best insight into the generalizability of effectiveness in actual clinical practice. We believe the clinical evidence that we have generated to date demonstrates the substantial benefits of OMNI across a range of adult POAG patients with various backgrounds, degrees of disease severity, and prior treatment histories. Since 2018, there have been 11 articles published in peer-reviewed journals for OMNI and its Sight Sciences predicate devices and procedures. Our robust clinical trial program for OMNI intends to include nearly 2,000 subjects across our trials, including: one completed multi-center study (ROMEO) that was used to support OMNI’s indication for use expansion in the U.S. in March 2021 and resulted in two published articles in peer-reviewed journals; an in-process prospective, multi-center, historical control, single-arm, U.S. study (GEMINI); one RCT ongoing in Europe versus the leading trabecular bypass stent (TRIDENT); an ongoing extension of our ROMEO multi-center study (ROMEO II); RCTs in the U.S. versus a leading trabecular bypass stent (PRECISION) and versus the leading glaucoma prescription medication eyedrop (JAEGER); and several additional studies currently in the planning phase.
Results from our recently completed ROMEO multi-center retrospective study, and published data from single surgeon datasets show a remarkable consistency in the IOP reduction observed with OMNI in both Standalone and Combination Cataract procedures. Figure 9 below presents data for mean IOP reduction observed following OMNI procedures (both Standalone and Combination Cataract) from four clinical studies in five peer-reviewed publications. Where preoperative IOP was at least 20 mmHg, a mean 8.5 to 10 mmHg decrease in IOP was observed in all four studies.
Figure 9. IOP Reduction Across OMNI Clinical Studies
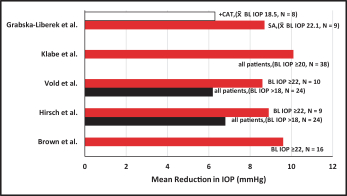
145
Table of Contents
Similarly, Figure 10 shows that, at the individual patient level, almost all patients (98 of 103, 95%) had an IOP decrease following treatment with OMNI, and three out of four (77 of 103, 75%) had at least a 20% decrease. For eyes with preoperative IOP of at least 15 mmHg, we observed lower postoperative IOP in 94 of 96 (98%) cases. These real-world patients also experienced substantial reductions in glaucoma medication usage following their OMNI procedures, a benefit not reflected in a number of “medication washout” trabecular bypass stent trials designed to isolate and thereby maximize IOP reduction in a non-real world manner. We believe consistent therapeutic outcomes are important for patients and surgeons alike. For patients, we believe the anxiety that may accompany the need for ocular surgery can be tempered with the knowledge that there is a high likelihood of success. For surgeons, consistent outcomes simplify the treatment choice and the decision to perform a procedure. We believe this is especially important for Standalone MIGS procedures which must deliver a very high consistency of efficacy and a very high degree of effectiveness to not only justify the procedure, but also provide surgeons with enough confidence to take patients to the operating room for a singular reason. We believe delivering consistently effective results will be crucial to unlocking the Standalone market, as well as capitalizing on the full potential of the Combination Cataract market.
Figure 10. Pre-operative versus Post-operative IOP for Patients
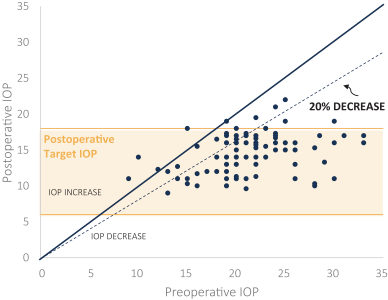
Vold et al., Hirsch et al., Brown et al., and Grabska-Liberek et al. A position below the solid diagonal reflects an IOP decrease post-operatively. These data represent cross-study observations under different conditions.
In March 2021, OMNI received FDA 510(k) clearance for an expanded indication for canaloplasty (microcatheterization and transluminal viscodilation of Schlemm’s canal) followed by trabeculotomy (cutting of trabecular meshwork) to reduce intraocular pressure in adult patients with POAG. As part of this process, the FDA reviewed our submission of clinical data from our ROMEO study that was collected through a real-world evidence approach evaluating use of OMNI for the reduction of IOP in adult POAG patients during the general practice of medicine.
We believe that OMNI’s recent clearance is one of few, if not the only, successful use of retrospective real-world data to support an expansion of an indication for use of an ophthalmic medical device. We believe the FDA’s reliance on this data to support the clearance speaks to the quality of the ROMEO clinical study data and that the expanded indication for use differentiates OMNI’s effectiveness and versatility from other MIGS
146
Table of Contents
devices. We believe that OMNI is the only device that has been authorized by the FDA specifically as an ab interno procedure to:
| • | Reduce IOP in adult patients with POAG across the spectrum of disease severity; |
| • | Be used in Mild-to-Moderate Combination Cataract or Standalone procedures; |
| • | Access 360 degrees of the diseased conventional outflow pathway through a single clear corneal incision; and |
| • | Facilitate two consecutive procedures, canaloplasty and trabeculotomy, that can comprehensively treat all three primary points of resistance in the conventional outflow pathway in a single operating room visit. |
147
Table of Contents
Table 2 below summarizes our completed, ongoing and planned clinical trials for OMNI.
Table 2: Sight Sciences OMNI Clinical Studies
Stage | Name | Study | Study Design | Subjects | Patients | N | Status / | |||||||
| ROMEO | Real world effectiveness and safety of OMNI Standalone or in Combination Cataract surgery | Retrospective, real-world, multi-center, stratified, U.S. study. 12 month | OMNI with Combination Cataract surgery; OMNI Standalone in pseudophakic eyes | Mild-to- Moderate OAG | 129 (81 Combination Cataract, 48 Standalone) | Vold et al. Hirsch et al. JCRS (2021). | |||||||
| GEMINI | Safety and effectiveness of OMNI in Combination Cataract surgery | Prospective, multi-center, historical control, single-arm, U.S. study 12-month | OMNI with Combination Cataract surgery; cataract surgery alone (historical control) | Mild-to-Moderate OAG | 145 | 12-month follow up complete; final database lock planned in 2H 2021 | ||||||||
| TRIDENT | Effectiveness as Standalone procedure versus trabecular bypass stent | Prospective, multi-center, randomized, active-controlled, EU/U.K. study. 12 month | (i) OMNI (canaloplasty + trabeculotomy) Standalone in Pseudophakic eyes; (ii) OMNI (canaloplasty only) Standalone in pseudophakic eyes; (iii) trabecular bypass stent in pseudophakic eyes | Mild-to- Moderate OAG | 459 | Initiated Q4 2020. Study completion expected 2025 | |||||||
| ROMEO II | Expand ROMEO database; collect longer-term data on original ROMEO cohort | Retrospective, real-world, multi-center, U.S. study. 12-month and longer follow-up | OMNI with Combination Cataract surgery; OMNI Standalone in pseudophakic. Preop IOP >18 mmHg | Mild-to- Moderate OAG | N/A | Initiated Q1 2021. Planned manuscript submission expected 1H 2022 | ||||||||
| TREY | Effectiveness in eyes previously treated with trabecular bypass stent | Retrospective, real-world, multi-center, U.S. post-market study. Available follow-up | OMNI in eyes previously treated with trabecular bypass stent | Mild-to- Advanced OAG, previously treated with trabecular bypass stent | 50 | Initiation expected 2H 2021 | |||||||
| ARTEMIS | Effectiveness in treating more advanced disease | Prospective, real-world, multi-center, U.S. post- market study. 12 month | OMNI in eyes with Moderate to Advanced / Severe glaucoma | Moderate-to- Severe POAG | 50 | Initiation expected 2023 | ||||||||
| GEMINI 2.0 | Long-term safety and effectiveness of OMNI in Combination Cataract surgery | Retrospective/ Prospective, multi-center, single-arm, U.S. post-market study; 24 month | OMNI with Combination Cataract surgery | Mild-to-Moderate OAG in Combination Cataract surgery minimum of 550 days prior to enrollment | up to 150 | Initiation expected 2H 2021 | ||||||||



148
Table of Contents
Stage | Name | Study | Study Design | Subjects | Patients | N | Status / | |||||||
| ORION 2.0 | Long-term safety and effectiveness of OMNI Standalone | Retrospective/ Prospective, multi-center, single-arm, observational; 24 month | Pseudophakic eyes | Mild-to-moderate POAG Standalone procedure; minimum of 150 days prior to enrollment | up to 100 | Initiation expected 2H 2021 | ||||||||
| JAEGER | Safety and effectiveness of OMNI Standalone in OAG versus medications | Prospective, multi-center, randomized, active-controlled, U.S. IDE study. 36 month | (i) OMNI (canaloplasty + trabeculotomy) Standalone; (ii) OMNI (canaloplasty only) Standalone; (iii) leading Glaucoma Medication | Mild-to-Moderate OAG | 459 | Initiation expected 1H 2022 | ||||||||
| PRECISION | Effectiveness in Combination Cataract surgery versus trabecular bypass stent | Prospective, multi-center, randomized, triple arm active-controlled, U.S. IDE study. 36 month | (i) OMNI (canaloplasty + trabeculotomy) with Combination Cataract surgery; (ii) OMNI (canaloplasty only) with Combination Cataract surgery; (iii) trabecular bypass stent with Combination Cataract surgery | Mild-to-Moderate OAG | 459 | Initiation expected 1H 2022 | ||||||||
There is a substantial body of historical clinical evidence supporting the effectiveness of circumferential, 360-degree surgical treatment of the conventional outflow pathway to reduce resistance to aqueous outflow and reduce intraocular pressure. Canaloplasty and trabeculotomy originated as invasive, “non-MIGS”, ab externo procedures requiring multiple conjunctival and scleral dissections to access the diseased outflow pathway. While the effectiveness of the invasive ab externo variants of circumferential angle surgery were compelling, these procedures are difficult to perform, traumatize the eye, have higher risk of intraoperative and post-operative complications and require longer patient recovery times. Moreover, the conjunctival and scleral dissections required during invasive surgery can limit future surgical options such as trabeculectomy or other filtering glaucoma procedures due to potential scarring.
The VISCO360 and TRAB360 predicates to OMNI could each be used to deliver small, controlled amounts of viscoelastic fluid (VISCO360) or cut the trabecular meshwork (TRAB360). Table 3 summarizes three IITs evaluating canaloplasty procedures performed using VISCO360 or OMNI. Table 4 summarizes two IITs evaluating trabeculotomy procedures using TRAB360. In one study, a series of 81 eyes with Refractory glaucoma, was observed to have a 34% mean reduction in IOP at 12 months following trabeculotomy with TRAB360. In another study, VISCO360 was used to treat 72 eyes where IOP was poorly controlled in patients with Mild-to-Moderate OAG. At 12 months, the mean IOP reduction was 41%. These ab interno canaloplasty and ab interno trabeculotomy single-center studies with open-label designs demonstrated substantial improvement in IOP control.
149
Table of Contents
Table 3: Published Sight Sciences Ab Interno Canaloplasty Investigator Initiated Trials
Reference | Diagnosis | N | Mean | Mean IOP and (length of | Percent Change | Medication Change | ||||||
| Ondrejka and Körber 2019* | POAG | IOP ³18 mmHg 72 | 24.6±7.1 | (12 month) 14.6±2.8 | -40.7 | -1.9 | ||||||
IOP <18 mmHg 34 | 14.9±1.8 | 13.6±2.3 | -8.7 | -1.6 | ||||||||
| Tracer et al. 2019* | OAG | IOP ³18 mmHg 111 | 22.0±5.5 | (12 month) 17.2±5.1 | -21.8 | no change | ||||||
IOP <18 mmHg 69 | 14.3±2.3 | 15.4±4.1 | +7.7 | -0.5 | ||||||||
| Hughes and Traynor 2020* | OAG | 89 | 24.5±8.3 | 15.8 ± 2.5 (18 month) | -35.5 | -0.8 |
| * | Sight Sciences supported independent research. |
Table 4: Published Sight Sciences Ab Interno Trabeculotomy Investigator Initiated Trials
Reference | Diagnosis | N | Baseline IOP and Range | Mean IOP at Last Follow-up and Range (length of follow-up) | Percent Change | Medication Change | ||||||||||
| Sarkisian et al. 2019* | POAG (83%) | 81 | 23.7±6.0† | 15.7±5.5† (12 month) | -33.8 | -0.6 | ||||||||||
| Areaux et al. 2020** | Pediatric PCG JOAG GANASDS GANOA GAAC GFCS | N 21 8 2 4 5 | | Success†† 81% 6 83% 50% 0% 50% 60% |
| 30.9 | 20.3 | -34 | -1.0 | |||||||
PCG: primary congenital glaucoma; JOAG: juvenile OAG; GANASDS: glaucoma associated with a nonacquired systemic disease or syndrome; GANOA: glaucoma associated with a nonacquired ocular anomaly; GAAC: glaucoma associated with an acquired condition; GFCS: glaucoma following cataract surgery. |
| † | Standard deviation estimated from error bars in published figure. |
| †† | Success defined as post-operative IOP £ 24 mmHg with or without medications and no additional surgery. |
| * | Sight Sciences supported independent research. |
| ** | No Sight Sciences funding. |
As much as these individual circumferential MIGS procedures had advantages over their more invasive, non-MIGS variants or the far less comprehensive trabecular bypass stents, neither procedure alone could completely and effectively address all three primary sources of resistance to aqueous outflow that may be present in the conventional outflow pathway in glaucoma patients. We believe that combining the two procedural mechanisms of action (ab interno canaloplasty and ab interno trabeculotomy) provides a comprehensive solution addressing all three potential primary points of resistance in the conventional outflow pathway. The clinical history described above and the focus on physically and procedurally optimizing the surgical treatment of the
150
Table of Contents
entire diseased conventional outflow pathway in glaucoma (titratable up to 360 degrees of trabecular meshwork, 360 degrees of Schlemm’s canal, 360 degrees of collector channels) is the genesis of OMNI.
ROMEO Study (Completed)
The ROMEO study was a multi-center retrospective study conducted from February 2018 through April 2020 and designed to assess safety and effectiveness of OMNI in reducing IOP and hypotensive medication usage in Mild-to-Moderate OAG patients at 12 months post-operation. This study evaluated the clinical effect of ab interno canaloplasty and trabeculotomy performed using OMNI in both Standalone and Combination Cataract procedures, the use of ocular hypotensive medications and safety in patients with OAG. Clinical data from ROMEO supported our March 2021 FDA 510(k) clearance for an expanded indication for use of OMNI.
The study evaluated two different groups of patients based on baseline IOP with different treatment goals: The Elevated IOP Group had a preoperative IOP greater than 18 mmHg and its treatment goal was IOP reduction. The Controlled IOP Group had a preoperative IOP less than or equal to 18 mmHg, with a treatment goal of IOP maintenance and medication reduction. The primary endpoint was defined as the proportion of subjects at 12 months post-operation with IOP between 6 mmHg and 18 mmHg or with a 20% or greater reduction from preoperative baseline IOP, on the same or fewer number of ocular hypotensive medications compared to the preoperative baseline, and with no additional IOP-lowering surgery or laser treatment. IOP of 18 mmHg or below is a well-established benchmark by the clinical community for control of POAG progression and is based on the belief that maintenance of IOP control should be considered a “success” for patients already controlled on medication. For patients not controlled on medication, a 20% reduction in IOP is the recommended primary efficacy endpoint according to FDA guidance for implantable MIGS devices, which we have relied upon in designing our retrospective nonimplantable device study. Safety endpoints included ocular adverse events, and efficacy endpoints included secondary surgical interventions.
The proportion of subjects meeting the success criteria overall and stratified by type of procedure and baseline IOP are presented below, in Table 5.
Table 5: Proportion of Subjects Meeting Success Criteria (Month 12)
Group | N | Number of Subjects Meeting Success Criteria | Proportion of Successes | 95% Confidence Interval | ||||||||
Combination Cataract | 81 | 65 | 80.2% | 71.4, 89.0 | ||||||||
Standalone | 48 | 35 | 72.9% | 60.1, 85.7 | ||||||||
p value Combination Cataract vs Standalone | 0.3855 | |||||||||||
Total | 129 | 100 | 77.5% | 70.1, 84.9 | ||||||||
151
Table of Contents
Mean preoperative IOP and at months one, six and 12 post-operation and mean preoperative medication usage and at month 12 post-operation for both the Elevated IOP Groups and the Controlled IPO Group of both Standalone and Combination Cataract cohorts are shown in Figures 11-18. Error bars are ± 95% confidence interval.
Figure 11. Mean IOP Over Time. Standalone Use of OMNI (Elevated IOP Group)
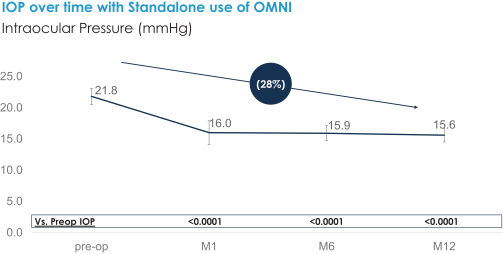
Figure 12. Mean IOP-lowering Medication Use. Standalone Use of OMNI (Elevated IOP Group)
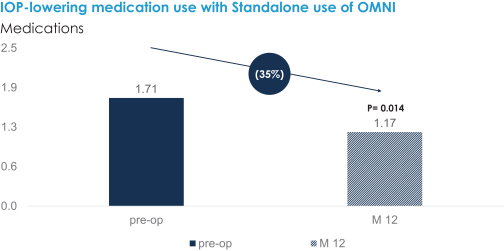
152
Table of Contents
Figure 13. Mean IOP Over Time. Standalone Use of OMNI (Controlled IOP Group)
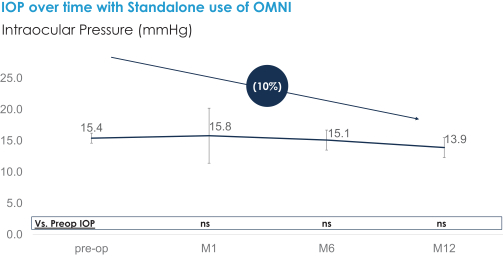
Figure 14. Mean IOP-lowering Medication Use. Standalone Use of OMNI (Controlled IOP Group)
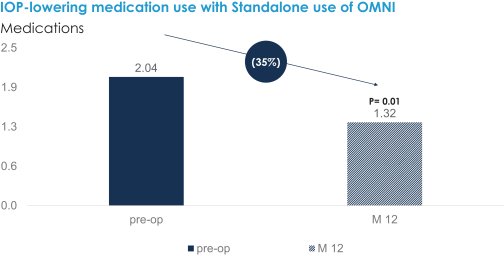
153
Table of Contents
Figure 15. Mean IOP Over Time. OMNI Combination Cataract Procedure (Elevated IOP Group)
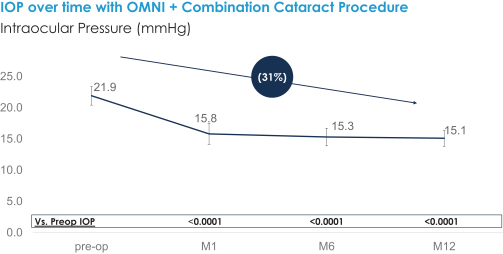
Figure 16. Mean IOP-lowering Medication Use. OMNI Combination Cataract Procedure (Elevated IOP Group)
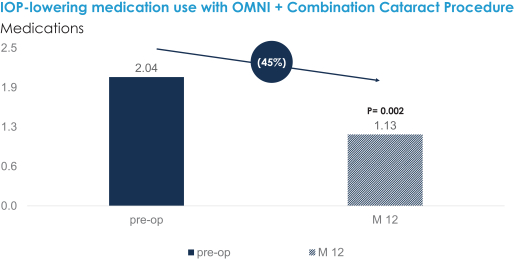
154
Table of Contents
Figure 17. Mean IOP Over Time. OMNI Combination Cataract Procedure (Controlled IOP Group)
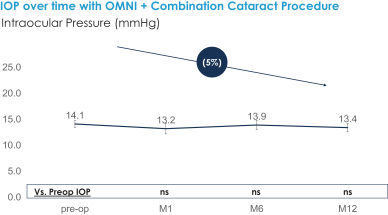
Figure 18. Mean IOP-lowering Medication Use. OMNI Combination Cataract Procedure (Controlled IOP Group)
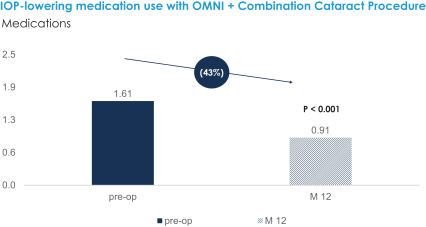
As shown in Figures 11 and 15, mean IOP was significantly reduced from baseline at all follow-up timepoints for both Standalone and Combination Cataract cohorts in the Elevated IOP Group. As shown in Figures 13 and 17, in the Controlled IOP Group, statistically significant differences with respect to mean IOP reductions from baseline were not observed either in the Standalone or Combination Cataract cohorts.
For all patients, in both Standalone and Combination Cataract cohorts, statistically significant (P<0.05) decreases in the mean number of medications compared to preoperative baseline were observed (Figures 12, 14, 16 and 18). In the Elevated IOP Group, mean medication usage decreased from 1.71 ± 1.31 to 1.17 ± 1.28 (P = .014), and from 2.04 ± 1.27 to 1.13 ± 1.09 (P = .002) for Standalone and Combination Cataract, respectively. Mean medication usage for Controlled IOP Group patients decreased from 2.04 ± 1.31 to 1.32 ± 1.26 (P = .001) and from 1.61 ± 1.25 to 0.91 ± 1.17 (P < .001), for Standalone and Combination Cataract, respectively.
Adverse Events, or AEs, observed in this study were generally mild, non-serious, transient in nature and consistent with expected events for the population under study. The most frequent AEs observed were posterior capsule opacity (15%), mild anterior chamber inflammation (11%), a rise in IOP greater than 10 mmHg above the baseline IOP at or after 30 days post-operation (4.7%), corneal edema (4.7%), and hyphema (3.9%). The incidence of these AEs were comparable to rates reported in studies of trabecular bypass stents. All of these AEs
155
Table of Contents
were observed to be temporary and mild. Nine subjects (7.0%) required a secondary surgical intervention for IOP control. Best corrected visual acuity was generally observed to have improved postoperatively overall.
GEMINI Study
GEMINI is an ongoing prospective, multi-center, single-arm, historic-controlled, interventional clinical trial designed to assess the safety and effectiveness of OMNI in Combination Cataract surgery in patients with
Mild-to-Moderate OAG at 12 months postoperatively. The GEMINI study initiated in February 2019, completed
enrollment in March 2020 (n=145) and completed final patient 12-month follow up by the end of April 2021. We plan to submit multiple articles based on data from GEMINI for publication in peer-reviewed journals and present the results at major ophthalmology conferences later in 2021.
All GEMINI patients underwent a complete ophthalmic screening prior to surgery, and postoperative follow-up examinations were performed at one day, one week, and one, three, six, and twelve months following treatment. GEMINI’s inclusion criteria closely followed the large pivotal trials of trabecular bypass stents with cataract surgery only (control arms) of these studies to be used as the control group in GEMINI. In conducting GEMINI we had initially described the trial as a post-market trial to the Institutional Review Board, or IRB, and in informed consent documents. Subsequently, we amended the study protocol and obtained informed consent for a revised description of the trial. The FDA has also granted us an expanded indication for use for OMNI, which is consistent with how we had initially described the trial to the IRB and in informed consent documents.
Additional Ongoing and Planned Sight Sciences OMNI Clinical Studies
We have two additional studies for OMNI ongoing. TRIDENT is a EU and U.K. 12-month, multi-center three arm RCT evaluating Standalone procedure patients with pseudophakic eyes (post-cataract surgery), treated with OMNI for canaloplasty and trabeculotomy, OMNI for canaloplasty alone, and a leading trabecular bypass stent. With ROMEO II, we plan to expand our retrospective data from ROMEO and extend follow up periods beyond the 12 month endpoint for ROMEO.
We also have six studies in planning stages: TREY, ARTEMIS, GEMINI 2.0, ORION 2.0, JAEGER and PRECISION, further demonstrating our ongoing commitment to developing complete and robust clinical data regarding OMNI. These studies will aim to evaluate the comparative effectiveness and safety of OMNI versus current treatment alternatives, such as leading trabecular bypass stents and leading topical pharmaceuticals, in both the Combination Cataract and Standalone settings, across the full spectrum of POAG severity.
Sight Sciences Supported OMNI Investigator Initiated Trial Program
There are also several completed or ongoing IITs of OMNI. Although we provide financial support for many of these studies, they are independent in conception, execution, and reporting. Investigators seeking support for their research submit a detailed study proposal, which is then reviewed by our IIT review committee for scientific merit and fit with company strategic goals, but without consideration for their associated commercial opportunities. There are currently two recently completed OMNI IITs and two ongoing. These are summarized in Table 6 below.
156
Table of Contents
Table 6: Sight Sciences OMNI Investigator Initiated Trials
Stage | Investigator | Study | Study Design | Treatment | Patients | N | Status / Publication | |||||||
| Matthew Traynor MD | Outcomes of canaloplasty as a Standalone or Combination Cataract surgery | Retrospective, single center, case series. 18 months of follow-up | Canaloplasty in Standalone or Combination Cataract surgery with either VISCO360 or OMNI | Mild-to-Moderate OAG | 89 | Hughes T, Traynor MP. Clinical Ophthalmology (2020) | |||||||
| Karsten Klabe MD | Outcomes for OMNI as a Standalone procedure in medically uncontrolled OAG | Retrospective single center case series. 12 months of follow-up | OMNI Standalone in either pseudophakic or phakic eyes | Mild-to-Moderate OAG | 38 | Submitted to Journal of Glaucoma | ||||||||
| Daniel Terveen MD | Safety and effectiveness of OMNI Standalone | Retrospective, multi- center, case series. 3 months of follow-up | OMNI standalone in pseudophakic eyes | Mild-to-Moderate OAG | 100 | Ongoing. Abstract submitted to ASCRS 2021 | |||||||
| Iwona Grabska-Liberek, MD | Outcomes for OMNI as Standalone procedure or Combination Cataract surgery | Prospective case-series; 24 months | Mild-to-Moderate OAG | 17 | Ongoing 12-month results published: Grabska-Liberek, European Journal of Ophthalmology (2021) | |||||||||
These IITs are retrospective case series in Mild-to-Moderate OAG patients, patients inadequately controlled on maximum tolerated medical therapy, Standalone procedures in both pseudophakic and phakic eyes and Combination Cataract procedures. We believe the investigators plan to present their results at major ophthalmic congresses, such as the American Academy of Ophthalmology and the American Society of Corneal and Refractive Surgery, and publish their results in peer-reviewed ophthalmology journals.
TearCare System
TearCare Clinical Program Overview
We designed TearCare to comprehensively address meibomian gland dysfunction, which we believe to be the primary underlying cause of evaporative DED. We have developed robust clinical data evaluating TearCare. We have completed one RCT for TearCare, have one RCT in the early stages of patient enrollment and have one additional study in the planning stage, as summarized in Table 7 below. In our completed OLYMPIA RCT, we observed significant improvements in the signs and all symptoms of DED as assessed by an array of measures including both functional and biologic markers, and patient-reported symptoms surveys. We observed TearCare to be safe and well tolerated, with only minor AEs that resolved without any further treatment. We have two additional ongoing and planned studies intended to evaluate the safety and effectiveness of TearCare in reducing signs and symptoms of DED due to MGD and plan to leverage the results of these studies to support FDA clearances to expand indications for use of TearCare and to support our patient access strategy.
The primary and secondary endpoints we used in OLYMPIA and plan to use in our ongoing or planned studies are homeostatic markers and patient-reported symptoms surveys used extensively in the study and diagnosis of DED. TBUT is a measure of the rate of evaporation of the tear film and is an indicator of tear film stability, according to the American Academy of Ophthalmology, and measurements below ten seconds are considered abnormal. Longer TBUT is desirable as it indicates a lower rate of evaporative loss. Corneal and conjunctival staining allows detection of corneal erosions and other ocular surface damage. MGSS is a measure of the quality and quantity of meibum secretion, which helps prevent evaporative loss of tears. Patient-reported
157
Table of Contents
symptoms surveys such as Ocular Surface Disease Index, or OSDI, Symptom Assessment in Dry Eye, or SANDE, and Eye Dryness Score, or EDS, are standard questionnaires designed to determine the severity of DED symptoms that are completed by patients and provide an overall score that increases with increased symptom severity.
Table 7: Sight Sciences TearCare Clinical Studies
Status | Name | Study Goals | Study Design | Treatment Groups | Patients | N | Status / | |||||||
| OLYMPIA | Safety and effectiveness of a single TearCare treatment compared to a single LipiFlow treatment to treat the signs and symptoms of DED in adult patients | Prospective, multi-center, randomized, active-controlled, U.S. abbreviated IDE study, 1 month | Single TearCare Tx vs Single LipiFlow Tx | Patients with moderate to severe dry eye associated with MGD | 235 | Pub1: Accepted by Cornea | |||||||
| SAHARA | Safety and effectiveness of TearCare treatments compared to Restasis to treat the signs and symptoms of DED in adult patients | Prospective, multi-center, randomized, active-controlled, U.S. abbreviated IDE study, 24 months | TearCare Tx vs Restasis Rx | Patients with moderate to severe dry eye associated with MGD | 300 | Initiated Q4 2020. Study completion expected 2025 | |||||||
 | RESTORE | Safety and effectiveness of TearCare to treat the signs and symptoms of DED in patients previously treated with Restasis or Xiidra | Retrospective, real-world, multi-center, U.S. post-market study | TearCare Tx | Patients with moderate to severe dry eye associated with MGD and history of Restasis or Xiidra and are treated with TC at least 4 weeks prior to enrollment | 300 | Initiation expected 2H 2021. Study completion expected 1H 2022 | |||||||
Tx = treatment, Rx = prescription eyedrop, MGD = meibomian gland dysfunction, TC = TearCare, CE = cataract extraction.
OLYMPIA Study (Completed)
Our OLYMPIA study was a masked, multi-center RCT conducted at ten U.S. sites designed to study the safety and effectiveness of a single treatment with TearCare in reducing the signs and symptoms of DED associated with MGD as compared to a single treatment with the LipiFlow Thermal Pulsation System (Johnson & Johnson), or LipiFlow.
Subjects with signs and symptoms of DED and MGD (N=235) were randomized 1:1 to a single treatment using either TearCare or LipiFlow. Key inclusion criteria were regular use of lubricating drops, OSDI score between 23 to 79 (moderate to severe), MGSS £ 12, TBUT of £ 7 seconds, and at least 15 expressible glands in each lower eyelid. The primary endpoint for the study was non-inferiority of TearCare to LipiFlow, as measured by TBUT, and MGSS scores at one month. Secondary endpoints included corneal and conjunctival staining and number of meibomian glands yielding clear liquid. To reduce potential bias in subjective endpoint assessments, the clinician performing the treatments did not perform the endpoint assessments and the clinician performing the endpoint assessment was blinded to which treatment the patient had received. Symptoms were recorded using OSDI, SANDE, and EDS questionnaires. Any AEs, either patient reported or observed by the investigators, were recorded to assess safety.
In OLYMPIA, the non-inferiority primary endpoint was met for all endpoints and a greater proportion of subjects in the TearCare group reported better symptomatic relief compared to the LipiFlow group assessed by
158
Table of Contents
OSDI; p<0.05 (Figure 18). Use of TearCare was associated with a statistically significant improvement in all assessed signs and symptoms of DED in subjects with MGD, including TBUT and MGSS, objective measurements of DED that were the trial’s primary endpoints, as well as patient-reported symptoms surveys, including EDS, OSDI and SANDE, at both two and four weeks following treatment. While statistically significant superiority differences between the TearCare and LipiFlow groups were not observed, in a post-hoc analysis, the TearCare group demonstrated consistently greater improvements in most signs and symptoms assessed. Statistically significant improvements in the primary endpoints of mean TBUT and MGSS from baseline were observed in both the TearCare group (3.0 ± 4.4 and 11.2 ± 11.1, respectively) and the LipiFlow group (2.6 ± 3.3 and 11.09 ± 10.4, respectively (p< .0001)). In the TearCare group, mean corneal and conjunctival staining were reduced from baseline by 0.3 ± 2.0 and 0.7 ± 2.3, respectively; the mean number of expressible glands and glands expressing clear liquid increased from baseline by 4.3 ± 3.6 and 1.8 ± 3.7, respectively. The TearCare group improved in mean SANDE (by 38.2 ± 31.0 from baseline), EDS (by 35.4 ± 34.1 from baseline), and OSDI scores (by 27.9 ± 20.5 from baseline). Although statistically significant differences between the TearCare and LipiFlow groups were not observed with respect to the primary endpoints, in a post-hoc analysis, the TearCare group had a statistically significantly higher proportion of subjects (72%) improving by at least one OSDI category than did the LipiFlow group (59%); p<0.05. A total of 11 AEs were reported in eight subjects treated with TearCare, nine of which were ocular AEs in seven subjects and only four (one chalazion, two superficial punctate keratitis, one blepharitis) of these were device-related AEs reported in three subjects. A total of 15 AEs were reported in 10 subjects treated with LipiFow, 13 of which were ocular AEs in eight subjects and seven (two blepharitis, three foreign body sensation, two dry eye disease) of these were device-related AEs reported in four subjects. No serious AEs were reported in either treatment group.
Figure 19. Change in OSDI at 1 month
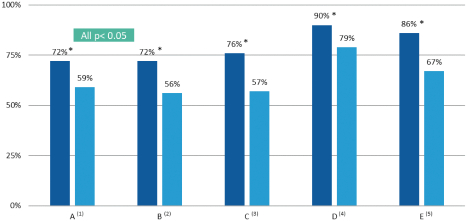
| * | Statistically significantly higher proportion of subjects showed clinically meaningful improvement in TearCare group compared with LipiFlow group |
| (1) | % Subjects improved at least by 1 OSDI category. |
| (2) | % Subjects who had severe OSDI at baseline and who improved at least by 1 OSDI category. |
| (3) | % Female subjects improved at least by 1 OSDI category. |
| (4) | Statistically significantly higher proportion of female subjects in TearCare group improved by Miller definition (7.4 point improvement in moderate OSDI and 10.4 point improvement in severe OSDI). |
| (5) | Statistically significantly higher proportion of female subjects who had TBUT <4.0 in TearCare group improved at least by 1 OSDI category. |
Additional Ongoing and Planned Clinical Studies
In addition to the above completed studies, we have two additional ongoing or planned studies to evaluate the safety and effectiveness of TearCare for the reduction of signs and symptoms of DED. Our SAHARA study
159
Table of Contents
is a multi-center RCT designed to compare TearCare treatments to Restasis, a current prescription eyedrop for DED, and to test the durability of TearCare treatments in 300 patients. We began recruiting subjects for SAHARA in the first quarter of 2021. SAHARA was designed specifically to provide key clinical data that we believe could support potential reimbursement decisions by third-party payors. RESTORE is a planned retrospective, multi-center study of TearCare in 50 patients with a history of using prescription eyedrops such as Restasis or Xiidra. We plan to leverage the results of these studies to seek further premarket clearances from the FDA for more robust indications for use of TearCare.
Sight Sciences TearCare Investigator Initiated Trials
We actively support independent study of TearCare through our IIT program. Dr. Thomas Chester completed a study of 134 eyes (both eyes of 67 patients) treated in his clinic with TearCare. The study compares pre- and post-treatment (8-12 weeks) dry eye symptoms as measured by the Standardized Patient Evaluation of Eye Dryness, or SPEED, questionnaire, and pre- and post-treatment meibomian gland expression scores. In this study, a single TearCare treatment was effective in reducing both the signs and symptoms of dry eye, as measured by meibomian gland expression and SPEED surveys, respectively.
Commercial Approach
Figure 20. OMNI in Use

We have built a world-class direct sales commercial organization that features professionals and executives with substantial leadership experience from leading ophthalmic product companies. In particular, we have recruited professionals with track records that include launching new technologies, growing primary demand and changing treatment paradigms. We believe this expertise is crucial to achieve our market development objectives for interventional Standalone MIGS and MGD treatment. Sales representatives typically have relevant experience across all facets of medical device and/or pharmaceutical sales focused on eyecare to ensure the development of a trusted consultative relationship with our ECPs. As we have continued to develop additional clinical data and brand recognition, we believe our team has differentiated our product offerings and gained commercial traction through exceptional, highly involved training, support and ongoing professional education. As of March 31, 2021, our overall commercial team consisted of over 100 professionals dedicated to sales, marketing, commercial support, training and professional relations.
160
Table of Contents
We created distinct sales, marketing, and training teams to sell OMNI and TearCare because the products are predominantly sold to different types of customers and require specialized product specific sales expertise and ECP training to integrate our products into their practices. We sell OMNI to facilities where ophthalmic surgeons perform outpatient procedures, mainly ASCs and HOPDs. We sell TearCare to optometry and ophthalmology practices.
Our marketing efforts are centered around increasing awareness share of our products and presenting clinical study results through leading medical publications and at-large industry and scientific meetings, both directly and through our advisors. We have also partnered with early-adopting ECPs to speak to peers on our behalf through educational forums either in-person or via virtual meetings. Clinical data that demonstrate the benefits of OMNI and TearCare for their authorized uses will continue to underpin our commercial efforts and we will continue to devote significant resources to conduct new clinical studies and publish articles in peer-reviewed journals.
OMNI
Since the commercial launch of OMNI in February 2018, we have pursued a three-part strategy to gain rapid commercial adoption and simultaneously expand its potential market:
(i) Target and train the over 3,000 high volume cataract surgeons who are already familiar with MIGS approaches (ab interno access techniques) and have a willingness to trial new technologies;
(ii) Leverage positive clinical experiences and outcomes to expand the utilization of OMNI among these MIGS-trained surgeons and drive adoption from additional surgeons and facilities; and
(iii) Promote interventional Standalone treatments with OMNI for the larger population of adult POAG patients for whom other leading MIGS devices are not indicated.
The majority of our OMNI sales representatives cover dedicated geographic territories or specialized customer segments, such as academic or government institutions, across the U.S. These sales representatives establish new accounts, train new surgeons and operating room personnel and nurture the continuing use of OMNI at existing accounts. In addition, we have positioned overlay sales representatives in our highest density customer markets to educate existing users of OMNI and primary care ECPs regarding the potential benefits of OMNI in interventional Standalone procedures in adult patients with POAG. The general ophthalmologists and optometrists who provide primary eyecare services are typically the first to diagnose POAG and deliver first line treatment. We aim to educate these primary ECPs regarding the clinical benefits and use cases for OMNI as they often have referral relationships with ophthalmic surgeons for patients who require advanced treatment. We seek to increase usage of OMNI among the ophthalmic surgeons who have already been trained and convert those who are not.
We believe our initial commercial efforts for OMNI have been successful and we plan to accelerate growth with the expansion of our team to cover more geographic territories and provide increased support to accounts, as well as roll-out large-scale marketing programs for the interventional Standalone opportunity in 2021. Although the vast majority of our sales are in the U.S., we have also begun to sell OMNI in select European countries both on a direct basis and through distributors. In 2020, we engaged an experienced international commercial leader to develop our European expansion plans and, in 2021, we hired this executive as a full-time employee and hired our first direct sales professionals in Europe. We expect to scale up our efforts in Europe and other regions over time.
TearCare
We implemented a controlled launch of TearCare in the U.S. in April 2019 with a limited sales effort. We have assembled a proprietary list of over 5,000 practices that are prime targets for our device and, as of April 30, 2021, we had sold TearCare to over 400 eyecare facilities.
161
Table of Contents
While the success of our initial launch has shown that a significant patient-pay market exists for TearCare, market research indicates that improving access to TearCare through Medicare and private payors will accelerate adoption of the product. Currently, no third-party payors have formal policies establishing coverage for procedures using TearCare, although we believe that some payors may agree to provide coverage outside of formal policy based on medical need. As an early step of a comprehensive long-term market development plan, our market access team is assisting key strategic accounts and their patients in the pursuit of prior authorization approvals and reimbursement claims for TearCare on a case-by-case basis. Simultaneously, we are also continuing to support our customers with patient-pay models, which remains a significant growth opportunity.
Our dedicated commercial team for TearCare consists of sales representatives and leaders, marketing professionals, dedicated trainers, and independent sales representatives. We intend to scale up this team to the extent we achieve key market development and patient access milestones, including completion of clinical trials and our pursuit of FDA clearances for more robust indications for use of TearCare. Our sales representatives collaborate with stakeholders across the practice to train doctors and staff, implement workflow processes and monitor operations to ensure proper integration. As we help customers incorporate the use of TearCare, we have gained insights that enable us to continually improve our selling model. We expect to add new accounts and increase utilization at existing accounts, as we methodically grow our commercial team dedicated to TearCare.
Reimbursement
There are three primary aspects of reimbursement in the United States: coding, coverage and payment. Each aspect is an important determinant of our customers’ ability to obtain reimbursement.
| • | Coding refers to the availability of billing codes for use by healthcare providers to report the provision of medical procedures, and the use of supplies and resources for specific patients, to insurance providers and organizations that make payments for healthcare, commonly referred to as third-party payors. The Healthcare Common Procedure Coding System, or HCPCS, is a national, standardized code set used by providers to capture and report healthcare services and products. This code set consists of two subsystems: Level I, Current Procedural Terminology, or CPT, codes, representing procedures performed, and Level II, commonly referred to as HCPCS codes, representing healthcare products (e.g. devices, drugs, durable medical equipment), supplies and services not captured in the CPT code set. CPT codes are published by the American Medical Association, or AMA, and are used to report medical services and procedures performed in the outpatient setting of care by or under the direction of physicians. HCPCS codes are established and maintained by the Centers for Medicare and Medicaid Services, or CMS, and identify items used in the course of care delivery. Health plans pay outpatient facilities and physicians for services based on submission of a claim using one or more CPT and/or HCPCS codes. CPT codes fall into one of three categories. |
| • | Category I CPT codes have been approved by the AMA as permanent procedure codes based on a number of factors, including the level of published clinical evidence. They are identified with a five-digit number and official code description. Approved Category I CPT codes have typically been endorsed by relevant medical specialty societies, are consistent with contemporary medical practice, and represent procedures performed by many physicians in clinical practice in multiple locations. Category I codes are only available to procedures for which the technology (e.g., device, drug, test) has been FDA approved/cleared when such a regulatory requirement exists. |
| • | Category II CPT Codes are supplemental tracking codes used for performance measurement. They are intended to facilitate data collection about quality of care by coding certain services and/or test results that support performance measures and that have been agreed upon as contributing to good patient care. Some codes in this category may relate to compliance by health care professionals with state or federal law. |
| • | Category III CPT codes are a temporary set of tracking codes for new and emerging technologies. These codes are designed to facilitate data collection for the assessment of new procedures. |
162
Table of Contents
Additionally, Category III codes provide a mechanism for payors to value a new procedure. Temporary codes are not automatically assigned Relative Value Units, or RVUs, or weights and, therefore, do not typically have a widely accepted payment rate methodology. To achieve Category III status, a new procedure is required to have either an approved protocol for a study of procedures being performed, support from the specialties that would use the procedure, availability of US peer-reviewed literature, or current clinical trials that outline the effectiveness of the procedure. Once granted, Category III CPT codes expire five years after the initial application was approved, although they can be extended beyond the five-year limit. |
| • | Level II HCPCS codes are alpha-numeric codes governed by CMS that identify medical products and items or services that are not appropriately designated by another code set (e.g., CPT). Criteria must be met in order to qualify for an HCPCS code, including such requirements as regulatory approval (if necessary), national programmatic need, and a distinct difference from existing HCPCS codes. |
| • | Coverage refers to decisions made by third-party payors as to whether there is sufficient published clinical evidence to support medical necessity, or to consider a healthcare item or service “reasonable and necessary” (as per Medicare guidelines). Coverage can be established by explicit medical policies that outline specific procedures and/or technologies, and under what conditions coverage is permitted, including specific diagnoses, clinical indications and therapeutic prerequisites. Coverage can also be implicit, as when payors are “silent” on a procedure or technology (i.e., no formal policy is developed). In the absence of formal policy, coverage may be granted one of two ways: (1) with no required review, as with long-standing established healthcare items or services, or (2) on a case-by-case basis via review of each patient’s circumstance, as may be the case with newer procedures/technologies. Each payor can make its own decision as to which procedures or technologies warrant formal policy. |
| • | Payment refers to the reimbursement rate for a healthcare item or service. The amount paid by third-party payors to providers, including facilities and doctors, for specific procedures and items (e.g., medical devices, drugs, ancillary supplies) is determined by each payor. Payments for professional services under CPT coding are generally determined by the RVUs of a specific billing code. These RVUs identify the time and intensity of the work required, the practice expense incurred and the level of risk related to the procedure. Payors can use their organization-specific formula or conversion factor to translate RVUs into payment rates, or may establish payment by reference to a national Medicare payment amount. Likewise, facility payments are weighted based on the resources (e.g., operating suite time, devices and supplies) needed for the procedure to be performed in the facility setting. Most payment rates are geographically adjusted, taking into account the cost of providing services in different wage index areas across the country. As with procedure payments, payments for healthcare items (e.g., products reported using HCPCS coding) are determined by individual health plans, often based on some form of manufacturer’s invoice or billed charges based on the provider’s mark-up methodology, or based on established fee schedule rates. It is important to recognize that not all reportable codes are separately payable. Some codes are bundled with related items or services and do not have a separate payment allowance. |
For further information regarding reimbursement, see “Risk Factors—We may not be able to maintain adequate levels of third-party coverage and payment for procedures in which OMNI is used, and third parties may rescind or modify their coverage related to OMNI. We may not be able to secure any, or adequate levels of, third-party coverage and payment for procedures in which TearCare is used, and even if third parties provide coverage they may rescind or modify their coverage related to TearCare”.
Our commercial activities are substantially within the United States. We sell OMNI primarily to ASCs and HOPDs, who in turn bill various third-party payors, such as Medicare and private health insurance plans for the healthcare services and resources rendered to treat a patient. TearCare is not currently covered or paid by Medicare or private payors under any formal policy, although some payors may agree to provide case-based coverage outside of a formal policy. Our market access team facilitates patient access to the OMNI and TearCare
163
Table of Contents
systems by engaging payors on coverage, coding and payment matters, and by providing support to patients and our customers as they seek reimbursement from payors that do not have positive coverage or those that do not have formal policies in place regarding our products.
Reimbursement for Uses of the OMNI Surgical System
Surgeons are able to use OMNI to sequentially perform two well-established glaucoma procedures, canaloplasty followed by trabeculotomy.
Canaloplasty and trabeculotomy are covered by Medicare outside of formal policy, based on a claim-by-claim adjudication. Widespread coverage is important for commercial adoption. Based on POAG prevalence, we estimate that currently over 70% of patients who receive glaucoma treatment using OMNI are covered by Medicare, and that this percentage may decline modestly over time as usage of OMNI expands to include patients with a broader range of OAG progression. Private payor coverage policies for canaloplasty and trabeculotomy vary. Some private payors, including Aetna and certain Blue Cross Blue Shield plans, have written policies that consider canaloplasty medically necessary for the treatment of glaucoma, though specific criteria for coverage may vary depending on the payor. Where coverage is less consistent or is limited, as is the case with certain private payors, our market access team works with payers directly and with customers to facilitate patient access to our solutions and verify that appropriate reimbursement can be obtained. We have established and continue to build a substantial library of clinical trial data and published articles to directly address the needs of some payors. We believe that the results from our nine completed, in progress and planned clinical trials and subsequent accompanying peer-reviewed articles will help to expand coverage of the use of OMNI. We estimate that, as of March 2021, 38% of the covered lives within the top nine national private payors (including commercial, Medicare Advantage and Medicaid Managed Care plans) cover the procedures performed using OMNI. The OMNI procedure is covered and reimbursed by all Medicare Administrative Contractors and numerous private insurers, covering an estimated 67% of U.S. POAG sufferers.
Virtually all sales of OMNI in the U.S. are to ASCs and HOPDs. Surgeons may use OMNI to perform canaloplasty and trabeculotomy sequentially, with CPT code 66174 used to report the procedure. Per Medicare and many private payor payment policies, when certain procedures are performed in the ASC setting, such as cataract surgery and canaloplasty, multiple procedure payment reduction rules apply. Therefore, when a canaloplasty is performed with cataract surgery are performed on the same patient on the same day, payment of the lower-cost procedure (most commonly the cataract procedure) is reduced by 50%. Multiple procedure payment reduction rules also typically apply to professional services. Physician payments are likely to be paid at a reduced rate for lower valued procedures when performed concomitantly. In the HOPD setting, Medicare procedures performed using OMNI as well as cataract procedures are paid under comprehensive ambulatory payment classifications (C-APCs). In this site of service, the highest valued code is paid at 100%, with payment for additional procedures performed during the same operative session bundled into the single highest payment rate. Many commercial payers use a similar payment methodology, but payment rules can vary across health plans, particularly across plan types (e.g., HMO, PPO, POS).
In the ASC setting, the 2021 Medicare national unadjusted average facility payment rate for CPT 66174 is $1,872.33. In the HOPD setting, the 2021 Medicare national unadjusted average facility payment rate for CPT 66174 is $3,917.74. These payments are classified as comprehensive C-APCs, therefore the highest valued code will be paid and other C-APC classified procedures will be bundled into the highest paid procedure. Regardless of facility setting, the Medicare national unadjusted physician payment rate for CPT 66174 is $947.70. Based on customer feedback, we believe the rates for facility and physician reimbursement in both settings reflect attractive and reasonable payments to cover all of our customers’ costs and economic needs related to glaucoma treatments using OMNI for both Standalone and Combination Cataract procedures.
While commercialization of OMNI has primarily been focused on the U.S., we have also begun international commercialization efforts. Outside the U.S., we have made the most progress in Germany where we
164
Table of Contents
have established and trained an ophthalmic distributor with successful experience commercializing the invasive form of canaloplasty. Although Germany employs a single-payor health system and a national MIGS procedure code which includes canaloplasty and trabeculotomy, coverage decisions are decentralized. Our distributor is working, and will work, with the decentralized Physician’s Associations (Kassenärztliche Vereinigung) to facilitate access to OMNI for patients and ECPs. As we expand into other countries, we will establish reimbursement strategies that are appropriate for each local market.
Reimbursement for Uses of the TearCare System
TearCare is not currently covered by Medicare or private payors via formal medical policy, although some payors may agree to provide coverage and subsequent payment outside of formal policy. We intend to seek FDA clearance of TearCare for an expanded indication for use in the second half of 2021. We believe that the current standard of care (representing over 95% of the existing market), which primarily consists of over-the-counter artificial tears or lubricating eyedrops, and prescription eyedrops, does not treat the root cause of MGD. We believe TearCare, if cleared by the FDA for an expanded indication for use, has the potential to offer a better standard of care for evaporative dry eye patients and reduced overall costs for payors.
Despite the presence of a large and growing patient-pay market for TearCare as shown in our controlled launch, we believe that improving access to TearCare through positive coverage decisions by Medicare and private payors will help grow the market for the device. We are pursuing a vigorous market development plan to convince Medicare and private payors to increase access to procedures using TearCare in the U.S.
In 2018, we applied for a Category III CPT code that describes the heating of meibomian glands using a wearable open-eye device and manual evacuation of meibomian glands. This new code, 0563T, was granted in 2019 and became effective January 1, 2020, allowing providers to pursue reimbursement claims and payors to establish payment rates for the procedure. Prior to formal coverage decisions or a permanent Category I code, third-party payors may cover procedures billed with temporary Category III codes that meet their coverage criteria.
We have already begun to generate clinical data to support positive coverage decisions from Medicare and private payors. In January 2021, an article discussing results from our OLYMPIA RCT was submitted to Cornea The Journal of Cornea and External Disease. This randomized controlled trial compared treatment using TearCare to the leading alternative MGD treatment device on the market. In the study, we observed that a single use of TearCare was associated with improvement in each of the signs and symptoms of DED within two weeks of treatment in subjects with MGD. In a post-hoc analysis we also observed that a greater proportion of subjects in the TearCare group reported better symptomatic relief relative to the comparator group as assessed by patient reported outcomes. We plan to submit additional articles discussing the results from our OLYMPIA RCT to The Ocular Surface and Clinical Ophthalmology in the near future.
Our comprehensive long term strategy to improve patient access to TearCare includes the following key initiatives:
| • | Demonstrate the effectiveness, safety and durability of TearCare with rigorous clinical data. Building on supportive data from completed studies, our upcoming clinical program for TearCare, including the SAHARA and RESTORE studies, aims to advance the development of TearCare for the signs and symptoms of DED due to MGD with comparative trial designs established to evaluate the effectiveness and durability of treatment with TearCare, which our research suggests would be the primary criteria for payors to decide coverage determinations. SAHARA, which will commence in 2021 and features a trial design directly informed by a masked panel of medical directors from eight payors, is a RCT of TearCare versus the leading DED prescription eyedrop, and will compare effectiveness and safety, as well as assess durability of effect through a 24-month follow up period. |
| • | Augment library of published articles on TearCare. We plan to facilitate publication of numerous articles describing the results of our studies of TearCare in peer-reviewed journals. We collaborate with |
165
Table of Contents
our advisors to design and conduct our studies, and ensure findings undergo the rigorous peer review process for publication in leading ophthalmology and optometry journals, recognizing that third-party payors base coverage decisions on reviews of the published medical literature. |
| • | Support coverage applications. Our market access team assists key strategic accounts in their submission of high quality reimbursement requests for uses of TearCare. Our market access team also works with customers and patients to navigate the reimbursement process with third-party payors, including prior authorization approvals and appeals for denial of coverage or low payment. As more claims for uses of TearCare are accepted, we will work with third-party payors to formalize coverage decisions to streamline the coverage and payment processes. |
| • | Convert to permanent Category I CPT code. We plan to leverage our clinical studies, peer-reviewed publications, society and medical community support, and utilization / real world reimbursement claims data to support conversion of our Category III CPT code for TearCare to a permanent Category I CPT code. Although Medicare and private payors may cover Category III CPT codes that meet their coverage criteria, we believe AMA approval of a permanent Category I CPT code for uses of TearCare, along with potential enhanced indications for use, will bolster our efforts to gain positive coverage determinations from Medicare and private payors. |
Competition
We believe our focus on developing and marketing intuitively designed products that are intended to restore the eye’s natural physiological function by addressing underlying causes of eye disease will be an important factor in our future success. The medical device and pharmaceutical industries are intensely competitive, subject to rapid change and significantly affected by new product introductions and other market activities of industry participants. We compete with medical device and pharmaceutical companies that develop and commercialize products for eye conditions. Notable competitors with approved MIGS products include Glaukos (iStent and iStent Inject), Ivantis (Hydrus Microstent) and AbbVie/Allergan (Xen), while AbbVie/Allergan (Restasis), Novartis (Xiidra), Johnson & Johnson (LipiFlow), and Alcon (iLux) have notable approved products to treat DED. Other competitors with approved ophthalmic products in glaucoma and DED include Alcon (Simbrinza), Novartis (Travatan, Duotrav), AbbVie/Allergan (Durysta, Lumigan, Combigan), Aerie Pharmaceuticals (Roclatan, Rhopressa), Bausch and Lomb (Vyzulta), MST (Trabectome and TrabEx), New World Medical (Kahook Dual Blade), Nova Eye (iTrack), Kala Pharmaceuticals (Eyesuvis) and Sun Pharmaceutical Industries (Cequa). Notable competitors seeking approval for new MIGS and sustained release glaucoma treatments include Glaukos (iDose), Ocular Therapeutix (OTX-TIC), and iSTARMedical (MINIject), and in pharmaceutical DED treatments include, among others, Aldeyra Therapeutics (Reproxalap), Bausch and Lomb (NOV03), Ocular Therapeutix (OTX-CSI), Oyster Point (OC-01) and Tarsus Pharmaceuticals (TP-03). Some of our competitors are larger, well-capitalized companies with greater market share and resources than us currently. Consequently, they are able to spend more on product development, marketing, sales and other product initiatives than we can. We also compete with a number of smaller medical device companies that have single products or a limited range of products. Some of our competitors have:
| • | Significantly greater name recognition; |
| • | Broader or deeper relations with healthcare professionals, customers and third-party payors; |
| • | More established distribution networks; |
| • | Additional lines of products and the ability to offer rebates or bundle products to offer greater discounts or other incentives to attract adoption; |
| • | Greater experience in conducting research and development, manufacturing, clinical trials, marketing and obtaining regulatory clearance or approval for products; and |
| • | Greater financial and human resources for product development, sales and marketing and patent and other intellectual property litigation. |
166
Table of Contents
We compete primarily on the basis that our medical devices are able to treat patients with prevalent eye diseases safely and effectively. Our continued success depends on our ability to:
| • | Develop innovative, proprietary technology and products that can cost-effectively address significant clinical needs; |
| • | Obtain and maintain regulatory clearances or approvals for the use of our products; |
| • | Obtain and maintain favorable reimbursement decisions relating to the use of our products; |
| • | Demonstrate clinical safety and effectiveness in our sponsored and third-party trials and studies; |
| • | Attract and retain skilled research and development and sales personnel; and |
| • | Successfully market and sell products. |
Manufacturing
From its launch in early 2018 until February 2021, OMNI was solely assembled and produced by Second Source Medical LLC, or SSM, a contract manufacturer based in San Jose, California on an individual purchase-order basis, pursuant to a regulatory and quality framework established by the Supplier Quality Agreement and Plan dated April 5, 2018.
On January 14, 2021, we entered into a Supply Agreement, or the Peter’s Supply Agreement, with Peter’s Technology (Suzhou) CO LTD., or PTCS, a Chinese subsidiary of Peter’s Co., Ltd., a Taiwan-based contract manufacturer. In February 2021, PTCS began to produce commercially saleable OMNI units for us at its Suzhou City, China production facility. Our objective is to transition OMNI production from SSM to Peter’s and an additional high-volume contract manufacturer with domestic U.S. production facilities by the end of the third quarter of 2021. The Peter’s Supply Agreement governs the assembly and supply of OMNI by PTCS, pursuant to which PTCS purchases components from our approved suppliers for assembly and we make purchases from PTCS on a purchase order basis. The initial term of the three year Peter’s Supply Agreement expires January 14, 2024. The Peter’s Supply Agreement automatically renews for additional one year periods if neither party provides notification that they intend to terminate the agreement within 90 days of the term ending. We have the right to terminate the agreement without cause during its term by providing 180 days’ advance written notice, or with 30 days’ written notice with any material agreement default by PTCS.
For the production of TearCare, we currently have supply arrangements with separate U.S. medical device manufacturers for the production of each of TearCare’s SmartLids and TearCare’s SmartHubs.
We directly engage with several third-party suppliers for key components used in our products. We believe that third-party suppliers will be adequate to meet our current and anticipated manufacturing needs. We do not currently plan to manufacture our products or any related components ourselves.
Manufacturing facilities that produce medical devices or their component parts intended for distribution world-wide are subject to regulation and periodic unannounced inspection by the FDA and other domestic and international regulatory agencies. In the United States, any products we sell are required to be manufactured in compliance with the FDA’s Quality System Regulation, which covers the methods used in, and the facilities used for, the design, testing, control, manufacturing, labeling, quality assurance, packaging, storage and shipping of our products.
The distribution of our products is handled directly through a third-party logistics provider. Our finished goods are shipped from our contract manufacturers to Sterigenics for gamma sterilization in Hayward, California after which they are shipped to distribution facilities and are distributed from there to customers.
167
Table of Contents
Intellectual Property
Our commercial success depends in part on our ability to obtain and maintain proprietary protection for our current and future products and product candidates, novel discoveries, product development technologies and know-how; to operate without infringing on the proprietary rights of others; and to prevent others from infringing our proprietary rights. Our policy is to seek to protect our proprietary position by, among other methods, seeking to obtain or in-licensing U.S. and foreign patents and patent applications related to our proprietary technology that are important to the development and implementation of our business. We seek to obtain domestic and international patent protection, and endeavor to promptly file patent applications for new commercially valuable inventions. We file new patent applications as we conduct research and development, initiate new programs, and monitor the activities of others. We also rely on other approaches to protecting our proprietary position, such as trademarks, trade secrets, know-how, and/or continuing technological innovation to develop and maintain our proprietary position.
The patent positions of medical device companies like us are generally uncertain and involve complex legal, scientific and factual questions. In addition, the coverage claimed in a patent may be challenged in courts after issuance. Moreover, many jurisdictions permit third parties to challenge issued patents in administrative proceedings, which may result in further narrowing or even cancellation of patent claims. We cannot predict whether the patent applications we are currently pursuing will issue as patents in any particular jurisdiction or at all, whether the claims of any patent applications, should they issue, will cover our products or product candidates, or whether the claims of any issued patents will provide sufficient protection from competitors or otherwise provide any competitive advantage.
We cannot be certain of the priority of inventions covered by our patents and pending patent applications, in part because patent applications in the United States and certain other jurisdictions are maintained in secrecy for 18 months or potentially even longer, and because publication of discoveries in the scientific or patent literature often lags behind actual discoveries and patent application filings. Accordingly, we may not have been the first to invent the subject matter disclosed in some of our patents and patent applications or the first to file patent applications covering such subject matter.
Patent Term
Generally, issued patents are granted a term of 20 years from the earliest claimed non-provisional filing date. In certain instances, U.S. patent term can be adjusted to recapture a portion of delay by the U.S. Patent & Trademark Office, or USPTO, in examining the patent application (patent term adjustment) or extended to account for term effectively lost as a result of the FDA regulatory review period (patent term extension), or both. In some cases, the term of a U.S. patent may be shortened by terminal disclaimer, such that its term is reduced to end with that of an earlier-expiring patent.
Trade Secrets
In addition to patents, we rely on or may in the future rely on trade secrets and know-how to develop and maintain our competitive position. We typically rely on or may in the future rely on trade secrets to protect aspects of our business that are not amenable to, or that we do not consider appropriate for, patent protection. It is our policy to protect trade secrets and/or know-how by establishing confidentiality agreements and invention assignment agreements with our employees, consultants, scientific advisors, contractors and collaborators. These agreements provide that all confidential information developed or made known during the course of an individual or entity’s relationship with us must be kept confidential during and after the relationship. These agreements also provide that all inventions resulting from work performed for us or relating to our business and conceived or completed during the period of employment or assignment, as applicable, shall be our exclusive property. In addition, we take other appropriate precautions, such as physical and technological security measures, to guard against misappropriation of our proprietary information by third parties.
168
Table of Contents
OMNI
As of April 30, 2021, we owned 19 issued U.S. patents, 25 issued patents outside the U.S. (which includes three issued European patents and their national validations), nine pending U.S. non-provisional patent applications, one pending U.S. provisional patent application and eight pending foreign patent applications in our OMNI portfolio. The issued patents include claims directed to devices and methods for canaloplasty and/or trabeculotomy, ocular implants, and related methods.
Subject to payment of required maintenance fees, annuities, and other charges, our issued U.S. patents in our OMNI Surgical System portfolio have expiration dates between 2027 and 2037, with six of our issued U.S. patents having expiration dates before 2030, 12 having expiration dates between 2031 and 2035, and the remaining one expiring in 2037, in each case exclusive of possible patent term extensions. Of the ten pending U.S. patent applications in our OMNI Surgical System portfolio, one was filed in 2015, four were filed in 2019, three, including our U.S. provisional patent application, were filed in 2020, and two were filed in 2021. Our pending U.S. non-provisional patent applications, if issued, have expected expiration dates between 2026 and 2040, exclusive of any possible patent term adjustments or patent term extensions.
The foreign jurisdictions where we own issued patents in our OMNI Surgical System portfolio include: Australia, China, France, Germany, Italy, Japan, Spain, Switzerland, and the United Kingdom. Subject to payment of required annuities and other charges, these foreign patents have expiration dates between 2027 and 2035. We have pending patent applications in our OMNI surgical system portfolio in Australia, Canada, China, Europe, Hong Kong, and Japan which, if issued, have expected expiration dates between 2032 and 2035.
TearCare
As of April 30, 2021, we owned eight issued U.S. patents, nine issued patents outside the U.S. (which includes one issued European patent and its national validations), seven pending U.S. non-provisional patent applications, seven pending foreign patent applications, and one pending Patent Cooperation Treaty, or PCT, patent application in our TearCare portfolio. The issued patents include claims directed to the TearCare apparatus and methods of using the TearCare apparatus, components of the TearCare apparatus (including the SmartHub and SmartLids) and methods of their use, the TearCare apparatus in combination with an eyelid compression instrument and methods of their use, and methods of using the TearCare apparatus with patients wearing contact lenses.
Subject to payment of required maintenance fees, annuities, and other charges, our issued U.S. patents in our TearCare portfolio have expiration dates in 2032, in each case exclusive of possible patent term extensions. Of the seven pending U.S. non-provisional patent applications in our TearCare portfolio, one was filed in 2016, one was filed in 2018, one was filed in 2019, two were filed in 2020, and two were filed in 2021. Any patents issuing from these pending U.S. non-provisional patent applications would have expected expiration dates between 2032 and 2040, exclusive of any possible patent term adjustments or patent term extensions.
The foreign jurisdictions where we own issued patents in our TearCare portfolio include: China, France, Germany, Italy, Japan, Spain, and the United Kingdom, all of which will expire in 2032. We have additional pending patent applications in our TearCare portfolio in Brazil, China, Europe, and Japan which, if issued, have expected expiration dates between 2032 and 2039. Our pending PCT patent application is not eligible to become an issued patent unless and until, among other things, we file a national stage patent application within 30 months from the earliest priority date of the PCT patent application in the countries in which we seek patent protection.
As of April 30, 2021, we owned eight U.S. trademark registrations, one German trademark registration and one pending E.U. trademark application.
For information regarding the risks related to our intellectual property, please see the section titled “Risk Factors—Risks Related to Our Intellectual Property.”
169
Table of Contents
Government Regulation
Our products and our operations are subject to extensive regulation by the U.S. Food and Drug Administration, or FDA, and other federal, state, and local authorities in the United States, as well as comparable authorities in foreign jurisdictions. Our products are subject to regulation as medical devices in the United States under the Federal Food, Drug, and Cosmetic Act, or FDCA, and its implementing regulations.
United States Regulation
The FDA regulates, among other things, the development, design, non-clinical and clinical testing, manufacturing, safety, effectiveness, labeling, packaging, storage, installation, servicing, recordkeeping, premarket clearance or approval, adverse event reporting, advertising, promotion, marketing and distribution, and import and export and post-marketing surveillance of medical devices in the United States to ensure that medical devices distributed domestically are safe and effective for their intended uses and otherwise meet the requirements of the FDCA.
FDA Premarket Clearance and Approval Requirements
Unless an exemption applies, each new or significantly modified medical device commercially distributed in the United States requires either FDA clearance of a 510(k) premarket notification, or approval of a premarket approval, or PMA, application. Both the 510(k) clearance and PMA processes can be resource intensive, expensive, and lengthy.
Under the FDCA, medical devices are classified into one of three classes—Class I, Class II or Class III—depending on the degree of risk associated with each medical device and the extent of manufacturer and regulatory control needed to ensure its safety and effectiveness. Class I devices are those for which safety and effectiveness can be assured by adherence to the FDA’s general controls for medical devices, which include compliance with the applicable portions of FDA’s current good manufacturing practices for devices, as reflected in the Quality System Regulation, or QSR, establishment registration and device listing, reporting of adverse medical events, and truthful and non-misleading labeling, advertising, and promotional materials. Some Class I devices, also called Class I reserved devices, also require premarket clearance by the FDA through the 510(k) premarket notification process described below. Most Class I devices are exempt from the premarket notification requirements.
Class II devices are subject to the FDA’s general controls, and any other special controls deemed necessary by the FDA to ensure the safety and effectiveness of the device. These special controls can include performance standards, special labeling requirements, post-market surveillance, patient registries and FDA guidance documents.
Most Class II devices are required to submit to the FDA a premarket notification under Section 510(k) of the FDCA requesting permission to commercially distribute the device. The FDA’s permission to commercially distribute a device subject to a 510(k) premarket notification is generally known as 510(k) clearance.
Class III devices include devices deemed by the FDA to pose the greatest risks, such as life sustaining, life supporting or some implantable devices, or devices that have a new intended use, or use advanced technology that is not substantially equivalent to that of a legally marketed device, requiring approval of a PMA. Due to the level of risk associated with Class III devices, the FDA’s general controls and special controls alone are insufficient to assure their safety and effectiveness. Devices placed in Class III general require the submission of a PMA application demonstrating the safety and effectiveness of the device, which must be approved by the FDA prior to marketing, or the receipt of a 510(k) de novo classification, which provides for the reclassification of the device in Class I or II. The PMA approval process is generally more costly and time consuming than the 510(k) process. Through the PMA application process, the applicant must submit data and information demonstrating
170
Table of Contents
reasonable assurance of the safety and effectiveness of the device for its intended use to the FDA’s satisfaction. Accordingly, a PMA application typically includes, but is not limited to, extensive technical information regarding device design and development, pre-clinical and clinical trial data, manufacturing information, labeling and financial disclosure information for the clinical investigators in device studies. The PMA application must provide valid scientific evidence that demonstrates to the FDA’s satisfaction a reasonable assurance of the safety and effectiveness of the device for its intended use.
If a new medical device does not qualify for the 510(k) premarket notification process because no predicate device to which it is substantially equivalent can be identified, the device is automatically classified into Class III. The Food and Drug Administration Modernization Act of 1997 established a new route to market for low to moderate risk medical devices that are automatically placed into Class III due to the absence of a predicate device, called the “Request for Evaluation of Automatic Class III Designation,” or the de novo classification process. This process allows a manufacturer whose novel device is automatically classified into Class III to request down-classification of its medical device into Class I or Class II on the basis that the device presents low or moderate risk, rather than requiring the submission and approval of a PMA. If the manufacturer seeks reclassification into Class II, the manufacturer must include a draft proposal for special controls that are necessary to provide a reasonable assurance of the safety and effectiveness of the medical device. The FDA may reject the reclassification petition if it identifies a legally marketed predicate device that would be appropriate for a 510(k) or determines that the device is not low to moderate risk and requires PMA or that general controls would be inadequate to control the risks and special controls cannot be developed.
Obtaining FDA marketing authorization, de novo down-classification, or approval for medical devices is expensive and uncertain, and may take several years, and generally requires significant scientific and clinical data.
Some pre-amendment devices are unclassified, but are subject to FDA’s premarket notification and clearance process in order to be commercially distributed. Our currently marketed OMNI products are regulated as Class II devices subject to 510(k) clearance. We currently market our TearCare product as a Class II, 510(k)-exempt powered heating pad.
Investigational Device Process
Clinical trials are almost always required to support a PMA and are sometimes required to support a 510(k) submission. In the United States, absent certain limited exceptions, human clinical trials intended to support medical device clearance or approval or to determine safety and effectiveness of a device for an investigational use must be conducted in accordance with the FDA’s investigational device exemption, or IDE, regulations which govern investigational device labeling, prohibit promotion of the investigational device, and specify an array of recordkeeping, reporting and monitoring responsibilities of study sponsors and study investigators. If the device presents a “significant risk,” to human health, as defined by the FDA, the FDA requires the device sponsor to submit an IDE application to the FDA, which must become effective prior to commencing human clinical trials. The IDE application must be supported by appropriate data, such as animal and laboratory testing results, showing that it is safe to test the device in humans and that the testing protocol is scientifically sound. The IDE application must be approved in advance by the FDA for a specified number of subjects. Generally, clinical trials for a significant risk device may begin once the IDE application is approved by the FDA and the study protocol and informed consent are approved by appropriate institutional review boards at the clinical trial sites. There can be no assurance that submission of an IDE will result in the ability to commence clinical trials, and although the FDA’s approval of an IDE allows clinical testing to go forward for a specified number of subjects, it does not bind the FDA to accept the results of the trial as sufficient to prove the product’s safety and effectiveness, even if the trial meets its intended success criteria.
If the device under evaluation does not present a significant risk to human health, then the device sponsor is not required to submit an IDE application to the FDA before initiating human clinical trials, but must still comply
171
Table of Contents
with abbreviated IDE requirements when conducting such trials. A significant risk device is one that presents a potential for serious risk to the health, safety or welfare of a patient and either is implanted, used in supporting or sustaining human life, substantially important in diagnosing, curing, mitigating or treating disease or otherwise preventing impairment of human health, or otherwise presents a potential for serious risk to a subject. An IDE application must be supported by appropriate data, such as animal and laboratory test results, showing that it is safe to test the device in humans and that the testing protocol is scientifically sound. The IDE will automatically become effective 30 days after receipt by the FDA unless the FDA notifies the company that the investigation may not begin. If the FDA determines that there are deficiencies or other concerns with an IDE for which it requires modification, the FDA may permit a clinical trial to proceed under a conditional approval.
Regardless of the degree of risk presented by the medical device, clinical studies must be approved by, and conducted under the oversight of, an Institutional Review Board, or IRB, for each clinical site. The IRB is responsible for the initial and continuing review of the IDE, and may pose additional requirements for the conduct of the study. If an IDE application is approved by the FDA and one or more IRBs, human clinical trials may begin at a specific number of investigational sites with a specific number of patients, as approved by the FDA. If the device presents a non-significant risk to the patient, a sponsor may begin the clinical trial after obtaining approval for the trial by one or more IRBs without separate approval from the FDA, but must still follow abbreviated IDE requirements, such as monitoring the investigation, ensuring that the investigators obtain informed consent, and labeling and record-keeping requirements. Acceptance of an IDE application for review does not guarantee that the FDA will allow the IDE to become effective and, if it does become effective, the FDA may or may not determine that the data derived from the trials support the safety and effectiveness of the device or warrant the continuation of clinical trials. An IDE supplement must be submitted to, and approved by, the FDA before a sponsor or investigator may make a change to the investigational plan that may affect its scientific soundness, study plan or the rights, safety or welfare of human subjects.
During a study, the sponsor is required to comply with the applicable FDA requirements, including, for example, trial monitoring, selecting clinical investigators and providing them with the investigational plan, ensuring IRB review, adverse event reporting, record keeping and prohibitions on the promotion of investigational devices or on making safety or effectiveness claims for them. The clinical investigators in the clinical study are also subject to FDA’s regulations and must obtain patient informed consent, rigorously follow the investigational plan and study protocol, control the disposition of the investigational device, and comply with all reporting and recordkeeping requirements. Additionally, after a trial begins, we, the FDA or the IRB could suspend or terminate a clinical trial at any time for various reasons, including the following:
| • | The FDA or other regulatory authorities do not approve a clinical trial protocol or a clinical trial, or place a clinical trial on hold; |
| • | Patients do not enroll in clinical trials at the rate expected; |
| • | Patients do not comply with trial protocols; |
| • | Patient follow-up is not at the rate expected; |
| • | Patients experience adverse events; |
| • | Patients die during a clinical trial, even though their death may not be related to the products that are part of the trial; |
| • | Device malfunctions occur with unexpected frequency or potential adverse consequences; |
| • | Side effects or device malfunctions of similar products already in the market that change the FDA’s view toward approval of new or similar PMAs or result in the imposition of new requirements or testing; |
| • | Institutional review boards and third-party clinical investigators may delay or reject the trial protocol; |
172
Table of Contents
| • | Third-party clinical investigators decline to participate in a trial or do not perform a trial on the anticipated schedule or consistent with the clinical trial protocol, investigator agreement, investigational plan, good clinical practices, the IDE regulations, or other FDA or IRB requirements; |
| • | Third-party investigators are disqualified by the FDA; |
| • | We or third-party organizations do not perform data collection, monitoring and analysis in a timely or accurate manner or consistent with the clinical trial protocol or investigational or statistical plans, or otherwise fail to comply with the IDE regulations governing responsibilities, records, and reports of sponsors of clinical investigations; |
| • | Third-party clinical investigators have significant financial interests related to us or our study such that the FDA deems the study results unreliable, or the company or investigators fail to disclose such interests; |
| • | Regulatory inspections of our clinical trials or manufacturing facilities, which may, among other things, require us to undertake corrective action or suspend or terminate our clinical trials; |
| • | Changes in government regulations or administrative actions; |
| • | The interim or final results of the clinical trial are inconclusive or unfavorable as to safety or effectiveness; or |
| • | The FDA concludes that our trial design is unreliable or inadequate to demonstrate safety and effectiveness. |
510(k) Clearance Process
Under the 510(k) process, the manufacturer must submit to the FDA a premarket notification submission demonstrating that the proposed device is “substantially equivalent,” as defined in the FDCA, to a legally marketed predicate device.
A predicate device is a legally marketed device that is not subject to premarket approval, i.e., a device that was legally marketed prior to May 28, 1976 (pre-amendments device) and for which a PMA is not required, a device that has been reclassified from Class III to Class II or I, or a device that was found substantially equivalent through the 510(k) process. A device is considered to be substantially equivalent if, with respect to the predicate device, it has the same intended use and has either (i) the same technological characteristics; or (ii) different technological characteristics, but the information provided in the 510(k) submission demonstrates that the device does not raise different questions of safety or effectiveness than the predicate device.
Before the FDA will accept a 510(k) premarket notification for substantive review, the FDA will first assess whether the submission satisfies a minimum threshold of acceptability. If the FDA determines that the 510(k) submission lacks necessary information for substantive review, the FDA will issue a “Refuse to Accept” letter which generally outlines the information the FDA believes is necessary to permit a substantive review and to reach a determination regarding substantial equivalence. An applicant must submit the requested information before the FDA will proceed with additional review of the submission. If a 510(k) submission is accepted for substantive review, the Medical Device User Fee Amendments sets a performance goal of 90 days for FDA review of a 510(k) submission, but the review time can be delayed if FDA raises questions or requests addition information during the review process. As a practical matter, clearance often takes longer, and clearance is never assured. Thus, as a practical matter, clearance often takes longer than 90 days. Although many 510(k) premarket notifications are cleared without clinical data, the FDA may require further information, including clinical data, to make a determination regarding substantial equivalence, which may significantly prolong the review process. If the FDA agrees that the device is substantially equivalent, it will grant clearance to commercially market the device.
If the FDA determines that the device is substantially equivalent to a predicate device, it will grant 510(k) clearance to commercially market the device. If the FDA determines that the device is “not substantially
173
Table of Contents
equivalent” to a previously cleared device, the device is automatically designated as a Class III device. The device sponsor must then fulfill more rigorous requirements of the PMA approval process, or can request a risk-based classification determination for the device in accordance with the “de novo” process, which is a route to market for certain novel medical devices that are low to moderate risk and are not substantially equivalent to a predicate device.
Medical devices can only be marketed for the indications for use for which they are cleared or approved. After a device receives 510(k) clearance, any modification that could significantly affect its safety or effectiveness, or that would constitute a major change or modification in its intended use, will require a new 510(k) clearance or, depending on the modification, PMA approval or de novo reclassification. The FDA requires each manufacturer to determine whether the proposed change requires submission of a 510(k), de novo request or a PMA in the first instance, but the FDA may review this determination to evaluate the regulatory status of the modified product at any time and may require the manufacturer to cease marketing and/or request the recall of the modified device until 510(k) marketing clearance or PMA approval is obtained or a de novo request is granted. Also, in these circumstances, the manufacturer may be subject to significant regulatory fines or penalties.
Over the last several years, the FDA has proposed reforms to its 510(k) clearance process, and such proposals could include increased requirements for clinical data and a longer review period, or could make it more difficult for manufacturers to utilize the 510(k) clearance process for their products. For example, in November 2018, FDA officials announced steps that the FDA intended to take to modernize the premarket notification pathway under Section 510(k) of the FDCA. Among other things, the FDA announced that it planned to develop proposals to drive manufacturers utilizing the 510(k) pathway toward the use of newer predicates. These proposals included plans to potentially sunset certain older devices that were used as predicates under the 510(k) clearance pathway, and to potentially publish a list of devices that have been cleared on the basis of demonstrated substantial equivalence to predicate devices that are more than 10 years old. These proposals have not yet been finalized or adopted, although the FDA may work with Congress to implement such proposals through legislation.
More recently, in September 2019, the FDA issued revised final guidance describing an optional “safety and performance based” premarket review pathway for manufacturers of “certain, well-understood device types” to demonstrate substantial equivalence under the 510(k) clearance pathway by showing that such device meets objective safety and performance criteria established by the FDA, thereby obviating the need for manufacturers to compare the safety and performance of their medical devices to specific predicate devices in the clearance process. The FDA has developed and maintains a list device types appropriate for the “safety and performance based” pathway and continues to develop product-specific guidance documents that identify the performance criteria for each such device type, as well as recommended testing methods, where feasible.
PMA Approval Process
Class III devices require PMA approval before they can be marketed, although some pre-amendment Class III devices for which FDA has not yet required a PMA are cleared through the 510(k) process. The PMA process is more demanding than the 510(k) premarket notification process. In a PMA, the manufacturer must demonstrate that the device is safe and effective for its intended use, and the PMA must be supported by extensive data, including data from preclinical studies and human clinical trials. The PMA must also contain a full description of the device and its components, a full description of the methods, facilities, and controls used for manufacturing, and proposed labeling. Following receipt of a PMA, the FDA conducts an administrative review to determine whether the application is sufficiently complete to permit a substantive review. If it is not, the agency will refuse to file the PMA. If FDA accepts the application for substantive review, it has 180 days under the FDCA to complete its review of a filed PMA application, although in practice, the FDA’s review often takes significantly longer, and can take up to several years. During this review period, the FDA may request additional information or clarification of information already provided, and the FDA may issue a major
174
Table of Contents
deficiency letter to the applicant, requesting the applicant’s response to deficiencies communicated by the FDA. The FDA considers a PMA or PMA supplement to have been voluntarily withdrawn if an applicant fails to respond to an FDA request for information (e.g., major deficiency letter) within a total of 360 days. Before approving or denying a PMA application, an advisory panel of experts from outside the FDA may be convened to review and evaluate the application and provide recommendations to the FDA as to whether the FDA should approve the submission, approve it with specific conditions, or not approve it. The FDA may or may not accept the panel’s recommendation. Prior to approval of a PMA, the FDA may conduct inspections of the clinical trial data and clinical trial sites, as well as conduct inspections of the applicant or its third-party manufacturers’ or suppliers’ manufacturing facility or facilities to, among other things, ensure compliance with the QSR. PMA applications are also subject to the payment of user fees, which for fiscal year 2021 includes a standard application fee of $365,657.
Overall, the FDA review of a PMA application generally takes between one and three years, but may take significantly longer. The FDA can delay, limit or deny approval of a PMA application for many reasons, including:
| • | The device may not be shown safe or effective to the FDA’s satisfaction; |
| • | The data from pre-clinical studies and/or clinical trials may be found unreliable or insufficient to support approval; |
| • | The manufacturing process or facilities may not meet applicable requirements; and |
| • | Changes in FDA approval policies or adoption of new regulations may require additional data. |
If the FDA evaluation of a PMA is favorable, the FDA will issue either an approval letter, or an approvable letter, the latter of which usually contains a number of conditions that must be met in order to secure final approval of the PMA. When and if those conditions have been fulfilled to the satisfaction of the FDA, the agency will issue a PMA approval letter authorizing commercial marketing of the device, subject to the conditions of approval and the limitations established in the approval letter. The FDA may approve a PMA with post-approval conditions intended to ensure the safety and effectiveness of the device, including, among other things, restrictions on labeling, promotion, sale and distribution, and collection of long-term follow-up data from patients in the clinical study that supported PMA approval or requirements to conduct additional clinical studies post-approval. The FDA may condition PMA approval on some form of post-market surveillance when deemed necessary to protect the public health or to provide additional safety and effectiveness data for the device in a larger population or for a longer period of use. In such cases, the manufacturer might be required to follow certain patient groups for a number of years and to make periodic reports to the FDA on the clinical status of those patients. Failure to comply with the conditions of approval can result in material adverse enforcement action, including withdrawal of the approval. If the FDA’s evaluation of a PMA application or manufacturing facilities is not favorable, the FDA will deny approval of the PMA or issue a not approvable letter. The FDA also may determine that additional tests or clinical trials are necessary, in which case the PMA approval may be delayed for several months or years while the trials are conducted and data is submitted in an amendment to the PMA, or the PMA is withdrawn and resubmitted when the data are available. The PMA process can be expensive, uncertain and lengthy and a number of devices for which the FDA approval has been sought by other companies have never been approved by the FDA for marketing.
Certain changes to an approved device, such as changes in manufacturing facilities, methods, quality control procedures, sterilization, packaging, expiration date, labeling, device specifications, ingredients, materials, or design of a device, or other changes which affect the safety or effectiveness of the device that has been approved through the PMA process require submission of a new PMA or PMA supplement. PMA supplements often require submission of the same type of information as a PMA, except that the supplement is limited to information needed to support any changes from the device covered by the original, approved PMA and may not require as extensive clinical data or the convening of an advisory panel, depending on the nature of the proposed change. Certain other changes to an approved device require the submission of a new PMA, such as when the
175
Table of Contents
design change causes a different intended use, mode of operation, and technical basis of operation, or when the design change is so significant that a new generation of the device will be developed, and the data that were submitted with the original PMA are not applicable for the change in demonstrating a reasonable assurance of safety and effectiveness. None of our products are currently marketed pursuant to a PMA.
Ongoing Regulation by the FDA
Even after the FDA permits a device to be marketed, numerous and pervasive regulatory requirements continue to apply. These include:
| • | Establishment registration and device listing with the FDA; |
| • | QSR requirements, which require manufacturers, including third-party manufacturers, to follow stringent design, testing, control, supplier/contractor selection, compliant handling, documentation and other quality assurance procedures during all aspects of the design and manufacturing process; |
| • | Labeling regulations, advertising and promotion requirements, restrictions on sale, distribution or sale of a device, each including the FDA prohibition against the promotion of products for any uses other than those authorized by the FDA, which are commonly known as “off-label” uses; |
| • | The Medical Device Reporting, or MDR, regulations, which require that a manufacturer report to the FDA if a device it markets may have caused or contributed to a death or serious injury, or has malfunctioned and the device or a similar device that it markets would be likely to cause or contribute to a death or serious injury, if the malfunction were to recur; |
| • | Medical device correction and removal reporting regulations, which require that manufacturers report to the FDA field corrections or removals if undertaken to reduce a risk to health posed by the device or to remedy a violation of the FDCA that may present a risk to health; |
| • | Recall requirements, including a mandatory recall if there is a reasonable probability that the device would cause serious adverse health consequences or death; |
| • | An order of repair, replacement, or refund; |
| • | Device tracking requirements; and |
| • | Post-market study and surveillance requirements. |
After a device receives 510(k) clearance, any modification that could significantly affects its safety or effectiveness, or that would constitute a major change in its intended use, will require a new 510(k) or possibly a PMA. The FDA requires each manufacturer to make this determination initially, but the FDA can review any such decision and can disagree with a manufacturer’s determination. If the FDA disagrees with our determination not to seek a new 510(k) clearance, the FDA may retroactively require us to seek 510(k) clearance or possibly a PMA. The FDA could also require us to cease marketing and distribution and/or recall the modified device until 510(k) clearance or a PMA is obtained. Also, in these circumstances, we may be subject to significant regulatory fines and penalties.
Some changes to an approved PMA device, including changes in indications, labeling, or manufacturing processes or facilities, require submission and FDA approval of a new PMA application or PMA supplement, as appropriate, before the change can be implemented. Supplements to a PMA often require the submission of the same type of information required for an original PMA application, except that the supplement is generally limited to that information needed to support the proposed change from the device covered by the original PMA. The FDA uses the same procedures and actions in reviewing PMA supplements as it does in reviewing original PMA applications.
FDA regulations require us to register as a medical device manufacturer with the FDA. Additionally, some states also require medical device manufacturers and/or distributors doing business within the state to register
176
Table of Contents
with the state or apply for a state license, which could subject our facility to state inspection as well as FDA inspection on a routine basis for compliance with the QSR and any applicable state requirements. These regulations require that we manufacture our products and maintain related documentation in a prescribed manner with respect to manufacturing, testing and control activities.
Manufacturing processes for medical devices are required to comply with the applicable portions of the QSR, which cover the methods and the facilities and controls for the design, manufacture, testing, production, processes, controls, quality assurance, labeling, packaging, distribution, installation and servicing of finished devices intended for human use. The QSR also requires, among other things, maintenance of a device master file, device history file, and complaint files. As a manufacturer, we are subject to periodic scheduled or unscheduled inspections by the FDA. Failure to maintain compliance with the QSR requirements could result in the shutdown of, or restrictions on, manufacturing operations and the recall or seizure of marketed products, which would have a material adverse effect on our business. The discovery of previously unknown problems with any of our products, including unanticipated adverse events or adverse events of increasing severity or frequency, whether resulting from the use of the device within the scope of its clearance or off-label by a physician in the practice of medicine, could result in restrictions on the device, including the removal of the product from the market or voluntary or mandatory device recalls.
The FDA has broad regulatory compliance and enforcement powers. If the FDA determines that a manufacturer has failed to comply with applicable regulatory requirements, it can take a variety of compliance or enforcement actions, which may result in any of the following sanctions:
| • | Warning letters, untitled letters, fines, injunctions, consent decrees and civil penalties; |
| • | Recalls, withdrawals, or administrative detention or seizure of our products; |
| • | Operating restrictions or partial suspension or total shutdown of production; |
| • | Refusing or delays in processing, clearing, or approving submissions or applications for new products or modifications to existing products; |
| • | Suspension or withdrawal of 510(k) clearances or PMA approvals that have already been granted; |
| • | FDA refusal to issue certification to foreign governments needed to export our products for sale in other countries; or |
| • | Criminal prosecution. |
Our facilities, records and manufacturing processes are subject to periodic unscheduled inspections by the FDA. Failure to comply with the applicable United States medical device regulatory requirements could result in, among other things, warning letters, untitled letters, fines, injunctions, consent decrees, civil penalties, unanticipated expenditures, repairs, replacements, refunds, recalls or seizures of products, operating restrictions, total or partial suspension of production, the FDA’s refusal to issue certificates to foreign governments needed to export products for sale in other countries, the FDA’s refusal to grant future premarket clearances or approvals, withdrawals or suspensions of current product clearances or approvals and criminal prosecution.
Regulation of Medical Devices in the European Union
The European Union, or EU, has adopted specific directives regulating the design, manufacture, clinical investigations, conformity assessment, labeling and adverse event reporting for medical devices. EU directives must be implemented into the national laws of the EU member states and national laws may vary from one member state to another.
In the EU, there is currently no premarket government review of medical devices. However, the EU requires that all medical devices placed on the market in the EU must meet the relevant essential requirements laid down
177
Table of Contents
in the Council Directive 93/42/EEC, or the Medical Devices Directive, and the Council Directive 90/385/EEC, or the Active Implantable Medical Devices Directive. The most fundamental essential requirement is that a medical device must be designed and manufactured in such a way that it will not compromise the clinical condition or safety of patients, or the safety and health of users and others. In addition, the device must achieve the performances intended by the manufacturer and be designed, manufactured, and packaged in a suitable manner. The European Commission has adopted various standards applicable to medical devices. These include standards governing common requirements, such as sterilization and safety of medical electrical equipment and product standards for certain types of medical devices. There are also harmonized standards relating to design and manufacture. While not mandatory, compliance with these standards is viewed as the easiest way to satisfy the essential requirements as a practical matter. Compliance with a standard developed to implement an essential requirement also creates a rebuttable presumption that the device satisfies that essential requirement.
To demonstrate compliance with the essential requirements laid down in Annex I to the Medical Devices Directive, medical device manufacturers must undergo a conformity assessment procedure, which varies according to the type of medical device and its (risk) classification. Conformity assessment procedures require an assessment of available clinical evidence, literature data for the product, and post-market experience in respect of similar products already marketed. Except for low-risk medical devices (Class I non-sterile, non-measuring devices), where the manufacturer can self-declare the conformity of its products with the essential requirements (except for any parts which relate to sterility or metrology), a conformity assessment procedure requires the intervention of a Notified Body. Notified Bodies are independent organizations designated by EU countries to assess the conformity of devices before being placed on the market. A Notified Body would typically audit and examine a product’s technical dossiers and the manufacturers’ quality system (which must, in particular, comply with ISO 13485:2016 related to Medical Devices Quality Management Systems). If satisfied that the relevant product conforms to the relevant essential requirements, the Notified Body issues a certificate of conformity, which the manufacturer uses as a basis for its own declaration of conformity. The manufacturer may then apply the CE Mark to the device, which allows the device to be placed on the market throughout the EU.
Notified Body certificates of conformity are valid for a fixed duration (which shall not exceed five years). Throughout the term of the certificate, the manufacturer will be subject to periodic surveillance audits to verify continued compliance with the applicable requirements. In particular, there will be a new audit by the Notified Body before it will renew the relevant certificate(s).
As a general rule, demonstration of conformity of medical devices and their manufacturers with the essential requirements must be based, among other things, on the evaluation of clinical data supporting the safety and performance of the products during normal conditions of use. Specifically, a manufacturer must demonstrate that the device achieves its intended performance during normal conditions of use, that the known and foreseeable risks, and any adverse events, are minimized and acceptable when weighed against the benefits of its intended performance, and that any claims made about the performance and safety of the device are supported by suitable evidence. All manufacturers placing medical devices into the market in the EU must comply with the EU medical device vigilance system. Under this system, incidents must be reported to the relevant authorities of the EU member states, and manufacturers are required to take Field Safety Corrective Actions, or FSCAs, to reduce a risk of death or serious deterioration in the state of health associated with the use of a medical device that is already placed on the market. An incident is defined as any malfunction or deterioration in the characteristics and/or performance of a device, as well as any inadequacy in the labeling or the instructions for use which, directly or indirectly, might lead to or might have led to the death of a patient or user or of other persons or to a serious deterioration in their state of health. An FSCA may include the recall, modification, exchange, destruction or retrofitting of the device. FSCAs must be communicated by the manufacturer or its legal representative to its customers and/or to the end users of the device through Field Safety Notices.
The advertising and promotion of medical devices is subject to some general principles set forth by EU directives. According to the Medical Devices Directive, only devices that are CE-marked may be marketed and advertised in the EU in accordance with their intended purpose. Directive 2006/114/EC concerning misleading
178
Table of Contents
and comparative advertising and Directive 2005/29/EC on unfair commercial practices, while not specific to the advertising of medical devices, also apply to the advertising thereof and contain general rules, for example requiring that advertisements are evidenced, balanced and not misleading. Specific requirements are defined at national level. EU member states laws related to the advertising and promotion of medical devices, which vary between jurisdictions, may limit or restrict the advertising and promotion of products to the general public and may impose limitations on promotional activities with healthcare professionals.
Many EU member states have adopted specific anti-gift statutes that further limit commercial practices for medical devices, in particular vis-à -vis healthcare professionals and organizations. Additionally, there has been a recent trend of increased regulation of payments and transfers of value provided to healthcare professionals or entities. In addition, many EU member states have adopted national “Sunshine Acts” which impose reporting and transparency requirements (often on an annual basis), similar to the requirements in the United States, on medical device manufacturers. Certain countries also mandate implementation of commercial compliance programs.
On May 25, 2017, Regulation 2017/745, or the EU Medical Devices Regulation, entered into force, which repeals and replaces the Medical Devices Directive and the Active Implantable Medical Devices Directive. Unlike directives, which must be implemented into the national laws of the EU member states, regulations are directly applicable, without the need for adoption of EU member state laws implementing them, in all EU member states and are intended to eliminate current differences in the regulation of medical devices among EU member states. The Medical Devices Regulation, among other things, is intended to establish a uniform, transparent, predictable and sustainable regulatory framework across the EU for medical devices and ensure a high level of safety and health while supporting innovation.
The Medical Devices Regulation was originally intended to become applicable three years after publication, but in April 2020 the transition period was extended by the European Parliament and the Council of the EU by an additional year – until May 26, 2021. Devices lawfully placed on the market pursuant to the Medical Devices Directive and the Active Implantable Medical Devices Directive prior to May 26, 2021 may generally continue to be made available on the market or put into service until May 26, 2025. Once applicable, the new regulations will among other things:
| • | Strengthen the rules on placing devices on the market and reinforce surveillance once they are available; |
| • | Establish explicit provisions on manufacturers’ responsibilities for the follow-up of the quality, performance and safety of devices placed on the market; |
| • | Improve the traceability of medical devices throughout the supply chain to the end-user or patient through a unique identification number; |
| • | Set up a central database to provide patients, healthcare professionals and the public with comprehensive information on products available in the European Union, or EU; and |
| • | Strengthen the rules for the assessment of certain high-risk devices, which may have to undergo an additional check by experts before they are placed on the market. |
The aforementioned EU rules are generally applicable in the European Economic Area, or EEA, which consists of the 27 EU member states plus Norway, Liechtenstein and Iceland. Other countries, such as Switzerland, have entered into Mutual Recognition Agreements and allow the marketing of medical devices that meet EU requirements.
The EU-UK Trade and Cooperation Agreement, or TCA, came into effect on January 1, 2021. The TCA does not specifically refer to medical devices. However, as a result of Brexit, the Medical Devices Regulation will not be implemented in the UK, and previous legislation that mirrored the Medical Devices Regulation in the UK law has been revoked. The regulatory regime for medical devices in the UK will continue to be based on the
179
Table of Contents
requirements derived from current EU legislation, and the UK may choose to retain regulatory flexibility or align with the Medical Devices Regulation going forward. CE markings will continue to be recognized in the UK, and certificates issued by EU recognized Notified Bodies will be valid in the UK, until June 30, 2023. For medical devices placed on the UK market after this period, the UK Conformity Assessment, or UKCA, marking will be mandatory. In contrast, UKCA marking and certificates issued by UK Notified Bodies will not be recognized on the EU market. The TCA does provide for cooperation and exchange of information in the area of product safety and compliance, including market surveillance, enforcement activities and measures, standardization related activities, exchanges of officials, and coordinated product recalls (or other similar actions). For medical devices that are locally manufactured but use components from other countries, the “rules of origin” criteria will need to be reviewed. Depending on which countries products will ultimately be sold in, manufacturers may start seeking alternative sources for components if this would allow them to benefit from no tariffs. The rules for placing medical devices on the Northern Ireland market will differ from those in the UK.
Healthcare Fraud and Abuse Laws
In the United States, we are subject to a number of federal and state healthcare regulatory laws that restrict business practices in the healthcare industry. These laws include, but are not limited to, federal and state anti-kickback, false claims, transparency and other healthcare fraud and abuse laws.
The U.S. federal Anti-Kickback Statute prohibits, among other things, any person or entity from knowingly and willfully offering, paying, soliciting, receiving or providing any remuneration, directly or indirectly, overtly or covertly, to induce or in return for purchasing, leasing, ordering, or arranging for or recommending the purchase, lease, or order of any good, facility, item or service reimbursable, in whole or in part, under Medicare, Medicaid or other federal healthcare programs. The term “remuneration” has been broadly interpreted to include anything of value, including cash, improper discounts, and free or reduced price items and services. Among other things, the Anti-Kickback Statute has been interpreted to apply to arrangements between medical device manufacturers on the one hand and prescribers and purchasers on the other. Although there are a number of statutory exceptions and regulatory safe harbors protecting some common activities from prosecution, the exceptions and safe harbors are drawn narrowly. The government can exercise enforcement discretion in taking action against unprotected activities. Further, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. The majority of states also have anti-kickback laws, which establish similar prohibitions, and in some cases may apply to items or services reimbursed by any third-party payor, including commercial insurers and self-pay patients.
The federal false claims, including the civil False Claims Act, prohibit, among other things, any person or entity from knowingly presenting, or causing to be presented, a false, fictitious or fraudulent claim for payment to, or approval by, the federal government, knowingly making, using, or causing to be made or used a false record or statement material to a false or fraudulent claim to the federal government, or knowingly making a false statement to avoid, decrease or conceal an obligation to pay money to the U.S. federal government. A claim includes “any request or demand” for money or property presented to the U.S. government. Actions under the civil False Claims Act may be brought by the Attorney General or as a qui tam action by a private individual in the name of the government. Moreover, a claim including items or services resulting from a violation of the U.S. federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal civil False Claims Act. In addition, various states have enacted false claim laws analogous to the federal False Claims Act, although many of these state laws apply where a claim is submitted to any third-party payor and not merely a federal healthcare program.
The federal Health Insurance Portability and Accountability Act of 1996 created additional federal criminal statutes that prohibit, among other actions, knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third-party payors, knowingly and willfully embezzling or stealing from a healthcare benefit program, willfully obstructing a criminal investigation of a healthcare offense, and knowingly and willfully falsifying, concealing or covering up a material fact or making
180
Table of Contents
any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Similar to the U.S. federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
The federal Physician Payments Sunshine Act requires certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program, with specific exceptions, to report annually to the Centers for Medicare & Medicaid Services, or CMS, information related to payments or other transfers of value made to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors), and teaching hospitals, and applicable manufacturers and applicable group purchasing organizations to report annually to CMS ownership and investment interests held by physicians and their immediate family members. Beginning in 2022, such obligations will include payments and other transfers of value provided in the previous year to additional healthcare professionals, including physician assistants, nurse practitioners, clinical nurse specialists, certified nurse anesthetists, anesthesiologist assistants and certified nurse midwives.
Violations of fraud and abuse laws, including federal and state anti-kickback and false claims laws, may be punishable by criminal and civil sanctions, including fines and civil monetary penalties, the possibility of exclusion from federal healthcare programs (including Medicare and Medicaid), disgorgement and corporate integrity agreements, which impose, among other things, rigorous operational and monitoring requirements on companies. Similar sanctions and penalties, as well as imprisonment, also can be imposed upon executive officers and employees of such companies.
Coverage and Reimbursement
In the United States, our currently cleared products are not separately reimbursed by any third-party payors and if covered, are paid for as part of the procedure in which the product is used. Outside of the United States, there are many reimbursement programs through private payors as well as government programs. In some countries, government reimbursement is the predominant program available to patients and hospitals. Our commercial success depends in part on the extent to which governmental authorities, private health insurers and other third-party payors provide coverage for and establish adequate reimbursement levels for the procedures in which our products are used. Failure by physicians, hospitals, ambulatory surgery centers and other users of our products to obtain coverage and adequate reimbursement from third-party payors for procedures in which our products are used, or adverse changes in government and private third-party payors’ coverage and reimbursement policies, may adversely impact demand for our products.
Based on our experience to date, third-party payors generally reimburse for the procedures in which our products are used only if the patient meets the established medical necessity criteria for surgery. Some payors are moving toward a managed care system and control their healthcare costs by establishing coverage policies that categorically restrict coverage of certain procedures, or by limiting authorization for procedures, including elective procedures using our devices. No uniform policy of coverage and reimbursement among payors in the United States exists and coverage and reimbursement for procedures can differ significantly from payor to payor. Third-party payors are increasingly auditing and challenging the prices charged for medical products and services with concern for upcoding, miscoding, using inappropriate modifiers, or billing for inappropriate care settings. Some third-party payors must approve coverage for new or innovative devices or procedures before they will reimburse healthcare providers who use the products or therapies. Even though a new product may have been cleared for commercial distribution by the FDA, we may find limited demand for our product unless reimbursement approval can be obtained and/or maintained from governmental and private third-party payors.
In addition to uncertainties surrounding coverage policies, there are periodic changes to reimbursement levels. Third-party payors regularly update reimbursement amounts and also from time to time revise the methodologies used to determine reimbursement amounts. This includes routine updates to payments to
181
Table of Contents
physicians, hospitals and ambulatory surgery centers for procedures during which our products are used. These updates could directly impact the demand for our products.
We believe the overall escalating cost of medical products and services being paid for by the government and private health insurance has led to, and will continue to lead to, increased pressures on the healthcare and medical device industry to reduce the costs of products and services. Third-party payors are developing increasingly sophisticated methods of controlling healthcare costs through prospective reimbursement and capitation programs, group purchasing, redesign of benefits, and exploration of more cost-effective methods of delivering healthcare. In the United States, some insured individuals enroll in managed care programs, which monitor and often require pre-approval of the services that a member will receive. Some managed care programs pay their providers on a per capita (patient) basis, which puts the providers at financial risk for the services provided to their patients by paying these providers a predetermined payment per member per month and, consequently, may limit the willingness of these providers to use our products.
In international markets, reimbursement and healthcare payment systems vary significantly by country, and many countries have instituted price ceilings on specific product lines and procedures. In the European Union, member states are facing increased pressure to limit public healthcare spending. There can be no assurance that procedures using our products will be covered for a specific indication, that our products will be considered cost-effective by third-party payors, that an adequate level of reimbursement will be available or that the third-party payors’ reimbursement policies will not adversely affect our ability to sell our products profitably. More and more, local, product specific reimbursement law is applied as an overlay to medical device regulation, which has provided an additional layer of clearance requirement.
Healthcare Reform
The United States and some foreign jurisdictions are considering or have enacted a number of legislative and regulatory proposals to change the healthcare system in ways that could affect our ability to sell our products profitably. Among policy makers and payors in the United States and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality or expanding access. Current and future legislative proposals to further reform healthcare or reduce healthcare costs may limit coverage of or lower reimbursement for the procedures associated with the use of our products. The cost containment measures that payors and providers are instituting and the effect of any healthcare reform initiative implemented in the future could impact our revenue from the sale of our products.
The implementation of the Affordable Care Act, or ACA, in the United States, for example, has changed healthcare financing and delivery by both governmental and private insurers substantially, and affected medical device manufacturers significantly. The ACA, among other things, provided incentives to programs that increase the federal government’s comparative effectiveness research, and implemented payment system reforms including a national pilot program on payment bundling to encourage hospitals, physicians and other providers to improve the coordination, quality and efficiency of certain healthcare services through bundled payment models. Additionally, the ACA expanded eligibility criteria for Medicaid programs and created a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research. Since its enactment, there have been judicial, executive and political challenges to certain aspects of the ACA. The U.S. Supreme Court is currently reviewing the constitutionality of the ACA in its entirety, although it remains unclear how the Supreme Court will rule.
In addition, other legislative changes have been proposed and adopted since the ACA was enacted. For example, the Budget Control Act of 2011, among other things, reduced Medicare payments to providers by 2% per fiscal year, effective on April 1, 2013 and, due to subsequent legislative amendments to the statute, will remain in effect through 2030, with the exception of a temporary suspension from May 1, 2020 through March 31, 2021, unless additional Congressional action is taken. Additionally, the American Taxpayer Relief Act of 2012, among other things, further reduced Medicare payments to several providers, including hospitals, and
182
Table of Contents
increased the statute of limitations period for the government to recover overpayments to providers from three to five years. The Medicare Access and CHIP Reauthorization Act of 2015 repealed the formula by which Medicare made annual payment adjustments to physicians and replaced the former formula with fixed annual updates and a new system of incentive payments that began in 2019 that are based on various performance measures and physicians’ participation in alternative payment models, such as accountable care organizations.
We expect additional state and federal healthcare reform measures to be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand for our products or additional pricing pressure.
Data Privacy and Security Laws
Numerous state, federal and foreign laws, including consumer protection laws and regulations, govern the collection, dissemination, use, access to, confidentiality and security of personal information, including health-related information. In the United States, numerous federal and state laws and regulations, including data breach notification laws, health information privacy and security laws, including HIPAA, and federal and state consumer protection laws and regulations (e.g., Section 5 of the FTC Act), that govern the collection, use, disclosure, and protection of health-related and other personal information could apply to our operations or the operations of our partners. In addition, certain state and non-U.S. laws, such as the CCPA, the CPRA and the GDPR, govern the privacy and security of personal information, including health-related information in certain circumstances, some of which are more stringent than HIPAA and many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts. Failure to comply with these laws, where applicable, can result in the imposition of significant civil and/or criminal penalties and private litigation. Privacy and security laws, regulations, and other obligations are constantly evolving, may conflict with each other to complicate compliance efforts, and can result in investigations, proceedings, or actions that lead to significant civil and/or criminal penalties and restrictions on data processing.
In Europe, the GDPR went into effect on May 25, 2018 and introduces strict requirements for processing the personal data of European Union data subjects. Companies that must comply with the GDPR face increased compliance obligations and risk, including more robust regulatory enforcement of data protection requirements and potential fines for noncompliance of up to €20 million or 4% of the annual global revenues of the preceding financial year of the noncompliant company, whichever is greater.
Among other requirements, the GDPR regulates transfers of personal data subject to the GDPR to third countries that have not been found to provide adequate protection to such personal data, including the United States, and the efficacy and longevity of current transfer mechanisms between the EU and the United States remains uncertain. For example, in 2016, the EU and United States agreed to a transfer framework for data transferred from the EU to the United States, called the Privacy Shield, but the Privacy Shield was invalidated in July 2020 by the Court of Justice of the European Union.
Further, from January 1, 2021, companies have to comply with the GDPR and also the United Kingdom General Data Protection Regulation, or the UK GDPR, which, together with the amended UK Data Protection Act 2018, retains the GDPR in UK national law. The UK GDPR mirrors the fines under the GDPR, i.e., fines up to the greater of €20 million (£17.5 million) or 4% of global turnover. The relationship between the United Kingdom and the European Union in relation to certain aspects of data protection law remains unclear, and it is also unclear how United Kingdom data protection laws and regulations will develop in the medium to longer term, and how data transfers to and from the United Kingdom will be regulated in the long term. Currently there is a four to six month grace period agreed in the EU and United Kingdom Trade and Cooperation Agreement, ending June 30, 2021 at the latest, whilst the parties discuss an adequacy decision. The European Commission published a draft adequacy decision on February 19, 2021. If adopted, the decision will enable data transfers from EU member states to the United Kingdom for a four-year period, subject to subsequent extensions.
183
Table of Contents
Facilities
Our corporate headquarters are located in Menlo Park, California, where we lease approximately 10,823 square feet of office, research and development, engineering and laboratory space pursuant to a sublease agreement which was effective as of September 17, 2019 and expires on July 31, 2021. Effective August 1, 2021, we will remain in the same space under a new lease agreement with the direct landlord to that space which will extend through August 31, 2024. We believe that our existing facilities are adequate to meet our business requirements for the near-term, and that additional space will be available on commercially reasonable terms, if required.
Human Capital
As of March 31, 2021, we had 169 full-time employees. Our highly qualified and experienced team includes scientists, physicians and professionals across sales, marketing, regulatory, finance and other important functions that are critical to our success. We believe that the success of our business will depend, in part, on our ability to attract and retain qualified personnel. None of our employees are represented by a labor union or are a party to a collective bargaining agreement and we believe that we have good relations with our employees.
Our human capital resources objectives include, as applicable, identifying, recruiting, retaining, incentivizing and integrating our existing and new employees, advisors and consultants. The principal purposes of our equity and cash incentive plans are to attract, retain and reward personnel through the granting of stock-based and cash-based compensation awards, in order to increase stockholder value and the success of our company by motivating such individuals to perform to the best of their abilities and achieve our objectives.
Legal Proceedings
We are not currently a party to any material legal proceedings. We may, however, in the ordinary course of business face various claims brought by third parties, and we may, from time to time, make claims or take legal actions to assert our rights, including intellectual property rights as well as claims relating to employment matters and the safety or effectiveness of our products. Any of these claims could subject us to costly litigation, and, while we generally believe that we have adequate insurance to cover many different types of liabilities, our insurance carriers may deny coverage, may be inadequately capitalized to pay on valid claims, or our policy limits may be inadequate to fully satisfy any damage awards or settlements. If this were to happen, the payment of any such awards could have a material adverse effect on our business, financial condition and results of operations. Additionally, any such claims, whether or not successful, could damage our reputation and business.
184
Table of Contents
Executive Officers and Directors
The following table sets forth the name, age and position of each of our executive officers and directors as of the date of this prospectus.
Name | Age | Position | ||||
Executive Officers | ||||||
Paul Badawi | 46 | President and Chief Executive Officer and Director | ||||
David Badawi, M.D. | 51 | Chief Technology Officer and Director | ||||
Jesse Selnick | 46 | Chief Financial Officer | ||||
Shawn O’Neil | 48 | Chief Commercial Officer | ||||
Sam Park | 60 | Chief Operating Officer | ||||
Jeremy Hayden | 51 | Chief Legal Officer | ||||
Directors | ||||||
Staffan Encrantz | 69 | Chairman of the Board of Directors | ||||
Mack Hicks | 40 | Director | ||||
Andrew Offer | 38 | Director | ||||
Erica Rogers | 58 | Director | ||||
Valeska Schroeder, Ph.D. | 48 | Director | ||||
Donald Zurbay | 53 | Director | ||||
| (1) | Member of the audit committee. |
| (2) | Member of the compensation committee. |
| (3) | Member of the nominating and corporate governance committee. |
Executive Officers
Paul Badawi is a co-founder of our Company and has served as our Chief Executive Officer and a member of our Board since the Company was founded in 2011. Mr. Badawi holds an M.B.A. from the University of California, Los Angeles and a B.S. in Biological Sciences from the University of Chicago. We believe that Mr. Badawi’s experience in the industry and knowledge of our Company qualify him to serve on our board of directors.
David Badawi, M.D. is a co-founder of our Company and has served as our Chief Technology Officer and a member of our Board since the Company was founded in 2011. Since 2012, Dr. Badawi has also served as the president and a practicing ophthalmologist at Central Eye Care Ltd, an ophthalmology practice. Dr. Badawi holds an M.D. from Georgetown University and a B.S. in Microbiology from the University of Maryland. We believe that Dr. Badawi’s medical experience and knowledge of our Company qualify him to serve on our board of directors.
Jesse Selnick has served as our Chief Financial Officer since January 2018. From March 2012 to March 2017, Mr. Selnick served as the Chief Financial Officer and a member of the board of Electric Lightwave (previously known as Integra Telecom), a telecom infrastructure company, until its purchase by Zayo Group Holdings, Inc. in March 2017. Prior to that, Mr. Selnick worked at The Blackstone Group from 2003 to February 2012, where he most recently served as Managing Director. Mr. Selnick holds an M.B.A. from Harvard Business School and a B.S. in Economics from the Wharton School at the University of Pennsylvania.
Shawn O’Neil has served as our Chief Commercial Officer since October 2017. From October 2003 to October 2017, Mr. O’Neil held various leadership positions at Alcon, Inc., a global leader in eye care, where he most recently served as the Head of Sales and Marketing, Surgical Glaucoma. Mr. O’Neil holds a B.A. in Economics from Princeton University.
185
Table of Contents
Sam Park has served as our Chief Operating Officer since March 2020. From March 2016 to May 2019, Mr. Park served as the founder and Chief Executive Officer of Park Medical, a medical device company. Mr. Park holds a B.S. in Mechanical Engineering from the University of California, Irvine.
Jeremy Hayden has served as our Chief Legal Officer since April 2020. From August 2017 to April 2020, Mr. Hayden served as General Counsel of Endologix, Inc. Prior to that, Mr. Hayden served as General Counsel and Vice President, Business Development at Cytori Therapeutics, Inc. from July 2015 to August 2017 and from May 2012 to July 2015 he served as Assistant General Counsel at Volcano Corporation, a publicly traded medical device company that was acquired by Royal Phillips in 2015. Mr. Hayden holds a J.D. from the University of Michigan Law School and an A.B. in Politics from Princeton University. Endologix, Inc. filed for Chapter 11 bankruptcy in July 2020.
Directors
Staffan Encrantz has served as a member of our Board since 2017. Mr. Encrantz is the founder of Allegro Investment Fund, L.P. and has served as its chairman since 1997. Mr. Encrantz holds a law degree from Uppsala University, Sweden. We believe that Mr. Encrantz’ financial and industry experience qualify him to serve on our board of directors.
Mack Hicks has served as a member of our Board since 2011. Since 2007, Mr. Hicks has been a Partner of Hicks Holdings LLC, an investment company. Prior to that, Mr. Hicks served as a research analyst at Halcyon Asset Management from 2005 to 2006 and worked at Credit Suisse in 2004. Mr. Hicks holds a B.A. in History from the University of Texas at Austin. We believe that Mr. Hicks’ financial and industry experience qualify him to serve on our board of directors.
Andrew Offer has served as a member of our Board since September 2020. Since 2007, Mr. Offer has held various positions, and currently serves as the Chief Executive Officer of Scientific Health Development, a healthcare investment company. From 2004 to 2007, Mr. Offer served as a senior analyst and associate at Value Management Group, a healthcare transaction advisory company. Mr. Offer holds a B.B.A. in Finance from the Mays School of Business at Texas A&M University. We believe that Mr. Offer’s experience in the healthcare industry qualifies him to serve on our board of directors.
Erica Rogers has served as a member of our Board since November 2019. Since October 2012, Ms. Rogers has served as President and Chief Executive Officer and a member of the board of Silk Road Medical, a medical device company. Ms. Rogers is also a director of Lucira Health, a diagnostics company, and currently serves as an advisor to Alydia Health and Venture Investors. Ms. Rogers holds a B.S. in Zoology from San Diego State University. We believe that Ms. Rogers’ experience in the medical device industry qualifies her to serve on our board of directors.
Valeska Schroeder, Ph.D. has served as a member of our Board since 2019. Since 2016, Dr. Schroeder has served as a Managing Director of KCK Medical Technologies, a single family evergreen fund that invests in medical technologies. From March 2014 to July 2016, Dr. Schroeder served as Senior Vice President, Product Management of Vital Connect, Inc., a wearable biosensor technology company. Dr. Schroeder holds a Ph.D., M.S. and B.S. in Materials Sciences and Engineering from the University of California at Berkeley. We believe that Dr. Schroeder’s experience in the healthcare industry qualifies her to serve on our board of directors.
Donald Zurbay has served as a member of our Board since July 2020. Since June 2018, Mr. Zurbay has served as the Chief Financial Officer of Patterson Companies, a global medical device company. Before that, from March 2004 to February 2017, Mr. Zurbay held various leadership positions at St. Jude Medical, Inc., where he most recently served as Vice President and Chief Financial Officer from August 2012 to January 2017. Mr. Zurbay currently serves on the board of Silk Road Medical. Mr. Zurbay holds a B.S. in Business Accounting from the University of Minnesota. We believe that Mr. Zurbay’s experience with publicly-traded healthcare companies and financial expertise qualify him to serve on our board of directors.
186
Table of Contents
Board Composition and Election of Directors
Director Independence
Our board of directors currently consists of members. Our board of directors has determined that, of our directors, , , , , and do not have a relationship that would interfere with the exercise of independent judgment in carrying out the responsibilities of a director and that each of these directors is “independent” as that term is defined under the rules of The Nasdaq Stock Market LLC, or the Nasdaq Rules. The Nasdaq Rules’ independence definition includes a series of objective tests, such as that the director is not, and has not been for at least three years, one of our employees and that neither the director nor any of his or her family members has engaged in various types of business dealings with us. In addition, as required by the Nasdaq Rules, our board of directors has made a subjective determination as to each independent director that no relationships exist that, in the opinion of our board of directors, would interfere with the exercise of independent judgment in carrying out the responsibilities of a director. In making these determinations, our board of directors reviewed information provided by the directors and us with regard to each director’s business and personal activities and relationships as they may relate to us and our management. There are no family relationships among any of our directors or executive officers.
Classified Board of Directors
In accordance with our restated certificate of incorporation that will go into effect upon the closing of this offering, our board of directors will be divided into three classes with staggered, three-year terms. At each annual meeting of stockholders, the successors to directors whose terms then expire will be elected to serve from the time of election and qualification until the third annual meeting following election. Effective upon the closing of this offering, our directors will be divided among the three classes as follows:
| • | The Class I directors will be , , and , and their terms will expire at our first annual meeting of stockholders following this offering; |
| • | The Class II directors will be , and , and their terms will expire at our second annual meeting of stockholders following this offering; and |
| • | The Class III directors will be , and , and their terms will expire at the third annual meeting of stockholders following this offering. |
Our restated certificate of incorporation that will go into effect upon the closing of this offering will provide that the authorized number of directors may be changed only by resolution of the board of directors. Any additional directorships resulting from an increase in the number of directors will be distributed among the three classes so that, as nearly as possible, each class will consist of one-third of the directors. The division of our board of directors into three classes with staggered three-year terms may delay or prevent a change of our management or a change in control of our company. Our directors may be removed only for cause by the affirmative vote of the holders of at least two-thirds of our outstanding voting stock entitled to vote in the election of directors.
Our directors were elected to and currently serve on the board pursuant to a voting agreement among us and several of our largest stockholders. See “Certain Relationships and Related Party Transactions—Voting Agreement.” This agreement will terminate upon the closing of this offering, after which there will be no further contractual obligations regarding the election of our directors.
Board Leadership Structure
Our board of directors is currently chaired by . Our corporate governance guidelines provide that, if the chairman of the board is a member of management or does not otherwise qualify as independent, the independent directors of the board may elect a lead director. The lead director’s responsibilities include, but are
187
Table of Contents
not limited to: presiding over all meetings of the board of directors at which the chairman is not present, including any executive sessions of the independent directors; approving board meeting schedules and agendas; and acting as the liaison between the independent directors and the chief executive officer and chairman of the board. Our corporate governance guidelines further provide the flexibility for our board of directors to modify our leadership structure in the future as it deems appropriate.
Role of the Board in Risk Oversight
One of the key functions of our board of directors is informed oversight of our risk management process. Our board of directors does not have a standing risk management committee, but rather administers this oversight function directly through our board of directors as a whole, as well as through various standing committees of our board of directors that address risks inherent in their respective areas of oversight. In particular, our board of directors is responsible for monitoring and assessing strategic risk exposure and our audit committee has the responsibility to consider and discuss our major financial risk exposures and the steps our management has taken to monitor and control these exposures, including guidelines and policies to govern the process by which risk assessment and management is undertaken. Our audit committee also monitors compliance with legal and regulatory requirements. Our nominating and corporate governance committee monitors the effectiveness of our corporate governance practices, including whether they are successful in preventing illegal or improper liability-creating conduct. Our compensation committee assesses and monitors whether any of our compensation policies and programs has the potential to encourage excessive risk-taking. While each committee is responsible for evaluating certain risks and overseeing the management of such risks, our entire board of directors is regularly informed through committee reports about such risks.
Board Committees
Our board of directors has established three standing committees—audit, compensation and nominating and corporate governance—each of which operates under a charter that has been approved by our board of directors. Upon our listing on The Nasdaq Global Market, each committee’s charter will be available under the Corporate Governance section of our website at www.sightsciences.com. The reference to our website address does not constitute incorporation by reference of the information contained at or available through our website, and you should not consider it to be a part of this prospectus.
Audit Committee
The audit committee’s responsibilities include:
| • | Appointing, approving the compensation of, and assessing the independence of our registered public accounting firm; |
| • | Overseeing the work of our registered public accounting firm, including through the receipt and consideration of reports from such firm; |
| • | Reviewing and discussing with management and the registered public accounting firm our annual and quarterly financial statements and related disclosures; |
| • | Coordinating our board of directors’ oversight of our internal control over financial reporting, disclosure controls and procedures and code of business conduct and ethics; |
| • | Discussing our risk management policies; |
| • | Meeting independently with our internal auditing staff, if any, registered public accounting firm and management; |
| • | Reviewing and approving or ratifying any related person transactions; and |
| • | Preparing the audit committee report required by Securities and Exchange Commission, or SEC, rules. |
188
Table of Contents
The members of our audit committee are , and . serves as the chairperson of the committee. All members of our audit committee meet the requirements for financial literacy under the Nasdaq Rules. Our board of directors has determined that and meet the independence requirements of Rule 10A-3 under the Exchange Act and the applicable Nasdaq Rules. Our board of directors has determined that is an “audit committee financial expert” as defined by applicable SEC rules and has the requisite financial sophistication as defined under the applicable Nasdaq Rules.
Compensation Committee
The compensation committee’s responsibilities include:
| • | Reviewing and approving, or recommending for approval by the board of directors, the compensation of our CEO and our other executive officers; |
| • | Overseeing and administering our cash and equity incentive plans; |
| • | Reviewing and making recommendations to our board of directors with respect to director compensation; |
| • | Reviewing and discussing annually with management our “Compensation Discussion and Analysis,” to the extent required; and |
| • | Preparing the annual compensation committee report required by SEC rules, to the extent required. |
The members of our compensation committee are , and . serves as the chairperson of the committee. Our board of directors has determined that each of , and is independent under the applicable Nasdaq Rules, including the Nasdaq Rules specific to membership on the compensation committee, and is a “non-employee director” as defined in Rule 16b-3 promulgated under the Exchange Act.
Nominating and Corporate Governance Committee
The nominating and corporate governance committee’s responsibilities include:
| • | Identifying individuals qualified to become board members; |
| • | Recommending to our board of directors the persons to be nominated for election as directors and to each board committee; |
| • | Developing and recommending to our board of directors corporate governance guidelines, and reviewing and recommending to our board of directors proposed changes to our corporate governance guidelines from time to time; and |
| • | Overseeing a periodic evaluation of our board of directors. |
The members of our nominating and corporate governance committee are , and . serves as the chairperson of the committee. Our board of directors has determined that , and are independent under the applicable Nasdaq Rules.
Compensation Committee Interlocks and Insider Participation
No member of our compensation committee is or has been our current or former officer or employee. None of our executive officers served as a director or a member of a compensation committee (or other committee serving an equivalent function) of any other entity, one of whose executive officers served as a director or member of our compensation committee during the fiscal year ended December 31, 2020.
189
Table of Contents
Code of Ethics and Code of Conduct
We have adopted a written code of business conduct and ethics that applies to our directors, officers and employees, including our principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. Upon our listing on The Nasdaq Global Market, our code of business conduct and ethics will be available under the Corporate Governance section of our website at www.sightsciences.com. In addition, we intend to post on our website all disclosures that are required by law or the Nasdaq Rules concerning any amendments to, or waivers from, any provision of the code. The reference to our website address does not constitute incorporation by reference of the information contained at or available through our website, and you should not consider it to be a part of this prospectus.
190
Table of Contents
EXECUTIVE AND DIRECTOR COMPENSATION
This section discusses the material components of the executive compensation program for our named executive officers. We are an “emerging growth company,” within the meaning of the JOBS Act, and have elected to comply with the reduced compensation disclosure requirements available to emerging growth companies under the JOBS Act. For 2020, our named executive officers and their positions were:
| • | Paul Badawi, President and Chief Executive Officer; |
| • | Shawn O’Neil, Chief Commercial Officer; and |
| • | Sam Park, Chief Operating Officer. |
This discussion may contain forward-looking statements that are based on our current plans, considerations, expectations and determinations regarding future compensation programs. Actual compensation programs that we adopt following the completion of this offering may differ materially from the currently planned programs summarized in this discussion.
2020 Summary Compensation Table
The following table sets forth all of the compensation awarded to or earned by or paid to our named executive officers during 2020.
Name and Principal Position | Year | Salary ($) | Option Awards ($)(2) | Non-Equity Incentive Plan Compensation ($)(3) | All Other Compensation ($) | Total | ||||||||||||||||||
Paul Badawi | 2020 | 360,000 | — | 136,710 | — | $ | 496,710 | |||||||||||||||||
President and Chief Executive Officer | ||||||||||||||||||||||||
Shawn O’Neil | 2020 | 300,000 | 143,886 | 90,628 | — | $ | 534,514 | |||||||||||||||||
Chief Commercial Officer | ||||||||||||||||||||||||
Sam Park(1) | 2020 | 332,326 | 165,406 | 113,925 | — | $ | 611,657 | |||||||||||||||||
Chief Operating Officer | ||||||||||||||||||||||||
| (1) | Mr. Park served as a consultant to the Company from January 1, 2020 until March 13, 2020, the date he commenced employment as our Chief Operating Officer. Amounts shown for Mr. Park include $93,672 in consulting fees and $238,654 in base salary earned as an employee. |
| (2) | Amounts reflect the full grant-date fair value of stock options granted during 2020 computed in accordance with ASC Topic 718, rather than the amounts paid to or realized by the named individual. We provide information regarding the assumptions used to calculate the value of the stock option awards made to named executive officers in Note 11 to the audited consolidated financial statements included in this prospectus. |
| (3) | Amounts represent bonuses earned by our named executive officers for 2020 under the Company’s annual incentive program. Refer to “—Annual Incentive Compensation” below for additional information regarding the Company’s annual incentive program for 2020. |
Narrative to Summary Compensation Table
Primary Elements of Our Executive Compensation Program
For 2020, the primary elements of our named executive officers’ compensation were base salary, annual cash incentive bonuses and long-term equity incentive compensation.
191
Table of Contents
Base Salaries
The base salaries of our named executive officers are an important part of their total compensation package and are intended to reflect their respective positions, duties and responsibilities. For 2020, the named executive officers’ annual base salaries were:
Named Executive Officer | Annual Base Salary | |||
Paul Badawi | $ | 360,000 | ||
Shawn O’Neil | $ | 300,000 | ||
Sam Park | $ | 300,000 | ||
Mr. Park served as a consultant to the Company from January 1, 2020 until March 13, 2020, the date he commenced employment as our Chief Operating Officer. While serving as a consultant, Mr. Park earned consulting fees at the rate of $325.00 per hour.
Annual Incentive Compensation
We maintain an annual bonus program for all employees who are not eligible for commissions, including our named executive officers. Participants in the bonus program may earn a performance-based cash bonus based on our achievement of specified performance goals. Performance goals for the 2020 bonus program generally related to specified commercial (weighted 50%), clinical (weighted 25%), research and development (weighted 10%), regulatory (weighted 7.5%) and financial (weighted 7.5%) objectives. For 2020, the named executive officers had the following target annual bonus amounts, expressed as a percentage of base salary received during the year:
Named Executive Officer | 2020 Bonus Target | |||
Paul Badawi | 35 | % | ||
Shawn O’Neil | 35 | % | ||
Sam Park | 35 | % | ||
In February 2021, our board of directors determined the bonus payments with respect to 2020. The actual amounts of the 2020 annual bonuses paid to our named executive officers are included in the “Non-Equity Incentive Plan Compensation” column of the 2020 Summary Compensation Table, above.
Equity Compensation
We generally offer stock options to our employees, including our named executive officers, as the long-term incentive component of our compensation program. Our stock options generally allow employees to purchase shares of our common stock at a price equal to the fair market value of our common stock on the date of grant, as determined by the board of directors. Stock options granted upon an employee’s commencing employment generally vest as to 25% of the underlying shares on the first anniversary of the date of grant and in equal monthly installments over the following three years. Subsequent grants to employees generally vest as to 1/48th of the shares underlying the stock option each month for four years following the date of grant. Historically, our stock options have been intended to qualify as “incentive stock options” to the extent permitted under the Internal Revenue Code.
Prior to this offering, we have granted equity awards under our 2011 Stock Incentive Plan, referred to below as the Existing Plan. We intend to adopt a 2021 Incentive Award Plan, referred to below as the 2021 Plan, in order to facilitate the grant of cash and equity incentives to directors, employees (including our named executive officers) and consultants of our company and certain of its affiliates and to enable our company and certain of its affiliates to obtain and retain services of these individuals. We expect that the 2021 Plan will be effective on the day prior to our first public trading date. Once the 2021 Plan becomes effective, we will cease making grants
192
Table of Contents
under the Existing Plan. However, the Existing Plan will continue to govern the terms and conditions of the outstanding awards granted under it. For additional information about the Existing Plan and the 2021 Plan, please see the section titled “Incentive Compensation Plans” below.
Retirement Plans and Other Employee Benefits
Our named executive officers are eligible to participate in our employee benefit plans and programs, including medical and dental benefits and life insurance, to the same extent as our other full-time employees, subject to the terms and eligibility requirements of those plans. We also sponsor a 401(k) defined contribution plan in which our named executive officers may participate, subject to limits imposed by the Code, to the same extent as our other full-time employees. We did not make any employer contributions to the 401(k) plan for 2020. We have not typically provided our executive officers with any perquisites, and none of the named executive officers received perquisites for 2020.
Employment, Severance or Change in Control Agreements
We have entered into employment offer letter agreements with our named executive officers that set forth certain terms and conditions of employment of each named executive officer, including initial base salary, annual bonus opportunity (for Messrs. O’Neil and Park) and equity grants and employee benefits eligibility. None of our named executive officers is currently entitled to any change in control or severance benefits. We expect to enter into new employment agreements with the named executive officers that supersede their existing agreements effective upon the effectiveness of the registration statement relating to this offering. The terms of these new agreements are not yet known.
Outstanding Equity Awards at 2020 Fiscal Year-End
The following table provides information about outstanding equity awards held by each of our named executive officers as of December 31, 2020. All awards were granted under the Existing Plan.
Name | Option Awards | |||||||||||||||||||
| Vesting Start Date | Number of Securities Underlying Unexercised Options (#) Exercisable | Number of Securities Underlying Unexercised Options (#) Unexercisable | Option Exercise Price ($) | Option Expiration Date | ||||||||||||||||
Paul Badawi(3) | — | — | — | — | — | |||||||||||||||
Shawn O’Neil | 9/18/2017 | 28,437 | 6,563 | (1) | $ | 0.69 | 11/28/2027 | |||||||||||||
| 3/18/2019 | 4,375 | 5,625 | (2) | $ | 1.24 | 4/16/2029 | ||||||||||||||
| 7/30.2020 | 2,604 | 22,396 | (2) | $ | 3.91 | 7/29/2030 | ||||||||||||||
Sam Park | 3/13/2020 | 0 | 40,000 | (1) | $ | 3.91 | 5/11/2030 | |||||||||||||
| 7/30/2020 | 833 | 7,167 | (2) | $ | 3.91 | 7/29/2030 | ||||||||||||||
| (1) | The option vests as to 25% of the underlying shares on the first anniversary of the vesting start date and in 36 equal monthly installments thereafter. |
| (2) | The option vests in 48 equal monthly installments following the vesting start date. |
| (3) | Mr. Badawi is a Company founder with significant beneficial ownership of our common stock. See the section titled “Principal Stockholders” in this prospectus for more information regarding Mr. Badawi’s beneficial ownership of our common stock. |
Director Compensation
We have entered into offer letter agreements with Ms. Rogers and Mr. Zurbay, our non-employee directors who are not affiliated with a significant stockholder, that provide for certain terms and conditions of their service
193
Table of Contents
on our board of directors, including annual retainers and the grant of equity awards. In 2020, we paid Ms. Rogers and Mr. Zurbay annual cash retainers equal to $50,000, prorated in the case or Mr. Zurbay for a partial year of service. In addition, in January 2020 and May 2020, Ms. Rogers received an option to purchase 15,000 shares and 20,000 shares, respectively, of our common stock, and in June 2020, Mr. Zurbay received an option to purchase 30,000 shares of our common stock. Ms. Rogers’ January 2020 option has an exercise price of $4.13 per share and the other options granted to Ms. Rogers and Mr. Zurbay have an exercise price of $3.91 per share, each of which our board of directors determined to be the fair market value per share of our common stock on the date of grant. All options granted to Ms. Rogers and Mr. Zurbay vest monthly in 48 equal installments and accelerate upon a Corporate Transaction (as defined in the Existing Plan).
None of our other non-employee directors received compensation for their service on our board of directors during 2020. Mr. Badawi, our Chief Executive Officer, and Dr. Badawi, our Chief Technology Officer, both served on our board of directors during 2020 but have not been included in the 2020 Director Compensation Table below because they did not receive any additional compensation for this service. Information regarding Mr. Badawi’s 2020 compensation is included in the 2020 Summary Compensation Table, Outstanding Equity Awards at 2020 Fiscal Year-End table and associated narrative disclosure above.
2020 Director Compensation Table
Name | Fees Earned or Paid in Cash ($) | Option Awards ($)(1) | Total ($) | |||||||||
Staffan Encrantz | — | — | — | |||||||||
Mack Hicks | — | — | — | |||||||||
Carter Meyer(2) | — | — | — | |||||||||
Andrew Offer | — | — | — | |||||||||
Erica Rogers | $ | 50,000 | $ | 102,111 | $ | 152,111 | ||||||
Valeska Schroeder | — | — | — | |||||||||
Don Zurbay(3) | $ | 27,466 | $ | 111,640 | $ | 139,106 | ||||||
| (1) | Amounts reflect the full grant-date fair value of stock options granted during 2020 computed in accordance with ASC Topic 718, rather than the amounts paid to or realized by the named individual. We provide information regarding the assumptions used to calculate the value of the option awards in Note 11 to the consolidated financial statements included in this prospectus. |
| (2) | Mr. Meyer resigned from our board of directors on October 2, 2020. |
| (3) | Mr. Zurbay joined our board of directors on June 16, 2020. |
The table below shows the aggregate numbers of option awards (exercisable and unexercisable) held as of December 31, 2020 by each non-employee director who was serving as of December 31, 2020. The non-employee directors did not hold any unvested stock awards as of December 31, 2020.
Name | Options Outstanding at Fiscal Year End | |||
Staffan Encrantz | — | |||
Mack Hicks | — | |||
Andrew Offer | — | |||
Erica Rogers | 35,000 | |||
Valeska Schroeder | — | |||
Don Zurbay | 30,000 | |||
We intend to adopt a compensation program for our non-employee directors that consists of annual retainer fees and long-term equity awards and that will become effective upon effectiveness of the registration statement relating to this offering. The terms of the program are not yet known.
194
Table of Contents
Incentive Compensation Plans
The following summarizes the material terms of the 2021 Plan and the 2021 Employee Stock Purchase Plan, which will be the long-term incentive compensation plans in which our directors and named executive officers will be eligible to participate following this offering, and the Existing Plan, under which we have historically made periodic grants of equity and equity-based awards to our directors and named executive officers.
2021 Incentive Award Plan
Effective the day prior to the first public trading date of our common stock, we intend to adopt and ask our stockholders to approve the 2021 Plan under which we may grant cash and equity-based incentive awards to eligible service providers in order to attract, retain and motivate the persons who make important contributions to the company. The material terms of the 2021 Plan, as it is currently contemplated, are summarized below. Our board of directors is still in the process of developing, approving and implementing the 2021 Plan and, accordingly, this summary is subject to change.
Eligibility and Administration. Our employees, consultants and directors, and employees and consultants of our subsidiaries will be eligible to receive awards under the 2021 Plan. The 2021 Plan will be administered by our board of directors with respect to awards to non-employee directors and by our compensation committee with respect to other participants, each of which may delegate its duties and responsibilities to committees of our directors and/or officers (referred to collectively as the plan administrator below), subject to the limitations that may be imposed under the 2021 Plan, Section 16 of the Exchange Act, stock exchange rules and other applicable laws, including Delaware law. The plan administrator will have the authority to take all actions and make all determinations under the 2021 Plan, to interpret the 2021 Plan and award agreements and to adopt, amend and repeal rules for the administration of the 2021 Plan as it deems advisable. The plan administrator will also have the authority to determine which eligible service providers receive awards, grant awards and set the terms and conditions of all awards under the 2021 Plan, including any vesting and vesting acceleration provisions, subject to the conditions and limitations in the 2021 Plan.
Shares Available. An aggregate of shares of our common stock will initially be available for issuance under the 2021 Plan. The number of shares initially available for issuance will be increased by an annual increase on January 1 of each calendar year beginning in 2022 and ending in and including 2031, equal to the lesser of (A) % of the shares outstanding on the final day of the immediately preceding calendar year and (B) a smaller number of shares as determined by our board of directors. No more than shares of common stock may be issued under the 2021 Plan upon the exercise of incentive stock options. Shares available under the 2021 Plan may be authorized but unissued shares, shares purchased on the open market or treasury shares.
If an award under the 2021 Plan or the Existing Plan expires, lapses or is terminated, exchanged for cash, surrendered, repurchased, or canceled without having been fully exercised or forfeited, any unused shares subject to the award will, as applicable, become or again be available for new grants under the 2021 Plan. Awards granted under the 2021 Plan in substitution for any options or other stock or stock-based awards granted by an entity before the entity’s merger or consolidation with us or our acquisition of the entity’s property or stock will not reduce the shares available for grant under the 2021 Plan, but will count against the maximum number of shares that may be issued upon the exercise of incentive stock options.
195
Table of Contents
Awards. The 2021 Plan provides for the grant of stock options, including incentive stock options, or ISOs, and nonqualified stock options, or NSOs, stock appreciation rights, or SARs, restricted stock, dividend equivalents, restricted stock units, or RSUs, and other stock or cash based awards. Certain awards under the 2021 Plan may constitute or provide for payment of “nonqualified deferred compensation” under Section 409A of the Code. All awards under the 2021 Plan will be set forth in award agreements, which will detail the terms and conditions of awards, including any applicable vesting and payment terms and post-termination exercise limitations. A brief description of each award type follows.
| • | Stock Options and SARs. Stock options provide for the purchase of shares of our common stock in the future at an exercise price set on the grant date. ISOs, by contrast to NSOs, may provide tax deferral beyond exercise and favorable capital gains tax treatment to their holders if certain holding period and other requirements of the Code are satisfied. SARs entitle their holder, upon exercise, to receive from us an amount equal to the appreciation of the shares subject to the award between the grant date and the exercise date. The plan administrator will determine the number of shares covered by each option and SAR, the exercise price of each option and SAR and the conditions and limitations applicable to the exercise of each option and SAR. The exercise price of a stock option or SAR will not be less than 100% of the fair market value of the underlying share on the grant date (or 110% in the case of ISOs granted to certain significant stockholders), except with respect to certain substitute awards granted in connection with a corporate transaction. The term of a stock option or SAR may not be longer than ten years (or five years in the case of ISOs granted to certain significant stockholders). |
| • | Restricted Stock and RSUs. Restricted stock is an award of nontransferable shares of our common stock that remain forfeitable unless and until specified conditions are met and which may be subject to a purchase price. RSUs are contractual promises to deliver shares of our common stock in the future, which may also remain forfeitable unless and until specified conditions are met and may be accompanied by the right to receive the equivalent value of dividends paid on shares of our common stock prior to the delivery of the underlying shares. The plan administrator may provide that the delivery of the shares underlying RSUs will be deferred on a mandatory basis or at the election of the participant. The terms and conditions applicable to restricted stock and RSUs will be determined by the plan administrator, subject to the conditions and limitations contained in the 2021 Plan. |
| • | Other Stock or Cash Based Awards. Other stock or cash based awards are awards of cash, fully vested shares of our common stock and other awards valued wholly or partially by referring to, or otherwise based on, shares of our common stock or other property. Other stock or cash based awards may be granted to participants and may also be available as a payment form in the settlement of other awards, as standalone payments and as payment in lieu of compensation to which a participant is otherwise entitled. The plan administrator will determine the terms and conditions of other stock or cash based awards, which may include any purchase price, performance goal, transfer restrictions and vesting conditions. |
Performance Criteria. The plan administrator may select performance criteria for an award to establish performance goals for a performance period. Performance criteria under the 2021 Plan may include, but are not limited to, the following: net earnings or losses (either before or after one or more of interest, taxes, depreciation, amortization, and non-cash equity-based compensation expense); gross or net sales or revenue or sales or revenue growth; net income (either before or after taxes) or adjusted net income; profits (including but not limited to gross profits, net profits, profit growth, net operation profit or economic profit), profit return ratios or operating margin; budget or operating earnings (either before or after taxes or before or after allocation of corporate overhead and bonus); cash flow (including operating cash flow and free cash flow or cash flow return on capital); return on assets; return on capital or invested capital; cost of capital; return on stockholders’ equity; total stockholder return; return on sales; costs, reductions in costs and cost control measures; expenses; working capital; earnings or loss per share; adjusted earnings or loss per share; price per share or dividends per share (or appreciation in or maintenance of such price or dividends); regulatory achievements or compliance; implementation, completion or attainment of objectives relating to research, development, regulatory,
196
Table of Contents
commercial, or strategic milestones or developments; market share; economic value or economic value added models; division, group or corporate financial goals; customer satisfaction/growth; customer service; employee satisfaction; recruitment and maintenance of personnel; human resources management; supervision of litigation and other legal matters; strategic partnerships and transactions; financial ratios (including those measuring liquidity, activity, profitability or leverage); debt levels or reductions; sales-related goals; financing and other capital raising transactions; cash on hand; acquisition activity; investment sourcing activity; and marketing initiatives, any of which may be measured in absolute terms or as compared to any incremental increase or decrease. Such performance goals also may be based solely by reference to the company’s performance or the performance of a subsidiary, division, business segment or business unit of the company or a subsidiary, or based upon performance relative to performance of other companies or upon comparisons of any of the indicators of performance relative to performance of other companies. When determining performance goals, the plan administrator may provide for exclusion of the impact of an event or occurrence which the plan administrator determines should appropriately be excluded, including, without limitation, non-recurring charges or events, acquisitions or divestitures, changes in the corporate or capital structure, events unrelated to the business or outside of the control of management, foreign exchange considerations, and legal, regulatory, tax or accounting changes.
Certain Transactions. In connection with certain corporate transactions and events affecting our common stock, including a change in control, or change in any applicable laws or accounting principles, the plan administrator has broad discretion to take action under the 2021 Plan to prevent the dilution or enlargement of intended benefits, facilitate the transaction or event or give effect to the change in applicable laws or accounting principles. This includes canceling awards for cash or property, accelerating the vesting of awards, providing for the assumption or substitution of awards by a successor entity, adjusting the number and type of shares subject to outstanding awards and/or with respect to which awards may be granted under the 2021 Plan and replacing or terminating awards under the 2021 Plan. In addition, in the event of certain non-reciprocal transactions with our stockholders, the plan administrator will make equitable adjustments to the 2021 Plan and outstanding awards as it deems appropriate to reflect the transaction. In the event of a change in control of the company (as defined in the 2021 Plan), to the extent that the surviving entity declines to continue, convert, assume or replace outstanding awards, then all such awards may become fully vested and exercisable in connection with the transaction. Individual award agreements may provide for additional accelerated vesting and payment provisions.
Provisions of the 2021 Plan Relating to Director Compensation. The 2021 Plan provides that the plan administrator may establish compensation for non-employee directors from time to time subject to the 2021 Plan’s limitations. Prior to commencing this offering, we intend to approve and implement a compensation program for our non-employee directors. Our board of directors or its authorized committee may modify the non-employee director compensation program from time to time in the exercise of its business judgment, taking into account such factors, circumstances and considerations as it shall deem relevant from time to time, provided that the sum of any cash compensation or other compensation and the grant date fair value of any equity awards granted under the 2021 Plan as compensation for services as a non-employee director during any fiscal year may not exceed $ , excluding cash and other compensation awarded prior to the commencement of this offering. The plan administrator may make exceptions to this limit for individual non-employee directors in extraordinary circumstances, as the plan administrator may determine in its discretion, subject to the limitations in the 2021 Plan.
Foreign Participants, Claw-Back Provisions, Transferability, and Participant Payments. The plan administrator may modify awards granted to participants who are foreign nationals or employed outside the United States or establish subplans or procedures to address differences in laws, rules, regulations or customs of such foreign jurisdictions. All awards will be subject to any company claw-back policy as set forth in such claw-back policy or the applicable award agreement. Except as the plan administrator may determine or provide in an award agreement, awards under the 2021 Plan are generally non-transferrable, except by will or the laws of descent and distribution, or, subject to the plan administrator’s consent, pursuant to a domestic relations order and are generally exercisable only by the participant. With regard to tax withholding obligations arising in
197
Table of Contents
connection with awards under the 2021 Plan and exercise price obligations arising in connection with the exercise of stock options under the 2021 Plan, the plan administrator may, in its discretion, accept cash, wire transfer or check, shares of our common stock that meet specified conditions, a promissory note, a “market sell order,” such other consideration as the plan administrator deems suitable or any combination of the foregoing.
Plan Amendment; Repricing and Termination. Our board of directors may amend or terminate the 2021 Plan at any time; however, no amendment, other than an amendment that increases the number of shares available under the 2021 Plan, may materially and adversely affect an award outstanding under the 2021 Plan without the consent of the affected participant and stockholder approval will be obtained for any amendment to the extent necessary to comply with applicable laws. Further, the plan administrator may, without the approval of our stockholders, amend any outstanding stock option or SAR to reduce its exercise price per share. The 2021 Plan will remain in effect until the tenth anniversary of its effective date, unless earlier terminated by our board of directors. No awards may be granted under the 2021 Plan after its termination.
2021 Employee Stock Purchase Plan
Effective the day prior to the first public trading date of our common stock, we intend to adopt and ask our stockholders to approve the 2021 Employee Stock Purchase Plan, or the 2021 ESPP, the material terms of which are summarized below.
The 2021 ESPP is comprised of two distinct components in order to provide increased flexibility to grant options to purchase shares under the 2021 ESPP to U.S. and to non-U.S. employees. Specifically, the 2021 ESPP authorizes (1) the grant of options to U.S. employees that are intended to qualify for favorable U.S. federal tax treatment under Section 423 of the Code, (the “Section 423 Component”), and (2) the grant of options that are not intended to be tax-qualified under Section 423 of the Code to facilitate participation for employees located outside of the U.S. who do not benefit from favorable U.S. federal tax treatment and to provide flexibility to comply with non-U.S. law and other considerations (the “Non-Section 423 Component”). Where permitted under local law and custom, we expect that the Non-Section 423 Component will generally be operated and administered on terms and conditions similar to the Section 423 Component.
Shares Available for Awards; Administration. A total of shares of our common stock will initially be reserved for issuance under the 2021 ESPP. In addition, the number of shares available for issuance under the 2021 ESPP will be annually increased on January 1 of each calendar year beginning in 2022 and ending in and including 2031, by an amount equal to the lesser of (A) % of the shares outstanding on the final day of the immediately preceding calendar year and (B) such smaller number of shares as is determined by our board of directors, provided that no more than shares of our common stock may be issued under the Section 423 Component. Our board of directors or a committee of our board of directors will administer and will have authority to interpret the terms of the 2021 ESPP and determine eligibility of participants. We expect that the compensation committee will be the initial administrator of the 2021 ESPP.
Eligibility. We expect that all of our employees will be eligible to participate in the 2021 ESPP. However, an employee may not be granted rights to purchase stock under our 2021 ESPP if the employee, immediately after the grant, would own (directly or through attribution) stock possessing 5% or more of the total combined voting power or value of all classes of our stock.
Grant of Rights. Stock will be offered under the 2021 ESPP during offering periods. The length of the offering periods under the 2021 ESPP will be determined by the plan administrator and may be up to twenty-seven months long. Employee payroll deductions will be used to purchase shares on each purchase date during an offering period. The purchase dates for each offering period will be the final trading day in the offering period. Offering periods under the 2021 ESPP will commence when determined by the plan administrator. The plan administrator may, in its discretion, modify the terms of future offering periods. In non-U.S. jurisdictions where participation in the 2021 ESPP through payroll deductions is prohibited, the plan administrator may provide that
198
Table of Contents
an eligible employee may elect to participate through contributions to the participant’s account under the 2021 ESPP in a form acceptable to the 2021 ESPP administrator in lieu of or in addition to payroll deductions.
The 2021 ESPP permits participants to purchase common stock through payroll deductions of up to a specified percentage of their eligible compensation. The plan administrator will establish a maximum number of shares that may be purchased by a participant during any offering period. In addition, no employee will be permitted to accrue the right to purchase stock under the Section 423 Component at a rate in excess of $25,000 worth of shares during any calendar year during which such a purchase right is outstanding (based on the fair market value per share of our common stock as of the first day of the offering period).
On the first trading day of each offering period, each participant will automatically be granted an option to purchase shares of our common stock. The option will expire at the end of the applicable offering period, and will be exercised at that time to the extent of the payroll deductions accumulated during the offering period. The purchase price of the shares, in the absence of a contrary designation, will be 85% of the lower of the fair market value of our common stock on the first trading day of the offering period or on the purchase date. Participants may voluntarily end their participation in the 2021 ESPP at any time during a specified period prior to the end of the applicable offering period, and will be paid their accrued payroll deductions that have not yet been used to purchase shares of common stock. Participation ends automatically upon a participant’s termination of employment.
A participant may not transfer rights granted under the 2021 ESPP, other than by will or the laws of descent and distribution, and rights granted under the 2021 ESPP are generally exercisable only by the participant.
Certain Transactions. In the event of certain non-reciprocal transactions or events affecting our common stock, the plan administrator will make equitable adjustments to the 2021 ESPP and outstanding rights. In the event of certain unusual or non-recurring events or transactions, including a change in control, the plan administrator may provide for (1) either the replacement of outstanding rights with other rights or property or termination of outstanding rights in exchange for cash, (2) the assumption or substitution of outstanding rights by the successor or survivor corporation or parent or subsidiary thereof, if any, (3) the adjustment in the number and type of shares of stock subject to outstanding rights, (4) the use of participants’ accumulated payroll deductions to purchase stock on a new purchase date prior to the next scheduled purchase date and termination of any rights under ongoing offering periods or (5) the termination of all outstanding rights.
Plan Amendment. The plan administrator may amend, suspend or terminate the 2021 ESPP at any time. However, stockholder approval will be obtained for any amendment that increases the aggregate number or changes the type of shares that may be sold pursuant to rights under the 2021 ESPP or changes the corporations or classes of corporations whose employees are eligible to participate in the 2021 ESPP.
Existing Plan
Our board of directors initially adopted, and our stockholders initially approved, the Existing Plan in September 2011. From and after the effective date of the 2021 Plan, no additional awards will be made under the Existing Plan. However, the Existing Plan will continue to govern the terms and conditions of the outstanding awards previously granted thereunder.
Outstanding Awards. As of , stock options covering shares with a weighted-average exercise price of $ per share were outstanding under the Existing Plan. If an option granted under the Existing Plan expires, lapses or is terminated, exchanged for cash, surrendered, repurchased, canceled without having been fully exercised or forfeited, in each case after effectiveness of the 2021 Plan, any unused shares subject to the option will become available for issuance under and in accordance with the terms of the 2021 Plan.
199
Table of Contents
Administration. Our board of directors or a committee delegated by our board of directors administers the Existing Plan. Subject to the terms of the Existing Plan, the administrator has the power to construe and interpret the plan and to take such actions are as the administrator determines are appropriate for the administration of the plan.
Options. Options granted under the Existing Plan are subject to terms and conditions generally similar to those described above with respect to options that may be granted under our 2021 Plan.
Changes to Capital Structure. Certain terms of awards outstanding under the Existing Plan will be proportionately adjusted, as determined appropriate by the administrator, in the event of certain increases or decreases in or transactions affecting our common stock.
Change in Control. In the event of certain corporate transaction or events, the administrator in its discretion may terminate awards that are not assumed in transaction or event or provide for the full or partial vesting and exercisability of awards, which may be conditioned upon a subsequent termination of employment.
Amendment. The Board may at any time amend the Existing Plan, subject to its terms. To the extent necessary to comply with applicable laws, the Company will obtain stockholder approval of any plan amendment in such a manner and to such a degree as required.
200
Table of Contents
CERTAIN RELATIONSHIPS AND RELATED PARTY TRANSACTIONS
The following includes a summary of transactions since January 1, 2018 to which we have been a party in which the amount involved exceeded or will exceed the lessor of (i) $120,000 or (ii) one percent of the average of our total assets at fiscal year end for our last two fiscal years, and in which any of our directors, executive officers or, to our knowledge, beneficial owners of more than 5% of our capital stock or any member of the immediate family of any of the foregoing persons had or will have a direct or indirect material interest, other than equity and other compensation, termination, change in control and other arrangements, which are described under “Executive and Director Compensation.” We also describe below certain other transactions with our directors, executive officers and stockholders.
Preferred Stock Financings
Series C Preferred Stock Financing. Between July 2017 and June 2018, we issued and sold to investors in private placements an aggregate of 2,342,857 shares of our Series C preferred stock at a purchase price of $9.4868 per share, for aggregate consideration of approximately $22.23 million.
Series D Preferred Stock Financing. In August 2019, we issued and sold to investors in private placements an aggregate of 2,447,818 shares of our Series D preferred stock at a purchase price of $12.5622 per share, for aggregate consideration of approximately $30.8 million.
Series E Preferred Stock Financing. In March 2020, we issued and sold to investors in private placements an aggregate of 1,899,847 shares of our Series E preferred stock at a purchase price of $15.8697 per share, for aggregate consideration of approximately $30.15 million.
Series F Preferred Stock Financing. In November 2020, we issued and sold to investors in private placements an aggregate of 1,062,716 shares of our Series F preferred stock at a purchase price of $21.8779 per share, for aggregate consideration of approximately $23.25 million.
The following table sets forth the aggregate number of shares of our capital stock acquired by beneficial owners of more than 5% of our capital stock in the financing transactions described above. Each share of our preferred stock identified in the following table will convert into shares of common stock immediately upon the closing of this offering.
Participants | Series C Preferred Stock | Series D Preferred Stock | Series E Preferred Stock | Series F Preferred Stock | ||||||||||||
5% or Greater Stockholders(1) | ||||||||||||||||
Entities associated with Allegro Investment Fund, L.P. | 977,881 | |||||||||||||||
D1 Master Holdco I LLC | 1,890,395 | 685,623 | ||||||||||||||
Entities associated with HH Sight Partners, L.P. | 431,724 | |||||||||||||||
KCK Ltd. | 2,388,116 | |||||||||||||||
Sight Sciences Angels, LP | 121,725 | |||||||||||||||
| (1) | Additional details regarding these stockholders and their equity holdings are provided in this prospectus under the caption “Principal Stockholders.” |
201
Table of Contents
Some of our directors and officers are associated with our principal stockholders as indicated in the table below:
Directors and Officers | Principal Stockholder | |
Staffan Encrantz | Allegro Investment Fund, L.P. | |
Allegro Investors LLC | ||
Mack Hicks | HH Sight Partners, L.P. | |
HH-IOP Partners, L.P. | ||
Valeska Schroeder | KCK Ltd. | |
Jesse Selnick | Sight Sciences Angels, LP |
Investors’ Rights Agreement
We entered into a Third Amended and Restated Investors’ Rights Agreement on November 23, 2020 with the holders of our preferred stock, including entities with which certain of our directors are related. The agreement provides for certain rights relating to the registration of such holders’ common stock, including shares issuable upon conversion of preferred stock, and a right of first refusal to purchase future securities sold by us. See “Description of Capital Stock—Registration Rights” for additional information.
Voting Agreement
We entered into a Third Amended and Restated Voting Agreement by and among us and certain of our stockholders, pursuant to which the following directors were initially designated to serve as members on our board of directors: Erica Rogers, Don Zurbay, and David Badawi. Paul Badawi was selected to serve on our board of directors in his capacity as our chief executive officer. Andrew Offer, Mack Hicks, Staffan Encrantz, and Valeska Schroeder were initially selected to serve on our board of directors as representatives of holders of our preferred stock, as designated by entities affiliated with Scientific Health Development II, Ltd., HH Sight Partners, L.P., Allegro Investment Fund, L.P., and KCK Ltd., respectively.
The voting agreement will terminate upon the closing of this offering, and directors previously elected to our board of directors pursuant to this agreement will continue to serve as directors until they resign, are removed or their successors are duly elected. The composition of our board of directors after this offering is described in more detail under “Management—Board Composition and Election of Directors.”
Right of First Refusal and Co-Sale Agreement
We entered into a Third Amended and Restated Right of First Refusal and Co-sale Agreement, or the First Refusal and Co-Sale Agreement, with certain holders of our common stock, or the Key Holders, and our redeemable convertible preferred stock, which includes certain of our directors and executive officers, pursuant to which we have a right of first refusal in respect of certain sales of securities by our Key Holders. To the extent we do not exercise such right in full, the holders of our redeemable convertible preferred stock are granted certain rights of first refusal and co-sale in respect of such sale. The First Refusal and Co-Sale Agreement will terminate immediately prior to the consummation of this offering.
Employment Agreements
We have entered into employment agreements with our named executive officers. For more information regarding the agreements with our named executive officers, see “Executive and Director Compensation—Executive Compensation Arrangements.”
We have also entered into an employment agreement with Dr. David Badawi, one of our directors and the brother of Paul Badawi, our chief executive officer and a director, to serve as our Chief Technology Officer. In connection with serving as our Chief Technology Officer, we paid Dr. Badawi $162,000 in each of the years ended December 31, 2018, 2019 and 2020.
202
Table of Contents
Indemnification Agreements
We intend to enter into indemnification agreements with each of our directors and executive officers. These agreements, among other things, require us or will require us to indemnify each director (and in certain cases their related venture capital funds) and executive officer to the fullest extent permitted by Delaware law, including indemnification of expenses such as attorneys’ fees, judgments, fines and settlement amounts incurred by the director or executive officer in any action or proceeding, including any action or proceeding by or in right of us, arising out of the person’s services as a director or executive officer. For further information, see “Executive and Director Compensation—Limitations of Liability and Indemnification.”
Stock Option Grants to Executive Officers and Directors
We have granted stock options to our executive officers and certain of our directors as more fully described in the section entitled “Executive and Director Compensation.”
Policies and Procedures for Related Person Transactions
Our board of directors has adopted a written related person transaction policy, to be effective upon the closing of this offering, setting forth the policies and procedures for the review and approval or ratification of related person transactions. This policy will cover, with certain exceptions set forth in Item 404 of Regulation S-K under the Securities Act, any transaction, arrangement or relationship, or any series of similar transactions, arrangements or relationships, in which we were or are to be a participant, where the amount involved exceeds $120,000 in any fiscal year and a related person had, has or will have a direct or indirect material interest, including without limitation, purchases of goods or services by or from the related person or entities in which the related person has a material interest, indebtedness, guarantees of indebtedness and employment by us of a related person. In reviewing and approving any such transactions, our audit committee is tasked to consider all relevant facts and circumstances, including, but not limited to, whether the transaction is on terms comparable to those that could be obtained in an arm’s length transaction and the extent of the related person’s interest in the transaction. All of the transactions described in this section occurred prior to the adoption of this policy.
203
Table of Contents
The following table sets forth information with respect to the beneficial ownership of our common stock, as of by:
| • | each person or group of affiliated persons known by us to beneficially own more than 5% of our common stock; |
| • | each of our named executive officers; |
| • | each of our directors; and |
| • | all of our executive officers and directors as a group. |
The number of shares beneficially owned by each stockholder is determined under rules issued by the Securities and Exchange Commission. Under these rules, beneficial ownership includes any shares as to which the individual or entity has sole or shared voting power or investment power. Applicable percentage ownership is based on 17,607,142 shares of common stock outstanding as of June 15, 2021. In computing the number of shares beneficially owned by an individual or entity and the percentage ownership of that person, shares of common stock subject to options, warrants or other rights held by such person that are currently exercisable or will become exercisable within 60 days of June 15, 2021 are considered outstanding, although these shares are not considered outstanding for purposes of computing the percentage ownership of any other person. Unless noted otherwise, the address of all listed stockholders is 4040 Campbell Ave, Suite 100, Menlo Park, CA 94025. Each of the stockholders listed has sole voting and investment power with respect to the shares beneficially owned by the stockholder unless noted otherwise, subject to community property laws where applicable. The table does not reflect any shares of our common stock that may be purchased in this offering by directors, executive officers or beneficial holders of more than 5% of our outstanding common stock, through our reserved share program described in “Underwriters—Reserved Share Program.”
| Shares Beneficially Owned Prior to Offering | Beneficially Owned After Offering | |||||||||||||||
Name of Beneficial Owner | Number | Percentage | Number | Percentage | ||||||||||||
5% or Greater Stockholders | ||||||||||||||||
Entities associated with Allegro Investment Fund, L.P.(1) | 1,801,263 | 10.2 | % | % | ||||||||||||
D1 Master Holdco I LLC(2) | 2,576,018 | 14.6 | ||||||||||||||
Entities associated with HH Sight Partners, L.P.(3) | 2,193,335 | 12.5 | ||||||||||||||
KCK Ltd.(4) | 2,388,116 | 13.6 | ||||||||||||||
Scientific Health Development II, Ltd.(5) | 1,177,531 | 6.7 | ||||||||||||||
Sight Sciences Angels, LP(6) | 1,109,784 | 6.3 | ||||||||||||||
Named Executive Officers and Directors | ||||||||||||||||
Paul Badawi(7) | 2,645,932 | 15.0 | ||||||||||||||
Jesse Selnick(6)(8) | 1,180,200 | 6.7 | ||||||||||||||
David Badawi, M.D.(9) | 884,764 | 5.0 | ||||||||||||||
Shawn O’Neil(10) | 47,082 | * | ||||||||||||||
Sam Park(11) | 17,832 | * | ||||||||||||||
Jeremy Hayden(12) | 15,958 | * | ||||||||||||||
Staffan Encrantz(1) | 1,801,263 | 10.2 | ||||||||||||||
Mack Hicks(3)(13) | 2,236,438 | 12.7 | ||||||||||||||
Andrew Offer(5)(14) | 1,179,112 | 6.7 | ||||||||||||||
Erica Rogers(15) | 12,500 | * | ||||||||||||||
Valeska Schroeder, Ph.D. | — | — | ||||||||||||||
Donald Zurbay(16) | 8,125 | * | ||||||||||||||
All executive officers and directors (12 persons) | 10,029,206 | 55.9 | ||||||||||||||
| * | Less than 1%. |
204
Table of Contents
| (1) | Consists of (i) 724,637 shares of common stock issuable upon the conversion of the Series A redeemable convertible preferred stock, (ii) 98,745 shares of common stock issuable upon the conversion of the Series B redeemable convertible preferred stock and (iii) 661,653 shares of common stock issuable upon the conversion of the Series C redeemable convertible preferred stock, held by Allegro Investment Fund, L.P. (Allegro Investment Fund”), and (iv) 316,228 shares of common stock issuable upon the conversion of the Series C redeemable convertible preferred stock held by Allegro Investors LLC (“Allegro Investors” and, together with Allegro Investment Fund, “Allegro”). Staffan Encrantz, a member of our Board of Directors, is the founder and Chairman of Allegro Investment Fund and a member of Allegro Investors and may be deemed to beneficially own the shares of common stock held by Allegro. The principal address for the entities affiliated with Allegro is 525 Middlefield Road, Suite 220, Menlo Park, California 94025. |
| (2) | Consists of (i) 1,890,395 shares of common stock issuable upon the conversion of the Series E redeemable convertible preferred stock and (ii) 685,623 shares of common stock issuable upon the conversion of the Series F redeemable convertible preferred stock, held by D1 Master Holdco I LLC. D1 Capital Partners L.P. is a registered investment adviser and serves as the manager of private investment vehicles and accounts, including D1 Capital Partners Master LP, the sole and managing member of D1 Master Holdco I LLC, and may be deemed to beneficially own the shares of common stock held by D1 Master Holdco I LLC. Daniel Sundheim indirectly controls D1 Capital Partners L.P. and may be deemed to beneficially own the shares of common stock held by D1 Master Holdco I LLC. The business address of each of D1 Capital Partners Master LP, D1 Master Holdco I LLC, D1 Capital Partners L.P. and Daniel Sundheim is 9 West 57th Street, 36th Floor, New York, New York 10019. |
| (3) | Consists of (i) 942,028 shares of common stock issuable upon the conversion of the Series A redeemable convertible preferred stock, (ii) 128,368 shares of common stock issuable upon the conversion of the Series B redeemable convertible preferred stock and (iii) 264,369 shares of common stock issuable upon the conversion of the Series C redeemable preferred stock, held by HH Sight Partners, L.P. (“HH Sight Partners”), and (iv) 691,215 shares of common stock issuable upon the conversion of the Series B redeemable convertible preferred stock and (v) 167,355 shares of common stock issuable upon the conversion of the Series C redeemable convertible preferred stock held by HH-IOP Partners, L.P. (“HHIOP” and, together with HH Sight Partners, “HH”). HEP Partners LLC is the investment manager for HH. Mack Hicks, a member of our Board of Directors, is an Executive Vice President of both HEP Partners LLC and Hicks Holdings LLC and may be deemed to have voting and dispositive power over the shares held by HH. The principal address for the entities affiliated with HH is 2200 Ross Avenue, Suite 5000, Dallas, Texas 75201. |
| (4) | Consists of 2,388,116 shares of common stock issuable upon the conversion of the Series D redeemable convertible preferred stock held by KCK Ltd. (“KCK”). The board of directors of KCK Ltd., consisting of Antoine Sacy, Kamal Kassar, and Nael Karim Kassar, has delegated its authority to vote or invest the shares to Nael Karim Kassar. As such, Nael Karim Kassar may also be deemed to have sole voting and investment with respect to the shares. KCK Medical Technologies (“KCK MedTech”) is a division of KCK-US Inc. (“KCK-US”), a wholly-owned subsidiary of KCK. Valeska Schroeder, Ph.D. is a Managing Director of KCK MedTech. The principal address for KCK MedTech is 368 E. Campbell Avenue, Suite 200, Campbell, California 95008. The principal address for KCK is Corner House 4th Floor, 20 Parliament Street, Hamilton, HM 12, Bermuda. |
| (5) | Includes (i) 64,655 shares of common stock, (ii) 1,086,956 shares of common stock issuable upon the conversion of the Series A redeemable convertible preferred stock and (iii) 25,920 shares of common stock issuable upon the conversion of the Series B redeemable convertible preferred stock held by Scientific Health Development II, Ltd. (“SHD II”). Scientific Health Development, LLC is the manager of SHD II. Andrew Offer is a member of our Board of Directors, the Chief Executive Officer of Scientific Health Development, LLC and may be deemed to beneficially own the shares of common stock held by SHD II. The principal address for the entities affiliated with SHD II is 2305 Cedar Springs Road, Suite 240, Dallas, Texas 75201. |
| (6) | Consists of (i) 869,565 shares of common stock issuable upon the conversion of the Series A redeemable convertible preferred stock, (ii) 118,494 shares of common stock issuable upon the conversion of the Series B redeemable convertible preferred stock and (iii) 121,725 shares of common stock issuable upon the |
205
Table of Contents
| conversion of the Series C redeemable convertible preferred stock, held by Sight Sciences Angels, LP (“Sight Sciences Angels”). Jesse Selnick, our Chief Financial Officer, is a Managing Member of the General Partner of Sight Sciences Angels and may be deemed to beneficially own the shares of common stock held by Sight Sciences Angels. The principal address for Sight Sciences Angels is 4040 Campbell Avenue, Suite 100, Menlo Park, California 94025. |
| (7) | Includes (i) 2,632,391 shares of common stock and (ii) 13,541 shares of common stock which Mr. Badawi has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
| (8) | Includes 70,416 shares of common stock which Mr. Selnick has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
| (9) | Includes (i) 720,598 shares of common stock and (ii) 164,166 shares of common stock which Dr. Badawi has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
| (10) | Includes 47,082 shares of common stock which Mr. O’Neil has the right to acquire pursuant to outstanding share options, including options that will be exercisable within 60 days of June 15, 2021. |
| (11) | Includes (i) 12,166 shares of common stock and (ii) 5,666 shares of common stock which Mr. Park has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
| (12) | Includes 15,958 shares of common stock which Mr. Hayden has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
| (13) | Includes 43,103 shares of common stock held by Mack H. Hicks, as Trustee of the MHH 2016 Descendants Trust. |
| (14) | Includes 1,581 shares of common stock issuable upon conversion of shares of convertible preferred stock held by Mr. Offer. |
| (15) | Includes 12,500 shares of common stock which Ms. Rogers has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
| (16) | Includes 8,125 shares of common stock which Mr. Zurbay has the right to acquire pursuant to outstanding share options that will be exercisable within 60 days of June 15, 2021. |
206
Table of Contents
General
The following description summarizes some of the terms of our restated certificate of incorporation and restated bylaws, each of which will become effective upon the closing of this offering, the investors’ rights agreement and of the Delaware General Corporation Law. Because it is only a summary, it does not contain all the information that may be important to you. For a complete description, you should refer to our restated certificate of incorporation, restated bylaws and amended and restated investors’ rights agreement, copies of which have been or will be filed as exhibits to the registration statement of which this prospectus is a part, as well as the relevant provisions of the Delaware General Corporation Law. The description of our common stock and preferred stock reflects changes to our capital structure that will occur upon the closing of this offering.
Following the closing of this offering, our authorized capital stock will consist of shares of common stock, par value $0.001 per share, and shares of preferred stock, par value $0.001 per share.
As of , 2021, there were shares of our common stock outstanding and shares of our common stock issuable upon the automatic conversion of all outstanding shares of our preferred stock in connection with this offering, held of record by stockholders.
Common Stock
Holders of our common stock are entitled to one vote for each share held on all matters submitted to a vote of stockholders and do not have cumulative voting rights. An election of directors by our stockholders shall be determined by a plurality of the votes cast by the stockholders entitled to vote on the election. Subject to the supermajority votes for some matters, other matters shall be decided by the affirmative vote of our stockholders having a majority in voting power of the votes cast by the stockholders present or represented and voting on such matter. Our restated certificate of incorporation and restated bylaws also provide that our directors may be removed only for cause and only by the affirmative vote of the holders of at least two-thirds in voting power of the outstanding shares of capital stock entitled to vote thereon. In addition, the affirmative vote of the holders of at least two-thirds in voting power of the outstanding shares of capital stock entitled to vote thereon is required to amend or repeal, or to adopt any provision inconsistent with, several of the provisions of our restated certificate of incorporation. See below under “—Anti-Takeover Effects of Delaware Law and Our Certificate of Incorporation and Bylaws—Amendment of Charter Provisions.” Holders of common stock are entitled to receive proportionately any dividends as may be declared by our board of directors, subject to any preferential dividend rights of any series of preferred stock that we may designate and issue in the future.
In the event of our liquidation or dissolution, the holders of common stock are entitled to receive proportionately our net assets available for distribution to stockholders after the payment of all debts and other liabilities and subject to the prior rights of any outstanding preferred stock. Holders of common stock have no preemptive, subscription, redemption or conversion rights. There are no sinking fund provisions applicable to our common stock. Our outstanding shares of common stock are, and the shares offered by us in this offering will be, when issued and paid for, validly issued, fully paid and nonassessable. The rights, preferences and privileges of holders of common stock are subject to and may be adversely affected by the rights of the holders of shares of any series of preferred stock that we may designate and issue in the future.
Preferred Stock
Under the terms of our restated certificate of incorporation that will become effective upon the closing of this offering, our board of directors is authorized to direct us to issue shares of preferred stock in one or more series without stockholder approval. Our board of directors has the discretion to determine the rights, preferences, privileges and restrictions, including voting rights, dividend rights, conversion rights, redemption privileges and liquidation preferences, of each series of preferred stock.
207
Table of Contents
The purpose of authorizing our board of directors to issue preferred stock and determine its rights and preferences is to eliminate delays associated with a stockholder vote on specific issuances. The issuance of preferred stock, while providing flexibility in connection with possible acquisitions, future financings and other corporate purposes, could have the effect of making it more difficult for a third-party to acquire, or could discourage a third-party from seeking to acquire, a majority of our outstanding voting stock. Upon the closing of this offering, there will be no shares of preferred stock outstanding, and we have no present plans to issue any shares of preferred stock.
Options
As of , 2021, options to purchase shares of our common stock were outstanding under our Existing Plan, of which were exercisable and of which were unvested as of that date.
Warrants
As of , 2021, warrants to purchase an aggregate of shares of our common stock were outstanding, with a weighted average exercise price of $ per share. On January 25, 2019, June 28, 2019 and November 23, 2020, we issued warrants to MidCap Funding XXVIII Trust, in connection with a loan and security agreement between us and Midcap Financial Services. Pursuant to the terms of the warrants, the number of shares for which the warrant is exercisable is determined by the total principal amount of loans made under the loan and security agreement. If unexercised, these warrants will expire on the tenth anniversary of their issuance dates.
The warrants will neither expire nor be automatically exercised upon the closing of this offering. The warrants provide that the holder thereof may elect to exercise the warrant on a net “cashless” basis at any time prior to the expiration thereof. Assuming the closing of this offering occurs, the fair market value of one share of our common stock in connection with any cashless exercise shall be the closing price or last sale price per share of our common stock on the or other public trading market on which our common stock is traded on the business day immediately prior to the date the holder elects to exercise the warrants on a cashless basis.
Registration Rights
Holders of shares of our common stock are entitled to certain rights with respect to the registration of such shares for public resale under the Securities Act, pursuant to an amended and restated investors’ rights agreement by and among us and certain of our stockholders, until the rights otherwise terminate pursuant to the terms of the investors’ rights agreement. The registration of shares of common stock as a result of the following rights being exercised would enable holders to trade these shares without restriction under the Securities Act when the applicable registration statement is declared effective.
Registration Rights
If at any time beginning 180 days after the closing date of this offering the holders of more than 50% of the registrable securities then outstanding request in writing that we effect a registration with respect to all or part of such registrable securities then outstanding and having an anticipated aggregate offering price of at least $20,000,000, net of expenses, we may be required to register their shares. We are obligated to effect at most two registrations in response to these demand registration rights. If the holders requesting registration intend to distribute their shares by means of an underwriting, the managing underwriter of such offering will have the right to limit the numbers of shares to be underwritten for reasons related to the marketing of the shares.
Piggyback Registration Rights
If at any time after this offering we propose to register any shares of our common stock under the Securities Act, subject to certain exceptions, the holders of registrable securities will be entitled to notice of the registration
208
Table of Contents
and to include their shares of registrable securities in the registration. If our proposed registration involves an underwriting, the managing underwriter of such offering will have the right to limit the number of shares to be underwritten for reasons related to the marketing of the shares.
Expenses and Indemnification
Ordinarily, other than underwriting discounts and commissions, we will be required to pay all expenses incurred by us related to any registration effected pursuant to the exercise of these registration rights. These expenses may include all registration and filing fees, printing expenses, fees and disbursements of our counsel, reasonable fees and disbursements of a counsel for the selling securityholders (not to exceed $25,000) and blue sky fees and expenses. Additionally, we have agreed to indemnify selling stockholders for damages, and any legal or other expenses reasonably incurred, arising from or based upon any untrue statement of a material fact contained in any registration statement, an omission or alleged omission to state a material fact in any registration statement or necessary to make the statements therein not misleading, or any violation or alleged violation by the indemnifying party of securities laws, subject to certain exceptions.
Termination of Registration Rights
Each of the foregoing registration rights terminate upon the earlier of five years after the effective date of the registration statement of which this prospectus is a part, the closing of a deemed liquidation event, as defined in our current certificate of incorporation, or as to any holder at such time as Rule 144 or another similar exemption under the Securities Act is available for the sale of all of such holders registrable securities without limitation during a three-month period without registration.
Anti-Takeover Effects of Delaware Law and Our Certificate of Incorporation and Bylaws
Some provisions of Delaware law, our restated certificate of incorporation and our restated bylaws could make the following transactions more difficult: an acquisition of us by means of a tender offer; an acquisition of us by means of a proxy contest or otherwise; or the removal of our incumbent officers and directors. It is possible that these provisions could make it more difficult to accomplish or could deter transactions that stockholders may otherwise consider to be in their best interest or in our best interests, including transactions which provide for payment of a premium over the market price for our shares.
These provisions, summarized below, are intended to discourage coercive takeover practices and inadequate takeover bids. These provisions are also designed to encourage persons seeking to acquire control of us to first negotiate with our board of directors. We believe that the benefits of the increased protection of our potential ability to negotiate with the proponent of an unfriendly or unsolicited proposal to acquire or restructure us outweigh the disadvantages of discouraging these proposals because negotiation of these proposals could result in an improvement of their terms.
Undesignated Preferred Stock
The ability of our board of directors, without action by the stockholders, to issue up to shares of undesignated preferred stock with voting or other rights or preferences as designated by our board of directors could impede the success of any attempt to change control of us. These and other provisions may have the effect of deferring hostile takeovers or delaying changes in control or management of our company.
Stockholder Meetings
Our restated bylaws provide that a special meeting of stockholders may be called only by our chairman of the board, chief executive officer or president (in the absence of a chief executive officer), or by a resolution adopted by a majority of our board of directors.
209
Table of Contents
Requirements for Advance Notification of Stockholder Nominations and Proposals
Our restated bylaws establish advance notice procedures with respect to stockholder proposals to be brought before a stockholder meeting and the nomination of candidates for election as directors, other than nominations made by or at the direction of the board of directors or a committee of the board of directors.
Elimination of Stockholder Action by Written Consent
Our restated certificate of incorporation eliminates the right of stockholders to act by written consent without a meeting.
Staggered Board
Our board of directors is divided into three classes. The directors in each class will serve for a three-year term, one class being elected each year by our stockholders. For more information on the classified board, see “Management—Board Composition and Election of Directors.” This system of electing and removing directors may tend to discourage a third-party from making a tender offer or otherwise attempting to obtain control of us, because it generally makes it more difficult for stockholders to replace a majority of the directors.
Removal of Directors
Our restated certificate of incorporation provides that no member of our board of directors may be removed from office by our stockholders except for cause and, in addition to any other vote required by law, upon the approval of the holders of at least two-thirds in voting power of the outstanding shares of stock entitled to vote in the election of directors.
Stockholders Not Entitled to Cumulative Voting
Our restated certificate of incorporation does not permit stockholders to cumulate their votes in the election of directors. Accordingly, the holders of a majority of the outstanding shares of our common stock entitled to vote in any election of directors can elect all of the directors standing for election, if they choose, other than any directors that holders of our preferred stock may be entitled to elect.
Delaware Anti-Takeover Statute
We are subject to Section 203 of the General Corporation Law of the State of Delaware, which prohibits persons deemed to be “interested stockholders” from engaging in a “business combination” with a publicly held Delaware corporation for three years following the date these persons become interested stockholders unless the business combination is, or the transaction in which the person became an interested stockholder was, approved in a prescribed manner or another prescribed exception applies. Generally, an “interested stockholder” is a person who, together with affiliates and associates, owns, or within three years prior to the determination of interested stockholder status did own, 15% or more of a corporation’s voting stock. Generally, a “business combination” includes a merger, asset or stock sale, or other transaction resulting in a financial benefit to the interested stockholder. The existence of this provision may have an anti-takeover effect with respect to transactions not approved in advance by the board of directors.
Choice of Forum
Our restated certificate of incorporation provides that, unless we consent in writing to the selection of an alternative form, the Court of Chancery of the State of Delaware will be the sole and exclusive forum for: (1) any derivative action or proceeding brought on our behalf; (2) any action asserting a claim of breach of a fiduciary duty or other wrongdoing by any of our directors, officers, employees or agents to us or our stockholders; (3) any
210
Table of Contents
action asserting a claim against us arising pursuant to any provision of the General Corporation Law of the State of Delaware or our certificate of incorporation or bylaws; (4) any action to interpret, apply, enforce or determine the validity of our certificate of incorporation or bylaws; or (5) any action asserting a claim governed by the internal affairs doctrine; provided that the exclusive forum provision will not apply to suits brought to enforce any liability or duty created by the Securities Act or the Exchange Act, or to any claim for which the federal courts have exclusive jurisdiction. For instance, the provision would not apply to actions arising under federal securities laws, including suits brought to enforce any liability or duty created by the Securities Act, Exchange Act, or the rules and regulations thereunder. Our restated certificate of incorporation further provides that, unless we consent in writing to the selection of an alternative forum, the federal district courts of the United States of America shall, to the fullest extent permitted by law, be the sole and exclusive forum for the resolution of any complaint asserting a cause of action arising under the Securities Act. Our restated certificate of incorporation also provides that any person or entity purchasing or otherwise acquiring any interest in shares of our capital stock will be deemed to have notice of and to have consented to this choice of forum provision. It is possible that a court of law could rule that the choice of forum provision contained in our restated certificate of incorporation is inapplicable or unenforceable if it is challenged in a proceeding or otherwise.
Amendment of Charter Provisions
The amendment of any of the above provisions, except for the provision making it possible for our board of directors to issue preferred stock and the provision prohibiting cumulative voting, would require approval by holders of at least two-thirds in voting power of the outstanding shares of stock entitled to vote thereon.
The provisions of Delaware law, our restated certificate of incorporation and our restated bylaws could have the effect of discouraging others from attempting hostile takeovers and, as a consequence, they may also inhibit temporary fluctuations in the market price of our common stock that often result from actual or rumored hostile takeover attempts. These provisions may also have the effect of preventing changes in the composition of our board and management. It is possible that these provisions could make it more difficult to accomplish transactions that stockholders may otherwise deem to be in their best interests
Transfer Agent and Registrar
The transfer agent and registrar for our common stock will be American Stock Transfer & Trust Company, LLC.
Stock Exchange Listing
We have applied to have our common stock listed on The Nasdaq Global Market under the symbol “SGHT.”
211
Table of Contents
SHARES ELIGIBLE FOR FUTURE SALE
Immediately prior to this offering, there was no public market for our common stock. Future sales of substantial amounts of common stock in the public market, or the perception that such sales may occur, could adversely affect the market price of our common stock.
Upon the closing of this offering, we will have outstanding an aggregate of shares of common stock, assuming the issuance of shares of common stock offered by us in this offering. Of these shares, all shares sold in this offering will be freely tradable without restriction or further registration under the Securities Act, except for any shares purchased by our “affiliates,” as that term is defined in Rule 144 under the Securities Act, whose sales would be subject to the Rule 144 resale restrictions described below, other than the holding period requirement.
The remaining shares of common stock will be “restricted securities,” as that term is defined in Rule 144 under the Securities Act. These restricted securities are eligible for public sale only if they are registered under the Securities Act or if they qualify for an exemption from registration under Rules 144 or 701 under the Securities Act, which are summarized below. We expect that substantially all of these shares will be subject to the 180-day lock-up period under the lock-up agreements described below. Upon expiration of the lock-up period, we estimate that approximately shares will be available for sale in the public market, subject in some cases to applicable volume limitations under Rule 144.
In addition, of the shares of our common stock that were subject to stock options outstanding as of , 2021, options to purchase shares of common stock were vested as of , 2021 and, upon exercise, these shares will be eligible for sale subject to the lock-up agreements described below and Rules 144 and 701 under the Securities Act.
Lock-Up Agreements
We and each of our directors and executive officers and holders of substantially all of our outstanding capital stock, have agreed that, without the prior written consent of Morgan Stanley & Co. LLC and BofA Securities, Inc., we and they will not, subject to certain exceptions, during the period ending 180 days after the date of this prospectus, offer, pledge, sell, contract to sell, sell any option or contract to purchase, purchase any option or contract to sell, grant any option, right or warrant to purchase, lend, or otherwise transfer or dispose of, directly or indirectly, any shares of our common stock or any securities convertible into or exercisable or exchangeable for common stock; or enter into any swap or other arrangement that transfers to another, in whole or in part, any of the economic consequences of ownership of our common stock, whether any transaction described above is to be settled by delivery of our common stock or such other securities, in cash or otherwise.
Upon the expiration of the applicable lock-up period, substantially all of the shares subject to such lock-up restrictions will become eligible for sale, subject to the limitations discussed above. For a further description of these lock-up agreements, please see “Underwriters.”
Rule 144
Affiliate Resales of Restricted Securities
In general, beginning 90 days after the effective date of the registration statement of which this prospectus is a part, a person who is an affiliate of ours, or who was an affiliate at any time during the 90 days before a sale, who has beneficially owned shares of our common stock for at least six months would be entitled to sell in “broker’s transactions” or certain “riskless principal transactions” or to market makers, a number of shares within any three-month period that does not exceed the greater of:
| • | 1% of the number of shares of our common stock then outstanding, which will equal approximately shares immediately after this offering; or |
212
Table of Contents
| • | the average weekly trading volume in our common stock on The Nasdaq Global Market during the four calendar weeks preceding the filing of a notice on Form 144 with respect to such sale. |
Affiliate resales under Rule 144 are also subject to the availability of current public information about us. In addition, if the number of shares being sold under Rule 144 by an affiliate during any three-month period exceeds 5,000 shares or has an aggregate sale price in excess of $50,000, the seller must file a notice on Form 144 with the Securities and Exchange Commission and The Nasdaq Global Market concurrently with either the placing of a sale order with the broker or the execution directly with a market maker.
Non-Affiliate Resales of Restricted Securities
In general, beginning 90 days after the effective date of the registration statement of which this prospectus is a part, a person who is not an affiliate of ours at the time of sale, and has not been an affiliate at any time during the three months preceding a sale, and who has beneficially owned shares of our common stock for at least six months but less than a year, is entitled to sell such shares subject only to the availability of current public information about us. If such person has held our shares for at least one year, such person can resell under Rule 144(b)(1) without regard to any other Rule 144 restrictions, including the 90-day public company requirement and the current public information requirement.
Non-affiliate resales are not subject to the manner of sale, volume limitation or notice filing provisions of Rule 144.
Rule 701
In general, under Rule 701, any of an issuer’s employees, directors, officers, consultants or advisors who purchases shares from the issuer in connection with a compensatory stock or option plan or other written agreement before the effective date of a registration statement under the Securities Act is entitled to sell such shares 90 days after such effective date in reliance on Rule 144. An affiliate of the issuer can resell shares in reliance on Rule 144 without having to comply with the holding period requirement, and non-affiliates of the issuer can resell shares in reliance on Rule 144 without having to comply with the current public information and holding period requirements.
The Securities and Exchange Commission has indicated that Rule 701 will apply to typical stock options granted by an issuer before it becomes subject to the reporting requirements of the Exchange Act, along with the shares acquired upon exercise of such options, including exercises after an issuer becomes subject to the reporting requirements of the Exchange Act.
Equity Plans
We intend to file one or more registration statements on Form S-8 under the Securities Act to register all shares of common stock subject to outstanding stock options and common stock issued or issuable under our stock plans. We expect to file the registration statement covering shares offered pursuant to our stock plans shortly after the date of this prospectus, permitting the resale of such shares by non-affiliates in the public market without restriction under the Securities Act and the sale by affiliates in the public market, subject to compliance with the resale provisions of Rule 144.
213
Table of Contents
Registration Rights
Upon the closing of this offering, the holders of shares of common stock, which includes all of the shares of common stock issuable upon the automatic conversion of our preferred stock upon the closing of this offering, or their transferees will be entitled to various rights with respect to the registration of these shares under the Securities Act. Registration of these shares under the Securities Act would result in these shares becoming fully tradable without restriction under the Securities Act immediately upon the effectiveness of the registration, except for shares purchased by affiliates. See “Description of Capital Stock—Registration Rights” for additional information. Shares covered by a registration statement will be eligible for sale in the public market upon the expiration or release from the terms of the lock-up agreement described above.
214
Table of Contents
MATERIAL U.S. FEDERAL INCOME TAX CONSEQUENCES TO NON-U.S. HOLDERS
The following discussion is a summary of the material U.S. federal income tax consequences to Non-U.S. Holders (as defined below) of the purchase, ownership, and disposition of our common stock issued pursuant to this offering, but does not purport to be a complete analysis of all potential tax effects. The effects of other U.S. federal tax laws, such as estate and gift tax laws, and any applicable state, local, or non-U.S. tax laws are not discussed. This discussion is based on the U.S. Internal Revenue Code of 1986, as amended, or the Code, Treasury Regulations promulgated thereunder, judicial decisions, and published rulings and administrative pronouncements of the U.S. Internal Revenue Service, or the IRS, in each case in effect as of the date hereof.
These authorities may change or be subject to differing interpretations. Any such change or differing interpretation may be applied retroactively in a manner that could adversely affect a Non-U.S. Holder. We have not sought and will not seek any rulings from the IRS regarding the matters discussed below. There can be no assurance the IRS or a court will not take a contrary position to that discussed below regarding the tax consequences of the purchase, ownership, and disposition of our common stock.
This discussion is limited to Non-U.S. Holders that hold our common stock as a “capital asset” within the meaning of Section 1221 of the Code (generally, property held for investment). This discussion does not address all U.S. federal income tax consequences relevant to a Non-U.S. Holder’s particular circumstances, including the impact of the Medicare contribution tax on net investment income or the alternative minimum tax. In addition, it does not address consequences relevant to Non-U.S. Holders subject to special rules, including, without limitation:
| • | U.S. expatriates and former citizens or long-term residents of the United States; |
| • | Persons holding our common stock as part of a hedge, straddle, or other risk reduction strategy or as part of a conversion transaction; |
| • | Banks, insurance companies, and other financial institutions; |
| • | Brokers, dealers, or traders in securities; |
| • | “Controlled foreign corporations,” “passive foreign investment companies,” and corporations that accumulate earnings to avoid U.S. federal income tax; |
| • | Partnerships or other entities or arrangements treated as partnerships for U.S. federal income tax purposes (and investors therein); |
| • | Tax-exempt organizations or governmental organizations; |
| • | Persons deemed to sell our common stock under the constructive sale provisions of the Code; |
| • | Tax-qualified retirement plans; and |
| • | “Qualified foreign pension funds” as defined in Section 897(l)(2) of the Code and entities all of the interests of which are held by qualified foreign pension funds. |
If an entity treated as a partnership for U.S. federal income tax purposes holds our common stock, the tax treatment of a partner in the partnership will depend on the status of the partner, the activities of the partnership, and certain determinations made at the partner level. Accordingly, partnerships holding our common stock and the partners in such partnerships should consult their tax advisors regarding the U.S. federal income tax consequences to them.
THIS DISCUSSION IS NOT TAX ADVICE. INVESTORS SHOULD CONSULT THEIR TAX ADVISORS WITH RESPECT TO THE APPLICATION OF THE U.S. FEDERAL INCOME TAX LAWS TO THEIR PARTICULAR SITUATIONS AS WELL AS ANY TAX CONSEQUENCES OF THE PURCHASE, OWNERSHIP, AND DISPOSITION OF OUR COMMON STOCK ARISING UNDER THE U.S. FEDERAL ESTATE OR GIFT TAX LAWS OR UNDER THE LAWS OF ANY STATE, LOCAL, OR NON-U.S. TAXING JURISDICTION OR UNDER ANY APPLICABLE INCOME TAX TREATY.
215
Table of Contents
Definition of Non-U.S. Holder
For purposes of this discussion, a “Non-U.S. Holder” is any beneficial owner of our common stock that is neither a “U.S. person” nor an entity treated as a partnership for U.S. federal income tax purposes. A U.S. person is any person that, for U.S. federal income tax purposes, is or is treated as any of the following:
| • | An individual who is a citizen or resident of the United States; |
| • | A corporation created or organized under the laws of the United States, any state thereof, or the District of Columbia; |
| • | An estate, the income of which is subject to U.S. federal income tax regardless of its source; or |
| • | A trust that (1) is subject to the primary supervision of a U.S. court and all substantial decisions of which are subject to the control of one or more “United States persons” (within the meaning of Section 7701(a)(30) of the Code), or (2) has a valid election in effect to be treated as a United States person for U.S. federal income tax purposes. |
Distributions
As described in the section of this prospectus titled “Dividend Policy,” we have never declared or paid cash dividends on our capital stock, and we do not currently intend to pay any cash dividends on our capital stock in the foreseeable future. However, if we do make distributions of cash or property on our common stock, such distributions will constitute dividends for U.S. federal income tax purposes to the extent paid from our current or accumulated earnings and profits, as determined under U.S. federal income tax principles. Amounts not treated as dividends for U.S. federal income tax purposes will constitute returns of capital and first be applied against and reduce a Non-U.S. Holder’s adjusted tax basis in its common stock, but not below zero. Any excess will be treated as capital gain and will be treated as described below under “—Sale or Other Taxable Disposition.”
Subject to the discussion below regarding effectively connected income, dividends paid to a Non-U.S. Holder will be subject to U.S. federal withholding tax at a rate of 30% of the gross amount of the dividends (or such lower rate specified by an applicable income tax treaty, provided the Non-U.S. Holder furnishes a valid IRS Form W-8BEN or IRS Form W-8BEN-E (or other applicable documentation) certifying qualification for the lower treaty rate). A Non-U.S. Holder that does not timely furnish the required documentation, but that qualifies for a reduced treaty rate, may obtain a refund of any excess amounts withheld by timely filing an appropriate claim for refund with the IRS. Non-U.S. Holders should consult their tax advisors regarding their entitlement to benefits under any applicable tax treaties.
If dividends paid to a Non-U.S. Holder are effectively connected with the Non-U.S. Holder’s conduct of a trade or business within the United States (and, if required by an applicable income tax treaty, the Non-U.S. Holder maintains a permanent establishment in the United States to which such dividends are attributable), the Non-U.S. Holder will be exempt from the U.S. federal withholding tax described above. To claim the exemption, the Non-U.S. Holder must furnish to the applicable withholding agent a valid IRS Form W-8ECI, certifying that the dividends are effectively connected with the Non-U.S. Holder’s conduct of a trade or business within the United States. Any such effectively connected dividends will be subject to U.S. federal income tax on a net income basis at the regular rates. A Non-U.S. Holder that is a corporation also may be subject to a branch profits tax at a rate of 30% (or such lower rate specified by an applicable income tax treaty) on such effectively connected dividends, as adjusted for certain items. Non-U.S. Holders should consult their tax advisors regarding any applicable tax treaties that may provide for different rules.
216
Table of Contents
Sale or Other Taxable Disposition
Subject to the discussion below regarding backup withholding, a Non-U.S. Holder will not be subject to U.S. federal income tax on any gain realized upon the sale or other taxable disposition of our common stock unless:
| • | The gain is effectively connected with the Non-U.S. Holder’s conduct of a trade or business within the United States (and, if required by an applicable income tax treaty, the Non-U.S. Holder maintains a permanent establishment in the United States to which such gain is attributable); |
| • | The Non-U.S. Holder is a nonresident alien individual present in the United States for 183 days or more during the taxable year of the disposition and certain other requirements are met; or |
| • | Our common stock constitutes a U.S. real property interest, or USRPI, by reason of our status as a U.S. real property holding corporation, or USRPHC, for U.S. federal income tax purposes. |
Gain described in the first bullet point above generally will be subject to U.S. federal income tax on a net income basis at the regular rates. A Non-U.S. Holder that is a corporation also may be subject to a branch profits tax at a rate of 30% (or such lower rate specified by an applicable income tax treaty) on such effectively connected gain, as adjusted for certain items.
A Non-U.S. Holder described in the second bullet point above will be subject to U.S. federal income tax at a rate of 30% (or such lower rate specified by an applicable income tax treaty) on gain realized upon the sale or other taxable disposition of our common stock, which may be offset by certain U.S.-source capital losses of the Non-U.S. Holder (even though the individual is not considered a resident of the United States), provided the Non-U.S. Holder has timely filed U.S. federal income tax returns with respect to such losses.
With respect to the third bullet point above, we believe we currently are not, and do not anticipate becoming, a USRPHC. Because the determination of whether we are a USRPHC depends, however, on the fair market value of our USRPIs relative to the fair market value of our non-U.S. real property interests and our other business assets, there can be no assurance that we currently are not a USRPHC or will not become one in the future. Even if we are or were to become a USRPHC, gain arising from the sale or other taxable disposition of our common stock by a Non-U.S. Holder will not be subject to U.S. federal income tax if our common stock is “regularly traded,” as defined by applicable Treasury Regulations, on an established securities market and such Non-U.S. Holder owned, actually and constructively, 5% or less of our common stock throughout the shorter of the five-year period ending on the date of the sale or other taxable disposition or the Non-U.S. Holder’s holding period.
Non-U.S. Holders should consult their tax advisors regarding any applicable tax treaties that may provide for different rules.
Information Reporting and Backup Withholding
Payments of dividends on our common stock will not be subject to backup withholding, provided the Non-U.S. Holder certifies its non-U.S. status, such as by furnishing a valid IRS Form W-8BEN, W-8BEN-E or W-8ECI, or otherwise establishes an exemption. However, information returns are required to be filed with the IRS in connection with any distributions on our common stock paid to the Non-U.S. Holder, regardless of whether any tax was actually withheld. In addition, proceeds of the sale or other taxable disposition of our common stock within the United States or conducted through certain U.S.-related brokers generally will not be subject to backup withholding or information reporting if the applicable withholding agent receives the certification described above or the Non-U.S. Holder otherwise establishes an exemption. Proceeds of a disposition of our common stock conducted through a non-U.S. office of a non-U.S. broker that does not have certain enumerated relationships with the United States generally will not be subject to backup withholding or information reporting.
217
Table of Contents
Copies of information returns that are filed with the IRS may also be made available under the provisions of an applicable treaty or agreement to the tax authorities of the country in which the Non-U.S. Holder resides or is established.
Backup withholding is not an additional tax. Any amounts withheld under the backup withholding rules may be allowed as a refund or a credit against a Non-U.S. Holder’s U.S. federal income tax liability, provided the required information is timely furnished to the IRS.
Additional Withholding Tax on Payments Made to Foreign Accounts
Withholding taxes may be imposed under Sections 1471 to 1474 of the Code (such Sections commonly referred to as the Foreign Account Tax Compliance Act, or FATCA) on certain types of payments made to non-U.S. financial institutions and certain other non-U.S. entities. Specifically, a 30% withholding tax may be imposed on dividends on, or (subject to the proposed Treasury Regulations discussed below) gross proceeds from the sale or other disposition of, our common stock paid to a “foreign financial institution” or a “non-financial foreign entity” (each as defined in the Code), unless (1) the foreign financial institution undertakes certain diligence and reporting obligations, (2) the non-financial foreign entity either certifies it does not have any “substantial United States owners” (as defined in the Code) or furnishes identifying information regarding each substantial United States owner, or (3) the foreign financial institution or non-financial foreign entity otherwise qualifies for an exemption from these rules. If the payee is a foreign financial institution and is subject to the diligence and reporting requirements in (1) above, it must enter into an agreement with the U.S. Department of the Treasury requiring, among other things, that it undertakes to identify accounts held by certain “specified United States persons” or “United States owned foreign entities” (each as defined in the Code), annually reports certain information about such accounts, and withholds 30% on certain payments to non-compliant foreign financial institutions and certain other account holders. Foreign financial institutions located in jurisdictions that have an intergovernmental agreement with the United States governing FATCA may be subject to different rules.
Under the applicable Treasury Regulations and administrative guidance, withholding under FATCA generally applies to payments of dividends on our common stock. While, beginning on January 1, 2019, withholding under FATCA would have applied also to payments of gross proceeds from the sale or other disposition of our common stock, proposed Treasury Regulations eliminate FATCA withholding on payments of gross proceeds entirely. Taxpayers generally may rely on these proposed Treasury Regulations until final Treasury Regulations are issued.
Prospective investors should consult their tax advisors regarding the potential application of withholding under FATCA to their investment in our common stock.
218
Table of Contents
Under the terms and subject to the conditions in an underwriting agreement dated the date of this prospectus, the underwriters named below, for whom Morgan Stanley & Co. LLC, BofA Securities, Inc., Citigroup Global Markets, Inc. and Piper Sandler & Co. are acting as representatives, have severally agreed to purchase, and we have agreed to sell to them, severally, the number of shares indicated below:
Name | Number of Shares | |||
Morgan Stanley & Co. LLC | ||||
BofA Securities, Inc. | ||||
Citigroup Global Markets, Inc. | ||||
Piper Sandler & Co. | ||||
|
| |||
Total: | ||||
The underwriters and the representatives are collectively referred to as the “underwriters” and the “representatives,” respectively. The underwriters are offering the shares of common stock subject to their acceptance of the shares from us and subject to prior sale. The underwriting agreement provides that the obligations of the several underwriters to pay for and accept delivery of the shares of common stock offered by this prospectus are subject to the approval of certain legal matters by their counsel and to certain other conditions. The underwriters are obligated to take and pay for all of the shares of common stock offered by this prospectus if any such shares are taken. However, the underwriters are not required to take or pay for the shares covered by the underwriters’ over-allotment option described below.
The underwriters initially propose to offer part of the shares of common stock directly to the public at the offering price listed on the cover page of this prospectus and part to certain dealers at a price that represents a concession not in excess of $ per share under the public offering price. After the initial offering of the shares of common stock, the offering price and other selling terms may from time to time be varied by the representatives.
We have granted to the underwriters an option, exercisable for 30 days from the date of this prospectus, to purchase up to additional shares of common stock at the public offering price listed on the cover page of this prospectus, less underwriting discounts and commissions. The underwriters may exercise this option solely for the purpose of covering over-allotments, if any, made in connection with the offering of the shares of common stock offered by this prospectus. To the extent the option is exercised, each underwriter will become obligated, subject to certain conditions, to purchase approximately the same percentage of the additional shares of common stock as the number listed next to the underwriter’s name in the preceding table bears to the total number of shares of common stock listed next to the names of all underwriters in the preceding table.
The following table shows the per share and total public offering price, underwriting discounts and commissions, and proceeds before expenses to us. These amounts are shown assuming both no exercise and full exercise of the underwriters’ option to purchase up to an additional shares of common stock.
| Total | ||||||||||||
| Per Share | No Exercise | Full Exercise | ||||||||||
Public offering price | $ | $ | $ | |||||||||
Underwriting discounts and commissions to be paid by us: | $ | $ | $ | |||||||||
Proceeds, before expenses, to us | $ | $ | $ | |||||||||
The estimated offering expenses payable by us, exclusive of the underwriting discounts and commissions, are approximately $ . We have agreed to reimburse the underwriters for expenses relating to clearance of this offering with the Financial Industry Regulatory Authority up to $ .
219
Table of Contents
The underwriters have informed us that they do not intend sales to discretionary accounts to exceed 5% of the total number of shares of common stock offered by them.
We have applied to list our common stock on the Nasdaq Global Market under the trading symbol “SGHT”.
We and all directors and officers and the holders of substantially all of our outstanding stock and stock options have agreed that, without the prior written consent of Morgan Stanley & Co. LLC and BofA Securities, Inc. on behalf of the underwriters, we and they will not, and will not publicly disclose an intention to, during the period ending 180 days after the date of this prospectus (the “restricted period”):
| • | Offer, pledge, sell, contract to sell, sell any option or contract to purchase, purchase any option or contract to sell, grant any option, right or warrant to purchase, lend or otherwise transfer or dispose of, directly or indirectly, any shares of common stock or any securities convertible into or exercisable or exchangeable for shares of common stock; |
| • | File any registration statement with the Securities and Exchange Commission relating to the offering of any shares of common stock or any securities convertible into or exercisable or exchangeable for common stock; or |
| • | Enter into any swap or other arrangement that transfers to another, in whole or in part, any of the economic consequences of ownership of the common stock, |
whether any such transaction described above is to be settled by delivery of common stock or such other securities, in cash or otherwise. In addition, we and each such person agrees that, without the prior written consent of Morgan Stanley & Co. LLC and BofA Securities, Inc. on behalf of the underwriters, we or such other person will not, during the restricted period, make any demand for, or exercise any right with respect to, the registration of any shares of common stock or any security convertible into or exercisable or exchangeable for common stock.
The restrictions described in the immediately preceding paragraph to do not apply to:
| (a) | the sale of shares to the underwriters; |
| (b) | the issuance by the Company of shares of common stock upon the exercise of an option or a warrant or the conversion of a security outstanding on the date of this prospectus of which the underwriters have been advised in writing; |
| (c) | transactions by any person other than us relating to shares of common stock or other securities acquired from the underwriters in this offering or open market transactions after the completion of the offering of the shares; provided that no filing under Section 16(a) of the Securities Exchange Act of 1934, as amended (the “Exchange Act”), is required or voluntarily made in connection with subsequent sales of the common stock or other securities acquired in this offering or such open market transactions; |
| (d) | transfers by any person other than us of shares of common stock or other securities convertible into or exercisable or exchangeable for common stock as a bona fide gift or for bona fide estate planning purposes; |
| (e) | transfers by any person other than us of shares of common stock or any security convertible into common stock to (i) a partnership, limited liability company or other entity which is controlled or managed by such person or the immediate family of such person or under common control of such person, (ii) to any trust for the direct or indirect benefit of such person or the immediate family of the such person or, if such person is a trust, to a trustor or beneficiary of the trust or to the estate of a beneficiary of such trust or (iii) if such person is a corporation, partnership, limited liability company, trust or other business entity, transfers to another corporation, partnership, limited liability company, trust or other business entity that is an affiliate (as defined in Rule 405 promulgated under the Securities Act of 1933, as amended) of such person, or to any investment fund or other entity |
220
Table of Contents
| controlling, controlled by, managing or managed by or under common control with such person or affiliates of such person (including, for the avoidance of doubt, where such person is a partnership, to its general partner or a successor partnership or fund, or any other funds managed by such partnership); |
| (f) | distributions of shares of common stock or any security convertible into common stock to limited partners or stockholders of such person; |
| (g) | transfers of shares of common stock or other securities convertible into or exercisable or exchangeable for common stock by operation of law, pursuant to a qualified domestic order, divorce settlement, divorce decree or separation agreement; |
| (h) | transfers to a nominee or a custodian of a person or entity to whom a disposition or transfer would be permissible under clauses (c) through (g) set forth above; |
| (i) | transfers to us by any person other than us of shares of common stock or any security convertible into or exercisable or exchangeable for common stock in connection with the repurchase by the Company from such person of shares of common stock or any security convertible into or exercisable or exchangeable for common stock pursuant to a repurchase right arising in connection with the termination of such person’s employment with or provision of services to the Company, provided that (i) any such shares of common stock or any such security are held by such person pursuant to an agreement or equity award granted under a stock incentive plan or other equity award plan, each such agreement or plan which is described in the prospectus and (ii) any public announcement or filing under the Exchange Act shall clearly indicate in the footnotes thereto that such transfer is being made pursuant to the circumstances described in this clause; |
| (j) | transfers to us by any person other than us of shares of common stock or any security convertible into or exercisable or exchangeable for common stock upon a vesting event of the Company’s securities, the settlement of restricted stock units, or the exercise of options or warrants to purchase the Company’s securities on a “cashless” or “net exercise” basis to the extent permitted by the instruments representing such options, restricted stock units or warrants (and any transfer to the Company necessary to generate such amount of cash needed for the payment of taxes, including estimated taxes, due as a result of such vesting, settlement or exercise whether by means of a “net settlement” or otherwise) so long as such “cashless exercise” or “net exercise” is effected solely by the surrender of outstanding options, warrants or restricted stock units (or the common stock issuable upon the exercise or settlement thereof) to us and our cancellation of all or a portion thereof to pay the exercise price and/or withholding tax and remittance obligations, provided that (i) any such shares of common stock received upon such exercise, vesting or settlement shall be subject to the terms of the lock-up agreement, (ii) any such restricted stock units, options, warrants or rights are held by such person pursuant to an agreement or equity award granted under a stock incentive plan or other equity award plan, each such agreement or plan which is described in this prospectus, and provided further that (iii) any public announcement or filing under the Exchange Act shall clearly indicate in the footnotes thereto that the filing relates to the circumstances described in this clause; |
| (k) | transfers by any person than us of shares of common stock or any security convertible into or exercisable or exchangeable for common stock pursuant to a bona fide third-party tender offer, merger, consolidation or other similar transaction that is approved by the board of directors and made to all holders of our capital stock involving a change of control, provided that in the event that such tender offer, merger, consolidation or other similar transaction is not completed, the common stock or securities convertible into or exercisable or exchangeable for common stock held by such person shall remain subject to the provisions of the lock-up agreement; or |
| (l) | facilitating the establishment of a trading plan on behalf of a shareholder, officer or director of the Company pursuant to Rule 10b5-1 under the Exchange Act for the transfer of shares of common stock, provided that (i) such plan does not provide for the transfer of common stock during the restricted period and (ii) to the extent a public announcement or filing under the Exchange Act, if any, is required |
221
Table of Contents
| of or voluntarily made by the Company regarding the establishment of such plan, such announcement or filing shall include a statement to the effect that no transfer of common stock may be made under such plan during the restricted period, |
provided that in the case of any transfer or distribution pursuant to clauses (d) through (h) above, (i) each donee, distributee or transferee shall sign and deliver a lock-up agreement substantially in the form of the agreement signed by the donor, distributor or transferor, (ii) such transfer or distribution shall not involve a disposition for value and (iii) any filing under the Exchange Act reporting a reduction in beneficial ownership of shares of common stock that is required to be made or shall be voluntarily made during the restricted period shall indicate by footnote disclosure or otherwise the nature of such transfer or disposition.
Morgan Stanley & Co. LLC and BofA Securities, Inc., in their sole discretion, may release the common stock and other securities subject to the lock-up agreements described above in whole or in part at any time.
In order to facilitate the offering of the common stock, the underwriters may engage in transactions that stabilize, maintain or otherwise affect the price of the common stock. Specifically, the underwriters may sell more shares than they are obligated to purchase under the underwriting agreement, creating a short position. A short sale is covered if the short position is no greater than the number of shares available for purchase by the underwriters under the over-allotment option described above. The underwriters can close out a covered short sale by exercising the over-allotment option or purchasing shares in the open market. In determining the source of shares to close out a covered short sale, the underwriters will consider, among other things, the open market price of shares compared to the price available under the over-allotment option. The underwriters may also sell shares in excess of the over-allotment option, creating a naked short position. The underwriters must close out any naked short position by purchasing shares in the open market. A naked short position is more likely to be created if the underwriters are concerned that there may be downward pressure on the price of the common stock in the open market after pricing that could adversely affect investors who purchase in this offering. As an additional means of facilitating this offering, the underwriters may bid for, and purchase, shares of common stock in the open market to stabilize the price of the common stock. These activities may raise or maintain the market price of the common stock above independent market levels or prevent or retard a decline in the market price of the common stock. The underwriters are not required to engage in these activities and may end any of these activities at any time.
We and the underwriters have agreed to indemnify each other against certain liabilities, including liabilities under the Securities Act.
A prospectus in electronic format may be made available on websites maintained by one or more underwriters, or selling group members, if any, participating in this offering. The representatives may agree to allocate a number of shares of common stock to underwriters for sale to their online brokerage account holders. Internet distributions will be allocated by the representatives to underwriters that may make Internet distributions on the same basis as other allocations.
Other Relationships
The underwriters and their respective affiliates are full service financial institutions engaged in various activities, which may include securities trading, commercial and investment banking, financial advisory, investment management, investment research, principal investment, hedging, financing and brokerage activities. Certain of the underwriters and their respective affiliates have, from time to time, performed, and may in the future perform, various financial advisory and investment banking services for us, for which they received or will receive customary fees and expenses.
In addition, in the ordinary course of their various business activities, the underwriters and their respective affiliates may make or hold a broad array of investments and actively trade debt and equity securities (or related
222
Table of Contents
derivative securities) and financial instruments (including bank loans) for their own account and for the accounts of their customers and may at any time hold long and short positions in such securities and instruments. Such investment and securities activities may involve our securities and instruments. The underwriters and their respective affiliates may also make investment recommendations or publish or express independent research views in respect of such securities or instruments and may at any time hold, or recommend to clients that they acquire, long or short positions in such securities and instruments.
Pricing of the Offering
Prior to this offering, there has been no public market for our common stock. The initial public offering price was determined by negotiations between us and the representatives. Among the factors considered in determining the initial public offering price were our future prospects and those of our industry in general, our sales, earnings and certain other financial and operating information in recent periods, and the price-earnings ratios, price-sales ratios, market prices of securities, and certain financial and operating information of companies engaged in activities similar to ours.
Reserved Share Program
At our request, an affiliate of , one of the underwriters, has reserved for sale, at the initial public offering price, up to 5% of the common stock offered by this prospectus for sale to certain individuals associated with us through a reserved share program. If these persons purchase reserved shares of common stock, it will reduce the number of shares of common stock available for sale to the general public. Any reserved shares of common stock that are not so purchased will be offered by the underwriters to the general public on the same terms as the other shares of common stock offered by this prospectus.
Selling Restrictions
Canada
The shares of our common stock may be sold only to purchasers purchasing, or deemed to be purchasing, as principal that are accredited investors, as defined in National Instrument 45-106 Prospectus Exemptions or subsection 73.3(1) of the Securities Act (Ontario), and are permitted clients, as defined in National Instrument 31-103 Registration Requirements, Exemptions and Ongoing Registrant Obligations. Any resale of the shares of our common stock must be made in accordance with an exemption from, or in a transaction not subject to, the prospectus requirements of applicable securities laws.
Securities legislation in certain provinces or territories of Canada may provide a purchaser with remedies for rescission or damages if this prospectus (including any amendment thereto) contains a misrepresentation, provided that the remedies for rescission or damages are exercised by the purchaser within the time limit prescribed by the securities legislation of the purchaser’s province or territory. The purchaser should refer to any applicable provisions of the securities legislation of the purchaser’s province or territory for particulars of these rights or consult with a legal advisor.
Pursuant to section 3A.3 (or, in the case of securities issued or guaranteed by the government of a non-Canadian jurisdiction, section 3A.4) of National Instrument 33-105 Underwriting Conflicts (NI 33-105), the underwriters are not required to comply with the disclosure requirements of NI 33-105 regarding underwriter conflicts of interest in connection with this offering.
European Economic Area
In relation to each Member State of the European Economic Area (each, a “Member State”), no securities have been offered or will be offered pursuant to the offering to the public in that Member State prior to the publication of a prospectus in relation to the securities which has been approved by the competent authority in
223
Table of Contents
that Member State or, where appropriate, approved in another Member State and notified to the competent authority in that Member State, all in accordance with the Prospectus Regulation, except that offers of securities may be made to the public in that Member State at any time under the following exemptions under the Prospectus Regulation:
| (a) | to any legal entity which is a qualified investor as defined in the Prospectus Regulation; |
| (b) | to fewer than 150 natural or legal persons (other than qualified investors as defined in the Prospectus Regulation), subject to obtaining the prior consent of the representatives; or |
| (c) | in any other circumstances falling within Article 1(4) of the Prospectus Regulation, |
provided that no such offer of shares shall require us or any of the representatives to publish a prospectus pursuant to Article 3 of the Prospectus Regulation or supplement a prospectus pursuant to Article 23 of the Prospectus Regulation and each person who initially acquires any shares or to whom any offer is made will be deemed to have represented, acknowledged and agreed to and with each of the representatives and us that it is a “qualified investor” as defined in the Prospectus Regulation.
In the case of any shares being offered to a financial intermediary as that term is used in Article 5 of the Prospectus Regulation, each such financial intermediary will be deemed to have represented, acknowledged and agreed that the shares acquired by it in the offer have not been acquired on a nondiscretionary basis on behalf of, nor have they been acquired with a view to their offer or resale to, persons in circumstances which may give rise to an offer of any shares to the public other than their offer or resale in a Member State to qualified investors as so defined or in circumstances in which the prior consent of the representatives has been obtained to each such proposed offer or resale.
For the purposes of this provision, the expression an “offer of shares to the public” in relation to any shares in any Member State means the communication in any form and by means of sufficient information on the terms of the offer and the shares to be offered so as to enable an investor to decide to purchase shares, the expression “Prospectus Regulation” means Regulation (EU) 2017/1129, as amended.
United Kingdom
In relation to the United Kingdom (“UK”), no Shares have been offered or will be offered pursuant to this offering to the public in the UK prior to the publication of a prospectus in relation to the Shares which has been approved by the Financial Conduct Authority in the UK in accordance with the UK Prospectus Regulation and the FSMA, except that offers of Shares may be made to the public in the UK at any time under the following exemptions under the UK Prospectus Regulation and the FSMA:
| a. | to any legal entity which is a qualified investor as defined under the UK Prospectus Regulation; |
| b. | to fewer than 150 natural or legal persons (other than qualified investors as defined under the UK Prospectus Regulation); or |
| c. | at any time in other circumstances falling within section 86 of the FSMA, |
provided that no such offer of Shares shall require the Issuer or any Manager to publish a prospectus pursuant to Section 85 of the FSMA or Article 3 of the UK Prospectus Regulation or supplement a prospectus pursuant to Article 23 of the UK Prospectus Regulation.
Notwithstanding the above, each person in the UK who initially acquires any Shares or to whom any offer is made will be deemed to have represented, acknowledged and agreed to and with the Company and the Managers that it is a qualified investor within the meaning of the UK Prospectus Regulation.
224
Table of Contents
In the case of any Shares being offered to a financial intermediary as that term is used in Article 5(1) of the UK Prospectus Regulation, each such financial intermediary will be deemed to have represented, acknowledged and agreed that the Shares acquired by it in the offer have not been acquired on a non-discretionary basis on behalf of, nor have they been acquired with a view to their offer or resale to, persons in circumstances which may give rise to an offer to the public other than their offer or resale in the UK to qualified investors, in circumstances in which the prior consent of the representatives has been obtained to each such proposed offer or resale.
The Company, the underwriters and their affiliates will rely upon the truth and accuracy of the foregoing representations, acknowledgements and agreements.
For the purposes of this provision, the expression an “offer to the public” in relation to any Shares in the UK means the communication in any form and by any means of sufficient information on the terms of the offer and any Shares to be offered so as to enable an investor to decide to purchase or subscribe for any Shares, the expression “UK Prospectus Regulation” means Regulation (EU) 2017/1129 as it forms part of domestic law by virtue of the European Union (Withdrawal) Act 2018, and the expression “FSMA” means the Financial Services and Markets Act 2000.
In connection with the offering, the underwriters are not acting for anyone other than the issuer and will not be responsible to anyone other than the issuer for providing the protections afforded to their clients nor for providing advice in relation to the offering.
Notice to Prospective Investors in Singapore
This prospectus has not been registered as a prospectus with the Monetary Authority of Singapore. Accordingly, the common stock was not offered or sold or caused to be made the subject of an invitation for subscription or purchase and will not be offered or sold or caused to be made the subject of an invitation for subscription or purchase, and this prospectus or any other document or material in connection with the offer or sale, or invitation for subscription or purchase, of the common stock, has not been circulated or distributed, nor will it be circulated or distributed, whether directly or indirectly, to any person in Singapore other than (i) to an institutional investor (as defined in Section 4A of the Securities and Futures Act (Chapter 289) of Singapore, as modified or amended from time to time (the “SFA”)) pursuant to Section 274 of the SFA, (ii) to a relevant person (as defined in Section 275(2) of the SFA) pursuant to Section 275(1) of the SFA, or any person pursuant to Section 275(1A) of the SFA, and in accordance with the conditions specified in Section 275 of the SFA, or (iii) otherwise pursuant to, and in accordance with the conditions of, any other applicable provision of the SFA.
Where the common stock is subscribed or purchased under Section 275 of the SFA by a relevant person which is:
| (a) | a corporation (which is not an accredited investor (as defined in Section 4A of the SFA)) the sole business of which is to hold investments and the entire share capital of which is owned by one or more individuals, each of whom is an accredited investor; or |
| (b) | a trust (where the trustee is not an accredited investor) whose sole purpose is to hold investments and each beneficiary of the trust is an individual who is an accredited investor, |
securities or securities-based derivatives contracts (each term as defined in Section 2(1) of the SFA) of that corporation or the beneficiaries’ rights and interest (howsoever described) in that trust shall not be transferred within six months after that corporation or that trust has acquired the common stock pursuant to an offer made under Section 275 of the SFA except:
| (a) | to an institutional investor or to a relevant person, or to any person arising from an offer referred to in Section 275(1A) or Section 276(4)(i)(B) of the SFA; |
| (b) | where no consideration is or will be given for the transfer; |
225
Table of Contents
| (c) | where the transfer is by operation of law; or |
| (d) | as specified in Section 276(7) of the SFA. |
Notice to Prospective Investors in Switzerland
The shares may not be publicly offered in Switzerland and will not be listed on the SIX Swiss Exchange (“SIX”) or on any other stock exchange or regulated trading facility in Switzerland. This document has been prepared without regard to the disclosure standards for issuance prospectuses under art. 652a or art. 1156 of the Swiss Code of Obligations or the disclosure standards for listing prospectuses under art. 27 ff. of the SIX Listing Rules or the listing rules of any other stock exchange or regulated trading facility in Switzerland. Neither this document nor any other offering or marketing material relating to the shares or the offering may be publicly distributed or otherwise made publicly available in Switzerland.
Neither this document nor any other offering or marketing material relating to the offering, the Company, the shares have been or will be filed with or approved by any Swiss regulatory authority. In particular, this document will not be filed with, and the offer of shares will not be supervised by, the Swiss Financial Market Supervisory Authority FINMA (FINMA), and the offer of shares has not been and will not be authorized under the Swiss Federal Act on Collective Investment Schemes (“CISA”). The investor protection afforded to acquirers of interests in collective investment schemes under the CISA does not extend to acquirers of shares.
Notice to Prospective Investors in Australia
No placement document, prospectus, product disclosure statement or other disclosure document has been lodged with the Australian Securities and Investments Commission (“ASIC”), in relation to the offering. This prospectus does not constitute a prospectus, product disclosure statement or other disclosure document under the Corporations Act 2001 (the “Corporations Act”), and does not purport to include the information required for a prospectus, product disclosure statement or other disclosure document under the Corporations Act.
Any offer in Australia of the common stock may only be made to persons (the “Exempt Investors”) who are “sophisticated investors” (within the meaning of section 708(8) of the Corporations Act), “professional investors” (within the meaning of section 708(11) of the Corporations Act) or otherwise pursuant to one or more exemptions contained in section 708 of the Corporations Act so that it is lawful to offer the common stock without disclosure to investors under Chapter 6D of the Corporations Act.
The common stock applied for by Exempt Investors in Australia must not be offered for sale in Australia in the period of 12 months after the date of allotment under the offering, except in circumstances where disclosure to investors under Chapter 6D of the Corporations Act would not be required pursuant to an exemption under section 708 of the Corporations Act or otherwise or where the offer is pursuant to a disclosure document which complies with Chapter 6D of the Corporations Act. Any person acquiring the common stock must observe such Australian on-sale restrictions.
This prospectus contains general information only and does not take account of the investment objectives, financial situation or particular needs of any particular person. It does not contain any securities recommendations or financial product advice. Before making an investment decision, investors need to consider whether the information in this prospectus is appropriate to their needs, objectives and circumstances, and, if necessary, seek expert advice on those matters.
Notice to Prospective Investors in the Dubai International Financial Centre
This prospectus relates to an Exempt Offer in accordance with the Offered Securities Rules of the Dubai Financial Services Authority (“DFSA”). This prospectus is intended for distribution only to persons of a type specified in the Offered Securities Rules of the DFSA. It must not be delivered to, or relied on by, any other
226
Table of Contents
person. The DFSA has no responsibility for reviewing or verifying any documents in connection with Exempt Offers. The DFSA has not approved this prospectus nor taken steps to verify the information set forth herein and has no responsibility for the prospectus. The common stock to which this prospectus relates may be illiquid and/or subject to restrictions on their resale. Prospective purchasers of the common stock offered should conduct their own due diligence on the common stock. If you do not understand the contents of this prospectus you should consult an authorized financial advisor.
Notice to Prospective Investors in Hong Kong
The common stock has not been offered or sold and will not be offered or sold in Hong Kong, by means of any document, other than (a) to “professional investors” as defined in the Securities and Futures Ordinance (Cap. 571) of Hong Kong and any rules made under that Ordinance; or (b) in other circumstances which do not result in the document being a “prospectus” as defined in the Companies Ordinance (Cap. 32) of Hong Kong or which do not constitute an offer to the public within the meaning of that Ordinance. No advertisement, invitation or document relating to the common stock has been or may be issued or has been or may be in the possession of any person for the purposes of issue, whether in Hong Kong or elsewhere, which is directed at, or the contents of which are likely to be accessed or read by, the public of Hong Kong (except if permitted to do so under the securities laws of Hong Kong) other than with respect to the common stock which are or are intended to be disposed of only to persons outside Hong Kong or only to “professional investors” as defined in the Securities and Futures Ordinance and any rules made under that Ordinance.
Japan
No registration pursuant to Article 4, paragraph 1 of the Financial Instruments and Exchange Law of Japan (Law No. 25 of 1948, as amended) (the “FIEL”) has been made or will be made with respect to the solicitation of the application for the acquisition of the shares of common stock.
Accordingly, the shares of common stock have not been, directly or indirectly, offered or sold and will not be, directly or indirectly, offered or sold in Japan or to, or for the benefit of, any resident of Japan (which term as used herein means any person resident in Japan, including any corporation or other entity organized under the laws of Japan) or to others for re-offering or re-sale, directly or indirectly, in Japan or to, or for the benefit of, any resident of Japan except pursuant to an exemption from the registration requirements, and otherwise in compliance with, the FIEL and the other applicable laws and regulations of Japan.
For Qualified Institutional Investors (“QII”)
Please note that the solicitation for newly-issued or secondary securities (each as described in Paragraph 2, Article 4 of the FIEL) in relation to the shares of common stock constitutes either a “QII only private placement” or a “QII only secondary distribution” (each as described in Paragraph 1, Article 23-13 of the FIEL). Disclosure regarding any such solicitation, as is otherwise prescribed in Paragraph 1, Article 4 of the FIEL, has not been made in relation to the shares of common stock. The shares of common stock may only be transferred to QIIs.
For Non-QII Investors
Please note that the solicitation for newly-issued or secondary securities (each as described in Paragraph 2, Article 4 of the FIEL) in relation to the shares of common stock constitutes either a “small number private placement” or a “small number private secondary distribution” (each as described in Paragraph 4, Article 23-13 of the FIEL). Disclosure regarding any such solicitation, as is otherwise prescribed in Paragraph 1, Article 4 of the FIEL, has not been made in relation to the shares of common stock. The shares of common stock may only be transferred en bloc without subdivision to a single investor.
227
Table of Contents
The validity of the shares of common stock offered hereby will be passed upon for us by Latham & Watkins LLP. Certain legal matters will be passed upon for the underwriters by Davis, Polk & Wardwell LLP. Latham & Watkins LLP and certain attorneys and investment funds affiliated with the firm own shares of our convertible preferred stock which will be converted into less than 1% of our common stock upon the completion of this offering.
The financial statements as of December 31, 2018, 2019 and 2020, and for each of the three years in the period ended December 31, 2020, included in this Registration Statement have been audited by Deloitte & Touche LLP, an independent registered public accounting firm, as stated in their report appearing herein. Such financial statements are included in reliance upon the report of such firm given upon their authority as experts in accounting and auditing.
WHERE YOU CAN FIND MORE INFORMATION
We have filed with the Securities and Exchange Commission a registration statement on Form S-1 under the Securities Act with respect to the shares of common stock offered hereby. This prospectus, which constitutes a part of the registration statement, does not contain all of the information set forth in the registration statement or the exhibits and schedules filed therewith. For further information about us and the common stock offered hereby, we refer you to the registration statement and the exhibits and schedules filed thereto. Statements contained in this prospectus regarding the contents of any contract or any other document that is filed as an exhibit to the registration statement are not necessarily complete, and each such statement is qualified in all respects by reference to the full text of such contract or other document filed as an exhibit to the registration statement. Upon completion of this offering, we will be required to file periodic reports, proxy statements, and other information with the Securities and Exchange Commission pursuant to the Securities Exchange Act of 1934. The Securities and Exchange Commission maintains an Internet website that contains reports, proxy statements and other information about registrants, like us, that file electronically with the Securities and Exchange Commission. The address of that site is www.sec.gov.
228
Table of Contents
SIGHT SCIENCES, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
F-1
Table of Contents
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the shareholders and the Board of Directors of Sight Sciences, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Sight Sciences, Inc. and subsidiary (the “Company”) as of December 31, 2020, 2019, and 2018, the related consolidated statements of operations and comprehensive loss, redeemable convertible preferred stock and stockholders’ deficit, and cash flows for each of the three years in the period ended December 31, 2020, and the related notes (collectively referred to as the “financial statements”). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2020, 2019 and 2018, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2020, in conformity with accounting principles generally accepted in the United States of America.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. As part of our audits, we are required to obtain an understanding of internal control over financial reporting but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion.
Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Deloitte & Touche LLP
San Jose, California
April 9, 2021
We have served as the Company’s auditor since 2019.
F-2
Table of Contents
(In thousands, except share and per share amounts)
| As of December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Assets | ||||||||||||
Current assets: | ||||||||||||
Cash and cash equivalents | $ | 4,242 | $ | 21,237 | $ | 61,511 | ||||||
Accounts receivable, net | 1,815 | 4,094 | 5,363 | |||||||||
Inventory, net | 486 | 2,244 | 2,598 | |||||||||
Prepaid expenses and other current assets | 621 | 426 | 1,161 | |||||||||
|
|
|
|
|
| |||||||
Total current assets | 7,164 | 28,001 | 70,633 | |||||||||
Property and equipment, net | 868 | 1,491 | 1,269 | |||||||||
Operating lease ROU assets | — | 1,081 | 518 | |||||||||
Other noncurrent assets | 62 | 168 | 386 | |||||||||
|
|
|
|
|
| |||||||
Total assets | $ | 8,094 | $ | 30,741 | $ | 72,806 | ||||||
|
|
|
|
|
| |||||||
Liabilities, redeemable convertible preferred stock, and Stockholders’ deficit | ||||||||||||
Current liabilities: | ||||||||||||
Accounts payable | $ | 1,879 | $ | 2,315 | $ | 2,158 | ||||||
Accrued compensation | 689 | 2,170 | 4,070 | |||||||||
Accrued and other current liabilities | 328 | 2,851 | 3,086 | |||||||||
|
|
|
|
|
| |||||||
Total current liabilities | 2,896 | 7,336 | 9,314 | |||||||||
Long-term debt | — | 12,855 | 31,955 | |||||||||
Other noncurrent liabilities | 7 | 977 | 3,055 | |||||||||
|
|
|
|
|
| |||||||
Total liabilities | 2,903 | 21,168 | 44,324 | |||||||||
|
|
|
|
|
| |||||||
Commitments and contingencies (Note 6) | ||||||||||||
Redeemable convertible preferred stock: | ||||||||||||
Convertible Preferred Stock, $0.001 par value; 7,413,965, 9,894,056, and 14,241,390 shares authorized as of December 31, 2018, 2019, and 2020, respectively; 7,356,822, 9,804,640, and 12,767,202 shares issued and outstanding as of December 31, 2018, 2019 and 2020, respectively; aggregate liquidation preference of $34.5 million, $65.2 million, and $118.6 million as of December 31, 2018, 2019, and 2020, respectively | 34,153 | 64,256 | 117,331 | |||||||||
Stockholders’ deficit: | ||||||||||||
Common stock par value of $0.001 per share—16,000,000 shares authorized at December 31, 2018, 17,000,000 shares authorized at December 31, 2019, and 21,831,000 shares authorized at December 31, 2020; 4,596,003 shares issued and outstanding at December 31, 2018, 4,659,733 shares issued and outstanding as of December 31, 2019, and 4,754,591 shares issued and outstanding as of December 31, 2020 | 5 | 5 | 5 | |||||||||
Additional paid-in capital | 512 | 660 | 1,187 | |||||||||
Accumulated deficit | (29,479 | ) | (55,348 | ) | (90,041 | ) | ||||||
|
|
|
|
|
| |||||||
Total stockholders’ deficit | (28,962 | ) | (54,683 | ) | (88,849 | ) | ||||||
|
|
|
|
|
| |||||||
Total liabilities, redeemable convertible preferred stock, and stockholders’ deficit | $ | 8,094 | $ | 30,741 | $ | 72,806 | ||||||
|
|
|
|
|
| |||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-3
Table of Contents
SIGHT SCIENCES, INC.
Consolidated Statements of Operations and Comprehensive Loss
(In thousands, except share and per share data)
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Revenue | $ | 7,530 | $ | 23,348 | $ | 27,640 | ||||||
Cost of goods sold | 2,338 | 6,544 | 9,209 | |||||||||
|
|
|
|
|
| |||||||
Gross profit | 5,192 | 16,804 | 18,431 | |||||||||
Operating expenses: | ||||||||||||
Research and development | 5,426 | 8,124 | 8,874 | |||||||||
Selling, general, and administrative | 14,063 | 32,719 | 41,745 | |||||||||
|
|
|
|
|
| |||||||
Total operating expenses | 19,489 | 40,843 | 50,619 | |||||||||
|
|
|
|
|
| |||||||
Loss from operations | (14,297 | ) | (24,039 | ) | (32,188 | ) | ||||||
Interest income | 1 | 174 | 30 | |||||||||
Interest expense | — | (1,961 | ) | (2,403 | ) | |||||||
Other income (expense), net | — | (35 | ) | (71 | ) | |||||||
|
|
|
|
|
| |||||||
Loss before income taxes | (14,296 | ) | (25,861 | ) | (34,632 | ) | ||||||
Provision (benefit) for income taxes | (6 | ) | 8 | 61 | ||||||||
|
|
|
|
|
| |||||||
Net loss and comprehensive loss | $ | (14,290 | ) | $ | (25,869 | ) | $ | (34,693 | ) | |||
|
|
|
|
|
| |||||||
Net loss per share outstanding attributable to common stockholders, basic and diluted | $ | (3.10 | ) | $ | (5.51 | ) | $ | (7.41 | ) | |||
|
|
|
|
|
| |||||||
Weighted-average common shares outstanding used in computing net loss per share attributable to common stockholders, basic and diluted | 4,611,325 | 4,693,534 | 4,678,109 | |||||||||
|
|
|
|
|
| |||||||
Pro forma net loss per share, basic and diluted (unaudited) | ||||||||||||
|
| |||||||||||
Weighted-average shares outstanding used in computing pro forma net loss per share, basic and diluted (unaudited) | ||||||||||||
|
| |||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-4
Table of Contents
SIGHT SCIENCES, INC.
Consolidated Statements of Redeemable Convertible Preferred Stock and Stockholders’ Deficit
(In thousands, except share amounts)
| Redeemable Convertible Preferred Stock | Common Stock | Additional Paid-In Capital | Accumulated Deficit | Total Stockholders’ Deficit | ||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||
Balances at January 1, 2018 | 6,068,061 | $ | 21,973 | 4,541,754 | $ | 5 | $ | 437 | $ | (15,189 | ) | $ | (14,747 | ) | ||||||||||||||
Issuance of Series C redeemable convertible preferred stock, net of issuance costs of $46 | 1,288,761 | 12,180 | — | — | — | — | — | |||||||||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 54,249 | — | 23 | — | 23 | |||||||||||||||||||||
Stock-based compensation expense | — | — | — | — | 52 | — | 52 | |||||||||||||||||||||
Net loss | — | — | — | — | — | (14,290 | ) | (14,290 | ) | |||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
Balances at December 31, 2018 | 7,356,822 | 34,153 | 4,596,003 | 5 | 512 | (29,479 | ) | (28,962 | ) | |||||||||||||||||||
Issuance of Series D redeemable convertible preferred stock, net of issuance costs of $647 | 2,447,818 | 30,103 | — | — | — | — | — | |||||||||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 63,730 | — | 30 | — | 30 | |||||||||||||||||||||
Stock-based compensation expense | — | — | — | — | 118 | — | 118 | |||||||||||||||||||||
Net loss | — | — | — | — | — | (25,869 | ) | (25,869 | ) | |||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
Balances at December 31, 2019 | 9,804,640 | 64,256 | 4,659,733 | 5 | 660 | (55,348 | ) | (54,683 | ) | |||||||||||||||||||
Issuance of Series E redeemable convertible preferred stock, net of issuance costs of $106 | 1,899,847 | 30,044 | — | — | — | — | — | |||||||||||||||||||||
Issuance of Series F redeemable convertible preferred stock, net of issuance costs of $219 | 1,062,715 | 23,031 | — | — | — | — | — | |||||||||||||||||||||
Issuance of common stock upon exercise of common stock warrants | — | — | 64,655 | — | 6 | — | 6 | |||||||||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 30,203 | — | 24 | — | 24 | |||||||||||||||||||||
Stock-based compensation expense | — | — | — | — | 497 | — | 497 | |||||||||||||||||||||
Net loss | — | — | — | — | — | (34,693 | ) | (34,693 | ) | |||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
Balances at December 31, 2020 | 12,767,202 | $ | 117,331 | 4,754,591 | $ | 5 | $ | 1,187 | $ | (90,041 | ) | $ | (88,849 | ) | ||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Table of Contents
SIGHT SCIENCES, INC.
Consolidated Statements of Cash Flows
(In thousands)
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Cash flows from operating activities | ||||||||||||
Net loss | $ | (14,290 | ) | $ | (25,869 | ) | $ | (34,693 | ) | |||
Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||||||
Depreciation | 63 | 295 | 554 | |||||||||
Accretion of debt discount and amortization of debt issuance costs | — | 525 | 574 | |||||||||
Stock-based compensation expense | 52 | 118 | 497 | |||||||||
Provision for doubtful accounts receivable | 58 | 41 | 209 | |||||||||
Provision for excess and obsolete inventories | — | 41 | 1,362 | |||||||||
Noncash operating lease expense | — | 137 | 563 | |||||||||
Change in fair value of redeemable convertible preferred stock warrant | — | 35 | 64 | |||||||||
Loss on disposal of property and equipment | — | 21 | 158 | |||||||||
Proceeds from Paycheck Protection Program loan | — | — | (2,246 | ) | ||||||||
Changes in operating assets and liabilities: | ||||||||||||
Accounts receivable | (1,415 | ) | (2,320 | ) | (1,477 | ) | ||||||
Inventory | (184 | ) | (1,799 | ) | (1,716 | ) | ||||||
Prepaid expenses and other current assets | (560 | ) | 196 | (735 | ) | |||||||
Other noncurrent assets | 5 | (106 | ) | (237 | ) | |||||||
Accounts payable | 1,003 | 168 | 448 | |||||||||
Accrued compensation | 503 | 1,481 | 1,900 | |||||||||
Accrued and other current liabilities | 289 | 1,826 | 1,987 | |||||||||
Other noncurrent liabilities | 1 | 213 | 614 | |||||||||
|
|
|
|
|
| |||||||
Net cash used in operating activities | (14,475 | ) | (24,997 | ) | (32,174 | ) | ||||||
|
|
|
|
|
| |||||||
Cash flows from investing activities | ||||||||||||
Purchases of property and equipment | (570 | )�� | (672 | ) | (953 | ) | ||||||
|
|
|
|
|
| |||||||
Net cash used in investing activities | (570 | ) | (672 | ) | (953 | ) | ||||||
|
|
|
|
|
| |||||||
Cash flows from financing activities | ||||||||||||
Proceeds from the issuance of debt (Term Loan) | — | 14,000 | 20,480 | |||||||||
Debt issuance costs | — | (1,469 | ) | (142 | ) | |||||||
Payments of costs related to initial public offering | — | — | (42 | ) | ||||||||
Proceeds from the issuance of Series C redeemable convertible preferred stock | 12,226 | — | — | |||||||||
Series C issuance costs | (46 | ) | — | — | ||||||||
Proceeds from the issuance of Series D redeemable convertible preferred stock | — | 30,750 | — | |||||||||
Series D issuance costs | — | (647 | ) | — | ||||||||
Proceeds from the issuance of Series E redeemable convertible preferred stock | — | — | 30,150 | |||||||||
Series E issuance costs | — | — | (106 | ) | ||||||||
Proceeds from the issuance of Series F redeemable convertible preferred stock | — | — | 23,250 | |||||||||
Series F issuance costs | — | — | (219 | ) | ||||||||
Proceeds from exercise of common stock warrants | — | — | 6 | |||||||||
Proceeds from exercise of stock options | 23 | 30 | 24 | |||||||||
|
|
|
|
|
| |||||||
Net cash provided by financing activities | 12,203 | 42,664 | 73,401 | |||||||||
|
|
|
|
|
| |||||||
Net change in cash and cash equivalents | (2,842 | ) | 16,995 | 40,274 | ||||||||
Cash and cash equivalents | ||||||||||||
Beginning of year | 7,084 | 4,242 | 21,237 | |||||||||
|
|
|
|
|
| |||||||
End of year | $ | 4,242 | $ | 21,237 | $ | 61,511 | ||||||
|
|
|
|
|
| |||||||
Supplemental disclosure of cash flow information | ||||||||||||
Cash paid for interest | $ | — | $ | 1,149 | $ | 1,286 | ||||||
Supplemental noncash disclosure | ||||||||||||
Acquisition of property and equipment included in accounts payable and accrued liabilities | $ | 237 | $ | 505 | $ | 41 | ||||||
Unpaid initial public offering costs in accounts payable and accrued liabilities | — | — | 325 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-6
Table of Contents
SIGHT SCIENCES, INC.
Notes to Consolidated Financial Statements
Note 1. Company and Nature of Business
Description of Business
Sight Sciences, Inc. (the “Company”) was incorporated in the state of Delaware in 2010. The Company is an ophthalmic medical device company focused on the development and commercialization of surgical and nonsurgical technologies for the treatment of prevalent eye diseases. The Company’s surgical glaucoma product portfolio features the OMNI Surgical System, a device that facilitates the performance of both trabeculotomy and canaloplasty with a single device and single corneal incision. The Company’s nonsurgical dry eye product portfolio consists of the TearCare system for ophthalmologists and optometrists. TearCare is a wearable eyelid technology that delivers highly targeted and adjustable heat to the meibomian glands of the eyelids.
The Company is located and headquartered in Menlo Park, California. The other office operated by the Company is in Southlake, Texas. All of the Company’s current operations are conducted in the United States.
Significant Risks and Uncertainties
Since inception, the Company has incurred losses and negative cash flows from operations. As of December 31, 2020, the Company had an accumulated deficit of $90.0 million and recorded a net loss of $34.7 million for the year then ended and expects to incur future additional losses. If the Company’s revenue levels from its products are not sufficient or if the Company is unable to secure additional funding when desired, the Company may need to delay the development of its products and scale back its business and operations.
The Company believes that its existing sources of liquidity will satisfy its working capital and capital requirements for at least 12 months from the issuance of its financial statements. Failure to generate sufficient revenues, achieve planned gross margins, or control operating costs will require the Company to raise additional capital through equity or debt financing. Such additional financing may not be available on acceptable terms, or at all, and could require the Company to modify, delay, or abandon some of its planned future expansion or expenditures or reduce some of its ongoing operating costs, which could harm its business, operating results, financial condition, and ability to achieve its intended business objectives.
On March 11, 2020, the World Health Organization declared the coronavirus disease 2019 (“COVID-19”) outbreak a global pandemic recommending containment measures worldwide. On March 16, 2020 the Company implemented alternative work arrangements for its employees and limited its employees’ travel activities to protect its employees and to comply with the provisions described within the local shelter in place order. Certain U.S. federal, state and local governmental authorities issued other orders and directives, including restrictions on elective procedures and therapies, aimed at minimizing the spread of COVID-19. As such, the COVID-19 pandemic impacted and is expected to continue to impact demand for the Company’s products, which are used in procedures and therapies that are considered elective. Although some of the governmental restrictions have since been lifted or scaled back, recent and future surges of COVID-19 may result in restrictions being re-implemented in response to efforts to reduce the spread of COVID-19.
The ultimate impact of the COVID-19 pandemic on the Company’s operations is unknown and will depend on future developments which are highly uncertain and cannot be predicted with confidence, including the duration and severity of the COVID-19 outbreak, the status of health and safety actions taken to contain its spread and any additional preventative and protective actions that governments, or the Company, may direct, any resurgence of COVID-19 that may occur and how quickly and to what extent economic and operating conditions normalize within the markets in which the Company operates. The COVID-19 pandemic could disrupt the operations of the Company’s third-party manufacturers and other suppliers. Although the Company has not experienced disruptions in its supply chain to date, it cannot predict how long the pandemic and measures
F-7
Table of Contents
intended to contain the spread of COVID-19 will continue and what effect COVID-19 and the associated containment measures will have on our suppliers and vendors, in particular for any of the Company’s suppliers and vendors that may not qualify as essential businesses and suffer more significant disruptions to their business operations. The Company is working closely with its manufacturing partners and suppliers to help ensure the Company is able to source key components and maintain appropriate inventory levels to meet customer demand.
Note 2. Summary of Significant Accounting Policies
Basis of Presentation
The consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (US GAAP). The Company’s consolidated financial statements include the accounts of the Company and its wholly owned subsidiary, Sight Sciences UK, Ltd. All intercompany balances and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of financial statements in conformity with US GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities, disclosure of contingent assets and liabilities at the date of the financial statements, and the reported amounts of revenues and expense during the reporting period. The most significant estimates related to inventory excess and obsolescence, the selection of useful lives of property and equipment, determination of the fair value of stock option grants, the fair value of the redeemable convertible preferred stock warrants, and provisions for income taxes and contingencies. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. These estimates are based on information available as of the date of the financial statements. Actual results could differ from these estimates and such differences could be material to the Company’s financial position and results of operations.
Unaudited Pro Forma Information
The unaudited pro forma basic and diluted net loss per share data has been computed to give effect to an adjustment to the denominator in the pro forma basic and diluted net loss per share calculation for the conversion of the redeemable convertible preferred stock into shares of common stock as of the beginning of the period or the date of issuance, if later. The numerator in the pro forma basic and diluted net loss per share calculation has been adjusted to remove gains or losses resulting from the remeasurement of the redeemable convertible preferred stock warrant liability.
Fair Value of Financial Instruments
The Company’s financial instruments consist of cash and cash equivalents, accounts receivable, accounts payable, accrued liabilities, redeemable convertible preferred stock, short-term and long-term debt and redeemable convertible preferred stock warrant liability. The Company states accounts receivable, accounts payable, and accrued and other current liabilities at their carrying value, which approximates fair value due to the short time to the expected receipt or payment. The carrying amount of the Company’s short-term debt approximates its fair value as the effective interest rate approximates market rates currently available to the Company. The redeemable convertible preferred stock warrant liability associated with the Company’s redeemable convertible preferred stock is carried at fair value based on unobservable market inputs.
Concentration of Credit Risk
Financial instruments that subject the Company to concentration of credit risk consist of cash and cash equivalents and accounts receivable. The Company’s cash and cash equivalents are deposited with a high-quality
F-8
Table of Contents
financial institution. Deposits at this institution may, at times, exceed federally insured limits. Management believes that this financial institution is financially sound and, accordingly, that minimal credit risk exists. The Company has not experienced any losses on its deposits of cash and cash equivalents.
The Company relies on third-party contract manufacturers for the manufacture of all of our commercial products currently available for sale. Disruption in production would have a negative impact on the Company’s financial position, results of operations and cash flows.
The Company provides for uncollectible amounts when specific credit problems are identified. In doing so, the Company analyzes historical bad debt trends, customer creditworthiness, current economic trends, and changes in customer payment patterns when evaluating the adequacy of the allowance for doubtful accounts.
The Company’s accounts receivable are due from a variety of health care organizations. At December 31, 2018, 2019 and 2020, no customer represented 10% or more of the Company’s accounts receivable. For the years ended December 31, 2018, 2019 and 2020, there were no customers that represented 10% or more of revenue.
Deferred Offering Costs
Deferred offering costs, consisting of legal, accounting and other fees and costs relating to the Company’s planned IPO, are capitalized and recorded on the balance sheet. The deferred offering costs will be offset against the proceeds received upon the closing of the planned IPO. In the event that the Company’s plans for an IPO are terminated, all of the deferred offering costs will be written off within operating expenses in the Company’s statements of operations and comprehensive loss. As of December 31, 2020, deferred offering costs of $0.4 million were capitalized and are included in “Other noncurrent assets”. There were no deferred offering costs capitalized as of December 31, 2018 and 2019.
Cash and Cash Equivalents
The Company considers all highly liquid investments with an original maturity of three months or less when purchased to be cash and cash equivalents. Cash and cash equivalents are recorded at cost, which approximate fair value. As of December 31, 2018, 2019 and 2020, cash consists primarily of checking and savings deposits. The Company’s cash balances exceed those that are federally insured. To date, the Company has not recognized any losses caused by uninsured balances.
Accounts Receivable and Provision for Doubtful Accounts
Accounts receivable are stated at invoiced amounts, net of estimated provisions for doubtful accounts. The majority of customers are not extended credit and, therefore, time to maturity for receivables is short. The Company makes estimates of the collectability of customer accounts and provisions based primarily on analysis of historical trends and experience and changes in customers’ financial condition. The Company uses its judgment, based on the best available facts and circumstances, and records a provision against amounts due to reduce the receivable to the amount that is expected to be collected. These specific provisions are reevaluated and adjusted as additional information is received that impacts the amount reserved. To date, the Company has not experienced material credit-related losses. The provision for doubtful accounts was $0.1 million, $0.1 million and $0.3 million as of December 31, 2018, 2019 and 2020, respectively.
Inventory
Inventory represents finished goods purchased from a third-party manufacturer and is valued at the lower of cost or net realizable value. Cost is determined using actual costs on a first-in, first-out basis for all inventory. Net realizable value is determined as the estimated selling prices in the ordinary course of business, less reasonably predictable costs of completion, disposal, and transportation. The Company regularly reviews
F-9
Table of Contents
inventory quantities in consideration of actual loss experiences, projected future demand, and remaining shelf life to record a provision for excess and obsolete inventory when appropriate. The Company’s policy is to write down inventory that has become obsolete, inventory that has a cost basis in excess of its expected lower of cost or net realizable value, and inventory in excess of expected requirements. The estimate of excess quantities is judgmental and primarily dependent on the Company’s estimates of future demand for the particular product.
Property and Equipment, net
Property and equipment are recorded at cost, less accumulated depreciation. Repairs and maintenance costs are expensed as incurred. Depreciation is calculated using the straight-line method over the estimated useful lives of the assets, typically two to five years. When assets are retired or otherwise disposed of, the cost and accumulated depreciation are removed from the balance sheet and any resulting gain or loss is reflected in operations in the period realized.
Construction-in-process assets consist primarily of tools and equipment that have not yet been placed in service. These assets are stated at cost and are not depreciated. Once the assets are placed into service, assets are reclassified to the appropriate asset class based on their nature and depreciated in accordance with the useful lives above.
Impairment of Long-Lived Assets
The Company assesses long-lived assets, including property and equipment, whenever events or changes in business circumstances indicate that the carrying amount of the assets may not be fully recoverable. If indicators of impairment exist, an impairment loss would be recognized when estimated undiscounted future cash flows expected to result from the use of the assets and their eventual disposition are less than their carrying amount. Impairment, if any, is measured as the amount by which the carrying amount of the long-lived assets exceeds their fair value. Fair value is determined through various valuation techniques, including discounted cash flow models, quoted market values, and third-party independent appraisals, as considered necessary. The Company did not record any impairment of long-lived assets for the years ended December 31, 2018, 2019 and 2020.
Leases
Contractual arrangements that meet the definition of a lease are classified as operating or finance leases and are recorded on the balance sheets as both a right-of-use asset (“ROU asset”) and lease liability, calculated by discounting fixed lease payments over the lease term at the Company’s incremental borrowing rate (“IBR”). Lease ROU assets and lease obligations are recognized based on the present value of the future minimum lease payments over the lease term at commencement date. The Company currently does not have any finance leases.
Operating lease ROU assets are adjusted for (i) payments made at or before the commencement date, (ii) initial direct costs incurred, and (iii) tenant incentives under the lease. As the implicit rates for the operating leases are not determinable, the Company uses an IBR based on the information available at the respective lease commencement dates to determine the present value of future payments. IBR represents the interest rate that the Company would expect to incur at lease commencement to borrow an amount equal to the lease payments on a collateralized basis with similar terms and payments, in an economic environment where the leased asset is located. The Company considers a lease term to be the noncancelable period that it has the right to use the underlying asset, including any periods where it is reasonably certain the Company will exercise any option to extend the contract.
Lease costs for minimum lease payments for operating leases are recognized on a straight-line basis over the lease term. Lease liabilities are increased by interest and reduced by payments each period, and the ROU asset is amortized over the lease term. Variable lease payments that do not depend on an index or rate are recognized as lease costs when incurred. In measuring the ROU assets and lease liabilities, the Company has elected to combine
F-10
Table of Contents
lease and non-lease components. The Company does not recognize ROU assets or lease liabilities for short-term leases, if any, having initial terms of 12 months or less at lease commencement as an accounting policy election, and recognizes rent expense on a straight-line basis over the lease term for these types of leases.
Redeemable Convertible Preferred Stock Warrants
The Company’s redeemable convertible preferred stock warrants require liability classification and accounting as the underlying redeemable convertible preferred stock is considered contingently redeemable and may obligate the Company to transfer assets to the holders at a future date upon occurrence of a deemed liquidation event. The warrants are recorded at fair value upon issuance and are subject to remeasurement to fair value at each balance sheet date, with any changes in fair value recognized as other expense in the statements of operations. The warrants liability is recorded as other noncurrent liabilities in the balance sheets. The Company will continue to adjust the warrant liability for changes in fair value until the earlier of the exercise or expiration of the redeemable convertible preferred stock warrants, occurrence of a deemed liquidation event, or conversion of redeemable convertible preferred stock into common stock. At that time, the liability associated with the redeemable convertible preferred stock warrants that are converted into warrants to purchase common stock will be reclassified to additional paid-in capital, while the liability associated with any expired warrants will be recognized as a gain within the statements of operations and comprehensive loss. As a result, the redeemable convertible preferred stock warrant liability will be settled and will no longer be subject to remeasurement.
Redeemable Convertible Preferred Stock
The Company records its redeemable convertible preferred stock at fair value on the dates of issuance, net of issuance costs. A redemption event will only occur upon the liquidation or winding-up of the Company, a greater than 50% change in control, or sale of substantially all of the assets of the Company. In the event of a change of control of the Company, proceeds received from the sale of such shares will be distributed in accordance with the liquidation preferences set forth in the Company’s amended and restated certificate of incorporation, unless the holders of redeemable convertible preferred stock otherwise agree or have converted their shares into shares of common stock. Therefore, redeemable convertible preferred stock is classified outside of stockholders’ equity in the balance sheets as events triggering the liquidation preferences are not solely within the Company’s control. The Company is not required to adjust the carrying values of the redeemable convertible preferred stock to the redemption value of such shares since it is uncertain whether or when a redemption event will occur. Subsequent adjustments to increase the carrying values to the redemption values will be made only when it becomes probable that such redemption will occur.
Common Stock Warrant
The Company’s common stock warrant is classified in equity as it meets all criteria for equity classification. The fair value of the common stock warrant was calculated using the BackSolve Method and is recorded at fair value upon issuance in additional paid-in capital in the consolidated balance sheets. The common stock warrant is not remeasured after the issuance date.
Revenue Recognition
The Company applies the following five steps in order to determine the appropriate amount of revenue to be recognized as it fulfills its obligations under each of its arrangements:
| • | Identify the contract with a customer, |
| • | Identify the performance obligations in the contract, |
| • | Determine the transaction price, |
| • | Allocate the transaction price to performance obligations in the contract, and |
| • | Recognize revenue as the performance obligations are satisfied. |
F-11
Table of Contents
The Company’s revenue is generated from the sale of its products from its surgical glaucoma product portfolio and its nonsurgical dry eye product portfolio to hospitals and medical centers in the United States and elsewhere through sales representatives and distributors. The Company’s contracts are in the form of a combination of signed agreements and/or purchase orders. The Company accounts for a contract with a customer when there is approval and commitment from both parties, the rights and obligations of the parties are identified, payment terms are identified, the contract has commercial substance, and it is probable that the Company will collect substantially all of the consideration to which it will be entitled.
Each of the Company’s surgical glaucoma and dry eye products specified in the contract represents a distinct good and is accounted for as separate performance obligation. Revenue is recognized when control of promised goods is transferred to a customer in amount that reflects the consideration that the Company expects to receive in exchange for those goods. Control of the Company’s products are transferred to its customers at a point in time, either upon shipment or delivery of the product to the customer under the Company’s standard terms and conditions. The customer is able to direct the use of, and obtain substantially all of the benefits from, the product at the time the product shipped or delivered. The Company considers control to have transferred upon shipment or delivery because the Company has a present right to payment at that time, the customer has legal title to the asset, the Company has transferred physical possession of the asset, the customer has accepted the asset, and the customer has significant risks and rewards of ownership of the asset.
Payment for the Company’s contracts are typically due within 30 days of transfer of control of the Company’s products to its customers. The Company excludes taxes assessed by governmental authorities on revenue-producing transactions from the measurement of the transaction price.
In the normal course of business, the Company does not accept product returns, unless the item is defective as manufactured. The Company establishes provisions for estimated returns and warranties. In addition, the Company does not typically provide customers with the right to a refund.
Practical Expedients and Exemptions
The Company’s contracts all have an original duration of one year or less. As a practical expedient, the Company does not consider the time value of money for such contracts. Further, because of the short duration of these contracts, the Company does not disclose the transaction price for the remaining performance obligations as of the end of each reporting period or the when the Company expects to recognize this revenue.
The Company expenses shipping and handling costs as incurred and includes them in the cost of goods sold. In those cases where the Company bills shipping and handling costs to customers, it will classify the amounts billed as a component of revenue.
As a practical expedient, the Company recognizes the incremental costs of obtaining contracts, such as sales commissions, as an expense when incurred since the amortization period of the asset the Company otherwise would have recognized is one year or less. Sales commissions are recorded within selling, general, and administrative expenses in the statements of operations.
Cost of Goods Sold
The Company purchases its products from third-party manufacturers. Cost of goods sold consists primarily of costs related to materials, manufacturing overhead costs, reserves for excess, and obsolete and non-sellable inventories. Cost of goods sold also includes depreciation expense for production equipment and certain direct costs, such as shipping and handling costs.
Research and Development
The Company expenses research and development costs as incurred. Research and development expenses consist primarily of product development, clinical studies to develop and support the Company’s products,
F-12
Table of Contents
regulatory expenses, medical affairs, and other costs associated with products and technologies that are in development. Research and development expenses include employee compensation, including stock-based compensation, supplies, consulting, prototyping, testing, materials, travel expenses, depreciation, and an allocation of facility overhead expenses.
Selling, General and Administrative
Selling, general and administrative expenses include compensation, employee benefits, and stock-based compensation for executive management, finance administration, and human resources; facility costs (including rent); bad debt costs; professional service fees; and other general overhead costs, including depreciation to support the Company’s operations.
Advertising Expense
The Company expenses advertising costs as incurred. Advertising expenses for fiscal years 2018, 2019 and 2020 were $1.0 million, $1.8 million and $0.8 million, respectively, included in selling, general, and administrative expenses in the statements of operations and comprehensive loss.
Accounting for Payroll Protection Program
In March 2020, Congress established the Paycheck Protection Program (“PPP”) to provide relief to small businesses during COVID-19 as part of the Coronavirus Aid, Relief, and Economic Security (“CARES”) Act. The legislation authorized the U.S. Treasury to use the Small Business Association’s (“SBA’s”) small business lending program to fund forgivable loans that qualifying businesses could spend to cover payroll, mortgage interest, rent, and utilities during the “Covered Period” defined as the 8-week period starting on the date the PPP loan proceeds are received. Upon meeting certain criteria as specified in the PPP program, the loans are eligible for partial or total forgiveness. In May 2020, the Company applied for and received a PPP loan for the amount $2.2 million from SBA. We believe we have satisfied all of the terms and conditions of the PPP loan and applied for loan forgiveness in September 2020. We expect a decision from the SBA on loan forgiveness in the second quarter of 2021.
U.S. GAAP does not contain authoritative accounting standards for forgivable loans provided by governmental entities to a for-profit entity. Absent authoritative accounting standards, interpretative guidance issued and commonly applied by financial statement preparers allows for the selection of accounting policies amongst acceptable alternatives. The Company determined it most appropriate to account for the PPP loan proceeds as an in-substance government grant by analogy to International Accounting Standards 20 (“IAS 20”) Accounting for Government Grants and Disclosure of Government Assistance. Under this guidance, a forgivable loan from government is treated as a government grant when there is reasonable assurance that the entity will meet the terms for forgiveness of the loan. While IAS 20 does not define “reasonable assurance”, this concept in practice is analogous to “probable” as defined in Financial Accounting Standards Board (“FASB”) ASC 450-20-20 under U.S. GAAP, which is the definition the Company has applied to its expectations of PPP loan forgiveness. Under IAS 20, government grants are recognized in earnings on a systematic basis over the periods in which the Company recognizes costs for which the grant is intended to compensate (i.e. qualified expenses). Further, IAS 20 permits for the recognition in earnings either separately under a general heading such as other income, or as a reduction of the related expenses.
The Company has elected to recognize this government grant income as a reduction of the related expenses, and recognized $0.1 million, $0.3 million and $1.8 million as a reduction of cost of revenue, research and development and selling, general and administrative expenses, respectively for the year ended December 31, 2020.
Stock-Based Compensation
The Company measures and records the expense related to stock-based payment awards based on the fair value of those awards as determined on the date of grant. The Company recognizes stock-based compensation
F-13
Table of Contents
expense over the requisite service period of the individual grant, generally equal to the vesting period and uses the straight-line method to recognize stock-based compensation, and accounts for forfeitures as they occur. The Company selected the Black-Scholes-Merton (“Black-Scholes”) option-pricing model as the method for determining the estimated fair value for stock options. The Black-Scholes option-pricing model requires the use of highly subjective and complex assumptions, which determine the fair value of share-based awards, including the option’s expected term, expected volatility of the underlying stock, risk-free interest rate and expected dividend yield.
Fair Value of Common Stock
The fair value of the Company’s common stock is determined by the board of directors with assistance from management and, in part, on input from an independent third-party valuation firm. The board of directors determines the fair value of common stock by considering a number of objective and subjective factors, including valuations of comparable companies, sales of redeemable convertible preferred stock, operating and financial performance, the lack of liquidity of the Company’s common stock and the general and industry-specific economic outlook.
Currency Remeasurement
Foreign currency transaction gains and losses are recorded in other expense, net in the Company’s statements of operations and such amounts have not been material for all periods presented.
Income Taxes
The Company uses the asset and liability method under ASC 740, Income Taxes, in accounting for income taxes. Deferred tax assets and liabilities are recognized for the estimated future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. Deferred tax expenses or benefits are the result of changes in the deferred tax assets and liabilities. Valuation allowances are established when necessary to reduce deferred tax assets to their net realizable value where it is more likely than not that the deferred tax assets will not be realized.
ASC 740 clarifies the accounting for uncertainty in income taxes recognized in the financial statements. ASC 740 provides that a tax benefit from an uncertain tax position may be recognized when it is more likely than not that the position will be sustained upon audit, including resolutions of any related appeals or litigation processes, based on the technical merits of the position.
The Company recognizes interest and penalties related to unrecognized tax benefits within the benefit for income taxes line in the accompanying statements of operations and comprehensive loss. Accrued interest and penalties are included within the related liability line in the balance sheets.
Comprehensive Loss
Comprehensive loss represents all changes in stockholders’ deficit except those resulting from distributions to stockholders. There have been no items qualifying as other comprehensive income (loss) and, therefore, for all periods presented, there was no difference between comprehensive loss and the Company’s reported net loss.
Net loss per share attributable to common stockholders
Basic and diluted net loss per share attributable to common stockholders is presented in conformity with the two-class method required for participating securities. The Company considers all series of its redeemable
F-14
Table of Contents
convertible preferred stock and restricted stock awards to be participating securities as the holders are entitled to receive dividends on a pari passu basis in the event that a dividend is paid on common stock. Under the two-class method, the net loss attributable to common stockholders is not allocated to the redeemable convertible preferred stock or restricted stock awards as the holders of the Company’s redeemable convertible preferred stock and restricted stock awards do not have a contractual obligation to share in losses.
Basic and diluted net loss per share attributable to common stockholders is computed by dividing the net loss attributable to common stockholders by the weighted-average number of common shares outstanding for the period without consideration of potentially dilutive securities. The Company’s potentially dilutive shares, which consist of outstanding common stock options, restricted stock awards, common stock warrants, redeemable convertible preferred stock and redeemable convertible preferred stock warrants were excluded in the computation of diluted net loss per share for the period as the result would be anti-dilutive.
Emerging growth company
The Company is an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012. As such the Company is eligible for exemptions from various reporting requirements applicable to other public companies that are not emerging growth companies, including reduced reporting and extended transition periods to comply with new or revised accounting standards for public business entities. The Company has elected to avail themselves of this exemption and, therefore, will not be subject to the timeline for adopting new or revised accounting standards for public business entities that are not emerging growth companies, and will follow the transition guidance applicable to private companies.
Recently Adopted Accounting Pronouncements
In May 2014, the FASB issued ASU No. 2014-09. Subsequently, the FASB also issued ASU No. 2015-14, Revenue from Contracts with Customers (Topic 606): Deferral of the Effective Date, which adjusted the effective date of ASU No. 2014-09; ASU No. 2016-08, Revenue from Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net), which amends the principal versus agent implementation guidance and illustrations in ASU No. 2014-09; ASU No. 2016-10, Revenue from Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing, which clarifies identifying performance obligation and licensing implementation guidance and illustrations in ASU No. 2014-09; and ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients, which addresses implementation issues and is intended to reduce the cost and complexity of applying the new revenue standard in ASU No. 2014-09 (collectively, the “Revenue ASUs”).
The Revenue ASUs provide an accounting standard for a single comprehensive model for use in accounting for revenue arising from contracts with customers and supersedes most current revenue recognition guidance. The accounting standard is effective for interim and annual periods beginning after December 15, 2019. The guidance permits two methods of adoption: retrospectively to each prior reporting period presented (the full retrospective method) or retrospectively with the cumulative effect of initially applying the guidance recognized at the date of initial application (the modified retrospective method). The Company performed a detailed review of its revenue agreements and assessed the differences in accounting for such contracts under this guidance compared with previous revenue accounting standards. On January 1, 2018, the Company early adopted ASU No. 2014-09 using the full retrospective method. The adoption of this standard did not have a material impact on the Company’s financial statements. Results for all periods presented are under ASC 606.
In March 2016, the FASB issued an ASU No. 2016-09, Compensation—Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting, to simplify several areas of accounting for share-based compensation arrangements, including the income tax impact and classification on the statements of cash flows. The Company adopted this update on January 1, 2018 and elected to record forfeitures as they occur. The adoption of this update was immaterial to the financial statements.
F-15
Table of Contents
In June 2018, the FASB issued an ASU No. 2018-07, Compensation—Stock Compensation (Topic 718): Improvements to Nonemployee Share-Based Payment Accounting, that expands the scope to include share-based payment transactions for acquiring goods and services from nonemployees. ASU No. 2018-07 simplifies the accounting for share-based payments to nonemployees by aligning it with the accounting for share-based payments to employees, with certain exceptions. This update is required to be applied through a cumulative effect adjustment to retained earnings as of the beginning of the fiscal year of adoption. This guidance is effective for fiscal years beginning after December 15, 2018, including interim periods within that fiscal year. Early adoption is permitted for any entity in any interim or annual period for which financial statements have not been issued or made available for issuance, but not before an entity adopts ASC 606. The Company early adopted the standard on January 1, 2018, which did not result in a material impact on its financial statements and related disclosures.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842). In July 2018, the FASB issued ASU No. 2018-10, Codification Improvements to Topic 842, Leases, which provides clarification to ASU No. 2016-02. These ASUs require an entity to recognize a lease liability and a ROU asset in the balance sheets for leases with lease terms of more than 12 months. Lessor accounting is largely unchanged, while lessees will no longer be provided with a source of off-balance-sheet financing. This guidance is effective for fiscal years beginning after December 15, 2021, and for interim periods within fiscal years beginning after December 15, 2022. In July 2018, the FASB issued ASU No. 2018-11, Leases (Topic 842): Targeted Improvements, which allows entities to elect a modified retrospective transition method where entities may continue to apply the existing lease guidance during the comparative periods and apply the new lease requirements through a cumulative effect adjustment in the period of adoptions rather than in the earliest period presented.
On January 1, 2019, the Company early adopted ASU No. 2016-02 and its associated amendments using the modified retrospective transition method by applying the new update to all leases existing at the date of initial application and not restating comparative periods. There was no cumulative effect adjustment recorded to retained earnings upon adoption. Under the update, a lessee is required to recognize a lease liability and ROU asset for all leases. The new guidance also modified the classification criteria and requires additional disclosures to enable users of financial statements to understand the amount, timing, and uncertainty of cash flows arising from leases. Consistent with current guidance, a lessee’s recognition, measurement, and presentation of expenses and cash flows arising from a lease continues to depend primarily on its classification. The Company elected the package of practical expedients permitted under the transition guidance, which allowed the Company to carry forward its historical lease classification, its assessment on whether a contract was or contains a lease, and its initial direct costs for any leases that existed prior to January 1, 2019. In addition, the Company elected the short-term lease exception and combined lease and non-lease components as practical expedients.
The adoption of this guidance did not materially impact the Company’s consolidated financial statements.
In August 2018, the FASB issued ASU No. 2018-13, Fair Value Measurement (Topic 820): Disclosure Framework—Changes to the Disclosure Requirements for Fair Value Measurement, which changed the disclosure requirements for fair value measurements by removing, adding, and modifying certain disclosures. The Company adopted this ASU beginning on January 1, 2020 which did not result in a material impact on the disclosures related to fair value measurements.
New Accounting Pronouncements Not Yet Adopted
In June 2016, the FASB issued ASU No. 2016-13, Financial Instruments—Credit Losses (Topic 326): Measurement of Credit Losses on Financial Instruments, which amends the impairment model by requiring entities to use a forward-looking approach based on expected losses to estimate credit losses on certain types of financial instruments, including trade receivables and available-for-sale debt securities. The guidance is effective for the Company beginning in the first quarter of 2023. The Company is evaluating the impact of adopting this guidance and does not expect to have a material impact on the Company’s financial statements and related disclosures.
F-16
Table of Contents
In December 2019, the FASB issued ASU No. 2019-12, Income Taxes (Topic 740): Simplifying the Accounting for Income Taxes, that simplifies the accounting for income taxes by eliminating certain exceptions related to the approach for intra-period tax allocation and modified the methodology for calculating income taxes in an interim period. It also clarifies and simplifies other aspects of the accounting for income taxes. The guidance is effective for the Company for fiscal years beginning after December 15, 2021, and interim periods within fiscal years beginning after December 15, 2022 with early adoption permitted. The Company is evaluating the effect this new guidance and does not expect it to have material impact on the Company’s financial statements.
In March 2020, the FASB issued ASU No. 2020-04, Reference Rate Reform (Topic 848): Facilitation of the Effects of Reference Rate Reform on Financial Reporting. The new guidance provides optional expedients and exceptions for applying generally accepted accounting principles to contract modifications and hedging relationships, subject to meeting certain criteria, that reference LIBOR or another reference rate expected to be discontinued. The guidance also establishes (1) a general contract modification principle that entities can apply in other areas that may be affected by reference rate reform and (2) certain elective hedge accounting expedients. The amendment is effective for all entities through December 31, 2022. LIBOR is used to calculate the interest on borrowings under the Company’s term loan and revolving line of credit with MidCap Financial Services. The Company is evaluating the effect this new guidance and does not expect it to have material impact on the Company’s financial statements.
Note 3. Fair Value Measurements
The Company reports all financial assets and liabilities and nonfinancial assets and liabilities that are recognized or disclosed at fair value in the financial statements on a recurring basis. Valuation techniques used to measure fair value must maximize the use of observable inputs and minimize the use of unobservable inputs. The authoritative guidance establishes a fair value hierarchy that prioritizes the inputs to valuation techniques used to measure fair value. The hierarchy gives the highest priority to unadjusted quoted prices in active markets for identical assets or liabilities (Level 1 measurements) and the lowest priority to measurements involving significant unobservable inputs (Level 3 measurements). The three levels of the fair value hierarchy are as follows:
Level 1—Inputs are quoted prices (unadjusted) in active markets for identical assets or liabilities that the Company has the ability to access at the measurement date.
Level 2—Inputs are observable, unadjusted quoted prices in active markets for similar assets or liabilities, unadjusted quoted prices for identical or similar assets or liabilities in markets that are not active, or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the related assets or liabilities.
Level 3—Inputs are unobservable inputs for the asset or liability. The level in the fair value hierarchy within which a fair value measurement in its entirety is based on the lowest-level input that is significant to the fair value measurement in its entirety.
The financial statements as of and for the years ended December 31, 2018, 2019 and 2020, do not include any nonrecurring fair value measurements relating to assets or liabilities.
The Company does not have any assets and liabilities that are measured at fair value on a recurring basis at December 31, 2018.
F-17
Table of Contents
The fair value measurements of liabilities that are measured at fair value on a recurring basis at December 31, 2019 and 2020, are as follows (in thousands):
| As of December 31, 2019 | ||||||||||||||||
| (Level 1) | (Level 2) | (Level 3) | Total | |||||||||||||
Liabilities | ||||||||||||||||
Redeemable convertible preferred stock warrants liabilities | $ | — | $ | — | $ | 236 | $ | 236 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Total liabilities measured at fair value | $ | — | $ | — | $ | 236 | $ | 236 | ||||||||
|
|
|
|
|
|
|
| |||||||||
| As of December 31, 2020 | ||||||||||||||||
| (Level 1) | (Level 2) | (Level 3) | Total | |||||||||||||
Liabilities | ||||||||||||||||
Redeemable convertible preferred stock warrants liabilities | $ | — | $ | — | $ | 2,112 | $ | 2,112 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Total liabilities measured at fair value | $ | — | $ | — | $ | 2,112 | $ | 2,112 | ||||||||
|
|
|
|
|
|
|
| |||||||||
The Company measures the redeemable convertible preferred stock warrants using Level 3 unobservable inputs within the Black-Scholes option-pricing model. The key assumptions include the fair value of redeemable convertible preferred stock, volatility, the risk-free interest rate, expected term (remaining contractual term of the warrants) and dividend yield. The Company has limited historical volatility information available, and the expected volatility was based on actual volatility for comparable public companies projected over the expected terms of the warrants. The Company did not apply a forfeiture rate to the warrants as there is not enough historical information available to estimate such a rate. The risk-free interest rate was based on the U.S. Treasury yield curve at the time of the grant over the expected term of the warrants. Refer to Note 9 for the assumptions used.
The Company measures the fair value of outstanding debt for disclosure purposes on a recurring basis. As of December 31, 2019 and 2020, total debt of $12.9 million and $31.9 million is reported at amortized cost, respectively. This outstanding debt is classified as Level 2 as it is not actively traded. The amortized cost of the outstanding debt approximates the fair value.
The Company determines the fair value of the redeemable convertible preferred stock warrants annually, with subsequent gains and losses from remeasurement of Level 3 financial liabilities recorded through the other expense, net in statements of operations and other comprehensive loss.
F-18
Table of Contents
A summary of the changes in the fair value of the Company’s Level 3 financial instruments at December 31, 2019 and 2020, is as follows (in thousands):
| Redeemable convertible preferred stock warrant liability | ||||
Balance—December 31, 2018 | $ | — | ||
Issuance of redeemable convertible preferred stock warrants | 201 | |||
Change in fair value | 35 | |||
|
| |||
Balance—December 31, 2019 | 236 | |||
Issuance of redeemable convertible preferred stock warrants | 1,812 | |||
Change in fair value | 136 | |||
Expiration of redeemable convertible preferred stock warrants | (72 | ) | ||
|
| |||
Balance—December 31, 2020 | $ | 2,112 | ||
Note 4. Balance Sheet Components
Property and Equipment, Net
Property and equipment, net consist of the following (in thousands):
| As of December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Tools and equipment | $ | 255 | $ | 1,498 | $ | 1,523 | ||||||
Computer equipment and software | 67 | 109 | 118 | |||||||||
Furniture and fixtures | 6 | 43 | 43 | |||||||||
Leasehold improvements | — | 29 | 30 | |||||||||
Construction in process | 630 | 162 | 298 | |||||||||
|
|
|
|
|
| |||||||
| 958 | 1,841 | 2,012 | ||||||||||
Less: Accumulated depreciation | (90 | ) | (350 | ) | (743 | ) | ||||||
|
|
|
|
|
| |||||||
Property and equipment, net | $ | 868 | $ | 1,491 | $ | 1,269 | ||||||
|
|
|
|
|
| |||||||
Depreciation expense for fiscal years 2018, 2019 and 2020 was $0.06 million, $0.3 million and $0.5 million, respectively.
Accrued and Other Current Liabilities
Accrued and other current liabilities consist of the following (in thousands):
| As of December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Accrued expenses | $ | 161 | $ | 1,767 | $ | 1,971 | ||||||
Current portion of lease liabilities | — | 557 | 395 | |||||||||
Short term interest payable | — | 119 | 274 | |||||||||
Other accrued liabilities | 167 | 408 | 446 | |||||||||
|
|
|
|
|
| |||||||
Total accrued and other current liabilities | $ | 328 | $ | 2,851 | $ | 3,086 | ||||||
|
|
|
|
|
| |||||||
F-19
Table of Contents
Other Noncurrent Liabilities
Other noncurrent liabilities consist of the following (in thousands):
| As of December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Noncurrent portion of lease liabilities | $ | — | $ | 528 | $ | 134 | ||||||
Redeemable preferred stock warrants liabilities | — | 236 | 2,112 | |||||||||
Long term interest payable | — | 213 | 465 | |||||||||
Other noncurrent liabilities | 7 | — | 344 | |||||||||
|
|
|
|
|
| |||||||
Total other noncurrent liabilities | $ | 7 | $ | 977 | $ | 3,055 | ||||||
|
|
|
|
|
| |||||||
Note 5. Debt
In January 2019, the Company entered into a loan and security agreement with MidCap Financial Services, which provided a maximum of $25.0 million credit facility consisting of a $20.0 million senior secured 2019 Term Loan and a $5.0 million 2019 Revolver (collectively, the “2019 MidCap Credit Facility”). In November 2020, the Company entered into a loan and security agreement with the same institution, which replaced the 2019 MidCap Credit Facility, and provided for a maximum of $40.0 million credit facility consisting of a $35.0 million senior secured 2020 Term Loan and a $5.0 million 2020 Revolver (collectively, the “2020 MidCap Credit Facility”).
2019 Term Loan
The 2019 Term Loan had a four-year term and had a stated floating interest rate which equates to reserve-adjusted LIBOR + 6.75%. The 2019 Term Loan was split into three tranches as follows: (i) the Tranche One Loans provided for $12.0 million in term loans, (ii) the Tranche Two Loans provided for up to $2.0 million in term loans, and (iii) the Tranche Three Loans provided for up to $6.0 million in term loans. The Company borrowed $14.0 million under the Tranche One Loans and Tranche Two Loans. While the conditions necessary to draw the Tranche Three Loans had been met as of December 31, 2019, the Company did not elect to draw the Tranche Three Term Loans. The 2019 Term Loan required 18 monthly interest-only payments, which began on January 31, 2019, followed by 30 equal monthly installments of principal, plus interest. The interest-only period was extended by an additional six months upon achievement of the Tranche Three Milestone.
The 2019 Term Loan had an effective interest rate of 14.52% per year. The 2019 Term Loan interest expense for the year ended December 31, 2019 and 2020 was $1.9 million and $2.0 million, respectively.
In conjunction with the funding of Tranche 1 and Tranche 2 under the 2019 Term Loan, the Company issued a 10-year warrant to the Lender to purchase 29,514 shares of the Company’s Series C redeemable convertible preferred stock (the “2019 Initial Warrant”) at an exercise price of $9.49 per share (the “Exercise Price”). Further, depending on the funding of the Term Loan Tranche 3, the Company was obligated to issue an additional Warrant to the Lender to purchase up to 12,649 shares of Series C redeemable convertible preferred stock at the Exercise Price (the “2019 Additional Warrant” and together with “2019 Initial Warrant” the “2019 Warrants”) (see Note 9).
The estimated fair value of the 2019 Warrants of $0.2 million upon draw down was based on the Black-Scholes option-pricing model and probability of future draw downs. The 2019 Warrants were recorded at the fair value as a debt discount and as a warrant liability. The debt discount is being accreted using the effective interest method as interest expense over the contractual period of four years for the Term Loan.
The Company incurred $1.5 million of issuance costs in conjunction with the 2019 Term Loan. The issuance costs have been netted against the borrowed funds in the consolidated balance sheet and is being accreted using the effective interest method as interest expense over the contractual period of four years for the 2019 Term Loan.
F-20
Table of Contents
The Company could voluntarily prepay the borrowings in full, with a prepayment premium beginning at 3% in the first year from tranche funding and declining to 2% in the second year from tranche funding, to 1% in the third year from tranche funding thereafter. In addition, a final payment fee of 5% of the amounts borrowed is payable at the end of the term or when the borrowings are repaid in full. A long-term liability was being accreted using the effective interest method for the final payment fee over the term of the loan agreement. The borrowings were collateralized by a security interest in substantially all of the Company’s assets.
The Company accrued $0.2 million as of December 31, 2019, related to accretion of final payment due at maturity per agreement using the effective interest rate method.
The Company was subject to financial covenants related to minimum trailing revenue targets that began on January 1, 2019, and are tested on a monthly basis. If only Tranche One Loans were funded, the Company had to achieve minimum net revenue of $7 million over a trailing 12-month period increasing to a maximum net revenue covenant of $35 million for the trailing 12-month period ending December 31, 2022, and thereafter. If only Tranche One Loans and Tranche Two Loans had been funded, the Company had to achieve minimum net revenue of $7 million over a trailing 12-month period increasing to a maximum net revenue covenant of $37.3 million for the 12-month period ending December 31, 2022, and thereafter. If Tranche Three Loans had been funded regardless of whether Tranche Two Loans have been funded, the Company had to achieve minimum net revenue of $15 million over a trailing 12-month period increasing to a maximum net revenue covenant of $46.7 million for the 12-month period ending December 31, 2022, and thereafter. As of December 31, 2019, the Company was in compliance with the applicable financial covenant.
On November 23, 2020, the 2019 Term Loan was replaced with 2020 Term Loan (see below).
2019 Revolver
The 2019 Revolver had a four-year term and has a stated floating interest rate which equates to reserve-adjusted LIBOR plus 4.25%. An unused line fee of 0.5% was payable monthly based on the average unused balance and a collateral management fee of 0.5% is payable monthly based on the outstanding balance of the Revolver. The Company can request to increase the 2019 Revolver commitment amount to $10.0 million under the term of the agreement. As of December 31, 2019, $4.0 million was available to be drawn under the 2019 Revolver.
The Company may voluntarily prepay the borrowings in full, with a prepayment premium equal to an amount determined by multiplying the Revolver commitment amount by 3.0% in the first year, 2.0% in year 2, and 1.0% thereafter.
The 2019 Revolver has not been drawn upon as of December 31, 2019. On November 23, 2020, the 2019 Revolver was replaced with the 2020 Revolver (see below).
2020 Term Loan
The 2020 Term Loan has a five-year term and has a stated floating interest rate which equates to reserve-adjusted LIBOR + 7.00%. The 2020 Term Loan is split into three tranches as follows: (i) the Tranche One Loans provide for $12.0 million in term loans which are deemed to have been converted from Tranche One Loans that were drawn and outstanding under the 2019 Term Loan immediately prior to entering into 2020 MidCap Credit Facility, (ii) the Tranche Two Loans provided for up to $2.0 million in term loans which are deemed to have been converted from Tranche Two Loans that were drawn and outstanding under the 2019 Term Loan immediately prior to entering into 2020 MidCap Credit Facility, and (iii) the Tranche Three Loans provided for up to $21.0 million in new term loans. The Company borrowed $21.0 million under the Tranche Three Loans in November 2020.
F-21
Table of Contents
The 2020 Term Loan requires 24 monthly interest-only payments, which began on December 1, 2020, followed by 36 equal monthly installments of principal, plus interest. The interest-only period can be extended by an additional 12 months provided that the Company is in compliance with the minimum trailing revenue targets (as described below), and has unrestricted cash and cash equivalents of at least 12 times of the amortization monthly cash burn amount, measured as defined in the 2020 Term Loan agreement (“First IO Extension”). If the First IO Extension conditions are satisfied, the interest-only period can be further extended by an additional 12 months, provided that the Company is in compliance with the minimum trailing revenue targets (as described below), has unrestricted cash and cash equivalents of at least 12 times of the amortization monthly cash burn amount, and has consummated an IPO in which the Company has received cash proceeds of at least $60.0 million.
The 2020 Term Loan has an effective interest rate of 13.59% per year. The 2020 Term Loan interest expense for the year ended December 31, 2020 was $0.4 million.
In conjunction with the entering the 2020 MidCap Credit Facility, the Company issued a 10-year warrant to the Lender to purchase 300,000 shares of the Company’s Series F redeemable convertible preferred stock (the “2020 Warrant”) at an exercise price of $21.88 per share (see Note 9). The estimated fair value at issuance of the 2020 Warrant of $1.8 million was based on the Option-Pricing Method with Discounts for Lack of Marketability for each class of security. In addition, the Company incurred $0.5 million of issuance costs paid to the Lender in conjunction with the 2020 Term Loan which represents a debt discount. The Company concluded that the 2020 Term Loan represented a modification of the 2019 Term Loan and accounted for the 2020 Term Loan as debt modification. The 2020 Warrants were recorded at the fair value as a debt discount and as a warrant liability. At each balance sheet date, the 2020 Warrants are remeasured to fair value with any changes in fair value recognized as other expense in the statements of operations. The debt discount is being amortized using the effective interest method as interest expense over the contractual period of five years for the 2020 Term Loan.
The Company can voluntarily prepay the borrowings in full, with a prepayment premium beginning at 3% in the first year from entering into the 2020 MidCap Credit facility and declining to 2% in the second year to 1% in the third year thereafter. In addition, a final payment fee of 6% of the amounts borrowed is payable at the end of the term or when the borrowings are repaid in full. A long-term liability is being accreted using the effective interest method for the final payment fee over the term of the loan agreement. The borrowings are collateralized by a security interest in substantially all of the Company’s assets.
The Company accrued $0.5 million as of December 31, 2020, related to accretion of final payment due at maturity per the agreement using the effective interest rate method. The final payment accrual is recorded in “Other noncurrent liabilities” on the balance sheets.
The Company is subject to financial covenants related to minimum trailing revenue targets that began on September 30, 2020 and are tested on a monthly basis. The Company has to achieve minimum net revenue of $20.0 million over a trailing 12-month period increasing to a maximum net revenue covenant of $84.8 million for the trailing 12-month period ending October 31, 2025. As of December 31, 2020, the Company was in compliance with the applicable financial covenant.
2020 Revolver
The 2020 Revolver has a four-year term and has a stated floating interest rate which equates to reserve-adjusted LIBOR plus 4.50%. An unused line fee of 0.5% is payable monthly based on the average unused balance and a collateral management fee of 0.5% is payable monthly based on the outstanding balance of the 2020 Revolver. The Company can request to increase the 2020 Revolver commitment amount to $15.0 million under the term of the agreement. As of December 31, 2020, $4.8 million was available to be drawn under the 2020 Revolver.
The 2020 Revolver has not been drawn upon as of December 31, 2020.
F-22
Table of Contents
Long-term and short-term debt was as follows (in thousands):
| As of December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Term Loan | $ | — | $ | 14,000 | $ | 35,000 | ||||||
|
|
|
|
|
| |||||||
Total principal payments due | — | 14,000 | 35,000 | |||||||||
|
|
|
|
|
| |||||||
Less: debt discount related to warrant liability and issuance costs | — | (1,145 | ) | (3,045 | ) | |||||||
Total amount outstanding | — | 12,855 | 31,955 | |||||||||
|
|
|
|
|
| |||||||
Less: Current portion | — | — | — | |||||||||
|
|
|
|
|
| |||||||
Long-term portion | $ | — | $ | 12,855 | $ | 31,955 | ||||||
|
|
|
|
|
| |||||||
The repayment schedule relating to the Company’s debt as of December 31, 2020, is as follows (in thousands):
| Amount | ||||
2021 | $ | — | ||
2022 | 1,944 | |||
2023 | 11,667 | |||
2024 | 11,667 | |||
2025 | 9,722 | |||
|
| |||
Total repayments | $ | 35,000 | ||
|
| |||
Note 6. Commitments and Contingencies
Operating Lease Obligations
The Company’s leases mainly include facility leases and storage leases. In September 2019, the Company entered into a noncancelable operating lease for approximately 10,823 square feet of primary office space, which expires on July 31, 2021, without the option to extend.
The Company recognizes rent expense on a straight-line basis over the noncancelable lease term. The Company’s rent expense was $0.2 million, $0.3 million and $0.7 million for the years ended December 31, 2018, 2019 and 2020, respectively.
The Company adopted Topic 842 as of January 1, 2019. In determining the present value of lease payments, the Company uses its incremental borrowing rate based on the information available at the lease commencement date if the rate implicit in the lease is not readily determinable. At the date of adoption of Topic 842, the Company determined the amounts of lease liability using a discount rate of 16.4%, which represents the Company’s incremental borrowing rate, which is based on the Company’s current borrowing rate adjusted for various factors including level of collateralization and term. As of December 31, 2020, the remaining lease term for the lease was 3.4 years.
Operating lease expense recognized and supplemental cash flow information related to operating leases for the year ended December 31, 2019 and 2020 were as follows (in thousands):
| Year Ended December 31, | ||||||||
| 2019 | 2020 | |||||||
Operating lease expense | $ | 197 | $ | 663 | ||||
Cash paid for operating leases | 193 | 694 | ||||||
New operating lease assets obtained in exchange for operating lease liabilities | 1,218 | — | ||||||
F-23
Table of Contents
During the year ended December 31, 2019 and 2020, the Company’s costs related to short-term lease arrangements and non-lease variable payments were immaterial.
Future minimum lease payments at December 31, 2018, under the noncancelable operating lease were as follows (in thousands):
| Amount | ||||
2019 | $ | 238 | ||
2020 | 41 | |||
2021 | 7 | |||
|
| |||
Total future minimum lease payments | $ | 286 | ||
|
| |||
Aggregate future minimum lease payments at December 31, 2019 and 2020, under these noncancelable operating leases were as follows (in thousands):
| As of December 31, | ||||||||
| 2019 | 2020 | |||||||
2020 | $ | 694 | $ | — | ||||
2021 | 440 | 440 | ||||||
2022 | 66 | 66 | ||||||
2023 | 68 | 68 | ||||||
2024 | 29 | 29 | ||||||
|
|
|
| |||||
Total future minimum lease payments | 1,297 | 603 | ||||||
Less: imputed interest | (212 | ) | (74 | ) | ||||
|
|
|
| |||||
Present value of future minimum lease payments | 1,085 | 529 | ||||||
Less: current portion of operating lease liability | (557 | ) | (395 | ) | ||||
|
|
|
| |||||
Operating lease liabilities—noncurrent | $ | 528 | $ | 134 | ||||
|
|
|
| |||||
Legal Proceedings
The Company is subject to claims and assessments from time to time in the ordinary course of business. Accruals for litigation and contingencies are reflected in the financial statements based on management’s assessment, including the advice of legal counsel, of the expected outcome of litigation or other dispute resolution proceedings, and/or the expected resolution of contingencies. Liabilities for estimated losses are accrued if the potential losses from any claims or legal proceedings are considered probable and the amounts can be reasonably estimated. Significant judgment is required in both the determination of probability of loss and the determination as to whether the amount can be reasonably estimated. Accruals are based only on information available at the time of the assessment due to the uncertain nature of such matters. As additional information becomes available, management reassesses potential liabilities related to pending claims and litigation and may revise its previous estimates, which could materially affect the Company’s results of operations in a given period. As of December 31, 2018, 2019 and 2020, the Company was not involved in any material legal proceedings.
Indemnification
In the normal course of business, the Company enters into contracts and agreements that contain a variety of representations and warranties and provide for general indemnifications. The Company’s exposure under these agreements is unknown because it involves claims that may be made against the Company in the future, but that have not yet been made. To date, the Company has not paid any claims or been required to defend any action related to its indemnification obligations. However, the Company may record charges in the future as a result of these indemnification obligations.
F-24
Table of Contents
The Company indemnifies each of its directors and officers for certain events or occurrences, subject to certain limits, while the director is or was serving at the Company’s request in such capacity, as permitted under Delaware law and in accordance with its certificate of incorporation and bylaws. The term of the indemnification period lasts as long as a director may be subject to any proceeding arising out of acts or omissions of such director in such capacity. The maximum amount of potential future indemnification is unlimited; however, the Company currently holds director liability insurance. This insurance allows the transfer of risk associated with the Company’s exposure and may enable it to recover a portion of any future amounts paid. The Company believes that the fair value of these indemnification obligations is minimal. Accordingly, the Company has not recognized any liabilities relating to these obligations as of December 31, 2018, 2019, and 2020.
Note 7. Redeemable Convertible Preferred Stock
The Company has the following redeemable convertible preferred stock issued and outstanding at December 31, 2018 (in thousands, except share and per share data):
Series | Shares Authorized | Shares Issued and Outstanding | Original Issuance Price | Liquidation Amount | Issuance Costs | Carrying Value | ||||||||||||||||||
Series A | 3,804,344 | 3,804,344 | $ | 1.38 | $ | 5,250 | $ | 9 | $ | 5,241 | ||||||||||||||
Series B | 1,209,621 | 1,209,621 | 5.79 | 7,000 | 106 | 6,894 | ||||||||||||||||||
Series C | 2,400,000 | 2,342,857 | 9.49 | 22,226 | 208 | 22,018 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
| 7,413,965 | 7,356,822 | $ | 34,476 | $ | 323 | $ | 34,153 | |||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
The Company has the following redeemable convertible preferred stock issued and outstanding at December 31, 2019 (in thousands, except share and per share data):
Series | Shares Authorized | Shares Issued and Outstanding | Original Issuance Price | Liquidation Amount | Issuance Costs | Carrying Value | ||||||||||||||||||
Series A | 3,804,344 | 3,804,344 | $ | 1.38 | $ | 5,250 | $ | 9 | $ | 5,241 | ||||||||||||||
Series B | 1,209,621 | 1,209,621 | 5.79 | 7,000 | 106 | 6,894 | ||||||||||||||||||
Series C | 2,372,371 | 2,342,857 | 9.49 | 22,226 | 208 | 22,018 | ||||||||||||||||||
Series D | 2,507,720 | 2,447,818 | 12.56 | 30,750 | 647 | 30,103 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
| 9,894,056 | 9,804,640 | $ | 65,226 | $ | 970 | $ | 64,256 | |||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
The Company has the following redeemable convertible preferred stock issued and outstanding at December 31, 2020 (in thousands, except share and per share data):
Series | Shares Authorized | Shares Issued and Outstanding | Original Issuance Price | Liquidation Amount | Issuance Costs | Carrying Value | ||||||||||||||||||
Series A | 3,804,344 | 3,804,344 | $ | 1.38 | $ | 5,250 | $ | 9 | $ | 5,241 | ||||||||||||||
Series B | 1,209,621 | 1,209,621 | 5.79 | 7,000 | 106 | 6,894 | ||||||||||||||||||
Series C | 2,372,371 | 2,342,857 | 9.49 | 22,226 | 208 | 22,018 | ||||||||||||||||||
Series D | 2,507,720 | 2,447,818 | 12.56 | 30,750 | 647 | 30,103 | ||||||||||||||||||
Series E | 1,921,902 | 1,899,847 | 15.87 | 30,150 | 106 | 30,044 | ||||||||||||||||||
Series F | 2,425,432 | 1,062,715 | 21.88 | 23,250 | 219 | 23,031 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
| 14,241,390 | 12,767,202 | $ | 118,626 | $ | 1,295 | $ | 117,331 | |||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
F-25
Table of Contents
The rights and preferences of holders of the redeemable convertible preferred stock are as follows:
Voting Rights
The holder of each share of redeemable convertible preferred stock has the voting rights equal to an equivalent number of shares of common stock into which it is convertible and votes together as a single class with common stock.
Election of Directors
The holders of a majority of the Shares of Series A, Series B, Series C and Series D redeemable convertible preferred stock, voting separately as a single class, are entitled to each elect one director of the Company. The holders of a majority of the shares of Series E and Series F redeemable convertible preferred stock, voting together as a single class, are entitled to elect one director of the Company.
Dividends
The holders of Series A, Series B, Series C, Series D, Series E and Series F redeemable convertible preferred stock are entitled to receive dividends declared by the board of directors in proportion to the numbers of shares of common stock, which are held by each holder if all shares of such series of redeemable convertible preferred stock were converted to common stock at the then-effective conversion rate of each series of redeemable convertible preferred stock. No dividends shall be paid on any common stock (other than dividends on shares of common stock payable in shares of common stock) until dividends to the holders of the redeemable convertible preferred stock have been paid. As of December 31, 2020, no dividends have been declared to date.
Liquidation Rights
In the event of any liquidation, dissolution, or winding-up of the Company, either voluntary or involuntary, the holders of Series F, Series E and Series D redeemable convertible preferred stock shall be entitled to receive on a pari passu basis among each other, prior to and in preference to any distribution of any of the assets to the holders of Series C redeemable convertible preferred stock, Series B redeemable convertible preferred stock, Series A redeemable convertible preferred stock, and the common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
After the payment of all preferential amounts required to be paid to the holders of Series D redeemable convertible preferred stock, the holders of Series C redeemable convertible preferred stock shall be entitled to receive, prior to and in preference to any distribution of any of the assets to the holders of Series B redeemable convertible preferred stock, Series A redeemable convertible preferred stock, and the common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
After the payment of all preferential amounts required to be paid to the holders of Series C redeemable convertible preferred stock, the holders of Series B shall be entitled to receive, prior to and in preference to any distribution of any of the assets to the holders of Series A redeemable convertible preferred stock and the common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
After the payment of all preferential amounts required to be paid to the holders of Series B redeemable convertible preferred stock, the holders of Series A shall be entitled to receive, prior to and in preference to any distribution of any of the assets to the holders of common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
F-26
Table of Contents
If upon the occurrence of such an event, the assets and funds distributed among the holders of the redeemable convertible preferred stock are insufficient to permit the payment to such holders of the redeemable convertible preferred stock, then the entire assets and funds of the Company legally available for distribution shall be distributed ratably among the holders of the redeemable convertible preferred stock in proportion to the full preferential amount each such holders are otherwise entitled to have received pursuant to the entitlement as noted above.
After the payment in full to holders of the redeemable convertible preferred stock as noted above, the remaining assets, if any, shall be distributed to the holders of the common and redeemable convertible preferred stock on a pro-rata as-if-converted basis.
Conversion rights
Each share of redeemable convertible preferred stock is convertible, at the option of the holder, at any time after the date of issuance of such share for such redeemable convertible preferred stock. Each share of redeemable convertible preferred stock shall be convertible into the number of shares of common stock determined by dividing the original issuance price by the conversion price. The initial conversion price for each share of redeemable convertible preferred stock is the original issuance price for such share of redeemable convertible preferred stock.
Each share of redeemable convertible preferred stock automatically converts into the number of shares of common stock at the conversion price on the earlier of (i) immediately prior to the closing of a firmly underwritten public offering in the aggregate gross proceeds received by the Company are not less than $75,000,000 and the Company’s valuation, represented by fair market value of the issued and outstanding shares of common stock (assuming conversion of all redeemable convertible preferred stock into common stock) immediately prior to giving effect to the issuance of any shares pursuant to such public offering, calculated based on the price per share at which the underwriters propose to sell such common stock to the public, is at least $425,000,000 on or before the 12-month anniversary of the initial purchase date of the Series F redeemable convertible preferred stock, and at least $475,000,000 after the twelve 12-month anniversary of the initial purchase date of the Series F redeemable convertible preferred stock (a “Qualified IPO”) or (ii) the date specified in a written request by the holders of a majority of the then outstanding shares of the Series E redeemable convertible preferred stock and the Series F redeemable convertible preferred stock, voting together as a separate class on an as-if converted basis.
As of December 31, 2020, the conversion ratio for each series of redeemable convertible preferred stock was one-for-one.
Redemption
The redeemable convertible preferred stock is recorded in mezzanine equity because, while it is not mandatorily redeemable, it will become redeemable at the option of the stockholders upon the occurrence of certain deemed liquidation events that are considered not solely within the Company’s control.
Note 8. Common Stock Warrants
In connection with the issuance of the Company’s Series A redeemable convertible preferred stock issuances in September 2011, the Company issued a warrant to purchase 64,655 shares of common stock to an investor who purchased Series A redeemable convertible preferred stock at an exercise price of $0.10 per share. The common stock warrant was exercised in December 2020 and is no longer outstanding.
F-27
Table of Contents
Note 9. Redeemable Convertible Preferred Stock Warrants
2019 Warrants
In conjunction with the funding of Tranche 1 and Tranche 2 under the 2019 Term Loan, the Company issued the 2019 Initial Warrant to purchase 29,514 shares of its Series C redeemable convertible preferred stock (see Note 5). The 2019 Initial Warrant is immediately exercisable, at an exercise price per share of $9.49, and expires 10 years from their date of issuance. The 2019 Initial Warrant will be automatically exercised upon the consummation or effective date of a change of control of the Company. Further, depending on the funding of the 2019 Term Loan Tranche 3, the Company was obligated to issue the 2019 Additional Warrant (together with the 2019 Initial Warrant to “2019 Warrants”) to the Lender to purchase up to 12,649 shares of Series C redeemable convertible preferred stock at the respective exercise price.
The estimated fair value of the 2019 Warrants on the date of issuance was $0.2 million. As of the issuance date, the fair value of the 2019 Warrants was calculated using the Black-Scholes option-pricing model and was based on a term of 10 years, a risk-free interest rate of 2.99%, expected volatility of 50.95%, and 0% expected dividend yield.
At initial recognition, the 2019 Warrants were recorded at their estimated fair values and were subject to remeasurement at each balance sheet date, with changes in fair value recognized as a component of net income. As of December 31, 2019 and 2020, the estimated fair values of the 2019 Warrants were $0.2 million and $0.3 million, respectively. The fair value of the 2019 Warrants as of December 31, 2019 and 2020 was calculated using the Black-Scholes option-pricing model with the following assumptions as of each reporting date:
| December 31, | ||||||||
| 2019 | 2020 | |||||||
Expected term (in years) | 9.1–10.0 | 8.1–8.5 | ||||||
Expected volatility | 50.63%–50.95% | 42.18%–42.63% | ||||||
Risk-free interest rate | 2.33%–2.49% | 2.33%–2.49% | ||||||
Dividend yield | — | — | ||||||
As of December 31, 2020, the 2019 Initial Warrant remained outstanding and the remaining term was 8.3 years. The 2019 Additional Warrant of 12,649 shares of series C redeemable convertible preferred stock was not legally issued and expired upon modification of the 2019 Term Loan.
2020 Warrants
In conjunction with entering the 2020 Term Loan agreement, the Company issued the 2020 Warrant to purchase 300,000 shares of its Series F redeemable convertible preferred stock (see Note 5). The 2020 Warrant is immediately exercisable, at an exercise price per share of $21.88, and expire 10 years from their date of issuance. The warrant will be automatically exercised upon the consummation or effective date of a change of control of the Company.
The estimated fair value of the 2020 Warrant on the date of issuance was $1.8 million. As of the issuance date, the fair value of the 2020 Warrant was calculated using an Option-Pricing Method with Discounts for Lack of Marketability for each class of security.
At initial recognition, the 2020 Warrant was recorded at its estimated fair values and was subject to remeasurement at each balance sheet date, with changes in fair value recognized as a component of net income. As of December 31, 2020, the estimated fair values of the 2020 Warrant was $1.8 million. The fair value of the 2020 Warrant as of December 31, 2020 was calculated using the Black-Scholes option-pricing model and was based on an Option-Pricing Method with Discounts for Lack of Marketability for each class of security.
As of December 31, 2020, the 2020 Warrant remained outstanding and the remaining term was 9.9 years.
F-28
Table of Contents
Note 10. Common Stock
At December 31, 2020, the Company’s certificate of incorporation, as amended and restated, authorizes the Company to issue up to 21,831,000 shares of common stock with $0.001 par value per share, of which 4,754,591 shares were issued and outstanding. The holders of common stock are also entitled to receive dividends whenever funds are legally available, when and if declared by the board of directors. As of December 31, 2020, no dividends have been declared to date. Each share of common stock is entitled to one vote.
At December 31, 2018, 2019 and 2020, the Company had reserved common stock for future issuances as follows:
| December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Conversion of Series A redeemable convertible preferred stock and warrants | 3,868,999 | 3,868,999 | 3,804,344 | |||||||||
Conversion of Series B redeemable convertible preferred stock | 1,209,621 | 1,209,621 | 1,209,621 | |||||||||
Conversion of Series C redeemable convertible preferred stock and warrants | 2,342,857 | 2,372,371 | 2,372,371 | |||||||||
Conversion of Series D redeemable convertible preferred stock | — | 2,447,818 | 2,447,818 | |||||||||
Conversion of Series E redeemable convertible preferred stock | — | — | 1,899,847 | |||||||||
Conversion of Series F redeemable convertible preferred stock | — | — | 1,362,715 | |||||||||
Exercise of options under stock plan | 4,596,003 | 4,659,733 | 4,754,591 | |||||||||
Issuance of options under plan | 921,468 | 993,988 | 1,568,888 | |||||||||
|
|
|
|
|
| |||||||
| 12,938,948 | 15,552,530 | 19,420,195 | ||||||||||
|
|
|
|
|
| |||||||
Note 11. Stock Option Plan
In 2011, the Company established its 2011 stock option plan (the “2011 Plan”) that provides for the granting of stock options to employees and nonemployees of the Company. Under the 2011 Plan, the Company has the ability to issue incentive stock options (ISOs), nonqualified stock options (NSOs), stock appreciation rights, dividend equivalent rights, restricted stock awards, and restricted stock unit awards. Options under the 2011 Plan may be granted for periods of up to 10 years. For incentive stock option granted to a grantee who, at the time the option is granted, owns stock representing more than 10% of the voting power of all classes of stock of the Company or any parent or subsidiary of the Company, the term of the incentive stock option may be granted for periods of up to five years. The ISOs and NSOs will be granted at a price per share not less than the fair value at the date of grant. The exercise price of an ISO granted to a 10% stockholder shall not be less than 110% of the estimated fair value of the shares on the date of grant, as determined by the board of directors. Options granted to new hires generally vest over a four-year period, with 25% vesting at the end of one year and the remaining vesting monthly thereafter; options granted as merit awards generally vest monthly over a four-year period. At December 31, 2018, 2019 and 2020, there were 25,377 shares, 830,938 shares and 225,835 shares, respectively, of common stock available for issuance under the 2011 Plan.
F-29
Table of Contents
The following table summarizes the Company’s stock option activity for the years ended December 31, 2018, 2019 and 2020:
| Options Outstanding | ||||||||||||||||||||
| Shares Available for Grant | Number of Options | Weighted- Average Exercise Price | Weighted- Average Remaining Contractual Term (In years) | Aggregate Intrinsic Value (in thousands) | ||||||||||||||||
Balances as of December 31, 2017 | 92,676 | 827,967 | $ | 0.37 | 7.2 | $ | 262 | |||||||||||||
Additional shares reserved | 80,451 | |||||||||||||||||||
Options granted | (164,500 | ) | 164,500 | $ | 0.69 | |||||||||||||||
Options forfeited/canceled | 16,750 | (16,750 | ) | $ | 0.61 | |||||||||||||||
Options exercised | — | (54,249 | ) | $ | 0.41 | |||||||||||||||
|
|
|
| |||||||||||||||||
Balances as of December 31, 2018 | 25,377 | 921,468 | $ | 0.42 | 6.6 | $ | 245 | |||||||||||||
Additional shares reserved | 941,811 | |||||||||||||||||||
Options granted | (154,000 | ) | 154,000 | $ | 1.24 | |||||||||||||||
Options forfeited/canceled | 17,750 | (17,750 | ) | $ | 0.66 | |||||||||||||||
Options exercised | — | (63,730 | ) | $ | 0.46 | |||||||||||||||
|
|
|
| |||||||||||||||||
Balances as of December 31, 2019 | 830,938 | 993,988 | $ | 0.54 | 6.1 | $ | 5,106 | |||||||||||||
Options granted | (624,950 | ) | 624,950 | $ | 3.94 | |||||||||||||||
Options forfeited/canceled | 19,847 | (19,847 | ) | $ | 2.45 | |||||||||||||||
Options exercised | — | (30,203 | ) | $ | 0.80 | |||||||||||||||
|
|
|
| |||||||||||||||||
Balances as of December 31, 2020 | 225,835 | 1,568,888 | $ | 1.87 | 6.8 | $ | 18,656 | |||||||||||||
|
|
|
| |||||||||||||||||
Vested and exercisable as of December 31, 2020 | 854,065 | $ | 0.74 | 4.9 | $ | 11,120 | ||||||||||||||
Expected to vest as of December 31, 2020 | 714,823 | $ | 3.22 | 8.9 | $ | 7,536 | ||||||||||||||
The weighted-average grant-date fair values of options granted in the years ended December 31, 2018, 2019 and 2020, were $0.1 million, $0.2 million and $2.9 million, respectively. The aggregate intrinsic value of options exercised were $0.1 million, $0.2 million and $0.2 million during the years ended December 31, 2018, 2019 and 2020, respectively. The aggregate intrinsic value was calculated as the difference between the exercise prices of the underlying options and the estimated fair value of the common stock on the date of exercise. As of December 31, 2020, the unrecognized stock-based compensation of unvested options was $2.6 million, which is expected to be recognized over a weighted-average period of 3.4 years.
The Company estimated the fair value of stock options using the Black-Scholes option-pricing model. The fair value of stock options is recognized on a straight-line basis over the requisite service periods of the awards. The fair value of stock options was estimated using the following weighted-average assumptions:
| December 31, | ||||||
| 2018 | 2019 | 2020 | ||||
Expected term (in years) | 6.08 | 5.00–6.08 | 5.85–6.08 | |||
Expected volatility | 55.13%–55.98% | 50.63%–51.00% | 48.27%–55.64% | |||
Risk-free interest rate | 2.80%–2.85% | 2.30%–2.49% | 0.33%–1.77% | |||
Dividend yield | — | — | — | |||
Expected Term
The expected term is calculated using the simplified method, which is available if there is insufficient historical data about exercise patterns and post vesting employment termination behavior. The simplified method
F-30
Table of Contents
is based on the vesting period and the contractual term for each grant or for each vesting tranche for awards with graded vesting. The midpoint of the vesting date and the maximum contractual expiration date is used as the expected term under this method. For awards with multiple vesting tranches, the time from grant until the midpoints for each of the tranches may be averaged to provide an overall expected term.
Expected Volatility
The Company used an average historical stock price volatility of a peer group of publicly traded companies to be representative of its expected future stock price volatility, as the Company did not have any trading history for its common stock. For purposes of identifying these peer companies, the Company considered the industry, stage of development, size, and financial leverage of potential comparable companies. For each grant, the Company measured historical volatility over a period equivalent to the expected term.
Risk-Free Interest Rate
The risk-free interest rate is based on the implied yield currently available on US Treasury zero-coupon issues with remaining terms equivalent to the expected term of a stock award.
Expected Dividend Rate
The Company has not paid, and does not anticipate paying, any dividends in the near future. Accordingly, the Company has estimated the dividend yield to be 0%.
The following is a summary of stock-based compensation expense by function (in thousands):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Cost of goods sold | $ | 2 | $ | 3 | $ | 20 | ||||||
Research and development | 22 | 42 | 84 | |||||||||
Selling, general and administrative | 28 | 73 | 393 | |||||||||
|
|
|
|
|
| |||||||
Total stock-based compensation expense | $ | 52 | $ | 118 | $ | 497 | ||||||
|
|
|
|
|
| |||||||
F-31
Table of Contents
Note 12. Income Taxes
Deferred Tax Assets and Liabilities
Deferred tax assets and liabilities reflect the net tax effect of temporary differences between carrying value of assets and liabilities for financial reporting purposes and the tax basis of these assets and liabilities as measured by income tax law. The income tax effect of temporary differences that give rise to deferred tax assets and (liabilities) consist of the following (in thousands):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Deferred tax assets: | ||||||||||||
Net operating loss carryforwards | $ | 7,229 | $ | 13,469 | $ | 22,208 | ||||||
Research and development credits | 505 | 775 | 1,071 | |||||||||
Operating lease liability | — | 270 | 138 | |||||||||
Deferred compensation | 84 | 362 | 899 | |||||||||
Provision for excess and obsolete inventories | — | — | 282 | |||||||||
Other | 21 | 44 | 94 | |||||||||
|
|
|
|
|
| |||||||
Total gross deferred tax assets | 7,839 | 14,920 | 24,692 | |||||||||
Less: Valuation allowance | (7,797 | ) | (14,365 | ) | (24,543 | ) | ||||||
|
|
|
|
|
| |||||||
Total net deferred tax assets | 42 | 555 | 149 | |||||||||
Deferred tax liabilities: | �� | |||||||||||
Operating lease right-of-use assets | — | (270 | ) | (135 | ) | |||||||
Fixed assets | (42 | ) | (285 | ) | (14 | ) | ||||||
|
|
|
|
|
| |||||||
Total deferred tax liabilities | (42 | ) | (555 | ) | (149 | ) | ||||||
|
|
|
|
|
| |||||||
Total net deferred taxes | $ | — | $ | — | $ | — | ||||||
|
|
|
|
|
| |||||||
The Company will continue to closely monitor the need for a valuation allowance against its existing deferred tax assets (“DTAs”) and any additional DTAs that are generated in each subsequent reporting period. The need for a valuation allowance can be affected by actual operating results, forecasted financial performance, variances between the two, and the rate at which future DTAs are generated.
Internal Revenue Code (IRC) Section 382 limits the use of federal net operating losses and income tax credit carryforwards in certain situations where changes occur in stock ownership of a company. If the Company should have an ownership change of more than 50% of the value of the Company’s capital stock, utilization of the carryforwards could be restricted.
The Company’s income tax provision for the years ended December 31, 2018, 2019 and 2020, consists of the following (in thousands):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Current: | ||||||||||||
Federal | $ | (6 | ) | $ | — | $ | 6 | |||||
State | — | 8 | 41 | |||||||||
|
|
|
|
|
| |||||||
Total current | (6 | ) | 8 | 47 | ||||||||
|
|
|
|
|
| |||||||
Provision (benefit) for income taxes | $ | (6 | ) | $ | 8 | $ | 47 | |||||
|
|
|
|
|
| |||||||
F-32
Table of Contents
The reconciliation of the statutory federal income tax rate to the Company’s effective tax rate is as follows (in thousands):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Tax at statutory federal rate | 21 | % | 21 | % | 21 | % | ||||||
State tax, net of federal benefit | 4 | % | 4 | % | 5 | % | ||||||
Research and development credit | — | 1 | % | 1 | % | |||||||
Change in valuation allowance | (25 | )% | (25 | )% | (27 | )% | ||||||
Other | — | (1 | )% | — | ||||||||
|
|
|
|
|
| |||||||
Effective tax rate | — | — | — | |||||||||
|
|
|
|
|
| |||||||
A valuation allowance is recorded when it is more likely than not that some portion of the deferred tax assets will not be realized. As of each reporting date, the Company’s management considers all evidence, both positive and negative, that could affect management’s view with regard to future realization of deferred tax assets. As of December 31, 2020, a full valuation allowance for deferred tax assets was recorded as management believes it is not more likely than not that all of the deferred tax assets will be realized. At December 31, 2018, 2019 and 2020, the Company has a net operating loss carryforward for federal income tax purposes of approximately $28.9 million, $54.1 million and $85.3 million, respectively. At December 31, 2018, 2019 and 2020, the Company has a net operating loss carryforward for state income tax purposes of approximately $29.1 million, $53.4 million and $ 83.5 million, respectively. Net operating losses prior to 2018 of $14.8 million will expire, if not utilized, beginning in 2032 for federal and state income tax purposes.
As of December 31, 2018, 2019 and 2020, the Company has federal and state research and development income tax credit carryforwards of approximately $0.3 million, $0.6 million and $0.8 million, respectively. As of December 31, 2018, 2019 and 2020, the Company has state research and development income tax credit carryforwards of approximately $0.5 million, $0.6 million and $0.9 million, respectively. The Federal income tax credits begin to expire in 2032. The Company has provided a valuation allowance of $0.4 million as of December 31, 2020 for deferred tax assets related to research and development income tax credits that are not expected to be utilized. The Company does not expect any significant change to the UTP balances in the next 12 months.
The following table summarizes the activity related to the unrecognized tax benefits (in thousands):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Unrecognized tax benefits at the beginning of the year | $ | — | $ | 200,089 | $ | 303,665 | ||||||
|
|
|
|
|
| |||||||
Additions based on tax positions related to the current year | 76,568 | 103,576 | 113,333 | |||||||||
Additions for tax positions of prior years | 123,521 | — | — | |||||||||
|
|
|
|
|
| |||||||
Unrecognized tax benefits at the end of the year | $ | 200,089 | $ | 303,665 | $ | 416,998 | ||||||
|
|
|
|
|
| |||||||
The Company does not have any material uncertain tax positions as of December 31, 2020 and does not expect any significant change to such balances in the next twelve months.
The Company currently has no federal or state tax examinations in progress nor has it had any federal or state tax examinations since its inception. Due to the history of net operating losses, the Company’s federal and state tax returns remain open to examination by the tax authorities.
F-33
Table of Contents
Note 13. Net loss per share attributable to common stockholders
Basic net loss per share is computed by dividing the net loss by the weighted-average number of common shares outstanding for the period. As the Company reported a net loss for 2018, 2019 and 2020, basic net loss per share is the same as diluted net loss per share as the inclusion of potentially dilutive shares would have been antidilutive if included in the calculation.
The following table sets forth the computation of basic and diluted net loss per share attributable to common stockholders (in thousands, except share and per share data):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Numerator: | ||||||||||||
Net loss attributable to common stockholders | $ | (14,290 | ) | $ | (25,869 | ) | $ | (34,693 | ) | |||
Denominator: | ||||||||||||
Weighted-average shares of common stock outstanding—basic and diluted | 4,611,325 | 4,693,534 | 4,678,109 | |||||||||
|
|
|
|
|
| |||||||
Net loss per share attributable to common stockholders—basic and diluted | $ | (3.10 | ) | $ | (5.51 | ) | $ | (7.41 | ) | |||
|
|
|
|
|
| |||||||
The following outstanding shares of potentially dilutive securities were excluded from the computation of diluted net loss per share attributable to common stockholders for the period presented because including them would have been antidilutive:
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Series A Redeemable Convertible Preferred Stock | 3,804,344 | 3,804,344 | 3,804,344 | |||||||||
Series B Redeemable Convertible Preferred Stock | 1,209,621 | 1,209,621 | 1,209,621 | |||||||||
Series C Redeemable Convertible Preferred Stock | 2,342,857 | 2,342,857 | 2,342,857 | |||||||||
Series D Redeemable Convertible Preferred Stock | — | 2,447,818 | 2,447,818 | |||||||||
Series E Redeemable Convertible Preferred Stock | — | — | 1,899,847 | |||||||||
Series F Redeemable Convertible Preferred Stock | — | — | 1,062,715 | |||||||||
Options to purchase common stock | 921,468 | 993,988 | 1,568,888 | |||||||||
Redeemable Convertible Preferred Stock Warrants | — | 42,163 | 329,514 | |||||||||
|
|
|
|
|
| |||||||
Total | 8,278,290 | 10,840,791 | 14,665,604 | |||||||||
|
|
|
|
|
| |||||||
Unaudited Pro Forma Net Loss per Share
Unaudited pro forma basic and diluted net loss per share were computed to give effect to the one-for-one conversion of all outstanding shares of the Company’s redeemable convertible preferred stock into shares of common stock in connection with the IPO, using the as-converted method as though the conversion had occurred as of the beginning of the period presented or the date of issuance, if later. Refer to Note 2 for further discussion.
F-34
Table of Contents
Unaudited pro forma basic and diluted loss per share is computed as follows (in thousands, except share and per share data):
| Year Ended December 31, 2020 | ||||
| Numerator: | ||||
Net loss attributable to common stockholders | $ | ( | ) | |
Adjust: change in fair value of redeemable convertible preferred stock warrants | ||||
|
| |||
Pro forma net loss | ||||
|
| |||
Denominator: | ||||
Weighted-average shares of common stock outstanding used in computing net loss per share attributable to common stockholder—basic and diluted | ||||
Adjust: conversion of redeemable convertible preferred stock | ||||
Adjust: conversion of common stock warrants | ||||
|
| |||
Weighted-average shares outstanding used in computing pro forma net loss per share—basic and diluted | ||||
|
| |||
Net loss per share attributable to common stockholders—basic and diluted | $ | ( | ) | |
|
| |||
Note 14. Defined Contribution Plan
The Company sponsors a defined contribution plan under Section 401(k) of the IRC of 1986, as amended, covering substantially all of its full-time US employees. Participating employees may contribute up to 100% of their eligible compensation up to the annual Internal Revenue Service’s contribution limit. For fiscal years 2018, 2019 and 2020, the Company did not match employee contributions.
Note 15. Segment Information
The Company has two reportable operating segments which are determined on the basis of product portfolio: Surgical Glaucoma and Dry Eye. The operating and reportable segments were determined based on how the Company’s Chief Executive Officer, its Chief Operating Decision Maker (“CODM”), views and evaluates the Company’s operations. The CODM allocates resources to and evaluates the financial performance of each operating segment primarily based on gross profit and gross profit margin.
Surgical Glaucoma segment includes sales of the Company’s OMNI® Surgical System and its predicate devices for use in minimally invasive glaucoma procedures. Dry Eye segment includes sales of the Company’s TearCare® System and related components.
F-35
Table of Contents
The following table summarizes select operating results information for each reportable segment (dollars in thousands):
| Years Ended December 31, | ||||||||||||
| 2018 | 2019 | 2020 | ||||||||||
Revenue | ||||||||||||
Surgical Glaucoma | $ | 7,530 | $ | 22,304 | $ | 26,000 | ||||||
Dry Eye | — | 1,044 | 1,640 | |||||||||
|
|
|
|
|
| |||||||
Total | 7,530 | 23,348 | 27,640 | |||||||||
Cost of goods sold | ||||||||||||
Surgical Glaucoma | 2,338 | 5,132 | 7,069 | |||||||||
Dry Eye | — | 1,412 | 2,140 | |||||||||
|
|
|
|
|
| |||||||
Total | 2,338 | 6,544 | 9,209 | |||||||||
Gross profit | ||||||||||||
Surgical Glaucoma | 5,192 | 17,172 | 18,931 | |||||||||
Dry Eye | — | (368 | ) | (500 | ) | |||||||
|
|
|
|
|
| |||||||
Total | 5,192 | 16,804 | 18,431 | |||||||||
Operating expenses | 19,489 | 40,843 | 50,619 | |||||||||
|
|
|
|
|
| |||||||
Loss from operations | (14,297 | ) | (24,039 | ) | (32,188 | ) | ||||||
Interest income | 1 | 174 | 30 | |||||||||
Interest expense | — | (1,961 | ) | (2,403 | ) | |||||||
Other income (expense), net | — | (35 | ) | (71 | ) | |||||||
|
|
|
|
|
| |||||||
Loss before income tax | $ | (14,296 | ) | $ | (25,861 | ) | $ | (34,632 | ) | |||
|
|
|
|
|
| |||||||
The Company does not allocate any income and expenses beyond revenue and cost of goods sold to the reportable operating segments in its reporting to the CODM. No asset information is provided for reportable operating segments because they are not reviewed by the CODM on segment basis. Substantially all of the Company’s revenue is generated from sales in the United States, and none of its property and equipment is located outside the United States.
Note 16. Subsequent Events
The Company evaluated subsequent events through April 9, 2021, the date on which the consolidated financial statements were available for issuance.
Lease renewal
On February 5, 2021, the Company entered into a lease to renew the corporate headquarters in Menlo Park, California. The lease commenced on August 1, 2021 and is for a term of 37 months from the commencement date. Total base rent is approximately $1.6 million under the lease agreement.
F-36
Table of Contents
SIGHT SCIENCES, INC.
Condensed Consolidated Balance Sheets
(In thousands, except share and per share amounts)
| As of December 31. | As of March 31, | |||||||
| 2020 | 2021 | |||||||
| (unaudited) | ||||||||
Assets | ||||||||
Current assets: | ||||||||
Cash and cash equivalents | $ | 61,511 | $ | 48,327 | ||||
Accounts receivable, net | 5,363 | 5,637 | ||||||
Inventory, net | 2,598 | 2,533 | ||||||
Prepaid expenses and other current assets | 1,161 | 1,040 | ||||||
|
|
|
| |||||
Total current assets | 70,633 | 57,537 | ||||||
Property and equipment, net | 1,269 | 1,224 | ||||||
Operating lease ROU assets | 518 | 362 | ||||||
Other noncurrent assets | 386 | 1,410 | ||||||
|
|
|
| |||||
Total assets | $ | 72,806 | $ | 60,533 | ||||
|
|
|
| |||||
Liabilities, redeemable convertible preferred stock, and Stockholders’ deficit | ||||||||
Current liabilities: | ||||||||
Accounts payable | $ | 2,158 | $ | 3,010 | ||||
Accrued compensation | 4,070 | 2,225 | ||||||
Accrued and other current liabilities | 3,086 | 4,063 | ||||||
|
|
|
| |||||
Total current liabilities | 9,314 | 9,298 | ||||||
Long-term debt | 31,955 | 32,124 | ||||||
Other noncurrent liabilities | 3,055 | 2,581 | ||||||
|
|
|
| |||||
Total liabilities | 44,324 | 44,003 | ||||||
|
|
|
| |||||
Commitments and contingencies (Note 6) | ||||||||
Redeemable convertible preferred stock: | ||||||||
Convertible Preferred Stock, $0.001 par value; 14,241,390 shares authorized as of December 31, 2020 and March 31, 2021; 12,767,202 shares issued and outstanding as of December 31, 2020 and March 31, 2021, respectively; aggregate liquidation preference of $118.6 million as of December 31, 2020 and March 31, 2021, respectively | 117,331 | 117,331 | ||||||
Stockholders’ deficit: | ||||||||
Common stock par value of $0.001 per share—21,831,000 shares authorized at December 31, 2020 and March 31, 2021; 4,754,591 shares issued and outstanding as of December 31, 2020, and 4,763,022 shares issued and outstanding at March 31, 2021 | 5 | 5 | ||||||
Additional paid-in capital | 1,187 | 1,475 | ||||||
Accumulated deficit | (90,041 | ) | (102,281 | ) | ||||
|
|
|
| |||||
Total stockholders’ deficit | (88,849 | ) | (100,801 | ) | ||||
|
|
|
| |||||
Total liabilities, redeemable convertible preferred stock, and stockholders’ deficit | $ | 72,806 | $ | 60,533 | ||||
|
|
|
| |||||
The accompanying notes are an integral part of these condensed consolidated financial statements.
F-37
Table of Contents
SIGHT SCIENCES, INC.
Condensed Consolidated Statements of Operations and Comprehensive Loss
(In thousands, except share and per share data)
| Three Months Ended March 31, | ||||||||
| 2020 | 2021 | |||||||
| (unaudited) | ||||||||
Revenue | $ | 6,496 | $ | 8,635 | ||||
Cost of goods sold | 2,128 | 2,301 | ||||||
|
|
|
| |||||
Gross profit | 4,368 | 6,334 | ||||||
Operating expenses: | ||||||||
Research and development | 2,400 | 3,440 | ||||||
Selling, general, and administrative | 10,678 | 14,550 | ||||||
|
|
|
| |||||
Total operating expenses | 13,078 | 17,990 | ||||||
|
|
|
| |||||
Loss from operations | (8,710 | ) | (11,656 | ) | ||||
Interest income | 27 | — | ||||||
Interest expense | (552 | ) | (1,084 | ) | ||||
Other income (expense), net | 91 | 552 | ||||||
|
|
|
| |||||
Loss before income taxes | (9,144 | ) | (12,188 | ) | ||||
Provision for income taxes | 31 | 52 | ||||||
|
|
|
| |||||
Net loss and comprehensive loss | $ | (9,175 | ) | $ | (12,240 | ) | ||
|
|
|
| |||||
Net loss per share outstanding attributable to common stockholders, basic and diluted | $ | (1.94 | ) | $ | (2.57 | ) | ||
|
|
|
| |||||
Weighted-average common shares outstanding used in computing net loss per share attributable to common stockholders, basic and diluted | 4,724,693 | 4,758,635 | ||||||
|
|
|
| |||||
Pro forma net loss per share, basic and diluted (unaudited) | ||||||||
|
| |||||||
Weighted-average shares outstanding used in computing pro forma net loss per share, basic and diluted (unaudited) | ||||||||
|
| |||||||
The accompanying notes are an integral part of these condensed consolidated financial statements.
F-38
Table of Contents
SIGHT SCIENCES, INC.
Condensed Consolidated Statements of Redeemable Convertible Preferred Stock and Stockholders’ Deficit
(In thousands, except share amounts, unaudited)
| Redeemable Convertible Preferred Stock | Common Stock | Additional Paid-In Capital | Accumulated Deficit | Total Stockholders’ Deficit | ||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||
Balances at December 31, 2019 | 9,804,640 | $ | 64,256 | 4,659,733 | $ | 5 | $ | 660 | $ | (55,348 | ) | $ | (54,683 | ) | ||||||||||||||
Issuance of Series E redeemable convertible preferred stock, net of issuance costs of $94 | 1,899,847 | 30,055 | — | — | — | — | — | |||||||||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 750 | — | 1 | — | 1 | |||||||||||||||||||||
Stock-based compensation expense | — | — | — | — | 61 | — | 61 | |||||||||||||||||||||
Net loss | — | — | — | — | (9,175 | ) | (9,175 | ) | ||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
Balances at March 31, 2020 | 11,704,487 | $ | 94,311 | 4,660,483 | $ | 5 | $ | 722 | $ | (64,523 | ) | $ | (63,796 | ) | ||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
| Redeemable Convertible Preferred Stock | Common Stock | Additional Paid-In Capital | Accumulated Deficit | Total Stockholders’ Deficit | ||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||
Balances at December 31, 2020 | 12,767,202 | $ | 117,331 | 4,754,591 | $ | 5 | $ | 1,187 | $ | (90,041 | ) | $ | (88,849 | ) | ||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 8,431 | — | 11 | — | 11 | |||||||||||||||||||||
Stock-based compensation expense | — | — | — | — | 277 | — | 277 | |||||||||||||||||||||
Net loss | — | — | — | (12,240 | ) | (12,240 | ) | |||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
Balances at March 31, 2021 | 12,767,202 | $ | 117,331 | 4,763,022 | $ | 5 | $ | 1,475 | $ | (102,281 | ) | $ | (100,801 | ) | ||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
The accompanying notes are an integral part of these condensed consolidated financial statements.
F-39
Table of Contents
SIGHT SCIENCES, INC.
Condensed Consolidated Statements of Cash Flows
(In thousands)
| Three Months Ended March 31, | ||||||||
| 2020 | 2021 | |||||||
Cash flows from operating activities | ||||||||
Net loss | $ | (9,175 | ) | $ | (12,240 | ) | ||
Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
Depreciation | 143 | 135 | ||||||
Accretion of debt discount and amortization of debt issuance costs | 140 | 170 | ||||||
Stock-based compensation expense | 61 | 277 | ||||||
Provision for doubtful accounts receivable | 127 | 27 | ||||||
Provision for excess and obsolete inventories | 382 | 211 | ||||||
Noncash operating lease expense | 132 | 156 | ||||||
Change in fair value of redeemable convertible preferred stock warrant | (91 | ) | (555 | ) | ||||
Loss on disposal of property and equipment | 5 | 4 | ||||||
Changes in operating assets and liabilities: | ||||||||
Accounts receivable | 188 | (301 | ) | |||||
Inventory | (210 | ) | (146 | ) | ||||
Prepaid expenses and other current assets | (176 | ) | 122 | |||||
Other noncurrent assets | — | (1,024 | ) | |||||
Accounts payable | 278 | 1,071 | ||||||
Accrued compensation | (1,149 | ) | (1,845 | ) | ||||
Accrued and other current liabilities | (329 | ) | 977 | |||||
Other noncurrent liabilities | 113 | 91 | ||||||
|
|
|
| |||||
Net cash used in operating activities | (9,561 | ) | (12,870 | ) | ||||
|
|
|
| |||||
Cash flows from investing activities | ||||||||
Purchases of property and equipment | (513 | ) | (104 | ) | ||||
|
|
|
| |||||
Net cash used in investing activities | (513 | ) | (104 | ) | ||||
|
|
|
| |||||
Cash flows from financing activities | ||||||||
Payments of costs related to initial public offering | — | (223 | ) | |||||
Proceeds from the issuance of Series E redeemable convertible preferred stock | 30,152 | — | ||||||
Series E issuance costs | (97 | ) | — | |||||
Proceeds from exercise of stock options | 1 | 13 | ||||||
|
|
|
| |||||
Net cash (used) and provided by financing activities | 30,056 | (210 | ) | |||||
|
|
|
| |||||
Net change in cash and cash equivalents | 19,982 | (13,184 | ) | |||||
Cash and cash equivalents | ||||||||
Beginning of period | 21,237 | 61,511 | ||||||
|
|
|
| |||||
End of period | $ | 41,219 | $ | 48,327 | ||||
|
|
|
| |||||
Supplemental disclosure of cash flow information | ||||||||
Cash paid for interest | $ | 310 | $ | 766 | ||||
Supplemental noncash disclosure | ||||||||
Acquisition of property and equipment included in accounts payable and accrued liabilities | $ | 55 | $ | 35 | ||||
Unpaid initial public offering costs in accounts payable and accrued liabilities | $ | — | 1,017 | |||||
The accompanying notes are an integral part of these condensed consolidated financial statements.
F-40
Table of Contents
SIGHT SCIENCES, INC.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Note 1. Company and Nature of Business
Description of Business
Sight Sciences, Inc. (the “Company”) was incorporated in the state of Delaware in 2010. The Company is an ophthalmic medical device company focused on the development and commercialization of surgical and nonsurgical technologies for the treatment of prevalent eye diseases. The Company’s surgical glaucoma product portfolio features the OMNI Surgical System, a device that facilitates the performance of both trabeculotomy and canaloplasty with a single device and single corneal incision. The Company’s nonsurgical dry eye product portfolio consists of the TearCare system for ophthalmologists and optometrists. TearCare is a wearable eyelid technology that delivers highly targeted and adjustable heat to the meibomian glands of the eyelids.
The Company is located and headquartered in Menlo Park, California. The other office operated by the Company is in Southlake, Texas.
Significant Risks and Uncertainties
Since inception, the Company has incurred losses and negative cash flows from operations. As of March 31, 2021, the Company had an accumulated deficit of $102.3 million and recorded a net loss of $12.2 million for the three months then ended and expects to incur future additional losses. If the Company’s revenue levels from its products are not sufficient or if the Company is unable to secure additional funding when desired, the Company may need to delay the development of its products and scale back its business and operations.
The Company believes that its existing sources of liquidity will satisfy its working capital and capital requirements for at least 12 months from the issuance of its financial statements. Failure to generate sufficient revenues, achieve planned gross margins, or control operating costs will require the Company to raise additional capital through equity or debt financing. Such additional financing may not be available on acceptable terms, or at all, and could require the Company to modify, delay, or abandon some of its planned future expansion or expenditures or reduce some of its ongoing operating costs, which could harm its business, operating results, financial condition, and ability to achieve its intended business objectives.
On March 11, 2020, the World Health Organization declared the coronavirus disease 2019 (“COVID-19”) outbreak a global pandemic recommending containment measures worldwide. On March 16, 2020 the Company implemented alternative work arrangements for its employees and limited its employees’ travel activities to protect its employees and to comply with the provisions described within the local shelter in place order. Certain U.S. federal, state and local governmental authorities issued other orders and directives, including restrictions on elective procedures and therapies, aimed at minimizing the spread of COVID-19. As such, the COVID-19 pandemic impacted and is expected to continue to impact demand for the Company’s products, which are used in procedures and therapies that are considered elective. Although some of the governmental restrictions have since been lifted or scaled back, recent and future surges of COVID-19 may result in restrictions being re-implemented in response to efforts to reduce the spread of COVID-19.
The ultimate impact of the COVID-19 pandemic on the Company’s operations is unknown and will depend on future developments which are highly uncertain and cannot be predicted with confidence, including the duration and severity of the COVID-19 outbreak, the status of health and safety actions taken to contain its spread and any additional preventative and protective actions that governments, or the Company, may direct, any resurgence of COVID-19 that may occur and how quickly and to what extent economic and operating conditions normalize within the markets in which the Company operates. The COVID-19 pandemic could disrupt the operations of the Company’s third-party manufacturers and other suppliers. Although the Company has not experienced disruptions in its supply chain to date, it cannot predict how long the pandemic and measures
F-41
Table of Contents
intended to contain the spread of COVID-19 will continue and what effect COVID-19 and the associated containment measures will have on our suppliers and vendors, in particular for any of the Company’s suppliers and vendors that may not qualify as essential businesses and suffer more significant disruptions to their business operations. The Company is working closely with its manufacturing partners and suppliers to help ensure the Company is able to source key components and maintain appropriate inventory levels to meet customer demand.
Note 2. Summary of Significant Accounting Policies
Basis of Presentation
The accompanying condensed consolidated financial statements are unaudited and have been prepared in accordance with accounting principles generally accepted in the United States (“GAAP”) applicable to interim periods. The condensed consolidated financial statements, in the opinion of management, include all normal and recurring adjustments necessary to present fairly the Company’s financial position and results of operations for the reported periods. These condensed consolidated financial statements have been prepared on a basis substantially consistent with, and should be read in conjunction with the audited financial statements for the year ended December 31, 2020 and notes thereto, the Company’s Annual Report on Form S-1 filed with the Securities and Exchange Commission (“SEC”) on April 9, 2021. Certain information and note disclosures normally included in the audited financial statements prepared in accordance with GAAP have been condensed or omitted from this report. The results of operations for any interim period are not necessarily indicative of the results for the year ending December 31, 2021, or for any future period.
The accompanying condensed consolidated financial statements reflect the operations of the Company and its wholly-owned subsidiaries. All intercompany accounts and transactions have been eliminated.
Use of Estimates
The preparation of financial statements in conformity with US GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities, disclosure of contingent assets and liabilities at the date of the financial statements, and the reported amounts of revenues and expense during the reporting period. The most significant estimates related to inventory excess and obsolescence, the selection of useful lives of property and equipment, determination of the fair value of stock option grants, the fair value of the redeemable convertible preferred stock warrants, and provisions for income taxes and contingencies. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. These estimates are based on information available as of the date of the financial statements. Actual results could differ from these estimates and such differences could be material to the Company’s financial position and results of operations.
Unaudited Pro Forma Information
The unaudited pro forma basic and diluted net loss per share data has been computed to give effect to an adjustment to the denominator in the pro forma basic and diluted net loss per share calculation for the conversion of the redeemable convertible preferred stock into shares of common stock as of the beginning of the period or the date of issuance, if later. The numerator in the pro forma basic and diluted net loss per share calculation has been adjusted to remove gains or losses resulting from the remeasurement of the redeemable convertible preferred stock warrant liability.
Fair Value of Financial Instruments
The Company’s financial instruments consist of cash and cash equivalents, accounts receivable, accounts payable, accrued liabilities, redeemable convertible preferred stock, short-term and long-term debt and
F-42
Table of Contents
redeemable convertible preferred stock warrant liability. The Company states accounts receivable, accounts payable, and accrued and other current liabilities at their carrying value, which approximates fair value due to the short time to the expected receipt or payment. The carrying amount of the Company’s short-term debt approximates its fair value as the effective interest rate approximates market rates currently available to the Company. The redeemable convertible preferred stock warrant liability associated with the Company’s redeemable convertible preferred stock is carried at fair value based on unobservable market inputs.
Deferred Offering Costs
Deferred offering costs, consisting of legal, accounting and other fees and costs relating to the Company’s planned IPO, are capitalized and recorded on the balance sheet. The deferred offering costs will be offset against the proceeds received upon the closing of the planned IPO. In the event that the Company’s plans for an IPO are terminated, all of the deferred offering costs will be written off within operating expenses in the Company’s statements of operations and comprehensive loss. As of December 31, 2020 and March 31, 20201 deferred offering costs of $0.4 million and $1.3 million, respectively, were capitalized and are included in “Other noncurrent assets.
Accounting for Payroll Protection Program
In March 2020, Congress established the Paycheck Protection Program (“PPP”) to provide relief to small businesses during COVID-19 as part of the Coronavirus Aid, Relief, and Economic Security (“CARES”) Act. The legislation authorized the U.S. Treasury to use the Small Business Association’s (“SBA’s”) small business lending program to fund forgivable loans that qualifying businesses could spend to cover payroll, mortgage interest, rent, and utilities during the “Covered Period” defined as the 8-week period starting on the date the PPP loan proceeds are received. Upon meeting certain criteria as specified in the PPP program, the loans are eligible for partial or total forgiveness. In May 2020, the Company applied for and received a PPP loan for the amount $2.2 million from SBA. We believe we have satisfied all of the terms and conditions of the PPP loan and applied for loan forgiveness in September 2020. We expect a decision from the SBA on loan forgiveness in the second quarter of 2021.
U.S. GAAP does not contain authoritative accounting standards for forgivable loans provided by governmental entities to a for-profit entity. Absent authoritative accounting standards, interpretative guidance issued and commonly applied by financial statement preparers allows for the selection of accounting policies amongst acceptable alternatives. The Company determined it most appropriate to account for the PPP loan proceeds as an in-substance government grant by analogy to International Accounting Standards 20 (“IAS 20”) Accounting for Government Grants and Disclosure of Government Assistance. Under this guidance, a forgivable loan from government is treated as a government grant when there is reasonable assurance that the entity will meet the terms for forgiveness of the loan. While IAS 20 does not define “reasonable assurance”, this concept in practice is analogous to “probable” as defined in Financial Accounting Standards Board (“FASB”) ASC 450-20-20 under U.S. GAAP, which is the definition the Company has applied to its expectations of PPP loan forgiveness. Under IAS 20, government grants are recognized in earnings on a systematic basis over the periods in which the Company recognizes costs for which the grant is intended to compensate (i.e. qualified expenses). Further, IAS 20 permits for the recognition in earnings either separately under a general heading such as other income, or as a reduction of the related expenses.
New Accounting Pronouncements Not Yet Adopted
In June 2016, the FASB issued ASU No. 2016-13, Financial Instruments—Credit Losses (Topic 326): Measurement of Credit Losses on Financial Instruments, which amends the impairment model by requiring entities to use a forward-looking approach based on expected losses to estimate credit losses on certain types of financial instruments, including trade receivables and available-for-sale debt securities. The guidance is effective for the Company beginning in the first quarter of 2023. The Company is evaluating the impact of adopting this guidance and does not expect to have a material impact on the Company’s financial statements and related disclosures.
F-43
Table of Contents
In December 2019, the FASB issued ASU No. 2019-12, Income Taxes (Topic 740): Simplifying the Accounting for Income Taxes, that simplifies the accounting for income taxes by eliminating certain exceptions related to the approach for intra-period tax allocation and modified the methodology for calculating income taxes in an interim period. It also clarifies and simplifies other aspects of the accounting for income taxes. The guidance is effective for the Company for fiscal years beginning after December 15, 2021, and interim periods within fiscal years beginning after December 15, 2022 with early adoption permitted. The Company is evaluating the effect this new guidance and does not expect it to have material impact on the Company’s financial statements.
In March 2020, the FASB issued ASU No. 2020-04, Reference Rate Reform (Topic 848): Facilitation of the Effects of Reference Rate Reform on Financial Reporting. The new guidance provides optional expedients and exceptions for applying generally accepted accounting principles to contract modifications and hedging relationships, subject to meeting certain criteria, that reference LIBOR or another reference rate expected to be discontinued. The guidance also establishes (1) a general contract modification principle that entities can apply in other areas that may be affected by reference rate reform and (2) certain elective hedge accounting expedients. The amendment is effective for all entities through December 31, 2022. LIBOR is used to calculate the interest on borrowings under the Company’s term loan and revolving line of credit with MidCap Financial Services. The Company is evaluating the effect this new guidance and does not expect it to have material impact on the Company’s financial statements.
Note 3. Fair Value Measurements
The Company reports all financial assets and liabilities and nonfinancial assets and liabilities that are recognized or disclosed at fair value in the financial statements on a recurring basis. Valuation techniques used to measure fair value must maximize the use of observable inputs and minimize the use of unobservable inputs. The authoritative guidance establishes a fair value hierarchy that prioritizes the inputs to valuation techniques used to measure fair value. The hierarchy gives the highest priority to unadjusted quoted prices in active markets for identical assets or liabilities (Level 1 measurements) and the lowest priority to measurements involving significant unobservable inputs (Level 3 measurements). The three levels of the fair value hierarchy are as follows:
Level 1—Inputs are quoted prices (unadjusted) in active markets for identical assets or liabilities that the Company has the ability to access at the measurement date.
Level 2—Inputs are observable, unadjusted quoted prices in active markets for similar assets or liabilities, unadjusted quoted prices for identical or similar assets or liabilities in markets that are not active, or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the related assets or liabilities.
Level 3—Inputs are unobservable inputs for the asset or liability. The level in the fair value hierarchy within which a fair value measurement in its entirety is based on the lowest-level input that is significant to the fair value measurement in its entirety.
The financial statements as of December 31, 2020 and March 31, 2021, do not include any nonrecurring fair value measurements relating to assets or liabilities.
F-44
Table of Contents
The fair value measurements of liabilities that are measured at fair value on a recurring basis at December 31, 2020 and March 31, 2021, are as follows (in thousands):
| As of December 31, 2020 | ||||||||||||||||
| (Level 1) | (Level 2) | (Level 3) | Total | |||||||||||||
Liabilities | ||||||||||||||||
Redeemable convertible preferred stock warrants liabilities | $ | — | $ | — | $ | 2,112 | $ | 2,112 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Total liabilities measured at fair value | $ | — | $ | — | $ | 2,112 | $ | 2,112 | ||||||||
|
|
|
|
|
|
|
| |||||||||
| As of March 31, 2021 | ||||||||||||||||
| (Level 1) | (Level 2) | (Level 3) | Total | |||||||||||||
Liabilities | ||||||||||||||||
Redeemable convertible preferred stock warrants liabilities | $ | — | $ | — | $ | 1,557 | $ | 1,557 | ||||||||
|
|
|
|
|
|
|
| |||||||||
Total liabilities measured at fair value | $ | — | $ | — | $ | 1,557 | $ | 1,557 | ||||||||
|
|
|
|
|
|
|
| |||||||||
The Company measures the redeemable convertible preferred stock warrants using Level 3 unobservable inputs within the Black-Scholes option-pricing model. The key assumptions include the fair value of redeemable convertible preferred stock, volatility, the risk-free interest rate, expected term (remaining contractual term of the warrants) and dividend yield. The Company has limited historical volatility information available, and the expected volatility was based on actual volatility for comparable public companies projected over the expected terms of the warrants. The Company did not apply a forfeiture rate to the warrants as there is not enough historical information available to estimate such a rate. The risk-free interest rate was based on the U.S. Treasury yield curve at the time of the grant over the expected term of the warrants. Refer to Note 9 for the assumptions used.
The Company measures the fair value of outstanding debt for disclosure purposes on a recurring basis. As of December 31, 2020 and March 31, 2021, total debt of $31.9 million $32.1 million is reported at amortized cost, respectively. This outstanding debt is classified as Level 2 as it is not actively traded. The amortized cost of the outstanding debt approximates the fair value.
The Company determines the fair value of the redeemable convertible preferred stock warrants annually, with subsequent gains and losses from remeasurement of Level 3 financial liabilities recorded through the other expense, net in statements of operations and other comprehensive loss.
A summary of the changes in the fair value of the Company’s Level 3 financial instruments for the three months ended March 31, 2020 and 2021, is as follows (in thousands):
| Redeemable convertible preferred stock warrant liability | ||||
Balance—December 31, 2019 | 236 | |||
Issuance of redeemable convertible preferred stock warrants | — | |||
Change in fair value | (92 | ) | ||
|
| |||
Balance—March 31, 2020 | $ | 144 | ||
F-45
Table of Contents
| Redeemable convertible preferred stock warrant liability | ||||
Balance—December 31, 2020 | 2,112 | |||
Issuance of redeemable convertible preferred stock warrants | — | |||
Change in fair value | (555 | ) | ||
|
| |||
Balance—March 31, 2021 | $ | 1,557 | ||
Note 4. Balance Sheet Components
Property and Equipment, Net
Property and equipment, net consist of the following (in thousands):
| As of December 31, | As of March 31, | |||||||
| 2020 | 2021 | |||||||
Tools and equipment | $ | 1,523 | $ | 1,582 | ||||
Computer equipment and software | 118 | 116 | ||||||
Furniture and fixtures | 43 | 43 | ||||||
Leasehold improvements | 30 | 29 | ||||||
Construction in process | 298 | 329 | ||||||
|
|
|
| |||||
| 2,012 | 2,099 | |||||||
Less: Accumulated depreciation | (743 | ) | (875 | ) | ||||
|
|
|
| |||||
Property and equipment, net | $ | 1,269 | $ | 1,224 | ||||
|
|
|
| |||||
Depreciation expense for the three months ended March 31, 2020 and 2021 was approximately $0.1 million each period.
Accrued and Other Current Liabilities
Accrued and other current liabilities consist of the following (in thousands):
| As of December 31, | As of March 31, | |||||||
| 2020 | 2021 | |||||||
Accrued expenses | $ | 1,971 | $ | 3,143 | ||||
Current portion of lease liabilities | 395 | 248 | ||||||
Short term interest payable | 274 | 274 | ||||||
Other accrued liabilities | 446 | 398 | ||||||
|
|
|
| |||||
Total accrued and other current liabilities | $ | 3,086 | $ | 4,063 | ||||
|
|
|
| |||||
F-46
Table of Contents
Other Noncurrent Liabilities
Other noncurrent liabilities consist of the following (in thousands):
| As of December 31, | As of March 31, | |||||||
| 2020 | 2021 | |||||||
Noncurrent portion of lease liabilities | $ | 134 | $ | 123 | ||||
Redeemable preferred stock warrants liabilities | 2,112 | 1,557 | ||||||
Long term interest payable | 465 | 556 | ||||||
Other noncurrent liabilities | 344 | 345 | ||||||
|
|
|
| |||||
Total other noncurrent liabilities | $ | 3,055 | $ | 2,581 | ||||
|
|
|
| |||||
Note 5. Debt
In January 2019, the Company entered into a loan and security agreement with MidCap Financial Services, which provided a maximum of $25.0 million credit facility consisting of a $20.0 million senior secured 2019 Term Loan and a $5.0 million 2019 Revolver (collectively, the “2019 MidCap Credit Facility”). In November 2020, the Company entered into a loan and security agreement with the same institution, which replaced the 2019 MidCap Credit Facility, and provided for a maximum of $40.0 million credit facility consisting of a $35.0 million senior secured 2020 Term Loan and a $5.0 million 2020 Revolver (collectively, the “2020 MidCap Credit Facility”).
2019 Term Loan
The 2019 Term Loan had a four-year term and had a stated floating interest rate which equates to reserve-adjusted LIBOR + 6.75%. The 2019 Term Loan was split into three tranches as follows: (i) the Tranche One Loans provided for $12.0 million in term loans, (ii) the Tranche Two Loans provided for up to $2.0 million in term loans, and (iii) the Tranche Three Loans provided for up to $6.0 million in term loans. The Company borrowed $14.0 million under the Tranche One Loans and Tranche Two Loans. While the conditions necessary to draw the Tranche Three Loans had been met as of December 31, 2019, the Company did not elect to draw the Tranche Three Term Loans. The 2019 Term Loan required 18 monthly interest-only payments, which began on January 31, 2019, followed by 30 equal monthly installments of principal, plus interest. The interest-only period was extended by an additional six months upon achievement of the Tranche Three Milestone.
The 2019 Term Loan had an effective interest rate of 14.52% per year. The 2019 Term Loan interest expense for the three months ended March 31, 2020 and 2021 was $0.6 million and nil, respectively.
In conjunction with the funding of Tranche 1 and Tranche 2 under the 2019 Term Loan, the Company issued a 10-year warrant to the Lender to purchase 29,514 shares of the Company’s Series C redeemable convertible preferred stock (the “2019 Initial Warrant”) at an exercise price of $9.49 per share (the “Exercise Price”). Further, depending on the funding of the Term Loan Tranche 3, the Company was obligated to issue an additional Warrant to the Lender to purchase up to 12,649 shares of Series C redeemable convertible preferred stock at the Exercise Price (the “2019 Additional Warrant” and together with “2019 Initial Warrant” the “2019 Warrants”) (see Note 9).
The estimated fair value of the 2019 Warrants of $0.2 million upon draw down was based on the Black-Scholes option-pricing model and probability of future draw downs. The 2019 Warrants were recorded at the fair value as a debt discount and as a warrant liability. The debt discount is being accreted using the effective interest method as interest expense over the contractual period of four years for the Term Loan.
The Company incurred $1.5 million of issuance costs in conjunction with the 2019 Term Loan. The issuance costs have been netted against the borrowed funds in the condensed consolidated balance sheet and was accreted using the effective interest method as interest expense over the contractual period of four years for the 2019 Term Loan.
F-47
Table of Contents
The Company could voluntarily prepay the borrowings in full, with a prepayment premium beginning at 3% in the first year from tranche funding, to 2% in the second year from tranche funding, to 1% in the third year from tranche funding thereafter. In addition, a final payment fee of 5% of the amounts borrowed is payable at the end of the term or when the borrowings are repaid in full. A long-term liability was being accreted using the effective interest method for the final payment fee over the term of the loan agreement. The borrowings were collateralized by a security interest in substantially all of the Company’s assets.
The Company was subject to financial covenants related to minimum trailing revenue targets that began on January 1, 2019, and are tested on a monthly basis. If only Tranche One Loans were funded, the Company had to achieve minimum net revenue of $7 million over a trailing 12-month period increasing to a maximum net revenue covenant of $35 million for the trailing 12-month period ending December 31, 2022, and thereafter. If only Tranche One Loans and Tranche Two Loans had been funded, the Company had to achieve minimum net revenue of $7 million over a trailing 12-month period increasing to a maximum net revenue covenant of $37.3 million for the 12-month period ending December 31, 2022, and thereafter. If Tranche Three Loans had been funded regardless of whether Tranche Two Loans have been funded, the Company had to achieve minimum net revenue of $15 million over a trailing 12-month period increasing to a maximum net revenue covenant of $46.7 million for the 12-month period ending December 31, 2022, and thereafter. As of December 31, 2019, the Company was in compliance with the applicable financial covenant.
On November 23, 2020, the 2019 Term Loan was replaced with 2020 Term Loan (see below).
2019 Revolver
The 2019 Revolver had a four-year term and has a stated floating interest rate which equates to reserve-adjusted LIBOR plus 4.25%. An unused line fee of 0.5% was payable monthly based on the average unused balance and a collateral management fee of 0.5% is payable monthly based on the outstanding balance of the Revolver. The Company could request to increase the 2019 Revolver commitment amount to $10.0 million under the term of the agreement. On November 23, 2020, the 2019 Revolver was replaced with the 2020 Revolver (see below).
2020 Term Loan
The 2020 Term Loan has a five-year term and has a stated floating interest rate which equates to reserve-adjusted LIBOR + 7.00%. The 2020 Term Loan is split into three tranches as follows: (i) the Tranche One Loans provide for $12.0 million in term loans which are deemed to have been converted from Tranche One Loans that were drawn and outstanding under the 2019 Term Loan immediately prior to entering into 2020 MidCap Credit Facility, (ii) the Tranche Two Loans provided for up to $2.0 million in term loans which are deemed to have been converted from Tranche Two Loans that were drawn and outstanding under the 2019 Term Loan immediately prior to entering into 2020 MidCap Credit Facility, and (iii) the Tranche Three Loans provided for up to $21.0 million in new term loans. The Company borrowed $21.0 million under the Tranche Three Loans in November 2020.
The 2020 Term Loan requires 24 monthly interest-only payments, which began on December 1, 2020, followed by 36 equal monthly installments of principal, plus interest. The interest-only period can be extended by an additional 12 months provided that the Company is in compliance with the minimum trailing revenue targets (as described below), and has unrestricted cash and cash equivalents of at least 12 times of the amortization monthly cash burn amount, measured as defined in the 2020 Term Loan agreement (“First IO Extension”). If the First IO Extension conditions are satisfied, the interest-only period can be further extended by an additional 12 months, provided that the Company is in compliance with the minimum trailing revenue targets (as described
F-48
Table of Contents
below), has unrestricted cash and cash equivalents of at least 12 times of the amortization monthly cash burn amount, and has consummated an IPO in which the Company has received cash proceeds of at least $60.0 million.
The 2020 Term Loan has an effective interest rate of 13.59% per year. The 2020 Term Loan interest expense for the three months ended March 31, 2020 and 2021 was nil and $1.1 million, respectively.
In conjunction with the entering the 2020 MidCap Credit Facility, the Company issued a 10-year warrant to the Lender to purchase 300,000 shares of the Company’s Series F redeemable convertible preferred stock (the “2020 Warrant”) at an exercise price of $21.88 per share (see Note 9). The estimated fair value at issuance of the 2020 Warrant of $1.8 million was based on the Option-Pricing Method with Discounts for Lack of Marketability for each class of security. In addition, the Company incurred $0.5 million of issuance costs paid to the Lender in conjunction with the 2020 Term Loan which represents a debt discount. The Company concluded that the 2020 Term Loan represented a modification of the 2019 Term Loan and accounted for the 2020 Term Loan as debt modification. The 2020 Warrants were recorded at the fair value as a debt discount and as a warrant liability. At each balance sheet date, the 2020 Warrants are remeasured to fair value with any changes in fair value recognized as other expense in the statements of operations. The debt discount is being amortized using the effective interest method as interest expense over the contractual period of five years for the 2020 Term Loan.
The Company can voluntarily prepay the borrowings in full, with a prepayment premium beginning at 3% in the first year from entering into the 2020 MidCap Credit facility and declining to 2% in the second year to 1% in the third year thereafter. In addition, a final payment fee of 6% of the amounts borrowed is payable at the end of the term or when the borrowings are repaid in full. A long-term liability is being accreted using the effective interest method for the final payment fee over the term of the loan agreement. The borrowings are collateralized by a security interest in substantially all of the Company’s assets.
The Company accrued $0.5 million and $0.6 million as of December 31, 2020 and March 31, 2021, respectively, related to accretion of final payment due at maturity per the agreement using the effective interest rate method. The final payment accrual is recorded in “Other noncurrent liabilities” on the balance sheets.
The Company is subject to financial covenants related to minimum trailing revenue targets that began on September 30, 2020 and are tested on a monthly basis. The Company has to achieve minimum net revenue of $20.0 million over a trailing 12-month period increasing to a maximum net revenue covenant of $84.8 million for the trailing 12-month period ending October 31, 2025. As of March 31, 2021, the Company was in compliance with the applicable financial covenant.
2020 Revolver
The 2020 Revolver has a four-year term and has a stated floating interest rate which equates to reserve-adjusted LIBOR plus 4.50%. An unused line fee of 0.5% is payable monthly based on the average unused balance and a collateral management fee of 0.5% is payable monthly based on the outstanding balance of the 2020 Revolver. The Company can request to increase the 2020 Revolver commitment amount to $15.0 million under the term of the agreement. As of March 31, 2021, $4.9 million was available to be drawn under the 2020 Revolver.
The 2020 Revolver has not been drawn upon as of March 31, 2021.
F-49
Table of Contents
Long-term and short-term debt was as follows (in thousands):
| As of December 31, | As of March, 31 | |||||||
| 2020 | 2021 | |||||||
Term Loan | $ | 35,000 | $ | 35,000 | ||||
|
|
|
| |||||
Total principal payments due | 35,000 | 35,000 | ||||||
|
|
|
| |||||
Less: debt discount related to warrant liability and issuance costs | (3,045 | ) | (2,876 | ) | ||||
Total amount outstanding | 31,955 | 32,124 | ||||||
|
|
|
| |||||
Less: Current portion | — | — | ||||||
|
|
|
| |||||
Long-term portion | $ | 31,955 | $ | 32,124 | ||||
|
|
|
| |||||
The repayment schedule relating to the Company’s debt as of March 31, 2021, is as follows (in thousands):
| Amount | ||||
2021 (remainder) | $ | — | ||
2022 | 1,944 | |||
2023 | 11,667 | |||
2024 | 11,667 | |||
2025 | 9,722 | |||
|
| |||
Total repayments | $ | 35,000 | ||
|
| |||
Note 6. Commitments and Contingencies
Operating Lease Obligations
The Company’s leases mainly include facility leases and storage leases. In September 2019, the Company entered into a noncancelable operating lease for approximately 10,823 square feet of primary office space, which expires on July 31, 2021, without the option to extend.
The Company recognizes rent expense on a straight-line basis over the noncancelable lease term. The Company’s rent expense was $0.2 million for the three months ended March 31, 2020 and 2021.
In determining the present value of lease payments, the Company uses its incremental borrowing rate based on the information available at the lease commencement date if the rate implicit in the lease is not readily determinable. At the date of adoption of Topic 842, the Company determined the amounts of lease liability using a discount rate of 16.4%, which represents the Company’s incremental borrowing rate, which was based on the Company’s current borrowing rate adjusted for various factors including level of collateralization and term. As of March 31, 2021, the remaining lease term for the lease was 3.2 years.
Operating lease expense recognized and supplemental cash flow information related to operating leases for the three months ended March 31, 2020 and 2021 were as follows (in thousands):
| Three Months Ended March 31, | ||||||||
| 2020 | 2021 | |||||||
Operating lease expense | $ | 175 | $ | 175 | ||||
Cash paid for operating leases | 172 | 177 | ||||||
New operating lease assets obtained in exchange for operating lease liabilities | — | — | ||||||
F-50
Table of Contents
During the three months ended March 31, 2020 and 2021, the Company’s costs related to short-term lease arrangements and non-lease variable payments were immaterial.
Aggregate future minimum lease payments at December 31, 2020 and March 31, 2021, under these noncancelable operating leases were as follows (in thousands):
| As of December 31, | As of March 31, | |||||||
| 2020 | 2021 | |||||||
2021 | $ | 440 | $ | 263 | ||||
2022 | 66 | 66 | ||||||
2023 | 68 | 68 | ||||||
2024 | 29 | 29 | ||||||
|
|
|
| |||||
Total future minimum lease payments | 603 | 426 | ||||||
Less: imputed interest | (74 | ) | (55 | ) | ||||
|
|
|
| |||||
Present value of future minimum lease payments | 529 | 371 | ||||||
Less: current portion of operating lease liability | (395 | ) | (248 | ) | ||||
|
|
|
| |||||
Operating lease liabilities—noncurrent | $ | 134 | $ | 123 | ||||
|
|
|
| |||||
Legal Proceedings
The Company is subject to claims and assessments from time to time in the ordinary course of business. Accruals for litigation and contingencies are reflected in the financial statements based on management’s assessment, including the advice of legal counsel, of the expected outcome of litigation or other dispute resolution proceedings, and/or the expected resolution of contingencies. Liabilities for estimated losses are accrued if the potential losses from any claims or legal proceedings are considered probable and the amounts can be reasonably estimated. Significant judgment is required in both the determination of probability of loss and the determination as to whether the amount can be reasonably estimated. Accruals are based only on information available at the time of the assessment due to the uncertain nature of such matters. As additional information becomes available, management reassesses potential liabilities related to pending claims and litigation and may revise its previous estimates, which could materially affect the Company’s results of operations in a given period. As of December 31, 2020 and March 31, 2021, the Company was not involved in any material legal proceedings.
Indemnification
In the normal course of business, the Company enters into contracts and agreements that contain a variety of representations and warranties and provide for general indemnifications. The Company’s exposure under these agreements is unknown because it involves claims that may be made against the Company in the future, but that have not yet been made. To date, the Company has not paid any claims or been required to defend any action related to its indemnification obligations. However, the Company may record charges in the future as a result of these indemnification obligations.
The Company indemnifies each of its directors and officers for certain events or occurrences, subject to certain limits, while the director is or was serving at the Company’s request in such capacity, as permitted under Delaware law and in accordance with its certificate of incorporation and bylaws. The term of the indemnification period lasts as long as a director may be subject to any proceeding arising out of acts or omissions of such director in such capacity. The maximum amount of potential future indemnification is unlimited; however, the Company currently holds director liability insurance. This insurance allows the transfer of risk associated with the Company’s exposure and may enable it to recover a portion of any future amounts paid. The Company believes that the fair value of these indemnification obligations is minimal. Accordingly, the Company has not recognized any liabilities relating to these obligations as of December 31, 2020 and March 31, 2021.
F-51
Table of Contents
Note 7. Redeemable Convertible Preferred Stock
The Company has the following redeemable convertible preferred stock issued and outstanding at March 31, 2021 and December 31, 2020 (in thousands, except share and per share data):
Series | Shares Authorized | Shares Issued and Outstanding | Original Issuance Price | Liquidation Amount | Issuance Costs | Carrying Value | ||||||||||||||||||
Series A | 3,804,344 | 3,804,344 | $ | 1.38 | $ | 5,250 | $ | 9 | $ | 5,241 | ||||||||||||||
Series B | 1,209,621 | 1,209,621 | 5.79 | 7,000 | 106 | 6,894 | ||||||||||||||||||
Series C | 2,372,371 | 2,342,857 | 9.49 | 22,226 | 208 | 22,018 | ||||||||||||||||||
Series D | 2,507,720 | 2,447,818 | 12.56 | 30,750 | 647 | 30,103 | ||||||||||||||||||
Series E | 1,921,902 | 1,899,847 | 15.87 | 30,150 | 106 | 30,044 | ||||||||||||||||||
Series F | 2,425,432 | 1,062,715 | 21.88 | 23,250 | 219 | 23,031 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
| 14,241,390 | 12,767,202 | $ | 118,626 | $ | 1,295 | $ | 117,331 | |||||||||||||||||
|
|
|
|
|
|
|
|
|
| |||||||||||||||
The rights and preferences of holders of the redeemable convertible preferred stock are as follows:
Voting Rights
The holder of each share of redeemable convertible preferred stock has the voting rights equal to an equivalent number of shares of common stock into which it is convertible and votes together as a single class with common stock.
Election of Directors
The holders of a majority of the Shares of Series A, Series B, Series C and Series D redeemable convertible preferred stock, voting separately as a single class, are entitled to each elect one director of the Company. The holders of a majority of the shares of Series E and Series F redeemable convertible preferred stock, voting together as a single class, are entitled to elect one director of the Company.
Dividends
The holders of Series A, Series B, Series C, Series D, Series E and Series F redeemable convertible preferred stock are entitled to receive dividends declared by the board of directors in proportion to the numbers of shares of common stock, which are held by each holder if all shares of such series of redeemable convertible preferred stock were converted to common stock at the then-effective conversion rate of each series of redeemable convertible preferred stock. No dividends shall be paid on any common stock (other than dividends on shares of common stock payable in shares of common stock) until dividends to the holders of the redeemable convertible preferred stock have been paid. As of March 31, 2021, no dividends have been declared to date.
Liquidation Rights
In the event of any liquidation, dissolution, or winding-up of the Company, either voluntary or involuntary, the holders of Series F, Series E and Series D redeemable convertible preferred stock shall be entitled to receive on a pari passu basis among each other, prior to and in preference to any distribution of any of the assets to the holders of Series C redeemable convertible preferred stock, Series B redeemable convertible preferred stock, Series A redeemable convertible preferred stock, and the common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
After the payment of all preferential amounts required to be paid to the holders of Series D redeemable convertible preferred stock, the holders of Series C redeemable convertible preferred stock shall be entitled to
F-52
Table of Contents
receive, prior to and in preference to any distribution of any of the assets to the holders of Series B redeemable convertible preferred stock, Series A redeemable convertible preferred stock, and the common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
After the payment of all preferential amounts required to be paid to the holders of Series C redeemable convertible preferred stock, the holders of Series B shall be entitled to receive, prior to and in preference to any distribution of any of the assets to the holders of Series A redeemable convertible preferred stock and the common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
After the payment of all preferential amounts required to be paid to the holders of Series B redeemable convertible preferred stock, the holders of Series A shall be entitled to receive, prior to and in preference to any distribution of any of the assets to the holders of common stock of the Company, an amount per share equal to the sum of the original issue price of the redeemable convertible preferred stock and all declared and unpaid dividends on such shares of redeemable convertible preferred stock.
If upon the occurrence of such an event, the assets and funds distributed among the holders of the redeemable convertible preferred stock are insufficient to permit the payment to such holders of the redeemable convertible preferred stock, then the entire assets and funds of the Company legally available for distribution shall be distributed ratably among the holders of the redeemable convertible preferred stock in proportion to the full preferential amount each such holders are otherwise entitled to have received pursuant to the entitlement as noted above.
After the payment in full to holders of the redeemable convertible preferred stock as noted above, the remaining assets, if any, shall be distributed to the holders of the common and redeemable convertible preferred stock on a pro-rata as-if-converted basis.
Conversion rights
Each share of redeemable convertible preferred stock is convertible, at the option of the holder, at any time after the date of issuance of such share for such redeemable convertible preferred stock. Each share of redeemable convertible preferred stock shall be convertible into the number of shares of common stock determined by dividing the original issuance price by the conversion price. The initial conversion price for each share of redeemable convertible preferred stock is the original issuance price for such share of redeemable convertible preferred stock.
Each share of redeemable convertible preferred stock automatically converts into the number of shares of common stock at the conversion price on the earlier of (i) immediately prior to the closing of a firmly underwritten public offering in the aggregate gross proceeds received by the Company are not less than $75,000,000 and the Company’s valuation, represented by fair market value of the issued and outstanding shares of common stock (assuming conversion of all redeemable convertible preferred stock into common stock) immediately prior to giving effect to the issuance of any shares pursuant to such public offering, calculated based on the price per share at which the underwriters propose to sell such common stock to the public, is at least $425,000,000 on or before the 12-month anniversary of the initial purchase date of the Series F redeemable convertible preferred stock, and at least $475,000,000 after the twelve 12-month anniversary of the initial purchase date of the Series F redeemable convertible preferred stock (a “Qualified IPO”) or (ii) the date specified in a written request by the holders of a majority of the then outstanding shares of the Series E redeemable convertible preferred stock and the Series F redeemable convertible preferred stock, voting together as a separate class on an as-if converted basis.
F-53
Table of Contents
As of March 31, 2021, the conversion ratio for each series of redeemable convertible preferred stock was one-for-one.
Redemption
The redeemable convertible preferred stock is recorded in mezzanine equity because, while it is not mandatorily redeemable, it will become redeemable at the option of the stockholders upon the occurrence of certain deemed liquidation events that are considered not solely within the Company’s control.
Note 8. Common Stock Warrants
In connection with the issuance of the Company’s Series A redeemable convertible preferred stock issuances in September 2011, the Company issued a warrant to purchase 64,655 shares of common stock to an investor who purchased Series A redeemable convertible preferred stock at an exercise price of $0.10 per share. The common stock warrant was exercised in December 2020 and is no longer outstanding.
Note 9. Redeemable Convertible Preferred Stock Warrants
2019 Warrants
In conjunction with the funding of Tranche 1 and Tranche 2 under the 2019 Term Loan, the Company issued the 2019 Initial Warrant to purchase 29,514 shares of its Series C redeemable convertible preferred stock (see Note 5). The 2019 Initial Warrant is immediately exercisable, at an exercise price per share of $9.49, and expires 10 years from their date of issuance. The 2019 Initial Warrant will be automatically exercised upon the consummation or effective date of a change of control of the Company. Further, depending on the funding of the 2019 Term Loan Tranche 3, the Company was obligated to issue the 2019 Additional Warrant (together with the 2019 Initial Warrant to “2019 Warrants”) to the Lender to purchase up to 12,649 shares of Series C redeemable convertible preferred stock at the respective exercise price.
The estimated fair value of the 2019 Warrants on the date of issuance was $0.2 million. As of the issuance date, the fair value of the 2019 Warrants was calculated using the Black-Scholes option-pricing model and was based on a term of 10 years, a risk-free interest rate of 2.99%, expected volatility of 50.95%, and 0% expected dividend yield.
At initial recognition, the 2019 Warrants were recorded at their estimated fair values and were subject to remeasurement at each balance sheet date, with changes in fair value recognized as a component of net income. As of December 31, 2020 and March 31, 2021, the estimated fair values of the 2019 Warrants were $0.3 million and $0.4 million, respectively. The fair value of the 2019 Warrants as of December 31, 2020 was calculated using the Black-Scholes option-pricing model with the following assumptions:
| December 31, | ||
| 2020 | ||
Expected term (in years) | 8.1–8.5 | |
Expected volatility | 42.18%–42.63% | |
Risk-free interest rate | 2.33%–2.49% | |
Dividend yield | — |
The fair value of the 2019 Warrants as of March 31, 2021 was calculated using a multi-scenario Option-Pricing Method with Discounts for Lack of Marketability for each class of security.
As of March 31, 2021, the 2019 Initial Warrant remained outstanding and the remaining term was 8.1 years. The 2019 Additional Warrant of 12,649 shares of series C redeemable convertible preferred stock was not legally issued and expired upon modification of the 2019 Term Loan.
F-54
Table of Contents
2020 Warrants
In conjunction with entering the 2020 Term Loan agreement, the Company issued the 2020 Warrant to purchase 300,000 shares of its Series F redeemable convertible preferred stock (see Note 5). The 2020 Warrant is immediately exercisable, at an exercise price per share of $21.88, and expires 10 years from its date of issuance. The warrant will be automatically exercised upon the consummation or effective date of a change of control of the Company.
The estimated fair value of the 2020 Warrant on the date of issuance was $1.8 million. As of the issuance date, the fair value of the 2020 Warrant was calculated using a multi-scenario Method with Discounts for Lack of Marketability for each class of security.
At initial recognition, the 2020 Warrant was recorded at its estimated fair values and was subject to remeasurement at each balance sheet date, with changes in fair value recognized as a component of net income. As of December 31, 2020 and March 31, 2021, the estimated fair values of the 2020 Warrant was $1.8 million and $1.2 million, respectively. The fair value of the 2020 Warrant as of December 31, 2020 and March 31, 2021 was calculated using a multi-scenario Method with Discounts for Lack of Marketability for each class of security.
As of March 31, 2021, the 2020 Warrant remained outstanding and the remaining term was 9.7 years.
The fair value of the redeemable convertible preferred stock warrants was determined using the following assumption as of each report date:
| December 31, 2020 | March 31, 2021 | |||
Term (in years) | 0.58-2.58 | 0.25-2.25 | ||
Expected volatility | 55.9%-65.6% | 46.8%-60.7% | ||
Risk-free interest rate | 0.08%-0.18% | 0.03%-0.21% |
Note 10. Common Stock
At March 31, 2021, the Company’s certificate of incorporation, as amended and restated, authorizes the Company to issue up to 21,831,000 shares of common stock with $0.001 par value per share, of which 4,763,022 shares were issued and outstanding. The holders of common stock are also entitled to receive dividends whenever funds are legally available, when and if declared by the board of directors. As of March 31, 2021, no dividends have been declared to date. Each share of common stock is entitled to one vote.
F-55
Table of Contents
At December 31, 2020 and March 31, 2021, the Company had reserved common stock for future issuances as follows:
| December 31, | March 31, | |||||||
| 2020 | 2021 | |||||||
Conversion of Series A redeemable convertible preferred stock | 3,804,344 | 3,804,344 | ||||||
Conversion of Series B redeemable convertible preferred stock | 1,209,621 | 1,209,621 | ||||||
Conversion of Series C redeemable convertible preferred stock and warrants | 2,372,371 | 2,372,371 | ||||||
Conversion of Series D redeemable convertible preferred stock | 2,447,818 | 2,447,818 | ||||||
Conversion of Series E redeemable convertible preferred stock | 1,899,847 | 1,899,847 | ||||||
Conversion of Series F redeemable convertible preferred stock | 1,362,715 | 1,362,715 | ||||||
Exercise of options under stock plan | 4,754,591 | 4,763,022 | ||||||
Issuance of options under plan | 1,568,888 | 1,655,878 | ||||||
|
|
|
| |||||
| 19,420,195 | 19,515,616 | |||||||
|
|
|
| |||||
Note 11. Stock Option Plan
In 2011, the Company established its 2011 stock option plan (the “2011 Plan”) that provides for the granting of stock options to employees and nonemployees of the Company. Under the 2011 Plan, the Company has the ability to issue incentive stock options (ISOs), nonqualified stock options (NSOs), stock appreciation rights, dividend equivalent rights, restricted stock awards, and restricted stock unit awards. Options under the 2011 Plan may be granted for periods of up to 10 years. For incentive stock option granted to a grantee who, at the time the option is granted, owns stock representing more than 10% of the voting power of all classes of stock of the Company or any parent or subsidiary of the Company, the term of the incentive stock option may be granted for periods of up to five years. The ISOs and NSOs will be granted at a price per share not less than the fair value at the date of grant. The exercise price of an ISO granted to a 10% stockholder shall not be less than 110% of the estimated fair value of the shares on the date of grant, as determined by the board of directors. Options granted to new hires generally vest over a four-year period, with 25% vesting at the end of one year and the remaining vesting monthly thereafter; options granted as merit awards generally vest monthly over a four-year period. At December 31, 2020 and March 31, 2021, there were 225,835 shares and 130,414 shares, respectively, of common stock available for issuance under the 2011 Plan.
F-56
Table of Contents
The following tables summarize the Company’s stock option activity for the three months ended March 31, 2021:
| Options Outstanding | ||||||||||||||||||||
| Shares Available for Grant | Number of Options | Weighted- Average Exercise Price | Weighted- Average Remaining Contractual Term (In years) | Aggregate Intrinsic Value (in thousands) | ||||||||||||||||
Balances as of December 31, 2020 | 225,835 | 1,568,888 | $ | 1.87 | 6.8 | $ | 18,656 | |||||||||||||
Options granted | (113,250 | ) | 113,250 | $ | 13.76 | |||||||||||||||
Options forfeited/canceled | 17,829 | (17,829 | ) | $ | 3.31 | |||||||||||||||
Options exercised | — | (8,431 | ) | $ | 1.60 | |||||||||||||||
|
|
|
| |||||||||||||||||
Balances as of March 31, 2021 | 130,414 | 1,655,878 | $ | 2.67 | 6.7 | $ | 28,121 | |||||||||||||
|
|
|
| |||||||||||||||||
Vested and exercisable as of March 31, 2021 | — | 929,354 | $ | 0.97 | 5.0 | $ | 17,359 | |||||||||||||
Expected to vest as of March 31, 2021 | — | 726,524 | $ | 4.84 | 8.9 | $ | 10,762 | |||||||||||||
The weighted-average grant-date fair values of options granted during the three months ended March 31, 2020 and 2021 was $4.13 and $13.76 per share, respectively. The aggregate intrinsic value of options exercised were $0.1 million during the three months ended March 31 2021. The aggregate intrinsic value was calculated as the difference between the exercise prices of the underlying options and the estimated fair value of the common stock on the date of exercise. As of March 31, 2021, the unrecognized stock-based compensation of unvested options was $3.4 million, which is expected to be recognized over a weighted-average period of 3.3 years.
The Company estimated the fair value of stock options using the Black-Scholes option-pricing model. The fair value of stock options is recognized on a straight-line basis over the requisite service periods of the awards. The fair value of stock options was estimated using the following weighted-average assumptions:
| March 31, 2021 | ||
Expected term (in years) | 5.00-6.07 | |
Expected volatility | 56.75%-57.69% | |
Risk-free interest rate | 0.48%-0.81% | |
Dividend yield | — |
Expected Term
The expected term is calculated using the simplified method, which is available if there is insufficient historical data about exercise patterns and post vesting employment termination behavior. The simplified method is based on the vesting period and the contractual term for each grant or for each vesting tranche for awards with graded vesting. The midpoint of the vesting date and the maximum contractual expiration date is used as the expected term under this method. For awards with multiple vesting tranches, the time from grant until the midpoints for each of the tranches may be averaged to provide an overall expected term.
Expected Volatility
The Company used an average historical stock price volatility of a peer group of publicly traded companies to be representative of its expected future stock price volatility, as the Company did not have any trading history for its common stock. For purposes of identifying these peer companies, the Company considered the industry, stage of development, size, and financial leverage of potential comparable companies. For each grant, the Company measured historical volatility over a period equivalent to the expected term.
F-57
Table of Contents
Risk-Free Interest Rate
The risk-free interest rate is based on the implied yield currently available on US Treasury zero-coupon issues with remaining terms equivalent to the expected term of a stock award.
Expected Dividend Rate
The Company has not paid, and does not anticipate paying, any dividends in the near future. Accordingly, the Company has estimated the dividend yield to be 0%.
The following is a summary of stock-based compensation expense by function (in thousands):
| Three Months Ended March 31, | ||||||||
| 2020 | 2021 | |||||||
Cost of goods sold | $ | 1 | $ | 7 | ||||
Research and development | 9 | 37 | ||||||
Selling, general and administrative | 51 | 233 | ||||||
|
|
|
| |||||
Total stock-based compensation expense | $ | 61 | $ | 277 | ||||
|
|
|
| |||||
Note 12. Net loss per share attributable to common stockholders
Basic net loss per share is computed by dividing the net loss by the weighted-average number of common shares outstanding for the period. As the Company reported a net loss for the three months ended March 31, 2020 and 2021, basic net loss per share is the same as diluted net loss per share as the inclusion of potentially dilutive shares would have been antidilutive if included in the calculation.
The following table sets forth the computation of basic and diluted net loss per share attributable to common stockholders (in thousands, except share and per share data):
| Three Months Ended March 31, | ||||||||
| 2020 | 2021 | |||||||
Numerator: | ||||||||
Net loss attributable to common stockholders | $ | (9,175) | $ | (12,240) | ||||
Denominator: | ||||||||
Weighted-average shares of common stock outstanding—basic and diluted | 4,724,693 | 4,758,635 | ||||||
|
|
|
| |||||
Net loss per share attributable to common stockholders—basic and diluted | $ | (1.94) | $ | (2.57) | ||||
|
|
|
| |||||
F-58
Table of Contents
The following outstanding shares of potentially dilutive securities were excluded from the computation of diluted net loss per share attributable to common stockholders for the period presented because including them would have been antidilutive:
| March 31, | ||||||||
| 2020 | 2021 | |||||||
Series A Redeemable Convertible Preferred Stock | 3,804,344 | 3,804,344 | ||||||
Series B Redeemable Convertible Preferred Stock | 1,209,621 | 1,209,621 | ||||||
Series C Redeemable Convertible Preferred Stock | 2,342,857 | 2,342,857 | ||||||
Series D Redeemable Convertible Preferred Stock | 2,447,818 | 2,447,818 | ||||||
Series E Redeemable Convertible Preferred Stock | 1,899,847 | 1,899,847 | ||||||
Series F Redeemable Convertible Preferred Stock | — | 1,062,715 | ||||||
Options to purchase common stock | 1,082,488 | 1,655,878 | ||||||
Redeemable Convertible Preferred Stock Warrants | 42,163 | 329,514 | ||||||
|
|
|
| |||||
Total | 12,829,138 | 14,752,594 | ||||||
|
|
|
| |||||
Unaudited Pro Forma Net Loss per Share
Unaudited pro forma basic and diluted net loss per share were computed to give effect to the one-for-one conversion of all outstanding shares of the Company’s redeemable convertible preferred stock into shares of common stock in connection with the IPO, using the as-converted method as though the conversion had occurred as of the beginning of the period presented or the date of issuance, if later. Refer to Note 2 for further discussion.
Unaudited pro forma basic and diluted loss per share is computed as follows (in thousands, except share and per share data):
| Three Months Ended March 31, 2021 | ||||
| Numerator: | ||||
Net loss attributable to common stockholders | $ | ( | ) | |
Adjust: change in fair value of redeemable convertible preferred stock warrants | ||||
|
| |||
Pro forma net loss | ||||
|
| |||
Denominator: | ||||
Weighted-average shares of common stock outstanding used in computing net loss per share attributable to common stockholder—basic and diluted | ||||
Adjust: conversion of redeemable convertible preferred stock | ||||
Adjust: conversion of common stock warrants | ||||
|
| |||
Weighted-average shares outstanding used in computing pro forma net loss per share—basic and diluted | ||||
|
| |||
Net loss per share attributable to common stockholders—basic and diluted | $ | ( | ) | |
|
| |||
F-59
Table of Contents
Note 13. Defined Contribution Plan
The Company sponsors a defined contribution plan under Section 401(k) of the IRC of 1986, as amended, covering substantially all of its full-time US employees. Participating employees may contribute up to 100% of their eligible compensation up to the annual Internal Revenue Service’s contribution limit. For the three months ended March 31, 2020 and 2021, the Company did not match employee contributions.
Note 14. Segment Information
The Company has two reportable operating segments which are determined on the basis of product portfolio: Surgical Glaucoma and Dry Eye. The operating and reportable segments were determined based on how the Company’s Chief Executive Officer, its Chief Operating Decision Maker (“CODM”), views and evaluates the Company’s operations. The CODM allocates resources to and evaluates the financial performance of each operating segment primarily based on gross profit and gross profit margin.
Surgical Glaucoma segment includes sales of the Company’s OMNI® Surgical System for use in minimally invasive glaucoma procedures. Dry Eye segment includes sales of the Company’s TearCare® System and related components.
The following table summarizes select operating results information for each reportable segment (dollars in thousands):
| Three Months Ended March 31, | ||||||||
| 2020 | 2021 | |||||||
Revenue | ||||||||
Surgical Glaucoma | $ | 6,100 | $ | 8,139 | ||||
Dry Eye | 396 | 496 | ||||||
|
|
|
| |||||
Total | 6,496 | 8,635 | ||||||
Cost of goods sold | ||||||||
Surgical Glaucoma | 1,514 | 1,858 | ||||||
Dry Eye | 614 | �� | 443 | |||||
|
|
|
| |||||
Total | 2,128 | 2,301 | ||||||
Gross profit | ||||||||
Surgical Glaucoma | 4,586 | 6,281 | ||||||
Dry Eye | (218) | 53 | ||||||
|
|
|
| |||||
Total | 4,368 | 6,334 | ||||||
Operating expenses | 13,078 | 17,990 | ||||||
|
|
|
| |||||
Loss from operations | (8,710) | (11,656) | ||||||
Interest income | 27 | — | ||||||
Interest expense | (552) | (1,084) | ||||||
Other income (expense), net | 91 | 552 | ||||||
|
|
|
| |||||
Loss before income tax | $ | (9,144) | $ | (12,188) | ||||
|
|
|
| |||||
The Company does not allocate any income and expenses beyond revenue and cost of goods sold to the reportable operating segments in its reporting to the CODM. No asset information is provided for reportable operating segments because they are not reviewed by the CODM on segment basis. Substantially all of the Company’s revenue is generated from sales in the United States, and none of its property and equipment is located outside the United States.
Note 16. Subsequent Events
The Company evaluated subsequent events through May 24, 2021, the date on which the condensed consolidated financial statements were available for issuance.
F-60
Table of Contents
Shares
Common Stock
P R O S P E C T U S
| Morgan Stanley | BofA Securities | |
| Citigroup | Piper Sandler | |
, 2021
Table of Contents
Part II
INFORMATION NOT REQUIRED IN PROSPECTUS
| Item 13. | Other Expenses of Issuance and Distribution. |
The following table indicates the expenses to be incurred in connection with the offering described in this registration statement, other than underwriting discounts and commissions, all of which will be paid by us. All amounts are estimated except the Securities and Exchange Commission registration fee, the Financial Industry Regulatory Authority, Inc., or FINRA, filing fee and the Nasdaq listing fee.
| Amount | ||||
Securities and Exchange Commission registration fee | $10,910 | |||
FINRA filing fee | 15,500 | |||
Initial listing fee | * | |||
Accountants’ fees and expenses | * | |||
Legal fees and expenses | * | |||
Blue Sky fees and expenses | * | |||
Transfer Agent’s fees and expenses | * | |||
Printing expenses | * | |||
Miscellaneous | * | |||
|
| |||
Total expenses | $ * | |||
|
| |||
| * | To be filed by amendment. |
| Item 14. | Indemnification of Directors and Officers. |
Section 102 of the General Corporation Law of the State of Delaware permits a corporation to eliminate the personal liability of directors of a corporation to the corporation or its stockholders for monetary damages for a breach of fiduciary duty as a director, except where the director breached his duty of loyalty, failed to act in good faith, engaged in intentional misconduct or knowingly violated a law, authorized the payment of a dividend or approved a stock repurchase in violation of Delaware corporate law or obtained an improper personal benefit. Our restated certificate of incorporation provides that no director of the Registrant shall be personally liable to it or its stockholders for monetary damages for any breach of fiduciary duty as a director, notwithstanding any provision of law imposing such liability, except to the extent that the General Corporation Law of the State of Delaware prohibits the elimination or limitation of liability of directors for breaches of fiduciary duty.
Section 145 of the General Corporation Law of the State of Delaware provides that a corporation has the power to indemnify a director, officer, employee, or agent of the corporation, or a person serving at the request of the corporation for another corporation, partnership, joint venture, trust or other enterprise in related capacities against expenses (including attorneys’ fees), judgments, fines and amounts paid in settlement actually and reasonably incurred by the person in connection with an action, suit or proceeding to which he was or is a party or is threatened to be made a party to any threatened, ending or completed action, suit or proceeding by reason of such position, if such person acted in good faith and in a manner he reasonably believed to be in or not opposed to the best interests of the corporation, and, in any criminal action or proceeding, had no reasonable cause to believe his conduct was unlawful, except that, in the case of actions brought by or in the right of the corporation, no indemnification shall be made with respect to any claim, issue or matter as to which such person shall have been adjudged to be liable to the corporation unless and only to the extent that the Court of Chancery or other adjudicating court determines that, despite the adjudication of liability but in view of all of the circumstances of the case, such person is fairly and reasonably entitled to indemnity for such expenses which the Court of Chancery or such other court shall deem proper.
Our restated certificate of incorporation provides that we will indemnify each person who was or is a party or threatened to be made a party to any threatened, pending or completed action, suit or proceeding (other than an
II-1
Table of Contents
action by or in the right of us) by reason of the fact that he or she is or was, or has agreed to become, a director or officer, or is or was serving, or has agreed to serve, at our request as a director, officer, partner, employee or trustee of, or in a similar capacity with, another corporation, partnership, joint venture, trust or other enterprise (all such persons being referred to as an “Indemnitee”), or by reason of any action alleged to have been taken or omitted in such capacity, against all expenses (including attorneys’ fees), judgments, fines and amounts paid in settlement actually and reasonably incurred in connection with such action, suit or proceeding and any appeal therefrom, if such Indemnitee acted in good faith and in a manner he or she reasonably believed to be in, or not opposed to, our best interests, and, with respect to any criminal action or proceeding, he or she had no reasonable cause to believe his or her conduct was unlawful. Our restated certificate of incorporation provides that we will indemnify any Indemnitee who was or is a party to an action or suit by or in the right of us to procure a judgment in our favour by reason of the fact that the Indemnitee is or was, or has agreed to become, a director or officer, or is or was serving, or has agreed to serve, at our request as a director, officer, partner, employee or trustee of, or in a similar capacity with, another corporation, partnership, joint venture, trust or other enterprise, or by reason of any action alleged to have been taken or omitted in such capacity, against all expenses (including attorneys’ fees) and, to the extent permitted by law, amounts paid in settlement actually and reasonably incurred in connection with such action, suit or proceeding, and any appeal therefrom, if the Indemnitee acted in good faith and in a manner he or she reasonably believed to be in, or not opposed to, our best interests, except that no indemnification shall be made with respect to any claim, issue or matter as to which such person shall have been adjudged to be liable to us, unless a court determines that, despite such adjudication but in view of all of the circumstances, he or she is entitled to indemnification of such expenses. Notwithstanding the foregoing, to the extent that any Indemnitee has been successful, on the merits or otherwise, he or she will be indemnified by us against all expenses (including attorneys’ fees) actually and reasonably incurred in connection therewith. Expenses must be advanced to an Indemnitee under certain circumstances.
We intend to enter into indemnification agreements with each of our directors and officers. These indemnification agreements may require us, among other things, to indemnify our directors and officers for some expenses, including attorneys’ fees, judgments, fines and settlement amounts incurred by a director or officer in any action or proceeding arising out of his or her service as one of our directors or officers, or any of our subsidiaries or any other company or enterprise to which the person provides services at our request.
We maintain a general liability insurance policy that covers certain liabilities of directors and officers of our corporation arising out of claims based on acts or omissions in their capacities as directors or officers.
In any underwriting agreement we enter into in connection with the sale of common stock being registered hereby, the underwriters will agree to indemnify, under certain conditions, us, our directors, our officers and persons who control us within the meaning of the Securities Act of 1933, as amended, or the Securities Act, against certain liabilities.
| Item 15. | Recent Sales of Unregistered Securities. |
Set forth below is information regarding shares of capital stock issued by us within the past three years. Also included is the consideration received by us for such shares and information relating to the section of the Securities Act, or rule of the Securities and Exchange Commission, under which exemption from registration was claimed.
(a) Issuance of Capital Stock.
Since January 1, 2018, the registrant issued an aggregate of (i) 1,288,761 shares of Series C preferred stock for an aggregate consideration of approximately $12.23 million to accredited investors, (ii) 2,447,818 shares of Series D preferred stock at for an aggregate consideration of approximately $30.8 million to accredited investors, (iii) 1,899,847 shares of Series E preferred stock at for an aggregate consideration of approximately $30.15 million to accredited investors and (vi) 1,062,716 shares of Series F preferred stock at for an aggregate consideration of approximately $23.25 million to accredited investors.
II-2
Table of Contents
In December 2020, the registrant issued 64,655 shares of common stock in connection with the exercise of a warrant to an accredited investor at an exercise price of $0.10 per share.
Each issuance was made pursuant to Section 4(a)(2) of the Securities Act and/or Rule 506 as a transaction not involving a public offering.
(b) Equity Grants.
Since January 1, 2018, the registrant granted stock options to purchase an aggregate of 2,112,950 shares of its common stock with exercise prices ranging between $0.69 and $21.92 per share to employees, non-employees, and directors in connection with services provided to the registrant by such parties.
Since January 1, 2018, the registrant issued an aggregate of 253,387 shares of its common stock to employees and consultants upon their exercise of stock options, for aggregate cash consideration of approximately $0.3 million.
The issuances of such stock options and the shares of common stock issuable upon the exercise of such options were issued pursuant to written compensatory plans or arrangements with the registrant’s employees, directors and consultants, in reliance on the exemption provided by Rule 701 promulgated under the Securities Act, or pursuant to Section 4(a)(2) under the Securities Act, relative to transactions by an issuer not involving any public offering, to the extent an exemption from such registration was required.
(c) Warrants.
On January 25, 2019, June 28, 2019 and November 23, 2020, the registrant issued (i) a warrant to purchase up to an aggregate of 25,298 shares of Series C preferred stock at an exercise price of $9.4868 per share; (ii) two warrants to purchase up to an aggregate of 4,216 shares of Series C preferred stock at an exercise price of $9.4868 per share; and (iii) a warrant to purchase up to an aggregate of 300,000 shares of Series F preferred stock at an exercise price of $21.8779 per share, respectively, to MidCap Funding XXVIII Trust, or its affiliates, pursuant to Section 4(a)(2) of the Securities Act or Rule 506 as a transaction not involving a public offering.
| Item 16. | Exhibits and Financial Statement Schedules. |
(a) Exhibits.
Exhibit | Description of Exhibit | |
| 1.1* | Underwriting Agreement | |
| 3.1 | Certificate of Incorporation of the Registrant, as amended (currently in effect) | |
| 3.2 | Bylaws of the Registrant (currently in effect) | |
| 3.3* | Form of Restated Certificate of Incorporation of the Registrant (to be effective upon the closing of this offering) | |
| 3.4* | Form of Restated Bylaws of the Registrant (to be effective upon the closing of this offering) | |
| 4.1 | Third Amended and Restated Investors’ Rights Agreement, dated as of November 23, 2020 | |
| 4.2* | Specimen Stock Certificate evidencing the shares of common stock | |
| 4.3 | Form of Warrant to Purchase Stock | |
| 5.1* | Opinion of Latham & Watkins LLP | |
| 10.1 | 2011 Stock Incentive Plan, as amended, and U.K. sub-plan and forms of agreements thereunder | |
| 10.2* | 2021 Incentive Award Plan and form of option agreements thereunder | |
| 10.3* | Non-Employee Director Compensation Program | |
| 10.4* | 2021 Employee Stock Purchase Plan | |
| 10.5* | Form of Indemnification Agreement for Directors and Officers | |
II-3
Table of Contents
| * | To be filed by amendment. |
(b) Financial Statement Schedules. Schedules not listed above have been omitted because the information required to be set forth therein is not applicable or is shown in the financial statements or notes thereto.
| Item 17. | Undertakings. |
The undersigned registrant hereby undertakes to provide to the underwriter, at the closing specified in the underwriting agreement, certificates in such denominations and registered in such names as required by the underwriter to permit prompt delivery to each purchaser.
Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of the registrant pursuant to the foregoing provisions, or otherwise, the registrant has been advised that in the opinion of the Securities and Exchange Commission such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by the registrant of expenses incurred or paid by a director, officer or controlling person of the registrant in the successful defense of any action, suit or proceeding) is asserted by such director, officer or controlling person in connection with the securities being registered, the registrant will, unless in the opinion of its counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
The undersigned hereby undertakes that:
| (1) | For purposes of determining any liability under the Securities Act of 1933, the information omitted from the form of prospectus filed as part of this registration statement in reliance upon Rule 430A and contained in a form of prospectus filed by the registrant pursuant to Rule 424(b)(1) or (4) or 497(h) under the Securities Act shall be deemed to be part of this registration statement as of the time it was declared effective. |
II-4
Table of Contents
| (2) | For the purpose of determining any liability under the Securities Act of 1933, each post-effective amendment that contains a form of prospectus shall be deemed to be a new registration statement relating to the securities offered therein, and the offering of such securities at that time shall be deemed to be the initial bona fide offering thereof. |
II-5
Table of Contents
SIGNATURES
Pursuant to the requirements of the Securities Act, the registrant has duly caused this registration statement to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Menlo Park, State of California, on this 23rd day of June, 2021.
SIGHT SCIENCES, INC. | ||
By: | /s/ Paul Badawi | |
Paul Badawi | ||
President and Chief Executive Officer | ||
SIGNATURES AND POWER OF ATTORNEY
We, the undersigned officers and directors of Sight Sciences, Inc., hereby severally constitute and appoint Paul Badawi and Jesse Selnick and each of them singly (with full power to each of them to act alone), our true and lawful attorneys-in-fact and agents, with full power of substitution and resubstitution in each of them for him and in his name, place and stead, and in any and all capacities, to sign any and all amendments (including post-effective amendments) to this registration statement (or any other registration statement for the same offering that is to be effective upon filing pursuant to Rule 462(b) under the Securities Act of 1933), and to file the same, with all exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing requisite or necessary to be done in and about the premises, as full to all intents and purposes as he might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact and agents or any of them, or their or his substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Act of 1933, this Registration Statement has been signed by the following persons in the capacities held on the dates indicated.
Signature | Title | Date | ||
/s/ Paul Badawi Paul Badawi | President, Chief Executive Officer and Director (principal executive officer) | June 23, 2021 | ||
/s/ Jesse Selnick Jesse Selnick | Chief Financial Officer (principal financial officer and principal accounting officer) | June 23, 2021 | ||
/s/ Staffan Encrantz Staffan Encrantz | Chairman of the Board of Directors | June 23, 2021 | ||
/s/ David Badawi, M.D. David Badawi, M.D. | Director | June 23, 2021 | ||
/s/ Mack Hicks Mack Hicks | Director | June 23, 2021 | ||
/s/ Andrew Offer Andrew Offer | Director | June 23, 2021 | ||
/s/ Erica Rogers Erica Rogers | Director | June 23, 2021 | ||
/s/ Valeska Schroeder, Ph.D. Valeska Schroeder, Ph.D. | Director | June 23, 2021 | ||
/s/ Donald Zurbay Donald Zurbay | Director | June 23, 2021 | ||
II-6