Exhibit 99.1

Chemomab Therapeutics Systemic Sclerosis Live WebinarNovember 3, 2021
This presentation contains "forward-looking statements" within the meaning of the Private Securities Litigation Reform Act. These forward-looking statements include, among other things, statements regarding the clinical development pathway for CM-101; the future operations of Chemomab and its ability to successfully initiate and complete clinical trials and achieve regulatory milestones; the nature, strategy and focus of Chemomab; the development and commercial potential and potential benefits of any product candidates of Chemomab; and that the product candidates have the potential to address high unmet needs of patients with serious fibrosis-related diseases and conditions. Any statements contained in this communication that are not statements of historical fact may be deemed to be forward-looking statements. These forward-looking statements are based upon Chemomab’s current expectations. Forward-looking statements involve risks and uncertainties.Because such statements deal with future events and are based on Chemomab’s current expectations, they are subject to various risks and uncertainties and actual results, performance or achievements of Chemomab could differ materially from those described in or implied by the statements in this presentation, including: the uncertain and time-consuming regulatory approval process; risks related to Chemomab’s ability to correctly manage its operating expenses and its expenses; Chemomab’s plans to develop and commercialize its product candidates, including CM-101; the timing of initiation of Chemomab’s planned clinical trials; the timing of the availability of data from Chemomab’s clinical trials; the timing of any planned investigational new drug application or new drug application; Chemomab’s plans to research, develop and commercialize its current and future product candidates; the clinical utility, potential benefits and market acceptance of Chemomab’s product candidates; Chemomab’s commercialization, marketing and manufacturing capabilities and strategy; Chemomab’s ability to protect its intellectual property position; and the requirement for additional capital to continue to advance these product candidates, which may not be available on favorable terms or at all. Additional risks and uncertainties relating to Chemomab’s and its business can be found under the caption “Risk Factors” and elsewhere in Chemomab’s filings and reports with the SEC. Chemomab expressly disclaims any obligation or undertaking to release publicly any updates or revisions to any forward-looking statements contained herein to reflect any change in Chemomab’s expectations with regard thereto or any change in events, conditions or circumstances on which any such statements are based. This presentation (“Presentation”) is for informational purposes only and does not constitute an offer to sell, solicitation of an offer to buy, or a recommendation to purchase any equity, debt or other financial instruments of Chemomab. The data contained herein is derived from various internal and external sources. No representation is made as to the reasonableness of the assumptions made within or the accuracy or completeness of any other information contained herein. All levels, prices and spreads are historical and do not represent current market levels, prices or spreads, some or all of which may have changed since the issuance of this document. Any data on past performance, modeling contained herein is not an indication as to future performance. Chemomab assume no obligation to update the information in this Presentation. Chemomab does not accept any liability whatsoever for any losses arising from the use of this Presentation or reliance on the information contained herein. Nothing herein shall be deemed to constitute investment, legal, tax, financial, accounting or other advice. This Presentation is being provided for use only by the intended recipient. Forward Looking Statements
Agenda Dr. Dale Pfost, CEO Introduction Dr. Adi Mor, CSO CM-101 Overview:A Novel CCL24 Neutralizing Monoclonal Antibody Dr. Dinesh Khanna, U MI Med. SchoolSystemic Sclerosis:OverviewClinical Trial & Endpoint Considerations Dr. Arnon Aharon, CMO Clinical Program: CM-101 Phase 2 in Systemic Sclerosis AllSpeakersQ&A

Discovery and development of innovative therapeutics for rare inflammatory and fibrotic diseases with high unmet need CM-101, a first-in-class CCL24 neutralizing monoclonal antibody targeting:Primary Sclerosing Cholangitis (PSC)Systemic Sclerosis (SSc)Liver fibrosis (MoA*) Conducting 2 Phase 2 clinical trials with 3rd Phase 2 trial in SSc expected to initiate in 1Q22First clinical readouts targeted for 2022 expected to drive multiple value inflections Global patent exclusivity through 2041. Granted composition of matter patent with multiple additional patents pending Cormorant Asset Management Cash and equivalents of $67M as of June 30, 2021 enabling runway through mid-2023 Focus CM-101:A Pipeline in A Product Near-Term Catalysts Robust IP Portfolio Top Tier Investors Solid Balance Sheet *MoA – Mechanism of Action Chemomab (Nasdaq: CMMB) Overview Clinical Stage Biotech Company Focused on Inflammatory-Fibrotic Diseases

CM-101 Overview: CCL24 Neutralizing Monoclonal Antibody for Treatment of Systemic Sclerosis & Other Fibrotic–Inflammatory diseases Dr. Adi MorChemomab CSO
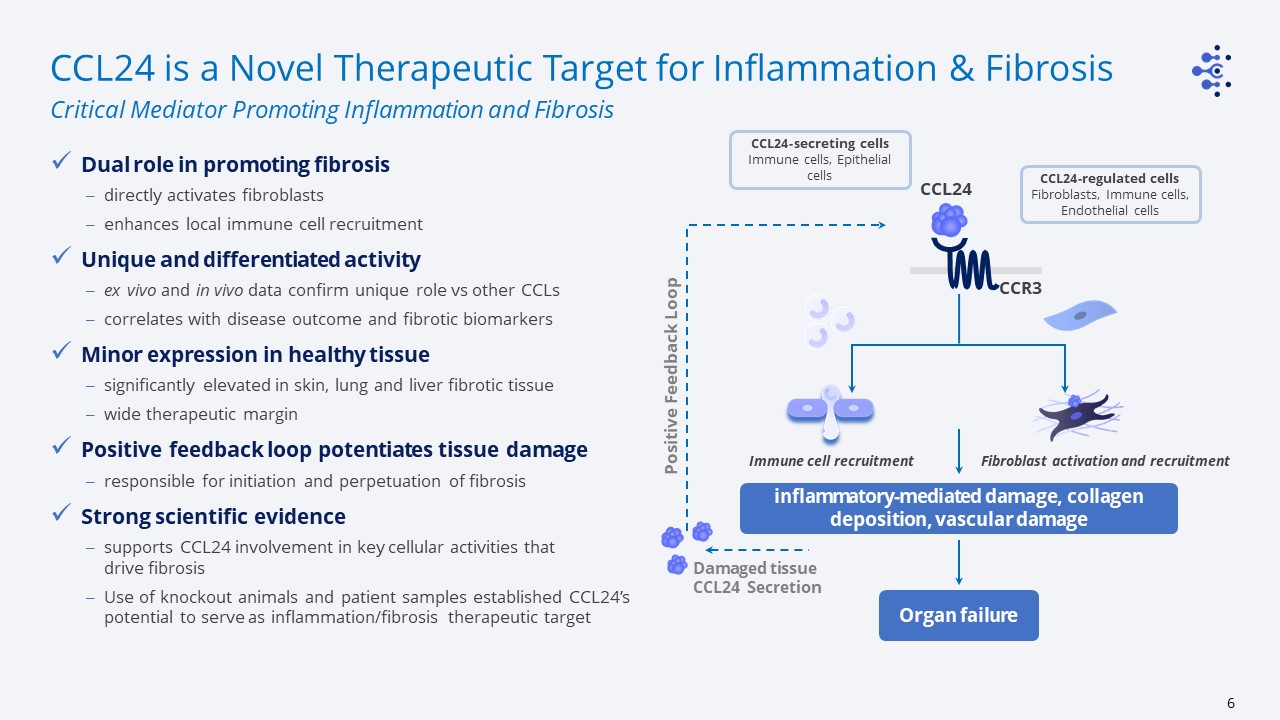
CCL24 is a Novel Therapeutic Target for Inflammation & Fibrosis Dual role in promoting fibrosisdirectly activates fibroblastsenhances local immune cell recruitmentUnique and differentiated activityex vivo and in vivo data confirm unique role vs other CCLscorrelates with disease outcome and fibrotic biomarkers Minor expression in healthy tissuesignificantly elevated in skin, lung and liver fibrotic tissue wide therapeutic margin Positive feedback loop potentiates tissue damageresponsible for initiation and perpetuation of fibrosisStrong scientific evidencesupports CCL24 involvement in key cellular activities that drive fibrosis Use of knockout animals and patient samples established CCL24’s potential to serve as inflammation/fibrosis therapeutic target Critical Mediator Promoting Inflammation and Fibrosis CCL24 CCR3 CCL24-secreting cellsImmune cells, Epithelial cells Immune cell recruitment Fibroblast activation and recruitment inflammatory-mediated damage, collagen deposition, vascular damage Positive Feedback Loop Organ failure Damaged tissue CCL24 Secretion CCL24-regulated cellsFibroblasts, Immune cells, Endothelial cells
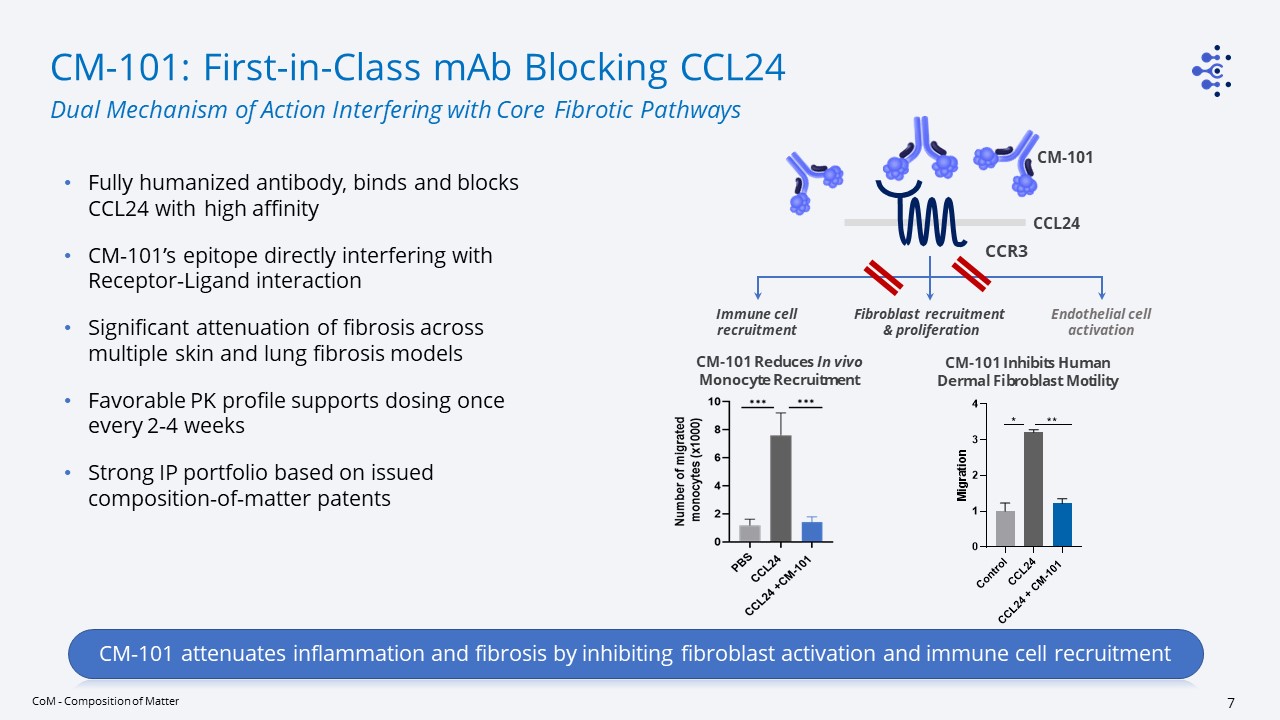
CM-101: First-in-Class mAb Blocking CCL24 Fully humanized antibody, binds and blocks CCL24 with high affinity CM-101’s epitope directly interfering with Receptor-Ligand interactionSignificant attenuation of fibrosis across multiple skin and lung fibrosis modelsFavorable PK profile supports dosing once every 2-4 weeksStrong IP portfolio based on issued composition-of-matter patents Dual Mechanism of Action Interfering with Core Fibrotic Pathways CoM - Composition of Matter CM-101 attenuates inflammation and fibrosis by inhibiting fibroblast activation and immune cell recruitment CCR3 Immune cell recruitment Fibroblast recruitment & proliferation CCL24 CM-101 Endothelial cell activation CM-101 Reduces In vivo Monocyte Recruitment CM-101 Inhibits Human Dermal Fibroblast Motility
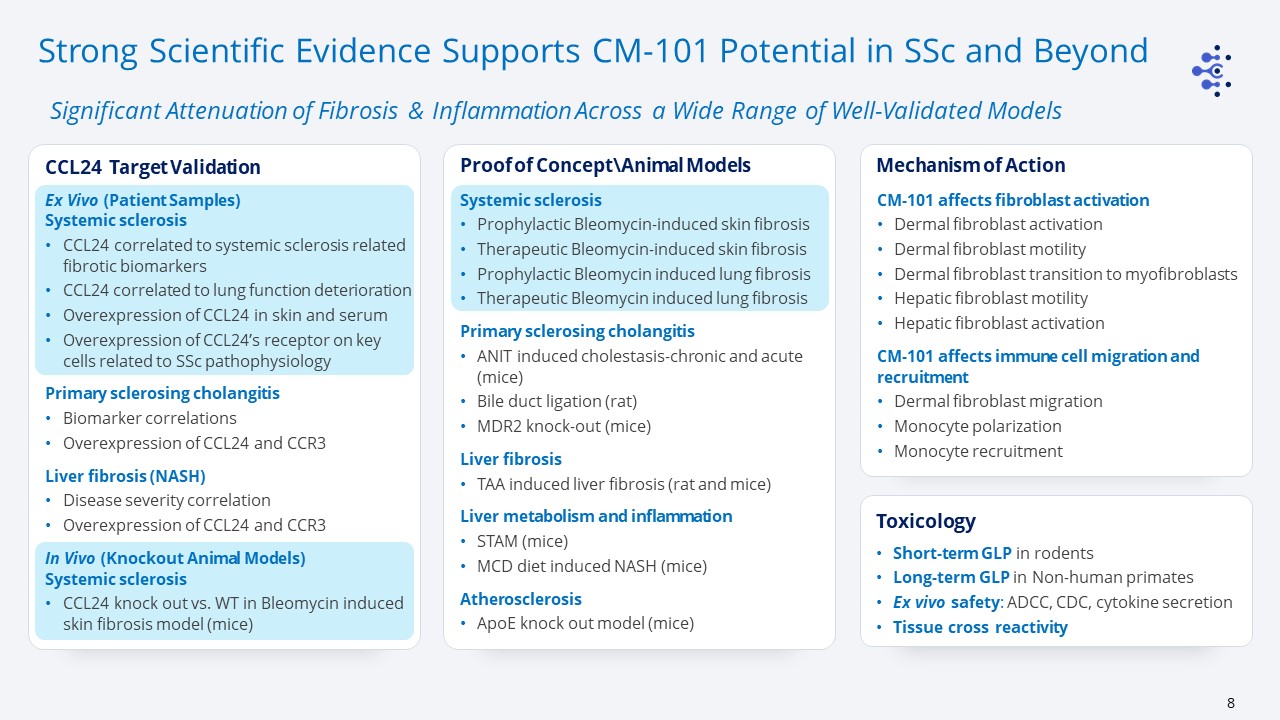
Systemic sclerosisProphylactic Bleomycin-induced skin fibrosisTherapeutic Bleomycin-induced skin fibrosisProphylactic Bleomycin induced lung fibrosisTherapeutic Bleomycin induced lung fibrosisPrimary sclerosing cholangitisANIT induced cholestasis-chronic and acute (mice)Bile duct ligation (rat)MDR2 knock-out (mice)Liver fibrosisTAA induced liver fibrosis (rat and mice)Liver metabolism and inflammationSTAM (mice)MCD diet induced NASH (mice)AtherosclerosisApoE knock out model (mice) Proof of Concept\Animal Models Mechanism of Action Ex Vivo (Patient Samples) Systemic sclerosisCCL24 correlated to systemic sclerosis related fibrotic biomarkersCCL24 correlated to lung function deterioration Overexpression of CCL24 in skin and serumOverexpression of CCL24’s receptor on key cells related to SSc pathophysiologyPrimary sclerosing cholangitisBiomarker correlationsOverexpression of CCL24 and CCR3Liver fibrosis (NASH)Disease severity correlationOverexpression of CCL24 and CCR3In Vivo (Knockout Animal Models)Systemic sclerosisCCL24 knock out vs. WT in Bleomycin induced skin fibrosis model (mice) CCL24 Target Validation Short-term GLP in rodentsLong-term GLP in Non-human primatesEx vivo safety: ADCC, CDC, cytokine secretionTissue cross reactivity Toxicology CM-101 affects fibroblast activationDermal fibroblast activationDermal fibroblast motilityDermal fibroblast transition to myofibroblastsHepatic fibroblast motilityHepatic fibroblast activation CM-101 affects immune cell migration and recruitmentDermal fibroblast migrationMonocyte polarizationMonocyte recruitment Strong Scientific Evidence Supports CM-101 Potential in SSc and Beyond Significant Attenuation of Fibrosis & Inflammation Across a Wide Range of Well-Validated Models
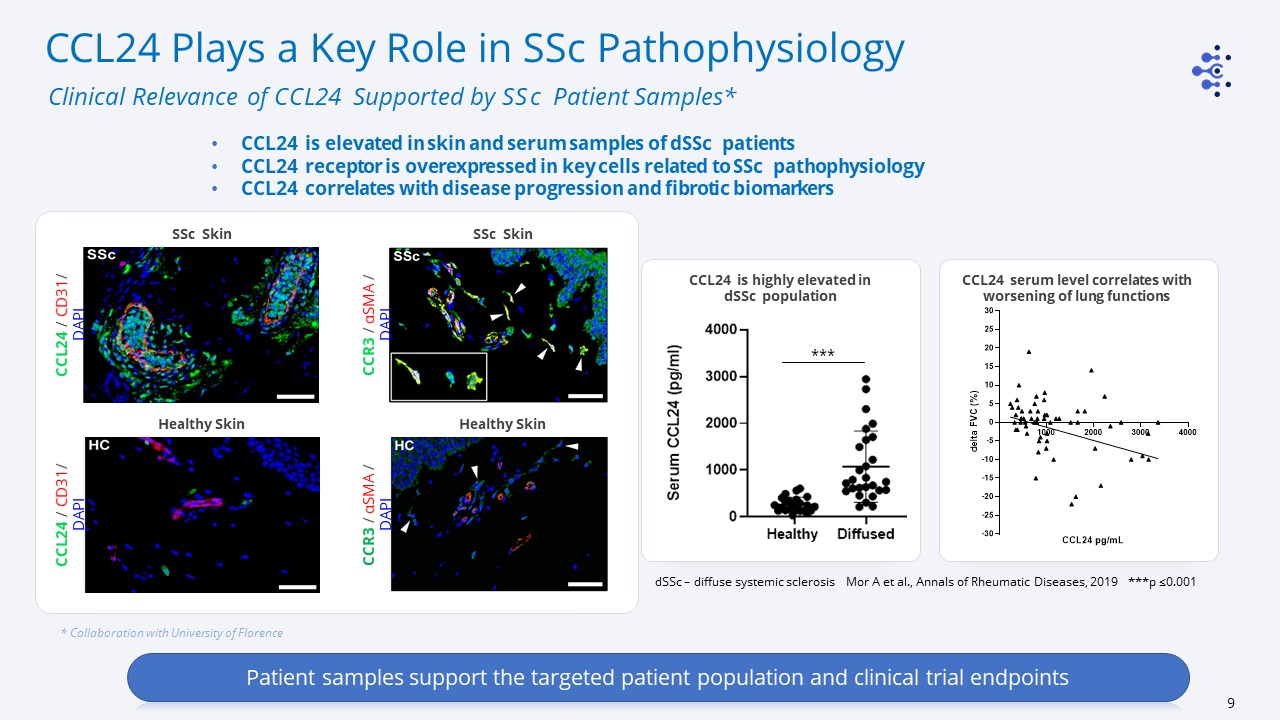
* Collaboration with University of Florence Patient samples support the targeted patient population and clinical trial endpoints CCL24 is elevated in skin and serum samples of dSSc patients CCL24 receptor is overexpressed in key cells related to SSc pathophysiology CCL24 correlates with disease progression and fibrotic biomarkers CCL24 Plays a Key Role in SSc Pathophysiology Clinical Relevance of CCL24 Supported by SSc Patient Samples* dSSc – diffuse systemic sclerosis Mor A et al., Annals of Rheumatic Diseases, 2019 ***p ≤0.001 *** CCL24 serum level correlates with worsening of lung functions CCL24 is highly elevated in dSSc population SSc Skin Healthy Skin CCR3 / αSMA / DAPI Healthy Skin SSc Skin CCL24 / CD31/ DAPI CCL24 / CD31/ DAPI CCR3 / αSMA / DAPI
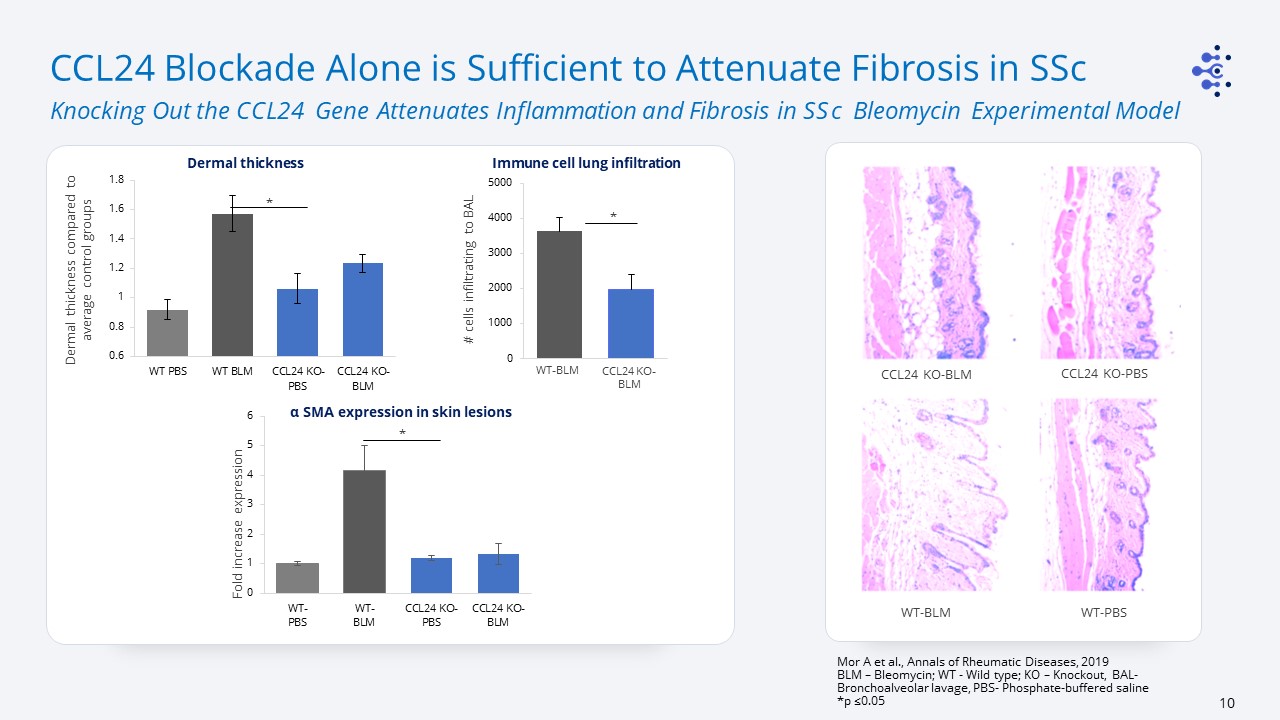
Fold increase expression Dermal thickness compared to average control groups * # cells infiltrating to BAL * WT-BLM CCL24 KO-BLM CCL24 Blockade Alone is Sufficient to Attenuate Fibrosis in SSc Knocking Out the CCL24 Gene Attenuates Inflammation and Fibrosis in SSc Bleomycin Experimental Model Mor A et al., Annals of Rheumatic Diseases, 2019BLM – Bleomycin; WT - Wild type; KO – Knockout, BAL- Bronchoalveolar lavage, PBS- Phosphate-buffered saline *p ≤0.05 WT-PBS CCL24 KO-PBS WT-BLM CCL24 KO-BLM * α SMA expression in skin lesions Dermal thickness Immune cell lung infiltration
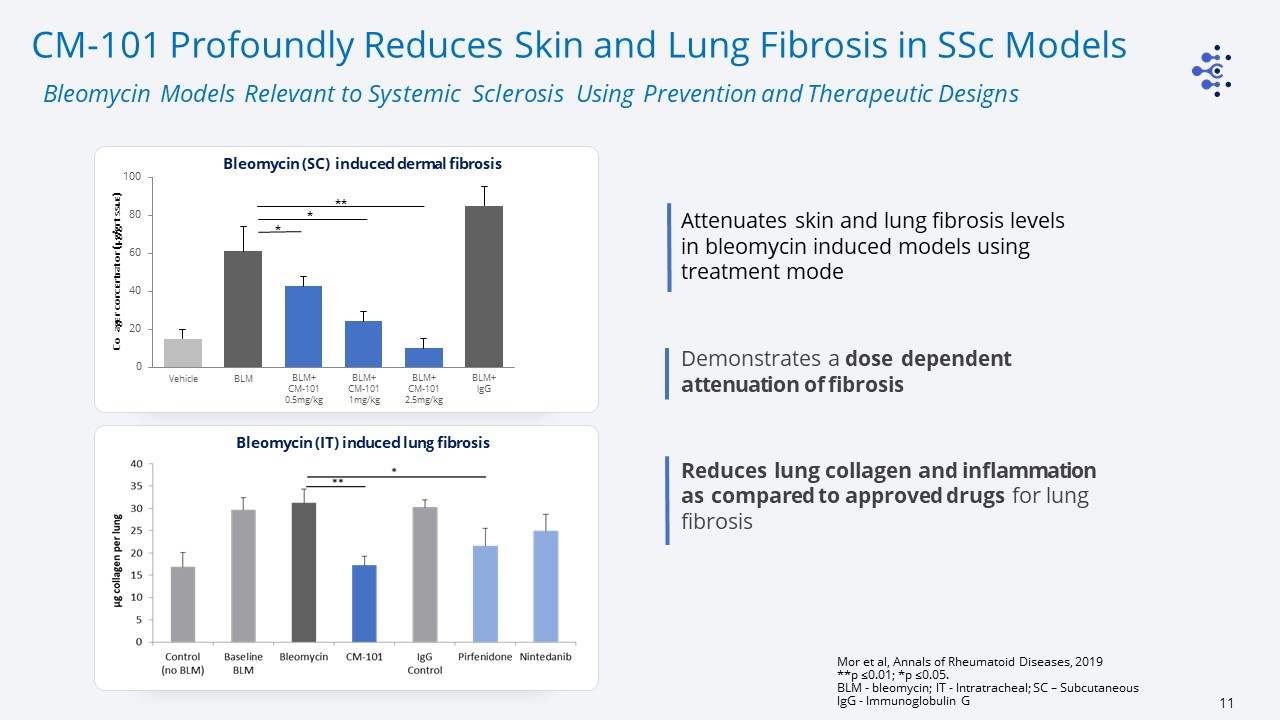
Collagen concentration (µg/gr tissue) Vehicle BLM BLM+CM-101 0.5mg/kg BLM+CM-101 1mg/kg BLM+CM-101 2.5mg/kg BLM+lgG * * ** Bleomycin (SC) induced dermal fibrosis Bleomycin (IT) induced lung fibrosis CM-101 Profoundly Reduces Skin and Lung Fibrosis in SSc Models Bleomycin Models Relevant to Systemic Sclerosis Using Prevention and Therapeutic Designs Mor et al, Annals of Rheumatoid Diseases, 2019**p ≤0.01; *p ≤0.05. BLM - bleomycin; IT - Intratracheal; SC – SubcutaneousIgG - Immunoglobulin G Attenuates skin and lung fibrosis levels in bleomycin induced models using treatment modeDemonstrates a dose dependent attenuation of fibrosisReduces lung collagen and inflammation as compared to approved drugs for lung fibrosis

PK-Target Engagement PK-PD 2.5mg/kg IV PK-PD 5mg/kg SC Liver Stiffness Relative change from baseline (%) Nordic Biosciences , Denmark Fibrotic Biomarkers Improved* FibroScan™ ProC4 *Concordant results across 6 relevant fibrotic markers TIMP1 Elastography Decreased Relative change from baseline (%) EOT EOT Phase 1: Excellent Safety Profile & 1st Confirmation of Anti-Fibrotic Effects CM-101 was safe and well tolerated in >42 healthy volunteers and patients across 3 Phase 1 studiesFavorable half-life supports long dosing interval (once every 2-4 weeks)Multiple administration 15-week study showed biomarker improvement with dose-dependent PK-Target engagement in NAFLD Patients ProC4-Procollagen 4; TIMP1- metallopeptidase inhibitor 1; EOT-End of Treatment
Systemic Sclerosis Overview: Clinical Trial & Clinical Endpoint Considerations Dr. Dinesh KhannaFrederick G. L. Huetwell Professor of RheumatologyProfessor of MedicineUniversity of Michigan khannad@umich.edu
Systemic Sclerosis Dinesh Khanna, MD, MSFrederick G. L. Huetwell Professor of RheumatologyProfessor of Medicine, University of Michigan khannad@umich.edu
Scleroderma The word “scleroderma” comes from two Greek words: “sclero” meaning hard, and “derma” meaning skin. There are approximately 200,000 patients in USApproximately 75,000-80,000 have systemic sclerosis (SSc) Scleroderma Localized Systemic Scleroderma or Systemic Sclerosis
SSc—Epidemiology Rare diseaseEstimated prevalence1 US 276/millionEurope 88-160/millionEstimated incidence 18.7 cases/ million/ year2 With US population at ~ 328 million people, there are ~ 6,000 new SSc cases diagnosed each year 1Chifflow H Semin Arthritis Rheum 37:223-235 2Mayes et al. Arthritis Rheum 2001 Peak age 30-50 years Female predominance of 3-5:1 High morbidity and highest mortality among rheumatic diseases Heterogeneous disease
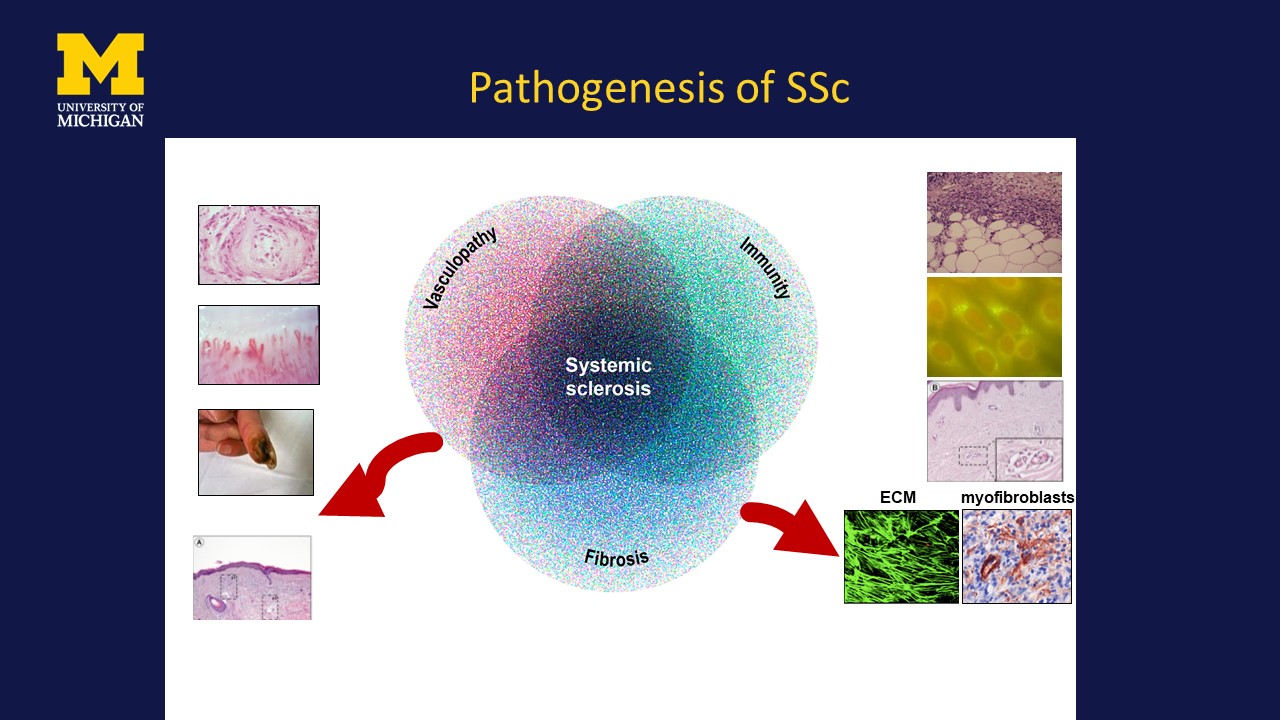
Fibroproliferative obliterationVascular remodelingDigital ischemiaLeaky capillaries Inflammation/autopimmunity ECM myofibroblasts Pathogenesis of SSc
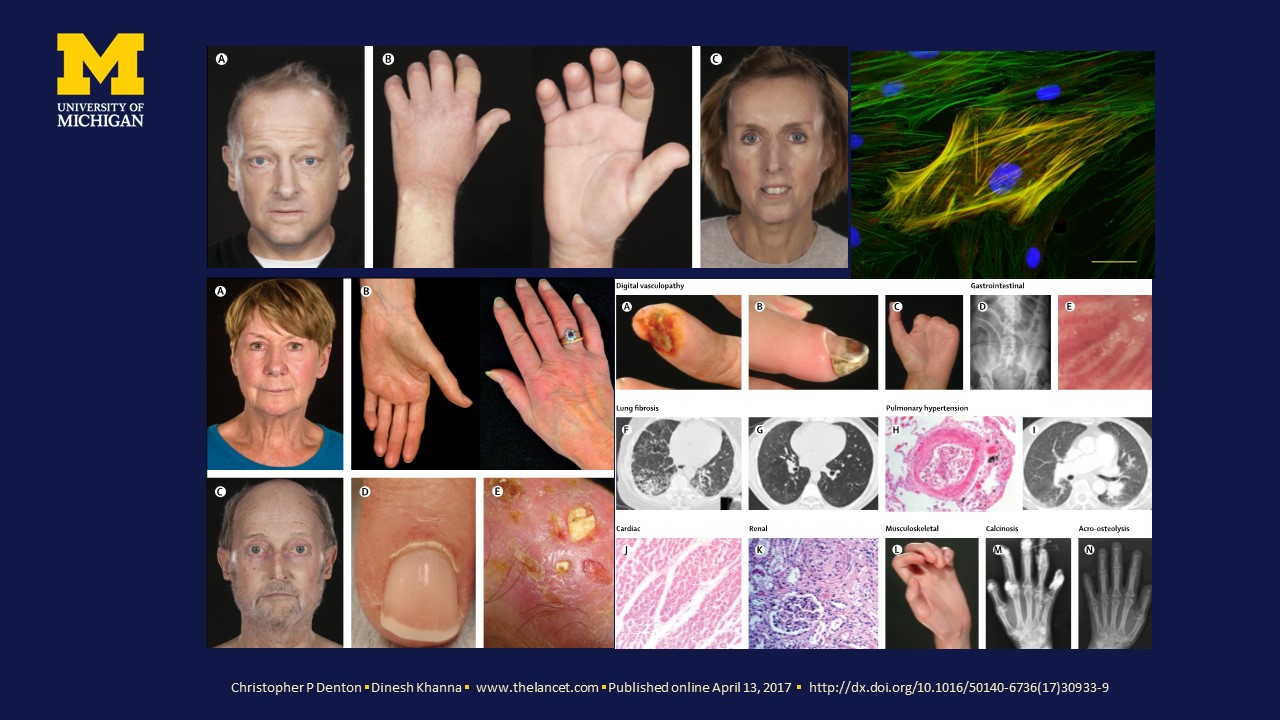
Christopher P Denton ▪ Dinesh Khanna ▪ www.thelancet.com ▪ Published online April 13, 2017 ▪ http://dx.doi.org/10.1016/50140-6736(17)30933-9
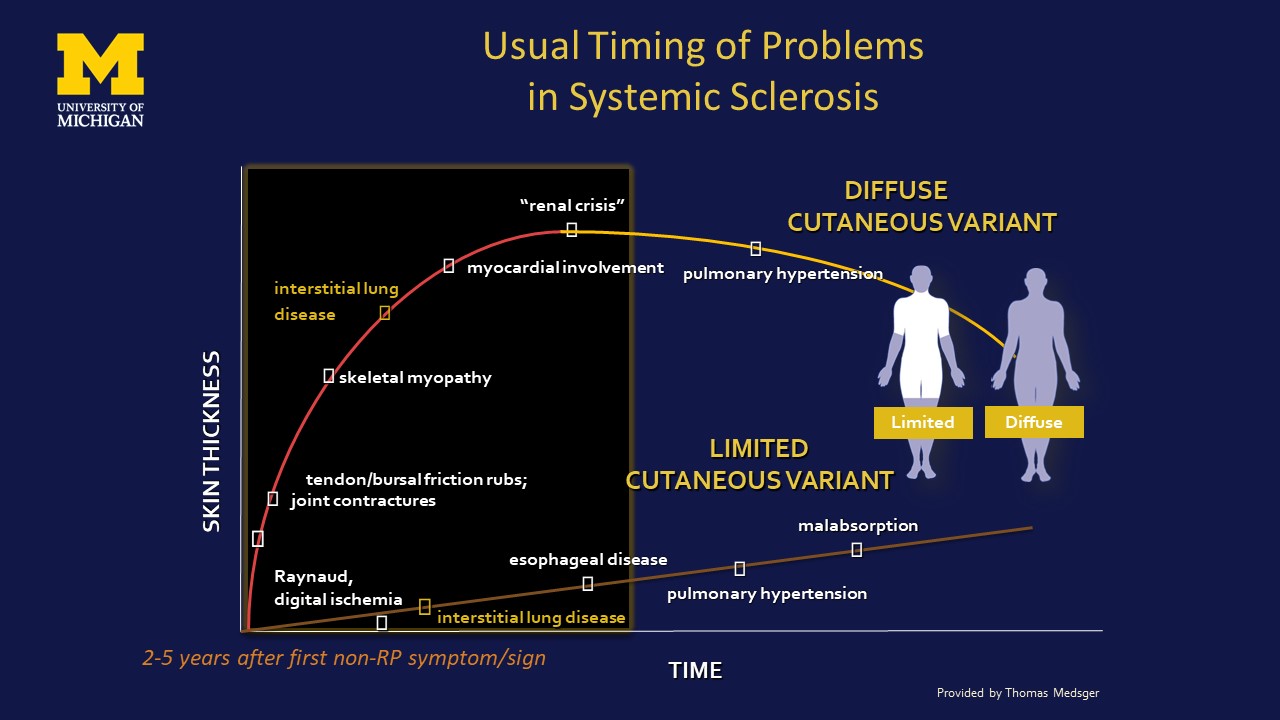
DIFFUSE CUTANEOUS VARIANT joint contractures skeletal myopathy interstitial lungdisease myocardial involvement esophageal disease pulmonary hypertension malabsorption LIMITEDCUTANEOUS VARIANT “renal crisis” TIME Raynaud, digital ischemia SKIN THICKNESS tendon/bursal friction rubs; interstitial lung disease pulmonary hypertension Provided by Thomas Medsger 2-5 years after first non-RP symptom/sign Usual Timing of Problems in Systemic Sclerosis Limited Diffuse
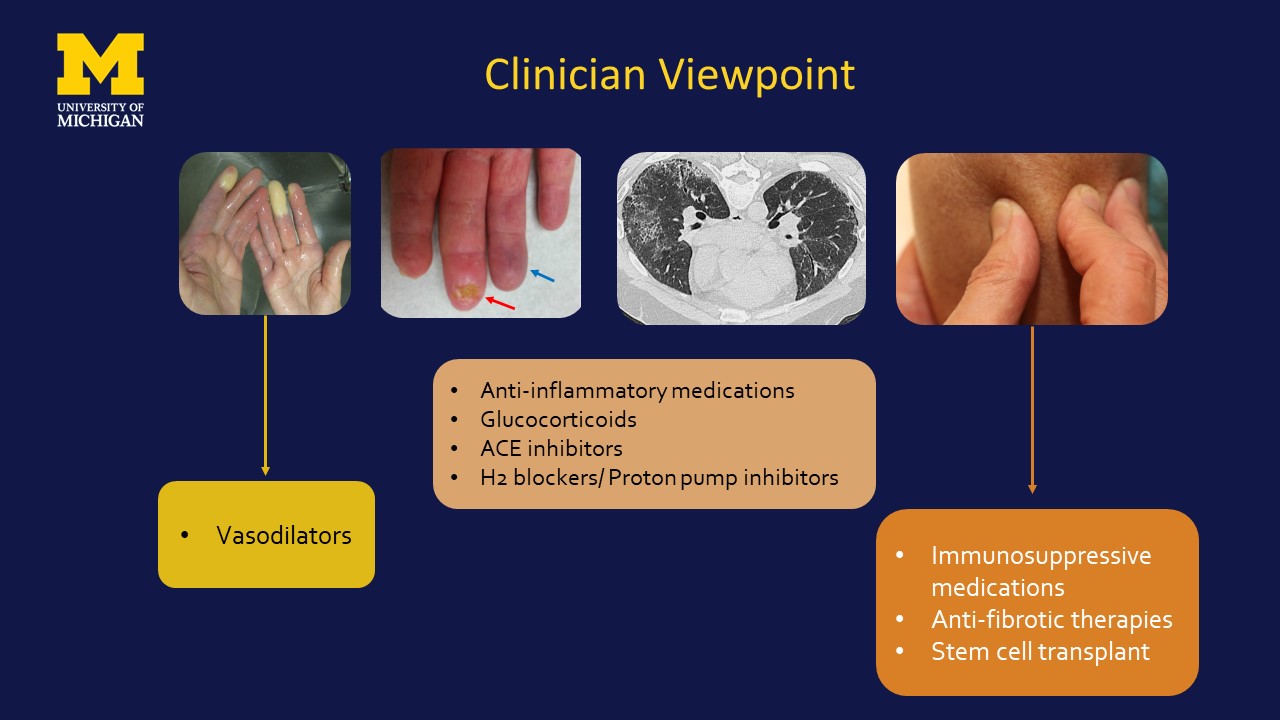
Clinician Viewpoint Vasodilators Anti-inflammatory medicationsGlucocorticoidsACE inhibitorsH2 blockers/ Proton pump inhibitors Immunosuppressive medicationsAnti-fibrotic therapiesStem cell transplant
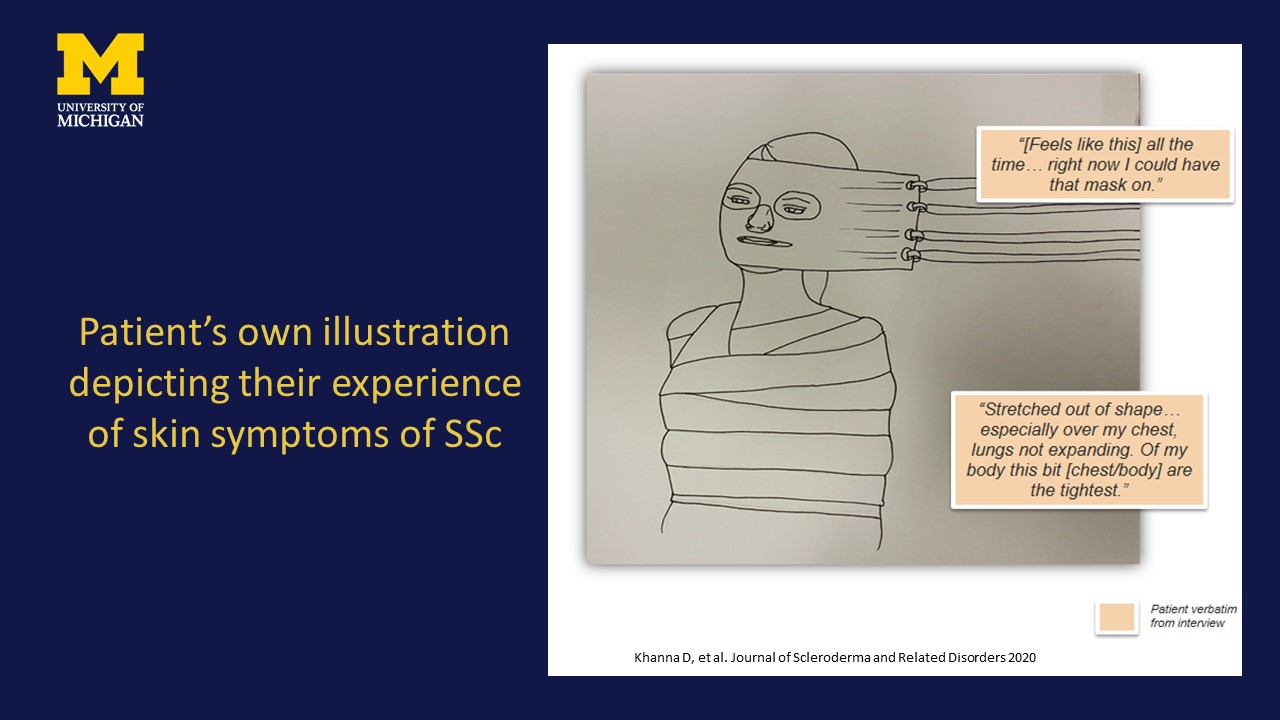
Patient’s own illustration depicting their experience of skin symptoms of SSc Khanna D, et al. Journal of Scleroderma and Related Disorders 2020
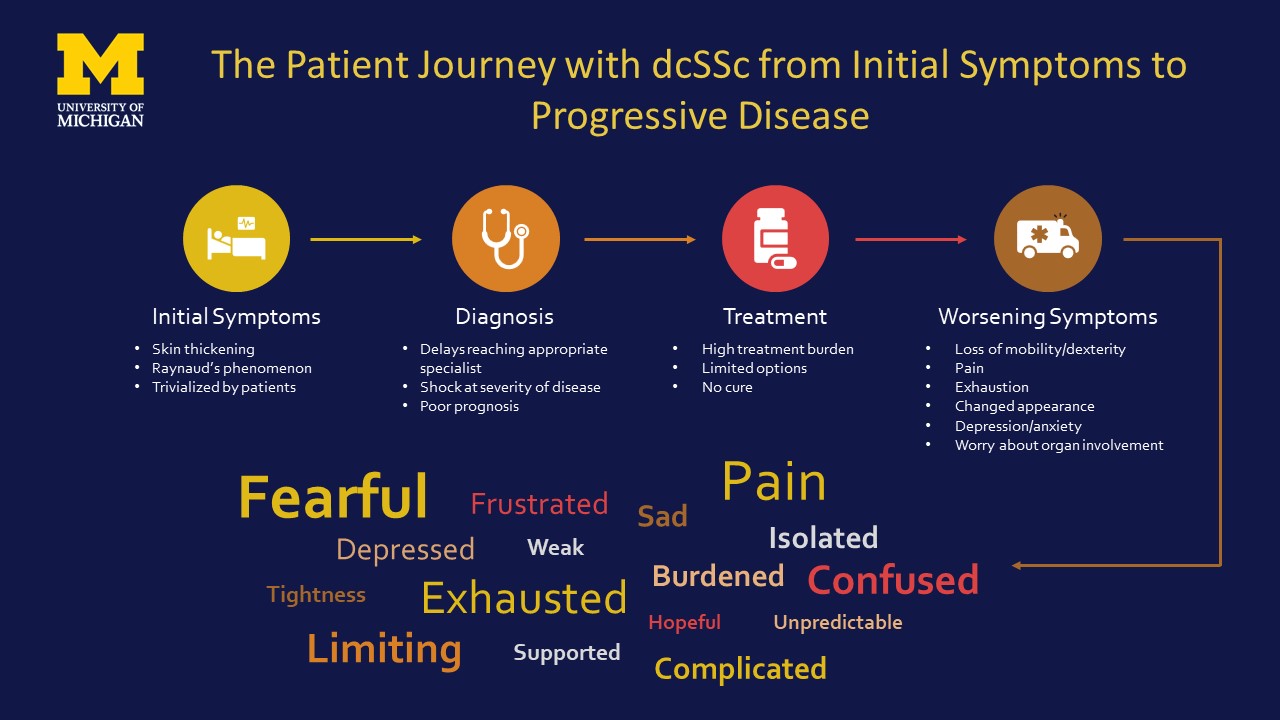
The Patient Journey with dcSSc from Initial Symptoms to Progressive Disease Initial SymptomsSkin thickeningRaynaud’s phenomenonTrivialized by patients DiagnosisDelays reaching appropriate specialist Shock at severity of diseasePoor prognosis TreatmentHigh treatment burdenLimited optionsNo cure Worsening SymptomsLoss of mobility/dexterityPainExhaustionChanged appearanceDepression/anxietyWorry about organ involvement Fearful Complicated Depressed Limiting Weak Unpredictable Sad Hopeful Burdened Isolated Exhausted Supported Tightness Confused Pain Frustrated
Unmet Need Lack of holistic approach to manage early SScCurrent management by a clinicianScreen for early organ involvementOrgan specific and supportive treatmentFDA approved therapyNintedanib and Tocilizumab for lung fibrosis PAH specific therapies as part of Group 1 PAH Off label treatments
Endpoints in Systemic Sclerosis End points for inflammatory/ fibrotic manifestationsModified Rodnan skin scoreForced Vital CapacityComposite IndexAmerican College of Rheumatology Composite Response Index (ACR CRISS)Revised CRISS

Modified Rodnan Skin Score (MRSS) Histological correlation of skin score Skin Score: 3 Skin Score: 1 Skin Score: 2 Face Upper arm Chest Forearm Hand Fingers Thigh Leg Foot Upper arm Abdomen Forearm Hand Fingers Thigh Leg Foot Total _____ / 51 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 1 3 2 0 Uninvolved Mild thickening Moderate thickening Severe thickening Date ID Hand Leg Calculating the MRSS

Forced Vital Capacity Physiological assessment of lung volumes Surrogate measure to assess for systemic sclerosis-associated interstitial lung disease
Why a Combined Response Index for SSc? SSc has validated outcomes for individual manifestations SSc is a multisystem disorderCombined indices successful in other complex systemic rheumatic diseases:RCTs FDA approval of new therapiesRA-ACR Responder Index/Disease activity index: joint count, HAQ, APRs, global assessmentsPsoriatic Arthritis--Responder index: joint count, HAQ-DI, APRs, global assessments We seek approaches to treat the underlying disease; thus, we want measures of overall disease ACR- American College of Rheumatology; HAQ-DI- Health Assessment Questionnaire, APR- Acute phase reactants

U.S. FDA Clinical Outcome Assessment (CoA) Center for Drug Evaluation and Research, U.S. Food & Drug Administration. Clinical Outcome Assessment (CoA) Compendium
ACR Response Criteria (Originally 20% but evolved to include 50% and 70%) BenefitsAcceptable FDA endpointLed to approval of multiple biologic therapiesUnderstood by regulators and physicians A decrease in both tender and swollen joint counts An improvement in at least 3 of the following 5 measures:- Patient Global- Patient Pain - Physician Global - HAQ-DI- Acute Phase Reactants
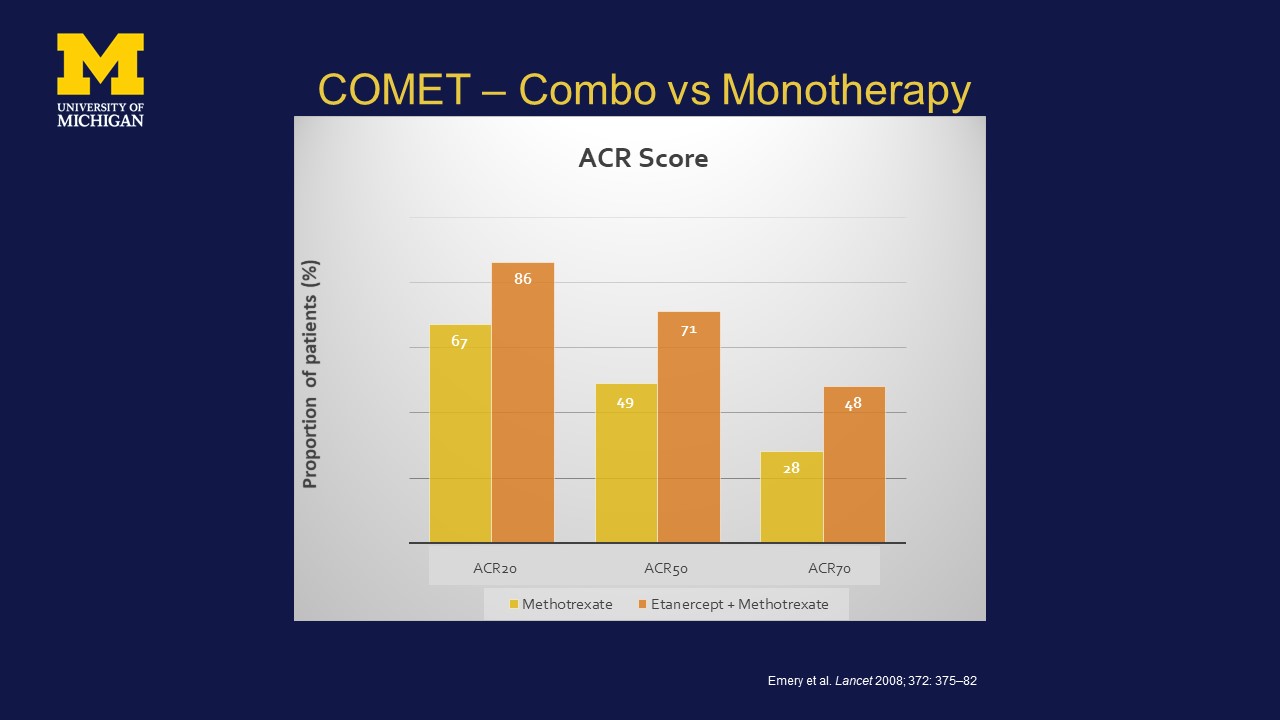
COMET – Combo vs Monotherapy Emery et al. Lancet 2008; 372: 375–82 ACR20 ACR50 ACR70

Composite End Point Revised CRISSCaptures global improvement in SSc 2-step process Ann Rheum Dis 2020;0:1-10. doi:10.1136/annrheumdis-2020-219100
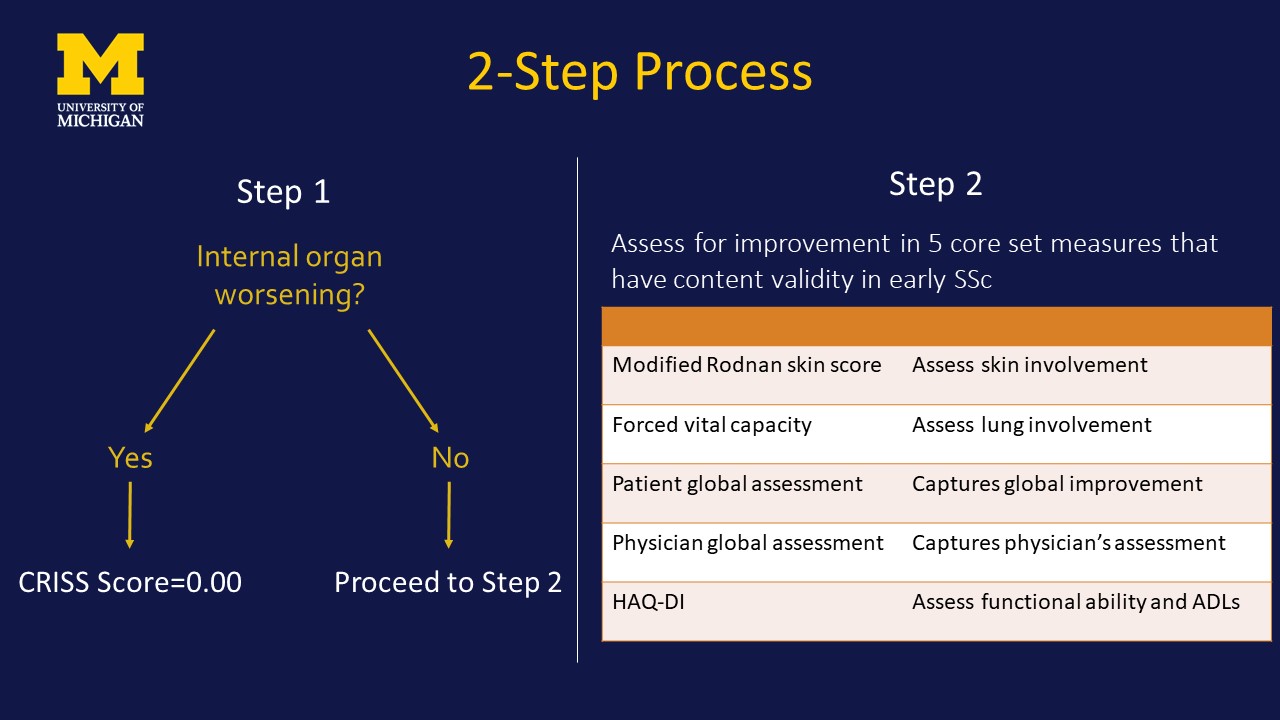
2-Step Process Step 1 Step 2 Internal organ worsening? No Yes CRISS Score=0.00 Proceed to Step 2 Modified Rodnan skin score Assess skin involvement Forced vital capacity Assess lung involvement Patient global assessment Captures global improvement Physician global assessment Captures physician’s assessment HAQ-DI Assess functional ability and ADLs Assess for improvement in 5 core set measures thathave content validity in early SSc
Revised CRISS Holistic measure that assesses internal organ involvement and improvement in 5 core set measures.Assessed as proportion of patients who achieved a certain improvement (as percent change) in ≥ 3 of 5 measures.This is similar to ACR response index for rheumatoid arthritis Acceptable endpoint by the FDAUnderstood by regulators and physiciansPrecedence with labeling claims
CM-101 Systemic Sclerosis Phase 2 Clinical Program Dr. Arnon Aharon Chemomab CMO

Phase 2 Trial in Diffuse Cutaneous Systemic Sclerosis (dcSSC) Territories: US, EU and Israel Number of sites: 100 sites globally Expected initiation – Q1/2022 Randomization 220 patients 1:1 Randomization ScreeningPeriod Treatment Period CM-101 10 mg/kg; I.V. Q3W Placebo; I.V. Q3W Week 45 EoT visit Week 48 Primary Endpoint Safety Follow-up Week 56 Diffuse Cutaneous Systemic Sclerosis Phase 2 Trial Design EoT- end of treatment; Q3W- once every 3 weeks; I.V. - Intravenous
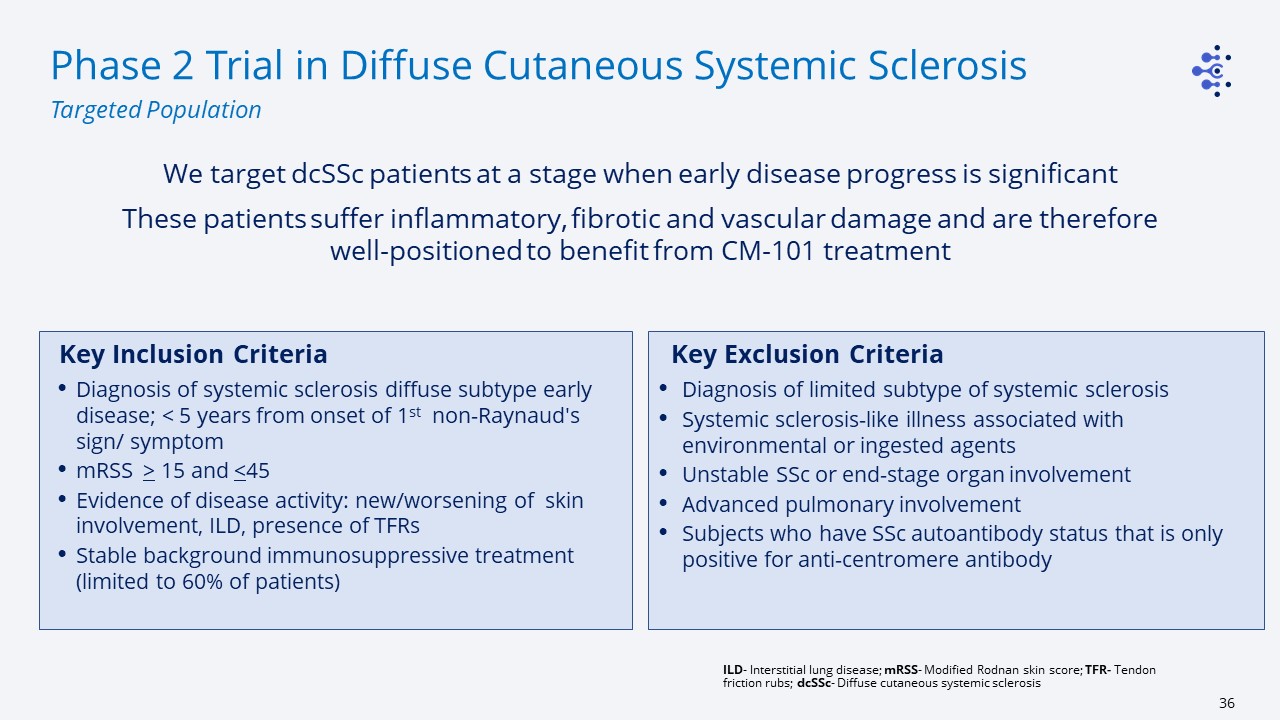
Phase 2 Trial in Diffuse Cutaneous Systemic Sclerosis Targeted Population Key Inclusion Criteria Diagnosis of systemic sclerosis diffuse subtype early disease; < 5 years from onset of 1st non-Raynaud's sign/ symptommRSS > 15 and <45Evidence of disease activity: new/worsening of skin involvement, ILD, presence of TFRsStable background immunosuppressive treatment (limited to 60% of patients) We target dcSSc patients at a stage when early disease progress is significant These patients suffer inflammatory, fibrotic and vascular damage and are therefore well-positioned to benefit from CM-101 treatment Key Exclusion Criteria Diagnosis of limited subtype of systemic sclerosisSystemic sclerosis-like illness associated with environmental or ingested agentsUnstable SSc or end-stage organ involvementAdvanced pulmonary involvementSubjects who have SSc autoantibody status that is only positive for anti-centromere antibody ILD- Interstitial lung disease; mRSS- Modified Rodnan skin score; TFR- Tendon friction rubs; dcSSc- Diffuse cutaneous systemic sclerosis
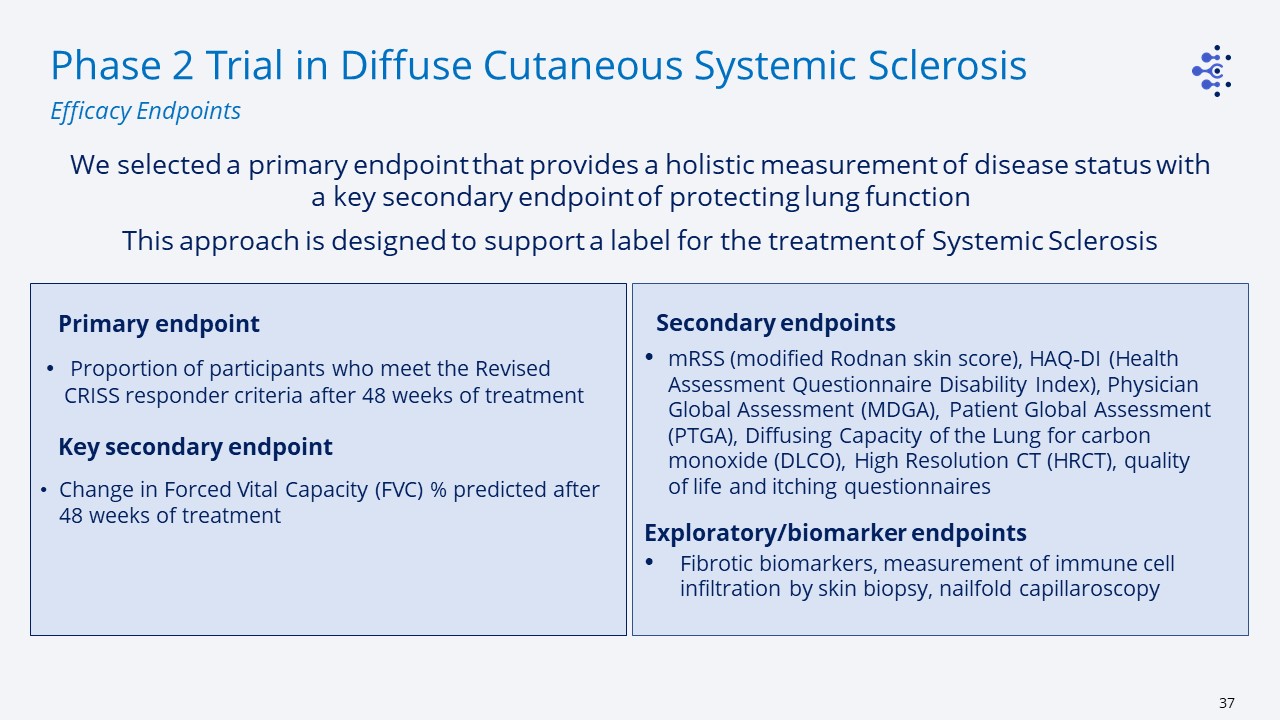
Phase 2 Trial in Diffuse Cutaneous Systemic Sclerosis Efficacy Endpoints Primary endpoint Proportion of participants who meet the Revised CRISS responder criteria after 48 weeks of treatment Key secondary endpoint Change in Forced Vital Capacity (FVC) % predicted after 48 weeks of treatment We selected a primary endpoint that provides a holistic measurement of disease status with a key secondary endpoint of protecting lung function This approach is designed to support a label for the treatment of Systemic Sclerosis Secondary endpointsmRSS (modified Rodnan skin score), HAQ-DI (Health Assessment Questionnaire Disability Index), Physician Global Assessment (MDGA), Patient Global Assessment (PTGA), Diffusing Capacity of the Lung for carbon monoxide (DLCO), High Resolution CT (HRCT), quality of life and itching questionnairesExploratory/biomarker endpointsFibrotic biomarkers, measurement of immune cell infiltration by skin biopsy, nailfold capillaroscopy
CM-101 in Systemic Sclerosis – Key Clinical Program Features CM-101 development program aimed at a label for the treatment of Systemic Sclerosis - Addressing high unmet medical need in Systemic Sclerosis - Leveraging unique dual MoA of CM-101 to support a disease modification label - Targeting the whole dcSSc population, not limited to subset of patients with specific organ damage - Focus on evaluating patient benefit as a whole, as well as effect on individual organs such as lung and skin Study was designed in collaboration with KOLs and incorporates input from regulators - Selected dose was proven efficacious in animal models of SSc, improving both skin and lung symptoms - Revised CRISS is a holistic composite primary endpoint that best matches CM-101 dual MoA - One-year study duration enables detection of improvement in both inflammatory and fibrotic disease - This trial could potentially serve as 1st adequate and well controlled study toward registration A switch to the subcutaneous formulation is planned prior to Phase 3 trial

Q&A: All Speakers