Exhibit 99.3

Appendix August 3, 2021 THERAVANCE BIOPHARMA ® , THERAVANCE ® , the Cross/Star logo and MEDICINES THAT MAKE A DIFFERENCE ® are registered trademarks of the Theravance Biopharma group of companies (in the U.S. and certain other countries). All third party trademarks used herein are the property of their respective owners. © 2021 Theravance Biopharma. All rights reserved.

Decades - long track record of driving innovative products to market for diseases of high unmet need Investment highlights 2 Innovative, commercial - stage biopharma with strong development track record Diversified pipeline of organ - selective medicines for rare disease, respiratory, GI and ocular indications Wholly - owned and partnered pipeline of differentiated assets Three major clinical readouts expected by early - 2022 Organ - selective approach serves as an engine for new opportunities Applying organ - selective expertise to biologically compelling pathways aiming to better serve patients Multiple near - term catalysts provide opportunity for value Underlying stream of derisked, long - tailed cash flow Strong base of cash flow, anchored by Yupelri and our economic interest in TRELEGY Multiple commercial and near - commercial products create growing revenue profile Topline growth poised for potential acceleration

Program Indication US Patients 1 Research Phase 1 Phase 2 Phase 3 Filed Marketed Collaborator Ampreloxetine (TD - 9855) NRI S ymptomatic nOH ~350k Wholly - owned Organ - Selective Izencitinib (TD - 1473) GI JAKi UC ~900k CD ~800k Janssen Biotech, Inc . TD - 5202 Irreversible JAK3i Celiac Disease UC CD ~5mm YUPELRI ® (revefenacin) LAMA COPD >8mm Nezulcitinib (TD - 0903) Inhaled JAKi Acute and chronic lung inflammation >32mm Wholly - owned TD - 8236 Inhaled JAKi Asthma ~25mm Inhaled ALK5i Idiopathic pulmonary fibrosis ~140k Program Indication Research Phase 1 Phase 2 Phase 3 Filed Marketed Rights Economic Interests TRELEGY 2 FF/UMEC/VI COPD >8mm GSK & Innoviva, Inc. Asthma ~25mm Skin - selective JAKi Dermatological diseases >8mm Key programs for large patient populations supported by proven development and commercial expertise 3 Phase 2 Phase 2 Phase 2b/3 Phase 1 Phase 3 Marketed Marketed Research Marketed Phase 1 Phase 2 1. TBPH estimate derived from integrating multiple data sources 2. TBPH holds 85% economic interest in upward - tiering royalty st ream of 6.5% – 10% payable by GSK (net of TRC expenses paid and the amount of cash, if any, expected to be used by TRC pursuant to the TRC Agreement over the next four fiscal quarters). 75% of TRC income received is p led ged to service outstanding notes, 25% of royalties received retained by TBPH. All statements concerning TRELEGY ELLIPTA based on publicly available information. ALK5i, transforming growth factor β receptor I kinase inhibitor; CD, Crohn’s di sease; COPD, chronic obstructive pulmonary disease; FF/UMEC/VI, fluticasone furoate/umeclidinium/ vilanterol; JAKi, Janus kinase inhibitor; LAMA, long - acting muscarinic receptor antagonist; nO H, neurogenic orthostatic hypotension; NRI, norepinephrine reuptake inhibitor; UC, ulcerative colitis.
Research and development portfolio of designed molecules: brain, lung, GI and eye 4 Molecular Design Biology Medicinal Chemistry DMPK Development and Commercial Symptomatic nOH (Neurogenic orthostatic hypotension) Asthma Lung Transplant Rejection IPF (idiopathic pulmonary fibrosis) COPD (chronic obstructive pulmonary disorder) — APPROVED COVID - 19 CD (Crohn’s disease) UC (ulcerative colitis) Celiac Disease DME (diabetic macular edema) DMPK, drug metabolism and pharmacokinetics; GI, gastrointestinal.
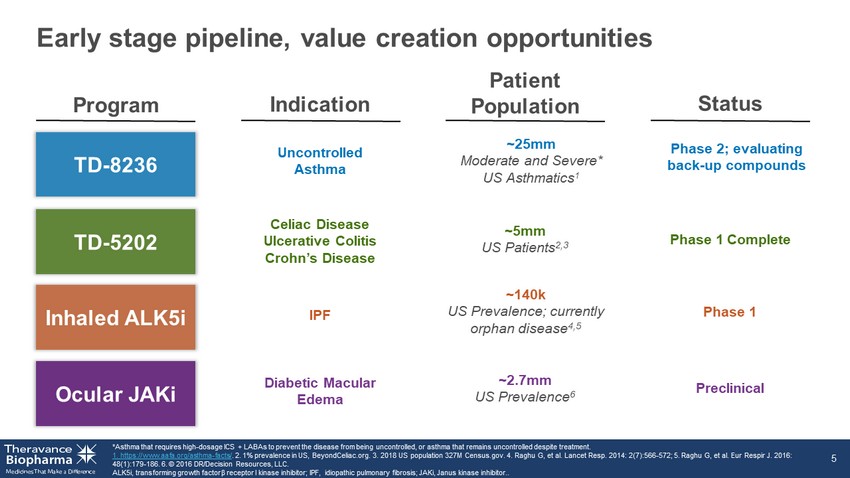
Early stage pipeline, value creation opportunities *Asthma that requires high - dosage ICS + LABAs to prevent the disease from being uncontrolled, or asthma that remains uncontrolle d despite treatment. 1. https://www.aafa.org/asthma - facts/ . 2. 1% prevalence in US, BeyondCeliac.org. 3. 2018 US population 327M Census.gov. 4. Raghu G, et al. Lancet Resp. 2014: 2(7) :56 6 - 572; 5. Raghu G, et al. Eur Respir J. 2016: 48(1):179 - 186. 6. © 2016 DR/Decision Resources, LLC. ALK5i, transforming growth factor β receptor I kinase inhibitor; IPF, idiopathic pulmonary fibrosis; JAKi , Janus kinase inhibitor.. 5 Program Patient Population Status Indication Uncontrolled Asthma TD - 8236 TD - 5202 Inhaled ALK5i Ocular JAKi Celiac Disease Ulcerative Colitis Crohn’s Disease ~25mm Moderate and Severe* US Asthmatics 1 Phase 2; evaluating back - up compounds ~5mm US Patients 2,3 Phase 1 Complete IPF ~140k US Prevalence; currently orphan disease 4,5 Phase 1 Diabetic Macular Edema ~2.7mm US Prevalence 6 Preclinical

Izencitinib (TD - 1473/JNJ - 8398) Oral gut - selective pan - JAK inhibitor to treat inflammatory bowel diseases

IBD represents an area of high unmet need Favorable Phase 1b data led to late - stage IBD studies Izencitinib: a novel approach to JAK inhibition for IBD 7 Izencitinib Preclinical and clinical data package represents a potential breakthrough approach for the treatment of IBD Oral, gut - selective agent Potent inhibition of Tyk2 Anti - inflammatory activity in disease model Low systemic exposure with high colonic concentrations Favorable Phase 1b data Phase 1b data 6 ‣ Demonstrated gut selectivity – High colonic concentration with low systemic drug exposures, consistent with pre - clinical data – For the goal of maximized therapeutic index ‣ Demonstrated numerically higher rates of clinical outcomes with reductions in biomarkers after only 4 weeks of treatment – Numerical improvements in rectal bleeding and mucosal healing IBD MARKET DYNAMICS 6.8mm global cases in 2017 1 1.6mm current US patients 2 ~780k current US Crohn’s patients 3 ~907k US Ulcerative Colitis patients 4 $16bn global IBD treatment market in 2018 5 $31bn US disease burden 2 Biologics have become mainstay of treatment in moderate - to - severe patients 1. GBD 2017 Inflammatory Bowel Disease Collaborators. Lancet 2020;5:17 - 30. 2. https://www.crohnscolitisfoundation.org/sites/default/files/2019 - 02/Updated%20IBD%20Factbook.pdf . 3. https://www.healthline.com/health/crohns - disease/facts - statistics - infographic 4. https://med.stanford.edu/news/all - news/2020/02/stanford - scientists - link - ulcerative - colitis - to - missing - gut - micro.html 5. https://www.transparencymarketresearch.com/inflammatory - bowel - disease.html 6. Sandborn et al. J Crohns Colitis;2020: 14:1202 - 13. IBD, inflammatory bowel disease; JAK, Janus kinase; Tyk, tyrosine kinase.

STAT - induced Inflammation α N UCLEUS STAT P STAT P STAT P STAT P STAT JAK β γ JAK JAK inhibitor JAK - STAT pathway: orchestrating signaling of multiple pro - inflammatory cytokines Clark JD, et al. J Med Chem 2014; 57:5023 - 5038. EPO, erythropoietin; GM - CSF, granulocyte - macrophage colony - stimulating factor; IFN, interferon; IL, interleukin; JAK, Janus kina se; STAT, signal transducer and activator of transcription; TPO, thrombopoietin; Tyk, tyrosine kinase. 8 γ c cytokines (IL - 2, IL - 4, IL - 7, IL - 9, IL - 15, IL - 21) Type 1 IFNs, IL - 10 family IL - 6, IL - 11, IL - 13, IL - 27, IL - 31, IL - 35 IFN γ IL - 12, IL - 23 EPO, TPO GM - CSF, IL - 3, IL - 5 α JAK1 β γ JAK3 α JAK1 β γ Tyk2 α JAK1 β γ JAK2 Tyk2 α JAK1 β γ JAK2 α JAK2 β γ Tyk2 α JAK2 β γ JAK2
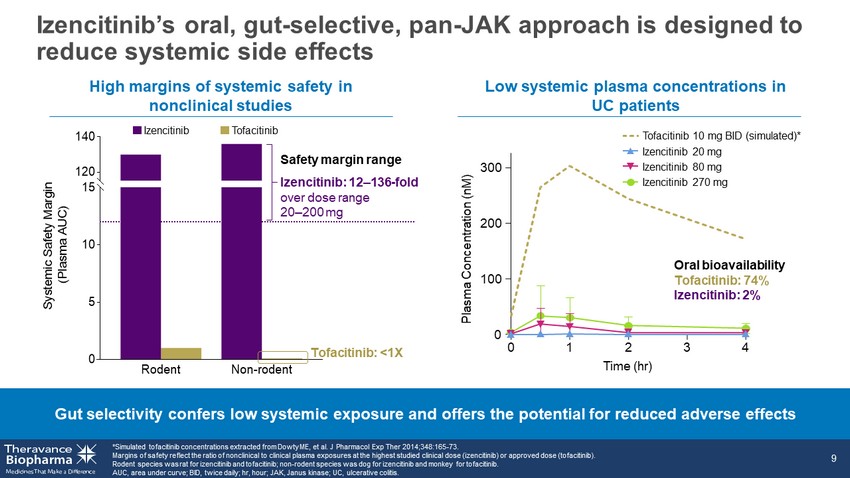
0 5 10 15 120 140 S y s t e m i c S a f e t y M a r g i n ( P l a s m a A U C ) Non-rodentRodent High margins of systemic safety in nonclinical studies Gut selectivity confers low systemic exposure and offers the potential for reduced adverse effects Low systemic plasma concentrations in UC patients Izencitinib’s oral, gut - selective, pan - JAK approach is designed to reduce systemic side effects *Simulated tofacitinib concentrations extracted from Dowty ME, et al. J Pharmacol Exp Ther 2014;348:165 - 73. Margins of safety reflect the ratio of nonclinical to clinical plasma exposures at the highest studied clinical dose (izencit ini b) or approved dose (tofacitinib). Rodent species was rat for izencitinib and tofacitinib; non - rodent species was dog for izencitinib and monkey for tofacitinib. AUC, area under curve; BID, twice daily; hr , hour; JAK, Janus kinase; UC, ulcerative colitis. 9 Tofacitinib 10 mg BID (simulated)* Izencitinib 20 mg Izencitinib 80 mg Izencitinib 270 mg 0 1 2 3 4 0 100 200 300 Plasma Concentration (nM) Time (hr) Oral bioavailability Tofacitinib: 74% Izencitinib: 2% Izencitinib Tofacitinib Izencitinib: 12 – 136 - fold over dose range 20 – 200 mg Tofacitinib: <1X Safety margin range

Izencitinib’s oral, gut - selective, pan - JAK approach is designed to maximize efficacy in IBD GI, gastrointestinal; IBD, inflammatory bowel disease; JAK, Janus kinase; UC, ulcerative colitis. 10 Vehicle treated control Izencitinib treatment CD3+ pan - T cells Blocks inflammation and penetrates deep within mouse colon The gut - selective approach is intended to maximize concentration where it matters, at the site of action in the GI tract Demonstrates improvement in UC patients in Phase 1b 0 44 20 30 30 70 18 73 0 20 40 60 80 100 Endoscopy Rectal Bleeding % of Patients Placebo (n=9) 20 mg (n=10) 80 mg (n=10) 270 mg (n=11) Izencitinib
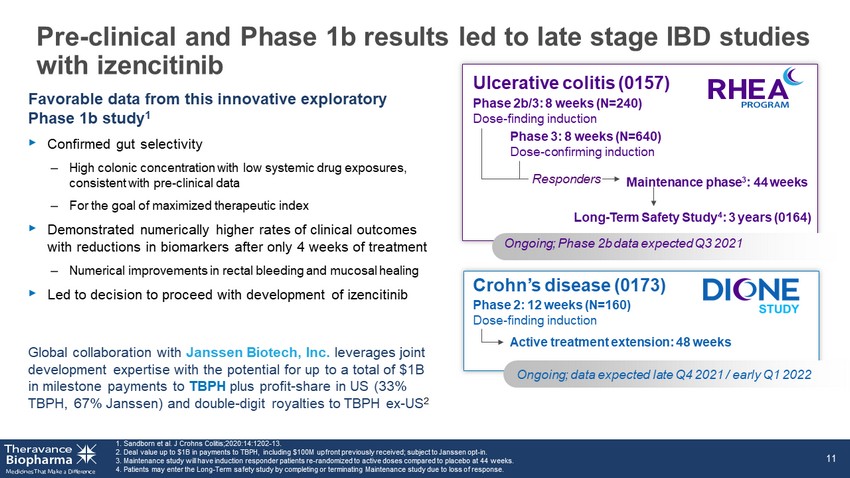
Favorable data from this innovative exploratory Phase 1b study 1 ‣ Confirmed gut selectivity – High colonic concentration with low systemic drug exposures, consistent with pre - clinical data – For the goal of maximized therapeutic index ‣ Demonstrated numerically higher rates of clinical outcomes with reductions in biomarkers after only 4 weeks of treatment – Numerical improvements in rectal bleeding and mucosal healing ‣ Led to decision to proceed with development of izencitinib Global collaboration with Janssen Biotech, Inc. leverages joint development expertise with the potential for up to a total of $1B in milestone payments to TBPH plus profit - share in US (33% TBPH, 67% Janssen) and double - digit royalties to TBPH ex - US 2 1. Sandborn et al. J Crohns Colitis;2020: 14:1202 - 13. 2. Deal value up to $1B in payments to TBPH, including $100M upfront previously received; subject to Janssen opt - in. 3. Maintenance study will have induction responder patients re - randomized to active doses compared to placebo at 44 weeks. 4. Patients may enter the Long - Term safety study by completing or terminating Maintenance study due to loss of response. 11 Phase 2: 12 weeks (N=160) Dose - finding induction Active treatment extension: 48 weeks Crohn’s disease (0173) Phase 2b/3: 8 weeks (N=240) Dose - finding induction Maintenance phase 3 : 44 weeks Phase 3: 8 weeks (N=640) Dose - confirming induction Responders Ulcerative colitis (0157) Long - Term Safety Study 4 : 3 years (0164) Ongoing; Phase 2b data expected Q3 2021 Pre - clinical and Phase 1b results led to late stage IBD studies with izencitinib Ongoing; data expected late Q4 2021 / early Q1 2022 11

Izencitinib: Phase 2 study in Crohn’s disease Endpoints ‣ Primary: Improvement in CDAI score at week 12 in patients with moderately to severely active CD ‣ Exploratory: – Clinical response measured by CDAI at 12 weeks – CDAI clinical remission at 12 weeks – SES - CD change from baseline to Week 12 – Endoscopic response [Time Frame: 12 weeks] – SFAP clinical remission [Time Frame: 12 weeks] *2 izencitinib doses. NCT03635112 CD, Crohn’s disease; CDAI, Crohn’s Disease Activity Index; SES - CD, Simple Endoscopic Score for Crohn's Disease; SFAP, Stool Freq uency and Abdominal Pain. 12 Key inclusion criteria: Age ≥18 y with moderately - to - severely active CD (CDAI 220 – 450) with corticosteroid dependence or failure of conventional or biologic therapy Geographies: South Africa, Asia, Australia, Europe, Middle East, New Zealand, UK, USA Study 0173 Program Status ‣ Ongoing Randomization Late Q4’21 Early Q1’22 Topline results Placebo Izencitinib* Ph 2 dose - finding induction: once - daily oral dose for 12 weeks Active treatment extension: once - daily oral dose for 48 weeks N=160 Izencitinib

Izencitinib: Phase 3 studies in ulcerative colitis Endpoints ‣ Primary: – Induction & Maintenance: clinical remission by aMS components at Week 8 and Week 44 ‣ Secondary: – Induction & Maintenance: endoscopic healing, symptomatic remission, clinical response by aMS, mucosal healing, maintenance of clinical response, corticosteroid - free remission, maintenance of clinical remission NCT03758443 aMS, adapted Mayo Score; UC, ulcerative colitis. 13 Program Status ‣ Phase 3 Induction study to begin post Phase 2b completion ‣ Phase 3 Maintenance study ongoing Study 0157 Randomization Placebo Izencitinib Ph 3 dose - confirming induction: once - daily oral dose for 8 weeks Responders from Ph 2b and Ph 3 Induction Placebo Izencitinib N=640 Ph 3 Induction Study starts after dose selection from Ph 2b Induction Ph 3 maintenance: once - daily oral dose for 44 weeks Key inclusion criteria: Age ≥18 y with moderately - to - severely active UC with corticosteroid dependence or failure of conventional or biologic therapy Geographies: South Africa, Asia, Australia, Europe , Middle East, North America, Japan
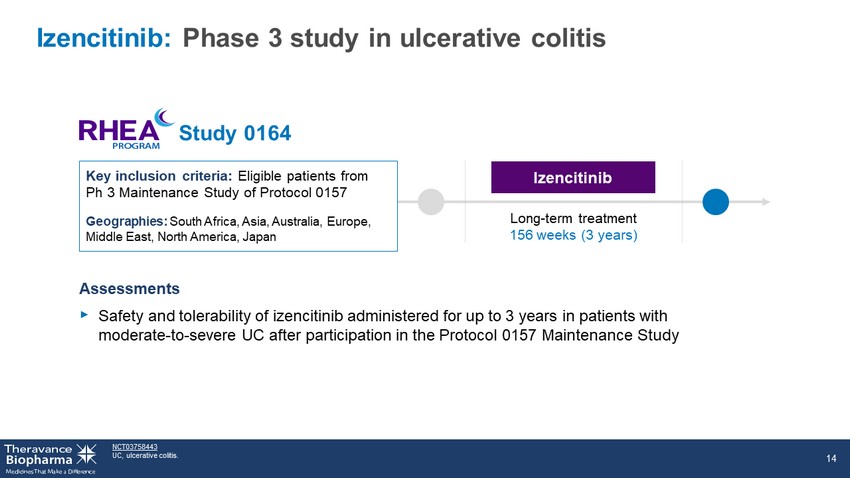
Izencitinib: Phase 3 study in ulcerative colitis Assessments ‣ Safety and tolerability of izencitinib administered for up to 3 years in patients with moderate - to - severe UC after participation in the Protocol 0157 Maintenance Study NCT03758443 UC, ulcerative colitis. 14 Key inclusion criteria: Eligible patients from Ph 3 Maintenance Study of Protocol 0157 Geographies: South Africa, Asia, Australia, Europe, Middle East, North America, Japan Long - term treatment 156 weeks (3 years) Izencitinib Study 0164

Month 6 0 5 10 15 20 F i r s t B P A R R a t e ( % ) Pan - JAK inhibitors can prevent transplant rejections ‣ JAK inhibition was superior to cyclosporine in prevention of acute and chronic rejections ‣ Serious infections increased with systemic JAK inhibitors including CMV 1. Vincenti F, et al. Am J Transplant 2015;15:1644 - 53. *p<0.001 vs CsA . BPAR, biopsy - proven acute rejection; CMV, cytomegalovirus; IF/TA, interstitial fibrosis/tabular atrophy; JAK, Janus kinase; SE, standard error. 15 Chronic Rejection Tofacitinib is superior to CsA in efficacy measures Acute Rejection Increased infection risk with tofacitinib over CsA CsA Tofacitinib 50 40 30 20 10 0 Month 12 * IF/TA (%) 24 5 53 25 0 20 40 60 Tofacitinib CsA CMV disease Serious infection 12 - month Kaplan - Meier estimates, % (SE) Noninferiority trial of tofacitinib vs cyclosporine (CsA) in kidney transplant recipients 1
Ampreloxetine (TD - 9855) Once - daily norepinephrine reuptake inhibitor to treat symptomatic neurogenic orthostatic hypotension

nOH profoundly impacts QoL Study 0169 primary endpoint: Change from baseline in OHSA Question 1 OHSA measures core nOH symptom: Dizziness / lightheadedness due to brain hypoperfusion Clinically significant endpoint: 1 - point OHSA improvement 1. https://www.parkinson.org/Understanding - Parkinsons/Statistics ; https://www.ninds.nih.gov/Disorders/Patient - Caregiver - Education/Fact - Sheets/Multiple - System - Atrophy . 2. Claassen DO, et al. BMC Neurol 2018;18:125 https://doi.org/10.1186/s12883 - 018 - 1129 - x . 3. Low PA. AMJC 2015;21:13,October 30 https://www.ajmc.com/view/ace0034_oct15_noh_low . 4. Not all patients are treated with prescription medication. MSA, multiple system atrophy; nOH, neurogenic orthostatic hypotension; OHSA, orthostatic hypotension symptom assessment; PD, Par kinson’s disease; QoL, quality of Life; Tx, treatment. Ampreloxetine: new approach in nOH 17 MARKET DYNAMICS ~350K US patients 1 : 70 – 80% of MSA patients 2 30 – 50% of PD patients 3 have nOH 4 Specialist network in place : concentrated group of neurologists/ cardiologists treat patients; ‘at risk’ patients already identified and managed by specialty institutions Physicians report urgency to treat due to high impact on patients’ QoL, high risk of injury from falls and caregiver burden Established nOH Tx paradigm: nOH included in medical treatment guidelines for PD/MSA patients; once diagnosed with nOH, patients prescribed drug SYMPTOMS IMPACT Depression Social isolation Poor QoL Falls (fractures/head trauma) Morbidity ‣ Dizziness or lightheadedness ‣ Fatigue ‣ Difficulty walking ‣ Weakness ‣ Impaired cognition ‣ Pain (back of head/neck/shoulders) ‣ Blurred vision ‣ Tremulousness ‣ Vertigo

Ampreloxetine: a once - daily, potent and selective norepinephrine reuptake inhibitor with a differentiated MOA for treating nOH Current nOH treatment options: ‣ No durable effect ‣ Multiple daily dosing ‣ Black box warning for SH 1. Kaufmann H, et al. Mov Disord. 2019;34(suppl 2). Poster presented at the 2019 International Congress of Parkinson’s and Mo vem ent Disorder Society. Note: a 1 - point change in the OHSA#1 score is considered clinically meaningful. MOA, mechanism of action; NE, norepinephrine; NET, norepinephrine transporters; nOH neurogenic orthostatic hypotension; OHSA #1, orthostatic hypotension symptom assessment question #1; SH, supine hypertension. 18 Ampreloxetine is designed to target and correct the norepinephrine imbalance… …and demonstrated a clinically meaningful and durable impact 1 Our goal: ampreloxetine to be the first treatment to demonstrate a sustained impact for patients managing the chronic and debilitating symptoms of nOH Change in OHSA #1 Efficacy Durability Withdrawal Study Week 0 - 1 - 4 - 7 4 20 24 Improvement Worsens back to baseline Vasoconstriction Blood pressure NE Release at Neurovascular Junction Ampreloxetine A XON TERMINAL D ENDRITE NE ~ 2 - fold increase Plasma NE Pre - dose Post - dose Reduction in syncope Normal …with potential for market differentiation…

Ampreloxetine: potential to provide meaningful and durable symptom improvement to underserved patients All subjects who complete Study 169 may enroll into 170; all subjects who complete 170 may enroll into extension study/171. Baseline OHSA #1 (Orthostatic Hypotension Symptom Assessment Question 1) >4 points. Negative change indicates improvement in sym ptoms; improvement of 1 point is defined as the MCID (minimal clinically important difference). Discontinuation rates for the Phase 3 trials as of Jan. 2020: 0169 – 5.3 percent; 0170 – 33.3 percent 19 Phase 3 registrational program ongoing; 4 - week efficacy data expected Q3 2021 Study 169: 4 weeks (N=188) Randomized, double - blind, placebo - controlled, parallel group Study 170: 22 weeks (N=254) Randomized 6 - week withdrawal phase Phase 3 Registrational Program Extension study: 3 years Completers

Ampreloxetine: Phase 3 registrational program Placebo - controlled, randomized withdrawal study *Negative change indicates improvement in symptoms; improvement of 1 point is defined as the MCID (minimal clinically importa nt difference). Discontinuation rates for the Phase 3 trials as of Jan. 2020: 0170 – 33.3%. NCT03829657 nOH, neurogenic orthostatic hypotension; OHDAS, orthostatic hypotension daily activities scale; OHSA, orthostatic hypotension sy mptom assessment; PGI - S, patient global impression of disease severity. 20 Key inclusion criteria: Age >30 y with symptomatic nOH with OHSA #1 score ≥4 Geographies: Argentina, Australia, Canada, Europe, New Zealand, Russia, UK, US Program Status ‣ Phase 3 registrational program ongoing ‣ All participants who complete Study 0170 are eligible for Extension Study 0171 Ampreloxetine Randomization Q3’22 Top - line results Ampreloxetine Placebo Open - label once - daily 10 mg oral dose: 16 weeks Once - daily 10 mg oral dose: 6 week withdrawal phase – PGI - S – % Time spent standing – Average no. of steps taken Study 0170 N=258 Objectives ‣ Primary: 1 - pt worsening from baseline in both OHSA #1 score* and PGI - S during withdrawal phase ‣ Secondary: Changes from baseline at Week 6 post - randomization – OHSA #1 – OHSA composite score – OHDAS composite score

Ampreloxetine: Phase 3 program 6 - month safety study + 3 - year optional extension Assessments ‣ Through Week 26: – Physical and neurological exams – Vital signs – ECGs – Clinical laboratory tests – Concomitant medications *Through week 26; for FDA filing NCT04095793 AE, adverse event; C - SSRS, Columbia Suicide Severity Rating Scale; ECG, electrocardiogram. 21 Program Status ‣ Includes patients who completed Study 0170 – AEs – Treatment compliance – Incidence of falls – Changes from baseline in C - SSRS Key inclusion criteria: patients who completed Study 0170 and, in investigator’s opinion, would benefit from long - term treatment with ampreloxetine Geographies: Argentina, Australia, Canada, Europe, New Zealand, Russia, UK, US Study 0171 Ampreloxetine Once - daily oral dose: 182 weeks Q3’22 Top - line results*
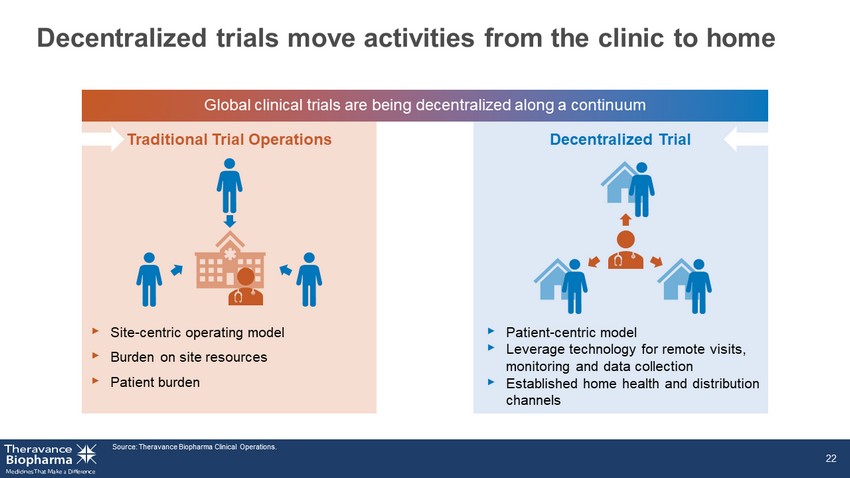
Decentralized trials move activities from the clinic to home ‣ Site - centric operating model ‣ Burden on site resources ‣ Patient burden Source: Theravance Biopharma Clinical Operations. 22 Global clinical trials are being decentralized along a continuum Traditional Trial Operations Decentralized Trial ‣ Patient - centric model ‣ Leverage technology for remote visits, monitoring and data collection ‣ Established home health and distribution channels

nOH is included in medical treatment guidelines for PD and MSA patients; once diagnosed, patients get on drug treatment quickly A concentrated group of neurologists and cardiologists treat patients with nOH; ‘at risk’ patients already identified and managed by specialty institutions TBPH’s infrastructure capable of commercializing ampreloxetine in the US with limited and targeted additions to current resources Physicians report high urgency to treat snOH due to the high impact on patients’ QoL, high risk of injury from falls and caregiver burden Meaningful value proposition will drive patient access; Ampreloxetine has the potential to improve the durability of treatment effect and thereby reduce costly events associated with nOH Strong message from PD and MSA advocacy groups that patients need new therapies to better manage nOH Ampreloxetine: has the potential to transform Theravance Biopharma into an independent commercial biopharma MSA, multiple system atrophy; nOH , neurogenic orthostatic hypotension; PD, Parkinson’s disease; QoL, quality of life; snOH, symptomatic neurogenic orthostatic hy potension. 23 Established disease, targeted market Established nOH treatment paradigm Specialist networks in place Manageable opportunity A strong value proposition An urgency to treat Understanding of current access barriers Established patient advocacy

Nezulcitinib (TD - 0903) Program Nebulized lung - selective pan - JAK inhibitor to treat: ► Acute hyperinflammation of the lung in COVID - 19 ► Chronic inflammation for the treatment and prevention of lung transplant rejection

Nezulcitinib (TD - 0903): breaking new ground with inhaled JAKi 1. https://www.kff.org/coronavirus - covid - 19/fact - sheet/coronavirus - tracker/ as of 4.29.21 2. https://coronavirus.jhu.edu/map.html as of 4.25.21 3. https://covid.cdc.gov/covid - data - tracker/#vaccinations as of 5.3.21 4. https://www.cdc.gov/coronavirus/2019 - ncov/transmission/variant.html as of 4.2.21 25 COVID - 19 MARKET DYNAMICS >149M COVID - 19 patients globally 1 ; >32M patients in US 2 56% of US population ≥1 vaccine dose; 40% fully vaccinated 3 Virus still surging in communities / parts of the world 1 5 variants of concern in US 4 Declining but substantial proportion of population refusing vaccination 5 Disproportionate burden on people of color 6 BUILDING A PIPELINE IN A PRODUCT Potential areas for exploration: ALI in COVID - 19 in hospitalized patients Preventing progression of lung hyperinflammation that leads to hospitalization Accelerated recovery of long - haul COVID - 19 patients Future applications for coronavirus and influenza inflammation Prevention of lung transplant rejection 5. https://www.aamc.org/news - insights/herd - immunity - closer - we - think as of 4.25.21 6. https://www.kff.org/coronavirus - covid - 19/issue - brief/latest - data - on - covid - 19 - vaccinations - race - ethnicity/ as of 4.25.21 7. https://www.medrxiv.org/content/10.1101/2021.03.09.21252944v1 , n=25 Focused execution in acute lung injury (ALI) driven by patient need Only therapeutic in development with nebulized lung - targeted approach Treatments needed for hospitalized COVID - 19 patients with acute lung injury TD - 0903 Dose finding placebo controlled data 7 ‣ Generally well - tolerated ‣ Low systemic exposure ‣ Positive trend in clinical status, reduced hospital stay ‣ No deaths in 3, 10 mg cohorts ‣ Improved oxygenation from baseline to Day 7 ‣ Improved inflammatory biomarkers

Nezulcitinib: Randomized, double - blind, placebo - controlled Ph 2 study in hospitalized patients with COVID - 19 requiring oxygen support Objectives ‣ Primary: Number of respiratory - free days from randomization through Day 28 ‣ Secondary: Tolerability, PK ‣ Exploratory : Clinical status, duration of hospitalization, repeat - dose safety *Loading dose (double the standard dose) administered on Day 1. NCT04402866 IMV, invasive mechanical ventilation; PK, pharmacokinetics; SARS - CoV - 2, Severe acute respiratory syndrome coronavirus 2; SOC, st andard of care, includes remdesivir, dexamethasone, anticoagulation. 26 Part 2 Study 0188 Key inclusion criteria: Hospitalized patients aged 18 – 80 y requiring supplemental oxygen to maintain >90% saturation (not requiring IMV) with positive SARS - CoV - 2 test <72 h prior to randomization and symptom onset >2 – 10 d prior to hospitalization Countries: South Africa, Europe, UK, USA Randomization Q2’21 Top - line results Nezulcitinib 3 mg* + SOC (n=99) Placebo + SOC (n=99) Double - blind once - daily nebulized treatment: 7 days Total observation: 28 days

Asymptomatic or pre - symptomatic Mild illness Moderate illness Severe illness Critical illness COVID recovery Features Positive SARS - CoV - 2 test; no symptoms Mild symptoms (e.g., fever, cough, or change in taste or smell); no dyspnea Clinical or radiographic evidence of LRT disease; oxygen saturation ≥94% Oxygen saturation <94%; respiratory rate ≥30 breaths/min; lung infiltrates >50% Respiratory failure, shock, and multiorgan dysfunction or failure Testing Screening test; if patient has known exposure, diagnostic test Diagnostic test Diagnostic test Diagnostic test Diagnostic test Isolation Yes Yes Yes Yes Yes Proposed disease pathogenesis Potential treatment Potential for nezulcitinib to improve lung immune system balance across disease progression LRT, lower respiratory tract; SARS - CoV - 2, Severe acute respiratory syndrome coronavirus 2. 27 Viral replication Inflammation Antiviral therapy Antibody therapy Systemic anti - inflammatory Nezulcitinib ongoing program Aid lung recovery Prevent progression

Nezulcitinib showed a trend of improvement in 28 - day all - cause mortality rate and time to mortality (ITT) 1. Hazard ratio (nezulcitinib vs placebo) and 95% CI calculated from Cox proportional hazards model adjusting for baseline ag e s trata (≤60 vs >60 years). 2. Unstratified log - rank p - value comparing distribution of nezulcitinib vs placebo. CI, confidence interval; HR, hazard ratio; ITT, intent - to - treat. 28 Nezulcitinib Placebo Deaths, n (%) 6 (5.7) 13 (12.5) HR (95% CI) 1 0.42 (0.16, 1.12) p - value 2 0.08 Cumulative Proportion Died Placebo (n=104) Nezulcitinib (n=106) Time from Randomization (days) 0 7 14 21 28 0.1 0.0 0.2 0.3
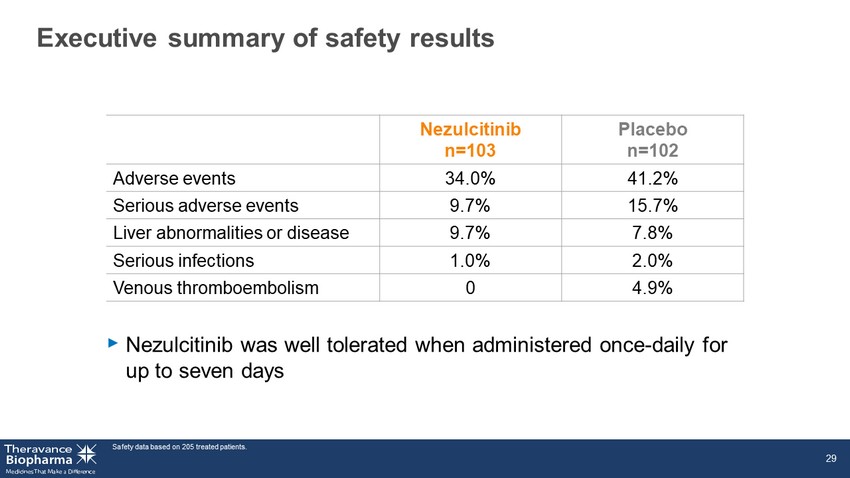
Executive summary of safety results Safety data based on 205 treated patients. 29 Nezulcitinib n=103 Placebo n=102 Adverse events 34.0% 41.2% Serious adverse events 9.7% 15.7% Liver abnormalities or disease 9.7% 7.8% Serious infections 1.0% 2.0% Venous thromboembolism 0 4.9% ‣ Nezulcitinib was well tolerated when administered once - daily for up to seven days

Nezulcitinib Phase 2 COVID - 19 trial summary ‣ Efficacy outcomes, n=210 (ITT) – Primary: No statistically significant difference between nezulcitinib and placebo for RFDs from randomization through Day 28 – Secondary: No difference in change from baseline at Day 7 in SaO 2 /FiO 2 ratio, proportion of patients in each category of the 8 - point Clinical Status scale, and proportion of patients alive and respiratory failure - free at Day 28 – A favorable trend in improvement for nezulcitinib when compared to placebo for 28 - day all - cause mortality and time to recovery ‣ Post - hoc analyses for baseline CRP, n=201 – CRP <150 mg/L (n=171): Nezulcitinib showed improvement in time to recovery and 28 - day all - cause mortality – CRP ≥150 mg/L (n=30): No differences between groups ‣ Nezulcitinib was well - tolerated when administered once - daily for up to seven days ‣ Plasma exposure was low, consistent with expectations for a lung - selective medicine CRP, C - Reactive protein; ITT, intent - to - treat; RFDs, Respiratory Failure - Free Days; SaO 2 /FiO 2 , percent oxygen saturation in arterial blood/fractional percentage of inspired oxygen. 30
TD - 8236 Potential first inhaled JAKi for asthma

High medical and economic burden in uncontrolled asthma *Asthma that requires high - dosage ICS + LABAs to prevent the disease from being uncontrolled) or asthma that remains uncontrolle d despite treatment. 1. World Health Organization; 2. https://www.aafa.org/asthma - facts/; 3. Sadatsafavi, M., et al. Can Respir J 2010;17:74 - 80. 4. N urmagambetov T, et al. Ann Am Thorac Soc 2018;15:348 - 56; 5. TBPH estimate based on multiple data sources. ICS, inhaled corticosteroids; IFN, interferon; IL, interleukin; JAK, Janus kinase; LABA, long - acting β2 agonists; LTRA, leukotriene receptor antagonist; OCS, oral corticosteroid; STAT, signal transducer and activator of transcription; T2, type 2; TSLP, thymic stromal lymphopoietin. 32 16 14 Severe* Moderate US asthma market (October 2020) 5 61 25 US cases 8% of adults 8% of children 2 Healthcare utilization 3 25M ~$15B P ATIENT P OPULATION C URRENT T REATMENT L ANDSCAPE S TRATEGIC O PPORTUNITY TD - 8236 Potential to transform the treatment of respiratory inflammation by treating moderate - to - severe asthma regardless of T2 phenotype, including patients who remain symptomatic despite compliance on high - dose ICS ICS + LABA (often fail to control disease) Approved biologics (affect subsets of patients) US medical costs 4 ~$58B T2 - high T2 - low IL - 4 IL - 23 /IL - 12 IL - 13 IL - 6 IL - 5 IL - 27 TSLP IFN - γ Bold: biologics in development or approved. JAK/STAT cytokines implicated in moderate - to - severe asthma • XOLAIR (omalizumab) • NUCALA (mepolizumab) • CINQAIR (reslizumab) • FASENRA (benralizumab) • DUPIXENT (dupilumab) Step - up for severe asthma: LTRAs, tiotropium, OCS, biologics cases worldwide 1 339M

TD - 8236: Phase 1 clinical trial design CXCL, chemokine (C - X - C motif) ligand; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; IFN, interferon; IgE, immunoglobulin E; IL, interleukin; ILC2, type 2 innate lymphoid cells; MAD, multiple - ascending dose; MoA, Mechanism of Action; PK, pharmacokinetic; PD, pharmacodynamic; pSTAT, phosphorylated signal transducer a nd activator of transcription; SAD, single - ascending dose; T2, type 2; Th2, T helper type 2; TSLP, thymic stromal lymphopoietin. 33 Parts A & B completed September 2019; Part C enrollment completed — data reported in Q4 2020 Part B: MAD (Mild asthmatics) Part A: SAD (Healthy volunteers) Safety, PK Safety, PK, PD (FeNO) All cohorts: N=6 active/2 Placebo 4500 µg 500 µg 1500 µg 150 µg 50 µg 4000 µg 1 2 3 4 5 6 7 D 150 µg 500 µg 1500 µg 1 2 3 4 5 6 7 D 1 2 3 4 5 6 7 D 1 2 3 4 5 6 7 D Part C: MoA Biomarkers (Moderate - to - severe asthmatics + ICS) N=16 active/8 placebo 1 2 3 4 5 6 7 D 1500 µg ‣ Goal: build confidence in compound, MoA and dose in early - development ‣ Endpoints: FeNO; pSTAT1 and pSTAT6 in bronchoalveolar lavage fluid; cytokines; epithelial gene expression T2 - dominant, n=8 Non - T2 - dominant, n=8 x x

TD - 8236: Positive Phase 1 trial in healthy subjects and patients with mild and moderate - to - severe asthma ‣ Biomarkers of JAK target engagement (pSTAT1 and pSTAT6) significantly reduced in lungs of T2 high and T2 low moderate/severe asthmatics on top of ICS ‣ Ongoing analysis of effect of TD - 8236 on additional biomarkers including cytokines and gene expression FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; JAK, Janus kinase; PD, pharmacodynamic; PK, pharmacokine tic ; pSTAT , phosphorylated signal transducer and activator of transcription; T2, type 2. 34 Phase 1 Profile Healthy Volunteer Single Dose (Part A) Mild Asthma Multiple Dose (Part B) Moderate - to - Severe Asthma [+ ICS] Multiple Dose (Part C) Generally well tolerated x x x Minimal systemic exposure x x x PK and PD profile consistent with once - daily dosing x x x Biologic activity in lungs of patients with asthma x ↓ FeNO x ↓ FeNO, pSTAT1, pSTAT6

-50 -40 -30 -20 -10 0 10 20 30 40 -0.4 -0.2 0.0 0.2 0.4 Favors Placebo Favors TD - 8236 Favors TD - 8236 Favors Placebo No impact of TD - 8236 on the Late Asthmatic Response (LAR) ‣ TD - 8236 was generally well tolerated as a single - daily dose administered for 14 consecutive days 35 Primary Endpoint: Weighted Mean Area Under the Curve, 3 – 8 h. CI, confidence interval; FeNO, fractional exhaled nitric oxide; LS, least - squares. % Change in FeNO Late Asthmatic Response Difference from Placebo, Liters (LS Means ± 95% CI) Difference from Placebo, % (LS Means ± 95% CI) 1500 µg 150 µg Day 14 Day 14 Day 7 - 0.01 n=22 - 0.04 n=20 4.28 n=22 - 20.16 n=24 - 3.72 n=22 - 26.87 n=23 Significant reductions in inflammation marker (FeNO) and favorable safety and tolerability
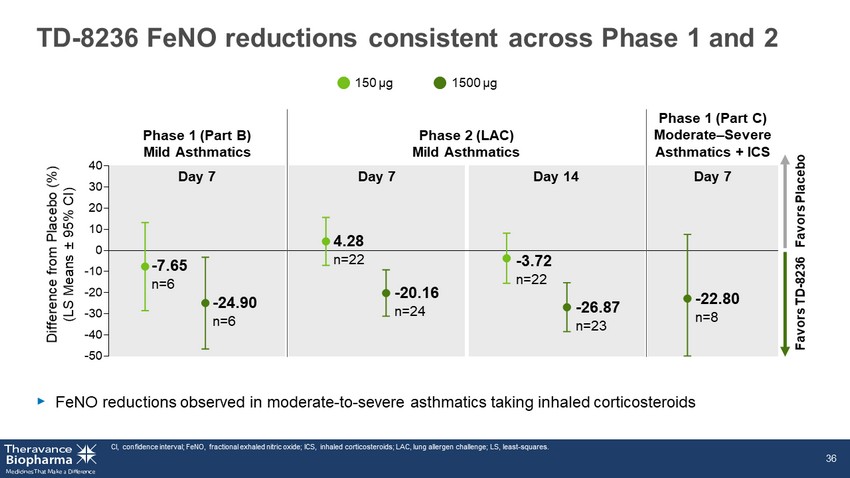
-50 -40 -30 -20 -10 0 10 20 30 40 TD - 8236 FeNO reductions consistent across Phase 1 and 2 ‣ FeNO reductions observed in moderate - to - severe asthmatics taking inhaled corticosteroids CI, confidence interval; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; LAC, lung allergen challenge; LS, least - squares. 36 Phase 1 (Part B) Mild Asthmatics Phase 2 (LAC) Mild Asthmatics Phase 1 (Part C) Moderate – Severe Asthmatics + ICS Difference from Placebo (%) (LS Means ± 95% CI) 1500 µg 150 µg Day 7 Day 7 Day 14 Day 7 - 7.65 n=6 - 24.90 n=6 4.28 n=22 - 20.16 n=24 - 3.72 n=22 - 26.87 n=23 - 22.80 n=8 Favors Placebo Favors TD - 8236

TD - 5202 Organ - gut selective irreversible JAK3 inhibitor to treat inflammatory intestinal diseases

Celiac disease has no current treatments and serious health consequences 38 1. http://www.drschaer - institute.com/us/celiac - disease/epidemiology - 1033.html ; 2. 1% prevalence in US, BeyondCeliac.org; 3. 2018 US population 327M Census.gov. 4. Reunala T, et al. Nutrients 2018;10;pii: E602; 5. Guandalini et al. Digestive Diseases Sciences 2016;61:2823 - 30; 6. Theravan ce Market Research. JAK, Janus kinase. S TRATEGIC O PPORTUNITY P ATIENT P OPULATION US patients 2,3 3.3M No approved treatment Only available intervention is strict life - long gluten - free diet 30% of diagnosed patients are poorly controlled despite best dietary efforts 6 TD - 5202 Organ - gut selective irreversible JAK3 inhibitor: potential to deliver significant value for both patients and payers increase in US over past 50 y 4 4 – 4.5x Global prevalence 1 1% higher healthcare costs than controls 5 >2x C URRENT T REATMENT L ANDSCAPE Celiac Normal

JAK3 - dependent cytokines play central role in pathogenesis of celiac disease ‣ Proof - of - relevance from recent positive Phase 2 data with systemic JAK3 inhibitor in alopecia areata, another T - cell mediated disease ‣ Localized JAK3 inhibition has the potential to avoid systemic immunosuppression (genetic JAK3 deficiency leads to severe immunodeficiency) Figure adapted from Jabri B and Sollid L. J Immunol 2017;198:3005 - 14. CD, Crohn’s disease; IE - CTL, intraepithelial cytotoxic lymphocyte; IEL, intraepithelial lymphocyte; IFN, interferon; IL, interle ukin; JAK, Janus kinase; STAT, signal transducer and activator of transcription; Th1, T helper 1 cells. 39 IL - 2, IL - 4, IL - 7, IL - 9, IL - 15, IL - 21 I MMUNE C ELL CD Pathogenesis α N UCLEUS STAT P STAT P STAT P STAT P STAT JAK1 β γ JAK3 P P P Gluten peptides G LUTEN - S PECIFIC T H 1 CELLS I NTESTINAL E PITHELIUM L AMINA P ROPIA I NTESTINAL L UMEN IFNγ IL - 2 IL - 21 IEL IE - CTL IL - 15

TD - 5202 First - in - human overall results summary ‣ No serious or severe AEs were reported ‣ All treatment - emergent AEs in TD - 5202 - treated subjects were mild in severity AE, adverse event; BID, twice daily; C max,ss , maximal steady - state concentration; ECG, electrocardiogram; IC 50 , inhibitory concentration at which 50% of JAK signaling is blocked; JAK, Janus kinase; IC 50 , NK, natural killer. 40 TD - 5202: generally well - tolerated (single dose ≤2000 mg, multiple doses ≤1000 mg BID) for 10 consecutive days in healthy subjects ‣ Systemic exposures were dose proportional from 100 to 1000 mg BID ‣ Low steady - state systemic exposures: mean C max,ss ~11 - fold below the protein - adjusted JAK IC 50 at the highest tested dose (1000 mg BID), consistent with a gut - selective approach ‣ No clinically significant changes from baseline in vital signs and ECG assessments ‣ No clinically significant changes in chemistry or hematology parameters – No changes in NK cell count

Inhaled ALK5i Potential best - in - disease therapy for the treatment of idiopathic pulmonary fibrosis (IPF)
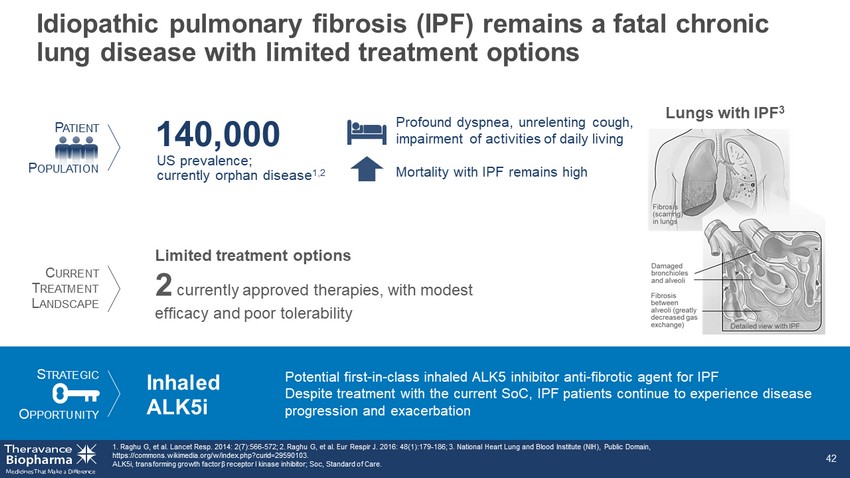
Limited treatment options 2 currently approved therapies, with modest efficacy and poor tolerability S TRATEGIC O PPORTUNITY P ATIENT P OPULATION Inhaled ALK5i Potential first - in - class inhaled ALK5 inhibitor anti - fibrotic agent for IPF Despite treatment with the current SoC, IPF patients continue to experience disease progression and exacerbation C URRENT T REATMENT L ANDSCAPE Idiopathic pulmonary fibrosis (IPF) remains a fatal chronic lung disease with limited treatment options 1. Raghu G, et al. Lancet Resp. 2014: 2(7):566 - 572; 2. Raghu G, et al. Eur Respir J. 2016: 48(1):179 - 186; 3. National Heart Lung and Blood Institute (NIH), Public Domain, https://commons.wikimedia.org/w/index.php?curid=29590103. ALK5i, transforming growth factor β receptor I kinase inhibitor; Soc, Standard of Care. 42 US prevalence; currently orphan disease 1,2 140,000 Lungs with IPF 3 Profound dyspnea, unrelenting cough, impairment of activities of daily living Mortality with IPF remains high

Significant opportunity remains for effective IPF treatments ‣ Mortality with IPF remains high – <50% alive 3 years after diagnosis 1 1. King TE, et al. Am J Respir Crit Care Med 2001;164:1171 - 81. IPF, idiopathic pulmonary fibrosis. 43 1.0 0.8 0.6 0.4 0.2 0.0 0 5 10 15 Years Probability of Survival Male Female To arrest disease progression with improved tolerability Goal

TGFβ, transforming growth factor β. 44 S CARRING TISSUES Collagen deposition Stimuli Genetic susceptibility Repetitive injury AEC damage TGF β A LVEOLAR E PITHELIAL C ELLS (AEC) T YPE 2 T YPE 1 Normal M YOFIBROBLASTS Fibrogenesis, proliferation Targeting the TGFβ pathway A core signaling pathway that drives fibrosis
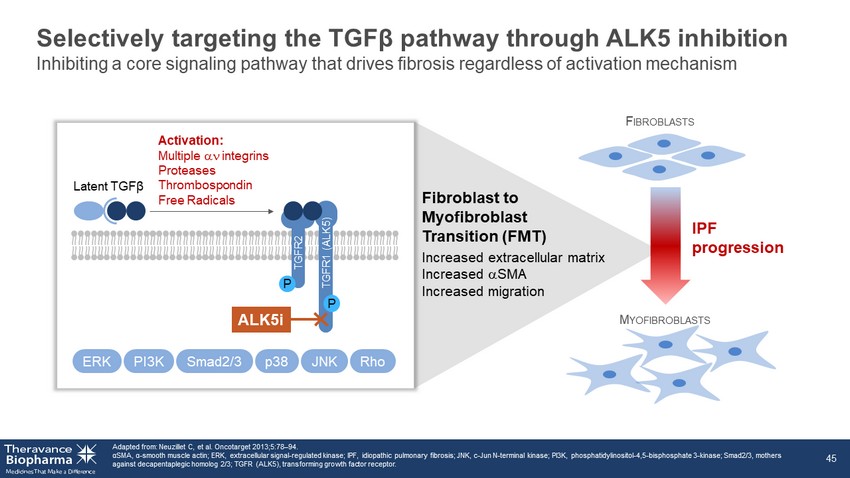
Selectively targeting the TGFβ pathway through ALK5 inhibition Adapted from: Neuzillet C, et al. Oncotarget 2013;5:78 – 94. α SMA, α - smooth muscle actin; ERK, extracellular signal - regulated kinase; IPF, idiopathic pulmonary fibrosis; JNK, c - Jun N - terminal kina se; PI3K, phosphatidylinositol - 4,5 - bisphosphate 3 - kinase; Smad2/3, mothers against decapentaplegic homolog 2/3; TGFR (ALK5), transforming growth factor receptor. 45 F IBROBLASTS M YOFIBROBLASTS Fibroblast to Myofibroblast Transition (FMT) Increased extracellular matrix Increased a SMA Increased migration ERK Smad2/3 PI3K p38 JNK Rho IPF progression P P ALK5i Activation: Multiple an integrins Proteases Thrombospondin Free Radicals TGFR2 Latent TGFβ TGFR1 (ALK5) Inhibiting a core signaling pathway that drives fibrosis regardless of activation mechanism

ALK5 inhibition directly interrupts FMT in IPF ALK5i, transforming growth factor β receptor I kinase inhibitor; α SMA, α - smooth muscle actin; FMT, fibroblast to myofibroblast transition. 46 Reference Standard ALK5i Log [M] % inhibition of α SMA - 9 - 8 - 7 - 6 - 5 0 50 100 150 FMT a SMA expressed a SMA reduced Negative control ALK5i treated
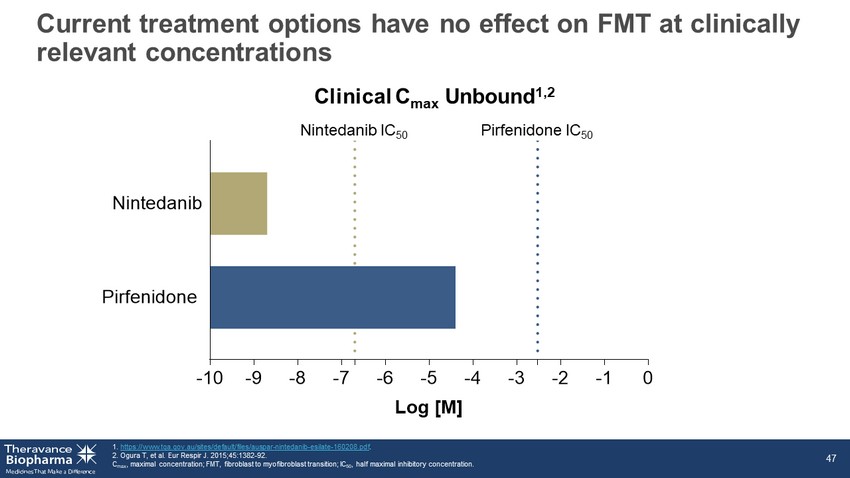
Current treatment options have no effect on FMT at clinically relevant concentrations 1. https://www.tga.gov.au/sites/default/files/auspar - nintedanib - esilate - 160208.pdf . 2. Ogura T, et al. Eur Respir J. 2015;45:1382 - 92. C max , maximal concentration; FMT, fibroblast to myofibroblast transition; IC 50 , half maximal inhibitory concentration. 47 -10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0 Pirfenidone Nintedanib Log [M] Nintedanib IC 50 Pirfenidone IC 50 Clinical C max Unbound 1,2

Wound repair Bone healing Cardiovascular homeostasis Tumor suppression Endocrine function Lung selectivity avoids unwanted systemic side effects Modified from: Akhurst RJ, Hata A. Nat Rev Drug Discov 2012;11:790 - 811. ALK5i, TGFβ receptor I kinase inhibitor; TGFβ, transforming growth factor β. 48 Maintaining key systemic regulatory roles of TGFβ Inhaled ALK5i Minimizing systemic inhibition of a cytokine essential for homeostasis
Ocular JAKi Potential best - in - disease, pan - JAK inhibitor with long - acting ocular anti - inflammatory activity
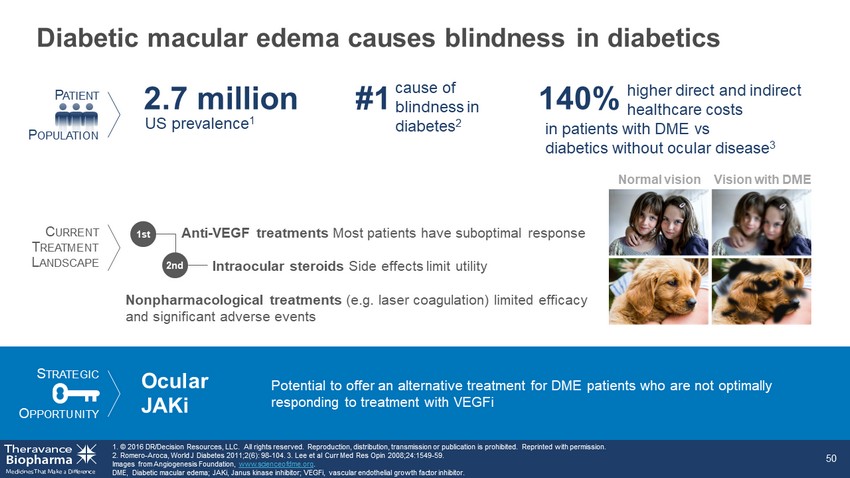
Diabetic macular edema causes blindness in diabetics 1. © 2016 DR/Decision Resources, LLC. All rights reserved. Reproduction, distribution, transmission or publication is prohibit ed. Reprinted with permission. 2. Romero - Aroca, World J Diabetes 2011;2(6): 98 - 104. 3. Lee et al Curr Med Res Opin 2008;24:1549 - 59. Images from Angiogenesis Foundation, www.scienceofdme.org . DME, Diabetic macular edema; JAKi, Janus kinase inhibitor; VEGFi, vascular endothelial growth factor inhibitor. 50 Vision with DME Normal vision US prevalence 1 2.7 million #1 Anti - VEGF treatments Most patients have suboptimal response S TRATEGIC O PPORTUNITY P ATIENT P OPULATION Ocular JAKi C URRENT T REATMENT L ANDSCAPE Potential to offer an alternative treatment for DME patients who are not optimally responding to treatment with VEGFi 140% higher direct and indirect healthcare costs in patients with DME vs diabetics without ocular disease 3 cause of blindness in diabetes 2 1st Intraocular steroids Side effects limit utility 2nd Nonpharmacological treatments (e.g. laser coagulation) limited efficacy and significant adverse events

Inflammation, not just VEGF, is a key driver of DME 51 1. Gonzalez VH, et al. Am J Ophthalmol 2016;172:72 - 79. DME, diabetic macular edema; VEGF, vascular endothelial growth factor. Current Pharmacological Treatments Intraocular steroids Hyperglycemia Disruption of blood - retinal barrier Vascular leakage DME VEGF Retinal capillary damage Inflammatory cytokines Need for broad, sustained release, anti - inflammatory with a safer side - effect profile ‣ High frequency of formation of cataracts and glaucoma ‣ One third do not respond to anti - VEGF while another third have a suboptimal response 1 ‣ Require frequent intravitreal injections Intraocular anti - VEGF agents
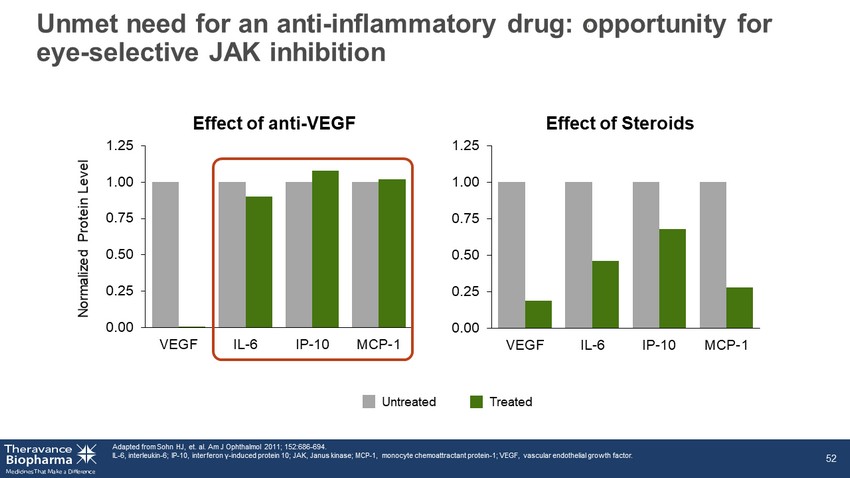
0.00 0.25 0.50 0.75 1.00 1.25 VEGF IL-6 IP-10 MCP-1 Unmet need for an anti - inflammatory drug: opportunity for eye - selective JAK inhibition Adapted from Sohn HJ, et. al. Am J Ophthalmol 2011; 152:686 - 694. IL - 6, interleukin - 6; IP - 10, interferon γ - induced protein 10; JAK, Janus kinase; MCP - 1, monocyte chemoattractant protein - 1; VEGF, vascular endothelial growth factor. 52 Effect of anti - VEGF Effect of Steroids 0.00 0.25 0.50 0.75 1.00 1.25 VEGF IL-6 IP-10 MCP-1 Untreated Treated Normalized Protein Level

Ocular pan - JAK inhibition has the potential to address key disease pathways in DME 53 DME, diabetic macular edema; IL - 6, interleukin - 6; IP - 10, interferon γ - induced protein 10; JAK, Janus kinase; MCP - 1, monocyte chemoattractant protein - 1; pSTAT, phosphorylated signal transducer and a ctivator of transcription; Tyk, tyrosine kinase; VEGF, vascular endothelial growth factor. TD - EyeJAKi inhibits key DME inflammatory pathways: JAK2 JAK1 IL - 6 Tyk2 JAK1 Interferons MCP - 1 IP - 10 TD - Eye JAKi ‣ IL - 6 and interferon signaling pathways in human primary cells ‣ IL - 6 induced pSTAT3 and interferon - induced IP - 10 in the back of the eye in vivo

0 1 2 3 0.000001 0.00001 0.0001 0.001 0.01 0.1 1 10 100 1000 Time (months) C o m p o u n d c o n c e n t r a t i o n ( g / m L o r g / g ) A pan - JAK inhibitor designed for eye selectivity with projected dosing interval of at least three months 54 JAK, Janus kinase. Single intravitreal injection of TD - Eye JAKi in Rabbits Vitreous humor (depot) Retina Plasma α STAT P STAT P STAT JAK β γ JAK N UCLEUS P STAT P STAT JAKi