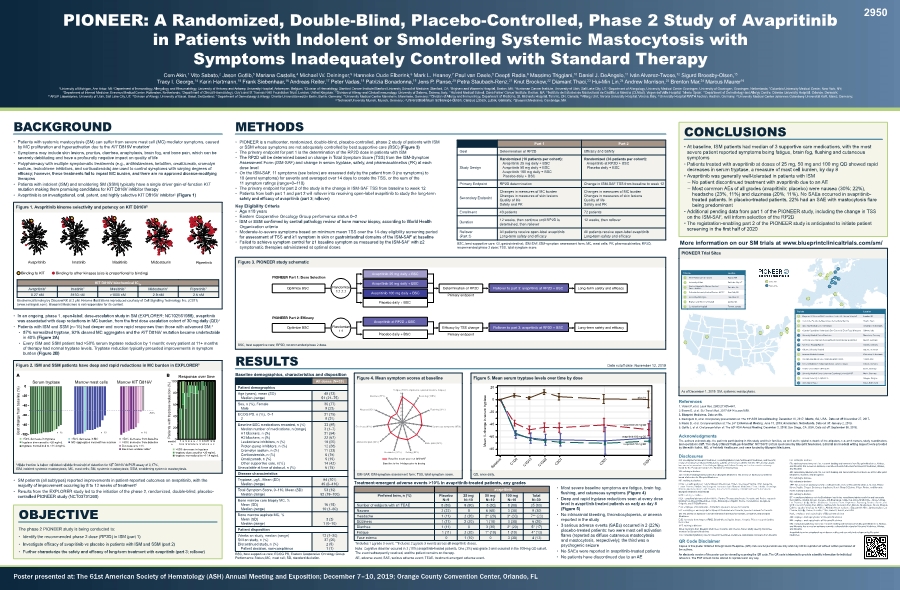
| 9 13 15 19 17 18 20 21 14 22 8 10 16 11 12 3 2 5 7 4 6 1 Active Site Planned Site QD, once daily. As of December 1, 2019. SM, systemic mastocytosis. ISM-SAF, ISM-symptom assessment form; TSS, total symptom score. • PIONEER is a multicenter, randomized, double-blind, placebo-controlled, phase 2 study of patients with ISM or SSM whose symptoms are not adequately controlled by best supportive care (BSC) • The primary endpoint for part 1 is the determination of the RP2D dose in patients with ISM • The RP2D will be determined based on change in Total Symptom Score (TSS) from the ISM-Symptom Assessment Form (ISM-SAF) and change in serum tryptase, safety, and pharmacokinetics (PK) at each dose level • On the ISM-SAF, 11 symptoms (see below) are assessed daily by the patient from 0 (no symptoms) to 10 (worst symptoms) for severity and averaged over 14 days to create the TSS, or the sum of the 11 symptom ratings (range=0–110) • The primary endpoint for part 2 of the study is the change in ISM-SAF TSS from baseline to week 12 • Patients from both part 1 and part 2 will rollover into receiving open-label avapritinib to study the long-term • • Eastern Cooperative Oncology Group performance status 0–2 • Organization criteria • Moderate-to-severe symptoms based on minimum mean TSS over the 14-day eligibility screening period • symptomatic therapies administered at optimal doses Age (years), mean (SD) Median (range) 51 (21–75) Sex, n (%), Female Male ECOG PS, n (%), 0–1 2 Baseline BSC medications recorded, n (%) Median number of medications, n (range) Leukotriene inhibitors, n (%) Proton pump inhibitors, n (%) Cromolyn sodium, n (%) Corticosteroids, n (%) Omalizumab, n (%) Other supportive care, n(%) Unavailable at time of datacut, n (%) 22 (67) 5 (15) 14 (42) 6 (15) Tryptase, µg/L, Mean (SD) Median (range) 45 (6–416) Total Symptom Score, 0–110, Mean (SD) Median (range) 52 (19–100) Bone marrow core biopsy MC, % Mean (SD) Median (range) 16 (15) 10 (1–60) Bone marrow aspirate MC, % Mean (SD) Median (range) 1 (0–10) Still on study, n (%) Discontinued study, n (%) Patient decision, non-compliance 2 (5) 1 (1) Cem Akin,1 Vito Sabato,2 Jason Gotlib, Mariana Castells,4 5 6 7 Paul van Daele, Deepti Radia,9 Massimo Triggiani,10 Daniel J. DeAngelo,11 Iván Alvarez-Twose,12 Sigurd Broesby-Olsen, Tracy I. George,14 15 Frank Siebenhaar,16 Andreas Reiter,17 Peter Vadas, Patrizia Bonadonna,19 Jens P. Panse,20 Petra Staubach-Renz,21 Knut Brockow,22 Diamant Thaci, 24 Andrew Morrison,24 Brenton Mar,24 Marcus Maurer16 1University of Michigan, Ann Arbor, MI; 2 4 5 6Department of Allergology, University Medical Center Groningen, University of Groningen, Groningen, Netherlands; 7Columbia University Medical Center, New York, NY; Department of Internal Medicine, Erasmus Medical Center, Rotterdam, Netherlands; 9 10Division of Allergy and Clinical Immunology, University of Salerno, Salerno, Italy; 11 12 14ARUP Laboratories, University of Utah, Salt Lake City, UT; 15Division of Allergy, University of Basel, Basel, Switzerland; 16Department of Dermatology & Allergy, Charité-Universätsmedizin Berlin, Berlin, Germany; 17University Medical Centre Mannheim, Mannheim, Germany; 19 20 21University Medical Center Johannes Gutenberg-Universität KöR, Mainz, Germany; 22Technical University Munich, Munich, Germany; 24Blueprint Medicines, Cambridge, MA • Patients with systemic mastocytosis (SM) can suffer from severe mast cell (MC) mediator symptoms, caused by MC proliferation and hyperactivation due to the 1 • Symptoms may include skin lesions, pruritus, diarrhea, anaphylaxis, brain fog, and bone pain, which can be severely debilitating and have a profoundly negative impact on quality of life • Polypharmacy with multiple symptomatic treatments (e.g., antihistamines, ketotifen, omalizumab, cromolyn sodium, leukotriene inhibitors, and corticosteroids) are used to control symptoms with varying degrees of therapies • Patients with indolent (ISM) and smoldering SM (SSM) typically have a single driver gain-of-function • 2 • 4 • Patients with ISM and SSM (n=15) had deeper and more rapid responses than those with advanced SM:5 • in 40% • Every ISM and SSM patient had >50% serum tryptase reduction by 1 month; every patient at 11+ months of therapy had normal tryptase levels. Tryptase reduction typically preceded improvements in symptom burden ISM, indolent systemic mastocytosis; MC, mast cells; SM, systemic mastocytosis; SSM, smoldering systemic mastocytosis. • SM patients (all subtypes) reported improvements in patient-reported outcomes on avapritinib, with the 6 • Results from the EXPLORER study led to the initiation of the phase 2, randomized, double-blind, placebo- BSC, best supportive care; RP2D, recommended phase 2 dose. Goal Determination of RP2D Study Design Avapritinib 25 mg daily + BSC Avapritinib 50 mg daily + BSC Avapritinib 100 mg daily + BSC Placebo daily + BSC Avapritinib at RP2D + BSC Placebo daily + BSC Primary Endpoint RP2D determination Change in ISM-SAF TSS from baseline to week 12 Secondary Endpoint Changes in measures of MC burden Changes in measures of skin lesions Quality of life Safety and PK Changes in measures of MC burden Changes in measures of skin lesions Quality of life Safety and PK Enrollment 40 patients 72 patients Duration 12 weeks, then continue until RP2D is determined, then rollover 12 weeks, then rollover Rollover All patients receive open-label avapritinib All patients receive open-label avapritinib BSC, best supportive care; GI, gastrointestinal; ISM-SAF, ISM-symptom assessment form; MC, mast cells; PK, pharmacokinetics; RP2D, recommended phase 2 dose; TSS, total symptom score. Avapritinib2 Imatinib2 Masitinib Midostaurin2 Ripretinib 0.27 nM >1000 nM 2.9 nM 2.6 nM (www.cellsignal.com). Blueprint Medicines is not responsible for its content. • symptoms • Patients treated with avapritinib at doses of 25 mg, 50 mg and 100 mg QD showed rapid • Avapritinib was generally well-tolerated in patients with ISM – No patient discontinued treatment with avapritinib due to an AE – being predominant • Additional pending data from part 1 of the PIONEER study, including the change in TSS on the ISM-SAF, will inform selection of the RP2D • The registration-enabling part 2 of the PIONEER study is anticipated to initiate patient The phase 2 PIONEER study is being conducted to: • Identify the recommended phase 2 dose (RP2D) in ISM (part 1) • • -100 -80 -60 -40 -20 0 >50% decrease in tryptase tryptase decreased to <20 ng/mL tryptase normalized to <11.4 ng/mL Serum tryptase <50% decrease from baseline Decreases to <1% >50% decrease from baseline Becomes undetectable* Response over time 0 20 40 60 80 100 months 1 3 5 7 9 1113 2 4 6 8 1012 n 1515 15 15 15 14 14 1313 13 9 8 8 Patients with tryptase reduction (%) >50% decrease in tryptase tryptase decreased to <20 ng/mL tryptase normalized to <11.4 ng/mL -100 -80 -60 -40 -20 0 n=15 n=13 -50% n=10 Marrow mast cells Marrow KIT D816V >50% decrease in MC MC aggregates cleared from marrow 1. Valent P, et al. 2. Evans E, et al. 2017;9(414):eaao1690. 4. DeAngelo D, et al. Oral plenary presentation at: The 59th 5. Radia D, et al. Oral presentation at: The 24th 6. Gotlib J, et al. Oral presentation at: The 60th The authors acknowledge the patients participating in this study and their families, as well as the global network of investigators, research nurses, study coordinators, CA: investigator for Blueprint Medicines; consulting/advisory role for Blueprint Medicines, and Novartis; board for the European Competence Network on Mastocytosis VS: nothing to disclose JG: research funding and honoraria from Blueprint Medicines; has served on advisory committees/ board of directors for Blueprint Medicines MC: nothing to disclose Blueprint Medicines and Takeda funding from Blueprint Medicines, Incyte, Bristol-Myers Squibb, Roche, Constellation, Deciphera, Celgene, and CTI BioPharma MT: has served on advisory committees/board of directors for Novartis, Deciphera, and Blueprint Medicines IA-T: nothing to disclose SB-O: honoraria from Blueprint Medicines, Novartis, and Thermo Fisher; study steering committee member for Blueprint Medicines TIG: consultancy/advisory role for Blueprint Medicines, Deciphera, and Allakos; honoraria from Novartis FS: advisory/consultancy role for, research funding and honoraria from Blueprint Medicines, Allakos, and Novartis; has served on advisory committees/board of directors for Blueprint Medicines, Allakos, and Novartis AR: consultancy/advisory role for, research funding and honoraria/travel reimbursement from Blueprint Medicines, Novartis, and Deciphera PV: nothing to disclose PB: nothing to disclose JPP: has served on advisory committees/board of directors for Blueprint Medicines, Alexion, Bristol- PS-R: nothing to disclose KB: nothing to disclose DT: consultancy/advisory role for Boehringer Ingelheim; consultancy/advisory role for and honoraria from AbbVie, Almiral, Amgen, Celgene, DS-Biopharma, Galderma, Glaxo-Smith Kline, Janssen-Cilag, UCB; research funding from AbbVie and Novartis; honoraria from Maruho, Medimmune, Merck Sharp & AM: employee and equity holder of Blueprint Medicines BM: employee and equity holder of Blueprint Medicines MM: consultancy/advisory roles for, research funding and honoraria from Blueprint Medicines, Allakos, and Novartis; has served on advisory committees/board of directors for Blueprint Medicines, Allakos, and Novartis Avapritinib is an investigational agent discovered by and currently in development by Blueprint Medicines. Copies of this poster obtained through Quick Response (QR) code are for personal use only and may not be reproduced without written permission of the authors. reference. The PDF should not be altered or reproduced in any way. 1 Dana-Farber Cancer Institute Boston, MA 2 University of Utah Salt Lake City, UT Cancer Institute Palo Alto, CA 4 New York, NY 5 University of Michigan Ann Arbor, M 6 Boston, MA 7 Toronto, Canada London, UK 9 Instituto de Estudios de Mastocitosis de Castilla la Mancha Toledo, Spain 10 University Medical Center Groningen Groningen, Netherlands 11 Salerno, Italy 12 University Medical Centre Mannheim Mannheim, Germany Technical University Munich, Department of Dermatology Biederstein Munich, Germany 14 Aachen, Germany 15 Odense, Denmark 16 Erasmus Medisch Centrum Rotterdam, Netherlands 17 Azienda Ospedaliera Universitaria Integrata Verona Verona, Italy 19 Charité-Universitätsmedizin Berlin Berlin, Germany 20 University Medical Center Johannes Gutenberg-Universität KöR Mainz, Germany 21 Edegem, Belgium 22 University of Basel Basel, Switzerland -80 -60 -40 -20 0 20 Mean % change in serum tryptase avapritinib 25 mg QD placebo avapritinib 100 mg QD avapritinib 50 mg QD • Most severe baseline symptoms are fatigue, brain fog, • Deep and rapid tryptase reductions seen at every dose • No intracranial bleeding, thrombocytopenia, or anemia reported in the study • placebo-treated patients: two were mast cell activation and mastocytosis, respectively); the third was a psychogenic seizure • No SAEs were reported in avapritinib-treated patients • No patients have discontinued due to an AE Data cutoff date: November 12, 2019 Baseline mean score on ISM-SAF 1 2 3 4 5 6 7 8 Fatigue (100% of patients reported baseline fatigue) Brain fog (100%) Flushing (92%) Cutaneous symptoms (97%) Bone pain (92%) Itching (92%) Headache (97%) Abdominal pain (95%) Dizziness (92%) Nausea (95%) Diarrhea (87%) Baseline is the 14-days prior to dosing 9 (90) Nausea 2 (22) 0 6 (60) 1 (11) 2 (20) 2* (20) Dizziness 1 (11) 2 (20) 1 (10) 6 (20) Diarrhea 1 (11) 0 2* (20) 5* (17) Fatigue 1 (11) 2 (20) 1* (10) 1 (10) Face edema 0 1 (10) 0 The event subsequently resolved, and the patient remains on therapy. AE, adverse event; SAE, serious adverse event; TEAE, treatment-emergent adverse event. BSC, best supportive care; ECOG PS, Eastern Cooperative Oncology Group Performance Status; MC, mast cell; SD, standard deviation. |