UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
| | | | | |
| (Mark One) | |
| ☒ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
| For the fiscal year ended December 31, 2019 | |
| or |
| ☐ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
| For the transition period from to | |
Commission File Number: 001-38468
Inspire Medical Systems, Inc.
(Exact name of registrant as specified in its charter)
| | | | | |
| Delaware | 26-1377674 |
| (State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) |
5500 Wayzata Blvd., Suite 1600 Golden Valley, MN | 55416 |
| (Address of principal executive offices) | (Zip Code) |
Registrant's telephone number, including area code: (844) 672-4357
____________________________________________________________________________
| | | | | | | | |
| Securities registered pursuant to Section 12(b) of the Act: | | |
| Common stock, $0.001 par value | Trading Symbol(s) | New York Stock Exchange |
| (Title of each class) | INSP | (Name of exchange on which registered) |
| | |
| Securities registered pursuant to Section 12(g) of the Act: | | |
| None | | |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☒ No ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of "large accelerated filer," "accelerated filer," "smaller reporting company," and "emerging growth company" in Rule 12b-2 of the Exchange Act.
| | | | | | | | | | | | | | | | | | | | | | | | | | |
Large accelerated filer ☒ | | Accelerated filer ☐ | | Non-accelerated filer ☐ | | Smaller reporting company ☐ | | Emerging growth company ☐ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐ No ☒
As of June 28, 2019, the last business day of the registrant's most recently completed second fiscal quarter, the aggregate market value of the registrant's common stock held by non-affiliates was approximately $1,071,122,062, based on the closing price of the registrant's common stock as reported on the New York Stock Exchange on such date.
As of February 18, 2020, the registrant had 24,129,656 shares of common stock, $0.001 par value per share, outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive proxy statement for its 2020 annual stockholders’ meeting, which is to be filed within 120 days of the registrant’s fiscal year ended December 31, 2019, are incorporated by reference into Part III of this Annual Report on Form 10-K.
TABLE OF CONTENTS
FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. We intend such forward-looking statements to be covered by the safe harbor provisions for forward-looking statements contained in Section 27A of the Securities Act of 1933, as amended (the "Securities Act") and Section 21E of the Securities Exchange Act of 1934, as amended (the "Exchange Act"). All statements other than statements of historical facts contained in this Annual Report on Form 10-K are forward-looking statements.
In some cases, you can identify forward-looking statements by terms such as ‘‘may,’’ ‘‘will,’’ ‘‘should,’’ ‘‘expect,’’ ‘‘plan,’’ ‘‘anticipate,’’ ‘‘could,’’ ‘‘intend,’’ ‘‘target,’’ ‘‘project,’’ ‘‘contemplate,’’ ‘‘believe,’’ ‘‘estimate,’’ ‘‘predict,’’ ‘‘potential’’ or ‘‘continue’’ or the negative of these terms or other similar expressions, although not all forward-looking statements contain these words. The forward-looking statements in this Annual Report on Form 10-K are only predictions and are based largely on our current expectations and projections about future events and financial trends that we believe may affect our business, financial condition, and results of operations. These forward-looking statements speak only as of the date of this Annual Report on Form 10-K and are subject to a number of known and unknown risks, uncertainties and assumptions, including, but not limited to:
•our history of operating losses and dependency on our Inspire system for revenues;
•commercial success and market acceptance of our Inspire therapy;
•our ability to achieve and maintain adequate levels of coverage or reimbursement for our Inspire system or any future products we may seek to commercialize;
•competitive companies and technologies in our industry;
•our ability to expand our indications and develop and commercialize additional products and enhancements to our Inspire system;
•future results of operations, financial position, research and development costs, capital requirements, and our needs for additional financing;
•our dependence on third-party suppliers and contract manufacturers;
•risks related to consolidation in the healthcare industry;
•our ability to accurately forecast customer demand for our Inspire system and manage our inventory;
•our ability to expand, manage, and maintain our direct sales and marketing organization, and to market and sell our Inspire system in markets outside of the United States;
•our ability to manage our growth;
•our ability to hire and retain our senior management and other highly qualified personnel;
•risks related to product liability claims and warranty claims;
•our ability to address quality issues that may arise with our Inspire system;
•our ability to successfully integrate any acquired companies;
•changes in global macroeconomic conditions;
•any failure of information technology systems, processes or sites or damage to our physical facilities;
•our ability to commercialize or obtain regulatory approvals for our Inspire therapy and system, or the effect of delays in commercializing or obtaining regulatory approvals;
•any violations of anti-bribery, anti-corruption, and anti-money laundering laws;
•risks related to our indebtedness;
•our ability to use our net operating losses and research and development carryforwards;
•the risk that we may be deemed to be an investment company under the Investment Company Act of 1940;
•U.S. Food and Drug Administration ("FDA") or other United States or foreign regulatory actions affecting us or the healthcare industry generally, including healthcare reform measures in the United States and international markets;
•our ability to establish and maintain intellectual property protection for our Inspire therapy and system or avoid claims of infringement;
•risks related to our ceasing to qualify as a smaller reporting company or an emerging growth company;
•risks related to our common stock; and
•other important factors that could cause actual results, performance or achievements to differ materially from those contemplated that are found in "Part I, Item 1. Business," "Part I, Item 1A. Risk Factors," and "Part I, Item 2. Management's Discussion and Analysis of Financial Condition and Results of Operations" of this Annual Report on Form 10-K.
Moreover, we operate in an evolving environment. New risk factors and uncertainties may emerge from time to time, and it is not possible for management to predict all risk factors and uncertainties.
Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise.
Unless the context requires otherwise, references to “Inspire,” the “Company,” “we,” “us,” and “our,” refer to Inspire Medical Systems, Inc.
PART I
Item 1. Business.
Overview
We are a medical technology company focused on the development and commercialization of innovative and minimally invasive solutions for patients with obstructive sleep apnea ("OSA"). Our proprietary Inspire system is the first and only FDA-approved neurostimulation technology that provides a safe and effective treatment for moderate to severe OSA. We have developed a novel, closed-loop solution that continuously monitors a patient’s breathing and delivers mild hypoglossal nerve stimulation to maintain an open airway. A significant body of clinical data, which includes a publication in the New England Journal of Medicine and more than 100 peer-reviewed publications, supports the safety and efficacy of Inspire therapy. Inspire therapy received premarket approval ("PMA") from the FDA in April 2014 and has been commercially available in certain European markets since November 2011. Inspire therapy is indicated for patients with moderate to severe OSA who do not have significant central sleep apnea and do not have a complete concentric collapse of the airway at the soft palate level. In addition, patients in the United States ("U.S.") must have been confirmed to fail or be unable to tolerate positive airway pressure ("PAP") treatments, such as continuous positive airway pressure ("CPAP"), and be 22 years of age or older, though there are no similar requirements for patients in Europe. Physicians have treated more than 7,800 patients with Inspire therapy at over 350 medical centers across the U.S. and Europe.
Sleep apnea is a serious and chronic disease that negatively impacts a patient’s sleep, health, and quality of life. OSA is the most common form of sleep apnea. OSA occurs when a person’s breathing is interrupted during sleep by a partially or completely blocked airway and affects patients of all ages, sexes, and body types. The severity of OSA is measured by the number of partial or complete airway blockages that a patient experiences in an hour, referred to as the apnea-hypopnea index ("AHI"). Moderate OSA patients have an AHI of 15 to 30 events per hour, while severe OSA patients have an AHI of 30 more events per hour. Left untreated, OSA increases the risk of high blood pressure, hypertension, heart failure, stroke, coronary artery disease, and other life-threatening diseases.
CPAP is the leading therapy for patients with moderate to severe OSA. CPAP is delivered through a face or nasal mask that connects through a hose to a bedside air pump. In order for CPAP to be most effective, the mask must form an airtight seal on the patient’s face or nose and the mask must be worn every night. The effectiveness of CPAP has been limited by low patient compliance as many patients find the mask or treatment cumbersome, uncomfortable, and loud. When CPAP fails or cannot be tolerated, patients’ remaining treatment options consist primarily of invasive surgical procedures developed to modify or remove existing tissue in an attempt to create free air flow. These invasive surgical procedures have limited or unpredictable clinical benefit, are irreversible, and can be extremely painful. We believe that there is both an urgent clinical need and a strong market opportunity for an alternative to CPAP that is effective and minimally invasive.
Inspire therapy is an innovative, closed-loop, minimally invasive solution that provides comfort and convenience, resulting in high compliance for patients with moderate to severe OSA. Once implanted, the Inspire system delivers electrical stimulation that causes a slight forward movement of the back of the tongue, which helps to maintain an open airway, enabling the patient to inhale freely without interruption. We believe our Inspire therapy provides the following benefits:
•Safe, effective, and durable treatment supported by compelling clinical data, including long-term efficacy results out to five years from initial treatment.
•Closed-loop system that uses a proprietary algorithm to continuously monitor patients’ breathing and provide electrical stimulation during the inspiratory phase.
•Comfortable and convenient therapy resulting in high patient satisfaction that was reported to be 93% at an average of 12 months from initial treatment in the first 1,017 patients in our ongoing global patient registry.
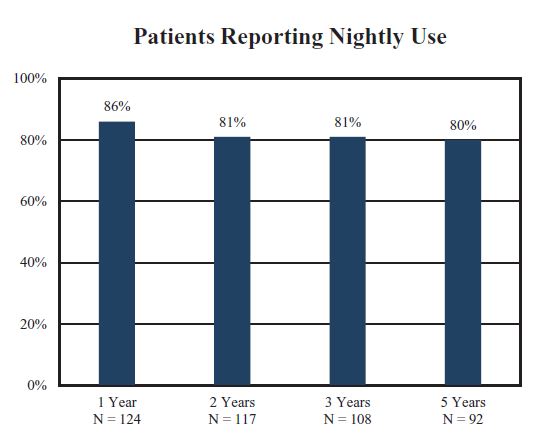
•Strong patient compliance, with 80% of patients reporting continued nightly use through five years from initial treatment in our Stimulation Therapy for Apnea Reduction ("STAR") trial.
•Minimally invasive outpatient procedure with short recovery time.
•Long-lasting solution with a battery designed to last approximately 11 years without charging or maintenance.
The results from multiple clinical trials, which include four sponsored and 19 independent clinical studies that evaluated approximately 2,000 patients, including approximately 960 patients evaluated in independent clinical studies, together with patient-reported outcomes, have shown that our Inspire therapy provides statistically significant and sustained reduction in the severity of patients’ OSA, improvement in sleep-related quality of life and reduction in snoring, as well as high patient compliance rates and a strong safety profile.
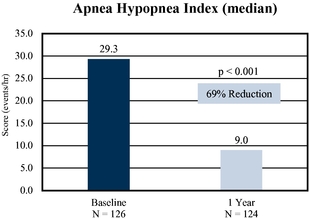
Our pivotal STAR trial was designed to demonstrate longitudinal therapy efficacy and included a randomized controlled therapy withdrawal study. The longitudinal study demonstrated an approximately 70% reduction in the median AHI in patients with moderate to severe OSA from a baseline of 29.3 events per hour to 9.0 events per hour at 12 months following initial treatment. STAR trial follow-up has shown results similar to the initial data at 18 months, three years, and five years. At five years, median AHI in patients with moderate to severe OSA remained low at 6.2 events per hour. The effectiveness of Inspire therapy was further demonstrated by the results of the randomized controlled therapy withdrawal study, in which patients in the therapy withdrawal group regressed to near-baseline AHI levels while patients in the control group that continued therapy experienced sustained therapeutic benefits.
We sell our Inspire system to hospitals and ambulatory surgery centers ("ASCs") in the U.S. and in select countries in Europe through a direct sales organization. As of December 31, 2019, we had 73 sales territories in the U.S. and eight in Europe. Our direct sales force engages in sales efforts and promotional activities focused on ear, nose and throat ("ENT") physicians, and sleep centers. In addition, we highlight our compelling clinical data and value proposition to increase awareness and adoption amongst referring physicians. We build upon this top-down approach with strong direct-to-patient marketing initiatives to create awareness of the benefits of our Inspire system and drive demand through patient empowerment. This outreach helps to educate thousands of patients on our Inspire therapy and frequently results in patient leads.
Our customers are reimbursed the cost of patient treatment by various third-party payors, such as commercial insurance providers and government agencies. We have secured positive coverage policies with 52 U.S. commercial payors, representing approximately 165 million covered lives. In parallel, a subset of our 14 person reimbursement team, which we refer to as our market access team, is focused on assisting patients and physicians in obtaining appropriate prior authorization approvals from commercial payors on a case-by-case basis in advance of treatment with our Inspire therapy. In addition, Medicare coverage for our procedure is determined on a case-by-case basis. All seven Medicare Administrative Contractors ("MACs") have drafted positive coverage policies for Inspire therapy and five of these MACs have since announced the formal release dates of either March 15, 2020 or April 1, 2020 for their final policies covering Inspire therapy. We expect the final two MACs will finalize their policies in 2020. We also have a U.S. government contract for patients who are treated by the Veterans Health Administration. We are in active discussions with commercial insurers to establish additional positive coverage policies to support reimbursement of Inspire therapy.
We generated revenue of $82.1 million, with a gross margin of 83.4% and a net loss of $33.2 million, for the fiscal year ended December 31, 2019, compared to revenue of $50.6 million, with a gross margin of 80.1% and a net loss of $21.8 million, for the fiscal year ended December 31, 2018, and revenue of $28.6 million, with a gross margin of 78.9% and a net loss of $17.5 million, for the fiscal year ended December 31, 2017. Our accumulated deficit as of December 31, 2019 was $180.2 million.
Our Competitive Strengths
We believe the continued growth of our company will be driven by the following competitive strengths:
•First to market with an innovative, closed-loop, minimally invasive solution. We have developed the first and only FDA-approved neurostimulation technology that provides a safe and effective treatment for patients with moderate to severe OSA who have been confirmed to fail or cannot tolerate PAP treatments, such as CPAP. We received a PMA from the FDA in April 2014 for our Inspire therapy. Unlike CPAP, which is limited by low patient compliance primarily due to patient discomfort with the mask or device, our innovative, closed-loop, minimally invasive solution is designed to provide comfort and convenience, resulting in high compliance for patients with moderate to severe OSA. We believe we have a significant first mover advantage and momentum over future competitors, as physicians have treated more than 7,800 patients with Inspire therapy.
•Significant body of strong clinical data. We have developed a significant body of clinical data that demonstrates the safety and effectiveness, therapy adherence, and long-term sustained benefits of our Inspire therapy. The benefits of treatment with Inspire therapy have been consistent across four sponsored and 19 independent clinical studies that evaluated approximately 2,000 patients, including approximately 960 patients evaluated in independent clinical studies, and have been highlighted in more than 100 peer-reviewed publications. Data reported in these clinical studies also demonstrated a high level of overall patient satisfaction. We believe this favorable data provides us with a significant competitive advantage and will continue to support increased adoption of our Inspire therapy.
•Holistic and targeted approach to market development and patient engagement. We have established a methodical approach to market development which centers on active engagement across three key stakeholders in the OSA treatment paradigm: physicians, sleep centers, and patients. Our sales force is focused on building long-lasting relationships with ENT physicians and sleep centers as we support physicians through all aspects of a case-from diagnosis to surgical support to patient follow-up. In addition, we are highlighting our compelling clinical data set and value proposition to increase awareness and adoption amongst referring physicians. We build upon this top-down approach with a strong direct-to-patient marketing initiative that further drives demand through patient empowerment. This outreach helps to educate thousands of patients on our Inspire therapy and frequently results in patient leads. We are confident that this holistic approach to engagement across multiple constituents will continue to drive increased awareness of and demand for our Inspire therapy.
•Dedicated team focused on providing market access for patients and providers. We have a highly efficient approach to advance patients, once identified, to placement of the Inspire system. Our dedicated market access team helps patients and providers work with payors to secure the appropriate prior authorization approvals in advance of initial treatment. In addition, this team proactively works with payors to establish positive coverage policies by highlighting the compelling clinical data and the value of our Inspire therapy. This highly leverageable team has been successful in helping to secure reimbursement from approximately 430 commercial payors to date, and positive coverage policies from 52 U.S. commercial payors, including several large national payors.
•Strong research and development capabilities and comprehensive intellectual property portfolio. Our commitment to driving innovation has allowed us to achieve continuous, significant improvements of our Inspire therapy. For example, in the U.S., in July 2017, and in Europe, in May 2018, we launched the fourth generation of our Inspire system, with a neurostimulator that is 40% smaller and 18% thinner than the neurostimulator in the previous generation, while maintaining an approximate 11-year battery life without needing to be recharged. Patients treated with this fourth generation device may now undergo an MRI scan of the head or extremities. In October 2018, the first implant of our new sensing lead was successfully completed in Germany, and in January 2019, the FDA approved the new sensing lead. This new lead has a significantly smaller profile, including a reduction in diameter of 49%, as compared to the prior design, and is intended to improve the patient’s comfort. It also incorporates several features to enable easier implanting and potentially reduce surgical time for an ENT surgeon. We have a comprehensive patent portfolio to protect our intellectual property and technology, with rights as of
December 31, 2019 to 28 issued U.S. patents, 26 issued foreign patents, 39 pending U.S. patent applications, and 47 pending foreign patent applications that cover aspects of our Inspire system and future product concepts.
Our Strategy
Our goal is to be a global leader in providing clinically proven innovative solutions that improve sleep, quality of life, and health of patients with moderate to severe OSA. We believe the following strategies will play a critical role in achieving this goal and our future growth:
•Promote awareness among patients, ENT physicians, sleep centers, and referring physicians. We believe that many patients who have failed or cannot tolerate CPAP are unaware of our Inspire therapy as a safe and effective alternative treatment for moderate to severe OSA. We intend to continue to promote awareness of our therapy through training and educating ENT physicians, sleep centers, key opinion leaders, and various medical societies on the proven clinical benefits of Inspire therapy. In addition, we intend to continue to publish additional clinical data in various industry and scientific journals and online, and to present at various industry conferences. We also plan to continue building patient awareness through our direct-to-patient marketing initiatives, which include paid online search, radio, social media, television, and online videos.
•Expand our U.S. sales and marketing organization to drive adoption of our Inspire therapy. We plan to expand our sales and marketing organization and seek to recruit and train exceptionally talented sales representatives in existing and new markets in the U.S. to help facilitate further adoption and broaden awareness of our Inspire therapy. Our success to date in developing new markets has been primarily due to our ability to identify new regions with high volume medical centers, educate ENT and sleep physicians, help generate steady patient demand, and provide sufficient support staff to our sales representatives. We believe investing in a scalable, efficient direct sales force and continuing the development of our marketing efforts will help us broaden adoption of our Inspire therapy and drive revenue growth.
•Leverage our prior authorization model while we work with payors to broaden coverage. Our dedicated in-house market access team will continue to assist patients and physicians in obtaining prior authorization approvals from commercial payors for treatment with our Inspire therapy. In parallel, we are in active discussions with commercial payors to establish positive coverage policies and continue to highlight our compelling and robust clinical data and our increased support from leading medical organizations and key opinion leaders. We believe increased positive payor coverage policies could substantially expand patient access by reducing hurdles to treatment.
•Invest in research and development to drive innovation and expand indications. Our foundational commitment to driving innovation and improving patient lives fuels our desire for continuous product development. We intend to invest in existing and next generation technologies to further improve our products and clinical outcomes, optimize patient acceptance and comfort and broaden the patient population that can benefit from our Inspire therapy. An example of our efforts to expand our label indications includes our clinical study that is evaluating the use of Inspire therapy in pediatric patients with Down syndrome.
•Further penetrate and expand into existing and new international markets. We plan to establish and strengthen our presence internationally. Our goal is to further increase sales of our Inspire therapy in existing international markets in Europe, including Germany and the Netherlands, and expand our reach to new markets, such as Japan and Australia. We plan to strategically invest in new markets based on our assessment of market size and opportunity and prospects for compelling reimbursement coding and coverage.
Our Solution for OSA
Overview of Inspire Therapy
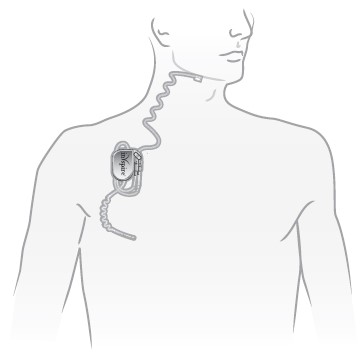
Our proprietary Inspire system is the first and only FDA-approved closed-loop neurostimulation technology that provides a safe and effective treatment for moderate to severe OSA. Our Inspire system consists of a remote control and three implantable components:
•a pressure sensing lead, which detects when the patient is attempting to breathe;
•a neurostimulator, which houses the electronics and battery power for the device; and
•a stimulation lead, which delivers electrical stimulation to the hypoglossal nerve.
The image below depicts the location of the Inspire system under the patient’s skin:
A pressure sensing lead is used to monitor the patient’s breathing. Our proprietary algorithm tracks breathing patterns and the neurostimulator delivers electrical stimulation at the start of inspiration. This electrical stimulation of the hypoglossal nerve causes a slight forward movement of the back of the tongue that helps maintain an open airway, thereby preventing obstructive events and enabling the patient to inhale freely.
To receive the Inspire system, patients undergo a short outpatient surgical procedure, typically lasting two hours, during which the neurostimulator, sensing lead, and stimulation lead are implanted. The procedure is minimally invasive and performed with a series of three small incisions. Patients typically recover quickly and are able to resume normal activities in just a few days. Initial activation of the system occurs 30 days after the implantation. After the initial activation, the patient is instructed to use the therapy each night by turning on their Inspire system before going to sleep using their remote control.
The following pictures depict the Inspire neurostimulator, shown with a quarter for scale, and the patient remote control, shown in hand for scale.
Patients turn their Inspire system on when they plan to go to sleep and turn it off when they awaken. The device has a programmed delay, typically 30 minutes, to allow patients to fall asleep naturally before the device activates. It then monitors the patient’s breathing and delivers mild stimulation to the hypoglossal nerve at the start of the inspiratory phase, causing a slight forward movement at the back of the tongue to maintain an open airway during the inspiratory phase of respiration. The therapy is designed to provide stimulation for each breath to prevent obstructive events.
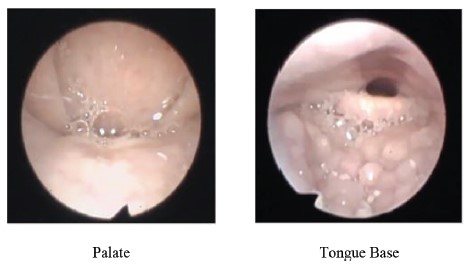
The following pictures depict the anatomy of a patient experiencing an OSA event. The patient’s soft palate and the base of the patient’s tongue are obstructing the patient’s airway and limiting airflow to the lungs.
Obstructed Airway
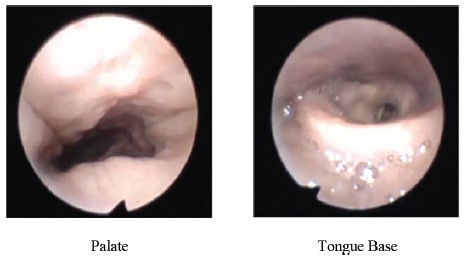
The following pictures depict the anatomy of the patient after mild stimulation of the hypoglossal nerve, which caused the patient's tongue to move forward slightly, opening the patient's airway and restoring airflow to the lungs.
Open Airway
The effectiveness of Inspire therapy to relieve OSA is objectively measured during a sleep study or polysomnogram. A sleep study records a patient’s breathing, airflow, and blood oxygen levels before and after activating the device. Before activation, the patient experiences multiple periods of interrupted breathing, and oxygen levels repeatedly drop before the patient experiences a transient arousal that allows air intake. The polysomnogram below shows that after activating Inspire therapy, the patient exhibited a more regular breathing pattern, higher and more consistent blood oxygen levels, and fewer or no transient arousals.
Polysomnogram Before and After Activation of Inspire System
Benefits of Inspire Therapy
We believe our Inspire therapy overcomes many of the limitations of CPAP and other current treatments of moderate to severe OSA by providing the following key benefits:
•Safe, effective, and durable treatment. Results from our clinical trials provide compelling safety and efficacy data regarding the clinical benefits of Inspire therapy as many as five years after initial treatment. The results from our STAR trial, a five-year follow-up phase III pivotal trial, demonstrated an approximately 70% reduction in the median AHI from a baseline of 29.3 events per hour to 9.0 events per hour at 12 months following initial treatment. STAR trial follow-up has shown similar results to the initial data at 18 months, three years, and five years. At five years, median AHI remained low at 6.2 events per hour.
•Closed-loop system. The Inspire system uses a proprietary algorithm to continuously monitor a patient’s breathing and provide electrical stimulation during the inspiratory phase, working with the body’s natural actions to keep the airway open during the breathing cycle.
•Comfortable and convenient therapy resulting in high patient satisfaction. Data reported on the first 1,017 patients in our ongoing ADHERE patient registry, which we established to follow patients who have been implanted with an Inspire system, demonstrated that these patients used Inspire therapy an average of 5.6 hours per night an average of 12 months after initial treatment, with overall patient satisfaction reported to be at 93%.
•Strong patient compliance. Results from our STAR trial demonstrated that 80% of patients continue to use Inspire therapy on a nightly basis five years after initial treatment.
•Minimally invasive outpatient procedure. The Inspire system’s implantable components are placed during an approximately two-hour outpatient procedure. The procedure is minimally invasive and performed with three small incisions. Patients typically recover quickly and are able to resume normal activities within a few days.
•Long-lasting solution. Our Inspire system uses a battery designed to last approximately 11 years without charging or maintenance.
Commercialization of Inspire Therapy
In the U.S., before we can market a new medical device, or a new use of, new claim for or significant modification to an existing product, we must first receive FDA clearance or approval. We obtained PMA approval for our Inspire system in 2014. Additionally, we received a CE mark for commercialization of our Inspire system in Europe in 2011, and in June 2018, Japan’s Ministry of Health, Labour and Welfare approved our Inspire therapy to treat moderate to severe OSA. We continue to work on the reimbursement process in Japan and hope to commercialize Inspire therapy there. To commercialize our Inspire system, both in the U.S. and Europe, we focus on physician and patient awareness and adoption of our Inspire therapy. To achieve this, our commercialization strategy primarily consists of our direct sales force engaging in sales efforts and promotional activities focused on ENT physicians and sleep centers and highlighting our compelling clinical data and value proposition. Our direct sales force utilizes strong direct-to-patient marketing initiatives to create awareness of the benefits of our Inspire system. We intend to make significant investments building our sales and marketing organization by increasing the number of U.S. sales representatives and continuing our direct-to-patient marketing efforts in existing and new markets throughout the U.S. and Europe.
In addition, a significant part of our commercialization effort consists of supporting our customers through the reimbursement process. Most commercial U.S. insurers now cover Inspire therapy. For those payors that do not have a positive policy, Inspire provides robust prior authorization support to our customers. Medicare has pending positive coverage for all states, which we expect will be finalized in 2020, and we have a U.S. government contract for patients who are treated by the Veterans Health Administration.
Treatment with Inspire Therapy
Patient Selection
Inspire therapy is indicated for patients with moderate to severe OSA (AHI of 15 to 65) who do not have significant central sleep apnea and do not have a complete concentric collapse of the airway at the soft palate level. Patients undergo a drug-induced sleep endoscopy performed by an ENT surgeon in order to confirm that they satisfy this anatomical requirement. In addition, patients in the U.S. must have been confirmed to fail or be unable to tolerate PAP treatments, such as CPAP, and be 22 years of age or older, though there are no similar requirements for patients in Europe. Patients who fail PAP are those that are not able to eliminate moderate to severe OSA despite PAP usage. Patients who cannot tolerate PAP treatments are those who either are unable to use PAP more than five nights per week for at least four hours per night, or who are unwilling to use PAP treatment. We have submitted a PMA supplement to the FDA to expand our indication in the U.S. to patients as young as 13 years of age, which is currently under review.
Implantation
The Inspire system is implanted under general anesthesia through three small incisions. One incision is under the lower jaw, where the stimulation lead is attached around a distal branch of the hypoglossal nerve that is responsible for forward movement of the tongue. A second incision in the upper right chest below the clavicle is used to implant the neurostimulator, which houses all the electronics and battery power for the device. The last incision is made near the ribs, where a pressure sensing lead is placed to monitor the breathing cycle. The functionality of the Inspire system is tested in the operating room to verify proper placement of the stimulation and pressure sensing leads. The wires for the electrodes are tunneled under the skin and the incisions are closed. The Inspire system is powered by a battery in the neurostimulator that is designed to last approximately 11 years without needing to be recharged. After this time, the neurostimulator is replaced during a simple outpatient procedure.
The implantation procedure is performed in an outpatient setting and surgery is completed in approximately two hours. Patients may experience mild discomfort and swelling at the incision sites for a few days that is usually managed with over-the-counter pain medications. Patients can return home and resume a normal diet shortly after completion of the procedure and resume most daily activities within a few days. The only restriction on their activity is to avoid strenuous activities until the incisions have had time to heal.
Activation
Patients are allowed to heal for a month before the Inspire system is activated through a wireless connection to the device in the clinician’s office. The initial activation is performed by the clinician using a programming tablet that is able to turn the system on as well as change various parameters such as the strength of the stimulating pulse, the sensitivity of the detection, the timing and length of the pulse, and which part of the stimulating electrode should be used. With the exception of pulse strength, the factory default settings are used in the majority of patients. The pulse strength is initially adjusted to the lowest level required to move the tongue out of the way without causing discomfort.
Patients receive a remote control that they use to turn their Inspire system on when they plan to go to sleep and to turn it off when they awaken. The device has a programmed delay, typically 30 minutes, to allow patients to fall asleep naturally before the device activates. It then delivers mild stimulation to the hypoglossal nerve, causing the tongue to move as the patient is inhaling. The remote enables patients to adjust the strength of the stimulation to optimize their therapy and comfort. The range of control given to patients is limited to avoid setting the strength of the stimulation to an ineffective or excessively high level. Patients also have the ability to temporarily pause therapy if they awaken during the night.
Clinical Results and Studies
A significant body of published clinical evidence, which includes four sponsored and 19 independent clinical studies that evaluated approximately 2,000 patients, including approximately 960 patients evaluated in
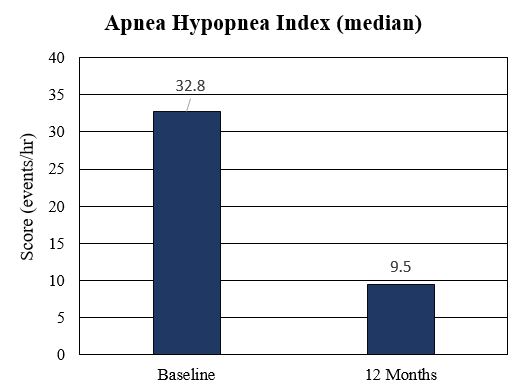
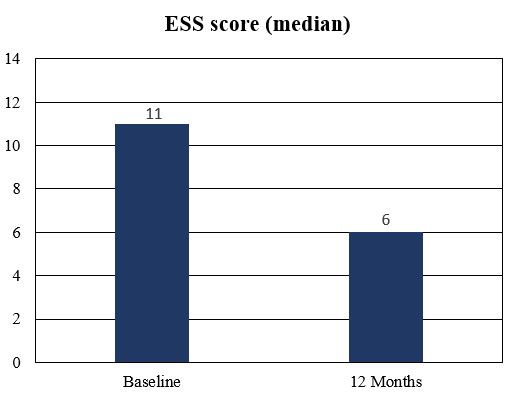
independent clinical studies, supports the safety and effectiveness of our Inspire therapy. The results of the STAR trial, our phase III pivotal clinical trial that served as the basis for the FDA approval of our PMA application, were published in the New England Journal of Medicine, and the results of additional clinical studies have been published in more than 100 peer-reviewed publications. We have established a global patient registry, which we refer to as our ADHERE patient registry, to collect data on safety, effectiveness, weekly usage, overall compliance, and satisfaction from patients who have been implanted with an Inspire system. The table below highlights key findings from certain of these studies and data from the first 1,017 patients in our ADHERE patient registry, including significant improvements in objective sleep measures and patient-reported quality of life measures, strong therapy compliance, and a favorable safety profile.
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| STAR Trial(1) | | | | German Post-Market Study(1) | | ADHERE Patient Registry(1) | | TJUH and UPMC Evaluation(2) |
| Number of Inspire therapy patients | 124 | | | 97 | | | 56 | | | 1,017 | | 48 / 49 |
| Time following implantation | 12 months | | 5 years | | 12 months | | 12 months | | 3 months |
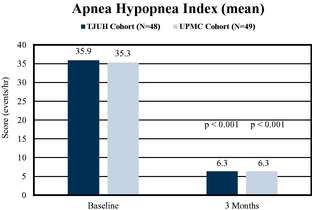
| AHI—Baseline | 29.3 | | | 29.3 | | | 28.6 | | | 32.8 | | | 35.9 / 35.3 |
| AHI—Therapy | 9.0 | | | 6.2 | | | 9.5 | | | 9.5 | | | 6.3 / 6.3 |
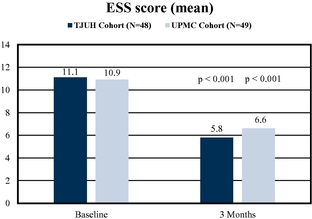
| ESS—Baseline | 11 | | | 11 | | | 13 | | | 11 | | | 11 / 11 |
| ESS—Therapy | 6 | | | 6 | | | 7 | | | 6 | | | 6 / 7 |
| FOSQ—Baseline | 14.6 | | | 14.6 | | | 13.7 | | | * | | * |
| FOSQ—Therapy | 18.2 | | | 18.7 | | | 18.6 | | | * | | * |
| Therapy compliance | 86% daily; 93% 5+ days weekly | | 80% daily | | Average 39 hours per week; 89% ≥20 hours per week | | Average 5.6 hours per night | | Average >45 hours per week; >75% ≥40 hours per week |
* Not measured
(1) Median results
(2) Mean results
STAR Trial
Overview
We sponsored the STAR trial, a multi-center, prospective, single-group, cohort design study that began in 2010 at 22 medical centers across the U.S. and Europe. We evaluated 126 patients who were confirmed to fail or were unable to tolerate positive airway treatments, such as CPAP. Of the 126 patients, 83% were men, the mean age was 54.5 years, and the mean body-mass index was 28.4.
The primary outcome measures were a reduction in AHI from baseline to 12 months of more than 50% along with final AHI being less than 20 events per hour, and a reduction from baseline to 12 months of more than 50% in oxygen desaturation index ("ODI") which measures the number of times per hour of sleep that the blood’s oxygen level drops by at least 4% below baseline. These are objective quantitative metrics that are measured during an in-office sleep study or polysomnogram, which also provides important objective measures of sleep quality.
Secondary outcome measures evaluated a patient’s quality of life using two standard and validated patient questionnaires, the Functional Outcomes of Sleep Questionnaire ("FOSQ") and the Epworth Sleepiness Scale ("ESS"). A clinically relevant improvement in FOSQ is 2.0 points from baseline, and a normalized patient has a FOSQ score greater than 17.9. ESS scores of 10 or greater reflect excessive daytime sleepiness. An additional secondary outcome measured the percentage of sleep time during which a patient’s blood oxygen saturation level was below 90%.
After 12 months, 46 consecutive patients who met the criteria of having a response to therapy were then included in a randomized, controlled therapy-withdrawal trial. These patients were randomly assigned, in a 1:1 ratio, to a therapy-withdrawal group, which had the device turned off for at least five days until a sleep study or polysomnogram was performed, or to a therapy-maintenance group, which continued nightly use of the device.
We have continued to follow patients from the STAR trial to collect data regarding long-term efficacy and utilization. See “-Long-Term Benefits of Inspire Therapy.”
Results
The results of the STAR trial were initially published in January 2014 in the New England Journal of Medicine. The trial met both of its primary endpoints at 12 months, as well as all secondary endpoints.
The median AHI for patients in the STAR trial decreased from 29.3 events per hour to 9.0 events per hour at 12 months (p<0.001). The median ODI decreased from 25.4 events per hour to 7.4 events per hour (p<0.001). Patients reported significantly improved quality of life based on the FOSQ, on which median scores increased from 14.6 to 18.2 out of a maximum score of 20 (p<0.001). Patients also had less daytime sleepiness as quantified by a decrease in the median ESS from 11.0 to 6.0 (p<0.001). In the trial, the percentage of sleep time during which a patient’s blood oxygen saturation levels was below 90% was reduced from 5.4% to 0.9% at 12 months (p=0.01).
Inspire therapy efficacy data from STAR trial at 12 months
After 12 months’ follow-up with 126 implanted patients, 124 patients (98%) remained active users of our Inspire therapy. One patient died unexpectedly due to an unrelated cause and one participant requested a device removal for personal reasons because the patient was a non-responder. Data at 12 months showed that 86% of patients (106 of 123) used the device daily and 93% (115 of 123) used the device at least five days a week, with data unavailable from one patient.
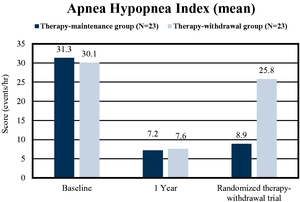
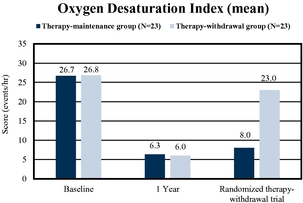
The effectiveness of Inspire therapy was further demonstrated by the results of the therapy-withdrawal portion of the trial, which showed a significant difference between the therapy-withdrawal group and the therapy-maintenance group with respect to the change in the AHI score from the assessment at 12 months of the cohort study to the assessment at the end of the therapy-withdrawal study. As illustrated in the charts below, a difference in change in mean scores of 16.4 events per hour was observed (p<0.001), and a similar effect was observed for the mean ODI scores.
Withdrawal of Inspire therapy results in reversal of therapeutic benefit as measured by AHI and ODI
Safety
Patients from the STAR trial reported various adverse events, typically mild and resolved within five days, which can be divided into two categories. The first category includes those occurring immediately subsequent to the implantation procedure. In this category, 26% of patients reported incision pain and 25% reported post-operative discomfort. There was only one report of a mild infection associated with the procedure. The second category includes device-related adverse events that were reported in the first 18 months after implantation. In this category, 47% of patients reported discomfort due to stimulation at some point during this period, which was generally resolved with programming adjustments to the device. Other common reports included tongue abrasion, headaches, and mouth dryness.
Explants and Revisions
Two patients out of 126 in the STAR trial did not complete the trial. One patient died unexpectedly due to an unrelated cause and one patient requested a device removal because the patient was a non-responder. Two other patients underwent revision surgeries to reposition the device to address patient discomfort.
Long-term Benefits of Inspire Therapy
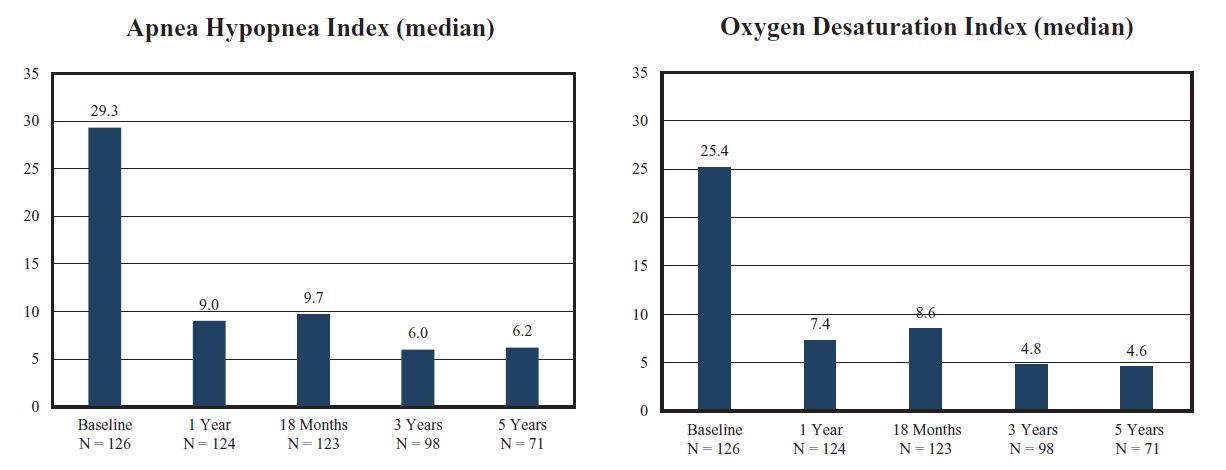
Patients receiving Inspire therapy in the STAR trial have been followed for long-term efficacy and utilization. The median AHI in these patients decreased from 29.3 events per hour to 9.0 events per hour after 12 months and the median ODI decreased from 25.4 events per hour to 7.4 events per hour after 12 months. After five years, the median AHI in these patients was 6.2 events per hour and the median ODI was 4.6 events per hour, as shown below.
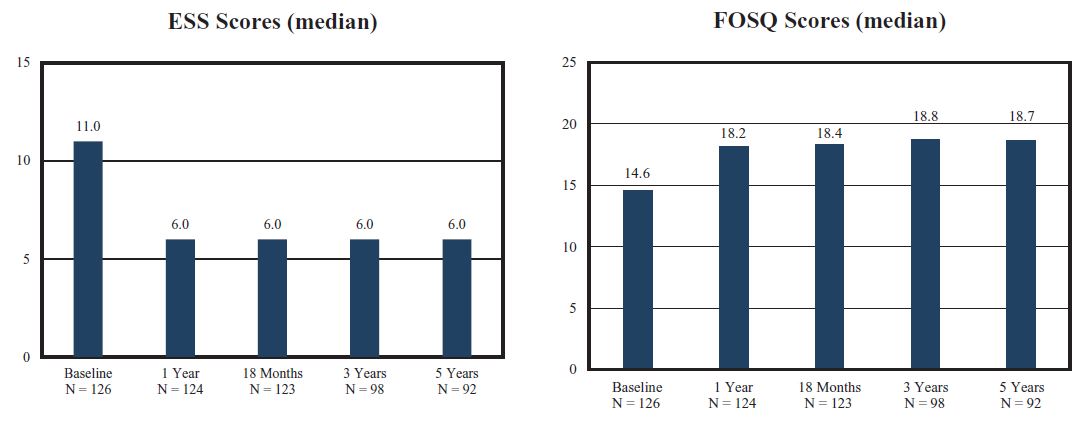
Patient-reported outcomes after five years also found a roughly 45% improvement and a roughly 28% improvement in daytime sleepiness as measured by ESS and FOSQ, respectively, and 80% of patients reported nightly usage. These results are shown below.
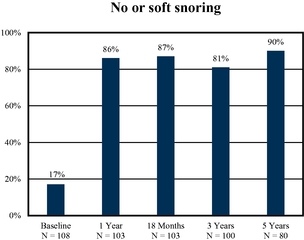
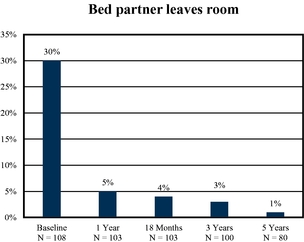
After five years, approximately 90% of patients reported no or only soft snoring, compared to only 17% at baseline. Before obtaining therapy, 30% of patients reported that their bed partners occasionally had to leave the room because of their snoring. After five years of therapy, this number decreased to 1%.
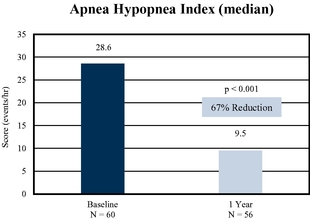
German Post-Market Study
We sponsored the German Post-Market Study, a multi-center post-approval study that evaluated 60 middle-aged, overweight patients, with measurements at two-, six-, and 12-month intervals. The results of this study, which were published in The Laryngoscope in 2017, were consistent with the outcomes demonstrated in our STAR trial and showed median AHI being reduced from a baseline of 28.6 events per hour to 9.5 events per hour in 56 patients measured after 12 months. Over the same period, median ESS score improved from a baseline of 13.0 to 6.5 and median FOSQ score improved from a baseline of 13.7 to 18.6. There were three patients lost to follow-up and one patient requested removal of the device for cosmetic and other personal reasons. There were no serious device-related adverse events.
ADHERE Patient Registry
We established our ADHERE patient registry to follow patients who have been implanted with an Inspire system, with a goal of collecting data on a group of at least 5,000 patients. Data gathered to date on the first 1,017 patients published in Laryngoscope in 2019 showed that patients used Inspire therapy an average of 5.6 hours per night when measured an average of 12 months after implantation. Median AHI was reduced from 32.8 events per hour to 9.5 events per hour and median ESS score improved from 11 to 6 over the same period. Overall satisfaction with Inspire therapy was reported by patients to be 93%, with 94% of patients reporting that they would choose the procedure again. In addition, 95% of patients reported a better experience than CPAP.
Independent Evaluations of Inspire Therapy
As the adoption of Inspire therapy continues to expand, many implanting centers have conducted and/or will conduct their own independent studies.
The effectiveness of our Inspire therapy has been documented by researchers at Thomas Jefferson University Hospital ("TJUH") and University of Pittsburgh Medical Center ("UPMC") who published their results in the Journal of Clinical Sleep Medicine in 2017. These researchers found that AHI decreased from a mean of over 35 events per hour to approximately six events per hour at both institutions after three months, in a group of 97 patients with a mean age of approximately 62 years and a mean body-mass index ("BMI") of approximately 28.5. Mean ESS scores also improved significantly at both institutions, as shown below. Patients at both institutions used the device for an average of more than 45 hours per week and more than 75% of patients used the device longer than 40 hours per week. One patient in the study requested removal of the device due to perceived lack of symptomatic improvement.
Positive results have been reported from a number of other independent studies to date, including:
•The University Hospitals Cleveland Medical Center reported in Clinical Otolaryngology on 20 patients who received Inspire therapy. The mean decrease of AHI was 30.2 events/hour and the mean increase of the minimum SpO2 was 4.3%. The mean therapy usage was 46 hours per week.
•Dr. Huntley et al reported a case-control, retrospective review of 153 patients who received Inspire therapy at two academic institutes in The Laryngoscope. The AHI reduced from 34.7 to 5.6 among patients with BMI less than 32, and from 41.0 to 6.5 among patients with BMI of more than 32, showing no difference in AHI response among patients with elevated BMI comparing with patients with lower BMI.
•Dr. Zhu et al reported in Respiratory Medicine the effect of age among 62 patients who received Inspire therapy. Among 31 patients younger than 65 years, AHI reduced from 28.7 to 4.9 and ESS reduced from 14.6 to 4.0. Among 31 patients older than 65 years, AHI reduced from 28.5 to 9.2 and ESS reduced from 12.0 to 5.5 at 12 months. There were no differences in therapy response between the two ago groups. Advanced age was not a limiting factor for patients to receive the benefit of Inspire therapy.
•At a non-academic hospital in San Diego, Dr. Weeks reported in in Laryngoscope Investigative Otolaryngology on 22 consecutive patients treated with Inspire therapy. Implant times for these patients averaged 171±40 minutes. All implantations were completed without complications and AHI reductions were consistent among patients, with all patients measured achieving a titrated AHI < 5. Average device use was 7.0±1.0 hours/night.
Comparison of Inspire Therapy and UPPP
Cleveland Clinic Study
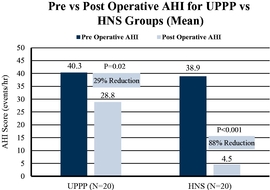
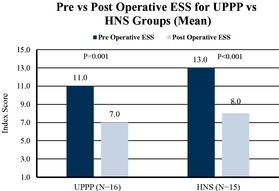
A retrospective study comparing the effectiveness of hypoglossal nerve stimulation ("HNS") therapy utilizing our Inspire system to the effectiveness of uvulopalatopharyngoplasty ("UPPP"), was conducted by researchers at the Cleveland Clinic on two cohorts of patients treated for OSA. A cohort of 20 patients, with a mean age at the time of surgery of 42.1 and mean BMI of 27.5, underwent traditional UPPP airway reconstructive surgery, while a cohort of 20 patients, with a mean age at the time of surgery of 62.4 and mean BMI of 28.0, were treated with
Inspire therapy. A higher percentage of patients who received Inspire therapy (65%) achieved reduction in AHI from the moderate to severe range into the normal range (defined as AHI <5) compared to patients who underwent UPPP (20%). Additionally, mean AHI for patients treated with Inspire therapy decreased by 88% while mean AHI for patients treated with UPPP decreased by 29%.
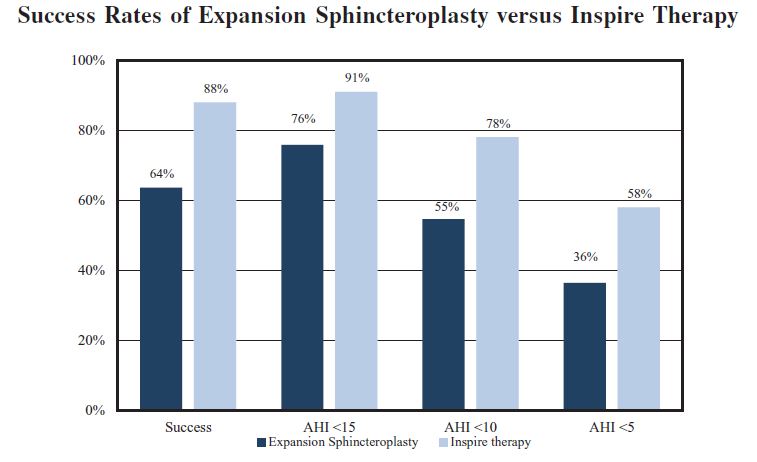
Thomas Jefferson University Hospital Study
An additional study comparing the effectiveness of our Inspire therapy to the effectiveness of UPPP was conducted by researchers at Thomas Jefferson University Hospital on two cohorts of patients treated for OSA. A cohort of 33 patients, with a mean age of 43.5 and mean BMI of 29.6, underwent expansion sphincteroplasty, a variant of UPPP, while a cohort of 90 patients, with a mean age of 61.2 and mean BMI of 29.8, were treated with Inspire therapy. A higher percentage of patients who received Inspire therapy (88%) were successfully treated compared to patients who received UPPP (64%), with successful treatment defined as a reduction in AHI of at least 50% from baseline and achieving an AHI of less than 20 events per hour.
Sales and Marketing
We have established a methodical approach to market development which centers on active engagement across three key stakeholders in the OSA treatment paradigm: patients, physicians, and sleep centers.
We sell our Inspire system through a direct sales force that primarily targets ENT physicians and sleep centers in the U.S. and Europe. The implant procedure for our Inspire therapy is typically performed by an ENT physician or in some cases by neurosurgeons. We also focus on sleep centers because they diagnose and manage large volumes of patients with sleep apnea and are often an important referral base for ENT physicians. In addition, because OSA is sometimes diagnosed during other procedures, we have developed programs to help educate
general practitioners and specialists in other fields, such as cardiovascular surgeons, electrophysiologists, and dentists, regarding our Inspire therapy.
We have 73 sales territories in the U.S. and eight in Europe. We seek to recruit sales representatives with strong sales backgrounds, direct experience developing markets with new technologies, and core knowledge of medical device coding, reimbursement, and the prior authorization process.
We also utilize direct communication channels to inform and educate patients about Inspire therapy and to enable them to connect with active clinical sites that offer our Inspire systems. Our primary methods of patient outreach are Facebook, Google ad placements, radio advertisements (either local or satellite), and television advertisements. The objective of this outreach is to bring patients to our website, where they can find educational materials and videos on sleep apnea and the use and benefits of our Inspire therapy, contact information for physicians and clinical sites, and information regarding community awareness events.
We believe our patient outreach efforts have been effective in bringing potential patients to our website and facilitating contact with our clinical sites. During 2019, we had approximately 4.5 million individual hits to our website and had over 2.0 million “engaged” visitors, defined as visitors who went to at least two pages or took an action while visiting our website. In 2019, we had nearly 520,000 visitors who used our website to find a physician in their area, more than 33,000 visitors contacted a clinical site to schedule an appointment, and about 10,000 visitors who signed up for a local Inspire informational event.
Commercial Activities Outside of the U.S.
We have eight sales territories in Europe, five of which are located in Germany. Our general practice is to limit commercial investments in European countries until such time as there is a determined reimbursement pathway. We provide consistent training in Europe as is conducted in the U.S. and have established a support team in Europe for patient outreach and education, implant support, and device programming. We expect to continue to scale our commercial activities in Europe as we continue to develop country-wide reimbursement in additional markets. We continue to work on the reimbursement process in Japan and hope to commercialize Inspire therapy there.
Third-Party Reimbursement
Our market access team is responsible for all of our reimbursement processes and initiatives. Our team includes 14 professionals who are focused on all key aspects of reimbursement, which include coding, payment, coverage, and prior authorization.
Coding and Payment
In the U.S., we sell our products to hospitals and ASCs. These customers in turn bill various third-party payors, such as commercial payors and government agencies, for the cost required to treat each patient.
Third-party payors require physicians and hospitals to identify the service for which they are seeking reimbursement by using Current Procedural Terminology ("CPT") codes, which are created and maintained by the American Medical Association ("AMA"). Implantation of our Inspire neurostimulator and stimulation lead is described by CPT code 64568, which is the code describing the implantation of a cranial nerve stimulator. Implantation of our Inspire pressure sensing lead is described by CPT code 0466T, a Category III code published by the AMA in January 2017.
Physician reimbursement under Medicare generally is based on a defined fee schedule, the Physician Fee Schedule, through which payment amounts are determined by the relative values of the professional service rendered. Medicare provides reimbursement to our hospital customers under the hospital outpatient prospective payment system ("HOPPS") which provides bundled amounts generally intended to reimburse the hospital for all facility costs related to procedures performed in the hospital outpatient setting. Under the HOPPS, the 2020 national average Medicare payment to the hospital for this procedure is approximately $29,000, which covers the hospitals’ costs for the device and the implantation procedure. The physician is issued a separate payment for the
professional service under the Medicare Physician Fee Schedule. Reimbursement rates from commercial payors vary depending on the procedure performed, the commercial payor, contract terms, and other factors.
Commercial Payor and Government Program Coverage
A core pillar of our reimbursement strategy involves broadening our third-party payor coverage. We continue to have active discussions with commercial payors to establish positive coverage policies by highlighting our compelling and robust clinical data, increased patient demand, and support from leading medical societies and key opinion leaders. We have been successful in obtaining prior authorization approvals from over 430 commercial payors for the Inspire device and procedure. Historically, commercial payors approve prior authorization requests for approximately 60% of Inspire implants in the U.S. We estimate that 70% of patients who meet the FDA indication for Inspire therapy are covered by commercial insurance companies and we have secured coverage policies with most major national commercial payors.
A number of other commercial payors currently consider hypoglossal nerve stimulation to be investigational, including procedures involving the Inspire system, and therefore do not have formal coverage policies.
Procedures involving our Inspire system may be reimbursed on a medical necessity basis for some Medicare patients, and all seven local MACs have published positive draft local coverage determinations for Inspire therapy. Five of these MACs have since announced the formal release dates of either March 15, 2020 or April 1, 2020 for their final policies covering Inspire therapy and we expect the final two MACs will finalize their policies in 2020. Medicare has historically accounted for approximately 30% of all Inspire system implantations in the U.S., although we expect this percentage to decrease over time as commercial policies are developed. In addition, we have a contract with the U.S. government that covers implantations of our Inspire system performed in Veterans Affairs and military hospitals, which account for approximately 10% of all Inspire system implantations historically in the U.S.
Prior Authorization Approval Process
A second pillar of our reimbursement strategy includes leveraging our market access team to assist patients and physicians in obtaining appropriate prior authorization approvals in advance of treatment on a case-by-case basis where positive coverage policies currently do not exist. We believe our market access team is highly effective in working with patients and physicians to obtain prior authorizations for our Inspire system including assisting with the appeals process. In 2019, we received multiple prior authorization approvals from most of the largest commercial payors, for example Anthem, Cigna, Blue Cross Blue Shield, and Humana. In addition, in 2019, market access team helped over 90% of patients who pursued the appeals process fully to secure prior authorizations with an average approval time of approximately two to three months, with less than 10% being denied external medical review approval while the remainder were lost to follow-up. Our market access team supported approximately 2,500 individual patient submissions in 2018 and approximately 3,000 individual patient submissions in 2019.
We believe we will continue to benefit from this efficient prior authorization process in the near-term and in the longer-term by expanding positive coverage policies. We intend to expand our market access team and increase the number of annual patient submissions as we grow our operations.
Reimbursement Outside of the U.S.
In Germany, the Institut für das Entgeltsystem im Krankenhaus, the German federal reimbursement agency, has granted the Neue Untersuchungs-und Behandlungsmethoden ("NUB") Status 1 coverage for our Inspire system. The NUB process allows for the introduction of new and innovative medical devices prior to reaching reimbursement eligibility and provides for a supplemental payment for new technologies in the German reimbursement system. NUB Status 1 is the highest of four levels and allows for full reimbursement for our Inspire system for the 113 hospitals that applied for therapy in 2019. Under NUB Status 1, payors at these hospitals are obligated to cover the gaps in treatment costs for the Inspire system.
In the Netherlands, the Zorginstituut, or the Dutch Health Institute, has approved Inspire therapy for conditional reimbursement within the basic package of all payors. This allows patients to receive the Inspire system in certain hospitals and within approved indications set by the Zorginstituut.
In Switzerland, Inspire therapy is covered by the public health insurance and hospitals receive reimbursement from the Swiss Diagnosis Related Groups ("DRG") system. This allows patients to receive the Inspire system in certain hospitals and within the indication covered by the Swiss DRG.
Reimbursement in other European countries is primarily provided by single center hospitals from their operating budgets or with generic payment codes, but we intend to continue to develop reimbursement in other European countries including Belgium, France, Italy, Spain, the Nordic region, and any other new market that we may enter in the future, such as Japan and Australia.
Research and Development
Product Evolution and Next Generation Products
The first Inspire device was developed by Medtronic Inc. (now Medtronic Public Limited Company), or Medtronic, in the early 1990s as a radio frequency controlled device that required an external apparatus to deliver electrical stimulation to the hypoglossal nerve. The first fully implantable, respiration-sensing, closed-loop Inspire system was developed shortly thereafter. Based on the initial clinical trial results, which were published in 2001, Medtronic began developing what became known as our Inspire II system, introducing a new, more durable stimulation lead and lower-power neurostimulator, and relocating the respiratory sensing lead to between the intercostal muscle layers.
After our inception and the spin-off of the Inspire business from Medtronic in 2007, our primary focus was to requalify the Inspire II system and resume clinical trial activity. We completed a phase I feasibility trial along with a phase II dosing or patient selection trial in 2009. In 2011, we began our phase III pivotal STAR trial. The STAR trial was completed and published in the New England Journal of Medicine in January 2014 and we received PMA approval in April 2014. Additionally, we received a CE mark for commercialization in Europe in 2011.
We continue to invest in advancing our Inspire system with the goal of providing patients more effective and less invasive therapy for OSA. In 2017, we released the Inspire IV neurostimulator, which is 40% smaller than the previous version while maintaining approximately 11 years of battery life. Patients with this version of the Inspire system are now able to undergo an MRI scan of the head or extremities. The Inspire IV device was launched in the U.S. in July 2017, and in Europe in the second quarter of 2018.
Our newly designed respiratory sensing lead was developed in 2017 and was approved by the FDA in January 2019. This lead was introduced in Europe in October 2018 and in the U.S. in March 2019. The lead has a significantly smaller profile, including a reduction in diameter of 49 percent as compared to the prior design. This smaller profile is intended to simplify surgical placement along with several other features to enable easier implanting, and potentially reduce surgical time for an ENT surgeon.
Our next generation of the Inspire neurostimulator is in development. We have launched a cloud-based patient management system called Inspire Cloud, which allows physicians to monitor patient compliance and more efficiently coordinate patient care.
Additional Indications
We have sought and continue to seek to expand the approved indications for our Inspire therapy. For instance, in January 2017, the FDA approved a PMA supplement expanding the indicated AHI range for our Inspire therapy from 20 to 65 events per hour to 15 to 65 events per hour.
We have submitted a PMA supplement to the FDA to expand our indication in the U.S. to patients as young as 13 years of age. This expanded indication would also allow pediatric patients with Down syndrome to be treated with Inspire therapy.
Patients born with Down syndrome have higher rates of OSA than the general pediatric population. The incidence rate can range from 30% to 60% in children with Down syndrome, compared to 1% in the general population. OSA remains a long-term disability in many of these individuals, and CPAP compliance in this patient population is significantly worse than in the general population. Results from a six-patient trial in adolescents with Down syndrome were published in 2017 in JAMA Otolaryngology-Head & Neck Surgery demonstrating the safety and efficacy of Inspire therapy for treating this patient population. Results from this investigator-initiated trial suggest that Inspire therapy may have therapeutic potential in Down syndrome patients.
Our research and development team focuses on the products currently under development, including our clinical trials, as well as feasibility studies in which we are evaluating different design configurations to enhance product functionality for future generations of the Inspire system.
Competition
Our industry is subject to rapid change from the introduction of new products and technologies and other activities of industry participants. We compete as a second-line therapy in the OSA treatment market for patients with moderate to severe OSA.
We consider our primary competition to be other neurostimulation technologies designed to treat OSA, though we are currently the only such technology approved for commercialization in the U.S. by the FDA. Outside the U.S., we compete with ImThera (now a part of LivaNova), which markets an open-loop neurostimulation device. ImThera is currently conducting clinical trials of its device in the U.S. We believe other emerging businesses are in the early stages of developing neurostimulation devices.
We also compete, both within and outside of the U.S., with invasive surgical treatment options such as UPPP, maxillomandibular advancement ("MMA") and robotic tongue reduction surgery, and, to a lesser extent, oral appliances, which are primarily used in the treatment of mild to moderate OSA. We do not believe we directly compete with CPAP or other types of PAP devices because in the U.S., Inspire therapy is only indicated for patients who have been confirmed to fail or cannot tolerate PAP treatments, such as CPAP.
We believe that the primary competitive factors in the OSA treatment market are:
•company, product, and brand recognition;
•product safety, reliability, and durability;
•quality and volume of clinical data;
•effective marketing to and education of patients, physicians, and sleep centers;
•product ease of use and patient comfort;
•sales force experience and access;
•product support and service;
•technological innovation, product enhancements, and speed of innovation;
•pricing and revenue strategies;
•procedure costs to patients;
•effectiveness of reimbursement teams and strategies; and
•dedicated practice development and clinical training teams.
Most of the other OSA treatments against which we compete have a greater penetration into the OSA treatment market. Oral appliances and other surgical treatments are better known to ENT physicians, sleep centers and the other physicians on whom we rely for referrals, but we believe physician awareness of our Inspire therapy is increasing.
We also compete with other medical technology companies to recruit and retain qualified sales, training and other personnel, including members of our in-house prior authorization team.
Intellectual Property
We rely on a combination of patent, copyright, trademark and trade secret laws, and confidentiality and invention assignment agreements to protect our intellectual property rights. As of December 31, 2019, we had rights to 28 issued U.S. patents, which will expire between 2020 and 2036 assuming all required fees are paid, 39 pending U.S. patent applications, 26 issued foreign patents, and 47 pending foreign patent applications. Our patents cover aspects of our current Inspire system and future product concepts. Some of the issued foreign patents and pending foreign patent applications preserve an opportunity to pursue patent rights in multiple countries.
There is no active patent litigation involving any of our patents and we have not received any notices of patent infringement.
As of December 31, 2019, we had 106 pending and registered trademark filings worldwide, some of which may apply to multiple countries.
We also rely, in part, upon unpatented trade secrets, know-how and continuing technological innovation, and may in the future rely upon licensing opportunities, to develop and maintain our competitive position. We protect our proprietary rights through a variety of methods, including confidentiality and assignment agreements with suppliers, employees, consultants, and others who may have access to our proprietary information.
Our pending patent applications may not result in issued patents, and we cannot assure you that any current or subsequently issued patents will protect our intellectual property rights or provide us with any competitive advantage. While there is no active litigation involving any of our patents or other intellectual property rights and we have not received any notices of patent infringement, we may be required to enforce or defend our intellectual property rights against third parties in the future. See Part I., "Item 1A. Risk Factors — Risks Related to Intellectual Property Matters” for additional information regarding these and other risks related to our intellectual property portfolio and their potential effect on us.
License Agreement with Medtronic
In November 2007, we entered into an assignment and license agreement with Medtronic ("the Assignment and License Agreement") pursuant to which Medtronic assigned certain patents and trademarks to us and granted to us a worldwide, royalty-free license to certain other patents and technical information to make, use, import and sell products, and to practice methods in the field of electrical stimulation of the upper airway for the treatment of OSA ("the Field"). We share co-exclusive rights with Medtronic under this license; however, Medtronic may not exercise its rights unless we make an assignment for the benefit of our creditors, file or have filed against us a bankruptcy petition or go into receivership. We also granted to Medtronic certain worldwide, royalty-free, exclusive licenses to the patents Medtronic assigned to us, as well as other intellectual property (including but not limited to Technical Information (as defined in the Assignment and License Agreement)) that applies to a device and methods with certain specifications for use in the Field, to make, use, import and sell products, and to practice methods outside of the Field. The licenses granted are perpetual and irrevocable.
Manufacturing and Supply
We rely on third-party suppliers to manufacture our Inspire system and its components. Outsourcing manufacturing reduces our need for capital investment and reduces operational expense. Additionally, outsourcing provides expertise and capacity necessary to scale up or down based on demand for our Inspire system. We select our suppliers to ensure that our Inspire system and its components are safe and effective,
adhere to all applicable regulations, are of the highest quality, and meet our supply needs. We employ a rigorous supplier assessment, qualification, and selection process targeted to suppliers that meet the requirements of the FDA and the International Organization for Standardization and quality standards supported by internal policies and procedures. Our quality assurance process monitors and maintains supplier performance through qualification and periodic supplier reviews and audits.
Certain components used in our Inspire system are supplied by single-source suppliers. Our suppliers manufacture the components they produce for us and test our components and devices to our specifications. We intend to maintain sufficient levels of inventory to enable us to continue our operations while we obtain another supplier in the event that one or more of our single-source suppliers were to encounter a delay in supply or end supply.
Government Regulation
Our products and our operations are subject to extensive regulation by the FDA and other federal and state authorities in the U.S., as well as comparable authorities in the European Economic Area ("EEA"). Our products are subject to regulation as medical devices under the Federal Food, Drug, and Cosmetic Act ("FDCA") as implemented and enforced by the FDA. The FDA regulates the development, design, non-clinical and clinical research, manufacturing, safety, efficacy, labeling, packaging, storage, installation, servicing, recordkeeping, premarket clearance or approval, import, export, adverse event reporting, advertising, promotion, marketing and distribution, and import and export of medical devices to ensure that medical devices distributed domestically are safe and effective for their intended uses and otherwise meet the requirements of the FDCA.
In addition to U.S. regulations, we are subject to a variety of regulations in the EEA governing clinical trials and the commercial sales and distribution of our products. Whether or not we have or are required to obtain FDA clearance or approval for a product, we will be required to obtain authorization before commencing clinical trials and to obtain marketing authorization or approval of our products under the comparable regulatory authorities of countries outside of the U.S. before we can commence clinical trials or commercialize our products in those countries. The approval process varies from country to country and the time may be longer or shorter than that required for FDA clearance or approval.
FDA Premarket Clearance and Approval Requirements
Unless an exemption applies, each medical device commercially distributed in the U.S. requires either FDA clearance of a 510(k) premarket notification or PMA approval. Under the FDCA, medical devices are classified into one of three classes-Class I, Class II, or Class III-depending on the degree of risk associated with each medical device and the extent of manufacturer and regulatory control needed to ensure its safety and effectiveness. Class I includes devices with the lowest risk to the patient and are those for which safety and effectiveness can be assured by adherence to the FDA’s General Controls for medical devices, which include compliance with the applicable portions of the QSR, facility registration and product listing, reporting of adverse medical events, and truthful and non-misleading labeling, advertising, and promotional materials. Class II devices are subject to the FDA’s General Controls, and special controls as deemed necessary by the FDA to ensure the safety and effectiveness of the device. These special controls can include performance standards, post-market surveillance, patient registries, and FDA guidance documents. While most Class I devices are exempt from the 510(k) premarket notification requirement, manufacturers of most Class II devices are required to submit to the FDA a premarket notification under Section 510(k) of the FDCA requesting permission to commercially distribute the device. The FDA’s permission to commercially distribute a device subject to a 510(k) premarket notification is generally known as 510(k) clearance. Under the 510(k) process, the manufacturer must submit to the FDA a premarket notification demonstrating that the device is “substantially equivalent” to either a device that was legally marketed prior to May 28, 1976, the date upon which the Medical Device Amendments of 1976 were enacted, or another commercially available device that was cleared to through the 510(k) process.
Devices deemed by the FDA to pose the greatest risks, such as life-sustaining, life-supporting or some implantable devices, or devices that have a new intended use, or use advanced technology that is not substantially equivalent to that of a legally marketed device, are placed in Class III, requiring approval of a PMA.
Some pre-amendment devices are unclassified, but are subject to the FDA’s premarket notification and clearance process in order to be commercially distributed.
Our currently marketed Inspire products are Class III devices which have received PMA approval.
PMA Approval Pathway
Class III devices require PMA approval before they can be marketed although some pre-amendment Class III devices for which the FDA has not yet required a PMA are cleared through the 510(k) process. The PMA process is more demanding than the 510(k) premarket notification process. In a PMA, the manufacturer must demonstrate that the device is safe and effective, and the PMA must be supported by extensive data, including data from preclinical studies and human clinical trials. The PMA must also contain a full description of the device and its components, a full description of the methods, facilities and controls used for manufacturing, and proposed labeling. Following receipt of a PMA, the FDA determines whether the application is sufficiently complete to permit a substantive review. If the FDA accepts the application for review, it has 180 days under the FDCA to complete its review of a PMA, although in practice, the FDA’s review often takes significantly longer, and can take up to several years. An advisory panel of experts from outside the FDA may be convened to review and evaluate the application and provide recommendations to the FDA as to the approvability of the device. The FDA may or may not accept the panel’s recommendation. In addition, the FDA will generally conduct a preapproval inspection of the applicant or its third-party manufacturers’ or suppliers’ manufacturing facility or facilities to ensure compliance with the Quality System Regulation ("QSR").
The FDA will approve the new device for commercial distribution if it determines that the data and information in the PMA constitute valid scientific evidence and that there is reasonable assurance that the device is safe and effective for its intended use(s). The FDA may approve a PMA with post-approval conditions intended to ensure the safety and effectiveness of the device, including, among other things, restrictions on labeling, promotion, sale and distribution, and collection of long-term follow-up data from patients in the clinical study that supported PMA approval or requirements to conduct additional clinical studies post-approval. The FDA may condition PMA approval on some form of post-market surveillance when deemed necessary to protect the public health or to provide additional safety and efficacy data for the device in a larger population or for a longer period of use. In such cases, the manufacturer might be required to follow certain patient groups for a number of years and to make periodic reports to the FDA on the clinical status of those patients. Failure to comply with the conditions of approval can result in material adverse enforcement action, including withdrawal of the approval.
Certain changes to an approved device, such as changes in manufacturing facilities, methods, or quality control procedures, or changes in the design performance specifications, which affect the safety or effectiveness of the device, require submission of a PMA supplement. PMA supplements often require submission of the same type of information as a PMA, except that the supplement is limited to information needed to support any changes from the device covered by the original PMA and may not require as extensive clinical data or the convening of an advisory panel. Certain other changes to an approved device require the submission of a new PMA, such as when the design change causes a different intended use, mode of operation, and technical basis of operation, or when the design change is so significant that a new generation of the device will be developed, and the data that were submitted with the original PMA are not applicable for the change in demonstrating a reasonable assurance of safety and effectiveness.
Clinical Trials
Clinical trials are almost always required to support a PMA and are sometimes required to support a 510(k) submission. All clinical investigations of investigational devices to determine safety and effectiveness must be conducted in accordance with the FDA’s investigational device exemption ("IDE") regulations which govern investigational device labeling, prohibit promotion of the investigational device, and specify an array of recordkeeping, reporting and monitoring responsibilities of study sponsors and study investigators. If the device presents a “significant risk” to human health, as defined by the FDA, the FDA requires the device sponsor to submit an IDE application to the FDA, which must become effective prior to commencing human clinical trials. A significant risk device is one that presents a potential for serious risk to the health, safety or welfare of a patient and either is implanted, used in supporting or sustaining human life, substantially important in diagnosing, curing,
mitigating or treating disease or otherwise preventing impairment of human health, or otherwise presents a potential for serious risk to a subject. An IDE application must be supported by appropriate data, such as animal and laboratory test results, showing that it is safe to test the device in humans and that the testing protocol is scientifically sound. The IDE will automatically become effective 30 days after receipt by the FDA unless the FDA notifies the company that the investigation may not begin. If the FDA determines that there are deficiencies or other concerns with an IDE for which it requires modification, the FDA may permit a clinical trial to proceed under a conditional approval.
In addition, the study must be approved by, and conducted under the oversight of, an Institutional Review Board ("IRB") for each clinical site. The IRB is responsible for the initial and continuing review of the IDE, and may pose additional requirements for the conduct of the study. If an IDE application is approved by the FDA and one or more IRBs, human clinical trials may begin at a specific number of investigational sites with a specific number of patients, as approved by the FDA. If the device presents a non-significant risk to the patient, a sponsor may begin the clinical trial after obtaining approval for the trial by one or more IRBs without separate approval from the FDA, but must still follow abbreviated IDE requirements, such as monitoring the investigation, ensuring that the investigators obtain informed consent, and labeling and record-keeping requirements. Acceptance of an IDE application for review does not guarantee that the FDA will allow the IDE to become effective and, if it does become effective, the FDA may or may not determine that the data derived from the trials support the safety and effectiveness of the device or warrant the continuation of clinical trials. An IDE supplement must be submitted to, and approved by, the FDA before a sponsor or investigator may make a change to the investigational plan that may affect its scientific soundness, study plan or the rights, safety or welfare of human subjects.
During a study, the sponsor is required to comply with the applicable FDA requirements, including, for example, trial monitoring, selecting clinical investigators and providing them with the investigational plan, ensuring IRB review, adverse event reporting, record keeping, and prohibitions on the promotion of investigational devices or on making safety or effectiveness claims for them. The clinical investigators in the clinical study are also subject to FDA regulations and must obtain patient informed consent, rigorously follow the investigational plan and study protocol, control the disposition of the investigational device, and comply with all reporting and recordkeeping requirements. Additionally, after a trial begins, we, the FDA or the IRB could suspend or terminate a clinical trial at any time for various reasons, including a belief that the risks to study subjects outweigh the anticipated benefits.
Post-market Regulation
After a device is cleared or approved for marketing, numerous and pervasive regulatory requirements continue to apply. These include:
•establishment registration and device listing with the FDA;
•QSR requirements, which require manufacturers, including third-party manufacturers, to follow stringent design, testing, control, documentation, and other quality assurance procedures during all aspects of the design and manufacturing process;
•labeling and marketing regulations, which require that promotion is truthful, not misleading, fairly balanced, provide adequate directions for use, and that all claims are substantiated, and also prohibit the promotion of products for unapproved or “off-label” uses and impose other restrictions on labeling; FDA guidance on off-label dissemination of information and responding to unsolicited requests for information;
•the federal Physician Sunshine Act and various state and foreign laws on reporting remunerative relationships with health care customers;
•the federal Anti-Kickback Statute (and similar state laws) prohibiting, among other things, soliciting, receiving, offering or providing remuneration intended to induce the purchase or recommendation of an item or service reimbursable under a federal healthcare program, such as Medicare or Medicaid. A person or entity does not have to have actual knowledge of this statute or specific intent to violate it to have committed a violation;
•the federal False Claims Act (and similar state laws) prohibiting, among other things, knowingly presenting, or causing to be presented, claims for payment or approval to the federal government that are false or fraudulent, knowingly making a false statement material to an obligation to pay or transmit money or property to the federal government or knowingly concealing, or knowingly and improperly avoiding or decreasing, an obligation to pay or transmit money to the federal government. The government may assert that claim includes items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the false claims statute;
•clearance or approval of product modifications to 510(k)-cleared devices that could significantly affect safety or effectiveness or that would constitute a major change in intended use of one of our cleared devices, or approval of a supplement for certain modifications to PMA devices;
•medical device reporting regulations, which require that a manufacturer report to the FDA if a device it markets may have caused or contributed to a death or serious injury, or has malfunctioned and the device or a similar device that it markets would be likely to cause or contribute to a death or serious injury, if the malfunction were to recur;
•correction, removal, and recall reporting regulations, which require that manufacturers report to the FDA field corrections and product recalls or removals if undertaken to reduce a risk to health posed by the device or to remedy a violation of the FDCA that may present a risk to health;
•complying with the new federal law and regulations requiring Unique Device Identifiers (UDI) on devices and also requiring the submission of certain information about each device to the FDA’s Global Unique Device Identification Database (GUDID);
•the FDA’s recall authority, whereby the agency can order device manufacturers to recall from the market a product that is in violation of governing laws and regulations; and
•post-market surveillance activities and regulations, which apply when deemed by the FDA to be necessary to protect the public health or to provide additional safety and effectiveness data for the device.
We may be subject to similar foreign laws that may include applicable post-marketing requirements such as safety surveillance. Our manufacturing processes are required to comply with the applicable portions of the QSR, which cover the methods and the facilities, controls for the design, manufacture, testing, production, processes, controls, quality assurance, labeling, packaging, distribution, installation, and servicing of finished devices intended for human use. The QSR also requires, among other things, maintenance of a device master file, device history file, and complaint files. As a manufacturer, our facilities, records, and manufacturing processes are subject to periodic scheduled or unscheduled inspections by the FDA. Our failure to maintain compliance with the QSR or other applicable regulatory requirements could result in the shut-down of, or restrictions on, our manufacturing operations and the recall or seizure of our products. The discovery of previously unknown problems with any of our products, including unanticipated adverse events or adverse events of increasing severity or frequency, whether resulting from the use of the device within the scope of its clearance or off-label by a physician in the practice of medicine, could result in restrictions on the device, including the removal of the product from the market or voluntary or mandatory device recalls.
The FDA has broad regulatory compliance and enforcement powers. If the FDA determines that we failed to comply with applicable regulatory requirements, it can take a variety of compliance or enforcement actions, which may result in any of the following sanctions:
•warning letters, untitled letters, fines, injunctions, consent decrees, and civil penalties;
•recalls, withdrawals, or administrative detention or seizure of our products;
•operating restrictions or partial suspension or total shutdown of production;
•refusing or delaying requests for 510(k) marketing clearance or PMA approvals of new products or modified products;
•withdrawing 510(k) clearances or PMA approvals that have already been granted;
•refusal to grant export or import approvals for our products; or
•criminal prosecution.
Regulation of Medical Devices in the EEA
There is currently no premarket government review of medical devices in the EEA (which is comprised of the 28 Member States of the European Union ("E.U.") plus Norway, Liechtenstein, and Iceland). However, all medical devices placed on the market in the EEA must meet the relevant essential requirements laid down in Annex I of Directive 93/42/EEC concerning medical devices ("the Medical Devices Directive"). There is also a directive specifically addressing Active Implantable Medical Devices (Directive 90/385/EEC). The most fundamental essential requirement is that a medical device must be designed and manufactured in such a way that it will not compromise the clinical condition or safety of patients, or the safety and health of users and others. In addition, the device must achieve the performances intended by the manufacturer and be designed, manufactured, and packaged in a suitable manner. The European Commission has adopted various standards applicable to medical devices. These include standards governing common requirements, such as sterilization and safety of medical electrical equipment and product standards for certain types of medical devices. There are also harmonized standards relating to design and manufacture. While not mandatory, compliance with these standards is viewed as the easiest way to satisfy the essential requirements as a practical matter. Compliance with a standard developed to implement an essential requirement also creates a rebuttable presumption that the device satisfies that essential requirement.
To demonstrate compliance with the essential requirements laid down in Annex I to the Medical Devices Directive, medical device manufacturers must undergo a conformity assessment procedure, which varies according to the type of medical device and its classification. Conformity assessment procedures require an assessment of available clinical evidence, literature data for the product, and post-market experience in respect of similar products already marketed. Except for low-risk medical devices (Class I non-sterile, non-measuring devices), where the manufacturer can self-declare the conformity of its products with the essential requirements (except for any parts which relate to sterility or metrology), a conformity assessment procedure requires the intervention of a Notified Body. Notified bodies are often separate entities and are authorized or licensed to perform such assessments by government authorities. The notified body would typically audit and examine a product’s technical dossiers and the manufacturers’ quality system. If satisfied that the relevant product conforms to the relevant essential requirements, the notified body issues a certificate of conformity, which the manufacturer uses as a basis for its own declaration of conformity. The manufacturer may then apply the CE Mark to the device, which allows the device to be placed on the market throughout the EEA. Once the product has been placed on the market in the EEA, the manufacturer must comply with requirements for reporting incidents and field safety corrective actions associated with the medical device.
In order to demonstrate safety and efficacy for their medical devices, manufacturers must conduct clinical investigations in accordance with the requirements of Annex X to the Medical Devices Directive ("MDD"), Annex 7 of the Active Implantable Medical Devices Directive ("AIMDD"), and applicable European and International Organization for Standardization standards, as implemented or adopted in the EEA member states. Clinical trials for medical devices usually require the approval of an ethics review board and approval by or notification to the national regulatory authorities. Both regulators and ethics committees also require the submission of serious adverse event reports during a study and may request a copy of the final study report.
On April 5, 2017, the European Parliament passed the Medical Devices Regulation (Regulation 2017/745), which repeals and replaces the E.U. Medical Devices Directive and the Active Implantable Medical Devices Directive. Unlike directives, which must be implemented into the national laws of the EEA member States, the regulations would be directly applicable, i.e., without the need for adoption of EEA member State laws implementing them, in all EEA member States and are intended to eliminate current differences in the regulation of medical devices
among EEA member States. The Medical Devices Regulation, among other things, is intended to establish a uniform, transparent, predictable, and sustainable regulatory framework across the EEA for medical devices and ensure a high level of safety and health while supporting innovation. The Medical Devices Regulation will only become applicable in May 2020, however CE certificates issued under the AIMDD or MDD framework that are in effect at that time will remain valid for the duration of that certificate provided significant changes are not made to the devices. Once applicable, the new regulations will among other things:
•strengthen the rules on placing devices on the market and reinforce surveillance once they are available;
•establish explicit provisions on manufacturers’ responsibilities for the follow-up of the quality, performance, and safety of devices placed on the market;
•improve the traceability of medical devices throughout the supply chain to the end-user or patient through a unique identification number;
•set up a central database to provide patients, healthcare professionals, and the public with comprehensive information on products available in the E.U.;
•strengthened rules for the assessment of certain high-risk devices, such as implants, which may have to undergo an additional check by experts before they are placed on the market.
We are subject to regulations and product registration requirements in many foreign countries in which we may sell our products, including in the areas of:
•design, development, manufacturing, and testing;
•product standards;
•product safety;
•product safety reporting;
•marketing, sales, and distribution;
•packaging and storage requirements;
•labeling requirements;
•content and language of instructions for use;
•clinical trials;
•record keeping procedures;
•advertising and promotion;
•recalls and field corrective actions;
•post-market surveillance, including reporting of deaths or serious injuries and malfunctions that, if they were to recur, could lead to death or serious injury;
•import and export restrictions;
•tariff regulations, duties, and tax requirements;
•registration for reimbursement; and
•necessity of testing performed in country by distributors for licensees.
The time required to obtain clearance required by foreign countries may be longer or shorter than that required for FDA clearance, and requirements for licensing a product in a foreign country may differ significantly from FDA requirements.
Federal, State, and Foreign Fraud and Abuse and Physician Payment Transparency Laws
In addition to FDA restrictions on marketing and promotion of drugs and devices, other federal and state laws restrict our business practices. These laws include, without limitation, foreign, federal, and state anti-kickback and false claims laws, as well as transparency laws regarding payments or other items of value provided to healthcare providers.
The federal Anti-Kickback Statute prohibits, among other things, knowingly and willfully offering, paying, soliciting or receiving any remuneration (including any kickback, bribe or rebate), directly or indirectly, overtly or covertly, in cash or in kind to induce or in return for purchasing, leasing, ordering or arranging for or recommending the purchase, lease or order of any good, facility, item or service reimbursable, in whole or in part, under Medicare, Medicaid or other federal healthcare programs. The term “remuneration” has been broadly interpreted to include anything of value, including stock, stock options, and the compensation derived through ownership interests.
Recognizing that the federal Anti-Kickback Statute is broad and may prohibit many innocuous or beneficial arrangements within the healthcare industry, the DHHS issued regulations in July 1991, which the Department has referred to as “safe harbors.” These safe harbor regulations set forth certain provisions which, if met in form and substance, will assure medical device manufacturers, healthcare providers, and other parties that they will not be prosecuted under the federal Anti-Kickback Statute. Additional safe harbor provisions providing similar protections have been published intermittently since 1991. Although there are a number of statutory exceptions and regulatory safe harbors protecting some common activities from prosecution, the exceptions and safe harbors are drawn narrowly. Our arrangements with physicians, hospitals, and other persons or entities who are in a position to refer may not fully meet the stringent criteria specified in the various safe harbors. Practices that involve remuneration that may be alleged to be intended to induce prescribing, purchases or recommendations may be subject to scrutiny if they do not qualify for an exception or safe harbor. Failure to meet all of the requirements of a particular applicable statutory exception or regulatory safe harbor does not make the conduct per se illegal under the federal Anti-Kickback Statute. Instead, the legality of the arrangement will be evaluated on a case-by-case basis based on a cumulative review of all its facts and circumstances. Several courts have interpreted the statute’s intent requirement to mean that if any one purpose of an arrangement involving remuneration is to induce referrals of federal healthcare covered business, the federal Anti-Kickback Statute has been violated. In addition, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. Moreover, a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal civil False Claims Act (described below).
Violations of the federal Anti-Kickback Statute may result in civil monetary penalties up to $100,000 for each violation, plus up to three times the remuneration involved. Civil penalties for such conduct can further be assessed under the federal False Claims Act. Violations can also result in criminal penalties, including criminal fines of up to $100,000 and imprisonment of up to 10 years. Similarly, violations can result in exclusion from participation in government healthcare programs, including Medicare and Medicaid. Liability under the federal Anti-Kickback Statute may also arise because of the intentions or actions of the parties with whom we do business. While we are not aware of any such intentions or actions, we have only limited knowledge regarding the intentions or actions underlying those arrangements. Conduct and business arrangements that do not fully satisfy one of these safe harbor provisions may result in increased scrutiny by government enforcement authorities. The majority of states also have anti-kickback laws which establish similar prohibitions and in some cases may apply more broadly to items or services covered by any third-party payor, including commercial insurers and self-pay patients.
The federal civil False Claims Act prohibits, among other things, any person or entity from knowingly presenting, or causing to be presented, a false or fraudulent claim for payment or approval to the federal government or
knowingly making, using or causing to be made or used a false record or statement material to a false or fraudulent claim to the federal government. A claim includes “any request or demand” for money or property presented to the U.S. government. The federal civil False Claims Act also applies to false submissions that cause the government to be paid less than the amount to which it is entitled, such as a rebate. Intent to deceive is not required to establish liability under the civil federal civil False Claims Act.
In addition, private parties may initiate “qui tam” whistleblower lawsuits against any person or entity under the federal civil False Claims Act in the name of the government and share in the proceeds of the lawsuit. Penalties for federal civil False Claim Act violations include fines for each false claim, plus up to three times the amount of damages sustained by the federal government and, most critically, may provide the basis for exclusion from the federally funded healthcare program. On May 20, 2009, the Fraud Enforcement Recovery Act of 2009 ("FERA") was enacted, which modifies and clarifies certain provisions of the federal civil False Claims Act. In part, the FERA amends the federal civil False Claims Act such that penalties may now apply to any person, including an organization that does not contract directly with the government, who knowingly makes, uses or causes to be made or used, a false record or statement material to a false or fraudulent claim paid in part by the federal government. The government may further prosecute conduct constituting a false claim under the federal criminal False Claims Act. The criminal False Claims Act prohibits the making or presenting of a claim to the government knowing such claim to be false, fictitious or fraudulent and, unlike the federal civil False Claims Act, requires proof of intent to submit a false claim. When an entity is determined to have violated the federal civil False Claims Act, the government may impose civil fines and penalties ranging from $11,181 to $22,363 for each false claim, plus treble damages, and exclude the entity from participation in Medicare, Medicaid, and other federal healthcare programs.
The Civil Monetary Penalty Act of 1981 imposes penalties against any person or entity that, among other things, is determined to have presented or caused to be presented a claim to a federal healthcare program that the person knows or should know is for an item or service that was not provided as claimed or is false or fraudulent, or offering or transferring remuneration to a federal healthcare beneficiary that a person knows or should know is likely to influence the beneficiary’s decision to order or receive items or services reimbursable by the government from a particular provider or supplier.
The Health Insurance Portability and Accountability Act of 1996 ("HIPAA") also created additional federal criminal statutes that prohibit among other actions, knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, including private third-party payors, knowingly and willfully embezzling or stealing from a healthcare benefit program, willfully obstructing a criminal investigation of a healthcare offense, and knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation.
Many foreign countries have similar laws relating to healthcare fraud and abuse. Foreign laws and regulations may vary greatly from country to country. For example, the advertising and promotion of our products is subject to E.U. directives concerning misleading and comparative advertising and unfair commercial practices, as well as other EEA Member State legislation governing the advertising and promotion of medical devices. These laws may limit or restrict the advertising and promotion of our products to the general public and may impose limitations on our promotional activities with healthcare professionals. Also, many U.S. states have similar fraud and abuse statutes or regulations that may be broader in scope and may apply regardless of payor, in addition to items and services reimbursed under Medicaid and other state programs.
Additionally, there has been a recent trend of increased foreign, federal, and state regulation of payments and transfers of value provided to healthcare professionals or entities. The federal Physician Payments Sunshine Act imposes annual reporting requirements on certain drug, biologics, medical supplies and device manufacturers for which payment is available under Medicare, Medicaid or CHIP for payments and other transfers of value provided by them, directly or indirectly, to physicians (including physician family members), certain other healthcare providers, and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members. A manufacturer’s failure to submit timely, accurately, and completely the required information for all payments, transfers of value or ownership or investment interests may result in civil monetary
penalties of $11,562 per failure up to an aggregate of $173,436 per year (or up to an aggregate of $1.128 million per year for “knowing failures”). Manufacturers must submit reports by the 90th day of each calendar year. Certain foreign countries and U.S. states also mandate implementation of commercial compliance programs, impose restrictions on device manufacturer marketing practices and require tracking and reporting of gifts, compensation, and other remuneration to healthcare professionals and entities.
Data Privacy and Security Laws
We are also subject to various federal, state, and foreign laws that protect personal information including certain patient health information, such as the E.U. General Data Protection Regulation (“GDPR”) and the California Consumer Privacy Act (“CCPA”) which became effective as of January 2020, and restrict the use and disclosure of patient health information by healthcare providers, such as HIPAA, as amended by HITECH, in the U.S.
HIPAA established uniform standards governing the conduct of certain electronic healthcare transactions and requires certain entities, called covered entities, to comply with standards that include the privacy and security of protected health information (“PHI”). HIPAA also requires business associates, such as independent contractors or agents of covered entities that have access to PHI in connection with providing a service to or on behalf of a covered entity, of covered entities to enter into business associate agreements with the covered entity and to safeguard the covered entity’s PHI against improper use and disclosure.
The HIPAA privacy regulations cover the use and disclosure of PHI by covered entities as well as business associates, which are defined to include subcontractors that create, receive, maintain, or transmit PHI on behalf of a business associate. They also set forth certain rights that an individual has with respect to his or her PHI maintained by a covered entity, including the right to access or amend certain records containing PHI, or to request restrictions on the use or disclosure of PHI. The security regulations establish requirements for safeguarding the confidentiality, integrity, and availability of PHI that is electronically transmitted or electronically stored. HITECH, among other things, established certain health information security breach notification requirements. A covered entity must notify any individual whose PHI is breached according to the specifications set forth in the breach notification rule. The HIPAA privacy and security regulations establish a uniform federal “floor” and do not supersede state laws that are more stringent or provide individuals with greater rights with respect to the privacy or security of, and access to, their records containing PHI or insofar as such state laws apply to personal information that is broader in scope than PHI as defined under HIPAA.
HIPAA requires the notification of patients, and other compliance actions, in the event of a breach of unsecured PHI. If notification to patients of a breach is required, such notification must be provided without unreasonable delay and in no event later than 60 calendar days after discovery of the breach. In addition, if the PHI of 500 or more individuals is improperly used or disclosed, we would be required to report the improper use or disclosure to the U.S. Department of Health and Human Services ("HHS") which would post the violation on its website, and to the media. Failure to comply with the HIPAA privacy and security standards can result in civil monetary penalties up to $58,490 per violation, not to exceed $1.75 million per calendar year for non-compliance of an identical provision, and, in certain circumstances, criminal penalties with fines up to $250,000 per violation and/or imprisonment.
HIPAA authorizes state attorneys general to file suit on behalf of their residents for violations. Courts are able to award damages, costs and attorneys’ fees related to violations of HIPAA in such cases. While HIPAA does not create a private right of action allowing individuals to file suit against us in civil court for violations of HIPAA, its standards have been used as the basis for duty of care cases in state civil suits such as those for negligence or recklessness in the misuse or breach of PHI. In addition, HIPAA mandates that the Secretary of HHS conduct periodic compliance audits of HIPAA covered entities, and their business associates for compliance with the HIPAA privacy and security standards. It also tasks HHS with establishing a methodology whereby harmed individuals who were the victims of breaches of unsecured PHI may receive a percentage of the civil monetary penalty paid by the violator.
In addition, California enacted the CCPA, effective January 1, 2020, which, among other things, creates new data privacy obligations for covered companies and provides new privacy rights to California residents, including the right to opt out of certain disclosures of their information. The CCPA also creates a private right of action with
statutory damages for certain data breaches, thereby potentially increasing risks associated with a data breach. Although the law includes limited exceptions, including for “protected health information” maintained by a covered entity or business associate, it may regulate or impact our processing of personal information depending on the context.
In the E.U. and EEA we are subject to laws which restrict our collection, control, processing, and other use of personal data (i.e. data relating to an identifiable living individual) including the GDPR (and any applicable national laws implementing the GDPR). We process personal data in relation to our operations, including clinical trials. We process data of our employees, contractors, suppliers, distributors, service providers, and our customers, as well as patient or clinical trial participants, including health and medical information of such participants. We need to ensure compliance with the GDPR (and any applicable national laws implementing the GDPR) in each E.U. and EEA jurisdiction where we are established or are otherwise subject to the GDPR (i.e., jurisdictions in which we are targeting or monitoring E.U. and EEA located individuals, or offering goods or services to E.U. located individuals.
The GDPR imposes onerous accountability obligations including: maintaining a record of data processing; implementing policies and a privacy governance framework; disclosing to data subjects how their personal data is to be used; limiting retention of personal data; mandatory data breach notification requirements; and high standards for data controllers to demonstrate that they have obtained valid consent for certain data processing activities. In addition, the GDPR permits E.U. Member State derogations for certain matters and, accordingly, we are also subject to E.U. national laws relating to the processing of genetic data, biometric data, and health data. We have a robust program that we believe ensures compliance with these obligations. Fines for certain breaches of the GDPR are significant: up to the greater of EUR 20 million or 4% of total global annual turnover. In addition to the foregoing, a breach of the GDPR could result in regulatory investigations, reputational damage, orders to cease/ change our use of data, enforcement notices, as well potential civil claims including class action type litigation where individuals suffer harm.
We are also subject to GDPR requirements with respect to cross-border transfers of personal data out of the E.U. and we need to ensure that such transfers are legitimized by valid transfer solutions and/or derogations under the GDPR (where required), including by entering into the E.U. Commission approved model contracts for the transfer of personal data to third countries (i.e., the standard contractual clauses). We note that there is ongoing litigation in the E.U. challenging the legitimacy of the standard contractual clauses. As such, there is a possibility that the standard contractual clauses may be invalidated as a compliant data transfer mechanism in the near future. In addition, the exit of the United Kingdom (“U.K.”) from the E.U. will mean that at some point that the U.K. will become a “third party” for the purposes of data transfers under the GDPR. We have enlisted the help of external advisors to implement a robust GDPR program that we believe achieves and maintains compliance with these obligations, but it is likely it will require us to expend additional capital and other resources for upcoming GDPR changes.
We depend on a number of third parties in relation to the operation of our business , a number of which process personal data on our behalf. With each new provider we perform security assessments and detailed due diligence, enter into contractual arrangements which require that they only process personal data according to our instructions, and which require that they have sufficient technical and organizational security measures in place. We have enlisted the help of external advisors to provide assistance in implementing these contractual arrangements with our existing providers. There is no assurance that these contractual measures and our own privacy and security-related safeguards will protect us from the risks associated with the third-party processing, storage, and transmission of such information. Any violation of data or security laws by our third party processors could have a material adverse effect on our business and result in the fines and penalties outlined above.
We are also subject to evolving E.U. privacy laws on cookies and e-marketing. The E.U. is in the process of replacing the E-Privacy Directive with a new set of rules in the form of a regulation, which will be directly implemented in the laws of each European Member State. The draft E-Privacy Regulation imposes strict opt-in marketing rules with limited exceptions for business-to-business communications, alters rules on third-party cookies, web beacons, and similar technology and significantly increases fining powers to the same levels as the GDPR (i.e. the greater of 20 million Euros or 4% of total global annual revenue for certain breaches). The e-Privacy Regulation is still going through the European legislative process and commentators expect it to be
agreed during 2020 or 2021, after which a two year transition period will follow before it is in force. We have enlisted the help of external advisors to implement a robust GDPR program that achieves and maintains compliance with these obligations, but it is likely it will require us to expend additional capital and other resources for upcoming GDPR changes.
Healthcare Reform
The U.S. and some foreign jurisdictions are considering or have enacted a number of legislative and regulatory proposals to change the healthcare system in ways that could affect our ability to sell our products profitably. Among policy makers and payors in the U.S. and elsewhere, there is significant interest in promoting changes in healthcare systems with the stated goals of containing healthcare costs, improving quality or expanding access. Current and future legislative proposals to further reform healthcare or reduce healthcare costs may limit coverage of or lower reimbursement for the procedures associated with the use of our products. The cost containment measures that payors and providers are instituting and the effect of any healthcare reform initiative implemented in the future could impact our revenue from the sale of our products.
The implementation of the Affordable Care Act in the U.S., for example, has changed healthcare financing and delivery by both governmental and private insurers substantially, and affected medical device manufacturers significantly. The Affordable Care Act imposed, among other things, a 2.3% federal excise tax, with limited exceptions, on any entity that manufactures or imports Class I, II, and III medical devices offered for sale in the U.S. that began on January 1, 2013. Through a series of legislative amendments, the tax was suspended, effective January 1, 2016, and subsequently repealed altogether on December 20, 2019. The Affordable Care Act also provided incentives to programs that increase the federal government’s comparative effectiveness research, and implemented payment system reforms including a national pilot program on payment bundling to encourage hospitals, physicians, and other providers to improve the coordination, quality, and efficiency of certain healthcare services through bundled payment models. Additionally, the Affordable Care Act has expanded eligibility criteria for Medicaid programs and created a new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research, along with funding for such research. We do not yet know the full impact that the Affordable Care Act will have on our business. There have been judicial and Congressional challenges to certain aspects of the Affordable Care Act, and we expect additional challenges and amendments in the future. Moreover, the Trump Administration and the U.S. Congress may take further action regarding the Affordable Care Act, including, but not limited to, repeal or replacement. Most recently, the Tax Cuts and Jobs Acts was enacted, which, among other things, removes penalties for not complying with the individual mandate to carry health insurance, beginning in 2019. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas, ruled that the Affordable Care Act’s individual mandate to carry insurance coverage is a critical and inseverable feature of the Affordable Care Act, and therefore, because it was repealed as part of the Tax Cuts and Jobs Act, the remaining provisions of the Affordable Care Act are invalid as well. On December 18, 2019, the U.S. Court of Appeals for the 5th Circuit upheld the District Court's decision that the individual mandate was unconstitutional but remanded the case back to the District Court to determine whether the remaining provisions of the Affordable Care Act are invalid as well. It is unclear how these decisions, subsequent appeals, and other efforts to challenge, repeal or replace the Affordable Care Act will impact the Act and our business.
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. For example, the Budget Control Act of 2011, among other things, included reductions to Medicare payments to providers of 2% per fiscal year, which went into effect on April 1, 2013 and, due to subsequent legislative amendments to the statute, will remain in effect through 2029 unless additional Congressional action is taken. Additionally, the American Taxpayer Relief Act of 2012, among other things, reduced Medicare payments to several providers, including hospitals, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years.
We expect additional state and federal healthcare reform measures to be adopted in the future, any of which could limit the amounts that federal and state governments will pay for healthcare products and services, which could result in reduced demand for our products or additional pricing pressure.
Anti-Bribery and Corruption Laws
Our U.S. operations are subject to the FCPA. We are required to comply with the FCPA, which generally prohibits covered entities and their intermediaries from engaging in bribery or making other prohibited payments to foreign officials for the purpose of obtaining or retaining business or other benefits. In addition, the FCPA imposes accounting standards and requirements on publicly traded U.S. corporations and their foreign affiliates, which are intended to prevent the diversion of corporate funds to the payment of bribes and other improper payments, and to prevent the establishment of “off books” slush funds from which such improper payments can be made. We also are subject to similar anticorruption legislation implemented in Europe under the Organization for Economic Co-operation and Development’s Convention on Combating Bribery of Foreign Public Officials in International Business Transactions.
Segment Information
We globally manage our business within one reportable segment. Segment information is consistent with how management reviews our business, makes investing and resource allocation decisions, and assesses our operating performance.
Seasonality
Historically, we have experienced seasonality in our first and fourth quarters, and we expect this trend to continue. In the U.S., we have experienced, and may in the future experience, higher sales in the fourth quarter as a result of patients having paid their annual insurance deductibles in full, thereby reducing their out-of-pocket costs. In the first quarter of each year in Europe, we have experienced, and may in the future experience, reduced demand for our Inspire therapy as Neue Untersuchungs-und-Behandlungsmethoden ("NUB") coverage status is being determined and as hospitals are establishing their budgets pertaining to allocation of funds to purchase our Inspire therapy.
Employees
As of December 31, 2019, we had 239 employees. None of our employees is subject to a collective bargaining agreement or represented by a trade or labor union. We consider our relationship with our employees to be good.
Corporate Information
We were incorporated in Delaware in November 2007 when our predecessor, Inspire Medical Systems, LLC, a Minnesota limited liability company, was spun-off from Medtronic. Inspire Medical Systems, LLC merged with us in November 2007, and we continued as the surviving entity.
Available Information
We file Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, proxy statements, amendments to such documents and other information with the SEC. Our SEC filings are available to the public over the Internet at the SEC's website at http://www.sec.gov. We also make these filings available, free of charge, under the Investor Relations section of our website at www.inspiresleep.com as soon as reasonably practicable after we electronically file such material with, or furnish such material to, the SEC. Our website and the information contained on or connected to that site are not incorporated into this Annual Report on Form 10-K or any other public filing made by us with the SEC.
Item 1A. Risk Factors.
Investing in our common stock involves a high degree of risk. These risks include, but are not limited to, those described below, each of which may be relevant to an investment decision. You should carefully consider the risks described below, together with the other information included or incorporated by reference in this Annual Report on Form 10-K. The realization of any of the following risks could have a significant adverse effect on our reputation, business, financial condition, results of operations, growth, and our ability to accomplish our strategic objectives. In that event, the trading price of our common stock could decline. Other events that we do not currently anticipate or that we currently deem immaterial may also affect our reputation, business, financial conditions, results of operations, growth, and our ability to accomplish our strategic objectives.
Risks Related to Our Business
We have incurred significant operating losses since inception, we expect to incur operating losses in the future and we may not be able to achieve or sustain profitability. We have limited history operating as a commercial company.
We have incurred net losses since our inception in 2007. For the years ended December 31, 2019, 2018, and 2017, we had net losses of $33.2 million, $21.8 million, and $17.5 million, respectively. As of December 31, 2019, we had an accumulated deficit of $180.2 million. To date, we have financed our operations primarily through sales of our Inspire system, private placements of our convertible preferred securities, amounts borrowed under our credit facility, the initial public offering of our common stock that closed in May 2018 ("IPO"), and the follow-on offering of our common stock that closed in December 2018 (our "follow-on offering"). We have devoted significant resources to research and development activities related to our Inspire system, including clinical and regulatory initiatives to obtain marketing approval, and sales and marketing activities.
We first commercialized our Inspire system in certain European markets in 2011 and in the U.S. in 2014 and therefore do not have a long history operating as a commercial company. Since 2011, our revenue has been derived, and we expect it to continue to be derived, primarily from sales of our Inspire system. Because of its recent commercial introduction, our Inspire system has limited product and brand recognition. In addition, demand for our Inspire system may decline or may not increase as quickly as we expect. Our ability to generate revenue from sales of our Inspire system, or from any products we may develop in the future, may not be sufficient to enable us to transition to profitability and generate positive cash flows.
We expect that our operating expenses will continue to increase as we continue to build our commercial infrastructure, invest in research and development, develop, enhance, and commercialize new products, and incur additional operational costs associated with being a public company, including as a result of no longer qualifying as an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012 (the “JOBS Act”). As a result, we expect to continue to incur operating losses for the foreseeable future and may never achieve profitability. Furthermore, even if we do achieve profitability, we may not be able to sustain or increase profitability on an ongoing basis. If we do not achieve or sustain profitability, it will be more difficult for us to finance our business and accomplish our strategic objectives, either of which would have a material adverse effect on our business, financial condition, results of operations, and cause the market price of our common stock to decline. In addition, failure of our Inspire system to significantly penetrate existing or new markets would negatively affect our business, financial condition, and results of operations.
Our revenue is primarily generated from sales of our Inspire system and we are therefore highly dependent on it for our success.
We began selling our Inspire system in 2011 in certain European countries and in 2014 in the U.S. Sales of our Inspire system accounted for primarily all of our revenue for the years ended December 31, 2019, 2018, and 2017. We expect that sales of our Inspire system will continue to account for the substantial majority of our revenue going forward. Our ability to execute our growth strategy and become profitable will therefore depend upon the adoption by patients, physicians, and sleep centers, among others, of our Inspire therapy to treat moderate to severe OSA in patients who are unable to use or get consistent benefit from CPAP. Some physicians
may have prior history with or a preference for other treatment options, such as positive airway pressure devices, surgical treatments or oral appliances, or may be reluctant to alter their practice patterns and undergo the training required to enable them to treat patients with our Inspire therapy. Patients may not adopt our Inspire therapy if, among other potential reasons, their airway anatomy would not allow for effective treatment with Inspire therapy, they are reluctant to receive an implantable device as opposed to an alternative, non-implantable treatment, they are worried about potential adverse effects of our Inspire system, such as infection, discomfort from the stimulation or tongue soreness or weakness, or they are unable to obtain adequate third-party coverage or reimbursement for our Inspire therapy.
We cannot assure you that our Inspire therapy will achieve broad market acceptance among physicians and patients. Any failure of the Inspire system to satisfy physician or patient demand or to achieve meaningful market acceptance will harm our business and future prospects.
If patients or physicians are not willing to change current practices to adopt our Inspire therapy to treat moderate to severe OSA, our Inspire therapy may fail to gain increased market acceptance, and our business will be adversely affected.
Our primary strategy to grow our revenue is to drive an increase in the adoption of our Inspire therapy to treat patients with moderate to severe OSA who are unable to use or get consistent benefit from CPAP. While the number of physicians prescribing our Inspire therapy has increased in recent years, there is a significant group of physicians who have not yet adopted our Inspire therapy, and additional physicians may choose not to adopt our Inspire therapy for a number of reasons, including:
•lack of availability of adequate third-party payor coverage or reimbursement;
•lack of experience with our products and with upper airway neurostimulation as a treatment alternative;
•our inability to convince key opinion leaders to provide recommendations regarding our Inspire therapy, or to convince physicians, patients, and healthcare payors that our Inspire therapy is an attractive alternative to other treatment options;
•perceived inadequacy of evidence supporting clinical benefits or cost-effectiveness of our Inspire therapy over existing alternatives;
•a perception among some physicians of patients’ inability to tolerate the surgical procedure required to implant our Inspire system;
•liability risks generally associated with the use of new products and procedures; and
•the training required to use new products.
We focus our sales, marketing, and training efforts primarily on ENT physicians and sleep physicians. However, physicians from other disciplines, including cardiologists, pulmonologists, electrophysiologists, and primary care physicians, as well as other medical professionals, such as dentists, nurse practitioners, and physician assistants, are often the initial point of contact for patients with OSA.
These physicians and other medical professionals commonly screen and treat patients with moderate to severe OSA, and are likely to prescribe more conventional second-line treatment methods for patients who are unable to use or obtain consistent benefit from CPAP. We believe that educating physicians in these disciplines and other medical professionals about the clinical merits and patient benefits of our Inspire therapy as a treatment for moderate to severe OSA is a key element of increasing the adoption of our Inspire therapy. If additional physicians or other medical professionals do not adopt, or existing physician customers cease prescribing our Inspire therapy for any reason, including those listed above, our ability to execute our growth strategy will be impaired, and our business may be adversely affected.
In addition, patients may not be able to adopt or may choose not to adopt our Inspire therapy if, among other potential reasons, their airway anatomy would not allow for effective treatment with Inspire therapy, they are reluctant to receive an implantable device as opposed to an alternative, non-implantable treatment, they are worried about potential adverse effects of our Inspire system, such as infection, discomfort from the stimulation or tongue soreness or weakness, or they are unable to obtain adequate third-party coverage or reimbursement.
If we are unable to achieve and maintain adequate levels of coverage or reimbursement for our Inspire system, or any future products we may seek to commercialize, our commercial success may be severely hindered.
We currently derive primarily all of our revenue from sales of our Inspire system and expect this to continue for the foreseeable future. The primary customers for our products are hospitals and ASCs. Our customers typically bill various third-party payors to cover all or a portion of the costs and fees associated with the procedures in which our products are used and bill patients for any deductibles or co-payments. Several third-party payors do not currently cover our products and the related procedures because they have determined that our products and the related procedures are experimental or investigational. When our products and the related procedures are reimbursed, they are reimbursed primarily on a per-patient prior authorization basis for patients covered by commercial insurers, on a case-by-case basis for patients covered by Medicare, and under U.S. government contract for patients who are treated by the Veterans Health Administration. Customers that perform the procedure may be subject to reimbursement claim denials upon submission of the claim. Customers may also be subject to recovery of overpayments if a payor makes payment for the claim and subsequently determines that the payor’s coding, billing or coverage policies were not followed. Our customers typically must directly bill patients enrolled with these third-party payors for the costs and fees associated with the procedures in which our products are used. Because there is often no separate reimbursement for supplies used in surgical procedures, the additional cost associated with the use of our products can affect the profit margin of the hospital or surgery center where the procedure is performed. Some of our target customers may be unwilling to adopt our products in light of the additional associated cost. Further, any decline in the amount payors are willing to reimburse our customers could make it difficult for existing customers to continue using or to adopt our products and could create additional pricing pressure for us. If we are forced to lower the price we charge for our products, our gross margins will decrease, which could have a material adverse effect on our business, financial condition, and results of operations, and impair our ability to grow our business.
Third-party payors, whether foreign or domestic, or governmental or commercial, are developing increasingly sophisticated methods of controlling healthcare costs. In addition, no uniform policy of coverage and reimbursement for procedures using our products exists among third-party payors. Therefore, coverage and reimbursement for procedures using our products can differ significantly from payor to payor. Payors continually review new and existing technologies for possible coverage and can, without notice, deny or reverse coverage for new or existing products and procedures. There can be no assurance that third-party payor policies will provide coverage for procedures in which our products are used. If we are not successful in reversing existing non-coverage policies, or if third-party payors that currently cover or reimburse our products and related procedures reverse or limit their coverage in the future, or if other third-party payors issue similar policies, this could have a material adverse effect on our business.
Further, we believe that future coverage and reimbursement may be subject to increased restrictions, such as additional prior authorization requirements, both in the U.S. and in international markets. Third-party coverage and reimbursement for procedures using our products or any of our products in development for which we may receive regulatory approval may not be available or adequate in either the U.S. or international markets, which could have an adverse effect on our business, financial condition and results of operations, and impair our ability to grow our business.
Third-party payors and physicians who do not cover or use our Inspire system may require additional clinical data prior to adopting or maintaining coverage of our Inspire system.
Our success depends on physician and third-party payor acceptance of our Inspire therapy as an effective treatment option for patients with moderate to severe OSA. If physicians or payors do not find our body of published clinical evidence and data compelling or wish to wait for additional studies, they may choose not to use
or provide coverage and reimbursement for our products. Currently, there are a number of large third-party payors that have determined upper airway neurostimulation to be experimental or investigational and therefore do not cover it at this time.
In addition, the long-term effects of upper airway neurostimulation with our Inspire system beyond five years are not yet known. Certain physicians, hospitals, ASCs, and payors may prefer to see longer-term safety and efficacy data than we have produced. We cannot provide assurance that any data that we or others may generate in the future will be consistent with that observed in our existing clinical studies.
The training required for physicians to use our Inspire system could reduce the market acceptance of our products.
As with any new method or technique, physicians must undergo a thorough training program before they are qualified to perform the surgery to implant our Inspire system. Physicians could experience difficulty with the technique necessary to successfully insert the device and may not achieve the technical competency necessary to complete the training program. Even after successfully completing the training program, physicians could still experience difficulty implanting our Inspire system and, as a result, limit its use significantly in their practice or cease utilizing it altogether.
In addition, we may experience difficulty growing the number of physicians who complete our training program if patient demand is low, if the length of time necessary to train each physician is longer than expected, if the capacity of our sales representatives to train physicians is less than expected or if we are unable to sufficiently grow our sales organization. All of these events would lead to fewer trained physicians qualified to implant our Inspire system, which could negatively affect our business, financial condition and results of operations, and impair our ability to grow our business.
We currently compete and will in the future continue to compete against other companies, some of which have longer operating histories, more established products or greater resources than we do, which may prevent us from achieving increased market penetration and improved operating results.
The medical technology industry is highly competitive, subject to change and significantly affected by new product introductions and other activities of industry participants. Our competitors have historically dedicated and will continue to dedicate significant resources to promoting their products or developing new products or methods to treat moderate to severe OSA. We consider our primary competition to be other neurostimulation technologies designed to treat OSA. Though we are currently the only such technology approved for commercialization in the U.S. by the FDA, we currently compete outside the U.S. with ImThera (now a part of LivaNova), which produces an open-loop neurostimulation device, and are aware that it is currently conducting clinical trials of its device in the U.S. We also believe other emerging businesses are in the early stages of developing neurostimulation devices designed to treat OSA. In addition, we also compete, both within and outside of the U.S., with invasive surgical treatment options such as UPPP and MMA and, to a lesser extent, oral appliances, which are primarily used in the treatment of mild to moderate OSA.
In addition, our Inspire therapy is approved for use as a second-line therapy in the treatment of moderate to severe OSA in patients who cannot use or obtain consistent benefit from CPAP. If one or more CPAP device manufacturers successfully develop a CPAP device that is more effective, better tolerated or otherwise results in better compliance by patients, or if improvements in other second-line therapies make them more effective, cost effective, easier to use or otherwise more attractive than our Inspire therapy, sales of our Inspire system could be significantly and adversely affected, which could have a material adverse effect on our business and financial condition and results of operations. In addition, if other companies are successful in developing neurostimulation devices that are approved for a broader range of indications than our Inspire system, we will be at a further competitive disadvantage, which could also affect our business, financial condition and results of operations.
Many of the companies against which we compete may have competitive advantages with respect to primary competitive factors in the OSA treatment market, including:
•greater company, product, and brand recognition;
•superior product safety, reliability, and durability;
•better quality and larger volume of clinical data;
•more effective marketing to and education of patients, physicians, and sleep centers;
•greater product ease of use and patient comfort;
•more sales force experience and greater market access;
•better product support and service;
•more advanced technological innovation, product enhancements, and speed of innovation;
•more effective pricing and revenue strategies;
•lower procedure costs to patients;
•more effective reimbursement teams and strategies;
•dedicated practice development; and
•more effective clinical training teams.
Most of the other OSA treatments against which we compete have a greater penetration into the OSA treatment market. Oral appliances and other surgical treatments are better known to ENT physicians, sleep centers, and the other physicians on whom we rely for referrals.
We also compete with other medical technology companies to recruit and retain qualified sales, training, and other personnel, including members of our in-house prior authorization team.
In addition, though there are currently no pharmacologic therapies approved to treat OSA, we may in the future face competition from pharmaceutical companies that develop such therapies. We also expect to experience increased competition in the future as other companies develop and commercialize competing neurostimulation devices. Any of these companies may also have the competitive advantages described above.
Our long-term growth depends on our ability to enhance our Inspire system, expand our indications, and develop and commercialize additional products.
It is important to our business that we continue to enhance our Inspire system and develop and introduce new products. Developing products is expensive and time-consuming and could divert management’s attention away from our core business. The success of any new product offering or product enhancements to our Inspire system will depend on several factors, including our ability to:
•properly identify and anticipate physician and patient needs;
•develop and introduce new products and product enhancements in a timely manner;
•avoid infringing upon the intellectual property rights of third-parties;
•demonstrate, if required, the safety and efficacy of new products with data from preclinical studies and clinical trials;
•obtain the necessary regulatory clearances or approvals for expanded indications, new products or product modifications;
•be fully FDA-compliant with marketing of new devices or modified products;
•provide adequate training to potential users of our products;
•receive adequate coverage and reimbursement for procedures performed with our products; and
•develop an effective and dedicated sales and marketing team.
If we are not successful in expanding our indications and developing and commercializing new products and product enhancements, our ability to increase our revenue may be impaired, which could have a material adverse effect on our business, financial condition, and results of operations.
Our financial results may fluctuate significantly and may not fully reflect the underlying performance of our business.
Our quarterly and annual results of operations may vary significantly in the future, and period-to-period comparisons of our operating results may not be meaningful. Accordingly, the results of any one quarter or period should not be relied upon as an indication of future performance. Our quarterly and annual financial results may fluctuate as a result of a variety of factors, many of which are outside our control and, as a result, may not fully reflect the underlying performance of our business. One such factor includes seasonal variations in our sales. We have experienced and may in the future experience higher sales in the fourth quarter as a result of patients having paid their annual insurance deductibles in full, thereby reducing their out-of-pocket costs. In the first quarter of each year in Europe, we have experienced and may in the future experience reduced demand for our Inspire therapy as NUB coverage status is being determined in Germany and as hospitals are establishing their budgets pertaining to allocation of funds to purchase our Inspire therapy.
Other factors that may cause fluctuations in our quarterly and annual results include:
•patient and physician adoption of our Inspire therapy;
•changes in coverage policies by third-party payors that affect the reimbursement of procedures using our products;
•timing of new product offerings, acquisitions, licenses or other significant events by us or our competitors;
•unanticipated pricing pressure;
•the hiring, retention, and continued productivity of our sales representatives;
•our ability to expand the geographic reach of our sales and marketing efforts;
•our ability to obtain regulatory clearance or approval for any products in development or for our current products for additional indications or in additional countries outside the U.S.;
•results of clinical research and trials on our existing products and products in development;
•delays in receipt of anticipated purchase orders;
•delays in, or failure of, component and raw material deliveries by our suppliers; and
•positive or negative coverage in the media or clinical publications of our products or products of our competitors or our industry.
Because our quarterly and annual results may fluctuate, period-to-period comparisons may not be the best indication of the underlying results of our business and should only be relied upon as one factor in determining
how our business is performing. These fluctuations may also increase the likelihood that we will not meet our forecasted performance, which could negatively affect the market price for our common stock.
Our results of operations could be materially harmed if we are unable to accurately forecast customer demand for our Inspire system and manage our inventory.
To ensure adequate inventory supply, we must forecast inventory needs and place orders with our suppliers based on our estimates of future demand for our Inspire system. Our ability to accurately forecast demand for our Inspire system could be negatively affected by many factors, including our failure to accurately manage our expansion strategy, product introductions by competitors, an increase or decrease in customer demand for our Inspire system or for products of our competitors, our failure to accurately forecast customer acceptance of new products, unanticipated changes in general market conditions or regulatory matters, and weakening of economic conditions or consumer confidence in future economic conditions. Inventory levels in excess of customer demand may result in inventory write-downs or write-offs, which would cause our gross margin to be adversely affected and could impair the strength of our brand. Conversely, if we underestimate customer demand for our Inspire system, our third-party contract manufacturers may not be able to deliver products to meet our requirements, and this could result in damage to our reputation and customer relationships. In addition, if we experience a significant increase in demand, additional supplies of raw materials or additional manufacturing capacity may not be available when required on terms that are acceptable to us, or at all, or suppliers or our third-party manufacturers may not be able to allocate sufficient capacity in order to meet our increased requirements, which could have an adverse effect on our ability to meet customer demand for our Inspire system and our results of operations.
We seek to maintain sufficient levels of inventory in order to protect ourselves from supply interruptions. As a result, we are subject to the risk that a portion of our inventory will become obsolete or expire, which could have a material adverse effect on our earnings and cash flows due to the resulting costs associated with the inventory impairment charges and costs required to replace such inventory.
We rely on a limited number of third-party suppliers and contract manufacturers for the manufacture and assembly of our products, and a loss or degradation in performance of these suppliers and contract manufacturers could have a material adverse effect on our business, financial condition, and results of operations.
We rely on third-party suppliers and contract manufacturers for the raw materials and components used in our Inspire system and to manufacture and assemble our products. The suppliers that provide certain materials and components, including Nortech Systems, Integer, and Cirtec Medical Systems, are sole suppliers. These sole suppliers, and any of our other suppliers or our third-party contract manufacturers, may be unwilling or unable to supply the necessary materials and components or manufacture and assemble our products reliably and at the levels we anticipate or that are required by the market. Our ability to supply our products commercially and to develop any future products depends, in part, on our ability to obtain these materials, components, and products in accordance with regulatory requirements and in sufficient quantities for commercialization and clinical testing. While our suppliers and contract manufacturers have generally met our demand for their products and services on a timely basis in the past, we cannot guarantee that they will in the future be able to meet our demand for their products, either because of acts of nature, the nature of our agreements with those manufacturers or our relative importance to them as a customer, and our manufacturers may decide in the future to discontinue or reduce the level of business they conduct with us. If we are required to change contract manufacturers due to any change in or termination of our relationships with these third parties, or if our manufacturers are unable to obtain the materials they need to produce our products at consistent prices or at all, we may lose sales, experience manufacturing or other delays, incur increased costs or otherwise experience impairment to our customer relationships. We cannot guarantee that we will be able to establish alternative relationships on similar terms, without delay or at all.
While we believe replacement suppliers and manufacturers exist for all materials, components, and services necessary to manufacture our Inspire system, establishing additional or replacement suppliers for any of these materials, components or services, if required, could be time-consuming and expensive, may result in interruptions in our operations and product delivery, may affect the performance specifications of our Inspire system or could require that we modify its design. Even if we are able to find replacement suppliers or third-party
contract manufacturers, we will be required to verify that the new supplier or third-party manufacturer maintains facilities, procedures, and operations that comply with our quality expectations and applicable regulatory requirements. Furthermore, our contract manufacturers could require us to move to another one of their production facilities or use alternative materials or components. Any of these events could require that we obtain a new regulatory authority approval before we implement the change, which could result in further delay and which may not be obtained at all. While we seek to maintain sufficient levels of inventory as discussed above, those inventories may not fully protect us from supply interruptions.
If our third-party suppliers fail to deliver the required commercial quantities of materials on a timely basis and at commercially reasonable prices, and we are unable to find one or more replacement suppliers capable of production at a substantially equivalent cost in substantially equivalent volumes and quality on a timely basis, the continued commercialization of our Inspire system, the supply of our products to customers, and the development of any future products will be delayed, limited or prevented, which could have material adverse effect on our business, financial condition, and results of operations.
Performance issues, service interruptions or price increases by our shipping carriers could adversely affect our business and harm our reputation and ability to provide our services on a timely basis.
Expedited, reliable shipping is essential to our operations. We rely heavily on providers of transport services for reliable and secure point-to-point transport of our Inspire system to our customers and for tracking of these shipments. Should a carrier encounter delivery performance issues such as loss, damage or destruction of any systems, it would be costly to replace such systems in a timely manner and such occurrences may damage our reputation and lead to decreased demand for our Inspire system and increased cost and expense to our business. Similarly, strikes, severe weather, natural disasters or other service interruptions affecting delivery services we use would adversely affect our ability to process orders for our Inspire system on a timely basis.
Consolidation in the healthcare industry or group purchasing organizations could lead to demands for price concessions, which may affect our ability to sell our products at prices necessary to support our current business strategies.
Healthcare costs have risen significantly over the past decade, which has resulted in or led to numerous cost reform initiatives by legislators, regulators, and third-party payors. Cost reform has triggered a consolidation trend in the healthcare industry to aggregate purchasing power, which may create more requests for pricing concessions in the future. Additionally, group purchasing organizations, independent delivery networks, and large single accounts may continue to use their market power to consolidate purchasing decisions for hospitals and ASCs. We expect that market demand, government regulation, third-party coverage, and reimbursement policies and societal pressures will continue to change the healthcare industry worldwide, resulting in further business consolidations and alliances among our customers, which may exert further downward pressure on the prices of our products.
We have limited experience marketing and selling our Inspire system, and if we are unable to expand, manage and maintain our direct sales and marketing organization we may not be able to generate revenue growth.
We began selling our Inspire system in certain European markets in 2011, and in the U.S. in 2014. As a result, we have limited experience marketing and selling our Inspire system. We currently sell our Inspire system through a direct sales force that targets ENT physicians and sleep centers in the U.S. and Europe, and also utilize various direct-to-patient marketing initiatives, including paid online search, radio, television, social media, and online videos. As of December 31, 2019, our direct sales and marketing organization, including reimbursement personnel, consisted of 186 employees, having increased from 40 employees as of December 31, 2015. Our operating results are directly dependent upon the efforts of these employees. If our direct sales force fails to adequately promote, market and sell our Inspire system, and obtain reimbursement for it, our revenue may be adversely affected.
In order to generate future revenue growth, we plan to expand the size and geographic scope of our direct sales organization. This growth may require us to split or adjust existing sales territories, which may adversely affect our
ability to retain customers in those territories. Additionally, our future success will depend largely on our ability to continue to hire, train, retain, and motivate skilled sales and reimbursement personnel with significant industry experience and technical knowledge of implantable devices and related products. Because the competition for their services is high, we cannot assure you we will be able to hire and retain additional personnel on favorable or commercially reasonable terms, if at all. Failure to hire or retain qualified sales and reimbursement personnel would prevent us from expanding our business and generating revenue. If we are unable to expand our sales and marketing capabilities, we may not be able to effectively commercialize our Inspire system, which could have an adverse effect on our business, financial condition, and results of operations.
To successfully market and sell our Inspire system in markets outside of the U.S., we must address many international business risks with which we have limited experience.
Sales in markets outside of the U.S. accounted for approximately 10.2%, 12.3%, and 15.0% of our revenue for the years ended December 31, 2019, 2018, and 2017, respectively. Our strategy is to increase our international presence in Europe, including Germany and the Netherlands, as well as other international markets, such as Japan and Australia, which may increase our revenue from markets outside the U.S. International sales are subject to a number of risks, including:
•difficulties in staffing and managing our international operations;
•increased competition as a result of more products and procedures receiving regulatory approval or otherwise free to market in international markets;
•longer accounts receivable payment cycles and difficulties in collecting accounts receivable;
•reduced or varied protection for intellectual property rights in some countries;
•export restrictions, trade regulations, and foreign tax laws;
•fluctuations in currency exchange rates;
•foreign certification and regulatory clearance or approval requirements;
•difficulties in developing effective marketing campaigns in unfamiliar foreign countries;
•customs clearance and shipping delays;
•political, social, and economic instability abroad, terrorist attacks, and security concerns in general;
•preference for locally produced products;
•potentially adverse tax consequences, including the complexities of foreign value-added tax systems, tax inefficiencies related to our corporate structure, and restrictions on the repatriation of earnings;
•the burdens of complying with a wide variety of foreign laws and different legal standards; and
•increased financial accounting and reporting burdens and complexities.
If one or more of these risks are realized, our business, financial condition, and results of operations could be adversely affected.
We rely on our own direct sales force for our Inspire system, which may result in higher fixed costs than our competitors and may slow our ability to reduce costs in the face of a sudden decline in demand for our products.
We rely on our own direct sales force, which as of December 31, 2019, consisted of 72 representatives in the U.S. and eight representatives in Europe, to market and sell our Inspire system. Some of our competitors rely predominantly on independent sales agents and third-party distributors. A direct sales force may subject us to higher fixed costs than those of companies that market competing products through independent third parties, due to the costs that we will bear associated with employee benefits, training, and managing sales personnel. As a result, we could be at a competitive disadvantage. Additionally, these fixed costs may slow our ability to reduce costs in the face of a sudden decline in demand for our Inspire system, which could have a material adverse effect on our business, financial condition, and results of operations.
We may be unable to manage our growth effectively.
Our past growth has provided, and our future growth may create, challenges for our organization. From December 31, 2015 to December 31, 2019, the number of our employees increased from 66 to 239. In the future, we expect to hire and train new personnel as we continue to grow and expand our operations. This growth may place significant strain on us. Successful growth is also dependent upon our ability to implement appropriate financial and management controls and systems and procedures, which have become more complex since we no longer qualify as an “emerging growth company” as defined in the Jumpstart Our Business Startups Act of 2012 (the “JOBS Act”) and smaller reporting company as defined under the Exchange Act rules. If we fail to manage these challenges effectively, there may be an adverse effect on our business, financial condition, and results of operations.
Our ability to maintain our competitive position depends on our ability to attract and retain senior management and other highly qualified personnel.
Our success depends in part on our continued ability to attract, retain, and motivate highly qualified management, clinical, and other personnel. We are highly dependent upon our management team, particularly our Chief Executive Officer and President and the rest of our senior management, and other key personnel. Although we have entered into employment letter agreements with all of our executive officers, each of them may terminate their employment with us at any time. The replacement of any of our key personnel likely would involve significant time and costs and may significantly delay or prevent the achievement of our business objectives and could therefore have an adverse effect on our business.
Many of our employees have own or will in the future own a substantial amount of our common stock or a number of common stock options. Our employees may be more likely to leave us if the shares they own have significantly appreciated in value relative to the original purchase prices of the shares, or if the exercise prices of the options that they hold are significantly below the market price of our common stock. Our future success also depends on our ability to continue to attract and retain additional executive officers and other key employees.
We face the risk of product liability claims that could be expensive, divert management’s attention and harm our reputation and business. We may not be able to maintain adequate product liability insurance.
Our business exposes us to the risk of product liability claims that are inherent in the testing, manufacturing and marketing of medical devices. This risk exists even if a device is cleared or approved for commercial sale by the FDA and manufactured in facilities licensed and regulated by the FDA or an applicable foreign regulatory authority. Our Inspire system is designed to affect, and any future products will be designed to affect, important bodily functions and processes. Any side effects, manufacturing defects, misuse or abuse associated with our Inspire system could result in patient injury or death. The medical device industry has historically been subject to extensive litigation over product liability claims, and we cannot offer any assurance that we will not face product liability suits. We may be subject to product liability claims if our Inspire system causes, or merely appears to have caused, patient injury or death. In addition, an injury that is caused by the activities of our suppliers, such as those who provide us with components and raw materials, may be the basis for a claim against us. Product liability claims may be brought against us by patients, healthcare providers or others selling or otherwise coming into
contact with our Inspire system, among others. If we cannot successfully defend ourselves against product liability claims, we will incur substantial liabilities and reputational harm. In addition, regardless of merit or eventual outcome, product liability claims may result in:
•costs of litigation;
•distraction of management’s attention from our primary business;
•the inability to commercialize our Inspire system or new products;
•decreased demand for our Inspire system;
•damage to our business reputation;
•product recalls or withdrawals from the market;
•withdrawal of clinical trial participants;
•substantial monetary awards to patients or other claimants; or
•loss of sales.
While we may attempt to manage our product liability exposure by proactively recalling or withdrawing from the market any defective products, any recall or market withdrawal of our products may delay the supply of those products to our customers and may impact our reputation. We can provide no assurance that we will be successful in initiating appropriate market recall or market withdrawal efforts that may be required in the future or that these efforts will have the intended effect of preventing product malfunctions and the accompanying product liability that may result. Such recalls and withdrawals may also be used by our competitors to harm our reputation for safety or be perceived by patients as a safety risk when considering the use of our products, either of which could have a material adverse effect on our business, financial condition and results of operations.
Although we have product liability and clinical study liability insurance that we believe is appropriate, this insurance is subject to deductibles and coverage limitations. Our current product liability insurance may not continue to be available to us on acceptable terms, if at all, and, if available, coverage may not be adequate to protect us against any future product liability claims. If we are unable to obtain insurance at an acceptable cost or on acceptable terms or otherwise protect against potential product liability claims, we could be exposed to significant liabilities. A product liability claim, recall or other claim with respect to uninsured liabilities or for amounts in excess of insured liabilities could have a material adverse effect on our business, financial condition and results of operations.
If the quality of our Inspire system does not meet the expectations of physicians or patients, then our brand and reputation or our business could be adversely affected.
In the course of conducting our business, we must adequately address quality issues that may arise with our Inspire system, including defects in third-party components included in our Inspire system. Although we have established internal procedures designed to minimize risks that may arise from quality issues, there can be no assurance that we will be able to eliminate or mitigate occurrences of these issues and associated liabilities. In addition, even in the absence of quality issues, we may be subject to claims and liability if the performance of our Inspire system does not live up to the expectations of physicians or patients as a result of the patient’s use of the product. For example, battery life will vary based on usage and therapy settings. Based on STAR trial therapy settings at the 12-month endpoint, the battery in our current generation neurostimulator is generally expected to last for approximately 11 years, but it may not last that long if a patient’s use of the device or chosen level of stimulation is greater than expected. The minimum estimated longevity based on STAR trial results is seven years. If the quality of our Inspire system does not meet the expectations of physicians or patients, then our brand and reputation with those physicians or patients, or our business, financial condition and results of operations, could be adversely affected.
If we choose to acquire new and complementary businesses, products or technologies, we may be unable to complete these acquisitions or to successfully integrate them in a cost-effective and non-disruptive manner.
Our success depends, in part, on our ability to continually enhance and broaden our product offerings in response to changing customer demands, competitive pressures and advances in technologies. Accordingly, although we have no current commitments with respect to any acquisition or investment, we may in the future pursue the acquisition of, or joint ventures relating to, complementary businesses, products or technologies instead of developing them ourselves. We do not know if we will be able to successfully complete any future acquisitions or joint ventures, or whether we will be able to successfully integrate any acquired business, product or technology or retain any key employees related thereto. Integrating any business, product or technology we acquire could be expensive and time-consuming, disrupt our ongoing business and distract our management. If we are unable to integrate any acquired businesses, products or technologies effectively, our business will be adversely affected. In addition, any amortization or charges resulting from the costs of acquisitions could increase our expenses.
Unfavorable global economic conditions could adversely affect our business, financial condition or results of operations.
Our results of operations could be adversely affected by general conditions in the global economy and in the global financial markets. The global financial crisis caused extreme volatility and disruptions in the capital and credit markets. A severe or prolonged economic downturn, such as the global financial crisis, could result in a variety of risks to our business, including weakened demand for our Inspire system, and our ability to raise additional capital when needed on acceptable terms, if at all. A weak or declining economy could also strain our manufacturers or suppliers, possibly resulting in supply disruption, or cause our customers to delay making payments for our services. Any of the foregoing could harm our business and we cannot anticipate all of the ways in which the economic climate and financial market conditions could adversely affect our business.
Failure of a key information technology system, process or site could have an adverse effect on our business.
We rely extensively on information technology systems to conduct our business. These systems affect, among other things, ordering and managing materials from suppliers, shipping products to customers, processing transactions, summarizing and reporting results of operations, complying with regulatory, legal or tax requirements, data security and other processes necessary to manage our business. If our systems are damaged or cease to function properly due to any number of causes, ranging from catastrophic events to power outages to security breaches, and our business continuity plans do not effectively compensate on a timely basis, we may experience interruptions in our operations, which could have an adverse effect on our business. Furthermore, any breach in our IT systems could lead to the unauthorized access, disclosure and use of non-public information, including information from our ADHERE patient registry or other patient information, which is protected by HIPAA and other laws. Any such access, disclosure, or other loss of information could result in legal claims or proceedings, liability under laws that protect the privacy of personal information, and damage to our reputation.
In addition, we accept payments for our sales through credit and debit card transactions, which are handled through a third-party payment processor. As a result, we are subject to a number of risks related to credit and debit card payments. As a result of these transactions, we pay interchange and other fees, which may increase over time and could require us to either increase the prices we charge for our Inspire system or experience an increase in our costs and expenses. In addition, as part of the payment processing process, we transmit our customers’ credit and debit card information to our third-party payment processor. We may in the future become subject to lawsuits or other proceedings for purportedly fraudulent transactions arising out of the actual or alleged theft of our customers’ credit or debit card information if the security of our third-party credit card payment processor is breached. We and our third-party credit card payment processor are also subject to payment card association operating rules, certification requirements and rules governing electronic funds transfers, which could change or be reinterpreted to make it difficult or impossible for us to comply. If we or our third-party credit card payment processor fail to comply with these rules or requirements, we may be subject to fines and higher transaction fees and lose our ability to accept credit and debit card payments from our customers, and there may be an adverse effect on our business.
If our facilities are damaged or become inoperable, we may be unable to continue to research, develop, and supply our Inspire system and, as a result, there could be an adverse effect on our business until we are able to secure a new facility and rebuild our inventory.
We do not have redundant facilities. We perform substantially all of our research and development and back office activity at a single location in Golden Valley, Minnesota. The majority of our finished goods inventory is maintained at a third party location in Tennessee. Our facility, equipment and inventory would be costly to replace and could require substantial lead time to repair or replace. These facilities may be harmed or rendered inoperable by natural or man-made disasters, including, but not limited to, tornadoes, flooding, fire and power outages, which may render it difficult or impossible for us to perform our research, development and commercialization activities for some period of time. The inability to perform those activities, combined with the time it may take to rebuild our inventory of finished product, may result in the loss of customers or harm to our reputation. Although we possess insurance for damage to our property and the disruption of our business, this insurance may not be sufficient to cover all of our potential losses and this insurance may not continue to be available to us on acceptable terms, or at all.
We are subject to anti-bribery, anti-corruption, and anti-money laundering laws, including the U.S. Foreign Corrupt Practices Act, as well as export control laws, customs laws, sanctions laws and other laws governing our operations. If we fail to comply with these laws, we could be subject to civil or criminal penalties, other remedial measures and legal expenses, which could adversely affect our business, results of operations and financial condition.
As we grow our international presence and global operations, we will have increasing obligations to comply with trade and economic sanctions and other restrictions imposed by the U.S., the European Union ("E.U.") and other governments and organizations. The U.S. Departments of Justice, Commerce, State and Treasury and other federal agencies and authorities have a broad range of civil and criminal penalties they may seek to impose against corporations and individuals for violations of economic sanctions laws, export control laws, the U.S. Foreign Corrupt Practices Act ("FCPA") and other federal statutes and regulations, including those established by the Office of Foreign Assets Control ("OFAC"). In addition, the U.K. Bribery Act of 2010 ("the Bribery Act") prohibits both domestic and international bribery, as well as bribery across both private and public sectors. An organization that “fails to prevent bribery” by anyone associated with the organization can be charged under the Bribery Act unless the organization can establish the defense of having implemented “adequate procedures” to prevent bribery. Under these laws and regulations, as well as other anti-corruption laws, anti-money laundering laws, export control laws, customs laws, sanctions laws and other laws governing our operations, various government agencies may require export licenses, may seek to impose modifications to business practices, including cessation of business activities in sanctioned countries or with sanctioned persons or entities and modifications to compliance programs, which may increase compliance costs, and may subject us to fines, penalties and other sanctions. A violation of these laws or regulations would negatively affect our business, financial condition and results of operations.
We have implemented policies and procedures designed to ensure compliance by us and our directors, officers, employees, representatives, consultants and agents with the FCPA, OFAC restrictions, the Bribery Act and other export control, anti-corruption, anti-money-laundering and anti-terrorism laws and regulations. We cannot assure you, however, that our policies and procedures are or will be sufficient or that directors, officers, employees, representatives, consultants and agents have not engaged and will not engage in conduct for which we may be held responsible, nor can we assure you that our business partners have not engaged and will not engage in conduct that could materially affect their ability to perform their contractual obligations to us or even result in our being held liable for such conduct. Violations of the FCPA, OFAC restrictions, the Bribery Act or other export control, anti-corruption, anti-money laundering and anti-terrorism laws or regulations may result in severe criminal or civil sanctions, and we may be subject to other liabilities, which could have a material adverse effect on our business, financial condition and results of operations.
Our indebtedness may limit our flexibility in operating our business and adversely affect our financial health and competitive position.
As of December 31, 2019, we had $24.5 million of indebtedness outstanding under our credit facility with Oxford Finance LLC ("Oxford Finance"). In order to service this indebtedness and any additional indebtedness we may incur in the future, we need to generate cash from our operating activities. Our ability to generate cash is subject, in part, to our ability to successfully execute our business strategy, as well as general economic, financial, competitive, regulatory and other factors beyond our control. We cannot assure you that our business will be able to generate sufficient cash flow from operations or that future borrowings or other financings will be available to us in an amount sufficient to enable us to service our indebtedness and fund our other liquidity needs. To the extent we are required to use cash from operations or the proceeds of any future financing to service our indebtedness instead of funding working capital, capital expenditures or other general corporate purposes, we will be less able to plan for, or react to, changes in our business, industry and in the economy generally. This will place us at a competitive disadvantage compared to our competitors that have less indebtedness.
In addition, the agreement governing the credit facility contains, and any agreements evidencing or governing other future indebtedness may contain, certain covenants that limit our ability to engage in certain transactions that may be in our long-term best interests. Subject to certain limited exceptions, these covenants limit our ability to, among other things:
•convey, sell, lease, transfer, assign, dispose of or otherwise make cash payments consisting of all or any part of our business or property;
•effect certain changes in our business, management, ownership or business locations;
•merge or consolidate with, or acquire all or substantially all of the capital stock or assets of, any other company;
•create, incur, assume or be liable for any additional indebtedness, or create, incur, allow or permit to exist any additional liens;
•pay cash dividends on, make any other distributions in respect of, or redeem, retire or repurchase, any shares of our capital stock;
•make certain investments; and
•enter into transactions with our affiliates.
While we have not previously breached and are not currently in breach of these or any of the other covenants contained in our credit agreement, there can be no guarantee that we will not breach these covenants in the future. Our ability to comply with these covenants may be affected by events and factors beyond our control. In the event that we breach one or more covenants, our lender may choose to declare an event of default and require that we immediately repay all amounts outstanding, terminate any commitment to extend further credit and foreclose on the collateral granted to it to collateralize such indebtedness. The occurrence of any of these events could have a material adverse effect on our business, financial condition and results of operations.
We bear the risk of warranty claims on our Inspire system.
We bear the risk of warranty claims on our Inspire system. We may not be successful in claiming recovery under any warranty or indemnity provided to us by our suppliers or vendors in the event of a successful warranty claim against us by a customer or that any recovery from such vendor or supplier would be adequate. In addition, warranty claims brought by our customers related to third-party components may arise after our ability to bring corresponding warranty claims against such suppliers expires, which could result in costs to us.
We may need substantial additional funding beyond our existing cash resources and may be unable to raise capital when needed, which could force us to delay or reduce our commercialization efforts or product development programs.
Our existing cash, cash equivalents, short-term investments and revenue will be sufficient to meet our capital requirements and fund our operations for at least 12 months. However, we have based these estimates on assumptions that may prove to be incorrect, and we could spend our available financial resources much faster than we currently expect. Any future funding requirements will depend on many factors, including:
•patient, physician and market acceptance of our Inspire therapy;
•the scope, rate of progress and cost of our current or future clinical studies;
•the cost of our research and development activities;
•the cost of filing and prosecuting patent applications and defending and enforcing our patent or other intellectual property rights;
•the cost of defending, in litigation or otherwise, any claims that we infringe third-party patents or other intellectual property rights;
•the cost and timing of additional regulatory clearances or approvals;
•the cost and timing of establishing additional sales and marketing capabilities;
•costs associated with any product recall that may occur;
•the effect of competing technological and market developments;
•the extent to which we acquire or invest in products, technologies and businesses, although we currently have no commitments or agreements relating to any of these types of transactions; and
•the costs of operating as a public company and losing our emerging growth company status.
Any additional equity or debt financing that we raise may contain terms that are not favorable to us or our stockholders. If we raise additional funds by selling additional shares of our common stock or other securities convertible into or exercisable or exchangeable for shares of our common stock, the issuance of such securities will result in dilution to our stockholders. The price per share at which we sell additional shares of our common stock, or securities convertible into or exercisable or exchangeable for shares of our common stock, in future transactions may be higher or lower than the price per share paid by investors in previous offerings of shares of our common stock. Furthermore, investors purchasing any securities we may issue in the future may have rights superior to the rights of a holder of our common stock.
In addition, any future debt financing into which we enter may impose upon us covenants that restrict our operations, including limitations on our ability to incur liens or additional debt, pay dividends, repurchase our common stock, make certain investments and engage in certain merger, consolidation or asset sale transactions. If we raise additional funds through collaboration and licensing arrangements with third-parties, it may be necessary to relinquish some rights to our technologies or our products, or grant licenses on terms that are not favorable to us.
Furthermore, we cannot be certain that additional funding will be available on acceptable terms, if at all. If we do not have, or are not able to obtain, sufficient funds, we may have to delay development or commercialization of our products or license to third-parties the rights to commercialize products or technologies that we would otherwise seek to commercialize. We also may have to reduce marketing, customer support or other resources devoted to our products or cease operations. Any of these factors could harm our business, financial condition and results of operations.
Our ability to use our net operating losses and research and development credit carryforwards to offset future taxable income may be subject to certain limitations.
In general, under Sections 382 and 383 of the Internal Revenue Code of 1986, as amended ("the Code"), a corporation that undergoes an “ownership change,” generally defined as a greater than 50% change by value in its equity ownership over a three-year period, is subject to limitations on its ability to utilize its pre-change net operating losses ("NOLs") and its research and development credit carryforwards to offset future taxable income. We have not performed a detailed analysis to determine whether an ownership change has occurred. Our existing NOLs and research and development credit carryforwards may be subject to limitations arising from previous ownership changes, and if we undergo an ownership change, our ability to utilize NOLs and research and development credit carryforwards could be further limited by Sections 382 and 383 of the Code. In addition, our ability to deduct net interest expense may be limited if we have insufficient taxable income for the year during which the interest is incurred, and any carryovers of such disallowed interest would be subject to the limitation rules similar to those applicable to NOLs and other attributes. Future changes in our stock ownership, some of which might be beyond our control, could result in an ownership change under Section 382 of the Code. For these reasons, in the event we experience a change of control, we may not be able to utilize a material portion of the NOLs, research and development credit carryforwards or disallowed interest expense carryovers, even if we attain profitability.
If we were deemed to be an investment company under the Investment Company Act of 1940, as amended (the “1940 Act”), applicable restrictions could make it impractical for us to continue our business as contemplated and could have a material adverse effect on our business, financial condition and results of operations.
Under Sections 3(a)(1)(A) and (C) of the 1940 Act, a company generally will be deemed to be an “investment company” for purposes of the 1940 Act if (1) it is, or holds itself out as being, engaged primarily, or proposes to engage primarily, in the business of investing, reinvesting or trading in securities or (2) it engages, or proposes to engage, in the business of investing, reinvesting, owning, holding or trading in securities and it owns or proposes to acquire investment securities having a value exceeding 40% of the value of its total assets (exclusive of U.S. government securities and cash items) on an unconsolidated basis. We do not believe that we are an “investment company,” as such term is defined in either of those sections of the 1940 Act.
We intend to conduct our operations so that we will not be deemed an investment company. However, if we were to be deemed an investment company, restrictions imposed by the 1940 Act, including limitations on our capital structure and our ability to transact with affiliates, could make it impractical for us to continue our business as contemplated and could have a material adverse effect on our business, financial condition and results of operations.
Risks Related to Government Regulation
Our products and operations are subject to extensive government regulation and oversight both in the U.S. and abroad, and our failure to comply with applicable requirements could harm our business.
We and our products are subject to extensive regulation in the U.S. and elsewhere, including by the FDA and its foreign counterparts. The FDA and foreign regulatory agencies regulate, among other things, with respect to medical devices: design, development and manufacturing; testing, labeling, content and language of instructions for use and storage; clinical trials; product safety; establishment registration and device listing; marketing, sales and distribution; pre-market clearance and approval; record keeping procedures; advertising and promotion; recalls and field safety corrective actions; post-market surveillance, including reporting of deaths or serious injuries and malfunctions that, if they were to recur, could lead to death or serious injury; post-market approval studies; and product import and export.
The regulations to which we are subject are complex and have tended to become more stringent over time. Regulatory changes could result in restrictions on our ability to carry on or expand our operations, higher than anticipated costs or lower than anticipated sales. The FDA enforces these regulatory requirements through
periodic unannounced inspections. We do not know whether we will pass any future FDA inspections. Failure to comply with applicable regulations could jeopardize our ability to sell our products and result in enforcement actions such as: warning letters; fines; injunctions; civil penalties; termination of distribution; recalls or seizures of products; delays in the introduction of products into the market; total or partial suspension of production; refusal to grant future clearances or approvals; withdrawals or suspensions of current approvals, resulting in prohibitions on sales of our products; and in the most serious cases, criminal penalties.
We may not receive the necessary approvals for our future products or expanded indications, and failure to timely obtain necessary approvals for our future products or expanded indications would adversely affect our ability to grow our business.
An element of our strategy is to continue to upgrade our products, add new features and expand the indications and uses for our current products. In the U.S., before we can market a new medical device, or a new use of, new claim for or significant modification to an existing product, we must first receive PMA from the FDA, In the process of obtaining PMA approval, which was required for our Inspire system, the FDA must determine that a proposed device is safe and effective for its intended use based, in part, on extensive data, including, but not limited to, technical, pre-clinical, clinical trial, manufacturing and labeling data. The PMA process is typically required for devices that are deemed to pose the greatest risk, such as life-sustaining, life-supporting or implantable devices.
Modifications to products that are approved through a PMA application generally require FDA approval. PMA approval can be expensive, lengthy and uncertain. The process of obtaining a PMA is costly and more uncertain than the 510(k) clearance process used for lower risk devices. PMA approvals generally take from one to three years, or even longer, from the time the application is filed with the FDA. In addition, a PMA often requires the performance of one or more clinical trials. Despite the time, effort and cost, a device may not be approved by the FDA. Any delay or failure to obtain necessary regulatory approvals could harm our business. Furthermore, even if we are granted regulatory approval, it may include significant limitations on the indicated uses for the device, which may limit the market for the device.
In the U.S., we have obtained approval of our Inspire system through the PMA pathway. Any modification to the Inspire system that has not been previously approved may require us to submit a new PMA or PMA supplement and obtain FDA approval prior to implementing the change. If the FDA requires us to go through a lengthier, more rigorous examination for future products or modifications to existing products than we had expected, product introductions or modifications could be delayed or canceled, which could adversely affect our ability to grow our business.
The FDA and other regulatory bodies outside the U.S. can delay, limit or deny approval of a device for many reasons, including:
•our inability to demonstrate to the satisfaction of the FDA or the applicable foreign regulatory entity or notified body that our products are safe or effective for their intended uses;
•the disagreement of the FDA or the applicable foreign regulatory body with the design or implementation of our clinical trials or the interpretation of data from pre-clinical studies or clinical trials;
•serious and unexpected adverse device effects experienced by participants in our clinical trials;
•the data from our pre-clinical studies and clinical trials may be insufficient to support approval, where required;
•our inability to demonstrate that the clinical and other benefits of the device outweigh the risks;
•the manufacturing process or facilities we use may not meet applicable requirements; and
•the potential for approval policies or regulations of the FDA or applicable foreign regulatory bodies to change significantly in a manner rendering our clinical data or regulatory filings insufficient for clearance or approval.
In addition, the FDA may change its approval policies, adopt additional regulations or revise existing regulations, or take other actions, which may prevent or delay approval of our future products under development or impact our ability to modify our currently cleared products on a timely basis. Such policy or regulatory changes could impose additional requirements upon us that could delay our ability to obtain new approvals, increase the costs of compliance or restrict our ability to maintain our current approval.
In order to sell our products in member countries of the European Economic Area ("EEA") our products must comply with the essential requirements of the Active Implantable Medical Devices Directive ("AIMDD") (Council Directive 90/385/EEC). Compliance with these requirements is a prerequisite to be able to affix the Conformité Européene ("CE") mark to our products, without which they cannot be sold or marketed in the EEA. To demonstrate compliance with the essential requirements we must undergo a conformity assessment procedure. A conformity assessment procedure requires the intervention of an organization accredited by a member state of the EEA to conduct conformity assessments ("Notified Body"). Depending on the relevant conformity assessment procedure, the Notified Body would typically audit and examine the technical file and the quality system for the manufacture, design and final inspection of our devices. The Notified Body issues a certificate of conformity following successful completion of a conformity assessment procedure conducted in relation to the medical device and its manufacturer and their conformity with the essential requirements. This certificate entitles the manufacturer to affix the CE mark to its medical devices after having prepared and signed a related EC Declaration of Conformity.
As a general rule, demonstration of conformity of medical devices and their manufacturers with the essential requirements must be based, among other things, on the evaluation of clinical data supporting the safety and performance of the products during normal conditions of use. Specifically, a manufacturer must demonstrate that the device achieves its intended performance during normal conditions of use, that the known and foreseeable risks, and any adverse events, are minimized and acceptable when weighed against the benefits of its intended performance, and that any claims made about the performance and safety of the device are supported by suitable evidence. If we fail to remain in compliance with applicable European laws and directives, we would be unable to continue to affix the CE mark to our products, which would prevent us from selling them within the EEA.
In addition, changes are being made to the regulatory framework in the E.U. Conformity assessments under the AIMDD will be replaced by conformity assessments pursuant to the new Medical Device Regulation ("MDR") (Regulation 2017/745). The MDR will implement changes to the E.U. regulatory process that will raise the requirements for clinical evidence on the specific device and be less accepting of claims of equivalence to other CE Marked devices in lieu of clinical evidence. The MDR will also centralize post-market surveillance and vigilance reporting. The MDR is a significant adjustment, not only for industry, but for the notified bodies reviewing the applications. While notified bodies and industry adjust to these new requirements review times for CE Mark applications will likely lengthen. As a result, product introductions or modifications could be delayed or canceled, which could adversely affect our ability to grow our business.
Modifications to our products may require us to obtain new PMA approvals or approvals of a PMA supplement, and if we market modified products without obtaining necessary approvals, we may be required to cease marketing or recall the modified products until required approvals are obtained.
Certain modifications to a PMA-approved device may require approval of a new PMA or a PMA supplement, or alternatively a notification or other submission to the FDA. The FDA may not agree with our decisions regarding whether a new PMA or PMA supplement is necessary. We may make modifications to our approved devices in the future that we believe do not require approval of a new PMA or PMA supplement. If the FDA disagrees with our determination and requires us to submit a new PMA or PMA supplement for modifications to our previously approved products, we may be required to cease marketing or to recall the modified product until we obtain approval, and we may be subject to significant regulatory fines or penalties. In addition, the FDA may not approve our products for the indications that are necessary or desirable for successful commercialization or could require clinical trials to support any modifications. Any delay or failure in obtaining required approvals would adversely affect our ability to introduce new or enhanced products in a timely manner, which in turn would harm our future growth.
Failure to comply with post-marketing regulatory requirements could subject us to enforcement actions, including substantial penalties, and might require us to recall or withdraw a product from the market.
Even though we have obtained approval for the Inspire system, we are subject to ongoing and pervasive regulatory requirements governing, among other things, the manufacture, marketing, advertising, medical device reporting, sale, promotion, registration, and listing of devices. For example, we must submit periodic reports to the FDA as a condition of PMA approval. These reports include safety and effectiveness information about the device after its approval. Failure to submit such reports, or failure to submit the reports in a timely manner, could result in enforcement action by the FDA. Following its review of the periodic reports, the FDA might ask for additional information or initiate further investigation.
In addition, the PMA approval for our Inspire system was subject to several conditions of approval, including a post-market long-term study. Though we believe we have complied with these conditions to date, any failure to comply with the conditions of approval could result in the withdrawal of PMA approval and the inability to continue to market the device. Failure to conduct the required studies in accordance with institutional review board ("IRB") and informed consent requirements, or adverse findings in these studies, could also be grounds for withdrawal of approval of the PMA.
The regulations to which we are subject are complex and have become more stringent over time. Regulatory changes could result in restrictions on our ability to continue or expand our operations, higher than anticipated costs, or lower than anticipated sales. Even after we have obtained the proper regulatory approval to market a device, we have ongoing responsibilities under FDA regulations and applicable foreign laws and regulations. The FDA, state and foreign regulatory authorities have broad enforcement powers. Our failure to comply with applicable regulatory requirements could result in enforcement action by the FDA, state or foreign regulatory authorities, which may include any of the following sanctions:
•untitled letters or warning letters;
•fines, injunctions, consent decrees and civil penalties;
•recalls, termination of distribution, administrative detention, or seizure of our products;
•customer notifications or repair, replacement or refunds;
•operating restrictions or partial suspension or total shutdown of production;
•delays in or refusal to grant our requests for future PMA approvals or foreign regulatory approvals of new products, new intended uses, or modifications to existing products;
•withdrawals or suspensions of our current PMA or foreign regulatory approvals, resulting in prohibitions on sales of our products;
•FDA refusal to issue certificates to foreign governments needed to export products for sale in other countries; and
•criminal prosecution.
Any of these sanctions could result in higher than anticipated costs or lower than anticipated sales and have a material adverse effect on our reputation, business, financial condition and results of operations.
Our products must be manufactured in accordance with federal and state regulations, and we or any of our suppliers or third-party manufacturers could be forced to recall our installed systems or terminate production if we fail to comply with these regulations.
The methods used in, and the facilities used for, the manufacture of our products must comply with the FDA’s Quality System Regulation ("QSR") which is a complex regulatory scheme that covers the procedures and
documentation of the design, testing, production, process controls, quality assurance, labeling, packaging, handling, storage, distribution, installation, servicing and shipping of medical devices. Furthermore, we are required to verify that our suppliers maintain facilities, procedures and operations that comply with our quality standards and applicable regulatory requirements. The FDA enforces the QSR through periodic announced or unannounced inspections of medical device manufacturing facilities, which may include the facilities of subcontractors. Our products are also subject to similar state regulations and various laws and regulations of foreign countries governing manufacturing.
Our third-party manufacturers may not take the necessary steps to comply with applicable regulations, which could cause delays in the delivery of our products. In addition, failure to comply with applicable FDA requirements or later discovery of previously unknown problems with our products or manufacturing processes could result in, among other things: warning letters or untitled letters; fines, injunctions or civil penalties; suspension or withdrawal of approvals; seizures or recalls of our products; total or partial suspension of production or distribution; administrative or judicially imposed sanctions; the FDA’s refusal to grant pending or future clearances or approvals for our products; clinical holds; refusal to permit the import or export of our products; and criminal prosecution of us or our employees.
Any of these actions could significantly and negatively affect supply of our products. If any of these events occurs, our reputation could be harmed, we could be exposed to product liability claims and we could lose customers and experience reduced sales and increased costs.
If treatment guidelines for OSA change or the standard of care evolves, we may need to redesign and seek new marketing authorization from the FDA for one or more of our products.
If treatment guidelines for OSA changes or the standard of care for this condition evolves, we may need to redesign the applicable product and seek new approvals from the FDA. Our PMA approvals from the FDA are based on current treatment guidelines. If treatment guidelines change so that different treatments become desirable, the clinical utility of one or more of our products could be diminished and our business could be adversely affected.
The misuse or off-label use of our Inspire system may harm our reputation in the marketplace, result in injuries that lead to product liability suits or result in costly investigations, fines or sanctions by regulatory bodies if we are deemed to have engaged in the promotion of these uses, any of which could be costly to our business.
Our Inspire system has been approved by the FDA for specific indications. We train our marketing personnel and direct sales force to not promote our Inspire system for uses outside of the FDA-approved indications for use, known as “off-label uses.” We cannot, however, prevent a physician from using our Inspire system off-label, when in the physician’s independent professional medical judgment he or she deems it appropriate. There may be increased risk of injury to patients if physicians attempt to use our Inspire system off-label. Furthermore, the use of our Inspire system for indications other than those approved by the FDA or approved by any foreign regulatory body may not effectively treat such conditions, which could harm our reputation in the marketplace among physicians and patients.
If the FDA or any foreign regulatory body determines that our promotional materials or training constitute promotion of an off-label use, it could request that we modify our training or promotional materials or subject us to regulatory or enforcement actions, including the issuance or imposition of an untitled letter, which is used for violators that do not necessitate a warning letter, injunction, seizure, civil fine or criminal penalties. It is also possible that other federal, state or foreign enforcement authorities might take action under other regulatory authority, such as false claims laws, if they consider our business activities to constitute promotion of an off-label use, which could result in significant penalties, including, but not limited to, criminal, civil and administrative penalties, damages, fines, disgorgement, exclusion from participation in government healthcare programs and the curtailment of our operations.
In addition, physicians may misuse our Inspire system or use improper techniques if they are not adequately trained, potentially leading to injury and an increased risk of product liability. If our Inspire system is misused or
used with improper technique, we may become subject to costly litigation by our customers or their patients. Similarly, in an effort to decrease costs, physicians may also reuse our Inspire system despite it being intended for a single use or may purchase reprocessed Inspire systems from third-party reprocessors in lieu of purchasing a new Inspire system from us, which could result in product failure and liability. As described above, product liability claims could divert management’s attention from our core business, be expensive to defend and result in sizable damage awards against us that may not be covered by insurance.
Our products may cause or contribute to adverse medical events or be subject to failures or malfunctions that we are required to report to the FDA, and if we fail to do so, we would be subject to sanctions that could harm our reputation, business, financial condition and results of operations. The discovery of serious safety issues with our products, or a recall of our products either voluntarily or at the direction of the FDA or another governmental authority, could have a negative impact on us.
We are subject to the FDA’s medical device reporting regulations and similar foreign regulations, which require us to report to the FDA when we receive or become aware of information that reasonably suggests that one or more of our products may have caused or contributed to a death or serious injury or malfunctioned in a way that, if the malfunction were to recur, it could cause or contribute to a death or serious injury. The timing of our obligation to report is triggered by the date we become aware of the adverse event as well as the nature of the event. We may fail to report adverse events of which we become aware within the prescribed timeframe. We may also fail to recognize that we have become aware of a reportable adverse event, especially if it is not reported to us as an adverse event or if it is an adverse event that is unexpected or removed in time from the use of the product. If we fail to comply with our reporting obligations, the FDA could take action, including warning letters, untitled letters, administrative actions, criminal prosecution, imposition of civil monetary penalties, revocation of our device approval, seizure of our products or delay in clearance or approval of future products.
The FDA and foreign regulatory bodies have the authority to require the recall of commercialized products in the event of material deficiencies or defects in design or manufacture of a product or in the event that a product poses an unacceptable risk to health. The FDA’s authority to require a recall must be based on a finding that there is reasonable probability that the device could cause serious injury or death. We may also choose to voluntarily recall a product if any material deficiency is found. A government-mandated or voluntary recall by us could occur as a result of an unacceptable risk to health, component failures, malfunctions, manufacturing defects, labeling or design deficiencies, packaging defects or other deficiencies or failures to comply with applicable regulations. Product defects or other errors may occur in the future.
Depending on the corrective action we take to redress a product’s deficiencies or defects, the FDA may require, or we may decide, that we will need to obtain new approvals for the device before we may market or distribute the corrected device. Seeking such approvals may delay our ability to replace the recalled devices in a timely manner. Moreover, if we do not adequately address problems associated with our devices, we may face additional regulatory enforcement action, including FDA warning letters, product seizure, injunctions, administrative penalties or civil or criminal fines.
Companies are required to maintain certain records of recalls and corrections, even if they are not reportable to the FDA. We may initiate voluntary withdrawals or corrections for our products in the future that we determine do not require notification of the FDA. If the FDA disagrees with our determinations, it could require us to report those actions as recalls and we may be subject to enforcement action. A future recall announcement could harm our reputation with customers, potentially lead to product liability claims against us and negatively affect our sales. Any corrective action, whether voluntary or involuntary, as well as defending ourselves in a lawsuit, will require the dedication of our time and capital, distract management from operating our business and may harm our reputation and financial results.
If we do not obtain and maintain international regulatory registrations or approvals for our products, we will be unable to market and sell our products outside of the U.S.
Sales of our products outside of the U.S. are subject to foreign regulatory requirements that vary widely from country to country. In addition, the FDA regulates exports of medical devices from the U.S. While the regulations of some countries may not impose barriers to marketing and selling our products or only require notification,
others require that we obtain the approval of a specified regulatory body. Complying with foreign regulatory requirements, including obtaining registrations or approvals, can be expensive and time-consuming, and we may not receive regulatory approvals in each country in which we plan to market our products or we may be unable to do so on a timely basis. The time required to obtain registrations or approvals, if required by other countries, may be longer than that required for FDA approval, and requirements for such registrations, clearances or approvals may significantly differ from FDA requirements. If we modify our products, we may need to apply for additional regulatory approvals before we are permitted to sell the modified product. In addition, we may not continue to meet the quality and safety standards required to maintain the authorizations that we have received. If we are unable to maintain our authorizations in a particular country, we will no longer be able to sell the applicable product in that country.
Regulatory approval by the FDA does not ensure registration, clearance or approval by regulatory authorities in other countries, and registration, clearance or approval by one or more foreign regulatory authorities does not ensure registration, clearance or approval by regulatory authorities in other foreign countries or by the FDA. However, a failure or delay in obtaining registration or regulatory clearance or approval in one country may have a negative effect on the regulatory process in others.
Legislative or regulatory reforms in the U.S. or the E.U. may make it more difficult and costly for us to obtain regulatory clearances or approvals for our products or to manufacture, market or distribute our products after clearance or approval is obtained.
From time to time, legislation is drafted and introduced in Congress that could significantly change the statutory provisions governing the regulation of medical devices. In addition, FDA regulations and guidance are often revised or reinterpreted by the FDA in ways that may significantly affect our business and our products. Any new statutes, regulations or revisions or reinterpretations of existing regulations may impose additional costs or lengthen review times of any future products or make it more difficult to obtain approval for, manufacture, market or distribute our products. We cannot determine what effect changes in regulations, statutes, legal interpretation or policies, when and if promulgated, enacted or adopted may have on our business in the future. Such changes could, among other things, require: additional testing prior to obtaining clearance or approval; changes to manufacturing methods; recall, replacement or discontinuance of our products; or additional record keeping.
On May 25, 2017, the new Medical Devices Regulation (2017/745 or “MDR”) entered into force. The MDR repeals and replaces the E.U. Medical Devices Directive and the Active Implantable Medical Devices Directive. Unlike directives, which must be implemented into the national laws of the EEA member states, the regulations would be directly applicable, i.e., without the need for adoption of EEA member state laws implementing them, in all EEA member states and are intended to eliminate current differences in the regulation of medical devices among EEA member States. The Medical Devices Regulation, among other things, is intended to establish a uniform, transparent, predictable and sustainable regulatory framework across the EEA for medical devices and ensure a high level of safety and health while supporting innovation.
The Medical Devices Regulation will, however, only become applicable three years after publication (in May 2020). Once applicable, the new regulations will among other things:
•strengthen the rules on placing devices on the market and reinforce surveillance once they are available;
•establish explicit provisions on manufacturers’ responsibilities for the follow-up of the quality, performance and safety of devices placed on the market;
•improve the traceability of medical devices throughout the supply chain to the end-user or patient through a unique identification number;
•set up a central database to provide patients, healthcare professionals and the public with comprehensive information on products available in the E.U.;
•strengthened rules for the assessment of certain high-risk devices, such as implants, which may have to undergo an additional check by experts before they are placed on the market.
These modifications may have an effect on the way we conduct our business in the EEA.
We are subject to certain federal, state and foreign fraud and abuse laws, health information privacy and security laws and transparency laws, which, if violated, could subject us to substantial penalties. Additionally, any challenge to or investigation into our practices under these laws could cause adverse publicity and be costly to respond to, and thus could harm our business.
There are numerous U.S. federal and state, as well as foreign, laws pertaining to healthcare fraud and abuse, including anti-kickback, false claims and physician transparency laws. Our business practices and relationships with providers are subject to scrutiny under these laws. We may also be subject to privacy and security regulation related to patient, customer, employee and other third-party information by both the federal government and the states and foreign jurisdictions in which we conduct our business. The healthcare laws and regulations that may affect our ability to operate include, but are not limited to:
•the federal Anti-Kickback Statute, which prohibits, among other things, persons and entities from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce either the referral of an individual or furnishing or arranging for a good or service, for which payment may be made, in whole or in part, under federal healthcare programs, such as Medicare and Medicaid. A person or entity does not need to have actual knowledge of the statute or specific intent to violate it to have committed a violation. The U.S. government has interpreted this law broadly to apply to the marketing and sales activities of manufacturers. Moreover, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal civil False Claims Act. Violations of the federal Anti-Kickback Statute may result in civil monetary penalties up to $100,000 for each violation, plus up to three times the remuneration involved. Civil penalties for such conduct can further be assessed under the federal False Claims Act. Violations can also result in criminal penalties, including criminal fines of up to $100,000 and imprisonment of up to 10 years. Similarly, violations can result in exclusion from participation in government healthcare programs, including Medicare and Medicaid;
•the federal civil and criminal false claims laws and civil monetary penalties laws, including the federal civil False Claims Act, which prohibit, among other things, individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid or other federal healthcare programs that are false or fraudulent. These laws can apply to manufacturers who provide information on coverage, coding, and reimbursement of their products to persons who bill third-party payers. Private individuals can bring False Claims Act “qui tam” actions, on behalf of the government and such individuals, commonly known as “whistleblowers,” may share in amounts paid by the entity to the government in fines or settlement. When an entity is determined to have violated the federal civil False Claims Act, the government may impose civil fines and penalties ranging from $11,181 to $22,363 for each false claim, plus treble damages, and exclude the entity from participation in Medicare, Medicaid and other federal healthcare programs;
•the federal Civil Monetary Penalties Law, which prohibits, among other things, offering or transferring remuneration to a federal healthcare beneficiary that a person knows or should know is likely to influence the beneficiary’s decision to order or receive items or services reimbursable by the government from a particular provider or supplier;
•HIPAA, which created additional federal criminal statutes that prohibit, among other things, executing a scheme to defraud any healthcare benefit program and making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it to have committed a violation;
•the federal Physician Sunshine Act under the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively referred to as the Affordable Care Act, which require certain applicable manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program ("CHIP") to report annually to the DHHS Centers for Medicare and Medicaid Services ("CMS") information
related to payments and other transfers of value to physicians, certain other healthcare providers, and teaching hospitals, and applicable manufacturers and group purchasing organizations, to report annually ownership and investment interests held by physicians and their immediate family members. Applicable manufacturers are required to submit annual reports to CMS. Failure to submit required information may result in civil monetary penalties of $11,562 per failure up to an aggregate of $173,436 per year (or up to an aggregate of $1.156 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately, and completely reported in an annual submission, and may result in liability under other federal laws or regulations;
•HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009 ("HITECH Act") and their respective implementing regulations, which impose requirements on certain covered healthcare providers, health plans and healthcare clearinghouses as well as their business associates that perform services for them that involve individually identifiable health information, relating to the privacy, security and transmission of individually identifiable health information without appropriate authorization, including mandatory contractual terms as well as directly applicable privacy and security standards and requirements. Failure to comply with the HIPAA privacy and security standards can result in civil monetary penalties up to $58,490 per violation, not to exceed $1.75 million per calendar year for non-compliance of an identical provision, and, in certain circumstances, criminal penalties with fines up to $250,000 per violation and/or imprisonment. State attorneys general can also bring a civil action to enjoin a HIPAA violation or to obtain statutory damages on behalf of residents of his or her state; and
•analogous state and foreign law equivalents of each of the above federal laws, such as anti-kickback and false claims laws which may apply to items or services reimbursed by any third-party payor, including commercial insurers or patients; state laws that require device companies to comply with the industry’s voluntary compliance guidelines and the applicable compliance guidance promulgated by the federal government or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; state laws that require device manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or marketing expenditures; consumer protection and unfair competition laws, which broadly regulate marketplace activities and activities that potentially harm customers, foreign and state laws, including the GDPR and CCPA governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts; and state laws related to insurance fraud in the case of claims involving private insurers.
These laws and regulations, among other things, constrain our business, marketing and other promotional activities by limiting the kinds of financial arrangements, including sales programs, we may have with hospitals, physicians or other potential purchasers of our products. Due to the breadth of these laws, the narrowness of statutory exceptions and regulatory safe harbors available, and the range of interpretations to which they are subject, it is possible that some of our current or future practices might be challenged under one or more of these laws.
To enforce compliance with the healthcare regulatory laws, certain enforcement bodies have recently increased their scrutiny of interactions between healthcare companies and healthcare providers, which has led to a number of investigations, prosecutions, convictions and settlements in the healthcare industry. Responding to investigations can be time-and resource-consuming and can divert management’s attention from the business. Additionally, as a result of these investigations, healthcare providers and entities may have to agree to additional compliance and reporting requirements as part of a consent decree or corporate integrity agreement. Any such investigation or settlement could increase our costs or otherwise have an adverse effect on our business. Even an unsuccessful challenge or investigation into our practices could cause adverse publicity, and be costly to respond to. If our operations are found to be in violation of any of the healthcare laws or regulations described above or any other healthcare regulations that apply to us, we may be subject to penalties, including administrative, civil and criminal penalties, damages, fines, exclusion from participation in government healthcare programs, such as Medicare and Medicaid, imprisonment, contractual damages, reputational harm, disgorgement and the curtailment or restructuring of our operations.
We are subject to U.S. federal, state, and foreign laws and regulations imposing obligations on how we collect, store and process personal information. Our actual or perceived failure to comply with such obligations could harm our business. Ensuring compliance with such laws could also impair our efforts to maintain and expand our customer base, and thereby decrease our revenue.
In the conduct of our business, we process personal data, including health-related personal data. The U.S. federal government and various states have adopted or proposed laws, regulations, guidelines and rules for the collection, distribution, use and storage of personal information of individuals. We may also be subject to U.S. federal rules, regulations and guidance concerning data security for medical devices, including guidance from the FDA. State privacy and security laws vary from state to state and, in some cases, can impose more restrictive requirements than U.S. federal law. Where state laws are more protective, we must comply with the stricter provisions. In addition to fines and penalties that may be imposed for failure to comply with state law, some states also provide for private rights of action to individuals for misuse of personal information.
The E.U. and EEA (and their member states) also have laws and regulations, including the GDPR, dealing with the collection, use and processing of personal data of individuals located in the E.U. or EEA, which are often more restrictive than those in the U.S., including, for example under the GDPR, mandatory data breach notification, new and strengthened rights for data subjects, detailed disclosures to data subjects, additional obligations when contracting with service providers and which restrict transfers of personal data from the E.U. or EEA to the U.S. (and other non-EEA countries unless deemed ‘adequate’ by the E.U. Commission) unless certain requirements are met. We are working with external advisers to undertake a robust program that we believe will ensure compliance with these obligations which is likely to require us to expend capital and other resources. Our obligations under the GDPR may conflict with the requirements of other privacy laws and regulations in other jurisdictions and our practices relating to personal data may differ globally in response to local requirements. In addition, these rules are from time to time under scrutiny. For example, there is ongoing litigation challenging the commonly used transfer mechanism under the GDPR, the E.U. Commission approved model clauses. It is possible that the model clauses (also called “standard contractual clauses”) will be invalidated by the European courts.
From May 25, 2018 onwards, we have been subject to the requirements of the GDPR (and national laws implementing the GDPR) because we are “established” in certain E.U. countries and we are processing personal data of individuals located in the E.U. and EEA in the context of these establishments, as well as offering of goods to, and/or monitoring the behavior of, individuals in the E.U. and EEA in connection with our clinical trials. We have enlisted the help of external advisors to provide assistance in implementing a robust program that we believe will ensure compliance with these obligations which is likely to require us to expend capital and other resources. If we do not comply with our obligations under the GDPR, we could be exposed to significant fines the greater of EUR 20 million or 4% of total global annual turnover for certain breaches. In addition to the foregoing, a breach of the GDPR could result in regulatory investigations, reputational damage, orders to cease/ change our use of data, enforcement notices, as well potential civil claims including class action type litigation where individuals suffer harm.
We are also subject to evolving E.U. and EEA privacy laws on cookies and e-marketing. The E.U. is in the process of replacing the E-Privacy Directive (2002/58/EC) with a new set of rules taking the form of a regulation, which will be directly implemented in the laws of each European Member State. The draft E-Privacy Regulation imposes strict opt-in marketing rules with limited exceptions for business-to-business communications, alters rules on third-party cookies, web beacons and similar technology and significantly increases fining powers to the same levels as the GDPR (i.e. the greater of EUR 20 million or 4% of total global annual turnover for certain breaches). The E-Privacy Regulation is expected to be agreed during 2020 or during 2021 and then a two year transition period will follow before it is in force. We have enlisted the help of external advisors to provide assistance in implementing a robust program that we believe will ensure compliance with these obligations which is likely to require us to expend capital and other resources.
Any actual or perceived failure by us, our employees or contractors, our partners, our service providers, or the third parties with whom we work, to comply with privacy or security laws, policies, legal obligations or industry standards, or any security incident that results in the unauthorized release or transfer of personal information, may result in governmental enforcement actions and investigations including by E.U. regulators and U.S. federal and
state regulatory authorities as well as fines and penalties, litigation, including by consumer advocacy groups, and/or adverse publicity and could cause our customers, their patients and other healthcare professionals to lose trust in us, which could harm our reputation and have a material adverse effect on our business, financial condition and results of operations.
Healthcare policy changes, including recently enacted legislation reforming the U.S. healthcare system, could harm our business, financial condition and results of operations.
In the U.S., there have been and continue to be a number of legislative initiatives to contain healthcare costs. In March 2010, the Affordable Care Act was enacted in the U.S., which made a number of substantial changes in the way healthcare is financed by both governmental and private insurers. Among other ways in which it may affect our business, the Affordable Care Act:
•imposed an annual excise tax of 2.3% on any entity that manufactures or imports medical devices offered for sale in the U.S., with limited exceptions (described in more detail below), although the effective rate paid may be lower. Through a series of legislative amendments, the tax was suspended , effective January 1, 2016, and subsequently repealed altogether on December 20, 2019;
•established a new Patient-Centered Outcomes Research Institute to oversee and identify priorities in comparative clinical effectiveness research in an effort to coordinate and develop such research;
•implemented payment system reforms including a national pilot program on payment bundling to encourage hospitals, physicians and other providers to improve the coordination, quality and efficiency of certain healthcare services through bundled payment models; and
•expanded the eligibility criteria for Medicaid programs.
We do not yet know the full impact that the Affordable Care Act will have on our business. The taxes imposed by the Affordable Care Act and the expansion in the government’s role in the U.S. healthcare industry may result in decreased profits to us, lower reimbursement by payors for our Inspire system, and/or reduced medical procedure volumes, all of which may have a material adverse effect on our business, financial condition and results of operations. The Trump Administration and the U.S. Congress may take further action regarding the Affordable Care Act, including, but not limited to, repeal or replacement. Most recently, the Tax Cuts and Jobs Act of 2017 was enacted, which, among other things, removes penalties for not complying with the individual mandate to carry health insurance. On December 14, 2018, a U.S. District Court Judge in the Northern District of Texas, ruled that the Affordable Care Act’s individual mandate to carry insurance coverage is a critical and inseverable feature of the Affordable Care Act, and therefore, because it was repealed as part of the Tax Cuts and Jobs Act, the remaining provisions of the Affordable Care Act are invalid as well. On December 18, 2019, the U.S. Court of Appeals for the 5th Circuit upheld the District Court's decision that the individual mandate was unconstitutional but remanded the case back to the District Court to determine whether the remaining provisions of the Affordable Care Act are invalid as well. It is unclear how these decisions, subsequent appeals, and other efforts to challenge, repeal or replace the Affordable Care Act will impact the Act or our business. Additionally, all or a portion of the Affordable Care Act and related subsequent legislation may be modified, repealed or otherwise invalidated through judicial challenge, which could result in lower numbers of insured individuals, reduced coverage for insured individuals and adversely affect our business.
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. On August 2, 2011, the Budget Control Act of 2011 was signed into law, which, among other things, reduced Medicare payments to providers by 2% per fiscal year, effective on April 1, 2013 and, due to subsequent legislative amendments to the statute, will remain in effect through 2029 unless additional Congressional action is taken. On January 2, 2013, the American Taxpayer Relief Act of 2012 was signed into law, which, among other things, reduced Medicare payments to several providers, including hospitals, and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. The Medicare Access and CHIP Reauthorization Act of 2015 ("MACRA") enacted on April 16, 2015, repealed the formula by which Medicare made annual payment adjustments to physicians and replaced the former formula with fixed annual updates and a new system of incentive payments began in 2019 that are based on various performance
measures and physicians’ participation in alternative payment models such as accountable care organizations. It is unclear what effect new quality and payment programs, such as MACRA, may have on our business, financial condition, results of operations or cash flows.
We expect additional state and federal healthcare policies and reform measures to be adopted in the future, any of which could limit reimbursement for healthcare products and services or otherwise result in reduced demand for our Inspire system or additional pricing pressure and have a material adverse effect on our industry generally and on our customers. Any changes of, or uncertainty with respect to, future coverage or reimbursement rates could affect demand for our Inspire system, which in turn could impact our ability to successfully commercialize our Inspire system and could have a material adverse effect on our business, financial condition and results of operations.
Our business involves the use of hazardous materials and our third-party manufacturers must comply with environmental laws and regulations, which may be expensive and restrict how we do business.
Our third-party manufacturers’ activities may involve the controlled storage, use and disposal of hazardous materials. Our manufacturers are subject to federal, state, local, and foreign laws and regulations governing the use, generation, manufacture, storage, handling and disposal of these hazardous materials. We currently carry no insurance specifically covering environmental claims relating to the use of hazardous materials. Although we believe the safety procedures of our manufacturers for handling and disposing of these materials and waste products comply with the standards prescribed by these laws and regulations, we cannot eliminate the risk of accidental injury or contamination from the use, storage, handling or disposal of hazardous materials. In the event of an accident, state or federal or other applicable authorities may curtail our manufacturers’ use of these materials and interrupt their business operations which could adversely affect our business.
The clinical trial process required to obtain regulatory approvals is lengthy and expensive with uncertain outcomes. If clinical studies of our future products do not produce results necessary to support regulatory clearance or approval in the U.S. or, with respect to our current or future products, elsewhere, we will be unable to expand the indications for or commercialize these products and may incur additional costs or experience delays in completing, or ultimately be unable to complete, the commercialization of those products.
We have obtained PMA approval for our Inspire system. In order to obtain PMA approval for a device, the sponsor must conduct well-controlled clinical trials designed to assess the safety and efficacy of the product candidate. Conducting clinical trials is a complex and expensive process, can take many years, and outcomes are inherently uncertain. We incur substantial expense for, and devote significant time to, clinical trials but cannot be certain that the trials will ever result in commercial revenue. We may experience significant setbacks in clinical trials, even after earlier clinical trials showed promising results, and failure can occur at any time during the clinical trial process. Any of our products may malfunction or may produce undesirable adverse effects that could cause us or regulatory authorities to interrupt, delay or halt clinical trials. We, the FDA, or another regulatory authority may suspend or terminate clinical trials at any time to avoid exposing trial participants to unacceptable health risks.
Successful results of pre-clinical studies are not necessarily indicative of future clinical trial results, and predecessor clinical trial results may not be replicated in subsequent clinical trials. Additionally, the FDA may disagree with our interpretation of the data from our pre-clinical studies and clinical trials, or may find the clinical trial design, conduct or results inadequate to prove safety or efficacy, and may require us to pursue additional pre-clinical studies or clinical trials, which could further delay the clearance or approval of our products. The data we collect from our pre-clinical studies and clinical trials may not be sufficient to support FDA clearance or approval, and if we are unable to demonstrate the safety and efficacy of our future products in our clinical trials, we will be unable to obtain regulatory clearance or approval to market our products.
In addition, we may estimate and publicly announce the anticipated timing of the accomplishment of various clinical, regulatory and other product development goals, which are often referred to as milestones. These milestones could include the obtainment of the right to affix the CE mark in the E.U.; the submission to the FDA of an IDE application to commence a pivotal clinical trial for a new product candidate; the enrollment of patients in clinical trials; the release of data from clinical trials; and other clinical and regulatory events. The actual timing of
these milestones could vary dramatically compared to our estimates, in some cases for reasons beyond our control. We cannot assure you that we will meet our projected milestones and if we do not meet these milestones as publicly announced, the commercialization of our products may be delayed and, as a result, our stock price may decline.
Clinical trials are necessary to support PMA applications and may be necessary to support PMA supplements for modified versions of our marketed device products. This would require the enrollment of large numbers of suitable subjects, which may be difficult to identify, recruit and maintain as participants in the clinical trial. The clinical trials supporting the PMA application for our Inspire system involved 126 randomized patients. Adverse outcomes in the post-approval studies could also result in restrictions or withdrawal of approval of the PMA. We will likely need to conduct additional clinical studies in the future to support new indications for our products or for approvals or clearances of new product lines, or for the approval of the use of our products in some foreign countries. Clinical testing is difficult to design and implement, can take many years, can be expensive and carries uncertain outcomes. The initiation and completion of any of these studies may be prevented, delayed, or halted for numerous reasons. We may experience a number of events during that could adversely affect the costs, timing or successful completion of our clinical trials, including:
•we may be required to submit an IDE application to FDA, which must become effective prior to commencing human clinical trials, and FDA may reject our IDE application and notify us that we may not begin investigational trials;
•regulators and other comparable foreign regulatory authorities may disagree as to the design or implementation of our clinical trials;
•regulators and/or IRBs, or other reviewing bodies may not authorize us or our investigators to commence a clinical trial, or to conduct or continue a clinical trial at a prospective or specific trial site;
•we may not reach agreement on acceptable terms with prospective contract research organizations ("CROs") and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites;
•clinical trials may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical trials or abandon product development programs;
•the number of subjects or patients required for clinical trials may be larger than we anticipate, enrollment in these clinical trials may be insufficient or slower than we anticipate, and the number of clinical trials being conducted at any given time may be high and result in fewer available patients for any given clinical trial, or patients may drop out of these clinical trials at a higher rate than we anticipate;
•our third-party contractors, including those manufacturing products or conducting clinical trials on our behalf, may fail to comply with regulatory requirements or meet their contractual obligations to us in a timely manner, or at all;
•we might have to suspend or terminate clinical trials for various reasons, including a finding that the subjects are being exposed to unacceptable health risks;
•we may have to amend clinical trial protocols or conduct additional studies to reflect changes in regulatory requirements or guidance, which we may be required to submit to an IRB and/or regulatory authorities for re-examination;
•regulators, IRBs, or other parties may require or recommend that we or our investigators suspend or terminate clinical research for various reasons, including safety signals or noncompliance with regulatory requirements;
•the cost of clinical trials may be greater than we anticipate;
•clinical sites may not adhere to the clinical protocol or may drop out of a clinical trial;
•we may be unable to recruit a sufficient number of clinical trial sites;
•regulators, IRBs, or other reviewing bodies may fail to approve or subsequently find fault with our manufacturing processes or facilities of third-party manufacturers with which we enter into agreement for clinical and commercial supplies, the supply of devices or other materials necessary to conduct clinical trials may be insufficient, inadequate or not available at an acceptable cost, or we may experience interruptions in supply;
•approval policies or regulations of FDA or applicable foreign regulatory agencies may change in a manner rendering our clinical data insufficient for approval; and
•our current or future products may have undesirable side effects or other unexpected characteristics.
Patient enrollment in clinical trials and completion of patient follow-up depend on many factors, including the size of the patient population, the nature of the trial protocol, the proximity of patients to clinical sites, the eligibility criteria for the clinical trial, patient compliance, competing clinical trials and clinicians’ and patients’ perceptions as to the potential advantages of the product being studied in relation to other available therapies, including any new treatments that may be approved for the indications we are investigating. For example, patients may be discouraged from enrolling in our clinical trials if the trial protocol requires them to undergo extensive post-treatment procedures or follow-up to assess the safety and efficacy of a product candidate, or they may be persuaded to participate in contemporaneous clinical trials of a competitor’s product candidate. In addition, patients participating in our clinical trials may drop out before completion of the trial or experience adverse medical events unrelated to our products. Delays in patient enrollment or failure of patients to continue to participate in a clinical trial may delay commencement or completion of the clinical trial, cause an increase in the costs of the clinical trial and delays, or result in the failure of the clinical trial.
Clinical trials must be conducted in accordance with the laws and regulations of the FDA and other applicable regulatory authorities’ legal requirements, regulations or guidelines, and are subject to oversight by these governmental agencies and IRBs at the medical institutions where the clinical trials are conducted. In addition, clinical trials must be conducted with supplies of our devices produced under current good manufacturing practice requirements and other regulations. Furthermore, we rely on CROs, and clinical trial sites to ensure the proper and timely conduct of our clinical trials and while we have agreements governing their committed activities, we have limited influence over their actual performance. We depend on our collaborators and on medical institutions and CROs to conduct our clinical trials in compliance with good clinical practice ("GCP") requirements. To the extent our collaborators or the CROs fail to enroll participants for our clinical trials, fail to conduct the study in accordance with GCP requirements or are delayed for a significant time in the execution of trials, including achieving full enrollment, we may be affected by increased costs, program delays or both. In addition, clinical trials that are conducted in countries outside the U.S. may subject us to further delays and expenses as a result of increased shipment costs, additional regulatory requirements and the engagement of non-U.S. CROs, as well as expose us to risks associated with clinical investigators who are unknown to the FDA, and different standards of diagnosis, screening and medical care.
Failure can occur at any stage of clinical testing. Our clinical studies may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical and non-clinical testing in addition to those we have planned. Our failure to adequately demonstrate the safety and efficacy of our system or any product we may develop in the future would prevent receipt of regulatory clearance or approval and, ultimately, the commercialization of that product or indication for use. Even if our future products are cleared or approved in the U.S., commercialization of our products in foreign countries would require approval by regulatory authorities in those countries. Approval procedures vary among jurisdictions and can involve requirements and administrative review periods different from, and greater than, those in the U.S., including additional preclinical studies or clinical trials. Any of these occurrences could have an adverse effect on our business, financial condition and results of operations.
Changes in funding for the FDA, the SEC and other government agencies could hinder their ability to hire and retain key leadership and other personnel, prevent new products and services from being developed or commercialized in a timely manner or otherwise prevent those agencies from performing normal functions on which the operation of our business may rely, which could negatively impact our business.
The ability of the FDA to review and approve new products or take action with respect to other regulatory matters can be affected by a variety of factors, including government budget and funding levels, ability to hire and retain key personnel and accept payment of user fees and statutory, regulatory and policy changes. Average review times at the agency have fluctuated in recent years as a result. In addition, government funding of the SEC and other government agencies on which our operations may rely, including those that fund research and development activities is subject to the political process, which is inherently fluid and unpredictable.
Disruptions at the FDA and other agencies may also slow the time necessary for new drugs to be reviewed or approved, or for other actions to be taken, by relevant government agencies, which would adversely affect our business. For example, over the last several years, including for 35 days beginning on December 22, 2018, the U.S. government has shut down several times and certain regulatory agencies, such as the FDA and the SEC, have had to furlough critical FDA, SEC and other government employees and stop critical activities. If a prolonged government shutdown occurs, it could significantly impact the ability of the FDA to timely review and process our regulatory submissions, which could have a material adverse effect on our business. Similarly, a prolonged government shutdown could prevent the timely review of our patent applications by the United States Patent and Trademark Office ("USPTO"), which could delay the issuance of any U.S. patents to which we might otherwise be entitled. Further, in our operations as a public company, future government shutdowns could impact our ability to access the public markets and obtain necessary capital in order to properly fund our business.
Risks Related to Intellectual Property Matters
If we are unable to adequately protect our intellectual property rights, or if we are accused of infringing on the intellectual property rights of others, our competitive position could be harmed or we could be required to incur significant expenses to enforce or defend our rights.
Our commercial success will depend in part on our success in obtaining and maintaining issued patents, trademarks and other intellectual property rights in the U.S. and elsewhere and protecting our proprietary technology. If we do not adequately protect our intellectual property and proprietary technology, competitors may be able to use our technologies or the goodwill we have acquired in the marketplace and erode or negate any competitive advantage we may have, which could harm our business and ability to achieve profitability.
Some of our intellectual property rights depend on a licensing agreement with a third party, and our patent coverage includes protection provided by licensed patents. Many of these licensed patents are over ten years old and the standard life of a patent is 20 years from its initial filing date. If in the future we no longer have rights to one or more of these licensed patents, our patent coverage may be compromised, which in turn could affect our ability to protect our Inspire system or defend against competitors.
We own numerous issued patents and pending patent applications that relate to our system. As of December 31, 2019, we had rights to 28 issued U.S. patents, 26 issued foreign patents, 39 pending U.S. patent applications, and 47 pending foreign patent applications. Assuming all required fees are paid, issued U.S. patents owned by us will expire between 2020 and 2036.
We cannot provide any assurances that any of our patents have, or that any of our pending patent applications that mature into issued patents will include, claims with a scope sufficient to protect our Inspire system, any additional features we develop for our Inspire system or any new products. Other parties may have developed technologies that may be related or competitive to our system, may have filed or may file patent applications and may have received or may receive patents that overlap or conflict with our patent applications, either by claiming the same methods or devices or by claiming subject matter that could dominate our patent position. The patent positions of medical device companies, including our patent position, may involve complex legal and factual questions, and, therefore, the scope, validity and enforceability of any patent claims that we may obtain cannot
be predicted with certainty. Patents, if issued, may be challenged, deemed unenforceable, invalidated or circumvented. Proceedings challenging our patents could result in either loss of the patent or denial of the patent application or loss or reduction in the scope of one or more of the claims of the patent or patent application. In addition, such proceedings may be costly. Thus, any patents that we may own may not provide any protection against competitors. Furthermore, an adverse decision in an interference proceeding can result in a third party receiving the patent right sought by us, which in turn could affect our ability to commercialize our products.
Though an issued patent is presumed valid and enforceable, its issuance is not conclusive as to its validity or its enforceability and it may not provide us with adequate proprietary protection or competitive advantages against competitors with similar products. Competitors could purchase our Inspire system and attempt to replicate some or all of the competitive advantages we derive from our development efforts, willfully infringe our intellectual property rights, design around our patents, or develop and obtain patent protection for more effective technologies, designs or methods. We may be unable to prevent the unauthorized disclosure or use of our technical knowledge or trade secrets by consultants, suppliers, vendors, former employees and current employees. The laws of some foreign countries do not protect our proprietary rights to the same extent as the laws of the U.S., and we may encounter significant problems in protecting our proprietary rights in these countries.
Our ability to enforce our patent rights depends on our ability to detect infringement. It may be difficult to detect infringers who do not advertise the components that are used in their products. Moreover, it may be difficult or impossible to obtain evidence of infringement in a competitor’s or potential competitor’s product. We may not prevail in any lawsuits that we initiate and the damages or other remedies awarded if we were to prevail may not be commercially meaningful.
In addition, proceedings to enforce or defend our patents could put our patents at risk of being invalidated, held unenforceable or interpreted narrowly. Such proceedings could also provoke third parties to assert claims against us, including that some or all of the claims in one or more of our patents are invalid or otherwise unenforceable. If any of our patents covering our Inspire system are invalidated or found unenforceable, or if a court found that valid, enforceable patents held by third parties covered one or more of our products, our competitive position could be harmed or we could be required to incur significant expenses to enforce or defend our rights.
The degree of future protection for our proprietary rights is uncertain, and we cannot ensure that:
•any of our patents, or any of our pending patent applications, if issued, will include claims having a scope sufficient to protect our Inspire system;
•any of our pending patent applications will issue as patents;
•we will be able to successfully commercialize our products on a substantial scale, if approved, before our relevant patents we may have expire;
•we were the first to make the inventions covered by each of our patents and pending patent applications;
•we were the first to file patent applications for these inventions;
•others will not develop similar or alternative technologies that do not infringe our patents; any of our patents will be found to ultimately be valid and enforceable;
•any patents issued to us will provide a basis for an exclusive market for our commercially viable products, will provide us with any competitive advantages or will not be challenged by third parties;
•we will develop additional proprietary technologies or products that are separately patentable; or
•our commercial activities or products will not infringe upon the patents of others.
We rely, in part, upon unpatented trade secrets, unpatented know-how and continuing technological innovation to develop and maintain our competitive position, which we seek to protect, in part, by confidentiality agreements with our employees and our collaborators and consultants. We also have agreements with our employees and consultants that obligate them to assign their inventions to us and have non-compete agreements with some, but not all, of our consultants. It is possible that technology relevant to our business will be independently developed by a person that is not a party to such an agreement. Furthermore, if the employees and consultants who are parties to these agreements breach or violate the terms of these agreements, we may not have adequate remedies for any such breach or violation, and we could lose our trade secrets through such breaches or violations. Further, our trade secrets could otherwise become known or be independently discovered by our competitors.
Litigation or other proceedings or third-party claims of intellectual property infringement could require us to spend significant time and money and could prevent us from selling our products or affect our stock price.
Our commercial success will depend in part on not infringing the patents or violating the other proprietary rights of others. Significant litigation regarding patent rights occurs in our industry. Our competitors in both the U.S. and abroad, many of which have substantially greater resources and have made substantial investments in patent portfolios and competing technologies, may have applied for or obtained or may in the future apply for and obtain, patents that will prevent, limit or otherwise interfere with our ability to make, use and sell our products. We do not always conduct independent reviews of patents issued to third parties. In addition, patent applications in the U.S. and elsewhere can be pending for many years before issuance, or unintentionally abandoned patents or applications can be revived, so there may be applications of others now pending or recently revived patents of which we are unaware. These applications may later result in issued patents, or the revival of previously abandoned patents, that will prevent, limit or otherwise interfere with our ability to make, use or sell our products. Third parties may, in the future, assert claims that we are employing their proprietary technology without authorization, including claims from competitors or from non-practicing entities that have no relevant product revenue and against whom our own patent portfolio may have no deterrent effect. As we continue to commercialize our products in their current or updated forms, launch new products and enter new markets, we expect competitors may claim that one or more of our products infringe their intellectual property rights as part of business strategies designed to impede our successful commercialization and entry into new markets. The large number of patents, the rapid rate of new patent applications and issuances, the complexities of the technology involved, and the uncertainty of litigation may increase the risk of business resources and management’s attention being diverted to patent litigation. We have, and we may in the future, receive letters or other threats or claims from third parties inviting us to take licenses under, or alleging that we infringe, their patents.
Moreover, we may become party to future adversarial proceedings regarding our patent portfolio or the patents of third parties. Such proceedings could include supplemental examination or contested post-grant proceedings such as review, reexamination, inter partes review, interference or derivation proceedings before the USPTO and challenges in U.S. District Court. Patents may be subjected to opposition, post-grant review or comparable proceedings lodged in various foreign, both national and regional, patent offices. The legal threshold for initiating litigation or contested proceedings may be low, so that even lawsuits or proceedings with a low probability of success might be initiated. Litigation and contested proceedings can also be expensive and time-consuming, and our adversaries in these proceedings may have the ability to dedicate substantially greater resources to prosecuting these legal actions than we can. We may also occasionally use these proceedings to challenge the patent rights of others. We cannot be certain that any particular challenge will be successful in limiting or eliminating the challenged patent rights of the third party.
Any lawsuits resulting from such allegations could subject us to significant liability for damages and invalidate our proprietary rights. Any potential intellectual property litigation also could force us to do one or more of the following:
•stop making, selling or using products or technologies that allegedly infringe the asserted intellectual property;
•lose the opportunity to license our technology to others or to collect royalty payments based upon successful protection and assertion of our intellectual property rights against others; incur significant legal expenses;
•pay substantial damages or royalties to the party whose intellectual property rights we may be found to be infringing;
•pay the attorney’s fees and costs of litigation to the party whose intellectual property rights we may be found to be infringing;
•redesign those products that contain the allegedly infringing intellectual property, which could be costly, disruptive and infeasible; and
•attempt to obtain a license to the relevant intellectual property from third parties, which may not be available on reasonable terms or at all, or from third parties who may attempt to license rights that they do not have.
Any litigation or claim against us, even those without merit, may cause us to incur substantial costs, and could place a significant strain on our financial resources, divert the attention of management from our core business and harm our reputation. If we are found to infringe the intellectual property rights of third parties, we could be required to pay substantial damages (which may be increased up to three times of awarded damages) and/or substantial royalties and could be prevented from selling our products unless we obtain a license or are able to redesign our products to avoid infringement. Any such license may not be available on reasonable terms, if at all, and there can be no assurance that we would be able to redesign our products in a way that would not infringe the intellectual property rights of others. We could encounter delays in product introductions while we attempt to develop alternative methods or products. If we fail to obtain any required licenses or make any necessary changes to our products or technologies, we may have to withdraw existing products from the market or may be unable to commercialize one or more of our products.
In addition, we generally indemnify our customers with respect to infringement by our products of the proprietary rights of third parties. Third parties may assert infringement claims against our customers. These claims may require us to initiate or defend protracted and costly litigation on behalf of our customers, regardless of the merits of these claims. If any of these claims succeed or settle, we may be forced to pay damages or settlement payments on behalf of our customers or may be required to obtain licenses for the products they use. If we cannot obtain all necessary licenses on commercially reasonable terms, our customers may be forced to stop using our products.
If we are unable to protect the confidentiality of our trade secrets, our business and competitive position could be harmed.
In addition to patent protection, we also rely upon copyright and trade secret protection, as well as non-disclosure agreements and invention assignment agreements with our employees, consultants and third parties, to protect our confidential and proprietary information. In addition to contractual measures, we try to protect the confidential nature of our proprietary information using commonly accepted physical and technological security measures. Such measures may not, for example, in the case of misappropriation of a trade secret by an employee or third party with authorized access, provide adequate protection for our proprietary information. Our security measures may not prevent an employee or consultant from misappropriating our trade secrets and providing them to a competitor, and recourse we take against such misconduct may not provide an adequate remedy to protect our interests fully. Unauthorized parties may also attempt to copy or reverse engineer certain aspects of our products that we consider proprietary. Enforcing a claim that a party illegally disclosed or misappropriated a trade secret can be difficult, expensive and time-consuming, and the outcome is unpredictable. Even though we use commonly accepted security measures, trade secret violations are often a matter of state law, and the criteria for protection of trade secrets can vary among different jurisdictions. In addition, trade secrets may be independently developed by others in a manner that could prevent legal recourse by us. If any of our confidential or proprietary information, such as our trade secrets, were to be disclosed or
misappropriated, or if any such information was independently developed by a competitor, our business and competitive position could be harmed.
We may be unable to enforce our intellectual property rights throughout the world.
The laws of some foreign countries do not protect intellectual property rights to the same extent as the laws of the U.S. Many companies have encountered significant problems in protecting and defending intellectual property rights in certain foreign jurisdictions. This could make it difficult for us to stop infringement of our foreign patents, if obtained, or the misappropriation of our other intellectual property rights. For example, some foreign countries have compulsory licensing laws under which a patent owner must grant licenses to third parties. In addition, some countries limit the enforceability of patents against third parties, including government agencies or government contractors. In these countries, patents may provide limited or no benefit. Patent protection must ultimately be sought on a country-by-country basis, which is an expensive and time-consuming process with uncertain outcomes. Accordingly, we may choose not to seek patent protection in certain countries, and we will not have the benefit of patent protection in such countries.
Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial costs and divert our efforts and attention from other aspects of our business. Accordingly, our efforts to protect our intellectual property rights in such countries may be inadequate. In addition, changes in the law and legal decisions by courts in the U.S. and foreign countries may affect our ability to obtain adequate protection for our technology and the enforcement of our intellectual property.
Third parties may assert ownership or commercial rights to inventions we develop.
Third parties may in the future make claims challenging the inventorship or ownership of our intellectual property. We have written agreements with collaborators that provide for the ownership of intellectual property arising from our collaborations. In addition, we may face claims by third parties that our agreements with employees, contractors or consultants obligating them to assign intellectual property to us are ineffective or in conflict with prior or competing contractual obligations of assignment, which could result in ownership disputes regarding intellectual property we have developed or will develop and interfere with our ability to capture the commercial value of such intellectual property. Litigation may be necessary to resolve an ownership dispute, and if we are not successful, we may be precluded from using certain intellectual property or may lose our exclusive rights in that intellectual property. Either outcome could harm our business and competitive position.
Third parties may assert that our employees or consultants have wrongfully used or disclosed confidential information or misappropriated trade secrets.
We employ individuals who previously worked with other companies, including our competitors or potential competitors. Although we try to ensure that our employees and consultants do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed intellectual property or personal data, including trade secrets or other proprietary information, of a former employer or other third party. Litigation may be necessary to defend against these claims. If we fail in defending any such claims or settling those claims, in addition to paying monetary damages or a settlement payment, we may lose valuable intellectual property rights or personnel. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Recent changes in U.S. patent laws may limit our ability to obtain, defend and/or enforce our patents.
Recent patent reform legislation could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents. The Leahy-Smith America Invents Act ("the Leahy-Smith Act") includes a number of significant changes to U.S. patent law. These include provisions that affect the way patent applications are prosecuted and also affect patent litigation. The USPTO recently developed new regulations and procedures to govern administration of the Leahy-Smith Act, and many of the substantive changes to patent law associated with the Leahy-Smith Act, and in particular, the first to file provisions, which became effective on March 16, 2013. The first to file provisions limit the rights of an inventor to
patent an invention if not the first to file an application for patenting that invention, even if such invention was the first invention. Accordingly, it is not clear what, if any, impact the Leahy-Smith Act will have on the operation of our business.
However, the Leahy-Smith Act and its implementation could increase the uncertainties and costs surrounding the enforcement and defense of our issued patents. For example, the Leahy-Smith Act provides that an administrative tribunal known as the Patent Trial and Appeals Board ("PTAB") provides a venue for challenging the validity of patents at a cost that is much lower than district court litigation and on timelines that are much faster. Although it is not clear what, if any, long-term impact the PTAB proceedings will have on the operation of our business, the initial results of patent challenge proceedings before the PTAB since its inception in 2013 have resulted in the invalidation of many U.S. patent claims. The availability of the PTAB as a lower-cost, faster and potentially more potent tribunal for challenging patents could increase the likelihood that our own patents will be challenged, thereby increasing the uncertainties and costs of maintaining and enforcing them.
Risks Related to Our Common Stock
The market price of our common stock may be volatile and fluctuate substantially, which could result in substantial losses for purchasers of our common stock
The market price of our common stock is likely to be highly volatile and may fluctuate substantially due to many factors, including:
•the volume and timing of sales of our products;
•the introduction of new products or product enhancements by us or others in our industry;
•disputes or other developments with respect to our or others' intellectual property rights;
•our ability to develop, obtain regulatory clearance or approval for, and market new and enhanced products on a timely basis;
•product liability claims or other litigation;
•quarterly variations in our results of operations or those of others in our industry;
•media exposure of our products or of those of others in our industry;
•changes in governmental regulations or in reimbursement;
•changes in earnings estimates or recommendations by securities analysts; and
•general market conditions and other factors, including factors unrelated to our operating performance or the operating performance of our competitors.
In recent years, the stock markets generally have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of those companies. Broad market and industry factors may significantly affect the market price of our common stock, regardless of our actual operating performance.
In addition, in the past, class action litigation has often been instituted against companies whose securities have experienced periods of volatility in market price. Securities litigation brought against us following volatility in our stock price, regardless of the merit or ultimate results of such litigation, could result in substantial costs, which would hurt our financial condition and operating results and divert management's attention and resources from our business.
We are no longer an emerging growth company or a smaller reporting company and, as a result, we now must comply with increased disclosure and compliance requirements which may increase our costs.
We no longer qualify as an “emerging growth company” under the Jumpstart Our Business Startups Act of 2012 (the “JOBS Act”) or a small reporting company as defined under the Exchange Act and, as a result, are subject to various disclosure and compliance requirements that did not previously apply, such as:
•the requirement that our independent registered public accounting firm attest to the effectiveness of our internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act of 2002;
•the requirement that we adopt new or revised accounting standards when they are applicable to public companies, instead of delaying their adoption until they are applicable to private companies;
•compliance with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor's report providing additional information about the audit and the financial statements;
•the requirement that we provide full and more detailed disclosures regarding executive compensation; and
•the requirement that we hold a non-binding advisory vote on executive compensation and obtain stockholder approval of any golden parachute payments not previously approved.
We expect that the loss of emerging growth company status and smaller reporting company status and compliance with these additional requirements will increase our legal and financial compliance costs and cause management and other personnel to divert attention from operational and other business matters to devote substantial time to public company reporting requirements. In addition, if we are not able to comply with changing requirements in a timely manner, the market price of our stock could decline and we could be subject to sanctions or investigations by the stock exchange on which our common stock is listed, the SEC or other regulatory authorities, which would require additional financial and management resources.
A significant portion of our total outstanding shares are eligible to be sold into the market. This could cause the market price of our common stock to drop significantly, even if our business is doing well.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that these sales may occur, could result in a decrease in the market price of our common stock. Subject to the restrictions set forth in the lock-up agreements entered into by each of our directors and officers and certain of our stockholders in connection with our follow-on offering, certain holders of our common stock have rights, subject to certain conditions, to require us to file registration statements covering shares of our common stock or to include such shares in registration statements that we may file for ourselves or other stockholders. We have also registered all shares of common stock that we may issue under our equity compensation plans. These shares can be freely sold in the public market subject to volume limitations applicable to affiliates. If any of these additional shares are sold, or if it is perceived that they will be sold, in the public market, the market price of our common stock could decline.
We have incurred and expect to continue to incur significant additional costs as a result of being a public company which may adversely affect our business, financial condition and results of operations.
We have incurred and expect to continue to incur costs associated with corporate governance requirements that are applicable to us as a public company, including rules and regulations of the SEC, under the Sarbanes-Oxley Act, the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010, and the Exchange Act, as well as the rules of the NYSE. These rules and regulations significantly increase our accounting, legal and financial compliance costs and make some activities more time-consuming. We also expect these rules and regulations to make it more expensive for us to maintain directors’ and officers’ liability insurance. As a result, it may be more difficult for us to attract and retain qualified persons to serve on our board of directors or as executive officers. Accordingly, increases in costs incurred as a result of being a publicly traded company may adversely affect our business, financial condition and results of operations.
If we fail to maintain proper and effective internal control over financial reporting, our ability to produce accurate and timely financial statements could be impaired, which could harm our operating results, investors' views of us and, as a result, the value of our common stock.
Pursuant to Section 404 of the Sarbanes-Oxley Act, our management is required to report upon the effectiveness of our internal control over financial reporting and, as we are no longer an emerging growth company, our independent registered public accounting firm is required to attest to the effectiveness of our internal control over financial reporting beginning with this Annual Report on Form 10-K. The rules governing the standards that must be met for our management and our independent registered public accounting firm to assess our internal control over financial reporting are complex and require significant documentation, testing and possible remediation. In connection with our and our independent registered public accounting firm’s evaluations of our internal control over financial reporting, we may need to upgrade our systems, including information technology; implement additional financial and management controls, reporting systems and procedures; and hire additional accounting and finance staff.
Any failure to implement required new or improved controls, or difficulties encountered in their implementation, could cause us to fail to meet our reporting obligations. In addition, any testing by us or our independent registered public accounting firm conducted in connection with Section 404 of the Sarbanes-Oxley Act may reveal deficiencies in our internal control over financial reporting that are deemed to be material weaknesses or that may require prospective or retroactive changes to our financial statements or identify other areas for further attention or improvement. Inferior internal controls could also cause investors to lose confidence in our reported financial information, which could have a negative effect on the trading price of our common stock. Internal control deficiencies could also result in a restatement of our financial results in the future. We could become subject to stockholder or other third-party litigation, as well as investigations by the SEC, the stock exchange on which our securities are listed, or other regulatory authorities, which could require additional financial and management resources and could result in fines, trading suspensions, payment of damages or other remedies.
Our disclosure controls and procedures may not prevent or detect all errors or acts of fraud.
We have designed our disclosure controls and procedures to provide reasonable assurance that information we must disclose in reports we file or submit under the Exchange Act is accumulated and communicated to management, and recorded, processed, summarized and reported within the time periods specified in the rules and forms of the SEC. We believe that any disclosure controls and procedures, no matter how well-conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met.
These inherent limitations include the realities that judgments in decision-making can be faulty, and that breakdowns can occur because of simple error or mistake. Additionally, controls can be circumvented by the individual acts of some persons, by collusion of two or more people or by an unauthorized override of the controls. Accordingly, because of the inherent limitations in our control system, misstatements due to error or fraud may occur and not be detected.
Provisions in our governing documents and under Delaware law could make an acquisition of us more difficult and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our amended and restated certificate of incorporation and our amended and restated bylaws may discourage, delay or prevent a merger, acquisition or other change in control of us that stockholders may consider favorable, including transactions in which stockholders might otherwise receive a premium for their shares. These provisions could also limit the price that investors might be willing to pay in the future for shares of our common stock, thereby depressing the market price of our common stock. In addition, these provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors. Because our board of directors is responsible for appointing the members of our management team, these provisions could in turn affect any attempt by our stockholders to replace current members of our management team. These provisions provide, among other things, that:
•our board of directors has the exclusive right to expand the size of our board of directors and to elect directors to fill a vacancy created by the expansion of the board of directors or the resignation, death or removal of a director, which prevents stockholders from being able to fill vacancies on our board of directors;
•our board of directors is divided into three classes, Class I, Class II and Class III, with each class serving staggered three-year terms, which may delay the ability of stockholders to change the membership of a majority of our board of directors;
•our stockholders may not act by written consent, which forces stockholder action to be taken at an annual or special meeting of our stockholders;
•a special meeting of stockholders may be called only by the chair of our board of directors, our chief executive officer or a majority of our board of directors, which may delay the ability of our stockholders to force consideration of a proposal or to take action, including the removal of directors;
•our amended and restated certificate of incorporation prohibits cumulative voting in the election of directors, which limits the ability of minority stockholders to elect director candidates;
•our board of directors may alter certain provisions of our bylaws without obtaining stockholder approval;
•the approval of the holders of at least two-thirds of the shares entitled to vote at an election of directors is required to adopt, amend or repeal our bylaws or repeal the provisions of our amended and restated certificate of incorporation regarding the election and removal of directors;
•stockholders must provide advance notice and additional disclosures in order to nominate individuals for election to the board of directors or to propose matters that can be acted upon at a stockholders’ meeting, which may discourage or deter a potential acquiror from conducting a solicitation of proxies to elect the acquiror’s own slate of directors or otherwise attempting to obtain control of our Company; and
•our board of directors is authorized to issue shares of preferred stock and to determine the terms of those shares, including preferences and voting rights, without stockholder approval, which could be used to significantly dilute the ownership of a hostile acquiror.
Moreover, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which prohibits a person who owns in excess of 15% of our outstanding voting stock from merging or combining with us for a period of three years after the date of the transaction in which the person acquired in excess of 15% of our outstanding voting stock, unless the merger or combination is approved in a prescribed manner.
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware will be the exclusive forum for substantially all disputes between us and our stockholders, which could limit our stockholders' ability to obtain a favorable judicial forum for disputes with us or our directors, officers or employees.
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware is the exclusive forum for (i) any derivative action or proceeding brought on our behalf, (ii) any action asserting a claim of breach of a fiduciary duty or other wrongdoing by any of our directors, officers, employees or agents to us or our stockholders, (iii) any action asserting a claim arising pursuant to any provision of the DGCL or our amended and restated certificate of incorporation or amended and restated bylaws or (iv) any action asserting a claim governed by the internal affairs doctrine. We believe this provision benefits us by providing increased consistency in the application of Delaware law by chancellors particularly experienced in resolving corporate disputes, efficient administration of cases on a more expedited schedule relative to other forums and protection against the burdens of multi-forum litigation. However, this provision may limit a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes with us or our directors, officers or other employees, which may discourage such lawsuits against us and our directors, officers and other employees. Alternatively, if a
court were to find the choice of forum provision contained in our amended and restated certificate of incorporation to be inapplicable or unenforceable in an action, we may incur additional costs associated with resolving such action in other jurisdictions.
Because we do not anticipate paying any cash dividends on our capital stock in the foreseeable future, capital appreciation, if any, will be your sole source of gain.
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the growth and development of our business. In addition, the agreement governing our credit facility precludes, and any future debt agreements may preclude, us from paying cash dividends. As a result, capital appreciation, if any, of our common stock will be your sole source of gain for the foreseeable future.
Securities analysts may not publish favorable research or reports about our business or may publish no information at all, which could cause our stock price or trading volume to decline.
The trading market for our common stock relies in part on the research and reports that securities or industry analysts publish about us or our business. We do not control these analysts. As a recently public company, we may be slow to attract research coverage and the analysts who publish information about our common stock will have had relatively little experience with us or our industry, which could affect their ability to accurately forecast our results and could make it more likely that we fail to meet their estimates. In the event we obtain securities or industry analyst coverage, if any of the analysts who cover us provide inaccurate or unfavorable research or issue an adverse opinion regarding our stock price, our stock price could decline. If one or more of the analysts covering our business downgrade our stock or change their opinion of our stock, our stock price would likely decline. In addition, if one or more of these analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which could cause our share price or trading volume to decline.
Item 1B. Unresolved Staff Comments.
None.
Item 2. Properties.
Our principal office is located in Golden Valley, Minnesota, where we lease approximately 45,000 square feet of office space. We currently sublease this space under a non-cancelable operating lease agreement that commenced January 15, 2019 and expires on November 30, 2020. In May 2019, we entered into a non-cancelable operating lease agreement for the same space that commences on December 1, 2020 and expires May 31, 2028 with an option to renew for one additional period of five years. We intend to add new facilities as we grow and we believe that suitable additional or substitute space will be available as needed to accommodate any such expansion of our operations.
Our former principal office was located in Maple Grove, Minnesota, where we leased approximately 9,500 square feet of office space. This lease terminated on March 31, 2019.
Item 3. Legal Proceedings.
We are not party to any material legal proceedings.
Item 4. Mine Safety Disclosures.
Not applicable.
PART II
Item 5. Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market Information
Our common stock began trading on the NYSE under the symbol “INSP” on May 3, 2018. Prior to that date, there was no established public trading market for our common stock.
Holders
As of February 18, 2020, there were approximately 27 holders of record of our common stock. This number does not include stockholders who are beneficial owners, but whose shares are held in street name by brokers and other nominees. This number of holders of record also does not include stockholders whose shares may be held in trust by other entities.
Recent Sales of Unregistered Securities
None.
Performance Graph
The following graph illustrates a comparison of the total cumulative stockholder return on our common stock with the total return for (i) the S&P Healthcare Equipment Select Industry Index and (ii) the NYSE Composite for the period from May 3, 2018 (the date our common stock commenced trading on the NYSE) through December 31, 2019. The graph assumes an investment of $100 in our common stock at market close on May 3, 2018 and the reinvestment of dividends, if any. The comparisons in the table are not intended to forecast or be indicative of possible future performance of our common stock. This graph shall not be deemed “soliciting material” or be deemed “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities under that Section, and shall not be deemed to be incorporated by reference into any of our filings under the Securities Act of 1933, as amended (the "Securities Act"), whether made before or after the date hereof and irrespective of any general incorporation language in any such filing.
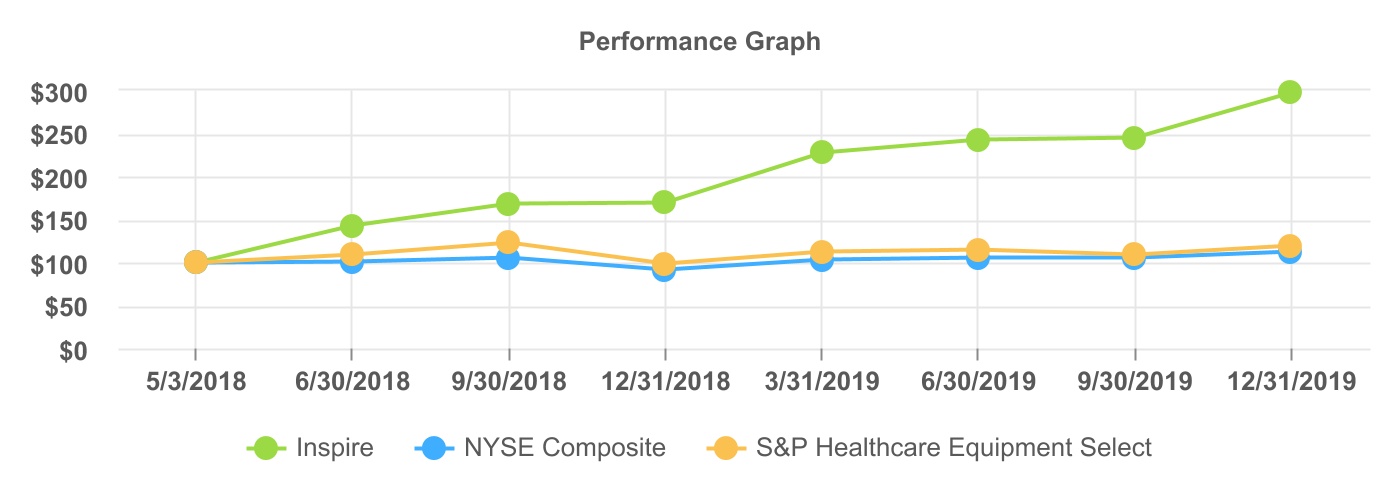
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | | 2018 | | | | | | | | 2019 | | | | | | |
| Stock or Index | | Ticker | | 5/3 | | 6/30 | | 9/30 | | 12/31 | | 3/31 | | 6/30 | | 9/30 | | 12/31 |
| Inspire | | INSP | | $ | 100.00 | | | $ | 142.75 | | | $ | 168.45 | | | $ | 169.14 | | | $ | 227.30 | | | | $ | 242.79 | | | | $ | 244.28 | | | | $ | 297.08 | |
| NYSE Composite | | NYA | | 100.00 | | | 100.90 | | | 105.57 | | | 91.78 | | | 102.46 | | | | 105.30 | | | | 104.94 | | | | 112.27 | |
| S&P Healthcare Equipment Select | | SPSIHE | | 100.00 | | | 108.94 | | | 122.20 | | | 97.68 | | | 111.86 | | | | 114.07 | | | | 108.89 | | | | 119.57 | |
Item 6. Selected Financial Data.
The following tables set forth, for the periods and as of the dates indicated, our selected historical financial data. The statements of operations data for the years ended December 31, 2019, 2018, and 2017 and the balance sheet data as of December 31, 2019 and 2018 are derived from our audited financial statements included elsewhere in this Annual Report on Form 10-K. The statements of operations data for the years ended December 31, 2016 and 2015 and the balance sheet data as of December 31, 2017, 2016, and 2015 are derived from our audited financial statements not included in this Annual Report on Form 10-K.
Our historical results are not necessarily indicative of the results that may be expected in the future. You should read the following information together with the more detailed information contained in "Management's Discussion and Analysis of Financial Condition and Results of Operations" and our financial statements and the related notes included elsewhere in this Annual Report on Form 10-K.
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year ended December 31, | | | | | | | | |
| | 2019 | | | 2018 | | | 2017 | | | 2016 | | | 2015 | |
| | (in thousands, except share and per share data) | | | | | | | | |
| Statement of Operations Data: | | | | | | | | | | |
| Revenue | | $ | 82,050 | | | $ | 50,593 | | | $ | 28,567 | | | $ | 16,427 | | | $ | 8,012 | |
| Cost of goods sold | | 13,643 | | | 10,056 | | | 6,018 | | | 3,905 | | | 2,809 | |
| Gross profit | | 68,407 | | | 40,537 | | | 22,549 | | | 12,522 | | | 5,203 | |
| Operating expenses: | | | | | | | | | | |
| Research and development | | 12,839 | | | 7,388 | | | 6,194 | | | 7,091 | | | 7,079 | |
| Selling, general and administrative | | 90,465 | | | 53,527 | | | 32,358 | | | 22,684 | | | 17,922 | |
| Total operating expenses | | 103,304 | | | 60,915 | | | 38,552 | | | 29,775 | | | 25,001 | |
| Operating loss | | (34,897) | | | (20,378) | | | (16,003) | | | (17,253) | | | (19,798) | |
| Other (income) expense: | | | | | | | | | | |
| Interest income | | (3,801) | | | (1,870) | | | (203) | | | (57) | | | (66) | |
| Interest expense | | 2,119 | | | 3,304 | | | 1,753 | | | 1,303 | | | 1,564 | |
| Other (income) expense, net | | (12) | | | 16 | | | (42) | | | 29 | | | 41 | |
| Total other (income) expense | | (1,694) | | | 1,450 | | | 1,508 | | | 1,275 | | | 1,539 | |
| Loss before income taxes | | (33,203) | | | (21,828) | | | (17,511) | | | (18,528) | | | (21,337) | |
| Income taxes | | 40 | | | — | | | — | | | — | | | — | |
| Net loss | | $ | (33,243) | | | $ | (21,828) | | | $ | (17,511) | | | $ | (18,528) | | | $ | (21,337) | |
| Net loss per share, basic and diluted | | $ | (1.40) | | | $ | (1.50) | | | $ | (14.88) | | | $ | (16.90) | | | $ | (20.74) | |
Weighted average common shares used to compute net loss per share, basic and diluted (1) | | 23,804,452 | | | 14,579,662 | | | 1,176,650 | | | 1,096,013 | | | 1,027,925 | |
(1) See Note 11 to our audited financial statements for an explanation of the method used to calculate our basic and diluted net loss per share.
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | As of December 31, | | | | | | | | |
| | 2019 | | | 2018 | | | 2017 | | | 2016 | | | 2015 | |
| | (in thousands) | | | | | | | | |
| Balance Sheet Data: | | | | | | | | | | |
| Cash, cash equivalents and investments | | $ | 155,741 | | | $ | 188,210 | | | $ | 16,143 | | | $ | 6,685 | | | $ | 12,127 | |
Working capital(1) | | 153,780 | | | 188,123 | | | 16,950 | | | 4,959 | | | 13,899 | |
| Total assets | | 181,253 | | | 200,080 | | | 25,091 | | | 13,116 | | | 18,294 | |
| Total long-term liabilities | | 24,562 | | | 24,926 | | | 16,617 | | | 12,434 | | | 15,705 | |
| Total stockholders' equity (deficit) | | 139,835 | | | 163,999 | | | 1,327 | | | (6,608) | | | (1,142) | |
(1) We define working capital as current assets less current liabilities.
Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion and analysis of our financial condition and results of operations should be read in conjunction with our financial statements and the related notes to those statements included elsewhere in this Annual Report on Form 10-K. In addition to historical financial information, the following discussion and analysis contains forward-looking statements that involve risks, uncertainties, and assumptions. Some of the numbers included herein have been rounded for the convenience of presentation. Our actual results may differ materially from those anticipated in these forward-looking statements as a result of many factors, including those discussed under Part I. "Item 1A. Risk Factors’’ and elsewhere in this Annual Report on Form 10-K.
Overview
We are a medical technology company focused on the development and commercialization of innovative and minimally invasive solutions for patients with OSA. Our proprietary Inspire system is the first and only FDA-approved neurostimulation technology that provides a safe and effective treatment for moderate to severe OSA. We have developed a novel, closed-loop solution that continuously monitors a patient’s breathing and delivers mild hypoglossal nerve stimulation to maintain an open airway. Inspire therapy is indicated for patients with moderate to severe OSA who do not have significant central sleep apnea and do not have a complete concentric collapse of the airway at the soft palate level. In addition, patients in the U.S. must have been confirmed to fail or be unable to tolerate positive airway pressure treatments, such as CPAP, and be 22 years of age or older, though there are no similar requirements for patients in Europe.
We sell our Inspire system to hospitals and ASCs in the U.S. and in select countries in Europe through a direct sales organization. Our direct sales force engages in sales efforts and promotional activities focused on ENT physicians and sleep centers. In addition, we highlight our compelling clinical data and value proposition to increase awareness and adoption amongst referring physicians. We build upon this top-down approach with strong direct-to-patient marketing initiatives to create awareness of the benefits of our Inspire system and drive demand through patient empowerment. This outreach helps to educate thousands of patients on our Inspire therapy and frequently results in patient leads. We increased the number of employees in our sales, marketing, and reimbursement organizations from 40 as of December 31, 2015 to 186 as of December 31, 2019.
Although our sales and marketing efforts are directed at patients and physicians because they are the primary users of our technology, we consider the hospitals and ASCs where the procedure is performed to be our customers, as they are the purchasing agents of our Inspire system. Our customers are reimbursed the cost required to treat each patient through various third-party payors, such as commercial payors and government agencies. Our Inspire system is currently reimbursed primarily on a per-patient prior authorization basis for patients covered by commercial payors, on a case-by-case basis for patients covered by Medicare, and under U.S. government contract for patients who are treated by the Veterans Health Administration. To date, more than 430 commercial payors have prior authorized for patients’ treatment with our Inspire therapy. We have currently secured positive coverage policies with 52 U.S. commercial payors, including most large national commercial insurers. In June 2018, Japan’s Ministry of Health, Labour and Welfare approved our Inspire therapy to treat
moderate to severe OSA, and we are currently seeking reimbursement coverage in Japan. For the year ended December 31, 2019, 89.8% of our revenue was derived in the U.S. and 10.2% was derived in Europe. No single customer accounted for more than 10% of our revenue.
We rely on third-party suppliers to manufacture our Inspire system and its components. Many of these suppliers are currently single source suppliers. We seek to maintain higher levels of inventory to protect ourselves from supply interruptions, and, as a result, we are subject to the risk of inventory obsolescence and expiration, which could lead to inventory impairment charges. In the U.S., our products are shipped directly to our customers on a purchase order basis, primarily by a third-party vendor with a facility in Tennessee, although we do ship some products from our facility in Minnesota. Warehousing and shipping operations for our European customers are handled by a third-party vendor with facilities located in the Netherlands. Customers do not have the right to return non-defective product, nor do we place product on consignment. Our sales representatives do not maintain trunk stock.
Since our inception in 2007, we have financed our operations primarily through sales of our Inspire system, private placements of our convertible preferred securities, amounts borrowed under our credit facility, the initial public offering of our common stock that closed in May 2018 (our "IPO"), and the offering of our common stock that closed in December 2018 (our "follow-on offering"). We have devoted significant resources to research and development activities related to our Inspire system, including clinical and regulatory initiatives to obtain marketing approval, and sales and marketing activities. For the year ended December 31, 2019, we generated revenue of $82.1 million with a gross margin of 83.4% and a net loss of $33.2 million compared to revenue of $50.6 million with a gross margin of 80.1% and a net loss of $21.8 million for the year ended December 31, 2018, and revenue of $28.6 million with a gross margin of 78.9% and a net loss of $17.5 million for the year ended December 31, 2017. Our accumulated deficit as of December 31, 2019 was $180.2 million.
We have invested heavily in product development. Our research and development activities have been centered on driving continuous improvements to our Inspire therapy. We have also made significant investments in clinical studies to demonstrate the safety and efficacy of our Inspire therapy and to support regulatory submissions. We intend to make significant investments building our sales and marketing organization by increasing the number of U.S. sales representatives and continuing our direct-to-patient marketing efforts in existing and new markets throughout the U.S. and in Europe. We also intend to continue to make investments in research and development efforts to develop our next generation Inspire systems and support our future regulatory submissions for expanded indications and for new markets such as Europe, Japan, and Australia. Because of these and other factors, we expect to continue to incur net losses for the next several years and we expect to require substantial additional funding, which may include future equity and debt financings.
On May 7, 2018, we completed our IPO by issuing 7,762,500 shares of common stock, at a public offering price of $16.00 per share, for net proceeds of approximately $112.0 million after deducting underwriting discounts and commissions and offering expenses payable by us. On December 11, 2018, we completed the follow-on offering that included our offer and sale of 1,875,000 shares of common stock and the selling stockholders' offer and sale of 1,000,000 shares of common stock, at a public offering price of $40.00 per share. We received net proceeds of approximately $69.8 million after deducting underwriting discounts and commissions and offering expenses. We received no proceeds from the sale of our common stock by the selling shareholders.
Components of Our Results of Operations
Revenue
We derive primarily all of our revenue from the sale of our Inspire system to hospitals and ambulatory service centers in the U.S. and select countries in Europe. Recent revenue growth has been driven by, and we expect continued growth as a result of, increased patient and physician awareness of the Inspire system, additional sales representatives, an increase in approvals of prior authorization submissions, and additional positive coverage policies. Any reversal in these recent trends, however, could have a negative impact on our future revenue. In addition, we have expanded our sales and marketing organization to help us drive and support revenue growth and intend to continue this expansion. Moreover, we expect that our revenue growth will be positively impacted by, and to the extent we obtain, additional positive coverage policies. Our revenue has fluctuated, and we expect
our revenue to continue to fluctuate, from quarter to quarter due to a variety of factors. For example, we have historically experienced seasonality in our first and fourth quarters.
Cost of Goods Sold and Gross Margin
Cost of goods sold consists primarily of acquisition costs for the components of the Inspire system, overhead costs, scrap, and inventory obsolescence, as well as distribution-related expenses such as logistics and shipping costs, net of costs charged to customers. The overhead costs include the cost of material procurement, depreciation expense for production equipment, warranty replacement costs, and operations supervision and management personnel, including employee compensation, stock-based compensation, supplies, and travel. We expect overhead costs as a percentage of revenue to continue to decrease as our sales volume increases. We expect cost of goods sold to increase in absolute dollars primarily as, and to the extent, our revenue grows.
We calculate gross margin as gross profit divided by revenue. Our gross margin has been and we expect it will continue to be affected by a variety of factors, including manufacturing costs, the average selling price of our Inspire system, the implementation of cost-reduction strategies, inventory obsolescence costs, which generally occur when new generations of our Inspire system are introduced, and to a lesser extent the sales mix between the U.S. and Europe as our average selling price in the U.S. tends to be higher than in Europe. Our gross margin may increase over the long term to the extent our production volumes increase and we receive discounts on the costs charged by our contract manufacturers, thereby reducing our per unit costs. However, our gross margin may fluctuate from quarter to quarter due to seasonality.
Research and Development Expenses
Research and development expenses consist primarily of product development, engineering, clinical studies to develop and support our products, regulatory expenses, testing, consulting services and other costs associated with the next generation versions of the Inspire system. These expenses include employee compensation, including stock-based compensation, supplies, materials, consulting, and travel expenses related to research and development programs. Additionally, these expenses include clinical trial management, payments to clinical investigators, data management and travel expenses for our various clinical trials. We expect research and development expenses to increase in the future as we develop next generation versions of our Inspire system and continue to expand our clinical studies to secure positive coverage policies from private commercial payors in the U.S. and enter into new markets including additional European countries, Japan, and Australia. We expect research and development expenses as a percentage of revenue to vary over time depending on the level and timing of initiating new product development efforts and new clinical development activities.
Selling, General and Administrative Expenses
Selling, general and administrative expenses consist primarily of compensation for personnel, including base salaries, stock-based compensation expense and commissions related to our sales organization, finance, information technology, and human resource functions, as well as spending related to marketing, sales operations, and training and reimbursement personnel. Other selling, general and administrative expenses include training physicians, travel expenses, advertising, direct-to-patient promotional programs, conferences, trade shows and consulting services, professional services fees, audit fees, insurance costs and general corporate expenses, including facilities-related expenses. We expect selling, general and administrative expenses to continue to increase as we expand our commercial infrastructure to both drive and support our planned growth in revenue and as we increase our headcount and expand administrative personnel to support our growth and operations as a public company including finance personnel and information technology services.
Additionally, we anticipate increased expenses related to audit, legal, and tax-related services associated with maintaining compliance with exchange listing and SEC requirements, director and officer insurance premiums and investor relations costs associated with being a public company. We also expect to see an increase in our stock-based compensation expense with grants of restricted stock or options and shares of our common stock purchased pursuant to our employee stock purchase plan.
Other (Income) Expense, Net
Other (income) expense, net consists primarily of interest expense payable under our credit facility and interest income. Other items include fair value adjustments related to convertible preferred stock warrants, which were accounted for as a liability and marked-to-market at each reporting period. Immediately prior to the closing of our IPO, our outstanding convertible preferred stock warrants automatically converted into warrants to purchase shares of our common stock.
Results of Operations
Year Ended December 31, 2019 Compared to Year Ended December 31, 2018
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | Change | | |
| | 2019 | | | 2018 | | | $ | | % |
| | (in thousands, except percentages) | | | | | | |
| Revenue | | $ | 82,050 | | | $ | 50,593 | | | $ | 31,457 | | | 62.2 | % |
| Cost of goods sold | | 13,643 | | | 10,056 | | | 3,587 | | | 35.7 | % |
| Gross profit | | 68,407 | | | 40,537 | | | 27,870 | | | 68.8 | % |
| Gross margin | | 83.4 | % | | 80.1 | % | | | | |
| Operating expenses: | | | | | | | | |
| Research and development | | 12,839 | | | 7,388 | | | 5,451 | | | 73.8 | % |
| Selling, general and administrative | | 90,465 | | | 53,527 | | | 36,938 | | | 69.0 | % |
| Total operating expenses | | 103,304 | | | 60,915 | | | 42,389 | | | 69.6 | % |
| Operating loss | | (34,897) | | | (20,378) | | | (14,519) | | | 71.2 | % |
| Other (income) expense, net | | (1,694) | | | 1,450 | | | (3,144) | | | (216.8) | % |
| Loss before income taxes | | (33,203) | | | | (21,828) | | | (11,375) | | | 52.1 | % |
| Income taxes | | 40 | | | | — | | | 40 | | | n/a | |
| Net loss | | $ | (33,243) | | | $ | (21,828) | | | $ | (11,415) | | | 52.3 | % |
Revenue
Revenue increased $31.5 million, or 62.2%, to $82.1 million for the year ended December 31, 2019 compared to the year ended December 31, 2018. The increase was attributable to an increase in sales of our Inspire system of $29.3 million in the U.S. and an increase of $2.2 million in Europe, primarily in Germany.
Revenue information by region is summarized as follows:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | | | | | | | |
| | 2019 | | | | | 2018 | | | | | Change | | |
| | Amount | | % of Revenue | | Amount | | % of Revenue | | $ | | % |
| | (in thousands, except percentages) | | | | | | | | | | |
| United States | | $ | 73,660 | | | 89.8 | % | | $ | 44,378 | | | 87.7 | % | | $ | 29,282 | | | 66.0 | % |
| Europe | | 8,390 | | | 10.2 | % | | 6,215 | | | 12.3 | % | | 2,175 | | | 35.0 | % |
| Total revenue | | $ | 82,050 | | | 100.0 | % | | $ | 50,593 | | | 100.0 | % | | $ | 31,457 | | | 62.2 | % |
Revenue generated in the U.S. was $73.7 million for the year ended December 31, 2019, an increase of $29.3 million or 66.0% over the year ended December 31, 2018. Revenue growth in the U.S. was due to increased market penetration in existing territories, the expansion into new territories, increased physician and patient awareness of our Inspire system, a greater number of prior authorization approvals, additional positive coverage policies and, to a lesser extent, an increase in our average selling price as a result of the introduction of the new sensing lead on the Inspire system to the U.S. market in February 2019.
Revenue generated in Europe was $8.4 million in the year ended December 31, 2019, an increase of $2.2 million or 35.0% over the year ended December 31, 2018. Revenue growth in Europe was primarily due to increased market penetration in existing territories, the expansion into new territories, and increased physician and patient awareness of our Inspire system.
Cost of Goods Sold and Gross Margin
Cost of goods sold increased $3.5 million, or 35.7%, to $13.6 million for the year ended December 31, 2019 compared to $10.1 million for the year ended December 31, 2018. The increase was primarily due to increased purchases of manufactured products due to higher sales volume of our Inspire system.
Gross margin was 83.4% for the year ended December 31, 2019 compared to 80.1% for the year ended December 31, 2018. Gross margin for the year ended December 31, 2019 was higher primarily due to the introduction of the new sensing lead on the Inspire system in the U.S. in February 2019 which has a higher gross margin than the previous sensor, as well as manufacturing efficiencies.
Research and Development Expenses
Research and development expenses increased $5.4 million, or 73.8%, to $12.8 million for the year ended December 31, 2019 compared to $7.4 million for the year ended December 31, 2018. This change was primarily due to an increase of $3.4 million for ongoing research and development costs, including initial development of the next generation Inspire therapy system and $2.0 million of compensation and employee-related expenses, mainly as a result of increased headcount.
Selling, General and Administrative Expenses
Selling, general and administrative expenses increased $37.0 million, or 69.0%, to $90.5 million for the year ended December 31, 2019 compared to $53.5 million for the year ended December 31, 2018. The primary driver of this increase was an increase of $22.5 million in compensation, including salaries, commissions, and stock-based compensation, travel and other employee-related expenses, mainly as a result of increased headcount. In addition, selling, general and administrative expenses increased by $3.9 million due to legal fees, financial audit fees, insurance costs, and other corporate costs which increased primarily as a result of being a public company during the entire year ended December 31, 2019 compared to being a public company during only part of the same prior year period, as well as out-sourced information technology services and facilities costs. Other drivers included an increase of $9.0 million of marketing, primarily consisting of direct-to-patient initiatives, and an increase of $1.6 million of regulatory and reimbursement costs, which increased primarily due to market access consulting services used to obtain positive coverage policies.
Other (Income) Expense, Net
Other (income) expense, net changed by $3.2 million, or 216.8%, to $1.7 million of income for the year ended December 31, 2019 compared to $1.5 million of expense for the year ended December 31, 2018. Interest income increased $1.9 million due to our higher cash, cash equivalents and investments balances. Interest expense decreased $1.2 million, primarily due to the lack of the $0.6 million fair value adjustment taken during the year ended December 31, 2018 on our previously outstanding convertible preferred stock warrants.
Year Ended December 31, 2018 Compared to Year Ended December 31, 2017
For a discussion of our results of operations for the year ended December 31, 2017, including a year-to-year comparison between 2018 and 2017, refer to Part II, Item 7, "Management's Discussion and Analysis of Financial Condition and Results of Operations" in our Annual Report Form 10-K for the year ended December 31, 2018.
Liquidity and Capital Resources
As of December 31, 2019, we had cash, cash equivalents and investments of $155.7 million and an accumulated deficit of $180.2 million, compared to cash, cash equivalents and investments of $188.2 million and an
accumulated deficit of $146.9 million as of December 31, 2018. As of December 31, 2019, we had $24.5 million of outstanding borrowings under our credit facility. No borrowings remain available under this credit facility.
On May 7, 2018, we completed our IPO by issuing 7,762,500 shares of common stock, at a public offering price of $16.00 per share, for net proceeds of approximately $112.0 million after deducting underwriting discounts and commissions and offering expenses payable by us. On December 11, 2018, we completed the follow-on offering that included our offer and sale of 1,875,000 shares of common stock and the selling stockholders' offer and sale of 1,000,000 shares of common stock, at a public offering price of $40.00 per share. We received net proceeds of approximately $69.8 million after deducting underwriting discounts and commissions and offering expenses. We received no proceeds from the sale of our common stock by the selling shareholders.
Our sources of capital have historically been from private placements of our convertible preferred securities, sales of our Inspire system, borrowings under credit facilities and registered offerings of our common stock. As of December 31, 2019, we had raised a total of $119.1 million in net proceeds from private placements of our convertible preferred securities and $181.8 million from registered equity offerings.
We believe that our existing cash resources will be sufficient to meet our capital requirements and fund our operations for at least the next 12 months. We may also seek liquidity through additional securities offerings or through borrowings under a new credit facility.
Cash Flows
The following table presents a summary of our cash flow for the periods indicated:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2019 | | 2018 | | 2017 |
| (in thousands) | | | | |
| Net cash provided by (used in): | | | | | |
| Operating activities | $ | (32,846) | | | $ | (18,694) | | | $ | (15,791) | |
| Investing activities | (43,559) | | | (83,389) | | | (7,600) | |
| Financing activities | 1,964 | | | 190,383 | | | 25,661 | |
| Effect of exchange rate on cash | 13 | | | 33 | | | — | |
| (Decrease) increase in cash and cash equivalents | $ | (74,428) | | | $ | 88,333 | | | $ | 2,270 | |
Operating Activities
Net cash used in operating activities was $32.8 million for 2019 and consisted of a net loss of $33.2 million, an increase in net operating assets of $6.6 million, and non-cash charges of $7.0 million. The non-cash charges consisted of stock-based compensation, accretion of the debt discount, non-cash lease expense, stock issued for services rendered, and depreciation and amortization, offset by the non-cash income related to the accretion of the investment discount, and other, net. Operating assets, which includes accounts receivable, inventories, and prepaid expenses and other current assets, increased generally due to increased revenues year-over-year. Operating liabilities, which includes accrued expenses and accounts payable, increased generally due to our increased business volume year-over-year and the costs to support the growth of our operations, including compensation and personnel-related costs.
Net cash used in operating activities was $18.7 million for 2018 and consisted of a net loss of $21.8 million, an increase in net operating assets of $0.9 million and non-cash charges of $2.3 million. Net operating assets consisted primarily of accrued expenses, accounts payable, accounts receivable, and prepaid expenses and other assets to support the growth of our operations. Non-cash charges consisted primarily of stock-based compensation, the change in fair value of preferred stock warrants, accretion of debt discount, and depreciation, offset by the non-cash income related to the accretion of the investment discount.
Net cash used in operating activities was $15.8 million in 2017 and consisted of a net loss of $17.5 million, a decrease in net operating assets of $0.8 million and non-cash charges of $0.9 million. Net operating assets
consisted primarily of accounts receivable and inventory to support the growth of our operations and accrued compensation as annual bonuses were paid. Non-cash charges consisted primarily of depreciation and stock-based compensation.
Investing Activities
Net cash used in investing activities for 2019 was $43.6 million and consisted primarily of purchases of investments of $178.1 million, partially offset by proceeds from sales or maturities of investments of $137.3 million. Purchases of property and equipment were $2.7 million.
Net cash used in investing activities for 2018 was $83.4 million and consisted primarily of purchases of investments of $115.5 million, offset by proceeds from sales or maturities of investments of $32.3 million. Purchases of property and equipment were $0.2 million.
Net cash used in investing activities for 2017 was $7.6 million and consisted primarily of purchases of investments of $9.0 million, offset by proceeds from sales or maturities of investments of $1.8 million. Purchases of property and equipment were $0.4 million.
Financing Activities
Net cash provided by financing activities was $2.0 million for 2019 and consisted of $1.4 million in proceeds from the issuance of common stock from the employee stock purchase plan and $1.1 million in proceeds from the exercise of stock options and warrants, partially offset by a $0.5 million final payment fee due upon the amendment of our credit facility.
Net cash provided by financing activities was $190.4 million for 2018 and consisted primarily of $181.8 million of net proceeds from public offerings of our common stock and borrowings of $8.0 million under our credit facility.
Net cash provided by financing activities was $25.7 million in 2017 and consisted primarily of $25.0 million of net proceeds from the issuance of Series F convertible preferred stock, borrowings of $1.0 million under our credit facility less $0.5 million of expenses and $0.2 million in proceeds from the exercise of stock options.
Indebtedness
In August 2015, we entered into a loan and security agreement with Oxford Finance LLC ("Oxford Finance"), as lender and collateral agent. The loan and security agreement initially provided for a term A loan facility in the amount of $15.5 million, which was fully funded on the closing date, and a term B loan facility in an amount of at least $3.5 million but no more than $10.0 million, to be available in the future subject to our achievement of certain revenue milestones. We refer to our term A loan facility and our term loan B facility together as our credit facility. In February 2017, we amended the loan and security agreement to, among other things, increase borrowings under the term A loan facility by $1.0 million, increase the minimum amount of the term B loan facility to $5.0 million and reduce the maximum amount of the term B loan facility to $9.0 million. In February 2018, we borrowed $8.0 million under the term B loan facility.
In March 2019, we amended the loan and security agreement. Following such amendment, outstanding borrowings under the credit facility bear interest at an annual rate equal to the sum of (i) the greater of (A) the 30 day U.S. LIBOR rate reported in The Wall Street Journal on the last business day of the month that immediately precedes the month in which the interest will accrue or (B) 2.50%, plus (ii) 5.10%; provided, however, under no circumstances will the basic rate be less than 7.60%. We are required to make monthly payments of interest only through April 1, 2022. Following the interest-only period, we will be required to make monthly payments of interest and principal in 24 consecutive monthly installments. Outstanding borrowings under the credit facility mature on March 1, 2024. On the maturity date, in addition to our regular monthly payments of principal and accrued interest, we will be required to make a payment of 3.50% of the total amount borrowed under the credit facility, which we refer to as the Final Payment, unless we have already made such payment in connection with an acceleration or prepayment of borrowings under the credit facility.
Borrowings under the facility are pre-payable at our option in whole, but not in part, together with all accrued and unpaid interest thereon and, if not previously made, the Final Payment, subject to a prepayment fee of 3.0% if such borrowings are prepaid prior to March 27, 2020, 2.0% if such borrowings are prepaid on or after March 27, 2020 but prior to March 27, 2021 and 1.0% if such borrowings are on or after March 27, 2021 and prior to maturity. We are also required to prepay the amounts outstanding under the credit facility upon the occurrence of certain customary events of default, as well as the occurrence of certain material adverse events. The credit facility also includes certain customary affirmative and negative covenants, but does not include any financial covenants. The credit facility is secured by substantially all of our personal property other than our intellectual property. We were in compliance with all covenants under the credit facility as of December 31, 2019.
In August 2015, we issued to Oxford Finance warrants to purchase 12,404 and 17,176 shares of our Series E convertible preferred stock, having an exercise price of $2.62 per share. In February 2017 and February 2018, we issued warrants to Oxford Finance to purchase 29,197 and 233,577 shares, respectively, of our Series F convertible preferred stock, having an exercise price of $1.37 per share. Each of the warrants described above has a term of 10 years.
Upon the closing of the IPO, the warrants to purchase 630,372 shares of preferred stock at a weighted average exercise price of $1.46 per share became exercisable to purchase 100,558 shares of common stock at a weighted average exercise price of $9.38 per share. Warrants to purchase 93,963 shares of common stock were exercised during 2018, and the warrants to purchase 6,595 shares of common stock were exercised during 2019. No warrants remain outstanding at December 31, 2019.
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements, as defined by applicable regulations of the SEC, that are reasonably likely to have a current or future material effect on our financial condition, results of operations, liquidity, capital expenditures or capital resources.
Contractual Obligations and Commitments
Our contractual obligations and commitments as of December 31, 2019 are summarized in the table below:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Payments Due by Year | | | | | | | | |
| ($ in thousands) | Total | | Less than 1 year | | 1 - 3 years | | 3 - 5 years | | More than 5 years |
| Recorded contractual obligations: | | | | | | | | | | | | | | | | | | |
Long-term debt (1) | $ | 24,500 | | | | $ | — | | | | $ | 9,188 | | | | $ | 15,312 | | | | $ | — | |
| Operating lease liabilities | 828 | | | | 828 | | | | — | | | | — | | | | — | |
| Unrecorded contractual obligations: | | | | | | | | | | | | | | | | | | |
Interest payments on long-term debt (2) | 6,219 | | | | 1,893 | | | | 3,539 | | | | 787 | | | | — | |
| Purchase obligations | 23,739 | | | | 23,739 | | | | — | | | | — | | | | — | |
Real estate obligation (3) | 7,425 | | | | 1 | | | | 651 | | | | 2,379 | | | | 4,394 | |
| Total contractual obligations | $ | 62,711 | | | $ | 26,461 | | | $ | 13,378 | | | $ | 18,478 | | | $ | 4,394 | |
(1) Represents principal payments only. See Note 5 to our audited financial statements for more information.
(2) Variable interest is assumed at December 31, 2019 rates. Under the terms of the credit facility, a final payment fee of 3.50% is due at the earlier of maturity or prepayment. This amount is not included in the table above.
(3) Real estate obligation represents the legally binding minimum lease payments for a lease signed but not yet commenced. See Note 4 to our audited financial statements for more information.
Critical Accounting Policies and Estimates
The preparation of the financial statements in conformity with accounting principles generally accepted in the U.S. requires management to make estimates and assumptions that affect the amounts reported in the audited financial statements and accompanying notes included elsewhere in this Annual Report on Form 10-K. We believe that such estimates have been based on reasonable and supportable assumptions and the resulting estimates are reasonable for use in the preparation of the audited financial statements. Actual results could differ from these estimates.
Significant areas requiring management estimates or judgments include the following key financial areas:
Revenue Recognition
We recognize revenue in accordance with Accounting Standards Codification ("ASC") Topic 606, Revenue from Contracts with Customers ("ASC 606"), which we adopted effective January 1, 2019 using the modified retrospective approach. The adoption of ASC 606 did not have a material impact on the amount and timing of revenue recognized in our financial statements.
Revenues from product sales are recognized when the customer obtains control of the product, which occurs at a point in time, either upon shipment of the product or receipt of the product, depending on shipment terms. Our standard shipping terms are free on board shipping point, unless the customer requests that control and title to the inventory transfer upon delivery. In those cases where shipping and handling costs are billed to customers, we classify the amounts billed as a component of cost of goods sold.
Revenue is measured as the amount of consideration we expect to receive, adjusted for any applicable estimates of variable consideration and other factors affecting the transaction price, which is based on the invoiced price, in exchange for transferring products. All revenue is recognized when we satisfy our performance obligations under the contract. The majority of our contracts have a single performance obligation and are short term in nature.
Sales taxes and value added taxes in foreign jurisdictions that are collected from customers and remitted to governmental authorities are accounted for on a net basis and therefore are excluded from net sales. Shipping and handling costs associated with outbound freight after control over a product has transferred to a customer are accounted for as a fulfillment cost and are included in cost of goods sold.
Variable consideration related to certain customer sales incentives is estimated based on the amounts expected to be paid based on the agreement with the customer using probability assessments.
We offer customers a limited right of return for our product in case of non-conformity or performance issues. We estimate the amount of our product sales that may be returned by our customers based on historical sales and returns. As our historical product returns to date have been immaterial, we have not recorded a reduction in revenue related to variable consideration for product returns.
Stock-Based Compensation
We maintain an equity incentive plan to provide long-term incentives for eligible employees, consultants, and members of the board of directors. The plan allows for the issuance of non-statutory and incentive stock options to employees and non-statutory stock options to consultants and directors. We also offer an employee stock purchase plan which allows participating employees to purchase shares of our common stock at a discount through payroll deductions.
We recognize equity-based compensation expense for awards of equity instruments to employees and directors based on the grant date fair value of those awards in accordance with ASC Topic 718, Stock Compensation ("ASC 718"). ASC 718 requires all equity-based compensation awards to employees and directors, including grants of restricted shares and stock options, to be recognized as expense in the statements of operations and comprehensive loss based on their grant date fair values. We estimate the fair value of stock options using the Black-Scholes option pricing model. The fair value of each purchase under the employee stock purchase plan is
estimated at the beginning of the offering period using the Black-Scholes option pricing model. We have not granted any restricted shares. We have not granted any stock-based awards to our consultants.
The Black-Scholes option pricing model requires the input of certain subjective assumptions, including (i) the expected share price volatility, (ii) the expected term of the award, (iii) the risk-free interest rate and (iv) the expected dividend yield. Due to the lack of a public market for the trading of our common stock and a lack of company-specific historical and implied volatility data, we have based our estimate of expected volatility on the historical volatility of a group of similar companies that are publicly traded. The historical volatility is calculated based on a period of time commensurate with the expected term assumption. The group of representative companies have characteristics similar to us, including stage of product development and focus on the life science industry. We use the simplified method, which is the average of the final vesting tranche date and the contractual term, to calculate the expected term for options granted to employees and directors as we do not have sufficient historical exercise data to provide a reasonable basis upon which to estimate the expected term. The risk-free interest rate is based on a U.S. government Treasury instrument whose term is consistent with the expected term of the stock options. We use an assumed dividend yield of zero as we have never paid dividends and have no current plans to pay any dividends on our common stock.
We expense the fair value of our equity-based compensation awards granted to employees and directors on a straight-line basis over the associated service period, which is generally the period in which the related services are received. We account for award forfeitures as they occur.
Inventories
Inventories are valued at the lower of cost or net realizable value, computed on a first-in, first out basis. We estimate the recoverability of our inventory by reference to internal estimates of future demands and product life cycles, including expiration of inventory prior to sale. We regularly review inventory quantities on-hand for excess and obsolete inventory and, when circumstances indicate, incur charges to write down inventories to their net realizable value. The determination of a reserve for excess and obsolete inventory involves management exercising judgment to determine the required reserve, considering future demand, product life cycles, introduction of new products and current market conditions. The reserve for excess and obsolete inventory was less than $0.1 million and $0.8 million as of December 31, 2019 and 2018, respectively.
Income Taxes
We account for income taxes using the liability method. Under this method, deferred tax assets and liabilities are determined based on the differences between the financial reporting and tax bases of assets and liabilities and are measured using the enacted tax rates that will be in effect when the differences are expected to reverse. Valuation allowances against deferred tax assets are established, when necessary, to reduce deferred tax assets to the amounts expected to be realized. As we have historically incurred operating losses, we have recorded a full valuation allowance against our net deferred tax assets, and there is no provision for income taxes other than the accrual for uncertain tax benefits recorded during the year ended December 31, 2019. Our policy is to record interest and penalties expense related to uncertain tax positions as other expense in the statements of operations and comprehensive loss.
Recent Accounting Pronouncements
A discussion of recent accounting pronouncements is included in Note 2 to our financial statements contained in this Annual Report on Form 10-K.
JOBS Act
Prior to December 31, 2019, we were an “emerging growth company” as defined by the JOBS Act. The JOBS Act provides that an emerging growth company can take advantage of the extended transition period for complying with new or revised accounting standards. This allows an emerging growth company to delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We elected to avail ourselves of this exemption prior to December 31, 2019, and as a result, our financial statements prior to
that date may not have been comparable to the financial statements of issuers who are required to comply with the effective dates for new or revised accounting standards that are applicable to public companies.
Subject to certain conditions, as an emerging growth company we also were able to rely on certain of the exemptions and reduced reporting requirements of the JOBS Act, including without limitation, from providing an auditor's attestation report on our system of internal control over financial reporting pursuant to Section 404(b) of the Sarbanes-Oxley Act of 2002 and from complying with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor's report providing additional information about the audit and the financial statements, known as the auditor discussion and analysis. Because we no longer qualify as an emerging growth company, we are no longer able to take advantage of the extended transition period for the adoption of certain accounting standards or of the reduced disclosure and other benefits available to emerging growth companies, including our exemption from providing our auditor’s attestation on our system of internal control over financial reporting, which is included in this Annual Report on Form 10-K.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk
The risk associated with fluctuating interest rates is primarily limited to our cash equivalents which are carried at quoted market prices and our short-term investments. If overall interest rates had decreased by 100 basis points during the year ended December 31, 2019, our interest income would have decreased by approximately $1.6 million. We do not currently use or plan to use financial derivatives in our investment portfolio.
The interest rate for our outstanding debt is variable. If overall interest rates had increased by 100 basis points during the year ended December 31, 2019 our interest expense would have increased by approximately $0.4 million.
Credit Risk
As of December 31, 2019 and 2018, our cash, cash equivalents, and investments were maintained with one financial institution in the U.S. We believe this institution has sufficient assets and liquidity to conduct its operations in the ordinary course of business with little or no credit risk to us, however our cash balances were in excess of insured limits.
The primary objective of our investment activities is to preserve our capital for the purpose of funding operations while at the same time maximizing the income we receive from our investments without significantly increasing risk or availability. To achieve these objectives, our investment policy allows us to maintain a portfolio of certain types of debt securities issued by the U.S. government and its agencies, corporations with investment-grade credit ratings, or commercial paper and money market funds issued by the highest quality financial and non-financial companies. We place restrictions on maturities and concentration by type and issuer. We are exposed to credit risk in the event of a default by the issuers of these securities to the extent recorded on the balance sheets. See Note 2 to our financial statements contained in this Annual Report on Form 10-K for additional information on our cash equivalents and available-for-sale marketable securities.
Our accounts receivable primarily relate to revenue from the sale of our Inspire system to hospitals in the U.S. and Europe, primarily in Germany. No single customer represented more than 10% of our accounts receivable as of December 31, 2019 or 2018.
Foreign Currency Risk
The majority of our business is currently conducted in U.S. dollars. Any transactions that may be conducted in foreign currencies are not expected to have a material effect on our results of operations, financial position or cash flows.
Inflation Risk
Inflationary factors, such as increases in our cost of goods sold and selling and operating expenses, may adversely affect our operating results. Although we do not believe that inflation has had a material impact on our financial position or results of operations to date, a high rate of inflation in the future may have an adverse effect on our ability to maintain and increase our gross margin and selling and marketing and operating expenses as a percentage of our revenue if the selling prices of our products do not increase as much as or more than these increased costs.
Item 8. Financial Statements and Supplementary Data.
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Inspire Medical Systems, Inc.
Opinion on the Financial Statements
We have audited the accompanying balance sheets of Inspire Medical Systems, Inc. (the Company) as of December 31, 2019 and 2018, the related statements of operations and comprehensive loss, stockholders' (deficit) equity and cash flows for each of the three years in the period ended December 31, 2019, and the related notes (collectively referred to as the "financial statements"). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2019 and 2018, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2019, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company's internal control over financial reporting as of December 31, 2019, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework), and our report dated February 25, 2020 expressed an unqualified opinion thereon.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company's financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matter
The critical audit matter communicated below is a matter arising from the current period audit of the financial statements that were communicated or required to be communicated to the audit committee and that: (1) relates to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective or complex judgments. The communication of the critical audit matter does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing a separate opinion on the critical audit matter or on the account or disclosure to which it relates.
| | | | | | | | |
| | Inventory valuation reserves |
| Description of the Matter | | At December 31, 2019, the Company’s net inventory balance was $5.8 million. As explained in Note 2 to the financial statements, the determination of a reserve for excess and obsolete inventory involves management exercising judgment to determine the required reserve, considering future demand, product life cycles, introduction of new products and current market conditions.
Auditing management’s estimate for excess and obsolete inventory involved subjective auditor judgment because the estimates and judgments used to calculate the inventory reserve, especially considering the timing of the introduction of new products and current market conditions. In particular, the excess and obsolete inventory calculations are sensitive to significant assumptions, including forecasted customer demand, technological and/or market obsolescence, and possible alternative uses. |
| | |
| How We Addressed the Matter in Our Audit | | We obtained an understanding, evaluated the design, and tested the operating effectiveness of controls over the Company's process to determine the amount of the Company’s reserve for excess and obsolete inventory. This included controls over the Company’s review of the significant assumptions underlying the reserve estimate.
To test the adequacy of the Company's inventory valuation reserve, we performed substantive audit procedures that included, among others, testing the accuracy and completeness of the underlying data used in the estimation calculations and evaluating significant assumptions (e.g., forecasted customer demand, technological and/or market obsolescence, and possible alternative uses) and the underlying data used in management's excess and obsolete inventory valuation assessment. We evaluated management’s ability to accurately estimate the excess and obsolete inventory by comparing actual write-off activity in recent years to the inventory valuation reserve estimated by the Company in prior years. We also audited management’s calculation of the inventory valuation reserve by testing the mathematical accuracy of the Company’s reserve calculation. |
/s/Ernst & Young LLP
We have served as the Company's auditor since 2015.
Minneapolis, Minnesota
February 25, 2020
INSPIRE MEDICAL SYSTEMS, INC.
BALANCE SHEETS
(in thousands, except share and per share amounts)
| | | | | | | | | | | |
| December 31, | | |
| 2019 | | 2018 |
| Assets | | | |
| Current assets: | | | |
| Cash and cash equivalents | $ | 22,860 | | | $ | 97,288 | |
| Investments, short-term | 126,605 | | | 90,922 | |
| Accounts receivable, net | 13,131 | | | 6,667 | |
| Inventories | 5,834 | | | 2,667 | |
| Prepaid expenses and other current assets | 2,206 | | | 1,734 | |
| Total current assets | 170,636 | | | 199,278 | |
| Investments, long-term | 6,276 | | | — | |
| Property and equipment, net | 3,045 | | | 802 | |
| Operating lease right-of-use asset | 915 | | | — | |
| Other non-current asset | 381 | | | — | |
| Total assets | $ | 181,253 | | | $ | 200,080 | |
| Liabilities and stockholders' equity | | | |
| Current liabilities: | | | |
| Accounts payable | $ | 4,459 | | | $ | 3,429 | |
| Accrued expenses | 12,397 | | | 7,726 | |
| | | |
| Total current liabilities | 16,856 | | | 11,155 | |
| Notes payable | 24,522 | | | 24,926 | |
| | | |
| Other non-current liability | 40 | | | — | |
| | | |
| Total liabilities | 41,418 | | | 36,081 | |
| Stockholders' equity | | | |
| Common Stock, $0.001 par value, 200,000,000 shares authorized at December 31, 2019 and 2018; 24,107,350 and 23,401,675 shares issued and outstanding at December 31, 2019 and 2018, respectively | 24 | | | 23 | |
| Additional paid-in capital | 319,865 | | | 310,941 | |
| Accumulated other comprehensive income (loss) | 102 | | | (52) | |
| Accumulated deficit | (180,156) | | | (146,913) | |
| Total stockholders' equity | 139,835 | | | 163,999 | |
| Total liabilities and stockholders' equity | $ | 181,253 | | | $ | 200,080 | |
The accompanying notes are an integral part of these financial statements.
INSPIRE MEDICAL SYSTEMS, INC.
STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS
(in thousands, except share and per share amounts)
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2019 | | 2018 | | 2017 |
| Revenue | $ | 82,050 | | | $ | 50,593 | | | $ | 28,567 | |
| Cost of goods sold | 13,643 | | | 10,056 | | | 6,018 | |
| Gross profit | 68,407 | | | 40,537 | | | 22,549 | |
| Operating expenses: | | | | | |
| Research and development | 12,839 | | | 7,388 | | | 6,194 | |
| Selling, general and administrative | 90,465 | | | 53,527 | | | 32,358 | |
| Total operating expenses | 103,304 | | | 60,915 | | | 38,552 | |
| Operating loss | (34,897) | | | (20,378) | | | (16,003) | |
| Other (income) expense: | | | | | |
| Interest income | (3,801) | | | (1,870) | | | (203) | |
| Interest expense | 2,119 | | | 3,304 | | | 1,753 | |
| Other (income) expense, net | (12) | | | 16 | | | (42) | |
| Total other (income) expense | (1,694) | | | 1,450 | | | 1,508 | |
| Loss before income taxes | (33,203) | | | (21,828) | | | (17,511) | |
| Income taxes | 40 | | | — | | | — | |
| Net loss | (33,243) | | | (21,828) | | | (17,511) | |
| Other comprehensive loss: | | | | | |
| Unrealized gain (loss) on investments | 154 | | | (52) | | | — | |
| Total comprehensive loss | $ | (33,089) | | | $ | (21,880) | | | $ | (17,511) | |
| Net loss per share, basic and diluted | $ | (1.40) | | | $ | (1.50) | | | $ | (14.88) | |
| Weighted average common shares used to compute net loss per share, basic and diluted | 23,804,452 | | | 14,579,662 | | | 1,176,650 | |
The accompanying notes are an integral part of these financial statements.
INSPIRE MEDICAL SYSTEMS, INC.
STATEMENTS OF STOCKHOLDERS' (DEFICIT) EQUITY
(in thousands, except share amounts)
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Common Stock | | | | | | | Convertible Preferred Stock | | | | | | | | |
| Shares | | Amount | | Additional paid-in capital | | | Shares | | Amount | | Accumulated Other Comprehensive Loss | | Accumulated Deficit | | Total Stockholders' (Deficit) Equity |
| Balance at December 31, 2016 | 1,145,238 | | | $ | 1 | | | $ | 6,827 | | | | 57,986,873 | | | $ | 94,138 | | | $ | — | | | $ | (107,574) | | | $ | (6,608) | |
| Stock options exercised | 127,122 | | | — | | | 235 | | | | — | | | — | | | — | | | — | | | 235 | |
| Sale of Series F convertible preferred stock, net issuance costs of $32 | — | | | — | | | — | | | | 18,248,177 | | | 24,968 | | | — | | | — | | | 24,968 | |
| Stock-based compensation expense | — | | | — | | | 243 | | | | — | | | — | | | — | | | — | | | 243 | |
| Net loss | — | | | — | | | — | | | | — | | | — | | | — | | | (17,511) | | | (17,511) | |
| Balance at December 31, 2017 | 1,272,360 | | | 1 | | | 7,305 | | | | 76,235,050 | | | 119,106 | | | — | | | (125,085) | | | 1,327 |
| Stock options and warrants exercised | 377,820 | | | — | | | 558 | | | | — | | | — | | | — | | | — | | | 558 | |
| Issuance of common stock | 2,285 | | | — | | | 95 | | | | — | | | — | | | — | | | — | | | 95 | |
| Sale of common stock from initial public offering, net of offering expenses | 7,762,500 | | | 8 | | | 112,032 | | | — | | | — | | | — | | | — | | | 112,040 | |
| Sale of common stock from follow-on public offering, net of offering expenses | 1,875,000 | | | 2 | | | 69,783 | | | | — | | | — | | | — | | | — | | | 69,785 | |
| Conversion of preferred stock to common stock | 12,111,710 | | | 12 | | | 119,094 | | | (76,235,050) | | | (119,106) | | | — | | | — | | | — | |
| Conversion of warrants to purchase preferred stock to warrants to purchase common stock | — | | | — | | | 855 | | | | — | | | — | | | — | | | — | | | 855 | |
| Stock-based compensation expense | — | | | — | | | 1,219 | | | | — | | | — | | | — | | | — | | | 1,219 | |
| Other comprehensive loss | — | | | — | | | — | | | | — | | | — | | | (52) | | | — | | | (52) | |
| Net loss | — | | | — | | | — | | | | — | | | — | | | — | | | (21,828) | | | (21,828) | |
| Balance at December 31, 2018 | 23,401,675 | | | 23 | | | 310,941 | | | | — | | | — | | | (52) | | | (146,913) | | | 163,999 | |
| Stock options and warrants exercised | 669,719 | | | 1 | | | | 1,139 | | | | | | — | | | | — | | | | — | | | | — | | | | 1,140 | |
| Issuance of common stock | 4,206 | | | — | | | | 233 | | | | | | — | | | | — | | | | — | | | | — | | | | 233 | |
| Issuance of common stock for employee stock purchase plan | 31,750 | | | — | | | | 1,355 | | | | | | — | | | | — | | | | — | | | | — | | | | 1,355 | |
| Stock-based compensation expense | — | | | — | | | | 6,197 | | | | | | — | | | | — | | | | — | | | | — | | | | 6,197 | |
| Other comprehensive income | — | | | — | | | — | | | | | | — | | | | — | | | | 154 | | | | — | | | | 154 | |
| Net loss | — | | | — | | | — | | | | | | — | | | | — | | | | — | | | | (33,243) | | | | (33,243) | |
| Balance at December 31, 2019 | 24,107,350 | | | $ | 24 | | | | $ | 319,865 | | | | $ | — | | | $ | — | | | | $ | 102 | | | | $ | (180,156) | | | | $ | 139,835 | |
The accompanying notes are an integral part of these financial statements.
INSPIRE MEDICAL SYSTEMS, INC.
STATEMENTS OF CASH FLOWS
(in thousands)
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2019 | | 2018 | | 2017 |
| Operating activities | | | | | |
| Net loss | $ | (33,243) | | | $ | (21,828) | | | $ | (17,511) | |
| Adjustments to reconcile net loss: | | | | | |
| Depreciation and amortization | 495 | | | 393 | | | 285 | |
| Accretion of investment discount | (983) | | | (648) | | | — | |
| Accretion of debt discount | 268 | | | 568 | | | 315 | |
| Non-cash lease expense | 904 | | | | — | | | | — | |
| Stock-based compensation expense | 6,197 | | | 1,219 | | | 243 | |
| Non-cash stock issuance for services rendered | 233 | | | 95 | | | — | |
| Change in the fair value of preferred stock warrants | — | | | 595 | | | 100 | |
| Other, net | (143) | | | 51 | | | — | |
| Changes in operating assets and liabilities: | | | | | |
| Accounts receivable | (6,480) | | | (2,836) | | | (1,767) | |
| Inventories | (3,167) | | | 1,003 | | | (315) | |
| Prepaid expenses and other assets | (905) | | | (1,326) | | | (308) | |
| Accounts payable | 1,034 | | | 439 | | | 1,825 | |
| Accrued expenses and other liabilities | 2,944 | | | 3,581 | | | 1,342 | |
| Net cash used in operating activities | (32,846) | | | (18,694) | | | (15,791) | |
| Investing activities | | | | | |
| Purchases of property and equipment | (2,739) | | | (250) | | | (412) | |
| Purchases of investments | (178,074) | | | (115,481) | | | (8,969) | |
| Proceeds from sales or maturities of investments | 137,254 | | | 32,342 | | | 1,781 | |
| Net cash used in investing activities | (43,559) | | | (83,389) | | | (7,600) | |
| Financing activities | | | | | |
| Proceeds from issuance of notes payable | — | | | 8,000 | | | 458 | |
| Payment of debt fees | (531) | | | | — | | | | — | |
| Proceeds from the exercise of stock options and warrants | 1,140 | | | 558 | | | 235 | |
| Proceeds from sale of common stock | — | | | 181,825 | | | — | |
| Proceeds from the issuance of common stock from employee stock purchase plan | 1,355 | | | | — | | | | — | |
| Proceeds from sale of preferred stock | — | | | — | | | 24,968 | |
| Net cash provided by financing activities | 1,964 | | | 190,383 | | | 25,661 | |
| Effect of exchange rate on cash | 13 | | | 33 | | | — | |
| (Decrease) increase in cash and cash equivalents | (74,428) | | | 88,333 | | | 2,270 | |
| Cash and cash equivalents at beginning of year | 97,288 | | | 8,955 | | | 6,685 | |
| Cash and cash equivalents at end of year | $ | 22,860 | | | $ | 97,288 | | | $ | 8,955 | |
| Supplemental cash flow information | | | | | |
| Cash paid for interest | $ | 2,033 | | | $ | 2,019 | | | $ | 1,323 | |
| Issuance of preferred stock warrants | — | | | 103 | | | 4 | |
The accompanying notes are an integral part of these financial statements.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
1. Organization
Description of Business
Inspire Medical Systems, Inc. is a medical technology company focused on the development and commercialization of innovative and minimally invasive solutions for patients with obstructive sleep apnea ("OSA"). Our proprietary Inspire system is the first and only United States ("U.S.") Food and Drug Administration ("FDA") approved neurostimulation technology that provides a safe and effective treatment for moderate to severe OSA. Inspire therapy received premarket approval ("PMA") from the FDA in April 2014 and has been commercially available in certain European markets since November 2011. In June 2018, Japan's Ministry of Health, Labour and Welfare approved Inspire therapy to treat moderate to severe OSA, and we are currently seeking reimbursement coverage in Japan.
2. Summary of Significant Accounting Policies
Basis of Presentation
The financial statements have been prepared in accordance with U.S. generally accepted accounting principles ("U.S. GAAP") and pursuant to the rules and regulations of the Securities and Exchange Commission ("SEC").
In the opinion of management, all adjustments, consisting of only normal recurring adjustments that are necessary to present fairly the financial position, results of operations, and cash flows have been made. The results of operations for the year ended December 31, 2019 are not necessarily indicative of the operating results for any future periods.
Reverse Stock Split
In connection with our initial public offering of common stock ("IPO"), our board of directors and stockholders approved a 1-for-6.650 reverse stock split of our common stock. The reverse stock split became effective on April 20, 2018. The par value of the common stock was not adjusted as a result of the reverse stock split. Adjustments corresponding to the reverse stock split were made to the ratio at which the convertible preferred stock converted into common stock immediately prior to the closing of the IPO. Accordingly, all share and per-share amounts for all periods presented in these financial statements and notes thereto have been adjusted retroactively, where applicable, to reflect the reverse stock split and adjustment of the conversion ratio of the convertible preferred stock.
Initial Public Offering
On May 7, 2018, we completed our IPO by issuing 7,762,500 shares of common stock, at an offering price of $16.00 per share, for net proceeds of approximately $112.0 million after deducting underwriting discounts and commissions and offering expenses payable by us. In connection with the IPO, our outstanding shares of convertible preferred stock were automatically converted into an aggregate of 12,111,710 shares of common stock, and our outstanding warrants to purchase shares of convertible preferred stock were automatically converted into warrants to purchase up to an aggregate of 100,558 shares of common stock, resulting in the reclassification of the related redeemable convertible preferred stock warrant liability of $0.9 million to additional paid-in capital ("APIC").
Follow-On Public Offering
On December 11, 2018, we completed a follow-on offering that included our offer and sale of 1,875,000 shares of common stock and the selling stockholders’ offer and sale of 1,000,000 shares of common stock, at a public offering price of $40.00 per share. We received net proceeds of approximately $69.8 million after deducting underwriting
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
discounts and commissions and offering expenses. We received no proceeds from the sale of our common stock by the selling stockholders.
Use of Estimates
The preparation of financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the amounts and disclosures reported in the financial statements. We use significant judgment when making estimates related to the allowance for doubtful accounts, inventory reserves, warranty reserves, and the valuations of our common stock prior to our IPO, stock-based awards, and certain of our previously outstanding preferred stock warrants. We base our estimates on historical experience and on various other assumptions that are believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results could differ from those estimates.
JOBS Act Accounting Election
Prior to December 31, 2019, we were an emerging growth company under the JOBS Act, and as a result we were eligible to take advantage of certain exemptions from various reporting requirements that are applicable to other public companies that are not emerging growth companies. We elected to take advantage of the extended transition period for adopting new or revised accounting standards that have different effective dates for public and private companies until such time as those standards apply to private companies. However, as we satisfy the definition of a “large accelerated filer” under the definition of the Securities Exchange Act of 1934, as amended, we no longer qualify as an emerging growth company as of December 31, 2019. Therefore we no longer are able to take advantage of the extended transition period for adopting new or revised accounting standards.
Cash and Cash Equivalents
We consider all highly liquid securities, readily convertible to cash, that mature within 90 days or less from the date of purchase to be cash equivalents. The carrying amount reported in the balance sheets for cash is cost, which approximates fair value.
Foreign Currency
Sales and expenses denominated in foreign currencies are translated at average exchange rates in effect throughout the year. Foreign currency transaction gains and losses are included in other (income) expense, net in the statements of operations and comprehensive loss. Assets and liabilities of foreign operations are remeasured at period-end exchange rates with the impacts of foreign currency remeasurement recognized in other (income) expense, net in the statements of operations and comprehensive loss.
Investments
At December 31, 2019 and 2018, our short-term investments consisted of commercial paper, corporate bonds, asset-backed securities, and U.S. government securities which are classified as available-for-sale and had maturities less than one year. Our long-term investments consisted of corporate bonds. Investments are reported at their estimated fair market value which approximates cost. Any unrealized gains and losses are reported as a separate component of accumulated other comprehensive income (loss). We had $0.1 million of unrecognized income and $0.1 million of unrecognized loss in accumulated other comprehensive income (loss) balance at December 31, 2019 and 2018, respectively. Any realized gains and losses are calculated on the specific identification method and reported net in other (income) expense. For both the years ended December 31, 2019 and 2018, we recognized less than $0.1 million of gains, net.
We review our investment portfolio periodically to assess for other-than-temporary impairment. Should we determine that any unrealized losses on the investments are other-than-temporary, the amount of that impairment to
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
be recognized in earnings will depend on whether we intend to sell the security or more likely than not will be required to sell the security before recovery of its amortized cost basis less any current period credit loss.
Fair Value of Financial Instruments
We measure certain financial assets and liabilities at fair value on a recurring basis, including cash equivalents, investments, and our previously outstanding preferred stock warrants. Fair value is an exit price, representing the amount that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants. As such, fair value is a market-based measurement that should be determined based on assumptions that market participants would use in pricing an asset or a liability. A three-tier fair value hierarchy is established as a basis for considering such assumptions and for inputs used in the valuation methodologies in measuring fair value:
Level 1—Observable inputs, such as quoted prices (unadjusted) for identical assets or liabilities in active markets.
Level 2—Other inputs that are based upon quoted prices for similar instruments in active markets, quoted prices for identical or similar instruments in markets that are not active, and model-based valuation techniques for which all significant inputs are observable in the market or can be derived from observable market data. Where applicable, these models project future cash flows and discount the future amounts to a present value using market-based observable inputs, including interest rate curves, foreign exchange rates, and credit ratings.
Level 3—Unobservable inputs that are supported by little or no market activities, which would require us to develop our own assumptions.
We use the methods and assumptions described below in determining the fair value of our financial instruments.
Money market funds: Fair values of money market funds are based on quoted market prices in active markets. These are included as Level 1 measurements in the tables below.
Commercial paper: Short-term, highly liquid investments are included as a Level 2 measurement in the tables below.
Corporate bonds: Consists of short- and long-term notes and bonds with various yields. These are included as a Level 2 measurement in the tables below.
Asset-backed securities: Consists of short-term, securitized investments backed by pools of credit card receivables. These are included as a Level 2 measurement in the tables below.
U.S. government securities: Consists of U.S. government Treasury bills with original maturities of less than one year. These are included as a Level 1 measurement in the table below.
The following tables sets forth by level within the fair value hierarchy our assets that are measured on a recurring basis and reported at fair value as of December 31, 2019 and 2018. Assets are classified in their entirety based on the lowest level of input that is significant to the fair value measurement.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Fair Value Measurements as of | | | | | | |
| | December 31, 2019 | | | | | | |
| | Estimated Fair Value | | Level 1 | | Level 2 | | Level 3 |
| Cash equivalents: | | | | | | | | |
| Money market funds | | $ | 18,429 | | | $ | 18,429 | | | $ | — | | | $ | — | |
| | | | | | | | |
| Total cash equivalents | | 18,429 | | | 18,429 | | | — | | | — | |
| Investments: | | | | | | | | |
| Commercial paper | | $ | 14,214 | | | $ | — | | | $ | 14,214 | | | $ | — | |
| Corporate bonds | | 32,485 | | | — | | | 32,485 | | | — | |
| Asset-backed securities | | 8,100 | | | — | | | 8,100 | | | — | |
| U.S. government securities | | 78,082 | | | 78,082 | | | — | | | — | |
| Total investments | | 132,881 | | | 78,082 | | | 54,799 | | | — | |
| Total cash equivalents and investments | | $ | 151,310 | | | $ | 96,511 | | | $ | 54,799 | | | $ | — | |
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Fair Value Measurements as of | | | | | | |
| | December 31, 2018 | | | | | | |
| | Estimated Fair Value | | Level 1 | | Level 2 | | Level 3 |
| Cash equivalents: | | | | | | | | |
| Money market funds | | $ | 94,700 | | | $ | 94,700 | | | $ | — | | | $ | — | |
| | | | | | | | |
| Total cash equivalents | | 94,700 | | | 94,700 | | | — | | | — | |
| Investments: | | | | | | | | |
| Commercial paper | | 27,898 | | | — | | | 27,898 | | | — | |
| Corporate bonds | | 28,012 | | | — | | | 28,012 | | | — | |
| Asset-backed securities | | 17,055 | | | — | | | 17,055 | | | — | |
| U.S. government securities | | 17,957 | | | 17,957 | | | — | | | — | |
| Total investments | | 90,922 | | | 17,957 | | | 72,965 | | | — | |
| Total cash equivalents and investments | | $ | 185,622 | | | $ | 112,657 | | | $ | 72,965 | | | $ | — | |
There were 0 transfers between Level 1, Level 2, or Level 3 during the years ended December 31, 2019 and 2018.
The recurring Level 3 fair value measurements of our preferred stock warrant liabilities used the Black-Scholes option pricing model and value of the respective class of our convertible preferred stock (see Note 7), which was unobservable. All other assumptions included in the model are observable Level 1 inputs.
The following table provides a reconciliation of the beginning and ending balances of our preferred stock warrant liabilities:
| | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | |
| | 2019 | | 2018 | | 2017 |
| Balance at beginning of period | | $ | — | | | $ | 157 | | | $ | 53 | |
| Initial fair value of preferred stock warrants issued | | — | | | 103 | | | 4 | |
| Reclassified to equity | | — | | | (855) | | | — | |
| Change in fair value of preferred stock warrants | | — | | | 595 | | | 100 | |
| Balance at end of period | | $ | — | | | $ | — | | | $ | 157 | |
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
Changes in the fair value of the preferred stock warrant liability were recorded in other expenses on the statements of operations and comprehensive loss. In connection with the closing of the IPO in May 2018, warrants to purchase shares of preferred stock automatically converted into warrants to purchase shares of common stock, resulting in the reclassification of the related convertible preferred stock warrant liability to APIC.
Concentration of Credit Risk
Financial instruments, which potentially subject us to concentrations of credit risk, consist principally of cash equivalents, investments, and accounts receivable.
Our investment policy limits investments to certain types of debt securities issued by the U.S. government and its agencies, corporations with investment-grade credit ratings, or commercial paper and money market funds issued by the highest quality financial and non-financial companies. We place restrictions on maturities and concentration by type and issuer. We are exposed to credit risk in the event of a default by the issuers of these securities to the extent recorded on the balance sheets. However, as of December 31, 2019 and 2018, we limited our credit risk associated with cash equivalents by placing investments with banks we believe are highly creditworthy.
We believe that the credit risk in our accounts receivable is mitigated by our credit evaluation process, relatively short collection terms, and dispersion of our customer base. We generally do not require collateral, and losses on accounts receivable have historically been within management's expectations.
Accounts Receivable and Allowance for Doubtful Accounts
Trade accounts receivable are recorded at the invoiced amount and do not bear interest. Customer credit terms are established prior to shipment with the general standard being net 30 days. Collateral or any other security to support payment of these receivables generally is not required. We record an allowance for doubtful accounts for accounts receivable deemed uncollectible. We evaluate the collectability of our accounts receivable based on known collection risks and historical experience. In circumstances where we are aware of a specific customer's inability to meet its financial obligations to us (e.g., bankruptcy filings or substantial downgrading of credit ratings), we record a specific allowance for bad debts against amounts due to reduce the carrying amount of accounts receivable to the amount we reasonably believe will be collected. Specific accounts receivable are written-off once a determination is made that the account is uncollectible. The allowance for doubtful accounts was less than $0.1 million as of each of December 31, 2019 and 2018.
Inventories
Inventories are valued at the lower of cost or net realizable value, computed on a first-in, first-out basis, and consisted of the following:
| | | | | | | | | | | | | | |
| | December 31, | | |
| | 2019 | | 2018 |
| Raw materials | | $ | 781 | | | $ | 802 | |
| Finished goods | | 5,053 | | | 1,865 | |
| Total inventories, net of reserves | | $ | 5,834 | | | $ | 2,667 | |
We regularly review inventory quantities on-hand for excess and obsolete inventory and, when circumstances indicate, incur charges to write down inventories to their net realizable value. The determination of a reserve for excess and obsolete inventory involves management exercising judgment to determine the required reserve, considering future demand, product life cycles, introduction of new products and current market conditions The reserve for excess and obsolete inventory was less than $0.1 million and $0.8 million as of December 31, 2019 and 2018, respectively.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
Property and Equipment
Property and equipment are stated at cost, less accumulated depreciation and amortization and consisted of the following:
| | | | | | | | | | | | | | |
| | December 31, | | |
| | 2019 | | 2018 |
| Computer equipment and software | | $ | 790 | | | $ | 333 | |
| | | | |
| Manufacturing equipment | | 1,050 | | | 925 | |
| Other equipment | | 68 | | | 34 | |
| Leasehold improvements | | 192 | | | 185 | |
| Construction in process | | 1,950 | | | 124 | |
| Property and equipment, cost | | 4,050 | | | 1,601 | |
| Less: accumulated depreciation and amortization | | (1,005) | | | (799) | |
| Property and equipment, net | | $ | 3,045 | | | $ | 802 | |
Depreciation is determined using the straight-line method over the estimated useful lives of the respective assets, generally three to five years. Leasehold improvements are amortized on a straight-line basis over the shorter of their estimated useful lives or the term of the lease. Depreciation and amortization expense was $0.5 million, $0.4 million and $0.3 million during the years ended December 31, 2019, 2018 and 2017, respectively.
Impairment of Long-lived Assets
Long-lived assets consist primarily of property and equipment and are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. If circumstances require that an asset be tested for possible impairment, we compare the undiscounted cash flows expected to be generated by the asset to the carrying amount of the asset. If the carrying amount of the asset is not recoverable on an undiscounted cash flow basis, we determine the fair value of the asset and recognize an impairment loss to the extent the carrying amount of the asset exceeds its fair value. We determine fair value using the income approach based on the present value of expected future cash flows or other appropriate measures of estimated fair value. Our cash flow assumptions consider historical and forecasted revenue and operating costs and other relevant factors. We did not record any material impairment charges on long-lived assets during the years ended December 31, 2019 and 2018.
Accrued Expenses
Accrued expenses consisted of the following:
| | | | | | | | | | | |
| December 31, | | |
| 2019 | | 2018 |
| Payroll related | $ | 10,304 | | | $ | 6,490 | |
| Interest | 160 | | | 195 | |
| Current operating lease liability | 828 | | | | — | |
| Other accrued expenses | 1,105 | | | 1,041 | |
| Total accrued expenses | $ | 12,397 | | | $ | 7,726 | |
Revenue Recognition
We recognize revenue in accordance with Accounting Standards Codification ("ASC") Topic 606, Revenue from Contracts with Customers ("ASC 606"), which we adopted effective January 1, 2019 using the modified
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
retrospective approach. The adoption of ASC 606 did not have a material impact on the amount and timing of revenue recognized in our financial statements.
Revenues from product sales are recognized when the customer obtains control of the product, which occurs at a point in time, either upon shipment of the product or receipt of the product, depending on shipment terms. Our standard shipping terms are free on board shipping point, unless the customer requests that control and title to the inventory transfer upon delivery. In those cases where shipping and handling costs are billed to customers, we classify the amounts billed as a component of cost of goods sold.
Revenue is measured as the amount of consideration we expect to receive, adjusted for any applicable estimates of variable consideration and other factors affecting the transaction price, which is based on the invoiced price, in exchange for transferring products. All revenue is recognized when we satisfy our performance obligations under the contract. The majority of our contracts have a single performance obligation and are short term in nature.
Sales taxes and value added taxes in foreign jurisdictions that are collected from customers and remitted to governmental authorities are accounted for on a net basis and therefore are excluded from net sales. Shipping and handling costs associated with outbound freight after control over a product has transferred to a customer are accounted for as a fulfillment cost and are included in cost of goods sold.
Variable consideration related to certain customer sales incentives is estimated based on the amounts expected to be paid based on the agreement with the customer using probability assessments.
We offer customers a limited right of return for our product in case of non-conformity or performance issues. We estimate the amount of our product sales that may be returned by our customers based on historical sales and returns. As our historical product returns to date have been immaterial, we have not recorded a reduction in revenue related to variable consideration for product returns.
See Note 10 for disaggregated revenue by geographic area.
Cost of Goods Sold
Cost of goods sold consists primarily of acquisition costs for the components of the Inspire system, overhead costs, scrap and inventory obsolescence, as well as distribution-related expenses such as logistics and shipping costs, net of costs charged to customers. The overhead costs include the cost of material procurement, depreciation expense for production equipment, warranty replacement costs, and operations supervision and management personnel, including employee compensation, stock-based compensation, supplies, and travel.
Research and Development
Research and development expenses consist primarily of product development, clinical and regulatory affairs, consulting services, and other costs associated with products and technologies in development. These expenses include employee compensation, stock-based compensation, supplies, travel, and facility costs. Clinical expenses include clinical trial design, clinical site reimbursement, data management, travel expenses, and the cost of manufacturing products for clinical trials.
Stock-Based Compensation
We maintain an equity incentive plan to provide long-term incentives for eligible employees, consultants, and members of the board of directors. The plan allows for the issuance of non-statutory and incentive stock options to employees and non-statutory stock options to consultants and directors. We also offer an employee stock purchase plan which allows participating employees to purchase shares of our common stock at a discount through payroll deductions.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
We recognize equity-based compensation expense for awards of equity instruments to employees and directors based on the grant date fair value of those awards in accordance with ASC Topic 718, Stock Compensation ("ASC 718"). ASC 718 requires all equity-based compensation awards to employees and directors, including grants of restricted shares and stock options, to be recognized as expense in the statements of operations and comprehensive loss based on their grant date fair values. We estimate the fair value of stock options using the Black-Scholes option pricing model. The fair value of each purchase under the employee stock purchase plan is estimated at the beginning of the offering period using the Black-Scholes option pricing model. We have not granted any restricted shares. We have not granted any stock-based awards to our consultants.
The Black-Scholes option pricing model requires the input of certain subjective assumptions, including (i) the expected share price volatility, (ii) the expected term of the award, (iii) the risk-free interest rate and (iv) the expected dividend yield. Due to the lack of a public market for the trading of our common stock and a lack of company-specific historical and implied volatility data, we have based our estimate of expected volatility on the historical volatility of a group of similar companies that are publicly traded. The historical volatility is calculated based on a period of time commensurate with the expected term assumption. The group of representative companies have characteristics similar to us, including stage of product development and focus on the life science industry. We use the simplified method, which is the average of the final vesting tranche date and the contractual term, to calculate the expected term for options granted to employees and directors as we do not have sufficient historical exercise data to provide a reasonable basis upon which to estimate the expected term. The risk-free interest rate is based on a U.S. government Treasury instrument whose term is consistent with the expected term of the stock options. We use an assumed dividend yield of 0 as we have never paid dividends and have no current plans to pay any dividends on our common stock.
We expense the fair value of our equity-based compensation awards granted to employees and directors on a straight-line basis over the associated service period, which is generally the period in which the related services are received. We account for award forfeitures as they occur.
Advertising Expenses
We expense the costs of advertising, including promotional expenses, as incurred. Advertising expenses were $18.0 million, $9.3 million and $6.3 million during the years ended December 31, 2019, 2018 and 2017, respectively.
Leases
Operating leases are included in operating lease right-of-use ("ROU") assets and current operating lease liabilities in our balance sheets. ROU assets represent our right to use an underlying asset for the lease term and lease liabilities represent our obligation to make lease payments arising from the lease. Operating lease ROU assets and liabilities are recognized at the lease commencement date based on the present value of lease payments over the lease term. In determining the present value of lease payments, we use our incremental borrowing rate based on the information available at the lease commencement date as the rate implicit in the lease is not readily determinable. The determination of our incremental borrowing rate requires management judgment based on information available at lease commencement. The operating lease ROU assets also include adjustments for prepayments, accrued lease payments and exclude lease incentives. Our lease terms may include options to extend or terminate the lease when it is reasonably certain that we will exercise such options. Operating lease cost is recognized on a straight-line basis over the expected lease term. Lease agreements entered into after the adoption of ASC 842 that include lease and non-lease components are accounted for as a single lease component. Lease agreements with a noncancelable term of less than 12 months are not recorded on our balance sheets.
Income Taxes
We account for income taxes using the liability method. Under this method, deferred tax assets and liabilities are determined based on the differences between the financial reporting and tax bases of assets and liabilities and are measured using the enacted tax rates that will be in effect when the differences are expected to reverse. Valuation
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
allowances against deferred tax assets are established, when necessary, to reduce deferred tax assets to the amounts expected to be realized. As we have historically incurred operating losses, we have recorded a full valuation allowance against our net deferred tax assets, and there is no provision for income taxes other than the accrual for uncertain tax benefits. Our policy is to record interest and penalties expense related to uncertain tax positions as other expense in the statements of operations and comprehensive loss.
Comprehensive Loss
Comprehensive loss consists of net loss and changes in unrealized gains and losses on investments classified as available-for-sale. Accumulated other comprehensive income (loss) is presented in the accompanying balance sheets as a component of stockholders' equity.
Loss Per Share
Basic net loss per share is computed by dividing the net loss by the weighted average number of shares of common stock outstanding during the period. Diluted net loss per share is computed by dividing the net loss by the weighted average number of shares of common stock and dilutive potential shares of common stock outstanding during the period. Because we have reported a net loss for all periods presented, diluted net loss per share is the same as basic net loss per share for those periods as all potentially dilutive shares consisting of convertible preferred stock, stock options and warrants were antidilutive in those periods.
Purchase Commitments
As of December 31, 2019, we had purchase commitments to suppliers for purchases totaling $23.7 million.
Recent Accounting Pronouncements
In February 2016, the FASB issued Accounting Standards Update ("ASU") 2016-02, Leases (Topic 842) ("ASU 2016-02"), which supersedes the existing guidance for lease accounting, Leases (Topic 840). ASU 2016-02 requires lessees to recognize a lease liability and a right-of-use asset for all leases with lease terms greater than 12 months. Lessor accounting remains largely unchanged. The original guidance required application on a modified retrospective basis with the earliest period presented in the financial statements. In August 2018, the FASB issued ASU 2018-11, Targeted Improvements to ASC 842, which includes an option to not restate comparative periods in transition and instead to elect to use the effective date of ASC 842, Leases, as the date of initial application of transition. We used the effective date of this standard as the date of initial application, which is January 1, 2019, with no retrospective adjustments to prior comparative periods. For leases that commenced before the effective date of ASC 842, we elected the transition package of three practical expedients permitted within ASC 842, which eliminates the requirements to reassess prior conclusions about lease identification, lease classification, and initial direct costs.
Until December 31, 2019, we were an emerging growth company as defined by the JOBS Act and previously disclosed that these amendments would become effective for us for interim and annual periods beginning after December 15, 2019. However, this ASU instead became effective for us in this Annual Report on Form 10-K for the fiscal year ended December 31, 2019 as we no longer qualify as an emerging growth company as of December 31, 2019. The adoption of this standard resulted in an increase of $0.9 million in the assets and $0.8 million in the liabilities recorded on our December 31, 2019 Balance Sheet. The adoption of this standard did not have a material impact on the Statements of Operations and Comprehensive Loss nor the Statements of Cash Flows. See Note 4 for further discussion of the adoption of ASC 842 and related disclosures.
In June 2016, the FASB issued ASU 2016-13, Financial Instruments - Credit Losses ("ASU 2016-13"), to require the measurement of expected credit losses for financial instruments held at the reporting date to be based on historical experience, current conditions, and reasonable forecasts. The ASU will become effective for us for interim and annual periods beginning January 1, 2020, and we will expand our financial statement disclosures in order to
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
comply with the guidance. We have determined that the adoption of ASU 2016-13 will not have a material impact on our results of operations, cash flows, or financial position.
We have reviewed and considered all other recent accounting pronouncements that have not yet been adopted and believe there are none that could potentially have a material impact on our business practices, financial condition, results of operations, or disclosures.
3. Investments
Our investments are classified as available-for-sale and consist of the following:
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | December 31, 2019 | | | | | | |
| | Amortized | | Unrealized Gross | | | | Aggregate |
| | Cost | | Gains | | Losses | | Fair Value |
| Short-Term: | | | | | | | | |
| Commercial paper | | $ | 14,214 | | | $ | — | | | $ | — | | | $ | 14,214 | |
| Corporate bonds | | 26,194 | | | 16 | | | (2) | | | 26,208 | |
| Asset-backed securities | | 8,097 | | | 5 | | | (1) | | | 8,101 | |
| U.S. government securities | | 78,017 | | | 65 | | | — | | | 78,082 | |
| Short-term investments | | 126,522 | | | 86 | | | (3) | | | 126,605 | |
| Long-Term: | | | | | | | | |
| Corporate bonds | | 6,258 | | | | 18 | | | | — | | | | 6,276 | |
| | | | | | | | |
| Long-term investments | | $ | 6,258 | | | | $ | 18 | | | | $ | — | | | | $ | 6,276 | |
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | December 31, 2018 | | | | | | |
| | Amortized | | Unrealized Gross | | | | Aggregate |
| | Cost | | Gains | | Losses | | Fair Value |
| Short-Term: | | | | | | | | |
| Commercial paper | | $ | 27,898 | | | $ | — | | | $ | — | | | $ | 27,898 | |
| Corporate bonds | | 28,043 | | | — | | | (31) | | | 28,012 | |
| Asset-backed securities | | 17,074 | | | | — | | | | (19) | | | | 17,055 | |
| U.S. government securities | | 17,959 | | | | — | | | | (2) | | | | 17,957 | |
| Short-term investments | | $ | 90,974 | | | $ | — | | | $ | (52) | | | $ | 90,922 | |
As of December 31, 2019 and 2018, we had 0 investments with a contractual maturity of greater than two years. Currently, we do not intend to sell the investments and it is not more likely than not that we will be required to sell the investments before recovery of their amortized cost bases, which may be maturity. We do not consider those investments to be other-than-temporarily impaired at December 31, 2019.
4. Leases
Adoption of ASC Topic 842, Leases
On December 31, 2019, Inspire adopted the new accounting standard ASC 842, Leases, which requires lessees to recognize a lease liability and a ROU asset for all leases with lease terms greater than 12 months. We used the effective date of this standard as the date of initial application, with no retrospective adjustments to prior comparative periods. We were an emerging growth company as defined by the JOBS Act until December 31, 2019
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
and therefore this guidance became effective for us in this Annual Report on Form 10-K for the fiscal year ended December 31, 2019 as we no longer qualify as an emerging growth company as of that date.
The impact of the adoption of ASC 842 on our balance sheet as of January 1, 2019 was as follows:
| | | | | | | | | | | | | | | | | | | | |
| | December 31, 2018 | | Adjustments due to the adoption of ASC 842 | | January 1, 2019 |
| Assets | | | | | | |
Prepaid expenses and other assets (1) | | $ | 1,734 | | | | $ | (8) | | | | $ | 1,726 | |
| Total current assets | | 199,278 | | | | (8) | | | | 199,270 | |
Operating lease right-of-use assets (1) | | — | | | | 22 | | | | 22 | |
| Total assets | | $ | 200,080 | | | | $ | 14 | | | | $ | 200,094 | |
| Liabilities and Stockholders' Equity | | | | | | | | | | | |
| Current liabilities: | | | | | | | | | | | |
Accrued expenses (2) | | $ | 7,726 | | | | $ | 14 | | | | $ | 7,740 | |
| Total current liabilities | | 11,155 | | | | 14 | | | | 11,169 | |
| | | | | | |
| Total liabilities | | 36,081 | | | | 14 | | | | 36,095 | |
| Total liabilities and stockholders' equity | | $ | 200,080 | | | | $ | 14 | | | | $ | 200,094 | |
(1) Upon the adoption of ASC 842, prepaid rent is included in the operating lease ROU assets
(2) Upon the adoption of ASC 842, deferred rent is included in the operating lease liabilities which is presented within accrued expenses on our balance sheets
Leases Overview
We previously rented approximately 9,500 square feet of office space under an operating lease that expired on March 31, 2019. In September 2018, we entered into a non-cancelable operating lease agreement to sublease approximately 45,000 square feet of office space for our corporate headquarters, which included real estate taxes and operating expenses in the base rent. This lease commenced January 15, 2019 and expires November 30, 2020. We recognized an additional ROU asset and lease liability of $1.8 million each on January 15, 2019.
In May 2019, we entered into a new, non-cancelable operating lease agreement for the same space directly with the landlord. The initial lease term commences on December 1, 2020 and expires May 31, 2028 with an option to renew for 1 additional period of five years at the then-prevailing market rate. The exercise of the lease renewal option is at our sole discretion and is not expected to be included in the lease term for the calculation of the ROU asset and lease liability when the lease commences on December 1, 2020 as it is not reasonably certain of exercise.
Beginning December 1, 2020, in addition to base rent, we will also pay our proportionate share of the operating expenses, as defined in the lease. These payments will be made monthly, and will be adjusted annually to reflect actual charges incurred for operating expenses, such as common area maintenance, taxes and insurance. In conjunction with this new lease, the landlord agreed to provide Inspire with a $0.6 million rent abatement and a refurbishment allowance in the amount of the cost of any leasehold improvements, not to exceed approximately $1.1 million upon Inspire providing the necessary documentation evidencing the costs of the leasehold improvements that are completed by May 31, 2022. However, the lease allows us to allocate the refurbishment allowance against base rent instead of taking a tenant improvement reimbursement. At this time, we intend to allocate the full amount of the refurbishment allowance against base rent. The total minimum lease payments related to this forward-starting lease is $7.4 million.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
The following table presents the lease balances within the balance sheets:
| | | | | | | | | | | | | | |
| Leases | | Classification | | December 31, 2019 |
| Assets | | | | | |
| Operating | | Operating lease right-of-use asset | | | | $ | 915 | |
| Liabilities | | | | | | | |
| Operating | | Accrued liabilities | | | | $ | 828 | |
The cost components of our operating lease were as follows for the year ended December 31, 2019:
| | | | | | | | |
| Operating lease cost | | $ | 1,021 | |
| Variable lease cost | | 29 | |
| Total lease cost | | $ | 1,050 | |
Variable lease costs consist primarily of taxes, insurance and common area maintenance costs on our prior corporate office lease, which expired March 31, 2019.
Prior to January 1, 2019, we recorded operating lease rent expense under ASC 840 on a straight-line basis over the period of the lease. Rent expense was $0.2 million during both of the years ended December 31, 2018 and 2017.
Maturities of our lease liability for our operating lease are as follows as of December 31, 2019 (1):
| | | | | | | | |
| 2020 | | $ | 828 | |
| | |
| | |
| | |
| | |
| | |
| Total undiscounted lease payments | | 828 | |
| Less: imputed interest | | (37) | |
| Present value of lease liability | | $ | 791 | |
(1) Excludes $7,425 of legally binding minimum lease payments for leases signed but not yet commenced
As of December 31, 2019, the remaining lease term was 0.9 years and the discount rate was 8.0%. For the year ended December 31, 2019, the operating cash outflows from our operating leases were $1.0 million.
5. Long-Term Debt
Credit Facility
In August 2015, we entered into a loan and security agreement, which provided for a term A loan facility in the amount of $15.5 million, the proceeds of which were used to refinance the $12.0 million of borrowings outstanding under our original credit facility, and a term B loan facility in an amount between $3.5 million and $10.0 million, subject to our achievement of certain revenue milestones. Amounts outstanding under the credit facility bore interest at a fixed rate of 7.95% per annum.
In February 2017, we amended the loan and security agreement. Under the loan and security agreement, as amended, and subject to the limitation noted below, amounts outstanding under the credit facility bear interest at a floating interest rate equal to the greater of 7.95% or LIBOR plus 6.9% per annum. Upon execution of the amendment, we borrowed an additional $1.0 million under the term A loan portion of the credit facility, receiving net proceeds of $0.5 million, net of expenses, for a total of $16.5 million outstanding under the credit facility and reduced borrowings available under the term B loan facility to $9.0 million. In connection with the execution of the amendment to the loan and security agreement, we issued 29,197 ten-year warrants to purchase Series F preferred shares of stock at an exercise price of $1.37 per share.
In February 2018, we borrowed an additional $8.0 million under the term B loan facility portion of the credit facility. After receipt of the $8.0 million, we had a total of $24.5 million outstanding under the credit facility, which bore
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
interest at a floating interest rate equal to the greater of 7.95% or LIBOR plus 6.9% per annum. All amounts borrowed under the credit facility were interest-only through March 1, 2020, after which monthly payments of principal and interest were due through February 1, 2022. In connection with this borrowing, we issued 233,577 ten-year warrants to purchase Series F preferred shares of stock at an exercise price of $1.37 per share.
On March 27, 2019, we amended the loan and security agreement. The amendment modified the terms of the loan and security agreement to: (1) extend the interest-only date from March 1, 2020 to April 1, 2022 and extend the maturity date from February 1, 2022 to March 1, 2024; (2) reduce the final payment percentage from 5.50% to 3.50%; (3) modify the basic rate to be a per annum rate of interest (based on a year of 360 days) equal to the sum of (i) the greater of (A) the 30 day U.S. LIBOR rate reported in The Wall Street Journal on the last business day of the month that immediately precedes the month in which the interest will accrue or (B) 2.50%, plus (ii) 5.10%; provided, however, under no circumstances will the basic rate be less than 7.60%; (4) provide a mechanism for determining an alternative interest rate to replace the U.S. LIBOR rate upon the occurrence of certain circumstances; and (5) revise the prepayment fee to be between 1.00% and 3.00% of the principal amount, depending on the timing of any prepayment. Upon closing the amendment to the loan and security agreement, payment of the previously accrued final payment under the credit facility was required.
In addition to the principal and interest payments, under the credit facility, we are required to pay a final payment fee of 3.50% on all amounts outstanding, which is being accreted using the effective interest rate method over the term of the loan and security agreement and shall be due at the earlier of maturity or prepayment. Borrowings are prepayable at our option in whole, but not in part, together with all accrued and unpaid interest thereon and, if not previously made, the final payment, subject to a prepayment fee of 3.00% if such borrowings are prepaid prior to March 27, 2020, 2.00% on or after March 27, 2020 but prior to March 27, 2021, and 1.00% if such borrowings are prepaid on or after March 27, 2021.
The credit facility includes affirmative and restrictive covenants and events of default, including the following events of default: payment defaults, breaches of covenants, judgment defaults, cross defaults to certain other contracts, certain events with respect to governmental approvals if such events could cause a material adverse change, a material impairment in the perfection or priority of the lender's security interest or in the value of the collateral, a material adverse change in the business, operations, or condition of us or any of our subsidiaries, and a material impairment of the prospect of repayment of the loans. Upon the occurrence of an event of default, a default increase in the interest rate of an additional 5.0% could be applied to the outstanding loan balance and the lender could declare all outstanding obligations immediately due and payable and take such other actions as set forth in the loan and security agreement.
Our obligations under the credit facility are secured by a first priority security interest in substantially all of our assets, other than our intellectual property. There are no financial covenants contained in the loan and security agreement. We were in compliance with the affirmative and restrictive covenants as of December 31, 2019.
Expected future principal payments for the credit facility are as follows:
| | | | | | | | |
Year ending December 31: | | |
| 2020 | | $ | — | |
| 2021 | | — | |
| 2022 | | 9,188 | |
| 2023 | | 12,250 | |
| 2024 | | 3,062 | |
| Total expected future principal payments | | $ | 24,500 | |
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
6. Employee Retirement Plan
We sponsor an employee retirement plan covering all of our full-time employees. The plan allows for eligible employees to defer a portion of their eligible compensation up to the maximum allowed by IRS Regulations. We may elect to make a voluntary contribution to the plan. We have not made contributions since inception.
7. Stockholders' Equity
Preferred Stock
As of December 31, 2018 and 2019, 0 preferred stock had been issued.
Preferred Stock Warrants and Common Stock Warrants
In connection with the borrowing completed in February 2018 (see Note 5), we issued 233,577 ten-year warrants to purchase Series F preferred shares of stock at an exercise price of $1.37 per share. Based on the Black-Scholes option pricing model, the value of each warrant was determined to be $0.44, for a total value of $0.1 million at the date of issuance and was fully expensed during the year ended December 31, 2018.
The preferred stock warrants issued in connection with the execution of the original credit facility and its subsequent amendments required re-measurement of the value of the preferred stock warrants each period, with changes in fair value recognized within other expenses on the statements of operations and comprehensive loss. The fair value of the preferred stock warrants was determined using the Black-Scholes option pricing model.
As of May 7, 2018, the date of the closing of our IPO, the following preferred stock warrants issued under the original credit facility and subsequent amendments were outstanding and exercisable:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| Issuance | | Expiration | | Series | | Exercise Price | | | | Warrants Outstanding at May 7, 2018 | | | | Initial Value | | | | Fair Value at May 7, 2018 | | |
| February 8, 2018 | | February 8, 2028 | | F | | | $ | 1.37 | | | | | 233,577 | | | | | $ | 103 | | | | | $ | 320 | | |
| February 24, 2017 | | February 24, 2027 | | F | | | $ | 1.37 | | | | | 29,197 | | | | | $ | 4 | | | | | $ | 40 | | |
| August 7, 2015 | | August 7, 2025 | | E | | | $ | 2.62 | | | | | 29,580 | | | | | $ | 33 | | | | | $ | 41 | | |
| June 27, 2014 | | June 27, 2024 | | E | | | $ | 2.62 | | | | | 76,334 | | | | | $ | 85 | | | | | $ | 174 | | |
| August 5, 2013 | | August 5, 2023 | | C | | | $ | 1.07 | | | | | 74,768 | | | | | $ | 39 | | | | | $ | 80 | | |
| November 16, 2012 | | November 16, 2022 | | C | | | $ | 1.07 | | | | | 186,916 | | | | | $ | 96 | | | | | $ | 200 | | |
| Total | | | | | | | | | | | 630,372 | | | | | | | | | $ | 855 | | |
In connection with the closing of the IPO in May 2018, the warrants to purchase shares of preferred stock automatically converted into warrants to purchase shares of common stock, resulting in the reclassification of the related convertible preferred stock warrant liability of $0.9 million to APIC. Upon the closing of the IPO, the warrants to purchase 630,372 shares of preferred stock at a weighted average exercise price of $1.46 per share became exercisable to purchase 100,558 shares of common stock at weighted average exercise price of $9.38 per share. During 2018, warrants for 93,963 shares were exercised through cashless exercises, resulting in the issuance of a net 76,762 shares of our common stock. During 2019, warrants for 6,595 shares were exercised through cashless exercises, resulting in the issuance of a net 5,102 shares of our common stock.
Warrants to purchase shares of our common stock are summarized below:
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
| | | | | | | | | | | | | | | | | | | | |
| | Common Stock Warrants | | Weighted Average Exercise Price | | Weighted Average Remaining Contractual Life (years) |
| Outstanding at December 31, 2017 | | — | | | $ | — | | | 0 |
| Preferred stock warrants converted to common stock warrants at IPO | | 100,558 | | | $ | 9.38 | | | |
| Exercised | | (93,963) | | | $ | 8.70 | | | |
| Outstanding at December 31, 2018 | | 6,595 | | | $ | 15.16 | | | 5.5 |
| Exercised | | (6,595) | | | $ | 15.16 | | | |
| Outstanding at December 31, 2019 | | — | | | $ | — | | | 0 |
8. Stock-Based Compensation
Stock Options
We adopted the 2007 Stock Incentive Plan (the "2007 Plan") in November 2007, which terminated in accordance with its terms on November 28, 2017; however, the outstanding stock options may continue to be exercised in accordance with their terms.
Immediately following the termination of the 2007 Plan, we adopted the 2017 Stock Incentive Plan (the "2017 Plan"), which contains substantially similar terms and conditions as the 2007 Plan. Upon the IPO, no further grants were made under the 2017 Plan and we adopted the 2018 Stock Incentive Plan (the "2018 Plan"). The purpose of the 2018 Plan is to promote the interest of our company and our stockholders by aiding in attracting and retaining employees, officers, consultants, independent contractors, and directors capable of assuring the future success of our business and to afford such persons an opportunity to acquire a proprietary interest in our company. The board of directors may amend, alter, suspend, discontinue, or terminate the 2018 Plan at any time with the approval of our stockholders. A total of 1,386,809 shares of common stock were initially reserved for issuance under the 2018 Plan, and this share reserve will automatically be supplemented each January 1, commencing on January 1, 2019 and ending on and including January 1, 2028, by an amount of shares equal to the lesser of: a) 739,631 shares, b) 4% of the shares outstanding on the final day of the immediately preceding fiscal year and c) such smaller number of shares as determined by the board of directors.
As of December 31, 2019, there were 2,124,819 shares reserved for issuance under the 2018 Plan, of which 548,868 shares were available for issuance. Prior to the IPO, the exercise price of stock options represented fair value of the common stock at the time of issuance and was determined by the board of directors with the assistance of a third-party valuation specialist. Post-IPO, options are granted at the exercise price, which is equal to the closing price of our stock on the date of grant. The stock options granted to employees include a four-year service period and 25% vest after the first year of service and the remainder vest in equal monthly installments over the next 36 months of service. The stock options granted to the board of directors vest in one, two, or three equal annual installments, in each case subject to the director's continuous services through the applicable vesting date. The stock options have a contractual life of ten years.
A summary of stock option activity and related information is as follows:
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Options | | Weighted Average Exercise Price | | | | Weighted average remaining contractual term (years) | | Aggregate intrinsic value (in thousands) |
| Outstanding at December 31, 2016 | | 1,497,511 | | | | $ | 1.76 | | | | 5.8 | | |
| Granted | | 721,763 | | | | $ | 0.94 | | | | | | |
| Exercised | | (127,122) | | | | $ | 1.85 | | | | | | |
| Forfeited | | (20,536) | | | | $ | 1.88 | | | | | | |
| Outstanding at December 31, 2017 | | 2,071,616 | | | | $ | 1.47 | | | | 5.9 | | |
| Granted | | 1,014,556 | | | | $ | 31.91 | | | | | | |
| Exercised | | (301,058) | | | | $ | 1.86 | | | | | | $ | 7,353 | |
| Forfeited | | (39,958) | | | | $ | 3.64 | | | | | | |
| Outstanding at December 31, 2018 | | 2,745,156 | | | | $ | 12.64 | | | | 7.4 | | $ | 81,453 | |
| Granted | | 809,454 | | | | $ | 67.43 | | | | | | |
| Exercised | | (664,617) | | | | $ | 1.71 | | | | | | $ | 35,305 | |
| Forfeited | | (45,829) | | | | $ | 36.39 | | | | | | |
| Outstanding at December 31, 2019 | | 2,844,164 | | | | $ | 30.41 | | | | 7.9 | | $ | 124,585 | |
| Exercisable at December 31, 2019 | | 1,232,204 | | | | $ | 8.88 | | | | 6.4 | | $ | 80,499 | |
The aggregate intrinsic value of options exercised is the difference between the estimated fair market value of our common stock at the date of exercise and the exercise price for those options. The aggregate intrinsic value of outstanding options is the difference between the closing price as of the date outstanding and the exercise price of the underlying stock options. The total grant date fair value of options vested during the year was $5.1 million, $0.2 million and $0.1 million for the years ended December 31, 2019, 2018 and 2017.
Total stock compensation recognized, before taxes, was as follows:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2019 | | 2018 | | 2017 |
| Cost of goods sold | $ | 121 | | | $ | 9 | | | $ | 9 | |
| Research and development | 689 | | | 51 | | | 43 | |
| Selling, general and administrative | 5,387 | | | 1,159 | | | 191 | |
| Total stock-based compensation | $ | 6,197 | | | $ | 1,219 | | | $ | 243 | |
As of December 31, 2019, the amount of unearned stock-based compensation currently estimated to be expensed from now through the year 2023 related to unvested employee and non-employee director stock-based awards is $33.9 million and the weighted average period over which the unearned stock-based compensation is expected to be recognized is 3.0 years. If there are any modifications or cancellations of the underlying unvested securities, we may be required to accelerate, increase, or cancel any remaining unearned stock compensation expense. Future stock-based compensation expense and unearned stock-based compensation will increase to the extent that we grant additional stock-based awards.
We estimate the fair value of stock-based awards on the date of grant using the Black-Scholes option pricing model using the fair market value of our common stock on the date of grant and a number of other complex and subjective assumptions. These assumptions include, but are not limited to, estimates regarding the expected term of the awards, estimates of the stock volatility over a duration that approximates the expected term of the awards, estimates of the risk-free rate, and estimates of expected dividend rates.
Due to our limited amount of historical exercise, forfeiture, and expiration activity, we have opted to use the "simplified method" for estimating the expected term of options, whereby the expected term equals the arithmetic average of the vesting terms and the original contractual term of the option. We will continue to analyze our
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
expected term assumption as more historical data becomes available. Due to our limited operating history and a lack of company specific historical and implied volatility data, we have based our estimate of expected volatility on the historical volatility of a group of similar companies that are publicly traded. When selecting these public companies on which we have based our expected stock price volatility, we generally selected companies with comparable characteristics to it, including enterprise value, stages of clinical development, risk profiles, position within the industry, and with historical share price information sufficient to meet the expected life of the stock-based awards. The historical volatility data was computed using the weekly closing prices for the selected companies' shares over historical periods that approximate calculated expected term of our stock-based awards. We will continue to analyze the historical stock price volatility assumption as more historical data for our common stock becomes available.
The risk-free rate assumption is based on the U.S. government Treasury instruments with maturities similar to the expected term of our stock options.
The expected dividend assumption is based on our history of not paying dividends and our expectation that we will not declare dividends for the foreseeable future.
The amount of stock-based compensation expense is recognized on a straight-line basis over the vesting term and is reduced by actual forfeitures as they occur.
The fair value of options granted to employees and directors during the years ended December 31, 2019, 2018, and 2017 was estimated as of the grant date using the Black-Scholes option pricing model using the following assumptions:
| | | | | | | | | | | | | | | | | |
| Year Ended December 31, | | | | |
| 2019 | | 2018 | | 2017 |
| Expected life (years) | 5.50 - 6.25 | | 5.50 - 6.25 | | 5.75 - 6.25 |
| Expected volatility | 43.1 - 50.6% | | 37.5 - 49.8% | | 37.5 - 41.5% |
| Risk-free interest rate | 1.39 - 2.63% | | 2.38 - 3.07% | | 1.88 - 2.32% |
| Dividend yield | —% | | | —% | | | —% | |
| Weighted average fair value | $30.69 | | | $16.20 | | | $0.40 | |
Employee Stock Purchase Plan
Our employee stock purchase plan (“ESPP”) allows participating employees to purchase shares of our common stock at a discount through payroll deductions. The plan is available to all of our U.S.-based full-time employees. Participating employees may purchase common stock, on a voluntary after-tax basis, at a price equal to 85% of the lower of the closing market price per share of our common stock on the first or last trading day of each stock purchase period. The plan provides for six-month purchase periods, beginning on January 1 and July 1 of each calendar year.
A total of 277,362 shares of common stock were initially reserved for issuance under the ESPP, and this share reserve will automatically be supplemented each January 1, commencing on January 1, 2019 and ending on and including January 1, 2028, by an amount of shares equal to the lesser of: a) 184,908 shares, b) 1% of the shares outstanding on the final day of the immediately preceding calendar year and c) such smaller number of shares as the board of directors may determine. During the year ended December 31, 2019, 31,750 shares were purchased under the ESPP, utilizing $1.4 million of employee contributions. As of December 31, 2019, 430,520 shares were available for future issuance under the ESPP. We recognized stock-based compensation expense associated with the ESPP of $0.5 million, $0, and $0 for the years ended December 31, 2019, 2018, and 2017, respectively.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
9. Income Taxes
Due to our cumulative net loss position, a valuation allowance has been required to be established for all deferred tax assets as of December 31, 2019, 2018, and 2017.
The components of our provision for income taxes are as follows:
| | | | | | | | | | | | | | | | | | | | |
| | December 31, | | | | |
| | 2019 | | 2018 | | 2017 |
| Current | | | | | | |
| Federal and state | | $ | — | | | $ | — | | | | $ | — | |
| Foreign | | 40 | | | — | | | | — | |
| Total current | | 40 | | | — | | | | — | |
| | | | | | |
| | | | | | |
| | | | | | |
| | | | | | |
| | | | | | |
| | | | | | |
| | | | | | |
| | | | | | |
| Total provision for income taxes | | $ | 40 | | | $ | — | | | | $ | — | |
The reconciliation of taxes at the federal statutory rate to our provision for income taxes are as follows:
| | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | |
| | 2019 | | 2018 | | 2017 |
| Tax at federal statutory rate | | 21.0 | % | | 21.0 | % | | 35.0 | % |
| State, net of federal benefit | | 4.3 | | | 4.0 | | | 3.0 | |
| Stock-based compensation | | 3.9 | | | 1.4 | | | (0.5) | |
| Research and development ("R&D") tax credit | | 1.0 | | | 1.3 | | | 1.2 | |
| Federal tax rate change | | — | | | — | | | (92.6) | |
| Other | | (0.6) | | | (1.4) | | | 0.5 | |
| Change in valuation allowance | | (29.7) | | | (26.3) | | | 53.4 | |
| Total | | (0.1) | % | | — | % | | — | % |
On December 22, 2017, the Tax Cuts and Jobs Act of 2017 ("the Act") was signed into law making significant changes to the Internal Revenue Code. Among other things, the Act reduced the corporate tax rate from 35% to 21% effective for tax years beginning after December 31, 2017. We accounted for the impact of the Act in our 2017 income tax provision, the period in which the legislation was enacted. The amount recorded related to the remeasurement of our deferred tax assets and liabilities, based on the lower tax rates at which they are expected to reverse in the future, was $16.2 million of expense. This tax expense was entirely offset by an income tax benefit related to the reduction of our deferred tax asset valuation allowance of the same amount, resulting in no net impact to tax expense or benefit. The amounts reported in 2017 were based on provisional estimates based on our understanding of the Act and guidance available as of the date of filing. In 2018, the accounting impact was finalized and no changes were required to adjust the provisional amounts recorded.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
Significant components of net deferred tax assets and liabilities were as follows:
| | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | |
| | 2019 | | 2018 | | 2017 |
| Deferred tax assets: | | | | | | |
| Net operating losses | | $ | 39,925 | | | $ | 31,120 | | | $ | 27,827 | |
| R&D tax credits | | 2,348 | | | 1,916 | | | 1,368 | |
| R&D expenditures, capitalized for tax | | 3,111 | | | 2,549 | | | 2,146 | |
| Interest expense carryforward | | — | | | 638 | | | — | |
| Accruals and other | | 1,330 | | | 1,194 | | | 319 | |
| Depreciation and amortization | | 221 | | | 311 | | | 431 | |
| Lease asset | | 202 | | | — | | | — | |
| Stock-based compensation | | 813 | | | 214 | | | 7 | |
| Other comprehensive loss | | — | | | 16 | | | — | |
| Total deferred tax assets | | 47,950 | | | 37,958 | | | 32,098 | |
| Deferred tax liabilities: | | | | | | |
| | | | | | |
| Lease liability | | (223) | | | — | | | — | |
| Other comprehensive income | | (25) | | | — | | | — | |
| Other | | (50) | | | (101) | | | — | |
| Total deferred tax liabilities | | (298) | | | (101) | | | — | |
| | | | | | |
| Net deferred tax assets | | 47,652 | | | 37,857 | | | 32,098 | |
| Valuation allowance | | (47,652) | | | (37,857) | | | (32,098) | |
| | $ | — | | | $ | — | | | $ | — | |
Deferred income taxes reflect the tax effects of net operating loss and tax credit carryforwards and the net temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes.
As of December 31, 2019, our gross federal net operating loss carryforwards of $160.9 million will expire at various dates beginning in 2028. In addition, net operating loss carryforwards for state income tax purposes of $347.1 million that include net operating losses that will begin to expire in 2028. We also have gross R&D credit carryforwards of $2.5 million as of December 31, 2019 of which will expire at various dates beginning in 2033.
Utilization of the net operating loss carryforwards may be subject to an annual limitation due to the ownership change limitations provided by Section 382 of the Internal Revenue Code of 1986 and similar state provisions. We have not performed a detailed analysis to determine whether an ownership change has occurred. Such a change of ownership would limit our utilization of the net operating losses and could be triggered by subsequent sales of securities by us or our stockholders.
Realization of the deferred tax assets is dependent upon the generation of future taxable income, if any, the amount and timing of which are uncertain. Based on available objective evidence and cumulative losses, we believe it is more likely than not that the deferred tax assets are not recognizable and will not be recognizable until we have sufficient taxable income. Accordingly, the net deferred tax assets have been fully offset by a valuation allowance. The valuation allowance increased by $9.8 million, increased by $5.8 million, and decreased by $9.4 million during the years ended December 31, 2019, 2018 and 2017, respectively.
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
The changes to our gross unrecognized tax benefits were as follows during the year ended December 31, 2019:
| | | | | | | | |
| Balance at December 31, 2018 | | $ | — | |
| Increase in balances related to current year tax positions | | 40 | |
| Balance at December 31, 2019 | | $ | 40 | |
We file income tax returns in the applicable jurisdictions. The 2015 to 2018 tax years remain open to examination by the major taxing authorities to which we are subject. We do not expect a significant change to our unrecognized tax benefits over the next 12 months.
Our policy is to record interest related to uncertain tax positions as interest expense and any penalties as other expense in our statements of operations and comprehensive loss. There was no interest or penalties accrued at December 31, 2019 and 2018.
10. Segment Reporting and Revenue Disaggregation
We operate our business as 1 operating segment. An operating segment is defined as a component of an enterprise for which separate discrete financial information is available and evaluated regularly by the chief operating decision maker, or decision-making group, in deciding how to allocate resources and in assessing performance. Segment information is consistent with how management reviews the business, makes investing and resource allocation decisions and assesses operating performance.
We sell our Inspire system to hospitals and ambulatory surgery centers in the U.S. and in select countries in Europe through a direct sales organization. Revenue by geographic region is as follows:
| | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | |
| | 2019 | | 2018 | | 2017 |
| United States | | $ | 73,660 | | | $ | 44,378 | | | $ | 24,293 | |
| Europe | | 8,390 | | | 6,215 | | | 4,274 | |
| Total revenue | | $ | 82,050 | | | $ | 50,593 | | | $ | 28,567 | |
All of our long-lived assets are located in the U.S.
11. Loss Per Share
Basic net loss per share is computed by dividing the net loss by the weighted average number of shares of common stock outstanding during the period. Diluted net loss per share is computed by dividing the net loss by the weighted average number of shares of common stock and dilutive potential shares of common stock outstanding during the period. Because we have reported a net loss for all periods presented, diluted net loss per share is the same as basic net loss per share for those periods as all potentially dilutive shares consisting of convertible preferred stock, convertible preferred stock warrants, convertible common stock warrants and common stock options were antidilutive in those periods.
The following potentially dilutive securities outstanding at the end of the periods presented have been excluded from the computations of diluted shares outstanding because such securities have an antidilutive impact due to losses reported:
Table of Contents
INSPIRE MEDICAL SYSTEMS, INC.
NOTES TO FINANCIAL STATEMENTS
(Table amounts in thousands, except share and per share amounts)
| | | | | | | | | | | | | | | | | | | | |
| | Year Ended December 31, | | | | |
| | 2019 | | 2018 | | 2017 |
| Convertible preferred stock outstanding | | — | | | — | | | 12,111,706 | |
| Convertible preferred stock warrants | | — | | | — | | | 423,784 | |
| Convertible common stock warrants | | — | | | 6,595 | | | — | |
| Common stock options outstanding | | 2,844,164 | | | 2,745,156 | | | 2,071,616 | |
| Total | | 2,844,164 | | | 2,751,751 | | | 14,607,106 | |
12. Quarterly Financial Information (Unaudited)
The following table provides selected quarterly financial data for the years ended December 31, 2019 and 2018.
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Three Months Ended | | | | | | | | | | | | | | |
| | Mar. 31, | | Jun. 30, | | Sep. 30, | | Dec. 31, | | Mar. 31, | | Jun. 30, | | Sep. 30, | | Dec. 31, |
| | 2019 | | | 2019 | | | 2019 | | | 2019 | | | 2018 | | | 2018 | | | 2018 | | | 2018 | |
| Revenue | | $ | 16,250 | | | $ | 18,032 | | | $ | 20,862 | | | $ | 26,906 | | | $ | 10,042 | | | $ | 10,938 | | | $ | 13,054 | | | $ | 16,559 | |
| Gross profit | | 13,396 | | | 14,938 | | | 17,406 | | | 22,667 | | | 7,748 | | | 8,836 | | | 10,587 | | | 13,366 | |
| Net loss | | (8,266) | | | (7,650) | | | (8,247) | | | (9,080) | | | (6,501) | | | (5,856) | | | (4,693) | | | (4,778) | |
Net loss per share, basic and diluted (1) | | $ | (0.35) | | | $ | (0.32) | | | $ | (0.34) | | | $ | (0.38) | | | $ | (5.05) | | | $ | (0.43) | | | $ | (0.22) | | | $ | (0.22) | |
| | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | |
(1) The summation of quarterly per share amounts may not equal the calculation for the full year, as each quarterly calculation is performed discretely.
Item 9. Changes in and Disagreements With Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2019. The term “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act, means controls and other procedures of a company that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure. Management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on the evaluation of our disclosure controls and procedures as of December 31, 2019, our Chief Executive Officer and Chief Financial Officer concluded that, as of such date, our disclosure controls and procedures were effective at the reasonable assurance level.
Changes in Internal Control over Financial Reporting
There was no change in the Company’s internal control over financial reporting, as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act, that occurred during the quarter ended December 31, 2019 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
Management Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Internal control over financial reporting is a process designed by, or under the supervision of, a company’s principal executive and principal financial officers, or persons performing similar functions, and effected by the company’s board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with U.S. generally accepted accounting principles. It includes those policies and procedures that:
•pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of the assets of the company;
•provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with U.S. generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and
•provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management conducted an assessment of the effectiveness of our internal control over financial reporting based on the criteria set forth in “Internal Control-Integrated Framework (2013)” issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this assessment, management concluded that, as of December 31, 2019, our internal control over financial reporting was effective.
Ernst & Young LLP, our independent registered public accounting firm, that audited the consolidated financial statements included in this Annual Report on Form 10-K, has issued an audit report on our internal control over financial reporting. See Report of Independent Registered Public Accounting Firm below.
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Inspire Medical Systems, Inc.
Opinion on Internal Control Over Financial Reporting
We have audited Inspire Medical Systems, Inc.’s internal control over financial reporting as of December 31, 2019, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework), (the COSO criteria). In our opinion, Inspire Medical Systems, Inc. (the Company) maintained, in all material respects, effective internal control over financial reporting as of December 31, 2019, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the accompanying balance sheets of Inspire Medical Systems, Inc. (the Company) as of December 31, 2019 and 2018, the related statements of operations and comprehensive loss, stockholders' (deficit) equity and cash flows for each of the three years in the period ended December 31, 2019, and the related notes and our report dated February 25, 2020 expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects.
Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk
that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/Ernst & Young LLP
Minneapolis, Minnesota
February 25, 2020
Item 9B. Other Information.
None.
PART III
Item 10. Directors, Executive Officers and Corporate Governance.
The information required by this Item is incorporated by reference to our definitive proxy statement for our 2020 annual meeting of stockholders to be filed with the SEC within 120 days of the fiscal year ended December 31, 2019.
Item 11. Executive Compensation.
The information required by this Item is incorporated by reference to our definitive proxy statement for our 2020 annual meeting of stockholders to be filed with the SEC within 120 days of the fiscal year ended December 31, 2019.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
The following table provides information as of December 31, 2019, regarding our common stock that may be issued under the Inspire Medical Systems, Inc. 2007 Incentive Award Plan, as amended (the "2007 Plan”), the Inspire Medical Systems, Inc. 2017 Incentive Award Plan, as amended (the “2017 Plan”), the Inspire Medical Systems, Inc. 2018 Incentive Award Plan (the “2018 Plan”) and the Inspire Medical Systems, Inc. 2018 Employee Stock Purchase Plan (the “2018 ESPP”).
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Number of Securities to be Issued Upon Exercise of Outstanding Options, Warrants, and Rights | | | | Weighted-Average Exercise Price of Outstanding Options, Warrants, and Rights | | | | Number of Securities Available for Future Issuance Under Equity Compensation Plans (excludes securities reflected in column (a)) | | |
| Plan category: | | (a) | | | | (b) | | | | (c) | | |
| Equity compensation plans approved by stockholders | | | | | | | | | | | | |
| 2007 Plan (1) | | | 1,071,544 | | | | | $ | 1.33 | | | | | — | | |
| 2017 Plan (1) | | | 196,669 | | | | | $ | 8.94 | | | | | — | | |
| 2018 Plan (2) | | | 1,575,951 | | | | | $ | 52.85 | | | | | 548,868 | | |
| 2018 ESPP (3) | | | — | | | | | $ | — | | | | | 430,520 | | |
| Equity compensation plans not approved by stockholders | | | — | | | | | $ | — | | | | | — | | |
| Total | | | 2,844,164 | | | | | $ | 30.41 | | | | | 979,388 | | |
(1) The 2007 Plan terminated in accordance with its terms on November 28, 2017. In connection with our IPO, we adopted the 2018 Plan and will not make future grants or awards under the 2017 Plan.
(2) Pursuant to the terms of the 2018 Plan, the number of shares of common stock available for issuance under the 2018 Plan automatically increases on each January 1, until and including January 1, 2028, by an amount equal to the lesser of (a) 739,631 shares, (b) 4% of the number of shares of common stock outstanding (on an as-converted basis) on the last day of the immediately preceding fiscal year, and (c) such smaller number of shares as is determined by our board of directors.
(3) Pursuant to the terms of the 2018 ESPP Plan, the number of shares reserved under the 2018 ESPP Plan will automatically be supplemented each January 1, until and including January 1, 2028, by an amount of shares equal to the lesser of a) 184,908 shares, b) 1% of the shares outstanding on the final day of the immediately preceding calendar year, and c) such smaller number of shares as the board of directors may determine.
Other
The remaining information required by this Item is incorporated by reference to our definitive proxy statement for our 2020 annual meeting of stockholders to be filed with the SEC within 120 days of the fiscal year ended December 31, 2019.
Item 13. Certain Relationships and Related Transactions, and Director Independence.
The information required by this Item is incorporated by reference to our definitive proxy statement for our 2020 annual meeting of stockholders to be filed with the SEC within 120 days of the fiscal year ended December 31, 2019.
Item 14. Principal Accounting Fees and Services.
The information required by this Item is incorporated by reference to our definitive proxy statement for our 2020 annual meeting of stockholders to be filed with the SEC within 120 days of the fiscal year ended December 31, 2019.
PART IV
Item 15. Exhibits, Financial Statement Schedules.
(a) List of documents filed as part of this Annual Report on Form 10-K:
(1) Financial Statements
The financial statements included in Part II, Item 8 of this document are filed as part of this Annual Report on Form 10-K.
(2) Financial Statement Schedules
All schedules are omitted because they are not applicable or the amounts are immaterial or the required information is presented in the consolidated financial statements and notes thereto in Part II, Item 8 above.
(3) Exhibits
The following documents are filed as exhibits to this Annual Report on Form 10-K.
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Exhibit
Number | | Description | | Form | | File No. | | Exhibit | | Filing
Date | | Filed/
Furnished
Herewith |
| 3.1 | | | | 8-K | | 001-38468 | | 3.1 | | | 5/7/2018 | | |
| 3.2 | | | | 8-K | | 001-38468 | | 3.2 | | | 5/7/2018 | | |
| 4.1 | | | | S-1 | | 333-224176 | | 4.1 | | 4/23/2018 | | |
| 4.2 | | | | S-1 | | 333-224176 | | 4.2 | | 4/6/2018 | | |
| 4.3 | | | | S-1 | | 333-224176 | | 4.3 | | 4/23/2018 | | |
| 4.4 | | | | S-1 | | 333-228668 | | 4.4 | | 12/4/2018 | | |
| 4.5 | | | | S-1 | | 333-228668 | | 4.5 | | 12/4/2018 | | |
| 4.6 | | | | | | | | | | | | * |
| 10.1 | | | | S-1 | | 333-224176 | | 10.1 | | 4/6/2018 | | |
| 10.2 | | | | S-1 | | 333-224176 | | 10.2 | | 4/6/2018 | | |
| 10.3 | | | | S-1 | | 333-224176 | | 10.3 | | 4/6/2018 | | |
| 10.4 | | | | S-1 | | 333-224176 | | 10.4 | | 4/6/2018 | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Exhibit
Number | | Description | | Form | | File No. | | Exhibit | | Filing
Date | | Filed/
Furnished
Herewith |
| 10.5 | | | | 8-K | | 001-38468 | | 10.1 | | 3/29/2019 | | |
| 10.6† | | | | S-1 | | 333-224176 | | 10.6 | | 4/6/2018 | | |
| 10.7† | | | | S-1 | | 333-224176 | | 10.7 | | 4/6/2018 | | |
| 10.8† | | | | S-1 | | 333-224176 | | 10.8 | | 4/6/2018 | | |
| 10.9† | | | | S-1 | | 333-224176 | | 10.9 | | 4/6/2018 | | |
| 10.10† | | | | S-1 | | 333-224176 | | 10.10 | | 4/6/2018 | | |
| 10.11† | | | | S-1 | | 333-224176 | | 10.11 | | 4/23/2018 | | |
| 10.12† | | | | S-1 | | 333-224176 | | 10.12 | | 4/23/2018 | | |
| 10.13† | | | | S-1 | | 333-224176 | | 10.13 | | 4/23/2018 | | |
| 10.14† | | | | S-1 | | 333-224176 | | 10.15 | | 4/23/2018 | | |
| 10.15† | | | | S-1 | | 333-224176 | | 10.17 | | 4/23/2018 | | |
| 10.16† | | | | S-1 | | 333-224176 | | 10.19 | | 4/23/2018 | | |
| 10.17† | | | | S-1 | | 333-224176 | | 10.21 | | 4/23/2018 | | |
| 10.18† | | | | S-1 | | 333-224176 | | 10.23 | | 4/6/2018 | | |
| 10.19† | | | | 10-Q | | 001-38468 | | 10.1 | | 8/6/2019 | | |
| 21.1 | | | | | | | | | | | | * |
| 23.1 | | | | | | | | | | | | * |
| 31.1 | | | | | | | | | | | | * |
| 31.2 | | | | | | | | | | | | * |
| 32.1 | | | | | | | | | | | | ** |
| 32.2 | | | | | | | | | | | | ** |
| 101.INS | | Inline XBRL Instance Document - the instance document does not appear in the Interactive Data File because its XBRL tags are embedded within the Inline XBRL document. | | | | | | | | | | * |
| 101.SCH | | Inline XBRL Taxonomy Extension Schema Document | | | | | | | | | | * |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Exhibit
Number | | Description | | Form | | File No. | | Exhibit | | Filing
Date | | Filed/
Furnished
Herewith |
| 101.CAL | | Inline XBRL Taxonomy Extension Calculation Linkbase Document | | | | | | | | | | * |
| 101.DEF | | Inline XBRL Taxonomy Extension Definition Linkbase Document | | | | | | | | | | * |
| 101.LAB | | Inline XBRL Taxonomy Extension Label Linkbase Document | | | | | | | | | | * |
| 101.PRE | | Inline XBRL Taxonomy Extension Presentation Linkbase Document | | | | | | | | | | * |
| 104 | | Cover Page Interactive Data File (formatted as Inline XBRL and contained in Exhibit 101) | | | | | | | | | | * |
* Filed herewith.
** Furnished herewith.
† Denotes a management contract or compensation plan or arrangement.
Certain agreements filed as exhibits to this Annual Report on Form 10-K contain representations and warranties that the parties thereto made to each other. These representations and warranties have been made solely for the benefit of the other parties to such agreements and may have been qualified by certain information that has been disclosed to the other parties to such agreements and that may not be reflected in such agreements. In addition, these representations and warranties may be intended as a way of allocating risks among parties if the statements contained therein prove to be incorrect, rather than as actual statements of fact. Accordingly, there can be no reliance on any such representations and warranties as characterizations of the actual state of facts. Moreover, information concerning the subject matter of any such representations and warranties may have changed since the date of such agreements.
Item 16. Form 10-K Summary.
None.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| | | | | | | | | | | | | | |
| | | | Inspire Medical Systems, Inc. |
| Date: | February 25, 2020 | By: | | /s/ TIMOTHY P. HERBERT |
| | | | Timothy P. Herbert
President and Chief Executive Officer
(principal executive officer) |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities indicated on February 25, 2020.
| | | | | | | | |
| Signature | | Title |
| | |
| /s/ TIMOTHY P. HERBERT | | Chief Executive Officer (principal executive officer), President and Director |
| Timothy P. Herbert | | |
| | |
| /s/ RICHARD BUCHHOLZ | | Chief Financial Officer (principal financial and accounting officer) |
| Richard Buchholz | | |
| | |
| /s/ MARILYN CARLSON NELSON | | Chair of the Board of Directors |
| Marilyn Carlson Nelson | | |
| | |
| /s/ GARY L. ELLIS | | Director |
| Gary L. Ellis | | |
| | |
| /s/ JERRY GRIFFIN, M.D. | | Director |
| Jerry Griffin, M.D. | | |
| | |
| /s/ MUDIT K. JAIN | | Director |
| Mudit K. Jain | | |
| | |
| /s/ CHAU KHUONG | | Director |
| Chau Khuong | | |
| | |
| /s/ DANA G. MEAD, JR. | | Director |
| Dana G. Mead, Jr. | | |
| | |
| /s/ SHAWN T MCCORMICK | | Director |
| Shawn T McCormick | | |
| | |
| /s/ CASEY TANSEY | | Director |
| Casey Tansey | | |