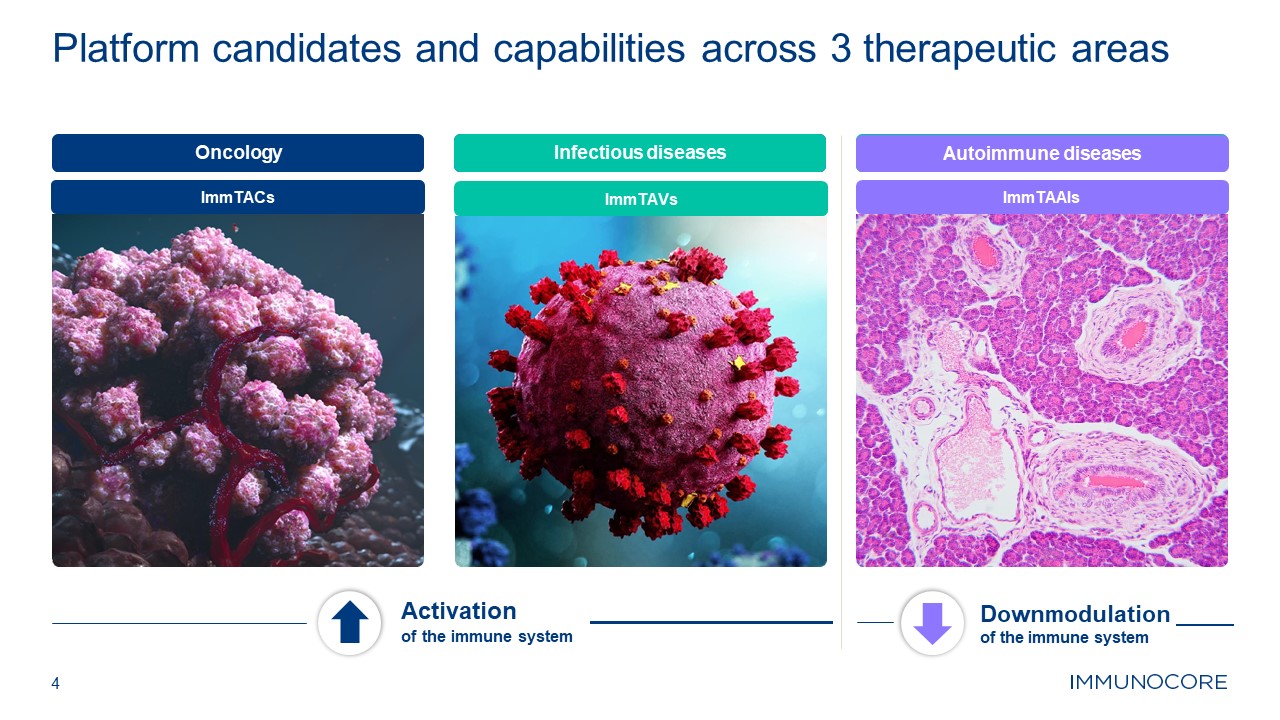
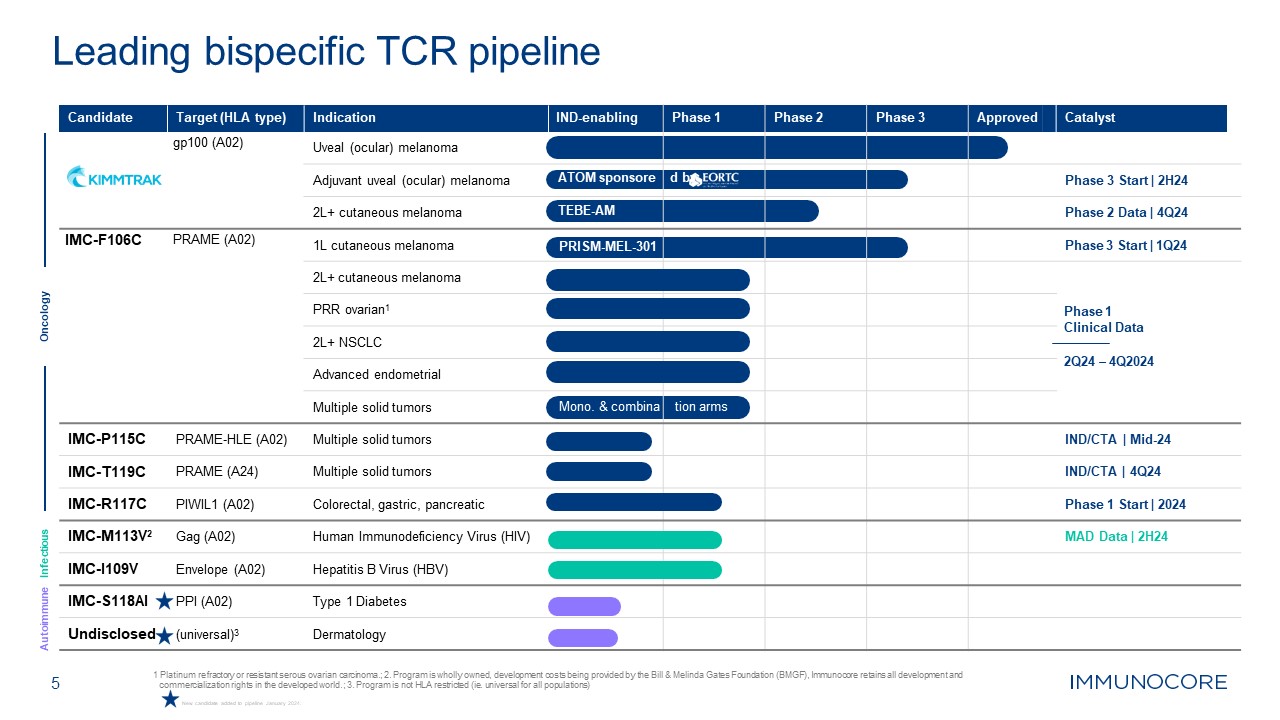
This presentation contains “forward-looking statements” within the meaning of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. Words such as “may”, “will”, “believe”, “expect”, “plan”, “anticipate” and similar expressions (as well as other words or expressions referencing future events or circumstances) are intended to identify forward-looking statements. All statements, other than statements of historical facts, included in this presentation are forward-looking statements. These statements include, but are not limited to, Immunocore’s capabilities across oncology, autoimmune and infectious disease therapeutic areas and its ability to grow and further development the PRAME franchise; the estimated market size and patient population for KIMMTRAK and Immunocore’s other product candidates; the three growth areas of KIMMTRAK including HLA-A02+ melanoma, metastatic cutaneous melanoma and adjuvant uveal melanoma; expected submission of investigational new drug applications or clinical trial applications; the potential regulatory approval, expected clinical benefits and availability of Immunocore’s product candidates; the commercial performance of KIMMTRAK including planned launches in additional countries, expanded access to KIMMTRAK in the United States and globally, and indication expansion; the ability to enter into pricing agreements and to translate such pricing agreement into a successful launch; the potential benefits and advantages KIMMTRAK and Immunocore’s other product candidates will provide for patients; the benefits of Immunocore’s collaboration with the European Organisation for Research and Treatment of Cancer (EORTC); expectations regarding the design, progress, timing, enrollment, scope, expansion, and results of Immunocore’s existing and planned clinical trials, those of Immunocore’s collaboration partners or the combined clinical trials with Immunocore’s collaboration partners; the timing and sufficiency of clinical trial outcomes to support potential approval of any of Immunocore’s product candidates or those of, or combined with, its collaboration partners; Immunocore’s goals to develop and commercialize product candidates based on its KIMMTRAK platform alone or with collaboration partners; Immunocore’s ability to develop new product candidates using its discovery engine; Immunocore’s ability to initiate CMC manufacturing for autoimmune candidates on the expected timeline, or at all; potential growth opportunities and trends, including in connection with product launches; and Immunocore’s preliminary unaudited cash and cash equivalents. Any forward-looking statements are based on management’s current expectations and beliefs of future events and are subject to a number of risks and uncertainties that could cause actual events or results to differ materially and adversely from those set forth in or implied by such forward-looking statements, many of which are beyond Immunocore’s control. These risks and uncertainties include, but are not limited to, the impact of worsening macroeconomic conditions on Immunocore’s business, financial position, strategy and anticipated milestones, including Immunocore’s ability to conduct ongoing and planned clinical trials; Immunocore’s ability to obtain a clinical supply of curr ent or future product candidates or commercial supply of KIMMTRAK or any future approved products, including as a result of health epidemics or pandemic, war in Ukraine, the conflict between Hamas and Israel, or global geopolitical tension; Immunocore’s ability to obtain and maintain regulatory approval of its product candidates, including KIMMTRAK; Immunocore’s ability and plans in continuing to establish and expand a commercial infrastructure and to successfully launch, market and sell KIMMTRAK and any future approved products; Immunocore’s ability to successfully expand the approved indications for KIMMTRAK or obtain marketing approval for KIMMTRAK in additional geographies in the future; the delay of any current or planned clinical trials, whether due to patient enrollment delays or otherwise; Immunocore’s ability to successfully demonstrate the safety and efficacy of its product candidates and gain approval of its product candidates on a timely basis, if at all; competition with respect to market opportunities; unexpected safety or efficacy data observed during preclinical studies or clinical trials; actions of regulatory agencies, which may affect the initiation, timing and progress of clinical trials or future regulatory approval; Immunocore’s need for and ability to obtain additional funding, on favorable terms or at all, including as a result of worsening macroeconomic conditions, including changes inflation and interest rates and unfavorable general market conditions, and the impacts thereon of the war in Ukraine, the conflict between Hamas and Israel, and global geopolitical tension; Immunocore’s ability to obtain, maintain and enforce intellectual property protection for KIMMTRAK or any product candidates it is developing; and the success of Immunocore’s current and future collaborations, partnerships or licensing arrangements. These and other risks and uncertainties are described in greater detail in the section titled "Risk Factors" in Immunocore’s filings with the Securities and Exchange Commission, including Immunocore’s most recent Annual Report on Form 20-F for the year ended December 31, 2022 filed with the Securities and Exchange Commission on March 1, 2023, as well as discussions of potential risks, uncertainties, and other important factors in Immunocore’s subsequent filings with the Securities and Exchange Commission. All forward looking statements contained in this presentation speak only as of the date on which they were made and should not be relied upon as representing its views as of any subsequent date. Except to the extent required by law, Immunocore undertakes no obligation to update such statements to reflect events that occur or circumstances that exist after the date on which they were made. Certain information contained in this presentation relates to or is based on studies, publications, surveys, and other data obtained from third party sources and Immunocore’s own internal estimates and research. While Immunocore believes these third party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy, or completeness of, any information obtained from third party sources. KIMMTRAK™ is a trademark owned or licensed to Immunocore. 2 Forward Looking Statements