Exhibit 99.1

IFX-1 C5a Controlling inflammation Corporate Presentation May 2019
Important Notice and Disclaimer THIS PRESENTATION HAS BEEN PREPARED BY INFLARX n.v. (“INFLARX”), a US-Nasdaq publicly listed Dutch company having its principle place of business in germany. THIS PRESENTATION IS MADE FOR INFORMATIONAL PURPOSES ONLY AND DOES NOT CONSTITUTE AN OFFER TO SELL OR A SOLICITATION OF AN OFFER TO BUY SECURITIES. THE INFORMATION SET FORTH HEREIN DOES NOT PURPORT TO BE COMPLETE OR TO CONTAIN ALL OF THE INFORMATION YOU MAY DESIRE. STATEMENTS CONTAINED HEREIN ARE MADE AS OF THE DATE OF THIS PRESENTATION UNLESS STATED OTHERWISE, AND NEITHER THE DELIVERY OF THIS PRESENTATION AT ANY TIME, NOR ANY SALE OF SECURITIES, SHALL UNDER ANY CIRCUMSTANCES CREATE AN IMPLICATION THAT THE INFORMATION CONTAINED HEREIN IS CORRECT AS OF ANY TIME AFTER SUCH DATE OR THAT INFORMATION WILL BE UPDATED OR REVISED TO REFLECT INFORMATION THAT SUBSEQUENTLY BECOMES AVAILABLE OR CHANGES OCCURRING AFTER THE DATE HEREOF.This presentation may contain forward-looking statements. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on our current beliefs, expectations and assumptions regarding the future of our business, future plans and strategies, our clinical results and other future conditions. All statements other than statements of historical facts contained in this presentation, including statements regarding future results of operations and financial position, business strategy, current and prospective product candidates, planned clinical trials and preclinical activities, product approvals, research and development costs, current and prospective collaborations, timing and likelihood of success, expectations regarding market acceptance and size, plans and objectives of management for future operations, and future results of anticipated product candidates, are forward-looking statements. These risks and uncertainties include those described under the caption “Risk Factors” in InflaRx's Registration Statement on Form F-1 and the accompanying prospectus filed with the Securities and Exchange Commission in connection with the company's initial public offering and other filings with the Securities and Exchange Commission. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. Although we believe the expectations reflected in such forward-looking statements are reasonable, we can give no assurance that such expectations will prove to be correct. Accordingly, readers are cautioned not to place undue reliance on these forward-looking statements. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements.Certain information contained in this presentation relates to or is based on studies, publications, surveys and other data obtained from third-party sources and InflaRx’s own internal estimates and research. While InflaRx believes these third-party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. In addition, all of the market data included in this presentation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Finally, while we believe our own internal research is reliable, such research has not been verified by any independent source. InflaRx n.v. - Winzerlaer Str. 2, 07745 Jena, Germany, Email: info@inflarx.com, Tel: +49-3641-508180, www.inflarx.com
About Inflarx: 3 Founded in Germany in 2008 Offices/Subsidiaries: JENA + Munich (Ger) & Ann Arbor + New York (USA) IPO on Nasdaq in November 2017 with GROSS proceeds of $106m strong balance sheet:$176 million as of Dec 31st 2018 Follow-on Financing round April 2018 with Gross proceeds of $117m

Investment highlights Leading anti-c5a ANTIBODY TECHNOLOGY Full and selective blockade of the biological activity of C5aStrong global IP protection Leading PROPRIETARY anti-c5a ANTIBODY TECHNOLOGY Leading anti-c5a ANTIBODY TECHNOLOGY Highly statistically significant C5a inhibition leaving MAC formation intactFavorable safety profile and excellent tolerability (n > 150 patients) Established Biological POC for lead drug IFX-1 Leading anti-c5a ANTIBODY TECHNOLOGY Established a pivotal role of C5a in HS with multi-bn market potential83% response rate on clinical response score (HiSCR) in severe HS patientsKey results of international phase IIb expected in Q2 2019 ifx-1 in hidradenitis Suppurativa (HS) Leading anti-c5a ANTIBODY TECHNOLOGY ANCA-associated vasculitis: US study ongoing, EU study approvedPipeline extension of IFX-1 in inflammatory diseases & oncologyIFX-1 s.c. and follow on anti-C5a mAb IFX-2 development in pipeline Broad applicability of anti-c5a TECHNOLOGY 4
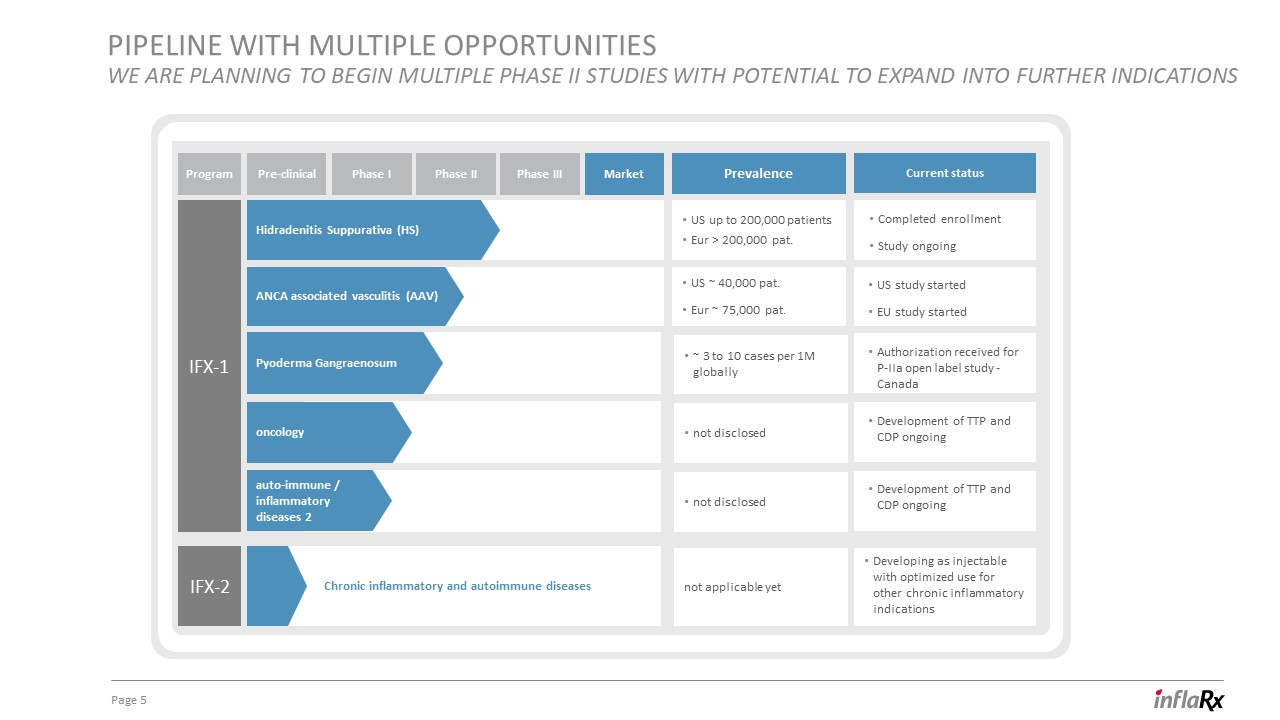
pipeline with multiple opportunitieswe are planning to begin multiple Phase ii studies with potential to expand into further indications 5 IFX-1 IFX-2 Current status Prevalence Pre-clinical Program Phase III Market Phase II Phase I Hidradenitis Suppurativa (HS) ANCA associated vasculitis (AAV) Pyoderma Gangraenosum Chronic inflammatory and autoimmune diseases US up to 200,000 patientsEur > 200,000 pat. Completed enrollmentStudy ongoing US ~ 40,000 pat.Eur ~ 75,000 pat. US study startedEU study started Authorization received for P-IIa open label study - Canada Developing as injectable with optimized use for other chronic inflammatory indications Development of TTP and CDP ongoing ~ 3 to 10 cases per 1M globally not disclosed oncology Development of TTP and CDP ongoing not disclosed not applicable yet auto-immune / inflammatory diseases 2

C5a as target & our PROPRIETARY anti-c5a TECHNOLOGY
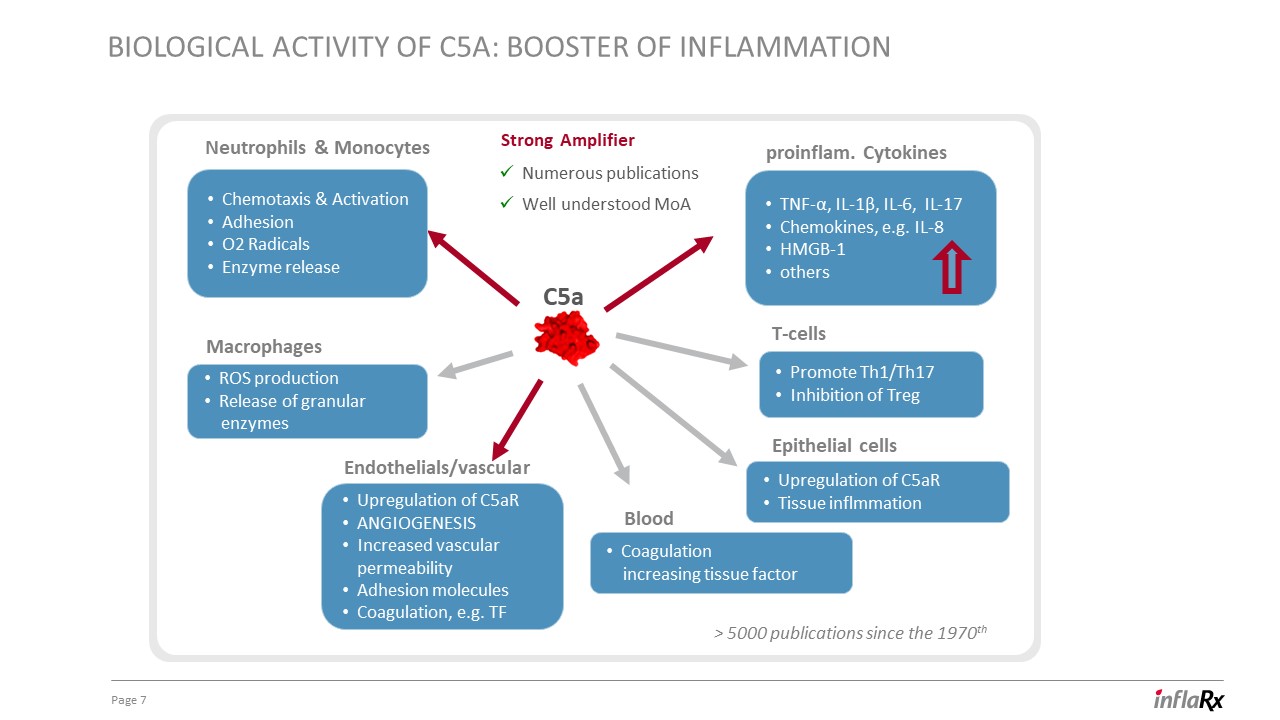
Biological activity of C5a: booster of inflammation 7 C5a Neutrophils & Monocytes proinflam. Cytokines > 5000 publications since the 1970th Endothelials/vascular Macrophages Epithelial cells Strong Amplifier Chemotaxis & ActivationAdhesionO2 RadicalsEnzyme release Upregulation of C5aRANGIOGENESISIncreased vascular permeabilityAdhesion moleculesCoagulation, e.g. TF Upregulation of C5aRTissue inflmmation Promote Th1/Th17Inhibition of Treg TNF-α, IL-1β, IL-6, IL-17Chemokines, e.g. IL-8HMGB-1others ROS production Release of granular enzymes Coagulation increasing tissue factor Blood Numerous publicationsWell understood MoA T-cells

C5a activation of neutrophils 8 Data Source: Prof. Peter Ward, University of Michigan Neutrophils , (4’600x enlarged) + C5a control C5a Mode of Action on Neutrophils:Chemotaxis of neutrophils (Shin et al 1968, Science 162,361-3)Enzyme release (Goldstein et al 1974, J. Immunol. 113, 1583-8)Production of O2-radicals in neutrophils (Sacks et al 1978, J Clin Invest 161, 1161-7)
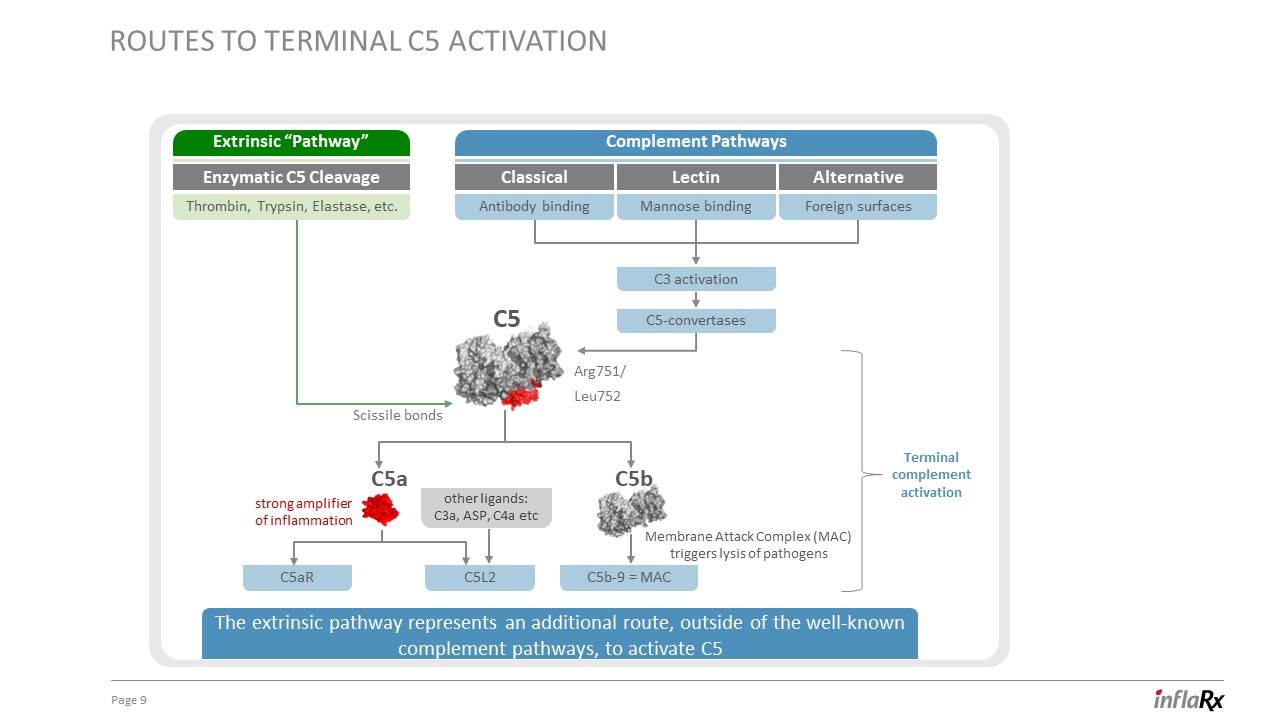
9 Routes to Terminal C5 activation Classical Lectin Alternative Complement Pathways Extrinsic “Pathway” Enzymatic C5 Cleavage Membrane Attack Complex (MAC)triggers lysis of pathogens strong amplifierof inflammation Antibody binding Mannose binding Foreign surfaces C3 activation C5aR C5b-9 = MAC C5-convertases C5L2 C5b C5a Terminalcomplementactivation C5 Thrombin, Trypsin, Elastase, etc. The extrinsic pathway represents an additional route, outside of the well-known complement pathways, to activate C5 Arg751/Leu752 Scissile bonds other ligands: C3a, ASP, C4a etc
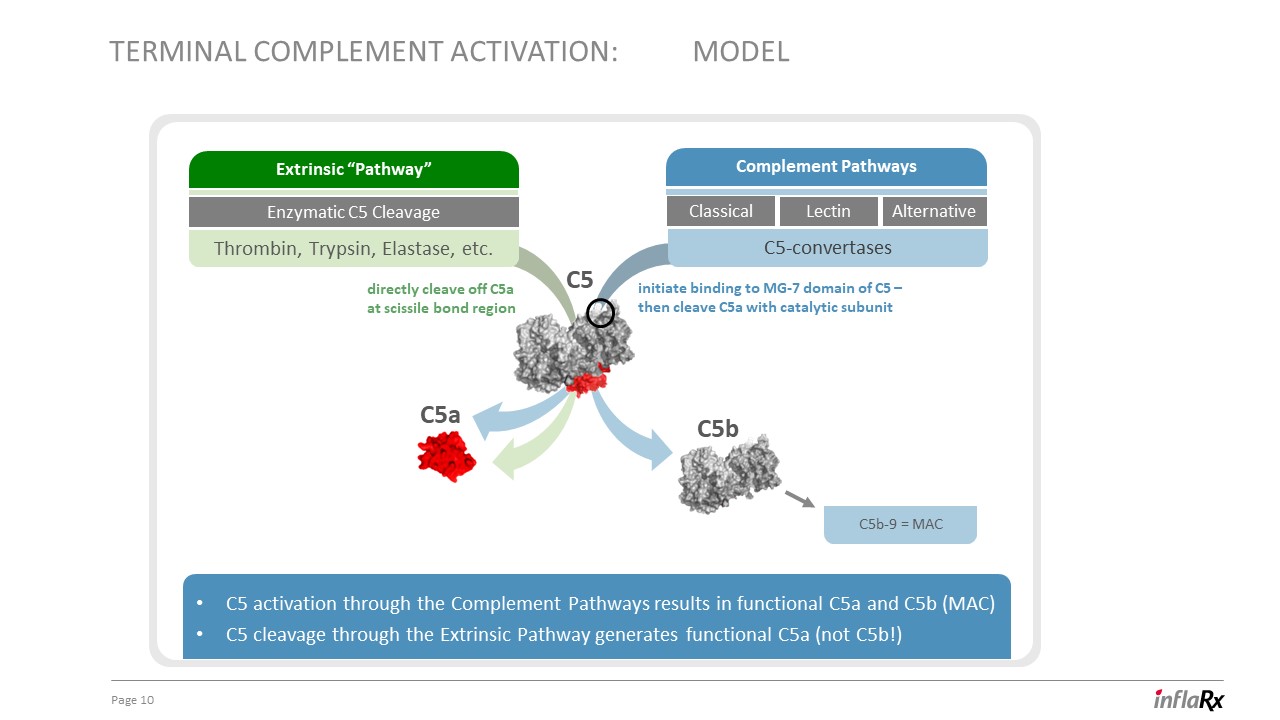
10 Terminal complement activation: model C5a C5 activation through the Complement Pathways results in functional C5a and C5b (MAC)C5 cleavage through the Extrinsic Pathway generates functional C5a (not C5b!) C5b C5 Classical Lectin Alternative Complement Pathways C5-convertases Extrinsic “Pathway” Enzymatic C5 Cleavage Thrombin, Trypsin, Elastase, etc. C5b-9 = MAC directly cleave off C5aat scissile bond region initiate binding to MG-7 domain of C5 –then cleave C5a with catalytic subunit
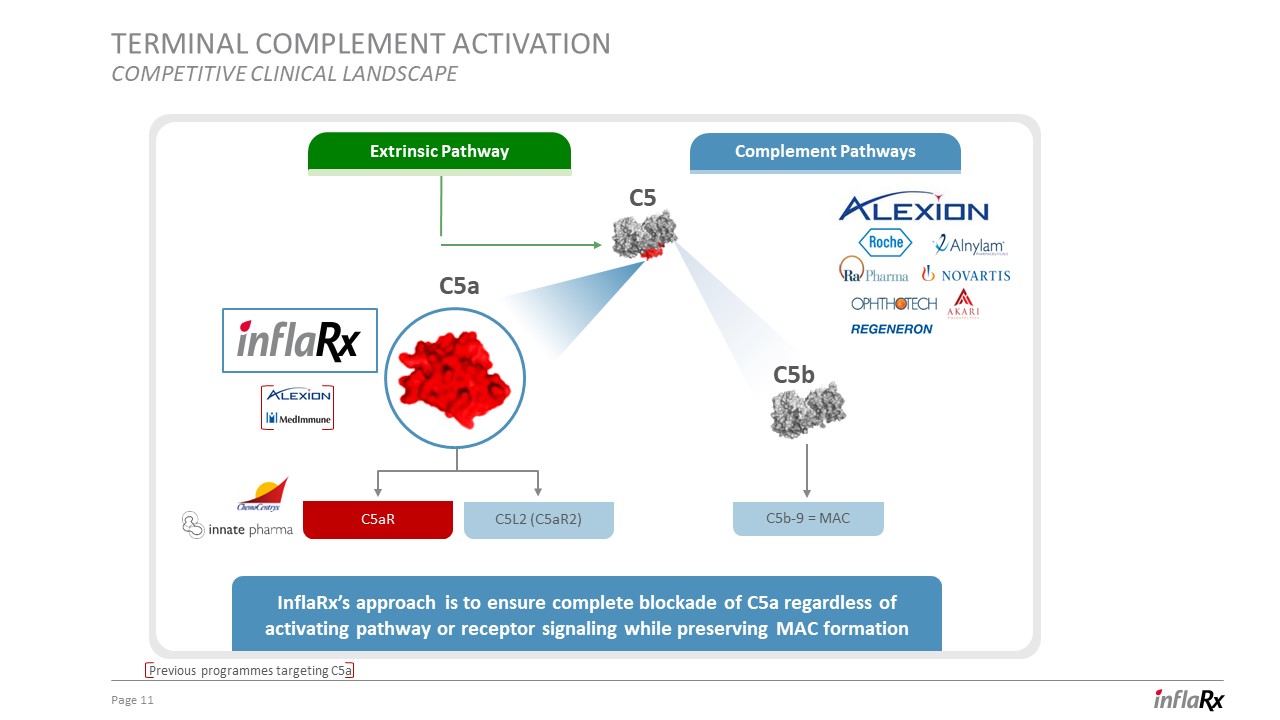
11 Terminal complement activationCompetitive clinical landscape Previous programmes targeting C5a Complement Pathways Extrinsic Pathway C5b-9 = MAC InflaRx’s approach is to ensure complete blockade of C5a regardless of activating pathway or receptor signaling while preserving MAC formation C5 C5a C5aR C5L2 (C5aR2) C5b

IFX-1 is a first-in-class anti-C5a monoclonal antibody 12 MAC lysis invading microorganisms C5b-9 = MAC C5b KEY FEATURES Blocks C5a biological effects up to 100% in human blood Leaves MAC formation intactBinds with high affinity to the discovered epitope C5 newepitope Cleavage of C5 through:Complement pathway activation, orDirectly through enzymes via “extrinsic” pathway C5a conformational change IFX-1 MAC lysis invading microorganisms C5b-9 = MAC
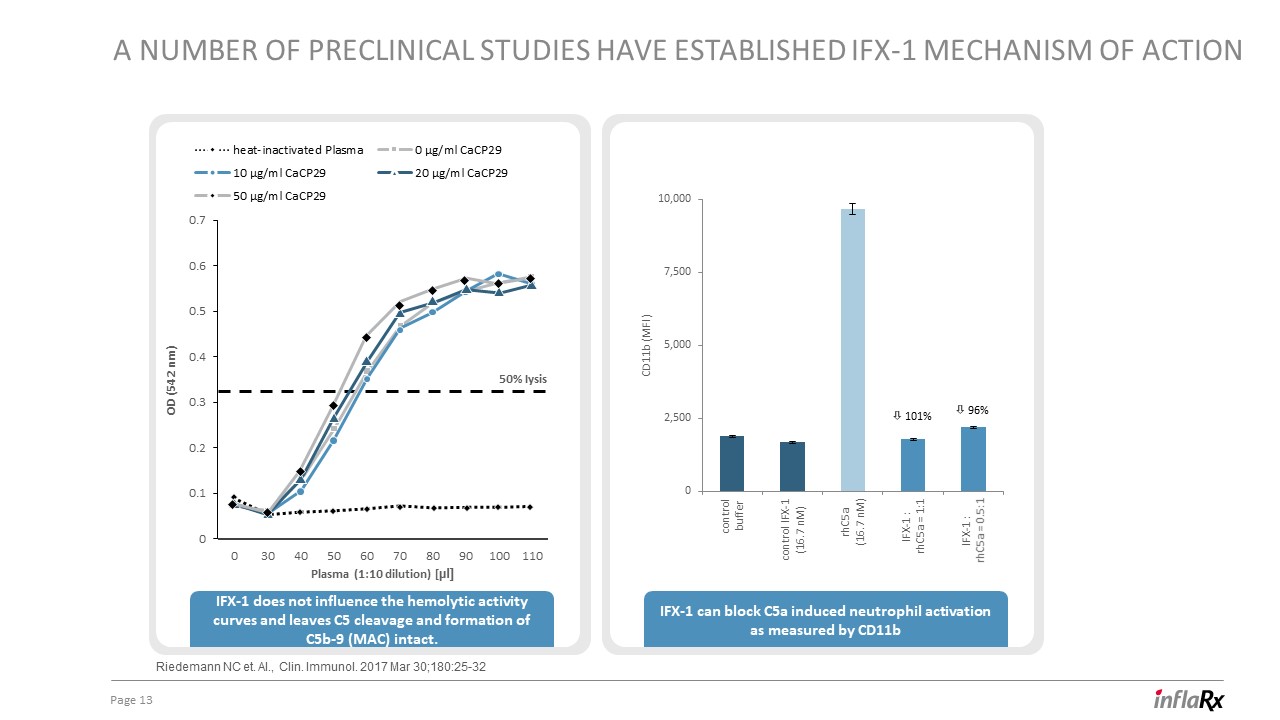
13 A number of preclinical studies have established ifx-1 mechanism of action Riedemann NC et. Al., Clin. Immunol. 2017 Mar 30;180:25-32 ò 101% ò 96% IFX-1 can block C5a induced neutrophil activation as measured by CD11b IFX-1 does not influence the hemolytic activity curves and leaves C5 cleavage and formation of C5b-9 (MAC) intact. Plasma (1:10 dilution) [µl] OD (542 nm) 50% Iysis

ifx-1 for hidradenitis Suppurativa
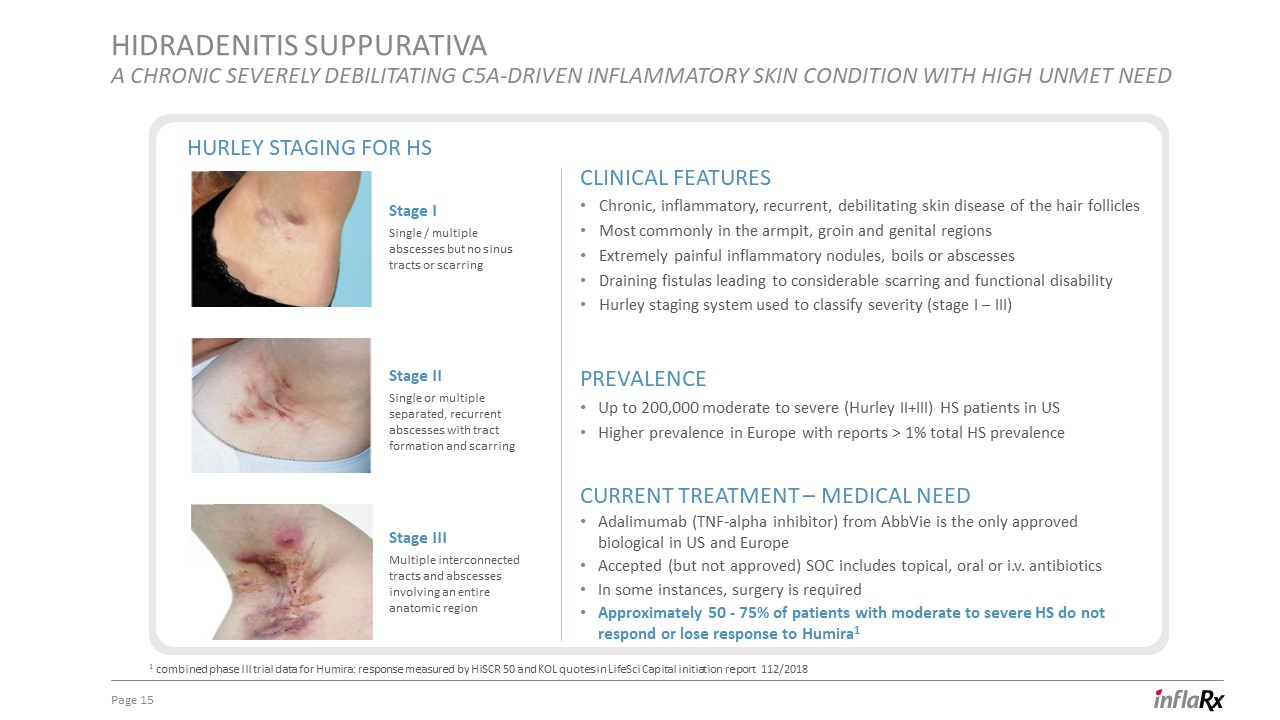
hidradenitis Suppurativaa chronic severely debilitating C5a-driven inflammatory skin condition with high unmet need 15 Clinical features Chronic, inflammatory, recurrent, debilitating skin disease of the hair follicles Most commonly in the armpit, groin and genital regionsExtremely painful inflammatory nodules, boils or abscessesDraining fistulas leading to considerable scarring and functional disability Hurley staging system used to classify severity (stage I – III) Current Treatment – Medical Need Adalimumab (TNF-alpha inhibitor) from AbbVie is the only approved biological in US and EuropeAccepted (but not approved) SOC includes topical, oral or i.v. antibioticsIn some instances, surgery is required Approximately 50 - 75% of patients with moderate to severe HS do not respond or lose response to Humira1 Prevalence Up to 200,000 moderate to severe (Hurley II+III) HS patients in USHigher prevalence in Europe with reports > 1% total HS prevalence Stage ISingle / multiple abscesses but no sinus tracts or scarring Stage IISingle or multiple separated, recurrent abscesses with tract formation and scarring Stage IIIMultiple interconnected tracts and abscesses involving an entire anatomic region Hurley staging for hs 1 combined phase III trial data for Humira: response measured by HiSCR 50 and KOL quotes in LifeSci Capital initiation report 112/2018
IFX-1 in Hidradenitis Suppurativa 16 HISCR – a validated endpoint Humira was approved based on HiSCR response – providing a potential pathway to approvalHiSCR defines 3 types of lesions:AbscessesInflammatory nodules Draining fistulasHiSCR response defined as:At least 50% reduction in total abscess and inflammatory nodule count (AN count)No increase in the number of abscesses from baselineNo increase in the number of draining fistulas from baseline

IFX-1 in Hidradenitis Suppurativa 17 InflaRx established that HS patients have significant complement activation with elevated C5a levels C5a is involved in several key pathophysiological mechanisms in HSNeutrophil activation is driven by C5aVarious C5a dependent players potentially involved (TNFa, IL-17, etc.)C5a is key neutrophil activator in HS patient plasma: HS patient plasma strongly provoked neutrophil activation in healthy donor blood, this effect could be completely blocked by the addition of IFX-1 Rationale for targeting C5a
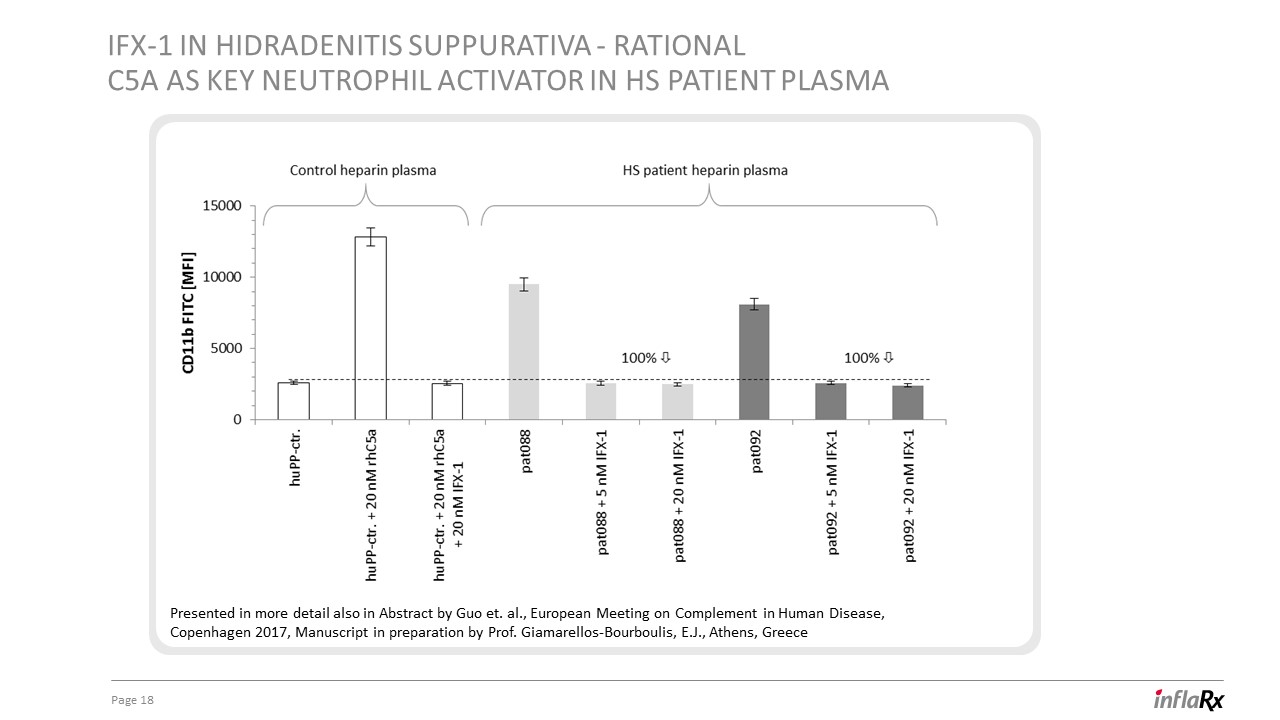
IFX-1 in Hidradenitis Suppurativa - rational C5a as key neutrophil activator in HS patient plasma 18 Presented in more detail also in Abstract by Guo et. al., European Meeting on Complement in Human Disease, Copenhagen 2017, Manuscript in preparation by Prof. Giamarellos-Bourboulis, E.J., Athens, Greece

19 Overview of IFX-1 Phase Iia study in HSStudy design and Patient characteristics 1 dose groupWeekly i.v., total of 8 doses Open labelSingle-center12 patientsKey inclusion: patients with moderate to severe HS with either primary or secondary failure to respond to biological treatment or not eligible for such treatment (adalimumab) Assessing safety and efficacy of IFX-1 in HSPrimary endpoint: safetySecondary endpoint:HiSCR response at different time points, various other secondary endpoints Study design FPFV: Q4 2016LPLV: Q2 2017First results: Q1 2017Final results: Q3 2017 Study design Male 8 (66.7%) Age [y] 48 ± 1550 (22; 69) Hurley Stage III 12 (100%) BMI 27.3 ± 4.926.6 (19.6; 34.5) Weight [kg] 82.2 ± 14.778.0 (63.0; 105.0) Duration of HS [y] 20 ± 920 (3; 35) AN count 6.4 ± 2.56 (3; 11) Failure to TNF-alpha blockade 9/12 Study objective Timelines Treatments Patient characteristics
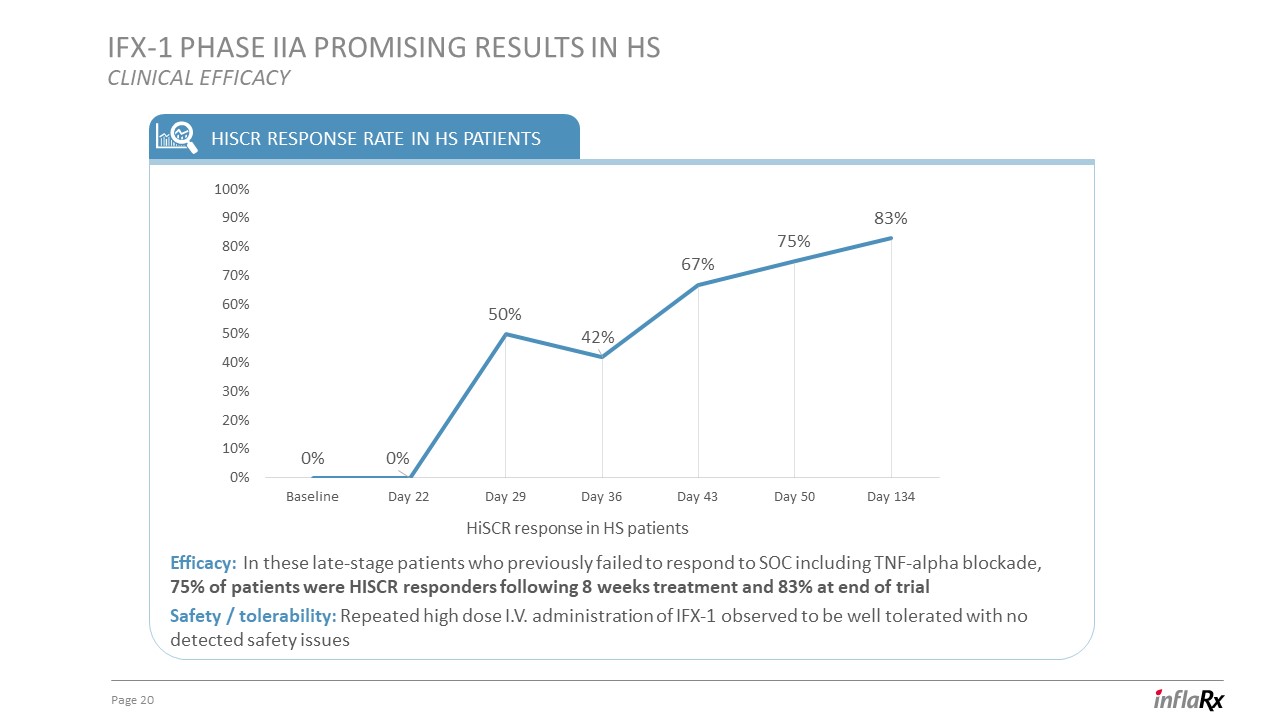
IFX-1 Phase Iia PROMISING Results in Hsclinical efficacy 20 HISCR response rate in HS patients HiSCR response in HS patients Efficacy: In these late-stage patients who previously failed to respond to SOC including TNF-alpha blockade, 75% of patients were HISCR responders following 8 weeks treatment and 83% at end of trial Safety / tolerability: Repeated high dose I.V. administration of IFX-1 observed to be well tolerated with no detected safety issues

21 IFX-1 Phase Iia Results in HsPHARMACODYNAMICS & C5A blocking activity of ifx-1 Mean c5a PLASMA LEVELS Data displayed in the F1 prospectus: Mean C5a levels (ng / ml) in HS patients at day 1 (pre-dosing), day 22 and day 50 (end of treatment) as well as on day 134 (at the end of the trial observation period). One sample was excluded from this analysis at day 50 (end of treatment) (as indicated with (+) above) from one patient in whom study drug infusion was discontinued prematurely after day 29 due to an unrelated adverse event

IFX-1 Phase Iia Results in HsSKIN REsPONSE EXAMPLES from treated patients 22 Day 1 Day 134 Visible improvement at the end of the trial Gluteal fold Right inguinal Day 1 Day 134

IFX-1 Phase Iib study in HS: SHINEStudy design 23 Responders Non Responders Placebo IFX-1 minimum dose IFX-1 low dose IFX-1 medium dose IFX-1 high dose IFX-1 low dose IFX-1 medium dose Screening Open Label Extension Period 28 Weeks Main Period (double blind)16 weeks 179 patients with moderate or severe HS – enrollment completedPrimary endpoint: dose response relationship based on HiSCR at week 16Secondary endpoints: Quality of Life, Safety, PK/PD substudy,Topline results expected in Q2 2019 TIMELINEs

IFX-1 Phase Iib study in HS: SHINE statistical Model MCP-mod 24 The Multiple comparison Procedure – Modelling (MCP-mod) What is this? novel and now more frequently used design for dose findingtests whether a new drug has a dose-response effect on an endpoint = MCP stepcalculates the dose-response relationship (curve fit) = mod step regulatory opinion and advantages? qualified and recommended by FDA and EMA1,2,3uses the available data better than pairwise comparisons with ANOVA (EMA written opinion3) HOW DO YOU SET THIS UP? make common assumptions (endpoint, effect sizes etc.)chose most suitable dose response relation (based on available information = other compounds, etc.) determine doses + scenarios for likely effect size and calculate sample size for desired power Bretz F et al (2005), Combining multiple comparisons and modeling techniques in dose-response studies. Biometrics 2005, 61(3), pp738-48. https://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/UCM508702.pdfhttps://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/qualification-opinion-mcp-mod-efficient-statistical-methodology-model-based-design-analysis-phase-ii_en.pdf

IFX-1 Phase Iib study in HS: SHINEstatistical analysis plan 25 SHINE Study MCP-mod set up dose placebo min dose low dose med dose high dose response ca. 25-30% 55% - 60% increasing response Main set up and assumptions dose groups: 4 + placeboplacebo HiSCR rate: 25% - 30%effective dose HiSCR rate: 55% - 60%power of trial (n=175) ca. 90% n=35 per group assumed dose-relationship (function) concave shape (emax)sigmoidal shape (logistic) Scenario basis number of patients per group power 90%

IFX-1 Phase Iib study in HS:mCP-mod outcome Simulated examples for illustration purposes only 26 26,7% 63,3% 56,7% 60% 66,7% Emax: p = 0.00256 logistic: p = 0.01994 36,7% 30% 43,3% 56,7% 73,3% Emax: p = 0.00608 logistic: p = 0.00172 30% 43,3% 43,3% 46,7% 33,3% Emax: p = 0.0787 logistic: p = 0.0719 Example 1: no curve fit = neg. p-value * Example 3: high placebo * Example 2: min dose highly efficacious * * depicted examples are for illustration purposes only based on freely invented figures with no relation to actual data in the SHINE study

ifx-1 for ANCA associated vasculitis

Anca associated vasculitis (AAV)A LIFE-THREATENING AUTOIMMUNE CONDITION 28 Rare, life-threatening autoimmune disease, characterized by necrotizing vasculitisLife-threatening flare phases affect organs leading to potentially fatal organ dysfunction and failure Predominantly affecting small vessels associated with anti-neutrophil cytoplasmic antibodies, or ANCADisease activity is assessed using Birmingham Vasculitis Activity Score v3 (BVAS) Clinical features Approx. 40,000 AAV patients in the USApprox. 75,000 AAV patients in EuropeOrphan drug market prevalence Source: Chen, Jayne and Zhao. Complement in ANCA-associated vasculitis: mechanism and implication for management Current Treatment – Medical Need Induction of remission critical during flare phases – induction treatment differs from maintenance therapy and consists of high dose corticosteroids plus either cyclophosphamide or RituximabInduction of remission therapy have significant side effects

IFX-1 in AAVClinical Poc established for role of C5a / C5aR pathway in AAV 29 rationale C5a/C5aR interaction is essential for development of MPA-ANCA crescentic glomerulonephritis in a mouse modelComplement activation in active AAV patients is significantChemocentryx’ CCX168 (small molecule, C5aR antagonist) data: C5aR inhibition results in a more rapid and consistent response in BVAS than high dose steroids (PoC of C5a / C5aR axis importance in humans) = successful reduction and replacement of steroid use for induction of remission Potential advantages of IFX-1 for AAV *Bekker, P., Jayne, D. et al., 2014 ACR/ARHP Annual Meeting Rapid onset of action: intravenous administration with fast onset of action, inhibiting C5a signaling completely protecting from C5a induced priming and activation of neutrophils potentially a) faster response rate and b) quicker induction of remission compared to the SOCPotential safety benefits: by blocking C5a and not its receptors, the properties of IFX-1 may allow it to avoid safety concerns arising from indirect off-target effects

IFX-1 in AAVComplement activation in AAV 30 Guo SI, 2012, Kid intl 83:127 C5a is significantly increased in patients with active AAV – but not in remission

IFX-1 in AAVC5a plays a key role in AAV 31 Van Timmeren, Curr. Opinion Rheumatol. 2012; 24:8 Role of c5a in AAV Chemotaxis of PMNsEnhancing IC effectsActivation of PMNsCytokine inductionEndothelial injury (enzymes & oxidative stress)Tissue factor releaseThrombo-inflammation & prolonged PMN life-span

32 IFX-1 – P2.6 Phase Ii study in AAV in the US (IXPLore)Study design Assessing safety and efficacy of IFX-1 in AAVPrimary endpoint: SafetySecondary endpoint: Response rate based on the Birmingham Vasculitis Score (BVAS), various other secondary endpoints Study objective Placebo + SOCGroup C (N=12) IFX-1 low dose + SOCGroup A (N=12) W 16 ScreeningW - 2 to -1 Remission Induction Phase:SOC = RTX/CYC+GC IFX-1 high dose + SOCGroup B (N=12) Randomization 1:1:1Day 1 Patients randomized 1:1:1 End of Study W 24 Treatment: 16 Weeks Follow up: 8 Weeks Remission Maintenance Phase: AZA/MTX/MMF/MPS+GC; or can remain RTX/CYC+GC W 20

group C: IFX-1 + no GC (N=33) group A: IFX-1 + reduced GC(N=15) Screening Remission Induction Phase:RTX/CYC group B: placebo + standard GC (N=15) Randomization 1:1 End of Study W 24 Treatment: 16 Weeks Follow up: 8 Weeks Remission Maintenance Phase: AZA/MTX/MMF/MPS; or can remain RTX/CYC W 16 W 8 W 2 W 4 W 20 Primary objective: efficacy of IFX-1 treatment as replacement for glucocorticoid (GC) therapy in GPA and MPA Secondary objectives: • To assess safety and tolerability of IFX-1 To compare toxicity of standard-dose GC with IFX-1To generate data for pharmacokinetic (PK) and pharmacodynamic (PD) modelling Day 1 group B: placebo + standard GC (N=18) part 1 part 2 Treatment: 16 Weeks Follow up: 8 Weeks W 16 W 8 W 2 W 4 W 20 GC = glucocorticoids Study objective 33 IFX-1 – P2.5 Phase Ii study in AAV in Europe (IXCHange)Study design
FiNancials & Strategic long term goals

Strong balance sheet to support clinical development 35 Financings $ Series D: $55m in Oct 2017NASDAQ IPO: $106m in Nov 2017 $15.00 per shareFollow-on: $117m in May 2018 $34.00 per share$63m gross proceeds for InflaRx$54m for selling shareholders J.P.Morgan Anupam RamaLeerink Joseph P. SchwartzBank of Montreal Matthew LuchiniSunTrust Robinson Humphrey Edward H. NashCredit Suisse Tiago FauthLifeSci Capital Sam SlutskyBaird Madhu KumarGuggenheim Yatin SuneyaRaymond James Steven Seedhouse Analysts Key Financials Cash position*: $176m (as of 31 Dec 2018) Exchange: Nasdaq, Ticker: IFRX Shares Outstanding: 25.97m (as of March 28) Price: $45.24 (as of May 1, 2019) Market Cap: ~ $1.17b (as of May 1, 2019) * cash equivalents plus securities and other investments
Our strategy 36 goal and strategy Advance our lead program IFX-1 for HS to commercialization and extent with additional IFX-1 s.c. development Our goal is to maintain and advance our leadership position within the anti-C5a complement space by leveraging full potential of our proprietary technology Commence / complete Phase II clinical development of IFX-1 for AAV, PG and within Oncology field Pursue the development of IFX-2 and continue to expand the breadth of our anti-C5a technology Commercialize IFX-1, if approved, either independently or with a partner Extend pipeline with initiation of clinical development of IFX-1 in other complement-mediated autoimmune / inflammatory diseases

InflaRx N.V.Winzerlaer Str. 207745 Jena, GermanyEmail: info@inflarx.comTel: +49-3641-508180Fax: +49-3641-508181www.inflarx.com Investor Relations InflaRx N.V.Jordan Silverstein Head of Corporate Development and Strategyjordan.silverstein[at]inflarx.de Page 37