Exhibit 99.3

Controlling inflammation SVB Leerink Global Healthcare Conference 2020

Important Notice and DisclaimerThis presentation has been prepared by InflaRx N.V. (“InflaRx”), a US-Nasdaq publicly listed Dutch company having its principle place of business in Germany. This presentation is made for informational purposes only and does not constitute an offer to sell or a solicitation of an offer to buy securities. The information set forth herein does not purport to be complete or to contain all of the information you may desire. Statements contained herein are made as of the date of this presentation unless stated otherwise, and neither the delivery of this presentation at any time, nor any sale of securities, shall under any circumstances create an implication that the information contained herein is correct as of any time after such date or that information will be updated or revised to reflect information that subsequently becomes available or changes occurring after the date hereof.This presentation may contain forward-looking statements. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based on our current beliefs, expectations and assumptions regarding the future of our business, future plans and strategies, our clinical results and other future conditions. All statements other than statements of historical facts contained in this presentation, including statements regarding future results of operations and financial position, business strategy, current and prospective product candidates, planned clinical trials and preclinical activities, product approvals, research and development costs, current and prospective collaborations, timing and likelihood of success, expectations regarding market acceptance and size, plans and objectives of management for future operations, and future results of anticipated product candidates, are forward-looking statements. These risks and uncertainties include those described under the caption “Risk Factors” in InflaRx's Registration Statement on Form F-1 and the accompanying prospectus filed with the Securities and Exchange Commission in connection with the company's initial public offering and other filings with the Securities and Exchange Commission. New risks and uncertainties may emerge from time to time, and it is not possible to predict all risks and uncertainties. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. Although we believe the expectations reflected in such forward-looking statements are reasonable, we can give no assurance that such expectations will prove to be correct. Accordingly, readers are cautioned not to place undue reliance on these forward-looking statements. No representations or warranties (expressed or implied) are made about the accuracy of any such forward-looking statements.Certain information contained in this presentation relates to or is based on studies, publications, surveys and other data obtained from third-party sources and InflaRx’s own internal estimates and research. While InflaRx believes these third-party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. In addition, all of the market data included in this presentation involves a number of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions. Finally, while we believe our own internal research is reliable, such research has not been verified by any independent source. InflaRx n.v. | Winzerlaer Str. 2, 07745 Jena, Germany, Email: info@inflarx.com, Tel: +49-3641-508180, www.inflarx.com

Investment Highlights 3 Complete and selective blockade of the biological activity of C5a in vitro and in vivoStrong patent coverage on anti-C5a technology until end of 2030 / 2035 with extension Proven anti-inflammatory effect in multiple Phase II studies Statistically significant reduction of inflammatory lesions in Phase IIb Hidradenitis Suppurativa study and impressive long-term efficacyFull data set analysis warrants continued development towards Phase III despite missing the primary endpoint (HiSCR) in Phase IIb studyFavorable safety profile and excellent tolerability (n > 300 patients) Ongoing Phase IIb studies in ANCA-associated vasculitis in the US and EUOngoing Phase IIa open label study in Pyoderma Gangraenosum in US and CanadaFollow-on anti-C5a mAb IFX-2 in pipeline (pre-clinical stage) Pipeline extension of IFX-1 in other inflammatory diseases & oncology Leading Proprietary Anti-C5a Technology Established Clinical Efficacy for Lead Drug IFX-1 Multiple ongoing studies and indication + Pipeline extension

Pipeline with Multiple Opportunities 4 We have multiple ongoing Phase II studies with potential to expand into further indications These compounds and/or uses of approved products are investigational and have not been approved by the FDA or any other regulatory agency for the uses under investigation. The safety and efficacy of these agents have not been established. Proposed Indications Prevalence Pre-Clinical Phase I Phase II Phase III Update IFX-1C5a Inhibitor Hidradenitis Suppurativa (HS) Up to 200,000patients in the USOver 200,000 patients in Europe Phase IIb completedPlanning for next steps ANCA-Associated Vasculitis ~40,000 patients in the US~75,000 patients in Europe Phase IIb enrollment ongoing in both Europe and US Pyoderma Gangraenosum ~50,000 patients in the US and Europe are affected Phase IIa open label enrollment ongoing in US and Canada Oncology Undisclosed Indication Development of TPP ongoing IFX-2C5a Inhibitor Undisclosed Chronic Inflammatory and Autoimmune Diseases Not applicable Developing as injectable with optimized use for other chronic inflammatory indications
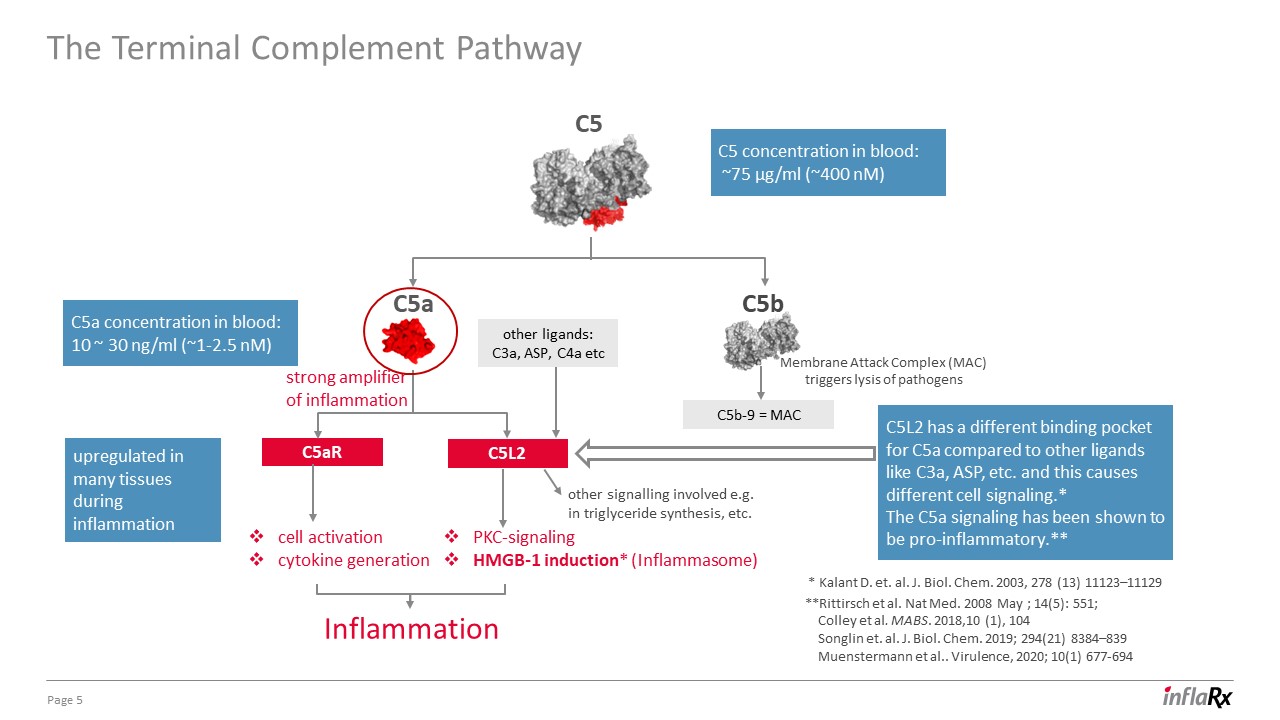
The Terminal Complement Pathway 5 Membrane Attack Complex (MAC)triggers lysis of pathogens strong amplifierof inflammation C5aR C5b-9 = MAC C5L2 C5b C5a C5 cell activationcytokine generation Inflammation PKC-signaling HMGB-1 induction* (Inflammasome) C5a concentration in blood: 10 ~ 30 ng/ml (~1-2.5 nM) C5 concentration in blood: ~75 µg/ml (~400 nM) other ligands: C3a, ASP, C4a etc upregulated in many tissues during inflammation **Rittirsch et al. Nat Med. 2008 May ; 14(5): 551; Colley et al. MABS. 2018,10 (1), 104 Songlin et. al. J. Biol. Chem. 2019; 294(21) 8384–839 Muenstermann et al.. Virulence, 2020; 10(1) 677-694 C5L2 has a different binding pocket for C5a compared to other ligands like C3a, ASP, etc. and this causes different cell signaling.* The C5a signaling has been shown to be pro-inflammatory.** * Kalant D. et. al. J. Biol. Chem. 2003, 278 (13) 11123–11129 other signalling involved e.g. in triglyceride synthesis, etc.

IFX-1 in HS: SHINE Study Details 6 Important Note: Patients entering the OLE were not unblinded to their initial therapy Test a dose-dependent effect of IFX-1 on HiSCR response at week 16 (primary endpoint) Assess long-term safety of IFX-1Test durability of response with lower maintenance therapy in open label extension period Main Goals Placebo IFX-1 minimal dose IFX-1 low dose IFX-1 medium dose IFX-1 high dose Screening 28 weeks (24 weeks treatment + 4 weeks observation) 16 weeks (double blind) Total treatment time: 9 months (week 40) + 1 month observation (week 44) Open Label Extension Period (OLE): n = 156 Main Period: n = 177 treated (400 mg q4w) (800 mg q4w) (800 mg q2w) (1200 mg q2w) Week 16 HiSCR Responders: IFX-1 low dose Week 16 HiSCR Non-Responders: IFX-1 medium dose (800 mg q4w) (800 mg q2w)

SHINE Study: Primary Outcome HiSCR at Week 16 versus AN Count Reduction 7 HiSCR response rate (%) week 16* * Full analysis set AN count score change (mean %) week 16* n = approx. 35/ group placebo minimum low medium high Treatment groups: Primary endpoint: HiSCR dose response signal not met but signal towards improved AN count
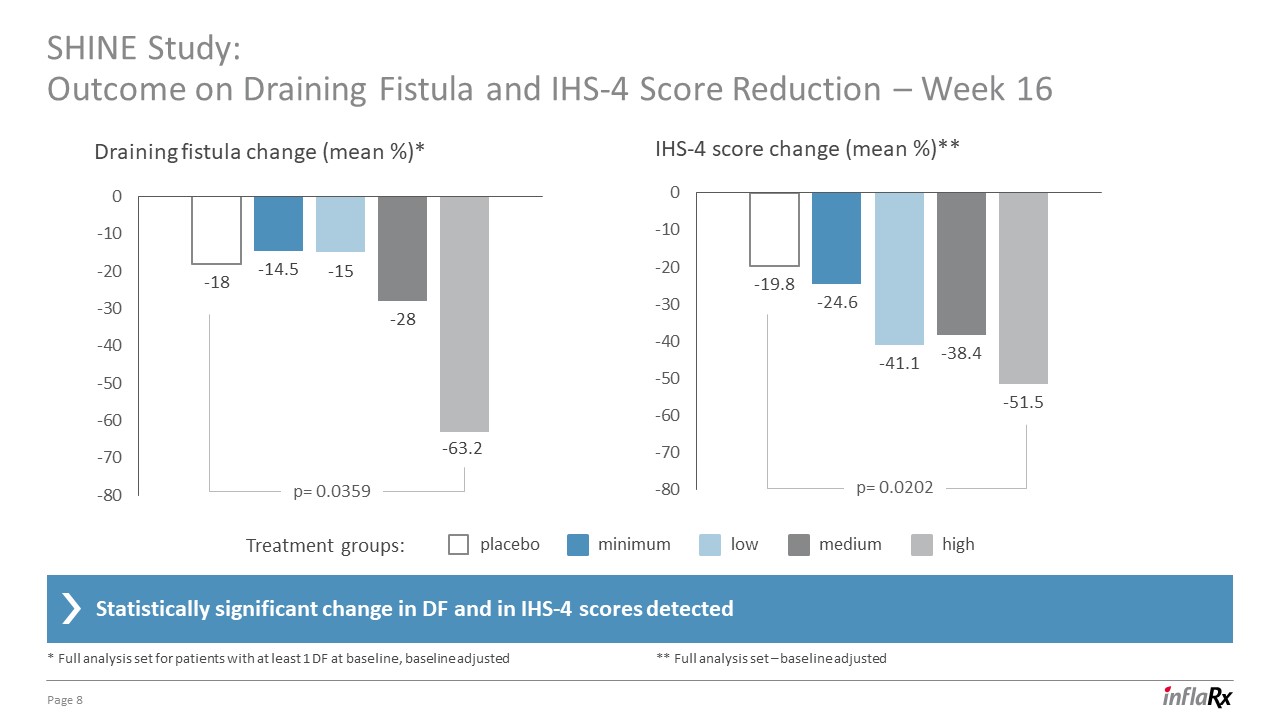
SHINE Study: Outcome on Draining Fistula and IHS-4 Score Reduction – Week 16 8 Draining fistula change (mean %)* IHS-4 score change (mean %)** placebo minimum low medium high Treatment groups: Statistically significant change in DF and in IHS-4 scores detected * Full analysis set for patients with at least 1 DF at baseline, baseline adjusted ** Full analysis set – baseline adjusted p= 0.0202 p= 0.0359
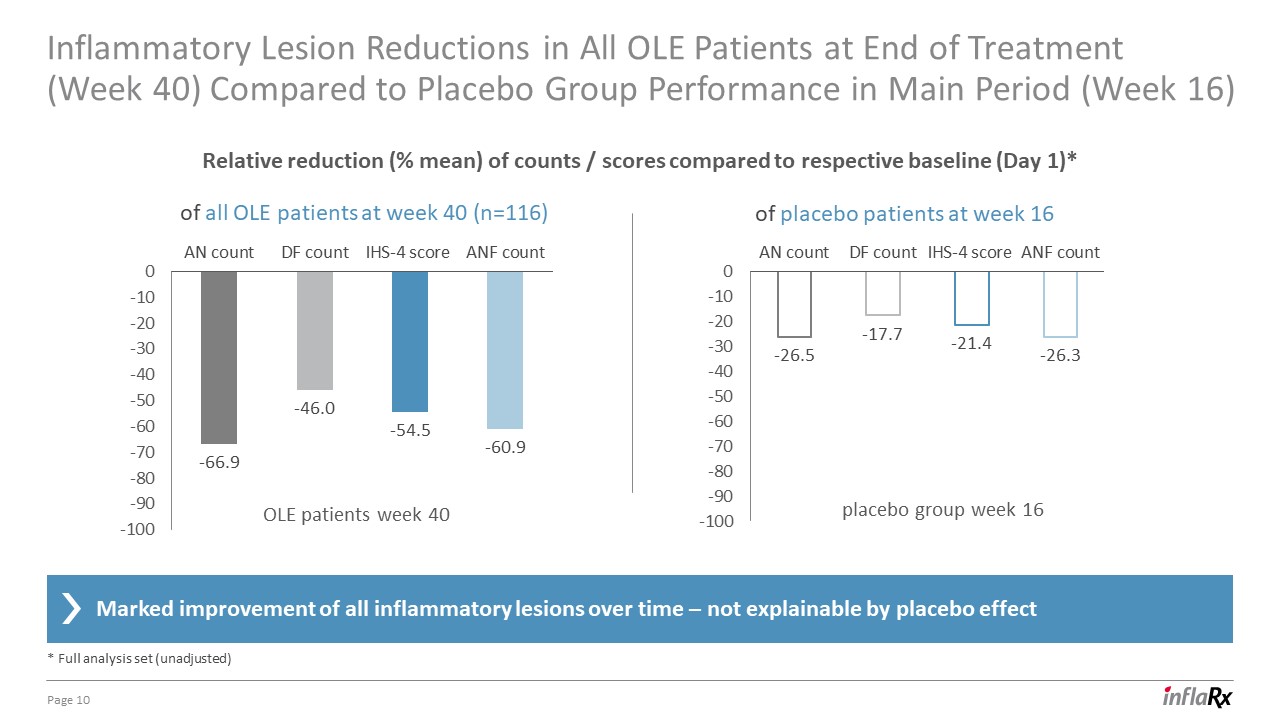
Inflammatory Lesion Reductions in All OLE Patients at End of Treatment (Week 40) Compared to Placebo Group Performance in Main Period (Week 16) 10 of all OLE patients at week 40 (n=116) of placebo patients at week 16 Marked improvement of all inflammatory lesions over time – not explainable by placebo effect * Full analysis set (unadjusted) Relative reduction (% mean) of counts / scores compared to respective baseline (Day 1)* placebo group week 16 OLE patients week 40

SHINE Study and Next Steps in HS Development 11 HiSCR is burdened by high variability (driven by AN count variability) and by a lack of capturing reduction of draining fistula Our conclusions Evidence for a high C5a turnover rate in HS, leading to increased dose requirements of IFX-1 IFX-1 leads to a marked reduction of all inflammatory lesions in HS with a durable long-term effect detected even at non-optimal doses IFX-1 long-term treatment was well tolerated, no drug related SAEs* in the open label extension phase * Serious adverse events Request End-of-Phase II FDA Meeting in Q1 2020 Next steps Discuss with FDA the path forward for regulatory approval towards a Phase III pivotal program Depending on meeting timing and feedback: define path forward by 2H 2020
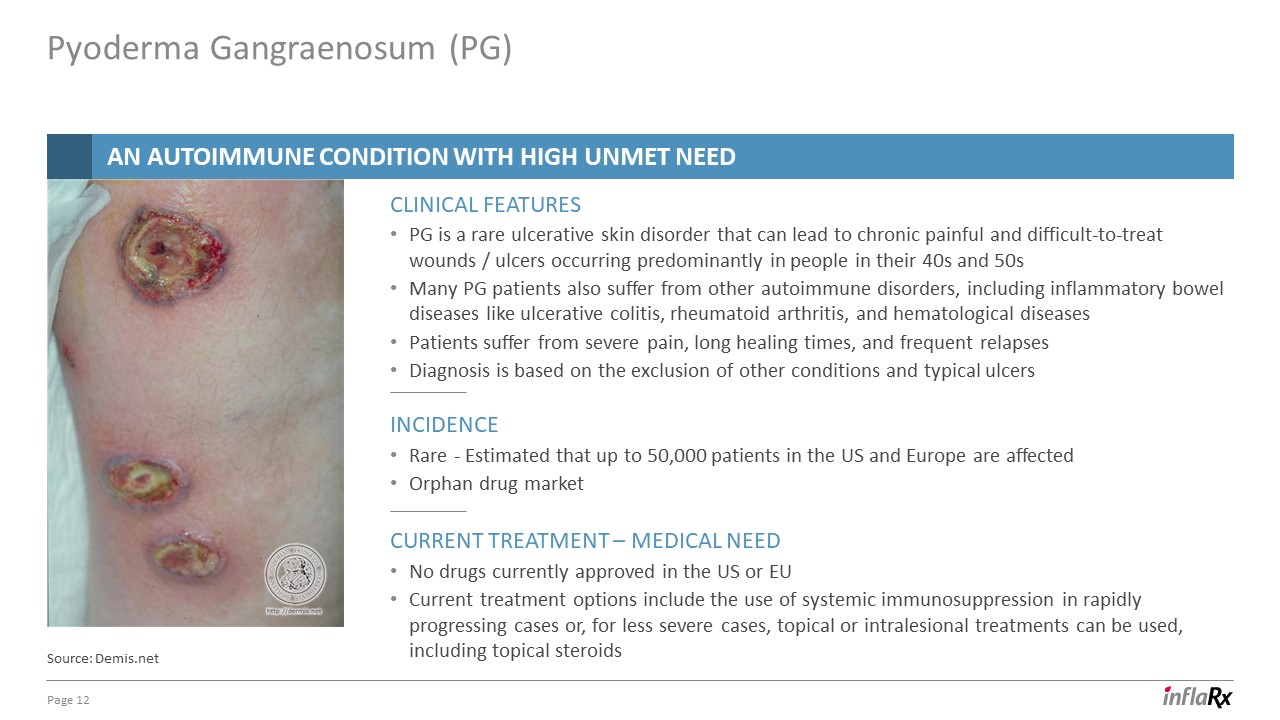
Pyoderma Gangraenosum (PG) 12 Source: Demis.net PG is a rare ulcerative skin disorder that can lead to chronic painful and difficult-to-treat wounds / ulcers occurring predominantly in people in their 40s and 50sMany PG patients also suffer from other autoimmune disorders, including inflammatory bowel diseases like ulcerative colitis, rheumatoid arthritis, and hematological diseases Patients suffer from severe pain, long healing times, and frequent relapsesDiagnosis is based on the exclusion of other conditions and typical ulcers Clinical features Current Treatment – Medical Need No drugs currently approved in the US or EUCurrent treatment options include the use of systemic immunosuppression in rapidly progressing cases or, for less severe cases, topical or intralesional treatments can be used, including topical steroids INCIDENCE Rare - Estimated that up to 50,000 patients in the US and Europe are affectedOrphan drug market An autoimmune condition with high unmet need

Overview of IFX-1 Phase IIa Study in PG - Study Design 13 Assessing safety and efficacy of IFX-1 in PGRationale: PG is associated with a neutrophilic leukocytosis, which is likely to be triggered by C5a. Pyoderma Gangraenosum lesions have pronounced neutrophilic infiltration and the expression of interleukin (IL)-1β, IL-17, tumor necrosis factor (TNF)-alpha, and their receptors are significantly elevated, indicating auto-inflammatory conditions.Primary endpoint: SafetyKey secondary endpoints:Responder rate defined as Physicians Global Assessment ≤3 of target ulcer at visits V4, V6, V10, and V16 (end of treatment); Time to complete closure of Pyoderma Gangraenosum target ulcer (investigator assessment) Open labelMulti-center in US and CanadaTarget enrollment – 18 patientsFirst patient dosed – June 2019 Trial started with 1 dose group: amendment approved to introduce a dose escalation to test 3 dose groupsSubjects receive IFX-1 dosing every other weekDose: 800 mg biweekly first 5 patients Study Objective Study Design Treatments

14 5 patients have been treated 2 out of the first 5 patients showed complete closure of the target ulcer with one patient in full disease remission and second in almost complete disease remissionIn one additional patient, initial wound healing activity was detected in the first 2-3 weeks of treatment – but no wound size decrease or closure detected2 additional patients with extensive disease (very large ulceration / ulcer reaching the entire circumference of the leg) did not heal the target ulcer and are still under treatmentThe “responders” have higher baseline C5a levelsPD analysis (C5a levels) warrants higher dosingDose escalation recently approved by relevant authorities STUDY UPDATE C5a Levels at Baseline responder responder Pyoderma Gangraenosum (PG)An AUTOIMMUNE CONDITION with high unmet need

Female patient with extensive genital PG disease and target ulcer on lower extremityVarious failed treatment attempts including high dose corticosteroids, etc.Significantly elevated baseline C5a levelsPatient completely healed of all PG lesions and off drug now for 2 months 15 day 1 day 18 Male patient with treatment resistant PG disease and Addison´s disease from high-dose GCSignificantly elevated baseline C5a levelsTarget ulcer is completely healed, and the patient is still on treatment (still one other lesion with minimal opening at different body location) day 43 Patient Example 1 day 1 day 30 day 131 Patient Example 2 Pyoderma Gangreaosum (PG)Two patients show complete wound closure with IFX-1 treatment
Our Strategy 16 Advance our lead program IFX-1 for HS towards Phase III / approval based on regulatory guidanceExplore application of IFX-1 for AAV, PG and within the oncology field in Phase II clinical developmentExtend pipeline with initiation of clinical development of IFX-1 in other complement-mediated autoimmune / inflammatory diseasesPursue the development of IFX-2 and continue to expand the breadth of our anti-C5a technologyContinue to explore broadening the R&D pipeline beyond anti-C5a technology as part of diversification strategy goalS and strategy We have a strong cash balance to pursue these activities (End of Q3 2019: US$151 million)

Winzerlaer Str. 207745 Jena, GermanyEmail: info@inflarx.comTel: +49-3641-508180Fax: +49-3641-508181www.inflarx.com Jordan ZwickGlobal Head of Business Development & Corporate StrategyEmail: jordan.zwick@inflarx.de InflaRx N.V. Investor Relations InflaRx N.V.