EXPLANATORY NOTE
This Post-Qualification Offering Circular Amendment No. 1 (this “Offering Circular Amendment No. 1”) amends the offering circular of Carolina Complete Health Network, Inc. qualified on March 12, 2018, and as may be further amended and supplemented from time to time (the “Offering Circular”), to add, update and/or replace information contained in the Offering Circular.
Post-Qualification Offering Circular Amendment No. 1
File No. 024-10799
PART II
OFFERING CIRCULAR DATED APRIL 26, 2018

Carolina Complete Health Network, Inc.
222 N. Person Street, Suite 010, Raleigh, NC 27601
919-719-4161
Up to 20,000 Shares of
Class P Common Stock
This Offering Circular relates to the offer and sale by Carolina Complete Health Network, Inc., a Delaware corporation (“CCHN,” “we,” “us” or “our”), of one, but not more than one, share of our Class P Common Stock, $0.01 par value per share (such class, the “Class P Common Stock” and the shares so offered, the “Provider Shares”), to each person who meets the eligibility criteria described herein, up to an aggregate amount of $15,000,000 (the “Offering”).
CCHN was formed as a wholly-owned subsidiary of the North Carolina Medical Society (the “NCMS”) in Delaware on May 19, 2016. CCHN’s primary purpose is to build and operate a network of health care professionals (the “Provider Network”) who will provide medical services under a patient-focused Medicaid health plan (the “Health Plan”) in response to the pending implementation of Medicaid reform in North Carolina. A North Carolina licensed insurance company, Carolina Complete Health, Inc. (“Carolina Complete Health”), will operate the Health Plan. The Health Plan will be owned and operated pursuant to a joint venture (the “Joint Venture”) among the NCMS, CCHN, Centene Corporation (“Centene”) and Centene Health Plan Holdings, Inc., a subsidiary of Centene (“Centene Sub,” and together with the NCMS, CCHN and Centene, the “Joint Venture Parties”). The closing of the Joint Venture transactions is expected to occur after September 1, 2018. See “The Joint Venture.” We maintain principal executive offices at 222 N. Person Street, Suite 010, Raleigh, NC 27601. The phone number for these offices is 919-719-4161. Our website address is www.cch-network.com.
The Provider Shares offered in the Offering represent in the aggregate a 46.5 percent direct equity interest in CCHN. The NCMS will at all times hold a 50 percent direct equity interest in CCHN through its ownership of Class M Common Stock, $0.01 par value per share (the “Class M Common Stock”). The subscription price for a Provider Share is $750.00. The Provider Shares are not listed on any national securities exchange or on the over-the-counter inter-dealer quotation system, and there is no market for the Provider Shares. See “Description of Capital Stock.”
Investment in a Provider Share involves significant risk, and you may be required to hold your investment for an indefinite period of time. You should purchase this security only if you can afford a complete loss of your investment. See “Risk Factors” beginning on page 6 of this Offering Circular.
We commenced the Offering of the Provider Shares promptly after the date this Offering Circular was qualified. The Offering will terminate at the earliest of (1) the date at which the total offering amount has been sold, (2) March 12, 2021, the date that is three years after this Offering was qualified by the Commission or (3) the date at which the Offering is earlier terminated by CCHN in our sole discretion. We may undertake one or more closings on a rolling basis. After each closing, funds tendered by investors will be available to us. After the initial closing of this Offering, we expect to hold closings on at least a quarterly basis.
The Offering is being conducted on a “best efforts” basis, which means our directors and officers are using their commercially reasonable best efforts in an attempt to sell the Provider Shares. Such persons are not receiving any commission or any other remuneration based either directly or indirectly on sales of the Provider Shares. In offering the Provider Shares on our behalf, such persons are relying on the safe harbor from broker-dealer registration set forth in Rule 3a4-1 under the Securities Exchange Act of 1934, as amended.
Purchase of the Provider Shares is limited to physicians, physician assistants and nurse practitioners licensed or approved to practice, as applicable, in North Carolina who participate in the Provider Network, reside in North Carolina, Georgia, South Carolina, Tennessee or Virginia and otherwise meet the eligibility criteria set forth herein (each, an “Eligible Investor”) (see “Offering Circular Summary—the Offering” and “Investor Suitability Requirements”). Each purchaser’s investment is limited to one, and only one, Provider Share. This Offering Circular shall not constitute an offer to sell or the solicitation of an offer to buy, nor shall there be any sales of these securities, in any state in which such offer, solicitation or sale would be unlawful, prior to registration or qualification under the laws of any such state.
We are following the “Offering Circular” format of disclosure under Regulation A.
IN MAKING AN INVESTMENT DECISION, INVESTORS MUST RELY ON THEIR OWN EXAMINATION OF CCHN AND THE TERMS OF THE OFFERING, INCLUDING THE MERITS AND RISKS INVOLVED. THESE SECURITIES HAVE NOT BEEN APPROVED OR DISAPPROVED BY ANY FEDERAL OR STATE SECURITIES COMMISSION OR REGULATORY AUTHORITY. FURTHERMORE, THESE AUTHORITIES HAVE NOT PASSED UPON THE ACCURACY OR ADEQUACY OF THIS OFFERING CIRCULAR. ANY REPRESENTATION TO THE CONTRARY IS A CRIMINAL OFFENSE.
THE UNITED STATES SECURITIES AND EXCHANGE COMMISSION DOES NOT PASS UPON THE MERITS OF OR GIVE ITS APPROVAL TO ANY SECURITIES OFFERED OR THE TERMS OF THE OFFERING, NOR DOES IT PASS UPON THE ACCURACY OR COMPLETENESS OF ANY OFFERING CIRCULAR OR OTHER SOLICITATION MATERIALS. THESE SECURITIES ARE OFFERED PURSUANT TO AN EXEMPTION FROM REGISTRATION WITH THE COMMISSION; HOWEVER, THE COMMISSION HAS NOT MADE AN INDEPENDENT DETERMINATION THAT THE SECURITIES OFFERED HEREUNDER ARE EXEMPT FROM REGISTRATION.
GENERALLY, NO SALE MAY BE MADE TO YOU IN THIS OFFERING IF THE AGGREGATE PURCHASE PRICE YOU PAY IS MORE THAN 10 PERCENT OF THE GREATER OF YOUR ANNUAL INCOME OR NET WORTH. DIFFERENT RULES APPLY TO ACCREDITED INVESTORS AND NON-NATURAL PERSONS. BEFORE MAKING ANY REPRESENTATION THAT YOUR INVESTMENT DOES NOT EXCEED APPLICABLE THRESHOLDS, WE ENCOURAGE YOU TO REVIEW RULE 251(d)(2)(i)(C) OF REGULATION A. FOR GENERAL INFORMATION ON INVESTING, WE ENCOURAGE YOU TO REFER TO WWW.INVESTOR.GOV.
Offering price to the public | Underwriting discounts and commissions | Proceeds to issuer(1) | Proceeds to other persons | |||||||||||||
| Per Share: | $ | 750 | N/A | $ | 750 | (2 | ) | |||||||||
| Total: | $ | 15,000,000 | N/A | $ | 13,957,000 | (2 | ) | |||||||||
| (1) | We estimate all expenses of the Offering to be approximately $1,043,000. |
| (2) | See “Plan of Distribution—Technology & Closing Services” for information regarding the fees payable to Folio Investments, Inc. with respect to its online investment platform. |
THIS OFFERING CIRCULAR CONTAINS ALL OF THE REPRESENTATIONS BY CCHN CONCERNING THE OFFERING. NO PERSON HAS BEEN AUTHORIZED TO GIVE ANY INFORMATION OR TO MAKE ANY REPRESENTATIONS OTHER THAN THOSE CONTAINED IN THIS OFFERING CIRCULAR, AND, IF GIVEN OR MADE, SUCH INFORMATION OR REPRESENTATIONS MUST NOT BE RELIED UPON AS HAVING BEEN AUTHORIZED BY CCHN.
THE PROVIDER SHARES HAVE NOT BEEN QUALIFIED UNDER THE SECURITIES LAWS OF ANY STATE OR JURISDICTION. WE MAY QUALIFY THE OFFERING WITH THE NORTH CAROLINA SECURITIES REGULATORY BODY AND THE SECURITIES REGULATORY BODIES OF OTHER STATES AS WE MAY DETERMINE FROM TIME TO TIME.
This summary highlights information contained in this Offering Circular. This summary is not complete and does not contain all of the information that you should consider before investing in a Provider Share. You should carefully read the entire Offering Circular, especially concerning the risks associated with the investment in the securities covered by this Offering Circular discussed under the “Risk Factors” section beginning on page 6. Some of the statements in this Offering Circular are forward-looking statements. See the section entitled “Special Note Regarding Forward-Looking Statements” on page 14.
The relationship among CCHN and the other entities having a direct or indirect interest in Carolina Complete Health, as well as the expected ownership of CCHN following this Offering, are illustrated in the following diagram (in which the darker shaded box identifies our company and the lighter shaded box identifies Eligible Investors who purchase a Provider Share in this Offering):
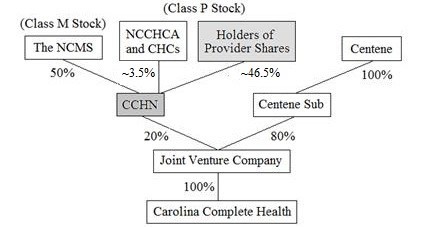
Our Company
CCHN was incorporated in Delaware on May 19, 2016 as a wholly-owned subsidiary of the NCMS. CCHN’s primary purpose is to build and operate the Provider Network for the Health Plan. See “Business.” The Health Plan will be operated by Carolina Complete Health and created in connection with the Joint Venture depicted above to offer a patient-focused Medicaid health plan in response to the pending implementation of Medicaid reform in North Carolina.
During the interim period until the closing of the Joint Venture transactions (which is expected to occur after September 1, 2018), we expect our operations to consist of recruiting and retaining providers to participate in the Provider Network. Following the closing of the Joint Venture transactions, our fundamental business will be recruiting, building, developing, managing, educating, operating and maintaining the Provider Network for the purposes of providing services to the Health Plan. In consideration for providing such services for the Health Plan, we will, pursuant to the terms of the Network License and Management Services Agreement with Carolina Complete Health (the “CCHN Services Agreement”), receive a monthly fee equal to a predetermined percentage of the projected net revenues of the Health Plan during such month, which percentage in any given month will depend in part upon the number of individuals who are participating providers in the Provider Network. Although we will be engaged in the Joint Venture with Centene and its subsidiary, Centene Sub, CCHN is a standalone business whose success is not controlled or guaranteed by Centene, any of its affiliates, the NCMS, the NCCHCA (as defined below under “—The Joint Venture”) or any CHC (as defined below under “—The Joint Venture”).
We maintain principal executive offices at 222 N. Person Street, Suite 010, Raleigh, NC 27601. The phone number for these offices is 919-719-4161. Our website address is www.cch-network.com.
1
The Health Plan and Carolina Complete Health
The Health Plan is designed to be a patient-focused Medicaid health plan in North Carolina. Carolina Complete Health is a North Carolina corporation and a wholly-owned subsidiary of the Joint Venture Company. Carolina Complete Health will be licensed as an insurer by the State of North Carolina and will operate the Health Plan.
Carolina Complete Health will operate the Health Plan with the goals of maintaining profitability, offering competitive health insurance products and maximizing the use of value-driven systems of care. Value-driven systems of care are collaborative arrangements that integrate care coordination, access to data, evidence-based quality standards and payments systems to help achieve the goals enumerated below and, ultimately, provide high-quality, cost-effective care for patients. Value-driven systems of care simultaneously pursue three goals as defined and discussed by the Institute for Healthcare Improvement: controlling costs across a defined population, improving the health of the defined population and improving the experience of care. In North Carolina, there is a fourth goal of improving provider engagement and support, which focuses on collaboration within the medical community (including providers, beneficiaries and other stakeholders) in order to provide innovative solutions to improve care and patient outcomes in North Carolina.
CCHN has already commenced operations in order to support Carolina Complete Health’s submission of a bid to obtain a contract to provide managed care services for North Carolina’s Medicaid program, which follows the enactment of Medicaid reform legislation by the North Carolina General Assembly in 2015. This first round of contracting is expected to occur in 2018, with a “go live” date for the Health Plan in July 2019. See “Business.”
The Joint Venture
The NCMS, CCHN, Centene and Centene Sub are parties to an Amended and Restated Joint Venture Agreement dated August 25, 2017 (the “Joint Venture Agreement”) to facilitate the creation and successful operation of the Health Plan. The NCMS is a professional member organization and is seeking to promote access to quality health care for all citizens in North Carolina and championing initiatives that seek to improve quality of care and promote patient safety. Centene is a diversified, multi-national health care enterprise that provides a portfolio of services to government sponsored and commercial health care programs, focusing on under-insured and uninsured individuals. Centene’s common stock is listed on the New York Stock Exchange under the symbol “CNC.” The North Carolina Community Health Center Association (the “NCCHCA”), a private, non-profit membership association that represents federally-qualified health centers and aspiring health centers (“CHCs”) across North Carolina, will also participate in the activities of the Joint Venture.
The joint venture entity, Carolina Complete Health Holding Company Partnership (the “Joint Venture Company”), has been established as a Delaware general partnership authorized to issue 400 Class A Partnership Units (the “Class A Partnership Units”) and 3,600 Class B Partnership Units (the “Class B Partnership Units”). CCHN currently holds one Class A Partnership Unit, representing 20 percent of the partnership interests in the Joint Venture Company, and Centene Sub currently holds four Class B Partnership Units, representing 80 percent of the partnership interests in the Joint Venture Company. See “The Joint Venture.”
The Offering
CCHN is offering for sale one, but not more than one, share of its Class P Common Stock, at a per share subscription price of $750.00, to North Carolina health care providers who meet certain eligibility criteria. As described under “Investor Suitability Requirements,” an Eligible Investor is a physician, physician assistant or nurse practitioner who (1) if a physician or physician assistant, is licensed, and if a nurse practitioner, has approval to practice, pursuant to Article I, Chapter 90 of the North Carolina General Statutes, (2) is a resident of North Carolina, Georgia, South Carolina, Tennessee or Virginia and (3) has executed a participating provider agreement (a “Participating Provider Agreement”) with CCHN and Carolina Complete Health or is bound as a “Contracted Provider” (as defined therein) by an existing Participating Provider Agreement between CCHN, Carolina Complete Health and a “Provider” (as defined therein) by which he or she is employed or with which he or she has a contractual relationship. While ownership of our securities is not required to participate in the Provider Network, ideally each Eligible Investor would elect to purchase a Provider Share and become a stockholder of CCHN.
2
The total number of authorized shares of CCHN’s capital stock is 40,001 shares, of which one share is Class M Common Stock, $0.01 par value per share, and 40,000 shares are Class P Common Stock, $0.01 par value per share. As of April 26, 2018, the NCMS held the sole outstanding share of Class M Common Stock, and there were 1,505 outstanding shares of Class P Common Stock. The rights and privileges of holders of CCHN’s Class M Common Stock and Class P Common Stock are apportioned based upon the number of “Common Stock Equivalents” held as follows: each holder of Class P Common Stock shall hold a number of Common Stock Equivalents equal to the number of shares of Class P Common Stock then held by such holder, and each holder of Class M Common Stock shall hold a number of Common Stock Equivalents equal to the number of shares of Class M Stock held by such holder multiplied by a fraction (1) the numerator of which is the aggregate number of shares of Class P Common Stock then outstanding (less, solely for the purposes of calculating Common Stock Equivalents for purposes of voting rights, the number of shares of Class P Common Stock that are then suspended from voting pursuant to the stockholders’ agreement between CCHN and the holders of Class P Common Stock (the “Stockholders’ Agreement”)) and (2) the denominator of which is the aggregate number of shares of Class M Common Stock then outstanding. Accordingly, at all times, the holder or holders of Class M Common Stock will retain 50 percent of the aggregate voting power of CCHN’s common stock and will have an interest in CCHN equal to the aggregate of all holders of Class P Common Stock. See “Description of Capital Stock.”
On January 19, 2018, CCHN completed a private placement to certain CHCs in North Carolina and the NCCHCA of 1,505 shares of Class P Common Stock at a purchase price of $750.00 per share for aggregate proceeds of approximately $1.13 million (the “Private Placement”). The Provider Shares issued in this Offering represent a 46.5 percent equity interest in CCHN.
Currently, we do not intend to pay dividends on the Provider Shares for the foreseeable future. We intend to invest our future earnings, if any, to repay our indebtedness and fund our growth.
Principal Terms of the Offering
The following table highlights the principal terms of the Offering and the Provider Shares. Before deciding to invest, please carefully review the other disclosures in this Offering Circular, including “Description of Capital Stock” and the forms of Participating Provider Agreement, Subscription Agreement (the “Subscription Agreement”) and Stockholders’ Agreement to be executed by each Eligible Investor who subscribes to purchase a Provider Share in this Offering. See “Investment Documents.”
| Issuer: | Carolina Complete Health Network, Inc.
|
| Class of Stock: | Class P Common Stock, $0.01 par value per share
|
| Size of Offering: | Up to 20,000 Provider Shares for up to $15,000,000 |
| Eligible Investors: | Any physician, physician assistant or nurse practitioner, in each case who: |
| ● | if a physician or physician assistant, is licensed, and if a nurse practitioner, has approval to practice, pursuant to Article I, Chapter 90 of the North Carolina General Statutes; | |
| ● | is a resident of North Carolina, Georgia, South Carolina, Tennessee or Virginia; and | |
| ● | has executed a Participating Provider Agreement with CCHN and Carolina Complete Health or is bound as a “Contracted Provider” (as defined therein) by an existing Participating Provider Agreement between CCHN, Carolina Complete Health and a “Provider” (as defined therein) by which he or she is employed or with which he or she has a contractual relationship. |
| See “Investor Suitability Requirements.” |
3
| Price Per Share: | $750.00 (the “Class P Original Purchase Price”) |
| Investment Limitation: | One Provider Share per Eligible Investor |
| Dividends: | No dividends shall be paid on CCHN’s Class M Common Stock (which is held by the NCMS) unless dividends are concurrently declared and paid on the Class P Common Stock (including the Provider Shares) on an equal basis according to the number of Common Stock Equivalents deemed to be held; all dividends will be as and if declared by CCHN’s Board of Directors (the “CCHN Board”). |
| Redemption: | Provider Shares will be subject to redemption by CCHN in the event that the holder no longer qualifies as an Eligible Investor or in the event of the holder’s death, in each case for an amount equal to the fair market value of a share of Class P Common Stock based on the most recent valuation of CCHN, which valuations are to occur at least annually, as determined by the CCHN Board. Provider Shares will be redeemed in the event that CCHN becomes obligated to sell all of its partnership units in the Joint Venture Company for an amount equal to the drag-along premium CCHN receives pursuant to the terms of the Amended and Restated Partnership Agreement of the Joint Venture Company divided by the number of shares of Class P Common Stock then outstanding. See also “—Termination of the Joint Venture” below. |
| Transfer Restrictions: | Provider Shares (or any interest therein) may not be transferred, assigned, pledged or otherwise disposed of or encumbered. |
| Liquidation Preference: | Holders of Class P Common Stock (including Provider Shares) will be entitled to share ratably in CCHN’s assets in proportion to the number of Common Stock Equivalents deemed to be held by them that are remaining after payment or provision for payment of all of CCHN’s debts and obligations. |
| Voting Rights: | Holders of Class P Common Stock (including Provider Shares) will have one vote per share. While each holder of a Provider Share will be entitled to only one vote, CHCs and the NCCHCA were permitted to purchase more than one share in the Private Placement, which means that each of them will have the number of votes equal to the number of shares of Class P Common Stock that they hold. On all matters submitted to CCHN’s stockholders, except with respect to certain amendments to CCHN’s Amended and Restated Certificate of Incorporation that relate solely to the terms of Class M Common Stock or as otherwise required by applicable law, holders of Class P Common Stock, subject to their continued status as Eligible Investors and provided that their license or approval to practice is not suspended by the North Carolina Medical Board, will vote together as one class with the holder or holders of Class M Common Stock. See “Description of Capital Stock.” |
Special Governance Rights:
| Holders of Provider Shares who are physicians licensed under Article I, Chapter 90 of the North Carolina General Statutes will be eligible to be nominated (1) by the CCHN Board to serve on the CCHN Board and (2) by the Nominating Committee of the Joint Venture Company to serve as a director of Carolina Complete Health. See “Governance.” |
4
| Use of Proceeds: | Pursuant to the Joint Venture Agreement, CCHN is permitted to retain 55 percent of the Net Offering Proceeds from the Offering and the Private Placement (collectively, the “Net Offering Proceeds”) and is obligated to use 45 percent of the Net Offering Proceeds to help fund CCHN’s portion of the initial capitalization of the Joint Venture Company upon the closing of the Joint Venture transactions. We intend to use the retained portion of Net Offering Proceeds for general working capital purposes, but we may also use such proceeds for certain other limited purposes. See “Use of Proceeds” for further explanation of how we use the defined term “Net Offering Proceeds” in this Offering Circular and our intended use of such Net Offering Proceeds. |
| Risk Factors: | You should carefully read and consider the information set forth under the heading “Risk Factors” and all other information set forth in this Offering Circular before deciding to invest in a Provider Share. |
Benefits of Investing in the Offering
Given that CCHN does not intend to pay dividends in the foreseeable future and that Eligible Investors are limited to purchasing one and not more than one Provider Share for an investment of $750.00, it is unlikely that an investment in the Offering will produce meaningful economic benefits, even if the value of Provider Shares appreciates over time. As such, Eligible Investors should consider the following non-economic benefits as the primary benefits of an investment in the Offering.
Eligible Investors who purchase Provider Shares in the Offering will gain the opportunity to contribute to the direction and guidance of the operations of the Provider Network and the Health Plan and be involved in decisions that impact the care provided to patients. Holders of Provider Shares who are licensed physicians under North Carolina law will be eligible to be nominated to serve on the CCHN Board, the Board of Directors of Carolina Complete Health (the “Carolina Complete Health Board”) and the Medical Affairs Committee of the Carolina Complete Health Board (the “Medical Affairs Committee”). One member of the Medical Affairs Committee of the Carolina Complete Health Board will also serve on the Financial Matters Committee of the Carolina Complete Health Board. In addition, all holders of Provider Shares, regardless of whether they are licensed physicians, will be eligible to serve on advisory subcommittees of the Medical Affairs Committee, the size, composition and existence of such subcommittees to be determined from time to time by the Medical Affairs Committee. The purpose of the advisory subcommittees is to analyze and provide advice and recommendations on issues related to medical policy development. See “Governance” for additional information about the governance structure of the Joint Venture and the involvement of the holders of Provider Shares therein.
The Joint Venture Parties have committed to ensure that each holder of Provider Shares has the opportunity to be engaged with respect to the operation and management of Carolina Complete Health, the Health Plan and the Provider Network by agreeing to invite all such holders to attend meetings, which will be held at least annually, at which such holders will receive information with respect to the performance and activities of CCHN, Carolina Complete Health, the Health Plan and the Provider Network. The Joint Venture Parties have also agreed to cooperate with each other on an ongoing basis to develop and implement programs aimed at incentivizing and benefiting holders of Provider Shares in connection with their participation in the Provider Network. We expect that incentives offered to such holders will include providing (1) access to the Medical Affairs Committee, (2) professional development training and resources and (3) other incentives and benefits that may encourage widespread participation in the Provider Network.
Termination of the Joint Venture
The consummation of the transactions contemplated by the Joint Venture Agreement (the “Joint Venture Closing”) is subject to a number of conditions, many of which are beyond our control. See “The Joint Venture—Conditions to Closing.” If the Joint Venture Closing does not occur, we are contractually required by the Stockholders’ Agreement to redeem all Provider Shares sold in this Offering for $750.00 per share, in which case Eligible Investors who purchase Provider Shares will not realize any financial benefit from their investment.
5
Investing in the Provider Shares involves a high degree of risk. In deciding whether to purchase a Provider Share, you should carefully consider the following risk factors. Any of the following risks could have a material adverse effect on the value of the Provider Share you purchase and could cause you to lose all or part of your investment.
Risks Related to Investing in the Provider Shares
Investors will not be able to transfer their respective Provider Shares.
Pursuant to the Stockholders’ Agreement, an investor will not be able to transfer, assign, pledge or otherwise dispose of or encumber his or her Provider Share. As a result, you should be prepared to hold the Provider Share that you purchase indefinitely, subject to your continued status as an Eligible Investor.
The Provider Shares will not be listed on any securities exchange, and no liquid market for the Provider Shares is expected to develop.
The Provider Shares will not be listed on any securities exchange or any other traditional trading platform. There is currently no trading market for the Provider Shares, and we do not expect a trading market will ever develop. We do not currently have plans to apply for or otherwise seek trading or quotation of the Provider Shares on an over-the-counter market, and we do not expect to seek a listing on any securities exchange. Any investment in the Provider Shares will be highly illiquid, and Eligible Investors who purchase Provider Shares may not be able to sell or otherwise dispose of their respective Provider Shares on a timely basis or at all. If you cease to qualify as an Eligible Investor or in the event of your death, your Provider Share will be subject to redemption by CCHN pursuant to the terms of the Stockholders’ Agreement. You should be prepared to hold the Provider Share that you purchase indefinitely, subject to your continued status as an Eligible Investor.
Currently, we do not intend to pay dividends on the Provider Shares for the foreseeable future, and you are limited to purchasing one Provider Share; consequently, your ability to achieve a financial return on your investment will depend solely on appreciation in the value of your Provider Share.
Currently, we do not intend to pay dividends on the Provider Shares for the foreseeable future. We intend to invest our future earnings, if any, to repay our indebtedness and fund our growth. Therefore, you are not likely to receive any dividends on your Provider Share for the foreseeable future, and the financial success of an investment in a Provider Share will depend solely upon any future appreciation in value. There is no guarantee that your Provider Share will appreciate in value or even maintain the price at which you purchase your Provider Share. Furthermore, each Eligible Investor may only purchase one Provider Share. For the foreseeable future, the financial return on your investment will be limited to the appreciation in value of your single Provider Share, if any. As a result of our intention to invest our future earnings rather than pay dividends on the Provider Shares, it is unlikely that an investment in the Offering will produce meaningful economic benefits, even if the value of Provider Shares appreciates over time.
If the Joint Venture Closing does not occur, CCHN will redeem your Provider Share, in which case you will not realize any financial benefit from the investment transaction.
The Offering is being made on a continuous basis, and Eligible Investors who purchase Provider Shares will receive such shares before the Joint Venture Closing. However, most of the benefits of holding a Provider Share, as further described in “Offering Circular Summary—The Offering,” will not accrue to holders of Provider Shares unless and until the Joint Venture Closing occurs and the Health Plan begins enrolling members. The Joint Venture Closing is subject to a number of conditions including, among other conditions, (1) Carolina Complete Health must have submitted a bid for, been awarded and accepted a capitated Medicaid contract with the State of North Carolina (an “N.C. Medicaid Contract”); (2) the number of Eligible Investors who purchase Provider Shares and the number of investors attributable to CHCs that subscribed in the Private Placement must be at least 10,000 in the aggregate prior to the earlier of (a) the date that is 10 business days prior to the deadline for submitting proposals for the contract with the State of North Carolina and (b) March 12, 2019, the date that is 12 months after the Offering Statement on Form 1-A, of which this Offering Circular is a part, was qualified by the Commission; and (3) on or prior to 10 business days before the deadline for submitting proposals for the contract with the State of North Carolina, the Provider Network must have satisfied the provider participation requirements established by the State of North Carolina with respect to network adequacy. If the Joint Venture Closing does not occur, we are contractually required by the Stockholders’ Agreement to redeem all Provider Shares sold in this Offering for $750.00 per share, in which case you will not realize any financial benefit from your investment.
6
You will experience dilution of your ownership interest if we issue additional shares of our capital stock in the future.
Each Eligible Investor may purchase only one Provider Share. Accordingly, if we issue any additional shares of our capital stock, no matter the series, you will experience dilution of your ownership interest. The CCHN Board may at any time authorize the issuance of additional common stock without common stockholder approval, subject only to the total number of authorized common shares set forth in our Amended and Restated Certificate of Incorporation. The terms of equity securities issued by us in future transactions may be more favorable to new investors, and may include dividend and/or liquidation preferences, superior voting rights and the issuance of warrants or other derivative securities, which may have a further dilutive effect. Furthermore, our Amended and Restated Certificate of Incorporation provides that each holder of Class M Common Stock will be deemed to hold a number of Common Stock Equivalents equal to the number of shares of Class M Common Stock held by such holder multiplied by a fraction (1) the numerator of which is the aggregate number of shares of Class P Common Stock then outstanding (less, solely for the purposes of calculating Common Stock Equivalents for purposes of voting rights, the number of shares of Class P Common Stock that are then suspended from voting pursuant to the Stockholders’ Agreement) and (2) the denominator of which is the aggregate number of shares of Class M Common Stock then outstanding. This provision ensures that the holder or holders of Class M Common Stock will retain 50 percent of the aggregate interest in CCHN, which will have a further dilutive effect on your ownership interest.
Risks Related to CCHN
We have a limited operating history in an evolving industry, which makes it difficult for you to evaluate our likely performance and this investment.
We were formed in May 2016 and have a limited operating history, which makes it difficult to accurately evaluate our capabilities and prospects. Our business is subject to the risks, expenses and difficulties frequently encountered by new ventures, including our reliance on other Joint Venture Parties, their key personnel and affiliates and outside consultants, among other factors. Our lack of history and the evolving nature of the market in which we operate make it likely that there are risks inherent in our business that are yet to be recognized by us or others, or not fully appreciated, and that could result in us earning less than we anticipate or even suffering further anticipated or unanticipated losses. Furthermore, our operations until the Joint Venture Closing will be primarily limited to recruiting and retaining providers to participate in the Provider Network. Since we will not gain significant experience or operating history until after the Joint Venture Closing occurs and the Health Plan begins enrolling members, the risks associated with our lack of experience and operations will not diminish until at least that time. It is possible that our inexperience will render us unable to efficiently and effectively perform services assigned to us pursuant to the Joint Venture Agreement. As a result of the foregoing, an investment in a Provider Share necessarily involves uncertainty about the stability of our earnings, cash flows and, ultimately, our ability to service and repay our debt and meet our other obligations.
We operate in an evolving industry that may not develop as expected. Assessing the future prospects of our business is challenging in light of both known and unknown risks and difficulties we may encounter. Growth prospects in our industry can be affected by a wide variety of factors, including, among others, competition from other companies, regulatory limitations on the services we can offer and the markets we can serve, changes in applicable laws and regulations and changes in underlying consumer behavior. We may not be able to successfully address these factors, which could negatively impact our growth and harm our business.
7
We have never generated revenue from operations, may never generate revenue from operations, are not currently profitable and may never become profitable.
We have incurred net losses since our formation. Although we are engaged in the Joint Venture, we operate and will continue to operate our own business, the results of which will not be controlled or guaranteed by any of the other participants in the Joint Venture. There are a number of events that must occur before we can generate revenue from operations, including the following: North Carolina’s application for Medicaid reform must receive federal approval; we must succeed in developing and maintaining the Provider Network; Carolina Complete Health must become licensed as an insurance company in North Carolina; and Carolina Complete Health must submit a bid for, be awarded and accept an N.C. Medicaid Contract. We cannot be certain that these events will occur, and even if they do, we may never generate revenue from operations that is significant enough to achieve profitability. We currently expect to begin generating revenue no earlier than mid-2019. Since we have no operating revenue, we expect to incur substantial losses and experience negative cash flow from operating activities until at least that time. In addition, there can be no assurance that we will be able to consummate our business strategy and plans or regarding whether financial, regulatory, market or other limitations may force us to modify, alter, significantly delay or significantly impede the implementation of such plans. Once we begin to generate revenue from operations, the payments we receive for our services to Carolina Complete Health will be the sole source of such revenue. If we cannot generate sufficient revenue based on our services to Carolina Complete Health, we may not achieve or maintain profitability. Furthermore, the amount of revenue that we generate from operations will directly correlate to the number of providers in the Provider Network and, as our service fees will be based on Carolina Complete Health’s revenues, will also depend on the number of members enrolled in the Health Plan and the per member per month fees set by the State of North Carolina. Accordingly, if we are unable to maintain a sufficiently sized Provider Network, or if there are a low number of members in the Health Plan or per member per month fees, it will negatively impact our revenue and may prevent us from having profitable operations. Our failure to achieve or maintain profitability would negatively impact the value of the Provider Shares and potentially require us to shut down our business, which would likely result in the loss of your investment.
We have substantial indebtedness and expect to incur additional substantial amounts of indebtedness in connection with the Joint Venture, which will affect our financial condition and may reduce the value of the Provider Shares.
Pursuant to the Second Amended and Restated Loan and Security Agreement dated August 25, 2017 between us and Centene (the “Centene Initial Loan Agreement”), Centene has funded our start-up costs with a multiple advance term loan in an amount up to $2.5 million, which amount may be increased in three increments of $500,000 up to an amount of $4.0 million upon the achievement of certain milestones related to this Offering (the “First Loan”). If Carolina Complete Health is awarded and accepts an N.C. Medicaid Contract, Centene has agreed to provide a secondary multiple advance term loan, which, based upon the amount of the Net Offering Proceeds, as well as our use of the Net Offering Proceeds, could provide us with up to an additional $3.0 million in funding, which amount may be increased up to $4.0 million if, in consultation with Centene and in Centene’s sole discretion, we have demonstrated good progress toward the establishment of the Provider Network (the “Second Loan” and, together with the First Loan, the “Initial Centene Loans”). We may use the Second Loan to fund our start-up costs, provided that the aggregate amount available under the Second Loan to fund our start-up costs will be reduced by an amount equal to 55 percent of the Net Offering Proceeds, less the amount of such proceeds applied by CCHN to capital calls for Carolina Complete Health or to repay principal borrowed from Centene under the Initial Centene Loans or the Loan and Security Agreement (as defined below). We may also use the Second Loan to repay amounts borrowed from Centene to fund a portion of our initial capital contribution to the Joint Venture Company at the Joint Venture Closing. Each of the First Loan and Second Loan bears interest at a rate of 6.75 percent and matures on the respective tenth anniversary of the first interest payment under such loan. All amounts drawn under the Initial Centene Loans are secured by all of our receivables from the CCHN Services Agreement and our partnership interest in the Joint Venture Company, and we are required under the Centene Initial Loan Agreement to remit 60 percent of our Excess Cash Flow (as defined in such agreement) to Centene in repayment of any amounts drawn.
8
Upon the Joint Venture Closing, we will enter into another Loan and Security Agreement with Centene (the “Loan and Security Agreement” and, together with the Centene Initial Loan Agreement, the “Loan Agreements”), pursuant to which Centene will provide us with multiple advance term loans in an aggregate amount of up to $40 million, $30 million of which will be incremental reserve funding that may be used by CCHN to (1) fund our portion of capital calls made for purposes of meeting Carolina Complete Health’s statutory reserve funding requirements, (2) fund a portion of our initial capital contribution to the Joint Venture Company at the Joint Venture Closing and (3) repay amounts borrowed from Centene to fund such portion of our initial capital contribution to the Joint Venture Company. The remaining $10 million will be a cushion loan in the event that we need assistance in funding our portion of capital calls made for purposes of (1) meeting Carolina Complete Health’s statutory reserve funding requirements; (2) satisfying operating losses incurred by Carolina Complete Health and/or (3) paying for any additional operating, capital or other expenses of Carolina Complete Health. Outstanding amounts under these facilities will bear interest at a rate of 5.00 percent over the three-month London Interbank Offered Rate and mature on the fifth anniversary of the date on which the initial term of the N.C. Medicaid Contract (excluding all renewals and extensions) expires or is terminated for any reason. We will not be permitted to use any borrowed funds to finance our own operations. The Loan and Security Agreement will contain an obligation to remit 60 percent of our Excess Cash Flows (as defined in such agreement) to Centene in repayment of any amounts drawn. Amounts drawn under the Loan and Security Agreement will be secured by all of our receivables from the CCHN Services Agreement and our partnership interest in the Joint Venture Company.
Our obligations under the Loan Agreements will reduce our available cash for re-investment, and therefore, may negatively impact our potential profitability until all drawn amounts are repaid. In addition, since the amounts drawn under the Loan Agreements are secured by our receivables from the CCHN Services Agreement and our partnership interest in the Joint Venture Company, if we default under either of them, you may lose the value of your investment. Our substantial indebtedness may also limit our ability to borrow additional funds or obtain additional financing in the future.
Upon the Joint Venture Closing, we will enter into an Amended and Restated Partnership Agreement with Centene Sub (the “Amended and Restated Partnership Agreement”), pursuant to which the parties have agreed that if the Joint Venture Company needs additional capital from CCHN in excess of the investment capital on-hand or available to CCHN, Centene will provide such additional capital that would otherwise be CCHN’s responsibility. If Centene were to provide such additional capital, it would dilute our partnership interest in the Joint Venture Company, and if necessary, Centene has the right to continue to provide such additional capital that can dilute our partnership interest in the Joint Venture Company from 20 percent down to a minimum partnership interest of 10 percent. Any dilution of our partnership interest in the Joint Venture Company may reduce the value of the Provider Shares. If we still require additional capital after our partnership interest in the Joint Venture Company has been reduced to 10 percent, any additional capital contribution from Centene may be reflected either as debt or preferred partnership units in the Joint Venture Company or Carolina Complete Health, which would further dilute our holdings and the value of the Provider Shares.
If we are required to raise capital through public or private financing or other arrangements, such financing may not be available on acceptable terms, or at all. Our failure to raise capital when needed could harm our business. If we raise additional funds through the issuance of equity or convertible debt securities, the percentage ownership of our stockholders could be significantly diluted, the newly-issued securities may have rights, preferences or privileges senior to those of existing stockholders and the value of the Provider Shares could be adversely affected. If we obtain additional debt financing, a substantial portion of our operating cash flow may be dedicated to the payment of principal and interest on such indebtedness, and the terms of the debt securities issued could impose significant restrictions on our operations.
9
Our ability to successfully build and operate the Provider Network and provide services to the Health Plan is substantially dependent upon our contractual arrangements with Centene, and any failure by Centene to perform its obligations under such contractual arrangements would have a material adverse effect on our business.
The success of our business is substantially dependent upon our contractual arrangements with Centene. In addition to providing us with necessary capital under the Loan Agreements, Centene has agreed to provide services necessary for operations in providing services to the Health Plan, including consulting services with respect to, among other things, the formation of our business and commencement of operations; recruitment and retention of health care providers to participate in the Provider Network; development of a business plan, financial plan and capitalization plan; and provision of access to data and analytics to facilitate implementation of value-based models of care on the broadest possible scale. Without the assistance to be provided by Centene, we would have to find a third party vendor to provide the necessary resources to build and operate the Provider Network effectively, which may or may not be available. Without such services, we would not be able to fulfill our obligations in the Joint Venture or continue our business. If Centene fails to perform its obligations under the contractual arrangements, we may have to incur substantial costs and expend additional resources to enforce such arrangements, and there can be no assurance that any such enforcement efforts would be effective.
We or Centene may also contract with various third parties to perform certain functions and services for us, including the provision of certain provider network services, information technology systems and other operational services and systems. Failure of any such third parties to perform their obligations could have a material adverse impact on our business.
Our success depends upon the participation in the Provider Network by health care providers serving North Carolina’s Medicaid beneficiaries.
We believe that the Health Plan will be one of the first physician-led Medicaid prepaid health plans (“PHPs”) offered in North Carolina. Our ability to build a sufficient Provider Network for the Health Plan and our ability to generate revenues will depend in part upon the willingness of North Carolina health care providers to participate in the Health Plan. Some physicians and other care providers have historically had negative opinions about managed care plans. We will need to undertake significant outreach and education efforts to sufficiently build the Provider Network. Even if North Carolina health care providers are willing to participate in a Medicaid health plan generally, there can be no assurance that they will view attributes of the Health Plan’s design favorably enough to join the Provider Network. Centene is not obligated to proceed with the Joint Venture and consummate the Joint Venture Closing if the Provider Network does not satisfy the applicable provider participation requirements established by the State of North Carolina with respect to network adequacy or if, by the applicable deadline, the number of Eligible Investors who purchase Provider Shares and the number of investors attributable to CHCs that subscribed in the Private Placement is not at least 10,000 in the aggregate. If the Joint Venture Closing does not occur, you will not realize any financial benefit from your investment. Furthermore, the revenues that we generate will depend in part upon the number of participating providers in the Provider Network; having fewer participating providers will decrease our revenues and negatively impact our financial condition.
There will be intense competition, both in the bid for an N.C. Medicaid Contract, without which the Joint Venture Closing will not occur, and also if Carolina Complete Health is awarded an N.C. Medicaid Contract, in the enrollment of members in the Health Plan.
In order to receive an N.C. Medicaid Contract, Carolina Complete Health must partake in a competitive bidding process. The State of North Carolina will offer three contracts for statewide PHPs, which may be awarded to either commercial plans or provider-led entities. Additionally, the State is authorized to award up to 12 regional PHP contracts, but only to provider-led entities. We anticipate that many companies will submit proposals in the bidding process for a statewide contract, one or more regional contracts, or both. If Carolina Complete Health is not awarded one of the available contracts, the Joint Venture Closing will not occur, and you will not realize any financial benefit from your investment.
If Carolina Complete Health is awarded an N.C. Medicaid Contract in the bidding process, there can be no guarantee that it will be one of the three statewide contracts. If Carolina Complete Health is awarded a regional N.C. Medicaid Contract, the scale of the Health Plan, and thus the scale of our operations, will be smaller, which may result in lower revenues and a longer timeframe until profitability. In addition, the Joint Venture Parties would face competition as they attempted to expand operations to serve other regions. Such competitive pressures in growing the scale of the Health Plan may impact our ability to successfully develop and operate the Provider Network. Regardless of which type of N.C. Medicaid Contract is awarded, if one is awarded, there will be competition for enrolling members in the Health Plan. Having too few members in the Health Plan would reduce Carolina Complete Health’s revenues, and in turn our revenues, perhaps below a profitable level.
10
Your ability to influence the outcome of matters submitted to our stockholders for a vote will be limited, and our influence over the actions of the Joint Venture Company will be limited.
Even though the CCHN Board ultimately will be composed of a majority of physicians, after the completion of the Offering, the NCMS will continue to hold 50 percent of the aggregate voting power of our securities. In addition, each Eligible Investor is limited to purchasing one Provider Share, whereas CHCs and the NCCHCA may have purchased more than one share of Class P Common Stock in the Private Placement. These circumstances will limit your ability to influence the outcome of matters submitted to our stockholders for a vote, including amendment of our Amended and Restated Certificate of Incorporation or our Amended and Restated Bylaws or the approval of any merger or other significant corporate transaction.
Additionally, the Offering will not impact the structure of the Joint Venture. CCHN and Centene Sub will own 20 percent and 80 percent of the partnership interests of the Joint Venture Company, respectively, which in turn, will continue to own 100 percent of Carolina Complete Health. In addition, although the Amended and Restated Partnership Agreement provides that only four of the 15 members of the Carolina Complete Health Board will be employees of Centene, eight of the 10 members of the management committee of the Joint Venture Company (the “Joint Venture Company Management Committee”) will be employees of Centene. Furthermore, under the Amended and Restated Partnership Agreement, our partnership units of the Joint Venture Company will be subject to certain “drag-along” rights in favor of Centene Sub. Accordingly, if Centene Sub elects to engage in a transaction with a third party purchaser that results in the sale of all of its partnership units of the Joint Venture Company or in the sale or other disposition of all or substantially all of the property and assets of the Joint Venture Company, Centene Sub may compel us to approve such transaction and, as applicable, sell our partnership units of the Joint Venture Company too. These governance and other provisions may restrict our ability to exert influence over and manage the business and operations of the Joint Venture Company.
We may pursue additional business opportunities that may not be successful.
Until such time as any and all amounts due and payable under any loan by Centene to CCHN, including the Initial Centene Loans, have been paid in full (the “Exclusivity Period”), CCHN is not permitted to provide network access and/or management services to any party other than Centene and Carolina Complete Health. Nonetheless, CCHN may explore and, prior to the expiration of the Exclusivity Period and with a waiver from Centene if needed, may enter into additional business opportunities with or without Centene and/or Carolina Complete Health, including, without limitation, providing services for the formation and operation of a health care plan or a network of health care providers, the provision of a Health Insurance Marketplace or Medicare Advantage product or other opportunities as they may arise.
Any opportunities that we may identify and pursue may involve risks, including the commitment of significant capital, the incurrence of additional indebtedness, the payment of advances, the acceleration of our proposed schedule of operations, the diversion of management’s attention and resources, litigation or other claims in connection with the endeavors, our lack of control over partnerships, joint ventures or other investment arrangements that facilitate the pursuit of those opportunities, the inability to successfully integrate any new businesses into our operations or even if successfully integrated, the risk of not achieving the intended results and the exposure to losses if the businesses are not successful. Additionally, pursuit of additional business opportunities may subject us to compliance with additional regulations depending on the nature of those businesses and our activities, which compliance may be burdensome and involve risks of liability and loss. If we do pursue new business opportunities, and those opportunities are not successful, we may not be able to offset their costs, which could have an adverse effect on our business, financial condition and operating results.
We may be unable to attract, retain or effectively manage the succession of key personnel.
We are highly dependent on our ability to attract and retain qualified personnel to operate our business. We currently have a very small management team, consisting of Jeffrey W. Runge, MD, an outside consultant serving as our President and Chief Executive Officer, Vincent T. Morgus, an employee of the NCMS serving as our Chief Operating Officer and Stephen W. Keene, an employee of the NCMS serving as our Secretary-Treasurer. We do not expect to hire employees until after the Joint Venture Closing. Until such time, we will rely exclusively on contracted assistance in connection with our preliminary activities related to building the Provider Network. If and when they are needed, our ability to find qualified individuals to serve as employees may be difficult and take an extended period of time because of the limited number of individuals in the managed care industry with the breadth of skills and experience required to operate and successfully expand a business such as ours. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these personnel. In addition, the unique nature of our capital and governance structure will preclude us from compensating personnel with equity securities, and it may be difficult for us to offer competitive levels of cash compensation. If we are unable to attract and retain and effectively manage the succession plans for key personnel, executives and senior management, our business and financial position, results of operations or cash flows could be harmed.
We may be subject to liability as a general partner of the Joint Venture Company.
CCHN is a general partner in the Joint Venture Company. As a general partner, we are potentially liable for all of the liabilities of the partnership, despite holding only a minority of the partnership interests in the Joint Venture Company. Therefore, our liability could far exceed the amount or value of investment we will have made in the partnership even though the Amended and Restated Partnership Agreement will contain indemnification and contribution provisions that require the general partners to bear their respective percentage interests of losses incurred by any partner with respect to partnership liabilities. If we incur liability in connection with our interest in the Joint Venture Company, our financial condition, results of operations and business prospects could suffer.
11
A failure in or breach of our operational or security systems or infrastructure, or those of third parties with which we do business, including as a result of cyber attacks, could have an adverse effect on our business.
Information security risks have significantly increased in recent years in part because of the proliferation of new technologies, the use of the internet and telecommunications technologies to conduct our operations, and the increased sophistication and activities of organized crime, hackers, terrorists and other external parties, including foreign state agents. Our operations rely on the secure processing, transmission and storage of confidential, proprietary and other information in our computer systems and networks.
Security breaches may arise from external or internal threats. External breaches include hacking personal information for financial gain, attempting to cause harm to our operations, or intending to obtain competitive information. We plan to maintain a rigorous system of preventive and detective controls through our security programs; however, our prevention and detection controls may not prevent or identify all such attacks. Internal breaches may result from inappropriate security access to confidential information by rogue future employees, consultants or third party service providers. Any security breach involving the misappropriation, loss or other unauthorized disclosure or use of confidential member information, provider information, financial data, competitively sensitive information or other proprietary data, whether by us or a third party, could have a material adverse effect on our business.
Recent U.S. tax legislation may adversely affect our financial condition, results of operations and cash flows.
Recently enacted U.S. tax legislation has significantly changed the U.S. federal income taxation of U.S. corporations, including by reducing the U.S. corporate income tax rate, limiting interest deductions, permitting immediate expensing of certain capital expenditures, and revising the rules governing net operating losses. Many of these changes are effective immediately, without any transition periods or grandfathering for existing transactions. The legislation is unclear in many respects and could be subject to potential amendments and technical corrections, as well as interpretations and implementation regulations by the U.S. Department of the Treasury and Internal Revenue Service, any of which could materially affect the impacts of the legislation. In addition, it is unclear how these U.S. federal income tax changes will affect state and local taxation, which often uses federal taxable income as a starting point for computing state and local tax liabilities.
While some of the changes made by the tax legislation may adversely affect us in one or more reporting periods and prospectively, other changes may be beneficial on a going forward basis. We continue to work with our tax advisors to determine the full impact of this legislation on us. See Note 6, “Income Taxes,” in the notes to our financial statements appearing elsewhere in this Offering Circular for additional information about our deferred tax assets and our provisional analysis of the income tax effects of this new legislation.
Risks Related to Compliance and Regulation
The activities undertaken in the performance of the Joint Venture will be highly regulated, and new laws or regulations or changes in existing laws or regulations or their enforcement or application could force us to change how we operate and could harm our business.
The business activities that will be undertaken in the course of the Joint Venture, particularly the activities of Carolina Complete Health, will be extensively regulated by the North Carolina and federal governments. In addition, the managed care industry has received negative publicity that has led to increased legislation, regulation, review of industry practices and private litigation. The operations of certain of the Joint Venture Parties will be regulated by the relevant insurance and health and human services departments charged with overseeing the activities of the PHPs selected to provide or arrange for services to Medicaid beneficiaries. For example, Carolina Complete Health will need to comply with minimum statutory capital and other financial solvency requirements, such as deposit and surplus requirements.
The frequent enactment of, changes to, or interpretations of laws and regulations could, among other things, force us to restructure our relationships with providers within the Provider Network; require us to implement additional or different programs and systems; restrict revenue and enrollment growth; increase Carolina Complete Health’s medical and administrative costs; impose additional capital and surplus requirements on Carolina Complete Health; and increase or change Carolina Complete Health’s liability to members in the event of malpractice by our contracted providers. In addition, changes in political party or administrations at the state or federal level may change the attitude towards health care programs.
Additionally, the taxes and fees paid to federal, state and local governments may increase due to several factors, including enactment of, changes to, or interpretations of tax laws and regulations, and audits by governmental authorities.
If awarded, Carolina Complete Health’s N.C. Medicaid Contract will include a minimum medical loss ratio (“MLR”), which will require Carolina Complete Health to expend a percentage of the premiums it receives from the State on health care services for beneficiaries. Failure to maintain the minimum MLR could result in the assessment of financial penalties or other sanctions against Carolina Complete Health. The N.C. Medicaid Contract may also require Carolina Complete Health to return premium to the State if the Health Plan generates profits that exceed established levels. The N.C. Medicaid Contract may also require Carolina Complete Health to meet certain performance and quality metrics in order to maintain its contract or receive additional or full contractual revenue. For Carolina Complete Health to meet or achieve these various requirements, CCHN may need to contribute additional capital to the Joint Venture Company, which could have a material adverse effect on our business and financial position.
12
Although we strive to comply with all existing regulations and to meet performance standards applicable to the Joint Venture’s business, failure to do so could result in financial penalties or other sanctions. In addition, if other Joint Venture Parties fail to comply with existing regulations and performance standards applicable to their respective operations, it would have a negative impact on the Joint Venture as a whole and could negatively impact our operations. Also, even if Carolina Complete Health is awarded an N.C. Medicaid Contract, North Carolina may not allow it to continue to participate in the Medicaid program, or it may fail to win future procurements to participate in such program, which may end our business.
If any of the applicable Joint Venture Parties or Carolina Complete Health fails to comply with applicable privacy, security and data laws, regulations and standards, including with respect to third-party service providers that utilize sensitive personal information on our behalf, our business, reputation, results of operations, financial position and cash flows could be materially and adversely affected.
As part of their normal operations, certain of the Joint Venture Parties and Carolina Complete Health will collect, process and retain confidential member information. They will be subject to various federal and state laws and rules regarding the use and disclosure of confidential member information, including the Health Insurance Portability and Accountability Act (“HIPAA”) and the Health Information Technology for Economic and Clinical Health Act (“HITECH”) and the Gramm-Leach-Bliley Act, which require the protection of the privacy of medical records and the safeguarding of personal health information that is maintained and used. Despite our best attempts to maintain adherence to information privacy and security best practices as well as compliance with applicable laws and rules, our facilities and systems, and those of our third party service providers, may be vulnerable to privacy or security breaches, acts of vandalism or theft, malware, misplaced or lost data including paper or electronic media, programming and/or human errors or other similar events. Data breaches could require us to expend significant resources to remediate any damage, interrupt our operations and damage our reputation, subject us to state or federal agency review and could also result in enforcement actions, material fines and penalties, litigation or other actions which could have a material adverse effect on our business. Similar occurrences that may be experienced by other Joint Venture Parties required to comply with HIPAA and HITECH or Carolina Complete Health could have a material adverse effect on the operations of the Joint Venture and thus on our business.
In addition, HIPAA broadened the scope of fraud and abuse laws applicable to health care companies. HIPAA created civil penalties for, among other things, billing for medically unnecessary goods or services. HIPAA established new enforcement mechanisms to combat fraud and abuse, including civil and, in some instances, criminal penalties for failure to comply with specific standards relating to the privacy, security and electronic transmission of protected health information. The HITECH Act expanded the scope of these provisions by mandating individual notification in instances of breaches of protected health information, providing enhanced penalties for HIPAA violations, and granting enforcement authority to states’ Attorneys General in addition to the HHS Office for Civil Rights. It is possible that Congress may enact additional legislation in the future to increase penalties and to create a private right of action under HIPAA, which could entitle patients to seek monetary damages for violations of the privacy rules. In addition, HHS has announced that it will continue its audit program to assess HIPAA compliance efforts by covered entities with a focus on security risk assessments. An audit resulting in findings or allegations of noncompliance could have a material adverse effect on our business.
If any of the applicable Joint Venture Parties or Carolina Complete Health fails to comply with the extensive federal and state fraud and abuse laws, our business could be materially and adversely affected.
Detection and prevention of fraud, waste and abuse in Medicaid has been a major focus of federal and state government in recent years. Recent federal regulations have strengthened program integrity requirements to state Medicaid agencies and Medicaid managed care organizations, and carry risk of sanctions for noncompliance. Areas of emphasis include provider screening and enrollment, claims processing, data collection and sound compliance programs designed to detect and prevent fraud. Another applicable law is the federal False Claims Act, which prohibits the known filing of a false claim or the known use of false statements to obtain payment from the federal government. Many states have false claim act statutes that closely resemble the federal False Claims Act. Federal and state governments have made investigating and prosecuting health care fraud and abuse a priority. In the event any of the applicable Joint Venture Parties or Carolina Complete Health fails to comply with the extensive federal and state fraud and abuse laws, our business could be materially and adversely affected.
The requirements of complying on an ongoing basis with Regulation A of the Securities Act of 1933, as amended (the “Securities Act”) may strain our resources and divert management’s attention.
Because we are conducting an offering pursuant to Regulation A of the Securities Act, we are subject to certain ongoing reporting requirements. Compliance with these rules and regulations will require legal and financial compliance costs, which may impose strain on our operating budget and divert management’s time and attention from operational activities. The requirements of Regulation A may also make it significantly more expensive for us to maintain director and officer liability insurance. These factors could also make it difficult for us to attract and retain qualified officers or members of the CCHN Board. Moreover, as a result of the disclosure of information in this Offering Circular and in other public filings we make, our business operations, operating results and financial condition have become and will continue to be more visible, including to competitors and other third parties.
13
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS
This Offering Circular contains forward-looking statements. In some cases, you can identify these statements by forward-looking words such as “believe,” “may,” “will,” “estimate,” “continue,” “anticipate,” “intend,” “could,” “would,” “project,” “plan,” “expect” or the negative or plural of these words or similar expressions. These forward-looking statements include, but are not limited to, statements concerning us, risk factors, plans and projections. You should not rely upon forward-looking statements as predictions of future events. These forward-looking statements are subject to a number of risks, uncertainties and assumptions, including those described in “Risk Factors.” In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed in this Offering Circular may not occur and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements.
Except as required by law, neither we nor any other person assumes responsibility for the accuracy and completeness of the forward-looking statements. We undertake no obligation to update publicly any forward-looking statements for any reason after the date of this Offering Circular to conform these statements to actual results or to changes in our expectations.
You should read this Offering Circular, and the documents that we reference in this Offering Circular and have filed with the Commission as exhibits to the Offering Statement on Form 1-A of which this Offering Circular is a part with the understanding that our actual future results, performance and events and circumstances may be materially different from what we expect.
INVESTOR SUITABILITY REQUIREMENTS
We are only offering the Provider Shares to Eligible Investors. To purchase a Provider Share in the Offering, you must be a physician, physician assistant or nurse practitioner who:
| ● | if a physician or physician assistant, is licensed, and if a nurse practitioner, has approval to practice, pursuant to Article I, Chapter 90 of the North Carolina General Statutes; |
| ● | resides in North Carolina, Georgia, South Carolina, Tennessee or Virginia; and |
| ● | has executed a Participating Provider Agreement with CCHN and Carolina Complete Health or is bound as a “Contracted Provider” (as defined therein) by an existing Participating Provider Agreement between CCHN, Carolina Complete Health and a “Provider” (as defined therein) by which he or she is employed or with which he or she has a contractual relationship. |
In addition, in order to invest, applicable securities laws require that either (1) you are an “accredited investor” as such term is defined in Rule 501 promulgated under the Securities Act (“Rule 501”) or (2) the purchase price that you pay for the Provider Share ($750.00) is no more than 10 percent of the greater of your annual income or net worth (as determined under Rule 501).
14
Executing a Participating Provider Agreement with CCHN and Carolina Complete Health or being bound as a “Contracted Provider” under a Participating Provider Agreement (as defined therein) is required to be an Eligible Investor. While ownership of our securities is not required to participate in the Provider Network, ideally each Eligible Investor would elect to purchase a Provider Share and become a stockholder of CCHN. In order to purchase a Provider Share, Eligible Investors must also execute a Subscription Agreement and the Stockholders’ Agreement. Forms of each of these documents are filed as exhibits to the Offering Statement on Form 1-A of which this Offering Circular is a part. You should read these forms in their entirety before deciding whether to invest in a Provider Share.
| ● | Participating Provider Agreement: In order to invest in a Provider Share, you must either execute a Participating Provider Agreement or be a Contracted Provider under a Participating Provider Agreement (as defined therein). The Participating Provider Agreement obligates you to, subject to the approval of Carolina Complete Health and/or its affiliates, participate as a health care provider for Carolina Complete Health under the Health Plan and such other programs or health benefit arrangements identified in such agreement. It also requires you to comply with the requirements, policies, programs and procedures of Carolina Complete Health (and/or its affiliates) and any payor entity, including, but not limited to, credentialing criteria and requirements; notification requirements; medical management programs; claims and billing, quality assessment and improvement, utilization review and management, disease management, case management, on-site reviews, referral and prior authorization, and grievance and appeal procedures; coordination of benefits and third party liability policies; carve-out and third party vendor programs; and data reporting requirements. The Participating Provider Agreement has a three-year initial term and automatically renews for successive annual terms subject to the termination provisions therein. |
| ● | Subscription Agreement: To purchase a Provider Share, you must execute a Subscription Agreement. In the Subscription Agreement, you will be required to make certain representations and warranties regarding your status as an Eligible Investor. You also acknowledge and agree that the Subscription Agreement will be signed by electronic signature and that all communications with respect to your investment in a Provider Share will be delivered electronically. |
| ● | Stockholders’ Agreement: In order to become a holder of a Provider Share, you must also execute the Stockholders’ Agreement, which governs certain rights and obligations in connection with holding Class P Common Stock of CCHN. The Stockholders’ Agreement describes the circumstances under which and procedures by which CCHN may redeem your Provider Share. See “Description of Capital Stock—Description of the Class P Common Stock.” The Stockholders’ Agreement also provides that you may not transfer your Provider Share and that you will be suspended from voting during any time that you no longer qualify as an Eligible Investor or following the date on which you have experienced an event that would trigger a redemption right for CCHN. |
In addition to executing the investment documents described above, you generally are required to have a brokerage account with Folio Investments, Inc. (“Folio”), as Provider Shares may only be purchased through Folio’s online investment platform. For more information about Folio and the procedures for subscribing for a Provider Share, see “Plan of Distribution.”
Pursuant to the Joint Venture Agreement, if the Joint Venture Closing occurs, we are permitted to retain 55 percent of the Net Offering Proceeds and are obligated to use 45 percent of the Net Offering Proceeds to help fund our portion of the initial capitalization to the Joint Venture Company at the Joint Venture Closing, which will be between 7.0 percent and 7.5 percent of the total initial cash capitalization of the Joint Venture Company. We expect to allocate the proceeds in this manner regardless of whether we sell all of the Provider Shares being offered in the Offering. We expect to use the retained Net Offering Proceeds for general working capital purposes, but we may also use such proceeds to fund capital calls for Carolina Complete Health or to repay principal owed by us to Centene under the Loan Agreements. The proceeds of the Offering will not be used to compensate or otherwise make payments to the officers or directors of CCHN or any of its subsidiaries prior to the Joint Venture Closing.
The Joint Venture Agreement generally defines Net Offering Proceeds to equal the sum of the aggregate gross proceeds from this Offering and the Private Placement, less expenses related to the Offering of up to $500,000. When we use the defined term “Net Offering Proceeds” in this Offering Circular in the context of our obligation to capitalize the Joint Venture Company, we have assumed that the expenses related to the Offering will not exceed $500,000. If expenses related to this Offering do exceed $500,000, the retained net proceeds used for working capital will decrease by the amount that the expenses increase.
We reserve the right to change the use of proceeds following the date of this Offering Circular; provided, however, that in any event, we are obligated to use 45 percent of the Net Offering Proceeds to make an initial capital contribution to the Joint Venture Company at the Joint Venture Closing. For a description of our obligation to capitalize the Joint Venture Company, including the amount of our capital contribution that will be financed through an advance under the Loan and Security Agreement, see “The Joint Venture—Capitalization of the Joint Venture Company.”
The Joint Venture Closing is subject to a number of conditions including, among other conditions, (1) Carolina Complete Health must have submitted a bid for, been awarded and accepted an N.C. Medicaid Contract; (2) the number of Eligible Investors who purchase Provider Shares and the number of investors attributable to CHCs that subscribed in the Private Placement must be at least 10,000 in the aggregate prior to the earlier of (a) the date that is 10 business days prior to the deadline for submitting proposals for the contract with the State of North Carolina or (b) March 12, 2019, the date that is 12 months after the Offering Statement on Form 1-A, of which this Offering Circular is a part, was qualified by the Commission; and (3) on or prior to 10 business days before the deadline for submitting proposals for the contract with the State of North Carolina, the Provider Network must have satisfied the provider participation requirements established by the State of North Carolina with respect to network adequacy. If the Joint Venture Closing does not occur, we are contractually required by the Stockholders’ Agreement to redeem all Provider Shares sold in this Offering for $750.00 per share.
15
The following table illustrates our estimated use of proceeds from this Offering as we currently expect to use them, assuming the sale of, respectively, 100 percent, 75 percent, 50 percent and 25 percent of the Provider Shares being offered:
| Assumed Percentage of Shares Sold | 100% | 75% | 50% | 25% (1) | ||||||||||||
| Shares sold | 20,000 | 15,000 | 10,000 | 5,000 | ||||||||||||
| Aggregate gross proceeds | $ | 15,000,000 | $ | 11,250,000 | $ | 7,500,000 | $ | 3,750,000 | ||||||||
| Assumed offering expenses (2) | $ | 500,000 | $ | 500,000 | $ | 500,000 | $ | 500,000 | ||||||||
| Net offering proceeds from this Offering (2) | 14,500,000 | 10,750,000 | 7,000,000 | 3,250,000 | ||||||||||||
| Amount used to capitalize the Joint Venture Company (3) | $ | 6,525,000 | $ | 4,837,500 | $ | 3,150,000 | $ | 1,462,500 | ||||||||
| Retained net proceeds (2) | 7,975,000 | 5,912,500 | 3,850,000 | 1,787,500 | ||||||||||||
| Proceeds used for working capital (2) | $ | 7,975,000 | $ | 5,912,500 | $ | 3,850,000 | $ | 1,787,500 | ||||||||
| (1) | As described in the preceding paragraph, if we only sell 25 percent of the Provider Shares being offered in this Offering, we will not meet the requisite threshold for subscribing Eligible Investors under the Joint Venture Agreement, and the Joint Venture Closing may not occur. If the Joint Venture Closing does not occur, we are contractually obligated to redeem all Provider Shares sold in this Offering for $750.00 per share and will have no retained net proceeds. |
| (2) | Our obligation to capitalize the Joint Venture Company depends upon our Net Offering Proceeds (generally defined in the Joint Venture Agreement as an amount equal to the sum of the aggregate gross proceeds from this Offering and the Private Placement, less expenses related to this Offering of up to $500,000). Throughout this Offering Circular, when we have used the defined term “Net Offering Proceeds” in the context of our ability to capitalize the Joint Venture Company, we have assumed that the expenses related to this Offering will not exceed $500,000. If expenses related to this Offering do exceed $500,000, the amount used to capitalize the Joint Venture Company will not change, but the retained net proceeds shown in this table (and therefore the proceeds used for working capital) will decrease by the amount that the expenses increase. We currently expect that offering expenses related to this Offering will be approximately $1,000,000. |
| (3) | Because we sold 1,505 shares of Class P Common Stock in the Private Placement for proceeds of $1,128,750, we are obligated to contribute to the capitalization of the Joint Venture Company an additional $507,938 in each of these scenarios. Further, our obligation to capitalize the Joint Venture Company includes, in addition to 45 percent of the Net Offering Proceeds, an amount drawn by us as an advance under the Loan and Security Agreement equal to 55 percent of the Net Offering Proceeds. The amount to be drawn in each scenario, taking into account the Private Placement proceeds of $1,128,750, is as follows: $8,595,813 in the event 100 percent of the shares are sold in this Offering; $6,533,313 in the event 75 percent of the shares are sold in this Offering; $4,470,813 in the event 50 percent of the shares are sold in this Offering; and $2,408,313 in the event 25 percent of the shares are sold in this Offering. |
Centene has funded the start-up costs of CCHN with the First Loan in an amount up to $2.5 million, which amount may be increased in three increments of $500,000 up to an amount of $4.0 million if certain milestones relating to the Offering are attained by CCHN. If Carolina Complete Health is awarded and accepts an N.C. Medicaid Contract, Centene has agreed to provide us with the Second Loan, which, based upon the amount of the Net Offering Proceeds, as well as our use of the Net Offering Proceeds, could provide us with up to an additional $3.0 million in funding, which amount may be increased up to $4.0 million if, in consultation with Centene and in Centene’s sole discretion, CCHN has demonstrated good progress toward the establishment of the Provider Network. We may use the Second Loan to fund our start-up costs, provided that the aggregate amount available under the Second Loan to fund our start-up costs will be reduced by an amount equal to 55 percent of the Net Offering Proceeds, less the amount of such proceeds applied by CCHN to capital calls for Carolina Complete Health or to repay principal borrowed from Centene under the Initial Centene Loans or the Loan and Security Agreement. We may also use the Second Loan to repay amounts borrowed from Centene to fund a portion of our initial capital contribution to the Joint Venture Company at the closing of the Joint Venture. See “The Joint Venture—Funding of CCHN.” On an ongoing basis, we expect that we will also use funds borrowed from Centene to satisfy our obligations to adequately capitalize the Joint Venture Company. See “The Joint Venture—Capitalization of the Joint Venture Company.”
Since CCHN’s inception on May 19, 2016, we have relied upon the sole stockholder of our Class M Common Stock, the NCMS, to provide us with both working capital and transaction-related cash advances, as needed, as well as the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct and perform CCHN’s activities. Working capital has been advanced by the NCMS to CCHN, which became due and payable as funds are borrowed under the First Loan. As funding is received under the First Loan, the outstanding working capital advance is settled.
As part of the Joint Venture discussions and transaction, CCHN incurred transaction-related outside advisor expenses that were ineligible for reimbursement under the First Loan. When certain of these expenses became due and payable to the outside advisors, the NCMS settled the transaction-related amounts due on behalf of CCHN. Also, since our inception, we have not had an employee. As such, CCHN has relied upon the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct and perform CCHN’s activities. The amount incurred for these expenses will be settled no earlier than the “go-live” date of the Health Plan, which is currently projected in July 2019.
Going forward, CCHN will continue to draw upon the NCMS professional and administrative staffs in the performance of CCHN’s activities, and as such, CCHN will incur additional costs associated with the staffs’ performance of these activities. These additional costs will be settled no earlier than the “go-live” date of the Health Plan, which is currently projected in July 2019.
16
The following table reflects our capitalization as of the most recent balance sheet date of December 31, 2017 (a) on an actual basis and (b) on an as-adjusted basis after giving effect to the Private Placement, in each case after deducting the estimated offering expenses payable by us. You should read this table together with “Management Discussion and Analysis” and our financial statements and the related notes appearing elsewhere in this Offering Circular.
| As of December 31, 2017 | ||||||||
| Actual | As-Adjusted | |||||||
| (audited) | (unaudited)(1) | |||||||
| Cash and Cash Equivalents(2) | $ | 1,009,613 | $ | 1,159,613 | ||||
| $ | 1,009,613 | $ | 1,159,613 | |||||
| Non-current Liabilities: | ||||||||
| Term Note(1a) | $ | 1,412,277 | $ | 1,469,277 | ||||
| Due to Stockholder | 906,822 | 906,822 | ||||||
| Accrued Interest | 39,068 | 39,068 | ||||||
| Total Non-Current Liabilities | $ | 2,358,167 | $ | 2,415,167 | ||||
| Common stock - Class M, $0.01 par value; 1 share authorized; 1 share issued and outstanding(3) | 1 | 1 | ||||||
| Common stock - Class P, $0.01 par value; 40,000 shares authorized; 1,505 shares issued and outstanding (3) | - | 15 | ||||||
| Additional Paid-in Capital | - | 1,128,735 | ||||||
| Stock Subscription Costs in Advance of Offering | (462,703 | ) | (462,703 | ) | ||||
| Accumulated Deficit | (2,120,592 | ) | (2,120,592 | ) | ||||
| Total Stockholder’s Deficit | $ | (2,583,294 | ) | $ | (1,454,544 | ) | ||
| Total Capitalization | $ | (225,127 | ) | $ | 960,623 | |||
| (1) | Reflects the Private Placement of 1,505 shares of Class P Common Stock to certain CHCs and the NCCHCA at a purchase price of $750.00 per share for an aggregate amount of approximately $1.13 million. The Private Placement closed on January 19, 2018. |
| (1a) | The $57,000 increase in the Term Note reflects the borrowing of funds in order to pay the Private Placement costs. |
| (2) | CCHN was holding $979,250 of funds received in advance from investors in the Private Placement of Class P Common Stock that closed on January 19, 2018, which advance is recorded in our audited financial statements as a current liability under “Advances from investors.” |
| (3) | On August 25, 2017, when CCHN had 100 shares of Class M Common Stock issued and outstanding, CCHN filed an Amended and Restated Certificate of Incorporation, in which the number of shares of all classes of stock that CCHN has the authority to issue is 40,001 shares, consisting of one share of Class M Common Stock, $0.01 par value per share, and 40,000 shares of Class P Common Stock, $0.01 par value per share, and which effected a 100-to-1 reverse stock split with respect to all outstanding shares of Class M Common Stock, resulting in one share of Class M Common Stock remaining issued and outstanding after the filing thereof. |
17
Overview
CCHN was formed as a wholly-owned subsidiary of the NCMS in Delaware on May 19, 2016. CCHN’s primary purpose is to build and operate a network of health care professionals who will provide medical services through the Health Plan, which we believe will be one of North Carolina’s first physician-led Medicaid PHPs. The NCMS, CCHN, Centene and Centene Sub will be engaged together in the Joint Venture to facilitate the creation and successful operation of the Health Plan in response to the pending implementation of Medicaid reform in North Carolina. See “—The Joint Venture” below. The relationship among the entities participating in the Joint Venture is illustrated in the following diagram (in which the darker shaded box identifies our company and the lighter shaded box identifies Eligible Investors who purchase a Provider Share in this Offering):
CCHN and the NCMS believe that partnering with a large insurance company to create a new health plan will enable the NCMS to help lead the Medicaid reform process in North Carolina and will provide physicians with an alternative to traditional managed care options that some providers have historically disfavored. The Joint Venture Parties have deliberately separated the Provider Network from Carolina Complete Health, seeking to design a structure that will offer an independent open channel for physicians to provide meaningful input in the design and implementation of the Health Plan. The aim is that such physician involvement will lead to greater provider satisfaction with managed care and participation in a groundbreaking managed care option that increases efficiency and creates better patient outcomes.
Medicaid Reform in North Carolina
Authorized by Title XIX of the Social Security Act of 1965 (the “Social Security Act”), Medicaid is an entitlement program providing medical coverage for low-income and disabled individuals, which is funded jointly by the federal and state governments and administered by the states. Each state establishes its own eligibility standards, benefit packages, payment rates and program administration within federal standards. Pursuant to the Social Security Act, the Secretary of Health and Human Services has the authority to approve experimental, pilot or demonstration projects that promote the objectives of the Medicaid program, thereby giving states additional flexibility to design Medicaid programs containing aspects that may differ from the federal standards in pursuit of improving care and patient outcomes, increasing efficiency and reducing costs.
18
In September 2015, the North Carolina legislature passed House Bill 372, S.L. 2015-245, a Medicaid reform bill with the stated purposes of ensuring (1) budget predictability through shared risk and accountability, (2) balanced quality, patient satisfaction and financial measures, (3) efficient and cost-effective administrative systems and structures and (4) a sustainable delivery system through the establishment of two types of PHPs: provider-led entities and commercial plans. To get the necessary federal approval of its proposed Medicaid reform plan, North Carolina submitted an application to the Centers for Medicare and Medicaid Services (“CMS”) requesting a waiver of certain portions of the Social Security Act under Section 1115 in June 2016 (as such application was amended on November 20, 2017 and as may be further amended, supplemented or replaced, the “Waiver Application”). In October 2016, the North Carolina legislature passed S.L. 2016-121 to address administrative and technical changes necessary to facilitate the ongoing implementation of the Medicaid reform project. The first formal discussion with the federal authority reviewing the Waiver Application occurred in October 2016. The review process was expected to take 12-18 months, with anticipated federal approval by April 2018.
If the federal government grants the request, North Carolina will move from its current traditional fee-for-service program to one of capitated contracts. Under capitated contracts, PHPs receive a fixed amount of money per member per unit of time, for which the plans generally finance all covered Medicaid services provided to members enrolled in those plans. The reformed system is designed to remove focus from individual services and instead incentivize improved patient outcomes, community health and cost containment. North Carolina’s proposed Medicaid program would allow eligible beneficiaries to choose from multiple PHPs, three of which will offer statewide coverage, and with the potential for one or two additional plans offering regional coverage in the beneficiary’s designated region of residence.
Medicaid reform in North Carolina would afford opportunities to offer new managed care solutions to providers and patients. Following federal approval of the Waiver Application, we expect the State of North Carolina to issue a request for proposal for new Medicaid PHPs – statewide and regional – in the Spring of 2018. Carolina Complete Health intends to submit a proposal for a new approach to managed care – a PHP led by physicians and community health centers – that gives providers more control over the plan and the care of the members enrolled in it.
The Health Plan
The Health Plan will be operated by Carolina Complete Health, a licensed insurance company in the State of North Carolina, with the goals of maintaining profitability, offering competitive health insurance products and maximizing the use of value-driven systems of care. Value-driven systems of care are collaborative arrangements that integrate care coordination, access to data, evidence-based quality standards and payments systems to help achieve the goals enumerated below and, ultimately, provide high-quality, cost-effective care for patients. Value-driven systems of care simultaneously pursue three goals as defined and discussed by the Institute for Healthcare Improvement: controlling costs across a defined population, improving the health of the defined population and improving the experience of care. In North Carolina, a fourth goal of improving provider engagement and support focuses on collaboration with the medical community, other providers, beneficiaries and other stakeholders to provide innovative solutions to improve care and patient outcomes.
We believe the Health Plan will have the following differentiating features that will improve care for North Carolina Medicaid beneficiaries:
| ● | Peer-selected physicians serving on board committees; |
| ● | Participating providers serving on advisory board subcommittees; |
| ● | Board committees that adopt peer-developed, evidence-based medical coverage and benefit policies; |
| ● | Relationships with North Carolina physicians, community health centers and other providers that value independent professional judgment and flexibility in care for their patients; |
| ● | Efforts to limit interference in the doctor-patient relationship; and |
| ● | Priorities of the reduction of paperwork and bureaucracy, as well as prompt and accurate payment of claims and processing of pre-approval and authorization requests. |
19
The Joint Venture
Together with the other Joint Venture Parties, we believe that the best health outcomes occur when there is appropriate clinical input into the medical policy and oversight of a health plan. The Joint Venture Parties also believe that Medicaid reform in North Carolina should incentivize physicians and other providers to consider the overall best approach to improving the health of the Medicaid population as a whole and of individual patients, emphasizing primary and preventative care and decreasing the burdens of coverage provided on a test and task basis. The goal of the Joint Venture Parties is to bring a health plan to North Carolina that provides physicians greater flexibility in caring for their patients and improves the effectiveness of the plan itself. The structure of the Joint Venture will result in physicians being able to actively participate in the Health Plan’s governance, which we believe will give them more control over the development and implementation of the Health Plan than more traditional plan structures.
We believe the strategy of the Joint Venture Parties will deliver on the objectives articulated by the State of North Carolina to ensure that costs are controlled across a defined population, the health of the defined population is improved and the experience of care is improved, making Carolina Complete Health more viable as a competitor for a PHP statewide contract. The Joint Venture unites the support of organizations respected in the North Carolina health care community with an organization that has significant financial resources and experience with establishing and maintaining Medicaid networks in other states. We believe that the Joint Venture Parties can create an innovative patient-focused Medicaid health plan that features a plan network that has its own management and governance, while also ensuring a role for health care providers in the plan’s governance.
The NCMS, which has been representing the interests of physicians and protecting the quality of patient care in North Carolina since 1849, has joined forces with Centene, with its financial resources and experience with regional and statewide Medicaid networks, to establish and serve the Health Plan. The NCMS is a professional member organization and is seeking to promote access to quality health care for all citizens in North Carolina and championing initiatives that seek to improve quality of care and promote patient safety. Centene is a diversified, multi-national health care enterprise that provides a portfolio of services to government sponsored and commercial health care programs focusing on under-insured and uninsured individuals. North Carolina’s CHCs, represented by the NCCHCA, will also play an important part in the Joint Venture as key providers of primary care services to Medicaid recipients in North Carolina. CHCs have a history of providing a broad spectrum of services to low-income and underserved populations, and we believe the Joint Venture will enable the CHCs to work more closely with physician specialists and health systems in their local communities to improve patient continuity of care, quality and cost.
The Joint Venture Parties have agreed to their respective operational roles and responsibilities with respect to the Health Plan in the Joint Venture Agreement. An affiliate of Centene Sub will manage the financial and daily operations of the Health Plan, while CCHN will provide services related to recruiting and retaining health care providers to participate in the Provider Network and oversight of programs and policies for such participating providers (see “—Business of CCHN” below). See “Joint Venture” and “Governance” for additional information about the structure, funding and management of the Joint Venture.
20
Anticipated Timeline to Launch
While the State of North Carolina’s process for Medicaid reform is underway, significant uncertainty remains about when many key events will occur, including approval of the Waiver Application, release of the request for proposal and the bidding process and the launch date for selected PHPs. Based upon the information available to and the current assumptions of the Joint Venture Parties, the following represents the anticipated time period until the launch of the Health Plan. However, many factors beyond the Joint Venture Parties’ collective control could cause the following timeline to vary. For example, if North Carolina’s Waiver Application is denied, it is unknown how the State would respond. If the State does not issue a request for proposal for PHPs to be offered, the Joint Venture Closing will not occur. Additionally, if Carolina Complete Health submits the proposal for the Health Plan and is not awarded an N.C. Medicaid Contract, the Joint Venture will not proceed, and in such case, we do not expect that any of the actions subsequent to the Joint Venture Closing will occur. If the Joint Venture Closing does not occur, we are contractually required by the Stockholders’ Agreement to redeem all Provider Shares sold in this Offering for $750.00 per share, in which case Eligible Investors who purchase Provider Shares will not realize any financial benefit from their investment. See “The Joint Venture—Conditions to Closing” and “The Joint Venture—Termination of the Joint Venture Agreement.”
| June 2016 | North Carolina submitted the Waiver Application to federal government |
| July 2017 | CCHN begins building the Provider Network |
| Spring 2018 | North Carolina receives approval of the Waiver Application |
| Spring-to-Summer 2018 | North Carolina issues a request for proposal for plans to be offered in the reformed Medicaid program |
| Summer-to-Fall 2018 | Carolina Complete Health submits the proposal for the Health Plan |
| Fall 2018 | North Carolina awards contracts to participate in the State’s Medicaid program; the Joint Venture Closing occurs |
| Fall-to-Winter 2018 | CCHN begins permanent employee hiring; North Carolina commences readiness review of the Health Plan |
| January-to-June 2019 | North Carolina concludes readiness review of the Health Plan; Medicaid beneficiaries enroll as members in Health Plan |
| July 2019 | Health Plan “goes live” |
Business of CCHN
Our Operations
The Joint Venture Parties have agreed to their roles and responsibilities with respect to the Health Plan in the Joint Venture Agreement. Our core responsibilities relate primarily to the Provider Network. During the interim period from the signing of the Joint Venture Agreement to the Joint Venture Closing, CCHN will conduct its activities by outsourcing its needed functions to NCMS professionals and staff, independent contractors, professional consultancy firms, third-party vendors or other such entities that can provide the capabilities required to recruit and retain providers to participate in the Provider Network.
After the Joint Venture Closing occurs and we retain individuals for a permanent CCHN workforce, our fundamental business will be recruiting, building, developing, managing, operating, educating and maintaining the Provider Network for the purposes of providing services to Carolina Complete Health and the members of the Health Plan. We will strive to build and enhance the Provider Network by, among other things, (1) continuing to recruit and retain providers to participate in the Provider Network, (2) maintaining and improving the Health Plan’s relationship with participating providers and provider employers, (3) facilitating the development, establishment and implementation of value-based models of care on the broadest possible scale, (4) providing ongoing education, enhancement and relations services to all participating providers and provider employers, and (5) developing, establishing and implementing incentive programs and benefit plans for holders of Provider Shares, other participating providers and provider employers.
We will also work to improve the efficiency and accuracy of case management and claims by, among other things, (1) using and providing qualified participating providers access to a platform for value-based arrangements to more effectively and efficiently coordinate case management services, (2) together with a management company affiliate of Centene, continually conduct educational and training programs to allow for accurate and efficient submission of claims, (3) assisting with updating participating provider files to facilitate eligibility verification and claims adjudication and the efficient and timely responses to inquiries from participating providers, and (4) together with a management company affiliate of Centene, providing and periodically updating materials for distribution to the participating providers with regard to billing procedures, payment for services, a schedule of covered plan benefits and applicable risk-sharing arrangements.
21
Pursuant to the terms of the CCHN Services Agreement, we will provide the above described services to Carolina Complete Health in exchange for a monthly fee equal to a predetermined percentage of the projected net revenues of the Health Plan during such month in connection with the plan’s operation. The revenue percentage in any given month will depend in part upon the number of individuals who are participating providers in the Provider Network. We will also be entitled to receive an annual performance-based award based upon our Provider Network’s ability to facilitate the Health Plan’s achievement of certain quality-of-care performance goals established by the Carolina Complete Health Board. These quality-of-care performance goals will be based on performance measures established by the State of North Carolina, the Healthcare Effectiveness Data and Information Set established by the National Committee for Quality Assurance on an annual basis and the recommendations of the Medical Affairs Committee. In addition, if the State of North Carolina makes a final determination that the Provider Network is adequate and has timely satisfied all applicable provider participation requirements and such other network adequacy standards and requirements as the State of North Carolina shall establish, we will also be entitled to receive a one-time performance-based award.
During the Exclusivity Period, CCHN is not permitted to provide network access and/or management services to any party other than Centene and Carolina Complete Health. Nonetheless, CCHN may explore and, prior to the expiration of the Exclusivity Period and with a waiver from Centene if needed, may enter into additional business opportunities, including, without limitation, providing services for the formation and operation of a health care plan or a network of health care providers, the provision of a Health Insurance Marketplace or Medicare Advantage product or other opportunities as they may arise. As CCHN’s first priority is building the Provider Network for the Health Plan, its primary consideration in pursuing any additional business opportunity will be the impact on the Provider Network and the Health Plan. While CCHN is open to exploring complementary businesses with or without Centene and/or Carolina Complete Health, it does not intend to pursue any opportunity that it believes will have a significant, long-term, adverse effect on its goal to build the Provider Network for one of the first physician-led Medicaid PHPs offered in North Carolina.
Involvement of Centene
Pursuant to the terms of a services agreement by and between Centene and CCHN, Centene has agreed to support our operations by, among other things, (1) consulting with us and our personnel in order to develop our business plan, financial plan and capitalization plan, (2) providing us with access to data and analytics to facilitate the implementation of value-based models of care on the broadest possible scale, and (3) marketing and advertising the Provider Network and the Health Plan. We have also entered into certain financial arrangements with Centene, as further described in “Joint Venture—Funding of CCHN.” We will continue to be a standalone business, and neither Centene nor any of its affiliates will control or act as a guarantor of our operations.
Following the Joint Venture Closing, Centene, like us, will also be providing services to the Health Plan, primarily focused on the day-to-day business operations of the Health Plan. A management company affiliate of Centene will provide management services to the Health Plan, including with respect to, among other things, (1) program planning and development, (2) management information systems, (3) financial systems and services, (4) claims administration, (5) enrollee services and records, (6) premium billing and collections, and, together with CCHN, (7) utilization review, (8) quality improvement and assurance and (9) provider services and records. In addition to this administrative support, initially, Centene will have primary responsibility for incorporating ancillary service providers into the Provider Network.
In connection with the creation, recruitment, building, development, management, operation, education and maintenance of the Provider Network, Centene has granted to CCHN a non-exclusive, nontransferable, revocable license within the State of North Carolina to all of Centene’s proprietary and/or confidential information, trade secrets (patentable or otherwise), materials, data, know-how, processes and expertise (1) related to the formation, development, operation and management of programs, services and health plans in connection with the provision of services to government-sponsored health care programs and (2) embodied in or otherwise made a part of the services being provided to CCHN under the services agreement by and between a management company affiliate of Centene and CCHN.
Competition
The State of North Carolina has authorized three statewide PHPs and up to 12 regional provider-led entities to offer care to Medicaid beneficiaries in North Carolina. Although we believe the Health Plan will be an innovative offering, Carolina Complete Health will face competition from several other companies that will be submitting proposals for plans to be offered, including Medicaid managed care organizations, national and regional commercial managed care organizations and other provider-led entities. In deciding whether to grant Carolina Complete Health the contract, the State of North Carolina will likely consider many factors, such as financial stability/solvency, ability to deliver services and establish adequate provider networks and infrastructure, commitment to value-based systems of care, ability to address social determinants of health and other factors identified in the request for proposal.
22
If Carolina Complete Health is awarded a regional N.C. Medicaid Contract rather than a statewide N.C. Medicaid Contract, the initial scale of the Health Plan, and thus the initial scale of our operations, will be smaller, but the Joint Venture Parties may work to expand the territories served. In competing for additional territories, there would likely be competition from other provider-led entities seeking entry or expansion into such regions, as well as competitors holding statewide contracts that wish to establish a presence in serving the populations we seek to reach.
There will also be competition to enroll new members to the Health Plan and to retain existing members. Beneficiaries wishing to enroll in a PHP or to change plans typically choose based on the quality of care and services offered, ease of access to services, whether a specific provider is part of the network and the availability of supplemental benefits. We and Carolina Complete Health will also compete with other PHPs to enter into contracts with physicians, physician groups and other providers, although such providers are not limited with respect to the number of contracts into which they may enter. We believe the factors that providers consider in deciding whether to contract with us include the opportunity to participate in this Offering, existing and potential member volume, reimbursement rates, medical management programs, speed of reimbursement and administrative service capabilities.
Regulation
The business activities of certain of the Joint Venture Parties, particularly the activities of Carolina Complete Health, will be regulated at both the state and federal level. Government regulation of the provision of health care products and services is a changing area of law, and regulatory agencies generally have discretion to issue regulations and interpret and enforce laws and rules.
Carolina Complete Health will be licensed to operate as an insurance company in the State of North Carolina and, together with CCHN, seeks to provide services as a PHP within the N.C. Medicaid program. The N.C. Department of Insurance (“NCDOI”) and the N.C. Department of Health and Human Services (“NCDHHS”) will share primary regulatory responsibility at the state level for the activities of PHPs providing or arranging to provide services to Medicaid enrollees. At the federal level, CMS will also exercise a significant ongoing oversight role in PHP performance and the N.C. Medicaid program generally. The Health Plan will also have continuing obligations under various other federal laws, including those relating to health information, which are discussed below.
NCDOI Regulations and Oversight
The process for obtaining licensure from NCDOI to operate as a health insurer is complex and will require Carolina Complete Health to satisfy the agency’s requirements for, among other things, organizational structure, financial resources and compliance procedures. Carolina Complete Health must comply with minimum statutory capital and other financial solvency requirements, such as minimum deposit and surplus levels. In addition, Carolina Complete Health will be required by NCDOI to file reports describing its capital structure, ownership, financial condition, intercompany transactions and general business operations. Carolina Complete Health will also need to meet certain criteria to secure NCDOI approval before implementing certain operational changes, including without limitation, changes to existing product offerings, the development of new product offerings, certain organizational restructurings or the expansion of geographical service areas.
CCHN may also be considered an insurance holding company under applicable North Carolina law and may be subject to certain regulatory provisions as a controlling person of an insurance company. Since the operational activities of CCHN will focus on building and maintaining the Provider Network, CCHN may also be required to comply with applicable operational regulations, including complying with utilization review requirements. In addition, depending on the size and nature of the transaction, there are various notice and reporting requirements that generally apply to transactions between insurance companies and their affiliates within an insurance holding company structure. Some insurance holding company laws and regulations require prior regulatory approval or, in certain circumstances, prior notice of certain material intercompany transfers of assets as well as certain transactions between insurance companies, their parent holding companies and affiliates.
Additionally, the holding company acts of North Carolina restrict the ability of any person to obtain control of an insurance company without prior regulatory approval. Under those statutes, without such approval or an exemption, no person may acquire any voting security of an insurance holding company, which controls an insurance company, or merge with such a holding company, if as a result of such transaction such person would “control” the insurance holding company. “Control” is generally defined as the direct or indirect power to direct or cause the direction of the management and policies of a company and is presumed to exist if a person directly or indirectly owns or controls 10 percent or more of the voting securities of a company.
NCDHHS Contract
In addition to insurance company licensure and oversight by NCDOI, Carolina Complete Health generally must bid for and be selected to receive a PHP contract with NCDHHS before the Health Plan may participate in the N.C. Medicaid program. The State will use a competitive, formal proposal process to evaluate applicants seeking to participate in the reformed Medicaid program. If awarded an N.C. Medicaid Contract, we expect Carolina Complete Health would receive monthly payments based on specified capitation rates determined on an actuarial basis. These rates are expected to differ by membership category, and will depend on state appropriations, as well as the specific benefits and policies that the State chooses to include in the PHP contract.
Throughout the contract term, NCDHHS will be responsible for administering the PHP contract and ensuring compliance with its provisions. In addition, the contract will be subject to regulation and oversight by CMS. For example, CMS has the right to audit Medicaid managed care organizations and their contracting health care providers and other vendors for the quality of care being rendered and the degree of compliance with CMS contracts and regulations.
23
Federal Medicaid Requirements
Title XIX of the Social Security Act of 1935, as amended, directs CMS to administer the Medicaid program in partnership with the states. Generally, CMS takes the lead role in providing funding, enacting regulations, and overseeing states that have been approved to implement Medicaid managed care programs.
In April 2016, CMS significantly revised its regulations relating to managed care programs under Title XIX with the “Medicaid and CHIP Managed Care Final Rule.” These regulations place extensive requirements on states and contracting Medicaid managed care organizations. Carolina Complete Health is expected to be subject to these regulatory provisions, which generally set forth the requirements for member eligibility; member enrollment and dis-enrollment processes; covered services; eligible providers; subcontractors; record-keeping and record retention; periodic financial and informational reporting; quality assurance; health education, wellness and prevention programs; timeliness of claims payments; financial standards; safeguarding of member information; fraud, waste and abuse detection and reporting; and appeals and grievances. Carolina Complete Health’s compliance with these requirements is expected to be subject to monitoring by state regulators and by CMS. Carolina Complete Health is also expected to be subject to periodic comprehensive quality assurance evaluations by a third-party reviewing organization, and potentially by NCDOI representatives as well.
Federal Requirements for Health Information
As part of their normal operations, certain of the Joint Venture Parties and Carolina Complete Health will collect, process and retain confidential member information. They will be subject to various federal and state laws and rules regarding the use and disclosure of confidential member information, including HIPAA, HITECH and the Gramm-Leach-Bliley Act, which require the protection of the privacy of medical records and the safeguarding of personal health information that is maintained and used. Privacy and security laws and regulations often change due to new or amended legislation, regulations or administrative interpretation. A variety of regulators enforce these laws, including but not limited to the U.S. Department of Health and Human Services (“HHS”), the Federal Trade Commission, the N.C. Attorney General and other state regulators.
HIPAA is designed to improve the portability and continuity of health insurance coverage, simplify the administration of health insurance through standard transactions and ensure the privacy and security of individual health information. Among the requirements of HIPAA are the Administrative Simplification provisions which include standards for processing health insurance claims and related transactions (“Transactions Standards”); requirements for protecting the privacy and limiting the use and disclosure of medical records and other personal health information (“Privacy Rule”); and standards and specifications for safeguarding personal health information which is maintained, stored or transmitted in electronic format (“Security Rule”).
HITECH amended certain provisions of HIPAA and enhanced data security obligations for covered entities and their business associates. HITECH also mandated individual notifications in instances of a data breach, provided enhanced penalties for HIPAA violations, and granted enforcement authority to states’ Attorneys General in addition to the HHS Office for Civil Rights. The HIPAA Omnibus Rule further enhanced the changes under the HITECH Act and the Genetic Information Nondiscrimination Act of 2008, which clarified that genetic information is protected under HIPAA and prohibited most health plans from using or disclosing genetic information for underwriting purposes. The Omnibus Rule enhances the privacy protections and strengthens the government’s ability to enforce the law. These regulations also establish significant criminal penalties and civil sanctions for non-compliance. The preemption provisions of HIPAA provide that the federal standards will not preempt state laws that are more stringent than the related federal requirements.
The Privacy and Security Rules and HITECH/Omnibus enhancements established requirements to protect the privacy of medical records and safeguard personal health information maintained and used by healthcare providers, health plans, healthcare clearinghouses and their business associates.
The Security Rule requires healthcare providers, health plans, healthcare clearinghouses and their business associates to implement administrative, physical and technical safeguards to ensure the privacy and confidentiality of health information electronically stored, maintained or transmitted. The HITECH Act and Omnibus Rule enhanced a federal requirement for notification when the security of protected health information is breached.
The requirements of the Transactions Standards apply to certain healthcare related transactions conducted using “electronic media.” Since “electronic media” is defined broadly to include “transmissions that are physically moved from one location to another using portable data, magnetic tape, disk or compact disk media,” many communications are considered to be electronically transmitted. Under HIPAA, health plans and providers are required to have the capacity to accept and send all covered transactions in a standardized electronic format. Penalties can be imposed for failure to comply with these requirements.
Employees
We do not currently have any part-time or full-time employees. Our executive officers are either NCMS employees or contracted consultants, and we do not intend to hire any employees until after the Joint Venture Closing.
Properties
Currently, we do not own any property. Our headquarters are located at 222 N. Person Street, Suite 010, Raleigh, NC 27601, within the NCMS building, in which we have been allocated specific office space to conduct our activities through the Joint Venture Closing. As described in “—Business of CCHN,” we do not anticipate conducting significant operations until the Joint Venture Closing.
24
THE JOINT VENTURE
We are only offering shares of Class P Common Stock in CCHN pursuant to this Offering Circular. The following disclosure describes arrangements between CCHN and the other Joint Venture Parties that you should consider in deciding whether to purchase a Provider Share. You will have limited, and in some cases no, control over the actions of the Joint Venture Parties. In addition to this section, you should carefully review the sections entitled “Risk Factors” and “Offering Circular Summary—The Offering” before deciding to purchase a Provider Share.
Overview
The NCMS, CCHN, Centene and Centene Sub entered into the Joint Venture Agreement to facilitate the creation and successful operation of a North Carolina licensed insurance company that is designed to offer a patient-focused Medicaid health plan in North Carolina in response to the pending implementation of Medicaid reform in that state. In addition to the Joint Venture Parties, the NCCHCA will participate in the activities of the Joint Venture. All of the equity securities of Carolina Complete Health are held by the Joint Venture Company, a general partnership held 20 percent by CCHN, which is a subsidiary of the NCMS, and 80 percent by Centene Sub, which is a subsidiary of Centene. See “Business—Overview” for a graphical depiction of the Joint Venture’s structure.
The Joint Venture Participants
The NCMS is the oldest professional member organization in North Carolina, representing physicians and physician assistants who practice in the state. Founded in 1849, the NCMS seeks to promote access to quality health care for all citizens in North Carolina and champions initiatives that seek to improve quality of care and promote patient safety. The NCMS strives to protect the importance of the patient-physician relationship, promote safe, cost-effective, patient-centered care, promote physician leadership at all levels of the health care delivery system, improve the health of North Carolina’s population, enhance patients’ and caregivers’ experience of care, promote physician wellness and minimize administrative burdens of the delivery of health care in order to achieve its goals.
Centene Corporation, a Fortune 100 company, is a diversified, multi-national healthcare enterprise that provides a portfolio of services to government sponsored and commercial healthcare programs, focusing on under-insured and uninsured individuals. Many receive benefits provided under Medicaid, including the State Children’s Health Insurance Program, as well as Aged, Blind or Disabled, Foster Care and Long-Term Services and Supports, in addition to other state-sponsored programs, Medicare (including the Medicare prescription drug benefit commonly known as “Part D”), dual eligible programs and programs with the U.S. Department of Defense and U.S. Department of Veterans Affairs. Centene also provides healthcare services to groups and individuals delivered through commercial health plans. Centene operates local health plans and offers a range of health insurance solutions. It also contracts with other healthcare and commercial organizations to provide specialty services including behavioral health management, care management software, correctional healthcare services, dental benefits management, in-home health services, life and health management, managed vision, pharmacy benefits management, specialty pharmacy and telehealth services. Centene’s common stock is listed on the New York Stock Exchange under the symbol “CNC.”
The NCCHCA is a private, non-profit membership association that represents CHCs across North Carolina, working to promote and support patient-governed community health care organizations and the populations they serve.
As noted above, the partnership interests of the Joint Venture Company are held by CCHN and Centene Sub. The Joint Venture Company does not and will not have operations and will solely serve as a holding company of Carolina Complete Health. Carolina Complete Health is a wholly-owned subsidiary of the Joint Venture Company. Carolina Complete Health is a North Carolina corporation and will be licensed as an insurer by the State of North Carolina.
25
Capitalization of the Joint Venture Company
The Joint Venture Company is authorized to issue 400 Class A Partnership Units and 3,600 Class B Partnership Units. We currently hold one Class A Partnership Unit, representing 20 percent of the partnership interests in the Joint Venture Company, and Centene Sub currently holds four Class B Partnership Units, representing 80 percent of the partnership interests in the Joint Venture Company. The issuance of additional partnership units in the Joint Venture Company is contingent upon the Joint Venture Closing, which will only occur if, among other things, Carolina Complete Health has been awarded and accepted an N.C. Medicaid Contract, the Provider Network satisfies the requirements established by the State of North Carolina with respect to network adequacy, and the number of Eligible Investors who purchase Provider Shares and the number of investors attributable to CHCs that subscribed in the Private Placement is at least 10,000 in the aggregate. Concurrently with the Joint Venture Closing, the Joint Venture Company will amend its Partnership Agreement to, among other things, authorize 2,000 undesignated preferred partnership units. If the Joint Venture Closing occurs, then at the Joint Venture Closing, CCHN and Centene Sub will capitalize the Joint Venture Company as follows:
| ● | As consideration for 199 Class A Partnership Units, CCHN (1) will contribute an amount equal to (a) 45 percent of the Net Offering Proceeds plus (b) an amount drawn by CCHN as an advance under the Loan and Security Agreement equal to 55 percent of the Net Offering Proceeds (collectively, the “CCHN Cash Contribution”) and (2) agree to provide certain services to Carolina Complete Health pursuant to the CCHN Services Agreement. |
| ● | As consideration for 796 Class B Partnership Units, Centene Sub will make a contribution of capital of an amount equal to the product of four multiplied by the sum of (1) the CCHN Cash Contribution plus (2) an agreed upon amount for each Eligible Investor who has purchased a Provider Share in this Offering existing as of the date of the Joint Venture Closing and for each investor attributable to CHCs subscribing in the Private Placement. The amount payable by Centene Sub in excess of the amount of the CCHN Cash Contribution would be funded when needed over the first 15 months of operations of the Health Plan, as requested by the Joint Venture Company Management Committee upon the determination of the Financial Matters Committee. |
| ● | In the event that it is determined that Carolina Complete Health is in need of additional funds (in excess of the initial funding provided by CCHN and Centene Sub) in order to meet and maintain statutory reserves at the 300 percent risk based capital ratio level, Centene will provide such incremental funding of reserves (the “Incremental Reserve Funding”) by (1) directly contributing 80 percent of such Incremental Reserve Funding to the Joint Venture Company and (2) pursuant to the terms of the Loan and Security Agreement, making a loan to CCHN, as necessary, in an amount not to exceed $30 million in the aggregate over the life of the loan to fund all or most of CCHN’s 20 percent share (the “Incremental Reserve Funding Loan”). The Incremental Reserve Funding Loan can only be used by CCHN to (i) fund its portion of capital calls made for purposes of meeting Carolina Complete Health’s statutory reserve funding requirements, (ii) fund a portion of its initial capital contribution to the Joint Venture Company at the Joint Venture Closing and (iii) repay amounts borrowed from Centene to fund such portion of its initial capital contribution to the Joint Venture Company. The Incremental Reserve Funding Loan would bear interest at a rate of 5.00 percent over the three-month London Interbank Offered Rate and mature on the fifth anniversary of the date on which the initial term of the N.C. Medicaid Contract (excluding all renewals and extensions) expires or is terminated for any reason. The Incremental Reserve Funding Loan would be secured by CCHN’s partnership interest in the Joint Venture Company and its receivables from the CCHN Services Agreement. During the time that any of CCHN’s obligations under the Loan and Security Agreement remain outstanding, CCHN will be required to remit 60 percent of its Excess Cash Flows (as defined in the Loan and Security Agreement) to repay the Incremental Reserve Funding Loan. |
| ● | Should Carolina Complete Health require additional capital to either maintain its reserves, fund its operating losses or pay for any additional operating, capital or other expenses, and if CCHN’s cash reserves and the remaining amount available under the Incremental Reserve Funding Loan to fund additional reserve requirements are collectively insufficient for CCHN to make its capital contribution to the Joint Venture Company, Centene will, pursuant to the terms of the Loan and Security Agreement, make an additional amount, not to exceed $10 million, available to CCHN through a loan by Centene to CCHN secured by the partnership interest held by CCHN in the Joint Venture Company and its receivables from the CCHN Services Agreement (the “Cushion Loan”). The Cushion Loan can be used by CCHN to fund its portion of capital calls made for purposes of (i) meeting Carolina Complete Health’s statutory reserve funding requirements, (ii) satisfying operating losses incurred by Carolina Complete Health and/or (iii) paying for any additional operating, capital or other expenses of Carolina Complete Health. The Cushion Loan would bear interest at a rate of 5.00 percent over the three-month London Interbank Offered Rate and mature on the fifth anniversary of the date on which the initial term of the N.C. Medicaid Contract (excluding all renewals and extensions) expires or is terminated for any reason. The Cushion Loan would be repaid from CCHN’s Excess Cash Flows (as defined in the Loan and Security Agreement). |
26
| ● | The NCMS will not be a guarantor or otherwise responsible for the repayment of any of CCHN’s obligations to Centene, including the Incremental Reserve Funding Loan or the Cushion Loan. |
| ● | To the extent that additional capital from CCHN is required beyond what CCHN can fund through its cash reserves, the Incremental Reserve Funding Loan and the Cushion Loan, Centene Sub may contribute such additional capital in exchange for additional Class B Partnership Units, which would dilute the partnership interest of CCHN in the Joint Venture Company from 20 percent down to an amount not less than 10 percent. |
If the partnership interest of CCHN in the Joint Venture Company has been diluted down to 10 percent, Centene Sub will solely determine the need for further additional capital for Carolina Complete Health to fund operating losses and/or capital reserve requirements. Any such additional capital contribution made by Centene or Centene Sub may be reflected either as a loan or preferred units in the Joint Venture Company or Carolina Complete Health and will be returned to Centene or Centene Sub in full with interest or other preferred return at a floating rate equal to the three month LIBOR plus 800 basis points (8.00 percent) before CCHN will be entitled to receive any distributions from the Joint Venture Company.
Funding of CCHN
Centene has funded the start-up costs of CCHN with the First Loan in an amount up to $2.5 million, secured by all of CCHN’s receivables from the CCHN Services Agreement and partnership interest in the Joint Venture Company and carrying an interest rate of 6.75 percent. The First Loan amount may be increased in three increments of $500,000 up to an amount of $4.0 million if certain milestones relating to the Offering are attained by CCHN.
In addition, if Carolina Complete Health is awarded and accepts an N.C. Medicaid Contract, Centene has agreed to provide CCHN with the Second Loan, which, based upon the amount of Net Offering Proceeds, as well as CCHN’s use of the Net Offering Proceeds, could provide CCHN with up to an additional $3.0 million in funding, which amount may be increased up to $4.0 million if, in consultation with Centene and in Centene’s sole discretion, CCHN has demonstrated good progress toward the establishment of the Provider Network. Any amounts drawn under the Second Loan will also be secured by all of CCHN’s receivables from the CCHN Services Agreement and its partnership interest in the Joint Venture Company. Each of the First Loan and Second Loan bear interest at a rate of 6.75 percent and matures on the respective tenth anniversary of the first interest payment under such loan. The proceeds of the First Loan have been, and the proceeds of the Initial Centene Loans may be, used for the following qualifying expenses: (1) personnel, consultants, third party service providers and other out-of-pocket operational, pre-operational and business development expenses of CCHN related to (a) conducting and administering the Offering and the Private Placement, (b) developing and retaining necessary operational capabilities, (c) ensuring regulatory compliance, (d) recruiting providers for the Provider Network and (e) compensating independent accountants and (2) legal expenses related to the Offering, the Private Placement and the development and review of provider agreements for the Health Plan. In addition, the proceeds of the Second Loan may be used to repay amounts borrowed from Centene under the Loan and Security Agreement to fund a portion of CCHN’s initial capital contribution to the Joint Venture Company at the Joint Venture Closing. The aggregate amount available under the Second Loan for payment of the qualifying expenses enumerated above will be reduced by an amount equal to 55 percent of the Net Offering Proceeds, less the amount of such proceeds applied by CCHN to capital calls for Carolina Complete Health or to repay principal borrowed from Centene under the Initial Centene Loans or the Loan and Security Agreement. During the time that any amount of principal or interest remains outstanding under the Initial Centene Loans, CCHN will remit 60 percent of its Excess Cash Flow (as defined in the Centene Initial Loan Agreement) to repay the Initial Centene Loans.
The NCMS is not a guarantor of the Initial Centene Loans.
27
Transfer of Partnership Units of the Joint Venture Company
Until the Joint Venture Closing or the earlier termination of the Joint Venture Agreement, neither Centene Sub nor CCHN may, directly or indirectly, transfer any of their respective partnership units of the Joint Venture Company and may not cause or otherwise permit the Joint Venture Company to, directly or indirectly, transfer its initial shares of Carolina Complete Health. Following the Joint Venture Closing, except for certain transfers permitted by the Amended and Restated Partnership Agreement, neither Centene Sub nor CCHN (nor any future unitholder of the Joint Venture Company) may transfer any of its partnership units of the Joint Venture Company or any of the rights associated therewith. Provided that the proposed transfer satisfies certain conditions, Centene Sub may transfer its partnership units of the Joint Venture Company to any of its affiliates, and any party may transfer its partnership units of the Joint Venture Company if approved in advance by at least seven members of the Joint Venture Company Management Committee, at least one of whom is elected by holders of Class A Partnership Units.
Subject to compliance with certain requirements, if Centene Sub (or any future unitholder holding more than 50 percent of the issued and outstanding common partnership units of the Joint Venture Company, each a “controlling partner”) agrees to consummate any transaction or series of related transactions with a third party purchaser resulting in (1) a sale of all, but not less than all, of the common partnership units of the Joint Venture Company held by such controlling partner or (2) the sale, lease, exchange, conveyance, transfer or other disposition of all or substantially all of the property and assets of the Joint Venture Company (whether by way of consolidation, conversion, merger, sale of common stock, sale of assets or other similar type of business combination), then such controlling partner may compel each other partner of the Joint Venture Company to participate in such sale (the “Drag-Along Right”). If Centene Sub (or any of its transferees, assigns or successors) exercises the Drag-Along Right, then at the closing of that sale, Centene Sub must pay a drag-along premium to CCHN based on the aggregate number of shares of Class P Common Stock of CCHN issued and outstanding as of the date on which Centene Sub notifies CCHN of its exercise of the Drag-Along Right. Pursuant to the Stockholder’s Agreement, CCHN has agreed to redeem each share of outstanding Class P Common Stock for a price equal to the aggregate drag-along premium received by it divided by the number of shares of Class P Common Stock outstanding. Any proceeds of a drag-along sale received by or otherwise allocable to CCHN that are in excess of the drag-along premium will be reduced by an amount equal to the amount of indebtedness (whether for principal, interest, fees or otherwise) of CCHN or its affiliates to Centene Sub or its affiliates outstanding as of the closing date of such sale, which amount will be paid or otherwise allocated to Centene Sub in repayment of such debt. If after this allocation of CCHN’s proceeds, there remains a principal balance outstanding of any indebtedness of CCHN or its affiliates to Centene Sub or any of its affiliates, then following the closing of a drag-along sale such indebtedness will be forgiven, subject to certain conditions described in the Amended and Restated Partnership Agreement. However, if after this allocation of CCHN’s proceeds such indebtedness is satisfied in full and there remain drag-along sale proceeds for the benefit of CCHN, these proceeds will belong to and may be retained by CCHN.
Subject to compliance with certain requirements, if Centene Sub (or any other controlling partner) proposes to transfer any of its common partnership units of the Joint Venture Company and does not exercise the Drag-Along Right, then each other partner of the Joint Venture Company will have the right to transfer up to its pro rata portion in such sale (the “Tag-Along Right”), and the number of partnership units to be sold by the controlling partner will be reduced by the aggregate amount of partnership units to be transferred by those exercising the Tag-Along Right. If a controlling partner transfers any of its common partnership units in violation of the tag-along provisions in the Amended and Restated Partnership Agreement, then each partner of the Joint Venture Company will have a right to sell to such controlling partner (and such controlling partner will have an obligation to purchase) the number of common partnership units of the Joint Venture Company that such partner would have had the right to sell according to its Tag-Along Right for a per partnership unit amount and form of consideration as agreed to by the controlling partner in connection with its sale, and the controlling partner must reimburse such partner for all reasonable out-of-pocket expenses, including reasonable legal fees and expenses, incurred in connection with exercising such partner’s rights.
28
If a Centene change of control (as defined in the Amended and Restated Partnership Agreement) occurs, CCHN will have the right, and if either the services agreement between Carolina Complete Health and a management company affiliate of Centene or the CCHN Services Agreement is terminated due to a fundamental breach (as such term is defined in such agreements), CCHN will have the obligation, to sell all, but not less than all, of its partnership units of the Joint Venture Company to Centene Sub pursuant to certain conditions under the Amended and Restated Partnership Agreement. Any partnership units sold pursuant to such provisions will be priced at an amount based on the fair market value per partnership unit of the Joint Venture Company at the time the event giving rise to the put right or obligation and will be reduced by an amount equal to the amount of indebtedness (whether for principal, interest, fees or otherwise) of CCHN or its affiliates to Centene Sub or its affiliates outstanding as of the closing date of such sale. If such sale occurs on or prior to the expiration of the initial term of Carolina Complete Health’s contract with the State of North Carolina, the amount for which the partnership units are sold will be further reduced by an amount based on (1) the number of Eligible Investors who have purchased Provider Shares in this Offering as of the date of the Joint Venture Closing and investors attributable to CHCs subscribing in the Private Placement, (2) the term of the contract with the State of North Carolina and (3) any committed contribution to the Joint Venture Company by Centene Sub that has not yet been made.
Conditions to Closing
The obligations of the Joint Venture Parties to consummate the Joint Venture Closing are subject to the satisfaction or prior written waiver by each party of the following conditions, among others:
| ● | no governmental authority with competent jurisdiction shall have (1) enacted any law that has the permanent effect of making the transactions contemplated by the Joint Venture illegal or otherwise preventing their completion, (2) repealed the North Carolina Medicaid reform legislation or (3) issued an order enjoining the completion of the transactions contemplated by the Joint Venture or otherwise preventing their completion; |
| ● | there shall not be any pending or threatened lawsuit or other legal proceeding seeking to prohibit, prevent, limit or otherwise restrain or to obtain damages with respect to the completion of the transactions contemplated by the Joint Venture; |
| ● | all material actions by or in respect of, or filings with, any governmental authority required to permit the completion of the transactions contemplated by the Joint Venture shall have been taken or made; |
| ● | Carolina Complete Health shall be duly registered as a licensed insurance company with the North Carolina Department of Insurance; and |
| ● | the Joint Venture Parties, by and on behalf of Carolina Complete Health, shall have, prior to the applicable deadline, submitted a formal response to North Carolina’s request for proposal to health insurance companies for plans to be offered in the reformed Medicaid program and, in response thereto, been awarded and accepted an N.C. Medicaid Contract. |
The obligations of Centene and Centene Sub to consummate the Joint Venture Closing are subject to the satisfaction or prior written waiver by Centene of the following conditions, among others:
| ● | the number of Eligible Investors who have purchased Provider Shares and the number of investors attributable to CHCs that subscribed in the Private Placement must be at least 10,000 in the aggregate prior to the earlier of (1) the date that is 10 business days prior to the deadline for submitting proposals for the contract with the State of North Carolina and (2) March 12, 2019, the date that is 12 months after the Offering Statement on Form 1-A, of which this Offering Circular is a part, was qualified by the Commission; and |
| ● | on or prior to the date that is 10 business days before the deadline for submitting proposals for the contract with the State of North Carolina, the Provider Network must have satisfied the provider participation requirements established by the State of North Carolina with respect to network adequacy. |
29
Termination of the Joint Venture Agreement
The Joint Venture Agreement may be terminated at any time prior to the Joint Venture Closing as provided therein, including, among others, at any time upon the mutual written agreement of the NCMS and Centene, or by either the NCMS or Centene in the event that:
| ● | any governmental authority with competent jurisdiction has (1) enacted any law that has the permanent effect of making the transactions contemplated by the Joint Venture illegal or otherwise preventing their completion, (2) repealed the North Carolina Medicaid reform legislation or (3) issued an order enjoining the completion of the transactions contemplated by the Joint Venture or otherwise preventing their completion, which order has become final and nonappealable; |
| ● | the Joint Venture Closing has not occurred by March 31, 2019; provided, however, that neither the NCMS nor Centene shall be permitted to terminate if their own failure to perform was the cause of the failure to close by March 31, 2019; |
| ● | Carolina Complete Health does not receive a contract with the State of North Carolina in connection with its response to the request for proposal; or |
| ● | they are not then in material breach of their respective provisions of the Joint Venture Agreement but there has been a material breach, inaccuracy in or failure to perform by the respective other Joint Venture Parties that would cause a condition to the Joint Venture Closing to be unsatisfied and is not cured within 10 business days of receiving written notice of such breach. |
Centene may terminate the Joint Venture Agreement upon written notice to the NCMS in the event that:
| ● | the number of Eligible Investors who have purchased Provider Shares and the number of investors attributable to CHCs that subscribed in the Private Placement does not equal at least 10,000 in the aggregate prior to the earlier of (1) the date that is 10 business days prior to the deadline for submitting proposals for the contract with the State of North Carolina and (2) March 12, 2019, the date that is 12 months after the Offering Statement on Form 1-A, of which this Offering Circular is a part, was qualified by the Commission; or |
| ● | on or prior to the date that is 10 business days before the deadline for submitting proposals for the contract with the State of North Carolina, the Provider Network fails to meet the provider participation requirements established by the State of North Carolina with respect to network adequacy. |
The NCMS may terminate the Joint Venture Agreement upon written notice to Centene if there has been a Centene Change in Control (as defined in the Amended and Restated Partnership Agreement) and, within two business days of such change in control, the acquiring or surviving entity has not (1) publicly affirmed its intent to complete the transactions contemplated by the Joint Venture Agreement and (2) signed a joinder or other similar contractual obligation to be bound by the Joint Venture Agreement and complete the transactions contemplated thereby.
If the Joint Venture Agreement terminates, the transactions contemplated by the Joint Venture Agreement will not occur. For information about the treatment of the Provider Shares in this event, see “The Offering Circular Summary—The Offering—Termination of the Joint Venture.”
30
GOVERNANCE
Governance of CCHN
Our Amended and Restated Bylaws provide that the CCHN Board may consist of up to nine individuals, one of whom is a designee of the NCMS and, if the CCHN Board consists of at least five individuals, one of whom is a representative of the CHCs. The CCHN Board is currently composed of four members, and we are actively searching for other qualified individuals to serve on the CCHN Board as we build the Provider Network.
Prior to the commencement of the Health Plan’s operations, we intend to amend and restate our Amended and Restated Bylaws (the “Proposed Bylaws”) to require the CCHN Board to be composed of the following:
| ● | five directors, one of whom will be a representative of the CHCs, who are physicians licensed under Article 1 of Chapter 90 of the North Carolina General Statutes and represent a mix of primary care physicians and specialists, practice settings and geographic regions of the States, to be initially selected and appointed by NCMS, and beginning at the first annual meeting of stockholders after the Health Plan first enrolls a member into the Health Plan, will be elected by the holders of Class P Common Stock and Class M Common Stock, voting together as a single class; |
| ● | two directors who are also members of the Board of Directors of Carolina Complete Health, who will be selected and appointed by Centene during the Exclusivity Period, and who will be elected by the holders of Class P Common Stock and Class M Common Stock, voting together as a single class, after the expiration of the Exclusivity Period; and |
| ● | two directors, one of whom will be designated by the NCMS, who are community leaders or representatives from other Medicaid provider groups, to be initially selected and appointed by the NCMS, and beginning at the first annual meeting of stockholders after the Health Plan first enrolls a member into the Health Plan, will be elected by the holders of Class P Common Stock and Class M Common Stock, voting together as a single class. |
Governance of the Joint Venture Company
Centene Sub is currently the Managing Partner of the Joint Venture Company. Pursuant to the Amended and Restated Partnership Agreement to be entered upon the Joint Venture Closing, the Joint Venture Company Management Committee will be established and be composed of 10 members, two of whom will be elected by the holders of the Joint Venture Company Class A Partnership Units, which are held solely by CCHN (each, a “Class A Manager”), and eight of whom will be elected by the holders of the Joint Venture Company Class B Partnership Units, which are held solely by Centene Sub.
As provided in the Amended and Restated Partnership Agreement, the following actions will require approval by at least seven members of the Joint Venture Company Management Committee, at least one of whom must be a Class A Manager:
| ● | amendment, modification or waiver of any of the governing documents of the Joint Venture Company or Carolina Complete Health, except as necessary to reflect the issuance of preferred partnership units authorized in the Amended and Restated Partnership Agreement; |
| ● | except as contemplated by the documents governing the Joint Venture, including the Joint Venture Agreement, the entry into any agreement or arrangement with (1) either of the NCMS or Centene or any of their respective affiliates or (2) for the direct or indirect benefit of any partnership unitholder of the Joint Venture Company or any officer, director, employee or consultant of the Joint Venture Company (or any members of their immediate families), or any affiliate thereof, other than for employment contracts, reimbursement or payment of business expenses or advances made in the ordinary course of business, in each case, consistent in nature, scope and magnitude with past practice; |
31
| ● | the entry into any strategic alliance, joint development or other relationship; |
| ● | the changing of the principal business of the Joint Venture Company or entry into new lines of business that are materially different from the Joint Venture Company’s principal business; |
| ● | except as otherwise provided in the Joint Venture Agreement, (1) the issuance, grant, delivery or sale or authorization of the issuance, grant, delivery or sale of any partnership units of the Joint Venture Company or other equity interests or investment interests convertible into, or subscriptions, rights, warrants or options to acquire, or other agreements or commitments of any character obligating it to issue any such partnership units or other equity interests of the Joint Venture Company or other convertible securities, (2) entry into or effecting any transaction or series of related transactions involving the repurchase, redemption or other acquisition of partnership units of the Joint Venture Company from any person or (3) initiation or consummation of any recapitalization, split or combination of partnership units, dividend of units or similar restructuring, including creating or issuing any new classes or series of Joint Venture Company partnership units or any options, warrants or rights convertible into or exercisable or exchangeable for any partnership units of Joint Venture Company; |
| ● | the initiation or consummation of any initial public offering, or the making of a public offering and sale of any partnership units or any other equity interests of the Joint Venture Company; |
| ● | the dissolution, winding-up or liquidation of the Joint Venture Company; and |
| ● | the commitment to, or agreement (in writing or otherwise) to taking, any of the actions described above. |
Upon the Joint Venture Closing, the Joint Venture Company will establish a Nominating Committee consisting of two representatives selected by Centene Sub and the two Class A Managers. The Nominating Committee will also contain an observer designated by the Board of Directors of the NCCHCA. The Nominating Committee will be charged with developing and recommending the proposed slate of candidates for the Carolina Complete Health Board (including without limitation the satisfaction of the director criteria outlined below under “—Governance of Carolina Complete Health”) to be elected by the Joint Venture Company as Carolina Complete Health’s sole shareholder.
Governance of Carolina Complete Health
Executive Officers
The executive team of Carolina Complete Health will have at least one member who is a physician, licensed under Article 1, Chapter 90 of the North Carolina General Statutes. The chief financial officer of Carolina Complete Health will be required to be an experienced insurance industry executive. The Carolina Complete Health Board will have the exclusive authority to appoint and remove the chief executive officer and chief medical officer of Carolina Complete Health.
Board of Directors
The Carolina Complete Health Board currently comprises two members, and, following the Joint Venture Closing, will consist of 15 members as follows, each to be elected by the Joint Venture Company in accordance with the recommendation of its Nominating Committee (as described below):
| ● | eight directors who are physicians licensed under Article 1, Chapter 90 of the North Carolina General Statutes and who are participants in the Provider Network, one of whom will be a representative of the CHCs and shall be selected by the Board of Directors of the NCCHCA (the “CCHN Directors”); |
| ● | four directors who are employees of Centene (the “Centene Directors”); and |
| ● | three directors who are North Carolina community leaders, one of whom will be a representative of the CHCs and shall be selected by the Board of Directors of the NCCHCA (the “Community Leader Directors”). |
32
As noted above, upon the Joint Venture Closing, the Joint Venture Company will establish a Nominating Committee to develop and recommend the proposed slate of candidates for the Carolina Complete Health Board. In voting for the nominees to the Carolina Complete Health Board, the Joint Venture Company may only approve or disapprove the slate recommended by the Nominating Committee and may not select a different slate of candidates for the Carolina Complete Health Board. In the event of a vacancy in the Carolina Complete Health Board, the Joint Venture Company will appoint a replacement director to serve the remainder of the term of a vacant directorship who has been nominated by the Nominating Committee and meets the same criteria (i.e., either a CCHN Director, Centene Director or Community Leader Director, as applicable) as the person who previously held the vacant directorship.
The Carolina Complete Health Board may not take the following actions unless approved by at least 12 directors (the “Supermajority Actions”):
| ● | sale, lease, license or exchange of all or substantially all of Carolina Complete Health’s assets; |
| ● | merger, consolidation or similar transaction involving Carolina Complete Health; |
| ● | change in the tax classification of Carolina Complete Health; |
| ● | redemption or repurchase of any shares (other than stock options or similar awards) of the capital stock of Carolina Complete Health; |
| ● | establishment of, or thereafter any variance from the previously approved, provider fee schedules or the parameters of value-based payment arrangements with providers; |
| ● | any transaction involving Carolina Complete Health and either the NCMS or Centene or an affiliate of either of them; |
| ● | any material asset acquisition by Carolina Complete Health; |
| ● | any material debt incurrence by Carolina Complete Health; |
| ● | entry into, or material modification or termination of, any material contract of Carolina Complete Health; |
| ● | any reverse stock split by Carolina Complete Health; |
| ● | addition of a new insurance product offering by Carolina Complete Health; |
| ● | any capital calls, except to meet the 300 percent risk based capital ratio for statutory surplus; |
| ● | issuance of additional shares of any existing class of capital stock, the creation or issuance of any additional class or series of capital stock, or an increase in the authorized number of shares of any class or series of capital stock, of Carolina Complete Health; |
| ● | reclassification, alteration or amendment of any existing security of Carolina Complete Health; |
| ● | any increase or decrease in the size of the Carolina Complete Health Board; |
| ● | any material modification to or departure from Carolina Complete Health’s business plan; |
33
| ● | liquidation, dissolution or winding-up of the business and affairs of Carolina Complete Health; |
| ● | any amendment, alteration, modification or change to the Articles of Incorporation or Bylaws of Carolina Complete Health, including, without limitation, the adoption of any new Bylaws or the repeal of any of the existing or later adopted Bylaws of Carolina Complete Health; |
| ● | any amendment or waiver of Carolina Complete Health’s rights under any agreement by and between Carolina Complete Health and Centene or any of its affiliates (except that the Centene Directors shall be recused due to conflict and the Supermajority Action shall be satisfied by the consent or vote of nine of the remaining directors); |
| ● | any amendment of or waiver of Carolina Complete Health’s rights under any agreement by and between Carolina Complete Health and the NCMS or any of its affiliates (except that the CCHN Directors shall be recused due to conflict and the Supermajority Action shall be satisfied by the vote of five of the remaining directors); |
| ● | the selection, initial hiring, retention at the end of an initial or renewal employment term or termination without cause of the chief executive officer/president or chief medical officer of Carolina Complete Health; |
| ● | selection of the chief executive officer and chief medical officer of Carolina Complete Health; |
| ● | any change in Carolina Complete Health’s auditor to an auditor that is not the auditor of Centene; and |
| ● | entering into any agreement, commitment or arrangement to affect any of the foregoing or granting the consent of Carolina Complete Health to any of the foregoing. |
Carolina Complete Health may not directly or indirectly, by amendment, merger, consolidation or otherwise, take any of the following actions without the written consent or affirmative vote of the Joint Venture Company in its capacity as the sole shareholder of Carolina Complete Health:
| ● | the sale, lease, license or exchange of all or substantially all of Carolina Complete Health’s assets; |
| ● | the merger, consolidation, conversion or similar transaction involving Carolina Complete Health; |
| ● | any amendment, alteration, modification or change to the Articles of Incorporation or Bylaws of Carolina Complete Health, including without limitation, the adoption of any new Bylaws or the repeal of any of the existing or later adopted Bylaws of Carolina Complete Health; |
| ● | the liquidation, dissolution or winding-up of the business and affairs of Carolina Complete Health; or |
| ● | entering into any agreement, commitment or arrangement to affect any of the foregoing or granting the consent of Carolina Complete Health to any of the foregoing. |
Financial Matters Committee
Upon the Joint Venture Closing, Carolina Complete Health will establish a Financial Matters Committee of the Carolina Complete Health Board to exercise the full authority of the Carolina Complete Health Board with respect to decisions directly affecting the capital or reserves of Carolina Complete Health or impacting Carolina Complete Health’s critical financial operations. The committee will consist of the four Centene Directors, two of the three Community Leader Directors (who will be appointed to the committee by a supermajority vote of the Carolina Complete Health Board) and one member of the Medical Affairs Committee described below (who will be selected by a majority vote of the CCHN Directors).
34
The Chairperson of the Financial Matters Committee will be one of the Centene Directors and must meet the requirements of an “audit committee financial expert” as defined in Item 407(d)(5) of Regulation S-K promulgated by the Commission. The presence of a majority of the members of the Financial Matters Committee, which majority must include at least three of the Centene Directors, will constitute a quorum for business. Once a quorum is present, any matter brought before the Financial Matters Committee will be determined by the affirmative vote of a majority of the members present at such meeting, which majority must include at least three of the Centene Directors. The Financial Matters Committee will have the authority to act for and bind the Carolina Complete Health Board with respect to the following items:
| ● | general oversight of Carolina Complete Health’s accounting and financial reporting processes, audits of the financial statements, and internal control and audit functions; |
| ● | adoption of the annual budget of Carolina Complete Health (provided that the proposed annual budget must have been first submitted to the full Carolina Complete Health Board for its review and input); |
| ● | investment policy of assets; |
| ● | chief executive officer and chief medical officer insurance coverage; and |
| ● | capital calls to maintain statutory surplus at the 300 percent risk based capital ratio level. |
Medical Affairs Committee
Upon the Joint Venture Closing, Carolina Complete Health will establish a Medical Affairs Committee of the Carolina Complete Health Board to exercise the full authority of the Carolina Complete Health Board with respect to certain decisions directly affecting medical issues and impacting patient care and overall medical management in connection with the organization, management and operation of the Health Plan. The Medical Affairs Committee will consist of seven Carolina Complete Health Directors who represent an appropriate composition of primary care physicians and specialists and of different practice settings and geographic regions (who will be appointed by a majority vote of the Carolina Complete Health Board) and one member who is also a member of the Financial Matters Committee (who will be appointed by a majority vote of the Centene Directors) (the “Financial Representative”).
The issues delegated to the Medical Affairs Committee for decision will include provider credentialing, quality assurance on medical issues, medical expertise in coverage, medical policy and other decisions impacting care, significant medical-related strategies and initiatives of Carolina Complete Health and the Health Plan and Carolina Complete Health’s medical strategies, policies and procedures. The Medical Affairs Committee will ensure appropriate medical expertise is involved in coverage, medical policy and other decisions that impact patient care. Any subcommittee established by the Medical Affairs Committee must include the Financial Representative.
The Medical Affairs Committee will have the authority to establish one or more various advisory subcommittees to analyze and provide advice and recommendations on issues related to the practice of medicine. Members of any such advisory subcommittee may, but are not required to, be members of the Carolina Complete Health Board or the Medical Affairs Committee; however, any member of any such advisory subcommittee must include only Eligible Investors who have purchased Provider Shares. The advisory subcommittees may consult with third party experts and make recommendations to the Medical Affairs Committee, but they may not bind Carolina Complete Health or the Medical Affairs Committee or otherwise take any formal action on behalf of Carolina Complete Health, the Carolina Complete Health Board or the Medical Affairs Committee.
35
MANAGEMENT DISCUSSION AND ANALYSIS
You should read the following discussion in conjunction with our financial statements and the related notes and the sections entitled “Business” and “The Joint Venture” elsewhere in this Offering Circular. This discussion contains forward-looking statements that involve risks and uncertainties. Actual results and the timing of events may differ materially from those contained in these forward-looking statements due to a number of factors, including but not limited to those discussed in the section entitled “Risk Factors” and elsewhere in this Offering Circular.
Overview
CCHN was incorporated on May 19, 2016 as a wholly-owned subsidiary of the NCMS and, to date, our operations have been limited.
During the interim period from the signing of the Joint Venture Agreement until the Joint Venture Closing, CCHN will conduct its activities by outsourcing its needed functions to NCMS professionals and staff, independent contractors, professional consultancy firms, third-party vendors or other such entities that can provide the capabilities required to recruit and retain providers to participate in the Provider Network. Until the commencement of the Health Plan’s operations, we do not expect to generate any revenue from operations. See “Business—Business of CCHN.”
The Joint Venture Closing is currently expected to occur after September 1, 2018, and the Health Plan is currently expected to “go live” around July 2019.
Results of Operations
For the year ended December 31, 2017
As of December 31, 2017, we have yet to generate any revenue from operations.
Beginning in January 2017, Centene has agreed to reimburse us up to $300,000 annually for certain launch, start-up and operational expenses incurred during fiscal years 2017 and 2018. For the year ended December 31, 2017, we recorded reimbursable expense revenue of $300,000 for such expenses incurred.
In 2017, we had no employees, and we relied exclusively on contracted assistance in connection with our preliminary activities related to building the Provider Network.
For the year ended December 31, 2017, we incurred total operating costs and expenses of $1,617,687, of which $1,232,348 were general and administrative expenses related to contracted resources as well as attorney fees, related-party services and other administrative expenses associated with establishing and running our company. Of these expenses, we incurred expenses of $441,495 from NCMS to engage the resources and related expenses of the NCMS’s professional and administrative staffs to conduct and perform activities on our behalf. Going forward, we will continue to draw upon the NCMS professional and administrative staffs in the performance of some of our activities, and as such, we will incur additional costs associated with the NCMS staffs’ performance of these activities. The remaining operating costs and expenses of approximately $385,339 were related to quality and development expenses incurred to recruit and retain a network of health care providers who will provide medical services under the Health Plan.
For the year ended December 31, 2017, we incurred $36,254 of interest expense under the Term Note “First Loan.”
As a result of the foregoing, net loss for the year ended December 31, 2017 was $1,353,010.
For the period from inception (May 19, 2016) through December 31, 2016
In 2016, we had no employees and relied exclusively on contracted assistance in connection with our preliminary activities related to building the Provider Network.
From inception through December 31, 2016, we incurred total operating costs and expenses of approximately $764,768, which were all general and administrative expenses related to organization costs as well as attorney fees, outside consultants, related-party services and other administrative expenses associated with setting up our company. Of these expenses, $162,221 of legal and consulting fees were incurred and paid directly on our behalf by the sole stockholder of our Class M Common Stock, the NCMS. We also incurred expenses of $303,106 from NCMS to engage the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct and perform activities on our behalf.
During 2016, we incurred $2,814 of interest expense under the First Loan.
As a result of the foregoing, net loss from inception through December 31, 2016 was $767,582.
36
Provision for Income Taxes
CCHN recognizes deferred tax assets to the extent that we believe that these assets are more likely than not to be realized. In making such a determination, we consider all available positive and negative evidence, including future reversals of existing taxable temporary differences, projected future taxable income, tax-planning strategies and results of recent operations. CCHN assessed the need for a valuation allowance against our net deferred tax assets and determined a full valuation allowance is required as of December 31, 2017 and 2016 due to uncertainty regarding future revenue generating activities. Therefore, a full valuation allowance of $414,052 and $224,138 was recorded for the year ended December 31, 2017 and the period May 19, 2016 through December 31, 2016, respectively.
On December 22, 2017, the United States enacted the Tax Cuts and Jobs Act (the “Tax Act”). The Tax Act, among other changes, lowers the general corporate income tax rate to 21 percent for tax years beginning after December 31, 2017. See Note 6, “Income Taxes,” in the notes to our financial statements appearing elsewhere in this Offering Circular for additional information about the impact of the Tax Act on CCHN.
CCHN does not have any uncertain tax positions. CCHN has not recorded any interest or penalties in the financial statements as of December 31, 2017 and 2016.
Liquidity and Capital Resources
As of December 31, 2016, we had established (1) a current payable due to outside vendors of $97,880, (2) a current amount due to the NCMS of $29,929, (3) a non-current amount due to the NCMS of $465,327 and (4) an outstanding amount under the First Loan of $171,632.
As of December 31, 2017, we had established (1) a current receivable for reimbursable expenses revenue of $52,016, (2) a current payable due to outside vendors of $278,481, (3) current accrued expenses for services provided of $37,570, (4) a current advance from investors of $979,250 for funds received for the purchase of Class P Common Stock in the Private Placement that occurred on January 19, 2018, (5) a non-current amount due to the NCMS of $906,822 and (6) an outstanding amount under the First Loan of $1,412,277.
Since CCHN’s inception on May 19, 2016, we have relied upon the sole stockholder of our Class M Common Stock, the NCMS, to provide us with both working capital and transaction-related cash advances, as needed, as well as the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct and perform CCHN’s activities. Working capital has been advanced by the NCMS to CCHN which became due and payable as funds are borrowed under the First Loan. As funding is received under the First Loan, the outstanding working capital advance is settled. At December 31, 2016, a $29,929 working capital advance had been recorded as a current liability, “Due to Stockholder.” As of December 31, 2017 there are no amounts outstanding as a current liability, “Due to Stockholder.”
As part of the Joint Venture discussions and transaction, CCHN incurred transaction-related outside advisor expenses that were ineligible for reimbursement under the First Loan. When these expenses became due and payable to the outside advisors, the NCMS settled the transaction-related amounts due on behalf of CCHN. The settlement of these transaction-related advances by the NCMS on behalf of CCHN had been recorded as a non-current liability, “Due to Stockholder,” and at December 31, 2016, CCHN had recorded $162,221 of such advances in the non-current liability, “Due to Stockholder.” As of December 31, 2017, this advanced amount remains outstanding, and it continues to be recorded in the non-current liability, “Due to Stockholder.”
Also, since our inception, we have not had an employee. As such, CCHN has relied upon the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct and perform CCHN’s activities. The cost of the NCMS staff time incurred to support CCHN has been calculated, and the staff time cost has been used as a basis for allocating the related expenses associated with the NCMS staff’s support. In 2016 and 2017, CCHN recorded $303,106 and $441,495, respectively, as the cost of the NCMS staff time incurred and related expenses as a “General and Administrative” expense.These amounts have been recorded as a non-current liability, “Due to Stockholder.” As of December 31, 2017, the total amount recorded as a non-current liability, “Due to Stockholder,” for the cost of NCMS staff time incurred and related expenses is $744,601.
Going forward, CCHN will continue to draw upon the NCMS professional and administrative staffs in the performance of CCHN’s activities, and as such, CCHN will incur additional costs associated with the staffs’ performance of these activities. The non-current liability, “Due to Stockholder,” amount will be settled no earlier than the “go-live” date of the Health Plan, which is currently projected in July 2019.
Beginning in January 2017, Centene has agreed to reimburse CCHN up to $300,000 annually for certain launch, start-up and operational expenses incurred during fiscal years 2017 and 2018. For the year ended December 31, 2017, we recorded reimbursable expense revenue of $300,000 for such expenses incurred.
In addition, Centene has provided CCHN with a First Loan in an amount up to $2.5 million, secured by all of CCHN’s receivables from the CCHN Services Agreement, if any, and the partnership interest in the Joint Venture Company. Borrowings under the term loan bear an interest rate of 6.75 percent. In addition, the First Loan requires CCHN to remit 60 percent of its Excess Cash Flows (as defined in the Centene Initial Loan Agreement) in repayment of amounts drawn. The loan amount may be increased in three increments of $500,000 up to an amount of $4.0 million if certain milestones are attained. The principal balance outstanding on the First Loan was $171,632 at December 31, 2016 with accrued interest of $2,814. As of December 31, 2017, the principal balance outstanding on the First Loan was $1,412,277 with accrued interest of $39,068.
37
On January 10, 2017, our loan agreement with Centene was amended and restated to include an additional funding provision that, if Carolina Complete Health is awarded and accepts an N.C. Medicaid Contract, Centene has agreed to provide CCHN with a secondary multiple advance term loan, which, based upon the amount of Net Offering Proceeds, as well as CCHN’s use of Net Offering Proceeds, could provide CCHN with the Second Loan of up to an additional $3.0 million in funding, which amount may be increased up to $4.0 million if, in consultation with Centene and in Centene’s sole discretion, CCHN has demonstrated good progress toward the establishment of the Provider Network.
On August 25, 2017, we entered the Centene Initial Loan Agreement, which amended and restated our prior loan agreement with Centene. Under the Centene Initial Loan Agreement, the aggregate amount available under the Second Loan for payment of the qualifying expenses enumerated below will be reduced by an amount equal to 55 percent of the Net Offering Proceeds, less the amount of such proceeds applied by CCHN to capital calls for Carolina Complete Health or to repay principal borrowed from Centene under the Initial Centene Loans or the Loan and Security Agreement.
The proceeds of the Initial Centene Loans have been, will be, and may be, used for the following qualifying expenses: (1) personnel, consultants, third party service providers and other out-of-pocket operational, pre-operational and business development expenses related to (a) conducting and administering financings, (b) developing and retaining necessary operational capabilities, (c) ensuring regulatory compliance, (d) recruiting providers for the Provider Network and (e) compensating independent accountants and (2) legal expenses related to any financing and the development and review of provider agreements for the proposed Health Plan. In addition, the proceeds of the Second Loan may be used to repay amounts borrowed from Centene under the Loan and Security Agreement to fund a portion of CCHN’s initial capital contribution to the Joint Venture Company at the Joint Venture Closing.
Based upon CCHN’s current operating plan, we believe, with the (1) continued deferral of payment for costs incurred for services provided to us by the NCMS, (2) up to $4.0 million currently available under the First Loan, (3) aggregate amount available under the Second Loan and (4) retention of an amount available from the Net Offering Proceeds, we will be able to sufficiently manage our activities and cash flow needs until September 2019.
On January 19, 2018, CCHN completed a Private Placement to certain CHCs and the NCCHCA of 1,505 shares of Class P Common Stock at a purchase price of $750.00 per share for an aggregate amount of approximately $1.13 million.
In connection with the Joint Venture Closing, we will be required to contribute 45 percent of the Net Offering Proceeds, together with an advance under the Loan and Security Agreement, to the capitalization of the Joint Venture Company. See “Use of Proceeds.” In addition, we will be required to commit capital to Carolina Complete Health to satisfy certain statutory requirements. If we are not generating sufficient revenue to cover such capital calls, Centene has agreed to provide additional funding in the form of additional loans as described in “The Joint Venture—Capitalization of the Joint Venture Company.”
Plan of Operations
CCHN’s core responsibilities relate primarily to the Provider Network. For the 12 months following the commencement of this Offering, we expect our operations to consist of recruiting and retaining providers to participate in the Provider Network. In order to conduct its operations, CCHN will outsource its needed functions to NCMS professionals and staff, independent contractors, professional consultancy firms, third-party vendors or other such entities that can provide the capabilities required.
Based upon CCHN’s current operating plan, we believe, with the (1) continued deferral of payment for costs incurred for services provided to us by the NCMS, (2) up to $4.0 million currently available under the First Loan, (3) aggregate amount available under the Second Loan and (4) retention of an amount available from the Net Offering Proceeds, we will be able to sufficiently manage our activities and cash flow needs until September 2019.
In connection with the Joint Venture Closing, we will be required to contribute 45 percent of the Net Offering Proceeds, together with an advance under the Loan and Security Agreement, to the capitalization of the Joint Venture Company.
Off-Balance Sheet Arrangements
We do not engage in any off-balance sheet financing activities. We do not have any interest in entities referred to as variable interest entities, which include special purpose entities and other structured finance entities.
38
Critical Accounting Policies and Estimates
Our discussion and analysis of our financial condition and results of operations are based upon our financial statements, which we prepared in accordance with accounting principles generally accepted in the United States (“U.S. GAAP”). The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, revenues and expenses and related disclosures of contingent assets and liabilities. “Critical accounting policies and estimates” are defined as those most important to the financial statement presentation and that require the most difficult, subjective or complex judgments. We base our estimates on various factors that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Under different assumptions and/or conditions, actual results of operations may materially differ. The most significant estimates impacting our financial statements relate to income taxes. We also have other policies that we consider key accounting policies, but these policies typically do not require us to make estimates or judgments that are difficult or subjective.
Income Taxes – CCHN follows the asset and liability method of accounting for income taxes. This method requires recognition of deferred tax assets and liabilities for the expected future tax consequences of temporary differences between the carrying amounts and the tax basis of assets and liabilities. If it is more likely than not that some portion of a deferred tax asset will not be realized, a valuation allowance is recorded.
CCHN recognizes the tax benefit or liability from uncertain tax positions only if it is more likely than not that the tax position will be sustained on examination by the tax authorities, based on the technical merits of the position. The tax benefit is measured based on the largest benefit that has a greater than 50 percent likelihood of being realized upon ultimate settlement. CCHN recognizes interest and penalties related to income tax matters in income tax expense if incurred.
Subsequent Events – Subsequent events are events or transactions that occur after the balance sheet date but before the financial statements are issued. CCHN recognizes in the financial statements the effects of all subsequent events that provide additional evidence about conditions that existed at the date of the balance sheet, including the estimates inherent in the process of preparing the financial statements. CCHN’s financial statements do not recognize subsequent events that provide evidence about conditions that did not exist at the date of the balance sheet but arose after the balance sheet date and before financial statements are available to be issued. CCHN has evaluated subsequent events through April 26, 2018, which is the date the financial statements were available to be issued.
39
Directors, Executive Officers and Significant Employees
| Name | Position | Age | Term of Office | Approximate Hours per Week | ||||
| Executive Officer: | ||||||||
| Jeffrey W. Runge, MD | Director, President and Chief Executive Officer | 62 | March 14, 2017 – present | 21 | ||||
| Vincent T. Morgus, MBA, CPA | Chief Operating Officer | 52 | April 27, 2017 – present | 40 | ||||
| Stephen W. Keene, MBA, JD, LLM | Secretary-Treasurer | 58 | May 19, 2016 – present | 24 | ||||
| Directors: | ||||||||
| John R. Mangum, MD | Director | 62 | March 15, 2017 – present | |||||
| John Jacob Meier IV, MD, MBA | Director | 53 | March 15, 2017 – present | |||||
Richard Hudspeth, MD | Director | 55 | January 24, 2018 – present | |||||
Biographies
Jeffrey W. Runge, MD,our Chief Executive Officer, serves on the Board of Directors of the NCMS and has been serving as the Chief Medical Officer for Biospatial, Inc., a national biosurveillance and preparedness company, since 2017 and as President of Biologue, Inc., a biodefense consulting company, since 2008. Dr. Runge has also served with The Chertoff Group, a homeland security business consulting organization, since 2009, as a Principal and now as a Senior Advisor. He served as the Director and Principal Investigator of the National Collaborative for Biopreparedness at the University of North Carolina at Chapel Hill through the project’s commercialization in 2017. Prior to that, he served as the head of two Federal government agencies, first as the Administrator of the National Highway Traffic Safety Administration (2001-2005) and as the Chief Medical Officer and Assistant Secretary for Health Affairs in the U.S. Department of Homeland Security (2005-2008). Prior to his government service, he served 17 years on the faculty of the Department of Emergency Medicine at Carolinas Medical Center in Charlotte, North Carolina in a variety of academic, clinical and administrative roles.
Vincent T. Morgus, MBA, CPA, our Chief Operating Officer, is an employee of the NCMS and has served for over 25 years in finance and corporate development leadership positions. From September 2015 to March 2017, Mr. Morgus served as Managing Partner of The Fahrenheit Group – Carolinas, a management consulting firm focused on advising growth-oriented organizations (“Fahrenheit”). In 2015, he served as the Chief Financial Officer and Treasurer of TyraTech, Inc., a life sciences company focused on nature-derived insect and parasite control products. He also served as Chief Financial Officer of Lulu Press, Inc., a self-publishing e-commerce company, from 2013 to 2014 and as Chief Financial Officer and Treasurer at Cornerstone Therapeutics, Inc., a specialty pharmaceutical company, from 2011 to 2012. Prior to his executive financial positions, Mr. Morgus served as the Senior Vice President of Corporate Development for Quintiles Transnational Holdings, Inc., a biopharmaceutical development and commercial outsourcing services company. Mr. Morgus received a B.S. in Accounting, with distinction, from Pennsylvania State University’s Smeal College of Business and an M.B.A. from the University of North Carolina’s Kenan-Flagler Business School.
Stephen W. Keene, MBA, JD, LLM,our Secretary-Treasurer, has served as General Counsel of the NCMS since 1999 and has served in the additional role of Chief Operating Officer of the NCMS since 2016. Mr. Keene joined the NCMS in 1994 as Director, Government Affairs and Medical Economics. Prior to his service at the NCMS, Mr. Keene held positions in a number of medical organizations, where he developed programs and policies to address health care legislation and economic issues affecting the practice of medicine. Mr. Keene received a B.B.A and an M.B.A. from Georgia Southern College, a J.D., cum laude, from North Carolina Central University School of Law and an L.L.M. from Loyola University Chicago School of Law.
40
John R. Mangum, MD has served as a family medicine physician with the Sanford Medical Group, a satellite of Pinehurst Medical Clinic that provides primary care and occupational health services, since 1984. He served on the Board of Directors of the NCMS from 2002 to 2012 and as President in 2010 and 2011. A member of the Board of Directors of The Carolinas Center for Medical Excellence since 2006, he served as Board Chair from 2011 to 2014. He received his M.D. at the University of North Carolina School of Medicine and completed his family medicine residency training at Carolinas Medical Center in Charlotte, North Carolina.
John Jacob Meier IV, MD, MBA, CPE, FAAP, FACP is a practicing internist and pediatrician in the Raleigh, North Carolina area. He serves on the Board of Directors of the NCMS, where he also actively participates with several working groups and committees, and of WakeMed Key Community Care, a Medicare Shared Savings Program participant and Accountable Care Organization, where he also serves as Treasurer, lead of the Finance Committee and a member of the Management and Operations Committees. Dr. Meier received his undergraduate degree from Princeton University and his M.B.A. from the University of Chicago Graduate School of Business. He held a variety of increasingly senior roles in the areas of operations, manufacturing and finance with a Fortune 100 company and served as the Executive Vice President and Chief Financial Officer for Kieffer Paper Mills and Kieffer Pulp Mills before returning to medical school and receiving his M.D. from the University of Chicago Pritzker School of Medicine. Dr. Meier completed his combined Internal Medicine and Pediatric residency at the University of North Carolina at Chapel Hill and served as the Medicine Chief Resident at WakeMed Hospital.
Richard Hudspeth, MDcurrently serves as the Chief Executive Officer (since April 2016) and Chief Medical Officer (since May 2015) of Blue Ridge Community Health Services, a non-profit community health center in Hendersonville, North Carolina. From October 2006 to June 2015, Dr. Hudspeth served as Medical Director of Community Care of Western North Carolina, a regional network of health care professionals based in Asheville, North Carolina. He has also served on the Clinical Faculty of the Hendersonville Family Medicine Residency Program since June 2005. Dr. Hudspeth received a B.A. from Duke University and an M.D. from the University of North Carolina School of Medicine, completed his family medicine residency at the University of Cincinnati and completed an obstetrics fellowship at the University of Utah.
Compensation of Our Management
Currently, our executive officers are either employees of the NCMS or contracted consultants, and we do not intend to directly hire any executive officers until the Joint Venture Closing. The Net Offering Proceeds will not be used to compensate or otherwise make payments to the officers or directors of CCHN prior to the Joint Venture Closing. The unique nature of our capital and governance structure will preclude us from compensating personnel with equity securities. Therefore, when we directly hire executive officers, we may need to offer substantial cash compensation to attract qualified individuals since we cannot include equity incentive awards as part of compensation packages.
The table below includes the annual compensation for the fiscal year ended December 31, 2017 of each of our current executive officers for services rendered to CCHN. We do not currently compensate our directors for their services.
| Name | Capacities in which compensation was received | Cash Compensation ($) | Other compensation ($) | Total compensation ($) | ||||||||||
| Jeffrey W. Runge, MD | President and Chief Executive Officer | $ | 261,537 | (1) | — | $ | 261,537 | |||||||
| Vincent T. Morgus, MBA, CPA | Chief Operating Officer | $ | 243,010 | (2) | $ | 4,000 | (4) | $ | 247,010 | |||||
| Stephen W. Keene, MBA, JD, LLM | Secretary-Treasurer | $ | 111,646 | (3) | — | $ | 111,646 | |||||||
| (1) | Pursuant to the Biologue Agreement (as defined below), this amount reflects professional fees paid of $171,546 and reimbursable expenses paid of $4,442 by CCHN to Biologue, Inc., as well as accrued professional fees of $83,328 and accrued expenses of $2,221. |
| (2) | Reflects payments by the NCMS to Fahrenheit for professional fees of $68,000 and to Mr. Morgus for reimbursable project-related expenses of $10 for Mr. Morgus’s financial consulting services to CCHN from January through March 2017. Of the remainder, $150,000 reflects payments by the NCMS, which are reimbursable by CCHN, to Mr. Morgus for his services as Chief Operating Officer of CCHN from April through December 2017, as well as an accrual of a bonus payment of $25,000 due to be paid to Mr. Morgus in 2018. These payments are more fully described below and in the section entitled “Interest of Management and Others in Certain Transactions.” |
| (3) | Reflects payments by the NCMS, which are reimbursable by CCHN, to Mr. Keene for his services as Secretary-Treasurer of CCHN. |
| (4) | Reflects payments by the NCMS as matching 401(k) contributions to Mr. Morgus’s 401(k) account. The amount is subject to a vesting schedule, and as of December 31, 2017, zero percent of the amount was vested. |
CCHN has entered into a master services agreement, effective January 2, 2017, with Biologue, Inc., pursuant to which Dr. Runge provides certain executive duties necessary for CCHN to build and operate the Provider Network (the “Biologue Agreement”). The Biologue Agreement provides that Dr. Runge will provide up to 84 hours of service per calendar month, with additional hours to be provided as agreed in advance by Dr. Runge and CCHN. CCHN has agreed to compensate Dr. Runge for his time at a rate of $248 per hour and has agreed to reimburse Dr. Runge for all reasonable out of pocket expenses incurred in the provision of his services, provided that expenses in excess of $250 are subject to prior approval of CCHN. The Biologue Agreement contains customary confidentiality provisions and indemnification obligations on behalf of CCHN and Dr. Runge and will continue until either party provides 30 days’ written notice of termination.
Each of Messrs. Morgus and Keene are employees of the NCMS. As such, the NCMS is solely responsible for the payment and provision of all wages, bonuses and commissions, employee benefits, including 401(k) matching contributions, severance and worker’s compensation, and the withholding and payment of applicable taxes relating to their employment. CCHN reimburses certain expenses incurred by the NCMS on CCHN’s behalf, including (1) a proportional share of the salary, health benefits and other employment-related expenses paid by the NCMS or on behalf of the NCMS for Messrs. Morgus and Keene and (2) reasonable travel, lodging, meals and other out-of-pocket expenses incurred by Messrs. Morgus and Keene in the performance of their services to CCHN.
We do not currently compensate our directors for their services. According to our Amended and Restated Bylaws, directors may be paid their expenses, if any, of attendance at each meeting of the CCHN Board and may be paid a fixed sum for attendance at each meeting of the CCHN Board, a fixed quarterly fee or a stated salary as a director.
41
The following table displays, as of April 26, 2018, the voting securities beneficially owned by (1) any individual director or officer who beneficially owns more than 10 percent of any class of our capital stock, (2) all executive officers and directors as a group and (3) any other holder who beneficially owns more than 10 percent of any class of our capital stock:
| Title of Class | Name and Address of Beneficial Owner | Amount and Nature of Beneficial Ownership | Percent of Class | Percent of CCHN Total Voting Power | ||||||||||
| Class M Common Stock | The NCMS (1) | 1 | 100.0 | % | 50.0 | % | ||||||||
| Class P Common Stock | Gaston Family Health Services (2) | 201 | 13.4 | % | 6.7 | % | ||||||||
| Class P Common Stock | The NCCHCA (3) | 334 | 22.2 | % | 11.1 | % | ||||||||
| Class P Common Stock | Stedman-Wade Health Services, Inc. (4) | 200 | 13.3 | % | 6.6 | % | ||||||||
| Class P Common Stock | Piedmont Health Services, Inc. (5) | 200 | 13.3 | % | 6.6 | % | ||||||||
| (1) | The business address of the NCMS is 222 N. Person Street, Raleigh, NC 27601. |
| (2) | The business address of Gaston Family Health Services is 200 E. Second Avenue, Gastonia, NC 28052. |
| (3) | The business address of the NCCHCA is 4917 Waters Edge Drive, Suite 165, Raleigh, NC 27606. |
| (4) | The business address of Stedman-Wade Health Services, Inc. is 7118 Main Street, Wade, NC 28395. |
| (5) | The business address of Piedmont Health Services, Inc. is 127 Kingston Drive, Chapel Hill, NC 27514. |
There is no person, including our officers or directors (either individually or as a group), who beneficially owns 10 percent or more of any class of capital stock other than as set forth in the table above. No options, warrants or other rights to purchase our securities are held by any person.
INTEREST OF MANAGEMENT AND OTHERS IN CERTAIN TRANSACTIONS
For a description of the arrangements between CCHN and each of Biologue, Inc., with respect to Dr. Runge’s service as President and Chief Executive Officer, and the NCMS, with respect to Mr. Morgus’s service as Chief Operating Officer and Mr. Keene’s service as Secretary-Treasurer, see “Management—Compensation of Our Management.”
Between July 2016 and March 2017, Mr. Morgus provided financial consulting services to the NCMS for the benefit of CCHN while serving as Managing Partner of Fahrenheit, pursuant to an agreement between Fahrenheit and the NCMS. The NCMS, the sole owner of the Class M Common Stock of CCHN, paid an aggregate of $167,375 to Fahrenheit for professional fees plus $922 for reimbursable project-related expenses that were reimbursed to Mr. Morgus.
Pursuant to the Biologue Agreement, as of December 31, 2017, CCHN has paid professional fees and reimbursable expenses in an aggregate of $175,988 to Biologue, Inc., of which Dr. Runge is the founder and President, and has incurred an additional aggregate of $85,549 that is to be paid to Biologue, Inc.
As of December 31, 2017, CCHN has incurred $179,000 for the services provided by Mr. Morgus to CCHN since becoming its Chief Operating Officer. CCHN has incurred $253,751 for the services provided by Mr. Keene to CCHN.
42
The total number of CCHN’s authorized shares of capital stock is 40,001 shares, of which one share is Class M Common Stock, $0.01 par value per share, and 40,000 shares are Class P Common Stock, $0.01 par value per share. As of April 26, 2018, the NCMS held the sole outstanding share of Class M Common Stock and there were 1,505 outstanding shares of Class P Common Stock.
The following summary of the capital stock and our Amended and Restated Certificate of Incorporation, Amended and Restated Bylaws and Proposed Bylaws does not purport to be complete and is qualified in its entirety by reference to the provisions of applicable law and to our Amended and Restated Certificate of Incorporation and Amended and Restated Bylaws, which are filed as exhibits to the Offering Statement on Form 1-A of which this Offering Circular is a part.
Description of the Class P Common Stock
Except as provided by law or in our governing documents, holders of Class P Common Stock are entitled to a number of votes per share equal to the number of Common Stock Equivalents held by them, voting together with the holders of Class M Common Stock as a single class, on all matters submitted to a vote of the stockholders. Each holder of Class P Common Stock will be deemed to hold a number of Common Stock Equivalents equal to the number of shares of Class P Common Stock held by such holder. Investors in Provider Shares may only hold one share and will therefore be entitled to only one vote, whereas CHCs and the NCCHCA were permitted to purchase more than one share of Class P Common Stock in the Private Placement and therefore have the number of votes equal to the number of shares of Class P Common Stock held by such holders. Except as otherwise required by law, holders of Class P Common Stock are not entitled to vote on any amendment to our Amended and Restated Certificate of Incorporation that relates solely to the terms of the Class M Common Stock if the holders of such affected class are entitled to vote thereon pursuant to our Amended and Restated Certificate of Incorporation or pursuant to the General Corporation Law of the State of Delaware (the “DGCL”). Pursuant to the Stockholders’ Agreement, holders of Class P Common Stock will not be entitled to vote if they no longer meet the criteria of an Eligible Investor or if their license or approval to practice is suspended by the North Carolina Medical Board. There are no cumulative voting rights.
Holders of Class P Common Stock are entitled to receive ratably in proportion to the number of Common Stock Equivalents held by them such dividends (payable in cash, stock or otherwise), if any, as may be declared from time to time by the CCHN Board out of funds legally available for dividend payments. Holders of Class P Common Stock will be deemed to hold a number of Common Stock Equivalents equal to the number of shares of Class P Common Stock held by them. The shares of Class P Common Stock to be issued upon completion of this Offering will be fully paid and non-assessable.
The holders of Class P Common Stock have no preferences or rights of conversion, exchange, pre-emption or other subscription rights. There are no redemption or sinking fund provisions applicable to Class P Common Stock, except that, pursuant to the Stockholders’ Agreement, (1) CCHN expects to redeem all shares of Class P Common Stock at the Class P Original Purchase Price if the Joint Venture Closing does not occur, (2) Provider Shares will be subject to redemption by CCHN in the event that the holder ceases to qualify as an Eligible Investor or in the event of the holder’s death, in each case for an amount equal to the fair market value of a share of Class P Common Stock based on the most recent valuation of CCHN, which valuations are to occur at least annually, as determined by the CCHN Board, (3) shares of Class P Common Stock purchased in the Private Placement will be subject to redemption by CCHN in the event that the holders thereof cease to satisfy the applicable eligibility criteria, for an amount equal to the fair market value of a share of Class P Common Stock based on the most recent valuation of CCHN, which valuations are to occur at least annually, as determined by the CCHN Board, and (4) in the event that Centene Sub exercises its Drag-Along Right causing CCHN to sell its partnership units of the Joint Venture Company, CCHN will redeem each outstanding share of Class P Common Stock for a per share amount equal to the aggregate drag-along premium paid by Centene Sub to CCHN divided by the number of shares of Class P Common Stock then outstanding.
Holders of Class P Common Stock may not transfer, assign, pledge or otherwise dispose of or encumber shares of Class P Common Stock (or any interest therein). In the event of any voluntary or involuntary liquidation, dissolution or winding-up of our affairs, holders of Class P Common Stock will be entitled to share ratably in our assets in proportion to the number of Common Stock Equivalents held by them that are remaining after payment or provision for payment of all of our debts and obligations.
43
Description of the Class M Common Stock
Except as provided by law or in our governing documents, holders of Class M Common Stock are entitled to a number of votes per share equal to the number of Common Stock Equivalents held by them, voting together with the holders of Class P Common Stock as a single class, on all matters submitted to a vote of the stockholders. Each holder of Class M Common Stock will be deemed to hold a number of Common Stock Equivalents equal to the number of shares of Class M Stock held by such holder multiplied by a fraction (1) the numerator of which is the aggregate number of shares of Class P Common Stock then outstanding (less, solely for the purposes of calculating Common Stock Equivalents for purposes of voting rights, the number of shares of Class P Common Stock that are then suspended from voting pursuant to any agreement between CCHN and the holders of Class P Common Stock) and (2) the denominator of which is the aggregate number of shares of Class M Common Stock then outstanding. Except as otherwise required by law, holders of Class M Common Stock are not entitled to vote on any amendment to our Amended and Restated Certificate of Incorporation that relates solely to the terms of the Class P Common Stock if the holders of such affected class are entitled to vote thereon pursuant to our Amended and Restated Certificate of Incorporation or pursuant to the DGCL. There are no cumulative voting rights.
Holders of Class M Common Stock are entitled to receive ratably in proportion to the number of Common Stock Equivalents held by them such dividends (payable in cash, stock or otherwise), if any, as may be declared from time to time by the CCHN Board out of funds legally available for dividend payments, provided that no dividends shall be paid on the Class M Common Stock unless the same dividend shall be concurrently declared and paid on CCHN’s Class P Common Stock. All outstanding shares of Class M Common Stock are fully paid and non-assessable.
The holders of Class M Common Stock have no preferences or rights of conversion, exchange, pre-emption or other subscription rights, and there are no redemption or sinking fund provisions applicable to Class M Common Stock. There are no restrictions on the transferability of Class M Common Stock subject to applicable securities laws. In the event of any voluntary or involuntary liquidation, dissolution or winding-up of our affairs, holders of Class M Common Stock will be entitled to share ratably in our assets in proportion to the number of Common Stock Equivalents held by them that are remaining after payment or provision for payment of all of our debts and obligations.
Limitation of Liability and Indemnification of Officers and Directors
OurAmended and Restated Certificate of Incorporationpermits us to provide indemnification ofdirectors and officers to the fullest extent permitted by law. Our Amended and Restated Bylaws provide that we must indemnify our directors and officers to the fullest extent permitted by Delaware law and that we may advance expenses to our directors and officers in connection with a legal proceeding.
44
The Provider Shares are being offered for purchase exclusively through our website, www.cch-network.com, and on the online investment platform of Folio Investments, Inc., a registered broker-dealer. The Provider Shares will be issued in book-entry electronic form only. CCHN does not intend to use commissioned sales agents or underwriters to help offer and sell the Provider Shares in this Offering. The Provider Shares will be offered only by us and by persons associated with us in reliance upon the exemption from registration contained in Rule 3a4-1 of the Securities Exchange Act of 1934, as amended (the “Exchange Act”). We intend to sell the Provider Shares through in-person meetings with providers, general advertising, electronic media and posting our Offering Circular and other materials on our website, www.cch-network.com, and on an online investment platform.
The Offering will terminate at the earliest of (1) the date at which the total offering amount has been sold, (2) March 12, 2021, the date that is three years after this Offering was qualified by the Commission or (3) the date at which the Offering is earlier terminated by CCHN in our sole discretion. We may undertake one or more closings on a rolling basis. After each closing, funds tendered by Eligible Investors will be available to us. After the initial closing of this Offering, we expect to hold closings on at least a quarterly basis.
CCHN is offering the Provider Shares only in North Carolina, Georgia, South Carolina, Tennessee and Virginia.
If you decide to purchase a Provider Share, the funds provided by you will be deposited by you into an account with Folio where they will stay until your subscription has been accepted or rejected by us on a closing date of the Offering. If we accept your subscription, the funds in your account will be delivered to us. If we do not accept your subscription, no funds will be provided to us, and the funds will stay in your account. We will be conducting this Offering on a continuous basis with no minimum offering amount, and there are no arrangements to return funds to you if a certain number of securities are not sold.
Technology & Closing Services
Folio will provide certain technology, brokerage, custody and closing services in connection with this Offering. We have agreed to pay Folio processing fees equal to 1.4 percent of the gross proceeds from the sale of the securities being offered, with a minimum non-refundable fee of $25,000 (“Folio Closing Fees”). We have also agreed to pay Folio platform fees in the amount of 0.6 percent of the gross proceeds from the sale of the securities being offered (“Folio Platform Fees”) and up to $10,000 for a third party due diligence report that was provided to Folio prior to the commencement of the Offering. Eligible Investors must pay in full for the Provider Share for which they subscribe prior to the closing in which they participate. Eligible Investors may subscribe for a Provider Share in this Offering by following the account opening instructions on the platform operated by Folio. Funds from subscriptions will be held by Folio in customer accounts for the exclusive benefit of its customers until such time as all conditions to each closing are met. Eligible Investors who meet the requirements and abide by the investment limitations described in this Offering Circular may subscribe for a Provider Share. All Eligible Investor funds will be held in accounts at Folio. When a closing occurs, Eligible Investor funds will be transferred from the Eligible Investors’ Folio accounts to the account of CCHN at Folio. This process complies with the requirements of Rule 15c2-4 of the Exchange Act pursuant to a no-action letter dated July 15, 2015 provided to Folio by the Commission.
Funds provided for the purchase of a Provider Share may not be withdrawn by Eligible Investors after they have been accepted by us on a closing date of the Offering.
Pricing Considerations
There is not an established public market for the Provider Shares. We determined the offering price of our common stock in this Offering based on current market conditions as well as other considerations, including the terms of the Joint Venture Agreement.
45
Investment Limitations
Generally, no sale may be made to you in this Offering if the aggregate purchase price you pay is more than 10 percent of the greater of your annual income or net worth. Different rules apply to accredited investors. Before making any representation that your investment does not exceed applicable thresholds, we encourage you to review Rule 251(d)(2)(i)(C) of Regulation A. For general information on investing, we encourage you to refer towww.investor.gov.
As a Tier 2, Regulation A offering, Eligible Investors must comply with the 10 percent limitation to investment in the Offering. The only Eligible Investors in this Offering exempt from this limitation are “Accredited Investors” as defined under Rule 501 of Regulation D. If you meet one of the following tests you should qualify as an Accredited Investor:
| ● | You are a natural person who has had individual income in excess of $200,000 in each of the two most recent years, or joint income with your spouse in excess of $300,000 in each of these years, and have a reasonable expectation of reaching the same income level in the current year; |
| ● | You are a natural person and your individual net worth, or joint net worth with your spouse, exceeds $1,000,000 at the time you purchase your Provider Share (where for purposes of calculating such net worth (1) your primary residence shall not be included as an asset, (2) indebtedness secured by your primary residence, up to the estimated fair market value of such residence at the time of the sale of the Provider Share, shall not be included as a liability (except that if the amount of such indebtedness outstanding at the time of the sale of the Provider Share exceeds the amount outstanding 60 days before such time, other than as a result of the acquisition of the primary residence, the amount of such excess shall be included as a liability); and (3) indebtedness that is secured by your primary residence in excess of the estimated fair market value of such residence at the time of the sale of the Provider Share shall be included as a liability); or |
| ● | You are an executive officer or director of CCHN. |
Procedures for Subscribing
Prior to purchasing a Provider Share, you should review this entire Offering Circular and any appendices, exhibits and supplements accompanying this Offering Circular. You will also need to either execute a Participating Provider Agreement or be a Contracted Provider under a Participating Provider Agreement (as defined therein) in order to participate in the Provider Network and invest in a Provider Share. Please contact CCHN by telephone at 919-719-4161 or by e-mail to investorrelations@cch-network.com to obtain a copy of the Participating Provider Agreement.
If you decide to subscribe for a Provider Share in this Offering, please go to cch-network.com, click on “Invest in CCHN” and follow the procedures as described.
| 1. | Set up a brokerage account on the platform operated by Folio; |
| 2. | Electronically receive, review, execute and deliver to us a Subscription Agreement and Stockholders’ Agreement; and |
| 3. | Deliver funds to your Folio account in the amount of the subscription price of $750.00. |
To invest in this Offering through the Folio platform, an Eligible Investor must have a brokerage account with Folio. When submitting the subscription request, an Eligible Investor is required to agree to various terms and conditions by checking boxes and to review and electronically sign certain necessary documents.
46
Right to Reject Subscriptions. After you have agreed to the Subscription Agreement and placed the funds required under the Subscription Agreement in the specified account, we have the right to review and accept (on a closing date of the Offering) or reject (at any time) your subscription in whole or in part, for any reason or for no reason. No funds will be provided to us from your account from rejected subscriptions.
Acceptance of Subscriptions. Upon processing our acceptance of your subscription on a closing date of the Offering, we will issue the Provider Share for which you subscribed. Once we have accepted your subscription on a closing date of the Offering, you may not revoke or change your subscription or request your subscription funds.
The validity of the Provider Shares offered hereby has been passed upon for us by Smith, Anderson, Blount, Dorsett, Mitchell & Jernigan, L.L.P.
The balance sheets of Carolina Complete Health Network, Inc. as of December 31, 2017 and December 31, 2016, and the related statements of operations, changes in stockholder’s deficit and cash flows for the year ended December 31, 2017 and the period from May 19, 2016 through December 31, 2016, and the related notes to the financial statements have been included herein in reliance on the report of Cherry Bekaert LLP, an independent public accounting firm, appearing elsewhere herein, and given upon its authority as experts in accounting and auditing.
WHERE YOU CAN FIND ADDITIONAL INFORMATION
We have filed the Offering Statement with the Commission with respect to the Provider Shares. This Offering Circular, which constitutes a part of the Offering Statement, does not contain all of the information set forth in the Offering Statement or the exhibits and schedules filed therewith. For further information about us and the Provider Shares, we refer you to the Offering Statement and the exhibits and schedules filed therewith. Statements contained in this Offering Circular regarding the contents of any contract or other document that is filed as an exhibit to the Offering Statement are not necessarily complete, and each such statement is qualified in all respects by reference to the full text of such contract or other document filed as an exhibit to the Offering Statement. We make available, free of charge, access on our website at www.cch-network.com to all information we file with the Commission, including our Offering Statement (as may be amended or supplemented from time to time) and our periodic reports, as soon as reasonably practicable after we electronically file such material with the Commission. The information we file with the Commission may also be obtained on the Commission’s website at www.sec.gov.
All communications or inquiries regarding CCHN or the Offering should be directed to Vincent T. Morgus by telephone at 919-719-4161 x102 or by e-mail to investorrelations@cch-network.com.
47
F-1
The Board of Directors and Stockholders of
Carolina Complete Health Network, Inc.
We have audited the accompanying financial statements of Carolina Complete Health Network, Inc. (the “Company”), which comprise the balance sheets as of December 31, 2017, and 2016, and the related statements of operations, changes in stockholder’s deficit and cash flows for the year ended December 31, 2017 and the period from May 19, 2016 through December 31, 2016, and the related notes to the financial statements.
Management’s Responsibility for the Financial Statements
Management is responsible for the preparation and fair presentation of these financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation, and maintenance of internal controls relevant to the preparation and fair presentation of financial statements that are free from material misstatement, whether due to fraud or error.
Auditors’ Responsibility
Our responsibility is to express an opinion on these financial statements based on our audits. We conducted our audits in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free from material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the financial statements. The procedures selected depend on the auditor's judgment, including the assessment of the risks of material misstatement of the financial statements, whether due to fraud or error. In making those risk assessments, the auditor considers internal controls relevant to the entity's preparation and fair presentation of the financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity's internal controls. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall presentation of the financial statements.
We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion.
Opinion
In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of Carolina Complete Health Network, Inc. as of December 31, 2017 and 2016, and the results of its operations and its cash flows for the year ended December 31, 2017 and the period from May 19, 2016 through December 31, 2016, in accordance with accounting principles generally accepted in the United States of America.
Emphasis of Matter
The accompanying financial statements have been prepared assuming that the Company will continue as a going concern. For the year ended December 31, 2017, the Company recognized a net loss of $1,353,010, and as of December 31, 2017, the Company had incurred an accumulated deficit of $2,120,592. Management’s plans regarding those matters are described in Note 1.
/s/ CHERRY BEKAERT LLP
Raleigh, North Carolina
April 26, 2018
F-2
Carolina Complete Health Network, Inc.
December 31, 2017 and 2016
| 2017 | 2016 | |||||||
| Assets: | ||||||||
| Current assets: | ||||||||
| Cash and cash equivalents | $ | 1,009,613 | $ | 1 | ||||
| Accounts receivable | 52,016 | - | ||||||
| Prepaid expenses and other | 8,545 | - | ||||||
| Total current assets | 1,070,174 | 1 | ||||||
| Total assets | $ | 1,070,174 | $ | 1 | ||||
| Liabilities and Stockholder’s deficit: | ||||||||
| Liabilities: | ||||||||
| Current liabilities: | ||||||||
| Accounts payable | $ | 278,481 | $ | 97,880 | ||||
| Accrued expenses and other | 37,570 | - | ||||||
| Advances from investors | 979,250 | - | ||||||
| Due to stockholder | - | 29,929 | ||||||
| Total current liabilities | 1,295,301 | 127,809 | ||||||
| Non-current liabilities: | ||||||||
| Term note | 1,412,277 | 171,632 | ||||||
| Due to stockholder | 906,822 | 465,327 | ||||||
| Accrued interest | 39,068 | 2,814 | ||||||
| Total non-current liabilities | 2,358,167 | 639,773 | ||||||
| Stockholder's deficit: | ||||||||
| Common stock - Class M, $0.01 par value; 1 share authorized; 1 share issued and outstanding | 1 | 1 | ||||||
| Stock subscription costs in advance of offering | (462,703 | ) | - | |||||
| Accumulated deficit | (2,120,592 | ) | (767,582 | ) | ||||
| Total stockholder's deficit | (2,583,294 | ) | (767,581 | ) | ||||
| Total liabilities and stockholder's deficit | $ | 1,070,174 | $ | 1 | ||||
The accompanying notes to the financial statements are an integral part of this statement.
F-3
Carolina Complete Health Network, Inc.
for the Year ended December 31, 2017 and for the Period from May 19, 2016 through December 31, 2016
| 2017 | 2016 | |||||||
| Revenue | ||||||||
| Reimbursable expenses | $ | 300,000 | $ | - | ||||
| Total revenue | 300,000 | - | ||||||
| Operating costs and expenses | ||||||||
| Quality and development | 385,339 | - | ||||||
| General and administrative | 1,232,348 | 764,768 | ||||||
| Total operating costs and expenses | 1,617,687 | 764,768 | ||||||
| Loss from operations | (1,317,687 | ) | (764,768 | ) | ||||
| Other income (expense) | ||||||||
| Interest, net | (35,323 | ) | (2,814 | ) | ||||
| Total other income (expense) | (35,323 | ) | (2,814 | ) | ||||
| Net loss | $ | (1,353,010 | ) | $ | (767,582 | ) | ||
| Weighted average common stock shares outstanding | ||||||||
| Basic and diluted | 1 | 1 | ||||||
| Net loss per common stock share basic and diluted | $ | (1,353,010 | ) | $ | (767,582 | ) | ||
The accompanying notes to the financial statements are an integral part of this statement.
F-4
Carolina Complete Health Network, Inc.
Statements of Changes in Stockholder’s Deficit
for the Year ended December 31, 2017 and for the Period from May 19, 2016 through December 31, 2016
| Common Stock | Stock subscription costs in advance of | Accumulated | Total Stockholder's | |||||||||||||||||
| Shares | Par Value | offering | deficit | Deficit | ||||||||||||||||
| Issuance of Common Stock - | ||||||||||||||||||||
| Class M at inception date of May 19, 2016 | 1 | $ | 1 | $ | - | $ | - | $ | 1 | |||||||||||
| Net loss | (767,582 | ) | (767,582 | ) | ||||||||||||||||
| Balances at December 31, 2016 | 1 | 1 | - | (767,582 | ) | (767,581 | ) | |||||||||||||
| Stock subscription costs in advance of offering | (462,703 | ) | (462,703 | ) | ||||||||||||||||
| Net loss | (1,353,010 | ) | (1,353,010 | ) | ||||||||||||||||
| Balances at December 31, 2017 | 1 | $ | 1 | $ | (462,703 | ) | $ | (2,120,592 | ) | $ | (2,583,294 | ) | ||||||||
The accompanying notes to the financial statements are an integral part of this statement.
F-5
Carolina Complete Health Network, Inc.
for the Year ended December 31, 2017 and for the Period from May 19, 2016 through December 31, 2016
| 2017 | 2016 | |||||||
| Cash flows from operating activities | ||||||||
| Net loss | $ | (1,353,010 | ) | $ | (767,582 | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities | ||||||||
| Change in operating assets and liabilities: | ||||||||
| Accounts receivable | (52,016 | ) | - | |||||
| Prepaid expenses and other current assets | (8,545 | ) | - | |||||
| Accounts payable | 180,601 | 97,880 | ||||||
| Accrued expenses and other | 37,570 | - | ||||||
| Accrued interest | 36,254 | 2,814 | ||||||
| Due to stockholder, current | (29,929 | ) | 29,929 | |||||
| Due to stockholder, non-current | 441,495 | 465,327 | ||||||
| Cash flows used in operating activities | (747,580 | ) | (171,632 | ) | ||||
| Cash flows from financing activities | ||||||||
| Borrowings on term note | 1,240,645 | 171,632 | ||||||
| Proceeds from issuance of Class M common stock | - | 1 | ||||||
| Advances from investors | 979,250 | - | ||||||
| Stock subscription costs in advance of offering | (462,703 | ) | - | |||||
| Cash flows provided by financing activities | 1,757,192 | 171,633 | ||||||
| Net increase in cash and cash equivalents | 1,009,612 | 1 | ||||||
| Cash and cash equivalents, beginning of period | 1 | - | ||||||
| Cash and cash equivalents, end of period | $ | 1,009,613 | $ | 1 | ||||
The accompanying notes to the financial statements are an integral part of this statement.
F-6
Note 1 – Description of Operations and Summary of Significant Accounting Policies
Operations– Carolina Complete Health Network, Inc.,(the “Company”), a Delaware corporation, was incorporated on May 19, 2016 as a wholly-owned subsidiary of the North Carolina Medical Society(the “NCMS”) in contemplation of the joint venture between the Company and a strategic partner. The joint venture is to be formed to facilitate the creation and successful operation of a patient-focused Medicaid health plan in North Carolina in response to pending Medicaid reform in North Carolina.
The Company will participate in the joint venture principally by building and operating a network of health care providers who will provide medical services under the health plan. During the interim period until the joint venture closes, the Company will conduct its activities by outsourcing its needed functions to NCMS professionals and staff, independent contractors, professional consultancy firms, third-party vendors or other such entities that can provide the capabilities required to recruit and retain providers to participate in the network of health care providers.
Once the joint venture closes, the Company’s fundamental business will be to continue recruiting, building, developing, managing, educating, operating, and maintaining the provider network for the purposes of providing services to the health plan.
The joint venture closing is currently expected to occur after September 1, 2018, and the health plan is currently expected to “go live” around July 2019.
Until the commencement of the health plan’s operations, the Company does not expect to generate any revenue from operations.
The Company’s headquarters are in Raleigh, North Carolina.
Liquidity and Uncertainty– The Company continues to be subject to the risks and challenges associated with other companies at a similar formative stage, including dependence on key outside consultants, successful development and marketing of its network and related services, successful collaborations with partners, and the ability to secure adequate financing to support future growth. As shown in the accompanying financial statements, the Company has incurred net losses and has an accumulated deficit of $2,120,592 and $767,582 at December 31, 2017 and 2016, respectively.
Since its inception on May 19, 2016, the Company’s sole stockholder, the NCMS, has provided to the Company its’ professional and administrative staffs to establish, conduct, and perform the Company’s activities. The cost of the NCMS staff time incurred to support the Company has been calculated, and the staff time cost has been used as a basis for allocating the related expenses associated with the NCMS staff’s support(see Note 4).
Going forward, the Company will continue to draw upon the NCMS professional and administrative staffs in the performance of the Company’s activities, and as such, the Company will incur additional costs associated with the staffs’ performance of these activities. Consistent with such costs incurred through December 31, 2017 and 2016, these additional costs will be settled no earlier than the health plan’s “go-live” date.
Also, a strategic partner has funded the Company with a multiple advance term loan in an amount up to $2.5 million, secured by all of the Company’s receivables, if any, and equity interest in the joint venture. Borrowings under the term loan bear an interest rate of 6.75 percent. In addition, the term loan requires the Company to remit a substantial percentage of its excess cash flow in repayment of amounts drawn and accrued interest. The loan amount may be increased in three increments of $500,000 up to an amount of $4.0 million if certain milestones are attained(see Note 3).
Once the health plan has been awarded and accepted a contract with the State of North Carolina, the strategic partner has agreed to provide an additional multiple advance term loan in an amount up to $3.0 million, which may be increased up to an amount of $4.0 million if, in consultation with the strategic partner and in its sole discretion, the Company has demonstrated good progress toward the establishment of the provider network. However, the aggregate amount available under the additional multiple advance term loan will be reduced by an amount equal to 55 percent of the net offering proceeds from the Company’s Regulation A offering of Class P Common Stock and the Company’s private placement of Class P Common Stock, less the amount of such proceeds applied by the Company to capital calls for the health plan company or to repay principal on borrowed funds. In addition, the proceeds of the additional multiple advance term loan may be used to repay amounts borrowed from the strategic partner to fund a portion of the Company’s initial capital contribution to the joint venture company at the joint venture closing.(see Notes 3 and 10).
F-7
The proceeds of the multiple advance term loan have been, will be, and may be, used for (i) personnel, consultants, third party service providers and other out-of-pocket operational, pre-operational and business development expenses related to (a) conducting and administering financings, (b) developing and retaining necessary operational capabilities, (c) ensuring regulatory compliance, (d) recruiting providers for the provider network and (e) compensating independent accountants and (ii) legal expenses related to any financing and the development and review of provider agreements for the proposed health plan.
Based upon the Company’s current operating plan, it believes with the i) continued deferral of payment for costs incurred for services provided to it by the NCMS, ii) up to $4.0 million currently available under the multiple advance term loan, iii) aggregate amount available under the additional multiple advance term loan and iv) retention of an amount available from the net offering proceeds, the Company will be able to sufficiently manage its activities and cash flow needs until September 2019(see Note 3). If the Company is unable to obtain a significant amount of capital on acceptable terms to finance its operations, the growth of the Company may be materially and adversely affected.
Basis of Accounting – The Company’s financial statements have been prepared using the accrual method of accounting.
Use of Estimates – The preparation of financial statements, in conformity with generally accepted accounting principles in the United States of America (U.S. GAAP), requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosures at the date of the financial statements and during the reporting period. The amounts ultimately realized from the assets or ultimately recognized as liabilities will depend on, among other factors, general business conditions, and could differ materially in the near-term from the carrying amounts reflected in the financial statements.
Reclassifications – Certain prior period amounts have been reclassified to conform to current classifications.
Cash and Cash Equivalents –The Company considers all highly liquid investments with an original maturity of three months or less at the date of purchase to be cash equivalents. The Company places its temporary cash investments with high credit quality financial institutions. At December 31, 2017, there were cash deposits of $759,613 in excess of amounts insured by the Federal Deposit Insurance Corporation.
At December 31, 2017, the Company was holding $979,250 of funds received in advance from investors for the purchase of Class P Common Stock in the Company’s private placement of Class P Common Stock that occurred on January 19, 2018(see Note 10).
Accounts Receivable- Accounts receivable is stated at the amount the Company expects to collect. Based on experience, management believes the amounts recorded are fully collectible. Therefore, no allowance for doubtful accounts has been recorded. In the event that an outstanding balance could not be collected, it would be written down with a charge against bad debt loss and a credit to the receivables balance. Past due status is determined based on contractual terms.
Income Taxes – The Company follows the asset and liability method of accounting for income taxes. This method requires recognition of deferred tax assets and liabilities for the expected future tax consequences of temporary differences between the carrying amounts and the tax basis of assets and liabilities. If it is more likely than not that some portion of a deferred tax asset will not be realized, a valuation allowance is recorded.
The Company recognizes the tax benefit or liability from uncertain tax positions only if it is more likely than not that the tax position will be sustained on examination by the tax authorities, based on the technical merits of the position. The tax benefit or liability is measured based on the largest benefit or liability that has a greater than 50 percent likelihood of being realized upon ultimate settlement. The Company recognizes interest and penalties related to income tax matters in income tax expense if incurred(see Note 6).
Reimbursable Expenses Revenue – Beginning in January 2017, the strategic partner agreed to reimburse the Company annually up to $300,000 for certain launch, start-up and operational expenses incurred during fiscal years 2017 and 2018.
F-8
Quality and Development Expenses – These expenses represent the costs incurred to recruit and retain a network of health care providers who will provide medical services under the health plan.
Subsequent Events – Subsequent events are events or transactions that occur after the balance sheet date but before the financial statements are issued. The Company recognizes in the financial statements the effects of all subsequent events that provide additional evidence about conditions that existed at the date of the balance sheet, including the estimates inherent in the process of preparing the financial statements. The Company’s financial statements do not recognize subsequent events that provide evidence about conditions that did not exist at the date of the balance sheet but arose after the balance sheet date and before financial statements are available to be issued. The Company has evaluated subsequent events through April 26, 2018, which is the date the financial statements were available to be issued(see Note 10).
Net Loss Attributable to Stockholder and Net Loss Per Common Stock Shares– Net earnings or loss per share is computed by dividing net income or loss by the weighted-average number of common shares outstanding during the period, excluding shares subject to redemption or forfeiture. The Company presents basic and diluted net earnings or loss per share. Basic and diluted net earnings or loss per share reflect the actual weighted average of common shares issued and outstanding during the period. There were no potentially dilutive securities as of December 31, 2017 and 2016.
Note 2 – Concentration with Vendors
At December 31, 2017, five vendors accounted for approximately 79 percent of the Company’s accounts payable. At December 31, 2016, two vendors accounted for 100 percent of the Company’s accounts payable.
Note 3 – Term Note
On May 20, 2016, the Company entered into a Loan and Security Agreement(the “Loan”) with its strategic partner. The strategic partner agreed to provide a multiple advance term loan in an amount up to $2.5 million, provided however, that upon the achievement of milestones, the amount of such Loan may be increased to an amount up to $4.0 million(the “First Loan”). The aggregate unpaid principal amount of all advances outstanding from time to time under the Loan bears interest at 6.75 percent per annum. Interest is due and payable quarterly in arrears, commencing on the first day of the fiscal quarter immediately following one of four Loan commitment termination dates available to the strategic partner, which dates are primarily tied to the State of North Carolina’s Medicaid proposal process, and then the first day of each succeeding fiscal quarter. Unless satisfied earlier, the Loan’s principal amount, all accrued interest and all other amounts due under the Loan agreement are due and payable on the tenth anniversary of the first interest payment date. The Loan is secured by all of the Company’s now owned or hereafter acquired receivables and equity of the joint venture companies.
On January 10, 2017, the parties agreed to an Amended and Restated Loan and Security Agreement(the “Amended Loan”). The Amended Loan provided for certain amendments and modifications to the Loan in order to provide for an additional multiple advance term loan in the amount of $3.0 million provided, however, that upon satisfaction of certain conditions in the sole discretion of the strategic partner, the amount may be increased to $4.0 million(the “Second Loan”).
On August 25, 2017, the parties agreed to a Second Amended and Restated Loan and Security Agreement(the “Second Amended Loan”). Under the Second Amended Loan, the aggregate amount available under the Second Loan will be reduced by an amount equal to 55 percent of the net offering proceeds from the Company’s Regulation A offering of Class P Common Stock and the Company’s private placement of Class P Common Stock(see Note 10), less the amount of such proceeds applied by the Company to capital calls for the health plan company or to repay principal owed by the Company under its Term Note. In addition, the proceeds of the Second Loan may be used to repay amounts borrowed from the strategic partner to fund a portion of the Company’s initial capital contribution to the joint venture company at the joint venture closing.
The principal balance outstanding on the First Loan was $1,412,277 and $171,632 at December 31 2017 and 2016, respectively. Accrued interest was $39,068 and $2,814 at December 31, 2017 and 2016, respectively, and interest expense for the year ended December 31, 2017 was $36,254 and $2,814 for the period May 19, 2016 through December 31, 2016.
F-9
Note 4 – Due to Stockholder
Since the Company’s inception on May 19, 2016, it has relied upon its sole stockholder, the NCMS, to provide it with both working capital and transaction-related cash advances, as needed, as well as the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct, and perform the Company’s activities.
Working capital is advanced by the NCMS to the Company, which becomes due and payable as funds become available and are borrowed under the First Loan. As funding is received under the First Loan, the outstanding working capital advance is settled. The working capital advance is recorded as a current liability, “Due to Stockholder”. The current liability, Due to Stockholder was zero and $29,929 at December 31, 2017 and 2016, respectively.
As part of the joint venture discussions and transaction, the Company incurred transaction-related outside advisor expenses that were ineligible for reimbursement under the Loan. When these expenses became due and payable to the outside advisors, the NCMS settled the transaction-related amounts due on behalf of the Company. The settlement of these transaction-related advances by the NCMS on behalf of the Company have been recorded as a non-current liability, “Due to Stockholder”, and at December 31, 2017 and 2016, the Company has recorded $162,221 of such advances in the non-current liability, Due to Stockholder.
Also, since its inception, the Company has not had an employee. As such, the Company has relied upon the resources and related expenses of the NCMS’s professional and administrative staffs to establish, conduct, and perform the Company’s activities. The cost of the NCMS staff time incurred to support the Company has been calculated, and the staff time cost has been used as a basis for allocating the related expenses associated with the NCMS staff’s support. In 2017, the Company has recorded $441,495 as the cost of the NCMS staff time incurred and related expenses, and for the period May 19, 2016 through December 31, 2016, the Company has recorded $303,106 as the cost of the NCMS staff time incurred and related expenses. These amounts have been recorded as a “General and Administrative” expense.
The non-current liability, Due to Stockholder was $906,822 and $465,327 at December 31, 2017 and 2016, respectively.
The non-current liability, Due to Stockholder amount will be settled no earlier than the “go-live” date of the health plan, which is currently projected in July 2019.
Note 5 – Common Stock and Stockholder’s Deficit
Common Stock– On August 25, 2017, the Company filed an Amended and Restated Certificate of Incorporation(the “Certificate”)with the Delaware Secretary of State in which the number of shares of all classes of stock the Company has the authority to issue is 40,001 shares, consisting of one share of Class M Common Stock, $0.01 par value per share, and 40,000 shares of Class P Common Stock, $0.01 par value per share. In addition, the Certificate effected a 100-to-1 reverse stock split with respect to all then outstanding shares of Class M Common Stock, resulting in one share of Class M Common Stock remaining issued and outstanding after the filing of the Certificate. The Company’s financial statements have been adjusted to reflect this reverse stock split.
The rights and privileges of holders of the Company’s Class M Common Stock and Class P Common Stock are apportioned based upon the number of “Common Stock Equivalents” held as follows: each holder of shares of Class P Common Stock shall be deemed to hold a number of Common Stock Equivalents equal to the number of shares of Class P Common Stock then held by such holder. Each holder of shares of Class M Common Stock shall be deemed to hold a number of Common Stock Equivalents equal to the number of shares of Class M Common Stock then held by such holder, multiplied by a fraction (i) the numerator of which is the aggregate number of shares of Class P Common Stock then outstanding (less, solely for the purposes of calculating Common Stock Equivalents pursuant to voting rights, the number of shares of Class P Common Stock that are then suspended from voting pursuant to any stockholders’ agreement entered into between the Company and the holders of Class P Common Stock), and (ii) the denominator of which is the aggregate number of shares of Class M Common Stock then outstanding. Accordingly, at all times, the holder or holders of Class M Common Stock will retain 50 percent of the aggregate voting power of the Company’s common stock and will have an interest in the Company equal to the aggregate of all holders of Class P Common Stock.
Except as otherwise required by law, holders of Class M Common Stock are not entitled to vote on any amendment to the Certificate that relates solely to the terms of the Class P Common Stock if the holders of such affected class are entitled to vote thereon pursuant to the Certificate or pursuant to the Delaware General Corporation Law. There are no cumulative voting rights.
F-10
The holders of Class M Common Stock have no preferences or rights of conversion, exchange, pre-emption or other subscription rights, and there are no redemption or sinking fund provisions applicable to Class M Common Stock.
There are no restrictions on the transferability of Class M Common Stock subject to applicable securities laws.
In the event of any voluntary or involuntary liquidation, dissolution or winding-up of the Company, holders of Class M Common Stock will be entitled to share ratably in the Company’s assets in proportion to the number of Common Stock Equivalents held by them that are remaining after payment or provision for payment of all of the Company’s debts and obligations.
Holders of Class P Common Stock will have one vote per share. On all matters submitted to the Company’s stockholders, except with respect to certain amendments to the Company’s Certificate that relate solely to the terms of Class M Common Stock or as otherwise required by applicable law, holders of Class P Common Stock will vote together as one class with the holder of Class M Common Stock.
In the event of any voluntary or involuntary liquidation, dissolution or winding-up of the Company, holders of Class P Common Stock will be entitled to share ratably in Company’s assets in proportion to the number of Common Stock Equivalents deemed to be held by them that are remaining after payment or provision for payment of all of the Company’s debts and obligations.
Class P Common Stock (or any interest therein) may not be transferred, assigned, pledged or otherwise disposed of or encumbered.
Class P Common Stock will be subject to redemption by the Company in the event that the holder no longer qualifies as an eligible investor(see Note 10) or in the event of the holder’s death, in each case for an amount equal to the fair market value of a share of Class P Common Stock based on the most recent valuation of the Company, which valuations are to occur at least annually, as determined by the Company’s Board of Directors. Class P Common Stock will be redeemed in the event that Company becomes obligated to sell all of its partnership units in the joint venture company.
No dividends shall be paid on Company’s Class M Common Stock unless dividends are concurrently declared and paid on the Class P Common Stock on an equal basis according to the number of Common Stock Equivalents deemed to be held; all dividends will be as and if declared by Company’s Board of Directors. There have been no dividends declared to date.
Note 6 – Income Taxes
Deferred taxes are recognized for temporary differences between the basis of assets and liabilities for financial statement and income tax purposes. The differences relate primarily to the treatment of organizational costs, start-up costs, and accrued expenses.
Significant components of the Company’s deferred tax assets and liabilities are as follows:
| 2017 | 2016 | |||||||
| Organizational and Start-up Costs | $ | 407,642 | $ | 223,181 | ||||
| Accrued Expenses | 8,204 | 957 | ||||||
| Valuation Allowance | (414,052 | ) | (224,138 | ) | ||||
| Deferred Tax Assets | $ | 1,794 | $ | - | ||||
| Prepaid Expenses | $ | (1,794 | ) | $ | - | |||
| Deferred Tax Liabilities | $ | (1,794 | ) | $ | - | |||
| Net Deferred Tax Assets | $ | - | $ | - | ||||
F-11
The Company recognizes deferred tax assets to the extent that it believes that these assets are more likely than not to be realized. In making such a determination, the Company considers all available positive and negative evidence, including future reversals of existing taxable temporary differences, projected future taxable income, tax-planning strategies, and results of recent operations. The Company assessed the need for a valuation allowance against its net deferred tax assets and determined a full valuation allowance is required as of December 31, 2017 and 2016 due to uncertainty regarding future revenue generating activities. Therefore, a full valuation allowance of $414,052 and $224,138 was recorded for the year ended December 31, 2017 and the period May 19, 2016 through December 31, 2016, respectively.
On December 22, 2017, the United States enacted the Tax Cuts and Jobs Act(the “2017 Tax Act”). The 2017 Tax Act, among other changes, lowers the general corporate income tax rate to 21% for tax years beginning after December 31, 2017. The Company has calculated its best estimate of the impact of the 2017 Tax Act in its income tax provision during the year ended December 31, 2017, in accordance with its understanding of the 2017 Tax Act and guidance available as of the date of this filing. The provisional amount related to the remeasurement of certain deferred tax assets and liabilities is based on the tax rates at which they are expected to reverse in the future.
The Company’s effective federal tax rate for the year ended December 31, 2017 and the period May 19, 2016 through December 31, 2016 differs from the statutory rate of 34% as follows:
| 2017 | 2016 | |||||||
| Expected Tax | $ | (460,023 | ) | $ | (260,978 | ) | ||
| Permanent Differences | 13,791 | 36,840 | ||||||
| Legislative Rate Change | 256,318 | - | ||||||
| Change in Valuation Allowance | 189,914 | 224,138 | ||||||
| Total | $ | - | $ | - | ||||
The Company does not have any uncertain tax positions. The Company has not recorded any interest or penalties in the financial statements as of December 31, 2017 and 2016.
Note 7 – Legal Proceedings
The Company may be subject to legal proceedings and litigation arising in the ordinary course of business, including, but not limited to, certain other third-party lawsuits, as well as other regulatory proceedings. The Company will record a liability when it believes that it is both probable that a loss has been incurred and the amount can be reasonably estimated. The Company periodically evaluates developments in its legal matters that could affect the amount of liability that it has previously accrued, if any, and makes adjustments as appropriate. Significant judgement is required to determine both the likelihood of there being, and the estimated amount of, a loss related to such matters, and the Company’s judgement may be incorrect. The outcome of any proceeding is not determinable in advance. Until the final resolution of any such matters that the Company may be required to accrue for, there may be an exposure to loss in excess of the amount accrued and such amounts could be material.
Note 8 - Joint Venture Agreement
On January 10, 2017, the NCMS announced that, working in conjunction with the North Carolina Community Health Center Association (the “NCCHCA”), it had signed a definitive agreement with a strategic partner to collaborate on a patient-focused health plan in response to pending Medicaid reform in the State of North Carolina.
Under that agreement, the parties will work together in a joint venture to establish, organize and operate a patient-focused Medicaid health plan to provide managed care services in North Carolina. A key feature of the joint venture will be the active participation of physicians in the ownership and governance of the health plan. The strategic partner will generally manage the health plan’s financial and daily operations. The Company will generally manage the provider network for the health plan.
F-12
The closing of the joint venture is subject to a number of conditions including, among other conditions, (i) the company operating the health plan having been awarded and accepted a capitated Medicaid contract with the State of North Carolina; (ii) the number of subscribing investors in the Company’s Offering (as defined in Note 10) and the number of investors attributable to subscribing investors in the Company’s Private Placement (as defined in Note 10) must be at least 10,000 in the aggregate prior to the earlier of (a) the date that is 10 business days prior to the deadline for submitting proposals for the contract with the State of North Carolina and (b) the date that is 12 months after the offering statement on Form 1-A for the Company’s public offering is qualified by the Securities and Exchange Commission; and (iii) on or prior to 10 business days before the deadline for submitting proposals for the contract with the State of North Carolina, the provider network must have satisfied the provider participation requirements established by the State of North Carolina with respect to network adequacy.
On August 25, 2017 the joint venture parties entered into an Amended and Restated Joint Venture Agreement(the “Amended Joint Venture Agreement”). Under the Amended Joint Venture Agreement, the Company will own a 20 percent general partnership interest of the joint venture company, which in turn, will own 100 percent of the health plan company.
Pursuant to the Amended Joint Venture Agreement, if the joint venture closing occurs, the Company is permitted to retain 55 percent of the Offering’s net proceeds and 55 percent of the Company’s Private Placement proceeds, and the Company is obligated to use 45 percent of the Offering’s net proceeds and 45 percent of the Private Placement proceeds to help fund its portion of the initial capitalization to the joint venture company at the joint venture closing. The Company expects to use the retained Offering’s net proceeds and Private Placement proceeds for general working capital purposes, but it may also use such proceeds to fund capital calls for the health plan company or to repay principal owed by the Company under its Term Note(see Note 10).
Note 9 - Related-Party Transactions
Under a Master Services Agreement with Biologue, Inc.(the “Biologue Agreement”), effective January 2, 2017, Dr. Jeffrey W. Runge provides certain executive duties necessary for the Company to build and operate a provider network. On March 14, 2017, Dr. Runge was appointed Chief Executive Officer and President of the Company and was appointed to the Company’s Board of Directors. The Biologue Agreement provides that Dr. Runge will provide up to 84 hours of service per calendar month, with additional hours to be provided as agreed in advance by Dr. Runge and the Company. The Company has agreed to compensate Dr. Runge for his time at a rate of $248 per hour and has agreed to reimburse Dr. Runge for all reasonable out of pocket expenses incurred in the provision of his services, provided that expenses in excess of $250 are subject to prior approval of the Company. The Biologue Agreement contains customary confidentiality and indemnification obligations on behalf of the Company and Dr. Runge, and the Biologue Agreement will continue until either party provides 30 days’ written notice of termination. At December 31, 2017 the amount due to Biologue, Inc was $85,549.
Note 10 – Subsequent Events
The Company has evaluated the impact of subsequent events through April 26, 2018, which is the date the financial statements were available to be issued.
Private Placement of Class P Common Stock – On January 19, 2018, the Company completed a private placement of 1,505 shares of Class P Common Stock to certain federally-qualified health centers and aspiring health centers in North Carolina and the North Carolina Community Health Center Association at a purchase price of $750.00 per share for aggregate proceeds of approximately $1.13 million(the “Private Placement”). The Class P Common Stock issued in the Private Placement represents a 50.0 percent equity interest in the Company. At the joint venture closing, the Company is permitted to retain 55 percent of the Private Placement’s net proceeds, and the Company is obligated to use 45 percent of the Private Placement’s net proceeds to help fund its portion of the initial capitalization to the joint venture company. The Company expects to use the retained Private Placement proceeds for general working capital purposes, but it may also use such proceeds to fund capital calls for the health plan company or to repay principal owed by the Company under its Term Note.
Regulation A Offering of Class P Common Stock– On March 12, 2018, the Securities and Exchange Commission(the “SEC”)qualified the Company’s offering statement on Form 1-A offering up to 20,000 shares of the Company’s Class P Common Stock pursuant to Regulation A of the Securities Act of 1933, as amended, on a continuous basis(the “Offering”). The Company is offering one, but not more than one, share of Class P Common Stock, for a subscription price per share of $750, solely to physicians, physician assistants and nurse practitioners licensed or approved to practice, as applicable, in North Carolina who (i) participate in the Company’s health care provider network, (ii) reside in North Carolina, Georgia, South Carolina, Tennessee or Virginia and (iii) meet certain other eligibility criteria. Pursuant to the Amended Joint Venture Agreement, at the joint venture closing, the Company is permitted to retain 55 percent of the Offering’s net proceeds, and the Company is obligated to use 45 percent of the Offering’s net proceeds to help fund its portion of the initial capitalization to the joint venture company. The Company expects to use the retained Offering’s net proceeds for general working capital purposes, but it may also use such proceeds to fund capital calls for the health plan company or to repay principal owed by the Company under its Term Note. The Class P Common Stock being offered in this Offering represents a 46.5 percent equity interest in the Company.
Term Note– The principal balance outstanding on the First Loan(see Note 3) was $1,908,750 at April 26, 2018. Accrued interest as of April 26, 2018 was $73,660.
F-13
PART III — EXHIBITS
Exhibit Index
* Previously filed.
+ To be entered into upon the closing of the Joint Venture.
# Schedules or similar attachments omitted pursuant to Item 17 of Form 1-A. CCHN will supplementallyfurnish a copy of any omitted schedule or similar attachment to the Commission upon request.
III-1
SIGNATURES
Pursuant to the requirements of Regulation A, the issuer certifies that it has reasonable grounds to believe that it meets all of the requirements for filing on Form 1-A and has duly caused this offering statement to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of Raleigh, State of North Carolina, on April 26, 2018.
| CAROLINA COMPLETE HEALTH NETWORK, INC. | ||
| By: | /s/ Jeffrey W. Runge | |
| Name: | Jeffrey W. Runge, MD | |
| Title: | President and Chief Executive Officer | |
This offering statement has been signed by the following persons in the capacities and on the dates indicated.
| Signature | Title | Date | ||
| /s/ Jeffrey W. Runge | Director, President and Chief Executive Officer | April 26, 2018 | ||
| Jeffrey W. Runge, MD | (Principal Executive Officer) | |||
| /s/ Vincent T. Morgus | Chief Operating Officer | April 26, 2018 | ||
| Vincent T. Morgus | (Principal Financial and Accounting Officer) | |||
| * | Director | April 26, 2018 | ||
| Richard Hudspeth, MD | ||||
| * | Director | April 26, 2018 | ||
| John R. Mangum, MD | ||||
| * | Director | April 26, 2018 | ||
| John Jacob Meier IV, MD |
| * By: | /s/ Jeffrey W. Runge | |
| Jeffrey W. Runge | ||
| Attorney-in-fact |