Exhibit 99.2
| CONFIDENTIAL Gene Therapy for the Treatment of Radiation-Induced Xerostomia: AAV-hAQP1 Program Update December 7, 2021 |
| CONFIDENTIAL 2 This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. All statements contained in this presentation that do not relate to matters of historical fact should be considered forward-looking statements, including, without limitation, statements regarding the development and efficacy of AAV-hAQP1, plans to advance AAV-hAQP1 into Phase 2 clinical trial and anticipated milestones regarding our clinical data and reporting of such data and the timing of results of data, including in light of the COVID-19 pandemic, as well as statements that include the words “expect,” “intend,” “plan,” “believe,” “project,” “forecast,” “estimate,” “may,” “should,” “anticipate” and similar statements of a future or forward-looking nature. These forward-looking statements are based on management’s current expectations. These statements are neither promises nor guarantees, but involve known and unknown risks, uncertainties and other important factors that may cause actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements, including, but not limited to, our incurrence of significant losses; any inability to achieve or maintain profitability, raise additional capital, identify additional and develop existing product candidates, successfully execute strategic priorities, bring product candidates to market, expansion of our manufacturing facilities and processes, successfully enroll patients in and complete clinical trials, accurately predict growth assumptions, recognize benefits of any orphan drug designations, retain key personnel or attract qualified employees, or incur expected levels of operating expenses; the impact of the COVID-19 pandemic on the status, enrollment, timing and results of our clinical trials and on our business, results of operations and financial condition; failure of early data to predict eventual outcomes; failure to obtain FDA or other regulatory approval for product candidates within expected time frames or at all; the novel nature and impact of negative public opinion of gene therapy; failure to comply with ongoing regulatory obligations; contamination or shortage of raw materials or other manufacturing issues; changes in healthcare laws; risks associated with our international operations; significant competition in the pharmaceutical and biotechnology industries; dependence on third parties; risks related to intellectual property; changes in tax policy or treatment; our ability to utilize our loss and tax credit carryforwards; litigation risks; and the other important factors discussed under the caption “Risk Factors” in our most recent quarterly report on Form 10-Q or annual report on Form 10-K or subsequent 8-K reports, as filed with the Securities and Exchange Commission. These and other important factors could cause actual results to differ materially from those indicated by the forward-looking statements made in this presentation. Any such forward-looking statements represent management’s estimates as of the date of this presentation. While we may elect to update such forward-looking statements at some point in the future, unless required by law, we disclaim any obligation to do so, even if subsequent events cause our views to change. Thus, one should not assume that our silence over time means that actual events are bearing out as expressed or implied in such forward-looking statements. These forward-looking statements should not be relied upon as representing our views as of any date subsequent to the date of this presentation. Unless otherwise stated or the context otherwise requires, the information herein is as of December 7, 2021. |
| CONFIDENTIAL 3 1. Introduction Zandy Forbes, PhD President & CEO MeiraGTx 2. Radiation-Induced Xerostomia: Disease Background and Unmet Medical Need Robert K. Zeldin, MD Chief Medical Officer MeiraGTx 3. AQUAx Phase 1 Study: Preliminary Data for AQUAx Cohorts 1 to 3 Zandy Forbes, PhD President & CEO MeiraGTx 4. Treating Physician Perspective: AAV-hAQP1 Treatment and Unmet Medical Need Michael Brennan, DDS, MHS, FDS RCSEd Professor and Chair, Department of Oral Medicine Director of the Sjögren’s Syndrome and Salivary Disorders Center Atrium Health’s Carolinas Medical Center, Charlotte, NC |
| Salivary Gland Gene Therapy Radiation-Induced Xerostomia Robert K. Zeldin, MD |
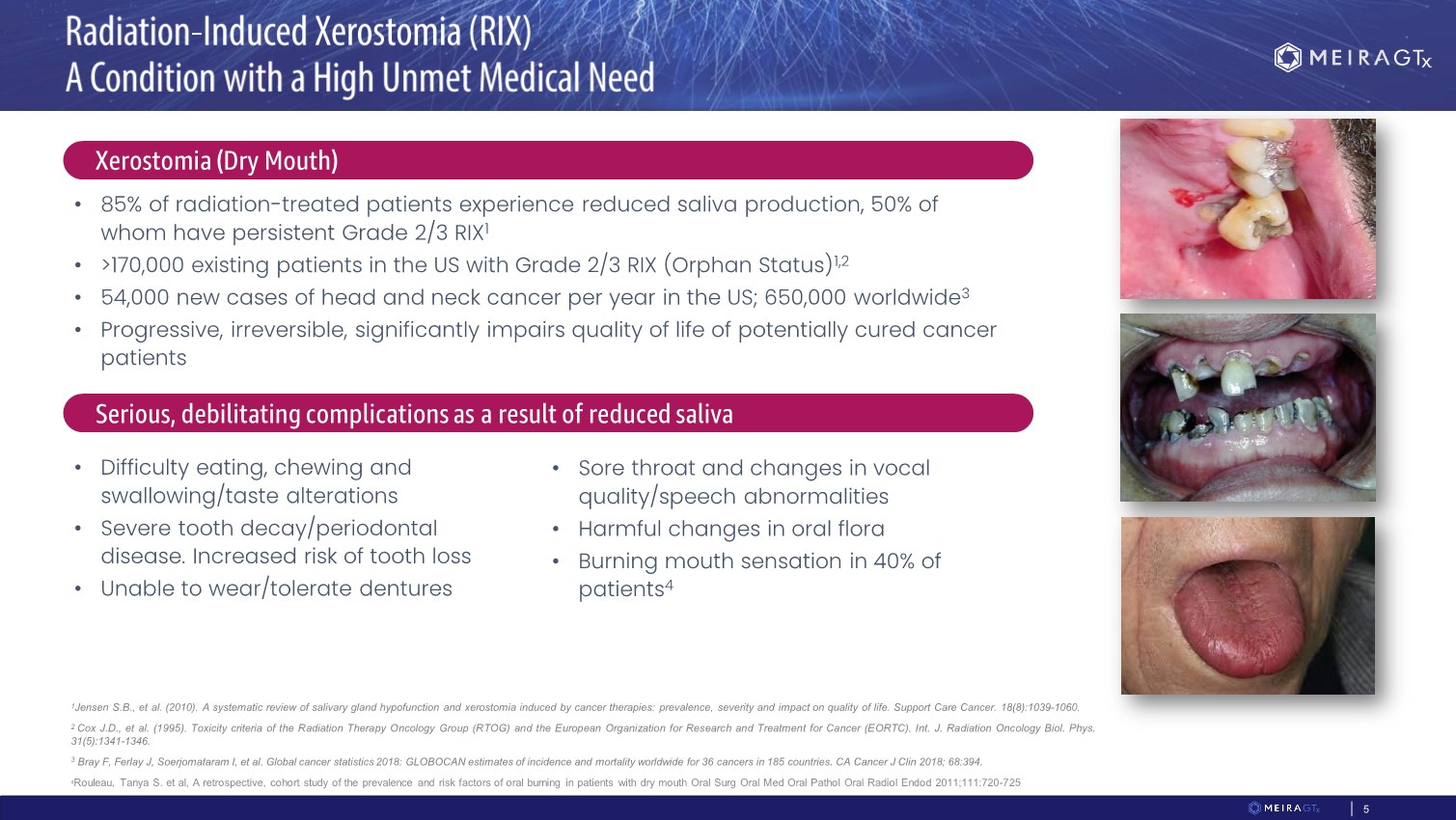
| CONFIDENTIAL • 85% of radiation-treated patients experience reduced saliva production, 50% of whom have persistent Grade 2/3 RIX1 • >170,000 existing patients in the US with Grade 2/3 RIX (Orphan Status)1,2 • 54,000 new cases of head and neck cancer per year in the US; 650,000 worldwide3 • Progressive, irreversible, significantly impairs quality of life of potentially cured cancer patients • Difficulty eating, chewing and swallowing/taste alterations • Severe tooth decay/periodontal disease. Increased risk of tooth loss • Unable to wear/tolerate dentures • Sore throat and changes in vocal quality/speech abnormalities • Harmful changes in oral flora • Burning mouth sensation in 40% of patients4 1Jensen S.B., et al.(2010).A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 18(8):1039-1060. 2 Cox J.D., et al.(1995). Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment for Cancer (EORTC). Int.J. Radiation Oncology Biol. Phys. 31(5):1341-1346. 3 Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394. 4Rouleau, Tanya S. et al, A retrospective, cohort study of the prevalence and risk factors of oral burning in patients with dry mouth Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:720-725 Xerostomia (Dry Mouth) Serious, debilitating complications as a result of reduced saliva 5 |
| CONFIDENTIAL 6 ❑ Saliva substitutes • Carboxymethyl cellulose and mucin • Short term benefit ❑ Mechanical and Gustatory stimulation • Not all patients tolerate frequent gum chewing • May exacerbate temporomandibular disorder symptoms ❑ Sialogogues: Pilocarpine (indicated for RIX) and Cevimeline (off-label) • Chronic, frequent dosing (x3 daily) • Do not improve salivary gland functionality • Not well tolerated • 20% of patients experience Grade 3 or higher side effects include flushing, upset stomach, sweating • Contraindicated in a variety of conditions ❑ Acupuncture • Some benefits to an extremely small subset of patients Treatment options for management of Grade 2/3 xerostomia are limited and have no effect on gland functionality. None are disease-modifying. No new treatments have been approved in 20 years – last drug approved was Cevimeline in 2000 |
| CONFIDENTIAL 7 Xerostomia-focused meeting hosted by a consortium of advocacy and patient care groups with guidance from the US FDA on August 19th, 2021 • The goal of Patient Focused Drug Development meetings is to systematically obtain the patient perspective on specific diseases and their treatments • The meeting provides a forum for the FDA to hear directly from patients, their families, caregivers, and patient advocates • Attendees included 16 individuals from the FDA and over 150 patients and caregivers from both the Head & Neck Cancer and Sjogren’s Disease advocacy communities • MeiraGTx was the corporate sponsor for the event |

| CONFIDENTIAL 8 “Sometimes the sticky saliva closes the back of my throat, and I can’t speak for up to a minute. My throat is just stuck, and I’m not able to get words out.” “Aside from painful swallowing, I’ve had a couple of incidents of almost choking due to food getting stuck in my throat.” “Along with the fear of cancer recurrence, I fear for my dental health, my nutrition, and most importantly – my sleep. These are important factors for a healthy life.” “Sometimes I feel a sense of panic, because the food blocks my airways and I struggle to clear.” “Weekly checks during my routine visits revealed serious weight loss, not surprising since extreme mouth dryness and sensitivity.“ “If there was one symptom of xerostomia that I could eliminate, it would be the dysphagia. I never know when I would start coughing and choking.” “Often my mouth becomes so dry I can’t enunciate clearly and my lips become stiff and cracked.” “Not having normal saliva production has affected me in several ways, the most negative being how it affected my sleep …. I wake up often during the night because of very uncomfortable and at times painful parched mouth and throat.” |
| AAV-hAQP1 MGT016 AQUAx Phase 1 Study |

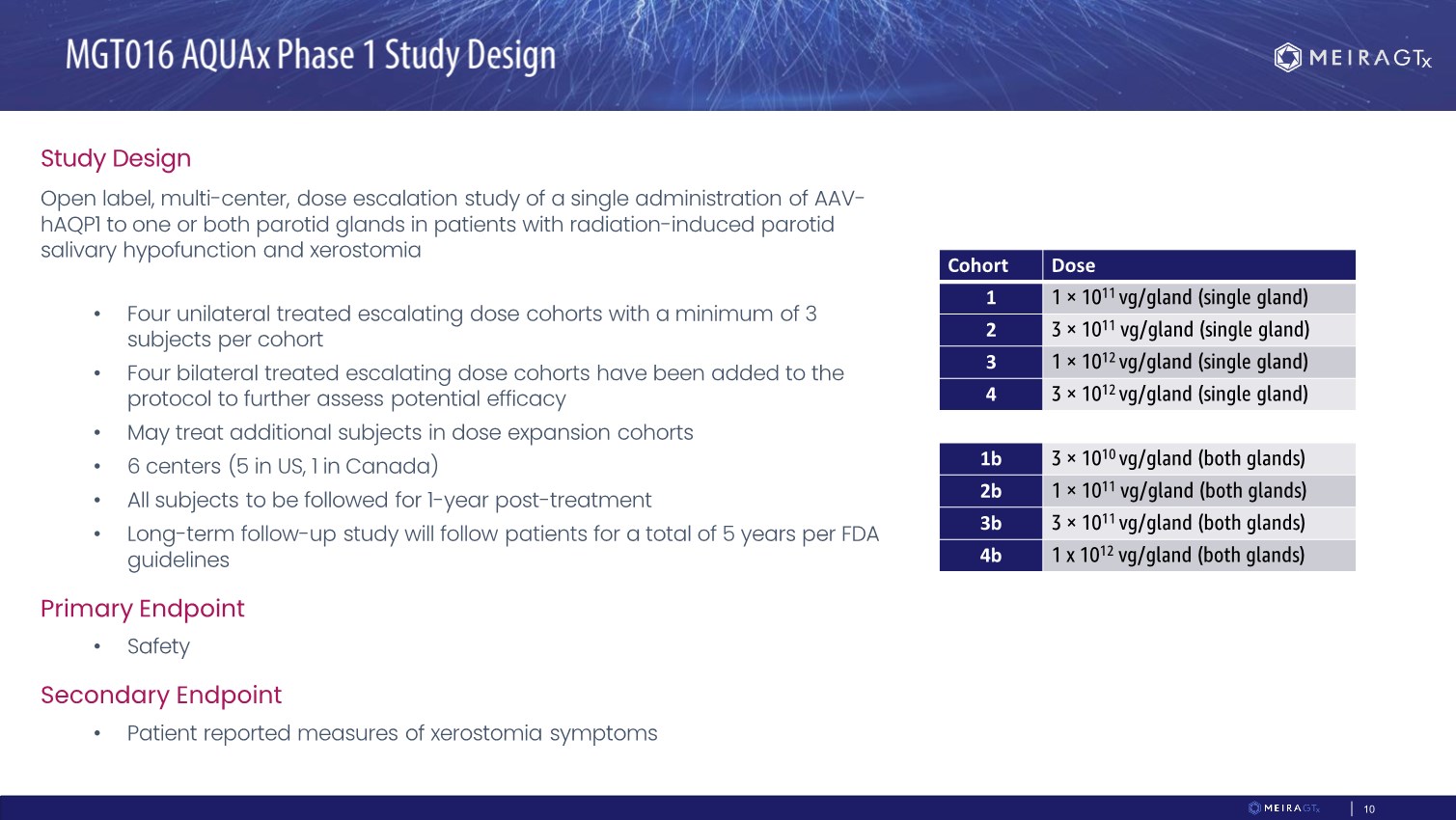
| CONFIDENTIAL 10 Study Design Open label, multi-center, dose escalation study of a single administration of AAV- hAQP1 to one or both parotid glands in patients with radiation-induced parotid salivary hypofunction and xerostomia • Four unilateral treated escalating dose cohorts with a minimum of 3 subjects per cohort • Four bilateral treated escalating dose cohorts have been added to the protocol to further assess potential efficacy • May treat additional subjects in dose expansion cohorts • 6 centers (5 in US, 1 in Canada) • All subjects to be followed for 1-year post-treatment • Long-term follow-up study will follow patients for a total of 5 years per FDA guidelines Primary Endpoint • Safety Secondary Endpoint • Patient reported measures of xerostomia symptoms Cohort Dose 1 1 × 1011 vg/gland (single gland) 2 3 × 1011 vg/gland (single gland) 3 1 × 1012 vg/gland (single gland) 4 3 × 1012 vg/gland (single gland) 1b 3 × 1010 vg/gland (both glands) 2b 1 × 1011 vg/gland (both glands) 3b 3 × 1011 vg/gland (both glands) 4b 1 x 1012 vg/gland (both glands) |
| CONFIDENTIAL 11 Study Status • All centers open for enrollment • All four unilateral dose cohorts treated (n=12) • One bilateral dose cohort treated (n=3) • Completion of enrollment of bilateral cohorts in the coming months 7 participants (3 each from Cohorts 1 & 2 and 1 from Cohort 3) have data available through Day 90 following treatment: • Treatment well tolerated • No dose limiting toxicity • No serious adverse events • Improvements observed in validated patient reported assessments of xerostomia symptoms |
| CONFIDENTIAL 12 Study Design: • Randomized, double-blind, placebo-controlled study • Two active doses of AAV2-hAQP1 Primary Endpoint: • McMaster Global Rate of Change at 12 months after treatment Secondary Endpoint: • Symptom-specific Xerostomia Questionnaire Exploratory: • Whole saliva volume |
| AAV-hAQP1 Clinical Development Program: Preliminary Data for AQUAx Cohorts 1 to 3 Zandy Forbes, PhD |
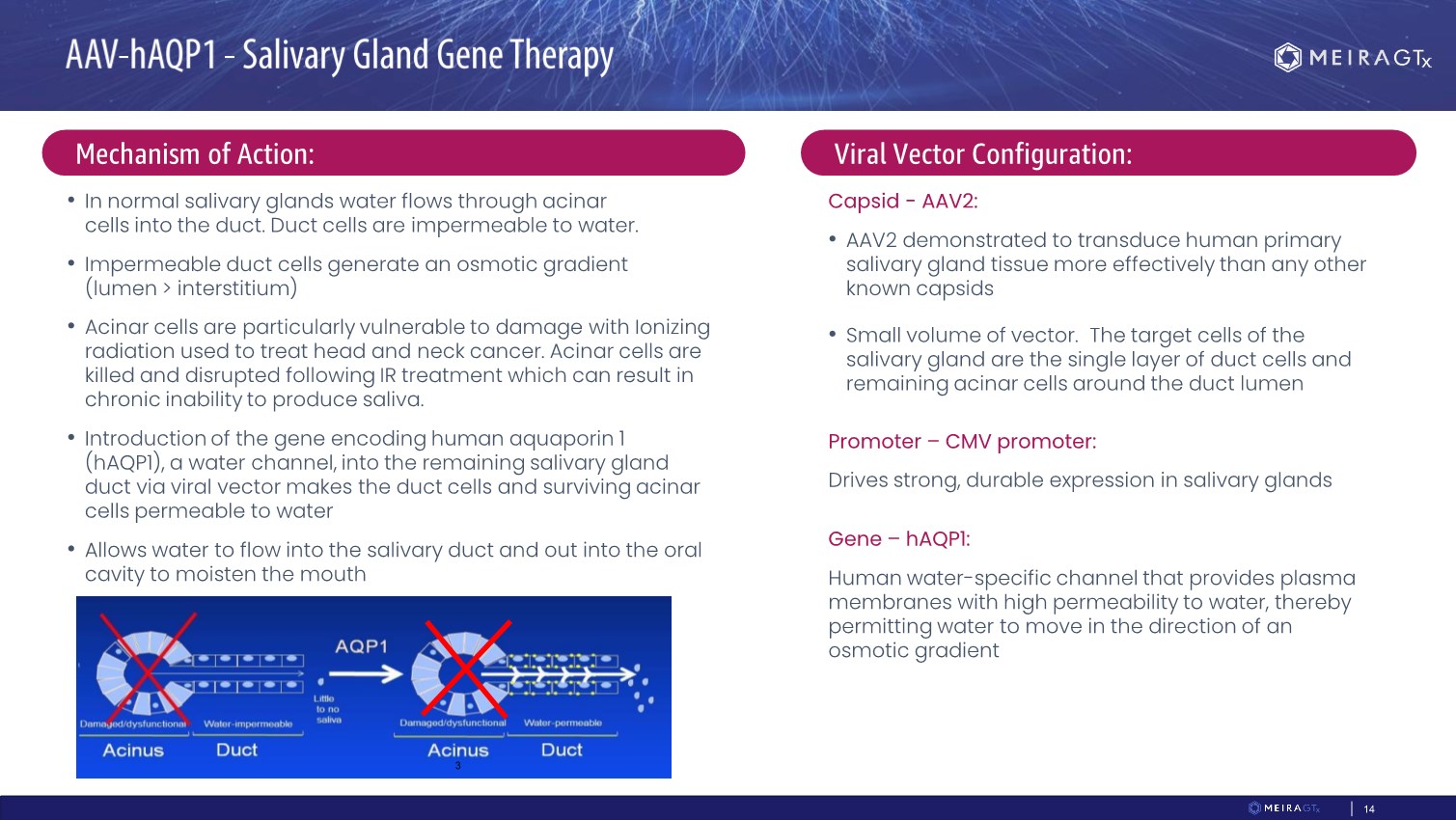
| CONFIDENTIAL 14 • In normal salivary glands water flows through acinar cells into the duct. Duct cells are impermeable to water. • Impermeable duct cells generate an osmotic gradient (lumen > interstitium) • Acinar cells are particularly vulnerable to damage with Ionizing radiation used to treat head and neck cancer. Acinar cells are killed and disrupted following IR treatment which can result in chronic inability to produce saliva. • Introduction of the gene encoding human aquaporin 1 (hAQP1), a water channel, into the remaining salivary gland duct via viral vector makes the duct cells and surviving acinar cells permeable to water • Allows water to flow into the salivary duct and out into the oral cavity to moisten the mouth 3 Mechanism of Action: Viral Vector Configuration: Capsid - AAV2: • AAV2 demonstrated to transduce human primary salivary gland tissue more effectively than any other known capsids • Small volume of vector. The target cells of the salivary gland are the single layer of duct cells and remaining acinar cells around the duct lumen Promoter – CMV promoter: Drives strong, durable expression in salivary glands Gene – hAQP1: Human water-specific channel that provides plasma membranes with high permeability to water, thereby permitting water to move in the direction of an osmotic gradient |
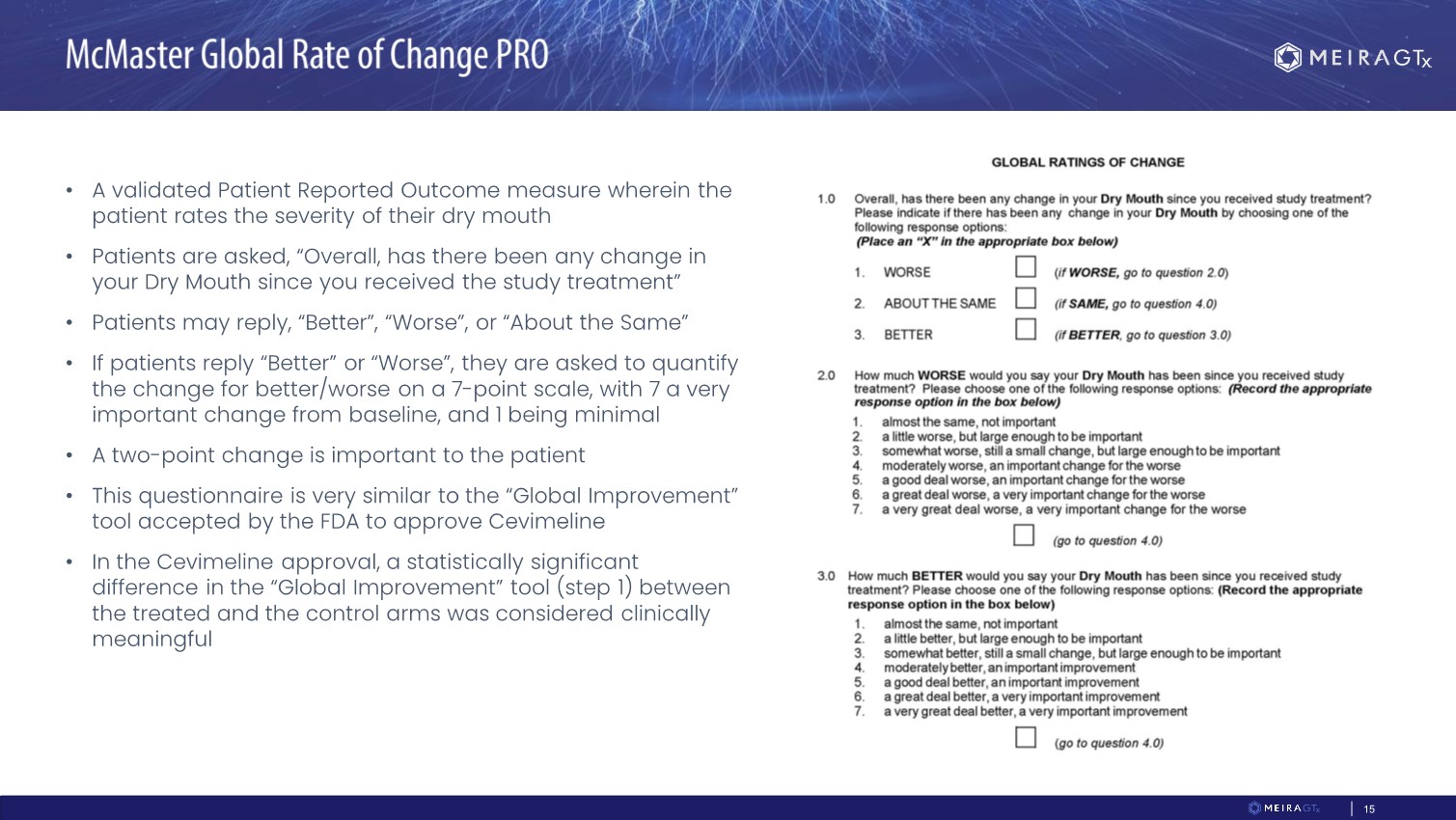
| CONFIDENTIAL 15 • A validated Patient Reported Outcome measure wherein the patient rates the severity of their dry mouth • Patients are asked, “Overall, has there been any change in your Dry Mouth since you received the study treatment” • Patients may reply, “Better”, “Worse”, or “About the Same” • If patients reply “Better” or “Worse”, they are asked to quantify the change for better/worse on a 7-point scale, with 7 a very important change from baseline, and 1 being minimal • A two-point change is important to the patient • This questionnaire is very similar to the “Global Improvement” tool accepted by the FDA to approve Cevimeline • In the Cevimeline approval, a statistically significant difference in the “Global Improvement” tool (step 1) between the treated and the control arms was considered clinically meaningful |
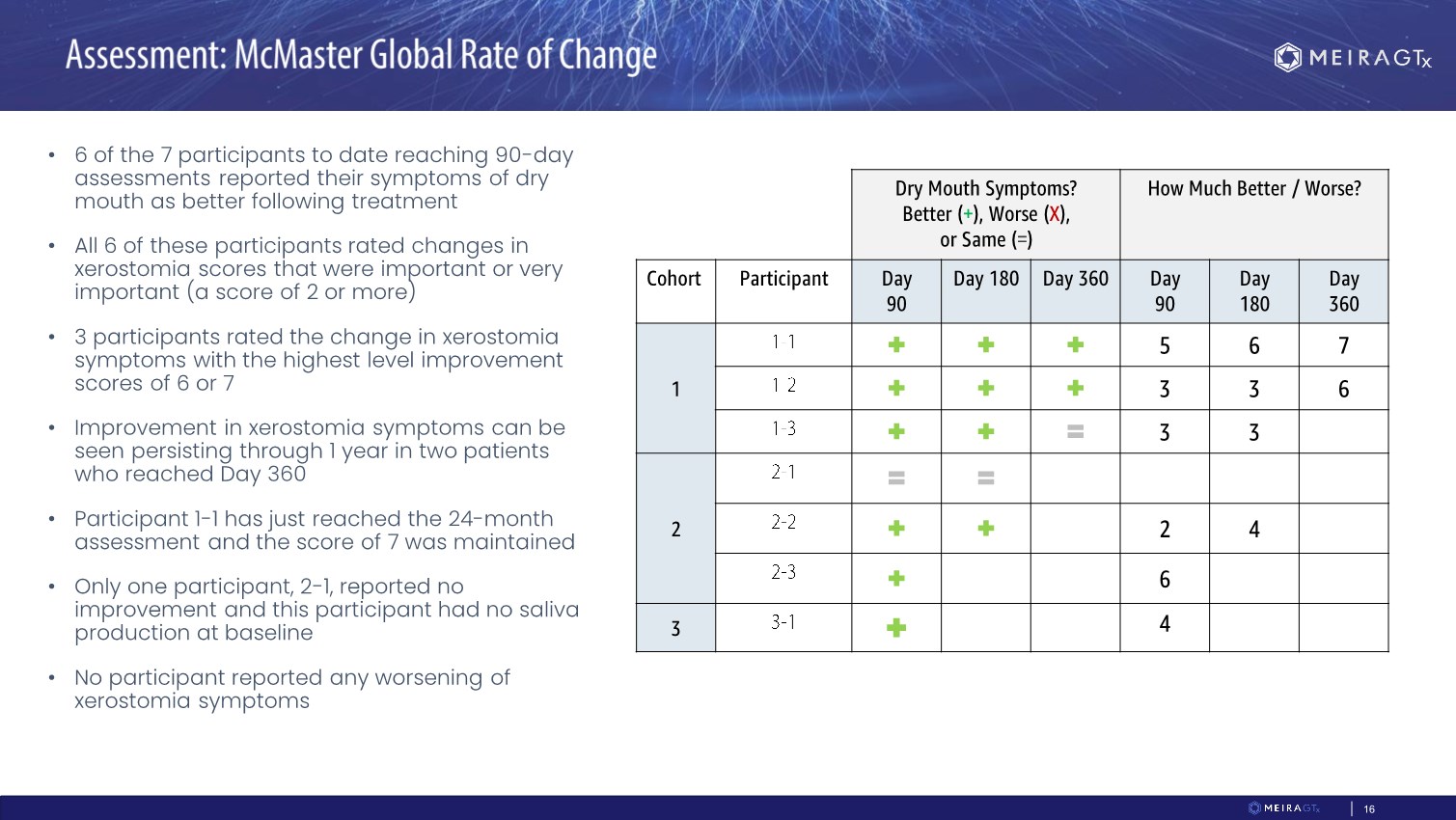
| CONFIDENTIAL 16 • 6 of the 7 participants to date reaching 90-day assessments reported their symptoms of dry mouth as better following treatment • All 6 of these participants rated changes in xerostomia scores that were important or very important (a score of 2 or more) • 3 participants rated the change in xerostomia symptoms with the highest level improvement scores of 6 or 7 • Improvement in xerostomia symptoms can be seen persisting through 1 year in two patients who reached Day 360 • Participant 1-1 has just reached the 24-month assessment and the score of 7 was maintained • Only one participant, 2-1, reported no improvement and this participant had no saliva production at baseline • No participant reported any worsening of xerostomia symptoms Dry Mouth Symptoms? Better (+), Worse (X), or Same (=) How Much Better / Worse? Cohort Participant Day 90 Day 180 Day 360 Day 90 Day 180 Day 360 1 + + + 5 6 7 + + + 3 3 6 + + = 3 3 2 = = + + 2 4 + 6 3 + 4 |
| CONFIDENTIAL 17 • A Patient Reported Outcome measure consisting of 8 symptom-specific questions wherein the patient rates each symptom from 0 (not present) to 10 (worst possible) • The responses are summed (0-80), providing an overall measure of disease burden • This is refined from the Xerostomia Inventory which consists of 11 questions and for which a 6- point change in disease burden is defined as a clinically meaningful improvement • In the AQUAx study, 6 of 7 participants reaching the 90-day assessment reported decreases in disease burden of 10 points or more on the XQ at 90 days – indicating a clinically meaningful alleviation in disease burden • More dramatic reductions of 19, 25, 26, and 41 points were reported by 4 of 7 participants at 90 days • In the subjects that reached additional timepoints, scores improved or stabilized at later timepoints • One participant reported complete resolution of symptoms at 12 months following treatment with no symptoms of xerostomia, a complete response |
| CONFIDENTIAL 18 Safety • AAV-hAQP1 treatment appears safe and well tolerated at each dose tested • No DLT or SAEs Efficacy • Improvements in xerostomia symptoms and disease burden reported in two different PRO tools validated for xerostomia • McMaster – which has been the basis of approval of other drugs for xerostomia • Xerostomia questionnaire – a higher bar than the McMaster • AAV-hAQP1 treatment response rate and effect size encouraging • 6 of the 7 participants through 90 days following treatment achieved clinically meaningful improvement in symptoms • One participant with the maximum response evaluable at 12 months has now reached 24 months and the same level of response/xerostomia symptom improvement is maintained Dosing in the unilateral dose escalation and first cohort of bilateral dosing phase completed Phase 2 double-blind randomized two dose study expected to initiate 2H 2022 |
| Clinical Perspective Michael Brennan, DDS, MHS, FDS RCSEd |

| CONFIDENTIAL 20 • Quick outpatient procedure • Non-invasive: allows local administration and avoids systemic exposure • Parotid gland is isolated and encapsulated, somewhat immune protected • Small volume of vector required Qualifying a patient for treatment with AAV-hAQP1 utilizes routine practices in oral medicine: • Oral exam • Sialometry (assessment of salivary flow rate) • Patient-reported measures of oral dryness Administration of AAV-hAQP1: • Non-invasive procedure • Easy to perform • Well tolerated by patients AAV-hAQP1 provides the potential for durable recovery of salivary function in patients with intractable radiation induced xerostomia in contrast to other treatments which are minimally effective |

| CONFIDENTIAL 21 • Serious debilitating condition with severe impact on health and daily living • Intractable disease with no treatment options • Large unmet need with >170,000 grade 2 and grade 3 xerostomia patients in the U.S. and 5,000-10,000 new patients annually • Patients are already in healthcare system under the regular care of physician • No competitive clinical programs to our knowledge • Small local dose, easy & non-invasive delivery • Appears safe and well tolerated at all doses tested • Preliminary signals of activity in two validated patient reported outcome assessments of xerostomia symptoms • Endpoints that have previously supported FDA approval • Response rate and effect size appear clinically meaningful and compare favorably with drugs approved for the treatment of xerostomia • Double blind, placebo-controlled multi-dose study expected to initiate 2H 2022 |
| Audience Q&A |
