
Exhibit 99.3 Day One Biopharmaceuticals Targeted therapies for people of all ages January 2025

Disclaimer This presentation and the accompanying oral commentary contain forward-looking statements that are based on our management’s beliefs and assumptions and on information currently available to our management. Forward-looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified. In some cases, you can identify forward-looking statements by terminology such as “may,” “will,” “should,” “could,” “expect,” “plan,” anticipate,” “believe,” “estimate,” “predict,” “intend,” “potential,” “would,” “continue,” “ongoing” or the negative of these terms or other comparable terminology. Forward-looking statements include all statements other than statements of historical fact contained in this presentation, including information concerning our future financial performance, including the sufficiency of our cash, cash equivalents and short-term investments to fund our operations, business plans and objectives, timing and success of our commercialization and marketing efforts, timing and success of our planned nonclinical and clinical development activities, the results of any of our strategic collaborations, including the potential achievement of milestones and provision of royalty payments thereunder, efficacy and safety profiles of our products and product candidates, the ability of OJEMDA (tovorafenib) to treat pediatric low-grade glioma (pLGG) or related indications, the potential therapeutic benefits and economic value of our products and product candidates, potential growth opportunities, competitive position, industry environment and potential market opportunities, our ability to protect intellectual property and the impact of global business or macroeconomic conditions, including as a result of inflation, changing interest rates, cybersecurity incidents, potential instability in the global banking system, changes in the U.S. presidential administration, uncertainty with respect to the federal debt ceiling and budget and potential government shutdowns related thereto and global regional conflicts, on our business and operations. Forward-looking statements are subject to known and unknown risks, uncertainties, assumptions and other factors. It is not possible for our management to predict all risks, nor can we assess the impact of all factors on our business or the extent to which any factor, or combination of factors, may cause actual results to differ materially from those contained in any forward-looking statements we may make. These factors, together with those that are described under the heading “Risk Factors” contained in our most recent Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission (SEC) and other documents we file from time to time with the SEC, may cause our actual results, performance or achievements to differ materially and adversely from those anticipated or implied by our forward-looking statements. In addition, statements that “we believe” and similar statements reflect our beliefs and opinions on the relevant subject. These statements are based upon information available to us as of the date of this presentation, and although we believe such information forms a reasonable basis for such statements, such information may be limited or incomplete, and our statements should not be read to indicate that we have conducted a thorough inquiry into, or review of, all potentially available relevant information. These statements are inherently uncertain and investors are cautioned not to unduly rely upon these statements. Furthermore, if our forward-looking statements prove to be inaccurate, the inaccuracy may be material. In light of the significant uncertainties in these forward-looking statements, you should not regard these statements as a representation or warranty by us or any other person that we will achieve our objectives and plans in any specified time frame, or at all. We undertake no obligation to publicly update any forward-looking statements, whether as a result of new information, future events or otherwise, except as required by law. This presentation also contains estimates and other statistical data made by independent parties and by us relating to market size and growth and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned not to give undue weight to such estimates. In addition, projections, assumptions and estimates of our future performance and the future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. 2

Inspired by the urgent needs of children, Day One creatively and intentionally develops new medicines for people of all ages with life- threatening diseases 3

Bringing life-changing medicines to patients sooner Who we are • Commercial-stage biopharmaceutical company • Our goal is to develop and provide access to targeted new medicines to patients of all ages as rapidly as possible • Focused on advancing first- or best-in-class medicines for childhood and adult diseases 2018 2021 2024 TM OJEMDA FOUNDED IPO APPROVAL Nasdaq: DAWN OJEMDA received approval in April 2024 and is indicated for the treatment of pediatric patients 6 months of age and older with relapsed or refractory pediatric low-grade glioma harboring a BRAF 4 fusion or rearrangement, or BRAF V600 mutation.

Compelling near-term opportunities to help patients are the foundation for long-term growth and sustainability Day One’s Future Potential Value creation Pillars to Support Growth • Continued revenue growth from OJEMDA globally 2024 accomplishments • Indication expansion in front-line pLGG with FIREFLY-2 ü Launched OJEMDA in the U.S., delivering growing revenues • Generate clinical POC data in DAY301 program ü Ex-U.S. commercial partnership Proven Track Record with Ipsen for OJEMDA • Fund pipeline expansion ü Acquisition of DAY301 (PTK7- • Focused capital allocation, Intentional in our approach targeted ADC) meaningfully leveraging our efficient operating expands our pipeline model to maintain strong financial • Expertise developing and position commercializing products ü Strong balance sheet with ~$532M 1 • Demonstrated ability to find and cash as of December 31, 2024 (no acquire first- or best-in-class debt) medicines 1 As used herein the term, “Cash” means our cash, cash equivalents and short-term investments (unaudited) as of December 31, 2024. Cash, cash equivalents and short-term investments as of December 31, 2024 5 5 were $531.7 million (unaudited). pLGG, pediatric low-grade glioma; POC, proof of concept; ADC, antibody-drug conjugate; PTK7, protein tyrosine kinase 7.

Our pipeline Our goal is to take aim at the gaps that have left patients and their families behind. Product Therapeutic Phase 3/ Recent & Anticipated Preclinical Phase 1 Phase 2 Approved Candidate Area Registrational Milestones 3 Tovorafenib FDA approval BRAF-altered April 2024 Type II RAF Inhibitor 2 relapsed FIREFLY-1 (pivotal Phase 2) Ex-U.S. license agreement pLGG OJEMDA brand July 2024 1 name in U.S. Ex-U.S. Rights: Front-line Enrollment completion expected FIREFLY-2 (pivotal Phase 3) RAF-altered 1H 2026 pLGG Adult and DAY301 First dose cohort cleared pediatric solid January 2025 PTK7-Targeted ADC tumors Adult and VRK1 Program In-licensed pediatric August 2023 VRK1 Inhibitor cancers 1 2 OJEMDA has received accelerated approval by the U.S. Food and Drug Administration. FIREFLY-1 is an open-label, pivotal Phase 2 trial. Ex-U.S. license agreement with Ipsen to commercialize OJEMDA (tovorafenib) 5 outside the U.S. DAY301 is a license agreement with MabCare Therapeutics for exclusive worldwide rights, excluding Greater China, for MTX-13/CB-002, a novel ADC targeting PTK7. VRK1 Program is a research collaboration and license agreement with Sprint Bioscience AB for exclusive worldwide rights to a research-stage program targeting VRK1. The safety and efficacy of investigational agents and/or investigational uses of approved products have not been established. pLGG, pediatric low-grade glioma. 6

OJEMDA Relapsed or refractory BRAF-altered pLGG Nora Living with pLGG 7

Pediatric low-grade glioma: The most common type of brain tumor in children A serious and life-threatening disease • For the majority of pLGG patients in the relapsed setting, there is no standard of care, and until recently, no approved therapies pLGGs are chronic and • Up to 75% of pLGGs have a BRAF alteration*, of those relentless, with patients ~80% are BRAF fusions and ~20% are BRAF V600 suffering profound tumor and 2-6 mutations treatment-associated morbidity that can impact their life • Despite surgery playing a significant role in treatment, 1 the vast majority of patients still require systemic trajectory over the long term 7,8 therapy • Due to high rate of disease recurrence, most patients will undergo multiple lines of systemic therapy over the course of their disease 1 2 *Incidence of BRAF alterations varies across pLGG subtypes. Sievert AJ, Fisher MJ. Pediatric low-grade gliomas. J Child Neurol. 2009;24(11):1397-1408. doi:10.1177/0883073809342005. Penman CL et al. Front Oncol. 3 4 5 6 2015;5:54. Cohen AR., N Engl J Med. 2020;386(20):1922-1931. Lassaletta A, et al. J Clin Oncol. 2017;35(25):2934-2941. Faulkner C, et al. J Neuropathol Exp Neurol. 2015;74(9):867-872. Packer RJ, et al. Neuro 7 8 8 Oncol. 2017;19(6):750-761. Ostrum QT et al., Neuro Oncol. 2015; 16(Suppl 10):x1-x36; De Blank P. et al., Curr Opin Pediatr. 2019 Feb; 31(1):21-27.
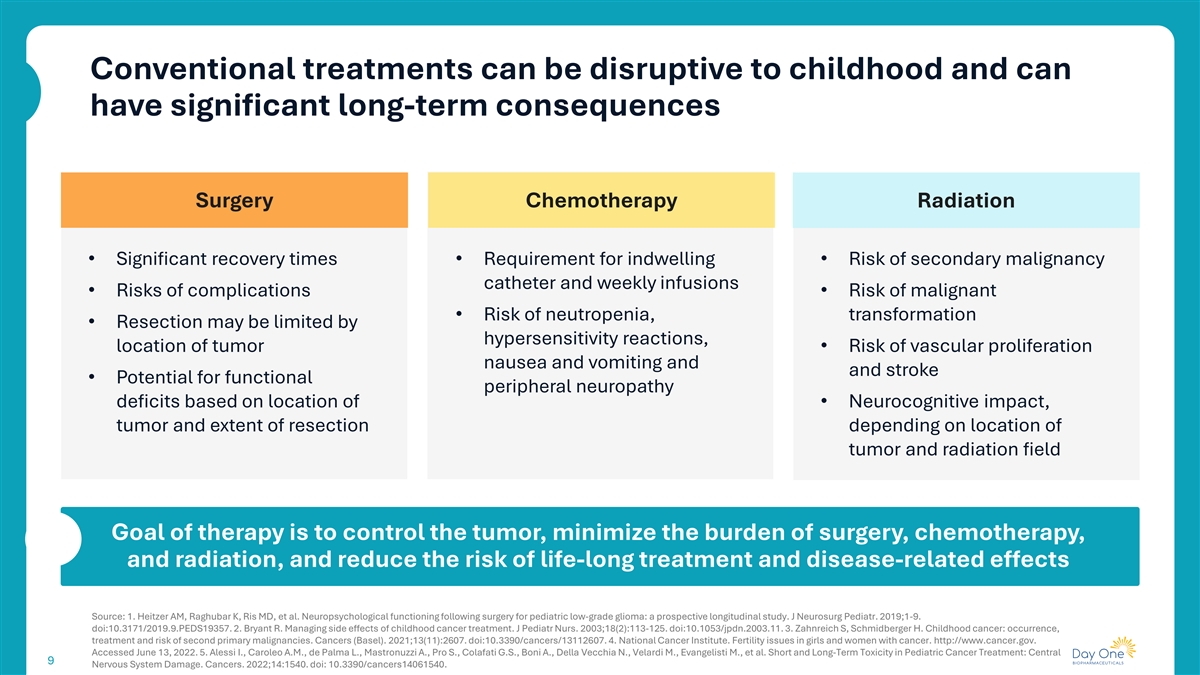
Conventional treatments can be disruptive to childhood and can have significant long-term consequences Surgery Chemotherapy Radiation • Significant recovery times • Requirement for indwelling • Risk of secondary malignancy catheter and weekly infusions • Risks of complications • Risk of malignant • Risk of neutropenia, transformation • Resection may be limited by hypersensitivity reactions, location of tumor • Risk of vascular proliferation nausea and vomiting and and stroke • Potential for functional peripheral neuropathy deficits based on location of • Neurocognitive impact, tumor and extent of resection depending on location of tumor and radiation field Goal of therapy is to control the tumor, minimize the burden of surgery, chemotherapy, and radiation, and reduce the risk of life-long treatment and disease-related effects Source: 1. Heitzer AM, Raghubar K, Ris MD, et al. Neuropsychological functioning following surgery for pediatric low-grade glioma: a prospective longitudinal study. J Neurosurg Pediatr. 2019;1-9. doi:10.3171/2019.9.PEDS19357. 2. Bryant R. Managing side effects of childhood cancer treatment. J Pediatr Nurs. 2003;18(2):113-125. doi:10.1053/jpdn.2003.11. 3. Zahnreich S, Schmidberger H. Childhood cancer: occurrence, treatment and risk of second primary malignancies. Cancers (Basel). 2021;13(11):2607. doi:10.3390/cancers/13112607. 4. National Cancer Institute. Fertility issues in girls and women with cancer. http://www.cancer.gov. Accessed June 13, 2022. 5. Alessi I., Caroleo A.M., de Palma L., Mastronuzzi A., Pro S., Colafati G.S., Boni A., Della Vecchia N., Velardi M., Evangelisti M., et al. Short and Long-Term Toxicity in Pediatric Cancer Treatment: Central 9 Nervous System Damage. Cancers. 2022;14:1540. doi: 10.3390/cancers14061540.

Overview U.S. prescribing information for OJEMDA Available in tablet formulation and pediatric- friendly powder for oral suspension Indication OJEMDA is indicated for the treatment of pediatric patients 6 months of age and older with relapsed or refractory pediatric low-grade glioma harboring a BRAF fusion or rearrangement, or BRAF V600 mutation Recommended Dose 2 380 mg/m administered orally once weekly (not to exceed a dose of 600mg once weekly); OJEMDA can be taken with or without food For full prescribing information, visit dayonebio.com * This indication is approved under accelerated approval based on response rate and duration of response. Continued approval for this indication may be contingent upon verification of clinical benefit in a confirmatory trial. 10 10

Efficacy summary from OJEMDA prescribing information RAPNO-LGG Response (IRC) n n (%) 95% CI 51% ORR, n (%) 76 39 (51) 40-63 BRAF fusion or rearrangement 64 33 (52) 39-64 BRAF V600 mutation 12 6 (50) 21-79 Overall response rate (RAPNO-LGG) Prior MAPKi use 45 22 (49) 31-64 in 76 evaluable patients MAPKi-naïve 31 17 (55) 36-73 † Median DOR, months 39 13.8 11.3-NR Median TTR, months 39 5.3 Range 1.6-11.2 June 5, 2023 data cutoff. CI, confidence interval; DOR, duration of response; IRC, independent radiology review committee; LGG, low-grade glioma; NR, not reached; ORR, overall response rate; RAPNO, Response Assessment † in Pediatric Neuro-Oncology; TTR, time to response; CR, complete response; PR, partial response; MR, minor response; SD, stable disease; PD, progressive disease. As of the data cutoff, 66% remain on tovorafenib. 11

Safety summary from OJEMDA prescribing information TEAEs (≥ 30% of patients [n=137]) Warnings and Precautions Preferred Term, n (%) Any Grade Grade ≥3 Any AE 137 (100) 86 (63) • Hemorrhage Hair color changes 104 (76) 0 Anemia 81 (59) 15 (11) • Skin toxicity, including photosensitivity Elevated CPK 80 (58) 16 (12) Fatigue 76 (55) 6 (4) • Hepatotoxicity Vomiting 68 (50) 6 (4) • Effect on growth Hypophosphatemia 64 (47) 0 Headache 61 (45) 2 (1) • Embryo-fetal toxicity Maculo-papular rash 60 (44) 11 (8) • Use in NF1- associated tumors Pyrexia 53 (39) 5 (4) Dry skin 49 (36) 0 Elevated LDH 48 (35) 0 Increased AST 47 (34) 4 (3) Constipation 45 (33) 0 Nausea 45 (33) 0 No boxed warnings or Upper RTI 43 (31) 2 (1) Dermatitis acneiform 42 (31) 1 (1) contraindications Epistaxis 42 (31) 1 (1) June 5, 2023 data cutoff. OJEMDA safety data (n=137). Treatment-emergent AEs ≥20% any grade in arms 1 & 2. AE, adverse event; AST, aspartate aminotransferase; CPK, creatine phosphokinase; LDH, lactate dehydrogenase; RTI, respiratory tract infection; TEAEs, treatment-emergent adverse events. 12
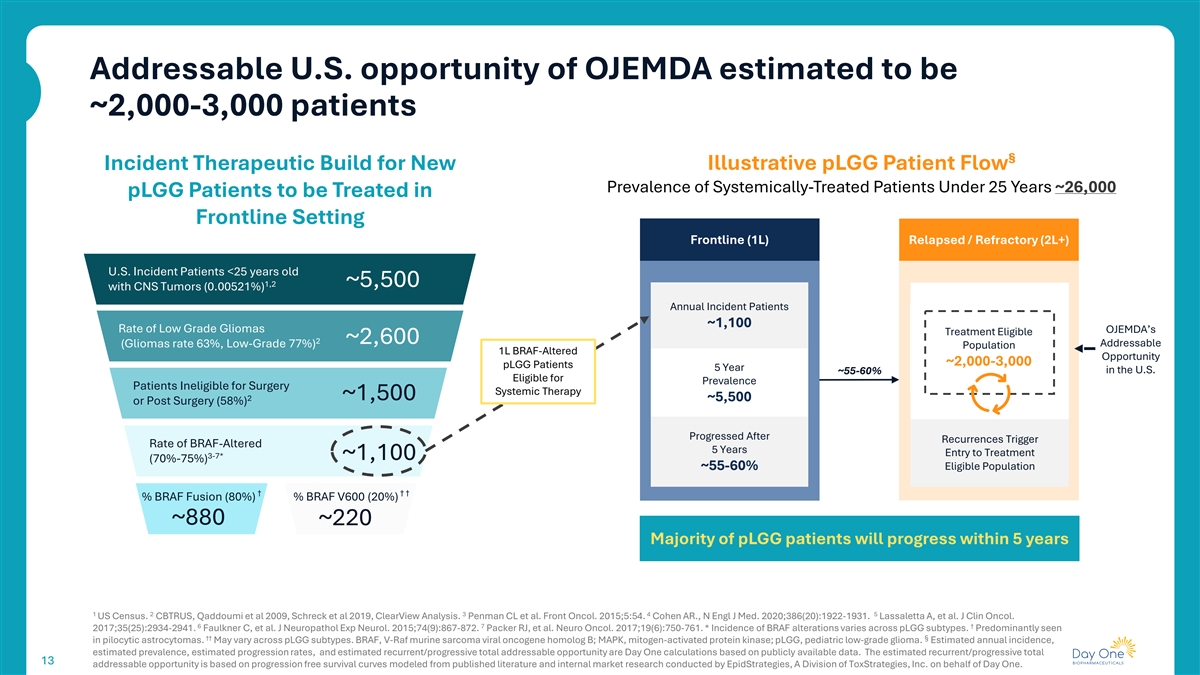
Addressable U.S. opportunity of OJEMDA estimated to be ~2,000-3,000 patients § Incident Therapeutic Build for New Illustrative pLGG Patient Flow Prevalence of Systemically-Treated Patients Under 25 Years ~26,000 pLGG Patients to be Treated in Frontline Setting Frontline (1L) Relapsed / Refractory (2L+) U.S. Incident Patients <25 years old 1,2 ~5,500 with CNS Tumors (0.00521%) Annual Incident Patients ~1,100 Rate of Low Grade Gliomas OJEMDA’s Treatment Eligible 2 ~2,600 Addressable (Gliomas rate 63%, Low-Grade 77%) Population 1L BRAF-Altered Opportunity ~2,000-3,000 pLGG Patients 5 Year in the U.S. ~55-60% Eligible for Prevalence Patients Ineligible for Surgery Systemic Therapy ~1,500 2 ~5,500 or Post Surgery (58%) Progressed After Recurrences Trigger Rate of BRAF-Altered 5 Years Entry to Treatment 3-7* ~1,100 (70%-75%) ~55-60% Eligible Population † † † % BRAF Fusion (80%) % BRAF V600 (20%) ~880 ~220 Majority of pLGG patients will progress within 5 years 1 2 3 4 5 US Census. CBTRUS, Qaddoumi et al 2009, Schreck et al 2019, ClearView Analysis. Penman CL et al. Front Oncol. 2015;5:54. Cohen AR., N Engl J Med. 2020;386(20):1922-1931. Lassaletta A, et al. J Clin Oncol. 6 7 † 2017;35(25):2934-2941. Faulkner C, et al. J Neuropathol Exp Neurol. 2015;74(9):867-872. Packer RJ, et al. Neuro Oncol. 2017;19(6):750-761. * Incidence of BRAF alterations varies across pLGG subtypes. Predominantly seen †† § in pilocytic astrocytomas. May vary across pLGG subtypes. BRAF, V-Raf murine sarcoma viral oncogene homolog B; MAPK, mitogen-activated protein kinase; pLGG, pediatric low-grade glioma. Estimated annual incidence, estimated prevalence, estimated progression rates, and estimated recurrent/progressive total addressable opportunity are Day One calculations based on publicly available data. The estimated recurrent/progressive total 13 13 addressable opportunity is based on progression free survival curves modeled from published literature and internal market research conducted by EpidStrategies, A Division of ToxStrategies, Inc. on behalf of Day One.
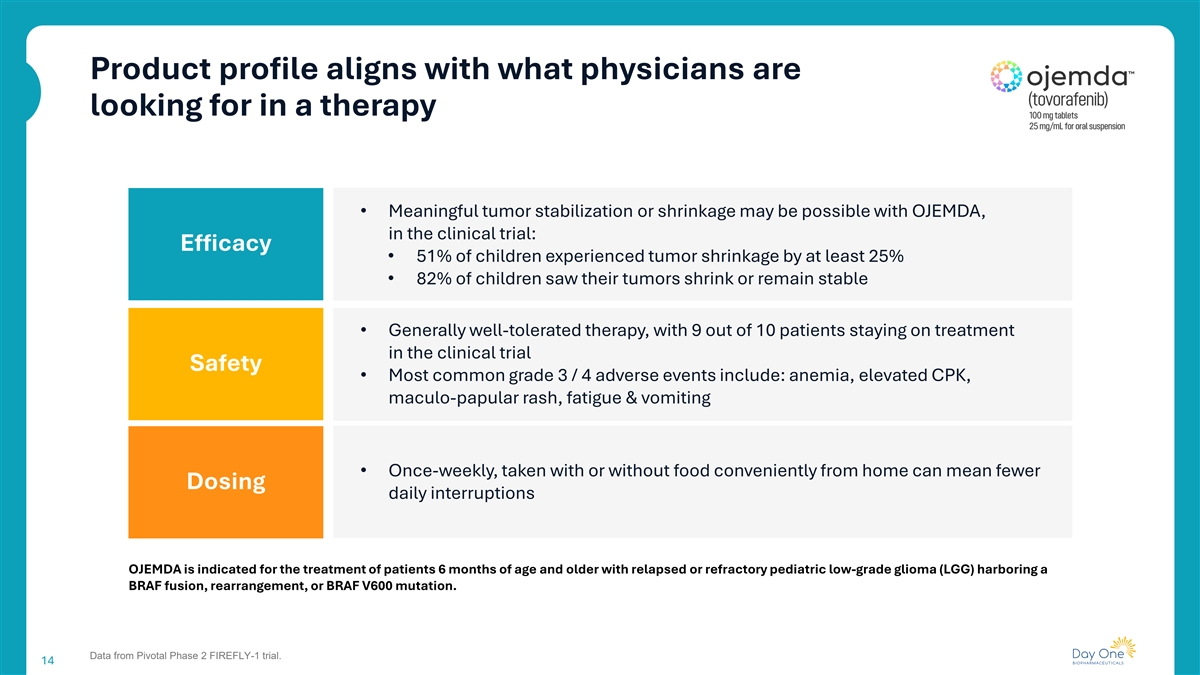
Product profile aligns with what physicians are looking for in a therapy • Meaningful tumor stabilization or shrinkage may be possible with OJEMDA, in the clinical trial: Efficacy • 51% of children experienced tumor shrinkage by at least 25% • 82% of children saw their tumors shrink or remain stable • Generally well-tolerated therapy, with 9 out of 10 patients staying on treatment in the clinical trial Safety • Most common grade 3 / 4 adverse events include: anemia, elevated CPK, maculo-papular rash, fatigue & vomiting • Once-weekly, taken with or without food conveniently from home can mean fewer Dosing daily interruptions OJEMDA is indicated for the treatment of patients 6 months of age and older with relapsed or refractory pediatric low-grade glioma (LGG) harboring a BRAF fusion, rearrangement, or BRAF V600 mutation. Data from Pivotal Phase 2 FIREFLY-1 trial. 14

Foundation for future growth through strong launch execution Our goal is to enable children with pLGG to live as normal of a childhood as possible, without interruptions Key factors expected to drive OJEMDA’s commercial opportunity • Profile aligned with prescriber and patient needs • Commercial execution driving awareness to increase breadth and depth of prescribers • Significant growth opportunity as we strengthen market position as the standard of care in 2nd line • Broad payer coverage established 15 15
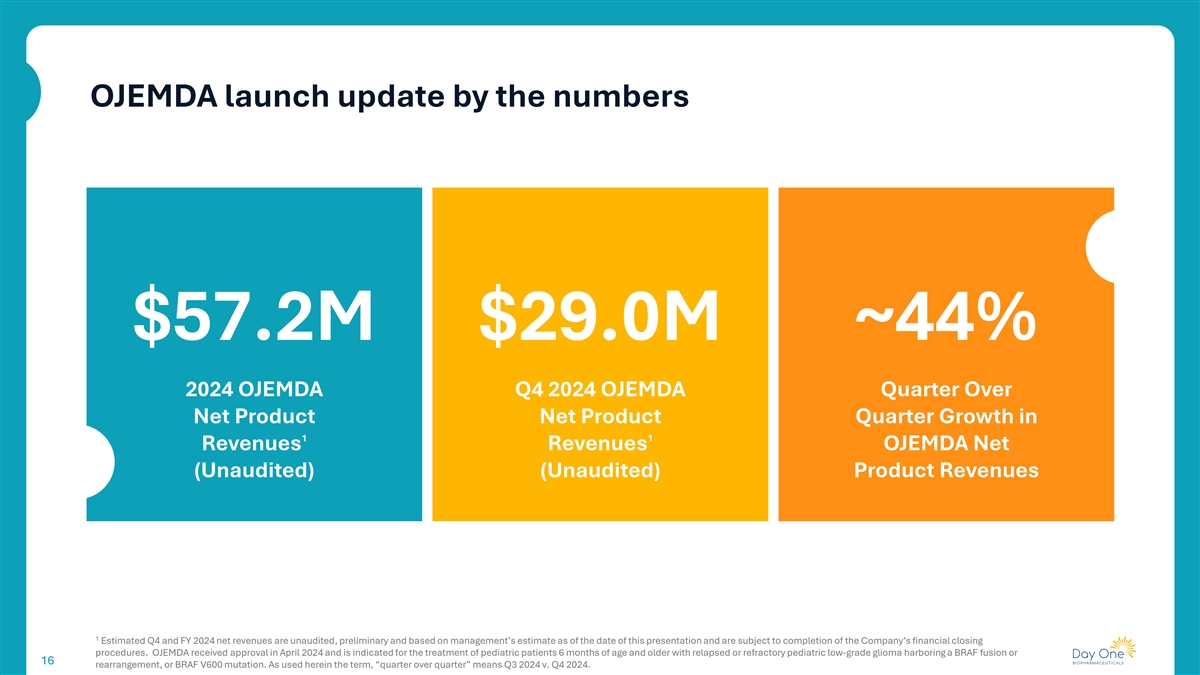
OJEMDA launch update by the numbers $57.2M $29.0M ~44% 2024 OJEMDA Q4 2024 OJEMDA Quarter Over Net Product Net Product Quarter Growth in 1 1 Revenues Revenues OJEMDA Net (Unaudited) (Unaudited) Product Revenues 1 Estimated Q4 and FY 2024 net revenues are unaudited, preliminary and based on management’s estimate as of the date of this presentation and are subject to completion of the Company’s financial closing procedures. OJEMDA received approval in April 2024 and is indicated for the treatment of pediatric patients 6 months of age and older with relapsed or refractory pediatric low-grade glioma harboring a BRAF fusion or 16 16 rearrangement, or BRAF V600 mutation. As used herein the term, “quarter over quarter” means Q3 2024 v. Q4 2024.
OJEMDA priorities to drive revenue growth in 2025 Continue to increase breadth and depth of prescribers Establish OJEMDA as standard of care in 2nd line relapsed or refractory BRAF-altered pLGG Support prescribers and patients to allow for optimal duration of treatment 17 17

FIREFLY-2 Pivotal Phase 3 trial of tovorafenib in front-line pLGG Bradon Living with pLGG since age 11 18

Expansion into front-line treatment represents a meaningful expansion opportunity for tovorafenib in pLGG Trial design Endpoints • Randomized, global, registrational Phase 3 trial of monotherapy tovorafenib • Primary endpoint: ORR based on RAPNO-LGG criteria, assessed by vs SoC chemotherapy blinded independent central review ‒ The ORR primary analysis is expected to occur ~12 months after the • Eligibility: Patients aged up to <25 years with LGG harboring a RAF alteration last patient randomized and requiring first-line systemic therapy • Key secondary endpoints: PFS and DoR by RAPNO-LGG criteria • Tovorafenib available as tablets and pediatric-friendly liquid suspension • Other secondary endpoints: changes in neurological and visual function, • Patients who progress after stopping tovorafenib may be re-challenged safety, and tolerability • Patients who progress in the SoC arm during or post-treatment may cross- • Key exploratory objectives: QoL and health utilization measures over to receive tovorafenib 2 Tovorafenib, 380mg/m QW Non-resectable or (not to exceed 600 mg) Stratified by sub-total resected LGG AND Long-term follow-up • Location of tumor Requiring first-line • Genomic alteration (48 months) systemic therapy Investigator's choice of • CDKN2A status vincristine/carboplatin* or N ≈ 400 • Infant CHG diagnosis vinblastine or monthly carboplatin * COG or SIOPe-LGG regimen. Abbreviations: CHG, chiasmatic, hypothalamic glioma; DoR, duration of response; LGG, low-grade glioma; ORR, objective response rate; QoL, quality of life; QW, once weekly; SoC, standard of care. 19 1:1 Randomization
DAY301 PTK7-targeted antibody-drug conjugate (ADC) 20
DAY301: Next generation ADC targeting PTK7 Substantial development PTK7: clinically- DAY301: potential first- and commercial potential validated ADC target in-class asset for DAY301 Anti-tumor activity of anti-PTK7 Novel ADC active in High PTK7 expression in ADC demonstrated in Phase 1b preclinical models, designed multiple adult and pediatric trial of Pfizer / Abbvie’s to maximize therapeutic tumor indications 1 cofetuzumab pelidotin window First dose cohort cleared January 2025 1 Cho BC, et al. Ann Oncol. (34; Suppl 2): S460-S461, 2023. 21

PTK7: A clinically-validated ADC target Potential opportunity for a next-generation PTK7 ADC with improved therapeutic index 1 • Clinical results for cofetuzumab pelidotin demonstrated proof of concept for PTK7-targeted ADCs • Cofetuzumab pelidotin activity seen in multiple tumor types: • Ovarian (Pt-resistant): ORR 27% (n=63) • TNBC: ORR 21% (n=29) • NSCLC: ORR 19% (n=31) • mDOR: 4.2-5.7m for Ovarian (Pt-resistant)/TNBC/NSCLC • mPFS: 1.5-2.9m for Ovarian (Pt-resistant)/TNBC/NSCLC • Aur0101 program limited by toxicity, resulting in reduced dose intensity and duration • A next generation product with optimized properties and a better therapeutic index may achieve greater clinical efficacy 1 Phase 1b study of PF-06647020/ABBV-647. 22

DAY301: Potential first-in-class asset DAY301 has been designed to maximize therapeutic index and overcome limitations of prior programs • Tumor regression at tolerable doses seen in multiple preclinical models • Higher HNSTD in cyno toxicology studies; payload with known safety profile • High cell permeability / bystander effect; low efflux (not a P-gp substrate) • Novel, highly hydrophilic, cleavable linker • Moderate-to-high affinity antibody with favorable stability and developability profile • Drug-antibody-ratio (DAR) of 8, shown to be effective for other ADCs in solid tumors • IP: Composition of Matter patent term expected 2044, once issued 1) Damelin M, et al. A PTK7-targeted antibody-drug conjugate reduces tumor-initiating cells and induces sustained tumor regressions. Sci Transl Med. 2017. HNSTD, Highest Non-Severely Toxic Dose; P-gp, P-glycoprotein. 23

DAY301: First-in-class potential Improved tumor regression activity demonstrated for DAY301 vs. benchmarks in multiple preclinical models PDX 362797 SCLC PDX 362310 TNBC PDX LD1-200615 HNSCC 2,400 H-score 210 H-score 255 H-score 120 3,000 4,000 2,000 1,600 3,000 2,000 1,200 2,000 800 1,000 400 1,000 0 0 0 20 40 60 80 14 21 28 35 0 0 7 Days Post Administration 0 7 Days Post A 14dministra21 tion 28 Days Post Administration Vehicle Control antibody + auristatin payload, 5 mg/kg Vehicle Cofetuzumab pelidotin, 10 mg/kg Cofetuzumab pelidotin, 5 mg/kg Control antibody + DAY301 payload Anti-DLL3 mAb + DAY301 payload, 10 mg/kg Control antibody + DAY301 payload, 10 mg/kg Control antibody + auristatin payload B7-H3 DXd ADC, 10 mg/kg Cofetuzumab mAb + DAY301 payload, 10 mg/kg Cofetuzumab pelidotin, 5 mg/kg Chemotherapy control DAY301, 5 mg/kg Cofetuzumab mAb + DAY301 payload DAY301, 10 mg/kg Control antibody + DAY301 payload DAY301, 10 mg/kg DAY301, 10 mg/kg Indicates when drug was administered Ref: Kong C, et al. MTX-13, a Novel PTK7-Directed Antibody–Drug Conjugate with Widened Therapeutic Index Shows Sustained Tumor Regressions for a Broader Spectrum of PTK7-Positive Tumors. Mol Cancer Ther. 2023 24 3 Tumor Volume (mm ) (Mean ± SEM) 3 Tumor Volume (mm ) (Mean ± SEM) *P 0.0435 3 Tumor Volume (mm ) (Mean ± SEM) *P 0.0316

DAY301: Encouraging development and commercial opportunities PTK7 U.S. Patient Population ORR at Median OS at Indication Expression (>1+) Cases/Deaths Relapse Relapse 2 3 7 7 Endometrial 100% 67,880/13,250 39% 9 months 1 3 4 4 Esophageal SCC 76% 22,370/16,130 5% 3 months 2 3 14 15 Gastric 35% 26,890/10,880 12% 6-14 months 1 3 5 5 Head & Neck SCC 75% 54,540/11,580 32% 7.8 months 2 3 8 9 NSCLC 50% 199,393/106,310 45-60% 7-12 months 2 3 3 6 Ovarian (platinum resistant) 30% (95%)* 19,710/13,270 20-35% 17.2 months 2 3 10 11 Small Cell Lung 50% 35,187/18,760 10-40% 9-12 months 2 3,16 12 13 TNBC 70% 46,608/12,675 5-35% 28 months Potential pediatric indications include: neuroblastoma, rhabdomyosarcoma and osteosarcoma 1 Kong et al, 2023; 2 Protein Atlas; 3 PDQ; 4 Parry et al, 2015; 5 Vermorken et al, 2010; 6 Sehouli et al, 2008; 7 Rutten et al, 2021; 8 Park et al, 2017; 9 Assi et al, 2023; 10 Abughanimeh et al, 2020; 11 Asai et al, 2014; 12 Bardia et al, 2021; 13 Cai et al, 2023; 14 Sym et al, 2008; 15 Ji et al, 2023; 16 Saraivaet al, 2017. * MabCare data 25

DAY301: Initial Phase1a/b clinical trial design Key design elements Adult & pediatric development • BOIN design for efficiency of dose escalation • Potential adult indications include platinum resistant ovarian cancer, squamous NSCLC, esophageal SCC, HNSCC, endometrial, and/or SCLC • Backfill active dose levels to generate additional safety data • Patients to be selected based on PTK7 expression clinical trial assay • Enroll tumor types with known high PTK7 expression • Pediatric dose confirmation and efficacy assessment to begin near/at the • Advance two recommended dose levels to Phase 1b end of adult dose escalation • Final dose optimization scheme and possible registrational path(s) pending • Initial target indications include neuroblastoma, osteosarcoma, discussions with FDA at end of dose escalation/expansion rhabdomyosarcoma Phase 1b: Monotherapy Dose Expansion and Optimization Phase 1a: Monotherapy Dose Escalation DL5 Go to dose Expand to a potential single-arm RD1 cohort RD1 optimization registrational trial for accelerated Simon 2-stage approval or randomized trial at DL4 design optimized dose RD2 cohort DL3 RD1 RD2 Phase 1: Pediatric DL2 Identify two recommended RD2 Monotherapy Dose Lower of the two dose levels for further RD1 adult RDs Confirmation DL1 evaluation, based on safety and anti-tumor activity FDA-cleared RD-1 starting dose DL, Dose Level; RD, Recommended Dose; BOIN, Bayesian Optimal Interval; HNSCC, Head and Neck Squamous Cell Carcinoma; SCLC, Small Cell Lung Cancer; SCC, Squamous-Cell Carcinoma; NSCLC, Non-Small Cell 26 Lung Cancer

Summary 27
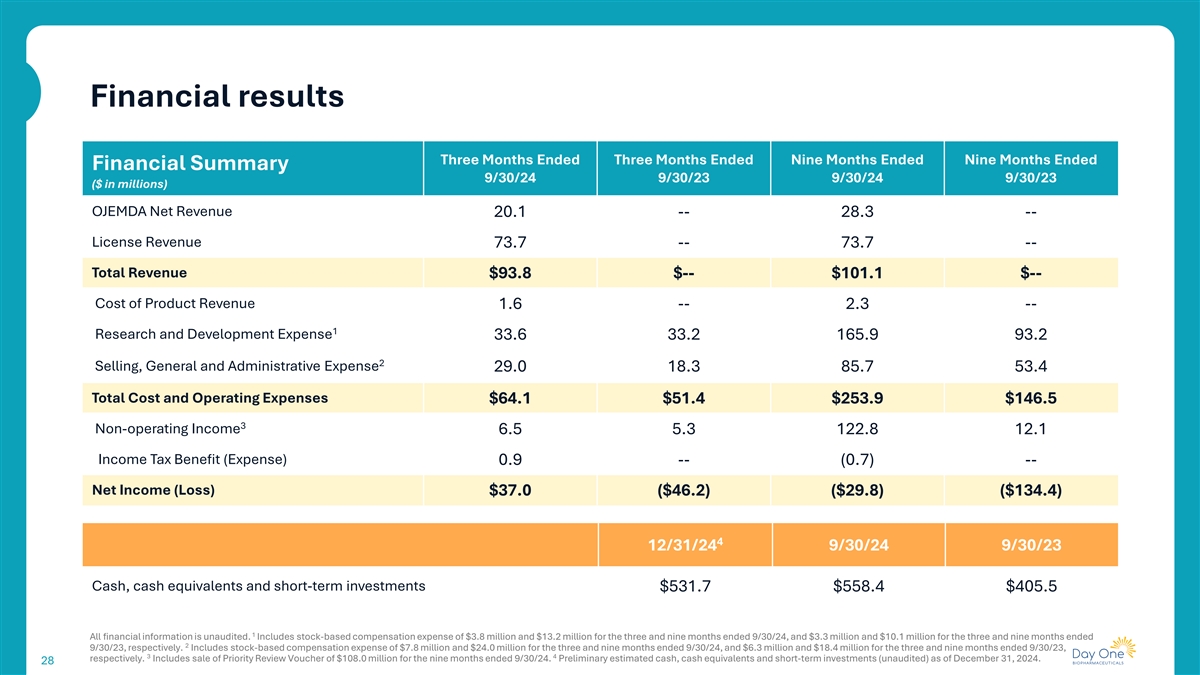
Financial results Three Months Ended Three Months Ended Nine Months Ended Nine Months Ended Financial Summary 9/30/24 9/30/23 9/30/24 9/30/23 ($ in millions) OJEMDA Net Revenue 20.1 -- 28.3 -- License Revenue 73.7 -- 73.7 -- Total Revenue $93.8 $-- $101.1 $-- Cost of Product Revenue 1.6 -- 2.3 -- 1 Research and Development Expense 33.6 33.2 165.9 93.2 2 Selling, General and Administrative Expense 29.0 18.3 85.7 53.4 Total Cost and Operating Expenses $64.1 $51.4 $253.9 $146.5 3 Non-operating Income 6.5 5.3 122.8 12.1 Income Tax Benefit (Expense) 0.9 -- (0.7) -- Net Income (Loss) $37.0 ($46.2) ($29.8) ($134.4) 4 12/31/24 9/30/24 9/30/23 Cash, cash equivalents and short-term investments $531.7 $558.4 $405.5 1 All financial information is unaudited. Includes stock-based compensation expense of $3.8 million and $13.2 million for the three and nine months ended 9/30/24, and $3.3 million and $10.1 million for the three and nine months ended 2 9/30/23, respectively. Includes stock-based compensation expense of $7.8 million and $24.0 million for the three and nine months ended 9/30/24, and $6.3 million and $18.4 million for the three and nine months ended 9/30/23, 3 4 respectively. Includes sale of Priority Review Voucher of $108.0 million for the nine months ended 9/30/24. Preliminary estimated cash, cash equivalents and short-term investments (unaudited) as of December 31, 2024. 28

Day One is well positioned for sustainable growth and long-term success Execute on clinical Drive OJEMDA development pipeline for revenue growth FIREFLY-2 and DAY301 Leverage our development and Maintain strong capital commercialization expertise to position while investing in further expand our multiple our pipeline asset portfolio 29 29

Appendix 30

Tovorafenib inhibits both BRAF fusions and BRAF V600 mutations MAPK RAS-independent activation of the Tovorafenib is an investigational, oral, pathway MAPK pathway selective, CNS-penetrant, type II RAF inhibitor that was designed to inhibit both monomeric and dimeric RAF kinase RAS • Activity in tumors driven by both RAF fusions and BRAF V600E mutations RAF RAF • Tablet and pediatric-friendly liquid RAF Tovorafenib suspension mutation fusion • Once weekly dosing Currently approved type I BRAF MEK inhibitors are indicated for use in patients with tumors bearing BRAF V600 mutations • Type I BRAF inhibitors cause ERK paradoxical MAPK activation in the setting of wild-type RAF, increasing the risk of tumor growth in BRAF fusion-driven Proliferation and survival Proliferation and survival Proliferation and survival Source: 1. Sun Y et al., Neuro Oncol. 2017; 19: 774–85; 2. Sievart AJ et al., PNAS. 2013; 110:5957-62; 3. Karajannis MA et al., Neuro Oncol 2014;16(10):1408-16. 31

Pivotal Phase 2 trial of monotherapy tovorafenib in relapsed or progressive pLGG (FIREFLY-1) Trial design Endpoints (pivotal arm 1) 1 • Three arm, open-label, global registrational phase 2 trial • Primary endpoint: ORR based on RANO-HGG , assessed by blinded independent central review • Pivotal Arm 1 (recurrent/progressive pLGG, n=77): harboring a KIAA1549- BRAF fusion or BRAF V600E mutation 2 • Secondary endpoints: ORR by RAPNO-LGG assessed by blinded independent • Arm 2 (expanded access recurrent/progressive LGG, n=60): harboring an central review; PFS, DoR; TTR, CBR; safety activating RAF alteration 3 • Exploratory analyses: ORR and CBR by RANO-LGG assessed by blinded • Arm 3 (extracranial solid tumors): harboring an activating RAF fusion independent central review rd Clinical and radiological evaluations at baseline, and every 3 Key Inclusion Criteria nd cycle for pLGG and every 2 cycle for solid tumors • 6 months – 25 years of age Day –28 to 0 • RAF-altered tumor Enrollment/ • ≥1 prior line of systemic Screening Baseline End of Trial Study Drug Administration After Cycle 27: patients may either C27D1 therapy with radiographic (C1D1) 2 continue treatment or enter drug 420mg/m QW (not to exceed 600mg), progression holiday period at any time (at QW in 28-day cycles discretion of investigator) • Prior use of MAPK pathway targeted therapy was permitted Eligibility evaluation Treatment period: minimum of 2 years or until progression or toxicity/intolerability 1 2 3 June 5, 2023 data cutoff. Wen PY, et al. J Clin Oncol. 2010;28(11):1963-1972. Fangusaro J, et al. Lancet Oncol. 2020;21(6):e305–316. van den Bent MJ, et al. Lancet Oncol. 2011;12(6):583-593. Abbreviations: CBR, clinical benefit rate; IRC, independent review committee; C, cycle; D, day; LGG, low-grade glioma; ORR, objective response rate; PFS, progression-free survival; DoR, duration of response; QW, once weekly; TTR, time to response; RANO, Response 32 Assessment in Neuro-Oncology; RAPNO, Response Assessment in Pediatric Neuro-Oncology; MAPK, mitogen-activated protein kinase. For more information, please refer to NCT04775485

FIREFLY-1 Data from pivotal phase 2 trial June 5, 2023 data cutoff 33

FIREFLY-1 baseline patient characteristics Characteristic Arm 1 (n=77) Location (n=77) Median age, years (range) 8 (2-21) Deep midline structures Optic pathway 12% 51% Sex, n (%) Male 40 (52) Other † Female 37 (48) 16% Cerebral hemisphere 8% Race, n (%) White 41 (53) Cerebellum Brain stem 6% Asian 5 (6) 8% Black 2 (3) Multiple 3 (4) Other 6 (8) BRAF alteration (n=77) Not specified 20 (26) Number of lines of prior systemic therapy Median (range) 3 (1-9) 17% 1, n (%) 17 (22) 2, n (%) 21 (27) ≥3, n (%) 39 (51) Prior MAPK pathway targeted therapy, n (%) 83% Prior MEK inhibitor 43 (56) Prior BRAF inhibitor 8* (10) ‡ Prior BRAF and MEK inhibitors 5 (7) BRAF V600E BRAF Fusion* Any MAPK inhibitor 46 (60) * † June 5, 2023 data cutoff. Includes 6 patients with BRAF duplication and 2 with BRAF rearrangement per fluorescence in situ hybridization or in situ hybridization. Includes tumors that were extending into multiple regions of the brain, leptomeningeal disease, and/or spinal disease. ‡The 5 patients that had previously received both a MEK inhibitor and also a BRAF inhibitor are recorded in both the “Prior MEK inhibitor” and “Prior BRAF inhibitor” groups. 34 MAPK, mitogen-activated protein kinase.
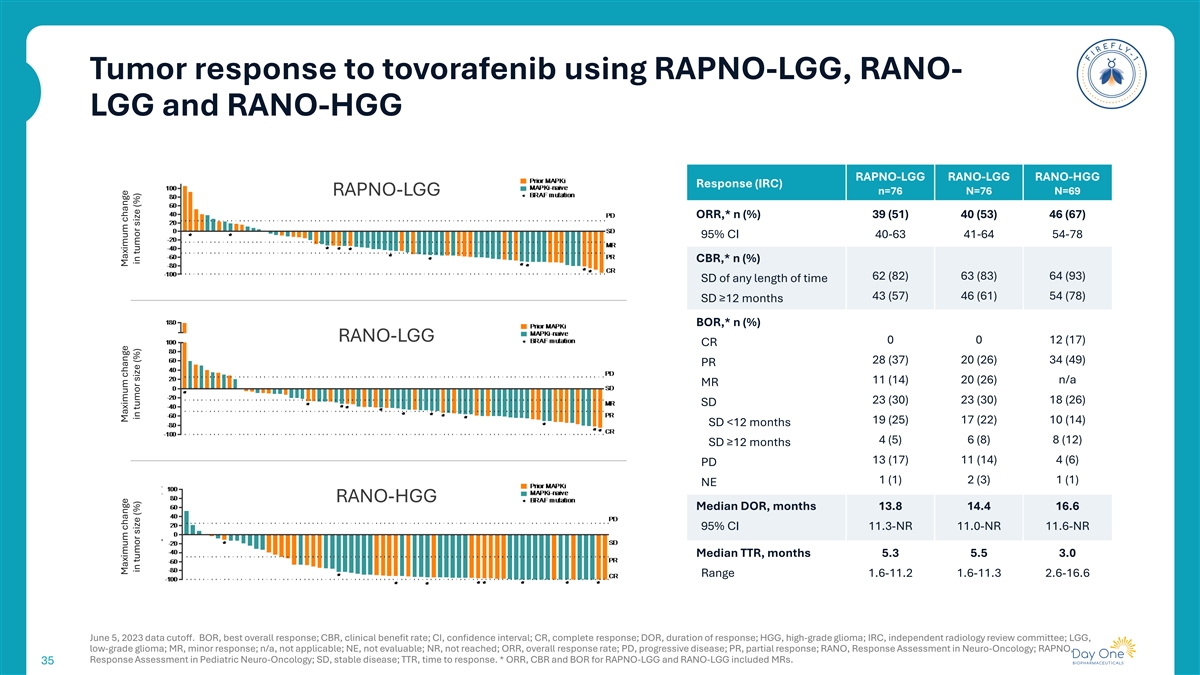
Tumor response to tovorafenib using RAPNO-LGG, RANO- LGG and RANO-HGG RAPNO-LGG RANO-LGG RANO-HGG Response (IRC) n=76 N=76 N=69 RAPNO-LGG ORR,* n (%) 39 (51) 40 (53) 46 (67) 95% CI 40-63 41-64 54-78 CBR,* n (%) 62 (82) 63 (83) 64 (93) SD of any length of time 43 (57) 46 (61) 54 (78) SD ≥12 months BOR,* n (%) RANO-LGG 0 0 12 (17) CR 28 (37) 20 (26) 34 (49) PR 11 (14) 20 (26) n/a MR 23 (30) 23 (30) 18 (26) SD 19 (25) 17 (22) 10 (14) SD <12 months 4 (5) 6 (8) 8 (12) SD ≥12 months 13 (17) 11 (14) 4 (6) PD 1 (1) 2 (3) 1 (1) NE RANO-HGG Median DOR, months 13.8 14.4 16.6 95% CI 11.3-NR 11.0-NR 11.6-NR Median TTR, months 5.3 5.5 3.0 Range 1.6-11.2 1.6-11.3 2.6-16.6 June 5, 2023 data cutoff. BOR, best overall response; CBR, clinical benefit rate; CI, confidence interval; CR, complete response; DOR, duration of response; HGG, high-grade glioma; IRC, independent radiology review committee; LGG, low-grade glioma; MR, minor response; n/a, not applicable; NE, not evaluable; NR, not reached; ORR, overall response rate; PD, progressive disease; PR, partial response; RANO, Response Assessment in Neuro-Oncology; RAPNO, Response Assessment in Pediatric Neuro-Oncology; SD, stable disease; TTR, time to response. * ORR, CBR and BOR for RAPNO-LGG and RANO-LGG included MRs. 35 Maximum change Maximum change Maximum change in tumor size (%) in tumor size (%) in tumor size (%)

Duration of tovorafenib therapy for all patients with RAPNO-LGG evaluable lesions 5.3 Median time to response Months Median duration of 13.8 treatment Months Overall treatment duration (months) June 5, 2023 data cutoff. 36 Patients

Duration of tovorafenib therapy for all patients with RANO- HGG evaluable lesions 3.0 Median time to response Months Median duration of 16.6 treatment Months Overall treatment duration (months) June 5, 2023 data cutoff. 37 Patients
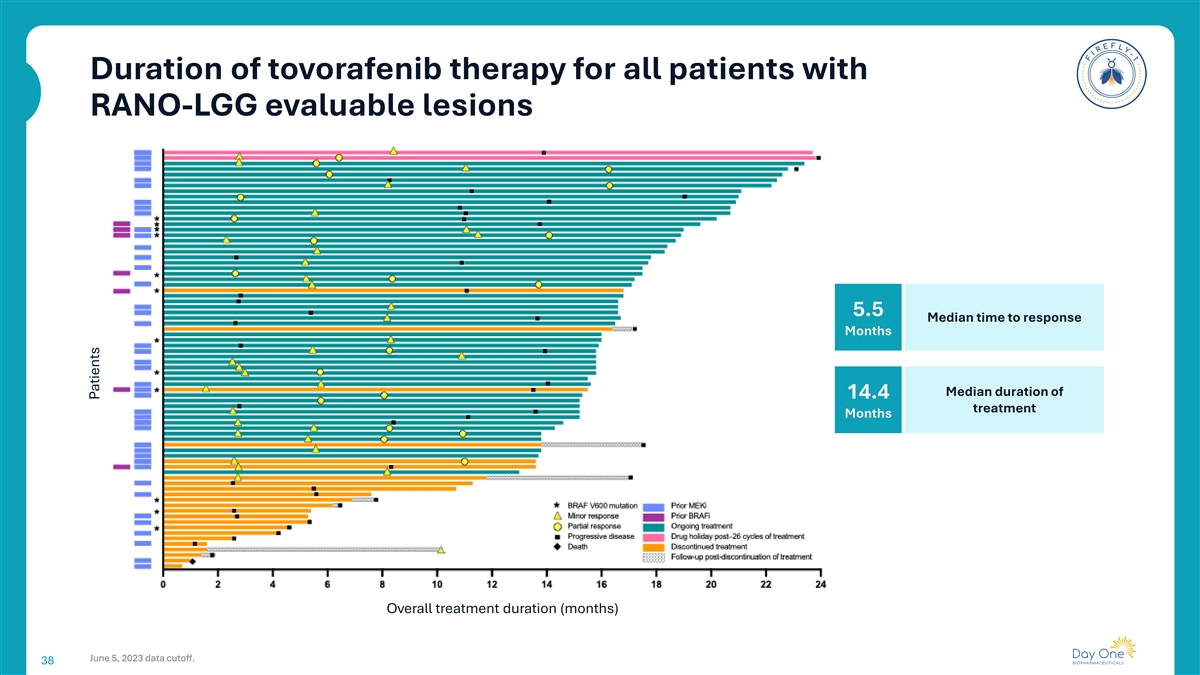
Duration of tovorafenib therapy for all patients with RANO-LGG evaluable lesions 5.5 Median time to response Months Median duration of 14.4 treatment Months Overall treatment duration (months) June 5, 2023 data cutoff. 38 Patients

Tumor response to tovorafenib across three assessment criteria were consistent across BRAF fusion and mutation patients, and patients with prior MAPK treament 2 3,4 1 RAPNO-LGG RANO-LGG RANO-HGG Response (IRC) n n n ORR,* n (%) 76 39 (51) 76 40 (53) 69 46 (67) BRAF fusion 64 33 (52) 64 33 (52) 59 41 (69) BRAF mutation 12 6 (50) 12 7 (58) 10 5 (50) Prior MAPKi 45 22 (49) 45 23 (51) 41 29 (71) MAPKi-naive 31 17 (55) 31 17 (55) 28 17 (61) CBR,* n (%) (SD of any length of time) 76 62 (82) 76 63 (83) 69 64 (93) BRAF fusion 64 53 (83) 64 53 (83) 59 55 (93) BRAF mutation 12 9 (75) 12 10 (83) 10 9 (90) Prior MAPKi 45 38 (84) 45 38 (84) 41 37 (90) MAPKi-naive 31 24 (77) 31 25 (81) 28 27 (96) CBR,* n (%) (SD ≥12 months) 76 43 (57) 76 46 (61) 69 54 (78) BRAF fusion 64 37 (58) 64 39 (61) 59 49 (83) BRAF mutation 12 6 (50) 12 7 (58) 10 5 (50) Prior MAPKi 45 25 (56) 45 26 (58) 41 33 (80) MAPKi-naive 31 18 (58) 31 20 (65) 28 21 (75) Median DOR, months (95% CI)** 39 13.8 (11.3-NR) 40 14.4 (11.0-NR) 46 16.6 (11.6-NR) BRAF fusion 33 13.8 (11.3-NR) 33 16.3 (11.0-NR) 41 16.8 (11.6-NR) BRAF mutation 6 NR (8.4-NR) 7 12.0 (8.4-NR) 5 15.1 (8.3-NR) Prior MAPKi 22 13.8 (11.3-NR) 23 12.0 (8.5-NR) 29 15.1 (9.0-16.8) MAPKi-naive 17 NR (8.4-NR) 17 16.3 (8.4-NR) 17 NR (11.6-NR) 1 2 3 June 5, 2023 data cutoff. Fangusaro J, et al. Lancet Oncol. 2020;21(6):e305–316. Fangusaro J, et al. Lancet Oncol. 2020;21(6):e305–316. van den Bent MJ, et al. Lancet Oncol. 2011;12(6):583-593. 4. Wen PY, et al. J. Clin Oncol. 39 2017;35(21),2439-2449. * ORR, CBR for RAPNO-LGG and RANO-LGG included MRs. ** the 95% CI were calculated using Kaplan-Meier method.
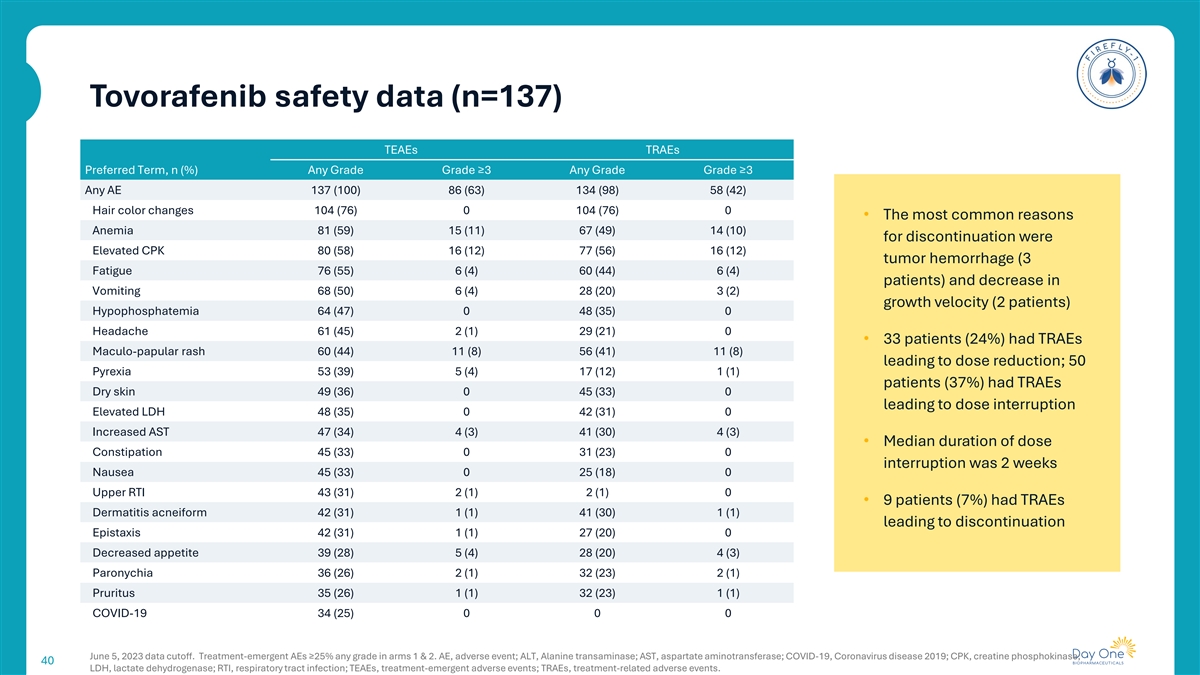
Tovorafenib safety data (n=137) TEAEs TRAEs Preferred Term, n (%) Any Grade Grade ≥3 Any Grade Grade ≥3 Any AE 137 (100) 86 (63) 134 (98) 58 (42) Hair color changes 104 (76) 0 104 (76) 0 • The most common reasons Anemia 81 (59) 15 (11) 67 (49) 14 (10) for discontinuation were Elevated CPK 80 (58) 16 (12) 77 (56) 16 (12) tumor hemorrhage (3 Fatigue 76 (55) 6 (4) 60 (44) 6 (4) patients) and decrease in Vomiting 68 (50) 6 (4) 28 (20) 3 (2) growth velocity (2 patients) Hypophosphatemia 64 (47) 0 48 (35) 0 Headache 61 (45) 2 (1) 29 (21) 0 • 33 patients (24%) had TRAEs Maculo-papular rash 60 (44) 11 (8) 56 (41) 11 (8) leading to dose reduction; 50 Pyrexia 53 (39) 5 (4) 17 (12) 1 (1) patients (37%) had TRAEs Dry skin 49 (36) 0 45 (33) 0 leading to dose interruption Elevated LDH 48 (35) 0 42 (31) 0 Increased AST 47 (34) 4 (3) 41 (30) 4 (3) • Median duration of dose Constipation 45 (33) 0 31 (23) 0 interruption was 2 weeks Nausea 45 (33) 0 25 (18) 0 Upper RTI 43 (31) 2 (1) 2 (1) 0 • 9 patients (7%) had TRAEs Dermatitis acneiform 42 (31) 1 (1) 41 (30) 1 (1) leading to discontinuation Epistaxis 42 (31) 1 (1) 27 (20) 0 Decreased appetite 39 (28) 5 (4) 28 (20) 4 (3) Paronychia 36 (26) 2 (1) 32 (23) 2 (1) Pruritus 35 (26) 1 (1) 32 (23) 1 (1) COVID-19 34 (25) 0 0 0 June 5, 2023 data cutoff. Treatment-emergent AEs ≥25% any grade in arms 1 & 2. AE, adverse event; ALT, Alanine transaminase; AST, aspartate aminotransferase; COVID-19, Coronavirus disease 2019; CPK, creatine phosphokinase; 40 LDH, lactate dehydrogenase; RTI, respiratory tract infection; TEAEs, treatment-emergent adverse events; TRAEs, treatment-related adverse events.