UNITED STATES SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2006
OR
| o | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from ____________ to __________
Commission file number 0-8527
DIALYSIS CORPORATION OF AMERICA |
| (Exact name of registrant as specified in its charter) |
| FLORIDA | 59-1757642 | |
| (State or other jurisdiction of | (I.R.S. Employer | |
| incorporation or organization) | Identification No.) |
| 1302 CONCOURSE DRIVE, SUITE 204, LINTHICUM, MARYLAND | 21090 | |
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code (410) 694-0500
Securities registered under Section 12(b) of the Act:
None
Securities registered under Section 12(g) of the Exchange Act:
| Title of each class |
| common stock, $.01 par value |
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act.
Yes o No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act.
Yes o No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer or a non-accelerated filer. Check One
Large accelerated filer o Accelerated filer x Non-accelerated filer o
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No x
The aggregate market value of the voting and non-voting common equity held by non-affiliates computed by reference to the closing price at which the common equity was sold on June 30, 2006 was approximately $81,912,000.
As of March 14, 2007, the Company had 9,573,596 shares of its common stock outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Registrant’s Registration Statement on Form SB-2 dated December 22, 1995, as amended February 9, 1996, April 2, 1996 and April 15, 1996, Registration No. 33-80877-A Part II, Item 27, Exhibits, incorporated in Part IV of this Annual Report.
Registrant’s Annual Report, Form 10-K for the years ended December 31, 1999 and 2005, Part IV, Exhibits, incorporated in Part IV of this Annual Report.
Registrant’s Registration Statement on Form S-4/A-1 dated June 3, 2005, as amended August 10, 2005, Registration No. 333-125515, Annex A to the Proxy Statement/Prospectus, incorporated in Part IV of this Annual Report.
Registrant’s Definitive Proxy Statement, Schedule 14A, dated April 26, 2006, Appendix A, incorporated in Part IV of this Annual Report.
Registrant’s former parent’s (Medicore, Inc.’s) Annual Report, Form 10-K for the year ended December 31, 1997, Part IV, Exhibits, incorporated in Part IV of this Annual Report.
Portions of Registrant’s Definitive Proxy Statement to be filed with the Securities and Exchange Commission in connection with its 2007 Annual Meeting of Shareholders are incorporated into Part III, Items 10-14 of this Annual Report.
DIALYSIS CORPORATION OF AMERICA
Index to Annual Report on Form 10-K
Year Ended December 31, 2006
| Page | ||||
PART I | ||||
| Cautionary Notice Regarding Forward-Looking Information | 1 | |||
| 2 | ||||
| 22 | ||||
| 30 | ||||
| 30 | ||||
| 32 | ||||
| 32 | ||||
PART II | ||||
| 32 | ||||
| 35 | ||||
| 36 | ||||
| 50 | ||||
| 50 | ||||
| 50 | ||||
| 50 | ||||
| 52 | ||||
i
| Page | ||||
PART III | ||||
| 52 | ||||
| 52 | ||||
| 53 | ||||
| 53 | ||||
| 53 | ||||
PART IV | ||||
| 54 | ||||
| 58 |
ii
Part I
The statements contained in this annual report on Form 10-K dated March 15, 2007 and the documents incorporated by reference in this annual report that are not historical are forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 as amended (the “Securities Act”), and Section 21E of the Securities Exchange Act of 1934 (the “Exchange Act”). In addition, from time to time, we or our representatives have made or may make forward looking statements, orally or in writing, and in press releases. The Private Securities Litigation Reform Act of 1995 contains certain safe harbors for forward-looking statements. Certain of the forward-looking statements include management’s expectations, intentions, beliefs and strategies regarding the growth of our company and our future operations, the character and development of the dialysis industry, anticipated revenues, our need for and sources of funding for expansion opportunities and construction, expenditures, costs and income, our business strategies and plans for future operations, potential business combinations, and similar expressions concerning matters that are not considered historical facts. Forward-looking statements also include our statements regarding liquidity, anticipated cash needs and availability, and anticipated expense levels in Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” Words such as “anticipates,” “estimates,” “expects,” “projects,” “intends,” “plans” and “believes,” and words and terms of similar substance used in connection with any discussions of future operating or financial performance identify forward-looking statements. Such forward-looking statements, like all statements about expected future events, are based on assumptions and are subject to substantial risks and uncertainties that could cause actual results or transactions to materially differ from those expressed in the statements, including general economic, market and business conditions, opportunities pursued or not pursued, competition, changes in federal and state laws or regulations affecting the company and our operations, and other factors discussed periodically in our filings. Many of the foregoing factors are beyond our control. Among the factors that could cause actual results to differ materially are the factors detailed in the risks discussed in Item 1A, “Risk Factors” section beginning on page 22 of this annual report on Form 10-K. If any of such events occur or circumstances arise that we have not assessed, they could have a material adverse effect upon our revenues, earnings, financial condition and business, as well as the trading price of our common stock, which could adversely affect your investment in our company. Accordingly, readers are cautioned not to place too much reliance on such forward-looking statements. All subsequent written and oral forward-looking statements attributable to us or persons acting on our behalf, are expressly qualified in their entirety by the cautionary statements contained in this annual report. You should read this annual report on Form 10-K, the exhibits attached and the documents incorporated by reference completely and with the understanding that the company’s actual results may be materially different from what we expect.
The forward-looking statements speak only as of the date of this annual report on Form 10-K, and except as required by law, we undertake no obligation to rewrite or update such statements to reflect subsequent events.
Item 1. Business
Historical
We are a Florida corporation organized in 1976. We develop and operate outpatient kidney dialysis centers that provide quality dialysis and ancillary services to patients suffering from chronic kidney failure, generally referred to as end stage renal disease, or ESRD. We also provide acute inpatient dialysis treatments in hospitals, homecare services and dialysis center management services. We currently operate 34 outpatient dialysis facilities including an unaffiliated center in Georgia, which we manage pursuant to a management services agreement. Pursuant to the exercise of a call option held by one of our subsidiaries, we are acquiring the assets of this center through that subsidiary which will operate the facility and in which we will have an 80% interest. See Note 7 and Note 17 to “Notes to Consolidated Financial Statements.” During 2006, we acquired three dialysis centers, one in Virginia and two in Maryland, as well as all of the interest of an Ohio facility in which we were previously the minority owner, and we opened three new dialysis centers, one in Georgia, one in Pennsylvania and one in South Carolina. We are in the process of developing two new centers, one each in Ohio and South Carolina. Subsequent to the completion of the company’s merger with Medicore, Inc., its former parent in September, 2005, the company also engages in medical product sales.
Our principal executive offices are located at 1302 Concourse Drive, Suite 204, Linthicum, Maryland 21090, and you may contact us as follows:
telephone: (410) 694-0500
fax: (410) 694-0596
email: info@dialysiscorporation.com
Our internet website can be found at www.dialysiscorporation.com. You may obtain through our internet website, free of charge, our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, amendments to those reports filed with the SEC, press releases, corporate profiles and corporate governance materials. We also make those documents available to shareholders free of charge upon request.
General
Management believes the company distinguishes itself on the basis of quality patient care, and a patient-focused, courteous, highly trained professional staff. In addition to outpatient facilities, we provide acute inpatient dialysis treatments that are conducted under contractual relationships. Currently we have such relationships with ten hospitals and medical centers located in areas and states serviced by our outpatient dialysis facilities. Our homecare services, primarily through the use of peritoneal dialysis, requires us to provide equipment and supplies, training, monitoring and follow-up assistance to patients who are able to perform their treatments at home.
Our medical services revenue is derived primarily from four sources: (i) outpatient hemodialysis services (54%, 52% and 46% of medical services revenue for 2006, 2005 and 2004, respectively); (ii) home dialysis services (6%, 7%, and 7% of medical services revenue for 2006, 2005 and 2004, respectively); (iii) inpatient hemodialysis services for acute patient care provided through agreements with hospitals and medical centers (3%, 5% and 5% of medical services revenue for 2006, 2005 and 2004, respectively); and (iv) ancillary services associated with dialysis treatments, primarily the administration of erythropoietin (“EPO”), a bio-engineered protein that stimulates the production of red blood cells (a deteriorating kidney loses its ability to regulate red blood cell count, resulting in anemia), (37%, 36% and 42% of medical services revenue for 2006, 2005 and 2004, respectively with EPO representing 28% of medical services revenue for each of 2006, 2005 and 2004). Dialysis is an ongoing and necessary therapy to sustain life for kidney dialysis patients. ESRD patients normally receive 156 dialysis treatments each year.
2
Essential to our operations and income is Medicare reimbursement which is a fixed rate determined by the Center for Medicare and Medicaid Services (“CMS”) of the Department of Health and Human Services (“HHS”). The level of our revenues and profitability may be adversely affected by future legislation that could result in rate cuts. Further, our operating costs tend to increase over the years in excess of increases in the prescribed dialysis treatment rates. From commencement of the Medicare ESRD program in 1972 through 1983, the ESRD composite rate was unchanged, and thereafter decreased over the years until January, 2000, when the rate was minimally increased by Congress, and further minimally increased in January, 2001. However, Congress approved a 1.6% composite rate increase for each of 2005 and 2006. For 2007, the drug add-on adjustment to the composite rate will increase .5%. In 2005, Medicare implemented an additional change in the manner it reimburses dialysis treatments, which includes a pricing revision to the current average wholesale price for separately billable drugs and biologicals. Effective January 1, 2006, payments for pharmaceuticals (including EPO) were set at the pharmaceutical’s average sales price as determined by the Inspector General of HHS, plus 6%, which will remain the same for 2007. Effective April, 2006, CMS implemented a policy for monitoring the dosage of EPO based upon the patient’s hematocrit level and for limiting the quantity of EPO that can be administered in any one month. Medicare has implemented a case mix payment system, adjusting the composite rate for a limited number of patient characteristics. The increase in the composite rate is intended to offset reductions in pharmaceutical reimbursements. See under this Item 1, “Operations - Medicare Reimbursement” and Item 1A, “Risk Factors.” Commercial third-party reimbursement rates, which have increased as a percentage of our revenues over the last two years, are also susceptible to reduction. See “Operations - Medicare Reimbursement.” The inpatient dialysis service agreements for treating acute kidney disease are not subject to government fixed rates, but rather are negotiated with hospitals. Typically these rates are at least equivalent to or higher than the government fixed rates on a per treatment basis.
Dialysis Industry
Kidneys act as a filter removing harmful substances and excess water from the blood, enabling the body to maintain proper and healthy balances of chemicals and water. Chronic kidney failure, ESRD, results from chemical imbalance and buildup of toxic chemicals, and is a state of kidney disease characterized by advanced irreversible renal impairment. ESRD is a likely consequence of complications resulting from diabetes, hypertension, advanced age, and specific hereditary, cystic and urological diseases. ESRD patients, in order to survive, must either obtain a kidney transplant, which procedure is limited due to lack of suitable kidney donors and the incidence of rejection of transplanted organs, or obtain dialysis treatments for the rest of their lives.
Based upon information published by CMS, the number of ESRD patients requiring dialysis treatments in the United States at December 31, 2004 was approximately 336,000, and continues to grow at a rate of approximately 3% to 4% a year. This is thought to be attributable primarily to the aging of the population, greater patient longevity as a result of improved dialysis technology, and better treatment and survival rates for illnesses that lead to chronic kidney disease. The statistics further reflect over 4,500 dialysis facilities, with a current annual cost for treating ESRD patients in the United States at approximately $32.5 billion at December, 2004, of which Medicare accounted for approximately $20.1 billion.
3
ESRD Treatment Options
Treatment options for ESRD patients include (1) hemodialysis, performed either at (i) an outpatient facility, or (ii) inpatient hospital facility, or (iii) the patient’s home; (2) peritoneal dialysis, either continuous ambulatory peritoneal dialysis or continuous cycling peritoneal dialysis; or (3) kidney transplant. A significant portion of ESRD patients receive treatments at non-hospital owned outpatient dialysis facilities (according to CMS, approximately 82%) with most of the remaining patients treated at home through hemodialysis or peritoneal dialysis. Patients treated at home are monitored by a designated outpatient facility.
The most prevalent form of treatment for ESRD patients is hemodialysis, which involves the use of an artificial kidney, known as a dialyzer, to perform the function of removing toxins and excess fluids from the bloodstream. This is accomplished with a dialysis machine, a complex blood filtering device which takes the place of certain functions of the kidney, and also controls external blood flow and monitors the toxic and fluid removal process. The dialyzer has two separate chambers divided by a semi-permeable membrane, and simultaneously with the blood circulating through one chamber; dialyzer fluid is circulated through the other chamber. The toxins and excess fluid pass through the membrane into the dialysis fluid. On the average, patients usually receive three treatments per week with each treatment taking three to five hours. Dialysis treatments are performed by teams of licensed nurses and trained technicians pursuant to the staff physician’s instructions.
Home hemodialysis treatment requires the patient to be medically suitable and have a qualified assistant. Additionally, home hemodialysis requires training for both the patient and the patient’s assistant, which usually encompasses four to eight weeks.
A second home treatment for ESRD patients is peritoneal dialysis. There are several variations of peritoneal dialysis, the most common being continuous ambulatory peritoneal dialysis and continuous cycling peritoneal dialysis. All forms of peritoneal dialysis use the patient’s peritoneal (abdominal) cavity to eliminate fluid and toxins from the patient. Continuous ambulatory peritoneal dialysis utilizes dialysis solution infused manually into the patient’s peritoneal cavity through a surgically-placed catheter. The solution is allowed to remain in the abdominal cavity for a three to five hour period and is then drained. The cycle is then repeated. Continuous cycling peritoneal dialysis is performed in a manner similar to continuous ambulatory peritoneal dialysis, but utilizes a mechanical device to cycle the dialysis solution while the patient is sleeping. Peritoneal dialysis is the third most common form of ESRD therapy following center hemodialysis and renal transplant.
While kidney transplantation, another treatment option for patients with ESRD, is typically the most desirable form of therapeutic intervention, the scarcity of suitable donors and possibility of donee rejection limits the availability of this surgical procedure as a treatment option.
Business Strategy
Dialysis Corporation of America has 30 years’ experience in developing and operating dialysis treatment facilities. Our priority is to provide quality patient care. We continue to establish alliances with physicians and hospitals and attempt to initiate dialysis service arrangements with nursing homes and managed care organizations.
4
We actively seek and negotiate with physicians and others to establish new outpatient dialysis facilities. We acquired three centers in early 2006 as well as opening three new centers that we developed. We acquired two centers in the first quarter of 2007, and we are in the process of developing two new dialysis centers. We are in different phases of negotiations with physicians for potential new facilities in a variety of states.
Same Center Growth
We endeavor to increase same center growth by adding quality staff and management and attracting new patients to our existing facilities. We seek to accomplish this objective by rendering high caliber patient care in convenient, safe and pleasant conditions. We believe that we have adequate space and stations within our facilities to accommodate greater patient volume and maximize our treatment potential. Same center growth relates to those centers that were operable during the entire prior year. During fiscal 2006, we experienced approximately 10% increase in dialysis treatments for our facilities that qualified to be included in same center growth compared to 3% during the preceding year.
Development and Acquisition of Facilities
One of the primary elements in developing or acquiring facilities is locating an area with an existing patient base under the current treatment of local nephrologists, since the proposed facility would primarily be serving such patients. Other considerations in evaluating development of a dialysis facility or a proposed acquisition are the availability and cost of qualified and skilled personnel, particularly nursing and technical staff, the size and condition of the facility and its equipment, the atmosphere for the patients, the area’s demographics and population growth estimates, state regulation of dialysis and healthcare services, and the existence of competitive factors such as existing outpatient dialysis facilities within reasonable proximity to the proposed center.
Expansion is either through the development of our own dialysis facilities, or acquisition of existing outpatient dialysis centers. While an acquisition of existing outpatient dialysis centers is a faster means for achieving operational status at that center, these transactions can be more costly, and , therefore, the company takes a selective approach to its acquisition strategy. The primary reason for physicians selling or participating in the development of centers is the avoidance of administrative and financial responsibilities, freeing their time to devote to their professional practice. Other motivating forces are the physician’s desire to be part of a larger organization allowing for economies of scale and the ability to realize a return on their investment if they have an interest in the dialysis entity.
To construct and develop a new facility ready for operation takes an average of six to eight months, and approximately 12 months or longer to generate income, all of which are subject to variables based on location, size and competitive elements. Some of our centers are in the developmental stage, since they have not reached the point where the patient base is sufficient to generate and sustain earnings. See Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” Construction of a 15 station facility, typically the size of our dialysis facilities, costs in a range of $750,000 to $1,000,000, including equipment and initial working capital requirements, depending on location, size and related services to be provided by the proposed facility. An acquisition of an existing facility is usually based primarily upon the patient base and earnings, and to a lesser extent, location and competition. As a result, the costs associated with an acquisition of a facility can be greater than that of a development. Nevertheless, we attempt to selectively identify potential acquisitions where the costs can be maintained within the range of development costs for a similar project. Any significant expansion, whether through acquisition or development of new facilities, is dependent upon existing funds or financing from other sources.
5
On October 24, 2005, we entered into a Credit Agreement with KeyBank National Association for a three year, $15,000,000 revolving credit facility intended to provide available funds for the development and acquisition of new dialysis facilities and for other general working capital and corporate purposes. This financing agreement is secured by our ownership interest in each of our subsidiaries. Additionally, each of our wholly-owned subsidiaries and any future wholly-owned subsidiary is and will be a guarantor of our obligation under the credit facility. Both base rate loans and LIBOR loans may be obtained with the interest rate to include the applicable margin based on the type of loan. We had $7,500,000 of outstanding borrowings under this financing agreement as of December 31, 2006. See Note 2 to “Notes to Consolidated Financial Statements.”
Inpatient Services
We also seek to increase acute dialysis treatments through contracts with hospitals for inpatient dialysis services. These contracts are sought with hospitals in areas serviced by our facilities. Hospitals are willing to enter into such inpatient care arrangements to eliminate the administrative burdens of providing dialysis services to their patients as well as the expense involved in maintaining dialysis equipment, supplies and personnel. We believe that these arrangements are beneficial to our operations, since the contract rates are individually negotiated with each hospital and are not fixed by government regulation as is the case with Medicare reimbursement fees for ESRD patient treatment.
There is no certainty as to when any additional centers or service contracts will be implemented, or, to the extent implemented, the number of dialysis stations or patient treatments these centers or service contracts may involve, or if they will ultimately be profitable. There is no assurance that we will be able to continue to enter into favorable relationships with physicians who would become medical directors of such proposed dialysis facilities, or that we will be able to acquire or develop any new dialysis centers within a favorable geographic area. Newly established dialysis centers, although contributing to increased revenues, also adversely affect results of operations due to their start-up costs and expenses and to their having a smaller and slower developing patient base. See “Business Strategy,” “Operations” and “Competition” of this Item 1, and Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
Operations
Location, Capacity and Use of Facilities
We operate 34 outpatient dialysis facilities in Georgia, Maryland, New Jersey, Ohio, Pennsylvania, Virginia and South Carolina including an unaffiliated center in Georgia which we manage. These dialysis facilities have a total designed capacity of 499 licensed stations.
6
Of our 34 dialysis facilities, 33 are owned by us through subsidiaries as follows: 19 wholly-owned subsidiaries, one of which owns two facilities, and 13 majority-owned subsidiaries in conjunction with the medical directors of those centers who hold minority interests. We also manage an unaffiliated dialysis center in Georgia. One of the Pennsylvania and one of the Georgia dialysis centers are located on properties that we own and lease to our subsidiaries. Our Cincinnati, Ohio dialysis center is leased from a corporation owned by the medical director of that center who, together with his wife, holds a minority interest in the subsidiary operating that center. Our Calhoun, Georgia dialysis center is leased from a group of local doctors. One of our Aiken, South Carolina dialysis centers is leased from an entity owned by the medical director of that center. Our York, Pennsylvania dialysis facility is leased from a limited partnership in which we have a 60% ownership interest with the remaining 40% owned by two doctors who are also affiliated with the entity that owns a 40% minority ownership in the subsidiary that operates that facility. See Item 2, “Properties.”
We had given the non-affiliated owner of the facility in Georgia that we manage a put option to sell to one of our subsidiaries all the assets of that Georgia dialysis facility. Our subsidiary held a call option to purchase the assets of the Georgia facility. The put option expired unexercised in September, 2005. The call option was extended until January 14, 2007, and our subsidiary exercised the option on January 11, 2007, pursuant to which we are acquiring the assets of this center through that subsidiary. At the conclusion of this acquisition we will hold an 80% interest in this facility and the former owner will hold the remaining 20% interest. See Note 7 and Note 17 to “Notes to Consolidated Financial Statements.”
Additionally, the company provides acute care inpatient dialysis services to ten hospitals in areas serviced by our dialysis facilities. We are in the process of negotiating additional acute dialysis services contracts in the areas surrounding our facilities, which we will also do in tandem with development of future proposed sites. Furthermore, most of our dialysis facilities have the capacity to provide training, supplies and on-call support services for home peritoneal patients. Dialysis Corporation of America provided approximately 219,000 hemodialysis treatments in 2006, an increase of approximately 40,000 treatments compared to fiscal 2005.
We estimate that on average our centers were operating at approximately 51% of capacity as of December 31, 2006, based on the assumption that a dialysis center is able to provide up to three treatments a day per station, six days a week. We believe we can increase the number of dialysis treatments at our centers without making significant additional capital expenditures.
Operations of Dialysis Facilities
Our dialysis facilities are designed specifically for outpatient hemodialysis and generally contain, in addition to space for dialysis treatments, a nurses’ station, a patient weigh-in area, a supply room, water treatment space used to purify the water used in hemodialysis treatments, a dialyzer reprocessing room (where, with both the patient’s and physician’s consent, the patient’s dialyzer is sterilized for reuse), staff work area, offices and a staff lounge. Most of our facilities have a designated area for training patients in home dialysis. Each facility also offers amenities for the patients, such as a color television with headsets for each dialysis station, to ensure the patients are comfortable and relaxed.
We maintain a team of dialysis specialists to provide for the individual needs of each patient. In accordance with participation requirements under the Medicare ESRD program, each facility retains a medical director qualified and experienced in the practice of nephrology and the administration of a renal dialysis facility. See “Physician Relationships” below. Each facility is overseen by an administrator who supervises the daily operations and the staff, which consists of registered nurses, licensed practical nurses, patient care technicians, a social worker to assist the patient and family to adjust to dialysis treatment and to provide help in financial assistance and planning, and a registered dietitian. In addition, there are independent consultants who visit with our dialysis patients. These individuals supervise the patient’s needs and treatments. See “Employees” below. In furtherance of our business strategy, we strive to attract and retain skilled nurses and other staff, competition for whom is intense.
7
Our dialysis facilities offer high-efficiency conventional hemodialysis, which, in our experience, provides the most viable treatment for most patients. We consider our dialysis equipment to be both modern and efficient, providing state of the art treatment in a safe and comfortable environment.
Our facilities also offer home dialysis, primarily continuous ambulatory peritoneal dialysis and continuous cycling peritoneal dialysis. Training programs for continuous ambulatory peritoneal dialysis or continuous cycling peritoneal dialysis generally encompass two to three weeks at the dialysis facility, and such training is conducted by the facility’s home training nurse. After the patient completes training, they are able to perform treatment at home with equipment and supplies provided by the company.
Inpatient Dialysis Services
We presently provide inpatient dialysis services to ten hospitals in Georgia, Ohio, Pennsylvania, and Virginia under agreements either with us or with one of our subsidiaries in the area. The agreements are for a term ranging from one to five years, with automatic renewal terms, subject to termination by notice of either party. Inpatient services are typically necessary for patients with acute kidney failure resulting from trauma or similar causes, patients in the early stages of ESRD, and ESRD patients who require hospitalization for other reasons.
Ancillary Services
Our dialysis facilities provide certain ancillary services to ESRD patients including the administration of certain prescription drugs, such as EPO, upon a physician’s prescription. EPO is a bio-engineered protein which stimulates the production of red blood cells and is used in connection with dialysis to treat anemia, a medical complication frequently experienced by ESRD patients. EPO decreases the necessity for blood transfusions in ESRD patients. Amgen is the only manufacturer of EPO in the United States. Although we have a good relationship with this manufacturer and have not experienced any problems in receipt of our supply of EPO, any loss or limitation of supply of this product could have a material adverse effect on our operating revenue and income.
Amgen has developed a new product, darbepoetin alfa, known as Aranesp®, which has been approved by the FDA. Aranesp® can be administered to patients less frequently than EPO, which is generally administered to the patient with each dialysis treatment. We are unable to predict to what extent this product will impact our revenues and income, although there has been no impact to date. See Item 1A ,”Risk Factors” below.
Physician Relationships
An integral element to the success of a facility is its association with area nephrologists. A dialysis patient generally seeks treatment at a facility near the patient’s home where the patient’s nephrologist has an established practice. Consequently, we rely on our ability to develop affiliations with area nephrologists.
The conditions of a facility’s participation in the Medicare ESRD program mandate that treatment at a dialysis facility be under the general supervision of a medical director who is a physician. We retain, by written agreement, qualified physicians or groups of qualified physicians to serve as medical directors for each of our facilities. Generally, the medical directors are board eligible or board certified in internal medicine by a professional board specializing in nephrology and have had at least 12 months of experience or training in the care of dialysis patients at ESRD facilities. The medical directors are typically a source of patients treated at the particular center served. Our dialysis centers are operated through subsidiaries, either corporations or limited liability companies. The medical directors of thirteen of our centers have a minority ownership interest in the center they service. We make every effort to comply with federal and state regulations concerning our relationship with the physicians and the medical directors treating patients at our facilities. See “Government Regulation” below.
8
Agreements with medical directors typically range from a term of five to ten years, with renewal provisions, usually two renewal options each for five years. Each agreement specifies the duties, responsibilities and compensation of the medical director. Under each agreement, the medical director or professional association maintains his, her or its own medical malpractice insurance. The agreements also typically provide for non-competition in a limited geographic area surrounding that particular dialysis center during the term of the agreement and upon termination for a limited period. These agreements, however, do not prohibit physicians providing services at our facilities from providing direct patient care services at other locations; and consistent with the federal and state law, such agreements do not require a physician to refer patients to our dialysis centers. Usually, physician’s professional fees for services are billed directly to the patient or to government payment authorities by the treating physician and paid directly to the physician or the professional association.
Our ability to establish and operate a dialysis facility in a particular area is substantially dependent on the availability of a qualified physician or nephrologist to serve as the medical director. The loss of a medical director who could not be readily replaced would have a material adverse effect on the operations of that facility, most likely resulting in closure. Compensation of medical directors is separately negotiated for each facility and generally depends on competitive factors, the size of the facility, and the fair market value of the services to be provided.
Quality Assurance
Dialysis Corporation of America implements a quality assurance program to maintain and improve the quality of dialysis treatment and care we provide to our patients in each facility. Quality assurance activities involve the ongoing examination of care provided, the identification of therapy deficiencies, the need for any necessary improvements in the quality of care, and evaluation of improved technology. Specifically, this program requires each center’s staff, including its medical director and nurse administrator, to regularly review quality assurance data and initiate programs for improvement, including dialysis treatment services, equipment, technical and environmental improvements, and staff-patient and personnel relationships. These evaluations are in addition to assuring regulatory compliance with CMS and the Occupational Safety and Health Administration. Our Vice President of Clinical Services, a certified nephrology nurse, oversees this program in addition to ensuring that we meet federal and state compliance requirements for our dialysis centers. See “Government Regulation” below.
Quality Clinical Results
Our goal is to provide consistent quality clinical care to our patients from caring and qualified doctors, nurses, patient care technicians, social workers and dieticians. We have demonstrated an unwavering commitment to quality renal care through our continuous quality improvement initiatives. We strive to maintain a leadership position as a quality provider in the dialysis industry and often set our goals higher than the national average standards.
9
Kt/V is a formula that measures the amount of dialysis delivered to the patient, based on the removal of urea, an end product of protein metabolism. Kt/V provides a means to determine an individual dialysis prescription and to monitor the effectiveness or adequacy of the dialysis treatment as delivered to the patient. It is critical to strive to achieve a Kt/V level of greater than 1.2 for as many patients as possible. 95.5% of our patients had a Kt/V level greater than 1.2, for 2006 and 94.5% for 2005.
Anemia is a shortage of oxygen-carrying red blood cells. Because red blood cells bring oxygen to all the cells in the body, anemia causes severe fatigue, heart disorders, difficulty concentrating, reduced immune function, and other problems. Anemia is common among renal patients, caused by insufficient erythropoietin, iron deficiency, repeated blood losses, and other factors. Anemia can be detected with a blood test for hemoglobin or hematocrit. It is ideal to have as many patients as possible with hemoglobin levels above 11. Approximately 81% of our patients had a hemoglobin level greater than 11 for 2006 and 2005.
Vascular access is the “lifeline” for hemodialysis patients. CMS has indicated that fistulas are the “gold standard” for establishing access to a patient’s circulatory system in order to provide life-sustaining dialysis. Approximately 48% and 43% of DCA patients were dialyzed with a fistula during 2006 and 2005, respectively.
Patient Revenues
A substantial amount of the fees for outpatient dialysis treatments are funded under the ESRD Program established by the federal government under the Social Security Act, and administered in accordance with rates set by CMS. A majority of dialysis patients are covered under Medicare. The balance of the outpatient charges are paid by private payors including the patient’s medical insurance, private funds or state Medicaid plans. The states in which we operate provide Medicaid or comparable benefits to qualified recipients to supplement their Medicare coverage.
Under the ESRD Program, payments for dialysis services are determined pursuant to Part B of the Medicare Act which presently pays 80% of the allowable charges for each dialysis treatment furnished to patients. The maximum payments vary based on the geographic location of the center. The remaining 20% may be paid by Medicaid if the patient is eligible, from private insurance funds or the patient’s personal funds. If there is no secondary payor to cover the remaining 20%, Medicare may reimburse us for part of that balance as part of our annual cost report filings. Medicare and Medicaid programs are subject to regulatory changes, statutory limitations and government funding restrictions, which may adversely affect dialysis services payments and, consequently, our revenues. See “Medicare Reimbursement” below.
The inpatient dialysis services are paid for by each contracted hospital pursuant to contractual pre-determined fees for the different dialysis treatments.
Medicare Reimbursement
We are reimbursed primarily by Medicare under a prospective reimbursement system for chronic dialysis services, and by third party payors including Medicaid and commercial insurance companies. Our dialysis facilities are certified to participate in the Medicare program. Under the Medicare system, the reimbursement rates are fixed in advance and limit the allowable charge per treatment, but provide us with predictable and recurring per treatment revenues and allows us to retain any profit earned. An established composite rate set by CMS governs the Medicare reimbursement available for a designated group of dialysis services, including dialysis treatments, supplies used for such treatments, certain laboratory tests and medications.
10
Other ancillary services and items are eligible for separate reimbursement under Medicare and are not part of the composite rate, including certain drugs such as EPO, for which the allowable rate for the fourth quarter of 2006 was $9.446 and for the first quarter of 2007 is $9.574 per 1000 units for amounts in excess of three units per patient per year, and certain physician-ordered tests provided to dialysis patients. Approximately 28% of our medical services revenue in 2006 was derived from providing dialysis patients with EPO. CMS limits the EPO reimbursement based upon patients’ hematocrit levels. CMS issued a new payment coverage policy for EPO, which became effective April 1, 2006. This policy restricts payments based on EPO doses and hemoglobin levels for certain patients and has affected physician prescription patterns. Other ancillary services, mostly other drugs, account for approximately an additional 9% of our medical services revenue. We submit claims monthly and are usually paid by Medicare within 14 days of the submission.
There have been a variety of proposals to Congress for Medicare reform. We are unable to predict what, if any, future changes may occur in the rate of reimbursement. Congress approved a 1.6% composite rate increase for each of 2005 and 2006. For 2007, the drug-add on adjustment to the composite rate will increase .5%. Medicare reimburses dialysis providers for the ten most utilized ESRD drugs at an amount equal to the cost of such drugs, and for other ESRD drugs Medicare reimburses at an amount equal to the average sale price of the drug as determined by the Inspector General of HHS, plus 6%, which will continue in 2007; and the composite rate has been increased by an amount estimated by HHS to be the dialysis provider’s average profit for these drugs. To make this change budget-neutral, a drug add-on composite has been included. Accordingly, CMS determined that the Medicare ESRD composite rate would increase by approximately 8.7% or $11 per treatment, and that payments for separately billable drugs would be reduced as described above. As of April 1, 2005, CMS reimburses providers using a case mix formula. CMS adjusted reimbursements based on predefined patient parameters such as patient height, weight and age. Congress has mandated a budget neutrality factor adjustment so that aggregate payments under the system equal payments that would have been made without the case mix adjustments and the add-on composite for reimbursement of the drugs. Management believes there has been minimal impact on its average Medicare revenue per treatment as a result of these changes in Medicare reimbursement. Any reduction in the Medicare composite reimbursement rate could have a material adverse effect on our business, revenues and net earnings.
Medicaid Reimbursement
Medicaid programs are state administered programs partially funded by the federal government. These programs are intended to provide coverage for patients whose income and assets fall below state defined levels and who are otherwise uninsured. The programs also serve as supplemental insurance programs for the Medicare co-insurance portion and provide certain coverages (e.g., oral medications) that are not covered by Medicare. State reimbursements generally follow Medicare reimbursement levels and coverages without any co-insurance amounts. Certain states, however, require beneficiaries to pay a monthly share of the cost based upon levels of income or assets. Pennsylvania and New Jersey have Medical Assistance Programs comparable to Medicaid, with primary and secondary insurance coverage to those who qualify. We are a licensed ESRD provider in Georgia, Maryland, New Jersey, Ohio, Pennsylvania, South Carolina and Virginia.
11
Sources of Medical Services Revenue
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Medicare | 52 | % | 51 | % | 48 | % | ||||
| Medicaid and Comparable Programs | 9 | % | 8 | % | 8 | % | ||||
| Hospital inpatient dialysis services | 3 | % | 5 | % | 6 | % | ||||
| Commercial and private payors | 36 | % | 36 | % | 38 | % | ||||
Management Services
Dialysis Corporation of America has a management services agreement with each of its subsidiaries, and with an unaffiliated Georgia dialysis center, providing each of them with administrative and management services, including, but not limited to, assisting in procuring capital equipment, preparing budgets, bookkeeping, accounting, data processing, and other corporate based information services, materials and human resource management, billing and collection, and accounts receivable and payable processing. These services are provided for a percentage of net revenues of each particular facility.
Corporate Integrity Program
Dialysis Corporation of America has developed a Corporate Integrity Program to assure it continues to achieve its goal of providing the highest level of care and service in a professional and ethical manner consistent with applicable federal and state laws and regulations. This program is intended to (i) reinforce our management’s, employees’ and professional affiliates’ awareness of their responsibilities to comply with applicable laws in the increased and complex regulatory environment relating to our operations, (ii) benefit the overall care and services for our dialysis patients, and (iii) assure our operations are in compliance with the law, which, in turn, should assist us in operating in a cost-effective manner, and accordingly, benefit our shareholders.
We have developed a Compliance Program to assure compliance with fraud and abuse laws, enhance communication of information, and provide a mechanism to quickly identify and correct any problems that may arise. This Compliance Program supplements and enhances our existing policies, including those applicable to claims submission, cost report preparation, internal audit and human resources.
Our board of directors has established an audit committee consisting of three independent members of the board who oversee audits, accounting, financial reporting, and who have established procedures for receipt, retention and resolution of complaints relating to those areas (none to date), among other responsibilities. The audit committee operates under a charter providing for its detailed responsibilities.
We also maintain disclosure controls and procedures and internal control over financial reporting to ensure the accuracy of our disclosure in our filings and our financial reporting and financial statements filed under the federal securities laws. Management provides a report on, and our independent accountants audit, management’s assessment of internal control over financial reporting. See Item 9A, “Controls and Procedures” and “Report of Independent Registered Public Accounting Firm,” page F-2 of this annual report on Form 10-K.
12
Code of Ethics
As part of our Corporate Integrity Program, we have established a Code of Ethics and Business Conduct covering management and all employees to assure all persons affiliated with our company and our operations act in an ethical and lawful manner. The Code of Ethics and Business Conduct covers relationships among and between affiliated persons, patients, payors, and relates to information processing, compliance, workplace conduct, environmental practices, training, education and development, among other areas. In our commitment to delivering quality care to dialysis patients, we have mandated rigorous standards of ethics and integrity.
Our Code of Ethics and Business Conduct is designed to provide:
| · | officers, directors and employees to be committed to the best interests of our company |
| · | ethical handling of actual or apparent conflicts of interest between personal and professional relationships |
| · | full, fair, accurate, timely, and understandable disclosure in reports and documents we file with the SEC and in our other public communications |
| · | compliance with applicable governmental laws, rules and regulations |
| · | prompt internal reporting of violations of the Code to an appropriate person identified in the Code |
| · | responsibilities of senior management with respect to related party transactions |
| · | accountability for adherence to the Code |
| · | non-waiver of policies and exception processes |
Our Code of Ethics and Business Conduct is posted on our website at www.dialysiscorporation.com under the caption “Investor Relations - Corporate Governance.” We will also provide the Code to any person without charge upon request to our corporate Secretary and counsel, Lawrence E. Jaffe, Esq., Jaffe & Falk, LLC, at 2337 West 76th Street, Hialeah, FL 33016, telephone (305) 364-1300, or email, lej@jaffefalkllc.com.
The Corporate Integrity Program is implemented, and reviewed and upgraded from time to time, to provide a highly professional work environment and lawful and efficient business operations to better serve our patients and our shareholders.
Potential Liability and Insurance
Participants in the health care industry are subject to lawsuits based upon alleged negligence, many of which involve large claims and significant defense costs. We currently have general and umbrella liability insurance, as well as professional and products liability. Our insurance policies provide coverage on an “occurrence” basis and are subject to annual renewal. A hypothetical successful claim against us in excess of our insurance coverage could have a material adverse effect upon our business and results of operations. The medical directors supervising our dialysis operations and other physicians practicing at the facilities are required to maintain their own professional malpractice insurance coverage.
13
Government Regulation
General
Regulation of healthcare facilities, including dialysis facilities, is extensive, with legislation continually proposed relating to safety, maintenance of equipment and proper records, quality assurance programs, reimbursement rates, confidentiality of medical records, licensing, patient care and other areas of operations. Each dialysis facility must be certified by CMS, and we must comply with certain rules and regulations established by CMS. Each dialysis facility is also subject to periodic inspections by federal and state agencies to determine if their operations meet the appropriate regulatory standards. Our operations are also subject to the Occupational Safety and Health Administration, known as OSHA, relating to workplace safety and employee exposure to blood and other potentially infectious material.
Many states have eliminated the requirement to obtain a certificate of need prior to the establishment or expansion of a dialysis center. There are no certificate of need requirements in the states in which we are presently operating.
Our record of compliance with federal, state and local governmental laws and regulations remains excellent. Nevertheless, we are unable to predict the scope and effect of any changes in government regulations, particularly any modifications in the reimbursement rate for medical services or requirements to obtain certification from CMS. Enforcement, both privately and by the government, has become more stringent, particularly in attempts to combat fraud and waste. Since our inception in 1976, we have maintained all of our licenses, including our Medicare and Medicaid and equivalent certifications. The loss of any licenses and certifications would have a material adverse effect on our operations, revenues and earnings.
We regularly review legislative and regulatory changes and developments and will restructure a business arrangement if we determine such might place our operations in material noncompliance with applicable laws or regulations. See “Fraud and Abuse” and “Stark II” below. To date, none of our business arrangements with physicians, patients or others have been the subject of investigation by any governmental authority. No assurance can be given, however, that our business arrangements will not be the subject of future investigation or prosecution by federal or state governmental authorities which could result in civil and/or criminal sanctions.
Certification and Reimbursement
Our dialysis centers must meet certain requirements, including, among others, those relating to patient care, patient rights, medical records, the physical set-up of the center, and personnel, in order to be certified by CMS, to be covered under the Medicare program and to receive Medicare reimbursement. See above under “Operations - Medicare Reimbursement.” Our dialysis centers are certified under the Medicare program, and are certified under applicable state Medicaid programs.
Fraud and Abuse
Certain aspects of our business are subject to federal and state laws governing financial relationships between health care providers and referral sources and the accuracy of information submitted in connection with reimbursement. These laws, collectively referred to as “fraud and abuse” laws, include the Anti-Kickback Statute, Stark II, other federal fraud laws, and similar state laws.
14
The fraud and abuse laws apply because our medical directors have financial relationships with the dialysis facilities and also refer patients to those facilities for items and services reimbursed by federal and state health care programs. Financial relationships with patients who are federal program beneficiaries also implicate the fraud and abuse laws. Other financial relationships which bear scrutiny under the fraud and abuse laws include relationships with hospitals, nursing homes, and various vendors.
Anti-Kickback Statutes
The federal Anti-Kickback Statute prohibits the knowing and willful solicitation, receipt, offer, or payment of any remuneration, directly or indirectly, in return for or to induce the referral of patients or the ordering or purchasing of items or services payable under the Medicare, Medicaid, or other federal health care program.
Sanctions for violations of the Anti-Kickback Statute include criminal penalties, such as imprisonment and fines of up to $25,000 per violation, and civil penalties of up to $50,000 per violation, as well as exclusion from Medicare, Medicaid, and other federal health care programs. Under U.S. Sentencing Guidelines, an individual may be fined up to $250,000 and an organization may be fined up to $500,000 upon conviction of offenses described in any federal statute. Individuals and entities convicted of violating the Anti-Kickback Statute are subject to mandatory exclusion from participation in Medicare, Medicaid and other federal healthcare programs for a minimum of five years.
The language of the Anti-kickback Statute has been construed broadly by the courts. Over the years, the federal government has published regulations that established “safe harbors” to the Anti-Kickback Statute. An arrangement that meets all of the elements of the safe harbor is immunized from prosecution under the Anti-Kickback Statute. The failure to satisfy all elements, however, does not necessarily mean the arrangement violates the Anti-Kickback Statute.
Some states have enacted laws similar to the Anti-Kickback Statute. These laws may apply regardless of payor source, may include criminal and civil penalties, and may contain exceptions that differ from the safe harbors to the Anti-Kickback Statute.
As required by Medicare regulations, each of our dialysis centers is supervised by a medical director, who is a licensed nephrologist or otherwise qualified physician. The compensation of our company’s medical directors, who are independent contractors, is fixed by a medical director agreement and reflects competitive factors in each respective location, the size of the center, and the physician’s professional qualifications. The medical director’s fee is fixed in advance, typically for periods of one to five years and does not take into account the volume or value of any referrals to the dialysis center. Thirteen of our outpatient dialysis centers are owned jointly between us and physicians who, in most cases, hold a minority position through a professional association. Other than for two facilities, these physicians also act as the medical directors for those facilities. We attempt to structure our arrangements with our physicians to comply with the Anti-Kickback Statute. Many of these physicians’ patients are treated at our facilities. We believe that the value of the minority interest in a subsidiary acquired by the physician has been consistent with the fair market value of the cash consideration paid, assets transferred to, and/or services performed by that physician for the subsidiary, and there is no intent to induce referrals to any of our centers. See “Business - Physician Relationships” above. We lease space for five of our centers from entities in which physicians hold ownership interests, and we sublease space to four of our medical directors at five of our dialysis centers. These arrangements must be in compliance with the Anti-Kickback Statute. We believe our arrangements with our medical directors are in material compliance with applicable law. Several states in which we operate have laws prohibiting physicians from holding financial interests in various types of medical facilities. If these statutes are interpreted to apply to relationships we have with our medical directors who hold a percentage ownership in our dialysis facilities, we would restructure our relationship with these physicians but could be subject to penalties.
15
Management believes that the Anti-Kickback Statute and other fraud and abuse laws are primarily directed at abusive practices that increase the utilization and cost of services covered by governmentally funded programs. The dialysis services we provide generally cannot, by their very nature, be over-utilized since dialysis treatment is not elective, and is only indicated when there is temporary or permanent kidney failure. Medical necessity is capable of being supported by objective documentation, drastically reducing the possibility of over-utilization. Additionally, there are safe harbors for certain arrangements. Nevertheless, while relationships created by medical director ownership of minority interests in our facilities satisfy many but not all of the criteria for the safe harbor, there can be no assurance that these relationships will not subject us to investigation or prosecution by enforcement agencies. In an effort to further our compliance with the law, we have adopted a corporate Compliance Program that addresses medical necessity and medical chart audits to confirm medical necessity of referrals.
With respect to our inpatient dialysis services, we provide hospitals with dialysis services, including qualified nursing and technical personnel, supplies, equipment and technical services. In certain instances, the medical director of our dialysis center who has a minority interest in that facility may refer patients to hospitals with which we have an inpatient dialysis services arrangement. We believe our acute inpatient hospital services are in compliance with the law. See “Stark II” below.
We endeavor in good faith to comply with all governmental regulations. However, there can be no assurance that we will not be required to change our practices or experience a material adverse effect as a result of any such potential challenge. We cannot predict the outcome of the rule-making process, enforcement procedures, or whether changes in the safe harbor rules will affect our position with respect to the Anti-Kickback Statute, but we will continue to make every effort to remain in compliance.
Stark II
The federal physician self referral law, commonly known as Stark II, prohibits a physician who has a financial relationship, or who has an immediate family member who has a financial relationship, with entities providing “designated health services” from referring Medicare or Medicaid patients to such entity for such services unless an exception applies. A “financial relationship” includes an ownership or investment interest in, or a compensation arrangement between the physician and the entity. For purposes of Stark II, “designated health services” include clinical laboratory services, durable medical equipment, parenteral and enteral nutrients, home health services, and inpatient and outpatient hospital services. Dialysis treatments are not “designated health services.”
The self-referral prohibition has numerous exceptions, including exceptions for personal service arrangements, leases of space and equipment, employment relationships and referrals within group practices.
16
An entity is prohibited from submitting Medicare or Medicaid claims for services furnished pursuant to an unlawful referral and must refund amounts received pursuant to prohibited referrals. Violators are subject to civil monetary penalties of up to $15,000 for each improper claim and may be excluded from participation in the Medicare and Medicaid programs. Unlike the federal Anti-Kickback Statute, intent to violate the law is not required. Knowing violations of Stark II may also serve as the basis for liability under the False Claims Act. See “False Claims Act” below.
HHS’ regulations to Stark II became effective in January, 2002. CMS adopted Phase II of its regulations under Stark II in March, 2004. These regulations exclude from covered designated health services and referral prohibitions, services included in the ESRD composite rate and EPO and other drugs required as part of dialysis treatments under certain conditions. Also excluded from “inpatient hospital services” are dialysis services provided by a hospital not certified by CMS to provide outpatient dialysis services, which would exclude our inpatient hospital services agreements from Stark II. Equipment and supplies used in connection with home dialysis are excluded from the Stark II definition of “durable medical equipment.”
Stark II regulations and the legislative history of Stark II indicate that the purpose behind the Stark II prohibition on physician referral is to prevent Medicare and Medicaid program and patient abuse. Since dialysis is a necessary medical treatment for those with temporary or permanent kidney failure, it is not highly susceptible to that type of abuse. We believe, based upon current rules and the industry practice, that Congress did not intend to include dialysis services and the services and items we provide that are incidental to dialysis services within the Stark II prohibitions.
If the provisions of Stark II were found to apply to our arrangements however, we believe that we would be in compliance. We compensate our nephrologist-physicians, or practices with which they are affiliated, as medical directors of our dialysis centers pursuant to medical director agreements, which we believe meet the exception for personal service arrangements under Stark II. Non-affiliated physicians who send their patients to or treat their patients at any of our facilities do not receive any compensation from the company.
Medical directors of our dialysis centers who hold a minority investment interest in the subsidiaries operating those centers may refer patients to hospitals with which we have an acute inpatient dialysis service arrangement. Although the regulations of Stark II may be interpreted to apply to these types of transactions, we believe that our contractual arrangements with hospitals for acute care inpatient dialysis services are in compliance with Stark II.
If CMS or any other government entity otherwise interprets the Stark II regulations, we may be required to restructure certain existing compensation or investment agreements with our medical directors, or, in the alternative, refuse to accept referrals for designated health services from certain physicians. Stark II prohibits Medicare or Medicaid reimbursement of items or services provided pursuant to a prohibited referral, and imposes substantial civil monetary penalties on facilities which submit claims for reimbursement. If such were to be the case, we could be required to repay amounts reimbursed for drugs, equipment and services that CMS determines to have been furnished in violation of Stark II, in addition to substantial civil monetary penalties, which could adversely affect our operations and financial results. We believe that if Stark II is interpreted by CMS or any other governmental entity to apply to our arrangements, it is possible that we could be permitted to bring our financial relationships with referring physicians into material compliance with the provisions of Stark II on a prospective basis. However, prospective compliance may not eliminate the amounts or penalties, if any, that might be determined to be owed for past conduct, and there can be no assurance that the costs and expenses associated with such prospective compliance, if permissible, would not have a material adverse effect on the company.
17
False Claims Act
The False Claims Act is the federal government’s primary civil remedy for improper or fraudulent claims. It applies to all federal programs, including Medicare and Medicaid. The False Claims Act prohibits, among other things, (1) knowingly presenting or causing to be presented a false or fraudulent claim, (2) knowingly making or using, or causing to be made or used, a false record or statement in order to have a false or fraudulent claim paid, (3) conspiring to defraud the government by getting a false or fraudulent claim allowed or paid, and (4) knowingly making or using, or causing to be made or used, a false record or statement to conceal, avoid, or decrease an obligation to pay the government.
“Knowingly” means that a person, with respect to information: (1) has actual knowledge of the information; (2) acts in deliberate ignorance of the truth or falsity of the information; or (3) acts in reckless disregard of the truth or falsity of the information. No proof of specific intent to defraud is required.
Penalties for violation of the False Claims Act include fines of $5,500 to $11,000 per false claim, plus treble damages.
Our Corporate Compliance Program is designed to address risks inherent in the submission of claims and other information in connection with the Medicare and Medicaid program and we are committed to ensuring the accuracy of all claims. There can be no assurance, however, that we will not be subject to an investigation or audit regarding the accuracy of any claim or other information submitted in connection with our operations.
HIPAA
The Health Insurance Portability and Accountability Act of 1996, known as HIPAA, provided for health insurance reforms which included a variety of provisions important to healthcare providers, such as significant changes to the Medicare and Medicaid fraud and abuse laws. HIPAA established two programs that coordinate federal, state and local healthcare fraud and abuse activities. Under these programs, these governmental entities undertake a variety of monitoring activities, including medical utilization and fraud review, cost report audits and secondary payor determinations. The Incentive Program for Fraud and Abuse Information rewards Medicare recipients 10% of the overpayment up to $1,000 for reporting Medicare fraud and abuse. HIPAA further created health care fraud crimes and extended their applicability to private health plans.
As part of the administrative simplification provisions of HIPAA, there are regulations governing electronic transactions relating to healthcare information. These regulations require a party transmitting or receiving healthcare transactions electronically to send and receive data in single format. This regulation applies to our submissions and processing of healthcare claims and also applies to many of our payors. We believe that we are in compliance with the transactions standards rule.
18
HIPAA also includes provisions relating to the privacy of healthcare information. HHS’ privacy rules cover all individually identifiable healthcare information known as “protected health information” and apply to healthcare providers, health plans, and healthcare clearing houses, known as “covered entities.” The regulations are quite extensive and complex, but basically require companies to: (i) obtain patient acknowledgement of receipt of a notice of privacy practices; (ii) obtain patient authorization before certain uses and disclosures of protected health information; (iii) respond to patient requests for access to their healthcare information; and (iv) develop policies and procedures with respect to uses and disclosures of protected health information. We expended significant resources to develop and implement policies and procedures to address privacy issues, and we believe we are in compliance with the HIPAA privacy rules.
HIPAA has security regulations governing the security of health information that is maintained or transmitted electronically. These regulations generally require implementation of safeguards for ensuring the confidentiality of electronic health information. Management believes it is currently in compliance with the HIPAA security standards.
HIPAA expressly prohibits four practices, namely (1) submitting a claim that the person knows or has reason to know is for medical items or services that are not medically necessary, (2) transferring remuneration to Medicare and Medicaid beneficiaries that is likely to influence such beneficiary to order or receive items or services, (3) certifying the need for home health services knowing that all of the coverage requirements have not been met, and (4) engaging in a pattern or practice of upcoding claims in order to obtain greater reimbursement.
As for criminal penalties, HIPAA adds healthcare fraud, theft, embezzlement, obstruction of investigations and false statements to the general federal criminal code with respect to federally funded health programs, thus subjecting such acts to criminal penalties. Persons convicted of these crimes face up to 10 years imprisonment and/or fines. Moreover, a court imposing a sentence on a person convicted of federal healthcare offense may order the person to forfeit all real or personal property that is derived from the criminal offense. The Attorney General is also provided with a greatly expanded subpoena power under HIPAA to investigate fraudulent criminal activities, and federal prosecutors may utilize asset freezes, injunctive relief and forfeiture of proceeds to limit fraud during such an investigation.
Although we believe we substantially comply with currently applicable state and federal laws and regulations and to date have not had any difficulty in maintaining our licenses and Medicare and Medicaid authorizations, the healthcare service industry is and will continue to be subject to substantial and continually changing regulation at the federal and state levels, and the scope and effect of such and its impact on our operations cannot be predicted. No assurance can be given that our activities will not be reviewed or challenged by regulatory authorities. We continue to work with our healthcare counsel in reviewing our policies and procedures and make every effort to comply with HIPAA and other applicable federal and state laws and regulations.
Any loss by us of our approval as a certified provider under the Medicare or Medicaid programs or our licenses under the laws of any state or other governmental authority from which a substantial portion of our revenues are derived or a change resulting from healthcare reform, a reduction of dialysis reimbursement or a reduction or complete elimination of coverage for dialysis services, would have a material adverse effect on our business.
19
Environmental and Health Regulations
Our dialysis centers are subject to various federal, state and local hazardous waste laws and non-hazardous medical waste disposal laws. Most of our waste is non-hazardous. We also follow OSHA’s Hazardous Waste Communications Policy, which requires all employees to be knowledgeable of the presence of and familiar with the use and disposal of hazardous chemicals in the facility. Medical waste of each facility is handled by licensed local medical waste sanitation agencies who are responsible for compliance with such laws.
There are a variety of regulations promulgated under OSHA relating to employees exposed to blood and other potentially infectious materials requiring employers, including dialysis centers, to provide protection. We adhere to OSHA’s protective guidelines, including regularly testing employees and patients for exposure to hepatitis B and providing employees subject to such exposure with hepatitis B vaccinations on an as-needed basis, protective equipment, a written exposure control plan and training in infection control and waste disposal.
Other Regulation
The company has received payments from Medicaid in 2006, in excess of $5 million. Accordingly, the company must and does comply with the employee education processes of the Deficit Reduction Act of 2005.
Certain states have Anti-Kickback legislation and laws dealing with self-referral provisions similar to the federal Anti-Kickback Statute and Stark II. We have no reason to believe that we are not in compliance with such state laws.
Dialysis Corporation of America has developed a Compliance Program as part of its Corporate Integrity Program, designed to assure compliance with fraud and abuse laws and regulations. See above under the caption “Corporate Integrity Program.” The establishment and implementation of our Compliance Program, coupled with our existing policies and internal controls, could have the effect of mitigating any civil or criminal penalties for potential violations, of which we have had none since our inception in 1976. We will continue to use our best efforts to fully comply with federal and state laws, regulations and requirements as applicable to our operations and business.
Medical Products
Subsequent to our merger in September, 2005, with our former parent company, Medicore, Inc., we became engaged in the distribution of medical products, primarily disposables and diabetic supplies, both domestically and internationally, to hospitals, blood banks, laboratories and retail pharmacies. We additionally distribute a line of blood lancets used to draw blood for testing. The lancets are distributed under the names Producers of Quality Medical Disposables™, Lady Lite™, our brand name Lite Touch, or under a private label if requested by the customer. Medical devices are required by the FDA, as a condition of marketing, to secure a 510(k) premarket notification clearance or a Premarket Approval Application. A product will be cleared by the FDA under a 510(k) if it is found to be substantially equivalent in terms of safety, effectiveness and intended use to another legally marketed product. We received 510(k) clearance for our blood lancet line and insulin syringes. Our medical products are subject to continuing FDA oversight, including labeling, “good manufacturing practices,” as defined in FDA regulations, and adverse event reporting, none of which adverse events have occurred to date. Although we hold three patents related to our lancets (see “Patents and Trade Names” below), and obtained required FDA approval relating to the production of lancets, we are no longer manufacturing these products. Marketing of medical products is conducted by independent manufacturer representatives and our employees.
20
Patents and Trade Names
We sell certain of our medical supplies and products under the trademark Medicore™. Certain of our lancets are marketed under the trademarks Providers of Quality Medical Disposables™ and Lady Lite™, and under the brand name Lite Touch. Although we hold three patents related to our lancets, we do not rely on patents or trademarks in our medical products division.
Competition
The dialysis industry is highly competitive. There are numerous providers who have dialysis centers in the same areas as our centers. Many are owned by larger corporations, which operate dialysis centers regionally, nationally and internationally. Our operations are small in comparison with those corporations. Some of our major competitors are large public companies, including Fresenius Medical Care, Inc., and DaVita, Inc. These companies have substantially greater financial resources, significantly more centers, patients and services than we do, and by virtue of such may have an advantage over us in competing for nephrologists and acquisitions of dialysis facilities in areas and markets we target. Moreover, competition for acquisitions has increased the cost of acquiring existing dialysis centers. Fresenius also manufactures and sells dialysis equipment and supplies, which may provide it with a greater competitive edge. We also face competition from hospitals and physicians that operate their own dialysis facilities.
Competitive factors most important in dialysis treatment are quality of care and service, convenience of location and pleasantness of the environment. Another significant competitive factor is the ability to attract and retain qualified nephrologists. These physicians are a substantial source of patients for the dialysis centers, are required as medical directors of the dialysis center for it to participate in the Medicare ESRD program, and are responsible for the supervision of the medical operations of the center. Our medical directors usually are subject to non-compete restrictions within a limited geographic area from the center they administer. Additionally, there is always substantial competition for obtaining qualified, competent nurses and technical staff at reasonable labor costs. There can be no assurance that we will compete effectively with any of our competitors.
Based upon advances in surgical techniques, immune suppression and computerized tissue typing, cross-matching of donor cells and donor organ availability, renal transplantation in lieu of dialysis is a competitive factor. It is presently the second most commonly used modality in ESRD therapy. With greater availability of kidney donations, currently the most limiting factor in the growth of this modality, renal transplantations could become a more significant competitive aspect to the dialysis treatments we provide. Although kidney transplant is a preferred treatment for ESRD, certain patients who have undergone such transplants have subsequently lost the functionality of the transplanted kidney and have returned to dialysis treatments.
The medical products industry is extremely competitive and our medical products operations are not a significant competitive factor in this area.
21
Employees
As of March 12, 2007, our company had 429 full time employees, including administrators, licensed practical nurses, registered nurses, technical specialists, patient care technicians, clerical employees, social workers, dietitians, corporate staff and four employees in the medical products operations. We retain 39 part-time employees consisting of registered nurses, patient care technicians and clerical employees. We also utilize 133 per diem personnel to supplement staffing.
We retain 26 independent contractors and sub-contractors who include social workers and dietitians at our Maryland, New Jersey, Ohio, Pennsylvania, Virginia and certain Georgia facilities. These contractors are in addition to the medical directors, who supervise patient treatment at each facility.
We believe our relationship with our employees is excellent and we have not suffered any strikes or work stoppages. None of our employees is represented by any labor union. We are an equal opportunity employer.
We have listed below certain of the risk factors relating to Dialysis Corporation of America and our securities. There may be other risks and uncertainties that we may face and of which we are currently unaware which could also adversely affect our business, operations and financial condition. If any of such risks or uncertainties arise, or the risks listed below occur, our operations, earnings and financial condition could be materially harmed, which, in turn, would most likely adversely affect the trading price of our common stock. Any such event could negatively impact a shareholder’s investment in the company.
Dialysis operations are subject to extensive government regulation
Our dialysis operations are subject to extensive federal and state government regulations, which include:
| · | licensing requirements for each dialysis center |
| · | government healthcare program participation requirements |
| · | reimbursement for patient services |
| · | patient referral prohibitions; broad federal and state Anti-Kickback regulations |
| · | false claims prohibitions for health care reimbursement and other fraud and abuse regulations |
| · | record keeping requirements |
| · | health, safety and environmental compliance |
| · | expanded protection of the privacy and security of personal medical data |
| · | standards for the exchange of electronic health information; electronic transactions and code sets; unique identifiers for providers |
| · | medical waste disposal regulations |
22
Many of these laws and regulations are complex and open to further judicial and legislative interpretations. If we are forced to change our method of operations because of these regulations, our earnings, financial condition and business could be adversely affected. The imposition of additional licensing and other regulatory requirements may, among other things, increase our cost of doing business. In addition, any violation of these governmental regulations could involve substantial civil and criminal penalties and fines, revocation of our licenses, closure of one or more of our centers, and our exclusion from participating in Medicare and Medicaid programs. Any loss of federal or state certifications or licenses would materially adversely impact our business.
In February, 2005, CMS published a proposed rule that would revise the conditions for coverage for dialysis facilities. The revised conditions would establish performance expectations and promote continuous quality improvement. These rules are subject to revision and would not become effective until issued in final form. Until the rules are finalized, it is impossible to predict what impact any revisions to the conditions of coverage will have on our business or our operating results.
Our arrangements with our physician medical directors do not meet the safe harbor provisions of federal and state laws, and may subject us to greater governmental scrutiny
Neither our arrangements with the medical directors of our facilities, typically retained by us as independent contractors under a fixed fee medical director agreement, nor the minority ownership interests of physicians in certain of our dialysis facilities meet all of the requirements of safe harbors to the Anti-Kickback Statute and similar state laws. These laws impose civil and criminal sanctions on persons who receive or make payments for referring a patient for treatment that is paid for in whole or in part by Medicare, Medicaid or similar state programs. Transactions that do not fall within a safe harbor may be subject to greater scrutiny by enforcement agencies.
Our operations are subject to Medicare and Medicaid audits with concurrent potential civil and criminal penalties for failure to comply
We are subject to periodic audits by the Medicare and Medicaid programs, which have various rights and remedies if they assert that we have overcharged the programs or failed to comply with program requirements. Rights and remedies available under these programs include repayment of any amounts alleged to be overpayments or in violation of program requirements, or making deductions from future amounts due to us. These programs may also impose fines, criminal penalties or program exclusions.
In the ordinary course of our business, we receive notices of deficiencies for failure to comply with various regulatory requirements. We review such notices and take appropriate corrective action. In most cases, we and the reviewing agency will agree upon the measures that will bring the center or services into compliance. In some cases or upon repeat violations, none of which we have experienced, the reviewing agency may take various adverse actions against a provider, including but not limited to:
| · | the imposition of fines; |
| · | suspension of payments for new admissions to the center; and |
| · | in extreme circumstances, decertification from participation in the Medicare or Medicaid programs and revocation of a center’s license. |
23
Any such regulatory actions could adversely affect a center’s ability to continue to operate, to provide certain services, and/or its eligibility to participate in Medicare or Medicaid programs or to receive payments from other payors. Moreover, regulatory actions against one center may subject our other centers, which may be deemed under our common control or ownership, to similar adverse remedies.
There has been increased governmental focus and enforcement with respect to anti-fraud initiatives as they relate to healthcare providers
State and federal governments are devoting increased attention and resources to anti-fraud initiatives against healthcare providers. Legislation has expanded the penalties for healthcare fraud, including broader powers to exclude providers from the Medicare and Medicaid programs. We have established policies and procedures that we believe are sufficient to ensure that our facilities will operate in substantial compliance with these anti-fraud requirements. While we believe that our business practices are consistent with Medicare and Medicaid criteria, those criteria are often vague and subject to change and interpretation. Anti-fraud actions could have an adverse effect on our financial position and results of operations.
Our revenues and financial stability are dependent on fixed reimbursement rates under Medicare and Medicaid
During 2004, 2005 and 2006, approximately 48% , 51% and 52%, respectively of our patient revenues was derived from Medicare reimbursement, and 8%, 8% and 9%, respectively, of our patient revenues in each of these years was derived from Medicaid and equivalent programs. Decreases in Medicare and Medicaid and equivalent rates and programs for our dialysis treatments would adversely affect our revenues and profitability.
Federal and state governments seek to maintain, if not reduce, costs, and any such actions in the healthcare industry could adversely affect our revenues and earnings, including the following:
| · | reductions in payments to us or government programs in which we participate |
| · | increases in labor and supply costs, which we do experience, without comparable governmental reimbursement rate increases |
| · | inclusion in the flat composite rate for dialysis treatments those ancillary services which we currently bill separately |
In November, 2005, CMS released the final physician fee schedule for 2006. A number of provisions contained in the fee schedule affects dialysis facilities. First, CMS revised the geographic designations and wage index adjustment applied to the composite payment rate. CMS eliminated the wage index cap, previously set at 1.3, and reduced the wage index floor for 2007 to .8423 from .85. Revisions to the geographic adjustments applicable to composite rate payments will be phased in over a four year period. For 2006, 75% of the wage adjusted composite rate reflected the old geographic adjustments and 25% reflected the revised adjustments. For 2007, the wage index blend will be 50%/50%.
24
CMS also revised its drug payment methodology, moving from average acquisition cost pricing to average sales price plus 6%. While these rates will result in lower payments for pharmaceuticals, the composite rate was concurrently increased with a revision to the drug add-on adjustment, for 2007 from 1.145 to 1.151. CMS is continuing the case mix adjustments finalized in 2005 whereby providers receive higher composite rate payments for certain patients based on age, body mass index and body surface area.
Management does not believe that in the aggregate these changes in Medicare reimbursement have significantly impacted our operations, expenses or earnings. Future changes in the structure of, and payment rates under, the Medicare program could substantially reduce our earnings.
Decreases in reimbursement payments from third-party, non-government payors could adversely affect our earnings
Any reduction in the rates paid by private insurers, hospitals and other non-governmental third-party organizations would adversely affect our business. Alternatively, any change in patient coverage, such as Medicare eligibility as opposed to higher private insurance coverage, would result in a reduction of revenue. We estimate approximately 44%, 41% and 39% of our patient revenues for 2004, 2005 and 2006, respectively, was obtained from sources other than Medicare or Medicaid and equivalent programs. We generally charge non-governmental organizations for dialysis treatment rates which exceed the fixed Medicare and Medicaid and equivalent rates. If private payors reduce their payments or we experience a shift in revenue mix toward Medicare or Medicaid reimbursement, then our revenue, cash flow and earnings would decrease, and our cash flow and profits would be disproportionately affected.
Any decrease in the availability of or the reimbursement rate of EPO would reduce our revenues and earnings
EPO, a bio-engineered drug used for treating anemia in dialysis patients, is currently available from a single manufacturer, Amgen, Inc. There currently is no alternative drug available to us for the treatment of anemia of our dialysis patients. The available supply of EPO could be delayed or reduced, whether by Amgen itself, through unforeseen circumstances, or as a result of excessive demand. In addition, Amgen could increase the price of EPO. This would adversely impact our revenues and profitability, since approximately 28% of our medical revenues in each of 2004, 2005 and 2006 were based upon the administration of EPO to our dialysis patients.
If government or private payors reduce reimbursement for EPO, then our revenues and earnings will decline. Most of our EPO reimbursement is from government programs. For 2006, Medicare and Medicaid reimbursement represented 64% of the total revenue derived from EPO. In 2005, CMS revised its rules for reimbursement of pharmaceuticals, including EPO, which resulted in a net reduction of average Medicare payment rates. In 2006, reimbursement for EPO was at the average sales price plus 6%, which will result in lower reimbursement for pharmaceuticals, but offset by the 1.6% composite rate increase.
Changes in Medicare reimbursement criteria may also impact EPO revenue. In 2005, CMS adopted a national monitoring policy for EPO claims. This policy, effective April, 2006, did not have an adverse impact on our net revenue and earnings. Under the new policy, CMS initiates monitoring when patient hematocrit levels reach a threshold of 39.0. CMS expects a reduction in the dosage of EPO for patients whose hemotocrit exceeds this threshold. If dosage is not reduced, payment will be made as if the reduction had occurred. The policy also limits the quantity of EPO that can be administered in a month, regardless of hematocrit levels. We have revised our protocols on anemia management to address this policy.
25
The implementation of the case-mix adjustment could adversely affect our revenues, profitability and cash flow.
In April, 2005, CMS adopted a case-mix adjustment for the ESRD composite rate, under which the Medicare composite rate is adjusted based on a patient’s age, body mass index and body surface area. This change is intended to link payment more closely to acuity and its impact on revenues will turn on our patient acuity mix. For 2006, case-mix adjustment has not adversely affected revenues or profitability.
New Amgen drug could affect use of EPO, adversely impacting our profitability.
Amgen is the sole manufacturer of EPO, which is administered in conjunction with dialysis treatments to address a patient’s anemia. Amgen has developed and obtained FDA approval for its new drug Aranesp®, used to treat anemia, and which is indicated to be effective for a longer period than EPO. Based on its longer lasting capabilities, potential profit margins on Aranesp® could be significantly lower than on EPO, and furthermore, Aranesp® could be administered by a dialysis patient’s physician, further eliminating potential revenues from the treatment of anemia in our dialysis patients. The introduction of Aranesp® as an anemia treatment for dialysis patients, could adversely impact our revenues and profitability.
Our ability to grow is subject to our resources and available locations
Other than four center acquisitions over the period 2002 through 2004, three centers acquired in the first quarter of 2006, and two centers acquired during the first quarter of 2007, expansion of our operations has been through construction of dialysis centers. We developed two dialysis centers and acquired one facility in 2003, opened five new centers and acquired a company with two dialysis facilities in 2004, opened three new centers in 2005, opened three new centers in 2006, acquired three centers in 2006, acquired two centers in the first quarter of 2007, and have two centers under development. We seek areas with qualified and cost-effective nursing and technical personnel and a sufficient population to sustain a dialysis center. These opportunities are limited and we compete with much larger dialysis companies for appropriate locations. The time period from the beginning of construction through commencement of operations of a dialysis center generally takes four to six months and sometimes longer. Once the center is operable, it generates revenues, but usually does not operate at full capacity, and may incur losses for approximately 12 months or longer. Our growth strategy based on construction also involves the risks of our ability to identify suitable locations to develop additional centers. Those we do develop may never achieve profitability, and additional financing may not be available to finance future development.
Our inability to acquire or develop dialysis centers in a cost-effective manner would adversely affect our ability to expand our business and as a result, our profitability.
Growth places significant demands on our financial and management skills. Inability on our behalf to meet the challenges of expansion and to manage any such growth would have an adverse effect on our results of operations and financial condition.
26
Our attempt to expand through development or acquisition of dialysis centers which are not currently identified entails risks which shareholders and investors will not have a basis to evaluate
We expand generally by seeking an appropriate location for a dialysis center and by taking into consideration the potential geographic patient base, and the availability of a physician nephrologist to be our medical director and a skilled work force. Construction, equipment and initial working capital costs for a new dialysis center with 15 stations, typically the size of our dialysis facilities, range from $750,000 to $1,000,000. While the cost of acquiring a center can be greater than the development costs of a similar center, we attempt to target our acquisitions such that those costs are in the range of costs we would expect to incur in a similar development project. We cannot assure you that we will be successful in developing or acquiring dialysis facilities, or otherwise successfully expanding our operations. We are negotiating with nephrologists and others to establish new dialysis centers, but we cannot assure you that these negotiations will result in the development of new centers. Furthermore, there is no basis for shareholders and investors to evaluate the specific merits or risks of any potential development or acquisition of dialysis facilities.
We depend on physician referrals, and the limitation or cessation of such referrals would adversely impact our revenues and earnings
Most dialysis facilities, including ours, are dependent upon referrals of ESRD patients for treatment by physicians, primarily those physicians specializing in nephrology. We retain by written agreement qualified physicians or groups of qualified physicians to serve as medical directors for each of our facilities. The medical directors are typically a source of patients treated at the particular facility served. There is no requirement for these physicians to refer their patients to us, and they are free to refer patients to any other dialysis facility. The loss of the patient base of the medical director or other physicians in the area of our facilities could result in a decline in our operations, revenues and earnings. We may not be able to renew or otherwise negotiate compensation under the medical director agreements with our medical director physicians which could terminate the relationship, and without a suitable medical director replacement could result in closure of the facility. Accordingly, the loss of these key physicians at a particular facility could have a material adverse effect on the operations of the facility and could adversely affect our revenues and earnings. Most of our medical director agreements range in terms of from five to ten years with renewals. We have had no difficulty in renewing agreements as they have expired. All the medical director agreements provide for noncompetition restrictions. We have never had to attempt to enforce such restrictions, but there is no assurance that a particular jurisdiction in which the agreement is applicable would uphold such noncompetition agreement, which would increase the potential for competition with affiliated dialysis centers and could adversely impact our revenues and earnings.
Some of our medical directors or the medical groups with whom they are associated own minority interests in certain of our subsidiaries which operate dialysis centers. If these interests are deemed to violate applicable federal or state law, these physicians may be forced to dispose of their ownership interests.
27
Industry changes could adversely affect our business
Healthcare organizations, public and private, continue to change the manner in which they operate and pay for services. Our business is designed to function within the current healthcare financing and reimbursement system. In recent years, the healthcare industry has been subject to increasing levels of government regulation of reimbursement rates and capital expenditures, among other things. In addition, proposals to reform the healthcare system have been considered by Congress, and still remain a priority issue. Any new legislative initiatives, if enacted, may (i) further increase government regulation of or other involvement in healthcare, (ii) lower reimbursement rates, and (iii) otherwise change the operating environment for healthcare companies. We cannot predict the likelihood of those events or what impact they may have on our earnings, financial condition or business.
Our business is subject to substantial competition, and we must compete effectively, otherwise our growth could slow
We are operating in a highly competitive environment in terms of operation, development and acquisition of existing dialysis centers. Our competition comes from other dialysis centers, many of which are owned by much larger companies, and from hospitals. The dialysis industry is rapidly consolidating, resulting in several very large dialysis companies competing for the acquisition of existing dialysis centers and the development of relationships with referring physicians. Many of our competitors have significantly greater financial resources, more dialysis facilities and a significantly larger patient base. In addition, technological advances by our competitors may provide more effective dialysis treatments than the services provided by our centers.
We also compete with physicians who open their own dialysis facilities. Competition for existing centers has increased the costs of acquiring such facilities. Competition is also intense for qualified nursing and technical staff as well as for nephrologists with an adequate patient base. Although we have exhibited growth over the last several years, we can provide no assurance that we will be able to compete effectively. Our failure to do so could impair our continued growth and profitability.
We could be subject to professional liability claims that may adversely affect us
Operation of dialysis centers and, in particular, the provision of dialysis treatments to ESRD patients, as is the case with most healthcare treatment services, entails significant risks of liability. Accordingly, we could be subject to various actions and claims of professional liability alleging negligence in the performance of our treatment and related services, as well as for the acts or omissions of our employees. As we grow and the number of our patients increases, so too does our exposure increase to potential malpractice, professional negligence, and other related legal theories and causes of action. These potential claims could seek substantial damages, possibly beyond our insurance coverage, and could subject us to the incurrence of significant fees and costs related to defending such potential claims. Such potential future claims for malpractice or professional liability, including any judgments, settlements or costs associated with such claims and actions, could have a material adverse effect on us.
28
Our insurance costs and deductibles have been substantially increasing over the last several years, and may not be sufficient to cover claims and losses
We maintain a program of insurance coverage against a broad range of risks in our business, including, and of primary importance, professional liability insurance, subject to certain deductibles. The premiums and deductibles under our insurance program have been steadily and significantly increasing over the last several years as a result of general business rate increases coupled with our continued growth and development of dialysis centers. We are unable to predict further increases in premiums and deductibles, but based on experience we anticipate further increases in this area, which would adversely impact earnings. The liability exposure of operations in the healthcare services industry has increased, resulting not only in increased premiums, but in limited liability on behalf of the insurance carriers. Our ability to obtain the necessary and sufficient insurance coverage for our operations upon expiration of our insurance policies may be limited, and sufficient insurance may not be available on favorable terms, if at all. Such insurance may not be sufficient to cover any judgments, settlements or costs relating to potential future claims, complaints or law suits. Our inability to obtain sufficient insurance for our operations, or if we obtain insurance which is limited, any future significant judgments, settlements and costs relating to future potential actions, suits or claims, could have an adverse effect on our company.
The loss of certain executive personnel without retaining qualified replacements could adversely affect our business operations, and as a result, our revenues and earnings could decline
We are dependent upon the services of Thomas K. Langbein, Chairman of the Board, and Stephen W. Everett, our President, Chief Executive Officer and a director. Mr. Langbein has been involved with us since we organized in 1976. Mr. Everett joined our company in November, 1998 as Vice President, became Executive Vice President in June, 1999, President on March 1, 2000, and Chief Executive Officer in May, 2003. Mr. Everett has been involved in the healthcare industry for 27 years. A new five-year employment agreement was entered into with Mr. Everett effective as of January 3, 2006. Among other things, the employment agreement contains a non-competition provision during the term of the agreement and for one year after termination. It would be very difficult to replace the services of these individuals, whose services, both individually and combined, if lost, would adversely affect our operations and earnings, and most likely as a result, the trading price of our common stock. There is no key-man life insurance covering any of our officers.
Shares eligible for future sale by restricted shareholders may adversely affect our stock price
Our officers and directors own 2,213,225 shares of our common stock and vested options exercisable into an additional 15,000 shares of common stock, for an aggregate of 2,228,225 shares or approximately 23% of our outstanding common stock. Most of the shares held by these officers and directors, upon satisfying the conditions of Rule 144 under the Securities Act, may be sold without complying with the registration provisions of the Securities Act. Rule 144 conditions include:
| · | holding the shares for one year from acquisition; |
| · | volume limits of selling every three months an amount of shares which does not exceed the greater of 1% of the outstanding common stock, or the average weekly volume of trading as reported by Nasdaq during the four calendar weeks prior to the sale; |
29
| · | filing Form 144 with the SEC; |
| · | the company continuing to timely file its reports under the Exchange Act; |
Our publicly tradable common stock, known as the float, is approximately 7,360,000 shares. Common stock of the company owned by our officers and directors represent approximately 30% of the float. Accordingly, the sale by such officers and directors under Rule 144 may have an adverse affect on the market price of our common stock, and may inhibit our ability to manage subsequent equity or debt financing.
Over the last year, our stock price has exhibited volatility, and any investment in our common stock may, therefore, decline for reasons unrelated to our performance
Our common stock trades on the Nasdaq Capital Market under the symbol “DCAI.” The market price of our common stock has exhibited volatility. For fiscal 2006, our per share price range was $9.64 to $14.69.
Other than the continued growth of the company, there was no information known to management that would cause significant fluctuation in the price of our common stock, or in the trading volume.
Other factors that could continue to cause fluctuation in our common stock include:
| · | changes in government regulation, whether legislative, enforcement or reimbursement rates |
| · | third party reports relating to the dialysis industry and our company (unsolicited by management) |
| · | announcements by management relating to the company’s performance or other material events |
| · | actions and announcements by our competitors |
| · | the outlook for the healthcare industry generally |
Investors should understand that in general, stock prices fluctuate for reasons unrelated to operating results. Any changes in the above discussed factors, the Medicare and Medicaid reimbursement rates in particular, or general economic, political, global and market conditions, could result in a decline in the market price and volume of trading in our common stock.
Item 1B. Unresolved Staff Comments
None.
Item 2. Properties
Dialysis Corporation of America owns a property in Easton, Maryland which consists of approximately 7,500 square feet, most of which is leased to a competitor under a 10-year lease through June 30, 2009 with two renewals of five years each. The lease is guaranteed by the tenant’s parent company.
30
Our Easton, Maryland property has a mortgage to secure a $700,000 development loan at an annual interest rate of prime rate, maturing in May 2026. This loan had a remaining principal balance of approximately $555,000 at December 31, 2006. See Item 7, “Management’s Discussions and Analysis of Financial Condition and Results of Operations” and Note 2 to “Notes to Consolidated Financial Statements.”
We also own a property in Lemoyne, Pennsylvania which consists of approximately 15,000 square feet and houses one of our dialysis centers, accounting for approximately 5,400 square feet, under a five year lease through December 22, 2008, with one additional renewal period of five years. The center is approved for 17 dialysis stations with space available for expansion. We use the remaining square footage of the Lemoyne property for administrative offices.
We acquired property in Valdosta, Georgia in 2000, subject to a five year $788,000 mortgage obtained in April, 2001, subsequently refinanced in April 2006, with interest at the prime rate, with a minimum rate of 5.75% and a maximum rate of 8%, maturing in April, 2011. This mortgage had a remaining principal balance of approximately $617,000 at December 31, 2006. We constructed a dialysis center at this property comprising approximately 6,000 square feet which we have leased to one of our subsidiaries for $90,600 per year under a 10-year lease, with two additional renewal periods of five years each.
For our Cincinnati, Ohio facility, we purchased the property, and completed the construction of an approximately 5,000 square foot dialysis facility at a cost of approximately $740,000. In February, 2003, we sold the property to a corporation owned by the medical director of that facility, which, in turn, leased the facility to our Cincinnati subsidiary for an initial term of 10 years from the commencement date of February 6, 2003, with two additional five-year renewal periods. Annual rental fees remain the same for the first four years of the lease, and thereafter increase annually based upon a percentage increase in the CPI for the Cincinnati, Ohio area.
In addition to our Lemoyne, Pennsylvania, Valdosta, Georgia and Cincinnati, Ohio facilities, we presently own or manage 30 other dialysis centers, that lease their respective facilities from unaffiliated parties, most under five to ten year initial terms, usually with two additional renewal periods of five years each, for space ranging from approximately 3,000 to 7,000 square feet. We sublet a minimal amount of space at five of our dialysis centers to the physicians who are our medical directors at those centers for their medical offices. The subleases are on a commercially reasonable basis and are structured to comply with the safe harbor provisions of the “Anti-Kickback Statute.” See Item 1, “Business – Government Regulation – Fraud and Abuse.”
In July, 2004, we moved our executive offices to Linthicum, Maryland, which comprise approximately 4,600 square feet and are leased for five years to July 11, 2009.
During 2005 we acquired undeveloped properties in Georgia, Pennsylvania and South Carolina where we subsequently constructed dialysis centers. The land purchase prices ranged from $150,000 to $205,000 and were paid in cash. In September, 2006, we completed a sale and leaseback transaction with an unaffiliated entity owned by a group of local doctors for the Georgia facility, similar to the arrangement at our Cincinnati, Ohio facility, and in February 2007 completed a similar sale and leaseback transaction for the South Carolina center with an entity owned by the medical director of that facility. We have another South Carolina center under development that may become subject to a similar arrangement when it is completed. In December, 2006, we sold the developed Pennsylvania facility to a 60% owned subsidiary limited partnership from which our operating subsidiary at this location is leasing the premises. We acquired three new centers, one in Virginia and two in Maryland in early 2006, that lease the facilities in which they operate. We continue to actively pursue the additional development and acquisition of dialysis facilities in other areas which would entail the acquisition or lease of additional property.
31
Dialysis stations at our centers are equipped with modern dialysis machines, which were largely financed under a 1996 master lease/purchase agreement until 2003 since which we have not utilized this financing agreement for additional equipment acquisitions. See Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
Most of our dialysis facilities do not operate at full capacity. See “Business – Operations – Location, Capacity and Use of Facilities” above. The existing dialysis facilities could accommodate greater patient volume, particularly if we increase hours and/or days of operation without adding additional dialysis stations or any additional capital expenditures. We also have the ability and space at most of our facilities to expand to increase patient volume subject to obtaining appropriate governmental approval.
We maintain executive offices at 1302 Concourse Drive, Suite 204, Linthicum, Maryland 21090, and administrative offices at 27 Miller Street, Suite 2, Lemoyne, Pennsylvania 17043, and 2337 West 76th Street, Hialeah, Florida 33016.
Item 3. Legal Proceedings
None.
Item 4. Submission of Matters to a Vote of Security Holders
No matter was submitted during the fourth quarter of our fiscal year ended December 31, 2006 to a vote of security holders through the solicitation of proxies or otherwise.
PART II
Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Price Range
Our common stock trades on the Nasdaq Capital Market under the symbol “DCAI.” The following table indicates the high and low bid prices for our common stock for each of the four quarters for the years ended December 31, 2005 and 2006 as reported by Nasdaq.
Bid Price | ||||||||
2005 | High | Low | ||||||
1st Quarter | $ | 34.60 | $ | 16.74 | ||||
2nd Quarter | 24.60 | 13.12 | ||||||
3rd Quarter | 27.98 | 11.93 | ||||||
4th Quarter | 14.71 | 9.14 | ||||||
32
Bid Price | ||||||||
2006 | High | Low | ||||||
1st Quarter | $ | 13.65 | $ | 9.64 | ||||
2nd Quarter | 13.90 | 10.49 | ||||||
3rd Quarter | 13.52 | 10.50 | ||||||
4th Quarter | 14.69 | 12.02 | ||||||
As of March 5, 2007, the high and low sales prices of our common stock were $13.62 and $13.31, respectively.
Bid prices represent prices between brokers, and do not include retail mark-ups, mark-downs or any commission, and may not necessarily represent prices in actual transactions.
Stockholders
At March 5, 2007, we had 1,021 shareholders of record as reported by our transfer agent. We have been advised by ADP, which organization holds securities for banks, brokers and depositories, that there are currently 3,400 beneficial owners of our common stock.
Dividend Policy
The company does not anticipate that it will pay dividends in the foreseeable future. The board of directors intends to retain earnings for use in the business. Future dividend policy will be at the discretion of the board of directors, and will depend on our earnings, capital requirements, financial condition and other similar relevant factors. Any determination to pay a dividend is also subject to the covenants in the KeyBank National Association credit facility (see Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” and Note 2 to “Notes to Consolidated Financial Statements”) which precludes the payment of any dividends (other than stock dividends), as does the mortgage on our Valdosta, Georgia property (see Item 2, “Properties”) which restricts the payment of dividends above 25% of our net worth.
Sale of Securities Not Registered Under the Securities Act
The only unregistered sales of our common stock during the fourth quarter of 2006 included: (i) 10,000 shares of common stock in November, 2006, upon retaining our interim Chief Operating Officer; (ii) 750 shares of common stock, 250 shares each to our three independent directors, which had vested on December 31, 2006, under a stock award granted in March, 2006 (previously reported in the company’s quarterly report on Form 10-Q for the first quarter ended March 31, 2006, Part II, Item 2); and (iii) 8,500 shares of common stock which had vested on December 31, 2006 pursuant to an aggregate grant of 64,000 stock awards to certain officers and key employees in the second quarter of 2006 (of which 30,000 shares were cancelled in November, 2006, upon resignation of an officer),, which stock awards vest in equal yearly increments through 2009, and which awards contain termination and acceleration provisions (previously reported on a current report on Form 8-K dated June 30, 2006). See Item 11, “Executive Compensation.”
33
The sales of our securities were exempt from the registration requirements of Section 5 of the Securities Act under the private placement exemptions of Section 4(2) and/or Regulation D of the Securities Act, based on the limited number of persons, each of whom are officers, directors and/or key employees knowledgeable concerning the affairs of the company. See Item 11, “Executive Compensation,” Item 12, “Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters,” and Note 6 to “Notes to Consolidated Financial Statements.” Other sales of common stock, which were not significant, during 2006, have been reported in our quarterly reports, Form 10-Q, for the periods ended March 31, 2006, June 30, 2006 and September 30, 2006.
Stock Repurchases
The company had a common stock repurchase plan which it terminated in the second quarter of 2005. The company has not made any repurchases of any equity securities during the fourth quarter months of October, November and December, 2006.
PERFORMANCE GRAPH
The following graph shows a five-year comparison of cumulative total shareholder returns for the company, the Nasdaq Market Index and the Dialysis Center Industry Index from December 31, 2001 through December 31, 2006. The cumulative total shareholder returns on our common stock was measured by dividing the difference between our share price at the end and the beginning of the measurement period by the share price at the beginning of the measurement period. The total shareholder return assumes $100 invested at the beginning of the period in our common stock, in the Nasdaq Market Index and the Dialysis Center Industry Index. We did not pay dividends on our common stock during the measurement period and the calculations of cumulative total shareholders return on the common stock did not include dividends. Our share price was adjusted to reflect a two-for-one stock split on January 28, 2004. This graph is presented in accordance with SEC requirements. You are cautioned against drawing any conclusions from this information, as past results are not necessarily indicative of future performance. This graph in no way reflects a forecast of future financial performance.
COMPARISON OF 5-YEAR CUMULATIVE TOTAL RETURN
AMONG DIALYSIS CORPORATION OF AMERICA,
NASDAQ MARKET INDEX AND SIC CODE INDEX
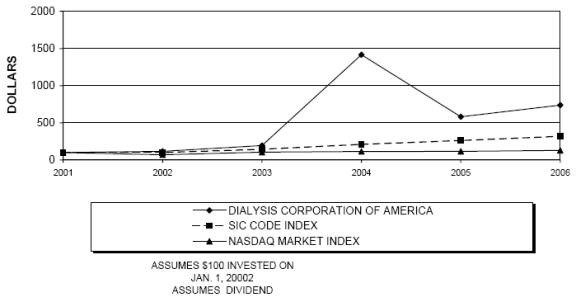
2001 | 2002 | 2003 | 2004 | 2005 | 2006 | ||||||||||||||
| Dialysis Corporation of America | 100.00 | 115.36 | 194.20 | 1,416.23 | 581.45 | 736.81 | |||||||||||||
| Kidney Dialysis Centers | 100.00 | 99.94 | 144.06 | 209.92 | 261.64 | 318.70 | |||||||||||||
| NASDAQ Market Index | 100.00 | 69.75 | 104.88 | 113.70 | 116.19 | 128.12 | |||||||||||||
The current composition of SIC Code 8092 – Kidney Dialysis Centers – is as follows:
Davita Inc.
Dialysis Corporation of America
Fresenius Med Care AG&Co.
34
The performance graph is furnished, not filed, and is not deemed to be soliciting material under the proxy rules or incorporated by reference into any company filing.
Item 6. Selected Financial Data
The following selected financial data for the five years ended December 31, 2006 is derived from the audited consolidated financial statements of the company and its subsidiaries. The consolidated financial statements and related notes for the three years ended December 31, 2006, together with the related Reports of Independent Certified Public Accountants, are included elsewhere in this annual report on Form 10-K. The data should be read in conjunction with the consolidated financial statements, related notes and other financial information included herein, and Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
Consolidated Statements of Operations Data (in thousands except per share amounts) Years Ended December 31, | ||||||||||||||||
| 2006 | 2005 | 2004 | 2003 | 2002 | ||||||||||||
| Revenues(1) | $ | 62,460 | $ | 45,392 | $ | 40,986 | $ | 29,997 | $ | 25,354 | ||||||
| Net income | 3,049 | 1,900 | 2,214 | 1,150 | 1,242 | |||||||||||
| Earnings per share(2) | ||||||||||||||||
| Basic | .32 | .22 | .27 | .15 | .16 | |||||||||||
| Diluted | .32 | .20 | .25 | .13 | .14 | |||||||||||
Consolidated Balance Sheet Data (in thousands) December 31, | ||||||||||||||||
| 2006 | 2005 | 2004 | 2003 | 2002 | ||||||||||||
| Working capital | $ | 17,098 | $ | 7,617 | $ | 3,644 | $ | 3,773 | $ | 4,593 | ||||||
| Total assets | 49,856 | 38,803 | 26,490 | 19,604 | 17,154 | |||||||||||
| Intercompany advance payable | ||||||||||||||||
| (receivable) from Medicore | ||||||||||||||||
| (non-current portion)(3) | — | — | 449 | 234 | — | |||||||||||
| Intercompany note and accrued interest | ||||||||||||||||
| payable to Medicore(3) | — | — | 1,462 | — | — | |||||||||||
| Long term debt, net of current portion | 8,618 | 635 | 1,586 | 2,097 | 2,727 | |||||||||||
| Stockholders’ equity | 29,061 | 25,613 | 13,330 | 10,970 | 9,727 | |||||||||||
| (1) | Prior year amounts have been reclassified to conform to current year presentation. |
| (2) | All share and per share data retroactively adjusted for two-for-one stock split effected January 28, 2004. |
| (3) | Pursuant to merger with former parent company, Medicore, Inc. in September, 2005, intercompany indebtedness was forgiven. |
35
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
Management’s Discussion and Analysis of Financial Condition and Results of Operations, commonly known as MD&A, is our attempt to provide a narrative explanation of our financial statements, and to provide our shareholders and investors with the dynamics of our business as seen through our eyes as management. Generally, MD&A is intended to cover expected effects of known or reasonably expected uncertainties, expected effects of known trends on future operations, and prospective effects of events that have had a material effect on past operating results. Our discussion of MD&A should be read in conjunction with our consolidated financial statements, including the notes, included elsewhere in this annual report on Form 10-K. Please also review the Cautionary Notice Regarding Forward-Looking Information on page one of this annual report.
Overview
Dialysis Corporation of America provides dialysis services, primarily kidney dialysis treatments through 34 outpatient dialysis centers, including three centers acquired in the first quarter of 2006, three centers opened during 2006, two centers acquired in the first quarter of 2007, and one unaffiliated dialysis center which it manages and is acquiring (see Note 7 and Note 17 to “Notes to Consolidated Financial Statements”), to patients with chronic kidney failure, also know as end-stage renal disease or ESRD. We provide dialysis treatments to dialysis patients of ten hospitals and medical centers through acute inpatient dialysis services agreements with those entities. We provide homecare services, including home peritoneal dialysis.
Quality Clinical Results
Our goal is to provide consistent quality clinical care to our patients from caring and qualified doctors, nurses, patient care technicians, social workers and dieticians. We have demonstrated an unwavering commitment to quality renal care through our continuous quality improvement initiatives. We strive to maintain a leadership position as a quality provider in the dialysis industry and often set our goals to exceed the national average standards. See Item 1, “Business - Operations - Quality Clinical Results.”
Patient Treatments
The following table shows the number of in-center, home peritoneal and acute inpatient treatments performed by us through the dialysis centers we operate, including one center we manage and one in which we had a 40% ownership interest until August 1, 2006, when this center was consolidated, in which center we subsequently acquired the other 60% interest in December, 2006, and those hospitals and medical centers with which we have inpatient acute service agreements for the periods presented:
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| In center | 197,628 | 155,130 | 127,293 | |||||||
| Home peritoneal | 15,486 | 16,942 | 13,311 | |||||||
| Acute | 6,350 | 7,100 | 8,387 | |||||||
| 219,464 | (1) | 179,172 | (1) | 148,991 | (1) | |||||
| (1) | Treatments by the managed Georgia center include: in-center treatments of 9,428; 8,888; and 7,532; respectively, for 2006, 2005 and 2004 and no home treatments or acute treatments. |
36
New Business Development
Dialysis Corporation of America’s future growth depends primarily on the availability of suitable dialysis centers for development or acquisition in appropriate and acceptable areas, and our ability to manage the development costs for these potential dialysis centers while competing with larger companies, some of which are public companies or divisions of public companies with greater numbers of personnel and financial resources available for acquiring and/or developing dialysis centers in areas targeted by us. Additionally, there is intense competition for qualified nephrologists who would serve as medical directors of dialysis facilities, and be responsible for the supervision of those dialysis centers. The company is currently constructing three dialysis centers and is in various stages of development with two others. There is no assurance as to when any new dialysis centers or inpatient service contracts with hospitals will be implemented, or the number of stations, or patient treatments such center or service contract may involve, or if such center or service contract will ultimately be profitable.
Start-up Losses
It has been our experience that newly established dialysis centers, although contributing to increased revenues, have adversely affected our results of operations in the short term due to start-up costs and expenses and a smaller patient base. These losses are typically a result of several months of pre-opening costs, and six to eighteen months of post opening costs, in excess of revenues. We consider new dialysis centers to be “start-up centers” through their initial twelve months of operations, or when they achieve consistent profitability, whichever is sooner. For the year ended December 31, 2006, we incurred an aggregate of approximately $1,423,000 in pre-tax losses for start-up centers compared to $744,000 for the preceding year.
EPO Utilization
We also provide ancillary services associated with dialysis treatments, including the administration of EPO for the treatment of anemia in our dialysis patients. EPO is currently available from only one manufacturer, and no alternative drug has been available to us for the treatment of anemia in our dialysis patients. If our available supply of EPO were reduced either by the manufacturer or due to excessive demand, our revenues and net income would be adversely affected. The manufacturer of EPO could implement price increases which would adversely affect our net income. This manufacturer developed another anemia drug that could possibly substantially reduce our revenues and profit from the treatment of anemia in our patients.
ESRD patients must either obtain a kidney transplant or obtain regular dialysis treatments for the rest of their lives. Due to a lack of suitable donors and the possibility of transplanted organ rejection, the most prevalent form of treatment for ESRD patients is hemodialysis through a kidney dialysis machine. Hemodialysis patients usually receive three treatments each week with each treatment lasting between three and five hours on an outpatient basis. Although not as common as hemodialysis in an outpatient facility, home peritoneal dialysis is an available treatment option, representing the third most common type of ESRD treatment after outpatient hemodialysis and kidney transplantation.
37
Reimbursement
Approximately 61% of our medical services revenue for 2006 was derived from Medicare and Medicaid reimbursement with rates established by CMS, and which rates are subject to legislative changes. Congress approved a 1.6% composite rate increase for each of 2005 and 2006. Medicare changed the way it reimburses dialysis providers, which includes revision of pricing for separately billable drugs and biologics, with an add-on component to make the change budget-neutral. Medicare also implemented a case mix payment system as an adjustment to the composite rate. See Item 1, “Business - Operations - Medicare Reimbursement.” Dialysis is typically reimbursed at higher rates from private payors, such as a patient’s insurance carrier, as well as higher payments received under negotiated contracts with hospitals for acute inpatient dialysis services.
The following table shows the breakdown of our revenues by type of payor for the periods presented:
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Medicare | 52 | % | 51 | % | 48 | % | ||||
| Medicaid and comparable programs | 9 | % | 8 | % | 8 | % | ||||
| Hospital inpatient dialysis services | 3 | % | 5 | % | 6 | % | ||||
| Commercial insurers and other private payors | 36 | % | 36 | % | 38 | % | ||||
| 100 | % | 100 | % | 100 | % | |||||
Our medical services revenue is derived primarily from four sources: outpatient hemodialysis services, home peritoneal dialysis services, inpatient hemodialysis services and ancillary services. The following table shows the breakdown of our medical services revenue (in thousands) derived from our primary revenue sources and the percentage of total medical service revenue represented by each source for the periods presented:
Year Ended December 31, | |||||||||||||||||||
2006 | 2005 | 2004 | |||||||||||||||||
| Outpatient hemodialysis services | $ | 32,856 | 54 | % | $ | 23,084 | 52 | % | $ | 18,599 | 46 | % | |||||||
| Home dialysis services | 3,625 | 6 | % | 3,198 | 7 | % | 2,691 | 7 | % | ||||||||||
| Inpatient hemodialysis services | 2,191 | 3 | % | 2,055 | 5 | % | 2,261 | 5 | % | ||||||||||
| Ancillary services | 22,467 | 37 | % | 16,350 | 36 | % | 16,899 | 42 | % | ||||||||||
| $ | 61,139 | 100 | % | $ | 44,687 | 100 | % | $ | 40,450 | 100 | % | ||||||||
Compliance
The healthcare industry is subject to extensive regulation by federal and state authorities. There are a variety of fraud and abuse measures to combat waste, including Anti-Kickback regulations and extensive prohibitions relating to self-referrals, violations of which are punishable by criminal or civil penalties, including exclusion from Medicare and other governmental programs. Unanticipated changes in healthcare programs or laws could require us to restructure our business practices which, in turn, could materially adversely affect our business, operations and financial condition. See Item 1, “Business - Government Regulation.” We have developed a Corporate Integrity Program to assure that we provide the highest level of patient care and services in a professional and ethical manner consistent with applicable federal and state laws and regulations. Among the different programs is our Compliance Program, which has been implemented to assure our compliance with fraud and abuse laws and to supplement our existing policies relating to claims submission, cost report preparation, initial audit and human resources, all geared towards a cost-efficient operation beneficial to patients and shareholders. See Item 1, “Business - Corporate Integrity Program.”
38
Results of Operations
The following table shows our results of operations (in thousands):
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Medical services revenue | $ | 61,139 | $ | 44,687 | $ | 40,450 | ||||
| Product sales | 891 | 207 | — | |||||||
Total sales | 62,030 | 44,894 | 40,450 | |||||||
| Other income | 430 | 498 | 536 | |||||||
| Total operating revenues | 62,460 | 45,392 | 40,986 | |||||||
| Cost of medical services | 36,969 | 27,860 | 23,546 | |||||||
| Cost of product sales | 549 | 119 | — | |||||||
Total cost of sales | 37,518 | 27,979 | 23,546 | |||||||
| Corporate selling, general and administrative expenses | 6,460 | 4,524 | 4,671 | |||||||
| Facility selling, general and administrative expenses | 8,988 | 7,183 | 5,919 | |||||||
Total selling, general and administrative expense | 15,448 | 11,707 | 10,590 | |||||||
| Stock compensation expense | 276 | — | — | |||||||
| Depreciation and amortization | 2,319 | 1,749 | 1,499 | |||||||
| Provision for doubtful accounts | 1,199 | 571 | 1,198 | |||||||
| Total operating costs and expenses | 56,760 | 42,006 | 36,833 | |||||||
| Operating income | 5,700 | 3,386 | 4,153 | |||||||
| Other income | 101 | 66 | 35 | |||||||
| Income before income taxes, minority interest | ||||||||||
| and equity in affiliate earnings | 5,801 | 3,452 | 4,188 | |||||||
| Income tax provision | 2,086 | 1,427 | 1,576 | |||||||
| Income before minority interest and | ||||||||||
| equity in affiliate earnings | 3,715 | 2,025 | 2,612 | |||||||
| Minority interest in income of | ||||||||||
| consolidated subsidiaries | (920 | ) | (454 | ) | (681 | ) | ||||
| Equity in affiliate earnings | 254 | 329 | 283 | |||||||
Net income | $ | 3,049 | $ | 1,900 | $ | 2,214 | ||||
2006 Compared to 2005
Medical services revenue increased approximately $16,452,000 (37%) for the year ended December 31, 2006, compared to the preceding year. Medical services revenue for 2006 includes approximately $688,000 of amounts previously included in excess insurance liability that was determined to be non-refundable compared to approximately $43,000 in the preceding year. See Note 1 to “Notes to Consolidated Financial Statements.” Dialysis treatments performed increased from 179,172 in 2005 to 219,464 in 2006, a 22% increase which includes treatments at managed facilities, one for which we acquired the 60% interest not already owned by the company in December, 2006, and one of which we are acquiring an 80% interest (see Note 7, Note 9, Note 14 and Note 17 to “Notes to Consolidated Financial Statements”). The increase in treatments includes treatments at the three new centers we opened during 2005 that were in operation throughout 2006, three centers acquired in the first quarter of 2006, and three new centers opened during 2006. Some of our patients carry commercial insurance which may require an out of pocket co-pay by the patient, which is often uncollectible by us. This co-pay is typically limited, and therefore may lead to our under-recognition of revenue at the time of service. We routinely recognize these revenues as we become aware that these limits have been met.
39
We record contractual adjustments based on fee schedules for a patient’s insurance plan except in circumstances where the schedules are not readily determinable, in which case rates are estimated based on similar insurance plans and subsequently adjusted when actual rates are determined. Out-of-network providers generally do not provide fee schedules and coinsurance information and, consequently, represent the largest portion of contractual adjustment changes. Estimated contractual adjustments for 2005 and prior years made during 2006 resulted in approximately a $65,000 reduction in revenues in 2006. Based on historical data we do not anticipate that a change in estimates would have a significant impact on our financial conditions or results of operations.
Operating income increased approximately $2,314,000 (68%) for the year ended December 31, 2006, compared to the preceding year, despite an increase in start-up costs associated with our new centers of $1,423,000 in 2006 compared to $744,000 in the preceding year.
Other operating income, representing management fee income pursuant to management services agreements with our Toledo, Ohio facility (until its consolidation effective August 1, 2006) and an unaffiliated Georgia center decreased approximately $68,000 during 2006 compared to the preceding year. This decrease largely resulted from the consolidation of our Toledo facility effective August 1, 2006 whereas that facility had previously been accounted for on the equity method with no revenue elimination in our consolidated financial statements. See Note 7, Note 9, Note 14 and Note 17 to “Notes to Consolidated Financial Statements.”
Cost of medical services sales as a percentage of sales decreased to 60% for the year ended December 31, 2006, compared to 62% for the preceding year, as a result of decreases in payroll costs and supply costs as a percentage of medical service sales.
Approximately 28% of our medical services revenue for the years ended December 31, 2006 and December 31, 2005 derived from the administration of EPO to our dialysis patients. Beginning in 2006, Medicare reimburses dialysis providers for the top ten most utilized ESRD drugs at an amount equal to the cost of such drugs as determined by the Inspector General of HHS, with complimentary increases in the composite rate. Management believes these changes have had little impact on the company’s average Medicare revenue per treatment. See Item 1, “Business – Operations – Medicare Reimbursement.”
Our medical products division was acquired pursuant to our merger with our former parent company in September, 2005. Operations of the medical products division are included in our operating results subsequent to the merger. These operations represent a minor portion of our operations with operating revenues of $891,000 during 2006, and $207,000 during 2005 (1.4% of total 2006 operating revenues and .5% of total 2005 operating revenues). Operating income for the medical products division was $69,000 for 2006 and $25,000 for 2005 (1.2% of total 2006 operating income and .7% of total 2005 operating income).
40
Cost of sales for our medical products division amounted to 62% of sales for the year ended December 31, 2006 and 58% of sales for the year ended December 31, 2005. Cost of sales for this division is largely related to product mix.
Selling, general and administrative expenses, those corporate and facility costs not directly related to the care of patients, including, among others, administration, accounting and billing, increased by approximately $3,741,000 (32%) for the year ended December 31, 2006, compared to the preceding year. This increase reflects operations of our new dialysis centers and increased support activities resulting from expanded operations. Included are expenses of new centers incurred prior to Medicare approval for which there were no corresponding medical services revenue. Selling, general and administrative expenses as a percentage of medical services revenue amounted to approximately 25% for the year ended December 31, 2006 compared to 26% for the preceding year.
Provision for doubtful accounts increased approximately $628,000 for year ended December 31, 2006, compared to the preceding year. The provision amounted to 2% of sales for the year ended December 31, 2006 compared to 1% for the preceding year. Medicare bad debt recoveries of $537,000 were recorded during the year ended December 31, 2006, compared to approximately $505,000 for the preceding year. Without the effect of the Medicare bad debt recoveries, the provision would have amounted to 3% of sales for the year ended December 31, 2006 compared to 2% for the preceding year. The provision for doubtful accounts reflects our collection experience with the impact of that experience included in accounts receivable presently reserved, plus recovery of accounts previously considered uncollectible from our Medicare cost report filings. The provision for doubtful accounts is determined under a variety of criteria, primarily aging of the receivables and payor mix. Accounts receivable are estimated to be uncollectible based upon various criteria including the age of the receivable, historical collection trends and our understanding of the nature and collectibility of the receivables, and are reserved for in the allowance for doubtful accounts until they are written off.
Days sales outstanding were 82 as of December 31, 2006 compared to 79 as of December 31, 2005. Days sales outstanding are impacted by the expected and typical slower receivable turnover at our new centers opened and by payor mix. Based on our collection experience with the different payor groups comprising our accounts receivable, our analysis indicates that our allowance for doubtful accounts reasonably estimates the amount of accounts receivable that we will ultimately not collect.
After a patient’s insurer has paid the applicable coverage for the patient, the patient is billed for the applicable co-payment or balance due. If payment is not received from the patient for its applicable portion, collection letters and billings are sent to that patient until such time as the patient’s account is determined to be uncollectible, at which time the account will be charged against the allowance for doubtful accounts. Patient accounts that remain outstanding four months after initial collection efforts are generally considered uncollectible.
Other non-operating income decreased approximately $117,000 for the year ended December 31, 2006, compared to the preceding year. This includes an increase in interest income of $94,000, an increase in rental income of $131,000, an increase in miscellaneous other income of $5,000 and an increase in interest expense to unrelated parties of $262,000 due to increased average non-inter-company borrowings and an increase in average interest rates and net litigation settlement expense of $85,000. Interest expense to our former parent, Medicore, Inc., decreased $158,000 for the year ended December 31, 2006 compared to the preceding year as a result of our merger with our former parent in September 2005. Both the intercompany advance payable and the demand promissory note payable, as well as accrued interest on the note, were forgiven in conjunction with our merger with our former parent. The prime rate was 8.25% at December 31, 2006, and 7.25% at December 31, 2005. See Notes 1, 2, 3, 4, 12, and 15 of “Notes to the Consolidated Financial Statements.”
41
Although operations of additional centers have resulted in additional revenues, certain of these centers are still in the start-up stage and, accordingly, their operating results will adversely impact our overall results of operations until they achieve a patient count sufficient to sustain profitable operations.
Minority interest represents the proportionate equity interests of minority owners of our subsidiaries whose financial results are included in our consolidated results. Equity in affiliate earnings represents our proportionate interest in the earnings of our Toledo, Ohio subsidiary until its consolidation effective August 1, 2006, prior to which it was accounted for on the equity method. See Note 1, Note 9 and Note 14 to “Notes to Consolidated Financial Statements.”
2005 Compared to 2004
Medical services revenue increased approximately $4,237,000 (10%) for the year ended December 31, 2005, compared to the preceding year. Dialysis treatments performed increased from 135,667 in 2004 to 163,689 in 2005, a 21% increase. The increase in treatments includes treatments at the five new centers we opened during 2004 which were in operation throughout 2005, the two Pennsylvania centers acquired in late August, 2004 which were in operation throughout 2005 and three new centers we opened during 2005. Some of our patients carry commercial insurance which may require an out of pocket co-pay by the patient, which is often uncollectible by us. This co-pay is typically limited, and therefore may lead to our under-recognition of revenue at the time of service. We routinely recognize these revenues as we become aware that these limits have been met.
We record contractual adjustments based on fee schedules for a patient’s insurance plan except in circumstances where the schedules are not readily determinable, in which case rates are estimated based on similar insurance plans and subsequently adjusted when actual rates are determined. Out-of-network providers generally do not provide fee schedules and coinsurance information and, consequently, represent the largest portion of contractual adjustment changes. Estimated contractual adjustments for 2004 and prior years made during 2005 resulted in approximately a $74,000 reduction in revenues in 2005. Based on historical data we do not anticipate that a change in estimates would have a significant impact on our financial conditions or results of operations.
Our medical products division was acquired pursuant to our merger with our former parent company in September, 2005. Operations of the medical products division are included in our operating results subsequent to the merger. These operations represent a minor portion of our operations with sales revenues of $207,000 during 2005 (.5% of total 2005 sales revenues).
Operating income decreased approximately $768,000 (18%) for the year ended December 31, 2005, compared to the preceding year, including the reflection of start-up costs associated with our new centers.
Other operating income decreased by approximately 7% for the year ended December 31, 2005, compared to the preceding year. Management fee income pursuant to management services agreements with our 40% owned Toledo, Ohio affiliate and an unaffiliated Georgia center increased $96,000. There was a gain on litigation settlement of $134,000 during 2004.
42
Cost of medical services sales as a percentage of sales increased to 62% for the year ended December 31, 2005, compared to 58% for the preceding year, as a result of increases in payroll costs and supply costs as a percentage of medical service sales.
Cost of sales for our medical products division amounted to 58% of sales. Cost of sales for this division is largely related to product mix.
Approximately 28% of our medical services revenue for the years ended December 31, 2005 and December 31, 2004 derived from the administration of EPO to our dialysis patients. Beginning this year, Medicare will reimburse dialysis providers for the top ten most utilized ESRD drugs at an amount equal to the cost of such drugs as determined by the Inspector General of HHS, with complimentary increases in the composite rate. Management believes these changes will have little impact on the company’s average Medicare revenue per treatment. See Item 1, “Business – Operations – Medicare Reimbursement.”
Selling, general and administrative expenses, those corporate and facility costs not directly related to the care of patients, including, among others, administration, accounting and billing, increased by approximately $1,367,000 (11%) for the year ended December 31, 2005, compared to the preceding year. This increase reflects operations of our new dialysis centers and increased support activities resulting from expanded operations. Included are expenses of new centers incurred prior to Medicare approval for which there were no corresponding medical services revenue. Selling, general and administrative expenses as a percentage of medical services revenue amounted to approximately 30% for the ended year December 31, 2005, and for the preceding year.
Provision for doubtful accounts decreased approximately $627,000 for year ended December 31, 2005, compared to the preceding year. The provision amounted to 1% of sales for the year ended December 31, 2005 compared to 3% for the preceding year. Medicare bad debt recoveries of $505,000 were recorded during the year ended December 31, 2005, compared to approximately $214,000 for the preceding year. Without the effect of the Medicare bad debt recoveries, the provision would have amounted to 2% of sales for the year ended December 31, 2005 compared to 3% for the preceding year. The provision for doubtful accounts reflects our collection experience with the impact of that experience included in accounts receivable presently reserved, plus recovery of accounts previously considered uncollectible from our Medicare cost report filings. The provision for doubtful accounts is determined under a variety of criteria, primarily aging of the receivables and payor mix. Accounts receivable are estimated to be uncollectible based upon various criteria including the age of the receivable, historical collection trends and our understanding of the nature and collectibility of the receivables, and are reserved for in the allowance for doubtful accounts until they are written off.
Days sales outstanding were 79 as of December 31, 2005 compared to 74 as of December 31, 2004. The 2004 collection delays resulting in the company’s Georgia dialysis facilities experiencing a deterioration in their accounts receivable aging were largely due to the State of Georgia Medicaid program’s implementation of a new computer system in 2003. Days sales outstanding were also impacted by the expected and typical slower receivable turnover at our new centers opened during 2005 and by payor mix. Based on our collection experience with the different payor groups comprising our accounts receivable, our analysis indicates that our allowance for doubtful accounts reasonably estimates the amount of accounts receivable that we will ultimately not collect.
After a patient’s insurer has paid the applicable coverage for the patient, the patient is billed for the applicable co-payment or balance due. If payment is not received from the patient for its applicable portion, collection letters and billings are sent to that patient until such time as the patient’s account is determined to be uncollectible, at which time the account will be charged against the allowance for doubtful accounts. Patient accounts that remain outstanding four months after initial collection efforts are generally considered uncollectible.
43
Medical Services
Accounts Receivable Aging Schedule
Fiscal 2006
Classification | December | November | October | September | August plus | Prepayments | Total | |||||||||||||||
| BLUE CROSS | $ | 778,345 | $ | 789,095 | $ | 562,097 | $ | 316,589 | $ | 1,581,192 | $ | (8,842 | ) | $ | 4,018,476 | |||||||
| COMMERCIAL | 732,511 | 846,980 | 560,484 | 301,350 | 212,464 | (4,874 | ) | 2,648,915 | ||||||||||||||
| HMO | 166,732 | 147,562 | 83,931 | 77,437 | 136,668 | 612,330 | ||||||||||||||||
| MEDICAID | 267,990 | 427,311 | 456,556 | 317,218 | 1,433,020 | (15,687 | ) | 2,886,408 | ||||||||||||||
| MEDICARE | 4,343,038 | 516,425 | 344,875 | 213,336 | 1,135,052 | (14,827 | ) | 6,537,899 | ||||||||||||||
| PRESUMPTIVE ELIGIBILITY | 549 | 1,314 | (22,475 | ) | 2,221 | 14,413 | (3,978 | ) | ||||||||||||||
| SELF PAY | 331 | 66,500 | 90,372 | 129,683 | 1,256,446 | (43,756 | ) | 1,499,576 | ||||||||||||||
| HOSPITAL | 146,185 | 182,089 | 29,120 | 1,446 | 9,744 | 368,584 | ||||||||||||||||
| Total | $ | 6,435,681 | $ | 2,977,276 | $ | 2,104,960 | $ | 1,359,280 | $ | 5,778,999 | $ | (87,986 | ) | $ | 18,568,210 | |||||||
Fiscal 2005
Classification | December | November | October | September | August plus | Prepayments | Total | |||||||||||||||
| BLUE CROSS | $ | 641,684 | $ | 680,315 | $ | 407,726 | $ | 212,608 | $ | 1,488,486 | $ | 0 | $ | 3,430,819 | ||||||||
| COMMERCIAL | 376,782 | 484,186 | 240,537 | 116,123 | 540,421 | 0 | 1,758,049 | |||||||||||||||
| HMO | 56,853 | 39,526 | 8,942 | 1,026 | (6,280 | ) | 0 | 100,067 | ||||||||||||||
| MEDICAID | 177,240 | 307,818 | 192,304 | 109,923 | 1,221,859 | 0 | 2,009,144 | |||||||||||||||
| MEDICARE | 2,821,902 | 261,276 | 156,261 | 203,381 | 673,578 | 0 | 4,116,398 | |||||||||||||||
| PRESUMPTIVE ELIGIBILITY | (7,913 | ) | 4,759 | (7,198 | ) | 5,180 | 20,149 | 0 | 14,977 | |||||||||||||
| SELF PAY | 3,534 | 39,221 | 59,803 | 58,320 | 481,831 | (45,116 | ) | 597,593 | ||||||||||||||
| HOSPITAL | 82,410 | 1,388 | (15,707 | ) | 64,627 | 192,991 | 0 | 325,709 | ||||||||||||||
| Total | $ | 4,152,492 | $ | 1,818,489 | $ | 1,042,668 | $ | 771,188 | $ | 4,613,035 | $ | (45,116 | ) | $ | 12,352,756 | |||||||
Other non-operating income (expense) increased approximately $131,000 for the year ended December 31, 2005, compared to the preceding year. This includes an increase in interest income of $64,000, an increase in rental income of $47,000, an increase in miscellaneous other income of $5,000 and a decrease in interest expense to unrelated parties of $15,000 with the effect of reduced average non-inter-company borrowings more than offsetting an increase in average interest rates. Interest expense to our former parent, Medicore, Inc., increased $102,000 for the year ended December 31, 2005 compared to the preceding year as a result of an increase in the intercompany advance payable to our former parent and borrowings under a demand promissory note payable to our former parent and increases in the average interest rates on these borrowings. Both the intercompany advance payable and the demand promissory note payable, as well as accrued interest on the note, were forgiven in conjunction with our merger with our former parent. The prime rate was 7.25% at December 31, 2005, and 5.25% at December 31, 2004. See Notes 1, 2, 3, 4, 12, and 15 of “Notes to the Consolidated Financial Statements.”
44
Although operations of additional centers have resulted in additional revenues, certain of these centers are still in the start-up stage and, accordingly, their operating results will adversely impact our overall results of operations until they achieve a patient count sufficient to sustain profitable operations.
Minority interest represents the proportionate equity interests of minority owners of our subsidiaries whose financial results are included in our consolidated results. Equity in affiliate earnings represents our proportionate interest in the earnings of our 40% owned Ohio affiliate until this company was consolidated effective August 1, 2006, due to a change in control, with the company stall having a 40% ownership interest until December, 2006, when it acquired the other 60% ownership. See Note 1, Note 9 and Note 14 to “Notes to Consolidated Financial Statements.”
Liquidity and Capital Resources
Working capital totaled approximately $17,098,000 at December 31, 2006, which reflected an increase of $9,481,000 (124%) during the current year. Included in the changes in components of working capital was an increase in cash and cash equivalents of $554,000, which included net cash provided by operating activities of $3,007,000; net cash used in investing activities of $10,992,000 (including additions to property and equipment of $5,197,000, payment of an employment contract liability of $1,960,000, payments of $4,161,000 on dialysis center acquisitions, and distributions of $164,000 received from our 40% owned Ohio affiliate); and net cash provided by financing activities of $8,539,000 (including borrowings of $7,500,000 under our line of credit, debt repayments of $340,000, distributions to subsidiary minority members of $306,000, receipts of $383,000 from the exercise of stock options, and capital contributions of $1,302,000 by subsidiary minority members).
Net cash provided by operating activities consists of net income before non-cash items consisting of depreciation and amortization of $2,319,000, bad debt expense of $1,199,000, a deferred income tax benefit of $331,000, deferred tax asset utilized of $1,190,000, income applicable to minority interest of $920,000, equity in affiliate earnings of $254,000 and non-cash stock compensation expense of $275,000, as adjusted for changes in components of working capital. Significant changes in components of working capital, in addition to the $554,000 increase in cash, included a decrease in refundable income taxes of $1,053,000, largely due to tax refunds received; an increase in accounts receivable of $5,604,000, an increase in prepaid expenses and other current assets of $1,307,000 including property to be sold of $626,000, a decrease in employment contract liability of $1,960,000 resulting from our merger with our former parent due to payment of the liability, a decrease in the current portion of long-term debt of $822,000 largely due to our refinancing our Georgia mortgage that matured April, 2006, a decrease of $380,000 in acquisition liabilities from the final payment due on our Keystone acquisition, and an increase in income taxes payable at $660,000. The major source of cash from operating activities is medical service revenue. The major uses of cash in operating activities are supply costs, payroll, independent contractor costs, and costs for our leased facilities.
Our Easton, Maryland building has a mortgage to secure a subsidiary development loan. This loan had a remaining principal balance of $555,000 at December 31, 2006 and $583,000 at December 31, 2005. In April, 2001, we obtained a $788,000 five-year mortgage on our building in Valdosta, Georgia which we refinanced upon maturity in April 2006 for an additional five years with a new maturity of April, 2011. This loan had an outstanding principal balance of approximately $617,000 at December 31, 2006 and $633,000 at December 31, 2005. See Note 2 to “Notes to Consolidated Financial Statements.”
45
We have an equipment financing agreement for kidney dialysis machines that had an outstanding balance of approximately $76,000 at December 31, 2006, and $371,000 at December 31, 2005. There was no additional equipment financing under this agreement during 2006. See Note 2 to “Notes to Consolidated Financial Statements.”
We opened centers in Calhoun, Georgia, Aiken, South Carolina (our second Aiken center) and York, Pennsylvania during 2006. We are in the process of developing a new dialysis center in each of South Carolina and Ohio. Payment of the final payment due of approximately $381,000 was made on our Keystone Kidney Care acquisition in August, 2006. See Note 10 to “Notes to Consolidated Financial Statements.”
Capital is needed primarily for the development of outpatient dialysis centers. The construction of a 15 station facility, typically the size of our dialysis facilities, costs in the range of $750,000 to $1,000,000, depending on location, size and related services to be provided, which includes equipment and initial working capital requirements. Acquisition of an existing dialysis facility is more expensive than construction, although acquisition would provide us with an immediate ongoing operation, which most likely would be generating income. Although our expansion strategy focuses primarily on construction of new centers, we have expanded through acquisition of dialysis facilities and continue to review potential acquisitions. Development of a dialysis facility to initiate operations takes four to six months and usually up to 12 months or longer to generate income. We consider some of our centers to be in the developmental stage since they have not developed a patient base sufficient to generate and sustain earnings.
We are seeking to expand our outpatient dialysis treatment facilities and inpatient dialysis care and are presently in different phases of negotiations with physicians and others for the development or acquisition of additional outpatient centers. Such expansion requires capital. We have been funding our expansion through internally generated cash flow and a revolving line of credit with KeyBank National Association. See Notes 3 and 5 to “Notes to Consolidated Financial Statements.” To assist with our future expansion we entered into a $15,000,000, 3 year credit agreement for a revolving line of credit with Key Bank National Association in October 2005. No amounts were financed under this new credit facility during 2005. We have outstanding borrowings of $7,500,000 under this credit facility as of December 31, 2006. No assurance can be given that we will be successful in implementing our growth strategy or that available financing will be adequate to support our expansion. See Item 1, “Business-Business Strategy.”
46
Aggregate Contractual Obligations
As of December 31, 2006, the Company’s contractual obligations (in thousands), including payments due by period, are as follows:
Payments due by period | ||||||||||||||||
Less than | More than | |||||||||||||||
Total | 1 year | 1-3 years | 3-5 years | 5 years | ||||||||||||
| Long-term debt | $ | 8,748,000 | $ | 128,000 | $ | 7,611,000 | $ | 119,000 | $ | 890,000 | ||||||
| Operating leases | 7,422,000 | 1,810,000 | 3,001,000 | 1,943,000 | 668,000 | |||||||||||
| Expected interest payments: | ||||||||||||||||
| Long-term debt | 1,660,000 | 655,000 | 597,000 | 155,000 | 253,000 | |||||||||||
| Purchase obligations: | ||||||||||||||||
| Medical services | 7,024,000 | 1,501,000 | 2,849,000 | 1,318,000 | 1,356,000 | |||||||||||
| Miscellaneous purchase obligations | 99,000 | 99,000 | — | — | — | |||||||||||
| Total purchase obligations | 7,123,000 | 1,600,000 | 2,849,000 | 1,318,000 | 1,356,000 | |||||||||||
| Total contractual obligations | $ | 24,953,000 | $ | 4,193,000 | $ | 14,158,000 | $ | 3,535,000 | $ | 3,167,000 | ||||||
Merger with Our Former Parent, Medicore, Inc.
Effective September 21, 2005, the company and Medicore, Inc., the company’s former parent, completed the merger of Medicore with and into the company pursuant to the provisions of the Agreement and Plan of Merger between the company and Medicore, dated June 2, 2005. In accordance with the terms of that Agreement, on September 21, 2005, the outstanding shares of Medicore common stock were deemed cancelled and converted into the right to receive .68 of a share of the company for each common share of Medicore outstanding on that date.
In connection with the merger there was a net issuance of approximately 449,000 common shares of the company resulting in approximately 9,116,000 common shares of the company outstanding after the merger. The net issuance gives effect to an aggregate of approximately 5,271,000 common shares issued by the company to former shareholders of Medicore based upon the .68 exchange ratio, and the cancellation of 4,821,244 common shares of the company owned by Medicore prior to the merger.
The merger enabled the control interest in the company to be in the hands of the public stockholders and provides the company with additional capital resources to continue its growth. See Note 1, Note 3, Note 4, Note 12, and Note 15 to “Notes to Consolidated Financial Statements.”
New Accounting Pronouncements
In June, 2006, the FASB issued FASB Interpretation No. 48 (“FIN 48”), “Accounting for Uncertainty in Income Taxes - an interpretation of FASB Statement No. 109, Accounting for Income Taxes,” which prescribes a recognition threshold and measurement attribute for financial statement recognition and measurement of tax position taken or expected to be taken in a tax return and provides guidance on derecognition, classification, interest and penalties, accounting in interim periods disclosure. The provisions of FIN 48 are effective for fiscal years beginning after December 15, 2006, with the cumulative effect of the change in accounting principle recorded as an adjustment to opening retained earnings. The company is evaluating the impact of adopting FIN 48, but does not expect FIN 48 to have a significant effect on its financial statements. See Note 1 to “Notes to Consolidated Financial Statements.”
47
In September, 2006, the FASB issued Statement of Financial Accounting Standards No. 157 (“SFAS 157”), “Fair Value Measurements”. SFAS 157 defines fair value, establishes a framework for measuring fair value in generally accepted accounting principles, and expands disclosures about fair value measurements. SFAS 157 will be effective for us beginning in 2009. The company is evaluating the impact on its financial statements of adopting SFAS 157. See Note 1 to “Notes to Consolidated Financial Statements.”
In September, 2006, the U.S. Securities and Exchange Commission (SEC) issued Staff Accounting Bulletin No. 108 (“SAB 108”), which provides interpretive guidance on how the effects of prior year misstatements should be considered in quantifying current year financial statement misstatements. SAB 108 is effective for fiscal years ending after November 15, 2006. SAB 108 has not had a significant effect on our financial statements. See Note 1 to “Notes to Consolidated Financial Statements.”
Critical Accounting Policies and Estimates
The SEC has issued cautionary advice to elicit more precise disclosure in this Item 7, MD&A, about accounting policies management believes are most critical in portraying our financial results and in requiring management’s most difficult subjective or complex judgments.
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make judgments and estimates. On an on-going basis, we evaluate our estimates, the most significant of which include establishing allowances for doubtful accounts, a valuation allowance for our deferred tax assets and determining the recoverability of our long-lived assets. The basis for our estimates are historical experience and various assumptions that are believed to be reasonable under the circumstances, given the available information at the time of the estimate, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily available from other sources. Actual results may differ from the amounts estimated and recorded in our financial statements.
We believe the following critical accounting policies affect our more significant judgments and estimates used in the preparation of our consolidated financial statements.
Revenue Recognition: Revenues are recognized net of contractual provisions at the expected collectable amount. We receive payments through reimbursement from Medicare and Medicaid for our outpatient dialysis treatments coupled with patients’ private payments, individually and through private third-party insurers. A substantial portion of our revenues are derived from the Medicare ESRD program, which outpatient reimbursement rates are fixed under a composite rate structure, which includes the dialysis services and certain supplies, drugs and laboratory tests. Certain of these ancillary services are reimbursable outside of the composite rate. Medicaid reimbursement is similar and supplemental to the Medicare program. Our acute inpatient dialysis operations are paid under contractual arrangements, usually at higher contractually established rates, as are certain of the private pay insurers for outpatient dialysis. We have developed a sophisticated information and computerized coding system, but due to the complexity of the payor mix and regulations, we sometimes receive more or less than the amount expected when the services are provided. We reconcile any differences at least quarterly.
48
In those situations where a patient’s insurance fee schedule cannot be readily determined, which typically occurs with out of network providers, we estimate fees based on our knowledge base of historical data for patients with similar insurance plans. Our internal controls, including an ongoing review and follow-up on estimated fees, allows us to make necessary changes to estimated fees on a timely basis. When the actual fee schedule is determined, we adjust the amounts originally estimated, and then use the actual fees to estimate fees for similar future situations. We adhere to the guidelines of SAB Topic 13 (SAB 104) in regard to recording reasonable estimates of revenue based on our historical experience and identifying on a timely basis necessary changes to estimates.
Allowance for Doubtful Accounts: We maintain an allowance for doubtful accounts for estimated losses resulting from the inability of our patients or their insurance carriers to make required payments. Based on historical information, we believe that our allowance is adequate. Changes in general economic, business and market conditions could result in an impairment in the ability of our patients and the insurance companies to make their required payments, which would have an adverse effect on cash flows and our results of operations. The allowance for doubtful accounts is reviewed monthly and changes to the allowance are updated based on actual collection experience. We use a combination of percentage of sales and the aging of accounts receivable to establish an allowance for losses on accounts receivable. We adhere to the guidelines of SFAS 5 in determining reasonable estimates of accounts for which uncollectibility is possible.
Valuation Allowance for Deferred Tax Assets: The carrying value of deferred tax assets assumes that we will be able to generate sufficient future taxable income to realize the deferred tax assets based on estimates and assumptions. If these estimates and assumptions change in the future, we may be required to adjust our valuation allowance for deferred tax assets which could result in additional income tax expense.
Long-Lived Assets: We state our property and equipment at acquisition cost and compute depreciation for book purposes by the straight-line method over estimated useful lives of the assets. In accordance with SFAS No. 144, “Accounting for the Impairment or Disposal of Long-Lived Assets,” long-lived assets are reviewed for impairment whenever events or changes in circumstances indicate the carrying amount of the asset may not be recoverable. Recoverability of assets to be held and used is measured by comparison of the carrying amount of an asset to the future cash flows expected to be generated by the asset. If the carrying amount of the asset exceeds its estimated future cash flows, an impairment charge is recognized to the extent the carrying amount of the asset exceeds the fair value of the asset. These computations are complex and subjective.
Goodwill and Intangible Asset Impairment: In assessing the recoverability of our goodwill and other intangibles we must make assumptions regarding estimated future cash flows and other factors to determine the fair value of the respective assets. This impairment test requires the determination of the fair value of the intangible asset. If the fair value of the intangible asset is less than its carrying value, an impairment loss will be recognized in an amount equal to the difference. If these estimates or their related assumptions change in the future, we may be required to record impairment charges for these assets. We adopted Statement of Financial Accounting Standards No. 142, “Goodwill and Other Intangible Assets,” (FAS 142) effective January 1, 2002, and are required to analyze goodwill and indefinite lived intangible assets for impairment on at least an annual basis.
49
Impact of Inflation
Inflationary factors have not had a significant effect on our operations. A substantial portion of our revenue is subject to reimbursement rates established and regulated by the federal government. These rates do not automatically adjust for inflation. Any rate adjustments relate to legislation and executive and Congressional budget demands, and have little to do with the actual cost of doing business. Therefore, dialysis services revenues cannot be voluntarily increased to keep pace with increases in nursing and other patient care costs. Increased operating costs without a corresponding increase in reimbursement rates may adversely affect our earnings in the future.
We do not consider our exposure to market risks, principally changes in interest rates, to be significant.
Sensitivity of results of operations to interest rate risks on our investments is managed by conservatively investing funds in liquid interest bearing accounts of which we held approximately
$3,351,000 at December 31, 2006.
Interest rate risk on debt is managed by negotiation of appropriate rates for equipment financing and other fixed rate obligations based on current market rates. There is an interest rate risk associated with our variable rate debt obligations, which totaled approximately $8,672,000 at December 31, 2006.
We have exposure to both rising and falling interest rates. Assuming a relative 15% decrease in rates on our period-end investments in interest bearing accounts and a relative 15% increase in rates on our period-end variable rate debt would have resulted in a negative impact of approximately $71,000 on our results of operations for the year ended December 31, 2006.
We do not utilize financial instruments for trading or speculative purposes and do not currently use interest rate derivatives.
The response to this item is submitted as a separate section to this annual report, specifically, Part IV, Item 15, “Exhibits, Financial Statement Schedules and Reports on Form 8-K,” subpart (a)1, “All Financial Statements - See Index to Consolidated Financial Statements,” and subpart (a)2, “Financial Statement Schedules - See Index to Consolidated Financial Statements,” and begins on page F-1 of this annual Report on Form 10-K.
None
Evaluation of Disclosure Controls and Procedures.
As of the end of the period covered by this areport on Form 10-K for the year ended December 31, 2006, we carried out an evaluation, under the supervision and with the participation of our management, including our President and CEO, and the Chief Financial Officer, of the effectiveness of the design and operation of our disclosure controls and procedures pursuant to Rule 13a-15 of the Exchange Act. These disclosure controls and procedures are designed to provide reasonable assurance that, among other things, information is accumulated and communicated to our management, including our President and CEO, and our Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure. Based upon such evaluation, our President and CEO, and our Chief Financial Officer have concluded that, as of the end of such period, our disclosure controls and procedures are effective in providing reasonable assurance that information required to be disclosed by our company in the reports that it files under the Exchange Act is recorded, processed, summarized and reported within required time periods specified by the SEC’s rules and forms.
50
Management’s Report on Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting that occurred during our fourth quarter ended December 31, 2006 that have materially affected, or are reasonably likely to materially affect, our control over financial reporting. During the year ended December 31, 2006, we retained independent consultants and additional personnel to continue to develop formal processes, review procedures and documentation standards for the accounting and monitoring of non-routine and complex transactions, and for the testing of our internal controls, and we anticipate continually improving our internal control over financial reporting.
Our management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Our internal control over financial reporting is a process designed by, or under the supervision of, our President and CEO and Chief Financial Officer and effected by our board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with accounting principles generally accepted in the United States of America. Internal control over financial reporting includes polices and procedures that:
| · | pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; |
| · | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with accounting principles generally accepted in the United States of America, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and |
| · | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of assets that could have a material effect on the consolidated financial statements |
All internal control systems, no matter how well designed, have inherent limitations and can provide only reasonable, not absolute, assurance that the objectives of the control system are met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations to all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, and none of which we are aware, within our company have been detected. Therefore, even those systems determined to be effective can provide only reasonable assurance with respect to financial statement preparation and presentation.
51
In connection with the preparation of our Form 10-K, our management assessed the effectiveness of our internal control over financial reporting as of December 31, 2006. In making that assessment, management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in “Internal Control-Integrated Framework.” Management’s assessment included an examination of the design of the company’s internal control over financial reporting and testing of the operating effectiveness of its internal control over financial reporting. Based on management’s assessment, management believes that, as of December 31, 2006, our internal control over financial reporting was effective based on those criteria. Management’s assessment of the effectiveness of the company’s internal control over financial reporting as of December 31, 2006, has been audited by Moore Stephens, P.C., an independent registered public accounting firm, as stated in their report attached to this annual report on Form 10-K, which expresses unqualified opinions with respect to management’s assessment and on the effectiveness of the company’s internal control over financial reporting as of December 31, 2006.
To the best of our knowledge, we have reported all information required to be disclosed in our current reports on Form 8-K during the fourth quarter of our fiscal year, 2006.
PART III
Directors and Executive Officers
Information concerning the company’s directors and executive officers is incorporated herein by reference to the company’s 2007 proxy statement* under the captions “Proposal No. 1: Election of Directors” and “Information About Directors and Executive Officers.”
Information relating to compliance with Section 16(a) of the Exchange Act is incorporated herein by reference to the company’s 2007 proxy statement* under the caption “Section 16(a) Beneficial Ownership Reporting Compliance.”
The company adopted a Code of Ethics that applies to our Chief Executive Officer, Chief Financial Officer, Principal Accounting Officer or Controller, and persons performing similar functions, as well as other employees. See Item 1, “Business - Corporate Integrity Program - Code of Ethics.” See also “Code of Ethics” in the company’s 2007 proxy statement* incorporated herein by reference.
Information concerning the audit, nominating and compensation committees and their charters and policies, and the audit committee report is incorporated herein by reference to the company’s 2007 proxy statement* under the captions “Corporate Governance” and “Report of the Audit Committee.”
Information concerning Compensation Discussion and Analysis, the Compensation Committee Report and management and director compensation is incorporated herein by reference to the company’s 2007 proxy statement* under the captions “Compensation Discussion and Analysis,” “Compensation Committee Report” and “Director Compensation.”
52
Information concerning security ownership of certain beneficial owners and management and securities authorized for issuance under equity compensation plans is incorporated herein by reference to the company’s 2007 proxy statement* under the caption “Security Ownership of Certain Beneficial Owners and Management.”
Information concerning certain relationships and related transactions is incorporated herein by reference to the company’s 2007 proxy statement* under the caption “Certain Relationships and Related Transactions, and Director Independence.” Reference is also made to Item 10, “Directors, Executive Officers and Corporate Governance.”
Information concerning fees and services of the company’s independent auditors is incorporated herein by reference to the company’s 2007 proxy statement* under the caption “Proposal No. 3: Ratification of the Appointment of the Independent Auditors.”
* The company’s definitive proxy statement relating to the upcoming annual meeting of shareholders will be filed within 120 days of the end of the company’s fiscal year, which is no later than April 30, 2007.
53
PART IV
| (a) | The following is a list of documents filed as part of this report. |
| 1. | All financial statements - See Index to Consolidated Financial Statements. |
| 2. | Financial statement schedules - See Index to Consolidated Financial Statements. |
| (b) | Exhibits + |
| 3.1 | Articles of Incorporation ‡ |
| 3.2 | By-Laws of the Company ‡ |
| 4 | Instruments defining the rights of equity holders, including indentures |
| 4.1 | Form of Common Stock Certificate of the Company ‡ |
| 4.2 | Form of Stock Option Certificate under the 1999 Stock Incentive Plan (May 21, 1999) (incorporated by reference to the Company’s Annual Report on Form 10-K for the year ended December 31, 1999, Part IV, Item 14(c)(10)(xxiv)). |
| 4.3 | Form of Restricted Stock Agreement (incorporated by reference to the Company’s Current Report on Form 8-K dated June 30, 2006, Item 9.01(d)(10) 10.1). |
| 10 | Material Contracts |
| 10.1 | 1999 Stock Incentive Plan of the Company, as amended (April, 2006) (incorporated by reference to the Company’s Proxy Statement dated April 26, 2006, Appendix A.* |
| 10.2 | Indemnity Deed of Trust from the Company to Trustees for the benefit of St. Michaels Bank dated December 3, 1999 (incorporated by reference to the Company’s Current Report on Form 8-K dated December 13, 1999 (“December Form 8-K”), Item 7(c)(99)(i)). |
| 10.3 | Guaranty Agreement from the Company to St. Michaels Bank dated December 3, 1999 (incorporated by reference to the Company’s December Form 8-K, Item 7(c)(99)(ii)). |
| 10.4 | Promissory Note by the Company to American Banking Company, dated April 3, 2006 (incorporated by reference to the Company’s Current Report on Form 8-K dated April 4, 2006, Item 9.01(d)(99) 99.1). |
| 10.5 | Debt Modification Agreement by DCA of Vineland, LLC(1) dated May 25, 2006 (incorporated by reference to the Company’s Current Report on Form 8-K, dated May 26, 2006 (“May 2006 Form 8-K”), Item 9.01(d)(99) 99.1). |
54
| 10.6 | Notice and Consent to Modification by Guarantor [the Company] dated May 25, 2006 (incorporated by reference to the Company’s May 2006 Form 8-K, Item 9.01 (d)(99) 99.2) |
| 10.7 | The Company’s Section 125 Plan effective September 1, 2002 (incorporated by reference to the Company’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2002, Part II, Item 6(99)). |
| 10.8 | Agreement of Lease by and between Copt Concourse, LLC and the Company dated March 31, 2004 (incorporated by reference to the Company’s Current Report on Form 8-K dated March 31, 2004, item 7(c)(10((i)). |
| 10.9 | Lease between Viragen, Inc.(2) [now Gesualdo and Rosanna Vitale(3)] and the Company dated December 8, 1992 (incorporated by reference to the Medicore, Inc.(4) Annual Report on Form 10-K for the year ended December 31, 1997 (“Medicore Form 10-K”), Part IV, Item 14(c)(10((xi)). |
| 10.10 | Addendum to Lease between Viragen, Inc.(2) [now Gesualdo and Rosanna Vitale(3)] and the Company dated January 15, 1993 (incorporated by reference to the Medicore(4) Form 10-K, Part IV, Item 14(c)(10)(xii)). |
| 10.11 | Lease Renewal Letter by the Company to Gesualdo Vitale(3) dated August 5, 2002 (incorporated by reference to Medicore, Inc.’s(4) Quarterly Report on Form 10-Q for the quarter ended September 30, 2002, Part II, Item 6(10)(i)). |
| 10.12 | Agreement and Plan of Merger By and Among Medicore, Inc.(2) and the Company dated June 2, 2005 (incorporated by reference to Annex A to the proxy statement/prospectus included in and made a part of the Company’s registration statement on Form S-4/A1 dated June 3, 2005, as amended on August 10, 2005, registration no. 333-125515). |
| 10.13 | Articles and Plan of Merger filed by the Company and Medicore, Inc.(2) dated September 21, 2005 (incorporated herein by reference to the Company’s Current Report on Form 8-K dated September 26, 2005, Item 9.01(c)3.1). |
| 10.14 | Credit Agreement between the Company and KeyBank National Association dated October 24, 2005 (incorporated by reference to the Company’s Current Report on Form 8-K dated October 27, 2005 (“October 2005 Form 8-K”), Item 9.01(d)(10)(i)). |
| 10.15 | Revolving Credit Note dated October 24, 2005 (incorporated by reference to the Company’s October 2005 Form 8-K, Item 9.01(d)(10)(ii)). |
| 10.16 | Guaranty of Payment by the Company’s Wholly-Owned Subsidiaries in favor of KeyBank National Association dated October 24, 2005 (incorporated by reference to the Company’s October 2005 Form 8-K, Item 9.01(d)(10)(iii)). |
| 10.17 | Pledge Agreement by the Company in favor of KeyBank National Association dated October 24, 2005 (incorporated by reference to the Company’s October 2005 Form 8-K, Item 9.01(d)(10)(iv). |
55
| 10.18 | Amendment No. 1 to Credit Agreement between the Company and KeyBank National Association dated December 15, 2005 (incorporated by reference to the Company’s Current Report on Form 8-K dated December 16, 2005, Item 9.01(d)(10)(i)). |
| 10.19 | Employment Agreement between the Company and Stephen W. Everett dated February 22, 2006 (incorporated by reference to the Company’s Current Report on Form 8-K dated February 28, 2006, Item 9.01(d)(10)10.1).* |
| 10.20 | Amendment No. 2 to Credit Agreement between the Company and KeyBank National Association dated as of February 14, 2006 (incorporated by reference to the Company’s Annual Report on Form 10-K for the year ended December 31, 2005, Part IV, Item 15, (10.19)). |
| 10.21 | Amendment No. 3 to Credit Agreement between the Company and KeyBank National Association dated April 7, 2006 (incorporated by reference to the Company’s Current Report on Form 8-K dated August 2, 2006). |
| 10.22 | Independent Contractor Agreement dated November 8, 2006 (incorporated by reference to the Company’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2006 (Part II, Item 10.1).* |
| 14 | Code of Ethics |
| 14.1 | Code of Ethics and Business Conduct, as amended, September 6, 2006 (incorporated by reference to the Company’s Current Report on Form 8-K dated September 12, 2006, Item 14.1). |
| 21 | Subsidiaries of the Company |
| 23 | Consent of experts and counsel |
| 23.1 | Consent of Moore Stephens, P.C. |
| 31 | Rule 13a-14(a)/15d-14(a) Certifications. |
| 31.1 | Certification of the Chief Executive Officer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934. |
| 31.2 | Certification of the Chief Financial Officer pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934. |
| 32 | Section 1350 Certifications |
| 32.1 | Certification of the Chief Executive Officer and the Chief Financial Officer pursuant to Rule 13a-14(b) of the Securities Exchange Act of 1934 and 18 U.S.C. Section 1350(5). |
* | Management contract or compensatory plan or arrangement. |
56
| + | Documents incorporated by reference not included in Exhibit Volume. |
| ‡ | Incorporated by reference to the company’s registration statement on Form SB-2 dated December 22, 1995 as amended February 9, 1996, April 2, 1996 and April 15, 1996, registration no. 33-80877-A, Part II, Item 27. |
(1) | 51% owned subsidiary. |
(2) | Former public subsidiary of the company; sold in 1993. |
(3) | Purchasers of the property from Viragen, Inc. in August, 2000. |
(4) | Former parent of the company. Merged into the company on September 21, 2005. |
(5) | In accordance with Release No. 34-47551, this exhibit is furnished to the SEC as an accompanying document and is not deemed to be “filed” for purposes of Section 18 of the Securities Exchange Act of 1934 or otherwise subject to the liabilities of that Section, and it shall not be deemed incorporated by reference into any filing under the Securities Act of 1933. |
| (c) | Financial Statement Schedules Required By Regulation S-X, Excluded From This Annual Report |
| None |
57
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| DIALYSIS CORPORATION OF AMERICA | ||
| | | |
| By: | /s/ STEPHEN W. EVERETT | |
Stephen W. Everett President and Chief Executive Officer | ||
March 15, 2007
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Signature | Title | Date | ||
| /s/ THOMAS K. LANGBEIN | Chairman of the Board of Directors | March 15, 2007 | ||
| Thomas K. Langbein | ||||
| /s/ STEPHEN W. EVERETT | President, Chief Executive Officer and Director | March 15, 2007 | ||
| Stephen W. Everett | ||||
| /s/ DANIEL R. OUZTS | Vice President of Finance, Chief Financial Officer, Chief Accounting Officer and Treasurer | March 15, 2007 | ||
| Daniel R. Ouzts | ||||
| /s/ PETER D. FISCHBEIN | Director | March 15, 2007 | ||
| Peter D. Fischbein | ||||
| /s/ ROBERT W. TRAUSE | Director | March 15, 2007 | ||
| Robert W. Trause | ||||
| /s/ ALEXANDER BIENENSTOCK | Director | March 15, 2007 | ||
| Alexander Bienenstock |
58
ANNUAL REPORT ON FORM 10-K
ITEM 8, ITEM 15(a) (1) and (2)
LIST OF FINANCIAL STATEMENTS AND FINANCIAL STATEMENT SCHEDULES
FINANCIAL STATEMENTS AND SUPPLEMENTAL DATA
FINANCIAL STATEMENT SCHEDULES
YEAR ENDED DECEMBER 31, 2006
DIALYSIS CORPORATION OF AMERICA
LINTHICUM, MARYLAND
FORM 10-K—ITEM 15(a)(1) and (2)
DIALYSIS CORPORATION OF AMERICA
LIST OF FINANCIAL STATEMENTS
The following consolidated financial statements of Dialysis Corporation of America and subsidiaries are included in Item 8 of the Annual Report on Form 10-K:
Page | ||
| F-2 | ||
| F-4 | ||
| F-5 | ||
| F-6 | ||
| F-7 | ||
| F-8 | ||
| The following financial statement schedule of Dialysis Corporation of America and subsidiaries is included in Item 15(a)(2): | ||
| F-34 | ||
All other schedules for which provision is made in the applicable accounting regulation of the Securities and Exchange Commission are not required under the related instructions or are inapplicable, and therefore have been omitted.
F-1
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders of
Dialysis Corporation of America
Linthicum, Maryland
We have audited the accompanying consolidated balance sheets of Dialysis Corporation of America and its subsidiaries as of December 31, 2006 and 2005, and the related consolidated statements of income, stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2006. We also have audited management’s assessment, included in the accompanying Report of Management’s Internal Control over Financial Reporting, that Dialysis Corporation of America maintained effective internal control over financial reporting as of December 31, 2006 based on criteria established in “Internal Control-Integrated Framework” issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Dialysis Corporation of America’s management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting. Our responsibility is to express an opinion on these consolidated financial statements, an opinion on management’s assessment, and an opinion on the effectiveness of the Company’s internal control over financial reporting based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, and whether effective internal control over financial reporting was maintained in all material respects. Our audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the consolidated financial statements. Our audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall consolidated financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, evaluating management’s assessment, testing and evaluating the design and operating effectiveness of internal control, and performing such procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that control may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
F-2
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the consolidated financial position of Dialysis Corporation of America and its subsidiaries as of December 31, 2006 and 2005, and the consolidated results of their operations and their cash flows for each of the three years in the period ended December 31, 2006, in conformity with accounting principles generally accepted in the United States of America.
Also in our opinion, management’s assessment that Dialysis Corporation of America maintained effective internal control over financial reporting as of December 31, 2006, is fairly stated, in all material respects, based on criteria established in “Internal Control - Integrated Framework” issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Furthermore, in our opinion, Dialysis Corporation of America maintained, in all material respects, effective internal control over financial reporting as of December 31, 2006, based on criteria established in “Internal Control - Integrated Framework” issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
MOORE STEPHENS, P. C. Certified Public Accountants. | ||
| | | |
Cranford, New Jersey February 23, 2007 | ||
F-3
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
December 31, 2006 | December 31, 2005 | ||||||
ASSETS | |||||||
| Current assets: | |||||||
| Cash and cash equivalents | $ | 3,491,569 | $ | 2,937,557 | |||
| Accounts receivable, less allowance | |||||||
| of $2,512,000 at December 31, 2006; | |||||||
| $1,886,000 at December 31, 2005 | 16,142,202 | 10,538,033 | |||||
| Inventories, less allowance for obsolescence | |||||||
| of $78,000 at December 31. 2006; $77,000 at December 31, 2005 | 1,985,415 | 1,457,566 | |||||
| Deferred income tax asset | 1,105,000 | 838,000 | |||||
| Prepaid expenses and other current assets | 2,731,888 | 1,425,112 | |||||
| Refundable income taxes | 174,174 | 1,227,306 | |||||
| Total current assets | 25,630,248 | 18,423,574 | |||||
| Property and equipment: | |||||||
| Land | 1,338,191 | 1,571,975 | |||||
| Buildings and improvements | 6,128,626 | 4,411,670 | |||||
| Machinery and equipment | 12,056,713 | 9,686,962 | |||||
| Leasehold improvements | 7,921,149 | 6,735,727 | |||||
| 27,444,679 | 22,406,334 | ||||||
| Less accumulated depreciation and amortization | 11,091,432 | 8,622,822 | |||||
| 16,353,247 | 13,783,512 | ||||||
| Deferred income taxes | 359,295 | 1,680,234 | |||||
| Goodwill | 6,681,160 | 3,649,014 | |||||
| Other assets | 831,776 | 1,266,789 | |||||
| Total other assets | 7,872,231 | 6,596,037 | |||||
| $ | 49,855,726 | $ | 38,803,123 | ||||
LIABILITIES AND STOCKHOLDERS’ EQUITY | |||||||
| Current liabilities: | |||||||
| Accounts payable | $ | 1,998,125 | $ | 1,775,352 | |||
| Accrued expenses | 5,744,348 | 5,739,266 | |||||
| Employment contract liability | — | 1,960,000 | |||||
| Income taxes payable | 660,092 | — | |||||
| Current portion of long-term debt | 130,000 | 952,000 | |||||
| Acquisition liabilities – current portion | — | 380,298 | |||||
| Total current liabilities | 8,532,565 | 10,806,916 | |||||
| Long-term debt, less current portion | 8,618,325 | 635,003 | |||||
| Total liabilities | 17,150,890 | 11,441,919 | |||||
| Minority interest in subsidiaries | 3,643,347 | 1,748,130 | |||||
| Commitments and Contingencies | |||||||
| Stockholders’ equity: | |||||||
Common stock, $.01 par value, authorized 20,000,000 shares: 9,564,346 shares issued and outstanding at December 31, 2006; 9,265,534 shares issued and outstanding at December 31, 2005 | 95,643 | 92,655 | |||||
| Additional paid-in capital | 15,729,206 | 15,332,975 | |||||
| Retained earnings | 13,236,640 | 10,187,444 | |||||
| Total stockholders’ equity | 29,061,489 | 25,613,074 | |||||
| $ | 49,855,726 | $ | 38,803,123 | ||||
See notes to consolidated financial statements.
F-4
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF INCOME
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Operating revenues: | ||||||||||
| Sales: | ||||||||||
| Medical services revenue | $ | 61,138,963 | $ | 44,686,579 | $ | 40,449,562 | ||||
| Product sales | 891,242 | 206,941 | — | |||||||
| Total sales revenues | 62,030,205 | 44,893,520 | 40,449,562 | |||||||
| Other income | 430,033 | 498,257 | 536,434 | |||||||
| 62,460,238 | 45,391,777 | 40,985,996 | ||||||||
| Cost and expenses: | ||||||||||
| Cost of sales revenues: | ||||||||||
| Cost of medical services | 36,968,682 | 27,859,804 | 23,545,586 | |||||||
| Cost of product sales | 549,590 | 119,327 | — | |||||||
| Total cost of sales revenues | 37,518,272 | 27,979,131 | 23,545,586 | |||||||
| Selling, general and administrative expenses | ||||||||||
| Corporate | 6,460,309 | 4,674,367 | 4,870,851 | |||||||
| Facility | 8,988,078 | 7,032,596 | 5,718,683 | |||||||
| Total | 15,448,387 | 11,706,963 | 10,589,534 | |||||||
| Stock compensation expense | 275,438 | — | — | |||||||
| Depreciation and amortization | 2,319,070 | 1,748,738 | 1,498,987 | |||||||
| Provision for doubtful accounts | 1,198,995 | 571,016 | 1,197,905 | |||||||
| 56,760,162 | 42,005,848 | 36,832,012 | ||||||||
| Operating income | 5,700,076 | 3,385,929 | 4,153,984 | |||||||
| Other income (expense): | ||||||||||
| Interest income officer/director note | — | 5,527 | 4,193 | |||||||
| Interest expense on note and advances | ||||||||||
| payable to parent | — | (157,591 | ) | (55,996 | ) | |||||
| Other income, net | 100,968 | 217,821 | 86,753 | |||||||
| 100,968 | 65,757 | 34,950 | ||||||||
| Income before income taxes, minority interest | ||||||||||
| and equity in affiliate earnings | 5,801,044 | 3,451,686 | 4,188,934 | |||||||
| Income tax provision | 2,085,874 | 1,426,552 | 1,576,292 | |||||||
| Income before minority interest and equity in | ||||||||||
| affiliate earnings | 3,715,170 | 2,025,134 | 2,612,642 | |||||||
| Minority interest in income | ||||||||||
| of consolidated subsidiaries | (919,739 | ) | (454,214 | ) | (681,385 | ) | ||||
| Equity in affiliate earnings | 253,765 | 328,732 | 282,946 | |||||||
| Net income | $ | 3,049,196 | $ | 1,899,652 | $ | 2,214,203 | ||||
| Earning per share: | ||||||||||
| Basic | .32 | $ | .22 | $ | .27 | |||||
| Diluted | .32 | $ | .20 | $ | .25 | |||||
| Weighted average shares outstanding: | ||||||||||
| Basic | 9,484,926 | 8,769,399 | 8,256,282 | |||||||
| Diluted | 9,575,733 | 9,266,905 | 8,783,857 | |||||||
See notes to consolidated financial statements.
F-5
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY
Capital in | ||||||||||||||||
Common | Excess of | Retained | Notes | |||||||||||||
Stock | Par Value | Earnings | Receivable | Total | ||||||||||||
| Balance December 31, 2003 | $ | 79,376 | $ | 5,238,952 | $ | 6,073,589 | $ | (421,600 | ) | $ | 10,970,317 | |||||
| Net income | — | — | 2,214,203 | — | 2,214,203 | |||||||||||
| Exercise of stock options for 712,446 | ||||||||||||||||
| shares of common stock, net of 72,375 | ||||||||||||||||
shares tendered in payment; includes tax effect of $119,611 (Notes 3 and 6) | 6,400 | 238,706 | — | — | 245,106 | |||||||||||
| Notes receivable paid with 91,800 | ||||||||||||||||
| shares of common stock (Note 6) | (918 | ) | (520,512 | ) | — | 421,600 | (99,830 | ) | ||||||||
| Balance December 31,2004 | 84,858 | 4,957,146 | 8,287,792 | — | 13,329,796 | |||||||||||
| Net income | — | — | 1,899,652 | — | 1,899,652 | |||||||||||
| Exercise of stock options for 330,616 | ||||||||||||||||
| shares of common stock | 3,306 | 329,329 | — | — | 332,635 | |||||||||||
| Merger with former parent | ||||||||||||||||
| (449,103 shares) (Note 16) | 4,491 | 10,046,500 | — | — | 10,050,991 | |||||||||||
| Balance December 31, 2005 | 92,655 | 15,322,975 | 10,187,444 | — | 25,613,074 | |||||||||||
| Exercise of stock options for 303,750 | ||||||||||||||||
| shares of common stock, net of 27,205 | ||||||||||||||||
| shares tendered in payment; includes | ||||||||||||||||
| tax effect of $31,000 (Notes 3 and 6) | 2,765 | 411,484 | — | — | 414,249 | |||||||||||
| Share compensation issued (22,250 shares) | 223 | 258,848 | — | — | 259,070 | |||||||||||
| Payment to dissenting merger shareholders | — | (2,100 | ) | — | — | (2,100 | ) | |||||||||
| Merger deferred tax adjustment | — | (272,000 | ) | — | — | (272,000 | ) | |||||||||
| Net income | — | — | 3,049,196 | — | 3,049,196 | |||||||||||
| Balance at December 31, 2006 | $ | 95,643 | $ | 15,729,206 | $ | 13,236,640 | $ | — | $ | 29,061,489 | ||||||
See notes to consolidated financial statements.
F-6
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Operating activities: | ||||||||||
| Net income | $ | 3,049,196 | $ | 1,899,652 | $ | 2,214,203 | ||||
Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||||
| Depreciation | 2,303,795 | 1,735,559 | 1,492,744 | |||||||
| Amortization | 15,275 | 13,179 | 6,243 | |||||||
| Bad debt expense | 1,198,995 | 571,016 | 1,197,905 | |||||||
| Deferred income tax provision (benefit) | (331,413 | ) | (63,930 | ) | 192,000 | |||||
| Deferred tax asset utilized | 1,190,000 | 1,309,283 | — | |||||||
| Stock compensation expense | 275,438 | — | — | |||||||
| Minority interest | 919,739 | 454,214 | 681,385 | |||||||
| Equity in affiliate earnings | (253,765 | ) | (328,732 | ) | (282,946 | ) | ||||
| Increase (decrease) relating to operating activities from: | ||||||||||
| Accounts receivable | (5,945,256 | ) | (2,462,593 | ) | (4,661,238 | ) | ||||
| Inventories | (411,557 | ) | 4,383 | (193,486 | ) | |||||
| Interest receivable on officer loan | — | 16,696 | (4,193 | ) | ||||||
| Prepaid expenses and other current assets | (716,821 | ) | (150,739 | ) | 85,183 | |||||
| Refundable income taxes | 1,053,132 | (1,111,929 | ) | — | ||||||
| Accounts payable | 161,266 | 95,809 | 330,112 | |||||||
| Accrued interest on note payable to former parent | — | 37,443 | 26,639 | |||||||
| Accrued expenses | (115,824 | ) | (96,676 | ) | 1,839,390 | |||||
| Income taxes payable | 614,444 | — | 90,662 | |||||||
| Net cash provided by operating activities | 3,006,644 | 1,922,635 | 3,014,603 | |||||||
| Investing activities: | ||||||||||
| Acquisition of former parent | — | 2,736,500 | — | |||||||
| Loans to physician affiliates | — | — | (125,000 | ) | ||||||
| Payments received on physician affiliate loans | 16,468 | 17,146 | 5,987 | |||||||
| Repayment of officer loan | — | 95,000 | — | |||||||
| Additions to property and equipment, net of minor disposals | (5,196,967 | ) | (5,482,338 | ) | (3,131,701 | ) | ||||
| Payment of employment contract liability | (1,960,000 | ) | — | — | ||||||
| Payment dissenting merger shareholders | (2,100 | ) | — | — | ||||||
| Acquisition of dialysis centers | (4,161,304 | ) | (380,297 | ) | (757,616 | ) | ||||
| Distributions from affiliate | 163,821 | 339,606 | 96,633 | |||||||
| Purchase of minority interests in subsidiaries | — | — | (670,000 | ) | ||||||
| Consolidation of former affiliate | 149,225 | — | — | |||||||
| Other assets | (1,264 | ) | (55,399 | ) | (23,389 | ) | ||||
| Net cash used in investing activities | (10,992,121 | ) | (2,729,782 | ) | (4,605,086 | ) | ||||
| Financing activities: | ||||||||||
| Advances from former parent | — | 161,929 | 215,023 | |||||||
| Notes payable to former parent | — | 3,096,000 | 1,435,008 | |||||||
| Line of credit borrowings | 7,500,000 | — | — | |||||||
| Payments on long-term debt | (339,582 | ) | (511,933 | ) | (715,037 | ) | ||||
| Exercise of stock options | 383,249 | 332,635 | 5,400 | |||||||
| Capital contributions by subsidiaries’ minority members | 1,301,884 | 434,000 | 172,000 | |||||||
| Distribution to subsidiary minority members | (306,062 | ) | (369,530 | ) | (435,510 | ) | ||||
| Net cash provided by financing activities | 8,539,489 | 3,143,101 | 676,884 | |||||||
| Increase (decrease) in cash and cash equivalents | 554,012 | 2,335,954 | (913,599 | ) | ||||||
| Cash and cash equivalents at beginning of year | 2,937,557 | 601,603 | 1,515,202 | |||||||
| Cash and cash equivalents at end of year | $ | 3,491,569 | $ | 2,937,557 | $ | 601,603 | ||||
See notes to consolidated financial statements.
F-7
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Business
The company is primarily engaged in kidney dialysis operations which include outpatient hemodialysis services, home dialysis services, inpatient dialysis services and ancillary services associated with dialysis treatments. The company owns 34 operating dialysis centers (including three centers acquired in the first quarter of 2006 and two centers acquired in the first quarter of 2007) located in Georgia, Maryland, New Jersey, Ohio, Pennsylvania, South Carolina and Virginia. The company also manages an unaffiliated Georgia center (see Note 7 and Note 17), has 3 dialysis facilities under development and has agreements to provide inpatient dialysis treatments to 10 hospitals. Subsequent to the completion of the company’s merger with Medicore, Inc., its former parent, the company also engages in medical product sales. The medical products operations are not a significant component of the company’s operations with operating revenues of $891,000 in 2006 and $207,000 in 2005 (1.4% and .5%, respectively of operating revenues) and operating income of $69,000 in 2006 and $25,000 in 2005 (1.2% and .7%, respectively of operating income). See “Consolidation” below in this Note 1, Note 3, Note 4, Note 12, and Note 15.
Medical Service Revenue
Our revenues by payor are as follows:
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Medicare | 52 | % | 51 | % | 48 | % | ||||
| Medicaid and comparable programs | 9 | 8 | 8 | |||||||
| Hospital inpatient dialysis services | 3 | 5 | 6 | |||||||
| Commercial insurers and other private payors | 36 | 36 | 38 | |||||||
| 100 | % | 100 | % | 100 | % | |||||
Our sources of revenue (in thousands) are as follows:
Year Ended December 31, | |||||||||||||||||||
2006 | 2005 | 2004 | |||||||||||||||||
| Outpatient hemodialysis services | $ | 32,856 | 54 | % | $ | 23,084 | 52 | % | $ | 18,599 | 46 | % | |||||||
| Home dialysis services | 3,625 | 6 | 3,198 | 7 | 2,691 | 7 | |||||||||||||
| Inpatient hemodialysis services | 2,191 | 3 | 2,055 | 5 | 2,261 | 5 | |||||||||||||
| Ancillary services | 22,467 | 37 | 16,350 | 36 | 16,899 | 42 | |||||||||||||
| $ | 61,139 | 100 | % | $ | 44,687 | 100 | % | $ | 40,450 | 100 | % | ||||||||
Consolidation
The consolidated financial statements include the accounts of Dialysis Corporation of America and its subsidiaries, collectively referred to as the “company.” All material intercompany accounts and transactions have been eliminated in consolidation. The company was formerly a majority owned subsidiary of Medicore, Inc., until the merger of Medicore into the company effected on September 21, 2005. See “Business” above in this Note 1, Note 3, Note 4, Note 12, and Note 15.
F-8
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
The company’s Toledo, Ohio subsidiary, which was 40% owned until December 2006, has been consolidated since August, 2006 due to the company taking control of this facility. This subsidiary was previously accounted for using the equity method of accounting. See Note 14.
Stock Split
On January 28, 2004, the company effected a two-for-one stock split. All share and per share data in the consolidated financial statements and notes have been adjusted to reflect the two-for-one split. See Note 13.
Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. Actual results could differ from those estimates.
The company’s principal estimates are for estimated uncollectible accounts receivable as provided for in our allowance for doubtful accounts, estimated useful lives of depreciable assets, and estimates for patient revenues from non-contracted payors. Our estimates are based on historical experience and assumptions believed to be reasonable given the available evidence at the time of the estimates. Actual results could differ from those estimates.
Vendor Volume Discounts
The company has contractual arrangements with certain vendors pursuant to which it receives discounts based on volume of purchases. These discounts are recorded in accordance with paragraph 4 of EITF 02-16 as a reduction in inventory costs resulting in reduced costs of sales as the related inventory is utilized.
Government Regulation
A substantial portion of the company’s revenues are attributable to payments received under Medicare, which is supplemented by Medicaid or comparable benefits in the states in which the company operates.
Reimbursement rates under these programs are subject to regulatory changes and governmental funding restrictions. Laws and regulations governing the Medicare and Medicaid programs are complex and subject to interpretation. The company believes that it is in compliance with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing. While no such regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation as well as significant regulatory action including fines, penalties, and exclusions from the Medicare and Medicaid programs.
F-9
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
Cash and Cash Equivalents
The company considers all highly liquid investments with a maturity of three months or less when purchased to be cash equivalents. The carrying amounts reported in the balance sheet for cash and cash equivalents approximate their fair values. Although cash and cash equivalents are largely not federally insured, the credit risk associated with these deposits that typically may be redeemed upon demand is considered low due to the high quality of the financial institutions in which they are invested.
Credit Risk
The company’s primary concentration of credit risk is with accounts receivable, which consist of amounts owed by governmental agencies, insurance companies and private patients. Receivables from Medicare and Medicaid comprised 45% of receivables at December 31, 2006 and December 31, 2005.
Inventories
Inventories, are valued at the lower of cost (first-in, first-out method) or market value and consist of supplies used in dialysis treatments and inventory of the company’s medical products division acquired pursuant to the company’s merger with its former parent. See “Consolidation” above in this Note 1, Note 3, Note 4, Note 12 and Note 15.
Prepaid Expenses and Other Current Assets
Prepaid expenses and other current assets is comprised as follows:
December 31, | |||||||
2006 | 2005 | ||||||
| Property to be sold (See Note 5) | $ | 625,716 | $ | ||||
| Prepaid expenses | 1,089,186 | 993,277 | |||||
| Other | 1,016,986 | 431,835 | |||||
| $ | 2,731,888 | $ | 1,425,112 | ||||
Accrued Expenses
Accrued expenses is comprised as follows:
December 31, | |||||||
2006 | 2005 | ||||||
| Accrued compensation | $ | 1,817,953 | $ | 1,059,791 | |||
| Excess insurance liability | 2,835,216 | 3,195,520 | |||||
| Other | 1,091,179 | 1,483,955 | |||||
| $ | 5,744,348 | $ | 5,739,266 | ||||
F-10
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
Excess insurance liability represents amounts paid by insurance companies in excess of the amounts expected by the company from the insurers. The company communicates with the payors regarding these amounts, which can result from duplicate payments, payments in excess of contractual agreements, payments as primary when payor is secondary, and underbillings by the company based on estimated fee schedules. These amounts remain in excess insurance liability until resolution. The company has identified approximately $536,000 of the excess insurance liability as of December 31, 2006, as relating to duplicate payments that will be refunded. Approximately $688,000 for 2006 and $43,000 for 2005 of amounts determined to be nonrefundable that had been included in excess insurance liability were recorded in medical services revenues.
Vendor Concentration
There is only one supplier of erythropoietin (EPO) in the United States. This supplier received FDA approval for an alternative product available for dialysis patients, which is indicated to be effective for a longer period than EPO. The alternative drug also could be administered by the patient’s physician. Accordingly, the use of this drug could reduce our revenues from our current treatment of anemia, thereby adversely impacting our revenues and profitability. There are no other suppliers of any similar drugs available to dialysis treatment providers. Revenues from the administration of EPO, which amounted to approximately $16,830,000 in 2006, $12,580,000 in 2005 and $11,381,000 in 2004, comprised 28% of medical services revenues in each of 2006, 2005 and 2004.
Property and Equipment
Property and equipment is stated on the basis of cost. Depreciation is computed for book purposes by the straight-line method over the estimated useful lives of the assets, which range from 5 to 34 years for buildings and improvements; 3 to 10 years for machinery, computer and office equipment, and furniture; and 5 to 10 years for leasehold improvements based on the shorter of the lease term or estimated useful life of the property. Replacements and betterments that extend the lives of assets are capitalized. Maintenance and repairs are expensed as incurred. Upon the sale or retirement of assets, the related cost and accumulated depreciation are removed and any gain or loss is recognized. See Note 8.
Long-Lived Asset Impairment
Pursuant to Financial Accounting Standards Board Statement No. 121, “Accounting for the Impairment of Long-Lived Assets to be Disposed of,” impairment of long-lived assets, including intangibles related to such assets, is recognized whenever events or changes in circumstances indicate that the carrying amount of the asset, or related groups of assets, may not be fully recoverable from estimated future cash flows and the fair value of the related assets is less than their carrying value. Financial Accounting Standards Board Statement No. 144, “Accounting for the Impairment of Disposal of Long-lived Assets” (FAS 144) clarified when a long-lived asset held for sale should be classified as such. It also clarifies previous guidance under FAS 121. The company, based on current circumstances, does not believe any indicators of impairment are present.
F-11
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
Comprehensive Income
The company follows Financial Accounting Standards Board Statement No. 130, “Reporting Comprehensive Income” (FAS 130) which contains rules for the reporting of comprehensive income and its components. Comprehensive income consists of net income.
Revenue Recognition
Net revenue is recognized as services are rendered at the net realizable amount from Medicare, Medicaid, commercial insurers and other third party payors. The company occasionally provides dialysis treatments on a charity basis to patients who cannot afford to pay. The amount is not significant, and the company does not record revenues related to these charitable treatments. Product sales are recorded pursuant to stated shipping terms.
Goodwill
Goodwill represents cost in excess of net assets acquired. The company adopted Statement of Financial Accounting Standards No. 142, “Goodwill and Other Intangible Assets” (FAS 142) effective January 1, 2002. Under FAS 142, goodwill and intangible assets with indefinite lives are no longer amortized but are reviewed annually (or more frequently if impairment indicators are present) for impairment, which testing indicated no impairment for goodwill. See Note 9.
Deferred Expenses
Deferred expenses, except for deferred loan costs, are amortized on the straight-line method over their estimated benefit period with deferred loan costs amortized over the lives of the respective loans. Deferred expenses of approximately $135,000 at December 31, 2006 and $67,000 at December 31, 2005 are included in other assets. Amortization expense was $15,275 for 2006, $13,179 for 2005 and $6,243 for 2004.
Income Taxes
Deferred income taxes are determined by applying enacted tax rates applicable to future periods in which the taxes are expected to be paid or recovered to differences between financial accounting and tax basis of assets and liabilities.
Stock-Based Compensation
The company measures compensation cost for stock award compensation arrangements based on grant date fair value to be expensed ratably over the requisite vesting period. Stock compensation expense for shares vesting during 2006 was approximately $275,000 with a related income tax benefit of approximately $105,000.
The company adopted Statement of Financial Statement of Financial Accounting Standards No. 123 (revised), “Share-Based Payment:” (“FAS 123(R)”) effective January 1, 2006. Provisions of FAS123(R) required companies to recognize the fair value of stock option grants as a compensation costs in their financial statements. In addition to stock options granted after the effective date, companies are required to recognize a compensation cost with respect to any unvested stock options outstanding as of the effective date equal to the grant date fair value of those options with the cost related to unvested options to be recognized over the vesting period of the options. The board of directors approved accelerated vesting of all unvested options as of December 31, 2005 resulting in there being no unvested options as of December 31, 2005.
F-12
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
Pro forma information regarding net income and earnings per share has been presented below for 2005 and 2004 as if the company had accounted for its employee stock options under the fair value method required by FAS 123(R). The fair value for these options was estimated at the date of grant using a Black-Scholes option pricing model with the following weighted-average assumptions for options granted during 2004, 2003, 2002 and 2001, respectively: risk-free interest rate of 3.83%, 1.44%, 3.73%, and 5.40%; no dividend yield; volatility factor of the expected market price of the company’s common stock of 1.31, 1.07, 1.15 and 1.14, and a weighted-average expected life of 5 years, 4.7 years, 5 years and 4 years.
The Black-Scholes option valuation model was developed for use in estimating the fair value of traded options which have no vesting restrictions and are fully transferable. In addition, option valuation models require the input of highly subjective input assumptions including the expected stock price volatility. Because the company’s employee stock options have characteristics significantly different from those of traded options, and because changes in the subjective input assumptions can materially affect the fair value estimate, in management’s opinion, the existing models do not necessarily provide a reliable measure of the fair value of its employee stock options.
For purposes of pro forma disclosures, the estimated fair value of options is amortized to expense over the options’ vesting period. The board of directors approved accelerated vesting of all unvested options with all outstanding options considered vested as of December 31, 2005. The effect of the accelerated vesting on 2005 pro forma results is reflected in the company’s pro forma information that follows:
2005 | 2004 | ||||||
| Net income, as reported | $ | 1,900,000 | $ | 2,214,000 | |||
| Stock-based employee compensation expense under fair value method, net of related tax effects | (430,000 | ) | (170,000 | ) | |||
| Pro forma net income | $ | 1,470,000 | $ | 2,044,000 | |||
| Earnings per share: | |||||||
| Basic, as reported | $ | .22 | $ | .27 | |||
| Basic, pro forma | $ | .17 | $ | .25 | |||
| Diluted, as reported | $ | .20 | $ | .25 | |||
| Diluted, pro forma | $ | .16 | $ | .23 | |||
F-13
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
Earnings per Share
Diluted earnings per share gives effect to potential common shares that were dilutive and outstanding during the period, such as stock options and warrants, calculated using the treasury stock method and average market price.
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Net income | $ | 3,049,196 | $ | 1,899,652 | $ | 2,214,203 | ||||
| Weighted average shares outstanding | 9,484,926 | 8,769,399 | 8,256,282 | |||||||
| Weighted average shares outstanding | 9,484,926 | 8,769,399 | 8,256,282 | |||||||
| Shares issuable for employee stock awards and director fees | 17,701 | — | — | |||||||
| Weighted average shares diluted computation | 9,502,627 | 8,769,399 | 8,256,282 | |||||||
| Effect of diluted stock options | 73,106 | 497,506 | 527,575 | |||||||
| Weighted average shares, as adjusted diluted computation | 9,575,733 | 9,266,905 | 8,783,857 | |||||||
| Earnings per share: | ||||||||||
| Basic | $ | .32 | $ | .22 | $ | .27 | ||||
| Diluted | $ | .32 | $ | .20 | $ | .25 | ||||
The company had various potentially dilutive outstanding stock options during the periods presented. See Note 6.
Other Income
Operating:
Other operating income is comprised as follows:
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Management fee income | $ | 430,033 | $ | 498,257 | $ | 402,251 | ||||
| Litigation settlement | — | — | 134,183 | |||||||
| $ | 430,033 | $ | 498,257 | $ | 536,434 | |||||
F-14
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
Non-operating:
Other non-operating income (expense) is comprised as follows:
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Rental income | $ | 369,888 | $ | 238,743 | $ | 191,350 | ||||
| Interest income | 193,429 | 99,300 | 35,402 | |||||||
| Interest expense | (409,676 | ) | (147,635 | ) | (162,791 | ) | ||||
| Other | 32,327 | 27,413 | 22,792 | |||||||
| Litigation settlement, net | (85,000 | ) | — | — | ||||||
| Other income, net | $ | 100,968 | $ | 217,821 | $ | 86,753 | ||||
Estimated Fair Value of Financial Instruments
The carrying value of cash, accounts receivable and debt in the accompanying financial statements approximate their fair value because of the short-term maturity of these instruments, and in the case of debt because such instruments either bear variable interest rates which approximate market or have interest rates approximating those currently available to the company for loans with similar terms and maturities.
Reclassification
Certain prior year amounts have been reclassified to conform with the current year’s presentation.
New Pronouncements
In June, 2006, the FASB issued FASB Interpretation No. 48 (“FIN 48”), “Accounting for Uncertainty in Income Taxes - an interpretation of FASB Statement No. 109, Accounting for Income Taxes,” which clarifies the accounting for uncertainty in income taxes. FIN 48 prescribes a recognition threshold and measurement attribute for financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return. FIN 48 requires that a company recognize in its financial statements, the impact of a tax position, if that position is more likely than not to be sustained on audit, based on the technical merits of the position. FIN 48 also provides guidance on de-recognition, classification, interest and penalties, accounting in interim periods and disclosure. The provisions of FIN 48 are effective for fiscal years beginning after December 15, 2006, with the cumulative effect of the change in accounting principle recorded as an adjustment to opening retained earnings. The company is evaluating the impact of adopting FIN 48, but does not expect FIN 48 to have a significant effect on its financial statements.
In September, 2006, the FASB issued Statement of Financial Accounting Standards No. 157 (“SFAS 157”), “Fair Value Measurements.” SFAS 157 defines fair value, establishes a framework for measuring fair value in generally accepted accounting principles, and expands disclosures about fair value measurements. SFAS 157 applies under other accounting pronouncements that require fair value measurement in which the FASB concluded that fair value was the relevant measurement, but does not require any new fair value measurements. SFAS 157 will be effective for the company beginning in 2009. The company is evaluating the impact on its financial statements of adopting SFAS 157.
F-15
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 1—SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES—Continued
In September, 2006, the U.S. Securities and Exchange Commission (SEC) issued Staff Accounting Bulletin No. 108 (“SAB 108”), which provides interpretive guidance on how the effects of prior year misstatements should be considered in quantifying current year financial statement misstatements. The interpretations by the SEC staff in SAB 108 were issued to address the diversity in the practice of quantifying financial statements misstatements and the potential for a build up of improper amounts on the balance sheet. The SEC staff indicated that companies should quantify errors using both a balance sheet and income statement approach and determine whether either approach results in material misstatement. SAB 108 is effective for fiscal years ending after November 15, 2006. SAB 108 has not had a significant effect on the company’s financial statements.
NOTE 2—LONG-TERM DEBT
Long-term debt is as follows:
December 31, | |||||||
2006 | 2005 | ||||||
| Revolving line of credit | $ | 7,500,000 | $ | — | |||
| Maturity of October 24, 2008. | |||||||
| See below for details. | |||||||
| Development loan secured by land and building | |||||||
| with a net book value of $378,000 at | |||||||
| December 31, 2006. Monthly principal | |||||||
payments of $2,402 plus interest at | |||||||
| prime with remaining balance due May 2, 2026. | 555,122 | $ | 582,979 | ||||
| Mortgage note secured by land and building | |||||||
| with a net book value of $823,000 at | |||||||
December 31, 2006. Interest of | |||||||
| prime with a rate floor of 5.75% and a | |||||||
| rate ceiling of 8.00%. Monthly | |||||||
| payments of $6,000 including principal and | |||||||
| interest with remaining balance due April, 2011. | 617,145 | 632,591 | |||||
| Equipment financing agreement secured by equipment | |||||||
| with a net book value of $168,000 at December 31, | |||||||
| 2006. Monthly payments totaling approximately $10,000 as of | |||||||
| December 31, 2006, including principal and interest, | |||||||
| as described below, pursuant to various schedules | |||||||
| extending through August, 2007 with interest at rates | |||||||
| ranging from 7.36% to 8.22%. | 76,058 | 371,433 | |||||
| 8,748,325 | 1,587,003 | ||||||
| Less current portion | 130,000 | 952,000 | |||||
| $ | 8,618,325 | $ | 635,003 | ||||
F-16
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 2—LONG-TERM DEBT—Continued
The company through its subsidiary, DCA of Vineland, LLC, pursuant to a December 3, 1999 loan agreement obtained a $700,000 development loan with interest at 8.75% through December 2, 2001, 1½% over the prime rate thereafter through December 15, 2002, 1% over prime until May 2006 and prime thereafter secured by a mortgage on the company’s real property in Easton, Maryland. The bank subsequently released DCA of Vineland, LLC’s assets as security leaving the company as the remaining obligor on this loan agreement. Outstanding borrowings were subject to monthly payments of interest only through December 2, 2001, with monthly payments thereafter of $2,917 principal plus interest through December 2, 2002, monthly payments thereafter of $2,217 plus interest until May 2006 when the loan was modified and $2,402 plus interest thereafter until maturity on May 2, 2026. This loan had an outstanding principal balance of approximately $555,000 at December 31, 2006 and $583,000 December 31, 2005.
In April 2001, the company obtained a $788,000 five-year mortgage through April, 2006, on its building in Valdosta, Georgia with interest at 8.29% until March, 2002, 7.59% thereafter until December 16, 2002, prime plus ½% with a minimum of 6.0% effective December 16, 2002 thereafter until April 2006 when the mortgage was refinanced, with a rate thereafter of prime with a rate floor of 5.75% and a rate ceiling of 8.00%. Payments are $6,000 including principal and interest commencing May, 2006, with a final payment consisting of a balloon payment and any unpaid interest due April, 2011. The remaining principal balance under this mortgage amounted to approximately $617,000 at December 31, 2006 and $633,000 at December 31, 2005.
The equipment financing agreement represents financing for kidney dialysis machines for the company’s dialysis facilities. There was no financing under this agreement in 2006, 2005 or 2004. Payments under the agreement are pursuant to various schedules extending through August, 2007. Financing under the equipment purchase agreement is a noncash financing activity, which is a supplemental disclosure required by Financial Accounting Standards Board Statement No 95, “Statement of Cash Flows.” The remaining principal balance under this financing amounted to approximately $76,000 at December 31, 2006 and $371,000 at December 31, 2005.
The prime rate was 8.25% as of December 31, 2006 and 7.25% as of December 31, 2005. For interest payments, see Note 12.
Scheduled maturities of long-term debt outstanding at December 31, 2006 are approximately:
| 2007 | $ | 130,000 | ||
| 2008 | 7,554,000 | |||
| 2009 | 56,000 | |||
| 2010 | 58,000 | |||
| 2011 | 61,000 | |||
| Thereafter | 889,000 | |||
| $ | 8,748,000 |
F-17
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 2—LONG-TERM DEBT—Continued
The company’s two mortgage agreements contain certain restrictive covenants that, among other things, restrict the payment of dividends, require lenders’ approval for a merger, sale of substantially all the assets, or other business combination of the company, and require maintenance of certain financial ratios. The company was in compliance with the debt covenants at December 31, 2006 and December 31, 2005.
On October 24, 2005, the company entered into a three year, $15,000,000 revolving line of credit with a maturity date of October 24, 2008. There was no financing under this agreement in 2005. Each of the company’s wholly-owned subsidiaries has guaranteed this credit facility, as will any future wholly-owned subsidiaries. Further, the obligation under the revolving line of credit is secured by the company’s pledge of its ownership in its subsidiaries. The credit facility, which has provisions for both base rate and LIBOR loans, is intended to provide funds for the development and acquisition of new dialysis facilities, to meet general working capital requirements, and for other general corporate purposes. Borrowings under the revolving line of credit accrue interest at a rate based upon the applicable margin for base rate and LIBOR loans plus the base rate for base rate loans and the LIBOR rate for LIBOR loans, as those terms are defined in the agreement. The LIBOR rate applicable to a LIBOR loan is determined by the interest period selected by the company for that particular loan, which represents the duration of the loan. The company has the right to convert the base rate loan to a LIBOR loan, and vice versa. The agreement contains customary reporting and financial covenant requirements for this type of credit facility. The company was in compliance with the requirements of this credit facility at December 31, 2006 and December 31, 2005.
The company has $7,500,000 in outstanding borrowings under its line of credit at December 31, 2006, including three LIBOR loans totaling $6,000,000, and a $1,500,000 in base rate loan. The LIBOR loans have an interest rate of 6.625%, including a LIBOR rate of 5.375% plus an applicable margin of 1.25%. The base rate loan has an interest rate of 8.25% as of December 31, 2006. The LIBOR loans are all three month loans including a $1,500,000 loan maturing January 3, 2007, a $3,500,000 loan maturing March 5, 2007 and a $1,000,000 loan maturing March 8, 2007. These loans have been renewed for the same terms.
NOTE 3—INCOME TAXES
The income tax provision consists of the following income tax expense (benefit) components:
2006 | 2005 | 2004 | ||||||||
Current: | ||||||||||
Federal | $ | 1,970,000 | $ | 1,241,000 | $ | 1,052,000 | ||||
State | 410,000 | 240,000 | 324,000 | |||||||
City | 37,000 | 10,000 | 8,000 | |||||||
| 2,417,000 | 1,491,000 | 1,384,000 | ||||||||
Deferred: | ||||||||||
Federal | (317,000 | ) | (156,000 | ) | 227,000 | |||||
State | (14,000 | ) | 92,000 | (35,000 | ) | |||||
| (331,000 | ) | (64,000 | ) | 192,000 | ||||||
| $ | 2,086,000 | $ | 1,427,000 | $ | 1,576,000 | |||||
F-18
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 3—INCOME TAXES—Continued
Deferred income taxes reflect the net tax effect of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Significant components of the company’s deferred tax liabilities and assets are as follows:
December 31, | |||||||
2006 | 2005 | ||||||
Deferred tax liabilities: | |||||||
Depreciation and amortization | $ | 640,000 | $ | 814,000 | |||
| Total deferred tax liabilities | 640,000 | 814,000 | |||||
Deferred tax assets: | |||||||
| Accrued expenses | 207,000 | 153,000 | |||||
| Bad debt allowance | 898,000 | 685,000 | |||||
| Startup costs and other intangibles | 64,000 | 141,000 | |||||
| Subtotal | 1,169,000 | 979,000 | |||||
Net operating loss carryforwards | 935,000 | 2,353,000 | |||||
| Total deferred tax assets | 2,104,000 | 3,332,000 | |||||
Net deferred tax asset | $ | 1,464,000 | $ | 2,518,000 | |||
No valuation allowance was recorded for deferred tax assets at December 31, 2006 or December 31, 2005, due to the company’s anticipated prospects for future taxable income in an amount sufficient to realize the deferred tax assets.
As a result of the company’s merger with its former parent, the company acquired a deferred tax asset of approximately $3,300,000, representing tax benefits from the former parent’s net operating loss carryforwards that the company can utilize to satisfy future income tax liabilities. The company has applied approximately $560,000 of the acquired deferred tax asset to offset a deferred income tax liability of the same amount, which would otherwise represent a future tax liability of the company. The company has also applied approximately $2,400,000 of the deferred tax asset toward its 2005 and 2006 tax liability. See Note 1, Note 4, Note 12 and Note 15.
The reconciliation of income tax (benefit) attributable to income (loss) before income taxes computed at the U.S. federal statutory rate is:
Year Ended December 31, | ||||||||||
2006 | 2005 | 2004 | ||||||||
Statutory tax rate (34%) applied to income (loss) | ||||||||||
before income taxes, minority interest and equity in affiliate earnings | $ | 1,972,000 | $ | 1,174,000 | $ | 1,424,000 | ||||
Adjustments due to: | ||||||||||
| State and city taxes, net of federal benefit | 295,000 | 193,000 | 218,000 | |||||||
| Change in valuation allowance | — | — | (18,000 | ) | ||||||
| Non-deductible items | 13,000 | 11,000 | 18,000 | |||||||
| Subsidiary minority ownership | (271,000 | ) | (131,000 | ) | (206,000 | ) | ||||
| Ownership in affiliate | 72,000 | 112,000 | 96,000 | |||||||
| Other | 5,000 | 68,000 | 44,000 | |||||||
| $ | 2,086,000 | $ | 1,427,000 | $ | 1,576,000 | |||||
F-19
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 3—INCOME TAXES—Continued
The company has equity positions in 30 limited liability companies (“LLC’s”), and one limited partnership (“LP”) each possessing a finite life. Based on their limited liability status, its members are not liable for the LLC’s and LP’s debts, liabilities, or obligations. Each LLC and LP has complied with the criteria for tax treatment as a partnership. As a result, taxable income or loss is to be reported on each member’s respective tax returns. Income and losses attributable to the company’s equity position in subsidiary LLC’s and LP’s are included in the company’s Consolidated Statements of Income with the minority interest in the results of operations of subsidiary LLC’s and LP’s shown separately on the Consolidated Statements of Income. Income attributable to the company’s equity position in its 40% owned affiliate (see Note 1 and Note 14) prior to the affiliate’s consolidation as a subsidiary effective August 1, 2006, is shown separately on the company’s Consolidated Statements of Income.
The exercise of 10,000 non-qualified stock options during 2006 and 70,348 non-qualified stock options during 2004 resulted in tax deductions of $84,000 and $304,000, respectively, corresponding to the difference in the market value of the shares obtained on exercise and the exercise price of the options. The reduction in income taxes payable of approximately $31,000 and $120,000, respectively, resulted in a corresponding increase in additional paid-in capital of approximately $31,000 and $120,000, respectively. This represents, a non cash financing activity, which is a supplemental disclosure required by Accounting Standards Board Statement No. 95 “Statement of Cash Flows”. See Note 12.
For income tax payments, see Note 12.
NOTE 4—TRANSACTIONS WITH FORMER PARENT
Our former parent provided certain financial and administrative services for us. Central operating costs were charged on the basis of time spent. In the opinion of management, this method of allocation is reasonable. The amount of expenses allocated by the former parent totaled approximately $150,000 for the year ended December 31, 2005, with this allocation ceasing when the company and its former parent merged (see Note 1, Note 3, Note 12 and Note 15) and $200,000 for the year ended December 31, 2004, which is included in selling, general and administrative expenses in the Consolidated Statements of Income.
We had an intercompany advance payable to our former parent of approximately $449,000 as of December 31, 2004, which bore interest at the short-term Treasury Bill rate. Interest expense on intercompany advances payable was approximately $9,000 and $5,000 for the years ended December 31, 2005 and 2004, respectively with the interest ceasing when the company and its former parent merged in September, 2005. Interest was included in the intercompany advance balance. The intercompany advance of approximately $611,000 was forgiven as a result of the company’s merger with its former parent. See Note 1, Note 3, Note 12 and Note 15.
F-20
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 4—TRANSACTIONS WITH FORMER PARENT—Continued
On March 17, 2004, the company issued a demand promissory note to its former parent for up to $1,500,000 of financing for equipment purchases with annual interest of 1.25% over the prime rate. The note was subsequently modified by increasing the maximum amount of advances that can be made to $5,000,000, and by adding to the purposes of the financing, working capital and other corporate needs. The outstanding note balance of approximately $4,531,000 was forgiven as a result of the company’s merger with its former parent. The weighted average interest rate on the note during the period it was outstanding during 2005 and 2004 was 7.58% and 5.84%, respectively. Interest expense on the note amounted to approximately $149,000 and $51,000 for the years ended December 31, 2005 and 2004 with the interest ceasing when the company and its former parent merged. Accrued interest on the note of approximately $64,000 was forgiven as a result of the company’s merger with its former parent. See Note 1, Note 3, Note 12, and Note 15.
NOTE 5—OTHER RELATED PARTY TRANSACTIONS
In May 2001, the company loaned its president $95,000 to be repaid with accrued interest at prime minus 1% (floating prime) on or before maturity on May 11, 2006. This demand loan was collateralized by all of the President’s stock options in the company, as well as common stock from exercise of the options and proceeds from sale of such stock. Interest income on the loan amounted to approximately $6,000 and $4,000 for 2005 and 2004, respectively. The note and accrued interest of approximately $22,000 were repaid in December, 2005.
Minority members in subsidiaries in certain situations have funded a portion of required capital contributions by issuance of an interest bearing note payable to the company which the minority members repay directly or through their portion of capital distributions of the subsidiary. The minority members did not fund any capital contributions through notes payable to the company during 2006 and funded in the aggregate approximately $15,000 in capital contributions through notes during 2005, and $324,000 during the preceding year, under notes accruing interest at prime plus 2%, with an aggregate of approximately $154,000 of distributions applied against the notes and accrued interest during 2006, $68,000 during 2005 and $74,000 during 2004. These represent non-cash investing activities, which is a supplemental disclosure required by Financial Accounts Standards Board Statement No. 95, “Statement of Cash Flows.” See Note 10 and Note 12.
The company has constructed and is constructing dialysis facilities, one of which is anticipated to be sold upon completion to a medical director of the company. The company’s subsidiary that will operate that dialysis facility will lease the facility from the purchaser on terms which are as favorable as could be obtained from unaffiliated parties. The cost of the land and construction costs are included in Prepaid Expenses and Other Current Assets. See Note 1.
NOTE 6—STOCK OPTIONS AND STOCK AWARDS
In January, 2001, the board of directors granted to the company’s Chief Executive Officer and President a five-year option for 330,000 shares exercisable at $.63 per share. In January, 2004, 56,384 of these options were exercised for $35,240 with the exercise price satisfied by a director bonus. In March, 2005, 150,000 of these options were exercised with the company receiving a $93,750 cash payment for the exercise price. In December, 2005, the remaining 123,616 of these options were exercised with the company receiving a $76,024 cash payment for the exercise price.
F-21
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 6—STOCK OPTIONS—Continued
In September, 2001, the board of directors granted five-year options for an aggregate of 150,000 shares exercisable at $.75 per share through September 5, 2006, to certain officers, directors and key employees. In 2003 and 2004, 8,146 of these options were exercised, with the exercise prices satisfied by director bonuses. These exercises represent non-cash investing activity, which is a supplemental disclosure required by Financial Accounting Standards Board Statement No. 95, “Statement of Cash Flows.” See Note 12. In January, 2004, 7,200 options were exercised. In February, 2005, 15,000 options were exercised for cash. 14,654 options were cancelled due to the resignation of a director in June, 2004. 100,000 options were exercised in March, 2006 and the balance of 5,000 options were exercised in April, 2006 with the company receiving cash payments totaling $78,750 for the exercise price.
In May, 2002, the board of directors granted five-year options for an aggregate of 21,000 shares to certain of the company’s employees. Options for 14,000 shares have been cancelled as a result of the termination of several employee option holders. During 2005, 7,000 of these options were exercised with the company receiving $14,350 cash payments for the exercise price.
In June, 2003, the board of directors granted to an officer a five-year option for 50,000 shares exercisable at $1.80 per share through June 3, 2008. These options were exercised in March, 2006 with the company receiving a $90,000 cash payment for the exercise price.
In August, 2003, the board of directors granted a three-year option to a director for 10,000 shares exercisable at $2.25 per share through August 18, 2006. These options were exercised in June, 2006 with the company receiving a $22,500 cash payment.
In January, 2004, the board of directors granted a five year option to an employee for 20,000 shares exercisable at $3.09 per share through January 12, 2009. In February, 2005, a portion of this option was exercised for 5,000 shares with the company receiving a cash payment of $15,425. 5,000 options were exercised in January, 2006 with the company receiving a cash payment of $15,425 for the exercise price, and the balance of 10,000 options were exercised in June, 2006 with the company receiving a $30,850 cash payment.
In June, 2004, the board of directors granted 160,000 stock options to officers, directors and a key employee exercisable at $4.02 per share through June 6, 2009. 3,750 options were exercised in July, 2005 with the company receiving a cash payment of $15,075 and an additional 13,750 options were exercised in December, 2005 with the company receiving $55,275 cash payments. 25,000 options were exercised in March, 2006 with the company receiving a $100,500 cash payment for the exercise price. An additional 87,500 options were exercised in March, 2006 with an exercise price of $351,750 that was satisfied through payment of 27,205 shares of company stock. 7,500 options were exercised in May and June, 2006 and 3,750 options were exercised in August, 2006 with the company receiving a total of $45,225 cash payments, leaving 18,750 options outstanding.
F-22
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 6—STOCK OPTIONS—Continued
In August, 2004, the board of directors granted 50,000 incentive stock options to an officer exercisable at $4.02 per share through August 15, 2009. The options were to vest 25% annually commencing August 16, 2005 with 12,500 vested options exercised in December, 2005 and the company receiving a cash payment of $50,250. The remaining 37,500 options were cancelled due to the officer’s resignation.
On June 8, 2006, the company’s shareholders approved an amendment to the company’s stock option plan to allow for the grant of stock awards in addition to options. The employment agreement of Stephen W. Everett, President, CEO and a director of the company, contains provisions for the receipt of up to 40,000 shares of the company’s company stock as described in Note 8, pursuant to which 10,000 shares were issued during 2006 resulting in $100,100 stock compensation expense, with an additional up to 10,000 performance based shares for 2006 not earned. See Note 7. The company granted stock awards of 1,000 shares each to each of its independent directors with the shares vesting in 250 share increments for each director at the end of each quarter of 2006, resulting in $37,560 stock compensation expense. On June 27, 2006, the company granted stock awards of 64,000 shares to officers and key employees with the awards vesting in equal yearly increments over four years commencing December 31, 2006. One of the June 2006 stock awards for 30,000 shares, which contained performance criteria, cancelled in November, 2006 upon resignation of the officer. 8,500 of the June 2006 stock awards vested during 2006 resulting in $94,180 stock compensation expense. In November, 2006, the company entered a six-month contract with an individual to serve as Chief Operating Officer for which the compensation is 10,000 shares of common stock to be earned over the six month period, with 3,333 shares earned during 2006 resulting in $43,598 stock compensation expense.
On January 28, 2004, the company affected a two-for-one stock split of its outstanding common stock. All option amounts and exercise prices have been adjusted to reflect the stock split. See Note 1. Split-adjusted option exercise prices resulting in a fraction of a cent have been rounded up to the nearest cent for purposes of these Notes.
F-23
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 6—STOCK OPTIONS—Continued
A summary of the company’s stock option activity and related information for the years ended December 31 follows:
2006 | 2005 | 2004 | |||||||||||||||||
Weighted- | Weighted- | Weighted- | |||||||||||||||||
Average | Average | Average | |||||||||||||||||
Options | Exercise Price | Options | Exercise Price | Options | Exercise Price | ||||||||||||||
| Outstanding-beginning of year | 322,500 | 694,616 | 1,191,716 | ||||||||||||||||
| Granted | — | — | 230,000 | $ | 3.94 | ||||||||||||||
| Cancellations | — | (41,500 | ) | $ | 3.83 | (14,654 | ) | $ | .75 | ||||||||||
| Exercised | (303,750 | ) | $ | 2.42 | (330,616 | ) | $ | 1.01 | (712,446 | ) | $ | .63 | |||||||
| Expired | — | — | — | ||||||||||||||||
| Outstanding-end of year | 18,750 | 322,500 | 694,616 | ||||||||||||||||
| Outstanding: | |||||||||||||||||||
| August 2004 options | — | — | 50,000 | $ | 4.02 | ||||||||||||||
| June 2004 options | 18,750 | $ | 4.02 | 142,500 | $ | 4.02 | 160,000 | $ | 4.02 | ||||||||||
| January 2004 options | — | 15,000 | $ | 3.09 | 20,000 | $ | 3.09 | ||||||||||||
| August 2003 options | — | 10,000 | $ | 2.25 | 10,000 | $ | 2.25 | ||||||||||||
| June 2003 options | — | 50,000 | $ | 1.80 | 50,000 | $ | 1.80 | ||||||||||||
| May 2002 options | — | — | 11,000 | $ | 2.05 | ||||||||||||||
| September 2001 options | — | 105,000 | $ | .75 | 120,000 | $ | .75 | ||||||||||||
| January 2001 options | — | — | 273,616 | $ | .63 | ||||||||||||||
| 18,750 | 322,500 | 694,616 | |||||||||||||||||
| Outstanding and exercisable end of year: | |||||||||||||||||||
| June 2004 options | 18,750 | $ | 4.02 | 142,500 | $ | 4.02 | 15,000 | $ | 4.02 | ||||||||||
| January 2004 options | — | 15,000 | $ | 3.09 | — | ||||||||||||||
| August 2003 | — | 10,000 | $ | 2.25 | 5,000 | $ | 2.25 | ||||||||||||
| June 2003 | — | 50,000 | $ | 1.80 | 12,500 | $ | 1.80 | ||||||||||||
| May 2002 | — | — | 11,000 | $ | 2.05 | ||||||||||||||
| September 2001 options | — | 105,000 | $ | .75 | 90,000 | $ | .75 | ||||||||||||
| January 2001 options | — | — | 207,616 | $ | .63 | ||||||||||||||
| 18,750 | 322,500 | 341,116 | |||||||||||||||||
| Weighted-average fair value of options granted during the year | $ | 3.88 | |||||||||||||||||
The remaining contractual life at December 31, 2006 is 2.4 years for the June, 2004 options.
The total exercise price for stock options exercised during 2006 was approximately $735,000 compared to a total stock value on the dates of exercise of approximately $3,923,000, resulting in an intrinsic value on these exercises of $3,188,000.
A summary of information on the company’s stock compensation and nonvested shares for the years ended December 31 follows:
2006 | 2005 | 2004 | ||||||||||||||||||||||||||
Shares | Total Fair Value | Weighted Average Fair Value | Shares | Total Fair Value | Weighted Average Fair Value | Shares | Total Fair Value | Weighted Average Fair Value | ||||||||||||||||||||
| Nonvested-beginning of year | — | $ | — | $ | — | — | $ | — | $ | — | — | $ | — | $ | — | |||||||||||||
| Issued | — | — | — | — | — | — | — | — | — | |||||||||||||||||||
| Unissued | — | $ | — | $ | — | — | $ | — | $ | — | — | $ | — | $ | — | |||||||||||||
| Shares granted: | ||||||||||||||||||||||||||||
| Issued | 22,250 | $ | 259,070 | $ | 11.64 | |||||||||||||||||||||||
| Unissued | 94,750 | 1,018,810 | $ | 10.75 | ||||||||||||||||||||||||
| 117,000 | $ | 1,277,880 | $ | 10.92 | ||||||||||||||||||||||||
| Shares vesting: | ||||||||||||||||||||||||||||
| Issued | (15,583 | ) | $ | (171,866 | ) | $ | 11.03 | — | $ | — | $ | — | — | $ | — | $ | — | |||||||||||
| Unissued | (9,250 | ) | (103,570 | ) | $ | 11.20 | — | — | $ | — | — | — | $ | — | ||||||||||||||
| (24,833 | ) | $ | (275,436 | ) | $ | 11.09 | — | $ | — | $ | — | — | $ | — | $ | — | ||||||||||||
| Shares forfeited: | ||||||||||||||||||||||||||||
| Issued | — | — | $ | 0.00 | ||||||||||||||||||||||||
| Unissued | (40,000 | ) | (432,500 | ) | $ | 10.81 | ||||||||||||||||||||||
| (40,000 | ) | (432,500 | ) | $ | 10.81 | |||||||||||||||||||||||
| Nonvested-end of year: | ||||||||||||||||||||||||||||
| Issued | 6,667 | $ | 87,204 | $ | 13.08 | — | $ | — | $ | — | — | $ | — | $ | — | |||||||||||||
| Unissued | 45,000 | 482,740 | $ | 10.61 | — | — | $ | — | — | — | $ | — | ||||||||||||||||
| 52,167 | $ | 569,944 | $ | 10.93 | — | $ | — | $ | — | — | $ | — | $ | — | ||||||||||||||
| Weighted average period over which nonvested | ||||||||||||||||||||||||||||
| compensation cost expected to be recognized: | ||||||||||||||||||||||||||||
| Issued shares | 0.33 years | |||||||||||||||||||||||||||
| Unissued shares: | ||||||||||||||||||||||||||||
| Performance based | 2.00 years | |||||||||||||||||||||||||||
| Nonperformance based | 3.00 years | |||||||||||||||||||||||||||
| Overall | 1.64 years | |||||||||||||||||||||||||||
The total grant date fair value of stock awards vesting during 2006 was approximately $275,000 compared to a total stock value on the dates of vesting of approximately $289,000 resulting in a fair value differential of $14,000.
As a result of board of director approval of accelerated vesting of remaining unvested options, all outstanding options at December 31, 2005 were vested.
F-24
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 6—STOCK OPTIONS—Continued
As of December 31, 2006, the company has 722,404 shares reserved for issuance, including: 18,750 shares for the June, 2004 options, and 45,500 outstanding non-vested stock awards. All options were issued at fair market value on date of grant.
The number and exercise price of outstanding options was adjusted based upon a two-for-one stock split affected by the company in February, 2004. See Note 1 and Note 13.
NOTE 7—COMMITMENTS
The company has leases on facilities housing its dialysis, administrative and medical operations and equipment leases. Total rent expense was approximately $1,727,000, $1,466,000 and $1,194,000 for the years ended December 31, 2006, 2005, and 2004, respectively. The aggregate lease commitments at December 31, 2006 for the company’s non-cancelable operating leases with a term of one year or more are approximately:
| 2007 | $ | 1,810,000 | ||
| 2008 | 1,633,000 | |||
| 2009 | 1,368,000 | |||
| 2010 | 1,143,000 | |||
| 2011 | 800,000 | |||
| Thereafter | 668,000 | |||
| $ | 7,422,000 |
Effective January 1, 1997, the company established a 401(k) savings plan (salary deferral plan) with an eligibility requirement of one year of service and 21 year old age requirement. The company and its former parent established a new 401(k) plan effective January, 2003, which allows employees, in addition to regular employee contributions, to elect to have a portion of bonus payments contributed. As an incentive to save for retirement, the company will match 10% of an employee’s contribution resulting from any bonus paid during the year and may make a discretionary contribution with the percentage of any discretionary contribution to be determined each year with only employee contributions up to 6% of annual compensation considered when determining employer matching. To date, employer matching expense has been minimal.
Stephen W. Everett, CEO, President and director of the company, had a five-year employment contract through December 31, 2005. The company and Mr. Everett finalized a new five-year employment agreement, agreed to in principle and effective January 3, 2006 with an initial annual salary of $275,000 and minimum increases of $10,000 per year thereafter. The agreement contains provisions for receipt of up to 40,000 shares of the company’s common stock of which 10,000 shares was granted upon shareholder approval in June, 2006. Issuance of the remaining 30,000 shares is based upon agreed upon performance criteria with the potential for 10,000 shares to be earned annually for 2006 - 2008. No performance shares were earned during 2006 since the performance criteria were not met. The agreement provides for certain fringe benefits, reimbursement of reasonable out-of-pocket expenses, and a non-competition agreement with the company during the term of the agreement and for one year after termination. See Note 6.
F-25
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 7—COMMITMENTS—Continued
A non-affiliated owner of a Georgia facility that is managed by the company held a put option to sell to a subsidiary of the company all the assets of that dialysis facility. The company’s subsidiary held a call option to purchase the assets of the Georgia facility. Each of the put and call options were exercisable through September, 2005. In August, 2005, our subsidiary notified the owner of the Georgia facility of its intent to exercise the call option and negotiate the acquisition of that facility’s assets. The parties agreed to extend the call option through December 31, 2006 with the option further extended until January 14, 2007. The call option was exercised on January 11,2007. See Note 17. The put option expired unexercised and was not extended.
NOTE 8—CAPITAL EXPENDITURES AND DEPRECIATION
| Capital expenditures and depreciation expense were as follows: | ||||||||||
2006 | 2005 | 2004 | ||||||||
| Capital expenditures | $ | 5,197,000 | $ | 5,482,000 | $ | 3,132,000 | ||||
| Depreciation expense | $ | 2,304,000 | $ | 1,736,000 | $ | 1,493,000 | ||||
NOTE 9—ACQUISITIONS
The company has made various acquisitions commencing in 2001, as further described below. These acquisitions were made either on the basis of existing profitability or expectation of future profitability for the interest acquired based on the company’s analysis of the potential for each acquisition, and the value of the relationship with the physician affiliated with the selling entity. Each acquisition was intended to either strengthen our market share within a geographic area or provide us with the opportunity to enter a new geographic area and market. Management also reviews the purchase price and any resulting goodwill based on established current per patient valuations for dialysis centers. Also considered are the synergistic effects of a potential acquisition, including potential costs integration and the effect of the acquisition on the overall valuation of the company.
These transactions resulted in an aggregate of approximately $6,681,000 of goodwill, representing the excess of the purchase price over the fair value of the net assets acquired. The goodwill is being amortized for tax purposes over a 15-year period with the exception of the goodwill on the acquisition of the stock of a Pennsylvania dialysis company in August 2004 as described below. Certain of the acquisition transactions were of minority interests held by medical directors of certain of our dialysis facilities.
In August, 2004, the company acquired a Pennsylvania dialysis company resulting in $1,358,000 of goodwill, the excess of the net purchase price over the estimated fair value of net assets acquired, including a valuation of an eight year non-competition agreement that will be amortized over the life of the agreement. The goodwill is not amortizable for tax purposes, since the transaction was a stock acquisition.
F-26
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 9—ACQUISITIONS—Continued
During the first quarter of 2006, the company acquired a Virginia dialysis center and a Maryland company with two dialysis centers. These transactions resulted in approximately $326,000 of goodwill amortizable over 15 years for tax purposes. In December, 2006, the company acquired the remaining 60% interest in its 40% owned Toledo, Ohio dialysis facility pursuant to a put option valued at $3,200,000 resulting in goodwill of approximately $2,707,000 for which the company has determined there is no impairment. See Note 14.
NOTE 10—LOAN TRANSACTIONS
The company has and may continue to provide funds in excess of capital contributions to meet working capital requirements of its dialysis facility subsidiaries, usually until they become self-sufficient. The operating agreements for the subsidiaries provide for cash flow and other proceeds to first pay any such financing, exclusive of any tax payment distributions. See Note 5 and Note 12.
NOTE 11—QUARTERLY FINANCIAL INFORMATION (Unaudited)
The following summarizes certain quarterly operating data (in thousands except per share data):
Year Ended December 31, 2006 | ||||||||||||||||
March 31 | June 30 | Sept. 30 | Dec.31 | Total | ||||||||||||
| Net sales | $ | 13,111 | $ | 14,281 | $ | 16,504 | $ | 18,134 | $ | 62,030 | ||||||
| Gross profit | 5,129 | 5,497 | 6,464 | 7,422 | 24,512 | |||||||||||
| Net income | 519 | 595 | 818 | 1,121 | 3,049 | |||||||||||
| Earnings per shares: | ||||||||||||||||
| Basic | $ | .06 | $ | .06 | $ | .09 | $ | .12 | $ | .32 | ||||||
| Diluted | $ | .05 | $ | .06 | $ | .08 | $ | .12 | $ | .32 | ||||||
Year Ended December 31, 2005 | ||||||||||||||||
March 31 | June 30 | Sept. 30 | Dec.31 | Total | ||||||||||||
| Net Sales | $ | 10,484 | $ | 11,022 | $ | 11,373 | $ | 12,015 | $ | 44,894 | ||||||
| Gross profit | 3,941 | 4,297 | 4,194 | 4,483 | 16,915 | |||||||||||
| Net income | 324 | 444 | 537 | 595 | 1,900 | |||||||||||
| Earnings per shares: | ||||||||||||||||
| Basic | $ | .04 | $ | .05 | $ | .06 | $ | .06 | $ | .22 | ||||||
| Diluted | $ | .04 | $ | .05 | $ | .06 | $ | .06 | $ | .20 | ||||||
Since the computation of earnings per share is made independently for each quarter using the treasury stock method, the total of four quarters’ earnings do not necessarily equal earnings per share for the year.
F-27
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 12—SUPPLEMENTAL CASH FLOW INFORMATION
The following amounts represent (rounded to the nearest thousand) non-cash financing and investing activities and other cash flow information in addition to information disclosed in Note 1, Note 2, Note 3, Note 4, Note 5, Note 6, Note 10, and Note 15:
2006 | 2005 | 2004 | ||||||||
| Interest paid (see Note 2) | $ | 395,000 | $ | 273,000 | $ | 204,000 | ||||
| Income taxes (refunded) paid (see Note 3) | (675,000 | ) | 1,301,000 | 1,350,000 | ||||||
Options exercise bonus (191,238 shares 2004; 159,284 shares 2003) (see Note 6) | — | — | 120,000 | |||||||
Subsidiary minority member capital contributions financing (see Note 5 and Note 10) | — | 15,000 | 324,000 | |||||||
Subsidiary minority member distributions applied against financing (see Note 5 and Note 10) | 154,000 | 68,000 | 74,000 | |||||||
| Share payment (2006—87,500 options exercised; 27,205 shares paid; 2005—514,008 options exercised, 72,375 shares paid) for stock option exercises (see Note 6) | 351,000 | — | 321,000 | |||||||
| Payment on note receivable with 91,800 shares of common stock (see Note 6) | — | — | 521,000 | |||||||
| Increase in additional paid-in capital from exercise of non-qualified stock options (see Note 3 and Note 6) | 31,000 | — | 120,000 | |||||||
| Net share issuance in merger with former parent (Note 1, Note 3, Note 4 and Note 15) | — | 10,051,000 | — | |||||||
NOTE 13—STOCK SPLIT
The board of directors declared a two-for-one stock split with respect to the company’s 3,968,772 shares of outstanding common stock. The record date of the split was January 28, 2004; the distribution date was February 9, 2004; and the date Nasdaq reported the adjusted price of the common stock was February 10, 2004. The two-for-one stock split increased the outstanding shares of common stock at that time to 7,937,544 shares. The split also required adjustment in the outstanding stock options by doubling the number of shares obtainable upon exercise, and halving the exercise price of the options. See Note 1 and Note 6.
F-28
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 14—PRO FORMA FINANCIAL INFORMATION FORMER AFFILIATE
The following amounts (in thousands) represent certain pro forma consolidated operating data reflecting consolidation of the company’s Toledo, Ohio subsidiary as if this subsidiary had been 100% owned and consolidated effective January 1, 2004. This subsidiary was consolidated as a 40% owned subsidiary for financial reporting purposes effective August 1, 2006, due to the company taking control of the facility, which was previously accounted for by the equity method and not consolidated and was consolidated as a 100% owned subsidiary upon payment for the put option exercised on the 60% interest owned by the former medical director in December, 2006. See Note 1 and Note 9:
2006 | 2005 | 2004 | ||||||||
| Operating revenues | $ | 64,106,000 | $ | 47,804,000 | $ | 43,049,000 | ||||
| Gross profit | $ | 25,477,000 | $ | 18,399,000 | $ | 18,148,000 | ||||
| Net income | $ | 3,088,000 | $ | 2,078,000 | $ | 2,352,000 | ||||
| Earnings per share: | ||||||||||
| Basic | $ | .33 | $ | .24 | $ | .28 | ||||
| Diluted | $ | .32 | $ | .22 | $ | .27 | ||||
The following amounts (in thousands) represent certain pro forma consolidated balance sheet data as if the company’s Toledo, Ohio subsidiary had been consolidated effective December 31, 2005:
December 31, 2005 | ||||
| ASSETS | ||||
Current assets | $ | 19,349 | ||
Property and equipment, net | 13,908 | |||
Other assets | 9,062 | |||
| $ | 42,319 | |||
| LIABILITES AND STOCKHOLDERS’ EQUITY | ||||
Current liabilities | $ | 11,023 | ||
Long-term debt, less current portion | 3,935 | |||
Minority and other equity interests | 1,748 | |||
Stockholders’ equity | 25,613 | |||
| $ | 42,319 | |||
NOTE 15—ACQUISITION OF FORMER PARENT COMPANY
On June 2, 2005, the company and its former parent, Medicore, Inc., which owned approximately 56% of the company, entered into an Agreement and Plan of Merger for Medicore to merge into the company for consideration consisting of approximately 5,271,000 shares of the company’s common stock. On September 21, 2005, the shareholders of Medicore and the company approved the merger, the articles of merger were filed, and the merger was completed. Each Medicore shareholder received .68 shares of the company’s common stock for each share of Medicore common stock, and Medicore’s ownership in the company of approximately 4,821,000 of the company’s common stock was retired resulting in approximately 9,116,000 shares of the company outstanding after the merger. See Note 1, Note 3, Note 4 and Note 12.
F-29
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 15—ACQUISITION OF FORMER PARENT COMPANY—Continued
The following table summarizes the merger transaction:
| Assets acquired: | ||||
| Cash | $ | 2,736,500 | ||
| Other current assets | 384,874 | |||
| Fixed assets, net | 1,042,849 | |||
| Deferred tax asset | 3,602,587 | |||
| Other assets | 5,831 | |||
| Total assets acquired | 7,772,641 | |||
| Forgiveness of intercompany | ||||
| indebtedness to former parent | 5,206,136 | |||
| 12,978,777 | ||||
| Liabilities assumed: | ||||
| Employment agreement liability | 1,960,000 | |||
| Accounts payable and accrued liabilities | 967,786 | |||
| Total liabilities assumed | 2,927,786 | |||
| Net assets acquired | $ | 10,050,991 | ||
A deferred tax asset of approximately $3,300,000 resulted from benefits from net operating loss carryforwards of the company’s former parent that can be utilized to satisfy future income tax liabilities of the company. Pursuant to Section 382 of the Internal Revenue Code, utilization of the acquired net operating losses are limited to certain amounts annually, though the company anticipates using all acquired net operating loss carryforwards prior to their expiration date. See Note 1 Note 3, Note 4 and Note 12.
In conjunction with the merger, a payment of $1,960,000 due pursuant to the employment agreement buyout of the CEO of the former parent, who is Chairman of the Board of the company, was deferred and reflected as a current liability on the company’s consolidated balance sheet at December 31, 2005. Payment of this liability was made in January, 2006.
The merger simplified the corporate structure and enabled the ownership of the control interest in the company to be in the hands of the public shareholders. The merger provided the company with additional capital resources to continue to build its dialysis business.
F-30
DIALYSIS CORPORATION OF AMERICA AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2006
NOTE 15—ACQUISITION OF FORMER PARENT COMPANY—Continued
The results of operations of the company’s former parent are included in the company’s consolidated operating results effective with the merger, September 21, 2005. Pro forma results of operations if the merger had completed as of January 1, 2004 are as follows (in thousands except per share data):
Year Ended December 31, | |||||||
2005 | 2004 | ||||||
| Operating revenues | $ | 46,008 | $ | 41,768 | |||
| Net income | $ | 2,093 | $ | 2,572 | |||
| Earnings per share: | |||||||
Basic | $ | .23 | $ | .29 | |||
Diluted | $ | .22 | $ | .28 | |||
NOTE 16—TRANSACTIONS WITH VIRAGEN, INC.
The company’s former parent, Medicore, Inc., had a royalty agreement with Viragen, Inc., a former subsidiary of Medicore pursuant to which it was to receive a royalty on Viragen’s gross sales of interferon and related products. The agreement provides for aggregate royalty payments of $2.4 million to be paid based on the following percentages of Viragen sales: 5% of the first $7 million, 4% of the next $10 million, and 3% of the next $55 million. The effective date of the agreement was November 15, 1994, with royalty payments due quarterly, commencing March 31, 1995. A payment of approximately $108,000, earned under a previous royalty agreement, is due as the final payment under the existing royalty agreement.
In August, 2002, Medicore initiated a legal action against Viragen for breach of the royalty agreement and for an accounting of sales pursuant to the royalty agreement. In July, 2003, Medicore reached an agreement with Viragen pursuant to mediation proceedings following its obtaining a partial summary judgment against Viragen in March, 2003, for amounts owed to it under the royalty agreement. Viragen remitted $30,000 on August 1, 2003, August 1, 2004 and August 1, 2005, with annual interest at 5% on the August, 2004 and 2005 payments. Viragen also agreed to commence remitting the quarterly royalty payments due under the royalty agreement. Pursuant to the company’s merger with its former parent, royalties are now payable to the company. See Note 1, Note 3, Note 4, Note 12 and Note 15.
NOTE 17—SUBSEQUENT EVENTS
Pursuant to a call option which it exercised on January 11, 2007, a subsidiary of the company is acquiring the assets of a Georgia dialysis facility that it has been managing pursuant to a management services agreement. The company will have an 80% interest in the facility to be operated through its subsidiary with the present owner to have a 20% interest. The company has determined that there will be no impairment of the goodwill that will result from this transaction. See Note 1 and Note 7.
F-31
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To The Board of Directors and Shareholders of
Dialysis Corporation of America
Our report on our audit of the basic consolidated financial statements of Dialysis Corporation of America and subsidiaries appears on page F-2. That audit was conducted for the purpose of forming an opinion on the basic financial statements taken as a whole. The supplemental schedule II is presented for purposes of complying with the Securities and Exchange Commission’s Rules and Regulations under the Securities Exchange Act of 1934 and is not otherwise a required part of the basic consolidated financial statements. Such information has been subjected to the auditing procedures applied in the audit of the basic consolidated financial statements, and in our opinion, is fairly stated in all material respects in relation to the basic consolidated financial statements taken as a whole.
MOORE STEPHENS, P.C. Certified Public Accountants | ||
| | | |
Cranford, New Jersey February 23, 2007 | ||
F-32
Schedule II - Valuation and Qualifying Accounts
Dialysis Corporation of America, Inc. and Subsidiaries
December 31, 2006
COL. A | COL. B | COL. C | COL. D | COL. E | ||||||||||||
Classification | Balance at Beginning Of Period | Additions (Deductions) Charged (Credited) to Cost and Expenses | Additions Charged to Other Accounts Describe | Other Changes Add (Deduct) Describe | Balance at End of Period | |||||||||||
| YEAR ENDED DECEMBER 31, 2006: | ||||||||||||||||
| Reserves and allowances deducted | ||||||||||||||||
| from asset accounts: | ||||||||||||||||
| Allowance for uncollectible accounts | $ | 1,886,000 | $ | 1,199,000 | $ | (573,000 | )(1) | $ | 2,512,000 | |||||||
| Reserve for inventory obsolescence | 77,000 | 1,000 | 78,000 | |||||||||||||
| $ | 1,963,000 | $ | 1,200,000 | $ | (573,000 | ) | $ | 2,590,000 | ||||||||
| YEAR ENDED DECEMBER 31, 2005: | ||||||||||||||||
| Reserves and allowances deducted | ||||||||||||||||
| from asset accounts: | ||||||||||||||||
| Allowance for uncollectible accounts | $ | 1,636,000 | $ | 571,000 | $ | (321,000 | )(1) | $ | 1,886,000 | |||||||
| Reserve for inventory obsolescence | — | — | 91,000 | (2) | 77,000 | |||||||||||
| (14,000 | )(3) | |||||||||||||||
| $ | 1,636,000 | $ | 571,000 | $ | (244,000 | ) | $ | 1,963,000 | ||||||||
| YEAR ENDED DECEMBER 31, 2004: | ||||||||||||||||
| Reserves and allowances deducted | ||||||||||||||||
| from asset accounts: | ||||||||||||||||
| Allowance for uncollectible accounts | $ | 785,000 | $ | 1,198,000 | $ | (347,000 | )(1) | $ | 1,636,000 | |||||||
| Valuation allowance for deferred tax asset | 52,000 | (52,000 | ) | — | — | |||||||||||
| $ | 837,000 | $ | 1,146,000 | $ | (347,000 | ) | $ | 1,636,000 | ||||||||
| (1) | Uncollectible accounts written off, net of recoveries. |
| (2) | Acquisition of former parent company. |
| (3) | Net write-offs against inventory reserves. |
F-33
Exhibit Index
DIALYSIS CORPORATION OF AMERICA
Annual Report on Form 10-K for the Fiscal Year Ended December 31, 2006
| 21 | Subsidiaries of the Company |
| 23.1 | Consent of Moore Stephens, P.C. |
| 31.1 | Certification of Chief Executive Officer Pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934 |
| 31.2 | Certification of Chief Financial Officer Pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934 |
| 32.1 | Certification of Chief Executive Officer and Chief Financial Officer Pursuant to Rule 13a-14(b) of the Securities Exchange Act of 1934 and 18 U.S.C. Section 1350 |