Use these links to rapidly review the document
TABLE OF CONTENTS
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
| | |
| (Mark one) | | |
ý |
|
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(D) OF THE SECURITIES
EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2014 |
or |
o |
|
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(D) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission File Number 000-15006
CELLDEX THERAPEUTICS, INC.
(Exact name of registrant as specified in its charter)
| | |
| Delaware | | 13-3191702 |
(State or other jurisdiction of
incorporation or organization) | | (I.R.S. Employer
Identification No.) |
Perryville III Building, 53 Frontage Road, Suite 220, Hampton, New Jersey 08827
(Address of principal executive offices) (Zip Code)
Registrant's telephone number, including area code:(908) 200-7500
Securities registered pursuant to Section 12(b) of the Act:
| | |
| Title of Class: | | Name of Each Exchange on Which Registered: |
|---|
| Common Stock, par value $.001 | | NASDAQ Global Market |
Securities registered pursuant to Section 12(g) of the Act:None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ý No o
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes o No ý
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ý No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ý No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this Chapter) is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ý
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See definitions of "large accelerated filer," "accelerated filer," and "smaller reporting company" in Rule 12b-2 of the Exchange Act. (Check one):
| | | | | | |
| Large accelerated filerý | | Accelerated filero | | Non-accelerated filero
(Do not check if a
smaller reporting company) | | Smaller Reporting Companyo |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes o No ý
The aggregate market value of the registrant's common stock held by non-affiliates as of June 30, 2014 was $1.5 billion. Exclusion of shares held by any person should not be construed to indicate that such person possesses the power, direct or indirect, to direct or cause the actions of the management or policies of the registrant, or that such person is controlled by or under common control with the registrant.
The number of shares of common stock outstanding at February 17, 2015 was 89,608,606 shares.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the definitive Proxy Statement for our 2015 Annual Meeting of Stockholders are incorporated by reference into Part III of this Report.
Table of Contents
CELLDEX THERAPEUTICS, INC.
ANNUAL REPORT ON FORM 10-K
YEAR ENDED DECEMBER 31, 2014
TABLE OF CONTENTS
| | | | | | |
| |
| | Page | |
|---|
Part I | | | | | | |
Item 1. | | Business | | | 1 | |
Item 1A. | | Risk Factors | | | 22 | |
Item 1B. | | Unresolved Staff Comments | | | 42 | |
Item 2. | | Properties | | | 43 | |
Item 3. | | Legal Proceedings | | | 43 | |
Item 4. | | Mine Safety Disclosures | | | 43 | |
Part II | | | | | | |
Item 5. | | Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | | | 44 | |
Item 6. | | Selected Financial Data | | | 45 | |
Item 7. | | Management's Discussion and Analysis of Financial Condition and Results of Operations | | | 47 | |
Item 7A. | | Quantitative and Qualitative Disclosures About Market Risk | | | 66 | |
Item 8. | | Financial Statements and Supplementary Data | | | 67 | |
Item 9. | | Changes in and Disagreements With Accountants on Accounting and Financial Disclosure | | | 95 | |
Item 9A. | | Controls and Procedures | | | 95 | |
Item 9B. | | Other Information | | | 96 | |
Part III | | | | | | |
Item 10. | | Directors, Executive Officers and Corporate Governance | | | 96 | |
Item 11. | | Executive Compensation | | | 96 | |
Item 12. | | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | | | 96 | |
Item 13. | | Certain Relationships and Related Transactions, and Director Independence | | | 96 | |
Item 14. | | Principal Accountant Fees and Services | | | 97 | |
Part IV | | | | | | |
Item 15. | | Exhibits, Financial Statement Schedules | | | 98 | |
Signatures | | | 103 | |
i
Table of Contents
Safe Harbor Statement under the Private Securities Litigation Reform Act of 1995: This Annual Report on Form 10-K contains forward-looking statements made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 under Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. Forward-looking statements include statements with respect to our beliefs, plans, objectives, goals, expectations, anticipations, assumptions, estimates, intentions and future performance, and involve known and unknown risks, uncertainties and other factors, which may be beyond our control, and which may cause our actual results, performance or achievements to be materially different from future results, performance or achievements expressed or implied by such forward-looking statements. All statements other than statements of historical fact are statements that could be forward-looking statements. You can identify these forward-looking statements through our use of words such as "may," "will," "can," "anticipate," "assume," "should," "indicate," "would," "believe," "contemplate," "expect," "seek," "estimate," "continue," "plan," "point to," "project," "predict," "could," "intend," "target," "potential" and other similar words and expressions of the future.
There are a number of important factors that could cause the actual results to differ materially from those expressed in any forward-looking statement made by us. These factors include, but are not limited to:
- •
- our ability to successfully complete research and further development, including animal, preclinical and clinical studies, and, if we obtain regulatory approval, commercialization of rindopepimut (also referred to as Rintega® and CDX-110), glembatumumab vedotin (also referred to as CDX-011), and other drug candidates and the growth of the markets for those drug candidates;
- •
- our ability to raise sufficient capital to fund our clinical studies and to meet our long-term liquidity needs, on terms acceptable to us, or at all. If we are unable to raise the funds necessary to meet our long-term liquidity needs, we may have to delay or discontinue the development of one or more programs, discontinue or delay on-going or anticipated clinical trials, license out programs earlier than expected, raise funds at significant discount or on other unfavorable terms, if at all, or sell all or part of our business;
- •
- our ability to manage multiple clinical trials for a variety of drug candidates at different stages of development, including ACT IV and ReACT for rindopepimut and METRIC for glembatumumab vedotin;
- •
- the cost, timing, scope and results of ongoing safety and efficacy trials of rindopepimut, glembatumumab vedotin, and other preclinical and clinical testing;
- •
- our ability to fund and complete the development and, if we obtain regulatory approval, to commercialize rindopepimut in North America and Europe ourselves;
- •
- the availability, cost, delivery and quality of clinical and commercial grade materials produced by our own manufacturing facility or supplied by contract manufacturers, suppliers and partners, who may be the sole source of supply;
- •
- the timing, cost and uncertainty of obtaining regulatory approvals for our drug candidates;
- •
- our ability to develop and commercialize products before competitors that are superior to the alternatives developed by such competitors;
- •
- our ability to negotiate strategic partnerships, where appropriate, for our programs, which may include, rindopepimut outside of North America and Europe, glembatumumab vedotin and varlilumab (also referred to as CDX-1127);
ii
Table of Contents
- •
- our ability to develop technological capabilities, including identification of novel and clinically important targets, exploiting our existing technology platforms to develop new product candidates and expand our focus to broader markets for our existing targeted immunotherapeutics;
- •
- our ability to adapt our proprietary antibody-targeted technology, or APC Targeting Technology™, to develop new, safe and effective therapeutics for oncology and infectious disease indications;
- •
- the availability, cost, delivery and quality of clinical management services provided by our clinical research organization partners;
- •
- our ability to protect our intellectual property rights, including the ability to successfully defend patent oppositions filed against a European patent related to technology we use in varlilumab, and our ability to avoid intellectual property litigation, which can be costly and divert management time and attention; and
- •
- the factors listed under "Risk Factors" in this Annual Report on Form 10-K.
All forward-looking statements are expressly qualified in their entirety by this cautionary notice. You are cautioned not to place undue reliance on any forward-looking statements, which speak only as of the date of this report or the date of the document incorporated by reference into this report. We have no obligation, and expressly disclaim any obligation, to update, revise or correct any of the forward-looking statements, whether as a result of new information, future events or otherwise. We have expressed our expectations, beliefs and projections in good faith and we believe they have a reasonable basis. However, we cannot assure you that our expectations, beliefs or projections will result or be achieved or accomplished.
iii
Table of Contents
PART I
Item 1. BUSINESS
Overview
Celldex Therapeutics, Inc., which we refer to as "Celldex," "we," "us," "our" or the "Company," is a biopharmaceutical company focused on the development and commercialization of several immunotherapy technologies for the treatment of cancer and other difficult-to-treat diseases. Our drug candidates are derived from a broad set of complementary technologies which have the ability to utilize the human immune system and enable the creation of therapeutic agents. We are using these technologies to develop targeted immunotherapeutics comprised of antibodies, adjuvants and monotherapies and antibody-drug conjugates that treat cancers and other diseases that induce undesirable activity by the body's own proteins or cells.
Our lead drug candidates include rindopepimut (also referred to as Rintega® and CDX-110) and glembatumumab vedotin (also referred to as CDX-011). Rindopepimut is a targeted immunotherapeutic in a pivotal Phase 3 study for the treatment of front-line glioblastoma and a Phase 2 study for the treatment of recurrent glioblastoma. Glembatumumab vedotin is a targeted antibody-drug conjugate in a randomized, Phase 2b study for the treatment of triple negative breast cancer and a Phase 2 study for the treatment of metastatic melanoma. We also have a number of earlier stage drug candidates in clinical development, including varlilumab (also referred to as CDX-1127), a fully human therapeutic monoclonal antibody for cancer indications, CDX-1401, a targeted immunotherapeutic aimed at antigen presenting cells, or APC, for cancer indications and CDX-301, an immune cell mobilizing agent and dendritic cell growth factor. Our drug candidates address market opportunities for which we believe current therapies are inadequate or non-existent.
We are building a fully integrated, commercial-stage biopharmaceutical company that develops important therapies for patients with unmet medical needs. Our program assets provide us with the strategic options to either retain full economic rights to our innovative therapies or seek favorable economic terms through advantageous commercial partnerships. This approach allows us to maximize the overall value of our technology and product portfolio while best ensuring the expeditious development of each individual product.
The following table includes the programs that we currently believe are significant to our business:
| | | | | | |
Product (generic) | | Indication/Field | | Partner | | Status |
|---|
| CLINICAL | | | | | | |
Rindopepimut | | Front-line glioblastoma | | — | | Phase 3 |
Glembatumumab vedotin | | Metastatic breast cancer | | — | | Phase 2b |
Rindopepimut | | Recurrent glioblastoma | | — | | Phase 2 |
Glembatumumab vedotin | | Metastatic melanoma | | — | | Phase 2 |
Varlilumab | | Lymphoma/leukemia and solid tumors | | — | | Phase 1 |
Varlilumab | | Multiple solid tumors | | — | | Phase 1/2 |
CDX-1401 | | Multiple solid tumors | | — | | Phase 1 |
CDX-301 | | Allogeneic Hematopoietic Stem Cell Transplantation | | — | | Phase 1 |
| PRECLINICAL | | | | | | |
CDX-014 | | Ovarian and renal cancer | | — | | Preclinical |
Our future success depends upon many factors, including our ability, and that of any licensees and collaborators that we may have, to successfully develop, obtain regulatory approval for and commercialize our drug candidates. We have had no commercial revenues from sales of our drug candidates and we have had a history of operating losses. It is possible that we may not be able to successfully develop, obtain regulatory approval for, or commercialize, our drug candidates, and we are
1
Table of Contents
subject to a number of risks that you should be aware of before investing in us. These risks are described more fully in "Item 1A. Risk Factors."
We are incorporated in Delaware. Our website is located athttp://www.celldex.com. On our website, investors can obtain, free of charge, a copy of our Annual Report on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and other reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act of 1934, as amended, as soon as reasonably practicable after we file such material electronically with, or furnish it to, the Securities and Exchange Commission, or SEC. None of the information posted on our website is incorporated by reference into this Annual Report.
Clinical Development Programs
Rindopepimut
Rindopepimut is an immunotherapeutic that targets the tumor-specific molecule epidermal growth factor receptor variant III, or EGFRvIII. EGFRvIII is a mutated form of the epidermal growth factor receptor, or EGFR, that is only expressed in cancer cells and not in normal tissue and can directly contribute to cancer cell growth. EGFRvIII is expressed in approximately 30% of glioblastoma multiforme, or GBM, tumors, the most common and aggressive form of brain cancer. Rindopepimut is composed of the EGFRvIII peptide linked to a carrier protein called Keyhole Limpet Hemocyanin, or KLH, and administered together with the adjuvant GM-CSF. The Food and Drug Administration, or FDA, and the European Medicines Agency, or EMA, have both granted orphan drug designation for rindopepimut for the treatment of EGFRvIII expressing GBM. The FDA has also granted Fast Track designation. In February 2015, the FDA granted rindopepimut Breakthrough Therapy Designation for the treatment of adult patients with EGFRvIII-positive glioblastoma.
The Phase 2a study of rindopepimut referred to as ACTIVATE was led by collaborating investigators at the Brain Center at Duke Comprehensive Cancer Center in Durham, North Carolina and at M.D. Anderson Cancer Center in Houston, Texas and enrolled 18 evaluable GBM patients. An extension of the Phase 2a study referred to as ACT II evaluated 22 additional GBM patients treated in combination with the current standard of care, maintenance temozolomide, or TMZ, at the same two institutions.
The Phase 2b study of rindopepimut referred to as ACT III combined rindopepimut with standard of care, TMZ, in patients with newly diagnosed GBM. The ACT III study provided for a multi-center, non-randomized dataset for rindopepimut in 65 patients at over 30 sites throughout the United States.
In November 2013, we announced the four- and five-year survival data from the 105 patients enrolled in the three Phase 2 rindopepimut clinical studies (ACTIVATE, ACT II and ACT III) in EGFRvIII-positive GBM. Across these three Phase 2 studies of rindopepimut, survival data remains consistent and suggests a continuing survival benefit in comparison to independent control datasets (see chart below) at the median and at all other time points evaluated.
Phase 2 Frontline Long-term Overall Survival Assessments
| | | | | | | | | | | | | | | | |
| | Median, Years
(95% CI) | | 2-year
rate | | 3-year
rate | | 4-year
rate | | 5-year
rate | |
|---|
Phase 2 rindopepimut studies (n=105) | | | 2.1 (1.8, 2.4 | ) | | 51 | % | | 30 | % | | 18 | % | | 14 | % |
Matched historical control (n=17)(1) | | | 1.3 (0.9, 1.7 | ) | | 6 | % | | 6 | % | | 0 | % | | 0 | % |
- (1)
- Patients treated at M.D. Anderson contemporaneously to ACTIVATE, matched for major eligibility requirements, including EGFRvIII-positive GBM, gross total resection and no disease progression through chemoradiation treatment.
2
Table of Contents
The pooled overall long-term survival results continue to be consistent with the ACT III Phase 2 study (18% for 4-years and 14% for 5-years).
In December 2011, we initiated ACT IV, a pivotal, randomized, double-blind, controlled Phase 3 study of rindopepimut in patients with surgically resected, EGFRvIII-positive GBM. Patients were randomized after the completion of surgery and standard chemoradiation treatment. The treatment regimen included a rindopepimut priming phase post-radiation followed by an adjuvant TMZ phase and a rindopepimut maintenance therapy phase. Patients are treated until disease progression or intolerance to therapy. The primary objective of the study is to determine whether rindopepimut plus adjuvant GM-CSF improves the overall survival of patients with newly diagnosed EGFRvIII-positive GBM with minimal residual disease post resection and traditional chemo-radiation when compared to treatment with TMZ and a control injection of KLH. KLH is a component of rindopepimut and was selected due to its ability to generate a similar injection site reaction to that observed with rindopepimut.
In December 2014, ACT IV completed enrollment. In total, over 4,800 GBM patients were screened for EGFRvIII status from more than 200 clinical trial sites across 22 countries and, consistent with prior studies, 30% were positive for the EGFRvIII mutation. The study enrolled 745 patients to reach the required 374 patients with minimal residual disease (assessed by central review) needed for analysis of the primary overall survival endpoint. All patients, including patients with disease that exceed this threshold, will be included in a secondary analysis of overall survival as well as analyses of progression-free survival, safety and tolerability, and quality of life. The timing of the overall survival primary endpoint data is event-driven. Interim analyses will be conducted by an independent Data Safety and Monitoring Board at 50% and 75% of events (deaths). The first interim analysis is expected in mid-2015. The second interim analysis is currently expected in late 2015 or early 2016 and the final data is expected by the end of 2016; although our expectations regarding the timing for the second interim analysis and final data read out may change based on event rates.
In December 2011, we also initiated ReACT, a Phase 2 study of rindopepimut in combination with Avastin® in patients with recurrent EGFRvIII-positive GBM. This study completed enrollment in 2014 and includes 3 groups. Group 1 consists of 72 patients who had not previously received Avastin and were randomized to receive either rindopepimut and Avastin or a control injection of KLH and Avastin in a blinded fashion. Group 2 includes 25 patients who are refractory to Avastin having received Avastin in either the frontline or recurrent setting with subsequent progression and who received rindopepimut plus Avastin in a single treatment arm. In August 2013, we announced the addition of an expansion cohort of up to 75 patients, called Group 2C, to better characterize the potential activity of rindopepimut in this refractory patient population. This decision was based on early evidence of anti-tumor activity, including stable disease, tumor shrinkage and investigator-reported response. In total, Group 2C enrolled 28 patients. The primary endpoint is six month progression-free survival rate (PFS-6) for groups 1 and 2 and objective response rate (ORR) for group 2C. Other study endpoints include PFS-6, ORR, PFS, overall survival, or OS and safety and tolerability.
In November 2014, we reported the following interim data from the ReACT study. Rindopepimut plus Avastin was very well tolerated (dosing up to 26+ months) and the results demonstrated clear signs of clinical activity in advanced patient populations, including evidence of anti-tumor activity (tumor shrinkage, objective response and stable disease). Strong immune response correlated with improved outcome. In Avastin-naïve patients treated with both rindopepimut and Avastin, a statistically significant survival benefit was seen compared to the control patients.
Group 1 Interim Data
- •
- PFS-6: PFS-6 by investigator read was 27% for patients treated with rindopepimut compared to 11% for control patients (p=0.048)
3
Table of Contents
- •
- Survival: The OS demonstrated a statistically significant benefit (p=0.0208) with a hazard ratio of 0.47 (0.25, 0.91) in favor of the rindopepimut treated patients. Median OS was 12.0 months for patients treated with rindopepimut compared to 8.8 months for control patients.
- •
- Response Rate: 7 out of 29 patients (24%) evaluable for response on the rindopepimut arm experienced a confirmed objective response versus 5 out of 30 patients (17%) evaluable for response on the control arm. Assessments of response were conducted by study investigators according to RANO criteria.
- •
- Other: All subgroup analyses, including performance status, steroid use and recent resection, show a hazard ratio in favor of rindopepimut treatment.
Group 2/2C Interim Data
- •
- Survival: Median OS was 5.1 months (95% CI 3.2, 6.5) for these heavily pretreated, refractory EGFRvIII-positive patients. 46% of patients in Group 2/2C were alive at 6 months.
- •
- Response Rate: Based on investigator assessment, two patients experienced complete response, of which one was unconfirmed, and two patients experienced partial response, of which one was unconfirmed, in Group 2. Two of these four patients did not meet the protocol defined definition of refractory in Group 2, the only two such patients enrolled. No additional objective responses were observed in Group 2C and the study did not meet the criteria (defined as two responses in the first 23 patients enrolled in Group 2C) for continued enrollment. Ten patients with measurable disease experienced objective tumor shrinkage across Group 2/2C.
Final data is anticipated by mid-year 2015 and we intend to present this data at a peer-reviewed medical meeting in this same time frame.
Glembatumumab Vedotin
Glembatumumab vedotin is an antibody-drug conjugate, or ADC, that consists of a fully-human monoclonal antibody, CR011, linked to a potent cell-killing drug, monomethyl-auristatin E, or MMAE. The CR011 antibody specifically targets glycoprotein NMB, referred to as gpNMB, that is over-expressed in a variety of cancers including breast cancer and melanoma. The ADC technology, comprised of MMAE and a stable linker system for attaching it to CR011, was licensed from Seattle Genetics, Inc. and is the same as that used in the marketed product Adcetris®. The ADC is designed to be stable in the bloodstream. Following intravenous administration, glembatumumab vedotin targets and binds to gpNMB and upon internalization into the targeted cell, glembatumumab vedotin is designed to release MMAE from CR011 to produce a cell-killing effect. The FDA has granted Fast Track designation to glembatumumab vedotin for the treatment of advanced, refractory/resistant gpNMB-expressing breast cancer.
Treatment of Breast Cancer: The Phase 1/2 study of glembatumumab vedotin administered intravenously once every three weeks evaluated patients with locally advanced or metastatic breast cancer who had received prior therapy (median of seven prior regimens). The study began with a bridging phase to confirm the maximum tolerated dose, or MTD, and then expanded into a Phase 2 open-label, multi-center study. The study confirmed the safety of glembatumumab vedotin at the pre-defined maximum dose level (1.88 mg/kg) in 6 patients. An additional 28 patients were enrolled in an expanded Phase 2 cohort (for a total of 34 treated patients at 1.88 mg/kg, the Phase 2 dose) to evaluate the PFS rate at 12 weeks. The 1.88 mg/kg dose was well tolerated in this patient population with the most common adverse events of rash, alopecia, and fatigue. The primary activity endpoint, which called for at least 5 of 25 (20%) patients in the Phase 2 study portion to be progression-free at 12 weeks, was met as 9 of 26 (35%) evaluable patients were progression-free at 12 weeks.
For all patients treated at the maximum dose level, tumor shrinkage was seen in 62% (16/26) and median PFS was 9.1 weeks. A subset of 10 patients had "triple negative disease," a more aggressive
4
Table of Contents
breast cancer subtype that carries a high risk of relapse and reduced survival as well as limited therapeutic options due to lack of over-expression of HER2/neu, estrogen and progesterone receptors. In these patients, 78% (7/9) had some tumor shrinkage, 12-week PFS rate was 70% (7/10), and median PFS was 17.9 weeks. Tumor samples from a subset of patients across all dose groups were analyzed for gpNMB expression. The tumor samples from most patients showed evidence of stromal and/or tumor cell expression of gpNMB.
In December 2012, we announced final results from the EMERGE study, a randomized, multi-center Phase 2b study of glembatumumab vedotin in 122 patients with heavily pre-treated, advanced, gpNMB positive breast cancer. Patients were randomized (2:1) to receive either glembatumumab vedotin or single-agent Investigator's Choice, or IC, chemotherapy. Patients randomized to receive IC were allowed to cross over to receive glembatumumab vedotin following disease progression. Activity endpoints included response rate, PFS and OS. The final results, as shown below, suggested that glembatumumab vedotin induces significant response rates compared to currently available therapies in patient subsets with advanced, refractory breast cancers with gpNMB over-expression (expression in greater than or equal to 25% of tumor cells) and in patients with triple negative breast cancer. The OS and PFS of patients treated with glembatumumab vedotin was also observed to be greatest in patients with triple negative breast cancer who also over-express gpNMB and all patients with gpNMB over-expression.
EMERGE: Overall Response Rate and Disease Control Data
| | | | | | | | | | | | | |
| | gpNMB Over-Expression | | Triple Negative
and gpNMB
Over-Expression | |
|---|
| | glembatumumab
vedotin | | Investigator
Choice | | glembatumumab
vedotin | | Investigator
Choice | |
|---|
| | (n=25) | | (n=8) | | (n=12) | | (n=4) | |
|---|
Response | | | 32 | % | | 13 | % | | 33 | % | | 0 | % |
Disease Control Rate | | | 64 | % | | 38 | % | | 75 | % | | 25 | % |
Responses per RECIST 1.1; IC = Investigator's Choice; glembatumumab vedotin arm includes 15 patients who crossed over to receive glembatumumab vedotin treatment after progression on IC. Analysis of best response excludes patients who discontinued from study without evaluable post-baseline radiographic imaging (n=15 for glembatumumab vedotin arm; n=5 for IC arm).
EMERGE: Progression Free Survival (PFS) and Overall Survival (OS) Data
| | | | | | | | | | | | | |
| | gpNMB
Over-Expression | | Triple Negative
and gpNMB
Over-Expression | |
|---|
| | glembatumumab
vedotin | | Investigator
Choice | | glembatumumab
vedotin | | Investigator
Choice | |
|---|
Median PFS (months) | | | 2.7 | | | 1.5 | | | 3.0 | | | 1.5 | |
| | | p=0.14 | | | p=0.008 | |
Median OS (months) | | |
10.0 | | |
5.7 | | |
10.0 | | |
5.5 | |
| | | p=0.18 | | | p=0.003
| |
When cross over patients are removed, median OS in patients with gpNMB over-expression is 10.0 months for glembatumumab vedotin vs 5.2 months for IC (p=0.05) and median OS in triple negative patients with gpNMB over- expression is 10.0 months for glembatumumab vedotin vs 5.2 months for IC (p=0.009).
In December 2013, we initiated METRIC, a randomized, controlled Phase 2b study of glembatumumab vedotin in patients with triple negative breast cancer that over-express gpNMB.
5
Table of Contents
To-date, 95 sites are open to enrollment across the United States, Canada and Australia. The study was originally designed to obtain accelerated approval. Feedback from clinical investigators conducting the study indicated that the eligibility criteria for study entry were limiting their ability to enroll patients they felt were clinically appropriate on study. In addition, we had spoken to country-specific members of the European Medicines Agency, or EMA, and believed a significant opportunity existed to expand the study into the EU. Based on these factors, in the fourth quarter of 2014, we amended the METRIC study and expanded patient entry criteria to position it for full marketing approval with global regulators, including the EMA, and to support improved enrollment in the study. The primary endpoint of the study is PFS as PFS is an established endpoint for full approval registration studies in this patient population in both the US and the EU. The sample size (n=300) and the secondary endpoint of OS remained unchanged. We implemented these changes in parallel to regulatory discussions to maintain momentum at open clinical trial sites. Since implementation, both the FDA and central European regulatory authorities have reviewed the protocol design and we believe the METRIC study could support marketing approval in both the US and Europe dependent upon data review. Based on current projections, we believe enrollment will be completed in 2016.
Treatment of Metastatic Melanoma: The Phase 1/2 open-label, multi-center, dose escalation study evaluated the safety, tolerability and pharmacokinetics of glembatumumab vedotin in 117 patients with un-resectable Stage III or Stage IV melanoma who had failed no more than one prior line of cytotoxic therapy. The MTD was determined to be 1.88 mg/kg administered intravenously once every three weeks. The study achieved its primary activity objective with an ORR in the Phase 2 cohort of 15% (5/34). Median PFS was 3.9 months. Glembatumumab vedotin was generally well tolerated, with the most frequent treatment-related adverse events being rash, fatigue, hair loss, pruritus, diarrhea and neuropathy. In the subset of patients with tumor biopsies, high levels of tumor expression of gpNMB appeared to correlate with favorable outcome. In the seven patients whose tumors were found to express high amounts of gpNMB, and who were treated at the maximum tolerated doses across all dosing schedules, median PFS was 4.9 months. The development of rash, which may be associated with the presence of gpNMB in the skin also seemed to correlate with greater PFS.
In December 2014, we initiated a single arm, open-label Phase 2 study of glembatumumab vedotin in patients with unresectable Stage III or IV melanoma. The study is expected to include approximately 10 sites in the United States and will enroll approximately 60 patients. The primary objective is to evaluate the anticancer activity of glembatumumab vedotin in advanced melanoma as measured by the ORR. Secondary endpoints include analyses of PFS, duration of response, OS, retrospective investigation of whether the anticancer activity of glembatumumab vedotin is dependent upon the degree of gpNMB expression in tumor tissue and safety.
We have completed the assay optimization and validation for a Phase 2 study in squamous cell lung cancer and expect the study will commence in 2015. We have also entered into a Cooperative Research and Development Agreement, or CRADA, with the National Cancer Institute, or NCI, under which NCI will sponsor two studies of glembatumumab vedotin—one in uveal melanoma and one in pediatric osteosarcoma.
Varlilumab
Varlilumab is a human monoclonal antibody that targets CD27, a potentially important target for immunotherapy of various cancers. We have entered into license agreements with the University of Southampton, UK for intellectual property related to uses of anti-CD27 antibodies and with Medarex (now a subsidiary of the Bristol-Myers Squibb Company, or BMS) for access to the UltiMab technology to develop and commercialize human antibodies to CD27.
CD27 acts downstream from CD40 and may provide a novel way to regulate the immune responses. CD27 is a co-stimulatory molecule on T cells and is over-expressed in certain lymphomas and leukemias. Varlilumab is an agonist antibody designed to have two potential therapeutic
6
Table of Contents
mechanisms. Varlilumab has been shown to activate immune cells that can target and eliminate cancerous cells in tumor-bearing mice and to directly kill or inhibit the growth of CD27 expressing lymphomas and leukemiasin vitro andin vivo. Both mechanisms have been seen even at low doses in appropriate preclinical models.
We are conducting an open label Phase 1 study of varlilumab in patients with selected malignant solid tumors or hematologic cancers at multiple clinical sites in the United States. Initial dose escalation cohorts were conducted to determine an optimal dose for future study and, to date, no maximum tolerated dose has been reached. The lymphoid malignancies dose escalation arm has completed enrollment (n=24) and a new cohort has been added to include evaluation of T cell malignancies. An expansion cohort has also been added at 0.3mg/kg dosed once every three weeks in patients with Hodgkin Lymphoma (n=15). The solid tumor arm, which included patients with various solid tumors, completed dose escalation in 2013. Two expansion cohorts were subsequently added at 3 mg/kg dosed weekly in metastatic melanoma (n=16) and renal cell carcinoma (n=15) to better characterize clinical activity and further define the safety profile in preparation for combination studies.
We presented updated data from this Phase 1 study in November 2014. Varlilumab was very well tolerated and induced immunologic activity in patients that is consistent with both its mechanism of action and preclinical models. A total of 86 patients have been dosed in the study. 55 patients have been dosed in dose escalation cohorts (various solid and hematologic B-cell tumors) and 31 patients have been dosed in the expansion cohorts (melanoma and RCC) at 3 mg/kg. In both the solid tumor and hematologic dose-escalations, the pre-specified maximum dose level (10 mg/kg) was reached without identification of a maximum tolerated dose. The majority of adverse events (AE) related to treatment have been mild to moderate (Grade 1/2) in severity, with only three serious AEs related to treatment reported. No significant immune-mediated adverse events (colitis, hepatitis, etc.) typically associated with check-point blockade have been observed. Two patients experienced objective responses including a complete response in Hodgkin Lymphoma and a partial response in renal cell carcinoma. Thirteen patients experienced stable disease with a range of 3-30.7+ months to-date. Based on the results observed in hematologic malignancies, an expansion cohort has been added to enroll up to 15 patients with Hodgkin Lymphoma and an abbreviated dose escalation in T cell hematologic malignancies is ongoing.
In May 2014, we entered into a clinical trial collaboration with Bristol-Myers Squibb Company, or BMS, to evaluate the safety, tolerability and preliminary efficacy of varlilumab and Opdivo®, BMS's PD-1 immune checkpoint inhibitor, in a Phase 1/2 study. Under the terms of this clinical trial collaboration, BMS made a one-time payment to us of $5.0 million and the companies amended the terms of our existing license agreement with Medarex (a subsidiary of BMS) related to our CD27 program whereby certain future milestone payments were waived and future royalty rates were reduced that may have been due from us to Medarex. In return, BMS was granted a time-limited right of first negotiation if we wish to out-license varlilumab. The companies also agreed to work exclusively with each other to explore anti-PD-1 antagonist antibody and anti-CD27 agonist antibody combination regimens. The clinical trial collaboration provides that the companies will share development costs and that we will be responsible for conducting the Phase 1/2 study.
The Phase 1/2 study was initiated in January of 2015 and is being conducted in adult patients with advanced non-small cell lung cancer, metastatic melanoma, colorectal cancer, ovarian cancer, and head and neck squamous cell carcinoma. The Phase 1 dose-escalation portion of the study will assess the safety and tolerability of varlilumab at varying doses when administered with Opdivo. Following dose escalation, a Phase 2 portion of the study will include five disease specific cohorts. The primary objective of the Phase 2 study is overall response rate. Secondary objectives include pharmacokinetics assessments, determining the immunogenicity of varlilumab when given in combination with Opdivo and further assessing the anti-tumor activity of combination treatment.
7
Table of Contents
In May 2014, we also entered into a clinical trial collaboration with Oncothyreon Inc. to evaluate the safety, tolerability and preliminary efficacy of varlilumab and ONT-10, Oncothyreon's therapeutic vaccine targeting the tumor-associated antigen MUC1, in a Phase 1b study. Under the terms of the clinical trial collaboration, the Phase 1b trial will be conducted and funded by Oncothyreon. Both companies will jointly own the data from the trial and will make any plans for potential future development of the combination therapy together. The Phase 1b study was initiated in November 2014 and is being conducted in up to 42 patients with advanced breast or ovarian cancer. The primary objective of the trial is to determine the safety and tolerability of the combined therapy. Additional objectives include evaluations of the impact of combination treatment on MUC1-specific humoral and cellular immune responses, T-cell activation markers and levels of regulatory T-cells, and anti-tumor effects.
Multiple efforts are underway to finalize designs and plans for additional Phase 2 combination studies of varlilumab, including but not limited to: a Phase 1/2 study of varlilumab and ipilumumab in patients with metastatic melanoma (plus CDX-1401 in NY-ESO positive patients); a Phase 1/2 of varlilumab plus sunitinib in renal cell carcinoma; and a Phase 1/2 study of varlilumab plus a mek pathway agent (followed sequentially by a checkpoint inhibitor) for patients with B-raf mutated metastatic melanoma. In addition to our sponsored studies and clinical trial collaborations, we anticipate that varlilumab's potential activity will also be explored in investigator sponsored studies at various academic institutions.
CDX-1401
CDX-1401, developed from our APC Targeting Technology, is a fusion protein consisting of a fully human monoclonal antibody with specificity for the dendritic cell receptor, DEC-205, linked to the NY-ESO-1 tumor antigen. In humans, NY-ESO-1 has been detected in 20% - 30% of all melanoma, lung, esophageal, liver, gastric, prostate, ovarian and bladder cancers, thus representing a broad opportunity. This product is intended to selectively deliver the NY-ESO-1 antigen to dendritic cells for generating robust immune responses against cancer cells expressing NY- ESO-1. We are developing CDX-1401 for the treatment of malignant melanoma and a variety of solid tumors which express the proprietary cancer antigen NY-ESO-1, which we licensed from the Ludwig Institute for Cancer Research in 2006. Preclinical studies have shown that CDX-1401 is effective for activation of human T cell responses against NY-ESO-1.
We have completed a Phase 1 study of CDX-1401 which assessed the safety, immunogenicity and clinical activity of escalating doses of CDX-1401 with TLR agonists (resiquimod and/or Poly ICLC) in 45 patients with advanced malignancies refractory to all available therapies. 60% of patients had confirmed NY-ESO expression in archived tumor sample. Thirteen patients maintained stable disease for up to 13.4 months with a median of 6.7 months. Treatment was well-tolerated and there were no dose limiting toxicities. Humoral responses were elicited in both NY-ESO-1 positive and negative patients. NY-ESO-1-specific T cell responses were absent or low at baseline, but increased post-vaccination in 53% of evaluable patients, including both CD4 and/or CD8 T cell responses. Robust immune responses were observed with CDX-1401 with resiquimod and Poly ICLC alone and in combination. Long-term patient follow up suggested that treatment with CDX-1401 may predispose patients to better outcomes on subsequent therapy with checkpoint inhibitors. Of the 45 patients in the Phase 1 study, eight went on to receive subsequent therapy of either ipilimumab or an investigational checkpoint inhibitor and six of these patients had objective tumor regression. Six patients with melanoma received ipilimumab within three months of treatment with CDX-1401 and four (67%) had objective tumor responses, including one complete response, which compares favorably to the overall response rate of 11% previously reported in metastatic melanoma patients treated with single-agent ipilimumab. In addition, two patients with non-small cell lung cancer received an investigational checkpoint blockade within two months of completing treatment with CDX-1401 and both achieved partial responses.
8
Table of Contents
The Phase 1 study identified a well-tolerated and immunogenic regimen to take forward into future studies. A Phase 2 study of CDX-1401 in combination with CDX-301 in metastatic melanoma is being conducted by the Cancer Immunotherapy Trials Network under a CRADA with the Cancer Therapy Evaluation Program of the NCI and is ongoing. In addition to our sponsored studies, we anticipate that CDX-1401's potential activity will also be explored in investigator sponsored studies at various academic institutions.
CDX-301
CDX-301 is a FMS-like tyrosine kinase 3 ligand, or Flt3L, stem cell mobilizer and dendritic cell growth factor. We licensed CDX-301 from Amgen Inc. in March 2009. CDX-301 is a potent hematopoietic cytokine that stimulates the expansion and differentiation of hematopoietic progenitor and stem cells. CDX-301 has demonstrated a unique capacity to increase the number of circulating dendritic cells in both laboratory and clinical studies. In addition, CDX-301 has shown impressive results in models of cancer, infectious diseases and inflammatory/autoimmune diseases. We believe CDX-301 may hold significant opportunity for synergistic development in combination with other proprietary molecules in our portfolio.
In February 2013, we announced final results from our dose-escalating Phase 1 study of CDX-301 in 30 healthy subjects in collaboration with Rockefeller University. The Phase 1 study evaluated seven different dosing regimens of CDX-301 to determine the appropriate dose for further development based on safety, tolerability, and biological activity. The data from the study were consistent with previous clinical experience and demonstrated that CDX-301 was well-tolerated and can effectively mobilize hematopoietic stem cell populations in healthy volunteers. In December 2013, we announced data from a preclinical combination study of CDX-301and Mozobil® (Plerixafor injection, formerly AMD3100) demonstrating that the combination of these agents significantly increases hematopoietic stem cell mobilization in mice. The data demonstrate a novel potent cell mobilization regimen combining CDX-301 and Mozobil®, which may have significant potential for use in autologous and allogeneic hematopoietic stem cell transplantation. Based on the safety profile and the clinical and preclinical data to date, we initiated a pilot clinical study of CDX-301 for the mobilization and transplantation of allogeneic hematopoietic stem cells in patients with hematological malignancies undergoing hematopoietic stem cell transplantation. The study will explore the utility of CDX-301 alone and in combination with Mozobil®. In addition to our sponsored studies and clinical trial collaborations, we anticipate that CDX-301's potential activity will also be explored in investigator sponsored studies at various academic institutions.
Preclinical Programs
CDX-014
CDX-014 is a fully-human monoclonal ADC that targets T-cell immunoglobulin and mucin domain 1, or TIM-1, a molecule that is upregulated in several cancers, including renal cell and ovarian carcinomas. TIM-1 is associated with kidney injury and the shedding of its ectodomain is a predictive biomarker for tumor progression. TIM-1 has very restricted expression in healthy tissues, making it a promising target for antibody mediated therapy. The TIM-1 antibody is linked to MMAE using Seattle Genetics' proprietary technology. The ADC is designed to be stable in the bloodstream, but to release MMAE upon internalization into TIM-1-expressing tumor cells, resulting in a targeted cell-killing effect. CDX-014 has shown potent activity in preclinical models of ovarian and renal cancer. We expect to complete manufacturing and IND-enabling studies by the end of 2015 to support the initiation of Phase 1 clinical studies in renal cell carcinoma and potentially other TIM-1 expressing tumors in 2016.
9
Table of Contents
Development Strategy
Immunotherapy Platform:
We believe there is untapped potential in immunotherapy that can be captured through the right combination and/or sequence of therapeutic agents. Immunotherapy approaches have encountered difficulties when following standard drug development. The mechanisms of action are complex, activity is generally not dependent on highest tolerated dose and patient response is highly variable. Our understanding of the immune system, cancer's effect on immune mediated mechanisms, and the impact of conventional therapies on the immune system provides a new rationale for combining therapies that may lead to significant clinical benefit for patients with cancer.
Our intent is to leverage this knowledge and the availability of good, tested products that may not have optimal clinical activity as a monotherapy, but which we believe may be very effective in combination approaches. Our goal is to design and develop targeted products that maximize the efficacy of immunotherapy regimens through combinations of therapeutic agents in significant and growing markets. We establish governmental and corporate alliances to fund development when appropriate and intend to commercialize our products either through our own direct selling efforts or, for products which we cannot develop ourselves through to commercialization, through corporate partners. This approach allows us to maximize the overall value of our technology and product portfolios while best ensuring the expeditious development of each individual product.
Factors that may significantly harm our commercial success, and ultimately the market price of our common stock, include but are not limited to, announcements of technological innovations or new commercial products by our competitors, disclosure of unsuccessful results of clinical testing or regulatory proceedings and governmental approvals, adverse developments in patent or other proprietary rights, public concern about the safety of products developed by us and general economic and market conditions. See "Item 1A. Risk Factors."
Partnerships
We plan to commercialize our lead drug candidate rindopepimut ourselves in North America and Europe. We may enter into co-development and commercialization partnerships for any of our programs where appropriate, including rindopepimut for commercialization outside of North America and Europe, glembatumumab vedotin and varlilumab. In the past, we have entered into collaborative partnership agreements with pharmaceutical and other companies and organizations that provided financial and other resources, including capabilities in research, development, manufacturing, and sales and marketing, to support our research and development programs and may enter into more of them in the future.
Partnership agreements may terminate without benefit to us if the underlying products are not fully developed. If we fail to meet our obligations under these agreements, they could terminate and we might need to enter into relationships with other collaborators and to spend additional time, money, and other valuable resources in the process. We cannot predict whether our collaborators will continue their development efforts or, if they do, whether their efforts will achieve success. Many of our collaborators face the same kinds of risks and uncertainties in their business that we face. A delay or setback to a partner will, at a minimum, delay the commercialization of any affected products, and may ultimately prevent it. Moreover, any partner could breach its agreement with us or otherwise not use best efforts to promote our products. A partner may choose to pursue alternative technologies or products that compete with our technologies or products. In either case, if a partner failed to successfully develop one of our products, we would need to find another partner. Our ability to do so would depend upon our legal right to do so at the time and whether the product remained commercially viable.
10
Table of Contents
TopoTarget A/S (TopoTarget)
Our agreement with TopoTarget provided for us to receive up to $6.0 million in either (i) potential commercial milestone payments related to future net sales of Belinostat or (ii) 10% of any sublicense income received by TopoTarget. We have no financial and operational responsibility for the clinical development of Belinostat under our agreement with TopoTarget. In February 2010, TopoTarget entered into a co-development and commercialization agreement for Belinostat with Spectrum Pharmaceuticals, Inc. During the years ended December 31, 2010 and 2014, we received $3.0 million and $3.0 million from TopoTarget, respectively. These payments are the last payments we were owed from TopoTarget.
Research Collaboration and License Agreements
We have entered into license agreements whereby we have received licenses or options to license technology, specified patents and/or patent applications. These license and collaboration agreements generally provide for royalty payments equal to specified percentages of product sales, annual license maintenance fees, continuing patent prosecution costs and potential future milestone payments to third parties upon the achievement of certain development, regulatory and/or commercial milestones.
Medarex, Inc., a subsidiary of Bristol-Myers Squibb (Medarex)
We and Medarex have entered into an assignment and license agreement, as amended, that provides for the assignment of certain patent and other intellectual property rights and a license to certain Medarex technology related to the Company's APC Targeting Technology™ and an anti-mannose receptor product. Under the terms of the agreement, we may be required to pay royalties in the low-single digits on any net product sale of a Licensed Royalty- Bearing Product or Anti-Mannose Product to Medarex until the later of (i) the expiration of the last to expire applicable patent and (ii) the tenth anniversary of the first commercial sale of such licensed product.
We and Medarex have also entered into a research and commercialization agreement, as amended, that provides us with certain rights to obtain exclusive commercial licenses to proprietary monoclonal antibodies raised against certain antigens utilizing the Medarex UltiMAb technology platform for generating antibodies until December 2015. Under the terms of the agreement, we may be required to pay Medarex milestones of up to $7.0 million upon obtaining first approval for commercial sale in a first indication of a product containing a licensed antibody and royalty payments in the low-to-mid single digits on any net product sales with respect to the development of any products containing such licensed antibodies until the later of (i) the expiration of the last to expire applicable patent and (ii) the tenth anniversary of the first commercial sale of such licensed product. In September 2010, we exercised an option under our agreement, whereby we licensed from Medarex access to the UltiMab technology to develop and commercialize human antibodies to CD27, including varlilumab. In connection with the clinical trial collaboration we entered into with BMS in May 2014, we and BMS agreed to waive certain future milestone payments and to reduce future royalty rates that we may have owed Medarex in connection with any CD27 program were reduced.
Rockefeller University (Rockefeller)
In November 2005, we and Rockefeller entered into a license agreement for the exclusive worldwide rights to human DEC-205 receptor, with the right to sublicense the technology. The license grant is exclusive except that Rockefeller may use and permit other nonprofit organizations to use the human DEC-205 receptor patent rights for educational and research purposes. We may be required to pay Rockefeller milestones of up to $3.8 million upon obtaining first approval for commercial sale in a first indication of a product targeting the licensed receptor and royalty payments in the low-to-mid single digits on any net product sales with respect to development and commercialization of the human DEC-205 receptor.
11
Table of Contents
Duke University Brain Tumor Cancer Center (Duke)
In September 2006, we and Duke entered into a license agreement that gave us access and reference to the clinical data generated by Duke and its collaborators in order for us to generate our own filing with the FDA relating to rindopepimut. We may be required to pay Duke milestones of up to $0.7 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of rindopepimut.
Ludwig Institute for Cancer Research (Ludwig)
In October 2006, we and Ludwig entered into an agreement for the nonexclusive rights to certain cancer tumor targets for use in combination with our APC Targeting Technology. We may be required to pay Ludwig milestones of up to $1.0 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of the technology licensed from Ludwig.
Alteris Therapeutics, Inc. (Alteris)
In October 2005, we completed the acquisition of the assets of Alteris, including the EGFRvIII molecule. We may be required to pay Alteris up to $5.0 million upon obtaining the first approval for commercial sale of a product containing EGFRvIII, including rindopepimut.
University of Southampton, UK (Southampton)
In November 2008, we entered into a license agreement with Southampton to develop human antibodies towards CD27, a potentially important target for immunotherapy of various cancers. We may be required to pay Southampton milestones of up to approximately $1.4 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of varlilumab.
Amgen Inc. (Amgen)
In March 2009, we entered into a license agreement with Amgen to acquire the exclusive rights to CDX-301 and CD40 ligand, or CD40L. CDX-301 and CD40L are immune modulating molecules that increase the numbers and activity of immune cells that control immune responses. We may be required to pay Amgen milestones of up to $1.0 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of the technology licensed from Amgen, including CDX-301.
Amgen Fremont (formerly Abgenix)
In connection with our acquisition of CuraGen Corporation in 2009, we assumed the license agreement between CuraGen and Amgen Fremont (successor in- interest to Abgenix) to develop fully-human monoclonal antibody therapeutics. In May 2009, an amendment to the license agreement was entered into related to CuraGen's exclusive rights to develop and commercialize glembatumumab vedotin, CDX-014 and antibodies to 10 other licensed antigens. Under the amendment, CuraGen and Amgen Fremont agreed to modify the terms of their existing cross-license of antigens whereby our amended license is fully paid-up and royalty-free.
Seattle Genetics, Inc. (Seattle Genetics)
In connection with our acquisition of CuraGen, we assumed the license agreement between CuraGen and Seattle Genetics whereby CuraGen acquired the rights to proprietary ADC technology, with the right to sublicense, for use with its proprietary antibodies for the potential treatment of cancer. Under the terms of the agreement, we have the responsibility of using commercially reasonable efforts
12
Table of Contents
to develop, commercialize and market such treatment. In furtherance of these responsibilities, technical assistance from Seattle Genetics is available to us as necessary. We may be required to pay Seattle Genetics milestones of up to $5.0 million and $9.0 million for glembatumumab vedotin and CDX-014, respectively, upon obtaining first approval for commercial sale in a first indication and royalty payments in the mid-single digits on any net product sales with respect to development and commercialization of these product candidates. The term of the agreement varies country to country and may be until the later of the expiration of the last relevant patent or the 10th anniversary of the first commercial sale. The agreement allows us to terminate with prior written notice, with both parties being able to terminate the agreement for an uncured material breach or insolvency of the other party.
Competition
The biotechnology and pharmaceutical industries are intensely competitive and subject to rapid and significant technological change. Many of the products that we are attempting to develop and commercialize will be competing with existing therapies. In addition, a number of companies are pursuing the development of pharmaceuticals that target the same diseases and conditions that we are targeting. We face competition from pharmaceutical and biotechnology companies both in the United States and abroad. Our competitors may utilize discovery technologies and techniques or partner with collaborators in order to develop products more rapidly or successfully than us or our collaborators are able to do. Many of our competitors, particularly large pharmaceutical companies, have substantially greater financial, technical and human resources than we do. In addition, academic institutions, government agencies and other public and private organizations conducting research may seek patent protection with respect to potentially competitive products or technologies and may establish exclusive collaborative or licensing relationships with our competitors.
We face intense competition in our development activities. We face competition from many companies in the United States and abroad, including a number of large pharmaceutical companies, firms specialized in the development and production of vaccines, adjuvants and vaccine and immunotherapeutic delivery systems and major universities and research institutions. The competitors of which we are aware that have initiated a Phase 3 study or have obtained marketing approval for a potentially competitive drug to rindopepimut for treatment of glioblastoma and/or glembatumumab vedotin for treatment of breast cancer include AbbVie, Arbor Pharmaceutics, Inc., AstraZeneca PLC, Bayer, Bristol-Myers Squibb, Celgene Corporation, Eisai Inc., Eli Lilly and Company, Medigene AG, Northwest Biotherapeutics, Inc., Novartis, Pfizer Inc., and Roche. Many other companies are developing or commercializing products in areas that we have targeted for product development. Some of these products use therapeutic approaches that may compete directly with our drug candidates. Most of our competitors possess substantially greater financial, technical and human resources than we possess. In addition, many of our competitors have significantly greater experience than we have in conducting preclinical and nonclinical testing and human clinical trials of drug candidates, scaling up manufacturing operations and obtaining regulatory approvals of drugs and manufacturing facilities. Accordingly, our competitors may succeed in obtaining regulatory approval for drugs more rapidly than we do. If we obtain regulatory approval and launch commercial sales of our drug candidates, we also will compete with respect to manufacturing efficiency and sales and marketing capabilities, areas in which we currently have limited experience.
We also face competition from pharmaceutical and biotechnology companies, academic institutions, government agencies and private research organizations in recruiting and retaining highly qualified scientific personnel and consultants and in the development and acquisition of technologies. Moreover, technology controlled by third parties that may be advantageous to our business may be acquired or licensed by our competitors, thereby preventing us from obtaining technology on commercially reasonable terms, if at all. We will also compete for the services of third parties that may have already developed or acquired internal biotechnology capabilities or made commercial arrangements with other
13
Table of Contents
biopharmaceutical companies to target the diseases on which we have focused both in the U.S. and outside of the U.S.
Our competitive position will also depend upon our ability to attract and retain qualified personnel, obtain patent protection or otherwise develop proprietary products or processes and secure sufficient capital resources for the often lengthy period between technological conception and commercial sales. We will require substantial capital resources to complete development of some or all of our products, obtain the necessary regulatory approvals and successfully manufacture and market our products. In order to secure capital resources, we anticipate having to sell additional capital stock, which would dilute existing stockholders. We may also attempt to obtain funds through research grants and agreements with commercial collaborators. However, these types of fundings are uncertain because they are at the discretion of the organizations and companies that control the funds. As a result, we may not receive any funds from grants or collaborations. Alternatively, we may borrow funds from commercial lenders, likely at high interest rates, which would increase the risk of any investment in us.
Manufacturing
We have limited experience in commercial manufacturing. We rely on contract manufacturing organizations, or CMOs, to manufacture drug substance and drug product for our late-stage clinical studies of rindopepimut and glembatumumab vedotin as well as for future commercial supplies. We also rely on CMOs for filling and packaging, storage and shipping of drug product. In order for us to establish our own commercial manufacturing facility, we would require substantial additional funds and would need to hire and retain significant additional personnel and comply with the extensive current Good Manufacturing Practices, or cGMP, regulations applicable to such a facility. The commercial manufacturing facility would also need to be licensed for the production of our drug candidates by the FDA. For our most advanced programs, we are working with CMOs under established manufacturing arrangements that comply with the FDA's requirements and other regulatory standards, although there is no assurance that the manufacturing will be successful.
We currently use rindopepimut drug product that was manufactured by Pfizer and Jubilant Hollister Stier, in the ACT IV and ReACT clinical studies. We have established a relationship with SAFC, a division of the Sigma Aldrich Corporation, and Patheon to manufacture and fill rindopepimut for late stage development and commercial supply. We rely on Biosyn and Ambiopharm for supplying suitable quantities of cGMP starting materials for the manufacture of rindopepimut. We also rely on Sanofi to supply suitable quantities of commercial quality GM-CSF which is co-administered with rindopepimut. Any manufacturing failures or delays by our rindopepimut contract manufacturers or suppliers of critical materials could cause delays in the ACT IV and ReACT studies and/or the commercial launch of rindopepimut.
To date, we have utilized contract manufacturing organizations for the manufacture of clinical trial supplies of glembatumumab vedotin. We have established a relationship with Lonza, AG to manufacture the CR-011 antibody and Piramal Healthcare UK Ltd. to conjugate the CR-011 antibody and stable linker with the MMAE toxin. We rely on SAFC for sourcing of suitable quantities of vcMMAE. Any manufacturing failures or delays by our glembatumumab vedotin contract manufacturers or suppliers of materials could cause delays in our glembatumumab vedotin clinical studies including the METRIC study and/or the commercial launch of glembatumumab vedotin.
We have established our own cGMP manufacturing facility in Fall River, Massachusetts, to produce clinical materials for our current and planned Phase 1 and Phase 2 clinical trials. Our Fall River manufacturing facility has up to 1000L bioreactor capacity and is able to manufacture in compliance with FDA regulations, allowing us to distribute potential products to clinical sites in the US for early clinical trials. We manufacture clinical materials of varlilumab, CDX-1401, CDX-301 and CDX-014 in our Fall River facility for our current and planned Phase 1 and Phase 2 clinical trials. The
14
Table of Contents
products are filled and packaged at CMOs. Any manufacturing failures or compliance issues at contract manufacturers could cause delays in our Phase 1 and Phase 2 clinical studies.
The manufacturing processes for our drug candidates and immunotherapeutic delivery systems utilize known technologies. We believe that the products we currently have under development can be scaled up to permit manufacture in commercial quantities. However, there can be no assurance that we will not encounter difficulties in scaling up the manufacturing processes.
While we believe that there is currently sufficient capacity worldwide for the production of our potential products through contract manufacturers, establishing long-term relationships with contract manufacturers and securing multiple sources for the necessary quantities of clinical and commercial materials required can be a challenge. Qualifying the initial source of clinical and ultimately commercial material is a time consuming and expensive process due to the highly regulated nature of the pharmaceutical/biotech industry. These costs may be mitigated by the economies of scale realized in commercial manufacture and product sale. The key difficulty in qualifying more than one source for each product is the duplicated time and expense in doing so without the potential to mitigate these costs if the secondary source is never utilized.
Use of third party manufacturers limits our control over and ability to monitor the manufacturing process. As a result, we may not be able to detect a variety of problems that may arise and may face additional costs in the process of interfacing with and monitoring the progress of our contract manufacturers. If third party manufacturers fail to meet our manufacturing needs in an acceptable manner, we would face delays and additional costs while we develop internal manufacturing capabilities or find alternate third party manufacturers. It may not be possible to have multiple third party manufacturers ready to supply us with needed material at all or without incurring significant costs.
Commercial Organization
Our strategy is to build a fully integrated, commercial stage biopharmaceutical company that would give us the opportunity to retain marketing rights to our product candidates and commercialize such products ourselves where we deem appropriate or pursue strategic partnerships to develop, sell, market and distribute our product candidates where we deem appropriate. We currently plan to commercialize rindopepimut in the United States and Europe ourselves, if regulatory approval is obtained, and to seek strategic partnerships to commercialize rindopepimut in other geographies. We may enter into strategic partnerships to develop, sell, market and distribute our other product candidates, including glembatumumab vedotin and varlilumab.
Over the past two years, we have begun to assemble key components of a commercial organization with a focus on preparation for the potential launch of rindopepimut, if regulatory approval is obtained. We are assembling a focused commercial team with broad experience in marketing, sales, distribution and product reimbursement. We have also developed the capability to provide current and future market insights to our research and development organization regarding glembatumumab vedotin, varlilumab and our earlier-stage product candidates.
We have been expanding our understanding of the glioblastoma market, developing our commercial strategy for the potential launch of rindopepimut, and planning the infrastructure necessary to support future commercial activities. Our understanding of the glioblastoma market in the United States and Europe incorporates information regarding the current standard of care as well as patient, health care provider and payer attitudes toward current and potential future therapies. Based on this information and the data obtained from our Phase 2 clinical trials of rindopepimut, we have begun developing our go-to-market strategy for rindopepimut, which we intend to update and refine as we obtain additional information regarding the potential commercial profile for rindopepimut. In particular, we plan to incorporate the information we obtain regarding the efficacy and safety of rindopepimut from our registration program into our marketing strategy.
15
Table of Contents
As we continue to prepare for a potential rindopepimut launch in the United States and Europe, we plan to expand our commercial organization over the next twelve to twenty-four months. This expansion will include implementation of internal systems and infrastructure in order to support commercial sales, incorporation of appropriate compliance policies and procedures, establishment of patient-focused programs and hiring and training a marketing and sales force to promote rindopepimut, if regulatory approval is obtained, to health care providers. There can be no assurance that we will be able to accomplish any of these activities or hire and train an effective marketing and sales force.
Patents, Licenses and Proprietary Rights
In general, our intellectual property strategy is to protect our technology by filing patent applications and obtaining patent rights covering our own technology, both in the United States and in foreign countries that we consider important to our business. In addition, we have acquired and will seek to acquire as needed or desired, exclusive rights of others through assignment or license to complement our portfolio of patent rights. We also rely on trade secrets, unpatented know-how and technological expertise and innovation to develop and maintain our competitive position.
Patents
The successful development and marketing of products by us will depend in part on our ability to create and maintain intellectual property, including patent rights. We are the owner or exclusive licensee to proprietary patent positions in the areas of immunotherapy technologies, vaccine technologies, antibody technologies and complement inhibitor technology. Although we continue to pursue patent protection for our products, no assurance can be given that any pending application will issue as a patent, that any issued patent will have a scope that will be of commercial benefit, or that we will be able to successfully enforce our patent position against infringers. We routinely review our patent portfolio and adjust our strategies for prosecution and maintenance of individual cases according to a number of factors including program priorities, stage of development, and patent term.
We own or license rights under more than 300 granted patents and national and regional patent applications in the U.S. and in major international territories covering inventions relating to our business. The key patents and patent applications owned by us or licensed to us that we consider important to our business include the following (the indicated and estimated patent expiry dates do not include any possible patent term extensions or supplementary protection certificates, if these may be secured in due course):
- •
- We have licensed rights from Duke University under an issued European patent, a patent application in the U.S. and patents and patent applications in other major international territories relating to uses of rindopepimut. If and where issued and maintained to full term in a form which covers commercial use of rindopepimut, the filings could potentially provide patent protection for the relevant use in the relevant territories to 2026. We also have patent applications in the U.S. and major international territories relating to methods of manufacture and formulation of rindopepimut, which, if issued in a form which covers manufacture and/or formulation of rindopepimut and maintained to full term in due course, would have estimated patent expiry dates in 2030.
- •
- Our patent portfolio for glembatumumab vedotin includes issued patents in the U.S., Europe and Australia and pending patent applications in Japan and Canada. If and where issued and maintained to full term in due course, these would have estimated patent expiry dates in 2025. In addition, patent rights relating to the toxin and conjugation technology used in glembatumumab vedotin have been licensed from Seattle Genetics. The patent rights from Seattle Genetics include issued patents and pending applications in Australia, Canada, Europe, the U.S. and Japan which include composition of matter claims relating to the toxin and conjugation technology. If maintained to full term in due course, the main Seattle Genetics
16
Table of Contents
There can be no assurance that patent applications owned by or licensed to us will result in granted patents or that, if granted, the resultant patents will afford protection against competitors with similar technology. It is also possible that third parties may obtain patents or other proprietary rights that may be necessary or useful to us. In cases where third parties are first to invent a particular product or technology, it is possible that those parties will obtain patents that will be sufficiently broad to prevent us from using important technology or from further developing or commercializing important drug candidates and immunotherapeutic systems. If licenses from third parties are necessary but cannot be obtained, commercialization of the covered products might be delayed or prevented. Even if these licenses can be obtained, they would probably require us to pay ongoing royalties and other costs, which could be substantial.
Although a patent has a statutory presumption of validity in the United States, the issuance of a patent is not conclusive as to validity or as to the enforceable scope of the patent claims. The validity or enforceability of a patent after its issuance by the Patent and Trademark Office can be challenged in litigation. As a business that uses a substantial amount of intellectual property, we face a heightened risk of intellectual property litigation. If the outcome of the litigation is adverse to the owner of the patent, third parties may then be able to use the invention covered by the patent without authorization
17
Table of Contents
or payment. There can be no assurance that our issued patents or any patents subsequently issued to or licensed by us will not be successfully challenged in the future. In addition, there can be no assurance that our patents will not be infringed or that the coverage of our patents will not be successfully avoided by competitors through design innovation.
We are aware that others, including universities and companies, have filed patent applications and have been granted patents in the United States and other countries which claim subject matter potentially useful or necessary to the commercialization of our products. The ultimate scope and validity of existing or future patents which have been or may be granted to third parties, and the availability and cost of acquiring rights in those patents necessary to the manufacture, use or sale of our products presently cannot be determined by us.
Third parties may have or may obtain valid and enforceable patents or proprietary rights that could block us from developing products using our technology, including:
- •
- certain patents and applications in the United States and Europe owned by Sanofi-Aventis, which relate to antibody-antigen conjugates and methods of their use for eliciting an immune response against the antigen;
- •
- certain patents and applications in the United States and foreign countries covering particular antigens and antigenic fragments targeted by our current drug candidates, including CDX-1401;
- •
- certain patents and pending applications related to particular receptors and other molecules on dendritic cells and macrophages that may be useful for generating monoclonal antibodies and can be employed in our APC Targeting Technology;
- •
- two United States patents and related foreign patents and applications covering methods of diagnosing gliomas by detecting the presence of the EGFRvIII (tumor specific splice variant) protein;
- •
- a United States patent relating to certain uses of GM-CSF;
- •
- a United States patent owned by Genentech, Inc., relating to the production of recombinant antibodies in host cells;
- •
- a United States patent owned by GlaxoSmithKline plc related to methods of culturing cells under certain conditions; and
- •
- certain patents held by third parties relating to antibody expression in particular types of host cells.
In addition to the patents referred to in the previous paragraphs, there may be other patent applications and issued patents belonging to competitors that may require us to alter our drug candidates and immunotherapeutic delivery systems, pay licensing fees or cease some of our activities. If our drug candidates conflict with patents that have been or may be granted to competitors, universities or others, the patent owners could bring legal action against us claiming damages and seeking to enjoin manufacturing and marketing of the patented products. If any of these actions is successful, in addition to any potential liability for damages, we could be required to obtain a license in order to continue to manufacture or market the affected products. There can be no assurance that we would prevail in any such action or that any license required under any such third party patent would be made available on acceptable terms or at all. We believe that there may be significant litigation in the biotechnology industry regarding patent and other intellectual property rights. If we become involved in that litigation, we could consume substantial resources.
Licenses
We have entered into several significant license agreements relating to technologies that are being developed by us. In general, these institutions have granted us an exclusive worldwide license (with right to sublicense) to make, use and sell products embodying the licensed technology, subject to the
18
Table of Contents
reservation by the licensor of a non-exclusive right to use the technologies for non-commercial research purposes. Generally, the term of each license is through the expiration of the last of the patents issued with respect to the technologies covered by the license. We have generally agreed to use reasonable efforts to develop and commercialize licensed products and to achieve specified milestones and pay license fees, milestone payments and royalties based on the net sales of the licensed products or to pay a percentage of sublicense income. If we breach our obligations, the licensor has the right to terminate the license, and, in some cases, convert the license to a non-exclusive license. Generally, we control and are responsible for the cost of defending the patent rights of the technologies that we license.
Proprietary Rights
We also rely on unpatented technology, trade secrets and confidential information, and no assurance can be given that others will not independently develop substantially equivalent information and techniques or otherwise gain access to our know-how and information, or that we can meaningfully protect our rights in such unpatented technology, trade secrets and information. We require each of our employees, consultants and advisors to execute a confidentiality agreement at the commencement of an employment or consulting relationship with us. The agreements generally provide that all inventions conceived by the individual in the course of employment or in providing services to us and all confidential information developed by, or made known to, the individual during the term of the relationship shall be the exclusive property of us and shall be kept confidential and not disclosed to third parties except in limited specified circumstances. There can be no assurance, however, that these agreements will provide meaningful protection for our information in the event of unauthorized use or disclosure of such confidential information.
Government Regulation
Our activities and products are significantly regulated by a number of governmental entities, including the FDA in the United States and by comparable authorities in other countries. These entities regulate, among other things, the manufacture, testing, safety, effectiveness, labeling, documentation, advertising and sale of our products. We must obtain regulatory approval from FDA and comparable authorities in other countries, as applicable, for our drug candidates before we can commercialize such drugs in the U.S. and foreign jurisdictions. Product development within this regulatory framework takes a number of years and involves the expenditure of substantial resources. Many products that initially appear promising ultimately do not reach the market because they are found to be unsafe or ineffective when tested. Our inability to commercialize a product would impair our ability to earn future revenues.
FDA Approval Process
In the United States, immunotherapeutics for human use are subject to FDA approval as "biologics" under the Public Health Service Act or as "drugs" under the Federal Food, Drug and Cosmetic Act. The steps required before a new product can be commercialized include: preclinical studies in animals, clinical trials in humans to determine safety and efficacy and FDA approval of the product for commercial sale.
Data obtained at any stage of testing is susceptible to varying interpretations, which could delay, limit or prevent regulatory approval. Moreover, during the regulatory process, new or changed drug approval policies may cause unanticipated delays or rejection of our product. We may not obtain necessary regulatory approvals within a reasonable period of time, if at all, or avoid delays or other problems in testing our products. Moreover, even if we received regulatory approval for a product, the approval may require limitations on use, which could restrict the size of the potential market for the product.
19
Table of Contents
The FDA provides that human clinical trials may begin thirty (30) days after receipt and review of an IND application, unless the FDA requests additional information or changes to the study protocol within that period. An IND must be sponsored and filed for each of our proposed products. Authorization to conduct a clinical trial in no way assures that the FDA will ultimately approve the product. Clinical trials are generally conducted in three sequential phases. In a Phase 1 trial, the product is given to a small number of healthy volunteers to test for safety (adverse effects). Phase 2 trials are conducted on a limited group of the target patient population; safety, optimal dosage and efficacy are studied. A Phase 3 trial is performed in a large patient population, generally over a wide geographic area to provide evidence for the safety and efficacy of the product. The FDA has ongoing oversight over all these trials and can order a temporary or permanent discontinuation if warranted. Such an action could materially harm us. Clinical trials are critical to the success of our products but are subject to unforeseen and uncontrollable delay, including delay in enrollment of patients. Any delay in clinical trials could delay our commercialization of a product.
A product's safety and effectiveness in one clinical trial is not necessarily indicative of its safety and effectiveness in another clinical trial. Moreover, we may not discover all potential problems with a product even after completing clinical trials on it. Some of our products and technologies have undergone only preclinical testing. As a result, we do not know whether they are safe or effective for humans. Also, regulatory authorities may decide, contrary to our findings, that a product is unsafe or not as effective in actual use as its clinical trial results indicated. This could prevent the product's widespread use, require its withdrawal from the market or expose us to liability.
The results of the clinical trials, nonclinical testing, and all supporting manufacturing data are submitted to the FDA for approval. A Biologics License Application (BLA) is submitted for a biologic product; a New Drug Application (NDA) for a drug product. The interval between IND filing and BLA/NDA filing is usually at least several years due to the length of the clinical trials, and the BLA/NDA review process can take over a year. During this time the FDA may request further testing or additional trials or may turn down the application. Even with approval, the FDA frequently requires post-marketing safety studies (known as Phase 4 trials) to be performed.
The FDA requires that the manufacturing facility that produces a licensed product meet specified standards, undergo an inspection and obtain an establishment license prior to commercial marketing. Subsequent discovery of previously unknown problems with a product or its manufacturing process may result in restrictions on the product or the manufacturer, including withdrawal of the product from the market. Failure to comply with the applicable regulatory requirements can result in fines, suspensions of regulatory approvals, product recalls, operating restrictions and criminal prosecution.
Expedited development and review programs
The FDA has a Fast Track program that is intended to expedite or facilitate the process for reviewing new drugs and biological products that meet certain criteria. Specifically, new drugs and biological products are eligible for Fast Track designation if they are intended to treat a serious or life-threatening condition and demonstrate the potential to address unmet medical needs for the condition. Fast Track designation applies to the combination of the product and the specific indication for which it is being studied. The sponsor of a new drug or biologic may request the FDA to designate the drug or biologic as a Fast Track product at any time during the clinical development of the product. Unique to a Fast Track product, the FDA may consider for review sections of the marketing application on a rolling basis before the complete application is submitted, if the sponsor provides a schedule for the submission of the sections of the application, the FDA agrees to accept sections of the application and determines that the schedule is acceptable, and the sponsor pays any required user fees upon submission of the first section of the application.
20
Table of Contents
Any product submitted to the FDA for marketing, including under a Fast Track program, may be eligible for other types of FDA programs intended to expedite development and review, such as priority review and accelerated approval. Under the Breakthrough Therapy program, products intended to treat a serious or life-threatening disease or condition may be eligible for the benefits of the Fast Track program when preliminary clinical evidence demonstrates that such product may have substantial improvement on one or more clinically significant endpoints over existing therapies. Additionally, FDA will seek to ensure the sponsor of a breakthrough therapy product receives timely advice and interactive communications to help the sponsor design and conduct a development program as efficiently as possible. Any product is eligible for priority review if it has the potential to provide safe and effective therapy where no satisfactory alternative therapy exists or a significant improvement in the treatment, diagnosis or prevention of a disease compared to marketed products. The FDA will attempt to direct additional resources to the evaluation of an application for a new drug or biological product designated for priority review in an effort to facilitate the review. Additionally, a product may be eligible for accelerated approval. Drug or biological products studied for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may receive accelerated approval, which means that they may be approved on the basis of adequate and well-controlled clinical studies establishing that the product has an effect on a surrogate endpoint that is reasonably likely to predict a clinical benefit, or on the basis of an effect on a clinical endpoint other than survival or irreversible morbidity. As a condition of approval, the FDA may require that a sponsor of a drug or biological product receiving accelerated approval perform adequate and well-controlled post-marketing clinical studies. In addition, the FDA currently requires as a condition for accelerated approval pre-approval of promotional materials, which could adversely impact the timing of the commercial launch of the product. Fast Track designation, Breakthrough Therapy designation, priority review and accelerated approval do not change the standards for approval but may expedite the development or approval process.
Orphan Drug
Under the Orphan Drug Act, the FDA may grant orphan drug designation to products intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States, or more than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making available in the United States a product for this type of disease or condition will be recovered from sales in the United States for that product. If a product that has orphan drug designation subsequently receives the first FDA approval for the disease for which it has such designation, the product is entitled to orphan product exclusivity, which means that the FDA may not approve any other applications to market the same product for the same indication, except in very limited circumstances, for seven years.
Post Approval
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory standards is not maintained or if problems occur after the product reaches the market. After approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further FDA review and approval. In addition, the FDA may require testing and surveillance programs to monitor the effect of approved products that have been commercialized, and the FDA has the power to prevent or limit further marketing of a product based on the results of these post-marketing programs.
Foreign Regulation
In addition to regulations in the United States, we will be subject to a variety of foreign regulations governing clinical trials, manufacture, and commercial sales and distribution of our
21
Table of Contents
products. Whether or not we obtain FDA approval for a product, we must obtain approval of a product by the comparable regulatory authorities of foreign countries before we can commence clinical trials or marketing of the product in those countries. The approval process varies from country to country and the time may be longer or shorter than that required for FDA approval. Approval by the FDA does not ensure approval by the regulatory bodies of other countries.
Under the European Union regulatory system, we will submit most of our marketing authorization applications under the centralized procedure. The centralized procedure is compulsory for medicines produced by biotechnology, or are for the treatment of cancer, or officially designated as 'orphan medicines'. The centralized procedure provides for the grant of a single marketing authorization that is valid for all European Union member states. As in the United States, we may apply for designation of our products as orphan drug for the treatment of a specific indication in the European Union before the application for marketing authorization is made. Orphan drugs in Europe enjoy economic and marketing benefits, including a 10-year market exclusivity period for the approved indication, but not for the same product, unless another applicant can show that its product is safer, more effective or otherwise clinically superior to the orphan-designated product.
Our collaborators are also subject to all of the above-described regulations in connection with the commercialization of products utilizing our technology.
Other Regulatory Processes
We are subject to a variety of financial disclosure and securities trading regulations as a public company in the U.S., including laws relating to the oversight activities of the SEC and the regulations of the NASDAQ Global Market, on which our shares are traded. We are also subject to regulation under other federal laws and regulation under state and local laws, including laws relating to occupational safety, laboratory practices, environmental regulations, and hazardous substance control.
Employees
As of December 31, 2014, we employed 161 employees (156 full-time, 2 part-time and 3 interns), 25 of whom have Ph.D. and/or M.D. degrees. Of these employees, 128 were engaged in or directly support research and development activities. We believe that our employee relations are good. We believe that our future success will depend in large part on our ability to attract and retain experienced and skilled employees.
Item 1A. RISK FACTORS
You should consider carefully these risk factors together with all of the information included or incorporated by reference in this Annual Report in addition to our financial statements and the notes to our financial statements. This section includes forward-looking statements.
The following is a discussion of the risk factors that we believe are material to us at this time. These risks and uncertainties are not the only ones facing us and there may be additional matters that we are unaware of or that we currently consider immaterial. All of these could adversely affect our business, results of operations, financial condition and cash flows.
Risks Related to our Financial Condition and Capital Requirements
We currently have no product revenue and will need to raise capital to operate our business.
To date, we have generated no product revenue and cannot predict when and if we will generate product revenue. We had an accumulated deficit of $463.8 million as of December 31, 2014. Until, and unless, we complete clinical trials and further development, and receive approval from the FDA and
22
Table of Contents
other regulatory authorities, for our drug candidates, we cannot sell our drugs and will not have product revenue. We expect to spend substantial funds to continue the research, development and testing of our products that are in the preclinical and clinical testing stages of development and to prepare to commercialize products in anticipation of FDA approval. Therefore, for the foreseeable future, we will have to fund all of our operations and development expenditures from cash on hand, equity or debt financings, licensing fees and grants. Additional financing will be required to meet our long term liquidity needs. If we do not succeed in raising additional funds on acceptable terms, we might not be able to complete planned preclinical and clinical trials or obtain approval of any drug candidates from the FDA and other regulatory authorities. In addition, we could be forced to discontinue product development, reduce or forego sales and marketing efforts, forego attractive business opportunities or curtail operations. Any additional sources of financing could involve the issuance of our equity securities, which would have a dilutive effect on our stockholders. No assurance can be given that additional financing will be available to us when needed on acceptable terms, or at all.
We cannot be certain that we will achieve or sustain profitability in the future. Failure to achieve profitability could diminish our ability to sustain operations, pay dividends on our common stock, obtain additional required funds and make required payments on our present or future indebtedness.
We expect to incur future losses and we may never become profitable.
We have incurred operating losses of $122.4 million, $81.4 million and $58.1 million during 2014, 2013 and 2012, respectively, and expect to incur an operating loss in 2015 and beyond. We believe that operating losses will continue in and beyond 2015 because we are planning to incur significant costs associated with the clinical development, manufacturing of commercial supply and building a commercial organization to prepare for the potential launch of rindopepimut and glembatumumab vedotin if regulatory approval is obtained. During the years ended December 31, 2014 and 2013, we incurred $45.6 million and $32.3 million in clinical trial expense and $20.9 million and $6.6 million in contract manufacturing expense. We anticipate clinical trial and contract manufacturing expense to increase over the next twelve months related to our rindopepimut, glembatumumab vedotin and varlilumab programs. In addition, we are planning to incur additional costs in the clinical development of CDX-1401 and CDX-301. Our net losses have had and will continue to have an adverse effect on, among other things, our stockholders' equity, total assets and working capital. We expect that losses will fluctuate from quarter to quarter and year to year, and that such fluctuations may be substantial. We cannot predict when we will become profitable, if at all.
We will need additional capital to fund our operations, including the development, manufacture and potential commercialization of our drug candidates. If we do not have or cannot raise additional capital when needed, we may be unable to develop and ultimately commercialize our drug candidates successfully.
We expect to incur significant costs as we develop our drug candidates. In particular, the continuing development and commercialization of rindopepimut, glembatumumab vedotin and our other drug candidates requires additional capital beyond our current resources. As of December 31, 2014, we had cash, cash equivalents and marketable securities of $201.0 million. We anticipate taking further steps to raise additional capital to fund our long-term liquidity needs. Our capital raising activities may include, but may not be limited to, one or more of the following:
- •
- licensing of drug candidates with existing or new collaborative partners;
- •
- possible business combinations;
- •
- issuance of debt; or
- •
- issuance of common stock or other securities via private placements or public offerings.
23
Table of Contents
While we may continue to seek capital through a number of means, there can be no assurance that additional financing will be available on acceptable terms, if at all, and our negotiating position in capital-raising efforts may worsen as existing resources are used. There is also no assurance that we will be able to enter into further collaborative relationships. Additional equity financing may be dilutive to our stockholders; debt financing, if available, may involve significant cash payment obligations and covenants that restrict our ability to operate as a business; and licensing or strategic collaborations may result in royalties or other terms which reduce our economic potential from products under development. If we are unable to raise the funds necessary to meet our long-term liquidity needs, we may have to delay or discontinue the development of one or more programs, discontinue or delay the build-out of our commercial infrastructure and our commercial planning and preparation activities, discontinue or delay on-going or anticipated clinical trials, license out programs earlier than expected, raise funds at significant discount or on other unfavorable terms, if at all, or sell all or part of our business.
Risks Related to Development and Regulatory Approval of Drug Candidates
Our long term success depends heavily on our ability to fund and complete the research and development activities for our program assets, including our lead drug candidates, rindopepimut and glembatumumab vedotin.
Our management team lacks significant experience in completing Phase 3 clinical trials and obtaining regulatory approval for a drug candidate. Only a small minority of all research and development programs ultimately result in commercially successful drugs. Clinical failure can occur at any stage of clinical development. Clinical trials may produce negative or inconclusive results, and we may decide, or regulators may require us, to conduct additional clinical or preclinical trials. In addition, data obtained from trials are susceptible to varying interpretations, and regulators may not interpret our data as favorably as we do, which may delay, limit or prevent regulatory approval. Success in preclinical testing and early clinical trials does not ensure that later clinical trials will generate the same results or otherwise provide adequate data to demonstrate the efficacy and safety of a drug candidate.
If we face delays, difficulties or unanticipated costs in completing the development of rindopepimut or glembatumumab vedotin, we will need substantial additional financing. Further, even if we complete the development of rindopepimut or glembatumumab vedotin and gain marketing approvals from the FDA and comparable foreign regulatory authorities in a timely manner, we cannot be sure that rindopepimut or glembatumumab vedotin will be commercially successful in the pharmaceutical market. If the results of clinical trials, the anticipated or actual timing of marketing approvals, or the market acceptance of rindopepimut or glembatumumab vedotin, if approved, do not meet the expectations of investors or public market analysts, the market price of our common stock would likely decline.
24
Table of Contents
We may be unable to manage multiple late stage clinical trials for a variety of drug candidates simultaneously.
As our current clinical trials progress, we may need to manage multiple late stage clinical trials simultaneously in order to continue developing all of our current products. Our management team does not have significant experience in completing late stage clinical trials and the management of late stage clinical trials is more complex and time consuming than early stage trials. Typically, early stage trials involve several hundred patients in no more than 10-30 clinical sites. Late stage (Phase 3) trials may involve up to several thousand patients in up to several hundred clinical sites and may require facilities in several countries. Therefore, the project management required to supervise and control such an extensive program is substantially larger than early stage programs. As the need for these resources is not known until some months before the trials begin, it is necessary to recruit large numbers of experienced and talented individuals very quickly. If the labor market does not allow this team to be recruited quickly, the sponsor is faced with a decision to delay the program or to initiate it with inadequate management resources. This may result in recruitment of inappropriate patients, inadequate monitoring of clinical investigators and inappropriate handling of data or data analysis. Consequently it is possible that conclusions of efficacy or safety may not be acceptable to permit filing of a BLA or NDA for any one of the above reasons or a combination of several.
We may enter into collaboration agreements for the licensing, development and ultimate commercialization of some of our drug candidates including, where appropriate, for our lead drug candidates. In such cases, we will depend greatly on our third-party collaborators to license, develop and commercialize such drug candidates, and they may not meet our expectations.
We may enter into co-development and commercialization partnerships for certain products, including rindopepimut for commercialization outside of North America and Europe, glembatumumab vedotin and varlilumab. The process of identifying collaborators and negotiating collaboration agreements for the licensing, development and ultimate commercialization of some of our drug candidates may cause delays and increased costs. We may not be able to enter into collaboration agreements on terms favorable to us or at all. Furthermore some of those agreements may give substantial responsibility over our drug candidates to the collaborator. Some collaborators may be unable or unwilling to devote sufficient resources to develop our drug candidates as their agreements require. They often face business risks similar to ours, and this could interfere with their efforts. Also, collaborators may choose to devote their resources to products that compete with ours. If a collaborator does not successfully develop any one of our products, we will need to find another collaborator to do so. The success of our search for a new collaborator will depend on our legal right to do so at the time and whether the product remains commercially viable.
If we enter into collaboration agreements for one or more of our lead drug candidates, the success of such drug candidates will depend in great part upon our and our collaborators' success in promoting them as superior to other treatment alternatives. We believe that our drug candidates can be proven to offer disease prevention and treatment with notable advantages over drugs in terms of patient compliance and effectiveness. However, there can be no assurance that we will be able to prove these advantages or that the advantages will be sufficient to support the successful commercialization of our drug candidates.
Our drug candidates are subject to extensive regulatory scrutiny.
All of our drug candidates are at various stages of development and our activities and drug candidates are significantly regulated by a number of governmental entities, including the FDA in the United States and by comparable authorities in other countries. These entities regulate, among other things, the manufacture, testing, safety, effectiveness, labeling, documentation, advertising and sale of drugs and drug candidates. We or our partners must obtain regulatory approval for a drug candidate in all of these areas before we can commercialize any of our drug candidates. Product development within
25
Table of Contents
this regulatory framework takes a number of years and involves the expenditure of substantial resources. This process typically requires extensive preclinical and clinical testing, which may take longer or cost more than we anticipate, and may prove unsuccessful due to numerous factors. Many drug candidates that initially appear promising ultimately do not reach the market because they are found to be unsafe or ineffective when tested. Companies in the pharmaceutical, biotechnology and immunotherapeutic drug industries have suffered significant setbacks in advanced clinical trials, even after obtaining promising results in earlier trials. Our inability to commercialize a drug candidate would impair our ability to earn future revenues.
If our drug candidates do not pass required tests for safety and effectiveness, we will not be able to obtain regulatory approval and derive commercial revenue from them.
In order to succeed, we will need to obtain regulatory approval for our drug candidates. The FDA has not approved our lead drug candidates, rindopepimut or glembatumumab vedotin, or any of our other products for sale to date. Our drug candidates are in various stages of preclinical and clinical testing. Preclinical tests are performed at an early stage of a product's development and provide information about a product's safety and effectiveness on laboratory animals. Preclinical tests can last years. If a product passes its preclinical tests satisfactorily, and we determine that further development is warranted, we would file an IND application for the product with the FDA, and if the FDA gives its approval we would begin Phase 1 clinical tests. Phase 1 testing generally lasts between 6 and 24 months. If Phase 1 test results are satisfactory and the FDA gives its approval, we can begin Phase 2 clinical tests. Phase 2 testing generally lasts between 6 and 36 months. If Phase 2 test results are satisfactory and the FDA gives its approval, we can begin Phase 3 pivotal studies. Phase 3 studies generally last between 12 and 48 months. Once clinical testing is completed and a new drug application is filed with the FDA, it may take more than a year to receive FDA approval.
In all cases we must show that a pharmaceutical product is both safe and effective before the FDA, or drug approval agencies of other countries where we intend to sell the product, will approve it for sale. Our research and testing programs must comply with drug approval requirements both in the United States and in other countries, since we are developing our lead products with the intention to, or could later decide to, commercialize them both in the U.S. and abroad. A product may fail for safety or effectiveness at any stage of the testing process. A major risk we face is the possibility that none of our products under development will come through the testing process to final approval for sale, with the result that we cannot derive any commercial revenue from them after investing significant amounts of capital in multiple stages of preclinical and clinical testing.
Product testing is critical to the success of our products but subject to delay or cancellation if we have difficulty enrolling patients.
As our portfolio of drug candidates moves from preclinical testing to clinical testing, and then through progressively larger and more complex clinical trials, we will need to enroll an increasing number of patients with the appropriate characteristics. At times we have experienced difficulty enrolling patients and we may experience more difficulty as the scale of our clinical testing program increases. The factors that affect our ability to enroll patients are largely uncontrollable and include principally the following:
- •
- the nature of the clinical test;
- •
- the size of the patient population;
- •
- patients' willingness to receive a placebo or less effective treatment on the control arm of a clinical study;
- •
- the distance between patients and clinical test sites; and
26
Table of Contents
- •
- the eligibility criteria for the trial.
If we cannot enroll patients as needed, our costs may increase or we may be forced to delay or terminate testing for a product.
We may have delays in completing our clinical trials and we may not complete them at all.
We have not completed the clinical trials necessary to obtain FDA approval to market rindopepimut, glembatumumab vedotin or any of our other products in development. Other than ACT IV and METRIC which is designed for approval, we have not initiated Phase 3 studies for any of our other products in development. Our management lacks significant experience in completing Phase 3 trials and bringing a drug through commercialization. ACT IV, METRIC and clinical trials for other products in development may be delayed or terminated as a result of many factors, including the following:
- •
- difficulty in enrolling patients in our clinical trials;
- •
- patients failing to complete clinical trials due to dissatisfaction with the treatment, side effects or other reasons;
- •
- failure by regulators to authorize us to commence a clinical trial;
- •
- suspension or termination by regulators of clinical research for many reasons, including concerns about patient safety or failure of our contract manufacturers to comply with cGMP requirements;
- •
- delays or failure to obtain clinical supply for our products necessary to conduct clinical trials from contract manufacturers, including commercial grade clinical supply for our Phase 3 clinical trials;
- •
- treatment candidates demonstrating a lack of efficacy during clinical trials;
- •
- inability to continue to fund clinical trials or to find a partner to fund the clinical trials;
- •
- competition with ongoing clinical trials and scheduling conflicts with participating clinicians; and
- •
- delays in completing data collection and analysis for clinical trials.
Any delay or failure to complete clinical trials and obtain FDA approval for our drug candidates could have a material adverse effect on our cost to develop and commercialize, and our ability to generate revenue from, a particular drug candidate.
Any delay in obtaining regulatory approval would have an adverse impact on our ability to earn future revenues.
It is possible that none of the drug candidates that we develop will obtain the regulatory approvals necessary for us to begin commercializing them. The time required to obtain FDA and other approvals is unpredictable but often can take years following the commencement of clinical trials, depending upon the nature of the drug candidate. Any analysis we perform of data from clinical activities is subject to confirmation and interpretation by regulatory authorities, which could delay, limit or prevent regulatory approval. Any delay or failure in obtaining required approvals could have a material adverse effect on our ability to generate revenues from the particular drug candidate including, but not limited to, loss of patent term during the approval period. Furthermore, if we, or our partners, do not reach the market with our products before our competitors offer products for the same or similar uses, or if we, or our partners, are not effective in marketing our products, our revenues from product sales, if any, will be reduced.
27
Table of Contents
We face intense competition in our development activities. We face competition from many companies in the United States and abroad, including a number of large pharmaceutical companies, firms specialized in the development and production of vaccines, adjuvants and vaccine and immunotherapeutic delivery systems and major universities and research institutions. The competitors of which we are aware that have initiated a Phase 3 study or have obtained marketing approval for a potentially competitive drug to rindopepimut for treatment of glioblastoma and/or glembatumumab vedotin for treatment of breast cancer include AbbVie, Arbor Pharmaceutics, Inc., AstraZeneca PLC, Bayer, Bristol-Myers Squibb, Celgene Corporation, Eisai Inc., Eli Lilly and Company, Medigene AG, Northwest Biotherapeutics, Inc., Novartis, Pfizer Inc., and Roche. Most of our competitors have substantially greater resources, more extensive experience in conducting preclinical studies and clinical testing and obtaining regulatory approvals for their products, greater operating experience, greater research and development and marketing capabilities and greater production capabilities than those of ours. These companies might succeed in obtaining regulatory approval for competitive products more rapidly than we can for our products, especially if we experience any delay in obtaining required regulatory approvals.
We have many competitors in our field and they may develop technologies that make ours obsolete.
Biotechnology, pharmaceuticals and therapeutics are rapidly evolving fields in which scientific and technological developments are expected to continue at a rapid pace. We have many competitors in the U.S. and abroad. The competitors of which we are aware that have initiated a Phase 3 study or have obtained marketing approval for a potentially competitive drug to rindopepimut for treatment of glioblastoma and/or glembatumumab vedotin for treatment of breast cancer include AbbVie, Arbor Pharmaceutics, Inc., AstraZeneca PLC, Bayer, Bristol-Myers Squibb, Celgene Corporation, Eisai Inc., Eli Lilly and Company, Medigene AG, Northwest Biotherapeutics, Inc., Novartis, Pfizer Inc., and Roche. Our success depends upon our ability to develop and maintain a competitive position in the product categories and technologies on which we focus. Many of our competitors have greater capabilities, experience and financial resources than we do. Competition is intense and is expected to increase as new products enter the market and new technologies become available. Our competitors may:
- •
- develop technologies and products that are more effective than ours, making ours obsolete or otherwise noncompetitive;
- •
- obtain regulatory approval for products more rapidly or effectively than us; and
- •
- obtain patent protection or other intellectual property rights that would block our ability to develop competitive products.
Risks Related to Commercialization of Our Drug Candidates
We may face delays, difficulties or unanticipated costs in establishing sales and distribution capabilities for the commercialization of rindopepimut, if regulatory approval is obtained, or any other of our drug candidates.
We are in the process of building a commercial organization which we believe will provide us with the strategic options to either retain full economic rights to our drug candidates or seek favorable economic terms through advantageous commercial partnerships. We plan to commercialize our lead drug candidate rindopepimut ourselves in North America and Europe. As a result, we may have full responsibility for commercialization of rindopepimut and our other drug candidates if and when they are approved for sale. We currently lack sufficient marketing, sales and distribution capabilities to carry out this strategy. If any of our drug candidates are approved by the FDA, we will need a drug sales force with technical expertise prior to the commercialization of any of our drug candidates. We will incur substantial additional expenses in developing, training and managing such an organization. We may be unable to build such a sales force, the cost of establishing such a sales force may exceed any
28
Table of Contents
product revenue, or our direct marketing and sales efforts may be unsuccessful. We may find it necessary to enter into strategic partnerships, co-promotion or other licensing arrangements and to the extent we enter into such strategic partnerships, co-promotion or other licensing arrangements, our product revenues are likely to be lower than if we directly marketed and sold such drugs, and some or all of the revenues we receive will depend upon the efforts of third parties, which may not be successful and may not be within our control. If we are unable to enter into such strategic partnerships, co-promotion or other licensing arrangements on acceptable terms or at all, we may not be able to successfully commercialize our existing and future drug candidates. If we are not successful in commercializing rindopepimut or any of our other drug candidates, either on our own or through collaborations with one or more third parties, our future product revenue will suffer and we may never achieve profitability or become unable to continue the operation of our business.
If rindopepimut or any other drug candidates for which we obtain regulatory approval do not achieve broad acceptance from physicians, patients and third-party payors, we may be unable to generate significant revenues, if any.
Even if we obtain regulatory approval for our drug candidates, our approved drugs may not gain market acceptance among physicians and patients. We believe that effectively marketing rindopepimut, if it is approved, and our other drug candidates, if any of them are approved, will require substantial efforts, both prior to launch and after approval. Physicians may elect not to prescribe our drugs, and patients may elect not to request or take them, for a variety of reasons including:
- •
- limitations or warnings contained in a drug's FDA-approved labeling;
- •
- changes in the standard of care or the availability of alternative drugs for the targeted indications for any of our drug candidates;
- •
- limitations in the approved indications for our drug candidates;
- •
- demonstrated clinical safety and efficacy compared to other drugs;
- •
- significant adverse side effects;
- •
- effectiveness of education, sales, marketing and distribution support;
- •
- timing of market introduction and perceived effectiveness of competitive drugs;
- •
- cost-effectiveness;
- •
- adverse publicity about our drug candidates or favorable publicity about competitive drugs; and
- •
- convenience and ease of administration of our drug candidates.
If our future drugs fail to achieve market acceptance, we will not be able to generate significant revenues and may never achieve profitability.
Reimbursement decisions by third-party payors may have an adverse effect on pricing and market acceptance of rindopepimut or any of our other drug candidates. If there is not sufficient reimbursement for our future drugs, it is less likely that such drugs will be widely used.
Market acceptance and sales of rindopepimut or any other drug candidates for which we obtain regulatory approval will depend on reimbursement policies and may be affected by future healthcare reform measures in both the United States and foreign jurisdictions. Government authorities and third-party payors, such as private health insurers and health maintenance organizations, decide which drugs they will cover and establish payment levels. In addition, government authorities and these third-party payors are increasingly attempting to contain health care costs by demanding price discounts or rebates and limiting both the types and variety of drugs that they will cover and the amounts that they will pay
29
Table of Contents
for these drugs. In addition, we might need to conduct post-marketing studies in order to demonstrate the cost-effectiveness of any future drugs to such payors' satisfaction. Such studies might require us to commit a significant amount of management time and financial and other resources.
Reimbursement rates may vary according to the use of the drug and the clinical setting in which it is used, may be based on payments allowed for lower-cost products that are already reimbursed, may be incorporated into existing payments for other products or services, and may reflect budgetary constraints and/or imperfections in Medicare or Medicaid data used to calculate these rates. Net prices for drugs may be reduced by mandatory discounts or rebates required by government health care programs. Such legislation, or similar regulatory changes or relaxation of laws that restrict imports of drugs from other countries, could reduce the net price we receive for any future marketed drugs. As a result, our future drugs might not ultimately be considered cost-effective.
We cannot be certain that reimbursement will be available for rindopepimut or any other drug candidates that we develop. Also, we cannot be certain that reimbursement policies will not reduce the demand for, or the price paid for, any future drugs. If reimbursement is not available or is available on a limited basis, we may not be able to successfully commercialize rindopepimut or any other drug candidates that we develop.
Other factors could affect the demand for and sales of any drug candidates that we may commercialize in the future.
In general, other factors that could affect the demand for and sales and profitability of our future drugs include, but are not limited to:
- •
- the timing of regulatory approval, if any, of competitive drugs;
- •
- our or any other of our partners' pricing decisions, as applicable, including a decision to increase or decrease the price of a drug, and the pricing decisions of our competitors;
- •
- government and third-party payer reimbursement and coverage decisions that affect the utilization of our future drugs and competing drugs;
- •
- negative safety or efficacy data from new clinical studies conducted either in the U.S. or internationally by any party could cause the sales of our future drugs to decrease or a future drug to be recalled;
- •
- the degree of patent protection afforded our future drugs by patents granted to or licensed by us and by the outcome of litigation involving our or any of our licensor's patents;
- •
- the outcome of litigation involving patents of other companies concerning our future drugs or processes related to production and formulation of those drugs or uses of those drugs;
- •
- the increasing use and development of alternate therapies;
- •
- the rate of market penetration by competing drugs; and
- •
- the termination of, or change in, existing arrangements with our partners.
In addition, some of our licensing and other agreements with third parties require or might require us to maintain product liability insurance. If we cannot maintain acceptable amounts of coverage on commercially reasonable terms in accordance with the terms set forth in these agreements, the corresponding agreements would be subject to termination, which could have a material adverse impact on our operations.
Any of these factors could have a material adverse effect on the sales of any drug candidates that we may commercialize in the future.
30
Table of Contents
Failure to obtain regulatory approvals in foreign jurisdictions will prevent us from marketing our products internationally.
We intend to seek approval for rindopepimut in Europe and may seek approval of our other drug candidates outside the United States and may market future products in international markets. In order to market our future products in the European Economic Area, or EEA, and many other foreign jurisdictions, we must obtain separate regulatory approvals. Specifically, in the EEA, medicinal products can only be commercialized after obtaining a Marketing Authorization, or MA.
Before granting the MA, the European Medicines Agency or the competent authorities of the member states of the EEA make an assessment of the risk-benefit balance of the product on the basis of scientific criteria concerning its quality, safety and efficacy.
The approval procedures vary among countries and can involve additional clinical testing, and the time required to obtain approval may differ from that required to obtain FDA approval. Clinical studies conducted in one country may not be accepted by regulatory authorities in other countries. Approval by the FDA does not ensure approval by regulatory authorities in other countries, and approval by one or more foreign regulatory authorities does not ensure approval by regulatory authorities in other foreign countries or by the FDA. However, a failure or delay in obtaining regulatory approval in one country may have a negative effect on the regulatory process in others. The foreign regulatory approval process may include all of the risks associated with obtaining FDA approval. We may not obtain foreign regulatory approvals on a timely basis, if at all. We may not be able to file for regulatory approvals and even if we file we may not receive necessary approvals to commercialize our products in any market.
If we obtain approval to commercialize any approved products outside of the United States, a variety of risks associated with international operations could materially adversely affect our business.
We plan to commercialize our lead drug candidate rindopepimut ourselves in Europe, if regulatory approval is obtained. If our other drug candidates are approved for commercialization outside of the United States, we may enter into agreements with third parties to market them on a worldwide basis or in more limited geographical regions. We expect that we will be subject to additional risks related to international operations and entering into international business relationships, including:
- •
- different regulatory requirements for drug approvals;
- •
- reduced protection for intellectual property rights, including trade secret and patent rights;
- •
- unexpected changes in tariffs, trade barriers and regulatory requirements;
- •
- economic weakness, including inflation, or political instability in particular foreign economies and markets;
- •
- compliance with tax, employment, immigration and labor laws for employees living or traveling abroad;
- •
- foreign taxes, including withholding of payroll taxes;
- •
- foreign currency fluctuations, which could result in increased operating expenses and reduced revenues, and other obligations incident to doing business in another country;
- •
- workforce uncertainty in countries where employment regulations are different than, and labor unrest is more common than, in the United States;
- •
- production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad;
31
Table of Contents
- •
- business interruptions resulting from geopolitical actions, including war and terrorism, or natural disasters including earthquakes, hurricanes, floods and fires; and
- •
- difficulty in importing and exporting clinical trial materials and study samples.
Risks Related to Reliance on Third Parties
We rely on third parties to plan, conduct and monitor our clinical tests, and their failure to perform as required would interfere with our product development.
We rely on third parties to conduct a significant portion of our clinical development activities. These activities include clinical patient recruitment and observation, clinical trial monitoring, clinical data management and analysis, safety monitoring and project management. We conduct project management and medical and safety monitoring in-house for some of our programs and rely on third parties for the remainder of our clinical development activities.
The significant third parties who we currently rely on for clinical development activities include Novella Clinical, a Quintiles company, for our ACT IV study and PPD Development, LLC for clinical studies including our METRIC study. If Novella or PPD Development is unable to perform in a quality and timely manner, and at a feasible cost, our clinical studies will face delays. Further, if any of these third parties fails to perform as we expect or if their work fails to meet regulatory standards, our testing could be delayed, cancelled or rendered ineffective.
We rely on contract manufacturers over whom we have limited control. Should the cost, delivery and quality of clinical and commercial grade materials manufactured by us in our Fall River facility or supplied by contract manufacturers vary to our disadvantage, our business operations could suffer significant harm.
We have limited experience in commercial manufacturing. We rely on contract manufacturing organizations, or CMOs, to manufacture drug substance and drug product for our late-stage clinical studies of rindopepimut and glembatumumab vedotin as well as for future commercial supplies. We also rely on CMOs for filling, packaging, storage and shipping of drug product. In order for us to establish our own commercial manufacturing facility, we would require substantial additional funds and would need to hire and retain significant additional personnel and comply with the extensive cGMP regulations applicable to such a facility. The commercial manufacturing facility would also need to be licensed for the production of our drug candidates by the FDA. For our most advanced programs, we are working with CMOs under established manufacturing arrangements that comply with the FDA's requirements and other regulatory standards, although there is no assurance that the manufacturing will be successful.
We currently use rindopepimut drug product that was manufactured by Pfizer and Jubilant Hollister Stier, in the ACT IV and ReACT clinical studies. We have established a relationship with SAFC, a division of the Sigma Aldrich Corporation, and Patheon to manufacture and fill rindopepimut for late stage development and commercial supply. We rely on Biosyn and Ambiopharm for supplying suitable quantities of cGMP starting materials for the manufacture of rindopepimut. We also rely on Sanofi to supply suitable quantities of commercial quality GM-CSF which is co-administered with rindopepimut. Any manufacturing failures or delays by our rindopepimut contract manufacturers or suppliers of critical materials could cause delays in the ACT IV and ReACT studies and/or the commercial launch of rindopepimut.
To date, we have utilized contract manufacturing organizations for the manufacture of clinical trial supplies of glembatumumab vedotin. We have established a relationship with Lonza, AG to manufacture the CR-011 antibody and Piramal Healthcare UK Ltd. to conjugate the CR-011 antibody and stable linker with the MMAE toxin. We rely on SAFC for sourcing of suitable quantities of vcMMAE. Any manufacturing failures or delays by our glembatumumab vedotin contract
32
Table of Contents
manufacturers or suppliers of materials could cause delays in our glembatumumab vedotin clinical studies including the METRIC study and/or the commercial launch of glembatumumab vedotin.
We have established our own cGMP manufacturing facility in Fall River, Massachusetts, to produce clinical materials for our current and planned Phase 1 and Phase 2 clinical trials. Our Fall River manufacturing facility has up to 1000L bioreactor capacity and is able to manufacture in compliance with FDA and EMEA regulations, allowing us to distribute potential products to clinical sites in both the US and EU for early clinical trials. We manufacture clinical materials of varlilumab, CDX-1401, CDX-301 and CDX-014 in our Fall River facility for our current and planned Phase 1 and Phase 2 clinical trials. The products are filled and packaged at CMOs. Any manufacturing failures or compliance issues at contract manufacturers could cause delays in our Phase 1 and Phase 2 clinical studies.
The manufacturing processes for our drug candidates and immunotherapeutic delivery systems utilize known technologies. We believe that the products we currently have under development can be scaled up to permit manufacture in commercial quantities. However, there can be no assurance that we will not encounter difficulties in scaling up the manufacturing processes.
Our leading drug candidates require specialized manufacturing capabilities and processes. We may face difficulty in securing commitments from U.S. and foreign contract manufacturers as these manufacturers could be unwilling or unable to accommodate our needs. Relying on foreign manufacturers involves peculiar and increased risks, including the risk relating to the difficulty foreign manufacturers may face in complying with cGMP requirements as a result of language barriers, lack of familiarity with cGMP or the FDA regulatory process or other causes, economic or political instability in or affecting the home countries of our foreign manufacturers, shipping delays, potential changes in foreign regulatory laws governing the sales of our product supplies, fluctuations in foreign currency exchange rates and the imposition or application of trade restrictions.
There can be no assurances that contract manufacturers will be able to meet our timetable and requirements. Further, contract manufacturers must operate in compliance with cGMP and failure to do so could result in, among other things, the disruption of product supplies. As noted above, non-U.S. contract manufacturers may face special challenges in complying with cGMP requirements, and although we are not currently dependent on non-U.S. collaborators or contract manufacturers, we may choose or be required to rely on non-U.S. sources in the future as we seek to develop stable supplies of increasing quantities of materials for ongoing clinical trials of larger scale. Our dependence upon third parties for the manufacture of our products may adversely affect our profit margins and our ability to develop and deliver products on a timely and competitive basis.
Our reliance on third parties requires us to share our trade secrets, which increases the possibility that a competitor will discover them.
Because we rely on third parties to develop our products, we must share trade secrets with them. We seek to protect our proprietary technology in part by entering into confidentiality agreements and, if applicable, material transfer agreements, collaborative research agreements, consulting agreements or other similar agreements with our collaborators, advisors, employees and consultants prior to beginning research or disclosing proprietary information. These agreements typically restrict the ability of our collaborators, advisors, employees and consultants to publish data potentially relating to our trade secrets. Our academic collaborators typically have rights to publish data, provided that we are notified in advance and may delay publication for a specified time in order to secure our intellectual property rights arising from the collaboration. In other cases, publication rights are controlled exclusively by us, although in some cases we may share these rights with other parties. We also conduct joint research and development programs which may require us to share trade secrets under the terms of research and development partnership or similar agreements. Despite our efforts to protect our trade secrets,
33
Table of Contents
our competitors may discover our trade secrets, either through breach of these agreements, independent development or publication of information including our trade secrets in cases where we do not have proprietary or otherwise protected rights at the time of publication. A competitor's discovery of our trade secrets would impair our competitive position.
Risks Related to Business Operations
We depend greatly on the intellectual capabilities and experience of our key executives and scientists and the loss of any of them could affect our ability to develop our products.
The loss of Anthony S. Marucci, our President and Chief Executive Officer, or other key members of our staff, including Avery W. Catlin, our Chief Financial Officer, Dr. Thomas Davis, our Chief Medical Officer, Dr. Tibor Keler, our Chief Scientific Officer or Dr. Ronald Pepin, our Chief Business Officer, could harm us. We entered into employment agreements with Messrs. Marucci, Catlin, Davis, Keler and Pepin although an employment agreement as a practical matter does not guarantee retention of an employee. We also depend on our scientific and clinical collaborators and advisors, all of whom have outside commitments that may limit their availability to us. In addition, we believe that our future success will depend in large part upon our ability to attract and retain highly skilled scientific, managerial and marketing personnel, particularly as we expand our activities in clinical trials, the regulatory approval process and sales and manufacturing. We routinely enter into consulting agreements with our scientific and clinical collaborators and advisors, key opinion leaders and heads of academic departments in the ordinary course of our business. We also enter into contractual agreements with physicians and institutions who recruit patients into our clinical trials on our behalf in the ordinary course of our business. Notwithstanding these arrangements, we face significant competition for this type of personnel from other companies, research and academic institutions, government entities and other organizations. We cannot predict our success in hiring or retaining the personnel we require for continued growth.
We expect to expand our clinical development, regulatory and sales and marketing capabilities, and as a result, we may encounter difficulties in managing our growth, which could disrupt our operations.
We expect that if our clinical drug candidates continue to progress in development, we will require significant additional investment in personnel, management systems and resources, particularly in the build out of our commercial capabilities. In preparation for potential approval of rindopepimut we are building the commercial organization that will be responsible for the commercial launch of rindopepimut in the United States and Europe, if it receives marketing approval in such jurisdictions. Over the next several years, we expect to experience significant growth in the number of our employees and the scope of our operations, particularly in the areas of drug development, regulatory affairs and sales and marketing. To manage our anticipated future growth, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and continue to recruit and train additional qualified personnel. Due to our limited financial resources and the limited experience of our management team in managing a company with such anticipated growth, we may not be able to effectively manage the expansion of our operations or recruit and train additional qualified personnel. The physical expansion of our operations may lead to significant costs and may divert our management and business development resources. Any inability to manage growth could delay the execution of our business plans or disrupt our operations.
We may not be able to successfully integrate our existing technology or to modify our technologies to create new immunotherapeutic drugs
If we are able to integrate our acquired and licensed assets with our immunotherapy technologies, we believe these assets will give our immunotherapeutic drugs a competitive advantage. However, if we are unable to successfully integrate licensed assets, or other technologies which we have acquired or
34
Table of Contents
may acquire in the future, with our existing technologies and potential products currently under development, we may be unable to realize any benefit from our acquisition of these assets, or other technologies which we have acquired or may acquire in the future and may face the loss of our investment of financial resources and time in the integration process.
We believe that our immunotherapy technology portfolio may offer opportunities to develop immunotherapeutic drugs that treat a variety of oncology, inflammatory and infectious diseases by stimulating a patient's immune system against those disease organisms. If our immunotherapy technology portfolio cannot be used to create effective immunotherapeutic drugs against a variety of disease organisms, we may lose all or portions of our investment in development efforts for new drug candidates.
Our internal computer systems, or those of our CROs or other contractors or consultants, may fail or suffer security breaches, which could result in a material disruption of our drug development programs.
Despite the implementation of security measures, our internal computer systems and those of our CROs and other contractors and consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. If such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our drug development programs and commercialization efforts. For example, the loss of clinical study data from completed or ongoing clinical studies for any of our drug candidates could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach were to result in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development or commercialization of our drug candidates could be delayed.
Our business requires us to use hazardous materials, which increases our exposure to dangerous and costly accidents.
Our research and development activities involve the use of hazardous chemicals, biological materials and radioactive compounds. Although we believe that our safety procedures for handling and disposing of hazardous materials comply with the standards prescribed by applicable laws and regulations, we cannot completely eliminate the risk of accidental contamination or injury from these materials. In the event of an accident, an injured party will likely sue us for any resulting damages with potentially significant liability. The ongoing cost of complying with environmental laws and regulations is significant and may increase in the future.
We face the risk of product liability claims, which could exceed our insurance coverage, and produce recalls, each of which could deplete our cash resources.
As a participant in the pharmaceutical, biotechnology and immunotherapeutic drug industries, we are exposed to the risk of product liability claims alleging that use of our drug candidates caused an injury or harm. These claims can arise at any point in the development, testing, manufacture, marketing or sale of our drug candidates and may be made directly by patients involved in clinical trials of our products, by consumers or healthcare providers or by individuals, organizations or companies selling our products. Product liability claims can be expensive to defend, even if the drug or drug candidate did not actually cause the alleged injury or harm.
Insurance covering product liability claims becomes increasingly expensive as a drug candidate moves through the development pipeline to commercialization. Under our license agreements, we are required to maintain clinical trial liability insurance coverage up to $15 million. However, there can be no assurance that such insurance coverage is or will continue to be adequate or available to us at a cost
35
Table of Contents
acceptable to us or at all. We may choose or find it necessary under our collaborative agreements to increase our insurance coverage in the future. We may not be able to secure greater or broader product liability insurance coverage on acceptable terms or at reasonable costs when needed. Any liability for damages resulting from a product liability claim could exceed the amount of our coverage, require us to pay a substantial monetary award from our own cash resources and have a material adverse effect on our business, financial condition and results of operations. Moreover, a product recall, if required, could generate substantial negative publicity about our products and business and inhibit or prevent commercialization of other products and drug candidates.
Risks related to Intellectual Property
We license technology from other companies to develop products, and those companies could influence research and development or restrict our use of it. In addition, if we fail to comply with our obligations in our intellectual property licenses with third parties, we could lose license rights that are important to our business.
Companies that license technologies to us that we use in our research and development programs may require us to achieve milestones or devote minimum amounts of resources to develop products using those technologies. They may also require us to make significant royalty and milestone payments, including a percentage of any sublicensing income, as well as payments to reimburse them for patent costs. The number and variety of our research and development programs require us to establish priorities and to allocate available resources among competing programs. From time to time we may choose to slow down or cease our efforts on particular products. If in doing so we fail to fully perform our obligations under a license, the licensor can terminate the licenses or permit our competitors to use the technology. Termination of these licenses or reduction or elimination of our licensed rights may result in our having to negotiate new or reinstated licenses with less favorable terms. Moreover, we may lose our right to market and sell any products based on the licensed technology. The occurrence of such events could materially harm our business.
Our ability to successfully develop and, if regulatory approval is obtained, commercialize our drug candidates may be materially adversely affected if we are unable to obtain and maintain effective intellectual property rights for our drug candidates and technologies.
Our success depends in part on our ability to obtain and maintain patent protection and other intellectual property protection for our drug candidates and proprietary technology. We have sought to protect our proprietary position by filing patent applications in the United States and abroad related to our drug candidates and technology that are important to our business. This process is expensive and time-consuming, and we may not be able to file and prosecute all necessary or desirable patent applications at a reasonable cost or in a timely manner. It is also possible that we will fail to identify patentable aspects of our research and development output before it is too late to obtain patent protection. Our existing patents and any future patents we obtain may not be sufficiently broad to prevent others from using our technologies or from developing competing drugs and technologies.
36
Table of Contents
Biotechnology patents involve complex legal, scientific and factual questions and are highly uncertain. To date, there is no consistent policy regarding the breadth of claims allowed in biotechnology patents, particularly in regard to patents for technologies for human uses like those we use in our business. We cannot predict whether the patents we or our licensors seek will issue. If such patents are issued, a competitor may challenge them and limit their scope. Moreover, our patents may not afford effective protection against competitors with similar technology. A successful challenge to any one of our patents could result in a third party's ability to use the technology covered by the patent. We also face the risk that others will infringe, avoid or circumvent our patents. Technology that we license from others is subject to similar risks and this could harm our ability to use that technology. If we, or a company that licenses technology to us, were not the first creator of an invention that we use, our use of the underlying product or technology will face restrictions, including elimination. For example, in September 2014, two European patent oppositions were filed against a University of Southampton European patent to which we have exclusive rights and which broadly supports one of our drug candidates, varlilumab. While we plan to defend the European patent vigorously in cooperation with the University of Southampton, we may be unsuccessful and the scope of such patent may be limited or the patent may be invalidated.
If we must defend against suits brought against us or prosecute suits against others involving intellectual property rights, we will incur substantial costs. In addition to any potential liability for significant monetary damages, a decision against us may require us to obtain licenses to patents or other intellectual property rights of others on potentially unfavorable terms. If those licenses from third parties are necessary but we cannot acquire them, we would attempt to design around the relevant technology, which would cause higher development costs and delays, and may ultimately prove impracticable.
We may be unable to protect the confidentiality of our trade secrets, thus harming our business and competitive position.
We rely upon trade secrets, including unpatented know-how, technology and other proprietary information to develop and maintain our competitive position, which we seek to protect, in part, by confidentiality agreements with our employees and our collaborators and consultants. We also have agreements with our employees that obligate them to assign their inventions to us. However, it is possible that technology relevant to our business will be independently developed by a person that is not a party to such an agreement. Furthermore, if the employees, consultants or collaborators that are parties to these agreements breach or violate the terms of these agreements, we may not have adequate remedies for any such breach or violation, and we could lose our trade secrets through such breaches or violations. Further, our trade secrets could be disclosed, misappropriated or otherwise become known or be independently discovered by our competitors. In addition, intellectual property laws in foreign countries may not protect our intellectual property to the same extent as the laws of the United States. If our trade secrets are disclosed or misappropriated, it would harm our ability to protect our rights and have a material adverse effect on our business.
We may become involved in lawsuits to protect or enforce our patents, which could be expensive, time-consuming and unsuccessful.
Competitors may infringe our patents. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time-consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours is invalid or unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation proceeding could put one or more of our patents at risk of being invalidated or interpreted narrowly. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a
37
Table of Contents
risk that some of our confidential information could be compromised by disclosure during this type of litigation.
Third parties may initiate legal proceedings alleging that we are infringing their intellectual property rights, the outcome of which would be uncertain and could have a material adverse effect on the success of our business.
Our commercial success depends upon our ability and the ability of our collaborators to develop, manufacture, market and sell our drug candidates and use our proprietary technologies without infringing, misappropriating or otherwise violating the proprietary rights or intellectual property of third parties. We may become party to, or be threatened with, future adversarial proceedings or litigation regarding intellectual property rights with respect to our drug candidates and technology. Third parties may assert infringement claims against us based on existing patents or patents that may be granted in the future. If we are found to infringe a third-party's intellectual property rights, we could be required to obtain a license from such third-party to continue developing our drug candidates and technology. However, we may not be able to obtain any required license on commercially reasonable terms or at all. Even if we were able to obtain a license, it could be non-exclusive, thereby giving our competitors access to the same technologies licensed to us. We could be forced, including by court order, to cease developing the infringing technology or product. In addition, we could be found liable for monetary damages. Claims that we have misappropriated the confidential information or trade secrets of third parties can have a similar negative impact on our business.
Third parties may assert that our employees or consultants have wrongfully used or disclosed confidential information or misappropriated trade secrets.
We employ individuals who were previously employed at universities or other diagnostic or biopharmaceutical companies, including our competitors or potential competitors. Although we try to ensure that our employees and consultants do not use the proprietary information or know-how of others in their work for us, we may be subject to claims that we or our employees, consultants or independent contractors have inadvertently or otherwise used or disclosed intellectual property, including trade secrets or other proprietary information, of a former employer or other third parties. Litigation may be necessary to defend against these claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management and other employees.
Regulatory Risks
If our processes and systems are not compliant with regulatory requirements, we could be subject to delays in submitting BLAs, NDAs or restrictions on marketing of drugs after they have been approved.
We currently are developing drug candidates for regulatory approval and are in the process of implementing regulated processes and systems required to obtain and maintain regulatory approval for our drug candidates. Certain of these processes and systems for conducting clinical trials and manufacturing material must be compliant with regulatory requirements before we can apply for regulatory approval for our drug candidates. These processes and systems will be subject to continual review and periodic inspection by the FDA and other regulatory bodies. If we are unable to achieve compliance in a timely fashion, or if compliance issues are identified at any point in the development and approval process, we may experience delays in filing for regulatory approval for our drug candidates, or delays in obtaining regulatory approval after filing. In addition, any later discovery of previously unknown problems or safety issues with approved drugs or manufacturing processes, or failure to comply with regulatory requirements, may result in restrictions on such drugs or manufacturing processes, withdrawal of drugs from the market, the imposition of civil or criminal
38
Table of Contents
penalties or a refusal by the FDA and/or other regulatory bodies to approve pending applications for marketing approval of new drugs or supplements to approved applications, any of which could have a material adverse effect on our business. In addition, we are a party to agreements that transfer responsibility for complying with specified regulatory requirements, such as filing and maintenance of marketing authorizations and safety reporting or compliance with manufacturing requirements, to our collaborators and third-party manufacturers. If our collaborators or third-party manufacturers do not fulfill these regulatory obligations, any drugs for which we or they obtain approval may be subject to later restrictions on manufacturing or sale, or may even risk withdrawal, which could have a material adverse effect on our business.
Even if we receive regulatory approval for a drug candidate, we will be subject to ongoing regulatory obligations and continued regulatory review, which may result in significant additional expense and subject us to penalties if we fail to comply with applicable regulatory requirements.
Once regulatory approval has been granted, the approved product and its manufacturer are subject to continual review by the FDA and/or non-U.S. regulatory authorities. Any regulatory approval that we or our collaboration partners receive for our drug candidates may be subject to limitations on the indicated uses for which the product may be marketed or contain requirements for potentially costly post-marketing follow-up studies to monitor the safety and efficacy of the product. In addition, if the FDA and/or non-U.S. regulatory authorities approve any of our drug candidates, we will be subject to extensive and ongoing regulatory requirements by the FDA and other regulatory authorities with regard to the labeling, packaging, adverse event reporting, storage, advertising, promotion and recordkeeping for our products. In addition, manufacturers of our drug products are required to comply with cGMP regulations, which include requirements related to quality control and quality assurance as well as the corresponding maintenance of records and documentation. Further, regulatory authorities must inspect and approve these manufacturing facilities before they can be used to manufacture our drug products, and these facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with cGMP regulations. If we or a third party discover previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where the product is manufactured, a regulatory authority may impose restrictions on that product, the manufacturer or us, including requiring withdrawal of the product from the market or suspension of manufacturing. If we, our drug candidates or the manufacturing facilities for our drug candidates fail to comply with regulatory requirements of the FDA and/or other non-U.S. regulatory authorities, we could be subject to administrative or judicially imposed sanctions, including the following:
- •
- warning letters;
- •
- civil or criminal penalties and fines;
- •
- injunctions;
- •
- consent decrees;
- •
- suspension or withdrawal of regulatory approval;
- •
- suspension of any ongoing clinical studies;
- •
- voluntary or mandatory product recalls and publicity requirements;
- •
- refusal to accept or approve applications for marketing approval of new drugs;
- •
- restrictions on operations, including costly new manufacturing requirements; or
- •
- seizure or detention of drugs or import bans.
39
Table of Contents
The regulatory requirements and policies may change and additional government regulations may be enacted for which we may also be required to comply. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the United States or in other countries. If we are not able to maintain regulatory compliance, we may not be permitted to market our future products and our business may suffer.
Health care reform and restrictions on reimbursement may limit our returns on potential products.
Because our strategy ultimately depends on the commercial success of our products, we assume, among other things, that end users of our products will be able to pay for them. In the United States and other countries, in most cases, the volume of sales of products like those we are developing depends on the availability of reimbursement from third-party payors, including national health care agencies, private health insurance plans and health maintenance organizations. Third-party payors increasingly challenge the prices charged for medical products and services. Accordingly, if we succeed in bringing products to market, and reimbursement is not available or is insufficient, we could be prevented from successfully commercializing our potential products.
The health care industry in the United States and in Europe is undergoing fundamental changes as a result of political, economic and regulatory influences. Reforms proposed from time to time include mandated basic health care benefits, controls on health care spending, the establishment of governmental controls over the cost of therapies, creation of large medical services and products purchasing groups and fundamental changes to the health care delivery system. We anticipate ongoing review and assessment of health care delivery systems and methods of payment in the United States and other countries. We cannot predict whether any particular reform initiatives will result or, if adopted, what their impact on us will be. However, we expect that adoption of any reform proposed will impair our ability to market products at acceptable prices and that uncertainty concerning future government regulation of consumer healthcare purchasing and insurance may result in difficulties for drug development companies, like us, in raising capital.
Changes in laws affecting the health care industry could adversely affect our business.
In the U.S., there have been numerous proposals considered at the federal and state levels to reform the health care industry and its cost, and it is likely that federal and state legislatures and health agencies will continue to focus on health care reform in the future. While additional health care reform may increase the number of patients who have insurance coverage for our products, it may also include cost containment measures that adversely affect reimbursement for our products. Congress has also considered legislation to change the Medicare reimbursement system for outpatient drugs, increase the amount of rebates that manufacturers pay for coverage of their drugs by Medicaid programs and facilitate the importation of lower-cost prescription drugs that are marketed outside the U.S. Some states are also considering legislation that would control the prices of drugs, and state Medicaid programs are increasingly requesting manufacturers to pay supplemental rebates and requiring prior authorization by the state program for use of any drug for which supplemental rebates are not being paid. Managed care organizations continue to seek price discounts and, in some cases, to impose restrictions on the coverage of particular drugs. Government efforts to reduce Medicaid expenses may lead to increased use of managed care organizations by Medicaid programs. This may result in managed care organizations influencing prescription decisions for a larger segment of the population and a corresponding constraint on prices and reimbursement for our products.
40
Table of Contents
We and our collaborators and partners operate in a highly regulated industry. As a result, governmental actions may adversely affect our business, operations or financial condition, including:
- •
- new laws, regulations or judicial decisions, or new interpretations of existing laws, regulations or decisions, related to health care availability, method of delivery and payment for health care products and services;
- •
- changes in the FDA and foreign regulatory approval processes that may delay or prevent the approval of new products and result in lost market opportunity;
- •
- changes in FDA and foreign regulations that may require additional safety monitoring, labeling changes, restrictions on product distribution or use, or other measures after the introduction of our products to market, which could increase our costs of doing business, adversely affect the future permitted uses of approved products, or otherwise adversely affect the market for our products;
- •
- new laws, regulations and judicial decisions affecting pricing or marketing practices; and
- •
- changes in the tax laws relating to our operations.
The enactment in the U.S. of health care reform, possible legislation which could ease the entry of competing follow-on biologics in the marketplace, new legislation or implementation of existing statutory provisions on importation of lower-cost competing drugs from other jurisdictions, and legislation on comparative effectiveness research are examples of previously enacted and possible future changes in laws that could adversely affect our business. In addition, the Food and Drug Administration Amendments Act of 2007 included new authorization for the FDA to require post-market safety monitoring, along with an expanded clinical trials registry and clinical trials results database, and expanded authority for the FDA to impose civil monetary penalties on companies that fail to meet certain commitments.
Risks Related to our Capital Stock
Our history of losses and uncertainty of future profitability make our common stock a highly speculative investment.
We have had no commercial revenue to date from sales of our drug candidates. We had an accumulated deficit of $463.8 million as of December 31, 2014. We expect to spend substantial funds to continue the research and development testing of our products candidates.
In anticipation of FDA approval of these products, we will need to make substantial investments to establish sales, marketing, quality control, regulatory compliance capabilities and commercial manufacturing alliances. These investments will increase if and when any of these products receive FDA approval. We cannot predict how quickly our lead products will progress through the regulatory approval process. As a result, we may continue to lose money for several years.
We cannot be certain that we will achieve or sustain profitability in the future. Failure to achieve profitability could diminish our ability to sustain operations, pay dividends on our common stock, obtain additional required funds and make required payments on our present or future indebtedness.
Our share price has been and could remain volatile.
The market price of our common stock has historically experienced and may continue to experience significant volatility. From January 2014 through December 2014, the market price of our common stock has fluctuated from a high of $33.33 per share in the first quarter of 2014, to a low of $10.76 per share in the second quarter of 2014. Our progress in developing and commercializing our products, the impact of government regulations on our products and industry, the potential sale of a
41
Table of Contents
large volume of our common stock by stockholders, our quarterly operating results, changes in general conditions in the economy or the financial markets and other developments affecting us or our competitors could cause the market price of our common stock to fluctuate substantially with significant market losses. If our stockholders sell a substantial number of shares of common stock, especially if those sales are made during a short period of time, those sales could adversely affect the market price of our common stock and could impair our ability to raise capital. In addition, in recent years, the stock market has experienced significant price and volume fluctuations. This volatility has affected the market prices of securities issued by many companies for reasons unrelated to their operating performance and may adversely affect the price of our common stock. In addition, we could be subject to a securities class action litigation as a result of volatility in the price of our stock, which could result in substantial costs and diversion of management's attention and resources and could harm our stock price, business, prospects, results of operations and financial condition.
Our ability to use our net operating loss carryforwards will be subject to limitation and, under certain circumstances, may be eliminated.
Utilization of our net operating loss and research and development credit carryforwards may be subject to substantial annual limitation due to ownership change limitations that have occurred previously or that could occur in the future provided by Section 382 of the Internal Revenue Code of 1986, or Section 382, as well as similar state provisions. In general, an ownership change, as defined by Section 382, results from transactions increasing the ownership of certain shareholders or public groups in the stock of a corporation by more than 50 percentage points over a three-year period.
In October 2007, June 2009 and in December 2009, we experienced a change in ownership as defined by Section 382 of the Internal Revenue Code. Historically, we have raised capital through the issuance of capital stock on several occasions which, combined with shareholders' subsequent disposition of those shares, has resulted in three changes of control, as defined by Section 382. As a result of the ownership change in October 2007, utilization of our Federal net operating loss carryforwards is subject to an annual limitation. Any unused annual limitation may be carried over to later years, and the amount of the limitation may, under certain circumstances, be subject to adjustment if the fair value of the our net assets are determined to be below or in excess of the tax basis of such assets at the time of the ownership change, and such unrealized loss or gain is recognized during the five-year period after the ownership change. Subsequent ownership changes, as defined in Section 382, could further limit the amount of net operating loss carryforwards and research and development credits that can be utilized annually to offset future taxable income.
We have not undertaken a study to assess whether an ownership change or multiple ownership changes has occurred for (i) AVANT or CuraGen prior to our acquisitions, (ii) the Company on the state level, (iii) the Company since October 2012, or (iv) research and development credits. If, based on such a study, we were to determine that there has been an ownership change at any time since its formation, utilization of net operating loss or tax credit carryforwards would be subject to an annual limitation under Section 382.
Refer to Note 15, "Income Taxes," in the accompanying notes to the consolidated financial statements for additional discussion on income taxes.
Item 1B. UNRESOLVED STAFF COMMENTS
None.
42
Table of Contents
Item 2. PROPERTIES
As of December 31, 2014, our significant leased properties are described below.
| | | | | | | |
Property Location | | Approximate
Square Feet | | Use | | Lease Expiration Date |
|---|
Hampton, New Jersey | | | 33,400 | | Headquarters, Office and Laboratory | | April 2019(1) |
Needham, Massachusetts | | | 35,200 | | Office and Laboratory | | April 2017(2) |
Fall River, Massachusetts | | | 23,400 | | Manufacturing Facility | | December 2017(3) |
Branford, Connecticut | | | 10,300 | | Office | | December 2019(4) |
- (1)
- Lease includes two renewal options of five years each.
- (2)
- Lease includes one renewal option of five years.
- (3)
- Lease includes two renewal options of five years each. Lease also includes provision for early termination in December 2015 upon prior notice of one year.
- (4)
- Lease includes two renewal options of three years. Lease also includes provision for early termination with 12 months notice.
Item 3. LEGAL PROCEEDINGS
We are not currently a party to any material legal proceedings.
Item 4. MINE SAFETY DISCLOSURES
Not applicable.
43
Table of Contents
PART II
Item 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Our common stock currently trades on the Nasdaq Global Market (NASDAQ) under the symbol "CLDX". The following table sets forth for the periods indicated the high and low sale prices per share for our common stock, as reported by NASDAQ.
| | | | | | | |
Fiscal Period | | High | | Low | |
|---|
Year Ended December 31, 2013 | | | | | | | |
First Quarter | | $ | 12.49 | | $ | 6.81 | |
Second Quarter | | | 16.48 | | | 10.73 | |
Third Quarter | | | 37.98 | | | 16.00 | |
Fourth Quarter | | | 38.84 | | | 20.85 | |
Year Ended December 31, 2014 | | | | | | | |
First Quarter | | $ | 33.33 | | $ | 16.58 | |
Second Quarter | | | 18.52 | | | 10.76 | |
Third Quarter | | | 18.30 | | | 11.93 | |
Fourth Quarter | | | 21.70 | | | 12.11 | |
As of February 17, 2015, there were approximately 366 shareholders of record of our common stock. On February 17, 2015 the closing price of our common stock, as reported by NASDAQ, was $21.44 per share. We have not paid any dividends on our common stock since our inception and do not intend to pay any dividends in the foreseeable future.
Equity Compensation Plan Information
The following table provides information as of December 31, 2014 regarding shares of our common stock that may be issued under our existing equity compensation plans, including our 2008 Stock Option and Incentive Plan (the "2008 Plan") and our 2004 Employee Stock Purchase Plan (the "2004 ESPP Plan").
| | | | | | | | | | |
| | Equity Compensation Plan Information | |
|---|
| | Number of securities
to be issued upon exercise
of outstanding options
and rights(1) | | Weighted Average
exercise price of
outstanding options
and rights | | Number of securities
remaining available for
future issuance under equity
compensation plan
(excluding securities
referenced in column (a)) | |
|---|
Equity compensation plans approved by security holders(2) | | | 7,015,350 | (3) | $ | 9.34 | | | 828,485 | (4) |
- (1)
- Does not include any Restricted Stock as such shares are already reflected in our outstanding shares.
- (2)
- Consists of the 2008 Plan, 2004 ESPP Plan, Celldex Research's 2005 Equity Incentive Plan and CuraGen's 2007 Stock Plan.
- (3)
- Does not include purchase rights accruing under the 2004 ESPP Plan because the purchase price (and therefore the number of shares to be purchased) will not be determined until the end of the purchase period.
- (4)
- Includes shares available for future issuance under the 2008 Plan and the 2004 ESPP Plan.
44
Table of Contents
CELLDEX THEAPEUTICS, INC., NASDAQ MARKET INDEX—U.S. AND
PEER GROUP INDICES
The graph below compares the cumulative total stockholder return on the common stock for the period from December 31, 2009 through December 31, 2014, with the cumulative return on (i) NASDAQ US Benchmark TR Index and (ii) NASDAQ Pharmaceutical (Subsector) Index. The comparison assumes investment of $100 on December 31, 2009 in our common stock and in each of the indices and, in each case, assumes reinvestment of all dividends. The points on the graph are as of December 31 of the year indicated.
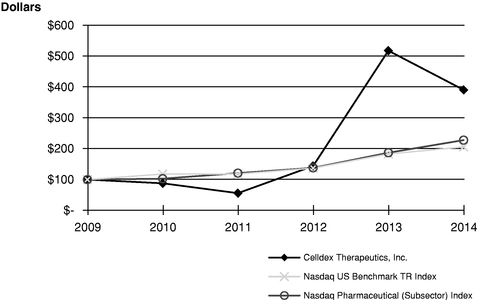
| | | | | | | | | | | | | | | | | | | |
| | 2009 | | 2010 | | 2011 | | 2012 | | 2013 | | 2014 | |
|---|
Celldex Therapeutics, Inc. | | $ | 100 | | $ | 88 | | $ | 56 | | $ | 144 | | $ | 518 | | $ | 391 | |
NASDAQ US Benchmark TR Index | | $ | 100 | | $ | 118 | | $ | 118 | | $ | 137 | | $ | 183 | | $ | 206 | |
NASDAQ Pharmaceutical (Subsector) Index | | $ | 100 | | $ | 103 | | $ | 121 | | $ | 138 | | $ | 187 | | $ | 228 | |
Item 6. SELECTED FINANCIAL DATA
The following selected consolidated financial data are derived from our financial statements. The consolidated statement of operations data for the years ended December 31, 2014, 2013 and 2012 and the consolidated balance sheet data as of December 31, 2014 and 2013 have been derived from our audited consolidated financial statements included in Item 8 of this Annual Report on Form 10-K. This data should be read in conjunction with our audited consolidated financial statements and related notes which are included elsewhere in this Annual Report on Form 10-K, and "Management's Discussion and Analysis of Financial Condition and Results of Operations" included in Item 7 below.
45
Table of Contents
CONSOLIDATED STATEMENTS OF OPERATIONS DATA
(In thousands, except per share amounts)
| | | | | | | | | | | | | | | | |
| | Year Ended December 31, | |
|---|
| | 2014 | | 2013 | | 2012 | | 2011 | | 2010 | |
|---|
REVENUE: | | | | | | | | | | | | | | | | |
Product Development and Licensing Agreements | | $ | 838 | | $ | 160 | | $ | 146 | | $ | 110 | | $ | 40,187 | |
Contracts and Grants | | | 2,748 | | | 1,617 | | | 281 | | | 36 | | | 220 | |
Product Royalties | | | — | | | 2,334 | | | 10,775 | | | 9,119 | | | 6,386 | |
| | | | | | | | | | | | | | | | | |
Total Revenue | | | 3,586 | | | 4,111 | | | 11,202 | | | 9,265 | | | 46,793 | |
| | | | | | | | | | | | | | | | | |
OPERATING EXPENSE: | | | | | | | | | | | | | | | | |
Research and Development | | | 104,381 | | | 67,401 | | | 47,398 | | | 32,439 | | | 27,650 | |
Royalty | | | — | | | 2,334 | | | 10,775 | | | 9,119 | | | 12,077 | |
Other Operating Expense | | | 21,635 | | | 15,818 | | | 11,106 | | | 11,106 | | | 13,521 | |
| | | | | | | | | | | | | | | | | |
Total Operating Expense | | | 126,016 | | | 85,553 | | | 69,279 | | | 52,664 | | | 53,248 | |
| | | | | | | | | | | | | | | | | |
Operating Loss | | | (122,430 | ) | | (81,442 | ) | | (58,077 | ) | | (43,399 | ) | | (6,455 | ) |
Investment and Other Income, Net | | | 4,350 | | | 819 | | | 530 | | | 396 | | | 5,259 | |
Interest Expense | | | — | | | (927 | ) | | (1,576 | ) | | (1,796 | ) | | (1,337 | ) |
| | | | | | | | | | | | | | | | | |
Net Loss | | $ | (118,080 | ) | $ | (81,550 | ) | $ | (59,123 | ) | $ | (44,799 | ) | $ | (2,533 | ) |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
Basic and Diluted Net Loss Per Common Share | | $ | (1.32 | ) | $ | (1.02 | ) | $ | (1.02 | ) | $ | (1.13 | ) | $ | (0.08 | ) |
| | | | �� | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
Shares Used in Calculating Basic and Diluted Net Loss Per Common Share | | | 89,399 | | | 79,777 | | | 57,713 | | | 39,501 | | | 31,868 | |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
CONSOLIDATED BALANCE SHEET DATA
(In thousands)
| | | | | | | | | | | | | | | | |
| | December 31, | |
|---|
| | 2014 | | 2013 | | 2012 | | 2011 | | 2010 | |
|---|
Working Capital | | $ | 180,494 | | $ | 284,839 | | $ | 67,429 | | $ | 40,386 | | $ | 42,739 | |
Total Assets | | | 248,014 | | | 347,095 | | | 125,541 | | | 97,994 | | | 109,943 | |
Long Term Liabilities | | | 11,863 | | | 6,950 | | | 12,082 | | | 14,974 | | | 14,480 | |
Accumulated Deficit | | | (463,759 | ) | | (345,679 | ) | | (264,129 | ) | | (205,006 | ) | | (160,207 | ) |
Total Stockholders' Equity | | | 211,660 | | | 319,795 | | | 95,774 | | | 68,722 | | | 75,255 | |
46
Table of Contents
Item 7. MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
OVERVIEW
We are a biopharmaceutical company focused on the development and commercialization of several immunotherapy technologies for the treatment of cancer and other difficult-to-treat diseases. Our drug candidates are derived from a broad set of complementary technologies which have the ability to utilize the human immune system and enable the creation of therapeutic agents. We are using these technologies to develop targeted immunotherapeutics comprised of antibodies, adjuvants and monotherapies and antibody-drug conjugates that prevent or treat cancer and other diseases that modify undesirable activity by the body's own proteins or cells.
Our lead drug candidates include rindopepimut (also referred to as Rintega® and CDX-110) and glembatumumab vedotin (also referred to as CDX-011). Rindopepimut is a targeted immunotherapeutic in a pivotal Phase 3 study for the treatment of front-line glioblastoma and a Phase 2 study for the treatment of recurrent glioblastoma. Glembatumumab vedotin is a targeted antibody-drug conjugate in a randomized, Phase 2b study for the treatment of triple negative breast cancer and a Phase 2 study for the treatment of metastatic melanoma. We also have a number of earlier stage drug candidates in clinical development, including varlilumab (also referred to as CDX-1127), a fully human therapeutic monoclonal antibody for cancer indications, CDX-1401, a targeted immunotherapeutic aimed at antigen presenting cells, or APC, for cancer indications and CDX-301, an immune cell mobilizing agent and dendritic cell growth factor. Our drug candidates address market opportunities for which we believe current therapies are inadequate or non-existent.
We are building a fully integrated, commercial-stage biopharmaceutical company that develops important therapies for patients with unmet medical needs. Our program assets provide us with the strategic options to either retain full economic rights to our innovative therapies or seek favorable economic terms through advantageous commercial partnerships. This approach allows us to maximize the overall value of our technology and product portfolio while best ensuring the expeditious development of each individual product.
The following table includes the programs that we currently believe are significant to our business:
| | | | | | |
Product (generic) | | Indication/Field | | Partner | | Status |
|---|
| CLINICAL | | | | | | |
Rindopepimut | | Front-line glioblastoma | | — | | Phase 3 |
Glembatumumab vedotin | | Metastatic breast cancer | | — | | Phase 2b |
Rindopepimut | | Recurrent glioblastoma | | — | | Phase 2 |
Glembatumumab vedotin | | Metastatic melanoma | | — | | Phase 2 |
Varlilumab | | Lymphoma/leukemia and solid tumors | | — | | Phase 1 |
Varlilumab | | Multiple solid tumors | | — | | Phase 1/2 |
CDX-1401 | | Multiple solid tumors | | — | | Phase 1 |
CDX-301 | | Allogeneic Hematopoietic Stem Cell Transplantation | | — | | Phase 1 |
| PRECLINICAL | | | | | | |
CDX-014 | | Ovarian and renal cancer | | — | | Preclinical |
The expenditures that will be necessary to execute our business plan are subject to numerous uncertainties. Completion of clinical trials may take several years or more, and the length of time generally varies substantially according to the type, complexity, novelty and intended use of a product candidate. It is not unusual for the clinical development of these types of product candidates to each take five years or more, and for total development costs to exceed $100 million for each product
47
Table of Contents
candidate. Our estimates that clinical trials of the type we generally conduct are typically completed over the following timelines:
| | |
Clinical Phase | | Estimated
Completion
Period |
|---|
Phase 1 | | 1 - 2 Years |
Phase 2 | | 1 - 5 Years |
Phase 3 | | 1 - 5 Years |
The duration and the cost of clinical trials may vary significantly over the life of a project as a result of differences arising during the clinical trial protocol, including, among others, the following:
- •
- the number of patients that ultimately participate in the trial;
- •
- the duration of patient follow-up that seems appropriate in view of results;
- •
- the number of clinical sites included in the trials;
- •
- the length of time required to enroll suitable patient subjects; and
- •
- the efficacy and safety profile of the product candidate.
We test potential product candidates in numerous preclinical studies for safety, toxicology and immunogenicity. We may then conduct multiple clinical trials for each product candidate. As we obtain results from trials, we may elect to discontinue or delay clinical trials for certain product candidates in order to focus our resources on more promising product candidates.
An element of our business strategy is to pursue the research and development of a broad portfolio of product candidates. This is intended to allow us to diversify the risks associated with our research and development expenditures. To the extent we are unable to maintain a broad range of product candidates, our dependence on the success of one or a few product candidates increases.
Regulatory approval is required before we can market our product candidates as therapeutic products. In order to proceed to subsequent clinical trial stages and to ultimately achieve regulatory approval, the regulatory agency must conclude that our clinical data is safe and effective. Historically, the results from preclinical testing and early clinical trials (through Phase 2) have often not been predictive of results obtained in later clinical trials. A number of new drugs and biologics have shown promising results in early clinical trials, but subsequently failed to establish sufficient safety and efficacy data to obtain necessary regulatory approvals.
Furthermore, our business strategy includes the option of entering into collaborative arrangements with third parties to complete the development and commercialization of our product candidates. In the event that third parties take over the clinical trial process for one of our product candidates, the estimated completion date would largely be under control of that third party rather than us. We cannot forecast with any degree of certainty which proprietary products, if any, will be subject to future collaborative arrangements, in whole or in part, and how such arrangements would affect our development plan or capital requirements. Our programs may also benefit from subsidies, grants, contracts or government or agency-sponsored studies that could reduce our development costs.
As a result of the uncertainties discussed above, among others, it is difficult to accurately estimate the duration and completion costs of our research and development projects or when, if ever, and to what extent we will receive cash inflows from the commercialization and sale of a product. Our inability to complete our research and development projects in a timely manner or our failure to enter into collaborative agreements, when appropriate, could significantly increase our capital requirements and could adversely impact our liquidity. These uncertainties could force us to seek additional, external sources of financing from time to time in order to continue with our business strategy. Our inability to raise additional capital, or to do so on terms reasonably acceptable to us, would jeopardize the future success of our business.
48
Table of Contents
During the past five years through December 31, 2014, we incurred an aggregate of $279.3 million in research and development expenses. The following table indicates the amount incurred for each of our significant research programs and for other identified research and development activities during the years ended December 31, 2014, 2013 and 2012. The amounts disclosed in the following table reflect direct research and development costs, license fees associated with the underlying technology and an allocation of indirect research and development costs to each program.
| | | | | | | | | | |
| | Year Ended
December 31, 2014 | | Year Ended
December 31, 2013 | | Year Ended
December 31, 2012 | |
|---|
| | (In thousands)
| |
|---|
Rindopepimut | | $ | 52,861 | | $ | 38,149 | | $ | 25,004 | |
Glembatumumab vedotin | | | 26,907 | | | 11,284 | | | 6,325 | |
Varlilumab | | | 9,459 | | | 9,376 | | | 4,020 | |
CDX-1401 | | | 4,144 | | | 612 | | | 1,032 | |
CDX-301 | | | 1,238 | | | 532 | | | 1,482 | |
CDX-014 | | | 3,722 | | | 937 | | | 1,071 | |
Other Programs | | | 6,050 | | | 6,511 | | | 8,464 | |
| | | | | | | | | | | |
Total R&D Expense | | $ | 104,381 | | $ | 67,401 | | $ | 47,398 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Clinical Development Programs
Rindopepimut
Rindopepimut is an immunotherapeutic that targets the tumor-specific molecule epidermal growth factor receptor variant III, or EGFRvIII. EGFRvIII is a mutated form of the epidermal growth factor receptor, or EGFR, that is only expressed in cancer cells and not in normal tissue and can directly contribute to cancer cell growth. EGFRvIII is expressed in approximately 30% of glioblastoma multiforme, or GBM, tumors, the most common and aggressive form of brain cancer. Rindopepimut is composed of the EGFRvIII peptide linked to a carrier protein called Keyhole Limpet Hemocyanin, or KLH, and administered together with the adjuvant GM-CSF. The Food and Drug Administration, or FDA, and the European Medicines Agency, or EMA, have both granted orphan drug designation for rindopepimut for the treatment of EGFRvIII expressing GBM. The FDA has also granted Fast Track designation. In February 2015, the FDA granted rindopepimut Breakthrough Therapy Designation for the treatment of adult patients with EGFRvIII-positive glioblastoma.
The Phase 2a study of rindopepimut referred to as ACTIVATE was led by collaborating investigators at the Brain Center at Duke Comprehensive Cancer Center in Durham, North Carolina and at M.D. Anderson Cancer Center in Houston, Texas and enrolled 18 evaluable GBM patients. An extension of the Phase 2a study referred to as ACT II evaluated 22 additional GBM patients treated in combination with the current standard of care, maintenance temozolomide, or TMZ, at the same two institutions.
The Phase 2b study of rindopepimut referred to as ACT III combined rindopepimut with standard of care, TMZ, in patients with newly diagnosed GBM. The ACT III study provided for a multi-center, non-randomized dataset for rindopepimut in 65 patients at over 30 sites throughout the United States.
In November 2013, we announced the four- and five-year survival data from the 105 patients enrolled in the three Phase 2 rindopepimut clinical studies (ACTIVATE, ACT II and ACT III) in EGFRvIII-positive GBM. Across these three Phase 2 studies of rindopepimut, survival data remains consistent and suggests a continuing survival benefit in comparison to independent control datasets (see chart below) at the median and at all other time points evaluated.
49
Table of Contents
Phase 2 Frontline Long-term Overall Survival Assessments
| | | | | | | | | | | | | | | | |
| | Median, Years
(95% CI) | | 2-year
rate | | 3-year
rate | | 4-year
rate | | 5-year
rate | |
|---|
Phase 2 rindopepimut studies (n=105) | | | 2.1 (1.8, 2.4 | ) | | 51 | % | | 30 | % | | 18 | % | | 14 | % |
Matched historical control (n=17)(1) | | | 1.3 (0.9, 1.7 | ) | | 6 | % | | 6 | % | | 0 | % | | 0 | % |
- (1)
- Patients treated at M.D. Anderson contemporaneously to ACTIVATE, matched for major eligibility requirements, including EGFRvIII-positive GBM, gross total resection and no disease progression through chemoradiation treatment.
The pooled overall long-term survival results continue to be consistent with the ACT III Phase 2 study (18% for 4-years and 14% for 5-years).
In December 2011, we initiated ACT IV, a pivotal, randomized, double-blind, controlled Phase 3 study of rindopepimut in patients with surgically resected, EGFRvIII-positive GBM. Patients were randomized after the completion of surgery and standard chemoradiation treatment. The treatment regimen included a rindopepimut priming phase post-radiation followed by an adjuvant TMZ phase and a rindopepimut maintenance therapy phase. Patients are treated until disease progression or intolerance to therapy. The primary objective of the study is to determine whether rindopepimut plus adjuvant GM-CSF improves the overall survival of patients with newly diagnosed EGFRvIII-positive GBM with minimal residual disease post resection and traditional chemo-radiation when compared to treatment with TMZ and a control injection of KLH. KLH is a component of rindopepimut and was selected due to its ability to generate a similar injection site reaction to that observed with rindopepimut.
In December 2014, ACT IV completed enrollment. In total, over 4,800 GBM patients were screened for EGFRvIII status from more than 200 clinical trial sites across 22 countries and, consistent with prior studies, 30% were positive for the EGFRvIII mutation. The study enrolled 745 patients to reach the required 374 patients with minimal residual disease (assessed by central review) needed for analysis of the primary overall survival endpoint. All patients, including patients with disease that exceed this threshold, will be included in a secondary analysis of overall survival as well as analyses of progression-free survival, safety and tolerability, and quality of life. The timing of the overall survival primary endpoint data is event-driven. Interim analyses will be conducted by an independent Data Safety and Monitoring Board at 50% and 75% of events (deaths). The first interim analysis is expected in mid-2015. The second interim analysis is currently expected in late 2015 or early 2016 and the final data is currently expected by the end of 2016, although our expectations regarding the timing for the second interim analysis and final data read out may change based on event rates.
In December 2011, we also initiated ReACT, a Phase 2 study of rindopepimut in combination with Avastin® in patients with recurrent EGFRvIII-positive GBM. This study completed enrollment in 2014 and includes 3 groups. Group 1 consists of 72 patients who had not previously received Avastin and were randomized to receive either rindopepimut and Avastin or a control injection of KLH and Avastin in a blinded fashion. Group 2 includes 25 patients who are refractory to Avastin having received Avastin in either the frontline or recurrent setting with subsequent progression and who received rindopepimut plus Avastin in a single treatment arm. In August 2013, we announced the addition of an expansion cohort of up to 75 patients, called Group 2C, to better characterize the potential activity of rindopepimut in this refractory patient population. This decision was based on early evidence of anti-tumor activity, including stable disease, tumor shrinkage and investigator-reported response. In total, Group 2C enrolled 28 patients. The primary endpoint is six month progression-free survival rate (PFS-6) for groups 1 and 2 and objective response rate (ORR) for group 2C. Other study endpoints include PFS-6, ORR, PFS, overall survival, or OS and safety and tolerability.
In November 2014, we reported the following interim data from the ReACT study. Rindopepimut plus Avastin was very well tolerated (dosing up to 26+ months) and the results demonstrated clear
50
Table of Contents
signs of clinical activity in advanced patient populations, including evidence of anti-tumor activity (tumor shrinkage, objective response and stable disease). Strong immune response correlated with improved outcome. In Avastin-naïve patients treated with both rindopepimut and Avastin, a statistically significant survival benefit was seen compared to the control patients.
Group 1 Interim Data
- •
- PFS-6: PFS-6 by investigator read was 27% for patients treated with rindopepimut compared to 11% for control patients (p=0.048)
- •
- Survival: The OS demonstrated a statistically significant benefit (p=0.0208) with a hazard ratio of 0.47 (0.25, 0.91) in favor of the rindopepimut treated patients. Median OS was 12.0 months for patients treated with rindopepimut compared to 8.8 months for control patients.
- •
- Response Rate: 7 out of 29 patients (24%) evaluable for response on the rindopepimut arm experienced a confirmed objective response versus 5 out of 30 patients (17%) evaluable for response on the control arm. Assessments of response were conducted by study investigators according to RANO criteria.
- •
- Other: All subgroup analyses, including performance status, steroid use and recent resection, show a hazard ratio in favor of rindopepimut treatment.
Group 2/2C Interim Data
- •
- Survival: Median OS was 5.1 months (95% CI 3.2, 6.5) for these heavily pretreated, refractory EGFRvIII-positive patients. 46% of patients in Group 2/2C were alive at 6 months.
- •
- Response Rate: Based on investigator assessment, two patients experienced complete response, of which one was unconfirmed, and two patients experienced partial response, of which one was unconfirmed, in Group 2. Two of these four patients did not meet the protocol defined definition of refractory in Group 2, the only two such patients enrolled. No additional objective responses were observed in Group 2C and the study did not meet the criteria (defined as two responses in the first 23 patients enrolled in Group 2C) for continued enrollment. Ten patients with measurable disease experienced objective tumor shrinkage across Group 2/2C.
Final data is anticipated by mid-year 2015 and we intend to present this data at a peer-reviewed medical meeting in this same time frame.
Glembatumumab Vedotin
Glembatumumab vedotin is an antibody-drug conjugate, or ADC, that consists of a fully-human monoclonal antibody, CR011, linked to a potent cell-killing drug, monomethyl-auristatin E, or MMAE. The CR011 antibody specifically targets glycoprotein NMB, referred to as gpNMB, that is over-expressed in a variety of cancers including breast cancer and melanoma. The ADC technology, comprised of MMAE and a stable linker system for attaching it to CR011, was licensed from Seattle Genetics, Inc. and is the same as that used in the marketed product Adcetris®. The ADC is designed to be stable in the bloodstream. Following intravenous administration, glembatumumab vedotin targets and binds to gpNMB and upon internalization into the targeted cell, glembatumumab vedotin is designed to release MMAE from CR011 to produce a cell-killing effect. The FDA has granted Fast Track designation to glembatumumab vedotin for the treatment of advanced, refractory/resistant gpNMB-expressing breast cancer.
Treatment of Breast Cancer: The Phase 1/2 study of glembatumumab vedotin administered intravenously once every three weeks evaluated patients with locally advanced or metastatic breast cancer who had received prior therapy (median of seven prior regimens). The study began with a bridging phase to confirm the maximum tolerated dose, or MTD, and then expanded into a Phase 2 open-label, multi-center study. The study confirmed the safety of glembatumumab vedotin at the
51
Table of Contents
pre-defined maximum dose level (1.88 mg/kg) in 6 patients. An additional 28 patients were enrolled in an expanded Phase 2 cohort (for a total of 34 treated patients at 1.88 mg/kg, the Phase 2 dose) to evaluate the PFS rate at 12 weeks. The 1.88 mg/kg dose was well tolerated in this patient population with the most common adverse events of rash, alopecia, and fatigue. The primary activity endpoint, which called for at least 5 of 25 (20%) patients in the Phase 2 study portion to be progression-free at 12 weeks, was met as 9 of 26 (35%) evaluable patients were progression-free at 12 weeks.
For all patients treated at the maximum dose level, tumor shrinkage was seen in 62% (16/26) and median PFS was 9.1 weeks. A subset of 10 patients had "triple negative disease," a more aggressive breast cancer subtype that carries a high risk of relapse and reduced survival as well as limited therapeutic options due to lack of over-expression of HER2/neu, estrogen and progesterone receptors. In these patients, 78% (7/9) had some tumor shrinkage, 12-week PFS rate was 70% (7/10), and median PFS was 17.9 weeks. Tumor samples from a subset of patients across all dose groups were analyzed for gpNMB expression. The tumor samples from most patients showed evidence of stromal and/or tumor cell expression of gpNMB.
In December 2012, we announced final results from the EMERGE study, a randomized, multi-center Phase 2b study of glembatumumab vedotin in 122 patients with heavily pre-treated, advanced, gpNMB positive breast cancer. Patients were randomized (2:1) to receive either glembatumumab vedotin or single-agent Investigator's Choice, or IC, chemotherapy. Patients randomized to receive IC were allowed to cross over to receive glembatumumab vedotin following disease progression. Activity endpoints included response rate, PFS and OS. The final results, as shown below, suggested that glembatumumab vedotin induces significant response rates compared to currently available therapies in patient subsets with advanced, refractory breast cancers with gpNMB over-expression (expression in greater than or equal to 25% of tumor cells) and in patients with triple negative breast cancer. The OS and PFS of patients treated with glembatumumab vedotin was also observed to be greatest in patients with triple negative breast cancer who also over-express gpNMB and all patients with gpNMB over-expression.
EMERGE: Overall Response Rate and Disease Control Data
| | | | | | | | | | | | | |
| | gpNMB Over-Expression | | Triple Negative and
gpNMB Over-Expression | |
|---|
| | glembatumumab
vedotin | | Investigator
Choice | | glembatumumab
vedotin | | Investigator
Choice | |
|---|
| | (n=25) | | (n=8) | | (n=12) | | (n=4) | |
|---|
Response | | | 32 | % | | 13 | % | | 33 | % | | 0 | % |
Disease Control Rate | | | 64 | % | | 38 | % | | 75 | % | | 25 | % |
Responses per RECIST 1.1; IC = Investigator's Choice; glembatumumab vedotin arm includes 15 patients who crossed over to receive glembatumumab vedotin treatment after progression on IC. Analysis of best response excludes patients who discontinued from study without evaluable post-baseline radiographic imaging (n=15 for glembatumumab vedotin arm; n=5 for IC arm).
52
Table of Contents
EMERGE: Progression Free Survival (PFS) and Overall Survival (OS) Data
| | | | | | | | | | | | | |
| | gpNMB
Over-Expression | | Triple Negative
and gpNMB
Over-Expression | |
|---|
| | glembatumumab
vedotin | | Investigator
Choice | | glembatumumab
vedotin | | Investigator
Choice | |
|---|
Median PFS (months) | | | 2.7 | | | 1.5 | | | 3.0 | | | 1.5 | |
| | | p=0.14 | | | p=0.008 | |
Median OS (months) | | |
10.0 | | |
5.7 | | |
10.0 | | |
5.5 | |
| | | p=0.18 | | | p=0.003
| |
When cross over patients are removed, median OS in patients with gpNMB over-expression is 10.0 months for glembatumumab vedotin vs 5.2 months for IC (p=0.05) and median OS in triple negative patients with gpNMB over- expression is 10.0 months for glembatumumab vedotin vs 5.2 months for IC (p=0.009).
In December 2013, we initiated METRIC, a randomized, controlled Phase 2b study of glembatumumab vedotin in patients with triple negative breast cancer that over-express gpNMB. To-date, 95 sites are open to enrollment across the United States, Canada and Australia. The study was originally designed to obtain accelerated approval. Feedback from clinical investigators conducting the study indicated that the eligibility criteria for study entry were limiting their ability to enroll patients they felt were clinically appropriate on study. In addition, we had spoken to country-specific members of the European Medicines Agency, or EMA, and believed a significant opportunity existed to expand the study into the EU. Based on these factors, in the fourth quarter of 2014, we amended the METRIC study and expanded patient entry criteria to position it for full marketing approval with global regulators, including the EMA, and to support improved enrollment in the study. The primary endpoint of the study is PFS as PFS is an established endpoint for full approval registration studies in this patient population in both the US and the EU. The sample size (n=300) and the secondary endpoint of OS remained unchanged. We implemented these changes in parallel to regulatory discussions to maintain momentum at open clinical trial sites. Since implementation, both the FDA and central European regulatory authorities have reviewed the protocol design and we believe the METRIC study could support marketing approval in both the US and Europe dependent upon data review. Based on current projections, we believe enrollment will be completed in 2016.
Treatment of Metastatic Melanoma: The Phase 1/2 open-label, multi-center, dose escalation study evaluated the safety, tolerability and pharmacokinetics of glembatumumab vedotin in 117 patients with un-resectable Stage III or Stage IV melanoma who had failed no more than one prior line of cytotoxic therapy. The MTD was determined to be 1.88 mg/kg administered intravenously once every three weeks. The study achieved its primary activity objective with an ORR in the Phase 2 cohort of 15% (5/34). Median PFS was 3.9 months. Glembatumumab vedotin was generally well tolerated, with the most frequent treatment-related adverse events being rash, fatigue, hair loss, pruritus, diarrhea and neuropathy. In the subset of patients with tumor biopsies, high levels of tumor expression of gpNMB appeared to correlate with favorable outcome. In the seven patients whose tumors were found to express high amounts of gpNMB, and who were treated at the maximum tolerated doses across all dosing schedules, median PFS was 4.9 months. The development of rash, which may be associated with the presence of gpNMB in the skin also seemed to correlate with greater PFS.
In December 2014, we initiated a single arm, open-label Phase 2 study of glembatumumab vedotin in patients with unresectable Stage III or IV melanoma. The study is expected to include approximately 10 sites in the United States and will enroll approximately 60 patients. The primary objective is to evaluate the anticancer activity of glembatumumab vedotin in advanced melanoma as measured by the ORR. Secondary endpoints include analyses of PFS, duration of response, OS, retrospective
53
Table of Contents
investigation of whether the anticancer activity of glembatumumab vedotin is dependent upon the degree of gpNMB expression in tumor tissue and safety.
We have completed the assay optimization and validation for a Phase 2 study in squamous cell lung cancer and expect the study will commence in 2015. We have also entered into a Cooperative Research and Development Agreement, or CRADA, with the National Cancer Institute, or NCI, under which NCI will sponsor two studies of glembatumumab vedotin—one in uveal melanoma and one in pediatric osteosarcoma.
Varlilumab
Varlilumab is a human monoclonal antibody that targets CD27, a potentially important target for immunotherapy of various cancers. We have entered into license agreements with the University of Southampton, UK for intellectual property related to uses of anti-CD27 antibodies and with Medarex (now a subsidiary of the Bristol-Myers Squibb Company, or BMS) for access to the UltiMab technology to develop and commercialize human antibodies to CD27.
CD27 acts downstream from CD40 and may provide a novel way to regulate the immune responses. CD27 is a co-stimulatory molecule on T cells and is over-expressed in certain lymphomas and leukemias. Varlilumab is an agonist antibody designed to have two potential therapeutic mechanisms. Varlilumab has been shown to activate immune cells that can target and eliminate cancerous cells in tumor-bearing mice and to directly kill or inhibit the growth of CD27 expressing lymphomas and leukemiasin vitro andin vivo. Both mechanisms have been seen even at low doses in appropriate preclinical models.
We are conducting an open label Phase 1 study of varlilumab in patients with selected malignant solid tumors or hematologic cancers at multiple clinical sites in the United States. Initial dose escalation cohorts were conducted to determine an optimal dose for future study and, to date, no maximum tolerated dose has been reached. The lymphoid malignancies dose escalation arm has completed enrollment (n=24) and a new cohort has been added to include evaluation of T cell malignancies. An expansion cohort has also been added at 0.3mg/kg dosed once every three weeks in patients with Hodgkin Lymphoma (n=15). The solid tumor arm, which included patients with various solid tumors, completed dose escalation in 2013. Two expansion cohorts were subsequently added at 3 mg/kg dosed weekly in metastatic melanoma (n=16) and renal cell carcinoma (n=15) to better characterize clinical activity and further define the safety profile in preparation for combination studies.
We presented updated data from this Phase 1 study in November 2014. Varlilumab was very well tolerated and induced immunologic activity in patients that is consistent with both its mechanism of action and preclinical models. A total of 86 patients have been dosed in the study. 55 patients have been dosed in dose escalation cohorts (various solid and hematologic B-cell tumors) and 31 patients have been dosed in the expansion cohorts (melanoma and RCC) at 3 mg/kg. In both the solid tumor and hematologic dose-escalations, the pre-specified maximum dose level (10 mg/kg) was reached without identification of a maximum tolerated dose. The majority of adverse events (AE) related to treatment have been mild to moderate (Grade 1/2) in severity, with only three serious AEs related to treatment reported. No significant immune-mediated adverse events (colitis, hepatitis, etc.) typically associated with check-point blockade have been observed. Two patients experienced objective responses including a complete response in Hodgkin Lymphoma and a partial response in renal cell carcinoma. Thirteen patients experienced stable disease with a range of 3-30.7+ months to-date. Based on the results observed in hematologic malignancies, an expansion cohort has been added to enroll up to 15 patients with Hodgkin Lymphoma and an abbreviated dose escalation in T cell hematologic malignancies is ongoing.
In May 2014, we entered into a clinical trial collaboration with Bristol-Myers Squibb Company, or BMS, to evaluate the safety, tolerability and preliminary efficacy of varlilumab and Opdivo®, BMS's PD-1 immune checkpoint inhibitor, in a Phase 1/2 study. Under the terms of this clinical trial
54
Table of Contents
collaboration, BMS made a one-time payment to us of $5.0 million and the companies amended the terms of our existing license agreement with Medarex (a subsidiary of BMS) related to our CD27 program whereby certain future milestone payments were waived and future royalty rates were reduced that may have been due from us to Medarex. In return, BMS was granted a time-limited right of first negotiation if we wish to out-license varlilumab. The companies also agreed to work exclusively with each other to explore anti-PD-1 antagonist antibody and anti-CD27 agonist antibody combination regimens. The clinical trial collaboration provides that the companies will share development costs and that we will be responsible for conducting the Phase 1/2 study.
The Phase 1/2 study was initiated in January of 2015 and is being conducted in adult patients with advanced non-small cell lung cancer, metastatic melanoma, colorectal cancer, ovarian cancer, and head and neck squamous cell carcinoma. The Phase 1 dose-escalation portion of the study will assess the safety and tolerability of varlilumab at varying doses when administered with Opdivo. Following dose escalation, a Phase 2 portion of the study will include five disease specific cohorts. The primary objective of the Phase 2 study is overall response rate. Secondary objectives include pharmacokinetics assessments, determining the immunogenicity of varlilumab when given in combination with Opdivo and further assessing the anti-tumor activity of combination treatment.
In May 2014, we also entered into a clinical trial collaboration with Oncothyreon Inc. to evaluate the safety, tolerability and preliminary efficacy of varlilumab and ONT-10, Oncothyreon's therapeutic vaccine targeting the tumor-associated antigen MUC1, in a Phase 1b study. Under the terms of the clinical trial collaboration, the Phase 1b trial will be conducted and funded by Oncothyreon. Both companies will jointly own the data from the trial and will make any plans for potential future development of the combination therapy together. The Phase 1b study was initiated in November 2014 and is being conducted in up to 42 patients with advanced breast or ovarian cancer. The primary objective of the trial is to determine the safety and tolerability of the combined therapy. Additional objectives include evaluations of the impact of combination treatment on MUC1-specific humoral and cellular immune responses, T-cell activation markers and levels of regulatory T-cells, and anti-tumor effects.
Multiple efforts are underway to finalize designs and plans for additional Phase 2 combination studies of varlilumab, including but not limited to: a Phase 1/2 study of varlilumab and ipilumumab in patients with metastatic melanoma (plus CDX-1401 in NY-ESO positive patients); a Phase 1/2 of varlilumab plus sunitinib in renal cell carcinoma; and a Phase 1/2 study of varlilumab plus a mek pathway agent (followed sequentially by a checkpoint inhibitor) for patients with B-raf mutated metastatic melanoma. In addition to our sponsored studies and clinical trial collaborations, we anticipate that varlilumab's potential activity will also be explored in investigator sponsored studies at various academic institutions.
CDX-1401
CDX-1401, developed from our APC Targeting Technology, is a fusion protein consisting of a fully human monoclonal antibody with specificity for the dendritic cell receptor, DEC-205, linked to the NY-ESO-1 tumor antigen. In humans, NY-ESO-1 has been detected in 20% - 30% of all melanoma, lung, esophageal, liver, gastric, prostate, ovarian and bladder cancers, thus representing a broad opportunity. This product is intended to selectively deliver the NY-ESO-1 antigen to dendritic cells for generating robust immune responses against cancer cells expressing NY- ESO-1. We are developing CDX-1401 for the treatment of malignant melanoma and a variety of solid tumors which express the proprietary cancer antigen NY-ESO-1, which we licensed from the Ludwig Institute for Cancer Research in 2006. Preclinical studies have shown that CDX-1401 is effective for activation of human T cell responses against NY-ESO-1.
We have completed a Phase 1 study of CDX-1401 which assessed the safety, immunogenicity and clinical activity of escalating doses of CDX-1401 with TLR agonists (resiquimod and/or Poly ICLC) in
55
Table of Contents
45 patients with advanced malignancies refractory to all available therapies. 60% of patients had confirmed NY-ESO expression in archived tumor sample. Thirteen patients maintained stable disease for up to 13.4 months with a median of 6.7 months. Treatment was well-tolerated and there were no dose limiting toxicities. Humoral responses were elicited in both NY-ESO-1 positive and negative patients. NY-ESO-1-specific T cell responses were absent or low at baseline, but increased post-vaccination in 53% of evaluable patients, including both CD4 and/or CD8 T cell responses. Robust immune responses were observed with CDX-1401 with resiquimod and Poly ICLC alone and in combination. Long-term patient follow up suggested that treatment with CDX-1401 may predispose patients to better outcomes on subsequent therapy with checkpoint inhibitors. Of the 45 patients in the Phase 1 study, eight went on to receive subsequent therapy of either ipilimumab or an investigational checkpoint inhibitor and six of these patients had objective tumor regression. Six patients with melanoma received ipilimumab within three months of treatment with CDX-1401 and four (67%) had objective tumor responses, including one complete response, which compares favorably to the overall response rate of 11% previously reported in metastatic melanoma patients treated with single-agent ipilimumab. In addition, two patients with non-small cell lung cancer received an investigational checkpoint blockade within two months of completing treatment with CDX-1401 and both achieved partial responses.
The Phase 1 study identified a well-tolerated and immunogenic regimen to take forward into future studies. A Phase 2 study of CDX-1401 in combination with CDX-301 in metastatic melanoma is being conducted by the Cancer Immunotherapy Trials Network under a CRADA with the Cancer Therapy Evaluation Program of the NCI and is ongoing. In addition to our sponsored studies, we anticipate that CDX-1401's potential activity will also be explored in investigator sponsored studies at various academic institutions.
CDX-301
CDX-301 is a FMS-like tyrosine kinase 3 ligand, or Flt3L, stem cell mobilizer and dendritic cell growth factor. We licensed CDX-301 from Amgen Inc. in March 2009. CDX-301 is a potent hematopoietic cytokine that stimulates the expansion and differentiation of hematopoietic progenitor and stem cells. CDX-301 has demonstrated a unique capacity to increase the number of circulating dendritic cells in both laboratory and clinical studies. In addition, CDX-301 has shown impressive results in models of cancer, infectious diseases and inflammatory/autoimmune diseases. We believe CDX-301 may hold significant opportunity for synergistic development in combination with other proprietary molecules in our portfolio.
In February 2013, we announced final results from our dose-escalating Phase 1 study of CDX-301 in 30 healthy subjects in collaboration with Rockefeller University. The Phase 1 study evaluated seven different dosing regimens of CDX-301 to determine the appropriate dose for further development based on safety, tolerability, and biological activity. The data from the study were consistent with previous clinical experience and demonstrated that CDX-301 was well-tolerated and can effectively mobilize hematopoietic stem cell populations in healthy volunteers. In December 2013, we announced data from a preclinical combination study of CDX-301and Mozobil® (Plerixafor injection, formerly AMD3100) demonstrating that the combination of these agents significantly increases hematopoietic stem cell mobilization in mice. The data demonstrate a novel potent cell mobilization regimen combining CDX-301 and Mozobil®, which may have significant potential for use in autologous and allogeneic hematopoietic stem cell transplantation. Based on the safety profile and the clinical and preclinical data to date, we initiated a pilot clinical study of CDX-301 for the mobilization and transplantation of allogeneic hematopoietic stem cells in patients with hematological malignancies undergoing hematopoietic stem cell transplantation. The study will explore the utility of CDX-301 alone and in combination with Mozobil®. In addition to our sponsored studies and clinical trial collaborations, we anticipate that CDX-301's potential activity will also be explored in investigator sponsored studies at various academic institutions.
56
Table of Contents
Preclinical Programs
CDX-014
CDX-014 is a fully-human monoclonal ADC that targets T-cell immunoglobulin and mucin domain 1, or TIM-1, a molecule that is upregulated in several cancers, including renal cell and ovarian carcinomas. TIM-1 is associated with kidney injury and the shedding of its ectodomain is a predictive biomarker for tumor progression. TIM-1 has very restricted expression in healthy tissues, making it a promising target for antibody mediated therapy. The TIM-1 antibody is linked to MMAE using Seattle Genetics' proprietary technology. The ADC is designed to be stable in the bloodstream, but to release MMAE upon internalization into TIM-1-expressing tumor cells, resulting in a targeted cell-killing effect. CDX-014 has shown potent activity in preclinical models of ovarian and renal cancer. We expect to complete manufacturing and IND-enabling studies by the end of 2015 to support the initiation of Phase 1 clinical studies in renal cell carcinoma and potentially other TIM-1 expressing tumors in 2016.
CRITICAL ACCOUNTING POLICIES AND ESTIMATES
Our significant accounting policies are described in Note 2 to the consolidated financial statements included in Item 8 of this Form 10-K. We believe our most critical accounting policies include accounting for revenue recognition, impairment of long-lived assets, research and development expenses and stock-based compensation expense.
The methods, estimates and judgments we use in applying our most critical accounting policies have a significant impact on the results we report in our consolidated financial statements. We evaluate our estimates and judgments on an on-going basis. We base our estimates on historical experience and on assumptions that we believe to be reasonable under the circumstances. Our experience and assumptions form the basis for our judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results may vary from what we anticipate and different assumptions or estimates about the future could materially change our reported results. We believe the following accounting policies are the most critical to us in that they are important to the portrayal of our financial statements and they require our most difficult, subjective or complex judgments in the preparation of our consolidated financial statements:
Revenue Recognition
We recognize revenue when all of the following criteria are met: persuasive evidence of an arrangement exists; delivery has occurred or services have been rendered; the seller's price to the buyer is fixed or determinable; and collectability is reasonably assured.
We have entered into and in the future may enter into biopharmaceutical product development agreements with collaborative partners for the research and development of therapeutic drug products. The terms of the agreements may include nonrefundable signing and licensing fees, funding for research, development and manufacturing, milestone payments and royalties on any product sales derived from collaborations. These multiple element arrangements are analyzed to determine whether the deliverables can be separated or whether they must be accounted for as a single unit of accounting. In accounting for these transactions, we allocate revenue to the various elements based on their relative fair value. The fair value of a revenue generating element can be based on current selling prices offered by us or another party for current products or our best estimate of a selling price for future products. Revenue allocated to an individual element is recognized when all other revenue recognition criteria are met for that element.
These collaborative and other agreements may contain milestone payments. Revenues from milestones, if they are considered substantive, are recognized upon successful accomplishment of the milestones. Determining whether a milestone is substantive involves judgment, including an assessment of our involvement in achieving the milestones and whether the amount of the payment is
57
Table of Contents
commensurate to our performance. If not considered substantive, milestones are initially deferred and recognized over the remaining period of the performance obligation.
Payments received to fund certain research activities are recognized as revenue in the period in which the research activities are performed. Revenue from contracts and grants is recognized as the services are performed and recorded as effort is expended on the contracted work and billed to the government or our contractual partner. Payments received in advance that are related to future performance are deferred and recognized as revenue when the research projects are performed.
Product royalty revenue consists of payments received from licensees for a portion of sales proceeds from products that utilize our licensed technologies and are recognized when the amount of and basis for such royalty payments are reported to us in accurate and appropriate form and in accordance with the related license agreement.
Impairment of Long-Lived Assets
We evaluate the recoverability of our long-lived assets, including property and equipment, and finite-lived intangible assets when circumstances indicate that an event of impairment may have occurred. Determination of recoverability is based on an estimate of undiscounted future cash flows resulting from the use of the asset and its eventual disposition. In the event that such cash flows are not expected to be sufficient to recover the carrying amount of the assets, the assets are written-down to their estimated fair values.
IPR&D assets acquired in a business combination initially are recorded at fair value and accounted for as indefinite-lived intangible assets. These assets are maintained on our consolidated balance sheets until either the project underlying them is completed or the assets become impaired. If a project is completed, the carrying value of the related intangible asset is amortized over the remaining estimated life of the asset beginning in the period in which the project is completed. If a project becomes impaired or is abandoned, the carrying value of the related intangible asset is written down to its fair value and an impairment charge is taken in the period in which the impairment occurs. IPR&D assets are tested for impairment on an annual basis during the third quarter, or earlier if impairment indicators are present. We performed an annual impairment test of the IPR&D assets as of July 1, 2014 and concluded that the IPR&D assets were not impaired.
Intangible assets acquired in a business combination with a finite life are recorded at fair value and amortized over the greater of economic consumption or on a straight-line basis over their estimated useful life.
The difference between the purchase price and the fair value of assets acquired and liabilities assumed in a business combination is recorded to goodwill. Goodwill is evaluated for impairment on an annual basis during the third quarter, or earlier if impairment indicators are present. We performed an annual impairment test of the goodwill asset as of July 1, 2014 and concluded that goodwill was not impaired.
Research and Development Expenses
Research and development costs, including internal and contract research costs, are expensed as incurred. Research and development expenses consist mainly of clinical trial costs, manufacturing of clinical material, toxicology and other preclinical studies, personnel costs, depreciation, license fees and funding of outside contracted research.
Clinical trial expenses include expenses associated with clinical research organizations, or CRO, services. Contract manufacturing expenses include expenses associated with contract manufacturing organizations, or CMO, services. The invoicing from CROs and CMOs for services rendered can lag several months. We accrue the cost of services rendered in connection with CRO and CMO activities based on our estimate of costs incurred. We maintain regular communication with our CROs and
58
Table of Contents
CMOs to assess the reasonableness of our estimates. Differences between actual expenses and estimated expenses recorded have not been material and are adjusted for in the period in which they become known.
Stock-Based Compensation Expense
We record stock-based compensation expense for all stock-based awards made to employees and directors based on the estimated fair values of the stock-based awards expected to vest at the grant date and is adjusted, if necessary, to reflect actual forfeitures. Compensation expense for all stock-based awards to employees and directors is recognized using the straight-line method over the term of vesting or performance.
We record stock-based compensation expense for stock options granted to non-employees based on the fair value of the stock options which is re-measured over the vesting term resulting in periodic adjustments to stock-based compensation expense.
RESULTS OF OPERATIONS
Year Ended December 31, 2014 compared with Year Ended December 31, 2013
| | | | | | | | | | | | | |
| | Year Ended
December 31, | |
| |
| |
|---|
| | Increase/
(Decrease)
$ | | Increase/
(Decrease)
% | |
|---|
| | 2014 | | 2013 | |
|---|
| | (In thousands)
| |
| |
|---|
Revenue: | | | | | | | | | | | | | |
Product Development and Licensing Agreements | | $ | 838 | | $ | 160 | | $ | 678 | | | 424 | % |
Contracts and Grants | | | 2,748 | | | 1,617 | | | 1,131 | | | 70 | % |
Product Royalties | | | — | | | 2,334 | | | (2,334 | ) | | (100 | )% |
| | | | | | | | | | | | | | |
Total Revenue | | $ | 3,586 | | $ | 4,111 | | $ | (525 | ) | | (13 | )% |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
Operating Expense: | | | | | | | | | | | | | |
Research and Development | | | 104,381 | | | 67,401 | | | 36,980 | | | 55 | % |
Royalty | | | — | | | 2,334 | | | (2,334 | ) | | (100 | )% |
General and Administrative | | | 20,622 | | | 14,805 | | | 5,817 | | | 39 | % |
Amortization of Acquired Intangible Assets | | | 1,013 | | | 1,013 | | | — | | | 0 | % |
| | | | | | | | | | | | | | |
Total Operating Expense | | | 126,016 | | | 85,553 | | | 40,463 | | | 47 | % |
| | | | | | | | | | | | | | |
Operating Loss | | | (122,430 | ) | | (81,442 | ) | | 40,988 | | | 50 | % |
Investment and Other Income, Net | | | 4,350 | | | 819 | | | 3,531 | | | 431 | % |
Interest Expense | | | — | | | (927 | ) | | (927 | ) | | (100 | )% |
| | | | | | | | | | | | | | |
Net Loss | | $ | (118,080 | ) | $ | (81,550 | ) | $ | 36,530 | | | 45 | % |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
Net Loss
The $36.5 million increase in net loss for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily the result of an increase in research and development and general and administrative expenses, partially offset by an increase in investment and other income.
Revenue
The $0.7 million increase in product development and licensing agreements revenue for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily related to our BMS agreement. In May 2014, we entered into a clinical trial collaboration with BMS whereby BMS
59
Table of Contents
made a one-time payment to us of $5.0 million which we are recognizing as revenue over our estimated performance period of five years. The $1.1 million increase in contracts and grants revenue for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily related to our Rockefeller University agreement pursuant to which we perform research and development services for Rockefeller. The agreement includes an approved project plan for the development services of $4.8 million and a term of three years. The $2.3 million decrease in product royalty revenue for the year ended December 31, 2014 compared to the year ended December 31, 2013 was due to the termination of our agreement with GlaxoSmithKline plc which occurred upon the expiration of the last relevant patent right covered by the agreement. The terminated retained interests in Rotarix® net royalties which were not sold to Paul Royalty Fund II, L.P. had been equal to the amount payable to Cincinnati Children's Hospital Medical Center and recognized as royalty expense by us.
Research and Development Expense
Research and development expenses consist primarily of (i) personnel expenses, (ii) laboratory supply expenses relating to the development of our technology, (iii) facility expenses, (iv) license fees and (v) product development expenses associated with our drug candidates as follows:
| | | | | | | | | | | | | |
| | Year Ended
December 31, | |
| |
| |
|---|
| | Increase/
(Decrease)
$ | | Increase/
(Decrease)
% | |
|---|
| | 2014 | | 2013 | |
|---|
| | (In thousands)
| |
| |
|---|
Personnel | | $ | 20,666 | | $ | 17,040 | | $ | 3,626 | | | 21 | % |
Laboratory Supplies | | | 3,598 | | | 3,247 | | | 351 | | | 11 | % |
Facility | | | 5,062 | | | 4,526 | | | 536 | | | 12 | % |
License Fees | | | 3,150 | | | 700 | | | 2,450 | | | 350 | % |
Product Development | | | 67,205 | | | 39,343 | | | 27,862 | | | 71 | % |
Personnel expenses primarily include salary, benefits, stock-based compensation and payroll taxes. The $3.6 million increase in personnel expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to increased headcount and higher stock-based compensation of $0.8 million. We expect personnel expenses to increase over the next twelve months as we plan to continue to increase our headcount, primarily to support our rindopepimut, glembatumumab vedotin and varlilumab programs.
Laboratory supply expenses include laboratory materials and supplies, services, and other related expenses incurred in the development of our technology. The $0.4 million increase in laboratory supply expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to higher manufacturing supply purchases. We expect supply expenses to remain relatively consistent over the next twelve months, although there may be fluctuations on a quarterly basis.
Facility expenses include depreciation, amortization, utilities, rent, maintenance, and other related expenses incurred at our facilities. The $0.5 million increase in facility expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to an increase in amortization expense related to the leasehold improvements made at our headquarters facility in Hampton, New Jersey. We expect facility expenses to remain relatively consistent over the next twelve months, although there may be fluctuations on a quarterly basis.
License fee expenses include annual license maintenance fees and milestone payments due upon the achievement of certain development, regulatory and/or commercial milestones. The $2.5 million increase in license fee expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to the one-time $2.5 million milestone incurred and paid to Seattle Genetics as a result of the METRIC initiation. We expect license fee expense to decrease over the next twelve months without this one-time milestone payment.
60
Table of Contents
Product development expenses include clinical investigator site fees, external trial monitoring costs, data accumulation costs, contracted research and outside clinical drug product manufacturing. The $27.9 million increase in product development expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily the result of an increase in clinical trial costs and contract manufacturing of $13.2 million and $14.3 million, respectively, primarily related to our rindopepimut and glembatumumab vedotin programs. We expect product development expenses to increase over the next twelve months primarily due to the increase in clinical trial and contract manufacturing expenses related to our rindopepimut, glembatumumab vedotin and varlilumab programs, although there may be fluctuations on a quarterly basis.
Royalty Expense
The $2.3 million decrease in royalty expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was due to the termination of our agreement with GlaxoSmithKline plc which occurred upon the expiration of the last relevant patent right covered by the agreement.
General and Administrative Expense
The $5.8 million increase in general and administrative expenses for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to higher stock-based compensation of $1.5 million, increased headcount and rindopepimut and glembatumumab vedotin commercialization planning costs. We expect general and administrative expense to increase over the next twelve months primarily due to increased commercial planning efforts for rindopepimut and glembatumumab vedotin, although there may be fluctuations on a quarterly basis.
Amortization Expense
Amortization expenses for the year ended December 31, 2014 were relatively consistent compared to the year ended December 31, 2013. We expect amortization expense of acquired intangible assets to remain relatively consistent over the next twelve months.
Investment and Other Income, Net
The $3.5 million increase in investment and other income, net for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to other income in 2014 of $3.0 million related to TopoTarget milestone payments. These payments are the last milestone payments we were owed from TopoTarget. Excluding the impact of the TopoTarget milestone payments, we anticipate investment income to remain relatively consistent over the next twelve months, although there may be fluctuations on a quarterly basis.
Interest Expense
The $0.9 million decrease in interest expense for the year ended December 31, 2014 compared to the year ended December 31, 2013 was primarily due to our election in May 2013 to prepay the Term Loan in full, pursuant to the terms of our loan agreement.
61
Table of Contents
Year Ended December 31, 2013 compared with Year Ended December 31, 2012
| | | | | | | | | | | | | |
| | Year Ended
December 31, | |
| |
| |
|---|
| | Increase/
(Decrease)
$ | | Increase/
(Decrease)
% | |
|---|
| | 2013 | | 2012 | |
|---|
| | (In thousands)
| |
| |
|---|
Revenue: | | | | | | | | | | | | | |
Product Development and Licensing Agreements | | $ | 160 | | $ | 146 | | $ | 14 | | | 10 | % |
Contracts and Grants | | | 1,617 | | | 281 | | | 1,336 | | | 475 | % |
Product Royalties | | | 2,334 | | | 10,775 | | | (8,441 | ) | | (78 | )% |
| | | | | | | | | | | | | | |
Total Revenue | | $ | 4,111 | | $ | 11,202 | | $ | (7,091 | ) | | (63 | )% |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
Operating Expense: | | | | | | | | | | | | | |
Research and Development | | | 67,401 | | | 47,398 | | | 20,003 | | | 42 | % |
Royalty | | | 2,334 | | | 10,775 | | | (8,441 | ) | | (78 | )% |
General and Administrative | | | 14,805 | | | 10,016 | | | 4,789 | | | 48 | % |
Amortization of Acquired Intangible Assets | | | 1,013 | | | 1,090 | | | (77 | ) | | (7 | )% |
| | | | | | | | | | | | | | |
Total Operating Expense | | | 85,553 | | | 69,279 | | | 16,274 | | | 23 | % |
| | | | | | | | | | | | | | |
Operating Loss | | | (81,442 | ) | | (58,077 | ) | | 23,365 | | | 40 | % |
Investment and Other Income, Net | | | 819 | | | 530 | | | 289 | | | 55 | % |
Interest Expense | | | (927 | ) | | (1,576 | ) | | (649 | ) | | (41 | )% |
| | | | | | | | | | | | | | |
Net Loss | | $ | (81,550 | ) | $ | (59,123 | ) | $ | 22,427 | | | 38 | % |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
Net Loss
The $22.4 million increase in net loss for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily the result of an increase in research and development and general and administrative expenses.
Revenue
The $1.3 million increase in contracts and grants revenue for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily related to our Rockefeller University agreement pursuant to which we perform research and development services for Rockefeller. The $8.4 million decrease in product royalty revenue for the year ended December 31, 2013 compared to the year ended December 31, 2012 was due to the termination of our agreement with GlaxoSmithKline plc upon the expiration of the last relevant patent right covered by the agreement.
Research and Development Expense
| | | | | | | | | | | | | |
| | Year Ended December 31, | |
| |
| |
|---|
| | Increase/
(Decrease)
$ | | Increase/
(Decrease)
% | |
|---|
| | 2013 | | 2012 | |
|---|
| | (In thousands)
| |
| |
|---|
Personnel | | $ | 17,040 | | $ | 13,465 | | $ | 3,575 | | | 27 | % |
Laboratory Supplies | | | 3,247 | | | 2,062 | | | 1,185 | | | 57 | % |
Facility | | | 4,526 | | | 4,457 | | | 69 | | | 2 | % |
Product Development | | | 39,343 | | | 24,426 | | | 14,917 | | | 61 | % |
62
Table of Contents
The $3.6 million increase in personnel expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily due to higher stock-based compensation of $1.2 million and increased headcount.
The $1.2 million increase in laboratory supply expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily due to higher manufacturing supply purchases.
The $0.1 million increase in facility expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily due to higher utility and maintenance expenses.
The $14.9 million increase in product development expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily the result of an increase in clinical trial costs and contract manufacturing of $9.0 million and $5.6 million, respectively, primarily related to our rindopepimut and glembatumumab vedotin programs.
Royalty Expense
The $8.4 million decrease in royalty expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was due to the termination of our agreement with GlaxoSmithKline plc upon the expiration of the last relevant patent right covered by the agreement.
General and Administrative Expense
The $4.8 million increase in general and administrative expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily due to higher stock-based compensation of $1.0 million, increased headcount and rindopepimut-related commercialization planning costs.
Amortization Expense
The $0.1 million decrease in amortization expenses for the year ended December 31, 2013 compared to the year ended December 31, 2012 was due to certain intangible assets becoming fully amortized during 2012.
Investment and Other Income, Net
The $0.3 million increase in investment and other income, net for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily due to higher levels of cash and investment balances compared to prior year and us recognizing $0.2 million and $0.1 million in other income related to our sale of New Jersey tax benefits during the years ended December 31, 2013 and 2012, respectively.
Interest Expense
The $0.6 million decrease in interest expense for the year ended December 31, 2013 compared to the year ended December 31, 2012 was primarily due to our election in May 2013 to prepay the Term Loan in full, pursuant to the terms of our loan agreement.
63
Table of Contents
LIQUIDITY AND CAPITAL RESOURCES
Our cash equivalents are highly liquid investments with a maturity of three months or less at the date of purchase and consist primarily of investments in money market mutual funds with commercial banks and financial institutions. We maintain cash balances with financial institutions in excess of insured limits. We do not anticipate any losses with respect to such cash balances. We invest our excess cash balances in marketable securities including municipal bond securities, U.S. government agency securities, and high-grade corporate bonds that meet high credit quality standards, as specified in our investment policy. Our investment policy seeks to manage these assets to achieve our goals of preserving principal and maintaining adequate liquidity.
The use of our cash flows for operations has primarily consisted of salaries and wages for our employees, facility and facility-related costs for our offices, laboratories and manufacturing facility, fees paid in connection with preclinical studies, clinical studies, contract manufacturing, laboratory supplies and services, consulting, legal and other professional fees. To date, the primary sources of cash flows from operations have been payments received from our collaborative partners and from government entities. The timing of any new collaboration agreements, government contracts or grants and any payments under these agreements, contracts or grants cannot be easily predicted and may vary significantly from quarter to quarter.
At December 31, 2014, our principal sources of liquidity consisted of cash, cash equivalents and marketable securities of $201.0 million. We incurred a loss of $118.1 million for the year ended December 31, 2014. Net cash used in operations for the year ended December 31, 2014 was $101.5 million. We believe that the cash, cash equivalents and marketable securities at December 31, 2014 are sufficient to meet estimated working capital requirements and fund planned operations through 2016, however, this could be impacted by our clinical data results from our rindopepimut program and their impact on our pace of commercial manufacturing and the rate of expansion of our commercial operations.
During the next twelve months, we may take further steps to raise additional capital to fund our long-term liquidity needs. Our capital raising activities may include, but may not be limited to, one or more of the following: the licensing of technology programs with existing or new collaborative partners, possible business combinations, issuance of debt, or the issuance of common stock or other securities via private placements or public offerings. While we may seek capital through a number of means, there can be no assurance that additional financing will be available on acceptable terms, if at all, and our negotiating position in capital-raising efforts may worsen as existing resources are used. There is also no assurance that we will be able to enter into further collaborative relationships. Additional equity financing may be dilutive to our stockholders; debt financing, if available, may involve significant cash payment obligations and covenants that restrict our ability to operate as a business; and licensing or strategic collaborations may result in royalties or other terms which reduce our economic potential from products under development.
Operating Activities
Net cash used in operating activities was $101.5 million for the year ended December 31, 2014 compared to $67.7 million for the year ended December 31, 2013. The increase in net cash used in operating activities was primarily due to an increase in net loss of $36.5 million. We expect that cash used in operating activities will continue to increase over the next twelve months primarily related to costs incurred on our rindopepimut, glembatumumab vedotin and varlilumab programs.
We have incurred and will continue to incur significant costs in the area of research and development, including preclinical and clinical trials and clinical drug product manufacturing as our drug candidates are developed. We plan to spend significant amounts to progress our current drug candidates through the clinical trial and commercialization processes as well as to develop additional
64
Table of Contents
drug candidates. As our drug candidates progress through the clinical trial process, we may be obligated to make significant milestone payments.
Investing Activities
Net cash used in investing activities was $41.0 million for the year ended December 31, 2014 compared to $77.4 million for the year ended December 31, 2013. The decrease in net cash used in investing activities was primarily due to net purchases of marketable securities for the year ended December 31, 2014 of $39.1 million as compared to $73.2 million for the year ended December 31, 2013. We expect that cash provided by investing activities will increase over the next twelve months as we fund our operations through the net proceeds from the sale and maturity of marketable securities, cash provided by financing activities and/or new partnerships, although there may be significant fluctuations on a quarterly basis.
Financing Activities
Net cash provided by financing activities was $1.2 million for the year ended December 31, 2014 compared to $289.6 million for the year ended December 31, 2013. Net proceeds from stock issuances, including stock issued pursuant to employee benefit plans, were $1.2 million during the year ended December 31, 2014 compared to $301.1 million for the year ended December 31, 2013. We paid $11.0 million in principal payments on our Term Loan during the year ended December 31, 2013.
Equity Offerings
In December 2013, we filed an automatic shelf registration statement with the Securities and Exchange Commission to register for sale any combination of the types of securities described in the shelf registration statement.
During the years ended December 31, 2013 and 2012, we issued 21,613,483 and 12,075,000 shares of our common stock in underwritten public offerings resulting in net proceeds to us of $278.6 million and $43.5 million, after deducting underwriting fees and offering expenses, respectively.
During the years ended December 31, 2013 and 2012, we issued 2,433,608 and 8,003,290 shares of our common stock under our controlled equity offering sales agreement with Cantor Fitzgerald & Co., as amended, resulting in net proceeds to us of $17.1 million and $40.1 million, after deducting commission and offering expenses, respectively.
AGGREGATE CONTRACTUAL OBLIGATIONS
We have entered into license agreements whereby we have received licenses or options to license technology, specified patents and/or patent applications. These license and collaboration agreements generally provide for royalty payments equal to specified percentages of product sales, annual license maintenance fees, continuing patent prosecution costs and potential future milestone payments to third parties upon the achievement of certain development, regulatory and/or commercial milestones. Because the achievement of these milestones had not occurred as of December 31, 2014, such contingencies have not been recorded in our financial statements. We expect to incur approximately $0.5 million of license and milestone payments in 2015.
The following table summarizes our contractual obligations (not including contingent royalty and milestone payments as described above) at December 31, 2014 and the effect such obligations and commercial commitments are expected to have on our liquidity and cash flow in future years. These
65
Table of Contents
obligations, commitments and supporting arrangements represent expected payments based on current operating forecasts, which are subject to change:
| | | | | | | | | | | | | | | | |
| | Total | | 2015 | | 2016 - 2017 | | 2018 - 2019 | | Thereafter | |
|---|
| | (In thousands)
| |
|---|
Contractual obligations: | | | | | | | | | | | | | | | | |
Operating lease obligations(1) | | $ | 8,720 | | $ | 2,793 | | $ | 4,875 | | $ | 1,052 | | $ | — | |
Other contractual obligations(2) | | | 15,352 | | | 13,251 | | | 2,101 | | | — | | | — | |
| | | | | | | | | | | | | | | | | |
Total contractual obligations | | $ | 24,072 | | $ | 16,044 | | $ | 6,976 | | $ | 1,052 | | $ | — | |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | |
- (1)
- Such amounts primarily consist of payments for our facility leases and do not assume the exercise of renewal terms or early termination provisions.
- (2)
- We enter into agreements in the normal course of business with contract research organizations for clinical trials, contract manufacturing organizations, vendors for preclinical research studies and other services and products for operating purposes. We have included obligations in the table above if the contracts are not cancelable at any time by us, generally upon 30 days prior written notice to the vendor.
RECENT ACCOUNTING PRONOUNCEMENTS
Refer to Note 2, "Summary of Significant Accounting Policies," in the accompanying notes to the consolidated financial statements for a discussion of recent accounting pronouncements.
OFF-BALANCE SHEET ARRANGEMENTS
None.
Item 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
We own financial instruments that are sensitive to market risk as part of our investment portfolio. Our investment portfolio is used to preserve our capital until it is used to fund operations, including our research and development activities. None of these market-risk sensitive instruments are held for trading purposes. We invest our cash primarily in money market mutual funds. These investments are evaluated quarterly to determine the fair value of the portfolio. From time to time, we invest our excess cash balances in marketable securities including municipal bond securities, U.S. government agency securities, and high-grade corporate bonds that meet high credit quality standards, as specified in our investment policy. Our investment policy seeks to manage these assets to achieve our goals of preserving principal and maintaining adequate liquidity. Because of the short-term nature of these investments, we do not believe we have material exposure due to market risk. The impact to our financial position and results of operations from likely changes in interest rates is not material.
We do not utilize derivative financial instruments. The carrying amounts reflected in the consolidated balance sheet of cash and cash equivalents, accounts receivables and accounts payable approximates fair value at December 31, 2014 due to the short-term maturities of these instruments.
66
Table of Contents
Item 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Stockholders of Celldex Therapeutics, Inc.
In our opinion, the accompanying consolidated balance sheets and the related consolidated statements of operations and comprehensive loss, of stockholders' equity, and of cash flows, present fairly, in all material respects, the financial position of Celldex Therapeutics, Inc. and its subsidiary at December 31, 2014 and December 31, 2013, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2014 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2014, based on criteria established inInternal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). The Company's management is responsible for these financial statements, for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in Management's Annual Report on Internal Control over Financial Reporting appearing under Item 9A. Our responsibility is to express opinions on these financial statements and on the Company's internal control over financial reporting based on our integrated audits. We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement and whether effective internal control over financial reporting was maintained in all material respects. Our audits of the financial statements included examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
A company's internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company's internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company's assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ PricewaterhouseCoopers LLP
Boston, Massachusetts
February 24, 2015
67
Table of Contents
CELLDEX THERAPEUTICS, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except share and per share amounts)
| | | | | | | |
| | December 31, 2014 | | December 31, 2013 | |
|---|
ASSETS | | | | | | | |
Current Assets: | | | | | | | |
Cash and Cash Equivalents | | $ | 28,020 | | $ | 169,402 | |
Marketable Securities | | | 173,023 | | | 133,581 | |
Accounts and Other Receivables | | | 427 | | | 489 | |
Prepaid and Other Current Assets | | | 3,515 | | | 1,717 | |
| | | | | | | | |
Total Current Assets | | | 204,985 | | | 305,189 | |
| | | | | | | | |
Property and Equipment, Net | | | 10,535 | | | 9,973 | |
Intangible Assets, Net | | | 21,807 | | | 22,820 | |
Other Assets | | | 1,722 | | | 148 | |
Goodwill | | | 8,965 | | | 8,965 | |
| | | | | | | | |
Total Assets | | $ | 248,014 | | $ | 347,095 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
LIABILITIES AND STOCKHOLDERS' EQUITY | | | | | | | |
Current Liabilities: | | | | | | | |
Accounts Payable | | $ | 2,603 | | $ | 2,243 | |
Accrued Expenses | | | 19,296 | | | 17,179 | |
Current Portion of Long-Term Liabilities | | | 2,592 | | | 928 | |
| | | | | | | | |
Total Current Liabilities | | | 24,491 | | | 20,350 | |
| | | | | | | | |
Other Long-Term Liabilities | | | 11,863 | | | 6,950 | |
| | | | | | | | |
Total Liabilities | | | 36,354 | | | 27,300 | |
| | | | | | | | |
Commitments and Contingent Liabilities (Notes 14 and 16) | | | | | | | |
Stockholders' Equity: | | | | | | | |
Convertible Preferred Stock, $.01 Par Value; 3,000,000 Shares Authorized; No Shares Issued and Outstanding at December 31, 2014 and 2013 | | | — | | | — | |
Common Stock, $.001 Par Value; 297,000,000 Shares Authorized; 89,592,779 and 89,246,832 Shares Issued and Outstanding at December 31, 2014 and 2013, respectively | | | 90 | | | 89 | |
Additional Paid-In Capital | | | 672,739 | | | 662,717 | |
Accumulated Other Comprehensive Income | | | 2,590 | | | 2,668 | |
Accumulated Deficit | | | (463,759 | ) | | (345,679 | ) |
| | | | | | | | |
Total Stockholders' Equity | | | 211,660 | | | 319,795 | |
| | | | | | | | |
Total Liabilities and Stockholders' Equity | | $ | 248,014 | | $ | 347,095 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
The accompanying notes are an integral part of the consolidated financial statements.
68
Table of Contents
CELLDEX THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS AND COMPREHENSIVE LOSS
(In thousands, except per share amounts)
| | | | | | | | | | |
| | Year Ended
December 31, 2014 | | Year Ended
December 31, 2013 | | Year Ended
December 31, 2012 | |
|---|
REVENUE: | | | | | | | | | | |
Product Development and Licensing Agreements | | $ | 838 | | $ | 160 | | $ | 146 | |
Contracts and Grants | | | 2,748 | | | 1,617 | | | 281 | |
Product Royalties | | | — | | | 2,334 | | | 10,775 | |
| | | | | | | | | | | |
Total Revenue | | | 3,586 | | | 4,111 | | | 11,202 | |
| | | | | | | | | | | |
OPERATING EXPENSE: | | | | | | | | | | |
Research and Development | | | 104,381 | | | 67,401 | | | 47,398 | |
Royalty | | | — | | | 2,334 | | | 10,775 | |
General and Administrative | | | 20,622 | | | 14,805 | | | 10,016 | |
Amortization of Acquired Intangible Assets | | | 1,013 | | | 1,013 | | | 1,090 | |
| | | | | | | | | | | |
Total Operating Expense | | | 126,016 | | | 85,553 | | | 69,279 | |
| | | | | | | | | | | |
Operating Loss | | | (122,430 | ) | | (81,442 | ) | | (58,077 | ) |
Investment and Other Income, Net | | | 4,350 | | | 819 | | | 530 | |
Interest Expense | | | — | | | (927 | ) | | (1,576 | ) |
| | | | | | | | | | | |
Net Loss | | $ | (118,080 | ) | $ | (81,550 | ) | $ | (59,123 | ) |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Basic and Diluted Net Loss Per Common Share | | $ | (1.32 | ) | $ | (1.02 | ) | $ | (1.02 | ) |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Shares Used in Calculating Basic and Diluted Net Loss per Share | | | 89,399 | | | 79,777 | | | 57,713 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
COMPREHENSIVE LOSS: | | | | | | | | | | |
Net Loss | | $ | (118,080 | ) | $ | (81,550 | ) | $ | (59,123 | ) |
Other Comprehensive Income (Loss): | | | | | | | | | | |
Foreign Currency Translation Adjustments | | | (5 | ) | | (3 | ) | | 2 | |
Unrealized (Loss) Gain on Marketable Securities | | | (73 | ) | | (74 | ) | | 91 | |
| | | | | | | | | | | |
Comprehensive Loss | | $ | (118,158 | ) | $ | (81,627 | ) | $ | (59,030 | ) |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
The accompanying notes are an integral part of the consolidated financial statements.
69
Table of Contents
CELLDEX THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
(In thousands, except share amounts)
| | | | | | | | | | | | | | | | | | | |
| | Common
Stock
Shares | | Common
Stock Par
Value | | Additional
Paid-In
Capital | | Accumulated
Other
Comprehensive
Income | | Accumulated
Deficit | | Total
Stockholders'
Equity | |
|---|
Balance at December 31, 2011 | | | 44,210,636 | | | 44 | | | 271,032 | | | 2,652 | | | (205,006 | ) | | 68,722 | |
Shares Issued under Stock Option and Employee Stock Purchase Plans | | | 70,587 | | | — | | | 163 | | | — | | | — | | | 163 | |
Shares Issued in Connection with Cantor Agreement | | | 8,003,290 | | | 8 | | | 40,130 | | | — | | | — | | | 40,138 | |
Shares Issued in Underwritten Offering | | | 12,075,000 | | | 12 | | | 43,471 | | | — | | | — | | | 43,483 | |
Share-Based Compensation | | | — | | | — | | | 2,298 | | | — | | | — | | | 2,298 | |
Foreign Currency Translation Adjustments | | | — | | | — | | | — | | | 2 | | | — | | | 2 | |
Unrealized Gains on Marketable Securities | | | — | | | — | | | — | | | 91 | | | — | | | 91 | |
Net Loss | | | — | | | — | | | — | | | — | | | (59,123 | ) | | (59,123 | ) |
| | | | | | | | | | | | | | | | | | | | |
Balance at December 31, 2012 | | | 64,359,513 | | | 64 | | | 357,094 | | | 2,745 | | | (264,129 | ) | | 95,774 | |
Shares Issued under Stock Option and Employee Stock Purchase Plans | | | 840,228 | | | 1 | | | 5,402 | | | — | | | — | | | 5,403 | |
Shares Issued in Connection with Cantor Agreement | | | 2,433,608 | | | 2 | | | 17,132 | | | — | | | — | | | 17,134 | |
Shares Issued in Underwritten Offering | | | 21,613,483 | | | 22 | | | 278,541 | | | — | | | — | | | 278,563 | |
Share-Based Compensation | | | — | | | — | | | 4,548 | | | — | | | — | | | 4,548 | |
Foreign Currency Translation Adjustments | | | — | | | — | | | — | | | (3 | ) | | — | | | (3 | ) |
Unrealized Losses on Marketable Securities | | | — | | | — | | | — | | | (74 | ) | | — | | | (74 | ) |
Net Loss | | | — | | | — | | | — | | | — | | | (81,550 | ) | | (81,550 | ) |
| | | | | | | | | | | | | | | | | | | | |
Balance at December 31, 2013 | | | 89,246,832 | | | 89 | | | 662,717 | | | 2,668 | | | (345,679 | ) | | 319,795 | |
Shares Issued under Stock Option and Employee Stock Purchase Plans | | | 193,775 | | | 1 | | | 1,170 | | | — | | | — | | | 1,171 | |
Shares Issued in Connection with Supply Agreement | | | 152,172 | | | — | | | 2,000 | | | — | | | — | | | 2,000 | |
Share-Based Compensation | | | — | | | — | | | 6,852 | | | — | | | — | | | 6,852 | |
Foreign Currency Translation Adjustments | | | — | | | — | | | — | | | (5 | ) | | — | | | (5 | ) |
Unrealized Losses on Marketable Securities | | | — | | | — | | | — | | | (73 | ) | | — | | | (73 | ) |
Net Loss | | | — | | | — | | | — | | | — | | | (118,080 | ) | | (118,080 | ) |
| | | | | | | | | | | | | | | | | | | | |
Balance at December 31, 2014 | | | 89,592,779 | | $ | 90 | | $ | 672,739 | | $ | 2,590 | | $ | (463,759 | ) | $ | 211,660 | |
| | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | |
The accompanying notes are an integral part of the consolidated financial statements.
70
Table of Contents
CELLDEX THERAPEUTICS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
| | | | | | | | | | |
| | Year Ended
December 31, 2014 | | Year Ended
December 31, 2013 | | Year Ended
December 31, 2012 | |
|---|
Cash Flows From Operating Activities: | | | | | | | | | | |
Net Loss | | $ | (118,080 | ) | $ | (81,550 | ) | $ | (59,123 | ) |
Adjustments to Reconcile Net Loss to Net Cash Used in Operating Activities: | | | | | | | | | | |
Depreciation and Amortization | | | 2,388 | | | 1,932 | | | 2,047 | |
Amortization of Intangible Assets | | | 1,013 | | | 1,013 | | | 1,090 | |
Amortization and Premium of Marketable Securities | | | 95 | | | (1,366 | ) | | (660 | ) |
Realized Gain on Sales and Maturities of Marketable Securities | | | (11 | ) | | — | | | (6 | ) |
Loss (Gain) on Sale or Disposal of Assets | | | 6 | | | (21 | ) | | (74 | ) |
Stock-Based Compensation Expense | | | 6,852 | | | 4,548 | | | 2,298 | |
Non-Cash Expense | | | 72 | | | 97 | | | 226 | |
Changes in Operating Assets and Liabilities: | | | | | | | | | | |
Accounts and Other Receivables | | | 62 | | | (445 | ) | | 126 | |
Prepaid and Other Current Assets | | | (2,026 | ) | | (706 | ) | | 33 | |
Other Assets | | | 65 | | | 276 | | | (95 | ) |
Accounts Payable and Accrued Expenses | | | 1,450 | | | 7,236 | | | 3,762 | |
Other Liabilities | | | 6,577 | | | 1,317 | | | 594 | |
| | | | | | | | | | | |
Net Cash Used in Operating Activities | | | (101,537 | ) | | (67,669 | ) | | (49,782 | ) |
| | | | | | | | | | | |
Cash Flows From Investing Activities: | | | | | | | | | | |
Sales and Maturities of Marketable Securities | | | 109,232 | | | 38,894 | | | 52,360 | |
Purchases of Marketable Securities | | | (148,314 | ) | | (112,118 | ) | | (69,255 | ) |
Acquisition of Property and Equipment | | | (1,929 | ) | | (4,219 | ) | | (303 | ) |
Proceeds from Sale or Disposal of Assets | | | — | | | 21 | | | 218 | |
| | | | | | | | | | | |
Net Cash Used in Investing Activities | | | (41,011 | ) | | (77,422 | ) | | (16,980 | ) |
| | | | | | | | | | | |
Cash Flows From Financing Activities: | | | | | | | | | | |
Net Proceeds from Stock Issuances | | | — | | | 295,697 | | | 83,784 | |
Proceeds from Issuance of Stock from Employee Benefit Plans | | | 1,171 | | | 5,403 | | | — | |
Payments of Term Loan | | | — | | | (11,029 | ) | | (3,971 | ) |
Payment of Other Liabilities | | | — | | | (472 | ) | | (55 | ) |
| | | | | | | | | | | |
Net Cash Provided by Financing Activities | | | 1,171 | | | 289,599 | | | 79,758 | |
| | | | | | | | | | | |
Effect of Exchange Rate Changes on Cash and Cash Equivalents | | | (5 | ) | | (3 | ) | | 2 | |
| | | | | | | | | | | |
Net Increase (Decrease) in Cash and Cash Equivalents | | | (141,382 | ) | | 144,505 | | | 12,998 | |
Cash and Cash Equivalents at Beginning of Period | | | 169,402 | | | 24,897 | | | 11,899 | |
| | | | | | | | | | | |
Cash and Cash Equivalents at End of Period | | $ | 28,020 | | $ | 169,402 | | $ | 24,897 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Supplemental Disclosure of Cash Flow Information | | | | | | | | | | |
Cash Paid for Interest | | $ | — | | $ | 1,209 | | $ | 1,384 | |
Non-cash Investing Activities | | | | | | | | | | |
Accrued construction in progress | | $ | 1,027 | | $ | — | | $ | — | |
The accompanying notes are an integral part of the consolidated financial statements.
71
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
(1) NATURE OF BUSINESS AND OVERVIEW
Celldex Therapeutics, Inc. (the "Company" or "Celldex") is a biopharmaceutical company focused on the development and commercialization of several immunotherapy technologies for the treatment of cancer and other difficult-to-treat diseases. The Company's lead drug candidates include rindopepimut (also referred to as Rintega® and CDX-110) and glembatumumab vedotin (also referred to as CDX-011). Rindopepimut is a targeted immunotherapeutic in a pivotal Phase 3 study for the treatment of front-line glioblastoma and a Phase 2 study for the treatment of recurrent glioblastoma. Glembatumumab vedotin is a targeted antibody-drug conjugate in a randomized, Phase 2b study for the treatment of triple negative breast cancer and a Phase 2 study for the treatment of metastatic melanoma. The Company has a number of earlier stage candidates in clinical development, including varlilumab (also referred to as CDX-1127), a fully human therapeutic monoclonal antibody for cancer indications, CDX-1401, a targeted immunotherapeutic aimed at antigen presenting cells for cancer indications and CDX-301, an immune cell mobilizing agent and dendritic cell growth factor
At December 31, 2014, the Company had cash, cash equivalents and marketable securities of $201.0 million. The Company incurred a loss of $118.1 million for the year ended December 31, 2014. Net cash used in operations for the year ended December 31, 2014 was $101.5 million. The Company believes that the cash, cash equivalents and marketable securities at December 31, 2014 will be sufficient to meet estimated working capital requirements and fund planned operations for at least the next twelve months.
During the next twelve months, the Company may take further steps to raise additional capital to meet its long-term liquidity needs. These capital raising activities may include, but may not be limited to, one or more of the following: the licensing of technology programs with existing or new collaborative partners, possible business combinations, issuance of debt, or the issuance of common stock or other securities via private placements or public offerings. While the Company may seek capital through a number of means, there can be no assurance that additional financing will be available on acceptable terms, if at all, and the Company's negotiating position in capital-raising efforts may worsen as existing resources are used. There is also no assurance that the Company will be able to enter into further collaborative relationships. Additional equity financings may be dilutive to the Company's stockholders; debt financing, if available, may involve significant cash payment obligations and covenants that restrict the Company's ability to operate as a business; and licensing or strategic collaborations may result in royalties or other terms which reduce the Company's economic potential from products under development.
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Basis of Presentation
The accompanying consolidated financial statements reflect the operations of the Company and its wholly-owned subsidiary. All intercompany balances and transactions have been eliminated in consolidation. On December 31, 2014, the Company's wholly-owned subsidiary, Celldex Research Corporation, merged into Celldex Therapeutics, Inc. The Company operates in one segment, which is the business of development, manufacturing and commercialization of novel therapeutics for human health care.
72
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
Use of Estimates
The preparation of the consolidated financial statements in conformity with accounting principles generally accepted in the United States of America (U.S. GAAP) requires management to make estimates and use assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the dates of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates.
Cash and Cash Equivalents
The Company considers all highly liquid investments purchased with a maturity date of 90 days or less at the date of purchase to be cash equivalents. Cash equivalents consist principally of money market funds and debt securities.
Marketable Securities
The Company invests its excess cash balances in marketable securities including municipal bond securities, U.S. government agency securities, and high-grade corporate bonds. The Company classifies all of its marketable securities as current assets on the consolidated balance sheets because they are available-for-sale and available to fund current operations. Marketable securities are stated at fair value with their unrealized gains and losses included as a component of accumulated other comprehensive income (loss), which is a separate component of stockholders' equity, until such gains and losses are realized. If a decline in the fair value is considered other-than-temporary, based on available evidence, the unrealized loss is transferred from other comprehensive income (loss) to the consolidated statements of operations. Realized gains and losses are determined on the specific identification method and are included in investment and other income, net.
Concentration of Credit Risk and of Significant Customers and Suppliers
Financial instruments that potentially subject the Company to concentrations of credit risk primarily consist of cash, cash equivalents, marketable securities and accounts receivable. The Company invests its cash, cash equivalents and marketable securities in debt instruments and interest bearing accounts at major financial institutions in excess of insured limits. The Company mitigates credit risk by limiting the investment type and maturity to securities that preserve capital, maintain liquidity and have a high credit quality. The Company has not historically experienced credit losses from its accounts receivable and therefore has not established an allowance for doubtful accounts.
Revenue from Rockefeller, BMS and Glaxo represented 75%, 20% and 0% for the year ended December 31, 2014, 35%, 0% and 57% for the year ended December 31, 2013, and 0%, 0% and 96% for the year ended December 31, 2012, of total Company revenue, respectively.
The Company relies on contract manufacturing organizations (CMO) to manufacture drug substance and drug product for its late-stage clinical studies of rindopepimut and glembatumumab vedotin as well as for future commercial supplies. The Company also relies on CMOs for supply of raw materials as well as filling, packaging, storage and shipping of drug product. These clinical studies would be adversely affected by a significant interruption in the supply of rindopepimut and glembatumumab vedotin.
73
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
Fair Value Measurements
The Company has certain assets and liabilities that are measured at fair value in the financial statements. The Company seeks to maximize the use of observable inputs (market data obtained from sources independent from the Company) and to minimize the use of unobservable inputs (the Company's assumptions about how market participants would price assets and liabilities) when measuring the fair value of its assets and liabilities. These assets and liabilities are classified into one of three levels of the following fair value hierarchy as defined by U.S. GAAP:
Level 1: Observable inputs such as quoted prices in active markets for identical assets or liabilities. An active market for an asset or liability is a market in which transactions for the asset or liability occur with sufficient frequency and volume to provide pricing information on an ongoing basis.
Level 2: Observable inputs other than Level 1 prices, such as quoted prices in active markets for similar assets or liabilities and quoted prices for identical assets or liabilities in markets that are not active.
Level 3: Unobservable inputs based on the Company's assessment of the assumptions that market participants would use in pricing the asset or liability.
Property and Equipment
Property and equipment is stated at cost and depreciated over the estimated useful lives of the related assets using the straight-line method. Laboratory equipment and office furniture and equipment are depreciated over five years and computer equipment is depreciated over three years. Manufacturing equipment is amortized over seven to ten years. Leasehold improvements are amortized over the shorter of the estimated useful life or the non-cancelable term of the related lease, including any renewals that are reasonably assured of occurring. Property and equipment under construction is classified as construction in progress and is depreciated or amortized only after the asset is placed in service. Expenditures for maintenance and repairs are charged to expense whereas the costs of significant improvements which extend the life of the underlying asset are capitalized. Upon retirement or sale, the cost of assets disposed of and the related accumulated depreciation are eliminated and any resulting gain or loss is reflected in the Company's consolidated statements of operations and comprehensive loss.
The treatment of costs to construct property and equipment depends on the nature of the costs and the stage of construction. Costs incurred in the project planning, design, construction and installation phases are capitalized as part of the cost of the asset. The Company stops capitalizing these costs when the asset is substantially complete and ready for its intended use. For manufacturing property and equipment, the Company also capitalizes the cost of validating these assets for the underlying manufacturing process. The Company completes the capitalization of validation costs when the asset is substantially complete and ready for its intended use. Costs capitalized include incremental labor and fringe benefits, and direct consultancy services.
74
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
Business Combinations
The Company records the fair value of the consideration transferred to acquire a business to the tangible assets and identifiable intangible assets acquired and liabilities assumed on the basis of their fair values at the date of acquisition. The Company assesses the fair value of assets, including intangible assets such as in-process research and development (IPR&D), using a variety of methods including present value models. Each asset is measured at fair value from the perspective of a market participant. The method used to estimate the fair values of IPR&D assets incorporates significant assumptions regarding the estimates a market participant would make in order to evaluate an asset, including a market participant's assumptions regarding the probability of completing IPR&D projects, which would require obtaining regulatory approval for marketing of the associated drug candidate; a market participant's estimates regarding the timing of and the expected costs to complete IPR&D projects; a market participant's estimates of future cash flows from potential product sales; and the appropriate discount rates for a market participant. Transaction costs and restructuring costs associated with the transaction are expensed as incurred.
Intangible Assets
IPR&D assets acquired in a business combination initially are recorded at fair value and accounted for as indefinite-lived intangible assets. These assets are maintained on the Company's consolidated balance sheets until either the project underlying them is completed or the assets become impaired. If a project is completed, the carrying value of the related intangible asset is amortized over the remaining estimated life of the asset beginning in the period in which the project is completed. If a project becomes impaired or is abandoned, the carrying value of the related intangible asset is written down to its fair value and an impairment charge is taken in the period in which the impairment occurs.
IPR&D assets are tested for impairment on an annual basis during the third quarter, or earlier if impairment indicators are present. As part of the annual impairment test of the IPR&D assets as of July 1, 2014, the Company bypassed the optional qualitative assessment and performed a calculation of the fair value of the asset. The Company concluded that the IPR&D assets were not impaired.
Intangible assets acquired in a business combination with a finite life are recorded at fair value and amortized over the greater of economic consumption or on a straight-line basis over their estimated useful life.
Goodwill
The difference between the purchase price and the fair value of assets acquired and liabilities assumed in a business combination is allocated to goodwill. Goodwill is evaluated for impairment on an annual basis during the third quarter, or earlier if impairment indicators are present. The Company has the option to assess qualitative factors to determine if it is more likely than not that goodwill might be impaired and whether it is necessary to perform the two-step goodwill impairment test required under U.S. GAAP. As part of its annual impairment test of the goodwill asset as of July 1, 2014, the Company bypassed the optional qualitative assessment and performed the two-step impairment test. The Company concluded that goodwill was not impaired.
75
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
Impairment of Long-Lived Assets
The Company evaluates the recoverability of its long-lived assets, including property and equipment, and intangible assets when circumstances indicate that an event of impairment may have occurred. Determination of recoverability is based on an estimate of undiscounted future cash flows resulting from the use of the asset and its eventual disposition. In the event that such cash flows are not expected to be sufficient to recover the carrying amount of the assets, the assets are written-down to their estimated fair values.
Revenue Recognition
The Company recognizes revenue when all of the following criteria are met: persuasive evidence of an arrangement exists; delivery has occurred or services have been rendered; the seller's price to the buyer is fixed or determinable; and collectability is reasonably assured.
The Company has entered into and in the future may enter into biopharmaceutical product development agreements with collaborative partners for the research and development of therapeutic drug products. The terms of the agreements may include nonrefundable signing and licensing fees, funding for research, development and manufacturing, milestone payments and royalties on any product sales derived from collaborations. These multiple element arrangements are analyzed to determine whether the deliverables can be separated or whether they must be accounted for as a single unit of accounting. In accounting for these transactions, the Company allocates revenue to the various elements based on their relative fair value. The fair value of a revenue generating element can be based on current selling prices offered by the Company or another party for current products or the Company's best estimate of a selling price for future products. Revenue allocated to an individual element is recognized when all other revenue recognition criteria are met for that element.
These collaborative and other agreements may contain milestone payments. Revenues from milestones, if they are considered substantive, are recognized upon successful accomplishment of the milestones. Determining whether a milestone is substantive involves judgment, including an assessment of the Company's involvement in achieving the milestones and whether the amount of the payment is commensurate to the Company's performance. If not considered substantive, milestones are initially deferred and recognized over the period of the remaining performance obligation.
Payments received to fund certain research activities are recognized as revenue in the period in which the research activities are performed. Revenue from contracts and grants is recognized as the services are performed and recorded as effort is expended on the contracted work and billed to the government or the Company's contractual partner. Payments received in advance that are related to future performance are deferred and recognized as revenue when the research projects are performed.
Product royalty revenue consists of payments received from licensees for a portion of sales proceeds from products that utilize the Company's licensed technologies and are recognized when the amount of and basis for such royalty payments are reported to the Company in accurate and appropriate form and in accordance with the related license agreement.
76
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
Research and Development Expenses
Research and development costs, including internal and contract research costs, are expensed as incurred. Research and development expenses consist mainly of clinical trial costs, manufacturing of clinical material, toxicology and other preclinical studies, personnel costs, depreciation, license fees and funding of outside contracted research.
Clinical trial expenses include expenses associated with clinical research organizations, or CRO, services. Contract manufacturing expenses include expenses associated with contract manufacturing organizations, or CMO, services. The invoicing from CROs and CMOs for services rendered can lag several months. The Company accrues the cost of services rendered in connection with CRO and CMO activities based on our estimate of costs incurred. The Company maintains regular communication with our CROs and CMOs to assess the reasonableness of its estimates. Differences between actual expenses and estimated expenses recorded have not been material and are adjusted for in the period in which they become known.
Patent Costs
Patent costs are expensed as incurred. Certain patent costs are reimbursed by the Company's product development and licensing partners. Any reimbursed patent costs are recorded as product development and licensing agreement revenues in the Company's financial statements.
Stock-Based Compensation
The Company records stock-based compensation expense for all stock-based awards made to employees and directors based on the estimated fair values of the stock-based awards expected to vest at the grant date and is adjusted, if necessary, to reflect actual forfeitures. Compensation expense for all stock-based awards to employees and directors is recognized using the straight-line method over the term of vesting or performance.
The Company records stock-based compensation expense for stock options granted to non-employees based on the fair value of the stock options which is re-measured over the graded vesting term resulting in periodic adjustments to stock-based compensation expense.
Foreign Currency Translation
Net unrealized gains and losses resulting from foreign currency translation are included in other comprehensive income (loss). At December 31, 2014 and December 31, 2013, accumulated other comprehensive income includes a net unrealized gain related to foreign currency translation of $2.6 million.
Income Taxes
The Company uses the asset and liability method to account for income taxes, including the recognition of deferred tax assets and deferred tax liabilities for the anticipated future tax consequences attributable to differences between financial statement amounts and their respective tax basis. Quarterly, the Company reviews its deferred tax assets for recovery. A valuation allowance is established when the Company believes that it is more likely than not that its deferred tax assets will
77
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
not be realized. Changes in valuation allowances from period to period are included in the Company's tax provision in the period of change.
The Company records uncertain tax positions in the financial statements only if it is more likely than not that the uncertain tax position will be sustained upon examination by the taxing authorities. The Company records interest and penalties related to uncertain tax positions in income tax expense.
Comprehensive Loss
Comprehensive loss is comprised of net loss and certain changes in stockholders' equity that are excluded from net loss. The Company includes foreign currency translation adjustments and unrealized gains and losses on marketable securities in other comprehensive loss. The consolidated statements of operations and comprehensive loss reflect total comprehensive loss for the years ended December 31, 2014, 2013 and 2012.
Net Loss Per Share
Basic net loss per common share is based upon the weighted-average number of common shares outstanding during the period, excluding restricted stock that has been issued but is not yet vested. Diluted net loss per common share is based upon the weighted-average number of common shares outstanding during the period plus additional weighted-average potentially dilutive common shares outstanding during the period when the effect is dilutive. The potentially dilutive common shares that have not been included in the net loss per common share calculations because the effect would have been anti-dilutive are as follows:
| | | | | | | | | | |
| | Year Ended December 31, | |
|---|
| | 2014 | | 2013 | | 2012 | |
|---|
Stock options | | | 7,015,350 | | | 5,770,544 | | | 5,349,810 | |
Restricted stock | | | 7,000 | | | 6,000 | | | 6,000 | |
| | | | | | | | | | | |
| | | 7,022,350 | | | 5,776,544 | | | 5,355,810 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Recent Accounting Pronouncements
From time to time, new accounting pronouncements are issued by the Financial Accounting Standards Board (FASB) or other standard setting bodies that are adopted by the Company as of the specified effective date. Unless otherwise discussed, the Company believes that the impact of recently issued standards that are not yet effective will not have a material impact on the Company's financial position or results of operations upon adoption.
78
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(2) SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES (Continued)
In May 2014, the FASB issued a new U.S. GAAP accounting standard that creates modifications to various other revenue accounting standards for specialized transactions and industries. The new U.S. GAAP accounting standard is intended to conform revenue accounting principles with a concurrently issued new standard under International Financial Reporting Standards, as well as, to enhance disclosures related to disaggregated revenue information. The updated guidance is effective for annual reporting periods beginning on or after December 15, 2016, and interim periods within those annual periods. The Company will further study the implications of this standard in order to evaluate the method of adoption and the expected impact on the consolidated financial statements.
In August 2014, the FASB issued a new U.S. GAAP accounting standard that provides guidance about management's responsibility to evaluate whether there is substantial doubt about an entity's ability to continue as a going concern and to provide related footnote disclosures. The new accounting standard requires management to assess an entity's ability to continue as a going concern by incorporating and expanding upon certain principles that are currently in U.S. auditing standards. The new accounting standard is effective for the annual period ending after December 15, 2016, and for annual periods and interim periods thereafter. Early application is permitted. The Company does not expect the adoption of this standard to have a material impact on the consolidated financial statements.
(3) COMPREHENSIVE LOSS
The changes in accumulated other comprehensive income (loss) by component for the years ended December 31, 2014 and 2013 are summarized below. No amounts were reclassified out of accumulated other comprehensive income during the years ended December 31, 2014, 2013 and 2012.
| | | | | | | | | | |
| | Unrealized Gain
(Loss) on
Marketable
Securities | | Foreign
Currency Items | | Total | |
|---|
| | (In thousands)
| |
|---|
Balance at December 31, 2013 | | $ | 82 | | $ | 2,586 | | $ | 2,668 | |
Other comprehensive loss before reclassifications | | | (73 | ) | | (5 | ) | | (78 | ) |
Amounts reclassified from other comprehensive income | | | — | | | — | | | — | |
| | | | | | | | | | | |
Net current-period other comprehensive loss | | | (73 | ) | | (5 | ) | | (78 | ) |
| | | | | | | | | | | |
Balance at December 31, 2014 | | $ | 9 | | $ | 2,581 | | $ | 2,590 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Balance at December 31, 2012 | | $ | 156 | | $ | 2,589 | | $ | 2,745 | |
Other comprehensive loss before reclassifications | | | (74 | ) | | (3 | ) | | (77 | ) |
Amounts reclassified from other comprehensive income | | | — | | | — | | | — | |
| | | | | | | | | | | |
Net current-period other comprehensive loss | | | (74 | ) | | (3 | ) | | (77 | ) |
| | | | | | | | | | | |
Balance at December 31, 2013 | | $ | 82 | | $ | 2,586 | | $ | 2,668 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
79
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(4) FAIR VALUE MEASUREMENTS
The following tables set forth the Company's financial assets subject to fair value measurements:
| | | | | | | | | | | | | |
| | As of
December 31, 2014 | | Level 1 | | Level 2 | | Level 3 | |
|---|
| | (In thousands)
| |
|---|
Money market funds and cash equivalents | | $ | 18,677 | | | — | | $ | 18,677 | | | — | |
Marketable securities | | $ | 173,023 | | | — | | $ | 173,023 | | | — | |
| | | | | | | | | | | | | | |
| | $ | 191,700 | | | — | | $ | 191,700 | | | — | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | |
| | As of
December 31, 2013 | | Level 1 | | Level 2 | | Level 3 | |
|---|
| | (In thousands)
| |
|---|
Money market funds and cash equivalents | | $ | 148,549 | | | — | | $ | 148,549 | | | — | |
Marketable securities | | $ | 133,581 | | | — | | $ | 133,581 | | | — | |
| | | | | | | | | | | | | | |
| | $ | 282,130 | | | — | | $ | 282,130 | | | — | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
There have been no transfers of assets or liabilities between the fair value measurement classifications. The Company's financial instruments consist mainly of cash and cash equivalents, marketable securities, short-term accounts receivable and accounts payable. The Company values its marketable securities utilizing independent pricing services which normally derive security prices from recently reported trades for identical or similar securities, making adjustments based on significant observable transactions. At each balance sheet date, observable market inputs may include trade information, broker or dealer quotes, bids, offers or a combination of these data sources. Short-term accounts receivable and accounts payable are reflected in the accompanying consolidated financial statements at cost, which approximates fair value due to the short-term nature of these instruments.
80
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(5) MARKETABLE SECURITIES
A summary of marketable securities is shown below:
| | | | | | | | | | | | | |
| | Amortized
Cost | | Gross
Unrealized
Gains | | Gross
Unrealized
Losses | | Fair
Value | |
|---|
| | (In thousands)
| |
|---|
December 31, 2014 | | | | | | | | | | | | | |
Marketable securities | | | | | | | | | | | | | |
U.S. government and municipal obligations | | | | | | | | | | | | | |
Maturing in one year or less | | $ | 44,580 | | $ | 30 | | $ | (6 | ) | $ | 44,604 | |
Maturing after one year through three years | | | 16,108 | | | 49 | | | (1 | ) | | 16,156 | |
| | | | | | | | | | | | | | |
Total U.S. government and municipal obligations | | $ | 60,688 | | $ | 79 | | $ | (7 | ) | $ | 60,760 | |
| | | | | | | | | | | | | | |
Corporate debt securities | | | | | | | | | | | | | |
Maturing in one year or less | | $ | 89,636 | | | 6 | | $ | (37 | ) | $ | 89,605 | |
Maturing after one year through three years | | | 22,690 | | | 3 | | | (35 | ) | | 22,658 | |
| | | | | | | | | | | | | | |
Total corporate debt securities | | $ | 112,326 | | $ | 9 | | $ | (72 | ) | $ | 112,263 | |
| | | | | | | | | | | | | | |
Total marketable securities | | $ | 173,014 | | $ | 88 | | $ | (79 | ) | $ | 173,023 | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
December 31, 2013 | | | | | | | | | | | | | |
Marketable securities | | | | | | | | | | | | | |
U.S. government and municipal obligations | | | | | | | | | | | | | |
Maturing in one year or less | | $ | 55,531 | | $ | 27 | | $ | (4 | ) | $ | 55,554 | |
Maturing after one year through three years | | | 18,234 | | | 56 | | | (4 | ) | | 18,286 | |
| | | | | | | | | | | | | | |
Total U.S. government and municipal obligations | | $ | 73,765 | | $ | 83 | | $ | (8 | ) | $ | 73,840 | |
| | | | | | | | | | | | | | |
Corporate debt securities | | | | | | | | | | | | | |
Maturing in one year or less | | $ | 38,973 | | $ | 9 | | $ | (9 | ) | $ | 38,973 | |
Maturing after one year through three years | | | 20,761 | | | 12 | | | (5 | ) | | 20,768 | |
| | | | | | | | | | | | | | |
Total corporate debt securities | | $ | 59,734 | | $ | 21 | | $ | (14 | ) | $ | 59,741 | |
| | | | | | | | | | | | | | |
Total marketable securities | | $ | 133,499 | | $ | 104 | | $ | (22 | ) | $ | 133,581 | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
The marketable securities held by the Company were high investment grade and there were no marketable securities that the Company considered to be other-than-temporarily impaired as of December 31, 2014.
81
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(6) PROPERTY AND EQUIPMENT, NET
Property and equipment include the following:
| | | | | | | |
| | December 31, 2014 | | December 31, 2013 | |
|---|
| | (In thousands)
| |
|---|
Laboratory Equipment | | $ | 4,223 | | $ | 3,699 | |
Manufacturing Equipment | | | 2,274 | | | 2,130 | |
Office Furniture and Equipment | | | 1,888 | | | 1,386 | |
Leasehold Improvements | | | 14,603 | | | 14,493 | |
Construction in Progress | | | 1,767 | | | 257 | |
| | | | | | | | |
Total Property and Equipment | | | 24,755 | | | 21,965 | |
Less Accumulated Depreciation and Amortization | | | (14,220 | ) | | (11,992 | ) |
| | | | | | | | |
| | $ | 10,535 | | $ | 9,973 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
Depreciation and amortization expense related to property and equipment was $2.4 million, $1.9 million and $2.0 million for the years ended December 31, 2014, 2013 and 2012, respectively.
(7) INTANGIBLE ASSETS AND GOODWILL
Intangible assets, net of accumulated amortization, and goodwill are as follows:
| | | | | | | | | | | | | | | | | | | | | |
| | December 31, 2014 | | December 31, 2013 | |
|---|
| | Estimated
Life | | Cost | | Accumulated
Amortization | | Net | | Cost | | Accumulated
Amortization | | Net | |
|---|
| |
| | (In thousands)
| |
|---|
Intangible Assets: | | | | | | | | | | | | | | | | | | | | | |
IPR&D | | Indefinite | | $ | 11,800 | | $ | — | | $ | 11,800 | | $ | 11,800 | | $ | — | | $ | 11,800 | |
Amgen Amendment | | 16 years | | | 14,500 | | | (4,708 | ) | | 9,792 | | | 14,500 | | | (3,812 | ) | | 10,688 | |
Core Technology | | 11 years | | | 1,296 | | | (1,081 | ) | | 215 | | | 1,296 | | | (964 | ) | | 332 | |
| | | | | | | | | | | | | | | | | | | | | | |
Total Intangible Assets | | | | $ | 27,596 | | $ | (5,789 | ) | $ | 21,807 | | $ | 27,596 | | $ | (4,776 | ) | $ | 22,820 | |
| | | | | | | | | | | | | | | | | | | | | | |
Goodwill | | Indefinite | | $ | 8,965 | | $ | — | | $ | 8,965 | | $ | 8,965 | | $ | — | | $ | 8,965 | |
| | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | |
The IPR&D intangible asset was recorded in connection with the acquisition of CuraGen and relates to the development of glembatumumab vedotin. At the date of acquisition and at December 31, 2014, glembatumumab vedotin had not yet reached technological feasibility nor did it have any alternative future use. Glembatumumab vedotin is in a randomized, Phase 2b study for the treatment of triple negative breast cancer and a Phase 2 study for the treatment of metastatic melanoma.
Amortization expense for intangible assets was $1.0 million, $1.0 million and $1.1 million for the years ended December 31, 2014, 2013 and 2012, respectively. The estimated future amortization expense of intangible assets for the years ending December 31, 2015, 2016, 2017, 2018 and 2019 is $1.0 million, $1.0 million, $0.9 million, $0.9 million and $0.9 million, respectively.
82
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(8) ACCRUED EXPENSES
Accrued expenses include the following:
| | | | | | | |
| | December 31,
2014 | | December 31,
2013 | |
|---|
| | (In thousands)
| |
|---|
Accrued Royalty and License Fees | | $ | — | | $ | 250 | |
Accrued Payroll and Employee Benefits | | | 4,284 | | | 3,515 | |
Accrued Research and Development Contract Costs | | | 12,696 | | | 11,840 | |
Accrued Professional Fees | | | 490 | | | 556 | |
Other Accrued Expenses | | | 1,826 | | | 1,018 | |
| | | | | | | | |
| | $ | 19,296 | | $ | 17,179 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
(9) OTHER LONG-TERM LIABILITIES
Other long-term liabilities include the following:
| | | | | | | |
| | December 31, 2014 | | December 31, 2013 | |
|---|
| | (In thousands)
| |
|---|
Deferred Rent | | $ | 482 | | $ | 419 | |
Net Deferred Tax Liability related to IPR&D | | | 4,661 | | | 4,661 | |
Deferred Income from Sale of Tax Benefits | | | 4,015 | | | 1,630 | |
Deferred Revenue | | | 5,297 | | | 1,168 | |
| | | | | | | | |
Total | | | 14,455 | | | 7,878 | |
Less Current Portion | | | (2,592 | ) | | (928 | ) |
| | | | | | | | |
Long-Term Portion | | $ | 11,863 | | $ | 6,950 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
In December 2014, January 2014, January 2013, January 2012 and January 2011, the Company received approval from the New Jersey Economic Development Authority and agreed to sell New Jersey tax benefits of $1.9 million, $1.1 million, $0.8 million, $0.8 million and $0.6 million to an independent third party for $1.8 million, $1.0 million, $0.8 million, $0.7 million and $0.5 million, respectively. Under the agreement, the Company must maintain a base of operations in New Jersey for five years or the tax benefits must be paid back on a pro-rata basis based on the number of years completed. During the years ended December 31, 2014 and 2013, the Company recorded $0.4 million and $0.2 million to other income related to the sale of these tax benefits, respectively.
In September 2013, the Company entered into an agreement with Rockefeller University pursuant to which the Company will perform research and development services for Rockefeller. The agreement includes an approved project plan for the development services of $4.8 million and a term of three years. The agreement included an upfront payment of $1.3 million which is being recognized as revenue over the term of the agreement. The Company bills Rockefeller quarterly for actual time and direct costs incurred and records those amounts to revenue in the quarter the services are performed. The Company recorded $2.7 million and $1.4 million in revenue related to the Rockefeller agreement during the years ended December 31, 2014 and 2013, respectively.
In May 2014, the Company entered into a clinical trial collaboration with Bristol-Myers Squibb Company ("BMS") to evaluate the safety, tolerability and preliminary efficacy of varlilumab and
83
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(9) OTHER LONG-TERM LIABILITIES (Continued)
Opdivo®, BMS's PD-1 immune checkpoint inhibitor, in a Phase1/2 study. Under the terms of this clinical trial collaboration, BMS made a one-time payment to the Company of $5.0 million and BMS and the Company amended the terms of the Company's existing license agreement with Medarex (a subsidiary of BMS) related to the Company's CD27 program whereby certain future milestone payments were waived and future royalty rates were reduced that may have been due from the Company to Medarex. In return, BMS was granted a time-limited right of first negotiation if the Company wishes to out-license varlilumab. The companies also agreed to work exclusively with each other to explore anti-PD-1 antagonist antibody and anti-CD27 agonist antibody combination regimens. The clinical trial collaboration provides that the companies will share development costs and that the Company will be responsible for conducting the ongoing Phase 1/2 study.
The Company has determined that its performance obligations under the BMS agreement, which primarily include performing research and development, supplying varlilumab and participating in the joint development committee, should be accounted for as a single unit of accounting and estimated that its performance period under the BMS agreement would be 5 years. Accordingly, the $5.0 million up-front payment was initially recorded as deferred revenue and is being recognized as revenue on a straight-line basis over the estimated 5-year performance period using the Contingency Adjusted Performance Model ("CAPM"). The BMS agreement also provides for BMS to reimburse the Company for 50% of the external costs incurred by the Company in connection with the clinical trial. These BMS payments will be recognized as revenue under the CAPM. The Company recorded $0.7 million in revenue related to the BMS agreement during the year ended December 31, 2014.
(10) TERM LOAN
In December 2010, the Company entered into a loan and security agreement pursuant to which the Company borrowed $10.0 million under a term loan. In March 2011, the Company amended the loan agreement and borrowed an additional $5.0 million. In May 2013, the Company elected to prepay the outstanding principal under the term loan in full, pursuant to the terms of its loan agreement, as amended, and paid $8.8 million in principal and $0.7 million in interest, prepayment and final payment fees. The Company's obligations under the loan agreement had been collateralized by a first priority security interest in substantially all of its assets, other than its intellectual property. In connection with the repayment of the term loan and the termination of the loan agreement, those security interests were released. Interest expense on the term loan was $0.8 million and $1.5 million for the years ended December 31, 2013 and 2012, respectively.
(11) STOCKHOLDERS' EQUITY
Common Stock
In December 2013, the Company filed an automatic shelf registration statement with the Securities and Exchange Commission to register for sale any combination of the types of securities described in the shelf registration statement.
During the years ended December 31, 2013 and 2012, Company issued 21,613,483 and 12,075,000 shares of its common stock in underwritten public offerings resulting in net proceeds to the Company of $278.6 million and $43.5 million, after deducting underwriting fees and offering expenses, respectively.
84
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(11) STOCKHOLDERS' EQUITY (Continued)
During the years ended December 31, 2013 and 2012, Company issued 2,433,608 and 8,003,290 shares of its common stock under our controlled equity offering sales agreement with Cantor Fitzgerald & Co., as amended, resulting in net proceeds to the Company of $17.1 million and $40.1 million, after deducting commission and offering expenses, respectively.
During the year ended December 31, 2014, the Company entered into an amended and restated supply agreement with Biosyn Corporation. Under the supply agreement, Biosyn will manufacture and supply keyhole limpet hemocyanin (KLH) to the Company for use in connection with the development, manufacture or commercial sale of rindopepimut. In connection with the supply agreement, the Company issued to Biosyn 152,172 shares of its common stock having a value of $2.0 million. The Company is recording the $2.0 million to research and development expense through August 2021, the current term of the supply agreement. At December 31, 2014, the Company recorded $0.3 million and $1.6 million to prepaid assets and other assets related to this stock issuance, respectively.
Convertible Preferred Stock
At December 31, 2014, the Company had authorized 3,000,000 shares of preferred stock all of which have been designated Class C Preferred Stock including 350,000 shares which have been designated Series C-1 Junior Participating Cumulative Preferred Stock (the "Series C-1 Preferred Stock").
(12) STOCK-BASED COMPENSATION
The Company has the following stock-based compensation plans: the 2004 Employee Stock Purchase Plan (the "2004 ESPP Plan"), the 2008 Stock Option and Incentive Plan (the "2008 Plan"), Celldex Research's 2005 Equity Incentive Plan (the "Celldex Research 2005 Plan") and CuraGen 2007 Stock Plan (the "CuraGen 2007 Plan"). There are no shares available for future grant under the Celldex Research 2005 Plan and CuraGen 2007 Plan.
Employee Stock Purchase Plan
At December 31, 2014, a total of 200,000 shares of common stock are reserved for issuance under the 2004 ESPP Plan. Under the 2004 ESPP Plan, each participating employee may purchase shares of common stock through payroll deductions at a purchase price equal to 85% of the lower of the fair market value of the common stock at either the beginning of the offering period or the applicable exercise date. During the years ended December 31, 2014 and 2013, the Company issued 10,798 and 11,823 shares under the 2004 ESPP Plan, respectively. At December 31, 2014, 153,326 shares were available for issuance under the 2004 ESPP Plan.
Employee Stock Option and Incentive Plan
The 2008 Plan permits the granting of incentive stock options (intended to qualify as such under Section 422A of the Internal Revenue Code of 1986, as amended), non-qualified stock options, stock appreciation rights, performance share units, restricted stock and other awards of restricted stock in lieu of cash bonuses to employees, consultants and non-employee directors.
At December 31, 2014, the 2008 Plan allowed for a maximum of 7,400,000 shares of common stock to be issued for grants of Stock Options and other Awards made prior to March 7, 2018 and grants of
85
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(12) STOCK-BASED COMPENSATION (Continued)
Incentive Stock Options made prior to October 20, 2017. The Company's board of directors determines the term of each option, option price, and number of shares for which each option is granted and the rate at which each option vests. Options generally vest over a period not to exceed four years. The term of each option cannot exceed ten years (five years for options granted to holders of more than 10% of the voting stock of the Company) and the exercise price of stock options cannot be less than the fair market value of the common stock at the date of grant (110% of fair market value for incentive stock options granted to holders of more than 10% of the voting stock of the Company). Vesting of all employee and non-employee director stock option awards is accelerated upon a change in control as defined in the 2008 Plan.
A summary of stock option activity for the year ended December 31, 2014 is as follows:
| | | | | | | | | | |
| | Shares | | Weighted
Average
Exercise
Price
Per Share | | Weighted
Average
Remaining
Contractual
Term (In Years) | |
|---|
Options Outstanding at December 31, 2013 | | | 5,770,544 | | $ | 8.17 | | | 7.0 | |
Granted | | | 1,456,800 | | $ | 13.69 | | | | |
Exercised | | | (169,977 | ) | $ | 6.00 | | | | |
Canceled | | | (42,017 | ) | $ | 13.10 | | | | |
| | | | | | | | | | | |
Options Outstanding at December 31, 2014 | | | 7,015,350 | | $ | 9.34 | | | 6.6 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Options Vested and Expected to Vest at December 31, 2014 | | | 6,963,570 | | $ | 9.31 | | | 6.6 | |
Options Exercisable at December 31, 2014 | | | 4,090,112 | | $ | 7.06 | | | 5.1 | |
Shares Available for Grant under the 2008 Plan | | | 675,159 | | | | | | | |
The total intrinsic value of stock options exercised during the years ended December 31, 2014, 2013 and 2012 was $2.7 million, $10.0 million and $0.2 million, respectively. The weighted average grant-date fair value of stock options granted during the years ended December 31, 2014, 2013 and 2012 was $8.82, $10.51 and $3.67, respectively. The total fair value of stock options vested during the years ended December 31, 2014, 2013 and 2012 was $5.7 million, $2.4 million and $2.1 million, respectively.
The aggregate intrinsic value of stock options outstanding at December 31, 2014 was $62.8 million. The aggregate intrinsic value of stock options vested and expected to vest at December 31, 2014 was $62.5 million. As of December 31, 2014, total compensation cost related to non-vested employee and non-employee director stock options not yet recognized was approximately $20.3 million, net of estimated forfeitures, which is expected to be recognized as expense over a weighted average period of 2.6 years.
86
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(12) STOCK-BASED COMPENSATION (Continued)
Restricted Stock
A summary of restricted stock activity under the 2008 Plan for the year ended December 31, 2014 is as follows:
| | | | | | | |
| | Shares | | Weighted
Average
Grant Date
Fair Value
(per share) | |
|---|
Outstanding and unvested at December 31, 2013 | | | 6,000 | | $ | 15.20 | |
Granted | | | 14,000 | | $ | 14.12 | |
Vested | | | (12,000 | ) | $ | 14.33 | |
Canceled | | | (1,000 | ) | $ | 13.45 | |
| | | | | | | | |
Outstanding and unvested at December 31, 2014 | | | 7,000 | | $ | 14.78 | |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
Valuation and Expenses Information
Stock-based compensation expense for the years ended December 31, 2014, 2013 and 2012 was recorded as follows:
| | | | | | | | | | |
| | 2014 | | 2013 | | 2012 | |
|---|
| | (In thousands)
| |
|---|
Research and development | | $ | 3,459 | | $ | 2,640 | | $ | 1,415 | |
General and administrative | | | 3,393 | | | 1,908 | | | 883 | |
| | | | | | | | | | | |
Total stock-based compensation expense | | $ | 6,852 | | $ | 4,548 | | $ | 2,298 | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
The fair values of employee stock options granted during the years ended December 31, 2014, 2013 and 2012 were valued using the Black-Scholes option-pricing model with the following assumptions:
| | | | | | |
| | Year Ended
December 31, 2014 | | Year Ended
December 31, 2013 | | Year Ended
December 31, 2012 |
|---|
Expected stock price volatility | | 70 - 72% | | 71 - 72% | | 70 - 72% |
Expected option term | | 6.0 Years | | 6.0 Years | | 6.0 Years |
Risk-free interest rate | | 1.9 - 2.2% | | 1.2 - 2.1% | | 0.9 - 1.4% |
Expected dividend yield | | None | | None | | None |
The Company estimates expected term based on historical exercise patterns. The Company uses its historical stock price volatility consistent with the expected term of grant as the basis for its expected volatility assumption. The risk-free interest rate is based upon the yield of U.S. Treasury securities consistent with the expected term of the option. The dividend yield assumption is based on the Company's history of zero dividend payouts and expectation that no dividends will be paid in the foreseeable future.
87
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(13) REVENUE
In 1997, the Company licensed its oral rotavirus strain to GlaxoSmithKline plc ("Glaxo") and Glaxo assumed responsibility for all subsequent clinical trials and all other development activities. The Company's licensed-in the rotavirus strain that was used to develop Glaxo's Rotarix rotavirus vaccine in 1995 and owed a license fee of 30% to Cincinnati Children's Hospital Medical Center ("CCH") on net royalties received from Glaxo. In May 2005, the Company entered into an agreement whereby an affiliate of Paul Royalty Fund II, L.P. ("PRF") purchased a 70% interest in the net royalties the Company received on worldwide sales of Rotarix. In December 2012, the Glaxo agreement expired automatically upon the expiration of the last relevant patent right covered by the Glaxo agreement. The Company's retained interests in Rotarix net royalties which were not sold to PRF are recorded as product royalty revenue and a corresponding amount that is payable to CCH is recorded as royalty expense. Product royalty revenue and royalty expense related to the Company's retained interest in Rotarix was $2.3 million and $10.8 million for the years ended December 31, 2013 and 2012, respectively.
(14) COLLABORATION AGREEMENTS
The Company has entered into license agreements whereby the Company has received licenses or options to license technology, specified patents or patent applications. The Company's licensing and development collaboration agreements generally provide for royalty payments equal to specified percentages of product sales, annual license maintenance fees, continuing patent prosecution costs and potential future milestone payments to third parties upon the achievement of certain developmental, regulatory and/or commercial milestones. Nonrefundable license fee expense of $3.2 million, $0.7 million and $0.7 million was recorded to research and development expense for the years ended December 31, 2014, 2013 and 2012, respectively.
Medarex, Inc., a subsidiary of Bristol-Myers Squibb (Medarex)
The Company and Medarex have entered into an assignment and license agreement, as amended, that provides for the assignment of certain patent and other intellectual property rights and a license to certain Medarex technology related to the Company's APC Targeting Technology™ and an anti-mannose receptor product. Under the terms of the agreement, the Company may be required to pay royalties in the low-single digits on any net product sale of a Licensed Royalty-Bearing Product or Anti-Mannose Product to Medarex until the later of (i) the expiration of the last to expire applicable patent and (ii) the tenth anniversary of the first commercial sale of such licensed product.
The Company and Medarex have also entered into a research and commercialization agreement, as amended, that provides the Company with certain rights to obtain exclusive commercial licenses to proprietary monoclonal antibodies raised against certain antigens utilizing the Medarex UltiMAb technology platform for generating antibodies until December 2015. Under the terms of the agreement, the Company may be required to pay Medarex milestones of up to $7.0 million upon obtaining first approval for commercial sale in a first indication of a product containing a licensed antibody and royalty payments in the low-to-mid single digits on any net product sales with respect to the development of any products containing such licensed antibodies until the later of (i) the expiration of the last to expire applicable patent and (ii) the tenth anniversary of the first commercial sale of such licensed product. In September 2010, the Company exercised an option under the agreement, whereby it licensed from Medarex access to the UltiMab technology to develop and commercialize human
88
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(14) COLLABORATION AGREEMENTS (Continued)
antibodies to CD27, including varlilumab. In connection with the clinical trial collaboration, the Company entered into with BMS in May 2014, certain future milestone payments were waived and future royalty rates that the Company may have owed Medarex in connection with any CD27 program were reduced.
Rockefeller University (Rockefeller)
In November 2005, the Company and Rockefeller entered into a license agreement for the exclusive worldwide rights to human DEC-205 receptor, with the right to sublicense the technology. The license grant is exclusive except that Rockefeller may use and permit other nonprofit organizations to use the human DEC-205 receptor patent rights for educational and research purposes. The Company may be required to pay Rockefeller milestones of up to $3.8 million upon obtaining first approval for commercial sale in a first indication of a product targeting the licensed receptor and royalty payments in the low-to-mid single digits on any net product sales with respect to development and commercialization of the human DEC-205 receptor.
Duke University Brain Tumor Cancer Center (Duke)
In September 2006, the Company and Duke entered into a license agreement that gave the Company access and reference to the clinical data generated by Duke and its collaborators in order for the Company to generate its own filing with the FDA relating to rindopepimut. The Company may be required to pay Duke milestones of up to $0.7 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of rindopepimut.
Ludwig Institute for Cancer Research (Ludwig)
In October 2006, the Company and Ludwig entered into an agreement for the nonexclusive rights to certain cancer tumor targets for use in combination with the Company's APC Targeting Technology. The Company may be required to pay Ludwig milestones of up to $1.0 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of the technology licensed from Ludwig.
Alteris Therapeutics, Inc. (Alteris)
In October 2005, the Company completed the acquisition of the assets of Alteris, including the EGFRvIII molecule. The Company may be required to pay Alteris up to $5.0 million upon obtaining the first approval for commercial sale of a product containing EGFRvIII, including rindopepimut.
University of Southampton, UK (Southampton)
In November 2008, the Company entered into a license agreement with Southampton to develop human antibodies towards CD27, a potentially important target for immunotherapy of various cancers. The Company may be required to pay Southampton milestones of up to approximately $1.4 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the
89
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(14) COLLABORATION AGREEMENTS (Continued)
low-single digits on any net product sales with respect to development and commercialization of varlilumab.
Amgen Inc. (Amgen)
In March 2009, the Company entered into a license agreement with Amgen to acquire the exclusive rights to CDX-301 and CD40 ligand (CD40L). CDX-301 and CD40L are immune modulating molecules that increase the numbers and activity of immune cells that control immune responses. The Company may be required to pay Amgen milestones of up to $1.0 million upon obtaining first approval for commercial sale in a first indication and royalty payments in the low-single digits on any net product sales with respect to development and commercialization of the technology licensed from Amgen, including CDX-301.
Seattle Genetics, Inc. (Seattle Genetics)
In connection with the acquisition of CuraGen, the Company assumed the license agreement between CuraGen and Seattle Genetics whereby CuraGen acquired the rights to proprietary antibody-drug conjugate (ADC) technology for use with the Company's proprietary antibodies for the potential treatment of cancer. The Company may be required to pay Seattle Genetics milestones of up to $5.0 million and $9.0 million for glembatumumab vedotin and CDX-014, respectively, upon obtaining first approval for commercial sale in a first indication and royalty payments in the mid-single digits on any net product sales with respect to development and commercialization of these product candidates.
(15) INCOME TAXES
The components of income tax expense attributable to continuing operations consist of the following:
| | | | | | | | | | |
| | Year Ended December 31, | |
|---|
| | 2014 | | 2013 | | 2012 | |
|---|
| | (In thousands)
| |
|---|
Income tax benefit (provision): | | | | | | | | | | |
Federal | | $ | 43,536 | | $ | 30,962 | | $ | 19,394 | |
State | | | 7,328 | | | 4,920 | | | 4,237 | |
Expiration of Net Operating Losses and Research & Development Tax Credits | | | (2,302 | ) | | (126 | ) | | (1,426 | ) |
| | | | | | | | | | | |
| | | 48,562 | | | 35,756 | | | 22,205 | |
Deferred tax valuation allowance | | | (48,562 | ) | | (35,756 | ) | | (22,205 | ) |
| | | | | | | | | | | |
| | $ | — | | $ | — | | $ | — | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
90
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(15) INCOME TAXES (Continued)
A reconciliation between the amount of reported income tax and the amount computed using the U.S. Statutory rate of 34% follows:
| | | | | | | | | | |
| | 2014 | | 2013 | | 2012 | |
|---|
| | (In thousands)
| |
|---|
Pre-tax loss | | $ | (118,080 | ) | $ | (81,550 | ) | $ | (59,123 | ) |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Loss at Statutory Rates | | | (40,147 | ) | | (27,727 | ) | | (20,102 | ) |
Research and Development Credits | | | (4,126 | ) | | (3,261 | ) | | — | |
State Taxes | | | (7,328 | ) | | (4,920 | ) | | (4,237 | ) |
Other | | | 737 | | | 26 | | | 708 | |
Expiration of Net Operating Losses and Research & Development Tax Credits | | | 2,302 | | | 126 | | | 1,426 | |
Change in Valuation Allowance | | | 48,562 | | | 35,756 | | | 22,205 | |
| | | | | | | | | | | |
Income tax (benefit) provision | | $ | — | | $ | — | | $ | — | |
| | | | | | | | | | | |
| | | | | | | | | | | |
| | | | | | | | | | | |
Deferred tax assets and liabilities are recognized based on temporary differences between the financial reporting and tax basis of assets and liabilities using future expected enacted rates. A valuation allowance is recorded against deferred tax assets if it is more likely than not that some or all of the deferred tax assets will not be realized.
The principal components of the deferred tax assets and liabilities at December 31, 2014 and 2013, respectively, are as follows:
| | | | | | | |
| | December 31,
2014 | | December 31,
2013 | |
|---|
| | (In thousands)
| |
|---|
Gross Deferred Tax Assets | | | | | | | |
Net Operating Loss Carryforwards | | $ | 95,577 | | $ | 79,558 | |
Tax Credit Carryforwards | | | 29,709 | | | 25,582 | |
Deferred Expenses | | | 85,889 | | | 61,370 | |
Stock-based Compensation | | | 5,556 | | | 3,926 | |
Fixed Assets | | | 1,882 | | | 1,638 | |
Deferred Revenue | | | 2,078 | | | 447 | |
Accrued Expenses and Other | | | 202 | | | 176 | |
| | | | | | | | |
| | | 220,893 | | | 172,697 | |
Gross Deferred Tax Liabilities | | | | | | | |
Other Acquired Intangibles | | | (3,749 | ) | | (4,115 | ) |
IPR&D Intangibles | | | (4,661 | ) | | (4,661 | ) |
| | | | | | | | |
| | | (8,410 | ) | | (8,776 | ) |
| | | | | | | | |
Total Deferred Tax Assets and Liabilities | | | 212,483 | | | 163,921 | |
Deferred Tax Assets Valuation Allowance | | | (217,144 | ) | | (168,582 | ) |
| | | | | | | | |
Net Deferred Tax Asset (Liability) | | $ | (4,661 | ) | $ | (4,661 | ) |
| | | | | | | | |
| | | | | | | | |
| | | | | | | | |
91
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(15) INCOME TAXES (Continued)
The net deferred tax liability of $4.7 million at December 31, 2014 and 2013 relates to the temporary differences associated with the IPR&D intangible assets acquired in the CuraGen acquisition, which are not deductible for tax purposes.
As of December 31, 2014, the Company had the following federal net operating loss ("NOL") carryforwards:
- •
- Prior to the merger of the Company and AVANT, $33.0 million was generated by the Company which expire at various dates starting in 2023 and going through 2028;
- •
- Prior to the merger of the Company and AVANT, $101.2 million, net of expirations and utilization, was generated by AVANT which expire at various dates starting in 2018 and going through 2028;
- •
- Following the merger of the Company and AVANT, $182 million was generated by the combined company which expire at various dates starting in 2028 and going through 2034; and
- •
- Prior to its acquisition by the Company, $518.3 million was generated by CuraGen.
As of December 31, 2014, the Company has an additional $8.0 million of federal and state net operating losses not reflected above, that are attributable to stock option exercises which will be recorded as an increase in additional paid in capital on the consolidated balance sheet once they are "realized" in accordance with ASC 718.
In general, an ownership change, as defined by Section 382 of the Internal Revenue Code, results from transactions increasing the ownership of certain shareholders or public groups in the stock of a corporation by more than 50 percentage points over a three-year period. Such ownership changes can significantly limit the amount of NOLs that may be utilized in future periods. The Company currently expects that it is remote that the CuraGen NOLs may be utilized and, as such, no related asset has been recorded for such losses. The Company has not completed an analysis of losses generated by AVANT, however, the Company believes it is remote that $60.8 million of the AVANT NOLs may be utilized in future periods and there may be substantial limitations on the Company's ability to use the remaining NOLs of $40.4 million. Following the merger of the Company and AVANT, the Company experienced changes in ownership as defined by Section 382 in June 2009 and December 2009. Further, prior to the AVANT merger, the Company as a stand alone company experienced a change in ownership in October 2007. As a result of the ownership change in October 2007, utilization of the Company's NOLs prior to October 2007 is subject to an annual limitation of $4.5 million on $28.3 million of NOLs generated before that date. As a result of the ownership changes in June 2009 and December 2009, there is an annual limitation amount of $6.0 million on $67.7 million NOLs. Any unused annual limitation may be carried over to later years, and the amount of the limitation may, under certain circumstances, be subject to adjustment if the fair value of the Company's net assets are determined to be below or in excess of the tax basis of such assets at the time of the ownership change, and such unrealized loss or gain is recognized during the five-year period after the ownership change.
Similar to the AVANT and CuraGen NOL carryforwards above, the Company believes that it is not more likely than not that federal and state research and development ("R&D") credits of $20.8 million and $14.4 million, respectively, will be utilized in the future periods. Further, the Company's ability to use the state NOLs of approximately $127.6 million and the remaining federal and state R&D credit carryforwards of approximately $23.6 million and $9.3 million, respectively, may be
92
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(15) INCOME TAXES (Continued)
substantially limited. These state NOLs and federal and state credits expire at various dates starting in 2016 going through 2034. The Company has not yet completed a study of these credits to substantiate the amounts. Until a study is completed, no amounts are being presented as an uncertain tax position.
Subsequent ownership changes, as defined in Section 382, could further limit the amount of net operating loss carryforwards and research and development credits that can be utilized annually to offset future taxable income.
The Company applies the authoritative guidance on account for and disclosure of uncertainty in income tax positions which requires the Company to determine whether an income tax position of the Company is more likely than not to be sustained upon examination, including resolution of any related appeals or litigation processes, based on the technical merits of the position. For income tax positions meeting the more likely than not threshold, the tax amount recognized in the financial statements is reduced to the largest benefit that has a greater than fifty perfect likelihood of being realized upon the ultimate settlement with the relevant taxing authority. At December 31, 2014 and 2013, we had no unrecognized tax benefits. A full valuation allowance has been provided against our deferred tax assets and liabilities and, if an adjustment is required, this adjustment would be offset by an adjustment to the valuation allowance. Thus, there would be no impact to the consolidated balance sheet or statement of operations if an adjustment were required.
Massachusetts, New Jersey and Connecticut are the three states in which the Company primarily operates or has operated and has income tax nexus. The Company is not currently under examination by these or any other jurisdictions for any tax year.
The Company has evaluated the positive and negative evidence bearing upon the realizability of its net deferred tax assets, which are comprised principally of net operating loss carryforwards, capitalized R&D expenditures and R&D tax credit carryforwards. The Company has determined that it is more likely than not that it will not recognize the benefits of federal and state deferred tax assets and, as a result, a full valuation allowance was maintained at December 31, 2014 against the Company's net deferred tax assets.
(16) COMMITMENTS AND CONTINGENCIES
The Company has facility and equipment leases that expire at various dates through 2019. Certain of these facility leases contain renewal options, early termination provisions, and provisions that escalate the base rent payments and require the Company to pay common area maintenance costs ("CAM") during the lease term. The following obligations for base rent and CAM costs under facility and other non-cancelable operating leases as of December 31, 2014 do not include the exercise of renewal terms or early termination provisions (in thousands):
| | | | |
2015 | | $ | 2,793 | |
2016 | | | 3,009 | |
2017 | | | 1,866 | |
2018 | | | 690 | |
2019 | | | 362 | |
Thereafter | | | — | |
| | | | | |
Total minimum lease payments | | $ | 8,720 | |
| | | | | |
| | | | | |
| | | | | |
93
Table of Contents
CELLDEX THERAPEUTICS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
(16) COMMITMENTS AND CONTINGENCIES (Continued)
The Company's total rent and CAM expense for all facility leases was $2.7 million, $2.7 million and $2.5 million for the years ended December 31, 2014, 2013 and 2012, respectively.
(17) RETIREMENT SAVINGS PLAN
The Company maintains a 401(k) Plan which is available to substantially all employees. Under the terms of the 401(k) Plan, participants may elect to contribute up to 15% of their compensation, or the statutory prescribed limits. The Company may make 50% matching contributions on up to 4% of a participant's annual salary. Benefit expense for the 401(k) Plan was $0.3 million, $0.3 million and $0.2 million for the years ended December 31, 2014, 2013 and 2012, respectively.
(18) SELECTED QUARTERLY FINANCIAL DATA (Unaudited)
| | | | | | | | | | | | | |
2014 | | Q1 2014 | | Q2 2014 | | Q3 2014 | | Q4 2014 | |
|---|
| | (In thousands, except per share amounts)
| |
|---|
Total revenue | | $ | 416 | | $ | 592 | | $ | 1,101 | | $ | 1,477 | |
Net loss | | | (29,903 | ) | | (28,274 | ) | | (28,082 | ) | | (31,821 | ) |
Basic and diluted net loss per common share | | | (0.33 | ) | | (0.32 | ) | | (0.31 | ) | | (0.36 | ) |
| | | | | | | | | | | | | |
2013 | | Q1 2013 | | Q2 2013 | | Q3 2013 | | Q4 2013 | |
|---|
| | (In thousands, except per share amounts)
| |
|---|
Total revenue | | $ | 2,414 | | $ | 97 | | $ | 980 | | $ | 620 | |
Net loss | | | (17,332 | ) | | (19,016 | ) | | (23,140 | ) | | (22,062 | ) |
Basic and diluted net loss per common share | | | (0.23 | ) | | (0.24 | ) | | (0.29 | ) | | (0.27 | ) |
94
Table of Contents
Item 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
Item 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
As of December 31, 2014, we evaluated, with the participation of our Chief Executive Officer and Chief Financial Officer, the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the "Exchange Act")). Based on that evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures were effective at the reasonable assurance level as of December 31, 2014. Our disclosure controls and procedures are designed to provide reasonable assurance that information required to be disclosed in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within time periods specified by the SEC's rules and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosure.
Management's Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over our financial reporting. Internal control over financial reporting is defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act as the process designed by, or under the supervision of, our Chief Executive Officer and Chief Financial Officer, and effected by our board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of our financial reporting and the preparation of our financial statements for external purposes in accordance with generally accepted accounting principles, and includes those policies and procedures that:
- •
- pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of assets;
- •
- provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures are being made only in accordance with the authorizations of management and directors; and
- •
- provide reasonable assurance regarding the prevention or timely detection of unauthorized acquisition, use or disposition of assets that could have a material effect on our financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the framework provided inInternal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this evaluation, our management concluded that our internal control over financial reporting was effective as of December 31, 2014.
95
Table of Contents
The effectiveness of our internal control over financial reporting as of December 31, 2014 has been audited by PricewaterhouseCoopers LLP, an independent registered public accounting firm, as stated in their report, which is included herein.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting during the three months ended December 31, 2014 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Item 9B. OTHER INFORMATION
None.
PART III
Item 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The information required by this Item 10 will be included in the definitive Proxy Statement for our 2015 Annual Meeting of Stockholders, or the 2015 Proxy Statement, under "Information Regarding the Current Directors and Executive Officers of Celldex Therapeutic, Inc.," "Section 16(a) Beneficial Ownership Reporting Compliance," "Code of Business Conduct and Ethics" and "The Board of Directors and Its Committees" and is incorporated herein by reference. If the 2015 Proxy Statement is not filed with the SEC within 120 days after the end of our most recent fiscal year, we will provide such information by means of an amendment to this Annual Report on Form 10-K.
Item 11. EXECUTIVE COMPENSATION
The information required by this Item 11 will be included in the 2015 Proxy Statement under "Executive Compensation," and "Compensation Committee Interlocks and Insider Participation," and is incorporated herein by reference. If the 2015 Proxy Statement is not filed with the SEC within 120 days after the end of our most recent fiscal year, we will provide such information by means of an amendment to this Annual Report on Form 10-K.
Item 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this Item 12 will be included in the 2015 Proxy Statement under "Security Ownership of Certain Beneficial Owners and Management" and "Equity Compensation Plan Information" and is incorporated herein by reference. If the 2015 Proxy Statement is not filed with the SEC within 120 days after the end of our most recent fiscal year, we will provide such information by means of an amendment to this Annual Report on Form 10-K.
Item 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this Item 13 will be included in the 2015 Proxy Statement under "Election of Directors" and "Approval of Related Person Transactions and Transactions with Related Persons" and is incorporated herein by reference. If the 2015 Proxy Statement is not filed with the SEC within 120 days after the end of our most recent fiscal year, we will provide such information by means of an amendment to this Annual Report on Form 10-K.
96
Table of Contents
Item 14. PRINCIPAL ACCOUNTING FEES AND SERVICES
The information required by this Item 14 will be included in the 2015 Proxy Statement under "Independent Registered Public Accounting Firm" and is incorporated herein by reference. If the 2015 Proxy Statement is not filed with the SEC within 120 days after the end of our most recent fiscal year, we will provide such information by means of an amendment to this Annual Report on Form 10-K.
97
Table of Contents
PART IV
Item 15. EXHIBITS, FINANCIAL STATEMENT SCHEDULES
- (A)
- The following documents are filed as part of this Form 10-K:
- (1)
- Financial Statements:
The Financial Statements and Supplementary Data are included in Part II Item 8 of this report.
- (2)
- Financial Statement Schedules:
Schedules are omitted since the required information is not applicable or is not present in amounts sufficient to require submission of the schedule, or because the information required is included in the Consolidated Financial Statements or Notes thereto.
| | | | | | | | | |
| |
| | Incorporated by Reference to |
|---|
| No. | | Description | | Form and
SEC File No. | | Exhibit
No. | | SEC
Filing Date |
|---|
| | Plan of Acquisition, Reorganization, Arrangement, Liquidation or Succession |
| | 2.1 | | Agreement and Plan of Merger, dated as of October 19, 2007, by and among AVANT, Celldex Merger Corporation, and Celldex Therapeutics, Inc. | | 8-K
(000-15006) | | 2.1 | | 10/22/07 |
|
2.2 |
|
Agreement and Plan of Merger, dated as of May 28, 2009, by and among Celldex Therapeutics, Inc., CuraGen Corporation and Cottrell Merger Sub, Inc. |
|
8-K
(000-15006) |
|
2.1 |
|
5/29/09 |
|
Articles of Incorporation and By-Laws |
| | 3.1 | | Third Restated Certificate of Incorporation | | S-4
(333-59215) | | 3.1 | | 7/16/98 |
|
3.2 |
|
Certificate of Amendment of Third Restated Certificate of Incorporation |
|
S-4
(333-59215) |
|
3.1 |
|
7/16/98 |
|
3.3 |
|
Second Certificate of Amendment of Third Restated Certificate of Incorporation |
|
S-4
(333-59215) |
|
3.2 |
|
7/16/98 |
|
3.4 |
|
Third Certificate of Amendment of Third Restated Certificate of Incorporation |
|
10-Q
(000-15006) |
|
3.1 |
|
5/10/02 |
|
3.5 |
|
Fourth Certificate of Amendment of Third Restated Certificate of Incorporation |
|
8-K
(000-15006) |
|
3.1 |
|
3/11/08 |
|
3.6 |
|
Fifth Certificate of Amendment of Third Restated Certificate of Incorporation |
|
8-K
(000-15006) |
|
3.2 |
|
3/11/08 |
|
3.7 |
|
Sixth Certificate of Amendment of Third Restated Certificate of Incorporation |
|
10-Q
(000-15006) |
|
3.7 |
|
11/10/08 |
|
3.8 |
|
Amended and Restated By-Laws, dated April 7, 2014 |
|
8-K
(000-15006) |
|
3.1 |
|
4/8/14 |
|
Instruments Defining the Rights of Security Holders |
| | 4.1 | | Specimen of Common Stock Certificate | | Filed herewith | | | | |
98
Table of Contents
| | | | | | | | | |
| |
| | Incorporated by Reference to |
|---|
| No. | | Description | | Form and
SEC File No. | | Exhibit
No. | | SEC
Filing Date |
|---|
|
4.2 |
|
Certificate of Designations, Preferences and Rights of a Series of Preferred Stock classifying and designating the Series C-1 Junior Participating Cumulative Preferred Stock |
|
8-A
(000-15006) |
|
3.1 |
|
11/8/04 |
|
Material Contracts—Leases |
| | 10.1 | | Commercial Lease Agreement of May 1, 1996 between the Company and Fourth Avenue Ventures Limited Partnership | | 10-Q/A
(000-15006) | | 10.11 | | 8/23/96 |
|
10.2 |
|
Extension of Lease Agreement of May 1, 1997 between the Company and DIV Needham 53 LLC (successor in interest to Fourth Avenue Ventures Limited Partnership) dated as of August 23, 2001 |
|
10-K
(000-15006) |
|
10.9 |
|
3/27/02 |
|
10.3 |
|
First Amendment to Lease by and between the Company and DIV Needham 53 LLC dated November 29, 2005 |
|
10-K
(000-15006) |
|
10.40 |
|
3/16/06 |
|
*10.4 |
|
Lease Agreement, by and between the Company and the Massachusetts Development Finance Agency, dated as of December 22, 2003 |
|
10-Q
(000-15006) |
|
10.1 |
|
4/30/04 |
|
10.5 |
|
First Amendment to Lease between Massachusetts Development Finance Agency and the Company dated March 17, 2005 |
|
10-K/A
(000-15006) |
|
10.6 |
|
12/23/10 |
|
10.6 |
|
Second Amendment to Lease by and between the Company and the Massachusetts Development Finance Agency dated as of November 4, 2005 |
|
10-K
(000-15006) |
|
10.41 |
|
3/16/06 |
|
10.7 |
|
Third Amendment to Lease between Massachusetts Development Finance Agency and the Company dated December 20, 2006 |
|
10-K/A
(000-15006) |
|
10.7 |
|
12/23/10 |
|
10.8 |
|
Fifth Amendment to Lease between Massachusetts Development Finance Agency and the Company dated October 3, 2008 |
|
10-K/A
(000-15006) |
|
10.8 |
|
12/23/10 |
|
10.9 |
|
Sixth Amendment to Lease between Massachusetts Development Finance Agency and the Company dated August 20, 2009 |
|
10-K/A
(000-15006) |
|
10.9 |
|
12/23/10 |
|
10.10 |
|
Seventh Amendment to Lease by and between the Company and the Massachusetts Development Finance Agency dated as of June 22, 2010 |
|
10-Q
(000-15006) |
|
10.1 |
|
8/5/10 |
|
10.11 |
|
Lease Agreement dated as of May 1, 2013 by and between Crown Perryville, LLC and the Company. |
|
10-Q
(000-15006) |
|
10.1 |
|
5/03/13 |
|
Material Contracts—License, Collaboration, Supply and Distribution Agreements |
| | *10.12 | | License Agreement dated as of November 1, 2005 by and between The Rockefeller University and the Company | | S-4
(333-148291) | | 10.2 | | 1/18/08 |
99
Table of Contents
| | | | | | | | | |
| |
| | Incorporated by Reference to |
|---|
| No. | | Description | | Form and
SEC File No. | | Exhibit
No. | | SEC
Filing Date |
|---|
| | *10.13 | | License Agreement dated September 1, 2006 by and between Duke University and the Company | | S-4
(333-148291) | | 10.3 | | 1/18/08 |
|
10.14 |
|
Amendment to License Agreement between Duke University and the Company dated April 2, 2008 |
|
10-K/A
(000-15006) |
|
10.5 |
|
12/23/10 |
|
*10.15 |
|
License Agreement between Duke University, The Johns Hopkins University and the Company dated December 31, 2003 |
|
10-K/A
(000-15006) |
|
10.11 |
|
12/23/10 |
|
*10.16 |
|
Amendment to License Agreement between Duke University, The Johns Hopkins University and the Company dated April 2, 2008 |
|
10-K/A
(000-15006) |
|
10.13 |
|
12/23/10 |
|
*10.17 |
|
Assignment and License Agreement, as amended, dated April 6, 2004 by and among Medarex, Inc., GenPharm International, Inc. and the Company |
|
S-4
(333-148291) |
|
10.4 |
|
1/18/08 |
|
*10.18 |
|
Research and Commercialization Agreement, as amended, dated as of April 6, 2004 by and among Medarex, Inc., GenPharm International, Inc. and the Company |
|
S-4
(333-148291) |
|
10.5 |
|
1/18/08 |
|
*10.19 |
|
Research Collaboration and Commercialization Agreement effective October 20, 2006 between the Company and the Ludwig Institute for Cancer Research |
|
10-K
(000-15006) |
|
10.45 |
|
3/2/09 |
|
*10.20 |
|
Exclusive Patent and Know-How License Agreement dated as of November 5, 2008 between the Company and the University of Southampton |
|
10-K
(000-15006) |
|
10.47 |
|
3/2/09 |
|
*10.21 |
|
License and Assignment Agreement, between Amgen Inc. and the Company dated March 16, 2009 |
|
10-K/A
(000-15006) |
|
10.1 |
|
12/23/10 |
|
*10.22 |
|
Collaboration Agreement dated June 18, 2004 between Seattle Genetics and CuraGen |
|
10-K
(000-15006) |
|
10.27 |
|
3/12/10 |
|
*10.23 |
|
Second Restated Collaboration Agreement dated April 12, 2004 and amended October 19, 2004 between Abgenix Inc. and CuraGen |
|
10-K
(000-15006) |
|
10.28 |
|
3/12/10 |
|
10.24 |
|
Amgen Letter Agreement, by and between CuraGen and Amgen Fremont, Inc. dated May 2, 2009 |
|
10-K
(000-15006) |
|
10.29 |
|
3/12/10 |
|
*10.25 |
|
Transfer and Termination Agreement, dated as of April 21, 2008 by and between TopoTarget A/S and CuraGen |
|
10-K
(000-15006) |
|
10.30 |
|
3/12/10 |
|
*10.26 |
|
License Agreement between Medarex and Company dated September 17, 2010 |
|
10-Q/A
(000-15006) |
|
10.3 |
|
12/23/10 |
|
10.27 |
|
Master Services Agreement dated March 29, 2010 by and between the Company and Prologue Research International, Inc. (Prologue) |
|
10-Q
(000-15006) |
|
10.2 |
|
11/3/11 |
100
Table of Contents
| | | | | | | | | |
| |
| | Incorporated by Reference to |
|---|
| No. | | Description | | Form and
SEC File No. | | Exhibit
No. | | SEC
Filing Date |
|---|
| | 10.28 | | Amendment to Master Services Agreement dated July 6, 2011 by and between the Company and Novella Clinical Inc. (formerly known as Prologue) | | 10-Q
(000-15006) | | 10.3 | | 11/3/11 |
|
10.29 |
|
Master Services Agreement dated May 6, 2013 by and between the Company and PPD Development, LLC |
|
10-Q
(000-15006) |
|
10.3 |
|
8/6/13 |
|
*10.30 |
|
Third Amended and Restated Supply Agreement dated October 15, 2014 between the Company and Biosyn Corporation |
|
10-Q
(000-15006) |
|
10.1 |
|
11/5/14 |
|
10.31 |
|
Subscription Agreement dated as of October 15, 2014 by and between the Company and Biosyn Corporation |
|
8-K
(000-15006) |
|
10.1 |
|
10/20/14 |
|
Material Contracts—Stock Purchase, Financing and Credit Agreements |
| | 10.32 | | Sales Agreement, dated January 6, 2011, between Celldex Therapeutics, Inc. and Cantor Fitzgerald & Co. | | 8-K
(000-15006) | | 10.1.3 | | 1/6/11 |
|
10.33 |
|
Amendment No. 1 to Sales Agreement, dated January 6, 2011, between Celldex Therapeutics, Inc. and Cantor Fitzgerald & Co., dated September 20, 2012 |
|
8-K
(000-15006) |
|
10.1 |
|
9/24/12 |
|
Material Contracts—Management Contracts and Compensatory Plans |
| | †10.34 | | 2008 Stock Option and Incentive Plan, as amended and restated | | 8-K
(000-15006) | | 10.1 | | 6/14/12 |
|
†10.35 |
|
2004 Employee Stock Purchase Plan, as amended and restated |
|
8-K
(000-15006) |
|
10.1 |
|
6/13/13 |
|
†10.36 |
|
Employment Agreement, dated as of January 1, 2013, by and between the Company and Anthony S. Marucci |
|
8-K
(000-15006) |
|
10.1 |
|
12/21/12 |
|
†10.37 |
|
Employment Agreement, dated as of January 1, 2013, by and between the Company and Avery W. Catlin |
|
8-K
(000-15006) |
|
10.2 |
|
12/21/12 |
|
†10.38 |
|
Employment Agreement, dated as of January 1, 2013, by and between the Company and Thomas Davis, MD |
|
8-K
(000-15006) |
|
10.3 |
|
12/21/12 |
|
†10.39 |
|
Employment Agreement, dated as of January 1, 2013, by and between the Company and Tibor Keler, Ph.D. |
|
8-K
(000-15006) |
|
10.4 |
|
12/21/12 |
|
†10.40 |
|
Employment Agreement, dated as of January 1, 2013, by and between the Company and Ronald A. Pepin, Ph.D. |
|
8-K
(000-15006) |
|
10.5 |
|
12/21/12 |
|
†10.41 |
|
Form of Stock Option Agreement |
|
8-K
(000-15006) |
|
10.1 |
|
1/25/10 |
|
†10.42 |
|
CuraGen 2007 Stock Incentive Plan, amended and restated |
|
10-K
(000-15006) |
|
10.41 |
|
3/12/10 |
|
†10.43 |
|
Form of Restricted Stock Award |
|
10-K
(000-15006) |
|
10.42 |
|
3/12/10 |
101
Table of Contents
| | | | | | | | | |
| |
| | Incorporated by Reference to |
|---|
| No. | | Description | | Form and
SEC File No. | | Exhibit
No. | | SEC
Filing Date |
|---|
| | 23.1 | | Consent of PricewaterhouseCoopers LLP, an Independent Registered Public Accounting Firm | | Filed herewith | | | | |
|
31.1 |
|
Certification of President and Chief Executive Officer |
|
Filed herewith |
|
|
|
|
|
31.2 |
|
Certification of Senior Vice President and Chief Financial Officer |
|
Filed herewith |
|
|
|
|
|
32 |
|
Section 1350 Certifications |
|
Furnished herewith |
|
|
|
|
|
101 |
|
XBRL Instance Document |
|
Filed herewith |
|
|
|
|
|
101 |
|
XBRL Taxonomy Extension Schema Document |
|
Filed herewith |
|
|
|
|
|
101 |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
Filed herewith |
|
|
|
|
|
101 |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
Filed herewith |
|
|
|
|
|
101 |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
Filed herewith |
|
|
|
|
|
101 |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
|
Filed herewith |
|
|
|
|
- *
- Confidential treatment has been requested for certain provisions of this Exhibit pursuant to Rule 24b-2 promulgated under the Securities Exchange Act of 1934, as amended.
- †
- Indicates a management contract or compensation plan, contract or arrangement.
102
Table of Contents
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| | | | |
| |
| |
|
|---|
| | CELLDEX THERAPEUTICS, INC. |
| | By: | | /s/ ANTHONY S. MARUCCI
|
Date | | | | Anthony S. Marucci |
February 24, 2015 | | | | President and Chief Executive Officer |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| | | | |
Signature | | Title | | Date |
|---|
|
|
|
|
|
/s/ ANTHONY S. MARUCCI
Anthony S. Marucci | | President, Chief Executive Officer, and Director
(Principal Executive Officer) | | February 24, 2015 |
/s/ AVERY W. CATLIN
Avery W. Catlin |
|
Senior Vice President, Chief Financial Officer and Treasurer
(Principal Financial and Accounting Officer) |
|
February 24, 2015 |
/s/ LARRY ELLBERGER
Larry Ellberger |
|
Director, Chairman of the Board of Directors |
|
February 24, 2015 |
/s/ HERBERT J. CONRAD
Herbert J. Conrad |
|
Director |
|
February 24, 2015 |
/s/ GEORGE O. ELSTON
George O. Elston |
|
Director |
|
February 24, 2015 |
/s/ HARRY H. PENNER, JR.
Harry H. Penner, Jr. |
|
Director |
|
February 24, 2015 |
/s/ KAREN L. SHOOS
Karen L. Shoos |
|
Director |
|
February 24, 2015 |
/s/ RICHARD A. VAN DEN BROEK
Richard A. van den Broek |
|
Director |
|
February 24, 2015 |
103