
JPMorgan
Healthcare Conference
January 7, 2008
Exhibit 99
1

The information contained in this presentation includes certain estimates, projections and
other forward-looking information that reflect our current views with respect to future events
and financial performance. These estimates, projections and other forward-looking
information are based on assumptions that HealthSouth believes, as of the date hereof, are
reasonable. Inevitably, there will be differences between such estimates and actual results,
and those differences may be material.
There can be no assurance that any estimates, projections or forward-looking
information will be realized.
All such estimates, projections and forward-looking information speak only as of the date
hereof. HealthSouth undertakes no duty to publicly update or revise the information
contained herein.
You are cautioned not to place undue reliance on the estimates, projections and other
forward-looking information in this presentation as they are based on current expectations
and general assumptions and are subject to various risks, uncertainties and other factors,
including those set forth in our Form 10-Q for the periods ended March 30, 2007, June 30,
2007 & Sept. 30, 2007, the Form 10-K for the fiscal year ended December 31, 2006 and
current report on Form 8-K dated March 30, 2007 and in other documents that we previously
filed with the SEC, many of which are beyond our control, that may cause actual results to
differ materially from the views, beliefs and estimates expressed herein.
Forward-Looking Statements
2

The “New” HealthSouth
With our turnaround complete and the regulatory uncertainty
resolved, our focus is now on executing our strategic plan and
growing EPS.
Our Goal: To be the preeminent specialty provider of inpatient
rehabilitative care in the U.S. through:
clinical, service and operational excellence;
growing market share in existing markets;
building new hospitals in new markets; and
acquiring, or joint-venturing with, competitors.
Longer term, we will evaluate expanding into other,
complementary post-acute services on an opportunistic basis.
3
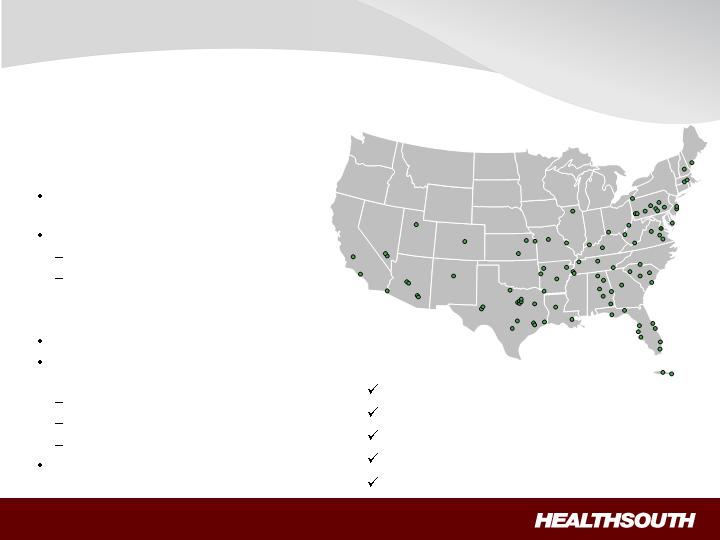
Current Portfolio and Services
Current Portfolio:
94 inpatient rehabilitation hospitals
(“IRH”)
Also have:
6 LTCH Hospitals
25 Licensed Home Health Agencies
Major IRH Services Offered:
Specialized nursing care (24/7)
Three-hours intensive therapy per day
(minimum)
Physical Therapy
Occupational Therapy
Speech Therapy
Physician (Medical Director) oversight
Key Investment Considerations:
Regulatory uncertainty resolved
Demand for services expected to grow
Leadership franchise in I/P rehabilitative care
Strong cash flows
EPS growth
* Adjusted Consolidated EBITDA - see appendix
4

Regulatory Uncertainty Resolved
75% “60% Rule”
Permanent regulatory relief (S.2499):
Threshold permanently “frozen” at 60% Positive Positive Positive
Co-morbidities permanently included N/A Positive Positive
Pricing “rolled back” to 3Q’07 levels Negative Negative N/A
Effective: April 1, 2008 until September
30, 2009
No pricing adjustments for hip/knee N/A N/A N/A
replacements or hip fractures
Implications at 60% vs Full
Implementation at 75%
’08 ’09 ’10
Anticipated HLS impact: While “freeze at 60% ” is a long-term positive, the
pricing “roll-back” will cause margin compression in ’08 & ’09.
Specific ’08 guidance will be included in February’s Earnings Release
Conference Call
5

Projected percentage of US population
65 years or older through 2050 (1)
(1) Source: US Census Bureau, 2004
(2) Source: Medicare Provider Analysis and Review File (2004); Claritas
Projected Medicare Compliant Case Growth (2)
+ 22%
Attractive Industry
Aging Demographics = Increased Demand
Demand for post-acute services will increase
as the U.S. population ages
“Compliant Cases” are expected to grow
~2% per year for the foreseeable future, creating
an attractive market.
6
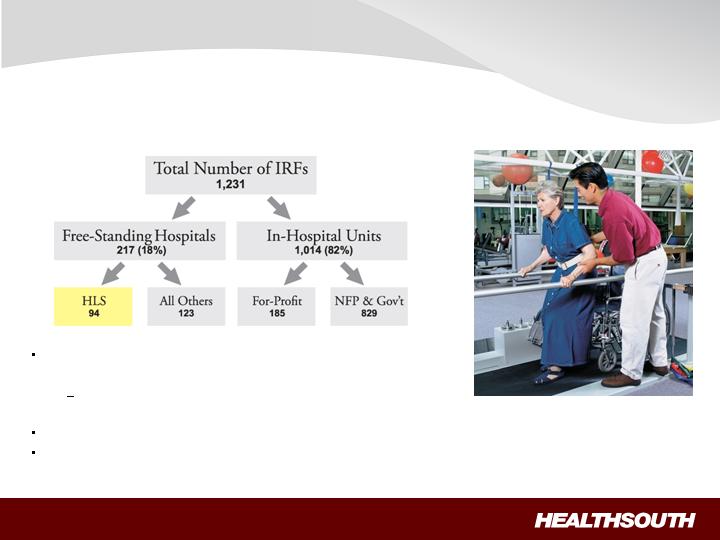
(1) Source: Report to Congress: Medicare Payment Policy; March 2007, MedPAC analysis of Providers of service files from CMS
(2) Typically a 15-30 bed unit/department of an acute care hospital
Inpatient rehabilitation is HLS’ core business -vs- one of many,
secondary services provided by acute-care hospitals
HLS not challenged by Bad Debt, CAPEX issues facing
acute-care hospitals
HLS can attract patients from multiple referral sources
Consolidation opportunities will be pursued
Attractive Industry
Fragmented Provider Base = Opportunities
1
2
7
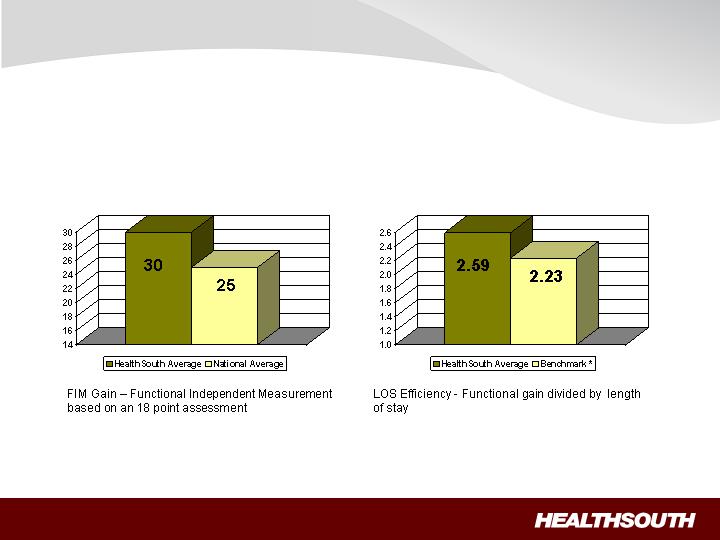
FIM Gains
LOS Efficiency
Source: UDSmr Database –On Demand
Reports - Q2 2007
*Benchmark = Risk Adjusted Expectancy
Leadership Franchise
Value Proposition = Quality of Care
8
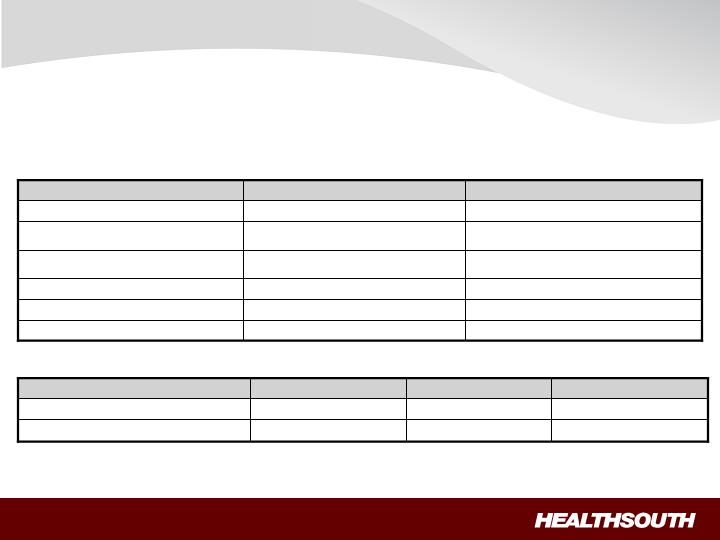
IRHs provide a Higher Level of Service…
Leadership Franchise
Differentiation = Better Outcomes at Comparable Costs
8 consecutive hours per day (min.)
24 hours per day
RN oversight and availability
None
Rehabilitation specialty expertise
Nursing training, expertise
2.5 – 4.0
5.0 to 7.5
Nursing hours per patient per day
Not required
Required
MD or DO designated as
Rehabilitation Director
Not required
Required
Multi-disciplinary team approach;
coordinated Program of Care
Once every 30 days (min.)
4+ times per week
Attending physician visits
Nursing Home
Inpatient Rehabilitation Hospital
Service
at Comparable Cost …
~$400
~$900
Average Cost/Day
~$12,000
~30
Nursing Home
~$13,500
~15
Inpatient Rehabilitation Hospital
Average Cost / Admission
Average LOS
9
Earnings Growth
“Roadmap” to EPS Growth
1. Pay down debt
2. Invest in existing IRH platform
Sales & Marketing
Non-Clinical Support Costs
Human Capital
Clinical
Service
Re-furbish existing hospitals
Add capacity (as warranted)
2008 2009 2010+
–
10
Earnings Growth
“Roadmap” to EPS Growth (cont’d)
3.
Develop “de-novo hospitals” in new
and existing markets
Goal: Launch 5/yr
CAPEX per 40-bed IRH:
HLS-financed = $15-20M
Off-Balance Sheet = $3-5M
Approx 18 mos. to permit/ build
+ 6 mos. to “ramp-up”
4.
Seek to consolidate existing markets
Goal: Consummate 3/yr
5.
Seek inpatient rehab acquisitions
6.
Expand into complementary post-
acute services
2008 2009 2010+
11
Earnings Growth
“Roadmap” to EPS Growth (cont’d)
Key Assumptions:
SS Discharges: 2+%/yr
Pricing: 2-3%/yr
SW&B: 3-4%/yr
G&A: 4.75% of Net Revenue
Other Op Expense: = Inflation
Interest Expense: $200-210M
(at current debt levels)
Federal Income Taxes: $0
(for foreseeable future)
Derivative Proceeds: TBD
“Restructuring”: $~25M in ‘08
Comments:
Primary operational focus (TeamWorks)
Beginning in Q409 (S.2499 “rolls-back” pricing
from Q208 thru Q309)
Higher in 2008 due to investment (“catch-up”) to
make Benefits competitive
Target: End-of-Year 2008
Operational focus (TeamWorks)
Cash payments are lower ($185-195M)
(at current debt levels)
NOL’s ($~2.5B)
Will be used to re-pay debt; expect in 2009
Fees related to pursuit of Derivative proceeds
(a)
(a) Targeted rate of 4.75% (not including 123R costs)
12

13
TAX LOSSES AVAILABLE FOR FUTURE YEARS ~ $2.5 BILLION
- No Federal Taxes for foreseeable future
Solid Financials
Strong Cash Flow
Significant turnaround from 2006
FCF = ($208M)
All Settlement Payments completed
by 12/31/07
FCF will be used for:
Reducing debt
Upgrading existing hospitals
Building new hospitals
Acquiring competitors
Note: Consolidations/JVs typically
do not require any CAPEX
Free Cash Flow
Nine Months ended 9/30/07
(a) Q3 Total of G&A to all revenues (continuing and discontinuing)
(b) Targeted rate of 4.75% (not including 123R costs)
(c) $190M cash run-rate post tax refund proceeds
(d) Before Preferred Stock Dividend
(in millions)
at 5.6%
(a)
of Rev.
at 5.2%
(b)
of Rev.
Adj. Consol. EBITDA
236.0
$
236.0
$
Source Medical Gain
(8.6)
(8.6)
Add: Normalization of G&A
33.6
38.9
Sub-total
261.0
$
266.3
$
Less: Capital expenditures (Maintenance)
(25.2)
(25.2)
Cash interest cost
(c)
(142.5)
(142.5)
Excess
(d)
93.3
$
98.6
$
Normalized
Gen & Admin Expense
Debt Balance
(in millions)
Debt Balance December 31, 2006 $3,402.3
Debt Balance September 30, 2007 $2,400.7
Post Sept 30, 2007:
Additional Proceeds from Outpatient Sale $ 23.0
Tax Refund (Portion used to pay down debt) $ 405.0
Final SEC & CMS/DOJ Payments ($ 47.3)
Derivative Proceeds from Litigation TBD
DEBT BALANCE POST SEPT 30, 2007 ~$2 BILLION
Solid Financials
Ongoing Debt Reduction
10.75% Senior Notes
Purchased ~$51M of
Notes during Sept/ Oct
timeframe at an average
price of 103.80
Will continue to
opportunistically look at
high cost debt to be
retired
14
Investment Considerations
Focused management: proven track record of achieving results
Attractive industry: demand for post-acute services expected to grow
(favorable demographics)
Leadership Franchise: largest specialty provider of inpatient rehabilitative care in
the U.S.
Differentiation through single specialty focus (quality)
Earnings growth: through organic and disciplined development initiatives
Strong cash flows: shareholder value enhanced through strategic use of FCF
Focus: Growing EPS
15

Appendix
16
Three Months Ended
September
30,
Nine Months Ended
September
30,
2007
2006
2007
2006
(In Millions)
Net income (loss)
$
287.6
$
(76.1)
$
699.2
$
(55
3.7)
(Income) loss from discontinued operations
(37.6)
18.0
(475.7)
35.4
Provision for income tax (benefit) expense
(281.1)
2.1
(288.2)
21.0
Loss on interest rate swap
21.4
28.7
6.8
13.9
Interest expense and amortization of debt discounts
and fees
60.2
56.8
177.9
176.8
Loss on early extinguishment of debt
2.2
–
19.9
365.6
Government, class action, and related settlements
3.9
28.4
(31.7)
49.9
Net noncash loss on disposal of assets
0.6
1.1
2.2
5.3
Impairment charges
0.
4
–
15.1
–
Depreciation and amortization
19.9
20.7
57.8
63.3
Professional fees
—
accounting, tax, and legal
9.2
23.1
44.3
99.4
Compensation expense under FASB Statement
No.
123(R)
2.0
3.6
8.1
11.6
Restructuring activities under FASB S
tatement No.
146
–
–
–
0.3
Sarbanes
-
Oxley related costs
–
0.9
0.3
4.2
Adjusted Consolidated EBITDA
(1)*
$
88.7
$
107.3
$
236.0
$
293.0
(1)
Adjusted Consolidated EBITDA is a non
-
GAAP financial measure. We believe it is useful to investors as it
is used in our
covenant calculations under our Credit Agreement.
Adjusted Consolidated EBITDA is not a measure of financial performance under accounting principles generally accepted
in the United States and should not be considered as an alternative to ne
t
income (
loss
)
or to cash flows from operating,
investing, or financing activities. Because Adjusted Consolidated EBITDA is not a measure determined in accordance with
generally accepted accounting principles and is susceptible to varying calculations, Ad
justed Consolidated EBITDA, as
presented, may not be comparable to other similarly titled measures presented by other companies.

Appendix (cont'd)
17
Our Credit Agreement allows certain items to be added to arrive at Adjusted Consolidated EBITDA that are viewed as not
being on
going costs once the Company has completed its restructuring.
After consummation of the divestitures of our surgery centers, outpatient, and diagnostic divisions, and in accordance with
our Credit Agreement, Adjusted Consolidated EBITDA is calculated to gi
ve effect to each divestiture, including adjustments
for the allocation of corporate overhead to each divested division.
However, these allocations are estimates and are not
necessarily indicative of the Adjusted Consolidated EBITDA that would have resulte
d had the applicable divisions been
divested as of the beginning of each period presented. Accordingly, t
hese adjustments are not included in the above table.
In
addition, we are allowed to add other income, including interest income, to the calculation of
Adjusted Consolidated
EBITDA under our Credit Agreement. This includes interest income associated with our federal income tax recovery. This
amount has not been included in the above calculation as it would not be indicative of our Adjusted Consolidated E
BITDA
for future periods.
Adjusted Consolidated EBITDA for the three and nine months ended September 30, 2007 includes an $8.6 million gain on
the
sale of our
remaining
investment in Source Medical Solutions, Inc. Adjusted Consolidated EBITDA for the three
and
nine months ended September 30, 2006 includes
a
$35.0 million recovery of incentive bonuses from Richard M. Scrushy,
our former chairman and chief executive officer.
*
Adjusted
Consolidated EBITDA includes general and administrative
expenses for all
divisions. G
eneral and administrative
expenses approximated
6.4
%
and
8.
2
%
of consolidated net operating revenues
for the three and
nine
months ended
September
30, 2007
, respectively
.
However,
these percentages decrease by 60 basis points and 260 basis poin
ts,
respectively
, if you include the revenues of the divisions reported in discontinued operations.