UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 for the fiscal year ended December 31, 2005 |
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission file number: 0-17821
ALLION HEALTHCARE, INC.
(Name of registrant as specified in its charter)
| | |
| Delaware | | 11-2962027 |
(State or other jurisdiction of incorporation or organization) | | (I.R.S. Employer Identification No.) |
1660 Walt Whitman Road, Suite 105, Melville, New York 11747
(Address of principal executive offices)
Registrant’s telephone number: (631) 547-6520
Securities Registered Pursuant to Section 12(b) of the Act:
| | |
Title of each class | | Name of each exchange on which registered |
| Common Stock, $0.001 par value | | NASDAQ |
Securities Registered Pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months, and (2) has been subject to such filing requirements for the past 90 days. Yes ¨ No x
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer an accelerated filer or a non-accelerated filer. See definition of “accelerated filer and large accelerated filer” in Rule 12b-2 of the Exchange Act.
Large accelerated filer ¨ Accelerated filer x Non-accelerated filer ¨
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2of the Act). Yes ¨ No x
The aggregate market value of the registrant’s voting and non-voting common equity held by non-affiliates of the registrant, computed by reference to the price at which the registrant’s common stock was last sold as of the last business day of the registrant’s most recently completed second fiscal quarter, was $169,924,500.
The number of shares of the registrant’s common stock outstanding as of March 13, 2006 was 16,131,816.
DOCUMENTS INCORPORATED BY REFERENCE: None
TABLE OF CONTENTS
2
INFORMATION RELATED TO FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K and certain information incorporated herein by reference contain forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. All statements included or incorporated by reference in this Annual Report on Form 10-K, other than statements that are purely historical are forward looking statements. Words such as “expects,” “anticipates,” “plans,” “believes,” “seeks,” “estimates,” and other similar expressions or variations of such words are intended to identify these forward-looking statements.
These forward-looking statements, which include statements about our strategy to expand our business, our ability to integrate past acquisitions and identify additional ones, our expectations regarding reimbursement rates and our eligibility for specific HIV/AIDS programs, our access to additional capital, the future demand for our services, expectations about future treatments for HIV/AIDS patients, and management’s expectations regarding future operating results are not guarantees of future performance and are subject to risks and uncertainties that could cause actual results to differ materially from the results contemplated by the forward-looking statements.
All forward-looking statements included or incorporated by reference in this Report are based on information available to us as of the date hereof, and we assume no obligation to update any such forward-looking statements. Readers of this Report are cautioned not to place undue reliance on such statements.
The forward-looking statements and any expectations based on such forward-looking statements are subject to risks and uncertainties and other important factors, including, without limitation, changes in reimbursement rates, our compliance with Medicare and Medicaid reimbursement regulations, our ability to market our services, our ability to successfully integrate acquisitions and other factors discussed under Item 1A of this Report under the heading “Risk Factors” and elsewhere in this Report. The reader also should consult the cautionary statements and risk factors listed from time to time in the other reports we file with the Securities and Exchange Commission (“SEC”).
PART I
Item 1. Business
Overview
We are a national provider of specialty pharmacy and disease management services focused on HIV/AIDS patients. In December 2005, we served 11,022 patients. We sell HIV/AIDS medications, ancillary drugs and nutritional supplies under our trade name MOMS Pharmacy. We work closely with physicians, nurses, clinics, AIDS Services Organizations (“ASO”), or with government and private payors, to improve clinical outcomes and reduce treatment costs for our patients. Most of our patients rely on Medicaid and other state-administered programs, such as AIDS Drug Assistance Programs or ADAP, to pay for their HIV/AIDS medications. Billing requirements for these programs are complex. We are one of a limited number of providers that has qualified for certain additional HIV/AIDS reimbursement programs under legislation enacted in California and New York.
We believe that the combination of services we offer to patients, healthcare providers and payors makes us an attractive source of specialty pharmacy and disease management services, contributes to better clinical outcomes and reduces overall healthcare costs. Our services include the following:
| | • | | Specialized MOMSPak prescription packaging that helps reduce patient error associated with complex combination therapies; |
| | • | | Reimbursement experience that assists patients and healthcare providers with the complex reimbursement processes of Medicaid and ADAP and that optimizes collection of payment; |
3
| | • | | Services that arrange for the timely delivery of medications as directed by our patients or their physicians in a discreet and convenient manner; |
| | • | | Specialized pharmacists who consult with patients, physicians, nurses and ASOs to provide education, counseling, treatment coordination, clinical information and compliance monitoring; and |
| | • | | Information systems and prescription automation solutions that make the provision of clinical data through Lab Tracker and the transmission of prescriptions more efficient and accurate. |
According to IMS Health, the United States market for HIV/AIDS anti-retroviral and co-morbidity medications totaled approximately $7.2 billion for the twelve-month period ended August 30, 2005, of that approximately $5.0 billion was anti-retroviral medications. According to the World Health Organization (“WHO”) and the Joint United Nations Programme on HIV/AIDS, or UNAIDS, as many as 1.6 million individuals living in the United States as of the end of 2004 were infected with HIV. Of this number, between 400,000 and 500,000 were receiving HIV/AIDS medications, according to the Cleveland Journal of Medicine. We believe approximately 44,000 new infections occur in the United States annually. Our distribution centers are located in or near metropolitan areas in those states where a majority of HIV/AIDS patients in the United States live, according to the Centers for Disease Control and Prevention, or CDC—New York, California, Florida, New Jersey and Washington.
We have grown through increases in our base-business, internal growth, and through acquisitions. We generated our internal growth primarily by increasing the number of patients we serve. In addition, the price of HIV/AIDS medications has increased, and we are filling more prescriptions per HIV/AIDS patient. In 2005, we completed four acquisitions in California which have increased the number of patients we serve. We will continue to evaluate acquisition opportunities as they arise, especially other specialty pharmacies that have established relationships with HIV/AIDS patients, clinics and hospitals. We will consider acquisitions in both our existing markets and in markets where we do not currently have operations.
HIV/AIDS
Human Immunodeficiency Virus, commonly known as HIV, is the virus that causes Acquired Immune Deficiency Syndrome, commonly known as AIDS. HIV is spread most commonly by sexual contact with an infected partner. HIV is also spread through contact with infected blood, including through the use of contaminated needles or syringes. Once inside a host body, HIV attacks the T cells, a major component of the immune system. The virus then takes over the cells’ reproductive machinery and reproduces itself causing the cells to weaken and eventually die. When the infected cells die, they release the recently created virus into the bloodstream. Other T cells are then invaded and die, and the body is left vulnerable to diseases that easily would have been fought off by a normally functioning immune system.
The demographic profile of HIV/AIDS patients has shifted since the disease was first diagnosed in 1981. Most HIV/AIDS patients now live in the inner-city of a major metropolitan area and are dependent on government programs to pay for the medications to treat HIV/AIDS. From 1981—2001, approximately 40,000 people per year were diagnosed with HIV, according to the CDC. According to a UNAIDS/WHO report, an estimated 44,000 people were infected with HIV in North America in 2004. Of the new HIV cases, it is estimated that 70% are male and 30% are female. A disproportionate number of these patients have been African Americans and Hispanics. The proportion of new cases in African Americans in the United States rose from 25% in 1981 to 50% in 2001. African American women accounted for approximately 72% of all new HIV diagnoses among women and 22% of the overall increase in new HIV cases in the United States in 2001. The proportion of Hispanics infected with HIV rose from 14% in 1981 to 20% in 2001. We believe that as more HIV/AIDS patients look to government programs, the government is likely to take a more active role regulating the pharmacies and other providers of HIV/AIDS medications.
4
The current standard of care for the treatment of HIV/AIDS involves complex treatment regimens of multiple drugs, or “combination therapies,” that consist of predominantly oral medications taken by a patient multiple times a day, typically outside a clinical setting. Combination therapies often require that a patient take variations of the multi-therapy regimens. For example, a patient may need to take certain medications either after meals or on an empty stomach, or, after high-fat or low-fat meals. The number of medications and varying dosages and schedules often can confuse and overwhelm patients. As a result, many patients lose confidence in their ability to adhere to their drug regimens and simply give up, while others lose track of which doses they have taken or inadvertently miss a dose because of their personal schedules. Alcohol and illicit drug use are also factors in causing non-compliance and may lead to an increasing amount of Medicaid fraud. Poor adherence or even slight or occasional deviations from a prescribed regimen can reduce the potency of therapy and lead to viral resistance. Given the ability of HIV to mutate rapidly in the absence of anti-retroviral medication, taking a combination therapy exactly as prescribed, without missing or reducing doses, is critical to effective treatment. Once resistance has developed in a patient, success rates of other HIV medications are often limited, particularly if the patient’s adherence issues are not resolved, and treatment options become greatly limited. Studies on adherence within the HIV/AIDS population have shown that if 95% of medication doses are not taken as prescribed, the medication may become ineffective or the patient may develop drug resistance to such medication, according to the AIDS Research Institute.
In the United States, HIV/AIDS-associated morbidity and mortality have declined significantly due to combination therapies. Before combination therapies, 50–60% of adults infected with HIV were diagnosed with AIDS within 10 years of infection, and 48% of them died after 10 years of infection, according to the U.S. Department of Health and Human Services. After increasing every year between 1987 and 1994 at an average annual rate of 16%, HIV mortality in the United States leveled off in 1995 and has since decreased, according to the CDC. In 1995, 19% of people living with HIV/AIDS in the United States died compared to 4% in 2003, according to the CDC. While HIV/AIDS remains life threatening, healthcare providers increasingly treat HIV/AIDS as more of a long-term chronic disease.
We are one of only a few specialty pharmacy and disease management service companies that primarily serve HIV/AIDS patients. Despite the special needs of the HIV/AIDS infected population, few national and regional pharmacies have focused on this patient population. Most of the pharmacies serving this market have been local or small regional providers located in a single urban market. These pharmacies often do not have the resources or sophistication to provide the specialty pharmacy and disease management services required by patients, healthcare providers and payors to maximize adherence to the treatment regimen. We also believe that neither the retail pharmacies nor the mail order pharmacies offer the range of specialty pharmacy and disease management services we provide.
Our Products and Services
We offer specialty pharmacy and disease management services to assist patients, healthcare providers and payors in managing HIV/AIDS. We sell HIV/AIDS medications, ancillary drugs and nutritional supplies. Patients or physicians generally initiate the prescription process by contacting us on our toll-free telephone number, through our facsimile number or through our electronic prescription writer. Some clinics have medication drop-off boxes in which physicians also may leave prescriptions for us to fill. A patient may also direct his or her physician to call, fax or electronically transmit a prescription. If requested by a patient, one of our pharmacists may contact the patient’s physician directly to obtain prescription information. Our pharmacists are required to validate and verify the completeness of each prescription, answer questions and, if appropriate, help coordinate support and training for patients. As soon as we receive a prescription, we also seek approval for reimbursement from the payor. Once the prescription is verified, the order is filled, shipped and delivered. Patients can also pick up their medications at our pharmacies.
5
We have designed our services to meet the following challenges that are of particular importance to HIV/AIDS patients, healthcare providers and payors:
Adherence
Packaging. We have designed our services to improve patient adherence to complex combination therapies. We dispense prescribed medications in a customized dose-by-dose package called a MOMSPak. We also dispense these medications in pre-filled pillboxes, at the patient’s request. Our customized packaging provides increased convenience to the patient and enhances patient adherence to complex combination therapies.
There recently has been increased attention to Medicaid fraud and the resale of HIV/AIDS medications on the black market. According to POZ, a leading HIV publication, the resale of unopened HIV medications on the black market has become a problem in New York. Additionally, some small pharmacies are reportedly repurchasing the medications they distribute to Medicaid patients. We believe the current problem is attributable to the availability of unopened HIV/AIDS medications. Our automated prescription packaging system requires us to open the original bottles before separating the medications into a MOMSPak, thereby reducing the likelihood of after-market resale of HIV/AIDS medications. Doctors can continue to write HIV medication prescriptions without fear of becoming complicit in Medicaid fraud if medication bottles are opened before distribution.
Delivery. We arrange for delivery of medications as directed by our patients or their physicians in a discreet, convenient and timely manner. We believe that this increases patient adherence as it eliminates the need to pick up medications at a local pharmacy. According to Wall Street Journal Reports and the National Association of Chain Drug Stores Economics Department, 30% of all refillable prescriptions are never refilled and up to 20% of new prescriptions are never filled.
Reimbursement Management
We have experience with the complex reimbursement processes of Medicaid and ADAP that optimizes collection of payment. As a result, we are able to manage efficiently the process of checking reimbursement eligibility, receiving authorization, adjudicating claims and confirming that payment is received.
We work with government and private payors to obtain appropriate reimbursement. Our billing and reimbursement specialists typically secure pre-approval from a payor before any shipment of medications. Our billing and reimbursement specialists also review such issues as pre-certification or other prior approval requirements, lifetime limits, pre-existing condition clauses and the availability of special state programs. Because the majority of our prescriptions are adjudicated through electronic submission, we are reasonably certain we will receive payment from the payor.
Due to the high cost and extended duration of the treatment of HIV/AIDS, the availability of adequate health insurance is an on-going concern for our patients and their families. We work closely with physicians and our patients to monitor coverage reductions or termination dates. Because of our ability to facilitate reimbursement from government and private payors, we can in many cases provide prescription medications to patients at lower initial out-of-pocket costs than they might obtain from other sources.
The two largest HIV/AIDS markets in the United States, California and New York, recently underwent fundamental changes in Medicaid reimbursement for HIV/AIDS medications. California recently approved a three-year HIV/AIDS Pharmacy Pilot Program, which provides additional reimbursement for HIV/AIDS medications for up to ten qualified pharmacies. We own two of the ten pharmacies that qualified for this program. In New York, we qualify for a higher reimbursement rate under the revised reimbursement rates of the state-mandated Medicaid program, which is in effect through March 31, 2006. The California Pilot Program is currently set to expire on January 1, 2008. If the legislation in New York or California is not renewed our revenue would be reduced.
6
Disease Management
The medications we distribute to our patients require timely delivery, may require temperature maintained distribution, and very often require dosage monitoring. Our employees have developed expertise in HIV/AIDS that allows them to provide customized care to our patients. By focusing on the HIV/AIDS community, we have been able to design our services to help patients better understand and manage their medication needs and schedules. We have named our disease management program MOMSCare.
Upon initiating service, we work closely with the patient and the patient’s physician and other healthcare providers to implement combination therapies and manage the following services:
| | • | | programs to monitor utilization compliance and outcomes; |
| | • | | clinical information and consultation regarding the patient’s illness, medications being used and treatment regimens; |
| | • | | educational information on the patient’s illness, including advancements in research, technology and combination therapies; |
| | • | | assistance in setting realistic expectations for a patient’s therapy, including challenges with adherence, and with anticipated outcomes and side effects; |
| | • | | systems for inventory management and record keeping; |
| | • | | assistance in coordinating treatment outside of the home / hospital setting; and |
| | • | | assistance in the formation of patient support groups, advocating legislation to advance the interests of the HIV/AIDS community, and participation in national and regional advocacy groups. |
We believe that these disease management services benefit government and private payors by helping our patients avoid costly episodes that can result from non-adherence to a prescribed care regimen. Improved patient adherence avoids costs for the payor by reducing the incidence of physician intervention, hospitalization and emergency room visits. Our staff works closely with patient care coordinators to routinely monitor the patient’s care regimen.
Information Systems and Prescription Automation Solutions
We have licensed and developed information systems that enable patients and healthcare providers to more effectively manage and treat HIV/AIDS. We believe the transmission of electronic prescriptions reduces confusion and potential medication errors. Our electronic prescription transmittal software enables healthcare providers to view their patients’ prescription histories, request new prescriptions, or renew prescriptions online, thereby saving physicians and their staff time that would otherwise be spent completing patient prescriptions. We have developed an interface between our pharmacy information system and the MOMSPak automated packaging system that allows for the efficient processing of prescriptions.
In July 2005, we acquired substantially all of the assets of Oris Medical Systems, Inc. As a result of this acquisition, we obtained Oris’ rights to theLabTracker—HIV ™ software system, which enables healthcare providers to record, track and analyze the outcomes of HIV/AIDS treatment. Oris’ rights include the exclusive right to licenseLabTracker to pharmacy providers and the right to develop a pharmacy interface withLabTracker’s existing system. We intend to integrate our electronic prescription writer, or that of Oris Medical, and the use of our specialty pharmacy services, with the functions ofLabTracker software.LabTracker has the ability to show the correlation between laboratory results and the medications prescribed to a HIV/AIDS patient. However, currently, healthcare providers that desire to use this feature are required to manually input prescription information. We expect that healthcare providers will be able to take prescription information that is transmitted to us electronically and import it directly into the provider’sLabTracker software. This will allow providers to produce reports that can correlate their patients’ laboratory results with the HIV/AIDS medications
7
prescribed and filled by our pharmacy. These reports contain more accurate, timely and comprehensive information about the interaction between a drug and the health of a HIV/AIDS patient. We believe this information allows healthcare providers to alter drug regimens as needed. Currently, more than 200 clinics and physician customers useLabTracker to help monitor approximately 100,000 HIV/AIDS patients.
Relationships with Pharmaceutical Companies
We actively pursue marketing and other business relationships with pharmaceutical manufacturers. We actively look to work with manufacturers of the leading HIV/AIDS medications to enhance their awareness of our services and to increase our opportunities to benefit from their significant sales teams and marketing efforts. The HIV/AIDS sales teams at pharmaceutical companies regularly make sales calls on the leading prescribers of HIV/AIDS medications. If these sales teams are aware of us, they will be in a position to inform the leading prescribers about our products and services, which can increase our visibility in the market.
We have entered into a specialized services agreement with Roche Laboratories Inc. (“Roche”) to receive product pricing discounts and we have agreed to provide Roche with blind patient data with respect toFUZEON, a HIV medication manufactured by Roche.FUZEON has an actual per patient cost per year in excess of $20,000. We believe that Roche has entered into this type of agreement with only a limited number of pharmacies.
Marketing
We intend to expand our business in the major metropolitan markets where the majority of HIV/AIDS patients live by enhancing our existing relationships and creating new relationships with HIV/AIDS clinics, hospitals and prescribing physicians through direct sales, outreach programs and community-based education programs. Our sales team markets to the leading prescribers of HIV/AIDS medications. We actively pursue relationships with the largest HIV/AIDS clinics, ASOs, and other groups focused on HIV/AIDS. We provide our services under the trade name of MOMS Pharmacy.
We have dedicated sales personnel who are working with clinics and physician customers who useLabTracker to migrate their patients to our pharmacies. We expect relationships we develop withLabTracker users to be an attractive opportunity to increase our customer base.
We believe MOMS Pharmacy is a recognized brand-name within the HIV/AIDS community. We have a website atwww.momspharmacy.com to directly market our products to the HIV/AIDS community and service organizations, which contains educational material and information of interest for the community. We do not intend the internet address to be an active link, and the contents of the website are not a part of this Report.
Suppliers
We deliver approximately 1,000 branded and generic prescription medications by purchasing the medications we use to fill prescriptions from wholesale distributors. In 2003, we entered into a five-year prime vendor agreement with AmerisourceBergen to provide us with the HIV/AIDS medications we sell. Pursuant to the agreement, we are obligated to purchase at least 95% of the medications we sell from AmerisourceBergen. As part of this agreement, we receive improved payment terms relative to the terms we could get from other pharmaceutical distributors. In addition, we agreed to purchase minimum dollar amounts of medications from AmerisourceBergen over the five-year term of the agreement which expires in September 2008. If we fail to meet these minimum purchase amounts, we will be required to make an additional payment equal to 0.2% of the un-purchased amount.
8
Competition
Our industry is highly competitive, fragmented and undergoing consolidation, with many public and private companies focusing on different products or diseases. Each of our competitors provides a different mix of products and services than we do. Some of our current and potential competitors include:
| | • | | specialty pharmacy distributors such as, Accredo Health, Inc. (acquired by Medco Health Solutions, Inc.), BioScrip, Inc., Curative Health Services, Inc., and Priority Healthcare Corp. (acquired by Express Scripts, Inc.); |
| | • | | pharmacy benefit management companies such as, Medco Health Solutions, Inc., Express Scripts, Inc. and Caremark, Rx, Inc.; |
| | • | | specialty pharmacy divisions of national wholesale drug distributors; |
| | • | | hospital-based pharmacies; |
| | • | | manufacturers that sell their products both to distributors and directly to clinics and physician offices; and |
| | • | | hospital-based care centers and other alternate site healthcare providers. |
Many of our existing and potential competitors have substantially greater financial, technical marketing and distribution resources than we do. Additionally, many of these companies have greater name recognition and more established relationships with HIV/AIDS patients. Furthermore, these competitors may be able to adopt more aggressive pricing policies and offer customers more attractive terms than we can.
Third Party Reimbursement, Cost Containment and Legislation
We generate the majority of our net sales from patients who rely on Medicaid and ADAP for reimbursement, both highly regulated government programs that are subject to frequent changes and cost containment measures. Medicaid is a state program partly funded by the federal government. In recent years, these programs have reduced reimbursement to providers.
Historically, many government payors, including Medicaid and ADAP programs which account for most of our net sales, paid us directly or indirectly for the medications we dispense at average wholesale price, or AWP, or a percentage of AWP. Private payors with whom we may contract also reimburse us for medications at AWP or a percentage of AWP. Federal and state governmental attention has been focused on the validity of using AWP as the basis for Medicaid medication payments, including payments for HIV/AIDS medications, and most state Medicaid programs now pay substantially less than AWP for the prescription drugs we dispense.
In January 2006, the Deficit Reduction Act (the “Reduction Act”) was enacted which established average manufacturer price (“AMP”) as the benchmark for prescription drug reimbursement in the Medicaid program, eliminating the previously used AWP standard. The Reduction Act also made changes to the federal upper payment limit for multiple source drugs. Payments to pharmacies for Medicaid-covered outpatient prescription drugs are set by the states. Federal reimbursements to states for the federal share of those payments are subject to a ceiling called the federal upper limit (“FUL”). Effective January 1, 2007, for multiple source drugs (i.e., generics), the FUL will be 250% of the AMP. We are reviewing the potential impact of the change in federal reimbursement rates on our business and are not yet in a position to fully assess its impact on our business or profitability. The FUL may have the effect of reducing the reimbursement rates for certain medications that we currently dispense or may dispense in the future.
As of September 1, 2004, as part of the passage of the State of California budget, reimbursement rates for pharmacy services provided under Medi-Cal were reduced. Under the changed reimbursement rate, prescriptions
9
are reimbursed at the AWP less 17%, and the provider is paid a $7.25 dispensing fee. The previous reimbursement rate was AWP less 10% with a $4.05 dispensing fee. On September 28, 2004, California approved a three-year HIV/AIDS Pharmacy Pilot Program bill that funds an additional $9.50 fee per prescription for qualified pharmacies that participate in the program. The payments are retroactive and apply to services rendered since September 1, 2004. We own two of the ten pharmacies that have qualified for the pilot program in California.
In New York, reimbursement rates for pharmacy services provided under Medicaid were reduced in September 2004. Under the changed reimbursement rate, prescriptions are reimbursed at the AWP less 12.75% for brand name pharmaceuticals and AWP less 16% for generic pharmaceuticals plus a dispensing fee for all prescriptions. The previous reimbursement rate was AWP less 12% plus a dispensing fee of $3.50 to $4.50. Approved specialized HIV pharmacies will continue to be reimbursed at AWP less 12% plus a dispensing fee. We have been approved as a specialized HIV pharmacy qualifying for the more favorable reimbursement rate. The legislation authorizing the more favorable reimbursement rate is currently effective until March 31, 2006.
As of January 1, 2004, Medicare adopted new pricing that reduced reimbursement for many drugs covered under Medicare Part B. In 2005, the agency that administers the Medicare and Medicaid Programs, the Centers for Medicare & Medicaid Services, known as CMS, changed reimbursement to be based on average sales price, or ASP rather than average wholesale price, or AWP. In 2006, reimbursement may be based on ASP or be administered under a competitive acquisition program. This change in pricing may result in reduced reimbursement amounts for drugs that we dispense.
Cost containment initiatives are a primary trend in the United States healthcare industry. The increasing prevalence of managed care, centralized purchasing decisions, consolidation among and integration of healthcare providers and competition for patients has affected, and continues to affect, pricing, purchasing, and usage patterns in healthcare. Efforts by payors to eliminate, contain or reduce costs through coverage exclusions, lower reimbursement rates, greater claims scrutiny, closed provider panels, restrictions on required formularies, mandatory use of generics, limitations on payments in certain therapeutic drug categories, claim delays or denials and other similar measures could erode our profit margins or materially harm the results of our operations.
We have entered into relationships with Prescription Drug Plans or PDPs (these plans service beneficiaries of the Medicare prescription drug plan or Medicare Part D) from whom we will receive reimbursement for our patients who are dual eligible and are enrolled with such PDPs. Medicare Part D became effective on January 1, 2006. We may not know the full impact of any reduction in the reimbursement rates we receive for the prescriptions we dispense to our dual eligible patients until the end of the first quarter of 2006.
Government Regulation
Marketing, repackaging, dispensing, selling and purchasing drugs is highly regulated and regularly scrutinized by state and federal government agencies for compliance with laws and regulations relating to the following topics:
| | • | | inducements for patient referrals; |
| | • | | manufacturer calculated and reported AWP and ASP amounts; |
| | • | | joint ventures and management agreements; |
| | • | | referrals from physicians with whom we have a financial relationship; |
| | • | | professional licensure; |
| | • | | repackaging, storing, and distributing prescription pharmaceuticals; |
| | • | | incentives to patients; and |
10
The laws and regulations are very complex and generally broad in scope resulting in differing interpretations and a lack of consistent court decisions. Compliance with laws continues to be a significant operational requirement for us. We believe that we currently comply in all material respects, and intend to continue to comply, with all laws and regulations with respect to our operations and conduct of business. However, the application of complex standards to the operation of our business always creates areas of uncertainty, and there can be no assurance that all of our business practices would be interpreted by the appropriate regulatory agency to be in compliance in all respects with the applicable requirements. Moreover, regulation of the healthcare industry is in a state of flux. Any failure or alleged failure to comply with applicable laws and regulations could have a material adverse effect on our business, financial condition and results of operations.
We are unable to predict or determine the future course of federal, state and local regulation, legislation or enforcement or what additional federal or state legislation or regulatory initiatives may be enacted in the future relating to our business or the healthcare industry in general, or what effect any such legislation or regulation might have on us. We cannot provide any assurance that federal or state governments will not impose additional restrictions or adopt interpretations of existing laws that could have a material adverse effect on our business or financial position. Consequently, any future change, interpretation or any violation (or alleged violation) of law and regulations could have a material adverse affect on our business, financial condition and results of operations. The following are particular areas of government regulation that apply to our business.
Medicare Legislation (Medicare Prescription Drug, Improvement and Modernization Act or MMA). On December 8, 2003, the MMA was signed into law. This complex legislation made many significant structural changes to the Federal Medicare program, including providing for a Medicare prescription drug benefit. Under the MMA, PDP sponsors were selected by CMS through a bidding process and beneficiaries will have a choice between at least two plans in the area in which they live. CMS announced the results of the bidding process and the selected PDPs through a press release on September 23, 2005. PDPs began marketing their services to eligible patients in October and beneficiaries began enrolling in PDPs on November 15, 2005.
Effective January 1, 2006 under the MMA, Medicaid coverage of prescription drugs for Medicaid beneficiaries who are also eligible for Medicare were shifted to the Medicare program. Medicaid drug coverage ended for people who also have or are eligible for Medicare on December 31, 2005. These enrollees are referred to as “dual eligibles.” In general, dual eligibles are persons who (1) have low income qualifying them for Medicaid benefits and (2) also qualify for Medicare because they have chronic illnesses and disabilities, or they are over age 65. Prior to January 1, 2006, Medicare only paid for basic health care services, like physician and hospital care, while Medicaid filled Medicare’s gaps and covers services and supplies, like prescription drugs, not covered by Medicare.
Dual eligibles may sign up for a PDP on their own, but if they do not do so, the Secretary of Health and Human Services is required to enroll them automatically in a PDP on a random basis. We have contracted with the auto enrollees plans to qualify us to provide pharmacy services to persons with HIV/AIDS in the regions surrounding our pharmacies. There is also an “any willing provider” requirement for pharmacy participation in Medicare Part D—a PDP must allow participation by any pharmacy that meets the terms and conditions for participation that the plan has established. We will be subject to the terms and conditions of each of the agreements we may negotiate with the PDPs. Termination of our agreements with PDPs could affect our profitability. We may not have a negotiated price with all of the PDPs in which our patients are enrolled or will be enrolled. Based on experience for several weeks of the first quarter, our reimbursement rates under Medicare Part D are lower than our historical reimbursement rates available under the various state Medicaid programs in which we participate.
As a result of shifting prescription drug coverage from Medicaid to Medicare, the MMA could affect our ability to provide pharmacy services to dual eligibles because we have no assurance that the patients we serve currently have enrolled in or have been assigned automatically to a PDP with which we have a negotiated
11
contract. Also, dual eligibles are permitted to switch plans each month, if they desire. Medicare Part D may not cover all medications we dispense for persons with HIV/AIDS. CMS has stated that its policy requiring all or substantially all anti-retrovirals available to patients as of January 1, 2006 to be included on all PDP formularies will be reevaluated in 2007. State Medicaid programs may at their discretion provide coverage for medications not covered by Medicare Part D, but we have no assurance that they will do so.
ADAP provides payment for certain items and services not covered by Medicare Part D. ADAP can cover Medicare PDP premiums, deductibles, coinsurance and co-pays. Certain ADAP recipients may also be Medicare beneficiaries and will need to enroll in a PDP to continue to be eligible for and supplement their ADAP coverage. We work with the various state ADAP and Medicaid programs to ensure coverage of our drugs, if possible.
We have described only those provisions of the MMA that we believe to be applicable to our business at this time. There may be other provisions of the legislation or the implementing regulations that may impact our business by decreasing net sales or increasing operational expenses. The impact of the MMA depends upon a variety of factors, including the nature of the implementing regulations. Because of the broad scope and phased-implementation of key provisions in the MMA, we are not in a position to fully assess its impact on our business or profitability. We are engaged in extensive and continuous evaluation of this legislation and the related regulations.
The MMA is a complex and new law that remains subject to interpretation from regulators in charge of overseeing its implementation including CMS. CMS is in the process of publishing guidance to both providers and beneficiaries. Because CMS is not a rulemaking body, it is uncertain whether all the guidance issued by CMS is enforceable. Accordingly, it is not possible to quantify fully the effect of potential legislative changes, the interpretation or administration of such legislation, or any other governmental initiatives on our business. We can provide no assurance that the impact of any future healthcare legislation or regulation will not adversely affect our business or profitability. There can be no assurance that payments under governmental and private third-party payor programs will be timely, or will remain at levels similar to present levels.
Reform. The U.S. healthcare industry continues to undergo significant change. Future changes in the nature of the health system could reduce our net sales and profits. We cannot provide any assurance as to the ultimate content, timing or effect of any healthcare reform legislation including sweeping changes to the Medicaid or Medicare programs, nor is it possible at this time to estimate the impact on us of potential legislation, which may be material. Further, although we exercise care in structuring our operations to comply in all material respects with all applicable laws and regulations, we can not assure you that (i) government officials charged with responsibility for enforcing such future laws will not assert that we or certain transactions in which we are involved are in violation thereof, and (ii) such future laws will ultimately be interpreted by the courts in a manner consistent with our interpretation. Therefore, it is possible that future legislation and regulation and the interpretation thereof could have a material adverse effect on us. We are unable to predict whether any such legislative proposals will be enacted.
Prescription Drug Marketing Act. This federal law exempts many drug and medical devices from federal labeling and packaging requirements, as long as they are not adulterated or misbranded and were prescribed by a physician. The law also prohibits the sale, purchase or trade of drug samples that are not intended for sale or intended to promote the sale of the drug. Records must be kept of drug sample distribution, and proper storage and maintenance methods used. To the extent that this law applies to us, we believe that we comply with the documentation, record keeping and storage requirements.
Liability Insurance. Providing healthcare services and products entails an inherent risk of liability. In recent years, participants in the healthcare industry have become subject to an increasing number of lawsuits, many of which involve large claims and significant defense costs. We may from time to time be subject to such suits as a result of the nature of our business. We maintain general liability insurance, including professional and product liability, in an amount deemed adequate by our management. There can be no assurance, however, that claims in
12
excess of, or beyond the scope of, our insurance coverage will not arise. In addition, our insurance policies must be renewed annually. Although, we have not experienced difficulty in obtaining insurance coverage in the past, there can be no assurance that we will be able to do so in the future on acceptable terms or at all.
Federal Food, Drug, and Cosmetic Act. This law, as amended by the Prescription Drug Marketing Act, imposes requirements for the labeling, packaging and repackaging, dispensing, advertising and promotion of prescription medication; and also prohibits, among other things, the distribution of unapproved, adulterated or misbranded drugs. In the past, the Food and Drug Administration, or the FDA, has viewed particular combination packaging arrangements as constituting new drugs that must be tested and labeled in the packaged combination. On occasion, the FDA also has sought to apply drug compounding guidance to analogous arrangements. We believe that sufficient legal authority, and pharmacy industry practice, supports our position that our activities in packaging the combination of drugs prescribed by physicians do not require the FDA approval or registration by us with the FDA as a manufacturer. However, the FDA may disagree with this interpretation and we could be required to defend our position and possibly to alter our practices; although no such action has ever been initiated against us. To the extent that this law applies to us, we believe that we comply with a reasonable interpretation of the repackaging, labeling, compounding, documentation, record-keeping and storage requirements. Finally, to the extent we engage in co-marketing arrangements with pharmaceutical manufacturers regulated by the FDA, we are required to maintain our independence to ensure that any reference to specific products used in combination does not constitute illegal off-label promotion in the view of the FDA.
Federal Controlled Substances Act. This federal law contains pharmacy registration, packaging and labeling requirements, as well as record-keeping requirements related to a pharmacy’s inventory and its receipt and disposition of all controlled substances. Each state has also enacted similar legislation governing pharmacies’ handling of controlled substances. We maintain federal and state controlled substance registrations for each of our facilities where applicable, and follow procedures intended to comply with all such record keeping requirements.
Federal Mail Order Provisions. Federal law imposes standards for the labeling, packaging and repackaging, advertising and adulteration of prescription drugs; and the dispensing of controlled substances and prescription drugs. The United States Postal Service and the Federal Trade Commission regulate mail order sellers, requiring truth in advertising, a reasonable supply of drugs to fill orders, the consumer’s right to a refund if an order cannot be filled within 30 days, and in certain cases, child-resistant packaging. To the extent applicable, we believe we substantially comply with these requirements.
Pharmacy Drug Use Review Law. Federal law requires that states offering Medicaid prescription drug benefits implement a drug use review program. The program requires “before and after” drug use reviews and the use of certain approved compendia and peer-reviewed medical literature as the source of standards for such drug use reviews. States offering Medicaid prescription drug benefits must develop standards for pharmacy patient counseling and record-keeping. These standards apply as well to non-resident pharmacies. We believe our pharmacists monitor these requirements, provide the necessary patient counseling and maintain the appropriate records.
Anti-Kickback Laws. We are subject to various laws that regulate our relationships with referral sources such as physicians, hospitals and other providers of healthcare services. Under the government payment programs for healthcare services (Medicare, Medicaid, ADAP, etc.), the federal government enforces the federal statute that prohibits the offer, payment, solicitation or receipt of any remuneration to or from any person or entity, directly or indirectly, overtly or covertly, in cash or in kind to induce or exchange for the referral of patients covered by the programs; or the purchasing, leasing, ordering, or arranging for or recommending the lease, purchase or order of any item, good, facility or service covered by the programs. Violations by individuals or entities are punishable by criminal fines, civil penalties, imprisonment or exclusion from participation in reimbursement programs, such as Medicaid.
13
States also have similar laws proscribing kickbacks, some of which are not limited to services for which government-funded payment may be made. State laws (and their respective exceptions or safe harbors) vary and are subject to interpretations of courts or regulatory agencies.
Anti-kickback laws are very broad in scope and are subject to modifications and variable interpretations. In an effort to clarify the federal anti-kickback law, the Department of Health and Human Services, or DHHS, has adopted a set of “safe harbor” rules, which specify various payment practices that are protected from civil or criminal liability. A practice that does not fall within a safe harbor is not necessarily unlawful, but may be subject to scrutiny and challenge. Failure to satisfy the requirements of a safe harbor requires an analysis of whether the parties intend to violate the anti-kickback law. In the absence of an applicable safe harbor, a violation of the anti-kickback law may occur even if only one purpose of a payment arrangement is to induce patient referrals or purchases or to induce the provision of a prescription drug reimbursable by a federal healthcare program such as Medicaid. Anti-kickback laws have been cited as a partial basis, along with the state consumer protection laws discussed below, for investigations and multi-state settlements relating to financial incentives provided by drug manufacturers to retail pharmacies in connection with pharmaceutical marketing programs. We review our business practices regularly to comply with the federal anti-kickback law and similar state laws. We have a variety of relationships with referral sources, such as physicians, clinics and hospitals. As we grow, we may pursue additional arrangements with such parties. Where applicable, we will attempt to structure these relationships to fit into the appropriate safe harbor; however, it is not always possible to meet all of the requirements of a safe harbor. While we believe that our relationships comply with the anti-kickback laws, if we are found to violate any of these laws, we could suffer penalties, fines, or possible exclusion from participation in federal and state healthcare programs, which could reduce our net sales and profits.
Health Insurance Portability and Accountability Act of 1996, or HIPAA. Among other things, HIPAA broadened the scope of the DHHS Secretary’s power to impose civil monetary penalties on healthcare providers, and added an additional category to the list of individuals and entities who may be excluded from participating in any federal healthcare program like Medicaid. HIPAA encourages the reporting of healthcare fraud by allowing reporting individuals to share in any recovery made by the government, and requires the DHHS Secretary to create new programs to control fraud and abuse and conduct investigations, audits and inspections. HIPAA also defined new healthcare fraud crimes including expanding the coverage of previous laws by, among other things, to include:
| | • | | knowingly and willfully attempting to defraud any healthcare benefit program (including government and private, commercial plans); and |
| | • | | knowingly and willfully falsifying, concealing, or covering up a material fact or making any materially false or fraudulent statements in connection with claims and payment for healthcare services by a healthcare benefit plan (including government and private, commercial plans). |
We believe that our business arrangements and practices comply with these HIPAA provisions. However, a violation could subject us to penalties, fines, or possible exclusion from Medicaid. Such sanctions could reduce our net sales or profits.
OIG Fraud Alerts and Advisory Opinions. The Office of Inspector General, or OIG, of DHHS periodically issues Fraud Alerts and Advisory Opinions identifying certain questionable arrangements and practices that it believes may implicate the federal fraud and abuse laws. In a December 1994 Special Fraud Alert relating to “prescription drug marketing schemes,” the OIG stated that investigation may be warranted when a prescription drug marketing activity involves the provision of cash or other benefits to pharmacists in exchange for such pharmacists’ performance of marketing tasks in the course of their pharmacy practice, including, for example, sales-oriented “educational” or “counseling” contacts or physician and/or patient outreach where the value of the compensation is related to the business generated. We believe that we have structured our business arrangements to comply with federal fraud and abuse laws. However, if we are found to have violated any of these laws, we could suffer penalties, fines or possible exclusion from the Medicaid or other government programs, which could adversely affect our operations.
14
State Unfair and Deceptive Trade Practices and Consumer Protection Laws. State laws regulating unfair and deceptive trade practices and consumer protection statutes have been used as bases for the investigations and multi-state settlements relating to pharmaceutical industry promotional drug programs in which pharmacists are provided incentives to encourage patients or physicians to switch from one prescription drug to another. We do not participate in any such programs. A number of states involved in these consumer protection driven enforcement actions have requested that the FDA exercise greater regulatory oversight in the area of pharmaceutical promotion activities by pharmacists. It is not possible to determine whether the FDA will act in this regard or what effect, if any, FDA involvement would have on our operations.
The Stark Law. Federal law prohibits physicians from making a referral for certain health items or services if they, or their family members, have a financial relationship with the entity receiving the referral. No bill may be submitted in connection with a prohibited referral. Violations are punishable by civil monetary penalties upon both the person making the referral and the provider rendering the service. Such persons or entities are also subject to exclusion from federal healthcare programs, such as Medicaid. In 1995, CMS published final regulations under the Stark Law, known as Stark I, which provide some guidance on interpretation of the scope and exceptions of the Stark Law as they apply to clinical laboratory services. In addition, CMS released Phase I of the Stark II final regulations which became effective, in large part on January 4, 2002, and which covers additional health services, including outpatient prescription drugs, and describes the parameters of the statutory exceptions in more detail and sets forth additional exceptions for physician referrals and physician financial relationships. Phase II of the Stark II final regulations became effective on July 26, 2004. Phase II clarifies portions of Phase I, addresses certain exceptions to the Stark Law not addressed in Phase I, and creates several new exceptions. As a result of the Phase II comment period and the fact that Phase II did not address application of the Stark Law to Medicaid, CMS plans to release Phase III regulations at a future date. Another feature of the Phase II regulations is that they include new provisions relating to indirect ownership and indirect compensation relationships between physicians and entities offering designated health services. These provisions are complex and have not been interpreted by the courts. We believe that we have structured our relationships with physicians to comply with these Phase II provisions.
Additionally, a number of states have enacted similar referral prohibitions, which may cover financial relationships between entities and healthcare practitioners other than physicians, as well. The Stark Law applies to our relationships with physicians and physician referrals for our products and services. We believe we have structured our relationships to comply with the Stark Law as well as the applicable state provisions similar to the Stark Law. However, if our practices are found to violate the Stark Law or a similar state prohibition, we may be subject to sanctions or be required to alter or discontinue some of our practices. This could reduce our net sales or profits.
Beneficiary Inducement Prohibition. The federal civil monetary penalty law prohibits the offering of remuneration or other inducements to beneficiaries of federal healthcare programs to influence the beneficiaries’ decision to seek specific governmentally reimbursable items or services, or to choose a particular provider. The federal civil monetary penalty law and its associated regulations exclude items provided to patients to promote the delivery of preventive care. However, permissible incentives do not include cash or cash equivalents. From time to time, we loan some items at no charge to our patients to assist them with adhering to their drug therapy regimen. Although these items are not expressly included on the list of excluded items set forth in the statute and regulations, we nevertheless believe that our provision of these items does not violate the civil monetary penalty law and regulations in part because we do not believe that providing these items is likely to influence patient choice of goods or services. A determination that we violated the statute or regulations, however, could result in sanctions that reduce our net sales or profits.
False Claims; Insurance Fraud Provisions. We are also subject to federal and state laws prohibiting individuals or entities from knowingly and willfully making claims for payment to Medicare, Medicaid, or other third-party payors that contain false or fraudulent information. These laws provide for both criminal and civil penalties, including exclusion from federal healthcare programs such as Medicaid, and being required to repay
15
previously collected amounts. The Federal False Claims Act contains a provision encouraging private individuals to file suits on behalf of the government against healthcare providers such as us. Federal false claims actions may be based on underlying violations of the kickback and/or self-referral prohibitions, as well. State law also proscribes fraudulent acts against third-party payors, including the ADAP and Medicaid programs. Healthcare providers who submit claims which they knew or should have known were false, fraudulent, or for items or services that were not provided as claimed, may be excluded from Medicaid, required to repay previously collected amounts, and subject to substantial civil monetary penalties.
Government Investigations. The government increasingly examines arrangements between healthcare providers and potential referral sources to determine whether they are designed to exchange remuneration for patient care referrals. Investigators are increasingly willing to look behind formalities of business transactions to determine the underlying purpose of payments. Enforcement actions have increased over the years and are highly publicized. The pharmaceutical industry continues to garner much attention from federal and state governmental agencies. In its Fiscal Year 2002 Work Plan, the OIG identified “pharmaceutical fraud” as one of its “special focus areas” and committed itself to conduct further assessments relating to Medicaid medication reimbursement issues. In the OIG’s 2003, 2004, and 2005 Work Plans, the OIG emphasized its continuing focus on pharmaceutical fraud. The Department of Justice has “identified prescription drug issues” (including product substitution without authorization, controlled substances controls, free goods/diversion, medication errors, sale of samples, and contracting with pharmacy benefit management companies) as being among the “top 10” areas in the healthcare industry meriting the Department’s attention.
The relationships between drug manufacturers and providers of healthcare, including pharmacies, physicians, and hospitals, are under increased government scrutiny. In 2003, the OIG published the Compliance Program Guidance for Pharmaceutical Manufacturers. Any relationships we develop with pharmaceutical companies should be consistent with such guidelines.
In addition to investigations and enforcement actions initiated by government agencies, we could be the subject of an action brought under the Federal False Claims Act by a private individual (such as a former employee, a customer or a competitor) on behalf of the government. Actions under the Federal False Claims Act, commonly known as “whistleblower” lawsuits, are generally filed under seal to allow the government adequate time to investigate and determine whether it will intervene in the action, and defendant healthcare providers are often without knowledge of such actions until the government has completed its investigation and the seal is lifted.
Privacy and Confidentiality; Electronic Transactions and Security. Many of our activities involve the receipt or use of confidential health information, including the transfer of the confidential information to a third-party payor program, such as Medicaid. DHHS has promulgated regulations implementing what are commonly referred to as the Administrative Simplification provisions of the Health Insurance Portability and Accountability Act of 1996, or HIPAA, concerning the maintenance, transmission, privacy and security of electronic health information, particularly individually identifiable information. Each state may also have similar, but more stringent statutes and regulations governing the maintenance, transmission, privacy and security of electronic health information, including individually identifiable information. Pursuant to the privacy provisions of HIPAA, DHHS promulgated regulations that had a compliance deadline of April 14, 2003 and that impose extensive requirements on the way in which healthcare providers, health plans and their business associates use and disclose protected health information. This final rule gives individuals significant rights to understand and control how their protected health information is used and disclosed. Direct providers, such as pharmacies, must obtain an acknowledgement from their patients that the patient has received the pharmacy’s Notice of Privacy Practices. For most uses and disclosures of protected health information that do not involve treatment, payment or healthcare operations, the rule requires that all providers and health plans obtain a valid individual authorization. In most cases, use or disclosure of protected health information must be limited to the minimum amount necessary to achieve the purpose of the use or disclosure. In addition, if we choose to distribute medications through new distribution channels such as the Internet, we will have to comply with government
16
regulations that exist now and that may be promulgated in the future. Standards are provided for removing all individually identifiable health information in order to produce de-identified data that may be transferred without obtaining the patient’s authorization. Sanctions for failing to comply with the privacy standards issued pursuant to HIPAA include criminal penalties and civil sanctions. We have implemented certain privacy protections with respect to HIPAA privacy regulations. However, we cannot provide assurance that we have complied with all of the HIPAA privacy requirements. Any failure to comply could subject us to enforcement actions, including civil and criminal penalties, and could cause us to incur expense in changing our medical records system or information management systems. In addition to the federal health information privacy regulations described above, most states have enacted confidentiality laws that limit the disclosure of confidential medical information. The final privacy rule under HIPAA does not preempt state laws regarding health information privacy that are more restrictive than HIPAA. The failure to comply with these federal and state provisions could result in the imposition of administrative or criminal sanctions.
On October 16, 2002 (which was extended to October 16, 2003 for those providers who submitted a “plan” describing how they will come into compliance) all healthcare providers who transmit certain protected health claims transactions electronically were required to comply with the HIPAA final regulations establishing transaction standards and code sets.
In addition, pursuant to HIPAA, in February 2003, DHHS issued regulations pursuant to HIPAA that govern the security of protected health information that is maintained or transmitted electronically. The compliance date for these regulations is April 20, 2005. The regulations impose additional administrative burdens on healthcare providers, such as pharmacies, relating to the storage and utilization of, and access to, health information. We believe that we have implemented reasonable measures to secure the protected health information that we maintain or transmit, however, we cannot provide assurance that we will be in compliance with all of the HIPAA security rule on April 20, 2005, and these HIPAA security regulations may require that we invest significant capital in upgrading information systems hardware, software and procedures. Any failure to comply could subject us to enforcement actions, including civil penalties.
On September 23, 2005, the Department of Health and Human Services published in the Federal Register a proposed rule that adds to the HIPAA transaction standards regulations and describes the requirements that health plans, covered health care providers, and health care clearinghouses would have to meet to comply with the statutory requirement to use standard codes and formats for electronic claims attachment transactions, and to facilitate the transmission of certain types of detailed clinical information to support an electronic health care claim. We are evaluating the applicability of this rule to our operations. There is no assurance that the rule will be adopted in its proposed form. If applicable, we will endeavor to comply with the rule. On January 23, 2004, CMS published a rule announcing the adoption of the National Provider Identifier as the standard unique health identifier for healthcare providers to use in filing and processing healthcare claims and other transactions. This rule was effective May 23, 2005 with a compliance date of May 23, 2007. In addition to those discussed here, from time to time, new standards and regulations may be adopted governing the use, disclosure and transmission of health information. We will endeavor to comply with all such requirements. We cannot, however, estimate the cost of compliance with such standards or determine if implementation of such standards will result in an adverse effect on our operations or profitability. Any failure to comply could subject us to enforcement actions, including civil penalties.
Developments in Health Information Technology. Healthcare providers are increasingly utilizing technology to make healthcare safer and more efficient. Health information technology initiatives include e-prescribing, which allows healthcare providers to transmit prescriptions electronically to a pharmacy rather than writing them on paper. E-prescribing products, services and arrangements must be compliant with numerous laws and regulations, including the final HIPAA security regulations, the federal anti-kickback law, and the Stark law. On October 11, 2005, the Department of Health and Human Services, Office of Inspector General, published a proposed rule establishing a safe harbor for providers who receive non-monetary remuneration necessary to set up and operate e-prescribing systems. Specifically, the proposed safe harbor would protect certain arrangements
17
involving hospitals, group practices, PDP sponsors and Medicare Advantage (MA) organizations that provide to specified recipients (such as prescribing health care professionals, pharmacies and pharmacists) certain non-monetary remuneration in the form of hardware, software or information technology and training services necessary and used solely to receive and transmit electronic prescription drug information. There can be no assurance that the proposed rule will be adopted as final. On October 11, 2005, CMS published a proposed rule to create an exception to the physician self-referral prohibition for certain arrangements in which a physician receives necessary non-monetary remuneration that is used solely to receive and transmit electronic prescription drug information. Regardless of how the safe harbor or self-referral exceptions are structured, we believe we will structure all such relationships to comply with the relevant statutes. However, if we are found to violate any of these laws, we could suffer penalties, fines, or possible exclusion from participation in federal and state healthcare programs, which could reduce our net sales and profits. If the safe harbor or self-referral exception were promulgated as proposed, we do not expect either to be available to the Company since the safe harbor will be available to hospitals, group practices, PDP plan sponsors and MA organizations and the self-referral exception will only apply to relationships between physicians and those entities.
Under the MMA, PDPs participating in Part D must comply with national standards to be developed by the Department of Health and Human Services for electronic prescriptions. The final rule adopting standards for an electronic prescription drug program under the MMA was announced on November 1, 2005. Compliance with the standards is voluntary for prescribers and pharmacies, except if such prescribers or pharmacies send or receive prescription-related information electronically for medications covered under Medicare Part D. We will endeavor to comply with all applicable standards for the transmission of electronic prescriptions as such standards are developed. We cannot, however, estimate the cost of compliance with such standards or if implementation of such standards will result in an adverse effect on our operations or profitability.
Regulation of the Practice of Pharmacy
State laws regulate the practice of pharmacy. Pharmacies and pharmacists must obtain state licenses to operate and dispense medications. Our pharmacists are licensed in those states where their activity requires it. Pharmacists must also comply with professional practice rules. We monitor our pharmacists’ practices for compliance with such state laws and rules. We do not believe that the activities undertaken by our pharmacists violate rules governing the practice of pharmacy or medicine. In an effort to combat fraud, New York State recently enacted emergency regulations requiring the use of an official New York State prescription for all prescribing done in-state. The emergency regulations are expected to become permanent. We are licensed to do business as a pharmacy in each state in which we operate a dispensing pharmacy.
Various states have enacted laws and adopted regulations requiring, among other things, compliance with all laws of the states into which the out-of-state pharmacy dispenses medications, whether or not those laws conflict with the laws of the state in which the pharmacy is located. To the extent that such laws or regulations are found to be applicable to our operations, and that such laws of other states where our pharmacies dispense medications are more stringent than those of the states in which our pharmacies are located, we would be required to comply with them. In addition, to the extent that any of these laws or regulations prohibit or restrict the operation of mail service pharmacies and are found to be applicable to us, they could have a harmful effect on our prescription mail service operations, if any. Some federal and state pharmacy associations and some boards of pharmacy have attempted to develop laws or regulations restricting the activity of out-of-state pharmacies.
Laws enforced by the federal Drug Enforcement Administration, as well as some similar state agencies, require our pharmacy locations to individually register in order to handle controlled substances, including prescription drugs. A separate registration is required at each principal place of business where the applicant manufactures, distributes, or dispenses controlled substances. Federal and state laws require that we follow specific labeling and record-keeping requirements for controlled substances. We maintain federal and state controlled substance registrations for each of our facilities that require it, and follow procedures intended to comply with all such record-keeping requirements.
18
Recent Events
On January 18, 2006, James B. Hoover resigned from our board effective immediately. Following Mr. Hoover’s resignation, our Board of Directors has five members, three of whom are independent. Mr. Hoover’s resignation letter of January 18, 2006 described concerns about certain matters, including making changes to the composition of two standing committees. This letter followed a December 23, 2005 letter that Mr. Hoover sent to our chairman and chief executive officer seeking to discuss his compensation as a non-employee director (and chairperson of the Audit Committee) and his concern about certain board procedures and board scheduling practices. We disagree with Mr. Hoover’s position and certain of his factual statements, as discussed in the Form 8-K filed by us on January 23, 2006. Mr. Hoover responded on January 25, 2006 with a letter that was included on an 8-K filed by us on January 26, 2006.
After receipt of Mr. Hoover’s resignation notice, our Board held a special meeting on January 19, 2006 and appointed John Colloton as a member of the Nominating and Corporate Governance Committee and determined that he qualifies as an “audit committee financial expert” as such term is defined by the SEC. At present, we have only two members on our Audit Committee. None of our remaining three directors satisfies the independence standards for service on the Audit Committee, pursuant to Rule 4350(d)(2) of the NASDAQ Marketplace Rules. While a vacancy exists on our Audit Committee, we will operate under an exemption available under Rule 4350(d)(4) of the NASDAQ Marketplace Rules and have properly notified the NASDAQ Stock Market of our intentions. Although we are not currently in compliance with Nasdaq listing standards, this exemption allows us to continue to be traded on the NASDAQ National Market until the earlier of our next annual meeting or one year from the date of Mr. Hoover’s resignation, at which time the Audit Committee will be required to have three members that satisfy the NASDAQ independence requirements. Our Nominating and Governance Committee has been charged with identifying an individual to serve on the Board and fill the vacancy created by Mr. Hoover’s resignation.
On January 25, 2006, we completed the sale of 5,101,922 common shares at the price of $12.83 per share, less an underwriting discount, for total gross proceeds of $61,857,488. The number of shares sold included 2,465,468 shares sold by us (665,468 shares through the over-allotment exercised by the underwriters after the offering) and 2,636,454 shares sold by certain selling stockholders. Allion Healthcare received total gross proceeds of $29,892,197 from the sale of its shares and did not receive any proceeds from the sale of shares by the selling stockholders.
On March 9, 2006, after discussion with our independent registered public accounting firm, BDO Seidman, LLP and consultation with management and our Board of Directors, we concluded that our financial statements for the three and six-months ended June 30, 2005, and the three and nine-months ended September 30, 2005 should no longer be relied upon and should be restated. We intend to restate previously issued financial statements for the above mentioned periods to correct a non-cash interest expense (below the “operating income” line) relating to warrants to purchase 140,000 shares of our common stock. Warrants for 100,000 shares were issued to John Pappajohn, one of our outside directors, in April 2005 in connection with the extension of a guarantee on our West Bank credit facility and warrants to purchase 40,000 shares of our common stock were issued to Crestview Capital Master, LLC in May 2005 in connection with a private placement loan. The total non-cash interest expense for both issuances of warrants was approximately $966,000, which will be recorded in the second quarter of 2005. We had previously booked $60,000 for the value of warrants. This is a one-time charge to the income statement and does not affect our operational results. We will file amendments, as needed, to our quarterly reports on Form 10-Q for the affected periods. The Board of Directors of the Company is conducting an inquiry into these matters.
On March 13, 2006, MOMS Pharmacy of Brooklyn, Inc., a New York corporation and wholly-owned subsidiary of Allion entered into and completed the transactions contemplated by an Asset Purchase Agreement with H.S. Maiman Rx, Inc., (“Maiman”), a Brooklyn, New York pharmacy with approximately $11.2 million in 2005 revenues as reported by its owners. Under the Asset Purchase Agreement, Moms Pharmacy of Brooklyn, Inc. paid $5.25 million and acquired Maiman’s right, title and interest in and to certain assets, including but not
19
limited to, its customer lists, inventory, books and records, files and goodwill used in connection with or related to its HIV/AIDS business, all in accordance with the terms and conditions of the Asset Purchase Agreement.
The Company
We were incorporated in Delaware in 1983 under the name The Care Group, Inc. In 1999, upon our exit from bankruptcy, we changed our name to Allion Healthcare, Inc. and focused our business principally on serving HIV/AIDS patients. Our principal executive offices are located at 1660 Walt Whitman Road, Suite 105, Melville, New York 11747, and our telephone number at that address is (631) 547-6520. We also maintain three websites, which can be located atwww.allionhealthcare.com, www.momspharmacy.com,andwww.orismed.com. We do not intend these internet addresses to be active links and the content of these websites are not part of this Report.
We make available free of charge, on or through our website, our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and amendments to those reports filed or furnished to the SEC pursuant to Section 13(a) or Section 15(d) of the Securities Exchange Act of 1934, as amended (the “Exchange Act”) as soon as reasonably practicable after we electronically file such material with, or furnish it to, the SEC. We are providing the address of our internet website solely for the information of investors. We do not intend the internet address to be an active link, and the contents of the website are not part of this Report.
Employees
As of February 15, 2006, we had 149 full-time employees and 21 part-time employees, all of whom were engaged in management, sales, marketing, pharmacy services, customer service, administration or finance. None of our employees are covered by a collective bargaining agreement. We have never experienced an employment-related work stoppage and consider our employee relations to be good.
20
Item 1A. Risk Factors
The occurrence of any of the following risks could materially harm our business and financial condition.
Risks Related to Our Company
If demand for our products and services is reduced, our business and ability to grow would be harmed.
A reduction in demand for HIV/AIDS medications would significantly harm our business as we would not be able to shift quickly our business to provide medications for other diseases. Reduced demand for our products and services could be caused by a number of circumstances, such as:
| | • | | a cure or vaccine for HIV/AIDS; |
| | • | | the emergence of a new strain of HIV that is resistant to available HIV/AIDS medications; |
| | • | | shifts to treatment regimens other than those we offer; |
| | • | | new methods of delivery of existing HIV/AIDS medications that do not require our specialty pharmacy and disease management services; |
| | • | | recalls of HIV/AIDS medications we sell; |
| | • | | adverse reactions caused by the HIV/AIDS medications we sell; |
| | • | | the expiration or challenge to the drug patents of the HIV/AIDS medications we sell; or |
| | • | | competing treatment from a new HIV/AIDS medication or a new use of an existing HIV/AIDS medication. |
Changes in reimbursement by third-party payors could harm our business.
The price we receive for our products depends primarily on the reimbursement rates paid by our government and private payors. In 2005, we generated approximately 87% of our net sales from patients who rely on Medicaid and ADAP, for reimbursement. In recent years, these programs have reduced reimbursement to providers. Changes to the programs themselves, the amounts the programs pay, or coverage limitations established by the programs for the medications we sell, may reduce our earnings. For example, these programs could revise their pricing methodology for the medications we sell, decide not to cover certain medications or cover only a certain number of units prescribed within a specified time period. We are likely to experience some form of revised drug pricing as ADAP and Medicaid expenditures for HIV/AIDS medications have garnered significant attention from government agencies during the past few years. Any reduction in amounts reimbursable by government programs for our services or changes in regulations governing such reimbursements could harm our business, financial condition and results of operations. In addition, if we are disqualified from participating in the state Medicaid programs of New York, New Jersey, California, Florida or Washington, our net sales and our ability to maintain profitability would be dramatically reduced.
We are also dependent on reimbursement from private payors. Many payors seek to limit the number of providers that supply drugs to their enrollees. From time to time, private payors with which we have relationships require that we and our competitors bid to keep their business, and there can be no assurance that we will be retained or that our margins will not be adversely affected when that rebidding occurs.
Our revenues could be adversely affected if our patients who are “dual-eligible” under the Medicare Modernization Act cease to use our services or if prescription drug plans, or PDPs, reduce reimbursement rates.
Part D of the Medicare Prescription Drug, Improvement and Modernization Act of 2003, or the MMA, presents a number of potential risks and uncertainties to our business and financial operations that we are
21
continuing to assess and for which we may not have better information until the end of the first quarter of 2006, after Part D takes effect and we have had several months to fill prescriptions for dual eligible patients. These risks include:
| | • | | Not being able to determine the exact number of patients we serve who currently receive Medicaid coverage and are also eligible for Medicare, or are “dual eligible;” |
| | • | | Reimbursement rates with PDPs may be less than the rates we have historically received for our services; |
| | • | | Having no assurance that all of our patients who are dual eligible will enroll in or be assigned automatically to PDPs with which we have a contract, or will choose our services over another pharmacy which has a contract with the PDP in which the patient is enrolled; |
| | • | | Regulations that strictly limit our ability to market to our current and new patients, which may limit our ability to maintain and grow our current patient base; |
| | • | | Disruption to our payments and services from the implementation of Part D; |
| | • | | The possibility that Part D may not cover all the medications or services needed for persons with HIV/AIDS, including those we have provided historically to our patients; and |
| | • | | Increased administrative expenses in implementing Part D and transitioning our dual eligible patients to PDPs with which we have a reimbursement agreement. |
We have a history of losses and may not be able to sustain profitability.
We achieved profitability for the first time in the first quarter of 2005 but we may not be able to maintain profitability on a regular basis. If we fail to maintain profitability, your investment in our stock could result in a significant or total loss. Our predecessor company, The Care Group, Inc., filed for protection under Chapter 11 of the Bankruptcy Code in September 1998. We emerged from bankruptcy in February 1999 and, since that time experienced operating losses prior to the first quarter of 2005.
If we do not continue to qualify for preferred reimbursement programs in California and New York, our net sales could decline.
We have qualified for additional reimbursement rates under a California pilot program for HIV/AIDS pharmacies that is effective until January 1, 2008 and have qualified as a specialty HIV pharmacy in New York and are eligible to receive preferred reimbursement rates for HIV/AIDS medications that we sell in New York until March 31, 2006.
As of September 1, 2004, reimbursement rates for pharmacy services provided under Medi-Cal, the Medicaid reimbursement program administered in California, were reduced as part of the passage of the State of California budget. On September 28, 2004, California approved an HIV/AIDS Pharmacy Pilot Program bill that funds an additional $9.50 fee per prescription for qualified and participating HIV pharmacies through January 1, 2008, unless extended.
In New York, reimbursement rates for pharmacy services provided under Medicaid were reduced in September 2004. Through March 31, 2006, we will continue to be reimbursed at the higher rate that was in place before the 2004 reimbursement reduction.
There can be no assurance that the California or New York legislatures will not change these programs in a manner adverse to us or will not terminate early or elect not to renew these programs. If either of these programs are not renewed or are terminated early, our net sales and profit could be adversely affected. Additionally, if either California or New York permits additional companies to take advantage of these additional reimbursement programs, our competitive advantage in these states could be adversely impacted.
22
If we are not able to market our services effectively to HIV/AIDS clinics, their affiliated healthcare providers and PDPs, we may not be able to grow our patient base as rapidly as we have anticipated.
Our success depends, in part, on our ability to develop and maintain relationships with HIV/AIDS clinics and their affiliated healthcare providers because each is an important patient referral source for our business. In addition, we will also have to maintain and continue to establish relationships with PDPs, so we can continue to fill prescriptions for our dual eligible customers who, beginning January 1, 2006, will now receive prescription drug coverage under Medicare Part D. If we are unable to market effectively our services to these clinics, healthcare providers and PDPs, or if our existing relationships with clinics and providers are terminated, our ability to grow our patient base will be harmed which could dramatically reduce our net sales and our ability to maintain profitability.
If we fail to manage our growth effectively, our business could be harmed.
If we are unable to manage our growth effectively, we could incur losses. How we manage our growth will depend, among other things, on our ability to adapt our operational, financial and management controls, reporting systems and procedures to the demands of a larger business. In addition, we may not be able to successfully hire, train and manage additional sales, marketing, customer support and pharmacists quickly enough to support our growth. To provide this support, we may need to open additional offices, which will result in additional burdens on our systems and resources and require additional capital expenditures.
If our credit terms with AmerisourceBergen become unfavorable or our relationship with AmerisourceBergen is terminated our business could be adversely affected.
In September 2003, we entered into a five-year prime vendor agreement with AmerisourceBergen under which we currently purchase almost 100% of our prescription medications. Pursuant to the agreement, we are obligated to purchase at least 95% of the medications we sell from AmerisourceBergen. We also depend on the existing credit terms from AmerisourceBergen to meet our working capital needs between the time we purchase medications from AmerisourceBergen and when we receive reimbursement or payment from third party payors. In the past, our ability to grow has been limited in part by our inability to negotiate favorable credit terms from our suppliers. We may become limited in our ability to continue to increase the volume of medications we need to fill prescriptions if we are unable to maintain adequate credit terms from AmerisourceBergen or, alternatively, if we are unable to obtain financing from third-party lenders to support the amount of prescription medications we need to purchase in the future.
There are only a few alternative wholesale distributors from whom we can purchase the medications we offer to HIV/AIDS patients. In the event that our prime vendor agreement with AmerisourceBergen terminates or is not renewed, we might not be able to enter into a new agreement with another wholesale distributor on a timely basis or on terms favorable to us. Our inability to enter into a new supply agreement may cause a shortage of the supply of medications we keep in stock or we may be required to accept pricing and credit terms from a vendor that are less favorable to us than those we have with AmerisourceBergen.
If we do not meet our minimum purchase requirements under our prime vendor agreement with AmerisourceBergen, we will be required to make an additional payment based on the un-purchased volume.
Our prime vendor agreement with AmerisourceBergen requires us to make minimum purchases during the five-year term of the agreement that will be no less than $400 million. If we do not meet the minimum purchase commitments as set forth in the agreement at the end of the term, we will be required to pay an amount equal to 0.20% of the un-purchased volume. We also would be required to pay this amount in the event we terminate our prime vendor agreement with AmerisourceBergen without cause or in the event we default under the agreement. If we were required to make this payment, we would incur a possibly significant expense without any corresponding net sales.
23
We will incur increased costs as a result of being a public company and, as a result, our financial results could be adversely affected.
As a public company, we are required to devote additional internal and external resources to various governance and compliance matters to comply with the laws, regulations and standards relating to corporate governance and public disclosure, including the Sarbanes-Oxley Act of 2002, Securities and Exchange Commission, or SEC, regulations and The NASDAQ National Market rules. As a result, we intend to invest resources to comply with evolving laws, regulations and standards, and in addition we expect to have increased general and administrative expenses. Because we have a relatively small corporate staff, we will rely heavily on outside professional advisers to assist us with these efforts. As a result, we expect to incur additional operating expenses in the future. These costs will include consulting and increased accounting-related fees associated with evaluating, testing and preparing the attestation report on our internal control over financial reporting as required under Section 404 of the Sarbanes-Oxley Act of 2002. The way in which these laws, regulations and standards are applied and implemented may change over time, which could result in even higher costs to address and implement revisions to compliance and governance practices. If our efforts to comply with new or changed laws, regulations and standards differ from the activities intended by regulatory or governing bodies due to ambiguities related to practice, our reputation may be harmed and we could be exposed to potential liability.
In addition, the corporate governance rules and regulations for public companies may make obtaining director and officer liability insurance more expensive, and we may be required to accept reduced policy limits and coverage or incur substantially higher costs to obtain the same or similar coverage. As a result, attracting and retaining qualified individuals to serve on our board of directors or as executive officers may be more difficult.
As required by Section 404 of the Sarbanes-Oxley Act of 2002, we are required to annually assess, test, and evaluate the design and operating effectiveness of our internal control over financial reporting, or ICFR. We have concluded that our ICFR was not effective as of December 31, 2005, as management identified a material weakness due to an omission of a non-cash interest expense (below the “operating income” line) relating to warrants to purchase 100,000 shares of the Company’s common stock that were issued to an outside director of the Company in April 2005 in connection with the extension of a guarantee on the Company’s West Bank credit facility and to warrants to purchase 40,000 shares of the Company’s common stock that were issued as part of a private placement with an institutional accredited investor in May 2005. As such, we will be required to change our ICFR to remediate this and potentially other deficiencies identified in the future, which may result in lost investor confidence in the reliability of our financial statements, and may subject us to investigation and/or sanctions, by regulatory authorities. Based on this and other factors, we cannot predict the outcome of our testing in future periods. In addition, if we fail to maintain the adequacy of our ICFR on a going forward basis, as such standards are modified, supplemented, or amended from time to time, we may not be able to ensure we can conclude on an ongoing basis that we have effective controls over financial reporting in accordance with Section 404, and our independent auditors may not be able to render the required attestation concerning our assessment and the effectiveness of our ICFR. If we fail to maintain an effective internal control environment or our independent auditors are unable to render the required attestation, it could have a material adverse effect on investor confidence in our reported financial information. Any such events could adversely affect our financial results and/or the market price of our common stock.
Our success in identifying and integrating acquisitions may impact our business and our ability to have effective disclosure controls.
As part of our strategy, we continually evaluate acquisition opportunities. There can be no assurance that we will complete any future acquisitions or that such transactions, if completed, will be integrated successfully or will contribute favorably to our operations and financial condition. The integration of acquisitions includes ensuring that our disclosure controls and procedures and our internal control over financial reporting effectively apply to and address the operations of newly acquired businesses. We may be required to change our disclosure controls and procedures or our internal control over financial reporting to accommodate newly acquired
24
operations, and we may also be required to remediate historic weaknesses or deficiencies at acquired businesses. For example, the auditors of Specialty identified certain material weaknesses in Specialty’s internal controls in connection with its audit of the 2004 financial statement of Specialty. The auditors stated that Specialty needed to implement an improved accounting system and implement better controls to segregate duties regarding the cash disbursements and cash receipts functions of Specialty. Based on this letter and our own evaluation of Specialty’s internal controls, we have taken a number of remedial steps, including increasing the number of persons (and making changes in the persons) who are primarily responsible for performing the accounting and financial duties at Specialty. Our review and evaluation of disclosure controls and procedures and internal controls over financial reporting of the companies we acquire may take time and require additional expense, and if they are not effective on a timely basis could adversely affect our business and the market’s perception of our company. In addition, acquisitions may expose us to unknown or contingent liabilities of the acquired businesses, including liabilities for failure to comply with healthcare or reimbursement laws. While we try to negotiate indemnification provisions that we consider to be appropriate for the transactions, there can be no assurance that liabilities relating to the prior operations of acquired companies will not have a material adverse effect on our business, financial condition and results of operations. Furthermore, future acquisitions may result in dilutive issuances of equity securities, incurrence of additional debt, and amortization of expenses related to intangible assets, any of which could have a material adverse effect on our business, financial condition and results of operations.
We may not be able to integrate successfully theLabTracker software into our business orLabTracker subscribers may choose not to use our services.
There is no guarantee that we will be able to interface theLabTracker software successfully with our and Oris Medical’s existing systems. There is also no guarantee that the physicians or clinics currently using theLabTracker software will use our services, and we cannot be certain that we will be able to attract new customers by marketing this software. Pursuant to the terms of the license agreement between Oris Medical and Ground Zero, we gained an exclusive right in the U.S. to develop and offer a pharmacy interface to users ofLabTracker, a leading patient monitoring software for physicians and clinics that treat HIV/AIDS patients. If the license is invalid or otherwise does not grant sufficient rights to continue to use the derivative works created by Oris from the underlyingLabTracker software, our business could be materially adversely affected.
As a result of our acquisition of Oris Medical, we are required to make royalty payments based on the number of our patients submitting their prescriptions throughLabTracker. If we fail to meet such payment obligations, the license to interface with theLabTracker software for HIV/AIDS may become nonexclusive or terminable by the licensor, and such a change could have a material adverse effect on our business, financial condition, results of operations, and cash flows.
We rely on third-party delivery services to deliver our products to the patients we serve. Price increases or service interruptions in our delivery services could adversely affect our results of operations and our ability to make deliveries on a timely basis.
Delivery is essential to our operations and represents a significant expense in the operation of our business that we cannot pass on to our customers. As a result, any significant increase in delivery rates, for example, as a result of an increase in the price of gasoline could have an adverse effect on our results of operations. Similarly, strikes or other service interruptions in these delivery services would adversely affect our ability to deliver our products on a timely basis. In addition, some of the medications we ship require special handling, including refrigeration to maintain temperatures within certain ranges. The spoilage of one or more shipments of our products could adversely affect our business or potentially result in damage claims being made against us.
We rely on a few key employees whose absence or loss could adversely affect our business.
Many key responsibilities within our business have been assigned to a small number of employees. The loss of their services could adversely affect our business. In particular, the loss of the services of our named executive officers—Michael P. Moran, our Chairman, Chief Executive Officer and President, James G. Spencer, our
25
Chief Financial Officer, Secretary and Treasurer, Mikelynn Salthouse, our Vice President, Oris Sales, or Robert Fleckenstein, our Vice President, Pharmacy Operations—could disrupt our operations. We do not have employment contracts with any of our named executives and none of Messrs. Moran, Spencer and Fleckenstein are restricted from competing with us if they cease working for us. Additionally, as a practical matter, any employment agreement we may enter into will not assure the retention of such employee. In addition, we do not maintain “key person” life insurance policies on any of our employees. As a result, we are not insured against any losses resulting from the death of our key employees. Further, as we grow we must be able to attract and retain other qualified technical operating and professional staff, such as pharmacists. If we cannot attract and retain, on acceptable terms, the qualified employees necessary for the continued development of our business, we may not be able to sustain our business or grow.
A prolonged malfunction of our MOMSPak automated packaging system could hurt our relationships with the patients we serve and our ability to grow.
We rely on our MOMSPak packaging system to create the MOMSPak for dispensing patient medication. We expect that prescriptions packaged in a MOMSPak will increase substantially in the future as more of the patients we serve switch to the MOMSPak from traditional packaging system pill boxes and as the number of patients and prescriptions we fill increases. We currently lease MOMSPak machines. If these machines fail to function properly for a prolonged period, we may have to fill prescriptions by hand using pill boxes or by otherwise sorting the various drug combinations into individual doses. Delays or failure to package medications by our MOMSPak packaging system could result in our loss of a substantial portion of our patients who receive their prescriptions in MOMSPaks.
Our financial results may suffer if we have to write-off intangible assets or goodwill.
As a result of our acquisitions, a significant portion of our total assets consist of intangible assets (including goodwill). Intangible assets, net of amortization, and goodwill together accounted for approximately 46% and 31% of the total assets on our balance sheet as of December 31, 2005 and December 31, 2004, respectively. Under current accounting standards we are able to amortize intangible assets over a period of five to fifteen years and do not amortize goodwill. We may not realize the full fair value of our intangible assets and goodwill. We expect to engage in additional acquisitions that may result in our recognition of additional intangible assets and goodwill. We evaluate on a regular basis whether all or a portion of our goodwill and those intangible assets may be impaired. Under current accounting rules, any determination that impairment has occurred would require us to write-off the impaired portion of goodwill and such intangible assets, resulting in a charge to our earnings. Such a write off could have a material adverse effect on our financial condition and results of operations.
We do not have patent or trademark protection for our MOMSPak or our automated prescription packaging system, or for our trade name, MOMS Pharmacy.
We believe that several components of our ability to compete effectively include our MOMSPak package, created by our MOMSPak automated prescription packaging system, and our trade name, MOMS Pharmacy. We developed our MOMSPak packaging system with software and other technology that we licensed from third- parties. We have not attempted to obtain patent protection for our MOMSPak packaging system, and we do not intend to do so in the future. As a consequence, our competitors may develop technology that is substantially equivalent to our MOMSPak system, and we could not prevent them from doing so. If our competitors or other third parties were able to recreate the MOMSPak, one of our competitive advantages in serving HIV/AIDS patients could be lost. In addition, we do not have trademark protections for either our automated packaging system, our MOMSPak package or our MOMS Pharmacy name, and there is no guarantee that if we were to decide to seek protection, we would be able to obtain it.
Unauthorized parties may attempt to use our name or copy or otherwise obtain and use our customized packaging solution or technology. We do not have any confidentiality agreements with any of our collaborative partners, employees or consultants that would prevent them from disclosing our trade secrets. There can be no
26
assurance that we will have adequate remedies for any misuse or misappropriation of our trade secrets. If we are not adequately protected, other companies with sufficient resources and expertise could quickly develop competing products which could materially harm our business, financial condition or results of operations.
A disruption in our telephone system or our computer system could harm our business.
We receive and take prescription orders over the telephone, by facsimile or through our electronic prescription writer. We also rely extensively upon our computer system to confirm payor information, patient eligibility and authorizations; to check on medication interactions and patient medication history; to facilitate filling and labeling prescriptions for delivery and billing; and, to help with the collection of payments. Our success depends, in part, upon our ability to promptly fill and deliver complex prescription orders as well as on our ability to provide reimbursement management services for our patients and their healthcare providers. Any continuing disruption in our telephone, facsimile or computer systems could adversely affect our ability to receive and process prescription orders, make deliveries on a timely basis and receive reimbursement from our payors. This could adversely affect our relations with the patients and healthcare providers we serve and potentially result in a partial reduction in orders from, or a complete loss of, these patients.
We may not be able to obtain insurance that is sufficient to protect our business from liability.
Our business exposes us to risks inherent in the provision of drugs and related services. Claims, lawsuits or complaints relating to our products and services may be asserted against us in the future. Although we currently maintain professional and general liability insurance, there can be no assurance that the scope of coverage or limits of such insurance will be adequate to protect us against future claims. In addition, there can be no assurance that we will be able to maintain adequate liability insurance in the future on acceptable terms or with adequate coverage against potential liabilities.
Risks Related To The Specialty Pharmacy Industry
There is substantial competition in our industry, and we may not be able to compete successfully.
The specialty pharmacy industry is highly competitive and is continuing to become more competitive. All of the medications, supplies and services that we provide are also available from our competitors. Our current and potential competitors may include:
| | • | | other specialty pharmacy distributors; |
| | • | | specialty pharmacy divisions of wholesale drug distributors; |
| | • | | pharmacy benefit management companies; |
| | • | | hospital-based pharmacies; |
| | • | | other retail pharmacies; |
| | • | | manufacturers that sell their products both to distributors and directly to clinics and physicians’ offices; and |
| | • | | hospital-based care centers and other alternate site healthcare providers. |
Many of our competitors have substantially greater resources and marketing staffs and more established operations and infrastructure than we have. A significant factor in effective competition will be our ability to maintain and expand relationships with patients, healthcare providers and government and private payors.
If we are found to be in violation of Medicaid and Medicare reimbursement regulations, we could become subject to retroactive adjustments and recoupments.
As a Medicaid and Medicare provider, we are subject to retroactive adjustments due to prior-year audits, reviews and investigations, government fraud and abuse initiatives, and other similar actions. Federal regulations also provide for withholding payments to recoup amounts payable under the programs. While we believe we are
27
in material compliance with applicable Medicaid and Medicare reimbursement regulations, there can be no assurance that we, pursuant to such audits, reviews, investigations, or other proceedings, will be found to be in compliance in all respects with such reimbursement regulations. A determination that we are in violation of any such reimbursement regulations could result in retroactive adjustments and recoupments of payments and have a material adverse effect on us. As a Medicaid and Medicare provider, we are also subject to routine, unscheduled audits that can have a material adverse impact on our results of operations should an audit result in a negative finding. There can be no assurance at this time as to the impact on us of future Medicaid and Medicare audits.
Our industry is subject to extensive government regulation, and noncompliance by us or our suppliers could harm our business.
The repackaging, marketing, sale and purchase of medications are extensively regulated by federal and state governments. If we fail or are accused of failing to comply with laws and regulations, our business, financial condition and results of operations could be harmed. Many of the HIV/AIDS medications that we sell receive greater attention from law enforcement officials than those medications that are most often dispensed by traditional pharmacies due to the high cost of HIV/AIDS medications and the potential for illegal use. In addition, we recognize that the Federal government has an interest in examining relationships between providers or between providers and other third parties relating to health technology services, including those that facilitate the electronic submission of prescriptions. For example, it is possible that our relationship withLabTracker/Oris Medical might invite inquiry from the Federal government. Part of the earn-out payment under our purchase agreement to acquire Oris Medical Systems, Inc. is based upon the number of patients who submit their prescriptions to our pharmacies through theLabTracker software system. These payments are made directly to the shareholders of Oris Medical and to Ground Zero Software, Inc., the owner ofLabTracker. The purchase agreement expressly prohibits the shareholders of Oris Medical and Ground Zero from marketing the Oris software system. In addition, we will charge each provider who licenses the Oris System a fair market value license fee. While we believe our relationships with the shareholders of Oris Medical and Ground Zero and with the users of Oris comply with the anti-kickback laws, if we are found to violate any of these laws, we could suffer penalties, fines, or possible exclusion from participation in federal and state healthcare programs, which would reduce our sales and profits.
Our business could also be harmed if the entities with which we contract or have business relationships, such as pharmaceutical manufacturers, distributors, physicians or HIV/AIDS clinics, are accused of violating laws or regulations. The applicable regulatory framework is complex and evolving, and the laws are very broad in scope. There are significant uncertainties involving the application of many of these legal requirements to our business. Many of the laws remain open to interpretation and have not been addressed by substantive court decisions that clarify their meaning. We are unable to predict what additional federal or state legislation or regulatory initiatives may be enacted in the future relating to our business or the healthcare industry in general, or what effect any such legislation or regulation might have on us. Further, we cannot provide any assurance that federal or state governments will not impose additional restrictions or adopt interpretations of existing laws that could increase our cost of compliance with such laws or reduce our ability to become profitable. If we are found to have violated any of these laws, we could be required to pay fines and penalties, which could materially adversely affect our profitability, and our ability to conduct our business as currently structured. Federal and state investigations and enforcement actions continue to focus on the healthcare industry, scrutinizing a wide range of items such as referral and billing practices, product discount arrangements, dissemination of confidential patient information, clinical drug research trials, pharmaceutical marketing programs, and gifts for patients. It is difficult to predict how any of the laws implicated in these investigations and enforcement actions may be interpreted to apply to our business. To our knowledge, we are not currently the subject of any investigation. Any future investigation may cause publicity that would cause potential patients to avoid us, reducing potential net sales and profits and cause our stock price to decline.
28
Recent changes in how Medicaid and other government payors calculate the amount we are paid for medications we sell could reduce our pricing and margins.
Historically, many government payors, including ADAP and Medicaid programs, which account for most of our net sales, paid us directly or indirectly for the medications we handle at average wholesale price, or AWP, or at a percentage of AWP. Private payors with whom we may contract also reimburse for medications at AWP or at a percentage of AWP. Federal and state governmental attention continues to focus on the validity of using AWP as the basis for Medicaid medication payments, including payments for HIV/AIDS medications, and most state Medicaid programs pay substantially less than AWP for drugs.
In January of 2006, the Reduction Act was enacted which established AMP as the benchmark for prescription drug reimbursement in the Medicaid program, eliminating the previously used AWP standard. This legislation also made changes to the federal upper payment limit for multiple source drugs. Payments to pharmacies for Medicaid-covered outpatient prescription drugs are set by the states. Federal reimbursements to states for the federal share of those payments are subject to FUL. Effective January 1, 2007, for multiple source drugs (i.e., generics), the FUL will be 250% of the AMP. We are reviewing the potential impact that the Reduction Act may have on our business and are not yet in a position to fully assess its impact on our business or profitability. Its effect may be to reduce reimbursement for certain medications that we dispense, either currently or in the future.
As of January 1, 2004, Medicare adopted new pricing that reduced reimbursement for many drugs covered under Medicare Part B. In 2005, the agency that administers the Medicare and Medicaid Programs, the Centers for Medicare & Medicaid Services, or CMS, changed reimbursement so that it will be based on average sales price, or ASP rather than AWP. In 2006, reimbursement may be based on ASP or administered under a competitive acquisition program. This change in pricing may result in reduced reimbursement for medications we dispense.
Our sales and profitability are affected by the efforts of healthcare payors to contain or reduce the cost of healthcare by lowering reimbursement rates, limiting the scope of covered services, and negotiating reduced or capitated pricing arrangements. Any changes which lower reimbursement levels under Medicaid, Medicare or private payors could also reduce our future revenue. Furthermore, other changes in these reimbursement programs or in related regulations could reduce our future revenue. These changes may include modifications in the timing or processing of payments and other changes intended to limit or decrease the growth of Medicaid, Medicare or third party expenditures. In addition, the failure, even if inadvertent, by us and/or our patients to comply with applicable reimbursement regulations could adversely affect our reimbursement under these programs and our ability to continue to participate in these programs. In addition, our failure to comply with these regulations could subject us to other penalties.
We have entered into relationships with PDPs from which we receive reimbursement for our patients who are dual eligible and enrolled with such PDPs. Part D became effective on January 1, 2006, and until the end of the first quarter of 2006, we may not know the number of patients we serve currently who do not enroll in a PDP with which we have a contract, or who are assigned automatically to a PDP with which we have a contract, or who choose another pharmacy with which the PDP has a contract. If we fail to comply with the terms and conditions of our agreements with the PDPs, our contracts with such PDPs may be terminated.
Our business could be affected by reforms in the healthcare industry.
Healthcare reform measures have been considered by Congress and other federal and state bodies during recent years. The intent of the proposals generally has been to reduce healthcare costs and the growth of total healthcare expenditures, and to eliminate fraud, waste and financial abuse. Comprehensive healthcare reform may be considered and efforts to enact reform bills are likely to continue. These changes are occurring on a fast-paced basis and it is impossible to predict the extent or substance of those changes. For example, Florida recently approved a sweeping change to its Medicaid program that shifts from the traditional Medicaid “defined benefit” plan to a “defined contribution” plan, under which the state sets a limit on spending for each recipient. Under the
29
new program, Medicaid enrollees will enroll in, or be automatically enrolled in, private health plans, which will have the authority to manage the Medicaid health care benefit. Other states are considering implementing such a change to the administration of their Medicaid programs. We are unable to predict the likelihood of any healthcare reform legislation or similar legislation being enacted into law or the effects that any such legislation would have on our business.
Item 1B. Unresolved Staff Comments
We have not received written comments regarding our periodic or current reports from the SEC staff that were issued 180 days or more preceding the end of our 2005 fiscal year and that remain unresolved.
Item 2. Properties
Our principal executive offices are located in Melville, New York, which we have leased through August 31, 2009. Both our executive offices and New York pharmacy operations are located at this site. We lease space in the following locations:
| | | | |
Location | | Principal Use | | Property Interest |
| | |
Melville, NY | | Pharmacy and Executive Offices | | Leased—expiring August 31, 2009 |
Gardena, CA | | Pharmacy | | Leased—expiring March 31, 2011 |
Van Nuys, CA | | Pharmacy | | Leased—expiring December 31, 2006 |
Miami, FL | | Pharmacy | | Leased—expiring November 30, 2008 |
La Jolla, CA | | Billing Center | | Leased—expiring July 1, 2008 |
San Francisco, CA | | Pharmacy | | Leased—expiring March 31, 2008 |
San Francisco, CA | | Pharmacy | | Leased—expiring February 28, 2007 |
San Diego, CA | | Administration (Oris) | | Leased—expiring June 30, 2008 |
San Diego, CA | | Pharmacy | | Leased—expiring January 31, 2009 |
Seattle, WA | | Pharmacy | | Leased—expiring May 31, 2006 |
At this time, we believe we have adequate space for our current operations. We plan to renew these leases prior to expiration or move to other comparable space.
Item 3. Legal Proceedings
New York Medicaid Audit. In May 2004, we were notified that MOMS Pharmacy Inc., our subsidiary in New York was the subject of an audit and review being conducted by the New York State Department of Health (the “Department”). As part of the audit, the Department withheld payment of certain Medicaid claims we had submitted. The Department refunded $800,000 of the $920,000 which it initially withheld. We settled this audit in July 2005 for approximately $120,000 and do not believe we have any continuing liability to the department.
In addition to the matter noted above, we are involved from time to time in legal actions arising in the ordinary course of our business. We currently have no pending or threatened litigation that we believe will result in an outcome that would materially affect our business. Nevertheless, there can be no assurance that future litigation to which we become a party will not have a material adverse effect on our business.
On March 9, 2006, we alerted the staff of the SEC’s Division of Enforcement to the issuance of our press release of that date. On March 13, 2006, we received a letter from the Division of Enforcement notifying us that the Division of Enforcement had commenced an informal inquiry and requested that we voluntarily produce certain documents and information. In that letter, the SEC also stated that the informal inquiry should not be construed as an indication that any violations of law have occurred. We are cooperating fully with the Division of Enforcement’s inquiry.
Item 4. Submission of Matters to a Vote of Security Holders
No matters were submitted to a vote of our security holders during the fourth quarter of 2005.
30
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
We completed our initial public offering on June 22, 2005; prior to that there was not public market for Allion’s common stock. The following table sets forth, for the periods indicated, the range of high and low sale prices for our common stock. Our common stock trades on the NASDAQ National Market under the symbol ALLI.
| | | | | | |
| | | High | | Low |
2005: | | | | | | |
Second quarter (beginning June 22, 2005) | | $ | 19.40 | | $ | 13.65 |
Third quarter | | $ | 20.25 | | $ | 15.26 |
Fourth quarter | | $ | 18.65 | | $ | 10.95 |
2006: | | | | | | |
First quarter (through March 13) | | $ | 17.40 | | $ | 10.90 |
The last reported sale price of our common stock on March 13, 2006 was $13.55 per share. As of March 13, 2006, there were approximately 147 holders of record and an estimated 230 beneficial owners of our common stock.
We have not declared or paid cash dividends on our common stock and we do not plan to pay cash dividends to our shareholders in the near future. We have not repurchased shares of our common stock and we do not currently have any share repurchase plans in place. There were no unregistered sales of our common stock during the fiscal year ended December 31, 2005. During 2004, we completed unregistered sales of two new classes of our preferred stock, both of which are convertible into shares of our common stock.
31
Item 6. Selected Financial Data
The following selected financial data should be read in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our Financial Statements and the Notes thereto included elsewhere in this Report. The selected financial data as of and for the fiscal years ended December 31 2001, 2002, 2003, 2004 and 2005 have been derived from our audited financial statements. The information set forth below is not necessarily indicative of the results of future operations.
| | | | | | | | | | | | | | | | | | | | |
| | | Years Ended December 31, | |
| | | 2001 | | | 2002 | | | 2003 | | | 2004 | | | 2005 | |
| | | (in thousands, except per share) | |
Statement of Operations Data: | | | | | | | | | | | | | | | | | | | | |
Net sales | | $ | 11,694 | | | $ | 21,441 | | | $ | 42,502 | | | $ | 60,080 | | | $ | 123,108 | |
Cost of sales | | | 10,070 | | | | 18,062 | | | | 37,036 | | | | 53,162 | | | | 103,246 | |
| | | | | | | | | | | | | | | | | | | | |
Gross profit | | | 1,624 | | | | 3,379 | | | | 5,466 | | | | 6,918 | | | | 19,862 | |
Operating expenses | | | | | | | | | | | | | | | | | | | | |
Selling, general and administrative expenses | | | 2,846 | | | | 3,718 | | | | 7,699 | | | | 9,163 | | | | 18,350 | |
Legal settlement (income) expense | | | — | | | | (150 | ) | | | 200 | | | | — | | | | — | |
| | | | | | | | | | | | | | | | | | | | |
Operating income (loss) | | | (1,222 | ) | | | (189 | ) | | | (2,433 | ) | | | (2,245 | ) | | | 1,512 | |
Other income | | | | | | | | | | | | | | | | | | | | |
Interest expense | | | (104 | ) | | | (69 | ) | | | (244 | ) | | | (233 | ) | | | (1,059 | ) |
Costs of withdrawn public offering and other | | | — | | | | (479 | ) | | | — | | | | — | | | | — | |
Other income | | | 445 | | | | — | | | | — | | | | 4 | | | | 317 | |
| | | | | | | | | | | | | | | | | | | | |
Income (loss) before income taxes and discontinued operations | | | (881 | ) | | | (737 | ) | | | (2,677 | ) | | | (2,474 | ) | | | 770 | |
Provision for taxes | | | 9 | | | | 35 | | | | 20 | | | | 76 | | | | 329 | |
| | | | | | | | | | | | | | | | | | | | |
Net income (loss) from continuing operations | | | (890 | ) | | | (772 | ) | | | (2,697 | ) | | | (2,550 | ) | | | 441 | |
Discontinued operations | | | (224 | ) | | | (267 | ) | | | (258 | ) | | | (130 | ) | | | (36 | ) |
| | | | | | | | | | | | | | | | | | | | |
Net Income (loss) | | | (1,114 | ) | | | (1,039 | ) | | | (2,955 | ) | | | (2,680 | ) | | | 405 | |
Deemed dividend on preferred stock | | | — | | | | — | | | | — | | | | — | | | | (1,338 | ) |
| | | | | | | | | | | | | | | | | | | | |
Net loss available to common stockholders | | $ | (1,114 | ) | | | (1,039 | ) | | | (2,955 | ) | | | (2,680 | ) | | $ | (933 | ) |
| | | | | |
Basic and diluted loss per common share | | | | | | | | | | | | | | | | | | | | |
Loss before discontinued operations | | $ | (0.29 | ) | | $ | (0.25 | ) | | $ | (0.87 | ) | | $ | (0.82 | ) | | $ | (0.11 | ) |
Loss from discontinued operations | | | (0.07 | ) | | | (0.09 | ) | | | (0.08 | ) | | | (0.04 | ) | | | 0.00 | |
| | | | | | | | | | | | | | | | | | | | |
Net loss per share | | $ | (0.36 | ) | | $ | (0.34 | ) | | $ | (0.95 | ) | | $ | (0.86 | ) | | $ | (0.11 | ) |
| | | | | |
Basic and diluted weighted average of common shares outstanding | | | 3,100 | | | | 3,100 | | | | 3,100 | | | | 3,100 | | | | 8,202 | |
| | | | | |
Balance Sheet Data: | | | | | | | | | | | | | | | | | | | | |
Cash and Cash Equivalents | | $ | 1,559 | | | $ | 213 | | | $ | 641 | | | $ | 6,980 | | | $ | 3,845 | |
Investments in short-term securities | | | — | | | | — | | | | — | | | | — | | | $ | 23,001 | |
Total Assets | | $ | 4,709 | | | $ | 4,622 | | | $ | 12,415 | | | $ | 19,996 | | | $ | 86,289 | |
Notes payable-subordinated | | | — | | | | — | | | $ | 1,150 | | | $ | 1,250 | | | $ | 1,358 | |
Total Liabilities | | $ | 4,414 | | | $ | 5,365 | | | $ | 10,022 | | | $ | 8,481 | | | $ | 18,946 | |
Total Stockholders’ Equity (Deficit) | | $ | 295 | | | $ | (744 | ) | | $ | 2,393 | | | $ | 11,514 | | | $ | 67,343 | |
32
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following discussion of our financial condition and results of operations should be read in conjunction with “Financial Data” and our Financial Statements and Notes thereto, which appear in Item 8 of this Report.
Overview
We are a national provider of specialty pharmacy and disease management services focused on HIV/AIDS patients. We sell HIV/AIDS medications, ancillary drugs and nutritional supplies under our trade name MOMS Pharmacy. We work closely with physicians, nurses, clinics and AIDS Service Organizations, or ASOs, and with government and private payors, to improve clinical outcomes and reduce treatment costs for our patients. Most of our patients rely on Medicaid and other state-administered programs, such as the AIDS Drug Assistance Program, or ADAP, to pay for their HIV/AIDS medications.
We operate our business as a single segment configured to serve key geographic areas most efficiently. As of December 31, 2005, we operated distribution centers in California, New York, Florida and Washington. These centers are in close proximity to major metropolitan markets in New York City, New York; San Francisco, California; Los Angeles, California; Seattle, Washington; and Miami, Florida. In discussing our results of operations, we address changes in the net sales contributed by each of these distribution centers because we believe this provides a meaningful indication of the historical performance of our business.
In March 2005, we decided to cease operating our Austin, Texas distribution center as of June 30, 2005. A significant portion of the operations of our Austin, Texas distribution center was dedicated to serving organ transplant and oncology patients, and consistent with our strategy of focusing on the HIV/AIDS market, we decided not to continue this business. We did not record any material expense associated with the discontinuance of these operations and the closing of our Austin, Texas facility. In 2004, our Austin, Texas distribution center contributed approximately $4,500,000 of net sales to our financial results. As a result of our decision to discontinue our Texas operations, we have presented the results of the Texas distribution center as “discontinued operations.” As required by generally accepted accounting principles, we have restated prior periods to reflect the presentation of the Texas facility as “discontinued operations,” so that period-to-period results are comparable.
Some of our patients are eligible for benefits under the MMA. Under the MMA, individuals who are eligible for benefits under both Medicaid and Medicare programs, known as “dual eligibles,” will receive prescription drug coverage through Medicare and will no longer have Medicaid prescription drug coverage for drugs covered under the MMA. Medicare began providing reimbursement for prescription drugs for eligible beneficiaries through private plans on January 1, 2006. In connection with the implementation of the MMA, all dual eligibles have the opportunity to enroll in a PDP that administers the Medicare drug benefit and will pay providers like us for providing drugs under the program. Dual eligible patients who did not voluntarily pick a PDP were automatically enrolled in a plan. This change in payor requires us to seek payment for our dual eligible patients from their PDP instead of the government. We may not have an agreement to receive reimbursement from all of the PDPs in which our patients are enrolled or will enroll. As a result, we may no longer be able to provide medications to some of our current patients. In addition, we may have to accept a lower reimbursement rate than we currently receive under Medicaid. Also, the MMA program may not cover all the drugs and services we currently provide to our dual eligible patients. Lower reimbursement rates or decreases in the patients we serve or prescriptions we fill may result in lower net sales and a lower gross profit for these dual eligible patients.
The key components of our financial results are our net sales, gross profit and operating expenses. Below we discuss each one of our key components.
Net Sales. We sell HIV/AIDS prescription and ancillary medications, and nutritional supplies. As of December 31, 2005, approximately 87% of our net sales came from payments from Medicaid, Medicare and ADAP. These are all highly regulated government programs that are subject to frequent changes and cost containment measures. We continually monitor changes in reimbursement for HIV/AIDS medications.
33
Gross Profit. Our gross profit reflects net sales less the cost of goods sold. Cost of goods sold is the cost of pharmaceutical products we purchase from wholesalers and is primarily dependent on contract pricing with our main wholesale provider, AmerisourceBergen. The amounts that we are reimbursed by government and private payors have historically increased as the price of the pharmaceuticals we purchase has increased. However, as a result of cost containment initiatives, government and private payors have reduced reimbursement rates, which prevents us from recovering the full amount of any price increases.
For the year ended December 31, 2005, we recorded net income of $441,095 from continuing operations. Prior to the first quarter of 2005, we had historically generated a net loss from operations. NAHH, which we acquired on January 4, 2005, has historically reported higher gross margins than our historical business and also reported net income. The higher gross margin for NAHH is due to a product mix that is reimbursed at higher amounts than the HIV/AIDS medications we sell. The purchasers of these higher margin products are primarily not HIV/AIDS patients. In light of our focus on serving HIV/AIDS patients, we expect that this higher margin business will become a smaller portion of our overall business over time. Consequently, we expect our gross margin to decline over time to levels more consistent with our historical HIV/AIDS operations. We, therefore, will depend on increases in the volume of business and sales of prescriptions to sustain our HIV/AIDS operations. There is no assurance that we will be able to achieve the increases needed to generate sufficient net sales and gross profit to result in net income.
While we believe that we now have a sufficient revenue base to operate profitably given our anticipated operating and other expenses, our business remains subject to uncertainties and potential changes that could result in losses. In particular, changes to reimbursement rates, unexpected increases in operating expenses, or declines in the number of patients we serve or the number of prescriptions we fill could adversely affect our future results.
Operating Expenses. Our operating expenses are made up of both variable and fixed costs. Our principal variable costs are labor and delivery, which vary with the number of prescriptions we fill. Our principal fixed costs are facilities, equipment and insurance, which do not vary directly with the number of prescriptions we fill. As we grow, subject to constraints such as facility size, we do not expect our fixed costs to increase as quickly as variable costs. We also believe that our existing fixed costs are sufficient to support additional growth in the number of patients we serve and the number of prescriptions we fill.
We have grown our business by acquiring other specialty pharmacies and expanding our existing business. We expect to continue to make acquisitions and to continue to expand our existing business
Critical Accounting Policies
Our critical accounting policies affect the amount of income and expense we record in each period as well as the value of our assets and liabilities and our disclosures regarding contingent assets and liabilities. In applying these critical accounting policies, we must make estimates and assumptions to prepare our financial statements that, if made differently, could have a positive or negative effect on our financial results. We believe that our estimates and assumptions are both reasonable and appropriate, in light of applicable accounting rules. However, estimates involve judgments with respect to numerous factors that are difficult to predict and are beyond management’s control. As a result, actual amounts could differ materially from estimates.
Management believes that the following accounting policies represent “critical accounting policies,” which the SEC defines as those that are most important to the portrayal of a company’s financial condition and results of operations and require management’s most difficult, subjective, or complex judgments, often because management must make estimates about uncertain and changing matters. We discuss these and other significant accounting policies related to our continuing operations in Note 2 of the notes to our consolidated financial statements included in Item 8 of this Report.
34
Revenue Recognition. Net sales refer to our sales of medications and nutritional supplements to patients and are reported at the amount billed to patients, government and private payors and others in the period when delivery to our patients is completed net of expected contractual allowances relating to the payor. Any customer can initiate the filling of prescriptions by having a doctor call in prescriptions to our pharmacists, faxing a prescription, or mailing prescriptions to one of our facilities. Once we have verified that the prescriptions are valid and have received authorization from a customer’s insurance company, the pharmacist then fills the prescriptions and ships the medications to the customers through our outside delivery service, an express courier service, or postal mail.
Allowance for Doubtful Accounts. We are reimbursed for the medications we sell by government and private payors. The net sales and related accounts receivable are recorded net of payor contractual discounts to reflect the estimated net billable amounts for the products delivered. We estimate the allowance for contractual discounts on a payor-specific basis, given our experience or interpretation of the contract terms if applicable. However, the reimbursement rates are often subject to interpretation that could result in payments that differ from our estimates. Additionally, updated regulations and contract negotiations occur frequently, necessitating our continual review and assessment of the estimation process. While management believes the resulting net carrying amounts for accounts receivable are fairly stated at each quarter-end and that we have made adequate provision for uncollectible accounts based on all available information, no assurance can be given as to the level of future provisions for uncollectible accounts, or how they will compare to the levels experienced in the past.
Intangible Asset Impairment. In assessing the recoverability of our intangible assets, we must make assumptions regarding estimated future cash flows and other factors to determine the fair value of the respective assets. If we determine that impairment indicators are present and that the assets will not be fully recoverable, their carrying values are reduced to estimated fair value. Impairment indicators include, among other conditions, cash flow deficits, a historic or anticipated decline in net sales or operating profit, adverse legal or regulatory developments, accumulation of costs significantly in excess of amounts originally expected to acquire the asset, and a material decrease in the fair value of some or all of the assets. Changes in strategy and/or market conditions could significantly impact these assumptions, and thus we may be required to record impairment charges for these assets. We adopted Statement of Financial Accounting Standards No. 144 “Accounting for the Impairment or Disposal of Long-Lived Assets” (“SFAS No. 144”) effective January 1, 2002, and the adoption of the Statement had no impact on our consolidated financial position or results of operations.
Goodwill and Other Intangible Assets. In accordance with Statement of Financial Accounting Standard (“FAS”) No. 141, “Business Combinations,” and No. 142, “Goodwill and Other Intangible Assets,” goodwill and intangible assets associated with acquisitions that are deemed to have indefinite lives are no longer amortized but are subject to annual impairment tests. Such impairment tests require the comparison of the fair value and carrying value of reporting units. Measuring fair value of a reporting unit is generally based on valuation techniques using multiples of sales or earnings, unless supportable information is available for using a present value technique, such as estimates of future cash flows. We assess the potential impairment of goodwill and other indefinite-lived intangible assets annually and on an interim basis whenever events or changes in circumstances indicate that the carrying value may not be recoverable. Some factors we consider important which could trigger an interim impairment review include the following:
| | • | | Significant underperformance relative to expected historical or projected future operating results; |
| | • | | Significant changes in the manner of our use of the acquired assets or the strategy for our overall business; and |
| | • | | Significant negative industry or economic trends. |
If we determine through the impairment review process that goodwill has been impaired, we record an impairment charge in our consolidated statement of income. Based on our 2005 impairment review process, we have not recorded any impairments during the year ended December 31, 2005.
35
Recently Issued Accounting Pronouncements
We describe recent accounting pronouncements applicable to us at Item 8 of this Report under Note 3 to our consolidated financial statements.
Results Of Operations
Years Ended December 31, 2005 and 2004
The following table sets forth the net sales and operating data for each of our distribution centers for the twelve months ended December 31, 2005 and 2004:
| | | | | | | | | | | | | | | |
| | | Year Ended December 31, |
| | | 2005 (3) | | 2004 (3) |
Distribution Region | | Net Sales | | | Prescriptions | | Patient
Months | | Net Sales | | Prescriptions | | Patient
Months |
California (1) | | $ | 75,396,306 | (4) | | 354,072 | | 75,603 | | $ | 21,803,119 | | 93,566 | | 13,634 |
New York | | | 42,904,453 | (5) | | 162,108 | | 22,995 | | | 36,507,850 | | 146,055 | | 21,536 |
Florida | | | 2,028,705 | | | 12,488 | | 1,486 | | | 1,769,034 | | 10,931 | | 1,247 |
Seattle (2) | | | 2,778,208 | | | 16,617 | | 2,867 | | | — | | — | | — |
| | | | | | | | | | | | | | | |
Total | | $ | 123,107,672 | | | 545,285 | | 102,951 | | $ | 60,080,003 | | 250,552 | | 36,417 |
| (1) | California operations for the twelve months ended December 31, 2005 included ten months of contribution from Specialty Pharmacies, Inc. five months of contribution from Frontier Pharmacies, Inc. (d/b/a PMW) and one month of contribution from Priority Pharmacy, Inc. |
| (2) | Seattle operations for the twelve months ended December 31, 2005 included ten months contribution from Specialty Pharmacies, Inc. |
| (3) | As required by generally accepted accounting principles, we have restated current and prior periods to reflect the presentation of the Austin, Texas facility as discontinued operations, so that period-to-period results are comparable. |
| (4) | California includes retroactive payments of $185,089 for periods prior to the 12 months ended December 31, 2005. |
| (5) | New York includes retroactive payments of $99,183 for periods prior to the 12 months ended December 31, 2005. |
The prescription and patient month data has been presented to provide additional data about our operations. A prescription typically represents a 30-day supply of medication for an individual patient. “Patient months” represents a count of the number of months during a period that a patient received at least one prescription. If an individual patient received multiple medications during each month for a year period, a count of twelve would be included in patient months irrespective of the number of medications filled each month.
Net Sales. Net sales in 2005 increased to $123,107,672 from $60,080,003 in 2004, an increase of 104.9%. Net sales in California increased by $53,593,188 for the year ended December 31, 2005 as compared to 2004, primarily because of our acquisitions in California completed during 2005 and increases in the number of prescriptions filled at the facilities that existed before the acquisitions. Our net sales growth in New York and Florida was due primarily to an increase in the number of prescriptions filled from our existing facilities. Net sales in New York increased by $6,396,602 for the year ended December 31, 2005, as compared to the same period in 2004. Net sales in Florida increased by $259,671 for the year ended December 31, 2005, as compared to the same period in 2004.
In 2004 revenue was reduced by reductions in reimbursement rates in California and New York for the last four months of the year. However, we have qualified for a pilot program in California and for additional reimbursement in New York under specialized reimbursement for HIV pharmacies. The legislation providing for
36
additional reimbursement in New York expires on March 31, 2006. We cannot be certain that this program will be renewed until New York passes its annual budget. In addition, we cannot be certain the pilot program in California will be renewed after it expires in January 2008. In the second quarter of 2005 we began recognizing revenue relating to premium reimbursement in California and New York. These revenues are estimated at the time service is provided and accrued. As of the end of 2005, we had $2,412,282 of accrued revenue relating to premium reimbursement in New York and California. As of February 15, 2006 we had received approximately $1.7 million of payments for revenue that had been accrued up to December 31, 2005. As of February 15, 2006, we had not received payment for these accrued revenues from New York. In addition, we have not received payment relating to the former operations of Specialty Pharmacies, Inc. We believe that we will receive payment for these accrued revenues during the first six months of 2006.
Gross Profit. Gross profit for the year ended December 31, 2005 increased to $19,861,782 from $6,917,802 for the year ended December 31, 2004, an increase of 187.1%, our gross margin increased to 16.1% for the year ended December 31, 2005 from 11.5% for the year ended December 31, 2004. Our overall gross margin for the year ended December 31, 2005 was approximately 460 basis points higher than the gross margin for the year ended December 31, 2004. This was primarily due to the acquisition of NAHH, which had a gross margin of 38% for the year ended December 31, 2005. NAHH predominantly fills prescriptions for enterals which is reimbursed at a higher gross margin. During 2005, we recognized revenue for periods prior to December 31, 2004 relating to retroactive premium reimbursement. This was in the amount of $283,665. Excluding this revenue, the gross margin would have been 15.9%. Our gross profit increased primarily due to an increase in net sales.
Selling, General and Administrative Expenses. Selling, general and administrative expenses for the year ended December 31, 2005 increased to $18,349,296 from $9,162,734 for the year ended December 31, 2004, but as a percentage of net sales they declined to 14.9% in 2005 from 15.3% in 2004. The increase was primarily due to increased expenses related to the acquisitions. The decrease as a percentage of net sales was primarily due to a reduction in labor and other general costs as a percentage of sales.
The main components of the increase in selling, general and administrative expenses of $9,186,563 for the year ended December 31, 2005 as compared to the same period in 2004 consisted of the following:
| | | |
Components of Selling, General and Administrative Expense | | Change ($) |
Labor costs | | $ | 5,278,340 |
Shipping and postage | | | 981,347 |
Consulting and accounting services relating to Sarbanes-Oxley 404 compliance | | | 528,586 |
Franchise and Property Taxes | | | 153,167 |
Supplies (pharmacy and office) | | | 151,283 |
Operating Income/(Loss). Operating income for the year ended December 31, 2005 was $1,512,486 as compared to an operating loss of $2,244,932 for the year ended December 31, 2004, which represented 1.2% and (3.7%) of net sales, respectively. The increase in operating income is attributable to an increase in gross profit of $12,943,980, partially offset by an increase in selling, general and administrative expenses of $9,186,563. The overall increase resulted primarily from the acquisitions in 2005 and growth at our existing pharmacies.
Interest Expense.Interest expense was $1,059,135 and $233,460 for the year ended December 31, 2005 and 2004, respectively. The increase in interest expense is primarily the result of a non-cash interest expense of $966,000 relating to warrants to purchase 140,000 shares of the Company’s common stock that were issued in two financing transactions in 2005 prior to the Company’s initial public offering, of which, 100,000 of these options were issued to a director of the Company.
Other Income. Other income was $316,744 of income for the year ended December 31, 2005 and a income of $4,466 for the year ended December 31, 2004. The increase in other income was primarily due to a gain
37
related to the extinguishment of mandatory redeemable warrants. In 2005 we repurchased warrants representing 175,719 shares of common stock that had been issued in connection with the acquisition of Specialty with proceeds from the initial public offering at a price of $9 per warrant.
Provision for Taxes. We recorded a provision for taxes in the amount of $329,000 for the year ended December 31, 2005. The provision relates primarily to state income tax and federal alternative minimum tax that would have been payable before income tax deductions relating to stock based compensation created a taxable loss and deferred taxes which relate to tax-deductible goodwill. Because the amount is not payable by the Company, the amount was credited to the additional paid in capital account. We recorded a tax provision for $76,202 for the year ended December 31, 2004, which related primarily to an increase in state tax payments.
Years Ended December 31, 2004 and 2003
The following table sets forth the net sales and operating data for each of our distribution centers for the twelve months ended December 31, 2004 and 2003:
| | | | | | | | | | | | | | |
| | | Year Ended December 31, |
| | | 2004(2) | | 2003(2) |
Distribution Region | | Net Sales | | Prescriptions | | Patient
Months | | Net Sales | | Prescriptions | | Patient
Months |
California (1) | | $ | 21,803,119 | | 93,566 | | 13,634 | | $ | 13,767,864 | | 60,262 | | 8,894 |
New York | | | 36,507,850 | | 146,055 | | 21,536 | | | 27,808,291 | | 121,845 | | 18,512 |
Florida | | | 1,769,034 | | 10,931 | | 1,247 | | | 926,402 | | 6,439 | | 689 |
| | | | | | | | | | | | | | |
Total | | $ | 60,080,003 | | 250,552 | | 36,417 | | $ | 42,502,557 | | 188,546 | | 28,095 |
| (1) | California operations for the twelve months ended December 31, 2003 included eight months of contribution from Medicine Made Easy, Inc. |
| (2) | As required by generally accepted accounting principles, we have restated current and prior periods to reflect the presentation of the Austin, Texas facility as “discontinued operations,” so that period-to-period results are comparable. |
The prescription and patient month data has been presented to provide additional data about our operations. A prescription typically represents a 30-day supply of medication for an individual patient. “Patient months” represents a count of the number of months during a period that a patient received at least one prescription. If an individual patient received multiple medications during each month for a year period, a count of twelve would be included in patient months irrespective of the number of medications filled each month.
Net Sales. Net sales for the year ended December 31, 2004 increased to $60,080,003 from $42,502,557 for the year ended December 31, 2003, an increase of 41.4%. Our net sales growth in New York and Florida was due primarily to an increase in the number of prescriptions filled from our existing facilities as a result of our customary sales and marketing initiatives. Net sales in New York increased by $8,699,560 for the year ended December 31, 2004, as compared to the same period in 2003. Net sales in Florida increased by $842,632 for the year ended December 31, 2004, as compared to the same period in 2003. Net sales in California increased by $8,035,254 for the year ended December 31, 2004 as compared to 2003, primarily because we operated in California for all of 2004, as compared to only eight months in 2003 (we acquired our initial California operation in May 2003), and due to improvements in operations and an increase in the number of prescriptions we fill in California.
Our net sales increases in 2004 were partially offset by reductions in reimbursement rates in California and New York for the last four months of the year. However, we have qualified for a pilot program in California and have qualified for additional reimbursement in New York for specialized HIV pharmacies.
38
Gross Profit. Gross profit for the year ended December 31, 2004 increased to $6,917,802 from $5,466,185 for the year ended December 31, 2003, an increase of 26.6%, but our gross margin declined to 11.5% for the year ended December 31, 2004 from 12.9% for the year ended December 31, 2003. Our gross profit increased primarily due to an increase in net sales. Our gross margin declined primarily due to a reduction in reimbursement rates by Medicaid and Medi-Cal, as discussed above.
Selling, General and Administrative Expenses. Selling, general and administrative expenses for the year ended December 31, 2004 increased to $9,162,733 from $7,698,701 for the year ended December 31, 2003, but as a percentage of net sales they declined to 15.3% in 2004 from 18.1% in 2003. The decrease as a percentage of net sales was primarily due to a reduction in labor costs as a percentage of sales, staff reductions in California, decreases in bad debt expense and a decrease in professional fees.
The main components of the increase in selling, general and administrative expenses of $1,464,032 for the year ended December 31, 2004 as compared to the same period in 2003 consisted of the following:
| | | |
Components of Selling, General and Administrative Expense | | Change ($) |
Labor costs | | $ | 467,000 |
Shipping (associated with acquisition of Medicine Made Easy) | | | 266,000 |
Insurance costs (commercial, employee medical and workers compensation) | | | 157,000 |
Rent, repair and maintenance (resulting from acquisition of Medicine Made Easy and relocation to our facility in Melville, NY) | | | 153,000 |
Legal and settlement expenses relating to New York Medicaid audit | | | 132,000 |
Travel expenses | | | 93,000 |
Operating Loss. Operating loss for the year ended December 31, 2004 decreased to $2,244,931 from $2,432,516 for the year ended December 31, 2003, which represented (3.7%) and (5.7%) of net sales, respectively. Operating loss in 2003 included a $200,000 expense associated with the settlement of a New Jersey Medicaid audit. The decline in operating loss (both in absolute dollars and as a percentage of sales) reflects the effect of a greater increase in sales (up 41.4% in 2004 from 2003) than in operating expenses (up 16.0% in 2004 from 2003, or 19.0% excluding the cost of settling the New Jersey Medicaid audit), partially offset by the decline in our gross margin, as discussed above.
Other Income (Expense). Other income (expense) decreased for the year ended December 31, 2004 to an expense of $228,994 from an expense of $243,882 for the year ended December 31, 2003. In 2004, other income (expense) was comprised primarily of interest expense of $233,460 and a gain of $4,466 from the disposal of an automobile. In 2003, other income (expense) included interest expense of $243,882. The decline in interest expense in 2004 from 2003 mainly reflected lower outstanding borrowing balances in 2004.
Provision for Taxes. We recorded a tax provision for $76,202 for the year ended December 31, 2004, as compared to a tax provision of $19,646 for the year ended December 31, 2003. The provision for taxes relates primarily to an increase in state tax payments. Because we operated at a loss in 2004 and 2003, we did not pay any income taxes and, thus, did not record any amount for income taxes owed.
Liquidity and Capital Resources
On June 22, 2005, we completed an initial public offering of our common stock. We sold 4,000,000 shares of our common stock at a price of $13.00 per share, less underwriting discounts and commissions of $0.91 per share. In addition, we granted the underwriters an option, exercisable until July 21, 2005, to purchase up to an additional 600,000 shares at the initial public offering price to cover over-allotments. On July 8, 2005, the over-allotment option was exercised at $13.00 per share, less underwriting discounts and commissions of $0.91 per share. We used the initial public offering proceeds to repay approximately $12 million of our debt on June 27, 2005. We used approximately $10.0 million of the initial public offering proceeds to purchase the assets of
39
PMW. In December 2005, we used approximately $6.9 million of the initial public offering proceeds to purchase certain assets of Priority (including inventory). Under the terms of the Asset Purchase Agreement with Priority, we may be obligated to pay Priority an additional $1.1 million of which we have subsequently paid during the first quarter of 2006.
On January 25, 2006, we completed the sale of 5,101,922 common shares at the price of $12.83 per share, less an underwriting discount, for total gross proceeds of $61,857,488. The number of shares sold included 2,465,468 shares sold by us (665,468 shares through the over-allotment exercised by the underwriters after the offering) and 2,636,454 shares sold by certain selling stockholders. Allion Healthcare received total gross proceeds of $29,892,197 from the sale of its shares and did not receive any proceeds from the sale of shares by the selling stockholders.
Operating Requirements—Our primary liquidity need is cash to purchase the medications that we require to fill prescriptions. Our primary vendor, AmerisourceBergen, requires payment within 31 days of delivery of the medications to us. We are reimbursed by third-party payors, on average, within 30 days after a prescription is filled and a claim is submitted in the appropriate format.
Our operations used $496,582 of cash during 2005, which was an improvement from the same period in 2004, when our operations used $2,396,121 of cash. During 2005 we recorded revenue of $2,412,282 relating to the premium reimbursement owed by New York and California that had not been paid by December 31, 2005, as the states set up systems to administer the premium reimbursement programs. Most of the accrued premium reimbursement was paid during the first quarter of 2006 and California has begun paying the premium reimbursement on a regular basis. California has not reimbursed us for the historical operations of Specialty Pharmacies, Inc. We believe that we will receive the premium reimbursement for Specialty Pharmacies, Inc. and the remainder of the 2005 premium reimbursement revenue in the first six months of 2006. Adjusting for the premium reimbursement revenue, the cash flow from operations would have been a positive cash flow of $1,915,700. The change in cash flow from operations in 2005 from 2004 resulted primarily from our net income in 2005 as compared to a net loss in 2004.
The five-year purchase agreement that we signed with AmerisourceBergen in September 2003 improved our supplier payment terms from 13 to 31 days. These payment terms improved our liquidity and enabled us to reduce our working capital. Since entering into that agreement, we have purchased nearly all of our medications from AmerisourceBergen, although we continue to purchase some medications from other wholesalers and from manufacturers on various payment terms. If we do not meet the aggregate minimum purchase commitments under our agreement with AmerisourceBergen by the end of the five-year term, we will be charged 0.2% of the un-purchased volume commitment. Pursuant to the terms of this agreement, AmerisourceBergen has a subordinated security interest in all of our assets.
Capital Resources—As of February 15, 2006, we had approximately $57 million in cash and short-term investments. We expect to use these capital resources to fund acquisitions and capital expenditures for at least the next 12 months. We have a revolving credit facility with GE HFS Holdings, Inc. f/k/a Heller Healthcare Financial for an amount up to a maximum of $6.0 million available to us for short-term borrowings, which expires in April 2006. Borrowings under the facility are based on our accounts receivable and bear interest at the “Prime Rate” plus 2%. At February 15, 2006, our borrowing capacity was approximately $6.0 million. Following completion of our initial public offering in June 2005, we reduced our borrowings to $0. GE Capital’s security interest in our assets is senior to the security interest granted to AmerisourceBergen, pursuant to the terms of an inter-creditor agreement between GE Capital and AmerisourceBergen. This facility expires in April 2006. The Company is currently evaluating renewing the facility and may allow it to expire.
We believe that our cash balances will be sufficient to provide us with the capital required to fund our working capital needs and operating expense requirements for at least the next 12 months.
40
Long-Term Requirements—We expect that the cost of additional acquisitions will be our primary long-term funding requirement. In addition, as our business grows, we anticipate that we will need to invest in additional capital equipment, such as the machines we use to create the MOMSPak for dispensing medication to our patients. We intend to acquire additional MOMSPak machines as we expand our business. We also may be required to expand our existing facilities or to invest in modifications or improvements to new or additional facilities. If our business results declined to where we were operating at a loss, we would need to use capital resources to fund losses.
We regularly review the availability of new or additional bank borrowing facilities. There is no assurance that we will be able to secure new or additional bank borrowings on favorable terms or at all. The failure to secure additional bank borrowings could limit our future growth.
Contractual Obligations—At December 31, 2005, our contractual cash obligations and commitments over the next five years were as follows:
| | | | | | | | | | | | | | | |
| | | Payments due by Period |
| | | Total | | Less than 1
year | | 1-3 years | | 4-5 years | | More than
5 years |
Long-Term Debt Obligation (1) | | $ | 1,357,710 | | $ | 675,000 | | $ | 682,710 | | $ | — | | $ | — |
Capital Lease Obligations (1) | | | 200,197 | | | 107,379 | | | 92,818 | | | — | | | — |
Operating Leases | | | 2,146,848 | | | 594,195 | | | 1,348,085 | | | 163,509 | | | 41,059 |
Purchase Commitments (2) | | | 231,831,000 | | | 32,956,000 | | | 198,875,000 | | | — | | | — |
| | | | | | | | | | | | | | | |
Total | | $ | 235,535,755 | | $ | 34,332,574 | | $ | 200,998,613 | | $ | 163,509 | | $ | 41,059 |
| (1) | Interest payments on these amounts will be approximately $80,262 over the next three years. |
| (2) | If we fail to satisfy the minimum purchase obligation under our purchase agreement with AmerisourceBergen, we would be required to pay an amount equal to 0.2% of the un-purchased commitments at the end of the five-year term of the contract. |
Off-Balance Sheet Arrangements—We do not have any off-balance sheet arrangements.
Item 7a. Quantitative and Qualitative Disclosure About Market Risk
Interest Rate Sensitivity—We have limited exposure to financial market risks, including changes in interest rates. At February 15, 2006, we had cash and cash equivalents of approximately $36 million and short-term investments of approximately $21 million. Cash and cash equivalents consisted of demand deposits, money market accounts and investment grade debt. Short-term investments consisted of highly liquid investments in debt obligations of the U.S. Government and other highly rated entities with maturities of one year or less. These investments are classified as available-for-sale and are considered short-term, because we expect to sell them within 12 months. These investments are subject to interest rate risk and will fall in value if market interest rates increase. If market interest rates continue to rise, the value of our short-term investments would decrease. We may sell these investments prior to maturity, and therefore, we may not realize the full value of these investments. We currently hold no derivative instruments and do not earn foreign-source income. We expect to invest only in short-term, investment grade, interest-bearing instruments and thus do not expect future interest rate risk to be significant. The interest rates on outstanding notes payable are not subject to change with changes in market interest rates. We have not hedged against our interest rate risk exposure for our cash, investments or the notes payable. As a result, our interest income will increase from increasing interest rates and our interest income will decrease from declining rates.
Other Market Risk—We are not subject to other market risks such as currency risk, commodity price risk or equity price risk.
41
Item 8. Financial Statements And Supplementary Data
The following financial statements are included in this Report.
Report of the Independent Registered Public Accounting Firm—Financial Audit
Report of the Independent Registered Public Accounting Firm—Audit of Internal Controls
Consolidated Balance Sheets as of December 31, 2005 and 2004
Consolidated Statements of Operations for the years ended December 31, 2005, 2004 and 2003
Consolidated Statements of Stockholders’ Equity for the years ended December 31, 2005, 2004 and 2003
Consolidated Statements of Cash Flows for the years ended December 31, 2005, 2004 and 2003
Notes to Consolidated Financial Statements
42
Report of Independent Registered Public Accounting Firm
Board of Directors and Stockholders
Allion Healthcare, Inc.
Melville, New York
We have audited the accompanying consolidated balance sheets of Allion Healthcare, Inc. as of December 31, 2005 and 2004 and the related consolidated statements of operations, stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2005. We have also audited the schedule listed in the accompanying index. These financial statements and schedule are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements and schedule based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements and schedule are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements and schedule, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements and schedule. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Allion Healthcare, Inc at December 31, 2005 and 2004, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2005, in conformity with accounting principles generally accepted in the United States of America.
Also, in our opinion, the schedule presents fairly, in all material respects, the information set forth therein.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the effectiveness of Allion Healthcare, Inc.’s internal control over financial reporting as of December 31, 2005, based on criteria established inIntegrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) and our report dated March 15, 2006 expressed an unqualified opinion on management’s assessment on the effectiveness of internal controls over financial reporting and an adverse opinion on the effectiveness of internal controls over financial reporting because of the existence of a material weakness.
/s/ BDO Seidman, LLP
43
Report of Independent Registered Public Accounting Firm
Board of Directors and Stockholders
Allion Healthcare, Inc.
Melville, New York
We have audited management’s assessment, included in the accompanying Management’s Report on Internal Control over Financial Reporting, that Allion Healthcare, Inc. did not maintain effective internal control over financial reporting as of December 31, 2005, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Allion Healthcare Inc.’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting. Our responsibility is to express an opinion on management’s assessment and an opinion on the effectiveness of the company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, evaluating management’s assessment, testing and evaluating the design and operating effectiveness of internal control, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
As indicated in the accompanying Management’s Report on Internal Control Over Financial Reporting, management’s assessment of and conclusion on the ineffectiveness of internal control over financial reporting did not include the internal controls of North American Home Supply, Inc., Specialty Pharmacies, Inc, Frontier Pharmacy & Nutrition, Inc., d/b/a PMW Pharmacy, and Priority Pharmacy, Inc., to the extent that their operations remain segregated which is included in the 2005 consolidated financial statements of Allion Healthcare, Inc. and constituted approximately 10% of consolidated assets at December 31, 2005 and 31% of consolidated revenues for the year ended December 31, 2005. Management did not assess the effectiveness of internal control over financial reporting at these entities because the Company acquired these entities during 2005. Refer to Note 5 of the consolidated financial statements for further discussion of these acquisitions and their impact on the Company’s consolidated financial statements. Our audit of internal control over financial reporting of Allion Healthcare, Inc. also did not include an evaluation of the internal control over financial reporting of the entities referred to above.
44
A material weakness is a significant deficiency, or a combination of significant deficiencies, that results in more than a remote likelihood that a material misstatement of the annual or interim financial statements will not be prevented or detected. The following material weakness has been identified and included in management’s assessment:
There existed a material weakness in internal controls over financial reporting due to an omission of a non-cash interest expense relating to warrants issued to an outside director of the Company in April 2005 in connection with the extension of a guarantee on the Company’s credit facility and to warrants issued to a third party in connection with the Company securing a bridge loan with an institutional accredited investor in May 2005. The correction of this omitted non-cash interest expense charge resulted in the need for the Company’s financial statements for the three and six months ended June 30, 2005, and three and nine months ended September 30, 2005 to be restated.
This material weakness was considered in determining the nature, timing, and extent of audit tests applied in our audit of the 2005 consolidated financial statements, and this report does not affect our report dated March 15, 2006 on those financial statements, which expressed an unqualified opinion.
In our opinion, management’s assessment that Allion Healthcare, Inc. did not maintain effective internal control over financial reporting as of December 31, 2005, is fairly stated, in all material respects, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Also in our opinion, because of the effects of the material weakness described above, Allion Healthcare, Inc. did not maintain, effective internal control over financial reporting as of December 31, 2005, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of Allion Healthcare, Inc. as of December 31, 2005 and December 31, 2004 and the related consolidated statements of operations, changes in stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2005 and our report dated March 15, 2006 expressed an unqualified opinion.
/s/ BDO Seidman, LLP
New York, New York
March 15, 2006
45
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
AS OF DECEMBER 31, 2005 AND 2004
| | | | | | | | |
| | | 2005 | | | 2004 | |
Assets | | | | | | | | |
Current Assets: | | | | | | | | |
Cash and cash equivalents | | $ | 3,845,037 | | | $ | 6,979,630 | |
Short term investments | | | 23,000,553 | | | | 0 | |
Accounts receivable, (net of allowance for doubtful accounts of $282,824 in 2005 and $296,320 in 2004) | | | 14,640,304 | | | | 4,678,596 | |
Inventories | | | 3,228,225 | | | | 733,581 | |
Prepaid expenses and other current assets | | | 762,466 | | | | 722,984 | |
| | | | | | | | |
Total Current Assets | | | 45,476,585 | | | | 13,114,791 | |
| | |
Property and equipment, net | | | 671,396 | | | | 561,732 | |
Goodwill | | | 19,739,035 | | | | 4,472,068 | |
Intangible assets, net | | | 20,314,866 | | | | 1,643,449 | |
Other assets | | | 87,123 | | | | 203,622 | |
| | | | | | | | |
Total Assets | | $ | 86,289,005 | | | $ | 19,995,662 | |
| | | | | | | | |
| | |
Liabilities And Stockholders’ Equity | | | | | | | | |
Current Liabilities: | | | | | | | | |
Accounts payable and accrued expenses | | $ | 17,205,977 | | | $ | 6,784,658 | |
Revolving credit line | | | — | | | | 1,154 | |
Notes payable-subordinated | | | 675,000 | | | | 1,250,000 | |
Current portion of capital lease obligations | | | 107,379 | | | | 130,640 | |
Other current liabilities | | | — | | | | 100,000 | |
| | | | | | | | |
Total Current Liabilities | | | 17,988,356 | | | | 8,266,452 | |
| | |
Long Term Liabilities: | | | | | | | | |
Notes payable—subordinated | | | 682,710 | | | | — | |
Capital lease obligations | | | 92,818 | | | | 193,306 | |
Deferred tax liability | | | 153,000 | | | | — | |
Other | | | 28,892 | | | | 21,409 | |
| | | | | | | | |
Total Liabilities | | | 18,945,776 | | | | 8,481,167 | |
| | | | | | | | |
Commitments And Contingencies | | | | | | | | |
| | |
Stockholders’ Equity | | | | | | | | |
Convertible preferred stock, $.001 par value, shares authorized 20,000,000; issued and outstanding -0- in 2005 and 4,570,009 in 2004 | | | — | | | | 4,570 | |
Common stock, $.001 par value; shares authorized 80,000,000; issued and outstanding 12,956,382 in 2005 and 3,100,000 in 2004 | | | 12,956 | | | | 3,100 | |
Additional paid-in capital | | | 78,778,705 | | | | 22,060,733 | |
Accumulated deficit | | | (11,486,985 | ) | | | (10,553,908 | ) |
Accumulated other comprehensive income | | | 38,553 | | | | — | |
| | | | | | | | |
Total stockholders’ equity | | | 67,343,229 | | | | 11,514,495 | |
| | | | | | | | |
Total Liabilities And Stockholders’ Equity | | $ | 86,289,005 | | | $ | 19,995,662 | |
| | | | | | | | |
See accompanying notes to consolidated financial statements.
46
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
YEARS ENDED DECEMBER 31, 2005, 2004 AND 2003
| | | | | | | | | | | | |
| | | 2005 | | | 2004 | | | 2003 | |
Statement of Operations Data: | | | | | | | | | | | | |
Net sales | | $ | 123,107,672 | | | $ | 60,080,003 | | | $ | 42,502,557 | |
Cost of goods sold | | | 103,245,890 | | | | 53,162,201 | | | | 37,036,372 | |
| | | | | | | | | | | | |
Gross profit | | | 19,861,782 | | | | 6,917,802 | | | | 5,466,185 | |
| | | |
Operating expenses: | | | | | | | | | | | | |
Selling, general and administrative expenses | | | 18,349,296 | | | | 9,162,734 | | | | 7,698,701 | |
Legal settlement expense | | | 0 | | | | 0 | | | | 200,000 | |
| | | | | | | | | | | | |
Operating income (loss) | | | 1,512,486 | | | | (2,244,932 | ) | | | (2,432,516 | ) |
| | | |
Other expense: | | | | | | | | | | | | |
Interest expense | | | 1,059,135 | | | | 233,460 | | | | 243,882 | |
Other income | | | (316,744 | ) | | | (4,466 | ) | | | — | |
| | | | | | | | | | | | |
Income (loss) before income taxes and discontinued operations | | | 770,095 | | | | (2,473,926 | ) | | | (2,676,398 | ) |
| | | |
Provision for taxes | | | 329,000 | | | | 76,202 | | | | 19,646 | |
| | | | | | | | | | | | |
Income (loss) from continuing operations | | | 441,095 | | | | (2,550,128 | ) | | | (2,696,044 | ) |
| | | |
Loss from discontinued operations | | | (36,125 | ) | | | (130,020 | ) | | | (258,124 | ) |
| | | | | | | | | | | | |
Net income (loss) | | $ | 404,970 | | | $ | (2,680,148 | ) | | $ | (2,954,168 | ) |
| | | |
Deemed dividend on preferred stock | | | 1,338,047 | | | | 0 | | | | 0 | |
| | | | | | | | | | | | |
Net loss available to common stockholders | | $ | (933,077 | ) | | $ | (2,680,148 | ) | | $ | (2,954,168 | ) |
| | | |
Basic and diluted loss per common share | | | | | | | | | | | | |
Loss before discontinued operations | | $ | (0.11 | ) | | $ | (0.82 | ) | | $ | (0.87 | ) |
Loss from discontinued operations | | $ | 0.00 | | | $ | (0.04 | ) | | $ | (0.08 | ) |
| | | | | | | | | | | | |
Net loss per share | | $ | (0.11 | ) | | $ | (0.86 | ) | | $ | (0.95 | ) |
| | | |
Basic and diluted weighted average of common shares outstanding | | | 8,201,565 | | | | 3,100,000 | | | | 3,100,000 | |
See accompanying notes to consolidated financial statements.
47
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY (DEFICIT)
YEARS ENDED DECEMBER 31, 2005, 2004 AND 2003
| | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | Preferred Stk. $.001 par value | | | Common Stk. $.001 par value | | Additional
Paid-In
Capital | | | Accumulated
Deficit | | | Accumulated
other
comprehensive
income | | Total | |
| | | Shares | | | Par Value | | | Shares | | Par Value | | | | |
Balance, December 31, 2002 | | 1,179,168 | | | $ | 1,179 | | | 3,100,000 | | $ | 3,100 | | $ | 4,171,725 | | | $ | (4,919,592 | ) | | $ | — | | $ | (743,588 | ) |
Net Loss | | — | | | | — | | | — | | | — | | | — | | | | (2,954,168 | ) | | | — | | | (2,954,168 | ) |
Issuance of Preferred Stock | | 1,235,000 | | | | 1,235 | | | — | | | — | | | 6,062,447 | | | | — | | | | — | | | 6,063,682 | |
Issuance of Warrants for Acquisition | | — | | | | — | | | — | | | — | | | 27,354 | | | | — | | | | — | | | 27,354 | |
| | | | | | | | |
Balance, December 31, 2003 | | 2,414,168 | | | | 2,414 | | | 3,100,000 | | | 3,100 | | | 10,261,526 | | | | (7,873,760 | ) | | | — | | | 2,393,280 | |
| | | | | | | | |
Net Loss | | — | | | | — | | | — | | | — | | | — | | | | (2,680,148 | ) | | | — | | | (2,680,148 | ) |
| | | | | | | | |
Issuance of Preferred Stock | | 2,155,841 | | | | 2,156 | | | — | | | — | | | 11,799,207 | | | | — | | | | — | | | 11,801,363 | |
| | | | | | | | |
Balance, December 31, 2004 | | 4,570,009 | | | | 4,570 | | | 3,100,000 | | | 3,100 | | | 22,060,733 | | | | (10,553,908 | ) | | | — | | | 11,514,495 | |
| | | | | | | | |
Comprehensive income: | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Unrealized gain on investments | | — | | | | — | | | — | | | — | | | — | | | | — | | | | 38,553 | | | 38,553 | |
| | | | | | | | |
Net income | | — | | | | — | | | — | | | — | | | — | | | | 404,970 | | | | — | | | 404,970 | |
Total comprehensive income | | — | | | | — | | | — | | | — | | | — | | | | — | | | | — | | | 443,523 | |
| | | | | | | | |
Issuance of warrants for: | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Acquisition | | — | | | | — | | | — | | | — | | | 241,760 | | | | — | | | | — | | | 241,760 | |
Services | | — | | | | — | | | — | | | — | | | 966,000 | | | | — | | | | — | | | 966,000 | |
| | | | | | | | |
Issuance of Common Stock: | | — | | | | — | | | — | | | — | | | — | | | | — | | | | — | | | — | |
Public Offering | | — | | | | — | | | 4,600,000 | | | 4,600 | | | 53,549,001 | | | | — | | | | — | | | 53,553,601 | |
Conversion of Preferred to Common Stock | | (4,570,009 | ) | | | (4,570 | ) | | 4,794,897 | | | 4,795 | | | 1,337,822 | | | | — | | | | — | | | 1,338,047 | |
Exercise of options | | — | | | | — | | | 213,000 | | | 213 | | | 448,387 | | | | — | | | | — | | | 448,600 | |
Exercise of warrants | | — | | | | — | | | 248,485 | | | 248 | | | 694 | | | | — | | | | — | | | 942 | |
| | | | | | | | |
Additional cost for prior year issuance of preferred shares | | — | | | | — | | | — | | | — | | | (1,692 | ) | | | — | | | | — | | | (1,692 | ) |
| | | | | | | | |
Deemed Dividend | | — | | | | — | | | — | | | — | | | — | | | | (1,338,047 | ) | | | — | | | (1,338,047 | ) |
| | | | | | | | |
Tax benefit from exercise of employee stock options | | — | | | | — | | | — | | | — | | | 176,000 | | | | — | | | | — | | | 176,000 | |
| | | | | | | | |
Balance, December 31, 2005 | | — | | | $ | — | | | 12,956,382 | | $ | 12,956 | | $ | 78,778,705 | | | $ | (11,486,985 | ) | | $ | 38,553 | | $ | 67,343,229 | |
See accompanying notes to consolidated financial statements.
48
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
| | | | | | | | | | | | |
| | | 2005 | | | 2004 | | | 2003 | |
CASH FLOWS FROM OPERATING ACTIVITIES | | | | | | | | | | | | |
Net income (loss) | | $ | 404,970 | | | $ | (2,680,148 | ) | | $ | (2,954,168 | ) |
Adjustments to reconcile net income (loss) to net cash used in operating activities: | | | | | | | | | | | | |
Depreciation and amortization | | | 1,935,442 | | | | 716,981 | | | | 606,057 | |
Deferred rent | | | 7,483 | | | | 21,409 | | | | — | |
Gain on redemption of mandatory redeemable warrants | | | (316,744 | ) | | | — | | | | — | |
Non-cash interest expense | | | 966,000 | | | | — | | | | — | |
Amortization of debt discount on acquisition notes | | | 33,963 | | | | — | | | | — | |
Provision for doubtful accounts | | | 128,000 | | | | (140,711 | ) | | | 266,851 | |
Loss on sale of asset | | | — | | | | — | | | | 5,575 | |
Tax benefit realized from the exercise of employee stock options | | | 176,000 | | | | | | | | | |
Deferred taxes | | | 153,000 | | | | — | | | | — | |
Changes in operating assets and liabilities exclusive of acquisitions: | | | | | | | | | | | | |
Accounts receivable | | | (6,161,188 | ) | | | (1,463,397 | ) | | | (346,869 | ) |
Inventories | | | (810,018 | ) | | | 563,075 | | | | (404,292 | ) |
Prepaid expenses and other assets | | | (458,243 | ) | | | (491,413 | ) | | | (140,918 | ) |
Accounts payable and accrued expenses | | | 3,444,753 | | | | 1,078,083 | | | | 272,919 | |
| | | | | | | | | | | | |
Net cash used in operating activities: | | | (496,582 | ) | | | (2,396,121 | ) | | | (2,694,845 | ) |
| | | |
CASH FLOWS USED IN INVESTING ACTIVITIES: | | | | | | | | | | | | |
Purchase of property and equipment | | | (329,457 | ) | | | (138,208 | ) | | | (117,183 | ) |
Sale of property and equipment | | | — | | | | 27,500 | | | | — | |
Investment in short term securities | | | (22,962,000 | ) | | | — | | | | — | |
Payments for acquisition of Medicine Made Easy | | | — | | | | — | | | | (2,257,146 | ) |
Payments for acquisition of North American | | | (5,409,360 | ) | | | — | | | | — | |
Payments for acquisition of Specialty Pharmacy | | | (5,060,661 | ) | | | — | | | | — | |
Payments for investment in Oris Medical’s Assets | | | (1,396,316 | ) | | | — | | | | — | |
Payments for acquisition of PMW | | | (9,997,144 | ) | | | — | | | | — | |
Payments for acquisition of Priority | | | (6,918,313 | ) | | | — | | | | — | |
| | | | | | | | | | | | |
Net cash used in investing activities | | | (52,073,251 | ) | | | (110,708 | ) | | | (2,374,329 | ) |
| | | |
CASH FLOWS FROM FINANCING ACTIVITIES: | | | | | | | | | | | | |
Net proceeds from sale of Preferred Stock -Net of fees | | | 103,554 | | | | 11,607,449 | | | | 6,063,682 | |
Net proceeds from line of credit | | | 43,252,082 | | | | 33,590,405 | | | | 20,725,000 | |
Repayment of line of credit | | | (43,253,236 | ) | | | (33,589,251 | ) | | | (21,190,081 | ) |
Payment of deferred financing costs | | | — | | | | — | | | | (101,564 | ) |
Net Proceeds from IPO | | | 53,553,601 | | | | — | | | | — | |
Net Proceeds—Exercise of Employee Stock Options and Warrants | | | 449,542 | | | | — | | | | — | |
Notes Payable and Warrants from Acquisitions | | | (2,982,840 | ) | | | — | | | | — | |
Repayment of Notes & Capital Leases | | | (4,983,584 | ) | | | (2,762,934 | ) | | | — | |
Proceeds from Notes Payable | | | 3,500,000 | | | | — | | | | — | |
Follow-on offering costs | | | (203,879 | ) | | | — | | | | — | |
| | | | | | | | | | | | |
Net cash provided by financing activities | | | 49,435,240 | | | | 8,845,669 | | | | 5,497,037 | |
NET (DECREASE) INCREASE IN CASH AND CASH EQUIVALENTS | | | (3,134,593 | ) | | | 6,338,840 | | | | 427,863 | |
CASH AND CASH EQUIVALENTS, BEGINNING OF YEAR | | | 6,979,630 | | | | 640,790 | | | | 212,927 | |
| | | | | | | | | | | | |
CASH AND CASH EQUIVALENTS, END OF YEAR | | $ | 3,845,037 | | | $ | 6,979,630 | | | $ | 640,790 | |
| | | | | | | | | | | | |
SUPPLEMENTAL DISCLOSURE | | | | | | | | | | | | |
Income Taxes Paid | | $ | — | | | $ | 75,407 | | | $ | 15,666 | |
Interest Paid | | | 537,398 | | | | 225,830 | | | | 227,216 | |
Assets acquired by capital lease | | | — | | | | 165,623 | | | | — | |
See accompanying notes to consolidated financial statements.
49
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Note 1. The Company
Allion Healthcare, Inc., referred to as the Company, is the parent corporation of several subsidiaries, which operate under the MOMS Pharmacy name as one reportable segment. These subsidiaries are located in New York, California, Florida and Washington. In March 2005, the Company decided to cease operations in Texas and these operations have been reflected as a discontinued operation in the statements of operations. The Company is a national provider of specialty pharmacy and disease management services focused on HIV/AIDS patients. The Company sells HIV/AIDS medications, ancillary drugs and nutritional supplies under its trade name MOMS Pharmacy. Most of the Company’s patients rely on Medicaid and other state-administered programs, such as the AIDS Drug Assistance Program, or ADAP, to pay for their HIV/AIDS medications.
Note 2. Summary of Significant Accounting Policies
Basis Of Presentation. The consolidated financial statements include the accounts of the Company and all of its subsidiaries. All significant inter-company accounts and transactions have been eliminated in consolidation.
Inventories. Inventories consist entirely of pharmaceuticals available for sale. Inventories are recorded at lower of cost or market, cost being determined on a first-in, first-out (“FIFO”) basis.
Use Of Estimates By Management. The preparation of the Company’s financial statements, in conformity with generally accepted accounting principles, requires the Company’s management to make certain estimates and assumptions that affect the amounts reported in these financial statements and accompanying notes. Such estimates primarily relate to accounts receivable, intangibles and deferred tax valuation. Actual results could differ from those estimates.
Property and Equipment. Property and equipment is stated at cost and depreciated using the straight-line method over the estimated useful life. Machinery and equipment under capital leases is amortized over the life of the respective lease or useful lives of the asset, whichever is shorter.
Revenue Recognition. Net sales are recognized as medications or products are received by customers. A substantial portion of the Company’s net sales are billed to third-party payors, including insurance companies, managed care plans and governmental payors. Net sales are recorded net of contractual adjustments and related discounts. Contractual adjustments represent estimated differences between billed net sales and amounts expected to be realized from third-party payors under contractual agreements.
Income Taxes. The Company recognizes deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the financial statements or tax returns. Under this method, deferred tax assets and liabilities are determined based on the difference between the financial statement and tax basis of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to reverse. Valuation allowances are established when necessary to reduce deferred tax assets to the amount currently estimated to be realized.
Cash Equivalents. For purposes of the consolidated statement of cash flows, the Company considers all highly liquid debt instruments purchased with a maturity of three months or less to be cash equivalents.
Short Term Investments. Our short term investments consist of certificates of deposit and available for sale securities (principally auction rate securities) which are carried at fair value. Unrealized gains and losses are reported as accumulated comprehensive income in stockholders equity until realized.
50
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Credit Risk. Financial instruments that potentially subject the Company to concentrations of credit risk consist principally of cash and cash equivalents and trade receivables. The Company places its cash equivalents with financial institutions. The Company has substantially all of its cash and short-term investments with two financial institutions. Such cash balances, at times, may exceed FDIC limits. The Company has not experienced any losses in such accounts. The Company’s trade receivables represent a broad customer base. The Company routinely assesses the financial strengths of its customers. As a consequence, concentrations of credit risk are limited.
Net Loss Per Share Information. Basic earnings per share are computed using the weighted average number of common shares outstanding during the period. Diluted earnings per share are adjusted for the impact of common stock equivalent using the treasury stock method when the effect is dilutive. For the year ended December 31, 2005 the fully diluted shares outstanding using this method would have been 12,053,280. For the years ended December 31, 2005, 2004 and 2003 diluted loss per share does not include the impact of common stock options and warrants then outstanding of 2,602,737, 2,830,137 and 2,359,973, respectively, as the effect of their inclusion would be anti-dilutive. Preferred stock convertible to common stock of -0- and 4,570,009 shares were outstanding at December 31, 2005 and 2004 respectively.
Stock-Based Compensation Plans.The Company accounts for its stock option awards to employees under the intrinsic value based method of accounting prescribed by Accounting Principles Board Opinion No. 25, “Accounting for Stock Issued to Employees.” Under the intrinsic value based method, compensation cost is the excess, if any, of the fair market value of the stock at grant date or other measurement date over the amount an employee must pay to acquire the stock. The Company makes pro forma disclosures of net income and earnings per share as if the fair value based method of accounting had been applied as required by Statement of Financial Accounting Standards No. 123 (“SFAS 123”, “Accounting for Stock-Based Compensation” and SFAS No. 148, “Accounting for Stock-Based Compensation—Transition and Disclosure”). The Company has not granted options below fair market value on the date of grant. Had compensation expenses been determined as provided by SFAS No. 123 using the Black-Scholes option pricing model, the pro forma effect on the Company’s net income (loss) per share would have been the following for the years ended December 31, 2005, 2004 and 2003, respectively.
| | | | | | | | | | | | |
| | | YEAR ENDED | |
| | | December 31,
2005 | | | December 31,
2004 | | | December 31,
2003 | |
Net loss available to common shareholders, as reported | | $ | (933,077 | ) | | $ | (2,680,148 | ) | | $ | (2,954,168 | ) |
Deduct: Total stock-based employee compensation expense determined under fair value method used | | | (361,270 | ) | | | (441,485 | ) | | | (72,725 | ) |
| | | | | | | | | | | | |
Net loss available to common stockholders, pro forma | | $ | (1,294,347 | ) | | $ | (3,121,633 | ) | | $ | (3,026,893 | ) |
| | | | | | | | | | | | |
Net loss per share: Basic & diluted, as reported | | $ | (0.11 | ) | | $ | (0.86 | ) | | $ | (0.95 | ) |
| | | | | | | | | | | | |
Net loss per share: Basic and diluted, as pro forma | | $ | (0.16 | ) | | $ | (1.01 | ) | | $ | (0.98 | ) |
| | | | | | | | | | | | |
The fair value of each option grant is estimated on the date of the grant using the Black-Scholes option-pricing model. The following range of weighted-average assumptions were used for grants during the years ended December 31, 2005, 2004 and 2003.
| | | | | | |
| | | 2005 | | 2004 | | 2003 |
Dividend yield | | 0.00% | | 0.00% | | 0.00% |
Volatility | | 20.00% | | 1.00% | | 1.00% |
Risk-free interest rate | | 3.96% | | 4.40% | | 4.02% |
Expected life | | Eight Years | | Eight Years | | Eight Years |
51
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The weighted average grant date fair value of options granted during 2005, 2004 and 2003 were $4.43, $1.76 and $0.38 respectively.
The Black-Scholes option valuation model was developed for use in estimating the fair value of traded options, which have no vesting restrictions and are fully transferable. In addition, option valuation models require the input of highly subjective assumptions including the expected stock price volatility. Because the Company’s stock options have characteristics significantly different from those of traded options, and because changes in the subjective input assumptions can materially affect the fair value estimate, in management’s opinion the existing models do not necessarily provide a reliable single measure of the fair value of its stock options.
Allowance For Doubtful Accounts. Management regularly reviews the collectibility of accounts receivable by tracking collection and write-off activity. Estimated write-off percentages are then applied to each aging category by payor classification to determine the allowance for estimated uncollectible accounts. The allowance for estimated uncollectible accounts is adjusted as needed to reflect current collection, write-off and other trends, including changes in assessment of realizable value. While management believes the resulting net carrying amounts for accounts receivable are fairly stated at each quarter-end and that the Company has made adequate provisions for uncollectible accounts based on all information available, no assurance can be given as to the level of future provisions for uncollectible accounts, or how they will compare to the levels experienced in the past. The Company’s ability to successfully collect its accounts receivable depends, in part, on its ability to adequately supervise and train personnel in billing and collection, and minimize losses related to system changes.
Shipping And Handling Costs. Shipping and handling costs that are incurred are not included in cost of sales. These costs are included in selling, general and administrative expenses. Shipping and handling costs were approximately $1,715,000, $819,400, and $597,300 in 2005, 2004 and 2003 respectively, excluding our Texas operations. Shipping and handling costs are not billed to customers.
Long-Lived Assets. Amortization of intangible assets is provided using the straight-line method over the estimated useful lives of the assets. The carrying values of intangible and other long-lived assets are periodically reviewed to determine if any impairment indicators are present. If it is determined that such indicators are present and the review indicates that the assets will not be fully recoverable, based on undiscounted estimated cash flows over the remaining amortization and depreciation period, their carrying values are reduced to estimated fair value. Impairment indicators include, among other conditions, cash flow deficits, a historic or anticipated decline in net sales or operating profit, adverse legal or regulatory developments, accumulation of costs significantly in excess of amounts originally expected to acquire the asset and a material decrease in the fair market value of some or all of the assets. Assets are grouped at the lowest level for which there are identifiable cash flows that are largely independent of the cash flows generated by other asset groups. No such impairment existed at December 31, 2005.
Goodwill And Other Indefinite-Lived Intangible Assets: In accordance with Statement of Financial Accounting Standard (“FAS”) No. 141, “Business Combinations,” and No. 142, “Goodwill and Other Intangible Assets,” goodwill and intangible assets associated with the Company’s acquisitions that are deemed to have indefinite lives are no longer amortized but are subject to annual impairment tests. Such impairment tests require the comparison of the fair value and carrying value of reporting units. Measuring fair value of a reporting unit is generally based on valuation techniques using multiples of sales or earnings, unless supportable information is available for using a present value technique, such as estimates of future cash flows. The Company assesses the potential impairment of goodwill and other indefinite-lived intangible assets annually and on an interim basis whenever events or changes in circumstances indicate that the carrying value may not be recoverable. Some factors considered important which could trigger an interim impairment review include the following:
| | • | | Significant underperformance relative to expected historical or projected future operating results; |
52
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| | • | | Significant changes in the manner of our use of the acquired assets or the strategy for our overall business; and |
| | • | | Significant negative industry or economic trends. |
If it is determined through the impairment review process that goodwill has been impaired, an impairment charge would be recorded in the consolidated statement of operations. Based on the 2005 impairment review process, there was no impairment charge.
Advertising Costs. Advertising costs are expensed as incurred. Advertising costs in 2005, 2004 and 2003 were approximately $30,000, $78,000, and $131,000, respectively and were included in selling, general and administrative expenses.
Reclassifications. Certain prior years’ balances have been reclassified to conform with the current years’ presentation.
Note 3. Recent Accounting Pronouncements
FAS 123R—On December 16, 2004, the Financial Accounting Standards Board (FASB) issued SFAS No. 123(R), Share-Based Payment, which is a revision of SFAS No. 123, Accounting for Stock-Based Compensation. SFAS No. 123(R) supersedes Accounting Principals Board (APB) Opinion No. 25, Accounting for Stock Issued to Employees, and amends SFAS No. 95, Statement of Cash Flows. Generally, the approach in SFAS No. 123(R) is similar to the approach described in SFAS No. 123. However, SFAS 123(R) requires all share-based payments to employees, including grants of employee stock options, to be recognized in the income statement based on their fair values. Pro forma disclosure is no longer an alternative. SFAS No. 123(R) permits public companies to adopt its requirements using one of two methods:
| | • | | “modified prospective” method in which compensation cost is recognized beginning with the effective date (a) based on the requirements of Statement 123(R) for all share-based payments granted after the effective date and (b) based on the requirements of SFAS No. 123 for all awards granted to employees prior to the effective date of statement 123(R) that remain unvested on the effective date. |
| | • | | “modified retrospective” method which includes the requirements of the modified prospective method described above, but also permits entities to restate based on the amounts previously recognized under SFAS No. 123 for purposes of pro forma disclosures either (a) all prior periods presented or (b) prior interim periods of the year of adoption. |
SFAS No. 123(R) must be adopted in the first annual period beginning after June 15, 2005, which in our case would be the quarterly period beginning January 1, 2006. Early adoption will be permitted in periods in which financial statements have not yet been issued. We will adopt Statement 123(R) on January 1, 2006.
As permitted by SFAS No. 123, we currently account for share-based payments to employees using the intrinsic value method prescribed in APB Opinion No. 25. Accordingly, the adoption of SFAS No. 123(R)’s fair value method may have a significant impact on our results of operations, although it will have no impact on our overall financial position. The impact of adoption of SFAS No. 123(R) cannot be predicted at this time because it will depend on levels of share-based payments granted in the future and on required changes in the method of computation of fair value. However, had we adopted SFAS No. 123(R) in prior periods, the impact of that standard would have approximated the impact of SFAS No. 123 as described in our disclosure of pro forma net income and earnings per share in Note 2 to our consolidated financial statements.
53
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 4. Discontinued Operations
In March 2005 the Company decided to cease its operations in Texas and completed the process in June 2005. In accordance with the provisions of Statement of Financial Accounting Standard, Accounting for the Impairment or Disposal of Long-Lived Assets (“SFAS No. 144”), the results of operations for the Company’s Texas operations have been classified as discontinued operations for all periods presented in the accompanying consolidated statements of operations. The Texas results for those periods are below.
| | | | | | | | | | | | |
| | | Year Ended December 31, | |
| | | 2005 | | | 2004 | | | 2003 | |
Revenue | | $ | 1,512,125 | | | $ | 4,525,719 | | | $ | 5,720,436 | |
Net loss | | $ | (36,125 | ) | | $ | (130,020 | ) | | $ | (258,124 | ) |
Note 5. Acquisitions
On January 4, 2005, MOMS Pharmacy, Inc., a California corporation and wholly-owned subsidiary of Allion Healthcare Inc., a Delaware corporation, entered into a stock purchase agreement with Michael Stone and Jonathan Spanier, who owned 100% of the stock of North American Home Health Supply, Inc. (“NAHH”), a California corporation. NAHH is engaged primarily in the pharmacy business in California. On the same day, MOMS Pharmacy acquired 100% of the stock of NAHH from Messrs. Stone and Spanier, in accordance with the terms of a stock purchase agreement.
In accordance with the terms of the Stock Purchase Agreement, on January 4, 2005 MOMS Pharmacy acquired 100% of the stock of NAHH in exchange for payment by Allion of the following consideration:
| | • | | $5,671,016 of cash paid, including $473,999 of direct acquisition costs (less cash acquired of $88,808); |
| | • | | promissory notes of MOMS Pharmacy, due January 1, 2006, in the aggregate principal amount of $675,000; |
| | • | | promissory notes of MOMS Pharmacy, due January 1, 2007, in the aggregate principal amount of $700,000; and |
| | • | | warrants issued by Allion to purchase an aggregate of 150,000 shares of Allion common stock, at an exercise price of $6.26 per share. |
The notes accrue interest at a rate of 2.78% per year. Allion unconditionally guaranteed the payment of the promissory notes by its MOMS Pharmacy subsidiary, pursuant to a guaranty, dated January 4, 2005, in favor of Messrs. Stone and Spanier. Under the guaranty, Allion is absolutely, irrevocably and unconditionally liable for the performance of each and every obligation of MOMS Pharmacy under the promissory notes.
The purchase price is subject to a post-closing adjustment based on the amount of NAHH’s working capital as of the closing date as well as cash collected from March 31, 2005 through December 31, 2005 in respect to accounts receivable as of the closing date. Through December 31, 2005, Allion has paid an additional $141,997 to Messrs. Stone and Spanier. The purchase price also is subject to reduction for changes in the Medi-Cal rules and regulations at any time after the closing date, which result in reduced reimbursement payments to North American for any enteral or nutritional products it sold in 2004. Any purchase price reduction due to changes in the Medi-Cal rules and regulations will be payable solely by offset against the outstanding principal amounts of the promissory notes issued in the transaction.
On February 28, 2005, MOMS Pharmacy, Inc., a California corporation and wholly-owned subsidiary of Allion Healthcare Inc., a Delaware corporation, entered into a stock purchase agreement with the owners (the
54
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
“Specialty Sellers”) of 100% of the stock of Specialty Pharmacies, Inc., a Washington corporation (“Specialty” or “SPI”). Specialty is engaged primarily in the business of providing HIV/AIDS pharmacy services in Washington and California. On the same day, MOMS Pharmacy acquired 100% of the stock of Specialty from the Specialty Sellers, in accordance with the terms of a stock purchase agreement.
Pursuant to the terms of the Stock Purchase Agreement, MOMS Pharmacy acquired 100% of the stock of Specialty for the following combination of cash and securities:
| | • | | $5,496,546 of cash paid, including $496,546 of direct acquisition costs; |
| | • | | promissory notes of MOMS Pharmacy, due February 28, 2006, in the aggregate principal amount of $1,900,000; and |
| | • | | warrants issued by Allion to purchase an aggregate of 351,438 shares of Allion common stock, at an exercise price of $6.26 per share. |
Allion unconditionally guaranteed the payment of the promissory notes issued to the Specialty Sellers by its MOMS Pharmacy subsidiary, pursuant to a guaranty, dated February 28, 2005, in favor of the Specialty Sellers. Under the guaranty, Allion is absolutely, irrevocably and unconditionally liable for the performance of the obligations of MOMS Pharmacy under the promissory notes. The promissory notes accrue interest at the prime rate plus 2% per annum. At the closing of Allion’s initial public offering the notes were paid-off.
The warrants have a fair market value of $1,898,215 and were recorded as a liability because the warrants were mandatorily redeemable upon the passage of time or upon a qualifying initial public offering. Allion paid $1,581,471 with proceeds from the IPO to repurchase 175,719 of the warrants issued to the Specialty Sellers and recognized a $316,744 gain that was recorded as other income. The purchase price is subject to a post-closing adjustment based on the amount of Specialty’s working capital as of the closing, which resulted in a $498,631 reduction in the purchase price. MOMS Pharmacy agreed to reimburse Specialty Sellers up to a maximum of $200,000, for any amounts received by Specialty from Medi-Cal relating to the California Pilot Program for prescriptions filled between September 1, 2004 and December 31, 2004.
On February 28, 2005, MOMS Pharmacy also acquired from Michael Tubb, pursuant to a Purchase Agreement signed on the same day, all rights he has to acquire capital stock of Specialty. Under the agreement, MOMS Pharmacy paid $1,200,000 to Mr. Tubb, consisting of $600,000 cash and a $600,000 one-year promissory note due February 28, 2006 and March 31, 2006. The contingent consideration of the $600,000 promissory note is treated as non-recurring compensation based on his continued employment for one year post acquisition. The Company is accruing $50,000 per month as compensation expense over the twelve month period of the agreement. This note accrues interest at a rate equal to the lowest applicable federal rate. These payments are expressly conditioned on (i) the fulfillment of the non-solicitation and non-competition provisions of the purchase agreement between MOMS Pharmacy and Mr. Tubb, and (ii) Mr. Tubb’s continued employment with Specialty and his use of best efforts, time and attention to and on behalf of Specialty.
On August 5, 2005, Medicine Made Easy, a California corporation and wholly-owned subsidiary of the Company, purchased certain assets of Frontier Pharmacy & Nutrition, Inc. d/b/a PMW Pharmacy (“PMW”), a California-based specialty pharmacy focused on HIV/AIDS pharmacy services in the Long Beach, California area. Under the terms of the asset purchase agreement between the Company and PMW, the Company acquired selected assets, including PMW’s customer list of HIV/AIDS patients and inventory, for the following:
| | • | | $8,875,379 of cash paid at closing, including $145,379 of direct acquisition costs; |
| | • | | $970,000 escrow payment paid 90 days after closing; and |
| | • | | $151,765 cash paid for inventories. |
55
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
On December 9, 2005, Medicine Made Easy, a California corporation and wholly-owned subsidiary of the Company, purchased certain assets of Priority Pharmacy, Inc. (“Priority”), a California-based specialty pharmacy focused on HIV/AIDS pharmacy services in the San Diego, California area. Under the terms of the asset purchase agreement between the Company and Priority, the Company acquired selected assets, including Priority’s customer list of HIV/AIDS patients and inventory, for the following:
| | • | | $6,539,121 of cash paid at closing, including $39,121 of direct acquisition costs; |
| | • | | $1,100,000 additional payment due in 3 equal payments monthly after closing; and |
| | • | | $379,192 cash paid for inventories. |
The results of operations from the acquisitions are included in Allion’s consolidated operating results as of the date the companies were acquired.
The goodwill recorded as the result of the NAHH acquisition will not be deductible for tax purposes. The goodwill recorded as the result of the Specialty, PMW and Priority acquisitions is expected to be deductible for tax purposes.
56
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The following tables describe the allocation of purchase price for these four acquisitions:
| | | | |
Purchase Price Paid for Specialty | | | | |
Cash paid | | $ | 5,000,000 | |
Notes Payable | | | 1,401,369 | |
Fair value of warrants issued | | | 1,898,215 | |
Direct acquisition costs | | | 496,546 | |
| | | | |
Total Purchase Price | | | 8,796,130 | |
plus: net liabilities | | | 415,149 | |
| | | | |
| | $ | 9,211,279 | |
| | | | |
Allocation of Purchase Price for Specialty | | | | |
Covenant Not to Compete (5 year life) | | $ | 75,000 | |
Covenant Not to Compete (3 year life) | | | 222,672 | |
Referral Lists (15 year life) | | | 4,153,386 | |
Workforce (part of goodwill) | | | 400,190 | |
Goodwill | | | 4,360,031 | |
| | | | |
| | $ | 9,211,279 | |
| | | | |
Purchase Price Paid for NAHH | | | | |
Cash paid | | $ | 5,141,996 | |
Notes Payable | | | 1,375,000 | |
Fair value of warrants issued | | | 241,760 | |
Direct acquisition costs | | | 473,999 | |
| | | | |
Total Purchase Price | | | 7,232,755 | |
less: net tangible assets | | | (243,630 | ) |
debt discount | | | (51,253 | ) |
| | | | |
| | $ | 6,937,872 | |
| | | | |
Allocation of Purchase Price for NAHH | | | | |
Covenant Not to Compete (5 year life) | | $ | 50,000 | |
Referral Lists (13 year life) | | | 4,514,331 | |
Goodwill | | | 2,373,541 | |
| | | | |
| | $ | 6,937,872 | |
| | | | |
Purchase Price Paid for PMW | | | | |
Cash Paid at closing | | $ | 8,730,000 | |
Escrow payment paid | | | 970,000 | |
Inventories | | | 151,765 | |
Direct acquisition costs | | | 300,000 | |
| | | | |
Total purchase price | | | 10,151,765 | |
less: net tangible assets | | | (151,765 | ) |
| | | | |
| | $ | 10,000,000 | |
| | | | |
Allocation of Purchase Price for PMW | | | | |
Referral list (15 year life) | | $ | 5,819,174 | |
Non compete—participating owner (3 year life) | | | 851,822 | |
Non compete—non-participating owner (3 year life) | | | 25,000 | |
Workforce (part of goodwill) | | | 110,350 | |
Goodwill | | | 3,193,654 | |
| | | | |
| | $ | 10,000,000 | |
| | | | |
57
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| | | | |
Purchase Price Paid for Priority | | | | |
Cash Paid | | $ | 6,500,000 | |
Additional payments due | | | 1,100,001 | |
Inventories | | | 379,192 | |
Direct acquisition costs | | | 250,000 | |
| | | | |
Total purchase price | | | 8,229,193 | |
less: net tangible assets | | | (379,192 | ) |
| | | | |
| | $ | 7,850,001 | |
| | | | |
Allocation of Purchase Price for Priority | | | | |
Referral list (15 year life) | | $ | 2,577,240 | |
Non compete—active owner (5 year life) | | | 418,561 | |
Non compete—inactive owner (5 year life) | | | 25,000 | |
Workforce (part of goodwill) | | | 118,661 | |
Goodwill | | | 4,710,539 | |
| | | | |
| | $ | 7,850,001 | |
| | | | |
The following pro forma results were developed assuming the acquisition of NAHH, Specialty, PMW and Priority occurred January 1, 2003. The pro forma results do not purport to represent what our results of operations actually would have been if the transactions set forth above had occurred on the date indicated or what our results of operations will be in future periods.
| | | | | | | | | | | |
| | | Year Ended December 31, | |
| | | 2005 | | | 2004 | | 2003 | |
Revenue | | $ | 160,403,708 | | | $ | 145,415,621 | | $ | 111,404,110 | |
Net income (loss) available to common stockholders | | $ | (818,491 | ) | | $ | 316,450 | | $ | (2,299,782 | ) |
Earning per common share: | | | | | | | | | | | |
Basic | | $ | (0.10 | ) | | $ | 0.10 | | $ | (0.74 | ) |
Diluted | | $ | (0.10 | ) | | $ | 0.05 | | $ | (0.74 | ) |
On June 30, 2005, Oris Health, Inc, a newly-formed California corporation and wholly-owned subsidiary of the Company, acquired, pursuant to an asset purchase agreement dated May 19, 2005, all right, title and interest in and to certain intellectual property and other assets owned, leased or held for use by Oris Medical System, Inc. (“Oris”) a development stage company incorporated in Washington, including an assignment of Oris’ license to use Ground Zero Software, Inc.’s computer software program knownas LabTracker—HIV™, and Oris System, an electronic prescription writing system. At the closing of the acquisition, Oris and Ground Zero were paid $850,000 and $150,000, respectively, in cash. In addition, pursuant to the terms of an earn-out formula set forth in the asset purchase agreement, Oris and Ground Zero may receive up to an additional $40,000,000 in the aggregate, paid on a quarterly basis, based on the net number of HIV patients of physician customers utilizing theLabTracker—HIV™ software or the Oris System to fill their prescriptions at MOMS Pharmacy, Inc. (“MOMS Pharmacy”) or an affiliate of MOMS Pharmacy. As of December 31, 2005 Allion had 297 patients on service from Oris/Lab Tracker. During the fourth quarter of 2005 we accrued and subsequently paid $123,000 for 123 new Oris/Lab Tracker patients. Oris’ and Ground Zero’s rights to these additional payments terminate 40 months after the closing of the acquisition and, under certain circumstances set forth in the asset purchase agreement, portions of these additional payments may be made in stock of the Company. Earn-out payments are recorded quarterly as earned. Payments made to Oris for the patients from existing clinics will be allocated to the clinic list and amortized over a fixed 15 year period beginning from when Oris was acquired, and from new clinics, will be expensed. Payments made to Ground Zero for patients from both new and existing clinics will be allocated to the exclusiveLabTracker license agreement and will be amortized over its remaining life. Oris does not qualify as a business so the transaction was accounted for as the acquisition of certain assets and liabilities of Oris.
58
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| | | | |
Purchase Price Paid for Oris’ Intangible Assets | | | | |
Cash paid | | $ | 1,000,000 | |
Earn out obligation | | | 168,000 | |
Operating expenses paid to seller | | | 250,000 | |
Employee severance payments | | | 72,520 | |
Direct acquisition costs | | | 41,156 | |
| | | | |
Total Purchase Price | | | 1,531,676 | |
less: net tangible assets | | $ | (29,000 | ) |
| | | | |
| | $ | 1,502,676 | |
| | | | |
| |
Allocation of Purchase Price for Oris’ Intangible Assets | | | | |
License agreement—LabTracker—exclusive rights (40 month life) | | $ | 1,084,005 | |
Clinic List (15 year life—from date of purchase) | | | 132,550 | |
Computer software (3 year life) | | | 86,121 | |
Non compete (40 month life) | | | 200,000 | |
| | | | |
| | $ | 1,502,676 | |
| | | | |
Note 6. Short-Term Investments
Investment in short term securities include certificates of deposit and available for sale securities, which are carried at fair value. The gross unrealized gain at December 31, 2005 is $38,553 and is recorded as a component of accumulated other comprehensive income. All of these investments mature within 12 months and consist of the following at December 31, 2005:
| | | |
Certificates of Deposit | | $ | 1,512,000 |
Auction Rate Securities | | | 21,488,553 |
| | | |
Total | | $ | 23,000,553 |
Note 7. Initial Public Offering
On June 22, 2005, the Company completed an initial public offering of its common stock. The Company sold 4,000,000 shares of its common stock at a price of $13.00 per share. In addition, the Company granted the underwriters an option, exercisable until July 21, 2005, to purchase up to an additional 600,000 shares at the initial public offering price. On July 8, 2005, the underwriters exercised their over-allotment option to purchase 600,000 shares of common stock at $13.00 per share, less an underwriting discount and commission of $0.91 per share. The Company used the proceeds from its initial public offering to repay approximately $12,000,000 of its debt on June 27, 2005. The Company received proceeds net of underwriters discount and commission of $48,360,000 from the initial public offering and $7,254,000 from the exercise of the over-allotment option, less costs incurred of $2,060,000.
59
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 8. Intangible Assets
Intangible assets as of December 31, 2005 and 2004 are as follows:
| | | | | | | | | | | | | | | | |
| | | Weighted
Average
Amortization
Period | | December 31, | |
| | | | 2005 | | | 2004 | |
| | | | Cost | | Accumulated
Amortization | | | Cost | | Accumulated
Amortization | |
Intangibles | | | | | | | | | | | | | | | | |
California License | | Perpetual | | $ | 478,616 | | $ | — | | | $ | 478,616 | | $ | — | |
Customer lists | | 60 Months | | | 2,155,256 | | | (1,480,442 | ) | | | 2,030,745 | | | (978,831 | ) |
Referral List | | 171 Months | | | 17,286,803 | | | (762,354 | ) | | | — | | | — | |
Non-Compete Covenant | | 43 Months | | | 1,792,390 | | | (308,650 | ) | | | 147,007 | | | (81,671 | ) |
Software | | 42 Months | | | 136,121 | | | (41,022 | ) | | | 50,000 | | | (16,667 | ) |
Lab tracker License | | 40 Months | | | 1,084,005 | | | (160,877 | ) | | | — | | | — | |
Clinic List | | 180 Months | | | 132,550 | | | (2,780 | ) | | | — | | | — | |
Other | | 60 Months | | | 45,000 | | | (39,750 | ) | | | 45,000 | | | (30,750 | ) |
| | | | | | | | | | | | | | | | |
Total | | 110 Months | | $ | 23,110,741 | | $ | (2,795,875 | ) | | $ | 2,751,368 | | $ | (1,107,919 | ) |
| | | | | | | | | | | | | | | | |
Amortization of intangible assets for the years ended December 31, 2005, 2004 and 2003 was approximately $1,613,000, $474,000 and $377,000, respectively. The estimated annual amortization expense, based on current intangible balances, for the next five fiscal years beginning January 1, 2006 is as follows:
| | | |
Years | | Amount |
2006 | | $ | 2,428,751 |
2007 | | $ | 2,292,727 |
2008 | | $ | 1,860,036 |
2009 | | $ | 1,260,262 |
2010 | | $ | 1,231,073 |
Note 9. Property and Equipment
| | | | | | | | |
| | | Useful
Lives in
Years | | December 31, |
| | | | 2005 | | 2004 |
Machinery and equipment under capital lease obligations | | 4 | | $ | 530,623 | | $ | 530,623 |
Machinery and equipment | | 3-5 | | | 685,679 | | | 345,607 |
Leasehold Improvements | | 1-5.5 | | | 162,316 | | | 191,535 |
Furniture and fixtures | | 3-7 | | | 122,754 | | | 38,333 |
| | | | | | | | |
| | | | | 1,501,372 | | | 1,106,098 |
| | | |
Less: accumulated depreciation and amortization | | | | | 829,976 | | | 544,366 |
| | | | | | | | |
| | | | $ | 671,396 | | $ | 561,732 |
| | | | | | | | |
Depreciation and amortization expense relating to property and equipment for the years ended December 31, 2005, 2004 and 2003 was approximately $322,000, $243,000 and $229,000 respectively.
60
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 10. Revolving Credit Line
The Company has an available short-term revolving credit facility for up to $6.0 million. At December 31, 2005, the Company’s borrowing capacity was approximately $6.0 million, there were no outstanding borrowings. This credit facility expires on April 21, 2006. Borrowings under the facility are based on the Company’s accounts receivable, bear interest at Prime + 2% and are collateralized by a perfected and primary security interest in all of the Company’s assets, accounts receivable, trademarks, licenses and values of any kind of the Company. The prime rate at December 31, 2005 was 7.25%. In connection with this credit line, the Company must comply with certain financial covenants. As of December 31, 2005, the Company was in compliance with its covenants under its revolving credit-facility.
Note 11. Issuance of Subordinated Notes
In May 2005, the Company completed a private placement with an institutional accredited investor pursuant to which the Company issued warrants to purchase 40,000 shares of common stock of the Company and issued subordinated notes in an amount equal to $2,000,000. The warrants expire in five years and have an exercise price of $13.00 per share. The notes and accrued interest were repaid with the proceeds of the Company’s initial public offering in June 2005. The Company paid placement agent fees and legal expenses of $176,000 and recorded $213,000 related to the value of the warrants in connection with the offering. These fees were recognized as interest expense in June 2005 when the notes were repaid.
Note 12. Notes Payable
As part of the acquisition of NAHH, the Company issued two notes. One note for $675,000 was paid on January 2, 2006. The second note for $700,000 is due on January 1, 2007. The notes accrue interest at an imputed rate of 5.25% per year. The unamortized discount as of December 31, 2005 was $17,290. The discount amortization reported as interest in 2005 was $33,963. Allion unconditionally guaranteed the payment of the promissory notes by its MOMS Pharmacy subsidiary, pursuant to a guaranty, dated January 4, 2005, in favor of Messrs. Stone and Spanier. Under the guaranty, Allion is absolutely, irrevocably and unconditionally liable for the performance of each and every obligation of MOMS Pharmacy under the promissory notes.
As part of the acquisition of Specialty, the Company issued promissory notes for $1,900,000. Allion unconditionally guaranteed the payment of the promissory notes issued to the former owners of Specialty by its MOMS Pharmacy subsidiary, pursuant to a guaranty, dated February 28, 2005, in favor of the former owners of Specialty. Under the guaranty, Allion is absolutely, irrevocably and unconditionally liable for the performance of the obligations of MOMS Pharmacy under the promissory notes. The promissory notes accrue interest at the prime rate plus 2% per annum. At the closing of the initial public offering the notes were paid-off.
As part of the acquisition of MME, the Company issued two notes. One note for $1,150,000 was paid on May 1, 2004. The second note for $1,250,000 was paid May 1, 2005. These notes accrued interest at Prime Rate plus 2% per annum. The Prime Rate as of December 31, 2004 and 2003 was 5.25% and 4.00%, respectively. These notes payable are secured by cash, cash equivalents, accounts receivable, inventory, fixed and other assets of the Company, and are subordinated to the Company’s senior debt.
61
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 13. Income Taxes
A reconciliation of the income tax expense (benefit) computed at the statutory Federal income tax rate to the reported amount follows:
| | | | | | | | | | | | |
| | | Year Ended December 31, | |
| | | 2005 | | | 2004 | | | 2003 | |
Federal statutory rate: | | | 34 | % | | | 34 | % | | | 34 | % |
Tax expense (benefit) at Federal statutory rates | | $ | 249,550 | | | $ | (885,342 | ) | | $ | (997,737 | ) |
Change in valuation allowance | | | (211,595 | ) | | | 938,894 | | | | 1,093,502 | |
Permanent differences | | | 214,485 | | | | 113,191 | | | | 77,833 | |
State income taxes | | | 76,560 | | | | (90,541 | ) | | | (153,952 | ) |
| | | | | | | | | | | | |
| | $ | 329,000 | | | $ | 76,202 | | | $ | 19,646 | |
At December 31, 2005, the Company had net operating loss carry forwards for tax purposes of approximately $8,758,000 expiring at various dates from 2006 through 2025.
Deferred tax assets (liabilities) comprise of the following:
| | | | | | | | |
| | | December 31, | |
| | | 2005 | | | 2004 | |
Deferred tax assets: | | | | | | | | |
Allowance for doubtful accounts | | $ | 99,000 | | | $ | 119,000 | |
Tax carry forwards | | | 3,508,000 | | | | 3,506,000 | |
Intangibles (tax basis difference) | | | 514,000 | | | | 165,000 | |
Non deductible accruals | | | 83,000 | | | | 18,000 | |
Inventory | | | 140,000 | | | | 19,000 | |
Warrants | | | 362,000 | | | | — | |
Book/Tax Depreciation Differences | | | (20,000 | ) | | | (25,000 | ) |
Investments | | | (15,000 | ) | | | — | |
| | | | | | | | |
Total deferred tax assets, net | | | 4,671,000 | | | | 3,802,000 | |
Valuation allowance | | | (4,671,000 | ) | | | (3,802,000 | ) |
| | | | | | | | |
| | $ | — | | | $ | — | |
Deferred tax liabilities: | | | | | | | | |
Deductible goodwill | | | (153,000 | ) | | | — | |
| | | | | | | | |
Total deferred tax liability | | $ | (153,000 | ) | | $ | — | |
| | | | | | | | |
The change in the valuation allowance per the above deferred tax schedule does not agree to the change in the valuation allowance per the reconciliation of income tax expense due to the fact that certain items, primarily warrant and option exercises, did not affect the Company’s pre-tax operating results.
Deferred tax assets related to net operating loss carry-forwards have been fully reserved by a valuation allowance. Pursuant to Section 382 of the Internal Revenue Code of 1986, as amended, future ownership changes and other limitations may apply to the utilization of this asset.
62
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The provisions for income taxes for the year ended December 31, 2005 consist of the following:
| | | |
Federal: | | | |
Current | | | 60,000 |
Deferred | | | 130,000 |
State: | | | |
Current: | | | 116,000 |
Deferred | | | 23,000 |
| | | |
Total | | $ | 329,000 |
| | | |
Note 14. Lease Commitments
The Company leases commercial as follows:
| | | | |
Location | | Principal Use | | Property Interest |
Melville, NY | | Pharmacy and Executive Offices | | Leased—expiring August 31, 2009 |
Gardena, CA | | Pharmacy | | Leased—expiring March 31, 2011 |
Van Nuys, CA | | Pharmacy | | Leased—expiring December 31, 2006 |
Miami, FL | | Pharmacy | | Leased—expiring November 30, 2008 |
La Jolla, CA | | Billing Center | | Leased—expiring July 1, 2008 |
San Francisco, CA | | Pharmacy | | Leased—expiring March 31, 2008 |
San Francisco, CA | | Pharmacy | | Leased—expiring February 28, 2007 |
San Diego, CA | | Administration (Oris) | | Leased—expiring June 30, 2008 |
San Diego, CA | | Pharmacy | | Leased—expiring January 31, 2009 |
Seattle, WA | | Pharmacy | | Leased—expiring May 31, 2006 |
At December 31, 2005, the Company’s lease commitments provide for the following minimum annual rentals.
| | | |
Year | | Minimum
Rent |
2006 | | $ | 594,195 |
2007 | | $ | 570,466 |
2008 | | $ | 505,744 |
2009 | | $ | 271,875 |
2010 | | $ | 163,509 |
2011 | | $ | 41,059 |
During the years ended December 31, 2005, 2004 and 2003, rental expense approximated to $573,459, $413,606 and $261,700 respectively.
Note 15. Contingencies—Legal Proceedings
New York Medicaid Audit. In May 2004, the Company was notified that MOMS Pharmacy, the Company’s New York wholly owned subsidiary, was the subject of an audit and review being conducted by the New York State Department of Health. As part of the audit, the Department of Health withheld payment of Medicaid claims to the Company but ceased withholding payments in December 2004. The Department returned the amount it withheld from the Company in the second quarter of 2005. The Company settled this audit in July 2005 for approximately $118,836 and the Company does not believe it has any continuing liability.
63
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
In addition to the matters noted above, the Company is involved from time to time in legal actions arising in the ordinary course of our business. The Company does not currently have any pending or threatened litigation that it believes will result in an outcome that would materially adversely affect the business. Nevertheless, there can be no assurance that future litigation, to which the company may become a party, will not have a material adverse effect on the business.
Note 16. Concentrations of Credit Risk And Major Customers
The Company provides prescription medications to its customers in the United States. Credit losses relating to customers historically have been minimal and within management’s expectations.
Federal and state third-party reimbursement programs represented approximately 87%, 88% and 87% of total sales for the years ended December 31, 2005, 2004 and 2003. At December 31, 2005 and 2004, the Company had an aggregate outstanding receivable from federal and state agencies of approximately $11,736,073 and $4,200,000, respectively. The increase was from the acquisitions and revenue accrued for the premium reimbursement payments from New York and California not yet paid.
Note 17. Capital Lease Obligation
Future minimum commitments under non-cancelable capital leases are as follows:
| | | | |
Leases | | Capital | |
2006 | | $ | 120,630 | |
2007 | | | 52,524 | |
2008 | | | 49,620 | |
| | | | |
Total minimum lease payments | | | 222,774 | |
Amounts representing interest | | | (22,577 | ) |
| | | | |
Present value of net minimum lease
payments (including current portion of $107,379) | | $ | 200,197 | |
| | | | |
Note 18. Stockholder’s Equity
A. Common shares reserved
Common shares reserved at December 31, 2005, are as follows:
| | |
Stock Option Plans | | 1,452,000 |
Warrants | | 1,150,737 |
B. Stock Options
Under the terms of the Company’s Stock Option Plans, the Board of Directors may grant incentive and nonqualified stock options to employees, officers, directors, agents, consultants and independent contractors of the Company. In connection with the 2002 and 1998 Stock Option Plans, 2,750,000 shares of common stock were reserved for issuance. The Company grants stock options with exercise prices equal to the fair market value of the common stock on the date of the grant, as determined by the Board of Directors. Options generally vest over a two to five year period and expire ten years from the date of the grant.
64
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
A summary of the status of the Company’s stock option plans as of December 31, 2005, 2004, 2003 and changes during the years then ended is presented below:
| | | | | | | | | | | | | | | | | | |
| | | 2005 | | 2004 | | 2003 |
Stock Options | | Shares | | | Weighted
Average
Exercise
Price | | Shares | | | Weighted
Average
Exercise
Price | | Shares | | | Weighted
Average
Exercise
Price |
Outstanding, beginning of year | | 1,682,750 | | | $ | 3.06 | | 1,365,200 | | | $ | 1.80 | | 1,341,700 | | | $ | 1.61 |
Granted | | 10,000 | | | | 13.00 | | 604,250 | | | | 6.02 | | 50,000 | | | | 5.00 |
Exercised | | (213,000 | ) | | | 2.11 | | — | | | | — | | — | | | | — |
Cancelled | | (27,750 | ) | | | 5.91 | | (286,700 | ) | | | 3.09 | | (26,500 | ) | | | 2.91 |
| | | | | | | | | | | | | | | | | | |
Outstanding, end of year | | 1,452,000 | | | $ | 3.21 | | 1,682,750 | | | $ | 3.06 | | 1,365,200 | | | $ | 1.80 |
Options exercisable at year end | | 1,110,195 | | | $ | 2.29 | | 1,133,758 | | | $ | 1.75 | | 1,001,268 | | | | 1.20 |
| | | | | | |
Weighted average fair value of options under the plan granted during the year | | | | | $ | 4.43 | | | | | $ | 1.76 | | | | | $ | 0.38 |
| | | | | | | | | | | | | | | | | | |
The following table summarizes information about stock options outstanding at December 31, 2005:
| | | | | | | | | | | | |
| | | Options Outstanding | | Options Exercisable |
Range of Exercise Price | | Number of
Outstanding | | Weighted
Average
Remaining
Contractual
Life | | Weighted
Average
Exercise
Price | | Number
Outstanding | | Weighted
Average
Exercise
Price |
$.17 - $.66 | | 500,000 | | 3.09 | | $ | .18 | | 500,000 | | $ | .18 |
$1.00 - $2.00 | | 154,000 | | 4.50 | | $ | 1.34 | | 154,000 | | $ | 1.34 |
$3.00 | | 4,000 | | 5.96 | | $ | 3.00 | | 4,000 | | $ | 3.00 |
$3.50 | | 175,000 | | 6.50 | | $ | 3.50 | | 175,000 | | $ | 3.50 |
$5.00 | | 50,000 | | 7.76 | | $ | 5.00 | | 41,667 | | $ | 5.00 |
$6.00 - 6.26 | | 559,000 | | 8.42 | | $ | 6.02 | | 235,528 | | $ | 6.01 |
$13.00 | | 10,000 | | 9.09 | | $ | 13.00 | | — | | $ | — |
| | 1,452,000 | | | | | | | 1,110,195 | | | |
C. Warrants
In January 2000, the Company issued 375,000 common stock warrants to a director of the Company, which have an exercise price of $1.00 per share. The warrants were issued as consideration for guarantying the Company’s facility with West Bank. These warrants expire ten years from the date of grant.
On May 1, 2003, the Company issued warrants to the previous owners of Medicine Made Easy. These warrants can be exercised to purchase 227,273 shares of the Company’s common stock for $11.00 a share and expire in May 2008. The fair value of the warrants was $27,354, and was included in the purchase price of MME.
In July 2003, the Company issued 125,000 warrants, which have an exercise price of $5.00 per share, to a director of the Company in connection with the extension of the guarantee for the West Bank credit facility. These warrants expire ten years from the date of grant.
In April and May 2004, the Company issued warrants to purchase 114,493 shares of common stock with an exercise price of $6.00 per share to the placement agents in conjunction with the Company’s Series D private placement. These warrants expire 5 years from the date of issue.
65
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
In December 2004 the Company issued warrants to purchase 53,121 shares of common stock, which have an exercise price of $6.25, in conjunction with the Company’s Series E convertible preferred stock to the placement agent. These warrants expire 5 years from the date of issue.
In January 2005 as part of a new acquisition the Company issued warrants to purchase 150,000 common shares, which have an exercise price of $6.26. These warrants expire five years from the date of issuance.
On February 28, 2005, pursuant to the terms of the stock purchase agreement, the Company issued warrants to purchase 351,438 common shares with exercise price of $6.26. Provisions on the warrants gave the Company rights to redeem and acquire 50% of these warrants under certain provisions. During June 2005 the Company exercised its rights and repurchased 175,719 of mentioned warrants. These warrants expire five years from the date of issuance.
In April 2005, the Company granted 100,000 warrants to a director for the extension of his guaranty of a $1.5 million line of credit. These warrants had an exercise price of $13.00 (equal to the stock price at the initial public offering). The fair value of the warrant was determined using Black Scholes pricing model. These warrants expire 10 years from the date of issuance.
In May 2005, the Company granted 40,000 warrants in connection with a private placement with an institutional accredited investor. (The placement is discussed in Note 11 above). These warrants had an exercise price of $13.00 (equal to the stock price at the initial public offering). The fair value of the warrant was determined using Black Scholes pricing model. These warrants expire five years from the date of issuance.
The fair value of the April and May 2005 warrants granted totaled $966,000 and was charged to interest expense for year ended December 2005.
A summary of the status of the Company’s warrants outstanding as of December 31, 2005, 2004, 2003 and changes during the years then ended is presented below:
| | | | | | | | | | | | | | | | |
| | | 2005 | | 2004 | | 2003 |
Warrants | | Shares | | | Weighted
Average
Exercise
Price | | Shares | | Weighted
Average
Exercise
Price | | Shares | | Weighted
Average
Exercise
Price |
Outstanding, beginning of year | | 1,162,387 | | | $ | 4.38 | | 994,773 | | $ | 4.09 | | 642,500 | | $ | 1.47 |
Granted | | 641,438 | | | | 7.73 | | 167,614 | | | 6.08 | | 352,273 | | | 8.87 |
Exercised | | (477,369 | ) | | | 7.66 | | — | | | — | | — | | | — |
Repurchased | | (175,719 | ) | | | 6.26 | | — | | | — | | — | | | — |
| | | | | | | | | | | | | | | | |
Outstanding and Exercisable, end of year | | 1,150,737 | | | $ | 4.60 | | 1,162,387 | | $ | 4.38 | | 994,773 | | $ | 4.09 |
D. Convertible Preferred Stock
The Company has authorized 20,000,000 shares of preferred stock, $.001 par value, which the Board of Directors has authority to issue from time to time in series. The Board of Directors also has the authority to fix, before the issuance of each series, the number of shares in each series and the designation, preferences, rights and limitations of each series. At the initial public offering in June 2005 all of the preferred stock was converted to common stock.
In March 2000, the Company sold 512,500 shares of Series A convertible preferred stock to a group of investors, the net proceeds to the Company were approximately $1,025,000.
66
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
In April 2001, the Company sold 333,334 shares of Series B convertible preferred stock to a group of investors. The net proceeds to the Company were approximately $988,000. In October 2001, the Company sold an additional 333,334 shares of Series B convertible preferred stock to a group of investors. The net proceeds to the Company were approximately $999,000.
In April 2003, the Company raised $6,063,682, net of costs of $111,318 related to this issuance in a private placement with several investors. The Company sold 1,235,000 shares of Series C convertible preferred stock at $5.00 per share. There will be no dividends payable on the shares, unless the Company, in its sole discretion declares a dividend. In the event of any liquidation, these shares shall share on a pari passu basis in liquidation with the Series A and B preferred stock outstanding. A portion of the proceeds of the sale of the Series C convertible preferred stock was used in connection with the Company’s $1,475,000 settlement of its lawsuit with Morris and Dickson. Approximately, $2,250,000 of the proceeds was used to fund the acquisition of Medicine Made Easy. $841,789 of the proceeds was used to repay Company indebtedness.
In April and May 2004, the Company raised an aggregate of $8,806,958 through the issuance of 1,491,828 shares of Series D convertible preferred stock at $6.00 per share in private placements with several investors. The terms and rights of the Series D convertible preferred shares are set forth in the Certificate of Designation of Series D Preferred Stock of the Company. There will be no dividends payable on these shares, unless the Company, in its sole discretion, declares a dividend with respect to the common stock. In the event of any liquidation, the shares shall share on a pari passu basis in liquidation with the Series A, B and C preferred stock outstanding. In conjunction with the offering and for services rendered, the Company issued 24,000 shares of Series D convertible preferred stock to a placement agent, issued warrants representing 114,759 shares of common stock with an exercise price of $6.00 per share to placement agents and paid fees of $745,198. The Company used $1,150,000 of the proceeds to pay off notes to the previous owners of MME (the acquisition discussed in Note 5 above) and the remaining balances of its revolving credit lines.
In December 2004 the Company completed a private placement of shares of its Series E convertible preferred stock, par value $.001 per share. The Company sold a total of 664,013 shares of Series E convertible preferred stock at a price of $6.25 per share to certain accredited investors for an aggregate purchase price of $4,150,081. The Company used a placement agent to assist it with the private placement. In connection with the placement, the Company paid a fee of $410,478 in cash, and it issued 5-year warrants to purchase 51,201 shares of Company common stock (representing 8% of the number of shares of Series E preferred stock). The warrants will have a per share exercise price of $6.25, subject to customary provisions regarding anti-dilution and “net issue” exercise.
The Series A, Series B, Series C, Series D and Series E preferred stock have senior preference and priority as to dividends, distributions and payments upon the liquidation, dissolution or winding up of affairs before any payments to holders of the common stock. Each share of Series A, Series B, Series C, Series D and Series E preferred stock is convertible, at the option of the holder at any time, into one share of common stock.
Deemed Dividend:In 2005, the Company recognized a deemed dividend of $1,338,047 for additional shares of common stock, par value $.001 per share, issued in connection with the conversion of preferred stock immediately prior to the Company’s initial public offering. These additional shares were issued in accordance with the terms of the Company’s Amended and Restated Certificate of Incorporation and the Certificate of Designation of Rights and Preferences for the Series D and Series E Preferred Stock as follows:
| | |
Series C | | 31,667 shares of common stock at $ 5.00 per share; |
Series D | | 113,151 shares of common stock at $ 6.00 per share; and |
Series E | | 80,129 shares of common stock at $ 6.25 per share. |
67
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Note 19. Related Party Transaction
In January 2000, the Company issued warrants to purchase 375,000 shares of common stock to John Pappajohn, a director, as consideration for his guarantee of a $1.5 million credit facility with West Bank. These warrants are exercisable at a price $1.00 per share. As consideration for the renewal of the guaranty, the Company issued warrants to purchase 125,000 shares of common stock to Mr. Pappajohn in July 2003, exercisable at a price per share of $5.00. In March 2005, when West Bank agreed to extend the maturity of its loan until September 2005, Mr. Pappajohn agreed to keep his guaranty in place through September 2005. As consideration for continuing his guaranty, in April 2005 the Company issued to Mr. Pappajohn warrants to purchase 100,000 shares of common stock exercisable at a price equal to our initial public offering price per share. The fair value of the warrants was $753,000 as calculated using the Black Scholes model. See Note 18 for a description of warrants issued.
Note 20. Major Suppliers
During the twelve months ended December 31, 2005 and 2004, the Company purchased approximately $99,437,000 and $55,707,000, respectively, from one major drug wholesaler and during the year ended December 31, 2003 the Company purchased approximately $40,268,000 from three major suppliers. Amounts due to this supplier at December 31, 2005 and 2004 were approximately $12,358,000 and $5,590,000, respectively.
In September 2003, the Company signed a five-year agreement with a drug wholesaler that requires certain minimum purchases. If the Company does not meet the minimum purchase commitments as set forth in the agreement, the Company will be charged a prorated amount of 0.20% of the projected volume remaining on the term of the Agreement. The agreement also provides that the Company’s minimum purchases during the term of the agreement will be no less than $400,000,000. The Company has purchased approximately $168,169,000 from this drug wholesaler since the beginning of the term of this agreement and believes it will be able to meet its minimum purchase obligations under this agreement.
Note 21. Supplemental Disclosure of Non-cash Financing Activities
Interest paid on credit facilities notes and capital leases for the twelve months ended December 31, 2005 and 2004 was $537,398 and $225,830, respectively. During 2005 the Company has made four acquisitions of assets with part of the consideration to be paid with notes payable or having a portion of the purchase price paid in months following the acquisition. The detail for these transactions can be found in Note 5.
NOTE 22. Fair value of financial instruments
The methods and assumptions used to estimate the fair value of the following classes of financial instruments were:
Current Assets and Current Liabilities:The carrying amount of cash, receivables and payables and certain other short-term financial instruments approximate their fair value.
Long-Term Debt:The fair value of the Company’s long term debt, including the current portions, was based on the Company’s assumed incremental borrowing rates for similar types of borrowing arrangements. The carrying amount of variable and fixed rate debt at December 31, 2005 approximates its fair value.
68
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
NOTE 23. Quarterly financial information (unaudited)
Quarterly financial information for the years ended December 31, 2005 and 2004 is summarized below (in thousands, except share data):
| | | | | | | | | | | | | | | | | | | | |
| | | 2005 | |
| | | First
Quarter | | | Restated*
Second
Quarter | | | Restated*
Third
Quarter | | | Fourth
Quarter | | | Total | |
| | | (In thousands, except per share data) | |
Net Sales | | $ | 22,696 | | | $ | 28,582 | | | $ | 33,984 | | | $ | 37,846 | | | $ | 123,108 | |
Gross Profit | | $ | 3,574 | | | $ | 4,141 | | | $ | 5,875 | | | $ | 6,272 | | | $ | 19,862 | |
Operating (Loss) Income | | $ | 125 | | | $ | 154 | | | $ | 714 | | | $ | 519 | | | $ | 1,512 | |
Discontinued Operations | | $ | (5 | ) | | $ | (5 | ) | | $ | (7 | ) | | $ | (19 | ) | | $ | (36 | ) |
Deemed Dividend on Preferred | | $ | — | | | $ | (1,338 | ) | | $ | — | | | $ | — | | | $ | (1,338 | ) |
Net (Loss) Income | | $ | 13 | | | $ | (2,233 | ) | | $ | 909 | | | $ | 378 | | | $ | (933 | ) |
Basic (Loss) Income per Common Share | | $ | 0.01 | | | $ | (0.55 | ) | | $ | 0.07 | | | $ | 0.03 | | | $ | (0.11 | ) |
Diluted (Loss) Income per Common Share | | $ | 0.00 | | | $ | (0.55 | ) | | $ | 0.06 | | | $ | 0.03 | | | $ | (0.11 | ) |
Basic weighted average shares | | | 3,100 | | | | 4,070 | | | | 12,635 | | | | 12,845 | | | | 8,202 | |
Diluted weighted average shares | | | 8,870 | | | | 4,070 | | | | 14,921 | | | | 14,890 | | | | 8,202 | |
| |
| | | 2004 | |
| | | First
Quarter | | | Second
Quarter | | | Third
Quarter | | | Fourth
Quarter | | | Total | |
Net Sales | | $ | 13,350 | | | $ | 14,476 | | | $ | 15,894 | | | $ | 16,360 | | | $ | 60,080 | |
Gross Profit | | $ | 1,564 | | | $ | 1,516 | | | $ | 1,973 | | | $ | 1,865 | | | $ | 6,918 | |
Operating loss | | $ | (535 | ) | | $ | (907 | ) | | $ | (297 | ) | | $ | (506 | ) | | $ | (2,245 | ) |
Discontinued Operations | | $ | (51 | ) | | $ | (90 | ) | | $ | (37 | ) | | $ | 48 | | | $ | (130 | ) |
Net loss | | $ | (677 | ) | | $ | (1,103 | ) | | $ | (370 | ) | | $ | (530 | ) | | $ | (2,680 | ) |
Basic and Diluted Loss per Common Share | | $ | (0.22 | ) | | $ | (0.36 | ) | | $ | (0.12 | ) | | $ | (0.17 | ) | | $ | (0.86 | ) |
Basic and Diluted weighted average shares | | | 3,100 | | | | 3,100 | | | | 3,100 | | | | 3,100 | | | | 3,100 | |
In the fourth quarter 2005 the Company recorded a provision for taxes of $329,000.
| * | As described below, the second and third quarters have been restated to reflect non-cash interest expense relating to warrants that were issued in the second quarter of 2005. |
On March 9, 2006, after discussion with our independent registered public accounting firm, BDO Seidman, LLP and consultation with management and our Board of Directors, we concluded that our financial statements for the three and six-months ended June 30, 2005, and the three and nine-months ended September 30, 2005 should no longer be relied upon and should be restated. We intend to restate previously issued financial statements for the above mentioned periods to correct a non-cash interest expense (below the “operating income” line) relating to warrants to purchase 140,000 shares of our common stock. Warrants for 100,000 shares were issued to John Pappajohn, one of our outside directors, in April 2005 in connection with the extension of a guarantee on our West Bank credit facility and warrants to purchase 40,000 shares of our common stock were issued to Crestview Capital Master, LLC in May 2005 in connection with a private placement loan. The total non-cash interest expense for both issuances of warrants was approximately $966,000, which will be recorded in the second quarter of 2005. We had previously booked $60,000 for the value of warrants in the third quarter of 2005. This is a one-time charge to the income statement and does not affect our operating results. We will file
69
ALLION HEALTHCARE, INC. AND SUBSIDIARIES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
amendments, as needed, to our quarterly reports on Form 10-Q for the affected periods. The Board of Directors of the Company is conducting an inquiry into these matters. Below we have presented the quarterly financials for the three months ended June 30, 2005 and September 30, 2005 as if the quarters had not been restated.
| | | | | | | | |
| | | 2005 | |
| | | Second
Quarter | | | Third
Quarter | |
| | | | | | | |
Net Sales | | $ | 28,582 | | | $ | 33,984 | |
Gross Profit | | $ | 4,141 | | | $ | 5,875 | |
Operating (Loss) Income | | $ | 154 | | | $ | 714 | |
Discontinued Operations | | $ | (5 | ) | | $ | (7 | ) |
Deemed Dividend on Preferred | | $ | (1,338 | ) | | $ | — | |
Net (Loss) Income | | $ | (1,267 | ) | | $ | 849 | |
Basic (Loss) Income per Common Share | | $ | (0.31 | ) | | $ | 0.07 | |
Diluted (Loss) Income per Common Share | | $ | (0.31 | ) | | $ | 0.06 | |
Basic weighted average shares | | | 4,070 | | | | 12,635 | |
Diluted weighted average shares | | | 4,070 | | | | 14,963 | |
NOTE 24. Subsequent events
On January 25, 2006, the Company completed the sale of 5,101,922 common shares at the price of $12.83 per share, less an underwriting discount and expenses, for total gross proceeds of $61,857,488. The number of shares sold included 2,465,468 shares sold by the Company (665,468 shares through the over-allotment exercised by the underwriters after the offering) and 2,636,454 shares sold by certain selling stockholders. The Company received total gross proceeds of $29,892,197 from the sale of its shares and did not receive any proceeds from the sale of shares by the selling stockholders.
On March 13, 2006, MOMS Pharmacy of Brooklyn, Inc., a New York corporation and wholly-owned subsidiary of the Company entered into and completed the transactions contemplated by an Asset Purchase Agreement with H.S. Maiman Rx, Inc., (“Maiman”), a Brooklyn, New York pharmacy with approximately $11.2 million in 2005 revenues as reported by its owners. Under the Asset Purchase Agreement, Moms Pharmacy of Brooklyn, Inc. paid $5.25 million and acquired Maiman’s right, title and interest in and to certain assets and liabilities, including but not limited to, its customer lists, inventory, books and records, files, lease and goodwill used in connection with or related to its HIV/AIDS business, all in accordance with the terms and conditions of the Asset Purchase Agreement.
70
Item 9. Changes in and disagreements with accountants on accounting and financial disclosure
None.
Item 9A. Controls and procedures
Evaluation of Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that information required to be disclosed in our Exchange Act reports is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure based on the definition of “disclosure controls and procedures” in Rule 13a-15(e). In designing and evaluating the disclosure controls and procedures, management recognized that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives, and management necessarily was required to apply its judgment in evaluating the cost-benefit relationship of possible controls and procedures.
As of the end of the period covered by this report, we carried out an evaluation, under the supervision and with the participation of our management, including our Chief Executive Officer and our Chief Financial Officer, of the effectiveness of the design and operation of our disclosure controls and procedures. Based upon that evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures were not effective as a result of a material weakness in internal control over financial reporting, as of December 31, 2005, as discussed below.
Management’s Annual Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting of the Company. Internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with accounting principles generally accepted in the United States of America.
The Company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with accounting principles generally accepted in the United States of America, and that receipts and expenditures of the Company are being made only in accordance with authorizations of management and directors of the Company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the Company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
A material weakness in internal controls is a significant deficiency (as defined by Public Company Accounting Oversight Board, Statement of Auditing Standard No. 2), or combination of significant deficiencies, that results in more than a remote likelihood that a material misstatement of the financial statements would not be prevented or detected on a timely basis by the Company.
Management conducted an evaluation of the effectiveness of internal control over financial reporting based on the framework in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. The acquisitions of North American Home Health Supply, Inc. on
71
January 4, 2005, Specialty Pharmacies, Inc. on February 28, 2005, and Priority Pharmacy on December 9, 2005 to the extent their operations remain segregated which is included in the 2005 consolidated financial statements of Allion Healthcare, Inc. and constituted approximately 10% of consolidated assets at December 31, 2005 and 31% of consolidated revenues for the year ended December 31, 2005, were excluded from the scope of management’s evaluation since their companies were acquired after December 31, 2004. Based on this evaluation, management concluded that the Company’s process related to controls over financial reporting was not effective as of December 31, 2005. In early 2006, Management identified a material weakness due to an omission of a non-cash interest expense (below the “operating income” line) relating to warrants to purchase 100,000 shares of the Company’s common stock that were issued to an outside director of the Company in April 2005 in connection with the extension of a guarantee on the Company’s West Bank credit facility and to warrants to purchase 40,000 shares of the Company’s common stock that were issued as part of a private placement with an institutional accredited investor in May 2005. Accordingly, after discussion with its independent registered public accounting firm, BDO Seidman, LLP and consultation with management and the Board of Directors, the Company concluded that the Company’s financial statements for the three and six months ended June 30, 2005, and three and nine months ended September 30, 2005 should be restated.
In order to immediately address and correct the deficiencies identified above, management has taken and will continue to take corrective actions including: improving training, education, accounting reviews and adding additional staff as necessary, all designed to ensure that all relevant personnel involved in non-routine stock based transactions understand and apply the appropriate accounting principles.
Management’s assessment of the Company’s internal control over financial reporting as of December 31, 2005 has been audited by BDO Seidman, LLP, an independent registered public accounting firm, as stated in their report, which is included herein.
Changes in Internal Control over Financial Reporting
There have been no significant changes in our internal control over financial reporting during the quarter ended December 31, 2005 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reports.
Item 9B. Other Information
None.
72
PART III
Item 10. Directors And Executive Officers Of The Registrant
The following table sets forth the names, ages and principal positions of our directors and executive officers as of February 15, 2006:
| | | | |
Name | | Age | | Position |
Michael P. Moran | | 45 | | Chairman, President and Chief Executive Officer |
John W. Colloton (1)(2)(3)(4) | | 75 | | Director |
John Pappajohn | | 77 | | Director |
Derace Schaffer, M.D (1)(2)(4) | | 58 | | Director |
Harvey Z. Werblowsky, Esq. (2)(4) | | 57 | | Director |
Robert E. Fleckenstein, R.Ph. | | 52 | | Vice President, Pharmacy Operations |
MikeLynn Salthouse | | 50 | | Vice President, Oris Sales |
James G. Spencer | | 37 | | Chief Financial Officer, Secretary and Treasurer |
| (1) | Member of the Audit Committee |
| (2) | Member of the Nominating and Corporate Governance Committee |
| (3) | Audit Committee Financial Expert |
| (4) | Member of Compensation Committee |
Michael P. Moran has served as our Chairman, Chief Executive Officer and President and as a member of our board of directors since 1997. From 1996 to 1997, Mr. Moran was a Regional Vice President at Coram Healthcare, Inc. From 1990 to 1996, Mr. Moran was a Regional Vice President for Chartwell Home Therapies, Inc. Prior to 1990, Mr. Moran held various sales and management positions at Critical Care America, Inc. Mr. Moran received a B.A. in management from Assumption College.
John W. Colloton has served as one of our directors since 2004. He is currently Director Emeritus of the University of Iowa Hospitals and Clinics, and serves as the lead director of Wellmark, Inc. (Iowa-South Dakota Blue Cross & Blue Shield). From 1989 to 2003, Mr. Colloton served as a director of Baxter International Inc. and from 1997 to 2002, he served as a director of Radiologix, Inc. From 1971 to 1993, Mr. Colloton served as the director of the University of Iowa Hospitals and Clinics, and from 1993 through the year 2000, he served as vice president of the University of Iowa for Statewide Health Services. Mr. Colloton received his B.A. in business administration from Loras College and a master’s degree in hospital administration from the University of Iowa.
John Pappajohnhas served as one of our directors since 1996. Since 1969, Mr. Pappajohn has served as the president and principal stockholder of Equity Dynamics, Inc., a financial consulting firm, and is the sole owner of Pappajohn Capital Resources, a venture capital firm. Mr. Pappajohn has served on the boards of directors of over 40 public companies and currently serves as a director of the following public companies: Healthcare Acquisition Corp., MC Informatics, Inc., PACE Health Management Systems, Inc. and Patient Infosystems, Inc. Mr. Pappajohn has been an active private equity investor in healthcare companies for more than 30 years. Mr. Pappajohn has been a founder in several public healthcare companies such as Caremark Rx, Inc., Quantum Health Resources, and Radiologix, Inc. Mr. Pappajohn received his B.A. in business from the University of Iowa.
Derace Schaffer, M.D. has served as one of our directors since 1996. Dr. Schaffer is the founder and Chief Executive Officer of The Lan Group, a venture capital firm specializing in healthcare and high technology investments. Dr. Schaffer currently serves as a director of the following public companies: Healthcare Acquisition Corp. and Patient Infosystems, Inc. He has served as chairman of several healthcare companies including, Radiologix, Inc. when the company was private. Dr. Schaffer served as Chief Executive Officer and Chairman of the Board of Imaging Group, P.C. from 1980 to 2001. Dr. Schaffer has served as a director on many healthcare services and technology companies. Dr. Schaffer received his postgraduate radiology training at Harvard Medical School and Massachusetts General Hospital, where he served as Chief Resident. Dr. Schaffer is currently also a Clinical Professor of Radiology at Weill Cornell Medical School.
73
Harvey Z. Werblowsky, Esq.has served as one of our directors since 2004. Since December 2003, he has been the general counsel of Kushner Companies, a real estate organization. From December 1990 until December 2003, Mr. Werblowsky was a partner at the law firm of McDermott Will & Emery LLP. Mr. Werblowsky received a B.A. from Yeshiva University and a J.D. from New York University School of Law.
Robert E. Fleckenstein, RPhhas served as our Vice President, Pharmacy Operations since December 2003 and is responsible for our national pharmacy operations. Mr. Fleckenstein has held positions in pharmacy management for 20 years, with over 10 of those years in specialty pharmacy. In 2003, he served as Account Manager for US Oncology, Inc. From 2000 to 2002, Mr. Fleckenstein served as Vice President of Operations for CVS ProCare at its Pittsburgh distribution center. From 1997 to 2000, he served as Director of Pharmacy Services for Stadtlanders Drug Company. Prior to 1997, Mr. Fleckenstein held various management level positions in specialty and hospital pharmacy companies. Mr. Fleckenstein received his B.S. in Pharmacy from the University of Pittsburgh and his M.B.A. from the Katz Graduate School of Business at the University of Pittsburgh.
MikeLynn Salthouse, RNhas served as our Executive Vice President, Oris Sales since November 2005 and, prior to that time, had served as our Vice President, HIV Sales since 2002. Ms. Salthouse has worked in the pharmaceutical industry for 20 years, including nine years with Stadtlanders and CVS ProCare, where she served as Vice President, Sales, and Vice President, Business Development. Prior to 1993, Ms. Salthouse held sales management positions with both Ivonyx and Clinical Homecare, infusion service companies, as well as various sales and management positions at McNeil Consumer Products, a division of Johnson & Johnson. Ms. Salthouse attended Loma Linda University and graduated from Riverside College, both in Southern California.
James G. Spencerhas served as our Chief Financial Officer, Secretary and Treasurer since 2004. From October 2003 to May 2004, Mr. Spencer served as a consultant to us until becoming Chief Financial Officer. From 2002 until 2003, Mr. Spencer served as a Vice President in the Health Care Investment Banking Group for Thomas Weisel Partners LLC. From 1999 to 2002, he served as Vice President in the Health Care Investment Banking Group for Credit Suisse First Boston. Prior to 1999, Mr. Spencer worked at Alex. Brown and Sons in Health Care Investment Banking. Mr. Spencer received his M.B.A. from The Wharton School of the University of Pennsylvania and his B.S. in Economics and Management Statistics from the University of Maryland.
A majority of our directors are “independent” in accordance with NASDAQ National Market requirements.
Election of Directors
Our restated certificate of incorporation provides that our board of directors shall initially consist of three directors and our third amended and restated bylaws give the board of directors the authority to fix the number of directors that constitutes the board of directors from time to time. Vacancies among the directors, whether caused by resignation, death, removal or an increase in the authorized number of directors may be filled by a majority of the directors, then in office. In accordance with the terms of our amended and restated certificate of incorporation, stockholders will elect each of our directors at the annual meeting of stockholders, or special meeting in lieu thereof. Each director serves until his successor is elected and qualified or until his earlier death, resignation or removal. The nominating and corporate governance committee is in the process of locating a replacement to fill the vacancy on the board created by Mr. Hoover’s resignation.
74
Board Committees
Our board of directors has an audit committee, a compensation committee and a nominating and corporate governance committee, each of which has the composition and responsibilities described below:
Audit Committee. The audit committee provides assistance to the board of directors in fulfilling its legal and fiduciary obligations in matters involving our accounting, auditing, financial reporting, internal controls and legal compliance functions by approving the services performed by our independent accountants and reviewing their reports regarding our accounting practices and systems of internal accounting controls. The audit committee also oversees the audit efforts of our independent accountants and determines whether the accountants are independent of management. The audit committee currently consists of Messrs. Colloton and Dr. Schaffer, each of whom is an independent member of our board of directors. Mr. Colloton serves as the chairperson of our audit committee, and our board of directors has determined that Mr. Colloton meets the definition of an “audit committee financial expert,” as defined by the SEC. The board of directors has also determined that Mr. Colloton is an audit committee financial expert and is independent of management, as required under Section 407 of the Sarbanes-Oxley Act of 2002. We believe Mr. Colloton is qualified to be an “audit committee financial expert” because he has the following attributes: (i) an understanding of generally accepted accounting principles, or GAAP, and financial statements, (ii) the ability to assess the general application of such principles in connection with accounting for estimates, accruals and reserves, (iii) experience preparing, auditing, analyzing or evaluating financial statements that represent a breadth and level of complexity and accounting issues that can reasonably be expected to be raised by our financial statements, or actively supervising one of more persons engaged in such activities, (iv) an understanding of internal control over financial reporting and (v) and understanding of audit committee functions. Mr. Colloton has acquired these attributes by means of having held various positions that provided the relevant experience, including having served as the chairman of the finance committee of Baxter International, Inc. and as lead director of Wellmark, Inc. We believe that the composition of our audit committee meets the criteria for independence under, and the functioning of our audit committee complies with, the applicable requirements of, the Sarbanes-Oxley Act of 2002, Rule 4350(d)(4) and other applicable rules and regulations of the NASDAQ National Market and SEC rules and regulations. Pursuant to Rule 4350(d)(4), the audit committee will be comprised solely of two independent directors until its next annual meeting of stockholders or one year from January 18, 2006.
Compensation Committee. The compensation committee determines our general compensation policies and the compensation provided to our directors and officers. The compensation committee also reviews and determines bonuses for our executive officers. In addition, the compensation committee reviews and determines equity-based compensation for our directors, officers, employees and consultants and administers our stock option plans. The current members of the compensation committee are Messrs. Werblowsky, Colloton and Dr. Schaffer, each of whom is an independent director. Mr. Werblowsky serves as the chairperson of our compensation committee. We believe that the composition of our compensation committee meets the criteria for independence under, and the functioning of our compensation committee complies with, the applicable requirements of, the Sarbanes-Oxley Act of 2002, the current rules of the NASDAQ National Market and SEC rules and regulations.
Nominating and Corporate Governance Committee. The nominating and corporate governance committee is responsible for making recommendations to the board of directors regarding candidates for directorships and the size and composition of the board. In addition, the nominating and corporate governance committee is responsible for overseeing our corporate governance guidelines and reporting and making recommendations to the board concerning corporate governance matters. The current members of the nominating and corporate governance committee are Messrs. Werblowsky, Colloton and Dr. Schaffer. Dr. Schaffer serves as the chairperson of our nominating and corporate governance committee. We believe that the composition of our nominating and corporate governance committee meets the criteria for independence under, and the functioning of our nominating and corporate governance committee complies with, the applicable requirements of the NASDAQ National Market and SEC rules and regulations.
75
The audit committee, the compensation committee and the nominating and corporate governance committee each has adopted a written charter that further describes its function and responsibilities. You may obtain copies of these charters by going to the “Investor Relations” section of our website located atwww.allionhealthcare.com. We do not intend this internet address to be an active link and the content of this website is not part of this Report.
We have adopted a Code of Ethics that applies to all of our directors, officers and employees including our senior financial officers. Our Code of Ethics has been filed with the SEC and is also available on our website located atwww.allionhealthcare.com. We do not intend this internet address to be an active link and the content of this website is not part of this Report.
Director Compensation
We do not have a formal policy regarding compensation of our directors for their service as directors. Historically, our non-employee directors have each been granted options to purchase 50,000 shares of common stock pursuant to our 1998 Stock Option Plan and 2002 Stock Incentive Plan as compensation for their initial term serving on our board of directors. These options have an exercise price ranging from $2.00 to $6.00 per share approximating the fair market value as of the date of grant, and vest monthly in equal amounts over either a two or three-year period, beginning one month following the date such option is granted, and cease vesting when a director ceases to serve on our board of directors. In 2004, we also granted our non-employee directors options to purchase 20,000 shares of common stock pursuant to our 1998 Stock Option Plan and our 2002 Stock Incentive Plan for the director’s re-election. These options have an exercise price approximating the fair market value as of the date of grant, and vest monthly in equal amounts over a one-year period. Our non-employee directors have not received any other compensation for their service as directors. We reimburse all directors for expenses incurred in connection with attending meetings. Directors who are employees or affiliates of ours have not received any compensation for their services as a director, other than Mr. Pappajohn, who may be deemed an affiliate. Accordingly, Mr. Moran has not been compensated for his services as a director.
Compensation Committee Interlocks and Insider Participation
No interlocking relationship exists between our board of directors or compensation committee and the board of directors or compensation committee of any other entity. Additionally, no member of our compensation committee was during 2005, or formerly, an officer or employee of ours or any of our subsidiaries.
Limitations on Directors’ Liability and Indemnification
Our amended and restated certificate of incorporation limits the liability of directors to the maximum extent permitted by Delaware law. Delaware law provides that directors of a corporation will not be personally liable for monetary damages for breach of their fiduciary duties as directors, except liability for:
| | • | | any breach of their duty of loyalty to the corporation or its stockholders; |
| | • | | acts or omissions not in good faith or which involve intentional misconduct or a knowing violation of law; |
| | • | | unlawful payments of dividends or unlawful stock repurchases or redemptions; or |
| | • | | any transaction from which the director derived an improper personal benefit. |
The limitation of liability does not apply to liabilities arising under the federal securities laws and does not affect the availability of equitable remedies such as injunctive relief or rescission.
Our third amended and restated bylaws provide that we will indemnify our directors and officers and may indemnify our employees and other agents to the fullest extent permitted by law. Our third amended and restated bylaws also permit us to secure insurance on behalf of any officer, director, employee or other agent for any liability arising out of his or her actions in his or her capacity as an officer, director, employee or other agent. We maintain liability insurance that insures our directors and officers against certain losses and that insures us against our obligation to indemnify our directors and officers.
76
The limited liability and indemnification provisions in our amended and restated certificate of incorporation and the third amended and restated by-laws may discourage stockholders from bringing a lawsuit against our directors for breach of their fiduciary duty and may reduce the likelihood of derivative litigation against our directors and officers, even though a derivative action, if successful, might otherwise benefit us and our stockholders. A stockholder’s investment in us may be adversely affected to the extent we pay the costs of settlement or damage awards against our directors and officers under these indemnification provisions.
At present, there is no pending litigation or proceeding involving any of our directors, officers or employees in which indemnification is sought, nor are we aware of any threatened litigation that may result in claims for indemnification. Insofar as indemnification for liabilities arising under the Securities Act may be permitted for directors, officers and controlling persons of us pursuant to the foregoing provisions or otherwise, we have been advised that in the opinion of the SEC such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable.
Item 11. Executive Compensation And Other Information
The following table sets forth certain elements of compensation paid by us during the years ended December 31, 2005, 2004 and 2003 to our Chief Executive Officer, and our three most highly compensated executive officers other than our Chief Executive Officer.
| | | | | | | | | | | | | |
| | | Annual Compensation | | Long-Term
Compensation
Awards |
Name and Principal Position | | Year | | Salary ($) | | Bonus ($)(1) | | Other Annual
Compensation
($)(2) | | Securities
Underlying
Options (#) |
Michael P. Moran, Chairman,
Chief Executive Officer
President | | 2005
2004
2003 | | $
$
$ | 250,000
251,924
247,483 | | $
$
$ | 125,000
100,000
100,000 | | $
$
$ | 0
0
0 | | 0
0
0 |
| | | | | |
James G. Spencer, (3) Chief Financial Officer
Secretary and Treasurer | | 2005
2004 | | $
$ | 200,000
151,538 | | $
$ | 70,000
20,000 | | $
$ | 8,876
2,513 | | 0
125,000 |
| | | | | |
MikeLynn Salthouse, (4) Executive Vice President,
Oris Sales | | 2005
2004
2003 | | $
$
$ | 175,000
169,204
150,000 | | $
$
$ | 5,000
10,000
0 | | $
$
$ | 7,200
7,200
7,200 | | 0
40,000
0 |
| | | | | |
Robert E. Fleckenstein, (5) RPh, Vice President,
Pharmacy Operations | | 2005
2004 | | $
$ | 130,000
131,000 | | $
$ | 35,000
18,750 | | $
$ | 0
0 | | 0
50,000 |
| (1) | Bonuses were paid at the discretion of the compensation committee from time to time based on merit-based performance. We do not have a written bonus plan. |
| (2) | For the years presented, perquisites and other personal benefits did not exceed the lesser of $50,000 or 10% of total annual salary and bonus for the named executive officer. |
| (3) | Mr. Spencer became our Chief Financial Officer on May 18, 2004. The amount shown in the table for 2004 represents the amount we paid Mr. Spencer from May 20 through December 31, 2004. In addition to the amount shown above, Mr. Spencer served as a consultant to us from January 1 until May 17, 2004, during which time he was paid a fee of $23,681. We pay 100% of the premiums for Mr. Spencer’s healthcare insurance plan in lieu of his participation in company-sponsored plans. We paid $8,876 and $2,513 for health insurance premiums for Mr. Spencer in 2005 and 2004, respectively. The amount we pay for Mr. Spencer’s coverage is less than the amount that we would be required to pay had he elected to be |
77
| | covered by the healthcare insurance that we make available to all of our employees. All of our other named executive officers except Mr. Spencer receive healthcare insurance that is identical to what we offer all of our employees. |
| (4) | The amounts shown for “Other Annual Compensation” reflect amounts paid to Ms. Salthouse for an annual automobile allowance. |
| (5) | Mr. Fleckenstein became our Vice President, Pharmacy Operations, in January 2004. |
Options Grants in Last Fiscal Year
During 2005 there were no stock options granted to our named executive officers.
| | | | | | | | | | | | | |
Name | | Number of
Securities
Underlying
Options | | Percentage of
Total Options
Granted to
Employees in
Fiscal Year
2005 | | | Exercise
Price | | Expiration
Date | | Potential Realizable Value
At Assumed Annual Rates
Of Stock Price
Appreciation For Option
Term |
| | | | | | 5% | | 10% |
Michael P. Moran | | 0 | | 0 | % | | — | | — | | — | | — |
James G. Spencer | | 0 | | 0 | % | | — | | — | | — | | — |
MikeLynn Salthouse | | 0 | | 0 | % | | — | | — | | — | | — |
Robert E. Fleckenstein | | 0 | | 0 | % | | — | | — | | — | | — |
Aggregated Stock Option Exercises in Last Fiscal Year and Fiscal Year-End Option Values
The following table provides information regarding the number and value of vested and unvested options held by each of our named executive officers as of December 31, 2005. There were no options exercised by the named executive officers in 2005. Dollar values in the table are calculated based upon an assumed per share price of $16.01, which was the closing price of our common stock on February 15, 2006, less the exercise price of the options, and multiplying the result by the number of shares.
| | | | | | | | | | |
Name | | Number of Securities Underlying
Unexercised Options at Fiscal Year-
End (#) | | Value of Unexercised In-the-Money Options at
Fiscal Year End Exercisable ($) |
| | Exercisable | | Unexercisable | | Exercisable | | Unexercisable |
Michael P. Moran | | 650,000 | | — | | $ | 10,044,000 | | $ | — |
James G. Spencer | | 62,500 | | 62,500 | | $ | 625,625 | | $ | 625,625 |
MikeLynn Salthouse | | 85,000 | | 30,000 | | $ | 1,038,350 | | $ | 300,300 |
Robert E. Fleckenstein | | 12,500 | | 37,500 | | $ | 125,125 | | $ | 375,375 |
Employment Agreements
Currently, we do not have any written employment agreements with any of our executive officers. The risks associated with not having employment agreements with our executive officers is discussed at Item 1A of this Report.
Compensation Committee Report On Executive Compensation
The Compensation Committee of the Board of Directors is responsible for determining the Company’s executive compensation policies, developing compensation incentive plans and programs, reviewing and approving the compensation of the Company’s chief executive officer and making grants of stock options.
Philosophy. The compensation philosophy of the Company is to develop and implement policies that will encourage and reward outstanding financial performance and increase the profitability of the Company, thereby increasing stockholder value. Maintaining competitive compensation levels in order to attract, retain and reward
78
executives who bring valuable experience and skills to the Company is also an important consideration. The Compensation Committee is composed of Harvey Werblowsky, John Colloton and Derace Schaffer, M.D. with Harvey Werblowsky serving as the Committee Chairperson. Working with the Company, the Compensation Committee develops and implements compensation arrangements for the Company’s executive officers.
Compensation Structure. There are three primary components of executive compensation for the Company’s executive officers: base salary, bonus and stock option grants. While the elements of compensation are considered separately, the Compensation Committee takes into account the total compensation package afforded by the Company to the individual executive.
Base Salary. Base salaries for the Company’s executive officers are determined initially by evaluating the responsibilities of the position held and the experience of the individual in light of the Company’s compensation philosophy described above. No specific formula is applied in setting an executive officer’s base salary, either with respect to the total amount of such base salary or the relative value such base salary should bear to the executive officer’s total compensation package. Salaries paid to executive officers (including the Chief Executive Officer) are reviewed annually by the Compensation Committee and proposed adjustments are based upon an assessment of the nature of the position and the individual’s contribution to the Company’s corporate goals, experience and tenure of the executive officer, comparable market salary data, growth in the Company’s size and complexity and changes in the executive’s responsibilities. The Compensation Committee approves all changes to executive officers’ salaries.
Bonus. The Compensation Committee, in its discretion, may award bonuses to executive officers. Such bonuses are based upon: an executive officer’s performance as well as the performance of the Company, such as the consummation of an important acquisition or financing, meeting or exceeding sales targets or recognition of superior performance. In 2005, the Compensation Committee approved all bonuses paid to the named executive officers. In addition to the bonuses paid to MikeLynn Salthouse and Robert Fleckenstein, the Compensation Committee approved performance bonuses to each of Mr. Moran, our Chief Executive Officer, and James Spencer, our Chief Financial Officer of $25,000 and $20,000, respectively, as well as bonuses paid in connection with the successful completion of the Company’s initial public stock offering of $100,000 and $50,000, respectively.
Stock Options. Stock options are designed to align the interests of executives with those of the Company’s stockholders. At this time, stock options are the only form of equity that an executive officer of the Company is entitled to receive. Stock option grants may be made to executive officers when one of the following events occurs: (i) upon initial employment, (ii) upon promotion to a new, higher position that entails increased responsibilities and accountability, (iii) for recognition of superior performance or (iv) as an incentive for continued service with the Company as well as continued superior performance. None of our named executive officers were granted stock options during 2005.
Chief Executive Officer Compensation. Mr. Moran does not have an employment agreement with the Company. In 2005, Mr. Moran received a salary of $250,000 and was eligible to participate in benefit plans generally available to all employees of the Company. The Compensation Committee awarded Mr. Moran a $25,000 performance bonus and a bonus of $100,000 based upon, among other things, the successful completion of the Company’s initial public stock offering. Mr. Moran did not receive an increase in salary nor did he receive any stock options during the year ended December 31, 2005. The Compensation Committee believes the relationship between the compensation paid to Mr. Moran and the Company’s performance is appropriate and serves stockholders’ interest. Going forward, the Compensation Committee may seek to negotiate the terms of an employment agreement with Mr. Moran.
Executive Officer Compensation. In addition to the factors mentioned above, the Compensation Committee’s general approach in setting executive officer compensation is to seek to be competitive with other companies in the Company’s industry and to get the best talent for the applicable management position. In determining bonuses, the Compensation Committee reviews the Company’s performance as a whole as well as all of the executive officer’s
79
achievements. No executive officers of the Company were employed by employment agreement during the year ended December 31, 2005. The Compensation Committee feels that actions taken regarding executive compensation are appropriate in view of the individual and corporate performance.
Policy Regarding Section 162(m) of the Internal Revenue Code. In the event total compensation for any named executive officer exceeds the $1 million threshold at which tax deductions are limited under Internal Revenue Code Section 162(m), the Compensation Committee intends to balance tax deductibility of executive compensation with its responsibility to retain and motivate executives with competitive compensation programs. As a result, the Compensation Committee may take such actions as it deems to be in the best interests of the stockholders, including (i) provide non-deductible compensation above the $1 million threshold; (ii) require deferral of a portion of the bonus or other compensation to a time when payment may be deductible by the Company; and/or (iii) modify existing programs to qualify bonuses and other performance-based compensation to be exempt from the deduction limit.
Submitted by the Compensation Committee of the Company’s board of directors
Harvey Z. Werblowsky, Esq.
John Colloton
Derace Schaffer, M.D.
80
Performance Graph
The following performance graph compares the cumulative total shareholder return on the Company’s common stock during the last seven months with the performance of a broad equity market indicator and the performance of a published industry index or peer group. The graph compares the cumulative total return on the Company’s common stock with (1) the NASDAQ Market Index and (2) with a peer group within NASDAQ Healthcare Services for the period from June 22, 2005 through December 31, 2005. Management believes the NASDAQ Healthcare Services peer group includes companies that are comparable to the Company in terms of their businesses.
The Company completed its initial public offering on June 22, 2005. Prior to June 23, 2005 the Company’s common stock did not trade on a public market. As a result, the cumulative total stockholder return on the common stock of the Company can not be provided for any period before that date. For purposes of preparing the graph, the Company assumed that an investment of $100 was made on June 22, 2005 with reinvestment of any dividends, if any, at the time they were paid.
The comparison in the graph below is based on historical data and is not intended to forecast the possible future performance of the Company’s common stock
Comparison of Cumulative Total Return Among The Company, NASDAQ Market Index and Peer Group of companies in NASDAQ Healthcare Services
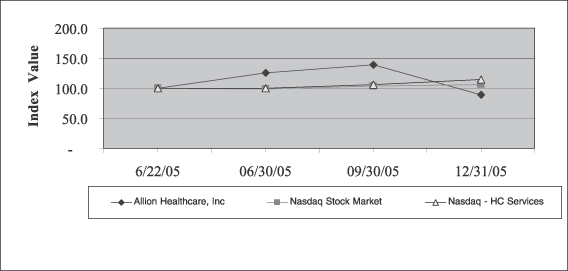
| | | | | | | | |
| | | 6/22/05 | | 06/30/05 | | 09/30/05 | | 12/31/05 |
Allion Healthcare, Inc | | 100.0 | | 126.2 | | 138.5 | | 89.6 |
NASDAQ Stock Market | | 100.0 | | 98.4 | | 104.0 | | 105.8 |
NASDAQ Healthcare Services | | 100.0 | | 99.4 | | 105.7 | | 114.8 |
Notwithstanding anything to the contrary set forth in any of the Company’s previous filings under the Securities Act of 1933, as amended, or the Exchange Act that may incorporate future filings, the stock performance graph shall not be incorporated by reference in any such filings.
81
Item 12. Security Ownership of Certain Beneficial Owners And Management And Related Stockholder Matters
The following table sets forth certain information as of February 15, 2005 regarding the beneficial ownership of our capital stock by (i) each person known by us to own more than five percent of the our outstanding capital stock; (ii) each of our directors and named executive officers and (iii) all of our directors and named executive officers as a group. Except as indicated in the footnotes to this table and under applicable community property laws, to our knowledge, the persons named in the table have sole voting and investment power with respect to all shares of common stock. Options exercisable on or before April 15, 2006, are included as shares beneficially owned. For the purposes of calculating percent ownership as of February 15, 2006, we had issued and outstanding 16,083,636 shares of our common stock. For any individual who beneficially owns shares represented by options exercisable on or before April 15, 2006 these shares were included for their calculation. These shares are treated as if outstanding for purposes of determining ownership of a particular class of our securities for that person, but not for any other person. Unless otherwise indicated, the address of each of the individuals and entities named below is: c/o Allion Healthcare, Inc., 1660 Walt Whitman Road, Suite 105, Melville, New York 11747.
Security Ownership Table
| | | | | |
| | | Shares Beneficially Owned | |
| | | Number | | Percent | |
Directors and Officers | | | | | |
John Pappajohn (1) | | 837,500 | | 5.1 | % |
Mike Moran (2) | | 455,000 | | 2.8 | % |
Derace Schaffer (3) | | 220,000 | | 1.4 | % |
Mikelynn Salthouse (4) | | 50,500 | | 0.3 | % |
Jim Spencer (5) | | 25,000 | | 0.2 | % |
John Colloton (6) | | 6,944 | | 0.0 | % |
Harvey Werblowsky (7) | | 6,944 | | 0.0 | % |
Robert Fleckenstein | | — | | 0.0 | % |
All directors and officers | | 1,601,888 | | 9.3 | % |
| | |
5% Stockholders | | | | | |
Next Century Growth Investors, LLC (8) | | 1,193,185 | | 7.4 | % |
Massachusetts Financial Services Co. (9) | | 895,500 | | 5.6 | % |
Arbor Capital Management, LLC (10) | | 891,700 | | 5.5 | % |
| (1) | The common stock owned includes 20,000 shares of Common Stock issuable upon exercise of options and 462,500 shares of common stock issuable upon exercise of warrants. |
| (2) | The common stock owned includes 455,000 shares of common stock issuable upon the exercise of options. |
| (3) | The common stock owned includes 120,000 shares of common stock issuable upon the exercise of options. |
| (4) | The common stock owned includes 50,500 shares of common stock issuable upon the exercise of options. |
| (5) | The common stock owned includes 25,000 shares of common stock issuable upon the exercise of options. |
| (6) | The common stock owned includes 6,944 shares of common stock issuable upon the exercise of options. |
| (7) | The common stock owned includes 6,944 shares of common stock issuable upon the exercise of options. |
| (8) | The address for Next Century Growth Investors, LLC is 5500 Wayzata Blvd, Suite 1275, Minneapolis, MN 55416. |
| (9) | The address for Massachusetts Financial Services Co. is 500 Boylston Street, Boston, MA 02116. |
| (10) | The address for Arbor Capital Management, LLC is One Financial Plaza, 120 South Sixth Street, Suite 1000, Minneapolis, MN 55402. |
82
Securities Authorized For Issuance Under Equity Compensation Plans
The following table sets forth certain information concerning compensation plans under which our equity securities are authorized for issuance:
| | | | | | | | |
Plan Category | | (a) Number of securities to be issued upon exercise of outstanding options, warrants and rights | | | (b) Weighted-average exercise price of outstanding options, warrants and rights | | (c) Number of securities remaining available under equity compensation plans (excluding securities reflected in column (a)) |
Equity compensation plans approved by security holders | | 1,452,000 | (1) | | $ | 3.21 | | 985,000 |
Equity compensation plans not approved by security holders | | 1,150,737 | (2) | | | 4.60 | | — |
| | | | | | | | |
Total | | 2,602,737 | | | $ | 3.82 | | 985,000 |
| (1) | Includes options granted pursuant to our 1998 Stock Option Plan and 2002 Stock Option Plan. |
| (2) | Includes warrants granted to individuals and corporations as consideration for services provided within the meaning of Statement of Financial Accounting Standards No. 123 and for purchase consideration for acquisitions. The warrants were granted by us upon authorization of our Board of Directors and were not issued pursuant to a single equity compensation plan that exists to grant warrants in exchange for goods and services. The terms of the warrants vary from grant to grant. |
Item 13. Certain Relationships And Related Transactions
In January 2000, we issued warrants to purchase 375,000 shares of common stock to John Pappajohn, a director, as consideration for his guarantee of a $1.5 million credit facility with West Bank. These warrants are exercisable at a price $1.00 per share. As consideration for the renewal of the guaranty, we issued warrants to purchase 125,000 shares of common stock to Mr. Pappajohn in July 2003, exercisable at a price per share of $5.00. In March 2005, when West Bank agreed to extend the maturity of its loan until September 2005, Mr. Pappajohn agreed to keep his guaranty in place through September 2005. As consideration for continuing his guaranty, in April 2005 we issued to Mr. Pappajohn warrants to purchase 100,000 shares of common stock exercisable at a price equal to our initial public offering price per share.
Item 14. Principal Accounting Fees And Services
The following table presents fees for professional audit services rendered by BDO Seidman, LLP for the audit of our financial statements for 2005 and 2004.
| | | | | | |
| | | 2005 | | 2004 |
Audit Fees (a) | | $ | 592,462 | | $ | 99,000 |
Audit related fees (b) | | | 47,719 | | | 11,292 |
Tax Fees (c) | | | 20,000 | | | 12,500 |
| | | | | | |
Total Fees | | $ | 660,181 | | $ | 122,792 |
a) Fees for audit services billed in 2004 and 2005 consisted of:
| | • | | Audit of the Company’s annual financial statements. |
| | • | | Reviews of the Company’s quarterly financial statements. |
| | • | | Fees for services rendered in connection with the Company’s Form S-1and Form S-8 filing. |
| | • | | Comfort letters, consents and other services related to Securities and Exchange Commission matters. |
| | • | | Audit of our internal control over financial reporting for compliance with Section 404 of the Sarbanes-Oxley Act of 2002. |
83
b) Fees for services relating to acquisition audits and reviews of filings on Form 8K/A.
c) Fees for tax services billed in 2005 consisted of review of our net operating losses.
No other professional services were rendered or fees were billed by BDO Seidman, LLP for the most recent fiscal year for the year ending December 31, 2005 and 2004.
Audit Committee Pre-Approval Policy
As required by Section 10A(i)(1) of the Exchange Act, all non-audit services to be performed by BDO Seidman, LLP our principal accountants must be approved in advance by the Audit Committee of the Board of Directors, subject to certain exceptions relating to non-audit services accounting for less than five percent of the total fees paid to its principal accountants which are subsequently ratified by the Audit Committee (the de minimus exception).
84
PART IV
Item 15. Exhibits And Financial Statement Schedules
The following documents are filed as part of this report.
Reports of Independent Registered Public Accounting Firm
Consolidated Balance Sheets as of December 31, 2004 and 2005
Consolidated Statements of Operations and Comprehensive Loss for the years ended December 31, 2003, 2004 and 2005
Consolidated Statements of Stockholders’ Equity for the years ended December 31, 2003, 2004 and 2005
Consolidated Statement of Cash Flows for the years ended December 31, 2003, 2004 and 2005
Notes to Consolidated Financial Statements
| (2) | Schedules. An index of Exhibits and Schedules follows below in this Report. Schedules other than those listed below have been omitted from this Report because they are not required, are not applicable or the required information is included in the financial statements or the notes thereon. |
Index To Financial Statements, Supplementary Data And Financial Statement Schedules
| | |
Schedules: | | Page
Numbering Form 10-K |
Valuation and Qualifying Accounts | | 92 |
| (3) | Exhibits. The exhibits listed in the accompanying Exhibit Index are filed or incorporated by reference as part of this Report |
85
SIGNATURES
In accordance with Section 13 or 15(d) of the Exchange Act, the registrant caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| | | | |
| | ALLION HEALTHCARE, INC. |
| | |
| Date: March 15, 2006 | | By: | | /S/ JAMES SPENCER |
| | | | James Spencer Secretary, Treasurer and Chief Financial Officer |
In accordance with the Exchange Act, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
/S/ MICHAEL P. MORAN |
Michael P. Moran, Chairman, President and Chief Executive Officer |
Date: March 15, 2006
|
/S/ JOHN PAPPAJOHN |
| John Pappajohn, Director |
Date: March 15, 2006
|
|
/S/ DERACE SCHAFFER |
| Derace Schaffer, M.D., Director |
Date: March 15, 2006
|
|
/S/ HARVEY WERBLOWSKY |
| Harvey Werblowsky, Director |
Date: March 15, 2006
|
|
/s/ JOHN COLLOTON |
| John Colloton, Director |
Date: March 15, 2006
86
Supplemental Information to be Furnished With Reports Filed
Pursuant to Section 15(d) of the Act by Registrants Which Have Not Registered
Securities Pursuant to Section 12 of the Act
Allion Healthcare, Inc. furnished a 2004 annual report to its stockholders in 2005 covering the 2004 fiscal year and intends to furnish a proxy statement and the 2005 annual report to its stockholders in 2006.
EXHIBIT INDEX
| | |
| 2.1 | | Confirmation Order dated February 1, 1999. (Incorporated by reference to Exhibit 2.1 to the Registrant’s Current Report on Form 8-K filed on October 10, 1999.) |
| |
| 2.2 | | First Amended Plan of Reorganization of The Care Group, Inc., et al. dated January 2, 1998. (Incorporated by reference to Exhibit 2.2 to the Registrant’s Current Report on Form 8-K filed on October 10, 1999.) |
| |
| 2.3 | | Stock Purchase Agreement, dated as of May 1, 2003, among MOMS Pharmacy, Inc., as buyer, Allion Healthcare, Inc. as parent, and Darin A Peterson and Allan H. Peterson collectively as sellers. (Incorporated by reference to Exhibit 2.1 to the Registrant’s Current Report on Form 8-K filed on May 16, 2003.) |
| |
| 2.4 | | Stock Purchase Agreement by and among MOMS Pharmacy, Inc. and Michael Stone and Jonathan Spanier dated as of January 4, 2005. (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on January 10, 2005.) |
| |
| 2.5 | | Stock Purchase Agreement by and among MOMS Pharmacy, Inc. and Pat Iantorno, Eric Iantorno, Jordan Iantorno, Jordan Iantorno A/C/F Max Iantorno, Michael Winters and George Moncada dated as of February 28, 2005. (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on March 4, 2005.) |
| |
| 2.6 | | Asset Purchase Agreement by and among MOMS Pharmacy, Inc. and Oris Medical Systems, Inc. dated as of May 19, 2005. (Incorporated by reference to Exhibit 2.6 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 2.7 | | Asset Purchase Agreement by and among Medicines Made Easy and Priority Pharmacy, Inc. dated as of December 9, 2005. (Incorporated by reference to Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on December 12, 2005.) |
| |
| 3.1 | | Amended and Restated Certificate of Incorporation of the Registrant. (Incorporated by reference to Exhibit A to the Registrant’s proxy statement filed on June 4, 2003.) |
| |
| 3.2 | | Certificate of Designation of Rights and Preferences of Series A Preferred Stock of Allion Healthcare, Inc. (Incorporated by reference to Exhibit 3.2 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
| |
| 3.3 | | Amended and Restated Certificate of Designation of Rights and Preferences of Series B Preferred Stock of Allion Healthcare, Inc. (Incorporated by reference to Exhibit 3.3 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
| |
| 3.4 | | Second Amended and Restated Bylaws of the Registrant. (Incorporated by reference to Exhibit 3.2 to the Registrant’s Annual Report on Form 10-KSB filed on April 15, 2003. |
| |
| 3.5 | | Certificate of Designation of Rights and Preferences of Series C Preferred Stock of Allion Healthcare, Inc. (Incorporated by reference to Exhibit 3.1 to the Registrant’s Annual Report on Form 10-KSB filed on April 16, 2003.) |
| |
| 3.6 | | Certificate of Designation of Rights and Preferences of Series D Preferred Stock of Allion Healthcare, Inc. (Incorporated by reference to Exhibit 3.2 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
87
| | |
| 3.7 | | Certificate of Designation of Rights and Preferences of Series E Preferred Stock of Allion Healthcare, Inc. (Incorporated by reference to Exhibit 3.1 to the Registrant’s Current Report on Form 8-K filed on December 20, 2004.) |
| |
| 3.8 | | Third Amended and Restated Bylaws of the Registrant. (Incorporated by reference to Exhibit 3.8 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 3.9 | | Certificate of Correction of Allion Healthcare, Inc., relating to the Certificate of Designation of Rights and Preferences of Series D Preferred Stock. (Incorporated by reference to Exhibit 3.9 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 3.10 | | Certificate of Correction of Allion Healthcare, Inc., relating to the Certificate of Designation of Rights and Preferences of Series E Preferred Stock. (Incorporated by reference to Exhibit 3.10 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 3.11 | | Certificate of Correction of Allion Healthcare, Inc., relating to the Certificate of Designation of Rights and Preferences of Series C Preferred Stock. (Incorporated by reference to Exhibit 3.11 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 3.12 | | Certificate of Correction of Allion Healthcare, Inc., relating to the Amended and Restated Certificate of Incorporation. (Incorporated by reference to Exhibit 3.12 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 4.1 | | Form of Warrant to Purchase Common Stock of Allion Healthcare, Inc. issued to the former owners of North American Home Health Supply, Inc., as of January 4, 2005. (Incorporated by reference to Exhibit 3.1 to the Registrant’s Current Report of Form 8-K filed on January 10, 2005.) |
| |
| 4.2 | | Form of Warrant to Purchase Common Stock of Allion Healthcare, Inc. issued to the former owners of Specialty Pharmacies Inc., as of February 28, 2005. (Incorporated by reference to Exhibit 3.1 to the Registrant’s Current Report of Form 8-K filed on March 4, 2005.) |
| |
| 4.3 | | Subordinated Secured Promissory Notes of Allion Healthcare, Inc., dated as of January 4, 2005, in the aggregate amount of $1,375,000, issued to the former owners of North American Home Health Supply, Inc. (Incorporated by reference to Exhibit 10.3 to the Registrant’s Current Report on Form 8-K filed on January 10, 2005.) |
| |
| 4.4 | | Guaranty given by Allion Healthcare, Inc. to and for the benefit of Michael Stone and Jonathan Spanier dated as of January 4, 2005. (Incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on January 10, 2005.) |
| |
| 4.5 | | Warrant to Purchase Common Stock of Allion Healthcare, Inc. issued to John Pappajohn on January 11, 2000. (Incorporated by reference to Exhibit 4.12 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 4.6 | | Warrant to Purchase Common Stock of Allion Healthcare, Inc. issued to John Pappajohn on October 1, 2003. (Incorporated by reference to Exhibit 4.13 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 4.7 | | Warrant to Purchase Common Stock of Allion Healthcare, Inc. issued to John Pappajohn on April 15, 2005. (Incorporated by reference to Exhibit 99.1 to the Registrant’s Current Report on Form 8-K filed on April 21, 2005.) |
| |
| 4.8 | | Warrant to purchase common stock of Allion Healthcare, Inc. issued to Crestview Capital Master, LLC on May 13, 2005. (Incorporated by reference to Exhibit 4.9 to the Registrant’s Quarterly Report on Form 10-Q filed on May 18, 2005.) |
| |
| 4.9 | | Form of Stock Certificate (Incorporated by reference to Exhibit 4.1 to the Registration Statement on Form S-1 filed on May 24, 2005). |
| |
| 10.1 | | Registration Rights Agreement, dated as of October 30, 2001, by and between Allion Healthcare, Inc. and Gainesborough, L.L.C. (Incorporated by reference to Exhibit 10.1 to the Registrant’s Annual Report on 10-KSB/A filed in May 2004.) |
88
| | |
| 10.2 | | Registration Rights Agreement issued to the holders of Series E convertible preferred stock, dated as of December 17, 2004 (Incorporated by reference to Exhibit 10.2 to the Registrant’s Current Report on Form 8-K filed on December 20, 2004.) |
| |
| 10.3 | | 1998 Stock Option Plan. (Incorporated by reference to Exhibit 10.3 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
| |
| 10.4 | | 2002 Stock Option Plan. (Incorporated by reference to Exhibit 10.4 to the Registrant’s Annual Report on Form 10-KSB filed on April 15, 2003.) |
| 10.5 | | Amendment No. 1 to the 1998 Stock Option Plan (Incorporated by reference to Exhibit 10.1 to the Registrant’s quarterly report on Form 10-Q filed on November 14, 2005). |
| |
| 10.6 | | Amended and Restated 2002 Stock Incentive Plan (Incorporated by reference to Exhibit 10.2 to the Registrant’s quarterly report on Form 10-Q filed on November 14, 2005). |
| |
| 10.7 | | Loan and Security Agreement, dated as of April 21, 1999, by and among the Registrant, The Care Group of Texas Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and HCFP Funding, Inc. (Incorporated by reference to Exhibit 10.6 to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 10.8 | | Amendment No. 1 to Loan and Security Agreement, executed as of July 27, 2001 and effective as of April 21, 2001, by and among the Registrant, The Care Group of Texas Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and Heller Healthcare Finance, Inc. (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.7 to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 10.9 | | Amendment No. 2 to Loan and Security Agreement, dated as of April 2002, by and among the Registrant, The Care Group of Texas, Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and Heller Healthcare Finance, Inc. (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.8 to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 10.10 | | Amendment No. 3 and Consent to Loan and Security Agreement, dated as of May 28, 2003, by and among the Registrant, The Care Group of Texas, Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and Heller Healthcare Finance, Inc. (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.9 to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 10.11 | | Amendment No. 4 to Loan and Security Agreement, dated as of September 2003, by and among the Registrant, The Care Group of Texas, Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and Heller Healthcare Finance, Inc. (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.10 to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 10.12 | | Agreement of Lease Between Reckson Operating Partnership, L.P and Allion Healthcare, Inc. (Incorporated by reference to Exhibit 10.11 to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 10.13 | | Amendment No. 5 to Loan and Security Agreement, dated as of January 2005, by and among the Registrant, The Care Group of Texas, Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and Heller Healthcare Finance, Inc. (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.12 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
| |
| 10.14 | | Amendment No. 6 to Loan and Security Agreement, dated as of February 2005, by and among the Registrant, The Care Group of Texas, Inc., Care Line of Houston, Inc., Mail Order Meds, Inc., Care Line of New York, Inc., Commonwealth Certified Home Care, Inc. and Heller Healthcare Finance, Inc. (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.13 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
89
| | |
| 10.15 | | AmerisourceBergen Prime Vendor Agreement dated September 15, 2003. (Incorporated by reference to Exhibit 10.14 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.)** |
| |
| 10.16 | | Registration Rights Agreement, dated as of January 4, 2005, by and between Allion Healthcare, Inc. and Michael Stone and Jonathan Spanier. (Incorporated by reference to Exhibit 10.16 to the Registrant’s Annual Report on Form 10-K filed on March 31, 2005.) |
| |
| 10.16A | | Amendment to Registration Rights Agreement dated as of May 19, 2005, between Allion Healthcare, Inc. and Michael Stone and Jonathan Spanier. (Incorporated by reference to Exhibit 10.15A to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 10.17 | | Registration Rights Agreement, dated as of April 4, 2003 issued to the holders of Series C convertible preferred stock. (Incorporated by reference to Exhibit 10.17 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| 10.18 | | Form of Registration Rights Agreement, dated as of April 16, 2004 issued to the holders of Series D convertible preferred stock. (Incorporated by reference to Exhibit 10.18 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 10.19 | | Form of Registration Rights Agreement, dated as of March 30, 2001 issued to the holders of Series A convertible preferred stock. (Incorporated by reference to Exhibit 10.19 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 10.20 | | Amendment No. 7 to Loan and Security Agreement, dated as of May 13, 2005 by and among Allion Healthcare, Inc., f/k/a The Care Group, Inc., Mail Order Meds of Texas, Inc., f/k/a Mail Order Meds, Inc., MOMS Pharmacy, Inc. (New York), f/k/a Mail Order Meds of New York, Inc., MOMS Pharmacy, Inc. (California), MOMS Pharmacy, LLC, Medicine Made Easy, North American Home Health Supply, Inc., Specialty Pharmacies, Inc. and GE HFS Holdings, Inc., f/k/a Heller Healthcare Finance, Inc., (f/k/a HCFP Funding, Inc.) (Incorporated by reference to Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed on May 18, 2005.) |
| |
| 10.21 | | Registration Rights Agreement dated as of May 13, 2005 by and between Allion Healthcare, Inc. and Crestview Capital Master, LLC. (Incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q filed on May 18, 2005.) |
| |
| 10.22 | | Amendment No. 8 to Loan and Security Agreement, dated as of May 17, 2005 by and among Allion Healthcare, Inc., f/k/a The Care Group, Inc., Mail Order Meds of Texas, Inc., f/k/a Mail Order Meds, Inc., MOMS Pharmacy, Inc. (New York), f/k/a Mail Order Meds of New York, Inc., MOMS Pharmacy, Inc. (California), MOMS Pharmacy, LLC, Medicine Made Easy, North American Home Health Supply, Inc., Specialty Pharmacies, Inc. and GE HFS Holdings, Inc., f/k/a Heller Healthcare Finance, Inc. (Incorporated by reference to Exhibit 10.23 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 10.23 | | Noncompetition agreement by and between Allion Healthcare, Inc. and Mikelynn Salthouse dated as of August 27, 2002. (Incorporated by reference to Exhibit 10.24 to the Registrant’s Registration Statement on Form S-1 filed on May 24, 2005.) |
| |
| 10.24 | | Asset Purchase Agreement by and among Medicine Made Easy and Frontier Pharmacy & Nutrition Inc. dated as of August 4, 2005. (Incorporated by reference to Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on August 15, 2005.) |
| |
| 10.25 | | Agreement with the California Department of Health Services dated as of August 2005. (Incorporated by reference to Exhibit 10.3 to the Registrant’s Quarterly Report on Form 10-Q filed on November 14, 2005.) |
| |
| 10.26 | | Waiver and Consent Agreement, dated as of August 4 by and among Allion Healthcare, Inc., f/k/a The Care Group, Inc., Mail Order Meds of Texas, Inc., f/k/a Mail Order Meds, Inc., MOMS Pharmacy, Inc. (New York), f/k/a Mail Order Meds of New York, Inc., MOMS Pharmacy, Inc. (California), MOMS Pharmacy, LLC, Medicine Made Easy, North American Home Health Supply, Inc., Specialty Pharmacies, Inc. and GE HFS Holdings, Inc., f/k/a Heller Healthcare Finance, Inc. (Incorporated by reference to Exhibit 10.4 to the Registrant’s Quarterly Report on Form 10-Q filed on November 14, 2005.) |
90
| | |
| 10.27 | | Amendment No. 9 to Loan and Security Agreement, dated as of September 29, 2005 by and among Allion Healthcare, Inc., f/k/a The Care Group, Inc., Mail Order Meds of Texas, Inc., f/k/a Mail Order Meds, Inc., MOMS Pharmacy, Inc. (New York), f/k/a Mail Order Meds of New York, Inc., MOMS Pharmacy, Inc. (California), MOMS Pharmacy, LLC, Medicine Made Easy, North American Home Health Supply, Inc., Specialty Pharmacies, Inc. and GE HFS Holdings, Inc., f/k/a Heller Healthcare Finance, Inc. (Incorporated by reference to Exhibit 10.5 to the Registrant’s Quarterly Report on Form 10-Q filed on November 14, 2005.) |
| |
| 10.28 | | Agreement of Sublease for 191 Golden Gate Avenue, San Francisco, CA 94102, dated as of February 25, 2005, by and between Tenderloin AIDS Resource Center and Specialty Pharmacies, Inc. (Incorporated by reference to Exhibit 10.6 to the Registrant’s Quarterly Report on Form 10-Q filed on November 14, 2005.) |
| |
| 10.29 | | Agreement of Lease for 19300 S. Hamilton Ave, Gardena, CA, dated as of August 23, 2005, by and between Kroeze Koncepts, Inc, and Medicine Made Easy. * |
| |
| 10.30 | | Agreement of Lease for 3940-58 Fourth Avenue, San Diego, CA, dated as of January 9, 2006, by and between Acadia Corporation and Medicine Made Easy. * |
| |
| 10.31 | | Asset Purchase Agreement among Medicine Made Easy and Priority Pharmacy, Inc., the David C. Zeiger Trust UTD 4/30/93, David C. Zeiger and Peter Ellman dated as of December 9, 2005.* |
| |
| 10.32 | | Asset Purchase Agreement Among MOMS Pharmacy of Brooklyn, Inc., H.S. Maiman Rx, Inc. Scott Maiman and Nancy Maiman, dated as of March 10, 2006. * |
| |
| 14.1 | | Code of Ethics. (Filed as an exhibit to the Registrant’s Annual Report on Form 10-KSB filed on April 14, 2004.) |
| |
| 21.1 | | Subsidiaries of the Registrant. * |
| |
| 23.1 | | Consent of BDO Seidman, LLP * |
| |
| 31.1 | | Certification of the Chief Executive Officer pursuant to Rule 13a-14(a) Section 302 of the Sarbanes-Oxley Act of 2002. * |
| |
| 31.2 | | Certification of the Chief Financial Officer pursuant to Rule 13a-14(a) Section 302 of the Sarbanes-Oxley Act of 2002. * |
| |
| 32.1 | | Certification by the Chief Executive Officer and Acting Chief Financial Officer pursuant to 18 U.S.C. § 1350 Section 906 of the Sarbanes-Oxley Act of 2002. *** |
| ** | - Certain portions of this document have been omitted pursuant to a request for confidential treatment. We have filed non-redacted copies of this agreement with the Securities and Exchange Commission. |
| *** | - These certifications are being furnished solely pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 and are not being filed as part this Annual Report on Form 10-K or as a separate disclosure document. |
91
SCHEDULE II—VALUATION AND QUALIFYING ACCOUNTS
| | | | | | | | | | |
| | | | | Additions | | | | |
| | | Balance at
beginning
of period | | Charge to Cost and
Expense | | Charged
to Other
Accounts | | Deductions
(1) | | Balance at
End of
period |
Deducted from asset accounts | | | | | | | | | | |
Year ended December 31, 2005: | | | | | | | | | | |
Allowance for doubtful accounts | | 296,320 | | 128,000 | | | | 141,496 | | 282,824 |
Valuation allowance on net deferred tax assets | | 3,802,000 | | 201,000 | | 668,000 | | | | 4,671,000 |
| | | | | | | | | | |
| | 4,098,320 | | 329,000 | | 668,000 | | 141,496 | | 4,953,824 |
| | | | | | | | | | |
Deducted from asset accounts | | | | | | | | | | |
Year ended December 31, 2004: | | | | | | | | | | |
Allowance for doubtful accounts | | 437,032 | | 80,200 | | | | 220,912 | | 296,320 |
Valuation allowance on net deferred tax assets | | 2,864,000 | | | | 938,000 | | | | 3,802,000 |
| | | | | | | | | | |
| | 3,301,032 | | 80,200 | | 938,000 | | 220,912 | | 4,098,320 |
| | | | | | | | | | |
Deducted from asset accounts | | | | | | | | | | |
Year ended December 31, 2003: | | | | | | | | | | |
Allowance for doubtful accounts | | 276,606 | | 236,558 | | | | 76,132 | | 437,032 |
Valuation allowance on net deferred tax assets | | 2,072,000 | | | | 792,000 | | | | 2,864,000 |
| | | | | | | | | | |
| | 2,348,606 | | 236,558 | | 792,000 | | 76,132 | | 3,301,032 |
| | | | | | | | | | |
| (1) | Consists primarily of recoveries of accounts previously deemed uncollectible. |
92