









Searchable text section of graphics shown above
Forward-Looking Statements
Statements in this presentation that are not historical facts are “forward-looking statements” that involve risks and uncertainties. Forward-looking statements can be identified by the use of words such as “may,” “will,” “should,” “anticipates,” “expects” or comparable terminology or by discussions of future events. Such forward looking statements include statements relating to the clinical development program for TPI 287, the anticipated activity of TPI 287 in taxanes resistant tumors, the safety and efficacy of TPI 287, the time tables for future development of TPI 287, and the company’s ability to continue to fund its development programs, either through existing resources or through new funding sources. Such statements involve known and unknown risks, uncertainties and other factors that may cause our actual results, performance or achievements to be materially different from the results, performance or achievements expressed or implied by such forward-looking statements. Such risks, uncertainties and other factors include risks that clinical trials for TPI 287 will be delayed due to institutional approvals, patient recruitment, formulation and manufacturing difficulties or other factors; and that human clinical trials may show that TPI 287 is unsafe and/or ineffective in treating cancer in human patients. General implementation risks associated with development of any of our products include the risk that we will be blocked or limited in the development or marketing because of the intellectual property rights of third parties; that we are limited in our ability to obtain, maintain and enforce our own intellectual property rights; that development of our product candidates is delayed or terminated because the costs of further development exceed the value of such candidates; and that the Company’s resources are insufficient to continue development and the Company will be unable to raise sufficient additional capital to continue operations and development. Additional risks, uncertainties and other information is contained in the Company’s reports filed from time to time with the Securities and Exchange Commission. Particular attention should be paid to information in such SEC reports under the captions “Risk Factors” and “Special Note Regarding Forward-Looking Statements.” The Company disclaims any intention or obligation to update publicly or revise any forward-looking statements contained in this presentation or any other disclosure, whether as a result of new or additional information, future events or otherwise.
[LOGO]
2
Tapestry Today
• Founded in 1991
• Located in Boulder, Colorado
• Clinical stage biopharmaceutical company focused on developing novel oncology compounds
• Experienced pre-clinical & clinical oncology development team
• Leading clinical oncology advisory team
• Novel third generation taxane (TPI 287-IV) active in a broad range of solid tumors
• Oral version of TPI 287 (TPI 287-Oral) has shown bioavailability in animals
3
Tapestry Financial Overview
As of 12/6/2005
• Price: $0.39
• 52 Week High/Low: $0.25 - $1.35
• Market Value: $13.39M
9 Months Ended 9/28/2005
• Cash and Short Term Investments: $17.57M
• Net Operating Loss: $14.52
• Number of Shares
• Primary: 34,238,995
• Diluted: 41,988,280
4
Senior Management
• Leonard Shaykin, Chairman and CEO
• Biotechnology entrepreneur, Venture capital, Private equity
• Martin Batt, COO
• Operations expertise in multiple industries including biotechnology, aerospace, computer software
• Gordon Link, CFO
• CPA plus over 15 years of biotechnology operations
• Michael Kurman, CMO
• Former Director of Clinical Research, Oncology and Allergy for Janssen Research Foundation; other positions at U.S. Biosciences and Quintiles
• David Emerson, VP of Cancer Biology
• 16 years in biopharmaceuticals; OSI, Gilead and GSK
• James McChesney, CSO
• Natural Products Chemistry specialist
• Gilles Tapolsky, VP of Product Development
• PhD with 16 years in biopharmaceuticals; FeRx, ViroTex, Rhone Poulenc Rorer and co-founder of Flamel Technologies
5
Staffing Summary
• 34 FTEs
• 29 Full time
• 9 Part time
• 4 Consultants
• 3 MDs, 8 PhDs
• 6 in clinical development and regulatory
6
Milestones
• Achieved
• Initial Public Offering in 1994
• Generic paclitaxel approved in US & 25 other countries, then…
• Paclitaxel business sold to Mayne Pharma for $70MM in 2003
• Filed first proprietary IND for TPI 287-IV in 2004
• Commenced Phase I clinical trial for TPI 287-IV in 2005
• Evidence of oral bioavailability of TPI 287-Oral
• Upcoming
• Oral PK study in humans
• Completion of Phase I clinical trial for TPI 287-IV (in 7 and 21 day dosing)
• Commencement of Phase II clinical trials for TPI 287-IV
7
TPI 287: A Third Generation Taxane
• Preclinical data shows that TPI 287 has more activity than paclitaxel or docetaxel in a variety of taxane-resistant human tumor cell lines
• TPI 287 has the potential to:
• circumvent expression of the drug efflux transporter, MDR-1 protein, seen in breast, lung and prostate cancers
• be active in tumor types currently not responsive to paclitaxel, (i.e., colon cancer)
• be active in tumor cells that express mutant tubulin
9
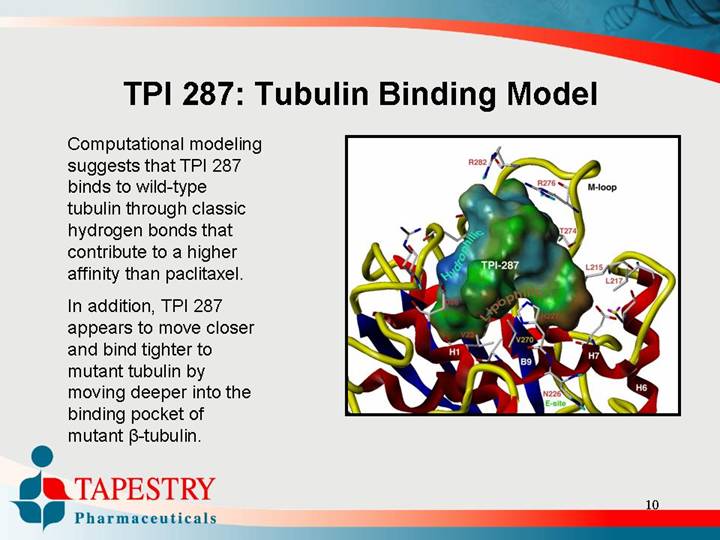
TPI 287: Tubulin Binding Model
Computational modeling suggests that TPI 287 binds to wild-type tubulin through classic hydrogen bonds that contribute to a higher affinity than paclitaxel.
In addition, TPI 287 appears to move closer and bind tighter to mutant tubulin by moving deeper into the binding pocket of mutant B-tubulin.
[GRAPHIC]
10
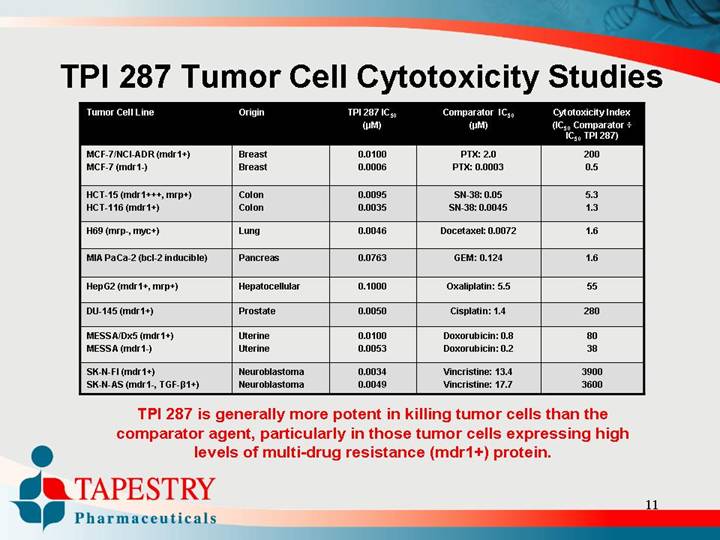
TPI 287 Tumor Cell Cytotoxicity Studies
Tumor Cell Line |
| Origin |
| TPI 287 IC50 |
| Comparator IC50 |
| Cytotoxicity Index |
|
|
|
| (µM) |
| (µM) |
| (IC50 Comparator ÷ |
|
|
|
|
|
|
|
| IC50 TPI 287) |
|
|
|
|
|
|
|
|
|
MCF-7/NCI-ADR (mdr1+) |
| Breast |
| 0.0100 |
| PTX: 2.0 |
| 200 |
MCF-7 (mdr1-) |
| Breast |
| 0.0006 |
| PTX: 0.0003 |
| 0.5 |
|
|
|
|
|
|
|
|
|
HCT-15 (mdr1+++, mrp+) |
| Colon |
| 0.0095 |
| SN-38: 0.05 |
| 5.3 |
HCT-116 (mdr1+) |
| Colon |
| 0.0035 |
| SN-38: 0.0045 |
| 1.3 |
|
|
|
|
|
|
|
|
|
H69 (mrp-, myc+) |
| Lung |
| 0.0046 |
| Docetaxel: 0.0072 |
| 1.6 |
|
|
|
|
|
|
|
|
|
MIA PaCa-2 (bcl-2 inducible) |
| Pancreas |
| 0.0763 |
| GEM: 0.124 |
| 1.6 |
|
|
|
|
|
|
|
|
|
HepG2 (mdr1+, mrp+) |
| Hepatocellular |
| 0.1000 |
| Oxaliplatin: 5.5 |
| 55 |
|
|
|
|
|
|
|
|
|
DU-145 (mdr1+) |
| Prostate |
| 0.0050 |
| Cisplatin: 1.4 |
| 280 |
|
|
|
|
|
|
|
|
|
MESSA/Dx5 (mdr1+) |
| Uterine |
| 0.0100 |
| Doxorubicin: 0.8 |
| 80 |
MESSA (mdr1-) |
| Uterine |
| 0.0053 |
| Doxorubicin: 0.2 |
| 38 |
|
|
|
|
|
|
|
|
|
SK-N-FI (mdr1+) |
| Neuroblastoma |
| 0.0034 |
| Vincristine: 13.4 |
| 3900 |
SK-N-AS (mdr1-, TGF-B1+) |
| Neuroblastoma |
| 0.0049 |
| Vincristine: 17.7 |
| 3600 |
TPI 287 is generally more potent in killing tumor cells than the comparator agent, particularly in those tumor cells expressing high levels of multi-drug resistance (mdr1+) protein.
11
TPI 287 Single Dose Toxicology Studies
• Intravenous or Intraperitoneal dose tolerance and MTD
• Maximum Tolerated Dose (MTD)
• Mouse – 80 mg/kg or 240 mg/m2
• Rat – 48 mg/kg or 288 mg/m2
• Dog – 12.5 mg/kg or 221 mg/m2
The toxicology profile and the maximum tolerated dose of TPI 287 is consistent to that routinely seen with other taxanes
12
TPI 287 Repeat Dose Toxicology Studies
• Maximum Tolerated Dose
• Mouse – 12 mg/kg or 36 mg/m2
• Rat – 14 mg/kg or 84 mg/m2
• Dog – 4 mg/kg or 71 mg/m2 (basis for human dosing)
The toxicology profile and the maximum tolerated dose of TPI 287 is consistent to that routinely seen with other taxanes
13
TPI 287: Preclinical Summary
• In Vitro Studies
• Evidence of activity in various cell lines including: breast, colon, lung, pancreas, prostate, and others
• Tumor Xenograft Studies
• Evidence of activity in breast, colon, lung, and prostate tumors models, including those tumors with expression of mdr-1 protein
• Toxicity
• Generally well-tolerated
• Key findings are GI in nature
• MTD based on dog repeat study is 4 mg/kg or 71 mg/m2
• Starting human dosing programs
• Based on 1/10 of MTD in dog
• Starting dose is 7 mg/m2
14
TPI 287 Additional Studies
• Studies comparing TPI 287 to epothilones and other new taxanes in clinical development
• Studies designed to investigate TPI 287 at alternative dosing regimens
• Studies designed to investigate combinations of TPI 287 with other anticancer drugs
• Studies designed to investigate sequencing of TPI 287 with other anticancer drugs
Tapestry is expanding its pre-clinical package in anticipation of additional clinical studies
15
Q7D Trial Sites and Investigators
• Lombardi Comprehensive Cancer Center at Georgetown University, Washington, D.C.
• John Marshall, M.D., Principal Investigator, Associate Professor of Oncology and Medicine at Georgetown University and Director of the Developmental Therapeutics program at the Lombardi Comprehensive Cancer Center.
• Westchester Medical Center, Valhalla, New York
• Tauseef Ahmed, M.D. Professor of Medicine and Chief of the Division of Oncology/Hematology at New York Medical College
17
Q7D Phase I Trial Objectives
Primary Objective:
• To determine the maximum tolerated dose of TPI 287
Secondary Objectives:
• To determine the safety of TPI 287
• To determine the antitumor activity of TPI 287
• To determine the pharmacokinetic profile of TPI 287
• To determine the pharmacodynamic profile of TPI 287
18
Q7D Phase I Trial Design - 1
• Open-Label
• Multicenter
• Sequential groups
• Dose-escalation until MTD
• Anticipated number of patients: up to 48
19
Q7D Phase I Trial Design - 2
• Maximum Tolerated Dose (MTD) = Dose Limiting Toxicity (DLT) - 1
• Enroll 4 patients at each dose level
• Escalate dose after 3 patients have completed one cycle
• If 0/3 with DLT, the next cohort will be enrolled at twice the previous dose
• If 1/3 with DLT, add 3 more patients at current dose
• If 1/6 with DLT, the next cohort will be enrolled at 1.25 the previous dose
• If 2/6 with DLT, stop escalation
• If 2/3 with DLT, stop escalation
20
Q7D Phase I Study Duration
• Patients will be treated until the following:
• Dose Limiting Toxicity
• Patient or Investigator decision
• Progressive disease
• Patient develops significant other illness
• If the study is not discontinued for above reasons, patients can remain enrolled in trial until disease progression
21
Q7D Status of Phase I Trial
(as of December 5, 2005)
• Completed third cohort (28 mg/m2)
• Currently dosing the fourth cohort (56 mg/m2)
• Types of cancers of patients enrolled to date include: breast, prostate, kidney, colorectal, basal cell, endometrial, glioblastoma and cervical cancers as well as osteosarcoma
22
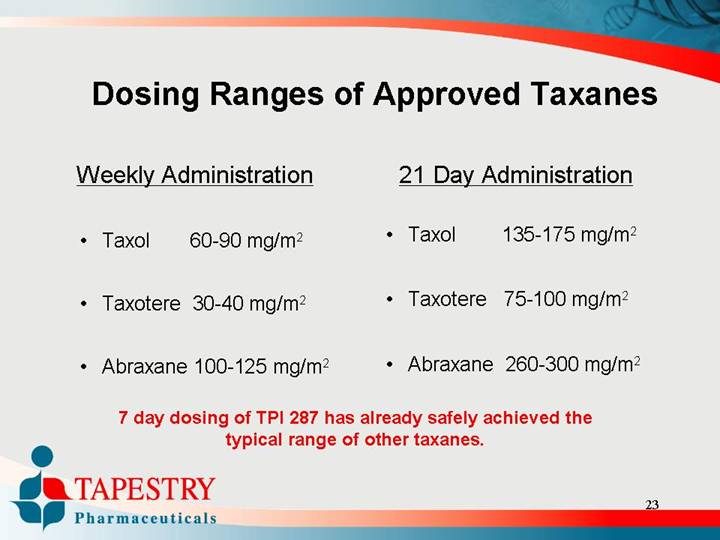
Dosing Ranges of Approved Taxanes
Weekly Administration |
| 21 Day Administration | ||||||||
|
|
|
|
|
|
|
|
| ||
• |
| Taxol |
| 60-90 mg/m2 |
| • |
| Taxol |
| 135-175 mg/m2 |
|
|
|
|
|
|
|
|
|
|
|
• |
| Taxotere |
| 30-40 mg/m2 |
| • |
| Taxotere |
| 75-100 mg/m2 |
|
|
|
|
|
|
|
|
|
|
|
• |
| Abraxane |
| 100-125 mg/m2 |
| • |
| Abraxane |
| 260-300 mg/m2 |
7 day dosing of TPI 287 has already safely achieved the typical range of other taxanes.
23
Q7D Phase I Timelines for TPI 287
• IND Submission Completed: December 2004
• First patient in Q7D Protocol Completed: May 2005
• Expected Q7D Phase I trial Completion: 2Q06
24
Differences between the Q7D and Q21D Phase I Studies
Q7D
• Q7 Day Administration one dose per week for three weeks followed by one week of rest
• Completed the third cohort (patients exposed to 84 mg/m2 in a 28 day period)
• Four patients per cohort, 3 of which must complete one cycle before the next cohort can be recruited
Q21D
• Q21 Day Administration one dose every 21 days
• First cohort starting at 7 mg/m2 in November 2005
• One patient per cohort until the first drug related Grade 2 or greater toxicity is seen, then three patients per cohort
26
Q21D Phase I Timelines for TPI 287
• Q21D Protocol Submission Completed: July 2005
• First patient in expected: December 2005
• Expected Q21D Phase I trial Completion : Mid-2006
27
Oral Program for TPI 287
• TPI 287 has been shown to have oral efficacy in mouse xenografts
• TPI 287 has been shown to have oral bioavailability in rats
• File a protocol amendment to TPI 287 IND for bioavailability study in man
• If oral bioavailability in man is sufficient, then Tapestry will file new IND to continue development of TPI 287-Oral
29
Oral Program for TPI 287
On November 16, 2005, at the AACR/NCI/EORTC International Conference on Molecular Targets and Cancer Therapeutics in Philadelphia, Tapestry presented supportive preclinical data on the oral bioavailability of TPI 287.
30
Intellectual Property for TPI 287
Composition of Matter:
• Pending patent claims cover the composition of matter and the methods of making TPI 287
• Various modifications on the sidechain and on some key positions on the taxane unit are the subject of a pending patent application
• A study done on possible combination therapies (using TPI 287 in combination with quassinoids) is the subject of a pending patent application
On-Going Work:
• Patent application is begin drafted to cover the new coupling methods (to provide key intermediates) generated. These new methods of manufacture demonstrated an efficient way of synthesizing this family of semi-synthetic taxanes, including paclitaxel, docetaxel and TPI 287
• Various side chain compositions and methods to synthesize taxanes are the subject of this new application
31
Board of Directors
• Leonard P. Shaykin
Chairman of the Board, Chief Executive Officer
• Stephen K. Carter, M.D.
Former Senior Vice President, Worldwide Clinical Research and Development, Bristol-Myers Squibb and Deputy Director, Division of Cancer Treatment, National Cancer Institute
• George M. Gould, Esq.
Attorney, Of Counsel, Gibbons, Del Deo, Dolan, Giffinger & Vecchione; formerly Vice President and Chief Patent Counsel of Hoffman-La Roche
• Arthur Hull Hayes, Jr., M.D.
President, MediScience Associates a pharmaceutical consulting company; Former FDA Commissioner
• The Honorable Richard N. Perle
Former U.S. Assistant Secretary of Defense; Director of Hollinger International, Inc.; Autonomy, PLC
• Patricia Pilia, Ph.D.
Executive VP, Secretary, Co-founder of Company
• Robert E. Pollack, Ph.D.
Professor of Biological Sciences and Director of the Center for the Study of Science and Religion at Columbia University
• Elliot M. Maza, J.D., C.P.A.
Chief Financial Officer of Emisphere Technologies, Inc.
32
Scientific Advisory Board
• Paul A. Bunn, Jr., M.D. (Chair)
Director of the University of Colorado Cancer Center, past president of American Society of Clinical Oncology (2002-2003), and former chairman of the Oncologic Drugs Advisory Committee (ODAC) for FDA
• S. Gail Eckhardt, M.D.
Professor of Medicine and Director of the Developmental Therapeutics and GI Malignancies Programs at the University of Colorado Health Sciences Center in Denver
• Robert E. Pollack, Ph.D.
Professor of Biological Sciences and Director of the Center for the Study of Science and Religion at Columbia University
• Eric K. Rowinsky, M.D.
Former Director of the Institute for Drug Development, Cancer Therapy and Research Center and Clinical Professor of Medicine at the University of Medicine at the University of Texas Health Science Center at San Antonio
• Daniel D. Von Hoff, M.D.
Professor of Medicine, Pathology, Molecular and Cellular Biology and the Director of the Arizona Health Sciences Center’s Cancer Therapeutics Program
33