UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended: December 31, 2020
OR
☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from to
Commission File Number: 0-24260

AMEDISYS, INC.
(Exact Name of Registrant as Specified in its Charter)
| Delaware | 11-3131700 | |||||||
| (State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) | |||||||
3854 American Way, Suite A, Baton Rouge, LA 70816
(Address of principal executive offices, including zip code)
(225) 292-2031 or (800) 467-2662
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Trading Symbol | Name of Each Exchange on Which Registered | ||||||||||||
| Common Stock, par value $0.001 per share | AMED | The NASDAQ Global Select Market | ||||||||||||
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☑ No ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ☐ No ☑
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☑ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☑ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and "emerging growth company" in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ☑ | Accelerated filer | ☐ | |||||||||||
| Non-accelerated filer | ☐ | Smaller reporting company | ☐ | |||||||||||
| Emerging growth company | ☐ | |||||||||||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☑
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ☐ No ☑
The aggregate market value of the voting and non-voting common stock held by non-affiliates of the registrant, based on the last sale price as quoted by the NASDAQ Global Select Market on June 30, 2020 (the last business day of the registrant’s most recently completed second fiscal quarter) was $5.5 billion. For purposes of this determination shares beneficially owned by executive officers, directors and ten percent stockholders have been excluded, which does not constitute a determination that such persons are affiliates.
As of February 19, 2021, the registrant had 32,848,547 shares of Common Stock outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive Proxy Statement for its 2021 Annual Meeting of Stockholders (the “2021 Proxy Statement”) to be filed pursuant to the Securities Exchange Act of 1934 with the Securities and Exchange Commission within 120 days of December 31, 2020 are incorporated herein by reference into Part III of this Annual Report on Form 10-K.
TABLE OF CONTENTS
SPECIAL CAUTION CONCERNING FORWARD-LOOKING STATEMENTS
When included in this Annual Report on Form 10-K, or in other documents that we file with the Securities and Exchange Commission (“SEC”) or in statements made by or on behalf of the Company, words like “believes,” “belief,” “expects,” “strategy,” “plans,” “anticipates,” “intends,” “projects,” “estimates,” “may,” “might,” "could," “would,” “should” and similar expressions are intended to identify forward-looking statements as defined by the Private Securities Litigation Reform Act of 1995. These forward-looking statements involve a variety of risks and uncertainties that could cause actual results to differ materially from those described therein. These risks and uncertainties include, but are not limited to the following: the impact of the novel coronavirus pandemic ("COVID-19"), including the measures that have been and may be taken by governmental authorities to mitigate it, on our business, financial condition and results of operations, changes in or our failure to comply with existing federal and state laws or regulations or the inability to comply with new government regulations on a timely basis, changes in Medicare and other medical payment levels, our ability to open care centers, acquire additional care centers and integrate and operate these care centers effectively, competition in the healthcare industry, changes in the case mix of patients and payment methodologies, changes in estimates and judgments associated with critical accounting policies, our ability to maintain or establish new patient referral sources, our ability to consistently provide high-quality care, our ability to attract and retain qualified personnel, our ability to keep our patients and employees safe, changes in payments and covered services by federal and state governments, future cost containment initiatives undertaken by third-party payors, our access to financing, our ability to meet debt service requirements and comply with covenants in debt agreements, business disruptions due to natural disasters or acts of terrorism, widespread protests or civil unrest, our ability to integrate, manage and keep our information systems secure, our ability to realize the anticipated benefits of acquisitions, changes in law or developments with respect to any litigation relating to the Company, including various other matters, many of which are beyond our control, and such other factors as discussed throughout Part I, Item 1A. "Risk Factors" of this Annual Report on Form 10-K.
Because forward-looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified, you should not rely on any forward-looking statement as a prediction of future events. We expressly disclaim any obligation or undertaking and we do not intend to release publicly any updates or changes in our expectations concerning the forward-looking statements or any changes in events, conditions or circumstances upon which any forward-looking statement may be based, except as required by law. For a discussion of some of the factors discussed above as well as additional factors, see Part I, Item 1A, “Risk Factors” and Part II, Item 7, “Critical Accounting Estimates” within “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
Unless otherwise provided, “Amedisys,” “we,” “us,” “our,” and the “Company” refer to Amedisys, Inc. and our consolidated subsidiaries and when we refer to 2020, 2019 and 2018, we mean the twelve month period then ended December 31, unless otherwise provided.
A copy of this Annual Report on Form 10-K for the year ended December 31, 2020 as filed with the SEC, including all exhibits, is available on our internet website at http://www.amedisys.com on the “Investors” page under the “SEC Filings” link.
1
PART I
ITEM 1. BUSINESS
Overview
Amedisys, Inc. is a leading healthcare services company committed to helping our patients age in place by providing clinically excellent care and support in the home. Our operations involve serving patients across the United States through our three operating divisions: home health, hospice and personal care. We deliver clinically distinct care that best suits our patients' needs, whether that is home-based recovery and rehabilitation after an operation or injury, care that empowers patients to manage a chronic disease, hospice care at the end of life or providing assistance with daily activities through our personal care division.
We are among the largest providers of home health and hospice care in the United States, with approximately 21,000 employees in 514 care centers in 39 states within the United States and the District of Columbia. Our employees deliver the highest quality care performing more than 11.5 million visits for more than 418,000 patients annually. Over 2,900 hospitals and 78,000 physicians nationwide have chosen us as a partner in post-acute care.
Due to the age demographics of our patient base, our services are primarily paid for by Medicare which has represented approximately 73% to 75% of our net service revenue over the last three years. We also remain focused on maintaining a profitable and strategically important managed care contract portfolio. We continuously work with our payors to structure innovative contracts which reward us for providing quality care to our patients.
Amedisys is headquartered in Baton Rouge, Louisiana, with an executive office in Nashville, Tennessee. Our common stock is currently traded on the NASDAQ Global Select Market under the trading symbol “AMED.” Founded and incorporated in Louisiana in 1982, Amedisys was reincorporated as a Delaware corporation prior to becoming a publicly traded company in August 1994.
Our strategy is to be the best choice for care wherever our patients call home. We accomplish this by providing clinically distinct care, being the employer of choice and delivering operational excellence and efficiency, which when combined, drive growth. Our mission is to provide best-in-class home health, hospice and personal care services allowing our patients to maintain a sense of independence, quality of life and dignity while delivering industry leading outcomes. We believe that our unwavering dedication to clinical quality and constant focus on both our patients and our employees differentiates us from our competitors.
Our Home Health Segment:
Amedisys Home Health provides compassionate healthcare to help our patients recover from surgery or illness, live with chronic diseases and prevent avoidable hospital readmissions. Our home health footprint includes 320 care centers located in 33 states within the United States and the District of Columbia. Within these care centers, we deploy our care teams which include skilled nurses who are trained, licensed and certified to administer medications, care for wounds, monitor vital signs and provide a wide range of other nursing services; rehabilitation therapists specialized in physical, speech and occupational therapy; and social workers and aides who assist our patients with completing important personal tasks.
We take an empowering approach to helping our patients and their families understand their medical conditions, how to manage them and how to maximize the quality of their lives while living with a chronic disease or other health condition. Our clinicians are trained to understand the whole patient – not just their medical diagnosis.
This commitment to clinical distinction is most evident in our clinical quality measures such as Star Ratings. In the Center for Medicare and Medicaid Services (“CMS”) reports for the October 2020 release, the Quality of Patient Care star average across all Amedisys providers is 4.33 with 92% of our providers at 4+ stars and 44 care centers rated at 5 stars. Our Patient Satisfaction average for the October 2020 release was 4.28, outperforming the industry average by 7%. CMS plans to hold the reported October 2020 release data constant until January 2022. Our goal is to have all care centers achieve a 4.0 Quality Star Rating, and we are implementing targeted action plans to continue to improve the quality of care we deliver for our patients and further our culture of quality.
Our Hospice Segment:
Hospice care is designed to provide comfort and support for those who are dealing with a terminal illness. It is a benevolent form of care that promotes dignity and affirms quality of life for the patient, family members and other loved ones. Individuals
2
with a terminal illness such as cancer, heart disease, pulmonary disease or Alzheimer’s may be eligible for hospice care if they have a life expectancy of six months or less.
Since 2019, we have acquired Compassionate Care Hospice ("CCH"), RoseRock Healthcare ("RoseRock"), Asana Hospice ("Asana") and AseraCare Hospice ("AseraCare"). With these acquisitions, Amedisys now owns and operates 180 hospice care centers in 35 states, providing care to more than 13,000 patients daily as the third largest hospice provider in the United States. Within these care centers, we deploy our care teams which include nurse practitioners and other skilled nurses, social workers, aides, bereavement counselors and chaplains.
Our focus is on building and retaining an exceptional team, delivering the highest quality care and service to our patients and their families and establishing Amedisys as the preferred and preeminent hospice provider in each community we serve. In order to realize these goals, we invest in tailored training, development and recognition programs for our employees, including medical record training, employee skills training and leadership development. This has led to our team’s consistent achievement at or above the national average in family satisfaction results and quality scores, as well as the trust of the healthcare community.
Another element of our approach is our outreach strategy to more fully engage the entire community of eligible patients. These outreach efforts have built our hospice patient population to more accurately represent the causes of death in the communities we serve, with a specific focus on heart disease, lung disease and dementia in order to address the historical underrepresentation of non-cancer diagnoses.
By working to accept every eligible patient who seeks end-of-life care, we fulfill our hospice mission and strengthen our standing in the community.
Our Personal Care Segment:
Personal care provides assistance with the essential activities of daily living. We believe that personal care services are highly synergistic with our core skilled home health and hospice businesses, and that by expanding these capabilities, we will be able to provide our patients and payor partners with a true continuum of care.
Amedisys acquired its first personal care company in 2016, an important step in executing our strategy of improving the continuity of care our patients receive as their clinical needs change. We continued our strategy to expand our personal care segment with four additional acquisitions. We currently operate 12 personal-care care centers in Massachusetts and one personal-care care center in each of Florida and Tennessee.
In July 2019, we signed an agreement with ClearCare, Inc. ("ClearCare"), the provider of the personal care industry’s leading software platform, representing 4,000 personal care agencies in every zip code in the United States. Our agreement with ClearCare creates an opportunity to establish a network partnership between Amedisys and the personal care agencies using ClearCare in order to better coordinate patient care. In August 2020, we signed a Care Coordination Agreement with BrightStar Care to add its agencies to the Amedisys personal care network, which helps facilitate the coordination of care between our home health and hospice care centers and a network of personal care partners. Long term, we believe these agreements will allow us to build a nation-wide network of personal care agencies and further our efforts to provide patients with a true care continuum in the home. These relationships will also help us as we continue to have innovative payment conversations with Medicare Advantage plans who have begun to recognize the value that combined home health, hospice and personal care services bring to their members and care delivery infrastructure.
Responding to the Changing Regulatory and Reimbursement Environment:
As the government continues to seek opportunities to refine payment models, we believe that our strategy of becoming a leader in providing a range of services across the at-home continuum positions us well for the future. Our ability to provide quality home health, hospice and personal care allows us to partner with health systems and managed care organizations to improve care coordination, reduce hospitalizations and lower costs.
Innovations:
As we continue to build our aging-in-place services, we intend to innovate around our core businesses to deliver new home based care models such as skilled nursing facilities in the home ("SNF@Home"). Additional innovation initiatives include the expansion of palliative care and telehealth which will also allow us to expand our primary businesses and accelerate our differentiated care delivery model.
3
Acquisitions:
On January 1, 2020, we acquired Asana Hospice, a hospice provider with eight locations in Pennsylvania, Ohio, Texas, Missouri and Kansas.
On March 1, 2020, we acquired the regulatory assets of a home health provider in Washington.
On April 18, 2020, we acquired the regulatory assets of a home health provider in Kentucky.
On June 1, 2020, we acquired Homecare Preferred Choice, Inc., doing business as AseraCare Hospice ("AseraCare"), a national hospice care provider with 44 locations.
Financial Information:
Financial information for our home health, hospice and personal care segments can be found in our consolidated financial statements included in this Annual Report on Form 10-K.
Human Capital
Our employees are critical to our vision to be the leading aging-in-place company. Taking care of our people is our top priority. Our success is directly correlated with our ability to continue to attract, develop and retain the most qualified and passionate employees. Our work is not just a job but a calling. Our workforce strategy emanates from our core values of SPIRIT - Service, Passion, Integrity, Respect, Innovation and Talent. We know that by taking care of our people, they can continue to provide industry leading patient care. Our mission has never been more important than has been demonstrated during this public health emergency.
As of February 19, 2021, we employed approximately 21,000 people throughout the United States. We also utilize contract employees in the normal course of our business.
Diversity and Inclusion:
Diversity and inclusion is a business imperative. We endeavor to create a culture of caregiving where our employees feel as cared for every day as our patients do. Success means all team members feel a sense of belonging, support and empowerment to be their best selves personally and professionally. We have committed to giving our employees a voice and have instituted numerous formal listening programs - quarterly pulse surveys, focus groups and town halls - to routinely gather feedback from our employees and address any concerns. Our commitment to diversity and inclusion is also broadly reflected across our policies and people practices. During 2020, we established an employee-led Diversity and Inclusion Council to address company policies and procedures that will facilitate a supportive, positive and inclusive work environment for all employees at Amedisys, and we invested in inclusion training for all leaders in the company.
We are also committed to having a diverse Board of Directors. Women currently comprise over half of the directors on our Board, and in December 2020, we expanded the Board to add a woman of color.
Talent Acquisition, Retention and Development:
We strive to hire, develop and retain top talent. The core of our care delivery model is dependent upon attracting high demand clinicians, predominately nurses. We compete for talent by offering a great culture, an opportunity to provide the highest quality clinical care and competitive market-based compensation. Our compensation plans are designed to deliver a competitive base pay as well as attractive incentive opportunities, primarily for leadership positions, but also to reward quality care. We provide significant opportunities for development and continuing education as we know that career development is a key component of attracting and retaining top talent. We continually monitor and assess employee metrics on hiring, retention and terminations to gain a deep understanding of our workforce and drive continuous improvement.
Health and Safety:
The health and well-being of our employees is of utmost importance to us. We offer a comprehensive benefit package that provides employees and their families with access to a variety of innovative, flexible and convenient health and wellness programs that support their physical and mental health by providing tools and resources to help them improve or maintain their health status.
Our focus on the health and safety of our employees became even more critical during the novel coronavirus pandemic (“COVID-19”), and Amedisys took action to help protect, educate and care for our employees. Measures taken to provide support during this pandemic include:
•Developed clinical protocols for COVID-19 testing, proper usage of personal protective equipment ("PPE"), caring for COVID-positive patients and maintaining safety measures in our care centers;
4
•Created a COVID-19 Resource Center available 24 hours a day, seven days a week for employees to access educational materials, safety documents, policies, clinical protocols and operational metrics. Our focus is now on resources to help our clinicians get vaccinated as quickly and easily as possible in each of the states we serve;
•Implemented up to 14 days of paid leave during any required quarantine periods;
•Awarded SPIRIT bonuses to our clinicians and caregivers who have seen patients during the pandemic;
•Completed an early cash pay-out of employee paid-time off;
•Instituted work-from-home arrangements for our corporate and administrative support employees;
•Allowed employees to temporarily suspend any 401(k) plan loan deductions and offered employees the option of making a withdrawal from their 401(k) plan for coronavirus-related distributions without incurring the additional 10% early withdrawal penalty;
•Granted access to Teladoc services to all employees;
•Provided access to COVID-19 self-test kits to all employees;
•Procured millions in PPE and created a centralized distribution center for all critical PPE, allowing us to flex our inventory on a care center by care center basis, based on need and demand as further described in Part II, Item 7, "Management's Discussion and Analysis of Financial Condition and Results of Operations: Overview - Novel Coronavirus Pandemic ("COVID-19")."
Payment for Our Services
Our revenues are derived in large part from governmental third-party payors. Governmental payment programs are subject to statutory and regulatory changes, retroactive rate adjustments, administrative or executive orders and government funding restrictions, all of which may materially increase or decrease the rate of program payments to us for our services. It is possible that future budget cuts in Medicare and Medicaid may be enacted by Congress and implemented by CMS. Therefore, we cannot assure you that payments from governmental or private payors will remain at levels comparable to present levels or will, in the future, be sufficient to cover the costs allocable to patients eligible for reimbursement pursuant to such programs. See Part II, Item 7, "Management's Discussion and Analysis of Financial Condition and Results of Operations: Overview - Payment" for additional information on the most recent regulations from CMS.
Home Health Medicare
The Medicare home health benefit is available both for patients who need home care following discharge from a hospital and patients who suffer from chronic conditions that require ongoing, but intermittent, care.
As a condition of participation under Medicare, beneficiaries must be homebound (meaning that the beneficiary is unable to leave his/her home without a considerable and taxing effort), require intermittent skilled nursing, physical therapy or speech therapy services, and receive treatment under a plan of care established and periodically reviewed by a physician. In order to provide greater flexibility during COVID-19, CMS has relaxed the definition of homebound status through the duration of the public health emergency. During the pandemic, a beneficiary is considered homebound if they have been instructed by a physician not to leave their house because of a confirmed or suspected COVID-19 diagnosis or if the patient has a condition that makes them more susceptible to contracting COVID-19. Therefore, if a beneficiary is homebound due to COVID-19 and requires skilled services, the services will be covered under the Medicare home health benefit.
Prior to January 1, 2020, Medicare payment rates were based on the severity of the patient’s condition, his or her service needs and other factors relating to the cost of providing services and supplies, bundled into 60-day episodes of care. An episode starts with the first day a billable visit is performed and ends 60 days later or upon discharge, if earlier. If a patient is still in treatment on the 60th day, a recertification assessment is undertaken to determine whether the patient needs additional care. If the patient’s physician determines that further care is necessary, another episode begins on the 61st day (regardless of whether a billable visit is rendered on that day) and ends 60 days later. The table below includes the 60-day base episode payment rates.
| Period | Base Episode Payment | ||||
| January 1, 2018 through December 31, 2018 | $ | 3,040 | |||
| January 1, 2019 through December 31, 2019 | $ | 3,154 | |||
| January 1, 2020 through December 31, 2020 (only applies to episodes beginning on December 31, 2019 or prior) | $ | 3,221 | |||
Effective January 1, 2020, CMS implemented a revised case-mix adjustment methodology, the Patient-Driven Groupings Model ("PDGM"), to better align payment with patient care needs and ensure that clinically complex and ill beneficiaries have
5
adequate access to home health care. PDGM uses a 30-day period of care rather than 60-day episodes of care as the unit of payment, eliminates the use of the number of therapy visits provided in determining payment and relies more heavily on clinical characteristics and other patient information. The table below includes the base 30-day payment rates.
| Period | Base 30-Day Payment | ||||
| January 1, 2020 through December 31, 2020 (only applies to episodes beginning on January 1, 2020 and thereafter) | $ | 1,864 | |||
| January 1, 2021 through December 31, 2021 | $ | 1,901 | |||
PDGM uses timing, admission source, functional impairment levels and principal and other diagnoses to case-mix adjust payments. The case mix adjusted payment for a 30-day period of care may be adjusted up or down as a result of one or more of the following: (a) an outlier payment if our patient’s care was unusually costly (capped at 10% of total reimbursement per provider number); (b) a low utilization payment adjustment (“LUPA”) if the number of visits provided was less than the established threshold, which ranges from two to six visits and varies for every case-mix group under PDGM; (c) a partial payment if a patient transferred to another provider or from another provider before completing the 30-day period of care; and (d) the applicable geographic wage index. Payments for routine and non-routine supplies, with limited exceptions, are now included in the 30-day payment rate.
As a Medicare provider, we are subject to periodic audits by the Medicare program, and that program has various rights and remedies against us if they assert that we have overcharged the program or failed to comply with program requirements. Home health providers are subject to pre- and post-payment reviews for compliance with Medicare coverage guidelines and medical necessity. Adjustments on this basis may include individual claims adjustments or overpayment determinations based on an extrapolated sample of claims. Medical necessity reviews evaluate whether services are clinically appropriate in terms of frequency, type, extent, site and duration. Technical billing and documentation reviews focus on documentation of services. Medicare and other payors may reject or deny claims for payment if the underlying paperwork does not support the medical necessity of services or fails to establish satisfaction of a coverage rule; such as if a provider is unable to perform periodic therapy assessments required by coverage criteria or cannot provide appropriate billing documentation, acceptable physician authorizations or face-to-face meeting documentation.
Medicare can reopen previously filed and reviewed claims and deny coverage of the services and require us to repay any overcharges, as well as make deductions from future amounts due to us. In the ordinary course of business, we appeal the Medicare and Medicaid program's denial of claims that we believe are inappropriate in an effort to recover the denied claims.
Home Health Non-Medicare
Payments from Medicaid and private insurance carriers are either a percentage of Medicare rates or per-visit rates depending upon the terms and conditions established with such payors. Reimbursements from our non-Medicare payors that are based on Medicare rates are paid in a similar manner and subject to the same adjustments as discussed above for Medicare; however, these rates can vary based upon negotiated terms which generally range from 90% to 100% of Medicare rates. Approximately 30% of our managed care contract volume affords us the opportunity to receive additional payment if we achieve certain quality or process metrics as defined in each contract.
Hospice Medicare
The Medicare hospice benefit is available when a physician and specific clinical findings support a diagnosis of a terminal condition where the patient has a terminal diagnosis of six months or less. Hospice care is evaluated in benefit periods; two 90-day benefit periods followed by an unlimited number of 60-day benefit periods. Payments are based on daily rates for each day a beneficiary is enrolled in the hospice benefit. The daily payment rates are intended to cover costs that hospices incur in furnishing services identified in patients' care plans, based on specific levels of care. Payments are adjusted by a wage index to reflect health care labor costs across the country and are established annually through federal legislation. Payments are made according to a fee schedule that has four different levels of care: routine home care, continuous home care, inpatient respite care and general inpatient care.
Medicare payment is provided for two separate payment rates for routine care: payments for the first 60 days of care and care beyond 60 days. In addition to the two routine rates, Medicare also reimburses for a service intensity add-on (“SIA”). The SIA is based on visits made in the last seven days of life by a registered nurse or medical social worker for patients in a routine level of care.
6
Adjustments for medical necessity and technical billing requirements may be made to Medicare revenue based on the same claims processing or medical necessity reviews described above for home health services when we find we are unable to obtain appropriate billing documentation, authorizations or face-to-face documentation and other reasons unrelated to credit risk.
Two caps limit the amount of payment that any individual hospice provider number can receive in a single year. Generally, each hospice care center has its own provider number; however, where we have created branch care centers to help our parent care centers serve a geographic location, the parent and branch have the same provider number.
•Inpatient Cap: The inpatient cap limits the number of days of inpatient care an agency may provide to not more than 20 percent of its total patient care days. The daily Medicare payment rate for any inpatient days of service that exceed the cap is set at the routine home care rate, and the provider is required to reimburse Medicare for any amounts it receives in excess of the cap.
•Overall Payment Cap: The overall payment cap is an absolute dollar limit on the average annual payment per beneficiary a hospice agency can receive. This cap is calculated by the Medicare administrative contractor at the end of each hospice cap period to determine the maximum allowable payments per provider number.
We estimate our potential cap exposure using information available for both inpatient day limits as well as per beneficiary cap amounts. The total cap amount for each provider is calculated by multiplying the number of beneficiaries electing hospice care during the period by a statutory amount that is indexed for inflation.
Payment rates for hospice care, the hospice cap amount and the hospice wage index are updated annually according to Section 1814(i)(1)(C)(ii)(VII) of the Social Security Act, which requires CMS to use the inpatient hospital market basket, adjusted for multifactor productivity and other adjustments as specified in the Social Security Act, to determine the hospice payment update percentage. The caps are subject to annual and retroactive adjustments, which can cause providers to be required to reimburse the Medicare program if such caps are exceeded. Our ability to stay within these caps depends on a number of factors, each determined on a provider number basis, including the average length of stay and mix in level of care.
Hospice Non-Medicare
Non-Medicare payors pay at rates that differ from established Medicare rates for hospice services, and are based on separate, negotiated agreements. We bill and are paid by these non-Medicare payors based on such negotiated agreements.
Personal Care Non-Medicare
Personal care payments are received from payor clients, including state and local governmental agencies, managed care organizations, commercial insurers and private consumers, based on rates that are either contractual or fixed by legislation.
Controls Over Our Business System Infrastructure
We establish and maintain processes and controls over coding, clinical operations, billing, patient recertifications and compliance to help monitor and promote adherence with Medicare requirements.
•Coding – Specified international classification of disease ("ICD") diagnosis codes are assigned to each of our patients based on their particular health conditions (such as diabetes, coronary artery disease or congestive heart failure). Because coding regulations are complex and are subject to frequent change, we maintain controls surrounding our coding process. To reduce the associated risk of coding failures, we provide annual update training to clinical managers, as needed training to care center directors and clinical managers and training during orientation for new employees to ensure accurate information is gathered and provided to our coding team. In addition, our electronic medical records system (Homecare Homebase) includes automated edits for home health and hospice based on pre-defined compliance metrics. For home health, we also provide monthly specialized coding education, obtain outside expert coding instruction and have certified clinician coders review all patient outcome and assessment information sets (“OASIS”) and assign the appropriate ICD code. Additional training for our home health coders, clinicians, office staff and business development teams occurred throughout 2019 and 2020 in connection with the implementation of PDGM.
•Clinical Operations – We provide education on coverage criteria and conditions of participation and utilize outside expert regulatory services if necessary. Regulatory requirements allow patients to be eligible for home health care benefits if through a face-to-face visit with a physician, they are considered homebound and it is determined that skilled nursing, physical therapy or speech therapy services are required. These clinical services may include: educating the patient about their disease, assessment and observation of disease status, delivery of clinical skills such
7
as wound care, administration of injections or intravenous fluids, management and evaluation of a patient’s plan of care, physical therapy services to assist patients with functional limitations and speech therapy services for speech or swallowing disorders. Patients eligible for hospice care are terminally ill (with a life expectancy of six months or less if the illness runs its normal course). Our hospice program provides care and support to our terminally ill patients with a 6-month prognosis and their families through services including medical care, counseling, spiritual care, pre-bereavement and bereavement support, medication management and needed equipment and supplies for the terminal illness and all related conditions.
•Billing – We maintain controls over our billing processes to help promote accurate and complete billing. We conduct annual billing compliance testing, use formalized billing attestations, limit access to billing systems, use automated daily billing operational indicators, and take prompt corrective action with employees who knowingly fail to follow our billing policies and procedures in accordance with a "zero tolerance" policy.
•Patient Recertification – In order to be recertified for an additional home health episode of care, a patient must continue to meet qualifying criteria and have a continuing medical need. Changes in the patient’s condition may require changes to the patient’s medical regimen or modified care protocols within the episode of care. The patient’s progress towards established goals is evaluated prior to recertification. As with the initial episode of care, a recertification requires orders from the patient’s physician. Before any employee recommends recertification to a physician, we conduct a care center level, multidisciplinary care team conference. Specific tools are used to ensure that the patient continues to meet coverage criteria prior to recertifying. Hospice recertification for additional benefit periods of care require continued demonstration of a terminal prognosis as determined by the hospice physician in collaboration with the attending physician and the interdisciplinary care team.
•Compliance – We develop, implement and maintain ethics and compliance programs as a component of the centralized corporate services provided to our home health, hospice and personal-care care centers. Our ethics and compliance program includes a Code of Conduct for our employees, officers, directors, contractors and affiliates and a disclosure program for reporting regulatory or ethical concerns to our compliance team through a confidential hotline, which is augmented by exit surveys of departing employees. We promote a culture of compliance within our company through educational presentations, regular newsletters and persistent messaging from our senior leadership to our employees stressing the importance of strict compliance with legal requirements and company policies and procedures. Additionally, we have mandatory compliance training and testing for all new employees upon hire and annually for all staff thereafter. We also maintain a robust compliance audit program focusing on key risk areas.
Our Regulatory Environment
We are highly regulated by federal, state and local authorities. The healthcare industry is subject to numerous laws, regulations and rules including, among others, those related to government healthcare participation requirements, various licensure and accreditations, reimbursement for patient services, health information privacy and security rules, and Medicare and Medicaid fraud and abuse prohibitions (including, but not limited to, federal statutes and regulations prohibiting kickbacks and other illegal inducements to potential referral sources, self-referrals by physicians and false claims submitted to federal health care programs). Regulations and policies frequently change, and we monitor changes through our internal government affairs department, as well as multiple trade and governmental publications and associations.
Our home health and hospice subsidiaries are certified by CMS and therefore are subject to the rules and regulations of the Medicare system. Additionally, all of our business lines are likewise subject to federal, state and local laws and regulations dealing with issues such as occupational safety, employment, medical leave, insurance, civil rights, discrimination, building codes, privacy and recordkeeping. We have set forth below a discussion of the regulations that we believe most significantly affect our home health and hospice businesses.
Licensure, Certificates of Need ("CON") and Permits of Approval ("POA")
Home health and hospice care centers operate under licenses granted by the health authorities of their respective states. Some states require health care providers (including hospice and home health agencies) to obtain prior state approval for the purchase, construction or expansion of health care locations, capital expenditures exceeding a prescribed amount, or changes in services. For those states that require a CON or POA, the provider must also complete a separate application process establishing a location and must receive required approvals.
Certain states, including a number in which we operate, carefully restrict new entrants into the market based on demographic and/or demonstrative usage of additional providers. These states limit the entry of new providers or services and the expansion
8
of existing providers or services in their markets through a CON process, which is periodically evaluated and updated as required by applicable state law.
To the extent that we require a CON or other similar approvals to expand our operations, our expansion could be adversely affected by the inability to obtain the necessary approvals, changes in the standards applicable to those approvals and possible delays and expenses associated with obtaining those approvals.
In every state where required, our care centers possess a license and/or CON or POA issued by the state health authority that determines the local service area for the home health or hospice care centers. Currently, state health authorities in 18 states and the District of Columbia require a CON or, in the State of Arkansas, a POA, in order to establish and operate a home health care center, and state health authorities in 9 states and the District of Columbia require a CON to operate a hospice care center.
We operate 228 home health care centers and 48 hospice care centers in the following CON/POA states as listed below.
| State | Home Health | Hospice | ||||||||||||
| Alabama | 30 | 11 | ||||||||||||
| Arkansas (POA) | 5 | — | ||||||||||||
| Florida | — | 6 | ||||||||||||
| Georgia | 60 | — | ||||||||||||
| Kentucky | 17 | — | ||||||||||||
| Maine | 2 | — | ||||||||||||
| Maryland | 9 | 3 | ||||||||||||
| Mississippi | 9 | — | ||||||||||||
| New Jersey | 2 | — | ||||||||||||
| New York | 4 | — | ||||||||||||
| North Carolina | 8 | 7 | ||||||||||||
| Rhode Island | 1 | — | ||||||||||||
| South Carolina | 22 | — | ||||||||||||
| Tennessee | 45 | 15 | ||||||||||||
| Washington | 2 | — | ||||||||||||
| West Virginia | 11 | 6 | ||||||||||||
| Washington, DC | 1 | — | ||||||||||||
| Total Care Centers in CON States | 228 | 48 | ||||||||||||
Medicare Participation: Licensing, Certification and Accreditation
Our care centers must comply with regulations promulgated by the United States Department of Health and Human Services and CMS in order to participate in the Medicare program and receive Medicare payments. Sections 1861(o) and 1891 of the SSA, 42 CFR 484.1 et seq., establish the conditions that a home health agency ("HHA") must meet in order to participate in the Medicare program. Section 1861(dd) of the SSA, 42 CFR 418.1, et seq., establishes the conditions that a hospice provider must meet in order to participate in the Medicare program. Among other things, these regulations, applicable to HHAs and hospices, respectively, known as conditions of participation (“COPs”), relate to the type of facility, its personnel and its standards of medical care, as well as its compliance with federal, state and local laws and regulations. Additional COPs applicable to HHAs, which went into effect on January 13, 2018, focus on the safe delivery of quality care provided to patients and the impact of that care on patient outcomes through the protection and promotion of patients' rights, care planning, delivery and coordination of services and streamlining of regulatory requirements.
CMS has adopted alternative sanction enforcement options which allow CMS (i) to impose temporary management, direct plans of correction or direct training and (ii) to impose payment suspensions and civil monetary penalties in each case on providers out of compliance with the COPs. CMS engages or has engaged a number of third party contractors, including Recovery Audit Contractors (“RACs”), Program Safeguard Contractors (“PSCs”), Zone Program Integrity Contractors (“ZPICs”), Uniform Program Integrity Contractors ("UPICs"), Medicaid Integrity Contractors (“MICs”) and Supplemental
9
Medical Review Contractors (“SMRCs”), to conduct extensive reviews of claims data and state and federal government health care program laws and regulations applicable to healthcare providers. These audits evaluate the appropriateness of billings submitted for payment. In addition to identifying overpayments, audit contractors can refer suspected violations of law to government enforcement authorities.
All providers are subject to compliance with various federal, state and local statutes and regulations in the U.S. and receive periodic inspection by state licensing agencies to review standards of medical care, equipment and safety. We have dedicated internal resources and utilize external parties when necessary to monitor and ensure compliance with the various applicable federal, state and local laws, rules and regulations.
If we fail to comply with applicable laws and regulations, we could be subjected to liabilities, including criminal penalties, civil penalties (including the loss of our licenses to operate one or more of our businesses) and exclusion of a facility from participation in the Medicare, Medicaid and other federal and state health care programs. If any of our facilities were to lose its accreditation or otherwise lose its certification under the Medicare and Medicaid programs, the facility may be unable to receive reimbursement from the Medicare and Medicaid programs and other payors. We believe our facilities are in substantial compliance with current applicable federal, state, local and independent review body regulations and standards. The requirements for licensure, certification and accreditation are subject to change and, in order to remain qualified, it may become necessary for us to make changes in our facilities, equipment, personnel and services in the future, which could have a material adverse impact on our operations.
Federal and State Anti-Fraud and Anti-Kickback Laws
As a provider under the Medicare and Medicaid systems, we are subject to various anti-fraud and abuse laws, including the federal health care programs’ anti-kickback statute and, where applicable, its state law counterparts. Affected government health care programs include any health care plans or programs that are funded by the United States government (other than certain federal employee health insurance benefits/programs), including certain state health care programs that receive federal funds, such as Medicaid.
Subject to certain exceptions, these laws prohibit any offer, payment, solicitation or receipt of any form of remuneration to induce or reward the referral of business payable under a government health care program or in return for the purchase, lease, order, arranging for, or recommendation of items or services covered under a government health care program. A related law forbids the offer or transfer of anything of value, including certain waivers of co-payment obligations and deductible amounts, to a beneficiary of Medicare or Medicaid that is likely to influence the beneficiary’s selection of health care providers, again, subject to certain exceptions. Violations of the federal anti-kickback statute can result in imprisonment, the imposition of penalties topping $100,000, plus three times the amount of the improper remuneration and potentially, exclusion from furnishing services under any government health care program. In addition, the states in which we operate generally have laws that prohibit certain direct or indirect payments or fee-splitting arrangements between health care providers where they are designed to obtain the referral of patients from a particular provider.
Stark Law
The Social Security Act includes a provision commonly known as the “Stark Law.” This law prohibits physicians from referring Medicare and Medicaid patients to entities for the provision of designated health services with which they or any of their immediate family members have a financial relationship, unless an exception to the law's prohibition is met. These types of referrals are known as “self-referrals.” Sanctions for violating the Stark Law include civil penalties up to $25,820 for each violation, up to $172,137 for schemes to circumvent the Stark restrictions and up to $10,000 for each day an entity fails to report required information and exclusion from the federal health care programs. There are a number of exceptions to the self-referral prohibition, including employment contracts, leases, and recruitment agreements that adhere to certain enumerated requirements.
Violations of the Stark Law result in payment denials and may also trigger civil monetary penalties and federal program exclusion. Several of the states in which we conduct business have also enacted statutes similar in scope and purpose to the federal anti-fraud and abuse laws and the Stark Law. These state laws may mirror the federal Stark Law or may be different in scope. The available guidance and enforcement activity associated with such state laws vary considerably.
We monitor all aspects of our business and have developed a comprehensive ethics and compliance program that is designed to ensure that Amedisys meets all applicable federal guidelines and industry standards. Nonetheless, because the law in this area is complex and constantly evolving, there can be no assurance that federal regulatory authorities will not determine that any of our arrangements with physicians violate the Stark Law.
10
Federal and State Privacy and Security Laws
The Health Insurance Portability and Accountability Act of 1996, or HIPAA, requires us to comply with standards for the exchange of health information within our company and with third parties, such as payors, business associates and patients. These include standards for common health care transactions, such as claims information, plan eligibility, payment information and the use of electronic signatures; unique identifiers for providers, employers, health plans and individuals; and security, privacy, breach notification and enforcement.
The HIPAA transaction regulations establish form, format and data content requirements for most electronic health care transactions, such as health care claims that are submitted electronically. The HIPAA privacy regulations establish comprehensive requirements relating to the use and disclosure of protected health information. The HIPAA security regulations establish minimum standards for the protection of protected health information that is stored or transmitted electronically. The HIPAA breach notification regulations establish the applicable requirements for notifying individuals, the U.S. Department of Health and Human Services (HHS), and the media in the event of a data breach affecting protected health information. Violations of the privacy, security and breach notification regulations are punishable by civil and criminal penalties.
The American Recovery and Economic Reinvestment Act of 2009 (“ARRA”) increased the amount of civil monetary penalties that can be imposed for violations of HIPAA, and the amounts are updated annually for inflation. For 2020, penalties for HIPAA violations can range from $119 to $1.785 million per violation with a maximum fine of $1.785 million for identical violations during a calendar year. In 2018, a nation-wide health benefit company paid $16 million to HHS following a data breach. Prior to this record payment, the largest HIPAA fine was $5.55 million. ARRA also authorized state attorneys general to bring civil enforcement actions under HIPAA, and attorneys general are actively engaged in enforcement. These penalties could be in addition to other penalties assessed by a state for a breach which would be considered reportable under the state’s data breach notification laws.
The Health Information Technology for Economic and Clinical Health (“HITECH”) Act was enacted in conjunction with ARRA. Among other things, the HITECH Act makes business associates of covered entities directly liable for compliance with certain HIPAA requirements, strengthens the limitations on the use and disclosure of protected health information without individual authorizations, and adopts the additional HITECH Act enhancements, including enforcement of noncompliance with HIPAA due to willful neglect. The changes to HIPAA enacted as part of ARRA reflect a Congressional intent that HIPAA’s privacy and security provisions be more strictly enforced. These changes have stimulated increased enforcement activity and enhanced the potential that health care providers will be subject to financial penalties for violations of HIPAA. In addition, the Secretary of HHS is required to perform periodic audits to ensure covered entities (and their business associates, as that term is defined under HIPAA) comply with the applicable HIPAA requirements, increasing the likelihood that a HIPAA violation will result in an enforcement action.
In addition to the federal HIPAA regulations, most states also have laws that protect the confidentiality of health information and other personal data. Certain of these laws grant individuals rights with respect to their information, and we may be required to expend significant resources to comply with these laws. Further, all 50 states and the District of Columbia have adopted data breach notification laws that impose, in varying degrees, an obligation to notify affected persons and/or state regulators in the event of a data breach or compromise, including when their personal information has or may have been accessed by an unauthorized person. Some state breach notification laws may also impose physical and electronic security requirements regarding the safeguarding of personal information, such as social security numbers and bank and credit card account numbers. Violation of state privacy, security, and breach notification laws can trigger significant monetary penalties. In addition, certain states’ privacy, security and data breach laws, including, for example, the California Consumer Privacy Act, include a private right of action that may expose us to private litigation regarding our privacy practices and significant damages awards or settlements in civil litigation.
The False Claims Act
The Federal False Claims Act ("FCA") prohibits false claims or requests for payment for health care services. Under the FCA, the government may penalize any person who knowingly submits, or participates in submitting, claims for payment to the Federal Government which are false or fraudulent, or which contain false or misleading information. Any person who knowingly makes or uses a false record or statement to avoid paying the Federal Government, or knowingly conceals or avoids an obligation to pay money to the Federal Government, may also be subject to fines under the FCA. Under the FCA, the term “person” means an individual, company or corporation.
The Federal Government has used the FCA to prosecute Medicare and other governmental program fraud in areas such as violations of the Federal anti-kickback statute or the Stark Laws, coding errors, billing for services not provided and submitting false cost reports. The FCA has also been used to prosecute people or entities that bill services at a higher reimbursement rate
11
than is allowed and that bill for care that is not medically necessary. In addition to government enforcement, the FCA authorizes private citizens to bring qui tam or “whistleblower” lawsuits, greatly extending the practical reach of the FCA. In 2018, the Department of Justice ("DOJ") announced that the FCA penalties would once again be increasing. The per-claim penalty range is between $11,665 and $23,331 (last updated 2020).
The Fraud Enforcement and Recovery Act of 2009 (“FERA”) amended the FCA with the intent of enhancing the powers of government enforcement authorities and whistleblowers to bring FCA cases. In particular, FERA attempts to clarify that liability may be established not only for false claims submitted directly to the government, but also for claims submitted to government contractors and grantees. FERA also seeks to clarify that liability exists for attempts to avoid repayment of overpayments, including improper retention of federal funds. FERA also included amendments to FCA procedures, expanding the government’s ability to use the Civil Investigative Demand process to investigate defendants, and permitting government complaints and intervention to relate back to the filing of the whistleblower’s original complaint. FERA is likely to increase both the volume and liability exposure of FCA cases brought against health care providers.
In the Patient Protection and Affordable Care Act, Congress enacted requirements related to identifying and returning overpayments made under Medicare and Medicaid. CMS finalized regulations regarding this so-called “60-day rule,” which requires providers to report and return Medicare and Medicaid overpayments within 60 days of identifying the overpayment. A provider who retains identified overpayments beyond 60 days may be liable under the FCA. “Identification” occurs when a person “has, or should have through the exercise of reasonable diligence,” identified and quantified the amount of an overpayment. The final rule also established a six-year lookback period, meaning overpayments must be reported and returned if a person identifies the overpayment within six years of the date the overpayment was received. Providers must report and return overpayments even if they did not cause the overpayment.
In addition to the FCA, the Federal Government may use several criminal statutes to prosecute the submission of false or fraudulent claims for payment to the Federal Government. Many states have similar false claims statutes that impose liability for the types of acts prohibited by the False Claims Act. As part of the Deficit Reduction Act of 2005 (the “DRA”), Congress provided states an incentive to adopt state false claims acts consistent with the federal FCA. Additionally, the DRA required providers who receive $5 million or more annually from Medicaid to include information on federal and state false claims acts, whistleblower protections and the providers’ own policies on detecting and preventing fraud in their written employee policies.
FDA Regulation
The U.S. Food and Drug Administration (“FDA”) regulates medical device user facilities, which include home health care providers. FDA regulations require user facilities to report patient deaths and serious injuries to the FDA and/or the manufacturer of a device used by the facility if the device may have caused or contributed to the death or serious injury of any patient. FDA regulations also require user facilities to maintain files related to adverse events and to establish and implement appropriate procedures to ensure compliance with the above reporting and recordkeeping requirements. User facilities are subject to FDA inspection, and noncompliance with applicable requirements may result in warning letters or sanctions including civil monetary penalties, injunction, product seizure, criminal fines and/or imprisonment.
The Improving Medicare Post-Acute Care Transformation Act
In October 2014, the Improving Medicare Post-Acute Care Transformation Act (“IMPACT Act”) was signed into law requiring the reporting of standardized patient assessment data for quality improvement, payment and discharge planning purposes across the spectrum of post-acute care providers (“PACs”), including skilled nursing facilities and home health agencies. The IMPACT Act requires PACs to report: (1) standardized patient assessment data at admission and discharge; (2) quality measures, including functional status, skin integrity, medication reconciliation, incidence of major falls and patient preference regarding treatment and discharge; and (3) resource use measures, including Medicare spending per beneficiary, discharge to community and hospitalization rates of potentially preventable readmissions. Failure to report such data when required would subject a facility to a two percent reduction in market basket prices then in effect.
The IMPACT Act further requires HHS and the Medicare Payment Advisory Commission (“MedPAC”), a commission chartered by Congress to advise it on Medicare payment issues, to study alternative PAC payment models, including payment based upon individual patient characteristics and not care setting, with corresponding Congressional reports required based on such analysis. The IMPACT Act also included provisions impacting Medicare-certified hospices, including: (1) increasing survey frequency for Medicare-certified hospices to once every 36 months; (2) imposing a medical review process for facilities with a high percentage of stays in excess of 180 days; and (3) updating the annual aggregate Medicare payment cap.
12
Pre-Claim Review Demonstration for Home Health Services
On June 8, 2016, CMS announced the implementation of a three-year Medicare pre-claim review ("PCR") demonstration for home health services provided to beneficiaries in the states of Illinois, Florida, Texas, Michigan and Massachusetts. The pre-claim review is a process through which a request for provisional affirmation of coverage is submitted for review before a final claim is submitted for payment. On April 1, 2017, CMS paused the PCR Demonstration for Home Health Services while CMS considered a number of changes. CMS revised the demonstration to incorporate more flexibility and choices for providers, as well as risk-based changes to reward providers who show compliance with Medicare home health policies.
On May 31, 2018, CMS issued a notice indicating its intention to re-launch an HHA pre-claim review demonstration project. The original program had drawn criticism that it created significant administrative burdens and reduced access to care. Now called the Review Choice Demonstration for Home Health Services ("RCD"), the revised demonstration will give HHAs in the demonstration states three options: pre-claim review of all claims, post-payment review of all claims, or minimal post-payment review with a 25% payment reduction for all home health services. Under the pre-claim review and post-payment review options, provider claims are reviewed for every episode of care until the appropriate claim approval rate (90% based on a minimum of ten pre-claim requests or claims submitted) is reached. Further, once the appropriate claim approval rate is reached, a provider can elect to opt-out of claim reviews except for a spot check of 5% of its claims to ensure continued compliance. The demonstration initially applies to HHA providers in Florida, Illinois, North Carolina, Ohio and Texas, with the option to expand after five years to other states in the Medicare Administrative Contractor Jurisdiction M (Palmetto). In April 2019, CMS announced a June 1, 2019 start date for RCD in Illinois. In July 2019, CMS announced a September 30, 2019 start date for RCD in Ohio. Thereafter, in an October 21, 2019 release, CMS announced that it will reschedule the next phase of its RCD to allow agencies in Texas, North Carolina and Florida time to transition to PDGM. Throughout the first few months of 2020, CMS made various announcements about new start dates for the remaining three states, including a March 2, 2020 start date in Texas and projected start date of May 4, 2020 for North Carolina and Florida. The Texas portion began as scheduled; however, due to the ongoing public health emergency, on March 31, 2020, CMS announced a voluntary pause of RCD for Illinois, Ohio and Texas and delay for beginning the demonstration in North Carolina and Florida. In July 2020, CMS announced its intention to resume the demonstration on August 30, 2020 for Illinois, Ohio and Texas and a voluntary phase-in for North Carolina and Florida. The voluntary phase-in was extended by CMS in October until January 1, 2021 and then again in December until March 31, 2021.
Home Health Value-Based Purchasing
On January 1, 2016, CMS implemented Home Health Value-Based Purchasing ("HHVBP"). The HHVBP model was designed to give Medicare-certified home health agencies incentives or penalties, through payment bonuses, to provide higher quality and more efficient care. HHVBP was rolled out to nine pilot states: Arizona, Florida, Iowa, Maryland, Massachusetts, Nebraska, North Carolina, Tennessee and Washington, seven of which Amedisys currently has home health operations. Bonuses and penalties began in 2018 with the maximum of plus or minus 3% growing to plus or minus 8% by 2022. Payment adjustments are calculated based on performance in a variety of measures which include current Quality of Patient Care and Patient Satisfaction star measures, as well as measures based on submission of data to a CMS web portal. The measures used may be subject to modification or change by CMS.
Under the demonstration, agencies with higher performance receive bonuses, while those with lower scores receive lower payments relative to current levels. Agency performance is evaluated against separate improvement and attainment scores, with payment tied to the higher of these two scores. CMS used 2015 as the baseline year for performance, with 2016 as the first year for performance measurement. The first payment adjustment began January 1, 2018, based on 2016 performance data. Between 2018 and 2022, the payment adjustment varies (upward or downward) from 3 percent to 8 percent.
In January 2021, CMS and the Center for Medicare and Medicaid Innovation announced its intention, through rulemaking, to expand HHVBP with an implementation date no earlier than January 2022.
Home Health Payment Reform
On February 9, 2018, Congress passed the Bipartisan Budget Act of 2018 ("BBA of 2018"), which funded government operations, set two-year government spending limits and enacted a variety of healthcare related policies. Specific to home health, the BBA of 2018 provides for a targeted extension of the home health rural add-on payment, a reduction of the 2020 market basket update, modification of eligibility documentation requirements and reform to the Home Health Prospective Payment System ("HHPPS"). The HHPPS reform included the following parameters: for home health units of service beginning on January 1, 2020, a 30-day payment system is to be applied; the transition to the 30-day payment system was to be budget neutral; and CMS was to conduct at least one Technical Expert Panel during 2018, prior to any notice and comment rulemaking process, related to the design of any new case-mix adjustment model.
13
The final HHA regulations introduced by CMS (CMS-1689-FC) updated the Medicare HHPPS and finalized the implementation of an alternative case-mix adjustment methodology, PDGM, that became effective on January 1, 2020. PDGM adjusts payments to home health agencies based on patient characteristics for 30-day periods of care and also eliminates the use of therapy visits in the determination of payments. While the changes were to be implemented in a budget neutral manner to the industry, the ultimate impact will vary by provider based on factors including patient mix and admission source. Additionally, CMS made assumptions about behavioral changes which were finalized in the Calendar Year 2020 Home Health Final Rule released on October 31, 2019 and resulted in a 4.36% reduction to reimbursement. The behavioral changes were related to coding practices, low utilization payment adjustment ("LUPA") management and co-morbidities. CMS is required by law to analyze data for calendar years 2020-2026, retrospectively, to determine the impact of the difference between assumed and actual behavior changes and to make any such payment changes as are necessary to offset or supplement the adjustments based on anticipated behavior. Additionally, in an effort to eliminate fraud risks, CMS reduced the upfront payment associated with requests for anticipated payment ("RAPs") to 20% in 2020 with the full elimination of RAPs in 2021.
Phase-Out of the Rural Add-On
The BBA of 2018 also mandated the implementation of a new methodology for applying rural add-on payments for home health services (“rural add-on”). Unlike previous rural add-ons, which were applied to all rural areas uniformly, the extension provided varying add-on amounts depending on the rural county (or equivalent area) classification by classifying each rural county (or equivalent area) into one of three distinct categories: (1) rural counties and equivalent areas in the highest quartile of all counties and equivalent areas based on the number of Medicare home health episodes furnished per 100 individuals who are entitled to, or enrolled for, benefits under Part A of Medicare or enrolled for benefits under Part B of Medicare only, but not enrolled in a Medicare Advantage plan under Part C of Medicare (the "high utilization" category); (2) rural counties and equivalent areas with a population density of 6 individuals or fewer per square mile of land area and are not included in the "high utilization" category (the "low population density" category); and (3) rural counties and equivalent areas not in either the "high utilization" or "low population density" categories (the "all other" category).
In the Calendar Year ("CY") 2019 Home Health Final Rule, CMS finalized policies for the rural add-on payments for CY 2019 through CY 2022, in accordance with section 50208 of the BBA of 2018. The CY 2019 proposed rule (83 FR 32373) described the provisions of the rural add-on payments and the methodology for applying the new payments and outlined how to categorize rural counties (or equivalent areas) based on claims data, the Medicare beneficiary summary file and census data.
The CY 2019 through CY 2022 rural add-on percentages outlined in the rule are shown in the table below.
| Rural Add-On Percentages, CYs 2019-2022 | ||||||||||||||
| Category | CY 2019 | CY 2020 | CY 2021 | CY 2022 | ||||||||||
| High utilization | 1.5% | 0.5% | None | None | ||||||||||
| Low population density | 4.0% | 3.0% | 2.0% | 1.0% | ||||||||||
| All other | 3.0% | 2.0% | 1.0% | None | ||||||||||
Civil Monetary Penalties
The United States Department of Health and Human Services may impose civil monetary penalties ("CMP") for a variety of civil offenses related to federal health care programs. They may be imposed upon any person or entity who presents, or causes to be presented, certain ineligible claims for medical items or services, for providing improper inducements to beneficiaries to obtain services, for payments to limit services to patients, and for offenses related to relationships with excluded individuals, among other things.
Maximum CMP amounts have been increased significantly as a result of the Bipartisan Budget Act of 2018, which was signed into law on February 9, 2018. The maximum CMP has increased to $104,330 for knowingly making or causing to be made a false statement, omission or misrepresentation of a material fact in any application, bid or contract to participate or enroll as a provider or supplier and to $58,832 for making or using a false record or statement that is material to a false or fraudulent claim.
14
Our Competitors
There are few barriers to entry in the home health and hospice jurisdictions that do not require certificates of need or permits of approval. Our primary competition in these jurisdictions comes from local privately and publicly-owned and hospital-owned health care providers. We compete based on the quality of services, the availability of personnel, expertise of visiting staff, and, in certain instances, on the price of our services. In addition, we compete with a number of non-profit organizations that finance acquisitions and capital expenditures on a tax-exempt basis or receive charitable contributions that are unavailable to us.
Available Information
Our company website address is www.amedisys.com. We use our website as a channel of distribution for important company information. Important information, including press releases, analyst presentations and financial information regarding our company, is routinely posted on and accessible on the Investor Relations subpage of our website, which is accessible by clicking on the tab labeled “Investors” on our website home page. Visitors to our website can also register to receive automatic e-mail and other notifications alerting them when new information is made available on the Investor Relations subpage of our website. In addition, we make available on the Investor Relations subpage of our website (under the link “SEC Filings”), free of charge, our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, ownership reports on Forms 3, 4 and 5 and any amendments to those reports as soon as reasonably practicable after we electronically file or furnish such reports with the SEC. Further, copies of our Certificate of Incorporation and Bylaws, our Code of Ethical Business Conduct, our Corporate Governance Guidelines and the charters for the Audit, Compensation, Quality of Care, Compliance and Ethics and Nominating and Corporate Governance Committees of our Board are also available on the Investor Relations subpage of our website (under the link “Governance”). Reference to our website does not constitute incorporation by reference of the information contained on the website and should not be considered part of this document.
Our electronically filed reports can also be obtained on the SEC’s internet site at http://www.sec.gov.
ITEM 1A. RISK FACTORS
The risks described below, and risks described elsewhere in this Form 10-K, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows and the actual outcome of matters as to which forward-looking statements are made in this Form 10-K. The risk factors described below and elsewhere in this Form 10-K are not the only risks faced by Amedisys. Our business and consolidated financial condition, results of operations and cash flows may also be materially adversely affected by factors that are not currently known to us, by factors that we currently consider immaterial or by factors that are not specific to us, such as general economic conditions.
If any of the following risks are actually realized, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected. In that case, the trading price of our common stock could decline.
You should refer to the explanation of the qualifications and limitations on forward-looking statements under “Special Caution Concerning Forward-Looking Statements.” All forward-looking statements made by us are qualified by the risk factors described below.
Risks Related to Reimbursement
Federal and state changes to reimbursement and other aspects of Medicare and Medicaid could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Our net service revenue is primarily derived from Medicare, which accounted for 75%, 74% and 73% of our revenue during 2020, 2019 and 2018, respectively. Payments received from Medicare are subject to changes made through federal legislation. When such changes are implemented, we must also modify our internal billing processes and procedures accordingly, which can require significant time and expense. These changes, as further detailed in Part I, Item 1, “Business: Payment for Our Services,” can include changes to base payments and adjustments for home health services, changes to cap limits and per diem rates for hospice services and changes to Medicare eligibility and documentation requirements or changes designed to restrict utilization. Any such changes, including retroactive adjustments, adopted in the future by the Center for Medicare and Medicaid Services (“CMS”) could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Section 6407 of the Affordable Care Act, as implemented by 42 CFR § 424.22, added new Medicare requirements for face-to-face encounters to support claims for home health services. The requirements for face-to-face encounters continue to be one of the most complex issues in the industry and can be the source of claims denials if not fulfilled. Section 6407(d) of the
15
Affordable Care Act also provided that the requirements for face-to-face encounters in the provisions described above shall apply in the case of physicians making certifications for home health services under title XIX of the Act (Medicaid) in the same manner and to the same extent as such requirements apply under title XVIII (Medicare).
There are continuing efforts to reform governmental health care programs that could result in major changes in the health care delivery and reimbursement system on a national and state level, including changes directly impacting the reimbursement systems for our home health and hospice care centers. Though we cannot predict what, if any, reform proposals will be adopted, health care reform and legislation may have a material adverse effect on our business and our financial condition, results of operations and cash flows through decreasing payments made for our services.
We could also be affected adversely by the continuing efforts of governmental payors to contain health care costs. We cannot assure you that reimbursement payments under governmental payor programs, including Medicare supplemental insurance policies, will remain at levels comparable to present levels or will be sufficient to cover the costs allocable to patients eligible for reimbursement pursuant to these programs. Any such changes could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Quality reporting requirements may negatively impact Medicare reimbursement.
Hospice quality reporting was mandated by the Patient Protection and Affordable Health Care Act and the Health Care and Education Reconciliation Act ("PPACA"), which directs the Secretary to establish quality reporting requirements for hospice programs. Failure to submit required quality data will result in a 2% reduction to the market basket percentage increase for that fiscal year. This quality reporting program is currently “pay-for-reporting,” meaning it is the act of submitting data that determines compliance with program requirements.
Similarly, in the Calendar Year 2015 Home Health Final Rule, CMS proposed to establish a new “Pay-for-Reporting Performance Requirement” with which provider compliance with quality reporting program requirements can be measured. Home health agencies that do not submit quality measure data to CMS are subject to a 2% reduction in their annual home health payment update percentage. Currently, home health agencies are required to report prescribed quality assessment data for a minimum of 90% of all patients.
The Improving Medicare Post-Acute Care Transformation Act of 2014 (the “IMPACT Act”) requires the submission of standardized data by home health agencies and other providers. Specifically, the IMPACT Act requires, among other significant activities, the reporting of standardized patient assessment data with regard to quality measures, resource use, and other measures. Failure to report data as required will subject providers to a 2% reduction in market basket prices then in effect.
There can be no assurance that all of our agencies will continue to meet quality reporting requirements in the future which may result in one or more of our agencies seeing a reduction in its Medicare reimbursements. Regardless, we, like other healthcare providers, are likely to incur additional expenses in an effort to comply with additional and changing quality reporting requirements.
Value-based purchasing may negatively impact Medicare reimbursement.
Both government and private payors are increasingly looking to value-based purchasing to contain costs. Value-based purchasing focuses on quality of outcomes and efficiency of care, rather than quantity of care. CMS currently has a pilot program for home health agencies in several states, which it may expand to other states. CMS may also create a similar plan for hospices in the future. Government and private payors’ implementation of value-based purchasing requirements could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
16
Any economic downturn, deepening of an economic downturn, continued deficit spending by the Federal Government or state budget pressures may result in a reduction in payments and covered services.
Adverse developments in the United States could lead to a reduction in Federal Government expenditures, including governmentally funded programs in which we participate, such as Medicare and Medicaid. In addition, if at any time the Federal Government is not able to meet its debt payments unless the federal debt ceiling is raised, and legislation increasing the debt ceiling is not enacted, the Federal Government may stop or delay making payments on its obligations, including funding for government programs in which we participate, such as Medicare and Medicaid. Failure of the government to make payments under these programs could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Further, any failure by the United States Congress to complete the federal budget process and fund government operations may result in a Federal Government shutdown, potentially causing us to incur substantial costs without reimbursement under the Medicare program, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. As an example, the failure of the 2011 Joint Select Committee to meet its Deficit Reduction goal resulted in an automatic reduction in Medicare home health and hospice payments of 2% beginning April 1, 2013.
Historically, state budget pressures have resulted in reductions in state spending. Given that Medicaid outlays are a significant component of state budgets, we can expect continuing cost containment pressures on Medicaid outlays for our services.
In addition, sustained unfavorable economic conditions may affect the number of patients enrolled in managed care programs and the profitability of managed care companies, which could result in reduced payment rates and could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Future cost containment initiatives undertaken by private third party payors may limit our future revenue and profitability.
Our non-Medicare revenue and profitability are affected by continuing efforts of third party payors to maintain or reduce costs of health care by lowering payment rates, narrowing the scope of covered services, increasing case management review of services and negotiating pricing. There can be no assurance that third party payors will make timely payments for our services, and there is no assurance that we will continue to maintain our current payor or revenue mix. We are continuing our efforts to develop our non-Medicare sources of revenue and any changes in payment levels from current or future third party payors could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Risks Related to our Operations
Our business may be materially adversely affected by the ongoing COVID-19 pandemic.
The outbreak of the COVID-19 pandemic has resulted in a general economic downturn and volatility in the stock market and has also caused and may continue to cause a decrease in our patient volumes and revenues, an increase in costs and an inability to access our patients and referral sources and could lead to staffing and medical supply shortages, any of which, or a combination of which, could have a material adverse effect on our business and financial results. The ultimate impact of COVID-19, including the impact on our liquidity, financial condition and results of operations, is uncertain and will depend on many factors and future developments, which are highly uncertain and cannot be predicted at this time, including the severity, scope and length of time that the pandemic continues, including regional surges in COVID-19 cases at various times, the impact of new variants of the virus, uncertainty regarding vaccine distribution timing and efficacy in slowing the spread of the virus, its impact on the national and global economy, its effect on the demand for our services, our ability to ensure the safety of our patients and employees and the actions taken by federal, state and local authorities to contain or treat the COVID-19 pandemic.
A shortage of qualified registered nursing staff and other clinicians, such as therapists and nurse practitioners, could materially impact our ability to attract, train and retain qualified personnel and could increase operating costs.
We compete for qualified personnel with other healthcare providers. Our ability to attract and retain clinicians depends on several factors, including our ability to provide these personnel with attractive assignments and competitive salaries and benefits. We cannot be assured we will succeed in any of these areas. In addition, there are shortages of qualified health care personnel in some of our markets. As a result, we may face higher costs of attracting clinicians and providing them with attractive benefit packages than we originally anticipated which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. In addition, if we expand our operations into geographic areas where health care providers historically have been unionized, or if any of our care center employees become unionized, being subject to a collective bargaining agreement may have a negative impact on our ability to timely and successfully recruit qualified personnel and may increase our operating costs. Generally, if we are unable to attract and retain clinicians, the quality of our services may decline and we could lose patients and referral sources, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
17
Because we are limited in our ability to control rates received for our services, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected if we are not able to maintain or reduce our costs to provide such services.
As Medicare is our primary payor and rates are established through federal legislation, we have to manage our costs of providing care to achieve a desired level of profitability. Additionally, non-Medicare rates are difficult for us to negotiate as such payors are under pressure to reduce their own costs. As a result, we manage our costs in order to achieve a desired level of profitability including, but not limited to, centralization of various processes, the use of technology and management of the number of employees utilized. If we are not able to continue to streamline our processes and reduce our costs, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected.
If we are unable to provide consistently high quality of care, our business will be adversely impacted.
Providing quality patient care is the cornerstone of our business. We believe that hospitals, physicians and other referral sources refer patients to us in large part because of our reputation for delivering quality care. Clinical quality is becoming increasingly important within our industry. Effective October 2012, Medicare began to impose a financial penalty upon hospitals that have excessive rates of patient readmissions within 30 days from hospital discharge. We believe this regulation provides a competitive advantage to home health providers who can differentiate themselves based upon quality, particularly by achieving low patient acute care hospitalization readmission rates and by implementing disease management programs designed to be responsive to the needs of patients served by referring hospitals. We are focused intently upon improving our patient outcomes, particularly our patient acute care hospitalization readmission rates. If we should fail to attain our goals regarding acute care hospitalization readmission rates and other quality metrics, we expect our ability to generate referrals would be adversely impacted, which could have a material adverse effect upon our business and consolidated financial condition, results of operations and cash flows.
Additionally, Medicare has established consumer-facing websites, Home Health Compare and Hospice Compare, that present data regarding our performance on certain quality measures compared to state and national averages. Failure to achieve or exceed these averages may affect our ability to generate referrals, which could have a material adverse effect upon our business and consolidated financial condition, results of operations and cash flows.
If we are unable to maintain relationships with existing patient referral sources, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected.
Our success depends on referrals from physicians, hospitals and other sources in the communities we serve and on our ability to maintain good relationships with existing referral sources. Our referral sources are not contractually obligated to refer patients to us and may refer their patients to other providers. Our growth and profitability depend, in part, on our ability to establish and maintain close working relationships with these patient referral sources and to increase awareness and acceptance of the benefits of home health and hospice care by our referral sources and their patients. Our loss of, or failure to maintain, existing relationships or our failure to develop new referral relationships could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Possible changes in the case mix of patients, as well as payor mix and payment methodologies, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Our revenue is determined by a number of factors, including our mix of patients and the rates of payment among payors. Changes in the case mix of our patients, payment methodologies or the payor mix among Medicare, Medicaid and private payors could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Our failure to negotiate favorable managed care contracts, or our loss of existing favorable managed care contracts, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
One of our strategies is to diversify our payor sources by increasing the business we do with managed care companies, and we strive to put in place favorable contracts with managed care payors. However, we may not be successful in these efforts. Additionally, there is a risk that the favorable managed care contracts that we put in place may be terminated. Managed care contracts typically permit the payor to terminate the contract without cause, on very short notice, typically 60 days, which can provide payors leverage to reduce volume or obtain favorable pricing. Our failure to negotiate and put in place favorable managed care contracts, or our failure to maintain in place favorable managed care contracts, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
18
Our industry is highly competitive, with few barriers to entry in certain states.
There are few barriers to entry in home health markets that do not require a CON or POA. Our primary competition comes from local privately-owned and hospital-owned health care providers. We compete based on the availability of personnel, the quality of services, expertise of visiting staff, and in certain instances, on the price of our services. Increased competition in the future may limit our ability to maintain or increase our market share.
Further, the introduction of new and enhanced service offerings by others, in combination with industry consolidation and the development of strategic relationships by our competitors (including mergers of competitors with each other and with insurers), could cause a decline in revenue or loss of market acceptance of our services or make our services less attractive. Additionally, we compete with a number of non-profit organizations that can finance acquisitions and capital expenditures on a tax-exempt basis or receive charitable contributions that are unavailable to us.
Managed care organizations and other third party payors continue to consolidate, which enhances their ability to influence the delivery of health care services. Consequently, the health care needs of patients in the United States are increasingly served by a smaller number of managed care organizations. These organizations generally enter into service agreements with a limited number of providers. Our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected if these organizations terminate us as a provider and/or engage our competitors as a preferred or exclusive provider. In addition, should private payors, including managed care payors, seek to negotiate additional discounted fee structures or the assumption by health care providers of all or a portion of the financial risk through prepaid capitation arrangements, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected.
If we are unable to react competitively to new developments, our operating results may suffer. State CON or POA laws often limit the ability of competitors to enter into a given market, are not uniform throughout the United States and are frequently the subject of efforts to limit or repeal such laws. If states remove existing CONs or POAs, we could face increased competition in these states. There can be no assurances that other states will not seek to eliminate or limit their existing CON or POA programs, which could lead to increased competition in these states. Further, we cannot assure you that we will be able to compete successfully against current or future competitors, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Our business depends on our information systems. A cyber-attack, security breach or our inability to effectively integrate, manage and keep our information systems secure and operational could disrupt our operations.
Most healthcare providers, including all who accept commercial insurance Medicare and Medicaid, must comply with the HIPAA regulations regarding the privacy and security of protected health information. All 50 states also maintain laws focused on the privacy, security and notification requirements with regard to personally identifiable information, including health information. The HIPAA regulations impose significant requirements on providers and our third party vendor business associates with regard to how such protected health information may be used and disclosed. Further, the regulations include extensive and complex regulations which require providers to establish reasonable and appropriate administrative, technical and physical safeguards to ensure the confidentiality, integrity and availability of protected health information. Providers are obligated under HIPAA and state law to notify individuals and the government if personal information is compromised as defined by the respective law. In addition to federal regulators, state attorneys general are also enforcing information security breaches. All 50 states have breach notification laws. In addition to state laws regarding confidentiality of medical information, several states are now focused on expanding state privacy laws regarding personal information. HIPAA directs the Secretary of HHS to provide for periodic audits to ensure covered entities (and their business associates, as that term is defined under HIPAA) comply with the applicable HIPAA requirements.
Our networks, systems and devices store sensitive information, including intellectual property, proprietary business information and personally identifiable information of our patients, partners, and employees. We have installed privacy protection systems and devices on our network, systems and point of care tablets in an attempt to prevent unauthorized access to information created, received, transmitted and maintained by us. However, our technology may fail to adequately secure the protected health information and personally identifiable information we create, receive, transmit and maintain in our databases. In such circumstances, we may be held liable to our patients and regulators, which could result in fines, litigation or adverse publicity that could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Even if we are not held liable, any resulting negative publicity could harm our business and distract the attention of management.
Our business depends on effective, secure and operational information systems which include systems provided by or hosted by external contractors, partners and other service providers. For example, our care centers depend upon our information systems
19
and software for patient care, accounting, billing, collections, risk management, quality assurance, human resources, payroll and other information considered to be confidential. We believe that our subcontractors and vendors take precautionary measures to prevent problems that could affect our business operations as a result of failure or disruption to their information systems or networks. However, there is no guarantee such efforts will be successful in preventing a disruption, and it is possible that we may be impacted by information system failures. The occurrence of any information system failures could result in interruptions, delays, breaches of protected health information and personally identifiable information, loss or corruption of data and cessations or interruptions in the availability of these systems and the information they create, receive, transmit or maintain. All of these events or circumstances, among others, could have an adverse effect on our business and consolidated financial position, results of operations and cash flows, and they could harm our business reputation.
In general, all information systems including those we host or have hosted by third parties are vulnerable to damage or interruption from fire, flood, power loss, telecommunications failure, human acts, break-ins and other intentional or unintentional events. Our business is at risk from and may be impacted by information security incidents, including ransomware, malware, viruses, phishing, social engineering, and other security events. Such incidents can range from individual attempts to gain unauthorized access to information technology systems to more sophisticated security threats. These events can also result from internal compromises, such as human error or malicious acts. These events can occur on our systems or on the systems of our partners and subcontractors.
Problems with, or the failure of, our technology and systems or any system upgrades or programming changes associated with such technology and systems could have a material adverse effect on our operations, patient care, data capture and integrity, medical documentation, billing, collections, assessment of internal controls and management and reporting capabilities. If we experience a reduction in the performance, reliability, or availability of our information systems, our operations and ability to produce timely and accurate reports could be materially adversely affected.
Our information systems and applications also require continual maintenance, upgrading and enhancement to meet our operational and security needs. Our acquisition activity requires transitions and integration of various information systems. We regularly upgrade and expand our information systems’ capabilities. If we experience difficulties with the transition and integration of information systems or are unable to implement, maintain, or expand our systems properly, we could suffer from, among other things, operational disruptions, regulatory investigations or audits and increases in administrative expenses.
As cyber threats continue to evolve, we may be required to expend significant capital and other resources to protect against the threat of security breaches or to mitigate and alleviate problems caused by breaches, including unauthorized access to protected health information and personally identifiable information stored in our information systems, and the introduction of computer viruses or other malicious software programs to our systems. Our security measures may be inadequate to prevent security breaches and our business operations could be materially adversely affected by federal and state fines and penalties, legal claims or proceedings, cancellation of contracts and loss of patients if security breaches are not prevented. The healthcare industry is currently a target for cyber criminals and therefore experiencing increased attention on compliance with regulations designed to safeguard protected health information and mitigate cyber-attacks on entities. There are significant costs associated with a breach, including investigation costs, remediation and mitigation costs, notification costs, attorney fees, litigation and the potential for reputational harm and lost revenues due to a loss in confidence in the provider. We cannot predict the costs to comply with these laws or the costs associated with a potential breach of protected health information, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows, and our business reputation.
If we are subject to cyber-attacks or security breaches in the future, this could result in harm to patients; business interruptions and delays; the loss, misappropriation, corruption or unauthorized access of data; litigation and potential liability under privacy, security and consumer protection laws or other applicable laws; reputational damage and federal and state governmental inquiries. Any such problems or failures and the costs incurred in correcting any such problems or failures, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Further, to the extent our external information technology contractors or other service providers have their own cyber-attack, security event or information technology failure, become insolvent or fail to support the software or systems we have licensed from them, our operations could be materially adversely affected. A failure to restore our information systems after the occurrence of any of these events could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Because of the protected health information we store and transmit, loss of electronically stored information for any reason could expose us to a risk of regulatory action and litigation and possible liability and loss.
We believe we have all the necessary licenses from third parties to use technology and software that we do not own. A third party could, however, allege that we are infringing its rights, which may deter our ability to obtain licenses on commercially
20
reasonable terms from the third party, if at all, or cause the third party to commence litigation against us. In addition, we may find it necessary to initiate litigation to protect our trade secrets, to enforce our intellectual property rights and to determine the scope and validity of any proprietary rights of others. Any such litigation, or the failure to obtain any necessary licenses or other rights, could materially and adversely affect our business.
Our insurance liability coverage may not be sufficient for our business needs.
As a result of operating in the home health industry, our business entails an inherent risk of claims, losses and potential lawsuits alleging incidents involving our employees that are likely to occur in a patient’s home. We maintain professional liability insurance to provide coverage to us and our subsidiaries against these risks. However, we cannot assure you claims will not be made in the future in excess of the limits of our insurance, nor can we assure you that any such claims, if successful and in excess of such limits, will not have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Our insurance coverage also includes fire, property damage and general liability with varying limits. We cannot assure you that the insurance we maintain will satisfy claims made against us or that insurance coverage will continue to be available to us at commercially reasonable rates, in adequate amounts or on satisfactory terms. Any claims made against us, regardless of their merit or eventual outcome, could damage our reputation and business.
We may be subject to substantial malpractice or other similar claims.
The services we offer involve an inherent risk of professional liability and related substantial damage awards. As of February 19, 2021, we have approximately 21,000 employees (10,800 home health, 6,500 hospice, 2,700 personal care and 1,000 corporate employees). In addition, we employ direct care workers on a contractual basis to support our existing workforce. Due to the nature of our business, we, through our employees and caregivers who provide services on our behalf, may be the subject of medical malpractice claims. A court could find these individuals should be considered our agents, and, as a result, we could be held liable for their acts or omissions. We cannot predict the effect that any claims of this nature, regardless of their ultimate outcome, could have on our business or reputation or on our ability to attract and retain patients and employees. While we maintain malpractice liability coverage that we believe is appropriate given the nature and breadth of our operations, any claims against us in excess of insurance limits, or multiple claims requiring us to pay deductibles, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
If we are unable to maintain our corporate reputation, our business may suffer.
Our success depends on our ability to maintain our corporate reputation, including our reputation for providing quality patient care and for compliance with Medicare requirements and the other laws to which we are subject. Adverse publicity surrounding any aspect of our business, including the death or disability of any of our patients due to our failure to provide proper care, or due to any failure on our part to comply with Medicare requirements or other laws to which we are subject, could negatively affect our Company’s overall reputation and the willingness of referral sources to refer patients to us.
A write off of a significant amount of intangible assets or long-lived assets could have a material adverse effect on our consolidated financial condition and results of operations.
A significant and sustained decline in our stock price and market capitalization, a significant decline in our expected future cash flows, a significant adverse change in the business climate or slower growth rates could result in the need to perform an impairment analysis under Accounting Standards Codification (“ASC”) Topic 350 “Intangibles – Goodwill and Other” in future periods in addition to our annual impairment test. If we were to conclude that a write down of goodwill is necessary, then we would record the appropriate charge, which could result in material charges that are adverse to our consolidated financial condition and results of operations. See Part II, Item 8, Note 5 – Goodwill and Other Intangible Assets, Net to our consolidated financial statements for additional information.
Because we have grown in part through acquisitions, goodwill and other acquired intangible assets represent a substantial portion of our assets. Goodwill was $932.7 million as of December 31, 2020 and if we make additional acquisitions, it is likely that we will record additional goodwill and intangible assets in our consolidated financial statements. We also have long-lived assets consisting of property and equipment and other identifiable intangible assets of $97.9 million as of December 31, 2020, which we review on a periodic basis as well as when events or circumstances indicate that the carrying amount of an asset may not be recoverable. If a determination that a significant impairment in value of our unamortized intangible assets or long-lived assets occurs, such determination could require us to write off a substantial portion of our assets. A write off of these assets could have a material adverse effect on our consolidated financial condition and results of operations.
21
Our operations could be impacted by natural disasters.
The occurrence of natural disasters in the markets in which we operate could not only impact the day-to-day operations of our care centers, but could also disrupt our relationships with patients, employees and referral sources located in the affected areas and, in the case of our corporate office, our ability to provide administrative support services, including billing and collection services. In addition, any episode of care that is not completed due to the impact of a natural disaster will generally result in lower revenue for the episode. For example, our corporate office and a number of our care centers are located in the southeastern United States and the Gulf Coast Region, increasing our exposure to hurricanes and flooding. Future hurricanes or other natural disasters may have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Risks Related to our Growth Strategies
Our growth strategy depends on our ability to acquire additional care centers and integrate and operate these care centers effectively. If our growth strategy is unsuccessful or we are not able to successfully integrate newly acquired care centers into our existing operations, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected.
We may not be able to fully integrate the operations of our acquired businesses with our current business structure in an efficient and cost-effective manner. Acquisitions involve significant risks and uncertainties, including difficulties in recouping partial episode payments and other types of misdirected payments for services from the previous owners; difficulties integrating acquired personnel and business practices into our business; the potential loss of key employees, referral sources or patients of acquired care centers; the delay in payments associated with change in ownership, control and the internal processes of the Medicare administrative contractors; and the assumption of liabilities and exposure to unforeseen liabilities of acquired care centers. Further, the financial benefits we expect to realize from many of our acquisitions are largely dependent upon our ability to improve clinical performance, overcome regulatory deficiencies, improve the reputation of the acquired business in the community and control costs. The failure to accomplish any of these objectives or to effectively integrate any of these businesses could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
The indemnification provisions of acquisition agreements by which we have acquired companies may not fully protect us and as a result we may face unexpected liabilities.
Certain of the acquisition agreements by which we have acquired companies require the former owners to indemnify us against certain liabilities related to the operation of the acquired company before we acquired it. In most of these agreements, however, the liability of the former owners is limited, and certain former owners may be unable to meet their indemnification responsibilities. We cannot assure you that these indemnification provisions will protect us fully or at all, and as a result, we may face unexpected liabilities that could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
State efforts to regulate the establishment or expansion of health care providers could impair our ability to expand our operations.
Some states require health care providers (including skilled nursing facilities, hospice care centers, home health care centers and assisted living facilities) to obtain prior approval, known as a CON or POA, in order to commence operations. See Part I, Item 1, “Our Regulatory Environment” for additional information on CONs and POAs. If we are not able to obtain such approvals, our ability to expand our operations could be impaired, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
22
Federal regulation may impair our ability to consummate acquisitions or open new care centers.
Changes in federal laws or regulations may materially adversely impact our ability to acquire care centers or open new start-up care centers. For example, the Social Security Act provides the Secretary with the authority to impose temporary moratoria on the enrollment of new Medicare providers, if deemed necessary to combat fraud, waste or abuse under government programs. While there are no active Medicare moratoria, there can be no assurance that CMS will not adopt a moratorium on new providers in the future. Additionally, in 2010, CMS implemented and amended a regulation known as the “36 Month Rule” that is applicable to home health care center acquisitions. Subject to certain exceptions, the 36 Month Rule prohibits buyers of certain home health care centers - those that either enrolled in Medicare or underwent a change in majority ownership fewer than 36 months prior to the acquisition - from assuming the Medicare billing privileges of the acquired care center. The 36 Month Rule may restrict bona fide transactions and potentially block new investments in home health agencies. These changes in federal laws and regulations, and similar future changes, may further increase competition for acquisition targets and could have a material detrimental impact on our acquisition strategy.
Risks Related to Laws and Government Regulations
We are subject to extensive government regulation. Any changes to the laws and regulations governing our business, or to the interpretation and enforcement of those laws or regulations, could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Our industry is subject to extensive federal and state laws and regulations. See Part I, Item 1, “Our Regulatory Environment” for additional information on such laws and regulations. Federal and state laws and regulations impact how we conduct our business, the services we offer and our interactions with patients, our employees and the public and impose certain requirements on us such as:
•licensure and certification;
•adequacy and quality of health care services;
•qualifications of health care and support personnel;
•quality and safety of medical equipment;
•confidentiality, maintenance and security associated with medical records and claims processing;
•relationships with physicians and other referral sources;
•operating policies and procedures;
•emergency preparedness risk assessments and policies and procedures;
•policies and procedures regarding employee relations;
•addition of facilities and services;
•billing for services;
•requirements for utilization of services;
•documentation required for billing and patient care; and
•reporting and maintaining records regarding adverse events.
These laws and regulations, and their interpretations, are subject to change. Changes in existing laws and regulations, or their interpretations, or the enactment of new laws or regulations could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows by:
•increasing our administrative and other costs;
•increasing or decreasing mandated services;
•causing us to abandon business opportunities we might have otherwise pursued;
•decreasing utilization of services;
•forcing us to restructure our relationships with referral sources and providers; or
•requiring us to implement additional or different programs and systems.
23
Additionally, we are subject to various routine and non-routine reviews, audits and investigations by the Medicare and Medicaid programs and other federal and state governmental agencies, which have various rights and remedies against us if they establish that we have overcharged the programs or failed to comply with program requirements. We are also subject to potential lawsuits under the federal False Claims Act and other federal and state whistleblower statutes designed to combat fraud and abuse in our industry. Violation of the laws governing our operations, or changes in interpretations of those laws, could result in the imposition of fines, civil or criminal penalties, and the termination of our rights to participate in federal and state-sponsored programs and/or the suspension or revocation of our licenses. If we become subject to material fines, or if other sanctions or other corrective actions are imposed on us, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected.
We face periodic and routine reviews, audits and investigations under our contracts with federal and state government agencies and private payors, and these audits could have adverse findings that may negatively impact our business.
As a result of our participation in the Medicare and Medicaid programs, we are subject to various governmental reviews, audits and investigations to verify our compliance with these programs and applicable laws and regulations. We also are subject to audits under various federal and state government programs in which third party firms engaged by CMS, including the Recovery Audit Contractors (“RACs”), Zone Program Integrity Contractors (“ZPICs”), Uniform Program Integrity Contractors ("UPICs"), Program Safeguard Contractors (“PSCs”), Medicaid Integrity Contractors (“MICs”) and Supplemental Medical Review Contractors (“SMRCs”), conduct extensive reviews of claims data and medical and other records to identify potential improper payments under the Medicare program. The Office of Inspector General-HHS ("OIG") also conducts audits and has included various home home health agency and hospice payment and quality issues in its current workplan. Additionally, private pay sources reserve the right to conduct audits. If billing errors are identified in the sample of reviewed claims, the billing error can be extrapolated to all claims filed which could result in a larger overpayment than originally identified in the sample of reviewed claims. Our costs to respond to and defend reviews, audits and investigations may be significant and could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Moreover, an adverse review, audit or investigation could result in:
•required refunding or retroactive adjustment of amounts we have been paid pursuant to the federal or state programs or from private payors;
•state or federal agencies imposing fines, penalties and other sanctions on us;
•loss of our right to participate in the Medicare program, state programs, or one or more private payor networks; or
•damage to our business and reputation in various markets.
These results could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
If a care center fails to comply with the conditions of participation in the Medicare program, that care center could be subjected to sanctions or terminated from the Medicare program.
Each of our care centers must comply with required conditions of participation in the Medicare program. If we fail to meet the conditions of participation at a care center, we may receive a notice of deficiency from the applicable state surveyor. If that care center then fails to institute an acceptable plan of correction to remediate the deficiency within the correction period provided by the state surveyor, that care center could be terminated from the Medicare program or subjected to alternative sanctions. CMS outlined its alternative sanction enforcement options for home health care centers through a regulation published in 2012; under the regulation, CMS may impose temporary management, direct a plan of correction, direct training or impose payment suspensions and civil monetary penalties, in each case, upon providers who fail to comply with the conditions of participation. Termination of one or more of our care centers from the Medicare program for failure to satisfy the program’s conditions of participation, or the imposition of alternative sanctions, could disrupt operations, require significant attention by management, or have a material adverse effect on our business and reputation and consolidated financial condition, results of operations and cash flows.
24
We are subject to federal and state laws that govern our financial relationships with physicians and other health care providers, including potential or current referral sources.
We are required to comply with federal and state laws, generally referred to as “anti-kickback laws,” that prohibit certain direct and indirect payments or other financial arrangements between health care providers that are designed to encourage the referral of patients to a particular provider for medical services. In addition to these anti-kickback laws, the Federal Government has enacted specific legislation, the physician self-referral prohibition, commonly known as the “Stark Law,” that prohibits certain financial relationships, specifically including ownership interests and compensation arrangements, between physicians (and the immediate family members of physicians) and providers of designated health services, such as home health care centers, to whom the physicians refer patients. Some of these same financial relationships are also subject to additional regulation by states. Although we believe we have structured our relationships with physicians and other actual or potential referral sources to comply with these laws where applicable, the laws are complex. It is possible that courts or regulatory agencies may interpret state and federal anti-kickback laws and/or the Stark Law and similar state laws regulating relationships between health care providers and physicians in ways that will adversely implicate our practices or that isolated instances of noncompliance may occur. Violations of federal or state Stark or anti-kickback laws could lead to criminal or civil fines or other sanctions, including repayment of federal health care program payments related to these arrangements, denials of government program reimbursement or even exclusion from participation in governmental health care programs, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. It is possible that a claim that results from a kickback or is made in violation of the Stark Law also may render it false or fraudulent, creating further potential liability under the federal False Claims Act, discussed above.
We may face significant uncertainty in the industry due to government health care reform.
The health care industry in the United States is subject to fundamental changes due to ongoing health care reform efforts and related political, economic and regulatory influences. In March 2010, comprehensive health care reform legislation was signed into law in the United States through the passage of PPACA, which calls for a number of changes to Medicare payment rates and the rebasing of the home health payment system to be made over time. PPACA has had and will likely continue to have a significant impact upon the health care delivery system. Implementation of the regulations and related initiatives as required by PPACA may increase our costs, decrease our revenues, expose us to expanded liability or require us to revise the ways in which we conduct our business.
Various health care reform proposals similar to the federal reforms have also emerged at the state level, including in several states in which we operate. We cannot predict with certainty what health care initiatives, if any, will be implemented at the state level, or what the ultimate effect of federal health care reform or any future legislation or regulation may have on us or on our business and consolidated financial condition, results of operations and cash flows.
In addition to impacting our Medicare businesses, PPACA may also significantly affect our non-Medicare businesses. PPACA makes many changes to the underwriting and marketing practices of private payors. The resulting economic pressures could prompt these payors to seek to lower their rates of reimbursement for the services we provide. PPACA may continue to have residual effects on our non-Medicare business.
Finally, efforts to repeal or substantially modify provisions of the PPACA continue in Congress and in the courts. The ultimate outcomes of legislative efforts to repeal, substantially amend, eliminate or reduce funding for the PPACA is unknown. In addition to the prospect for legislative repeal or revision, administrative action, including revised regulation and other Executive Branch action, could impose changes on how the law is applied. The effect of any major modification or repeal of the PPACA on our business, operations or financial condition cannot be predicted, but could be materially adverse.
Risks Related to Liquidity
Delays in payment may cause liquidity problems.
Our business is characterized by delays from the time we provide services to the time we receive payment for these services. If we have difficulty in obtaining documentation, such as physician orders, experience information system problems or experience other issues that arise with Medicare or other payors, we may encounter additional delays in our payment cycle.
In addition, timing delays in billings and collections may cause working capital shortages. Working capital management, including prompt and diligent billing and collection, is an important factor in achieving our financial results and maintaining liquidity. It is possible that documentation support, system problems, Medicare or other payor issues or industry trends may extend our collection period, which may materially adversely affect our working capital, and our working capital management procedures may not successfully mitigate this risk.
25
On May 29, 2018, CMS issued a notice indicating its intention to re-launch a home health agency pre-claim review demonstration project. Now called the Review Choice Demonstration for Home Health Services, the revised demonstration will give home health agencies in the demonstration states three initial options: pre-claim review of all claims, post-payment review of all claims, or minimal post-payment review with a 25% payment reduction for all home health services. Reduced review options are available for home health agencies that demonstrate compliance. The demonstration initially applies to home health providers in Florida, Illinois, North Carolina, Ohio, and Texas, with staggered start dates beginning in 2019 and extending into 2021. Compliance with this process could result in increased administrative costs or delays in reimbursement for home health services in states subject to the demonstration.
Additionally, our hospice operations may experience payment delays. We have experienced payment delays when attempting to collect funds from state Medicaid programs in certain instances. Delays in receiving payments from these programs may also materially adversely affect our working capital.
Changes in units of payment for home health agencies could reduce our Medicare home health reimbursement levels.
Pursuant to the Bipartisan Budget Act of 2018 and final rules issued in October of 2019, PDGM changed the unit of payment for home health agencies from a 60-day episode of care to 30-day periods of care, effective January 1, 2020. Although this change was to be implemented in an overall budget neutral manner, the ultimate impact will vary by provider based on factors including patient mix and admission source. Additionally, CMS made assumptions about behavioral changes which resulted in a 4.36% reduction to reimbursement. Accordingly, the adoption of PDGM had a negative impact on our Medicare revenue per episode in 2020 and could negatively impact our rates of reimbursement in future years and have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. See Part I, Item 1, “Our Regulatory Environment - Home Health Payment Reform” for additional information on PDGM.
The volatility and disruption of the capital and credit markets and adverse changes in the United States and global economies could impact our ability to access both available and affordable financing, and without such financing, we may be unable to achieve our objectives for strategic acquisitions and internal growth.
While we intend to finance strategic acquisitions and internal growth with cash flows from operations and borrowings under our revolving credit facility, we may require sources of capital in addition to those presently available to us. Uncertainty in the capital and credit markets may impact our ability to access capital on terms acceptable to us (i.e. at attractive/affordable rates) or at all, and this may result in our inability to achieve present objectives for strategic acquisitions and internal growth. Further, in the event we need additional funds, and we are unable to raise the necessary funds on acceptable terms, our business and consolidated financial condition, results of operations and cash flows could be materially adversely affected.
Our indebtedness could impact our financial condition and impair our ability to fulfill other obligations.
As of December 31, 2020, we had total outstanding indebtedness of approximately $215.1 million. Our level of indebtedness could have a material adverse effect on our business and consolidated financial position, results of operations and cash flows and could impair our ability to fulfill other obligations in several ways, including:
•it could require us to dedicate a portion of our cash flow from operations to payments on our indebtedness, which could reduce the availability of cash flow to fund acquisitions, start-ups, working capital, capital expenditures and other general corporate purposes;
•it could limit our ability to borrow money or sell stock for working capital, capital expenditures, debt service requirements and other purposes;
•it could limit our flexibility in planning for, and reacting to, changes in our industry or business;
•it could make us more vulnerable to unfavorable economic or business conditions; and
•it could limit our ability to make acquisitions or take advantage of other business opportunities.
In the event we incur additional indebtedness, the risks described above could increase.
The agreements governing our indebtedness contain various covenants that limit our discretion in the operation of our business and our failure to satisfy requirements in these agreements could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
The agreements governing our indebtedness (the “Debt Agreements”) contain certain obligations, including restrictive covenants that require us to comply with or maintain certain financial covenants and ratios and restrict our ability to:
•incur additional debt;
26
•redeem or repurchase stock, pay dividends or make other distributions;
•make certain investments;
•create liens;
•enter into transactions with affiliates;
•make acquisitions;
•enter into joint ventures;
•merge or consolidate;
•invest in foreign subsidiaries;
•amend acquisition documents;
•enter into certain swap agreements;
•make certain restricted payments;
•transfer, sell or leaseback assets; and
•make fundamental changes in our corporate existence and principal business.
Our Debt Agreements also limit our ability to reinvest the net cash proceeds from asset sales or subordinated debt issuances in certain circumstances. For example, in the event we or any of our subsidiaries receive more than $5 million in net cash proceeds from an asset sale, disposition or involuntary disposition, our Debt Agreements require us to prepay our term loan facility and revolving credit facility with all of such net cash proceeds, unless we elect to reinvest the net cash proceeds in fixed or capital assets related to our business.
In addition, events beyond our control could affect our ability to comply with the Debt Agreements. Any failure by us to comply with or maintain all applicable financial covenants and ratios and to comply with all other applicable covenants could result in an event of default with respect to the Debt Agreements. If we are unable to obtain a waiver from our lenders in the event of any non-compliance, our lenders could accelerate the maturity of any outstanding indebtedness and terminate the commitments to make further extensions of credit (including our ability to borrow under our revolving credit facility). Any failure to comply with these covenants could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
The potential cessation or modification of LIBOR may increase our interest expense or otherwise adversely affect us.
Our credit facility carries a floating interest rate which is tied to the Eurodollar rate (i.e., LIBOR) and the prime rate. On July 27, 2017, the United Kingdom’s Financial Conduct Authority, which regulates LIBOR, announced that it intends to stop persuading or compelling banks to submit LIBOR quotations after 2021 (the “FCA Announcement”). The FCA Announcement indicates that the continuation of LIBOR on the current basis cannot and will not be assured after 2021, and LIBOR may cease to exist or otherwise be unsuitable for use as a benchmark. Recent proposals for LIBOR reforms may result in the establishment of new methods of calculating LIBOR or the establishment of one or more alternative benchmark rates. Although our credit facility provides for alternative base rates, some of those alternative base rates are related to LIBOR, and the consequences of any potential cessation, modification or other reform of LIBOR cannot be predicted at this time. If LIBOR ceases to exist, we most likely will need to amend the credit facility, and we cannot predict what alternative interest rate(s) will be negotiated with our counterparties. As a result, our interest expense may increase, our ability to refinance some or all of our existing indebtedness may be impacted and our available cash flow may be adversely affected.
Risks Related to Ownership of Our Common Stock
The price of our common stock may be volatile.
The price at which our common stock trades may be volatile. The stock market from time to time experiences significant price and volume fluctuations that impact the market prices of securities, particularly those of health care companies. The market price of our common stock may be influenced by many factors, including:
•our operating and financial performance;
•variances in our quarterly financial results compared to research analyst expectations;
•the depth and liquidity of the market for our common stock;
27
•future purchases or sales of common stock by the Company or large stockholders or the perception that such purchases or sales could occur;
•investor, analyst and media perception of our business and our prospects;
•developments relating to litigation or governmental investigations;
•changes or proposed changes in health care laws or regulations or enforcement of these laws and regulations, or announcements relating to these matters;
•departure of key personnel;
•changes in the Medicare, Medicaid and private insurance payment rates for home health and hospice;
•the operating and stock price performance of other comparable companies;
•announcements by us or our competitors of significant contracts, acquisitions, strategic partnerships, joint ventures or capital commitments;
•market and business conditions related to COVID-19;
•general economic and stock market conditions; or
•other factors described in this "Risk Factors" section and elsewhere in this Annual Report on Form 10-K.
In addition, the stock market in general, and the NASDAQ Global Select Market (“NASDAQ”) in particular, has experienced price and volume fluctuations that we believe have often been unrelated or disproportionate to the operating performance of health care provider companies. These broad market and industry factors may materially reduce the market price of our common stock, regardless of our operating performance. Securities class-action cases have often been brought against companies following periods of volatility in the market price of their securities. Such litigation, if instituted against us, could result in substantial costs and a diversion of management's attention and resources.
The activities of short sellers could reduce the price or prevent increases in the price of our common stock. “Short sale” is defined as the sale of stock by an investor that the investor does not own. Typically, investors who sell short believe the price of the stock will fall, and anticipate selling shares at a higher price than the purchase price at which they will buy the stock. As of December 31, 2020, investors held a short position of approximately 0.6 million shares of our common stock which represented 2% of our outstanding common stock. The anticipated downward pressure on our stock price due to actual or anticipated sales of our stock by some institutions or individuals who engage in short sales of our common stock could cause our stock price to decline.
Our Board of Directors may use anti-takeover provisions or issue stock to discourage a change of control.
Our certificate of incorporation currently authorizes us to issue up to 60,000,000 shares of common stock and 5,000,000 shares of undesignated preferred stock. Our Board of Directors may cause us to issue additional stock to discourage an attempt to obtain control of our company. For example, shares of stock could be sold to purchasers who might support our Board of Directors in a control contest or to dilute the voting or other rights of a person seeking to obtain control. In addition, our Board of Directors could cause us to issue preferred stock entitling holders to vote separately on any proposed transaction, convert preferred stock into common stock, demand redemption at a specified price in connection with a change in control, or exercise other rights designed to impede a takeover.
The issuance of additional shares may, among other things, dilute the earnings and equity per share of our common stock and the voting rights of common stockholders.
We have implemented other anti-takeover provisions or provisions that could have an anti-takeover effect, including advance notice requirements for director nominations and stockholder proposals, no cumulative voting for directors, requirement that director vacancies are filled by remaining directors (including vacancies resulting from removal), and the number of directors is fixed by the Board of Directors, and the Board of Directors can increase or decrease the size of the Board of Directors without stockholder approval (within the range set forth in our Certificate of Incorporation and Bylaws). These provisions, and others that our Board of Directors may adopt hereafter, may discourage offers to acquire us and may permit our Board of Directors to choose not to entertain offers to purchase us, even if such offers include a substantial premium to the market price of our stock. Therefore, our stockholders may be deprived of opportunities to profit from a change of control.
28
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
ITEM 2. PROPERTIES
Our executive office is located in Nashville, Tennessee in a leased property consisting of 25,097 square feet; our corporate headquarters is located in Baton Rouge, Louisiana in a leased property consisting of 85,955 square feet. We believe we have adequate space to accommodate our corporate staff located in these locations for the foreseeable future.
In addition to our executive office and corporate headquarters, we also lease facilities for our home health, hospice and personal-care care centers. Generally, our leases have an initial term of five years, but range from one to ten years. Most of our leases also contain early termination options and renewal options. The following table shows the location of our 320 Medicare-certified home health care centers, 180 Medicare-certified hospice care centers and 14 personal-care care centers at December 31, 2020:
| State | Home Health | Hospice | Personal Care | State | Home Health | Hospice | Personal Care | |||||||||||||||||||||||||||||||||||||
| Alabama | 30 | 11 | — | New Jersey | 2 | 7 | — | |||||||||||||||||||||||||||||||||||||
| Arkansas | 5 | — | — | Nebraska | — | 7 | — | |||||||||||||||||||||||||||||||||||||
| Arizona | 3 | 1 | — | New York | 4 | — | — | |||||||||||||||||||||||||||||||||||||
| California | 4 | 4 | — | New Hampshire | 3 | 4 | — | |||||||||||||||||||||||||||||||||||||
| Connecticut | 1 | 1 | — | North Carolina | 8 | 7 | — | |||||||||||||||||||||||||||||||||||||
| Delaware | 2 | 2 | — | Ohio | 1 | 5 | — | |||||||||||||||||||||||||||||||||||||
| Florida | 18 | 6 | 1 | Oklahoma | 6 | 1 | — | |||||||||||||||||||||||||||||||||||||
| Georgia | 60 | 10 | — | Oregon | 3 | 1 | — | |||||||||||||||||||||||||||||||||||||
| Illinois | 3 | 1 | — | Pennsylvania | 7 | 22 | — | |||||||||||||||||||||||||||||||||||||
| Indiana | 5 | 6 | — | Rhode Island | 1 | 2 | — | |||||||||||||||||||||||||||||||||||||
| Iowa | — | 1 | — | South Carolina | 22 | 8 | — | |||||||||||||||||||||||||||||||||||||
| Kansas | — | 1 | — | South Dakota | — | 2 | — | |||||||||||||||||||||||||||||||||||||
| Kentucky | 17 | — | — | Tennessee | 45 | 15 | 1 | |||||||||||||||||||||||||||||||||||||
| Louisiana | 9 | 5 | — | Texas | 2 | 13 | — | |||||||||||||||||||||||||||||||||||||
| Massachusetts | 5 | 10 | 12 | Virginia | 13 | 6 | — | |||||||||||||||||||||||||||||||||||||
| Maine | 2 | 4 | — | Washington | 2 | — | — | |||||||||||||||||||||||||||||||||||||
| Maryland | 9 | 3 | — | West Virginia | 11 | 6 | — | |||||||||||||||||||||||||||||||||||||
| Michigan | — | 1 | — | Wisconsin | 1 | 3 | — | |||||||||||||||||||||||||||||||||||||
| Minnesota | — | 1 | — | Washington, D.C. | 1 | — | — | |||||||||||||||||||||||||||||||||||||
| Mississippi | 9 | 1 | — | Total | 320 | 180 | 14 | |||||||||||||||||||||||||||||||||||||
| Missouri | 6 | 2 | — | |||||||||||||||||||||||||||||||||||||||||
ITEM 3. LEGAL PROCEEDINGS
See Part II, Item 8, Note 11 – Commitments and Contingencies for information concerning our legal proceedings.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
29
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information and Holders
Our common stock trades on the NASDAQ Global Select Market under the trading symbol “AMED.” As of February 19, 2021, there were approximately 483 holders of record of our common stock. This number of holders of record does not represent the actual number of beneficial owners of our common stock because shares are frequently held in “street name” by securities dealers and others for the benefit of individual owners who have the right to vote their shares.
Dividend Policy
We have not declared or paid any cash dividends on our common stock or any other of our securities and do not expect to pay cash dividends for the foreseeable future. We currently intend to retain our future earnings, if any, to fund the development and growth of our business. Future decisions concerning the payment of dividends will depend upon our results of operations, financial condition, capital expenditure plans and debt service requirements, as well as such other factors as our Board of Directors, in its sole discretion, may consider relevant. In addition, our outstanding indebtedness restricts, and we anticipate any additional future indebtedness may restrict, our ability to pay cash dividends; provided, however, that we may pay dividends (i) payable solely in our equity securities and (ii) if (1) no default or event of default under the Amended Credit Agreement shall have occurred and be continuing at the time of such dividend or would result therefrom, (2) we demonstrate that, upon giving pro forma effect to such dividend, our consolidated leverage ratio (as defined in the Amended Credit Agreement) is less than 2.0 to 1.0 and (3) we demonstrate a minimum liquidity of $50 million upon giving effect to such dividend.
Purchases of Equity Securities
The following table provides the information with respect to purchases made by us of shares of our common stock during each of the months during the three-month period ended December 31, 2020:
| Period | (a) Total Number of Shares (or Units) Purchased | (b) Average Price Paid per Share (or Unit) | (c) Total Number of Shares (or Units) Purchased as Part of Publicly Announced Plans or Programs | (d) Maximum Number (or Approximate Dollar Value) of Shares (or Units) That May Yet Be Purchased Under the Plans or Programs (2) | |||||||||||||||||||||||||
| October 1, 2020 to October 31, 2020 | 1,275 | $ | 251.64 | — | $ | — | |||||||||||||||||||||||
| November 1, 2020 to November 30, 2020 | — | — | — | — | |||||||||||||||||||||||||
| December 1, 2020 to December 31, 2020 | — | — | — | — | |||||||||||||||||||||||||
| 1,275 | (1) | $ | 251.64 | — | $ | — | |||||||||||||||||||||||
(1)Includes shares of common stock surrendered to us by certain employees to satisfy tax withholding obligations in connection with the vesting of non-vested stock previously awarded to such employees under our 2008 and 2018 Omnibus Incentive Compensation Plans.
(2)On December 23, 2020, we announced that our board of directors authorized a stock repurchase program, under which we may repurchase up to $100 million of our outstanding common stock through December 31, 2021. We did not repurchase any shares pursuant to this stock repurchase program.
Stock Performance Graph
The Performance Graph below compares the cumulative total stockholder return on our common stock, $0.001 par value per share, for the five-year period ended December 31, 2020, with the cumulative total return on the NASDAQ composite index and an industry peer group over the same period (assuming the investment of $100 in our common stock, the NASDAQ composite index and the industry peer group on December 31, 2015 and the reinvestment of dividends). The peer group we selected is comprised of: Addus Homecare Corporation ("ADUS"), Chemed Corporation ("CHE"), Encompass Health Corporation ("EHC"), LHC Group, Inc. (“LHCG”) and National Healthcare Corporation (“NHC”). The cumulative total stockholder return on the following graph is historical and is not necessarily indicative of future stock price performance. No cash dividends have been paid on our common stock.
30
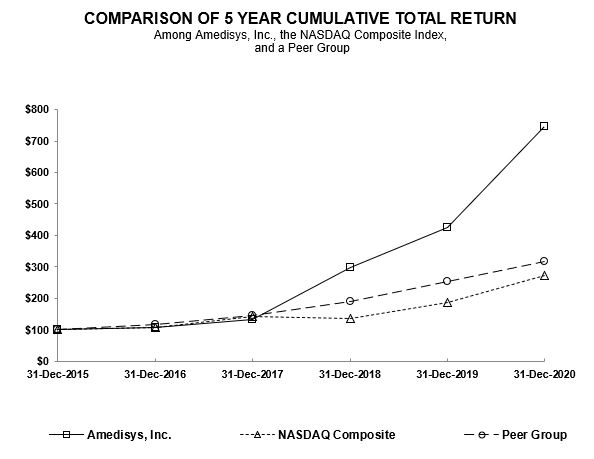
| 12/31/2015 | 12/31/2016 | 12/31/2017 | 12/31/2018 | 12/31/2019 | 12/31/2020 | ||||||||||||||||||||||||||||||
| Amedisys, Inc. | $ | 100.00 | $ | 108.42 | $ | 134.05 | $ | 297.84 | $ | 424.52 | $ | 746.01 | |||||||||||||||||||||||
| NASDAQ Composite | $ | 100.00 | $ | 108.87 | $ | 141.13 | $ | 137.12 | $ | 187.44 | $ | 271.64 | |||||||||||||||||||||||
| Peer Group | $ | 100.00 | $ | 116.30 | $ | 146.71 | $ | 189.28 | $ | 253.37 | $ | 318.07 | |||||||||||||||||||||||
This stock performance information is “furnished” and shall not be deemed to be “soliciting material” or subject to Regulation 14A under the Securities Exchange Act of 1934 (the “Exchange Act”), shall not be deemed “filed” for purposes of Section 18 of the Exchange Act or otherwise subject to the liabilities of that section, and shall not be deemed incorporated by reference in any filing under the Securities Act of 1933, as amended, or the Exchange Act, whether made before or after the date of this report and irrespective of any general incorporation by reference language in any such filing, except to the extent we specifically incorporate the information by reference.
31
ITEM 6. SELECTED FINANCIAL DATA
The selected consolidated financial data presented below is derived from our audited consolidated financial statements for the five-year period ended December 31, 2020. The financial data for the years ended December 31, 2020, 2019 and 2018 should be read together with our consolidated financial statements and related notes included in Item 8, “Financial Statements and Supplementary Data” and the information included in Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations” herein.
| 2020 (1) | 2019 | 2018 | 2017 (2) | 2016 (3) | |||||||||||||||||||||||||
| (Amounts in thousands, except per share data) | |||||||||||||||||||||||||||||
| Income Statement Data: | |||||||||||||||||||||||||||||
| Net service revenue | $ | 2,071,519 | $ | 1,955,633 | $ | 1,662,578 | $ | 1,511,272 | $ | 1,419,261 | |||||||||||||||||||
| Operating income | $ | 219,268 | $ | 177,472 | $ | 155,148 | $ | 78,524 | $ | 57,340 | |||||||||||||||||||
| Net income attributable to Amedisys, Inc. | $ | 183,608 | $ | 126,833 | $ | 119,346 | $ | 30,301 | $ | 37,261 | |||||||||||||||||||
| Net income attributable to Amedisys, Inc. per basic share | $ | 5.64 | $ | 3.95 | $ | 3.64 | $ | 0.90 | $ | 1.12 | |||||||||||||||||||
| Net income attributable to Amedisys, Inc. per diluted share | $ | 5.52 | $ | 3.84 | $ | 3.55 | $ | 0.88 | $ | 1.10 | |||||||||||||||||||
(1)During 2020, we recorded a $24.0 million income tax benefit in connection with the stock option exercise by Paul B. Kusserow, President, Chief Executive Officer and Chairman of the Board of Amedisys.
(2)During 2017, we recorded charges related to the Securities Class Action Lawsuit settlement and related legal fees in the amount of $29.8 million ($18.1 million, net of tax). Additionally, we recorded a charge in the amount of $21.4 million as the result of H.R. 1 (Tax Cuts and Jobs Act) enacted on December 22, 2017.
(3)During 2016, we recorded Homecare Homebase (“HCHB”) implementation costs in the amount of $8.4 million ($5.1 million, net of tax) and recognized a non-cash charge to write off assets as a result of our conversion to the HCHB platform in the amount of $4.4 million ($2.7 million, net of tax).
| 2020 | 2019 | 2018 | 2017 | 2016 | ||||||||||||||||||||||||||||
| (Amounts in thousands) | ||||||||||||||||||||||||||||||||
| Balance Sheet Data: | ||||||||||||||||||||||||||||||||
| Total assets | $ | 1,567,198 | $ | 1,262,745 | $ | 717,118 | $ | 813,482 | $ | 734,029 | ||||||||||||||||||||||
| Total debt, including current portion | $ | 215,007 | $ | 242,183 | $ | 7,387 | $ | 88,841 | $ | 93,029 | ||||||||||||||||||||||
| Total Amedisys, Inc. stockholders’ equity | $ | 809,224 | $ | 640,450 | $ | 481,582 | $ | 515,321 | $ | 460,203 | ||||||||||||||||||||||
| Cash dividends declared per common share | $ | — | $ | — | $ | — | $ | — | $ | — | ||||||||||||||||||||||
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion and analysis provides information we believe is relevant to an assessment and understanding of our results of operations and financial condition for 2020, 2019 and 2018. This discussion should be read in conjunction with our audited financial statements included in Item 8, “Financial Statements and Supplementary Data” and Part I, Item 1, “Business” of this Annual Report on Form 10-K. The following analysis contains forward-looking statements about our future revenues, operating results and expectations. See “Special Caution Concerning Forward-Looking Statements” for a discussion of the risks, assumptions and uncertainties affecting these statements as well as Part I, Item 1A, “Risk Factors.”
Overview
We are a provider of high-quality in-home healthcare and related services to the chronic, co-morbid, aging American population, with approximately 75%, 74% and 73% of our revenue derived from Medicare for 2020, 2019 and 2018, respectively.
32
Our operations involve servicing patients through our three reportable business segments: home health, hospice and personal care. Our home health segment delivers a wide range of services in the homes of individuals who may be recovering from an illness, injury or surgery. Our hospice segment provides care that is designed to provide comfort and support for those who are facing a terminal illness. Our personal care segment provides patients assistance with the essential activities of daily living. As of December 31, 2020, we owned and operated 320 Medicare-certified home health care centers, 180 Medicare-certified hospice care centers and 14 personal-care care centers, including unconsolidated joint ventures, in 39 states within the United States and the District of Columbia.
Care Centers Summary (Includes Unconsolidated Joint Ventures)
| Home Health | Hospice | Personal Care | |||||||||||||||
| At December 31, 2017 | 323 | 83 | 15 | ||||||||||||||
| Acquisitions/Start-Ups/Denovos | 1 | 1 | 1 | ||||||||||||||
| Closed/Consolidated | (1) | — | (4) | ||||||||||||||
| At December 31, 2018 | 323 | 84 | 12 | ||||||||||||||
| Acquisitions/Start-Ups/Denovos | 3 | 59 | — | ||||||||||||||
| Closed/Consolidated | (5) | (5) | — | ||||||||||||||
| At December 31, 2019 | 321 | 138 | 12 | ||||||||||||||
| Acquisitions/Start-Ups/Denovos | 4 | 54 | 2 | ||||||||||||||
| Closed/Consolidated | (5) | (12) | — | ||||||||||||||
| At December 31, 2020 | 320 | 180 | 14 | ||||||||||||||
When we refer to “same store business,” we mean home health, hospice and personal-care care centers that we have operated for at least the last twelve months and start-ups that are an expansion of a same store care center; when we refer to “acquisitions,” we mean home health, hospice and personal-care care centers that we acquired within the last twelve months; and when we refer to “denovos,” we mean home health, hospice and personal-care care centers opened by us in the last twelve months which are not an expansion of a same store care center. Once a care center has been in operation for a twelve month period, the results for that particular care center are included as part of our same store business from that date forward.
2020 Developments
•Achieved the highest Quality of Patient Care Star Score in the Home Health industry in the October 2020 Home Health Compare ("HHC") release of 4.33 stars with 95% of our care centers at 4+ Stars.
•Outperformed the industry on all Hospice Item Set ("HIS") measures.
•Performed over 11.5 million visits.
•Acquired and successfully integrated Asana Hospice ("Asana") and AseraCare Hospice ("AseraCare") making Amedisys the third largest hospice company in the United States, exceeding 13,000 in hospice average daily census.
•Successfully procured personal protective equipment ("PPE") and implemented protocols to ensure the safety of our employees and patients during the novel coronavirus pandemic as discussed in further detail under Novel Coronavirus Pandemic ("COVID-19") below.
•Ended the year with overall voluntary turnover of 18.3% and reduced our early exit rate by 6% over 2019, ending 2020 at 11.9%.
•Successfully piloted several tools and data analytics platforms of Medalogix, a predictive data and analytics company, helping to further optimize our current business and positioning us to work more closely with Medicare Advantage payors.
•Implemented pay practice changes and staffing model efficiencies to further drive operational excellence.
•Successfully navigated the transition to the Patient-Driven Groupings Model ("PDGM") while continuing to deliver operational efficiencies through margin expansion.
•Executed a Care Coordination Agreement with BrightStar Care to facilitate the coordination of care between home health and hospice care centers and a network of personal care partners.
33
•Increased operating income 24%.
•Expanded home health gross margin as a percentage of revenue by 320 basis points.
•Delivered $289 million in cash flow from operations.
2021 Strategy
•Further advance our industry leading Quality of Patient Care Star scores in home health.
•Drive best-in-class hospice quality while continuing to integrate acquired hospice assets.
•Advance our culture and sense of belonging through diversity and inclusion initiatives.
•Build a learning culture through world class leadership development.
•Reduce turnover in critical clinician roles.
•Continue our success in operating under PDGM.
•Expand our analytics capabilities internally and through our Medalogix investment.
•Deliver above industry average growth rates in all three lines of business.
•Pursue consolidations in the home health industry via a regional-based acquisition strategy.
•Incrementally innovate around our core business to deliver new home based care models such as Skilled Nursing Facility ("SNF") at Home.
Financial Performance
Results for the year ended December 31, 2020 were impacted by acquisitions, COVID-19, the suspension of sequestration and the transition to PDGM. On a consolidated basis, we increased operating income $42 million on a $116 million increase in net service revenue.
Our home health care centers experienced growth in volumes and improvement in utilization and clinician mix which, combined with our variable cost structure and sequestration relief, mitigated a significant portion of our estimated COVID-19 impact and led to the segment delivering a $26 million increase in operating income.
Our hospice segment completed the acquisitions of Asana and AseraCare in 2020. These acquisitions contributed approximately $13 million in operating income to the hospice segment.
Our personal care segment contributed approximately $6 million in operating income during 2020.
Economic and Industry Factors
Our home health, hospice and personal care segments operate in a highly fragmented and highly competitive industry. The degree of competitiveness varies based upon whether our care centers operate in states that require a certificate of need ("CON") or permit of approval ("POA"). In such states, expansion by existing providers or entry into the market by new providers is permitted only where determination is made by state health authorities that a given amount of unmet healthcare need exists. Currently, 71% and 27% of our home health and hospice care centers, respectively, operate in CON/POA states.
As the Federal government continues to debate a reduction in expenditures and a reform of the Medicare system, our industry continues to face reimbursement pressures. These reform efforts could result in major changes in the health care delivery and reimbursement system on a national and state level, including changes directly impacting the reimbursement systems for our home health and hospice care centers.
Payment
Hospice
On July 31, 2020, the Centers for Medicare and Medicaid Services ("CMS") issued a final rule to update hospice payment rates and the wage index for fiscal year 2021 effective for services provided beginning October 1, 2020. CMS estimates hospices serving Medicare beneficiaries would see an estimated 2.4% increase in payments. This increase is the result of a 2.4% market basket adjustment as required under the Patient Protection and Affordable Health Care Act and the Health Care and Education Reconciliation Act (collectively, "PPACA"). The rule also changed the hospice wage index by adopting the most recent Office
34
of Management and Budget statistical area delineations with a five percent cap on wage index decreases. Finally, CMS increased the aggregate cap amount by 2.4% to $30,684. Based on our analysis of the final rule, we expect our impact to be in line with the 2.4% increase.
Home Health
On October 31, 2019, CMS issued the Calendar Year 2020 Home Health Final Rule, which confirmed the implementation of PDGM effective January 1, 2020 as well as a change in the unit of payment from a 60-day episode of care to a 30-day period of care. Additionally, in an effort to reduce fraud risks, CMS reduced requests for anticipated payment ("RAPs") for 2020 to 20% with the full elimination in 2021. CMS estimated that the final rule would result in a 1.3% increase in payments to home health providers. The increase is the result of a statutorily mandated 1.5% market basket increase pursuant to the Bipartisan Budget Act of 2018, reduced by 0.2% for the rural add-on. In calculating the impact, CMS also assumed that the industry would make certain behavioral changes related to coding practices, low utilization payment adjustment ("LUPA") management and co-morbidities. As a result, CMS reduced reimbursement by 4.36%. The impact of the final rule on us was a 2.8% reduction in revenue for 2020.
On October 29, 2020, CMS issued the Home Health Final Rule for Medicare home health providers for calendar year 2021. CMS estimates that the final rule will result in a 1.9% increase in payments to home health providers. The increase is the result of a 2.0% market basket adjustment reduced by 0.1% for the rural add-on. Based on our analysis of the final rule, we expect our impact to be in line with the 1.9% increase. Additionally, CMS made permanent the telehealth flexibilities that were announced in the Interim Final Rule (Emergency Rule) for COVID-19 in March 2020. These flexibilities allow home health agencies to provide certain care via telehealth if it is clinically appropriate and included in the plan of care. Telehealth visits still do not count as visits for purposes of patient eligibility or payment.
The following payment adjustments are effective for each of the years indicated based on CMS’s final rules:
| Home Health | Hospice | ||||||||||||||||||||||||||||||||||
| 2021 | 2020 | 2019 | 2021 (1) | 2020 | 2019 | ||||||||||||||||||||||||||||||
| Market Basket Update | 2.0 | % | 1.5 | % | 3.0 | % | 2.4 | % | 3.0 | % | 2.9 | % | |||||||||||||||||||||||
| Rural Add-On Adjustment | (0.1) | (0.2) | — | — | — | — | |||||||||||||||||||||||||||||
| PPACA Adjustment | — | — | — | — | — | (0.3) | |||||||||||||||||||||||||||||
| Productivity Adjustment | — | — | (0.8) | — | (0.4) | (0.8) | |||||||||||||||||||||||||||||
| Behavioral Assumptions | — | (4.4) | — | — | — | — | |||||||||||||||||||||||||||||
| Estimated Industry Impact Including Behavioral Assumptions | 1.9 | % | (3.1 | %) | 2.2 | % | 2.4 | % | 2.6 | % | 1.8 | % | |||||||||||||||||||||||
Estimated Company-Specific Impact (2) | 1.9 | % | (2.8 | %) | 1.2 | % | 2.4 | % | 0.5 | % | 1.6 | % | |||||||||||||||||||||||
(1)Effective for services provided from October 1, 2020 to September 30, 2021.
(2)Our company-specific impact of the home health final rule could differ depending on differences in the wage index, our patient case mix and other factors, such as LUPAs or outliers, which are described in more detail under Critical Accounting Estimates below. Our company-specific impact of the hospice final rule could differ based on our mix of patients and differences in the wage index.
Novel Coronavirus Pandemic ("COVID-19")
Our operations and financial performance for the year ended December 31, 2020 have been impacted by COVID-19. The impacts on our operations began during the second week of March 2020, as we experienced declines in referral volumes and an increase in missed visits. Our home health segment experienced a referral low-point the week of April 5th. Since that time, we have seen a steady recovery in referral volumes and a corresponding drop in missed visits. In our hospice segment, our referrals hit their low-point the week of March 22nd. While hospice admission volumes have improved significantly, the slowdown in March has impacted our average daily census and has been most significant in our facility-based census. Additionally, we have seen a decline in our hospice average daily census as a result of a significant increase in deaths, an increase in the discharge rate of same-month admissions and a delay in the timing of patients coming onto service resulting in a shorter length of stay. The financial impacts of COVID-19 during the year ended December 31, 2020 are discussed in further detail under "Results of Operations" below.
While we currently believe that we have a reasonable view of operations, the uncertainty created by COVID-19 could alter our outlook of the pandemic's impact on our consolidated financial condition, results of operations or cash flows. The following factors could potentially impact our performance: the continued increase or decrease in the number of COVID-19 cases nationwide, the severity and impacts of new variants of the virus, uncertainty regarding vaccine distribution timing and
35
efficiency, the utilization of elective procedures, the return of patient confidence to enter a hospital or a doctor's office, the ability to have access to our patients in their homes and in facilities, cost normalization around PPE and any future or prolonged shelter-in-place orders and other federal, state and local requirements. Potential impacts of COVID-19 on our results include lower revenue, higher salary and wage expense related to quarantine pay and training and increased supply costs related to PPE and COVID-19 testing. The impacts to revenue may consist of the following:
•lower volumes due to interruption of the operations of our referral sources, patients' unwillingness to accept services and restrictions on access to facilities for hospice services;
•lower reimbursement due to missed visits resulting in an increase in LUPAs and lost billing periods; and
•lower hospice average daily census due to a decline in average length of stay and an increase in deaths.
On March 27, 2020, the bipartisan Coronavirus Aid, Relief, and Economic Security Act ("CARES Act") was signed into legislation. The CARES Act provides for the following:
•$175 billion to healthcare providers, including hospitals on the front lines of the COVID-19 pandemic. Of this total allocated amount, $30 billion was distributed immediately to providers based on their proportionate share of Medicare fee-for-service reimbursements in 2019. Healthcare providers were required to sign an attestation confirming receipt of the Provider Relief Fund ("PRF") funds and agree to the terms and conditions of payment. Our home health and hospice segments received approximately $100 million from the first $30 billion of funds distributed to healthcare providers in April 2020, which is inclusive of $2 million related to our joint venture care centers (equity method investments). We also acquired approximately $6 million of PRF funds in connection with the acquisition of AseraCare. Consistent with the terms and conditions for receipt of the payment, we are allowed to use the funds to cover lost revenues and health care costs related to COVID-19, and we are required to properly and fully document the use of these funds in reports to the U.S. Department of Health and Human Services ("HHS").
For our wholly-owned subsidiaries, we have decided to only utilize PRF funds to the extent we have qualifying COVID-19 expenses, which totaled $33 million for our home health and hospice segments during the year ended December 31, 2020. Accordingly, for our wholly-owned subsidiaries, we will not be using the funds to cover lost revenues resulting from COVID-19. In September 2020, HHS issued new guidance noting that PRF funds can be used through June 30, 2021. We do not believe that we will fully utilize the funds received; therefore, we have recorded a liability related to the funds that we do not expect to utilize totaling $60 million which is reflected in the Provider Relief Fund Advance account in current liabilities within our consolidated balance sheet. Funds that we intend to use in the future to cover COVID-19 expenses, which we have estimated to be approximately $12 million, have been recorded to a deferred liability account within accrued expenses in our consolidated balance sheet. These estimates may change as our ability to utilize and retain the funds will depend on the magnitude, timing and nature of the impact of the pandemic.
•The temporary suspension of the automatic 2% reduction of Medicare claim reimbursements ("sequestration") for the period May 1 through December 31, 2020. The impact was an increase to our 2020 net service revenue of approximately $23 million. In December 2020, Congress passed additional COVID-19 relief legislation as part of the Consolidated Appropriations Act, 2021. This legislation extended the suspension of sequestration through March 31, 2021.
•The deferral of the employer share of social security tax (6.2%), effective for payments due after the enactment date. Fifty percent is due on December 31, 2021 with the remaining amounts due on December 31, 2022. As of December 31, 2020, we have deferred approximately $55 million of social security tax which has increased our cash flow from operations by the same amount; approximately $28 million is reflected in each of payroll and employee benefits and other long-term obligations within our consolidated balance sheet.
•The temporary suspension of Medicare patient coverage criteria and documentation and care requirements and the expansion of providing home health and hospice care to patients via telehealth.
•The ability for non-physician practitioners to certify for home health, order home health services, establish and review plans of care and certify and recertify eligibility.
The well-being of our employees has been one of our top priorities during this pandemic. We have taken the following steps to support our employees: implemented up to 14 days of paid leave during any required quarantine periods; awarded SPIRIT bonuses to our clinicians and caregivers who have seen patients during the pandemic; completed an early cash pay-out of employee paid-time-off; instituted work-from-home arrangements for our corporate and administrative support employees; allowed employees to temporarily suspend any 401(k) plan loan deductions and offered employees the option of making a
36
withdrawal from their 401(k) plan for coronavirus-related distributions without incurring the additional 10% early withdrawal penalty; granted access to Teladoc services to all employees; provided access to COVID-19 self-test kits to all employees and created a COVID-19 Resource Center, available 24 hours a day, seven days a week for employees to access educational materials, safety documents, policies, clinical protocols and operational metrics.
The safety of our clinicians and patients has also been a focus, and as a result, we have made the following business changes: developed clinical protocols for COVID-19 testing, proper usage of PPE, caring for COVID-positive patients and maintaining safety measures in our care centers; researched each state's vaccination plan to develop a state by state protocol to work with local health departments and other health systems to obtain vaccine appointments for our clinical staff; implemented software enabling us to track staff that have been vaccinated; procured millions in PPE and created a centralized distribution center for all critical PPE, allowing us to flex our inventory on a care center by care center basis, based on need and demand. We have had success in utilizing both traditional and non-traditional suppliers for our PPE needs. While we were very fortunate to secure the supplies needed, we faced significantly higher per unit costs for the purchase of PPE.
Network Developments
In August 2020, we signed a Care Coordination Agreement with BrightStar Care to add its agencies to the Amedisys personal care network, which helps facilitate the coordination of care between our home health and hospice care centers and a network of personal care partners.
In July 2019, we signed an agreement with ClearCare, Inc. ("ClearCare"), the provider of the personal care industry’s leading software platform, representing 4,000 personal care agencies in every zip code in the United States. Our agreement with ClearCare creates an opportunity to establish a network partnership between Amedisys and personal care agencies using ClearCare in order to better coordinate patient care.
Long term, we believe these agreements will allow us to build a nation-wide network of personal care agencies and further our efforts to provide patients with a true care continuum in the home. These relationships will also help us as we continue to have innovative payment conversations with Medicare Advantage plans who have begun to recognize the value that combined home health, hospice and personal care services bring to their members and care delivery infrastructure.
Governmental Inquiries and Investigations and Other Litigation
See Item 8, Note 11 – Commitments and Contingencies to our consolidated financial statements for additional information regarding the subpoena and civil investigative demands issued by the U.S. Department of Justice and the South Carolina and Florida Zone Program Integrity Contractor audits. No assurances can be given as to the timing or outcome of these items.
37
Results of Operations
Consolidated
The following table summarizes our consolidated results of operations (amounts in millions):
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Net service revenue | $ | 2,071.5 | $ | 1,955.6 | $ | 1,662.6 | |||||||||||
| Other operating income | 34.4 | — | — | ||||||||||||||
| Cost of service, excluding depreciation and amortization | 1,185.4 | 1,150.3 | 992.9 | ||||||||||||||
| Gross margin, excluding depreciation and amortization | 920.5 | 805.3 | 669.7 | ||||||||||||||
| % of revenue | 44.4 | % | 41.2 | % | 40.3 | % | |||||||||||
| Other operating expenses | 668.2 | 607.9 | 501.3 | ||||||||||||||
| % of revenue | 32.3 | % | 31.1 | % | 30.1 | % | |||||||||||
| Depreciation and amortization | 28.8 | 18.4 | 13.3 | ||||||||||||||
| Asset impairment charge | 4.2 | 1.5 | — | ||||||||||||||
| Operating income | 219.3 | 177.5 | 155.1 | ||||||||||||||
| Total other (expense) income, net | (8.4) | (7.1) | 3.8 | ||||||||||||||
| Income tax expense | (25.6) | (42.5) | (38.8) | ||||||||||||||
| Effective income tax rate | 12.2 | % | 24.9 | % | 24.4 | % | |||||||||||
| Net income | 185.2 | 127.9 | 120.1 | ||||||||||||||
| Net income attributable to noncontrolling interests | (1.6) | (1.1) | (0.8) | ||||||||||||||
| Net income attributable to Amedisys, Inc. | $ | 183.6 | $ | 126.8 | $ | 119.3 | |||||||||||
Year Ended December 31, 2020 Compared to the Year Ended December 31, 2019
On a consolidated basis, our operating income increased approximately $42 million on a revenue increase of $116 million. COVID-19 resulted in significant impacts to all of our segments; however, we experienced a significant increase in our gross margin as a percentage of revenue which drove our improvement over 2019. Our results were also impacted by acquisitions, the suspension of sequestration, the transition to PDGM, a reduction in revenue adjustments, severance associated with reductions in staffing levels, primarily within our home health segment and an asset impairment charge related to our acquired names intangibles.
Our 2020 results include the acquisitions of Asana and AseraCare, which contributed revenue of $88 million and an operating loss of $12 million, which is inclusive of acquisition and integration costs totaling $10 million and intangibles amortization totaling $9 million. Our results also reflect one additional month of revenue and operating income from Compassionate Care Hospice ("CCH"), which was acquired on February 1, 2019, and three additional months of revenue and operating income from RoseRock Healthcare ("RoseRock"), which was acquired on April 1, 2019.
COVID-19 disrupted both net service revenue and costs during 2020. The most significant impact occurred in the second quarter during which we experienced a $30 million decline in net service revenue over prior year due to COVID-19. Our variable cost structure helped us mitigate a significant portion of the revenue impact. Our home health segment, which was the most heavily impacted by COVID-19, recovered quickly and returned to year over year growth in volumes during the third and fourth quarters. Our hospice segment experienced declines in admissions during the second quarter but saw an overall slower decline in average daily census, which is the main driver of hospice revenue. While we have experienced strong admission growth during the third and fourth quarters, a significant increase in deaths, an increase in the discharge rate of same-month admissions and a delay in the timing of patients coming onto service has driven down our length of stay resulting in average daily census growth of only 1% year over year. Based on our current projections, we are anticipating a decline in average daily census early in 2021 despite strong growth in admissions. We expect that our length of stay will return to normal levels during 2021.
Our 2020 operating results were positively impacted by the suspension of sequestration effective May 1, 2020, which resulted in an increase to net service revenue of approximately $23 million ($13 million home health, $10 million hospice) but negatively impacted by the change in reimbursement under PDGM, which resulted in a $23 million reduction in net service revenue. We were able to significantly mitigate the PDGM rate cut and expand margin in our home health segment by
38
delivering improvements in clinician utilization and discipline mix and by reducing our revenue adjustments. Additionally, we experienced an expansion in our hospice gross margin resulting from lower costs associated with a decline in visit volumes due to access restrictions imposed by facilities as well as a reduction in revenue adjustments; prior year results included a $7 million reduction to revenue related to settlement discussions with the U.S. Department of Justice (See Item 8, Note 11 – Commitments and Contingencies to our consolidated financial statements for additional information).
Each of our segments incurred incremental costs related to COVID-19. As noted above, for our wholly-owned subsidiaries, we have elected to use the CARES Act Provider Relief Funds to cover COVID-19 expenses incurred by our home health and hospice segments which totaled $33 million during 2020. Our personal care segment received funds from the Mass Home Care ASAP COVID-19 Provider Sustainability Program totaling $1 million. We have used these funds to cover COVID-19 expenses as well. We have recorded income associated with both of these programs totaling $34 million in other operating income within our consolidated statement of operations.
Our operating results reflect a 1.2% increase in our other operating expenses as a percentage of revenue compared to prior year; this increase is due to the addition of resources to support growth (primarily business development employees), investments related to PDGM and planned wage increases, partially offset by overall reductions in spend during the pandemic and lower acquisition and integration costs.
Last, we recorded a $4 million asset impairment charge related to acquired names which are no longer in use (see Item 8, Note 5 – Goodwill and Other Intangible Assets, Net to our consolidated financial statements for additional information).
Total other (expense) income, net includes the following items (amounts in millions):
| For the Years Ended December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Interest income | $ | 0.3 | $ | 0.1 | |||||||
| Interest expense | (11.0) | (14.5) | |||||||||
| Equity in earnings from equity method investments | 4.0 | 5.3 | |||||||||
| Miscellaneous, net | (1.7) | 2.0 | |||||||||
| $ | (8.4) | $ | (7.1) | ||||||||
Interest expense decreased $4 million in 2020 from 2019 as a result of a decrease in borrowings under our Amended Credit Agreement (see Item 8, Note 8 – Long-Term Obligations to our consolidated financial statements for additional information regarding our Amended Credit Agreement). Miscellaneous, net includes a $3 million loss from the sale of our investment in the Heritage Healthcare Innovation Fund, LP during 2020 (see Item 8, Note 1 - Nature of Operations, Consolidation and Presentation of Financial Statements to our consolidated financial statements for additional information).
Year Ended December 31, 2019 Compared to the Year Ended December 31, 2018
Overall, our operating income increased $22 million on a revenue increase of $293 million. Our 2019 operating results include the acquisitions of CCH and RoseRock which contributed approximately $174 million in revenue and an operating loss of approximately $5 million, which is inclusive of $14 million in acquisition and integration costs and $6 million in intangibles amortization.
Additionally, our operating income was negatively impacted by a $7 million accrual related to settlement discussions with the U.S. Department of Justice (see Item 8, Note 11 - Commitments and Contingencies to our consolidated financial statements for additional information) and a $2 million asset impairment charge related to our acquired names (see Item 8, Note 5 - Goodwill and Other Intangible Assets, Net to our consolidated financial statements for additional information).
Our year-to-date performance reflects growth and operating improvement in all three segments of our legacy operations. We expanded gross margin as a percentage of revenue in our home health and personal care segments. Both segments benefited from rate increases with home health also delivering improvements in clinician utilization and discipline mix. Our hospice segment's gross margin as a percentage of revenue decreased due to our acquisition activity. Additionally, our other operating expenses as a percentage of revenue increased only 1% compared to 2018; this increase is inclusive of approximately $16 million in acquisition and integration costs. Excluding the acquisition and integration costs, our other operating expenses as a percentage of revenue remained relatively flat compared to 2018 despite planned wage increases and the addition of resources to support growth.
39
Total other (expense) income, net includes the following items (amounts in millions):
| For the Years Ended December 31, | |||||||||||
| 2019 | 2018 | ||||||||||
| Interest income | $ | 0.1 | $ | 0.3 | |||||||
| Interest expense | (14.5) | (7.4) | |||||||||
| Equity in earnings from equity method investments | 5.3 | 7.7 | |||||||||
| Miscellaneous, net | 2.0 | 3.2 | |||||||||
| $ | (7.1) | $ | 3.8 | ||||||||
Interest expense increased $7 million in 2019 from 2018 as a result of an increase in borrowings under our Amended Credit Agreement (see Item 8, Note 8 – Long-Term Obligations to our consolidated financial statements for additional information regarding our Amended Credit Agreement). Equity in earnings from equity method investments includes gains of $2 million and $5 million for 2019 and 2018, respectively.
Home Health Division
The following table summarizes our home health segment results of operations:
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
Financial Information (in millions): | |||||||||||||||||
| Medicare | $ | 847.3 | $ | 859.2 | $ | 830.8 | |||||||||||
| Non-Medicare | 401.9 | 397.2 | 343.7 | ||||||||||||||
| Net service revenue | 1,249.2 | 1,256.4 | 1,174.5 | ||||||||||||||
| Other operating income | 20.2 | — | — | ||||||||||||||
| Cost of service | 729.9 | 754.1 | 722.1 | ||||||||||||||
| Gross margin | 539.5 | 502.3 | 452.4 | ||||||||||||||
| Asset impairment charge | 3.4 | 1.5 | — | ||||||||||||||
| Other operating expenses | 311.1 | 301.4 | 279.8 | ||||||||||||||
| Operating income | $ | 225.0 | $ | 199.4 | $ | 172.6 | |||||||||||
| Same Store Growth (1): | |||||||||||||||||
| Medicare revenue | (1 | %) | 4 | % | 6 | % | |||||||||||
| Non-Medicare revenue | 1 | % | 16 | % | 18 | % | |||||||||||
| Total admissions | 1 | % | 7 | % | 5 | % | |||||||||||
| Total volume (2) | 2 | % | 5 | % | 7 | % | |||||||||||
| Key Statistical Data - Total (3): | |||||||||||||||||
| Admissions | 331,354 | 328,693 | 309,325 | ||||||||||||||
| Recertifications | 181,195 | 172,568 | 168,509 | ||||||||||||||
| Total volume | 512,549 | 501,261 | 477,834 | ||||||||||||||
| Medicare completed episodes (6) | 301,856 | 306,520 | 301,701 | ||||||||||||||
| Average Medicare revenue per completed episode (4) (6) | $ | 2,836 | $ | 2,853 | $ | 2,799 | |||||||||||
| Medicare visits per completed episode (5) (6) | 14.9 | 17.0 | 17.4 | ||||||||||||||
| Visiting Clinician Cost per Visit | $ | 89.62 | $ | 83.11 | $ | 81.88 | |||||||||||
| Clinical Manager Cost per Visit | $ | 9.17 | $ | 8.04 | $ | 8.01 | |||||||||||
| Total Cost per Visit | $ | 98.79 | $ | 91.15 | $ | 89.89 | |||||||||||
| Visits | 7,388,549 | 8,273,308 | 8,033,654 | ||||||||||||||
40
(1)Same store information represents the percent change in our Medicare, Non-Medicare and Total revenue, admissions or volume for the period as a percent of the Medicare, Non-Medicare and Total revenue, admissions or volume of the prior period. Effective July 1, 2019, same store is defined as care centers that we have operated for at least the last twelve months and startups that are an expansion of a same store care center.
(2)Total volume includes all admissions and recertifications.
(3)Total includes acquisitions and denovos.
(4)Average Medicare revenue per completed episode is the average Medicare revenue earned for each Medicare completed episode of care. Average Medicare revenue per completed episode for the year ended December 31, 2020 reflects the transition to PDGM effective January 1, 2020 and the suspension of sequestration effective May 1, 2020.
(5)Medicare visits per completed episode are the home health Medicare visits on completed episodes divided by the home health Medicare episodes completed during the period.
(6)Prior year amounts have been recast to conform to the current year calculation.
Year Ended December 31, 2020 Compared to the Year Ended December 31, 2019
Operating Results
Overall, our operating income increased $26 million on a $7 million decrease in net service revenue. Our results for the year ended December 31, 2020 were impacted by COVID-19, the suspension of sequestration, the transition to PDGM, severance associated with reductions in staffing levels and a reduction in revenue adjustments. Despite the decrease in net service revenue, we saw significant improvement in our operating performance driven by improvements in our clinician utilization and discipline mix, both of which have contributed to year over year gross margin expansion.
COVID-19 resulted in disruption to our home health volumes beginning at the end of the first quarter through most of the second quarter and amplified the negative impact of the PDGM rate cut on our Medicare revenue per episode. Volumes significantly improved during the third and fourth quarters and our efforts to operationalize PDGM reduced the impact of the PDGM rate cut in the second half of the year. While we are very encouraged by the improvement in volumes and Medicare revenue per episode that we have experienced, we will continue to closely monitor COVID-19 cases and the potential impacts on our operating results.
Our operating results were also impacted by incremental costs totaling $20 million related to COVID-19, which were offset by the recognition of income totaling $20 million associated with the CARES Act Provider Relief Fund, and severance totaling $5 million related to reductions in staffing levels.
Net Service Revenue
Our net service revenue decreased $7 million primarily due to the impacts of COVID-19 and the 2020 change in reimbursement under PDGM. The combination of these resulted in lower volumes than anticipated and lower Medicare revenue per episode for the year ended December 31, 2020. COVID-19 significantly increased the number of missed visits which increased the number of LUPA episodes and the number of episodes with lost billing periods (i.e. episodes with no visits during one of the 30-day billing periods), leading to a decline in our Medicare revenue per episode. Additionally, the implementation of PDGM resulted in a $23 million reduction in net service revenue during the year ended December 31, 2020. This reduction was partially offset by $13 million resulting from the suspension of sequestration effective May 1, 2020.
We have seen significant increases in both volumes and Medicare revenue per episode in the second half of the year as the impacts of COVID-19 have moderated and as we have been able to refocus our efforts on operationalizing PDGM. We have provided additional training, increased our focus on OASIS accuracy and coding and also completed the rollout of Medalogix Care to all of our home health care centers, all of which have resulted in higher case mix and functional impairment scores for our patients. Additionally, we have seen a reduction in our revenue adjustments year over year.
41
Other Operating Income
Other operating income consists of the recognition of funds received from the CARES Act Provider Relief Fund. In accordance with the terms and conditions, these funds can be used to cover lost revenues as well as costs directly attributable to COVID-19. For our wholly-owned subsidiaries, we have elected to utilize the funds to cover COVID-19 related costs only, and therefore, have recognized income equal to the amount of COVID-19 costs incurred to date totaling $20 million. These costs are associated with the purchase of personal protective equipment, bonuses paid to our clinicians, clinician training, quarantine pay and COVID-19 testing. Of the $20 million of COVID-19 costs incurred to date, $19 million has been recorded to cost of service and $1 million has been recorded to other operating expenses.
Cost of Service, Excluding Depreciation and Amortization
Our cost of service consists of costs associated with direct clinician care in the homes of our patients as well as the cost of clinical managers who monitor the overall delivery of care. Overall, our total cost of service decreased 3% on an 11% decrease in total visits. Lower costs associated with a decline in volumes driven by COVID-19, improvements in clinician utilization as evidenced by a decline of 2.1 visits per completed episode year over year and optimization of discipline mix were partially offset by an 8% increase in our total cost per visit, which was driven by planned wage increases, an increase in the utilization of contractors to supplement clinician visits in certain areas, new hire pay, a change in the mix of our visits, costs directly attributable to COVID-19 totaling approximately $19 million and severance totaling $5 million related to a reduction in staffing levels. While we compensate our clinicians on a per visit basis, there is a fixed cost component of our cost structure which resulted in an increase in our cost per visit as we had a significant decline in visits.
Other Operating Expenses
Other operating expenses increased approximately $10 million primarily due to planned wage increases, the addition of resources to support volume growth, investments related to PDGM and approximately $1 million of costs directly attributable to COVID-19. These increases were partially offset by a reduction in travel and training expense and an overall reduction in spend during the pandemic.
Year Ended December 31, 2019 Compared to the Year Ended December 31, 2018
Operating Results
Overall, our operating income increased $27 million on an $82 million increase in net service revenue. Our gross margin as a percentage of revenue was positively impacted by the 2019 changes in reimbursement, growth in volumes, the acuity level of our patients, improved utilization and a focus on discipline mix. The impact of the 2019 change in reimbursement was an increase in net service revenue and gross margin of approximately $12 million.
Net Service Revenue
Our revenue increased $82 million (7%) on a 5% increase in total volume and a 2% increase in Medicare revenue per episode. The volume growth was driven by a 7% increase in admissions offset by lower recertification volume. The increase in Medicare revenue per episode is the result of a 1.2% increase in reimbursement with the remainder due to an increase in the acuity level of our patients. Additionally, our non-Medicare (per visit and episodic) rates increased approximately 3% which is a combination of rate increases and increases in the acuity level of our patients. Revenue was also positively impacted by a reduction in our revenue adjustments.
Cost of Service, Excluding Depreciation and Amortization
Our cost of service increased 4% on a 3% increase in total visits. Our total cost per visit increased approximately 1% as improvements in clinician utilization and optimization of discipline mix partially offset planned wage increases. Additionally, changes in our home health care center staffing resulted in a shift of some office staff from cost of service to other operating expenses totaling approximately $4 million.
42
Other Operating Expenses
Other operating expenses increased approximately $22 million primarily due to an increase in salaries and benefits expense as a result of the addition of resources to support volume growth, planned wage increases and the home health staffing shifts referenced above.
Hospice Division
The following table summarizes our hospice segment results of operations:
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
Financial Information (in millions): | |||||||||||||||||
| Medicare | $ | 710.0 | $ | 586.6 | $ | 390.2 | |||||||||||
| Non-Medicare | 40.1 | 30.6 | 20.7 | ||||||||||||||
| Net service revenue | 750.1 | 617.2 | 410.9 | ||||||||||||||
| Other operating income | 13.1 | — | — | ||||||||||||||
| Cost of service | 400.6 | 335.1 | 212.0 | ||||||||||||||
| Gross margin | 362.6 | 282.1 | 198.9 | ||||||||||||||
| Asset impairment | 0.8 | — | — | ||||||||||||||
| Other operating expenses | 177.6 | 139.1 | 85.7 | ||||||||||||||
| Operating income | $ | 184.2 | $ | 143.0 | $ | 113.2 | |||||||||||
| Same Store Growth (1): | |||||||||||||||||
| Medicare revenue | 4 | % | 7 | % | 11 | % | |||||||||||
| Hospice admissions | 6 | % | 4 | % | 8 | % | |||||||||||
| Average daily census | 1 | % | 7 | % | 11 | % | |||||||||||
| Key Statistical Data - Total (2): | |||||||||||||||||
| Hospice admissions | 49,694 | 40,194 | 27,596 | ||||||||||||||
| Average daily census | 13,081 | 11,164 | 7,588 | ||||||||||||||
| Revenue per day, net | $ | 156.69 | $ | 151.47 | $ | 148.36 | |||||||||||
| Cost of service per day | $ | 83.67 | $ | 82.24 | $ | 76.53 | |||||||||||
| Average discharge length of stay | 99 | 98 | 100 | ||||||||||||||
(1)Same store information represents the percent change in our Medicare revenue, Hospice admissions or average daily census for the period as a percent of the Medicare revenue, Hospice admissions or average daily census of the prior period. Effective July 1, 2019, same store is defined as care centers that we have operated for at least the last twelve months and startups that are an expansion of a same store care center.
(2)Total includes acquisitions and denovos.
Year Ended December 31, 2020 Compared to the Year Ended December 31, 2019
Operating Results
Our operating results for 2020 include the results of the acquisition of Asana on January 1, 2020 (8 hospice care centers) and AseraCare on June 1, 2020 (44 hospice care centers). Acquisitions are included in our consolidated financial statements from their respective acquisition dates. As a result of our acquisitions, our hospice segment operating results for 2020 and 2019 are not fully comparable.
Overall, our operating income increased $41 million on a $133 million increase in net service revenue. Our 2020 results include the acquisitions of Asana and AseraCare, which contributed revenue of $88 million and operating income of $13 million. Our results also reflect one additional month of revenue and operating income from CCH and three additional months of revenue and operating income from RoseRock. Additionally, our operating results were favorably impacted by the following: 1% growth in average daily census, changes in reimbursement, which resulted in an increase in net service revenue and gross margin of approximately $6 million and $3 million, respectively, lower revenue adjustments, the suspension of sequestration effective May 1, 2020 and lower visit volumes due to facility access restrictions.
43
Net Service Revenue
Our net service revenue increased $133 million, approximately $88 million of which is attributable to our Asana and AseraCare acquisitions during 2020. The remaining increase in net service revenue is the result of one additional month of revenue from our 2019 acquisition of CCH (approximately $15 million), three additional months of revenue from our 2019 acquisition of RoseRock (approximately $2 million), growth in our average daily census, the suspension of sequestration effective May 1, 2020 ($9 million excluding acquisitions), a 0.5% increase in reimbursement effective October 1, 2019 ($3 million), a 2.4% increase in reimbursement effective October 1, 2020 ($3 million, excluding acquisitions) and lower revenue adjustments as prior year results included a $7 million reduction to revenue related to settlement discussions with the U.S. Department of Justice (see Note 11 – Commitments and Contingencies to our consolidated financial statements for additional information).
While COVID-19 significantly impacted our admission volumes during the second quarter, our hospice admissions rebounded quickly, resulting in strong year over year growth in admissions during the third and fourth quarters. Our same store admissions growth was up 6% year over year; however, our average daily census, which is the main driver of hospice revenue, was up only 1%. Generally, changes in average daily census lag changes in admission volumes; however, we have not seen an increase in our average daily census growth due to a significant increase in the number of deaths, an increase in the discharge rate of same-month admissions and a delay in the timing of patients coming onto service resulting in a lower length of stay. This lower length of stay resulted in a declining census as we exited 2020. Based on our current projections, we expect this trend to continue into 2021.
Other Operating Income
Other operating income consists of the recognition of funds received from the CARES Act Provider Relief Fund. In accordance with the terms and conditions, these funds are intended to cover lost revenues as well as costs directly attributable to COVID-19. For our wholly-owned subsidiaries, we have elected to utilize the funds to cover COVID-19 related costs only, and therefore, have recognized income equal to the amount of COVID-19 costs incurred to date totaling $13 million. These costs are associated with the purchase of personal protective equipment, bonuses paid to our clinicians, clinician training, quarantine pay and COVID-19 testing. Of the $13 million of COVID-19 costs incurred to date, $12 million has been recorded to cost of service and $1 million has been recorded to other operating expenses.
Cost of Service, Excluding Depreciation and Amortization
Our hospice cost of service increased $66 million, approximately $52 million of which is attributable to our Asana and AseraCare acquisitions during 2020. The remaining increase is primarily due to one additional month of costs from our 2019 acquisition of CCH, three additional months of costs from our 2019 acquistion of RoseRock, a 1% increase in average daily census, planned wage increases, COVID-19 costs totaling $12 million and an increase in our general inpatient and respite facility costs as the majority of the reimbursement increase, which became effective October 1, 2019, was passed through to these facilities. These increases were offset by a decline in visits performed by our hourly licensed practical nurses and hospice aides due to facility access restrictions as well as lower transportation costs.
Other Operating Expenses
Other operating expenses increased $39 million, approximately $25 million of which is related to our Asana and AseraCare acquisitions during 2020. The remaining increase is due to the addition of resources to support census growth and planned wage increases, partially offset by a decrease in travel and training expense.
Year Ended December 31, 2019 Compared to the Year Ended December 31, 2018
Operating Results
On February 1, 2019, we acquired CCH, which owned and operated 53 hospice care centers. On April 1, 2019, we acquired RoseRock, which owned and operated one hospice care center. Acquisitions are included in our consolidated financial statements from their respective acquisition dates. As a result, our hospice segment operating results for 2019 and 2018 are not fully comparable.
Overall, our operating income increased $30 million on a $206 million increase in net service revenue. Our operating income was negatively impacted by a $7 million reduction to revenue and gross margin related to settlement discussions with the U.S. Department of Justice (see Item 8, Note 11 - Commitments and Contingencies to our consolidated financial statements for
44
additional information). Our operating results were positively impacted by changes in reimbursement, which resulted in an increase in net service revenue and gross margin of approximately $7 million and $6 million, respectively. The majority of the revenue increase associated with the 2020 change in reimbursement, which became effective October 1, 2019, was passed through to our general inpatient and respite facilities. Our operating results were also positively impacted by continued growth and by our acquisitions which contributed approximately $174 million in net service revenue and $22 million in operating income to our hospice segment's results for the year ended December 31, 2019.
Net Service Revenue
Our hospice revenue increased $206 million; approximately $174 million of which is attributable to our acquisition activities. The remaining $32 million increase is the result of a 7% increase in our average daily census and increases in reimbursement totaling 1.6% and 0.5% effective for services provided from October 1, 2018 and October 1, 2019, respectively, partially offset by an increase in our revenue adjustments, which include a $7 million reduction to revenue and gross margin related to the U.S. Department of Justice matter noted above.
Cost of Service, Excluding Depreciation and Amortization
Our hospice cost of service increased $123 million, approximately $110 million of which is attributable to our acquisition activity. The remaining $13 million increase is primarily due to a 7% increase in average daily census, planned wage increases and an increase in our general inpatient and respite facility costs as the majority of the reimbursement increase, which became effective October 1, 2019, was passed through to these facilities. Our cost of service per day increased 7%, largely driven by our acquisitions as our same store cost of service per day remained relatively flat.
Other Operating Expenses
Other operating expenses increased $53 million; approximately $42 million of the increase is related to our acquisition activity. The remaining $11 million increase is due to increases in other care center related expenses, primarily salaries and benefits expense due to the addition of resources to support census growth and planned wage increases, professional fees and travel and training expense.
Personal Care Division
The following table summarizes our personal care segment results of operations:
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
Financial Information (in millions): | |||||||||||||||||
| Medicare | $ | — | $ | — | $ | — | |||||||||||
| Non-Medicare | 72.2 | 82.0 | 77.2 | ||||||||||||||
| Net service revenue | 72.2 | 82.0 | 77.2 | ||||||||||||||
| Other operating income | 1.1 | — | — | ||||||||||||||
| Cost of service | 54.9 | 61.1 | 58.8 | ||||||||||||||
| Gross margin | 18.4 | 20.9 | 18.4 | ||||||||||||||
| Other operating expenses | 12.6 | 12.5 | 13.1 | ||||||||||||||
| Operating income | $ | 5.8 | $ | 8.4 | $ | 5.3 | |||||||||||
| Key Statistical Data - Total (1): | |||||||||||||||||
| Billable hours | 2,730,121 | 3,308,338 | 3,248,304 | ||||||||||||||
| Clients served | 15,019 | 17,364 | 17,981 | ||||||||||||||
| Shifts | 1,177,586 | 1,488,175 | 1,468,541 | ||||||||||||||
| Revenue per hour | $ | 26.45 | $ | 24.80 | $ | 23.75 | |||||||||||
| Revenue per shift | $ | 61.31 | $ | 55.13 | $ | 52.54 | |||||||||||
| Hours per shift | 2.3 | 2.2 | 2.2 | ||||||||||||||
(1)Total includes acquisitions.
45
Year Ended December 31, 2020 Compared to the Year Ended December 31, 2019
Operating income related to our personal care segment decreased approximately $3 million on a $10 million decrease in net service revenue. The decrease in net service revenue is due to the impact of COVID-19 partially offset by rate increases. The impact of COVID-19 was mitigated by a reduction in costs as most of our personal care employees are paid on an hourly basis and rate increases which were intended to address market pressures and incremental costs related to the pandemic. Our personal care segment incurred approximately $2 million of COVID-19 costs related to the purchase of PPE, bonuses paid to our employees and quarantine pay. Additionally, our personal care segment received funds totaling $1 million under the Mass Home Care ASAP COVID-19 Provider Sustainability Program. These funds were used to cover COVID-19 related costs and are recorded to other operating income within our consolidated statement of operations.
Year Ended December 31, 2019 Compared to the Year Ended December 31, 2018
Operating income related to our personal care segment increased $3 million on a $5 million increase in net service revenue. These results are inclusive of the acquisitions of East Tennessee Personal Care Services (May 2018) and Bring Care Home (October 2018). As a result, our personal care operating results for 2019 and 2018 are not fully comparable.
Gross margin as a percentage of revenue increased 170 basis points as the segment benefited from rate increases combined with operating cost controls. Additionally, other operating expenses decreased approximately $1 million resulting in an increase in operating income.
Corporate
The following table summarizes our corporate results of operations:
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
Financial Information (in millions): | |||||||||||||||||
| Other operating expenses | $ | 173.2 | $ | 160.9 | $ | 127.6 | |||||||||||
| Depreciation and amortization | 22.5 | 12.4 | 8.4 | ||||||||||||||
| Total operating expenses | $ | 195.7 | $ | 173.3 | $ | 136.0 | |||||||||||
Corporate expenses consist of costs relating to our executive management and administrative support functions, primarily information services, accounting, finance, billing and collections, legal, compliance, risk management, procurement, marketing, clinical administration, training, human resources and administration.
Year Ended December 31, 2020 Compared to the Year Ended December 31, 2019
Corporate total operating expenses increased approximately $22 million during the year ended December 31, 2020 compared to 2019. Our 2020 acquisitions of Asana and AseraCare added approximately $15 million which is inclusive of $9 million related to intangibles amortization. The remaining $7 million increase is primarily due to one additional month of corporate support costs from our 2019 acquisition of CCH, planned wage increases, the addition of corporate support staff, an increase in employer payroll taxes associated with employee stock option exercises, incentive compensation accruals, fees related to our ClearCare partnership and lower gains on the sale of fleet vehicles in 2020 as compared to 2019; these items were partially offset by decreases in travel and training expense and acquisition and integration costs.
Year Ended December 31, 2019 Compared to the Year Ended December 31, 2018
During 2019, corporate operating expenses increased $37 million; approximately $27 million of which is attributable to the CCH acquisition: $7 million relates to CCH corporate and administrative support functions, $6 million relates to CCH intangibles amortization and approximately $14 million relates to CCH acquisition and integration costs. Excluding the impact of the CCH acquisition, corporate operating expenses increased $10 million which represents 3% of our $293 million increase in revenue. This increase is primarily due to increases in salaries and benefits expense and information technology expense which were partially offset by decreases in professional fees and legal settlements as well as gains on the sale of fleet vehicles.
46
Liquidity and Capital Resources
Cash Flows
The following table summarizes our cash flows for the periods indicated (amounts in millions):
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Cash provided by operating activities | $ | 289.0 | $ | 202.0 | $ | 223.5 | |||||||||||
| Cash used in investing activities | (287.1) | (352.9) | (22.2) | ||||||||||||||
| Cash (used in) provided by financing activities | (15.0) | 227.2 | (267.4) | ||||||||||||||
| Net (decrease) increase in cash, cash equivalents and restricted cash | (13.1) | 76.3 | (66.1) | ||||||||||||||
| Cash, cash equivalents and restricted cash at beginning of period | 96.5 | 20.2 | 86.4 | ||||||||||||||
| Cash, cash equivalents and restricted cash at end of period | $ | 83.4 | $ | 96.5 | $ | 20.2 | |||||||||||
Cash provided by operating activities for 2020, 2019 and 2018 have provided sufficient liquidity to finance our capital expenditures, both routine and non-routine, and acquisitions. Changes in our cash provided by operating activities during the past three years were primarily the result of fluctuations in our net income, the collections of our accounts receivable and the timing of payments of accrued expenses. Additionally, our cash provided by operating activities for 2020 also includes the deferral of payroll taxes as provided for in the CARES Act totaling $55.4 million and the receipt of Provider Relief Funds, which we expect to retain, totaling $38.5 million, partially offset by the payment of COVID-19 related expenses.
Our cash used in investing activities primarily consists of the purchase of property and equipment, investments in equity method investees and acquisitions. Additionally, during 2020, our cash flows from investing activities includes proceeds from the sale of our investment in the Heritage Healthcare Innovation Fund, LP (see Item 8, Note 1 - Nature of Operations, Consolidation and Presentation of Financial Statements to our consolidated financial statements for additional information). Cash used in investing activities decreased $65.8 million during 2020 compared to 2019 as a result of a reduction in acquisition spend. Cash used in investing activities increased $330.7 million during 2019 compared to 2018 primarily due to the acquisitions of CCH and RoseRock.
Our financing activities primarily consist of borrowings under our term loan and/or revolving credit facility, repayments of borrowings, the remittance of taxes associated with shares withheld on non-cash compensation and proceeds related to the exercise of stock options and the purchase of stock under our employee stock purchase plan. Additionally, during 2020, our financing activities included the receipt of Provider Relief Funds, which we do not expect to retain, totaling $60 million (see Note 3 - Novel Coronavirus Pandemic ("COVID-19") to our consolidated financial statements for additional information). Cash used in financing activities totaled $15.0 milling during 2020 primarily due to repayments of borrowings and the remittance of tax withholding obligations related to non-cash compensation and stock option exercises (see Item 8, Note 10 - Capital Stock and Share-Based Compensation to our consolidated financial statements for additional information), partially offset by the receipt of Provider Relief Funds totaling $60.0 million. Cash provided by financing activities totaled $227.2 million during 2019 and is primarily related to our borrowings under our Amended Credit Agreement to fund acquisitions. Cash used in financing activities totaled $267.4 million in 2018 and is primarily related to our repurchase of company stock and the repayments of borrowings.
Liquidity
Typically, our principal source of liquidity is the collection of our patient accounts receivable, primarily through the Medicare program. In addition to our collection of patient accounts receivable, from time to time, we can and do obtain additional sources of liquidity by the incurrence of additional indebtedness.
During 2020, we spent $5.3 million in capital expenditures compared to $7.9 million and $6.6 million during 2019 and 2018, respectively. Our capital expenditures for 2021 are expected to be approximately $6.0 million to $8.0 million, excluding the impact of any future acquisitions.
As of December 31, 2020, we had $81.8 million in cash and cash equivalents and $470.2 million in availability under our $550.0 million Revolving Credit Facility. Our cash and cash equivalents include $60.0 million related to CARES Act funds that we do not expect to utilize and have recorded as a liability within our consolidated balance sheet as of December 31, 2020.
47
Based on our operating forecasts and our debt service requirements, we believe we will have sufficient liquidity to fund our operations, capital requirements and debt service requirements.
Outstanding Patient Accounts Receivable
Our patient accounts receivable increased $17.5 million from December 31, 2019 to December 31, 2020 due to our acquisition activity which added $19.6 million to accounts receivable and the reduction in RAP payments under PDGM, partially offset by a reduction in days revenue outstanding which decreased 0.7 days despite an estimated negative impact of 2.7 days related to the transition to PDGM. Our cash collection as a percentage of revenue was 106% and 105% for the twelve-month periods ended December 31, 2020 and 2019, respectively. Our days revenue outstanding, net at December 31, 2020 was 40.2 days which is a decrease of 0.7 days from December 31, 2019.
Our patient accounts receivable includes unbilled receivables and are aged based upon the initial service date. We monitor unbilled receivables on a care center by care center basis to ensure that all efforts are made to bill claims within timely filing deadlines. Our unbilled patient accounts receivable can be impacted by acquisition activity, probe edits or regulatory changes which result in additional information or procedures needed prior to billing. The timely filing deadline for Medicare is one year from the date the episode was completed, varies by state for Medicaid-reimbursable services and varies among insurance companies and other private payors.
The following schedules detail our patient accounts receivable, by payor class, aged based upon initial date of service (amounts in millions, except days revenue outstanding):
| 0-90 | 91-180 | 181-365 | Over 365 | Total | |||||||||||||||||||||||||
| At December 31, 2020: | |||||||||||||||||||||||||||||
| Medicare patient accounts receivable | $ | 156.2 | $ | 5.4 | $ | 2.1 | $ | 0.8 | $ | 164.5 | |||||||||||||||||||
| Other patient accounts receivable: | |||||||||||||||||||||||||||||
| Medicaid | 20.7 | 1.7 | 1.5 | — | 23.9 | ||||||||||||||||||||||||
| Private | 58.4 | 6.4 | 1.9 | — | 66.7 | ||||||||||||||||||||||||
| Total | $ | 79.1 | $ | 8.1 | $ | 3.4 | $ | — | $ | 90.6 | |||||||||||||||||||
| Total patient accounts receivable | $ | 255.1 | |||||||||||||||||||||||||||
| Days revenue outstanding (1) | 40.2 | ||||||||||||||||||||||||||||
| 0-90 | 91-180 | 181-365 | Over 365 | Total | |||||||||||||||||||||||||
| At December 31, 2019: | |||||||||||||||||||||||||||||
| Medicare patient accounts receivable | $ | 115.2 | $ | 13.8 | $ | 6.8 | $ | 1.0 | $ | 136.8 | |||||||||||||||||||
| Other patient accounts receivable: | |||||||||||||||||||||||||||||
| Medicaid | 22.6 | 5.7 | 4.0 | — | 32.3 | ||||||||||||||||||||||||
| Private | 60.0 | 6.3 | 2.2 | — | 68.5 | ||||||||||||||||||||||||
| Total | $ | 82.6 | $ | 12.0 | $ | 6.2 | $ | — | $ | 100.8 | |||||||||||||||||||
| Total patient accounts receivable | $ | 237.6 | |||||||||||||||||||||||||||
| Days revenue outstanding (1) | 40.9 | ||||||||||||||||||||||||||||
(1)Our calculation of days revenue outstanding, net is derived by dividing our ending net patient accounts receivable at December 31, 2020 and 2019 by our average daily net patient service revenue for the three-month periods ended December 31, 2020 and 2019, respectively.
Indebtedness
First Amendment to Amended and Restated Credit Agreement
On February 4, 2019, we entered into the First Amendment to the Credit Agreement (as amended by the First Amendment, the “Amended Credit Agreement”). The Amended Credit Agreement provides for a senior secured credit facility in an initial aggregate principal amount of up to $725.0 million, which includes the $550.0 million Revolving Credit Facility under the Credit Agreement, and a term loan facility with a principal amount of up to $175.0 million (the “Term Loan Facility” and collectively with the Revolving Credit Facility, the “Credit Facility”), which was added by the First Amendment.
48
We borrowed the entire principal amount of the Term Loan Facility on February 4, 2019 in order to fund a portion of the purchase price of the CCH acquisition, with the remainder of the purchase price and associated transactional fees and expenses funded by proceeds from the Revolving Credit Facility.
Our weighted average interest rate for borrowings under our $175.0 million Term Loan Facility was 2.2% for the period ended December 31, 2020 and 3.8% for the period February 4, 2019 to December 31, 2019. Our weighted average interest rate for borrowings under our $550.0 million Revolving Credit Facility was 2.2% for the period ended December 31, 2020 and 4.0% for the period ended December 31, 2019.
As of December 31, 2020, our consolidated leverage ratio was 0.6, our consolidated interest coverage ratio was 25.6 and we are in compliance with our covenants under the Amended Credit Agreement.
As of December 31, 2020, our availability under our $550.0 million Revolving Credit Facility was $470.2 million as we have $51.0 million outstanding in borrowings and $28.8 million outstanding in letters of credit.
See Item 8, Note 8 - Long Term Obligations to our consolidated financial statements for additional details on our outstanding long-term obligations.
Share Repurchases
2021 Stock Repurchase Program
On December 23, 2020, we announced that our Board of Directors authorized a stock repurchase program, under which we may repurchase up to $100 million of our outstanding common stock through December 31, 2021.
Under the terms of the program, we are allowed to repurchase shares from time to time through open market purchases, unsolicited or solicited privately negotiated transactions, an accelerated stock repurchase program, and/or a trading plan in compliance with Exchange Act Rule 10b5-1. The timing and the amount of the repurchases will be determined by management based on a number of factors, including but not limited to share price, trading volume and general market conditions, as well as on working capital requirements, general business conditions and other factors.
We did not repurchase any shares pursuant to this stock repurchase program during the year ended December 31, 2020.
2019 Stock Repurchase Program
On February 25, 2019, we announced that our Board of Directors authorized a stock repurchase program, under which we could repurchase up to $100 million of our outstanding common stock through March 1, 2020. We did not repurchase any shares pursuant to this stock purchase program during 2019 or 2020. The stock repurchase plan expired on March 1, 2020.
2018 Share Repurchase
On June 4, 2018, we purchased 2,418,304 of our common shares from affiliates of KKR Credit Advisors (US) LLC ("KKR"), representing one-half of KKR's then current holdings in the Company and 7.1% of the aggregate outstanding shares of the Company's common stock for a total purchase price of $181.4 million including related direct costs. The Company repurchased the shares at $73.96 which represents 96% of the closing stock price of the Company's common stock on June 4, 2018. The repurchased shares are classified as treasury shares.
49
Contractual Obligations
Our future contractual obligations at December 31, 2020 were as follows (amounts in millions):
| Payments Due by Period | |||||||||||||||||||||||||||||
| Total | Less than 1 Year | 1-3 Years | 4-5 Years | After 5 Years | |||||||||||||||||||||||||
| Long-term obligations | $ | 215.1 | $ | 8.8 | $ | 20.8 | $ | 185.5 | $ | — | |||||||||||||||||||
| Interest on long-term obligations (1) | 8.5 | 3.3 | 5.0 | 0.2 | — | ||||||||||||||||||||||||
| Finance leases | 2.7 | 1.8 | 0.9 | — | — | ||||||||||||||||||||||||
| Operating leases | 97.6 | 32.2 | 42.9 | 17.9 | 4.6 | ||||||||||||||||||||||||
| Purchase obligations (2) | 19.3 | 8.7 | 9.9 | 0.7 | — | ||||||||||||||||||||||||
| Uncertain tax positions | 2.7 | — | 2.7 | — | — | ||||||||||||||||||||||||
| $ | 345.9 | $ | 54.8 | $ | 82.2 | $ | 204.3 | $ | 4.6 | ||||||||||||||||||||
(1)Interest on debt with variable rates was calculated using the current rate for that particular debt instrument at December 31, 2020.
(2)Purchase obligations are primarily related to information technology contracts and software licenses.
Critical Accounting Estimates
The discussion and analysis of our financial condition and results of operations is based upon our consolidated financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles (“U.S. GAAP”). The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, revenue and expenses and related disclosures of contingent assets and liabilities. On an ongoing basis, we evaluate our estimates, including those related to revenue recognition, collectability of accounts receivable, reserves related to insurance and litigation, business combinations, goodwill, intangible assets, income taxes and contingencies. We base these estimates on our historical experience and various other assumptions that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results experienced may vary materially and adversely from our estimates. To the extent there are material differences between our estimates and the actual results, our future results of operations may be affected.
We believe the following critical accounting policies represent our most significant judgments and estimates used in the preparation of our consolidated financial statements.
Revenue Recognition
We account for revenue from contracts with customers in accordance with Accounting Standards Codification ("ASC") 606, Revenue from Contracts with Customers, and as such, we recognize revenue in the period in which we satisfy our performance obligations under our contracts by transferring our promised services to our customers in amounts that reflect the consideration to which we expect to be entitled in exchange for providing patient care, which are the transaction prices allocated to the distinct services. The Company's cost of obtaining contracts is not material.
Revenues are recognized as performance obligations are satisfied, which varies based on the nature of the services provided. Our performance obligation is the delivery of patient care services in accordance with the nature and frequency of services outlined in physicians' orders, which are determined by a physician based on a patient's specific goals.
The Company's performance obligations relate to contracts with a duration of less than one year; therefore, the Company has elected to apply the optional exemption provided by ASC 606 and is not required to disclose the aggregate amount of the transaction price allocated to performance obligations that are unsatisfied or partially unsatisfied as of the end of the reporting period. The unsatisfied or partially unsatisfied performance obligations are generally completed when the patients are discharged, which generally occurs within days or weeks of the end of the reporting period.
We determine the transaction price based on gross charges for services provided, reduced by estimates for contractual and non-contractual revenue adjustments. Contractual revenue adjustments are recorded for the difference between our standard rates and the contracted rates to be realized from patients, third party payors and others for services provided. Non-contractual revenue adjustments include discounts provided to self-pay, uninsured patients or other payors, adjustments resulting from payment reviews and adjustments arising from our inability to obtain appropriate billing documentation, authorizations or face-
50
to-face documentation. Subsequent changes to the estimate of the transaction price are recorded as adjustments to net service revenue in the period of change.
Non-contractual revenue adjustments are recorded for self-pay, uninsured patients and other payors by major payor class based on our historical collection experience, aged accounts receivable by payor and current economic conditions. The non-contractual revenue adjustments represent the difference between amounts billed and amounts we expect to collect based on our collection history with similar payors. The Company assesses its ability to collect for the healthcare services provided at the time of patient admission based on the Company's verification of the patient's insurance coverage under Medicare, Medicaid, and other commercial or managed care insurance programs. Medicare represents approximately 75% of the Company's consolidated net service revenue.
Amounts due from third-party payors, primarily commercial health insurers and government programs (Medicare and Medicaid), include variable consideration for retroactive revenue adjustments due to settlements of audits and payment reviews. We determine our estimates for non-contractual revenue adjustments related to payment reviews based on our historical experience and success rates in the claim appeals and adjudication process.
We determine our estimates for non-contractual revenue adjustments related to our inability to obtain appropriate billing documentation, authorizations, or face-to-face documentation based on our historical experience which primarily includes a historical collection rate of over 99% on Medicare claims. Revenue is recorded at amounts we estimate to be realizable for services provided.
Home Health Revenue Recognition
Medicare Revenue
Effective January 1, 2020, CMS implemented a revised case-mix adjustment methodology, PDGM, to better align payment with patient care needs and ensure that clinically complex and ill beneficiaries have adequate access to home health care. PDGM uses 30-day periods of care rather than 60-day episodes of care as the unit of payment, eliminates the use of the number of therapy visits provided in determining payment and relies more heavily on clinical characteristics and other patient information.
Net service revenue is recorded based on the established Federal Medicare home health payment rate for a 30-day period of care. ASC 606 notes that if an entity has a right to consideration from a customer in an amount that corresponds directly with the value of the entity’s performance completed to date, the entity may recognize revenue in the amount to which the entity has a right to invoice. We have elected to apply the "right to invoice" practical expedient and therefore, our revenue recognition is based on the reimbursement we are entitled to for each 30-day payment period. We utilize our historical average length of stay for each 30-day period of care as the measure of progress towards the satisfaction of our performance obligation.
PDGM uses timing, admission source, functional impairment levels and principal and other diagnoses to case-mix adjust payments. The case-mix adjusted payment for a 30-day period of care is subject to additional adjustments based on certain variables including, but not limited to: (a) an outlier payment if our patient’s care was unusually costly (capped at 10% of total reimbursement per provider number); (b) a low utilization payment adjustment (“LUPA”) if the number of visits provided was less than the established threshold, which ranges from two to six visits and varies for every case-mix group under PDGM; (c) a partial payment if a patient transferred to another provider or from another provider before completing the 30-day period of care; and (d) the applicable geographic wage index. Payments for routine and non-routine supplies are now included in the 30-day payment rate.
Medicare can also make various adjustments to payments received if we are unable to produce appropriate billing documentation or acceptable authorizations. We estimate the impact of such adjustments based on our historical experience, which primarily includes a historical collection rate of over 99% on Medicare claims, and record this estimate during the period in which services are rendered to revenue and a corresponding reduction to patient accounts receivable.
Amounts due from Medicare include variable consideration for retroactive revenue adjustments due to settlements of audits and payment reviews. We determine our estimates for non-contractual revenue adjustments related to payment reviews based on our historical experience and success rates in the claim appeals and adjudication process.
51
The Medicare home health benefit requires that beneficiaries be homebound (meaning that the beneficiary is unable to leave his/her home without a considerable and taxing effort), require intermittent skilled nursing, physical therapy or speech therapy services, and receive treatment under a plan of care established and periodically reviewed by a physician. In order to provide greater flexibility during the novel coronavirus pandemic ("COVID-19"), CMS has relaxed the definition of homebound status through the duration of the public health emergency. During the pandemic, a beneficiary is considered homebound if they have been instructed by a physician not to leave their home because of a confirmed or suspected COVID-19 diagnosis or if the patient has a condition that makes them more susceptible to contracting COVID-19. Therefore, if a beneficiary is homebound due to COVID-19 and requires skilled services, the services will be covered under the Medicare home health benefit.
All Medicare contracts are required to have a signed plan of care which represents a single performance obligation, comprised of the delivery of a series of distinct services that are substantially similar and have a similar pattern of transfer to the customer. Accordingly, the Company accounts for the series of services ("episode") as a single performance obligation satisfied over time, as the customer simultaneously receives and consumes the benefits of the goods and services provided. An episode starts the first day a billable visit is performed and ends 60 days later or upon discharge, if earlier, with multiple continuous episodes allowed.
A portion of reimbursement from each Medicare episode, referred to as a request for anticipated payment ("RAP") is billed near the start of each 30-day period of care, and cash is typically received before all services are rendered. Any cash received from Medicare for a RAP for a 30-day period of care that exceeds the associated revenue earned is recorded to accrued expenses within our consolidated balance sheets. CMS reduced the upfront payment for RAPs to 20% for 2020 and has fully eliminated payments associated with RAPs in 2021.
Non-Medicare Revenue
Episodic-based Revenue. We recognize revenue in a similar manner as we recognize Medicare revenue for amounts that are paid by other insurance carriers, including Medicare Advantage programs; however, these amounts can vary based upon the negotiated terms which generally range from 90% to 100% of Medicare rates.
Non-episodic based Revenue. Gross revenue is recorded on an accrual basis based upon the date of service at amounts equal to our established or estimated per-visit rates. Contractual revenue adjustments are recorded for the difference between our standard rates and the contracted rates to be realized from patients, third parties and others for services provided and are deducted from gross revenue to determine net service revenue. We also make non-contractual revenue adjustments to non-episodic revenue based on our historical experience to reflect the estimated transaction price. We receive a minimal amount of our net service revenue from patients who are either self-insured or are obligated for an insurance co-payment.
Hospice Revenue Recognition
Hospice Medicare Revenue
Gross revenue is recorded on an accrual basis based upon the date of service at amounts equal to the estimated payment rates. The estimated payment rates are predetermined daily or hourly rates for each of the four levels of care we deliver. The four levels of care are routine care, general inpatient care, continuous home care and respite care. Routine care accounted for 97% of our total Medicare hospice service revenue for each of 2020, 2019 and 2018, respectively. There are two separate payment rates for routine care: payments for the first 60 days of care and care beyond 60 days. In addition to the two routine rates, we may also receive a service intensity add-on (“SIA”). The SIA is based on visits made in the last seven days of life by a registered nurse or medical social worker for patients in a routine level of care.
The performance obligation is the delivery of hospice services to the patient, as determined by a physician, each day the patient is on hospice care.
We make adjustments to Medicare revenue for non-contractual revenue adjustments, which include our inability to obtain appropriate billing documentation or acceptable authorizations and other reasons unrelated to credit risk. We estimate the impact of these non-contractual revenue adjustments based on our historical experience, which primarily includes a historical collection rate of over 99% on Medicare claims, and record it during the period services are rendered.
Additionally, our hospice service revenue is subject to certain limitations on payments from Medicare which are considered variable consideration. We are subject to an inpatient cap limit and an overall Medicare payment cap for each provider number. We monitor these caps on a provider-by-provider basis and estimate amounts due back to Medicare if we estimate a cap has been exceeded. We record these adjustments as a reduction to revenue and an increase in accrued expenses within our consolidated balance sheets. Providers are required to self-report and pay their estimated cap liability by February 28th of the following year. As of December 31, 2020, we have settled our Medicare hospice reimbursements for all fiscal years through
52
October 31, 2013. As of December 31, 2020, we have recorded $9.3 million for estimated amounts due back to Medicare in accrued expenses for the Federal cap years ended October 31, 2014 through September 30, 2021; approximately $2.0 million of this balance was acquired with the AseraCare acquisition. As of December 31, 2019, we had recorded $5.7 million for estimated amounts due back to Medicare in accrued expenses for the Federal cap years ended October 31, 2013 through September 30, 2020.
Hospice Non-Medicare Revenue
Gross revenue is recorded on an accrual basis based upon the date of service at amounts equal to our established rates or estimated per day rates, as applicable. Contractual revenue adjustments are recorded for the difference between our standard rates and the contractual rates to be realized from patients, third party payors and others for services provided and are deducted from gross revenue to determine our net service revenue. We also make non-contractual adjustments to non-Medicare revenue based on our historical experience to reflect the estimated transaction price.
Personal Care Revenue Recognition
Personal Care Revenue
We generate net service revenues by providing our services directly to patients based on authorized hours, visits or units determined by the relevant agency, at a rate that is either contractual or fixed by legislation. Net service revenue is recognized at the time services are rendered based on gross charges for the services provided, reduced by estimates for contractual and non-contractual revenue adjustments. We receive payment for providing such services from payors, including state and local governmental agencies, managed care organizations, commercial insurers and private consumers. Payors include the following elder service agencies: Aging Services Access Points ("ASAPs"), Senior Care Options ("SCOs"), Program of All-Inclusive Care for the Elderly ("PACE") and the Veterans Administration ("VA").
Business Combinations
We account for acquisitions using the acquisition method of accounting in accordance with ASC 805, Business Combinations. Acquisitions are accounted for as purchases and are included in our consolidated financial statements from their respective acquisition dates. Assets acquired and liabilities assumed, if any, are measured at fair value on the acquisition date using the appropriate valuation method. Goodwill generated from acquisitions is recognized for the excess of the purchase price over tangible and identifiable intangible assets. In determining the fair value of identifiable intangible assets, we use various valuation techniques including discounted cash flow analysis, the income approach, the cost approach and the market approach. These valuation methods require us to make estimates and assumptions surrounding projected revenues and costs, future growth and discount rates.
Goodwill and Other Intangible Assets
Goodwill represents the amount of the purchase price in excess of the fair values assigned to the underlying identifiable net assets of acquired businesses. Goodwill is not amortized, but is subject to an annual impairment test. Tests are performed more frequently if events occur or circumstances change that would more likely than not reduce the fair value of the reporting unit below its carrying amount. These events or circumstances include, but are not limited to, a significant adverse change in the business environment, regulatory environment or legal factors, or a substantial decline in the market capitalization of our stock.
U.S. GAAP allows for impairment testing to be done on either a quantitative or qualitative basis. During 2020, we utilized a qualitative analysis for our annual impairment test and determined that there were no triggering events that would indicate that it is "more likely than not" that the carrying values of our reporting units are higher than their respective fair values. As a result, we did not record any goodwill impairment charges and none of the goodwill associated with our various reporting units was considered at risk of impairment as of October 31, 2020. Since the date of our last annual goodwill impairment test, there have been no material developments, events, changes in operating performance or other circumstances that would cause management to believe it is more likely than not that the fair value of any of our reporting units would be less than their carrying amounts.
Intangible assets consist of certificates of need, licenses, acquired names and non-compete agreements. We amortize non-compete agreements and acquired names that we do not intend to use indefinitely on a straight-line basis over their estimated useful lives, which is generally two to three years for non-compete agreements and up to three years for acquired names. Our indefinite-lived intangible assets are reviewed for impairment annually or more frequently if events occur or circumstances change that would more likely than not reduce the fair value of the intangible asset below its carrying amount. During 2020, we performed a qualitative assessment of our indefinite-lived intangible assets; as a result of this analysis, we wrote off approximately $4.2 million of acquired names that are no longer in use. There have been no material developments, events,
53
changes in operating performance or other circumstances that would cause management to believe it is more likely than not that the fair value of any of our remaining intangible assets would be less than their carrying amounts.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
We are exposed to market risk from fluctuations in interest rates. Our Term Loan and Revolving Credit Facility carry a floating interest rate which is tied to the Eurodollar rate (i.e. LIBOR) and the Prime Rate and therefore, our consolidated statements of operations and our consolidated statements of cash flows are exposed to changes in interest rates. As of December 31, 2020, the total amount of outstanding debt subject to interest rate fluctuations was $215.1 million. A 1.0% interest rate change would cause interest expense to change by approximately $2.2 million annually, assuming the Company makes no principal repayments.
54
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
Report of Independent Registered Public Accounting Firm
To the Stockholders and Board of Directors
Amedisys, Inc.:
Opinion on the Consolidated Financial Statements
We have audited the accompanying consolidated balance sheets of Amedisys, Inc. and subsidiaries (the Company) as of December 31, 2020 and 2019, the related consolidated statements of operations, comprehensive income, stockholders’ equity, and cash flows for each of the years in the three-year period ended December 31, 2020, and the related notes (collectively, the consolidated financial statements). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2020 and 2019, and the results of its operations and its cash flows for each of the years in the three-year period ended December 31, 2020, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company’s internal control over financial reporting as of December 31, 2020, based on criteria established in Internal Control – Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission, and our report dated February 25, 2021 expressed an unqualified opinion on the effectiveness of the Company’s internal control over financial reporting.
Change in Accounting Principle
As discussed in Note 1 to the consolidated financial statements, the Company has changed its method of accounting for leases as of January 1, 2019 due to the adoption of Accounting Standards Update (ASU) 2016-02, Leases (Topic 842); ASU 2018-01, Land Easement Practical Expedient for Transition to Topic 842; ASU 2018-10, Codification Improvements to Topic 842, Leases; and ASU 2018-11, Targeted Improvements (collectively, Topic 842).
Basis for Opinion
These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these consolidated financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the consolidated financial statements that were communicated or required to be communicated to the audit committee and that: (1) relate to accounts or disclosures that are material to the consolidated financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing separate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
55
Acquisition of AseraCare Hospice – Evaluation of the fair value of certain intangible assets
As discussed in Notes 2 and 4 to the consolidated financial statements, the Company accounts for business combinations using the acquisition method of accounting. The Company acquired Homecare Preferred Choice, Inc., doing business as AseraCare Hospice (AseraCare), on June 1, 2020. Intangible assets acquired in connection with this transaction included licenses, acquired names and non-compete agreements.
We identified the evaluation of the fair value of certain intangible assets, which consisted of licenses, acquired names, and non-compete agreements, acquired in the AseraCare transaction as a critical audit matter. Subjective auditor judgment was required to evaluate the identification of intangible assets acquired and significant assumptions used in the valuation of certain intangible assets. Specifically, the significant assumptions included projected revenue growth rates, projected earnings before interest, taxes, depreciation and amortization (EBITDA), and the weighted average cost of capital (WACC). Changes to these assumptions could have had a significant effect on the Company’s estimate of fair value of the intangible assets.
The following are the primary procedures we performed to address this critical audit matter. We evaluated the design and tested the operating effectiveness of certain internal controls over the Company’s acquisition accounting process, including controls over the identification of intangible assets acquired and the development of the significant assumptions used in the valuation of the intangible assets. We read the purchase agreement to identify the significant terms, conditions, and intangible assets acquired and compared them to the Company’s analysis of intangible assets acquired. We evaluated the Company’s projected revenue growth rates by comparing such assumptions to those of AseraCare’s peers and to industry reports. We evaluated the Company’s projected EBITDA by comparing such assumptions to those of AseraCare’s peers. Additionally, we compared the Company’s projected revenue growth rates and projected EBITDA to AseraCare’s and the Company’s historical actual results. We involved valuation professionals with specialized skills and knowledge, who assisted in:
•evaluating the Company’s identification of intangible assets acquired
•evaluating the WACC, which was used by the Company to determine the discount rate, by comparing the Company's inputs to the WACC to publicly available data for comparable entities and assessing the resulting WACC.
Evaluation of the non-contractual revenue adjustment estimates for Home Health and Hospice
As discussed in Note 2 to the consolidated financial statements, the Company determines the transaction price for revenue contracts based on gross charges for services provided, reduced by contractual revenue adjustments and an estimate for non-contractual revenue adjustments. Non-contractual revenue adjustments are recorded for self-pay, uninsured patients, and other payors by major payor class based on historical collection experience, evaluated for current economic conditions. Adjustments resulting from payment reviews and adjustments arising from the inability to obtain appropriate billing documentation, authorizations, or face-to-face documentation are factors that are relevant to the estimate of ultimate collection. The non-contractual revenue adjustments represent the difference between amounts billed and amounts the Company expects to collect based on its collection history with similar payors.
We identified the evaluation of the non-contractual revenue adjustment estimates noted above for the Home Health and Hospice segments as a critical audit matter. Subjective and complex auditor judgment was required to evaluate the method and historical collection experience used by the Company when developing the non-contractual revenue adjustment estimate. Specifically, the significant judgments related to evaluating the relevance of historical collection experience to the determination of the estimate, which included evaluation of current conditions, trends, historical adjustment experience, and other factors.
The following are the primary procedures we performed to address this critical audit matter. We evaluated the design and tested the operating effectiveness of certain internal controls related to the Company’s revenue process, including controls over the method and significant judgments for estimating non-contractual revenue adjustments noted above. We assessed the outcome of the estimation of non-contractual revenue adjustments in the prior period to identify circumstances or conditions that are relevant to the determination of the current year estimate. To assess the current year method and the relevance of the historical collection experience, we also evaluated current conditions, trends, historical adjustment experience, and other factors relevant to the estimation of non-contractual revenue adjustments.
56
/s/ KPMG LLP
We have served as the Company's auditor since 2002.
Baton Rouge, Louisiana
February 25, 2021
57
AMEDISYS, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
(Amounts in thousands, except share data)
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| ASSETS | |||||||||||
| Current assets: | |||||||||||
| Cash and cash equivalents | $ | 81,808 | $ | 30,294 | |||||||
| Restricted cash | 1,549 | 66,196 | |||||||||
| Patient accounts receivable | 255,145 | 237,596 | |||||||||
| Prepaid expenses | 10,217 | 8,243 | |||||||||
| Other current assets | 13,265 | 8,225 | |||||||||
| Total current assets | 361,984 | 350,554 | |||||||||
| Property and equipment, net of accumulated depreciation of $95,024 and $96,137 | 23,719 | 28,113 | |||||||||
| Operating lease right of use assets | 93,440 | 84,791 | |||||||||
| Goodwill | 932,685 | 658,500 | |||||||||
| Intangible assets, net of accumulated amortization of $22,973 and $7,044 | 74,183 | 64,748 | |||||||||
| Deferred income taxes | 47,987 | 21,427 | |||||||||
| Other assets | 33,200 | 54,612 | |||||||||
| Total assets | $ | 1,567,198 | $ | 1,262,745 | |||||||
| LIABILITIES AND EQUITY | |||||||||||
| Current liabilities: | |||||||||||
| Accounts payable | $ | 42,674 | $ | 31,259 | |||||||
| Payroll and employee benefits | 146,929 | 120,877 | |||||||||
| Accrued expenses | 166,192 | 137,111 | |||||||||
| Provider relief fund advance | 60,000 | 0 | |||||||||
| Current portion of long-term obligations | 10,496 | 9,927 | |||||||||
| Current portion of operating lease liabilities | 30,046 | 27,769 | |||||||||
| Total current liabilities | 456,337 | 326,943 | |||||||||
| Long-term obligations, less current portion | 204,511 | 232,256 | |||||||||
| Operating lease liabilities, less current portion | 61,987 | 56,128 | |||||||||
| Other long-term obligations | 33,622 | 5,905 | |||||||||
| Total liabilities | 756,457 | 621,232 | |||||||||
| Commitments and Contingencies – Note 11 | 0 | 0 | |||||||||
| Equity: | |||||||||||
| Preferred stock, $0.001 par value, 5,000,000 shares authorized; NaN issued or outstanding | 0 | 0 | |||||||||
| Common stock, $0.001 par value, 60,000,000 shares authorized; 37,470,212 and 36,638,021 shares issued; and 32,814,278 and 32,284,051 shares outstanding | 38 | 37 | |||||||||
| Additional paid-in capital | 698,287 | 645,256 | |||||||||
| Treasury stock at cost, 4,655,934 and 4,353,970 shares of common stock | (319,092) | (251,241) | |||||||||
| Accumulated other comprehensive income | 0 | 15 | |||||||||
| Retained earnings | 429,991 | 246,383 | |||||||||
| Total Amedisys, Inc. stockholders’ equity | 809,224 | 640,450 | |||||||||
| Noncontrolling interests | 1,517 | 1,063 | |||||||||
| Total equity | 810,741 | 641,513 | |||||||||
| Total liabilities and equity | $ | 1,567,198 | $ | 1,262,745 | |||||||
The accompanying notes are an integral part of these consolidated financial statements.
58
AMEDISYS, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
(Amounts in thousands, except per share data)
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Net service revenue | $ | 2,071,519 | $ | 1,955,633 | $ | 1,662,578 | |||||||||||
| Other operating income | 34,372 | 0 | 0 | ||||||||||||||
| Cost of service, excluding depreciation and amortization | 1,185,369 | 1,150,337 | 992,863 | ||||||||||||||
| General and administrative expenses: | |||||||||||||||||
| Salaries and benefits | 449,448 | 394,452 | 316,522 | ||||||||||||||
| Non-cash compensation | 26,730 | 25,040 | 17,887 | ||||||||||||||
| Other | 192,122 | 188,434 | 166,897 | ||||||||||||||
| Depreciation and amortization | 28,802 | 18,428 | 13,261 | ||||||||||||||
| Asset impairment charge | 4,152 | 1,470 | 0 | ||||||||||||||
| Operating expenses | 1,886,623 | 1,778,161 | 1,507,430 | ||||||||||||||
| Operating income | 219,268 | 177,472 | 155,148 | ||||||||||||||
| Other income (expense): | |||||||||||||||||
| Interest income | 292 | 78 | 278 | ||||||||||||||
| Interest expense | (11,038) | (14,515) | (7,370) | ||||||||||||||
| Equity in earnings from equity method investments | 3,966 | 5,338 | 7,692 | ||||||||||||||
| Miscellaneous, net | (1,669) | 2,037 | 3,240 | ||||||||||||||
| Total other (expense) income, net | (8,449) | (7,062) | 3,840 | ||||||||||||||
| Income before income taxes | 210,819 | 170,410 | 158,988 | ||||||||||||||
| Income tax expense | (25,635) | (42,503) | (38,859) | ||||||||||||||
| Net income | 185,184 | 127,907 | 120,129 | ||||||||||||||
| Net income attributable to noncontrolling interests | (1,576) | (1,074) | (783) | ||||||||||||||
| Net income attributable to Amedisys, Inc. | $ | 183,608 | $ | 126,833 | $ | 119,346 | |||||||||||
| Basic earnings per common share: | |||||||||||||||||
| Net income attributable to Amedisys, Inc. common stockholders | $ | 5.64 | $ | 3.95 | $ | 3.64 | |||||||||||
| Weighted average shares outstanding | 32,559 | 32,142 | 32,791 | ||||||||||||||
| Diluted earnings per common share: | |||||||||||||||||
| Net income attributable to Amedisys, Inc. common stockholders | $ | 5.52 | $ | 3.84 | $ | 3.55 | |||||||||||
| Weighted average shares outstanding | 33,268 | 32,990 | 33,609 | ||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
59
AMEDISYS, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF COMPREHENSIVE INCOME
(Amounts in thousands)
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Net income | $ | 185,184 | $ | 127,907 | $ | 120,129 | |||||||||||
| Other comprehensive income | 0 | 0 | 0 | ||||||||||||||
| Comprehensive income | 185,184 | 127,907 | 120,129 | ||||||||||||||
| Comprehensive income attributable to non-controlling interests | (1,576) | (1,074) | (783) | ||||||||||||||
| Comprehensive income attributable to Amedisys, Inc. | $ | 183,608 | $ | 126,833 | $ | 119,346 | |||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
60
AMEDISYS, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY
(Amounts in thousands, except common stock shares)
| Total | Common Stock | Additional Paid-in Capital | Treasury Stock | Accumulated Other Comprehensive Income | Retained Earnings | Noncontrolling Interests | |||||||||||||||||||||||||||||||||||||||||
| Shares | Amount | ||||||||||||||||||||||||||||||||||||||||||||||
| Balance, December 31, 2017 | $ | 516,426 | 35,747,134 | $ | 35 | $ | 568,780 | $ | (53,713) | $ | 15 | $ | 204 | $ | 1,105 | ||||||||||||||||||||||||||||||||
| Issuance of stock – employee stock purchase plan | 2,429 | 38,961 | — | 2,429 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Issuance of stock – 401(k) plan | 9,232 | 129,451 | — | 9,232 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Issuance/(cancellation) of non-vested stock | 0 | 174,044 | 1 | (1) | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Exercise of stock options | 5,953 | 162,690 | — | 5,953 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Non-cash compensation | 17,887 | — | — | 17,887 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Surrendered shares | (6,570) | — | — | — | (6,570) | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Shares repurchased | (181,402) | — | — | — | (181,402) | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Noncontrolling interest distribution | (1,090) | — | — | — | — | — | — | (1,090) | |||||||||||||||||||||||||||||||||||||||
| Repurchase of noncontrolling interest | (361) | — | — | (614) | — | — | — | 253 | |||||||||||||||||||||||||||||||||||||||
| Net income | 120,129 | — | — | — | — | — | 119,346 | 783 | |||||||||||||||||||||||||||||||||||||||
| Balance, December 31, 2018 | 482,633 | 36,252,280 | 36 | 603,666 | (241,685) | 15 | 119,550 | 1,051 | |||||||||||||||||||||||||||||||||||||||
| Issuance of stock – employee stock purchase plan | 3,187 | 30,483 | — | 3,187 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Issuance of stock – 401(k) plan | 9,753 | 79,056 | — | 9,753 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Issuance/(cancellation) of non-vested stock | 0 | 189,134 | 1 | (1) | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Exercise of stock options | 3,611 | 87,068 | — | 3,611 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Non-cash compensation | 25,040 | — | — | 25,040 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Surrendered shares | (9,556) | — | — | — | (9,556) | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Noncontrolling interest distribution | (1,062) | — | — | — | — | — | — | (1,062) | |||||||||||||||||||||||||||||||||||||||
| Net income | 127,907 | — | — | — | — | — | 126,833 | 1,074 | |||||||||||||||||||||||||||||||||||||||
| Balance, December 31, 2019 | 641,513 | 36,638,021 | 37 | 645,256 | (251,241) | 15 | 246,383 | 1,063 | |||||||||||||||||||||||||||||||||||||||
| Issuance of stock – employee stock purchase plan | 3,562 | 21,561 | — | 3,562 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Issuance of stock – 401(k) plan | 3,057 | 18,312 | — | 3,057 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Issuance/(cancellation) of non-vested stock | 0 | 169,489 | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Exercise of stock options | 6,325 | 622,829 | 1 | 6,324 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Non-cash compensation | 26,730 | — | — | 26,730 | — | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Surrendered shares | (54,493) | — | — | 13,358 | (67,851) | — | — | — | |||||||||||||||||||||||||||||||||||||||
| Noncontrolling interest distribution | (1,122) | — | — | — | — | — | — | (1,122) | |||||||||||||||||||||||||||||||||||||||
| Write-off of other comprehensive income | (15) | — | — | — | — | (15) | — | — | |||||||||||||||||||||||||||||||||||||||
| Net income | 185,184 | — | — | — | — | — | 183,608 | 1,576 | |||||||||||||||||||||||||||||||||||||||
| Balance, December 31, 2020 | $ | 810,741 | 37,470,212 | $ | 38 | $ | 698,287 | $ | (319,092) | $ | 0 | $ | 429,991 | $ | 1,517 | ||||||||||||||||||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
61
AMEDISYS, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
(Amounts in thousands)
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Cash Flows from Operating Activities: | |||||||||||||||||
| Net income | $ | 185,184 | $ | 127,907 | $ | 120,129 | |||||||||||
| Adjustments to reconcile net income to net cash provided by operating activities: | |||||||||||||||||
| Depreciation and amortization | 28,802 | 18,428 | 13,261 | ||||||||||||||
| Non-cash compensation | 26,730 | 25,040 | 17,887 | ||||||||||||||
| Non-cash 401(k) employer match | 0 | 10,509 | 8,976 | ||||||||||||||
| Amortization and impairment of operating lease right of use assets | 39,140 | 35,905 | 0 | ||||||||||||||
| (Gain) loss on disposal of property and equipment | (30) | 141 | 714 | ||||||||||||||
| Loss on sale of equity method investment | 2,980 | 0 | 0 | ||||||||||||||
| Write-off of other comprehensive income | (15) | 0 | 0 | ||||||||||||||
| Deferred income taxes | (26,560) | 13,466 | 20,271 | ||||||||||||||
| Equity in earnings from equity method investments | (3,966) | (5,338) | (7,692) | ||||||||||||||
| Amortization of deferred debt issuance costs/debt discount | 869 | 873 | 797 | ||||||||||||||
| Return on equity investment | 5,444 | 4,955 | 6,158 | ||||||||||||||
| Asset impairment charge | 4,152 | 1,470 | 0 | ||||||||||||||
| Changes in operating assets and liabilities, net of impact of acquisitions: | |||||||||||||||||
| Patient accounts receivable | 2,114 | (24,146) | 12,224 | ||||||||||||||
| Other current assets | (7,181) | (2,682) | 8,679 | ||||||||||||||
| Other assets | 31 | 832 | 2,947 | ||||||||||||||
| Accounts payable | 1,941 | (11,329) | 3,165 | ||||||||||||||
| Accrued expenses | 39,839 | 42,096 | 13,524 | ||||||||||||||
| Other long-term obligations | 27,717 | (329) | 2,443 | ||||||||||||||
| Operating lease liabilities | (34,695) | (32,295) | 0 | ||||||||||||||
| Operating lease right of use assets | (3,544) | (3,503) | 0 | ||||||||||||||
| Net cash provided by operating activities | 288,952 | 202,000 | 223,483 | ||||||||||||||
| Cash Flows from Investing Activities: | |||||||||||||||||
| Proceeds from sale of deferred compensation plan assets | 101 | 448 | 715 | ||||||||||||||
| Proceeds from the sale of property and equipment | 80 | 162 | 54 | ||||||||||||||
| Purchases of property and equipment | (5,332) | (7,888) | (6,558) | ||||||||||||||
| Investments in equity method investees | (875) | (210) | (7,144) | ||||||||||||||
| Proceeds from sale of equity method investment | 17,876 | 0 | 0 | ||||||||||||||
| Acquisitions of businesses, net of cash acquired | (298,958) | (345,460) | (9,260) | ||||||||||||||
| Net cash used in investing activities | (287,108) | (352,948) | (22,193) | ||||||||||||||
| Cash Flows from Financing Activities: | |||||||||||||||||
| Proceeds from issuance of stock upon exercise of stock options | 6,325 | 3,611 | 5,953 | ||||||||||||||
| Proceeds from issuance of stock to employee stock purchase plan | 3,562 | 3,187 | 2,429 | ||||||||||||||
| Shares withheld to pay taxes on non-cash compensation | (54,493) | (9,556) | (6,570) | ||||||||||||||
| Non-controlling interest distribution | (1,122) | (1,062) | (1,090) | ||||||||||||||
| Proceeds from borrowings under term loan | 0 | 175,000 | 0 | ||||||||||||||
| Proceeds from borrowings under revolving line of credit | 684,200 | 262,500 | 138,000 | ||||||||||||||
| Repayments of borrowings under revolving line of credit | (703,200) | (200,000) | (130,500) | ||||||||||||||
| Principal payments of long-term obligations | (10,249) | (5,624) | (91,450) | ||||||||||||||
| Debt issuance costs | 0 | (847) | (2,433) | ||||||||||||||
| Provider relief fund advance | 60,000 | 0 | 0 | ||||||||||||||
| Purchase of company stock | 0 | 0 | (181,402) | ||||||||||||||
| Repurchase of noncontrolling interest | 0 | 0 | (361) | ||||||||||||||
| Net cash (used in) provided by financing activities | (14,977) | 227,209 | (267,424) | ||||||||||||||
| Net (decrease) increase in cash, cash equivalents and restricted cash | (13,133) | 76,261 | (66,134) | ||||||||||||||
| Cash, cash equivalents and restricted cash at beginning of period | 96,490 | 20,229 | 86,363 | ||||||||||||||
| Cash, cash equivalents and restricted cash at end of period | $ | 83,357 | $ | 96,490 | $ | 20,229 | |||||||||||
| Supplemental Disclosures of Cash Flow Information: | |||||||||||||||||
| Cash paid for interest | $ | 6,207 | $ | 9,628 | $ | 3,522 | |||||||||||
| Cash paid for income taxes, net of refunds received | $ | 50,721 | $ | 29,522 | $ | 14,278 | |||||||||||
| Supplemental Disclosures of Non-Cash Financing Activity: | |||||||||||||||||
| Note payable issued for software licenses | $ | 0 | $ | 0 | $ | 418 | |||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
62
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
1. NATURE OF OPERATIONS, CONSOLIDATION AND PRESENTATION OF FINANCIAL STATEMENTS
Amedisys, Inc., a Delaware corporation (together with its consolidated subsidiaries, referred to herein as “Amedisys,” “we,” “us,” or “our”), is a multi-state provider of home health, hospice and personal care services with approximately 75%, 74% and 73% of our revenue derived from Medicare for 2020, 2019 and 2018, respectively. As of December 31, 2020, we owned and operated 320 Medicare-certified home health care centers, 180 Medicare-certified hospice care centers and 14 personal-care care centers in 39 states within the United States and the District of Columbia.
Recently Adopted Accounting Pronouncements
On January 1, 2020, the Company adopted Accounting Standards Update ("ASU") 2016-13, Financial Instruments - Credit Losses (Topic 326), which provides guidance for measuring credit losses on financial instruments. Our adoption of this standard did not have a material effect on our consolidated financial statements.
During the fourth quarter of 2020, the Company adopted ASU 2019-12, Income Taxes (Topic 740) - Simplifying the Accounting for Income Taxes, which eliminates certain exceptions related to the approach for intraperiod tax allocation, the methodology for calculating taxes during the interim periods and the recognition of deferred tax liabilities for outside basis differences. This guidance also simplifies aspects of the accounting for franchise taxes, enacts changes in tax laws or rates and clarifies the accounting for transactions that result in a step-up in the tax basis of goodwill. The guidance is effective for interim and annual periods beginning after December 15, 2020, with early adoption permitted. Our adoption of this standard on a prospective basis was not material to the Company’s consolidated financial statements.
On January 1, 2019, the Company adopted Accounting Standards Codification ("ASC") 842, Leases, using a modified retrospective transition approach, which requires the new standard to be applied to all leases existing at the date of initial application. Under ASC 842, lessees are required to recognize a lease liability and right-of-use asset ("ROU asset") for all leases with a term greater than twelve months and to disclose key information about leasing arrangements. Additionally, leases are classified as either financing or operating; the classification determines the pattern of expense recognition and classification within the statement of operations. We used the standard's effective date as our date of initial application. Consequently, our financial information was not updated and the disclosures required under the new standard are not provided for dates and periods prior to January 1, 2019. The new standard provides several optional practical expedients that can be adopted at transition. We elected the "package of practical expedients," which allows us to not reassess our prior conclusions regarding lease identification, lease classification and initial direct costs. We did not elect the use-of-hindsight or the practical expedient pertaining to land easements; the latter not being applicable to us. The most significant effects related to this adoption relate to (1) the recognition of new ROU assets and lease liabilities on our balance sheet for our real estate and fleet operating leases; and (2) significant new disclosures about our leasing activities. Upon adoption, we recognized approximately $80 million in operating leases liabilities with corresponding ROU assets of approximately the same amount. The new standard also provides practical expedients for an entity’s ongoing accounting. We have elected the practical expedient that allows us to not separate lease and non-lease components for all of our leases.
On January 1, 2019, the Company adopted ASU 2018-07, Compensation - Stock Compensation (Topic 718): Improvements to Nonemployees Share-Based Payment Accounting, which expands the scope of Topic 718 to include share-based payments issued to nonemployees for goods or services. Our adoption of this standard did not have an effect on our consolidated financial statements.
On January 1, 2018, the Company adopted ASC 606, Revenue from Contracts with Customers, using the full retrospective method. ASC 606 outlines a single comprehensive model to use in accounting for revenue arising from contracts with customers. The standard supersedes existing revenue recognition requirements and eliminates most industry-specific guidance from U.S. Generally Accepted Accounting Principles ("U.S. GAAP"). The core principle of the revenue recognition standard is to require an entity to recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which it expects to be entitled in exchange for those goods or services. As a result of the Company's adoption of ASC 606, the revenue and related estimated uncollectible amounts owed to us by non-Medicare payors that were historically classified as provision for doubtful accounts are now considered a revenue adjustment in determining net service revenue. Accordingly, the Company reports estimated uncollectible balances due from third-party payors and uncollectible balances associated with patient responsibility as a reduction of the transaction price and therefore, as a reduction in net service revenue (or as it relates to Hospice room and board, an increase in cost of service, excluding depreciation and amortization) when historically these amounts were classified as provision for doubtful accounts within operating expenses within our consolidated statements of operations. In addition, the adoption of ASC 606 resulted in increased disclosure,
63
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
including qualitative and quantitative disclosures about the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers.
On January 1, 2018, the Company adopted ASU 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business, which provides guidance to assist entities with evaluating whether transactions should be accounted for as an acquisition (or disposal) of assets or a business. We adopted this ASU on a prospective basis. The impact on our consolidated financial statements and related disclosures will depend on the facts and circumstances of any specific future transactions as evaluated under the new framework.
On January 1, 2018, the Company adopted ASU 2017-04, Intangibles - Goodwill and Other (Topic 350) - Simplifying the Test for Goodwill Impairment, which eliminates the requirement to calculate the implied fair value of goodwill to measure a goodwill impairment charge (Step 2 of the goodwill impairment test). Instead, impairment will be measured using the difference between the carrying amount and the fair value of the reporting unit. The ASU is effective for annual and interim periods beginning after December 15, 2019, with early adoption permitted. We adopted this ASU on a prospective basis and will apply this guidance to our future tests of goodwill impairment.
On January 1, 2018, the Company adopted ASU 2016-15, Statement of Cash Flows (Topic 230): Classification of Certain Cash Receipts and Cash Payments, which provides specific guidance on eight cash flow classification issues not specifically addressed by U.S. GAAP. The ASU is effective for annual and interim periods beginning after December 15, 2017. The standard should be applied using a retrospective transition method unless it is impractical to do so for some of the issues. In such case, the amendments for those issues would be applied prospectively as of the earliest date practicable. Our adoption of this standard using a retrospective transition method for each period presented did not have an effect on our consolidated financial statements.
Recently Issued Accounting Pronouncements
On March 12, 2020, the FASB issued ASU 2020-04, Reference Rate Reform (Topic 848): Facilitation of the Effects of Reference Rate Reform on Financial Reporting, which provides optional expedients and exceptions for applying U.S. GAAP to contract modifications and hedging relationships that reference LIBOR or another reference rate expected to be discontinued, subject to meeting certain criteria. The amendments in this ASU were effective beginning on March 12, 2020 and may generally be applied prospectively through December 31, 2022. This standard will not have an effect on our consolidated financial statements.
Use of Estimates
Our accounting and reporting policies conform with U.S. GAAP. In preparing the consolidated financial statements, we are required to make estimates and assumptions that impact the amounts reported in the consolidated financial statements and accompanying notes. Actual results could materially differ from those estimates.
Principles of Consolidation
These consolidated financial statements include the accounts of Amedisys, Inc. and our wholly owned subsidiaries. All significant intercompany accounts and transactions have been eliminated in our accompanying consolidated financial statements, and business combinations accounted for as purchases have been included in our consolidated financial statements from their respective dates of acquisition. In addition to our wholly owned subsidiaries, we also have certain equity investments that are accounted for as set forth below.
Investments
We consolidate investments when the entity is a variable interest entity and we are the primary beneficiary or if we have controlling interests in the entity, which is generally ownership in excess of 50%. Third party equity interests in our consolidated joint ventures are reflected as noncontrolling interests in our consolidated financial statements. During 2016, we sold a 30% interest in one of our care centers while maintaining a controlling interest in the newly formed joint venture; we repurchased the 30% interest during 2018.
We account for investments in entities in which we have the ability to exercise significant influence under the equity method if we hold 50% or less of the voting stock and the entity is not a variable interest entity in which we are the primary beneficiary. During 2020, we sold our investment in the Heritage Healthcare Innovation Fund, LP via a secondary transaction for $17.9 million which resulted in a $3.0 million loss which is reflected in miscellaneous, net within our consolidated statement of
64
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
operations for the year ended December 31, 2020. The Company's original investment was made in 2010 and no longer fit within our strategic areas of focus. Proceeds from the sale were used to pay down debt and fund operations. During 2018, we made a $7.0 million investment in a healthcare analytics company; this investment is accounted for under the equity method. The book value of investments that we account for under the equity method of accounting totaled $14.2 million and $35.7 million as of December 31, 2020 and 2019, respectively, and is reflected in other assets within our consolidated balance sheets.
2. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
Revenue Recognition
We account for revenue from contracts with customers in accordance with ASC 606, Revenue from Contracts with Customers, and as such, we recognize revenue in the period in which we satisfy our performance obligations under our contracts by transferring our promised services to our customers in amounts that reflect the consideration to which we expect to be entitled in exchange for providing patient care, which are the transaction prices allocated to the distinct services. The Company's cost of obtaining contracts is not material.
Revenues are recognized as performance obligations are satisfied, which varies based on the nature of the services provided. Our performance obligation is the delivery of patient care services in accordance with the nature and frequency of services outlined in physicians' orders, which are determined by a physician based on a patient's specific goals.
The Company's performance obligations relate to contracts with a duration of less than one year; therefore, the Company has elected to apply the optional exemption provided by ASC 606 and is not required to disclose the aggregate amount of the transaction price allocated to performance obligations that are unsatisfied or partially unsatisfied as of the end of the reporting period. The unsatisfied or partially unsatisfied performance obligations are generally completed when the patients are discharged, which generally occurs within days or weeks of the end of the reporting period.
We determine the transaction price based on gross charges for services provided, reduced by estimates for contractual and non-contractual revenue adjustments. Contractual revenue adjustments are recorded for the difference between our standard rates and the contracted rates to be realized from patients, third-party payors and others for services provided. Non-contractual revenue adjustments include discounts provided to self-pay, uninsured patients or other payors, adjustments resulting from payment reviews and adjustments arising from our inability to obtain appropriate billing documentation, authorizations or face-to-face documentation. Subsequent changes to the estimate of the transaction price are recorded as adjustments to net service revenue in the period of change.
Non-contractual revenue adjustments are recorded for self-pay, uninsured patients and other payors by major payor class based on our historical collection experience, aged accounts receivable by payor and current economic conditions. The non-contractual revenue adjustments represent the difference between amounts billed and amounts we expect to collect based on our collection history with similar payors. The Company assesses its ability to collect for the healthcare services provided at the time of patient admission based on the Company's verification of the patient's insurance coverage under Medicare, Medicaid, and other commercial or managed care insurance programs. Medicare represents approximately 75% of the Company's consolidated net service revenue.
Amounts due from third-party payors, primarily commercial health insurers and government programs (Medicare and Medicaid), include variable consideration for retroactive revenue adjustments due to settlements of audits and payment reviews. We determine our estimates for non-contractual revenue adjustments related to payment reviews based on our historical experience and success rates in the claim appeals and adjudication process.
We determine our estimates for non-contractual revenue adjustments related to our inability to obtain appropriate billing documentation, authorizations, or face-to-face documentation based on our historical experience which primarily includes a historical collection rate of over 99% on Medicare claims. Revenue is recorded at amounts we estimate to be realizable for services provided.
65
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Revenue by payor class as a percentage of total net service revenue is as follows:
| As of December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Home Health: | |||||||||||||||||
| Medicare | 41 | % | 44 | % | 50 | % | |||||||||||
| Non-Medicare - Episodic-based | 7 | % | 9 | % | 9 | % | |||||||||||
| Non-Medicare - Non-episodic based | 13 | % | 12 | % | 12 | % | |||||||||||
| Hospice (1): | |||||||||||||||||
| Medicare | 34 | % | 30 | % | 23 | % | |||||||||||
| Non-Medicare | 2 | % | 1 | % | 1 | % | |||||||||||
| Personal Care | 3 | % | 4 | % | 5 | % | |||||||||||
| 100 | % | 100 | % | 100 | % | ||||||||||||
(1) Acquired Compassionate Care Hospice on February 1, 2019, RoseRock Healthcare on April 1, 2019, Asana Hospice on January 1, 2020 and AseraCare Hospice on June 1, 2020.
Home Health Revenue Recognition
Medicare Revenue
Effective January 1, 2020, the Centers for Medicare and Medicaid Services ("CMS") implemented a revised case-mix adjustment methodology, the Patient-Driven Groupings Model ("PDGM"), to better align payment with patient care needs and ensure that clinically complex and ill beneficiaries have adequate access to home health care. PDGM uses 30-day periods of care rather than 60-day episodes of care as the unit of payment, eliminates the use of the number of therapy visits provided in determining payment and relies more heavily on clinical characteristics and other patient information.
Net service revenue is recorded based on the established Federal Medicare home health payment rate for a 30-day period of care. ASC 606 notes that if an entity has a right to consideration from a customer in an amount that corresponds directly with the value of the entity’s performance completed to date, the entity may recognize revenue in the amount to which the entity has a right to invoice. We have elected to apply the "right to invoice" practical expedient and therefore, our revenue recognition is based on the reimbursement we are entitled to for each 30-day payment period. We utilize our historical average length of stay for each 30-day period of care as the measure of progress towards the satisfaction of our performance obligation.
PDGM uses timing, admission source, functional impairment levels and principal and other diagnoses to case-mix adjust payments. The case-mix adjusted payment for a 30-day period of care is subject to additional adjustments based on certain variables including, but not limited to: (a) an outlier payment if our patient’s care was unusually costly (capped at 10% of total reimbursement per provider number); (b) a low utilization payment adjustment (“LUPA”) if the number of visits provided was less than the established threshold, which ranges from 2 to 6 visits and varies for every case-mix group under PDGM; (c) a partial payment if a patient transferred to another provider or from another provider before completing the 30-day period of care; and (d) the applicable geographic wage index. Payments for routine and non-routine supplies are now included in the 30-day payment rate.
Medicare can also make various adjustments to payments received if we are unable to produce appropriate billing documentation or acceptable authorizations. We estimate the impact of such adjustments based on our historical experience, which primarily includes a historical collection rate of over 99% on Medicare claims, and record this estimate during the period in which services are rendered to revenue with a corresponding reduction to patient accounts receivable.
Amounts due from Medicare include variable consideration for retroactive revenue adjustments due to settlements of audits and payment reviews. We determine our estimates for non-contractual revenue adjustments related to payment reviews based on our historical experience and success rates in the claim appeals and adjudication process.
The Medicare home health benefit requires that beneficiaries be homebound (meaning that the beneficiary is unable to leave his/her home without a considerable and taxing effort), require intermittent skilled nursing, physical therapy or speech therapy services, and receive treatment under a plan of care established and periodically reviewed by a physician. In order to provide greater flexibility during the novel coronavirus pandemic ("COVID-19"), CMS has relaxed the definition of homebound status through the duration of the public health emergency. During the pandemic, a beneficiary is considered homebound if they have been instructed by a physician not to leave their home because of a confirmed or suspected COVID-19 diagnosis or if the patient has a condition that makes them more susceptible to contracting COVID-19. Therefore, if a beneficiary is homebound due to COVID-19 and requires skilled services, the services will be covered under the Medicare home health benefit.
66
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
All Medicare contracts are required to have a signed plan of care which represents a single performance obligation, comprised of the delivery of a series of distinct services that are substantially similar and have a similar pattern of transfer to the customer. Accordingly, the Company accounts for the series of services ("episode") as a single performance obligation satisfied over time, as the customer simultaneously receives and consumes the benefits of the goods and services provided. An episode starts the first day a billable visit is performed and ends 60 days later or upon discharge, if earlier, with multiple continuous episodes allowed.
A portion of reimbursement from each Medicare episode, referred to as a request for anticipated payment ("RAP"), is billed near the start of each 30-day period of care, and cash is typically received before all services are rendered. Any cash received from Medicare for a RAP for a 30-day period of care that exceeds the associated revenue earned is recorded to accrued expenses within our consolidated balance sheets. CMS reduced the upfront payment for RAPs to 20% for 2020 and has fully eliminated payments associated with RAPs in 2021.
Non-Medicare Revenue
Episodic-based Revenue. We recognize revenue in a similar manner as we recognize Medicare revenue for amounts that are paid by other insurance carriers, including Medicare Advantage programs; however, these amounts can vary based upon the negotiated terms which generally range from 90% to 100% of Medicare rates.
Non-episodic based Revenue. Gross revenue is recorded on an accrual basis based upon the date of service at amounts equal to our established or estimated per-visit rates. Contractual revenue adjustments are recorded for the difference between our standard rates and the contracted rates to be realized from patients, third parties and others for services provided and are deducted from gross revenue to determine net service revenue. We also make non-contractual revenue adjustments to non-episodic revenue based on our historical experience to reflect the estimated transaction price. We receive a minimal amount of our net service revenue from patients who are either self-insured or are obligated for an insurance co-payment.
Hospice Revenue Recognition
Hospice Medicare Revenue
Gross revenue is recorded on an accrual basis based upon the date of service at amounts equal to the estimated payment rates. The estimated payment rates are predetermined daily or hourly rates for each of the four levels of care we deliver. The four levels of care are routine care, general inpatient care, continuous home care and respite care. Routine care accounted for 97% of our total Medicare hospice service revenue for each of 2020, 2019 and 2018, respectively. There are two separate payment rates for routine care: payments for the first 60 days of care and care beyond 60 days. In addition to the two routine rates, we may also receive a service intensity add-on (“SIA”). The SIA is based on visits made in the last seven days of life by a registered nurse or medical social worker for patients in a routine level of care.
The performance obligation is the delivery of hospice services to the patient, as determined by a physician, each day the patient is on hospice care.
We make adjustments to Medicare revenue for non-contractual revenue adjustments, which include our inability to obtain appropriate billing documentation or acceptable authorizations and other reasons unrelated to credit risk. We estimate the impact of these non-contractual revenue adjustments based on our historical experience, which primarily includes a historical collection rate of over 99% on Medicare claims, and record it during the period services are rendered.
Additionally, our hospice service revenue is subject to certain limitations on payments from Medicare which are considered variable consideration. We are subject to an inpatient cap limit and an overall Medicare payment cap for each provider number. We monitor these caps on a provider-by-provider basis and estimate amounts due back to Medicare if we estimate a cap has been exceeded. We record these adjustments as a reduction to revenue and an increase in accrued expenses within our consolidated balance sheets. Providers are required to self-report and pay their estimated cap liability by February 28th of the following year. As of December 31, 2020, we have settled our Medicare hospice reimbursements for all fiscal years through October 31, 2013. As of December 31, 2020, we have recorded $9.3 million for estimated amounts due back to Medicare in accrued expenses for the Federal cap years ended October 31, 2014 through September 30, 2021; approximately $2.0 million of this balance was acquired with the AseraCare Hospice ("AseraCare") acquisition. As of December 31, 2019, we had recorded $5.7 million for estimated amounts due back to Medicare in accrued expenses for the Federal cap years ended October 31, 2013 through September 30, 2020.
67
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Hospice Non-Medicare Revenue
Gross revenue is recorded on an accrual basis based upon the date of service at amounts equal to our established rates or estimated per day rates, as applicable. Contractual revenue adjustments are recorded for the difference between our standard rates and the contractual rates to be realized from patients, third party payors and others for services provided and are deducted from gross revenue to determine our net service revenue. We also make non-contractual adjustments to non-Medicare revenue based on our historical experience to reflect the estimated transaction price.
Personal Care Revenue Recognition
Personal Care Revenue
We generate net service revenues by providing our services directly to patients based on authorized hours, visits or units determined by the relevant agency, at a rate that is either contractual or fixed by legislation. Net service revenue is recognized at the time services are rendered based on gross charges for the services provided, reduced by estimates for contractual and non-contractual revenue adjustments. We receive payment for providing such services from payors, including state and local governmental agencies, managed care organizations, commercial insurers and private consumers. Payors include the following elder service agencies: Aging Services Access Points ("ASAPs"), Senior Care Options ("SCOs"), Program of All-Inclusive Care for the Elderly ("PACE") and the Veterans Administration ("VA").
Government Grants
In the absence of specific guidance to account for government grants under U.S. GAAP, we have decided to account for government grants in accordance with International Accounting Standard ("IAS") 20, Accounting for Government Grants and Disclosure of Government Assistance, and as such, we recognize grant income on a systematic basis in line with the recognition of expenses or the loss of revenues for which the grants are intended to compensate. We recognize grants once both of the following conditions are met: (1) we are able to comply with the relevant conditions of the grant and (2) the grant will be received. See Note 3 - Novel Coronavirus Pandemic ("COVID-19") for additional information on our accounting for government funds received under the Coronavirus Aid, Relief and Economic Security Act ("CARES Act") and the Mass Home Care ASAP COVID-19 Provider Sustainability Program.
Cash, Cash Equivalents and Restricted Cash
Cash and cash equivalents include certificates of deposit and all highly liquid debt instruments with maturities of three months or less when purchased. Our cash balance as of December 31, 2020 includes approximately $77 million associated with the CARES Act Provider Relief Fund ("PRF"). We separated the PRF funds into their own account and as of December 31, 2020, we have only transferred funds used during the nine-month period ended September 30, 2020 to our operating account. We will transfer funds used during the three-month period ended December 31, 2020 to our operating account in 2021. Restricted cash includes cash that is not available for ordinary business use. As of December 31, 2020, we had $1.5 million of restricted cash that was placed into an escrow account related to the indemnity provisions within the Asana Hospice purchase agreement. As of December 31, 2019, we had $66.2 million of restricted cash that was placed into an escrow account to fund the acquisition of Asana Hospice on January 1, 2020.
The following table summarizes the balances related to our cash, cash equivalents and restricted cash (amounts in millions):
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Cash and cash equivalents | $ | 81.8 | $ | 30.3 | |||||||
| Restricted cash | 1.5 | 66.2 | |||||||||
| Cash, cash equivalents and restricted cash | $ | 83.3 | $ | 96.5 | |||||||
68
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Patient Accounts Receivable
We report accounts receivable from services rendered at their estimated transaction price, which includes contractual and non-contractual revenue adjustments based on the amounts expected to be due from payors. Our patient accounts receivable are uncollateralized and consist of amounts due from Medicare, Medicaid, other third-party payors and patients. The Company's non-Medicare third-party payor base is comprised of a diverse group of payors that are geographically dispersed across the country. As of December 31, 2020, there is no single payor, other than Medicare, that accounts for more than 10% of our total outstanding patient receivables. Thus, we believe there are no other significant concentrations of receivables that would subject us to any significant credit risk in the collection of our patient accounts receivable. We write off accounts on a monthly basis once we have exhausted our collection efforts and deem an account to be uncollectible. We believe the collectibility risk associated with our Medicare accounts, which represent 64% and 58% of our net patient accounts receivable at December 31, 2020 and 2019, respectively, is limited due to our historical collection rate of over 99% from Medicare and the fact that Medicare is a U.S. government payor.
We do not believe there are any significant concentrations of revenues from any payor that would subject us to any significant credit risk in the collection of our accounts receivable.
Medicare Home Health
For our home health patients, our pre-billing process includes verifying that we are eligible for payment from Medicare for the services that we provide to our patients. Our Medicare billing begins with a process to ensure that our billings are accurate through the utilization of an electronic Medicare claim review. We submit a RAP for 20% of our estimated payment for each 30-day period of care. The RAP received for that billing period is then deducted from our final payment. If a final bill is not submitted within the greater of 90 days from the start of the 30-day period of care, or 60 days from the date the RAP was paid, any RAPs received for that billing period will be recouped by Medicare from any other claims in process for that particular provider number. The RAP claim must then be resubmitted. CMS has mandated the full elimination of all upfront payments associated with RAPs in 2021.
Medicare Hospice
For our hospice patients, our pre-billing process includes verifying that we are eligible for payment from Medicare for the services that we provide to our patients. Our Medicare billing begins with a process to ensure that our billings are accurate through the utilization of an electronic Medicare claim review. We bill Medicare on a monthly basis for the services provided to the patient.
Non-Medicare Home Health, Hospice, and Personal Care
For our non-Medicare patients, our pre-billing process primarily begins with verifying a patient’s eligibility for services with the applicable payor. Once the patient has been confirmed for eligibility, we will provide services to the patient and bill the applicable payor. Our review and evaluation of non-Medicare accounts receivable includes a detailed review of outstanding balances and special consideration to concentrations of receivables from particular payors or groups of payors with similar characteristics that would subject us to any significant credit risk.
Property and Equipment
Property and equipment is stated at cost and depreciated on a straight-line basis over the estimated useful lives of the assets or life of the lease, if shorter. Additionally, we have internally developed computer software for our own use. Additions and improvements (including interest costs for construction of qualifying long-lived assets) are capitalized. Maintenance and repair expenses are charged to expense as incurred. The cost of property and equipment sold or disposed of and the related accumulated depreciation are eliminated from the property and related accumulated depreciation accounts, and any gain or loss is credited or charged to other general and administrative expenses.
We assess the impairment of a long-lived asset group whenever events or changes in circumstances indicate that the asset’s carrying value may not be recoverable. Factors we consider important that could trigger an impairment review include but are not limited to the following:
•A significant change in the extent or manner in which the long-lived asset group is being used.
•A significant change in the business climate that could affect the value of the long-lived asset group.
•A significant change in the market value of the assets included in the asset group.
69
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
If we determine that the carrying value of long-lived assets may not be recoverable, we compare the carrying value of the asset group to the undiscounted cash flows expected to be generated by the asset group. If the carrying value exceeds the undiscounted cash flows, an impairment charge is indicated. An impairment charge is recognized to the extent that the carrying value of the asset group exceeds its fair value.
We generally provide for depreciation over the following estimated useful service lives.
| Years | |||||
| Building | 39 | ||||
| Leasehold improvements | Lesser of lease term or expected useful life | ||||
| Equipment and furniture | 3 to 7 | ||||
| Vehicles | 5 | ||||
| Computer software | 2 to 7 | ||||
| Finance leases | 3 | ||||
The following table summarizes the balances related to our property and equipment for 2020 and 2019 (amounts in millions):
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Building and leasehold improvements | $ | 9.0 | $ | 8.7 | |||||||
| Equipment and furniture | 53.1 | 55.6 | |||||||||
| Finance leases | 5.9 | 5.2 | |||||||||
| Computer software | 50.7 | 54.7 | |||||||||
| 118.7 | 124.2 | ||||||||||
| Less: accumulated depreciation | (95.0) | (96.1) | |||||||||
| $ | 23.7 | $ | 28.1 | ||||||||
Depreciation expense for 2020, 2019 and 2018 was $12.1 million, $11.6 million and $10.8 million, respectively.
Business Combinations
We account for acquisitions using the acquisition method of accounting in accordance with ASC 805, Business Combinations. Acquisitions are accounted for as purchases and are included in our consolidated financial statements from their respective acquisition dates. Assets acquired and liabilities assumed, if any, are measured at fair value on the acquisition date using the appropriate valuation method. Goodwill generated from acquisitions is recognized for the excess of the purchase price over tangible and identifiable intangible assets. In determining the fair value of identifiable intangible assets, we use various valuation techniques including discounted cash flow analysis, the income approach, the cost approach and the market approach. These valuation methods require us to make estimates and assumptions surrounding projected revenues and costs, future growth and discount rates.
Goodwill and Other Intangible Assets
Goodwill represents the amount of the purchase price in excess of the fair values assigned to the underlying identifiable net assets of acquired businesses. Goodwill is not amortized, but is subject to an annual impairment test. Tests are performed more frequently if events occur or circumstances change that would more likely than not reduce the fair value of the reporting unit below its carrying amount. These events or circumstances include, but are not limited to, a significant adverse change in the business environment, regulatory environment or legal factors, or a substantial decline in the market capitalization of our stock.
Each of our operating segments described in Note 14 – Segment Information is considered to represent an individual reporting unit for goodwill impairment testing purposes. We consider each of our home health care centers to constitute an individual business for which discrete financial information is available. However, since these care centers have substantially similar operating and economic characteristics and resource allocations and since significant investment decisions concerning these businesses are centralized and the benefits broadly distributed, we have aggregated these care centers and deemed them to constitute a single reporting unit. We have applied this same aggregation principle to our hospice and personal-care care centers and have also deemed each of them to be a single reporting unit.
70
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
During 2020, we performed a qualitative assessment to determine if it is more likely than not that the fair value of the reporting units are less than their carrying values by evaluating relevant events and circumstances including financial performance, market conditions and share price. Based on this assessment, we did not record any goodwill impairment charges and none of the goodwill associated with our various reporting units was considered at risk of impairment as of October 31, 2020. Since the date of our last annual goodwill impairment test, there have been no material developments, events, changes in operating performance or other circumstances that would cause management to believe it is more likely than not that the fair value of any of our reporting units would be less than their carrying amounts.
Intangible assets consist of certificates of need, licenses, acquired names and non-compete agreements. We amortize non-compete agreements and acquired names that we do not intend to use indefinitely on a straight-line basis over their estimated useful lives, which are generally two to three years for non-compete agreements and up to three years for acquired names. Our indefinite-lived intangible assets are reviewed for impairment annually or more frequently if events occur or circumstances change that would more likely than not reduce the fair value of the intangible asset below its carrying amount. During 2020, we performed a qualitative assessment of our indefinite-lived intangible assets; as a result of this analysis, we wrote off approximately $4.2 million of acquired names that are no longer in use. During 2019, we also performed a qualitative assessment of our indefinite-lived intangible assets; as a result of this analysis, we wrote off approximately $1.5 million of acquired names. There have been no material developments, events, changes in operating performance or other circumstances that would cause management to believe it is more likely than not that the fair value of any of our remaining intangible assets would be less than their carrying amounts.
Debt Issuance Costs
During 2019, we recorded $0.8 million in deferred debt issuance costs as a reduction to long-term obligations, less current portion in our consolidated balance sheet in connection with our entry into the Amended Credit Agreement (See Note 8 - Long-Term Obligations). As of December 31, 2020 and 2019, we had unamortized debt issuance costs of $2.7 million and $3.5 million, respectively, recorded as a reduction to long-term obligations, less current portion in our accompanying consolidated balance sheets. We amortize deferred debt issuance costs related to our long-term obligations over the term of the obligation through interest expense, unless the debt is extinguished, in which case unamortized balances are immediately expensed. The unamortized debt issuance costs of $2.7 million at December 31, 2020 will be amortized over a weighted-average amortization period of 3.1 years.
Fair Value of Financial Instruments
The following details our financial instruments where the carrying value and the fair value differ (amounts in millions):
| Fair Value at Reporting Date Using | |||||||||||||||||||||||
| Financial Instrument | Carrying Value as of December 31, 2020 | Quoted Prices in Active Markets for Identical Items (Level 1) | Significant Other Observable Inputs (Level 2) | Significant Unobservable Inputs (Level 3) | |||||||||||||||||||
| Long-term obligations | $ | 215.1 | $ | 0 | $ | 217.7 | $ | 0 | |||||||||||||||
The fair value hierarchy is based on three levels of inputs, of which the first two are considered observable and the last unobservable, that may be used to measure fair value. The three levels of inputs are as follows:
•Level 1 – Quoted prices in active markets for identical assets and liabilities.
•Level 2 – Inputs other than Level 1 that are observable, either directly or indirectly, such as quoted prices for similar assets or liabilities, quoted prices in markets that are not active or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities.
•Level 3 – Unobservable inputs that are supported by little or no market activity and are significant to the fair value of the assets or liabilities.
Our deferred compensation plan assets are recorded at fair value and are considered a level 2 measurement. For our other financial instruments, including our cash and cash equivalents, patient accounts receivable, accounts payable, payroll and employee benefits and accrued expenses, we estimate the carrying amounts approximate fair value.
71
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Income Taxes
We use the asset and liability approach for measuring deferred tax assets and liabilities based on temporary differences existing at each balance sheet date using currently enacted tax rates. Our deferred tax calculation requires us to make certain estimates about future operations. Deferred tax assets are reduced by a valuation allowance when we believe it is more likely than not that some portion or all of the deferred tax assets will not be realized. The effect of a change in tax rate is recognized as income or expense in the period that includes the enactment date. As of December 31, 2020 and 2019, our net deferred tax assets were $48.0 million and $21.4 million, respectively.
Management regularly assesses the ability to realize deferred tax assets recorded in the Company’s entities based upon the weight of available evidence, including such factors as the recent earnings history and expected future taxable income. In the event future taxable income is below management’s estimates or is generated in tax jurisdictions different than projected, we could be required to increase the valuation allowance for deferred tax assets. This would result in an increase in our effective tax rate.
Share-Based Compensation
We record all share-based compensation as expense in the financial statements measured at the fair value of the award. We recognize compensation cost on a straight-line basis over the requisite service period for each separately vesting portion of the award. Share-based compensation expense for 2020, 2019 and 2018 was $26.7 million, $25.0 million and $17.9 million, respectively, and the total income tax benefit recognized for these expenses was $4.7 million, $4.6 million and $4.3 million, respectively.
Weighted-Average Shares Outstanding
Net income per share attributable to Amedisys, Inc. common stockholders, calculated on the treasury stock method, is based on the weighted average number of shares outstanding during the period. The following table sets forth, for the periods indicated, shares used in our computation of weighted-average shares outstanding, which are used to calculate our basic and diluted net income attributable to Amedisys, Inc. common stockholders (amounts in thousands):
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Weighted average number of shares outstanding – basic | 32,559 | 32,142 | 32,791 | ||||||||||||||
| Effect of dilutive securities: | |||||||||||||||||
| Stock options | 420 | 545 | 502 | ||||||||||||||
| Non-vested stock and stock units | 289 | 303 | 316 | ||||||||||||||
| Weighted average number of shares outstanding – diluted | 33,268 | 32,990 | 33,609 | ||||||||||||||
| Anti-dilutive securities | 25 | 117 | 50 | ||||||||||||||
Advertising Costs
We expense advertising costs as incurred. Advertising expense for 2020, 2019 and 2018 was $8.0 million, $8.5 million and $7.0 million, respectively.
3. NOVEL CORONAVIRUS PANDEMIC ("COVID-19")
In March 2020, the World Health Organization declared COVID-19 a pandemic. As a healthcare at home company, we have been and will continue to be impacted by the effects of COVID-19; however, we remain committed to carrying out our mission of caring for our patients. We will continue to closely monitor the impact of COVID-19 on all aspects of our business, including the impacts to our employees, patients and suppliers; however, at this time, we are unable to estimate the ultimate impact the pandemic will have on our consolidated financial condition, results of operations or cash flows.
On March 27, 2020, the CARES Act was signed into legislation. The CARES Act provides for $175 billion to healthcare providers, including hospitals on the front lines of the COVID-19 pandemic. Of this total allocated amount, $30 billion was distributed immediately to providers based on their proportionate share of Medicare fee-for-service reimbursements in 2019. Healthcare providers were required to sign an attestation confirming receipt of the Provider Relief Fund ("PRF") funds and agree to the terms and conditions of payment. Our home health and hospice segments received approximately $100 million from the first $30 billion of funds distributed to healthcare providers in April 2020, which is inclusive of $2 million related to our joint venture care centers (equity method investments). We also acquired approximately $6 million of PRF funds in
72
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
connection with the acquisition of AseraCare. Under the terms and conditions for receipt of the payment, we are allowed to use the funds to cover lost revenues and health care costs related to COVID-19, and we are required to properly and fully document the use of these funds in reports to the U.S. Department of Health and Human Services ("HHS").
For our wholly-owned subsidiaries, we have decided to only utilize PRF funds to the extent we have qualifying COVID-19 expenses, which totaled $33 million for our home health and hospice segments during the year ended December 31, 2020. Accordingly, for our wholly-owned subsidiaries, we will not be using PRF funds to cover lost revenues resulting from COVID-19. The grant income associated with the COVID-19 expenses incurred to date is reflected in other operating income within our consolidated statement of operations.
HHS issued new guidance in September 2020 noting that PRF funds can be used towards lost revenues or expenses attributable to COVID-19 through June 30, 2021. We do not believe that we will fully utilize the funds received; therefore, we recorded a liability related to the funds that we do not expect to utilize totaling $60 million which is reflected in the Provider Relief Fund Advance account in current liabilities within our consolidated balance sheet. Funds that we intend to use in the future to cover COVID-19 expenses, which we have estimated to be approximately $12 million, have been recorded to a deferred liability account within accrued expenses in our consolidated balance sheet. These estimates may change as our ability to utilize and retain the funds will depend on the magnitude, timing and nature of the impact of the pandemic. In summary, the total funds that we have received from the CARES Act PRF as of December 31, 2020 consist of the following (amounts in millions):
| Amount | |||||
| Funds utilized during the year ended December 31, 2020 | $ | 33.3 | |||
| Estimated funds to be utilized January 2021 through June 2021 | 11.6 | ||||
| Estimated funds to be repaid to the government | 60.0 | ||||
| Funds received by unconsolidated joint ventures | 1.9 | ||||
| $ | 106.8 | ||||
On April 24, 2020, HHS distributed an additional $18 billion in funds to healthcare providers. We did not receive, nor apply, for any additional funds from this second distribution. On October 1, 2020, HHS announced $20 billion in new funding to healthcare providers under the Phase 3 general distribution. We did not apply for any additional funds from this distribution.
The CARES Act also provides for the temporary suspension of the automatic 2% reduction of Medicare claim reimbursements (sequestration) for the period May 1 through December 31, 2020 and the deferral of the employer share of social security tax (6.2%), effective for payments due after the enactment date. Fifty percent of the deferred payroll taxes are due on December 31, 2021 with the remaining amounts due on December 31, 2022. As of December 31, 2020, we have deferred $55 million of social security taxes; approximately $28 million is reflected in each of payroll and employee benefits and other long-term obligations within our consolidated balance sheet.
In December 2020, Congress passed additional COVID-19 relief legislation as part of the Consolidated Appropriations Act, 2021. This legislation extended the suspension of sequestration through March 31, 2021.
Our personal care segment did not receive funds under the CARES Act; however, they did receive funds from the Mass Home Care ASAP COVID-19 Provider Sustainability Program, which are intended to cover costs related to the public health emergency. The grant income associated with the funds received, which totaled $1 million during the year ended December 31, 2020, is reflected in other operating income within our consolidated statement of operations.
4. ACQUISITIONS
We complete acquisitions from time to time in order to pursue our strategy of increasing our market presence by expanding our service base and enhancing our position in certain geographic areas as a leading provider of home health, hospice and personal care services. The purchase price paid for acquisitions is negotiated through arm’s length transactions, with consideration based on our analysis of, among other things, comparable acquisitions and expected cash flows. Acquisitions are accounted for as purchases and are included in our consolidated financial statements from their respective acquisition dates. Goodwill generated from acquisitions is recognized for the excess of the purchase price over tangible and identifiable intangible assets because of the expected contributions of the acquisitions to our overall corporate strategy. We typically engage outside appraisal firms to assist in the fair value determination of identifiable intangible assets for significant acquisitions. The preliminary purchase price allocation is adjusted, as necessary, up to one year after the acquisition closing date if management obtains more information regarding asset valuation and liabilities assumed.
73
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
2020 Acquisitions
Home Health Division
On March 1, 2020, we acquired the regulatory assets of a home health provider in Washington for a purchase price of $3.0 million. The purchase price was paid with cash on hand on the date of the transaction. We recorded goodwill of $2.8 million and other intangibles (certificate of need) of $0.2 million in connection with the acquisition.
On April 18, 2020, we acquired the regulatory assets of a home health provider in Kentucky for a purchase price of $0.7 million. The purchase price was paid with cash on hand on the date of the transaction. We recorded goodwill of $0.5 million and other intangibles (certificate of need) of $0.2 million in connection with the acquisition.
Hospice Division
On January 1, 2020, we acquired Asana Hospice ("Asana"), a hospice provider with 8 locations in Pennsylvania, Ohio, Texas, Missouri and Kansas for a purchase price of $66.3 million, net of cash acquired of $0.7 million. Under the purchase agreement, the purchase price was subject to a net working capital adjustment, whereby the purchase price would be adjusted to the extent the actual net working capital of Asana as of the closing differed from the required net working capital under the purchase agreement. The net working capital adjustment, which was finalized during the three-month period ended June 30, 2020, reduced the purchase price by $0.7 million, from $66.3 million to $65.6 million.
The Company has finalized its valuation of the assets acquired and liabilities assumed. The total estimated consideration of $65.6 million has been allocated to assets acquired and liabilities assumed as of the acquisition date as follows (amounts in millions):
| Amount | |||||
| Patient accounts receivable | $ | 4.6 | |||
| Property and equipment | 0.2 | ||||
| Operating lease right of use assets | 0.9 | ||||
| Intangible assets | 5.6 | ||||
| Total assets acquired | 11.3 | ||||
| Accounts payable | (3.2) | ||||
| Payroll and employee benefits | (1.5) | ||||
| Accrued expenses | (0.5) | ||||
| Operating lease liabilities | (0.9) | ||||
| Total liabilities assumed | (6.1) | ||||
| Net identifiable assets acquired | 5.2 | ||||
| Goodwill | 60.4 | ||||
| Total estimated consideration | $ | 65.6 | |||
Intangible assets acquired include licenses ($2.0 million), acquired names ($1.3 million) and non-compete agreements ($2.3 million). The acquired names and non-compete agreements will be amortized over a weighted-average period of 2.0 years.
Asana contributed approximately $23.4 million in net service revenue and an operating loss of $3.3 million (inclusive of acquisition and integration costs totaling $2.0 million and intangibles amortization totaling $2.6 million) during the year ended December 31, 2020.
We expect the entire amount of goodwill recorded for this acquisition to be deductible for income tax purposes over approximately 15 years.
On June 1, 2020, we acquired Homecare Preferred Choice, Inc., doing business as AseraCare Hospice ("AseraCare"), a national hospice care provider with 44 locations, for an estimated purchase price of $230.4 million, net of cash acquired and inclusive of a $32 million tax asset. The closing payment for the purchase price included estimates for cash, working capital and various other items. Under the purchase agreement, the purchase price was subject to a closing payment adjustment for any differences between estimated amounts included in the closing payment and actual amounts at close, not to exceed $1.0 million. The
74
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
closing payment adjustment, which was finalized in October 2020, reduced the purchase price by $0.8 million, from $230.4 million to $229.6 million.
The Company is in the process of reviewing the fair value of the assets acquired and liabilities assumed. During the year ended December 31, 2020, we recorded measurement period adjustments based on changes to management's estimates and assumptions related to the assets acquired and liabilities assumed. The final valuation of the assets acquired and liabilities assumed was not complete as of December 31, 2020, but will be finalized within the allowable measurement period. Based on the Company's preliminary valuation, the total estimated consideration of $229.6 million has been allocated to assets acquired and liabilities assumed as of the acquisition date as follows (amounts in millions):
| Amount | |||||
| Patient accounts receivable | $ | 15.0 | |||
| Prepaid expenses | 0.7 | ||||
| Property and equipment | 0.6 | ||||
| Operating lease right of use assets | 5.9 | ||||
| Intangible assets | 24.3 | ||||
| Other assets | 0.1 | ||||
| Total assets acquired | 46.6 | ||||
| Accounts payable | (5.8) | ||||
| Payroll and employee benefits | (5.9) | ||||
| Accrued expenses | (10.4) | ||||
| Operating lease liabilities | (5.4) | ||||
| Total liabilities assumed | (27.5) | ||||
| Net identifiable assets acquired | 19.1 | ||||
| Goodwill | 210.5 | ||||
| Total estimated consideration | $ | 229.6 | |||
Intangible assets acquired include licenses ($8.7 million), certificates of need ($0.7 million), acquired names ($5.7 million) and non-compete agreements ($9.2 million). The acquired names will be amortized over a weighted-average period of 2.0 years and the non-compete agreements will be amortized over a weighted-average period of 1.7 years.
AseraCare contributed approximately $64.5 million in net service revenue and an operating loss of $8.2 million (inclusive of acquisition and integration costs totaling $7.6 million and intangibles amortization totaling $6.0 million) during the year ended December 31, 2020.
We expect the entire amount of goodwill recorded for this acquisition to be deductible for income tax purposes over approximately 15 years.
The following table contains unaudited pro forma condensed consolidated statement of operations information for the years ended December 31, 2020 and 2019 assuming that the AseraCare acquisition closed on January 1, 2019 (amounts in millions, except per share data). The pro forma financial information includes various assumptions, including those related to the preliminary purchase price allocation of assets acquired and liabilities assumed. The pro forma financial information may vary in future quarters based on the final valuations and analysis of the fair value of the assets acquired and liabilities assumed.
| For the Years Ended December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Net service revenue | $ | 2,120.1 | $ | 2,077.0 | |||||||
| Operating income | 218.0 | 167.5 | |||||||||
| Net income attributable to Amedisys Inc. | 180.6 | 112.3 | |||||||||
| Basic earnings per share | 5.55 | 3.49 | |||||||||
| Diluted earnings per share | 5.43 | 3.40 | |||||||||
75
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
The pro forma information presented above includes adjustments for (i) amortization of identifiable intangible assets, (ii) interest on additional debt required to fund the AseraCare acquisition, (iii) non-recurring transaction costs and (iv) income taxes based on the Company's statutory tax rate. This pro forma information is presented for illustrative purposes only and may not be indicative of the results of operations that would have actually occurred. In addition, future results may vary significantly from the results reflected in the pro forma information.
2019 Acquisitions
Hospice Division
On February 1, 2019, we acquired Compassionate Care Hopsice ("CCH"), a national hospice care provider headquartered in New Jersey, for a purchase price of $327.9 million, net of cash acquired of $6.7 million.
The Company has finalized its valuation of the assets acquired and liabilities assumed. The total consideration of $327.9 million has been allocated to assets acquired and liabilities assumed as of the acquisition date as follows (amounts in millions):
| Amount | |||||
| Patient accounts receivable | $ | 24.5 | |||
| Prepaid expenses | 0.8 | ||||
| Other current assets | 0.1 | ||||
| Property and equipment | 0.2 | ||||
| Intangible assets | 27.2 | ||||
| Operating lease right of use assets | 3.4 | ||||
| Other assets | 1.1 | ||||
| Total assets acquired | 57.3 | ||||
| Accounts payable | (14.9) | ||||
| Payroll and employee benefits | (11.7) | ||||
| Accrued expenses | (11.7) | ||||
| Deferred tax liability | (0.9) | ||||
| Operating lease liabilities | (3.4) | ||||
| Total liabilities acquired | (42.6) | ||||
| Net identifiable assets acquired | 14.7 | ||||
| Goodwill | 313.2 | ||||
| Total estimated consideration | $ | 327.9 | |||
Intangible assets acquired include licenses, certificates of need, acquired names and non-compete agreements. The acquired names and non-compete agreements will be amortized over a weighted-average period of 2.0 and 2.3 years, respectively.
CCH contributed approximately $167.4 million in net service revenue and an operating loss of $5.6 million (inclusive of acquisition and integration costs totaling $14.5 million) during the year ended December 31, 2019.
We expect $278.8 million of goodwill recorded for this acquisition to be deductible for income tax purposes over approximately 15 years.
The following table contains unaudited pro forma condensed consolidated statement of operations information for the years ended December 31, 2019 and 2018 assuming that the CCH acquisition closed on January 1, 2018 (amounts in millions, except per share data):
76
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
| For the Years Ended December 31, | |||||||||||
| 2019 | 2018 | ||||||||||
| Net service revenue | $ | 1,971.7 | $ | 1,852.8 | |||||||
| Operating income | 183.8 | 175.7 | |||||||||
| Net income attributable to Amedisys, Inc. | 130.5 | 124.6 | |||||||||
| Basic earnings per share | 4.06 | 3.80 | |||||||||
| Diluted earnings per share | $ | 3.96 | $ | 3.71 | |||||||
The pro forma information presented above includes adjustments for (i) amortization of identifiable intangible assets, (ii) interest on additional debt required to fund the CCH acquisition, (iii) non-recurring transaction costs and (iv) income taxes based on the Company’s statutory tax rate. This pro forma information is presented for illustrative purposes only and may not be indicative of the results of operations that would have actually occurred. In addition, future results may vary significantly from the results reflected in the pro forma information.
On April 1, 2019, we acquired RoseRock Healthcare ("RoseRock"), an Oklahoma based hospice provider, for a purchase price of $17.5 million. The purchase price was paid with cash on hand on the date of the transaction. We recorded goodwill ($15.8 million) and other intangibles including acquired names ($1.0 million) and non-compete agreements ($0.7 million). The acquired names and non-compete agreements will each be amortized over a weighted-average period of 3.0 years. RoseRock contributed approximately $6.8 million in net service revenue and $0.8 million in operating income for the year ended December 31, 2019. We expect the entire amount of goodwill recorded for this acquisition to be deductible for income tax purposes over approximately 15 years.
5. GOODWILL AND OTHER INTANGIBLE ASSETS, NET
During 2020, 2019 and 2018, we did not record any goodwill impairment charges as a result of our annual impairment test and none of the goodwill associated with our various reporting units was considered at risk of impairment as of October 31st of each respective year (the date of our annual goodwill impairment test). Since the date of our last annual goodwill impairment test, there have been no material developments, events, changes in operating performance or other circumstances that would cause management to believe it is more likely than not that the fair value of any of our reporting units would be less than their carrying amounts.
The following table summarizes the activity related to our goodwill for 2020 and 2019 (amounts in millions):
| Goodwill | |||||||||||||||||||||||
| Home Health | Hospice | Personal Care | Total | ||||||||||||||||||||
| Balances at December 31, 2018 (1) | $ | 87.1 | $ | 199.3 | $ | 43.1 | $ | 329.5 | |||||||||||||||
| Additions | 0 | 329.0 | 0 | 329.0 | |||||||||||||||||||
| Balances at December 31, 2019 | 87.1 | 528.3 | 43.1 | 658.5 | |||||||||||||||||||
| Additions | 3.3 | 270.9 | 0 | 274.2 | |||||||||||||||||||
| Balances at December 31, 2020 | $ | 90.4 | $ | 799.2 | $ | 43.1 | $ | 932.7 | |||||||||||||||
(1)Net of prior years' accumulated impairment losses of $733.7 million, which is inclusive of write-offs related to the sale and closure of care centers.
During 2020, we recorded a non-cash other intangible assets impairment charge of $4.2 million related to acquired names which are no longer in use; additionally, we recorded amortization of $2.4 million related to certificates of need and licenses associated with care centers that were closed. During 2019, we recorded a non-cash other intangible assets impairment charge of $1.5 million related to acquired names which are no longer in use or are associated with care centers that were closed.
77
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
The following table summarizes the activity related to our other intangible assets, net for 2020 and 2019 (amounts in millions):
| Other Intangible Assets, Net | |||||||||||||||||||||||||||||
| Certificates of Need and Licenses | Acquired Names -Unamortizable | Acquired Names -Amortizable (4) | Non-Compete Agreements (4) | Total | |||||||||||||||||||||||||
| Balances at December 31, 2018 (1) | $ | 23.9 | $ | 19.6 | $ | 0 | $ | 0.6 | $ | 44.1 | |||||||||||||||||||
| Additions | 13.7 | 0 | 10.0 | 5.2 | 28.9 | ||||||||||||||||||||||||
| Write-off (2) | 0 | (1.5) | 0 | 0 | (1.5) | ||||||||||||||||||||||||
| Amortization | 0 | 0 | (4.4) | (2.4) | (6.8) | ||||||||||||||||||||||||
| Balances at December 31, 2019 | 37.6 | 18.1 | 5.6 | 3.4 | 64.7 | ||||||||||||||||||||||||
| Additions | 11.8 | 0 | 7.0 | 11.5 | 30.3 | ||||||||||||||||||||||||
| Write-off (2) | 0 | (4.2) | 0 | 0 | (4.2) | ||||||||||||||||||||||||
| Amortization (3) | (2.4) | 0 | (7.1) | (7.1) | (16.6) | ||||||||||||||||||||||||
| Balances at December 31, 2020 | $ | 47.0 | $ | 13.9 | $ | 5.5 | $ | 7.8 | $ | 74.2 | |||||||||||||||||||
(1)Net of prior years' accumulated amortization of $0.7 million for non-compete agreements.
(2)Write-offs are related to our acquired names that are no longer in use or that were associated with care centers that are closed.
(3)Amortization of certificates of need and licenses is related to care centers that were closed during 2020.
(4)The weighted average remaining amortization period of our amortizable acquired names and non-compete agreements is 1.3 years and 1.2 years, respectively.
See Note 4 – Acquisitions for further details on additions to goodwill and other intangible assets, net.
The estimated aggregate amortization expense related to intangible assets for each of the five succeeding years is as follows (amounts in millions):
| Intangible Asset Amortization | |||||
| 2021 | $ | 10.6 | |||
| 2022 | 2.7 | ||||
| 2023 | 0 | ||||
| 2024 | 0 | ||||
| 2025 | 0 | ||||
| $ | 13.3 | ||||
78
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
6. DETAILS OF CERTAIN BALANCE SHEET ACCOUNTS
Additional information regarding certain balance sheet accounts is presented below (amounts in millions):
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Other current assets: | |||||||||||
| Payroll tax escrow | $ | 6.3 | $ | 1.5 | |||||||
| Income tax receivable | 0.2 | 2.0 | |||||||||
| Due from joint ventures | 2.3 | 2.0 | |||||||||
| Other | 4.5 | 2.7 | |||||||||
| $ | 13.3 | $ | 8.2 | ||||||||
| Other assets: | |||||||||||
| Workers’ compensation deposits | $ | 0.3 | $ | 0.2 | |||||||
| Health insurance deposits | 0.5 | 0.5 | |||||||||
| Other miscellaneous deposits | 1.2 | 1.0 | |||||||||
| Indemnity receivable | 13.6 | 13.6 | |||||||||
| Equity method investments | 14.2 | 35.7 | |||||||||
| Other | 3.4 | 3.6 | |||||||||
| $ | 33.2 | $ | 54.6 | ||||||||
| Accrued expenses: | |||||||||||
| Health insurance | $ | 15.1 | $ | 15.8 | |||||||
| Workers’ compensation | 35.8 | 33.4 | |||||||||
| Florida ZPIC audit, gross liability | 17.4 | 17.4 | |||||||||
| Legal settlements and other audits | 24.4 | 19.0 | |||||||||
| Income tax payable | 0 | 0.5 | |||||||||
| Charity care | 3.6 | 2.7 | |||||||||
| Estimated Medicare cap liability | 9.3 | 5.7 | |||||||||
| Hospice accruals (room and board, general in-patient and other) | 29.2 | 24.4 | |||||||||
| Patient liability | 8.4 | 9.4 | |||||||||
| Deferred operating income (CARES Act) | 11.6 | 0 | |||||||||
| Other | 11.4 | 8.8 | |||||||||
| $ | 166.2 | $ | 137.1 | ||||||||
| Other long-term obligations: | |||||||||||
| Reserve for uncertain tax positions | $ | 3.3 | $ | 3.1 | |||||||
| Deferred compensation plan liability | 1.0 | 1.0 | |||||||||
| Non-current social security taxes (deferred under CARES Act) | 27.7 | 0 | |||||||||
| Other | 1.6 | 1.8 | |||||||||
| $ | 33.6 | $ | 5.9 | ||||||||
7. LEASES
We determine whether an arrangement is a lease at inception. We have operating leases, primarily for offices and fleet, that expire at various dates over the next eight years. We also have finance leases covering certain office equipment that expire at various dates over the next three years. Our leases do not contain any restrictive covenants.
Our office leases generally contain renewal options for periods ranging from one to five years. Because we are not reasonably certain to exercise these renewal options, the options are not considered in determining the lease term, and payments associated with the option years are excluded from lease payments. Our office leases also generally include termination options, which allow for early termination of the lease after the first one to three years. Because we are not reasonably certain to exercise these termination options, the options are not considered in determining the lease term; payments for the full lease term are included in lease payments. Our office leases do not contain any material residual value guarantees.
Our fleet leases include a term of 367 days with monthly renewal options thereafter. Our fleet leases also include terminal rental adjustment clauses (“TRAC”), which provide for a final rental payment adjustment at the end of the lease, typically based on the amount realized from the sale of the vehicle. The TRAC is structured such that it will almost always result in a significant
79
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
payment by us to the lessor if the renewal option is not exercised. Based on the significance of the TRAC adjustment at the initial lease expiration, we believe that it is reasonably certain that we will exercise the monthly renewal options; therefore, the renewal options are considered in determining the lease term, and payments associated with the renewal options are included in lease payments.
For our fleet and office equipment leases, we use the implicit rate in the lease as the discount rate. For our office leases, the implicit rate is typically not available, so we use our incremental borrowing rate as the discount rate. Our lease agreements include both lease and non-lease components. We have elected the practical expedient that allows us to not separate lease and non-lease components for all of our leases.
Payments due under our operating and finance leases include fixed payments as well as variable payments. For our office leases, variable payments include amounts for our proportionate share of operating expenses, utilities, property taxes, insurance, common area maintenance and other facility-related expenses. For our vehicle and equipment leases, variable payments consist of sales tax.
The components of lease cost for the years ended December 31, 2020 and 2019 are as follows (amounts in millions):
| For the Years Ended December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Operating lease cost: | |||||||||||
| Operating lease cost | $ | 38.6 | $ | 35.0 | |||||||
| Impairment of operating lease ROU assets | 0.5 | 0.9 | |||||||||
| Total operating lease cost | 39.1 | 35.9 | |||||||||
| Finance lease cost: | |||||||||||
| Amortization of ROU assets | 2.0 | 1.7 | |||||||||
| Interest on lease liabilities | 0.2 | 0.2 | |||||||||
| Total finance lease cost | 2.2 | 1.9 | |||||||||
| Variable lease cost | 3.0 | 2.6 | |||||||||
| Short-term lease cost | 0 | 0.2 | |||||||||
| Total lease cost | $ | 44.3 | $ | 40.6 | |||||||
Amounts reported in the consolidated balance sheets as of December 31, 2020 and 2019 for our operating leases are as follows (amounts in millions):
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Operating lease ROU assets | $ | 93.4 | $ | 84.8 | |||||||
| Current portion of operating lease liabilities | 30.0 | 27.8 | |||||||||
| Operating lease liabilities, less current portion | 62.0 | 56.1 | |||||||||
| Total operating lease liabilities | $ | 92.0 | $ | 83.9 | |||||||
Amounts reported in the consolidated balance sheets as of December 31, 2020 and 2019 for finance leases are included in the table below. The finance lease ROU assets are recorded within property and equipment, net of accumulated depreciation within our consolidated balance sheets. The finance lease liabilities are recorded within current portion of long-term obligations and long-term obligations, less current portion within our consolidated balance sheets.
80
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Finance lease ROU assets | $ | 5.9 | $ | 5.2 | |||||||
| Accumulated amortization | (3.3) | (1.8) | |||||||||
| Finance lease ROU assets, net | $ | 2.6 | $ | 3.4 | |||||||
| Current installments of obligations under finance leases | $ | 1.7 | $ | 1.7 | |||||||
| Long-term portion of obligations under finance leases | 0.9 | 1.7 | |||||||||
| Total finance lease liabilities | $ | 2.6 | $ | 3.4 | |||||||
Supplemental cash flow information and non-cash activity related to our leases are as follows (amounts in millions):
| For the Years Ended December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Cash paid for amounts included in the measurement of lease liabilities and ROU assets: | |||||||||||
| Operating cash flow from operating leases | $ | (38.2) | $ | (35.8) | |||||||
| Financing cash flow from finance leases | (2.0) | (1.7) | |||||||||
| ROU assets obtained in exchange for lease obligations: | |||||||||||
| Operating leases | 38.5 | 116.0 | |||||||||
| Finance leases | 1.2 | 2.9 | |||||||||
| Reductions to ROU assets resulting from reductions to lease obligations: | |||||||||||
| Operating leases | (1.1) | (1.7) | |||||||||
| Finance leases | 0 | 0 | |||||||||
Amounts disclosed for ROU assets obtained in exchange for lease obligations include amounts added to the carrying amount of ROU assets resulting from lease modifications and reassessments.
Weighted average remaining lease terms and discount rates for our leases as of December 31, 2020 and 2019 are as follows:
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Weighted average remaining lease term (years): | |||||||||||
| Operating leases | 3.7 | 3.9 | |||||||||
| Finance leases | 1.7 | 2.1 | |||||||||
| Weighted average discount rate: | |||||||||||
| Operating leases | 3.1 | % | 3.9 | % | |||||||
| Finance leases | 5.3 | % | 5.3 | % | |||||||
81
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Maturities of lease liabilities as of December 31, 2020 are as follows (amounts in millions):
| Operating Leases | Finance Leases | ||||||||||
| 2021 | $ | 32.2 | $ | 1.8 | |||||||
| 2022 | 25.3 | 0.7 | |||||||||
| 2023 | 17.6 | 0.2 | |||||||||
| 2024 | 11.7 | 0 | |||||||||
| 2025 | 6.2 | 0 | |||||||||
| Thereafter | 4.6 | 0 | |||||||||
| Total undiscounted lease payments | 97.6 | 2.7 | |||||||||
| Less: Imputed interest | (5.6) | (0.1) | |||||||||
| Total lease liabilities | $ | 92.0 | $ | 2.6 | |||||||
8. LONG-TERM OBLIGATIONS
Long-term debt consists of the following for the periods indicated (amounts in millions):
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| $175.0 million Term Loan; interest rate at Base Rate plus Applicable Rate or Eurodollar Rate plus the Applicable Rate (1.7% at December 31, 2020); due February 4, 2024 | $ | 164.1 | $ | 171.7 | |||||||
| $550.0 million Revolving Credit Facility; interest only payments; interest rate at Base Rate plus Applicable Rate or Eurodollar Rate plus the Applicable Rate (3.8% at December 31, 2020); due February 4, 2024 | 51.0 | 70.0 | |||||||||
| Promissory notes | 0 | 0.6 | |||||||||
| Finance leases | 2.6 | 3.4 | |||||||||
| Principal amount of long-term obligations | 217.7 | 245.7 | |||||||||
| Deferred debt issuance costs | (2.7) | (3.5) | |||||||||
| 215.0 | 242.2 | ||||||||||
| Current portion of long-term obligations | (10.5) | (9.9) | |||||||||
| Total | $ | 204.5 | $ | 232.3 | |||||||
Maturities of debt as of December 31, 2020 are as follows (amounts in millions):
| Long-term obligations | |||||
| 2021 | $ | 10.5 | |||
| 2022 | 9.4 | ||||
| 2023 | 12.3 | ||||
| 2024 | 185.5 | ||||
| 2025 | 0 | ||||
| $ | 217.7 | ||||
Credit Agreement
On June 29, 2018, we entered into our Amended and Restated Credit Agreement ("Credit Agreement") which provided for a senior secured revolving credit facility in an initial aggregate principal amount of up to $550.0 million (the "Revolving Credit Facility"). The Revolving Credit Facility provided for and included within its $550.0 million limit a $25.0 million swingline facility and commitments for up to $60.0 million in letters of credit. Upon lender approval, we could increase the aggregate loan amount under the Revolving Credit Facility by $125.0 million plus an unlimited amount subject to a leverage limit of 0.5x under the maximum allowable consolidated leverage ratio which was 3.0x per the Credit Agreement.
The final maturity of the Revolving Credit Facility was June 29, 2023 and there was no mandatory amortization on the outstanding principal balances which were payable in full upon maturity. The Revolving Credit Facility was used to provide
82
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
ongoing working capital and for general corporate purposes of the Company and our subsidiaries, including permitted acquisitions, as defined in the Credit Agreement.
First Amendment to Amended and Restated Credit Agreement
On February 4, 2019, we entered into the First Amendment to the Credit Agreement (as amended by the First Amendment, the “Amended Credit Agreement”). The Amended Credit Agreement provides for a senior secured credit facility in an initial aggregate principal amount of up to $725.0 million, which includes the $550.0 million Revolving Credit Facility under the Credit Agreement, and a term loan facility with a principal amount of up to $175.0 million (the “Term Loan Facility” and collectively with the Revolving Credit Facility, the “Credit Facility”), which was added by the First Amendment.
We borrowed the entire principal amount of the Term Loan Facility on February 4, 2019 in order to fund a portion of the purchase price of the CCH acquisition, with the remainder of the purchase price and associated transactional fees and expenses funded by proceeds from the Revolving Credit Facility.
The loans issued under the Credit Facility bear interest on a per annum basis, at our election, at either: (i) the Base Rate plus the Applicable Rate or (ii) the Eurodollar Rate plus the Applicable Rate. The “Base Rate” means a fluctuating rate per annum equal to the highest of (a) the federal funds rate plus 0.50% per annum, (b) the prime rate of interest established by the Administrative Agent, and (c) the Eurodollar Rate plus 1% per annum. The “Eurodollar Rate” means the quoted rate per annum equal to the London Interbank Offered Rate ("LIBOR") or a comparable successor rate approved by the Administrative Agent for an interest period of one, two, three or six months (as selected by us). The “Applicable Rate” is based on the consolidated leverage ratio and is presented in the table below. As of December 31, 2020, the Applicable Rate is 0.25% per annum for Base Rate Loans and 1.25% per annum for Eurodollar Rate Loans. We are also subject to a commitment fee and letter of credit fee under the terms of the Amended Credit Agreement, as presented in the table below.
| Pricing Tier | Consolidated Leverage Ratio | Base Rate Loans | Eurodollar Rate Loans | Commitment Fee | Letter of Credit Fee | ||||||||||||||||||||||||
| I | ≥ 3.00 to 1.0 | 1.00 | % | 2.00 | % | 0.35 | % | 1.75 | % | ||||||||||||||||||||
| II | < 3.00 to 1.0 but ≥ 2.00 to 1.0 | 0.75 | % | 1.75 | % | 0.30 | % | 1.50 | % | ||||||||||||||||||||
| III | < 2.00 to 1.0 but ≥ 0.75 to 1.0 | 0.50 | % | 1.50 | % | 0.25 | % | 1.25 | % | ||||||||||||||||||||
| IV | < 0.75 to 1.0 | 0.25 | % | 1.25 | % | 0.20 | % | 1.00 | % | ||||||||||||||||||||
The final maturity date of the Credit Facility is February 4, 2024. The Revolving Credit Facility will terminate and be due and payable as of the final maturity date. The Term Loan Facility, however, is subject to quarterly amortization of principal in the amount of (i) 0.625% for the period commencing on February 4, 2019 and ending on March 31, 2020, (ii) 1.250% for the period commencing on April 1, 2020 and ending on March 31, 2023, and (iii) 1.875% for the period commencing on April 1, 2023 and ending on February 4, 2024. The remaining balance of the Term Loan Facility must be paid upon the final maturity date. In addition to the scheduled amortization of the Term Loan Facility, and subject to customary exceptions and reinvestment rights, we are required to prepay the Term Loan Facility, first, and the Revolving Credit Facility, second, with 100% of all net cash proceeds received by any loan party or any subsidiary thereof in connection with (a) any asset sale or disposition where such loan party receives net cash proceeds in excess of $5 million or (b) any debt issuance that is not permitted under the Amended Credit Agreement.
The Amended Credit Agreement requires maintenance of two financial covenants: (i) a consolidated leverage ratio of funded indebtedness to Earnings Before Interest, Taxes, Depreciation and Amortization ("EBITDA"), as defined in the Amended Credit Agreement, and (ii) a consolidated interest coverage ratio of EBITDA to cash interest charges, as defined in the Amended Credit Agreement. Each of these covenants is calculated over rolling four-quarter periods and also is subject to certain exceptions and baskets. The Amended Credit Agreement also contains customary covenants, including, but not limited to, restrictions on: incurrence of liens, incurrence of additional debt, sales of assets and other fundamental corporate changes, investments, and declarations of dividends. These covenants contain customary exclusions and baskets as detailed in the Amended Credit Agreement. In connection with our entry into the Amended Credit Agreement, we recorded $0.8 million in deferred debt issuance costs as long-term obligations, less current portion within our consolidated balance sheet during the year ended December 31, 2019.
The Revolving Credit Facility is guaranteed by substantially all of our wholly-owned direct and indirect subsidiaries. The Amended Credit Agreement requires at all times that we (i) provide guarantees from wholly-owned subsidiaries that in the aggregate represent not less than 95% of our consolidated net revenues and adjusted EBITDA from all wholly-owned subsidiaries and (ii) provide guarantees from subsidiaries that in the aggregate represent not less than 70% of consolidated adjusted EBITDA, subject to certain exceptions.
83
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Our weighted average interest rate for borrowings under our $175.0 million Term Loan Facility was 2.2% for the period ended December 31, 2020 and 3.8% for the period February 4, 2019 to December 31, 2019. Our weighted average interest rate for borrowings under our $550.0 million Revolving Credit Facility was 2.2% for the period ended December 31, 2020 and 4.0% for the period ended December 31, 2019.
As of December 31, 2020, our consolidated leverage ratio was 0.6, our consolidated interest coverage ratio was 25.6 and we are in compliance with our covenants under the Amended Credit Agreement. In the event we are not in compliance with our debt covenants in the future, we would pursue various alternatives in an attempt to successfully resolve the non-compliance, which might include, among other things, seeking debt covenant waivers or amendments.
As of December 31, 2020, our availability under our $550.0 million Revolving Credit Facility was $470.2 million as we have $51.0 million outstanding in borrowings and $28.8 million outstanding in letters of credit.
Joinder Agreement
In connection with the CCH acquisition, we entered into a Joinder Agreement, dated as of February 4, 2019 (the “CCH Joinder”), pursuant to which CCH and its subsidiaries were made parties to, and became subject to the terms and conditions of, the Amended Credit Agreement, the Amended and Restated Security Agreement, dated as of June 29, 2018 (the “Amended and Restated Security Agreement”), and the Amended and Restated Pledge Agreement, dated as of June 29, 2018 (the “Amended and Restated Pledge Agreement”). In connection with the AseraCare acquisition, we entered into a Joinder Agreement, dated as of June 12, 2020, pursuant to which the AseraCare entities were made parties to, and became subject to the terms and conditions of, the Amended Credit Agreement, the Amended and Restated Security Agreement and the Amended and Restated Pledge Agreement (the “AseraCare Joinder,” and together with the CCH Joinder, the “Joinders”). Pursuant to the Joinders, the Amended and Restated Security Agreement and the Amended and Restated Pledge Agreement, CCH and its subsidiaries and the AseraCare entities granted in favor of the Administrative Agent a first lien security interest in substantially all of their personal property assets and pledged to the Administrative Agent each of their respective subsidiaries' issued and outstanding equity interests. CCH and its subsidiaries and the AseraCare entities also guaranteed our obligations, whether now existing or arising after the respective effective dates of the Joinders, under the Amended Credit Agreement pursuant to the terms of the Joinders and the Amended Credit Agreement.
Finance Leases
Our finance leases outstanding of $2.6 million relate to leased equipment and bear interest rates ranging from 5.3% to 5.8%.
9. INCOME TAXES
Income taxes attributable to continuing operations consist of the following (amounts in millions):
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Current income tax expense/(benefit): | |||||||||||||||||
| Federal | $ | 41.6 | $ | 24.2 | $ | 16.4 | |||||||||||
| State and local | 10.6 | 4.8 | 2.1 | ||||||||||||||
| 52.2 | 29.0 | 18.5 | |||||||||||||||
| Deferred income tax expense/(benefit): | |||||||||||||||||
| Federal | (22.5) | 9.5 | 14.5 | ||||||||||||||
| State and local | (4.1) | 4.0 | 5.8 | ||||||||||||||
| (26.6) | 13.5 | 20.3 | |||||||||||||||
| Income tax expense | $ | 25.6 | $ | 42.5 | $ | 38.8 | |||||||||||
84
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Total income tax expense for the years ended December 31, 2020, 2019 and 2018 was allocated as follows (amounts in millions):
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Income from continuing operations | $ | 25.6 | $ | 42.5 | $ | 38.8 | |||||||||||
| Interest expense | 0.2 | 0.3 | 0.1 | ||||||||||||||
| Goodwill | 0 | 0.9 | 0 | ||||||||||||||
| Total | $ | 25.8 | $ | 43.7 | $ | 38.9 | |||||||||||
A reconciliation of significant differences between the reported amount of income tax expense and the expected amount of income tax expense that would result from applying the U.S. federal statutory income tax rate of 21% to income before income taxes is as follows:
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Income tax expense at U.S. federal statutory rate | 21.0 | % | 21.0 | % | 21.0 | % | |||||||||||
| State and local income taxes, net of federal income tax benefit (1) | 2.4 | 4.8 | 4.8 | ||||||||||||||
| Excess tax benefits from share-based compensation (1) | (12.7) | (2.2) | (1.8) | ||||||||||||||
| Non-deductible executive compensation | 2.1 | 1.6 | 0.4 | ||||||||||||||
| Other items, net (2) | (0.6) | (0.3) | 0 | ||||||||||||||
| Income tax expense | 12.2 | % | 24.9 | % | 24.4 | % | |||||||||||
(1)On August 10, 2020, Paul B. Kusserow, President, Chief Executive Officer and Chairman of the Board of Amedisys, exercised 500,000 stock options previously awarded to him under our 2008 Omnibus Incentive Compensation Plan. We recognize compensation expense for stock option awards on a straight-line basis over the requisite service period for each separately vesting portion of the award in accordance with ASC 718, Compensation: Stock Compensation; however, the income tax deduction related to stock options is not recognized until the stock option exercise date. As a result, for awards that are expected to result in a tax deduction, a deferred tax asset is created as the entity recognizes compensation expense for U.S. GAAP purposes. If the tax deduction exceeds the cumulative U.S. GAAP compensation expense for the award, the tax benefit associated with any excess deduction is recognized as an income tax benefit in the statement of operations, resulting in a reduction of the effective tax rate. Mr. Kusserow's stock option exercise produced a $92.1 million tax deduction in excess of U.S. GAAP compensation expense, resulting in a $19.4 million federal income tax benefit and a $4.6 million state and local income tax benefit for the year ended December 31, 2020.
(2)Includes various items such as non-deductible expenses, non-taxable income, tax credits, valuation allowance, uncertain tax positions and return-to-accrual adjustments.
As of December 31, 2020 and 2019, the Company had income taxes receivable of $0.2 million and $2.0 million, respectively, included in other current assets within our consolidated balance sheets.
85
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Deferred tax assets (liabilities) consist of the following components (amounts in millions):
| As of December 31, | |||||||||||
| 2020 | 2019 | ||||||||||
| Deferred tax assets: | |||||||||||
| Accrued payroll & employee benefits | $ | 15.9 | $ | 15.1 | |||||||
| Workers’ compensation | 9.6 | 9.0 | |||||||||
| Share-based compensation | 5.1 | 7.9 | |||||||||
| Legal & compliance matters | 7.0 | 4.8 | |||||||||
| Lease liability | 25.2 | 23.1 | |||||||||
| Provider relief fund advance (1) | 15.6 | 0 | |||||||||
| Deferred social security taxes (2) | 14.3 | 0 | |||||||||
| Net operating loss carryforwards | 2.4 | 3.7 | |||||||||
| Tax credit carryforwards | 2.9 | 3.1 | |||||||||
| Other | 0.6 | 0.5 | |||||||||
| Gross deferred tax assets | 98.6 | 67.2 | |||||||||
| Less: valuation allowance | (0.1) | (0.4) | |||||||||
| Net deferred tax assets | 98.5 | 66.8 | |||||||||
| Deferred tax liabilities: | |||||||||||
| Property and equipment | (3.8) | (4.3) | |||||||||
| Amortization of intangible assets | (11.8) | (0.3) | |||||||||
| Deferred revenue | (9.0) | (13.5) | |||||||||
| Investment in partnerships | 0 | (3.3) | |||||||||
| Right-of-use asset | (24.9) | (22.8) | |||||||||
| Other liabilities | (1.0) | (1.2) | |||||||||
| Gross deferred tax liabilities | (50.5) | (45.4) | |||||||||
| Deferred income taxes | $ | 48.0 | $ | 21.4 | |||||||
(1)In April 2020, approximately $100 million was provided to the Company through the healthcare Provider Relief Fund established under the CARES Act. As of December 31, 2020, the Company recorded a liability related to the funds that we do not expect to utilize totaling $60 million, which is reflected in the Provider Relief Fund Advance account in current liabilities within our consolidated balance sheet. For income tax purposes, the Company recognized the $60 million as income upon receipt, resulting in a deferred tax asset as of December 31, 2020. The company will recognize an income tax deduction when the liability is paid during the year ended December 31, 2021.
(2)The CARES Act provides for the deferral of the employer share of social security tax (6.2%), effective for payments due after the enactment date through December 31, 2020. Fifty percent of the deferred payroll taxes are due on December 31, 2021 with the remaining amounts due on December 31, 2022. As of December 31, 2020, the Company has deferred $55.4 million of social security tax payments; $27.7 million of this amount is reflected in each payroll and employee benefits and other long-term obligations within our consolidated balance sheet. For income tax purposes, the deferred social security taxes will be deductible when paid on December 31, 2021 and December, 31, 2022, resulting in a deferred tax asset at December 31, 2020.
As of December 31, 2020, we have state net operating loss ("NOL") carryforwards of $47.5 million that are available to reduce future taxable income and $3.7 million of various state tax credits available to reduce future state income taxes. The state NOL and tax credit carryforwards expire at various times.
As of December 31, 2020 and 2019, the valuation allowance for deferred tax assets, which is primarily related to certain state NOLs and state tax credit carryforwards, was $0.1 million and $0.4 million, respectively. The net change in the total valuation allowance for the years ended December 31, 2020 and 2019 was a decrease of $0.3 million.
In assessing the realizability of deferred tax assets, management considers whether it is more likely than not that some portion or all of the deferred tax assets will not be realized. The ultimate realization of deferred tax assets is dependent upon the generation of future taxable income in those jurisdictions during the periods in which those temporary differences become deductible. Management considers the scheduled reversal of deferred tax liabilities (including the impact of available carryback and carryforward periods), projected future taxable income, and tax-planning strategies in making this assessment. In order to fully realize the deferred tax assets, the Company will need to generate future taxable income before the expiration of the
86
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
carryforwards governed by the tax code. Based on the current level of pretax earnings, the Company will generate the minimum amount of future taxable income needed to support the realization of the deferred tax assets. As a result, as of December 31, 2020, management believes that it is more likely than not that we will realize the benefits of these deferred tax assets, net of the existing valuation allowances. The amount of the deferred tax asset considered realizable, however, could be reduced in the near term if estimates of future taxable income during the carryforward period are reduced.
Uncertain Tax Positions
We account for uncertain tax positions in accordance with the authoritative guidance for uncertain tax positions. A reconciliation of the beginning and ending amount of unrecognized tax benefits is as follows (amounts in millions):
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Balance at beginning of period | $ | 2.7 | $ | 2.7 | $ | 2.7 | |||||||||||
| Additions for tax positions related to current year | 0 | 0 | 0 | ||||||||||||||
| Additions for tax positions related to prior year | 0 | 0 | 0 | ||||||||||||||
| Reductions for tax positions related to prior years | 0 | 0 | 0 | ||||||||||||||
| Lapse of statute of limitations | 0 | 0 | 0 | ||||||||||||||
| Settlements | 0 | 0 | 0 | ||||||||||||||
| Balance at end of period | $ | 2.7 | $ | 2.7 | $ | 2.7 | |||||||||||
As of December 31, 2020 and 2019, there is $2.7 million of unrecognized tax benefits recorded in other long-term obligations within the consolidated balance sheets that, if recognized in future periods, would impact our effective tax rate.
We recognized $0.2 million, $0.3 million and $0.1 million of interest as components of interest expense in connection with our reserve for uncertain tax positions during the years ended December 31, 2020, 2019 and 2018, respectively. Interest related to uncertain tax positions included in the consolidated balance sheets at December 31, 2020 and 2019 was $0.6 million and $0.4 million, respectively.
We are subject to income taxes in the U.S. and in many individual states, with significant operations in Louisiana, South Carolina, Alabama, Georgia, Massachusetts and Tennessee. We are open to examination in the U.S. and in various individual states for tax years ended December 31, 2014 through December 31, 2020. We are also open to examination in various states for the years ended 2007 through 2020 resulting from NOLs generated and available for carryforward from those years.
10. CAPITAL STOCK AND SHARE-BASED COMPENSATION
We are authorized by our Certificate of Incorporation to issue 60,000,000 shares of common stock, $0.001 par value and 5,000,000 shares of preferred stock, $0.001 par value. As of December 31, 2020, there were 37,470,212 and 32,814,278 shares of common stock issued and outstanding, respectively, and 0 shares of preferred stock issued or outstanding. Our Board of Directors is authorized to fix the dividend rights and terms, conversion and voting rights, redemption rights and other privileges and restrictions applicable to our preferred stock.
87
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Share-Based Awards
On March 29, 2018, our Board of Directors and the Compensation Committee approved, subject to stockholder approval, the Amedisys, Inc. 2018 Omnibus Incentive Compensation Plan (the “2018 Plan”). On June 6, 2018, our stockholders approved the 2018 Plan at the Company's annual meeting of stockholders. The 2018 Plan replaces our 2008 Omnibus Incentive Compensation Plan (the “2008 Plan”), which terminated on June 6, 2018 when the stockholders approved the 2018 Plan. The 2018 Plan authorizes the grant of various types of equity-based awards, such as stock awards, restricted stock units, stock appreciation rights and stock options to eligible participants, which include all of our employees and all employees of our 50% or more owned subsidiaries, our non-employee directors and certain consultants. The vesting terms of the awards may be tied to continued employment (or, for our non-employee directors, continued service on the Board of Directors) and/or achievement of certain pre-determined performance goals. We refer to stock awards subject to service-based vesting conditions as “non-vested stock” and restricted stock units subject to service-based or a combination of service-based and performance-based vesting conditions as “non-vested stock units.” The 2018 Plan is administered by the Compensation Committee of our Board of Directors, which determines, within the provisions of the 2018 Plan, those eligible participants to whom, and the times at which, awards shall be granted. The Compensation Committee, in its discretion, may delegate its authority and duties under the 2018 Plan to specified officers; however, only the Compensation Committee may approve the terms of awards to our executive officers.
Equity-based awards may be granted for a number of shares not to exceed, in the aggregate, approximately 2.5 million shares of common stock. We had approximately 2.0 million shares available at December 31, 2020. The price per share for stock options shall be no less than the greater of (a) 100% of the fair value of a share of common stock on the date the option is granted or (b) the aggregate par value of the shares of our common stock on the date the option is granted. If a stock option is granted to any owner of 10% or more of the total combined voting power of us and our subsidiaries, the price is to be at least 110% of the fair value of a share of our common stock on the date the award is granted. Each equity-based award vests ratably over a one year to four year period, with the exception of those issued under contractual arrangements that specify otherwise, and may be exercised during a period as determined by our Compensation Committee or as otherwise approved by our Compensation Committee. The contractual terms of stock options exercised shall not exceed ten years from the date such option is granted. The Company analyzes historical data of forfeited awards to develop an estimated forfeiture rate that is applied to the Company's non-cash compensation expense; however, all non-cash compensation expense is adjusted to reflect actual vestings and forfeitures.
Employee Stock Purchase Plan (“ESPP”)
We have a plan whereby our eligible employees may purchase our common stock at 85% of the market price at the time of purchase. On June 7, 2012, our stockholders ratified an amendment adopted by our Board of Directors to increase the total number of shares of our common stock authorized for issuance under our ESPP from 2,500,000 shares to 4,500,000 shares, and as of December 31, 2020, there were 1,328,627 shares available for future issuance. The following is a detail of the purchases that were made under the plan:
| Employee Stock Purchase Plan Period | Shares Issued | Price | |||||||||
| 2018 and Prior | 3,122,983 | $ | 15.92 | ||||||||
| January 1, 2019 to March 31, 2019 | 7,181 | 104.77 | |||||||||
| April 1, 2019 to June 30, 2019 | 8,230 | 103.20 | |||||||||
| July 1, 2019 to September 30, 2019 | 7,216 | 111.36 | |||||||||
| October 1, 2019 to December 31, 2019 | 6,063 | 141.88 | |||||||||
| January 1, 2020 to March 31, 2020 | 5,295 | 156.01 | |||||||||
| April 1, 2020 to June 30, 2020 | 5,414 | 168.76 | |||||||||
| July 1, 2020 to September 30, 2020 | 4,789 | 200.97 | |||||||||
| October 1, 2020 to December 31, 2020 | 4,202 | 249.33 | |||||||||
| 3,171,373 | |||||||||||
ESPP expense included in general and administrative expense in our accompanying consolidated statements of operations was $0.6 million, $0.6 million and $0.5 million for 2020, 2019 and 2018, respectively.
88
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Stock Options
On August 10, 2020, Paul B. Kusserow, President, Chief Executive Officer and Chairman of the Board of Amedisys, exercised 500,000 stock options previously awarded to him under the 2008 Plan. In connection with the exercise, Mr. Kusserow surrendered 231,683 shares of common stock to us to satisfy tax withholding and strike price obligations and elected to hold the net 268,317 shares issued to him. The surrendered shares are classified as treasury shares. This transaction resulted in a cash outflow of $40.4 million, reflected within financing activities in our consolidated statement of cashflows, related to the remittance of tax withholding obligations. In addition, Mr. Kusserow's stock option exercise resulted in a $24.0 million income tax benefit that was recorded in our consolidated statement of operations during the year ended December 31, 2020. We recognize compensation expense for stock option awards on a straight-line basis over the requisite service period for each separately vesting portion of the award in accordance with ASC 718, Compensation: Stock Compensation; however, the income tax deduction related to stock options is not recognized until the stock option exercise date. As a result, for awards that are expected to result in a tax deduction, a deferred tax asset is created as the entity recognizes compensation expense for U.S. GAAP purposes. If the tax deduction exceeds the cumulative U.S. GAAP compensation expense for the award, the tax benefit associated with any excess deduction is recognized as an income tax benefit in the statement of operations.
We use the Black-Scholes option pricing model to estimate the fair value of our stock options. There were 43,249, 142,122 and 163,666 options granted during 2020, 2019 and 2018, respectively. Stock option compensation expense included in general and administrative expense in our accompanying consolidated statements of operations was $4.3 million, $6.2 million and $5.7 million for 2020, 2019 and 2018, respectively.
The fair values of the awards were estimated using the following assumptions for 2020, 2019 and 2018:
| For the Years Ended December 31, | |||||||||||||||||
| 2020 | 2019 | 2018 | |||||||||||||||
| Risk Free Rate | 0.38% - 1.51% | 1.44% - 2.53% | 2.56% - 3.04% | ||||||||||||||
| Expected Volatility | 40.15% - 42.80% | 42.46% - 43.83% | 42.00% - 45.32% | ||||||||||||||
| Expected Term | 6.25 years | 6.00 - 6.25 years | 4.12 - 6.25 years | ||||||||||||||
| Weighted Average Fair Value | $86.72 | $54.42 | $42.48 | ||||||||||||||
| Dividend Yield | 0% | 0% | 0% | ||||||||||||||
We used the simplified method to estimate the expected term for the stock options granted during 2020, 2019 and 2018 as adequate historical experience is not available to provide a reasonable estimate.
The following table presents our stock option activity for 2020:
| Number of Shares | Weighted Average Exercise Price | Weighted Average Contractual Life (Years) | |||||||||||||||
| Outstanding options at January 1, 2020 | 875,974 | $ | 49.62 | 6.26 | |||||||||||||
| Granted | 43,249 | 209.41 | |||||||||||||||
| Exercised | (622,829) | 31.60 | |||||||||||||||
| Canceled, forfeited or expired | (18,353) | 103.89 | |||||||||||||||
| Outstanding options at December 31, 2020 | 278,041 | $ | 111.27 | 7.68 | |||||||||||||
| Exercisable options at December 31, 2020 | 89,429 | $ | 76.40 | 6.75 | |||||||||||||
The aggregate intrinsic value of our outstanding options and exercisable options at December 31, 2020 was $50.6 million and $19.4 million, respectively. Total intrinsic value of options exercised was $121.1 million, $7.3 million and $9.7 million for 2020, 2019 and 2018, respectively. The tax benefit from stock options exercised during the period amounted to $27.9 million, $1.3 million and $1.6 million for 2020, 2019 and 2018, respectively.
89
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
The following table presents our non-vested stock option activity for 2020:
| Number of Shares | Weighted Average Grant Date Fair Value | ||||||||||
| Non-vested stock options at January 1, 2020 | 305,750 | $ | 41.66 | ||||||||
| Granted | 43,249 | 86.72 | |||||||||
| Vested | (142,233) | 34.84 | |||||||||
| Forfeited | (18,154) | 47.66 | |||||||||
| Non-vested stock options at December 31, 2020 | 188,612 | $ | 56.55 | ||||||||
At December 31, 2020, there was $4.8 million of unrecognized compensation cost related to stock options that we expect to be recognized over a weighted-average period of 1.9 years.
Non-Vested Stock
We issue shares of non-vested stock with a vesting term of one year. The compensation expense is determined based on the market price of our common stock at the date of grant applied to the total number of shares that are anticipated to fully vest. Non-vested stock compensation expense included in general and administrative expenses in our accompanying consolidated statements of operations was $0.8 million, $1.2 million and $1.4 million for 2020, 2019 and 2018, respectively.
The following table presents our non-vested stock activity for 2020:
| Number of Shares | Weighted Average Grant Date Fair Value | ||||||||||
| Non-vested stock at January 1, 2020 | 9,859 | $ | 119.12 | ||||||||
| Granted | 1,560 | 158.72 | |||||||||
| Vested | (11,419) | 124.53 | |||||||||
| Canceled, forfeited or expired | 0 | 0 | |||||||||
| Non-vested stock at December 31, 2020 | 0 | $ | 0 | ||||||||
The weighted average grant date fair value of non-vested stock granted was $158.72, $119.12 and $80.54 in 2020, 2019 and 2018, respectively.
At December 31, 2020, there was no unrecognized compensation cost related to non-vested stock awards; we currently do not have any outstanding awards.
Non-Vested Stock Units
We issue non-vested stock unit awards that are service-based, performance-based or a combination of both with vesting terms ranging from one to four years. Based on the terms and conditions of these awards, we determine if the awards should be recorded as either equity or liability instruments. The compensation expense is determined based on the market price of our common stock at the date of grant, applied to the total number of units that are anticipated to vest, unless the award specifies differently. We account for such awards similar to our non-vested stock awards; however, no shares of stock are issued to the recipient until the stock unit awards have vested and after the pre-determined delivery date has occurred.
Non-Vested Stock Units – Service-Based
Service-based non-vested stock unit compensation expense included in general and administrative expenses in our accompanying consolidated statements of operations was $7.5 million, $8.7 million and $4.5 million for 2020, 2019 and 2018, respectively.
90
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
The following table presents our service-based non-vested stock units activity for 2020:
| Number of Shares | Weighted Average Grant Date Fair Value | ||||||||||
| Non-vested stock units at January 1, 2020 | 231,418 | $ | 91.87 | ||||||||
| Granted | 34,429 | 206.10 | |||||||||
| Vested | (89,074) | 78.15 | |||||||||
| Canceled, forfeited or expired | (19,227) | 97.36 | |||||||||
| Non-vested stock units at December 31, 2020 | 157,546 | $ | 123.92 | ||||||||
The weighted average grant date fair value of service-based non-vested stock units granted was $206.10, $123.70 and $95.14 in 2020, 2019 and 2018, respectively.
At December 31, 2020, there was $9.3 million of unrecognized compensation cost related to our service-based non-vested stock units that we expect to be recognized over a weighted average period of 1.8 years.
Non-Vested Stock Units – Service-Based and Performance-Based Awards
During 2020, we awarded performance-based awards to certain employees. The target level established by the award, which is based on the Company’s 2020 adjusted earnings before interest, taxes, depreciation and amortization (“Adjusted EBITDA”), provided for the recipients to receive an aggregate of 81,183 non-vested stock units if the target was achieved. For a select group of employees, if the target objective is surpassed to the point of achieving the projected maximum payout, the recipients will receive an additional aggregate of 11,633 non-vested stock units during the three-month period ending March 31, 2021. The target number of shares to be potentially awarded has been reduced by forfeitures as indicated in the table below. Performance-based non-vested stock units compensation expense included in general and administrative expenses in our consolidated statements of operations was $13.5 million, $8.4 million and $5.8 million for 2020, 2019 and 2018, respectively.
The following table presents our performance-based non-vested stock units activity for 2020:
| Number of Shares | Weighted Average Grant Date Fair Value | ||||||||||
| Non-vested stock units at January 1, 2020 | 207,424 | $ | 97.55 | ||||||||
| Granted | 85,727 | 201.90 | |||||||||
| Vested | (78,856) | 83.12 | |||||||||
| Canceled, forfeited or expired | (18,008) | 101.40 | |||||||||
| Non-vested stock units at December 31, 2020 | 196,287 | $ | 148.16 | ||||||||
The weighted average grant date fair value of performance-based non-vested stock units granted was $201.90, $128.89 and $79.59 in 2020, 2019 and 2018, respectively.
At December 31, 2020, there was $17.3 million in unrecognized compensation costs related to our performance-based non-vested stock units that we expect to be recognized over a weighted average period of 1.8 years.
11. COMMITMENTS AND CONTINGENCIES
Legal Proceedings – Ongoing
We are involved in the following legal actions:
Subpoena Duces Tecum and Civil Investigative Demands Issued by the U.S. Department of Justice
On May 21, 2015, we received a Subpoena Duces Tecum (“Subpoena”) issued by the U.S. Department of Justice. The Subpoena requests the delivery of information regarding 53 identified hospice patients to the United States Attorney’s Office for the District of Massachusetts. It also requests the delivery of documents relating to our hospice clinical and business operations and related compliance activities. The Subpoena generally covers the period from January 1, 2011 through May 21, 2015. We are fully cooperating with the U.S. Department of Justice with respect to this investigation.
On November 3, 2015, we received a civil investigative demand (“CID”) issued by the U.S. Department of Justice pursuant to the federal False Claims Act relating to claims submitted to Medicare and/or Medicaid for hospice services provided through designated facilities in the Morgantown, West Virginia area. The CID requests the delivery of information to the United States
91
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Attorney’s Office for the Northern District of West Virginia regarding 66 identified hospice patients, as well as documents relating to our hospice clinical and business operations in the Morgantown area. The CID generally covers the period from January 1, 2009 through August 31, 2015. We are fully cooperating with the U.S. Department of Justice with respect to this investigation.
On June 27, 2016, we received a CID issued by the U.S. Department of Justice pursuant to the federal False Claims Act relating to claims submitted to Medicare and/or Medicaid for hospice services provided through designated facilities in the Parkersburg, West Virginia area. The CID requests the delivery of information to the United States Attorney’s Office for the Southern District of West Virginia regarding 68 identified hospice patients, as well as documents relating to our hospice clinical and business operations in the Parkersburg area. The CID generally covers the period from January 1, 2011 through June 20, 2016. We are fully cooperating with the U.S. Department of Justice with respect to this investigation.
Based on our analysis of sample claims data in connection with preliminary settlement discussions with the U.S. Department of Justice regarding the above matters, we have recorded a total of $6.5 million to accrued expenses in our consolidated balance sheets related to this matter. Due to the ongoing nature of the investigations and current stage of the settlement discussions, we are unable to estimate a range of potential loss at this time, and we cannot predict the timing or outcome of these investigations.
In addition to the matters referenced in this note, we are involved in legal actions in the normal course of business, some of which seek monetary damages, including claims for punitive damages. Based on information available to us as of the date of this filing, we do not believe that these normal course actions, when finally concluded and determined, will have a material impact on our consolidated financial condition, results of operations or cash flows.
Legal fees related to all legal matters are expensed as incurred.
Other Investigative Matters – Completed
Corporate Integrity Agreement
On May 5, 2020, the Company received notice from the Office of Inspector General-HHS ("OIG") that the Company's five-year corporate integrity agreement ("CIA") with the OIG has been completed. On April 23, 2014, with no admissions of liability on our part, we entered into a settlement agreement with the U.S. Department of Justice relating to certain of our clinical and business operations. Concurrently with our entry into this agreement, we entered into a CIA with the OIG. The CIA formalized various aspects of our already existing ethics and compliance programs and contained other requirements designed to help ensure our ongoing compliance with federal health care program requirements. Among other things, the CIA required us to maintain our existing compliance program, executive compliance committee and compliance committee of the Board of Directors; provide certain compliance training; continue screening new and current employees to ensure they are eligible to participate in federal health care programs; engage an independent review organization ("IRO") to perform certain audits and reviews and prepare certain reports regarding our compliance with federal health care programs, our billing submissions to federal health care programs and our compliance and risk mitigation programs; and provide certain reports and management certifications to the OIG. Additionally, the CIA specifically required that we report substantial overpayments that we discovered we had received from federal health care programs, as well as probable violations of federal health care laws. The corporate integrity agreement had a term of five years that ended on April 21, 2019. We filed our final annual report on July 19, 2019.
Compassionate Care Hospice Corporate Integrity Agreement
On January 8, 2021, the Company received notice from the OIG that the Company's five-year CIA with the OIG has been completed. On January 30, 2015, CCH entered into a CIA with the OIG. The CIA required that CCH provide annual on-site compliance training; develop and implement policies to ensure compliance with federal health care program requirements; screen new and current employees to ensure that they are eligible to participate in federal health care programs; establish a compliance committee that contains both a Compliance Officer and a Chief Quality Officer; retain a Governing Authority expert who will periodically complete a compliance program review; and retain an IRO to complete claims review for hospice services rendered in New York. The OIG waived the claims review for the final year of the CCH CIA based on the closure of the New York operations. Additionally, the CIA required that CCH report substantial overpayments that CCH discovered it received from federal health care programs, as well as probable violations of federal criminal, civil or administrative health care laws. Upon breach of the CIA, CCH could have become liable for payment of certain stipulated penalties, or could have been excluded from participation in federal health care programs. The CIA had a term of five years that ended on January 30, 2020. We filed our final annual report on March 25, 2020.
92
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Third Party Audits – Ongoing
From time to time, in the ordinary course of business, we are subject to audits under various governmental programs in which third party firms engaged by CMS, including Recovery Audit Contractors (“RACs”), Zone Program Integrity Contractors (“ZPICs”), Uniform Program Integrity Contractors (“UPICs”), Program Safeguard Contractors (“PSCs”), Medicaid Integrity Contractors (“MICs”) and Supplemental Medical Review Contractors (“SMRCs”), conduct extensive reviews of claims data to identify potential improper payments. We cannot predict the ultimate outcome of any regulatory reviews or other governmental audits and investigations.
In July 2010, our subsidiary that provides hospice services in Florence, South Carolina received from a ZPIC a request for records regarding a sample of 30 beneficiaries who received services from the subsidiary during the period of January 1, 2008 through March 31, 2010 (the “Review Period”) to determine whether the underlying services met pertinent Medicare payment requirements. We acquired the hospice operations subject to this review on August 1, 2009; the Review Period covers time periods both before and after our ownership of these hospice operations. Based on the ZPIC’s findings for 16 beneficiaries, which were extrapolated to all claims for hospice services provided by the Florence subsidiary billed during the Review Period, on June 6, 2011, the Medicare Administrative Contractor ("MAC") for the subsidiary issued a notice of overpayment seeking recovery from our subsidiary of an alleged overpayment. We dispute these findings, and our Florence subsidiary has filed appeals through the Original Medicare Standard Appeals Process, in which we are seeking to have those findings overturned. An administrative law judge ("ALJ") hearing was held in early January 2015. On January 18, 2016, we received a letter dated January 6, 2016 referencing the ALJ hearing decision for the overpayment issued on June 6, 2011. The decision was partially favorable with a new overpayment amount of $3.7 million with a balance owed of $5.6 million including interest based on 9 disputed claims (originally 16). We filed an appeal to the Medicare Appeals Council on the remaining 9 disputed claims and also argued that the statistical method used to select the sample was not valid. No assurances can be given as to the timing or outcome of the Medicare Appeals Council decision. As of December 31, 2020, Medicare has withheld payments of $5.7 million (including additional interest) as part of their standard procedures once this level of the appeal process has been reached. In the event we are not able to recoup this alleged overpayment, we are entitled to be indemnified by the prior owners of the hospice operations for amounts relating to the period prior to August 1, 2009. On January 10, 2019, an arbitration panel from the American Health Lawyers Association determined that the prior owners' liability for their indemnification obligation was $2.8 million. This amount is recorded as an indemnity receivable within other assets in our consolidated balance sheets.
In July 2016, the Company received a request for medical records from SafeGuard Services, L.L.C (“SafeGuard”), a ZPIC, related to services provided by some of the care centers that the Company acquired from Infinity Home Care, L.L.C. The review period covers time periods both before and after our ownership of the care centers, which were acquired on December 31, 2015. In August 2017, the Company received Requests for Repayment from Palmetto GBA, LLC (“Palmetto”) regarding Infinity Home Care of Lakeland, LLC, (“Lakeland Care Centers”) and Infinity Home Care of Pinellas, LLC, (“Clearwater Care Center”). The Palmetto letters are based on a statistical extrapolation performed by SafeGuard which alleged an overpayment of $34.0 million for the Lakeland Care Centers on a universe of 72 Medicare claims totaling $0.2 million in actual claims payments using a 100% error rate and an overpayment of $4.8 million for the Clearwater Care Center on a universe of 70 Medicare claims totaling $0.2 million in actual claims payments using a 100% error rate.
The Lakeland Request for Repayment covers claims between January 2, 2014 and September 13, 2016. The Clearwater Request for Repayment covers claims between January 2, 2015 and December 9, 2016. As a result of partially successful Level I and Level II Administrative Appeals, the alleged overpayment for the Lakeland Care Centers has been reduced to $26.0 million and the alleged overpayment for the Clearwater Care Center has been reduced to $3.3 million. The Company has now filed Level III Administrative Appeals, and will continue to vigorously pursue its appeal rights, which include contesting the methodology used by the ZPIC contractor to perform statistical extrapolation. The Company is contractually entitled to indemnification by the prior owners for all claims prior to December 31, 2015, for up to $12.6 million.
At this stage of the review, based on the information currently available to the Company, the Company cannot predict the timing or outcome of this review. The Company estimates a low-end potential range of loss related to this review of $6.5 million (assuming the Company is successful in seeking indemnity from the prior owners and unsuccessful in demonstrating that the extrapolation method used by SafeGuard was erroneous). The Company has reduced its high-end potential range of loss from $38.8 million (the maximum amount Palmetto claims has been overpaid for both the Lakeland Care Centers and the Clearwater Care Center, of which $12.6 million is subject to indemnification by the prior owners) to $29.3 million based on the partial success achieved by the Company in prosecuting its Level I and II Administrative Appeals.
As of December 31, 2020, we have an accrued liability of approximately $17.4 million related to this matter. We expect to be indemnified by the prior owners for approximately $10.9 million of the total $12.6 million available indemnification related to this matter and have recorded this amount within other assets in our consolidated balance sheets. The net of these two amounts,
93
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
$6.5 million, was recorded as a reduction in revenue in our consolidated statements of operations during 2017. As of December 31, 2020, $1.5 million of net receivables have been impacted by this payment suspension.
Insurance
We are obligated for certain costs associated with our insurance programs, including employee health, workers’ compensation and professional liability. While we maintain various insurance programs to cover these risks, we are self-insured for a substantial portion of our potential claims. We recognize our obligations associated with these costs, up to specified deductible limits in the period in which a claim is incurred, including with respect to both reported claims and claims incurred but not reported. These costs have generally been estimated based on historical data of our claims experience. Such estimates, and the resulting reserves, are reviewed and updated by us on a quarterly basis.
The following table presents details of our insurance programs, including amounts accrued for the periods indicated (amounts in millions) in accrued expenses in our consolidated balance sheets. The amounts accrued below represent our total estimated liability for individual claims that are less than our noted insurance coverage amounts, which can include outstanding claims and claims incurred but not reported.
| As of December 31, | |||||||||||
| Type of Insurance | 2020 | 2019 | |||||||||
| Health insurance | $ | 15.1 | $ | 15.8 | |||||||
| Workers’ compensation | 35.8 | 33.4 | |||||||||
| Professional liability | 4.9 | 5.1 | |||||||||
| 55.8 | 54.3 | ||||||||||
| Less: long-term portion | (1.2) | (1.3) | |||||||||
| $ | 54.6 | $ | 53.0 | ||||||||
Our health insurance has an exposure limit of $1.3 million for any individual covered life. Our workers compensation insurance has a retention limit of $1.0 million per incident and our professional liability insurance has a retention limit of $0.3 million per incident.
Severance
We have commitments related to our severance plans applicable to a number of our senior executives and senior management, as well as the employment agreement entered into with our Chief Executive Officer, all of which generally commit us to pay severance benefits under certain circumstances.
Other
We are subject to various other types of claims and disputes arising in the ordinary course of our business. While the resolution of such issues is not presently determinable, we believe that the ultimate resolution of such matters will not have a significant effect on our consolidated financial condition, results of operations and cash flows.
12. EMPLOYEE BENEFIT PLANS
401(k) Benefit Plan
We maintain a plan qualified under Section 401(k) of the Internal Revenue Code for all employees who have reached 21 years of age, effective the first month after their hire date. Under the plan, eligible employees may elect to defer a portion of their compensation, subject to Internal Revenue Service limits.
Our match of contributions to be made to each eligible employee contribution is $0.44 for every $1.00 contributed up to the first 6% of their salary. The match is discretionary and thus is subject to change at the discretion of management. Effective January 1, 2020, our match of contributions is made in the form of cash. During 2019 and 2018, matching contributions were made in the form of our common stock, valued based upon the fair value of the stock as of the end of each calendar quarter end. We expensed approximately $12.9 million, $10.5 million and $9.0 million related to our 401(k) benefit plan for 2020, 2019 and 2018, respectively.
94
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
Deferred Compensation Plan
We had a Deferred Compensation Plan for additional tax-deferred savings for a select group of management or highly compensated employees. Amounts credited under the Deferred Compensation Plan were funded into a rabbi trust, which is managed by a trustee. The trustee has the discretion to manage the assets of the Deferred Compensation Plan as deemed fit, thus, the assets are not necessarily reflective of the same investment choices that would have been made by the participants.
Effective January 1, 2015, all prospective salary deferrals ceased. Participants will be allowed to make transactions with any remaining account balances as they wish per plan guidelines.
13. SHARE REPURCHASES
2021 Stock Repurchase Program
On December 23, 2020, we announced that our Board of Directors authorized a stock repurchase program, under which we may repurchase up to $100 million of our outstanding common stock through December 31, 2021.
Under the terms of the program, we are allowed to repurchase shares from time to time through open market purchases, unsolicited or solicited privately negotiated transactions, an accelerated stock repurchase program, and/or a trading plan in compliance with Exchange Act Rule 10b5-1. The timing and the amount of the repurchases will be determined by management based on a number of factors, including but not limited to share price, trading volume and general market conditions, as well as on working capital requirements, general business conditions and other factors.
We did not repurchase any shares pursuant to this stock repurchase program during the year ended December 31, 2020.
2019 Stock Repurchase Program
On February 25, 2019, we announced that our Board of Directors authorized a stock repurchase program, under which we could have repurchased up to $100 million of our outstanding common stock through March 1, 2020. We did not repurchase any shares pursuant to this stock repurchase program during 2019 or 2020. The stock repurchase program expired on March 1, 2020.
2018 Share Repurchase
On June 4, 2018, we purchased 2,418,304 of our common shares from affiliates of KKR Credit Advisors (US) LLC ("KKR"), representing one-half of KKR's then current holdings in the Company and 7.1% of the aggregate outstanding shares of the Company's common stock for a total purchase price of $181.4 million including related direct costs. The Company repurchased the shares at $73.96 which represents 96% of the closing stock price of the Company's common stock on June 4, 2018. The repurchased shares are classified as treasury shares.
14. SEGMENT INFORMATION
Our operations involve servicing patients through our 3 reportable business segments: home health, hospice and personal care. Our home health segment delivers a wide range of services in the homes of individuals who may be recovering from surgery, have a chronic disability or terminal illness or need assistance with completing important tasks. Our hospice segment provides palliative care and comfort to terminally ill patients and their families. Our personal care segment provides patients with assistance with the essential activities of daily living. The “other” column in the following tables consists of costs relating to executive management and administrative support functions, primarily information services, accounting, finance, billing and collections, legal, compliance, risk management, procurement, marketing, clinical administration, training, human resources and administration.
Management evaluates performance and allocates resources based on the operating income of the reportable segments, which includes an allocation of corporate expenses attributable to the specific segment and includes revenues and all other costs directly attributable to the specific segment. Segment assets are not reviewed by the company’s chief operating decision maker and therefore are not disclosed below (amounts in millions).
95
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
| For the Year Ended December 31, 2020 | |||||||||||||||||||||||||||||
| Home Health | Hospice | Personal Care | Other | Total | |||||||||||||||||||||||||
| Net service revenue | $ | 1,249.2 | $ | 750.1 | $ | 72.2 | $ | 0 | $ | 2,071.5 | |||||||||||||||||||
| Other operating income | 20.2 | 13.1 | 1.1 | 0 | 34.4 | ||||||||||||||||||||||||
| Cost of service, excluding depreciation and amortization | 729.9 | 400.6 | 54.9 | 0 | 1,185.4 | ||||||||||||||||||||||||
| General and administrative expenses | 307.2 | 175.4 | 12.4 | 173.2 | 668.2 | ||||||||||||||||||||||||
| Depreciation and amortization | 3.9 | 2.2 | 0.2 | 22.5 | 28.8 | ||||||||||||||||||||||||
| Asset impairment charge | 3.4 | 0.8 | 0 | 0 | 4.2 | ||||||||||||||||||||||||
| Operating expenses | 1,044.4 | 579.0 | 67.5 | 195.7 | 1,886.6 | ||||||||||||||||||||||||
| Operating income (loss) | $ | 225.0 | $ | 184.2 | $ | 5.8 | $ | (195.7) | $ | 219.3 | |||||||||||||||||||
| For the Year Ended December 31, 2019 | |||||||||||||||||||||||||||||
| Home Health | Hospice | Personal Care | Other | Total | |||||||||||||||||||||||||
| Net service revenue | $ | 1,256.4 | $ | 617.2 | $ | 82.0 | $ | 0 | $ | 1,955.6 | |||||||||||||||||||
| Cost of service, excluding depreciation and amortization | 754.1 | 335.1 | 61.1 | 0 | 1,150.3 | ||||||||||||||||||||||||
| General and administrative expenses | 297.2 | 137.5 | 12.3 | 160.9 | 607.9 | ||||||||||||||||||||||||
| Depreciation and amortization | 4.2 | 1.6 | 0.2 | 12.4 | 18.4 | ||||||||||||||||||||||||
| Asset impairment charge | 1.5 | 0 | 0 | 0 | 1.5 | ||||||||||||||||||||||||
| Operating expenses | 1,057.0 | 474.2 | 73.6 | 173.3 | 1,778.1 | ||||||||||||||||||||||||
| Operating income (loss) | $ | 199.4 | $ | 143.0 | $ | 8.4 | $ | (173.3) | $ | 177.5 | |||||||||||||||||||
| For the Year Ended December 31, 2018 | |||||||||||||||||||||||||||||
| Home Health | Hospice | Personal Care | Other | Total | |||||||||||||||||||||||||
| Net service revenue | $ | 1,174.5 | $ | 410.9 | $ | 77.2 | $ | 0 | $ | 1,662.6 | |||||||||||||||||||
| Cost of service, excluding depreciation and amortization | 722.1 | 212.0 | 58.8 | 0 | 992.9 | ||||||||||||||||||||||||
| General and administrative expenses | 276.3 | 84.6 | 12.8 | 127.6 | 501.3 | ||||||||||||||||||||||||
| Depreciation and amortization | 3.5 | 1.1 | 0.3 | 8.4 | 13.3 | ||||||||||||||||||||||||
| Operating expenses | 1,001.9 | 297.7 | 71.9 | 136.0 | 1,507.5 | ||||||||||||||||||||||||
| Operating income (loss) | $ | 172.6 | $ | 113.2 | $ | 5.3 | $ | (136.0) | $ | 155.1 | |||||||||||||||||||
15. UNAUDITED SUMMARIZED QUARTERLY FINANCIAL INFORMATION
| Net Income Attributable to Amedisys, Inc. Common Stockholders (1) | |||||||||||||||||||||||
| Net Service Revenue | Net Income Attributable to Amedisys, Inc. | Basic | Diluted | ||||||||||||||||||||
| 2020 | |||||||||||||||||||||||
| 1st Quarter | $ | 491.7 | $ | 31.8 | $ | 0.98 | $ | 0.96 | |||||||||||||||
| 2nd Quarter | 485.0 | 34.7 | 1.07 | 1.04 | |||||||||||||||||||
| 3rd Quarter | 544.1 | 72.0 | 2.20 | 2.16 | |||||||||||||||||||
| 4th Quarter | 550.7 | 45.1 | 1.38 | 1.36 | |||||||||||||||||||
| $ | 2,071.5 | $ | 183.6 | $ | 5.64 | $ | 5.52 | ||||||||||||||||
| 2019 | |||||||||||||||||||||||
| 1st Quarter | $ | 467.3 | $ | 31.3 | $ | 0.98 | $ | 0.95 | |||||||||||||||
| 2nd Quarter | 493.0 | 33.7 | 1.05 | 1.02 | |||||||||||||||||||
| 3rd Quarter | 494.6 | 34.1 | 1.06 | 1.03 | |||||||||||||||||||
| 4th Quarter | 500.7 | 27.7 | 0.86 | 0.83 | |||||||||||||||||||
| $ | 1,955.6 | $ | 126.8 | $ | 3.95 | $ | 3.84 | ||||||||||||||||
(1)Because of the method used in calculating per share data, the quarterly per share data may not necessarily total to the per share data as computed for the entire year.
96
AMEDISYS, INC. AND SUBSIDIARIES
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2020
16. RELATED PARTY TRANSACTIONS
During 2018, we made a $7.0 million investment in Medalogix, a healthcare predictive data and analytics company; this investment is accounted for under the equity method. During the years ended December 31, 2020 and 2019, we incurred costs of approximately $3.9 million and $0.5 million, respectively, in connection with the usage of Medalogix's analytics platforms. We believe that the terms of these transactions are consistent with those negotiated at arm’s length.
On June 4, 2018, we purchased 2,418,304 of our common shares from affiliates of KKR, representing one-half of KKR's holdings in the Company and 7.1% of the aggregate outstanding shares of the Company's common stock for a total purchase price of $181.4 million including related direct costs. The Company repurchased the shares at $73.96 which represents 96% of the closing stock price of the Company's common stock on June 4, 2018. At the time of the transaction, KKR held approximately 14.2% of the Company's outstanding shares of common stock.
97
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
We have established disclosure controls and procedures which are designed to provide reasonable assurance of achieving their objectives and to ensure that information required to be disclosed in our reports filed under the Exchange Act is recorded, processed, summarized, disclosed and reported within the time periods specified in the SEC’s rules and forms. This information is also accumulated and communicated to our management, including our principal executive officer and principal financial officer, and Board of Directors to allow timely decisions regarding required disclosure.
In connection with the preparation of this Annual Report on Form 10-K, as of December 31, 2020, under the supervision and with the participation of our principal executive officer and principal financial officer, our management conducted an evaluation of the effectiveness of our disclosure controls and procedures, as such term is defined under Rules 13a-15(e) and 15d-15(e) promulgated under the Exchange Act.
Based on this evaluation, our principal executive officer and principal financial officer concluded that our disclosure controls and procedures were effective at a reasonable assurance level as of December 31, 2020, the end of the period covered by this Annual Report on Form 10-K.
Management’s Annual Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over our financial reporting, as such term is defined in Rules 13a-15(f) and 15d-15(f) promulgated under the Exchange Act. Under the supervision and with the participation of our principal executive officer and our principal financial officer, our management conducted an evaluation of the effectiveness of our internal control over financial reporting based on the framework in Internal Control – Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this evaluation under the framework in Internal Control – Integrated Framework (2013), our management concluded our internal control over financial reporting was effective as of December 31, 2020.
Under guidelines established by the SEC, companies are allowed to exclude acquisitions from their assessment of internal control over financial reporting during the first year of an acquisition while integrating the acquired company. Accordingly, our assessment of internal controls excluded our acquisition of AseraCare Hospice ("AseraCare"), completed on June 1, 2020. See Item 8, Note 4 - Acquisitions to our consolidated financial statements for additional information on our acquisition of AseraCare. Operations from this acquisition represented approximately 3% of total assets and 3% of total revenue as of and for the year ended December 31, 2020.
KPMG LLP, the independent registered public accounting firm that audited our consolidated financial statements included in this Form 10-K, has issued a report on our internal control over financial reporting, which is included herein.
Changes in Internal Controls
There were no changes in our internal control over financial reporting (as defined in Exchange Act Rule 13a-15(f)) that have occurred during the quarter ended December 31, 2020 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
98
Inherent Limitations on Effectiveness of Controls
Our management, including our principal executive officer and principal financial officer, does not expect that our disclosure controls or our internal controls over financial reporting will prevent or detect all errors and all fraud. A control system, no matter how well designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. The design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Further, because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that misstatements due to error or fraud will not occur or that all control issues and instances of fraud, if any, have been detected. These inherent limitations include the realities that judgments in decision-making can be faulty and that breakdowns can occur because of simple error or mistake. Controls can also be circumvented by the individual acts of some persons, by collusion of two or more people, or by management override of the controls. The design of any system of controls is based in part on certain assumptions about the likelihood of future events, and there can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions. Projections of any evaluation of controls’ effectiveness to future periods are subject to risks. Over time, controls may become inadequate because of changes in conditions or deterioration in the degree of compliance with policies and procedures. Our disclosure controls and procedures are designed to provide reasonable assurance of achieving their objectives and, based on an evaluation of our controls and procedures, our principal executive officer and our principal financial officer concluded our disclosure controls and procedures were effective at a reasonable assurance level as of December 31, 2020, the end of the period covered by this Annual Report.
99
Report of Independent Registered Public Accounting Firm
To the Stockholders and Board of Directors
Amedisys, Inc.:
Opinion on Internal Control Over Financial Reporting
We have audited Amedisys, Inc. and subsidiaries' (the Company) internal control over financial reporting as of December 31, 2020, based on criteria established in Internal Control – Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2020, based on criteria established in Internal Control – Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the consolidated balance sheets of the Company as of December 31, 2020 and 2019, the related consolidated statements of operations, comprehensive income, stockholders’ equity, and cash flows for each of the years in the three-year period ended December 31, 2020, and the related notes (collectively, the consolidated financial statements), and our report dated February 25, 2021 expressed an unqualified opinion on those consolidated financial statements.
The Company acquired Homecare Preferred Hospice, Inc., doing business as AseraCare Hospice during 2020, and management excluded from its assessment of the effectiveness of the Company’s internal control over financial reporting as of December 31, 2020, Homecare Preferred Hospice, Inc., doing business as AseraCare Hospice’s internal control over financial reporting associated with 3% of total assets and 3% of total revenues included in the consolidated financial statements of the Company as of and for the year ended December 31, 2020. Our audit of internal control over financial reporting of the Company also excluded an evaluation of the internal control over financial reporting of Homecare Preferred Hospice, Inc., doing business as AseraCare Hospice.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Annual Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audit also included performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
100
/s/ KPMG LLP
Baton Rouge, Louisiana
February 25, 2021
101
ITEM 9B. OTHER INFORMATION
None.
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The information required by this item is incorporated by reference to the 2021 Proxy Statement to be filed with the SEC within 120 days after the end of the year ended December 31, 2020.
Code of Conduct and Ethics
We have adopted a code of ethics that applies to all of our directors, officers and employees, including our principal executive officer, principal financial officer and principal accounting officer. This code of ethics, which is entitled Code of Ethical Business Conduct, is posted at our internet website, http://www.amedisys.com. Any amendments to, or waivers of, the code of ethics will be disclosed on our website promptly following the date of such amendment or waiver.
ITEM 11. EXECUTIVE COMPENSATION
The information required by this item is incorporated by reference to the 2021 Proxy Statement to be filed with the SEC within 120 days after the end of the year ended December 31, 2020.
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this item is incorporated by reference to the 2021 Proxy Statement to be filed with the SEC within 120 days after the end of the year ended December 31, 2020.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this item is incorporated by reference to the 2021 Proxy Statement to be filed with the SEC within 120 days after the end of the year ended December 31, 2020.
ITEM 14. PRINCIPAL ACCOUNTANT FEES AND SERVICES
The information required by this item is incorporated by reference to the 2021 Proxy Statement to be filed with the SEC within 120 days after the end of the year ended December 31, 2020.
102
PART IV
ITEM 15. EXHIBITS AND FINANCIAL STATEMENT SCHEDULES
| (a) | 1. | Financial Statements | ||||||||||||
| All financial statements are set forth under Part II, Item 8 of this report. | ||||||||||||||
| 2. | Financial Statement Schedules | |||||||||||||
| There are no financial statement schedules included in this report as they are either not applicable or included in the financial statements. | ||||||||||||||
| 3. | Exhibits | |||||||||||||
| The Exhibits are listed in the Exhibit Index required by Item 601 of Regulation S-K preceding the signature page of this report. | ||||||||||||||
ITEM 16. FORM 10-K SUMMARY
None.
103
EXHIBIT INDEX
The exhibits marked with the cross symbol (†) are filed and the exhibits marked with a double cross (††) are furnished with this Form 10-K. Any exhibits marked with the asterisk symbol (*) are management contracts or compensatory plans or arrangements filed pursuant to Item 601(b)(10)(iii) of Regulation S-K. The registrant agrees to furnish to the Commission supplementally upon request a copy of any schedules or exhibits omitted pursuant to Item 601(a)(5) of Regulation S-K of any exhibit set forth below.
| Exhibit Number | Document Description | Report or Registration Statement | SEC File or Registration Number | Exhibit or Other Reference | ||||||||||||||||||||||
| 2.1 | The Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2016 | 0-24260 | 2.1 | |||||||||||||||||||||||
| 2.2 | The Company’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2018 | 0-24260 | 10.1 | |||||||||||||||||||||||
| 2.3 | The Company's current Report on Form 8-K filed on June 4, 2018 | 0-24260 | 2.1 | |||||||||||||||||||||||
| 2.4 | The Company’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2018 | 0-24260 | 2.1 | |||||||||||||||||||||||
| 2.5 | The Company's Current Report on Form 8-K filed on April 27, 2020 | 0-24260 | 2.1 | |||||||||||||||||||||||
| 3.1 | The Company’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2007 | 0-24260 | 3.1 | |||||||||||||||||||||||
| 3.2 | The Company’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2019 | 0-24260 | 3.2 | |||||||||||||||||||||||
| 4.1 | The Company’s Registration Statement on Form S-3 filed August 20, 2007 | 333-145582 | 4.8 | |||||||||||||||||||||||
| 4.2 | The Company's Annual Report on Form 10-K for the year ended December 31, 2019 | 0-24260 | 4.2 | |||||||||||||||||||||||
| 10.1 | The Company’s Annual Report on Form 10-K for the year ended December 31, 2008 | 0-24260 | 10.1 | |||||||||||||||||||||||
| 10.2* | The Company’s Current Report on Form 8-K filed June 8, 2012 | 0-24260 | 10.1 | |||||||||||||||||||||||
104
| Exhibit Number | Document Description | Report or Registration Statement | SEC File or Registration Number | Exhibit or Other Reference | ||||||||||||||||||||||
| 10.3* | The Company's Annual Report on Form 10-K for the year ended December 31, 2019 | 0-24260 | 10.3 | |||||||||||||||||||||||
| 10.4* | The Company’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2008 | 0-24260 | 10.3 | |||||||||||||||||||||||
| 10.5* | The Company’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2008 | 0-24260 | 10.4 | |||||||||||||||||||||||
| 10.6* | The Company’s Annual Report on Form 10-K for the year ended December 31, 2014 | 0-24260 | 10.6 | |||||||||||||||||||||||
| 10.7* | The Company’s Annual Report on Form 10-K for the year ended December 31, 2014 | 0-24260 | 10.7 | |||||||||||||||||||||||
| 10.8* | The Company’s Annual Report on Form 10-K for the year ended December 31, 2014 | 0-24260 | 10.8 | |||||||||||||||||||||||
| 10.9* | The Company’s Annual Report on Form 10-K for the year ended December 31, 2014 | 0-24260 | 10.9 | |||||||||||||||||||||||
| 10.10* | The Company's Annual Report on Form 10-K for the year ended December 31, 2018 | 0-24260 | 10.10 | |||||||||||||||||||||||
| 10.11* | The Company's Annual Report on Form 10-K for the year ended December 31, 2018 | 0-24260 | 10.11 | |||||||||||||||||||||||
| 10.12* | The Company's Annual Report on Form 10-K for the year ended December 31, 2018 | 0-24260 | 10.12 | |||||||||||||||||||||||
105
| Exhibit Number | Document Description | Report or Registration Statement | SEC File or Registration Number | Exhibit or Other Reference | ||||||||||||||||||||||
| 10.13* | The Company’s Current Report on Form 8-K filed on October 3, 2018 | 0-24260 | 10.1 | |||||||||||||||||||||||
| 10.14* | The Company's Quarterly Report on Form 10-Q for the quarter ended September 30, 2019 | 0-24260 | 10.1 | |||||||||||||||||||||||
| 10.15* | The Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2018 | 0-24260 | 10.1 | |||||||||||||||||||||||
| †10.16* | ||||||||||||||||||||||||||
| 10.17 | The Company’s current Report on Form 8-K filed on July 2, 2018 | 0-24260 | 10.1 | |||||||||||||||||||||||
| 10.18 | The Company’s current Report on Form 8-K filed on July 2, 2018 | 0-24260 | 10.2 | |||||||||||||||||||||||
106
| Exhibit Number | Document Description | Report or Registration Statement | SEC File or Registration Number | Exhibit or Other Reference | ||||||||||||||||||||||
| 10.19 | The Company’s current Report on Form 8-K filed on July 2, 2018 | 0-24260 | 10.3 | |||||||||||||||||||||||
| 10.20 | The Company’s Annual Report on Form 10-K for the year ended December 31, 2015 | 0-24260 | 10.27 | |||||||||||||||||||||||
| 10.21 | The Company’s Annual Report on Form 10-K for the year ended December 31, 2015 | 0-24260 | 10.28 | |||||||||||||||||||||||
| 10.22 | The Company’s Current Report on Form 8-K filed on February 4, 2019 | 0-24260 | 10.1 | |||||||||||||||||||||||
107
| Exhibit Number | Document Description | Report or Registration Statement | SEC File or Registration Number | Exhibit or Other Reference | ||||||||||||||||||||||
| 10.23 | The Company’s Current Report on Form 8-K filed on February 4, 2019 | 0-24260 | 10.2 | |||||||||||||||||||||||
| 10.24 | The Company’s Current Report on Form 8-K filed on February 19, 2019 | 0-24260 | 10.1 | |||||||||||||||||||||||
| 10.25 | The Company's Current Report on Form 8-K filed on June 15, 2020 | 0-24260 | 10.1 | |||||||||||||||||||||||
| †10.26* | ||||||||||||||||||||||||||
| †21.1 | ||||||||||||||||||||||||||
| †23.1 | ||||||||||||||||||||||||||
| †31.1 | ||||||||||||||||||||||||||
| †31.2 | ||||||||||||||||||||||||||
| ††32.1 | ||||||||||||||||||||||||||
| ††32.2 | ||||||||||||||||||||||||||
108
| Exhibit Number | Document Description | Report or Registration Statement | SEC File or Registration Number | Exhibit or Other Reference | ||||||||||||||||||||||
| †101.INS | Inline XBRL Instance - The instance document does not appear in the Interactive Data File because its XBRL tags are embedded within the Inline XBRL document. | |||||||||||||||||||||||||
| †101.SCH | Inline XBRL Taxonomy Extension Schema Document | |||||||||||||||||||||||||
| †101.CAL | Inline XBRL Taxonomy Extension Calculation Linkbase Document | |||||||||||||||||||||||||
| †101.DEF | Inline XBRL Taxonomy Extension Definition Linkbase | |||||||||||||||||||||||||
| †101.LAB | Inline XBRL Taxonomy Extension Labels Linkbase Document | |||||||||||||||||||||||||
| †101.PRE | Inline XBRL Taxonomy Extension Presentation Linkbase Document | |||||||||||||||||||||||||
| 104 | Cover Page Interactive Data File (formatted as Inline XBRL and contained in Exhibit 101) | |||||||||||||||||||||||||
109
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, as amended, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
AMEDISYS, INC. | ||||||||
| By: | /S/ PAUL B. KUSSEROW | |||||||
| Paul B. Kusserow, | ||||||||
| Chief Executive Officer and | ||||||||
| Chairman of the Board | ||||||||
Date: February 25, 2021
110
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the date indicated:
| Signature | Title | Date | ||||||||||||
/S/ PAUL B. KUSSEROW | Chief Executive Officer and Chairman of the Board (Principal Executive Officer) | February 25, 2021 | ||||||||||||
| Paul B. Kusserow | ||||||||||||||
/S/ SCOTT G. GINN | Executive Vice President and Chief Financial Officer (Principal Financial Officer and Principal Accounting Officer) | February 25, 2021 | ||||||||||||
| Scott G. Ginn | ||||||||||||||
/S/ VICKIE L. CAPPS | Director | February 25, 2021 | ||||||||||||
| Vickie L. Capps | ||||||||||||||
/S/ MOLLY COYE, MD | Director | February 25, 2021 | ||||||||||||
| Molly Coye, MD | ||||||||||||||
/S/ JULIE D. KLAPSTEIN | Director | February 25, 2021 | ||||||||||||
| Julie D. Klapstein | ||||||||||||||
/S/ TERESA L. KLINE | Director | February 25, 2021 | ||||||||||||
| Teresa L. Kline | ||||||||||||||
/S/ RICHARD A. LECHLEITER | Lead Independent Director | February 25, 2021 | ||||||||||||
| Richard A. Lechleiter | ||||||||||||||
/S/ BRUCE D. PERKINS | Director | February 25, 2021 | ||||||||||||
| Bruce D. Perkins | ||||||||||||||
/S/ JEFFREY A. RIDEOUT, MD | Director | February 25, 2021 | ||||||||||||
| Jeffrey A. Rideout, MD | ||||||||||||||
/S/ IVANETTA D. SAMUELS | Director | February 25, 2021 | ||||||||||||
| Ivanetta D. Samuels | ||||||||||||||
111