Exhibit 99.1

Clinical Profile, Quality
Controls and Survey Results
www.amedisys.com
Clinical Profile Of Patients Serviced
Amedisys services an elderly population with many poly-pharmacy needs, clinical co-morbidities and functional debilities. Detailed below are some key statistics regarding the company’s patient population.
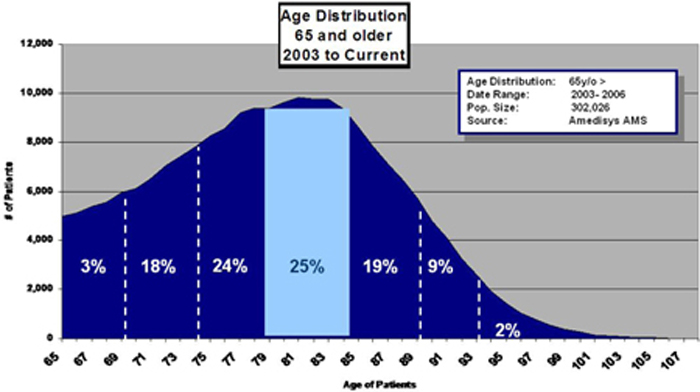
Amedisys’ average age patient is 82 year olds. Twenty five percent of the population (the largest component) is between the age of 80 and 84 years old. The Company primarily provides care to the more senior Medicare recipient as opposed to the newly benefited eligible.
www.amedisys.com
Three Year Trend of Case Mix Weights
The case mix weight in homecare is a combined score of the patients’ clinical status, functional condition and service level requirements. It is essentially a singular number reflecting the acuity or sickness of a represented population.
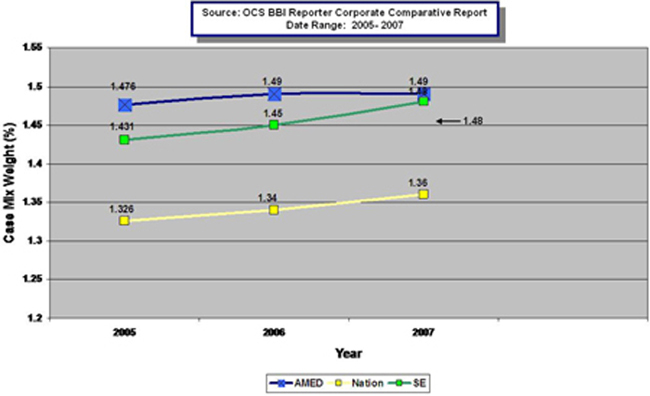
Outlined above is a three year trend of case mix weight scores for Amedisys, the national average and the southeastern average.
www.amedisys.com

A Review of Patient Risk
Prepared by OCS, Inc.
One of the most challenging parts of health care is the diversity of patients. Every patient brings a multitude of characteristics that ultimately impacts that patient’s ability to heal. Severity and risk have broad implications in health care. Not only do they present more of a clinical challenge, but higher risk patients are often more resource-intensive and costly to care for. In addition, they are patients who are more likely to require unplanned services, such as ER visits and hospital admissions, presenting burdens to both the provider and the healthcare system.
It is a critical part of a clinician’s job to be able to assess patients and their characteristics, to understand each patient’s overall severity and the risks his condition presents and plan appropriate levels of care accordingly. The challenge is that the process of assessing patients’ risk is difficult – people are complex. Clinical conditions, the acuity of the ailments, physical and mental impairments, and a patient’s history all make each individual inherently more or less likely to achieve certain outcomes. In home health, clinicians are presented with even more of a challenge, because factors including the home environment and caregivers also impact the course of a patient’s health.
OCS has developed a risk modeling tool that assesses and categorizes individual patients’ risk of hospitalization or emergent care at admission, based on more than 100 patient clinical, functional, and environmental characteristics. We have applied the model to millions of cases of home health patient care in our proprietary database, examining trends and the impact of high risk patients.
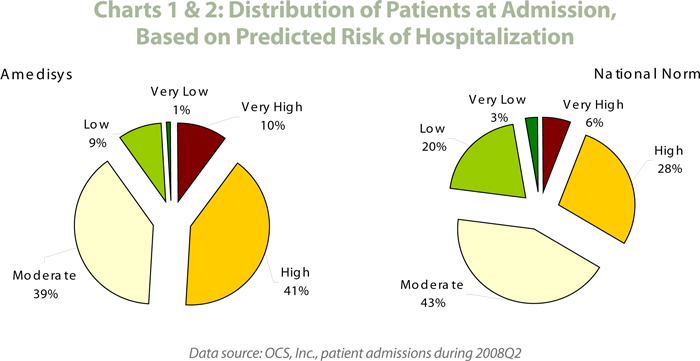
One of the most enlightening discoveries of our analyses is the difference in distribution of risk at the provider level. Not all providers have a patient risk profile that matches the national norm. Some have a higher distribution of lower risk patients; others have patient populations disproportionately representative of higher risk patients.
Amedisys is a clear example of a home health provider with a higher distribution of patients on the high-end of the risk scale. More than one-half (51%) of all patients admitted by Amedisys home health agencies are predicted to be of high or very high risk of hospitalization, compared to just one-third (34%) of patients nation-wide (see charts 1 and 2). Conversely, only 10% of Amedisys patients are assessed as low or very low risk, compared to 23% of patients nationally.
OCS -Leading Healthcare Insight
(continued)
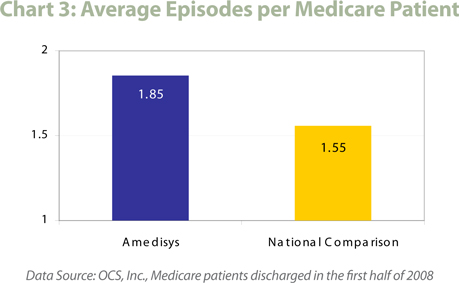
Another indicator of overall patient severity is length of stay, with higher severity patients requiring more days of service as a general rule. As patient length of stay increases, hospitalization rates also increase and many measures of patient outcomes decrease. The higher severity of Amedisys patients is also demonstrated by a length of stay longer than the national benchmarks (see chart 3). The average Medicare patient requires approximately 1.55 60-day episodes of care; the average Amedisys Medicare patient receives almost 1.9 episodes of care. Similarly, almost half of all Amedisys PPS episodes that started during the first half of 2008 were recertification episodes, where the patient was continuing home health service, rather than a new admission. Nationally, only about one-third of all PPS episodes were patients continuing on service during the same time frame.
OCS -Leading Healthcare Insight
(continued)
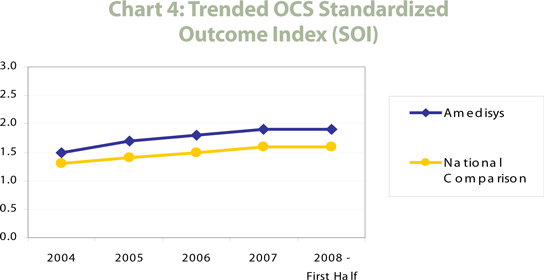
The logical result of a high risk patient population is overall lower quality outcome scores. Yet despite caring for a patient population that is considerably higher risk and requires a longer length of stay than the national norm, Amedisys has shown consistently higher overall quality of care as measured by the OCS Standardized Outcome Index (SOI), a proprietary measure that offers a single number representative of overall quality. As shown in Chart 4, Amedisys not only has a higher SOI than the national database, but an increasing SOI score over the past several years.
OCS -Leading Healthcare Insight
(continued)
The effects of a high risk patient population could reach into virtually every area of agency management – from outcome measures to clinical management to the use of technology to financial performance. Agencies that have a well-developed understanding of the risk profile of their patient population, and clear plans for managing that risk from all angles, will be best positioned to weather the challenges of higher risk patients, providing high quality care and maintaining a positive bottom-line.
Amedisys clearly excels in this complicated care management environment, as evidenced by their higher quality patient outcomes, despite caring for a patient population with greater risk and a longer length of care than national norms.
OCS -Leading Healthcare Insight
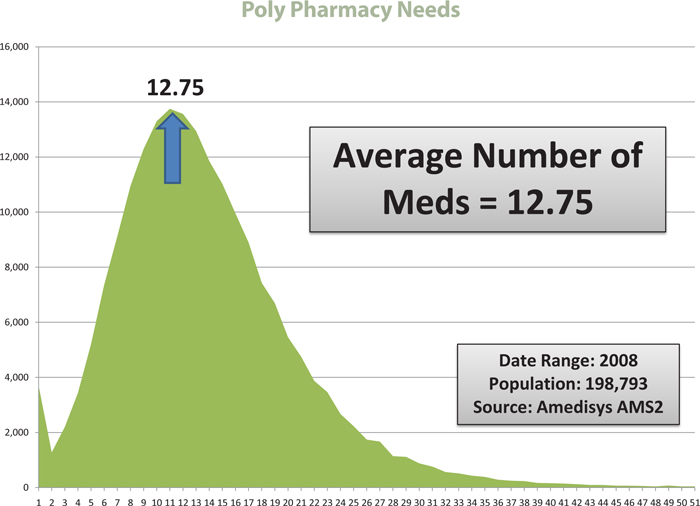
Distribution of Average Medication
Amedisys’ elderly population has many medical conditions requiring pharmaceutical management. Medications are prescribed by physicians, not Amedisys. In 2006 the company’s patients were on an average of 8 medications per day. In 2007 this average increased to 9 medications per day. In 2008, our patient population is now taking on average 12 medications per day. The average for 2008 (through Q3) has increased to 12.75 medications per day.
www.amedisys.com
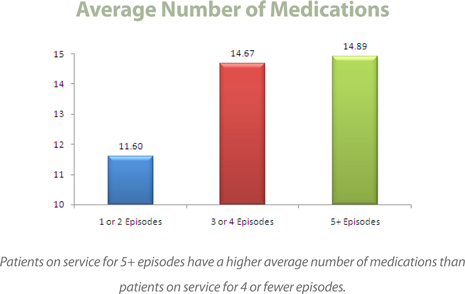
Distribution Breakdown—Average Meds/Average Episode
The data below represents all Amedisys patients with completed Medicare episodes that started and completed in 2008 (through Q3). This data validates the higher clinical acuity of our long-term, chronic, co-morbid population.
www.amedisys.com
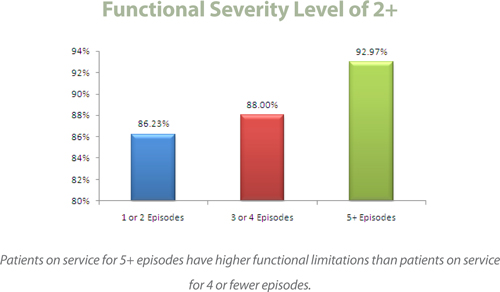
Three Year Trend of Functional Scorings
The graph below represents a visual trend of the functional debility levels of the patients served by Amedisys over the last three year period. The admission document in home care, known as the OASIS assessment, generates what is known as a functional score. Ranging from F0 (fully functional-no deficits) to F4 (potentially bed bound), this scoring gives the organization insight into how debilitated the population is on a year over year period.
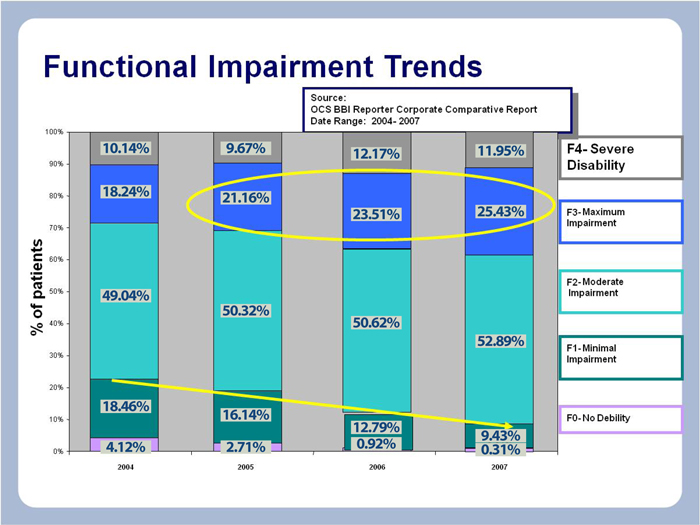
Over a three year period, the organization has experienced an increasing trend of patients admitted with higher function debilities (F2 to F4) each year and at the same time a decreasing percentage of patients with small or minimal functional deficits entering the system of care (F0 to F1).
www.amedisys.com
Distribution Breakdown—Average F2 Scorings/Average Episode
The data below represents all Amedisys patients with completed Medicare episodes that started and completed in 2008 (through Q3). This data validates the higher clinical acuity of our long-term, chronic, co-morbid population.
www.amedisys.com
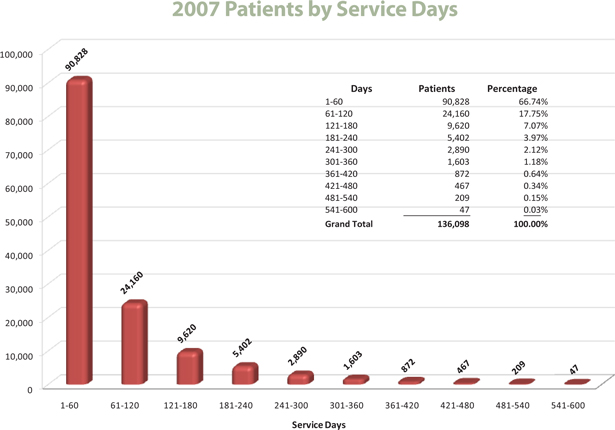
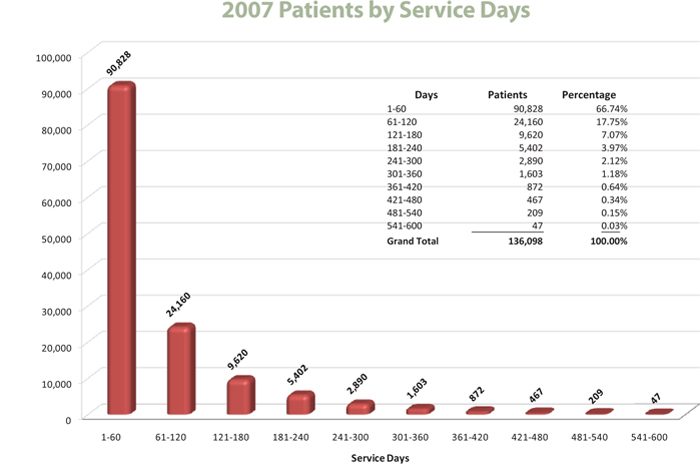
Patients on Service Graphical Breakdown
Distribution of Admitted Patients
To allow investors the opportunity to further understand our patient service levels, detailed below is a time on service breakdown of our patients in 2007.
www.amedisys.com
Clinical Research—Therapy Wound Modalities
References for Amedisys Wound Care Clinical Programs can be found below.
| 1. | PT Practice Settings: Electrophysiology and Wound Management |
By Chris Hayhurst
This article can be found at www.aptasce.com.
| 2. | Electrical Stimulation |
Author: Carrie Sussman, PT
This paper on electrical stimulation for wound healing has been excerpted from: Chapter 16, Sussman, C and Byl, N, Electrical Stimulation for Wound Healing, Wound Care Collaborative Practice Manual for Physical Therapists and Nurses, Sussman, C. And Bates-Jensen, BM, Aspen Publishers 1998.
| 3. | Effects of Electrical Stimulation on Wound Healing in Patients with Diabetic Ulcers |
LL Baker, R Chambers, SK DeMuth and F VillarDepartment of Biokinesiology and Physical Therapy, University of Southern California, Los Angeles 90033, USA. llbaker@hsc.usc.edu Diabetes Care, Vol 20, Issue 3 405-412, Copyright © 1997 by American Diabetes Association
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 4. | Ultrasound for Cutaneous Wound Healing |
Author: Ernst E.
Ultrasound for cutaneous wound healing. Phlebology 1995; 10:2-4.
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 5. | Ultrasound in Wound Healing |
Author: Joseph McCulloch, PT, PhD
LSU Medical Center, Director of the Physical Therapy Department
To obtain this article please contact the author directly at the LSU Medical Center Physical Therapy Department.
www.amedisys.com
Clinical Research—Therapy Wound Modalities (continued)
| 6. | Therapeutic Ultrasound for Venous Leg Ulcers |
Al-Kurdi D, Bell-Syer SEM, Flemming K. Cochrane
Database of Systematic Reviews 2008, Issue 1. Art. No.: CD001180. DOI: 10.1002/14651858.CD001180.pub2.
This article can be accessed through the Cochrane Library at www.cochrane.org/reviews.
| 7. | Electrical Stimulation for Chronic Wounds: Cochrane Database |
Fernandez-ChimenoM, Houghton PE, Holey L. Electrical Stimulation for Chronic Wounds. Cochrane
Database of Systematic Reviews 2004, Issue 1. Art. No.: CD004550. DOI: 10.1002/14651858.CD004550.
This article can be accessed through the Cochrane Library at www.cochrane.org/reviews.
| 8. | Effect of Electrical Stimulation on Chronic Leg Ulcer Size and Appearance |
Authors: Pamela E Houghton, Cynthia B Kincaid, Marge Lovell, Karen E Campbell, David H Keast, M Gail Woodbury, Kenneth A Harris
Physical Therapy, Volume 83, Number 1. January 2003
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 9. | Restoration of Sensation, Reduced Pain, and Improved Balance in Subjects With Diabetic Peripheral Neuropathy |
A double-blind, randomized, placebo-controlled study with monochromatic near-infrared treatment
Authors: DAVID R. LEONARD, MD, FACEM. HAMED FAROOQI, MD, FACESARA MYERS, RN
Diabetes Care, Volume 27, Number 1, January 2004 clinical rehabilitation 2004; 18: 76–83
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
Our references to these articles and the websites in which they appear should not be construed as the sponsorship of these articles or websites by Amedisys. Amedisys provides this information merely for your convenience and reference.
www.amedisys.com
Clinical Research—Vestibular Balance Retaining
References for Amedisys Balance for Life program can be found below.
| 1. | Efficacy of Vestibular Rehabilitation on Chronic Unilateral Vestibular Dysfunction |
Oya Topuz Department of Physical Medicine and Rehabilitation, Bülent Topuz, F Necdet Ardiç Department of Otolaryngology, Merih Sarhus, Department of Physical Medicine and Rehabilitation, Gülsen Ögmen Department of Otolaryngology and Füsun Ardiç Department of Physical Medicine and Rehabilitation, Pamukkale University, School of Medicine, Turkey
Received 15th January 2003; returned for revisions 23rd April 2003; revised manuscript accepted 20th July 2003.
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 2. | Exercise for Improving Balance in Older People (Review ) |
Authors: Howe TE, Rochester L, Jackson A, Banks PMH, Blair VA
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2007, Issue 4.
This article can be accessed through the Cochrane Library at www.cochrane.org/reviews.
| 3. | Falls in Patients with Vestibular Deficits |
*Susan J. Herdman, †Philip Blatt, *Michael C. Schubert, and ‡Ronald J. Tusa
The American Journal of Otolog, 21:847–851© 2000, The American Journal of Otology, Inc
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 4. | Reversal of Diabetic Peripheral Neuropathy with Phototherapy (MIRE™) Decreases Falls and the Fear of Falling and Improves Activities of Daily Living in Seniors |
Author: MARK W. POWELL DALE H. CARNEGIE2, THOMAS J. BURKE
Age and Ageing 2006; 35: 11–16 _ The Author 2005. Published by Oxford University Press on behalf of the British Geriatrics Society.
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
www.amedisys.com
Clinical Research—Vestibular Balance Retaining (continued)
| 5. | Vestibular Rehabilitation: For Whom and How? A Systematic Review |
Author: EVA EKVALL HANSSON
Lund University, Department of Clinical Sciences in Malmo¨/General Practice, Clinical Research Centre, Malmo¨ University.
Hospital, 205 02 Malmo, Swed Advances in Physiotherapy. 2007; 9: 106_116
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 6. | Efficacy of the Epley Maneuver for Posterior Canal BPPV: A Long-Term, Controlled Study of 81 Patients |
Authors: Wietske Richard, MD; Tjasse D. Bruintjes, MD, PhD; Peter Oostenbrink; Roeiand B. van Leeuwen
Ear, Nose and Throat Journal, Volume 84, Number 1
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
| 7. | Canalith Repositioning for Benign Paroxysmal Positional Vertigo |
*Judith White, †Panos Savvides, ‡Neil Cherian, and §John Oas
Otology & Neurotology, 26:704–710 _ 2005, Otology & Neurotology, Inc.
*Section of Vestibular and Balance Disorders, Head and Neck Institute, The Cleveland Clinic, Cleveland, Ohio; *‡Department of Neurology, The Cleveland Clinic, Cleveland, Ohio; †University Hospital, Case.
This article can be found through the pubmed.gov search engine by typing in the search bar the last name of the first author then the first initial of the first name.
Our references to these articles and the websites in which they appear should not be construed as the sponsorship of these articles or websites by Amedisys. Amedisys provides this information merely for your convenience and reference.
www.amedisys.com
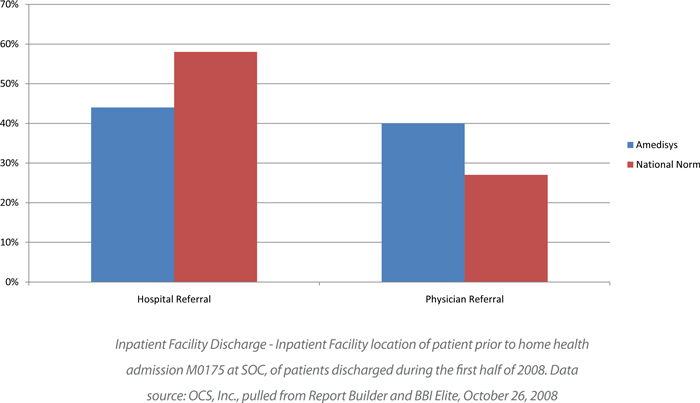
External Benchmark Referral Source Statistics
Amedisys receives more Physician direct referrals for home health than the national norm and fewer hospital direct referrals than the national norm. Patients from Physician direct referrals have not had a recent hospitalization that would assist in stabilizing the patient’s health status prior to the home health admission.
www.amedisys.com
Business Systems Infrastructure
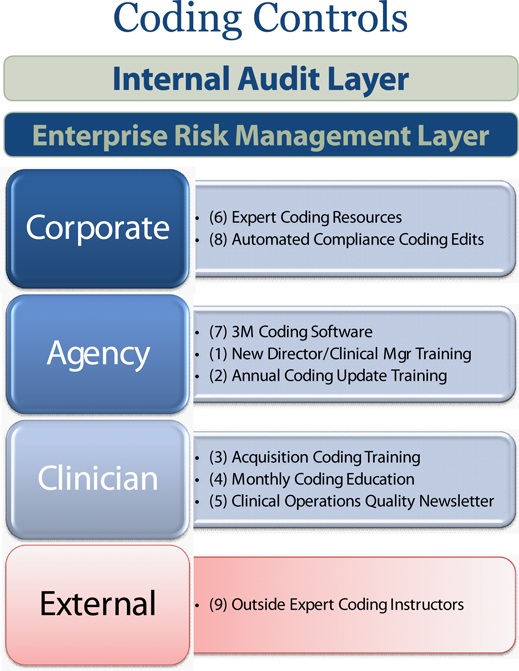
Coding Controls
www.amedisys.com
Coding Controls (continued)
It’s important for investors to understand that coding regulations are extremely complex. They change each year and require intense recurrent clinical education. Amedisys employs many resources with a view toward ensuring proper coding.
| 1. | New Directors/CM Coding Training |
Clinical Managers (CM’s) work at the agency level locally with visiting clinicians to determine the most appropriate clinical coding. All clinical managers need specific, in depth coding education. It is also important for our agency Directors to understand coding principles. For this reason, we have developed three Learn Center Computer Based Instruction courses (approximately 4 hours of learning time) that cover coding regulatory practices and home health coding compliance principles. These sessions are required for all new Director’s and CM’s, and are also used for specialized training as needed. Coding tests are electronically administered and a passing score of 80 must be obtained for certification of completion of the course.
| 2. | Director/CM Annual Coding Update Training |
Each year in October, the International Classification of Diseases (Revision 9) [ICD-9], updates select codes by adding and deleting certain diagnosis codes. This includes deletions, additions, and adjustments of more specificity to currently utilized diagnosis codes. For this reason, Amedisys conducts annual coding training via Learn Center Computer Based Instruction for the organization’s Clinical Managers and Directors. Coding tests are electronically administered and a passing score of 80 must be obtained for certification of completion of the course.
| 3. | Acquisition Orientation Coding Training |
Employees who join Amedisys via acquisitions receive monthly Centra web based training with a live presenter on diagnosis selection training. This presentation is focused on selecting the proper diagnosis that is the focus of care in accordance with home health regulatory principles. All acquisition home health clinicians down to the field staff level are required to attend these training sessions. Coding tests are electronically administered and a passing score must be obtained for certification of completion of the course.
www.amedisys.com
Coding Controls (continued)
| 4. | Monthly Specialized Coding Education |
In addition to new position and new agency coding training, specialized live web based Centra or teleconference training is performed for requesting agencies and field staff at a minimum of monthly. These are offered on a recurrent basis both as a refresher course for experienced coders and as an introductory session for clinicians new to the system.
| 5. | Clinical Operations Quality Newsletter |
The Clinical Operations Department routinely publishes a clinical newsletter. Each edition has a dedicated coding education section in which the top educational topics related to coding are published. This newsletter goes out to all clinicians within the organization.
| 6. | Expert Coding Resources |
It’s imperative for clinicians to have on-going access to expert coding resources. As stated above, coding regulations are complex and change annually. In 2003, we added central coding experts who are certified in homecare coding. These coding experts are nationally certified and most hold multiple additional certifications.
| 7. | Coding Software |
Imbedded in the company’s point of care system is an outside third party application known as 3M Coding software. This industry recognized software assists our Clinical Managers, who process our assessments, in managing the complex rules and terminology of ICD-9 coding. This software follows all important rules, principles, and guidelines for coding and is updated annually with any regulatory or ICD-9 changes.
| 8. | Automated “compliance” coding edits |
The organization has developed centralized automated coding compliance edits. Since locations are all connected via a Wide Area Network, the company developed global sweep reports. This program sweeps all coded assessments weekly and as needed and generates exception reports by agency that are used to identify assessments that may have been coded improperly.
www.amedisys.com
Coding Controls (continued)
These automated compliance edits are designed to ensure the organization does not have an agency or individual purposefully upcoding volumes of assessments. Most often assessments coded improperly are attributable to a knowledge deficit as opposed to any willful intent. If any location has a trend of volumes of assessments coded improperly, it is reported to the Compliance Department. However to date, the organization has not discovered any trend of exception reporting in mass from multiple agencies. All locations understand the company has this exception based compliance programming. This infrastructure provides a deterrent to improper coding.
In studies of agencies in every region of the country, Fazzi and Associates, found that significant inconsistencies were discovered in each of the case mix domains, that impacted quality measures, financial reimbursement and OBQI risk scoring (3 M National Integrity Project, 2003). All homecare organizations experience coding and OASIS documentation inconsistencies.
Coding regulations are difficult to understand, change annually, and all new clinicians and key management must receive constant coding education. The organizations intent is to provide ongoing coding education to all key individuals, expert coding resources, and automated coding compliance edits to ensure proper controls are maintained.
| 9. | Outside expert coding instructions |
The Company utilizes regulatory coding and OASIS experts for credentialing its staff. The OASIS Certificate and Competency Board is utilized for third party OASIS certification. Lisa Selman-Holeman and Associates is utilized for third party coding certification. Both are recognized as experts in the industry.
www.amedisys.com
Business Systems Infrastructure
Clinical Audit Controls
www.amedisys.com
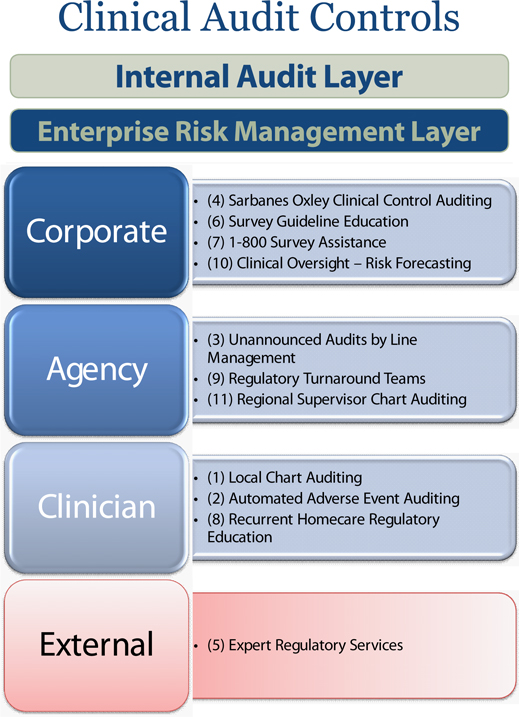
Clinical Audit Controls (continued)
Clinical Auditing Controls
Regulatory requirements allow patients to be admitted to homecare only if they meet certain criteria. Patients essentially must be considered “homebound” and must require certain clinical services in order to qualify for the Medicare benefit.
Homebound Status
To be considered homebound a patient must only leave their residence for anintermittent period of timethat isshort in durationand the absence must require a “taxing effort”.Taxing effort comes in the form of patients having to use an assistive device such as a walker, cane, or person helping them while leaving the home. Being homebound is an eligibility requirement for Medicare home health services. Aside from the homebound rule, patients must also require the need for the provision of certain clinical “skills”:
| 1. | Teaching or retraining on their disease. |
| 2. | Assessment or observation skills provided by a clinician. |
| 3. | Technical skills provided by a clinician (e.g. wound care, shots, intravenous fluids) |
| 4. | Management/Evaluation of a patient’s Care Plan. |
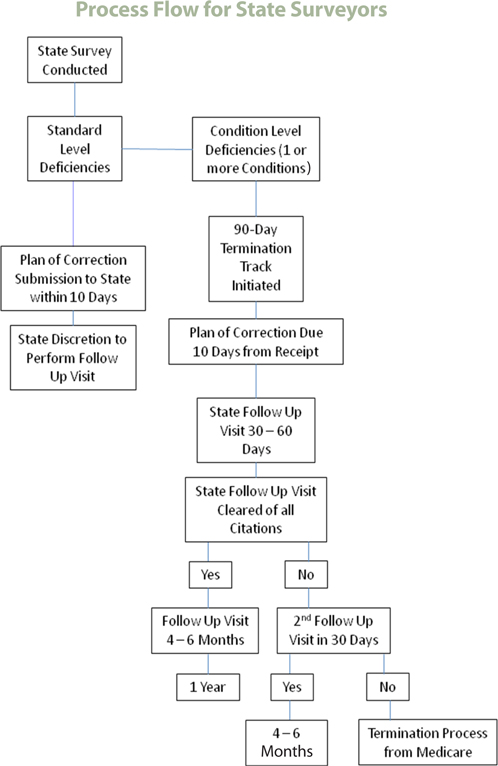
Reimbursement risk is created in homecare when an agency’s medical records do not adequately reflect homebound documentation or clinical skill delivery. The records should clearly identify why an agency is providing the service. A state surveyor can place a provider number on a termination track if they find the location to be noncompliant with any of the Conditions of Participation (Medicare guidelines). If the identified issues are not corrected within a 45 to 90 day time period, the agency and provider number could be terminated from participating in the Medicare program. The majority of Home Health agencies are surveyed at least every 24-36 months. However, state agencies may use their discretion in surveying more or less often.
An agency can be placed on a 12 month survey cycle if the following criteria are present:
The Home Health agency has been Medicare approved for less than 3 years.
The Home Health agency has had a Change of Ownership since the previous standard survey.
The Home Health agency has had a condition-level deficiency cited within 24 months.
The Home Health agency has had a complaint survey resulting in deficiency citations.
The Home Health agency has been reviewed by any state, regional, or national fraud & abuse initiatives.
www.amedisys.com
Clinical Audit Controls (continued)
www.amedisys.com
Clinical Audit Controls (continued)
Amedisys agencies are routinely audited by external surveyors on a monthly basis.
Because growth naturally increases survey frequency, the organization has implemented many proactive clinical controls.
| 1. | Local agency chart auditing |
Each agency must self-audit a minimum of 10% of its census quarterly. This is part of the Medicare Conditions of Participation. Agencies use these audit results to develop clinical improvement plans on an on-going basis.
| 2. | Automated adverse event auditing |
An adverse event is a clinical event that must be clinically reviewed to determine if there is a problem with an agencies care delivery. For example, an intra episode hospital admission due to a wound infection while under the care of an agency may be listed out as a potential adverse event. In this case, the agency is responsible for reviewing this case to determine if there was a problem with their care delivery. If a problem with their care delivery exists, the agency is responsible for developing an improvement plan to address this area. All adverse events are audited to determine if a true adverse event exist. Based on the audits, the agency then educates the clinical staff on best practices and documentation accordingly.
www.amedisys.com
Clinical Audit Controls (continued)
| 3. | Unannounced Audits by Line Management Regional Staff |
The company has operational and clinical support teams with assigned regions who are responsible for conducting unannounced random clinical audits, developing agency action plans to address any risk area they find, educating all locations on changes in regulations, and providing education as needed.
| 4. | Sarbanes Oxley auditing |
The Internal Audit Division is made up of credentialed auditing staff and conducts chart audits annually on randomly selected agencies. In 2004 an independent SOX team was added. This group also conducts annual clinical audits.
Based on the findings of the audits from both teams, education is provided by the Clinical Oversight Division and Line Management, and action plans are developed. No material weaknesses related to the company’s local agency controls have been reported.
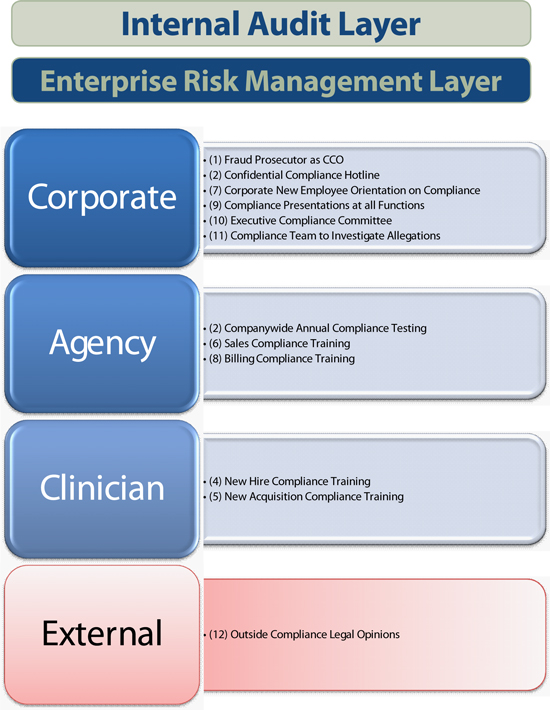
| 5. | Outside expert regulatory services |
The organization utilizes outside, third party legal consultants on an ad hoc basis. These attorneys are experts in Home Care and Medicare regulatory requirements. The company often seeks regulatory opinions regarding its processes, procedures or practices.
| 6. | Survey guideline education |
New agency Directors sometimes have a learning curve related to understanding regulations and available resources. For this reason the organization has developed Survey Guideline Education. This education guides a new Director through what actions to take to ensure the agency remains in compliance.
www.amedisys.com
Clinical Audit Controls (continued)
| 7. | 1-800-Survey assistance |
Surveyors often ask specific policy or corporate level questions during the survey process. A 1-800-Survey hotline has been established as a resource to our locations. The hotline is a direct call to our Clinical Oversight Division. This division develops policies, procedures, forms and protocols, and conducts extensive research on State regulatory requirements. They are also available to assist any Director during the survey process.
| 8. | Recurrent homecare regulatory education |
The company’s Talent Management Division has developed a Learn Center which houses educational sessions for all home care staff as well as Orientation and Skills Competencies for Clinical Staff and Home Health Aides.
The educational components include Disease Management programs, Regulatory education – Home Care 101, Best Practices, up to date Wound Care treatments, Medicare Coding, as well as the basics of homecare regulations and required documentation. This is a critical part of our regulatory education controls and has been incorporated into our new employee orientation.
| 9. | Regulatory “turn around teams” |
If an agency receives a multiple citation survey, the organization sends in a regulatory “turn around team”. In the event an agency has a poor survey, an agency is required to submit an action plan to the state showing its strategy for improvement.
For the return survey, the agency must demonstrate improvement in key areas. Showing improvement in a short time requires intense visiting nurse education and operational process restructuring. The turnaround teams provide extra resources at the local level to ensure compliance with state action plans.
www.amedisys.com
Clinical Audit Controls (continued)
| 10. | Risk forecasting methodologies (Clinical Oversight Auditing) |
Known variables create regulatory risk and subsequent poor surveys in homecare. The Clinical Oversight Division employs statistical forecasting methodologies which provide early warning signals to identify at-risk agencies before they receive a poor survey.
This is a proactive mechanism used across the organization on a recurrent basis every six (6) months. All at-risk agencies identified are placed on required action plans similar to the methodology used by external state surveyors.
| 11. | Direct line supervisor chart auditing |
Once the Clinical Oversight Division statistically identifies focus agencies, direct line supervisors at the Area Vice President (AVP) and Vice President (VP) level audit those locations. The supervisors then identify the specific areas in which an agency needs to show improvement. This process occurs across throughout the organization every six (6) months.
www.amedisys.com
Business Systems Infrastructure
Billing Controls
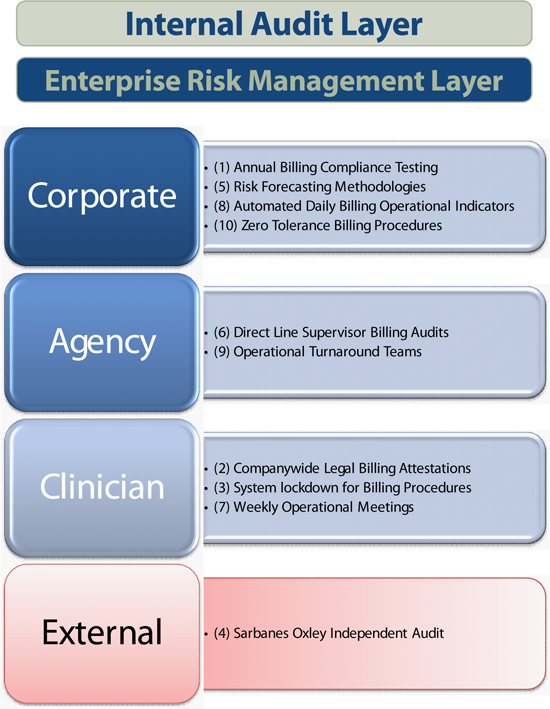
Billing Controls
www.amedisys.com
Billing Controls (continued)
Investors should note the organization’s emphasis on recurrent proactive processes. It is the company’s belief that in order to remain successful in an environment of growth, a proactive recurrent infrastructure should be in place to provide a proper control environment. That control environment should also include multiple resources to inspect, oversee and ensure regulatory compliance on an ongoing basis.
| 1. | Companywide annual billing compliance testing |
There are select positions identified within the company that should always have to complete billing compliance testing. On an annual basis companywide, all agency Directors-the individuals who lead our offices, Business Office Managers (BOMs)-the individuals who run the operations within the agencies, and Schedulers go through billing compliance testing. These are the key positions within our organization that potentially touch the local billing process. New hires into these positions are also required to complete this training prior to 90 days of employment and annually thereafter. A score of 100 percent is required on this test.
| 2. | Legal billing attestations company wide |
The organization requires that all agency Directors, BOMs, and Schedulers sign a legal attestation related to the billing procedures. It delineates clearly our zero tolerance policy and clearly defines that any individual found to be violating billing procedures os subject to termination.
| 3. | System lock down for billing individuals |
Only those holding key positions involved in the billing process in each location are allowed access to billing systems. Each individual who has access to our billing system has to go through billing compliance testing, pass the post test successfully and sign the legal attestation.
| 4. | Sarbanes Oxley outside auditing |
The intent of Sarbanes Oxley is to ensure the internal controls that touch a company’s revenue stream are adequate and without material weaknesses. Our independent accounting firm has audited both the clinical and the billing internal control procedures since Sox inception in 2004. No material weaknesses have been reported in the companies billing internal controls.
www.amedisys.com
Billing Controls (continued)
| 5. | Risk forecasting methodologies |
The Clinical Oversight Division conducts forecast extrapolations every six (6) months to determine both clinical and billing survey risk.
| 6. | Direct line supervisor billing audits |
Vice Presidents and Area Vice Presidents conduct billing audits every six (6) months, on our agencies that we determine to have higher risk. If warranted, improvement plans are required. We believe that the combination of outside clinical audits and direct supervisor audits has been successful in reducing clinical risk and improving our state survey results.
| 7. | Weekly operational meetings |
It’s important for homecare agencies to have sound operational processes to ensure all agency functions run smoothly. In homecare, operational risk and subsequent state survey risk is created when an agency’s clinical side and operational side do not work in sync.
For this reason, we conduct standardized operations meetings. Agencies review the operational metrics and address/resolve any outstanding paperwork or credentialing. We have found these meetings to be extremely beneficial to promote sound agency operations.
| 8. | Automated Daily Billing Operational Indicators |
All locations are connected via a Wide Area Network. This connection provides many compliance advantages. Through remote monitoring we are able to better understand the efficiencies and/or inefficiencies in all of our locations. For example, we can determine if any agency has a lot of outstanding paperwork which is often a good indication that operations personnel are not working in sync with clinical personnel.
We have isolated eight (8) operational indicators that we believe are a good reflection of an efficiently operating agency. We believe there is a direct correlation between sound homecare operational processes and reduced survey and regulatory risk.
www.amedisys.com
Billing Controls (continued)
Each week, the system automatically generates a report inclusive of all agencies and lists each of the 8 indicators. This information is published weekly for the agency Directors and BOM’s to review. Once a month, at a minimum, the Vice President of Office Operations reviews the data and identifies any agencies that have elevated trends. Those agencies are required to submit a plan of action to the Vice President of Office Operations and to their Area Vice President.
Daily Billing Indicators
| 1. | SYSDC’S/SYS60’S– System generated holds for billing that are evaluated thru Daily Billing to look at SYS holds greater than 3 days old that have a “frequency” or “absent data only” issue. |
| 2. | Logging – Daily Billing evaluates logging for the prior week to monitor timely logging of visits/supplies. |
| 3. | Late Oasis– Daily Billing evaluates locked Oasis Assessments for the prior week to monitor the number of assessments locked late (greater than 7 days). |
| 4. | Outstanding Orders – Daily Billing evaluates the number of unsigned orders that are due to be resubmitted to MD that have not been resubmitted. |
| 5. | Timely D/C’s– Daily Billing evaluates the number of potential D/C’s that have not been entered/processed thru the system. |
| 6. | Past Due Recerts – Daily Billing evaluates the number of potential Recerts that have not been entered/processed thru the system. |
| 7. | SYSAU’s – System generated holds for billing where visits were logged and payor required an authorization that wasn’t in the system. Daily Billing evaluates SYSAU’s greater than 5 days old. |
| 8. | Weekly Frequency – Daily Billing evaluates the number of patients for the prior week that had a discrepancy between what was logged and what was scheduled. |
www.amedisys.com
Billing Controls (continued)
Through continued monitoring and evaluation, if at any time the Vice President of Office Operations is concerned with an agency’s indicators, a conference call is scheduled to discuss the status of the agency and to formulate an action plan. The attendees on the call include, but are not limited to, the Vice President of Office Operations, Vice President of Clinical Operations, the SVP, VP, and AVP of the agency. Subsequent conference calls are scheduled as needed until all parties are satisfied with the performance of the agency.
This process is one of the company’s agency billing key controls for Sarbanes Oxley. It has been tested annually and found to be free of any significant deficiencies or material weaknesses.
| 9. | Operational turn around teams |
Each SVP and Vice President has a clinical and operational team. The SVP/VP will send an operational “Turn Around Team” to locations with poor operational indicator scores. This team will focus on improving processes, ensuring any backlog of paperwork is processed, and interviewing/hiring/orienting new employees.
If a turnaround team has been dispatched to an agency, that site’s leadership is closely evaluated. Statistical evaluations reveal that staffing shortages in the clinical side and office positions have the potential to create risk. The company also tracks this indicator in conjunction with other operational indicators to understand where best to allocate resources.
| 10. | Zero Tolerance Billing Policy |
In July, 2006, Amedisys adopted a Zero Tolerance Policy regarding billing compliance. This policy states that if at any time an employee is found not following proper billing procedures, he or she will be terminated immediately. This Zero Tolerance Policy is strictly enforced.
www.amedisys.com
Business Systems Infrastructure
Compliance Controls
Compliance Controls
www.amedisys.com
Compliance Controls (continued)
| 1. | Department of Justice Prosecutor as Chief Compliance Officer |
Jeffrey Jeter was hired in 2001 to head the company’s compliance division. Jeffrey worked as an attorney with the Department of Justice prosecuting healthcare fraud. He has been instrumental in establishing a multi-layered compliance infrastructure based upon the OIG’s recommendations for healthcare entities.
| 2. | Confidential Compliance Hotline |
Since 2001 a confidential hotline has been in place throughout the company to ensure employees they can anonymously report any potential wrongdoing. Jeffrey Jeter personally manages and investigates all complaints that are confidentially reported. All complaints are reported to the Board of Directors to ensure transparency and in keeping with our organizational commitment to compliance.
| 3. | Annual Compliance Testing |
All employees are required to attend annual compliance training and must successfully pass post-training testing. This requirement began in 2001 and was a key step in ingraining compliance into our culture.
Amedisys has recognized that the most effective deterrent to fraud and abuse is having a rigorous, recurrent training schedule for staff. Recurrent training ensures that all employees understand the rules, pitfalls, and the processes for compliance. Therefore, all staff, regardless of position within the company, are required to undergo a series of training dedicated solely to compliance.
| 4. | New Hire Compliance Training |
Upon hire, all staff are required to view a compliance training video and complete a post-training test demonstrating their mastery of the concepts. The video was produced in-house, and therefore, is narrowly tailored to the specific compliance risks encountered by Amedisys. This training video also details the company’s Zero Tolerance Policy with respect to fraud and abuse and explains the incident reporting hotline available to all staff. Furthermore, when completing this training,all staff are required to certify, in writing, that they have received training, understand the company’s policies, and will report any known incidents of fraud.
www.amedisys.com
Compliance Controls (continued)
| 5. | New Acquisition Compliance Training |
When Amedisys acquires a new agency, all newly-acquired staff receive the same compliance training, which is conducted within the first few months of the acquisition.
| 6. | Sales Compliance Training |
All newly-hired business development employees (Account Executives, Account Managers, and Regional Directors of Business Development) as well as newly-hired agency Directors must attend a separate Business Development Orientation training, which includes several hours of compliance training conducted by the Company’s Chief Compliance Officer. In these presentations, state and federal laws concerning kickbacks and illegal remuneration are discussed. In addition, the sessions focus on proper and improper marketing activities. The audience is also afforded the opportunity to ask questions and pose hypotheticals to ensure that the Company has addressed all of their unresolved issues with respect to conducting business development in a legal and ethical manner.
| 7. | One Day Corporate Orientation—Compliance |
Moreover, since the beginning of 2004, all new employees are required to attend a one-day corporate orientation, which is held six (6) times a year in regional locations. During this orientation, senior management meets with employees to discuss the company’s mission and values and culture. Included in this orientation is a separate compliance presentation. This presentation explains the company’s expectations with respect to compliant conduct by all staff, as well as the consequences for fraudulent conduct and the avenues available for reporting compliance concerns. Attendees must also certify their receipt of training and adherence to the Company’s compliance plan.
| 8. | Billing Compliance Training |
The Company conducts separate compliance training annually for staff responsible for billing and coding. A separate Billing Compliance training manual and video has been created and disseminated to the field. This training covers the policies, processes, and procedures required for billing and explains how each ties back to key internal controls for compliance. This training, which was jointly created by Clinical Operations and the Company’s Chief Compliance Officer, is mandatory for all staff involved in billing and coding.
www.amedisys.com
Compliance Controls (continued)
All staff involved in billing have also been required to participate in a separate Billing Compliance training meeting tied with the Company’s Sarbanes Oxley compliance. During this meeting, the Chief Compliance Officer presents a training session on Billing and Coding Compliance. Again, all attendeesmust certify their attendance and adherence in writing.
| 9. | Compliance Presentations at all Company Functions |
All formal Company meetings include a specific session on compliance presented by the Chief Compliance Officer. These annual meetings bring together the company’s operational and sales leadership. The compliance presentations focus on the important role of compliance, potential fraud schemes to be avoided, and the compliance policies of the company.
A sample of recent compliance presentations includes the following:
| • | “Chocolate Covered Compliance”—New Employee Orientation |
| • | “Beware of HHAs Bearing Gifts”—Business Development Training |
| • | “King of the Compliance Mountain”—Billing compliance training |
| • | “A Few Good Docs”—Compliance training for Amedisys’ medical directors |
| • | “Abracadabra ... Compliance”—Compliance training for Amedisys operators and sales staff |
| • | “Mission: Compliance”—Compliance training used for both Amedisys’ medical directors and company leadership |
| • | “Swimming with the Fishes”—Compliance training for Amedisys’ medical directors |
| • | “Compliance Building Blocks for Agency Success”—Compliance training for Amedisys’ operators and sales staff |
| • | “Time=Money: Care Plan Oversight Compliance”—Business Development Training |
| • | “Compliance Survivor: Outwit, Outplay, Outlast”—Compliance training for Amedisys’ leadership |
| • | “Confessions of a 400 Pound Gorilla”—Compliance training for Amedisys’ operators and sales staff |
www.amedisys.com
Compliance Controls (continued)
| 10. | Executive Compliance Committee |
In the OIG’s compliance guidance for home health, it was recommended that providers “designate an appropriate body, e.g. a corporate compliance committee, charged with the responsibility for operating and monitoring the compliance program.” The OIG’s guidance contemplated that such a committee would report directly to the CEO and governing body of the agency, and in so doing would reflect a good faith and meaningful commitment to compliance by the agency’s administration as well as its governing body and CEO.
Based on this guidance, Amedisys has created a Compliance Committee comprised of the following persons: (1) the Chief Compliance Officer; (2) the Chief Executive Officer; (3) the Chief Operating Officer; (3) the Chief Financial Officer; (4) the Chief Information Officer, (5) the Senior Vice President of Clinical Operations; (6) the Senior Vice President of Human Resources; and (7) the Vice President of Compliance.
The Amedisys Corporate Compliance Committee meets at least bi-annually, and more often as circumstances warrant. It is important to note that Amedisys’ Compliance Committee is comprised of all senior-level management in the company.
It is critical that compliance oversight be vested at the highest levels of an organization. In so doing, there is not a committee report to senior management, where issues could be overlooked or buried in a report; rather, senior management is an active participant in the compliance process.
The Compliance Committee is responsible for setting compliance policies, reviewing compliance problems, and ensuring the overall compliance climate of the Company.
Issues that are typically discussed in Corporate Compliance Committee meetings include: (a) compliance hotline calls; (b) review of compliance audits; (c) changes in legislation or regulations; (d) changes to company policies; and (e) current risk areas for fraud and abuse.
In addition, all compliance problems are vetted to both the Chief Executive Officer and the Chief Financial Officer each quarter in advance of the release of financial statements in accordance with the provisions of the Sarbanes Oxley legislation.
www.amedisys.com
Business Systems Infrastructure
Patient Recertification Controls
Patient Recertification Controls
www.amedisys.com
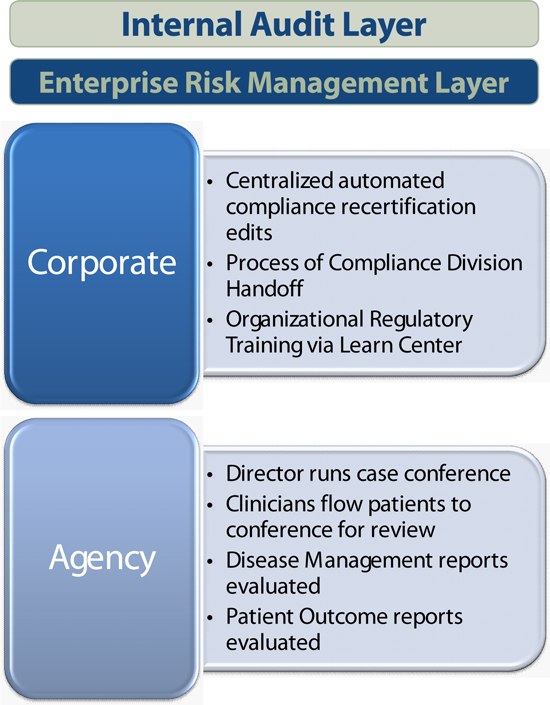
Patient Recertification Controls (continued)
Decentralized Agency based Care Conference Process
In homecare, patients can be recertified into another episode of care if they meet certain regulatory standards. As discussed previously in Clinical Audit controls, patients must have a continuing medical need that essentially meets the admission criteria in home care. Medical necessity within the episode of care takes the form of a continuing skilled clinical need, changes to the patient’s medical regimen or modified care protocols within the episode period.
Each site Director runs their weekly patient care conference and makes a patient-by patient clinical decision on discharge or recertification. Visiting clinicians who believe a patient is ready for discharge will follow that patient up through weekly case conference. It is during that meeting where our disease Directors then run select Disease Management Reports and review them to ensure their clinicians have addressed all aspects of the patient’s disease and if the patient is compliant with self-management measures. These reports are designed to ensure the organization delivers the appropriate level of outcome based care.
If the patient is trending successfully with his disease management compliance and outcomes, the agency will begin the discharge planning process. If the patient still has a knowledge or compliance deficit or his outcomes are trending negatively and he continues to have a qualifying skill, the agency will recertify that patient and focus its care delivery on those specific non-compliant areas. The organization recertification rate is the result of standardized clinical management processes in our locations and applying disease management principles to the homecare industry. We believe the company’s outcomes are a direct reflection of the standardized care management model implemented throughout the organization.
www.amedisys.com
Patient Recertification Controls (continued)
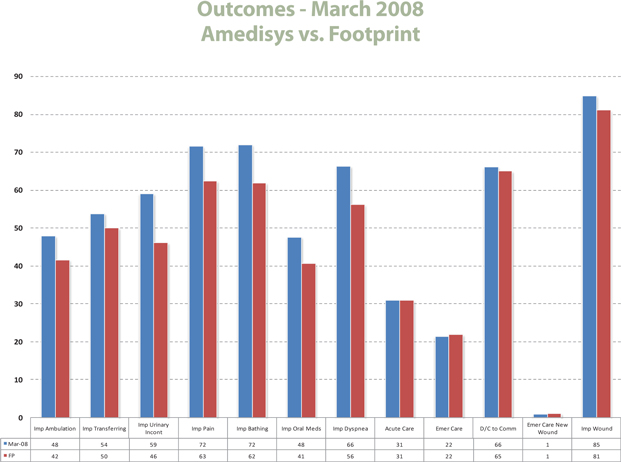
Detailed above is where the organization stands related to its current foot print of competitors on publically reported patient outcomes.
Centralized Automated Compliance Recert Edits
Using the same methodology as our automated compliance coding edits, the company developed centralized automated compliance recertification edits. A global program sweeps all monthly recertifications to ensure that patients have had either changes to their medication regimen, changes to their physician orders during the original care episode or clinical variants on their disease management clinical tracks.
www.amedisys.com
Patient Recertification Controls (continued)
These monthly automated compliance recertification edits are designed to ensure we don’t have multiple locations that are purposefully recertifying patients in mass that do not meet Medicare criteria. If locations have a trend of recertifications without a regulatory basis, this is reported to the Compliance Department. As is the case with our automated compliance coding edits, to date, the company has not discovered any trend of agencies recertifying patients in mass without a Medicare reimbursable need or reporting unjustifiable clinical changes in condition.
Distribution of Admitted Patients
To allow investors the opportunity to further understand our patient service levels, detailed below is a time on service breakdown of our patients in 2007.

www.amedisys.com
Patient Recertification Controls (continued)
It is a regulatory requirement that homecare agencies case conference on their patients. The organization has standardized this process and applied disease management principles in order to make the right clinical decision on each.
In 2004, Amedisys was awarded the National OCS Vision Quality Award for the care management processes the organization applied to the homecare industry. We routinely receive compliments from our state surveyors regarding our clinical management review processes. The organizations commitment to a disease management care delivery model reduces risk, improves outcomes, and is a direct compliance control.
www.amedisys.com
Business Systems Infrastructure
Summary of Clinical Auditing and Trends
The organization audits its clinical care delivery frequently and on a recurrent basis. Annual clinical auditing is broken down into (6) categories:
| 1. | Clinical Oversight Audit |
| 2. | Quality Improvement Clinical Audits |
| 3. | Sarbanes Oxley/IA Clinical Audits |
| 4. | Compliance Clinical Audits |
| 5. | State Surveyor Clinical Audits |
| 6. | Fiscal Intermediary Clinical Audits |
Clinical Oversight Audits
Two times a year all homecare locations nationwide are risk stratified. This stratification is not based upon poor clinical survey results from regulatory bodies, but rather it is a proactive stratification to identify locations that have the potential for future clinical risk. All higher scoring locations are proactively placed upon clinical improvement plans.
This recurrent audit infrastructure ensures the organization deploys its resources in a proactive manner designed to prevent poor clinical survey results from occurring.
Year | Locations Assessed | Charts Audited | ||||
2006 | 261 | 2,700 | ||||
2007 | 325 | 1,300 | ||||
2008 | 500 | * | 540 | * |
| * | Projected by year end |
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
Quality Improvement Clinical Audits
The organizationsQuality Improvement Planrequires that all locations audit a minimum ten percent of their census quarterly. These audits are uploaded into a system wide web site for aggregation, trending and submission of improvement plans. This is a further layer of proactive clinical auditing the company employs to ensure clinical standards are maintained.
Year | Locations Assessed | Charts Audited | ||||
2006 | 261 | 8,292 | ||||
2007 | 325 | 11,135 | ||||
2008 | 500 | * | 12,062 | * |
| * | Projected by year end |
Sarbanes Oxley Clinical Audits
Each year the organization is responsible for performing clinical audits to determine if there exists any control breakdowns in the form of significant deficiencies or material weaknesses in its billing or clinical practices. These revenue assurance audits are performed by a combination of outside consultants, the Internal Audit division and the Company’s Sox division.
Below summaries the clinical information to date:
Year | Charts Audited | Significant Deficiency | Material Weakness | |||
2006 | 920 | No | No | |||
2007 | 501 | No | No | |||
2008* | 300 | TBD | TBD | |||
Total | 1,701 |
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
Compliance Clinical Investigations
The Compliance division conducts a combination of clinical investigations. These are conducted as the result of confidential inquires phoned into the compliance hotline, a risk-based screening process and focused clinical reviews based upon requests from the Operational line.
Outlined below are the totals of by year.
Year | Charts Audited | |
2006 | 87 | |
2007 | 58 | |
2008 | 74 YTD | |
Total | 219 |
State Surveyor Clinical Audits
External audits are conducted on an annual recurrent basis by the individual state regulatory bodies. These regulatory bodies typically audit a sample of 10 records or more per site to determine if services are being provided according to stated Medicare guidelines.
If poor survey results are not improved by the surveyors’ return assessment date, the state regulatory entity has the legislative authority to bar the provider from participating in the Medicare program. In its twenty five year history, the organization has never had any location closed by a regulatory body due to poor survey results or inadequate clinical standards.
Year | Locations | Number Surveys | Chart Samples | |||
2005 | 208 | 57 | 570 | |||
2006 | 261 | 96 | 950 | |||
2007 | 325 | 121 | 1,210 | |||
| Total | 2,730 |
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
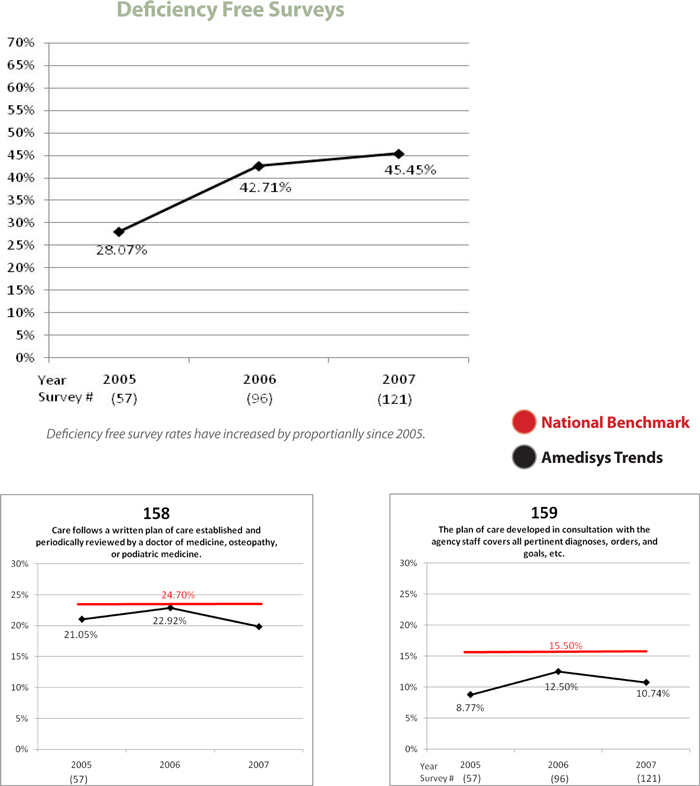
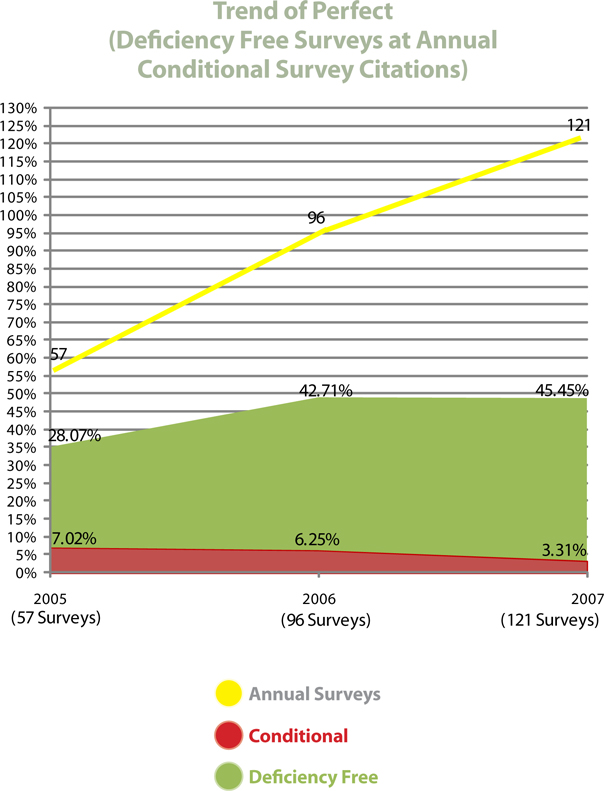
External State Survey Result Trends
The organization has experienced year over year improvements in its external state survey results. The percentage of deficiency-free surveys (perfect surveys with no citations) has increased proportionally. We believe these results can be attributed to the roll out of our Point of Care system which contains embedded compliance controls and the volume of proactive clinical auditing the organization performs.
For explanation, state surveyors issue deficiency citations for items such as missing documentation or policy/process errors. These items, by nature, are lower risk citations. More serious citations are known as condition level deficiencies and can put the provider number at risk, if problems are not addressed.
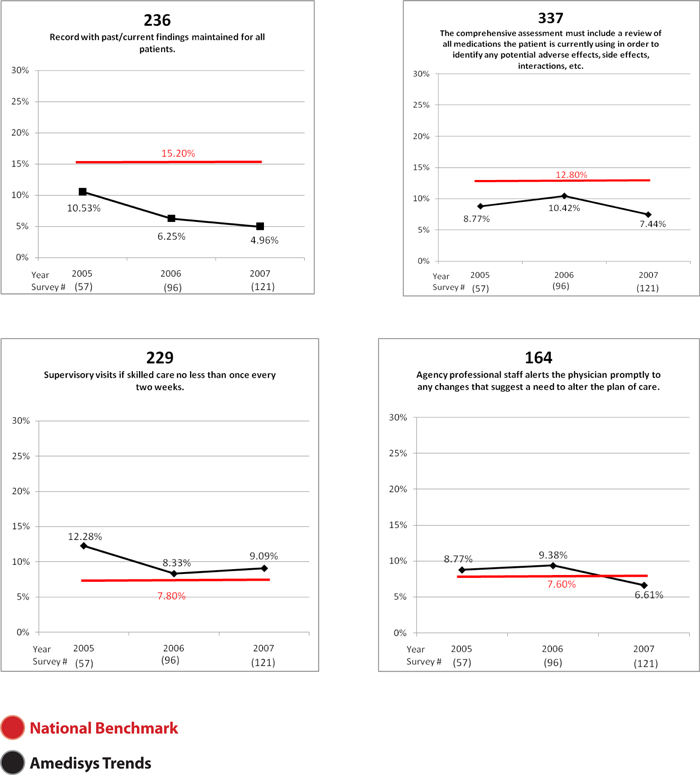
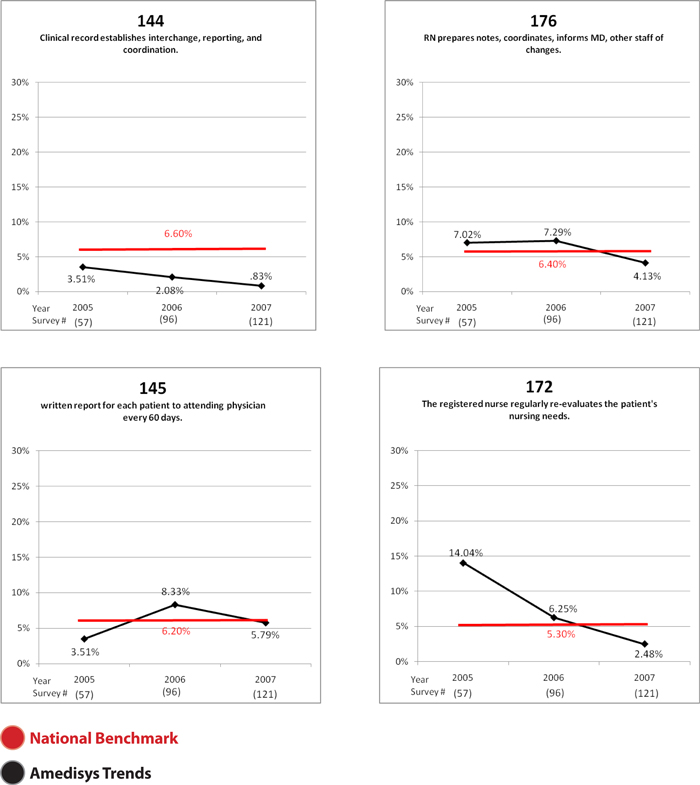
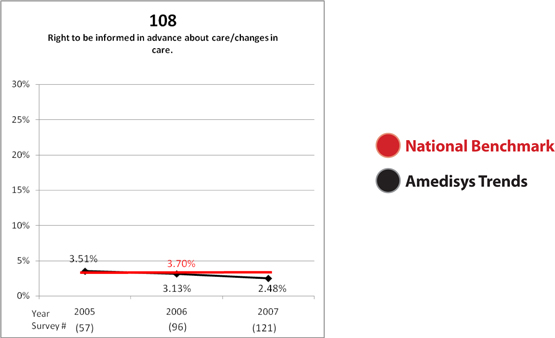
Outlined below is where the organization ranks related to CMS self reported survey deficiency/citation rates. Out of the top 15 citations reported by CMS, Amedisys survey citation rate is less than the national average in 14 of 15 categories.
| CMS Top 15 Survey Deficiencies | Indicates less than national average of citations | [GRAPHIC APPEARS HERE] | ||||||
Deficiency | Description | National Deficiency% | Amedisys Deficiency% | |||
G0158 | Written plan of care established & periodically reviewed | 24.7 | 19.8 | |||
G0159 | Plan of care covers diagnoses, required services, visits, etc. | 15.5 | 10.7 | |||
G0236 | Record with past/current findings maintained for all patients | 15.2 | 5.0 | |||
G0337 | Assessment includes review of all medications | 12.8 | 7.4 | |||
G0229 | Supervisory visits if skilled care no less than once every two weeks | 7.8 | 9.1 | |||
G0164 | Alert physician to changes that suggest need to alter plan | 7.6 | 6.6 | |||
G0143 | Coordination of patient services | 7.6 | 5.0 | |||
G0165 | Drugs & treatment administered only as ordered by physician | 7.3 | 4.1 | |||
G0121 | Compliance with accepted professional standards/principles | 6.7 | 3.3 | |||
G0170 | Skilled nursing services furnished in accordance with plan of care | 6.7 | 3.3 | |||
G0144 | Clinical record establishes interchange, reporting & coordination | 6.6 | 0.8 | |||
G0176 | RN prepares notes, coordinates, informs MD, other staff of changes | 6.4 | 4.1 | |||
G0145 | Written report for each patient to attending physician every 60 days | 6.2 | 5.8 | |||
G0172 | RN regularly re-evaluates patient nursing needs | 5.3 | 2.5 | |||
G0108 | Right to be informed in advance about care/changes in care | 3.7 | 2.5 | |||
Source: CMS
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)

www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
Fiscal Intermediary Clinical Audits
The external organizations contractually responsible for processing Medicare payments on the governments’ behalf conduct annual recurrent clinical audits to determine if organizations are billing for services appropriately. These audits are known as Focused Medicare Reviews (FMRs).
Providers are placed on FMR for a quarter duration at a time. Clinical records are requested and reviewed by the external entity. If a provider’s payment denial rate is less than 10 percent by quarter end, they are removed from the edit. If the denial rate is greater than 10 percent, the edit will be extended into subsequent quarters.
If a provider’s FMR status has been extended beyond four quarters in duration, the Fiscal Intermediary has the regulatory authority to request that a sample methodology be applied to the homecare provider. In this case, a sample of records is requested, a payment denial is determined through a clinical audit process and that payment denial percentage is applied to the provider’s annual Medicare revenue for a specified year and/or multiple years.
In its twenty five year history, the organization has never had a sampling methodology applied to any of its provider numbers.
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
Clinical audit tally by year
Outlined below are both internal and external audits combined.
| 2006 | 2007 | 2008 | |||||
Clinical Oversight | 2,700 | 1,330 | 540 | * | |||
Quality Improvement | 8,292 | 11,135 | 12,062 | ||||
Sarbanes Oxley/IA | 920 | 501 | 300 | * | |||
Compliance | 87 | 58 | 74 | (YTD) | |||
External State Surveyor | 960 | 1,200 | 1,050 | (YTD) | |||
Total annual clinical audits | 12,959 | 14,224 | 14,026 |
| * | Estimate |
Summary
Organizational trends from 2006 to present reflect the following clinical/compliance dynamics:
| • | The company’s recurrent clinical auditing processes have provided it with an infrastructure designed to proactively identify and mitigate clinical risk before receiving a poor survey from a regulatory body. |
| • | The point of care technology rolled out companywide in 2007 enhanced many documentation controls. |
| • | State surveyor citations have significantly reduced from 2006 to present. |
| • | Surveys without deficiencies have increased proportionally. |
| • | Using CMS self reported survey deficiency percentages as a benchmark, Amedisys is better than national citation percentages in 14 of the top 15 categories. |
| • | Using CMS publically reported clinical outcomes as a benchmark, Amedisys is better than national averages in 10 of the top 12 categories. |
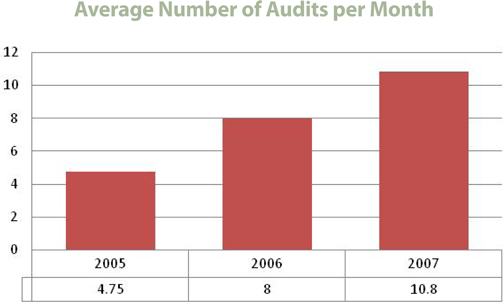
External audits by outside regulatory bodies have increased from 5 per month to in excess of 10 per month over the last three (3) years. During that timeframe the organization has experienced both an increase in deficiency-free (perfect) surveys and a corresponding decrease in condition level surveys.
www.amedisys.com
Summary of Clinical Auditing and Trends (continued)
Amedisys plans to continue to focus on enhancing its proactive controls with processes, procedures and automation designed to provide an effective control environment.
www.amedisys.com