[LETTERHEAD OF BUREAU VERITAS UK LTD]
AstraZeneca PLC
Legal & Secretary’s Department
2 Kingdom Street
London
W2 6BD
For the attention of Adrian Kemp
By fax 020 7604 8151 & by post
25 March, 2013
Dear Ladies and Gentlemen
BUREAU VERITAS STATEMENT OF ASSURANCE FOR ANNUAL REPORT AND FORM 20-F INFORMATION 2012
In connection with the anticipated filing by AstraZeneca PLC (“AstraZeneca”) of a Form 20-F with the US Securities and Exchange Commission, Bureau Veritas hereby authorizes AstraZeneca to refer to Bureau Veritas’s external assurance on corporate responsibility related information as stated on page 49 and identified (highlighted in yellow) on the pages of the Annual Report and Form 20-F Information for the fiscal year ended December 31, 2012 (the “Annual Report”) annexed as Exhibit A, which is incorporated by reference in the registration statements No. 33-83774 for AstraZeneca and Zeneca Wilmington Inc. and No. 333-145848, No. 333-114165 and No. 333-171306 for AstraZeneca, each on Form F-3, and in the registration statements No. 333-09060, No. 333-09062, No. 33-65362, No, 33-65366, No. 333-12310, No. 333-12426, No. 333-12428, No. 333-13328, No. 333-13918, No. 333-124689, No. 333-152767 and No. 333-170381 on Form S-8 for AstraZeneca.
Our authorization is subject to AstraZeneca’s acknowledgement and agreement that:
| | 1) | Bureau Veritas has undertaken an independent review of the corporate responsibility information disclosed in the Annual Report and provided an opinion as to the accuracy and reliability of the information subject to the scope, objectives and limitations defined in the full assurance statement posted on AstraZeneca’s responsibility website; |
| | 2) | AstraZeneca acknowledges and agrees that Bureau Veritas shall not be deemed an “Expert” in respect of AstraZeneca’s securities filings, and AstraZeneca agrees that it shall not characterize Bureau Veritas as such; and |
| | 3) | AstraZeneca accepts full responsibility for the disclosure of all information and data, including that relating to Bureau Veritas, set forth in the Annual Report as filed with the SEC and agrees to indemnify Bureau Veritas from any third party claims that may arise therefrom. |
Please indicate your agreement to the foregoing by signing in the space indicated below. Our authorization will not become effective until accepted and agreed by AstraZeneca.
Very truly yours,
/s/ Rachel Noel
Rachel Noel, Principal Consultant (Assurance Services)
For and on behalf of Bureau Veritas UK Ltd
ACCEPTED AND AGREED
this 25th day of March 2013
AstraZeneca PLC
/s/ Adrian Kemp
Name: Adrian Kemp
Title: Company Secretary
Exhibit A
In 2012, there was Core R&D expenditure of $4.5 billion in our R&D organisation (2011: $5 billion; 2010: $4.2 billion). In addition, $5,228 million was spent on acquiring product rights (such as in-licensing) (2011: $189 million; 2010: $1,017 million) and we invested approximately $791 million on the implementation of our R&D restructuring strategy. The allocations of spend by early development and late-stage activities are presented in the R&D spend analysis table opposite.
R&D ethics
We want to be recognised for our high quality science and for the impact we can make on serious diseases, and to be trusted for the way we work. Our standards of R&D ethics are global and apply to all AstraZeneca research activity, in all locations, whether conducted by us or on our behalf by third parties.
Clinical trials†
Our commitment:to deliver consistently high standards of ethical practice and scientific conduct in all our trials worldwide and to public transparency on registration and results of all clinical trials, whether positive or negative.
Our objective:to be recognised as an industry leader in the publication and sharing of clinical trial information.
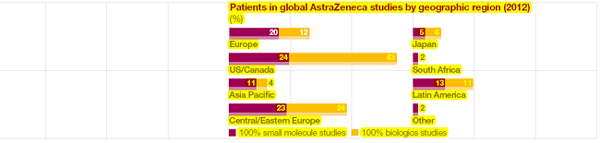
We conduct clinical trials at multiple sites in several different countries/regions as shown in the chart above. A broad geographic span helps us to ensure that those taking part in our studies reflect the diversity of patients around the world for whom the new medicine is intended. This approach also helps to identify the types of people for whom the treatment may be most beneficial.
Our global governance process for determining where we place clinical trials provides the framework for ensuring a consistent approach worldwide. We take several factors into account, including the availability of experienced and independent ethics committees and a robust regulatory regime, as well as sufficient numbers of trained healthcare professionals and patients willing to participate in a trial.
Before a trial begins, we work to make sure that those taking part understand the nature and purpose of the research and that proper procedure for gaining informed consent is followed (including managing any special circumstances, such as different levels of literacy). Protecting participants throughout the trial process is a core priority and we have strict procedures in place to ensure that they are not exposed to any unnecessary risks.
All our clinical studies are conceptually designed and finally interpreted in-house but a percentage of them are run for us by contract research organisations (CROs). In 2012, around 31% of patients in our small molecule studies and around 87% of patients in our biologics studies were monitored by CROs on our behalf. We contractually require CROs to work to our global standards and we conduct risk-based audits to monitor compliance.
Animal research†
Our commitment: to embrace, promote and embed scientific and technical best practice in animal research.
Our objective: to drive continuous improvement internally and engage with external providers on the implementation of AstraZeneca global standards for non-human primate housing and care. These include the following targets:
| > | roll-out of AstraZeneca Good Statistical Practice (GSP) global standard and associated compliance monitoring |
| > | more than 80% of external providers of AstraZeneca non-human primate research studies are operating to AstraZeneca standards. |
We remain committed to minimising our use of animals in our research without compromising the quality of the research data. Wherever possible, we use non-animal methods, such as computer modelling, that eliminate the need to use animals early in drug development or reduce the number required. We also work to refine our existing methods. This replacement, reduction and refinement of animal studies is known as ‘the 3Rs’. To support our drive for
continuous improvement, we work both within AstraZeneca and the wider scientific community to share the 3Rs knowledge and learning.
The number of animals we use will continue to vary because it depends on a number of factors, including the amount of pre-clinical research we are doing, the complexity of the diseases under investigation and regulatory requirements. We believe that, without our active commitment to the 3Rs, our animal use would be much greater. In 2012, we used approximately 304,000 animals in-house (2011: 381,000). In addition, approximately 14,000 animals were used by external CROs on our behalf (2011: 17,000). Against our 2012 target of more than 80%, 85% of our externally-placed non-human primate studies met AstraZeneca standards in 2012. We will continue to progress towards our 2013 target of 100% of our studies being conducted in facilities meeting AstraZeneca required standards.
The welfare of the animals we use continues to be a top priority and our Bioethics Policy applies worldwide. We routinely have inspections by government authorities of our internal animal research facilities. External CROs that conduct animal studies on our behalf are required to comply with our global standards and we undertake audits to ensure our expectations are being met.
During 2012, we developed, launched and began implementation of standard operating procedures and guidance documents to underpin our new GSP global standard, developed in 2011. These apply to our internal animal research and the launch included extensive training programmes for relevant scientists, technical staff and managers across the organisation.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found in the Responsible Business section from page 48 and on our website, astrazeneca.com/responsibility. |

| | |
| AstraZeneca Annual Report and Form 20-F Information 2012 | | 33 |
Performance |Business Review
Patient safety†
Our commitment: the safety of the patients who take our medicines is of fundamental importance to us.
Our objective: to enhance pharmacovigilance awareness – including the use of collaborative programmes to share and use our knowledge and best practice in order to improve reporting and patient safety in developing countries.
All drugs have potential side effects and we aim to minimise the risks and maximise the benefits of each of our medicines throughout the whole life-cycle of a medicine. We continually monitor the use of all our medicines to ensure that we become aware of any side effects not identified during the development process. This is known as pharmacovigilance and is core to our ongoing responsibility to patients. We have comprehensive and rigorous systems in place for detecting and rapidly evaluating such effects,
including mechanisms for highlighting those that require immediate attention. We also work to ensure that accurate, well-informed and up-to-date information concerning the safety profile of our drugs is provided to regulators, doctors, other healthcare professionals and, where appropriate, patients.
A pharmacovigilance awareness programme was developed in 2012 and circulated to marketing companies, together with guidance about how the information should be shared with regulatory authorities in readiness for external enquiry. One such opportunity arose when SFDA (the Chinese health authority) met UMC (WHO Uppsala Monitoring Centre) and we were able to share our experience and thoughts around signal management.
We have an experienced, in-house team of clinical patient safety professionals dedicated to the task of ensuring that we meet our commitment to patient safety.
At a global level, every medicine in development and on the market is allocated a Global Safety Physician and a team of patient safety scientists. In each of our markets we also have dedicated safety managers with responsibility for patient safety at a local level.
Our Chief Medical Officer has overall accountability for the benefit/risk profiles of the products we have in development and those on the market. He provides medical oversight and ensures that appropriate risk assessment processes are in place to enable informed decisions to be made about safety as quickly as possible.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found in the Responsible Business section from page 48 and on our website, astrazeneca.com/responsibility. |
Clinical trial transparency
AstraZeneca has a long-standing commitment to making information about our clinical research publicly available to enhance the scientific understanding of how our medicines work and in the medical interest of patients. By the end of 2012, we had registered 2,050 clinical trials and posted the results of 1,360 trials on a range of public websites including our own dedicated clinical trials website, astrazenecaclinicaltrials.com.
We publish information on the registration and results of all new and ongoing AstraZeneca-sponsored clinical trials for all products in all phases, including marketed medicines, drugs in development and drugs whose further development has been discontinued. We post results, irrespective of whether they are favourable or unfavourable to AstraZeneca.
| > | Our disclosure policy goes beyond legal requirements, which currently require publication for Phase II studies onwards only. |
| > | From 15 January 2013, we are voluntarily disclosing the research protocol for our clinical trials on astrazenecaclinicaltrials.com once a manuscript relating to an investigational or approved product is published in a peer-reviewed medical journal. |
These disclosure requirements are set out in our Bioethics Policy and compliance is mandatory across the Group.
We consider requests for patient-level data from other parties on a case-by-case basis, following consistent criteria to establish if, and how, the information provided will be used for valid scientific purposes and to benefit patients.
Calls for ‘open access’ to clinical data raise complex practical, legal and ethical issues around full disclosure of patient information. Decision makers, as well as academia and industry, have a duty to consider all the implications that could arise from such proposals. These include ensuring scientific rigour, safeguarding patient privacy and protecting innovation and medical progress. We are engaging with regulators, legislators, industry, and medical and scientific bodies to discuss the issues raised by the proposals to routinely publish full clinical trial and patient data so we can collectively identify practicable solutions that deliver real benefits to medical science and patients.
| | |
| 34 | | AstraZeneca Annual Report and Form 20-F Information 2012 |
Performance |Business Review
Global strategies tailored to meet local needs
We focus on developing global strategies tailored to meet local needs and recognise that our commercial capabilities must evolve to meet future market requirements. The pace and degree of change in global economies and intensifying regulatory and access challenges have led us to look at ways of better and more efficiently addressing the changing needs and preferences of payers, prescribers and patients. In 2012, this effort included completing the regional consolidation of our Commercial organisation announced in 2011. Our streamlined operating model includes integrating our smaller local marketing companies into area clusters, allowing them to benefit from global resources while staying local and concentrating on meeting local customer needs.
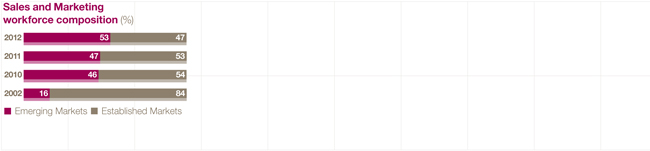
All our markets have a role to play in delivering our commercial strategy. We continue to prioritise investment and allocate our resources in the most cost-effective way. This allows us to identify those markets of major significance to us, those that will become more important drivers of our business in the future and highlight those Established Markets where we need to refocus our approach to deliver sustained success. Our footprint continues to evolve to reflect declining sales in Established Markets and increasing sales in Emerging Markets. For example, in 2012 we enhanced our presence in Asia with the opening of the Zhangjiang Park Regional Hub Headquarters in Shanghai.
Changing customer needs
In most countries, our sales are made through wholly-owned local marketing companies. In other countries, we sell through distributors or local representative offices. Our products are marketed primarily to primary care and specialist doctors. Our efforts are directed towards explaining the therapeutic as well as the economic benefits of our products to doctors, governments and others who pay for healthcare.
Historically, our commercial model has been based on the use of face-to-face marketing techniques. This is now changing to reflect the changing profile of the prescribers of our medicines. For example, primary care physicians tend to be younger on average than previously, a greater proportion is female, and more work part-time. Primary care physicians want to interact with pharmaceutical companies in different ways. Driven by experience from innovative approaches piloted and implemented in North America and Europe, we have changed the way we work. Improvements include the introduction of office-based sales teams, which include physicians and dedicated customer service staff, and expanded use of digital channels. These selling channels have now been rolled out in more than 30 countries and across a range of products. Evidence to date suggests these channels are appreciated by those who use them and are an efficient and effective way of driving value for our business. We are accelerating the roll-out and adoption of the new model in the majority of markets in which we operate.
Pricing our medicines
Our challenge is to deliver innovative medicines that improve health for patients, bring benefits to society and provide an appropriate return on our investment. Our global pricing policy provides the framework to ensure appropriate patient access while optimising the profitability of all our products in a sustainable way. When setting the price of a medicine, we take into consideration its full value to patients, to those who pay for healthcare and to society in general. We also pursue a flexible approach to the pricing of our medicines. For example, we support the concept of differential pricing, provided that appropriate safeguards are in place to ensure that differentially priced products are not diverted from patients who need them to be sold and used in more affluent markets.
Delivering value for payers
Our medicines play an important role in treating unmet medical need. In doing so, they bring economic as well as therapeutic benefits. Effective treatments can help to lower healthcare costs by reducing the need for more expensive care, such as hospital stays or surgery, or through preventing patients from developing more serious or debilitating diseases that are costly to treat. They also contribute to increased productivity by reducing or preventing the incidence of diseases that keep people away from work.
As outlined in the Pricing pressure section on page 18, there is continued downward pressure on drug pricing and, in the current difficult economic environment, payers expect us to be able to define the value our medicines create. We are acutely aware of the challenges facing those who pay for healthcare and are committed to delivering value, which will allow us to bring our medicines to the patients that need them. Therefore, we work with payers and healthcare providers to understand their priorities and requirements and generate evidence regarding how our products offer value and support cost-effective healthcare delivery.
Increasing access to healthcare†
Our commitment: to increase access to healthcare for under-served patient populations in a sustainable way.
Our objective:to roll-out our access to healthcare strategy within the business and further develop the framework for implementation, including non-financial performance indicators for monitoring our performance across all our initiatives.
Sales of medicines in our Established Markets enable us to generate the revenue we need to provide our shareholders with a return, invest in continued innovation and pursue other opportunities to expand the availability of our medicines. Increasing that availability and increasing access to healthcare for under-served patient
| | |
| 38 | | AstraZeneca Annual Report and Form 20-F Information 2012 |
populations in a sustainable way is a significant global challenge and, in March 2012, we announced our access to healthcare strategy to help in that process. The strategy framework is explained on our website, astrazeneca.com/responsibility. It seeks to take account of the different barriers to healthcare around the world and is tailored locally to meet the needs of different patient populations. We are pursuing a range of initiatives, including broadening affordability of our medicines, across these populations to understand what works best and in what context.
During the year, we rolled out our access to healthcare framework within our Global Sales and Marketing Organisation to support further development of our existing approach and to enable us to capture ongoing ‘broadening affordability’ commercial initiatives. For example, our work to expand patient access to healthcare in countries such as Brazil, Romania and Ukraine continues with a range of different commercial approaches being adopted. In China, we are pursuing our strategy to reach patients in the broader market, beyond the big hospitals in the big cities, by developing new commercial channels for reaching emerging hospitals and community health centres. Best practice will be shared and replicated. In addition, in 2012, we acquired Guangdong BeiKang Pharmaceutical Company Limited, a generics manufacturing company in China which gave us access to a portfolio of injectable medicines used to treat infections. First launches are planned for 2013 and underscore our intention to serve the health needs of Chinese patients through our innovative medicines and, increasingly, high quality branded generic treatments that are locally produced to global standards. You can read more about our strategy and the accessinitiatives we have under way on our website, astrazeneca.com.
We are making progress on the development of non-financial indicators for monitoring our performance and these are included in our 2013 Responsible Business Plan.
Sales and marketing ethics†
Our commitment:to deliver consistently high ethical standards of sales and marketing practice worldwide.
Our objective:to focus on ensuring compliance with our Ethical Interactions Policy and report on the:
| > | number of confirmed breaches of external sales and marketing codes |
| > | number of instances of failure to meet our standards in the Global Commercial Organisation, including contract staff |
| > | number of corrective actions for breaches of our Code of Conduct or supporting policies by Commercial employees, including contract staff. |
During 2012, we continued to provide training for employees on our global standards that govern the way that we conduct our business around the world. We have comprehensive processes in place for monitoring compliance with our Code of Conduct and global policies, including dedicated compliance professionals who support our line managers locally in monitoring their staff activities. We also have a network of nominated signatories who review our promotional materials against all applicable requirements. Additionally, in 2012, audit professionals have conducted compliance audits of a selection of our marketing companies.
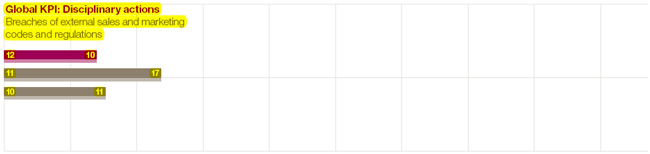
As shown in the Global KPI: Disciplinary actions chart opposite, we identified a total of 10 confirmed breaches of external sales and marketing regulations or codesglobally in 2012 (17 in 2011). There were 1,932 instances, including contract staff, of failure to comply with AstraZeneca’s Code of Conduct and global policies in our Global Commercial Organisation, the majority of which were minor (1,292 in 2011, including external breaches). We believe that the movement in both numbers reflects our enhanced management oversight and compliance monitoring.
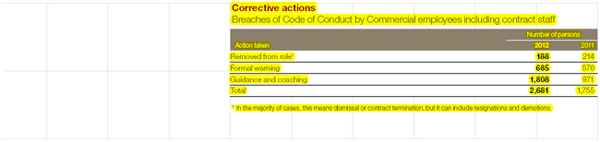
As shown in the Corrective actions table above, in relation to these breaches (and it is important to note that a single breach can involve more than one person failing to meet the standards required), we removed 188 people from their role, formally warned 685 people and provided further guidance or coaching on our policies for 1,808 people. The most serious breaches are raised with the Audit Committee.
US Corporate Integrity Agreement reporting
In April 2010, AstraZeneca signed an agreement with the US Department of Justice to settle an investigation relating to the sales and marketing ofSeroquel IR. The requirements of the associated Corporate Integrity Agreement between AstraZeneca and the Office of the Inspector General of the US Department of Health and Human Services (OIG) include a number of active monitoring and self-reporting obligations that differ from self-reporting required by authorities in the rest of the world. To meet these obligations, AstraZeneca provides notices to the OIG describing the outcomes of particular investigations potentially relating to violations of certain laws, as well as a separate annual report to the OIG summarising monitoring and investigation outcomes relevant to Corporate Integrity Agreement requirements.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found in the Responsible Business section from page 48 and on our website, astrazeneca.com/responsibility. |
| | |
| AstraZeneca Annual Report and Form 20-F Information 2012 | | 39 |
Performance |Business Review
Working with suppliers†
Our commitment:to integrate AstraZeneca ethical standards into our procurement activities and decisions worldwide.
Our objective: to monitor compliance through our ongoing assessment and programmes with focus on areas experiencing highest challenges; to address challenges with our suppliers and promote improvement through collaboration.
Our Global Responsible Procurement Standard defines one of the key business processes for integrating our ethical standards into our procurement activity and decision making worldwide. It includes detailed expectations of suppliers. The process is based on an escalating set of risk-based due diligence activities, applied in a pragmatic way. The same initial assessment process is used for all suppliers and more detailed, focused assessments are then made, relevant to the service provided. Since the programme began in 2009, we have completed 5,661 assessments of new and existing suppliers, which accounts for approximately two-thirds of our spend on suppliers.
We categorise suppliers as high, medium or low risk. We focus our auditing efforts on high and medium risk rated suppliers but we also audit some suppliers that we consider to be lower risk, to confirm our performance expectations across all suppliers we do business with. In 2012, we continued our audit activity with 482 audits across 52 countries (751 audits in 2011) as set out in the table on the previous page.
Forty-three percent of suppliers audited demonstrated standards that met our expectations, with a further 53% implementing improvements to address minor non-compliances. We monitor progress across all corrective actions and 4% of suppliers audited this year will require significant follow up to confirm they will make the improvements we require. We will not use suppliers who are unable or unwilling to meet our expectations in a timely way. During 2012, we removed eight suppliers from our supply chain.
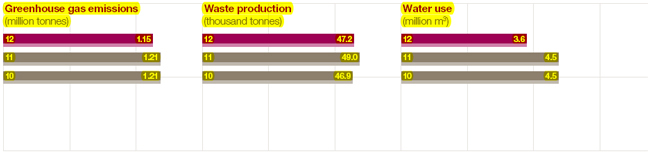
Environmental impact†
Our commitment:to minimise the environmental impact of our operations by reducing the carbon footprint and natural resource demands of our own and our suppliers’ business activities.
Our targets for 2012‡ included reducing:
| > | operational greenhouse gas footprint to 890 kilo tonnes CO2 e/yr |
| > | hazardous waste to 0.70 tonnes/$m sales and non-hazardous waste to 0.52 tonnes/employee |
| > | water use to 4.0 million m3. |
Our SHE strategy and associated objectives and targets for 2011 to 2015 provide the framework for driving our environmental sustainability going forward. This section includes summary information about certain key areas of the framework. Full details of our strategy, objectives and targets are available on our website, astrazeneca.com/responsibility.
We work to reduce our greenhouse gas emissions by, among other things, improving our energy efficiency and pursuing lower-carbon alternatives to fossil fuels at our sites. We strive to ensure that our travel and transport activities are as efficient as possible. Our carbon footprint is also affected by some of our respiratory therapies, specifically our pressurised metered-dose inhalers that rely on hydrofluoroalkane (HFA) propellants to deliver the medicine to a patient’s airways. While HFAs have no ozone depletion potential and a third or less of the global warming potential than the chlorofluorocarbons (CFCs) they replace, they are still greenhouse gases. Our target is to reduce our operational greenhouse gas footprint (excluding emissions from patient use of our inhaler therapies) by 20% from our 2011 levels by 2015. In 2012, our gross greenhouse gas emissions (from all sources) totalled 1.15 million tonnes (41 tonnes/$m indexed to Group revenue).
The management of waste is another key aspect of our commitment and we have a 2015 target of a 15% reduction in hazardous and non-hazardous waste from our 2011 levels. Our primary focus is waste prevention, but where this is not practical, we concentrate on waste minimisation and appropriate treatment or disposal to maximise the reuse and recycling of materials and minimise disposal to landfill. In 2012, our total waste was 47,000 tonnes with a tonnes/$m index of 1.7.
We recognise the need to use water responsibly and, where possible, to minimise the use of water in our facilities. To support the delivery of our target to reduce water use by 25% from our 2011 levels by 2015, we now have water conservation plans at our largest sites. In 2012, our water use was 3.6 million m3 with a m3/$m index of 130.
We are also working to ensure that we measure and report the impact of our external manufacturing activity on the environment, and that our suppliers have appropriate environmental improvement targets.
Our continued commitment to product stewardship is underpinned by our ongoing work to integrate environmental considerations into a medicine’s complete life-cycle, from discovery and development, through manufacturing, marketing and to its ultimate disposal. Further information is available on our website, astrazeneca.com/ responsibility, including environmental risk assessment data for our medicines.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found in the Responsible Business section from page 48 and on our website, astrazeneca.com/responsibility. |
| ‡ | The following figures have been revised from those previously published to incorporate our biologics capabilities into our targets. |
| | |
| 42 | | AstraZeneca Annual Report and Form 20-F Information 2012 |
Performance |Business Review
Further developing leadership and management capabilities
We encourage and support our people in achieving their full potential by providing a range of learning and development (L&D) programmes. These are designed to build the capabilities and encourage the behaviours needed to deliver our business strategy.
We have a global approach, supported by the creation of our global talent and development organisation, to ensure that high standards of L&D practice are applied across AstraZeneca. We continue to develop and deploy instructor-led and online development resources, which we aim to make available to all employees to increase access to learning and to support self-development.
We recognise the importance of good leadership and its critical role in stimulating high levels of performance and engagement. Our leadership development frameworks are focused on the core capabilities that we believe are essential for strong and effective leadership. These capabilities are defined for each level in the organisation and apply to all our employees. We complement our leadership capabilities with a set of manager accountabilities, which define what we expect from our managers. These manager accountabilities are further enabled across all markets through the deployment of our global HR platform.
Alongside judicious hiring of new leaders into critical senior roles, the development of an internal pipeline of future global leaders is a high priority. We identify individuals with
the potential for more senior and complex roles. These talent pools provide succession candidates for a range of leadership roles across
AstraZeneca. We regard these individuals as key assets to the organisation and we proactively support them to reach their potential through, for example, global talent development programmes and targeted development opportunities.
Changes to the Senior Executive Team announced in January 2013 included the promotion of six internal candidates and demonstrate our commitment to the development of senior leaders.
We remain committed to making full use of the talents and resource of all our people. We have policies in place to avoid discrimination, including on the grounds of disability. Our policies cover recruitment and selection, performance management, career development and promotion, transfer, and training (including re-training, if needed, for people who have become disabled) and reward.
Improving the strength and diversity of the talent pipeline†
Our commitment:to build an inclusive, open and trusting organisation embracing the skills, knowledge and unique ability of our employees.
Our objective:to accelerate diversity and inclusion appropriately throughout the business, build accountability and track progress. Our target for 2015 is to improve female representation:
| > | at senior manager level and above from 38% (2010) to 43% (2015) |
| > | in the global talent pool from 33% (2010) to 38% (2015). |
Our global workforce provides a diversity of skills, capabilities and creativity, and we value the benefits that such diversity brings to our business. We aim to foster a culture of respect and fairness where individual success depends solely on ability, behaviour, work performance and demonstrated potential. As we continue to reshape our organisation and geographic footprint, our challenge is to ensure that diversity in its broadest sense is reflected in our workforce and leadership, and integrated into our business and people strategies. Within this context, we support the representation of women at the highest
levels in our business. Women make up 50% of our global workforce, giving us a real opportunity to develop female leaders. Indeed, there are currently three women on our Board (25%) and, below Board level, women account for 40% of senior management.
Under the leadership of a global Diversity & Inclusion steering group chaired by a member of the SET and comprising senior leaders from across the business and geographies, we are driving change in three key areas: ‘leadership & management capability’; ‘transparency in talent management & career progression’; and ‘work-life challenges’. In March 2012, we launched our Global Insight Exchange programme as a direct result of the work of the steering group. This programme, which consists of peer-to-peer mentoring of over 30 ‘learning pairs’ of identified talent from different functional areas and geographies within our organisation, is designed to accelerate the development of our leadership culture and talent pipeline through the exchange of diversity of thought and experience. In addition, we track gender representation at different levels of the organisation and country of origin representation of our senior leaders to measure progress over the medium term.
Driving employee engagement
We use a variety of global leadership communication channels to engage employees in our business strategy. These include face-to-face meetings, video conferencing and Yammer (a social media tool) to encourage two-way dialogue to take place. For the third year in a row our annual global employee survey (FOCUS) included an open text feedback mechanism, with around 25,000 comments made on a variety of topics.
| | |
| 44 | | AstraZeneca Annual Report and Form 20-F Information 2012 |
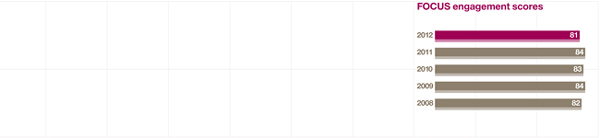
In 2012, 91% of our employees participated in the survey, which measures levels of employee engagement and considers the effectiveness of our organisational, leadership and management capabilities, and satisfaction in terms of employees’ working environment. Our employee engagement score decreased by three percentage points this year and our leadership communications and work-life balance scores also decreased. The survey took place at a challenging time for the Group and the scores were disappointing. We remained ahead of external pharmaceutical industry norms in areas such as motivation, willingness to put in more effort than would normally be expected, line management, and operating with integrity and ethics. However, we recognise that we have more work to do in important areas, such as strategic understanding and reducing organisational complexity, to ensure AstraZeneca is a great place to work. Local leadership teams have also identified actions designed to target any concerns specific to their organisational area.
A key element of our people strategy is the continued development of a performance culture across the organisation. By strengthening our focus on setting high quality objectives aligned to our business strategy, and ongoing coaching and feedback, we strive to ensure that performance at all levels of the organisation delivers value. The Board is responsible for setting our high-level strategic objectives and monitoring performance against them (see the Operation of the Board section on page 111). Managers across AstraZeneca are accountable for working with their teams to develop individual and team performance targets, and for ensuring that employees understand how they contribute to overall business objectives.
We will continue to empower our leaders to drive performance, to hold our managers accountable for understanding and delivering against the standards required, and to provide the tools necessary to reward outstanding contributions.
Our focus on optimising performance is reinforced by performance-related bonus and incentive plans. AstraZeneca also encourages employee share ownership by offering the opportunity to participate in various employee share plans, some of which are described in the Directors’ Remuneration Report from page 122 and also in Note 24 to the Financial Statements from page 179.
Human rights†
Our commitment:to respect and promote international human rights in our operations and our sphere of influence.
Our objective:to ensure that human rights considerations are appropriately integrated into our policies, processes and practices.
As reported in 2011, we have carried out labour reviews in 106 countries in which we have employees. The reviews focused on International Labour Organization (ILO) core areas, including freedom of association and collective bargaining, child labour, discrimination, working hours and wages. The framework for the review was provided by an adaptation of the employment section of the Danish Institute for Human Rights assessment tool for pharmaceutical companies, which was developed with our industry’s help and launched in 2010. Results showed that our practices are generally consistent across all countries, based on our mandate that our global standards areapplied when external national standards do not meet our minimum requirements. Some gaps to ILO standards have been identified and are being addressed as part of the review of our Global People Policy, which is planned for 2014.
Managing change
Recruitment in our Emerging Markets continues to be accompanied by headcount reductions in our Established Markets as a result of our continuing strategic drive to improve efficiency and effectiveness. Reductions have come about through restructuring in R&D, supply and manufacturing, support functions and our sales and marketing workforce. The net effect of these changes since the end of 2006 has been to reduce our total headcount by some 15,100 from 66,800 to 51,700. This decrease includes a reduction of 2,600 positions in 2010, 5,000 in 2011 and a further 6,300 in 2012, which resulted from our business change plans announced since 2010.
We are committed to ensuring that AstraZeneca’s core values, robust people policies, consultation infrastructure and prior experience were integrated into this multi-faceted business transformation. Trade unions and employee representative groups were involved throughout the restructuring process. With significant investment in outplacement support, high levels of success have been achieved in finding employees alternative opportunities outside AstraZeneca. Further details are set out in the Our strategy section from page 20.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found in the Responsible Business section from page 48 and on our website, astrazeneca.com/responsibility. |
| | |
| AstraZeneca Annual Report and Form 20-F Information 2012 | | 45 |
Performance |Business Review
Managing employee relations
We work to ensure a level of global consistency in managing employee relations, while allowing enough flexibility to support the local markets in building good relations with their workforces, taking into account local laws and circumstances. To that end, relations with trade unions are nationally determined and managed locally in line with the applicable legal framework and standards of good practice. However, each change programme has its unique challenges and a standard solution may not always be appropriate. Where this is the case, the appropriate solution is developed through consultation with employee representatives or, where applicable, trade unions, with the aim of retaining key skills and mitigating job losses.
Early in 2012, we implemented our Global Employment Standards, which are linked to our Global People Policy. Our Global Employment Standards serve to provide common and consistent expectations concerning the way in which our employees will be managed globally and cover matters including attendance, employee concerns, flexible working, leaving AstraZeneca, misconduct, performance improvement, redeployment and redundancy, and work-life balance.
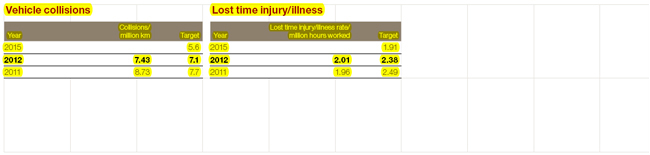
Safety, health and wellbeing†
Our commitment:to promote a safe, healthy and energising work environment in which our people, and those from third parties working closely with us, are able to express their talents, drive innovation and improve business performance.
Our targets for 2012 included:
| > | combined lost time injury/illness rate per million hours worked of 2.38 |
| > | 7.1 collisions per million kilometres driven. |
Driver safety remains our highest priority for improvement and our focus is on promoting driver safety among our sales forces, collectively the single largest group of employees who drive on AstraZeneca business. Driver safety targets are included in regional and local scorecards. Performance is monitored centrally to assess progress and identify areas for improvement. In 2012, we missed our annual target for collisions per million kilometres driven. We remain on track to achieve our 2015 target.
We regret that during 2012, two members of the public were killed in two separate road traffic accidents involving AstraZeneca drivers in Russia and Turkey. Detailedinvestigations into both accidents have been carried out. For the Russian accident, an action plan was formulated to respond to the findings of the investigation and those actions are being tracked. The investigation report for the Turkish accident, which occurred in October, has not yet been finalised. Learning from the investigations into both accidents will be shared widely across the Group.
In 2012, the lost time injury/illness rate increased by 3% from 2011. However, we remain on track to achieve our 2015 target of a 25% reduction in the lost time injury/illness rate from the 2010 baseline, with an overall 21% reduction achieved so far.
Work-related stress has been a particular focus for us in recent years; in 2012 we achieved a significant (59%) reduction in the number of reportable cases compared to 2011. We are continuing our efforts in this area, using a risk-based approach, including wellbeing risk assessment tools, to identify high-risk areas and target interventions effectively.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found in the Responsible Business section from page 48 and on our website, astrazeneca.com/ responsibility. |
| | |
| 46 | | AstraZeneca Annual Report and Form 20-F Information 2012 |
of 23 criteria in 2011) including marketing practices, supply chain management and human capital development. While these scores are encouraging, we lost ground in some areas including innovation management and health outcomes contribution. To better understand these lower scores, we commissioned an in-depth external benchmark survey and the analysis will be used to inform our improvement planning.
Responsible business governance
The Board is responsible for our responsible business framework and Non-Executive Director, Nancy Rothwell, oversees implementation and reporting to the Board.
The SET and senior managers throughout the Group are accountable for operating responsibly within their areas taking into account national, functional and site issues and priorities. Line managers are accountable for ensuring that their teams understand the requirements and that people are clear about what is expected of them as they work to achieve AstraZeneca’s business goals.
Our Responsible Business Council (the Council) is chaired by our Executive Vice-President of Human Resources & Corporate Affairs, and members include senior leaders from each relevant SET area. Its agenda is focused on driving long-term value creation by agreeing, among other things:
| > | responsible business priorities for the Group in line with strategic business objectives |
| > | managing and monitoring the annual process of setting responsible business objectives and targets recorded in the Responsible Business Plan, as well as reviewing performance against KPIs |
| > | appropriate policy positions to support AstraZeneca’s business objectives and reputation management. |
The Council is supported by a Responsible Business Working Group (the Working Group) of SET area representatives. Among other things, the Working Group continuously reviews external issues with the potential to impact AstraZeneca and, as appropriate, prepares management and measurement proposals for the Council’s consideration.
External assurance
Bureau Veritas has provided external assurance on the responsible business information contained within this Annual Report on pages 33-34, 38-39, 42, 44-46 and below, and of the performance related content of the Responsibility section of our website. Based on the evidence provided and subject to the scope, objectives and limitations defined in the full assurance statement, nothing has come to the attention of Bureau Veritas causing them to believe that the responsible business information included within this Annual Report is materially misstated. The full assurance statement, which contains detailed scope, methodology, overall opinion and recommendations can be found on our website, astrazeneca.com/responsibility. Bureau Veritas is an independent professional services company that specialises in quality, health, safety, social and environmental management with a long history of providing independent assurance services.
Community investment†
Our commitment:to meet our responsibility as a global corporation to support the wider community, maximising the benefit of our investment for all stakeholders, through focused investment and by embracing current best practice.
Our objective:to extend the geographic reach of our Young
Health Programme (YHP). Our target was to have 15 YHP country programmes running by the end of 2012 with a total target reach of 500,000 adolescents by 2015.
In 2012, we spent a total of $1.18 billion (2011: $1.06 billion*) on community investment sponsorships, partnerships and charitable donations worldwide, including our product donation and patient assistance programmes which make our medicines available free of charge or at reduced prices. Through our three patient assistance programmes in the US we donated products valued at an average wholesale price of over $1.12 billion (2011: $938 million). We also donated products worth over $5.8 million, valued at average wholesale price, to charitable organisations Americares and Direct Relief International.
Our global community investment strategy focuses on two key areas, healthcare in the community and science in education. In 2012, we continued to expand our YHP country programme. This is designed to help young people in need around the world deal with the health issues they face so they can improve their chances of living a better life. We currently have 15 country programmes under way around the world.
Through YHP, we have reached over 250,000 young people in communities across five continents with health information. Over 3,000 of these young people have been trained to share this health information with their peers and with the community, and over 2,700 frontline health providers have completed training programmes in adolescent health. We are on track to meet our Clinton Global Initiative commitment to reach 500,000 young people by the end of 2015. Initial findings from the Wellbeing of Adolescents in Vulnerable Environments study being undertaken by Johns Hopkins Bloomberg School of Public Health as part of YHP were presented at the World Health Summit in Berlin, Germany in October. As part of our best practice sharing, our dedicated online resource (younghealthprogrammeYHP.com) enables those working with young people to access information and resources created by the YHP partners.
Our support for science education takes a number of forms. For example, in 2011, we entered a three year partnership with Career Academies UK to support increased participation by 16 to 19-year-olds in Science, Technology, Engineering and Maths (STEM) subjects, with a target that one-third of Career Academies have a STEM theme by the 2014/15 academic year. By the 2012/13 academic year, the proportion was almost one-quarter, representing 48 Career Academies. Our work with Career Academies UK complements the involvement we have had since 2003 with the STEM ambassador programme.
| † | Extract from 2012 Responsible Business Plan. |
| | Further information on AstraZeneca’s approach to responsible business can be found above and on our website, astrazeneca.com/responsibility. |
| * | Figures re-stated to correct product donation data capture error in 2011. |
| | |
| AstraZeneca Annual Report and Form 20-F Information 2012 | | 49 |