UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
________________________________
FORM 10-Q
________________________________
CHECK ONE:
|
| |
| ý | QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the Quarterly Period Ended: March 31, 2017
OR
|
| |
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to .
Commission file No.: 1-12996
________________________________
Diversicare Healthcare Services, Inc.
(exact name of registrant as specified in its charter)
________________________________
|
| | |
| Delaware | | 62-1559667 |
(State or other jurisdiction of incorporation or organization) | | (IRS Employer Identification No.) |
1621 Galleria Boulevard, Brentwood, TN 37027
(Address of principal executive offices) (Zip Code)
(615) 771-7575
(Registrant’s telephone number, including area code)
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ý No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ý No ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and a “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
|
| | | | | |
| Large accelerated filer | | ¨ | Accelerated filer | | ¨ |
| | | | |
| Non-accelerated filer | | ¨(do not check if a smaller reporting company) | Smaller reporting company | | ý |
| | | | Emerging growth company | | ¨ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act.
| | ¨
|
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No ý
6,458,836
(Outstanding shares of the issuer’s common stock as of May 1, 2017)
Part I. FINANCIAL INFORMATION
ITEM 1 – FINANCIAL STATEMENTS
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
INTERIM CONSOLIDATED BALANCE SHEETS
(in thousands)
|
| | | | | | | |
| | March 31,
2017 | | December 31,
2016 |
| | (Unaudited) | | |
| CURRENT ASSETS: | | | |
| Cash and cash equivalents | $ | 3,931 |
| | $ | 4,263 |
|
| Receivables, less allowance for doubtful accounts of $10,824 and $10,326, respectively | 66,916 |
| | 62,152 |
|
| Other receivables | 1,149 |
| | 1,193 |
|
| Prepaid expenses and other current assets | 3,115 |
| | 3,623 |
|
| Income tax refundable | — |
| | 431 |
|
| Current assets of discontinued operations | 28 |
| | 28 |
|
| Total current assets | 75,139 |
| | 71,690 |
|
| PROPERTY AND EQUIPMENT, at cost | 131,038 |
| | 128,822 |
|
| Less accumulated depreciation and amortization | (71,389 | ) | | (69,022 | ) |
| Property and equipment, net | 59,649 |
| | 59,800 |
|
| OTHER ASSETS: | | | |
| Deferred income taxes | 20,785 |
| | 21,185 |
|
| Deferred lease and other costs, net | 180 |
| | 193 |
|
| Other noncurrent assets | 3,588 |
| | 3,108 |
|
| Acquired leasehold interest, net | 6,979 |
| | 7,075 |
|
| Total other assets | 31,532 |
| | 31,561 |
|
| | $ | 166,320 |
| | $ | 163,051 |
|
The accompanying notes are an integral part of these interim consolidated financial statements.
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
INTERIM CONSOLIDATED BALANCE SHEETS
(in thousands, except share and per share amounts)
(continued)
|
| | | | | | | |
| | March 31,
2017 | | December 31,
2016 |
| | (Unaudited) | | |
| CURRENT LIABILITIES: | | | |
| Current portion of long-term debt and capitalized lease obligations | $ | 7,715 |
| | $ | 7,715 |
|
| Trade accounts payable | 13,913 |
| | 12,972 |
|
| Current liabilities of discontinued operations | 430 |
| | 427 |
|
| Income tax payable | 61 |
| | — |
|
| Accrued expenses: | | | |
| Payroll and employee benefits | 18,538 |
| | 20,108 |
|
| Self-insurance reserves, current portion | 10,157 |
| | 9,401 |
|
| Provider taxes | 2,535 |
| | 3,114 |
|
| Other current liabilities | 3,863 |
| | 4,432 |
|
| Total current liabilities | 57,212 |
| | 58,169 |
|
| NONCURRENT LIABILITIES: | | | |
| Long-term debt and capitalized lease obligations, less current portion and deferred financing costs, net | 75,648 |
| | 72,145 |
|
| Self-insurance reserves, noncurrent portion | 11,685 |
| | 11,766 |
|
| Other noncurrent liabilities | 9,133 |
| | 9,551 |
|
| Total noncurrent liabilities | 96,466 |
| | 93,462 |
|
| COMMITMENTS AND CONTINGENCIES |
| |
|
| SHAREHOLDERS’ EQUITY: | | | |
| Common stock, authorized 20,000,000 shares, $.01 par value, 6,691,000 and 6,592,000 shares issued, and 6,459,000 and 6,361,000 shares outstanding, respectively | 67 |
| | 66 |
|
| Treasury stock at cost, 232,000 shares of common stock | (2,500 | ) | | (2,500 | ) |
| Paid-in capital | 22,044 |
| | 21,935 |
|
| Accumulated deficit | (7,301 | ) | | (8,276 | ) |
| Accumulated other comprehensive loss | 332 |
| | 195 |
|
| Total shareholders’ equity | 12,642 |
|
| 11,420 |
|
| | $ | 166,320 |
| | $ | 163,051 |
|
The accompanying notes are an integral part of these interim consolidated financial statements.
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
INTERIM CONSOLIDATED STATEMENTS OF OPERATIONS
(in thousands, except per share amounts, unaudited)
|
| | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| PATIENT REVENUES, net | $ | 141,500 |
| | $ | 97,945 |
|
| EXPENSES: | | | |
| Operating | 110,667 |
| | 78,618 |
|
| Lease and rent expense | 13,743 |
| | 7,252 |
|
| Professional liability | 2,670 |
| | 2,066 |
|
| General and administrative | 8,973 |
| | 6,734 |
|
| Depreciation and amortization | 2,487 |
| | 2,003 |
|
| Total expenses | 138,540 |
| | 96,673 |
|
| OPERATING INCOME | 2,960 |
| | 1,272 |
|
| OTHER INCOME (EXPENSE): | | | |
| Equity in net income of unconsolidated affiliate | — |
| | 33 |
|
| Gain on sale of investment in unconsolidated affiliate | 733 |
| | — |
|
| Interest expense, net | (1,483 | ) | | (1,070 | ) |
| Debt retirement costs | — |
| | (351 | ) |
| Total other expense | (750 | ) | | (1,388 | ) |
| INCOME (LOSS) FROM CONTINUING OPERATIONS BEFORE INCOME TAXES | 2,210 |
| | (116 | ) |
| BENEFIT (PROVISION) FOR INCOME TAXES | (862 | ) | | 42 |
|
| INCOME (LOSS) FROM CONTINUING OPERATIONS | 1,348 |
| | (74 | ) |
| LOSS FROM DISCONTINUED OPERATIONS: | | | |
| Operating loss, net of tax benefit (expense) of ($9) and $21, respectively | (15 | ) | | (37 | ) |
| NET INCOME (LOSS) | $ | 1,333 |
| | $ | (111 | ) |
| NET INCOME (LOSS) PER COMMON SHARE: | | | |
| Per common share – basic | | | |
| Continuing operations | $ | 0.22 |
| | $ | (0.01 | ) |
| Discontinued operations | — |
| | (0.01 | ) |
| | $ | 0.22 |
| | $ | (0.02 | ) |
| Per common share – diluted | | | |
| Continuing operations | $ | 0.21 |
| | $ | (0.01 | ) |
| Discontinued operations | — |
| | (0.01 | ) |
| | $ | 0.21 |
| | $ | (0.02 | ) |
| COMMON STOCK DIVIDENDS DECLARED PER SHARE OF COMMON STOCK | $ | 0.055 |
| | $ | 0.055 |
|
| WEIGHTED AVERAGE COMMON SHARES OUTSTANDING: | | | |
| Basic | 6,233 |
| | 6,160 |
|
| Diluted | 6,440 |
| | 6,160 |
|
The accompanying notes are an integral part of these interim consolidated financial statements.
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
INTERIM CONSOLIDATED STATEMENTS OF COMPREHENSIVE INCOME
(in thousands and unaudited)
|
| | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| NET INCOME (LOSS) | $ | 1,333 |
| | $ | (111 | ) |
| OTHER COMPREHENSIVE INCOME: | | | |
| Change in fair value of cash flow hedge, net of tax | 254 |
| | 311 |
|
| Less: reclassification adjustment for amounts recognized in net income | (117 | ) | | (144 | ) |
| Total other comprehensive income | 137 |
| | 167 |
|
| COMPREHENSIVE INCOME | $ | 1,470 |
| | $ | 56 |
|
The accompanying notes are an integral part of these interim consolidated financial statements.
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
INTERIM CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands and unaudited)
|
| | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| CASH FLOWS FROM OPERATING ACTIVITIES: | | | |
| Net income (loss) | $ | 1,333 |
| | $ | (111 | ) |
| Discontinued operations | (15 | ) | | (37 | ) |
| Income (loss) from continuing operations | 1,348 |
| | (74 | ) |
| Adjustments to reconcile income (loss) from continuing operations to net cash provided by (used in) operating activities: | | | |
| Depreciation and amortization | 2,487 |
| | 2,003 |
|
| Provision for doubtful accounts | 1,970 |
| | 1,640 |
|
| Deferred income tax provision (benefit) | 354 |
| | (35 | ) |
| Provision for self-insured professional liability, net of cash payments | (83 | ) | | 1,013 |
|
| Stock-based compensation | 241 |
| | 252 |
|
| Equity in net income of unconsolidated affiliate, net of investment | — |
| | (33 | ) |
| Gain on sale of unconsolidated affiliate | (733 | ) | | — |
|
| Debt retirement costs | — |
| | 351 |
|
| Deferred bonus | 500 |
| | — |
|
| Other | 32 |
| | (254 | ) |
| Changes in assets and liabilities affecting operating activities: | | | |
| Receivables, net | (6,518 | ) | | 2,085 |
|
| Prepaid expenses and other assets | 1,081 |
| | (275 | ) |
| Trade accounts payable and accrued expenses | (1,468 | ) | | (1,438 | ) |
| Net cash provided by (used in) continuing operations | (789 | ) | | 5,235 |
|
| Discontinued operations | (67 | ) | | (1,862 | ) |
| Net cash provided by (used in) operating activities | (856 | ) | | 3,373 |
|
| CASH FLOWS FROM INVESTING ACTIVITIES: | | | |
| Purchases of property and equipment | (2,237 | ) | | (8,492 | ) |
| Change in restricted cash | — |
| | 1,658 |
|
| Net cash used in continuing operations | (2,237 | ) | | (6,834 | ) |
| Discontinued operations | — |
| | — |
|
| Net cash used in investing activities | (2,237 | ) | | (6,834 | ) |
| CASH FLOWS FROM FINANCING ACTIVITIES: | | | |
| Repayment of debt obligations | (9,193 | ) | | (57,885 | ) |
| Proceeds from issuance of debt | 12,567 |
| | 62,566 |
|
| Financing costs | (10 | ) | | (1,833 | ) |
| Issuance and redemption of employee equity awards | (94 | ) | | (95 | ) |
| Payment of common stock dividends | (346 | ) | | (342 | ) |
| Payment for preferred stock restructuring | (163 | ) | | (158 | ) |
| Net cash provided by financing activities | 2,761 |
| | 2,253 |
|
| Discontinued operations | — |
| | — |
|
| Net cash provided by financing activities | $ | 2,761 |
| | $ | 2,253 |
|
The accompanying notes are an integral part of these interim consolidated financial statements.
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
INTERIM CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands and unaudited)
(continued)
|
| | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| NET DECREASE IN CASH AND CASH EQUIVALENTS | $ | (332 | ) | | $ | (1,208 | ) |
| CASH AND CASH EQUIVALENTS, beginning of period | 4,263 |
| | 4,585 |
|
| CASH AND CASH EQUIVALENTS, end of period | $ | 3,931 |
| | $ | 3,377 |
|
| SUPPLEMENTAL INFORMATION: | | | |
| Cash payments of interest | $ | 1,231 |
| | $ | 919 |
|
| Cash payments of income taxes | $ | 6 |
| | $ | 229 |
|
The accompanying notes are an integral part of these interim consolidated financial statements.
DIVERSICARE HEALTHCARE SERVICES, INC. AND SUBSIDIARIES
NOTES TO INTERIM CONSOLIDATED FINANCIAL STATEMENTS
MARCH 31, 2017 AND 2016
Diversicare Healthcare Services, Inc. (together with its subsidiaries, “Diversicare” or the “Company”) provides long-term care services to nursing center patients in ten states, primarily in the Southeast, Midwest, and Southwest. The Company’s centers provide a range of health care services to their patients and residents that include nursing, personal care, and social services. Additionally, the Company’s nursing centers also offer a variety of comprehensive rehabilitation services, as well as nutritional support services. The Company's continuing operations include centers in Alabama, Florida, Indiana, Kansas, Kentucky, Mississippi, Missouri, Ohio, Tennessee, and Texas.
As of March 31, 2017, the Company’s continuing operations consist of 76 nursing centers with 8,453 licensed nursing beds. The Company owns 17 and leases 59 of its nursing centers. Our nursing centers range in size from 48 to 320 licensed nursing beds. The licensed nursing bed count does not include 496 licensed assisted and residential living beds.
| |
| 2. | CONSOLIDATION AND BASIS OF PRESENTATION OF FINANCIAL STATEMENTS |
The interim consolidated financial statements include the operations and accounts of Diversicare Healthcare Services and its subsidiaries, all wholly-owned. All significant intercompany accounts and transactions have been eliminated in consolidation. The Company had one equity method investee, which was sold during the fourth quarter of 2016. The Company's share of the profits and losses from this investment are reported as equity in earnings of investment in an unconsolidated affiliate and the proceeds received from the sale are reported under the heading "Gain on sale of investment in unconsolidated affiliate" in the accompanying interim consolidated statement of operations. The sale resulted in a $1,366,000 gain in the fourth quarter of 2016. Subsequently, we recognized an additional gain of $733,000 for the three-month period ended March 31, 2017, related to the liquidation of remaining assets affiliated with the partnership.
The interim consolidated financial statements for the three month periods ended March 31, 2017 and 2016, included herein have been prepared by the Company, without audit, pursuant to the rules and regulations of the Securities and Exchange Commission. Certain information and footnote disclosures normally included in financial statements prepared in accordance with accounting principles generally accepted in the United States of America have been condensed or omitted pursuant to such rules and regulations. In the opinion of management of the Company, the accompanying interim consolidated financial statements reflect all normal, recurring adjustments necessary to present fairly the Company’s financial position at March 31, 2017, and the results of operations for the three month periods ended March 31, 2017 and 2016, and cash flows for the three month periods ended March 31, 2017 and 2016. The Company’s balance sheet information at December 31, 2016, was derived from its audited consolidated financial statements as of December 31, 2016.
The results of operations for the periods ended March 31, 2017 and 2016 are not necessarily indicative of the operating results that may be expected for a full year. These interim consolidated financial statements should be read in connection with the audited consolidated financial statements and notes thereto included in the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2016.
| |
| 3. | RECENT ACCOUNTING GUIDANCE |
In May 2014, the Financial Accounting Standards Board ("FASB") issued Accounting Standards Update ("ASU") No. 2014-09, Revenue from Contracts with Customers (Topic 606), which requires an entity to recognize the amount of revenue to which it expects to be entitled for the transfer of promised goods or services to customers. In March 2016, the FASB issued an update to ASU No. 2014-09 in the form of ASU No. 2016-08, which amended the principal-versus-agent implementation guidance and illustrations in the new revenue guidance. The update clarifies that an entity should evaluate whether it is the principal or the agent for each specified good or service promised in a contract with a customer. In April 2016, the FASB issued another update to the new revenue standard in the form of ASU No. 2016-10, which amends the guidance on identifying performance obligations and the implementation guidance on licensing. In May 2016, ASU No. 2016-12 was issued, which amends the new revenue recognition guidance on transition, collectability, noncash consideration and the presentation of taxes. The new revenue standard (including updates) will be effective for annual and interim reporting periods beginning after December 15, 2017, with early adoption permitted only as of annual reporting periods beginning after December 15, 2016. The Company will adopt the requirements of this standard effective January 1, 2018. We are in the early stages of evaluating the expected adoption method of ASU No. 2014-09, and we are analyzing whether enhancements are needed to our business and accounting systems.
In November 2015, the FASB issued ASU No. 2015-17, Balance Sheet Classification of Deferred Taxes, which changes how deferred taxes are classified on the Company's balance sheets. The Company adopted ASU No. 2015-17 as of January 1, 2017,
and the new standard was applied on a retrospective basis. The adoption of this guidance resulted in a $7,644,000 reclassification between current deferred income taxes and non-current deferred income taxes.
In February 2016, the FASB issued ASU No. 2016-02, Leases. The new standard establishes a right-of-use (ROU) model that requires a lessee to record a ROU asset and a lease liability on the balance sheet for all leases with terms longer than 12 months. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the income statement. The new standard is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. A modified retrospective transition approach is required for lessees for capital and operating leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements, with certain practical expedients available. Disclosures will be required to meet the objective of enabling users of financial statements to assess the amount, timing, and uncertainty of cash flows arising from leases. We anticipate this standard will have a material impact on our consolidated financial statements. While we are continuing to assess all potential impacts of the standard, we currently believe the most significant impact relates to our accounting for building and equipment operating leases and will result in a significant increase in the assets and liabilities on the consolidated balance sheet.
In March 2016, the FASB issued ASU No. 2016-09, Compensation - Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting. The ASU was issued as part of the FASB Simplification Initiative and involves several aspects of accounting for shared-based payment transactions, including the income tax consequences and classification on the statement of cash flows. We adopted this standard as of January 1, 2017. The adoption did not have a material impact on our financial position, results of operations or cash flows.
In June 2016, the FASB issued ASU No. 2016-13, Measurement of Credit Losses on Financial Instruments. This update is intended to improve financial reporting by requiring timelier recognition of credit losses on loans and other financial instruments that are not accounted for at fair value through net income, including loans held for investment, held-to-maturity debt securities, trade and other receivables, net investment in leases and other such commitments. This update requires that financial statement assets measured at an amortized cost be presented at the net amount expected to be collected, through an allowance for credit losses that is deducted from the amortized cost basis. This standard is effective for the fiscal year beginning after December 15, 2019 with early adoption permitted. The Company is in the initial stages of evaluating the impact from the adoption of this new standard on the consolidated financial statements and related notes.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows (Topic 230). The ASU provides clarification regarding how certain cash receipts and cash payments are presented and classified in the statement of cash flows. The guidance addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The ASU is effective for annual and interim periods beginning after December 15, 2017, which will require the Company to adopt these provisions in the first quarter of fiscal 2018 using a retrospective approach. Early adoption is permitted. The Company is currently evaluating the impact this standard will have on our consolidated financial statements.
In November 2016, the FASB issued ASU No. 2016-18, Statement of Cash Flows (Topic 230): Restricted Cash, which requires that the Statement of Cash Flows explain the changes during the period of cash and cash equivalents inclusive of amounts categorized as Restricted Cash. As a result, amounts generally described as restricted cash and restricted cash equivalents should be included with cash and cash equivalents when reconciling the beginning-of-period and end-of-period total amounts shown on the statement of cash flows. The standard is effective for periods beginning after December 15, 2017. The Company plans to adopt this standard on January 1, 2018, and is currently evaluating the impact this standard will have on our consolidated financial statements.
| |
| 4. | LONG-TERM DEBT AND INTEREST RATE SWAP |
The Company has agreements with a syndicate of banks for a mortgage term loan ("Original Mortgage Loan") and the Company’s revolving credit agreement ("Original Revolver"). On February 26, 2016, the Company executed an Amended and Restated Credit Agreement (the "Credit Agreement") which modified the terms of the Original Mortgage Loan and the Original Revolver Agreements dated April 30, 2013. The Credit Agreement increases the Company's borrowing capacity to $100,000,000 allocated between a $72,500,000 Mortgage Loan ("Amended Mortgage Loan") and a $27,500,000 Revolver ("Amended Revolver"). The Amended Mortgage Loan consists of a $60,000,000 term loan facility and a $12,500,000 acquisition loan facility. Loan acquisition costs associated with the Amended Mortgage Loan and the Amended Revolver were capitalized in the amount of $2,162,000 and are being amortized over the five-year term of the agreements.
Under the terms of the amended agreements, the syndicate of banks provided the Amended Mortgage Loan with an original principal balance of $72,500,000 with a five-year maturity through February 26, 2021, and a $27,500,000 Amended Revolver through February 26, 2021. The Amended Mortgage Loan has a term of five years, with principal and interest payable monthly based on a 25-year amortization. Interest on the term and acquisition loan facilities is based on LIBOR plus 4.0% and 4.75%, respectively. A portion of the Amended Mortgage Loan is effectively fixed at 5.79% pursuant to an interest rate swap with an initial notional amount of $30,000,000. As of March 31, 2017, the interest rate related to the Amended Mortgage Loan was 5.0%. The Amended Mortgage Loan balance was $63,679,000 as of March 31, 2017, consisting of $58,390,000 on the term loan facility
and $5,289,000 on the acquisition loan facility. The Amended Mortgage Loan is secured by seventeen owned nursing centers, related equipment and a lien on the accounts receivable of these centers. The Amended Mortgage Loan and the Amended Revolver are cross-collateralized and cross-defaulted. The Company’s Amended Revolver has an interest rate of LIBOR plus 4.0% and is secured by accounts receivable and is subject to limits on the maximum amount of loans that can be outstanding under the revolver based on borrowing base restrictions.
Effective October 3, 2016, the Company entered into the Second Amendment to the Third Amended and Restated Revolver ("Second Amendment"). The Second Amendment increased the Amended Revolver capacity from the $27,500,000 in the Amended Revolver to $52,250,000; provided that the maximum revolving facility be reduced to $42,250,000 on August 1, 2017.
On December 29, 2016, the Company executed a Third Amendment to the Third Amended and Restated Revolver ("Third Amendment"). The Third Amendment modifies the terms of the Amended Mortgage Loan Agreement by increasing the Company’s letter of credit sublimit from $10,000,000 to $15,000,000.
As of March 31, 2017, the Company had $20,000,000 borrowings outstanding under the Amended Revolver compared to $15,000,000 outstanding as of December 31, 2016. The outstanding borrowings on the revolver were used primarily to compensate for accumulated Medicaid and Medicare receivables at recently acquired facilities as these facilities proceed through the change in ownership process with Centers for Medicare & Medicaid Services (“CMS”). Annual fees for letters of credit issued under the Amended Revolver are 3.00% of the amount outstanding. The Company has twelve letters of credit with a total value of $12,352,000 outstanding as of March 31, 2017. Considering the balance of eligible accounts receivable, the letters of credit, the amounts outstanding under the revolving credit facility and the maximum loan amount of $46,308,000, the balance available for borrowing under the Amended Revolver was $9,456,000 at March 31, 2017.
The Company’s debt agreements contain various financial covenants, the most restrictive of which relates to debt service coverage ratios. The Company is in compliance with all such covenants at March 31, 2017.
Interest Rate Swap Transaction
As part of the debt agreements entered into in April 2013, the Company entered into an interest rate swap agreement with a member of the bank syndicate as the counterparty. The Company designated its interest rate swap as a cash flow hedge and the earnings component of the hedge, net of taxes, is reflected as a component of other comprehensive income (loss). In conjunction with the February 26, 2016 amendment to the Credit Agreement, the Company amended the terms of its interest rate swap. The interest rate swap agreement has the same effective date and maturity date as the Amended Mortgage Loan, and has an amortizing notional amount that was $29,125,000 as of March 31, 2017. The interest rate swap agreement requires the Company to make fixed rate payments to the bank calculated on the applicable notional amount at an annual fixed rate of 5.79% while the bank is obligated to make payments to the Company based on LIBOR on the same notional amount.
The Company assesses the effectiveness of its interest rate swap on a quarterly basis, and at March 31, 2017, the Company determined that the interest rate swap was highly effective. The interest rate swap valuation model indicated a net liability of $8,000 at March 31, 2017. The fair value of the interest rate swap is included in “other noncurrent liabilities” on the Company’s interim consolidated balance sheet. The liability related to the change in the interest rate swap included in accumulated other comprehensive loss at March 31, 2017 is $5,000, net of the income tax benefit of $3,000. As the Company’s interest rate swap is not traded on a market exchange, the fair value is determined using a valuation based on a discounted cash flow analysis. This analysis reflects the contractual terms of the interest rate swap agreement and uses observable market-based inputs, including estimated future LIBOR interest rates. The interest rate swap valuation is classified in Level 2 of the fair value hierarchy, in accordance with the FASB guidance set forth in ASC 820, Fair Value Measurement.
| |
| 5. | COMMITMENTS AND CONTINGENCIES |
Professional Liability and Other Liability Insurance
The Company has professional liability insurance coverage for its nursing centers that, based on historical claims experience, is likely to be substantially less than the claims that are expected to be incurred. Effective July 1, 2013, the Company established a wholly-owned, offshore limited purpose insurance subsidiary, SHC Risk Carriers, Inc. (“SHC”), to replace some of the expiring commercial policies. SHC covers losses up to specified limits per occurrence. All of the Company's nursing centers in Florida, and Tennessee are now covered under the captive insurance policies along with most of the nursing centers in Alabama, Kentucky, and Texas. The SHC policy provides coverage limits of either $500,000 or $1,000,000 per medical incident with a sublimit per center of $1,000,000 and total annual aggregate policy limits of $5,000,000. The remaining nursing centers are covered by one of seven claims made professional liability insurance policies purchased from entities unaffiliated with the Company. These policies provide coverage limits of $1,000,000 per claim and have sublimits of $3,000,000 per center, with varying self-insured retention levels per claim and varying aggregate policy limits.
Reserve for Estimated Self-Insured Professional Liability Claims
Because the Company’s actual liability for existing and anticipated professional liability and general liability claims will likely exceed the Company’s limited insurance coverage, the Company has recorded total liabilities for reported and estimated future claims of $19,839,000 as of March 31, 2017. This accrual includes estimates of liability for incurred but not reported claims, estimates of liability for reported but unresolved claims, actual liabilities related to settlements, including settlements to be paid over time, and estimates of legal costs related to these claims. All losses are projected on an undiscounted basis and are presented without regard to any potential insurance recoveries. Amounts are added to the accrual for estimates of anticipated liability for claims incurred during each period, and amounts are deducted from the accrual for settlements paid on existing claims during each period.
The Company evaluates the adequacy of this liability on a quarterly basis. Semi-annually, the Company retains a third-party actuarial firm to assist in the evaluation of this reserve. Since May 2012, Merlinos & Associates, Inc. (“Merlinos”) has assisted management in the preparation of the appropriate accrual for incurred but not reported general and professional liability claims based on data furnished as of May 31 and November 30 of each year. Merlinos primarily utilizes historical data regarding the frequency and cost of the Company's past claims over a multi-year period, industry data and information regarding the number of occupied beds to develop its estimates of the Company's ultimate professional liability cost for current periods.
On a quarterly basis, the Company obtains reports of asserted claims and lawsuits incurred. These reports, which are provided by the Company’s insurers and a third-party claims administrator, contain information relevant to the actual expense already incurred with each claim as well as the third-party administrator’s estimate of the anticipated total cost of the claim. This information is reviewed by the Company quarterly and provided to the actuary semi-annually. Based on the Company’s evaluation of the actual claim information obtained, the semi-annual estimates received from the third-party actuary, the amounts paid and committed for settlements of claims and on estimates regarding the number and cost of additional claims anticipated in the future, the reserve estimate for a particular period may be revised upward or downward on a quarterly basis. Any increase in the accrual decreases results of operations in the period and any reduction in the accrual increases results of operations during the period.
As of March 31, 2017, the Company is engaged in 68 professional liability lawsuits. Ten lawsuits are currently scheduled for trial or arbitration during the next twelve months, and it is expected that additional cases will be set for trial or hearing. The Company’s cash expenditures for self-insured professional liability costs from continuing operations were $2,071,000 and $613,000 for the three months ended March 31, 2017 and 2016, respectively.
Although the Company adjusts its accrual for professional and general liability claims on a quarterly basis and retains a third-party actuarial firm semi-annually to assist management in estimating the appropriate accrual, professional and general liability claims are inherently uncertain, and the liability associated with anticipated claims is very difficult to estimate. Professional liability cases have a long cycle from the date of an incident to the date a case is resolved, and final determination of the Company’s actual liability for claims incurred in any given period is a process that takes years. As a result, the Company’s actual liabilities may vary significantly from the accrual, and the amount of the accrual has and may continue to fluctuate by a material amount in any given period. Each change in the amount of this accrual will directly affect the Company’s reported earnings and financial position for the period in which the change in accrual is made.
Civil Investigative Demand ("CID")
In July 2013, the Company learned that the United States Attorney for the Middle District of Tennessee (DOJ) had commenced a civil investigation of potential violations of the False Claims Act (FCA).
In October 2014, the Company learned that the investigation was started by the filing under seal of a false claims action against the two facilities that were the subject of the original CID. In connection with this matter, between July 2013 and early February 2016, the Company has received three civil investigative demands (a form of subpoena) for documents and information relating to our practices and policies for rehabilitation, and other services, our preadmission evaluation forms ("PAEs") required by TennCare and our Pre-Admission Screening and Resident Reviews ("PASRRs"). The DOJ has also issued CID's for testimony from current and former employees of the Company. The DOJ’s civil investigation of the Company's practices and policies for rehabilitation now covers all of the Company’s centers, but thus far only documents from six of our centers have been requested.
In June 2016, the Company received an authorized investigative demand (a form of subpoena) for documents in connection with a criminal investigation by the DOJ related to our practices with respect to PAEs and PASRRs. The Company has responded to this subpoena and the CID's and continues to provide additional information as requested. The Company cannot predict the outcome of these investigations or the related lawsuits, and the outcome could have a materially adverse effect on the Company, including the imposition of treble damages, criminal charges, fines, penalties and/or a corporate integrity agreement. The Company is committed to provide caring and professional services to its patients and residents in compliance with applicable laws and regulations.
Other Insurance
With respect to workers’ compensation insurance, substantially all of the Company’s employees became covered under either an indemnity insurance plan or state-sponsored programs in May 1997. The Company is completely self-insured for workers’ compensation exposures prior to May 1997. The Company has been and remains a non-subscriber to the Texas workers’ compensation system and is, therefore, completely self-insured for employee injuries with respect to its Texas operations. From June 30, 2003 until June 30, 2007, the Company’s workers’ compensation insurance programs provided coverage for claims incurred with premium adjustments depending on incurred losses. For the period from July 1, 2007 until June 30, 2008, the Company is completely self-insured for workers' compensation exposure. From July 1, 2008 through March 31, 2017, the Company is covered by a prefunded deductible policy. Under this policy, the Company is self-insured for the first $500,000 per claim, subject to an aggregate maximum of $3,000,000. The Company funds a loss fund account with the insurer to pay for claims below the deductible. The Company accounts for premium expense under this policy based on its estimate of the level of claims subject to the policy deductibles expected to be incurred. The liability for workers’ compensation claims is $515,000 at March 31, 2017. The Company has a non-current receivable for workers’ compensation policies covering previous years of $1,138,000 as of March 31, 2017. The non-current receivable is a function of payments paid to the Company’s insurance carrier in excess of the estimated level of claims expected to be incurred.
As of March 31, 2017, the Company is self-insured for health insurance benefits for certain employees and dependents for amounts up to $175,000 per individual annually. The Company provides reserves for the settlement of outstanding self-insured health claims at amounts believed to be adequate. The liability for reported claims and estimates for incurred but unreported claims is $1,488,000 at March 31, 2017. The differences between actual settlements and reserves are included in expense in the period finalized.
| |
| 6. | STOCK-BASED COMPENSATION |
Overview of Plans
In December 2005, the Compensation Committee of the Board of Directors adopted the 2005 Long-Term Incentive Plan (“2005 Plan”). The 2005 Plan allows the Company to issue stock options and other share and cash based awards. Under the 2005 Plan, 700,000 shares of the Company's common stock have been reserved for issuance upon exercise of equity awards granted thereunder. All grants under this plan expire 10 years from the date the grants were authorized by the Board of Directors.
In June 2008, the Company adopted the Advocat Inc. 2008 Stock Purchase Plan for Key Personnel (“Stock Purchase Plan”). The Stock Purchase Plan provides for the granting of rights to purchase shares of the Company's common stock to directors and officers and 150,000 shares of the Company's common stock has been reserved for issuance under the Stock Purchase Plan. The Stock Purchase Plan allows participants to elect to utilize a specified portion of base salary, annual cash bonus, or director compensation to purchase restricted shares or restricted share units (“RSU's”) at 85% of the quoted market price of a share of the Company's common stock on the date of purchase. The restriction period under the Stock Purchase Plan is generally two years from the date of purchase and during which the shares will have the rights to receive dividends, however, the restricted share certificates will not be delivered to the shareholder and the shares cannot be sold, assigned or disposed of during the restriction period. In June 2016, our shareholders approved an amendment to the Stock Purchase Plan to increase the number of shares of our common stock authorized under the Plan from 150,000 shares to 350,000 shares. No grants can be made under the Stock Purchase Plan after April 25, 2028.
In April 2010, the Compensation Committee of the Board of Directors adopted the 2010 Long-Term Incentive Plan (“2010 Plan”), followed by approval by the Company's shareholders in June 2010. The 2010 Plan allows the Company to issue stock appreciation rights, stock options and other share and cash based awards. Under the 2010 Plan, 380,000 shares of the Company's common stock have been reserved for issuance upon exercise of equity awards granted. In April 2017, the Board amended the 2010 Plan, subject to shareholder approval, to increase the shares under the plan to 680,000 and to extend the 2010 Plan to May 31, 2027.
Equity Grants and Valuations
During the three months ended March 31, 2017 and 2016, the Compensation Committee of the Board of Directors approved grants totaling approximately 88,000 and 83,000 shares of restricted common stock to certain employees and members of the Board of Directors, respectively. The fair value of restricted shares are determined as the quoted market price of the underlying common shares at the date of the grant. The restricted shares typically vest 33% on the first, second and third anniversaries of the grant date. Unvested shares may not be sold or transferred. During the vesting period, dividends accrue on the restricted shares, but are paid in additional shares of common stock upon vesting, subject to the vesting provisions of the underlying restricted shares. The restricted shares are entitled to the same voting rights as other common shares. Upon vesting, all restrictions are removed. Summarized activity of the equity compensation plans is presented below:
|
| | | | | | |
| | | | Weighted |
| | Options/ | | Average |
| | SOSARs | | Exercise Price |
| Outstanding, December 31, 2016 | 231,000 |
| | $ | 6.97 |
|
| Granted | — |
| | — |
|
| Exercised | — |
| | — |
|
| Expired or cancelled | (16,000 | ) | | 11.59 |
|
| Outstanding, March 31, 2017 | 215,000 |
| | $ | 6.64 |
|
| | | | |
| Exercisable, March 31, 2017 | 210,000 |
| | $ | 6.56 |
|
|
| | | | | | |
| | | | Weighted |
| | | | Average |
| | Restricted | | Grant Date |
| | Shares | | Fair Value |
| Outstanding, December 31, 2016 | 153,000 |
| | $ | 9.47 |
|
| Granted | 88,000 |
| | 9.98 |
|
| Dividend Equivalents | 1,000 |
| | 10.48 |
|
| Vested | (74,000 | ) | | 9.03 |
|
| Cancelled | — |
| | — |
|
| Outstanding, March 31, 2017 | 168,000 |
| | $ | 9.94 |
|
Summarized activity of the Restricted Share Units for the Stock Purchase Plan is as follows:
|
| | | | | | |
| | | | Weighted |
| | | | Average |
| | Restricted | | Grant Date |
| | Share Units | | Fair Value |
| Outstanding, December 31, 2016 | 54,000 |
| | $ | 11.10 |
|
| Granted | 26,000 |
| | 9.98 |
|
| Dividend Equivalents | 1,000 |
| | 10.48 |
|
| Vested | (37,000 | ) | | 12.11 |
|
| Cancelled | — |
| | — |
|
| Outstanding, March 31, 2017 | 44,000 |
| | $ | 9.58 |
|
Prior to 2016, the Compensation Committee of the Board of Directors also approved grants of Stock Only Stock Appreciation Rights (“SOSARs”) and Stock Options at the market price of the Company's common stock on the grant date. The SOSARs and Options vest 33% on the first, second and third anniversaries of the grant date, and expire 10 years from the grant date. The SOSARs and Options were valued and recorded in the same manner, and will be settled with issuance of new stock for the difference between the market price on the date of exercise and the exercise price. The Company estimated the total recognized and unrecognized compensation related to SOSARs and stock options using the Black-Scholes-Merton equity grant valuation model.
In computing the fair value estimates using the Black-Scholes-Merton valuation model, the Company took into consideration the exercise price of the equity grants and the market price of the Company's stock on the date of grant. The Company used an expected volatility that equals the historical volatility over the most recent period equal to the expected life of the equity grants. The risk free interest rate is based on the U.S. treasury yield curve in effect at the time of grant. The Company used the expected dividend yield at the date of grant, reflecting the level of annual cash dividends currently being paid on its common stock.
While no SOSARs or Options were granted during 2017 and 2016, previously granted SOSARs and Options remain outstanding as of March 31, 2017. The following table summarizes information regarding stock options and SOSAR grants outstanding as of March 31, 2017:
|
| | | | | | | | | | | | | | | | | | |
| | | Weighted | | | | | | | | |
| | | Average | | | | Intrinsic | | | | Intrinsic |
| Range of | | Exercise | | Grants | | Value-Grants | | Grants | | Value-Grants |
| Exercise Prices | | Prices | | Outstanding | | Outstanding | | Exercisable | | Exercisable |
| $10.21 to $10.88 | | $ | 10.64 |
| | 46,000 |
| | $ | 4,000 |
| | 41,000 |
| | $ | 3,000 |
|
| $2.37 to $6.21 | | $ | 5.55 |
| | 169,000 |
| | $ | 833,000 |
| | 169,000 |
| | $ | 833,000 |
|
| | | | | 215,000 |
| | | | 210,000 |
| | |
Stock-based compensation expense is non-cash and is included as a component of general and administrative expense or operating expense based upon the classification of cash compensation paid to the related employees. The Company recorded total stock-based compensation expense of $241,000 and $252,000 in the three month periods ended March 31, 2017 and 2016, respectively.
| |
| 7. | EARNINGS (LOSS) PER COMMON SHARE |
Information with respect to basic and diluted net income (loss) per common share is presented below in thousands, except per share:
|
| | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| Net income (loss) | | | |
| Income (loss) from continuing operations | $ | 1,348 |
| | $ | (74 | ) |
| Loss from discontinued operations, net of income taxes | (15 | ) | | (37 | ) |
| Net income (loss) | $ | 1,333 |
| | $ | (111 | ) |
|
| | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| Net income (loss) per common share: | | | |
| Per common share – basic | | | |
| Income (loss) from continuing operations | $ | 0.22 |
| | $ | (0.01 | ) |
| Loss from discontinued operations | — |
| | (0.01 | ) |
| Net income (loss) per common share – basic | $ | 0.22 |
| | $ | (0.02 | ) |
| Per common share – diluted | | | |
| Income (loss) from continuing operations | $ | 0.21 |
| | $ | (0.01 | ) |
| Loss from discontinued operations | — |
| | (0.01 | ) |
| Net income (loss) per common share – diluted | $ | 0.21 |
| | $ | (0.02 | ) |
| Weighted Average Common Shares Outstanding: | | | |
| Basic | 6,233 |
| | 6,160 |
|
| Diluted | 6,440 |
| | 6,160 |
|
The effects of 46,000 and 62,000 SOSARs and options outstanding were excluded from the computation of diluted earnings per common share in the three months ended March 31, 2017 and 2016, respectively, because these securities would have been anti-dilutive.
8. EQUITY METHOD INVESTMENT
The Company had one equity method investee, which was sold during the fourth quarter of 2016. The Company's share of the net profits and losses of the unconsolidated affiliate are reported as equity in net earnings or losses of unconsolidated affiliate in our statement of operations. For the three-month period ended March 31, 2017, the equity in the net income of an unconsolidated affiliate was zero compared to $33,000 for the three-month period ended March 31, 2016. The proceeds received from the sale are considered in the calculation of the gain on sale of investment in unconsolidated affiliate in our statement of operations. For the three-month period ended March 31, 2017, the gain on the sale of investment in unconsolidated affiliate was $733,000, related to the liquidation of remaining assets affiliated with the partnership.
| |
| 9. | BUSINESS DEVELOPMENTS AND OTHER SIGNIFICANT TRANSACTIONS |
Golden Living Transaction
On August 15, 2016, the Company entered into an Operation Transfer Agreement with Golden Living (the "Lessor") to assume the operations of 22 centers in Alabama and Mississippi.
On October 1, 2016, the Company entered into a Master Lease Agreement (the "Lease") with Golden Living to directly lease eight centers located in Mississippi from the Lessor, which include: (i) a 152-bed skilled nursing center known as Golden Living Center - Amory; (ii) a 130-bed skilled nursing center known as Golden Living Center - Batesville; (iii) a 58-bed skilled nursing center known as Golden Living Center - Brook Manor; (iv) a 119-bed skilled nursing center known as Golden Living Center - Eupora; (v) a 140-bed skilled nursing center known as Golden Living Center - Ripley; (vi) a 140-bed skilled nursing center known as Golden Living Center - Southaven; (vii) a 120-bed skilled nursing center known as Golden Living Center - Eason Blvd; (viii) a 60-bed skilled nursing center known as Golden Living Center - Tylertown. The Lease is triple net and has an initial term of ten years with two separate five year options to extend the term. The Company also assumed the individual leases of a 120-bed center known as Broadmoor Nursing Home, with an initial lease term of ten years with first year rent of $540,000, escalating to $780,000 in the second year, and 2% annually thereafter, and a 99-bed skilled nursing center known as Leake County Nursing Home, with a lease term of two years with annual rent of $300,000.
On November, 1 2016, the Company amended and restated the Lease ("Amended Lease") with the Lessor to directly lease an additional twelve centers located in Alabama from the Lessor, which include: (i) a 87-bed skilled nursing center known as Golden Living Center - Arab; (ii) a 180-bed skilled nursing center known as Golden Living Center - Meadowood; (iii) a 132-bed skilled nursing center known as Golden Living Center - Riverchase; (iv) a 100-bed skilled nursing center known as Golden Living Center - Boaz; (v) a 154-bed skilled nursing center known as Golden Living Center - Foley; (vi) a 50-bed skilled nursing center known as Golden Living Center - Hueytown; (vii) a 85-bed skilled nursing center known as Golden Living Center - Lanett; (viii) a 138-bed skilled nursing center known as Golden Living Center - Montgomery; (ix) a 120-bed skilled nursing center known as Golden Living Center - Oneonta; (x) a 173-bed skilled nursing center known as Golden Living Center - Oxford; (xi) a 94-bed skilled nursing center known as Golden Living Center - Pell City; (xii) a 123-bed skilled nursing center known as Golden Living Center - Winfield. The Amended Lease is triple net and has an initial term of ten years with two separate five years options to extend the term. Base rent for the amended lease is $24,675,000 for the first year and escalates 2% annually thereafter.
2016 Acquisitions
On February 26, 2016, the Company exercised its purchase options to acquire the real estate assets for Diversicare of Hutchinson in Hutchinson, Kansas and Clinton Place in Clinton, Kentucky for $4,250,000 and $3,300,000, respectively. The Company has operated these facilities since February 2015 and April 2012, respectively. Hutchinson is an 85-bed skilled nursing facility, and Clinton is an 88-bed skilled nursing facility. As a result of the consummation of the Agreements, the Company allocated the purchase price and acquisition costs between the assets acquired. The allocation of the purchase price was determined with the assistance of HealthTrust LLC, a third-party real estate valuation firm. The allocation for the assets acquired is as follows:
|
| | | | | | |
| | Hutchinson | Clinton Place |
| Purchase Price | $ | 4,250,000 |
| $ | 3,300,000 |
|
| Acquisition Costs | 43,000 |
| 34,000 |
|
| | $ | 4,293,000 |
| $ | 3,334,000 |
|
| | | |
| Allocation: | | |
| Buildings | 3,443,000 |
| 2,898,000 |
|
| Land | 365,000 |
| 267,000 |
|
| Furniture, Fixtures and Equipment | 485,000 |
| 169,000 |
|
| | $ | 4,293,000 |
| $ | 3,334,000 |
|
2016 Lease Termination
On May 31, 2016, the Company entered into an Agreement with Avon Ohio, LLC to amend the original lease agreement, thus terminating the Company's right of possession of the facility. As a result, the Company incurred lease termination costs of $2,008,000 in the second quarter of 2016. Under the amended agreement, the Company is required to pay $300,000 per year through the term of the original lease agreement, July 31, 2024. For accounting purposes, this transaction was not reported as a discontinued operation, which is in accordance with the modified authoritative guidance for reporting discontinued operations, effective January 1, 2015. A disposal is now required to be reported in discontinued operations only if the disposal represents a strategic shift that has (or will have) a major effect on the Company's operations and financial results.
2016 Sale of Investment in Unconsolidated Affiliate
On October 28, 2016, the Company and its partners entered into an asset purchase agreement to sell the pharmacy joint venture. The sale resulted in a $1,366,000 gain in the fourth quarter of 2016. Subsequently, we recognized an additional gain of $733,000 for the three-month period ended March 31, 2017, related to the final liquidation of remaining net assets affiliated with the partnership.
ITEM 2 – MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
Overview
Diversicare Healthcare Services, Inc. (together with its subsidiaries, “Diversicare” or the “Company”) provides long-term care services to nursing center patients in ten states, primarily in the Southeast, Midwest, and Southwest. The Company’s centers provide a range of health care services to their patients and residents that include nursing, personal care, and social services. Additionally, the Company’s nursing centers also offer a variety of comprehensive rehabilitation services, as well as nutritional support services. The Company's continuing operations include centers in Alabama, Florida, Indiana, Kansas, Kentucky, Mississippi, Missouri, Ohio, Tennessee, and Texas.
As of March 31, 2017, the Company’s continuing operations consist of 76 nursing centers with 8,453 licensed nursing beds. The Company owns 17 and leases 59 of its nursing centers. Our nursing centers range in size from 48 to 320 licensed nursing beds. The licensed nursing bed count does not include 496 licensed assisted living and residential beds.
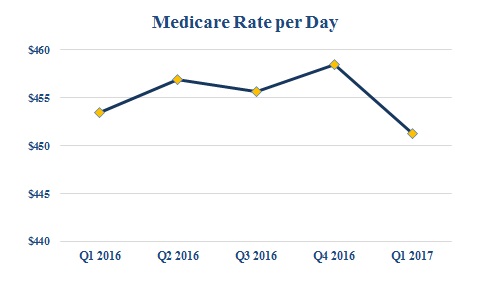
Strategic Operating Initiatives
We identified several key strategic objectives to increase shareholder value through improved operations and business development. These strategic operating initiatives include: improving skilled mix in our nursing centers, improving our average Medicare rate, implementing and maintaining Electronic Medical Records (“EMR”) to improve Medicaid capture, and completing strategic acquisitions. We have experienced success in these initiatives and expect to continue to build on these improvements.
Improving skilled mix and average Medicare rate:
Our strategic operating initiatives of improving our skilled mix and our average Medicare rate required investing in nursing and clinical care to treat more acute patients along with nursing center-based marketing representatives to attract these patients. These initiatives developed referral and Managed Care relationships that have attracted and are expected to continue to attract payor sources for patients covered by Medicare and Managed Care. The Company's skilled mix for the periods ending March 31, 2017 and 2016 was 15.7% and16.3%, respectively. The graph below illustrates our success with increasing our average Medicare rate per day:
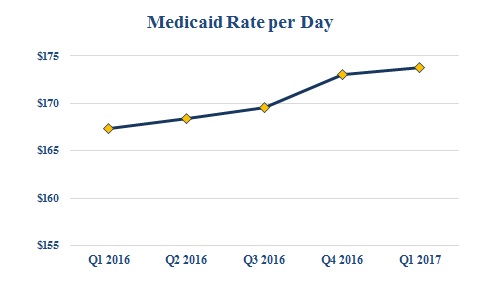
Implementing Electronic Medical Records to improve Medicaid capture:
As another part of our strategic operating initiatives, we implemented EMR to improve Medicaid acuity capture, primarily in our states where the Medicaid payments are acuity based. We completed the implementation of EMR in all our nursing centers in December 2011, on time and under budget, and since implementation, have increased our average Medicaid rate despite rate cuts in certain acuity based states by accurate and timely capture of care delivery. The graph below illustrates our success with increasing our average Medicaid rate per day since implementation:
Completing strategic acquisitions and dispositions:
Our strategic operating initiatives include a renewed focus on completing strategic acquisitions. We continue to pursue and investigate opportunities to acquire, lease or develop new centers, focusing primarily on opportunities within our existing geographic areas of operation.
On October 1, 2016 and November 1, 2016, we assumed the operations of ten centers in Mississippi and 12 centers in Alabama, respectively, which is further discussed in Note 9 to the interim consolidated financial statements. The completion of this acquisition brings the Company's operations to 76 nursing centers with 8,453 skilled nursings beds. These acquired facilities are expected to contribute in excess of $185 million in annual revenues.
As part of our strategic efforts, we have also performed thorough analysis on our existing centers in order to determine whether continuing operations within certain markets or regions was in line with the short-term and long-term strategy of the business. As a result, in May 2016, we ceased operations at our Avon, Ohio, facility, thus terminating our lease with Avon Ohio, LLC. This transaction was not reported as a discontinued operation as described in Note 9 to the interim consolidated financial statements.
Basis of Financial Statements
Our patient revenues consist of the fees charged for the care of patients in the nursing centers we own and lease. Our operating expenses include the costs, other than lease, professional liability, depreciation and amortization expenses, incurred in the operation of the nursing centers we own and lease. Our general and administrative expenses consist of the costs of the corporate office and regional support functions. Our interest, depreciation and amortization expenses include all such expenses across the range of our operations.
Critical Accounting Policies and Judgments
A “critical accounting policy” is one which is both important to the understanding of our financial condition and results of operations and requires management’s most difficult, subjective or complex judgments often involving estimates of the effect of matters that are inherently uncertain. Actual results could differ from those estimates and cause our reported net income or loss to vary significantly from period to period. Our critical accounting policies are more fully described in our 2016 Annual Report on Form 10-K.
Revenue Sources
We classify our revenues from patients and residents into four major categories: Medicaid, Medicare, Managed Care, and Private Pay and other. Medicaid revenues are composed of the traditional Medicaid program established to provide benefits to those in need of financial assistance in the securing of medical services. Medicare revenues include revenues received under both Part A and Part B of the Medicare program. Managed Care revenues include payments for patients who are insured by a third-party entity, typically called a Health Maintenance Organization, often referred to as an HMO plan, or are Medicare beneficiaries who assign
their Medicare benefits to a Managed Care replacement plan often referred to as Medicare replacement products. The Private Pay and other revenues are composed primarily of individuals or parties who directly pay for their services. Included in the Private Pay and other payors are patients who are hospice beneficiaries as well as the recipients of Veterans Administration benefits. Veterans Administration payments are made pursuant to renewable contracts negotiated with these payors.
The following table sets forth net patient and resident revenues related to our continuing operations by payor source for the periods presented (dollar amounts in thousands):
|
| | | | | | | | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 |
| Medicaid | $ | 72,873 |
| | 51.5 | % | | $ | 47,206 |
| | 48.2 | % |
| Medicare | 38,011 |
| | 26.9 |
| | 28,021 |
| | 28.6 |
|
| Managed Care | 10,806 |
| | 7.6 |
| | 7,401 |
| | 7.6 |
|
| Private Pay and other | 19,810 |
| | 14.0 |
| | 15,317 |
| | 15.6 |
|
| Total | $ | 141,500 |
| | 100.0 | % | | $ | 97,945 |
| | 100.0 | % |
The following table sets forth average daily skilled nursing census by payor source for our continuing operations for the periods presented:
|
| | | | | | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | 2016 |
| Medicaid | 4,649 |
| | 68.7 | % | | 3,087 |
| | 66.5 | % |
| Medicare | 792 |
| | 11.7 |
| | 574 |
| | 12.4 |
|
| Managed Care | 273 |
| | 4.0 |
| | 180 |
| | 3.9 |
|
| Private Pay and other | 1,056 |
| | 15.6 |
| | 804 |
| | 17.2 |
|
| Total | 6,770 |
| | 100.0 | % | | 4,645 |
| | 100.0 | % |
Consistent with the nursing home industry in general, changes in the mix of a facility’s patient population among Medicaid, Medicare, Managed Care, and Private Pay and other can significantly affect the profitability of the facility’s operations.
Health Care Industry
The health care industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government health care program participation requirements, reimbursement for patient services, quality of patient care and Medicare and Medicaid fraud and abuse. Over the last several years, government activity has increased with respect to investigations and allegations concerning possible violations by health care providers of fraud and abuse statutes and regulations, false claims statutes, HIPAA violations, as well as laws and regulations governing quality of care issues in the skilled nursing profession in general. Violations of these laws and regulations could result in exclusion from government health care programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed. Compliance with such laws and regulations is subject to ongoing government review and interpretation, as well as regulatory actions in which government agencies seek to impose fines and penalties. The Company is involved in regulatory actions of this type from time to time.
Health care and health insurance reform.
In March 2010, significant legislation concerning health care and health insurance was passed, including the “Patient Protection and Affordable Care Act” (“Patient Protection Act”), along with the “Health Care and Education Reconciliation Act of 2010” (“Reconciliation Act”), collectively defined as the “Legislation.” We expect this Legislation to impact our Company, our employees and our patients in a variety of ways. Some aspects of these new laws have been implemented while others will be phased in over the next several years when all mandates become effective. This Legislation significantly changes the future responsibility of employers with respect to providing health care coverage to employees in the United States. We have not estimated the financial impact of the Legislation and the costs associated with complying with the increased levels of health insurance we will be required to provide our employees and their dependents in future years. We expect the Legislation will result in increased operating expenses.
We also anticipate this Legislation will continue to impact our Medicaid and Medicare reimbursement as well, though the timing and ultimate level of that impact is currently unknown as we anticipate that many of the provisions of the Legislation may be subject to further clarification and modification through the rule making process. The Legislation expands the role of home-based and community services, which may place downward pressure on our sustaining population of Medicaid patients. These reforms
include the possible modifications to the conditions of qualification for payment, bundling of payments to cover both acute and post-acute care and the imposition of enrollment limitations on new providers. The provisions of the Legislation discussed above are examples of recently-enacted federal health reform provisions that we believe may have a material impact on the long-term care industry and on our business. However, the foregoing discussion is not intended to constitute, nor does it constitute, an exhaustive review and discussion of the Legislation.
Skilled nursing centers are required to bill Medicare on a consolidated basis for certain items and services that they furnish to patients, regardless of the cost to deliver these services. This consolidated billing requirement essentially makes the skilled nursing center responsible for billing Medicare for all care services delivered to the patient during the length of stay.
CMS has instituted a number of new exploratory test programs designed to extend the reimbursement and financial responsibilities under consolidated billing beyond the traditional discharge date to include a broader set of bundled services. Such examples may include, but are not exclusive to, home health, durable medical equipment, home and community based services, and the cost of re-hospitalizations during a specified bundled period. Today, these test programs for bundled reimbursement are confined to a small set of clinical conditions. This bundled form of reimbursement could be extended to a broader range of diagnosis related conditions in the future. Because of the untested nature of this new form of reimbursement, the potential impact on skilled nursing center utilization and reimbursement is currently unknown. The process for defining bundled services has not been fully determined by CMS and therefore is subject to change during the rule making process.
Health Insurance Portability and Accountability Act of 1996 Compliance.
The Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) has mandated an extensive set of regulations to standardize electronic patient health, administrative and financial data transactions and to protect the privacy of individually identifiable health information. We have a HIPAA compliance committee and designated privacy and security officers.
The HIPAA transaction standards are intended to simplify the electronic claims process and other healthcare transactions by encouraging electronic transmission rather than paper submission. These regulations provide for uniform standards for data reporting, formatting and coding that we must use in certain transactions with health plans. The HIPAA security regulations establish detailed requirements for safeguarding protected health information that is electronically transmitted or electronically stored. Some of the security regulations are technical in nature, while others are addressed through policies and procedures. We implemented or upgraded computer and information systems as we believe necessary to comply with the new regulations.
The HIPAA regulations related to privacy establish comprehensive federal standards relating to the use and disclosure of individually identifiable health information (“protected health information”). The privacy regulations establish limits on the use and disclosure of protected health information, provide for patients' rights, including rights to access, to request amendment of, and to receive an accounting of certain disclosures of protected health information, and require certain safeguards for protected health information. In addition, each covered entity must contractually bind individuals and entities that furnish services to the covered entity or perform a function on its behalf, and to which the covered entity discloses protected health information, to restrictions on the use and disclosure of that protected health information. In general, the HIPAA regulations do not supersede state laws that are more stringent or grant greater privacy rights to individuals. Thus, we must reconcile the HIPAA regulations and other state privacy laws.
Although we believe that we are in material compliance with these HIPAA regulations, inadvertent violations of these regulations may occur in the course of our business. For this and other reasons, the HIPAA regulations are expected to continue to impact us operationally and financially and may pose increased regulatory risk.
Self-Referral and Anti-Kickback Legislation.
The health care industry is subject to state and federal laws which regulate the relationships of providers of health care services, physicians and other clinicians. These self-referral laws impose restrictions on physician referrals to any entity with which they have a financial relationship, which is a broadly defined term. We believe our relationships with physicians are in compliance with the self-referral laws. Failure to comply with self-referral laws could subject us to a range of sanctions, including civil monetary penalties and possible exclusion from government reimbursement programs. There are also federal and state laws making it illegal to offer anyone anything of value in return for referral of patients. These laws, generally known as “anti-kickback” laws, are broad and subject to interpretations that are highly fact dependent. Given the lack of clarity of these laws, there can be no absolute assurance that any health care provider, including us, will not be found in violation of the anti-kickback laws in any given factual situation. Strict sanctions, including fines and penalties, exclusion from the Medicare and Medicaid programs and criminal penalties, may be imposed for violation of the anti-kickback laws.
Reporting Obligations under Section 111 of the Medicare, Medicaid and SCHIP Extension Act of 2007 (“MMSEA”).
Since January 1, 2010, we have reported specific information regarding all claimants and claim settlements involving Medicare participants so CMS can recover Medicare funds expended to provide healthcare treatment to the claimant. The requirements are to ensure that CMS is notified so that it may recoup the amounts paid for services from the settlement proceeds. This does not
result in us making additional payments to CMS for these services provided and does not result in an incremental cost to us. Strict sanctions, including fines and penalties, exclusion from the Medicare and Medicaid programs and criminal penalties, may be imposed for non-compliance with these reporting obligations.
Medicare and Medicaid Reimbursement
A significant portion of our revenues are derived from government-sponsored health insurance programs. Our nursing centers derive revenues under Medicaid, Medicare, Managed Care, Private Pay and other third party sources. We employ third-party specialists in reimbursement and also use these services to monitor regulatory developments to comply with reporting requirements and to ensure that proper payments are made to our operated nursing centers.
Medicare
Medicare is a federally-funded and administered health insurance program for the aged and for certain chronically disabled individuals. Part A of the Medicare program covers certain services furnished by skilled nursing centers and other institutional providers and inpatient hospital services. Part B covers physician services, durable medical equipment, various outpatient services and certain ancillary services. Medicare generally covers skilled nursing center services for beneficiaries who require nursing care or rehabilitation services after a qualifying hospital stay. Medicare pays a per diem rate for each beneficiary, adjusted for patient acuity and additional factors such as geographic differences in wage rates. The payment rates are set forth under a prospective payment system that uses nursing and therapy indexes to assign a payment rate to each beneficiary. The Centers for Medicare & Medicaid Services (“CMS”) updates the rates annually. The payment rates cover all services to be provided to a beneficiary, including room and board, skilled nursing care, therapy, and medications.
In July 2016, CMS issued its final rule outlining Medicare payment rates and policies for skilled nursing centers for federal fiscal year 2017, which began October 1, 2016. CMS projects that aggregate payments to skilled nursing centers will increase by a net 2.4% for fiscal year 2017. This reflects a 2.7% market basket increase, reduced by a 0.3% multi-factor productivity adjustment required by Patient Protection and Affordable Care Act ("PPACA"). The payment rates for fiscal year 2016, which were projected to increase aggregate payments to skilled nursing centers by 1.2%, reflected a 0.6% forecast error reduction and the 0.5% productivity reduction required by PPACA. For fiscal year 2018, the Medicare Access and CHIP Reauthorization Act of 2015 (“MACRA”) requires the payment update for skilled nursing centers to be 1%.
In addition to the adjustments described above, payment rates are reduced pursuant to ongoing sequestration. The Budget Control Act of 2011 (“BCA”) requires automatic spending reductions to reduce the federal deficit, including Medicare spending reductions of up to 2% per fiscal year, with a uniform percentage reduction across all Medicare programs. CMS began imposing a 2% reduction on Medicare claims in April of 2013. These reductions have been extended through 2025.
CMS has increasingly introduced policies intended to shift Medicare to value-based payment methodologies, tying reimbursement to quality of care rather than quantity. For example, CMS has implemented the Quality Reporting Program, under which skilled nursing centers are required to report quality data. Beginning in fiscal year 2018, skilled nursing centers that fail to submit required data will be subject to a 2% reduction to the annual market basket update. The Skilled Nursing Facility Value-Based Purchasing (“SNF VBP”) Program, which begins on October 1, 2018, will make incentive payments available to skilled nursing centers based on their past performance on a specified quality measure. The first measure under this program is the 30-day potentially preventable readmission measure, which assesses the rate of unplanned, potentially preventable hospital readmissions for skilled nursing center patients within 30 days of discharge from a prior admission to a hospital. CMS will fund the SNF VPB Program incentive payment pool by withholding and then redistributing 2% of skilled nursing center payments, beginning in fiscal year 2019.
In addition, CMS has established the Five-Star Quality Rating System to assist the public in choosing a skilled care provider. Each nursing home is given a rating between 1 and 5 stars, which is published on the Nursing Home Compare website. The overall star rating is determined by three components: information from the last three years of health inspections, staffing information, and quality measures. The rating is based, in part, on the quality data nursing centers are required to report. For example, nursing centers must report the percentage of short-stay residents who are successfully discharged into the community and the percentage who had an outpatient emergency department visit. We remain diligent in continuing to provide outstanding patient care to achieve high rankings for our centers, as well as assuring that our rankings are correct and appropriately reflect our quality results.
Therapy Services. Reimbursement for physical therapy, occupational therapy, and speech-language pathology services covered under Medicare Part B is determined according to the Medicare Physician Fee Schedule (“MPFS”), which is updated annually. If a beneficiary receives multiple therapy treatments in one day, Medicare Part B pays the full rate for the therapy unit of service that has the highest Practice Expense (“PE”) component. A multiple procedure payment reduction is applied to the second and subsequent therapy units, reducing reimbursement to 50% of the applicable PE component.
Therapy services covered under Medicare Part B are subject to an annual dollar-amount payment cap per beneficiary. These limitations on reimbursement are determined on a calendar year basis. For 2017, the limit on incurred expenses is $1,980 per patient for physical and speech therapy services combined, and a separate $1,980 per patient limit applies for occupational therapy
services. Deductible and coinsurance amounts paid by the beneficiary for therapy services count toward the amount applied to the limit.
A temporary two-tier exceptions process permits providers to request reimbursement of therapy services beyond the caps in certain situations. The MACRA extended the exceptions process through December 31, 2017. The first tier, the automatic exceptions process, can be used for claims beyond the caps, up to a $3,700 threshold. The second tier, a targeted review process, may apply when a beneficiary’s incurred expenses exceed a $3,700 threshold. MACRA eliminated a previous requirement for manual medical review of all claims exceeding the $3,700 threshold, instead providing for a targeted post-payment reviews to be conducted by Supplemental Medical Review Contractors. These claim reviews focus on providers with a high percentage of patients receiving therapy beyond the threshold and on therapy provided in specified settings, including skilled nursing centers.
MACRA also provides for a 0.5% increase to the MPFS rates each calendar year through 2019, subject to other adjustments. It required the establishment of the Quality Payment Program (“QPP”), a payment methodology intended to reward high-quality patient care. Beginning in 2017, physicians and certain other clinicians are required to participate in one of two QPP tracks, which will affect Medicare payments in 2019. The Advanced Alternative Payment Model (“Advanced APM”) track makes incentive payments available for participation in specific innovative payment models approved by CMS. A provider with sufficient participation in an Advanced APM is exempt from the reporting requirements and payment adjustments imposed under the second track, the Merit-Based Incentive Payment System (“MIPS”). Providers electing to participate in MIPS will tie payment to performance with respect to clinical quality, resource use, clinical improvement activities, and meaningful use of electronic health records. MIPS will consolidate components of three existing incentive programs, including the Value-Based Payment Modifier program and the Physician Quality Reporting System.
Medicaid
Medicaid is a medical assistance program for the indigent that is funded jointly by the federal and state governments and administered by the states. Federal law requires states to cover certain nursing center services for Medicaid-eligible individuals when other payment options are unavailable. However, Medicaid eligibility requirements and benefits vary by state, and states may impose limitations on nursing services. States may also establish levels of service or payment methodologies by acuity or specialization of a nursing center.
PPACA, as currently structured, requires states to expand Medicaid coverage by adjusting eligibility requirements such as income thresholds. However, the future of the Medicaid expansion is uncertain as a result of the 2016 federal elections. Further, a number of states have opted out of the Medicaid expansion provisions. Some states that opted out of the expansion provisions are evaluating alternatives such as waiver plans to extend or replace existing supplemental payment programs.
For example, effective February 1, 2015, the Company began participating in Indiana's Upper Payment Limit ("UPL") supplemental payment program, which provides supplemental Medicaid payments for skilled nursing centers that are licensed to non-state government entities such as county hospital districts. One skilled nursing center previously operated by the Company entered into a transaction with one such hospital district participating in the UPL program, providing for the transfer of the license from the Company to the hospital district. The Company's operating subsidiary retained the management of the center on behalf of the hospital district. The agreement between the hospital district and the Company is terminable by either party. Termination would fully restore the prior license status.
We receive the majority of our annual Medicaid rate increases during the third quarter of each year. The rate changes received in 2016 and 2015, along with increased Medicaid acuity in our acuity based states, were the primary contributor to our 3.8% increase in average rate per day for Medicaid patients in 2017 compared to 2016. Based on the rate changes received during the third quarter of 2016, we expect a favorable impact to our rate per day for Medicaid patients in 2017 due to modest rate increases in many of the states within which we operate.
Several states in which we operate face budget shortfalls, which could result in reductions in Medicaid funding for nursing centers. Pressures on state budgets are expected to continue in the future. Certain of the states in which we operate are actively seeking ways to reduce Medicaid spending for nursing center care by such methods as capitated payments and substantial reductions in reimbursement rates. Some states are promoting alternatives such as community and home-based services. We are unable to predict what, if any, reform proposals or reimbursement limitations will be implemented in the future, or the effect such changes would have on our operations. For the three months ended March 31, 2017, we derived 26.9% and 51.5% of our total patient revenues related to continuing operations from the Medicare and Medicaid programs, respectively. Any health care reforms that significantly limit rates of reimbursement under these programs could, therefore, have a material adverse effect on our financial position and profitability.
Licensure and Other Health Care Laws
All of our nursing centers must be licensed by the state in which they are located in order to accept patients, regardless of payor source. In most states, nursing centers are subject to certificate of need laws, which require us to obtain government approval for the construction of new nursing centers or the addition of new licensed beds to existing centers. Our nursing centers must comply with detailed statutory and regulatory requirements on an ongoing basis in order to qualify for licensure, as well as for certification as a provider eligible to receive payments from the Medicare and Medicaid programs. Generally, the requirements for licensure and Medicare/Medicaid certification are similar and relate to quality and adequacy of personnel, quality of medical care, record keeping, dietary services, patient rights, and the physical condition of the center and the adequacy of the equipment used therein. Each center is subject to periodic inspections, known as “surveys” by health care regulators, to determine compliance with all applicable licensure and certification standards. Such requirements are both subjective and subject to change. If the survey concludes that there are deficiencies in compliance, the center is subject to various sanctions, including, but not limited to, monetary fines and penalties, suspension of new admissions, non-payment for new admissions and loss of licensure or certification. Generally, however, once a center receives written notice of any compliance deficiencies, it may submit a written plan of correction and is given a reasonable opportunity to correct the deficiencies. There can be no assurance that, in the future, we will be able to maintain such licenses and certifications for our facilities or that we will not be required to expend significant sums in order to comply with regulatory requirements.
Contractual Obligations and Commercial Commitments
We have certain contractual obligations of continuing operations as of March 31, 2017, summarized by the period in which payment is due, as follows (dollar amounts in thousands):
|
| | | | | | | | | | | | | | | | | | | |
| Contractual Obligations | Total | | Less than 1 year | | 1 to 3 Years | | 3 to 5 Years | | After 5 Years |
Long-term debt obligations (1) | $ | 100,135 |
| | $ | 12,422 |
| | $ | 31,641 |
| | $ | 56,072 |
| | $ | — |
|
Settlement obligations (2) | 1,779 |
| | 1,779 |
| | — |
| | — |
| | — |
|
Elimination of Preferred Stock Conversion feature (3) | 1,030 |
| | 687 |
| | 343 |
| | — |
| | — |
|
Operating leases (4) | 1,117,318 |
| | 57,237 |
| | 117,431 |
| | 121,522 |
| | 821,128 |
|
Required capital expenditures under operating leases (5) | 11,522 |
| | 1,262 |
| | 2,515 |
| | 2,511 |
| | 5,234 |
|
| Total | $ | 1,231,784 |
| | $ | 73,387 |
| | $ | 151,930 |
| | $ | 180,105 |
| | $ | 826,362 |
|
| |
| (1) | Long-term debt obligations include scheduled future payments of principal and interest of long-term debt and amounts outstanding on our capital lease obligations. Our long-term debt obligations increased $4.9 million between December 31, 2016 and March 31, 2017, which is related to assumption of operation for the Golden Living centers. See Note 4, "Long-Term Debt and Interest Rate Swap," to the interim consolidated financial statements included in this report for additional information. |
| |
| (2) | Settlement obligations relate to professional liability cases that are expected to be paid within the next twelve months. The professional liabilities are included in our current portion of self-insurance reserves. |
| |
| (3) | Payments to Omega Health Investors ("Omega"), from which we lease 35 nursing centers, for the elimination of the preferred stock conversion feature in connection with restructuring the preferred stock and master lease agreements. Monthly payments of approximately $57,000 will be made through the end of the initial lease period that ends in September 2018. |
| |
| (4) | Represents lease payments under our operating lease agreements. Assumes all renewal periods are enacted. Our operating lease obligations decreased $14.5 million between December 31, 2016 and March 31, 2017. |
| |
| (5) | Includes annual expenditure requirements under operating leases.Our required capital expenditures decreased $1.7 million between December 31, 2016 and March 31, 2017. |
We have employment agreements with certain members of management that provide for the payment to these members of amounts up to two times their annual salary in the event of a termination without cause, a constructive discharge (as defined therein), or upon a change of control of the Company (as defined therein). The maximum contingent liability under these agreements is approximately $1,843,000 as of March 31, 2017. The terms of such agreements are for one year and automatically renew for one year if not terminated by us or the employee. In addition, upon the occurrence of any triggering event, those certain members of management may elect to require that we purchase equity awards granted to them for a purchase price equal to the difference in the fair market value of our common stock at the date of termination versus the stated equity award exercise price. Based on the closing price of our common stock on March 31, 2017, the potential contingent liability for the repurchase of the equity grants is $469,000.
Results of Operations
The following tables present the unaudited interim statements of operations and related data for the three month periods ended March 31, 2017 and 2016:
|
| | | | | | | | | | | | | | | |
| (in thousands) | Three Months Ended March 31, |
| | 2017 | | 2016 | | Change | | % |
| PATIENT REVENUES, net | $ | 141,500 |
| | $ | 97,945 |
| | $ | 43,555 |
| | 44.5 | % |
| EXPENSES: | | | | | | | |
| Operating | 110,667 |
| | 78,618 |
| | 32,049 |
| | 40.8 | % |
| Lease and rent expense | 13,743 |
| | 7,252 |
| | 6,491 |
| | 89.5 | % |
| Professional liability | 2,670 |
| | 2,066 |
| | 604 |
| | 29.2 | % |
| General and administrative | 8,973 |
| | 6,734 |
| | 2,239 |
| | 33.2 | % |
| Depreciation and amortization | 2,487 |
| | 2,003 |
| | 484 |
| | 24.2 | % |
| Total expenses | 138,540 |
| | 96,673 |
| | 41,867 |
| | 43.3 | % |
| OPERATING INCOME | 2,960 |
| | 1,272 |
| | 1,688 |
| | 132.7 | % |
| OTHER INCOME (EXPENSE): | | | | | | | |
| Equity in net income of unconsolidated affiliate | — |
| | 33 |
| | (33 | ) | | (100.0 | )% |
| Gain on sale of investment in unconsolidated affiliate | 733 |
| 0.005180212014 |
| — |
| | 733 |
| | 100.0 | % |
| Interest expense, net | (1,483 | ) | | (1,070 | ) | | (413 | ) | | (38.6 | )% |
| Debt retirement costs | — |
| | (351 | ) | | 351 |
| | (100.0 | )% |
| | (750 | ) | | (1,388 | ) | | 638 |
| | 46.0 | % |
| INCOME FROM CONTINUING OPERATIONS BEFORE INCOME TAXES | 2,210 |
| | (116 | ) | | 2,326 |
| | (2,005.2 | )% |
| BENEFIT (PROVISION) FOR INCOME TAXES | (862 | ) | | 42 |
| | (904 | ) | | 2,152.4 | % |
| INCOME (LOSS) FROM CONTINUING OPERATIONS | $ | 1,348 |
| | $ | (74 | ) | | $ | 1,422 |
| | (1,921.6 | )% |
|
| | | | | | |
| Percentage of Net Revenues | Three Months Ended March 31, |
| | 2017 | | 2016 |
| PATIENT REVENUES, net | 100.0 | % | | 100.0 | % |
| EXPENSES: | | | |
| Operating | 78.2 |
| | 80.3 |
|
| Lease and rent expense | 9.7 |
| | 7.4 |
|
| Professional liability | 1.9 |
| | 2.1 |
|
| General and administrative | 6.3 |
| | 6.9 |
|
| Depreciation and amortization | 1.8 |
| | 2.0 |
|
| Total expenses | 97.9 |
| | 98.7 |
|
| OPERATING INCOME | 2.1 |
| | 1.3 |
|
| OTHER INCOME (EXPENSE): | | | |
| Equity in net losses of unconsolidated affiliate | — |
| | — |
|
| Gain on sale of investment in unconsolidated affiliate | 0.5 |
| — |
| — |
|
| Interest expense, net | (1.0 | ) | | (1.1 | ) |
| Debt retirement costs | — |
| | (0.4 | ) |
| | (0.5 | ) | | (1.5 | ) |
| INCOME (LOSS) FROM CONTINUING OPERATIONS BEFORE INCOME TAXES | 1.6 |
| | (0.2 | ) |
| BENEFIT (PROVISION) FOR INCOME TAXES | (0.6 | ) | | — |
|
| INCOME (LOSS) FROM CONTINUING OPERATIONS | 1.0 | % | | (0.2 | )% |
Three Months Ended March 31, 2017 Compared With Three Months Ended March 31, 2016
Patient Revenues
Patient revenues were $141.5 million and $97.9 million for the three months ended March 31, 2017 and 2016, respectively, an increase of $43.6 million. The following table summarizes the revenue fluctuations attributable to our portfolio growth (in thousands):
|
| | | | | | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 | | Change |
| Same-store revenue | $ | 95,821 |
| | $ | 97,945 |
| | $ | (2,124 | ) |
| 2016 acquisition revenue | 45,679 |
| | — |
| | 45,679 |
|
| Total revenue | $ | 141,500 |
| | $ | 97,945 |
| | $ | 43,555 |
|
The overall increase in revenues of $43.6 million is primarily attributable to revenue contributions from the acquisition of the Golden Living operations in Alabama and Mississippi during the fourth quarter of 2016 of $45.7 million. The increase from the acquisition activity was partially offset by a decrease in same-store revenue of $2.1 million which is explained in more detail below.
For same-store centers, the first quarter of 2017 experienced one less day of operations compared to the first quarter of 2016, resulting in a decrease in revenue of $1.0 million or 1.1%.
On a same-store basis, our Medicare and Private Pay average daily census for the first quarter of 2017 decreased compared to the first quarter of 2016, resulting in decreases in revenue of $1.9 million and $0.4 million, respectively, or 8.0% and 3.9%, respectively. The average Medicare and Medicaid rate per patient day for same-store centers in first quarter of 2017 increased $0.7 million and $0.5 million, respectively, or 2.8% and 1.0%, respectively.
The following table summarizes key revenue and census statistics for continuing operations for each period:
|
| | | | | | | | | | | |
| | Three Months Ended March 31, | | |
| | 2017 | | | | 2016 | | |
| Skilled nursing occupancy | 80.1 | % | | | | 76.7 | % | | |
| As a percent of total census: | | | | | | | |
| Medicare census | 11.7 | % | | | | 12.4 | % | | |
| Medicaid census | 68.7 | % | | | | 66.5 | % | | |
| Managed Care census | 4.0 | % | | | | 3.9 | % | | |
| As a percent of total revenues: | | | | | | | |
| Medicare revenues | 26.9 | % | | | | 28.6 | % | | |
| Medicaid revenues | 51.5 | % | | | | 48.2 | % | | |
| Managed Care revenues | 7.6 | % | | | | 7.6 | % | | |
| Average rate per day: | | | | | | | |
| Medicare | $ | 451.26 |
| | | | $ | 453.51 |
| | |
| Medicaid | $ | 173.75 |
| | | | $ | 167.34 |
| | |
| Managed Care | $ | 381.54 |
| | | | $ | 394.92 |
| | |
Operating Expense
Operating expense increased in the first quarter of 2017 to $110.7 million as compared to $78.6 million in the first quarter of 2016. Operating expense decreased as a percentage of revenue at 78.2% for the first quarter of 2017 as compared to 80.3% for the first quarter of 2016. The following table summarizes the expense increases attributable to our portfolio growth (in thousands):
|
| | | | | | | | | | | |
| | Three Months Ended March 31, |
| | 2017 | | 2016 | | Change |
| Same-store operating expense | $ | 75,383 |
| | $ | 78,618 |
| | $ | (3,235 | ) |
| 2016 acquisition expense | 35,284 |
| | — |
| | 35,284 |
|
| Total expense | $ | 110,667 |
| | $ | 78,618 |
| | $ | 32,049 |
|
The overall increase in operating expense of $32.1 million is primarily attributable the acquisition of the Golden Living operations in Alabama and Mississippi during the fourth quarter of 2016 of $35.3 million.
On a same-store center basis, operating expenses decreased by $3.2 million, which is primarily attributable to a provider tax refund of $2.2 million from the state of Kentucky. Additionally, our bad debt expense and nursing and ancillary costs decreased by $0.6 million and $0.4 million, respectively, in first quarter of 2017 compared to the first quarter of 2016.
One of the largest components of operating expenses is wages, which increased to $65.0 million during the first quarter of 2017 as compared to $45.1 million in the first quarter of 2016, which consistent with above is due to acquisition activity.
Lease Expense
Lease expense increased in the first quarter of 2017 to $13.7 million as compared to $7.3 million in the first quarter of 2016. The increase in lease expense was primarily attributable to the 22 newly leased centers in Alabama and Mississippi, which occurred during the fourth quarter of 2016.
Professional Liability
Professional liability expense was $2.7 million and $2.1 million in the first quarters of 2017 and 2016, respectively. Our cash expenditures for professional liability costs of continuing operations were $2.1 million and $0.6 million for the first quarters of 2017 and 2016, respectively. Professional liability expense and cash expenditures fluctuate from year to year based respectively on the results of our third-party professional liability actuarial studies and on the costs incurred in defending and settling existing claims. See “Liquidity and Capital Resources” for further discussion of the accrual for professional liability.
General and Administrative Expense
General and administrative expense was $9.0 million in the first quarter of 2017 as compared to $6.7 million in the first quarter of 2016, an increase of $2.3 million, but conversely a decrease as a percentage of revenue from 6.9% in 2016 to 6.3% in 2017. The increase in general and administrative expense is primarily attributable to an increase in wages, travel and consulting fees by $1.7 million, $0.1 million and $0.2 million, respectively, which is due to the acquisition of 22 new centers during the fourth quarter of 2016.
Depreciation and Amortization
Depreciation and amortization expense was approximately $2.5 million in the first quarter of 2017 as compared to $2.0 million in 2016. The increase in depreciation expense relates to fixed assets at the newly leased centers.
Gain on sale of investment in unconsolidated affiliate
Gain on the sale of investment in unconsolidated affiliate was $0.7 million for the three months ended March 31, 2017. The Company and its partners entered into an asset purchase agreement to sell the pharmacy joint venture in the fourth quarter of 2016. A gain of $1.4 million was recognized for the period ended December 31, 2016. The additional gain recognized in the first quarter of 2017 is related to the final liquidation of remaining net assets affiliated with the partnership.
Interest Expense, Net
Interest expense was $1.5 million in the first quarter of 2017 and $1.1 million in the first quarter of 2016, an increase of $0.4 million. The increase was primarily attributable to higher debt balances in 2017 as a result of the change in ownership processes for the newly leased Alabama and Mississippi centers.
Income (loss) from Continuing Operations before Income Taxes; Income (loss) from Continuing Operations per Common Share
As a result of the above, continuing operations reported income of $2.2 million before income taxes for the first quarter of 2017 as compared to a loss of $0.1 million for the first quarter of 2016. The provision for income taxes was $0.9 million for the first quarter of 2017, and was inconsequential for the first quarter of 2016. The basic and diluted income per common share from continuing operations was $0.22 and $0.21, respectively, for the first quarter of 2017 as compared to both basic and diluted loss per common share from continuing operations of $0.01 in the first quarter of 2016.
Liquidity and Capital Resources
Liquidity
Our primary source of liquidity is the net cash flow provided by the operating activities of our centers. We believe that these internally generated cash flows will be adequate to service existing debt obligations, fund required capital expenditures as well as provide cash flows for investing opportunities. In determining priorities for our cash flow, we evaluate alternatives available to us and select the ones that we believe will most benefit us over the long-term. Options for our cash include, but are not limited to, capital improvements, dividends, purchase of additional shares of our common stock, acquisitions, payment of existing debt obligations, preferred stock redemptions as well as initiatives to improve nursing center performance. We review these potential uses and align them to our cash flows with a goal of achieving long-term success.
Net cash used in operating activities of continuing operations totaled $0.8 million in the three months ended March 31, 2017, compared to net cash provided by operating activities of continuing operations of $5.2 million in the same period of 2016. One primary driver of the decline in cash provided by operating activities from continuing operations is the acquisition activity that occurred during the fourth quarter of 2016. The Company is required to complete a Change in Ownership ("CHOW") process for each of the nursing centers for which we assumed operations which results in limited cash inflows from the operations at these centers during this initial process.
Our cash expenditures related to professional liability claims of continuing operations were $2.1 million and $0.6 million for three months ended March 31, 2017 and 2016, respectively. Although we work diligently to limit the cash required to settle and defend professional liability claims, a significant judgment entered against us in one or more legal actions could have a material adverse impact on our cash flows and could result in our being unable to meet all of our cash needs as they become due.
Investing activities of continuing operations used cash of $2.2 million and $6.8 million in 2017 and 2016, respectively. The fluctuation is primarily attributable to the asset purchases of Hutchinson and Clinton in February 2016.
Financing activities of continuing operations provided cash of $2.8 million in 2017 primarily due to draws on the Company's revolving credit facility. In 2016, financing activities of continuing operations provided cash of $2.3 million primarily due to the new debt associated with the Company's refinance in February 2016.
Dividends
On April 28, 2017, the Board of Directors declared a quarterly dividend of $0.055 per common share payable to shareholders of record as of June 30, 2017, to be paid on July 14, 2017. While the Board of Directors intends to pay quarterly dividends, the Board will make the determination of the amount of future cash dividends, if any, to be declared and paid based on, among other things, the Company’s financial condition, funds from operations, the level of its capital expenditures and its future business prospects and opportunities.
Professional Liability
The Company has professional liability insurance coverage for its nursing centers that, based on historical claims experience, is likely to be substantially less than the claims that are expected to be incurred. Effective July 1, 2013, the Company established a wholly-owned, offshore limited purpose insurance subsidiary, SHC Risk Carriers, Inc. (“SHC”), to replace some of the expiring commercial policies. SHC covers losses up to specified limits per occurrence. On a per claim basis, coverage for losses in excess of those covered by SHC is maintained through unaffiliated commercial reinsurance carriers. All of the Company's nursing centers in Florida and Tennessee are now covered under the captive insurance policies along with most of the nursing centers in Alabama, Kentucky, and Texas. The insurance coverage provided for these centers under the SHC policy include coverage limits of $0.5 million or $1.0 million per medical incident with a sublimit per center of $1.0 million and total annual aggregate policy limits of $5.0 million. All other centers within the Company’s portfolio are covered through various commercial insurance policies which provide coverage limits of $1.0 million per claim and have sublimits of $3.0 million per center, with varying aggregate policy limits and deductibles.
As of March 31, 2017, we have recorded total liabilities for reported and settled professional liability claims and estimates for incurred, but unreported claims of $19.8 million. Our calculation of this estimated liability is based on an assumption that the Company will not incur a severely adverse judgment with respect to any asserted claim; however, a significant judgment could be entered against us in one or more of these legal actions, and such a judgment could have a material adverse impact on our financial position and cash flows.
Capital Resources
As of March 31, 2017, we had $85.5 million of outstanding long-term debt and capital lease obligations. The $85.5 million total includes $1.8 million in capital lease obligations and $20.0 million currently outstanding on the revolving credit facility. The balance of the long-term debt is comprised of $63.7 million owed on our mortgage loan, which includes $58.4 million on the term loan facility and $5.3 million on the acquisition loan facility.
On February 26, 2016, the Company executed an Amended and Restated Credit Agreement (the "Credit Agreement") which modified the terms of the Original Mortgage Loan and the Original Revolver Agreements dated April 30, 2013. The Credit Agreement increases the Company's borrowing capacity to $100.0 million allocated between a $72.5 million Mortgage Loan ("Amended Mortgage Loan") and a $27.5 million Revolver ("Amended Revolver"). The Amended Mortgage Loan consists of a $60 million term loan facility and a $12.5 million acquisition loan facility. Loan acquisition costs associated with the Amended Mortgage Loan and the Amended Revolver were capitalized in the amount of $2.2 million and are being amortized over the five-year term of the agreements.
Under the terms of the amended agreements, the syndicate of banks provided the Amended Mortgage Loan with an original balance of $72.5 million with a five-year maturity through February 26, 2021, and a $27.5 million Amended Revolver through February 26, 2021. The Amended Mortgage Loan has a term of five years, with principal and interest payable monthly based on a 25-year amortization. Interest on the term and acquisition loan facilities is based on LIBOR plus 4.0% and 4.75%, respectively. A portion of the Amended Mortgage Loan is effectively fixed at 5.79% pursuant to an interest rate swap with an initial notional amount of $30.0 million. As of March 31, 2017, the interest rate related to the Amended Mortgage Loan was 5.00%. The Amended Mortgage Loan is secured by seventeen owned nursing centers, related equipment and a lien on the accounts receivable of these centers. The Amended Mortgage Loan and the Amended Revolver are cross-collateralized and cross-defaulted. The Company’s Amended Revolver has an interest rate of LIBOR plus 4.0% and is secured by accounts receivable and is subject to limits on the maximum amount of loans that can be outstanding under the revolver based on borrowing base restrictions.
Effective October 3, 2016, the Company entered into the Second Amendment to the Third Amended and Restated Revolver ("Second Amendment"). The Second Amendment increased the Amended Revolver capacity from the $27,500,000 in the original Amended Revolver to $52,250,000; provided that the maximum revolving facility be reduced to $42,250,000 on August 1, 2017. The Amended Mortgage Loan balance was $63.7 million as of March 31, 2017, consisting of $58.4 million on the term loan facility and $5.3 million on the acquisition loan facility.
On December 29, 2016, the Company executed a Third Amendment to the Third Amended and Restated Revolver ("Third Amendment"). The Third Amendment modifies the terms of the Loan Agreement by increasing the Company’s letter of credit sublimit from $10.0 million to $15.0 million.
As of March 31, 2017, the Company had $20.0 million borrowings outstanding under the Amended Revolver compared to $15.0 outstanding as of December 31, 2016. The outstanding borrowings on the revolver primarily compensate for accumulated Medicaid and Medicare receivables at recently acquired facilities as these facilities proceed through the change in ownership process with CMS. Annual fees for letters of credit issued under the Amended Revolver are 3.00% of the amount outstanding. The Company has twelve letters of credit with a total value of $12.4 million outstanding as of March 31, 2017. Considering the balance of eligible accounts receivable, the letters of credit, the amounts outstanding under the revolving credit facility and the maximum loan amount of 46.3 million, the balance available for borrowing under the Amended Revolver was $9.5 million at March 31, 2017.
Our lending agreements contain various financial covenants, the most restrictive of which relates to debt service coverage ratios. We are in compliance with all such covenants at March 31, 2017.
Our calculated compliance with financial covenants is presented below:
|
| | | |
| | Requirement | | Level at March 31, 2017 |
| Minimum fixed charge coverage ratio | 1.05:1.00 | | 1.18:1.00 |
| Minimum adjusted EBITDA | $10.0 million | | $13.5 million |
| EBITDAR (mortgaged centers) | $10.0 million | | $14.5 million |
| Current ratio (as defined in agreement) | 1.00:1.00 | | 1.43:1.00 |
As part of the debt agreements entered into in February 2016, we amended our interest rate swap agreement with a member of the bank syndicate as the counterparty. The interest rate swap agreement has the same effective date and maturity date as the Amended Mortgage Loan, and carries an initial notional amount of $30.0 million. The interest rate swap agreement requires us to make fixed rate payments to the bank calculated on the applicable notional amount at an annual fixed rate of 5.79% while the bank is obligated to make payments to us based on LIBOR on the same notional amounts. We entered into the interest rate swap agreement to mitigate the variable interest rate risk on our outstanding mortgage borrowings.
Receivables
Our operations could be adversely affected if we experience significant delays in reimbursement from Medicare, Medicaid or other third-party revenue sources. Our future liquidity will continue to be dependent upon the relative amounts of current assets (principally cash, accounts receivable and inventories) and current liabilities (principally accounts payable and accrued expenses). In that regard, accounts receivable can have a significant impact on our liquidity. Continued efforts by governmental and third-party payors to contain or reduce the acceleration of costs by monitoring reimbursement rates, by increasing medical review of bills for services, or by negotiating reduced contract rates, as well as any delay by us in the processing of our invoices, could adversely affect our liquidity and financial position.
Accounts receivable attributable to patient services of continuing operations totaled $77.8 million at March 31, 2017 compared to $72.5 million at December 31, 2016, representing approximately 45 days and 47 days revenue in accounts receivable, respectively. The decrease in accounts receivable is due to an increase in Medicaid collections from the centers undergoing the change in ownership process.
The allowance for bad debt was $10.8 million at March 31, 2017 as compared to $10.3 million at December 31, 2016. We continually evaluate the adequacy of our bad debt reserves based on patient mix trends, aging of older balances, payment terms and delays with regard to third-party payors, collateral and deposit resources, as well as other factors. We continue to evaluate and implement additional procedures to strengthen our collection efforts and reduce the incidence of uncollectible accounts.
Off-Balance Sheet Arrangements
We have twelve letters of credit outstanding with an aggregate value of approximately $12.4 million as of March 31, 2017. Eleven of these letters of credit serve as a security deposits for certain center leases, while one was issued in conjunction with the initial funding of our wholly-owned captive insurance company. These letters of credit were issued under our revolving credit facility. Our accounts receivable serve as the collateral for this revolving credit facility.
Forward-Looking Statements
The foregoing discussion and analysis provides information deemed by management to be relevant to an assessment and understanding of our consolidated results of operations and financial condition. This discussion and analysis should be read in conjunction with our interim consolidated financial statements included herein. Certain statements made by or on behalf of us, including those contained in this “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere, are forward-looking statements as defined in the Private Securities Litigation Reform Act of 1995. Actual results could differ materially from those contemplated by the forward-looking statements made herein. Forward-looking statements are predictive in nature and are frequently identified by the use of terms such as "may," "will," "should," "expect," "believe," "estimate," "intend," and similar words indicating possible future expectations, events or actions. In addition to any assumptions and other factors referred to specifically in connection with such statements, other factors, many of which are beyond our ability to control or predict, could cause our actual results to differ materially from the results expressed or implied in any forward-looking statements including, but not limited to, our ability to successfully integrate the operations of our new nursing centers in Alabama, Mississippi, Kansas and Kentucky, as well as successfully operate all of our centers, our ability to increase census at our centers, changes in governmental reimbursement, including the impact of the CMS final rule that has resulted in a reduction in Medicare reimbursement and our ability to mitigate the impact of the revenue reduction, government regulation, the impact of the recently adopted federal health care reform or any future health care reform, any increases in the cost of borrowing under our credit agreements, our ability to extend or replace our current credit facility, our ability to comply with covenants contained in those credit agreements, the outcome of professional liability lawsuits and claims, our ability to control ultimate professional liability costs, the accuracy of our estimate of our anticipated professional liability expense, the impact of future licensing surveys, the outcome of proceedings alleging violations of state or Federal False Claims Acts, laws and regulations governing quality of care or other laws and regulations applicable to our business including HIPAA and laws governing reimbursement from government payors, impacts associated with the implementation of our electronic medical records plan, the costs of investing in our business initiatives and development, our ability to control costs, changes to our valuation of deferred tax assets, changes in occupancy rates in our centers, changing economic and competitive conditions, changes in anticipated revenue and cost growth, changes in the anticipated results of operations, the effect of changes in accounting policies as well as others. Investors also should refer to the risks identified in this
“Management's Discussion and Analysis of Financial Condition and Results of Operations” as well as risks identified in “Part I. Item 1A. Risk Factors” in our annual report on Form 10-K for the year ended December 31, 2016, for a discussion of various risk factors of the Company and that are inherent in the health care industry. Given these risks and uncertainties, we can give no assurances that these forward-looking statements will, in fact, transpire and, therefore, caution investors not to place undue reliance on them. These assumptions may not materialize to the extent assumed, and risks and uncertainties may cause actual results to be different from anticipated results. These risks and uncertainties also may result in changes to the Company’s business plans and prospects. Such cautionary statements identify important factors that could cause our actual results to materially differ from those projected in forward-looking statements. In addition, we disclaim any intent or obligation to update these forward-looking statements.
ITEM 3. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
The chief market risk factor affecting our financial condition and operating results is interest rate risk. As of March 31, 2017, we had outstanding borrowings of approximately $83.7 million, $54.4 million of which was subject to variable interest rates. In connection with our February 2016 financing agreement, we entered into an interest rate swap with an initial notional amount of $30.0 million to mitigate the floating interest rate risk of a portion of such borrowing. In the event that interest rates were to change 1%, the impact on future pre-tax cash flows would be approximately $0.5 million annually, representing the impact of increased or decreased interest expense on variable rate debt.
ITEM 4. CONTROLS AND PROCEDURES
As required by Rule 13a-15(b) of the Securities Exchange Act of 1934, as amended (the Exchange Act), our management, including our chief executive officer and chief financial officer, conducted an evaluation of the effectiveness of the design and operation of our disclosure controls and procedures (as defined in Exchange Act Rule 13a-15(e)) as of March 31, 2017. Disclosure controls and procedures include controls and procedures designed to ensure that information required to be disclosed in our reports filed or submitted under the Exchange Act, such as this Quarterly Report on Form 10-Q, is properly recorded, processed, summarized and reported within the time periods required by the Securities and Exchange Commission’s rules and forms. Management necessarily applied its judgment in assessing the costs and benefits of such controls and procedures that, by their nature, can provide only reasonable assurance regarding management’s control objectives. Management does not expect that its disclosure controls and procedures will prevent all errors and fraud. A control system, irrespective of how well it is designed and operated, can only provide reasonable assurance, and cannot guarantee that it will succeed in its stated objectives.
Based on an evaluation of the effectiveness of the design and operation of disclosure controls and procedures, our chief executive officer and chief financial officer concluded that, as of March 31, 2017, our disclosure controls and procedures were effective in reaching a reasonable level of assurance that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time period specified in the Securities and Exchange Commission’s rules and forms.
PART II — OTHER INFORMATION
ITEM 1. LEGAL PROCEEDINGS.
The provision of health care services entails an inherent risk of liability. Participants in the health care industry are subject to lawsuits alleging malpractice, negligence, violations of false claims acts, product liability, or related legal theories, many of which involve large claims and significant defense costs. Like many other companies engaged in the long-term care profession in the United States, we have numerous pending liability claims, disputes and legal actions for professional liability and other related issues. It is expected that we will continue to be subject to such suits as a result of the nature of our business. Further, as with all health care providers, we are periodically subject to regulatory actions seeking fines and penalties for alleged violations of health care laws and are potentially subject to the increased scrutiny of regulators for issues related to compliance with health care fraud and abuse laws and with respect to the quality of care provided to residents of our facilities. Like other health care providers, in the ordinary course of our business, we are also subject to claims made by employees and other disputes and litigation arising from the conduct of our business.
As of March 31, 2017, we are engaged in 68 professional liability lawsuits. Ten lawsuits are currently scheduled for trial or arbitration during the next twelve months, and it is expected that additional cases will be set for trial or hearing. The ultimate results of any of our professional liability claims and disputes cannot be predicted. We have limited, and sometimes no, professional liability insurance with regard to most of these claims. A significant judgment entered against us in one or more of these legal actions could have a material adverse impact on our financial position and cash flows.
In July 2013, the Company learned that the United States Attorney for the Middle District of Tennessee ("DOJ") had commenced a civil investigation of potential violations of the False Claims Act ("FCA").
In October 2014, the Company learned that the investigation was started by the filing under seal of a false claims action against the two centers that were the subject of the original civil investigative demand ("CID"). In connection with this matter, between July 2013 and early February 2016, the Company has received three civil investigative demands (a form of subpoena) for documents and information relating to our practices and policies for rehabilitation, and other services, our preadmission evaluation forms ("PAEs") required by TennCare and our Pre-Admission Screening and Resident Reviews ("PASRRs"). The DOJ has also issued CID’s for testimony from current and former employees of the Company. The DOJ’s civil investigation of the Company’s practices and policies for rehabilitation now covers all of the Company’s centers, but thus far only documents from six of our centers have been requested.
In June 2016, the Company received an authorized investigative demand (a form of subpoena) for documents in connection with a criminal investigation by the DOJ related to our practices with respect to PAEs and PASRRs. The Company has responded to this subpoena and the CID's and continues to provide additional information as requested. The Company cannot predict the outcome of these investigations or the related lawsuits, and the outcome could have a materially adverse effect on the Company, including the imposition of treble damages, criminal charges, fines, penalties and/or a corporate integrity agreement. The Company is committed to provide caring and professional services to its patients and residents in compliance with applicable laws and regulations.
In January 2009, a purported class action complaint was filed in the Circuit Court of Garland County, Arkansas against the Company and certain of its subsidiaries and Garland Nursing & Rehabilitation Center (the “Center”). The complaint alleges that the defendants breached their statutory and contractual obligations to the patients of the Center over the five-year period prior to the filing of the complaints. The lawsuit remains in its early stages and has not yet been certified by the court as a class action. The Company intends to defend the lawsuit vigorously.
We cannot currently predict with certainty the ultimate impact of any of the above cases on our financial condition, cash flows or results of operations. Our reserve for professional liability expenses does not include any amounts for the pending DOJ investigation or the purported class action against the Arkansas centers. An unfavorable outcome in any of these lawsuits or any of our professional liability actions, any regulatory action, any investigation or lawsuit alleging violations of fraud and abuse laws or of elderly abuse laws or any state or Federal False Claims Act case could subject us to fines, penalties and damages, including exclusion from the Medicare or Medicaid programs, and could have a material adverse impact on our financial condition, cash flows or results of operations.
ITEM 1A. RISK FACTORS.
In addition to the other information contained in this Quarterly Report, the risks and uncertainties that we believe could materially affect our business, financial condition or future results and are most important for you to consider are discussed in Part I, “Item 1A. Risk Factors” in our Annual Report on Form 10-K filed with the SEC on March 2, 2017. Additional risks and uncertainties which are not presently known to us, which we currently deem immaterial or which are similar to those faced by other companies in our industry or business in general, may also materially and adversely affect any of our business, financial position or future results.
ITEM 2. UNREGISTERED SALES OF EQUITY SECURITIES AND USE OF PROCEEDS.
None.
ITEM 3. DEFAULTS UPON SENIOR SECURITIES.
None.
ITEM 4. MINE SAFETY DISCLOSURE.
Not applicable.
ITEM 5. OTHER INFORMATION.
None.
ITEM 6. EXHIBITS
The exhibits filed as part of this report on Form 10-Q are listed in the Exhibit Index immediately following the signature page.
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
|
| | | |
| | | | |
| | Diversicare Healthcare Services, Inc. |
| | | |
| May 4, 2017 | | | |
| | | |
| | By: | | /s/ Kelly J. Gill |
| | | | Kelly J. Gill |
| | | | President and Chief Executive Officer, Principal Executive Officer and |
| | | | An Officer Duly Authorized to Sign on Behalf of the Registrant |
| | | |
| | By: | | /s/ James R. McKnight, Jr. |
| | | | James R. McKnight, Jr. |
| | | | Executive Vice President and Chief Financial Officer and |
| | | | An Officer Duly Authorized to Sign on Behalf of the Registrant |
|
| | | |
| | | |
Exhibit Number | | Description of Exhibits |
| 3.1 |
| | Certificate of Incorporation of the Registrant (incorporated by reference to Exhibit 3.1 to the Company’s Registration Statement No. 33-76150 on Form S-1). |
| | |
| 3.2 |
| | Certificate of Designation of Registrant (incorporated by reference to Exhibit 3.5 to the Company’s quarterly report on Form 10-Q for the quarter ended September 30, 2006). |
| | |
| 3.3 |
| | Bylaws of the Company (incorporated by reference to Exhibit 3.2 to the Company’s Registration Statement No. 33-76150 on Form S-1). |
| | |
| 3.4 |
| | Bylaw Amendment adopted November 5, 2007 (incorporated by reference to Exhibit 3.4 to the Company’s annual report on Form 10-K for the year ended December 31, 2007). |
| | |
| 3.5 |
| | Amendment to Certificate of Incorporation dated March 23, 1995 (incorporated by reference to Exhibit A of Exhibit 1 to the Company’s Form 8-A filed March 30, 1995). |
| | |
| 3.6 |
| | Certificate of Designation of Registrant (incorporated by reference to Exhibit 3.4 to the Company’s quarterly report on Form 10-Q for the quarter ended March 31, 2001). |
| | |
| 3.7 |
| | Certificate of Ownership and Merger of Diversicare Healthcare Services, Inc. with and into Advocat Inc. (incorporated by reference to Exhibit 3.1 to the Company's current report on Form 8-K filed March 14, 2013). |
| | | |
| 3.8 |
| | Amendment to Certificate of Incorporation dated June 9, 2016 (incorporated by reference to Exhibit 3.8 to the Company's quarterly report on Form 10-Q for the quarter ended June 30, 2016). |
| | | |
| 3.9 |
| | Bylaw Second Amendment adopted April 14, 2016. |
| | | |
| 4.1 |
| | Form of Common Stock Certificate (incorporated by reference to Exhibit 4 to the Company's Registration Statement No. 33-76150 on Form S-1). |
| | | |
| 31.1 |
| | Certification of Chief Executive Officer pursuant to Rule 13a-14(a) or Rule 15d-14(a). |
| | |
| 31.2 |
| | Certification of Chief Financial Officer pursuant to Rule 13a-14(a) or Rule 15d-14(a). |
| | |
| 32 |
| | Certification of Chief Executive Officer and Chief Financial Officer pursuant to Rule 13a-14(b) or Rule 15d-14(b). |
| | |
| 101.INS |
| | XBRL Instance Document |
| | |
| 101.SCH |
| | XBRL Taxonomy Extension Schema Document |
| | |
| 101.CAL |
| | XBRL Taxonomy Extension Calculation Linkbase Document |
| | |
| 101.LAB |
| | XBRL Taxonomy Extension Labels Linkbase Document |
| | |
| 101.PRE |
| | XBRL Taxonomy Extension Presentation Linkbase Document |